“Every human being deserves dignified health care. Where you were born should not determine whether you live or die.”
FEATURES
12 Lost in the Maze of Cancer
BY ILANA YURKIEWICZ
Can cancer survivorship be transformed for both patients and physicians?
20 A Lifetime of Discovery
BY ALLISON ECK
Immunologists Arlene Sharpe and Gordon Freeman have shared a long journey of scientific exploration.
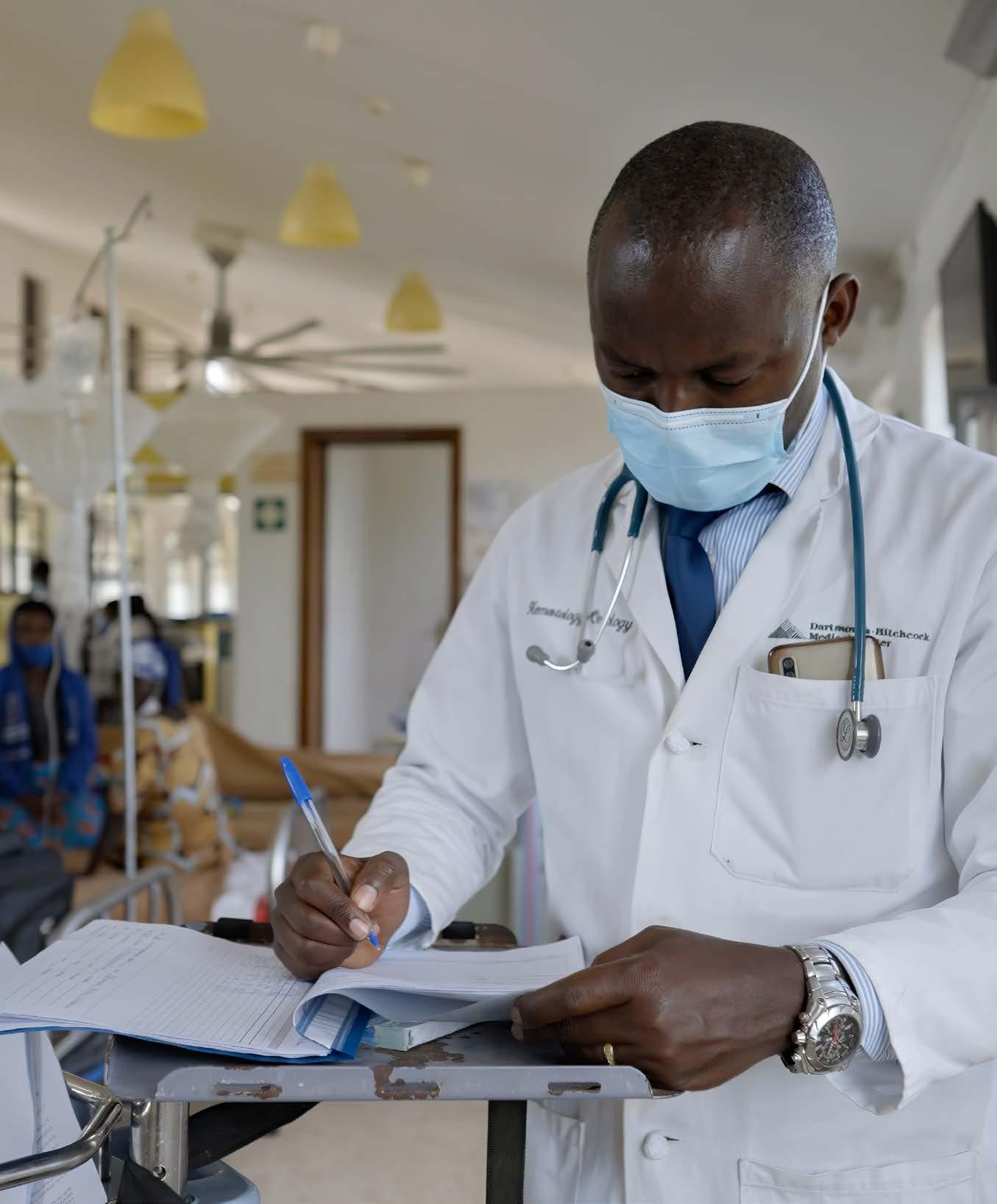
28 Cancer Care from the Ground Up
BY JAKE MILLER
Thanks to the Butaro Cancer Center of Excellence, a cancer diagnosis is no longer a death sentence in Rwanda.
34 Cancer’s Unlikely Accomplice
BY MOLLY MCDONOUGH
Scientists are making surprising discoveries about connections between cancer and the nervous system.
42 From Hype to Health
BY DANIELLE BITTERMAN
What will it take to implement generative AI effectively in clinical settings?
DEPARTMENTS
2 COMMENTARY
A letter from the dean
3 ON CAMPUS
Research and news from Harvard Medical School
9 CLIMATE IN THE CLINIC
BY STEPHANIE DUTCHEN
Preparing Hospitals for a Storm Surge
46 FIVE QUESTIONS
BY EKATERINA PESHEVA
Jessica Whited on the potential of regeneration in salamanders and humans
48 ROOTS
BY CATHERINE CARUSO
Levi Garraway on asking the right questions in cancer research
49 STUDENT LIFE
BY MIKE CAMPBELL AND STEPHANIE M. MCPHERSON
Match Day — plus members of the Class of 2025 on their experiences at HMS
52 ROUNDS
Alumni recall the people and experiences that shaped their careers
“I
saw how living with or after cancer is given short shrift compared to treating cancer — both with health care dollars and cultural norms.”
HARVARD
medicine
Reminders of Our Mission in an Uncertain Time
Today, Harvard Medical School, and all of academic medicine, face extraordinary uncertainty. The freezing of billions of dollars in federal funding to Harvard threatens the HMS budget, but the proposed 40 percent cut to the NIH budget threatens the very foundation of biomedical science in the United States. The termination of grants that is occurring not just at Harvard but across the country will stifle innovation, crucial research, and the training of the next generation of scientists. These developments raise urgent questions about the future of discovery in the United States and the long-standing partnership between the federal government and academic institutions.
Amid this uncertainty, I am grateful to the members of the HMS community who share their stories in this issue. They remind us of the vast scientific progress that has been made, what is at stake, and what we know to be true.
We know that investing in talented scientists who can pursue their curiosity leads to breakthroughs that save lives. The distinguished careers of Arlene Sharpe, MD ’82 PhD ’81, and Gordon Freeman, PhD ’79, offer powerful examples. Their desire to understand the mechanisms of the immune system provided essential contributions to the development of immune checkpoint inhibitors. These therapies, made possible after decades of persistent inquiry, have transformed cancer treatment for many patients.
We know that similar breakthroughs await if investments in biomedical research continue. In the young field of cancer neuroscience, researchers such as William Hwang, MD ’15 PhD ’13, Humsa Venkatesh, and Richard Wong, MD ’94, are extending the boundaries of knowledge. The full impact of their efforts may not be known for years, but their discoveries are already upending old beliefs about how tumors interact with the nervous system and opening up new possibilities for targeted therapies.
We know that HMS alumni and faculty will continue to lead efforts to improve patient care. Work with cancer survivors by Ilana Yurkiewicz, MD ’15, exemplifies the dedication of our community to filling gaps in the health care system. As cancer therapies continue to improve, more and more people find themselves facing both the day-to-day challenges of living with cancer and the existential questions that battling cancer can raise. Yurkiewicz is helping to provide better answers to the question of how to help these patients thrive. Likewise, we know that everyone deserves to benefit from medical advances. Fifteen years ago, there was essentially no cancer care available in Rwanda. But now the Butaro Cancer Center of Excellence treats thousands of patients each year, providing a remarkable example of efforts to ensure that improvements in cancer care reach all those in need, wherever they are.
There is no easy solution to the challenges we face, but I take heart in the strength of the HMS community. Now, as ever, we remain committed to our mission in service to humanity. Thank you for standing with us.
Scientists at HMS have contributed to mapping a critical component of the Nipah virus, a highly lethal bat-borne pathogen that has caused outbreaks in humans almost every year since it was identified in the late 1990s. The advance brings scientists a step closer to developing muchneeded medicines. Currently, there are no vaccines to prevent or mitigate infection with the Nipah virus and no effective treatments for the disease other than supportive care. In the new study, researchers provided a detailed three-dimensional picture of the polymerase complex and its key features. Understanding the structure and behavior of this critical piece of the viral machinery illuminates how the pathogen multiplies inside its hosts.
Hu S, et al., Cell, February 2025
NEUROSCIENCE
How the brain balances risk and reward
Every day, our brain makes thousands of decisions, big and small. Any of these decisions may result in a better or worse outcome — from the least consequential, such as picking a restaurant, to the more important, such as pursuing a different career or moving to a new city.
How does the brain gauge risk and reward in making these calls? The answer to this question continues to puzzle scientists, but a new study carried out by researchers at HMS and Harvard University offers intriguing clues.
The research incorporated machinelearning concepts into mouse experiments to study the brain circuitry that supports reward-based decisions. In the study, Jan Drugowitsch, an associate professor of neurobiology in the Blavatnik Institute at HMS, teamed up with co-senior author Naoshige Uchida, a professor of molecular and cellular biology at Harvard. The researchers trained mice to associate different odors with rewards of varying magnitudes — in essence, teaching mice the range of possible outcomes of a choice. They then presented the mice with odors and observed licking behavior (mice lick more in anticipation of better rewards) while recording neural activity in the ventral striatum.
The team identified two distinct groups of neurons in the brain: one that helps mice learn about better-than-expected outcomes and another tied to worsethan-expected outcomes. Together, the experiments showed, these cells allow the brain to gauge the full range of possible rewards associated with a choice.
“You can think of this as having an optimist and a pessimist in your brain, both giving you advice on what to do next,” Drugowitsch explains.
When the researchers silenced the “optimistic” neurons, the mice exhibited behavior suggesting that they anticipated a less appealing reward. Conversely, when the researchers silenced the “pessimistic” neurons, the mice behaved as if they expected a higher value treat.
“These two groups of brain cells work together to form a representation of the full distribution of potential rewards for a decision,” Drugowitsch says.
The researchers see many future directions for their work, including how
the brain makes decisions when there is more uncertainty about what each initial option represents and how their findings apply to more general reasoning about the world.
Drugowitsch notes that more research is needed to confirm the results in humans and to adapt the findings to the complexity of human decision-making. However, based on the parallels between mouse and human brains, he believes the work may already shed some light on how humans assess risk in decisions and why people with certain conditions such as depression or addiction may struggle with such assessments.
AS, et al., Nature, February 2025
NEUROBIOLOGY
The sound of touch
Ludwig van Beethoven began to lose his hearing at age 28 and was deaf by age 44. Despite his hearing loss, he never ceased to compose music, likely because he was able to sense the vibrations of musical instruments and “hear” music through the sense of touch.
A study by HMS researchers could help explain what enabled Beethoven to develop an exquisitely refined sense of touch after losing his hearing. The findings offer a clue to how and why the diminishment of one sense augments the other and add a surprising twist to our understanding of how the brain and the body work in synchrony to process multiple sensations at the same time.
The research shows that an area in the midbrain called the inferior colliculus — so far studied mostly for its role in processing sound — is also involved in processing touch signals, including mechanical vibrations detected by nerve endings on the skin. The team’s experiments reveal that highfrequency mechanical vibrations picked up by ultra-sensitive mechanoreceptors in the skin called Pacinian corpuscles are not exclusively channeled into the somatosensory cortex — the area of the brain where bodily sensations are processed. Instead, the study found, these signals are mainly routed from the body to the inferior colliculus.
“This is a very surprising finding that counters the canonical view of where and how tactile sensation is processed in the brain,” says David Ginty, senior author of the study, who is chair of the Department
Lowet
of Neurobiology in the Blavatnik Institute at HMS and the Edward R. and Anne G. Lefler Professor of Neurobiology.
In future studies, the researchers are excited to explore whether these findings are a clue to the brain’s capacity for adaptation, specifically researching whether organisms develop enhanced sensitivity to vibration sensing as a compensatory mechanism in instances of hearing loss.
Huey EL, et al., Cell, January 2025
GENETICS
Challenging interpretations
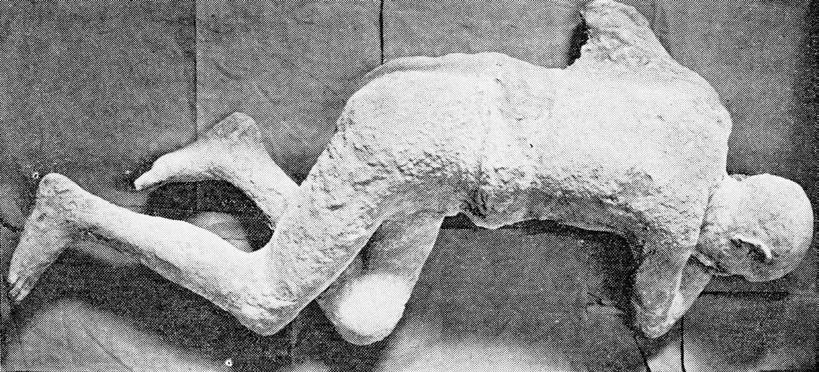
A genetic study of the remains of five people who died in the eruption of Mt. Vesuvius in 79 CE and were cast in plaster calls into question long-held beliefs about the individuals’ sexes and family relationships.
A team led by scientists at HMS, the University of Florence, and the Max Planck Institute for Evolutionary Anthropology retrieved DNA from the individuals in conjunction with the Archaeological Park of Pompeii during restoration of 86 damaged casts in 2015. The results reveal that some of the stories told for decades, which were based on the casts’ physical appearance and other archaeological evidence, are either incorrect or oversimplified.
For example, an adult with a golden bracelet and a child on their lap, often interpreted as mother and son or daughter, turned out to be a genetic male and a biologically unrelated child. Three of four presumed family members at one site had no genetic ties to one another, at least up to the third degree. (The team wasn’t able to analyze DNA from the remains of the fourth
ARCHEOLOGICAL INTERPRETATIONS BASED ON PLASTER CASTS OF PEOPLE KILLED BY THE ERUPTION IN 79 CE OF MT. VESUVIUS HAVE BEEN CALLED INTO QUESTION BY DNA ANALYSIS.
person.) And two individuals lying in a position frequently seen as an embrace — previously hypothesized to be sisters, mother and daughter, or lovers — include at least one genetic male, excluding two of the three common interpretations.
“The findings demonstrate the importance of integrating genetic analysis with archaeological and historical information to enrich or correct narratives constructed based on limited evidence,” says study co-senior author Alissa Mittnik, a former research fellow in genetics at HMS who is now a group leader at the Max Planck Institute.
The authors note that such narratives often reflect the worldviews and biases of researchers and other storytellers at the time. In the case of the Pompeii individuals, the genetic insights should serve as a caution not to make deductions about characteristics like sex and kinship based on evidence like jewelry and physical proximity.
Further complicating the picture is that the remains themselves had been moved into different positions and the plaster casts likely “creatively restored” in the past, the authors write. They also note that some groups of casts reflect the different aesthetic preferences of the historical periods in which they were made.
The authors warn against making similar mistakes based on the new DNA findings.
“Instead of establishing new narratives that might also misrepresent these people’s experiences, the genetic results encourage reflection on the dangers of making up stories about gender and family relationships in past societies based on present-day expectations,” says co-senior author David Reich, a professor of genetics in the Blavatnik Institute at HMS and professor of human evolutionary biology at Harvard University.
The analysis does corroborate previous evidence that ancient Pompeiians largely
descended from people who had immigrated from the eastern Mediterranean.
“This underscores the cosmopolitanism of the Roman Empire in this period,” says Reich.
Pompeii Park has included ancient DNA analysis of humans and animals in its study protocols for years, says director Gabriel Zuchtriegel — augmenting other types of data to form a comprehensive, updated interpretation of the site’s archaeological findings and to develop new research methods that advance understanding of the past.
Pilli E, et al., Current Biology, November 2024
IMMUNOLOGY
Immunity on the mind
Immune cells called regulatory T cells have long been known for their role in countering inflammation. In the setting of infection, these “Tregs” restrain the immune system to ensure it doesn’t go into overdrive and mistakenly attack the body’s own organs.
Recently, HMS scientists discovered a distinct population of Tregs dwelling in the protective layers of the brains of healthy mice with a repertoire much broader than inflammation control. The research shows that these specialized Tregs not only control access to the inner regions of the brain but also ensure the proper renewal of nerve cells in an area of the brain where shortterm memories are formed and stored.
The research represents an important step toward untangling the interplay of immune cells in the brain. If replicated in animal studies and confirmed in humans, the research could open up avenues for averting or mitigating inflammation in the brain.
“We found a thus-far uncharacterized, unique compartment of regulatory T cells residing in the meninges surrounding the brain and involved in an array of protective functions, acting as gatekeepers for other immune cells and involved in nerve cell regeneration,” says study senior author Diane Mathis, the Morton Grove-Rasmussen Professor of Immunohematology in the Blavatnik Institute at HMS.
The work adds to research showing that Tregs go above and beyond their immuneregulatory duties and act as tissue-specific guardians of health, the researchers say.
Marin-Rodero M, et al., Science Immunology, February 2025
Fact and Fiction About the HMS Endowment
A CONVERSATION WITH HMS CHIEF FINANCIAL OFFICER JULIE JONCAS
ASK ANYONE WHICH university has the largest endowment in the world and most will guess correctly that the answer is Harvard. They also will likely have opinions on what Harvard could do with that money. What people may not know is that there are restrictions on how much of these funds an institution can spend each year and what it can spend them on. Just ask Julie Joncas, chief financial officer at HMS since 2022.
In a conversation, Joncas explains some misconceptions about the Harvard University and HMS endowments, reasons behind the current strategy for drawing funds from the endowment, and what that means for the School’s research, education, and community goals, particularly at a time when federal funding for research is at risk.
What is the Harvard University endowment and how does it support Harvard Medical School?
The Harvard University endowment, which had a market value of just over $53 billion as of June 2024, is the sum of more than 14,000 endowment funds given to specific schools, often for specific purposes, since the University’s founding. That amount includes approximately 1,400 gifts, worth about $5.4 billion, that have been given specifically to HMS. These constitute the HMS endowment.
Most of the HMS endowment is designated for financial aid and professorships to support research and teaching. About a third of the gifts to HMS have terms that require the money be used at one of our affiliated hospitals in a clinical setting or for a specific type of research that is
done only at a hospital. In those cases, we act as stewards on behalf of our hospital affiliates. Other gifts have unique terms, such as supporting our library collections.
What are the biggest misconceptions about the Harvard or HMS endowment?
There’s a perception that the endowment is a checking account that can be spent at our discretion. That is not true.
People contribute to an endowment specifically so the gift lasts in perpetuity and continues to support the University and the schools long past when any of us is still here. We never actually touch the original gift. Instead, we invest it and spend only a portion of the income that is generated.
Even then, donors are often very specific about the intent of their contributions, and they put restrictions on those gifts. About 80 percent of Harvard’s endowment funds and about 90 percent of HMS’s endowment funds are subject to donor restrictions, which means we are only allowed to spend the income according to the terms of the gift. That makes it challenging to fund something completely new because there typically isn’t an unrestricted endowment that isn’t already being used elsewhere. It is hard for leadership to pivot quickly if they want to change their strategic course because any new project requires fundraising from scratch. This is why other sources of revenue are important and why we are so grateful to the donors who support new ideas and programs that allow us to remain on the forefront of research and education.
There are so many energetic faculty, postdocs, staff, and students at HMS with endless talent and wonderful ideas, and we will never be able to support all of them through our endowment. We have to be thoughtful about how we spend our resources and be responsible about the pace of spending so we don’t overspend. It’s important to keep in mind as well that endowment income is one part of the
complete picture of University and HMS income. Endowment distributions cover just over 25 percent of HMS’s annual operating expenses. The remaining threequarters have come from other sources, including federal and non-federal research grants, education revenue, and gifts from alumni, parents, and friends.
How are things looking right now?
Unfortunately, it looks like our costs may grow faster than our endowment revenue over the next several years. So, we are exploring a number of ways to keep costs from increasing as much as we expect by identifying ways to use our financial, physical, and technological resources more effectively.
We are not stopping investments in new initiatives, but we need to be thoughtful about what is time sensitive and critical to our strategy. One example of a strategic focus for the medical school
is investing in artificial intelligence, particularly around generative AI.
Why can’t Harvard or HMS use some of the endowment to help during difficult financial times?
Endowment gifts are intended by their donors to benefit both current and future generations of students and scholars. As a result, Harvard is obligated to preserve the purchasing power of these gifts by spending only a fraction of their value each year. Spending significantly more than that over time, for any reason, and even if it were within the restrictions of the gifts, would privilege the present over the future in a manner inconsistent with an endowment’s fundamental purpose of maintaining intergenerational equity. In addition to donor restrictions, the Massachusetts endowment law, which is governed by the Uniform Prudent Management of Institutional Funds Act
HMS SOURCES OF OPERATING REVENUE (FY 2024)
(UPMIFA), outlines rules for managing endowment funds and limits the use of the principal of the endowment.
Harvard has gone through many financial downturns over its history, including market crashes, pandemics, and wartime depression. If, during each of these periods, leaders had spent down the endowment instead of making decisions to reduce spending and programming until income was sufficient to grow again, we would not have the resources we have today.
Although it may seem like a simple solution during challenging financial times to look to the endowment for relief, in order for HMS to remain the number one medical school in the world for another hundred years, we need a strong financial foundation and continued fiscal discipline. It takes all of us making difficult tradeoffs now, in the best interest of the institution, to protect its future for generations to come.
Noteworthy
Risks to funding
Harvard University is responding to announcements and actions by the government that threaten federal research funding at Harvard and other academic institutions.
In early February, the National Institutes of Health (NIH) announced it would cap facilities and administration costs (often referred to as indirect costs) at 15 percent of the value of a grant. Indirect costs typically vary from one institution to another based on location, research facilities, and other factors.
For both Harvard as a whole and HMS, the negotiated rate has typically been 69 percent. Harvard received $488 million in NIH funding over the past year and could lose more than $100 million in annual revenue as a result of the change. John Shaw, Harvard’s vice provost for research, noted in a Harvard Gazette interview that indirect costs received from the NIH do not cover the full costs of research.
The implementation of the cuts was halted by a temporary restraining order issued by a federal judge in response to multiple lawsuits brought by attorneys general of twenty-two states, the Association of American Medical Colleges, and the Association of American Universities, among others. Harvard filed a declaration of support for the AAU lawsuit.
The government has also sought to cut funding to Harvard specifically. On March 31, the administration announced that in response to concerns about antisemitism, it would review nearly $9 billion in federal research funding to Harvard, including that controlled by HMS-affiliated hospitals.
In a community email that evening, President Alan Garber wrote: “If this funding is stopped, it will halt life-saving research and imperil important scientific research and innovation.... For the past fifteen months, we have devoted considerable effort to addressing antisemitism ... and we will continue to combat antisemitism and to foster a campus culture that includes and supports every member of our community.”
On April 11, government officials issued demands that Harvard would need to meet to maintain funding. These included making changes to governance and to admissions and hiring practices; discontinuing all diversity, equity, and inclusion programs; and allowing extensive government oversight of academic matters.
Harvard rejected the demands in a response sent on April 14. In his community email, Garber wrote that “No government — regardless of which party is in power — should dictate what private universities can teach, whom they can admit and hire, and which areas of study and inquiry they can pursue.”
In response, the administration announced it would freeze $2.2 billion in multiyear federal grants and contracts to Harvard. On April 21, Harvard filed a lawsuit to halt the government’s funding freeze.
In early May, the U.S. Department of Education asserted that Harvard would no longer be eligible for new federal grants, and by mid-May, HMS and the University received a large number of grant terminations from the federal government, stopping lifesaving research and, in some cases, causing the loss of years of work.
On May 14, Garber and Provost John Manning reiterated their support for Harvard’s research community and announced that the University would initially dedicate $250 million of central funding to complement School-based resources and strategies to support research affected by the recent grant suspensions and cancellations.
Financial sustainability
HMS is implementing financial sustainability measures to address the challenges caused by overlapping factors, including preexisting budget deficits and threats to federal research funding, which accounts for the largest portion of the School’s annual revenues.
On March 10, in solidarity with guidance issued by the University, HMS announced
“If this funding is stopped, it will halt life-saving research and imperil important scientific research and innovation.”
ALAN GARBER, HARVARD PRESIDENT
a freeze on hiring, School-funded travel, and renovation projects and improvement requests until July 1, later extended to at least September 1. Academic and administrative units were also asked to submit permanent budget cuts of 15 percent beginning with fiscal year 2026.
“Recent uncertainty around the future of federal research funding, coupled with ongoing cost inflation, increased labor costs, and reduced funding for programs and activities, has prompted the need for preemptive measures to ensure the continuation of our education and research mission and core values,” wrote Dean George Q. Daley, MD ’91, and Lisa Muto, executive dean for administration, in their email to the HMS community.
Presidential task forces
On April 29, Harvard released two reports from presidential task forces focused on combating bias on campus: one on antisemitism and anti-Israeli bias, the other on anti-Muslim, anti-Arab, and anti-Palestinian bias. These efforts build on fifteen months of work.
President Garber reaffirmed Harvard’s strong resolve to continuing to take action on recommendations put forward by both task forces. This work is focused on nurturing a widespread sense of belonging and promoting respectful dialogue; revising and implementing policies, procedures, and training; and strengthening academic and residential life.
Many of Harvard’s actions and initiatives began last academic year, guided by the task forces’ preliminary recommendations, released in June 2024. Harvard will continue to advance this work in alignment with the final recommendations.
The full reports are available online, along with Garber’s message about the new University action plan and more information on the steps Harvard has taken to date to respond to the concerns, information, and recommendations.
Preparing Hospitals for a Storm Surge
PROVIDING CARE IN THE AGE OF CLIMATE CHANGE REQUIRES ATTENTION TO PHYSICAL INFRASTRUCTURE
NEW YORK CITY HEALTH care systems did their best to prepare for Hurricane Sandy in 2012. Some had built flood barriers that could handle a storm tide of up to twelve feet — more than two feet higher than had ever been recorded in the area. Then the storm hit, and the tide crested to fourteen feet. Water gushed into hospital buildings and stalled backup generators; the power went out. Staff had to evacuate an estimated 6,500 patients. Five hospitals in the city closed.
Sandy became a regional wake-up call about the need to shore up the physical infrastructure of health care facilities against climate-driven extreme weather events. Hospitals can’t provide needed care if storms or heat waves knock out power, winds tear off the roof, plunging temperatures freeze pipes, or wildfires choke clinics with smoky air.
“Making sure the walls are intact can help your patient’s health, just like giving them an inhaler for their asthma,” says Tess Wiskel, an HMS instructor in emergency medicine at Beth Israel Deaconess
Medical Center. “Thinking about the infrastructure and resilience of health systems will improve patient care and prevent unnecessary morbidity and mortality.”
Climate change already raised the risk of damage to hospitals’ physical infrastructures by 41 percent worldwide and 38 percent in the United States between 1990 and 2020, according to an analysis by XDI (the Cross Dependency Initiative), part of a group of companies committed to quantifying and communicating the costs of climate change. The report estimates that one in twelve hospitals will be at high risk of partial or total shutdown from extreme weather events by the end of the century, including 477 in the United States. Researchers are also documenting hospital damage from extreme weather events and calculating the interrupted care in the months that follow.
“I do think health care systems are waking up to this,” says Gregory Ciottone, HMS associate professor of emergency medicine at Beth Israel, founding direc-
HURRICANE KATRINA DEVASTATED AREAS ALONG THE GULF COAST IN 2005, INCLUDING CAUSING EXTENSIVE DAMAGE TO HEALTH CARE FACILITIES.
tor of the BIDMC fellowship in disaster medicine, and a global expert on medical preparedness for disasters. “The conversation is intensifying as we see dramatic weather-related events in the United States and globally.”
The action, however, does not yet reflect the stakes.
“I think it is essential for hospital leaders to examine what mitigation efforts are necessary to ensure their facilities do not fail during climate emergencies and become unable to serve their communities,” says Paul Biddinger, chief preparedness and continuity officer at Mass General Brigham and an HMS associate professor of emergency medicine. “Unfortunately, I don’t think this issue is receiving adequate attention yet.”
Facilities that receive Medicare and Medicaid funds are required to run hazard vulnerability analyses each year, but studies suggest that only about 20 percent of U.S. health care systems have assessed climate threats to their infrastructure, Biddinger says. Plus, hazard calculations based on historical weather data fail to account for the climate of the present and future, as Biddinger and colleagues — including first author Joshua Baugh, MD ’15, an HMS assistant professor of emergency medicine — wrote in the Rhode Island Medical Journal in 2021.
Given the importance of the issue, HMS community members have taken leadership roles in raising awareness, crafting guidance for medical centers, and building and retrofitting with climate change in mind.
Learning from the front lines
Toolkits, reports, and other materials can help health systems by centering the problem and sharing information and best practices.
Faculty and students at HMS and the Center for Climate, Health, and the Global Environment (C-CHANGE) at Harvard T.H. Chan School of Public Health, including Wiskel, partnered with
the nonprofit Americares to conduct a national survey and produce the Climate Resilience for Frontline Clinics Toolkit, updated in August 2024. Cambridge Health Alliance is among the pilot sites. The Health Care Climate Council, which counts Mass General Brigham among its members, includes infrastructure in its publication Climate Action: A Playbook for Hospitals. Groups such as the WHO, U.S. Department of Health and Human Services, and National Oceanic and Atmospheric Administration have also provided alarm raising and advice.
HMS-authored papers offer further data and case studies. In the last year alone, Ciottone and colleagues published best practices incorporating lessons learned from the Los Angeles wildfires (in The Lancet), Hurricane Helene (in JAMA), and extreme heat, droughts, and fires (in the European Journal of Emergency Medicine).
Recommendations run the gamut, including acquiring backup power and communications systems; raising critical infrastructure above likely flood heights; installing particulate filtration; hiring a disaster medicine expert or naming a weather resilience lead who can advise on risk and infrastructure improvements; procuring emergency supplies in advance in case of medical supply chain failures, such as those that followed Hurricanes Maria and Helene; and procedures for repairing and reentering facilities after weather-related damage.
The need for action extends to Boston. Alexandra Tarabochia-Gast, MD ’17, coauthored a 2022 study in GeoHealth that quantified flood risks to hospitals along the Eastern seaboard. Greater Boston ranked third for predicted impact of a Category 2 hurricane, after only the Miami and New York metro areas. Ciottone cites recent summer droughts, small-scale local wildfires, and smoke that reached the city from Canada as local examples of climate-related challenges. The Boston Globe reported that four emergency departments in the city
had to turn away patients during a historically cold weekend in February 2023 after pipes froze and burst, flooding the facilities.
Building for the future
Partners HealthCare (now Mass General Brigham) took into account the destruction Hurricane Katrina wreaked on health care facilities along the Gulf Coast in 2005 when it designed and constructed the new Spaulding Rehabilitation Hospital, completed in 2013. The hospital’s essential mechanical and electrical equipment, including backup generators, are on the roof. Its first floor was installed thirty inches above the five-hundred-year flood line in preparation for projected sea level rise during the eighty-year life of the building. Triple-glazed windows and sunshades insulate against extreme heat and cold, and they can be unlocked for ventilation in an emergency. Berms, drainage systems, and a green roof can mitigate heavy rain and flooding. There is storage for at least four days of essential supplies. These and other innovations led the Health Care Climate Council to call Spaulding “one of the most sustainable and resilient hospitals in the country.” Partners made the full request for proposal used for the design available for others to adapt.
The effects of Hurricane Sandy in the New York metro area motivated Partners to commission a study of its vulnerabilities to Boston’s future climate, and Mass General Brigham continues to incorpo -
“The U.S. hospital system is already beyond capacity in many places, and if one hospital fails in a crisis, others are severely affected.”
rate findings into its decision-making. Several hospitals began redesigning their HVAC systems to handle higher cooling loads and increase redundancy in case of a power grid failure; others retrofitted facades and roofs to withstand wind speeds previously relegated to places like Miami but now expected in New England.
“Some of the projections were startling and resulted in construction principles we would otherwise have never employed,” Baugh, Biddinger, and their coauthors wrote in their 2021 paper.
A clinical building being erected at Mass General is designed to withstand predicted increases in sea level, precipitation, and days over 90 degrees in the next fifty years. It can also operate selfsufficiently for up to four days and double its occupancy to absorb patients from older, less resilient parts of the hospital during an emergency, Biddinger says.
Boston hospitals also learn from other health systems’ successes. Mass General Brigham is considering procuring the same flood barrier that Tampa General Hospital used to protect itself during Hurricanes Helene and Milton.
Protecting infrastructure requires money, and it must compete with hospitals’ other financial priorities. Yet experts cite several reasons to invest.
First, they reiterate that climate change is inescapable and, as in patient care, prevention is cheaper than postdisaster repairs.
“Crossing your fingers and hoping something doesn’t happen is not a good disaster preparedness strategy,” says Ciottone.
Wiskel learned to change people’s thinking by changing their verbs: “not ‘floods could do this to our hospital,’ but ‘floods will.’”
Second, costs may not be as high as feared if they’re incorporated into plans early. Spaulding estimates its climate resilience features accounted for as little as 0.3 percent of the construction total because they were embedded in the initial design.
Third, individual health care systems do not need to prepare for all eventualities all at once. They can identify the climate risks that apply to their region
and prioritize them by likelihood, expected impact, and what the facility is currently prepared to handle, experts advise. Decisions can be slated for the short or long term and for retrofitting or new construction.
Finally, preparing for climate and other emergencies — including but not limited to infrastructure considerations — raises hospitals’ financial, operational, and energy efficiency, says Ciottone.
Such preparedness involves considering the infrastructure that allows staff and patients to get to hospitals, planning and practicing emergency procedures, and coordinating with other health care institutions and local government. It’s all part of bolstering a health care system that is both crucial and fragile.
“The U.S. hospital system is already beyond capacity in many places, and if one hospital fails in a crisis, others are severely affected,” says Biddinger. “We are all extremely interdependent.”
STEPHANIE DUTCHEN IS EDITORIAL DIRECTOR IN THE HMS OFFICE OF COMMUNICATIONS AND EXTERNAL RELATIONS.
THE DESIGN OF SPAULDING REHABILITATION HOSPITAL TOOK INTO ACCOUNT CLIMATE PROJECTIONS.
LOST CANCER MAZE OF IN THE
A growing number of patients living with and after cancer are shuffled between oncology and primary care. Can survivorship be transformed for both patients and physicians?
By Ilana Yurkiewicz, MD ’15
illustration by mark weaver photographs by winni wintermeyer
Kate is a software engineer, mom, and cancer survivor — though she might hesitate to define herself with that last term. After a hike one summer day her hip began to ache. Soon the pain was so searing it woke her from sleep. An X-ray showed it wasn’t bursitis, as her primary doctor initially suspected, but a rare bone tumor called osteosarcoma. She underwent a seven-hour surgery that removed a good portion of her femur and replaced it with a prosthetic. This was flanked by six cycles of grueling chemotherapy. She slept fourteen hours a day, vomited frequently, and was hospitalized several times to receive IV fluids.
Six months later, a chest CT to ensure she was in remission caught the tip of her adrenal glands. There looked to be a mass, the radiologist noted. Kate felt numb. She knew osteosarcoma could metastasize even after all the treatment she had received. She tried to remain calm as she methodically went through the next steps. Another CT scan focused on her adrenal glands, and there it was: a tumor the size of a grapefruit. Her surgeon conferred with her oncologist and decided to go straight to surgery, as a biopsy could spread cancer cells with the needle. When the pathology results came back, there was good news and bad news. The good: It wasn’t metastatic sarcoma. The bad: It was a new, second cancer, adrenal carcinoma.
“I SAW HOW LIVING WITH OR AFTER CANCER IS GIVEN SHORT SHRIFT COMPARED TO TREATING CANCER — BOTH WITH HEALTH CARE DOLLARS AND CULTURAL NORMS.”
It was then that her oncologist referred her for genetic testing. Kate had two rare cancers before her fortieth birthday. Did cancer run in the family? Kate didn’t know — she wasn’t close with her family. The genetic test came back positive for Li-Fraumeni syndrome, an inherited condition involving a mutation in a gene called TP53. Colloquially called the guardian of the genome, TP53 is responsible for repairing genetic errors that could lead to cancers. With that mechanism impaired, the lifetime risk of cancer is over 90 percent. Many, like Kate, are diagnosed young. Many develop more than one cancer.
I met Kate in Stanford’s Primary Care for Cancer Survivorship program, a clinic I codirect that provides comprehensive primary care for patients along the cancer continuum. My clinic is a landing pad for four groups: 1) survivors of childhood cancers who have reached adulthood, 2) survivors of adult cancers who have
Cancer Survivors by Age Group (2022)
completed treatment, 3) adults receiving ongoing cancer-directed therapies, including those living with metastatic disease, and 4) “previvors” — people who haven’t been diagnosed with cancer but who carry an inherited genetic mutation, such as Li-Fraumeni, conferring elevated risk for developing it. In addition to the primary care practice, I see survivors and previvors in a consultative role, where I help bridge the gaps between their cancer care and primary care.
At our first visit, Kate came with many questions. Her hip still ached, her brain felt foggy, and chemotherapy had pushed her into an accelerated menopause. Were the drenching night sweats she was experiencing related to that or suggestive of something more sinister? Her abdomen felt numb over the surgical scar — would it stay that way forever? When should she test her children, now 8 and 6, for LiFraumeni syndrome?
As we got to know each other, more
Ilana Yurkiewicz codirects Stanford’s Primary Care for Cancer Survivorship program.
concerns bubbled to the surface. She took stock of all the radiation she received before she learned about her genetic risk and ruminated on what cancers might have been provoked. Her relationship with her husband was fraying, she feared, as the emotional energy flowed one way since cancer entered their lives. The medical bills hit right as she had to cut back at work.
And, there was the question underlying all the others: How should she live, knowing cancer could strike again at any moment?
Becoming a champion
I never envisioned a career where I could provide comprehensive, ongoing medical care to patients like Kate. In residency I was torn between primary care and oncology. Both encompass the medicine I value most: care for the whole patient, diagnostic complexity, a mix of emergencies and longer-term follow-up, and space for hard conversations. I pursued fellowship in hematology and oncology because I imagined becoming an oncologist was as close as I could get to being a primary doctor for patients with cancer.
But oncologists, I learned, are very much specialists whose expertise lies in treatment. When new problems landed in gray zones, I watched as oncologists advised patients to see their primary care physicians while primary care physicians told patients to ask their oncologists. I saw patients suppress concerns because of external and internalized pressures to celebrate cancer-free scans. I didn’t have the language of cancer survivorship at the time. What I saw were unmet needs. I was independently discovering what the literature has been sounding the alarm on since 2006, when the Institute of Medicine (IOM) published the report From Cancer Patient to Cancer Survivor: Lost in Transition. The report recognized survivorship as a distinct phase of the cancer spectrum, acknowledged the need to improve education of providers
about survivorship, and called for the dissemination of survivorship care plans to inform patients about what to expect after treatment.
Even earlier, in 1986, the advocacy organization National Coalition for Cancer Survivorship (NCCS) generated the language for survivorship we still use today. A cancer survivor, the NCCS said, is any individual who has experienced cancer from the day of diagnosis. Notably, family members, friends, and caregivers were also included in the definition.
Other papers delineated the gaps between oncology and primary care. “I have not found a provider who understands both sides of my current needs,” one survivor was quoted as saying in a 2010 study. “Internists do not understand my cancer and oncologists do not understand my noncancer health maintenance needs, such as monitoring cholesterol and blood pressure.”
But despite these clarion calls in the literature, I found that survivorship in practice was limited and ad hoc. I saw
how living with or after cancer is given short shrift compared to treating cancer — both with health care dollars and cultural norms. “It takes a champion,” one physician who led a successful program advised me.
After completing my fellowship in 2021, I wanted to leverage my expertise in medical oncology, hematology, and internal medicine to be a one-stop shop for the cancer survivor and previvor. A few years earlier, a primary care physician and my now codirector, Jennifer Kim, under the guidance of Stanford’s Director of Cancer Survivorship, Lidia Schapira, piloted survivorship visits in the primary care setting. I joined the Stanford Primary Care faculty to establish my clinic with a slightly different practice model. I drew inspiration from geriatrics; just as a geriatrician is a primary care physician with a focus on older adults, I would be a primary care physician with a focus on patients with cancer. The only similar model I could find was the Primary Care for Cancer Survivors Program at Johns
Cancer Survivors by Years Since Diagnosis (2022)
Hopkins. Its founder, Kimberly Peairs, kindly walked me through the lessons they had learned.
I quickly built a clinic of about three hundred cancer survivors and previvors within my approximately thousandpatient primary care practice. I treat more than one hundred others in my consultative role, where I continue to see new patients weekly. I see patients with all cancer types, from the most common breast and colon cancers to the rarest leukemias and sarcomas. I see entire families with hereditary cancer syndromes such as BRCA and Lynch syndrome. My work is both reactive — evaluating any new symptoms patients notice and interpreting them within the context of their cancer history — and proactive — reviewing that history and laying out plans to catch issues before they become problems. Survivorship means untangling what was caused by cancer or its treatment from what is not. It means improving what can be improved, while helping people navigate a new normal.
There is the 63-year-old writer who survived breast cancer. For two years she followed her oncologist’s advice to the letter and took a daily hormone blocker that kept her cancer in remission but also torpedoed her productivity and mood. She was advised to continue for five years total, but could she really take another three years of this? We reviewed her early stage, low-grade cancer and calculated her 10-year chances of survival to be 87 percent without the medication and 89 percent with it. With that data in hand, she felt empowered to stop. We monitor closely with mammograms and physical exams. Energy restored, she recently finished writing her fourth book.
There is the 50-year-old athlete who completed months of surgery, radiation, and chemotherapy for breast cancer. Monitoring her overall health meant keeping an eye on lung nodules noted incidentally on one of her many scans. One afternoon her CT scan revealed not only nodules but enlarged lymph nodes.
“HOW CAN WE TRANSFORM CANCER SURVIVORSHIP FROM AN AD HOC NETWORK OF CHAMPIONS INTO A FORMAL BRANCH OF MEDICINE WITH TRAINING, STANDARDS, AND ACCESS?”
I asked how she was feeling. “Not great,” she admitted. For the past few weeks, she had felt exhausted by her usual bike ride. Then she noticed gum bleeding. I immediately ordered lab tests. When two blood cell lines returned abnormally low, I called my patient and told her to go straight to the emergency department. The next day, the flow cytometry I ordered confirmed my fears: an aggressive leukemia called t-AML (therapy-related acute myeloid leukemia), precipitated by the very treatment that cured her breast cancer. Her life is radically changed after surviving her secondary cancer, but, miraculously, she is back to biking ten miles a day.
There is the 22-year-old lymphoma survivor who — haunted by a long ICU stay, countless lumbar punctures, and not knowing whether he’d live to see his high school graduation — stopped coming to medical appointments entirely. Just walking into a medical building like mine caused him tremendous anxiety. His sleep was wrecked. Once worried about being underweight, he was now fifty pounds overweight. I connected him with a support group, and he agreed to try antidepressants. With the energy to tackle other issues, we scheduled a litany of vaccines that he needed to redo after his bone marrow transplant. Now we’re working on weight; we figured out that radiation to the neck had caused hypothyroidism, making it difficult to drop pounds. We have reduced the number of specialists he sees from four to one, eliminating at least one obstacle that made recovery after cancer so daunting.
In each case, I imagine the alternative. What if our clinic did not exist? Perhaps the first patient would have accepted a major professional hit as par for the course for clean mammograms. The second may have been referred to a hematologist as an outpatient, resulting in dangerous delays that could have caused a life-threatening bleed. The third might have continued to suffer alone, in more ways than one. Of course, I can’t say any of this for sure. But I can imagine, because
I’ve seen similar outcomes in those who lack survivorship care. And they are often missed by quality metrics in oncology that focus on remission and longevity, as well as those in primary care that use a one-size-fits-all approach to things like vaccines and cancer screenings.
Studying the model
After about a year in practice, I knew the only way to improve the new model of primary care and survivorship wrapped into one clinic was to put it under a microscope. I assembled a team to help me study the clinic’s successes and shortcomings. Where were we helping, and what continued to be missed?
Step one was creating a database. My colleague Natasha Steele and I formulated a list of common survivorship issues: cancer-related fatigue, neuropathy, cognitive changes, bone health, fertility, sexual health, cardiovascular risk, goals-of-care discussions, genetic testing, immunizations, surveillance for the original cancer, screening for secondary cancers, lifestyle counseling, and mental health. Then we scoured charts to see if those needs were being met. We published data showing the feasibility of the combined primary care–survivorship model. Long-term effects — defined as those that began during cancer treatment and persisted — and late effects — defined as those that cropped up later — were addressed in 87 percent of patients, while at least one other primary care issue was managed in 96 percent.
Next we parsed data by group. My colleague Maya Ramachandran led an analysis of geriatric patients. We learned that 28 percent of patients in the clinic are over age 65; among those, 40 percent have active cancer. They average 2.8 visits per year split between in person (61 percent) and video (29 percent) or phone (10 percent), representing multiple avenues to engage a patient population requiring more touch points.
A senior resident, Ellen Zhang, MD ’23,
compared survivorship needs addressed among patients with blood cancers to those with solid tumors. We learned that cardiovascular risk, fertility, and cancerrelated fatigue were addressed significantly more often, while sexual health was managed less often.
Why that is remains to be determined. But just seeing these results led to a partial fix. For example, I updated my note template to broach sexual health in blood cancer survivors, and I make sure we offer phone calls and video visits to older patients. We are currently working on an analysis of adolescents and young adults compared to adult survivors. We are also in the midst of a quality improvement project studying how survivors in the clinic navigate their care. We designed a questionnaire that asks: Do patients feel empowered to manage long-term symptoms? Do they know when to seek care for new ones? Do they know who to call?
From champions to programs
To me, these health systems gaps remain the most motivating ones. Patients must know who to call, and, on the other end, we need a workforce to pick up the receiver. The National Cancer Institute projects that there will be 26 million cancer survivors by 2040. Many of these will be young people, who are getting diagnosed at higher rates now compared to previous generations.
Recently, I was interviewing medical students applying to residency at Stanford. Over and over again I spoke to applicants interested in cancer survivorship as a career. I was happily stunned. These students were speaking a language I had barely heard until my fellowship. That there’s this much interest so early in the pipeline means something in our public messaging is working. Yet I tell them the truth: There is still no career path. I invite them to join me in my clinic, where I frequently host residents. I echo the line I was told: that it takes a champion. Then I ponder — how can we transform cancer
survivorship from an ad hoc network of champions into a formal branch of medicine with training, standards, and access?
I have some ideas: a one-year, nationally accredited cancer survivorship fellowship that teaches the subject directly, rather than as a Post-it note tacked onto an oncology fellowship. Elective rotations for junior and senior residents. And, at the bare minimum, a billing code — as of 2025, there remain no survivorshipspecific codes to ensure these visits get covered. Then there are more ambitious goals, including team-based survivorship clinics — a model we know works in medicine more broadly — with important players such as a nutritionist, social worker, and physical therapist working together to help survivors.
We must also find creative ways to support general practitioners who see cancer survivors every day. Last year my codirector Jennifer Kim and I teamed up with Regina Jacob from Northwell Health and gave a workshop on survivorship pearls at the Society of General Internal Medicine Annual Meeting, one of the largest national conferences for internists. I regularly teach high-yield survivorship concepts at Stanford along the training spectrum from medical students through residents and fellows to attendings. This year we are piloting “e-consults,” where we will guide providers through chart review and remote care.
I recognize the obstacles. Working within the U.S. health care system means navigating a wider ecosystem of fragmented care; we wrestle with barriers such as unshared medical records, payment models that reward short visits, and hyperspecialization (something I wrote much more about in my 2023 book Fragmented: A Doctor’s Quest to Piece Together American Health Care). Primary care desperately needs to delegate bureaucratic tasks so that the important work of caring for survivors does not feel like another chore that busy doctors have no time to do. But even as we advocate for broad systemic change, there is
much we can do now to embed a survivorship lens into routine medical care.
Take Kate. While fear of cancer’s return may prevent her from ever fully identifying as a survivor, she has found a way to live. She learned to walk the tightrope of staying aware of new symptoms while not letting thoughts of cancer consume her. She let herself plan ahead — first in months, then in years. Together, we speak candidly about living in uncertainty. We interpret unexpected findings on MRIs. We triage new problems within the context of her medical story.
The last we met, that new problem was headaches. Three days earlier she stood too quickly and struck her head against an open freezer. She had the welt to prove it, and the pain was throbbing and persistent. I did a focused neurologic exam. I recommended Tylenol and ice packs, and she recovered well at home. I quietly picture what might have happened if our clinic didn’t exist. I could see an urgent care or primary care doctor sending Kate straight to the emergency department for a head CT — something relatively benign for most but dangerous for someone with Li-Fraumeni syndrome.
But then I imagine more hopeful alternatives. What if a survivorship e-consult offered time-sensitive advice to a primary care doctor? What if an experienced nurse practitioner on a survivorship team evaluated Kate and carefully weighed a CT scan’s risks and benefits? The world of cancer survivorship is facing a unique moment with a combination of rising demand and supply; we must match them. The what-ifs no longer just trouble me about the worst-case scenarios. They give me hope for the best.
ILANA YURKIEWICZ, MD ’15, IS A CLINICAL ASSISTANT PROFESSOR AT STANFORD UNIVERSITY SCHOOL OF MEDICINE, CODIRECTOR OF STANFORD’S PRIMARY CARE FOR CANCER SURVIVORSHIP PROGRAM, AND AUTHOR OF THE BOOK FRAGMENTED: A DOCTOR’S QUEST TO PIECE TOGETHER AMERICAN HEALTH CARE (W.W. NORTON, 2023). SHE GRADUATED CUM LAUDE FROM HMS IN 2015. DISCLOSURES: NAMES AND CERTAIN IDENTIFYING DETAILS WERE ALTERED TO PROTECT PATIENT CONFIDENTIALITY. THE AUTHOR IS A STRATEGIC ADVISOR TO PREVIVOR EDGE AND A CONSULTANT TO ONCOVERYCARE.
“I KNEW THE ONLY WAY TO IMPROVE THE NEW MODEL OF PRIMARY CARE AND SURVIVORSHIP WRAPPED INTO ONE CLINIC WAS TO PUT IT UNDER A MICROSCOPE.”
For more than forty years, immunologists arlene sharpe and gordon freeman have shared a journey of scientific exploration
A LIFETIME OF DISCOVERY
B y ALLISON ECK
Illustration by DANA SMITH
Photographs by JASON GROW
Picture two scientists, giants in their field, traipsing around the United Kingdom on a scenic adventure.
First, they stop at Stonehenge on the summer solstice and marvel with the thousands of others gathered to greet the rising sun. Next, they wander through the rolling hills, browse the charming shops, and admire the famous yew trees of the Cotswolds. They could easily be mistaken for ordinary, enchanted tourists.
Then they stop at Dr. Jenner’s House, a museum dedicated to educating the public about the life of Gloucestershire scientist Edward Jenner. In 1796, Jenner inoculated an eight-year-old boy against smallpox with a sample collected from a cowpox sore on the hand of a milkmaid. In the following years, Jenner helped popularize vaccination, essentially founding the field of immunology.
On this day in 2023, the museum is closed. But when the scientists find a staff member and explain why the visit is so important to them, they receive a private tour of the house and grounds. That’s because the tourists, Arlene Sharpe, MD ’82 PhD ’81, and Gordon Freeman, PhD ’79, are not just scientists but immunologists. Indeed, if Edward Jenner was the “father of immunology,” as he is often called, Sharpe and Freeman are among the heirs to his legacy.
For Sharpe and Freeman, the museum is one stop in a lifetime of scientific exploration. Sharpe, the chair of the Harvard Medical School Department of Immunology and Kolokotrones University Professor, and Freeman, an HMS professor of medicine at Dana-Farber Cancer Institute, have been married for forty-seven years and professional collaborators for almost as long. All the while, they’ve brought complementary skills and insights to the study of the immune system: Freeman through his expertise in molecular biology, and Sharpe through her use of knockout technologies, genetic engineering techniques used to inactivate or remove specific genes in an organism. Their research on cell communication systems involved in immune responses has led to a fusion of their two approaches that directly contributed to the development of immune checkpoint inhibitors — a form of immunotherapy that stimulates the immune system’s natural defenses to ward off cancer.
Their work has contributed to the development of an entirely new class of cancer therapies and to a deeper understanding of how the immune system works, opening new portals to discovery. Together, their careers represent a journey through a highly productive period in the history of American biomedical research.
From the Heartland to Harvard
As a child growing up in northwest Indiana in the 1950s and ’60s, Sharpe conducted hydroponics experiments in her living room. Though she remembers succeeding only in growing mold, her parents supported her curiosity.
When Sharpe was fifteen, her mother died of cancer, a loss that left a deep impression. That experience motivated her to pursue a career in science. In high school, she took part in the Westinghouse Science Talent Search, a prestigious nationwide competition, working on a project analyzing samples at a local water company. When she graduated, Sharpe headed east to Harvard to take the next step toward becoming a scientist,
As a high-schooler in a suburb of Fort Worth, Texas, Freeman also took part in the Westinghouse competition, becoming a finalist two years before Sharpe entered it. In his high school, a science teacher had built a lab where students could do research, funded by a National Science Foundation (NSF) grant to encourage scientific education. “It was one of these old ramshackle wooden buildings behind the high school, but it had a complete biology lab with spectrophotometers, a dark room, and autoclaves,” Freeman says. The same teacher convinced him to apply to a summer research program at the University of Texas funded by the NSF. Freeman was accepted, helping prepare him to pursue science when he arrived at Harvard as an undergraduate.
It wasn’t just a coincidence that Sharpe and Freeman both had opportunities to explore their scientific interests at a
young age. This was the post-Sputnik era, when the United States was obsessed with keeping up with the Soviet Union — not just militarily but scientifically and technologically. Sharpe and Freeman were among the many children and teenagers who benefited from a massive influx of funding for science education. Over just one year, from 1958 to 1959, NSF funding more than doubled, increasing from $52 million to $138 million. By 1975, NSF funding surpassed $800 million.
Sharpe and Freeman met when they took the same German class at Harvard.
“At that point in my life, I was a very, very late-night person,” Freeman says. “It would be two hours of sleep and then German class. Sometimes I didn’t make it.”
“Gordon would come over and ask what the assignments were,” Sharpe says. “After a while, I realized he was interested in more than just the assignments.”
Freeman says Sharpe’s “animation and curiosity” piqued his interest. And the University as a whole — not just Freeman
— embraced her intellectual eagerness.
“I was the Indiana girl,” Sharpe says. “Coming to Harvard and Radcliffe was life-changing because I met other women who had similar aspirations.”
After graduation, Sharpe planned to attend medical school. She contemplated attending Yale School of Medicine instead of continuing at Harvard. Wanting to make sure they stayed together, Freeman proposed, and they remained in Boston.
The family business
After earning their bachelor’s degrees, Sharpe and Freeman pursued their separate but related scientific interests — Sharpe as an MD-PhD student and Freeman as a graduate student in the HMS Department of Microbiology and Molecular Genetics. For her graduate work in the lab of Bernard Fields, Sharpe studied how viruses cause diseases in their target hosts, with a focus on reoviruses, a type of RNA virus that
Right: Freeman (fifth from left) on the steps of the U.S. Capitol with fellow finalists in the 1969 Westinghouse Science Competition. Opposite: Sharpe and Freeman in Bermuda in the early 1980s.
“I WOULD BE GOING BACK AND FORTH TO THE LAB AND HOME, WORKING ON EXPERIMENTS, TRYING TO WRITE PAPERS. IT WAS AN EXCITING BUT CHALLENGING TIME.”
is a versatile model for studying pathogenesis. This experience later inspired Sharpe to pursue pathology as a resident at Brigham and Women’s Hospital.
As a postdoctoral fellow, Sharpe worked with Rudolph Jaenisch at the Whitehead Institute during the early days of knockout approaches — which can be thought of as precursors to CRISPR-Cas9 gene editing. At that time, “every step of making a knockout was a Nature paper,” Sharpe says.
Freeman went in a different direction. During his postdoctoral fellowship at Dana-Farber, he explored gene cloning, a new technology at the time, working alongside Harvey Cantor (now the Baruj Benacerraf Professor of Immunology at Dana-Farber) and later Lee Nadler, MD ’73 (now the HMS Virginia and D.K. Ludwig Professor of Medicine at Dana-Farber). “Molecular biology really blossomed” in concert with the advent of gene cloning, Freeman says. It allowed scientists to identify and manipulate specific immune-related genes, whereas in the past, immunology had relied on observational studies and broader analy-
ses of immune responses.
One gene Freeman cloned in 1989 codes for the B7 protein (also known as CD80), which has a critical role in the immune system. When a pathogen infects the body, there may be just fifty to one hundred T cells capable of recognizing that specific pathogen. B7 contributes to expanding that T cell population from fifty to perhaps fifty million, creating “an effective fighting force,” as Freeman describes it. B7 has the same role in expanding cancerfighting cells.
Freeman and his colleagues at DanaFarber tried inserting B7 into cancer cells to see if it would stimulate an immune response against the cancer. This worked in mice but not in human trials. Rather than abandon B7, he turned to Sharpe’s expertise in knockout technology. She developed a mouse model that lacked B7, a fortuitous step that led to the discovery of genes related to B7, including B7-2 (also known as CD86). Their 1993 paper in Science describing this work was their first joint publication and launched what Freeman likes to call “the family busi-
ness.” They then extended their studies to the functions of additional members of the B7 family.
Sharpe and Freeman embarked on another type of family business around the same time: parenthood. Their children, Sam and Suzanne, were born as Sharpe and Freeman were ramping up their early discovery work. Sharpe joined the HMS faculty as an assistant professor of pathology in 1991, and Freeman started his lab as an HMS assistant professor of medicine at Dana-Farber in 1994.
Balancing the demands of childcare and the complexities of biomedical research proved difficult. “I would be going back and forth to the lab and home, working on experiments, trying to write papers,” Sharpe says. “It was an exciting but challenging time.”
One of Sharpe’s mentors, pathologist Ramzi Cotran — with whom she had worked during residency — wasn’t shy about asking her what she needed. “He said, ‘I can’t pretend to know what you’re going to need to navigate this, but we have other women faculty who have done this. Let me introduce you to them,’” Sharpe says.
Cotran’s introductions were crucial. It wasn’t easy for women faculty to meet other women faculty. Elizabeth Petri Henske, MD ’85, now an HMS professor of medicine at Brigham and Women’s, remembers being a junior faculty member in the 1990s and seeing Sharpe in the halls of the hospital.
“I could go a month and never even pass in the hallway a woman senior to me,” Henske says. “There were just so few of them.”
At the time Sharpe and Freeman were exploring B7, cancer immunology “hadn’t produced cures,” Freeman says, “just promise.” Indeed, over the course of the twentieth century, sentiment regarding even the possibility of co-opting the immune system to fight cancer vacillated between optimism and skepticism.
About a century before Sharpe and Freeman were establishing their
labs, New York surgeon William Coley reported remarkable success in treating cancer by injecting Streptococcus bacteria (“Coley’s Toxins”) into more than a thousand patients over the course of several decades. But attempts to replicate his findings failed, and interest waned as more effective treatments such as chemotherapy and radiation emerged.
The 1970s saw a surge of interest nationally in cancer research. President Nixon announced the War on Cancer in 1971, and the National Cancer Institute (NCI) budget more than doubled from 1970 to 1972. But it would be quite some time before the scientific community reawakened to the potential of cancer immunotherapy. As recently as the early 2000s, the NCI and biopharmaceutical companies were largely focused on targeted kinase inhibitors (drugs that block enzymes called kinases in cancer cells, impeding their growth).
But the fact remained: Existing cancer treatments — chemotherapy, radiation, surgery, and even kinase inhibitors — were neither sufficient nor practical for many patients.
Immunologist and Nobel Laureate Baruj Benacerraf, Dana-Farber’s president from 1980 to 1992, attracted top scientific talent and raised funding through philanthropy, leading the institution through a period of significant growth. Under his leadership, Dana-Farber became an “immunologically focused place,” Freeman says. “It was good about keeping a wide range of possibilities in play.”
That commitment — plus consistent funding for basic science research from the National Institute of Allergy and Infectious Diseases and, later, the NCI — put Sharpe and Freeman in the right place at the right time.
Lock and key
A breakthrough in a new approach to harnessing the immune system against cancer came in 1996, when James Allison, a scientist who was then at the University
“THEIR TECHNICAL EXPERTISE IS VERY COMPLEMENTARY, AND THEY’RE BOTH DEEP THINKERS AND OUTSTANDING SCIENTISTS.”
of California, Berkeley, demonstrated that antibodies against the CTLA-4 protein could eliminate tumors in mice. Around the same time, Sharpe developed a mouse model that lacked CTLA-4 and revealed that CTLA-4 acts as a brake on T cells. These findings focused attention on other similar targets, including one called PD-1, which had been discovered by Japanese scientist Tasuku Honjo in 1992 and would soon prove to be pivotal.
In the late 1990s, Sharpe and Freeman became intrigued by a member of the B7 family Freeman identified called PD-L1 (originally called B7-H1). In collaboration with others, Freeman’s lab discovered that, unlike other well-studied members of the B7 family, PD-L1 suppressed — rather than stimulated — the immune system by interacting with PD-1.
The critical finding, published in 2000 in the Journal of Experimental Medicine, was this: When PD-L1 binds to PD-1 receptors on T cells, it activates an inhibitory pathway that puts the brakes on T-cell activity. This is why immunologists refer to PD-1 as an immune checkpoint protein. Freeman and Sharpe showed that when PD-1 is engaged by PD-L1 (or its sibling, PD-L2), PD-1 curbs T cells’ supercharged powers so they don’t act as aggressors
toward the body’s own tissues and organs.
“This was the lock and key to turn off the immune system,” Freeman says.
He and Sharpe demonstrated in subsequent years — along with Honjo and others — that blocking the PD-1/PD-L1 interaction could trigger an antitumor response. Further research revealed the inner workings of this lock-and-key system: By cloaking themselves in PD-L1, cancer cells render T cells inert and helpless, ensuring the cancer cells’ survival. To make matters worse, a 2002 discovery showed that when T cells recognize a tumor, they produce a protein called interferon-gamma, which raises PD-L1 levels — thereby inadvertently pressing on the brakes even harder.
But disrupting the interaction between PD-1 and PD-L1 with antibodies could disable cancer cells’ sneaky tactics and restore the power of T cells to destroy them. Hence the fundamental principle of checkpoint blockade immunotherapy: By blocking the inhibitory pathways of PD-1/PD-L1, the brakes on T-cell activity could be released, and a full-fledged attack on cancer could commence.
Dana-Farber licensed patents on Freeman’s and Sharpe’s discoveries nonexclusively, meaning multiple companies
Right: Sharpe and Freeman with Lee Nadler in 1993. Freeman was a postdoctoral fellow in Nadler’s lab before joining the HMS faculty. Opposite: Sharpe and Freeman with their son, Sam, in 1989.
could try their hand at developing PD-1/ PD-L1 antibodies.
At the 2014 meeting of the American Society of Clinical Oncology in Chicago, Sharpe gave the opening keynote address about PD-1 biology, and then representatives from pharmaceutical companies Bristol Myers Squibb, Genentech, and Merck reported clinical trial results for their PD-1/PD-L1 antibodies — which have since been approved by the U.S. Food and Drug Administration as the drugs nivolumab, atezolizumab, and pembrolizumab, respectively. Whereas just one year before, checkpoint blockade had only been successful in advanced melanoma (through the drug ipilimumab, which inhibits CTLA-4 and was approved by the FDA in 2011), the new results indicated a watershed moment, with success in non-small cell lung cancer, renal cell carcinoma, and urothelial bladder cancer.
“People were literally crying and hugging each other,” Sharpe says.
Freeman agrees. “It was an electric atmosphere. You knew the revolution had arrived.”
Immune checkpoint inhibitors are now approved for more than twenty-five types of cancer. For melanoma patients, checkpoint blockade has radically changed outcomes. Before these therapies, few people survived metastatic melanoma for more than two years. But in a recent clinical trial, about half of patients with advanced melanoma who were treated with a combination of checkpoint inhibitors were still alive after ten years.
The drugs that treat these patients are among the best-selling in the world, and they are built on the premise that a patient’s own immune system is the strongest medicine.
It’s a beautiful message, and yet, cancer immunotherapies aren’t foolproof; about 14 percent of patients treated with PD-1 or PD-L1 inhibitors experience a serious adverse event. Nevertheless, the advantages of immunotherapy over chemotherapy, for example, are stark: Side effects are, in general, less severe with immune
“GORDON WOULD COME OVER AND ASK WHAT THE ASSIGNMENTS WERE. AFTER A WHILE, I REALIZED HE WAS INTERESTED IN MORE THAN JUST THE ASSIGNMENTS.”
checkpoint inhibitors than with chemotherapy and, overall, the treatment is more durable and has a higher success rate.
“Chemotherapy is one of the great dreads of the latter stage of American life,” Freeman says. “Immunotherapy is kinder and gentler.”
The ultimate journey
To bring the benefits of immunotherapy to more people, Sharpe and Freeman are studying so-called combination approaches. That is, they’re looking into why certain combinations of immunotherapy and other therapeutic options, as well as the blockade of multiple inhibitory pathways at once, work well in some patients and not others. They’re also analyzing the complexities of the tumor microenvironment, including the effects of the microbiome on patient responses to immunotherapy. Finally, they’re teaming up with colleagues to understand how their immunological insights can inform autoimmunity, aging, and tissue inflammation. These are all topics of relevance to the new Gene Lay Institute of Immunology and Inflammation, a collaboration among Brigham and Women’s, Massachusetts General Hospital, and HMS that has Sharpe as a vice director.
Meanwhile, they’ve also gained tremendous respect from their peers.
“Arlene and Gordon are incredibly insightful, energetic, and enthusiastic scientists, collaborators, and educators,” says Dennis Kasper, the William Ellery Channing Professor of Medicine and a professor of immunology at HMS. “They each bring a unique skill set to their work, and the synergy of their efforts results in important contributions impacting all of medicine and science.”
“Their technical expertise is very complementary,” says Rafi Ahmed, PhD ’81, who went to graduate school with Sharpe and is now a professor in the department of microbiology and immunology at Emory University. “And they’re both deep thinkers and outstanding scientists.”
More than fifty years after arriving at Harvard as undergraduates, Sharpe and Freeman continue their investigations into the immune system.
Just as Sharpe and Freeman’s lockand-key collaborations have spurred an extraordinary wave of new research, they know the journey won’t end when they someday hang up their lab coats. Nurturing the next generation is critical — not just because mentorship is good for trainees’ career growth, but because it’s the way of science.
“Our students and postdocs can be human bridges to create new fields,” says Sharpe, who has been a staunch advocate for the value of mentorship.
“Arlene was always the first person I would turn to when facing tough moments in my career,” says Kristen Pauken, an assistant professor in the department of immunology at the University of Texas MD Anderson Cancer Center and a former postdoc in Sharpe’s lab. “She’s a one-in-a-million kind of mentor.”
Henske, who studies tuberous sclerosis complex, a rare genetic disorder that causes tumors to form in various organs, feels indebted to Sharpe and Freeman for their basic science discoveries.
“They weren’t trying to treat a disease,” Henske says. “They and others were trying to understand: How is the activity of T cells regulated? Now this work on immune checkpoints is benefitting many people who are living with cancer. And it wouldn’t have happened without people like Arlene and Gordon revealing the basic mechanisms.”
For Sharpe and Freeman, curiosity and a love of discovery are evident in all aspects of their life together. Besides the Cotswolds, recent trips include the Galapagos — Darwin’s famous scientific playground — and the Lyngen Alps in Norway to see the aurora borealis.
They both know, however, that science itself is the ultimate adventure.
“Funding curiosity-driven science is so important,” Sharpe says. “It takes you down avenues you could never have imagined.”
Butaro Hospital opened in 2011, and a year later work on Butaro Cancer Center of Excellence was completed. Today, the hospital provides comprehensive cancer care and serves as a teaching hospital.
Cancer Care from the Ground Up
FIFTEEN YEARS AGO, A CANCER DIAGNOSIS WAS ESSENTIALLY A DEATH SENTENCE IN RWANDA. TODAY, THE COUNTRY’S BUTARO CANCER CENTER OF EXCELLENCE IS A MODEL FOR GLOBAL CANCER CARE.
BY JAKE MILLER
2011, Cyprien Shyirambere was working as a pediatrician at a teaching hospital in southern Rwanda, where he occasionally saw children who had been diagnosed with cancer. There wasn’t much he could do to help them, recalls Shyirambere, who is now the director of oncology for the nongovernmental organization Partners In Health in Rwanda. Sometimes he would be able to get access to enough chemotherapy to put a child’s cancer into remission for a month, but the hospital didn’t have the resources to do much more than that. His young patients inevitably, heartbreakingly, died.
At the time, there was essentially no cancer care available anywhere in Rwanda. That meant that for most of the 11 million residents of the nation, a cancer diagnosis was almost certainly a death sentence. But that year, the government of Rwanda invited the DanaFarber Brigham Cancer Center and Partners In Health to work together to establish a cancer center in Butaro, in Rwanda’s Northern Province. The goal from the very beginning was to create a comprehensive cancer center, which would make it the first such center in East Africa.
PIH, including its cofounder Paul Farmer, MD ’90 PhD ’90, had worked in Rwanda since 2005, contributing to progress in treating HIV, malaria, and other leading causes of premature death. But Farmer saw a gap in cancer care.
The Butaro Cancer Center of Excellence opened in 2012, and within its first year more than 1,000 patients were treated there. In the years since, the center has seen more than 18,000 patients, saved thousands of lives, built and tested key elements of robust national cancer screening and preven-
tion programs, and trained a generation of clinicians who are proving that effective cancer care is possible anywhere.
Harvard Medicine talked with a few of the people involved in the early years of the center about their experiences helping to build an effective, sustainable cancer program.
Establishing the foundation
When Lawrence Shulman, MD ’75, first visited Rwanda in 2011, he was already a veteran of several campaigns to build new systems for treating cancer. Now the codirector of the Center for Global Oncology at the University of Pennsylvania, Shulman started his career as a medical oncologist before most hospitals, even in the United States, had oncology departments. He recalls mixing chemotherapy drugs on the desk in his office in the 1970s, when he was working at Beth Israel Hospital.
Shulman met Farmer and PIH cofounder Jim Kim, MD ’91 PhD ’93, when Farmer and Kim were interns at Brigham and Women’s Hospital. When Farmer was in Haiti in the early days of PIH, he enlisted Shulman’s help to treat cancer patients. At first, they practiced a sort of ad hoc telemedicine, with Farmer calling Shulman to talk about diagnoses and figure out how to get chemotherapy drugs delivered from Boston to rural Haiti (often by packing them in Farmer’s suitcase). Later, they worked together to help build a robust cancer program that continues today at Mirebalais Hospital.
When Shulman started working on a plan for cancer care in Rwanda, he knew it would be a challenging experience. “When we first went in 2011, we were starting from zip,” he says. “There was essentially no cancer care in the country, and if you got cancer, you died.”
There were no medical oncologists, no radiation therapy facilities, a single, part-time pathology lab, and just one CT scanner in the entire country, Shulman recalls.
PIH opened a 150-bed community hospital in Butaro in 2011 that served as a medical hub for a network of small clinics staffed by nurses. As work on the cancer center progressed, PIH put the fundamental elements of a cancer treatment system in place. General surgeons at the hospital learned to perform basic cancer surgeries, and the cancer center was staffed with an internist, general practitioners, and nurses. PIH also began to explore possibilities for integrating cancer care into the district’s health and primary care systems.
Shulman spent time on the wards at Butaro, delivering care; training the local clinical staff; working with visiting doctors, researchers, and trainees from HMS; and developing detailed instructions to support care for the most common cancer types that they could treat with the resources at hand.
“The other thing that we committed to from day one was that we would keep careful records of what we were doing so that we would know exactly what we were accomplishing, where the gaps in our care were, and where we could do better,” Shulman says.
Continuous improvement
Temidayo Fadelu became the associate director of oncology for PIH in Rwanda after completing his internal medicine residency at the University of Pennsylvania. He grew up in Nigeria and knew he wanted to help meet the rising demand for cancer care in Africa.
One of the many challenges of delivering cancer care in any setting is the capacity to be emotionally present but not let it immobilize you, says Fadelu, who is now an HMS assistant professor of medicine and an oncologist at the DanaFarber Cancer Institute Center for Global Cancer Medicine. That was especially difficult in his early days in Butaro.
“The amount of tragedy I saw every day while I was in Butaro initially was not easy to cope with,” he says. “We need to
Butaro Cancer Center of Excellence is in a rural district in northern Rwanda.
“Every human being deserves dignified health care. Where you were born should not determine whether you live or die.”
CYPRIEN SHYIRAMBERE
be present with the patient in front of us so that they get what they need in that particular moment. We also need to be able to close the chapter on that patient when we go see a different patient.”
Fadelu emphasizes the importance of taking a similar in-the-moment approach to improving cancer care systems. You have to start where you are and do the best you can with the available tools and look for little ways to improve the situation quickly whenever you can, he says.
For example, when the center first opened there were no pathologists, so clinicians sent whole biopsy samples to Boston for processing. Over time, staff in Butaro traveled to Brigham and Women’s and Dana-Farber for training. Once they learned to process biopsies, they were able to send images of the prepared samples for review instead of whole samples. And now, with two histopathologists on site, 90 percent of samples are read in Butaro.
Fadelu still runs a weekly tumor board — either in person or remotely — with the team in Butaro, discussing patients and
“We need to be present with the patient in front of us so that they get what they need in that particular moment.”
samples to help with tricky diagnoses and continue to train clinicians at the center.
Progress through research
In the months before the Butaro Cancer Center opened, Lydia Pace was already in Rwanda helping to treat patients with cancer at Butaro Hospital. Pace, now an HMS associate professor of medicine at Brigham and Women’s, started working at Butaro Hospital in 2011, after finishing her residency.
During her time in Rwanda, Pace helped identify gaps that were leading to a startling number of diagnoses of advanced breast cancer in young women. Through her research, she discovered that many women, community health workers, and clinicians weren’t aware of the early signs of cancer or how to respond to them. Many women also worried that treatment might be unaffordable and that even when the care was free, the time required could prevent them from working.
One of her early research projects
Lawrence Shulman (middle) on the wards at Butaro Hospital in 2011 with hospital staff and race car driver Jeff Gordon (to the right of Shulman), whose foundation contributed to the opening of the cancer center.
found that women faced 15-month delays from the onset of breast cancer symptoms to diagnosis. “It was the longest documented delay in the literature anywhere in the world,” Pace says. That research helped secure funding for a pilot project to improve early detection. “Working with this team taught me that research can be a powerful tool for bringing understanding of an issue and helping direct resources to solutions,” Pace says.
The goal of the research was always to try to improve care. For one project, Pace and her colleagues created a strategy for building capacity for early breast cancer diagnosis in a country with no mammography machines and very few radiologists. Pace recruited a group of breast radiologists from Brigham and Women’s to train general practitioners, nurses, and nurse midwives in Rwanda to use ultrasound for breast cancer diagnosis. They established regular breast clinics staffed with trained clinicians and saw dramatic increases in patients seeking care and earlier cancer diagnoses, even without specialist radiologists or oncologists on site. Pace notes that the breast cancer early diagnosis program has now been scaled up by the Rwandan government to include 60 percent of Rwanda’s districts.
Essential health workers
In 2009, when Emmanuel Kamanzi gave up a prestigious job at the University of Rwanda to work for PIH at a rural hospital in southeastern Rwanda, his friends asked him why he would leave his comfortable life in the city to live in a place with no internet and no running water.
“I wanted to be there because I thought it was the best place to work on the root causes of health disparities,” Kamanzi says. “I realized that I was driven by a passion for helping people.”
In 2010, Kamanzi moved to northern Rwanda to oversee PIH’s projects there, including the construction of the cancer center and an oncology support center with housing and spaces for families to
cook. Before long, demand for treatment outgrew the space available at the center, and Kamanzi managed the construction of the new Ambulatory Cancer Center.
Kamanzi says that instead of hiring skilled workers from Kigali to do the work, PIH hired master builders from the capital to train workers in Butaro. These workers have used their newfound skills to help build the growing community, and in their own way, each is making Rwanda a healthier place. “We’re all essential health workers,” he says.
More recently, Kamanzi decided to return to school and is now a student in the HMS master of medical science in global health delivery program, where his mentors include Lydia Pace. For his thesis project, Kamanzi plans to conduct a formative study to adapt new World Health Organization guidelines for patient navigation programs for the current clinical and social context in Rwanda.
The work continues
About 70 percent of the 10 million deaths worldwide from cancer each year occur in
BUTARO BY THE NUMBERS:
1,000+
Number of patients seen within the first year of operation at Butaro Cancer Center (2012-2013)
18,000+
Number of patients seen since Butaro Cancer Center opened
15 Months The median delay between the development of symptoms and diagnosis for patients with breast cancer in Rwanda in 2015, the longest reported anywhere at the time
low- and middle-income countries like Rwanda, and both the number of deaths from cancer and the percentage occurring in these countries are expected to increase. In the years since its founding, Butaro Cancer Center has transformed the diagnosis and treatment of cancer in Rwanda and become a much-needed model for delivering cancer care in a resource-limited setting.
Still, many challenges remain, including potentially fatal delays in diagnosis and treatment, high costs for necessary drugs, and a lack of specialist surgeons.
As an example of both the progress that has been made and the work that remains, Shulman points out that the survival rate for Hodgkin’s lymphoma in Rwanda is now up to 50 percent, a dramatic improvement over the years before the Butaro Cancer Center opened, and work continues to improve results. But, he adds, “in the U.S., it’s 90 percent.”
This is also a precarious time for global health efforts that depend on funding from the U.S. government. The National Institutes of Health has provided crucial funding for pilot programs, research, and
training for some of the work at Butaro. Rwanda’s health initiatives have received funding from USAID programs and the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR), among others. Some of these programs have already been cut, and others are in jeopardy.
Shyirambere has seen the benefits of the years of work firsthand. Not long after he first arrived in Butaro, in 2014, a child he knew from his time in southern Rwanda developed cancer and came to Butaro Cancer Center. The child had B-cell acute lymphoblastic leukemia, a common cancer with a high survival rate when treated, and received treatment in Butaro for 32 months. On a recent visit to the south, Shyirambere ran into the child’s father and learned that the boy was doing well.
“Every human being deserves dignified health care,” Shyirambere says. “Where you were born should not determine whether you live or die.”
Cyprien Shyirambere has practiced at Butaro Cancer Center since 2014.
Cancer’s
Scientists are making surprising discoveries about the connections between cancer and the nervous system
Unlikely
By Molly McDonough
illustration by dominic kesterton
Ofthe many tumor slides William Hwang, MD ’15 PhD ’13, has seen, there’s one in particular that is seared into his memory. He encountered it as a medical student while on a rotation caring for an elderly patient with pancreatic cancer. “What struck me as the most horrible part of the experience for them was the pain,” he recalls.
Hwang wanted to understand where that intractable pain was coming from. So, he asked Mari Mino-Kenudson, an HMS professor of pathology at Massachusetts General Hospital, to walk him through the patient’s tissue slides under a microscope. That’s when he saw a nerve encased within a tumor, being prodded and compressed by cancer cells. The patient was suffering from perineural invasion, a painful phenomenon in which malignant cells surround and invade nerves.
“I remember thinking that it looked like something out of a horror film,” says Hwang, who is now an HMS assistant professor of radiation oncology at Mass General. “I wondered why cancer cells would form such intimate connections with nerves. What do they derive from this relationship, and how can we intervene?”
Hwang dug into the literature and found that perineural invasion was documented as early as 1897, when a urologist named Hugh Young used methylene blue staining to examine tumors and noticed something curious: bundles of nerve fibers creeping into many of his samples. Although nearly half of the tumors he examined showed connections with nerves, Young expressed surprise that no other researchers had yet investigated such links. “The question of the relation of nerves to tumors … is practically terra incognita,” he wrote in the Journal of Experimental Medicine
It remained that way for nearly a century, with the presence of nerves in tumors passed off as coincidental. “If you look at all the components of a tumor, not everything is playing an active role,” says
Hwang. “Some elements are just bystanders: wrong place, wrong time. Only more recently have people started to see the important biological connections.”
One of the first scientists to do so was pathologist Gustavo Ayala, who, in the early 2000s at Baylor College of Medicine, grew nerve and cancer cells together in lab dishes. The results were striking: Mouse-derived spinal nerve cells seemed to stretch out toward human prostate cancer cells, beckoning them. As the cells intermingled, the cancer cell colonies blossomed.
Around the same time, cancer researchers started appreciating the importance of the tumor microenvironment: the ecosystems of cells, molecules, and blood vessels that surround tumors. At the Albert Einstein College of Medi-
cine, oncologist Claire Magnon and her team wondered what would happen to tumors in the absence of nearby nerves. When they grafted human tumors into mice and destroyed the sympathetic nerves around them, they found that the tumors stopped growing. Inhibiting the parasympathetic nervous system reduced the ability of tumors to spread and metastasize. Other researchers noted that a greater density of nerves around tumors in the prostate, breast, colon, and elsewhere could help to predict whether a tumor would be more likely to grow or recur. More recently, Hwang’s research involving patients with twelve types of cancer found that perineural invasion predicts worse outcomes.
Studies like these have fueled a growing realization that the nervous system may
William Hwang works with graduate student Ella Perrault in Hwang’s lab at Massachusetts General Hospital.
not be the innocent bystander in cancer that it was once considered to be. Instead, it likely plays a role in everything from tumor initiation and growth to metastasis and response to treatment. Perineural invasion is just one dimension of an emerging field, known as cancer neuroscience, that Hwang and a new generation of researchers are bringing into the spotlight. The communication signals they are discovering between cancer cells and nerves are opening up new possibilities for therapies that act on these links to treat the disease.
Yet cancer neuroscience “is still an early field, almost in its infant stages,” cautions Richard Wong, MD ’94, chief of head and neck surgery at Memorial Sloan Kettering Cancer Center. “People are only just starting to realize how important it is.”
Co-opted by cancer
Wong’s interest in cancer neuroscience is in part a matter of practicality. Since he started performing ear, nose, and throat surgeries in the 1990s during an otolaryngology residency at Massachusetts Eye and Ear, he’s been drawn to the “elegant” challenge of uprooting tumors while keeping nerves in the head and neck intact — nerves he describes as “critical to a person’s persona.” The invasion of nerves by cancers is a reality of his daily life. “Yesterday, I spent hours trying to peel a tumor off of a tiny nerve that enables a person to speak,” he says. Such encounters are what first drew Wong’s attention to cancers that seem to track nerves, almost like the nerves are “highways for more extensive invasion,” he says. Around 2010, his lab at Memorial
Sloan Kettering published one of the first studies to probe why this happens. The researchers studied interactions between nerve cells and pancreatic cancer cells in petri dishes and in mouse models and found that cancer cells migrated toward a protein called glial cell line–derived neuro trophic factor (GDNF) that is released by the nerves. This study showed that the nerves were actually inviting and enabling cancer spread.
Wong’s lab co-cultured cancer and nerve cells in petri dishes and took time-lapse videos, which showed cancer cells latching onto and moving along the nerves. That’s how Sylvie Deborde, a biologist in Wong’s lab, first noticed a mysterious, skinny cell darting between cancer and nerve cells, as if it were “grabbing and pulling the cancer cells toward the nerves, like pathfinders,” Wong says.
The researchers figured out that those skinny cells were Schwann cells. In a healthy peripheral nervous system, Schwann cells usually wrap around nerves and protect them; if a nerve gets injured, they “wake up” and get to work on repair. Wong and Deborde learned that these activated Schwann cells also attract cancer cells and create channels for the cancer to spread through. They’ve also found that pancreatic cancer patients with activated Schwann cells tend to have worse outcomes. “We believe that this Schwann cell behavior enables more aggressive cancer behavior,” Wong says.
These findings hint at a wider trend: Cancer seems to have an uncanny ability to co-opt the nervous system’s own maintenance processes. “A theme we see repeatedly is that cancer is kind of like a traumatic event,” Wong says. “It destroys tissues around it and creates trauma in the area. And then it triggers and utilizes these innate programs in the host, in the environment, that try to repair the injury. But paradoxically, these repair mechanisms may actually promote cancer progression.”
Hwang’s research has revealed similar themes. For example, a 2021 study found that tumors with perineural invasion tend
to express genes related to axonal guidance. These genes are typically activated when the nervous system is first developing, so the expression of the genes by tumors indicates that cancer cells could be hijacking normal growth processes to interact with and invade nerves.
A traditional approach to studying a tumor has been to blend its cells together and analyze the aggregate gene expression. But Hwang is instead using spatial transcriptomics — an approach that combines advanced imaging with RNA sequencing and complex algorithms analyzing massive data sets — to pinpoint the genes that are expressed within individual cells in different areas of a tumor.
“The areas of a tumor that feature interactions between cancer cells and nerves are often sparse, so if you don’t isolate them in space and analyze the tumor in its entirety, you’ll never pick up on the relevant signals,” he says. The methods that his group and other researchers have pioneered in spatial biology only really emerged in the last few years, but they now enable scientists to identify differences between tumor
cells that are engaged with nerves and those that aren’t.
Hwang’s team recently used these spatial methods to uncover hints that pancreatic cancer cells spreading along and into nerves are more likely to express genes associated with a family of molecules called platelet-derived growth factor, or PDGF, which is usually involved in cell growth, tissue repair, and blood vessel development. By growing genetically engineered cancer cells with nerves in dishes, they confirmed that when cancer cells produce high levels of specific forms of PDGF, nerves are more likely to grow toward a tumor and help the cancer cells invade the nerves. They also found that targeting PDGF signaling may reduce perineural invasion, potentially improving outcomes — something that they are now actively testing in preclinical models.
While chipping away at the causes of perineural invasion is important, Wong says that the interactions he is studying in the peripheral nervous system are just a “small subset” of all the relationships scientists are exploring between cancer cells and nerves. Some of the most compelling nerve-cancer links are emerging in the central nervous system, where aggressive and deadly brain cancers grow in close proximity to dense networks of neurons and the cells that support them.
Electric findings
While working as a postdoctoral fellow in the Stanford laboratory of Michelle Monje in 2017, Humsa Venkatesh, now an HMS assistant professor of neurology at Brigham and Women’s, was exploring how neural activity might affect the growth of gliomas, the most common type of brain tumor. She had adopted an unconventional approach, taking tools traditionally used in neuroscience, such as optogenetics — using light to control the activity of genetically modified neurons to study and manipulate neural circuits — and applying them to study cancer.
Humsa Venkatesh
“THESE REPAIR MECHANISMS MAY ACTUALLY PROMOTE CANCER PROGRESSION.”
By implanting cells from human gliomas into the brains of mice, Venkatesh was able to activate the mice’s brain cells and see how they were communicating. She vividly remembers the moment when she came to an important realization: Brain cancer cells were directly exchanging electrical signals with neurons. She became one of the first scientists to witness this phenomenon as she watched tumor cells pulsate with green light on a computer screen. Her work showed that the glioma cells were exchanging signals with neurons — and with one another — by forming a kind of synapse, similar to the way neurons communicate in healthy brains.
The surprising finding showed that cancer doesn’t only connect with the nervous system via chemical messages
For one study, Hwang and colleagues grew genetically engineered cancer cells in the form of tumoroids (green structures) alongside neurons that formed interconnected highways between them (pink). They used this model to test how certain genes influence cancer-nerve interactions.
or third parties, like Schwann cells. It can also integrate into neural circuits more directly, and this electrical communication can help it grow. And it happens in a feedback loop: Venkatesh found that the more the neurons fired signals, the more the tumors grew; the more the tumors grew, the more excitable the surrounding neurons became.
Venkatesh also found that the increased electrical activity she’d induced in the mouse brains was stimulating the production of certain proteins, including one called neuroligin-3. That protein normally helps the brain with cell growth and communication between neurons, but it also helped glioma cells to grow. When her team prevented the production of neuroligin-3 in mice, the cancer stopped in its tracks.
“We often find these proteins that are growth factors — they’re a dime a dozen,” she says. “But we were able to knock out just one of them and saw a complete stagnation of growth. It was unlike anything we ever see in cancer research.” A treatment based on these findings that suppresses production of neuroligin-3, led to a clinical trial.
Gliomas can be especially tricky to treat. Even after they are removed surgically, they tend to recur, sometimes in distant parts of the brain. In a study published in December 2024 from the labs of Bernardo Sabatini and Marcia Haigis in the Blavatnik Institute at HMS, neuro-oncologist Annie Hsieh helped to explain these recurrences by tracing the paths of neurons that form synapses with glioma cells. Using an
injected rabies virus engineered to light up cells of interest in the brains of mice, Hsieh was able to capture images of all the glowing neurons leading to a glioma, providing visual proof that gliomas integrate into existing wiring patterns that extend across the brain.
These and other recent findings piggyback on Venkatesh’s research to illustrate that cancer’s synaptic connections with neurons are important and widespread, arising from different brain regions. “We’re not thinking about this from a local perspective, because of the way neurons work together. We know from neuroscience that they’re highly interconnected,” Venkatesh says.
That interconnectedness spreads to the peripheral nervous system as well. “Neural circuits are extensively connected throughout the whole body, from the brain to the periphery,” says Venkatesh. “So we’re trying to look at it from a systems perspective.”
Her lab has more recently been exploring whether cancers outside the brain with a high propensity to metastasize — such as skin, lung, and breast cancers — could be forming electrical connections with nerves similar to what she has seen in the brain, and whether that could help them travel to the central nervous system and grow there.
In a study that is currently undergoing peer review, for example, Venkatesh found that not only do connections with nearby nerves appear to encourage small cell lung cancer tumor formation in the lungs but also that the cancer cells can sense and respond to electrical signals from neurons. When the researchers exposed the cancer cells to neurons in the lab, the behavior and appearance of those cancer cells began to shift; some of them looked more like neurons that integrated into existing circuits, whereas others behaved more like neuron-supporting brain cells called astrocytes — indicating that neurons can help cancer cells adapt to the environment of the brain as cancer spreads.
“I SPENT HOURS TRYING TO PEEL A TUMOR OFF OF A TINY NERVE THAT ENABLES A PERSON TO SPEAK.”
Interactions and interventions
Although it’s taken time for the nervous system’s role in cancer to be appreciated, Venkatesh says the connections are logical. “The nervous system is so powerful in driving tumor growth, I think, because it is the master regulator of almost every process in the human body,” she says, “from the function of every organ to the function of every cell.”
That fact could complicate the development of treatments that target the crosstalk between cancer cells and nerves. “It’s difficult because the body has evolved these mechanisms over however many years to serve a purpose,” says Wong. “Maybe you can disable these Schwann cell repair mechanisms and slow cancer progression in a mouse. But if you disable them in a person, is that acceptable? Could it lead to problems with nerve function?”
Wong says it will take time for researchers to overcome such hurdles. But he’s encouraged by the scientists entering the field who are willing to take risks and ask big questions. “In the past, it was clinicians like me who were
interested in the relationship between nerves and cancer because we deal with them in the operating room,” he says.
“But now there are a lot of young, talented scientists like Humsa and William who are making major discoveries and starting new labs.” As interest in cancer neuroscience grows, so does the range of questions being asked. Some researchers are exploring how cancer and nerve cells interact with the immune system, for example; others are focused on how chemotherapy affects cognition or how stress modulates tumor growth.
Scientists will need to decode many different specific neuron-to-malignantcell interactions, which are likely to vary across the subclasses of neurons and branches of the nervous system — as well as the different organs and tissues where cancers grow. “It won’t be a onesize-fits-all mechanism,” Venkatesh says. “We need to be really smart about how we assess these interactions.”
But, she adds, because there are many different ways that tumors exploit existing mechanisms of neuroplasticity, there may be many different targets for treatment. There are likely also drugs that modulate neural circuits that have already gone through FDA approval — treatments for epilepsy, seizures, or depression, for instance — that could help thwart some of the interactions between cancer cells and nerves.
“What’s so interesting is that we’ve gotten a lot of clues about how these tumor cells will respond based on normal development, because they’re just rehashing the processes that already exist in the body,” Venkatesh says.
In other words, insights from neurology about how nervous systems help human bodies function, heal, and grow could inform interventions in oncology when those same processes promote cancer. “It’s this double-edged sword,” says Wong. “And it’s fascinating.”
MOLLY MCDONOUGH IS THE ASSOCIATE EDITOR OF HARVARD MEDICINE
Above: Richard Wong. Opposite: Cancer cells migrate along nerve fibers to invade nerve cell bodies.
What will it take to implement generative AI effectively in clinical settings?
From Hype to Health
By Danielle Bitterman
illustration by valerie chiang
WHEN I DECIDED TO join a natural language processing lab during my residency in radiation oncology, I encountered some skepticism from colleagues. Natural language processing (NLP) is a field of artificial intelligence (AI) that focuses on “teaching” computers to understand and process human language, and it falls outside the continuum of basic science to clinical research that residents in my field typically focus on. “Why not leave computer science to the engineers?” I was often asked. “Can’t we clinicians just use the tools they create?”
I joined the lab — Guergana Savova’s clinical NLP lab in the Computational Health Informatics Program at Boston Children’s Hospital — in 2018, right around the time that Google released its groundbreaking model BERT, the predecessor of today’s large language models (LLMs). The impressive performance of BERT and similar models on many traditionally challenging NLP tasks captured the attention of the computer science community, drawing new scientists to the field. But it wasn’t until 2022, when OpenAI released ChatGPT, that the public really began to interact with, understand, and envision the potential of LLMs. By that time, I had established my own lab — focused on translating AI into the clinic — within the Department of Radiation Oncology at Brigham and Women’s Hospital/Dana-Farber Cancer Institute.
LLMs are now nearly synonymous with AI in the general vernacular, and the rapid advances in their development have played a major role in driving research on and investments in AI. These technologies undoubtedly hold the potential to advance human health, but the enthusiasm surrounding them often overshadows the on-the-ground reality of translating them into clinical care. Within months of ChatGPT’s release, studies reported that LLMs could pass benchmark biomedical exams, including the United States Medical Licensing Exam (USMLE), implying that they had the ability to conduct clinical reasoning.
These reports received a lot of media attention and spurred efforts to employ the models for patient portal messaging, ambient documentation, and other uses.
At the same time, my research group and others found that these models fell short when moving from multiplechoice exams to more realistic use cases that require deeper clinical reasoning, such as responding to patient messages or answering patients’ questions about their cancer care. For example, we found in one study that while ChatGPT almost always recommended at least one correct component of multimodal treatment, one-third of responses also included an inappropriate modality, such as surgery and radiotherapy for noncurative diagnoses or newer systemic therapies such as targeted therapies and immunotherapies in diagnoses where they are not indicated. More recently, clinical pilots using LLMs to help clinicians respond to patients’ questions have failed to produce the anticipated efficiency gains, although other use cases, such as for ambient documentation, have shown more promise.
This gap between the hype surrounding AI and the reality of its role in health care is impeding the translation of AI advances into practical, user-centered applications that are actually needed by health care institutions, clinicians, and — most importantly — patients. My field of radiation oncology has a long history of close collaborations between clinicians, engineers, and physicists to develop technologies that address significant clinical challenges, such as stereotactic radiosurgery. We need to foster that type of translational expertise in the development of AI technologies to ensure they are grounded in real health care needs.
Better benchmarks
One step in this direction is to develop benchmarks that reflect real-world goals. For developers, benchmarks and leaderboards play a major role in driving com-
petition and innovation. A benchmark is a dataset that can be used to score a model’s performance. Leaderboards track and rank model performance across a group of benchmarks as a proxy for performance in a given domain or task. For example, the Open Medical-LLM Leaderboard includes the USMLE as well as other datasets pertaining to biomedicine that were mostly generated from existing multiple-choice biomedical exams. Developers use such leaderboards to demonstrate their model’s strength in the domain of health care.
These benchmarks are already having a real effect on accelerating the integration of LLMs into health care, but the clinical community is not usually included in constructing them and may not even be aware that they exist. This focus on benchmark performance inadvertently marginalizes the voices of clinicians and patients. Chasing leaderboards leads to the development of LLMs that are really good at answering questions found in the benchmark exams, but it’s not clear how this kind of performance relates to clinical use. My research group has shown that popular benchmarks are not always reliable and may not demonstrate generalizable knowledge or understanding. For example, we found in one study that using the brand name of a medication in a prompt to a model can result in different answers than using the generic name. The result of this focus on existing benchmarks is a mismatch between the purported clinical performance of a model and its actual performance, risks, and utility. More realistic benchmarks require close collaboration between clinicians and computer scientists — neither can do this alone. Clinicians can identify the clinically relevant task for a model to perform, create the dataset that models will be scored against, and determine threshold performance metrics needed to proceed to clinical testing. Computer scientists can ensure benchmarks effectively stress-test models and are evaluable, accessible, secure, and robust.
Testing, testing
A second step is to address the tension between the speed of AI advances and the time needed to implement and evaluate new approaches in the clinic. Although we don’t want unnecessary delays, uptake of AI tools based on insufficient, inadequately aligned testing and anecdotal experiences risks early harms and loss of trust, which over the long term could slow implementation. Benchmarks can’t model the complexities of clinical care or of the interaction between humans and AI. To understand the full spectrum of risks and benefits, we need realistic preclinical simulations and lower-risk applications where there is a human expert in the loop to oversee and fix errors.
For example, my research group found that use of LLMs to respond to simulated patient questions about cancer care led to responses that contained more educational content than responses written by clinicians alone, and clinicians felt more efficient. These results indicate that using an LLM could improve health literacy and mitigate burnout. But responses drafted by the models also sometimes included errors, and clinicians exhibited automation bias when given the drafts written by models — that is, clinicians were likely to accept the model’s output even when they would have answered differently if writing the response on their own.
These results indicate that clinical decision-making was affected and that errors could make their way to patients if clinicians aren’t vigilant. There were also a few severe errors that resulted when models inadequately communicated urgency, a critical type of error that is not tested in biomedical exam benchmarks. This straightforward study provided a path for us to improve models for our use case, develop more realistic, safety-focused benchmarks, and explore strategies to better support clinicians to oversee AI output.
Approaches to evaluating AI can draw on existing standards for medical research,
“WE NEED TO MAKE IT EASIER FOR CLINICIANS AND COMPUTER SCIENTISTS TO COLLABORATE.”
ethics, and regulation. Like all medical technologies, AI should be evaluated in a risk-stratified manner suited to the clinical domain, specific use case, and implementation strategy. Research focused on understanding where and how to integrate new AI technologies into the clinical workflow will ensure that we don’t miss an otherwise promising technology that was suboptimally implemented. At a more transformative level, clinical expertise is needed to reimagine how medical data is entered and used in order to realize the true potential of AI in health care.
Clinicians’ role
DANIELLE BITTERMAN IS AN HMS ASSISTANT PROFESSOR IN THE DEPARTMENT OF RADIATION ONCOLOGY AT BRIGHAM AND WOMEN’S HOSPITAL/DANA-FARBER CANCER INSTITUTE AND A FACULTY MEMBER IN THE AI IN MEDICINE PROGRAM AT MASS GENERAL BRIGHAM. SHE IS A CLINICAL LEAD FOR DATA SCIENCE/AI AT MASS GENERAL BRIGHAM DIGITAL.
As a third step, we need to make it easier for clinicians and computer scientists to collaborate. I have worked with many talented computer scientists who are passionate about developing safe, ethical AI innovations to improve the lives of patients and clinicians. But most work outside of health care and do not have easy access to the clinical expertise and datasets needed to build tools that address pressing medical needs.
Computer scientists and clinicians
largely exist in separate academic spheres. When I attend NLP or broader AI conferences, I am often one of only a handful of clinicians present, even at conferences with special sessions and workshops dedicated to AI in health care. Computer scientists rarely attend clinical conferences, even those that have strong communities of clinical and biomedical informatics researchers. We also publish our research in different venues and might not even know where to find one another’s papers. There is a lot we can learn from other translational research fields. We can improve collaboration via joint conferences, collaborative journals, and interdisciplinary research teams. Such efforts could be incentivized by multidisciplinary funding opportunities, promotion criteria, and requirements for meaningful engagement between clinicians and developers who want to bring their models to the clinic. I urge my colleagues interested in health care AI to consider attending AI conferences. You will certainly meet many scientists interested in using their skills to improve health care, and you might even find you have an outsized voice in aligning technical advances with clinical needs.
AI is becoming more accessible, but the nuanced understanding of clinical contexts remains a critical, nonautomatable asset unique to clinicians. As clinicians, we can take a leadership role in identifying high-value use cases; overseeing clinically appropriate and reproducible evaluations that demonstrate value for patients, the workforce, and payers; advocating for transparency about AI models we’re using; and ensuring that patients are included in decisions about AI strategies. Bringing AI to the clinic requires critical evaluation under uncertainty, balancing risks and benefits, and navigating and communicating new information quickly. We practice these skills every day. We are well-equipped to partner with our computer science colleagues to move beyond the hype cycle toward genuine improvements in health care.
Danielle Bitterman
We still share most of our genes with salamanders, which hints at a genetic program that could be reawakened in a human.”
A CONVERSATION WITH JESSICA WHITED, ASSOCIATE PROFESSOR OF STEM CELL AND REGENERATIVE BIOLOGY
You study axolotl salamanders. Why?
Axolotls can do things humans can’t — they can regrow body parts, and they do it with precision. Although scientists have known this for a couple hundred years, no one’s cracked the molecular details of how they do it. Doing so could offer a blueprint for understanding how limbs can be regenerated. An axolotl is the best model among salamanders because it has the shortest generation time — about a year from egg to adult — and you can do real genetics on axolotls. You can knock a gene out and, in a few years, see what the real effect is. There are a lot of new tools developed to study axolotl genetics that do not exist for other salamanders.
The ultimate goal of your efforts is to enable limb regeneration in humans. What about human biology hints that this is even possible?
First, some 350 million years ago, humans and salamanders shared an ancestor that was likely able to regenerate limbs. We think this based on genetic analysis but also on fossils of ancient salamander pre -
cursors, some of which were fossilized while regenerating body parts. It’s a clue that in our ancient shared evolutionary history, the common ancestor likely had the ability to regenerate. We still share most of our genes with salamanders, which hints at a genetic program that could be reawakened in a human.
Second, our lab has uncovered a role for a body-wide cell proliferation response to amputation in the salamander, and we show it can promote regeneration. Another lab has shown something similar happens in mice, and mice don’t regenerate limbs. But if we consider the mouse closer to humans, then I would predict humans have this systemic activation response that’s intimately tied to the ability to regenerate. I would guess human amputees are taking the first molecular steps toward regeneration, but our organism is genetically blocked from taking the next steps in most cases, with the exception of digit tips, which can regrow.
Third, one of the most common effects of limb loss in humans is something called a neuroma, which is the spot where the nerves that service an amputee’s limb continue to grow, because humans have intrinsic peripheral nerve regeneration capabilities. These growing nerves no longer have a limb to go into, but it’s yet another clue that some regeneration is happening in human amputees. Peripheral innervation is critical to salamander limb regeneration. If we are ever able to provoke limb regeneration in humans, peripheral innervation will be a key ingredient in that recipe.
Why did humans lose their ability to regenerate? That’s the big question. Some of the work that’s come out of invertebrates shows trade-offs to the overall growth of the organism, but I think there’s more to the story. I think it probably has something to do with the real-world pressures faced by different species, such as the likelihood of losing a limb to predation. Other factors probably include the ability to heal wounds quickly to avoid blood loss and molecular mechanisms to
prevent tumor growth. The same insults that would cause a tumor in a mammal will induce an extra limb to grow in a salamander. There is some mysterious and important biology at the interface of cancer and regeneration.
How did you end up in science and how did you choose regenerative biology?
I’m the first scientist in my family. I come from a blue-collar family in Michigan. Most of my male relatives and my grandparents worked in factories. My father worked on the assembly line at General Motors for nearly thirty years. My mother, who is brilliant, had me very young, at 18. She was an amazing teacher, even though she hadn’t yet been trained to do that when I was a small kid. We didn’t have a lot of money, so our entertainment was the outdoors. She got me into the woods and collecting butterflies in fields. Later in life, she went to college, and she’s a second-grade teacher now. But back then, this is what we spent our free time doing. I attribute my interest in biology to her.
My dad pursued side gigs because there was a lot of downtime when people were laid off. He would take on odd jobs, and one of them was to raise earthworms to sell to the tackle shop in Michigan, so he built a worm breeding colony in our backyard. When it would rain, we would accompany him into a big field across from the house, where the earthworms would come up — we called them night crawlers — and we would help him collect night crawlers to seed the farm and sell to the bait shop for extra money.
I didn’t realize you could make a career out of science until college. I dualmajored in philosophy and biological sciences. I was very much into philosophy, but even then, I sensed some trepidation about the job market, and coming from a blue-collar family, I had to think about that. My philosophy professor told me that he’d give his left big toe to be a biologist in this era.
What brings you the greatest joy in this line of work?
That moment when you know something no other human has ever known before, which could turn out to be a really important secret in the natural world. I love that. That’s the adrenaline rush that comes from doing research. Very closely tied to this is mentoring, and I’ve had some great mentors myself. The sheer joy of influencing the next generation of scientists is why I do what I do. It’s a way to touch the trajectory of science as a whole but also to influence individual lives and career paths. This can take many forms. It’s the postdoc who’s been here for nine years because she came in as a PhD student. It could be an undergraduate having their first science experience in my lab. Later today, I am meeting a fourth-grader who wrote me about helping her with a school project.
How do you cope with disappointment or failure?
I have a high tolerance for failure and delayed gratification. My grandfather had several amputations for his peripheral artery disease before he passed away, and this too motivates my long-term objective, even if I don’t live to see it come true. Of course, sometimes I get bummed out, but I try to remember it’s the long game that matters. If I’m really stressed, almost the only thing that can cure me is getting in the woods. The other is perspective.
I think one of the reasons why I have higher tolerance for failure is having the perspective of where I came from. When I get frustrated about something, I ask myself: “What was expected of me given where I started from in Monroe, Michigan, which is a town that is pretty bleak from many vantage points?” Getting to where I am on this campus, I really can’t get too depressed. My twin boys are almost 16 and doing well. They have a normal life. They’re healthy. I remember those things and I’m like, “It’s OK.”
—EKATERINA PESHEVA
A Prepared Mind
Throughout his career as a physician-scientist, first studying cancer genomics in academia and now pushing forward new therapies in industry, Levi Garraway, MD ’99 PhD ’99, has embraced a simple tenet: Chance favors the prepared mind. “The idea is that you come curious and ready to work and immerse yourself in interesting problems,” Garraway says. “Part of it is chance, but you also have to understand how to ask the right questions.”
Garraway arrived at HMS intending to study infectious diseases, but his plans changed when his father was diagnosed with an aggressive form of prostate cancer. “I found myself in the library spending as much time reading about what was happening in cancer research as I was on my PhD thesis topic,” he recalls. As he realized that very little of the research was being translated into better cancer therapies, his curiosity turned into what he describes as “vexing frustration.” This frustration helped convince him to devote his career to studying cancer, with the goal of improving treatments.
Garraway finished his training at the perfect time to join the field of cancer genomics. “For the first time, it was possible to look at cancers at a whole-genome level,” he says. “We didn’t know what we were going to learn, but we were quite certain that there would be something important.”
In the early 2000s, Garraway and colleagues in his lab at Dana-Farber Cancer Institute used genomic tools to map various cancers. In the process, they made discoveries about the genes that drive cancer and the genetic mechanisms that enable tumor cells to resist treatment. “The progression of the field has been breathtaking, and the technology continues to expand at a remarkable rate,” Garraway says.
In 2013, Dana-Farber established the Joint Center for Cancer Precision Medicine with Garraway as its founding director. His work there, he says, was “a great opportunity to create a bridge between the cancer genetics insights and key clinical questions.”
As Garraway’s interest in the therapeutic side of cancer research continued to grow, he eventually made the leap from academia to industry, moving first to Eli Lilly and then to Roche, where he is now the head of global product development and chief medical officer.
Garraway has what he describes as his “dream job,” overseeing late-stage drug development for five disease areas, including cancer. “I spend a lot of my time gathering information to help us make decisions about bringing new medicines forward,” Garraway says, adding that the process draws daily on his experiences as both a scientist and a physician.
Garraway considers his work to be equal parts humbling and thrilling — humbling when lab research doesn’t translate into humans as expected and thrilling when it finally does. “Developing a therapy that improves survival can mean one more wedding or anniversary or season of college football,” Garraway says. “It’s meaningful for patients and families, and that’s what gets me up in the morning.”
—CATHERINE CARUSO
Match Day 2025
On March 21, joyful shouts filled the lobby of the New Research Building on the HMS campus as 164 graduating students tore open the envelopes of longawaited letters containing the momentous news of where they will begin their clinical training.
Dean for Students Fidencio Saldaña, MD ’01, had just led a countdown to noon and rung the bell signifying that students could open their Match Day letters.
Faculty, family, and friends joined the students to celebrate the next steps in their careers.
Emily Rencsok
MD-PHD PROGRAM
HEALTH SCIENCES AND TECHNOLOGY TRACK (HST)
How her grandmother’s double knee replacement sparked an interest in medicine: “It was night and day,” Rencsok says. “She was having trouble walking and was in a lot of pain, and within a couple days, she was up and walking around…. I wanted to design devices so people could walk better or do tissue engineering so people could have better cartilage repair.”
What led her to study epidemiology: During a gap year between college and HMS, Rencsok conducted research with one of her college professors, interviewing people who had moved out of Baltimore City with the help of government-subsidized housing vouchers. She worked for a STEM pipeline program for middle schoolers in West Baltimore and at Thread, a community impact
organization supporting young people in Baltimore, which taught her about the diverse factors that affect people’s well-being.
What she focused on for her graduate research: Rencsok pursued her doctorate at the Harvard T.H. Chan School of Public Health with Lorelei Mucci, a professor of epidemiology, as her advisor. Less than six months in, Mucci invited her to travel to Nigeria to present on IRONMAN, an international registry of men with advanced prostate cancer. “Lorelei was a superstar in terms of giving me those sorts of opportunities, connecting me to people I wouldn’t have met otherwise,” she says.
“She became truly like family to me.” For her dissertation, Rencsok studied racial disparities in quality-of-life outcomes for patients with prostate cancer.
“The
opportunities we get as part of HST are just wild.”
How HMS impressed her: “The opportunities we get as part of HST are just wild,” she says. She was invigorated by the approach to studying disease and thrilled by the “glimpse into how medicine might change over the next twenty to thirty years.”
What’s next: Rencsok will pursue her residency in physical medicine and rehabilitation at Spaulding Rehabilitation Hospital.
Final thoughts: “I’ve tried to expose myself to a lot of different things and not worry too much about what people want me to be or think an MD-PhD should be,” she says. “I think that’s given me the opportunity to find what I can contribute to the world.”
—MIKE CAMPBELL
How football led to psychiatry:
Jowan Watson was playing football at Georgetown University when a major knee injury knocked him out during his sophomore season. He was jarred to discover that “there wasn’t a lot of work being done around preparing athletes for the possibility of losing that huge aspect of their identity.” Watson has worked to change the narrative by creating a first-of-its-kind residency training curriculum in sports psychiatry so future doctors can better help athletes in similar situations.
Why faith is so important to him: “Faith is the most important thing in my life,” he says. “It’s helped me in navigating patient conversations, respecting individuals’ perspectives and values and beliefs. It informs the way I interact with people at all levels.”
“I wouldn’t be here without the individuals who have come before me.”
How he hopes to repay his mentors by being a mentor himself:
“I wouldn’t be here without the individuals who have come before me, both in general in terms of my ancestors and my family and also those who have decided to pour into me as a learner,” he says. He became a mentor with the MV3 Foundation, which empowers Black undergraduates interested in health and biomedical sciences, and an executive board member of Hope Medical Scholars, an HMS student-founded organization that provides an immersion program for underrepresented minority and first-generation students in New England.
What he does outside the classroom and clinic: Watson and his wife enjoy playing video games and trying new restaurants. Football continues to
be a passion. He has played guitar since he was a child, inspired by the musicians on stage in his local church, and has kept that interest alive by teaching others to play.
What’s next: Watson will pursue his residency in psychiatry at Brigham and Women’s Hospital.
Final thoughts: “I hope that the way I navigate relationships, including patient and collegial interactions, reminds people that life is incredible, that they are worth it, and that it is truly important to just be kind to everyone,” he says.
—STEPHANIE
M. MCPHERSON
Jowan Watson MD PROGRAM PATHWAYS TRACK
DETAILS, UPDATES, AND OBSERVATIONS FROM ALUMNI
WHAT EXPERIENCES, PERSONAL OR OTHERWISE, LED YOU TO HMS?
Stephen Smith, MD ’63
I spent the summer following my undergraduate sophomore year with my uncle, a physician in California. That experience led me to choose a career in medicine.
Kenneth Bridges, MD ’76
Alvin Poussaint was key to my choice of HMS. As a first-to-college African American, I was uncertain of the reception I would receive at an elite Ivy League medical school. Dr. Poussaint’s openness about the medical school experience in general and HMS in particular gave me confidence both in the quality of the education and the ambience of the environment. His impact on me was life-changing.
Mary McCarthy-Tiella, MSc ’21
As a hospice nurse I am challenged daily with ethical dilemmas. The confluence of the opioid epidemic, the pandemic, and decreasing resources for families caring for loved ones dying at home required a fresh approach to combat moral distress. I found support and knowledge at HMS at the Center for Bioethics graduate program.
Benjamin Rix Brooks, MD ’70
In 1954, my cousin’s U.S. Navy officer husband developed bulbar poliomyelitis, leading to an early experience in the polio ward in the White Building at MGH. Later, in college, I stumbled upon a description of poliomyelitis in a book I found in Harvard Square on motor neuron disease that crystallized my interest in neurovirology. At HMS, I worked in the John F. Enders lab as a student with many who were developing the measles vaccine and others. Prior to the Salk vaccine, polio was a common influence on us all.
Stephanie Pincus, MD ’68
In summer 1964 I was working at a research laboratory when I received a letter admitting me from the HMS waiting list. I knew almost nothing about Harvard and had never been to Boston, but the laboratory head said
it was a good place to go and an easy place to transfer from. So I jumped into the unknown and never regretted it.
Jose Giron, MD ’75
Superb reputation and great depth in research and clinical experience.
Edward Walkley, MD ’70
Three years undergrad at Dartmouth. I did my first two years of medical school at Dartmouth Medical School. It had small classes with great faculty and clinical correlation from day one. Then I transferred to HMS for the unrivaled clinical base and teaching.
Cheryl Warner, MD ’79
My father was a family practitioner and Holocaust survivor. As an immigrant from what was then Czechoslovakia, he restarted his life and career in the United States, grateful to be here with an opportunity to provide patientcentered, empathic care for his working-class patients. At retirement he received hundreds of cards and local news articles praising him. He encouraged me to aim high and remain committed to my personal goals.
Kenneth Chin, MD ’74
My first plane flight to Boston was for a research project I was involved in while in college. I liked the “town”!
Tsontcho Ianchulev, MD ’99 Providence.
Claire Broome, MD ’75
Thanks to all who shared their thoughts. We welcome responses to our future Rounds questions at alumni. hms.harvard.edu/ rounds. Submissions will appear in print, online, or both in the coming months.
Kenneth Walker, MD ’50
I applied and was so very lucky to be accepted. And fortunate to be both a surgeon and syndicated medical journalist. I traveled the world as a journalist interviewing great scientists. In the process I’ve learned that great discoveries often go unnoticed.
Pablo LaPuerta, MD ’89
I was interested in both research and practice. I knew other medical schools would give me great clinical experience. I felt Harvard could add world-class research to that. My laboratory work in medical school eventually led to my involvement in drug development.
Johnson Lightfoote, MD ’76
I was blessed by a deep exposure to the sciences from Phillips Academy and Harvard College. I only wish that I would have given back more.
Richard Peinert, MD ’73
Easy. I was accepted!
Richard Hannah, MD ’66
I strongly considered the offer Case Western Reserve School of Medicine tendered me. However, it is tough to ignore Harvard Medical School. Was my choice to attend HMS rather than Western Reserve wise? I can only wonder. Harvard was quite good.
Herbert Dan Adams, MD ’65
I spent the year after college in Colombia on a traveling fellowship loosely centered on public health, experiencing a very different culture and figuring out what to do with my life. I had two revelations — I wanted to contribute to global development, and I had to bring expertise to the table. HMS was the source of expertise, although the structure of the first year of med school was a huge challenge. I learned later how I had bored my friends talking about life in the barrio.
My dad (HMS ’29) had told me of its challenge and excellence. Thus, I believed HMS was the toughest test, and I loved that concept. HMS almost killed me ... LOL.
Kathryn Glatter, MD ’93
I got accepted to both Stanford and Harvard Medical Schools. I liked Harvard, but I really loved Stanford. The weather there was great, and the students were playing hacky sack, which I had never seen before. Coming from the Midwest, both places seemed fantastic. My father said, “Well, Harvard is Harvard,” so I enrolled to
get the Harvard name on my resume. I loved it and was later able to do my electrophysiology fellowship and get married at Stanford.
Stephen Grund, MD ’91
While doing postdoctoral research at Children’s Hospital, I met so many smart, dedicated physicians from HMS — riding in the elevator with Judah Folkman, for example. They inspired me to change careers from research to medicine. I knew that HMS provided the best teaching and training, which would allow me to become the best physician I was capable of. There was nowhere else I wanted to go.
Ichiro Ikuta, MMSc ’12
I was looking to gain a better understanding of radiation exposure from medical imaging after seeing one of my patients get many CT head exams. I found great mentorship at HMS from Drs. Katherine Andriole, Aaron Sodickson, and Alexa McCray. An HMS postdoctoral fellowship in biomedical informatics gave me the foundation for better research and has made me a better doctor.
Bliss Chang, MD ’20
A second look solidified my desire to attend HMS. While the resources at HMS are outstanding, there are many places with sufficient resources to launch an excellent medical career. What really struck me about HMS was the collegiality and openness to sharing diverse viewpoints. The true advantage of HMS is exposure to unique life experiences and viewpoints that one would never encounter otherwise. Essentially, this is a fast track to accumulating the currency of life.
John Bullock, MD ’68
When I was in the first grade, I decided that I wanted to be a doctor. My best friend’s father had gone to Dartmouth College and Harvard Law School, so I decided to go to Dartmouth and HMS. Fortunately, I did!
JOHN SOARES
Alvin Poussaint was a legendary figure at HMS, inspiring generations of students. “His impact on me was life-changing,” notes Kenneth Bridges, MD ’76. Poussaint died on February 24.
In Memoriam
1940s
1949
Jesse H. Jampol, MD October 25, 2024
1950s
1951
David Hayes, MD February 14, 2025
1954
Thomas F. O’Brien, MD December 9, 2024
Thomas F. Stallings, MD December 6, 2024
1955
David S. Fischer, MD December 8, 2024
Thomas G. Gabuzda, MD November 21, 2024
Leston B. Nay, MD November 14, 2024
Robert L. Parsons, MD September 18, 2024
Peter W. Rand, MD November 18, 2024
1956
Guy Octo Barnett, MD June 30, 2020
1957
George P. Baker, MD December 17, 2024
Donald E. Dickerson, MD November 4, 2024
Francis X. Rockett, MD December 26, 2024
Philip R. Sullivan, MD September 26, 2024
1958
John F. Barlow, MD September 20, 2024
Gunes N. Ege, MD January 8, 2025
Martin Kantor, MD 2024
Howard M. Kremen, MD December 4, 2024
Joseph C. Todd, MD November 27, 2024
1959
James E. Colberg, MD September 11, 2024
Cavin P. Leeman, MD November 2, 2024
Kilmer S. McCully, MD February 21, 2025
Joseph Garretson Pittman, MD November 6, 2024
Paul E. Sapir, MD December 24, 2024
1960s
1960
Robert B. Greer III, MD
March 27, 2025
1961
Ruben Altman, MD
January 5, 2025
1962
David W. Dain, MD
November 16, 2024
Charles B. Smith, MD December 23, 2024
1963
Rudolf G. Bickel, MD March 23, 2025
Michael N. Oxman, MD January 15, 2025
David S. Papermaster, MD October 12, 2024
1964
Roger P. Bernard, MD September 28, 2024
Alexander R. Irvine, MD September 14, 2024
1965
William G. Couser, MD February 27, 2025
1968
Robert A. Marshall, MD November 28, 2024
1969
Bryan J. Arling, MD March 12, 2025
Ronald E. DeCesare, MD February 26, 2025
William E. Hinkley, MD November 13, 2024
1970s
1973
Joseph Rogers Simpson, MD October 24, 2024
1974
Thomas Najarian, MD November 17, 2024
Frank M. Torti, MD October 14, 2024
1978
Patricia E. Meadow, MD December 29, 2024
1980s
1989
Michael S. Aronow, MD March 11, 2025
This listing includes alumni whose notices of death were received between September 10, 2024, and May 4, 2025.
PRESIDENT’S REPORT
Winter 2025 Meeting
For HMS, as for other medical schools, 2025 got off to a challenging start. Proposed cuts to federal funding of research, particularly to so-called indirect research costs, would be felt across the institution. At the winter Alumni Council meeting, held virtually in mid-February, we learned more about how these cuts might affect HMS and talked about how alumni might help to respond.
At HMS, as elsewhere, patients, students, faculty, postdocs, and staff could all be affected. That the impact would be felt across the enterprise illustrates the often invisible yet crucial interrelationships of the school’s educational, clinical, and research missions.
We came to consensus on several points during our discussion. Most importantly, we affirmed that medicine is and should remain a service-focused caring profession and that any actions should be guided by that perspective. HMS’s primary concerns must always be patients, trainees, and the staff that make the system work. There was also agreement that the institution would (and perhaps should) change in response to potential revenue loss.
There are many ways that alumni can support HMS and ensure its survival for future generations as the outstanding school we experienced. Actions include contacting legislators and respectfully educating friends and acquaintances outside of medicine about the interconnectivity of research and patient care and the critical role of the NIH in making such essential, nonpartisan work possible. Donations of time, expertise, or money can be directed to areas of alumni passion or offered for use in areas of greatest need. With even a spare thirty to sixty minutes, alumni can log onto the new HMS platform MD Connect to support current students concerned about their futures in this time of upheaval.
The people of HMS were and are remarkable; let’s do what we can to ensure that doesn’t change.
2025 Distinguished Service Award for HMS Alumni
Michael Rosenblatt, MD ’73, will be honored at the Harvard Medical Alumni Association’s annual meeting on June 13 for his extraordinary dedication to HMS over five decades. As a member of the Board of Fellows and the Advisory Council on Education, as well as a past president of the Alumni Council, he has provided invaluable leadership — championing debt-free MD education and fostering stronger alumni ties. His efforts to engage industry alumni, mentor students, and lead class reunions have helped build a more vibrant and tightly knit HMS community. Learn more at alumni.hms.harvard.edu/service-award.
Meet Seven New Alumni Council Members
MD graduates will elect seven new members to the Alumni Council by acclamation during the Harvard Medical Alumni Association’s annual meeting on June 13. Representing the Third Pentad (classes of 2010–2014) is Robert “Bobby” Daly, MD ’10. David J. Brown, MD ’97 (Class of 1996), will represent the Sixth Pentad (classes of 1995–1999). Tessa Gardner, MD ’72, will represent the Tenth and Beyond Pentads (classes of 1979 and beyond). Tamara R. Fountain, MD ’88, has been appointed as the council’s president-elect. R. Sonia Batra, MD ’00, will serve as a councilor-at-large representing all classes. Jay Chyung, MD ’06 PhD ’04 (Class of 2003), will serve as a Harvard Alumni Association graduate school director representing HMS. Martin Burke, MD ’05 PhD ’04 (Class of 2002), will assume the position of chair of annual giving. Learn more about the new representatives at alumni.hms. harvard.edu/election.
Proposed HMAA Constitutional Amendment
At the Harvard Medical Alumni Association’s annual meeting on June 13, come vote on proposed constitutional changes that would grant voting rights to the chairs of alumni relations and alumni giving. Learn more at alumni.hms.harvard.edu/election.
Let’s MD Connect
We invite MD alumni to create a profile on this innovative platform to connect with fellow alumni and students seeking advice on student life, career paths, identity-based connections, and professional networking. Connect today at aad.hms.harvard.edu. You will need your HarvardKey to access MD Connect.
Reunion and Alumni Days
Registration for Reunion 2025 is open for MD classes ending in “0” or “5.” Events will be held June 12–14 for the 20th through 60th classes and June 13–14 for the 5th through 15th classes. Register today to join us for engaging discussions, campus tours, the Party on the Quad, and more. Visit alumni.hms.harvard.edu/ reunion for further details. Additionally, all alumni are invited to participate in activities June 13–14. Learn more at alumni.hms.harvard.edu/alumni-days.
LOUISE ARONSON, MD ’92, IS PROFESSOR EMERITUS AT THE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO, AND VISITING SCHOLAR AT THE STANFORD CENTER ON LONGEVITY.
FUTURE OF DISCOVERY
Bold ideas, transformative education, and lifesaving breakthroughs begin with academic freedom—and with you.
With national investment in biomedical discovery and education under threat, philanthropy plays a critical role in empowering Harvard Medical School to pursue the most urgent, audacious, and unexpected ideas—no matter where they come from.
It’s how breakthroughs happen. It’s how the next great discovery begins.
And how tomorrow’s physician-leaders are trained to heal, innovate, and serve.
Your gift funds more than medicine. It fuels the freedom to lead and learn.
25 Shattuck Street
Boston, Massachusetts 02115
Electronic Service Requested
(RE)GENERATION WHY
About 350 million years ago, humans and salamanders likely shared an ancestor that could regenerate limbs. Salamanders retain this ability. Humans, not so much. The study of axolotl salamanders provides clues as to why that is and hints at the possibility of reawakening regeneration (page 46).