Gavin Finkelstein President, Haemophilia Foundation Australia
As we head into spring, we have a lot happening, with both Bleeding Disorders Awareness Month and the Australian Bleeding Disorders Conference.
HEPATITIS C
You will read an update in this issue of National Haemophilia about our current work in the hepatitis C space. Hepatitis C has had an immense impact on the bleeding disorders community. You may be aware of our survey for people affected by hepatitis C earlier this year and some of you have been asking about our findings. We have reported on the survey results about current needs and priorities and our steps in pursuing this with government. At the same time, we need to remain active on the health of our community affected by hepatitis C, even if they have been cured, and I invite you to share the key messages in our World Hepatitis Day campaign with family, friends and your wider connections.
CAMBODIA TWINNING
In August 2025, Executive Director, Natashia Coco, and HFNSW President, Dan Credazzi visited the Cambodia Hemophilia Association (CHA) in Phnom Penh to conduct an assessment for a potential World Federation of Hemophilia (WFH) Twinning starting 2026, together with Hazri Aris, WFH Regional Manager – South East Asia & Western Pacific. We met the local haemophilia foundation committee and visited the Haemophilia Treatment Centre in Phnom Penh to gauge how HFA can help CHA and develop a year 1 plan. This was funded by WFH.
The WFH Twinning programs enable established and emerging haemophilia organisations and Haemophilia Treatment Centres around the world to share their knowledge and help to improve treatment and care.
We look forward to a formal announcement at the end of the year.
From the President
Haemophilia Foundation Australia and Cambodia Hemophilia Association representatives.
L-R: Ny Channaroon, Hun Chhay, Natashia Coco, Dan Credazzi, Vorlek Nuon, Soung Somaly, Senghenh Nuon, Hazri Aris
L-R: Dan Credazzi, Hazri Aris, Natashia Coco
AUSTRALIAN BLEEDING DISORDERS CONFERENCE
The Conference will take place on 16-18 October 2025 and I look forward to seeing some familiar and new faces there. The program has been released. Take a look – you will find it as an insert in this edition of National Haemophilia and it’s also available online. I’m amazed at the range of topics that will be covered and the really innovative approaches in the sessions. Some great international and Australian speakers will be presenting. I expect there will be some robust discussions!
Our conference is a time when community, health professionals and other stakeholders come together and have open forums on where we are going in the future. I encourage you to consider coming to Brisbane and being part of it.
Youth program
It’s also an opportunity for young people to connect and have some fun together as well as participating in the Conference program. Alan Dursun, who recently attended the WFH Youth Leadership training and Ben Inglis from Victoria will run the youth program, starting on Thursday afternoon with rock climbing at Kangaroo Point.
See the HFA website for more information –www.haemophilia.org.au/conference-2025
NEW HFA LOGO
You might have seen on our website and communications that HFA has a new, inclusive logo! Designed as an evolution on our previous logo, the new logo sports the same look and feel but with a brand new tagline: For all bleeding disorders. It was important for us at HFA to demonstrate that we recognise – and represent – people with all bleeding disorders. Haemophilia is and always will be a big part of who we are, but we are also a community that includes other bleeding disorders–from the not-so-rare, such as von Willebrand disease (VWD), to the exceedingly rare, like Glanzmann thrombasthenia. Highlighting this in our logo is a way of being proud of our diverse community and encouraging connection and support.
STAY UP-TO-DATE
With so much happening and changing very quickly, it’s important to stay up to date with what’s new. You can register for the HFA e-newsletter by signing up at https://www.haemophilia.org.au/helpful/sign-up-toour-enews/. This will give you the latest news about bleeding disorders and HFA activities, with updates on events.
Meeting with Dr Chean Sophal and patients at National Paediatric Hospital in Phnom Penh
HFA and hepatitis C
For more than 20 years Haemophilia Foundation Australia (HFA) has conducted hepatitis C advocacy campaigns for our bleeding disorders community. These campaigns have aimed to address significant impacts on our community: recognition, financial and support needs, treatment product safety and a cure. After new hepatitis C treatments became available to all Australians in 2016 and most people with bleeding disorders have now been cured of hep C, the landscape has changed.1
It has been important to understand the priorities of our affected community now and HFA conducted a snapshot survey in January 2025 to hear from people with bleeding disorders affected by hep C. The results of this survey have helped to guide HFA’s current approach to hep C.
HEPATITIS C AND BLEEDING DISORDERS
In Australia many people with bleeding disorders acquired hepatitis C virus (HCV) from their plasmaderived clotting factor treatment products or other blood products before 1993. Plasma-derived concentrates were a particularly high risk as each batch was manufactured from the pooled donations of thousands of donors and one HCV infection could infect the entire batch. In 2004 the Australian Red Cross Blood Service estimated that approximately 1350 Australians with bleeding disorders had hepatitis C.2
Several safety measures were introduced by 1993 and the risk of bloodborne viruses from plasmaderived clotting factor products in Australia is now considered to be extremely low:
1990 HCV testing of the blood supply commenced
1990 factor VIII (8) products manufactured using HCV inactivation measures became available
1993 factor IX (9) products manufactured using HCV inactivation measures became available
2004 universal access to recombinant clotting factor products (created in a laboratory and virus-free) for Australians with haemophilia.
In 2020 the HFA Getting older with a bleeding disorder needs assessment found that, although the greater majority of surviving people with bleeding disorders and hepatitis C have now been cured, there are ongoing health, financial and support issues for many.
This includes:
• Ongoing monitoring for people with cirrhosis to check for complications such as liver cancer.
• Careful medical liaison between hepatitis specialists and Haemophilia Treatment Centres for those with advanced liver disease.
• Some people with mild bleeding disorders and women who carry the gene may not be aware that they were at risk for hepatitis C and have not been tested or treated for hepatitis C. >>
• Being exposed to hepatitis C and the continuing impact on their life has been a traumatic experience for affected people with bleeding disorders. This needs to be acknowledged and support provided, even if they have been cured
• Living with a bleeding disorder and hepatitis C has had a cumulative impact on increasing health care costs and reduced income over a lifetime, making affected people increasingly vulnerable in their senior years
• Financial assistance is also needed for out-ofpocket health and community care costs.3
Australian governments contributed to HCV litigation settlement schemes for eligible people who contracted HCV via the blood supply in Australia between
WHAT HAS HFA DONE SO FAR?
1985 and 1991, before the introduction of reliable screening tests for hepatitis C virus. However, to be eligible, an individual needed to link their source of infection to a single donor with hepatitis C.
HFA believes that nearly all people with bleeding disorders were excluded from eligibility as they had many treatments during this period and usually with plasma-derived concentrates and they could not identify a particular treatment batch or a single donor. Apart from a small ex-gratia payment that was made by the ACT government to people with bleeding disorders who acquired hepatitis C through the blood supply, there have been no other government financial recompense schemes for people with bleeding disorders in Australia.4
The HFA hepatitis C strategy page on our website gives more information about the issues and the work HFA has done over more than 20 years to advocate for affected community members. This page also includes links to our previous community consultation reports: www.haemophilia.org.au/hfa-hepcstrategy
2004 Senate Inquiry
• HFA presented all of our known hep C evidence to the 2004 Australian Government Senate Inquiry into Hepatitis C and the Blood Supply in Australia. The Inquiry recommended a scheme for case management and financial support for health and community care costs of those who acquired hepatitis C through the blood supply, but it was never carried out.2
Recognition
• HFA’s Getting Older report recommended an acknowledgement: ‘That the traumatic experience of being exposed to HIV and hepatitis C and the ongoing impact on the life of affected people with bleeding disorders is acknowledged by Australian governments, even if they have been cured of hepatitis C.’
Financial and support needs
• HFA conducted advocacy campaigns for a no fault (ex gratia) recompense scheme in 2003-04 and 2010-11 on moral grounds.
• In 2011 HFA began advocating for the Senate Inquiry recommendation that was never carried out: a scheme for case management and financial support for health and community care costs.
Treatment product safety and a cure
• HFA conducted an advocacy campaign for recombinant factor VIII and IX therapy for all Australians (not manufactured from human blood) – achieved 2004.
• From 2014 HFA advocated for new DAA hep C treatments as a cure - cure was the highest priority in the HFA Double Whammy consultation (2007-9). These treatments became available for all Australians in 2016.
2025 HFA HEPATITIS C SNAPSHOT SURVEY
In January 2025, HFA asked our community with hepatitis C about their current priorities and issues. Results from the HFA hepatitis C snapshot survey confirmed that hepatitis C remains a concern for many of those affected in our community.
76 Australians with bleeding disorders affected by hepatitis C responded to the survey.
50% reported ongoing liver health issues.
Please describe any liver health issues you currently experience n = 38
Symptoms: Elevated LFTs, fatigue, nausea, pain
Cirrhosis/advanced liver disease
Liver transplant +outcomes
Liver cancer
No/unsure symptoms: Elevated LFTs
Serious liver damage; waiting for test results
Very reactive to medications/can’t have some
The survey asked participants what would help and their priorities.
What would improve your life re: hep C?
Needs identified n = 45 - 1 priority per person
Financial assistance/support
Treatment/support for liver health issues
Full inquiry/Royal commission
Apology/acknowledgment
Mental health/PTSD support
How important are these outcomes to you?
‘Very important - Work is getting harder to do (work part-time).’
‘Very - in the past I have had to pay for some CT scans. Currently I am bulk billed.’
‘Very. I am still hurting emotionally from my diagnosis despite being treated and of course my liver continues to have issues.’
‘Extensively, due to the great impact it has had on my life and that of my family’s.’
‘Very important, many haemophiliacs cannot move forward in life with proper acknowledgement of what occurred.’
Mental health
People with bleeding disorders are often stoic and the mental health impact of hepatitis C is often unrecognised.
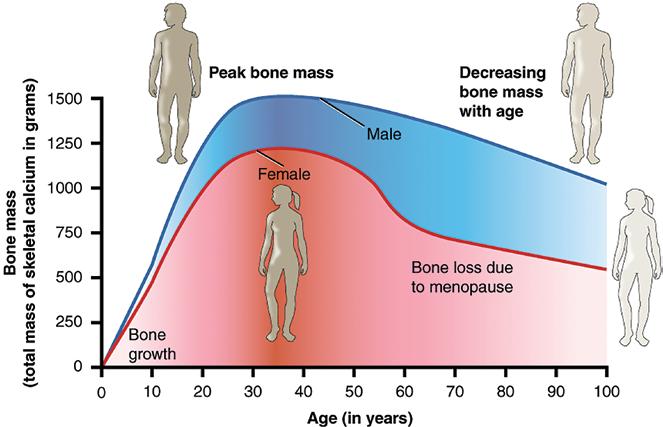
Although only 7% in the survey identified a need for mental health support, the HFA 2020 PROBE (Patient Reported Outcomes Burdens and Experiences)
Australia Study found that older men with haemophilia, who were nearly all affected by hep C, had twice the rate of clinically diagnosed depression and anxiety as those without a bleeding disorder, who did not have hep C.3 In the Getting Older report, Haemophilia Treatment Centre health professionals saw mental health as an issue for all of those affected by bloodborne viruses.3 This is consistent with overseas studies, which have found high scores for depression, stress and emotional distress in people with haemophilia affected by hepatitis C.5
Going forward it will be important to acknowledge the mental health impact of hepatitis C and provide services and support to all those affected.
Highest priorities
The outcomes given the highest priority were (in order of popularity):
• Financial compensation/assistance
• Support services
• Better access to liver health care (monitoring, management and treatment)
• Recognition/apology.
WHAT NEXT?
The 2025 snapshot survey results have confirmed that it is a priority for HFA to move forward to address the health, support and financial needs of Australians with bleeding disorders affected by hepatitis C.
HFA has prepared our case and revisited costings with the generous support of individuals in the community who provided case studies. A potential scheme has been prepared that aims to address the needs described in the survey and the HFA Getting Older report. This has been approved by HFA Council. While we are not able to share the scheme with you at this point, it has been based on evidence from our consultation, drawing on real experiences, case studies and research data.
In June 2025, we re-started the conversation about the effects hepatitis C has had on the bleeding disorders community and current needs with different departments in the Australian government. We have presented the potential scheme and aim to have further discussions in the coming months.
We are grateful to the community members who have shared their personal stories about the impact of hepatitis C for our advocacy in the past, and may be looking for others in the future who are willing to share their experiences.
We will keep the community updated on developments and any requests like this.
To keep up-to-date, make sure you are registered for the HFA e-news by signing up at: www.haemophilia.org.au/helpful/sign-up/.
REFERENCES
1. Unpublished Australian Haemophilia Centre Directors’ Organisation Project Report. Current health status of Australian patients with Hepatitis C and bleeding disorders. Melbourne: AHCDO, 2020.
2. Australia. Senate Community Affairs References Committee. Hepatitis C and the blood supply in Australia. Canberra: Senate Community Affairs References Committee Secretariat, 2004.
4. Chapter 5, ‘Compensation arrangements’ in Australia. Senate Community Affairs References Committee. Hepatitis C and the blood supply in Australia. Canberra: Senate Community Affairs References Committee Secretariat, 2004.
5. Schmidt A, Tomschi F, Möllers P, et al. Factors influencing symptoms of depression, anxiety and stress in patients with haemophilia. Haemophilia, 2025;0:1–9. https://doi.org/10.1111/hae.70079
World Hepatitis Day 2025
World Hepatitis Day is held annually on 28 July. In 2025 we come together globally to share the message It’s time for action: hepatitis C and liver health remain important issues for our community and acting now is vital.
Your liver can’t wait. You can’t either. DON’T DELAY. TAKE ACTION TODAY.
Are you at risk? Do you know your hep C status? Find out if you don’t know
Hep C can be cured. Treatment is simple
Do you need ongoing liver health monitoring? Ask your doctor.
A healthy liver is vital to us all. Take steps to look after your liver health. A healthy liver is important to everyone, whether we have had hep C or not. Your liver has a lot of different jobs to do to keep your body working well.
Find out 5 ways to keep your liver healthy at: www.haemophilia.org.au/healthy-liver.
HEP C AND BLEEDING DISORDERS
You may be aware that in Australia many people with bleeding disorders acquired hepatitis C from treatment with blood products before 1993. Several safety measures were introduced by 1993 and the risk of hep C or HIV from plasma-derived clotting factor products in Australia is now considered to be extremely low. But many people in our community live on with the consequences of those early infections.
WHO IS AT RISK?
Are you over 30 years of age and have a bleeding disorder, or carry the gene? If you had a blood product before 1993 – even once – you could be at risk.
Nearly 1 in 5 Australians with hepatitis C have never been diagnosed and don’t know they have hep C. Symptoms are not always obvious. >>
You can have a free hep C blood test to find out your hep C status if you don’t know – your GP or your HTC can organise it. Current hep C treatments are simple and easy - a once-daily tablet, with few if any side-effects and very high cure rates.
CURED OF HEP C? HAS YOUR LIVER RECOVERED?
Most Australians with bleeding disorders and hep C have now had treatment and been cured – but some need ongoing care for their liver health. Although you might think it’s all OK, you may not notice liver disease symptoms. Ignoring your liver health can have serious consequences.
It’s important to know the status of your liver health when you were cured. This determines whether you will need ongoing monitoring.
If you don’t know, take the time today to contact your hepatitis doctor or your GP to check your liver test results. Find out if you need ongoing follow-up with a liver specialist.
Remember: If you had cirrhosis or extensive scarring before being cured of hep C, you will still need to have a liver ultrasound scan every 6 months long-term.
Sadly, some people with bleeding disorders have very advanced liver disease due to long term hep C infection. Close liaison between liver specialists and Haemophilia Treatment Centres is important for treatment and care. Research into management of advanced liver disease is ongoing.
Q: Can I have gene therapy if I’ve had hep C?
A: Yes - as long as you have been cured or you are HCV PCR negative (no active virus in your blood) and your liver is showing signs that it is functioning normally.
Talk to your doctor about this and they may refer you to a liver specialist for some tests to show that your liver is healthy:
• a liver assessment with an ultrasound
• a fibrosis assessment via FibroScan® or another non-invasive assessment such as shear wave elastography or ARFI (Acoustic Radiation Force Impulse)
• and blood tests.
If you are treated with gene therapy for haemophilia, your liver function will be monitored as part of routine care. There are things you can do to prepare your liver for gene therapy. Visit https://tinyurl.com/HFA-healthy-liver to find out more.
Advice from hepatitis specialists Associate Professors Simone Strasser and Joe Sasadeusz and the Australian Haemophilia Centre Directors’ Organisation (AHCDO).
FOR MORE INFORMATION
Visit:
• www.worldhepatitisday.org.au
• The HFA World Hepatitis Day page: www.haemophilia.org.au/world-hep-day
As a Partner in the national World Hepatitis Day Campaign, HFA works with Hepatitis Australia and the state and territory Haemophilia Foundations on the awareness campaign for the bleeding disorders community and is committed to making a difference on hepatitis C in Australia.
In October 2025, we are once again raising awareness of bleeding disorders in Australia with Bleeding Disorders Awareness Month. This is an opportunity for individuals, families, Haemophilia Foundations, Haemophilia Treatment Centres and other organisations to raise awareness in your local community.
Our theme this year is Teamwork - Pushing the Boundaries, which is in line with our Australian Bleeding Disorders Conference, also taking place in October 2025.
Teamwork - Pushing the Boundaries highlights the power of collaboration in advancing care, treatment, and support for people living with a bleeding disorder. By working together, we can break down barriers, share knowledge, and explore new possibilities for better health outcomes.
WHAT’S ON FOR THE MONTH?
Find out more about Bleeding Disorders Awareness Month: www.haemophilia.org.au/BDAM
Throughout the month we’ll share personal stories, fast facts and bust some myths about bleeding disorders. There will also be activities for kids, including word finds, scavenger hunts and our national colouring-in competition.
The last week of October will be Red Week. During the week organise an activity with your family or friends around something red – wear red to school, bake red cupcakes, red hair day – the ideas are endless!!
LOCAL EVENTS
Meet up with your local community. Attend state/territory Foundation events, including walks, trivia nights, and more. Reach out to your local Foundation for more details or head to our website closer to the date for a full list of events.
GET INVOLVED!
Help raise awareness. Host an event through your workplace, school, or with family and friends. Whether it’s an information session, morning tea, ‘wear red’ day, or red cupcake sale, HFA offers a range of promotional items to help you raise awareness for all bleeding disorders.
PROMOTIONAL ITEMS
What’s available for your events?
• posters
• colouring-in sheets
• toy cars
• jibbitz (croc charms)
• stickers, pens, balloons
• and more!
To order your promotional items, complete the online form via our website: www.haemophilia.org.au/BDAMorder
Please note, these items are free of charge, however quantities are limited. Place your order as soon as possible. All orders will be posted out in midSeptember.
FIND OUT MORE
To keep up to date with HFA and Bleeding Disorders Awareness Month, make sure you
• are registered for our eNews: www.haemophilia.org.au/helpful/sign-up
• and follow us on social media. HFA is active on Facebook, Instagram and LinkedIn – find us: @haemophiliafoundationaustralia
FOR MORE INFORMATION
visit www.haemophilia.org.au/BDAM or contact: hfaust@haemophilia.org.au or call HFA on 03 9885 7800
The Australian Bleeding Disorders Conference is just around the corner.
Being held in Brisbane from 16-18 October 2025, it is a fantastic opportunity to bring together people with bleeding disorders and their families and carers, health professionals, policy makers, and industry.
Our Conference Program Committee has been working together to bring you a comprehensive program with current and emerging issues, personal stories, panel sessions, and more.
To view the latest program, visit: www.haemophilia.org.au/conference-2025
What previous attendees have said:
‘It is making me feel more connected to people with bleeding disorders. It has also helped me build on my confidence to advocate for my son.’
‘As a health care professional, I found hearing the patient stories very motivating but also inspiring that we still need to do better. Opportunity to network is always invaluable professionally.’
‘We have come back from the conference feeling validated, more confident and connected. We wish that we had been attending previously.’ www.haemophilia.org.au/conference-2025
A unique Conference –thoughts from the Co-Chairs
What’s special about the Australian Bleeding Disorders Conference?
HFA interviewed the Co-Chairs of the 2025 Conference, Dr Simon Brown and Dr Jane Mason.
HFA: What makes the Australian Bleeding Disorders Conference unique or different from other events?
Dr Simon Brown: I’ve always found that conferences like HFA and WFH are most impactful when individuals with bleeding disorders share their personal experiences. These perspectives offer invaluable insight. In the medical field, it’s easy to become entrenched in a clinical or ‘medicalised’ view of the world. Hearing directly from those living with these conditions challenges that mindset in meaningful ways. Their stories often spark new lines of inquiry - ones that might otherwise remain unexplored.
Dr Jane Mason: What truly sets this conference apart is its remarkable inclusivity - clinicians and patients stand together, side by side, as equal contributors. This shared space sparks genuine collaboration, where the lived experiences of patients are not just heard but celebrated. Their stories are powerful, often deeply moving, and serve to remind us all of the real-world impact of our work.
Equally, the multidisciplinary nature of the meeting enriches every conversation. It’s not unusual to come away with a fresh insight from a physiotherapist, nurse or social worker—perspectives that prompt reflection and, on occasion, lead to meaningful changes in my own clinical practice. This dynamic blend of voices and expertise is what makes the event so vibrant and transformative.
Dr Simon Brown
Dr Jane Mason
‘What truly sets this conference apart is its remarkable inclusivity - clinicians and patients stand together, side by side, as equal contributors.’ Dr Jane Mason
HFA: What are you most excited to talk about at the Conference?
Dr Simon Brown: The evolution of comprehensive care for bleeding disorders is entering a transformative phase. Emerging therapies are challenging long-standing treatment paradigms, prompting critical conversations about how we fund these innovations and adapt our models of care. As we move toward the next generation of treatments, we must reimagine not only how care is delivered, but also how it remains accessible, sustainable, and patient-centred.
Dr Jane Mason: This year, I have the privilege of both speaking and chairing in the minor procedures session - a segment that has direct relevance to daily life with a bleeding disorder. Our focus will be on the seemingly routine interventions that many encounter throughout life: dental extractions, minor surgeries, colonoscopies or even simple biopsies. While these procedures might sound unremarkable, for someone with a bleeding disorder, they can present significant risks if not carefully managed.
We want to emphasise just how critical it is to inform your Haemophilia Treatment Centre ahead of time and work together to develop a tailored plan. A proactive approach, with clear communication and preparation, can transform what might otherwise become a complicated ordeal into a smooth, safe experience. It’s often the ordinary, ‘minor’ procedures - those we might be tempted to overlook - that pose the greatest threats if the appropriate treatments aren’t in place.
By sharing insights from both clinicians and patients who have navigated these situations, we hope to equip everyone with practical strategies, foster a sense of empowerment, and, ultimately, prevent avoidable complications.
‘To me, teamwork is a cornerstone of care for individuals with bleeding disorders. It extends far beyond the staff within a Treatment Centre - encompassing clinical decision-making, government policy, and collaboration among colleagues at both national and international levels.’
Dr Simon Brown
HFA: How does the Conference help build connections and foster teamwork within the bleeding disorders community?
Dr Simon Brown: To me, teamwork is a cornerstone of care for individuals with bleeding disorders. It extends far beyond the staff within a Treatment Centre - encompassing clinical decision-making, government policy, and collaboration among colleagues at both national and international levels. Delivering safe and effective therapies requires a unified effort across all these domains.
Meetings like this one offer a valuable opportunity to strengthen those connections and align our collective focus on the shared goal of optimal patient outcomes. On several occasions, I’ve reached out to international colleagues - such as Cedric Hermans - for guidance on complex clinical scenarios, or to industry partners regarding potential therapies for unique cases. Teamwork truly permeates every aspect of clinical care.
Dr Jane Mason: Teamwork truly lies at the heart of haemophilia care. Over the years, I’ve been continually inspired by the insights shared by fellow clinicians - these exchanges often spark new
HFA: This year marks our 23rd Conference! What are you looking forward to as a Chair?
Dr Simon Brown: As you know, I was especially keen for the Conference to be held in Brisbane, as it marks the 25th anniversary of the Haemophilia Centres in Queensland - a milestone worth celebrating. I’m deeply grateful to the HFA team for helping make this vision a reality. I hope the conference not only honours this achievement, but also offers attendees a chance to enjoy the Queensland sunshine and the vibrant spirit of our community.
Dr Jane Mason: To be honest, casting my mind back to my very first conference is a challenge - I have to admit, the details are a bit hazy! If memory serves, it was in 2015, at a time when I was a senior registrar with aspirations for a future in bleeding disorders care.
collaborations, leading us to co-author research and develop innovative approaches together.
What I find especially powerful is witnessing the diverse ways colleagues tackle familiar challenges. Sometimes, it’s a subtle shift in protocol or a new tool for patient engagement that makes all the difference. By embracing these fresh perspectives and learning from one another, we create space for improvement, ensuring our care evolves. This collective spirit of learning and adaptation is what drives our field forward, making it possible for us to deliver safer, more effective outcomes - together.
Since then, my journey has been full of growth and opportunity: I’ve moved on to become Director of Haemophilia at the Royal Brisbane and Women’s Hospital and am now privileged to care for people across the whole lifespan, holding appointments at both Queensland Children’s Hospital and the Royal Brisbane and Women’s Hospital. The path has also given me the chance to dive into research and form collaborations with haemophilia clinicians worldwide, continually learning from peers near and far and contributing, in some small way, to the progress of our field.
HFA: What do you think will have the biggest impact on people with bleeding disorders in the next 10 years?
Dr Simon Brown: If you had asked me this question back in 1999, when I began my first consultant appointment at The Katharine Dormandy Centre in London, my answer would have been gene therapy. And today, my response remains the same. Yet, it’s now tempered by a broader awareness: despite the remarkable progress we’ve made, many individuals with bleeding disorders around the world remain undiagnosed or lack access to essential therapies.
Looking ahead, one of the most meaningful advancements over the next decade would be to redress these global disparities. Ensuring equitable access to care and treatment for all - regardless of geography - would be a truly transformative achievement.
Dr Jane Mason: Without question, the further advancement of novel therapies will shape the future of care for those living with bleeding disorders. Having had the privilege to witness firsthand the effects of gene therapy clinical trials - and to
personally administer this therapy to more than ten individuals - I see enormous promise on the horizon. Yet, the journey is far from over. The goal remains a reliable, safe, and durable gene therapy option accessible to everyone, regardless of background or circumstance.
However, we must not lose sight of a deeper challenge - the glaring inequity in diagnosis and access to care. With an estimated two-thirds of people with bleeding disorders globally still undiagnosed or unable to receive appropriate treatment, bridging this gap stands to make the greatest impact of all. Progress in science is vital, but progress in equity is essential; only by addressing both can we ensure that the benefits of innovation reach every corner of our community.
Dr Simon Brown is the Haemophilia Treatment Centre Director at Queensland Children’s Hospital, Brisbane.
Dr Jane Mason is the Haemophilia Treatment Centre Director at the Royal Brisbane & Women’s Hospital, Queensland.
ISTH 2025 – emerging therapies in haemophilia and VWD
Ashley Fletcher
The International Society on Thrombosis and Haemostasis (ISTH) 2025 Congress, held in Washington D.C. in June 2025, brought together leading experts, researchers, and clinicians to share the latest advances in bleeding and clotting disorders. This summary highlights emerging therapies in haemophilia and von Willebrand disease (VWD), focusing on innovative treatments that aim to improve patient outcomes and quality of life.
These therapies are currently being tested in clinical trials and are not available yet.
Treatments for bleeding disorders are evolving rapidly and researchers are always looking for new ways to advance treatment.
If you have a bleeding disorder, it’s important that you stay in touch with your HTC and discuss your treatment options regularly to determine what would best suit you and your situation and if new options are available.
Ashley with his poster at ISTH 2025
WHAT ARE CLINICAL TRIAL PHASES?
Phase 1 is a very early stage clinical trial.
• Testing a new treatment in a small group of people
• Testing safety and possible side effects.
Phase 2 is the next stage.
• Testing a new treatment in a larger group of people
• Testing a new treatment in large groups –hundreds to thousands of people
• Comparing the treatment to other treatments
• Monitoring side effects and safety information.
Phase 4 is a ‘real world’ study.
• Monitoring what happens when the treatment is prescribed for the wider population with the condition
• Monitoring side effects over a longer period of time
• May test the treatment for another health condition or in combination with another treatment.1
proteins that block TFPI, an anti-clotting protein, and increase how much thrombin the body makes, which then increases clotting connect two clotting factor proteins at once, helping clotting to occur imitating the function of a clotting factor, eg factor VIII (8) laboratory made proteins that imitate human antibodies in the immune system bind only to one site by mouth treatment administered regularly to prevent bleeds treatments that ‘silence’ the clotting protein antithrombin, which then allows thrombin production to increase and help with clotting under the skin
a protein that helps with clotting
1.Australian Government. Australian Clinical Trials. What is a clinical trial? 8 November 2023. https://www.australianclinicaltrials.gov.au/about/what-is-a-clinical-trial
Information on this page supplied by Haemophilia Foundation Australia, September 2025
KEY THERAPIES BY CLASS Haemophilia
Inno8
The first oral bispecific antibody 1
For: haemophilia A
How it works: oral FVIIIa (factor 8a)-mimetic bispecific antibody (imitating FVIIIa).
Bridges FIXa (factor 9a) and FX (factor 10)
Status: Phase 1 (VOYAGER1; NCT06649630) – in humans
Key points:
• Delivered orally using an absorption enhancer.
• High potency.
• Half-life is approx. 113 hrs (albumin binding).
• Potentially a daily tablet.
Significance: Very early days but potentially the first oral prophylaxis therapy for haemophilia A.
NXT007
Next generation emicizumab-like bispecific antibody 2
For: haemophilia A (with or without inhibitors)
How it works: Bispecific antibody with enhanced FVIIIa (8a)-mimetic activity (imitating FVIIIa)
Status: Phase 2
Key points:
• It’s built to do the same job as emicizumab.
• Quite potent.
• Maintains steady normal FVIII (factor 8)-equivalent levels.
• Subcutaneous dosing every 4 weeks or longer.
Significance: Improved bleed protection with extended length of time between doses.
Mim8
Potent next generation FVIII (factor 8)-mimetic 3
For: haemophilia A with or without inhibitors
How it works: subcutaneous FVIII-mimetic bispecific antibody (imitating FVIII)
Status: Phase 3 (FRONTIER 2)
Key points:
• It works for people who have never had haemophilia treatment before and for those changing over from emicizumab.
For: haemophilia A and B with or without inhibitors
How it works: subcutaneous monoclonal antibody inhibiting TFPI and enabling more thrombin to be produced to help clotting.
Status: Phase 3 (explorer8 – in extension phase until 2028)
Key points:
• Significantly reduces the number of bleeds in a year.
• Effective in patients with target joints.
• Can be stored at room temperature for 28 days.
Significance: non-factor therapy option for a broad haemophilia population
Fitusiran
small interfering RNA (siRNA)-based antithrombin suppression 5
For: haemophilia A and B with or without inhibitors
How it works: it’s a type of genetic medicine that tells the liver to make less of a natural clot-blocking protein (antithrombin), so blood can clot more easily.
Status: Phase 3 (ATLAS studies)
Key points:
• Monthly subcutaneous injection.
• Bleed rates reduced across all populations.
• Can be given at a lower dose, improving the safety profile.
• Can be stored at room temperature for 3 months.
Significance: Durable, long-acting prophylaxis; a long-lasting preventative treatment that’s showing a good balance between benefits and side effects.
Altuviiio (efanesoctocog alfa)
Extended Half-Life (EHL) FVIII (factor 8) 6, 7
For: haemophilia A
How it works: it’s a lab-made clotting protein that’s been modified with special attachments so it stays in the body longer, meaning fewer infusions are needed.
Status: XTEND-ed Study Phase 3 trial and approved in the USA (FDA 2023); new real-world data presented at ISTH 2025.
Key points:
• Once-weekly intravenous dosing.
• The drug keeps clotting factor levels much higher than the usual low point between doses, giving stronger ongoing protection from bleeding.
• Excellent bleed protection in adults and children.
Significance: good EHL-FVIII product; strong real-world uptake >>
Von Willebrand disease (VWD)
HMB-002
monovalent antibody 8, 9
For: von Willebrand disease (VWD) – all types
How it works: prophylaxis therapy designed to increase and extend the half-life of von Willebrand factor (VWF) in the bloodstream.
Status: early clinical Proof-of-Mechanism data presented (does it work in the human body as it is meant to); ongoing development.
Key points:
• A therapy that is first in its class aimed at sustained elevation of VWF levels.
• Potential to provide longer-lasting protection against bleeds for patients.
Significance: offers promise for improved bleeding control with less frequent dosing, enhancing patient quality of life.
VGA039 monoclonal antibody 10
For: von Willebrand disease (VWD)
How it works: targets Protein S, a crucial cofactor in coagulation, enhancing thrombin generation
Status: A large Phase 3 trial will begin in late 2025 to confirm how well it works and how safe it is in people with VWD.
Key points: Current treatments for VWD often require frequent IV (intravenous) infusions. VGA039 could become the first simple, under-the-skin option for routine prevention of bleeding.
Significance: This could greatly improve convenience, quality of life, and treatment consistency for people living with VWD.
Advanced diagnostic tools for VWD 11,
12
For: diagnostic evaluation and management of von Willebrand disease
How it works: new assays (laboratory tests) measuring platelet binding activity of VWF to improve the classification of VWD subtypes and the assessment of severity.
Status: emerging diagnostic tools undergoing evaluation and validation.
Key points:
• Enhanced ability to characterize VWD more accurately.
• Supports personalised treatment decisions.
Significance: Improves diagnosis and guides tailored therapies, potentially optimising outcomes for patients.
FINAL TAKEAWAYS
• haemophilia A is experiencing rapid therapeutic expansion: oral (Inno8), next-generation bispecifics (Mim8, NXT007), siRNA (Fitusiran), gene therapy, and weekly factor therapy (Altuviiio) are all viable and increasingly personalised.
• haemophilia B has reliable gene therapy and broader non-factor options like concizumab and fitusiran.
• von Willebrand disease has emerging therapies focussing on extending treatment durability, improving bleeding control, and enhancing diagnostic precision offering hope for more effective, personalised care for patients.
These innovative therapies represent important progress in reducing treatment burdens and enhancing quality of life for people living with haemophilia and von Willebrand disease. As research continues to evolve, collaboration with healthcare professionals remains essential to tailor these advances to individual patient needs and ensure the best outcomes.
REFERENCES
1. Lund J, Jensen K, Ezban M. In vitro activity of Inno8 in global hemostatic assays alone and with other hemostatic agents. [abstract OC39.5] ISTH 2025 Congress, 21-25 June 2025, Washington.
2. Shima M, You C-W, Park Y-S, et al. NXT007 prophylaxis in emicizumabnaive persons with hemophilia A without inhibitor: phase I/II study. [abstract OC20.3] ISTH 2025 Congress, 21-25 June 2025, Washington.
3. Oldenburg J, Benson G, Chowdary P, et al. FRONTIER5 direct switch study: safety of initiating Mim8 prophylaxis without washout of emicizumab. [abstract OC20.4] ISTH 2025 Congress, 21-25 June 2025, Washington.
4. Wheeler A, Angchaisuksiri P, Apte S, et al. Annualized bleeding rates in hemophilia A/B and target joints: concizumab Explorer8 study. [abstract OC59.2] ISTH 2025 Congress, 21-25 June 2025, Washington.
5. Young G, Kavakli K, Shen M-C, et al. Association of antithrombin levels with efficacy of fitusiran prophylaxis in people with hemophilia A or B with and without inhibitors: a predictive modeling approach. [abstract OC59.3] ISTH 2025 Congress, 21-25 June 2025, Washington DC.
6. Malec L, Königs C, Dunn A, et al. Treatment of bleeding episodes with efanesoctocog alfa in children: XTEND-ed second interim analysis. [abstract OC20.5] ISTH 2025 Congress, 21-25 June 2025, Washington DC.
7. Khoo L, Klamroth R, von Drygalski A, et al. Major surgical outcomes with efanesoctocog alfa: 4 years’ experience in the XTEND clinical program. [abstract OC64.4] ISTH 2025 Congress, 21-25 June 2025, Washington DC.
8. Raheja P, Tsiamita O, Knott A, et al. VELORA Pioneer: first-in-human safety and PK/PD study of HMB-002 in Type 1 Von Willebrand disease. [abstract LB 01.4] ISTH 2025 Congress, 21-25 June 2025, Washington DC.
9. Haeger M, Zivkovic M, Gandhi PS, et al. HMB-002: elevating von Willebrand Factor for prophylactic treatment of Von Willebrand Disease. [abstract OC 08.4] ISTH 2025 Congress, 21-25 June 2025, Washington DC.
10. Moser M, Leong L, Kovacevic-Miljevic K, et al. The anti-Protein S antibody VGA039 enhances ex vivo coagulation as assessed by thromboelastometry. [abstract PB0111] ISTH 2025 Congress, 21-25 June 2025, Washington DC.
11. Miller AP, Smith J, Lee K, et al. Furthering understanding of VWF copy number variants in patients with von Willebrand disease. [abstract OC28.3] ISTH 2025 Congress, 21-25 June 2025, Washington DC.
12. Christopherson P, Nguyen T, Patel R, et al. The value of VWF plateletand factor VIII-binding assays versus genetic testing in diagnosing type 2 von Willebrand disease. [abstract OC 56.3] ISTH 2025 Congress, 21-25 June 2025, Washington DC.
Stock picture background - Zeksheuskaya for Pexels.com; Ali Pazani for Pexels.com
Ashley Fletcher is the AHCDO Australian Bleeding Disorders Registry (ABDR) Senior Research Fellow.
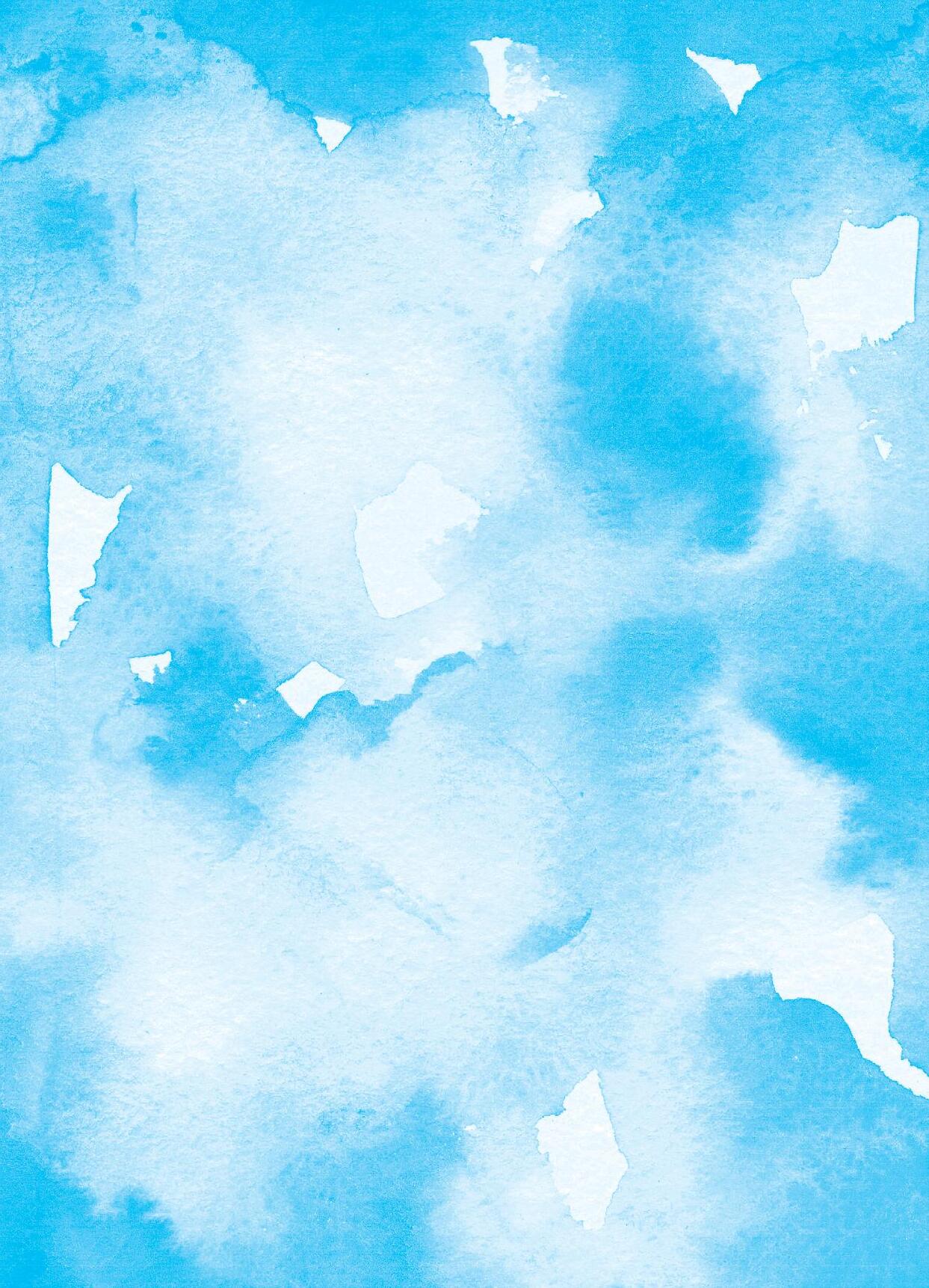
Haemophilia, fractures and bone density
Abi Polus
Why is low bone density and osteoporosis an issue for people with haemophilia? Will that mean they are more likely to have fractures? What can be done about it?
Haemophilia physiotherapist Abi Polus explains bone density in humans, how it is measured and why people with haemophilia are more vulnerable to low bone density and the risk of osteoporosis. She walks through the options for preventing and managing low bone density and osteoporosis in people with haemophilia.
SOME TERMINOLOGY
A fracture is a discontinuity in the bone cells caused due to either trauma OR poor structural integrity of the bone.
Osteoporosis is a term that refers to the fragility of a bone, usually due to reduced bone density and affected bone architecture.
UNDERSTANDING BONE
What is bone density?
Let’s go back a step – what is bone? Bone is a living tissue of cells called osteocytes that are composed of collagen, (plus some carbohydrates, water and proteins), and have (non-living, or inorganic) minerals within.
Bone (architectural) structure
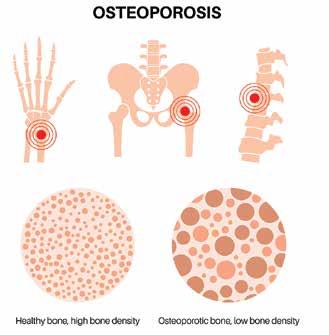
Mature (fully formed) bone cells are termed osteocytes: these are cells embedded in the bone matrix. Osteoblasts (Bone Builders) are cells that form bones and help lay down new bone matrix, to repair damage and re-model the bone. Osteoclasts (Bone cleaners) are cells that reabsorb the bone that is old or has damage so that new bone (the osteoblasts) can repair and lay down new bone. Bone cells are in a constant state of turnover throughout life. Bone mass is primarily developed in childhood and adolescence with Peak Bone Mass occurring typically in early 20s for females and late 20s for males. Genetics, diet, exercise and lifestyle at those ages may influence bone density throughout life. Nutrition is important for bone health, with adequate intake of calcium and vitamin D, as well as magnesium, protein, potassium being important. Alcohol and smoking have been proven to negatively affect bone health. As ageing occurs, in general, less osteoblast than osteoclast action occurs. Hormonal changes can also affect bone density, predominantly in females as oestrogen declines.1
BONE MINERALS
Minerals, such as calcium and phosphate ions, are deposited into the bone matrix in high levels as hydroxyapatite (termed ‘calcification’). This allows the bone to have both strength and flexibility, in order to absorb impact and prevent breakage.
Bone density measures the amount of the bone minerals within the bone tissue. Low bone density indicates an increased risk of fracture if the bone is stressed, e.g. during a fall.
Bone mineral density measures the levels of calcium and other minerals in your bones. This is usually measured with a DEXA scan which uses radiation to measure the levels of calcium and you are often given a ‘T-score’ or a ‘Z-score’. These scores measure levels against what a normal level of bone mineral density in a young healthy adult is. This is used in postmenopausal women and men aged over 50 years. There are a few common areas that are measured most often the hip and spine.
Osteopenia is a stage of low bone density. If left and not addressed, it may progress to lower level of bone density called osteoporosis. Osteoporosis is diagnosed in adults if there has been a fracture
with minimal trauma or have a low T- or Z-score. If osteoporosis is present the risk of a fracture with minimal trauma is higher. Osteoporosis is suggested to affect up to 10% of the male population, and often is only identified after a fracture.
HAEMOPHILIA AND LOW BONE MASS DENSITY
There is a strong correlation between haemophilia and low bone mass density throughout the age ranges, not just in the older age populations. 3,4,5
People with haemophilia may be more vulnerable to low bone mass density and increased osteopenia and osteoporosis. A 2023 study compared men with haemophilia and compared them with agematched controls without haemophilia and found a significant decrease in bone mass density in those with haemophilia. 3 This has also been demonstrated in earlier studies. 4,5 It is suggested that may factors may contribute to this which include, but are not limited to, reduced physical activity, haemophilic arthropathy, periods of immobility, muscle atrophy, hepatitis C and/or HIV infection,
Bone mass changes with age Image licensed via Creative Commons2
and vitamin D deficiency. 5,6 There has been some research presented that low bone mass density could also be due to the lack of coagulation factor itself on bone metabolism and bleeding into an area may affect the bone architecture. 3
There have been some studies looking at haemophilia and bone density and osteoporosis risk. A study in 2012 found that adolescent boys with haemophilia have a lower trabecular (architectural bone cell matrix) density suggesting that peak bone mass may not be achieved in this population at this time. This could be due to lifestyle factors, or enforced rest if bleeds occurred which would decrease weightbearing at an essential time of growth. 4 It is interesting that this study was conducted before novel therapies were available, and a more current study may have different results. It is relevant to our current middle-aged and older populations due to lower levels of activity as people with haemophilia were historically encouraged to do less physical activity due to lack of treatment if they were to have an injury (something we have completely changed our suggestions on with the available treatment nowadays).
Another consideration is that ‘normal’ peak bone density may not have ever occurred during the critical times of childhood and adolescence. 3 For example, if you had recurrent bleeds in a weightbearing joint and had frequent periods of offloading (not putting weight or only partial weight) through that joint then you may not have laid down the full potential bone mass and density that would be reflected in the figures for an individual who had. When this is tested later on (or now) it may then show a ‘below average’ score, however this may not be due to decreasing bone density, but actually may be normal for you as you never had it. It is of more relevance to see if your bone mass is decreasing over time (problematic) or if it is stable (optimal). In patients who are now ageing, this then has the double impact of potentially less original bone mass density with now less osteoblastic action (laying down bone cells). This is why screening is encouraged.
BONE DENSITY SCREENING
The World Federation of Hemophilia (WFH) recommends screening for osteoporosis in people with haemophilia with ‘additional risk factors’ 7 , however the 2016 Australian guidelines for the
management of haemophilia in Australia advised all people with haemophilia should be screened according to local guidelines. 8 Australian national guidelines on osteoporosis prevention state that all post-menopausal women and men over 50 years of age with one major risk factor (of which haemophilia could be counted) should be screened.9 A DEXA scan is recommended for people with haemophilia. These can be arranged through your general practitioner (GP) or rheumatology or orthopaedic clinics via your Haemophilia Treatment Centre. A vitamin D level is also advised as this impacts directly on bone mass density.
An increased risk of falls and of fractures has also been identified in people with haemophilia. Although the majority of fractures in the general population occur in those over 65 years, 81% of fractures in people with haemophilia occur below 50 years with an average of 28-30 years old. 4 This is more prevalent in people with severe haemophilia than in those with mild or moderate haemophilia. For this reason we advise bone mass density DEXA scans to identify risks, but also strongly encourage exercise and activities to address risk of falls and maintenance of general fitness. There is a plethora of evidence to demonstrate that healthy and strong muscles, and balance and proprioception work can prevent falls. This includes the WFH guidelines and the Australian guidelines. 3 Weight-bearing exercise specifically increases bone mass density and is recommended throughout the age ranges. At any age you can increase osteoclast formation (to increase bone mass density) with weightbearing exercise. Feel free to contact you HTC physiotherapist or local physiotherapist for a program.
In Australia a registry, the haemophilia osteoporosis registry (THOR), has been created so that data in individuals with and without haemophilia can be compared. 3
WHAT CAN WE DO?
MANAGEMENT OF LOW BONE DENSITY
Alongside weight bearing exercises and exercise programs targeting healthy movement and promoting good balance and falls prevention, there are various medications used to prevent osteopenia and osteoporosis if identified as a risk. Cessation of smoking, minimising alcohol and a healthy diet are
also advised. If identified early and managed, this can prevent the risk of a fracture if a trauma was to occur.
The medical treatments may include calcium treatments and supplements for vitamin D if deficient.
There are anti-resorptive options these days, which slow down or prevent bone loss. The main differences are the mechanism of action and formulation, e.g. IV (intravenous) annual injection versus a weekly oral tablet. There are numerous options now which give patients choice due to suitability, preference and side effects. Your rheumatologist or GP are best placed to discuss this with you.
The WFH guidelines state that anti-osteoporosis medication should be used with people with haemophilia and osteoporosis and those with osteopenia should commence bisphosphonates as appropriate. 6 The 2016 Australian guidelines stated bisphosphonates may be appropriate in some people with haemophilia. 7
PREVENTION IS BETTER THAN CURE
Take home messages
It is recommended that children and adolescents should be doing regular, daily weight-bearing exercise to maximise peak bone mass.
Adults should also be doing regular, daily weight-bearing exercise to maintain their bone mass. Balance, proprioception and strength exercises will help to prevent falls and the risk of trauma and potentially fracture.
In addition to lifestyle and nutrition these are all factors we can individually contribute towards better bone health to protect ourselves from fractures.
Bone density should be regular screened in people with haemophilia.
If a decrease in bone mass density is identified it should be medically managed.
With thanks to Dr Ryan Moore, Rheumatology Registrar, The Alfred hospital, Melbourne for the pharmacological advice.
REFERENCES
1. Radhakrishnan S, d’Oiron R. Ageing and women with bleeding disorders. The Journal of Haemophilia Practice. 2022;9(1):126-131. https://doi.org/10.2478/jhp-2022-0016
2. Anatomy & Physiology, Connexions Web site. File: 615_Age_and_ Bone_Mass.jpg. http://cnx.org/content/col11496/1.6/, Jun 19, 2013. Licensed under Creative Commons by 3.0 <https://creativecommons.org/licenses/by/3.0>, via Wikimedia Commons
3. Petkovic MJ, Tran HA, Ebeling PR, Zengin A. Osteoporosis management and falls prevention in patients with haemophilia: review of haemophilia guidelines. Haemophilia. 2022;28:388–396. https://doi.org/10.1111/hae.14540
4. Biernat MM, Jędrzejuk D, Urbaniak-Kujda D, et al. Association of bone mineral density and potential risk factors for osteoporosis in patients with severe haemophilia A. Haemophilia. 2024;30:130–139 https://doi.org/10.1111/hae.14903
5. Kempton CL, Antun A, Antoniucci DM, et al. Bone density in haemophilia: a single institutional cross-sectional study. Haemophilia. 2014;20(1):121-128. https://doi.org/10.1111/hae.12240
6. Gerstner G, Damiano ML, Tom A, et al. Prevalence and risk factors associated with decreased bone density in patients with haemophilia. Haemophilia. 2009;15(2):559-565. https://doi.org/10.1111/j.1365-2516.2008.01963.x
7. Srivastava A, Santagostino E, Dougall A, et al. WFH Guidelines for the Management of Hemophilia, 3rd edn. Haemophilia. 2020: 26(Suppl 6): 1-158. https://doi.org/10.1111/hae.14046
8. Australian Haemophilia Centre Directors’ Organisation. Guidelines for the management of haemophilia in Australia. Canberra: National Blood Authority, 2016.
9. The Royal Australian College of General Practitioners and Osteoporosis Australia. Osteoporosis prevention, diagnosis and management in postmenopausal women and men over 50 years of age. 2nd ed. East Melbourne, Vic: RACGP, 2017.
Stock images: Freepik; Osteoporosis: user19987712 for Freepik
Abi Polus is Senior Clinical Physiotherapist - Haemophilia at the Ronald Sawers Haemophilia Centre, Alfred Health, Melbourne, Victoria.
Navigating factor X deficiency: a nursing perspective
Jen Dowbnia and Lara Olson
WHAT IS FACTOR X (10) DEFICIENCY?
While people with haemophilia are familiar with deficiencies in factor VIII/8 (haemophilia A) and factor IX/9 (haemophilia B), factor X/10 deficiency is much rarer and less commonly discussed. It is estimated that 1 in 1,000,000 people are diagnosed worldwide, with approximately 30 people diagnosed in Australia.
Factor X deficiency is a rare bleeding disorder that may be inherited or acquired. It can lead to symptoms ranging from easy bruising and nosebleeds to severe joint or internal bleeding, particularly in the severe form of the condition. Factor X deficiency affects male and females equally and can range from mild to severe, with severe patients requiring prophylaxis (preventive treatment).
FROM A NURSE’S PERSPECTIVE: HOW WE MANAGE IT
As haemophilia nurses in Australia, we work within a multidisciplinary comprehensive care model. That means we coordinate with haematologists, general practitioners, social workers, physiotherapists, and sometimes genetic counsellors to ensure holistic care for patients with bleeding disorders - including rare ones like factor X deficiency.
Diagnosis and monitoring
Most patients are referred to Haemophilia Treatment Centres (HTCs) across Australia after abnormal bleeding episodes or family history leads to further investigation. Blood tests such as prothrombin time (PT) and activated partial thromboplastin time (aPTT), along with specific factor assays, confirm the diagnosis.
As haemophilia nurses, we help:
• Coordinate testing
• Educate patients and families about what the diagnosis means
• Support emotional wellbeing post-diagnosis
• Order and coordinate factor replacement and consumables
Treatment options in Australia
The mainstay of treatment for moderate to severe factor X deficiency is plasma-derived factor X concentrate, currently available in a multiple factor Prothrombin Complex Concentrate/PCC (eg, Beriplex AU®). This treatment is provided at no cost to patients through the National Blood Authority (NBA), which sources and supplies blood products to HTCs on behalf of Australian and state/territory governments.
Other treatments may include:
• Fresh frozen plasma (FFP) or other Prothrombin Complex Concentrates (PCCs) in emergencies or if Beriplex AU® is not available
• Recombinant factor X concentrates if available
• Antifibrinolytics like tranexamic acid for minor bleeds
Researchers are always looking for new ways to treat bleeding disorders and treatments are advancing rapidly. It’s important that people with factor X deficiency stay in touch with their HTC and discuss their treatment options to determine which one would best suit them and if new options are available.
As nurses, we ensure:
• Patients and carers are educated in administration techniques, especially if home infusions are required
• Bleed logs and infusion records are maintained
• We assist in managing treatment plans for surgeries or dental work, where clotting support is needed in advance
THE AUSTRALIAN APPROACH: EQUITY AND ACCESS
Australia is fortunate to have a well-structured bleeding disorders network, with HTCs located in major cities and support from Haemophilia Foundations - Haemophilia Foundation Australia (HFA) and state/territory Foundations. Access to factor replacement therapy is funded by the government, and some delivery options reduce the burden on rural or remote patients.
However, challenges still exist:
• Delayed diagnosis due to rarity and lack of awareness
• Access to specialists in rural and remote areas
• Psychosocial impacts of living with a rare disorder
• Consumables are not included with PCCs. Patients requiring prophylaxis may need to rely on the goodwill of local health services to supply if not living near an HTC.
Nurses play a key role in advocating for timely referrals and bridging care gaps, particularly through telehealth, which has grown significantly since the COVID-19 pandemic. >>
BEL’S STORY
I was born with factor X deficiency, a rare genetic bleeding disorder that affects the blood’s ability to clot. Every week, I give myself an injection to prevent spontaneous bleeds. It’s a non-negotiable part of my routine, even when the rest of life feels chaotic.
As a child, I never thought much of it. It was just my ‘normal’. But as I became a teenager and started wanting more independence, I struggled. Like many young people, I pushed boundaries and resisted treatment.
As an adult now, I still have days where I can’t be bothered doing treatment and wish I didn’t have to, but I learned pretty quickly what happens when I skip it and end up with a bleed. I’m also very lucky that my husband knows how to do my treatment and can help me. His support has been especially important during my period, when I
have days that are quite heavy due to the condition.
I’ve been fortunate to travel, work remotely on the mines, and do pretty much everything I’ve wanted without being held back. My travel bags might be a little fuller than most, but I’ve never had any problems bringing my supplies on holidays or on mine sites.
Having factor X has even opened up opportunities I wouldn’t have had otherwise. I’ve met likeminded people, been involved in youth work, and attended haemophilia camps, all of which have added real value to my life.
Over time, I’ve come to accept that this is something I’ll live with for the rest of my life. It’s just part of my routine now. Having a strong support system, including my Haemophilia Treatment Centre, as well as my family and friends, has made all the difference.
LIVING WELL WITH FACTOR X DEFICIENCY
Although it can be daunting to receive a rare diagnosis, patients in Australia are not alone. With the support of knowledgeable healthcare providers, including nurses who specialise in bleeding disorders, it is possible to live a full and active life.
Top nursing tips:
1. Report all unusual bleeding or bruising –even if it seems minor
2. Keep an updated bleeding disorder management plan
3. Wear a medical alert ID and carry ABDR card in wallet
4. Inform your healthcare team (GP, dentist, physio) about your diagnosis
5. Stay connected with peer support groups through HFA and your local Foundation.
Factor X deficiency may be rare, but in Australia, we have the infrastructure, expertise, and compassion to manage it effectively. As nurses, our mission is to empower patients with knowledge, confidence, and a safety net of care—no matter how rare the condition. For more information or support, contact your local Haemophilia Treatment Centre or visit Haemophilia Foundation Australia. Contact details can be found at www.haemophilia.org.au.
REFERENCES
Australian Bleeding Disorders Registry Annual Report 2023-2024. National Blood Authority: Canberra, 2024. Accessed 14 August 2025. https://www.blood.gov.au/australian-bleeding-disorders-registryannual-report
Stock images: Gustavo Fring for Pexels.com; Prostock Studio Freepik
Jen Dowbnia and Lara Olson are Haemophilia Clinical Nurses at the Haemophilia & Haemostatis Centre, Fiona Stanley Hospital, Perth, WA.
Don’t get lost in transition
Angela McGill and Emma Wells
An interview on moving from paediatric to adult haemophilia care
Transitioning from paediatric to adult haemophilia care isn’t just a medical change - it’s a major life shift. So how do young people make the leap without falling through the cracks?
Social Workers Angela McGill and Emma Wells and Ash, a young person with haemophilia who recently made the move to adult care, talk about this question. Together, they share insights, tips, and firsthand experience to help others make the transition with confidence.
Q: Why is the transition from paediatric to adult care such a big deal?
Angela and Emma: It’s a really vulnerable time. In paediatrics, care is very family-focused with lots of support from your whole team – doctor, Clinical Nurse Specialist, physiotherapist, child life therapists and social worker – some Haemophilia Treatment Centres also have a clinical psychologist. But once you enter adult services, the expectation is that you take chargemanaging appointments, medications, emergencies, and all communication. If we don’t prepare young people well, they can become ‘lost in transition,’ which can lead to delayed treatment, missed doses, or even serious complications.
Q: Ash, what was it like for you?
Ash: At first, I was overwhelmed. I’d gone from having Mum speak for me at appointments to suddenly needing to explain my treatment plan and log everything myself. I didn’t feel ready - but luckily, my team started talking about transition when I was around 13 or 14, so I had time to adjust.
Q: When should transition planning actually begin?
Angela and Emma: Ideally, between 12 and 14 years old. It’s not a one-time event - it’s a gradual process. At that stage, we start introducing developmentally appropriate education and encourage young people to ask more questions. For example, ‘What do I do during a bleed?’ or ‘What’s my treatment regimen?’ They should begin learning how to explain their condition to others, too.
Q: What practical steps should young people take in the middle stage — say, between 14 and 16?
Angela and Emma: That’s when we encourage independence. Young people should:
• Start taking charge of their healthcare — organising appointments, tracking treatments.
• At 15 years of age, a young person can apply for a tax file number, access their immunisation history, open their own bank account and get their own Medicare card.
• Understand what Medicare covers — including their factor products.
• From 16 years of age a young person can set up a myGov account and link it to their online Centrelink account.
• At 16 years of age, apply to Centrelink for an Ex-Carer Allowance Health Care Card application, if eligible.
• Maintain a summary of their diagnosis, treatment plan, and emergency contacts.
• Learn to manage anxiety and stress in healthy ways. >>
Ash: The myABDR app was a lifesaver. I got used to logging infusions and bleeds before I fully transitioned. It made me feel more in control. Make sure you have a good list of emergency contacts, especially afterhours and check out the HFA website for support and information.
Q: What happens in the final phase, around ages 16 to 18?
Angela and Emma: This is where we focus on hands-on skills. Teens should:
• Learn how to self-infuse, manage prescriptions, and recognise early signs of complications.
• Visit their adult Haemophilia Treatment Centre ahead of their first appointment.
• Attend joint transition clinics — where the paediatric and adult teams meet the patient together.
Ash: Visiting my new Centre helped a lot. I asked things like, ‘How do you book appointments here?’ and ‘What happens if I have a bleed on the weekend?’ Knowing the answers before I needed them made me feel safer.
Q: Is it just about the medical stuff?
Angela and Emma: Not at all. It’s also about identity and confidence. Teenagers are figuring out who they are while learning to live with a chronic condition. That’s why emotional support is critical. We encourage families to support their child’s independence while still being in the background - offering help when needed but not taking over.
Ash: I had a few rough patches. Honestly, it helps to talk to a social worker or a peer mentor who’s been through it. You’re not alone, even if it feels that way.
Q: Any last words of advice?
Angela and Emma: Yes - ask for a written transition plan. It should include your handover summary, emergency protocols, and contact info for your new team. Also, don’t transition during high-stress times like final exams or a treatment change. Timing matters.
One more suggestion, you know what works well for you – build on this to ensure your long-term good health and well-being!
Ash: Start early, ask questions, and get familiar with your care. I felt lost at first, but now I’m more independent than I thought I could be. I would remind families that they often know what works best for them. Be confident in asking for things and discussing what has worked in the past.
USEFUL LINKS
Transition to adulthood: www.haemophilia.org.au/youth/transition (Factored In - Haemophilia Foundation Australia)
Mental health and support: https://www.haemophilia.org.au/wp-content/uploads/ 2024/03/NH-Mar24-Mental-health-and-support.pdf (Crollini N, National Haemophilia Mar 2024;225:16-17)
Teenagers with chronic health conditions: moving to adult care: https://tinyurl.com/RCN-Teens-adult-care (Raising Children Network)
3 Sentence Health Summary: https://tinyurl.com/CHEO-3-sentence (CHEO: Children’s Hospital of East Ontario, Canadawww.cheo.on.ca)
Services Australia: www.servicesaustralia.gov.au
Stock images: Pavel Danilyuk for Pexels.com; Freepik
Angela McGill is Haematology Social Worker at Calvary Mater Hospital, Newcastle, NSW. Emma Wells is Paediatric Social Worker at John Hunter Children’s Hospital, Newcastle, NSW.
Supporting our children with bleeding disorders in sport
Nicola’s story
OUR EARLY JOURNEY WITH HAEMOPHILIA
My name is Nicola. I am William’s mum. William has moderate haemophilia A. From the very beginning Will was a happy, busy and energetic boy; always keeping his twin sister on her toes. Will and his sister grew up together, running everywhere from the moment they could walk.
Will had many bleeds in his early life: trampoline incidents, constantly running into something and hitting his head. We spent a lot of time at the children’s hospital. Times were tough. I often wondered what his life would turn out to be. The more he grew up, the more he wanted to play sport, run around with his friends and be a complete dare devil! He never held back from rough play and, later, from giving his all on the soccer field.
Nicola’s story beautifully captures the courage and resilience of families living with haemophilia. With the remarkable advances in treatment and care including non-factor therapies, children today can grow up chasing their dreams - whether that’s on the sports field, in the classroom, or beyond.
Just as important is the support of HFV (Haemophilia Foundation Victoria) and HFA (Haemophilia Foundation Australia) which brings families together, provides guidance, and reminds us all that no one has to face the journey of having a bleeding disorder alone.
Stories like Will’s show us that with the right care, encouragement, and community, children with bleeding disorders can truly thrive and live life to the fullest.
Dr Chris Barnes, Haemophilia Treatment Centre Director, The Royal Children’s Hospital, Melbourne
BALANCING RISK AND PASSION
Will always had so much energy, so we knew early on that he would need sport in his life. He always had a passion for it. He started playing basketball when he was 5 years old but constantly got finger bleeds or was knocked, ending up on the couch for the rest of the weekend resting, icing, and elevating. There were calls back and forth to the Haemophilia Treatment Centre (HTC) at the children’s hospital, sometimes a visit for the night, even a week or so for factor VIII (8) infusions, immobilisation, and rehabilitation.
Will and his sister
Hospital trips were extremely hard for him as he was so scared of needles. It was also very hard for his sister; being his twin and so close to him, she would always want to be by his side. Will’s dad, Chris and I always questioned ourselves: were we doing the right thing allowing him to play a lot of sport? Should we tell him to take it easy out on the court, hold him back from giving it his all? Take that courageous spirit out of him? We wondered what other families did, how did they cope?
FINDING COMMUNITY AND CONFIDENCE
So, off to the Haemophilia Foundation family camp we went - to meet other families. I think Chris and I were more scared and nervous than the kids. What were we going to have to face? We had only ever seen the hard, sad times of other patients as well as Will at the hospital. The Foundation family camp has been the best thing we ever did! There were so many amazing
families who had to find resilience and bravery just like us. Families that had faced so much in their lives but were all so positive, encouraging, and inspirational. Will’s new friends at camp gave him the courage to treat himself after they all showed him how they did it. He met some exceptional camp leaders who changed his whole perspective on life with haemophilia. One camp leader showed him that building strength in your body keeps you fit and healthy. To this day, I know he finds inspiration from him. Family camp did not only help Will, it gave Chris and I a newfound hope that we are all going to be ok, that there are so many ways a bleeding disorder can change your life but that’s ok, you can find ways of fulfilling your dreams. Family camp changed our lives forever; the families we meet at our first camp are now our family that we get through life with.
SUPPORT FROM HTC AND HOME TREATMENT
There were still tough times right from the very beginning of our journey with haemophilia but the doctors, nurses and physiotherapist at the HTC were our guiding light. The doctors always encouraged us to let Will live his life to his fullest and we would deal with a bleed when it happened. They taught us how to use appropriate risk assessment while encouraging Will to go forth and follow his dreams.
The physiotherapists were always so supportive as well as informative. Our amazing physio has taught Will so much about how his body works - how to stretch
Recovering from a bleed in hospital
Overcoming challenges at camp
Learning to infuse with the haemophilia nurse
and keep his muscles and body fit. We slowly began to understand through their guidance that keeping fit and strong actually helped to prevent bleeds and maintain joint health.
With the help of our haemophilia nurse - her patience, kindness, and care at times when we felt defeated after a second or sometimes third bleed in a row - we slowly built our confidence to face haemophilia as something that we could all live through, and that Will could actually thrive in ways we never could have imagined. Her connection with Will and all the boys is something that gives them the belief in themselves to always look forward and keep going.
When Will was about 8 years old, it was time for us as a family to decide that we were going to do our treatment at home. This way, Will could get on with his life and do what he loves the most; play sport! So with our nurse’s guidance, we learnt how to treat at home. Dad was the best, never missing a vein and always being an eager patient for Will to practise on.
CHOOSING SOCCER AND EMBRACING INDEPENDENCE
It was at this time that Will decided to try soccer. I think every family’s journey with haemophilia is so unique and everyone makes their own educated decisions on what sport their child plays. I decided early on that Will wouldn’t play AFL football. Partly because of some of the bleeds he had already endured - including some head bleeds - and partly because of how hard he goes into contact on the field. I felt at the time that soccer may be a safer option.
He was still playing basketball but now also added soccer to his weekly love of sport. So, we watched as our brave, resilient, amazing young boy fall in love with a game that has become his life; training for his club as well as earning a place in an elite soccer academy for his age.
Has there been bleeds? Yes. Have there been difficult times? Yes, but they seem to be all the less painful when Will knew he had to work through a bleed, rest and do his physio so that he could get back out on the field; always icing injuries straight away, resting his injury and calling the hospital for further advice and extra factor treatment if needed. With this drive to always be fit and ready to play, came an understanding that if he wanted to play, he needed to have his treatment. That is when he became dedicated to his treatment times.
That resilience and bravery out on the field is what pushed him to decide to find his own vein and treat himself at 9-years-old. This independence changed his life and gave him a new belief in himself. He began treating two times a week, including every Saturday morning before basketball and soccer.
THRIVING IN COMPETITIVE SPORT
When Will was 13 years old, he tried out for the National Premiers League team for his local soccer club. When he made the team, training times stepped up and games became more physical and intense, which did not slow Will down. He had also started at a new grammar school where it is compulsory to play Saturday sports and train during the week. So, he added another soccer team to his playing schedule.
This is when all our learning, guidance from the HTC as well as life experience from past bleeds and inspiration from family camp, came together to prepare Will for a level of sport that I never thought would be a possibility in his lifetime.
At this time, the new non-factor subcutaneous treatment emicizumab (Hemlibra®) came along and changed Will’s life. No more finding veins, no more regular needles and even more of an opportunity
Will playing for the local Academy league
for Will to play sport at level that we know he dreamed about but never thought possible.
Through Will’s hard work and determination, he has played every season of soccer since he was 9 years old; three years of those seasons at a National Premier League level for different clubs as well as for his grammar school in the AGSV (Associated Grammar Schools of Victoria) competition. Last year he was invited to try out for the First team for his grammar school to play with the top boys in the state from different grammar schools and made the team. This year as a 16-year-old he is currently playing up a level in the under 17 team for his local National Premiers League team and the club have also asked him to play in their Reserves side which is made up of 18–21-year-olds before they go into senior soccer. He now plays three games of soccer a weekend and some of his opponents are a lot bigger and stronger than him, being much older and developed than him.
But he is dedicated to keeping fit, training four times a week with his different teams as well as building strength through gym sessions. He also always makes sure he is warmed up with stretching before games and after games he stretches down.
Will playing in the National Premier League
MANAGING UPS AND DOWNS
Will is still working on recognising a bleed from a sporting injury, but we guide him through each decision. We have a process of Rest, Ice, Compression and Elevate after a game if he thinks he might be having a bleed. Once he learnt to understand that the sooner he recognises a bleed and gets treatment, the
sooner he will be back out on that soccer field.
Bad bleeds do still happen and they can be really hard to deal with both physically and emotionally, but Will’s resilience, bravery and courage never cease to amaze. Will and I have many chats about his life with haemophilia; one day we discussed that it is haemophilia that has made him the brave, resilient person he is today and gives him a constant awareness of how lucky he is to be doing what he loves - playing soccer. That bravery, courage and determination is extended out on that soccer field and that is what makes Will such an exceptional player.
While every person’s experience with a bleeding disorder is unique and personal, with guidelines from our amazing doctors, nurses and physios, everyone can have hope for a bright future and follow their dreams. Using the tools we are given such as Rest, Ice, Compress, Elevate - knowing when to rest and rehabilitate and when to use our treatment when needed, a life of health and fitness and passion for sport is now possible moving into a bright future for kids with bleeding disorders.
A final word from Will:
‘Don’t be scared, scared of having a bleed because is just what comes with having haemophilia. You can always deal with the bleed when it comes to the time.’
For more information on competitive sport for teenagers with bleeding disorders,
• visit the Factored In Youth section on the Haemophilia Foundation Australia website: www.haemophilia.org.au/youth
• speak to the team at your Haemophilia Treatment Centre.
This article was originally published in The Missing Factor Spring 2025, magazine of Haemophilia Foundation Victoria (www.hfv.org.au) and has been adapted with permission.
Images provided by Nicola and reproduced with permission.
Nicola is a community member from Victoria, Australia.
PROBE Australia Study update
Thank you for the fantastic support you have given to the PROBE Australia Study. This is a very important study for HFA and a big project! We have been recruiting for more than a year but are not quite there yet.
We still need about 90 men WITHOUT a bleeding disorder to complete the survey.
Family, friend, colleague – it can be any male in Australia who is 18 years or older. It will only take them around 10 mins to complete the survey.
Why? For credible data, we need to compare the lives of a similar number of people WITH haemophilia and WITHOUT a bleeding disorder.
By the way, you are also welcome to complete the survey if you are a male or female affected by haemophilia and haven’t done the survey since 2020! Please consider sharing the study with people you know.
ANY QUESTIONS?
Visit www.haemophilia.org.au/probe Or contact Suzanne at HFA: socallaghan@haemophilia.org.au
HOW TO DO THE PROBE SURVEY
It’s very easy!
Go to:
• myprobe.org for the web version
• Or download the myPROBE app from Apple Store or Google Play (Android)
• Or ask HFA for a print survey pack
Playing competition sport
What’s one goal you’re proud of reaching in your sport so far?
A goal that I am very proud of is playing soccer at a senior level in a reserves side at the age of 16. And also playing a year up in NPL (National Premier Leagues) for under 17s as well as playing first AGSV (Associated Grammar Schools of Victoria) through my school.
How do you feel after a good practice or game?
After a good game I am full of confidence and it makes me feel like all of my hard work and dedication has paid off giving me a greater sense of purpose and belief in myself.
Is there anything you wish more people understood about playing sports with haemophilia?
I would like people to know that having haemophilia does not impact how I play and also others with haemophilia should not be scared and that getting bleeds from sport is just part of our life.
Hi, my name is Will. I am 16 years old, I have haemophilia A and I love to play soccer.
Will spoke to Haemophilia Foundation Victoria about taking on the challenge of playing competition soccer and what has supported him to follow his passion.
I would like people to know that having haemophilia does not impact how I play.
Have you found any routines that help you stay safe while playing?
A large part of it is staying fit, healthy and building strength to keep my joints healthy to avoid having a bleed. Before and after every training and game I try to stretch and warm up my muscles to also prevent any bleeds.
A large part is staying fit, healthy and building strength to keep my joints healthy to avoid having a bleed.
How has your HTC (Haemophilia treatment Centre) helped with this?
My HTC physio has provided me with stretches and techniques to keep fit during injuries and when I am healthy playing sport almost every day. She always guides me through my injuries when I am struggling taking it step by step no matter how long the recovery is.
My HTC doctor has provided me with confidence and self-belief to follow my passion and never stop chasing it. Also it is great to have in the back of mind knowing I have a great haematologist on call to speak to at any time.
My HTC nurse has been a great support my whole life always being there whenever something happens. She supports and guides me through all of my bleeds and even helped start me off doing my own needles.
What would you tell other young people with bleeding disorders about sport?
I would tell others not to be afraid and to never stop chasing your passion. Also don’t think about what others might think or say about our situation. If you put in enough hard work and dedication you are guaranteed to thrive.
Never stop chasing your passion
A part of playing sport with haemophilia can include difficult times, such as the possibility of having multiple bleeds in a row, but you must always try to stay positive and know that with good management and working with the Haemophilia team you will always get back on track. A good athlete with or without haemophilia will always go through tough times of injury.
Find out more
To read more about sport and personal stories from young people with bleeding disorders, visit the FACTORED IN youth section on the HFA website - www.haemophilia.org.au/youth/
Talk to your team at the Haemophilia Treatment Centre about the sports you are interested in and how to manage them to help you make the right decisions and plans based on your individual health and situation.
This article was originally published in The Missing Factor Spring 2025, magazine of Haemophilia Foundation Victoria (www.hfv.org.au) and has been adapted with permission. Images provided by Will and his parents and reproduced with permission.
Stock image: Engin Akyurt for Pexels.com
CALENDAR
Bleeding Disorders Awareness Month
October 2025
www.haemophilia.org.au/BDAM
Australian Bleeding Disorders Conference, Brisbane
16-18 October 2025
www.haemophilia.org.au/conferences
World Haemophilia Day
17 April 2026
wfh.org/world-hemophilia-day
WFH World Congress 2026
Kuala Lumpur, Malaysia
19-22 April 2026
wfh.org
ACKNOWLEDGEMENTS
Haemophilia Foundation Australia (HFA) acknowledges funding grants received from the Australian Government.
We thank the individuals, service clubs, philanthropic trusts and businesses that have made donations to HFA. We acknowledge the education and awareness grants and/or conference sponsorship from the following pharmaceutical companies:
CSL BEHRING | NOVO NORDISK | PFIZER AUSTRALIA ROCHE | SANOFI GENZYME | TAKEDA
See the HFA website for more information: www.haemophilia.org.au/BDAM or email: hfaust@haemophilia.org.au
NATIONAL HAEMOPHILIA is a publication of Haemophilia Foundation Australia. Every effort is taken to ensure accurate and relevant content, however opinions expressed in NATIONAL HAEMOPHILIA do not necessarily reflect those of the Foundation or the editor, nor is any information intended to take the place of advice from a qualified medical practitioner or health professional.
Haemophilia Foundation Australia does not endorse or assure the products, programs or services featured in NATIONAL HAEMOPHILIA and does not make specific recommendations for any products, programs or services.
We welcome reproduction of articles or quotations from NATIONAL HAEMOPHILIA on the understanding that acknowledgement is made of NATIONAL HAEMOPHILIA as the source.
Haemophilia Foundation Australia acknowledges the Traditional Owners and Custodians of Country throughout Australia, the land, waters and community where we walk, live, meet and work. We pay our respects to Elders past, present and emerging and extend that respect to all Aboriginal and Torres Strait Islander peoples.