This year’s MedSoc committee is proud to present the 2024-2025 annual publication of MedMag This year, we fuse history from the past, with innovation of the future, showing you medicine at its most vulnerable and most complex, as we accelerate into an age fuelled by technological advancement and input
This year’s magazine weaves stories about pharmacogenetics, hypertension and personalised medicine, to name but a few, into an interlinked web, allowing for connections and correlations to be drawn about illnesses, prevention, and even cure
As an aspiring doctor, this magazine to me, shows the varying specialities within the medical field but also the disciplines hunger to accelerate in its approach to improving patient safety and outcome, so doctors can deliver holistic revolutionary care, regardless of the environment
I would like to thank all those who have contributed, aspiring medics and healthcare researchers alike All the writers have put incredibly hard work into making academically curious, exciting and sound articles, showing their commitment to the profession and a future of lifelong learning
This review has been a pleasure to lead, it is fulfilling to see the drive of future doctors and an array of inputs, excited by our common interest
Please enjoy the articles within. I hope they inspire and provoke response
Introductionto Pharmacogenomics
George Vasylevch
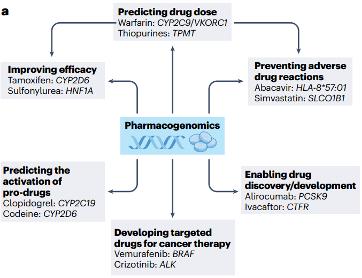
The human body is an incredibly complex organism, unique to each individual. This distinction explains the large variation in drug response in different people: effective doses for some individuals are ineffective or result in adverse drug reactions (ADRs) in others. This variation can be caused by many factors such as age, health, size, and interactions with other medications. On the whole, pharmacogenomics can be defined as the study of how a person’s genetic make-up affects their response to a drug. It is used for the development of novel drugs, the optimisation of drug dose and tailoring treatment for a patient's genetic profile to maximise efficacy and minimise toxicity (Fig 1)
Fig 1 | The aim of pharmacogenomics in moving away from ‘one drug fits all’ or ‘one dose fits all’ strategies (e g predicting dose of warfarin based on variation in the CYP2C9 gene) (Pirmohamed, 2023).
The concept of ‘inborn errors of metabolism’ was first developed by Sir Archibald Garrold in 1908, where he speculated about the abnormal response to food and drugs caused by inherited problems in metabolism However, it was not until the 1940s when scientists described the first instances of genetically-determined ADRs, such as haemolytic anaemia in African-American soldiers exposed to anti-malarials. This haemolytic response is now known to be caused by a G6PD gene mutation, which leads to glucose-6-phosphate dehydrogenase deficiency Specifically, GP6D helps red blood cells to work correctly and its lack of, can have tragic consequences. The term ‘pharmacogenomics’ was introduced by Arno Motulsky and Werner Kalow and became popular in the 1990s as the Human Genome Project progressed.
To be identifiable in science, a star nomenclature is used by pharmacogeneticists (e g CYP2C19*2) to describe genetic variation in determining drug response (also known as pharmacogenes).
Basis of drug-gene associations
The two pathways that describe an organism’s overall response to a drug are Pharmacokinetics and Pharmacodynamics Pharmacokinetics can be described as what the body does to a drug, referring to the variability in the processes regulating the delivery, removal of a drug and active metabolites from their target site. It deals with the four main processes - absorption, distribution, metabolism and excretion. Pharmacodynamics covers biochemical, physiological and molecular effects: this can include the variability in the interaction of an active drug with its effector molecules Such variability is often determined by multiple genes and biological processes in the organism, which complicates interpretation and prediction of pharmacodynamic pathways.
Dose, Safety and Efficacy
Large effects in drug response can be caused by single gene variants, which can be shown most clearly, in two scenarios:
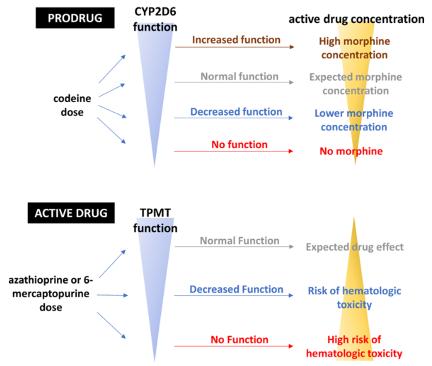
The first scenario involves administration of a prodrug, a compound with little or no pharmacological activity, which needs to be metabolised in the body to activate its therapeutic effects The drugs bioactivation pathways usually involve a single metabolising enzyme, which may show significant variability in pharmacokinetics due to genetic variation A good example is codeine which is bioactivated to morphine by CYP2D6; the activity of this enzyme determines both safety and efficacy of the drug (Fig 2, top). Heterozygotes for lossof-function polymorphisms (e g CYP2D6*4) will have a decreased morphine concentration as they still have noticeable CYP2D6 activity, whilst homozygotes will result in no active drug concentration. On the other hand, gain-of-function variants can lead to morphine toxicity caused by dangerously high concentrations. The exact enzyme reaction stimulated, can have a lethal effect
The second situation shows how single gene variants can cause drastic effects during administration of an active drug. The anticancer drug 6-mercaptopurine is broken down by thiopurine-S-methyltransferase (TPMT) In individuals who are heterozygotes for faulty TPMT, the drug isn’t broken down properly, leading to dangerously high levels and harmful side effects. People with two copies of the loss-of-function gene will suffer from life-threatening bone marrow toxicity caused by the usual drug doses (Fig 2, bottom).
Fig 2 | Two scenarios that show how gene variants for drug metabolising enzymes in homo and heterozygotes influence safety and efficacy of a drug (Roden et al , 2019)
In all the instances, a polymorphism that increases or reduces the activity of the relevant enzyme in bioactivation or bioinactivation of a drug can result in unusual drug responses However, the clinical relevance of such reactions depends on multiple factors, including the drug’s metabolic pathways and therapeutic range (i.e difference between effective and toxic doses). For example, drugs with a wide therapeutic range which are metabolised by a single enzyme can show a significant variability in pharmacokinetics due to genetic variation, but are less susceptible to serious ADRs because of the wide theraupetic margain
Genomics in Drug Discovery
Drug discovery and development is a very costly, time consuming and risky process, with over 90% of candidate drugs not achieving regulatory approval. Use of genomic data to genetically support drug targets has been shown to increase the success rates in clinical trials and marketing Approaches such as genome-wide association studies (GWAS) are used to identify genes and their variants which are associated with a disease These code for target proteins, providing the basis for new drug development.
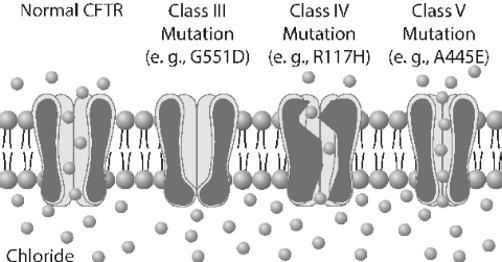
An example of a genetically identified drug target is the CFTR protein in cystic fibrosis, a genetic disease caused by a mutation in cystic fibrosis transmembrane conductance regulator (CFTR) gene. The CFTR protein is an ion channel, which allows chloride ions inside the cell to move to the outside. In cystic fibrosis, mutations can result in CFTR proteins being misfolded, altering their conductance (Fig 3) Patients with genetic variants for poor chloride ion conductance took part in clinical trials for Ivacaftor, a drug which bind to a defective protein at the cell surface allowing ions to flow.
Fig 3 | Genetic variants affecting the folding of CFTR proteins, altering the conductance.
(Condren and Bradshaw, 2013)
The integration of computational tools like Bioinformatics has made a positive effect on drug discovery by accelerating the discovery and regulatory process, increasing success rates and reducing costs. One of the main roles of bioinformatics is drug target identification. Drugs are usually developed when a potential target site has been identified and studied. Once the drug target is identified, bioinformatics helps to confirm if the target is therapeutically associated with a disease of interest. This process is known as drug target validation, it aims to reduce the potential for failure in the future clinical trials, making the overall process more costeffective.
Final thoughts
Despite the increasing availability of human genomic data, the implementation of pharmacogenomics into clinical practice has been very slow due to limited awareness and knowledge on the relationship between genetic variants and drug response To determine which drug is most suited for a patient, doctors will have to implement an extra diagnostic step and all prescribing physicians will need a better knowledge on genetics, regardless of their speciality Furthermore, there is a need to study the genetic profile of each individual to obtain a bigger picture on drug-gene associations, since many genes are likely to influence the response. The field of pharmacogenomics faces many challenges, overcoming which will determine the future improvement of human health.
Fertility Preservationin ChildhoodCancer
Josh Alexander
Introduction
Due to major advancements in oncology treatment in children and young adults over the last two decades, the survival rate of children with cancer has risen to over 85%. As this has improved, the clinicians’ challenge has shifted to minimise the effects that the cancer treatment has on patients once they are cured The challenges of maintaining a patient’s quality of life, after intense treatment and minimising the lasting effect that could arise is now a primary focus of clinical medicine. The last ten years of paediatric oncology has shifted some focus into minimising the late effects of treatment around fertility. Internationally, the practice of oncofertility this article divulges into, is considered to be part of the expected standard of care, as shown by recent NICE regulation
Background
How does Chemotherapy affect fertility in prepubescent children?
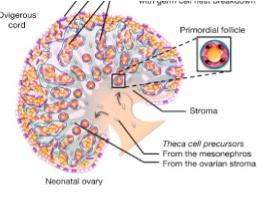
Females are born with their lifetime supply of primitive oocytes (eggs) around 7,000 at birth. This number drops over time, and by the time a woman has less than 300 oocytes, menopause takes effect This means that if these primitive gametes are significantly affected by chemotherapy there is no chance that fertility can be restored, as no new unaffected gametes will be produced.
1: The Ovary demonstrating oocytes around the cortex. (Nicol and Yao, 2017)
Chemotherapy most commonly, fights cancer by attacking rapidly dividing cells As a consequence, stem sperm cells ( called spermatogonia), which are found in males and produce sperm cells in post-pubescent males but lay dormant in prepubescent males, are often significantly affected This results in the inability to produce sperm (infertility). Specifically, within the male testis, there are three populations of cells: spermatogonia, Leydig and Sertoli cells All these cells are affected by chemotherapy, but the Leydig and Sertoli cells, which are responsible for hormone production, do recover. This means that the young people who are exposed to chemotherapeutic agents still go through puberty but are infertile in later life.
Figure
Some chemotherapies don’t produce any side effects with regards to infertility in both genders, however most of the common treatments can be gonadotoxic (harmful to sperm and egg) For example, platinum-containing agents prevent rapidly dividing cells from multiplying, by binding to DNA. However, whilst effective on cancer, it also binds to the DNA in spermatogonia resulting in significantly high rates of infertility in patients.
Options for fertility preservation
It is now mandatory that all patients undergoing chemotherapy discuss the effects of it on their future fertility before starting, in order to be best informed of any dangers and risks. If these effects are minimal, then the patient can proceed with planned cancer treatment If, however, patients are considered at high risk of infertility, then they must be offered the option of preservation. Historically, the only group who were able to be offered this opportunity, were post pubertal males, who could produce a sperm sample, which could be stored for later use
Now, post pubertal girls are also able to store eggs, through egg retrieval. This process takes a couple of months of cycles of hormone treatment, to produce the eggs in the ovaries, which can be extracted Although this seems like a robust mechanism, practically children’s cancers are aggressive and need treatments to start almost immediately from diagnosis. This means that egg storage in children’s cancer is practically impossible.
Over the last ten years, gonadal tissue cryopreservation, has been introduced and implemented as part of a collaborative international program. It is now possible to harvest ovarian and testicular tissue to preserve potential fertility. This approach is more suited to children and adolescents.
Ovarian cryopreservation
Prepubertal and post pubertal females have all their primitive follicles arranged around the outside of the ovary, in the cortex Using keyhole surgery/laparoscopy female patients who are at high risk of infertility can have a single ovary harvested before the treatment starts.
Once the ovary is extracted, it is transported directly to the National Biobank, where the cortex is dissected off the ovary and sectioned into strips with primitive oocytes inside These strips are then frozen slowly in a process called cryopreservation, in such a way that no ice crystals are formed in the process.
Figure 2(a): Ovarian harvest of a threemonth-old (NHS training video)
Figure 2(b): Ovarian harvest of a twelveyear-old (NHS training video)
When the patient requires their tissue to restore fertility as an adult, some of these small pieces are inserted into the remaining ovary In this way, the pieces of ovary generate a blood supply by being rejoined with the paired ovarian arteries, and the patient will ovulate.
There have been four hundred live births worldwide using this method and the UK had its first two live births in 2023 If there was not a contralateral ovary left, researchers can implant these pieces of tissue into the pelvic sidewall, or even in distant sites such as the arm, from where eggs can be harvested.
This technique of ovarian tissue preservation can be done rapidly and at any age, thereby providing a robust method of preserving fertility. This tissue preservation can be extended to women who are older, but beyond the age of approximately 26 it is believed that the egg density in the cortex is no longer sufficient for this to be a viable option
Testicular cryopreservation
In prepubertal boys, or post pubertal boys who are unable to produce a sperm sample, fertility specialists are now able to preserve testicular tissue through performing a wedge biopsy of one of the testes. This wedge biopsy contains all three populations of cells, as described above; spermatogonia, Leydig and Sertoli cells. Unlike in women, the whole sexual organ is not taken as this would be cosmetically obvious The procedure involves opening the testis, extracting the biopsy and then closing the testis leaving it with a slightly reduced mass
The biopsy is taken to the Biobank and the testis is made into strips and frozen in the same manner as for the ovary, as mentioned before. Unlike in females, there have been no reimplantation of these pieces back into patients yet. This is because the patients who have undergone cryopreservation are younger and therefore have yet to reach the age where they require fertility There is an international trial that started in 2024, to reinsert testicular biopsy tissue back into patients, in London (UK) and Michigan (USA). Primate studies doing the same procedure have yielded births already, however.
Conclusion
Paediatric cancer treatment can be both a stressful and traumatic experience, mentally and physically for patients and their families Minimising the long-term late effects of cancer treatment can lead to a better quality of life for the patient and a return to normality To that end, the preservation of fertility is critical for the patients’ long term mental and physical health. This article has covered all the current, cutting-edge methods that have greatened our ability to offer long term, sustainable fertility preservation to cancer survivors Today, oncofertility is a leading area of development within clinical research
Figure 4(a), 4(b), 4(c): Testicular cryopreservation (NHS training video)
Nitish Nandakumar
Evolutionof Radiology
Introduction
Radiology is the branch of medicine centred around creating and analysing images of organs and organ systems for purposes of enabling doctors to diagnose disease and injury, such as arthritis or broken bones Different imaging techniques, including radiography and computed tomography are used for various purposes of diagnosing different diseases The main application in radiography involves capturing radiographs to aid in conducting diagnostic studies. Blood clots, tumours, and bone fractures are displayed by CT scanning. Additionally, DEXA scanning is undergone to evaluate the density of bones to study the risk of osteoporosis Major milestones that have been accomplished within the 128 years that radiology has been used, have managed to help doctors to detect and recognise the possibility of interconnected conditions and injuries, such as a fractured arm or broken wrist, with efficiency which has in turn benefited patient care.
Röntgen and the birth of radiology
Radiology’s origins date back to the year 1895, when German engineer and physicist Wilhelm Conrad Röntgen discovered X-rays. He had experimented in his laboratory for a few weeks to produce these "strange rays" which he termed as " x " , when he later figured out that when objects of varied thicknesses were placed in the path of the rays there was a visible, variable transparency on a photographic plate. He asked his wife, Anna Bertha, to lend him her left hand which he lay in the path of the rays, indicating that the bones of her left hand were more permeable to the rays, as they scattered a less dense shadow. It was this discovery that he wrote about in his paper "on a new kind of rays" that won him his first Noble Prize in Physics in 1901. This "phenomenon" sparked worldwide interest and, within weeks of Röntgen's announcement, many hospitals around the world established X-ray rooms This gave way to the first radiology departments. The British Röntgen society was opened two years later after Röntgens discovery in 1895 after an increase in global interest, and over the next few years, the society carried out further studies into the use of X-rays and the results of radiation on the human body. While further studies were still being carried out, the first clinical use of radiology took place two weeks after Röntgens discovery, by John HallEdwards on the 11th of January 1896 in Birmingham, where he radiographed a needle that was embedded in his associate's hand.
Figure 1: First X-ray image of Anna Bertha's left hand (Bakalar, 2009)
Early 20th Century and initial research
Whilst the initial excitement of Röntgen’s discovery spurred both interests and concern, the early 20th century saw the transition of radiology from what people perceived as an art to more of a critical medical tool. The incorporation of radiographs into clinical particles was swift and by the 1920s, they were no longer reserved to research institutions, becoming visible in many hospitals and practices
The early 20th century also saw significant technological advancements, most notably, the development of the Coolidge tube in 1913 by William Coolidge The Coolidge tube, which later became the prototype for the modern x-ray tube, was an incredibly important development in the history of radiology, improving the reliability of previous X-ray equipment as well as proving to be vital in cancer treatment The tube used a heated cathode as the source of the electrons, with a tungsten anode on the opposite end. When a high voltage was transmitted, electrons were accelerated across the tube into the tungsten anode, which produced Xrays. These X-rays then passed through the glass envelope where it could become discoloured as a result. The Coolidge tube was much safer and more reliable than its predecessors, as it allowed the X-ray output to be controlled which in turn reduced radiation exposure to patients and operators. The ability to reduce the exposure of ionising radiation was significant in establishing radiology as a vital solution to the difficulties in diagnosing certain infections and injuries, whilst also responding to the underlying concern of the dangers of long X-ray exposure.
War
Radiology played a pivotal role during the world wars. Its newly discovered ability to locate bullets, shrapnel and foreign objects in soldiers alongside providing detailed images to surgeons was one of the main reasons as to why doctors were able to remove the objects without the risk of infection. X-rays were also used to monitor the progress of healing wounds and detect infections such as osteomyelitis, a bone infection that causes serious leg pain, as well as providing doctors and surgeons with quality radiographs enabling them to assess the effectiveness of treatments
Figure 3: Marie Curie's portable X-ray machines in ambulances (Jorgensen, 2017)
Figure 4: Fluoroscopy (CDC, 2024)
Both wars saw major developments in the field of radiology including the introduction of portable X-ray machines and the use of fluoroscopy. Portable X-ray machines were one of the most important developments during the First World War and played a key role in the Second World War as well Both Marie Curie and her daughter, Irène, played a crucial role in equipping vehicles with X-ray machines and training doctors in how to use them The vehicles allowed X-ray services to be brought directly to the battlefield giving way for rapid diagnosis of wounds and infections. Additionally, fluoroscopy, a type of imaging that uses several pulses of an X-ray beam to take real time (moving) footage of the tissues within the body, was invaluable for examining various body parts such as the oesophagus and the stomach as well as the arteries and spinal cord. This imaging allowed doctors to assess the condition of certain body parts as well as diagnose patients with conditions such as infertility.
Introduction of CT and MRI Scanning
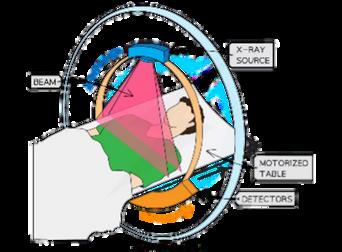
From the 1960s to the 1980s, radiology experienced a period of remarkable progress characterised by the discoveries of Godfrey Hounsfield and Raymond Damadian Their research which resulted in the emergence of computed tomography (CT) scanning and magnetic resonance imaging (MRI) revolutionised the medical imaging field, allowing for accurate diagnosis. In the late 1960s, British electric engineer, Godfrey Hounsfield began investigating into an improved form of diagnostic imaging that would use an X-ray scanner to rotate around the patient’s head, imaging thin “slices” of the patient’s skull and brain, these slices were imported into a computer where they would produce a high-resolution threedimensional image of greater detail than the other conventional X-rays.
The patient would lie down on a table, this table would slide into the scanner and the scanner would spin extremely quickly, producing signals that would be processed by the machine’s computer to produce a cross-sectional image of the patient’s head. It was this invention that later won Hounsfield the Nobel Prize in 1979 which he shared with Allan MacLeod Cormack for his endeavours in the production of the first CT scanner.
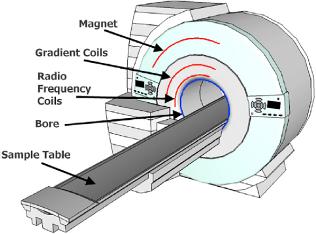
The late 1970s saw another major breakthrough in radiology with the production of the first MRI scanner. It was invented to provide a safer method of imaging the internal structures of the body without the use of ionising radiation like X-rays An MRI scanner is a large tube that contains powerful magnets, during the scan, the patient lies inside the tube and the scanner uses strong magnetic fields and radio waves to produce detailed images of the inside of the patient’s body. When you lie under the scanner magnets, the protons in your body all line up in the same direction Then, short bursts of radio waves are sent to certain areas of the body, which knock the protons out of alignment and when the radio waves are turned off, the protons realign. The signals from the protons are combined to create a detailed images of inside the body.
Figure 3: MRI Scanner (Researchgate.net, 2024)
Figure 4: CT Scanner (Save My Exams, n.d.)
Late 20th Century and the disaster of Chernobyl
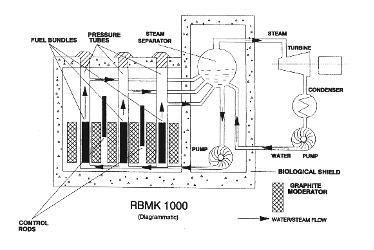
Figure 5: The structural design of Chernobyl reactor four (World Nuclear Association, 2024)
The late 20th century saw notable developments in the radiology field such as the introduction of computed radiography and imaging to store images of the internal structures of the body. The development of computed imaging meant that image acquisition and processing was immediate, reducing wait times for patients and doctors, alongside allowing enhancement in the quality of radiographs, meaning that radiation dosage could decrease, and doctors could easily detect abnormalities. The use of computer radiography made collaboration easier, digital images could be stored electronically and so as a result, sharing and accessing images with other doctors was much easier.
However, in 1986, an event that took place in Ukraine would impact radiology massively In the site of Chernobyl, the number four RBMK reactor went out of control during testing leading to an explosion which caused a fire that destroyed the reactor building, releasing large amounts of radiation throughout the city. As a result, many extensive studies were carried out into the effects of radiation exposure and increased incidences of thyroid cancer As well as this, a revision of safety guidelines to protect those who lived close to nuclear power stations occurred .
2000s - present day (using AI)
Over the last 25 years, a major collaboration has significantly advanced the healthcare field as well as the radiology field. Since the introduction of AI in the 1950s, doctors and surgeons have researched into possibilities to incorporate AI within healthcare, and since the 1990s, AI has been trialled with radiology in detecting cancer and neurological abnormalities.
The first known use was in 1992, when AI was used to detect micro-calcifications in a mammogram, which are tiny deposits of calcium in a patient’s breasts that when the specks cluster together, can indicate that cancer may be present. Since the integration of artificial intelligence in the work of radiologists, there have been many scenarios where surgeons and doctors have been able to deliver accurate medical services
One such situation is the classification of brain tumours. When dealing with brain tumours, it can be very time-consuming, it takes up to 40 minutes to classify a tumour and only after that can the doctor decide on further action and treatment
Using MRI images and machine learning, brain tumours can be identified within minutes and with high accuracy. A recent study used convoluted neural networks with MRI scans as the inputted image and it achieved an accuracy of 98 56% in classifying brain tumour types Using AI in mammograms has enabled doctors to accurately detect breast cancer AI tools can enhance the mammograms obtained because of breast screening, making them much more detailed and easier to diagnose.
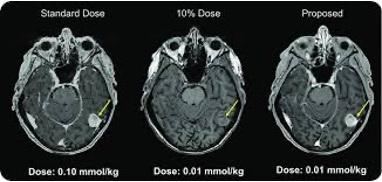
Figure 6: Using AI to limit ionising radiation dosage (Sajid, 2022)
A study carried out by the Radiology Society of North America examined mammograms to detect breast cancer and 87.6% of the AI detected cancer. In the conclusion of their research, they added that AI will be of great value in the future when screening and examining mammograms One of the most important applications of AI in radiology is its ability to optimise radiation dosage To get a detailed MRI scan, the patient must be exposed to harmful radiation, however, whilst the longer the scan, the more detailed the image, it can be harmful to children as high doses have the possibility to change DNA patterns and cause cancer Artificial intelligence models such as those that upscale images, can help to create detailed images which in turn, lead to doctors requiring less dosage to comfortably diagnose conditions and injuries.
Conclusion
The evolution of radiology over the past 128 years, has enabled doctors to provide improved patient care. From Wilhelm Conrad Röntgen's sparking discovery of X-rays to the much more accurate imaging techniques we use today, radiology has positively advanced, enhancing the ability for doctors and surgeons to accurately detect fractures and diseases such as cancer The integration of artificial intelligence has and will further advance the field of medicine by helping analyse radiographs and enhance images whilst acting to minimise radiation exposure In the future, the integration of AI with medicine holds great potential for enabling healthcare providers to supply patients with precise, and accurate diagnoses, strengthening the need for radiology in the world today. The evolution of radiology mirrors not only the progress of scientific research but also the commitment of doctors to better improve healthcare as it is today.
Alpha-Foldand ProteinStructure Prediction
Ravjoth Brar
In 1972, Christian Anfinsen was awarded a Nobel Prize for his research which demonstrated that it should be possible to determine a protein’s 3D shape based on the sequence of the amino acids which comprise it This problem is more commonly known as the ‘protein folding problem’, and remained, gathering dust, for just under 50 years – then AlphaFold knocked on the door.
Proteins are involved in essentially every important activity that happens inside every organism: digesting food, muscle contraction, moving oxygen through your body, your immune system, your hormones, even your hair. The famed biologist Arthur Lesk stated – ‘In the drama of life at a molecular scale, proteins are where the action is’. Their importance cannot be underestimated Proteins themselves are comprised of a string of amino acids and can range from a few dozen to several thousand amino acids in length But proteins do not stay like this. To function, they must fold into a 3D shape. Each specific shape correlates to its purpose, and through understanding the shapes proteins fold into, it enables us to better understand how organisms function, and ultimately how life itself works Therefore, solving the protein folding problem would be a monumental milestone for the field of biology as a whole and thus, CASP (the Critical Assessment of (techniques for protein) Structure Prediction) was born.
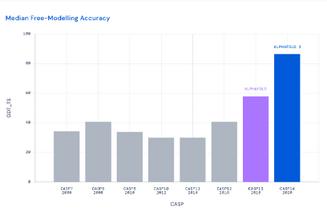
Every two years after this, teams gathered from across the world to predict, using purely computers, the 3D structures of hundreds of proteins, from their amino acid sequence alone. Simultaneously, the 3D structures were being painstakingly worked out in the lab using traditional techniques such as X-ray crystallography which while accurate, was extremely time-consuming and challenging X-ray crystallography determined the 3D structure of molecules by analysing how X-rays diffracted when passed through a crystallised sample. The entire process for even one protein took months or years to complete. Thus, when considering that each given protein can adopt 10^300 different configurations, and that there are billions of known protein sequences, demonstrated the possibilities were quite literally, almost endless. When AlphaFold 2 was first showcased in CASP 2020, its performance was historic. On average, AlphaFold 2 successfully predicted protein’s 3D shapes to within the width of a singular atom! The CASP organisers themselves declared that the protein folding problem had been solved
Figure 1: Graph detailing the huge increase in accuracy that AlphaFold brought to the CASP conference.
GDT TS is the measure of similarity between two protein structures with known correspondence. (Putting the Power of AlphaFold into the World’s Hands)
AlphaFold itself is a Machine Learning (ML) model, and for any ML model the key component always remains the training data. AlphaFold was trained on predominantly publicly available datasets: most specifically the Protein Data Bank (PDB) which contains 180,000 3D structures and amino acids sequence for human and non-human proteins Another database, UniProt, contains the amino acid sequences (without the 3D structure) for another 200,000,000 more proteins. The model itself is built on Transformers, a revolutionary neural network architecture pioneered by Google in 2017 which ChatGPT, Gemini, and many other major AI models use However, the AlphaFold team designed their own transformer to work specifically with 3D structures known as Invariant Point Attention (IPA).
Vigo Magnusson
IPA works in various steps Firstly, each amino acid in the protein sequence is assigned a random point in 3D space Each of these vectors might also include some contextual information about the amino acid such as its type and local environment. Essentially providing more factors for the model to take into consideration, improving its accuracy. Next, the model computes each possible pairing relationship between each of the points This includes: the Euclidean distance between the two points, the orientation between the two points, and any differences in contextual information (the actual computation here can be done by hand by using Pythagoras’ Theorem, but the model automates it extremely quickly). The Euclidean distance is the shortest distance along a straight-line between two points This next step is where all the magic of IPA happens, IPA ensures that the model’s attention mechanism is not affected by the orientation of the protein structure. This is achieved by the model focusing on features that will remain consistent even if the shape drastically changes, these are known as inherently invariant features Imagine you have two points, A and B, in 3D space If you rotate the entire space, the co-ordinates of A and B will change respectively, but the distance between them remains the same.
This distance is an example of an inherently invariant feature and the Euclidean distance between the two points is the core feature that IPA relies on Similarly, consider three points A, B, and C. The angles formed by the vectors AB and AC will stay constant even under transformations. Features derived from these angles (like its sine or cosine) would thus also be inherently invariant These all aid the model in learning the spatial relationships between different points of the structure This leads to the model being quite robust, ensuring that predictions are less likely to be affected by irrelevant changes in the orientations of the amino acids and result instead, in the same 3D protein structure, with the inherently invariant features constant This architecture puts AlphaFold’s IPA technology parsecs beyond all its possible competitors
AlphaFold has brought about a paradigm shift in biology, leaving a permanent mark on multiple different fronts Before AlphaFold we knew the 3D structure of about 17% of the 20,000 proteins in the human body, these had been painstakingly worked out in the laboratory across decades through tediously long experimental methods. Thanks to AlphaFold, we now have the 3D structures for almost all proteins in the human body (98.5%). Perhaps the best thing about AlphaFold is that it is open-source and easy for anyone, anywhere to use, simply through the following link you can predict the 3D structure of proteins: https://alphafold.ebi.ac.uk/. AlphaFold has displayed its accuracy, most famously, in the COVID-19 outbreak. AlphaFold shared its most up-to-date predictions for the 5 SARSCoV-2 targets and their first prediction had the correct topology and their second prediction was spot on The correct topology is absolutely necessary to vaccine development as it helps scientist to understand how the virus functions, how it interacts with host cells, and which components are crucial for it to be infectious. This conveys how AlphaFold may become even more important in the future as more disease outbreaks occur. AlphaFold’s most anticipated usage is drug discovery AlphaFold provides structural insights into target proteins which can aid designing more effective drugs, hopefully, in the future, combating illnesses such as cancer, Alzheimer’s, and infectious diseases.
In conclusion, AlphaFold represents the first, and certainly not the last time AI has and will significantly improve humanity’s scientific knowledge. The possibilities with AI’s usage in biology are quite literally endless, and the vast field of proteins has changed forever. The impacts will not come today nor tomorrow, but the long-term impact will be transformative. I, for one, cannot wait to witness what AI will change next
DementiaandIts EffectontheBrain
Issie Ridgway
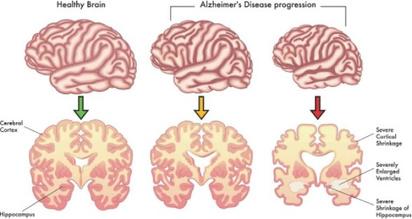
Dementia is a general term for the loss of memory, language, problem solving and other thinking abilities, that are severe enough to affect someone’s day-to-day life Dementia is an umbrella term, that encompasses many different conditions (such as Alzheimer's disease, vascular dementia and more). Alzheimer’s disease is the most common cause of dementia accounting for 60 to 80 percent of cases worldwide.
An adult brain contains approximately 86 billion neurones, connected by branches known as the ‘neuron forest’. All our thoughts, feelings, sensations and memories are formed by signals travelling through this forest, which are later stored. These impulses are transferred by electrical impulses and then neurotransmitters, which move across the synapse (the place where neurons connect and communicate), before carrying their potential to other cells. Alzheimer’s affects this communication between cells, and it eventually causes cell death and tissue loss, which can be observed under a microscope.
Scientists believe that plaques and tangles are the main reason for this loss of tissue in the brain. Plaque are abnormal clusters of protein, that block communication between cells. Tangles are twisted strands of another protein, that are found in dead/dying nerve cells. Specifically, beta-amyloid is a protein fragment that is deposited in the brain, it is chemically sticky, which causes a build up into plaque People with Alzheimer’s over-produce amyloidbeta which causes abnormal amounts of this naturally occurring protein to form clumps (plaques) in the brain which block cell to cell communications, cause inflammation, neuronal death and eventually dementia Tangles are made of another naturally occurring protein called tau Normally, tau proteins are found on the inside of neurons axons, but in people with dementia these tau proteins become detached and damaged from their axons. Now able to move freely these tau proteins clump together to form tangles. Tau is toxic to neurons, so it causes them to die, and this, as a result, disrupts neuron communication chains which causes difficulty delivering messages through the brain This is why people with Alzheimer’s commonly struggle to make informed decisions and often have to rely on carers.
Plaques and tangles spread through the cortex, and in serious cases, most of the cortex is seriously damaged This causes the brain to shrink due to widespread cell death The hippocampus is typically the first part of the brain to be affected by the dying cells, which is why patients often loose memories and the ability to learn in the earlier stages of Alzheimer’s. Eventually, this damage affects areas of the brain that control the body, causing systems to go wrong, shut down, leading to death
Figure 1: The progression of Alzheimer’s Disease on cell death of brain tissue.
(SHEIKH, 2022)
After Alzheimer’s, vascular dementia is the second most common cause of dementia. Vascular dementia is caused by a lack of blood supply to the brain. This means that cells in the brain are not getting the required nutrients and oxygen which eventually causes cells in the brain to die There are many reasons why this might happen Small vessel disease is one reason This is when walls inside small vessels deep inside your brain narrow, or clog This is typically a result of atherosclerosis (build of fatty tissue in your arteries). Another reason could be a stroke, which causes blood supply to part of your brain to suddenly be cut off and could cause a blood clot or haemorrhage The final major cause of vascular dementia could be mini strokes (transient ischaemic attacks) The main difference between a stroke and TIA, is the duration and severity (for example you often don’t realise when you have a mini stroke). During a mini-stroke areas of your brain are damaged, and you may not even realise. But over time the damage builds up, which can lead to cell death
While Alzheimer’s disease originally affects the hippocampus, vascular dementia causes widespread damage to white matter beneath the cortex. The nerve fibres here carry signals between different parts of the cortex including the frontal lobe Unlike Alzheimer’s disease, which is mainly linked to memory loss, vascular dementia tends to affect people’s speed of thinking and problem solving.
There is no known cure for any kind of dementia at the moment, and since dementia is caused by a variety of disease there will likely never be just one cure However, you can slow down the progression of dementia. For patients with vascular dementia, they are often given medicine to help control high blood pressure or high cholesterol levels, as these factors often contribute to the condition, so controlling them can help slow down the progression of the disease Patients with Alzheimer’s are often given medication that helps with cell communication in the brain, such as acetylcholinesterase, which is commonly associated with the creation of action potentials within the brain.
In October 2024, the UK’s National Institute for Health and Care Excellence (NICE) declined to approve donanemab, a new Alzheimer’s drug, citing concerns over its cost-effectiveness relative to its quality-of-life benefits. Donanemab is designed to target and clear amyloid plaques in the brain, which are clumps of beta-amyloid protein associated with the neural damage seen in Alzheimer’s disease By reducing plaque buildup, donanemab has shown promise in slowing cognitive decline, especially in early stages of Alzheimer’s, potentially extending the time patients can remain independent.
However, while it offers hope for slowing disease progression, the high cost and uncertain long-term impact on patients' quality of life has raised concerns. This decision underscores the ongoing balancing act in Alzheimer's care prioritizing treatments that can extend or improve life quality while considering costs and the varying responses of patients to these therapies
JunkDNA
Karis Lau
In 1972, Susumu Ohno suggested that at least 90% of DNA is nonfunctional, coining the term "junk DNA." By 1980, influential biologists published research in Nature, asserting that evolutionary theory implies our DNA should be predominantly junk They argued it was "folly" to search for functionalities in non-coding DNA, stating that natural selection would result in excess genetic material. Supporting this theory, The Human Genome Project, completed in the early 2000s, revealed that only 1-2% of our DNA codes for proteins essential for survival. This led to the assumption that the remaining 98% was largely useless Richard Dawkins articulated in 1976 that the primary purpose of DNA is survival. He suggested surplus DNA could even be viewed as parasitic. By 2004, creationists began questioning why a creator would place genomes with untranslated pseudogenes and repetitive sequences. By 2009, it was proposed that up to 95% of the human genome might as well be absent, given its perceived lack of impact.
With all this research, society believed Junk DNA was simply a waste of space in the body, as many prominent evolutionary scientists did However, proponents of Intelligent Design (ID) offered a contrasting perspective. Since the ID movement's emergence in the 1990s, supporters predicted much of this junk would turn out functional. They argued the divine deity is created purposefully, suggesting that non-coding DNA should serve specific functions. This links to a rather interesting aspect of scientific research: religion The podcast “Evolution’s Junk DNA”, debates these Christian views on the discovery of Junk DNA with scientific.
Today, evolutionists believe, body parts such as the appendix and tonsils are obsolete and were a result of our primitive development as mammals To draw perspective, Genesis 1:2627 (NIV), states, "Then God said, 'Let us make mankind in our image, in our likeness...' So, God created mankind in his own image, in the image of God he created them; male and female he created them” Here, even now, Christians argue God made mankind perfect in reflection of Him, showing differing evolutionary views of humans and scientific evidence
The podcast furthermore discusses how over the years as science has developed our knowledge of our human bodies, we have found even these body parts are useful For example, the appendix contains a high concentration of immune lymphoid tissue and probiotics important in helping the immune system fight and produce B lymphocytes which help in the maturation and guiding of these lymphocytes to different parts of the body. Additionally, according to Luke University in the US, the appendix is also a reserve for good bacteria Research has also shown each tonsil consists of a network of cryptical bits that store white blood cells used to fight infection and diseases such as influenza. This proves tonsils are not useless and are instead the first act of defense against bacteria.
One of the earliest ID predictions came from Forest Mims in 1994, who cautioned against dismissing junk DNA as useless. Although Science declined to publish his letter, the discussion continued; and in 1998, William Dembski contended that the term "junk DNA" discouraged scientific inquiry, masking ignorance with a veneer of certainty He argued that if organisms are designed, we should expect their DNA to exhibit functionality These debates led many excellent researchers to publish work of their research in this aspect, such as in 2011 when Wells published The Myth of Junk DNA, citing numerous studies demonstrating functions for non-coding regions
A groundbreaking article from the ENCODE project in 2012 reported that about 80% of DNA exhibits functional biochemical activity. However, lead researcher Yan Ruan noted that this study examined only a subset of human cells, suggesting that future research could reveal additional functions The implications were significant: Science magazine declared that ENCODE had "written the eulogy for junk DNA," indicating a shift in consensus among biologists. A 2021 paper stated that the days of junk DNA are over, identifying over 130,000 specific functions for previously labeled junk DNA Some functions consist of forming telomeres, centromeres, and higher-order nuclear structures, binding cohesion to chromosomes, chromatin condensation, DNA repair, etc. James Shapiro from the University of Chicago argued that the notion of abundant selfish DNA in complex genomes is fundamentally flawed
Recent studies, including a 2023 paper in BioEssays, have highlighted a paradigm shift away from the concept of junk DNA. What was once dismissed as junk is now recognized for its roles in gene regulation, cellular responses, and other vital functions This evolving understanding illustrates how the predictions of Intelligent Design proponents have advanced scientific inquiry, revealing the limitations of long-held evolutionary assumptions. Junk DNA still holds a lot of potential for inquiries and discoveries in new ideas in the field of genetics and DNA Current research uncovers the functional roles of previously dismissed genetic material, it challenges long-held assumptions, demonstrating the need to keep an open mind and move away from conceptions of “Junk DNA”.
In full, this topic comments on the value of a religious perspective in medicine but also the need for innovation and understanding, which will help enable the care of patients and the creation of an innovative health service.
GutMicrobiota andMentalHealth
Arjuna Shankar
Introduction
For decades, mental health conditions such as anxiety, depression, and in general pathophysiology were all perceived to be rooted and embedded within the neurological system solely, fuelled by genetic causes, substance abuse, trauma from youth, and other factors. However, in recent years, the gastrointestinal system, often overlooked by healthcare professionals, is becoming spotlighted, specifically the gut microbiota that harbour it Gut microbiota consists of trillions of microorganisms, primarily, fungi, archaea, viruses, and bacteria which are split into two different phyla, Bacteroidetes and Firmicutes. Bacteroidetes are primarily involved in energy production, amino acid transport and metabolism while firmicutes are most recognised for activity in carbohydrate metabolism Studies have proven that these gut microbiota can influence cognitive function and psychological state, through a relationship most notably referred to as the Gut-Brain Axis, a bidirectional communication system connecting the enteric nervous system to the central nervous system with the aid of nerves, hormone signals, and immune signals This interrelationship can be a revolutionary discovery since it grants us the potential for new, possibly more advanced cures for the evergrowing issue of mental health. Problems that are ubiquitous in the 21st century.
The rudiments of the Gut-Brain Axis
The association of psychiatric and neurodevelopmental disorders with the gut microbiome is through the passageway of the Gut-Brain Axis. Such a connection was first revealed by a study in 1998 when the bacterium, Campylobacter jejuni, was orally administered to mice within a controlled environment. This further triggered a reaction of anxiety and seemingly unhinged nature, yet an auto-immune response was not generated.
The Gut-Brain Axis can depict how our ingested food can affect our cognitive state Following mechanical digestion, the churning of the stomach, and the roles of many other organs along the alimentary canal, our digested food particles travel to the small intestine coated with villi and microvilli along its surface. The villi consists primarily of two different cells, goblet cells, and enterocyte cells, the enterocytes are unique since they are neuropod cells. Specialised cells that are necessary for sensory transmissions to the brain.
Originally, neuropod cells were thought to solely be utilised for communication through hormones, however it has been uncovered that they synapse with nerves such as the vagus nerve. These neuropod cells can detect mechanical, thermal, and chemical stimuli, within these cells, and can propagate signals to the vagus nerve by converting said signals into electrical impulses that convert into neurotransmitters along synapses. The vagus nerve cells can intermittently carry this information to the brain stem
Moreover, the Gut-Brain Axis has another critical role, in the transport and regulation of serotonin. On the epithelial lining of the lumen, specialised cells known as Enterochromaffin cells produce approximately 90% of serotonin Serotonin is released in response to stimuli as a result of the food we eat. Amino acids like tryptophan are essential in this production. Our gut microbiota plays a vital part in this as bacteria like bifidobacteria and lactobacilli can increase the availability of tryptophan. Following its production, serotonin can decisively control mood, when it is at its standard levels, ideally one would experience a more emotionally stable state of tranquillity and elation. Serotonin is also a biosynthetic precursor to melatonin, which is a necessity for healthy and regulated levels of sleep.
The role of Gut microbiota in mental disorders
Intestinal dysbiosis, meaning a varied, abnormal number of microorganisms within intestines, has been proven to influence behavioural tendencies which has subsequently shed light upon gut microbiota and its role in mental health.
An interesting mental disorder that has successfully been linked to gut microbiota is attention deficit hyperactivity disorder ADHD is a disorder, most commonly diagnosed from an early age yet can affect the entirety of one’s lifespan. It is characterised by symptoms of inability to focus and impulsiveness in correlation to age. ADHD can be a result of dysbiosis within gut bacteria causing insufficiencies of neurotransmitters. Insufficiencies of neurotransmitters such as dopamine, serotonin, and norepinephrine can be caused by gut microbes stimulating inflammatory responses through endotoxins or by exerting neuroprotective effects on dopaminergic levels. Nevertheless, with a low concentration of dopamine, a complex hormone associated with feelings of reward and pleasure, patients can become restless. Additionally with low concentrations of norepinephrine and serotonin, memory problems, headaches (possibly to the extent of migraines), depression and anxiety can spurt.
Another mental disorder related and intertwined with gut microbiota is Schizophrenia. Schizophrenia is a complex heterogenous neurodevelopmental disorder This term is often reserved for the portion of the psychosis spectrum that is on a severe end. The glutamate hypothesis of schizophrenia shows how the pathological mechanisms involved in schizophrenia are linked to glutamatergic signalling, this hypothesis suggests that reduced NMDA receptor function leads to an excess of glutamate release, which can contribute to psychosis and cognitive deficits.
NMDA receptor antagonists like ketamine and phencyclidine can mimic schizophrenia symptoms, and these NMDA receptor antagonists can be varied by gut microbiota. There is also a potential link between gut microbiota and schizophrenia as researchers have found evidence that antibiotic minocycline which can cause changes in gut microbiota can aid in enhancing the effects of anti-psychotic drug.
Finally, gut microbiota can affect autism spectrum disorders (ASD). Patients with ASD have been found to contain strange, abnormal configurations of their gut microbiota. The link has primarily been with higher levels of (primarily) Bacteroidetes and lower levels of Firmicutes. This difference in concentration gradient between these two counteragents means that more pro-inflammatory properties are exhibited due to endotoxins and cytokine production. This can cause neuroinflammation which has the potential to disrupt neural connectivity and communication. However, this study was conducted with a smaller sample size when conducted so no official link between correlation and causation can be made
Ameliorative regulation of gut microbiota for mental disorders
There are very promising ways of modifying gut microbiota to aid in the treatment of these mental disorders, the principal, foremost methods being: faecal transplantation, proper dieting, and probiotics.
A faecal transplant is an operation of transferring a sample of helpful, healthy microbiota. One trial conveyed major improvements following the operation on a person affected with autism as he experienced a heavily reduced amount of problems such as constipation and diarrhoea. Many autistic people often also suffer from bowel problems and stool movements due to them having a higher risk of IBD (inflammatory bowel disease) than non-autistic people Additionally, this case study continued to show reduced levels of bipolar tendencies and improvements in social interactions, but a larger sample size is required to confirm these conceptions.
Penultimately, proper dieting can also play a heavy factor in decreasing the risk of falling prey to mental health issues, as diets high in a surplus of processed foods can negatively affect one’s cognitive state, as it can lead to inflammation through the alimentary canal and potentially the brain. Additionally, a study conducted by Public Health Nutrition presents how individuals with a diet saturated with commercially baked goods and fast food have a 51% higher chance of becoming a victim of depression and anxiety.
Finally, probiotics have the ability to counteract the repercussions of a poor diet. Probiotics are supplements of live microorganisms designed to stabilise or uplift the normal microflora (“healthy” bacteria). Animal studies on mice and other organisms have portrayed positive reactions and acceptance, with this decreasing anxiety and regulating a serene state, however, this could be variable/interchangeable with humans.
Conclusion
In summary, gut microbiota have recently become spotlighted and made headlines within the medical world due to their revolutionary potential solutions to mental disorders that our population is teeming with. However, to put these into place we must continue trialling and investigating these cures intermittently with larger sample sizes, to prevent misinformation or misconceptions. The gut microbiota’s linkage through the Gut-Brain Axis opens a world of possibilities and new medicinal approaches that can change the course of our understanding of the gastrointestinal system. It also brings about a wider message about how significant our diet is and treating our body correctly We must promote healthier lifestyles to the public as it brings a more holistic approach to health. Ultimately, gut microbiota holds the potential to prodigiously improve the lifestyles of individuals with mental health issues and alleviate them of inflammatory issues regarding bowel movement.
AssistedDyingBill
Ben Loebinger
Assisted dying allows a person to end their life, with the help of others, usually a healthcare professional at a time of their choosing and in a circumstance of their choosing, when their physical or psychological suffering is unbearable. In the UK, assisted dying is currently illegal, however a new assisted dying bill was formally introduced to the House of Commons in October 2024 This was debated on November 29th, 2024, with the potential of legalisation of assisted dying in certain circumstances, having passed initial voting
The bill was introduced by Kim Leadbeater, a Labour MP. Leadbeater said that the law would cover those who were terminally ill and suffering at the end of their life and in the final stage of palliative care The law would therefore cover only certain diseases, for example Motor Neurone Disease (MND), a terminal disease affecting one’s motor neurones. Another more common example, but nevertheless ethically complex, that could be applied to this new law may be dementia, most commonly associated with the degradation of brain cells This bill would require adults who want the assistance to end their lives to have 6 months or fewer to live, within the last stages of palliative care.
From the perspective of the four medical ethic pillars the question to legalise assisted dying is incredibly complex The legalisation would uphold the autonomy pillar This allows patients to be entitled to their own opinion, refuse treatment and decide what treatment they want, provided the doctor sees it as within their best interest. The legalisation of assisted dying would give the patient autonomy, as they are allowed to decide whether to end their suffering or not Furthermore, the bill ensures that the patients are in the right state of mind to make their decision and have capacity to give informed consent. Former Labour ‘Justice Secretary’ Lord Falconer told the BBC that his bill would apply only to people ‘mentally able to make the decision ’
To have the capacity to consent the patient must be able to understand the information, retain it, repeat it and be free from coercion. Their choice would also need to be approved by two doctors and potentially the high court, ensuring that the patient has capacity to give consent For the beneficence (duty to do good) and non-maleficence (doing no harm to the patient) pillars, the arguments are more complicated. Some argue that assisted dying would not uphold these pillars, as the doctors are inflicting harm by ending the patients’ lives and thus not doing right by others However, some believe that assisted dying does uphold these pillars, as they think that it is more harmful to keep the patient suffering while alive compared to peacefully ending their life. If the patient is truly suffering, then sometimes ending their life will also be in their best interest.
This is particularly true for those with terminal illnesses, as it allows them to die peacefully rather than in suffering. The pillar of justice asserts this view, as it is undignified to not give the patient an opportunity to end their pain and moreover, would allow the patients care to be stopped, allowing others to benefit from NHS funds. Although, it is complicated, this demonstrates how assisted dying can uphold the four pillars of medical ethics, and therefore it can be the right path to take in certain scenarios.
The legalisation of assisted dying may save the NHS money and release higher quality organs which could be used for transplants End of Life Care is also very costly for the NHS, costing them in the range of 1.8 billion pounds to 4.5 billion pounds a year, roughly 3% of the NHS’s annual budget. The introduction of assisted dying in the UK could save the NHS lots of money, as less of it would have to go towards palliative care. Researchers argue that up to 74 million pounds could be saved if just one third of the costs involved in caring for those with cancer were cut by vulnerable cancer patients opting for assisted suicide. This demonstrates the financial benefits that the introduction of assisted dying could have on the NHS.
Although the pillars suggest that it can be the ethically right decision in some circumstances many doctors and public figures may still disagree with the decision to legalise assisted dying Many argue that this practice would turn ‘doctors into executioners,’ thus defeating their purpose to save lives. Some believe that the bill being passed could lead to ‘a slippery slope,’ where the law could be changed more to apply to a wider group people, thus allowing it to become a popular practice in the UK, increasing death rates across the country
Many believe that this legislation sends out a message to the public, that where quality of life is hindered in some conditions it is not worth preserving that life. This paves way for assisted dying to be allowed in more vulnerable groups like those with disabilities and mental illnesses Moreover, patients may feel bullied and pressured to spare their carers the burden of looking after themselves, thus choosing death. Furthermore, although the pillar of autonomy is upheld, patients are still not allowed to demand treatment, and doctors can still refuse treatment if they believe that it is not in the patient’s best interest This demonstrates how although assisted dying can be medically ethical, there are many arguments that show how its legalisation can be immoral and wrong, displaying the more complicated decision that must be made with a multi-disciplinary team setting. Assisted dying may also provide a psychological challenge to doctors, with doctors actively helping a patient end their life instead of saving it, having a negative impact on the doctors themselves
Within the community of physicians’ people’s opinions are also quite split. A BMA survey in February 2020 demonstrated how 50% of members thought it should be supported, 39% of members thought it should be opposed and 11% were undecided This demonstrates the complicated nature of implementation, as many doctors’ opinions are differing and controversial. Since, the BMA has said it will only accept an OPT-out system for its doctors.
1: Sarco Euthanasia Pod (Wakefield, 2021)
In other countries around the world, assisted dying is legal, these include Canada, the USA, Australia, Belgium, The Netherlands, France and Switzerland This demonstrates how the law can work in the UK, as it works in other countries across the globe, however in some more successfully than others.
Furthermore, if the law was legalised in the UK, it would prevent others from travelling to another country to try and access assisted dying (which is also considered a form of murder within UK courts).
This thus presents another argument for the bill to be passed (in order to upscale regulation) for UK citizens. Countries that allow assisted dying, use a variety of different methods to conduct the practice. The most common one is with lethal drugs. The drug that is usually used is pentobarbital in high doses. In overdose the drug rapidly leads to sedation and depression of medullary centres leading to respiratory and cardiovascular depression, which progresses to coma, apnoea and death. In July 2024 a group of people used the ‘sarco’ pod in Switzerland. This is a suicide pod which fills with nitrogen gas to kill the patient through inert gas asphyxiation. The nitrogen decreases oxygen levels rapidly which prevents panic and a sense of suffocation before unconsciousness This allows the patient to die peacefully Although this method may have been effective, it is illegal in Switzerland, as the process of assisted dying is strictly regulated, resulting in multiple arrests being made.
Figure
Assisted dying is a very relevant topic in the UK currently, with the new bill to pass a law allowing the practice, recently having been introduced to the House of Commons, which is to be debated frequently in the near future This article has explored the bill further and demonstrated medical and ethical arguments for and against the laws legalisation, highlighting the complicated nature surrounding the topic. Personally, I think if introduced, the assisted dying act and the usage of it by doctors, would require some very careful balancing to ensure proper capacity is used and prevent avoidable loss of life in an over-worked system
An assisted dying bill would not result in more people dying, but in fewer people
suffering...
Campaign for Dignity in Dying
Shravan Senthilkumar
3DPrintingin Cardiology
Introduction
3D printing is a technology typically associated within the realms of engineering and design creation, but it also plays a vital role in the field of medicine, especially in the specialty of cardiology, which deals with diseases and abnormalities of the heart and its vessels.
3D printing in simple terms involves the creation of 3D structures from digital models that are geometrically defined, created using a printing material which varies based on the models' contextual use. This technology holds many applications within cardiology such as interventional cardiology (a specialty that diagnoses and treats heart and blood vessel conditions using small tubes called catheters) and cardiovascular surgery Today, it is still undergoing regulatory approval and innovation, to ensure patient safety
Using 3D printing, applications such as different approaches to understanding circulatory illnesses or methods of visualising anatomy have been made possible by 3D heart models Though the technology has been around for almost 30 years, 3D printing has steadily made its way into the medical field from the technology sector during the last 20 years, especially in surgical practice. The complex procedure of 3D printing in cardiology can be separated into two key stages which this article will delve into However further, we will look towards prospects and advancements in care
Process of application
Step 1 (medical imaging data acquisition, image segmentation, and mesh generation):
In medicine a wide range of imaging techniques have been made available due to years of medical advancements In the field of cardiology, the following methods are most used when assessing internal structures of the cardiovascular system for later 3D printing
Magnetic resonance imaging, or CMR (non-invasive examination of the cardiovascular system's structures), and computed tomography, or CT (3D images created using X-rays that are projected at the object at various positions to generate a topographic image), are the most used imaging techniques for 3D printing in cardiology. It is estimated that around 90% of printed models of cardiovascular systems are made using these applications, signifying their popularity within the field as they are non-invasive and therefore more comfortable for a patient
Another example is ultrasound which is widely accessible, reasonably priced, and radiationfree, and is therefore also used Examples include the 3D transoesophageal echocardiography, or TEE (which visualises the heart from inside the oesophagus, avoiding sonographic interference from the lungs and chest). These procedures are invasive and are therefore less frequently used although the lack of radiation would help reduce the chance of cell mutations which for example can lead to cancer due to rapid multiplication. The lack of interference, due to the images being from within the oesophagus, is significantly reduced which would help produce a much more accurate replication of the heart's intricate internal structures, which some would say is necessary for the best surgical outcomes.
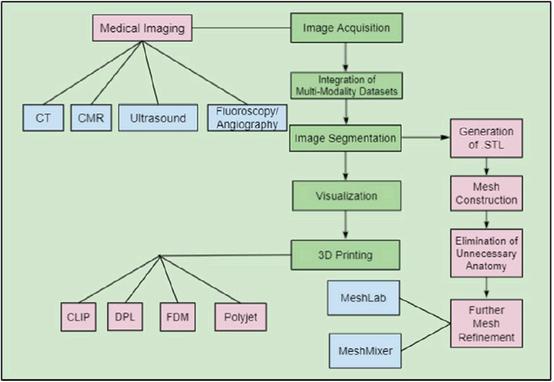
Once the medical images have been acquired, key heart structures of relevance and interest are chosen and transformed into digital models using four main processes:
1) Segmentation uses techniques to isolate and identify important features, which is translated into a STL (stereolithography) file
2) The creation of digital meshes (an online structure which comprises of polygon shapes).
- During mesh production, surface meshes involving triangulation are made to create a sealed shape or volume (also known as tessellation) MeshLab and Mesh Mixer are examples of the software used
3) The elimination of unnecessary anatomy (also known as the removal of 'noise').
4) Finally, the model may undergo final refinements using software.
Step 2 (Use of 3D printing technologies):
The final procedure in the production of 3D printed models, involves the creation of the physical models itself, which is carried out in a variety of ways based on the models’ needs and requirements
One example is fused deposition modelling (FDM). A filament (which is made of thermoplastics) is first heated to its melting point and then extruded (process of forcing a material through a fixed profile) into separate layers through a printer nozzle The model finally cools down itself. FDM can create highly complex prototypes and models.
Another method used is Polyjet which prints models' layer by layer however uses ultraviolet (UV) light to cure and harden each polymer layer Polyjet is perfect for patient-specific cardiovascular models because it allows for the creation of multicoloured and multi-material models allowing for intricate designs such as walls with different thickness, as this would help to for example differentiate between different blood vessels such as arteries, veins and capillaries
A case study by Valverde et al. on ‘the impact of 3D printed models on surgical planning for complex CHD surgery’ used FDM with polyurethane filament The models represented the medical images with great accuracy, with the study concluding that ‘96% of surgeons agreed that the models provided a better understanding of CHD’ and almost half of the 40 cases adapted the original planned biventricular repair due to the 3D models findings for improved surgical correction
Fig. 1. Flowchart outlining the process of 3D printing in cardiology from image acquisition to 3D printing (Lindquist et al., 2021)
Uses of 3D printing in Cardiology
Making accurate, patient-specific heart models using medical pictures from MRI or CT scans is one of the applications of 3D printing in cardiology. By customising the treatment for each patient, this enables medical professionals to practise personalised medicine. Additionally, it helps cardiologists and surgeons better understand complex anatomy, which can lead to more effective surgery planning, lowering associated risks and improving patient outcomes. Additionally, it helps practitioners to better communicate with patients because models can be utilised to demonstrate a patient's situation, which could result in a proposed surgical strategy which both the practitioner and patient agree upon without miscommunication
Another use of 3D printing is its usability in an education setting. In contrast to traditional education, which relied on animal models that frequently don't reflect the complexity of the human heart because whole human bodies and heart dissections are less common, medical experts can now make lifelike models of the heart using 3D printing. These models can serve several uses in education, including teaching anatomy or serving as a framework for low-risk interventional surgical practice. Realistic heart replicas can help medical students prepare better and ensure they have the skills necessary for a successful medical career
Due to its high levels of accuracy and precision, 3D printing may also be used to produce specifically designed valves, stents, and prosthetic devices that fit a patient's anatomy precisely Standard production uses standard forms and sizes, which might result in issues like heart valve leaks or incorrect stent placement. Replicating a patient's size and condition in devices can improve performance and lower the chance of complications following surgery.
‘3D Bioprinting’, which involves printing functional heart tissues, is a potential future development, but one that is primarily in the research stage. Researchers are investigating the viability of printing whole organs or replacing damaged cardiac tissue using living heart cells. Although full organ printing is a long-term objective, certain early uses have been discovered, such as patching damaged heart regions in patients who have experienced myocardial infarction, also referred to as a "heart attack," which has assisted in tissue regeneration and function restoration.
The practice of 3D printing in medicine is only going to get more common, and as we move towards a more patient-centric, personalised approach, its frequency of usage will increase, and in turn, so will outcomes for patients.
AntibioticResistance
Advait Tripathi
Antibiotic resistance is a growing global health concern that threatens to override decades of medical work in the treatment of bacterial infections It is defined as the ability of bacteria to resist the effects of antibiotics that were previously effective against them Antibiotic resistance has emerged as a critical issue, driven largely by the overuse and misuse of these lifesaving medicines. According to the World Health Organization (WHO), antibiotic resistance makes for around 700,000 deaths yearly, a number that might rise to 10 million by 2050 if current trends continue This alarming rise shows the important need for thorough and effective strategies to fight the mutation. In this essay, we will explore the history of antibiotic use, look at the primary causes of antibiotic resistance, discuss the large consequences it has on public health and the economy, and show some effective solutions to tackle the problem
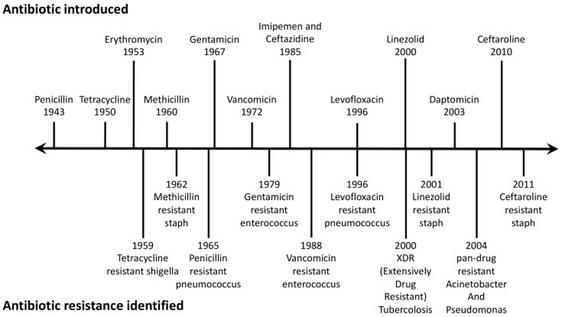
The use of antibiotic producing microbes has gone on for millennia. In Serbia, China, Greece and Egypt, more than 2000 years ago mouldy bread was used to treat open wounds The Eber's papyrus is the world's oldest preserved medical document and inside its list of remedies is mouldy bread, alongside medicinal soil and numerous others. However, the development of the antibacterial drugs we use today, originated from Paul Ehrlich, who developed Sarvasan over 100 years ago in an effort to treat Treponema pallidum (Treponema pallidum caused syphilis which was an infectious disease which could spread to organs quickly). In 1928, Alexander Fleming discovered Penicillin on a petri dish, and since, it was worked on by colleagues at Oxford, before being successfully taken to the clinic as a medicine in 1941. Antibiotics helped massively in curing previously deadly illnesses after WW2, saving numerous lives and revolutionizing surgical techniques But due to their early effectiveness, antibiotics were often overused in both human treatment and agriculture. Because of this over-reliance, bacteria were exposed to antibiotics in ways that allowed them to adapt and survive, which led to the creation of antibiotic resistance. Healthcare professionals started to notice concerning resistance patterns by the late 20th century, and these trends have only gotten worse since the 21st century.
Figure 1: Antibiotic resistance timeline, the top is when the antibiotic was introduced, the bottom is when a resistant strain was identified. (Source: National Library of Medicine USA)
In many healthcare areas, antibiotics are overprescribed in sections where they are not needed, like for the common cold or the flu. This unnecessary use exposes the bacteria to antibiotics allowing resistant strains to arise. Apart from the overprescription of antibiotics, there are numerous other ways antibiotic resistance can spread One of these is use of antibiotics on livestock. In total, around 80% of total consumption of medically important antibiotics is in the animal industry, largely for growth promotion in healthy animals. The widespread use of antibiotics in farming pushes the selection pressure on bacteria, making for the development of resistant strains that can be transmitted to humans through food or environmental exposure. Patient non-compliance is another reason for antibiotic resistance. For example, when patients do not finish the prescribed antibiotic course, some bacteria can survive and become resistant strains. Hence why, despite feeling better, doctors insist you complete a regulated dose
Antibiotic resistance has severe impacts going well beyond individual health. The increase of these resistant strains has led to higher mortality rates, as regular, common bacterial infections have become harder to treat Patients with resistant strains often must stay in hospitals for longer and have more complicated treatment which puts higher pressure on hospitals, not just with rising in-patient figures but with costs and finance management. More money is being spent on antimicrobial-resistant infections instead of preventative care or other essential health care services Alongside this, antibiotic resistance raises new challenges for procedures like organ transplants, surgeries or chemotherapy where doctors rely on antibiotics to prevent infections. Addressing the drastic issues of antibiotic resistance is key not just for public health or the economy but also for modern day medical practises. As resistance increases, the risk of surgical site infections rises This complicates recovery and increases the likelihood of severe complications or fatality. As a result, doctors may be more reluctant to perform elective surgeries and may undermine the success of treatments for chronic diseases, ultimately impacting patient outcomes and healthcare delivery.
The real question now is how to solve this issue of antibiotic resistance.
Some researchers are working on a way to impair antibiotic resistant bacteria that cause diseases like E Coli, by inhibiting a protein that drives the formation of the resistant abilities in the bacteria. Another method being employed by scientists is searching sea sponges in an attempt to find new antibiotics in the microbiome of organisms deep beneath the surface of the ocean, as researchers believe that there are diverse populations of cultivatable bacteria in such The sponges thrive in extreme environments which may have allowed them to develop new defences to bacteria and pathogens. Researchers collect samples from different depths and analyse the compounds to see how they potentially inhibit bacterial growth. By isolating, and then testing these substances, scientists hope to discover new antibiotics, which can combat resistant infections The whole process highlights how important marine research is to medicine.
Alongside this, there have been attempts made to develop new types of antibiotics, and some areas have tried to implement diagnostic tests to determine whether an infection is bacterial, and which antibiotic will be effective. Potential strategies against antibiotic resistance include implementing strict guidelines for healthcare providers on when to provide antibiotics, educate patients to only take antibiotics when prescribed and only when necessary, encouraging vaccinations to treat infections that may require more antibiotic usage, regulation of antibiotics in agriculture, especially for use of promoting growth on livestock, and overall global cooperation on the matter. Global cooperation on antibiotic resistance would allow key research and data to be shared between countries allowing for progress to be made faster. Combating antibiotic resistance requires a multifaceted approach which would involve not just researchers but also pharmacists and the public Simply, it is imperative that a greater understanding is created on the topic to prevent further growth of resistant strains.
In summary, antibiotic resistance is a pressing global challenge which stems from factors such as overuse of antibiotics, inadequate infection control, uses of antibiotics in agriculture and more. The consequences are dire, leading to a drastic increase in mortality rate, complications to medical procedures, and severe economic burdens. Addressing this issue requires the need for a comprehensive approach on both research and development, alongside public education As a call to action, individuals can contribute by adhering to prescribed antibiotic regimes and supporting vaccination efforts. Healthcare providers should implement antibiotic stewardship programs and educate patients about the risks of antibiotic misuse, and overuse. Policymakers must prioritize regulations that limit unnecessary antibiotic use in agriculture and invest in research for new treatment options
Ultimately, addressing antibiotic resistance is not only imperative for the health of the current public, but also for future generations. By committing to these strategies, we can ensure that antibiotics remain a useful tool to fight bacteria and cure illnesses
"I would like to sound one note of warning... It is not difficult to make microbes resistant to penicillin in the laboratory by exposing them to concentrations not sufficient to kill them, and the same thing has occasionally happened in the body"
Alexander Fleming in his 1945 Noble Prize Acceptance Speech
Bacteriophages
Sonny Shastri
Figure 1: A Bacteriophage (Wikipedia Contributors, 2019)
Bacteria are infected by viruses called bacteriophages An estimated 10 million trillion of them exist on the planet, making them the most abundant microorganism we know exist, with a population two times as large as bacteria In 1917, French-Canadian microbiologist Félix D'Hérelle characterised them and recognised that they might be used to cure bacterial illnesses; in a process known as phage therapy Historically, bacteriophages were initially discovered in 1915, only two years earlier, by Frederick William Twort, a British scientist. He kept discovering clear patches of dead bacteria while attempting to cultivate the vaccinia bacteria that were used to make the smallpox vaccine. Twort hypothesised that the bacteria might be being killed by a virus, however, his research halted due to the impending war.
In the same year, while D’Herelle was employed by the Pasteur Institute in Paris and working in Tunisia, he discovered something similar to Twort while cultivating a bacillus to use against locusts. He discovered similar patches in a dysentery bacillus culture back in Paris in 1917. D'Herelle thought it was a virus and named it a bacteriophage (bacteria-eater) because it was evident that something was actively attacking those microorganisms. For a while, no one was sure what a bacteriophage was. Some thought it was a chemical, whereas D'Hérelle thought it was a bacterium. Quickly, he recognised the medical potential of phage’s and that they could certainly treat some infections if they could kill bacteria. D'Hérelle tested it on himself and was able to treat a number of patients with dysentery in Paris in 1919. He quickly replicated his success in treating the Indochina plague and the cholera pandemic in India. Phages were very quickly being applied to medical practice using phage therapy, specifically a "cocktail" of phages designed to overwhelm the bacteria in case they become resistant to one type
However, other researchers discovered that they couldn't duplicate D’Hérelle's accomplishment, and scepticism over the efficacy of phage therapy started to grow
2a: Félix d'Hérelle (lnorkin2013, 2015)
2b: Georgi Eliava (ResearchGate , 2024)
Figure
Figure
Microbiologist, Georgi Eliava pioneered phage development in the Soviet Union (USSR) in the 1930s and soon after, D’Herelle travelled there to work with him, before Eliava was abruptly put to death in 1937 for being an enemy of the people. The USSR adopted phage therapy, unlike the West, as a vital tool to use against bacterial diseases, since it lacked access to the antibiotics available in Europe and the US Today, it is still widely used there as a way to combat the rise of antimicrobial resistance, leading the advancement towards alternate healthcare.
Importantly however, the enormous biological and medical significance of phages was only shown properly during the late 1930’s. Phage groups played a key role in the discovery of the structure of DNA, led by the renowned Phage Group of Scientists established in Cold Spring Harbour, USA, in 1940 In 1952, Martha Chase and Alfred Hershey utilised them to demonstrate that DNA is the genetic material of life, which was an immense scientific achievement.
As research has continued, two methods by which phages take over bacterial cells have been identified by researchers When killing bacterial cells, the phage's tail fibres adhere to the cell wall and then pierce it to introduce the double-stranded DNA genome into the cell. During the "lytic" cycle, the phage repeatedly replicates until the cell bursts by using the resources of the cell and in the "lysogenic" cycle, the DNA remains dormant within the cell and replicates when the host cell divides, causing little harm to the host, but attaching within the DNA
Phage treatment has regained popularity due to bacteria developing antibiotic resistance, and as a result numerous trials are currently in progress The phage’s rapid rate of reproduction and capacity to be able to target particular bacteria are two important advantages. Phages could also potentially be utilised to produce antibodies which can fight diseases such as rheumatism and gastrointestinal disorders, as well as to test for infections. Applications continue to be developed today in multiple different avenues of research as well, however Phage therapy is being used to treat some forms of cancer in human cells and a vector for biological research. These microorganisms have a huge range of application and the potential to innovate medical research
An example of bacteriophages being used in medicine is in 2017, when phages were successfully used in London to treat a 15-year-old patient for a bacterial infection after a double lung transplant The patient had developed antibiotic resistance due to exposure mutation After sending a sample of the patient’s bacteria over to a lab, Graham Hatfull (a professor at the University of Pittsburgh) searched a collection of 15,00 phages he had assembled with his students. Hatfull identified one that would be good at killing the bacterium, Mycobacterium abscessus, which was the bacterium causing the patient’s infection The phage has complimentary receptors on its membrane to attach to the target cell, and no inherent toxicity to humans, making it ideal for usage.
Though not yet approved for routine use, promising UK trials with NICE support highlight bacteriophage therapy's potential to transform treatment for resistant infections Now is the moment to advance this research, building on early successes to make phage therapy a viable, accessible and innovative option, bringing new hope to patients within the NHS.
Figure 3: Lytic and lysogenic cycle (Biotech Tutorials, 2022)
Hypertension
Riaan Prakashan
What is Hypertension?
Hypertension is a chronic medical condition which is usually characterised by elevated blood pressure. Hypertension can contribute to significant health risks such as strokes and cardiovascular disease, and is usually exacerbated by modifiable factors like diet and exercise (more commonly known as lifestyle choices)
Blood pressure is the pressure exerted on the walls of blood vessels by blood. It is signified by two numbers Systolic pressure is the pressure when the heart beats and muscle contracts Diastolic pressure oppositely is the pressure when the heart rests between beats and the atria/ventricle refills with blood. It is calculated by doing the systolic pressure divided by the diastolic pressure and is measured in millimetres of mercury (mmHg).
NHS England stipulates: “If you're under 80 years of age, you're usually considered to have high blood pressure if your reading is either... 140/90 or higher when checked by a healthcare professional, or 135/85 or higher when checked at home.”
Hypertension is classified into two categories, both of which are severe and can lead to comorbidities, or worse healthcare outcomes.
Primary Hypertension
Primary hypertension accounts for approximately 90% of cases and does not have a single identifiable cause. It develops over many years and is influenced by lifestyle and genetic factors. Some causes are not limited to, coding within the DNA, obesity, diet, physical inactivity and stress For example, obesity is correlated with increased blood pressure due to a greater resistance to insulin (caused by overexposure in insulin receptors) and higher levels of fat which can block arteries and increases blood pressure. High fat, alcohol and generally “junk” food such as foods which are high in calories, salt, unhealthy fats, and sugars are dietary factors that contribute to hypertension
Foods high in sodium, such as chips and processed meats, cause the body to retain water, leading to an increase in blood pressure. This occurs because the higher blood volume forces the heart to pump more blood, requiring it to work harder, which can contribute to hypertension. Likewise, sugary foods and drinks, such as soft drinks, candy and chocolates can cause spikes in blood sugar, and can cause promote insulin resistance, affecting the kidneys, as they may not be able to regulate the blood pressure properly. Over prolonged periods of time blood pressure can increase as the body’s metabolic system can be overworked, in what can be considered a positive feedback loop.
Similarly, elevated levels of stress can cause temporary increases in blood pressure and can contribute to hypertension This is because, when we experience stress, the body releases adrenaline and cortisol, produced in the adrenal gland. The hormone, adrenaline causes an increased heart rate and makes the heart pump a larger volume of blood faster which causes a rise in blood pressure. Its mechanism for this is by binding to β₁-adrenergic receptors located on the heart's muscle cells (cardiomyocytes)
Stress hormones also cause blood vessels to constrict, which raises the blood pressure To be specific, cortisol has long-lasting effects such as prompting the kidneys to retain sodium, leading to water retention and a higher blood volume. Chronic stress keeps the stress response activated, causing a frequently elevated blood pressure and often leads to poor lifestyle habits like unhealthy eating and lack of exercise
Secondary Hypertension
This type of elevated blood pressure accounts for 10% of cases and comes from specific medical conditions. It is commonly caused by kidney disease, hormonal disorders, and medications.
Conditions like Renal Artery Stenosis and Cushing’s Syndrome can lead to increased blood pressure whilst medications like oral contraceptives can also cause hypertension.
Renal Artery Stenosis
Renal artery stenosis is a condition where one or both arteries supplying blood to the kidneys narrow which reduces blood flow, usually due to atherosclerosis (plaque buildup). In response, the kidneys release the hormone renin, which starts a cascade that activates the renin-angiotensin-aldosterone system (RAAS) This system raises blood pressure by causing vasoconstriction and increasing sodium and water retention. As a result, renal artery stenosis can lead to secondary hypertension and wide-scale body effects.
Cushing’s Syndrome
Cushing’s syndrome can be caused by chronic exposure to elevated levels of cortisol, often due to an adrenal or pituitary tumour. Excess cortisol raises blood pressure through several mechanisms: it raises blood volume by promoting sodium and water retention, and can lead to weight gain, which further stresses the cardiovascular system. The prolonged high cortisol levels in Cushing’s Syndrome contribute to secondary hypertension, which is often severe and difficult to control, which can lead to complications like heart disease if left untreated.
Figure 1: Renal Artery Stenosis (NIDDK, 2014)
Figure 2: Cushing Disease (Oregon Health & Science University, 2023)
Consequences of Hypertension
If hypertension is left untreated it can lead to major consequences such as cardiovascular disease, kidney damage, vision loss and cognitive decline
Cardiovascular disease is associated with hypertension, as high blood pressure can damage artery walls and cause the development of atherosclerosis. In hypertension, the force exerted on the arterial walls is consistently elevated, leading to microscopic tears in the endothelium (the inner lining of blood vessels) These tears provide entry points for cholesterol, fats, and other substances circulating in the blood to accumulate, forming plaques. Over time, these plaques grow and harden, causing the arteries to narrow (atherosclerosis) The restricted arteries mean the heart has to work even harder to pump blood through the body, which increases blood pressure Additionally, hardened arteries lose their ability to dilate effectively, which is crucial for regulating blood flow during physical activity. This restricted blood flow can starve the heart muscle of oxygen, especially if a plaque ruptures and forms a blood clot, which may fully block an artery If this blockage occurs in one of the coronary arteries supplying the heart, a heart attack can be induced. Thus, the cycle of hypertension and atherosclerosis significantly raises the risk of cardiovascular disease.
Hypertension can lead to kidney damage by placing strain on blood vessels, especially the delicate vessels in the kidneys. The high pressure can damage the kidney’s filtering units (glomerulus), impairing their ability to filter waste from the blood effectively and leading to chronic kidney disease
Vision loss can be caused by hypertension as it can also damage blood vessels in the retina. This is typically because vessels walls cannot withstand large amount of pressure, and is a commonly associated symptom of diabetes
Hypertension contributes to cognitive decline by damaging the brain's blood vessels which leads to reduced blood flow and oxygen delivery to brain tissues. This strain on the blood vessels can result in vascular damage, particularly in small arteries and capillaries within the brain, impairing cognitive function The reduced blood flow can also cause lesions or small areas of damage which disrupts communication between different parts of the brain. These changes are strongly linked to cognitive decline and are a major factor in the development of dementia
Hypertension can also increase the risk of strokes, which can cause direct damage to areas of the brain responsible for memory, attention, and function. Repeated strokes can accumulate and cause cognitive decline Moreover, hypertension in midlife has been identified as a risk factor for Alzheimer's disease, due to mechanisms like increased inflammation and damage to the blood-brain barrier. Managing blood pressure is crucial to prevent these harmful effects and reduce the risk of dementia, as studies have shown that effectively controlling hypertension can delay the onset of cognitive decline and lower the risk of dementia later in life
Managing Hypertension
Managing Hypertension can lead to reduced risk of complications Some steps that can be taken for this is to maintain a healthy and full diet to include fruits, vegetables and low-fat dairy which can lower blood pressure. Physical activity, especially aerobic exercises like walking, running, or swimming, can help reduce blood pressure by improving cardiovascular efficiency When the heart becomes stronger through consistent exercise, it pumps a larger volume of blood with each beat. This allows the heart to pump more effectively while lowering the number of beats per minute, which reduces overall stress on the heart and lowers blood pressure.
Exercise also enhances the flexibility of blood vessels, making it easier for them to expand and accommodate the increased blood flow that occurs during physical activity. Over time, this improved vasodilation helps maintain lower blood pressure even when at rest Additionally, aerobic exercise reduces the activity of the sympathetic nervous system, which controls the body’s stress response. By lowering the production of stress hormones like adrenaline and cortisol, exercise helps prevent spikes in blood pressure associated with stress.
Furthermore, regular physical activity aids in weight management, which is crucial for controlling blood pressure. Excess weight forces the heart to work harder, raising blood pressure. By maintaining a healthy weight, the cardiovascular system faces less strain, contributing to a decrease in blood pressure
Conclusion
Hypertension is a serious health condition that affects millions of people around the world It does not have a cure and can only be managed by looking at your diet, physical activity, and stress levels. Eating fewer fatty foods and working out intensely, can reduce blockages in blood vessels, which reduces blood pressure and strengthens the heart.
In developed countries, hypertension is a leading cause of heart attack in the obese population and with wider access to fat foods and a general decrease in people doing exercise, elevated blood pressure among the general population is considered a standard of life As a result, every year, the NHS spends around £2 1bn on hypertension related illnesses, a figure that is increasing, as people use healthcare to get around being held accountable and acting on their own poor health.
TheHuman GenomeProject
Aayan Kureshi
Introduction
The Human Genome project, launched in October of 1990 and completed in April 2003, is arguably one of the most significant scientific feats in history. Scientists from all around the globe set out to comprehensively study the entirety of the genomes of a selection of organisms. In total, the project cost approximately 3 billion dollars. However, the greatest achievement of this project was arguably the mapping of the entire human genome- a feat that can help in the prevention of genetic diseases, as well as serving to aid us in understanding the past of humans, for example, exploring and mapping human migration patterns through history, and how these patterns resulted in the variety of the human species we experience today.
The official National Human Genome Research Institute claims that the projects aims were to sequence the entire genomes of humans, E. coli bacteria, baker's yeast, fruit flies, nematodes and the mouse, in order to gain a richer understand of diversity among organisms.
Which human's genome was sequenced? The final Human Genome Project was composed of a blend of the DNAs of 20 people. 30% of the data was provided from 19 individuals with mostly European ancestry, while the rest of the 70% was mapped from 1 individual with blended ancestry. The identities of individuals were intentionally made anonymous to protect their privacy Their DNA was collected from blood samples
What is a genome?
A genome is the complete genetic information of an organism, determined by the sequence of DNA found in their cells. A genome is fully responsible for many of the physical traits of an organism as the DNA sequences in genes code for specific proteins that, in turn result in physical properties, for example eye colour or hair colour. It is also deeply involved in many other physical aspects in combination with external factors, for example, the total genetic potential size of an organism is determined by their genome, but whether or not it reaches that size is also heavily dependent on aspects like nutrition and physical environment.
Genomes of organisms can vary in size, with different numbers of nucleotides (the chemical components of DNA) but all serve the same purpose, which is to "construct and maintain a living example of that organism".
A Short History of the Human Genome Project
January 1984 to December 1986 - Early summits take place to assess the feasibility of the Human Genome Project. The Genome Sequencing Workshop in Sante Fe, New Mexico, held by the US Department of Energy (DOE) and their Office of Health and Environmental Research discusses the further possibility of the project
February 1988 to 1st March - NIH Director James Wyngaarden assembles scientists, administrators and policy expert in Virginia to lay out the plan for the project
October 1988 - NIH (National Institute of Health) and the DOE sign a "memorandum of understanding" to co-ordinate activities surrounding the Human Genome.
October 1988 - Department of Human Health and Services creates the "National Centre for Human Genome Research", the NCHGR. The first appointed director was James D. Watson.
April 1990 - NIH and DOE publish the first five years of a supposed fifteen-year plan that outlined the aims of the project: to map all 3.2 billion letters of the human genome, as well as the genomes of other organisms, to develop technologies to analyse DNA.
October 1990 - The project officially begins as the first funds are allocated
September 1994 - The Human Genome Project meets one of its first major goals as a "comprehensive human genetic linkage map" The map shows approximate spacing and relative order of certain DNA patterns It was completed a full year ahead of schedule and was the projects first tool that could be used to locate disease causing genes.
February 1996 - An International Strategy Meeting on Human Genome Sequencing is held in Bermuda by the leaders of the project and "The Bermuda Principles" are drafted They detail that any and all human genomic sequencing information should be made free and available to the public, contrasting the general scientific practice of information coming out exclusively after publishing This step was taken to further emphasise the societal benefit of the project as a priority
October 1998 - NIH-DOE new five-year plan was published, anticipated completion of the project in 2003, 2 years ahead of schedule One of the main aims was to create a "working draft" of the human genome by 2001
March 1999 - The project completes the pilot phase of sequencing the human genome and launches the full-scale effort to sequence all 3 billion letters of the human genome
December 1999 – An international team of researchers unravels the genetic code of Chromosome 22 - a massive scientific milestone.
June 2000 - The Human Genome Sequencing Consortium announces it has completed the working draft of the Human Genome, one year ahead of schedule.
February 2001 - The draft sequence is published The total number of genes at this time is estimated to be around 35,000 It is found that the DNA sequences of 2 humans are 99 9% identical.
March 2003 - The Telomere-to-Telomere consortium announced they had filled all the gaps in the sequence, and the first truly complete human genome sequence was produced
April 2003 - The Human Genome Project is announced to be completed.
October 2004 - The Human Genome Sequencing Consortium publishes the scientific description of the finished human genome sequence.
Technology involved in the Human Genome Project
The Human Genome Project was only possible due to contemporary technology that allowed scientists to dive deep into the structure of the genome. In this section I will be exploring the technologies involved and responsible for the project, as well as how they work.
Sanger DNA sequencing
Modern genetic studies are founded on the principle of DNA sequencing, which involves the ability to determine the composition and order of nucleic acids in a strand of DNA or RNA Before Fred Sanger and his colleagues developed Sanger sequencing, analytical chemistry methods were used to determine nucleic acid composition, involving chemical tests to determine chemical compositions of the bases Fred Sanger and his colleagues in 1977, created a new technique to sequence DNA that determines the exact order of nucleotides in a DNA strand. It is based on incorporating dideoxynucleosides (ddNTP) into the process of DNA synthesis, which stops the formation of a complete strand of DNA, producing fragments that can be analysed
After the collection of all the short strands of DNA, gel electrophoresis can take place. This process separates fragments based on size and charge as they are placed in gel, and an electric current is applied This causes negatively charged DNA fragments to move towards the positive electrode through the gel Smaller DNA fragments travel faster, so they move further, resulting in the sample being separated by size.
Finally, the fragments pass through a detector The labelled ddNTP, which is marked fluorescently before the sequencing, revealing the identity of the nucleotide at each position, as different ddNTPs terminate the strand formation at different points. The sequence is read from shortest to the longest, providing the DNA sequence.
This method was labour intensive and time consuming, as only 500 - 100 base pairs could be sequenced at a time, so sequencing the entire human genome would take a very long time. However, the process of DNA sequencing continued to evolve as the Human Genome Project continued, eventually leading to Capillary DNA sequencing
Capillary DNA Sequencing
Capillary sequencing could produce 4 times as many samples as the gel method used in the previously used Sanger sequencing
The process of fragmenting DNA using ddNTPs remained the same, but rather than placing the fragments in a gel, capillary sequencing involved passing them down a capillary tube filled with a polymer solution Similar to before, molecules with less mass would travel faster The fluorescent endings of the ddNTPs would be read by a fluorescent detecting laser. The colour of the fluorescence would be picked up by a camera and a graph would be produced, containing different peaks with different colours
The small diameter of the capillary meant that high electric fields could be applied to the molecules in the solution to rapidly separate them. Furthermore, the automation of the process allowed one individual to oversee the sequencings of multiple machines - since this process could be totally automated, conserving labour and time for the scientists working on the project.
Benefits of the Human Genome Project
While the project is undoubtedly very interesting, the question of its significance and benefit can be raised. The project advanced international medicine surrounding disease diagnosis, risk prediction, gene therapy, drug development. On top of this, it simply grants scientist more insight into biological history, in our relation to other species and more general biological processes.
The project enabled the modern identification of genes associated with certain genetic disorders, leading to early detection and treatment for conditions like Alzheimer's or cystic fibrosis. Furthermore, the more detailed understanding of the human genome allows for medicine to be more personalised to individuals, so that medicinal institutes can avoid situations like adverse reactions to medicinal drugs more often.
Building on this, the pharmaceutical industry can use knowledge of the human genome to more efficiently design substances, as less trial and error must be used, decreasing the money lost in the developments of drugs that do not pass the testing stage Now, drugs will be more likely to pass testing as they will be tailored according to the human genome. By streamlining the development process of new medicinal drugs, less money is wasted and less time is taken to produce medicines of equal quality.
Ethical issues of the Human Genome Project
While the Human Genome Project undoubtedly benefits society in many aspects, as mentioned above, the project does also raise a number of ethical concerns, due to the sheer amount of information about an individual their genome contains, as the Human Genome Project advanced genetic testing to the point where it could be used commonly in hospitals.
Patients need to be completely informed on the implications of genetic testing, as results for genetic testing can be emotionally distressing, particularly surrounding genetic diseases and conditions.
Patient confidentiality also raises a large ethical concern, as genetic information can be misused. An example of this would be if a patient with a predisposition to a certain genetic condition were to have their information leaked - the individual could face far higher insurance prices or outright denial of coverage from insurance companies.
Another ethical concern arises surrounding the potential for the use of genetic information in state surveillance and control, as well as law enforcement. A state could use genetic testing to potentially enforce and police an apartheid state by using DNA testing to identify members of a discriminated race Forensic data has often been used in the past to resolve criminal cases, but this raises ethical concerns around the consent of subjects of forensic tests- many believe that it is unethical to use the genetic information of individuals in forensic testing without the consent of the individual.
Likewise, future development may see the creation of, so called, designer babies, as the human genome is further understood and manipulated. Here, parents may choose to edit their genome artificially to give their children recognised traits for sport or academia.
Conclusion
In conclusion, the Human Genome Project was a massive project that spanned over more than a decade, with involvement from scientists all across the globe It utilised incredible technology, and advanced later gene sequencing technology It provided the basis for vast progress in the pharmaceutical and wider medicinal field, while also raising several interesting and pressing ethical concerns surrounding the management of the genetic information of individuals
Motor-Neurone Disease:IsthereaCure?
Saanidh Bhatt
Motor neurone disease, known as MND for short, refers to a group of diseases, in which nerves, known as motor neurons, degenerate and die It affects 1 in every 300 people in the UK, and 6 people are killed every day by it in the UK. Motor neurons are the nerves that send signals to our body and muscles to move, and they are found in the brain and the spinal cord. As they degenerate, they are less able to pass instructions from the brain to the muscle, leading to weakness in muscles, and, as the numbers of motor neurons further decrease, eventually paralysis.
There are six main types of MND One of them is commonly known as Lou Gehrig’s disease but its scientific name is amyotrophic lateral sclerosis. When someone is suffering from ALS, they lose control of their muscles very quickly causing paralysis at a rapid rate. ALS is also the disease that Stephen Hawking, one of the most famous people to have lived with MND, had. There are five other main types of MND, one of which is progressive muscular atrophy (PMA), which is largely similar to ALS, but in PMA the limbs are affected before the rest of the body. Another is progressive bulbar palsy (PBP), which mainly affects facial movement, especially the jaw, making things such as speaking, chewing, and swallowing hard. This can lead to tube feeding, which is extended on later in this article. Primary lateral sclerosis (PLS) is a different type of MND PLS causes weakness in the arms, legs, and face. Additionally, there is Kennedy's disease, also known as spinal and bulbar muscular atrophy (SBMA). In Kennedy’s disease most of the body becomes weak and sometimes slightly paralysed, but it happens gradually, normally starting with weakness in the hands. Finally, there is post-polio Syndrome, (PPS) PPS is an infectious viral disease, which can happen anywhere between 15 and 40 years after a person has had polio. It also leads to muscle weakness. The main thing that all of these variations of Motor Neurone Disease have in common, is that the motor neurons degenerate, causing weakness in parts of the body, eventually leading to paralysis
Causes of MND
We do not know the causes of MND, but there are multiple theories on why it happens One of the most prevalent theories on the cause of motor neurone disease, is that it happens due to an error in our genes. 20% of cases are linked with a genetic cause, where someone who is diagnosed with the disease has a close relative who has previously suffered from the disease Another theory is that MND comes from high exposure to chemicals and toxins, particularly agricultural ones such as pesticides. Additional causes of the disease, as stated by the MNDA (Motor Neurone Disease Association), could be mechanical trauma, military service, high levels of exercise, and exposure to a variety of heavy metals. However, as the MNDA further state, ‘the evidence of these has often been conflicting and clear conclusions cannot be given’.
However, we can identify trends in the type of people who have been diagnosed with MND. One of these trends is that a lot of rugby players are getting it such as the late Rob Burrow. This helps us understand potential causes for MND, and, as research has shown, there is potential that multiple concussions can lead to a higher likelihood of being diagnosed with the disease. As reported by the BBC, sports people who have had 5 or more concussions in their career, which leads to higher protein levels in the brain, something which is common in rugby, are more likely to suffer from diseases such as Alzheimer’s and MND This is confirmed by research conducted by Durham University, that pitted 30 retired sportsmen with a history of 5 or more concussions, against 26 other sportsmen, with less than five previous concussions. The results showed that the concussion-prone subjects seemed to have higher levels of proteins in their brain, which leads to diseases such as MND or Alzheimer’s These higher levels of protein can cause abnormal clumps of protein, called aggregates, to develop inside motor neurons and hence they disrupt the motor neurons. Aggregates can also indicate that a motor neuron is under stress, which is highly common in MND. Abnormal proteins are also commonly found in genetic instances of MND. Specific proteins can also be mutated and one of these mutated proteins that is commonly found in MND, is Superoxide dismutase1 (SOD1). SOD1 usually protects cells, but, if mutated, the protein could turn toxic, and therefore harm the nerves within the body.
Symptoms of MND
There are numerous symptoms of MND. The following are the ones which are stated by the MNDA:
The most obvious ones are muscle weakness and pains, along with other symptoms such as muscle twitching, pins and needles, numbness in hands, feet or limbs, slurred speech, dropping things due to weak hands, tripping often and legs getting thinner (due to reduced muscle mass) Overall, signs of MND revolve around weakness, especially if in multiple areas, and a typical diagnosis begins at a GP, within the UK, who refers and escalates to a neurological unit once confirmed.
Medication with MND
When a person is diagnosed with MND, they need to take lots of medication. Some of the general medication that MND patients take are:
Tube feeding: When patients find it hard to chew and swallow food and liquids doctors insert tubes into the body, to make sure vital nutrients are given to the patient. For short term illnesses, nasogastric tubing is used. In nasogastric tubing, a tube is inserted through your nose, and it leads to your stomach, where food and drink can enter it However, in longer term illnesses, such as MND, gastronomies are offered to the patients. In, a gastronomy a small operation is performed, where a tube is inserted into your abdomen leading to your stomach. A gastronomy offers the advantage of not having to remove the tube every time it is used, so can be seen as slightly easier
Breathing support: With MND, extra oxygen is not always a must, as too much can upset the balance between oxygen and carbon dioxide in the body. However, when patients with MND have low levels of oxygen, extra oxygen can be used carefully This oxygen can be administered by a nasal canula, oxygen mask or it can be added to one of the CPAP or the BiPAP, (depending on which the patient has). Ventilation is another form of breathing support. In ventilation, a machine is used to support intake of air, but not specifically oxygen There are two types of ventilation, non-invasive, where a machine supports intake of air through a mask, and tracheostomy, where a tube is inserted in the windpipe and a machine helps breathing through the tube.
Therapies: When a patient loses full control of a part of their body, there are numerous exercises and therapies that the patient can do such as physiotherapy, occupational therapy, communication support and psychological support
Riluzole- Riluzole is a common drug that people with MND take to help their survival. Glutamate is a sugar in the body that causes damage in nerves when an excess amount is produced. It is a neurotransmitter, which means it sends message between neurons in the brain, exciting and stimulating them in the process, allowing for messages to be sent easily. However, when there is excess glutamate, it can overstimulate these nerve cells and damage the brain. When too much glutamate is in the body, Riluzole is used. Riluzole is thought to reduce the amount of glutamate produced, therefore prolonging the life span of nerves
Cures for MND
MND was first discovered in the late 19th century Since then, we have still not found a cure for it, and instead treat it with multiple medicines that try to prolong the patient’s life. However, as funding and knowledge about it increases, numerous organisations are trying to find ways to cure it.
One of these organisations is the University of Sheffield. They have a very advanced neuroscience department called SiTraN, who are constantly working on different medicines for a cure. They also claim that the cure will almost certainly be ‘Sheffield made’. On the 3rd of November 2023, a new research institute was launched by the University of Sheffield, in partnership with Kings College. Called the UK Motor Neurone Disease Research Institute, it researches around patients with MND, in the aim of finding a new drug that can help patients with MND, or even cure them.
Another organisation researching a cure for the disease, is the University of Sydney. The University is using a multi-arm drug trial, where patients can be administered multiple drugs at the same time, speeding up progress in research. The university reports ‘A cure for the genetic forms of MND is close, probably 3 years away, and we are hoping for a cure for the sporadic forms within the decade.
Along with these, numerous other organisations are also researching and testing a cure for MND
One of the drugs researched as a cure for MND is known as Tegoprubart (AT-1051). Tegoprubart is an antibody, which binds to a harmful protein called CD40 ligand, which prevents the protein from reaching its target Tegoprubart mainly acts in the spinal cord, and delays the CD40L from damaging the body. The outcome of the trail for this drug yielded positive results, with it being deemed safe and also that it achieved its intention. However, the drug has not been rolled out for general use yet, with no detail about when this will happen.
Another drug being tested as a cure is called ILB. ILB is a pleiotropic molecule, which means it has numerous effects on the body. Its active component is called dextran sulphate, and instead of targeting juts one pathway like Tegoprubart, it targets numerous pathways. It is administered by and injection under the skin The study also yielded positive results, with the drug being well tolerated by the test subjects, and therefore deemed to be safe. Now, the University of Birmingham has reported that Swedish company TikoMed is conducting larger studies to find out whether ILB works as a cure for MND.
Finally, the MNDA are constantly updating development in MND research on their website, with details able to be found on the following website:
Personal implications and organisations that help
When someone is suffering from Motor Neurone Disease, they need lots of care, not only from doctors in a holistic environment, but also from family When a family member suffers from MND, it can have numerous personal implications on that family, specifically in the area of taking care of that diagnosed person. As the person does not have control over certain parts of their body, they need help from their family to perform certain day-to-day tasks, such as eating, excretion, and shaving, to name a few Therefore, as there is still no cure for MND, numerous things can/are being done to help those with MND lead better lives
Examples include foundations such as the My Name’5 Doddie Foundation, established under the oversight of another rugby great, Doddie Weir, before he sadly passed away from MND in November 2022 Recently, the foundation donated five-hundred-million pounds in research for the cure. There are other similar organisations, where people generously donate to the cause, and then that money goes toward research for a cure. Worldwide organisations such as the MNDA also donate money for research into cures Furthermore, caretakers and GP’s also help the diagnosed person and their family
Overall, Motor Neurone Disease is an, as of now, incurable disease. However, we are progressing rapidly with research, due to new technology and massive funding boosts. Some organisations say a cure for some forms of MND is likely to only take a couple of years However, I still believe that a cure will take longer, as no cures have been proven to work spectacularly yet, and, even if one is found in the near future, it will unlikely be available for general use for numerous years after being found, due to both clinical testing and safety regulation, meaning it will take numerous years for a cure for MND to be globally accessible
MND kills six people per day in the UK...
DementiaandOther AgingConditions...
Sanhith Dandeniya
Dementia, medically known as major cognitive disorder, is a syndrome related to the deterioration of brain functioning It is one of the most common conditions people get as they age. Specifically, it is when neurons in the brain, which were once healthy, stop working and lose connections with other brain cells and eventually, they die. Some symptoms include memory loss, slow thinking speed, low mental sharpness, difficulty with language, trouble with understanding, trouble with judgement, radical or unusual mood changes, some difficulty in movement and some difficulties in doing daily activities Dementia is prevalent in elderly people, and statistics show that cases are generally diagnosed between the ages of 45 and 65.
When diagnosed, dementia is almost like a spectrum, with seven stages, where stage 1 is the mildest and stage 7 is the most severe. Doctors typically diagnose patients with dementia when it reaches stage 4, as the symptoms are not severe enough to diagnose. Dementia is divided into three phases They are:
Pre-phase / Early-phase Dementia
- Stage 1 (No Cognitive Impairment): Brain function is normal; no detectable symptoms, so diagnosis is nearly impossible
- Stage 2 (Very Mild Cognitive Decline): Age-related memory lapses, such as trouble recalling recent acquaintances or where items were placed, affect about 40% of people over 65 Only 1% progress to dementia
- Stage 3 (Mild Cognitive Decline): Memory and behaviour changes become more noticeable Symptoms include frequent forgetting, difficulty with speech, and trouble managing complex tasks or remembering recent plans.
Moderate / Middle-phase Dementia
- Stage 4 (Moderate Cognitive Decline): Clear enough symptoms allow for diagnosis. Patients experience emotional variability, decreased cognitive sharpness, difficulty with recent events, and may deny memory issues
- Stage 5 (Moderately Severe Cognitive Decline): Care is recommended as disorientation increases, and previous symptoms worsen significantly.
Severe / Late-phase Dementia
- Stage 6 (Severe Cognitive Decline): Patients need full-time care. They may struggle with sleep, become more aggressive or anxious, and lose recognition of even familiar people
- Stage 7 (Very Severe Cognitive Decline): This final stage brings severe physical and cognitive decline. Patients may sleep extensively, lose bodily control, and require total assistance, with life expectancy typically ranging from 2–5 years.
Progression timelines differ between individuals, and not everyone advances to the extreme stages, largely depending on care and treatment quality.
However, dementia is not the only problem elderly people face Other ageing conditions include hearing loss, visual impairment and arthritis Almost all elderly people develop at least one of these three conditions. Also, elderly people can develop diseases, relative to ageing. One such disease, which is growing more common, is Alzheimer’s disease. In fact, diagnosis rates in both dementia itself and other ageing conditions, including Alzheimer’s disease, are increasing This piece of data leads to one question: is there a link between dementia and all these other ageing conditions and if so, what can be done?
Link Between Visual Impairment and Dementia
Investigations to understand the link between dementia and visual impairments in elderly people prove to show that the two are connected. Studies show that uncorrected vision, especially from the youth, including near and far sightedness as well as other conditions like cataracts, which is where the lens of the eye gets clouded, and glaucoma, which is where the optic nerve gets damaged, provides increased risk for dementia. The link was identified by a study that used 3,000 US citizens, all over the age of 71, with ranging conditions, including dementia and vision loss The study found out that those people with vision loss also had dementia In fact, people with more vision loss had more severe dementia, and people with less vision loss had less severe dementia, and people with no vision loss had no or little dementia. Although a likely link has been identified, reasons as to why this may be the case have been trickier to discover Scientists believe that there are two main possibilities:
- Diabetes
- “Shared pathways”
Diabetes, which is not classified as an ageing condition, causes problems in vision This is because blood vessels with high concentrations of sugar can damage the retina, a part of the eye, causing problems in vision and therefore creates a higher risk of dementia. Therefore, if someone has diabetes, it possibly means that they will develop dementia and vision loss at the same rate Some people in the study did have diabetes, and scientists have identified this link.
Another possibility is described as a ‘shared pathway’, which implies that a common factor causes deterioration in the brain that directly affects vision and memory at the same time Therefore, a correlation has been identified between dementia and vision loss, and although the reasons are not yet clarified, scientists believe that a medical reason must be present.
Link Between Hearing Loss and Dementia
Scientists have also been investigating whether there is a link between dementia and hearing loss. Studies show that people who have problems with hearing, during the ages of 40-65, have a higher risk of dementia Hearing loss is classified as an early symptom of dementia. Studies have also proven that using hearing aids to reduce your hearing loss will also reduce your risk of dementia.
They also identify that if you have more intense hearing loss, for a longer period of time, you will have an increased risk of developing dementia. The main reason for this is because your auditory cortex, the part of the brain that understands speech and language, must work harder to understand language because of the hearing loss present. Because this part of the brain must work harder This overwhelms it to an extent that changes in the brain occur, which affect the part of the brain relating to memory, specifically within the hippocampus, an organ located in the temporal lobe. A study in 2011 used 2,413 adults, half over the age of 80, with a range of conditions. This study showed that adults with moderate or high levels of hearing loss, who also had presence of dementia was 61% more than those who had presence of dementia but did not have hearing loss. Also, in the 853 participants who had some form of hearing loss, 32% had a lower presence of dementia with the use of a hearing aid. Therefore, another link has been identified between hearing loss and dementia, and this is because of changes in how the brain works because of hearing loss
Link Between Arthritis and Dementia
Researchers have also been investigating whether there is a link between dementia and a type of arthritis There are two types of arthritis: osteoarthritis and rheumatoid arthritis Osteoarthritis is the most common type, which starts to develop from the age of 45. It is where smooth cartilage is worn down, which causes difficulty in movement, pain and swelling. The tendons and ligaments of the joint have to work harder. This can cause swelling and osteophytes can form Great loss of cartilage can lead to friction between two bones, or the shape of the joint can change.
Rheumatoid arthritis is less common. It starts when someone is between 30 and 50, and women are more likely to be affected than men Rheumatoid arthritis is caused when the immune system targets joints, which leads to swelling and pain. It firsts affects the synovium and then spreads to the rest of the joint. This can cause further swelling and alter the shape of the joint. This can lead to the wear and tear of bone and cartilage.
A study of 388,252 adults, with ranging conditions has shown that there is a link between dementia and osteoarthritis. This study concluded that adults have a 36% higher chance of getting dementia as an elderly person with arthritis than without. One definite reason scientists have concluded on, is that the long-term pain patients experience through osteoarthritis caused dementia, as long-term pain gradually shrinks the prefrontal cortex and the frontal lobe, which are involved in memory and understanding language. Another possible reason scientists have identified is that inflammatory cytokines, which are small, secreted proteins that affect the interactions between cells, can release damage-associated molecular patterns (DAMPs), which are found in the brain and can cause dementia. The study also shows that if you treat osteoarthritis from an early stage, this will reduce the risk of dementia by around 15%. Therefore, there is a correlation between arthritis (specifically osteoarthritis) and dementia, in that if you have osteoarthritis, you are more likely to get dementia, of which, treatment can prevent.
Link Between Brain Diseases and Dementia
Finally, diseases, which not all elderly people contract, such as Alzheimer’s disease, have been investigated to see whether there is a link with dementia. Alzheimer’s and dementia often get interchanged; however, this is not correct. Alzheimer’s is a brain disease, but dementia is a syndrome Alzheimer’s is actually the most common type of dementia. They both have the same effects of affecting memory, thinking and understanding things. Alzheimer’s disease is where the proteins in the brain do not function like they usually would. This causes brain cells to shrink and eventually die. The unusual build-up of two proteins, amyloid and tau, which over time kill brain cells Therefore, there is a direct correlation between Alzheimer’s and dementia. Alzheimer’s directly causes dementia, as Alzheimer’s effectively kills brain cells over a period, which causes dementia.
Why is it important to identify these links?
It is important to identify these links because it means you can try and find ways to reduce the severity or even cure dementia. This has already been identified by scientists, as studies show For example, correcting vision loss at an early stage will help reduce the risk of you getting dementia in the future. Also, wearing a hearing aid frequently in an effort to correct your hearing loss will similarly reduce the risk of dementia by a lot. This is extremely important as you can reduce the severity of dementia in your elder years by a lot, reducing the stages by bringing it down from a potential stage 7 to a stage 4 or a stage 5, which is much easier to live with. This can also help doctors in geriatrics ward, help guide elder people so that they can live a better end to their lives, without suffering from severe dementia. Also, if you have temporary remedies to reduce how intense something is, this can act as a basis for scientists to try and find a cure for dementia, by identifying what is similar and trying to replicate that in a different way.
In conclusion, dementia poses some significant health challenges as the aging population continues to rise. This condition, characterised by the progressive deterioration of brain function, is closely linked with other age-related conditions such as visual impairment, hearing loss, arthritis, and neurodegenerative diseases like Alzheimer’s disease Emerging research highlights the potential for these conditions to exacerbate or contribute to dementia, with vision and hearing loss shown to increase the risk, while osteoarthritis may promote cognitive decline through chronic pain and inflammatory mechanisms. Alzheimer’s disease, on the other hand, is directly implicated in causing dementia through the accumulation of amyloid and tau proteins, leading to neuronal death
Understanding these links offers valuable insights into potential interventions that can mitigate dementia risk Early correction of vision and hearing impairments, as well as effective management of osteoarthritis, could reduce dementia severity, promoting better quality of life for aging individuals. These findings underscore the importance of interdisciplinary approaches in geriatric care, where addressing coexisting conditions can play a crucial role in slowing the progression of dementia Further research into these connections may also pave the way for novel preventive and therapeutic strategies, potentially altering the trajectory of cognitive decline and enhancing the management of dementia in elderly populations.
Personalised Medicine:Scienceor Fiction?
Boran Sahin
Through the other articles in this publication, you will likely have read about and hopefully learnt about some of modern medicine’s most promising breakthroughs, some of which you may have already been familiar with, others not For the contemporary scientist interested in the life sciences, the advent of technologies such as CRISPR-Cas9 and targeted therapies for cancer have opened our eyes to a branch of healthcare that is a world away from the sweeping, top-down approach we have traditionally taken mass prescribing the same treatments to patients with vastly different individual experiences However, these examples are just a glimpse into the much larger shift occurring in medicine today. This shift is driven by the increasing recognition that no two patients are identical, neither in their biology nor in how they respond to treatments.
In contrast, personalised medicine focuses on the molecular and genetic basis of individual diseases and aims to tailor medical interventions to the unique genetic, molecular, and environmental profile of each individual. This shift towards precision healthcare is enabled by advancements in molecular biology, genomics, and bioinformatics Personalised medicine allows us to move beyond traditional, rigid treatment regimens, emphasising targeted interventions that are informed by specific biomarkers, genetic variations, and environmental factors.
One of the most significant developments in this field is the rise of pharmacogenomics, which combines pharmacology with genomics to understand how an individual’s genetic makeup influences their response to drugs. Research has shown that certain genetic variants can impact drug metabolism, efficacy, and toxicity A key example is the anticoagulant warfarin, whose dosing is influenced by genetic variations in the CYP2C9 and VKORC1 genes. Pharmacogenomic testing for these variants has become a standard practice in some healthcare systems to optimise treatment and minimise adverse reactions. Where testing for the CYP2C9 and VKORC1 genes has been implemented, adverse reactions to the anticoagulant have been significantly reduced, with studies indicating a decrease in major bleeding events by up to 30%.
Another area where personalised medicine has made remarkable strides is in the treatment of cancer. Targeted therapies such as trastuzumab (Herceptin) for HER2-positive breast cancer and vemurafenib for BRAF V600E-mutant melanoma have revolutionised cancer treatment by specifically targeting the genetic mutations that drive cancer growth, rather than treating cancer as a monolithic disease Studies have demonstrated that these therapies significantly improve survival rates when compared to traditional chemotherapies, prompting their use as a priority. These treatments are tailored to the patient’s tumour genotype, allowing the healthcare provider to alter the approach taken to treatment, shaping therapeutic decisions and providing oncologists with more precise tools to achieve optimal outcomes For instance, trastuzumab has been shown to increase the overall survival rate for HER2-positive breast cancer by approximately 33% when used in combination with chemotherapy, while vemurafenib has demonstrated a median overall survival benefit of 13.6 months compared to 9 7 months with traditional chemotherapy for patients with BRAF V600E-mutant melanoma.
The use of CRISPR-Cas9 gene-editing technology also holds enormous potential in personalised medicine. CRISPR allows for precise modifications to the genome, enabling the correction of genetic mutations that cause inherited diseases One promising application is in the treatment of sickle cell anaemia (SCA), which causes a mutation in the haemoglobin molecule, making it abnormally ‘sticky’ and prone to clumping together. This results in red blood cells taking on a sickle shape, losing their flexibility, and getting stuck in small blood vessels due to their altered structure Early clinical trials have demonstrated that patients with sickle cell disease can be treated by editing their haemoglobin gene to produce haemoglobin without this mutation.
Moreover, the human microbiome has emerged as a critical factor influencing drug response Once completely overlooked, we now understand that microbial composition can affect drug metabolism, efficacy, and even toxicity. Research has shown that the microbiome can alter the response to drugs like checkpoint inhibitors used in cancer immunotherapy. As our understanding of the microbiome expands, chemists and clinicians are beginning to consider microbiome profiling as part of the personalised medicine approach, offering more tailored and hopefully more effective treatments.
In summary, personalised medicine represents a profound shift in how we approach healthcare By integrating molecular, genetic, and environmental data, we can strive to optimise treatments for individual patients, increasing efficacy and reducing adverse effects. Chemists play a crucial role in this transformation, particularly through drug discovery, formulation, and the development of novel therapies based on genetic and molecular understanding The future of personalised medicine holds enormous promise, and it is the collaborative efforts between chemists, geneticists, and clinicians that will bring these advancements to fruition.
TheLifesavingGap
Nathan Wolfson
The doors to the emergency department swing open, alarms beep, orders are barked, and teams gather around your cardiac arrest patient. CPR is commenced, pads are positioned, and the trauma lead warns everyone to remain clear, so as to deliver a lifesaving shock It is the ultimate emergency, a last-ditch attempt to bring someone back to life, to restore the flow of blood to vital organs, and to prevent neurological damage, that is otherwise impossible to fix.
Cardiac arrest is defined, by the British Heart Foundation, as when your heart suddenly stops pumping blood around your body. Specifically, because of irregular electrical activity which prevents contraction of the myogenic tissue. Within a pre-hospital environment, first aiders are taught it is recognisable by immediate collapse, lack of breathing and consciousness This is when the timer starts This is the make or break
In a cardiac arrest, you are taught about as an advanced first aider, a sequence of events known as
The Chain of Survival
1 Early Recognition
2 Early CPR
3. Early Defibrillation
4. Post-resuscitation (advanced) care
This sequence is what gives patients the best chance of survival, the ability to hopefully see family again and continue life as they had before. Yet usually that isn’t the case. This article seeks to go into the reasoning and explanation to why cardiac arrest care is so shockingly low in society. Despite the advancement in critical technology, worldwide, we remain incredibly primitive in our approach to basic life support (BLS) within pre-hospital environments. A study done in January 2024 by the University of Warwick, revealed that less than one in twelve patients survive 30 days after experiencing an out-of-hospital cardiac arrest. The review goes onto say despite 70% being given some form of CPR (cardiopulmonary resuscitation), the use of publicly accessible defibrillators remains fewer than one in ten. So where are we going wrong?
Cardiopulmonary Resuscitation
Cardiopulmonary Resuscitation is an invasive, critical treatment option, that is necessary to carry out when someone’s breathing or heartbeat has stopped. It is done, to physically pump the heart by providing compressions to the chest, between the nipples. This moves minimal oxygen (still left in the blood) around the body so as to prolong a patients survival chance, giving time for an ambulance crew or defibrillator to arrive.
However, whilst CPR is widely known and administered, emergency department staff make a key differentiation between effective and ineffective CPR For effective CPR to occur, trained individuals are advised to compress at a rate of 120bpm, in a ratio of 30:2 compressions to breaths. In those who are trained, these breaths are an opportunity to move the approximately, 16% oxygen and 79% nitrogen composition of your exhaled breath to the lungs of the patients, to diffuse through the alveoli and into body cells
Contrary to belief, CPR is not a treatment, it is not an outcome, it is an act of desperation. By itself CPR does not improve a patient’s condition, it buys time. To restart the heart, you need more costly, less publicly available and more comprehensive equipment including emergency drugs like adrenaline and access to automatic external defibrillators, as this review will present.
An article published by the Emergency Medical Journal of the BMJ Group, in 2020 detailed specifically within the United States, the large proportion of patients and their families who overestimated CPR success The article detailed patients thought survival with CPR was as high as 75% and that for around 500 respondents who took a survey into CPR education, television was their main source of information. This review did prudently mention 64% of the respondents had taken a CPR course at some point in their life, however it also accepted that within just 30 days of a first aid course, skills fade exponentially and must be continually kept up to date, which for many, just isn’t an option. So, is education the only issue?
The Use of a Publically Accessible Defibrillator
When going to the shops or the park, you might have noticed large yellow boxes labelled with a heart and lightning sign. These are defibrillators, lifesaving, regularly maintained and electrically powered devices that deliver an electrical shock to a patient, to restore a regular heartbeat (from extreme tachycardia or bradycardia) or restart the heart
To be used correctly, pads must be placed, depending on a patient’s size, and shocks should be delivered depending on a patients age or weight. In adults, positioning takes the form of a pad on the right chest (near the collarbone) and above the left waist, so that if a line was drawn between them, it would pass straight through the heart
In the UK, currently there are over 100,000 registered publicly accessible defibrillators for usage however, their location is not either communicated by emergency services, or the devices are simply too far away for the trip to be beneficial If a first aider knows a device is near, it is advised that it is collected in preference to the delivery of CPR, if you are on your own. Recent studies show that without quick usage, every minute, chance of survival without a defibrillator decreases by 10%, so that after 10 minutes without critical intervention, chances of a successful outcome are depressingly low
This is incredibly frightening and considering many aren’t trained in its usage. A death wish for society, which must be remedied
Inequalities & Socioeconomic Barriers
This review finds it prudent to investigate further the causes and implications of treatment for OHCA (out-of-hospital cardiac arrests) To do so, I have chosen two key areas to investigate
1. Location disparities of AEDs within England
2 Bystander willingness to use an AED
Location disparities of AEDs within England
To be explicit, during cardiac arrest, the heart can present in two rhythms, those that are classified as shockable and those classified as non-shockable The importance of early defibrillation is to deliver a charge to the heart when it still has a shockable rhythm. Once this degenerates to a non-shockable rhythm, the heart is largely unresponsive to treatment. Of those who present with OHCA’s, approximately 85% present with a shockable rhythm showing early defibrillation has a disproportionate effect on survival outcomes and the ability to help.
Prior to EMS arrival, around 5% of patients have already received a defibrillator shock This stems from fundamental and structural barriers that limit PAD usage as only a minority of OHCA’s occur near defibrillators. The European Resuscitation Council suggests an AED should be in an area where an OHCA has occurred in the past 3-5 years however, generally within the UK, defibrillators are placed by ad-hoc local initiatives and fundraisers and not matching metrics like those suggested to benefit the most people This has led to paradoxical and political AED placement, with availability widely greater in affluent areas.
A study in 2022, analysed the location of 32,332 AEDs in England focusing on distribution within different neighbourhoods It concluded that AEDs were found predominately in areas with a lower residential population density and higher working population density These areas had a higher percentage of older individuals, individuals in management occupations, and with a greater proportion of individuals that had higher education qualifications.
The review showed regional and socio-economic disparities were evident, with the NorthEast having the lowest coverage at 19.5%, while East Midlands had the highest at 63.7%. The variation in AED density ranged from 0.08/km² in the North-East to 2.97/km² in London. Areas in more deprived deciles (lower Index of Multiple Deprivation) had the lowest AED coverage, with only 27 4% of these areas containing an AED Notably, rural areas exhibited a higher proportion of AEDs relative to urban areas, with 76.4% of rural areas having at least one AED.
Bystander willingness to use an AED
Figure 1: The percentage of lower layer super output areas (LSOA) within each deprivation decile that contain a public access defibrillator (PAD) in 2019 (1 = most deprived, 10 = least deprived) (Brown et al , 2022)
A September 2024 review published by the National Institutes of Health explored the impact of the bystander effect during an OHCA The bystander effect is characterised as a social, psychological theory, that people are less likely to help in the presence of others. It aimed to identify what would potentially hinder someone from helping in an emergency, including the addition of competent staff like security personnel or station staff. The review surveyed all 47 prefectures in Japan by web-based questionnaire, to discuss and research potential issues
Key Hypotheses:
Hypothesis 1: The greater the number of bystanders, the less likely individuals are to intervene in an emergency.
Hypothesis 2: The presence of competent parties (station staff, security guards, etc.) will decrease bystanders' willingness to initiate a rescue.
The investigation resulted in 1123 responses to a scenario of a cardiac arrest in a crowded and sparse station environment. Willingness to intervene ranged from running and calling for help (basic intervention) to using an AED as the most critical action. 65% who responded were men, and 65 6% had no prior AED training The results showed a significant statistical difference in those who intervened during sparse and crowded conditions, and this was most often seen in the 40-49 and >60 age groups. Meanwhile, both trained and untrained individuals were less likely to intervene properly in crowded conditions, however in trained individuals this was more because of a lack of confidence (which resulted in lower defibrillator usage), than a lack of intervention at all, suggesting the bystander effect was not as prominent.
Conclusion
Within schools nowadays, and communities around the UK, defibrillator usage and CPR training is delivered infrequently and insufficiently to ensure good outcomes. In many cases, a lack of confidence can be cited, as well as legal concerns and potential imprisonment if incorrect intervention CPR training is incredibly costly and without implementation into the school curriculum and wider workplace, gaps, socioeconomically and politically, will continue to be created, preventing successful outcomes.
As a country, we need to do better, for each other, to improve the system and standardisation of care and awareness. Lifesaving must be prioritised and until it isn’t, the over 30,000 OHCA’s each year, will lead to diminishing returns, and loved ones lost.
References
George Vasylevych
Cecchin, E. and Stocco, G. (2020). Pharmacogenomics and Personalized Medicine. Genes, [online] 11(6), p.679. doi:https://doi.org/10.3390/genes11060679.
Condren, M.E. and Bradshaw, M.D. (2013). Ivacaftor: A Novel Gene-Based Therapeutic Approach for Cystic Fibrosis. The Journal of Pediatric Pharmacology and Therapeutics, [online] 18(1), pp.8–13. doi:https://doi.org/10.5863/1551-677618.1.8.
Katara, P. (2013). Role of bioinformatics and pharmacogenomics in drug discovery and development process. Network Modeling Analysis in Health Informatics and Bioinformatics, 2(4), pp.225–230. doi:https://doi.org/10.1007/s13721-013-0039-5.
Pirmohamed, M. (2023). Pharmacogenomics: current status and future perspectives. Nature Reviews Genetics, 24. doi:https://doi.org/10.1038/s41576-022-00572-8.
Roden, D.M., McLeod, H.L., Relling, M.V., Williams, M.S., Mensah, G.A., Peterson, J.F. and Van Driest, S.L. (2019). Pharmacogenomics. The Lancet, [online] 394(10197), pp.521–532. doi:https://doi.org/10.1016/s0140-6736(19)31276-0.
Shapiro, A. (2017). From Severe Depression to Treatment and the Role of Genetic Testing: Kristen’s Story. [online] HuffPost. Available at: https://www.huffpost.com/entry/from-severe-depression-to-treatment-and-the-roleof b 59c55f7ce4b0b7022a646a3d [Accessed 5 Aug. 2024].
Smith, Y. (2015). Pharmacogenetics: past, present and future. [online] NewsMedical.net. Available at: https://www.news-medical.net/health/Pharmacogeneticspast-present-andfuture.aspx#:~:text=The%20first%20recorded%20association%20with.
Somogy, A. (2008). Evolution of pharmacogenomics. Proceedings of the Western Pharmacology Society, [online] 51, pp.1–4. Available at: https://pubmed.ncbi.nlm.nih.gov/19544663/.
Josh Alexander
Font-Gonzalez, A. et al. (2016) ‘Fertility preservation in children, adolescents, and young adults with cancer: Quality of clinical practice guidelines and variations in recommendations’, Cancer, 122(14). Available at: https://doi.org/10.1002/cncr.30047.
Logan, S. et al. (2019) ‘Systematic review of fertility-related psychological distress in cancer patients: Informing on an improved model of care ’ , Psycho-Oncology. Available at: https://doi.org/10.1002/pon.4927.
Tian En, L. et al. (2020) ‘Impacts of platinum-based chemotherapy on subsequent testicular function and fertility in boys with cancer ’ , Human Reproduction Update, 26(6). Available at: https://doi.org/10.1093/humupd/dmaa041.
Nicol, B. and Yao, H.H.-C. (2017). Cellular and Structural Aspects of Fetal Ovarian Differentiation. Elsevier eBooks, [online] pp.52–56. doi: https://doi.org/10.1016/b978-0-12-801238-3.64627-5.
Nitish Nandakumar
MTMI. (n.d.). The History of Radiology. [online] Available at: https://www.mtmi.net/blog/history-of-radiology.
John Hopkins Medicine (2023). Computed Tomography (CT) Scan. [online] www.hopkinsmedicine.org. Available at: https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/computedtomography-ct-scan.
NHS Choices (2019). Overview - Bone density scan (DEXA scan). [online] NHS. Available at: https://www.nhs.uk/conditions/DEXA-scan/.
https://www.facebook.com/cgdclarke (2019). A brief history of radiology - Radiology Cafe. [online] Radiology Cafe. Available at: https://www.radiologycafe.com/blog/abrief-history-of-radiology [Accessed 20 Oct. 2024].
Faculty of Medicine, Dentistry and Health Sciences Museums at The University of Melbourne Collection Online. (2017). Coolidge X-ray tube. [online] Available at: https://collections.mdhs.unimelb.edu.au/objects/28210/coolidge-x-ray-tube [Accessed 20 Oct. 2024].
Bell, D. (2020). William D Coolidge. Radiopaedia.org. doi:https://doi.org/10.53347/rid-84503.
Martin, N.L. (n.d.). Radiology at Base Hospital #28 in France During WW1. [online] www.kumc.edu. Available at: https://www.kumc.edu/school-ofmedicine/academics/departments/history-and-philosophy-ofmedicine/archives/wwi/base-hospital-28/clinical-services/radiology.html.
Barnsleyhospital.nhs.uk. (2024). Fluoroscopy | Barnsley Hospital NHS Foundation Trust. [online] Available at: https://www.barnsleyhospital.nhs.uk/services/fluroscopy [Accessed 20 Oct. 2024].
www.invent.org. (n.d.). NIHF Inductee Godfrey Hounsfield, Who Invented the CT Scan. [online] Available at: https://www.invent.org/inductees/godfrey-newboldhounsfield.
Sajid, H. (2022). AI in Radiology: Pros & Cons, Applications, and 4 Examples. [online] www.v7labs.com. Available at: https://www.v7labs.com/blog/ai-inradiology.
Cowen, L. (2023). How Artificial Intelligence Is Driving Changes in Radiology. [online] Inside Precision Medicine. Available at: https://www.insideprecisionmedicine.com/news-and-features/how-artificialintelligence-is-driving-changes-in-radiology/.
Bakalar, N. (2009). X-Rays, 1896. The New York Times. [online] 15 Jun. Available at: https://www.nytimes.com/2009/06/16/health/16firs.html.
Jorgensen, T. (2017). How Marie Curie Brought X-Ray Machines To the Battlefield. [online] Smithsonian. Available at: https://www.smithsonianmag.com/history/howmarie-curie-brought-x-ray-machines-to-battlefield-180965240/.
CDC (2024). Facts About Fluoroscopy. [online] Radiation and Your Health. Available at: https://www.cdc.gov/radiation-health/data-research/factsstats/fluoroscopy.html.
Save My Exams. (n.d.). 10.5.6 The CT Scanner | AQA A Level Physics Revision Notes 2017. [online] Available at: https://www.savemyexams.com/alevel/physics/aqa/17/revision-notes/10-medical-physics/10-5-x-ray-imaging/10-5-6the-ct-scanner/.
World Nuclear Association (2024). Chernobyl Accident 1986 - World Nuclear Association. [online] world-nuclear.org. Available at: https://worldnuclear.org/information-library/safety-and-security/safety-of-plants/chernobylaccident.
Sajid, H. (2022). AI in Radiology: Pros & Cons, Applications, and 4 Examples. [online] www.v7labs.com. Available at: https://www.v7labs.com/blog/ai-inradiology.
Ravjoth Brar alphafold.ebi.ac.uk. (n.d.). AlphaFold Protein Structure Database. [online] Available at: https://alphafold.ebi.ac.uk.
Google DeepMind. (2022). Putting the power of AlphaFold into the world’s hands. [online] Available at: https://deepmind.google/discover/blog/putting-the-power-ofalphafold-into-the-worlds-hands/.
Google DeepMind. (2024). Computational predictions of protein structures associated with COVID-19. [online] Available at: https://deepmind.google/discover/blog/computational-predictions-of-proteinstructures-associated-with-covid-19 [Accessed 21 Oct. 2024].
Jumper, J., Evans, R., Pritzel, A., Green, T., Figurnov, M., Ronneberger, O., Tunyasuvunakool, K., Bates, R., Žídek, A., Potapenko, A., Bridgland, A., Meyer, C., Kohl, S.A.A., Ballard, A.J., Cowie, A., Romera-Paredes, B., Nikolov, S., Jain, R., Adler, J. and Back, T. (2021). Highly Accurate Protein Structure Prediction with Alphafold. Nature, 596(7873), pp.583–589. doi:https://doi.org/10.1038/s41586-02103819-2.
One of biology’s biggest mysteries ‘largely solved’ by AI. (2020). BBC News. [online] 30 Nov. Available at: https://www.bbc.co.uk/news/science-environment-55133972.
Senior, A.W., Evans, R., Jumper, J., Kirkpatrick, J., Sifre, L., Green, T., Qin, C., Žídek, A., Nelson, A.W.R., Bridgland, A., Penedones, H., Petersen, S., Simonyan, K., Crossan, S., Kohli, P., Jones, D.T., Silver, D., Kavukcuoglu, K. and Hassabis, D. (2020). Improved Protein Structure Prediction Using Potentials from Deep Learning. Nature, 577(7792), pp.706–710. doi:https://doi.org/10.1038/s41586-019-1923-7.
Toews, R. (2021). AlphaFold Is The Most Important Achievement In AI—Ever. [online] Forbes. Available at: https://www.forbes.com/sites/robtoews/2021/10/03/alphafold-is-the-mostimportant-achievement-in-ai-ever/.
Tunyasuvunakool, K., Adler, J., Wu, Z., Green, T., Zielinski, M., Žídek, A., Bridgland, A., Cowie, A., Meyer, C., Laydon, A., Velankar, S., Kleywegt, G.J., Bateman, A., Evans, R., Pritzel, A., Figurnov, M., Ronneberger, O., Bates, R., Kohl, S.A.A. and Potapenko, A. (2021). Highly accurate protein structure prediction for the human proteome. Nature, [online] 596(596), pp.1–9. doi:https://doi.org/10.1038/s41586021-03828-1.
Issie Ridgway
Alzheimer's Association (2019). Inside the Brain: A tour of how the mind works. [online] Alzheimer’s Disease and Dementia. Available at: https://www.alz.org/alzheimers-dementia/what-is-alzheimers/brain tour part 2.
Alzheimer's Society (2019). Dementia Symptoms and Areas of the Brain. [online] Alzheimer’s Society. Available at: https://www.alzheimers.org.uk/aboutdementia/symptoms-and-diagnosis/how-dementia-progresses/symptoms-brain.
British Heart Foundation (2023). Vascular dementia. [online] Bhf.org.uk. Available at: https://www.bhf.org.uk/informationsupport/conditions/vascular-dementia.
Clarkson, J. (2021). Amyloid and tau: the Proteins Involved in Dementia DPUK. [online] www.dementiasplatform.uk. Available at: https://www.dementiasplatform.uk/news-and-media/blog/amyloid-and-tau-theproteins-involved-in-dementia.
National Institute on Aging (2024). What Happens to the Brain in Alzheimer’s Disease? [online] National Institute on Aging. Available at: https://www.nia.nih.gov/health/alzheimers-causes-and-risk-factors/what-happensbrain-alzheimers-disease.
SHEIKH, N. (2022). Advanced Stages of Alzheimer’s: Understanding the StagesAltoida. [online] Altoida. Available at: https://altoida.com/blog/advanced-stages-ofalzheimers-understanding-the-stages/.
www.stroke.org.uk. (n.d.). What is vascular dementia? | Stroke Association. [online] Available at: https://www.stroke.org.uk/stroke/effects/vascular-dementia.
Karis Lau
Discovery Science (2024). The MYTH of Junk DNA (Long Story Short, Ep. 12). [online] YouTube. Available at: https://www.youtube.com/watch?v=7gyp1QnTJvY [Accessed 12 Oct. 2024].
Anderson, R. (2024). Evolution’s Junk DNA. [online] Spotify.com. Available at: https://open.spotify.com/episode/0F7LUINyzr7iPDtiNOHuOq?si=0dabb716d6f44b03 [Accessed 12 Oct. 2024].
Arjuna Shankar
Appleton, J. (2018). The Gut-Brain Axis: Influence of Microbiota on Mood and Mental Health. Integrative Medicine: A Clinician’s Journal, [online] 17(4), p.28. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC6469458/.
Bohorque, D. (2018). The Gut-Brain Connection. YouTube. Available at: https://www.youtube.com/watch?v=oym87kVhqm4.
Chong, C., Bloomfield, F. and O’Sullivan, J. (2018). Factors Affecting Gastrointestinal Microbiome Development in Neonates. Nutrients, [online] 10(3), p.274. doi: https://doi.org/10.3390/nu10030274.
Gkougka, D., Mitropoulos, K., Tzanakaki, G., Panagouli, E., Psaltopoulou, T., Thomaidis, L., Tsolia, M., Sergentanis, T.N. and Tsitsika, A. (2022). Gut microbiome and attention deficit/hyperactivity disorder: a systematic review. Pediatric Research. doi: https://doi.org/10.1038/s41390-022-02027-6.
Hamamah, S., Aghazarian, A., Nazaryan, A., Hajnal, A. and Covasa, M. (2022). Role of Microbiota-Gut-Brain Axis in Regulating Dopaminergic Signaling. Biomedicines, 10(2), p.436. doi: https://doi.org/10.3390/biomedicines10020436.
intermountainhealthcare.org. (2024). Nutrition and depression link. [online] Available at: https://intermountainhealthcare.org/blogs/fast-food-depression-link.
Jandhyala, S.M. (2015). Role of the Normal Gut Microbiota. World Journal of Gastroenterology, 21(29), p.8787. doi: https://doi.org/10.3748/wjg.v21.i29.8787.
Kelly, J.R., Minuto, C., Cryan, J.F., Clarke, G. and Dinan, T.G. (2020). The role of the gut microbiome in the development of schizophrenia. Schizophrenia Research. doi: https://doi.org/10.1016/j.schres.2020.02.010.
Lange, K.W., Lange, K.M., Nakamura, Y. and Kanaya, S. (2020). Is there a role of gut microbiota in mental health? Journal of Food Bioactives, 9. doi: https://doi.org/10.31665/jfb.2020.9213.
Scaccia, A. (2016). Serotonin: Functions, Normal Range, Side Effects, and More. [online] Healthline. Available at: https://www.healthline.com/health/mentalhealth/serotonin#functions.
Sonuga-Barke, E.J.S., Brandeis, D., Cortese, S., Daley, D., Ferrin, M., Holtmann, M., Stevenson, J., Danckaerts, M., van der Oord, S., Döpfner, M., Dittmann, R.W., Simonoff, E., Zuddas, A., Banaschewski, T., Buitelaar, J., Coghill, D., Hollis, C., Konofal, E., Lecendreux, M. and Wong, I.C.K. (2013). Nonpharmacological Interventions for ADHD: Systematic Review and Meta-Analyses of Randomized Controlled Trials of Dietary and Psychological Treatments. American Journal of Psychiatry, [online] 170(3), pp.275–289. doi: https://doi.org/10.1176/appi.ajp.2012.12070991.
Thursby, E. and Juge, N. (2017). Introduction to the Human Gut Microbiota. Biochemical Journal, [online] 474(11), pp.1823–1836. doi: https://doi.org/10.1042/bcj20160510.
University of Washington School of Medicine (2023). The Gut Microbiome with Chris Damman, MD, MA. [online] YouTube. Available at: https://www.youtube.com/watch?v=ch2KsDGoH0Y [Accessed 18 Oct. 2024].
Woese, C.R. (2004). A New Biology for a New Century. Microbiology and Molecular Biology Reviews, 68(2), pp.173–186. doi: https://doi.org/10.1128/mmbr.68.2.173186.2004.
Ben Loebinger
NHS (2023). Euthanasia and Assisted Suicide. [online] NHS. Available at: https://www.nhs.uk/conditions/euthanasia-and-assisted-suicide/.
Spina, B. (1998). ETHICAL JUSTIFICATIONS FOR VOLUNTARY ACTIVE EUTHANASIA. [online] Available at: https://scholarship.richmond.edu/cgi/viewcontent.cgi?article=1031&context=jolpi.
The Medic Portal (2021). Euthanasia and Assisted Dying. [online] The Medic Portal. Available at: https://www.themedicportal.com/application-guide/medical-schoolinterview/nhs-hot-topics/euthanasia-and-assisted-dying/.
Keohan, M. (2024). Assisted dying idea is dangerous, Bishop of Dover warns. BBC News. [online] 22 Oct. Available at: https://www.bbc.co.uk/news/articles/c0r8r4yz087o [Accessed 23 Oct. 2024].
Whannel, K. (2024). Assisted dying bill introduced in House of Lords. [online] BBC News. Available at: https://www.bbc.co.uk/news/articles/c3g9yvdrxzzo.
Parliament.uk. (2024). Assisted Dying for Terminally Ill Adults Bill [HL]Parliamentary Bills - UK Parliament. [online] Available at: https://bills.parliament.uk/bills/3741.
Sherwood, H. (2024). England and Wales assisted dying bill formally launched in House of Commons. [online] the Guardian. Available at: https://www.theguardian.com/society/2024/oct/16/england-and-wales-assisteddying-bill-formally-launched-in-house-of-commons.
Dignity in Dying. (2016). Assisted dying - Dignity in Dying. [online] Available at: https://www.dignityindying.org.uk/assisted-dying/.
BBC News (2019). What’s the difference between assisted suicide and euthanasia? BBC News. [online] 8 Feb. Available at: https://www.bbc.co.uk/news/uk-47158287.
Wakefield, J. (2021). Maker of Suicide Pod Plans to Launch in Switzerland. BBC News. [online] 9 Dec. Available at: https://www.bbc.co.uk/news/technology59577162.
Shravan Senthilkumar
Diment, L.E., Thompson, M.S. and Bergmann, J.H.M. (2017). Clinical efficacy and effectiveness of 3D printing: a systematic review. BMJ Open, [online] 7(12), p.e016891. doi:https://doi.org/10.1136/bmjopen-2017-016891.
Gharleghi, R., Dessalles, C.A., Lal, R., McCraith, S., Sarathy, K., Jepson, N., Otton, J., Barakat, A.I. and Beier, S. (2021). 3D Printing for Cardiovascular Applications: From End-to-End Processes to Emerging Developments. Annals of Biomedical Engineering, 49(7), pp.1598–1618. doi:https://doi.org/10.1007/s10439-021-02784-1.
HUBS (2024). What is FDM 3D printing? [online] Hubs. Available at: https://www.hubs.com/knowledge-base/what-is-fdm-3d-printing/.
Lindquist, E.M., Gosnell, J.M., Khan, S.K., Byl, J.L., Zhou, W., Jiang, J. and Vettukattil, J.J. (2021). 3D Printing in Cardiology: A Review of applications and roles for advanced cardiac imaging. Annals of 3D Printed Medicine, p.100034. doi:https://doi.org/10.1016/j.stlm.2021.100034.
Shabbak, A., Masoumkhani, F., Fallah, A., Amani-Beni, R., Mohammadpour, H., Shahbazi, T. and Bakhshi, A. (2024). 3D Printing for Cardiovascular Surgery and Intervention: A Review Article. Current Problems in Cardiology, [online] 49(1, Part B), p.102086. doi:https://doi.org/10.1016/j.cpcardiol.2023.102086.
Society for Cardiovascular Magnetic Resonance. (2024). Why CMR | Society for Cardiovascular Magnetic Resonance. [online] Available at: https://scmr.org/whycmr/ [Accessed 17 Oct. 2024].
Vukicevic, M., Mosadegh, B., Min, J.K. and Little, S.H. (2017). Cardiac 3D Printing and its Future Directions. JACC: Cardiovascular Imaging, [online] 10(2), pp.171–184. doi:https://doi.org/10.1016/j.jcmg.2016.12.001.
Zhang, X., Yi, K., Xu, J.-G., Wang, W.-X., Liu, C.-F., He, X.-L., Wang, F.-N., Zhou, G.-L. and You, T. (2024). Application of three-dimensional printing in cardiovascular diseases: a bibliometric analysis. International Journal of Surgery, [online] 110(2), p.1068. doi:https://doi.org/10.1097/JS9.0000000000000868. Advait Tripathi
American Chemical Society (2023). Alexander Fleming Discovery and Development of Penicillin - Landmark. [online] American Chemical Society. Available at: https://www.acs.org/education/whatischemistry/landmarks/flemingpenicillin.html.
Annunziato, G. (2019). Strategies to Overcome Antimicrobial Resistance (AMR) Making Use of Non-Essential Target Inhibitors: A Review. International Journal of Molecular Sciences, [online] 20(23). doi:https://doi.org/10.3390/ijms20235844.
Dadgostar, P. (2019). Antimicrobial Resistance: Implications and Costs. [online] Infection and Drug Resistance. Available at: https://www.dovepress.com/antimicrobial-resistance-implications-and-costs-peerreviewed-fulltext-article-IDR.
Duncan, C. (2022). Scientists discover new approach to fighting antibiotic resistance | Imperial News | Imperial College London. [online] Imperial News. Available at: https://www.imperial.ac.uk/news/234060/scientists-discover-approach-fightingantibiotic-resistance/.
Habboush, Y. and Guzman, N. (2023). Antibiotic Resistance. [online] National Library of Medicine. Available at: https://www.ncbi.nlm.nih.gov/books/NBK513277/.
Hutchings, M.I., Truman, A.W. and Wilkinson, B. (2019). Antibiotics: past, Present and Future. Current Opinion in Microbiology, [online] 51(1), pp.72–80. doi:https://doi.org/10.1016/j.mib.2019.10.008.
Llor, C. and Bjerrum, L. (2014). Antimicrobial resistance: risk associated with antibiotic overuse and initiatives to reduce the problem. Therapeutic Advances in Drug Safety, [online] 5(6), pp.229–241. doi:https://doi.org/10.1177/2042098614554919.
University of Plymouth. (n.d.). How do we solve the antibiotic resistance crisis? [online] Available at: https://www.plymouth.ac.uk/discover/how-do-we-solve-the-antibiotic-resistance-crisis.
Xu, C., Kong, L., Gao, H., Cheng, X. and Wang, X. (2022). A Review of Current Bacterial Resistance to Antibiotics in Food Animals. Frontiers in Microbiology, 13. doi:https://doi.org/10.3389/fmicb.2022.822689.
Institut Pasteur. (2024). Félix d’Hérelle, discoverer of bacteriophages. [online] Available at: https://www.pasteur.fr/en/institut-pasteur/history/felix-herellediscoverer-bacteriophages.
Kasman, L.M. and Porter, L.D. (2022). Bacteriophages. [online] National Library of Medicine. Available at: https://www.ncbi.nlm.nih.gov/books/NBK493185/.
World (2024). Building evidence for the use of bacteriophages against antimicrobial resistance. [online] Who.int. Available at: https://www.who.int/europe/news/item/25-06-2024-building-evidence-for-the-useof-bacteriophages-against-antimicrobial-resistance.
Wikipedia Contributors (2019). Bacteriophage. [online] Wikipedia. Available at: https://en.wikipedia.org/wiki/Bacteriophage.
lnorkin2013 (2015). Felix d’Herelle, the Discovery of Bacteriophages, and Phage Therapy. [online] Leonard Norkin Virology Site. Available at: https://norkinvirology.wordpress.com/2015/05/20/felix-dherelle-the-discovery-ofbacteriophages-and-phage-therapy/.
Biotech Tutorials (2022). Lytic and Lysogenic cycle of λ Bacteriophage and Regulation - Biotech MCQ. [online] Biotech MCQ. Available at: https://biotechnologymcq.com/life-cycles-of- [Accessed 23 Oct. 2024].
Riaan Prakashan
Chobanian, AV., Bakris, GL., Black, HR., et al. (2003) 'The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: The JNC 7 Report', Journal of the American Medical Association, 289(19), pp. 2560-2572.
Cornelissen, VA. & Smart, NA. (2013) 'Exercise Training for Blood Pressure: A Systematic Review and Meta-Analysis', Journal of the American Heart Association, 2(1), e004473.
Mills, KT., Bundy, JD., Kelly, TN., et al. (2016) 'Global and Regional Prevalence of Hypertension and its Control', Journal of the American Medical Association, 317(2), pp. 165-182.
Nerenberg, KA., et al. (2018) 'Hypertension in the Elderly: The Current State of Management', Canadian Journal of Cardiology, 34(5), pp. 688-696.
Sacks, FM., Svetkey, LP., Vollmer, WM., et al. (2001) 'Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet', New England Journal of Medicine, 344(1), pp. 3-10.
Whelton, PK., Carey, RM., Aronow, WS., et al. (2018) '2017 Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines', Hypertension, 71(6), e13-e115.
World Health Organization (2021) 'Hypertension'. Available at: https://www.who.int/news-room/fact-sheets/detail/hypertension (Accessed: 21 October 2024).
NIDDK (2014). Renal Artery Stenosis | NIDDK. [online] National Institute of Diabetes and Digestive and Kidney Diseases. Available at: https://www.niddk.nih.gov/health-information/kidney-disease/renal-artery-stenosis.
Aayan Kureshi
Brown, T.A. (2002). The Human Genome. [online] www.ncbi.nlm.nih.gov. Wiley- Liss. Available at: https://www.ncbi.nlm.nih.gov/books/NBK21134/#A5306.
FuseSchool - Global Education (2020). The Human Genome Project | Genetics | Biology | FuseSchool. YouTube. Available at: https://www.youtube.com/watch?v=hryHoTIHak.
LWW. (2019). THE HUMAN GENOME PROJECT RAISES ETHICAL ISSUES THAT DESERVE ... : Neurology Today. [online] Available at: https://journals.lww.com/neurotodayonline/Fulltext/2001/07000/The Human Gen ome Project Raises Ethical Issues.3.aspx.
National Human Genome Research Institute (2020). The Human Genome Project. [online] National Human Genome Research Institute. Available at: https://www.genome.gov/human-genome-project.
Sigma Aldrich (2024). Blue-White Screening & Protocols for Colony Selection. Merck, [online] 1(1). Available at: https://www.sigmaaldrich.com/MX/en/technicaldocuments/technical-article/genomics/cloning-and-expression/blue-white-screening.
www.yourgenome.org. (n.d.). What was sequencing like before the Human Genome Project? [online] Available at: https://www.yourgenome.org/theme/what-wassequencing-like-before-the-human-genome-project/.
Saanidh Bhatt
Motor neurone disease (MND) (2022) healthdirect. Available at: https://www.healthdirect.gov.au/motor-neuron/e-disease-mnd (Accessed: 31 August 2024).
Durham researchers find concussions may raise risk of MND (2024) BBC News. Available at: https://www.bbc.com/news/articles/cx024wl9lpxo (Accessed: 01 September 2024).
Early signs of MND (2023) MND Association. Available at: https://www.mndassociation.org/about-mnd/mnd-explained/early-signs-of-mnd (Accessed: 01 September 2024).
What causes MND? (2023) MND Association. Available at: https://www.mndassociation.org/about-mnd/mnd-explained/what-causes-mnd (Accessed: 31 August 2024).
What is MND? (2023) MND Association. Available at: https://www.mndassociation.org/about-mnd/mnd-explained/what-ismnd#: :text=MND%20is%20the%20short%20term,a%20wide%20range%20of%20sym ptoms. (Accessed: 31 August 2024).
Treatments and medication (2024) MND Association. Available at: https://www.mndassociation.org/support-and-information/health-and-social-careservices/treatments-and-medication (Accessed: 06 September 2024).
Khalil, S.T. et al. (2017) Outcomes of infants with home tube feeding: Comparing nasogastric vs gastrostomy tubes, JPEN. Journal of parenteral and enteral nutrition. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5727911/#:~:text=While%20NG%20 tubes%20are%20easier,to%20prevent%20potential%20respiratory%20complications.& text=Alternatively%2C%20G%2Dtubes%20may%20be,%2C%20infection%2C%20and% 20wound%20issues. (Accessed: 06 September 2024).
Weekley, M.S. (2023) Oxygen Administration, StatPearls [Internet]. Available at: https://www.ncbi.nlm.nih.gov/books/NBK551617/# (Accessed: 06 September 2024).
Making MND history (2024) The University of Sheffield. Available at: https://www.sheffield.ac.uk/future/mnd (Accessed: 08 September 2024).
Fighting Motor Neurone Disease on all fronts (n.d.) The University of Sydney. Available at: https://www.sydney.edu.au/brain-mind/about/our-stories/patientstories/fighting-mnd-on-allfronts.html#: :text=A%20cure%20for%20the%20genetic,for%20the%20first%20nine% 20months. (Accessed: 08 September 2024).
Latest research news (2024) MND Association. Available at: https://www.mndassociation.org/research/latest-news (Accessed: 08 September 2024).
New Research Institute to accelerate the search for a cure for MND (2023) The University of Sheffield. Available at: https://www.sheffield.ac.uk/news/new-research-institute-accelerate-search-cure-mnd (Accessed: 08 September 2024).
Motor neuron diseases | National Institute of Neurological Disorders and stroke (2024a) national institute of neurological disorders and strokes. Available at: https://www.ninds.nih.gov/health-information/disorders/motor-neuron-diseases (Accessed: 08 September 2024).
Abnormal protein could be a common link between all forms of motor neurone disease (2022) The University of Sydney. Available at: https://www.sydney.edu.au/newsopinion/news/2022/08/12/abnormal-protein-could-be-a-common-link-between-allforms-of-mot.html (Accessed: 24 October 2024).
(2024) Motor neurone disease (MND) | NHS inform. Available at: https://www.nhsinform.scot/illnesses-and-conditions/brain-nerves-and-spinalcord/motor-neurone-disease-mnd/ (Accessed: 24 October 2024).
professional, C.C. medical (2024) Glutamate: What it is & function, Cleveland Clinic. Available at: https://my.clevelandclinic.org/health/articles/22839-glutamate (Accessed: 24 October 2024).
Treatment trials. (n.d.). MND Association. Available at: https://www.mndassociation.org/research/clinical-trials/treatment-trials(Accessed: 18 November 2024).
Sanhith Dandeniya
Alzheimer’s Society (2024). Hearing loss and the risk of dementia | Alzheimer’s Society - Connected Content. [online] www.alzheimers.org.uk. Available at: https://www.alzheimers.org.uk/about-dementia/managing-the-risk-ofdementia/reduce-your-risk-of-dementia/hearing-loss.
Alzheimer’s society (2024). Vision loss and the risk of dementia. [online] Alzheimer’s Society. Available at: https://www.alzheimers.org.uk/about-dementia/managing-therisk-of-dementia/reduce-your-risk-of-dementia/vision-loss-and-risk [Accessed 17 Oct. 2024].
Alzheimer's Association (2024). What is Alzheimer’s Disease? [online] Alzheimer’s Disease and Dementia. Available at: https://www.alz.org/alzheimers- dementia/what-is-alzheimers.
Alzheimer's Disease International (2020). Dementia Statistics. [online] Alzheimer’s Disease International. Available at: https://www.alzint.org/about/dementia-factsfigures/dementia-statistics/.
Campellone, J. (2024). Dementia: MedlinePlus Medical Encyclopedia. [online] medlineplus.gov. Available at: https://medlineplus.gov/ency/article/000739.htm.
CDC (2024). Vision Loss and Diabetes. [online] Diabetes. Available at: https://www.cdc.gov/diabetes/diabetes-complications/diabetes-and-vision-loss.html.
Guo, R., Ou, Y.-N., Ma, L.-Y., Tang, L., Yang, L., Feng, J.-F., Cheng, W., Tan, L. and Yu, J.-T. (2024). Osteoarthritis, osteoarthritis treatment and risk of incident dementia: a prospective cohort study based on UK Biobank. Age and Ageing, 53(8). doi:https://doi.org/10.1093/ageing/afae167.
Hallstrom, L. (2022). The 7 Stages of Dementia & Symptoms. [online] www.aplaceformom.com. Available at: https://www.aplaceformom.com/caregiverresources/articles/dementia-stages.
Huang, A., Jiang, K., Lin, F., Reed, N. and Deal, J. (2023). New Study Links Hearing Loss With Dementia in Older Adults | Johns Hopkins | Bloomberg School of Public Health. [online] publichealth.jhu.edu. Available at: https://publichealth.jhu.edu/2023/new-study-links-hearing-loss-with-dementia-inolder-adults.
Johns Hopkins Medicine (2019). Cataracts. [online] Johns Hopkins Medicine. Available at: https://www.hopkinsmedicine.org/health/conditions-and-diseases/cataracts.
Johns Hopkins Medicine (2024). Brain Anatomy and How the Brain Works. [online] Johns Hopkins Medicine. Available at: https://www.hopkinsmedicine.org/health/conditions-and-diseases/anatomy-of-thebrain.
LaMotte, S. (2023). Dementia risk rises if you live with chronic pain, study says. [online] CNN. Available at: https://edition.cnn.com/2023/02/20/health/dementiachronic-pain-wellness/index.html [Accessed 17 Oct. 2024].
Mayo Clinic (2023). Alzheimer’s disease - symptoms and causes. [online] Mayo Clinic. Available at: https://www.mayoclinic.org/diseases-conditions/alzheimersdisease/symptoms-causes/syc-20350447.
National Health Service (2023). What is dementia. [online] nhs.uk. Available at: https://www.nhs.uk/conditions/dementia/about-dementia/what-is-dementia/.
National Institute on Aging (2022). What Is Dementia? Symptoms, Types, and Diagnosis. [online] What Is Dementia? Symptoms, Types, and Diagnosis. Available at: https://www.nia.nih.gov/health/alzheimers-and-dementia/what-dementiasymptoms-types-and-diagnosis.
NHS (2021). Glaucoma. [online] NHS. Available at: https://www.nhs.uk/conditions/glaucoma/.
NHS (2022). Overview - Arthritis. [online] NHS. Available at: https://www.nhs.uk/conditions/arthritis/.
NHS (2023a). Causes of dementia. [online] nhs.uk. Available at: https://www.nhs.uk/conditions/dementia/about-dementia/causes/.
NHS (2023b). Symptoms of dementia. [online] NHS. Available at: https://www.nhs.uk/conditions/dementia/symptoms-and-diagnosis/symptoms/.
NHS (2024). Alzheimer’s Disease. [online] NHS. Available at: https://www.nhs.uk/conditions/alzheimers-disease/.
Office for National Statistics (2019). Living longer - Office for National Statistics. [online] Ons.gov.uk. Available at:https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriage s/ageing/articles/livinglongerhowourpopulationischangingandwhyitmatters/201903-15.
Purves, D., Augustine, G.J., Fitzpatrick, D., Katz, L.C., Anthony-Samuel LaMantia, McNamara, J.O. and S Mark Williams (2016). The Auditory Cortex. [online] Nih.gov. Available at: https://www.ncbi.nlm.nih.gov/books/NBK10900/.
Rani, V., Verma, R., Kumar, K. and Chawla, R. (2023). Role of pro-inflammatory cytokines in Alzheimer’s disease and neuroprotective effects of pegylated self- assembled nanoscaffolds. Role of pro-inflammatory cytokines in Alzheimer’s disease and neuroprotective effects of pegylated self-assembled nanoscaffolds, 4(36593925), pp.100149–100149. doi:https://doi.org/10.1016/j.crphar.2022.100149.
Sanganee, A. (2024). New evidence linking sight loss to dementia - Alzheimer’s Research UK. [online] Alzheimer’s Research UK. Available at: https://www.alzheimersresearchuk.org/news/new-evidence-linking-sight-loss-todementia/[Accessed 17 Oct. 2024].
Seladi-Schulman, J. (2020). Frontal Lobe Function, Location in Brain, Damage, More. [online] Healthline. Available at: https://www.healthline.com/health/frontal- lobe.
Weber, A., Mak, S. hung, Berenbaum, F., Sellam, J., Zheng, Y.-P., Han, Y. and Wen, C. (2019). Association between osteoarthritis and increased risk of dementia. Medicine, [online] 98(10), p.e14355.
doi:https://doi.org/10.1097/md.0000000000014355.
World Health Organization (2024). Ageing and health. [online] World Health Organization. Available at: https://www.who.int/news-room/factsheets/detail/ageing-and-health.
Zhang, J.-M. and An, J. (2007). Cytokines, Inflammation, and Pain. International Anesthesiology Clinics, [online] 45(2), pp.27–37. doi:https://doi.org/10.1097/AIA.0b013e318034194e.
Boran Sahin
Baselga, J., Cortés, J., Kim, S.B., Im, Y.H., Hegg, R., et al., 2012. ‘Pertuzumab plus trastuzumab in HER2-positive breast cancer ’ , New England Journal of Medicine, 366(2), pp. 109-119.
Frangoul, H., Altshuler, D., Cappellini, M.D., Dever, D.P., et al., 2020. ‘CRISPRCas9 gene editing for sickle cell disease and β-thalassemia’, New England Journal of Medicine, 383(3), pp. 251-260.
Gage, B.F., Eby, C., Johnson, J.A., et al., 2008. ‘Improved warfarin dosing with pharmacogenetic-based clinical algorithms’, Clinical Pharmacology & Therapeutics, 84(3), pp. 326-332.
Gopalakrishnan, V., Spencer, C.N., Nezi, L., Reuben, A., et al., 2018. ‘Gut microbiome modulates response to anti–PD-1 immunotherapy in melanoma patients’, Science, 359(6371), pp. 97-103.
Larkin, J., Ascierto, P.A., Dreno, B., Atkinson, V., et al., 2014. ‘Combined vemurafenib and cobimetinib in BRAF-mutated melanoma’, New England Journal of Medicine, 371(20), pp. 1867-1876.
Nicholson, J.K., Holmes, E., Kinross, J., Burcelin, R., et al., 2012. ‘Host-gut microbiota metabolic interactions’, Science, 336(6086), pp. 1262-1267.
Ritchie, M.D., Denny, J.C., Crawford, D.C., Weiner, J.S., et al., 2016. ‘Pharmacogenomic discovery and clinical implementation: Lessons learned from the eMERGE Network’, Clinical Pharmacology & Therapeutics, 99(3), pp. 344-347.
Nathan Wolfson
BMJ Group - Helping doctors make better decisions. (2020). Patients overestimate the success of CPR - BMJ Group. [online] Available at: https://bmjgroup.com/patients-overestimate-the-success-of-cpr/.
British Heart Foundation (2023). Cardiac Arrest. [online] Bhf.org.uk. Available at: https://www.bhf.org.uk/informationsupport/conditions/cardiac-arrest.
Brown, T.P., Perkins, G.D., Smith, C.M., Deakin, C.D. and Fothergill, R. (2022). Are there disparities in the location of automated external defibrillators in England? Resuscitation, 170, pp.28–35. doi:https://doi.org/10.1016/j.resuscitation.2021.10.037. byjus.com. (n.d.). What is percentage of Various gases in exhaled and inhaled air ..... [online] Available at: https://byjus.com/question-answer/what-is-percentage-ofvarious-gases-in-exhaled-and-inhaled-air/.
Kono, H., Takaishi, K., Onuma, M., Fukushima, M. and Takeuchi, R. (2024). Bystanders’ willingness to assist using automated external defibrillators during cardiac arrest. Heliyon, [online] 10(17), p.e37316. doi:https://doi.org/10.1016/j.heliyon.2024.e37316.
Resuscitation Council UK (2024). New data reveals decrease in out-of-hospital cardiac arrest survival rates in England. [online] Resuscitation Council UK. Available at: https://www.resus.org.uk/about-us/news-and-events/new-data-revealsdecrease-out-hospital-cardiac-arrest-survival-rates.
Resuscitation Council UK. (2022). Case Study: Asad - ‘From the football pitch to a coma in a matter of hours’. [online] Available at: https://www.resus.org.uk/aboutus/news-and-events/case-study-asad-football-pitch-coma-matter-hours [Accessed 16 Feb. 2025].
Scotland, S.J. (2025). Public Access Community Defibrillators | St John Scotland. [online] St John Scotland. Available at: https://www.stjohnscotland.org.uk/home/defibrillators [Accessed 16 Feb. 2025].
Uny, I., Angus, K., Duncan, E. and Dobbie, F. (2022). Barriers and Facilitators to Delivering Bystander Cardiopulmonary Resuscitation in Deprived communities: a Systematic Review. Perspectives in Public Health, 143(1), p.175791392110554. doi:https://doi.org/10.1177/17579139211055497.
Stock Images
All unreferenced images are courtesy of photographers of Unsplash (https://unsplash.com), and are licensed for free commercial usage.
“I wouldn't be here today if it were not for the NHS. I have received a large amount of high-quality treatment without which I would not have survived.”
Stephen Hawking
“The NHS will last as long as there are folk left with faith to fight for it.”
“No society can legitimately call itself civilized if a sick person is denied medical aid because of lack of means. ”
Aneurin Bevan
“Anyone who works in the NHS has superpowers. It’s a miracle, it is magic.”