
Quality Account 2022/23

Page 2 of 87 Contents 1 Our Commitment to Quality 3 1.1 Chief Executive’s Welcome.......................................................................................... 3 1.2 Quality Assurance at GMMH 6 1.3 Quality Improvement at GMMH (QI Strategy) 7 1.4 Accolades and Developments 9 1.5 Equality, Diversity and Inclusion at GMMH ................................................................ 12 2 Statements of Assurance from the Board for 2022/23 ................................................. 14 2.1 Review of Services 14 2.2 Participation in Clinical Audits and National Confidential Enquiries 15 2.3 Participation in Clinical Research 19 2.4 Commissioning for Quality and Innovation (CQUIN) .................................................. 23 2.5 Registration with the Care Quality Commission (CQC) 25 2.6 CQC Mental Health Act Monitoring 27 2.7 Data Quality 27 2.8 Information Governance............................................................................................. 28 2.9 Clinical Coding........................................................................................................... 28 2.10 Department of Health Mandatory Quality Indicators 29 2.11 Freedom to Speak Up 50 2.12 Increasing Community Mental Health Services Capacity 51 3 Review of Quality Performance in 2022/23.................................................................... 54 3.1 Delivery of Quality Improvement Priorities in 2022/2023 54 3.2 Performance against Quality Indicators Selected 61 3.3 Performance against Key National Priorities 65 3.4 Improvement Priorities for 2023/2024 ........................................................................ 66 3.5 Monitoring our Quality Improvement Priorities............................................................ 69 3.6 ANNEX 1 – Feedback from Key Stakeholders 70 3.7 ANNEX 2 Statement of Directors’ Responsibilities in Respect of the Quality Account 77 3.8 ANNEX 3 Equality Impact Assessment 78 3.9 ANNEX 4 Local Clinical Audits Reviewed in 2022/23................................................. 79 3.10 ANNEX 5 Glossary of Terms 83
1 Our Commitment to Quality
1.1 Chief Executive’s Welcome
On behalf of the Trust Board, I would like to present our Quality Account for 2022/23. This describes the steps taken during what have been extraordinary and challenging times to improve the quality of the care we offer at Greater Manchester Mental Health NHS Foundation Trust (GMMH).
2022 was an extremely challenging year for GMMH. Emerging from the COVID-19 pandemic, with unprecedented pressures on the entire NHS, and with demand for mental health services at record levels, we faced an additional set of difficulties of our own making
During 2022/23, care and treatment failures were identified at GMMH via the BBC Panorama programme. The documentary shocked us all and shamed the vast majority of our hard-working colleagues, for whom patient care and safety is fundamental and absolute. On behalf of the Board, I am truly sorry for the distress that this caused to our service users, and their families.
Soon after, the Trust was placed into Segment 4 of NHS England’s Oversight Framework and placed into the National Recovery Support Programme. We absolutely welcome this support. The Trust Board accepted responsibility for, and sought to understand the root causes of, these multiple and serious failures. We commissioned a number of clinical reviews and other investigations, conducted by independent and expert bodies, alongside those commissioned by our regulators. Some of these are still underway and will report their findings in the coming months.
In November 2022, the Care Quality Commission (CQC) published their report, following their inspection of services at our Trust earlier that year. The report identified a series of failings and led to our CQC rating being suspended As a Board, we accept the findings of the CQC’s inspection of our Trust and are committed to making the changes and improvements that our service users deserve. The CQV also issued a number of warning notices to GMMH. Further details regarding these are included in section 2.5 of this report.
The report made for challenging reading and raised a number of areas in which the Trust must urgently improve. This was incredibly disappointing, but was no reflection on the hard work, commitment and dedication shown by the large majority of our staff who have faced unprecedented pressures in recent years. It is also important to note that the CQC did report and recognise some good care and management in several services, with staff and managers displaying the values of the Trust and working well together.
In addition to those challenges, the demand for our services remains higher than ever and, like many NHS trusts, workforce challenges continue to be a major issue. This inevitably has had an impact on our teams and leaders, as well as their capacity to assess and support service users effectively.
Page 3 of 87
This has affected staff resilience, health, and wellbeing. This is a challenging time, but the Board continues to be proud of the care, support and dedication the vast majority of colleagues show to our service users. On behalf of the Board, I thank our staff for their continued hard work and dedication.
The Trust Board is fully committed to rectifying these issues. Work is already underway in order to build better and more sustainable services. The NHS England Recovery Support Programme (RSP) has provided us with access to additional expertise and resource to ensure that sustainable improvements are made as quickly as possible. The pressing need for immediate –and long-term - change within our organisation is clear, and we have already taken a number of steps to strengthen our current approach to quality and safety. This has included working with our external partners to improve our governance and oversight arrangements, and beginning a programme of work to build a dynamic quality oversight framework that aims to provide assurance at all levels across the Trust.
We have prioritised early work to establish a trust-wide safe staffing group, in line with recommendations received from the NHS Clinical Workforce Lead to strengthen our end to end safe staffing processes. We have also commenced a significant programme of work to focus on fire safety, smoke free premises and ligature safety, following concerns raised by the CQC.
We have now completed work with Health Education England and our local universities across GMMH to develop and agree robust plans to return student nurses and trainees nursing assistants back to our adult forensic services. We have also commenced plans to design and deliver an effective ‘report and support’ process to address incidents of bullying, harassment, discrimination, abuse, violence or hate across our services.
In addition, our Care Groups have now established forums where learning from incidents is routinely discussed, accompanied by mechanisms for cascading learning to relevant teams throughout GMMH.

The Board has recognised the scale of the challenge ahead and understands it will not be a simple or straightforward task. But we are firmly committed to remedying the problems that have so clearly emerged over the past year, and improving outcomes and experiences for our service users, their families and our staff. We are also committed to doing so in a spirit of openness and collaboration.
With this in mind, we have been working hard to produce our improvement plan, which has been in development since last autumn and includes a number of immediate actions to tackle the most urgent quality and safety issues. This sits alongside a comprehensive set of long-term ambitions to improve everything we do at the Trust, grouped into five themes
We recognise clearly that our improvement journey will only succeed if the views of our service users, their families, and carers, alongside those of our staff and stakeholders, are central to the development and implementation of our detailed plans and have embarked on a robust engagement programme to help us to achieve this
Page 4 of 87
The engagement was key in ensuring that we identified the right areas for initial action and the ways in which these needed to be prioritised. Going forward, continued engagement and collaboration throughout our journey will also guide our shared vision into meaningful action, as we start to deliver these bold, long-term ambitions and measure the impact of the changes we make
Looking ahead, 2023/24 promises to be another challenging year with some uncertain times. However, we will continue with our efforts to ensure that we do everything we can to improve outcomes and experiences for our service users, their families and our staff, in a spirit of openness and collaboration
Finally, I am pleased to inform you that the Board of Directors has reviewed this 2022/23 Quality Account and confirm that this is an accurate and fair reflection of our quality and performance.
As Chief Executive of Greater Manchester Mental Health NHS Foundation Trust (GMMH), I can confirm that, to the best of my knowledge, the information contained in this report is accurate. The ‘Statement of Directors’ Responsibilities’ at Annex 2 summarises the steps we have taken to develop this Quality Account and external assurance is provided in the form of statements from our commissioners, local HealthWatch organisations and Scrutiny Committees in Annex 1.
Neil Thwaite, Chief Executive
30 May 2022

5 of 87
Page
1.2 Quality Assurance at GMMH
The Trust has reflected on the concerns identified specifically with regards to quality assurance and commenced work to establish a robust integrated governance and quality management system, that enables the Board of Directors to have effective oversight of quality and safety concerns and to use information about risks, performance and outcomes to identify emerging issues and improve care.
This revised governance and assurance system will be underpinned by an inclusive and positive culture of continuous learning and improvement and will support compliance with Regulation 17: Good Governance of the Health and Social Care Act 2008 (Regulated Activities Regulations) (Part three).
In addition to the Trusts governance and assurance system, on the 15 September 2022 the Trust was supported by NHS England in line with the National Guidance on Quality Risk Response and Escalation in Integrated Care Systems. NHSE convened an initial Rapid Quality Review (RQR) a multi-stakeholder meeting that provided a collaborative, system-focused approach for supporting providers with the toughest challenges. It provided support to help strengthen Trusts to be able to use all their levers to address complex, deep-seated problems and embed lasting quality and financial solutions.
The Rapid Quality Review meeting facilitated rapid diagnosis of the quality concerns at Edenfield Unit and established from a diverse group of stakeholders a wider picture of concerns for the Trust. It also gained assurance with regard to GMMH immediate response to the recent concerns and to agree next steps including the development of and arrangements for the monitoring of a comprehensive Improvement Plan for the organisation.
On the 22 November 2022, the Trust was placed into NHSE Oversight Framework Segment 4, as outlined in the NHSE Oversight Framework 2022/23 and therefore started to receive support from the Recovery Support Programme (RSP). This is a nationally led programme providing mandated focused assistance to organisations and systems facing the most acute challenges.
As a result, the national and regional teams have been working collaboratively with GMMH and our system partners to agree the key drivers of the concerns that need to be resolved and to better understand GMMH support needs, reach agreement on clear and timely exit criteria, and agree interventions, undertakings and oversight arrangements.
These oversight arrangements include a System Improvement Board chaired by the NHS England regional director. The principal purpose of the Improvement Board is:
• To oversee development and delivery of an improvement plan which addresses the key concerns of the CQC and other arm’s length bodies.
• To agree Recovery Support Programme exit criteria.
Page 6 of 87
• To ensure there is a system response and support from system partners to address the issues and concerns raised and to assist the Trust in achieving the Recovery Support Programme exit criteria.
• To ensure that any changes and improvements made are embedded and sustainable.
The Improvement Board (IB) has agreed a work plan and the appropriate collective oversight of the delivery of actions to ensure the required pace of improvement. It works with the Trust Board, ensuring that the ownership of the improvements and associated governance sits with the Trust Board. The IB will provide appropriate confirm and challenge in terms of aspiration and the collective contributions, including improvement support. It will also agree the process for unblocking any issues which delay progress or reduce the quantum of progress either internally or across the wider health care system.
The GMMH Quality Improvement Committee (QIC), which is a subcommittee of the Trust Board, is chaired by a non-executive director and has representation from the Board, lead clinicians from all services and from corporate leads with responsibility for quality. QIC provides leadership and oversight for the Trust’s quality and integrated governance framework. It maintains a strategic overview of our approach to quality assurance and ensures that it encompasses a robust range of programmes that reflect our local and regulatory requirements.
The structure, membership and business of the QIC, including its assurance function, will be strengthened and developed further throughout the coming year as part of our goal to establish a robust integrated governance and quality management system, within a culture of continuous improvement
1.3 Quality Improvement at GMMH (QI Strategy)
Since its launch, the QI strategy has aimed to play a key role in ensuring that there is clear focus, profile and identity for the improvement agenda across GMMH. Throughout 2022/23, there has been increased focus on building an improvement culture across GMMH, and in the continued development of capacity and capability for QI.
Our QI strategy currently incorporates three key enablers which have driven our approach to continuous improvement, supported the delivery of our quality improvement priorities and our wider vision for QI. These are as follows:
1. Supporting staff to deliver QI - building capacity and capability.
2. Identifying improvement methodology to complement workflow.
3. The development of improvement orientated data throughout the organisation, from Board to team/ward
Page 7 of 87
To continue to build QI capacity and capability, we have focussed on the provision of highquality training, to support our staff to have the capability, enthusiasm, and motivation to make, sustain and spread QI across GMMH. Building capability in this way will enable us to create a culture, where staff members are trained and empowered to focus on where they can make improvements to the work, they do, whether that is in clinical care, governance, financial systems, estates and facilities or human resources.
Throughout 2023/24, we will ensure all QI work is aligned to the improvement plan priorities and supports delivery of the Trusts Exit criteria. We will continue to focus on the development and delivery of our in-house programme, which will be available to all staff including our service users across GMMH. Our aim for 2023/24 is to introduce a gold level training package, which will be aimed at improving Leaders involved in complex change programmes.
During 2022/23, the QI Team has provided training at different levels to promote capacity and capability. In total, over 1220 attendances have been recorded across each different training programme. The information below summarises current training activities delivered by the team.
To date, progress has been made against each of the Quality Improvement Programmes, but there is much more to do. Each achievement reflects the immense commitment of our staff, services users, and carers to continually improving quality. Please refer to section 3.1 of this Quality Account for further information.
8 of 87
Page
Quality Improvement Courses An introduction to quality improvement 361 Introduction to Statistical Process Control (SPC) charts 147 Quality Improvement (Bronze) 265 Quality Improvement (Bronze for leaders) 200 Quality Improvement (Silver) 189 Introduction to Lean 25 Quality Improvement (Bronze for service users) 26 Quality Improvement (Bronze + for service users) 10
1.4 Accolades and Developments
Whilst 2022/23 has seen a range of care and treatment failures and regulatory improvement actions, we have also received local and national recognition for our achievements.
These include:
• In April 2022 a study using virtual reality (VR) to treat mental health problems trialled in Manchester was hailed as a breakthrough success. A national study, delivered by nine NHS Trusts, including GMMH, found that automated VR technology can successfully help people recover from mental health problems.

Dr Elizabeth Murphy, gameChange Trial Coordinator and Research Clinical Psychologist
• GMMH was rated ‘Good’ in all areas of our education and training programme for apprentices, following an inspection by Ofsted in May 2022.
• A partnership between GMMH, Greater Manchester Police and the North-west Ambulance Service, aimed at improving care for people experiencing a mental health crisis, was hailed a success. Just six months in (May 2022), over 1,100 cases had been diverted from frontline NWAS and GMP services, with quality NHS mental health support being provided instead.
• A Research Unit dedicated to researching inequalities in mental and physical healthcare was launched by GMMH during Equality, Diversity and Human Rights Week in May 2022.
Page 9 of 87
• The Greater Manchester Universities Student Mental Health Service which is a partnership between GMMH, NHS Greater Manchester and the region’s five universitieswas hailed a success in July 2022.

• In July 2022, an external evaluation found that the Trust’s Achieve Service’s approach to partnership-working is effective in supporting recovery from substance misuse, and could be rolled out in other geographical areas. Addiction services for Bolton, Bury, Salford and Trafford were praised in an evaluation report, undertaken by SQW, an independent research and consultancy organisation.
• An evaluation of Living Well Salford in August 2022 found that the service has supported people to achieve improved outcomes. The service offers support co-designed by people with lived experience of mental health problems and was also shortlisted for ‘Mental Health Innovation of the Year’ in the prestigious national Health Service Journal awards 2022.
Living Well Salford
• In October 2022, GMMH became the first mental health trust to install state of the art CPR training technology. The technology, called Brayden Online, combines a traditional mannequin with an iOS application which uses a cloud server, allowing staff to undertake CPR training at a time, date and location that is flexible for them.
• We were proud to be an NHS Partner of a bid for Greater Manchester awarded its largest ever research funding in October 2022 to tackle health inequalities and drive health improvements across the city region. This investment supports the delivery of important research into mental health care and treatment at the Biomedical Research Centre in Manchester.
• Ceramicists from our Recovery Pathways service contributed to the Manchester City Council’s Be Proud Awards 2022 by creating a series of sculptures as prizes for winners.
Some of our fantastic colleagues continued to be recognised for their excellent work at various local and national awards ceremonies.
Page 10 of 87
Here are some examples of where staff were shortlisted or won prestigious awards:
• Sophie Parker, Director of Youth Mental Health Research Unit and Consultant Clinical Psychologist at GMMH was recognised for her contribution to clinical psychology and research in the area of adolescent mental health by the Manchester Academic Health Science Committee (MAHSC). The Committee awards honorary appointments to individuals who have made a major contribution to their clinical speciality.
• Dr Eleanor Swift, Speciality Trainee Six Doctor in General Adult Psychiatry, was awarded Higher Trainee of the Year; and Dr Aaron McMeekin, Consultant Perinatal Psychiatrist, won the Psychiatric Trainer of the Year Award at the RCPsych North West Division Awards 2022.
• The Greater Manchester Liaison and Diversion Service was commended in the ‘Liaison and Diversion’ category for their Out of Court Disposal Pathway in partnership with Greater Manchester Police in the Penal Reform Community Awards 2022.
• Adele McKie, GMMH Assistant Director of Finance won the John Andrews Award. This award recognises a finance colleague who has shown care and compassion to support the health and well-being of colleagues during the 12 months preceding the award.
• GMMH's Finance team were shortlisted in the Public Finance Awards 2022 for Finance Team of the Year.
• The Marketing and Communications team were Highly Commended in the NHS Communicate Awards 2022 for Best Use of Digital Communications and Engagement Award.
• Dr Hannah Cappleman, Consultant Psychiatrist was shortlisted in the 2022 Royal College of Psychiatrists Awards in the ‘Psychiatric Educator of the Year’ category.
• Filippo Varese, Head of the Complex Trauma and Resilience Research Unit (C-TRU), a collaboration between GMMH and the University of Manchester, was awarded the May Davidson Award by The British Psychological Society (BPS). The award recognises individuals who have made an outstanding contribution to the development of clinical psychology within the first ten years post qualification.
• A project run by GMMH using a technology called ‘Management and Supervision Tool’ (MaST) to support clinical care and patient safety in Community Mental Health Teams (CMHTs), was recognised in the National Positive Practice in Mental Health Awards 2022.
• Miriam Avery, an NIHR Clinical Doctoral Research Fellow at GMMH, was named the winner in the ‘Exceptional Research Delivery Leadership’ category in the Greater Manchester Health and Care Research Awards for her work as a Clinical Research Nurse on the Biohaven OCD study, a trial investigating the effectiveness of the medication Troriluzole in the treatment of OCD. Motiv8, a weight management programme for people in secure mental health settings was also a finalist in the ‘Best Public Engagement’ category.
Page 11 of 87
• Jemima Lacey, a Nursing Support Worker was a finalist in the Nursing Support Worker category of the RCN Nursing Awards 2022.
• Dr Azza Aglan, Consultant Clinical Psychologist was shortlisted for The Caroline Flack Mental Health Hero award. She who works at an allergy clinic to provide mental health support to people with severe allergies.

• Paula St-John, Senior Practitioner for Personality Disorder at Ramsgate House in Salford, was recognised as being highly commended in the Key Worker category for the BBC Radio Manchester #MakeADifference awards!
1.5 Equality, Diversity and Inclusion at GMMH
At GMMH, we recognise that we serve a diverse population, and that our workforce reflects the diverse communities who access our care and treatment. The Trusts Advancing Equalities Strategy 2022/25, which was ratified by the board in June 2022, adopts a quality improvement (QI) approach in so doing making a firm commitment ‘to understanding and reducing variation and inequalities and ensuring that everybody has access to high-quality care and outcomes’.
The broad aim of the Advancing Equalities strategy is to advance equality in the delivery of mental health services and address the systemic inequalities that people face, by supporting our workforce and services to be inclusive and meet the needs of the populations they serve. The strategy sets the key principles that will underpin our approach and outlines four equality objectives and twelve priorities that will help us to meet our overall aim. Our Advancing Equalities Action Plan 2023 identifies the immediate actions that will be taken to support our approach.
Page 12 of 87
Dr Azza Aglan, Consultant Clinical Psychologist
The Business Case to accompany the strategy was agreed by the Strategic Delivery Group (SDG) in August 2022. This secured investment for a central Equality Diversity and Inclusion Team, which was established in February 2023. The Trust has become a partner of the Royal College of Psychiatrists (RCP) Advancing Mental Health Equality (AMHE) QI Collaborative and the three-year project began in October 2022.
In January 2023 we produced guidance on Advancing Equalities through the Business Planning Framework for 2023/24 and areas have been asked to identify accountable officers to drive change at a local level. This will focus on data and intelligence, inclusive integrated services and inclusive accessible audits, as sumamrised below.
Data and Intelligence
In collaboration with the Greater Manchester Integrated Care Board (GM ICB), we are implementing the NHS Equality Delivery System (EDS) focusing on children and young people’s services, and Interpretation Services for 2023/24, supporting the NHS England’s (NHSE) Core20PLUS5 approach to tackling health inequalities for children and young people,
Inclusive Integrated Services
The Trust continue to support the NHSE to develop and test the Patient and Carers Race Equality Framework (PCREF) and important part of the NHS Advancing Mental Health Equalities Strategy As part of this we have worked in partnership with the GM ICB and the Greater Manchester Voluntary, Community, and Social Enterprise (GM VCSE) sector to help establish and deliver the GM ICB Culturally Appropriate Services Fund (CASF) 22/23 (Year One), which aims to improve access, experience and outcomes for people that experience racial inequalities. The fund has commissioned 31 community and voluntary organisations, that support people that experience racial inequalities, to deliver services to adults or older adults from those communities. We have secured investment through the NIHR Mental Health Improvement Network (MHIN) to undertake an 18-month evaluation of the GM ICB Culturally Appropriate Services Fund (CASF) 2022/23 to 2023/24 (Year One/Two).
Inclusive Accessible Environments
The You Report We Support Steering Group aims to increase the percentage of staff who feel we offer a safe and healthy place to work by developing effective prevention strategies, in the short-term increasing the number of people who report unacceptable behaviours and get support, in the long-term decreasing the number of incidents that take place. If you are interested in learning more about our Equality, Diversity and Inclusion programme at GMMH, please contact:
Cath Prescott, Head of Equality, Diversity and Inclusion
Email: cath.prescott@gmmh.nhs.uk
Page 13 of 87
2 Statements of Assurance from the Board for 2022/23
This section of our Quality Account includes mandated information common across all organisations’ Quality Accounts. This information demonstrates that we are performing to essential standards; measuring clinical processes and performance; and are involved in national initiatives aimed at improving quality.
2.1 Review of Services
During 2022/23 Greater Manchester Mental Health NHS Foundation Trust provided and/or subcontracted a wide range of relevant health services to support treatment and recovery of mental health and/or substance misuse problems for our service users and carers. This includes community services in the localities we cover and within a range of specialist services.
Services provided include:
• Community and inpatient mental health services.
• Inpatient Child and Adolescent mental health services
• Community Child and Adolescent mental health services.
• Talking Therapies – primary care psychology (previously known as IAPT).
• Mental Health Practitioners working within Primary Care Networks
• Rehabilitation services.
• Adolescent forensic mental health services.
• Adult forensic mental health services
• Perinatal Mental Health In-Patient and Community services including parent and infant services.
• Deaf mental health services.
• Prison healthcare and in-reach services.
• Community and inpatient addiction services.
• Supporting services for people with a gambling addiction.
• A wide variety of VCSE contracts with a range of partners across GM.
• Mental health and homelessness services.
Further detail on the services provided by us can be found on our website –www.gmmh.nhs.uk
Page 14 of 87
2.2 Participation in Clinical Audits and National Confidential Enquiries
During 2022/23, There were two national clinical audits and two national confidential enquiries covering relevant health services that GMMH provides. During that period, GMMH participated in 100% of the national clinical audits and 100% of the national confidential enquiries which it was eligible to participate in.
The national clinical audits and national confidential enquiries that GMMH was eligible to participate in during 2022/23 are as follows:
• Prescribing Observatory for Mental Health: Prescribing of High Dose and Combined Antipsychotics
• Prescribing Observatory for Mental Health: Valproate prescribing in Adult Mental Health Service
• National Audit of Psychosis – Spotlight Audit
• National Confidential Inquiry (NCI) into Suicide and Safety into Mental Health
The national clinical audits and national confidential enquiries that GMMH participated in and for which data collection was completed during 2022/23, are listed below alongside the number of cases submitted to each audit or inquiry as a percentage of registered cases required of that audit or enquiry (list and percentages are in the table below).
National Clinical Audits:
Information about the Audits
Prescribing Observatory for Mental Health: Valproate prescribing in Adult Mental Health Service (topic 20b).
Report due: April 2023.
Page 15 of 87
Audit Title Participation % of cases Submitted National Clinical Audit of Psychosis Yes 100% National Confidential Enquiry into Suicide and Safety into Mental health Yes 100% Prescribing Observatory for Mental Health: Prescribing of High Dose and Combined Antipsychotics Yes 100% Prescribing Observatory for Mental Health: Valproate prescribing in Adult Mental Health Service Yes 100%
POMH Valproate
100 audit tools completed for this programme The national report is due to be received at the Trust during May 2023. The audit team carried out a summary of the results, which at this stage indicate that practice standards and treatment targets are not always routinely met. As a result, one of the likely actions will include that consideration must be given to how improvements can be made to increase the awareness and the documenting of each of the following for patient’s prescribed valproate.
Other likely actions at this stage currently include:
• Documenting the clinical reason/indication/target symptoms for valproate treatment.
• If “off label” it should be documented that this has been explained to the patient.
• Pre-treatment screening to be carried out prior to initiating treatment with valproate.
• Screening review to be carried out within the first three months of valproate treatment.
• An annual review of risk-benefit balance to be undertaken
• Conditions of ‘prevent’ the pregnancy prevention programme to be fulfilled, as ARA forms are not routinely initialled.
The national report is due to be published and received at the Trust during May 2023. This will help to fine tune the proposed set of recommendations and improvement actions. In the meantime, an audit summary has been provided to the GMMH pharmacy team to review the proposed key actions and make recommendations for others, based on the initial results.
A report will also be taken to the GMMH Valproate Steering Group in April 2023, to discuss the early results and identify any immediate next steps to improve practice, ahead of the publication of the formal report
Prescribing Observatory for Mental Health: Prescribing of High Dose and Combined Antipsychotics (Topic 1h and 3e)
Report: September 2022
The standards are derived from the Prescribing Observatory for Mental health Topic 1h and 3e.: recognition and the audit will look at eligible patients currently prescribed antipsychotic medication as inpatients, under the care of adult mental health services, including forensic services
Practice standards:
• Documentation of the target symptoms/behaviours for such a treatment regimen
• Regular reviews of the clinical response
• Monitoring of side effects/tolerability
Page 16 of 87
If prescription of oral PRN antipsychotic and/or Benzodiazepine medication:
• There should be a clear description of symptoms/behaviours for which PRN medication is indicated.
• the maximum daily dose that can be administered should be specified.
• The continuity needs for a prescription and regular reviews.
NCAP EI audit
This audit explores the use of Cognitive Behavioural Therapies, work education and training, supported employment programmes and Family Interventions. In addition, physical health screening and intervention is also audited.
Data entry for this audit closed on 31 March 2023 – It is a new process this year as the NCAP team will be providing a dashboard once all data has been entered and analysed by the NCAP team. This is currently being tested by the NCAP team and they will confirm once the dashboards are available.
National Clinical Audit of Psychosis
The National Clinical Audit of Psychosis (NCAP) aims to improve the quality of care that NHS mental health trusts in England and Health Boards in Wales provide to people with psychosis.
The audit focused on whether the following physical health indicators have been monitored within the past 12 months such as Physical health monitoring, use of tobacco and/or alcohol, substance misuse, measure of glucose control and health history in members of the service user’s family.
When monitoring within the past 12 months has indicated a need for intervention, the service user has been offered an intervention or the treating clinician has made a referral to the appropriate services.
• Access and waiting times (time from referral to assessment/offer of treatment), receiving NICE concordant care within 14 days
• Offer and uptake of NICE concordant interventions for first episode psychosis (CBTp, psychosis focussed family interventions, education, and employment support)
• Identification, assessment, and delivery of evidence-based interventions for at-risk mental states (ARMS)
• Prescribing practices (nature and duration of prescribing)
• Outcomes (clinician and patient reported experience measures (PREMs) and outcome measures (PROMs))
The audit also looked at the offer of supported employment programmes to service users who wish to find or return to work.
Page 17 of 87
National Confidential Inquiry (NCI) into Suicide and Safety into Mental Health (NCI/NCISH)
The National Confidential Inquiry into Suicide and Safety into Mental Health examines people who have been in contact with secondary and specialist mental health services in the preceding 12 months. Previous findings of the Inquiry have informed recommendations and guidelines produced by the National Institute for Clinical Excellence (NICE), the National reporting and learning system (NRLS) and the Inquiry itself aimed at improving outcomes and reducing suicides rates for individuals with mental illness.
The reports of four national clinical audits were reviewed by GMMH in 2022/23 and GMMH intends to take the following actions to improve the quality of healthcare provided as per the table below:
Key Actions from National Audits
Audit Title
Prescribing Observatory for Mental Health: Prescribing of High Dose and Combined Antipsychotics
Prescribing Observatory for Mental Health: Valproate prescribing in Adult Mental Health Service
National Clinical Audit of Psychosis.
Key Actions
• GMMH is currently awaiting publication of this report, and will summarise key actions once received within the organisation
• GMMH is currently awaiting publication of this report, and will summarise key actions once received within the organisation
• GMMH is currently awaiting publication of this report, and will summarise key actions once received within the organisation
We also undertook and reviewed the reports of 59 local trust clinical audits in 2022/23. A full list of these local audits is included in Annex Five. Recommendations and action plans for each local audit has been agreed and shared with relevant people/services in line with our Clinical Audit Policy. If you are interested in learning more about the actions, we are taking to improve the quality of healthcare provided based on the outcomes of these audits, please contact:
Patrick Cahoon, Head of Quality Improvement
Email: Patrick.cahoon@gmmh.nhs.uk
of 87
Page 18
National confidential inquiry Questionnaires received from NCI 2022/2023 Questionnaires completed and returned back to NCI % Suicide 80 74 93%
2.3 Participation in Clinical Research
The NHS Constitution for England requires us to inform service users of any research opportunities that are available to them through which they may be able to improve potential outcomes for themselves and others. The level of research activity within GMMH continues to set us apart from many mental health Trusts nationally and this is illustrated by the ongoing success in obtaining external funding from the National Institute for Health and Care Research (NIHR) to carry out ground-breaking research led by Manchester researchers.
Research Funding
Our total NIHR grant income for 2022/23 for all active NIHR grants was £7,611,095 and this illustrates a year-on-year increase in NIHR income since the Trust was created in 2017 and a significant increase since last year which relates in part to multiple variations to contract due to COVID-19 delays.
Page 19 of 87
0 1,000,000 2,000,000 3,000,000 4,000,000 5,000,000 6,000,000 7,000,000 8,000,000 2017/18 2018/19 2019/20 2020/21 2021/22 2022/23
Total NIHR Grant and Fellowship income by year (£)
We have also received notification of six successful NIHR grant awards since April 2022 including funding for a randomised controlled looking at a novel dialogical therapy (Talking with Voices) led by one of our very successful postdoctoral lived experience researchers, Dr Eleanor Longden. All of these awards will run over the next three to five years:
A novel dialogical therapy (Talking With Voices) in comparison to treatment as usual in adults with distressing and persistent auditory hallucinations: A randomised controlled trial to investigate the efficacy of a treatment strategy targeted at trauma-related mechanisms
NIHR grant income also generates Research Capability Funding (RCF) from the NIHR which enables us to support research growth across the Trust. In 2022/23 the Trust received £1,473,755 which has enabled us to support essential growth of our research support service and the continuation of support for our 10 established Research Units.
Page 20 of 87
Lead Title Funding Stream Value Dr Peter Taylor Cognitive Analytic Therapy for SelfInjury: A feasibility trial Research for Patient Benefit £210,232 Dr Lora Capobianco Cardiac Rehabilitation for Young People: A Single-Blind Randomised Acceptability and Feasibility Study of an Integrated Physical and Mental Health Approach Research for Patient Benefit £257,430 Dr Lynsey Gregg Parenting Intervention for Parents with Psychosis in Adult Mental Health Services (PIPPA): An acceptability and feasibility trial Research for Patient Benefit £249,346 Prof Bernadka Dubicka BAY: Behavioural Activation for Young people with depression in specialist child and adolescent mental health services. Health Technology Assessment £2,089,442 Dr Cintia Fajia Co-developing
Therapies
long-term
patients
and anxiety Research for Patient Benefit £149,316 Eleanor Longden
Improving Access to Psychological
(IAPT) services to improve
benefits for
with depression
Efficacy and Mechanism Evaluation £1,413,526
Each unit has committed to submitting applications for further research funding as well as demonstrating service user involvement, integration with clinical services, opportunities for service users to participate in research and a commitment to ensuring equal access to research across the communities we serve.


Research Delivery
During 2022/23, over 1,500 service users, staff, relatives, and carers participated in externally funded research projects approved by the Health Research Authority in GMMH. This is a decrease compared to 2021/22 however GMMH is ranked 5th out of 46 NHS Trusts recruiting to mental health studies and 9th of 45 NHS Trusts recruiting to dementia studies (Quarter 3 data from GM Clinical Research Network).
Throughout the year, we have been able to offer our communities the opportunity to participate in over 85 research studies with many studies adapted to allow full or partial delivery of the research remotely as a result of new ways of working following the pandemic. Our study portfolio includes 37 interventional trials including 12 Clinical Trials of Investigational Medicinal Products and 15 studies sponsored by GMMH. This demonstrates an increase in all categories compared to 2021/22.
Page 21 of 87
Anxiety, Depression and Psychological Therapies Research Unit (ADePT-RU) Team
Bringing Research to our Service Users
Research in GMMH is not just about study participation but involvement in every aspect of the research process. Research and Innovation is at the heart of everything we do at GMMH. It is a key part of the NHS constitution and a strategic priority for the Trust.
We want to make sure that our staff, service users and carers have every opportunity to take part in and benefit from research and innovation. We want to use research and innovation to help close the inequalities gap and improve clinical services and outcomes. And we want to empower staff with the latest information about evidence-based practice.
Service user involvement is central to our 2021/24 Research and Innovation strategy and is a key deliverable for all Research Units. This allows our service users to contribute to the development of research questions and the design, conduct and dissemination of all research studies including clinical trials.
Alongside well-established Service User Reference Groups and Lived Experience Advisory Panels within our Research Units, the Research and Innovation workforce is enhanced by people in post who have been employed on the basis of their lived experience or who use their lived experience to lead their own research or grant/fellowship applications. This will be enhanced in 2023/24 by a Lived Experience Mental Health Research Involvement Officer.
Impact of Research and Innovation
Our established Research Units continue to support Trust-wide quality improvements, specifically in relation to implementation of trauma informed care, access to psychological therapies for service users with serious mental health conditions (psychosis, bipolar, personality disorder), physical health initiatives, equality, diversity and inclusion workstreams, and digital workstreams
Following successful delivery of a randomised controlled trial in GMMH testing automated virtual reality cognitive therapy for patients with fears in everyday social situations (the gameChange Trial – led by Oxford Health), an implementation project is delivering the gameChange virtual reality intervention within three GMMH Early Intervention Teams and two Community Mental Health Teams. GMMH is the only site nationally to have overcome the initial barriers to implementation and to have commenced real-world implementation. Preliminary analyses suggest this brief intervention, delivered by peer support workers and assistant psychologists, is resulting in large, clinically significant reductions in agoraphobic avoidance. For further information about our Research and Innovation work streams please contact:
 Sarah Leo, Head of Research and Innovation Office
Sarah Leo, Head of Research and Innovation Office
Email: sarah.leo@gmmh.nhs.uk or researchoffice@gmmh.nhs.uk
Page 22 of 87
2.4 Commissioning for Quality and Innovation (CQUIN)
For 2022/23, zero proportion of GMMH’s income was conditional upon achieving quality improvement and innovation goals agreed between GMMH and any person or body they entered into a contract, agreement or arrangement with for the provision of relevant health services, through the Commissioning for Quality and Innovation (CQUIN) payment framework.
There are two categories of CQUINs in 2022/23 – national CCG commissioned services CQUINs and NHS England commissioned service CQUINs. These CQUINs are for a twelvemonth period (April 2022 to March 2023) and are summarised below: -
National CCG/ICB indicators
CCG1:Staff Flu Vaccinations
The aim of this CQUIN is to achieve a 90% uptake of flu vaccinations by frontline clinical staff. Staff flu vaccinations are a crucial lever for reducing the spread of flu during the winter months, where it can significantly impact on the health of patients, staff, their families and the overall running of NHS services. GMMH ran a comprehensive flu campaign with dedicated flu fighters and incentives to promote vaccination. The position as at Q4 was 29%, which is below target. However, we know additional staff have received the vaccination in the community (from their GPs or local pharmacies) and not all of this activity is able to be captured.
CCG9: Cirrhosis and fibrosis tests
for alcohol dependent patients
NICE Guidance recommends that people who are alcohol dependent should receive a test for fibrosis and cirrhosis. This proposal aims to support the consistent delivery of that pathway of care and it can be delivered without additional investment or training, and within existing pathways. This CQUIN has a target to achieve 35%. This CQUIN is not being pursued due to the lack of onward pathway for people whose scan suggests ongoing care is needed.
CCG10: Outcome measure across specified mental health services
CCG10a: Routine outcome monitoring in Children and Young People (CYP) and perinatal mental health services
Achieving 40% of children and young people and women in the perinatal period accessing mental health services, having their outcomes measured at least twice. The achievement of this CQUIN is improving but remains a challenge. At Q4, both CYP at 13% and perinatal services at 11% were below the target.
CCG10b: Routine outcome monitoring in community mental health services
Achieving 40% of adults and older adults accessing select Community Mental Health Services (CMHSs), having their outcomes measure recorded at least twice. In order to meet the requirements of this indicator, Patient Reported Outcome Measures (PROMs) data is submitted (either in combination with Clinician Reported Outcome Measures (CROMs), or only PROMs)
Page 23 of 87
as part of the numerator for this CQUIN during the financial year. The position as at quarter four shows GMMH below target at 33%.
CCG11: Use of anxiety disorder specific measures in IAPT
Achieving 65% of referrals with a specific anxiety disorder problem descriptor finishing a course of treatment having paired scores recorded on the specified Anxiety Disorder Specific Measure (ADSM). GMMH achieved the 65% target for this CQUIN at Q4
CCG12: Biopsychosocial assessments by MH liaison services
Achieving 80% of self-harm referrals receiving a biopsychosocial assessment concordant with NICE guidelines. The target for this CQUIN has been met as at Q4
NHS England Indicators
These CQUIN schemes apply to our specialist services commissioned by NHS England
PSS6: Delivery of formulation or review within six weeks of admission, as part of a dynamic assessment process for admissions within Tier 4 CYPMH settings
The proportion of inpatients with a formulation or review that has been shared in the appropriate format with the young person, carers and community key workers as part of a dynamic assessment process. Performance is reported with a slight time lag, but latest figures show the target was achieved in Q4
PSS7: Supporting QI in the use of restrictive practice in Tier 4 CYPMH settings
The MHSDS RI CQUIN score. This is an overall assessment of data quality for each provider, based on a list of key MHSDS data items listed. The MHSDS RI CQUIN score is defined as the mean of all the data item scores for percentage valid and complete, multiplied by a coverage score for the MHSDS. Position against target has improved during the year, and work continues to increase compliance further. The latest available data for this indicator shows GMMH compliance at 60.8% against an 80% target. A related CQUIN is in operation for 2023/24 to support an increase in compliance in this area.
PSS8: Outcome measurement in perinatal inpatient services
The proportion of women accessing perinatal Mental Health services within Specialised Mother and Baby Units (MBUs) having paired scores recorded on the specific outcome measures required. At Quarter 4, GMMH compliance was at 78% against a 95% target for the clinically reported outcome measure (CROM) and at 5.6% against a 55% target for the patient reported outcome measure (PROM). Whilst there have been significant improvements in the CROM, there has been a poor compliance with the PROM which has not shown sustained improvement. A review has shown that in several cases, additional patients have had the paired CROM, but the paired one has occurred within a few days of discharge. Work is underway with the team to ensure that the paired rating is completed before the episode of care is closed.
Page 24 of 87
Further details and information in relation to the CQUIN schemes that relate to GMMH services can be provided by contacting:
Ali Rehman, Deputy Director of
Email: Ali.Rehman@gmmh.nhs.uk
Performance and Business Intelligence
2.5 Registration with the Care Quality Commission (CQC)
GMMH received the following warning notices throughout 2022/23:
In November 2022, the CQC published a report following an inspection of services provided by GMMH. Unannounced inspections were carried out at the following services in June after CQC received concerns about the safety and quality of care being provided:
• Acute wards for adults of working age and psychiatric intensive care units (PICU)
• Forensic inpatient and secure wards
• Mental health crisis services and health-based places of safety.
CQC also carried out an announced inspection in July of how well-led the trust is overall. However, due to concerns about services provided by the trust - including community mental
Page 25 of 87
Service/Area of Focus Date of Issue Date Action Required By Community-based mental health services for Adults of Working Age – Central Manchester CMHTs 27/04/2022 31/07/2022 Fire and ligature safety – Acute Wards for Adults of Working Age and PICU and Forensic Inpatients or Secure Wards 06/07/2022 31/07/2022 Medicines management - HMP Wymott 30/08/2022 25/10/2022 Safe staffing and governance 23/09/2022 31/12/2022 – Safe Staffing 31/03/2023 – Governance Community-based mental health services for Adults of Working Age – Central Manchester CMHTs 04/11/2022 04/01/2023 Woodlands Hospital 20/12/2022 31/01/2023 30/03/2023
health services, prison services and older people’s services - which came to light since this inspection, it was necessary to conduct further inspections, and the overall trust rating including for well-led has been suspended as a result. The rating suspension will remain in place until CQC returns to the trust to carry out a further trust-wide well-led inspection.
Following the June inspection, the overall rating for the acute wards for adults and PICUs deteriorated from good to inadequate. The safe and well led domains also dropped to inadequate. The ratings for effective, caring and responsive moved from good to requires improvement.
The overall rating for forensic inpatient and secure wards dropped from good to inadequate, as have the safe and well-led ratings. How effective, caring and responsive the service is has declined from good to requires improvement. However, the mental health crisis services and health-based places of safety remained rated as good overall and for being safe, effective, caring, responsive and well-led.
As a result of these inspections CQC took enforcement action, serving the trust with six Section 29A warning notices - one relating to ligature and fire risks, and another relating to staffing and governance, requiring significant improvements within a set timescale. A further inspection has been carried out to ensure action has been taken to comply with the warning notices. CQC will continue to monitor the progress of the other areas for improvement through the system improvement board and their usual inspection regime
CQC have also recently carried out inspections at other GMMH services including HMP Wymott and HMP Garth. Both services were inspected by CQC to follow up on information received regarding concerns around medicines management. CQC also inspected communitybased mental health services for adults of working age to follow up on previous enforcement action, and an inspection of wards for older people with mental health needs was carried out in response to receiving whistleblowing concerns.
Following the inspections in June and July, the undercover footage regarding the Edenfield Centre was broadcast by the BBC. In response CQC has been working with the trust, the local authority safeguarding team, NHS England and Greater Manchester Police as well as other partners to ensure patients were safe. The trust carried out clinical reviews of people affected, and they immediately suspended and subsequently dismissed a number of staff. CQC suspended the trust’s ratings for forensic inpatient and secure wards until this report was published, due to concerns about the quality and safety of services. CQC will continue to work closely with NHS England, as well as other partners to ensure urgent improvements are made and embedded.
Page 26 of 87
2.6 CQC Mental Health Act Monitoring
The CQC have now resumed ‘in-person’ visits to undertake CQC Mental Health Act Reviews of inpatient services following the ending of the interim methodology introduced during the period of the Coronavirus pandemic.
Between 1 April 2022 and 31 March 2023, the CQC undertook Mental Health Act reviews for the following GMMH wards:
• Salford – Eagleton, Loweswater Ward (MacColl), Delamere Ward, Chaucer Unit,
• Manchester
• SSN – John Denmark Unit, Gardener Unit, Derwent Ward, Borrowdale Ward, Dovedale Ward, Griffin Ward, Eskdale Ward.
• Trafford – Bollin and Greenway, Brook Ward, Beech Ward
• Wigan – Prospect Ward, Priestner’s Unit, Sovereign Ward
• Bolton – Oak Ward,
• Rehab – Honeysuckle Lodge
2.7 Data Quality
The Trust recognises that accurate, complete, and timely information is vital to support both the delivery of safe and efficient patient care and the management, planning, and monitoring of its services.
GMMH submitted records during 2022/23 to the Secondary Uses Service (SUS) via the MHSDS for inclusion in the Hospital Episodes Statistics, which are included in the latest published data (October 2022).
The percentage of records in the published data:
• Which included the patients valid NHS Number was: 100%
• Which included the patient’s valid General Medical Practice Code was: 100%
During 2022/23 GMMH has continued to build on the improvements of previous years, to ensure that the importance of accurate data quality and effective collection processes are fully embedded across the organisation.
This is achieved by:
• Including a specific sub workstream on data quality and visibility as part of the Trusts Improvement plan and receiving support from the National Making Data Count team
Page 27 of 87
• Reviewing all Information Quality Assurance policies and procedures every three years as required as part of our assurance processes for the Data Security and Protection Toolkit.
• Providing constructive and supportive feedback to colleagues when data quality errors are identified.
• Undertaking a proactive programme of audits throughout the year, the findings of which inform the Trust on areas of strengths and weaknesses and ultimately guide ongoing developments.
• Continuing to communicate key messages regarding accurate recording of clinical activity.
2.8 Information Governance
At GMMH, we aim to deliver excellence in Information Governance by ensuring that information is collated, stored, used, transferred, and disposed of, securely, efficiently, and effectively and that all our processes adhere to national mandates and legal requirements.
This ensures that information is accessible when needed, to support the delivery of the best possible care to our service users. All our Information Governance polices are reviewed every three years and the Trust is fully compliant with the Data Security and Protection (DS&P) toolkit which outlines the management requirements of all service user, staff, and organisational information in terms of the Data Protection Act (2018), GDPR and all other relevant legislation. The DS&P toolkit sets national standards for achievement to ensure that organisations maintain high levels of security and confidentiality of information at all times. The timeline for submission of the annual DS&P is end of June 2023.
Due to the timing of the quality account and the final submission date of the DS&P, we are currently unable to update the outcome of the submission for 2022/23, however, indications suggest previous years standards have been maintained.
2.9 Clinical Coding
GMMH outsources its clinical coding processes. This arrangement is audited for accuracy annually by an external expert as part of the Data Security and Protection toolkit submission. During 2022/23 the audit report confirmed an accuracy level of 98% for primary diagnosis and 84.3% for secondary diagnosis against a sample of 51 randomly selected patient records. This has reaffirmed Trust’s confidence in the existing system. GMMH will continue to work with clinicians to maintain the high levels of clinical coding accuracy.
Page 28 of 87
2.10 Department of Health Mandatory Quality Indicators
2.10.1 Preventing People from Dying Prematurely - Seven Day Follow-Up
As above please note that the national KPI is in relation to seven day follow up has now been retired. The Trust has continued to report locally on this indicator at Board and team level.
GMMH achieved the Long-Term Plan for Mental Health target of >80% of patients who were followed up within 72 hours after discharge from psychiatric inpatient care.
The latest available local figures are as at the end of Q4 and are set out as follows:
The performance set out above demonstrates that GMMH achieved the 80% target set out in the Long-Term Plan for mental health for 72 hour follow up in Q4. The Trust has continued to report on the seven day follow up target through local commissioner reporting. All our staff understand the clinical evidence underpinning this target and are committed to improving clinical outcomes for patients. GMMH continue to take the following actions to consolidate this performance, and in doing so, the quality of our services:
• Review individual breaches to ensure best practice can be shared and identify learning opportunities to minimise breaches wherever possible.
• Identify any potential training issues as they arise, and provide training to address these issues, particularly for new staff.
• Review our operational and data quality policies and procedures to ensure they reflect quality and safety best practice for service users and provide clear guidance for staff.
Page 29 of 87
Performance 72-hour Follow-Up YTD Q4 2022-23 GMMH 84.3% Performance Seven Day Follow-Up YTD Q4 2022-23 GMMH 93.1%
2.10.2 Enhancing Quality of Life for People with Long-term Conditions –Gatekeeping
As above please note that the national reporting for Gatekeeping has now been retired. GMMH have continued to report locally on this indicator, which is included in commissioner reporting.
GMMH achieved the target of >95% of admissions to acute wards for which the Crisis Resolution Home Treatment Team acted as a gatekeeper during the reporting period.
The latest available local figures are as at the end of Q4 and are set out as follows:
Gatekeeping
Performance
YTD Q4 2022-2023
GMMH 95.4%
GMMH achieved this target in Q4
All our staff are committed to improving clinical outcomes for patients. Individual breaches are reviewed to ensure best practice can be shared and learning opportunities identified.
2.10.3 Ensuring that People have a Positive Experience of Care – Staff Survey

The GMMH National Staff Survey results were published and widely shared earlier this year. We used the NHS People Promise as our foundation for engagement and employee experience and aligned the National Staff Survey results to these themes. It is vitally important to us that we know how things really are for our staff, and by encouraging our colleagues to complete the Staff Survey, the quarterly pulse survey and attending our internal Listening Labs, this is helping us to do this. The NHS staff survey is conducted annually.
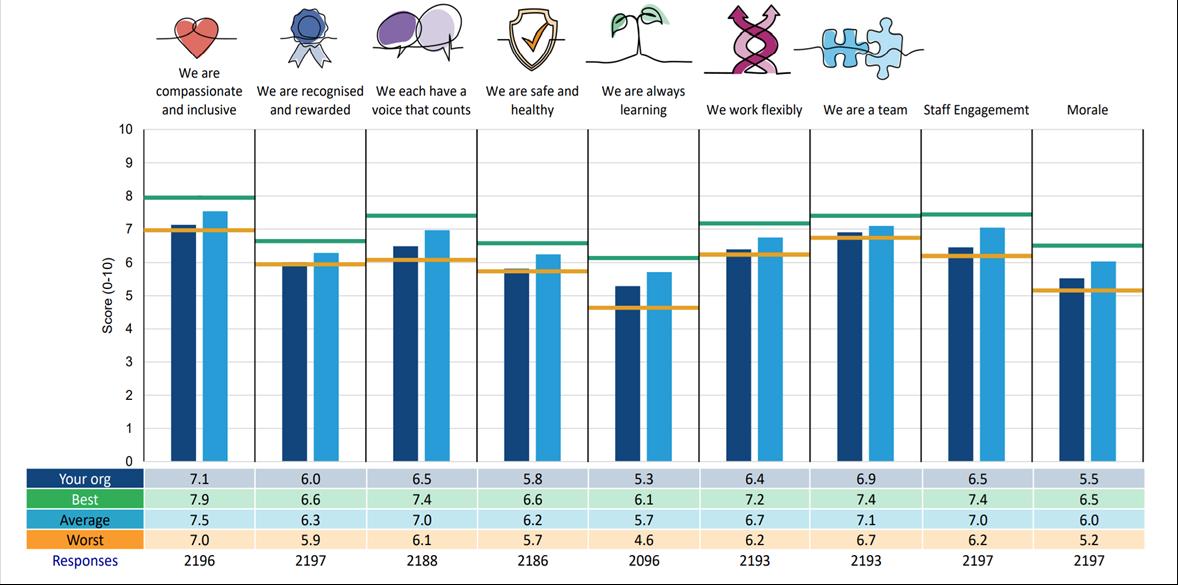
For 2022/23 the survey questions continue to align to the seven elements of the NHS ‘People Promise’ and retain the two previous themes of engagement and morale. These replaced the ten indicator themes used in previous years. All indicators are based on a score out of 10 for specific questions with the indicator score being the average of those.
The response rate to the 2022/23 survey among trust staff was 36% compared to 47% in 2021/22.
Page 30 of 87
2022/23 and 2021/22 Survey Data
2.10.3 Ensuring that People have a Positive Experience of Care – Staff Survey
The GMMH National Staff Survey results were published and widely shared earlier this year. We used the NHS People Promise as our foundation for engagement and employee experience and aligned the National Staff Survey results to these themes. It is vitally important to us that we know how things really are for our staff, and by encouraging our colleagues to complete the Staff Survey, the quarterly pulse survey and attending our internal Listening Labs, this is helping us to do this.
The NHS staff survey is conducted annually. For 2022/23 the survey questions continue to align to the seven elements of the NHS ‘People Promise’ and retain the two previous themes of engagement and morale. These replaced the ten indicator themes used in previous years. All indicators are based on a score out of 10 for specific questions with the indicator score being the average of those.
The response rate to the 2022/23 survey among trust staff was 36% compared to 47% in 2021/22.
2022/23 and 2021/22 Survey Data
Scores for each indicator together with that of the survey benchmarking group (other Mental Health, Mental Health & Learning Disability and Learning Disability & Community Trusts) are presented below:
The chart below shows how the Trusts scores compare to the best, worst and average scores in each of the themes within the people promise for the 2022 Staff Survey.
Page 31 of 87
Indicators (‘People Promise’ elements and themes) 2022/23 2021/22 Trust score Benchmarking group score Trust score Benchmarking group score People Promise: We are compassionate and inclusive 7.1 7.5 7.4 7.5 We are recognised and rewarded 6.0 6.3 6.3 6.3 We each have a voice that counts 6.5 7.0 6.8 7.0 We are safe and healthy 5.8 6.2 6.0 6.2 We are always learning 5.3 5.7 5.5 5.6 We work flexibly 6.4 6.7 6.6 6.7 We are a team 6.9 7.1 7.0 7.1 Staff engagement 6.5 7.0 6.8 7.0 Morale 5.5 6.0 5.8 6.0
All of the People Promise elements, themes and sub-scores are scored on a 0-10 scale, where a higher score is more positive than a lower score.
2020/21 Survey Data (For comparison)
Scores for each indicator together with that of the survey benchmarking group (other Mental Health, Mental Health & Learning Disability and Learning Disability & Community Trusts) are presented below.
2020/21 staff survey scores – benchmarked
Page 32 of 87
Category Trust score Benchmarking group score Equality, Diversity and Inclusion 9.0 9.1 Health and Wellbeing 6.2 6.4 Immediate Managers 7.4 7.3 Morale 6.3 6.4 Quality of Care 7.3 7.5 Safe Environment – Bullying and Harassment 8.1 8.3 Safe Environment – Violence 9.2 9.5 Safety Culture 6.8 6.9 Staff Engagement 7.0 7.2 Team Working 6.8 7.0
There is no question, that this last year has been very tough for us at GMMH. The engagement results reflect just how tough it has been. Some of the results are a difficult read, however, what our staff have told us is being both recognised and heard.
We are committed to making things better where we can, and where we might not be able to change things, we will explain why we can’t.
In a nutshell, we know we must ensure that our purpose and focus is clear, and that we act to support our aim that patient care truly is at the heart of what we do. We also know that we must act on concerns raised and provide our staff with a safe environment to do so, that we must support our staff to feel better in work, and that we do all we can to help manage burnout. We absolutely must also demonstrate our appreciation for the valuable contribution and commitment our staff make to our patients and our Trust – we really do recognise the incredible work they do, and we know at a senior level, and want to get better at showing this.
Our staff survey this year also highlighted several areas that we were very proud to read, this includes feedback that local line management is supportive and overall, there is good recognition given to staff from their immediate leaders, and that teams locally, work well together and overall have positive working relationships. We are currently undertaking further analysis on the results and will be working with Care Group/Divisional senior leaders to roll out the local results and develop tailored action plans.
2.10.4 Ensuring People have a Positive Experience of Care – Community Mental Health Patient Survey
The 2022 survey of people who use community mental health services involved 53 providers of NHS mental health services in England. People aged 18 and over were eligible for the survey if they (1) had received specialist care or treatment for a mental health condition, (2) had at least one contact between 1 September and 30 November 2021, as well as at least one other contact either before, during or after the sampling period, and (3) were not a current inpatient.
The Care Quality Commission will use the results from this survey in their regulation, monitoring and inspection of NHS trusts in England. They will use data from the survey in CQC Insight, which provides inspectors with an assessment of performance in areas of care within an NHS trust. They also include survey data in the evidence appendices that they produce for inspections.
This year saw the addition of the following questions to the survey:
• ‘Thinking about the last time you contacted this person; did you get the help you needed?’
• ‘How do you feel about the length of time it took you to get through to this person or team?’
Page 33 of 87
In addition, a new category of questions around ‘responsive care’ was added with the below questions included:
• ‘In the last 12 months, have you and someone from NHS mental health services agreed how your care and treatment will be delivered?’
• ‘Have you received your care and treatment in the way you agreed?’
This year saw the removal of the following questions from the survey:
• ‘In the last 12 months, were care and services available when you needed them?’
• ‘Were you informed how the care and treatment you were receiving would change due to the coronavirus pandemic?’
Response Rate
For 2022, 219 responses were provided to the 1250 questionnaires for GMMH, which is a decrease on the 243 responses from 2021. This represents a response rate of 18%, which is a reduction on the response rate for the 2021 survey programme (20.2%). Additional information and posters have been developed in order to encourage service users to complete the survey. These have been distributed to Community Mental Health Team offices across GMMH. For next year’s survey programme, Care Coordinators will also be asked to encourage service users to complete a copy of the questionnaire, if they have received one.
The following table provides a summary of thematic scores highlighting the results for the 2022 community mental health survey. For each question in the survey, the individual (standardised) responses are converted into scores on a scale from zero to 10. A score of 10 represents the best possible response and a score of zero the worst. The higher the score for each question, the better the trust is performing. Thematic scoring takes into account the scores for each individual question, and then averages these to provide a single overall score.
The table also highlights the 2022 scores for GMMH, in comparison to the 53 providers of NHS mental health services in England, who participated in this year’s programme.
Page 34 of 87
Thematic section 2020 score 2021 score 2022 score Score in comparison to other trusts 1. Health and Social Care Workers 7.2 7.0 7.0 About the same 2. Organising Care 8.7 8.4 8.2 About the same 3. Planning Care 6.9 6.6 6.9 About the same 4. Reviewing Care 7.7 7.3 7.0 About the same 5. Crisis Care 7.0 6.9 6.2 About the same 6. Medicines 7.1 7.1 6.9 About the same
As the above table highlights, GMMH scored highest in relation to organising care (as in 2021), and lowest in relation to feedback (as in 2021).
High Level Summary
The section that follows provides an overall summary of all questions included within the 2022 survey programme. The below table includes a comparison to other mental health trusts, showing where GMMH scores were better, about the same, or worse.
Page 35 of 87
7. NHS Therapies 7.7 7.6 7.7 About the same 8. Support and Wellbeing 5.4 5.0 4.6 About the same 9. Feedback 2.4 2.1 2.0 About the same 10. Overall Views of Care and Services 7.6 7.2 7.0 About the same 11. Overall Experience 7.3 6.7 6.7 About the same 12. Responsive Care N/A N/A 7.7 About the same Category: Your Health and Social care Workers Question: 2020 score 2021 score 2022 score National comparison Were you given enough time to discuss your needs and treatment? 7.6 7.1 7.0 About the same Did the person or people you saw understand how your mental health needs affect other areas of your life? 7.0 6.8 6.9 About the same Did the person or people you saw appear to be aware of your treatment history? 6.9 7.0 7.0 About the same Category: Organising Care Question: 2020 score 2021 score 2022 score National comparison Have you been told who is in charge of organising your care and services? 7.6 7.8 7.1 About the same Do you know how to contact this person if you have a concern about your care? 9.9 9.5 9.5 About the same How well does this person organise the care and services you need? 8.5 8.0 8.4 About the same Thinking about the last time you contacted this person, did you get the help you needed? N/A N/A 8.0 About the same
Have you agreed with someone from NHS mental health services what care you will receive?
Were you involved as much as you wanted to be in agreeing what care you will receive?
Does this agreement on what care you will receive take your personal circumstances into account?
In the last 12 months have you had a formal meeting with someone from NHS mental health services to discuss how your care is working?
Did you feel that decisions were made together by you and the person you saw during this discussion?
Do you know who to contact out of office hours within the NHS if you have a crisis?
Thinking about the last time you tried to contact this person or team, did you get the help you needed?
How do you feel about the length of time it took you to get through to this person or team?
Page 36 of 87 Category: Planning Care Question: 2020 score 2021 score 2022 score National comparison
5.9 6.0 5.6 About the same
7.5 7.2 7.9
better
Somewhat
than expected
7.3 6.7 7.1 About the same Category:
Question: 2020 score 2021 score 2022 score National comparison
Reviewing Care
7.5 6.9 6.1 About the same
7.9 7.7 7.9 About the same Category: Crisis Care Question: 2020 score 2021 score 2022 score National comparison
7.0 7.1 6.6 About the same
7.0 6.7 6.8 About the same
N/A N/A 5.3 About the same
Has the purpose of your medicines ever been discussed with you?
Have the possible side-effects of your medicines ever been discussed with you?
In the last 12 months, has an NHS mental health worker checked with you about how you are getting on with your medicines?
Were these NHS therapies explained to you in a way you could understand?
Were you involved as much as you wanted to be in deciding what NHS therapies to use?
In the last 12 months, did NHS mental health services support you with your physical health needs (this might be an injury, a disability, or a condition such as diabetes, epilepsy etc?)
In the last 12 months, did NHS mental health services give you any help or advice with finding support for financial advice or benefits?
In the last 12 months, did NHS mental health services give you any help or advice with finding support for finding or keeping work?
Have NHS mental health services involved a member of your family or someone else close to you as much as you would like?
Page 37 of 87 Category:
Question: 2020 score 2021 score 2022 score National comparison
Medicines
7.7 7.7 8.0 About
same
the
5.8 5.7 5.8 About
same
the
7.9 7.9 6.8 About the same Category:
Question: 2020 score 2021 score 2022 score National comparison
NHS Therapies
8.3 8.1 7.9 About the same
7.0 7.0 7.5 About the same Category:
and
Question: 2020 score 2021 score 2022 score National comparison
Support
Wellbeing
5.6 5.3 4.8 About the same
4.9 4.4 3.7 About the same
4.2 3.4 3.4 About the same
7.1 7.1 6.6 About the same
Aside from in this questionnaire, in the last 12 months, have you been asked by NHS mental health services to give your views on the quality of your care?
Overall Views of Care and Services
In the last 12 months, do you feel you have seen NHS mental health services often enough for your needs?
Overall, in the last 12 months, did you feel that you were treated with respect and dignity by NHS mental health services?
In the last 12 months, have you and someone from NHS mental health services agreed how your care and treatment will be delivered?
Have you received your care and treatment in the way you agreed?
Page 38 of 87 Category:
Question: 2020 score 2021 score 2022 score National comparison
Feedback
2.4 2.1 2.0 About the same Category:
Question: 2020 score 2021 score 2022 score National comparison
6.8 6.3 6.0 About the same
8.4 8.3 8.1 About the same Category:
Question: 2020 score 2021 score 2022 score National comparison Overall, I had a very good experience. 7.3 6.7 6.7 About the same Category: Responsive Care Question: 2020 score 2021 score 2022 score National comparison
Overall Experience
N/A N/A 6.9 About the same
N/A N/A 8.5 About the same
During 2023/24, GMMH will ensure that we maintain momentum around the Trust feedback agenda. Text messaging has been in place during the year, and steps were taken to introduce ‘Share Your Views’ QR codes on all appointment letters, easy read posters in services and the launch of the GMMH You Said, We Did campaign.
Developments relating to feedback will also feed through Support and Well Being findings to the Trust Community Transformation Workforce Strategy Group to look at training needs and skill mix of staff including AHP’s.
2.10.5 Ensuring that People have a Positive Experience of Care – Friends and Family Test (FFT)
During 2022/23 we have reviewed our governance processes for measuring people’s experiences of care which now include monthly, quarterly and annual reporting to care groups and QIC that triangulate feedback received from FFT, experience surveys, compliments, concerns and complaints as well as that that is received anecdotally via service user engagement activities, ward and community meetings and that received via third parties e.g. Healthwatch, advocacy and the VCSE.
Feedback received via FFT and experience surveys has increase fourfold and now averages 1430 per quarter with 85% representing a positive experience of care. Our results in the 2022 CMHS tally with our experience surveys in that we have improved people’s experiences of engagement in their care, however, people need more support with wider health and social care needs. These findings have been fed through to our workforce committee in terms of skill mix of staff and community transformation team in terms of the models of care, and will subsequently feed through to the Improvement Plan Steering Group and respective workstreams.
Experience received from service users and carers via complaints and engagement activities tells us that we need to improve people’s experience of care, predominantly with regards to: communication, compassion and being trauma informed; working with families; access to and consistent care; least restrictive practices and transfer of care including partnership working. Again, all of these themes reach care groups and Trust level committees and the new Improvement Plan will quite rightly hold us to account in terms of setting SMART objectives, improving performance and involving service users and carers in these service improvements.
We have developed a draft plan for strengthening the voice of our service users and carers throughout the organisation and the inter relationship between improvement workstreams and committees will be key to ensuring that all improvements are informed by lived experience of mental health and service provision.
Page 39 of 87
2.10.6 Treating and Caring for People in a Safe Environment and Protecting them from Avoidable Harm – Patient Safety Incidents:

Information within this section of the Quality Account highlights the number and, where available, rate of patient safety incidents reported by GMMH to NHS Improvement via the National Reporting and Learning System (NRLS). There are a number of CQC improvement actions relating to this area. The data below includes the number and percentage of patient safety incidents that resulted in severe harm or death and compares this data against the national average along with the highest and lowest incidents reported by other mental health organisations.
Patient Safety
GMMH is committed to maintaining an open, honest, and timely reporting culture when incidents occur. In our improvement plan, referenced throughout this quality report, we have included a dedicated section with a robust set of actions linked to being an open and listening organisation. Timeliness for the reporting and reviewing of incidents is critical in enabling us to respond quickly to concerns that are identified to ensure the care we deliver is safe and of a high standard. The National Patient Safety Strategy, which was published in July 2019 which sits alongside the NHS Long Term Plan and Implementation Framework highlights that ‘those organisations who identify, contain and recover from errors as quickly as possible will be alert to the possibilities of learning and continuous improvement’.
Although there has been some delay in implementing the Strategy nationally, GMMH has identified Patient Safety Specialists who are registered with the National Patient Safety Team and who directly lead and support patient safety activity across the Trust. These identified specialists are part of a national and regional network who link together to share learning and good practice
The specialists have undertaken level one and two training in the national patient safety syllabus, and this is now available on the Learning Hub for all staff to access. Since May 2022, the Patient Safety Team have also developed and publish a monthly newsletter which promotes the training and includes any National updates. The Trust Patient Safety Practitioners, introduced in 2019, are linked into Care Groups and Senior Leadership Teams and work closely with operational staff so that information and learning in relation to the patient safety agenda can be shared. The Patient Safety Practitioners continue to work collaboratively with all our commissioners in relation to further strengthening the Trust Incident management and review processes.
Improving our in-patient environments has always been a key priority for GMMH. GMMH has included a dedicated section on patient safety, which will be a key focus of our improvement plan, as referenced throughout this report. The Trust is working in close collaboration with
Page 40 of 87
system partners to build further upon its environmental risk improvement and audit programme that takes place on an annual basis in partnership with our Risk and Safety Team, Facilities team, and Ward Managers from across the organisation. Any environmental risks identified during the annual audit programme are then escalated to senior managers and the board through the Trusts risk register and Board Assurance Framework for consideration of further action. The Trust SharePoint system has been adapted to enable our ward teams quick and easy access to their local environmental risk audits and action plans. Every ward induction checklist has been strengthened to include the location of identified environmental risks which will assist new staff and agency staff who work across our in-patient areas in maintaining the safety of service users.
During 2022/23 the Self-Harm Toolkit and Trust Self-harm Policy were reviewed and strengthened to reflect a Trauma Informed Care approach and updated with reference to Trauma Informed Care and ligature care plans.
To equip our staff with the skills to assess the risks of our service users to self and others the Trust clinical risk training package was reviewed and updated to include some of the learning from serious incident reviews and make it deliverable via Teams.
Some of the changes included involving carers in risk assessment and management plans and when to breach confidentiality, the use of professional curiosity when assessing risk and the use of protective factors, the things that may reduce someone’s risk level and ensuring these are individualised and put into context.
The Trust Clinical Risk Policy has been updated to reflect these changes and each Division has clinical risk training leads and a programme of training in place. Additionally, the risk tool currently in use is being developed to have a greater focus on risk formulation and capturing a services user’s story, the pilot for the new risk tool is likely to be implemented towards the latter part of 2023.
The data below indicates that the number of patient safety incidents resulting in severe harm or death is low in comparison to the number of patient safety incidents reported. This has been a consistent picture for the Trust year on year and demonstrates a culture of reporting and learning from incidents.
41 of 87
Page
Data Source: National Reporting and Learning System (NRLS). The data reported only includes data released by the NRLS in October 2022. This data includes the period of April 2018 to March 2022.
Page 42 of 87
Reporting period No of incidents occurring Rate per 1000 bed days No of incidents reported as severe harm % of incidents reported as severe harm No of incidents reported as death % of incidents reported as death Greater Manchester Mental Health NHS Foundation Trust Apr 2021March 2022 16874 52.4 25 0.1 56 0.3 Apr 2020March 2021 14485 Data not available 31 0.2 66 0.5 April 2019March 2020 13974 Data Not Available 30 n/a 51 n/a April 18March 2019 9517 Data not available 13 n/a 45 n/a Total number of incidents for mental health organisations Apr 2021March 2022 440969 Data not available 1658 0.4 2807 0.6 Apr 2020March 2021 424986 Data not available 1590 0.4 2864 0.7 April 2019March 2020 412371 Data not available 1449 n/a 2469 n/a April 18March 2019 356537 Data not available 1104 n/a 2598 n/a
Page 43 of 87 Highest value reported from any mental health organisation Apr 2021March 2022 21097 73.3 478 2.3 283 2.6 Oct 2019March 2020 20749 n/a 333 17.6 328 41.2 April 2019March 2020 7014 130.8 207 n/a 113 n/a April 18March 2019 18262 n/a 247 n/a 187 n/a Lowest value reported from any mental health organisation Apr 2021March 2022 8 n/a 0 n/a 0 n/a Oct 2019March 2020 34 21.4 0 0 0 0 April 2019March 2020 17 n/a 0 0 0 0 April 18March 2019 1189 n/a 0 0 0 0
*Please note that the data source for this data (NRLS) will be closing in September 2023 and will be replaced by the LFPSE system. This will mean the data for next year’s report will include both the historical NRLS figures and the LFPSE data.
*Benchmarking data reports from the NRLS continue to highlight that there is a positive and consistent incident reporting culture within the organisation. In accordance with the NRLS reporting criteria only deaths of current service users where the death is suspected to be as a result of an accident or suspected suicide are reported to the NRLS.
In the latest reporting period, there was an increase in total number of incidents in comparison to the last reporting period which can be attributed to the addition of Wigan Services in April 2021. However, the degree of harm has maintained with similar number of severe harm and deaths and over 95% of incidents reported being low harm or no harm and therefore required no further review.
Incident Reporting and Reviewing Processes
During 2021/22 the Trust’s Incident, Accident and Near Miss, policy and processes were audited by Mersey Internal Audit Authority (MIAA). The overall objective of the audit was to review the systems and processes in place relating to serious incidents, ensuring that controls are established and operating effectively and that policies and procedures relating to serious incidents comply with the Serious Incidents Framework, 2015.
Whilst the Trust received substantial assurance that showed that there is a good system in place to identify, manage and learn from serious incidents, we have seen from recent regulatory feedback and improvement work that we have more to do in respect of this. We are therefore undertaking a system review of our incident process in 2023/24.
2.10.7 Learning from Deaths Supporting Carers and Families
The Trust introduced a Bereavement Liaison Practitioner in 2018 to provide timely support to families and staff following an unexpected service user’s death. The role has provided direct support to families throughout the Trust internal review process and supported families during the coroner’s inquest process. The Bereavement Practitioner has delivered Grief awareness workshops to staff across the Trust on how to support families following a death including bespoke sessions for student nurses and staff working in perinatal services, further training workshops took place over 2022/23
The Trust is hoping to further develop the Bereavement Practitioner support as we recognise how critical this role is in supporting families and staff who are affected or bereaved in the event of all service user deaths and not only deaths by suicide The Trust records the death of all patients and reviews each thoroughly to ensure that the circumstances leading up to
Page 44 of 87
the patient’s death are clarified and any learning for the Trust is identified. The systems in place to do this continued throughout the COVID-19 pandemic.
During 1April 2022 to 31 March 2023 a total of 1203 GMMH patients died of these 28 are COVID-19 related. This is shown as number of deaths, which occurred in each quarter of that reporting period: There has been an increase of 84 deaths from 1119 total deaths reported in 2021/22 which can be attributed to the addition of Wigan Services in April 2021.
There is an increase of expected and unexpected outpatient deaths with little to no variation for inpatient deaths in comparison to 2021/22:
• Unexpected outpatient deaths show an increase of 20 (COVID-19 related has reduced by 20)
• Unexpected inpatient deaths show a decrease of one (COVID-19 related have remained at 0)
• Expected Outpatient’s deaths show an increase of 65 (COVID-19 related reduced by 11)
• Expected inpatient deaths remain the same (COVID-19 related has reduced by three)
• 326 deaths in the first quarter
• 298 deaths in the second quarter
• 342 deaths in the third quarter
• 237 deaths in the fourth quarter
*Inpatient deaths refer to those service users who are inpatient or former inpatients who died within three months of discharge.
During 1 April 2022 to 31 March 2023, 71 RCA’s have been commissioned in response to the above deaths reported (Please note that for more recent incidents these may not have been through the SI Panel process as of yet for decision on onward investigation). The data
Page 45 of 87
Quarter Unexpected Outpatient Unexpected Inpatient Expected Outpatient Expected Inpatient Total 1 169 6 147 4 326 2 176 6 109 7 298 3 196 6 138 2 342 4 130 1 103 3 237 Total: 671 19 497 16 1203
highlights a reduction in commissioned RCAs compared to the previous year of 81 RCAs commissioned for 2021/22 following the implementation of Facilitated Learning Events to share learning Division/Trust Wide.
The Trust ‘Learning from Deaths’ policy highlights to staff that all deaths should be reported through the GMMH Incident Risk Management System. All deaths including deaths of service users with an identified learning disability are reported and are then reviewed by the Trust Patient Safety Team. A 72-hour review is requested by the service for all unexpected deaths and for those expected deaths where care concerns have been identified by the service during the service users end of life pathway.
Where a completed 72-hour review has indicated significant care delivery concerns and areas for learning, further review will be carried out in the form of a Root Cause Analysis Investigation or Structured Judgement Review will be commissioned. Data relating to service user deaths is reviewed by the Trust Mortality Review Group and presented to the Trust Board of Directors meeting through the Trust quarterly Mortality Dashboard in accordance with the National Learning from Deaths Framework.
• 21 serious incident root cause analysis investigations, four case record reviews* in the first quarter.
• 27 serious incident root cause analysis investigations, 0 case record reviews* in the second quarter.
• 12 serious incident root cause analysis Investigations, three case record reviews* in the third quarter.
• 11 serious incident root cause analysis Investigations, 0 case note reviews* in the fourth quarter.
*Structured Judgement Reviews are referred to as ‘case record reviews’.
Zero representing 0% of the patient deaths during the reporting period are judged to be more likely than not to have been due to problems in the care provided to the patient.
As mandated, this is broken down by quarter as follows:
• Zero representing 0% in the first quarter.
• Zero representing 0% in the second quarter.
• Zero representing 0% in the third quarter.
• Zero representing 0% in the fourth quarter.
The National Quality Board Learning from Deaths Guidance published in March 2017 set out the key requirements ensuring organisations have mechanisms in place to effectively respond to, learn from and review all patient deaths. GMMH currently uses Root Cause
Page 46 of 87
Analysis as its primary investigatory methodology, in line with the requirements of the National Serious Incident Framework 2015 to review unexpected deaths. The Learning from Deaths Guidance also highlights the use by Trusts of the Structured Judgement Review (SJR) process as another method of reviewing deaths.
The SJR approach requires reviewers to make safety and quality judgements over six elements and phases of care accessed by a service user. In 2018 training for approximately 40 staff was delivered by the Yorkshire and Humber improvement academy who adapted the SJR Tool for mental health Trusts. More of this training will be commissioned during 2022 to ensure there are sufficient staff with the skills required to carry out these reviews.
Although most deaths that occur in the Trust are reviewed using the RCA methodology, the trust will use the SJR process where a 72-hour review has identified problems in care that may relate to treatment and management plans for those incidents relating to for example pressure ulcers, falls, some medication errors and VTEs. The SJR process helps to understand the reasons for poor care and define further action or learning for the organisation.
The SJR process was used to review all the expected inpatient deaths of people from COVID-19 to ensure the care they received was of good quality and adhered to guidelines in place at that time.
All reviews completed into a service user death are presented and reviewed by the Trust Serious Incident Review (SIR) panel or Post Incident Review (PIR) Panel. One of the significant functions of both the SIR and PIR panels is to review the findings from all reviews and ensure recommendations made within the serious Incident report address the overall root causes and key areas for action by the Trust to reduce the likelihood for further similar incidents to occur.
Learning from Serious Incidents
This workstream has received significant regulatory focus during 2022/23. The Trust continues to explore new methods of how learning from serious Incidents is effectively shared across the organisation. To support a positive, open and learning culture across GMMH a learning event is held following the completion of a serious incident review. Some learning events are held locally within the team or division that the incident occurred. Over the course of the year, GMMH has introduced larger Trust wide learning events where the details of either one incident or a group of similar incidents is shared with staff across the Trust. These continued to be held throughout 2022/23 on a monthly basis and are well received by staff in the Trust.
The Executive led Post Incident Review (PIR) Panel identify individual incidents or themes of incidents to be presented at the learning event, which occurs monthly. PIR panel members attend to introduce the learning event and to present any themes from incidents and what actions have been taken across the Trust in response to identified themes.
Page 47 of 87
Following the event, the Patient Safety Team summarise the incident and learning event in a briefing which is shared with all Care Groups and made available on the Trust Patient Safety Intranet page.
During 2022/23, there have been two learning events focusing on individual incidents and other events focusing on themes including CMHT zoning, prescribing and monitoring of clozapine, safeguarding, neglect and capacity and managing the deteriorating patient. These meetings have generated very positive feedback and have been really well attended, with between 120 to 150 people attending each event.
The Patient Safety Team has developed a ‘Lessons Learned’ newsletter that shares learning from incidents and reviews of incidents. The newsletter was launched in February 2021, is available on the intranet as well as being shared in the weekly Trust staff bulletin. Following feedback of this quarterly briefing it was developed into a briefer monthly newsletter in April 2022 In addition, lessons learned briefings continue to be used to provide a short briefing to staff regarding a particular subject. These briefings provide a mixture of new information such as learning from serious incidents or a reminder of information for teams to think about the application to practice within their teams such as Duty of Candour, self-harm, and red flags.
The Trust has adopted the principles of a ‘Just Culture’, a term that acknowledges that we are human and refers to a culture that demonstrates the fair treatment of staff who make errors and supports a culture of fairness, openness and learning in the NHS by making staff feel confident to speak up when things go wrong, rather than fearing blame.
The serious incident investigation training now incorporates how to use the Just Culture guide and a briefing has been produced to explain the process to staff. The Trust is also testing out alternative reviews to ascertain learning from incidents as outlined in the Patient Safety Strategy.
The Trust will be delivering a programme of work during 2023/24 to both improve on how we manage our serious incident processes and in how we learn from these. To ensure these approaches can become embedded, the patient safety team will work with the Care Group Leadership and provide support and training to staff across the Divisions.
Datix is the risk management system used by the Trust. This system is used to report and manage incidents, and on average there are 100 to 120 incidents reported daily. When an incident is reported it sits in a holding area until it is reviewed by the manager of the service. The work we are undertaking will help us to improve timeliness and ensure that this happens as soon as is possible.
Actions to support delivery of this will include developing process flowcharts on the management of incidents through Datix clarifying role of incident manager, and developing training for managers on how to record and manage an incident. GMMH will ensure steps are taken to share this process with all appropriate staff with timeframes for completion, offering support and/or training from the patient safety and incident teams.
Page 48 of 87
The Trust’s Incident team will check all incidents daily to ensure any serious incident are identified. The Trust will also ensure all Corporate Services have identified managers to regularly review incidents, and that all Corporate Managers are provided with bespoke incident management training
GMMH will also undertake a programme of work during 2023/24 to reduce the number of outstanding 72-hour reviews whilst ensuring that any serious incidents are identified to have further review undertaken by end June 2023. To support this, the trust will develop a process flowchart and escalation process for 72-hour reviews. Training will be put in place and delivered to all appropriate staff, with oversight from the staff through Associate Director’s of Quality and Health Professionals. The patient safety team will appraise all overdue 72-hour reviews to see what can be stepped down or closed and identify how many 72-hour reviews require further investigation so that this can be progressed within clear, agreed timescales.
The Trust will also take steps to reduce the number of outstanding Root Cause Analysis Investigations (RCA’s) by the end of June 2023 and ensure that timeframes are adhered to for the completion of 80% of RCA’s by end September 2023. To achieve this, GMMH will identify any delays for any open RCA’s, including what support is required to complete the RCA within an expected completion date. We will review and update RCA flowcharts to include escalation processes. We will compile a list of all RCA trained staff, highlighting current role, and professional background, to include any obstacles to completing RCA. We will also deliver RCA training to identified staff/staff groups and develop a standard operating procedure and evaluation framework for a pilot investigation team.
Monitoring for these developments will include weekly progress reports to each Division and Care group leadership team, progress monitored in Serious Incident Panel (SIP), and a monthly report to the GMMH Audit Committee.
Learning and Dissemination of Good Practice Review 2022 – Mersey Internal Audit Agency (MIAA)
In June 2022, MIAA carried out a review of how the Trust learns and disseminates good practice. The report findings were published in September 2022, and identified that the Trust has established and well documented processes and controls, to ensure that actions identified as a result of serious incidents are monitored to completion and that lessons learned are identified and appropriately disseminated.
Discussions confirmed that there is no Trust wide Learning Lessons Framework in place, however, they were advised that the Trust will be implementing the Patient Safety Incident Response Framework (PSIRF) introduced by NHS England in August 2022 and details of the new process is regularly being reported to the Trust Board. It was however noted that on a Trust wide level, assurances regarding lessons learned are regularly received by the Serious Incident Panel (SIP) Panel, Post Incident Review Panel (PIR) Panel and the Quality Improvement Committee (QIC) and ultimately by the Trust Board.
Page 49 of 87
Hate Crime
At GMMH, we have taken a number of steps to help tackle racism and launched our first Hate Crime Protocol in October 2020 as part of National Hate Crime Awareness Week. We are committed to protecting and safeguarding all our employees, service users and visitors within our Trust from hate crimes.
The key priority of the organisation is to raise awareness and enhance society's perception and understanding of what constitutes a hate crime, to challenge inequality and to celebrate the diverse make up of our society. The hate crime group won the award for Creating a Diverse and Inclusive Place to Work at the annual GMMH staff awards in December for the work done on developing the protocol and online training for staff. To support this a hate crime button has been located on the Trust intranet and internet pages to enable people to report a hate crime to the police or to report online hate material.
2.11 Freedom to Speak Up
GMMH has adopted the national ‘Freedom to Speak Up’ Policy to promote an open culture across the Trust to ensure staff feel safe to report incidents and raise concerns, this means that staff are encouraged to speak up in a variety of forums, whether that be directly to their line manager, a more senior manager or to the Trust’s Freedom to Speak Up Guardians. We recognise that this is a key area for the Trust.
The Trust has a nationally registered Freedom to Speak up Guardian and a deputy whose roles are to support and enable staff to raise concerns. The guardians are championed by three trust board members, the CEO, the Chair and a Non-executive director. The Freedom to Speak Up Guardians report directly to this group and meet on a quarterly basis with them.
In line with the national policy, staff are encouraged to raise concerns with line managers and line managers are encouraged to listen and act on staff’s concerns. It is appreciated that, at times, staff may not feel able to do this and the role of the Freedom to Speak Up Team is widely promoted through a variety of methods including through the Corporate Welcome Day, as a continual feature on the Intranet Site, posters, and wide coverage within operational meetings held throughout the organisation.
The Trust reports quarterly to the National Guardian’s Office on the number of speaking up cases, and in addition reports twice a year directly to the Trust Board. These reports contain information in relation to the number of cases, and locally the themes of cases to encourage organisational learning.
The Freedom to Speak Up Team work closely with Trade Union Representatives and others in trusted roles. They have also taken recent steps to refresh the role of the “Freedom to Speak Up Champions” following the new National Guardian’s office guidance on this role and to expand their numbers to create a network that covers the whole Trust. The champions will act as advocates for the Freedom to Speak Up process and guide staff accordingly when concerns may arise. The Trust is committed to ensuring that staff do not
Page 50 of 87
suffer any detriment as a result of speaking up. Any indicator of such detriment will be dealt with immediately at the highest levels of the Trust.

Freedom to Speak Up is regularly promoted through engagement visits to Wards and other work areas within the organisation to ensure that staff know there is still a process for hearing their concerns if they are not being heard in their part of the trust.
Once the Freedom to speak up team have met with a staff member, they will seek to feedback action responses in way best suited to the staff member raising the concern. The team will then maintain contact with the member of staff until they feel their concern has been heard and acted upon. The Trust improvement plan has actions which focus on the expansion of the freedom to speak up team, provision of an anonymous feedback route, freedom to speak up training for all staff, and cultural developments to promote more openness and safety to raise concerns
2.12 Increasing Community Mental Health Services Capacity
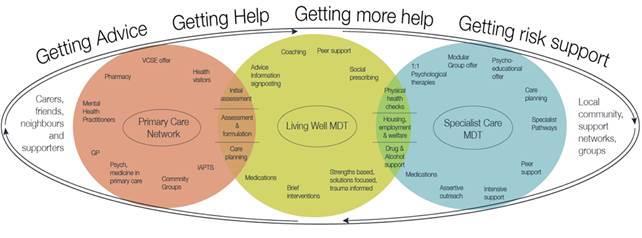
The national strategic vision is “to address the gap and achieve radical change in the design of community mental health care by moving away from siloed, hard-to-reach services towards joined up care and whole population approaches and establishing a revitalised purpose and identity for community mental health services.” The approach to delivery is as outlined in the Community Mental Health Framework for Adults and Older Adults (NHSE/I and NCCMH, 2019) and the Greater Manchester Community Mental Health Transformation prospectus (GMHSCP, February 2021).
The programme of work under Community Transformation is in response to The Community Mental Health Framework (NHSE 2019). The overall aim is to increase continuity of care by increasing capacity in the system across primary and secondary care, and by moving away from CPA care coordination towards a MDT approach that will mean team members share cases, manage risk together, can address a wider range of needs, and individual staff can deepen their own clinical practice.
The Community Mental Health Transformation Programme provides the opportunity for the planning and delivery of integrated and effective place-based care, working across the GM footprint. The GM Community Mental Health Transformation Programme model is summarised below.
Living Well MDT progress summary:
Location Summary
Salford Live in Broughton PCN and Ordsall and Claremont PCN. Citywide rollout to be complete by end of March 2023.
Bolton
The Living Well Hub One prototype in Farnworth and Kearsley PCN went live in June 2022 and is progressing well. Prototyping has commenced in three neighbourhoods with further roll out planned from April 2023. Full model to be implemented by April 2024
Manchester
Prototype MDT staffing model agreed by the planning group and is awaiting financial sign off. Projected commencement of prototypes May 2023
Trafford Prototyping to commence in North and Central PCNs in February 2023
Wigan Prototyping to commence in Hindley in March 2023.
Specialist Care Redesign
The Community Mental Health Transformation programme provides a unique opportunity to change the way services are designed and delivered alongside addressing persistent areas of concern. The timing and successful redesign of the Specialist Care MDT phase is interdependent on the LW systems being in place.
GMMH have recently commenced the Specialist Care MDT element of the programme. The scale of the programme and design process presents some unique challenges and is viewed as an opportunity to achieve significant change that has not been experienced in community services for more than twenty years. The implementation of this work is being supported in the first instance by the NHS Transformation Unit.
Page 52 of 87
Please see below for an overall view of the programme and wider transformation projects which are already underway or at the established phase.
The Community Transformation programme also includes workstreams delivering the service offers of Community Rehabilitation, Complex Emotional Relational Needs (previously known as SCM now CERN), Community Eating Disorders, Physical Health for those with SMI and Independent Placement Support.
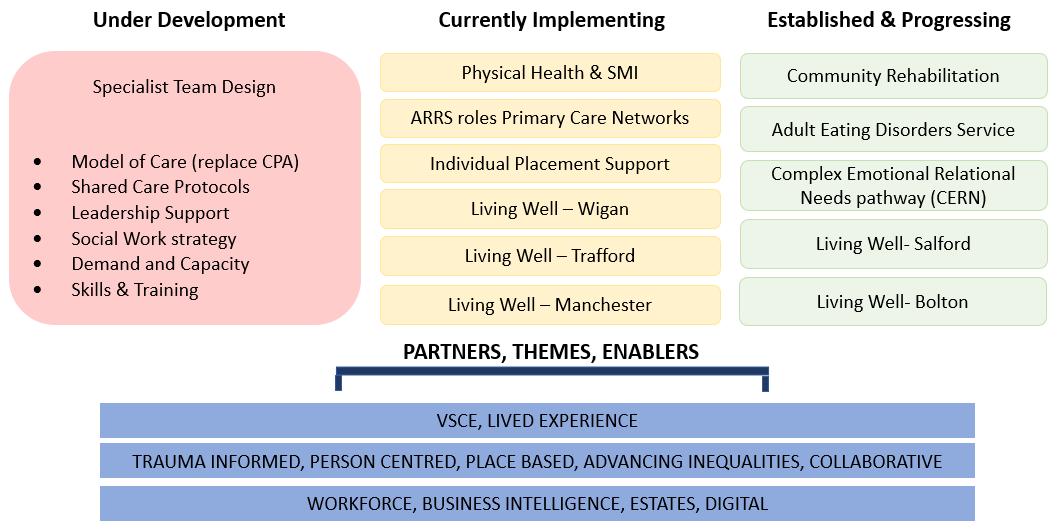
Page 53 of 87
GMMH Transformation Programme Overview
3 Review of Quality Performance in 2022/23
3.1 Delivery of Quality Improvement Priorities in 2022/2023
As referenced in section 1.3 of this Quality Account, we have made significant progress against all our 2022/23 priorities for improvement.
Summaries of our key achievements from our main GMMH QI programmes are detailed in this section. Each achievement reflects the immense commitment of our staff, services users, and carers to continually improving quality. We have provided summaries along with evidence of our key achievements, within the section that follows:
Page 54 of 87
Improvement Priority One: To Improve Outcomes
Quality
QI Project: Multi Professional Clinical Staff – Strengthening Preceptorship Clinical Microsystem
The aim of the Preceptorship Clinical Microsystem is that 100% of newly registered Nurses/RNA’s across GMMH from September 2021 will receive an Individualised preceptorship which will be aligned to 11 agreed standards by 31 July 2022.
Ten teams were recruited to participate in this programme to identify and test change ideas to create a nurse pathway to substantive employment, creating a live tracker, introducing and aligning PARE system to GMMH current systems, induction booklet, Training, and Nurse forums. This has been tested using PDSA cycles and has subsequently been implemented Trustwide. Outcomes include a more streamlined recruitment process of Mental Health Nurses and Allied Health Professionals.
The next phase of this work is will look at the Policy and the preceptorship portfolio to build to be field specific for Nurses and AHP’s.
Phase 2 of the improvement project will include a wider multi-Professional team to innovate, create and test change ideas linked to strengthening preceptorship across GMMH.
Improving Supervision
Nine Innovation teams were recruited from across the Trust including: Safeguarding, Patient Safety, Community Addiction Services, Salford Community Team, Trafford Inpatient and Community Clinical team, Health & Justice, Capital Estates and Facilities, Occupational Therapists (South Manchester) and Social Workers.
The aims of the project are to improve the quality of supervision based on an appropriate set of standards developed by Innovation Teams, and to achieve and sustain 85% compliance on the frequency of supervision. The project was paused temporarily prior to the Celebration event due to challenges conflicting priorities. We intend to re-launch this project in Q1 of 2023.
However, innovation teams have continued refining tests of change leading to implementation of those tests that have evidenced improvement and this is continuing. The aims of the project remain as above but will also include piloting an electronic upgraded system. This is now being piloted across inpatient wards at Bolton.
Key areas of focus for the next phase are the quality of supervision including safeguarding, line management and clinical. There will be a focus on qualitative reporting and the workforce having access to their supervision records. There is a priority piece of work to be included that
Page 55 of 87
supports the NHS people plan to focus upon our people and their wellbeing.
Building an Improvement Culture (Adult Forensic service and North Manchester community services)
Phase 2 of this Breakthrough Series Collaborative began in December 2021. It was expanded to include 28 teams across AFS and North Manchester inpatients and North Manchester Community services. Change ideas included QI training for patients delivered by patients, development of junior staff, mug of the month, improving handover, top tips for administrators, rate my shift and new starters group amongst many others. Improvements are measured through responses to a questionnaire which has been re-designed by both Phase 1 and 2 teams along with a revised Driver Diagram. The project aims were to improve baseline scores on ‘4 cultural’ metrics from the questionnaire by December 2022.
The outcomes of the final questionnaire revealed that improvements were made across three cultural metrics and analysis subsequently found that teams identifying themselves as a ‘real team’ as opposed to a pseudo team had improved by 11%. The project was paused in September 2022 due to challenges and conflicting priorities across services. The project has not yet proceeded into a Phase Three, due to emerging quality and safety priorities within the GMMH improvement plan. This will be reviewed again during quarter one.
Quality Improvement Priority One: To Deliver the Safest Care
Page 56 of 87
Reducing Restrictive Practice Falls Reduction
Phase 2 of this Breakthrough Series
Collaborative project began in April 2022 with an aim to reduce the use of restraint by 10% by 31 March 2023. There are 13 teams involved across the Trust including a variety of different wards and the Positive and Safe team.
Change ideas include increasing ward-based activities, improving staff wellbeing, postincident debriefs, sensory integration, self-harm management, and increased protected time for 1:1s with patients.
The importance and aims of this project are aligned with the Mental Health Units (Use of Force) Act 2018, which has a goal of reducing the use of restrictive interventions and delivering care which has a trauma-informed approach and a focus on human rights.
The project was paused due to staffing issues and changes in Leadership teams across Innovation teams. The re-launch of the Reducing Restrictive Practice BTS collaborative will take place in Q2 of 2023 and will feed into the new Reducing Restrictive Practice Clinical Excellence Network for oversight A new tool will be tested by Innovation teams which has been drafted by colleagues from NHSE/I. Teams will adapt the tool as necessary and start testing during Q2.
Eight Innovation wards were recruited including Later Life wards across the Trust and CBU Detox Unit wards. Innovation wards have progressed with testing ideas using PDSA cycles which have demonstrated an improvement in reducing the number of Inpatient falls and subsequent harm.
We have achieved a 26% reduction in Inpatient falls and subsequent harm by December 2021 and therefore surpassed our aim. From January 22 to December 2022 there has been an increase in the number of falls by 11%.
This is likely due to organizational pressures and competing priorities as we had to delay the launch of the Trustwide change package and did not build in our sustainability plans for this work.
In addition, there has been a slight increase in moderate and minor harm, but major harm has decreased.
A change package has been compiled along with implementation of a sustainability plan to spread at scale by the end of Q2 2023.
Page 57 of 87
Reducing Violence and Aggression and Increasing Perception of Safety on North Manchester wards Clinical Microsystem
The seven acute and PICU wards at North Manchester are involved in a Clinical Microsystem project with the aim of reducing the violence and aggression on the wards and increasing feelings of safety for staff. The main aim is to improve the baseline response to “I feel safe when I’m at work” on the Safety Evaluation questionnaire by 31 October 2022. The questionnaire was redistributed in October 2022 and the results showed a slight increase in staff not feeling safe at work. Outcomes have been measured using violence and aggression average monthly incidents data as well as the staff safety survey. There has been an increase in violence and aggression incidents across all wards apart from a slight decrease on Mulberry ward.
There has been a 12% reduction in staff experiencing assault whilst at work in the last six months. Change ideas include implementing a twilight shift, developing staff skills, debriefing incidents, and partnering with other wards to cover breaks. This project was started in response to a number of serious incidents on the wards in order to improve the experience of being on the wards for staff and patients. This project has now been concluded.
Quality Improvement Priority Three: To Integrate Care Around the Person
Trauma Informed Care
Phase 1 of the Trauma-Informed Care Breakthrough Series Collaborative ended in October 2022.
This project included inpatient and community teams and had involvement from the MDT and lived experience experts. The aim of the project was to improve the responses to the questions “Is the service you currently work in trauma-informed?” and “How confident are you in how to implement trauma-informed care?” on the TIC Questionnaire by 30 September 2022 across GMMH, which was achieved.
Improving Physical Health for people with serious mental illness
The Deteriorating Patient project has now been renamed to “Improving Physical Health for people with serious mental illness” there has been a delay due to organisational pressures but this work has commenced in April 2023. Key themes have been identified as a priority for Phase 1 of this work. The priorities are: To develop a Competency Framework, to review the PHITT tool (screening), Escalation Pathways – referrals, Identification and management of the deteriorating patient. Data analysis is complete and innovation teams will be selected and recruited during Q2 of 2023
Change ideas tested include increasing the understanding of trauma-informed care in relation to self-harm for carers, ensuring
Measurements for this project will include NEWS2 and VTE training compliance, timely completion of assessments,
Page 58 of 87
supervision is trauma-informed, empowering staff to routinely enquire about a patient’s trauma history, and many more. Results were analysed at the end of Phase 1 of the project and showed improvement against the main aims.
This project is linked with ongoing Trustwide implementation of Trauma-Informed Care throughout the organisation and will be included in Trauma-Informed Care policy and strategy.
appropriate escalation of deteriorating patients and the formation of pathways.
A draft driver diagram has been developed. Next steps are to confirm Terms of Reference and diarise meetings and learning events. An initial workshop was held in April 2023 to focus on creating a Competency Framework for Physical Health which was well attended by Physical Health colleagues across the trust and identified service user/lived experience peers.
Quality Improvement Priority Three: To Integrate Care Around the Person
Clinical Risk tool re-design AFS Care Plans
A rapid improvement group was established during Q2 of 2023 to consider improving the current risk tool STARV2. A draft ToR for this group has been circulated. The overall aim of the project is to develop an alternative to the current trust risk management tool. It has been agreed that when the draft tool has been completed that it will be initially tested in Bolton and Trafford with an evaluation taking place after the testing cycles before this is considered to be rolled out across the trust.
An MDT project group was established during Q4 2022 across Edenfield to consider re-designing the current Care Plans used across Adult Forensic Services to ensure that this was co-designed with patients and carers to support service users in their journey through mental health services and improves accessibility for the wider MDT. Initial focus of this work was to review the Women’s service care plan. However, during Q1 of 2023 a refocus to include both a female and male ward to co-create a care plan. A draft care plan has now been created and PDSA cycle testing has commenced. It is anticipated that the testing will be complete by the end of May and an evaluation will take place.
Quality Improvement Priority One: To Improve Outcomes
Page 59 of 87
Handover QI Project Mental Health QI Programme
The Handover QI project commenced Q2 2023. The aim of the project is to develop a standardised handover process and procedures to ensure safe and effective handover of clinical information, risks associated to individual service users, and environmental risk such as ligature risk, fire risks, with clear management plans to support the care and treatment of all service users who are admitted to an inpatient setting. The group reports into the Workstream 2 of the Trust Improvement Plan. A questionnaire is being developed to be distributed across teams to establish a baseline.
A project group has been identified including representation from the MHA team, QI and three wards across the trust which are: Redwood, Borrowdale and Phoenix to participate in a National QI programme supported by The PSC. The project aims to support improvements in culture and practice to meet the aims of the Mental Health Act reforms.
This is a two-year programme and will commence in May 2023.
AQuA Regional Medication Management collaborative
Teams across Health & Justice have been recruited to participate in this learning collaborative which commences in Q2 of 2023. This nine-month programme will bring together individuals from across health and social care systems and settings to share experiences and challenges. H&J teams will focus on controlled drug management at two sites, HMP Wymott and HMP Garth. Participants will include members of the nursing and support staff along with patients/carers input
If you are interested in learning more about the GMMH QI methodology, or our QI programmes, please contact:
Patrick Cahoon, Head of Quality Improvement
Email: Patrick.cahoon@gmmh.nhs.uk
Page 60 of 87
3.2 Performance against Quality Indicators Selected
This section of our Quality Account provides an overview of quality as demonstrated by a range of indicators. The indicators cover the three domains of quality (experience, effectiveness, and safety).
We have continued to use a number of the same indicators as our previous years’ quality accounts.
Please note that due to the COVID-19 pandemic, national collection of a number of these indicators were suspended as from Quarter 4 of 2019/20. GMMH have continued to report locally where possible at Board and team level. The below statement and comparison use local figures were available to indicate level of achievement. Figures reflect the latest available position.
National published figures for comparison purposes are not available where national reporting has been suspended.
The latest available local figures are as at the end of January 2022 and are set out as follows:
Page 61 of 87
Patient Experience 2021/22 2022/23
PLACE inspections. The assessment evaluates cleanliness, condition/ appearance, privacy and dignity and food.
Not Available Cleanliness domain: 96.33%
Food Domain: 81.95%
Organisation Food domain: 91.01%
Ward Food domain: 77.07%
Privacy domain: 89.62%
Condition, Appearance and Maintenance domain: 95.53%
Dementia domain: 7.61%
Disability domain: 76.83%
Comments
Please note PLACE inspections were suspended during 2020 and 2021 due to the COVID-19 pandemic hence scores not available.
https://digital.nhs.uk/data-andinformation/publications/statistical/patient-ledassessments-of-the-care-environment-place
Latest figures for 2022 published on 31 March 2023
Source:
PARIS/RIO and Datix 2021/22 (April 2021 to March 2022) to 2022/23 (April 2022 to March 2023)
Source: PARIS/RIO and Datix 2021/22 (April 2021 to March 2022) to 2022/23 (April 2022 to March 2023)
of
Page 62
87
Complaints – total number of complaints received per 10,000 recorded service user contacts. 4.95 5.22
Compliments – total number of compliments received per 10,000 recorded service user contacts. 20.31 20.97
Comments
*CQC Community Survey 2021, Q36, Rank 7-10 as % of Ranks 0-10)
**CQC Community Survey 2022, Q37, Rank 7-10 as % of Ranks 0-10
Source: Friends and Family Service Users Submission to Unify. (YTD As at March 2023)
*Please note: Due to COVID-19, the Friends and Family Service Users Submission was suspended between March 2020 and April 2021.
Source: Electronic Staff Record (ESR) - (April 2022 to March 2023 position)
Average sickness rate for Mental Health / Learning Disability Trusts in England is 6.59%*.
Average sickness rate for All Trusts in the North West is 7.43%*.
*Source: NHS Sickness Absence Rates - NHS Digital
Latest Version: December 2022 Provisional
Page 63 of 87 Clinical Effectiveness 2021/22 2022/23
Community Mental Health Survey - % of responses that rated the services received from our Trust as good, very good or excellent. 58.4%* 60%**
Friends and Family Test –Service Users – % of Service Users who responded as “Extremely Likely” or “Likely”. 83.7% 85.4%
Total staff sickness absence (%) – rolling 12-month position 7.17% 6.96%
Comments
Source: Datix (April 2022 to March 2023)
Further information on this indicator can be found in Section 2.10.7 of this Quality Account.
Source: Datix (Apr 2022 to Mar 2023)
Source: PARIS/RIO 2021/22 (April 2021 to March 2022) to 2022/23 (April 2022 to March 2023)
Page 64 of 87 Safety 2021/22 2022/23
Degree of harm incurred by service users in incidents reported to the National Patient Safety Agency - % of all incidents reported that resulted in no obvious harm 70.35% 72.24%
% of all patient safety incidents that resulted in severe harm or death 1.47% 1.86%
Number of under 18s admitted to our adult mental health inpatient wards 18 4
3.3 Performance against Key National Priorities
GMMH are registered with NHSE/I the regulatory body for Foundation Trusts and have consistently achieved all required targets and standards for continued registration.
Similarly, we are registered with CQC without conditions, complying with all regulations. We have established robust mechanisms for monitoring compliance against all the outcomes detailed in the CQC Compliance Guidance to provide ongoing registration assurances. We are compliant with the NHS Quality Risk Management Litigation Authority Standards.
The mental health metrics for providers are set out by NHS England and Improvement (NHSI) in the System Oversight Framework and Long-Term Plan for Mental health. The System Oversight Framework guidance and metrics were updated in June 2022 to reflect the new system wide approach to performance and quality across commissioners, integrated care systems and providers. GMMH work hard to deliver all relevant national priorities and targets as a provider and support our Greater Manchester system in system wide achievement. A summary of some of these metrics for providers are set out as follows:
1. People with a first episode of psychosis begins. treatment with a NICE recommended package of care within two weeks of referral (SDCS and MHSDS)
2. Data Quality Maturity Index (DQMI) – MHSDS Dataset Score.
3. Improving Access to Psychological Therapies (IAPT)/Talking Therapies (from IAPT minimum dataset):
3a. Proportion of people completing treatment who move to recovery (from IAPT minimum dataset)
3b. Waiting time to begin treatment within six weeks of referral
Page 65 of 87
Indicator Target 2021/22 2022/23 Comments inc. 2022/23 time point
60% 77.8% 68.8% April 2022 to March 2023.
Source: Board Performance Report
97% 98.3%* 97.2%** *Position as of March 2022
Figure
2022
**Latest Published
December
50% 45.8% 44.2% April 2022 to March 2023.
Board Performance Report
Source:
75% 86.9% 84.3% April 2022 to March 2023.
Board Performance Report
Source:
The above reflects good performance in the majority of areas when compared to previous years. The IAPT recovery target has not been met however it should be noted that in Salford and Manchester GMMH only provide the Step three IAPT services. This impacts on our recovery rates for these services as the recovery target is linked to the delivery of the whole stepped-care IAPT pathway. The Step two IAPT services in these areas contribute to the achievement of the target at a CCG pathway level.
During 2022/23 improving patient flow and supporting people as close to home as possible has continued to be a key priority for the Trust. This has remained challenging to address given the ongoing impact of recovery from COVID-19 on the wider system. A Healthier Patient Pathway project has been ongoing during 2022/23. The work includes promoting timely discharges and developing alternatives to admissions in collaboration with the whole system including third sector partners and voluntary agency support.
3.4 Improvement Priorities for 2023/2024
This section of the Quality Account sets out our priorities for improvement that we intend to deliver during 2023/24. As referenced within section 1:1 of this Quality Account, we have produced our improvement plan, which has been in development since last autumn and includes a number of immediate actions to tackle the most urgent quality and safety issues This sits alongside a comprehensive set of long-term ambitions to improve everything we do at the Trust, grouped into five themes
The Quality Improvement focus for 2023/24, will therefore focus on the following themes and immediate priorities, as outlined within our improvement plan. These are summarised as follows:
Page 66 of 87
Waiting time to
treatment within 18 weeks of referral 95% 98.8% 97.7% April 2022 to March 2023. Source: Board Performance Report
Inappropriate
placements for
mental health services –external and internal. (Total number of bed days) 0 2150 4434* Ambition to achieve 0 by the end of Q3 2021/22. * 2022-23 (April 2022 to March 2023).
Board Performance Report Proportion of discharges from hospital followed up within 72 hours days 80% 80.9% 84.3% April 2022 to March 2023 position
3c.
begin
4.
out of area
adult acute
Source:
1. Patient Safety
Our approach to care and treatment will focus on maximising the things that go right and minimising the things that go wrong. We will protect all of our service users from avoidable harm and create the conditions in which our staff can deliver care safely.
Our immediate priorities:
• Safe Staffing – making sure there are enough qualified, competent, skilled and experienced staff who feel supported and able to develop in their roles and deliver high standards of care.
• Reducing Restrictive Practices – prevent the need to use restrictive practices through the implementation of reduction strategies and the promotion of a human rights approach. This will include looking at alternatives to restraint, seclusion, rapid tranquilisation and blanket rules in our clinical services.
• Medicines Management – promote the safe and effective use of medicines including how we prescribe, handle and administer them to service users.

• Sexual Safety – protect our service users from any unwanted and inappropriate behaviour of a sexual nature and ensure they feel safe from sexual harm.

• Safe and Therapeutic Environments - making sure our environments are always safe, clean and regularly monitored so that any issues are dealt with quickly and effectively.
2. Clinical Strategy and Professional Standards
We will create a safe and supportive working environment for all staff. Of utmost importance will be their wellbeing and development. We will foster open communication, set clear direction and enable our staff to play a vital part in improving both the service they work in and the Trust as a whole.
Our immediate priorities:
• Ensuring the safety of our staff – both physically and mentally – through direct safety interventions and easy access to learning and development. We will support our leaders to lead with compassion and make the development of staff their focus.
• Making access to education and training accessible to all staff and ensuring that staff personal development plans are meaningful and supported.
• Developing leaders who will uphold the values of the Trust and provide a safe and supportive working environment. We will support them to focus on the fundamental standards of care.
Page
of 87
67
3. People
We will make sure that the care, treatment and support we provide meets need and achieves positive outcomes for our service users. We will set clear standards for ourselves, that are shaped by service users and clinicians and based on best practice and evidence.
Our immediate priorities:
• Working together with different professional groups, service users and carers and our partners to reshape and improve the way we deliver care.
• Being clear about what we expect
• Developing leaders who will uphold the values of the Trust and provide a safe and supportive working environment. We will support them to focus on the fundamental standards of care.
4. Culture
We want to be a collaborative, inclusive and compassionate organisation that actively engages with our service users and carers, staff, the public and other stakeholders and involves them in building a more positive future for the Trust.

Our immediate priorities:
• Creating opportunities to empower the staff voice across the organisation, with the Trust Board playing a visible and pro-active leadership role.
• Building more open and collaborative ways in which our service users and carers can provide feedback and play a part in shaping and improving our services.
5. Leadership and Governance
We want service users, carers, staff and the public to have confidence in our leaders and the systems and processes we have in place to help us achieve our goals. We want to promote and share learning and be able to evidence delivery of all our agreed standards of care.

Our immediate priorities:
• Reviewing and strengthening our corporate and quality governance arrangements, ensuring they promote fairness, transparency and responsibility and are supported by good quality data.
• Improving Trust Board and Committee effectiveness by undertaking targeted development work with all existing Trust Board members. We will recruit to the current executive vacancies and revise how we assess and manage key risks.
• Increasing Board and Senior Leader visibility and connectivity to frontline clinical services.

Page 68 of 87
Our stakeholders have engaged with us in an extensive consultation programme to help us to develop these ambitions quality improvement plans Going forward, this continued engagement throughout our journey will also guide our shared vision into meaningful action, as we start to deliver these bold, long-term ambitions and measure the impact of the changes we make. Our improvement plan and journey will only succeed if the views of our service users, their families and carers, alongside those of our staff and stakeholders, are central to its implementation.
Updates on the implementation of this improvement plan will be provided within the Quality Account for 2023/24.
For further information on the GMMH Quality Improvement strategy and programmes, please contact:
Patrick Cahoon, Head of Quality Improvement
Email: Patrick.cahoon@gmmh.nhs.uk
3.5 Monitoring our Quality Improvement Priorities
These Quality Improvement Priorities will be subject to robust monitoring during 2023/24. Each priority area has a designated executive director lead, along with dedicated support from across relevant GMMH teams and departments, as well as the QI team.
Leads are required to produce regular summaries for assurance, which will be reported to our Quality Improvement Committee and received at our Trust Board.
This Quality Account provides an overarching picture of some of the work we have completed within 2022/23, and describes our priorities for improvement in the future as part of a much wider comprehensive quality agenda. This ensures that our services are provided to the highest possible quality standards and continue to meet changing needs in a person-centred way.
Please feel free to contact us if you would like to know more about any of the priorities for 2023/24 or any other quality improvement activity at the Trust.
69 of 87
Page
3.6 ANNEX 1 – Feedback from Key Stakeholders
Feedback from Councillor Green, Chair of the Manchester City Council Health Scrutiny Committee, received on 06/06/23:
Page 70 of 87
Feedback from Healthwatch Bolton, Healthwatch Salford, Healthwatch Trafford, Healthwatch Wigan and Leigh, received on 20/06/23.
Page
Page 72 of 87
Feedback from Healthwatch Bolton, Healthwatch Salford, Healthwatch Trafford, Healthwatch Wigan and Leigh, received on 20/06/23:
Page 73 of 87
Page 74 of 87
Feedback from Mark Fisher, Chief Executive of the NHS Greater Manchester Integrated Care Board, received on 21/06/23:
Page
of 87
75
Page 76 of 87
3.7 ANNEX 2 Statement of Directors’ Responsibilities in Respect of the Quality Account
The directors are required under the Health Act 2009 and the National Health Service (Quality Accounts) Regulations to prepare Quality Accounts for each financial year. NHS Improvement has issued guidance to NHS foundation trust boards on the form and content of annual quality reports (which incorporate the above legal requirements) and on the arrangements that NHS foundation trust boards should put in place to support the data quality for the preparation of the quality report. In preparing the Quality Report, directors are required to review:
• The Quality Report presents a balanced picture of the NHS foundation trust’s performance over the period covered.
• The performance information reported in the Quality Report is reliable and accurate.
• There are proper internal controls over the collection and reporting of the measures of performance included in the Quality Report, and these controls are subject to review to confirm that they are working effectively in practice.
• The data underpinning the measures of performance reported in the Quality Report is robust and reliable, conforms to specified data quality standards and prescribed definitions, is subject to appropriate scrutiny and review.
• The Quality Report has been prepared in accordance with NHS Improvement’s annual reporting manual and supporting guidance (which incorporates the Quality Accounts regulations) as well as the standards to support data quality for the preparation of the Quality Report.
The directors confirm to the best of their knowledge and belief they have complied with the above requirements in preparing the Quality Report. Greater Manchester Mental Health NHS Foundation Trust
By order of the board:
 Bill McCarthy – Chairman Neil Thwaite - Chief Executive
Bill McCarthy – Chairman Neil Thwaite - Chief Executive
Page 77 of 87
3.8 ANNEX 3 Equality Impact Assessment
1. Does the Quality Account affect a group with a protected characteristic less or more favourably than another on the basis of:
• Age
• Disability
• Gender Re-assignment
• Marriage and Civil Partnership
• Pregnancy and Maternity
•
2. Has the Quality Account taken into consideration any privacy and dignity or same sex accommodation requirements that may be relevant?
Yes
Please see comments below
3. Is there any evidence that some groups are affected differently? No
4. If you have identified potential discrimination, are any exceptions valid, legal and/or justifiable?
Not Applicable
This was taken into account as part of the planning and production of the Quality Account. No specific issues have been identified throughout the production stages of this Quality Account.
There is no evidence that any groups are adversely affected as a result of the Quality Account. Monitoring and consideration will remain ongoing.
No valid, legal, or justifiable discrimination has been identified throughout the production of this Quality Account.
Page 78 of 87
Consideration Yes/No Comments
Race
Religion
Belief
Sex • Sexual Orientation No No No No No No No No No N/A N/A N/A N/A N/A N/A N/A N/A N/A
•
or
•
5. Is the impact of the Quality Account likely to be negative?
6. If so, can the impact be avoided?
7. What alternatives are there to achieving the Quality Account without impact?
Not Applicable
Not Applicable
8. Can we reduce the impact by taking a different action? Not Applicable
The impact of the Quality Account is not likely to be negative.
This does not apply as no negative impact has been identified
This does not apply as no negative impact has been identified
This does not apply as no negative impact has been identified
3.9 ANNEX 4 Local Clinical Audits Reviewed in 2022/23
Audits from the GMMH clinical audit programme 2022/2023 completed Patient experience/safety audits, health and safety audits 1
(previously
Page 79 of 87
Consideration Yes/No Comments
No
Ligature
Ligature
Audit of Seclusion
Re-audit of Seclusion
Infection Prevention
Hand Hygiene re-audit
Mattress re-audit
Transfer of Care – Use of
Cutter Audit 2
Environmental Audit 3
4
5
-
6
7
Intervention
8 CPA - Risk Assessment/Risk Management plans
risk assessment in AOTs) 9 National Patient Safety Alert. Use of Oxygen where patients do not have access to medical gas pipeline system
Mental capacity/mental health act audits
10 Re-audit Consent to Treatment (T2 and T3)
11 Re-audit Patient’s Rights
Medicines management audits
12 Medicines Handling (Duthie) Audit
13 Re-audit New Prescription Card
14 Medicines Management (Covert Medicines)
Audits completed within each service
Trust wide and multi–site audits
15 Audit on Admission Consent to Treatment in all Later Life Inpatient Ward
Bolton services
16 Use of Sodium Valproate in women with childbearing potential in LD Team in Bolton
Manchester services
17 Timely completion MHA assess by AMHP and IC after MHA recommendation from HBTT South
18 DLB – diagnosis rates vs national rates and implementation of QIP 19 Improving MDT handover implementation of I-PASS
Page 80 of 87
20 Audit of complete SCP in a timely manner to GP 21 Process of triage assessment within the Manchester Psychotherapy service 22 VTE Risk Assessment Audit in Older Adult In-Patients 23 Dementia and driving
24 Safe sleep guidance or advice within the Specialist Perinatal Service
25 Physical health monitoring in later life patients receiving long-acting antipsychotic depot injections
Page 81 of 87 26 Medication prescribing and monitoring within the MHLT at MRI 27 Re-Gatekeeping Review in HBTT North 28 Driving advice for inpatients on Park House Wards 29 Carer participation in ward rounds for admissions to Andersen Ward 30 Carer participation in ward rounds for admissions to Andersen Ward 31 Maple ward In-patient MDT documentation 32 Safe sleep guidance or advice within the Specialist Perinatal Service 33 Physical health monitoring in later life patients receiving long-acting antipsychotic depot injections 34 Medication prescribing and monitoring within the MHLT at MRI 35 Re-Gatekeeping Review in HBTT North 36 Driving advice for inpatients on Park House Wards 37 Carer participation in ward rounds for admissions to Andersen Ward Rehab services 38 Factors of delayed discharges from mental health rehabilitation units 39 Audit on quality of PHIT tool and physical health care plans 40 Treatment with Clozapine in treatment resistant schizophrenia 41 Factors of delayed discharges from mental health rehabilitation units Salford services 42 Performance of urine drug screen for substance misuse in patients admitted with psychotic symptoms on Eagleton ward 43 Audit on standard care template on community mental health team clinic letter 44 Use of Valproate in women with childbearing potential in Ramsgate House CMHT 45 Physical Health Workup and documentation prior to initiating anti-psychotic medication 46 An audit on prescription chart documentation at Woodlands Hospital
47 Performance of urine drug screen for substance misuse in patients admitted with psychotic symptoms on Eagleton ward
48 Audit on standard care template on community mental health team clinic letter
49 Use of Valproate in women with childbearing potential in Ramsgate House CMHT
Specialist Network services
50 Weight monitoring of inpatients at the Lowry Low Secure Unit
51 Re-audit of Compliance of the physiological observations (NEWs) frequency on inpatient acute male forensic wards at Edenfield unit
52 review of initial assessments
53 Adapting an anxiety management group intervention for deaf patients at the John Denmark Unit
54 STARV2 Risk Formulation in Medium Secure
55 Weight monitoring of inpatients at the Lowry Low Secure Unit
56 Re-audit of physical health monitoring for inpatients on antipsychotic medication on Pegasus ward, Phoenix ward and the Gardener Unit
Trafford services
57 Increasing the number inpatients receiving baseline physical investigations
58 Physical Health Monitoring for High-Dose Antipsychotic Medication Central CMHT
59 Patient Medical review within 7 days of admission to Trafford HBTT
Page 82 of 87
3.10 ANNEX 5 Glossary of Terms
A&E Accident and Emergency hospital services
ACE 111
The Addenbrooke’s Cognitive Examination are neuropsychological tests used to identify cognitive impairment in conditions such as dementia
Achieve Drug and alcohol recovery services
AIMS Accreditation for Inpatient Mental Health Services
ADSM Anxiety Disorder Specific Measures
AQuA Advancing Quality Alliance
ARMS At Risk Mental State
BAME Black and Minority Ethnic
BD Bipolar Disorder
BMI Body Mass Index
BNF British National Formulary
BP Blood Pressure
BSL British Sign Language
CAARMS Comprehensive Assessment of at-Risk Mental States
CAMHS Child and Adolescent Mental Health Services
Care Co-ordinator
Carer
The professional who, irrespective of their ordinary professional role, has responsibility for co-ordinating care, keeping in touch with the service user, and ensuring the care plan is delivered and reviewed as required.
An individual who provides or intends to provide support to someone with a mental health problem. A carer may be a relative, partner, friend or neighbour, and may or may not live with the person cared for.
CBT Cognitive Behavioural Therapy
CBU Chapman Barker Unit, specialist service for those with substance misuse needs on the Prestwich site
CG Clinical Guideline
CA&QS Clinical Audit and Quality Standards Group
CMHT Community Mental Health Team
COASSIST Children with OCD: Identifying Accessible Support Strategies for Parents
CTIMP’s Clinical Trials of Investigational Medicinal Products
CoG Council of Governors
Page 83 of 87
CPA
Care Programme Approach - a framework for assessing service users’ needs, planning ways to meet needs and checking that needs are being met.
CQC
The Care Quality Commission is the independent regulator of all health and adult social care in England and has responsibility for protecting the rights of individuals detained under the Mental Health Act.
CQUIN Commissioning for Quality and Innovation framework, which allows commissioners to link income to the achievement of quality improvement goals
CRN:GM Clinical Research Network: Greater Manchester
CROM Clinician Reported Outcome Measures
DATIX The Trust’s Integrated Risk Management Software
DH Department of Health
DS&P Data Security and Protection
DNAR Do not attempt resuscitation
ECG Electrocardiography
EDI Equality, Diversity and Inclusion
EDIE Early detection and intervention evaluation for people at risk of psychosis
e-GFR Estimated Glomerular Filtration Rate
EI Early Intervention
EIP Early Intervention in Psychosis
EQUIP
‘Enhancing the quality of user involved care planning in mental health services. A collaborative project between the University of Manchester, University of Nottingham, Nottinghamshire Healthcare NHS Trust and Greater Manchester Mental Health NHS Foundation Trust to examine ways to improve user and carer involvement in care planning in mental health services.
FFT Friends and Family Test
GDPR General Data Protection Regulation
GM Greater Manchester
GMMH Greater Manchester Mental Health NHS Foundation Trust
GMP Greater Manchester Police
GM: CRN Greater Manchester Clinical Research Network
GP General Practitioner
HAELO Innovation and Improvement Science Centre in Salford
HBT Home Based Treatment
Page 84 of 87
HealthWatch
HealthWatch is an independent consumer champion. It was created to listen and gather the public and patient’s experiences of using local health and social care services. Local Health Watches were set up in every local authority area to help put patients and the public at the heart of service delivery and improvement across the NHS and care services.
HEE Health Education England
HinM Health Innovation Manchester
HMP Her Majesty’s Prison
HoNOS Health of Nation Outcome Scales
HR Human Resources
HSJ Health Service Journal
IAPT
Improving Access to Psychological Therapies: National programme aiming to improve access to evidence-based talking therapies in the NHS through an expansion of the psychological therapy workforce and supporting services.
ICB Integrated Care Board
ICO Integrated Care Organisation
iESE Improvement and Efficiency Social Enterprise
IM Intra-muscular
IMHA Independent Mental Health Advocate
JDR Join Dementia Research
JDU John Denmark Unit - Inpatient unit for deaf mental health services on the Prestwich site
Junction 17 Inpatient unit for child and adolescent mental health services on the Prestwich site
KPI Key Performance Indicator
LeDeR Learning Disabilities Mortality Review
Lester Tool
Downloadable resource used in a range of healthcare settings to improve screening and to ensure a person’s physical and mental health conditions are jointly addressed providing a systematic framework for screening and recommendations for treatment and support.
LGBTQI
Umbrella term for people who identify as Lesbian, Gay, Bisexual, Transsexual. The “Q” stands for those who are questioning or in a state of flux with their gender and/or sexual identity
LQAF Library Quality Assurance Framework
MATS Memory Assessment Services
Page 85 of 87
MBU Mother and Baby Unit
MDT Multi-Disciplinary Team
MH Mental Health
MHSDS Mental Health Services Data Set
MIAA Mersey Internal Audit Agency
MSK Musculoskeletal
NCI National Confidential Inquiry
NCISH National Confidential Inquiry into Suicide and Homicide
NCSCT National Centre for Smoking Cessation and Training
NG NICE Guidelines
NHS National Health Service
NICE The National Institute for Health and Care Excellence
NIHR National Institute for Health Research: The NIHR commissions and funds a range of NHS and social care research programmes
NRLS National Reporting and Learning System
NWAS North West Ambulance Service
OPS Operations
OCD Obsessive compulsive disorder
OF Oversight Framework
PAM Assist People Asset Management Assistance
PARIS PARIS: GMMH current electronic patient record system.
PbR Payment by Results
PIR Post Incident Review panel
PCFT Pennine Care NHS Foundation Trust
PCMIS Clinical information system used in Manchester
PHIT Physical Health Improvement Tool used in PARIS
PICU Psychiatric Intensive Care Unit
PLACE Patient-Led Assessments of the Care Environment
PLAN Psychiatric Liaison Accreditation Network
PMVA Prevention and Management of Violence and Aggression
PREM Patient Reported Experience Measures
PROM Patient Reported Outcome Measures
Page 86 of 87
PRN Pro Re Natum (as the need arises)
PRU Psychosis Research Unit
PSI’s Psychological Interventions
QIC Quality Improvement Committee
QIODG Quality Improvement Operational Delivery Group
QI Quality Improvement
QIP’s Quality Improvement Priorities
QPR Questionnaire about Process of Recovery
R&D Research and Development
R&I Research and Innovation
RAG Red, Amber Green
RCA Root Cause Analysis investigation
RCF Research Capability Funding
SPC Statistical Process Control
SQI The Sustainability and Quality Improvement Group
SUS Secondary Uses Service
STORM Skills based suicide prevention training in risk assessment and safety planning for frontline staff
SJR Structured Judgement Review
SIR Serious Incident Review
THOMAS Those on the margins of society
WRES Workforce Race Equality Standard
WDES Workforce Disability Equality Standard
Page 87 of 87
