

CBEBC BENEFIT GUIDE EFFECTIVE: 09/01/2023 - 8/31/2024 WWW.CBEBC.COM 2023 - 2024 Plan Year 1

HOW TO ENROLL PG. 4 How to Enroll 4-5 Annual Benefit Enrollment 6-10 1. Annual Enrollment 6 2. Section 125 Cafeteria Plan Guidelines 7 3. Eligibility Requirements 8 4. Helpful Definitions 9 5. Health Savings Account (HSA) vs. Flexible Spending Account (FSA) 10 Medical 11-12 Health Savings Account (HSA) 13-14 Hospital Indemnity 15 Telehealth 16 Dental 17 Vision 18-19 Disability 20-22 Cancer 23-24 Accident 25-26 Voluntary Life and AD&D 27 Critical Illness 28-29 Identity Theft 30 Emergency Medical Transportation 31 Flexible Spending Account (FSA) 32-33 FBS Benefits App Group # Index 34 2
Table of Contents FLIP TO... SUMMARY PAGES PG. 6 YOUR BENEFITS PG. 11
Benefit Contact Information
CBEBC BENEFITS MEDICAL HEALTH SAVINGS ACCOUNT (HSA)
Financial Benefit Services (469) 385-4685
www.cbebc.com
Texas Schools Health Benefits Program (TSHBP) (888) 803-0081
All Plans: www.tshbp.org
Pharmacy Benefits: SouthernScripts Group #50000
https://tshbp.info/DrugPham
EECU (817) 882-0800
www.eecu.org
HOSPITAL INDEMNITY TELEHEALTH DENTAL

Lincoln Financial Group (800) 423-2765
www.lfg.com
MD Live (888) 365-1663
www.consultmdlive.com
Lincoln Financial Group (800) 423-2765
https://www.lfg.com
VISION DISABILITY CANCER
Unum
Group #440116 (866) 679-3054
www.unum.com
Cigna Group #SLH100006 (800) 244-6224
www.cigna.com
ACCIDENT UNIVERSAL LIFE
Chubb (888) 409-0425
www.chubb.com
Texas Republic Life (572) 330-0099
Lincoln Financial Group (800) 423-2765
www.lfg.com
www.texasrepubliclife.com
American Public Life Group #127 (800) 256-8606
www.ampublic.com
VOLUNTARY LIFE AND AD&D
Unum
BASIC: Group #657216
VOLUNTARY: Group #292000 (866) 679-3054
www.unum.com
CRITICAL ILLNESS IDENTITY THEFT EMERGENCY MEDICAL TRANSPORT
Lincoln Financial Group (800) 423-2765
www.lfg.com
FLEXIBLE SPENDING ACCOUNTS (FSA)
National Benefit Services (800) 274-0503
www.nbsbenefits.com
Experian (855) 797-0052
www.experian.myfinancialexpert.com/ login
MASA Group #MCKBEBC (800) 423-3226
www.masamts.com
3


OR SCAN App Group #: Go to PAGE 34 to find your district’s group # Employee benefits made easy through the FBS Benefits App! All Your BenefitsOne App Text “FBS CBEBC” to (800) 583-6908 Text “FBS CBEBC” to (800) 583-6908 and get access to everything you need to complete your benefits enrollment: • Benefit Resources • Online Enrollment • Interactive Tools • And more! 4
1 www.cbebc.com How to Log In CLICK LOGIN 3 ENTER USERNAME & PASSWORD Login Credentials vary by district. Please review the instructions on the login page for your district, as your instructions may have changed. 2 5
Annual Benefit Enrollment
Annual Enrollment
During your annual enrollment period, you have the opportunity to review, change or continue benefit elections each year. Changes are not permitted during the plan year (outside of annual enrollment) unless a Section 125 qualifying event occurs.
• Changes, additions or drops may be made only during the annual enrollment period without a qualifying event.
• Employees must review their personal information and verify that dependents they wish to provide coverage for are included in the dependent profile. Additionally, you must notify your employer of any discrepancy in personal and/or benefit information.
• Employees must confirm on each benefit screen (medical, dental, vision, etc.) that each dependent to be covered is selected in order to be included in the coverage for that particular benefit.
New Hire Enrollment
All new hire enrollment elections must be completed in the online enrollment system within the first 30 days of benefit eligibility employment. Failure to complete elections during this timeframe will result in the forfeiture of coverage.
Q&A
Who do I contact with Questions?
For supplemental benefit questions, you can contact your Benefits/HR department or you can call Financial Benefit Services at 866-914-5202 for assistance.
Where can I find forms?
For benefit summaries and claim forms, go to your benefit website: www.cbebc.com. Click the benefit plan you need information on (i.e., Dental) and you can find the forms you need under the Benefits and Forms section.
How can I find a Network Provider?
For benefit summaries and claim forms, go to the CBEBC benefit website: www.cbebc.com. Click on the benefit plan you need information on (i.e., Dental) and you can find provider search links under the Quick Links section.

When will I receive ID cards?
If the insurance carrier provides ID cards, you can expect to receive those 3-4 weeks after your effective date. For most dental and vision plans, you can login to the carrier website and print a temporary ID card or simply give your provider the insurance company’s phone number and they can call and verify your coverage if you do not have an ID card at that time. If you do not receive your ID card, you can call the carrier’s customer service number to request another card.
If the insurance carrier provides ID cards, but there are no changes to the plan, you typically will not receive a new ID card each year.
Don’t Forget!
• Login and complete your benefit enrollment from 05/08/2023 - 08/17/2023 (Dates vary by district)
• Enrollment assistance is available by calling Financial Benefit Services at (866) 914-5202.
• Update your information: home address, phone numbers, email, and beneficiaries.
• REQUIRED!! Due to the Affordable Care Act (ACA) reporting requirements, you must add your dependent’s CORRECT social security numbers in the online enrollment system. If you have questions, please contact your Benefits Administrator.
SUMMARY PAGES
6
Annual Benefit Enrollment
Section 125 Cafeteria Plan Guidelines
A Cafeteria plan enables you to save money by using pre-tax dollars to pay for eligible group insurance premiums sponsored and offered by your employer. Enrollment is automatic unless you decline this benefit. Elections made during annual enrollment will become effective on the plan effective date and will remain in effect during the entire plan year.
Changes in benefit elections can occur only if you experience a qualifying event. You must present proof of a qualifying event to your Benefit Office within 30 days of your qualifying event and meet with your Benefit/HR Office to complete and sign the necessary paperwork in order to make a benefit election change. Benefit changes must be consistent with the qualifying event.
CHANGES IN STATUS (CIS): QUALIFYING EVENTS
Marital Status
Change in Number of Tax Dependents
Change in Status of Employment Affecting Coverage Eligibility
Gain/Loss of Dependents’ Eligibility Status
A change in marital status includes marriage, death of a spouse, divorce or annulment (legal separation is not recognized in all states).
A change in number of dependents includes the following: birth, adoption and placement for adoption. You can add existing dependents not previously enrolled whenever a dependent gains eligibility as a result of a valid change in status event.
Change in employment status of the employee, or a spouse or dependent of the employee, that affects the individual’s eligibility under an employer’s plan includes commencement or termination of employment.
An event that causes an employee’s dependent to satisfy or cease to satisfy coverage requirements under an employer’s plan may include change in age, student, marital, employment or tax dependent status.
Judgment/ Decree/Order
Eligibility for Government Programs
If a judgment, decree, or order from a divorce, annulment or change in legal custody requires that you provide accident or health coverage for your dependent child (including a foster child who is your dependent), you may change your election to provide coverage for the dependent child. If the order requires that another individual (including your spouse and former spouse) covers the dependent child and provides coverage under that individual’s plan, you may change your election to revoke coverage only for that dependent child and only if the other individual actually provides the coverage.
Gain or loss of Medicare/Medicaid coverage may trigger a permitted election change.
SUMMARY PAGES
7
Annual Benefit Enrollment
Employee Eligibility Requirements
Supplemental Benefits: Eligible employees must work 20 or more regularly scheduled hours each work week.
Eligible employees must be actively at work on the plan effective date for new benefits to be effective, meaning you are physically capable of performing the functions of your job on the first day of work concurrent with the plan effective date. For example, if your 2023 benefits become effective on September 1, 2023, you must be actively-at-work on September 1, 2023 to be eligible for your new benefits.
Dependent Eligibility Requirements
Dependent Eligibility: You can cover eligible dependent children under a benefit that offers dependent coverage, provided you participate in the same benefit, through the maximum age listed below. Dependents cannot be double covered by married spouses within the district as both employees and dependents.
Please note, limits and exclusions may apply when obtaining coverage as a married couple or when obtaining coverage for dependents.
Potential Spouse Coverage Limitations: When enrolling in coverage, please keep in mind that some benefits may not allow you to cover your spouse as a dependent if your spouse is enrolled for coverage as an employee under the same employer. Review the applicable plan documents, contact Financial Benefit Services, or contact the insurance carrier for additional information on spouse eligibility.
FSA/HSA Limitations: Please note, in general, per IRS regulations, married couples may not enroll in both a Flexible Spending Account (FSA) and a Health Savings Account (HSA). If your spouse is covered under an FSA that reimburses for medical expenses then you and your spouse are not HSA eligible, even if you would not use your spouse’s FSA to reimburse your expenses. However, there are some exceptions to the general limitation regarding specific types of FSAs. To obtain more information on whether you can enroll in a specific type of FSA or HSA as a married couple, please reach out to the FSA and/or HSA provider prior to enrolling or reach out to your tax advisor for further guidance.
Potential Dependent Coverage Limitations: When enrolling for dependent coverage, please keep in mind that some benefits may not allow you to cover your eligible dependents if they are enrolled for coverage as an employee under the same employer. Review the applicable plan documents, contact Financial Benefit Services, or contact the insurance carrier for additional information on dependent eligibility.
Disclaimer: You acknowledge that you have read the limitations and exclusions that may apply to obtaining spouse and dependent coverage, including limitations and exclusions that may apply to enrollment in Flexible Spending Accounts and Health Savings Accounts as a married couple. You, the enrollee, shall hold harmless, defend, and indemnify Financial Benefit Services, LLC from any and all claims, actions, suits, charges, and judgments whatsoever that arise out of the enrollee’s enrollment in spouse and/or dependent coverage, including enrollment in Flexible Spending Accounts and Health Savings Accounts.
If your dependent is disabled, coverage may be able to continue past the maximum age under certain plans. If you have a disabled dependent who is reaching an ineligible age, you must provide a physician’s statement confirming your dependent’s disability. Contact your HR/Benefit Administrator to request a continuation of coverage.
PLAN MAXIMUM AGE Accident To age 26 Cancer To age 26 Critical Illness To age 26 Dental To age 26 Identity Theft To age 26 Individual Life To age 26 Hospital Indemnity To age 26 Telehealth To age 26 Vision To age 26 Voluntary Life and AD&D To age 26
SUMMARY PAGES
8
Helpful Definitions
Actively-at-Work
You are performing your regular occupation for the employer on a full-time basis, either at one of the employer’s usual places of business or at some location to which the employer’s business requires you to travel. If you will not be actively at work beginning 9/1/2023 please notify your benefits administrator.
Annual Enrollment
The period during which existing employees are given the opportunity to enroll in or change their current elections.
Annual Deductible
The amount you pay each plan year before the plan begins to pay covered expenses.
Calendar Year
January 1st through December 31st
Co-insurance
After any applicable deductible, your share of the cost of a covered health care service, calculated as a percentage (for example, 20%) of the allowed amount for the service.
Guaranteed Coverage
The amount of coverage you can elect without answering any medical questions or taking a health exam. Guaranteed coverage is only available during initial eligibility period. Actively-at-work and/or preexisting condition exclusion provisions do apply, as applicable by carrier.
In-Network
Doctors, hospitals, optometrists, dentists and other providers who have contracted with the plan as a network provider.
Out-of-Pocket Maximum
The most an eligible or insured person can pay in coinsurance for covered expenses.
Plan Year
September 1st through August 31st
Pre-Existing Conditions
Applies to any illness, injury or condition for which the participant has been under the care of a health care provider, taken prescriptions drugs or is under a health care provider’s orders to take drugs, or received medical care or services (including diagnostic and/or consultation services).
SUMMARY PAGES
9
Health Savings Account (HSA) (IRC Sec. 223)
Flexible Spending Account (FSA) (IRC Sec. 125)
Description
Approved by Congress in 2003, HSAs are actual bank accounts in employee’s names that allow employees to save and pay for unreimbursed qualified medical expenses tax-free.
Allows employees to pay out-of-pocket expenses for copays, deductibles and certain services not covered by medical plan, taxfree. This also allows employees to pay for qualifying dependent care tax- free. Employer
Permissible Use Of Funds
Cash-Outs of Unused Amounts (if no medical expenses)
Year-to-year rollover of account balance?
Does the account earn interest?
Employees may use funds any way they wish. If used for non-qualified medical expenses, subject to current tax rate plus 20% penalty.
Permitted, but subject to current tax rate plus 20% penalty (penalty waived after age 65).
Yes, will roll over to use for subsequent year’s health coverage.
Reimbursement for qualified medical expenses (as defined in Sec. 213(d) of IRC).
Not permitted
No. Access to some funds may be extended if your employer’s plan contains a 2 1/2-month grace period or $610 rollover provision.
Eligibility
All employers Contribution Source Employee and/or employer Employee and/or employer Account Owner Individual Employer Underlying Insurance Requirement High deductible health plan None Minimum Deductible $1,500 single (2023) $3,000 family (2023) N/A Maximum Contribution $3,850 single (2023) $7,750 family (2023) $3,050 (2023)
A qualified high deductible health plan.
Yes No
No FLIP TO FOR HSA INFORMATION FLIP TO FOR FSA INFORMATION PG. 13 PG. 32 SUMMARY PAGES HSA
10
Portable? Yes, portable year-to-year and between jobs.
vs. FSA
Medical Insurance Texas Schools Health Benefits Program EMPLOYEE BENEFITS
ABOUT TSHBP
The TSHBP is proud to offer a variety of plans and benefits to meet school district needs. All plans are designed so members can easily navigate through their health medical needs.
For full plan details, please visit your benefit website: www.cbebc.com
Directed Care Highlights
The TSHBP Directed Care Plans utilize a national network to provide physician and ancillary services access to all members. Enrolled school districts will access the HealthSmart practitioner and ancillary only network to gain access to over 502,309 providers in over 1,421,000 unique locations across the United States.

Please note, hospitals are excluded from the PPO networks. All hospital and other medical facility-based services are accessed via an assigned Care Coordinator.
It is easy to look up providers in your area by looking up providers in your area by clicking on the link below. https://tshbp.info/HSNetwork
Hinge Health
Hinge Health is a digital musculoskeletal management program with custom physical therapy programs designed by physicians and led by board certified Health coaches. You and your eligible family members get free access to Hinge Health’s programs for back, knee, hip, shoulder, or neck pain, which may include: a free tablet computer and wearable sensors, unlimited 1-on-1 health coaching, personalized exercise therapy, etc.
TSHBeFit
TSHBeFit is a Wellness Program, powered by WellRight, is available for members to achieve their personal health and well-being through a collection of holistic activities and is no additional cost to members.

PPO Deductible Credits

Aetna Network Highlights

You want a network that is comprehensive, is easy to use and can help you save on costs. Look no further. You can now find support through our Aetna Signature Administrators® preferred provider organization network. Discover provider options and reduced costs.

With our network, you now have access to over 1.2 million participating doctors, 8,700 hospitals, and strong, negotiated discounts.
We know quality care is important. So we make sure our doctors successfully complete our credentialing requirements. Our credentialing process meets industry standards, as well as state and federal requirements.

You’ll also have access to over 600 Institutes of Excellence™ facilities and Institutes of Quality® facilities. We measure these publicly recognized institutes by clinical performance, outcomes and efficiency. Then, we pass this guidance along to you—so you can choose the best facility.
Ready to search our network? Just visit http://aetna.com/asa
With the Aetna PPO plan, if you choose to utilize the services of a Care Coordinator for a procedure or admission to a facility, you may receive up to a $500 credit toward your deductible. If you have already met your deductible, the $500 credit will apply to your out-of-pocket maximum!
Scan the QR code with your mobile device or visit tshbp.org/myrates to view your rates! 11
Medical Insurance Texas Schools Health Benefits Program
EMPLOYEE BENEFITS PLAN SUMMARY DIRECTED CARE PLANS AETNA NETWORK PLAN TSHBP - HD Plan TSHBP CoPay Plan Aetna Signature Directed Care Plan • Use Care Coordinator for Hospital/ Surgical Services • Compatible with an HSA • Embedded Deductible - no coinsurance • Out-of-Network Benefits Directed Care Plan • Use Care Coordinator for Hospital/ Surgical Services • Co-payments for Services • Reduce Out-of-Pocket • Out-of-Network Benefits Traditional PPO Plan • PPO Network for all physician/hospital services • Brand Drug Deductible • Care Coordinator is an optional benefit Coverage In-Network Coverage In-Network Coverage In-Network Only Network HealthSmart - National HealthSmart AETNA Plan Deductible Feature Deductible, then Plan pays 100% Copayments, then Plan pays 100% Deductible, then Plan pays 70% Individual/Family Deductible $3,500/$10,500 $0/$0 $4,000/$8,000 Coinsurance None - Plan Pays 100% after deductible None - Plan Pays 100% after deductible You pay 30% after deductible Individual/Family Maximum Out-ofPocket $3,500/$10,500 $4,000/$11,000 $10,000/$20,000 Health Savings Account (HSA) Eligible Yes No No Required - Primary Care Provider (PCP) No No No Required - PCP Referral to Specialist No No No Doctor Visits Preventive Care Yes - $0 copay Yes - $0 copay Yes - $0 copay Virtual Health - Teladoc $30 per consultation $0 per consultation $0 per consultation Primary Care Deductible, then Plan pays 100% $45 copay $45 copay Specialist Deductible, then Plan pays 100% $70 copay $70 copay Office Services Allergy Injections Deductible, then Plan pays 100% $5 copay You pay 30% after deductible Allergy Serum Deductible, then Plan pays 100% $35 copay You pay 30% after deductible Chiropractic Services Deductible, then Plan pays 100% $35 copay $70 copay Office Surgery Deductible, then Plan pays 100% $110 copay You pay 30% after deductible MRI's, Cat Scans, and Pet Scans Deductible, then Plan pays 100% $275 copay You pay 30% after deductible Care Facilities Urgent Care Facility Deductible, the Plan pays 100% $75 copay $75 copay Freestanding Emergency Room Deductible, the Plan pays 100% $500 copay You pay $500 copay + 30% after ded Hospital Emergency Room Deductible, the Plan pays 100% $500 copay You pay 30% after deductible Ambulance Services Deductible, the Plan pays 100% $275 copay You pay 30% after deductible Outpatient Surgery Deductible, the Plan pays 100% $650 copay You pay 30% after deductible Hospital Services Deductible, the Plan pays 100% $650 copay You pay 30% after deductible Surgeon Fees Deductible, the Plan pays 100% $200 copay You pay 30% after deductible Maternity and Newborn Services Maternity Charges (prenatal and postnatal care) Deductible, the Plan pays 100% $500 copay You pay 30% after deductible Routine Newborn Care Deductible, the Plan pays 100% $250 copay You pay 30% after deductible Rehabilitation/Therapy Occupational/Speech/Physical Deductible, the Plan pays 100% $55 copay $30 copay Cardiac Rehabilitation Deductible, the Plan pays 100% $110 copay You pay 30% after deductible Chemotherapy, Radiation, Dialysis Deductible, the Plan pays 100% $110 copay You pay 30% after deductible Home Health Care Deductible, the Plan pays 100% $55 copay You pay 30% after deductible Skilled Nursing Deductible, the Plan pays 100% $500 copay You pay 30% after deductible Prescription Drug Benefits Drug Deductible Intergrated into Medical No Drug Deductible $500 brand deductible Generic Deductible, the Plan pays 100%; $0 for certain generics $0 copay CVS/HEB/Walmart/Costco/Sam’s | $10 copay All other net Pharmacies $15/$45 copay; $0 for certain generics Preferred Brand Deductible, the Plan pays 100% $35 copay or 50% copay whichever is greater (max $100) You pay 25% after deductible Non-Preferred Deductible, the Plan pays 100% $70 copay or 50% copay whichever is greater (max $200) You pay 50% after deductible Specialty Full Coverage - PAP Required - Deductible then plan pays 100% Full Coverage - PAP Required - 50% copay (max $500) Full Coverage - PAP Required - You pay 50% after deductible 12
Health Savings Account (HSA)
ABOUT HSA
A Health Savings Account (HSA) is a personal savings account where the money can only be used for eligible medical expenses. Unlike a flexible spending account (FSA), the money rolls over year to year however only those funds that have been deposited in your account can be used. Contributions to a Health Savings Account can only be used if you are also enrolled in a High Deductible Health Care Plan (HDHP).
For full plan details, please visit your benefit website: www.cbebc.com
A Health Savings Account (HSA) is more than a way to help you and your family cover health care costs – it is also a taxexempt tool to supplement your retirement savings and cover health expenses during retirement. An HSA can provide the funds to help pay current health care expenses as well as future health care costs.
A type of personal savings account, an HSA is always yours even if you change health plans or jobs. The money in your HSA (including interest and investment earnings) grows tax-free and spends tax-free if used to pay for qualified medical expenses. There is no “use it or lose it” rule — you do not lose your money if you do not spend it in the calendar year — and there are no vesting requirements or forfeiture provisions. The account automatically rolls over year after year.
HSA Eligibility
You are eligible to open and contribute to an HSA if you are:
• Enrolled in an HSA-eligible HDHP (High Deductible Health Plan)
• Not covered by another plan that is not a qualified HDHP, such as your spouse’s health plan
• Not enrolled in a Health Care Flexible Spending Account, nor should your spouse be contributing towards a Health Care Flexible Spending Account
• Not eligible to be claimed as a dependent on someone else’s tax return
• Not enrolled in Medicare or TRICARE
• Not receiving Veterans Administration benefits
You can use the money in your HSA to pay for qualified medical expenses now or in the future. You can also use HSA funds to pay health care expenses for your dependents, even if they are not covered under your HDHP.
Maximum Contributions
Your HSA contributions may not exceed the annual maximum amount established by the Internal Revenue Service. The annual contribution maximum for 2023 is based on the coverage option you elect:
• Individual – $3,850
• Family (filing jointly) – $7,750
You decide whether to use the money in your account to pay for qualified expenses or let it grow for future use. If you are 55 or older, you may make a yearly catch-up contribution of up to $1,000 to your HSA. If you turn 55 at any time during the plan year, you are eligible to make the catch-up contribution for the entire plan year.

EECU EMPLOYEE
13
BENEFITS
Health Savings Account (HSA)
Opening an HSA
If you meet the eligibility requirements, you may open an HSA administered by EECU. You will receive a debit card to manage your HSA account reimbursements. Keep in mind, available funds are limited to the balance in your HSA.
Important HSA Information
• Always ask your health care provider to file claims with your medical provider so network discounts can be applied. You can pay the provider with your HSA debit card based on the balance due after discount.
• You, not your employer, are responsible for maintaining ALL records and receipts for HSA reimbursements in the event of an IRS audit.
You may open an HSA at the financial institution of your choice, but only accounts opened through EECU are eligible for automatic payroll deduction and company contributions.
How to Use your HSA
• Online/Mobile: Sign-in for 24/7 account access to check your balance, pay bills and more.
• Call/Text: (817) 882-0800. EECU’s dedicated member service representatives are available to assist you with any questions. Their hours of operation are Monday through Friday from 8:00 a.m. to 7:00 p.m. CT, Saturday 9:00 a.m. –1:00 p.m. CT and closed on Sunday.
• Lost/Stolen Debit Card: Call the 24/7 debit card hotline at (800) 333-9934
• Stop by a local EECU financial center for in-person assistance; find EECU locations & service hours at www.eecu.org/ locations
EECU
14
EMPLOYEE BENEFITS
Hospital Indemnity Lincoln Financial Group
ABOUT HOSPITAL INDEMNITY
This is an affordable supplemental plan that pays you should you be inpatient hospital confined. This plan complements your health insurance by helping you pay for costs left unpaid by your health insurance.
For full plan details, please visit your benefit website: www.cbebc.com
Benefits at a glance
If you or a covered family member have to go to the hospital for an accident or injury, hospital indemnity insurance provides a lump-sum cash benefit to help you take care of unexpected expenses — anything from deductibles to childcare to everyday bills. Because you’re selecting this coverage through your company, you can take advantage of group rates. You don’t have to answer medical questions to receive coverage; this is guaranteed coverage.
admission - For the initial day of admission to a hospital for treatment of a sickness/ an injury. per day for one day per calendar year
Hospital confinement - For each day of confinement in a hospital as a result of a sickness/an injury. per day for 30 days per calendar year starting on the first day of confinement
Hospital intensive care unit (ICU) admission- For the initial day of admission to an ICU for treatment as the result of a sickness/an injury. per day for one day per calendar year
Hospital ICU confinement - For each full or partial day of confinement in an ICU as a result of a sickness/an injury. per day for 30 days per calendar year starting the first day of confinement
• If admitted to a hospital or ICU within 90 days after being discharged from a preceding stay for the same or related cause, the subsequent admission will be considered part of the first admission.
• If both hospital and ICU admission or hospital and ICU confinement become payable for the same day, only the larger of the two benefits will be paid. If the amount of the benefits is the same, only one will be paid. Additional confinement benefits

Newborn care - For each day of confinement to a hospital for routine post-natal care following birth. per day for two days per calendar year
• If a newborn baby is confined for treatment of an illness, infirmity, disease, or injury, we will pay the Hospital or ICU confinement benefit instead of the Newborn care benefit.
Hospital Indemity Insurance Monthly Premiums
As an employee, you can take advantage of this accident insurance plan. Plus, you can add loved ones to the plan for just a little more.
Questions? Call (800) 423-2765 and mention ID: CBEC
Core hospital benefits Low Plan High Plan
$1,000 $3,000
Hospital
$100
$200
$2,000 $6,000
$200 $400
Included Included
Complications of pregnancy
Low Plan High Plan
$500 $500
Hospital Indemnity Low Plan High Plan Employee Only $16.57 $32.42 Employee and Spouse $31.45 $65.48 Employee and Child(ren) $25.44 $51.04 Employee and Family $40.32 $84.10
EMPLOYEE BENEFITS 15
ABOUT TELEHEALTH
Telehealth provides 24/7/365 access to board-certified doctors via telephone or video consultations that can diagnose, recommend treatment and prescribe medication. Telehealth makes care more convenient and accessible for non-emergency care when your primary care physician is not available.

For full plan details, please visit your benefit website: www.cbebc.com
Alongside your medical coverage is access to quality telehealth services through MDLIVE. Connect anytime day or night with a board-certified doctor via your mobile device or computer. While MDLIVE does not replace your primary care physician, it is a convenient and cost-effective option when you need care and:
• Have a non-emergency issue and are considering a convenience care clinic, urgent care clinic or emergency room for treatment
• Are on a business trip, vacation or away from home
• Are unable to see your primary care physician
When to Use MDLIVE:
At a cost that is the same or less than a visit to your physician, use telehealth services for minor conditions such as:
• Sore throat
• Headache
• Stomach ache
• Cold
• Flu
• Allergies
• Fever
• Urinary tract infections
Do not use telemedicine for serious or life-threatening emergencies.
Registration is Easy
Register with MDLIVE so you are ready to use this valuable service when and where you need it.
• Online – www.mdlive.com/fbsbh
• Phone – (888) 365-1663
• Mobile – download the MDLIVE mobile app to your smartphone or mobile device
• Select –“MDLIVE as a benefit” and “FBS” as your Employer/Organization when registering your account.
Telehealth
Employee $8.00
Employee + Family $16.00
Check with your district to see if your employer offers this benefit at no cost to you and your family.
16
Telehealth MDLive EMPLOYEE BENEFITS
Dental Insurance Lincoln Financial Group
ABOUT DENTAL
Dental insurance is a coverage that helps defray the costs of dental care. It insures against the expense of routine care, dental treatment and disease.
For full plan details, please visit your benefit website: www.cbebc.com
Plans Effective 09/01/2023:
• Plan cover many preventive, basic, and major dental care services. (See Below)
• Both plans allow you to choose any dentist you wish, though you can lower your out-of-pocket costs by selecting a contracting dentist.
• Does not make you and your dependents wait six months between routine cleanings.
• More information available to you at www.lfg.com
Deductibles are combined for basic and major Contracting Dentists’ services. Deductibles are combined for basic and major Non-Contracting Dentists’ services.
Maximums are combined for preventive, basic, and major services
Orthodontic Coverage is available for dependent children to age 19.
Waiting Period There are no benefit waiting periods for any service types
You can also go to www.lfg.com and register/login to access your account and Downloand the Lincoln Dental Mobile App.
• Find a network dentist near you in minutes
• Have an ID card on your phone
• Customize the app to get details of your plan
• Find out how much your plan covers for checkups and other services
• Keep track of your claims
You can request your dental ID card by contacting Lincoln Financial Dental directly at (800) 423-2765.
Benefit Highlights High Plan Low Plan Contracting Dentists Non-Contracting Dentists Contracting Dentists Non-Contracting Dentists Calendar
Deductible Individual: $50 Family: $150 Waived for Preventive Individual: $50 Family: $150 Waived for Preventive Individual: $50 Family: $150 Waived for Preventive Individual: $50 Family: $150 Waived for Preventive
(Annual)
Annual Maximum $2,000 $2,000 $1,000 $1,000 Annual
Lifetime Orthodontic Max $1,000 $1,000 $1,000 $1,000
Dental High Plan Low Plan Employee Only $33.20 $17.96 Employee and Spouse $63.86 $35.90 Employee and Child(ren) $65.61 $39.43 Employee and Family $92.53 $57.38 17
EMPLOYEE BENEFITS
Vision Insurance Unum
ABOUT VISION
Vision insurance provides coverage for routine eye examinations and can help with covering some of the costs for eyeglass frames, lenses or contact lenses.
EMPLOYEE BENEFITS
For full plan details, please visit your benefit website: www.cbebc.com
Monthly Premiums
Employee Only $6.51
Employee and Spouse $12.92
Employee and Child(ren) $12.65
Employee and Family $19.27
Plan features:
Our network offers members access to convenient, quality care with more than 40,000 vision access points1, including independent optometrists and retail stores like Walmart, Sam’s Club, JCPenney, Sear’s Optical, America’s Best and many more!
• Find an in-network provider at unumvisioncare.com
• Manage benefits online with AlwaysAssist.com and onthe go with the AlwaysAssist mobile app.
Covered benefits:
Exam: Each member is entitled to a comprehensive vision exam. An exam co-pay applies and is outlined in the grid below.
All Participating Providers Out-of-Network Exam (1 per 12 month) $10 Co-pay Up to $42
Vision Care Services
Materials $25 Co-pay See Below
Standard Plastic Lenses: (1 per 12 month)
Single Vision Bifocal Trifocal
Lenticular Progressive
Premium Progressive
Ultra Progressive
Lens Options: Scratch resistant coating Polycarbonate Lenses for children to age 19
Frames: (1 per 12 months)
Members choose from any frame available at provider locations.
Contact Lenses3: (1 per 12 months)
(Includes fit4, follow-up and materials)
Elective
Medically Necessary
Covered by Co-pay
Covered by Co-pay
Covered by Co-pay
Covered by Co-pay
Covered by Co-pay
Covered by Co-pay + additional $60 Co-pay $110 allowance (20% discount on overages at VA and SP providers)
Covered at Wal-Mart only Covered
Up to $32 Up to $46 Up to $61 Up to $84 Up to $46 Up to $46
Up to $46 N/A N/A
Up to $130 allowance Up to $68 retail
$0 Co-pay Up
allowance Covered
Materials: Each member may purchase eyewear in the form of an eyeglass frame and lenses, or contact lenses. Purchases are subject to benefit frequencies and co-pays. Plan features include:
• Frame benefit: You may choose any frame within a provider’s collection, subject to the retail frame allowance listed below. If the cost is greater than the plan’s benefits, you are responsible for the difference.
• Eyeglass lens benefit: Standard plastic (CR-39 Plastic Material) single vision, bifocal and trifocal lenses are generally covered after any applicable materials copay. Plan allowances are listed below for specialty lenses. If the cost is greater than the plan’s benefits, you are responsible for the difference.
• Contact lens benefit: Members electing contact lenses instead of glasses may apply the contact lens allowance to any lenses in the provider’s collection. If the cost is greater than the plan’s benefits, you are responsible for the difference.
Laser vision correction: Discounts are available with participating surgery providers across the country (not an insured benefit)
to $130
$25
$100
$210
Standard contact lens fitting Exam Fee* Specialty contact lens fitting Exam Fee** Not Covered 18
Co-pay $50 allowance Up to
Up to
Not Covered
Vision Insurance Unum
Dependent children: Dependent age guidelines vary by state. Please refer to your policy certificate or contact customer service at (888) 400-9304.
Services not listed: If you expect to require a vision service not included on this brochure, it may still be covered. Please contact customer service at (888) 400-9304, to confirm your exact benefits.
This is a primary vision care benefit and is intended to cover only eye examinations and corrective eyewear. Medical or surgical treatment of eye disease or injury is not provided under this plan. Coverage may not exceed the lesser of actual cost of covered services and materials or the limits of the policy. Some providers at optical and/or retail chains, such as Walmart, may charge for a contact lens fit and evaluation separately and apart from your contact lens allowance, leaving the entire allowance for materials. Covered materials that are lost or broken will be replaced only at normal service intervals indicated in the Plan Design; however, these materials and any items not covered below may be purchased at Preferred Pricing from a Participating Provider. In addition, benefits are payable only for expenses incurred while the Group and individual Member coverage is in force.
This plan will not cover:
• Orthoptics or vision training and any supplemental testing; Plano (non- prescription) lenses; or two pair of eyeglasses in lieu of bifocals or trifocals;
• Medical or surgical treatment of the eyes;
• An eye exam or corrective eye wear required by an employer as a condition of employment;
• Any injury or illness covered under Workers’ Compensation or similar law, or which is work related;
• Plain or prescription sunglasses or tinted lenses, and no-line bifocals and blended lenses (subject to allowance);
• Sub-normal vision aids;
• Services rendered or materials purchased outside the U.S. or Canada, unless: the insured resides in the U.S. or Canada, and the charges are incurred while on a business or pleasure trip;
• Charges in excess of Usual and Customary for services and materials; Experimental or non-conventional treatments or devices;
• Safety eyewear;
• Spectacle lens styles, materials, treatments or “add-ons” not shown in the Schedule of Benefits.
Laser vision correction network
Membership provides access to preferred pricing. Transactions are handled directly between members and providers. Refractive surgery is an elective procedure and may involve potential risks to patients. This is not an insured benefit. Unum cannot and does not guarantee the outcome of any refractive surgical procedure or a total elimination of the need for glasses or contacts. Providers may not be available in all metropolitan areas. Login to www.alwaysassist.com for a list of participating laser vision correction providers.
19
EMPLOYEE BENEFITS
Disability Insurance Cigna | LFG EMPLOYEE BENEFITS
ABOUT DISABILITY
Disability insurance protects one of your most valuable assets, your paycheck. This insurance will replace a portion of your income in the event that you become physically unable to work due to sickness or injury for an extended period of time.
For full plan details, please visit your benefit website: www.cbebc.com
SUMMARY OF BENEFITS
If you had an unexpected illness of injury and were unable to work, how long would you be able to pay your bills? Long-term disability pays a portion of your salary if you’re unable to work due to a covered disability. Eligibility
All active Full-time Employees of the Employer who are citizens or permanent resident aliens of the United States and working a minimum of 20 hours per week in the United States.
Select Monthly Benefit: Flat dollar benefit in $100 increments between $200 and $7,500 that cannot exceed 662/3% of your current monthly earnings
0 days/7 days*
14 days/14 days*
30 days/30 days*
60 days/60 days
90 days/90 days
180 days/180 days
Please refer to the “Maximum Benefit Period” Schedules below for more details
*If because of your disability, you are hospital confined an inpatient, benefits begin on the first day of inpatient confinement
Employee’s Monthly Cost of Coverage
you are unable to perform the material duties of any occupation for which you are (or may reasonably become) qualified by education, training or experience, and you are unable to earn 60% or more of your indexed earnings. We will require proof of earnings and continued disability.
Covered Earnings–“Covered Earnings” means your wages or salary, not including bonuses, commissions, and other extra compensation.
Important Definitions and Policy Provisions:
Disability– “Disability” or “Disabled” means that, solely because of a covered injury or sickness, you are unable to perform the material duties of your regular occupation and you are unable to earn 80% or more of your indexed earnings from working in your regular occupation. After benefits have been payable for 24 months, you are considered disabled if solely due to your injury or sickness,
When Benefits Begin– You must be continuously Disabled for your elected benefit waiting period before benefits will be payable for a covered Disability. For any selected Benefit Waiting Period of 30 days or less, the Benefit Waiting Period will end of the date you are admitted as an inpatient in a hospital if that date is before the end of the time period specified.
Maximum Benefit Period– Once you qualify for benefits under this plan, you continue to receive them until the end of the benefit or until you no longer qualify for benefits,
Disability - per $100 in benefit Elimination Period Plan 1 0/7 $3.70 14/14 $3.14 30/30 $2.72 60/60 $2.22 90/90 $1.28 180/180 $0.92
Gross
Benefit1 Maximum Gross Monthly Benefit Benefit Waiting Period Maximum Benefit Period
Monthly
Employee Options
$7,500
Select from Four Options: Accident/Sickness
20
Disability Insurance
whichever occurs first. Should you remain Disabled, your benefits continue according to one of the following schedules, depending on your age at the time you become Disabled and the plan you select.
Pre-existing Condition Waiver: The Insurance Company will waive the Pre-Existing Condition Limitation for the first month of Disability even if the Employee has a Pre-Existing Condition. The Disability Benefits as shown in the Schedule of Benefits will continue beyond 1 month only if the Pre-Existing Condition Limitation does not apply.
Pre-existing Condition Limitation: Benefits are not payable for medical conditions for which you incurred expenses, took prescription drugs, received medical treatment, care or services (including diagnostic measures,) during the 3 months just prior to the most recent effective date of insurance. Benefits are not payable for any disability resulting from a pre- existing condition unless the disability occurs after you have been insured under this plan for at least 12 months after your most recent effective date of insurance.
When Coverage Takes Effect– Your coverage takes effect on the later of the policy’s effective date, the date you become eligible, the date we receive your completed enrollment form, or the date you authorize any necessary payroll deductions. If you’re not actively at work on the date your coverage would otherwise take effect, your coverage will take effect on the date you return to work. If you have to submit evidence of good health, your coverage takes effect on the date we agree, in writing, to cover you.
Benefit Reductions, Conditions, Limitations and Exclusions:
Effects of Other Income Benefits: This plan is structured to prevent your total benefits and post-disability earnings from equaling or exceeding pre-disability earnings. Therefore, we reduce this plan’s benefits by Other Income Benefits payable to you, your dependents, or a qualified third party on behalf of you or your dependents. Disability benefits maybe reduced by amounts received through Social Security disability benefits payable to you, your dependents, or a qualified third party on behalf of you or your dependents. Your disability benefits will not be reduced by any Social Security disability benefits you are not receiving as long as you cooperate fully in efforts to obtain them and agree to repay any overpayment when and if you do receive them. Disability benefits will also be reduced by amounts received through other government programs, sick leave, employer’s sabbatical leave, employer’s assault leave plan, employer funded retirement benefits, workers’ compensation, franchise/group insurance, auto no-fault, and damages for wage loss. For details, see your outline of coverage, policy certificate, or your employer’s summary plan description. Note: Some of the Other Income Benefits, as defined in the group policy, will not be considered until after disability benefits are payable for 6 months.
Earnings While Disabled: During the first 24 months that benefits are payable, benefits will be reduced if benefits plus income from employment exceeds 100% of pre-disability Covered Earnings. After that, benefits will be reduced by 50% of earnings from employment.
Limited Benefit Period: Disabilities caused by or contributed to by any one or more of the following conditions are subject to a lifetime limit of 24 months for outpatient treatment: Anxiety-disorders, delusional (paranoid) or depressive disorders, eating disorders, mental illness, somatoform disorders (including psychosomatic illnesses), alcoholism, drug addiction or abuse. Benefits are payable during periods of hospital confinement for these conditions for hospitalizations lasting more than 14 consecutive days that occur before the 24-month lifetime outpatient limit is exhausted.
Termination of Disability Benefits: Your benefits will terminate when your Disability ceases, when your benefit duration period is exceeded, or on the following events: (1) the date you earn from any occupation more than 80% of your Covered Earnings, or the date you fail to cooperate with us in a rehabilitation plan, or transitional work arrangement, or the administration of the claim.
Rehabilitation Requirement: To be eligible for Disability benefits under this plan, you may be required to participate in a rehabilitation plan at the sole discretion and expense of the insurance company or company administering benefits under this plan. If you fail to fully cooperate with the rehabilitation plan, no Disability benefits will be paid, and coverage will end. For details, see your Certificate of Insurance.
Exclusions: This plan does not pay benefits for a Disability which results, directly or indirectly, from any of the following:
• Suicide, attempted suicide, or intentionally self-inflicted injury while sane or insane.
• war or any act of war, whether or not declared.
• active participation in a riot.
• commission of a felony.
• the revocation, restriction, or non-renewal of an Employee’s license, permit or certification necessary to perform the duties of his or her occupation unless due solely to Injury or Sickness otherwise covered by the Policy.
• any cosmetic surgery or surgical procedure that is not Medically Necessary.
• an Injury or Sickness for which the Employee is entitled to benefits from Workers’ Compensation or occupational disease law.
• an Injury or Sickness that is work related.
In addition, the plan does not pay disability benefits any period of Disability during which you are incarcerated in a penal or corrections institution.
Maximum Benefit Period Schedule Age at Disability Duration of Payments (Accident and Sickness) Prior to age 60 To age 65, but not less than 5 years Age 60 through 64 5 years Age 65 through 69 To age 70, but not less than 1 year Age 70 and over 1 year
LFG EMPLOYEE BENEFITS 21
Cigna |
Disability Cigna | LFG
Traditional LTD and STD Disability - Definitions
What is disability insurance? Disability insurance protects one of your most valuable assets, your paycheck. This insurance will replace a portion of your income in the event that you become physically unable to work due to sickness or injury for an extended period of time.
Pre-Existing Condition Limitations - Please note that all plans will include pre-existing condition limitations that could impact you if you are a first-time enrollee in your employer’s disability plan. This includes during your initial new hire enrollment. Please review your plan details to find more information about pre-existing condition limitations.
How do I choose which plan to enroll in during my open enrollment?
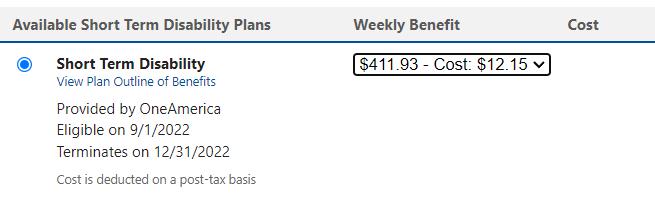
You will enroll in Long Term and Short Term Disability on two separate pages during your open enrollment walkthrough. Generally your short term coverage and long term coverage work together so that once your short term coverage ends, at that time your long term coverage would begin if you are still disabled and approved to remain on your claim. In other words, your short term coverage may continue for up to 12 weeks and your long term coverage begins the 13th week.
Your short term coverage will generally be a weekly benefit. This is the maximum amount of money you will receive from the carrier on a weekly basis once your disability claim is approved by the carrier. This is generally a flat percentage of your salary.
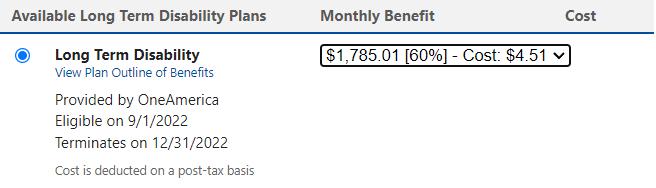
Your long term coverage will generally be a monthly benefit. This is the maximum amount of money you will receive from the carrier on a monthly basis once your disability claim is approved by the carrier. This is generally a flat percentage of your salary.
EMPLOYEE
BENEFITS
22
ABOUT CANCER
Cancer insurance offers you and your family supplemental insurance protection in the event you or a covered family member is diagnosed with cancer. It pays a benefit directly to you to help with expenses associated with cancer treatment.

For full plan details, please visit your benefit website: www.cbebc.com
Limited Benefit Group Specified Disease Cancer Indemnity Insurance
THE INSURANCE POLICY UNDER WHICH THIS CERTIFICATE IS ISSUED IS NOT A POLICY OF WORKERS’ COMPENSATION INSURANCE. YOU SHOULD CONSULT YOUR EMPLOYER TO DETERMINE WHETHER YOUR EMPLOYER IS A SUBSCRIBER TO THE WORKERS’ COMPENSATION SYSTEM.
Per
Summary of Benefits Low High Cancer Treatment Policy Benefits Level 1 Level 4 Radiation Therapy, Chemotherapy, Immunotherapy - Maximum per 12-month period $10,000 $20,000 Hormone Therapy
Maximum
12 treatments per calendar year $50 per treatment Experimental Treatment paid
maximums
benefit Cancer Screening Rider Benefits Level 1 Level 1 Diagnostic Testing - 1 test per calendar year $50 per test $50 per test Follow-Up Diagnostic Testing - 1 test per calendar year $100 per test Medical Imaging - per calendar year $500 per test/ 1 per calendar year $500 per test/ 1 per calendar year Surgical Rider Benefits Level 1 Level 4 Surgical $30 unit dollar amount Max $3,000 per operation $45 unit dollar amount Max $4,500 per operation Anesthesia 25% of amount paid for covered surgery Bone Marrow Transplant - Maximum per lifetime $6,000 $9,000 Stem Cell Transplant - Maximum per lifetime $600 $900 Prosthesis - Surgical Implantation/Non-Surgical (not Hair Piece) 1 device per site, per lifetime $1,000 / $100 $2,000 / $200 Patient Care Rider Benefits Level 1 Level 4 Hospital Confinement
-
of
in same manner and under the same
as any other
day of Hospital Confinement (1-30 days)
day
Eligible Dependent Children (1-30
Confinement (31+ days) Per day for Eligible Dependent Children (31+ days) $100 $200 $100 $200 $300 $600 $600 $1,200 Outpatient Facility - Per day surgery is performed $200 $600 Attending Physician - Per day of Hospital Confinement $30 $50 Dread Disease - Per day of Hospital Confinement (1-30 days / 31+ days) $100/$100 $300/$600 Extended Care Facility - Up to
of Hospital Confinement Days $100 per day $300 per day
Per
for
days) Per day of Hospital
the same number
Cancer
APL EMPLOYEE BENEFITS 23
Insurance
Cancer Insurance APL EMPLOYEE BENEFITS
of 45 days per Confinement for any combination of
Should you need to file a claim contact APL at (800)256-8606 or online at www.ampublic.com
You can find additional claim forms and materials at www.cbebc.com
Patient Care Rider Benefits (cont’d) Level 1 Level 4 Donor $100 per day $300 per day Home Health Care - Up to the same number of Hospital Confinement Days $100 per day $300 per day Hospice Care - Up to maximum of 365 days per lifetime $100 per day $300 per day US Government, Charity Hospital or HMO - Per day of Hospital Confinement (1-30 days / 31+ days) $100/$100 $300/$600 Miscellaneous Care Rider Benefits Level 1 Level 2 Cancer Treatment Center Evaluation or Consultation - 1 per lifetime Not Included $750 Evaluation or Consultation Travel and Lodging - 1 per lifetime Not Included $350 Second / Third Surgical Opinion - per diagnosis of cancer $300 / $300 $300 / $300 Drugs and Medicine - Inpatient / Outpatient (maximum $150 per month) $150 per confinement / $50 per prescription Hair Piece (Wig) - 1 per lifetime $150 $150 Transportation - Maximum 12 trips per calendar year for all modes of transportation combined Travel by bus, plane, or train Travel by car Lodging - up to a maximum of 100 days per calendar year actual coach fare or $0.40 per mile $0.40 per mile $50 per day actual coach fare or $0.75 per mile $0.75 per mile $100 per day Family Transportation - Maximum 12 trips per calendar year for all modes of transportation combined Travel by bus, plane or train Travel by car Family Lodging - up to a maximum of 100 days per calendar year actual coach fare or $0.40 per mile $0.40 per mile $50 per day actual coach fare or $0.75 per mile $0.75 per mile $100 per day Blood, Plasma and Platelets $300 per day Ambulance - Ground/Air - Maximum of 2 trips per Hospital Confinement for all modes of transportation combined $200 / $2,000 per trip Inpatient Special Nursing Services - per day of Hospital Confinement $150 per day Outpatient Special Nursing Services - Up to same number of Hospital Confinement days $150 per day Medical Equipment - Maximum of 1 benefit per calendar year Not Included $150 Physical, Occupational, Speech, Audio Therapy & Psychotherapy / Maximum per calendar year $25 per visit / $1,000 Waiver of Premium Waive Premium Internal Cancer First Occurrence Rider Benefits Level 1 Level 1 Lump Sum Benefit - Maximum 1 per Covered Person per lifetime $2,500 $2,500 Lump Sum for Eligible Dependent Children - Maximum 1 per Covered Person per lifetime $3,750 $3,750 Heart Attack/Stroke First Occurrence Rider Benefits Level 1 Level 1 Lump Sum Benefit - Maximum 1 per Covered Person per lifetime $2,500 Lump Sum for Eligible Dependent Children - Maximum 1 per Covered Person per lifetime $3,750 Hospital Intensive Care Unit Rider Benefits Intensive Care Unit $600 per day
Down Unit
Care Unit
$300 per day
Step
- Maximum
Intensive
or Step Down Unit
Cancer Low High Employee Only $17.10 $33.20 Employee and Spouse $31.20 $58.80 Employee and Child(ren) $23.60 $45.40 Employee and Family $31.20 $58.80 24
Accident Insurance Chubb EMPLOYEE BENEFITS
ABOUT ACCIDENT
Do you have kids playing sports, are you a weekend warrior, or maybe accident prone? Accident plans are designed to help pay for medical costs associated with accidents and benefits are paid directly to you.

For full plan details, please visit your benefit website: www.cbebc.com
Cash Benefits Paid in Addition to Any Other Coverage You Have
You do everything you can to stay active and healthy, but accidents happen every day, including sports-related accidents. An injury that hurts an arm or a leg can hurt your finances too. That’s where Chubb Accident can help. Chubb Accident pays cash benefits directly to you regardless of any other coverage you have. Benefits are designed to cover health plan gaps for out-ofpocket expenses like deductibles, copays, and coinsurance. Let Chubb Accident help take care of your bills so you can take care of yourself and your family.
Per visit, up to three visits
Per visit, up to three visits
Lodging
For treatment 100 miles or more away; per night, up to 30 nights
Major Diagnostic Exam (CT, MRI, etc.)
Physical, Occupational, or Speech
Per visit, up to 10 visits
Prosthetics
Surgery: Abdominal, Cranial, & Thoracic Tendon, Ligament or Rotator Cuff
For treatment 100 miles or more away; per trip, up to three trips
Accident Low High Employee Only $6.94 $10.73 Employee and Spouse $10.92 $16.89 Employee and Child(ren) $11.52 $17.82 Employee and Family $17.99 $29.08 Schedule of Benefits — 24-Hour Coverage Initial Care Low High Ambulance Ground Air Emergency Room Initial Doctor’s Office Visit Urgent Care Emergency Dental Crown Extraction Dentures Implants $500 $1,500 $150 $100 $100 $200 $50 $200 $200 $750 $2,000 $200 $150 $150 $450 $50 $450 $450 Hospital and Rehabilitation Low High Hospital Admission ICU Admission Hospital Confinement Per day, up to 365 days ICU Confinement Per day, up to 30 days Rehabilitation Confinement Per day, up to 30 days Recovery Per day, up to seven days $1,000 $1,000 $200 $400 $150 $25 $1,500 $2,000 $400 $600 $300 $25 Follow-up Care & Treatment Low High Appliances $100 $200 Follow-up Care & Treatment (cont’d) Low High Blood, Plasma, Platelets Chiropractic Care
Follow-up Treatment
Therapy
Surgery Transportation
X-ray $200 $25 $75 $125 $100 $50 $500 $2,000 $400 $400 $100 $200 $50 $100 $150 $300 $75 $1,500 $3,000 $400 $400 $150 Injuries Low High Burns 2nd/3rd Degree,
Skin Graft Coma Dislocations, up to Eye Injury $10,000 25% $10,000 $4,000 $500 $15,000 50% $15,000 $8,000 $800 25
up to
Accident Insurance Chubb
Knee Cartilage (Torn) Surgery
Loss of Hands, Feet or Sight, up to Loss of Fingers or Toes, up to Paralysis
For each child in a child care center: Per day, up to 30 days
Sports Package Benefit
Increases total benefit by 25% when accident is due to participation in organized sports. Up to $1,000 per person per year.
Injuries (cont’d) Low High Fractures,
Herniated
up to
Disc
Lacerations
Two limbs Four limbs Traumatic Brain Injury $8,000 $400 $400 $30-$500 $50,000 $5,000 $5,000 $7,500 $150 $10,000 $1,200 $400 $60-$1,000 $50,000 $5,000 $7,500 $10,000 $200 Additional Benefits Low High
Accident
Family Care
First
(Once per policy)
Elbow
Knee
Joint Replacement
Hip
Shoulder
Outpatient Physician Treatment & Preventative Care Benefit
$100 $25 $750 $1,500 $2,000 $900 $50 $100 $35 $1,500 $3,000 $4,000 $1,800 $50
EMPLOYEE
26
BENEFITS
Voluntary Life and AD&D Unum
ABOUT LIFE AND AD&D
Group term life is the most inexpensive way to purchase life insurance. You have the freedom to select an amount of life insurance coverage you need to help protect the well-being of your family.
Accidental Death & Dismemberment is life insurance coverage that pays a death benefit to the beneficiary, should death occur due to a covered accident. Dismemberment benefits are paid to you, according to the benefit level you select, if accidentally dismembered.
For full plan details, please visit your benefit website: www.cbebc.com
How does it work?
You choose the amount of coverage that’s right for you, and you keep coverage for a set period of time, or “term.” If you die during that term, the money can help your family pay for basic living expenses, final arrangements, tuition and more. AD&D Insurance is also available, which pays a benefit if you survive an accident but have certain serious injuries. It pays an additional amount if you die from a covered accident.
Why is this coverage so valuable?
If you previously purchased coverage, you can increase it up to $250,000 to meet your growing needs — with no health questions or exams.
Who can get Term Life coverage?
If you are actively at work at least 20 hours per week, you may apply for coverage for:
• You: Choose from $10,000 to $500,000 in $10,000 increments, up to 7 times your earnings. If you previously purchased coverage, you can increase it up to $250,000, your guaranteed issue amount, with no health questions. If you previously declined coverage, you may have to answer some health questions.
• Your spouse: Get up to $500,000 of coverage in $5,000 increments. Spouse coverage cannot exceed 100% of the coverage amount you purchase for yourself. If you previously purchased coverage for your spouse, they can increase their coverage up to $50,000, their guaranteed issue amount, with no health questions or exams, if eligible (see delayed effective date). If you previously declined spouse coverage, some health questions may be required.

• Your children: Get up to $10,000 of coverage in $2,000 increments if eligible (see delayed effective date). One policy covers all of your children until their 26th birthday. The maximum benefit for children live birth to 6 months is $100.
Who can get Accidental Death & Dismemberment (AD&D) coverage?
• You: Get up to $500,000 of AD&D coverage for yourself in $10,000 increments to a maximum of 7 times your earnings.
• Your spouse:50% of your AD&D coverage amount to a max
of $250,000 for your Spouse, if eligible (see delayed effective date).
• Your children: 10% of your AD&D coverage amount to a max of $50,000
What else is included?
A ‘Living’ Benefit — If you are diagnosed with a terminal illness with less than 12 months to live, you can request 50% of your life insurance benefit (up to $750,000) while you are still living. This amount will be taken out of the death benefit and may be taxable. These benefit payments may adversely affect the recipient’s eligibility for Medicaid or other government benefits or entitlements and may be taxable. Recipients should consult their tax attorney or advisor before utilizing living benefit payments.
Waiver of premium — Your cost may be waived if you are totally disabled for a period of time.
Portability — You may be able to keep coverage if you leave the company, retire, or change the number of hours you work. Employees or dependents who have a sickness or injury having a material effect on life expectancy at the time their group coverage ends are not eligible for portability.
Voluntary Group Life - per $1,000
in coverage Age Employee or Spouse 18-29 $0.048 30-34 $0.067 35-39 $0.076 40-44 $0.095 45-49 $0.143 50-54 $0.228 55-59 $0.371 60-64 $0.561 65-69 $1.083 70-74 $1.758 75+ $2.48 Child(ren) Voluntary Group Life - per $10,000 in coverage 0-26 $1.60 Spouse rates based on Employee's age. EMPLOYEE
BENEFITS
27
Critical Illness Insurance
Lincoln Financial Group EMPLOYEE BENEFITS
ABOUT CRITICAL ILLNESS
Critical illness insurance can be used towards medical or other expenses. It provides a lump sum benefit payable directly to the insured upon diagnosis of a covered condition or event, like a heart attack or stroke. The money can also be used for non-medical costs related to the illness, including transportation, child care, etc.

For full plan details, please visit your benefit website: www.cbebc.com
The Critical Illness Insurance Plan:
• Provides cash benefits if you or a covered family member is diagnosed with a critical illness or event
• Benefits are paid in addition to what is covered under your health insurance
• Features group rates for employees
• Includes access to a personal health advocate who can assist you in managing healthcare services for you and your entire family
• There are no waiting periods or overall plan maximums Group
Coverage for you
Critical Illness Insurance | Employee
Guaranteed coverage amount $40,000
Maximum Coverage Amount $40,000 (in increments of $5,000)
Minimum coverage amount $10,000
Guaranteed coverage amounts
• You can choose from the coverage amount
Maximum coverage amount
• You can choose from the coverage amount of $40,000 (in increments of $5,000).
Coverage for your spouse
You can secure Critical Illness Insurance for your spouse when you choose coverage for yourself.
Critical Illness Insurance | Spouse
Guaranteed coverage amount $40,000
Maximum Coverage Amount 100% of the employee coverage amount up to $40,000 maximum in increments of $5,000
Minimum coverage amount $5,000
Guaranteed coverage amount
• You can choose from the coverage amount up to $40,000 for your spouse
Maximum coverage amount
• You can choose a coverage amount up to 100% of your coverage amount ($40,000 maximum) for your spouse
Coverage for your dependent children
Your dependent children automatically receive 50% of your coverage amount at no extra cost.
Critical Illness Insurance | Children
Guaranteed coverage amount $20,000 (up to 50% of the employee coverage amount)
Rates
Employee Age Range (Attained Age) Critical Illness Premium Rate per $1,000 0-29 $0.260 30-39 $0.424 40-49 $0.646 50-59 $1.182 60-69 $3.183 70+ $3.183
Rates for Your Spouse Employee Age Range (Attained Age) Critical Illness Premium Rate per $1,000 0-29 $0.260 30-39 $0.424 40-49 $0.646 50-59 $1.182 60-69 $3.183 70+ $3.183
for You
Group
28
Critical Illness Insurance Lincoln Financial Group EMPLOYEE
You receive a cash benefit every year you and any of your covered family members complete a single covered exam, screening or immunization
Level: $50
Benefits Covered Conditions Benefit Percentage Heart attack 100% Sudden cardiac arrest resulting in death 100% Stroke 100% Invasive Cancer 100% End Stage Renal (kidney) Failure 100% Major organ failure (heart, lung, liver, pancreas, or intestine) 100% Arterial/vascular disease 25% Mitral or aortic valve disease 10% Noninvasive cancer (in situ) 25% Skin Cancer (other than melanoma $500 per lifetime Supplemental Conditions 100% Advanced Huntington’s disease 100% Advanced COPD 100% AIDS 100% Advanced ALS/Lou Gehrig’s disease 100% Advanced Alzheimer’s disease 100% Advanced Parkinson’s disease 100% Advanced multiple sclerosis 25% Benign brain tumor 100% Loss of sight, hearing and/or speech 25% Accidental Injuries Benefit Benefit Percentage Severe burns, permanent paralysis or traumatic brain injuries (includes coma) 100% Additional Childhood Conditions Benefit Percentage Cerebral palsy 100% Cleft lip, cleft palate 100% Cystic Fibrosis 100% Down syndrome 100% Muscular dystrophy 100% Spina bifida 100% Type 1 Diabetes 100%
Core
Health Assessment / Wellness Benefit Your Cash Benefit
29
BENEFITS
Identity Theft Experian EMPLOYEE BENEFITS
ABOUT IDENTITY THEFT PROTECTION
Identity theft protection monitors and alerts you to identity threats. Resolution services are included should your identity ever be compromised while you are covered.
For full plan details, please visit your benefit website: www.cbebc.com
My Financial Expert: Elite Plan
Financial Wellness & Identity Protection
Achieve your credit & financial goals sooner with unique insights With features like Digital Financial Management you will have tools to help manage your finances and credit profile in a single experience.
Digital Financial Management
360° view of financial accounts
Link your financial accounts to generate unique insights that can help improve your financial health and build good credit habits. Stay on top of your daily spending with recommended budgets powered by AI and machine learning of past transactional behavior.
Exclusive credit insights
Combine the power of financial transaction and credit data to unlock 50+ unique insights and recommendations to help achieve financial goals. Insights are displayed in your personalized feed and categories include account activity, spending and budgeting, VantageScore®* improvements, financial updates, and more.
Industry leading monitoring & alerts
Consistent monitoring of your Experian® credit report and VantageScore* can help you better understand your current credit profile and personal finances. Financial Alerts will notify you, via push notifications and emails, when certain financial events are detected.
Features to assist you with:
• Budgeting & cashflow
• Tracking spending
• Investments & net worth
Identity protection for the whole family
As identity theft continues to increase, an evolving suite of identity products helps you monitor any potential threats to your identity and alerts you if there are any areas of concern. In addition, you’ll have access to a suite of proactive digital privacy tools to help you keep passwords and other personal information private and secure while surfing the web.
An evolving suite of identity products to help you guard against the rising threat of fraud.
• Identity Restoration: Get back on track with support from an expert restoration agent that will walk you through the process of reclaiming what’s rightfully yours.
• Dark Web Monitoring: If we detect any threats on the thousands of websites and millions of data points we scan, we’ll alert you so you can keep your family’s personal information safe.
• Medical Identity Monitoring: If your insurance information is used to receive medical care or fill prescriptions, we’ll send you an alert to verify the service or act if you suspect identity theft.
• Experian CreditLock™: Block fraudsters from using your information to get new credit and act quickly to help prevent identity theft. Unlock it when you want to apply for credit.
Proactive Digital Privacy features to help keep your family’s personal data secure and reduce the threat of potential fraud
• Secure VPN: Helps to prevent people and companies from seeing and collecting your data.
• Password Manager: Safely store and protect your logins and payment information in one place.
• Safe Browser: Get alerted of unsafe websites, block ads and help prevent the tracking of your data.

Identity Theft Elite Plan Individual $7.00 Family $14.00 30
Emergency Medical Transport MASA
ABOUT MEDICAL TRANSPORT
Medical Transport covers emergency transportation to and from appropriate medical facilities by covering the out-of-pocket costs that are not covered by insurance. It can include emergency transportation via ground ambulance, air ambulance and helicopter, depending on the plan.
For full plan details, please visit your benefit website: www.cbebc.com
A MASA MTS Membership provides the ultimate peace of mind at an affordable rate for emergency ground and air transportation service within the United States and Canada, regardless of whether the provider is in or out of a given group healthcare benefits network. If a member has a high deductible health plan that is compatible with a health savings account, benefits will become available under the MASA membership for expenses incurred for medical care (as defined under Internal Revenue Code (“IRC”) section 213 (d)) once a member satisfies the applicable statutory minimum deductible under IRC section 223(c) for high-deductible health plan coverage that is compatible with a health savings account.
Emergent Air Transportation
In the event of a serious medical emergency, Members have access to emergency air transportation into a medical facility or between medical facilities.
Emergent Ground Transportation
In the event of a serious medical emergency, Members have access to emergency ground transportation into a medical facility or between medical facilities.

Non-Emergency Inter-Facility Transportation
In the event that a member is in stable condition in a medical facility but requires a heightened level of care that is not available at their current medical facility, Members have access to nonemergency air or ground transportation between medical facilities.
Repatriation/Recuperation
Suppose you or a family member is hospitalized more than 100-miles from your home. In that case, you have benefit coverage for air or ground medical transportation into a medical facility closer to your home for recuperation.
Should you need assistance with a claim contact MASA at (800)643-9023. You can find full benefit details at: www.cbebc.com.
EMPLOYEE BENEFITS Plan Features Emergent Plus Membership Platinum Membership Emergency Air Transportation x x Emergent Ground Transportation x x Non-Emergency InterFacility Transportation x x Repatriation/ Recuperation x x Escort Transportation x Visitor Transportation x Return Transportation x Mortal Remains Transportation x Minor Return x Organ Retrieval/Organ Recipient Transportation x Vehicle Return x Pet Return x Worldwide Coverage x 31
Flexible Spending Account (FSA)
ABOUT FSA
A Flexible Spending Account allows you to pay for eligible healthcare expenses with a pre-loaded debit card. You choose the amount to set aside from your paycheck every plan year, based on your employer’s annual plan limit. This money is use it or lose it within the plan year (unless your plan contains a $610 rollover or grace period provision).

For full plan details, please visit your benefit website: www.cbebc.com
Health Care FSA
The Health Care FSA covers qualified medical, dental and vision expenses for you or your eligible dependents. You may contribute up to $3,050 annually to a Health Care FSA and you are entitled to the full election from day one of your plan year. Eligible expenses include:
• Dental and vision expenses
• Medical deductibles and coinsurance
• Prescription copays
• Hearing aids and batteries
You may not contribute to a Health Care FSA if you enrolled in a High Deductible Health Plan (HDHP) and contribute to a Health Savings Account (HSA).
How the Health Care FSAs Work
You can access the funds in your Health Care FSA two different ways:
• Use your NBS Debit Card to pay for qualified expenses, doctor visits and prescription copays.
• Pay out-of-pocket and submit your receipts for reimbursement:
• Fax – (844) 438-1496
• Email – service@nbsbenefits.com
• Online – my.nbsbenefits.com
• Call for Account Balance: (855) 399-3035
• Lost or Stolen Debit Cards Replacement Fee $5.00 (taken from account balance)
• Mail: PO Box 6980 West Jordan, UT 84084
Contact NBS
• Hours of Operation: 6:00 AM – 6:00 PM MST, Mon-Fri
• Phone: (800) 274-0503
• Email: service@nbsbenefits.com
• Mail: PO Box 6980 West Jordan, UT 84084
Dependent Care FSA
This account helps pay for expenses associated with caring for elder or child dependents so you or your spouse can work or attend school full time. You can use the account to pay for day care or baby sitter expenses for your children under age 13 and qualifying older dependents, such as dependent parents.
NBS EMPLOYEE
32
BENEFITS
Flexible Spending Account (FSA)
Important FSA Rules
The maximum per plan year you can contribute to a Health Care FSA is $3,050. The maximum per plan year you can contribute to a Dependent Care FSA is $5,000 when filing jointly or head of household and $2,500 when married filing separately.
• You cannot change your election during the year unless you experience a Qualifying Life Event.
• You can continue to file claims incurred during the plan year for another 30 days (up until date).
• Your Health Care or Limited Purpose FSA debit card can be used for health care expenses only. It cannot be used to pay for dependent care expenses.
• The IRS has amended the “use it or lose it rule” to allow you to carry-over up to $610 in your Health Care FSA into the next plan year. The carry-over rule does not apply to your Dependent Care FSA.
Over-the-Counter (OTC) Item Rule
Health care reform legislation requires that certain over-the-counter (OTC) items require a prescription to qualify as an eligible Health Care FSA expense. You will only need to obtain a one-time prescription for the current plan year. You can continue to purchase your regular prescription medications with your FSA debit card. However, the FSA debit card may not be used as payment for an OTC item, even when accompanied by a prescription.
Flexible Spending Accounts
Health Care FSA
Dependent Care FSA
FSAstore.Com
Most medical, dental and vision care expenses that are not covered by your health plan (such as copayments, coinsurance, deductibles, eyeglasses and doctorprescribed over-the-counter medications)
Dependent care expenses (such as day care, afterschool programs or elder care programs) so you and your spouse can work or attend school full-time
$3,050
$5,000 single $2,500 if married and filing separate tax returns
Saves on eligible expenses not covered by insurance, reduces your taxable income
Reduces your taxable income
Check out the FSAstore at: https://fsastore.com. It offers thousands of FSA-eligible products and services to purchase using your FSA Debit Card or any major credit card. Competitive pricing and free shipping on orders over $50 can save you up to 40% using your FSA pretax dollars.
Account Type Eligible Expenses Annual Contribution Limits Benefit
NBS
33
EMPLOYEE BENEFITS
CBEBC Mobile App Login Group #’s
District
Agua Dulce ISD
Banquete ISD
Beeville ISD
Ben Bolt-Palito Blanco ISD
Benavides ISD
Bloomington ISD
Brooks County ISD
Cuero ISD
Dr M L Garza Gonzales Charter
Driscoll ISD
Ezzell ISD
Freer ISD
Hallettsville ISD
Horizon Montessori Public Schools
Ingleside ISD
Kenedy ISD
Kenedy County Wide CSD
La Villa ISD
Louise ISD
Lyford CISD
District GROUP #
Meyersville ISD
Monte Alto ISD
Odem-Edroy ISD
Odyssey Academy Inc.
Orange Grove ISD
Pettus ISD
Port Aransas ISD CBEBCW
Ramirez CSD
Refugio ISD
Ricardo ISD
Riviera ISD
San Perlita ISD CBEBCAC
Santa Gertrudis ISD CBEBCAD
Sinton ISD
Skidmore-Tynan ISD
St. Marys Academy Charter School
Three Rivers ISD
Waelder ISD
Webb CISD
CBEBCAE
CBEBCAF
CBEBCAG
CBEBCAQ
CBEBCAR
CBEBCAH
GROUP
#
CBEBCA
CBEBCB
CBEBCC
CBEBCD
CBEBCE
CBEBCF
CBEBCAJ
CBEBCH
CBEBCI
CBEBCJ
CBEBCK
CBEBCAN
CBEBCL
CBEBCAM
CBEBCM
CBEBCN
CBEBCAP
CBEBCAK
CBEBCP
CBEBCQ
CBEBCR
CBEBCAL
CBEBCS
CBEBCT
CBEBCU
CBEBCV
CBEBCX
CBEBCY
CBEBCZ
CBEBCAA
34
Use your District’s group # to login to the FBS Benefits app.
35
Notes
Enrollment Guide General Disclaimer: This summary of benefits for employees is meant only as a brief description of some of the programs for which employees may be eligible. This summary does not include specific plan details. You must refer to the specific plan documentation for specific plan details such as coverage expenses, limitations, exclusions, and other plan terms, which can be found at the CBEBC Benefits Website. This summary does not replace or amend the underlying plan documentation. In the event of a discrepancy between this summary and the plan documentation the plan documentation governs. All plans and benefits described in this summary may be discontinued, increased, decreased, or altered at any time with or without notice.

Rate Sheet General Disclaimer: The rate information provided in this guide is subject to change at any time by your employer and/or the plan provider. The rate information included herein, does not guarantee coverage or change or otherwise interpret the terms of the specific plan documentation, available at the CBEBC Benefits Website, which may include additional exclusions and limitations and may require an application for coverage to determine eligibility for the health benefit plan. To the extent the information provided in this summary is inconsistent with the specific plan documentation, the provisions of the specific plan documentation will govern in all cases.
WW W.CBEBC.COM 2023 - 2024 Plan Year
36
