

High tech EYE TECH May 2021 | Vol 26 Issue 5 SPECIAL FOCUS CATARACT & REFRACTIVE TECHNOLOGIES CATARACT & REFRACTIVE | CORNEA | RETINA | GLAUCOMA PAEDIATRIC OPHTHALMOLOGY
www.escrs.org RAI Amsterdam, The Netherlands 8 – 11 October 2021
Publisher
Carol Fitzpatrick
Executive Editor
Colin Kerr
Editors
Sean Henahan
Paul McGinn
Managing Editor
Caroline Brick
Content Editor
Aidan Hanratty
Senior Designer
Lara Fitzgibbon
Designer
Ria Pollock
Circulation Manager
Angela Morrissey
Contributing Editors
Howard Larkin
Dermot McGrath
Roibeard Ó hÉineacháin
Contributors
Maryalicia Post
Leigh Spielberg
Gearóid Tuohy
Priscilla Lynch
Soosan Jacob
Colour and Print
W&G Baird Printers
Advertising Sales
Amy Bartlett
ESCRS
Tel: 353 1 209 1100
email: amy.bartlett@escrs.org
Published by the European Society of Cataract and Refractive Surgeons, Temple House, Temple Road, Blackrock, Co Dublin, Ireland. No part of this publication may be reproduced without the permission of the managing editor.
Letters to the editor and other unsolicited contributions are assumed intended for this publication and are subject to editorial review and acceptance.
ESCRS EuroTimes is not responsible for statements made by any contributor. These contributions are presented for review and comment and not as a statement on the standard of care. Although all advertising material is expected to conform to ethical medical standards, acceptance does not imply endorsement by ESCRS EuroTimes. ISSN 1393-8983
18 ‘The Pandemic’: The latest television sensation: Dr Conor Lyons’s shortlisted essay for the John Henahan writing prize
19 People with clinically significant cataract have a higher mortality rate
20 Synchronisation: Dr Khayam Naderi’s shortlisted essay for the John Henahan writing prize
21 Allied healthcare professional participation can increase efficiency of ISBC
22 Mobile laminar air flow device allows hospital to treat patients safely
23 JCRS Highlights
CORNEA
24 Corneal transplantation can be performed safely in this COVID-19 era
26 Cross-linking alone shows promise as treatment in microbial keratitis
27 Intrastromal implantation for keratoconus patients
28 Tracking the role of genetic analysis in diagnosing corneal diseases

P.36
As certified by ABC, the EuroTimes average net circulation for the 10 issues distributed between January and December 2020 was 46,748
29 Bowman’s technique offers potential to avoid DALK or PK
P.25 CONTENTS A EUROPEAN OUTLOOK ON THE WORLD OF OPHTHALMOLOGY www.eurotimes.org RETINA 30 Advances in technology have expanded the possibilities for imaging in pathologic myopia 31 Postoperative posture after retinal detachment surgery - up or down? GLAUCOMA 33 ‘Alphabet soup’ trials have expanded clinical knowledge PAEDIATRIC OPHTHALMOLOGY 34 Remote screening can reduce blindness from retinopathy of prematurity REGULARS 36 Inside Ophthalmology 37 Industry News 39 Calendar SPECIAL FOCUS CATARACT & REFRACTIVE TECHNOLOGIES 4 What are the most significant technological advancements in cataract surgery? 6 Protection from violent assaults and infection top practice safety lists 7 COVID-19 has pushed teleophthalmology to the fore 8 An endothelial implant is a possible paradigm shift for corneal transplants 9 AI can improve the management of anterior segment diseases 11 Live streaming of surgery could help trainees CATARACT & REFRACTIVE 12 Immediate sequential bilateral cataract surgery is on the rise 13 Two different IOLs provide similar visual outcomes 14 What have we been missing?: Dr Diana Dragnea’s shortlisted essay for the John Henahan writing prize 15 Cataract surgery can induce wet AMD in a minority of dry AMD patients 16 Complications in phaco for small eyes
EUROTIMES | MAY 2021
MEDICAL EDITORS
INTERNATIONAL EDITORIAL BOARD
Noel Alpins (Australia), Bekir Aslan (Turkey), Roberto Bellucci (Italy), Hiroko Bissen-Miyajima (Japan), John Chang (China), Béatrice Cochener-Lamard (France), Oliver Findl (Austria), Nino Hirnschall (Austria), Soosan Jacob (India), Vikentia Katsanevaki (Greece), Daniel Kook (Germany), Boris Malyugin (Russia), Marguerite McDonald (USA), Cyres Mehta (India), Sorcha Ní Dhubhghaill (Ireland)
Rudy Nuijts (The Netherlands), Leigh Spielberg (The Netherlands), Sathish Srinivasan (UK), Robert Stegmann (South Africa), Ulf Stenevi (Sweden), Marie-José Tassignon (Belgium), Manfred Tetz (Germany), Carlo Enrico Traverso (Italy)
A
PhD
Guiding progress
It is with great pleasure that I write this editorial for the May issue of EuroTimes. This issue has a special focus on the use of technology in cataract and refractive surgery. Cataract surgery has improved significantly in terms of visual outcomes, complications and ease of the procedure. Our patients benefited from improvements in surgical technique and the development of more advanced phaco machines, OVDs and intraocular lenses with advanced optical characteristics.
I believe that recent advances are also based on improvements in optical biometry and the inclusion of factors such as posterior corneal power in IOL formulae. The use of these newer formulae including those based on artificial intelligence is also helping to improve accuracy. Some of them may be particularly useful for post-refractive surgery cases and extremely long or short axial lengths.
There have also been major advances in intraoperative imaging technologies such as 3D and OCT. The latter helped us to better understand the fluidics and anatomical causes of Infusion Misdirection Syndrome (IMS). Typical characteristics of IMS are the posterior capsule bulging forward, accumulation of lens particles behind the PC and anterior chamber flattening at the final steps of phacoemulsification and during irrigation-aspiration. That is not infrequent in eyes with advanced and mature cataracts and loose zonules and coming from irrigation fluid accumulating behind the posterior capsule due to the Wieger’s ligament rupture.
Since the outbreak of the COVID-19 pandemic, we have also had to re-evaluate the way we perform our surgeries and deal with our patients. In future years, we can look forward to more exciting developments in the field of telemedicine.
In this issue of EuroTimes Dr Iain Livingstone discusses his experience helping to set up a pioneering virtual emergency teleophthalmology programme covering a large part of Scotland in response to the COVID-19 emergency.

In conclusion, let me leave a final reflection from my friend and colleague, Professor Rudy MMA Nuijts, President of the ESCRS.





In the EuroTimes Cover Story Prof Nuijts points out that whatever the future holds, the focus must continue to be on addressing patient needs. He asks will it make sense to continue to push visual outcomes within 0.5D of target beyond the 80-85% achievable today? “I have not seen any study that addresses that,” he says.
With limited resources and difficulties to eye care access in many countries we really are in great need of breakthrough innovations that will increase our efficiency and the quality of care for the many patients in need.
EDITORIAL 2
EDITORIAL
GUEST
Emanuel Rosen Chief Medical Editor
José Güell
Boris Malyugin
Thomas Kohnen
Paul Rosen
Cataract surgery has improved significantly in terms of visual outcomes, complications and ease of the procedure
WORD FROM BORIS MALYUGIN MD,
Whatever the future holds, we must address patient needs
EUROTIMES | MAY 2021
Boris Malyugin is Professor of Ophthalmology, Cataract and Implant Surgery Department, and Chief, S.Fyodorov Microsurgery Complex, Moscow, Russia
Research Education Innovation
ESCRS’s vision is to educate and help our peers excel in our field. Together, we are driving the field of ophthalmology forward.

High tech EYE TECH
Meeting patient needs drives adoption of new cataract technologies. Howard Larkin reports
It is often said that technology innovation drives cataract surgery progress, and to a large extent this is true. But of the multitude of technological innovations over the past quarter century, which are most significant?
For Rudy MMA Nuijts MD, PhD, the answer is simple: the ones that have the most favourable effects on patients. And by that definition the most significant change was already well under way when he trained in the late 1980s – the transition from extracapsular cataract extraction to phacoemulsification.
“You didn’t have the sutures so there was an immediate beneficial effect in terms of the speed of restoration of visual acuity because of the smaller incision. Crucial to the adoption of new technology is, what does it do for the patient? If the patient experience is not dramatically changed, adoption will be very difficult,” said Prof Nuijts, of Maastricht University Medical Centre, The Netherlands.
Prof Nuijts offered laser-assisted cataract surgery and trifocal lenses as two examples of technologies that have not caught on as well. For routine cases, laser-assisted surgery has not been shown to improve
outcomes over manual phaco, while issues such as haloes and glare continue to hold back multifocal diffractive lenses. “In my experience, patients are often willing to trade off a little less spectacle independence for less visual side-effects and greater predictability.”
PAST AND FUTURE PROGRESS
Applying the same standard to technologies on the horizon, Prof Nuijts sees eliminating antibiotic and anti-inflammatory eye drops after surgery through the use of intracameral
EUROTIMES | MAY 2021 SPECIAL FOCUS: CATARACT & REFRACTIVE TECHNOLOGIES 4
and periocular injections, and druginfused IOLs as one of most likely to improve patient experience. The effect of subconjunctival injection of antiinflammatory drugs is the subject of the ongoing EPICAT study sponsored by ESCRS. In addition to improving outcomes and relieving patient burden, dropless cataract surgery would reduce the expense of home care for the 9% or so of patients who require it. At €70 per day, its cost can exceed the total professional fee for surgery, he pointed out.
Prof Nuijts sees same-day bilateral cataract surgery as another change that will greatly enhance patient experience and reduce the time and cost of follow-up. Already nearly half of his procedures are bilateral, up from next to nothing two years ago. “It’s word of mouth; ‘can you do both eyes for me?’ Patients actively ask for it.”
Similarly, accelerated by COVID-19, phone and video technology have cut in person follow-up visits from four to one. Development of artificial intelligence routines may make remote follow-up even more efficient. These procedural changes will also reduce the environmental impact of cataract surgery, he added.
That said, cataract surgery has improved significantly in terms of visual outcomes, complications and ease of the procedure thanks to many incremental technical improvements. For example, as recently as 2006, the UK National Health Service benchmark for post-cataract surgery refractive outcomes in normal eyes was 55% within 0.5D of target and 85% within 1.0D. A recent study involving 10 centres in The Netherlands reached 80% within 0.5D using the Barrett Universal II intraocular lens (IOL) power formula, Prof Nuijts said. “That is 10% higher than before.” With such accuracy cataract surgery has truly become a refractive procedure.
These recent advances are due in part to improvements in optical biometry and the inclusion of factors such as posterior corneal power in IOL formulae, said Boris Malyugin MD, PhD, of the S. Fyodorov Eye Microsurgery Federal State Institution in Moscow, Russia. Incorporating artificial intelligence into formulae is further increasing their accuracy and may be particularly useful for post-refractive surgery and extremely long or short axial lengths.
Dr Malyugin sees integration of imaging technology into surgical microscopes as a significant step forward for the future, particularly for handling complex cases. For example, OCT imaging has revealed that much of the anterior chamber flattening in eyes with mature cataracts and loose zonules comes from irrigation fluid accumulating behind the posterior capsule due to rupture of the anterior hyaloid, pushing the capsule forward. Understanding this complication, which was previously unknown, helps avoid and manage it.
Improved tomographers and a better understanding of astigmatism have
also improved IOL power prediction, said Soosan Jacob MS, FRCS, DNB, of Dr Agarwal’s Refractive and Cornea Foundation and Dr Agarwal’s Group of Eye Hospitals, Chennai, TN, India. She sees even better prediction of IOL power and preoperative assessment of visual needs using technologies such as SimVis (2Eyesvision) as ways to customise and improve visual outcomes.
Improvements in surgical technique, particularly reducing incision size, have also contributed to better outcomes, Dr Malyugin said. “At around 2.0mm, slightly less or slightly more, it looks like we have reached the sweet spot and do not need to decrease it further. These incisions are truly astigmatically neutral and reduce surgical trauma significantly.”
Improvements in phaco machines also helped, Dr Malyugin said. The introduction of alternatives to longitudinal ultrasound vibration, such as Ozil (Alcon) torsional and Ellips (Johnson & Johnson) elliptical vibration, improved the effectiveness and reduced ultrasound energy required for dissolving cataracts. Smaller needles and stiffer tubing allowed higher vacuum with stable fluid flow, while advanced sensors interrupted suction instantaneously. This not only enhances chamber stability, reducing the risk of corneal endothelial cell and iris damage, it can help reduce cystoid macular oedema and posterior vitreous detachment, he added.
ADDRESSING GLOBAL BLINDNESS
For David F. Chang MD, access to affordable cataract surgery in the developing world is perhaps the most significant unmet eye care need. According to the World Health Organization, an estimated 94 million people worldwide have moderate or severe vision impairment or blindness due to unaddressed cataract, with prevalence four times higher in low-and middle-income regions than in highincome areas.
But advanced surgical technology is not the solution, said Dr Chang, a clinical professor at the University of CaliforniaSan Francisco, USA, and co-chair of the ASCRS Foundation. Certain surgical technologies are not practical in many low-resource countries for reasons ranging from cost to the reliability of electrical power and equipment maintenance.
The increasing backlog of global cataract blindness is due in large part to the lack of enough skilled surgeons who can execute more sustainable and cost-effective procedures such as manual small-incision cataract surgery (MSICS).
Enlisting visiting ophthalmologists to operate or teach in low- to middleincome countries is neither a sufficient nor scalable approach, Dr Chang added. Instead, the focus should be
on developing and improving local ophthalmology training programs.
“This is potentially where new technology can really help – by enabling and supporting remote learning and virtual consultation,” said Dr Chang. Applications such as Zoom can already allow experienced surgeons to virtually teach, mentor and provide clinical consultation to ophthalmologists and trainees anywhere in the world in real time, even as they perform surgery.
“Having the high-speed networking infrastructure to deliver these services is essential and new technology that can harness remote volunteers to help train and provide virtual consultation can accelerate the improvement of eye care in resource limited settings,” he noted.
According to Dr Chang, a leading example is Orbis’ Cybersight, which offers free online training courses and live webinars in all of the major sub-specialty areas in ophthalmology. The Cybersight platform is already virtually linking ophthalmologists in lower resource settings with volunteer consultants who can provide clinical answers and support within hours.
Cybersight’s networking technology allows a surgeon in the US to remotely monitor the live surgical microscope view of someone operating in Africa. Or they could remotely supervise a trainee using a networked surgical microscope in a wet lab.
Telemedicine holds the promise that ophthalmologists anywhere in the world could access AI-driven interpretation of uploaded fundus images.
“In addition, we’ve learned during COVID that virtual meetings, such as the ESCRS Congress, can be attended by international ophthalmologist that would not otherwise be able to travel for meetings,” Dr Chang said.
Finally, Orbis is working on an affordable surgical simulator for MSICS. Simulators are an effective and proven training adjunct, but the technology remains too expensive for most global settings. The Orbis project seeks to utilise existing gaming technology to develop surgical simulation systems that are portable, more affordable, and truly scalable, Dr Chang noted. Both he and the ASCRS Foundation have contributed support to this project.
PATIENT NEEDS RESEARCH
Whatever the future holds the focus must continue to be on addressing patient needs, Dr Nuijts said. Doing so will require research into exactly what those needs are. For example, will it make sense to continue to push visual outcomes within 0.5D of target beyond the 80-85% achievable today?
“I have not seen any study that addresses that.” In a world of limited resources, better defining the goals will be increasingly important to guide further progress.
SPECIAL FOCUS: CATARACT & REFRACTIVE TECHNOLOGIES 5 EUROTIMES | MAY 2021
Staying safe
Protection from violent assaults and infection top practice safety lists. Howard Larkin reports
Doctors being abused and attacked over COVID-19 concerns.” “Second wave brings new reports of ‘awful’ abuse against nurses.”
These are some of the headlines in the news today, said Christopher Teng MD, associate professor of ophthalmology and visual science at Yale School of Medicine, New Haven, Connecticut, USA. Protecting your practice staff and yourself against an increase in violent activity is emerging as a concern during the pandemic, according to Dr Teng and others on a disaster preparedness panel at AAO 2020 Virtual.
In a recent survey by the UK’s Medical Protection Society, more than one-third of doctors reported they had suffered verbal or physical abuse from patients during the COVID-19 outbreak, including being assaulted and shouted at in the street, Dr Teng said.
But while the pandemic has played a role in shortening fuses, even before the 2020 outbreak violence against doctors was a significant problem. Indeed, healthcare is one of the more dangerous occupations, said Ranya Habash MD, medical director for technology innovation at Bascom Palmer Eye Institute, Miami, USA.
Nearly half of emergency department physicians reported being assaulted in the emergency room and 71% have witnessed an assault, according to studies by the American College of Emergency Physicians and the US Bureau of Labour Statistics. And healthcare workers are about four times more likely to suffer violence at work than construction workers.
PANIC BUTTON
Dr Teng recommends taking precautions. A few years ago, a colleague in his practice was assaulted. “We were not fully prepared. Silent alarms were not active, we did not know how to optimally handle the situation, there was no safe room.
“Since then, we have implemented
de-escalation trainings, activated alarms at the front desk, installed keyboard alarm systems and created a locked area,” Dr Teng said. “Ask yourself this question: what if there were a violent act in my office against a staff member or doctor? What would I do?”
Dr Teng recommended talking about the risk of violence with partners, associates and staff, and coming up with a plan. Take training courses. Create an exit plan or safe area. Know when to run, hide or fight.
“Our exams are in closed-door rooms. Consider outfitting every room with panic buttons or alarms, keyboard buttons, silent alarms or even airhorns. You can never be overprepared.”
Installing alarms can be as simple as downloading an app, said Dr Habash, who is also chief medical officer for Everbridge, a safety technology concern. The firm’s software offerings include a tracking programme with a virtual panic button. It can instantly tell event managers and security personnel where an incident is taking place.
“We have had a lot of success with that in large health systems.” Often, assaults take place outside or in parking area, and mobile security devices are especially helpful for these, Dr Habash noted.
PROTECTING STAFF & PATIENTS
When patients must be seen after hours, consider having a second team member come to help ensure safety, log into an app, or have patients be seen in an emergency department, though this may be less convenient for some patients such as postoperative patients, Dr Teng said. At Bascom Palmer, patients are almost always seen by telemedicine first both outside and inside the hospital, and residents are typically sent to in-person visits whenever appropriate to reduce exposure for older doctors at higher risk of infection, Dr Habash said.
At the Eye Clinic of Florida in Zephyrhills, Florida, USA, in addition to the usual wipe-downs, masks and other hygiene measures, a robot with ultraviolet lights

is sent in to help sanitise rooms between patients, said Ahad Mahootchi MD. The clinic publishes pictures of staff hugging the robot as part of an overall effort to communicate to patients that the clinic takes their safety seriously. “I think that really breaks the ice with a lot of people who are scared to come in.” The message is also reinforced in phone calls to patients before visits, and helps reduce cancellations, which currently run about 15%, Dr Mahootchi said. Assessing and documenting steps you take to keep patients and staff safe are essential for ongoing success, said Steven Yeh MD, professor of ophthalmology at the Truhlsen Eye Institute, University of Nebraska Medical Center, Omaha, Nebraska, USA. He recommended that clinics develop a leadership task force to identify personnel for decision-making, implementation and communication of protocols to keep the clinic safe during a public health emergency.
In addition, Dr Yeh recommends a thorough review of processes as an institution to assess clinic performance and response and to identify areas where new knowledge or procedures are needed to improve responses to emergencies of all kinds.
“We clearly need to anticipate infectious disease outbreaks as they can affect our collective global health and vision health communities,” Dr Yeh said.
EUROTIMES | MAY 2021 SPECIAL FOCUS: CATARACT & REFRACTIVE TECHNOLOGIES 6
We were not fully prepared. Silent alarms were not active, we did not know how to optimally handle the situation...
Christopher Teng MD
A robot with UV lights is sent in to help sanitise rooms between patients at the Eye Clinic of Florida in Zephyrhills, Florida, USA
Courtesy of Ahad Mahootchi MD
Pioneering telemedicine project
Scottish tele-ophthalmology project points to the future of eye care. Dermot McGrath reports
Telemedicine offers rich potential to serve dispersed populations in rural areas, reduce crowded clinics and avoid unnecessary hospital visits for patients, according to a presentation at the 25th Winter Meeting of the ESCRS.
In a wide-ranging talk, Iain Livingstone MD discussed his experience helping to set up a pioneering virtual emergency teleophthalmology programme covering a large part of Scotland in response to the COVID-19 emergency. The innovative network uses inexpensive equipment and a live video feed to securely connect doctors, opticians and patients and ensure that patients with serious eye problems can be immediately diagnosed and treated.
“We have been using digital mobile technologies and leveraging them for decision support since around 2017. However, the technology really came into its own when the COVID-19 pandemic struck and completely disrupted traditional eye care,” said Dr Livingstone.
The tele-ophthalmology system was developed in collaboration between the University of Strathclyde in Scotland and NHS Forth Valley, which is one of the “health boards” that make up the Scotland National Health Service (NHS), explained Dr Livingstone.
A network of optometrists in different regions of Scotland was enlisted to attend to urgent eye problems, meaning that only cases that need secondary care were directed to hospitals. The system works well with screenshare from any video slit lamp, but can also be achieved with four basic components: a slit-lamp microscope, a 3D-printed bracket mount for stability, an iPad or webcam to provide a live video feed between the patient, the on-site clinician and the remote ophthalmologist and a telemedicine platform, such as Attend Anywhere, a Chrome-based web platform in the case of NHS Scotland.
“The paradigm basically involved interposing a webcam or iPad into the slit lamp that enables video consultation whereby we could see through the optical equipment and give more nuanced advice
and often prevent an escalation to hospital. The system essentially means that an eye specialist is able to review patients at the moment advice is needed, offering decision support to the optometrist and ensuring any follow-up treatment is more streamlined,” he said.
Since first using the system to diagnose and grade a chemical injury of a patient in 2017, Dr Livingstone said that its utility really came to the fore during the COVID-19 pandemic when a lot of routine healthcare ground to a halt in Scotland.
“In March 2020, NHS Scotland changed the way that it handles acute eye care. The population was told to stay home, and in several NHS boards, including my own, optometric practices were only opened if there were going to be providing exclusively acute eye care. Using the teleophthalmology system, we activated one optometrist per 100,000 population. In my NHS board, we had three optometric practices for a population of around 320,000,” he said.
The goal was to massively increase the remit of what optometrists could typically do by giving them the digital tools to include experts directly in their consultations as needed, said Dr Livingstone.
“Whether it was viewing the OCT in a live way that we could see the volume scans and discuss with them and the patient at the same time, or whether it was through the video slit-lamp and looking at a cornea, the system meant that we could get much more nuanced plans. We would typically receive up to nine calls a day for consultations,” he said.
Using this approach, the experts were able to successfully manage between 50 and 70% of cases at a distance without the need
for a second consultation for the patient.
“We use NHS Near Me, powered by Attend Anywhere, which is a Google Chrome-based video conferencing platform specifically designed to embody a virtual clinical workspace. We found that the level of escalations before lockdown was decreased significantly. In about 64% of all the video calls, we felt at least one appointment was saved and that increased to 86% during the first lockdown,” he said.
Dr Livingstone said that the system has also proven its worth in enabling emergency consultations directly from the patient’s home in certain instances.
He cited the example of one patient whose optometrist forwarded a photo of possible COVID-19 conjunctivitis to the experts for a second opinion.
“These optometrists were in harm’s way at the time as there was limited personal protective equipment available. So, we agreed to set up a video call with the patient and we were able to examine the eye and perform a visual acuity test. It became clear this was not conjunctivitis but a pupil-involving orbital problem, causing proptosis and limitation of eye movements. The patient went directly for a CT scan without seeing an optometrist or ophthalmologist face to face. It turned out he had a fistula and went straight to the neurosurgeon,” he said.
Going forward, Dr Livingstone said that ongoing advances in technology and increasing pressure on healthcare systems to make better use of resources will further spur demand for tele-ophthalmology.
“I honestly think that this kind of system is going to be the heart of a forwardlooking ophthalmic service in 2021 and beyond,” he concluded.
EUROTIMES | MAY 2021 SPECIAL FOCUS: CATARACT & REFRACTIVE TECHNOLOGIES 7
...the technology really came into its own when the COVID-19 pandemic struck and completely disrupted traditional eye care
Iain Livingstone MD
Deceptive NORMALITY
Quick and reliable early detection of normal tension glaucoma


Glaucoma is only young once, making its early detection and treatment all the more important. However, glaucoma is especially often overlooked in eyes with normal IOP. Here’s where the OCULUS Corvis ® ST with its glaucoma screening software comes in useful.
Novel corneal implant in trials
Endothelial implant a possible paradigm shift for corneal transplants.

Dermot McGrath reports
The first in-human trials of a novel artificial implant designed to replace dysfunctional corneal endothelium have shown the device to be safe and well-tolerated, according to a study presented at the 25th ESCRS Winter Meeting online.
“The initial results of the EndoArt (EyeYon Medical) are very promising indeed,” said Ruth Lapid-Gortzak MD, PhD, Amsterdam University Medical Centre in the Netherlands. “There were no device-related adverse events over the 12 months’ follow-up and technically the implantation of the EndoArt is simpler and easier than surgery with donor tissue. In the first four patients, the implant was safely attached throughout the study period and in most patients the corneal thickness decreases without pathological thinning,” she said.
Visual acuity also improved in two patients even though that was not a primary goal of the study.
The gold standard for treating corneal endothelial failure is human donor tissue, but there are an estimated 13 million patients currently waiting for corneal tissue globally. A safe and effective artificial endothelium implant would address a fundamental medical need, said Dr Lapid-Gortzak.
With a thickness of 30-50 microns, a diameter of 5-8mm and a curvature of 8mm, the EndoArt is an optically clear dome-shaped flexible disc that is biocompatible and biostable. It works by partially sealing the posterior cornea, decreasing the flow of liquid and establishing a new equilibrium to maintain metabolism.
This initial study had two principal goals, explained Dr Lapid-Gortzak: to demonstrate the adherence of the EndoArt to the cornea and establish a thinner cornea over the follow-up period. The inclusion criteria were eyes with endothelial cell failure with a guarded visual prognosis for non-corneal reasons and with good vision in the other eye.
Of the four patients implanted with EndoArt, all were complex eyes (complicated cataract, distorted pupil, severe atopia, glaucoma, nanophthalmos) with very thick corneas. The vision improved in two patients postoperatively and central corneal thickness decreased in three out of four patients.
“In the one patient where it did not decrease, we think it was due to using an implant that was too small in diameter,” noted Dr Lapid-Gortzak.
The next steps for the device are to confirm its safety according to protocol, improve the implantation technique, reduce re-bubbling and build a nomogram for the sizing of the implant.
“Theoretically, the EndoArt has clear benefits as no tissue or tissue bank is needed, and there are no rejection issues or transmission of infections to worry about. The technique will be cost-effective, scalable and may also provide a temporising measure in case one would like to perform a DMEK at a later stage – for example during the recent COVID epidemic when there was no tissue available,” she concluded.
www.oculus.de
The internal pressure was completely normal, yet still the balloon burst. Why?
Eurotimes Corvis ST Deceptive Normality 93x266 e 4c 03.21 v2.indd 1 06.04.2021 13:17:40
EUROTIMES | MAY 2021 SPECIAL FOCUS: CATARACT & REFRACTIVE TECHNOLOGIES 8
There were no device-related adverse events over the 12 months’ follow-up...
Ruth Lapid-Gortzak MD, PhD
AI and corneal diseases

While retinal disease has led the way in the application of artificial intelligence (AI) in ophthalmology, there are also many opportunities for using AI technology to improve the evaluation and management of anterior segment diseases, said Jodhbir S Mehta MD, PhD. Speaking at the ESCRS 2020 Virtual meeting, Dr Mehta focused on AI applications for corneal dystrophies.
“Artificial intelligence is a platform technology that can be employed for multiple purposes in any field where there is a large dataset and good images. The promise of AI is from its capability to see things that we cannot interpret clinically,” said Dr Mehta, Distinguished Professor of Clinical Innovation, Singapore National Eye Centre, Singapore.
MULTIPLE USES
Dr Mehta reported that his research group has developed and validated AI software for segmenting granular lesions in images from individuals with granular corneal dystrophy type 2.
“We know that the transforming growth factor β-induced (TGFBI) protein dystrophies are cumulative disorders in which the mutant TGFBI protein aggregates and accumulates in the cornea with time. However, patients with the same genotype can present with different phenotypes because the protein aggregates can develop in a different form depending on ethnicity, age at presentation, and other factors. In addition, patients with different genotypes can present with the same phenotype. Furthermore, patients with a TGFBI protein dystrophy who undergo transplantation are at risk for recurrence, but the risk varies depending on the underlying mutation,” Dr Mehta explained.
He proposed that the software could be used in clinical practice as a longitudinal monitoring tool in primary patients who have been diagnosed with a TGFBI-associated corneal dystrophy, and to check for protein aggregate recurrence in patients being followed after corneal transplantation. In addition, the AI algorithm could have a role in research to evaluate the effect of novel therapies for the protein aggregation disorder, such as osmolytes, chaperones and gene therapies.
Dr Mehta reported that the AI deep learning algorithm for analysing corneal images from patients with granular corneal dystrophy type 2 was developed by binarising the images into a black background with white spots representing the aggregates. The algorithm was trained and validated using a set of 806 “ideal” slit-lamp photographs from patients with granular corneal dystrophy type 2 and an internal testing set of 201 highquality slit-lamp photographs. The software was also shown to have good reproducibility when applied to images from a smaller series of cases.
Next, it was applied to an external testing set of 140 “realworld” photographs that were of poorer quality but considered representative of images that might be obtained in clinical practice.
In that application, the AI algorithm outperformed human raters who undertook segmenting of the stromal lesions by hand.
“As expected, the software did not perform as well when analysing the ‘real-world’ slitlamp pictures as it did with the ideal images. However, our deep learning algorithm still did much better compared to the human rater values for this external dataset,” Dr Mehta said.
GUTTAE GRADING IN EYES WITH FUCHS’
Similarly, Dr Mehta and colleagues have used AI to develop an automated tool for analysing corneal guttae in eyes with Fuchs’ endothelial corneal dystrophy [Soh YQ, et al. Am J Ophthalmol 2020 Jul 27:S0002-9394(20)30387-1]. The algorithm’s performance was validated through comparison with a manual approach to guttae identification and shown to have good agreement with the conventional Krachmer grading scale. In addition, the reproducibility of its results was demonstrated through repeated testing in a subgroup of patients.
Explaining the clinical application of this tool, Dr Mehta suggested it has the potential to improve the outcomes of transplantation surgery.
“An improved disease grading system for eyes with Fuchs’ dystrophy that is able to identify anatomic subregions of the cornea that are most affected by dense Descemet membrane guttae could potentially help guide planning of descemetorhexis zones when performing Descemet stripping only or Descemet membrane transplantation.
FAST-TRACKING THERAPEUTIC DEVELOPMENT
Dr Mehta also highlighted the power of using AI as a drug discovery platform when designing therapeutics for corneal dystrophies. He discussed published work from his group that involved a conventional approach to developing pharmacotherapy for TGFBI-corneal dystrophy [Venkatraman A, et al. J Adv Res. 2020;24:529-543.]. He reviewed the steps that were used in the drug screening process for identifying candidate compounds able to bind with high affinity to the mutant protein, beginning with the need to characterise the folding and shape of the protein itself.
“The conventional approach to drug discovery is cumbersome. In fact, according to one paper, it could take 13.8 billion years to figure out all of the possible configurations of a typical protein. Artificial intelligence with deep learning could potentially enable the search for therapeutic targets for new drugs by fast-tracking the process of protein structure and binding prediction,” he predicted.
Technology holds promise as diagnostic and drug development tool. Cheryl Guttman Krader reports
EUROTIMES | MAY 2021 SPECIAL FOCUS: CATARACT & REFRACTIVE TECHNOLOGIES 9
• Reduced Registration Fees for ESCRS Congresses
• Subscription to Journal of Cataract & Refractive Surgery
• Access to ESCRS Grants, Bursaries and Research Awards
Access to:
• ESCRS iLearn
Online CME accredited interactive courses
• ESCRS On Demand

Online library of presentations from ESCRS Congresses
• EUREQUO
European Registry of Quality Outcomes for Cataract and Refractive Surgery
• ECCTR
European Cornea and Cell Transplantation Registry
5 year membership for trainees Join today. www.escrs.org
ESCRS Membership FREE
Live streaming of cataract surgery











Live streaming of cataract surgery could help deliver safe enhanced experiential learning to undergraduate ophthalmology teaching during the COVID-19 pandemic, according to a Free Paper presented at the 35th ESCRS Winter Meeting Virtual 2021.




In his paper “Live Streaming Cataract Surgery - A Unique Solution To Reduced Theatre Opportunities For Medical Students”, Dr Murad Khan, a Clinical Teaching Fellow at UCL and Basildon University Hospital, UK, pointed out that the global COVID-19 pandemic has caused considerable disruption to teaching.

“Opportunities to observe operations were typically scarce prior to the pandemic, and given social distancing rules and concerns over transmission of the coronavirus these chances have been reduced even further. Experiential learning can help medical students solidify experiences and engage in reflective practice,” he said.
Dr Khan, working with Mr James Myerscough and the Ophthalmology Department in Southend University Hospital, reported what they described as a novel, inexpensive method of live-streaming cataract surgery to enable medical students to engage in experiential learning during the pandemic.
For their research, they used a consumer-level laptop, an inexpensive video capture cable and free video conferencing software. The video signal from the operating microscope was relayed to the laptop, where the screen was then livestreamed 13 miles away to medical students in the University Hospital. Recording of the operation to the cloud was also done simultaneously.
“We found our method to be simpler and cheaper than those previously reported in the literature,” said Dr Khan. “We did not require any additional expensive equipment to record the videos or convert the video output” he said.
“I think one really important fact is that the theatre environment wasn’t that different to what it would be on any given day with the clinical staff on hand to answer questions from the medical students and there wasn’t any undue pressure on the operating surgeon given the set-up that we had,” said Dr Khan.
Dr Khan concluded that with the advent of 5G, HD and 4K, live-streaming resolution is now possible given the strengthening of the digital infrastructure during the global pandemic. “This technique would be of interest to ophthalmologists who wish to deliver safe enhanced experiential learning to undergraduate ophthalmology teaching during the COVID-19 pandemic,” he said.

















Are you facing aphakia without capsular or zonular support? Artisan Aphakia IOL offers a Safe, Fast & Simple Solution to prevent or correct IOL dislocation or subluxation. www.ophtec.com
Cataract surgery live streaming could assist medical students.
Colin Kerr reports
EUROTIMES | MAY 2021 SPECIAL FOCUS: CATARACT & REFRACTIVE TECHNOLOGIES 11
I think one really important fact is that the theatre environment wasn’t that different to what it would be on any given day...
Dr Murad Khan
Bilateral surgery
European study underscores trend towards immediate sequential bilateral cataract surgery. Dermot McGrath reports
Immediate sequential bilateral cataract surgery (ISBCS) offers comparable safety and efficacy to delayed sequential bilateral cataract surgery (DSBCS) and may confer other cost advantages as well, according to a major Dutch study presented at the 25th ESCRS Winter Meeting.
“The clear take-home message is that ISBCS shows comparable safety and effectiveness versus DSBCS. There are also lower costs for ISBCS, but we still need more analysis to determine the true cost-effectiveness of the procedure,” said Rudy MMA Nuijts MD, PhD, Professor of Ophthalmology, Vice-Chairman, and Director of the Cornea Clinic and the Centre for Refractive Surgery at the University Eye Clinic Maastricht, Maastricht Medical University, The Netherlands.
Prof Nuijts presented data from the bilateral cataract surgery in the Netherlands (BICAT-NL), a multicentre randomised controlled trial with non-inferiority design carried out at 10 hospitals in the Netherlands, with 865 patients randomised for either ISBCS or DSBCS.
The primary outcome of the study was to evaluate whether ISBCS is non-inferior to DSBCS, with effectiveness defined as the proportion of patients with a postoperative refraction within 1.0D of target refraction.
“This outcome was chosen because it is an indicator for insurance companies in the Netherlands to evaluate how well cataract surgery has been performed,” explained Prof Nuijts.
Secondary objectives included the proportion of patients with a postoperative refraction within 0.5D of target refraction, postoperative visual acuity, patient satisfaction using patient-reported outcome measures (PROMs), incidence of complications and cost-effectiveness.
The guidelines followed for surgery were in line with the ISBCS General Principles for Excellence, said Prof Nuijts, with strict separation of procedure, instruments and intraocular medication for right and left eye.
Turning to the results, the number of eyes within 1.0D of target refraction was around 97% for both groups and there was no statistical difference either for eyes within 0.5D in both groups. The uncorrected and best-corrected visual acuity outcomes were also similar between the two groups, said Prof Nuijts.
In terms of adverse events, there were no cases of endophthalmitis, one case of bilateral
corneal decompensation (DSBCS patient) which developed six weeks after surgery, one case of bilateral uveitis (ISBCS patient) which developed at 10.5 weeks after surgery and one case of bilateral macular oedema (DSBCS patient), which developed at 4.5 weeks after surgery. There were also comparable mild adverse events for ISBCS versus DSBCS such as dry eye and dysphotopsias.
For total operating room (OR) time, there was not a lot of difference between the two groups.
“This was a bit surprising to us as we expected there to be less time for ISBCS, yet only one centre showed a clear advantage for ISBCS. I think this shows that most centres have organised their patient flow very efficiently in the Netherlands,” he said.
Costs were also less for ISBCS, with a difference of around 620 euros per procedure coming from reduced day admission costs, visits to ophthalmologists and eye drops, he said.
Prof Nuijts said that the outcomes of the study reflect the growing interest in ISBCS at a time of shrinking healthcare budgets and increased demographic pressure on practitioners to deliver quality eyecare as efficiently as possible.
“The COVID-19 pandemic has sparked a lot of interest in ISBCS over the past year and we have seen a lot of debate in the academic journals concerning the pros and cons of this approach,” he said.
Prof Nuijts cited a recent editorial in Ophthalmology (Ahmed I et al., Ophthalmology 2021 Jan;128(1):13-14) arguing that ISBCS is less expensive, more efficient and provides faster visual recovery than traditional delayed bilateral surgery. They also argue that the cost efficiency is greater due to less patient costs for travel, less home care and decreased absence from work.

“They reported no cases of bilateral endophthalmitis or TASS in a series
of over 95,000 ISBCS surgeries. The refractive outcomes were enhanced when using the latest generation formulas such as the Barrett Universal II. In their opinion patients should be given an informed option between ISBCS and DSBCS,” he said.
The counter argument outlined in another editorial by Samuel Masket (Masket S. Ophthalmology 2021;128(1):11-12) is that ISCBS poses a risk for potentially blinding complications such as endophthalmitis or TASS and there is no justification for placing the surgeon at greater medicolegal risk with ISBCS.
“He also suggests there is a risk of a wrong power IOL as the first eye cannot be properly evaluated before second eye surgery. There is also a greater risk of negative dysphotopsia in both eyes. He argues that the benefits disappear if second eye surgery is performed within two days. There are also adoption hurdles: surgeons are financially penalised for ISBCS, leaving the bulk of the benefit to third-party payers,” said Prof Nuijts.
Although guidelines in the Netherlands officially prohibit ISBCS, the reality is that some surgeons are already performing such procedures and the demand is growing, said Prof Nuijts.
“We performed a survey last year in the Netherlands and some 26% said they currently perform ISBCS for a small percentage of cases despite the fact that it is not officially allowed. When we asked if they would consider performing ISBCS in the near future, the answer was yes for 46%, which underlines the interest in the procedure,” he said.
Rudy MMA Nuijts: rudy.nuijts@mumc.nl
Lindsay Spekreijse: lindsay.spekreijse@mumc.nl
12
EUROTIMES | MAY 2021 CATARACT & REFRACTIVE
...we expected there to be less time for ISBCS, yet only one centre showed a clear advantage for ISBCS. I think this shows that most centres have organised their patient flow very efficiently in the Netherlands
Rudy MMA Nuijts MD, PhD
Phakic IOL comparison
The implantable phakic contact lens (IPCL, Care Group) and the implantable collamer lens (ICL, Staar Surgical) provide similar visual outcomes with similar refractive predictability and safety in the correction of moderate-to-high myopia with or without astigmatism, according to a study presented by Suphi Taneri MD, FEBOS-CR, Ruhr-University Bochum, Germany.
The observational consecutive case series study included 111 eyes that underwent implantation of the IPCL and 115 eyes that underwent implantation of the ICL. Eyes with an internal anterior chamber depth of less than 2.8mm and a central endothelial cell count of less than 2000/cm2 were excluded from the study, Dr Taneri told the 25th ESCRS Winter Meeting.
He noted that the lenses have similar designs with regard to their dimensions, haptic design and the inclusion of a central hole to allow flow of the aqueous. They differ slightly in their lens material and in the available power range (IPCL: +15 to -30D, Cylinder up to 12D; ICL: +10 to -20D, Cylinder up to 6D) and sizes (IPCL: 13 sizes from 11.0 to 14.0mm; ICL: four sizes from 12.1 to 13.7mm).
At three months’ follow-up, uncorrected distance visual acuity among eyes targeted for plano was the same or better than preoperative corrected distance visual acuity in 86% of eyes in the IPCL group and 91% of the ICL group. Furthermore, 35% and 38%, respectively, gained one or more lines in corrected distance acuity, Dr Taneri said.
In eyes undergoing correction of up to -20D of myopia, the spherical equivalent was within 1.0D of target refraction in 92% of the IPCL group and 94% of the ICL group. Furthermore, postoperative cylinder was less than 1.0D in 97% and 95% of the IPCL and ICL group, respectively. Moreover, refraction was stable throughout one year of follow-up with both lenses.
Dr Taneri noted that a review of all ICLs and IPCLs implanted over the past 10 years at his centre indicates that postoperative re-rotation was necessary in five of 58 toric IPCL implanted from 2017 to February 2021, compared to two eyes of 64 toric ICLs implanted from 2011 to 2019. However, he pointed out that vaulting was perfect in all cases where rotation occurred and he speculated that iris factors may be at fault.
He also reported that there was no significant endothelial cell loss with either lens at two years’ follow-up. Intraocular pressure returned to preoperative levels after a spike in the first hours after implantation, while cataracts occurred in one eye in the IPCL group and two eyes in the ICL group.
The new OS 4 marks the beginning of the next generation of retina, glaucoma and cataract surgery. The all-in-one platform has received numerous exciting features that provide even more comfort, precision and safety.
Laser integration: More safety, fully automated user protection filter
Light: 45% more power*, maximum visibility
Pedal: Multifunctional with over 100 setting options
Phaco: Speedier readiness, greater controllability
User comfort: Even more userfriendly and communicative
Make the difference –with the new OS 4: www.oertli-instruments.com

13
EYE SURGERY. SWISS MADE.
Not available for sales in the US *Oertli data on file
NEW FEATURE Anzeige_OS4-The next generation_93x266mm_print.indd 1 06.04.2021 15:13:19
OS 4TM THE NEXT GENERATION
Two different posterior capsule IOLs show comparable performance. Roibeard Ó hÉineacháin reports
EUROTIMES | MAY 2021 CATARACT & REFRACTIVE
...the lenses have similar designs with regard to their dimensions, haptic design and the inclusion of a central hole to allow flow of the aqueous
Suphi Taneri MD
What have we been missing?
In her shortlisted essay for the 2021 John Henahan Prize, Dr Diana Dragnea says the COVID-19 pandemic may be a reminder of what we missed long before it started
Has COVID-19 changed long-term clinical practice?
Definitely, at least on an individual level. Over the past 10 years I have noticed a gradual and striking change in myself. I became aware of many things I had learned in the previous years and often wondered: How come I didn’t know these obvious things before? But in 2020 I initially thought that my personal development had stopped.
WHEN THE BODY PUNISHES YOU
I was in a constant loop. Waking up > driving to the clinic > driving back > having dinner >working on my computer > going to bed > waking up... I was stuck in a constant state of fatigue and stuffiness. My body began to protest giving me neck and back pain. I ignored it. It increased. After a while it turned into a kind of numbness mixed with episodes of severe ache. The problem worsened on OR days, as in full concentration I would completely forget the pain which helped me to hold whatever position I wanted. Immediately after surgery, my body would start screaming.
A friend said to me one day: “Just because you have a Ferrari doesn’t mean you have to drive it full speed’’. Very slowly I came to realise that working at that pace was making me sick and this was also affecting the quality of care I was giving to my patients. Finding peace of mind even in hard times is crucial. But this is a long process.
DEATH
During the first lockdown I realised that as ophthalmologists we are far from being exposed to death. I only spent a week in a COVID ward and I still remember vividly the first patient who died. I was standing in the staff kitchen, staring at the monitor and suppressing as much as I could. The monitor showed from above a man who was agonising alone in his bed. I was somehow calm as this was a story from another dimension that I could turn off at any moment. The black and white screen was also helping. All the actors from black
and white movies are dead by now and I feel no tragedy in that. But the thing that really saddened me was that his family decided not to pay him a visit. They were given the option of going in with full protection for a short time or staying with him as long as they wanted, but to remain in quarantine as well. The answer was no. I became much more aware of my patients’ fears and anxieties and decided to listen more.
YOU DON’T KNOW WHAT YOU HAVE UNTIL YOU LOSE IT
It was never difficult for me to distance myself because I was never particularly “that warm” with my patients. Not because I didn’t want to put my hand on their shoulders, but because I was taught that it might be inappropriate. In the midst of the pandemic, while accompanying an 88-year-old lady who thought I was a student, I witnessed a somewhat natural lapse that reminded me of what I had been missing even before that. She was abiding by hospital rules and, despite her age and the sudden onset of double vision the previous evening, had brought no relatives and remained alone in the waiting room with her mask fallen under her mouth. The moment I asked her to follow me for consultation, she immediately approached and slipped her hands under my arm as if it were the most natural thing in the world. My righteousness was instantly disturbed. But I immediately began to feel an immense warmth fill my heart as I slowly guided her to the doctor’s room. She said smiling to me: “Don’t worry, I had my injection this morning.’’ ... She must have felt my rigidity. Since she had partial gaze palsy in downward direction, I called my orthoptist colleague to do a full examination of her eye movements. During the examination, the lady reminded me that if I hadn’t started university yet, I should consider staying in the department as it is a great place to learn. With the suspicion of a brain stem insult, she had to be sent to the emergency department for possible admission to neurology. Instead of calling the transport
service, I decided to personally bring her down two floors so I could enjoy a few extra minutes arm in arm with her.
Maybe this pandemic is a reminder of what we missed long before it started. Some of our humanity and care for ourselves and others.
Because of my upbringing and exposure, I never paid much attention to small physical closeness with patients (except when a Polish patient wanted to kiss me for joy), but now I long for it and want to experience it more once our lives are safe again. As well as taking better care of myself and listening to my patients more. These will be long-term changes in my individual clinical practice. And perhaps in many others.
Dr Diana Dragnea is pursuing a PhD and a fellowship in anterior segment surgery at the University Hospital of Antwerp (UZA), Belgium

14
EUROTIMES | MAY 2021 CATARACT & REFRACTIVE
...as ophthalmologists we are far from being exposed to death. I only spent a week in a COVID ward and I still remember vividly the first patient who died
AMD and cataract

Cataract patients with AMD require close follow-up. Roibeard
Ó hÉineacháin
reports
Cataract surgery can induce wet age-related macular degeneration (AMD) in a minority of dry AMD patients and may reactivate the condition in patients in whom the condition is quiescent. Patients with previously diagnosed or suspected AMD therefore require close follow-up after cataract procedures, suggests Kavita Aggarwal MBBS, MSc, FRCOpth, John Radcliffe Hospital, Oxford, UK.
In a retrospective cohort study, Dr Aggarwal and her associates reviewed all patients who underwent cataract surgery and were receiving intravitreal anti-vascular endothelial growth factor injections from December 1 2017 to November 30 2018 at Amersham/Stoke Mandeville hospitals. During that period 4,133 cataract operations and 6,149 injections for AMD were performed, Dr Agarwal told the 25th ESCRS Winter Meeting.
In total, 106 patients received injections for wet AMD at any time, either preceding or after cataract surgery. Of those patients, eight (7.5%) developed wet AMD following cataract surgery, having never previously received intravitreal injections preoperatively. The mean time to activation was 75.38 days (range 31-183 days). Average time from suspicion of wet AMD to injection was 11.6 days (range 0-28), she said. Of the patients with previously treated but stable wet AMD there were 18 in whom cataract surgery did not reactivate the condition over a follow-up of at least 12 months postoperatively, Dr Aggarwal said. Of those patients, eight had received injections over a period of more than six months and 10 had received the injection over a period less than six months. In four patients with stable wet AMD and who had not required injections for more than
six months, the condition returned after a mean of 165 days (range 48-423 days). In addition, 71.7% required more intravitreal injections postoperatively. The average interval between injections decreased from 7.15 weeks preoperatively to 6.7 weeks postoperatively.
Dr Aggarwal noted that visual acuity improved by a mean value of -0.13 logMAR with a range of change -0.88 to +0.44. In addition, BCVA at presentation of reactivation wet AMD was logMAR 0.40 compared to a preoperative acuity of logMAR 0.47.
“In this cohort, preoperative dry AMD patients who do reactivate are appropriately treated within 14 days according to the Royal College of Ophthalmologists guidelines for wet AMD. Telephone and virtual follow-up may affect this in the future as demand increases,” Dr Aggarwal added.
LENSTAR MYOPIA Your Companion for Myopia Management
State-of-the-art Myopia Management and Patient Education
Introduce and expand your myopia management capabilities and join the fight against myopia with precise measurements for early detection of myopia onset and state-of-the-art myopia management with graphical visualisations for easy education and consultation of patients and parents with «Lenstar Myopia».
Well Established Biometry - Lenstar 900
«Lenstar Myopia» consists of our well established Lenstar 900 optical biometer and the corresponding EyeSuite software «EyeSuite Myopia». Aside from precise axial length measurements, Lenstar 900 contributes to other indispensable myopia management factors such as keratometry, thus placing a wide range of data at your disposal for making accurate predictions of the myopia’s onset and progression.
www.haag-streit.com

15
EUROTIMES | MAY 2021 CATARACT & REFRACTIVE
_ADV_Lenstar_Myopia_Eurotimes_halfpage_horizontaly.indd 1 23.03.2021 18:05:55
Complications in phacoemulsification for small eyes
Small eyes can lead to a range of problems in surgery.
Soosan Jacob MS, FRCS, DNB reports


Small eyes can be classified as microphthalmos [short anterior chamber (AC) depth and short axial length], relative anterior microphthalmos (short AC depth and normal axial length) and axial hyperopia (normal AC depth with short axial length).
Microphthalmic eyes may be short but otherwise normal (nanophthalmos) or may have associated abnormalities like coloboma, glaucoma, corneal opacity or other complex malformations.
Nanophthalmos is bilateral with affected patients having small eye, microcornea, small anterior segment, normal or increased lens thickness, convex iris, shallow and crowded AC, high hypermetropic errors (+8 to +20DS) and axial length <20.5mm. Blindness may occur if left untreated and even after successful cataract surgery, retinal problems such as macular hypoplasia can limit vision.
Problems encountered during cataract surgery are secondary to small size, peripheral anterior synechiae, chronic angle closure glaucoma (CACG), poorly dilating pupil and thickened choroid and sclera. Spontaneous as well as postoperative uveal effusions and exudative retinal detachments may occur.
Microphthalmic eyes with choroidal coloboma may require retinal laser preoperatively and those with iris coloboma may require iridoplasty together with cataract surgery. Additional surgery for glaucoma or corneal opacity may be required in complex cases. Postoperative vision may be limited by associated ocular comorbidity.
In relative anterior microphthalmos, the normal sized lens causes crowded anterior segment, shallow AC and CACG. It is not associated with scleral abnormalities or uveal effusions.
Cataract surgery in small eyes has the benefit of decreasing anterior chamber crowding. Preoperatively, pupillary
dilatation can precipitate angle closure and prophylactic YAG peripheral iridectomy may be necessary. Fundus evaluation to look for uveal effusions and B-scan to measure thickness of choroid and sclera are important.
The eye should be softened with oral acetazolamide and/or glycerol, IV mannitol and ocular pressure with Pinkie ball/ Honan balloon before surgery. Well-constructed tunnels prevent iris prolapse. Pupillary dilatation techniques such as mydriatics, viscomydriasis, synechiolysis, pupil stretch, mini-sphincterotomies or pupil expanders are used if indicated. Lack of manoeuvring space within the AC may be a challenge.
Rhexis with high molecular weight cohesive viscoelastics and microinstruments passed through a partially opened incision is generally successful. Bimanual phaco may be preferable in very small eyes.
Arshinoff’s soft shell technique maintains space and protects endothelium. Soft nuclei may be partially hydroprolapsed and emulsified in parts. However, hard nuclei are often encountered because both patient and surgeon tend to delay surgery. Debulking by shaving away epinucleus followed by divide and conquer or crater and chop techniques are helpful. Manoeuvring space can be maintained by increasing bottle height or by using pressurised air infusion.
Loose or defective zonules cause vitreous hydration and further AC shallowing. Limited dry anterior vitrectomy with highspeed 25-gauge vitrector helps deepen AC. However, pars plana dimensions may be different from normal eyes and sclerotomies should be placed carefully. High-powered IOLs are difficult to inject and the incision may need to be enlarged. Prophylactic sclerotomies or sclerectomies may be placed in microphthalmic eyes for decompression of vortex veins and allow fluid drainage without causing uveal effusions. Sudden changes in intraocular pressure should be avoided.
Phacoemulsification can generally be carried out using normal techniques but with extra care in eyes with axial hyperopia. In these eyes, surgery may be done for cataractous lens or alternatively as refractive lens exchange for correction of the refractive error; a good choice in older hyperopic patients who have started to lose accommodation. Surgery is generally easy as the nucleus is soft and can easily be hydroprolapsed out of the capsular bag and aspirated.
Patients should be counselled regarding increased risk of surgery and poor visual prognosis secondary to any associated retinal abnormalities or amblyopia. Risk of posterior capsular rent (PCR) and endothelial damage are higher in these eyes because of positive vitreous pressure
16
EUROTIMES | MAY 2021 CATARACT & REFRACTIVE
Problems encountered during cataract surgery are secondary to small size, peripheral anterior synechiae, chronic angle closure glaucoma (CACG), poorly dilating pupil and thickened choroid and sclera
and lack of surgical space. Uveal effusion, suprachoroidal haemorrhage, aqueous misdirection syndrome and prolonged uveitis are other complications. In case of a PCR, secondary IOL fixation may be done using a glued IOL (using small diameter optic and with trimmed haptics for tucking) or other preferred technique.
IOL power calculation is difficult in these eyes with a higher chance of errors as small errors in axial length measurements and estimation of ELP can get magnified. Ultrasound biometric machines are calibrated for normal eyes with fixed anatomical proportions and this may affect accuracy in microphthalmic eyes where the normal sized lens takes up a larger volume. Both immersion and optical biometry should be used and repeated measurements taken. The Holladay 2, Kane, EVO 2.0, Barrett Universal II, Hill-RBF, Haigis and Hoffer Q formulae are better relied on. It is advisable to calculate using different formulae before deciding final IOL power. Intra-operative aberrometry (ORA Inc, Wavetec Vision) can also be useful.
For lower degrees of hyperopia, standard choices may be made but higher degrees require customised special highpowered IOLs.

An alternative option is to piggyback an IOL in the same sitting or at a second sitting after checking residual refractive error and available space in the sulcus. The power may be calculated by using the Gills nomogram: {(1.5 x Spherical equivalent) +1}. Placing two IOLs in the bag should be avoided as this can lead to interlenticular fibrosis, decrease in vision and late hyperopic shift. It should, however, be remembered that many of these small eyes may not have enough space or may not tolerate two IOLs with resultant crowding, uveitisglaucoma-hyphema syndrome etc. Also, interlenticular membranes may still develop even with one IOL in the bag and
other in the sulcus and even if made of different materials. Hyperopic eyes may have a large angle kappa and multifocal IOLs should be avoided in such eyes. IOL implantation may be deferred in very severe microcornea where the IOL optic may cause crowding.


FEMTOSECOND LASER ASSISTED CATARACT SURGERY (FLACS)

FLACS can be useful in shallow anterior chambers where manoeuvring space is less. Longer tunnels should be programmed
and positioned carefully to prevent iris prolapse. A femtosecond-created rhexis decreases the chances of a runaway and is a major advantage. Pre-treatment of a dense nucleus with femtosecond can break the nucleus into smaller fragments, thus making removal easier and thereby decrease possible endothelial damage.
Dr Soosan Jacob is Director and Chief of Dr Agarwal’s Refractive and Cornea Foundation at Dr Agarwal’s Eye Hospital, Chennai, India and can be reached at dr_soosanj@hotmail.com
17
EUROTIMES | MAY 2021 CATARACT & REFRACTIVE EuroTimes is your magazine! Contact EuroTimes Executive Editor Colin Kerr at colin@eurotimes.org Do you have ideas for any stories that might be of interest to our readers?
A: Microcornea
C; Iris coloboma
D; Repaired iris coloboma
B: Choroidal coloboma
‘The Pandemic’ THE LATEST TELEVISION SENSATION
As I left my house on the way to work one morning a few weeks ago I noticed my next door neighbour Mr Morris shuffling up the street on his zimmer frame trying to catch my eye.
“Morning Doctor Lyons, I was wondering if you had a minute, I’d like a word.”
“Morning, Mr Morris what’s up?” I said, feeling a little apprehensive. The previous week he had chastised me for not bringing my dustbin in promptly after collection.
“What’s your opinion on the AstraZeneca vaccine?” Slightly bemused I reverted to my standard, “The vaccines have been proven to be safe, the risk of serious complications is very small.”
Somewhat annoyed Mr Morris interrupted. “Yes, yes of course, I was wondering if you felt it was effective in over sixty-fives? I read that the EU is considering limiting it to younger people. Would it be better to wait for the Pfizer vaccine? Would it create more antibodies?”
“Uh well, you see,” I parried, stalling for time. “The Pfizer vaccine is difficult to transport,” he continued eagerly, “what if it’s defrosted too early, will it still work?”
Flashbacks of being put on the spot in medical school ward rounds assailed me. I immediately struggled to form a coherent thought. Mr Morris looked at me expectantly as the seconds ticked by.
“Ehm, I’m actually not really sure Mr Morris” I mumbled, cheeks reddening and hurried to the car.
Surprised at his knowledge and very aware of the limitations of mine I was relieved as I closed the car door and sped off to work, committed to reading up on vaccines later.
Later that same day in casualty I encountered a lady who presented with a very uncomfortable, red eye. I examined the eye and diagnosed her with episcleritis. I mentioned that since it’s severe I’d treat it with a steroid drop and review in a couple of weeks for a pressure check. We also discuss the self limiting nature of the condition. As I started to prescribe the steroid she stopped me, “If it’s going to get better either way, I’d prefer to tough it out.”
“If that’s what you want” I started to reply when she interjected, “I heard
steroids cause you to gain muscle anyway.”
Both incidents demonstrate patients taking a proactive role in their health and an eagerness to take the lead in the decision making. Most patients are no longer passive consumers, readily taking their doctor’s word as law. Of course this change has been occurring organically over many years. Since the pandemic I feel the number of patients with this approach is increasing as exponentially as the virus itself.
As people have sheltered, cocooned and shielded in their homes this past year they have been bombarded with twentyfour seven rolling news coverage of every aspect of the outbreak. ‘The Pandemic’ seems to be the most fervently watched soap opera of all time. The butcher who had previously paid attention to the cricket trials now only cares about vaccine trials. The hairdresser who formerly dedicated her time to creating the perfect curls, now debates the best way to flatten the curve. This new fascination with all things medical has spilled over into ophthalmology. More and more of my patients are presenting to the ophthalmology clinic better informed and motivated to understand every aspect of their healthcare. This brings both opportunities and challenges.
COVID-19 has forced people to think about their health and healthcare needs more than ever before. Patients who previously complained about their early cataracts are now happy to defer their surgery till it’s absolutely necessary. Apart from the risks of catching the virus I’ve noticed that patients are more tentative, keen to know as much as possible about all risks and complications. Recently they have seen that medicine and doctors are fallible. Patients are less and less likely to blindly follow doctors’ advice without making sure they have all the information.
Moving on from the pandemic, the doctor’s role is shifting to guiding patients in the right direction. Patients are more knowledgeable than before but many will harbour half truths and misconceptions. Like my patient with episcleritis and her fear of developing bulging biceps from Betnesol eye drops, many patients will
turn up to the clinic with medical myths we need to dispel. Conversely, with so much information available online, there is a distinct possibility that other patients may end up knowing more about their condition than us. I have experience of a patient mentioning a new treatment or trial that Google alerted them to that I was ignorant about. As I realised with my neighbour and his vaccine admitting your own ignorance can be a humbling (but important) experience for doctors.
Reflecting on the effect of COVID-19 in clinical practice is overwhelming. It has altered the most basic aspects of our work, such as how we dress at work; to the most complex, like which sight-saving surgery should be prioritised. In many departments it has cost colleagues their health or even their lives. Trying to find a silver lining to the pandemic is difficult. My hope is that going forward the pandemic will serve as a stimulus for honest, effective and synergistic dialogue between patients and healthcare staff.
Dr Conor Lyons is an ophthalmology resident at Royal Gwent Hospital, Newport, Wales

18
In his shortlisted essay for the 2021 John Henahan Prize, Dr Conor Lyons says he hopes that the pandemic will serve as a stimulus for effective dialogue between patients and healthcare staff
EUROTIMES | MAY 2021 CATARACT & REFRACTIVE
As people have sheltered [and] cocooned they have been bombarded with twenty-four seven rolling news coverage
Cataract and mortality
Mortality from vascular and renal disease significantly higher among cataract patients. Roibeard Ó hÉineacháin reports
People with clinically significant cataract have a higher mortality rate, both in general and more especially with regard to vascular and renal diseases, according to the findings of a large study reported by Yifan Chen BM BCh, Medical Sciences Division, University of Oxford, Oxford, UK at the 25th ESCRS Winter Meeting.
“The pathological causes underlying cataract are not fully understood. Therefore, a comprehensive understanding of the relationship between cataract and specific causes of death may provide insights into its pathogenesis or help to provide relevant health screening programmes,” Dr Chen said.
The study used data from the 19992008 cycles of the National Health and Nutrition Examination Survey (NHANES), a programme of studies designed to assess health-related and nutritional status of a nationally representative sample of the US civilian population. History of cataract surgery was used as a surrogate for clinically significant cataract because of the increasing rate of cataract surgery and increasingly lower threshold of visual acuity loss required for the procedure, Dr Chen explained.
The study based patient survival on the duration between the NHANES interview and the date of death or 31 December 2015, whichever came first. They confirmed mortality data from the National Death Index and classified the underlying causes of death according to the International Classification of Diseases, Tenth Revision (ICD-10), a globally used diagnostic tool for epidemiology, health management and clinical purposes. In their analysis, they identified deaths from all causes, including vascular disease, cancer, accidents, Alzheimer’s disease/ respiratory disease/renal disease and others.
The researchers also considered a wide range of confounding variables including sociodemographic characteristics such as age, gender, ethnicity, education and income, smoking status and alcohol consumption. They also considered comorbidities such as diabetes, hypertension and hypercholesteremia, chronic kidney disease pathology, as well as body mass index and self-reported health status.
In total, the study included data from 14,918 participants aged 40 years and older with a mean age 56.8 years. They had a weighted prevalence of clinically significant cataract of 9.61% (n=2009). After a median follow-up of 10.8 years 3966 participants had died.
The study showed that after multiple adjustments, all-cause mortality remained significantly higher among those who reported a history of clinically significant cataract compared to those without it, with a hazard ratio (HR) of 1.11 (95% CI, p=0.036).
For cause-specific mortality, multivariable Cox models showed that a history of cataract predicted a 34% higher risk of vascular disease-related mortality (p=0.044) and an 85% higher risk of renal diseaserelated mortality (p=0.028). No significant association was observed between cataract and cancer, respiratory disease, Alzheimer’s disease, accident or other causes for mortality after multiple adjustments
Many previous studies have investigated the association between cataract and all-cause mortality, but the results are conflicting, Dr Chen said. Moreover, very few studies to date have explored the associations between cataract and causespecific mortalities and these studies have mainly focused on only a few specific causes such as cancer and vascular diseases
Dr Chen noted that the finding of an association of clinically significant cataract with higher all-cause mortality compared to those without was consistent with most previous large-scale prospective studies. Previous studies also suggested different strengths of the associations between cataracts and mortality depending on the type of cataract. However, the present study was unable to confirm those findings as the
data on cataract type was unavailable.
She added that a few previous studies have also shown an association between cataract and vascular mortality, suggesting the possibility of common pathogenesis pathways. Some hypotheses that have been proposed include a potential role of cumulative oxidative stress and crystallins degeneration, which is a biomarker for ageing and systemic disorders.
Dr Chen also pointed out that no previous studies to her knowledge have reported a significant association between cataract and renal disease-related mortality, whereas in the present study participants with clinically significant cataract had an almost two-fold increase in renal diseaserelated mortality risk, compared to those without clinically significant cataract.
She noted that hypocalcaemia and urea sequestration secondary to renal insufficiency may both contribute to the higher incidence of cataract. In addition, increased oxidative stress is implicated in the pathogenesis of both chronic kidney disease and cataract.
She added that the strengths of the study included its large sample size, its relatively long duration of follow-up, its detailed enumeration of specific causes of death and the multiple adjustments made for confounding variables. The study’s weaknesses included its potential for recall bias because of its dependence on a self-reported history of cataract surgery. In addition, there may be residual confounding factors and there was no information on the types of cataracts that patients had.
“Further studies are needed to confirm the associations we found between cataract and cause-specific mortality and to investigate the mechanisms behind these associations,” she concluded.
19 EUROTIMES | MAY 2021 CATARACT & REFRACTIVE
...the strengths of the study included its large sample size, its relatively long duration of follow-up, its detailed enumeration of specific causes of death and the multiple adjustments made for confounding variables
Yifan Chen BM BCh
Synchronisation
Ismile at my patient as I explain that her next follow-up appointment in our clinic will be in six months’ time.
“Can you make sure it does not clash with my other eye clinic appointment dear?”
“Let’s see what I can do,” I reply as I accompany her to the front desk. With the help of my administrator colleague, we somehow manage to arrange her next two clinic appointments at staggered times on the same morning. A small effort for which she is very grateful for.
I trot back to my desk with an extra bounce in my step as I reflect on how I have managed to save my patient an extra hospital visit. However, it soon dawns on me that there are many such patients requiring multi-specialty input and I will not be able to synchronise future clinic visits for all of them!
Avoiding unnecessary hospital visits for our patients has always been something to strive for during the best of times. But as I ponder (yet again) on how a simple journey to hospital can now expose my patients to a deadly virus, minimising extra visits where possible is more important than ever before.
Could it be that rather than merely changing practice, COVID-19 has simply reminded us to re-evaluate how we deliver patient-centred care?
JACK OF ALL TRADES OR MASTER OF (MORE THAN) ONE?
There are growing calls for the return of the general ophthalmologist, amplified by the hurdles that we continue to face one year into a pandemic. Rather than addressing a single ailment during a visit, managing a second condition where possible would go a long way to reducing additional clinic appointments and meeting patient expectations. This may sometimes mean nipping down the corridor to consult with a colleague. But those extra few minutes spent will lead to happier patients. I sometimes have to remind myself that most patients do not identify with the ‘retina clinic’ or the ‘cornea clinic’. They simply attend the ‘eye clinic’ and hope that their needs are addressed in a single sitting. We must structure our clinic lists accordingly and
set aside extra time for those patients requiring multiple clinical tests. A big shout out for the ‘double slot’.
Some of our patients will indeed require expert specialist care for which there can be no substitute. A few will even need referral to tertiary centres for complex treatments. But on the whole, it is not farfetched to claim that a notable proportion of our patients can be managed safely in a general ophthalmology clinic. A step back into the past when an ophthalmology consultant was expected to be the ultimate multi-specialist!
In recent years, sub-specialisation has been the ultimate long-term goal of many ophthalmology residents. Having crossed the halfway stage of my residency training, I have narrowed down my choice of future subspecialties following much contemplation. But I have recently started asking myself: do I have to settle on just the one specialty for the rest of my career?
Becoming dual-trained will equip me with a larger skillset and allow me to expertly manage a larger cohort of patients. Plus, it will keep things more interesting in the long run. This will likely mean prolonging of my training time. But isn’t medicine all about lifelong learning anyway? The pandemic has pushed us to not only re-evaluate our clinical practice, but our training pathways as well.
THE SOCIALLY-DISTANCED CONSULTATION
But do we always need to see each patient in person? As a progressive specialty, we have been quick to take advantage of new technology in ophthalmology.
Use of virtual clinics continue to expand in glaucoma and medical retina. Mobile apps can detect wet AMD. Breakthroughs in deep-learning algorithms in the management of medical retina conditions appear promising. The utilisation of telemedicine continues to gather pace in many subspecialties, including oculoplastics.
The time and money saved by adopting innovative strategies alongside the traditional face-to-face clinic approach is a no-brainer. We were already making use of such approaches before the emergence of COVID-19. The pandemic has simply shed even more
light on their respective potentials. At the time of writing where global vaccination programs appear to have given healthcare services the upper hand in the battle against COVID-19, we must pause before we declare our intentions to get back to ‘normality’. Things will never be quite the same again. We must reflect on the lessons of the pandemic and prepare even better for future challenges which may be around the corner. Sometimes, this can mean looking at past practices which have worked. Sometimes, we may have to combine the ‘old-school’ with the ‘new kids on the block’. The results may pleasantly surprise us all.
Dr Khayam Naderi is a UK ophthalmology trainee, currently undertaking an MD (Res) at St.Thomas’ Hospital and King’s College London, UK

20
In his shortlisted essay for the 2021 John Henahan Prize, Dr Khayam Naderi says that in responding to the COVID-19 pandemic we may have to combine the ‘old-school’ with the ‘new kids on the block’
EUROTIMES | MAY 2021 CATARACT & REFRACTIVE
Avoiding unnecessary hospital visits for our patients has always been something to strive for during the best of times
Maximising efficiency
Increased allied healthcare professional participation can increase efficiency of ISBCS. Roibeard ÓhÉineacháin reports
Immediate simultaneous bilateral cataract surgery (ISBCS) combined with an optimum participation of allied healthcare professionals can greatly increase the number of procedures performed in a theatre session and reduce costs for both patients and medical facilities, reports Professor David O’Brart MBBS, MD, FRCS, FRCOphth, Guy’s and St Thomas’ NHS Foundation Trust, King’s College London.
“With the current COVID-19 pandemic and increasing cataract burden we need higher volume surgical models and ISBCS is potentially more efficient with Time and motion study modelling.”
Time and motion study (TMS), widely used in industry, was first introduced by Winslow Frederick Taylor in the early 20th Century as a means of standardising the amount of time a task should take and optimising work methods in order to increase productivity. In previous research, Prof O’Brart and his associates performed a TMS of cataract theatre lists at five UK institutions, recording individual tasks and their duration for every member of staff during 140 cataract procedures performed over the course of 18 theatre sessions (Roberts et al, BJO 2018;102:1259-1267).
The study showed that there was an inverse correlation between the duration of surgery and the number of allied healthcare professionals (AHPs) participating and the number of tasks they performed (p<0.001). That is, surgical time was reduced by 0.95 minutes for every additional AHP, 0.38 minutes for every additional task an AHP performed and 0.19 minutes for each additional minute spent by AHPs performing tasks.
In addition, there was a similar inverse correlation between the amount of time patients spent in theatre and the time AHPs took to perform key tasks (p<0.001). That is, patients’ time in theatre was reduced by 0.75 minutes for each task performed by AHPs and by 0.19 minutes for each minute
AHPs spent performing tasks.
“Basically, what this study showed is that by having enough allied healthcare professionals in the theatre supporting the surgeon you could increase the numbers of surgeries by about 70% in a four-hour period, even with high-volume surgical models. I always like to use the aircraft analogy where you wouldn’t expect your pilot on a flight from London to New York to suddenly stop in Greenland to serve the dinners and then take off again. And that’s what we tend to do with cataract procedures in the public health sector, where we have surgeons doing multiple tasks in the operating room which can be performed by other staff members instead of performing surgery,” Prof O’Brart said.
TMS MODELLING
In a subsequent study, Prof O’Brart re-analysed their findings from their TMS study to construct a hypothetical model where all except one patient underwent ISBCS to calculate the gains in efficiency that could be achieved through optimal participation of AHPs.
They found that with TMS modelling they could expect a mean 16% reduction (range 9.8-17.8%) in the time taken for two cataract operations. That, in turn would translate into a mean 54% increase (range 38-67%) in the number of cases currently performed per list and a mean 18% increase (range 9-28%) even if the number of unilateral cases per list had been fully maximised. An average number of four ISBCS cases per list (range 3-6) were required to achieve sufficient time savings to allow an extra unilateral surgery to be conducted.
Prof O’Brart noted that randomised prospective studies have shown that there is no difference between the outcomes with ISBCS and delayed sequential bilateral cataract surgery (DSBCS) in terms of postoperative acuity or refractive predictability. Research also shows that
patients have lower quality of life scores when they have to wait for second-eye surgery compared to when they undergo ISBCS. Furthermore, ISBCS has cost advantages compared to DSBCS for both patients and medical facilities in terms of decreased travel time and decreased hospital visits as well as reduced visual recovery time.
He added that although there might be some concerns about the possibility of bilateral sight-threatening complications, there have to date been only five reports of endophthalmitis following ISBCS among the millions of such surgeries performed, and in all of those cases there was breakdown in the usual high aseptic standards.
“Therefore, on the basis of the current public scientific literature, I think most cataract services are happy to perform ISBCS. It also has the possibility to improve surgical efficiency, especially in the public health sector by reducing patient turnover,” he said.
GAINING PATIENTS’ CONFIDENCE
There is still some ground to be gained in terms of improving patients’ understanding and acceptance of ISBCS, he noted. When he and his associates contacted 265 patients awaiting surgery and asked them if they would be willing to undergo ISBCS, 45% said they were happy to do so, but 50% expressed concern about the risk of bilateral simultaneous ocular complications and 23% said they were not familiar with concept of ISBCS.
“Patients are open to ISBCS but they require more information and education about the option, which will hopefully bring more patients on board,” Prof O’Brart added.

CATARACT & REFRACTIVE
21 EUROTIMES | MAY 2021
Therefore, on the basis of the current public scientific literature, I think most cataract services are happy to perform ISBCS
David O’Brart MBBS, MD, FRCS, FRCOphth
...by having enough allied healthcare professionals in the theatre supporting the surgeon you could increase the numbers of surgeries by about 70% in a four-hour period
David O’Brart MBBS, MD, FRCS, FRCOphth
Improving cataract surgery workflow
Laminar air device ensures safe patient flow during COVID pandemic. Dermot McGrath reports
The introduction of a mobile laminar air flow device has enabled one hospital in the United Kingdom to overhaul its cataract surgery workflow and continue to treat patients safely and effectively during the COVID-19 pandemic, according to a study presented at the 25th ESCRS Winter Meeting.
“We know that delaying surgeries can lead to worsening of patients’ condition and an increased risk of complications, so our goal was to restart cataract surgery safely in our UK district hospital. We created an outpatient pathway to reduce the time spent in the department, eliminated the need for a waiting room and prevent increased transmission of COVID-19,” said Dr Radhika Patel, Victoria Eye Unit, Hereford County Hospital, United Kingdom.
This was done by creating a streamlined pathway, a one-way system through the department where patients were booked in for surgery, administered dilating agents and then asked to wait in their car with a buzzer, explained Dr Patel.
“Once ready they were called back to the hospital, examined and seen by the surgeon, and taken straight into the clean room for their operation. After the postoperative care was explained to them, they were then discharged home,” she said.
The key to a successful reorganisation of the cataract service was the deployment of the Operio Mobile (Toul Meditech), an innovative device that circulates ambient air through a HEPA filter to
clean the air from bacteria and maintain a sterile environment around the patient at all times during the surgery.
“The machine is not difficult to use at all,” Dr Patel told EuroTimes. “It has an air filter that produces ultra-clean laminar air flow of a higher standard than most operating theatres, with an inbuilt foldable instrument tray. The sterile air produced by the unit is continually blown over the instrument tray and an operating field, and the sterile area is demarcated by a visible laser light. The portable nature of the equipment makes it very versatile and its use within an outpatient clean room makes the overall costs of surgery considerably less than in an operating theatre,” she said.
Mr Simon Madge, a co-author and one of the five surgeons who participated in the study, agreed that the mobile air unit performed very effectively.
“From a scientific perspective, we need as a profession to remember that our historic obsessions with ‘airflow’ and ‘changes’ simply represent surrogate markers for air quality, which is far more important in reducing infection rates. In cataract and lens surgery, in many units such as our own, patients wear their own clothes and shoes into our procedure room and for the procedure; the Operio Mobile allows clean air where it is needed, with clearly no need to try and provide sterile air to the rest of the patient,” he said.
An additional benefit, he added and a major advantage over conventional systems, is a new clean filter every time the machine is turned on.
“This gives surgeons incredible peace-ofmind for their patients and surgical results. The device is compatible with the Royal College of Ophthalmologists guidelines as a mobile laminar air flow device within a clean room setting,” he said.
The study included a total of 515 patients undergoing phacoemulsification and IOL insertion using the same equipment in two clean rooms. Five experienced surgeons performed the operations which had varying surgical difficulty and included patients with a range of co-morbidities (22% diabetes, 10% glaucoma and 10% dense cataract).
The results showed that the time spent in the department was well below the target of 90 minutes in patients with unilateral cataracts, with a total average time of 74.3 minutes, and 93.1 for bilateral cataracts. No intraoperative or postoperative complications were noted in 515 patients.
The first 100 patients were contacted by telephone two weeks after surgery and no patients reported any complications or any COVID-19 symptoms. There was also a very high patient satisfaction score of 9.5 from 53 patients on the Likert scale of 1 to 10. Most of the feedback was that the process was smooth, efficient and that they felt safe and enjoyed individual treatment.
Dr Patel told EuroTimes that the study had been undertaken between May and July 2020 as the UK was recovering from the first COVID-19 peak.
“It is difficult to say what the incidence of the COVID was at the time as community testing had not been rolled out to current levels but we were significantly affected with several admissions as a hospital during the first peak similar to the rest of the UK and also had a significant number of staff infected with the virus at the start of the pandemic. Therefore, it was very encouraging to have no cases during the two weeks after each treatment and no staff infections, as it meant that we had sufficient infection control,” she said.
EUROTIMES | MAY 2021
CATARACT & REFRACTIVE 22
It has an air filter that produces ultra-clean laminar air flow of a higher standard than most operating theatres
Dr Radhika Patel
It is difficult to say what the incidence of the COVID was at the time as community testing had not been rolled out to current levels
Dr Radhika Patel
THOMAS KOHNEN European Editor of JCRS

JCRS HIGHLIGHTS
VOL: 47 ISSUE: 3 MONTH: MARCH 2021
TREATING KERATOCONUS AND CATARACT


A new treatment algorithm aims to optimise refractive outcomes for keratoconus patients undergoing cataract surgery. Australian researchers describe an approach that involves cataract extraction with small aperture IOL insertion using an IC-8 IOL (Acufocus). The next step is to perform topography-guided photorefractive keratectomy (PRK) with simultaneous corneal collagen cross-linking (CXL). The PRK is performed using the Schwind excimer laser, aiming for low myopia. CXL follows, using the LIGHTLink system (Lightmed). Results of a retrospective case series analysis showed that all eyes achieved rigid gas permeable contact lens independence, with improved corrected and uncorrected distance visual acuity. Postoperative uncorrected near visual acuity ranged from N.8 to N.12. L Northey et al., “A new treatment algorithm for keratoconus and cataract, small aperture intraocular lens insertion with sequential topography guided photorefractive keratectomy and simultaneous accelerated corneal collagen crosslinking”, March 18, 2021, Published ahead of print, doi: 10.1097/j.jcrs.0000000000000642.

CHANGING PRACTICE PATTERNS IN EUROPE

The latest results from the EUREQUO database suggest that cataract surgery is being performed in younger patients with better preoperative visual acuity. A review of more than two million cataract procedures performed between January 1, 2008 and December 31, 2017 shows a decline in the rate of surgical complications with patients experiencing better predicted refractions and visual outcomes. Researchers attribute these improvements to refinements in surgical techniques IOLS, as well as better machines and improved intraocular lenses. The researchers note that the 30-day follow-up used in the EUREQUO protocol would not represent late complications such as posterior capsule opacification. While endophthalmitis rates did appear to decline over time, the current study would also not catch cases that occurred after the 30-day period. M Lundström et al., “Changing practice patterns in European cataract surgery as reflected in the European Registry of Quality Outcomes for Cataract and Refractive Surgery 2008 to 2017”, Vol. 47, #3, p 373-378.

PREOPERATIVE TELEMEDICINE
Preoperative telephone screening of patients undergoing ophthalmic surgery can streamline an otherwise cumbersome and lengthy process, saving patients both time and money, a US study concludes. Researchers conducted a retrospective cohort study at a single ophthalmic ambulatory surgery centre to evaluate the efficacy of preoperative telephone medical clearance for patients undergoing ophthalmic surgery. All patients receiving non-laser ophthalmic surgery were initially screened by phone. A vast majority, 97.76%, were cleared for surgery. Cardiovascular conditions were a common cause for referral for further preoperative medical clearance. The same-day surgery cancellation rate was only 0.19% with telemedicine clearance. AG Miller et al., “Preoperative Telephone Medical Clearance for Ophthalmic Surgeries”, March 9, 2021, published ahead of print, doi: 10.1097/j.jcrs.0000000000000548.
ASCRS’ PREMIER EVENT for Education, Networking, and Inspiration 2021 ASCRS ANNUAL MEETING July 23–27, 2021 | Las Vegas, Nevada Featuring ASCRS Subspecialty Day July 23, 2021 For registration and more information, visit: AnnualMeeting.ASCRS.org
CATARACT & REFRACTIVE 23 JCRS is the official journal of ESCRS and ASCRS EUROTIMES | MAY 2021
Corneal transplanation
The COVID-19 pandemic created logistical challenges for maintaining corneal transplantation activity and raised questions about the risk of transmitting the SARS-CoV-2 virus to graft recipients.
In a EuCornea Educational Webinar moderated by Jesper Hjortdal MD, PhD, Aarhus, Denmark, speakers reported data on European corneal donor procurement and transplantation procedures during the pandemic and discussed research designed to support evidence-based strategies for maintaining the safety of corneal grafting.
A concluding remark from Diego Ponzin MD, aptly summarised the key message. He said: “Corneal transplantation can be performed in this COVID-19 era if done properly with the current safe procedures.”
Characterising the pandemic’s impact Mor Dickman MD, PhD, Maastricht, The Netherlands, and Gilles Thuret MD, PhD, Saint-Etienne, France, presented findings from surveys sent to European eye banks to gather information on corneal procurement, assignment and donor selection algorithms. Results from
a first survey, which was returned by 64 of 110 eye banks, showed overall transplantation activity during March through May 2020 decreased by 50% when compared to the same period in the previous two years. Overall procurement decreased significantly in March and April and increased in May, but there

EUROTIMES | MAY 2021
Corneal transplantation can be performed in this COVID-19 era if done properly with the current safe procedures.
Cheryl Guttman Krader reports
CORNEA 24
Ilaria Zorzi MD performs a nasopharyngeal swab on an employee at The Veneto Eye Bank Foundation, Venice, Italy, as a surveillance measure against COVID-19
The utility of this systematic testing seems to be very low. Very few donors were found to be positive, probably because donors are clinically selected as being asymptomatic and having no contact with positive cases
Gilles Thuret MD, PhD
Courtesy of Diego Ponzin MD
were significant disparities between eye banks such that the increases were only observed in small eye banks with few donors, reported Dr Dickman.
The surveys also showed significant differences in donor screening algorithms between countries that correlated mainly with the stringency of national recommendations for donor selection and not according to pandemic severity in each country.
Dr Thuret presented initial findings from a second survey covering the months of June through December 2020 that analysed responses received from 48 eye banks. He reported that the results showed major differences between the first and second waves of the pandemic, indicating that the corneal transplantation chain was able to adapt rapidly to the impact of COVID-19.
Similar to the findings of the first survey, there was large variation among eye banks that was mainly related to eye bank size. A quarter of the responding eye banks indicated that their algorithm for donor selection changed after May 30, 2020, and the changes occurred at different dates in different countries. Two-thirds of the eye banks reported doing systematic PCR testing on donors.

“The utility of this systematic testing seems to be very low. Very few donors were found to be positive, probably because donors are clinically selected as being asymptomatic and having no contact with positive cases,” Dr Thuret said.
EYE BANK SURVEY
The findings of the first survey were reflected by data from the Veneto Eye Bank, Venice, Italy, that were presented by its medical director, Dr Ponzin. He also shared some of the measures his eye bank used to address the challenges created by COVID-19.
Dr Ponzin said that to prolong the storage time for procured tissue, his eye bank adopted a previously described dehydration process. In addition, he cited a study investigating various biocidal agents for inactivating the coronavirus as providing reassuring evidence for his eye bank’s existing practice of using povidoneiodine to disinfect the enucleation site and donor eye.
RESEARCH ON VIRAL TRANSMISSION
Dr Ponzin described a study investigating viral infectivity in corneal transplants using tissue from donors that had recovered from COVID-19. He reported that although genomic SARS-CoV-2 RNA was detected, subgenomic RNA was absent, indicating absence of replicative potential.
Dr Thuret presented findings from a series of laboratory studies designed to investigate whether the ocular surface can host the virus ex vivo. The results
showed that a minority of corneas from COVID-19 positive donors (3/14, 21%) were positive for the virus by RT-PCR. In no case did both corneas from any one donor test positive, indicating that unilateral contamination is very likely, Dr Thuret said.
Additional studies investigated the presence of viral receptor and activators in the corneal, limbal and conjunctival epithelium and the ability of SARS-CoV-2 to infect and proliferate in corneal and scleral tissues ex vivo. Dr Thuret reported that proteins for SARS-CoV-2 infectious routes were present in the ocular surface, but the complete set of molecules for both the internal and external routes of infection were present only in the conjunctiva.
Using supraoptimal conditions to induce ocular surface infection, viral replication was obtained in the conjunctiva and to a lesser extent in the cornea.
“It is very important to understand that we infected the tissue with a very high viral load and kept the virus in contact with tissue for 30 minutes. These conditions are probably not compatible with what is occurring in real life,” said Dr Thuret.
“Furthermore, whether the virus isolated in these tissues could infect another person remains to be proven.”
ADDRESSING PATIENT CONCERNS
Dr Dickman observed that cornea transplant patients are asking whether it is safe to get the COVID-19 vaccine.

“The answer is categorically yes,” he said.
Dr Dickman mentioned that as a precautionary measure, Drs Francis and Marian Price, Indianapolis, USA, suggest increasing the use of topical steroid treatment to four times daily beginning two days before vaccination and continuing for two weeks. He also advised informing patients about “RSVP”.
“Patients should know to consult their ophthalmologist if they develop Redness, Sensitivity to light, Visual blurring or Pain,” Dr Dickman said.
CORNEA
25 EUROTIMES | MAY 2021
Dr. Davide Camposampiero searches the SARS CoV 2 antigen in a nasal sample, as a surveillance measure against Covid-19 (The Veneto Eye Bank Foundation, Venice, I)
Courtesy
Ponzin MD Courtesy of
Ponzin MD
The disinfection of the donor eye with I-PVP reduces the viral load of the SARS CoV2 that could be present on the ocular surface
of Diego
Diego
CXL vs antimicrobials
Photo-activated chromophore for infectious keratitiscorneal cross-linking (PACK-CXL) appears to be as effective as antimicrobial agents as a standalone treatment for infectious corneal infiltrates and early corneal ulcers, according to the results of a phaseIII clinical trial presented by Emilio Torres-Netto MD PhD, at the 25th ESCRS Winter Meeting.
“Our findings challenge the dogma that antimicrobials should always be used as a first line of treatment in microbial keratitis and show that PACK-CXL could be a viable alternative,” said Dr Torres-Netto, University of Zurich, Zurich, Switzerland.
The prospective, multi-centre, randomised controlled trial involved 39 patients with infectious keratitis. Participants were recruited from five centres in Egypt, India, Iran, Israel and China. All had infiltrates and early ulcers up to 4.0mm in diameter and 350μm in depth. In 28 cases the infections were due to bacteria, with Gram-positive cocci being the most commonly identified pathogens. There were also 11 cases of filamentous fungal keratitis associated with Aspergillus species, Fusarium species and also Candida albicans.
Dr Torres–Netto – on behalf of the PACK-CXL Working Group – randomised patients to undergo standard antimicrobial treatment or PACK-CXL. Those who were already receiving antibiotic or antifungal therapy stopped their treatment at least one day before undergoing their assigned treatment. Prior to treatment, there was no significant difference between the medication group and the PACK-CXL group in terms of the mean infiltrate size, 2.3mm and 2.7mm, respectively. Median corrected distance visual acuity (CDVA) were also similar, logMAR 0.73 and logMAR 0.76, respectively.
In the PACK-CXL group, the researchers removed the epithelium around the borders of the ulcerations and then applied riboflavin and irradiated the corneal infiltrates or ulcers with UV-A using a total energy up to 7.2J/cm2, Dr TorresNetto explained. They excluded four cases due to treatment failure. This included two eyes in the Medication group that required corneal transplantation due to descemetocele and corneal perforation and two eyes in PACK-CXL group that needed additional antimicrobial therapy.
He noted that the mean time to re-epithelialisation was 7.0 days the both treatment groups. In addition, there was no significant difference in terms of improvement in BCVA, with a final median BDVA of logMAR 0.54 in the medication group and logMAR 0.53 in the PACK-CXL group. Furthermore, the cumulative distribution favoured PACK-CXL in terms of re-epithelialisation. Moreover, even when including the cases excluded from the analysis there was an 89% healing rate among eyes in the PACK-CXL group without antimicrobial treatment.
NEED FOR ALTERNATIVES TO ANTIMICROBIALS
Dr Torres-Netto noted that infectious keratitis due to corneal infection is a major cause of global blindness and severe visual impairment, with immense socioeconomic costs. In addition, antibiotic resistance has become a global problem and the development of new antibiotics has been at a virtual standstill for decades.
“Even though in different circumstances, in some series, our group has already found fourth-generation fluoroquinolone-resistant bacteria in up to 50% of our patients receiving a chronic prophylactic regime with moxifloxacin ( American Journal of Ophthalmology, 2018),” he said.
He noted that PACKCXL does not require the massive expense involved in the development of new antibiotics and their manufacture, but instead is fairly simple technology requiring only vitamin B2 solution and a light source. Moreover, the combination of UV-A+ riboflavin has already been used as for disinfectant purposes in blood banks and also as a method to purify water in some remote areas of the world.
Dr Torres-Netto explained that there are three hypotheses for the potential mechanisms by which PACK-CXL achieves its effect in infectious keratitis. First there is the oxidative stress the treatment induces which would cause a disruption in cell membranes, second, there is the direct damage to microbial genes through the intercalation of their DNA and RNA, and third, there is steric hindrance that may increase the corneal collagen’s resistance to digestion by microbial enzymes.
He noted that PACK-CXL is more effective in bacterial keratitis than in fungal keratitis but he pointed out that studies showing very poor results with fungal keratitis have used low UV-A energy (Ophthalmology, 2021). However, recently published in vivo studies he and his associates have carried out show that the germicidal efficacy increases as fluence is increased (Cornea, 2020).
In fact, they were able to demonstrate that using fluence rates of 15 J/mm2 resulted in a 99% kill rate of some strains of bacteria. Although that is approximately three times the fluence used in the Dresden CXL protocol, there are now many studies reporting good results with acceptable safety using 15 J/mm2 at the thinnest area of the cornea in customised CXL treatments for keratoconus.
“PACK-CXL might be an alternative first-line treatment for infectious corneal infiltrates and early corneal ulcers. While the results of this multi-centre randomised controlled trial are promising, a larger sample is needed to further investigate the efficacy and safety of this treatment modality, especially in fungal infections,” he concluded.
References on request
Emilio Torres-Netto: emilioatorres@me.com
EUROTIMES | MAY 2021
Corneal cross-linking alone shows promise as a first-line treatment in microbial keratitis. Roibeard Ó hÉineacháin reports
CORNEA 26
PACK-CXL might be an alternative firstline treatment for infectious corneal infiltrates and early corneal ulcers
Emilio Torres-Netto MD PhD
Our findings challenge the dogma that antimicrobials should always be used as a first line of treatment in microbial keratitis
Emilio Torres-Netto MD PhD
Intrastromal implantation of donor lenticules that are decellularised or recellularised with autologous adipose-derived autologous stem cells (ADASc) results in improvements in keratoconus parameters without loss of corneal transparency and with no evidence of rejection or any inflammatory reaction at three years’ follow-up, according to a preliminary study presented by Mona Zarif PhD and Prof Jorge Alió MD, PhD, FEBO, Universidad Miguel Hernandez, Alicante, Spain.
“All patients in our study had moderate improvements in visual acuity and no patient lost lines. There was also great improvement in stromal thickness parameters and corneal cellularity,” Prof Alió told the 38th Congress of the ESCRS.
The phase I study randomised 14 advanced keratoconus patients into three treatment groups. The first group underwent injection of ADASc into a femtosecond lasercreated intrastromal pocket. The second group underwent intrastromal implantation of a 120µm thick decellularised human donor lenticule, and the third group underwent implantation of a decellularised human donor lenticule that had been recellularised with autologous ADASc.
By 36 months months postoperatively, the corneas in all eyes were transparent. In addition, anterior segment optical coherence tomography showed that corneal thickness had increased by 14.5µm (NS) in the ADASc group and by 117.34µm (p=0.008) in the lenticule groups.
Visual acuity improved by a mean of 2.1 lines in the group receiving the ADASc alone (p=0.07) over the first month followed by a stabilisation. In the lenticule groups there was an initial worsening followed by progressive improvement after one month (p=0.04).
In terms of refraction, sphere was stable in the stem cell alone group and improved slightly in eyes receiving lenticule implants (p=0.23). Cylinder values deteriorated by -0.563 D in the ADASc alone group (p=0.21) and improved by 0.17D in the stromal lenticule groups(p=-0.46).
Mean keratotomy remained stable in the ADASc alone group (p=0.14) but improved significantly by -1.82D (p=0.05) in the stromal lenticule groups. Kmax was also stable in the ADASc alone group with a nonsignificant change of +2.02 D (p=0.14) but improved by -3.04D in the stromal lenticule groups.
Confocal microscopy showed that in the ADASc group the stem cells changed progressively to a normal keratocyte-like appearance during the six-month period after surgery. In patients with decellularised lenticules, the lamina remained acellular in the first postoperative month but became recellularised with native keratocytes, after around three months. Recellularised lenticules had a greater number of keratocytes than in the decellularised lenticules at six, 12 and 36 months.
This study confirms the feasibility and safety of stem cell advance therapy of corneal stromal diseases as keratoconus. The study is ongoing and a new multi-centre clinical investigation will start in five clinical centres in Spain along this year.
Jorge Alió: jlalio@vissum.com
CORNEA
www.registries.escrs.org One-stop-shop Registries in Ophthalmology ECCT R EURE QU O EuRe CC a Patient Care Research Benchmark Accountability Outcome & Risks 27 EUROTIMES | MAY 2021
Implantation of stromal lenticule yields promising results for keratoconus. Roibeard Ó hÉineacháin reports
Stem cells and lenticules
GENETIC TESTING for inherited diseases
Tracking the role of genetic analysis in diagnosing corneal disease. Dermot McGrath reports
Genetic analysis is playing an increasingly valuable role in the diagnosis of a broad range of inherited corneal diseases, according to Joni A.
Turunen MD, PhD, FEBO.
Speaking at the 11th EuCornea Virtual Congress, Dr Turunen said that considerable progress has been made in recent years in elucidating the molecular genetic basis of corneal dystrophies and paving the way for novel treatment strategies for these rare eye diseases.
“Genetic tests with high specificity and sensitivity are now commercially available to screen for genetic mutations in the genes responsible for the development of a number of corneal dystrophies,” he said.
Diagnosing inherited corneal disease is a complex process, as the disease may present with other ocular conditions such as developmental eye defects in megalocornea, microphthalmia, anterior segment dysgenesis or congenital cataracts. Systemic genetic syndromes such as Meretoja disease, familial amyloid polyneuropathy type IV and cryopyrin-associated periodic syndromes may also have ocular manifestations, noted Dr Turunen, an ophthalmologist at Helsinki University Hospital and group leader at Folkhälsan Research Center, Helsinki, Finland.
When considering genetic testing for corneal diseases, it is important to understand the kind of inherited diseases present in the specific population group, he said.
“Of course, this is getting more difficult nowadays because almost every country now has more mixed populations. We need to consider the family history of eye diseases and possible inheritance factors, to check for systemic diseases or symptoms and to carry out detailed clinical examinations and imaging,” he said.
Dr Turunen also stressed the importance of genetic counselling to advise patients and their families and to help them understand and adapt to the medical, psychological and familial implications of genetic contributions to disease.
“Genetic testing can be done in one variant at a time when we already know the variant in the family or doing whole-gene sequencing or using targeted gene panels, usually utilising exome sequencing,” he said.
The responsible genes for most corneal dystrophies have been identified in the recent update of the International Classification of Corneal Dystrophies (IC3D) and grouped into four distinct categories, explained Dr Turunen: epithelial and subepithelial dystrophies; epithelial stromal transforming growth factor betainduced (TGFBI) dystrophies; stromal dystrophies; and endothelial dystrophies.
A lot of research has been conducted into TGFBI-associated corneal dystrophies, with more than 70 different TGFBI mutations described to date. These mutations cause a spectrum of different dystrophies, including granular corneal dystrophy type 1 and 2 (previously designated as Avellino corneal dystrophy), epithelial basement membrane dystrophy (EBMD), lattice corneal dystrophy, ReisBücklers corneal dystrophy and ThielBehnke corneal dystrophy.
“There is a great deal of clinical heterogeneity and the diagnosis is often unclear especially in younger individuals. Some of the mutations are very certain while others are only suspect. No doubt much of this is because mutations in the TGFBI gene are also responsible for at least five inheritable corneal dystrophies” he said.
The success rate of gene testing depends on quite a few variables, noted Dr Turunen.
“As an indication, a recent poster study from Blueprint Genetics reported that the causative variant for corneal dystrophies
was successfully identified in 71% of patients,” he said.
Dr Turunen’s own research in this area has recently focused on two dystrophies: recurrent corneal erosion dystrophy (ERED) and keratoendotheliitis fugax hereditaria. ERED is an autosomal dominant dystrophy characterised by recurrent corneal erosions presented in the first decades of life, leading to diffuse subepithelial opacities and fibrosis.
“It was reported recently that at least a subset of the patients harbour a mutation of a collagen type XVII alpha 1 chain gene (COL17A1). In our clinical research we have found five families from Finland with ERED carrying the same mutation in COL17A1. Our finding of the same variant in yet another population strengthens the evidence that this variant is a frequent cause of ERED,” he said.
Keratitis fugax hereditaria is another autosomal dominant corneal disease characterised by unilateral attacks of corneal inflammation starting at a median age of 11 years. Symptoms are redness, pain and photophobia, which typically flare up several times a year. Over time, these repeated attacks can cause corneal opacities and reduced vision.
Genetic analysis by Dr Turunen and co-workers identified a pathogenic variant c.61G>C in the NLRP3 gene, encoding cryopyrin, of 34 tested patients affected by keratis fugax hereditaria. “Given that the variant is present in both Finnish and Swedish populations at a frequency of about 0.02% and 0.01%, respectively, we have good reason to suspect that this disease also affects other populations of Scandinavian origin,” he said.
Joni A. Turunen: joni.turunen@helsinki.fi
CORNEA 28 EUROTIMES | MAY 2021
There is a great deal of clinical heterogeneity and the diagnosis is often unclear especially in younger individuals Joni A. Turunen MD, PhD, FEBO
Bowman’s layer grafting
Intrastromal implantation of Bowman’s membrane graft in eyes with moderate and advanced progressive keratoconus can result in an immediate flattening of the corneal curvature that is sustained over the longer term, according to Isabel Dapena MD, The Netherlands Institute for Innovative Ocular Surgery, Rotterdam, The Netherlands.
“Bowman’s layer intrastromal grafting does not compromise the corneal surface and has a lower risk for complications than penetrating keratoplasty or deep anterior lamellar keratoplasty and theoretically diminishes the risk for allograft rejection,” Dr Dapena told the 38th Congress of the ESCRS.
The technique involves obtaining the complete Bowman’s layer from donor corneas and creating a scleral pocket through a scleral tunnel at 50% depth with a lamellar spatula. The donor Bowman’s membrane is then inserted in the pocket with a glide and with the injection of liquid carefully unfolding the membrane with a cannula, she explained.
Dr Dapena presented the results obtained in a series of 35 keratoconus cases who underwent Bowman’s layer intrastromal implantation. The patients had a mean age of 32 years, a Kmax greater than 69 in 26 of the patients and thin corneas with a mean thinnest pachymetry of 349 microns. They included 26 advanced keratoconus cases and nine moderate cases.

Immediately after surgery there was an important flattening of the cornea maintained largely unchanged throughout a follow-up of seven-to-eight years, she noted. There was an average flattening of the cone of 5.0D. In addition, the best spectacle-corrected visual acuity improved slightly and the vision with contact lenses remained stable.
Complications included corneal hydrops in five eyes (14%), which occurred between four and seven years postoperatively. Four of those with hydrops occurred among the advanced keratoconus cases and one occurred in a moderate keratoconus case. In addition, five eyes (14%) showed continued corneal steepening, three of which occurred among the advanced cases and two of which occurred among the moderate cases.
“This technique achieved flattening of cornea curvature and stabilisation of progressive keratoconus in 83 and 63% of cases at five and eight years, respectively, with preservation of the visual acuity. It may postpone or even completely avoid the need for deep anterior lamellar keratoplasty or penetrating keratoplasty,” Dr Dapena added.
She noted that she and her associates have also achieved good results of a new technique, Bowman’s layer onlay grafting, in a series of five patients with progressive advanced keratoconus. The new technique has the advantage of being a completely extraocular approach without risk for micro-perforation in very thin corneas.
• ESCRS Research Study Portals (ESCRS-funded research projects)
• ESCRS Podcasts
• EyeJC (The ESCRS Journal Club)
• Case Studies
• EBO – ESCRS Examination
• ESCRS Media Player
• ESCRS On Demand
• ESCRS iLearn
• Astigmatism Double Angle Plot Tool
CORNEA
29
Continue
education all year with our range of online resources Visit education.escrs.org Ready when you are.
Bowman’s technique offers potential to avoid DALK or PK. Roibeard Ó hÉineacháin reports
your
and more... EUROTIMES | MAY 2021
Isabel Dapena MD
Future of imaging
How far can we see into the future? Or rather, can we catch a glimpse of what the future of imaging will look like for patients with pathologic myopia?
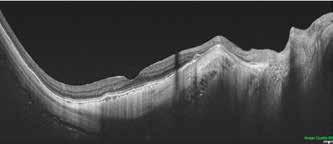
Gemmy Cheung MBBS, FRCOphth, FAMS, MCI, Singapore National Eye Centre, Singapore, sought to answer this question during her presentation at the EURETINA 2020 Virtual Conference. “Imaging in Myopia: Seeing Far into the Future” gave us insight into the present state of the art in myopia imaging techniques, and what we can expect soon.
Professor Cheung started her lecture by reviewing two important classification systems for high myopia. First, the META-PM (metaanalysis for pathologic myopia) international classification for myopic maculopathy, which was published in 2015. Second, the ATN classification, published in 2019. These classification systems are intended to clarify research into this highly complex disease and improve clinical follow-up of patients who suffer from it.
The META-PM incorporates both OCT and colour fundus photography to describe not only retinal changes, but also those in the choroid, Bruch’s membrane and the RPE. This classification system defines five categories of myopic maculopathy: “no myopic retinal degenerative lesion” (Category 0), “tessellated fundus” (Category 1), “diffuse chorioretinal atrophy” (Category 2), “patchy chorioretinal atrophy” (Category 3), and “macular atrophy” (Category 4). Three additional features to supplement these categories were defined as “plus” lesions: lacquer cracks, myopic choroidal neovascularisation, and Fuchs spot. Posterior staphyloma was considered as a further, important sign of myopic retinopathy. The intra-observer agreement for this system is ≥85%.
A more recently developed system, the ATN classification, takes three factors into account: atrophy, traction and neovascularisation. This system has led to the discovery that, for example, the pathogenesis of myopic tractional myopathy is different from that of myopic atrophic maculopathy and myopic neovascular maculopathy.
After completing this review of classification systems, Prof Cheung switched to the imaging systems themselves, where great advances have been made in terms of speed and resolution as well as scan width and depth. Swept-source OCT (SS-OCT) represents the latest such advance. It boasts longer wavelengths and higher scanning speed, which results in images that are longer in width and deeper in penetration than those of previous generations.
“These properties of SS-OCT are particularly useful in evaluating eyes with posterior staphyloma,” she said. “In some eyes, we can look even further, right at the sclera. We are now adopting these imaging techniques in children and teenagers undergoing
atropine treatment, and the pattern of progression will no doubt bring new insights into the development of pathologic myopia and staphyloma.”
Prof Cheung then showed an example of an SS-OCT-derived 3D-reconstruction of the posterior eye wall, in which we can clearly visualise two deep staphylomas on either side of the optic nerve.
“In the next few years, we can anticipate further advances in SS-OCT with increasingly faster scan speed and higher resolution,” she concluded.
After displaying a series of impressive SS-OCT images, Prof Cheung moved on to the advances in OCT angiography (OCT-A).
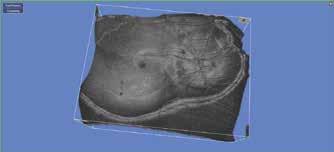
“OCT-A allows us to see and detect choroidal neovascularisation with high sensitivity and specificity, which will enable their incorporation into diagnostic algorithms used in clinical practices as a screening tool,” she said.
This might make fluorescein angiography unnecessary for this indication. One limitation, however, is that the flow signal produced by the neovascularisation may persist even with treatment. Hence retreatment decisions should not be made with OCT-A in isolation, but together with structural OCT.
OCT-A can also be used to evaluate changes in the choriocapillaris and choroid. “However, these very thin structures make it difficult to achieve quantification, particularly because of their susceptibility to inaccurate automated segmentation,” said Prof Cheung.
Despite this limitation, Prof Cheung referred to a paper in which a wide-field, whole-eye OCT system could not only scan the posterior pole with great resolution, but can produce a topographic curvature map of the posterior pole. With longitudinal data, these types of quantitative techniques will be extremely valuable in our ability to assess changes in the posterior eye wall.
Finally, using dynamic evaluation of the eye shape during different gaze positions, some groups have looked at the potential mechanical forces involved in the development of staphyloma, vitreomacular traction and intra-choroidal cavitation.
In summary, there have been many significant advances in imaging technologies, which have in turn expanded the possibilities for imaging in pathologic myopia. These improvements will enable clinicians to evaluate myopic pathology and its pathogenesis in new ways,
“The new imaging techniques allow us to see and think and imagine in a three-dimensional fashion, not only at one tissue layer but in multiple, specific layers,” she said.
These imaging data will further complement clinical data, longitudinal follow-up as well as both serum and ocular biomarkers to further our understanding of the development and progression of myopia and its complications.
EUROTIMES | MAY 2021
Advances in technology have expanded the possibilities for imaging in pathologic myopia. Leigh Spielberg MD reports
RETINA 30
A 3D reconstruction of the posterior eye curvature based on swept-source OCT. The complex shape of the posterior staphyloma can be appreciated in the 3D reconstruction
Swept-source OCT through the fovea of the same eye
Courtesy of Gemmy Cheung MBBS, FRCOphth, FAMS, MCI
Post-op patient posturing
Facing up to face down posturing after detachment surgery?
Leigh Spielberg MD reports
The latest Amsterdam Retina Debate, presented online by EURETINA 2020 Virtual, was a vitreoretinal battle on the topic of postoperative care after retinal detachment surgery. The question was: do we know how to correctly posture these patients in order to prevent retinal displacement and macular folds?
The debate, hosted by Sarit LesnikOberstein MD, Amsterdam, The Netherlands, was an entirely British affair between David Yorston MD, Glasgow, Scotland, and Rumana Hussain MD, Liverpool, England. Pre-debate polling indicated that 72% of the online audience members were convinced that we already know how to posture correctly, while 28% had their doubts. Dr Yorston might have had a difficult time defending that initial advantage.
Dr Yorston began with a defence of the utility of posturing. As one of the authors of the PostRD trial, he might be considered an expert on the topic. The PostRD trial was a randomised controlled trial that compared the effect of face-down positioning versus support-the-break positioning on retinal displacement and distortion after macula-involving retinal detachment (RD) repair in 239 patients.
“Our study shows that face-down positioning is associated with a reduction in the rate and amplitude of postoperative retinal displacement after macula-involving RD repair and a reduction in binocular diplopia,” he said.
No association was found with visual acuity or postoperative distortion. However, the study “was not powered to show changes in function, only in anatomical changes”, he added.
“In practice, I posture everyone facedown for four hours,” he added. “What’s more important than the length of time for posturing is the immediacy of the posturing, because there’s always some residual subretinal fluid, regardless of the surgical technique.”
Dr Hussain made a strong case for the argument that we really don’t know how best to posture our retinal detachment patients in the immediate postoperative period.
“Why do we posture our patients immediately postoperatively?” asked Dr Hussain. “The only reason is the prevention of macular folds, which occurs because there’s some residual subretinal fluid with redundant pliable retina, which gets trapped during fluid-air exchange and pinches the posterior pole.”
When macular folds occur, it’s “a bit of a disaster”, she continued, but the incidence is difficult to ascertain. Based on a review of the literature, Dr Hussain concluded that it is an uncommon complication.
A Japanese paper suggests that it is more common in outpatients than inpatients.
“This was due to the reduced posturing compliance of face-down posturing in outpatients. However, the problem with all of these papers is that they talk about the posturing but do not mention whether there was residual subretinal fluid, whether heavy liquids were used during surgery or whether posterior or anterior retinotomies were used for drainage of subretinal fluid. So, we don’t really know the rate of folds, especially after different procedures, like scleral buckling or vitrectomy,” she observed.
What complicates matters is the presence of subclinical retinal displacement, as visualised on postoperative autofluorescence imaging, and the recent study suggesting that up to 88% of macula-off retinal detachment patients experience symptomatic metamorphopsia, so this may be a bigger issue than we previously realised.
“So, how do prevent this from happening?” she asked. “Well, these shifts and folds result from residual subretinal fluid, with a big gas bubble splinting the redundant retina at the posterior pole.”
The question remains: “Who do we posture? All retinal detachment patients? Only those with visible residual subretinal fluid? Only patients with bullous retinal detachments? Or maybe only those with macula-off or fovealsplitting detachments? And then there are the questions of how to posture: face-down, supine, temporal down or steam roller, not to mention the serious question of compliance.”
“The PostRD Trial, as my opponent
mentioned, showed a significant difference in the retinal displacement measured; however, subjective results were approximately the same between groups,” she pointed out. So, what’s the point? “Maybe we shouldn’t be treating scans and images and autofluorescence, but rather patients’ symptoms and satisfaction.”
So, what are Dr Hussain’s suggestions to prevent this disastrous complication?
“If you want to prevent retinal folds, intraoperative prevention is what makes the difference. This includes stringent drainage of all the subretinal fluid. Do we know how to posture our retinal detachment patients? The answer is no!”
In the end, both debaters could agree on two important features of postoperative posturing. First: rapid posturing in the immediate postoperative period. Second: limitation of movement in the hours thereafter, so that the posture that is assumed remains stable for about four hours.
Dr Yorston joked that the number one threat to postoperative posturing is the friendly nurse who comes to offer the patient a nice cup of tea an hour after surgery, thus interrupting the posturing.
Dr Hussain, however, had the last laugh, as the post-debate poll showed that nearly about 50% of online viewers polled remained convinced that the issue of postoperative posturing could be laid to rest.
RETINA 31
EUROTIMES | MAY 2021
The only reason is the prevention of macular folds, which occurs because there’s some residual subretinal fluid with redundant pliable retina
Rumana Hussain MD
10-12 September www.euretina.org Programme and Registration information available on the website
‘Alphabet soup’ expands clinical knowledge
Randomised controlled trials (RCTs) have transformed the understanding of nature of glaucoma and changed the goal of treating the condition, said Prof Anders Heijl MD, Malmö University Hospital, Lund University, Sweden, in the inaugural Jules François lecture delivered at the 14th European Glaucoma Society Congress.
Prof Heijl noted that in particular, RCTs published over the last few decades have greatly cleared up the confusion regarding the role of intraocular pressure (IOP) in glaucoma pathology. The normal values for IOP were first determined in the 1950s following a large population study, which showed that normal IOP had an upper limit of around 20mmHg. From this finding, many assumed that patients with higher levels either had glaucoma or would develop the condition in a relatively short amount of time.
However, subsequent studies in the 1960s showed that, to the contrary, patients with ocular hypertension generally had a good prognosis most of them not developing manifest glaucoma, while at the same time, many glaucoma patients had IOP within the normal range. These findings raised important questions about who should be treated, when they should be treated and how they should be treated.
ALPHABET SOUP
To address those questions researchers at several centres around the world conducted randomised studies in the 1980s to evaluate whether IOP reduction was useful in glaucoma by investigating whether it could reduce the incidence of glaucoma damage in patients with ocular hypertension. However, the studies had contradictory results, and some had design flaws, leaving the questions unanswered. This triggered several crucial studies that started in the 1990s.
Knowledge increased dramatically with the publication of the “alphabet soup” of RCTs published in the early years of this century, including the collaborative normal tension glaucoma study (CNTGS), the early manifest glaucoma trial (EMGT), the ocular hypertension study (OHTS), Collaborative Initial Glaucoma Treatment Study (CIGTS), the advanced Glaucoma Intervention Study (AGIS) and, later, the UK Glaucoma Treatment Study (UKGTS) .
The EMGT showed that IOP reduction reduced the risk of progression of open-angle glaucoma, including normal tension glaucoma. The OHTS study showed that timolol reduced the risk of progression to glaucoma in eyes with ocular hypertension. The CIGTS trial showed that initial surgery was more effective than medication in eyes with advanced glaucoma and the UKGTS study showed that latanoprost reduced the risk of progression in eyes with openangle glaucoma, including normal-tension glaucoma (NTG).
The studies also revealed important risk factors for glaucoma such as higher IOP, exfoliation, older age and worse
glaucoma status as expressed by the mean deviation value. The OHTS study showed similar risk factors, but also showed thinner central corneas to be an independent risk factor for progression to glaucoma.
“The large glaucoma RCTs dramatically increased our knowledge about glaucoma, showing that IOP lowering actually works, that 21mmHg is not low enough, but pressure sensitivity varies a lot among eyes. Some progression occurs in the majority of glaucoma patients, even if IOP is always “normal”. Rates of progression vary a lot among patients – even with identical IOP levels.
“Nobody discussed rate of progression before the results of these large RCTs. But, since progression is the rule, we no longer consider any progression a failure and a reason to step up treatment. Now we instead consider whether the observed progression is acceptable, or whether it poses a threat to the patient's visual function and quality of life,” Prof Heijl said.
The clinical implications of this were quickly understood by the EGS, Prof Heijl noted. For example, the third edition of the EGS guidelines introduced the recommendation that all newly diagnosed glaucoma patients should be tested with standard automated perimetry (SAP) three times per year during the first two years after diagnosis. In this way, rate of progression can be determined early, and rapidly progressing eyes be revealed with great certainty.
OTHER IMPORTANT RCTS
Several subsequent RCTs have also provided valuable information regarding glaucoma management. For example, at the beginning of this century, it was generally believed among glaucoma specialists that short-wave automated perimetry (SWAP) could detect glaucomatous field loss earlier than SAP. However, a Dutch study published in 2010 proved definitively that SWAP was actually inferior to SAP in that regard.
Similarly, much hope was placed in the neuroprotective potential of memantine as a means of protecting the optic nerve from glaucomatous damage. However, despite a wealth of non-clinical data supporting that conjecture, two 48-month prospective RCTs involving 2,298 patients showed that treatment did not prevent glaucoma progression.
“These study results clearly demonstrate one of the really great advantages of RCTs – they give us the right answer even if we do not understand the mechanisms. RCTs, therefore, almost always give results that are clinically relevant,” Prof Heijl said.
The EGS introduced the Jules François lecture at its 14th Congress to mark the 40th anniversary of the society’s founding and is named in honour of the founding president of the society.
Randomised controlled studies with clinically relevant outcome criteria have a crucial role in determining appropriate management. Roibeard Ó hÉineacháin reports
GLAUCOMA 33 EUROTIMES | MAY 2021
Telemedicine for ROP
Paediatric ophthalmologists share experiences and insights for success. Cheryl Guttman Krader reports
Telemedicine for remote screening can reduce blindness from retinopathy of prematurity (ROP) and has been facilitated by advances in imaging technology. A successful programme requires close collaboration among neonatal intensive care unit (NICU) staff, well-trained imaging personnel and examining ophthalmologists combined with a detailed protocol describing image acquisition, interpretation and follow-up are critical for success.
These were the take-home messages shared by speakers during a recent World Society of Paediatric Ophthalmology and Strabismus World Wide Webinar. The programme was moderated by Andrea Zin MD, Instituto Brasileiro de Oftalmologica, Rio de Janeiro, Brazil, and Manca Tekavcic Pompe MD, University Eye Clinic, Lbubljana, Slovenia, and featured an international faculty.
Alejandra Daruich-Matet MD, PhD, Necker Enfants Maladies University Hospital, Paris, France, discussed her group’s experience using the Panocam digital camera system for telemedicine ROP screening and treatment.
“Findings from available studies show that photographic screening using contact widefield cameras can detect treatment- and/or referral-warranted ROP at a rate that is safe and comparable to screening with binocular indirect ophthalmoscopy (BIO). Most of the studies, however, compared BIO against the RetCam. No study has been performed with the Panocam, which we have used
since 2018,” Dr Daruich-Matet said. Describing the technology, she explained that her department has both the Panocam Pro, which is kept in the operating room, and the totally portable Panocam Solo, which resides in the consultation office.
Dr Daruich-Matet said that the system allows detection of treatment- and/ or referral-warranted ROP. Its main limitation is that when used to image eyes with a dark pigmented fundus, details of the periphery are hard to identify because the image appears blue. The problem is worse when the infant has a small palpebral fissure that prevents adequate contact between the cornea and the camera, she said.
Mangat Ram Dogra MD discussed telescreening of ROP in middle-income group countries. He gave credit to Anand Vinekar MD, Narayana Nethralaya Eye Institute Bangalore, India, who pioneered the Karnataka Internet Assisted Diagnosis of ROP (KIDROP) programme that was the focus of his talk.
Implemented in 2008, KIDROP brought ROP screening to underserved areas using non-physician graders and smartphone reporting with fast turnaround time. Imaging was initially done with the RetCam Shuttle. Now, the 3nethra Neo, is being used that compared with the RetCam is more portable, less expensive, and has higher resolution.
“Teleimaging works well, but camera cost has been a big problem,” Dr Dogra said.
“Dr Vinekar calculated the impact of expanding telemedicine screening for ROP in India and concluded that that implementation of a KIDROP-like model in other low resource settings with similar demographics could prevent over $US 100 million of blindness burden annually. His model is being replicated in most states in India, and it is good that we have an affordable camera so it can be done in other areas.”
RETCAM SYSTEM
Matthew S. Pihlblad MD, University of Pittsburgh, USA, described his institution’s ROP telemedicine program that serves a NICU in a hospital located about two hours away. He presented the screening protocol, which follows the 2018 screening guidelines from the AAP/AAPOS/AAO/AACO. Images are
acquired with a RetCam system and sent via secure email for interpretation.
Dr Pihlblad reported that in the 12-month period beginning March 1, 2020, 26 babies underwent 53 examinations. At birth, the babies’ mean gestational age was 29.3 weeks and their mean weight was 1,242g.
“These babies tended to be larger – almost two-thirds were at least 28 weeks and at least 1,250g – and they may be ideal for telemedicine because their risk for ROP is lower and ideally they will not require transfer for further evaluation,” he commented.
Only five of the 53 examinations generated inadequate images that needed to be repeated, and only one baby needed referral for ROP and eventually needed treatment.
“Considering that the estimated cost for ambulance transfer is $5,800, this small telemedicine program saved $145,000 in a year by avoiding transfer of the other 25 babies,” Dr Pihlblad said.
Polly Quiram, MD, PhD, said that the ROP service she directs at Children’s Minnesota – St Paul Hospital, St Paul, USA, is involved in a ROP telemedicine program with six local hospitals. All infants who meet screening criteria at the outside hospitals are imaged by trained staff using the Phoenix Icon camera, which Dr Quiram described as very lightweight, easy to use, and featuring convenient software.
She noted that the infants in the NICUs she services are often just 21-to23 weeks gestational age and weigh between 300 and 400g.
“We still see some babies with ‘garden variety’ ROP that is treated with laser, but more babies have aggressive posterior ROP that can rapidly progress and is treated with intravitreal bevacizumab based on the BEAT-ROP study,” Dr Quiram said.
She cautioned that close follow-up is critical after injection.
“Anti-VEGF treatment can buy us time, but we can’t just inject and forget because there is a risk for late reactivation of ROP that can progress to retinal detachment if left untreated. Continued monitoring through telemedicine enables us to provide the best high-quality care,” Dr Quiram said.
EUROTIMES | MAY 2021
PAEDIATRIC OPHTHALMOLOGY 34
...this small telemedicine program saved $145,000 in a year by avoiding transfer of the other 25 babies
Matthew S. Pihlblad MD
at a Glance 46,748 * * Average net circulation for the 10 issues circulated between 1 January 2020 to 31 December 2020. See www.abc.org.uk Reach 10 issues per year 27 Members on the editorial board 6 Subspecialities Available online 169 Countries eTIMES newsletter Years in print 25
Decision time
Dealing with the here and now and looking to the future. Dr Clare Quigley reports
I'll take the lens please.”
Lyndon, the scrub nurse, handed me the lens injector. I was relieved to be at the end of the case; this cataract had been a white marble. The patient was under anaesthetic, as he could not lie still for surgery; his pre-op vision had been reduced to hand movements. His procedure had gone smoothly with the help of vision blue dye and intracameral phenylephrine initially, a good volume of viscoat to protect the endothelium and then a stop and chop approach to the phaco. Throughout, there was a medical student by my side, tracking my every move in the eye.
As I watched the lens implant unfold in the bag, my heart sank. There, towards the centre of the optic, was a jagged dark line. A full thickness crack in the lens.
“There's a problem,” I exhaled. “The lens has a scratch.” At least the patient was asleep, and he did not have to listen to this. I took the BSS and used it as a pointer, indicating with the cannula tip the irregular scratch visible in the optic, showing it to Lyndon and the medical student.
“There's
“The lens has a scratch.” At least the patient was asleep, and he did not have to listen to this
“Ooh, I see it,” said Lyndon. “You'll need the lens cutter, and holder?”
“Yes... and a new lens, another twenty-three point five,” Nicola, the circulating nurse, went to fetch the lens and the explantation instruments.
Waiting for her to come back, I recalled a recent discussion I'd had with one of my Consultant trainers in cornea, Billy Power, on lens explantation. He had talked about a nice approach to improve the safety of removing a lens; make a scaffold. First, fill the eye with plenty of viscoelastic, and dial the lens for explantation up into the anterior chamber. Leave this lens for now. Next, insert your new lens into the bag, directly underneath the old one, which is still in the anterior chamber. At this point you have two lenses in the eye; your lens for removal, but also your new lens that is in the bag now, that will act as a barrier scaffold, keeping the bag distended back and out of the way. You can cut and remove the lens from the anterior chamber, without worry that your scissor could nick the capsule. It sounded like a neat technique.
Dialling up the cracked lens into the AC was straightforward – it flopped up out of the bag, and then on top of the iris after
I nudged it up and out with a drysdale. Next, I enlarged the wound slightly, and got the fresh lens injector. There was a tense moment while I pushed the plunger, and watched the new lens emerge; it slid in under the damaged lens, into the bag, no problem. Nice clean optic. But now I had two intraocular lenses in the eye, one of which I did not want.
Actually cutting and removing the cracked lens was the more awkward task to complete – I held the lens with the forceps, and started cutting with the scissors, but the forceps grip was not strong enough, and the pressure from the scissor blades were causing it to slip away in the anterior chamber. At this point my Consultant trainer Barry Quill, who was watching my movements on the screen, gave me a useful pointer – I could take the Sinskey hook to stabilise the lens from the opposite end. With the hook giving counter-traction, I was able bite down on the lens with the scissors, without it sliding away from me. I was elated when I finally cut through and pulled the slices of the cracked lens from the eye.
Between theatres and clinics, we are happy to be back to a more normal pace of work. The country is still in level 5 lockdown, but the Royal Victoria Eye and Ear is a specialist hospital where we look after only eye and ENT problems, and all the staff are now vaccinated. That means we are able to see patients, including routine cases and emergencies. People are presenting with a miscellany of different eye problems in the emergency department, a mix of more serious problems than pre-COVID. That's because the nurses now do a telephone triage of those wanting to come in – to ensure that they really do need to be seen – meaning less blepharitis and dry eye, more traumas and retinal detachments.
I see those in the year ahead of me getting ready to leave for fellowship jobs. Next year that will be me, which means I should really start applying soon. I find that it is not such an easy decision, considering the range of excellent specialty options we have in ophthalmology. Some of my colleagues have known from the start – definite VR. Definite paeds... Not me. But decision time is nigh.
a problem,” I exhaled.
INSIDE OPHTHALMOLOGY 36 EUROTIMES | MAY 2021
Clare Quigley is a resident at the Royal Victoria Eye and Ear Hospital, Dublin, Ireland
Illustration by Eoin Coveney
INDUSTRY NEWS
FDA Clearance
The new OCULUS Pentacam® AXL Wave has received the 510(k) clearance of the US Food and Drug Administration (FDA). “The Pentacam® AXL Wave represents the continued development of the successful and time-proven Pentacam® portfolio,” said an Oculus spokeswoman. “The established functions of anterior segment tomography and optical biometry have been complemented by retroillumination and a Hartman-Shack sensor for total eye wavefront and objective refraction,” she said.

Oculus say the Pentacam® AXL Wave incorporates intuitive reports based on clinical studies, with guaranteed network compatibility and full operability of all Pentacam® software and examinations. A new examination routine guides the user through the imaging process. The measuring process is straightforward, user-independent, fast and patient-friendly. The intuitive guide allows both eyes to be examined in less than five minutes. www.pentacam.com
COMPREHENSIVE REFRACTION SYSTEMS
NIDEK has launched the RT-6100 CB for Windows, an optional control software for the RT-6100 Intelligent Refractor and the TS-610 Tabletop Refraction System.
“This software adapts to the varying needs of patients and operators. Additionally, the software allows refractions that meet social distancing needs.





RT-6100 CB for Windows simultaneously offers convenience and safety.” said Motoki Ozawa, President and CEO of NIDEK CO., LTD. “We are committed to providing comprehensive refraction systems that maintain patient and operator comfort while adapting to changing clinical requirements,” he said.
www.nidek.com
OPHTHALMIC GEL


















Santen has launched PURALID LIPOGEL, an ophthalmic gel for blepharitis that soothes and cleanses the eyelids and periocular area.
“Blepharitis is a common and symptomatic disease and it has no established cure. It’s therefore crucial that we recognise that this condition needs a careful diagnostic approach and personalised management, and that we continue to educate patients on the value of lid hygiene, such as using warm compresses and cleansing the eyelids daily,” said Professor Edoardo Villani, University of Milan, Italy.
www.santen.eu


forum.escrs.org A library of symposia, interviews, video discussions, supplements, articles and presentations Spotlight on: Toric IOLs and Presbyopia Glaucoma Ocular Surface Disease Corneal Therapeutics
Refractive IOL Patient Journey
Phaco Fundamentals EUROTIMES | MAY 2021 INDUSTRY NEWS
37
The OCULUS Pentacam AXL Wave

Belong to something impressive. Join us. Reach the peak. Visit www.escrs.org for information about membership & benefits
Due to the COVID-19 virus, a number of meetings have been cancelled or rescheduled. The information in this calendar is correct at the time of going to print; please check the meeting website or email the conference organisers to confirm all meeting dates.
↙ LAST CALL
MAY 2021
ARVO 2021
Virtual Meeting
1 – 7 May
https://www.arvo.org/
COPHy Global 2021
Virtual Meeting
21 – 22 May
https://cophy-global.comtecmed.com/
JUNE
AECOS 2021
European Symposium
3 – 6 June
Florence, Italy

https://aecosurgery.org/ 2021-european-symposium/
46th Meeting of the European Paediatric Ophthalmological Society
– EPOS 2021
Virtual Meeting
18 –19 June https://epos2021.dk/
JULY
AECOS 2021 Summer Symposium
15 – 18 July
Utah, USA
https://aecosurgery.org/2021-summersymposium/
2021 ASCRS Annual Meeting
23 – 27 July
Las Vegas, Nevada https://annualmeeting.ascrs.org/
18 ↙ CALENDAR 39 EUROTIMES | MAY 2021
The AECOS 2021 European Symposium will take place in Florence, Italy
JULY
33rd APACRS–
SNEC 30th Anniversary
Joint Meeting
Virtual Meeting
30 – 31 July
https://apacrs-snec2020.org/
SEPTEMBER
49th European Contact
Lens and Ocular Surface Congress (ECLSO)
Virtual Meeting
4 September
https://www.eclso.eu/
EURETINA 2021 Virtual
10 – 12 September
https://www.euretina.org/
OCTOBER
39th Congress of the ESCRS
8 – 11 October
Amsterdam, The Netherlands
https://www.escrs.org/
Joint event: 14th National Congress of Bulgarian Society of Ophthalmology and Conference
Innovation in Ophthalmology 2021
14 – 17 October
Borovets, Bulgaria
https://mareamedical.com/en/events/ ophthalmology_oct_2021_english/
NOVEMBER
AAO 2021
12 – 15 November
New Orleans, USA

https://www.aao.org/ annual-meeting
DECEMBER
SOE Congress 2021
2 – 4 December
Prague, Czech Republic
https://soe2021.soevision.org/
CALENDAR 40 EUROTIMES | MAY 2021 Watch the latest video content from ESCRS and EuroTimes, FREE on the ESCRS Player Eye Contact Interviews Video of the Month Video Journal of Cataract & Refractive Surgery Young Ophthalmologists Videos: “My Early Surgeries”
Online Museum player.escrs.org
AAO 2021 will take place in New Orleans, USA
The 39th Congress of the ESCRS in Amsterdam, The Netherlands
TRIFOCAL SULCUS TECHNOLOGY






SULCUS-BASED ENHANCEMENT OF VISUAL QUALITY

ET Supplement export@medicontur.com

For indications, contraindications and warnings please refer to the relevant product’s instruction for use. © 2019 Alcon. 09/19 EMEA-VIV-1900035 1.AcrySof® IQ Vivity® Extended Vision IOL Directions for Use. 2. Alcon Data on File. TDOC-0055576. 29-Mar-2019 3. Alcon Data on File. Optical Evaluations of Alcon Vivity®, Symfony*, and Zeiss* AT LARA* IOLs *Trademarks are the property of their respective owners. Adva ncing CATARACT SURGERY LEAVE HALOS & GLARE BEHIND1-3 With the visual disturbance profile of a monofocal IOL, the AcrySof ® IQ Vivity® lens is the clear choice for delivering an extended range of vision with minimal halos and glare.1-3 See the difference it can make for your patients. Move Presbyopia Correction Forward














