Radiology

Review of ECR 2024
Maureen Kohi and Susan Shelmerdine discuss innovations in interventional radiology Interviews

Rise in Chronic Diseases: Will Radiology Survive? Feature
1 emjreviews.com
Volume 5.1 April 2024
4 Editorial Board 7 Welcome 9 Foreword Congress Review 10 Review of the European Congress of Radiology (ECR) 2024, 28ᵗʰ February-3ʳᵈ March 2024 Congress Features 12 Cancer Screening and Detection: Can AI Change The Game? Helena Bradbury 15 Changing the Game: Interventional Radiology's Growing Impact on Imaging Victoria Antoniou Abstract Reviews 19 Quantitative CT Analysis of Hepatocellular Carcinoma Nodules in Liver Transplant Candidates: Impact of Volume of Interest and Contrast Phase on Recurrence Prediction Rizzetto et al. 22 Acute and Chronic Complications of Caesarean Section: A Pictorial Review McNeil et al. 24 Radiogenomics Relationship of Non-small Cell Lung Cancer: Preliminary Results Belfiore et al. 25 A Proposal for a New Fluoroscopy Severity Assessment in Achalasia: The In Vivo Assessment of Achalasia Score Fontanella et al. 27 Revision of Diagnostic Reference Levels in Radiotherapy: A Road to Dose Optimisation Borrelli et al. Contents 2 T Area ● Month 2023 ● Creative Commons Attribution-Non Commercial 4.0 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0
29 Abstract Highlights Congress Interviews 36 Andrea Rockall 40 Aad van der Lugt Interviews 44 Maureen Kohi 47 Susan Shelmerdine Infographic 50 Understanding Micro-CT Scanning Feature 52 Rise in Chronic Diseases: Will Radiology Survive? England Articles 56 Editor's Pick: Risk Stratification Using Cardiac Imaging: A Comprehensive Review King et al. 65 Imaging Features of Myometrial Necrosis in a Patient Due to Uterine Compression Sutures Varrior et al. 71 Imaging Innovations in the Screening, Diagnosis, and Monitoring of Systemic Autoimmune Disease-Related Interstitial Lung Disease Nagaraja et al. 82 Cardiac MRI Imaging Features of Erdheim–Chester Disease: A Case Review Aher et al. 87 Imaging Gigantic Small Bowel Gastrointestinal Stromal Tumours Through Different Radiological Lenses: A Case Report Driver et al. Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 3 reative
Editorial Board
Editor-in-Chief
Yasmeen Malik St George’s University of London, UK
Editorial Board
Prof Jean de la Rosette Academic Medical Center (AMC), the Netherlands
Prof Eduard Ruiz-Castañé Fundació Puigvert, Spain
Prof Christian Jürgens BG Trauma Hospital Hamburg, Germany
Dr Olusola Michael Adeleke NHS Clinical Entrepreneur Fellow, UK
Prof Roger Dmochowski Vanderbilt University Medical Center, USA
Dr Sophie Willis Health Education England, Cambridge, UK
Prof Aad van der Lugt Erasmus University Medical Center, the Netherlands
Dr Çetin Erol Ankara University, Türkiye
Dr Luke Dixon Imperial College Healthcare NHS Trust, UK
Dr Sanjog Kalra Einstein Medical Center, USA
Dr Paul Bezzina University of Malta, Malta
Dr Nicholas Kipshidze New York Cardiovascular Research, USA
4 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0
Aims and Scope
EMJ is an online only, peer-reviewed, open access general journal, targeted towards readers in the medical sciences. We aim to make all our articles accessible to readers from any medical discipline.
EMJ allows healthcare professionals to stay abreast of key advances and opinions across Europe.
EMJ aims to support healthcare professionals in continuously developing their knowledge, effectiveness, and productivity. The editorial policy is designed to encourage discussion among this peer group.
EMJ is published quarterly and comprises review articles, case reports, practice guides, theoretical discussions, and original research.
EMJ also publishes 18 therapeutic area journals, which provide concise coverage of salient developments at the leading European congresses. These are published annually, approximately 6 weeks after the relevant congress. Further details can be found on our website: www.emjreviews.com
Editorial Expertise
EMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors are recognised authorities from their respective fields.
• Peer review, which is conducted by EMJ’s Peer Review Panel as well as other experts appointed due to their knowledge of a specific topic.
• An experienced team of editors and technical editors.
Peer Review
On submission, all articles are assessed by the editorial team to determine their suitability for the journal and appropriateness for peer review.
Editorial staff, following consultation with either a member of the Editorial Board or the author(s) if necessary, identify three appropriate reviewers, who are selected based on their specialist knowledge in the relevant area.
All peer review is double blind. Following review, papers are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected.
Editorial staff have final discretion over any proposed amendments.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects.
We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial.assistant@emjreviews.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in EMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
EMJ is distributed through controlled circulation to healthcare professionals in the relevant fields across Europe.
Indexing and Availability
EMJ is indexed on DOAJ, the Royal Society of Medicine, and Google Scholar®; selected articles are indexed in PubMed Central®.
EMJ is available through the websites of our leading partners and collaborating societies.
EMJ journals are all available via our website: www.emjreviews.com
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
This Publication
ISSN 2633-9978
EMJ Radiology is published once a year. For subscription details please visit: www.emjreviews.com
All information obtained by EMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, EMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. EMJ is completely independent of the review event (ESR 2024) and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever.
Front cover and contents photograph: Vienna, Austria home of the ECR 2024 ©Andrew Mayovskyy / stock.adobe.com
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 5
EMJ Podcasts
The EMJ Podcast aims to provoke conversations around the latest trends and innovations in healthcare, provide engaging and educational content for healthcare professionals, and hosts conversations with physician entrepreneur, Jonathan Sackier.
Listen today www.emjreviews.com

6 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0
Welcome letter
Editor
Evgenia Koutsouki
Editorial Managers
Anaya Malik, Darcy Richards
Copy Editors
Noémie Fouarge, Kirsty Hewitt, Katheeja Imani, Jenna Lorge
Editorial Co-ordinators
Natasha Meunier-McVey, Abigail Craig
Editorial Assistants
Victoria Antoniou, Ada Enesco, Helena Bradbury
Creative Director
Tim Uden Design Manager
Stacey Rivers
Senior Designer
Roy Ikoroha Designers
Steven Paul, Owen Silcox
Junior Designers
Dillon Benn Grove, Shanjok Gurung
Head of Sales
Robert Hancox
Senior Project Manager
Michael Stevenson
Marketing Director
Kristina Mestsaninova
Chief Content Officer
Justin Levett
Chief Operating Officer
Dan Scott
Chief Commercial Officer
Dan Healy
Founder and Chief Executive Officer
Spencer Gore
Dear Readers,

Evgenia Koutsouki Editor
I am delighted to welcome you to our 2024 issue of EMJ Radiology, featuring key highlights from the European Congress of Radiology (ECR), which, this year, took place in Vienna, Austria. Artificial intelligence (AI) and robots dominated this year’s congress, as Ameca, the world’s most advanced human-shaped robot, was present at the congress. Equally captivating was the live discussion with an AI assistant during the plenary lectures, a real-time showcase of AI’s strengths and limitations in radiology practice.
We have handpicked some of the most engaging sessions from ECR to bring to you, discussing the role that AI can play in cancer detection, as well as the evolution of interventional radiology and its impact on imaging. Of course, our issue would not be complete without summaries of key research abstracts from the congress, giving you a taste of the most important advancements in the field, and exclusive interviews with highly respected experts from the congress.
We are proud to include a compelling feature article that discusses the impact of chronic diseases on radiology practice, and the need for a medium- and long-term vision in appropriately planning and resourcing radiological diagnostics. Our Editor’s Pick is a review that explores imaging modalities for coronary artery disease, highlighting the value of combining clinical experience with established guidelines.
I would like to take this opportunity to thank our authors and interviewees for their fantastic contribution to this issue, and our reviewers and Editorial Board for their commitment to excellence. We eagerly anticipate next year’s congress, as every ECR so far has been nothing short of fantastic. Until then, we hope you enjoy reading through this journal!
Contact us Editorial enquiries: editor@emjreviews.com Sales opportunities: salesadmin@emjreviews.com Permissions and copyright: accountsreceivable@emjreviews.com Reprints: info@emjreviews.com Media enquiries: marketing@emjreviews.com
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 7

Stay up to date with new advancements across European healthcare Visit EMJ for our comprehensive collection of peerreviewed research articles, latest interviews, and features across a range of therapeutic disciplines. Visit EMJ www.emjreviews.com

are taking the place of surgeons, and how technology will continue to develop, altering how healthcare professionals go about everything from operations to training curricula.
In addition to covering these key topics, EMJ Radiology 5.1 features several fascinating articles on a wide range of topics and conditions, from a detailed review of the innovations in screening and treating interstitial lung disease, to a gripping case study on the imaging features of myometrial necrosis, to our Editor’s Pick, which delves into the imaging modalities of coronary artery disease.
Moreover, in the following pages you can find enlightening interviews with expert radiologists, each of whom are paving the way in innovations and clinical trials in their respective specialities. Andrea Rockall gives her thoughts on sustainability in the field and the future of ECR, and Susan Shelmerdine details her innovative work in perinatal autopsy, as well as much more.
Lastly, I would like to take this opportunity to thank everyone who has contributed to this spectacular issue, including all the authors, peer reviewers, interviewees, and the Editorial Board. I hope you enjoy reading this journal.
April 2024 ● Radiology 9
ECR 2024
Review of the European Congress of Radiology (ECR) 2024
Location: Vienna, Austria
Date: 28th February–3rd March 2024
Citation:
EMJ Radiol. 2024;5[1]:10-11. https://doi.org/10.33590/emjradiol/EDRW5064.
THE most advanced robotic humanoid in the world; gravity-defying stunts in bedazzled costumes; mind-bending science fiction stories. These were the themes that kicked off this year’s European Congress of Radiology (ECR) with a bang. Taking place once again in Vienna, Austria, home to great minds such as Mozart and Freud, and even greater foods, such as schnitzel and sachertorte, ECR 2024 welcomed thousands of world-renowned specialists in a wide range of disciplines, from 127 different countries. The congress featured interactive demonstrations, groundbreaking research presentations, and several eye-opening plenary lectures delivered by some of the brightest minds in radiology today.
Wednesday evening saw the marvel that was the opening ceremony, featuring a captivating performance by Austrian dance troop Zurcaroh. This was followed by an unmissable entrance by Ameca, the world’s most advanced humanoid powered by artificial intelligence (AI), who introduced this year’s theme of ‘Next Generation Radiology’. Assisting Ameca in her welcome was ECR President, Carlo Catalano, Sapienza University of Rome, Italy, who reflected on the rapid and immense advancements which have been made in medical imaging throughout history. Looking to the future, Catalano rejected the idea held by so many young professionals
entering the field, that AI will one day take over the role of radiologists, and emphasised instead its potential as the perfect companion. The next generation of radiologists will need to adapt to this changing landscape, to revolutionise radiology, and to lead innovation in medicine, all with the help of AI. This is reflected in the new ECR slogan, ‘Advancing radiology, advancing you’.
To illustrate the immense potential of AI, a short film was played throughout the opening ceremony, split into three parts: GENESIS, RAGNAROK, and SYMBIOSIS. Part one portrayed the creation and introduction of AI, its power, and the possibilities which come with it.
Following his introduction, Catalano welcomed Nino Bogveradze, Department of Biomedical Imaging at the Medical University of Vienna, Austria, and the face of the next generation of radiologists. Bogveradze detailed her impressive journey into radiology, and the challenges she faced throughout, such as the difficulties of facing motherhood whilst pursuing an academic career, and the ways in which she had to balance life and work. Bogveradze concluded her speech by encouraging young radiologists to work hard, to persist, and to believe that anything is possible.
"Congress featured interactive demonstrations, groundbreaking research presentations, and several eye-opening plenary lectures."
Congress Review ● ECR 2024 10 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0
Honorary membership to the European Society of Radiology (ESR) was awarded to three of radiology’s most significant contributors: Matthew A. Mauro, University of North Carolina, Chapel Hill, USA; Takamichi Murakami, Kobe University, Japan; and Alair Sarmet Santos, Fluminense Federal University, Rio de Janeiro, Brazil. Each of the new members expressed their gratitude and hopes for the future of radiology.
"AI cannot currently compete with over 100 years of experience held by radiologists."
Part two of the short film, RAGNAROK, followed, demonstrating not only the power of AI, but its ability to progress, to grow, and to perform tasks we have not yet even considered.
More awards followed, with gold medals going to Deniz Akata, Hacettepe University, Ankara, Türkiye; Boris Brkljačić, University Hospital Dubrava, Zagreb, Croatia; and Valérie Vilgrain, University Hospital Beaujon, Clichy, France.
Catalano closed the ceremony by thanking his mentors, looking back on previous congresses, and marvelling at how far ECR has come, with all of the experts now involved in making it the event it is today. He implored everyone to glimpse into, and help to mould, the radiology of the future, to embrace the new developments, and to not fear the future of AI. As Ameca went on to point out, AI cannot currently compete with over 100 years of experience held by radiologists, and nobody knows what the future of radiology and AI will look like. For now, we must continue to innovate, to explore, and to learn.
The final part of the ECR short film, SYMBIOSIS, emphasised the potential held by the future of radiology and AI, and the wonders that may stem from their relationship. The future is uncertain, it points out, but is undoubtedly full of hope, and something to look forward to.
Read on for more key insights into ECR 2024, and make sure to come back next year for updates at ECR 2025, taking place in Vienna, Austria, from 26th February–2nd March 2025. ●

ECR 2024 ● Congress Review Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 11
Authors:
Citation:
Cancer Screening and Detection: Can AI Change The Game?
Helena Bradbury, EMJ, London, UK
EMJ Radiol. 2024;5[1]:12-14. https://doi.org/10.33590/emjradiol/LZIE6219.
“We recognise that cancer detection is one of the main pillars of how to take care of the population today,” remarked Luis Marti-Bonmati, Le Fe Polytechnic and University Hospital, Valencia, Spain, who chaired a session at the European Congress of Radiology (ECR). In a timely conversation, the role of artificial intelligence (AI) in the screening, early detection, and depiction of tumours was explored at the annual ECR congress, which took place in Vienna, Austria, from the 28th February–3rd March 2024.
AI AND BREAST CANCER SCREENING
Sarah J. Vinnicombe, Cheltenham General Hospital, UK, opened her presentation citing a particularly concerning statistic; it is estimated that by 2027, there will be a 40% reduction in consultant breast radiologists within the UK. AI could alleviate this potential workforce crisis by shortening reading time, improving workflow efficacy, and thus reducing radiologists’ workload.
The traditional cancer screening workflow involves consultation between two readers, followed by arbitration. Within this process, AI could replace the second reader, acting as an aid for both radiologists, or as a pre-screening triage tool. Despite the improved resolution and image quality digital breast tomosynthesis offers over traditional mammograms, it takes almost twice as long, slowing down the efficiency of radiologists’ workflow. Referencing a 2022 study, Vinnicombe proposed that AI could act as complimentary tool to digital breast tomosynthesis, with 17–91% of digital mammogram scans being able to be read by AI alone, missing only 0–7% of cancer cases.
Interval cancer is defined as breast cancer detected during the 3 years after a normal result, and before the next screening appointment. Characteristically, interval cancers are aggressive and are associated with a poor prognosis.
Drawing on novel research, Vinnicombe stated that AI flags 20–50% of interval cancers at the prior screen, which were incorrectly deemed negative by human readers. Operating at a 99% specificity, a 2022 study also concluded that AI could correctly localise 27.5% of false negatives, and 12.0% of cases with minimal signs, at the prior screen. The ability of machine learning to not only localise potential tumours, but also correct human misreading is highly significant, elevating the predictive properties of screening.
In her concluding remarks, Vinnicombe detailed the current barriers and facilitators in breast cancer screening. According to a review, which analysed 107 papers looking at the implementation of AI in clinical radiology, the common limitations are data size, variability, quality, model transparency, and meaningful clinical evaluation. Conversely, the majority of papers consistently concluded that AI mainly aids in diagnostic performance and clinical workflow.
"It is estimated that by 2027 there will be a 40% reduction in consultant breast radiologists within the UK."
12 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Congress Feature ● ECR 2024

AI AND LUNG CANCER SCREENING
Bram Van Ginneken, Radboudumc, Nijmegen, the Netherlands, discussed the current challenges in lung cancer screening, notably the occurrence of false positives, leading to overdiagnosis and overtreatment. Like Vinnicombe, Ginneken too was optimistic that AI could help minimise false readings, workload, and overall expenditure.
Several trials have demonstrated the use of low-dose chest CT as a diagnostic tool for lung cancer, namely the NLST, and more recently, the Dutch-Belgian NELSON trial. Ginneken summarised a study, assessing the performance of a computer aided detection (CAD) algorithm, to recognise abnormal nodules, and classify their malignancy risk based on volume. Unsurprisingly, the average reading time per scan was less than 1 second, compared to 60 seconds for a radiologist, and CAD successfully matched the malignancy risk of 70% of scans to the recommended NELSON criteria.
Ginneken emphasised the variability in performance between radiologists, but even between scans of an individual, and explained how AI offers, in comparison, consistent high performance. Looking to the future, he advocated for greater responsibility and tasks to be assigned to AI, allowing it to detect abnormalities across entire scans, and training it to identify rarer manifestations of the disease.
AI AND PANCREATIC CANCER
Vincenza Granata, Istituto Nazionale Tumori di Napoli, IRCCS G. Pascale, Naples, Italy, opened her presentation sharing the startling 5-year survival rate for pancreatic cancer in the USA (12%). With this statistic increasing to 44% with early detection, she stressed the importance of early intervention and screening techniques. The current guidelines, provided by the International Cancer of the Pancreas Screening (CAPS) consortium, recommend screening to start at 50–55 years for those who meet the familial risk criteria, and 40 years for patients with Peutz–Jeghers syndrome, a familial atypical mole, or melanoma syndrome.
"As the third leading cause of cancer deaths, PDAC is a significant global health concern."
Granata addressed several research initiatives set up to train and validate the use of deep learning models in the detection of pancreatic cancer, specifically pancreatic ductal adenocarcinoma (PDAC). As the third leading cause of cancer deaths, PDAC is a significant global health concern, with less than 20% of patients eligible for surgery at the time of diagnosis. The Felix project, for instance, is a multidisciplinary research collaboration, funded by the Lustgarten Foundation, New York, USA,
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 13
ECR 2024 ● Congress Feature
comprised of experts in medical imaging, pathology, cancer research, and computer science. Conducted at Johns Hopkins Hospital, Baltimore, Maryland, USA, it assessed the specificity and sensitivity of AI PDAC detection from CT scans. The preliminary results of this project, using 156 PDAC and 300 normal cases, were highly promising, with AI yielding a 94.1% sensitivity and 98.5% specificity for PDAC detection. Additionally, the artificial neural network (ANN) was developed, trained, and subsequently tested using the health data of 800,114 respondents, captured in the National Health Interview Survey (NHIS) and Pancreatic Lung, Colorectal and Ovarian Cancer (PLCO) datasets. Interestingly, ANN exhibited exceptional sensitivity and specificity, 87.3 and 80.3, respectively, with an area under the receiver operating curve of 0.85.
In her closing remarks, Grenata drew attention to several barriers preventing full integration of AI into clinical practice. Firstly, the training and validation of these models requires large datasets and multicentre studies, across various institutions and populations, to prevent opportunistic bias. She explained that the accuracy of AI detection is solely dependent on the image quality of CT scans, a factor that can be variable, especially in heterogenous, multicentre datasets. Finally, she highlighted the extensive collaboration between several specialists, such as radiation oncologists, surgeons, and researchers, as well as policy makers, before the implementation of these predictive tools in patient care, and pancreatic cancer detection, can be a reality.
AI AND PROSTATE CANCER DETECTION
“MRI offers high sensitivity, approximately 91%, but lower specificity (37%) and moderate
reproducibility,” stated Olivier Rouvière, Centre Hospitalier Universitaire de Lyon, France, shifting the focus to the use of AI in prostate cancer detection. He outlined two fully automated systems, CADe and CADx, utilised in the detection and diagnosis of prostate cancer, respectively. Whilst CADe analyses MRI scans and highlights possible lesions, CADx quantifies the degree of suspicion of said lesions.
Although current research indicates exceptional detection capabilities in these systems, Rouvière cautiously noted some considerations when reading said literature. He put into question the definition of ‘external cohort’, a term mentioned frequently in validation studies. He explained that if the cohort AI is being tested on is too similar to the training dataset, the model will undoubtedly perform well, invalidating the study, and lending to opportunistic bias. As a combative effort, he called for large-scale external validation studies on multicentre, multivendor, multi-scanner, multiprotocol cohorts, to ensure thorough testing of the robustness of algorithms for prostate cancer detection. Finally, he touched on the potential shifts in sensitivity/specificity balance of predefined diagnostic thresholds.
CONCLUSION
With the ever-growing demand on diagnostic services, coupled with the deficit in clinical radiologists, the emergence of AI could not have come at a better time. By training computer models to detect abnormalities in scans, tasks traditionally performed by radiologists can be shared out, alleviating the workforce crisis, and revolutionising detection technology. However, as alluded to by the experts, cancer diagnosis is a complex process, and before AI can be routinely implemented into clinical practice, it must be thoroughly validated first. ●
14 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Congress Feature ● ECR 2024
Changing the Game: Interventional Radiology's Growing Impact on Imaging
Authors: Victoria Antoniou, EMJ, London, UK
Citation:
EMJ Radiol. 2024;5[1]:15-18. https://doi.org/10.33590/emjradiol/CWOB3604.
THIS YEAR’s European Congress of Radiology (ECR) took place in Vienna, Austria, from 28ᵗʰ February–3ʳᵈ March, and featured a gripping Innovation in Focus session that delved into the various ways interventional radiology (IR) is changing imaging today. Chaired by Jurgen Fütterer, University of Twente, Enschede, the Netherlands, the session featured talks discussing the evolution of interventional radiology from past to present, and where it will take us next.
THE EVOLUTION OF INTERVENTIONAL RADIOLOGY
“Interventional radiology is based on the integration of disruptive technologies and disruptive approaches, and [we] need to keep this approach if [we] want to survive.” This was how Gilles Soulez from the University of Montréal, Canada, began his presentation on the evolution of the ever-transforming field which is IR. The work of Charles Dotter, who performed the first angioplasty, and Andreas Grüntzig, who first thought to use a balloon to do so, was discussed, and their revolutionary contributions to IR were acknowledged as a basis for many more decades of innovation.
Soulez went on to discuss multiple other innovative radiologists, and their significant ideas, which have changed how the field operates today. Ideas alone were not their main reason for success, however, emphasised Soulez; successful innovation in IR is the result of the ability to bridge unmet clinical needs, with the conception of a new device. Each of these pioneers used collaborative, transdisciplinary methods in their approach to innovation, utilising
biomedical engineering, physics, and surgery, in addition to IR. Experts from various fields collaborating instead of competing is also vital, as are supportive institutions and sheer persistence, explained Soulez.
Whether or not these factors will make up the recipe for success in IR innovation in the future is uncertain, however. More stringent regulations in today’s medical scene mean less room for progression, and the now-mature nature of the once-new imaging capabilities, on which so many innovations were dependent, may result in fewer changes to the field. Soulez anticipated that the next disruptive technologies will stem from the various ‘omics’: genomics, transcriptomics, proteomics, metabolomics, and a range of others.
Consequently, Soulez emphasised the need for change in the industry, so as not to fall behind. He underscored the need to reinvest in imaging, to reach targets, better select patients, and advance technology; pointed out the need for collaboration with basic scientists; and lastly, highlighted the importance of more randomised, cost-efficient studies. Radiotheranostics and radiomics were given as examples of
"Interventional radiology is based on the integration of disruptive technologies and disruptive approaches."
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 15 ECR 2024 ● Congress Feature

technologies which can go on to evolve in the near future with these approaches, and the potential for developments in drug delivery and simulation for training were explored.
NEW TECHNOLOGIES: WHICH SURGERIES WILL BE REPLACED NEXT?
As IR continues to develop, more procedures are being handled by interventional radiologists. Roberto Luigi Cazzato, Hôpitaux Universitaires de Strasbourg, France, discussed the areas in which IR is taking over surgery in his institution. He began his talk by exploring the latest developments in liver tumour microwave ablation. The goal of this procedure is a large ablation with large safety margins to prevent recurrence of local disease. Today, liver ablations can be achieved with a single antenna working at high power, and the organs around the liver can be protected almost entirely. Larger ablations run the risk of injuring the diaphragm, pericardium, gallbladder, and stomach; however, modern materials allow interventional radiologists to avoid this. To achieve these results, a combination of fluoroscopy and CT guidance is needed, in order to see precisely how far the needle can go in the liver, and to erase any uncertainty throughout the procedure. Furthermore, with this method, multiple lesions
can be treated in the same session, and complications such as bleeding can be dealt with immediately. Cazzato emphasised the value of precise angio-CT imaging over conventional CT or ultrasound in procedures like liver ablation, for improved progression-free survival.
Cazzato went on to describe how other procedures, such as cryoablation for kidney tumours and desmoid tumours, have a higher safety profile and better outcomes than other forms of treatment. He highlighted, however, that cryoablation for desmoid tumours often results in both minor and major complications, due to the size of the tumours being treated. Should the tumours be ablated earlier, when they are smaller, the risk of complication would lessen. This is what Cazzato and colleagues are aiming to prove in a Phase II, multicentre, randomised trial, in which patients with these tumours are observed until they start to grow or become symptomatic, when they will be treated with standard treatment (chemotherapy) or cryoablation. Cazzato expressed his hope that cryoablation will have the ability to entirely destroy the tumour, instead of simply stopping the growth, as other therapies do.
With these examples from his own work, Cazzato demonstrated the potential for improvement in IR and interventional oncology, highlighting which surgeries are already being replaced
16 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Congress Feature ● ECR 2024

by interventional procedures. He additionally emphasised the importance of remaining clinical as this happens. In his closing remarks, he pointed out that progress happens when radiologists interact with their patients; when patients can speak to their clinicians, and know who is performing their treatment.
THE FUTURE OF TRAINING IN INTERVENTIONAL RADIOLOGY
Development, innovation, and progress are all dependent on the future generations entering the field. Training, therefore, is a vital aspect of IR, and one which will need to adapt and evolve with the technology if radiologists are to keep up. Elif Can, Freiburg University Hospital, Germany, began her presentation on the future of training in IR by pointing out the high mortality rates in hospitals across Europe and the USA due to medical errors. This is especially prevalent in IR, due to the repetitive nature of a radiologist’s work and the steep learning curve that comes with such work. We know, however, that trainees are far more likely to earn actively, remembering 90% of what they do but only 50% of what they hear. In addition to this, effective teamwork, communication, and technical skills are all essential in learning environments.
One way to achieve this in IR is through simulation and virtual reality (VR). Can presented data to support the use of these methods in training, demonstrating that simulation-based training reduces procedure time, improves procedure performance ratings, and reduces errors and complications. Simulation-based training has also been shown to improve the retention of high-level skills in trainees. The same can be said for the use of VR; studies have shown that use of VR amongst training interventional radiologists reduced both major and minor errors, increasing the procedure safety. This was proven across multiple institutions with multiple procedures, including fluoroscopy and angiography.
Financially, VR has proven to be more costeffective than animal lab training in several cases. The initial costs, however, are still high, and Can pointed out that a potential limitation of using VR in training may be its inaccessibility in resource-limited settings. Moreover, the lack of realism may be a cause of doubt, as VR may not completely mimic the physical experience of
"Can emphasised the effectiveness and benefits of simulation and VR in IR training."
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 17 ECR 2024 ● Congress Feature
being in an operating room. The quality of the simulations and VR used in different institutions may also vary, which would significantly impact training. Many have pointed out that, although VR aids the clinician in learning technical skills, it could lead to neglect of other aspects of practice, such as interpersonal skills. Lastly, Can pointed out that there is also a reluctance to moving over to a new, VR-based model of training in many university hospitals, as a result of the long-standing traditions and bureaucracy in medical training.
Ultimately, Can emphasised the effectiveness and benefits of simulation and VR in IR training, at the same time acknowledging their drawbacks
and challenges. She concluded her talk by stressing the need for further research and continuous improvement in these technologies, as they have great potential to help with the future of training new radiologists.
FINAL REMARKS AND QUESTIONS
This illuminating session drew to a close with a panel discussion where the speakers answered questions and discussed the future of education, the applications of AI in the field and why ‘AI’ may be too vague a term, as well as the implementations of robotics today and in the future. ●
Congress Feature ● ECR 2024 18 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0
Abstract Reviews
Dive into the latest findings in radiology, from novel abstracts presented by experts from institutions around the world at the European Congress of Radiology (ECR) 2024. Read on for insights into the cutting edge field of radiology.
Quantitative CT Analysis of Hepatocellular Carcinoma Nodules in Liver Transplant Candidates: Impact of Volume of Interest and Contrast Phase on Recurrence Prediction
Authors: *F. Rizzetto,1 R. Manzini,1 L. Centonze,2 C.B. Monti,1 S. Garziano,1 J. Di Napoli,1 L.A. Carbonaro,1 A. Vanzulli1,3
1. Department of Radiology, ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy
2. Department of General Surgery and Transplantation, ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy
3. Department of Oncology and Hemato-Oncology, Università degli Studi di Milano, Milan, Italy *Correspondence to francesco.rizzetto@unimi.it
Disclosure: The authors have declared no conflicts of interest.
Keywords: Contrast, hepatocellular carcinoma, liver, recurrence, radiomics, segmentation, transplant, variability.
Citation: EMJ Radiol. 2024;5[1]:19-21. https://doi.org/10.33590/emjradiol/LYFS8578.
BACKGROUND AND AIMS
Liver transplantation is the primary treatment for patients with early-stage hepatocellular carcinoma (HCC), which is not eligible for resection.1 However, even when Milan criteria are met, disease recurrence occurs in up to 16% of cases, resulting in a decrease in disease-free survival to 40%.2
Therefore, having preoperative knowledge of the likelihood of recurrence would assist in selecting the most suitable liver transplant recipients, potentially avoiding unnecessary surgeries, and improving patient prognosis and organ allocation. In this context, radiomics, which involves high-throughput data extraction from medical images, holds great promise.3 However, there is ongoing debate regarding the optimal data selection strategy, as factors such as the choice of contrast phase and volume of interest (VOI) can significantly impact radiomic analysis results.4-6 Therefore, the authors’ study aimed to investigate how these factors influence radiomic features (RF), to identify the optimal combination for predicting HCC recurrence in liver transplant candidates.
MATERIALS AND METHODS
Liver transplant candidates from 2010–2019, with waitlist placement CT scans showing nodules suspicious for HCC, according to the Liver Reporting and Data System (LI-RADS) criteria7 (LR-4/-5), and histologically confirmed after the transplant, were retrospectively included. Patients who had previously undergone locoregional procedures, exhibited tumour in vein, or had poor image quality were excluded from the analysis. HCC nodules were contoured
Abstract ● ECR 2024 Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 19
Redundancy: InterVOI: 14–26%



Interphase: 16–34%
Autocorrelation: 4%
AP: arterial phase; AUC: area under the curve; CI: confidence interval; DP: delayed phase; No: number; PVP: portal venous phase; RF: radiomic features.
Segmentation Feature Selection Modelling Arterial phase Portal venous phase Delayed phase = Nodule = +5 mm (PT_5) = +10 mm (PT_10) = +15 mm (PT_15) = Background Nodule AP-PVP PVP-DP AP-DP 0% 0% 20% 20% 40% 40% 60% 60% 80% 80% 100% InterVOI MRC >10% Interphase MRC >10% 100% PT_5 PT_10 PT_15 AUC (CI: 95%) P value Pseudo-R2 No. of RFs AP_Nodule 0.77 (0.65–0.90) 0.020 0.23–0.32 8 AP_PT_5 0.90 (0.83–0.97) <0.001 0.33–0.44 8 AP_PT_15 0.88 (0.76–1.00) <0.001 0.36–0.46 12 AP_Nodule_Norm 0.87 (0.75–0.98) <0.001 0.34–0.44 9 DP_Nodule_Norm 0.86 (0.77–0.95) <0.001 0.24–0.35 11 AP_PT_5_Norm 0.88 (0.80–0.97) <0.001 0.31–0.44 8 PVP_PT_10_Norm 0.88 (0.77–0.99) <0.001 0.35–0.45 8 PVP_PT_15_Norm 0.77 (0.65–0.89) 0.002 0.13–0.24 5
Figure 1: Workflow and results from the radiomic analysis of hepatocellular carcinoma nodules and peritumoural regions extracted from the waitlist placement CT scans of liver transplant candidates to predict disease recurrence.
■ = Arterial ■ = Delayed ■ = Portal
Abstract ● ECR 2024 20 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0
■ = Nodule ■ = PT_10 ■ = PT_15 ■ = PT_5
across arterial, venous, and delayed phases, with or without peritumoral region of 5, 10, and 15 mm. An area of ‘background’ liver parenchyma, distant from the lesions, was also segmented in each phase.
A total of 107 RFs, both directly extracted from segmentations, and normalised for the ‘background’ parenchyma, were obtained using PyRadiomics (Python Software Foundation, Beaverton, Oregon, USA). The normalisation was conducted by calculating the ratio between the RFs extracted from the VOI, and those extracted from the background segmentation. These features were then compared with each other for inter-VOIs and inter-phase relative change, while autocorrelation was assessed using Spearman’s rank correlation coefficient. RFs with relative change <10% and rank correlation coefficient >0.90 were considered non-informative. Informative RFs with different distribution in patients with and without posttransplant recurrence were selected to build multiple logistic regression models. Prediction of post-transplant recurrence was assessed by comparing the areas under the curve from receiver operating characteristic analysis and goodness-of-fit, expressed as the value range of Tjur’s, McFadden’s, and Nagelkerke’s R2 .
RESULTS
The CT scans of 53 patients were selected, resulting in a total of 1,032 segmentations from 86 nodules, with eight (15%) recurrence cases. When varying VOIs and phases, the proportion of noninformative RFs, indicating insignificant differences between the VOI and liver background, were 14–26% and 16–34%, respectively, while 4% of RFs showed autocorrelation >0.90.
The selected informative RFs allowed the building of eight predictive models with adequate performance and goodness-of-fit,
each comprising 5–12 RFs, with an area under the curve of 0.77–0.90 (p<0.02) and pseudo-R2 values of 0.13–0.46. A predominance of models derived from the arterial phase was observed, utilising the nodule with or without a 5 mm peritumoral region as the VOI, followed by the venous phase, including a 10–15 mm margin after normalisation (Figure 1).
CONCLUSION
Selection of optimal VOI and contrast phase combination is critical to maximise post-liver transplant HCC recurrence prediction using quantitative CT imaging. Specifically, segmenting the nodule, eventually including a 5 mm peritumoral region, during the arterial phase, or the nodule with a 10-15 mm margin during the venous phase after normalisation against the liver background, appeared to be the most promising strategy.●
References
1. Galle PR et al.; European Association for the Study of the Liver (EASL). EASL Clinical Practice Guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182-236.
2. Al-Ameri A et al. Predictors of post-recurrence survival in hepatocellular carcinoma patients following liver transplantation: systematic review and meta-analysis. Transplant Rev (Orlando). 2022;36(1):100676.
3. Nie P et al. Incremental value of radiomics-based heterogeneity to the existing risk criteria in predicting recurrence of hepatocellular carcinoma after liver transplantation. Eur Radiol. 2023;33(9):6608-18.
4. Wang F et al. Use of radiomics containing an effective peritumoral area to predict early recurrence of solitary hepatocellular carcinoma ≤5 cm in diameter. Front Oncol. 2022;12:1032115.
5. Escudero Sanchez L et al. Robustness of radiomic features in CT images with different slice thickness, comparing liver tumour and muscle. Sci Rep. 2021;11(1):8262.
6. Rizzetto F et al. Impact of interreader contouring variability on textural radiomics of colorectal liver metastases. Eur Radiol Exp. 2020;4(1):62.
7. Chernyak V et al. Liver imaging reporting and data system (li-rads) version 2018: imaging of hepatocellular carcinoma in at-risk patients. Radiology. 2018;289(3):816-30.
Abstract ● ECR 2024 Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 21
Acute and Chronic Complications of Caesarean Section: A Pictorial Review
Authors: *Kirsty McNeil,1 Magdalena Szewczyk-Bieda,1 Thiru Sudarshan1
1. NHS Tayside, Dundee, UK
*Correspondence to kirsty.mcneil@nhs.scot
Disclosure: The authors have declared no conflicts of interest.
Acknowledgements: The authors would like to thank their patients for contributing their cases.
Keywords: Caesarean, complications, obstetrics.
Citation: EMJ Radiol. 2024;5[1]:22-23. https://doi.org/10.33590/emjradiol/PONH7215.
BACKGROUND AND AIMS
Caesarean section, where a baby is delivered via an incision to the abdomen, is currently the most prevalent surgical procedure among patients aged 15–59 years in the UK.1 Globally, rates of Caesarean section deliveries vary, with an average estimated rate of 21%, higher in less developed countries. This number continues to increase, and is projected to reach 30% by 2032.2
While Caesarean sections are generally considered safe, there are a range of associated complications. With the increasing frequency of Caesarean sections, a corresponding rise in the incidence of complications can be expected. Therefore, it is important to ensure that radiologists can effectively identify the most common complications and their features across different imaging modalities.
The purpose of this pictorial review is to depict the various complications associated with Caesarean sections, and their appearances on different imaging modalities using local cases.
RESULTS
The complications identified in this local review of Caesarean section cases align with the recognised complications documented in the literature.
Acute complications included injury to adjacent organs, bleeding, and haemorrhage, along with the risks associated with anaesthesia, typical of acute complications seen with most surgical procedures. The organs most at risk during a Caesarean section are the bladder, ureters, and bowel, due to their proximity to the uterus. Most of the postoperative collections observed were located anterior to the uterus in the uterovesical space, or wound infections in the subcutaneous tissue.
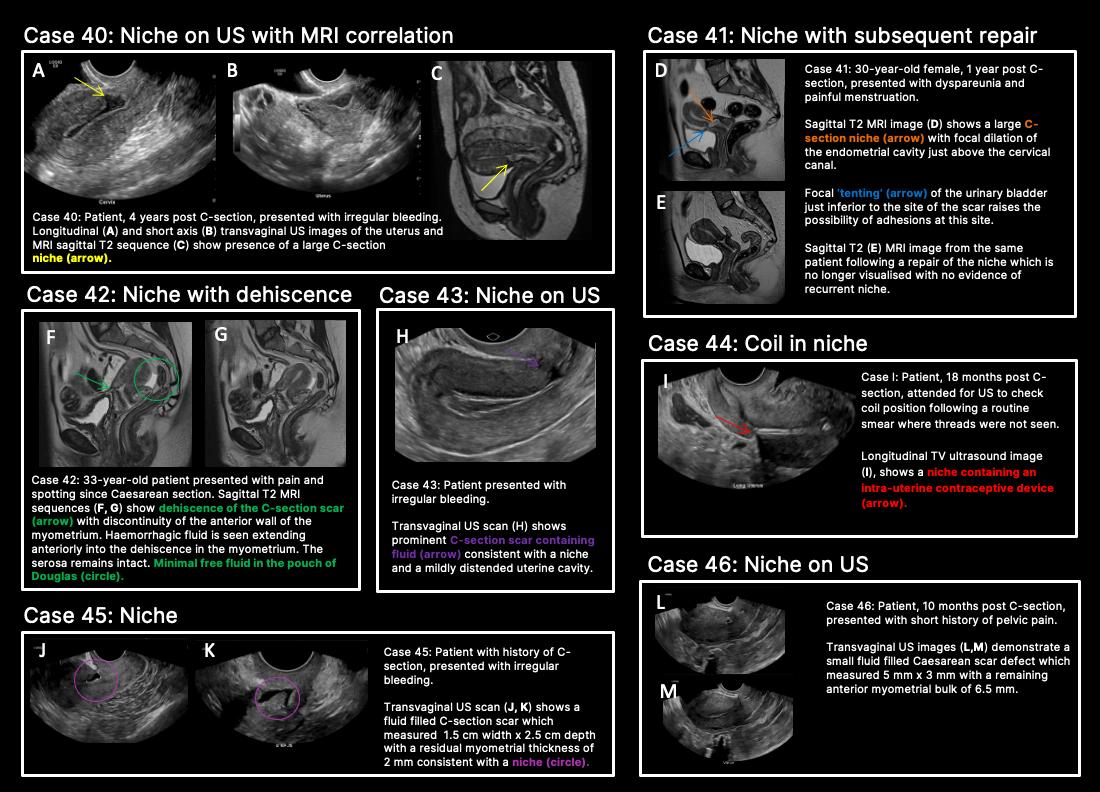
In contrast to acute complications, chronic complications are generally more unique to the Caesarean section itself, and are not typically seen with other surgical procedures, with the exception of incisional hernia. Caesarean scar niche was identified as an important cause of pain and irregular bleeding (Figure 1).
CONCLUSION
Familiarisation with the complications of Caesarean sections and their imaging appearances is important for radiologists and sonographers in identification and interpretation, and to assist clinicians in the ongoing management of patients. ●
Abstract ● ECR 2024 22 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0
C-section: Caesarean section; US: ultrasound.
References
1. Fowler AJ et al. Age of patients undergoing surgery. Br J Surg. 2019;106(8):1012-18.
2. Betran AP et al. Trends and projections of Caesarean section rates: global and regional estimates. BMJ Global Health. 2021;6:e005671:1-8.
A B C D E F G H J K L M I Abstract ● ECR 2024 Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 23
Figure 1: Caesarean scar niche.
Radiogenomics Relationship of Nonsmall Cell Lung Cancer: Preliminary Results
Authors: M.P. Belfiore,1 M. Sansone,1 V. Patanè,1 R. Monti,1 F. Grassi,1 G. Ciani,1 R. Grassi,1 S. Cappabianca1
1. Precision Medicine Department, Campania University Luigi Vanvitelli, Naples, Italy
*Correspondence to mariapaolabelfiore@gmail.com
Disclosure: The authors report no conflicts of interest.
Keywords: Cancer, lung, radiogenomics, radiology.
Citation: EMJ Radiol. 2024;5[1]:24-25. https://doi.org/10.33590/emjradiol/10304578.
BACKGROUND AND AIMS
Radiomics, an emerging paradigm in medical imaging, entails the quantitative analysis of tumour features, and has exhibited potential in predicting treatment responses and outcomes. Furthermore, within the domain of -omics assessments, the significance of comprehensive genetic evaluation in non-small cell lung cancer (NSCLC) is on the rise, influenced by both biological and therapeutic considerations.
The aim of this study was to correlate radiomics features with the genetic results obtained from liquid biopsy in patients with lung tumours. The prediction of tumour genetics in radiomics relies on the presumption of conducting a non-invasive evaluation of molecular characteristics in tumour tissues, which can be challenging in certain tumour types, such as NSCLC. Therefore, in this context, the authors considered it pertinent to explore and generate hypotheses regarding the technical feasibility of identifying associations between genomics acquired through liquid biopsy assessments and radiomics.
MATERIALS AND METHODS
This observational, prospective study integrated radiomic perspectives using CT and genomic perspectives, through next-generation sequencing applied to liquid biopsies.
The authors included 62 patients with NSCLC who underwent pre-surgery CT (Revolution™ 128 MDCT, GE HealthCare, Chicago, Illinois, USA) at the Radiology Department of Campania University Luigi Vanvitelli, Naples, Italy. Every patient for whom liquid biopsy was performed gave informed consent for the genetic analysis. For the radiomic analysis, image processing CT volumes were manually delineated using ITK-SNAP 3.8.0 (University of Pennsylvania, Philadelphia, USA). Radiomics features (first order: Gray Level Co-occurrence Matrix, Gray Level Run Length Matrix, Gray Level Size Zone, Gray Level Dependence Matrix, and Neighbouring Gray Tone Difference Matrix) were computed using Pyradiomics1 in Python 3.7 (Python Software Foundation, USA) environment.
Radiomic features were derived from CT images, and genetic assessments were performed using a comprehensive panel targeting 523 cancerrelated genes. For the statistical analysis, association between radiomic features and gene mutations were assessed using feature importance based on receiver operating characteristic curve analysis; moreover, a machine learning approach based on support vector machine was used to evaluate the ability of radiomic features to predict gene mutations.
Associations between radiomic features and genetic mutations were established using the area under the receiver operating characteristic curve. Machine learning techniques, including support vector machine classification, aimed to predict genetic mutations based on radiomic features. The prognostic impact of selected gene variants was assessed using Kaplan–Meier curves and log-rank tests.
RESULTS
Sixty-two patients underwent screening, with 53 being comprehensively characterised radiomically and genomically. This group was predominantly male (68.4%), and adenocarcinoma was the prevalent histological type (73.7%). Most patients exhibited ECOG Performance Status of 0 or 1 (87.7%), and 91.2% had a history of former or current smoking. Disease staging was distributed across I–II (38.6%), III (31.6%), and IV (29.8%). Significant correlations were identified with mutations
Abstract ● ECR 2024 24 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0
of ROS1 p.Thr145Pro (shape_Sphericity), ROS1 p.Arg167Gln (glszm_ZoneEntropy, firstorder_TotalEnergy), ROS1 p.Asp2213Asn (glszm_GrayLevelVariance, firstorder_ RootMeanSquared), and ALK p.Asp1529Glu (glcm_Imc1). Patients with the ROS1 p.Thr145Pro variant demonstrated markedly shorter median survival compared to the wild-type group (9.7 months versus not reached; p=0.0143; hazard ratio: 5.35; 95% confidence interval: 1.39–20.48).
CONCLUSION
This study contributes to advancing the prediction of cancer genetics through the application of non-invasive radiomic techniques. The prediction of tumour genetics in radiomics hinges on the assumption of conducting a non-invasive assessment of molecular characteristics in tumour tissues, which can pose challenges in certain tumour types, such as NSCLC. Therefore, within this context, the authors deemed it relevant to explore and formulate hypotheses regarding the technical feasibility of identifying associations between genomics obtained through liquid biopsy assessments and radiomics.
Specific radiomic features illustrate the capability to predict non-synonymous mutations of ROS1 and ALK in patients with NSCLC. Investigating the prediction of cancer genetics using non-invasive radiomic techniques represents an innovative frontier in scientific research, which is currently undergoing extensive investigation. Research on the use of conventional CT features and CT image-based radiomic features to predict the gene mutation status of lung cancer is still in its nascent stages.
The integration of radiomic techniques in predicting cancer genetics holds potential, but is constrained by cost and technological limitations. Despite these challenges, the authors’ study explores the relationships between genomics and radiomics, revealing specific genetic variants associated with radiomic features. While acknowledging limitations, particularly the small sample size and the lack of actionable mutations, this research lays the groundwork for broader investigations aiming to link radiomics and genomics in NSCLC. The ultimate objective is to improve prognostic accuracy and refine therapeutic strategies. ●
References
1. Pyradiomics. Homepage. Available at: https://pyradiomics.readthedocs.io/en/latest/. Last accessed: 1 March 2024.
A Proposal for a New Fluoroscopy Severity Assessment in Achalasia: The In Vivo Assessment of Achalasia Score
Authors: *Giovanni Fontanella,1 Simona Borrelli,2 Barbara Brogna3
1. Ospedale Sacro Cuore di Gesù FBF, Benevento, Italy
2. Hillman Cancer Center Villa Maria, Mirabella Eclano, Italy
3. A.O.R.N. 'S.G.MoscaG’, Avellino, Italy
*Correspondence to fontanella.giovanni@fbfbn.it
Disclosure: The authors have declared no conflicts of interest.
Keywords: Achalasia, barium, barium swallow, fluoroscopy, gastrointestinal, radiology.
Citation: EMJ Radiol. 2024;5[1]:25-26. https://doi.org/10.33590/emjradiol/NMKL9036.
BACKGROUND AND AIMS
The aim of the study was to establish a quali-quantitative fluoroscopic severity assessment for achalasia, comparable to the equivalent clinical Eckhard scoring system (ESS).
Abstract ● ECR 2024 Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 25
MATERIALS AND METHODS
From September 2020–August 2022, 69 patients already diagnosed with achalasia, and scored with ESS, were recruited and evaluated with the authors’ fluoroscopy barium protocol. The anteroposterior (AP) sequence was used to divide the oesophagus into nine segments, according to Brombart's classic description, plus the gastro-oesophageal junction. Three scoring items were chosen, after a profiling study of achalasia, to depict the features, some mutually exclusive, of the three clinical subtypes: lumen dilation, stasis, and spasm. Each oesophageal segment was scored for the three items (1 point given if the item was present; 0 points given if no item). The In Vivo Assessment of Achalasia (IVA) score was calculated by summing points up, until a maximum of 20 points for each subtype was reached. IVA scores were then normalised on a 0–12 scale to be compared to ESS.
RESULTS
IVA and ESS scores were not found to be statistically diverging in 60/69 patients (86.95%; p=0.05). IVA scores were diverging, and superior to ESS in 6/69 patients (8.69%); in this group of patients, the ESS 'chest pain' and 'weight loss' items were found to be biasing factors. IVA scores were inferior to ESS in just 3/69 patients (4.34%). In all patients with a diverging IVA score (9/9), ESS scores were found to be lower than 6/12.
CONCLUSION
IVA score was found to be consistent and compatible with ESS scores, especially in patients with moderate-to-severe achalasia.
The apparent superiority of imaging scores in a small proportion of patients might instead be used as a revealing tool to call out patients in which the ESS does not reflect the disease's severity, due to internal biases. ●
References
1. Fontanella G et al. A proposal for a new prognostic grading system in achalasia using dynamic barium swallow: the FBF score. EMJ Radiol. 2021;2[1]:34-6.
2. Bredenoord AJ et al.; International High Resolution Manometry Working Group. Chicago classification criteria of esophageal motility disorders defined in high resolution esophageal pressure topography. Neurogastroenterol Motil. 2012;24(Suppl 1):57-65.
3. Pandolfino JE, Gawron AJ. Achalasia: a systematic review. JAMA. 2015;313(18):1841-52.
4. Goldblum JR et al. Achalasia: a morphologic study of 42 resected specimens. Am J Surg Pathol. 1994;18(4):327-37.
5. Clayton SB et al. Functional and anatomic esophagogastric junction outflow obstruction: manometry, timed barium esophagram findings, and treatment outcomes. Clin Gastroenterol Hepatol. 2016;14:907-11.
6. de Oliveira JM et al. Timed barium swallow: a simple technique for evaluating esophageal emptying in patients with achalasia. AJR Am J Roentgenol. 1997;169:473-9.
7. Vaezi MF et al. Assessment of esophageal emptying post- pneumatic dilation: use of the timed barium esophagram. Am J Gastroenterol. 1999;94:1802-7.
8. Vaezi MF et al. Timed barium oesophagram: better predictor of long term success after pneumatic dilation in achalasia than symptom assessment. Gut. 2002;50:765-70.
9. Fontanella G, Morphodynamic Imaging in Achalasia (2023), Boca Raton: CRC Press.
10. Fontanella G et al. End-stage, Chicago/FBF Type I achalasia in a patient with long-standing untreated dysphagia: case report and pictorial essay. JCRC. 2022;DOI/10.33140/JCRC.07.02.01.
Abstract ● ECR 2024 26 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0
Revision of Diagnostic Reference Levels in Radiotherapy: A Road to Dose Optimisation
Authors: *Simona Borrelli,1 Giuliana Russo,1 Stefania Caponigro,1 Debora Diminico,1 Francesca Cavallo,1 Natascia Gennuso,1 Serena Romolo,1 Velia Forte,1 Ivana Russo,1 Piercarlo Gentile2
1. UPMC Villa Maria, Mirabella Eclano, Italy
2. UPMC San Pietro FBF, Rome, Italy
*Correspondence to borrellis@upmc.it
Disclosure: The authors have disclosed no conflicts of interest.
Keywords: CT, dosimetry, oncology, quality assurance, radiotherapy techniques, radiation therapy.
Citation: EMJ Radiol. 2024;5[1]:27-28. https://doi.org/10.33590/emjradiol/WXCD8245.
BACKGROUND AND AIMS
The aim of the work is the possibility of respecting diagnostic reference levels (DRL) for CT simulations, preserving a good image resolution required for radiotherapy planning activities.1
MATERIALS AND METHODS
The dosimetric indexes of simulation CT scans were examined in comparison to Italian and European standards. Dose length product and CT dose index values of 80 simulation CT scans of different anatomical districts, acquired in the period of October–November 2022, were collected. Dose length product values exceeded, in particular for head and neck, brain, and pelvis CT scans, the reference values (Figure 1). Following the analysis of the causes, CT acquisition parameters, such as scan field of view, display field of view, pitch, and modulation interval, were modified, and new CT protocols were implemented.2
An initial evaluation of the results was performed on 80 CT scans acquired in January–February 2023. The changes in CT protocols were then further discussed in terms of dosimetric impact and image quality and resolution. The final observation was performed on 80 scans acquired in April–May 2023, with the final protocols.
RESULTS
During the second analysis, the acquisition parameters were further refined, to optimise the results obtained in quantitative and qualitative terms. For example, for the head and neck district, the previous parameters were restored in favour of a better image resolution, although the DRLs were not respected.3
CONCLUSION
In many cases, it is possible to respect the DRLs alongside clinical/therapeutic requirements, while maintaining good image quality, and reducing the dose delivered to the patient.
LIMITATIONS
CT acquisitions for radiotherapy do not overlap with diagnostic ones, so DRLs are not an absolutely applicable standard. Compliance with these guidelines is, in fact, not mandatory for radiotherapy. ●
Abstract ● ECR 2024 Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 27
Figure 1: How the average dose length product changed during the periods under review, with reference to EU and ITA regulations.
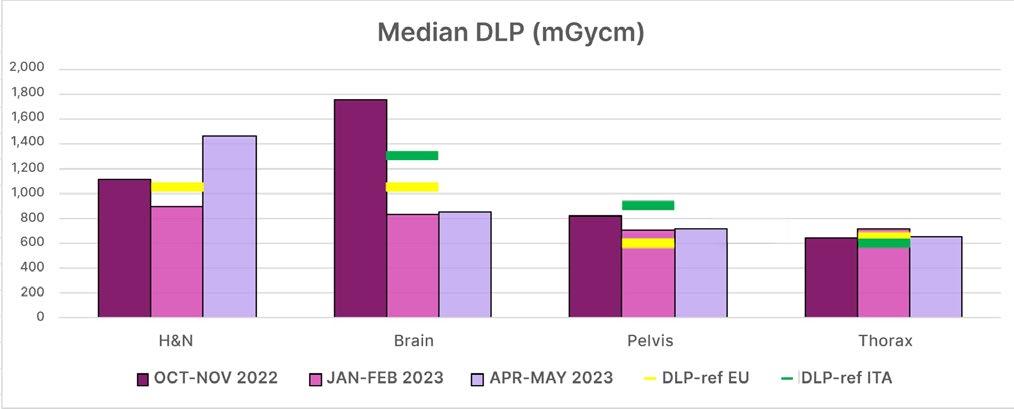
DLP: dose length product; EU: European Union; H&N: head and neck; ITA: Italy.
References
1. Vañó E et al. ICRP Publication 135: Diagnostic reference levels in medical imaging. Ann IRCP. 2017;46(1):1-144.
2. Dawd JE et al. A review of diagnostic reference levels in computed tomography. Curr Med Imaging. 2022;18(6):623-32.
3. Tabesh J et al. Determination of diagnostic reference level (DRL) in common computed tomography examinations with the modified quality controlbased dose survey method in four university centers: a comparison of methods. J Biomed Phys Eng. 2021;11(4):447-58.
Abstract ● ECR 2024 28 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0
Abstract Highlights
The following highlights spotlight selected abstracts presented at the European Congress of Radiology (ECR) 2024. Covering a range of topics, from deep learning applications in neurological disorders to using a single cranial CT slice for identifying deceased individuals, these highlights present the latest cutting-edge developments in radiology.
Citation:
EMJ Radiol. 2024;5[1]:29-35.
https://doi.org/10.33590/emjradiol/SEFB6923.

Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 29 ECR 2024 ● Abstract Highlights

A Comprehensive Approach to Reading Paediatric Chest X-rays
CHEST X-RAY is the most frequently ordered radiological investigation in paediatric health facilities; thus, errors in interpretation must be minimised. A systematic, comprehensive approach to reading paediatric chest X-rays, aimed at Paediatric and Radiology residents, was recently presented at ECR 2024, held from 28th February–3rd March in Vienna, Austria.
In this educational session, the authors emphasised that interpretation of paediatric chest X-rays is a taught skill that requires a multistep approach. Firstly, they highlighted some preliminary steps to follow, including checking the patient’s clinical history, as this will be interrelated with the chest X-ray findings; and the patient's age, which is correlated with the presence or absence of the thymus, and the expected signs of bony maturity.
The authors also stressed the importance of recognising suboptimal technical factors, which may degrade the quality of chest X-rays, and lead to misinterpretations. For instance, they noted that poor inspiration is associated with
false cardiomegaly and diffuse opacification of the lungs, and a high degree of film rotation may lead to false hyperlucency of the lung, a pseudo mass, or false positive impression of cardiomegaly. Radiologist should aim for central positioning, where clavicles are symmetrically shaped, and the trachea is centrally positioned between the right and left pedicles.
The authors then detailed how to interpret a normal paediatric chest X-ray, by providing an analysis of eleven structures: the abdomen, diaphragm, costophrenic angle, chest wall soft tissue, bones, thymus, airway, heart, aorta, hila, and lungs. For each structure, they presented a checklist to aid in evaluation of the X-ray.
Finally, the study emphasised the common variants, and the unconventional appearance of normal structures, on a paediatric chest X-ray. The authors explained that this could be especially helpful for residents who are accustomed to reading adult chest X-rays, and are new to paediatric chest X-rays.●
"In this educational session, the authors emphasised that interpretation of paediatric chest X-rays is a taught skill that requires a multistep approach."
30 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Abstract Highlights ● ECR 2024
The Broad Imaging Spectrum of Adenomyosis: Beyond the Junctional Zone Thickening
ADENOMYOSIS is a widespread benign gynaecological condition, in which the uterine lining penetrates the muscular wall of the uterus. Symptoms commonly include painful menstruation (dysmenorrhoea), chronic pelvic pain, and heavy bleeding during menstruation, known as menorrhagia. In new research presented at ECR 2024, held from 28th February–3rd March in Vienna, Austria, the highlights and pitfalls of MRI as a diagnostic tool for adenomyosis were explored.
As discussed in the session, the pathogenesis of adenomyosis is as follows: endometrial basalis cells will migrate and proliferate within the myometrium, forming an adenomyotic lesion. Alternatively, an ectopic endometrium will form by de novo metaplasia of stem cells, or implantation of stem cells through retrograde menstruation and invasion of the outer myometrium, known as ‘outside-to-inside invasion’. MRI images the innermost layer in the myometrium, called the junctional zone (JZ), and the classification and subsequent reporting as internal or external adenomyosis was described. For instance, if JZ thickness is over 12 mm, it is classed as internal adenomyosis, whereas a thickness of less than 8 mm is external adenomyosis. The size of the affected area also determines classification as focal or diffuse.
Researchers emphasised how the pseudothickening of the JZ during the menstrual phase can sometimes lead to a misdiagnosis of adenomyosis, with the recommendation to avoid MRI scanning during this time. It was additionally stressed that whilst JZ thickness is generally a reliable marker for adenomyosis diagnosis, hormone conditions, such as pregnancy and pre-menarcheal age, can affect the JZ. The JZ also may not be measurable in approximately 30% of postmenopausal uteruses, and in females using contraceptive drugs. It was additionally noted that several other benign conditions and malignant tumours have also shown to exhibit similar JZ characteristics to adenomyosis, such as uterine and JZ enlargement. Conditions mentioned included lymphoma, low-grade endometrial stromal sarcoma, myometrial involvement by pelvic endometriosis, and transient myometrial contraction.
The study concluded that adenomyosis can be accurately diagnosed by using MRI; however, it is imperative to be aware of both the typical and atypical features of adenomyosis, as well as other possible conditions that exhibit a similar phenotype. ●
"Pseudo-thickening of the JZ during the menstrual phase can sometimes lead to a misdiagnosis of adenomyosis."

Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 31 ECR 2024 ● Abstract Highlights
Deep Learning Applications for Alzheimer’s Disease
ALGORITHMS based on deep learning, with applications for diagnosis, developing prediction models, and treatment research, were outlined in an abstract presented at ECR 2024. The abstract was intended to inform neuroimaging prediction in radiologists.
Dementia affects over 55 million people worldwide, and as the seventh global cause of death, approximately 65% of cases are attributable to Alzheimer’s disease (AD). The significant burden this has on patients, caretakers, and the economy is vast, but emerging research aims to combat the progressive decline in cognition, and severe impairment caused by the condition. Early intervention can delay this decline, and improve quality of life. Modern neuroimaging techniques, aided by emerging AI and deep learning models, allow rapid and accurate assessment of key markers, such as brain atrophy, the accumulation of neurotoxic proteins, and synaptic disruptions.
The emergence of these AI and deep learningguided algorithms has provided solutions for semi-automated and automated brain segmentation and morphometry. Highly detailed reports are used, and a novel tool for AD detection and mild cognitive impairment prognostic has been developed, relying on lifespan trajectories of brain structures. This Hippocampal-AmygdaloVentricular Alzheimer score (HAVAs) is based on lifespan models of normal population, and patients with AD. After validation, it has shown great capability in detecting patients with AD, compared to control subjects. The probability score has shown considerable accuracy, both in diagnosis and prognosis.
From this abstract, and the other research shared at ECR 2024, it is clear that AI-based solutions are rapidly finding their way into AD clinical practice, and are set to improve patients’ quality of life dramatically. Neuroimaging plays a key role in the diagnosis and monitoring of AD, and the new software outlined provides automated and time-saving solutions, which will significantly aid neuroradiologists in identifying disease earlier, staging this, and monitoring both evolution and treatment response. ●
"AI and deep learning models allow rapid and accurate assessment of key markers."
32 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Abstract Highlights ● ECR 2024
Videofluoroscopic Swallow Study in Diagnosing Dysphagia
DYSPHAGIA, a debilitating condition, can lead to severe complications, including malnutrition, dehydration, aspiration pneumonia, and even death. Dysphagia is commonly a result of various medical conditions and their associated treatment complications, with prevalence increasing with age. Research presented at ECR 2024 explored the diagnosis of this condition.
The gold standard investigation for diagnosing dysphagia is the videofluoroscopic swallow study (VFSS), a dynamic fluoroscopic study. VFSS is often performed by collaboration between speech therapists and radiologists, and through the use of fluoroscopy, clinicians can visualise bolus flow through the aerodigestive tract in relation to structural changes. Overall, this enables real-time evaluation of the patient's swallowing physiology, specifically enabling the detection of any penetration/aspiration, underlying functional and/or structural abnormalities, and the observation of the effects of different bolus consistencies/volumes on swallowing.
Commonly, patients present with a combination of swallowing pathologies across different phases of swallowing. However, these pathologies may be difficult to identify, as swallowing occurs rapidly in real-time. Viewing these pathologies in slow motion is helpful to ensure abnormalities are not missed, and enables the identification of subsequent individualised rehabilitative therapy.
"VFSS is often performed by collaboration between speech therapists and radiologists."
VFSS allows the comprehensive assessment of oropharyngeal dysphagia and risk of aspiration, and is a useful tool in providing a preliminary evaluation of oesophageal motility. A good understanding of swallow physiology is important in identifying the underlying cause of dysphagia, before also guiding rehabilitation and management. ●

ECR 2024 ● Abstract Highlights 33 Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology

Advantages of Photon-Counting CT
PHOTON-COUNTING CT is an emerging imaging technique that promises a vast array of advantages for radiologists, as explored in new research presented at ECR 2024, held from 28th February–3rd March in Vienna, Austria.
Conventional CT, despite its widespread use and availability, continues to struggle with challenges in radiation exposure, image noise, and limited tissue differentiation, according to the study’s authors. Photon-counting CT may be the solution to many of these issues, with the potential for enhanced spatial resolution, reduced radiation noise, and improved characterisation of tissues. This new technology promises success, as photon-counting detectors (PCD) consist of a single layer of a semiconductor diode with applied voltage, and therefore do not need a separate layer to convert X-rays into light in the way of energy-integrating detectors. In a PCD, the authors explained, an X-ray is absorbed, generating positive and negative charges separated rapidly, and creating an electrical pulse in attached wires, which is then registered by an electronic readout circuit.
As a result of its unique operating method, photon-counting CT provides several clinical benefits to radiographers. This emerging
technology may improve the ways in which cardiac imaging is performed, increasing spatial resolution in coronary angiography, and reducing radiation noise in cardiac CT imaging. The authors went on to describe the ways in which photon-counting CT may also improve neuroimaging, and tumour detection and imaging, particularly when applied to small tumours and lesions.
"This emerging technology may improve the ways in which cardiac imaging is performed."
The study concluded that photon-counting CT has the potential to surpass conventional CT, as it provides improved spatial resolution, noise elimination, and efficient dose usage. PCD additionally may benefit larger patients, as it addresses artifacts like calcium blooming. Photon-counting CT has a wide range of applications in various areas of medicine, and therefore provides a promising future for radiography. ●
34 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Abstract Highlights ● ECR 2024
Identifying Deceased Individuals Using Single Cranial CT Slice
AUTOMATIC identification of unknown deceased individuals has been achieved with single cranial CT (CCT) slices, using a novel computer vision (CV)-based method. This research was presented at ECR 2024.
Orthopantograms (OPG) are often used in the identification of unknown persons; however, these are difficult to acquire post-mortem. As such, CT is the preferred post-mortem imaging modality. Considering the lack of literature exploring the use of CCT imaging to identify deceased individuals, researchers extended an automatic CV-based identification method used to extract CV features from OPGs to individual CCT images.
Using OPGs as a reference, a total of 819 CCT scans from 772 individuals aged between 10–99 years (321 females; 452 males; and 46 unknown), obtained between November 2016–May 2023, were retrospectively analysed across six defined regions: lower row of teeth, upper row of teeth, end of maxilla, cervical spine, maximal representation of maxillary sinus, and maximal representation of eye structures.
In instances where large metal or movement artifacts were present, accurate location of these six regions was not achievable, and thus, specific images for these areas could not be exported to aid identification. Subsequently, a further 1,771 OPGs from these individuals between December 2000–May 2023 were included. CV features were extracted from imaging using the AKAZE algorithm.
To enable individual identification, 50–69 CT slices per region from individuals with at least two examinations were compared with up to 818 database entries, and a further 410 OPGs were matched with 1,759 OPGs from the same individuals. Following this, calculation of a CV feature matching concordance metric was performed (matching points/number of key points) [%]).
"The highest success was seen in the maxillary sinus region."
Identification was achieved for 72–87% (rank: 1–10) of the identities using CT images. Sameindividual identification across all six CT regions achieved a concordance metric score of 12.04±0.86%, compared to 2.15±0.40% for different individuals. This difference could be a result of metal artifacts or lower image resolution. The highest success was seen in the maxillary sinus region, with identification rates of 72%, 80%, and 87% for rank 1, 5, and 10, respectively.
The study concluded that a single CCT slice can be used to identify unknown individuals, and that future research assessing CT abdomen and thorax imaging for other distinctive CV features to further improve identification success rates, should be explored. ●

Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 35 ECR 2024 ● Abstract Highlights
Congress Interviews
The following interviews highlight the latest developments in radiology, covered at the European Congress of Radiology (ECR) 2024, held in Vienna, Austria, from 28th February–3rd March 2024. Andrea Rockall, ECR First Vice President, discusses her plans for the future of the congress, and Aad van der Lugt, Erasmus University Medical Center, Rotterdam, the Netherlands, discusses how the industry is changing for young radiologists.
Featuring: Andrea Rockall and Aad van der Lugt

Citation:
Q1
Andrea Rockall
Clinical Chair of Radiology, Imperial College London, UK; European Society of Radiology (ESR) First Vice-President
EMJ Radiol. 2024;5[1]:36-39. https://doi.org/10.33590/emjradiol/SCDS7604.
What originally inspired you to pursue a career in radiology?
Well, it gives away my age a little bit, but when I had just qualified as a medical doctor, and I was doing what in England are called ‘house jobs’, MRI was actually just coming in. I can remember seeing the images, and actually being struck by this incredibly beautiful thing that we could demonstrate. CT was already gaining a lot of traction, but it was still relatively new, and MRI was really new. I loved the combination of trying to solve a puzzle: “What is the diagnosis, and what has happened to the patient based on their symptoms?”, and then having these fantastic new tools at our disposal.
In addition, there were developments happening in interventional radiology, and it just seemed
to me like a very, very exciting speciality to go into. I actually did my exams in internal medicine, which was, at that time, quite standard within the UK. You did your internal medicine, or your Membership of the Royal Colleges of Physicians (MRCP), or your Fellowship of the Royal Colleges of Physicians (FRCS) in surgery, and then you would apply for radiology. So, I had this period of time when I was a houseman, where I could see all of the imaging developments that were happening in the tumour boards, with the images coming in; it just really looked fantastic.
"The pace of innovation in radiology has been really dramatic over the last decades."
36 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Interview ● ECR 2024

Q2
You chaired, and took part in, several presentations and sessions at the European Congress of Radiology (ECR) this year, in Vienna, Austria. Which sessions did you most enjoy attending?
Rick Abramson’s plenary, on the digital AI interface, was really spectacular. It was looking at where we've come from, and where we're going. If I think of my own journey, going from when MRI was emerging as a new technology, and now we're in this era of artificial intelligence (AI), you can see the pace of innovation in radiology has been really dramatic over the last decades. There are limits at the moment with what AI can offer us, but nonetheless, there are some benefits that we can potentially gain from having AI tools there. However, there are still lots of challenges in understanding the health economic arguments, the safety side, the benchmarking of tools, and what have you. There's a lot of work for us to be doing. But nonetheless, the opportunities are very exciting; we will be facing a big change in our careers, as AI-supported radiology becomes a reality, and that will change the way that we practice. That was one session that I just loved. It was brilliant. It was inspirational.
Of course, because it's my area of passion, there are also the sustainability sessions. I spoke in a session on the ‘green hospital’, and we kicked
off with how departments can identify resource savings from implementing green policies. We also had a talk on contrast media: how we need to be careful about our use of contrast media, making sure that we get good images, but at the same time using as little contrast as we can, in order to get that vivid image. And then, how do we dispose of those? That session was actually packed out. We had a very full discussion at the end, which was lovely.
Q3
As First Vice-President of ESR, and future President, what changes do you hope to implement in the society in the coming years, and what have you already been working on?
There have been some really exciting changes in just the past few months that many of us have been pushing for, which I'm really pleased about. We implemented a new vertical young committee, and within that, we have the sustainability subcommittee, and an Equity, Diversity, and Inclusion subcommittee. I think these are really important to our community, and they fill a gap in our executive council. This is a new development, and I am really looking forward to working with the committee and subcommittee chairs to really build those areas of ESR commitment. We also have another new subcommittee, which is digital AI and emerging
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 37 ECR 2024 ● Interview
technologies. The AI will shift across from the quality and safety committee over a period of time; it hasn't gone straight away, but that's our overarching plan. This also allows us to have a committee that really focuses on emerging technologies, as we've seen this incredible change that we are continuously going through; how do we adapt to the changes of things like photon counting CT, for example? So, those things have come in.
One of the things I would love to bring to the ESR, in order to really reach out to our members and encourage engagement, is find a way for people to be able to indicate that they're interested in getting involved in subcommittees and committees. I'm trying to see if we can have some kind of volunteering portal, where people can say, actually I'm really interested in, say, sustainability. They can let us know about their motivations, and send across their CVs, and then when places come up, the subcommittee and committee chairs will already have a list of people that have indicated that they'd really like to work with us. They can then evaluate the applicants, and invite people to join. So, I'd love to have some kind of system for our members to be able to volunteer, get involved, and take part.
Q4
Much of your work focuses on sustainability in healthcare, particularly in medical imaging, which contributes significantly to global emissions. How do you think radiology can improve to become a more sustainable practice?
It is very important for us to make this transition, and we have to make it relatively quickly. This is why I really feel strongly about taking a leadership role in trying to help the process. There are some things that are easy to do, which will actually save money in departments; there are a lot of energy saving tips and tricks to do with the automated switch-off of large and small machinery, and laptops. There are simple solutions for waste management that can actually dramatically impact carbon usage; for example, the correct waste disposal of plastic tubing. A lot of it often
ends up in the sharps bin, but if you put it in the appropriate waste stream, and just put the sharp aspect in the sharps bin, you can reduce your carbon imprint. In our department, two CT scanners have a project like that, and they have reduced our sharps bin waste by 98%. That actually saved the department a lot of money, because the sharps bin waste is very costly.
I think there's a real mission to educate. What can we do now in our departments, with really very little effort? But then, there is another whole package which is more complex; for example, pathways of care. Can we make sure, for example, that the patient has one journey to the hospital, instead of three, for their diagnostic tests? In a lifecycle assessment of the CT scanner, we found that 60% of our emissions were related to patient travel. So, if we can co-ordinate outpatient appointments, imaging, and diagnostic blood tests, this will have a big impact; this may be in the medium term, and is a little bit more difficult to impact.
Also in the medium term, although I wish it was in the short-term, is embedding a decision support software, so that we can image the patient with the right test the first time. We don't want the patient to have the wrong test, to say, “oh no, you shouldn't have had that one. You should have had this one,” and then they have to come back again. All of the resources that are used for that low-value imaging have really been wasted; not only for spaces on the scanner, waiting lists, etc. We have all of the downstream effects: all of the scans will be stored on a server, creating carbon for another 20 years. None of this benefits the patient's care. So, I think decision support, and some of the care pathways, are medium term. When we're doing procurement, we need to have sustainability as one of the scoring factors, so I need to look at asking our industry partners: do they have a recycling system when they take the equipment back? Do they have anything that's actually been refurbished? Can they refurbish our systems as we upgrade? There are different levels of difficulty.
"In a lifecycle assessment of the CT scanner, we found that 60% of our emissions were related to patient travel."
38 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Interview ● ECR 2024

Q5 In 2020, you participated in an interview discussing the role of AI in breast cancer diagnosis. Four years on, to what extent do you believe AI has been implemented in the field?
In the UK, interestingly, it's difficult to know how many implementations there are. This is why we've developed a registry for deployed AI tools, because there is a registry of tools that have permission to be marketed and sold, but we don't have a registry of where they're deployed. We're developing this registry so that we can know who has deployed what, and where. I think there is very limited actual clinical deployment in the UK. But there is a current a very large study going on, funded by the National Institutes for Health and Care Research (NIHR), a multicentre, multi-vendor study, led by Fiona Gilbert from the University of Cambridge, UK. This study will hopefully provide a strong, independent evidence base, to allow the National Health Service (NHS) to say, “actually, this now has good evidence for implementation, and we can sign that off.” I am sure there are a lot of other breast products that will be going on, for breast density and things like that, but I think the big health economic impact is going to be that, if you can use AI as a second reader, that frees up a radiologist. This therefore makes a really strong economic argument for efficiency.
Q6 What, in your opinion, are some of the biggest challenges facing radiology today, in the UK and globally?
Number one is workforce shortages. At first, I thought it was just within the UK, but I think everywhere is having workforce shortages. How do we train enough radiologists quickly enough to expand into this growing field? Of course, those that are working in the field need to have the time to train those that are coming through. We also have huge waiting lists. How do we manage the waiting lists versus the workforce and training aspects? There is a hope, of course, as I said with the breast, that if you can have some AI tools that can help with this, this may help us with second reading, for example. AI may also help us in some of the workflow, with the rapid triage of cases, etc. However, I think that workforce is definitely the biggest issue.
Another big issue that we have is that we're in a period of massive change, which can be stressful for people, especially when they're already stretched from workforce shortages. So, bringing in AI will be a big transformation for us in terms of how we work. Also, with regard to sustainability, we've got to crack that nut. ●
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 39 ECR 2024 ● Interview
Q1

Citation:
Aad van der Lugt
Professor and Chair Department of Radiology & Nuclear Medicine at Erasmus University Medical Center, Rotterdam, the Netherlands
EMJ Radiol. 2024;5[1]:40-43. https://doi.org/10.33590/emjradiol/VLXJ1549.
What was it that inspired you to first begin a career in radiology, specifically neuroradiology?
I have to confess that I did not choose radiology because I found it to be a fantastic job. In the 1980s, there was a labour crisis, and there were actually no available vacancies for residency programmes. My PhD supervisor stepped in and helped me to get a position as a resident in radiology. It took me 2 years to appreciate the profession, but after those initial years, I became committed to radiology for two reasons. The main reason was that I had a hunger for knowledge. Radiology offered an environment with continuous developments in the technical domain. Besides knowledge on imaging physics, we also had to become familiar with various diseases, to interpret the images accurately. In addition, it is not just reporting an exam; you have to know what the relevance is of the abnormalities. In the end, I had to become familiar with two knowledge domains: medicine and physics. So that was, for me, one of the reasons why I truly began to love radiology.
The second reason was that I was exposed to experts in the field, and they were real role models. My supervisor in neuroradiology was consulted frequently to solve difficult cases, and he was so important for the clinical decision-making process. He motivated me to reach the same level in neuroradiology. Thereafter, I was a neuroradiologist, and I was very lucky to have a department chair who was focusing on international development, so he brought in a lot of new trends. He was a great promotor of scientific research and he gave me the opportunity to start my own research
programme. I was surrounded by nice, smart people, who actually told me, “come on, try and you can reach the same expert level.” I've followed their advice all my life.
Q2
You moderated a talk at the European Congress of Radiology (ECR) this year, in Vienna, Austria, on implementing quantitative imaging biomarker protocols in lung cancer screening. Can you give our readers a little bit of information on the European Union (EU)'s lung cancer screening programme decision and implementation plans?
I'm a neuroradiologist, and a head and neck radiologist, so why do I have an interest in lung cancer screening? That's because I'm Chairman of the European Imaging Biomarker Alliance (EIBALL), which is a subcommittee of the European Society of Radiology (ESR). Our main task is to promote the use of quantitative imaging biomarkers, which are measurements extracted from images, like size, volume, and density. The problem in measuring biomarkers is the variability. When you measure a lung nodule today and tomorrow, it will not have the same size or the same volume, as there is an inherent variability. This variability is increased when you use, for example, a different scan protocol, another scanner, or software. The question arises of how to deal with this variability when the lung cancer screening guidelines propose to
"Radiology offered an environment with continuous developments in the technical domain."
40 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Interview ● ECR 2024

"When you measure a lung nodule today and tomorrow, it will not have the same size or the same volume, as there is an inherent variability."
do a follow-up exam when the lung nodule size is smaller than 6 mm. EIBALL is dealing with that problem, and trying to solve it.
My main message in the EIBALL session was that, when you start implementing lung cancer screening, you should be aware of the variability, and you should take measures to reduce it, because that will strengthen the study you are performing, and also strengthen the screening programme. We had three presenters: a pulmonologist and a radiologist actively involved in lung cancer screening programmes, and an expert on the imaging biomarker problems. We brought them together and said, “let's discuss that, and inform the audience about the problems and the solutions.” I was really surprised that the topic was appreciated: the session ran at 8 a.m., and I was little bit afraid that only 10 people would show up. But in the end, it was fully booked!
Q3 Could you explain a bit more what EIBALL is, and what its aims are?
Around 10 years ago, in Europe and the USA, we realised that historically, we have used imaging just to diagnose disease. We described the disease, whether it was a round lesion, or an irregular lesion, and we linked these descriptors to biology or outcome. At a certain moment
in time, we realised we could also extract measurements: for example the severity of vascular stenosis or the size of the lesion. We felt this was important for radiology and patient care, but we experienced that the measurement had a significant variability, and we realised there was a problem. So, we started trying to quantify the size of the problem. Was it really a problem? Could we reduce the variability in measurements? It would be silly, of course, to do that in every country or professional society; a more harmonised approach would lead to better results. We have collaborated extensively with the USA’s version of EIBALL, the Quantitative Imaging Biomarker Alliance (QIBA), founded by RSNA. We have tried to advocate a common methodology in measuring the variability, and also in solving and reducing variability. I wouldn't say we are there yet, but progress has been made.
Q4
You chaired a session on EIBALL at last year’s ECR. What key developments have taken place in the alliance since then?
So-called metrics have been developed, which help to measure the variability in such a way that you can compare measurements between different sides. Papers have been published on how to do this properly. Of course, this has
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 41 ECR 2024 ● Interview

not fully penetrated the imaging domain yet, but a lot of radiologists and researchers are using these types of metrics. Studies have also been performed to explain how to reduce the variability. With regard to clinical application, studies have been performed that demonstrate that the use of an imaging biomarker is important in the clinical decision-making process. For example, in lung cancer screening, it is clear that you need the measurement of lung nodule size to make a decision about what to do, and that is already a step forward. So, we are trying to increase the evidence base for the use of imaging biomarkers. It is possible to extract multiple biomarkers from an image, and it is important to find out which one is relevant. Artificial intelligence (AI) is also helping us to have a more precise, or fast, measurement of disease characteristics in the image.
Q5 What new developments in the field of radiology are you most excited about at the moment?
That’s a very difficult question. Each of us has a narrow view of their own, and an area of expertise, so having a broad view is difficult. However, surprising new developments pop up in many domains. In the image acquisition domain,
we have seen CT scanners with photoncounting detectors becoming an exciting topic in the last 2 years, as they provided an increased resolution, a lower dose, and spectral imaging. New contrast agents have popped up in MRI. Sometimes I have the feeling that the field hasn’t changed for 5 years, and nothing new is on the horizon, and suddenly we see exciting new developments, not realising that companies have been working on a topic for more than 20 years before it has reached the imaging community. In image analysis, you can really see that AI is revolutionising the process, not only in the extraction of quantitative imaging biomarkers, but also in detecting disease, aiding diagnosis, and helping to speed up the workflow. For the moment that is the most exciting development, to be honest. But we should not forget the progress in imaging physics and technology!
Q6 Speaking of AI, how is the everincreasing use of AI influencing your practice, research, and teaching as a radiologist and professor?
I have to admit that AI looks like a promising paradise. But it will take years before we will see the fruits of it, because we are still in the process where everyone is trying to pick low-hanging
"Artificial intelligence (AI) is also helping us to have a more precise, or fast, measurement of disease characteristics in the image."
42 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Interview ● ECR 2024
"The ESR serves as an important vehicle for radiological education, enabling us to stay up-to-date."
fruit. As an academic radiologist, I have an inborn critical approach, so I like to see the evidence that AI will result in value for patients and society, especially before we invest money. Of course, there are areas where we see improvements in workflow or diagnostic accuracy, but we can't expand that yet to all domains in radiology. In the coming years, I think there will be a steady progress of penetration of AI in radiology and nuclear medicine.
Q7
What do you hope to see ESR and EIBALL achieve in the coming years?
The ESR serves as an important vehicle for radiological education, enabling us to stay upto-date. Amid our busy daily routines, finding time to extract information from research papers, journals, and websites can be challenging. With the ECR, ESR makes it easy for us to get a quick overview on the current status of radiology. Furthermore, connecting with colleagues and drawing inspiration from these interactions is essential. ESR is also instrumental in harmonising radiology across Europe. By fostering research, ESR is crucial in providing evidence for the important role of imaging in daily clinical care. I sincerely hope that ESR continues to play this crucial role. For EIBALL, I hope that AI and other innovative techniques will significantly enhance biomarker extraction. Overall, I hope that ESR helps us to strive for a future where diagnostic advancements not only improve patient care, but also make our professional lives more fulfilling and enjoyable.
Q8 What do you think are the biggest challenges facing young radiologists starting out in the field today?
Feeling overwhelmed. While I acknowledge my own hunger for knowledge, I recognise that many residents may find themselves in a similar situation, but unsure of where to begin. As a radiologist, I often encounter young colleagues who question their abilities and wonder if they can truly reach higher levels of expertise. My message to them is unequivocal: yes, you can. Being selected for a training programme signifies that others believe in your potential. However, it’s essential to understand that progress doesn’t come without effort. Merely sitting in a room and passively listening won’t suffice. Professional growth demands active participation, mental investment, and time. This approach may seem old-fashioned, but it remains effective. As a physician specialising in imaging, you may forget that your commitment extends beyond technical skills. Patient care should remain at the core. Embrace this commitment, invest in your development, and maintain unwavering focus. It’s not merely a hobby; it’s a fulfilling journey. The satisfaction comes when you find yourself in a pivotal role: people seeking your advice, making decisions based on your insights. That, indeed, is rewarding.
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 43 ECR 2024 ● Interview
Q1
Interviews


This year, EMJ is thrilled to have the pleasure of introducing key opinion leaders Maureen Kohi and Susan Shelmerdine, whose interviews detail their impressive careers, as well as the latest exciting innovations in radiology today. Discussions touch on diversity in interventional radiology, current clinical trials in the field, artificial intelligence in radiology, and much more.

Citation:
Maureen Kohi
Ernest H. Wood Distinguished Professor and Chair, Department of Radiology, University of North Carolina (UNC) at Chapel Hill, USA
EMJ Radiol. 2024;5[1]:44-46. https://doi.org/10.33590/emjradiol/10302707.
Having read about your extensive work in the field, what led you to focus on interventional radiology (IR) as opposed to other areas of healthcare?
During medical school, I found myself gravitating towards procedural specialties, such as surgery. What attracted me to IR was the innovative nature of the field. I was fascinated by how we could treat complex diseases through a minimally invasive approach, with fewer complications, quicker recovery, and at times, better results compared to surgery. I fell in love with the diversity of the procedures and the elegant techniques.
Q2
Our readers may find it interesting to hear that much of your work is centred around female health. What are your primary interests in that field, and what was it that made you want to work in that space specifically?
I have been fortunate to have a very broad practice in IR, taking care of patients with a variety of diseases.
However, in the field of IR research, my focus has been on female health and interventions. I have learned a great deal by leading clinical trials comparing different minimally invasive therapies for uterine fibroids, uterine vascular anomalies, and morbidly adherent placenta, or evaluating the different sex-based outcomes of interventions for peripheral arterial disease. I also feel that there is still a need for robust data to support the role of minimally invasive therapies to promote female health. Let’s take uterine fibroids, for example. This is the most common benign disease of the premenopausal female pelvis, and yet the most common reason for hysterectomy in the USA is uterine fibroids. We take out an entire organ for a benign disease. Think of how rarely we do this for other processes; we do not take out somebody's lung because they have a pulmonary arteriovenous malformation, we embolise it. You do not take out a kidney because somebody has angiomyolipoma, you embolise it. So, why is it that for a female, so long as they are done with childbearing, they are relegated to a hysterectomy? What if they don’t want to have their uterus removed?
44 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Interview
It was that kind of advocacy for female health that got me started in female health research. It’s fascinating to run a clinical trial, and show that one therapy is superior to another for a disease state, and help to impact the lives of people who have commonly been neglected, which in most cases in medicine includes females, children, and underrepresented minorities.
Q3
Do you think that underrepresentation and the nonchalant approach to female health in general are the most significant areas that are still lacking in clinical care and radiology?
Absolutely! The COVID-19 pandemic opened up people’s eyes to health disparity. There were so many people that suffered and died from COVID, and so many people who didn't. When you looked at it, you realised that if you're affluent and have access to healthcare, you are likely to do better than someone who has a lot of comorbidities, hasn’t had proper preventative care, or doesn’t have access to healthcare. Many of us have known that disparities have existed in every field of medicine for years.
I think that one of the reasons we haven't really dived deeply into this matter has been the quality of our clinical trials, preventing patients who are underrepresented, or don't speak English, from being included in the trials. For example, diversity of patient population and backgrounds has long been lacking in the makeup of nearly all peripheral arterial disease clinical trials. This lack of diversity was not only restricted to the patients, but also included the clinical trial leadership and research coordinators, etc. If the trial leadership is not representative of our patient population and there is no emphasis on diverse patient recruitment strategies, then chances are that the trial will not recruit diverse patients. As a result, we will be left with trial results from a certain group of patients, i.e., White males or adult patients, which we will extrapolate to our female, underrepresented minorities, and paediatric patients. This is not the best way of practising medicine.
"The COVID-19 pandemic opened up people’s eyes to health disparity."
Q4
What is being done to increase diversity in radiology and clinical trials?
The main issue is that we don't have diversity in the field of radiology as practitioners. Diagnostic radiology in America is composed of around 25% female specialists. So, one-quarter of radiologists in America are female, and in interventional radiology, it's about 10%. That number may have increased a little bit.
What we are doing to address the lack of diversity, as it applies in the gender gap, at least, is to try to recruit more females into the field of interventional radiology. In the latest data I was looking at just recently, about 20% of the applicants to interventional radiology are female, which is fantastic! I hope we continue to see more females enter the field of interventional radiology.
We're not seeing that much of an increase in diagnostic radiology, unfortunately, so we have some work to do. We need more females, and more underrepresented minorities, because patients want to see people who look like them. This also validates the trust in the clinical trial; if we have more females in the fields of radiology and interventional radiology, then we can teach them to become physician scientists, and then they can be the next generation of principal investigators running the clinical trials. They can go in with the mindset of recruiting a more diverse patient population into the clinical trial. The first step is outreach; we have to try to create pathway programmes to get medical students, college students, and high school students educated and excited about the field of interventional radiology.
Q5
What do you think are the most exciting new developments in radiology and female health taking place at the moment, and how will they impact clinical care in the future?
I'm super excited about a new prospective, randomised controlled trial (RCT) called Embolize, that hopefully will open in the next few months. Embolize is going to be a pivotal landmark clinical trial, because it's prospective, randomised, sham controlled, and it addresses pelvic venous disease.
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 45 Interview
This is a condition that has been neglected in females for years, and now, we're doing an RCT, to try to show that embolisation is a safe and effective therapy for the management of this condition. We need this RCT to get insurance coverage for this procedure, because even though we have a lot of single arm clinical trials and case series, most insurance companies in the USA still consider embolisation for pelvic venous disease to be experimental.
I think in the world of radiology, what's really exciting is artificial intelligence, and how we can leverage deep learning pathways to improve our efficiency and clinical excellence. I'm very excited about the future of artificial intelligence and its integration into diagnostic and interventional radiology. Ultimately, I feel it will help us take better care of our patients.
Q6
What is next for you and your research in interventional radiology at the University of North Carolina (UNC)?
I really love being a Department Chair and being an integral part of a distinguished school of medicine and healthcare system. However, regardless of how busy I may be in my administrative role, I will still want to be an interventional radiologist and take care of patients, and continue to contribute to the field with scholarly activities. I deeply believe in the tripartite mission of compassionate clinical care, research innovation, and educational excellence. It’s incredibly rewarding to take care of patients, to teach a resident or convince a medical student that interventional radiology is the best field, and run a clinical trial that will change the way medicine is practised in the future. I love each of these components and can’t imagine a future without them. ●
"I'm very excited about the future of artificial intelligence and its integration into diagnostic and interventional radiology."

46 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Interview
Q1

Citation:
Susan Shelmerdine
Paediatric Radiology Consultant, Great Ormond Street Hospital, London, UK
EMJ Radiol. 2024;5[1]:47-49.
https://doi.org/10.33590/emjradiol/10305013.
You now work in paediatric radiology, and have previously worked in paediatric post-mortem radiology. What led you to specialise in these areas instead of other aspects of the field?
I've always loved working with children, and ever since my medical training, I felt that children’s hospitals were a very upbeat, positive, and friendly environment to work. You might think it's strange that I then transitioned to learning about post-mortem imaging, which may not sound so upbeat and positive. However, I felt that it was a part of imaging that wasn't being addressed properly. Children on the whole don't have serious illnesses, and don't die on the same scale as adults. Some do, but on the whole, they're pretty healthy. However, there is a huge population of perinatal deaths that we don't see, hear, or talk about. Throughout the world, every year, approximately 2 million babies are stillborn, and 23 million miscarriages happen. Many parents suffer from not knowing how or why this has happened. In the past, the best we could offer them was either a full autopsy or nothing, and many parents suffered in isolation. They don't want an autopsy, because it's very invasive and emotional, but they do want answers. Imaging has become something we can now offer, allowing us to scan babies and children who have died, and potentially find some reasons as to why this has happened. We can give some closure to parents, or even help understand whether or not this is likely to happen again if we find a genetic or recurrent problem. I was interested in this research, because not many people were doing it, and I felt it was an area of need, to offer more understanding for a part of the population that doesn’t get a huge amount of attention.
"There is a huge population of perinatal deaths that we don't see, hear, or talk about."
Q2
You developed the INTACT biopsy procedure for perinatal autopsy. Could you tell our readers a little about the procedure and its applications?
Although we try our best to move from something invasive to non-invasive with imaging, there are times when you want to investigate a death, where having tissue samples from the deceased would be helpful. For example, when you want to look at the cell makeup of a particular tumour that you see on the imaging, or you want information on genetics, metabolomics, infection, or microbiology. Whilst we try our best to image and not do anything invasive, occasionally, a small sample from the patient would be helpful. How do we do this in the most minimally invasive way possible? In live patients, we do biopsies of things that we think look abnormal, rather than a full operation. The whole idea of the INTACT biopsy was trying to do that but for the deceased, and in children in particular. INTACT stands for INcisionless TArgeted Core Tissue biopsy. What I was trying to do with this was to take tissue samples from a perinatal death without making any incisions to the body at all, keeping it as intact as possible. We do this by using a needle biopsy tool directed through the umbilical cord. Through this one entry point, we’ve managed to take tissue samples from the lungs, the heart, the kidneys, the liver, and the spleen. Because babies are quite small, with a long enough needle, you can actually target multiple organs through that one area
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 47 Interview
that's central in the body, without having to make extra incisions anywhere else. We found that it was quite effective, and over 75% of the time, the tissue biopsies were suitable for analysis by the pathologist. You will probably think, “well, biopsies aren't something new, people were doing biopsies before,” and the truth is, people were doing biopsies, but they were often doing this blinded by using body landmarks, feeling bones, and then targeting the needle underneath the bone where they thought the organs would be, which was less than 50% successful. Sometimes they were also using ultrasound guidance, but making multiple incisions and holes in the body. With the INTACT biopsy, we were doing it under ultrasound guidance, and only through one particular entry point. So, even though you've taken lots of samples of tissues, when you return the baby to the parents, it doesn't look like anything has been done to them, and we have more information than we would with just imaging alone.
Q3
A popular topic in all aspects of medicine, but particularly radiology, at the moment is artificial intelligence (AI). How are you already applying new AI technology in your practice?
I feel very lucky to be a radiologist because I feel like we are at the cutting edge of using AI technology in healthcare. There are more AI tools available in radiology than any other medical specialty right now, so it’s an exciting time to be a radiologist! Unfortunately, paediatric radiology AI is probably a little more behind than adult imaging. However, in my hospital, we are using one tool called BoneXpert to help us look at hand X-rays from children and predict their bone age, which is really important for children who are having hormone treatment, have hormonal problems, or are too short for their age, to investigate whether they have delayed growth or some other problem. This, I believe, is the most commonly used AI tool internationally. I've previously done a survey of paediatric radiologists internationally, asking them questions about how they are using AI in their practice. I would say the top tools they use are for bone age prediction. In some places, AI also has uses in cardiac imaging, although that's a very subspecialist part of paediatric radiology, not your ‘bread and butter’ imaging. In my practice, as an academic radiologist, we are working with AI companies in many ways to
try to develop and test AI tools for children, so that they are not left behind with this brand new technology that others benefit from. My particular research is trying to develop an algorithm that can detect bone fractures in children's bones, which look different to adults, because they're still growing, and children of different ages have very different looking bones. But we are also testing commercially available tools that exist for adults on this and seeing how accurate they are in children. We are working with other AI collaborators on how we can look for emergency findings on chest X-rays, for example, abnormal line and tube placement, and our intensive care colleagues are very keen to push that forward.
"There are more AI tools available in radiology than any other medical specialty right now."
Q4
In what ways do you believe AI will change paediatric imaging in the future?
It's really hard to predict the future, especially when AI is so fast moving and so many new developments are happening all the time. Because children as a population are a little bit smaller in number than adults, we have to work with the most common things in children if we want to use AI, because we need enough cases to train an AI to detect problems. For things like bone fractures, which are common, or tube placements, which are also very common, I do think these tasks may become automated in some way in the future. But I also think the most useful AI is what I call ‘boring AI’. It is working in the background, and helping things get processed without you even knowing it is there. I feel that is going to be a big part of AI for all specialties, but particularly paediatrics in the future. I don't think flashy, in your face, lifesaving AI will take the headlines, but rather things that really speed up our processes in a paediatric hospital. For example, we have children that cannot sit still for their scans, so there is motion on the imaging. AI will correct that. AI will help reduce the time it takes to scan a whole body from half an hour to maybe 5 minutes. It speeds up MRI acquisition, so children don't need to have sedation or a general anaesthetic to tolerate these scans. It will probably be AI that helps reduce the amount of radiation we impart to a
48 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0
Interview

child having repeated scans for cancer follow-up. It will be things that speed up processes, reduce appointment times, or make sure we don't have to recall patients to have repeated imaging, which then blocks up our backlog of appointments. I think AI that helps us with that will be more useful, and we will see immediate effects. The problem with so much AI right now that detects things on imaging is that, whilst it looks fancy and flashy, and it can diagnose a problem, there is very little evidence at the moment that it actually improves patient outcomes or that it is cost effective. That will take a lot longer and timelier studies to find out. It will be much easier to prove the efficiency and cost savings for a hospital for things that speed up processes.
Q5
Do you think that AI will be a large part of every radiologist’s practice in the near future?
Absolutely. I don't think it will replace radiologists, but I do think it will replace certain tasks that radiologists do. For example, when someone requests a scan, we have to vet them, say whether they're appropriate or inappropriate, and then say what kind of imaging would be best suited for the problem that the patient-facing doctor wants answered. I think some of those things could be automated with AI. It might save us time if we don't have to protocol and vet scans quite so frequently, and only for the very unusual cases where our opinion is needed. That can speed up processes, and help book patients onto appropriate scanners faster with the appropriate type of imaging protocols. I think a few aspects in our jobs won't have to happen quite so much, but I don't think our jobs will be replaced, at least not for the very near future.
Q6
Could you share with our readers what you think is the most exciting development happening in paediatric or forensic radiology at the moment?
There are two things that I think are exciting, one more academic and the other organisational. The organisational thing is that more people are interested in wanting to take it up as a service. When I started doing it, I was seen as someone who was quite strange, who wanted to do this niche project and specialty. Now we have proven the benefit of it, and patients really want it, there aren't enough imaging experts who are experienced in this subarea to be able to offer that service. I see many people wanting to offer it, learn about it, talk about it, and get their hands on exposure to this kind of imaging. I think it is really exciting to be able to see multiple new services for post-mortem imaging developing across the country and internationally, because I think it will benefit so many parents and families, and hopefully patients, if we can find a problem during the pregnancy and stop that from happening again with a future pregnancy. The second thing is in forensic imaging, where we’re now seeing the rise of new imaging techniques. One that I’ve been involved with is micro-CT scanning, which is like a CT scanner, except it sees images in very high resolution, up to 10 microns in resolution, which is amazing considering the usual CT scanner is just under 1 mm. We're now using this to scan bone specimens as well as some pathological specimens, to try to get a sense as to whether or not there are very subtle fractures in particular bones of patients. This can be really important for forensic investigations about injuries and trauma. These things can be very hard to detect both by the pathologist and by the radiologist, but hopefully, harnessing this new technology gives us that extra bit of information to help put the pieces together for a challenging case. Not many places have a micro-CT scanner, but more and more of them that are currently being used for animal studies are being repurposed for this particular research area. I think that's an exciting area of development. ●
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 49 Interview
Understanding Micro-CT Scanning
EMJ Radiol. 2024;5[1]:50-51. https://doi.org/10.33590/emjradiol/11000016.
What Is It?
Microfocus CT utilises X-rays to see, slice-by-slice, within an object.
Similar to regular CT scanning, but on a smaller scale with higher resolution.
• Samples can be imaged with pixel sizes as small as 100 nm
• Objects can be scanned as large as 200 mm in diameter.
Applications of Micro-CT
Perinatal autopsy
• This is a recent use of micro-CT, but one which shows a lot of promise.
• Useful for imaging early gestational fetuses, as they are very small.
• Non-invasive, therefore less distressing for the parents when seeing their child.
• Gives an indication as to whether a full autopsy is needed.
• Imaging feasibility as low as 7 weeks’ gestation has been reported.
Evaluation of bone quality, structure, and microdamage
• Micro-CT imaging can assess the strain associated with the damage.
• Can be used to study metabolic bone diseases, such as osteoporosis.
• Can additionally be used to test the efficacy of anti-resorptive and anabolic therapeutics for such diseases.
References
1. Micro Photonics Inc. What is micro-CT? An introduction. Available at: https://www.microphotonics.com/what-is-micro-ct-an-introduction/.
2. Micro Photonics Inc. How does a micro-CT scanner work? Available at: https://www.microphotonics.com/how-does-a-microct-scanner-work/.
3. Alsop K et al. Advantages of micro-CT in the case of a complex dismemberment. J Forensic
4. Shelmerdine SC et al. Postmortem microfocus computed tomography for noninvasive autopsies:
5. Nagaraja S et al. Spatial correlations of trabecular bone microdamage with local stresses and
6. Boerckel JD et al. Microcomputed tomography: approaches and applications in bioengineering.
7. Keklikoglou K et al. Micro-CT for biological and biomedical studies: a comparison of imaging
8. Shelmerdine SC et al. Novel usage of microfocus computed tomography (micro-CT) for visualisation
100 nm 10 μm 200 mm 10 mm DNA Strand Ladybird Average human hand Red Blood Cell
How Does It Work?
• X-rays are emitted from an X-ray generator.
• These travel through the sample.
• A detector on the other side records these to produce a radiograph.
• The sample is then rotated by a fraction of a degree, and another projection image is taken.
• This process is repeated until the sample has been rotated either 180 or 360 degrees, producing a series of projection images.
Benefits
• This gives radiologists the ability to distinguish between materials of different densities.
• Non-destructive, which means that the sample can be preserved for any reason.
• Concerns have been raised regarding the harmful impact of X-rays on genetic material; however, studies have shown no damage thus far.
Complex dismemberment
• Non-destructive and clear visual representation of the skeletal wounds.
• Leads to shorter investigative process in court cases.
Bone remodelling and adaptation
• This may go on to help cases of strain and fracture of bones.
https://www.microphotonics.com/what-is-micro-ct-an-introduction/. Last accessed: 16 January 2024. https://www.microphotonics.com/how-does-a-microct-scanner-work/. Last accessed: 16 January 2024. Sci. 2022;67(3):1258-66.
autopsies: experience in >250 human fetuses. Am J Obstet Gynecol. 2021;224(1):103.e1-15. and strains using rigid image registration. J Biomech Eng. 2011;133(6):064502. bioengineering. Stem Cell Res Ther. 2014;5(6):144. techniques. J Imaging. 2021;7(9):172. visualisation of human embryonic development-Implications for future non-invasive post-mortem investigation. Prenat Diagn. 2018;38(7):538-42.
here to download X-ray generator Sample Rotation Table Detector
the dismemberment
Radiograph
Click
Approximate locations of
sites
Authors:
Rise in Chronic Diseases: Will Radiology Survive?
*Andrew England1
1. Discipline of Medical Imaging & Radiation Therapy, University College Cork, Ireland
*Correspondence to aengland@ucc.ie
Disclosure:
England is President of the European Federation of Radiographer Societies (EFRS), Chair of the RoClub Radiographers’ International Advisory Board, and Member of the ECR 2024/25 Programme Planning Committee.
Received: 13.02.24
Accepted: 26.02.24
Keywords:
Citation:
Capacity, chronic disease, radiology challenges, workload.
EMJ Radiol. 2024;5[1]:52-55.
https://doi.org/10.33590/emjradiol//HHEU2045.
The global population continues to rise, and by 2050, it is predicted that 2.1 billion people will be aged 60 years and over.1 With a rise in the population of older people comes an increase in the prevalence of chronic disease and disability.2,3 Within the healthcare community, there can be large variation in definition of the term chronic disease.4 The World Health Organization (WHO) definition of chronic disease is diseases that are not passed on from person to person. They are of long duration, and generally have a slow progression. The four main types are cardiovascular diseases, cancers, chronic respiratory diseases, and diabetes.5
Increases in the number of older people who live longer will exacerbate the burden of chronic disease, and place a higher demand on healthcare services.6 Based on current figures, it is estimated that 50% of the population of the USA have a chronic disease, which disproportionately accounts for 86% of healthcare costs.7 Radiology has not escaped these additional pressures. Wang et al.8 highlight that due to an ageing baby boom population, utilisation of diagnostic imaging has increased significantly compared to other healthcare services.8 Utilisation of imaging resources does
not necessarily follow a linear relationship with population change. Gaget et al.9 reported that between 2009–2019, the Australian population aged over 65 years old increased by 39%, yet the utilisation of radiography in this age group unproportionally increased by 63%.9
Further commentary suggests that chronic disease definitions should acknowledge that they usually originate from complex causality, can be multifactorial in origin, and develop over a long period. Chronic diseases are also associated with a prolonged course of illness, which may be associated with other health complications, and can lead to functional impairment or disability.4 Osteoporosis and osteoarthritis have also been highlighted as chronic diseases, which again tend to arise in the later years of life.10,11 Transition between disease states has also been noted; for example, from acute to chronic or chronic to terminal disease states. Rates of chronic disease are a function of age, but also other factors, including lifestyle choices, such as tobacco and alcohol consumption.12-15 Access to healthcare also has a strong relationship between the incidence of chronic disease and clinical outcomes.16,17
52 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Feature
Predicting the impact of changes in chronic disease rates on radiology is paramount. Over the past few decades, the contribution of radiology into modern medical practice has increased substantially.18 Radiology plays a clear and essential role in the investigation and management of many chronic conditions, and their resultant acute presentations.19 With the advent of minimally invasive procedures, radiology also plays an important and everincreasing role in providing procedural guidance. 20
Moving forward is not simply about understanding overall chronic disease prevalence and likely future trends. Changes in the proportions of individual chronic diseases, and the evolution of clinical pathways for how diseases are diagnosed and managed are important. It is widely acknowledged that the proportion of different diseases within the overall category of ‘chronic disease’ will evolve. Radiology is also likely to contribute differently to diagnosis and management in the future. By way of example, since 1990, global smoking prevalence has declined by 27% for males and 38% for females.21
Trends continue to vary by region, with decline being limited in low- and middle-income countries. The impact of these trends should be modelled when predicting the future requirements for radiological imaging; for example, thoracic CT examinations, and the need for lung cancer screening. Lung cancer screening is broadly believed to be cost-effective for highrisk populations, yet has not been implemented in many European countries.22 Ischaemic heart disease is a leading cause of death worldwide, and management is guided by understanding the physiological significance of the coronary artery stenosis. Traditionally, the physiological significance of a stenosis can be estimated by invasive coronary angiography, and by determining the fractional flow reserve. Overall, this is a safe procedure, but is associated with arterial injury in <1% of cases.23 Non-invasive imaging of the heart, and the assessment of the physiological significance of a stenosis is now possible, and such examinations are on the rise.24,25 Several authors now argue that non-invasive imaging methods are equivalent to invasive catheter angiography, and thus, there are likely to be further increased demands on radiology, and less so on cardiology.26-28
In view of the significance of changes in the prevalence of chronic diseases, modelling by academic groups and policymakers is in operation. Within England, The Health Foundation have estimated that between 2019–2040, we will see rises in dementia (45%), chronic obstructive pulmonary disease (37%), heart failure (92%), chronic kidney disease (34%), cancer (31%), and diabetes (49%).29 Such disease groups rely on heavy involvement from radiology, but this has been known to change rapidly and significantly; for example, the rise in the use of PET-CT in cancer staging.30 This can be illustrated by comparing Australia to the UK; Australia has a population of approximately 26 million, and in 2017 had 46 PET-CT scanners.31 The UK, by contrast, has a population more than double (around 67 million), and in 2017 had 54 PET-CT scanners.31
Access to radiology is not without problems, and this precious resource is, regardless of healthcare system, not infinite.32 Even where access to physical imaging equipment is in abundance, there can be challenges in providing image acquisition, and with reporting. Shortages of radiographers and radiologists have been widely reported within the literature.33,34 Within the UK, a recent workforce census estimates that there is a 43% deficit in the number of required radiologists.34 Support from artificial intelligence (AI) has demonstrated potential in reducing some of these uncertainties. There are, however, still many examples of difficulties in successfully implementing AI within routine clinical practice.35 Growth in referrals, when combined with human resource challenges, is likely to further exacerbate problems in imaging chronic diseases over the short- to mid-term.
Access to appropriate and timely radiology when investigating chronic disease has demonstrated a positive impact on patient outcomes.36 Prompt access to radiology in the early stages of disease has, in many instances, demonstrated economic advantages, both for healthcare budgets but also society more widely. Changes in the way healthcare is being delivered have also demonstrated the effects of the utilisation of radiology services. A USA-based study in 2017 demonstrated that more fragmented care was independently associated with higher rates of radiology and other diagnostic tests than less fragmented care.36
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 53 Feature
The benefit from prompt radiological imaging is likely to increase with developments in imaging technology, and improvements in the safety profile of diagnostic examinations. Such possibilities are readily visible in terms of lowdose CT acquisitions, possibly with the same radiation doses as conventional radiographs. For example, emerging studies have documented paranasal CT sinuses examinations with doses as low as 0.08 mGy.37 Discussions on whether abdominal radiography could be substituted with ultra-low dose CT are progressing.38 Quantitative image analysis, for example, from dual-energy CT scanning, will increase radiology’s ability to contribute to the characterisation of disease, for example, in determining the composition of renal stones.39 Modern software algorithms have also permitted the minimisation of artefacts from metallic prostheses, i.e., total hip replacements.40 Not only will there be more patients to scan; more of them will have chronic disease, but the indications and contribution of radiology will also expand. With increases in the number of imaging examinations come a greater frequency of incidental findings. Studies evaluating brain MRI scans in older people have reported incidental findings in approximately 5% of patients.41 Identification of an unexpected finding can trigger additional medical care, including further diagnostic procedures and treatments, which, in some cases, may pose an additional risk to the patient.42
References
1. World Health Organization (WHO). Ageing and health. 2022. Available at: https://www.who.int/newsroom/fact-sheets/detail/ageingand-health. Last accessed: 6 March 2024.
2. Mitra S, Brucker D. Disability and aging: from successful aging to wellbeing through the capability and human development lens. Disabil Health J. 2020;13(4):100924.
3. Fong J. Disability incidence and functional decline among older adults with major chronic diseases. BMC Geriatr. 2019;19(1):323.
4. Bernell S, Howard S. Use your words carefully: what is a chronic disease? Front Public Health. 2016;4:159.
5. World Health Organization (WHO). Noncommunicable Diseases.
Challenges are undoubtedly ahead for radiology when contributing to the care of patients with chronic diseases. Radiologists, radiographers, other healthcare professionals, and funders must collaborate effectively to carefully plan and resource radiological diagnostics appropriately. Short-term decisions are required, but the problem will only get greater without an ambitious medium- and long-term vision. Such discussions are happening; for example, at the European Congress of Radiology (ECR) in Vienna, Austria, in February and March 2024. The theme of ECR’s 2024 congress was next-generation radiology, and it is fitting that the role of radiology in chronic disease was a significant part of the agenda. For over a century, radiology has been strongly based around key developments in technology. AI, robotics, cloud-based computing, and big data are just some of the current initiatives, which will continue to shape how we practise radiology. Radiology is also moving outside of traditional hospital-based departments. In the future, more and more chronic diseases will be imaged in the community, away from hospitals. Such endeavours are likely to increase the visibility of radiology, increase access, and again, strengthen demand.
2024. Available at: https://www. who.int/data/gho/data/themes/ noncommunicable-diseases. Last accessed: 6 March 2024.
6. de Carvalho I et al. Organizing integrated health-care services to meet older people's needs. Bull World Health Organ. 2017;95(11):756-63.
7. Holman H. The relation of the chronic disease epidemic to the health care crisis. ACR Open Rheumatol. 2020;2(3):167-73.
8. Wang L et al. Utilization patterns of diagnostic imaging across the late life course: A populationbased study in Ontario, Canada. Int J Technol Assess Health Care. 2008;24(4):384-90.
9. Gaget V et al. Trends in utilisation of plain X-rays by older Australians (2010–2019). BMC Geriatr. 2022;22(1):100.
10. Sözen T et al. An overview and management of osteoporosis. Eur J Rheumatol. 2017;4(1):46-56.
11. Di Nicola V. Degenerative osteoarthritis a reversible chronic disease. Regen Ther. 2020;15:14960.
12. Centers for Disease Control and Prevention (CDC); National Centre for Chronic Disease Prevention and Health Promotion; Office on Smoking and Health, How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease [Internet] (2010) Centers for Disease Control and Prevention (US). Available at: https:// www.ncbi.nlm.nih.gov/books/ NBK53017/. Last accessed: 6 March 2024.
13. Johannsen A et al. Smoking and inflammation: evidence for a synergistic role in chronic disease. Periodontol 2000. 2014;64(1):111-
54 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Feature
26.
14. Erhardt L. Cigarette smoking: an undertreated risk factor for cardiovascular disease. Atherosclerosis. 2009;205(1):2332.
15. Shield K et al. Chronic diseases and conditions related to alcohol use. Alcohol Res. 2013;35(2):15573.
16. Bindman A et al. Preventable hospitalizations and access to health care. JAMA. 1995;274(4):305-11.
17. Christopher A et al. Access to care and chronic disease outcomes among medicaid-insured persons versus the uninsured. Am J Public Health. 2016;106(1):63-9.
18. Ko C-H et al. Demands for medical imaging and workforce size: a nationwide population-based study, 2000–2020. Eur J Radiol. 2024;172:111330.
19. Brady A et al. Radiology in the era of value-based healthcare: a multi-society expert statement from the ACR, CAR, ESR, IS3R, RANZCR, and RSNA. Radiology. 2021;298(3):486-91.
20. Doherty M. Value of interventional radiology: past, present, and future. Semin Intervent Radiol. 2019;36(1):26-8.
21. Dai X et al. Evolution of the global smoking epidemic over the past half century: strengthening the evidence base for policy action. Tob Control. 2022;31(2):129-37.
22. Grover H et al. Systematic review of the cost-effectiveness of screening for lung cancer with low dose computed tomography. Lung Cancer. 2022;170:20-33.
23. Ahmed N et al. Safety of guidewire-based measurement of fractional flow reserve and the index of microvascular resistance using intravenous adenosine in patients with acute or recent myocardial infarction. Int J Cardiol. 2016;202:305-10.
24. Sirajuddin A et al. Ischemic heart disease: noninvasive
imaging techniques and findings. Radiographics. 2021;41(4):9901021.
25. Natale L et al. Cardiac radiology in Europe: status and vision by the European Society of Cardiovascular Radiology (ESCR) and the European Society of Radiology (ESR). Eur Radiol. 2023;33(8):5489-97.
26. Weberling LD et al. Coronary computed tomography vs. cardiac magnetic resonance imaging in the evaluation of coronary artery disease. Diagnostics (Basel). 2022;13(1):125.
27. Kofoed K et al. Comparative effectiveness of initial computed tomography and invasive coronary angiography in women and men with stable chest pain and suspected coronary artery disease: multicentre randomised trial. BMJ. 2022;379:e071133.
28. Bolognese L, Reccia M. Computed tomography to replace invasive coronary angiography? The DISCHARGE trial. Eur Heart J Suppl. 2022;24(Suppl I):I25-8.
29. The Health Foundation. Health in 2040: projected patterns of illness in England. 2023. Available at: https://reader.health.org.uk/ projected-patterns-of-illness-inengland. Last accessed: 7 March 2024.
30. Paydary K et al. The evolving role of FDG-PET/CT in the diagnosis, staging, and treatment of breast cancer. Mol Imaging Biol. 2019;21(1):1-10.
31. Lynch C et al. A comparative analysis: international variation in PET-CT service provision in oncology-an international cancer benchmarking partnership study. Int J Qual Health Care. 2021;33(1):mzaa166.
32. da Silva R et al. Dynamic capacity allocation in a radiology service considering different types of patients, individual no-show probabilities, and overbooking. 2021;21(1):968.
33. Konstantinidis K. The shortage of radiographers: a global crisis in
healthcare. J Med Imaging Radiat Sci. 2023;S1939-8654(23):018775. [Epub ahead of print].
34. Kalidindi S, Gandhi S. Workforce crisis in radiology in the UK and the strategies to deal with it: is artificial intelligence the saviour? Cureus. 2023;15(8):e43866.
35. Bizzo B et al. Addressing the challenges of implementing artificial intelligence tools in clinical practice: principles from experience. J Am Coll Radiol 2023;20(3):352-60.
36. Kern L et al. Healthcare fragmentation and the frequency of radiology and other diagnostic tests: a cross-sectional study. 2017;32(2):175-81.
37. Grunz JP et al. Ultra-low-dose photon-counting CT imaging of the paranasal sinus with tin prefiltration: how low can we go? Invest Radiol. 2022;57(11):728-33.
38. Gavrielli S et al. Ultra-low dose CT abdomen and pelvis for the detection of acute abdominal pathology in the emergency room: initial experience from an academic hospital. Emerg Radiol. 2021;28(1):15-21.
39. Ogawa N et al. Evaluation of urinary stone composition and differentiation between urinary stones and phleboliths using single-source dual-energy computed tomography. Acta Med Okayama. 2017;71(2):91-6.
40. Conti D et al. Dual-energy computed tomography applications to reduce metal artifacts in hip prostheses: a phantom study. Diagnostics (Basel). 2022;13(1):50.
41. Sarah E et al. Incidental findings on brain imaging and blood tests: results from the first phase of Insight 46, a prospective observational substudy of the 1946 British birth cohort. BMJ Open. 2019;9(7):e029502.
42. Lumbreras B et al. Incidental findings in imaging diagnostic tests: a systematic review. Br J Radiol. 2010;83(988):276-89.
FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 55 Feature
Risk Stratification Using Cardiac Imaging: A Comprehensive Review
Editor's Pick
My Editor’s Pick for this year’s edition of EMJ Radiology is an insightful review article, in which the authors explore the different imaging modalities for coronary artery disease. King et al. emphasise the importance of understanding the options in light of patients’ clinical presentations, and choosing the correct modality based on this analysis. The authors highlight the value of combining clinical experience with existing guidelines.
Yasmeen Malik
St George’s University of London, UK
Authors:
Disclosure:
*David J. King,1 Shishir Gupta,1 Shailen Shah,1 Rushi Patel,1 Sohum Sheth,2 Marco Foreman,2 Sean Hyunchang Kwak,2 Jonathan Harder,1 Noah Blaker,1 Jay Talati,2 Mitchell Bourne,1 Madeline Smoot,1 David E. Winchester3
1. Department of Medicine, University of Florida, Gainesville, USA
2. College of Medicine, University of Florida, Gainesville, USA
3. Division of Cardiovascular Medicine, University of Florida, Gainesville, USA
*Correspondence to david.king@medicine.ufl.edu
Winchester reports a leadership role with the American Society of Nuclear Cardiology (ASNC) Board of Directors. All other authors report no conflicts of interest.
Received: 18.12.23
Accepted: 14.02.24
Keywords:
Citation:
Abstract
Cardiac magnetic resonance imaging, coronary artery calcium score (CACS), coronary artery disease (CAD), coronary CT angiography (CCTA), CT-fractional flow reserve, intravascular ultrasound, optical coherence tomography (OCT), risk stratification, stress echocardiography.
EMJ Radiol. 2024;5[1]:56-64.
https://doi.org/10.33590/emjradiol/10308328.
There are numerous cardiac imaging modalities which aid in the diagnosis and management of coronary artery disease (CAD). Each modality has variable efficacy in detecting stenosis and stratifying risk among those with CAD. Clinicians must evaluate these methods in light of their patients’ clinical presentations, to choose the most appropriate imaging technique. Understanding the unique benefits and indications of each modality aids in the selection of high-value imaging. Following is a review of the available cardiac imaging methods for the identification and risk stratification of CAD.
56 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
Key Points
1. When screening for obstructive coronary disease, and risk stratifying those with known stenosis, there are multiple imaging modalities available to the clinician; however, the indications and benefits of each are not always readily apparent.
2. This review article describes and compares the techniques used for the evaluation of stable coronary disease, taking into account their unique risks, benefits, and the current guidelines.
3. While guidelines and expert recommendations are necessary to consider when choosing the most appropriate screening technique, they must be utilised alongside clinical acumen, informed by an accurate understanding of the available imaging modalities.
INTRODUCTION
There are numerous cardiac imaging modalities which aid in the diagnosis and management of coronary artery disease (CAD). Each modality has variable efficacy in detecting stenosis and stratifying risk among those with CAD. Clinicians must evaluate these methods in light of their patients’ clinical presentations, to choose the most appropriate imaging technique. However, deciding between tests can be challenging. Guidelines determined by expert panels can suggest if one test modality is clinically superior, or whether imaging is indicated at all.1 As with most areas of clinical medicine, discrepancies exist between the guidelines of professional societies.2 Some experts have advocated that imaging modalities can adequately fulfil multiple roles, including diagnosis and risk stratification, serving as a ‘one-stop shop’.3 Others assert that a combination of several techniques can provide highly effective screening.4 In light of these disparate views, the American College of Cardiology (ACC) and American Heart Association (AHA) published updated guidelines on the appropriate use of imaging for patients with stable chest pain, based primarily on clinical risk stratification, which guides recommended testing.5 Understanding the unique benefits and indications of each modality in accordance with these guidelines elucidates the selection of high-value imaging. Following is a review of the available cardiac imaging methods for the identification and risk stratification of CAD.
CORONARY ARTERY CALCIUM SCORE
The coronary artery calcium score (CACS), also called the Agatston score, is an application of CT imaging which quantifies calcified plaque in the coronary arteries, allowing for measurement of atherosclerotic burden. A positive CACS has a sensitivity of 98%, specificity of 40%, negative predictive value (NPV) of 93%, and positive predictive value of 68% for detecting the presence of >50% stenosis.6 Given these statistics, some clinicians have argued that a CACS of zero does not warrant further cardiac evaluation; however, a subgroup analysis of the CORE64 study showed an NPV of 68%, concluding that a CACS score of zero could not exclude coronary disease. Further, a subgroup of the CONFIRM registry demonstrated coronary stenosis in 3.5% of patients with CACS of 0.7 In combination with the Framingham risk score (FRS), which predicts a patient’s 10-year cardiovascular event risk, coronary calcium scoring can assist with this clinical decision. For individuals who fall within the intermediate-risk category (FRS >10%), assessing their CACS can predict for elevated risk. In fact, CACS was predictive of risk among patients with an FRS higher than 10% (P<0.001). For patients with FRS of 5.0–7.5%, an elevated CACS can reclassify their risk up or down, clarifying the necessity for statin therapy.8
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 57 Article
CORONARY CT ANGIOGRAPHY
Coronary CT angiography (CCTA) is another noninvasive technique that visualises the coronary arteries. The 2021 ACC/AHA guidelines for the evaluation and diagnosis of chest pain gives a Class 1A recommendation for intermediate-risk patients with acute chest pain and no known CAD.5 Diagnosing CAD via CCTA has a sensitivity ranging from 90–98%, and specificity of 70–95%, with values increasing as slice resolution increases.9-13 These sensitivities and specificities are comparable to invasive coronary angiography (ICA). CCTA thereby decreases procedural risk by excluding patients without significant lesions, and allows for the rapid, early detection of CAD.14 However, limitations exist, including radiation exposure, administration of contrast, and difficulty visualising heavily calcified vessels.
CCTA findings of ≥50% and ≥70% stenosis, as well as stenosis in the left main and proximal left anterior descending arteries, are predictors of all-cause mortality in patients with chest pain (P<0.0001).15 In addition, vulnerable plaque characteristics, such as low-attenuation plaque, positive remodelling, napkin-ring sign, and spotty calcium pattern of calcification are also predictors of major adverse cardiac events (MACE).16 Of note, in the PROMISE trial, a strategy of initial CCTA as compared with functional testing did not improve clinical outcomes.17 This implies more than anatomical data from CCTA is needed, which is where CCTA-fractional flow reserve (FFR) plays a role.
CT FRACTIONAL FLOW RESERVE
FFR, the index measuring functional severity of coronary artery stenosis, is calculated as the ratio of the maximum achievable blood flow through a stenotic artery, to the maximum achievable blood flow in the absence of that stenosis. Traditionally, FFR is assessed during ICA to identify haemodynamically significant lesions, in addition to visual assessment. Studies have shown reductions of the composite endpoint of death, myocardial infarction (MI), and need for revascularisation with FFR-guided percutaneous coronary intervention (PCI).18,19
CT-FFR is a newer technology that utilises CCTA images and advanced computational modelling techniques to create an anatomic model with
FFR values of the entire coronary tree. It should be noted that, as CT-FFR is a function of CCTA imaging, it has similar efficacy in identifying CAD. Compared to the diagnostic value of CCTA alone, CT-FFR is noted to have increased accuracy per vessel and specificity in identifying significant stenosis.20,21 When comparing CT-FFR to invasive FFR, the accuracy of detecting an abnormal invasive FFR was only 50% for CT-FFR in the range of 0.76–0.80, whereas it was 75% in the range of 0.71–0.75, and 100% for CT-FFR <0.7.22
Data from CT-FFR registries demonstrate this tool’s prognostic ability, with patients of CT-FFR values of >0.80 having an excellent prognosis with no adverse events at 30 days, or 1 year.23
STRESS ECHOCARDIOGRAPHY
Stress echocardiography utilises variability of endocardial wall motion to assess global and regional cardiac function, thereby assisting in the diagnosis and management of clinically significant CAD. Induction of stress may be physiologic, through exercise (e.g., treadmill or bicycle ergometer), or pharmacologic, through dobutamine or dipyridamole, with both agents carrying a strong evidence base for prognostic evaluation. The implications of normal stress echocardiography results have been well evaluated, and carry a low risk of subsequent cardiac events, with a cardiac event rate of <1% per year.24 In comparison to stress myocardial perfusion imaging, the negative predictive value of normal test results was similar in metaanalyses,24-26 highlighting the role of stress echocardiography as a cost-effective gatekeeper for more invasive strategies.
In patients with known or suspected CAD, peak wall motion stress index (WMSI) was able to effectively stratify patients into low (WMSI: 1.0; 0.9% per year), intermediate (WMSI: 1.1–1.7; 3.1% per year), and high (WMSI: >1.7%; 5.2% per year) risk of cardiac death, in both univariate (P=0.0001), and multivariate analysis (P=0.04). Furthermore, left ventricular ejection fraction (LVEF) during testing could also independently stratify patients into low-to-intermediate-risk (LVEF >45%), or high-risk (LVEF ≤45%) for cardiac events.27
In the context of post-acute MI, regional systolic function assessed by WMSI yields significant
58 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
prognostic utility. In a large retrospective study on 767 patients post-MI, both WMSI (P<0.0001), and LVEF (P<0.0001), were strongly predictive of all-cause mortality.28 By univariate analysis, WMSI proved to be an independent predictor of both death (P<0.0001) and hospitalisation for congestive heart failure (P=0.002) in this population.28 LVEF did not provide additional prognostic information in this study when combined with WMSI, suggesting WMSI may be more valuable in risk stratification.28 Notably, the impact of stress echocardiography in risk stratification can be applied to all subsets of patient populations, irrespective of age, sex, and comorbidities such as diabetes.29 However, abnormal stress echocardiography test results should be analysed in the context of factors including patient comorbidities; the extent of dysmotility; presence of prior scar; ischaemic threshold; and in combination with additional testing, such as the Duke Treadmill Score.
STRAIN AND STRAIN RATE ECHOCARDIOGRAPHY
Myocardial strain and strain rate (SR) echocardiography are newer imaging modalities that offer additive value over traditional echocardiography, which neglects the longitudinal and circumferential components of myocardial deformation. Strain and strain rate represent the magnitude and rate of myocardial deformation, respectively. Abnormalities of myocardial deformation are observed early in various cardiovascular disease states, and may be useful for identifying preclinical disease, or those at risk for developing a cardiac condition.30 For patients with clinical suspicion for CAD, strain echocardiography provides a sensitivity of 86%, and specificity of 73%, for detecting significant coronary stenosis.31,32 Segmental left ventricular longitudinal strain specifically has been demonstrated to provide accurate localisation of stenotic vessels.31
Strain and SR echocardiography can provide important insights into various cardiovascular diseases, including CAD, detection of viable myocardium, sequelae of MI, and response to reperfusion. Although strain imaging has multiple applications, perhaps its most significant role is in the detection of ischaemic heart disease. For example, in patients with a normal LVEF
at increased risk of atherosclerotic disease, a progressive impairment of 2D global strain and SR correlated with increasing severity of CAD.33 In another study of 2D strain imaging, peak systolic longitudinal SR and early diastolic SR predicted significant (>70%) arterial stenosis.34 Furthermore, 2D peak systolic longitudinal strain of the left ventricle has been shown to discriminate severe triple vessel or left main disease from lesser CAD,35 demonstrating the utility of SR echocardiography in cardiac risk-stratification.
SINGLE-PHOTON EMISSION CT MYOCARDIAL PERFUSION IMAGING
Single-photon emission CT (SPECT) myocardial perfusion imaging (MPI) utilises gamma rays to evaluate the flow-dependent selective uptake of a radioactive tracer, typically thallium-201 or technetium (sestamibi or tetrofosmin). SPECT MPI is typically done both at rest and with stress, to assess for inducible ischaemia, giving qualitative or semi-quantitative assessment of myocardial perfusion. Physiologically, myocardial arterioles distal to a significant epicardial coronary stenosis are autoregulated and dilated at rest to maintain myocardial blood flow. Under stress, normal vascular beds dilate more than abnormal vascular beds, leading to relative differences in tracer uptake, referred to as ‘perfusion defects’. Stress and rest images are compared in transverse, vertical, and horizontal axes, and perfusion defects are described in a standardised model of the left ventricle, allowing semi-quantitative scoring of defects.36 It is the most commonly used imaging modality in nuclear cardiology, as it is able to evaluate for the physiologic presence, extent, and degree of myocardial ischaemia or infarction, and assists with prognostication in patients with suspected or known CAD. The sensitivity and specificity of SPECT has been measured at 88% and 76%, respectively, when compared with ICA.37 SPECT MPI also assesses viability of myocardial tissue when evaluating for further interventions.36
With regard to prognostication, SPECT adds independent and incremental value to predict cardiac death or non-fatal MI, even when accounting for exercise tolerance testing, clinical, and angiographic variables.38 SPECT has a high negative prognostic value, with
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 59 Article
a meta-analysis indicating that a normal or low-risk stress MPI is associated with a 0.6% annual MACE rate, approaching that of a normal age-matched population, and a population of patients with normal coronary angiography.39 This persists even in patients with strongly positive exercise electrocardiogram testing, or angiographically significant coronary disease.40 The prognosis seems to be sustained for up to 3 years in one meta-analysis, indicating a negative predictive value for MI and cardiac death at 98.8% over 36 months.25 On the other hand, if SPECT MPI is abnormal, the extent and severity of the abnormal findings are able to predict progressively higher annual cardiac death rates.40 Even when a study is mildly abnormal, high-risk features can help with risk stratification, including transient or persistent left ventricular cavity dilation, LVEF <45%, and defects in more than one coronary vascular territory, with any of these indicating a higher annual mortality rate.39 Because of this feature, SPECT MPI is commonly used for patients pre-operatively at intermediate risk, to help with risk stratification. Additionally, SPECT can help guide treatment decisionmaking and prognosis following treatment. Studies have suggested that revascularisation may be favoured when >10% of the myocardium is ischaemic.39 Some limitations of the modality include the inability to distinguish global blood flow reduction due to balanced perfusion defects during stress; the exposure of the patient to radiation; limited off-hours availability; inability to measure absolute myocardial blood flow; and attenuation artifacts from surrounding soft tissues, the diaphragm, or extracardiac radioisotope uptake. The use of ECG-gating and attenuation correction software is able to improve the accuracy of the study, and help with alleviating some of these limitations.
PET MYOCARDIAL PERFUSION IMAGING
PET MPI utilises positron emitting radiotracers (rubidium-82 or nitrogen-13 ammonia) administered under rest and stressed conditions. Detection and distribution of these radiotracers allows for 3D mapping of cardiac perfusion.41
PET MPI image quality is superior to most SPECT MPI set-ups, although widespread adoption of PET MPI is limited by equipment cost, expertise, reimbursement, and a number
of other factors.42 A particular strength of this method over other modalities is the ability to measure coronary flow reserve (CFR).43-46
For detecting CAD with at least one coronary artery with >50% stenosis, PET MPI has an average sensitivity of 90%, and an average specificity of 80%, yielding a positive predictive value of 94%, and NPV of 73%.47 It is notable that, for the purpose of predicting cardiac death, all cause death, and MACE in patients with known or suspected CAD, other studies have found an NPV of 98%.48 Multiple studies have shown that a normal PET MPI confers a <1% annual cardiac event rate, while there is incrementally increasing risk of MI and death based on the extent of cardiac involvement.43,44 Similar to SPECT, risk of MACE after PET MPI is often classified by the percentage defect size, low risk with <5% involvement of the myocardium, intermediate risk involving 5–10%, and high risk involving >10%.49 Patients with high risk findings are suitable to be referred for left heart catheterisation.50 One advantage of PET MPI is the use of PET-derived CFR, which can further risk stratify patients; there is evidence of elevated risk of MACE with poor CFR, independent of the size of the perfusion defect.44,45 One study found a 5.6-fold higher risk of cardiac mortality in the lowest tertile as compared to the highest.46 When comparing PET to SPECT MPI, multiple studies have shown similar patient outcomes and rates of diagnostic failure.51,52 One additional advantage of PET MPI over SPECT is the lower radiation exposure of 3.7 mSv, much lower than the equivalent test using SPECT with a mean exposure of 12.8 mSV, due to the short half-lives of the radiotracers administered.53,54
CARDIAC MRI
Cardiac magnetic resonance imaging (CMR) is a reliable clinical technique for the evaluation of myocardial structure, function, perfusion, and viability, serving as an important predictor of MACE.55,56 Meta-analysis has demonstrated that CMR can detect CAD of ≥50% with a sensitivity of 89%, and specificity of 72%, increasing to 95% and 80%, respectively, with utilisation of contrast material and 3T magnets. Additionally, elevated plaque-to-myocardium signal intensity ratios of ≥1.4 obtained via CMR have been shown as significant predictors of coronary
60 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
events at 2-year follow-up.57,58 Compared to another anatomic imaging technique, CCTA has excellent spatial resolution that permits robust coronary plaque composition analysis,59 while CMR resolution is often limited to the presence or absence of clinically significant CAD.60
CMR also provides valuable prognostic information for individuals with ischaemic and non-ischaemic cardiomyopathy, through measurement of late gadolinium enhancement (LGE).61 Elevated LGE has been found by metaanalysis to be associated with appropriate implantable cardioverter-defibrillator discharges, aborted sudden cardiac death, and sudden cardiac death events.62 Arrhythmic MACE occurs in 23.9% of patients with positive LGE for an annualised event rate of 8.6%, while only 4.9% of individuals with negative LGE results experienced arrhythmic MACE at an annualised event rate of 1.7%.63 However, as LGE detects fibrotic scars, it may be limited in the evaluation of progressive non-ischaemic cardiomyopathies.61 The use of other CMR-derived values, including extracellular volume quantification, bridges this gap, as elevated extracellular volume quantification values indicate strong association with MACE in NICM.
OPTICAL COHERENCE TOMOGRAPHY
Optical coherence tomography (OCT) is an imaging modality that is often used during ICA with planned intervention, including stent placement, suction thrombectomy, and balloon angioplasty. It allows the operator to visualise high resolution intracoronary images and assess coronary plaques, thereby optimising coronary interventions.64 Data on the routine use of OCT outside of PCI is limited.65 In the acute setting, there is clear description that OCT helps to prevent complications related to stent placement and other procedural-based complications, as it provides a superior assessment of fibrous cap, intracoronary thrombus, and plaque morphology.65 Operators’ decision-making can be altered by OCT findings.
Despite no current application in the preventative risk assessment setting, OCT offers improved visualisation of the coronary lumen, including visualisation of the vessel, the plaque, and the coronary thrombus, if present. Prior work has
shown that OCT can be used to detect plaque areas with thin fibrous caps and lipid cores with high sensitivity.66 These are the areas thought to be primarily responsible for acute rupture and coronary vessel occlusion.66 Further work needs to be conducted in order to determine if there is a role for OCT in other settings, including if use impacts long-term clinical outcomes for patients.67
INTRAVASCULAR ULTRASOUND
Although ICA allows for prompt evaluation of CAD and vessel patency, diagnostic information is limited to 2D fluoroscopy acquired from multiple sequential angles with contrast dye administration. Similar to OCT, intravascular ultrasound (IVUS) is an adjunct tool that is used during ICA for the real-time assessment of coronary artery vessel architecture. IVUS can elucidate multiple lesion characteristics, including numeric dimensions and the composition of surrounding coronary plaque/thrombosis, offering up to two- to three-times the axial resolution of angiography alone.68 IVUS is useful during PCI, as it can help guide stent placement, and enable precise deployment without the use of radiation via fluoroscopy. Additionally, its ability to provide useful information to operators about the presence of dissection, thrombus, and calcium burden enables them to use situation-specific therapies, including distal embolic protective devices and atherectomy, as needed.69
Direct intravascular visualisation has been shown to improve outcomes in patients undergoing IVUS-guided stent placement versus angiographically-guided stent placement.70
Although the use of IVUS has been increasing in recent years, only a minority (<20%) of ICAs are performed with IVUS.71 The 2021 AHA Guideline for Coronary Artery Revascularization gives IVUS a Class 2a indication for assessing the severity of left main coronary artery stenosis, but there are sparse data from large trials demonstrating its impact on long-term clinical outcomes.68
Near-infrared spectroscopy technology can be used in conjunction with IVUS to detect the presence of lipid-rich coronary plaques, which are associated with higher incidence of MACE and cardiac-related deaths.72 With continued research and newer clinical adaptations of IVUS, its use may likely increase over the coming years.
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 61 Article
CONCLUSION
In summary, each modality discussed offers unique benefits in the correct clinical circumstance. CACS is an effective anatomic evaluation for screening out young patients with low risk for obstructive CAD. CCTA provides similar benefit for intermediate- to high-risk individuals without known CAD, as well as to evaluate stent patency in those with known obstructive disease. Based on local availability, patient characteristics, and individual contraindications, the stress imaging modalities, including stress echocardiography, SPECT/PET MPI, and CMR, effectively assess for significant obstructive lesions. When management remains unclear, CT-FFR in combination with stress imaging or positive CCTA results can determine the presence of functionally highgrade stenosis. Lastly, IVUS and OCT provide
References
1. Winchester DE et al. ACC/AHA/ ASE/ASNC/ASPC/HFSA/HRS/ SCAI/SCCT/SCMR/STS 2023 multimodality appropriate use criteria for the detection and risk assessment of chronic coronary disease. J Am Coll Cardiol. 2023;81(25):2445-67.
2. Winchester DE et al. Discordance between appropriate use criteria for nuclear myocardial perfusion imaging from different specialty societies: a potential concern for health policy. JAMA Cardiol. 2016;1(2):207-10.
3. Cerqueira MD. Nuclear cardiology: finally a one-stop shop for diagnosis, risk stratification, and management of coronary artery disease. Clin Cardiol. 2006;29(9 Suppl 1):I26-33.
4. Rana JS et al. Combination of myocardial perfusion imaging and coronary artery calcium scanning: potential synergies for improving risk assessment in subjects with suspected coronary artery disease. Curr Atheroscler Rep. 2011;13(5):381-9.
valuable information during PCI to direct stent placement, and delineate further high-risk characteristics of culprit lesions.
The clinician’s role is to choose the most appropriate imaging modality for each scenario, with the assistance of expert guidelines and decision-making tools, including appropriate use criteria. Granted, this task is more complicated than simply selecting the recommended test; as evidenced by Bayes’ theorem, false positive and false negative testing, especially in low-risk populations, can significantly impact the value of these tests and the clinical courses for many patients. Factors including local availability, radiation exposure, contrast administration, procedural risk, and cost must be weighed as well. An understanding of each modality, its indications, and its shortcomings allows the clinician to offer patients the highest value cardiovascular imaging.
6. Neves PO et al. Coronary artery calcium score: current status. Radiol Bras. 2017;50(3):182-9.
7. Gottlieb I et al. The absence of coronary calcification does not exclude obstructive coronary artery disease or the need for revascularization in patients referred for conventional coronary angiography. J Am Coll Cardiol. 2010;55(7):627-34.
8. Greenland P et al. Coronary calcium score and cardiovascular risk. J Am Coll Cardiol. Jul 24 2018;72(4):434-47.
9. Mansour HH et al. The diagnostic accuracy of coronary computed tomography angiography in patients with and without previous coronary interventions. J Med Imaging Radiat Sci. 2022;53(1):816.
10. Gatti M et al. Diagnostic accuracy of coronary computed tomography angiography for the evaluation of obstructive coronary artery disease in patients referred for transcatheter aortic valve implantation: a systematic review and meta-analysis. Eur Radiol. 2022;32(8):5189-200.
11. Yin X et al. Diagnostic performance of coronary computed tomography angiography versus exercise electrocardiography for coronary artery disease: a systematic review and meta-analysis. J Thorac Dis.
5. Writing Committee Members; Gulati M et al. 2021 AHA/ACC/ ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2021;78(22):e187-285.
2016;8(7):1688-96.
12. Barbero U et al. 64 slice-coronary computed tomography sensitivity and specificity in the evaluation of coronary artery bypass graft stenosis: a meta-analysis. Int J Cardiol. 2016;216:52-7.
13. Budoff MJ et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (assessment by coronary computed tomographic angiography of individuals undergoing invasive coronary angiography) trial. J Am Coll Cardiol. 2008;52(21):1724-32.
14. Lu MT et al. Safety of coronary CT angiography and functional testing for stable chest pain in the PROMISE trial: a randomized comparison of test complications, incidental findings, and radiation dose. J Cardiovasc Comput Tomogr. 2017;11(5):373-82.
15. Zheng J, Lu B. Current progress of studies of coronary CT for risk prediction of major adverse cardiovascular event (MACE). J Cardiovasc Imaging. 2021;29(4):301-15.
16. Williams MC et al. Coronary artery plaque characteristics associated with adverse outcomes in the
62 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
SCOT-HEART study. J Am Coll Cardiol. 2019;73(3):291-301.
17. Douglas PS et al.; PROMISE Investigators. Outcomes of anatomical versus functional testing for coronary artery disease. N Engl J Med. 2015;372(14):1291300.
18. Pijls NH et al.; FAME Study Investigators. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention in patients with multivessel coronary artery disease: 2-year follow-up of the FAME (fractional flow reserve versus angiography for multivessel evaluation) study. J Am Coll Cardiol. 2010;56(3):177-84.
19. van Nunen LX et al. Fractional flow reserve versus angiography for guidance of PCI in patients with multivessel coronary artery disease (FAME): 5-year follow-up of a randomised controlled trial. Lancet. 2015;386(10006):1853-60.
20. Koo B-K et al. Diagnosis of ischemia-causing coronary stenoses by noninvasive fractional flow reserve computed from coronary computed tomographic angiograms. Results from the prospective multicenter DISCOVER-FLOW (diagnosis of ischemia-causing stenoses obtained via noninvasive fractional flow reserve) study. J Am Coll Cardiol. 2011;58(19):1989-97.
21. Nørgaard BL et al.; NXT Trial Study Group. Diagnostic performance of noninvasive fractional flow reserve derived from coronary computed tomography angiography in suspected coronary artery disease: the NXT trial (analysis of coronary blood flow using CT angiography: next steps). J Am Coll Cardiol. 2014;63(12):1145-55.
22. Mathew RC et al. Computed tomography fractional flow reserve to guide coronary angiography and intervention. Interv Cardiol Clin. 2018;7(3):345-54.
23. Patel MR et al. 1-year impact on medical practice and clinical outcomes of FFRCT: the ADVANCE registry. JACC Cardiovasc Imaging. 2020;13(1 Pt 1):97-105.
24. McCully RB et al. Outcome after normal exercise echocardiography and predictors of subsequent cardiac events: follow-up of 1,325 patients. J Am Coll Cardiol. 1998;31(1):144-9.
25. Metz LD et al. The prognostic value of normal exercise myocardial perfusion imaging and exercise echocardiography: a
meta-analysis. J Am Coll Cardiol. 2007;49(2):227-37.
26. Marwick TH. Stress echocardiography. Heart. Jan 2003;89(1):113-8.
27. Yao SS et al. Practical applications in stress echocardiography: risk stratification and prognosis in patients with known or suspected ischemic heart disease. J Am Coll Cardiol. 2003;42(6):1084-90.
28. Møller JE et al. Wall motion score index and ejection fraction for risk stratification after acute myocardial infarction. Am Heart J. 2006;151(2):419-25.
29. Senior R et al.; British Society of Echocardiography. Stress echocardiography for the diagnosis and risk stratification of patients with suspected or known coronary artery disease: a critical appraisal. Supported by the British Society of Echocardiography. Heart. 2005;91(4):427-36.
30. Hoit BD. Strain and strain rate echocardiography and coronary artery disease. Circ Cardiovasc Imaging. 2011;4(2):179-90.
31. Pastore MC et al. Speckle tracking echocardiography: early predictor of diagnosis and prognosis in coronary artery disease. Biomed Res Int. 2021;2021:6685378.
32. Dandel M et al. Strain and strain rate imaging by echocardiography - basic concepts and clinical applicability. Curr Cardiol Rev. 2009;5(2):133-48.
33. Nucifora G et al. Incremental value of subclinical left ventricular systolic dysfunction for the identification of patients with obstructive coronary artery disease. Am Heart J. 2010;159(1):148-57.
34. Liang H-Y et al. Usefulness of two-dimensional speckle strain for evaluation of left ventricular diastolic deformation in patients with coronary artery disease. Am J Cardiol. 2006;98(12):1581-6.
35. Choi J-O et al. Longitudinal 2D strain at rest predicts the presence of left main and three vessel coronary artery disease in patients without regional wall motion abnormality. Eur J Echocardiogr. 2009;10(5):695-701.
36. Li DL, Kronenberg MW. Myocardial perfusion and viability imaging in coronary artery disease: clinical value in diagnosis, prognosis, and therapeutic guidance. Am J Med. 2021;134(8):968-75.
37. Varga-Szemes A et al. CT
myocardial perfusion imaging. AJR Am J Roentgenol. 2015;204(3):487-97.
38. Mowatt G et al. Systematic review of the prognostic effectiveness of SPECT myocardial perfusion scintigraphy in patients with suspected or known coronary artery disease and following myocardial infarction. Nucl Med Commun. 2005;26(3):217-29.
39. Berman DS et al. Comparative use of radionuclide stress testing, coronary artery calcium scanning, and noninvasive coronary angiography for diagnostic and prognostic cardiac assessment. Semin Nucl Med. 2007;37(1):2-16.
40. Papaioannou GI, Heller GV. Risk assessment by myocardial perfusion imaging for coronary revascularization, medical therapy, and noncardiac surgery. Cardiol Rev. 2003;11(2):60-72.
41. Nakazato R et al. Myocardial perfusion imaging with PET. Imaging Med. 2013;5(1):35-46.
42. Dorbala S, Di Carli MF. Cardiac PET perfusion: prognosis, risk stratification, and clinical management. Semin Nucl Med. 2014;44(5):344-57.
43. Dorbala S et al. Prognostic value of stress myocardial perfusion positron emission tomography: results from a multicenter observational registry. J Am Coll Cardiol. 2013;61(2):176-84.
44. Yoshinaga K et al. What is the prognostic value of myocardial perfusion imaging using rubidium-82 positron emission tomography? J Am Coll Cardiol. 2006;48(5):1029-39.
45. Ziadi MC et al. Impaired myocardial flow reserve on rubidium-82 positron emission tomography imaging predicts adverse outcomes in patients assessed for myocardial ischemia. J Am Coll Cardiol. 2011;58(7):740-8.
46. Murthy VL et al. Improved cardiac risk assessment with noninvasive measures of coronary flow reserve. Circulation. 2011;124(20):2215-24.
47. Al-Mallah MH et al. Assessment of myocardial perfusion and function with PET and PET/CT. J Nucl Cardiol. 2010;17(3):498-513.
48. Chen A et al. Prognostic value of normal positron emission tomography myocardial perfusion imaging in patients with known or suspected coronary artery disease: a meta-analysis. Br J Radiol. 2017;90(1074):20160702.
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 63 Article
49. Patel MR et al. ACC/AATS/AHA/ ASE/ASNC/SCAI/SCCT/STS 2017 appropriate use criteria for coronary revascularization in patients with stable ischemic heart disease: a report of the American College of Cardiology Appropriate Use Criteria Task Force, American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2017;69(17):221241.
50. Patel MR et al. ACCF/SCAI/ AATS/AHA/ASE/ASNC/HFSA/ HRS/SCCM/SCCT/SCMR/STS 2012 appropriate use criteria for diagnostic catheterization: a report of the American College of Cardiology Foundation
Appropriate Use Criteria Task Force, Society for Cardiovascular Angiography and Interventions, American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society of Critical Care Medicine, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2012;59(22):1995-2027.
51. Patel KK et al. Randomized comparison of clinical effectiveness of pharmacologic SPECT and PET MPI in symptomatic CAD patients. JACC Cardiovasc Imaging. 2019;12(9):1821-31.
52. Siebelink HM et al. No difference in cardiac event-free survival between positron emission tomography-guided and singlephoton emission computed tomography-guided patient management: a prospective, randomized comparison of patients with suspicion of jeopardized myocardium. J Am Coll Cardiol. 2001;37(1):81-8.
53. Cerqueira MD et al. Recommendations for reducing radiation exposure in myocardial
perfusion imaging. J Nucl Cardiol. 2010;17(4):709-18.
54. Desiderio MC et al. Current status of patient radiation exposure of cardiac positron emission tomography and single-photon emission computed tomographic myocardial perfusion imaging. Circ Cardiovasc Imaging. 2018;11(12):e007565.
55. Constantine G et al. Role of MRI in clinical cardiology. Lancet. 2004;363(9427):2162-71.
56. Holdsworth DA et al. Cardiac MRI improves cardiovascular risk stratification in hazardous occupations. J Cardiovasc Magn Reson. 2019;21(1):48.
57. Korosoglou G et al. Cardiac magnetic resonance and computed tomography angiography for clinical imaging of stable coronary artery disease. Diagnostic classification and risk stratification. Front Physiol. 2014;5:291.
58. Noguchi T et al. High-intensity signals in coronary plaques on noncontrast T1-weighted magnetic resonance imaging as a novel determinant of coronary events. J Am Coll Cardiol. 2014;63(10):98999.
59. Di Leo G et al. Diagnostic accuracy of magnetic resonance angiography for detection of coronary artery disease: a systematic review and meta-analysis. Eur Radiol. 2016;26(10):3706-18.
60. Li M et al. Diagnostic accuracy of myocardial magnetic resonance perfusion to diagnose ischemic stenosis with fractional flow reserve as reference: systematic review and meta-analysis. JACC Cardiovasc Imaging. 2014;7(11):1098-105.
61. Porcari A et al. Arrhythmic risk stratification by cardiac magnetic resonance tissue characterization: disclosing the arrhythmic substrate within the heart muscle. Heart Fail Rev. 2022;27(1):49-69.
62. Kamp NJ et al. Risk stratification using late gadolinium enhancement on cardiac magnetic resonance imaging in patients with hypertrophic cardiomyopathy: a systematic review and metaanalysis. Prog Cardiovasc Dis. 2021;66:10-16.
63. Disertori M et al. Myocardial fibrosis assessment by LGE Is a powerful predictor of ventricular tachyarrhythmias in ischemic and nonischemic LV dysfunction: a meta-analysis. JACC Cardiovasc Imaging. 2016;9(9):1046-55.
64. Karimi Galougahi K et al. Optical coherence tomography in acute coronary syndromes. Interv Cardiol Clin. 2021;10(3):323-32.
65. McCabe JM, Croce KJ. Optical coherence tomography. Circulation. 2012;126(17):2140-3.
66. van Soest G et al. Imaging atherosclerotic plaque composition with intracoronary optical coherence tomography. Neth Heart J. 2009;17(11):448-50.
67. Häner JD et al. Impact of intracoronary optical coherence tomography in routine clinical practice: a contemporary cohort study. Cardiovasc Revasc Med. 2022;38:96-103.
68. Lawton JS et al. 2021 ACC/AHA/ SCAI guideline for coronary artery revascularization: a report of the American College of Cardiology/ American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145(3):e18-114.
69. Shammas NW et al. The role of precise imaging with intravascular ultrasound in coronary and peripheral interventions. Vasc Health Risk Manag. 2019;15:28390.
70. Gao X-F et al. 3-year outcomes of the ULTIMATE trial comparing intravascular ultrasound versus angiography-guided drugeluting stent implantation. JACC Cardiovasc Interv. 2021;14(3):24757.
71. Hannan EL et al. Percutaneous coronary intervention with and without intravascular ultrasound for patients with complex lesions: utilization, mortality, and target vessel revascularization. Circ Cardiovasc Interv. 2022;15(6):e011687.
72. Waksman R et al.; LRP Investigators. Identification of patients and plaques vulnerable to future coronary events with near-infrared spectroscopy intravascular ultrasound imaging: a prospective, cohort study. Lancet. 2019;394(10209):1629-37.
FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM 64 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
Imaging Features of Myometrial Necrosis in a Patient Due to Uterine Compression Sutures
Authors:
Disclosure:
Padma Vikram Badhe,1 *Ajith Varrior,1 Moinuddin Sultan,2 Swapnil Moharkar1
1. Department of Radiology, Seth GS Medical College and KEM Hospital, Mumbai, India
2. Department of Radiology, Vedantaa Institute of Medical Sciences, Dahanu, India
*Correspondence to ajithvarrior@gmail.com
The authors have declared no conflicts of interest.
Acknowledgements: Informed consent was obtained from the patient.
Received: 06.12.23
Accepted: 29.01.24
Keywords: B-Lynch, hysterectomy, myometrial necrosis, postpartum haemorrhage, uterine compression sutures.
Citation:
Abstract
EMJ Radiol. 2024;5[1]:65-70.
https://doi.org/10.33590/emjradiol/10300182.
Postpartum haemorrhage (PPH) is a significant cause of maternal morbidity and mortality. The management includes a spectrum ranging from mechanical and pharmacological to surgical methods. The authors report a case of a 24-year-old primigravida who presented with complaints of abdominal pain, distension, fever, and diarrhoea a few days after her delivery. She had postpartum haemorrhage, for which compression sutures were applied. On radiological investigations, she was diagnosed with myometrial necrosis, following which she underwent a subtotal hysterectomy. Myometrial necrosis is a common complication encountered in the setting of postpartum haemorrhage secondary to compressive sutures. An early diagnosis and an appropriate management requires adequate radiological investigations.
Key Points
1. Myometrial necrosis is an expected complication with compression sutures for postpartum haemorrhage. The choice of compression sutures must be based on the clinical status of the patient, and the surgeon’s expertise.
2. Radiological features of myometrial necrosis include avascularity on colour Doppler and CT. Air foci might be encountered in the setting of infection.
3. Constant vigilance is necessary in patients who are high-risk for myometrial necrosis, in the form of clinical symptoms and appropriate radiological investigations.
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 65 Case Report
INTRODUCTION
Postpartum haemorrhage (PPH) is a significant cause of maternal morbidity and mortality. PPH affects approximately 2% of all females who give birth. It is associated not only with nearly one-quarter of all maternal deaths globally, but is also the leading cause of maternal mortality in most low-income countries.1 PPH needs a rampant diagnosis, and adequate management. The management includes a spectrum ranging from mechanical and pharmacological to surgical methods. Physiological means of prevention of blood loss include the anatomical arrangement of the uterine muscular layer, which constricts the uterine vasculature during contraction;2 and the release of oxytocin during breastfeeding, which is a physiological uterotonic agent.3,4 Although the first-line management includes mechanical compression and the use of pharmacological agents, many patients require additional measures. Depending on the haemodynamic parameters, the patient may be offered compression sutures or uterine artery embolisation if vitally stable. If unstable, or if all other methods have failed to achieve haemostasis, they may be directly taken up for hysterectomy. Apart from managing the blood loss, it is equally important to watch out for complications associated with the measures adopted for haemostasis. One such dreaded complication is uterine myometrial necrosis, which requires hysterectomy as its management. Myometrial necrosis has been reported as a complication of embolisation and compression sutures for PPH, a sequelae to endometritis, and rarely post-Caesarean section.5,6 Clinically, it presents with abdominal pain, fever, diarrhoea, or vaginal discharge. The authors report a case of myometrial necrosis, following compression suture surgery for atonic PPH.
CLINICAL CASE
A 24-year-old primigravida (G1P0L0) was admitted to a secondary referral centre for safe confinement. After a trial of labour, she was taken up for emergency lower segment Caesarean section (LSCS) due to obstructed labour. LSCS was carried out under spinal anaesthesia. The baby was delivered headfirst, cried immediately after birth, and was handed over to the paediatrician. The placenta and
membranes were expelled spontaneously and completely. The uterus was atonic, resulting in primary postpartum haemorrhage. The patient was administered uterotonic agents, failing which B-lynch compression sutures were applied with No. 1 Vicryl suture (Johnson & Johnson MedTech, New Brunswick, New Jersey, USA) for refractory PPH. Both the uterine arteries were ligated with absorbable sutures for controlling haemorrhage. The uterus was well contracted post-compression sutures, and haemostasis was confirmed. The abdomen was closed in layers. The patient was transfused with packed cell volume and fresh frozen plasma.
On postoperative Day 3, the patient developed five-to-six episodes of loose stools and vomiting, with gradually increasing abdominal distension. On postoperative Day 5, she developed occasional fever spikes, and was shifted to the ICU for paralytic ileus. CT on postoperative Day 7 showed dilated small bowel loops with bulky uterus, and few air foci in the uterine cavity. Ultrasonogram of the abdomen on postoperative Day 11 showed 100 cc of collection anterior and posterior to the uterus, with dilated small bowel loops. The patient developed daily fever spikes up to 102 oF, and was started on antibiotics.
The patient was referred to the Seth GS Medical College and KEM Hospital, Mumbai, India, for further management. On admission, the patient was afebrile and vitally stable, with soft and non-tender abdomen. On local examination, there was a wound gape of 2x1 cm (up to the muscular layer) with purulent discharge. Ultrasonogram of the abdomen showed a bulky uterus of size 17x15x9 cm with heterogenous echotexture and ill-defined endomyometrial junction, with multiple air foci in the endometrial cavity (Figure 1A), extending up to the scar site, suggestive of scar dehiscence. There was no vascularity in the myometrium on colour Doppler (Figure 1B). There was a heterogeneously hypoechoic collection of approximately 50 cc seen superior to the bladder, with no collection at the suture site. Contrast-enhanced CT scan of the abdomen showed enlarged postpartum uterus with multiple air foci in the endometrial cavity, with loss of endomyometrial junction and non-enhancing myometrium (Figures 2A and 2B). There was dehiscence in the anterior wall of the uterus at the LSCS site, with focal bulge contained by overlying serosa (Figure 2B). There
66 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Case Report
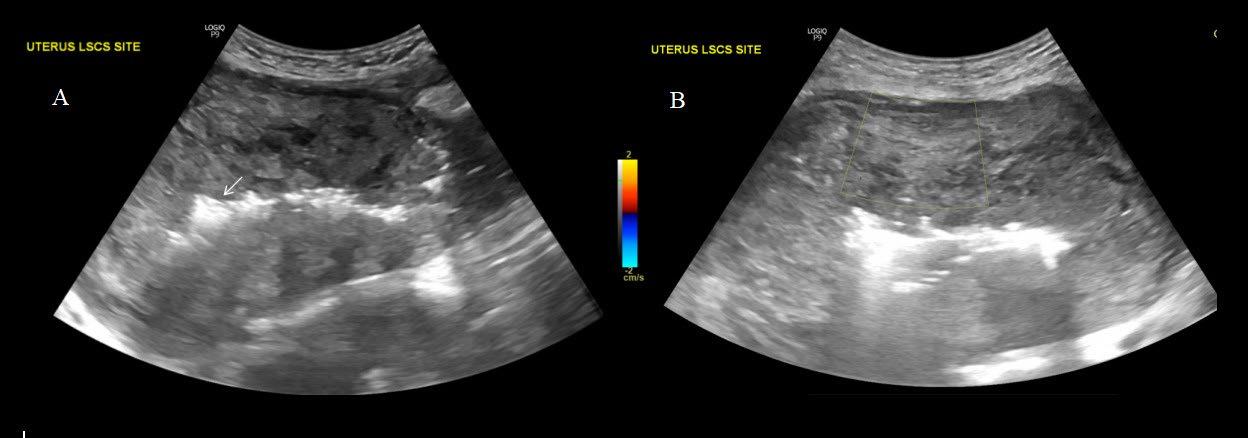
A)
a bulky
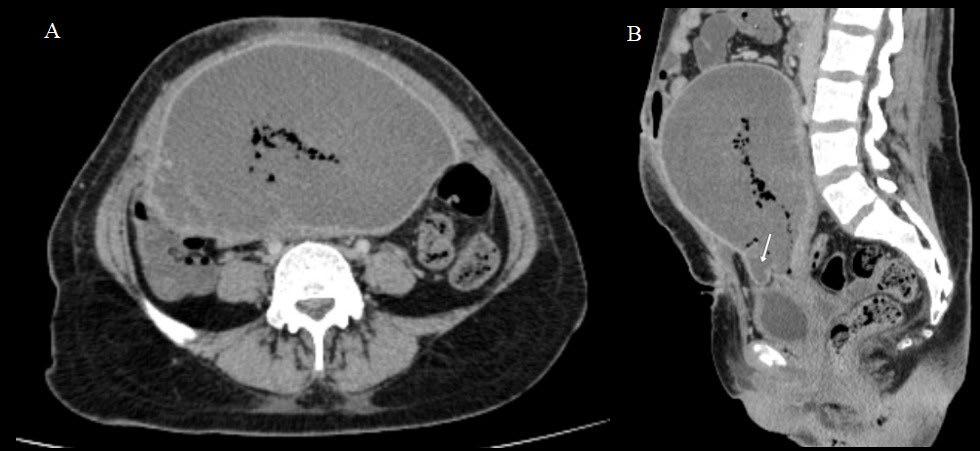 Ultrasound of the abdomen in the longitudinal section shows
postpartum uterus with heterogenous echotexture of the myometrium. There are air foci with dirty post-acoustic shadowing in the endometrium (arrow). B) Axial sections of the abdomen show no vascularity in the myometrium on colour Doppler with minimal scale.
Figure 1: Ultrasound findings in myometrial necrosis.
Figure 2: CT findings in myometrial necrosis.
Ultrasound of the abdomen in the longitudinal section shows
postpartum uterus with heterogenous echotexture of the myometrium. There are air foci with dirty post-acoustic shadowing in the endometrium (arrow). B) Axial sections of the abdomen show no vascularity in the myometrium on colour Doppler with minimal scale.
Figure 1: Ultrasound findings in myometrial necrosis.
Figure 2: CT findings in myometrial necrosis.
A B A B Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 67 Case Report
A) Axial sections of the abdominal CT in the venous phase show lack of myometrial enhancement. The mean Hounsfield unit of the myometrium in post-contrast phase is 33. B) Sagittal section of the abdominal CT in the venous phase shows a bulge in the serosa at the scar site (arrow).

was a collection measuring 4.4x2.6x2.3 cm in the pouch of Douglas.
The patient underwent obstetric subtotal hysterectomy (Figure 3), in view of myometrial necrosis. After a stable course in the ward, the patient was discharged from the hospital.
DISCUSSION
The most common cause of PPH is uterine atony.7 Appropriate timely intervention is required to stem the haemorrhage. Physiological factors responsible for haemostasis following delivery might sometimes fall short, and might warrant the use of various pharmacological or surgical options. In the authors’ case, the bleeding could not be controlled with pharmacological agents, and the patient was subjected to uterine compression sutures and uterine artery ligation.
Various types of compression sutures commonly used for the management of PPH include B-Lynch sutures, Hayman sutures, and Cho square sutures.8-11 The B-Lynch technique was first introduced in 1997,12 and has since gained popularity as an effective means of achieving haemostasis in cases of atonic PPH. It involves the apposition of the anterior and
the posterior uterine walls, with vertical sutures put around the uterus.13 B-Lynch, Hayman, and Pereira sutures are used to compress the uterine body. Cho square sutures are more useful in lower segment bleeding.14,15 Another variant of compression sutures is a simple U suture, which is easy to perform, and has lesser complications.8,9 Although these compression sutures are lifesaving and fertility-preserving, they do sometimes come with the cost of certain complications, including synechiae formation, haematometra, pyometra, and myometrial necrosis.16,17 Complications are more frequently encountered with Cho square sutures.14 The choice of sutures depends on the bleeding site, severity, disorders causing PPH, and the experience of the obstetric surgeon.14 Ligation of the uterine arteries and the internal iliac arteries may achieve adequate haemostasis, preserving fertility.18-20 The choice between uterine artery ligation and uterine compression sutures depends primarily on the preference of the surgeon. Both may be used as a first step in controlling bleeding refractory to medical management. Either of the methods may be used first, and if this fails, the other method can be implemented.21
68 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Case Report
Figure 3: The specimen of the bulky postpartum uterus with areas of necrosis (arrows) post-subtotal hysterectomy.
The involution of the postpartum uterus ensures that the pressure created by the sutures is dynamic, and, as the uterus shrinks in size, the tension reduces. This, combined with the increased uterine vascularity and a rich anastomotic network, minimises the possibility of myometrial necrosis.22,23 The concomitant use of uterine compression sutures with devascularisation increases the risk of complications, compared to adopting the compression sutures alone.24,25 The setting of uterine necrosis can be explained by the lack of collateral supply to the uterus postdevascularisation. Incorrectly placed sutures can also pave the way for necrosis. Both arterial and venous infarction have been postulated as causes of myometrial necrosis. This was complicated by the presence of infection, as in the authors’ case. By the time the patient was referred to the authors’ centre, there was a significant delay, and a hysterectomy was done to prevent septicaemia, further morbidity, and mortality.
Radiology plays a vital role in diagnosing the cause, and also the complications encountered during the management of PPH. Ultrasound as the first line of imaging modality can diagnose retained products of conception as the cause of PPH, and can guide clinicians during curettage, ensuring adequate removal of products. Myometrial necrosis can be seen post-compression sutures, or post-uterine artery embolisation. It presents with complaints such as
References
1. World Health Organization (WHO). WHO recommendations for the prevention and treatment of postpartum haemorrhage. World Health Organisation. 2012. Available at: https:// www.who.int/publications/i/ item/9789241548502. Last accessed: 14 February 2024.
2. De Tourris T. [Contribution to the study of structure of the uterine cervix.] Gynecol Prat. 1964;15(6):463-5. (In French).
3. Abedi P et al. Breastfeeding or nipple stimulation for reducing postpartum haemorrhage in the third stage of labour. Cochrane Database Syst Rev. 2016;2016(1):CD010845.
4. Irons DW et al. A simple alternative to parenteral oxytocics for the
abdominal or pelvic pain, abdominal distension, fever, metrorrhagia, and vaginal discharge.26-28 It can be diagnosed on ultrasound, wherein the myometrium shows no internal vascularity on colour Doppler, as well as on CT, where the myometrium shows lack of enhancement in post-contrast sequences. Although rarely used, an MRI may also confirm the findings of myometrial necrosis. The necrosed myometrium shows intermediate-to-high signal intensity on T1-weighted images, and high signal intensity on T2-weighted images, along with a lack of early and delayed enhancement.29
Postoperatively, the patient should be under constant vigilance for myometrial vascularity. One must look for the signs and symptoms of necrosis as described above, and an ultrasound must be carried out at the earliest opportunity to detect the vascularity status.
CONCLUSION
Postpartum haemorrhage is a significant cause of mortality, and warrants rampant measures for its diagnosis and management. The choice of compression sutures should be tailored according to the status of the patient. Myometrial necrosis following compression sutures is a known complication, and early detection and appropriate management require adequate radiological investigations.
third stage of labor. Int J Gynaecol Obstet. 1994;46:15‐8.
5. Eboué C et al. [Nécrose utérine et ovarienne après embolisation des artères utérines pour hémorragie de la délivrance.] J Gynecol Obstet Biol Reprod. 2007;36(3):298-301. (In French.)
6. Cottier JP et al. Uterine necrosis after arterial embolization for postpartum hemorrhage. Obstet Gynecol. 2002;100(Suppl 5 Pt 2):1074-77.
7. Evensen A et al. Postpartum hemorrhage: prevention and treatment. Am Fam Physician. 2017;95(7):442-9.
8. Al Riyami N et al. Uterine compression sutures as an effective treatment for postpartum
hemorrhage: case series. AJP Rep. 2011;1(1):47-52.
9. Hackethal A et al. Uterine compression U-sutures in primary postpartum hemorrhage after Cesarean section: fertility preservation with a simple and effective technique. Hum Reprod. 2008;23:74-9.
10. Cho JH et al. Hemostatic suturing technique for uterine bleeding during cesarean delivery. Obstet Gynecol. 2000;96(1):129-31.
11. Allam MS, B-Lynch C. The B-Lynch and other uterine compression suture techniques. Int J Gynaecol Obstet. 2005;89(3):236-41.
12. B-Lynch C et al. The B-Lynch surgical technique for the control of massive postpartum haemorrhage: an alternative
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 69 Case Report
to hysterectomy? Five cases reported. Br J Obstet Gynaecol. 1997;104:372-5.
13. Begum J et al. B-lynch: a technique for uterine conservation or deformation? A case report with literature review. J Clin Diagn Res. 2014;8(4):OD01-3.
14. Matsubara S et al. Uterine compression sutures for postpartum hemorrhage: an overview. Acta Obstet Gynecol Scand. 2013;92(4):378-85.
15. Palacios-Jaraquemada JM. Efficacy of surgical techniques to control obstetric hemorrhage: analysis of 539 cases. Acta Obstet Gynecol Scand. 2011;90:1036-42.
16. Treloar EJ et al. Uterine necrosis following B-Lynch suture for primary postpartum haemorrhage. 2006;113(4):486-8.
17. Gottlieb AG et al. Uterine necrosis: a complication of uterine compression sutures. Obstet Gynecol. 2008;112(Suppl 2 Pt 2):429-31.
18. O'Leary JL. Uterine artery ligation in the control of intractable postpartum hemorrhage. Am J Obstet Gynecol. 1966;94(7):920-4.
19. Waters EG et al. Surgical management of postpartum hemorrhage with particular reference to ligation of uterine arteries. Am J Obstet Gynecol. 1952;64(5):1143-48.
20. Evans S, McShane P. The efficacy of internal iliac artery ligation in obstetric hemorrhage. Surg Gynecol Obstet. 1985;160(3):2503.
21. Bouchghoul H et al. Uterinesparing surgical procedures to control postpartum hemorrhage. Am J Obstet Gynecol. 2022;19:S0002-9378(22)00465-3.
22. Benkirane S et al. Uterine necrosis following a combination of uterine compression sutures and vascular ligation during a postpartum hemorrhage: a case report. Int J Surg Case Rep. 2017;38:5-7.
23. El-Hamamy E. Partial ischemic necrosis of the uterus following a uterine brace compression suture. BJOG. 2005;112(1):126.
24. Luo L et al. Uterine necrosis, infection, and subinvolution: complications observed after combined application of modified B-Lynch suture and
vascular ligation. J Int Med Res. 2021;49(5):3000605211010730.
25. Lodhi W et al. Uterine necrosis following application of combined uterine compression suture with intrauterine balloon tamponade. J Obstet Gynaecol. 2012;32(1):30-1.
26. Yoshikawa M et al. A case of preeclampsia with uterine necrosis after uterine artery embolization for postpartum hemorrhage. Case Rep Obstet Gynecol. 2022;2022:2859766.
27. Poujade O et al. Uterine necrosis following pelvic arterial embolization for post-partum hemorrhage: review of the literature. Eur J Obstet Gynecol Reprod Biol. 2013;170(2):309-14.
28. Tseng JJ et al. Uterine necrosis associated with acute suppurative myometritis after angiographic selective embolization for refractory postpartum hemorrhage. Am J Obstet Gynecol. 2011;204(6):e4-6.
29. Torigian DA et al. MRI of uterine necrosis after uterine artery embolization for treatment of uterine leiomyomata. Am J Roentgenol. 2005;184(2):555-9.
FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM 70 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Case Report
Imaging Innovations in the Screening, Diagnosis, and Monitoring of Systemic Autoimmune DiseaseRelated Interstitial Lung Disease
Authors:
Disclosure:
Clinton Jokerst,1 Kavitha Yaddanapudi,2 Sachin Chaudhary,3 Ana C. Zamora,4 *Vivek Nagaraja5
1. Department of Radiology, Mayo Clinic Arizona, Phoenix, USA
2. Department of Radiology, University of Arizona, Tucson, USA
3. Division of Pulmonary Critical Care and Sleep Medicine, University of Arizona, Tucson, USA
4. Division of Pulmonary and Sleep Medicine, Mayo Clinic Arizona, Phoenix, USA
5. Division of Rheumatology, Mayo Clinic Arizona, Scottsdale, USA
*Correspondence to nagaraja.vivek@mayo.edu
Chaudhary received an investigator initiated grant from Boehringer Ingelheim; and consulting and speaking fees from Boehringer Ingelheim and Veracyte. Nagaraja has served on the advisory board of activities, and received a consulting fee from Boehringer Ingelheim. All other authors have declared no conflicts of interest.
Received: 02.02.24
Accepted: 14.02.24
Keywords: CT scan, diagnosis, imaging, interstitial lung disease (ILD), screening.
Citation: EMJ Radiol. 2024;5[1]:71-81.
https://doi.org/10.33590/emjradiol/11000033.
Abstract
Interstitial lung disease (ILD) is a common and serious complication of systemic autoimmune rheumatic diseases (SARD). The prevalence and prognosis of ILD vary depending on the type and severity of the underlying SARD. Recently, two drugs have been approved by the U.S. Food and Drug Administration (FDA) for the treatment of ILD in SARD, and the American College of Rheumatology (ACR) has issued guidelines for the screening and monitoring of these patients. Therefore, it is essential to detect and manage ILD in SARDs as early as possible. High-resolution CT of the chest is the current gold standard test for diagnosis of ILD, yet, it is not uniformly performed as an initial diagnostic test. This review discusses the latest advances in imaging techniques for the diagnosis, assessment, and follow-up of SARD-ILDs.
Key Points
1. High-resolution CT scan of the chest is widely recognised as a screening imaging tool for interstitial lung disease (ILD), and is more available.
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 71 Article
2. There is a role for innovatively repurposing existent imaging modalities, such as ultrasound, MRI, or PET-CT, to better characterise ILD and assess for progression.
3. Incorporation of artificial intelligence and machine learning models can serve as an important tool to consistently quantify and characterise ILD by radiologists.
INTRODUCTION
Interstitial lung disease (ILD) is a relatively frequent manifestation of systemic autoimmune rheumatic disorders (SARD), including systemic sclerosis (SSc), rheumatoid arthritis (RA), idiopathic inflammatory myopathies (IIM), primary Sjögren’s syndrome (pSS), anti-neutrophil cytoplasmic antibody-associated vasculitis, and rarely, systemic lupus erythematosus (SLE). ILD in SARD (SARD-ILD) is considered to be a serious end-organ complication, and has a significant impact on morbidity, work productivity, quality of life, and mortality.1 The natural history, in terms of onset and progression, is variable between SARDs, and even among the same patients with SARDs. The ILD manifestation of a given SARD may precede, coincide, or succeed the extrapulmonary manifestation. The screening for ILD may vary between SARDs, depending on risk factors. When suspected, high resolution CT (HRCT) of the chest remains the centre piece to confirm the diagnosis, besides obtaining pulmonary function tests (PFT), and testing the exercise capacity with hall walk testing.2 This review focuses on key factors in screening, diagnosis, and imaging innovations of SARD-ILD.
CLINICAL RELEVANCE OF THIS REVIEW
Therapeutic options, although limited, continue to grow in the management of patients with SARD-ILD. Alongside, there are major advancement in the imaging techniques for earlier detection of ILD. This review describes key and recent developments in imaging to screen and monitor SARD-ILD. Through this review, the authors project what the future may hold in the application of the imaging innovation in different phases of ILD care (Figure 1).
SCREENING AND DIAGNOSIS FOR INTERSTITIAL LUNG DISEASE IN SYSTEMIC AUTOIMMUNE RHEUMATIC DISEASES
When Should Screening Be Considered?
Often, ILD develops after a diagnosis of SARD. However, subclinical ILD in SARDs like SSc, confirmed by HRCT, can precede, or appear concomitantly.3 The prevalence estimates vary by study, and by type of SARD. Most studies report higher prevalence in SSc, mixed connective tissue disease, RA, and IIM (30–60%), with lower prevalence in pSS and SLE.4-11 ILD is one of the leading causes of death in SSc and RA,12-15 and because of the high prevalence of ILD in SSc, all patients with SSc should be screened at the time of their diagnosis, even if they are asymptomatic.16 Male African-American patients, patients positive for the anti-Scl-70 antibody, with diffuse cutaneous SSc subset, reflux/ dysphagia symptoms, and cardiac involvement, are at high risk for developing progressive ILD.17
In patients with RA, ILD is the second leading cause of death after cardiovascular complications. The timing of ILD development is unclear. In one study, approximately one-third of patients developed ILD in the first year of RA diagnosis, and under one-fifth of them between 1–5 years of RA diagnosis.6 A few known risk factors for the development of ILD are old age, male sex, smoking, positive rheumatoid factor or anti-citrullinated peptide antibodies, and high RA disease activity.6,18 Besides these risk factors, screening for ILD should be considered in patients with RA showing respiratory symptoms (persistent cough or shortness of breath) and Velcro crackles on physical exam.18,19
In patients with IIM, ILD prevalence is variable, and has been reported to be upwards of 70% in longitudinal follow-up.20 The presence of anti-synthetase antibodies and anti-MDA5
72 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
Figure 1: Screening and monitoring for interstitial lung disease in patients with systemic autoimmune rheumatic diseases: current tools and future directions.
Screen for SARD-ILD Monitoring for SARD-ILD
SARD with risk factors or pulmonary symptoms
Current Tools and Approaches
Future Directions
• HRCT (required)
• +PFT
• +6 MWT
• +Ambulatory desaturation testing
• Integrating the innovations in the HRCT modalities (PCCT+ DLIR+AI)
• 68Ga-FAPI-PET (differentiate fibrosis from alveolitis)
• Lung ultrasound (in resource-limited settings)
Established SARD-ILD
• PFT
• HRCT
• Ambulatory desaturation testing
• SARD-specific considerations (based on risk factors of progression)
• For quantification and progression
• Integrating the innovations in the HRCT modalities (PCCT+DLIR+AI)
• Lung ultrasound for low-cost and radiation-free monitoring
• 68Ga-FAPI-PET (differentiate fibrosis from alveolitis)
• MRI characterisation of GGO (differentiate fibrotic versus inflammatory)
AI: artificial intelligence; DLIR: deep learning image reconstruction; GGO: ground-glass opacity; HRCT: high-resolution CT; PCCT: photon-counting CT; PFT: pulmonary function test; SARD-ILD: systemic autoimmune rheumatic disease-related interstitial lung disease; 6MWT: 6-minute walk test; 68Ga-FAPI-PET: gallium 68–labelled fibroblast activation protein inhibitor positron emission tomography.
antibodies is considered high risk, and should necessitate screening irrespective of pulmonary symptoms.21,22 In other SARDs, namely pSS, anti-neutrophil cytoplasmic antibody-associated vasculitis, and SLE, screening for ILD is based upon patient symptomatology.
Current Screening and Diagnostic Modalities
Screening for ILD should involve a comprehensive clinical history in order to identify symptoms, risk factors, and potential exposures. A detailed physical examination involves lung auscultation for crackles, clubbing, and any physical signs suggesting underlying autoimmune diseases. The gold standard for screening ILD is HRCT.23 Other essential evaluations include pulmonary function testing (including diffusing capacity for carbon monoxide [DLCO], PFT), assessment of exercise capacity (such as the 6-minute walk distance), and ambulatory desaturation testing.
Pulmonary function testing involves measurement of forced expiratory volume, forced vital capacity, total lung capacity, residual volume, and DLCO. PFT is a vital tool in screening patients with SARD in conjunction with HRCT. While 6-minute walk distance and ambulatory desaturation testing are needed as a part of comprehensive diagnostic evaluation, they should not be used in isolation for screening purposes.24
HRCT is optimised to enhance spatial resolution by using reconstruction (recon) algorithms to enhance edge detail, and by using thin (1–2 mm) slice recons to better detect and more accurately characterise subtle abnormalities of the lung parenchyma. In addition to standard supine inspiratory scanning, an HRCT protocol often includes additional prone imaging (to help differentiate between atelectasis and fibrosis), and expiratory imaging (to detect air trapping). HRCT protocols are usually obtained without intravenous contrast, which does not add to pulmonary parenchymal evaluation.
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 73 Article
According to the proposed 2023 guidelines by the American College of Rheumatology (ACR), for people with SARDs at increased risk of developing ILD, it is recommended against screening with surgical lung biopsy or transbronchial biopsy.24 In certain instances, patients may require a biopsy for a more definitive diagnosis. In such situations, less invasive options could be explored, like transbronchial biopsy or cryobiopsy. More invasive surgical lung biopsy should only be considered in select situations for diagnostic purposes. The decision to undergo a biopsy should be taken after a collaborative consensus driven by multidisciplinary discussion.
Once Diagnosed, What Is the Role Of Imaging in Interstitial Lung Disease Monitoring?
Studies in patients with SSc-ILD provide the most robust guidance on monitoring in patients with subclinical or clinical SARD-ILD. The ACR 2023 ILD guidelines have provided guidance on monitoring, and vary by the SARD.24 Periodic assessment of symptoms, PFTs, and ambulatory desaturation (every 3–12 months) is considered essential in monitoring. Repeating an HRCT should be considered when clinically indicated. In patients with either IIM-ILD or SSc-ILD, PFTs are recommended every 3–6 months for the first year, then less frequently once stable. In patients with RA-ILD, pSS-ILD, and mixed connective tissue disease ILD, PFTs are recommended every 3–12 months for the first year, then less frequently once stable.
INNOVATIONS IN IMAGING FOR SCREENING AND MONITORING OF INTERSTITIAL LUNG DISEASE IN SYSTEMIC AUTOIMMUNE RHEUMATIC DISEASES
CT: Technical Innovations
HRCT has been an important modality for imaging-based detection, characterisation, and quantification of ILD for nearly 5 decades.25 Since its arrival in the 1980s, incremental advances in CT technology have increased the role of HRCT in the detection, diagnosis, and management of ILD. For example, the shift from second-generation CT towards third-generation helical multidetector CT dropped the scanning time, making single-
breath-hold chest CT a reality. This also allowed for a volumetric (as opposed to axial ‘step-andshoot’) scanning mode. The ensuing benefits include improved image quality, decreased radiation exposure, and obviation of the need to choose between total lung coverage versus high spatial resolution reconstructions. All chest CT scans could now be high-resolution.26
Photon-Counting CT Detector Technology
The maturation of photon-counting CT (PCCT) detector technology is a significant technological shift in the field of HRCT. The ILD-relevant improvements that PCCT brings to the application of HRCT include improved spatial resolution (through new detector design), and decreased image noise (through inherent detector spectral sensitivity).27 PCCT scanners are now a reality in clinical practice, with the first U.S. Food and Drug Administration (FDA)-approved PCCT system made available in 2021.8 Pre-PCCT scanners have a detector size of 0.500–0.625 mm, with one notable exception,28 which limits the spatial resolution of standard CT technology. With PCCT, the discreet detector element, which must be optically isolated from surrounding elements, is replaced by a semiconductor detector element with associated pixellated anodes.27 The size of the anode determines the spatial resolution of the system; these anodes can be made smaller more easily than the scintillation crystals used in non-PCCT. PCCT can reconstruct slices as thin as 0.2 mm, resulting in significant improvements in spatial resolution, which is a game changer for better characterising ILD.
A variety of CT findings characterise ILD, including reticulation, traction bronchiectasis/ bronchiolectasis, consolidation, ground glass, nodules, airway thickening, air-trapping, peribronchovascular versus peripheral distribution, etc.29 All these findings are easier to accurately detect and characterise with better spatial resolution. In short, PCCT results in much better HRCT image quality, which allows radiologists to detect more subtle initial presence, or more subtle interval changes in pattern and extent of ILD over time.30 When integrated with machine learning-based tools for detection, categorisation, and quantification, CT findings from ILD will be more accurate, and will allow for better and faster segmentation/quantification.
74 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
Better image quality with CT usually comes at the cost of increased radiation exposure, and the associated risks to the patient.31 This tradeoff does not apply to PCCT, where a better image quality is obtained at a lower radiation exposure.32 This is because the spectral capabilities of PCCT allow it to identify lowenergy scattered photons (noise). Removing noise from the system results in improved signal-to-noise performance of PCCT.27 Studies with use of PCCT demonstrate improved characterisation of ILD with radiation doses 28–32% lower compared to standard CT.33 The utility of low-dose HRCT techniques has been established with traditional CT systems.34 The additional denoising capabilities of PCCT may facilitate better-quality low-dose HRCT protocols, hopefully leading to increased utilisation of HRCT for surveillance of SARD-ILD.
CT Imaging Reconstruction
There has been a shift in CT image recon techniques utilising machine learning to improve the speed and quality of CT recons. These ‘deep learning image reconstructions’ (DLIR) provide a way to denoise CT images. Like PCCT, this results in improved image quality, and enables the use of lower radiation doses for HRCT. For example, Zhao et al.35 compared standard-dose, standard-recon HRCT with low dose HRCT (38% of dose of standard-dose exam) using DLIR, in a population of 70 prospectively enrolled patients with ILD. Despite the significant reduction in dose, the use of DLIR resulted in significantly better recognition of ground glass, architectural distortion, bronchiolectasis, and honeycombing.
The aggregate effects of the incorporation of both PCCT and DLIR into HRCT imaging techniques will have a multitude of benefits. Firstly, it will improve CT sensitivity, resulting in detection of more subtle disease (higher sensitivity) and more confident determination of ILD stability versus progression (hence, impacting management). Secondly, it improves accuracy of characterisation of CT findings related to ILD (more accurate imaging-based ILD pattern recognition and prognostication). Thirdly, lowering the cumulative radiation dose means less hesitation in use of HRCT for screening, diagnosis, and follow-up, especially for younger females, who make up a large portion of the SARD-ILD patient population.
CT: Artificial Intelligence
In recent years, there have been significant developments in the use of artificial intelligence (AI) for CT-based characterisation and quantification of ILD. Machine learning holds the promise of a more reproducible and quantifiable approach to what has traditionally been a very qualitative endeavour, the interpretation of HRCT.
In this portion of the review, representative work in the areas of disease detection (screening), pattern recognition (diagnosis), and quantification (management) will be discussed. Although it is expedient to group the applications of AI this way, machine learning algorithms can be trained to ‘do it all’ at one point in time.
In the area of early detection, the merging of AI into CT technology dates back to 2011, when a computer program capable of detecting and quantifying ILD on HRCT was developed and validated in a patient cohort with familial pulmonary fibrosis or RA (with or without ILD).36 This program used segmentation, texture analysis, training, classification, and grading to score ILD, and was able to consistently identify mild ILD. In a recent study, a fully convolutional network was used for semantic segmentation of several ILD patterns.37 After training the algorithm, it was used to analyse HRCT data from two separate databases. Despite some limitations, the study proved the feasibility of creating a fully automated software for detecting the presence of pulmonary fibrosis.
ILD pattern recognition on HRCT is of prognostic value. For example, in patients with SARD-ILD, the presence of a usual interstitial pneumonia (UIP) pattern on HRCT is associated with decreased survival, compared to patients without typical UIP features.38 Recently, deep learning methodologies were innovatively tested to predict histopathologic diagnosis. A custom DL model was evaluated to explore the non-invasive diagnosis of UIP, and compared to histopathologic diagnosis. The researchers trained the DL model with 894 CT cases, where each case was assigned a label based on histopathologic diagnosis (UIP or non-UIP). The deep learning model was subsequently validated in another 198 cases. The model’s reproducibility was compared against intra-rater and interrater radiologist reproducibility. Deep learning performance was superior to visual analysis in predicting histopathologic diagnosis (area under
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 75 Article
the receiver operating characteristic curve: 0.87 versus 0.80, respectively; P<0.05) with a significantly greater reproducibility compared to radiologist inter-rater and intrarater reproducibility39
HRCT plays an important role in the ongoing care of patients with SARD-ILD, as serial quantification of HRCT findings assists in determining ILD behaviour as stable versus progressive. A post-processing tool called Computer-Aided Lung Informatics for Pathology Evaluation and Ratings (CALIPER) uses HRCT information, such as texture analysis, to identify and quantify CT features predictive of mortality and forced vital capacity decline.40,41 CALIPER increases radiologist confidence as to whether HRCT findings of SARD-ILD are stable or progressing on follow-up CT (Figure 2),

which impacts management decisions. When a radiologist with access to CALIPER encounters a case where quantitative analysis may be useful, the axial thin supine reconstruction is sent to the CALIPER server. Within minutes, results are available with a map of the lung volume segmentation (upper versus mid versus lower, and central versus peripheral), a colour-coded reconstruction of the pulmonary findings, and a glyph summarising the distribution and relative abundance of findings, such as emphysema, normal lung, ground glass, reticulation, and honeycombing (Figure 3). Such representation of CALIPER-based parameters is shown to be better than traditional functional parameters for assessing outcomes and mortality in patients with SARD-ILD.42
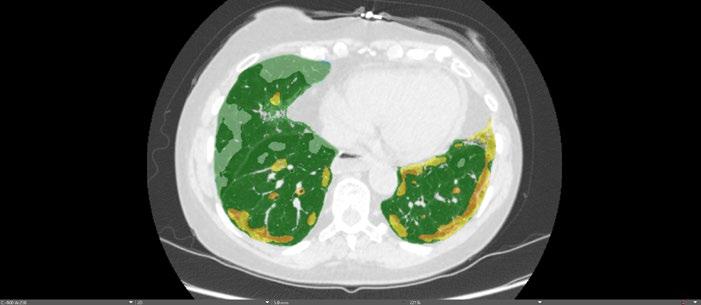
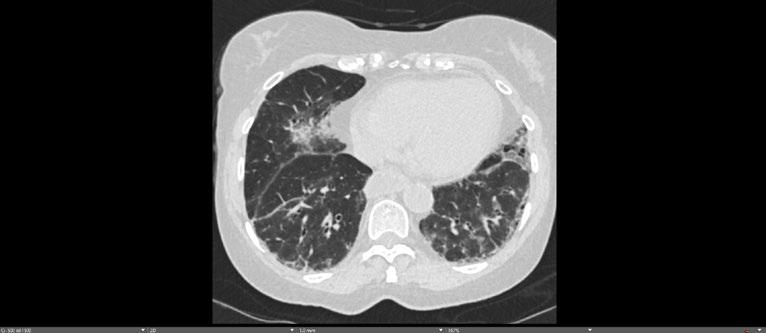
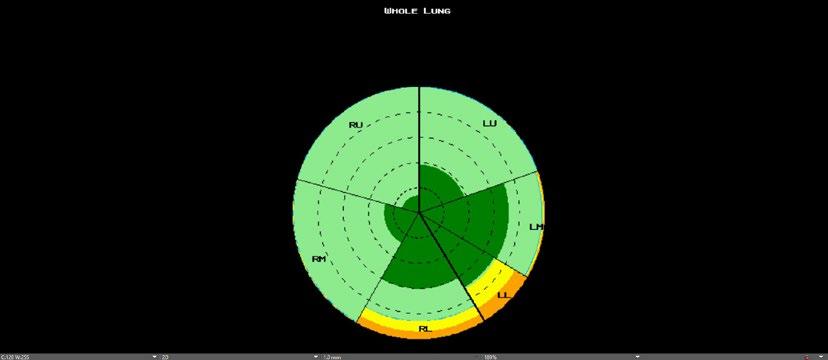
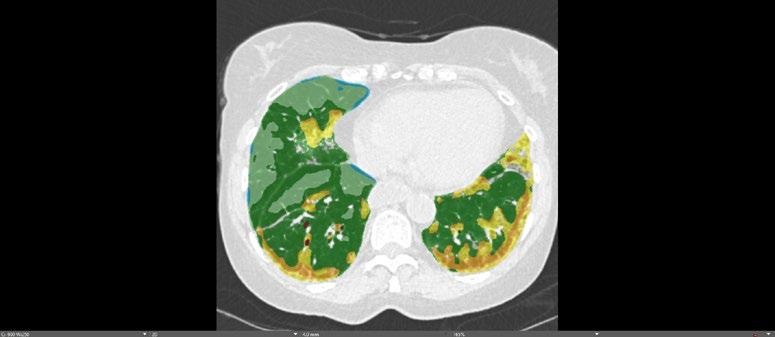
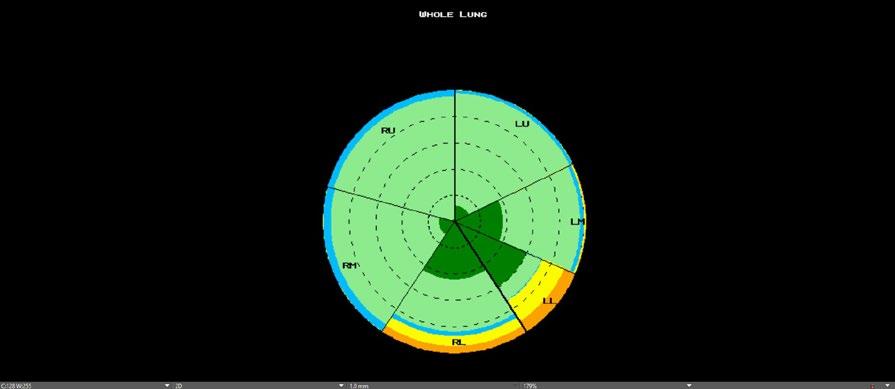
Baseline axial CT image (A); axial image with color-coded CALIPER overlay (B); and summary CALIPER
Glyph (C) from a young female with systemic sclerosis and interstitial lung disease, compared to a 6-month follow-up HRCT (D, E, F).
Subjective comparison of the baseline (A) and follow-up (D) CT images suggests some possible ILD progression; however, the fact that the ILD has progressed is much easier to appreciate when comparing the colour-coded CALIPER images (B versus E). Note the patulous oesophagus (A, arrow), a classic CT finding for patients with SSc-ILD.
HRCT: high-resolution CT; ILD: interstitial lung disease; SSc-ILD: systemic sclerosis-related ILD.
D E F
A B C
Figure 1
E F
D 76 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
Figure 2: Application of artificial intelligence to high-resolution CT in assessing disease progression.
A
B C
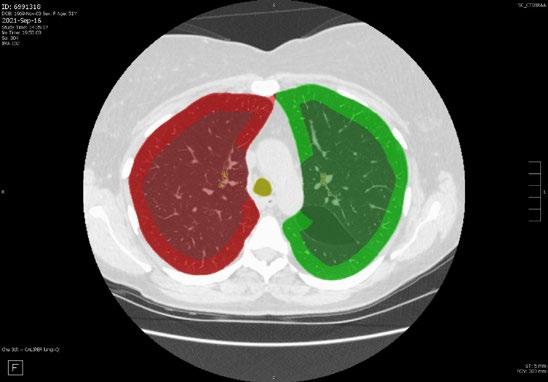
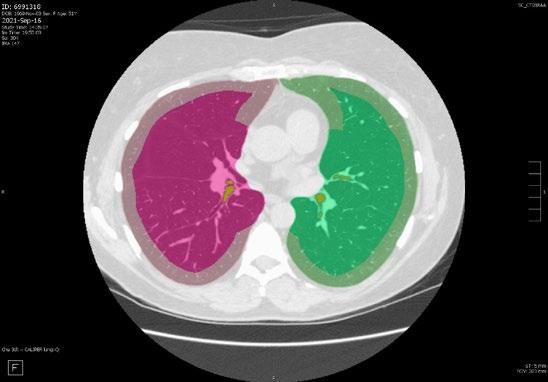

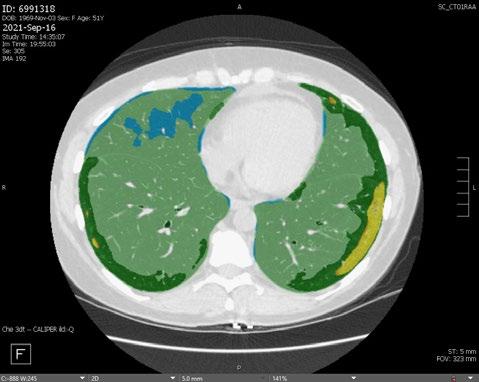
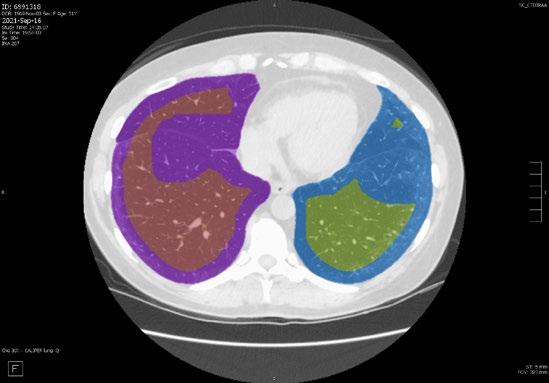
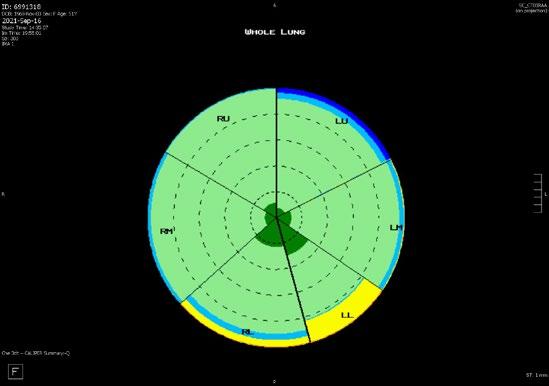
Colour-coded representative axial CT images from CALIPER demonstrating central versus peripheral segmentation in the upper (A), mid (B), and lower (C) lung zones. Axial CT images without (D) and with (E) colour-coded CALIPER overlay demonstrating subtle peripheral areas of ground-glass (yellow) in a patient with SARD-ILD. The darker green peripheral areas (E) often go on to develop into ground glass, suggesting future disease progression. A summary CALIPER Glyph (F) demonstrates the relative distribution of HRCT findings.
SARD-ILD: systemic autoimmune rheumatic disease-related interstitial lung disease.
Positron Emission Tomography-CT: New Tracers
The use of positron emission tomography with CT (PET/CT) to assess ILD activity has, thus far, been based on the use of 2-deoxy-2-[fluorine-18] fluoro-D-glucose PET with CT (FDG PET/CT). This tracer, while useful for a variety clinical applications, is limited to assessing the degree of inflammation rather than fibrotic activity/pulmonary remodelling in the setting of ILD.43 Persistent activation and local accumulation of myofibroblasts play a key role in the development of fibrotic diseases of the lung.44,45 Fibroblast activation protein α (FAP) is induced in activated fibroblasts, and is negligible in resting fibroblasts.
An advancement in molecular imaging is the development of radiolabelled quinoline-based PET tracers that bind to FAP, such as 68Ga-FAPinhibitor (68Ga-FAPI), which demonstrate tracer uptake in various tumour entities, and in fibrotic diseases.46 A study in 21 patients with SSc-ILD reported the use of 68Ga-FAPI-04 PET/CT, and showed that FAP imaging directly visualised activated fibroblasts in vivo 47 Increased 68GaFAPI-04 uptake at baseline was associated with progression of ILD, independently of extent of involvement on HRCT scans, and of the forced vital capacity on baseline PFTs. Moreover, changes in 68Ga-FAPI-04 uptake were concordant with the observed response to the fibroblast-targeting antifibrotic drug nintedanib.47 These new PET/CT tracers may play an important role in managing SARD-ILDs in the near future.
A B C D E F
Figure 2
A E F B C D Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 77 Article
Figure 3: Characterisation of lung parenchymal changes using artificial intelligence incorporated high-resolution CT.
MRI
MRI for evaluation of SARD-ILD, although desirable due to a lack of ionising radiation and due to superior tissue characterisation, has not become a mainstream tool for the diagnosis and management of ILD. Relative to HRCT, major drawbacks of lung MRI include lower spatial resolution (related to low proton density in lungs), and long acquisition times (resulting in respiratory motion artefacts exacerbated by poor breath-holding in the ILD population). Advances in lung MRI sequences, such as ultrashort echo time sequences, which are faster, with less signal decay and higher resolution, have increased investigation of MRI as a potential tool for imaging ILD.
Recently, ultrashort echo time MRI has shown near-perfect inter-method agreement compared to HRCT for ILD changes, in terms of assessing extent, severity, and pattern (reticulation, traction bronchiectasis, and honeycombing) of disease.48,49 An area of limitation with HRCT is the ability to consistently differentiate inflammatory ground-glass opacities (GGO) from fibrotic GGO. In this regard, MRI tissue characterisation has been shown to differentiate active alveolitis from fibrosis based on the higher water content in active inflammation. T2 weighted imaging helps identify active alveolitis by high T2 signal and early enhancement in patients with nonspecific interstitial pneumonia and UIP. On the other hand, fibrosis has low T2, and a more delayed pattern of enhancement.46 This MRI-based differentiation could potentially be a useful predictor of treatment response of active alveolitis. MRI could also aid in deciding the need for, and choice of, immunosuppressive therapy, depending on the presence or absence of alveolitis in chronic infiltrative lung disease.50,51
In specific SARD-ILDs, like SSc-ILD, recent studies have shown good agreement between lung MRI and HRCT in the assessment of ILD in SSc, with 100% sensitivity of MRI relative to HRCT.52 Lung MRI demonstrated good diagnostic performance and correlation with forced vital capacity and DLCO; however, MRI underestimated disease extent relative to HRCT.53 Short tau inversion recovery MRI, on the other hand, was a good indicator for disease progression independent of HRCT. In this same study, both T1 and sort tau inversion recovery values were significantly different between normal and abnormal lung parenchyma.54
The limitation of conventional MRI in evaluating the lung parenchyma is due to its low proton density, resulting in low contrast images of the lungs on magnetic resonance images. The magnetic resonance signal may be further degraded by air-tissue interfaces, respiratory motion, and blood flow in the vasculature.55 To overcome this limitation, functional MRI using hyperpolarised gases has been an advancement. For example, O2-enhanced MRI may aid early evaluation of ILD, and serve as a marker for disease progression.56 O2-enhanced MRI was found to be comparable to CT in SARD-ILD in assessing pulmonary function loss and disease severity.57 In another study, hyperpolarised helium 3 (3He) diffusion-weighted (DW) MRI was used to demonstrate reproducibility with chest CT findings of sub-pleural and basilar fibrotic changes in patients with ILD.58 Further, 3HeDWMRI being a functional study, the elevated DW MRI metrics correlated with the diffusing capacity of the lungs for carbon monoxide, consistent with deteriorating alveolar gas transfer. MRI, with its detection of active inflammation, ability to predict response to treatment, and newer functional assessment tools, has a lot of potential for the evaluation of SARD-ILD.
Lung Ultrasound
Lung ultrasound (LUS) has been studied in the setting of ILD for more than a decade, and has the advantage of being radiation free, noninvasive, portable, and low cost.59 Convex and linear probes have both been used in LUS, with frequencies ranging from 3.5–10.0 MHz, depending on the transducer used. Limited scanning of the posterobasal chest, between the scapula and diaphragm, has been proposed as a sensitive and quick screening tool for ILD evaluation60.
B-lines and pleural abnormalities are the two main diagnostic criteria used in LUS for ILD.60 B-lines are reverberation artefacts, which are caused by the reflection of ultrasound waves by interlobar septal thickening from fibrosis. They appear as hyperechoic lines that extend from pleural surface to edge of field, and move synchronously with lung sliding. As a screening tool, B lines have a high sensitivity and negative predictive value.61 Total B-line cut-offs have been reported in SSc-ILD and RA-ILD with high sensitivity.62,63 Total B-lines have also significantly differentiated ILD versus no ILD, and
78 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
anterior B-lines have differentiated extensive ILD from limited ILD.64 LUS as a follow-up tool has been shown to detect new onset ILD in known SSc and worsening ILD.65 In a patient with amyopathic dermatomyositis, a combination of LUS B-lines and KL-6 were applied successfully in the ongoing follow-up of a patient with known ILD on immunosuppressive therapy.66
Pleural abnormalities can be detected on LUS in the setting of ILD, and are easily identifiable and reproducible. In SSc-ILD, pleural abnormalities on LUS include pleural thickening (≥3 mm) and granularity, defects in pleural surface, or pleural irregularity. A preliminary prospective investigation using the pleural abnormalities for diagnosis of ILD had high sensitivity, specificity, and excellent inter-reader agreement.67 The sensitivity of B-lines increases when paired with pleural abnormalities for diagnosis.
A major limitation of LUS is that it cannot distinguish between the various types of pulmonary fibrotic findings, such as reticulation, GGO, or honeycombing; nor can it identify the pattern of fibrosis as nonspecific interstitial pneumonia or UIP.60 Also, using B-lines in the setting of ILD has its own limitations. B-lines can be a nonspecific sign of an interstitial process, and are seen with interstitial oedema. B-lines can also be seen in areas of decreased aeration,
References
1. Fischer A, du Bois R. Interstitial lung disease in connective tissue disorders. Lancet. 2012;380(9842):689-98.
2. Raghu G et al. Idiopathic pulmonary fibrosis (an update) and progressive pulmonary fibrosis in adults: an official ATS/ERS/JRS/ ALAT clinical practice guideline. Am J Respir Crit Care Med. 2022;205(9):e18-e47.
3. Jaafar S et al. Clinical characteristics, visceral involvement, and mortality in at-risk or early diffuse systemic sclerosis: a longitudinal analysis of an observational prospective multicenter US cohort. Arthritis Res Ther. 2021;23(1):170.
4. Bergamasco A et al. Epidemiology of systemic sclerosis and systemic sclerosis-associated interstitial lung disease. Clin Epidemiol. 2019;11:257-73.
posing a problem for the evaluation of the lung bases.60 B-lines are difficult to quantify, and can be dependent on machine settings, which affect reproducibility. There is currently no consensus in LUS for definition of lesions, standard acquisition parameters, areas to be scanned, quantification, scoring systems, or transducers used. Overall, LUS can be a sensitive and accessible radiationfree screening tool for SARD-ILD, when in the right hands, but the modality needs further validation and standardisation with larger prospective studies.
Figure 1 depicts the potential future role of the imaging innovations reviewed in this manuscript in screening and monitoring of SARD-ILDs.
CONCLUSION
HRCT has been a pivotal imaging development in the past two decades, and has become the mainstay in the diagnosis of ILD in patients with SARDs. There have been significant innovations in imaging in the past decade, as described in this article, with compelling evidence to support the integration of these innovations into mainstream clinical practice. While larger scale validation of these modalities is required, the future holds promise in terms of costs without compromising quality.
5. Graney BA, Fischer A. Advocating for early interstitial lung disease detection in mixed connective tissue disease. Rheumatology (Oxford). 2018;57(2):204-5.
6. Hyldgaard C et al. A populationbased cohort study of rheumatoid arthritis-associated interstitial lung disease: comorbidity and mortality. Ann Rheum Dis. 2017;76(10):17006.
7. Reiseter S et al. Progression and mortality of interstitial lung disease in mixed connective tissue disease: a long-term observational nationwide cohort study. Rheumatology (Oxford). 2018;57(2):255-62.
8. Administation FaD. FDA clears first major imaging device advancement for computed tomography in nearly a decade. 2021. Available at: https://www.fda.gov/newsevents/press-announcements/ fda-clears-first-major-imagingdevice-advancement-computed-
tomography-nearly-decade. Last accessed: 5 December 2023.
9. Hannah JR, D'Cruz DP. Pulmonary complications of systemic lupus erythematosus. Semin Respir Crit Care Med. 2019;40(2):227-34.
10. Luppi F et al. Interstitial lung disease in Sjogren's syndrome: a clinical review. Clin Exp Rheumatol. 2020;38 Suppl 126(4):291-300.
11. Raimundo K et al. Rheumatoid arthritis-interstitial lung disease in the United States: prevalence, incidence, and healthcare costs and mortality. J Rheumatol. 2019;46(4):360-9.
12. Mira-Avendano I et al. Interstitial lung disease and other pulmonary manifestations in connective tissue diseases. Mayo Clin Proc. 2019;94(2):309-25.
13. Cottin V, Brown KK. Interstitial lung disease associated with systemic sclerosis (SSc-ILD). Respir Res. 2019;20(1):13.
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 79 Article
14. Marigliano B et al. Lung involvement in connective tissue diseases: a comprehensive review and a focus on rheumatoid arthritis. Autoimmun Rev. 2013;12(11):1076-84.
15. Steen VD, Medsger TA. Changes in causes of death in systemic sclerosis, 1972-2002. Ann Rheum Dis. 2007;66(7):940-4.
16. Makol A et al. Recent innovations in the screening and diagnosis of systemic sclerosis-associated interstitial lung disease. Expert Rev Clin Immunol. 2023;19(6):613-26.
17. Rahaghi FF et al. Expert consensus on the management of systemic sclerosis-associated interstitial lung disease. Respir Res. 2023;24(1):6.
18. Garrote-Corral S et al. Screening of interstitial lung disease in patients with rheumatoid arthritis: a systematic review. Reumatol Clin (Engl Ed). 2022;18(10):587-96.
19. Narvaez J et al. Screening criteria for interstitial lung disease associated to rheumatoid arthritis: expert proposal based on Delphi methodology. Reumatol Clin (Engl Ed). 2023;19(2):74-81.
20. Fathi M et al. Interstitial lung disease in polymyositis and dermatomyositis: longitudinal evaluation by pulmonary function and radiology. Arthritis Rheum. 2008;59(5):677-85.
21. Andersson H et al. Pulmonary involvement in the antisynthetase syndrome: a comparative crosssectional study. J Rheumatol. 2016;43(6):1107-13.
22. Radic M et al. Delphi-based consensus on interstitial lung disease screening in patients with connective tissue diseases (Croatian National-Based Study). Biomedicines. 2022;10(12):3291.
23. Travis WD et al. An official American Thoracic Society/ European Respiratory Society statement: update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. 2013;188(6):733-48.
24. Rheumatology ACo. 2023 Interstitial Lung Disease Guidelines. 2023. Available at: https://rheumatology.org/ interstitial-lung-disease-guideline. Last accessed: 4 February 2024.
25. Bergin CJ, Muller NL. CT in the diagnosis of interstitial lung disease. AJR Am J Roentgenol. 1985;145(3):505-10.
26. Hsieh J, Flohr T. Computed tomography recent history and future perspectives. J Med Imaging (Bellingham). 2021;8(5):052109.
27. Willemink MJ et al. Photoncounting CT: technical principles and clinical prospects. Radiology. 2018;289(2):293-312.
28. Boedeker K. Aquilion precision ultra-high resolution CT: quantifying diagnostic image quality. 2018. Available at: https:// global.medical.canon/publication/ ct/2018WP_Aquilion_Precision_ Ultra-High_Resolution. Last accessed: 5 December 2023.
29. Pagano AM et al. Evaluation of interstitial lung disease: an algorithmic review using ILD-RADS. Clin Imaging. 2022;88:45-52.
30. Inoue A et al. Estimating the clinical impact of photon-countingdetector CT in diagnosing usual interstitial pneumonia. Invest Radiol. 2022;57(11):734-41.
31. Lin EC. Radiation risk from medical imaging. Mayo Clin Proc. 2010;85(12):1142-6;quiz 1146.
32. Rajendran K et al. First clinical photon-counting detector CT system: technical evaluation. Radiology. 2022;303(1):130-8.
33. Van Ballaer V et al. Impact of ultra-high-resolution imaging of the lungs on perceived diagnostic image quality using photoncounting CT. Eur Radiol. 2023.
34. Koo CW et al. Prospective machine learning CT quantitative evaluation of idiopathic pulmonary fibrosis in patients undergoing antifibrotic treatment using low- and ultra-low-dose CT. Clin Radiol. 2022;77(3):e208-e14.
35. Zhao R et al. Can deep learning improve image quality of lowdose CT: a prospective study in interstitial lung disease. Eur Radiol. 2022;32(12):8140-51.
36. Rosas IO et al. Automated quantification of high-resolution CT scan findings in individuals at risk for pulmonary fibrosis. Chest. 2011;140(6):1590-7.
37. Agarwala S et al. Deep learning for screening of interstitial lung disease patterns in highresolution CT images. Clin Radiol. 2020;75(6):481 e1-8.
38. Walsh SL et al. Connective tissue disease related fibrotic lung disease: high resolution computed tomographic and pulmonary function indices as prognostic determinants. Thorax. 2014;69(3):216-22.
39. Bratt A et al. Predicting usual interstitial pneumonia histopathology from chest CT imaging with deep learning. Chest. 2022;162(4):815-23.
40. Bartholmai BJ et al. Quantitative computed tomography imaging of interstitial lung diseases. J Thorac Imaging. 2013;28(5):298-307.
41. Jacob J et al. Predicting outcomes in idiopathic pulmonary fibrosis using automated computed tomographic analysis. Am J Respir Crit Care Med. 2018;198(6):767-76.
42. Jacob J et al. Evaluation of computer-based computer tomography stratification against outcome models in connective tissue disease-related interstitial lung disease: a patient outcome study. BMC Med. 2016;14(1):190.
43. Chen DL et al. Quantification of lung PET images: challenges and opportunities. J Nucl Med. 2017;58(2):201-7.
44. Distler JHW et al. Shared and distinct mechanisms of fibrosis. Nat Rev Rheumatol. 2019;15(12):705-30.
45. Schmidkonz C. Perspective on fibroblast activation proteinspecific PET/CT in fibrotic interstitial lung diseases: imaging fibrosis-a new paradigm for molecular imaging? J Nucl Med. 2022;63(1):125-6.
46. Lindner T et al. Development of quinoline-based theranostic ligands for the targeting of fibroblast activation protein. J Nucl Med. 2018;59(9):1415-22.
47. Bergmann C et al. 68Ga-FAPI-04 PET-CT for molecular assessment of fibroblast activation and risk evaluation in systemic sclerosisassociated interstitial lung disease: a single-centre, pilot study. Lancet Rheumatol. 2021;3(3):e185-e94.
48. Ohno Y et al. Pulmonary highresolution ultrashort TE MR imaging: comparison with thinsection standard- and low-dose computed tomography for the assessment of pulmonary parenchyma diseases. J Magn Reson Imaging. 2016;43(2):512-32.
49. Landini N et al. Advanced and traditional chest MRI sequence for the clinical assessment of systemic sclerosis related interstitial lung disease, compared to CT: disease extent analysis and correlations with pulmonary function tests. Eur J Radiol. 2023;170:111239.
50. Muller NL et al. Value of MR imaging in the evaluation of chronic infiltrative lung diseases:
80 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
comparison with CT. AJR Am J Roentgenol. 1992;158(6):1205-9.
51. Yi CA et al. 3-T MRI for differentiating inflammation- and fibrosis-predominant lesions of usual and nonspecific interstitial pneumonia: comparison study with pathologic correlation. AJR Am J Roentgenol. 2008;190(4):878-85.
52. Muller CS et al. Pulmonary magnetic resonance imaging is similar to chest tomography in detecting inflammation in patients with systemic sclerosis. Rev Bras Reumatol Engl Ed. 2017;57(5):41924.
53. Pinal-Fernandez I et al. Fast 1.5 T chest MRI for the assessment of interstitial lung disease extent secondary to systemic sclerosis. Clin Rheumatol. 2016;35(9):233945.
54. Gargani L et al. Lung magnetic resonance imaging in systemic sclerosis: a new promising approach to evaluate pulmonary involvement and progression. Clin Rheumatol. 2021;40(5):1903-12.
55. Altes TA, Flors L. Detection of longitudinal microstructural changes in idiopathic pulmonary fibrosis with hyperpolarized (3)he diffusion-weighted MRI. Radiology. 2019;291(1):230-1.
56. Lonzetti et al. Magnetic resonance imaging of interstitial lung diseases: a state-of-the-art review. Respir Med. 2019;155:7985.
57. Ohno Y et al. Oxygen-enhanced MRI for patients with connective tissue diseases: comparison with thin-section CT of capability for pulmonary functional and disease severity assessment. Eur J Radiol. 2014;83(2):391-7.
58. Chan HF et al. Airway microstructure in idiopathic pulmonary fibrosis: assessment at hyperpolarized (3)He diffusionweighted MRI. Radiology. 2019;291(1):223-9.
59. Gargani L et al. Ultrasound lung comets in systemic sclerosis: a chest sonography hallmark of pulmonary interstitial fibrosis. Rheumatology (Oxford). 2009;48(11):1382-7.
60. Gargani L et al. Lung ultrasound B-lines in systemic sclerosis: cut-off values and methodological indications for interstitial lung disease screening. Rheumatology (Oxford). 2022;61(SI):SI56-64.
61. Barskova T et al. Lung ultrasound for the screening of interstitial lung disease in very early systemic sclerosis. Ann Rheum Dis. 2013;72(3):390-5.
62. Di Carlo M et al. Lung ultrasound in patients with rheumatoid arthritis: definition of significant interstitial lung disease. Clin Exp Rheumatol. 2022;40(3):495-500.
63. Gargani L et al. Prognostic value of lung ultrasound B-lines in systemic sclerosis. Chest. 2020;158(4):151525.
64. Bruni C et al. Lung ultrasound B-lines in the evaluation of the extent of interstitial lung disease in systemic sclerosis. Diagnostics (Basel). 2022;12(7):1696.
65. Gasperini ML et al. The predictive role of lung ultrasound in progression of scleroderma interstitial lung disease. Clin Rheumatol. 2020;39(1):119-23.
66. Wang Y et al. Utilize lung ultrasound B-lines and KL-6 to monitor anti-MDA-5 antibodypositive clinically amyopathic dermatomyositis-associated interstitial lung disease: a case report and literature review. Clin Rheumatol. 2019;38(5):1433-6.
67. Fairchild R et al. Development and assessment of novel lung ultrasound interpretation criteria for the detection of interstitial lung disease in systemic sclerosis. Arthritis Care Res (Hoboken). 2021;73(9):1338-42.
FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 81 Article
Cardiac MRI Imaging Features of Erdheim–Chester Disease: A Case Review
Authors:
Disclosure:
*Pritish Aher,1 Aman Aher,2 Sarv Priya,3 Chris Schettino1
1. Miller School of Medicine, University of Miami, Florida, USA
2. Bharati Vidyapeeth Medical College, Pune, India
3. Department of Radiology, University of Iowa Hospitals & Clinics, Iowa City, USA
*Correspondence to pritishaher@hotmail.com
The authors have declared no conflicts of interest.
Received: 04.06.23
Accepted: 12.12.23
Keywords:
Citation:
Abstract
Blood, BRAF V600E mutation, cardiac MRI, Erdheim–Chester disease (ECD), non-Langerhans cell histiocytosis, oncology.
EMJ Radiol. 2024;5[1]:82-86.
https://doi.org/10.33590/emjradiol/10308930.
Erdheim–Chester disease (ECD) is a disease of non-Langerhans cell histiocyte multisystemic proliferation. The pathogenesis is related to accumulation of histiocytes across the body, leading to multiple organ failure, and thus necessitating an early diagnosis. In all ECD cases, BRAF and RAS mutations are critical. Clinical manifestations affect individuals between the fourth and seventh decades of life. The most common symptoms reported are central nervous system involvement with functional disability, and bone pain with osteosclerosis of long bones. Other reported symptoms are skin involvement with xanthelasma, diabetes insipidus, cardiovascular involvement with pericardial effusion and tamponade, perivascular thickening, and right atrial and atrioventricular grove infiltration, leading to heart failure. Females may develop galactorrhoea due to deposition in the pituitary gland, with or without menstrual irregularities. Only few publications address the cardiac MRI findings of ECD. The authors present a case of cardiac involvement of ECD and associated cardiac MRI findings. The patient presented with multisystemic disease with bone pain, diplopia, cardiac arrythmia, and dyspnoea.
Key Points
1. Erdheim–Chester disease is a disease of non-Langerhans cell histiocytosis and clonal disorder, with BRAF V600E mutation and chronic uncontrolled inflammation. In all ECD cases, BRAF and RAS mutations are critical.
2. Clinical manifestations involve the central nervous system, cardiovascular system, bones, skin, and eyes. In cases of cardiovascular involvement, patients present with arrhythmias, valvular heart disease, ischaemia, or heart failure. Some patients are asymptomatic. Patients with renal artery involvement present with hypertension.
82 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
3. MRI imaging of the heart and bones is important for diagnosis. Cardiac imaging with contrastenhanced MRI shows late gadolinium enhancement involving the cardiac wall, cardiac valve, aortic root, and aortic wall. Cardiac MRI volumetric evaluation helps in the diagnosis of heart failure.
CASE REPORT
A 54-year-old female with a history of suspected IgG4-related sclerosing disease, who had been struggling with multisystem symptoms for approximately 4 years, presented with worsening diplopia, fever, bone pain, acute kidney disease, arrythmia, and dyspnoea. Patient blood panel revealed haemoglobin of 10.4 g/ dL. Urine analysis and infection panel were normal. Immunological studies of serum IgG4 level were normal (16 mg/dL), and serum β2 microglobulin levels were raised (10.2 mg/L). Positron emission tomography (PET) and CT scans revealed hypermetabolic disease in the right kidney, bilateral femurs, and periaortic and pericardial regions. The patient underwent orbitotomy. Mutational analysis showed a BRAF V600E mutation. Femur and renal biopsies were performed, which diagnosed Erdheim–Chester disease (ECD). The patient also developed recurrent pericardial effusions that further confirmed the authors’ suspicions. Cardiac MRI was performed on the MAGNETOM Sola 1.5T MRI system (Siemens Healthineers, Erlangen, Germany), which revealed hyperintense signal within the atrioventricular groove surrounding the right coronary artery, right atrium walls, interatrial septum, and periadventitial region of the ascending aorta. Cardiac MRI also demonstrated diffuse periatrial and periventricular late gadolinium enhancement with atrioventricular groove soft tissue enhancement, and periaortic thickening (‘coated aorta’). Native T1 mapping images showed increased native T1 values at 1,390 (Figure 1). On functional cardiac MRI measurements, left ventricular ejection fraction was reduced due to reduced global systolic function. No significant valvular abnormality was detected. The cardiac involvement in this case was pericardial effusion, detected on chest CT scan (Figure 2). PET imaging identified diffuse pericardiac and periaortic fluorodeoxyglucose uptake (Figure 3).
DISCUSSION
ECD infiltration usually affects individuals between 40–70 years of age. 1,2 The most common symptom reported is central nervous system involvement, with functional disability and bilateral upper and lower extremity bone pain. More than 50% of patients with ECD present with these symptoms, but some may never experience bone pain. Patients may develop skin manifestations with xanthelasma, hypertension due to renal artery involvement, and diabetes insipidus. Females may develop galactorrhoea due to deposition in the pituitary gland, with or without menstrual irregularities.3,4 The presentation of cardiac involvement by ECD infiltration can be variable, from being asymptomatic to having multiple cardiac symptoms. Patients may present with palpitations due to arrhythmias, valvular heart disease, chest pain due to ischaemia, tamponade, or cardiac failure. Pericardial disease in ECD infiltration can present with pericardial thickening, pericardial effusion, and/or cardiac tamponade. Incidence of cardiac tamponade in patients with ECD infiltration is 13–24%. However, pericardial calcification is rare, and can be seen in up to 4% of patients.5,6 Myocardial infiltration occurs in 25–31% of patients, most commonly affecting the right atrium and right atrioventricular groove, with development of a right atrial pseudotumour.2,3 Another common clinical finding in ECD infiltration is hypertension, secondary to renal artery involvement. ECD causes renal artery infiltration progression to stenosis. In this case report, the patient presented with diplopia and retro-orbital masses. Diplopia was a rare presenting symptom, along with palpitations, dyspnoea, and bone pain.5,7
Pathogenesis reveals a BRAF V600E mutation in most patients, leading to oncogenic alteration. Patients with ECD infiltration also have an oncologic NRAS Q61R mutation, which highlights mitogen-activated protein kinase signalling. The absence of BRAF V600E mutation does not necessarily rule out ECD. ECD infiltration is a
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 83 Article
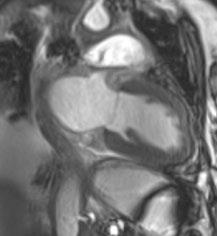
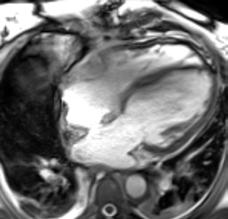
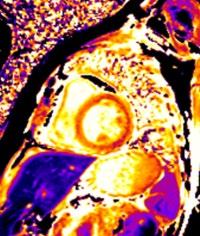
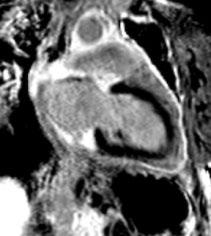
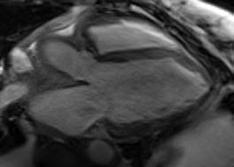
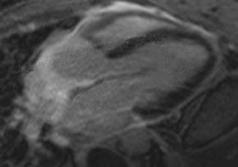
A) SSFP non-contrast two-chamber view, with hyperintense soft tissue around left atrium and ventricle.
B) SSFP non-contrast two-chamber view, with post-gadolinium soft tissue enhancement around left atrium, and ventricle with minimal intramyocardial enhancement at apical region. C) SSFP three-chamber view, with periaortic soft tissue. D) SSFP post-contrast three-chamber view, with thickened soft tissue enhancement around aortic root. E) SSFP four-chamber white blood image, with hyperintense soft tissue density mass at right atrioventricular groove, around right atrium and ventricle, and pericardial effusion. F) SSFP fourchamber post-gadolinium, with atrioventricular soft tissue enhancement, and diffuse enhancement in the soft tissue around the right atrium and right ventricle. G) SSFP short axis images, with soft tissue thickening around the right ventricle and inferior wall. H) SSFP short axis postcontrast image, with soft tissue enhancement around the right ventricle and inferior wall. I) and J) Pre-contrast short-axis T1 mapping, with regions of interest drawn in the septum native myocardial T1.
SSFP: steady-state free precession.
A E F G H B C D I J 84 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
Figure 1: Steady-state free precession cardiac MRI images.
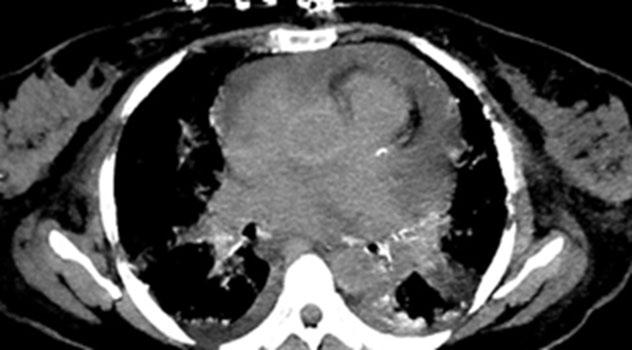
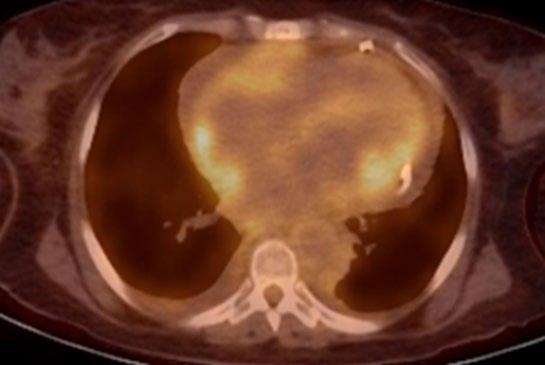
purely pathological diagnosis, that is aided by radiological imaging studies. Tissue biopsies classically show an infiltration of bland appearing histiocytes, characterised by abundant foamy cytoplasm with surrounding fibrosis and inflammation. Touton giant cells are frequently present. Immunohistochemistry of histiocytes shows positive staining for CD68, CD163, Factor XIIIa, and S100 (variable); however, does not show expression of CD1a and langerin. Serum analysis of patients with ECD consists of elevated interferon-α, IL-12, and monocyte chemotactic protein-1, as well as decreased IL-4
and IL-7. The case presented here also showed a BRAF V600E mutation, and histopathology of retroorbital masses, which confirmed the diagnosis of ECD.3,4
Imaging Findings
Cardiac and vascular ECD lesions develop due to periadventitial infiltration of the pericardium, myocardium, and coronary arteries, with incidence of 40%. Guidelines for baseline evaluation of ECD now recommend cardiac MRI in all patients, to identify involvement and
Figure 2: Chest CT (non-contrast study) showing pericardial effusion.
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 85 Article
Figure 3: Diffuse fluorodeoxyglucose avid soft tissue around right heart, and focal area of avidity around left ventricle.
delineate the extent of disease. The typical appearance of cardiac MRI is a hyperintense mass on T1-weighted images, and hypointense on T2-weighted images, with heterogeneous enhancement following gadolinium administration. Periarterial infiltration of the coronary arteries has been described in up to one-third of patients with ECD, most commonly affecting the right coronary artery, and may cause vascular stenosis and territorial ischaemia. Valvular involvement in ECD is also reported, with the most common valve involved being the mitral valve. It can present with thickening and stenosis of the valve, and progress to valvular insufficiency.4 Myocardial infiltration in ECD is rare, but can lead to cardiac dysfunction, arrhythmias, and heart failure. Patchy late gadolinium enhancement of the myocardium in patients with ECD may also be visualised in a non-coronary distribution. The myocardial infiltration in ECD involves the right atrium, and presents as an ill-defined, heterogeneous mass with variable signal intensity, and can mimic malignancy. Cardiac MRI, in the authors’ case, showed diffuse infiltration in the right atrial, right ventricle myocardium, and aortic root. On functional cardiac MRI, systolic function was impaired, with reduced ejection fraction.5-8
References
1. Haroche J et al. High prevalence of BRAF V600E mutations in ErdheimChester disease but not in other non-Langerhans cell histiocytoses. Blood. 2012;120(13):2700-3.
2. Blombery P et al. Erdheim-Chester disease harbouring the BRAF V600E mutation. J Clin Oncol. 2012;30(32):e331-2.
3. Diamond E et al. Consensus guidelines for the diagnosis and clinical management of Erdheim-Chester disease. Blood. 2014;124(4):483-92.
4. Mazor R et al. Erdheim-Chester disease: a comprehensive review of the literature. Orphanet J Rare Dis. 2013;8:137.
5. Gupta A et al. Erdheim-Chester disease with prominent pericardial
Other radiological imaging findings can be seen with plain radiographs, showing bilateral and symmetric long bone cortical osteosclerosis. Increased fluorodeoxyglucose uptake can be seen on PET imaging around the middle and ends of the long bones, especially in the femur and tibia, present in 95% of patients with ECD.9
The treatment for cardiac involvement in ECD is challenging, and there is currently no standard of care for cardiac involvement. Treatment options include corticosteroids, immunomodulatory agents, and chemotherapy. In some cases, radiation therapy or surgery may be considered. For pericardial effusion, pericardiocentesis or pericardiectomy may be performed. For valvular involvement, valve replacement or repair may be necessary. The prognosis for ECD is generally poor, with a median survival of around 5 years, and cardiac involvement can significantly affect the survival rate.3,10-12
The differential diagnosis for ECD involves pericardial metastasis (e.g., lung, breast), pericarditis, connective tissue disorders, infections (e.g., tuberculosis, fungal, pyogenic), pericardial or cardiac tumour (e.g., myxoma, lipoma, and angiosarcoma), and Rosai–Dorfman disease.3,4
involvement: clinical, radiologic, and histologic findings. Am J Med Sci. 2002;324(2):96-100.
6. Jain P et al. Erdheim-Chester disease presenting with large pericardial effusion: a mimic of disseminated malignancy. Intern Med J. 2011;41(3):291-3.
7. Haroche J et al. Images in cardiovascular medicine. Cardiac involvement in Erdheim-Chester disease: magnetic resonance and computed tomographic scan imaging in a monocentric series of 37 patients. Circulation. 2009,119(25):e597-8.
8. Quinaglia-Silva T et al. Cardiac involvement in Erdheim-Chester disease. Circ Cardiovasc Imaging. 2018;11(12):e008531.
9. Arnaud L et al. 18F-fluorodeoxyglucose-positron emission tomography scanning is more useful in follow up than in the initial assessment of patients with Erdheim-Chester disease. Arthritis Rheum. 2009;60(10):3128-38.
10. Hervier B et al. Treatment of Erdheim-Chester disease with long-term high-dose interferonalpha. Semin Arthritis Rheum. 2012;41(6):907-13.
11. Courcoul A et al. Successful treatment of Erdheim-Chester disease by interleukin-1 receptor antagonist protein. Joint Bone Spine. 2014;81(2):175-7.
12. Yano S et al. A case of ErdheimChester disease effectively treated by cyclophosphamide and prednisolone. Nihon Kokyuki Gakkai Zasshi. 2007;45(1):43-8.
FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM 86 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Article
Gigantic Small Bowel Gastrointestinal Stromal Tumours Through Different Radiological Lenses: A Case Report
Authors:
Disclosure:
Padma V. Badhe,1 Moinuddin Sultan,2 *Zubin Driver1
1. Department of Radiology, Seth GS Medical College and KEM Hospital, Mumbai, India
2. Department of Radiology, Vedantaa Institute of Medical Sciences, Dahanu, India
*Correspondence to driverzubin9@gmail.com
The authors have declared no conflicts of interest. Informed, written consent was obtained from the patient for the publication of this case report, and any accompanying images.
Received: 10.02.24
Accepted: 05.03.24
Keywords:
Citation:
Abstract
Conventional imaging, cross-sectional imaging, gastrointestinal stromal tumours (GIST), KIT gene.
EMJ Radiol. 2024;5[1]:87-92.
https://doi.org/10.33590/emjradiol/MYDG8219.
Gastrointestinal stromal tumours (GIST) account for 1–3% of all the gastrointestinal (GI) neoplasms. It is the most common mesenchymal tumour in the Gl tract. The majority of GISTs are KIT gene positive; however, it is necessary to diagnose them pre-operatively. Here, the authors report the case of a 65-year-old male who presented with pain and a lump in the umbilical region for the last 2 years. On abdominal ultrasound, there was a heterogeneously hypoechoic mass in the umbilical region, with lobulated margins and central necrotic areas. On small bowel series, the core of the mass showed faint contrast opacification. Contrastenhanced CT of the abdomen showed a heterogeneously enhancing, lobulated exophytic lesion arising from the small bowel loops, the central core of the lesion demonstrating an air-contrast level. Under ultrasound guidance, the lesion was biopsied. Histopathological findings were suggestive of a spindle cell tumour. The sample was c-KIT positive. Hence, the diagnosis of GIST was confirmed. The patient was given imatinib after resection of the mass. Usually, a GIST of larger size has higher malignant and metastatic potential; however, this article shows a gigantic small bowel GIST with cavitation and heterogeneity in different imaging modality, and still has no metastasis on imaging or high mitotic activity, and nuclear atypia on histopathology. A radiologist should also know the imaging pattern on conventional imaging and ultrasound, apart from usual cross-sectional imaging.
Imaging
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 87 Case Report
Key Points
1. Although CT is the imaging modality of choice, and presence of the c-KIT gene on immunohistochemistry confirms the diagnosis, this case report emphasises the role of ultrasound and conventional imaging.
2. Small bowel series and ultrasound can prove to be useful along with CT, to confirm the origin of air foci within a lesion.
3. Gastrointestinal stromal tumours (GIST) >5 cm usually show lobulated margins, central cavitation, and heterogenous enhancement on venous phase. Larger GIST tends to be malignant and metastasise to the liver, which was not seen in this case.
INTRODUCTION
Accounting for 1–3% of all gastrointestinal (GI) tumours, the most common mesenchymal tumour of the GI tract, which originates from the interstitial cells of Cajal in the myenteric plexus of the muscularis layer, is GI stromal tumour (GIST).1,2 Apart from CT, ultrasonogram, radiographs, and barium study, there are other multimodality imaging options, with which a radiologist should be well-versed. Here, the authors report a case of a 65-year-old male patient with a large small bowel GIST, highlighting the role of imaging in GIST and its management.
CASE PRESENTATION
A 65-year-old male presented with pain and a lump in the umbilical region for the last 2 years. He also had anorexia and weight loss for 2 months. He did not have fever, jaundice, or history of any previous surgeries. Clinical examination of the abdomen revealed a large abdominal lump in the umbilical region, spanning both the lumbar quadrants and measuring approximately 15x10 cm in size. The mass was palpated distinctly from the liver. A routine ultrasound of abdomen was requested. On ultrasound (Figure 1) the mass was heterogeneously hypoechoic, with well-defined lobulated margins, central necrotic areas, and size of 13.7x10.9 cm. Linear hyperechoic areas with dirty posterior shadowing were also seen in the core of the lesion, suggestive of air. On colour Doppler study, the lesion demonstrated


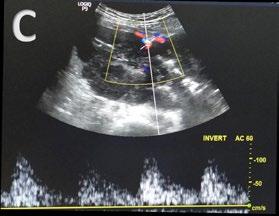
A) These show a well-defined, heterogeneously hypoechoic, lobulated solid lesion, with central necrotic areas. B) There are linear hyperechoic areas with dirty posterior acoustic shadowing in the core of lesion, suggestive of luminal air. C) Colour doppler shows vascularity within the lesion.
A B C 88 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Case Report
Figure 1: Ultrasonography images.
both arterial and venous vascularity. To confirm if the origin of air foci within the lesion was from the bowel loops, a small bowel series was done.
On pre-contrast radiograph (Figure 2A), there was a large abnormal soft tissue opacity of size 15x10 cm in the umbilical and right lumbar quadrant, with a central lucent area. On small bowel series (Figure 2B), gastric distensibility and emptying was normal. The core of the mass showed faint contrast opacification. The mass had displaced the ileal loops to the left. To radiologically confirm the diagnosis, and plan surgical resection of the mass, a contrastenhanced CT (CECT) abdomen with oral contrast was performed. Axial sections of the CECT abdomen (Figure 3A) showed a large, welldefined, heterogeneously enhancing, lobulated exophytic mass, with the central necrotic area arising from the small bowel loops occupying the umbilical and both lumbar quadrants. The central core of the lesion demonstrated contrast filling with air-contrast level. There were no calcifications. There were no enlarged surrounding mesenteric or retroperitoneal lymph
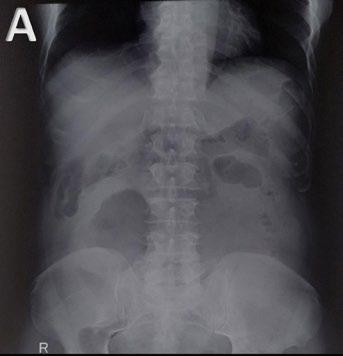
nodes. Under ultrasound guidance, the lesion was biopsied.
Histopathology (Figure 3B) revealed spindled shaped cells arranged in sheets, whorls, and vague storiform pattern. Individual spindle cells had ovoid to elongated, blunt ended pleomorphic nuclei, with prominent nucleoli. The cells also showed a moderate amount of fibrillary eosinophilic cytoplasm and vacuolations. There were abundant blood vessels in the surrounding stroma. Histopathological findings were suggestive of a spindle cell tumour. The sample was c-KIT positive. Hence, the diagnosis of GIST was confirmed. The patient was given imatinib after the surgical excision of the mass.
DISCUSSION
Nearly half of the benign tumours in the stomach and small bowel are mesenchymal in origin, arising from the muscularis propria, and 90% of them are GIST. Other submucosal lesions are lipomas, haemangiomas, neurofibroma,


A) Reveals a large soft tissue radio-opacity of approximate size 15x10 cm in right lumbar and umbilical quadrants with a central lucent area. B) Small bowel series show normal gastric distensibility and emptying. There is faint opacification in the core of lesion. The mass is displacing ileal loops to the left.
inflammatory fibroid polyps, Brunner’s gland hamartoma, ectopic pancreatic rests, and duplication cysts.3,4 The most common site for GIST is the stomach in two-thirds of cases,
followed by small bowel in 30% of cases. Other rare sites are the colon, oesophagus, appendix, and extra GI (omentum, mesentery, and retroperitoneum).2,5-7 Extra-GI stromal
Figure 2: Pre-contrast radiograph of the abdomen.
A B
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 89 Case Report

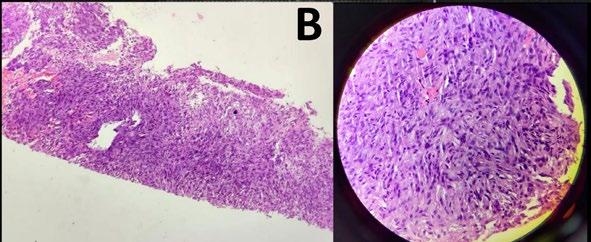
A) Shows a large, well-defined, heterogeneously enhancing, lobulated exophytic mass, with central necrotic area, arising from the small bowel loops and occupying the umbilical and both lumbar quadrants. There is contrast filling within core of the lesion with air contrast level. B) On histopathology, there are spindled shaped cells arranged in sheets, whorls, and vague storiform pattern. Individual spindle cells have ovoid to elongated, blunt-ended pleomorphic nuclei with prominent nucleoli. The cells also show moderate amount of fibrillary eosinophilic cytoplasm and vacuolations. There are abundant blood vessels in the surrounding stroma.
tumours are similar to GIST with respect to histology and immunophenotype; however, they are more aggressive, and similar to small intestinal GIST.7,8 Patients with GIST present with vague abdominal pain, distention, or bleeding (haematemesis, malaena, haematochezia). Other rare presentations are obstructive jaundice (duodenal GIST), and bowel obstruction (due to endophytic growth causing intussusception or lumen narrowing, or mesenteric growth causing volvulus).2,5,6
Histologically, GIST are classified into three types: spindle, epithelioid, and mixed pattern, of which the spindle variety is more common.2,9 Eighty-five percent of GIST are associated with KIT gene mutation, while 5–10% of cases are due to platelet-derived growth factor receptor A (PDGFRA) mutation.2,10 A product of the c-KIT gene, CD117, is present on the interstitial cells
of Cajal, which helps to differentiate GIST from other mesenchymal tumours.6,8 The basic pathology behind the development of GIST mutation in the KIT or PDGFRA gene, leads to increased tyrosine kinase activity and unchecked growth on the tumour. To combat this, various targeted molecular therapies have been approved for GIST, such as imatinib.11,12 Imatinib competitively inhibits KIT, BCR-ABL, and PDGFRA or B 2,9,11,12 Others, like sunitinib and regorafenib, are also in clinical use for patients with GIST who are resistant to imatinib therapy, or have recurrence of disease or metastasis.5
The single-most prognostic factor to determine the malignant potential is the tumour size; however, GIST of any size should not be considered as a benign entity.9 Other features are the location of tumour in the bowel, and high mitotic activity.5,11 Endoscopic ultrasound helps to
90 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Case Report
Figure 3: Axial sections of contrast-enhanced CT abdomen.
A B
determine the layer from which the submucosal lesions originate, apart from its endoscopic findings.12-15 However, exophytic lesions are not easily detected on endoscopy; in such cases, transabdominal ultrasound is the first modality to diagnose the GIST. Plus, core particles obtained from transabdominal ultrasound-guided biopsy are superior to endoscopic ultrasoundguided biopsy to assess the mitotic index, and determine risk for malignant potential.13 On transabdominal ultrasound, GIST are welldefined hypoechoic masses with smooth or lobulated margins. Small tumours are round while large tumours are oval or ovoid. Echogenicity is similar to that of the muscular layer of stomach or bowel.4,16,17
Two patterns are frequently encountered on ultrasound. Homogeneous solid mass is the most common pattern, and has low mitotic activity. Another pattern is heterogenous mass, with a central area of low echogenicity, which corresponds to fluid filled cavities of blood or necrosis.14 These tumours are usually large, and have high mitotic activity. Sometimes a fistula develops due to mucosal erosion in the central necrotic cavity of large tumours. They appear as linear hyperechoic areas with dirty post acoustic shadowing. If the tumour bleeds, acute haematomas are hyperechoic. Metastatic or advanced GIST post-treatment with tyrosine kinase inhibitors, typically have cystic appearance.18
On small bowel series, endophytic lesions show intraluminal defects. Exophytic lesions, unless large, are difficult to detect; they show mild luminal protrusion, and displacement of the adjacent bowel loops.3 Rarely, calcification is seen, showing irregular streaks or clumps of mottled calcification (mucinous adenocarcinoma of the stomach shows punctate calcification).3 Areae gastricae is normal in GIST, while it is obliterated in the mucosal disease.3 On profile view, barium study with the patient in upright position shows that the lesion has smooth margins, forming an obtuse angle with the GI wall, and a barium stalactite is seen draping down from the inferior surface.19 The same barium stalactite when viewed en face appears like a central-filled cavity within a lobulated submucosal lesion, due to ulceration. The ulceration or cavitation within the mass has direct communication with the bowel lumen. This
characteristic appearance is described as target or bull’s eye lesions.2,3
Exophytic lesion shows a central dimple or spicule at the apex of mass, as a result of traction in the gastric or bowel wall by the base of mass, thus helping to differentiate it from the extrinsic lesion.3 Findings on CT (the primary modality of choice for GIST): small GIST (<5 cm) show homogeneous enhancement and are round in morphology, while large GIST (>5 cm) are lobulated with heterogeneous enhancement, and are associated with degenerative changes, like necrosis, haemorrhage, and very rarely, calcification and metastasis as well.2,6,19,20
Irrespective of the tumour size, there is mucosal ulceration which leads to GI bleeding. Cavitation is also seen in GIST, which leads to air entrapment in the necrotic ulcer (Torricelli–Bernoulli sign). Necrosis and ulceration are common as it outgrows the blood supply, or if the endophytic growth causes thinning and stretching of the overlying mucosa layer.3
Gastric GIST shows an intermediate pattern of enhancement, while small bowel GIST shows marked arterial phase enhancement. ‘Tumour vessel’ sign, a feature of small bowel GIST due to early venous return and prominence of the draining vein, helps in tracing the origin of the tumour. A nodule within the mass is a sign of recurrence.1 Treatment of choice for resectable GIST is surgery, although neoadjuvant imatinib is given to reduce the tumour size, and postsurgery imatinib is administered to prevent recurrence of the disease for at least 3 years. In case of metastasis or recurrence, imatinib is a first line drug.4,10,11,20
CONCLUSION
Although CT is the modality of choice for GIST, it is imperative for a radiologist to be wellacquainted with various other non-cross section imaging, such as radiographs, small bowel series, and ultrasound, to increase the level of confidence in radiological diagnosis before histopathology and immunohistochemistry confirms it.
Creative Commons Attribution-Non Commercial 4.0 ● April 2024 ● Radiology 91 Case Report
References
1. Inoue A et al. Gastrointestinal stromal tumors: a comprehensive radiological review. Jpn J Radiol. 2022;40(11):1105-20.
2. Levy AD et al. Gastrointestinal stromal tumors: radiologic features with pathologic correlation. Radiographics. 2003;23(2):283304.
3. Gore RM et al. "Benign tumors," Levine MS, Gore RM (eds.), Textbook of Gastrointestinal Radiology Volume One (1994), Philadelphia: Saunders, pp.4358;640-4.
4. Udina EL, Fisher KL. Sonographic detection of a gastrointestinal stromal tumor of the stomach. J Diagn Med Sonogr. 2016;32(4):211-6.
5. Sandrasegaran K et al. Gastrointestinal stromal tumors: clinical, radiologic, and pathologic features. AJR Am J Roentgenol. 2005;184(3):803-11.
6. Nishida T, Hirota S. Biological and clinical review of stromal tumors in the gastrointestinal tract. Histol Histopathol. 2000;15(4):1293-301.
7. Miettinen M et al. Gastrointestinal stromal tumors/smooth muscle tumors (GISTs) primary in the omentum and mesentery: clinicopathologic and
immunohistochemical study of 26 cases. Am J Surg Pathol. 1999;23(9):1109-18.
8. Reith JD et al. Extragastrointestinal (soft tissue) stromal tumors: an analysis of 48 cases with emphasis on histologic predictors of outcome. Mod Pathol. 2000;13(5):577-85.
9. Hong X et al. Gastrointestinal stromal tumor: role of CT in diagnosis and in response evaluation and surveillance after treatment with imatinib. Radiographics. 2006;26(2):481-95.
10. Tirumani SH et al. Update on gastrointestinal stromal tumors for radiologists. Korean J Radiol. 2017;18(1):84-93.
11. Joensuu H et al. Management of malignant gastrointestinal stromal tumours. Lancet Oncol. 2002;3(11):655-64.
12. Rubin BP et al. Gastrointestinal stromal tumour. Lancet. 2007;369(9574):1731-41.
13. Dietrich CF et al. Imaging of gastrointestinal stromal tumours with modern ultrasound techniques− a pictorial essay. Gastroenterologe. 2012;50(5):457-67.
14. Seven G et al. Correlation of endoscopic ultrasonography features with the mitotic index in
2-to 5-cm gastric gastrointestinal stromal tumors. J Dig Dis. 2022;40(1):14-22.
15. Kim MN et al. Prediction of risk of malignancy of gastrointestinal stromal tumors by endoscopic ultrasonography. Gut Liver. 2013;7(6):642-7.
16. Chan KP. What’s the mass? The gist of point-of-care ultrasound in gastrointestinal stromal tumors. Clin Pract Cases Emerg Med. 2018;2(1):82-5.
17. Pinto V et al. Gastrointestinal stromal tumors mimicking gynecological masses on ultrasound: a report of two cases. Ultrasound Obstet Gynecol. 2007;30(3):359-61.
18. Wronski M et al. Gastrointestinal stromal tumors: ultrasonographic spectrum of the disease. J Ultrasound Med. 2009;28(7):941-8.
19. Vernuccio F et al. Imaging of gastrointestinal stromal tumors: from diagnosis to evaluation of therapeutic response. Anticancer Res. 2016;36(6):2639-48.
20. King DM. The radiology of gastrointestinal stromal tumours (GIST). Cancer Imaging. 2005;5(1):150-6.
FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM 92 Radiology ● April 2024 ● Creative Commons Attribution-Non Commercial 4.0 Case Report

Receive our free newsletters and alerts Get the latest updates on all our upcoming journals and receive first-class insights into ground-breaking news and advancements in medicine across multiple therapeutic areas. www.emjreviews.com Join our mailing list
