41 Influence of Potassium Intake on the Renoprotective Response to Sodium Restriction and Hydrochlorothiazide in Patients with Diabetic Nephropathy
van Lieshout et al.
44 Interaction of General Obesity and Abdominal Obesity, and Frailty in Patients with Chronic Kidney Disease
Yang et al.
45 Continuous Blood Pressure Monitoring with a Finger Cuff is Unsuitable for Intradialytic Blood Pressure Monitoring
Chaara et al.
47 Impact and Interest of Implementing the EKFC Formula over CKD-EPI for Estimating Glomerular Filtration Rate in Automated Estimated Glomerular Filtration Rate Reporting Within Laboratory Practice
Derain Dubourg et al.
Congress Interviews
49 Peter Stenvinkel
53 Jeroen de Baaij
57 Jasper Callemeyn
59 Elisabet Van Loon Feature
61 Is Lack of Consensus on the Management of Chronic Active Antibody-Mediated Rejection Harming Renal Transplant Recipients?
Rostaing Articles
64 Immune Complex-Mediated Membranoproliferative Glomerulonephritis Secondary to Primary Biliary Cholangitis: A Rare Case Report
Intas et al.
70 Accessibility and Affordability Issues for Renal Replacement Therapy Remain Challenges in Resource-Limited Healthcare Settings: A Case Report and Critique of Literature for Chronic Kidney and End-Stage Renal Disease
Nzayikorera
81 End-Stage Renal Disease and Neurological Connection
Choudhary et al.
"Rethinking kidney health and transforming kidney care was the theme for the 61st European Renal Association (ERA) Congress"
Editorial Board
Editor-in-Chief
Dr Angela Yee-Moon Wang Duke-NUS Medical School, Singapore
Professor Angela Yee-Moon Wang has a strong track record in clinical and academic nephrology, having served at the Department of Medicine, Queen Mary Hospital, the University of Hong Kong, SingHealth Duke-NUS Academic Medical Centre, and Department of Renal Medicine, Singapore General Hospital. Professor Wang is world recognised for her research in cardiovascular-kidney-metabolic health, trials, and innovations in biomarker research for personalised care.
Dr Sanjay Agarwal
Marengo Asia Group of Hospitals, India
Dr Ahmed Akl
Mansoura University, Egypt
Dr Mufti Baleegh
Khyber Medical College and Khyber Teaching Hospital, Pakistan
Prof Sebastjan Bevc University of Maribor, Slovenia
Dr Juliette Hadchouel
Hôpital Tenon, France
Prof Wolfgang Jelkmann University of Lübeck, Germany
Prof Djalila Mekahli University Hospitals Leuven, Belgium
Prof Harun Ur Rashid Kidney Foundation Hospital and Research Institute, Bangladesh
Prof Maurizio Salvadori Careggi University Hospital Florence, Italy
Dr Arjun Sekar
Rochester General Hospital, New York, USA
Dr Ankur Shah Brown University, Rhode Island, USA
Aims and Scope
EMJ Nephrology is an open access, peer-reviewed eJournal committed to all aspects of renal function and disease to help elevate the quality of nephrology healthcare.
The journal is published annually, six weeks after the European Renal Association (ERA) Congress, and features highlights from this congress, alongside interviews with experts in the field, reviews of abstracts presented at the congress, as well as in-depth features on congress sessions. EMJ Nephrology also covers advances within the clinical and pharmaceutical arenas by publishing sponsored content from congress symposia, which is of high educational value for healthcare professionals. This undergoes rigorous quality control checks by independent experts and the in-house editorial team.
EMJ Nephrology also publishes peer-review ed research papers, review articles, and case reports in the field. In addition, the journal welcomes the submission of features and opinion pieces intended to create a discussion around key topics in the field and broaden readers’ professional interests. The journal is managed by a dedicated editorial team that adheres to a rigorous double-blind peer-review process, maintains high standards of copy editing, and ensures timely publication.
EMJ Nephrology endeavours to enhance knowledge, stimulate discussion, and contribute to a better understanding of renal diseases. Our focus is on research that is relevant to all healthcare professionals in the field. We do not publish veterinary science papers or laboratory studies not linked to patient outcomes. We have a particular interest in topical studies that advance knowledge and inform of the coming trends affecting clinical practice in nephrology.
Further details on coverage can be found here: www.emjreviews.com
Editorial Expertise
EMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors who are recognised authorities in their respective fields.
• Peer review, which is conducted by expert reviewers who are invited by the Editorial team and appointed based on their knowledge of a specific topic.
• An experienced team of editors and technical editors.
Peer Review
On submission, all articles are assessed by the editorial team to determine their suitability for the journal and appropriateness for peer review.
Editorial staff, following consultation with either a member of the Editorial Board or the author(s) if necessary, identify three appropriate reviewers, who are selected based on their specialist knowledge in the relevant area.
All peer review is double blind. Following review, papers are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected.
Editorial staff have final discretion over any proposed amendments.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects. We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial.assistant@emjreviews.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in EMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
EMJ is distributed through controlled circulation to healthcare professionals in the relevant fields across Europe.
Indexing and Availability
EMJ is indexed on DOAJ, the Royal Society of Medicine, and Google Scholar®; selected articles are indexed in PubMed Central®
EMJ is available through the websites of our leading partners and collaborating societies. EMJ journals are all available via our website: www.emjreviews.com
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
All information obtained by EMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, EMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. EMJ is completely independent of the review event (ERA 2024) and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever. The cover photo is of Stockholm, Sweden, the location of ERA 2024.
Enesco, Laith Gergi, Katrina Thornber, Aleksandra Zurowska
Creative Director
Tim Uden
Design Manager
Stacey Rivers
Senior Designers
Roy Ikoroha, Steven Paul
Designer Owen Silcox
Junior Designers
Dillon Benn Grove, Shanjok Gurung
Business Unit Leader
Billy Nicholson
Marketing Director
Kristina Mestsaninova
Chief Content Officer
Justin Levett
Chief Commercial Officer
Dan Healy
Founder and Chief
Executive Officer
Spencer Gore
Welcome
Dear Readers,
I am thrilled to welcome you to the 2024 issue of EMJ Nephrology, covering key highlights from the 61st European Renal Association (ERA) Congress, which took place in Stockholm, Sweden. The focal point of this year's programme were the clinical trial sessions, presenting updates from multiple landmark trials.
Our Congress features explore the current advances and clinical trial landscape for IgA nephropathy and membranous nephropathy, and managing hypertension in individuals with kidney disease. We are proud to feature interviews with local Congress President, Peter Stenvinkel, as well as three of the ERA Young Investigators Award Winners, for their research in basic and translational science.
Make sure not to miss a feature discussing chronic active antibodymediated rejection in patients who have undergone renal transplantation, focusing on the underuse of diagnostic protocols and lack of treatment options beyond immunosuppression.
This issue spans diverse nephrology topics, hoping to offer something for everyone. I would like to thank our Editorial Board, authors, peer reviewers, and interviewees for their contributions in helping to bring this compelling issue to life. I would also like to invite you, our valued readers, to engage with us by providing feedback on our content via our website. This will be pivotal in helping us to shape the future direction of the journal, and deliver relevant, timely, and high-quality content.
We look forward to the 2025 issue, but until then, we hope you enjoy reading EMJ Nephrology 12.1!
Editorial enquiries: editor@emjreviews.com
Sales opportunities: salesadmin@emjreviews.com
Permissions and copyright: accountsreceivable@emjreviews.com
Editor
Reprints: info@emjreviews.com
Media enquiries: marketing@emjreviews.com
Evgenia Koutsouki
Foreword
I am honoured to welcome you to the latest issue of EMJ Nephrology. Firstly, I would like to thank the commitment and efforts of all authors, peer reviewers, and Editorial Board members who have made the publication of the most upto-date research in this journal possible.
This year’s issue comprises a selection of original peer-reviewed articles, features, and interviews, alongside a comprehensive review of the 61st European Renal Association (ERA) Congress 2024, which took place in person in Stockholm, Sweden, between the 23rd–26th of May. The overarching theme for this year’s congress was ‘Rethinking Kidney Health and Transforming Kidney Care’. Specifically, the congress drew attention to looking to nature for solutions to human health and disease, and saw Barbara Natterson-Horowitz, University of California, Los Angeles (UCLA) School of Medicine, USA, deliver a fascinating plenary on this topic. The congress also spotlighted research on early detection, targeted screening programs, and educating the community about kidney disease risk factors and lifestyle changes.
For those who were unable to attend, our review of the ERA 2024 Congress includes coverage of late-breaking news on cutting edge clinical trial data, including the FLOW Study and the SELECT, ALIGN, and APPEAR-C3G trials, as well as research abstract reviews and topical features from key congress sessions.
The articles in this year’s issue cover important topics, including membranoproliferative glomerulonephritis secondary to autoimmunity, and neurological complications in end-stage renal disease.
You will also find a fascinating feature article by Lionel Rostaing, CHU Grenoble Alpes, France, which explores how an absence of expert consensus on managing chronic active antibody-mediated rejection is holding back kidney transplantation advancements. Other featured articles explore how the accessibility and affordability of renal replacement therapy represent a significant challenge in resource-limited healthcare settings.
Finally, I would like to express my appreciation for your continued support. I hope that you enjoy this issue of EMJ Nephrology and find it a valuable resource in shaping your daily practice.
The congress drew attention to looking to nature for solutions to human health and disease
Angela Yee-Moon Wang
Clinical Professor and Senior Consultant, Duke-National University of Singapore (NUS) Academic Medical Centre, Singapore General Hospital, Singapore
ERA 2024
We can pave the way for innovative, natural approaches to prevention, diagnosis, and treatment of kidney disease
Review of the 61st European Renal Association (ERA) Congress Congress Review
RETHINKING kidney health and transforming kidney care was the theme for the 61st European Renal Association (ERA) Congress, which took place in Stockholm, Sweden, between the 23rd–26th May. As the location of the first Nobel Prizes in Physics, Chemistry, Physiology or Medicine, and Literature; Stockholm provided an ideal backdrop for the event.
This year, the congress saw an attendance of 7,448 delegates. The programme comprised 47 main symposia and 26 free communication sessions; with over 2,200 abstracts from 82 countries submitted. With a programme dedicated to improving kidney health and the education around lifestyle and risk factors, the seven main tracks for the Congress were physiology, cell biology, and genetic diseases; glomerular and tubule-interstitial diseases; chronic kidney disease (CKD); dialysis; kidney transplantation; hypertension and diabetes; and acute kidney injury and critical care nephrology.
The Welcome Ceremony saw local Congress President, Peter Stenvinkel, welcome delegates and deliver a thoughtprovoking speech on the progress made in nephrology, and how planetary health and interconnectedness could help shed light on further understanding kidney disease and developing novel therapeutic targets.
Stenvinkel discussed that despite being known as the discipline of negative trials for many years, new understanding has paved the way for remarkable advances, including over 12 clinical trials in IgA nephritis at
present. He drew focus to the late-breaking clinical trials sessions, emphasising to the audience that: “We are part of the most exciting times in nephrology.”
Considering the focus on planetary health, Stenvinkel spoke on the contribution of global warming and air pollution in causing new cases of kidney disease globally, and that worldwide CKD prevalence is a barometer of planetary health; noting that the environment is an emerging concern for the field of nephrology. He explained that planetary health is the science of interconnectedness and stressed that healthcare professionals need to learn how to connect the dots and embrace interdisciplinary collaboration. Understanding of the interconnectedness and influence of multiple factors, including diet, lifestyle, genetics, and the environment on kidney health, will help to elucidate novel pathways underlying kidney disease development and progression. Stenvinkel implored that researchers can harness the butterfly effect by adopting a comprehensive approach to studying kidney disease and examining how seemingly unrelated factors interact to uncover novel insights into disease
mechanisms and potential novel therapeutic targets. He stated: “By acknowledging the interconnected nature of biological systems and environmental factors, we can pave the way for innovative, natural approaches to prevention, diagnosis, and treatment of kidney disease.”
Worldwide CKD prevalence is a barometer of planetary health
Following this, Stenvinkel invited His Royal Highness, Prince Daniel, Prince of Sweden and Duke of Vastergotland, to join the stage. Prince Daniel reflected on his own personal experience as a renal transplant recipient and discussed the enormous burden CKD has on healthcare systems, which is of particular importance as the global prevalence rises. He highlighted global inequalities in access to treatment, which underscores the urgent need for continued efforts in research, education, and policy advocacy, and also stressed that the environmental factors that impact kidney disease (climate change, pollution, and water shortages) must be addressed. He concluded by expressing gratitude to those who dedicate their lives to improving
opportunities for patients, before leaving the stage.
The Welcome Ceremony then saw ERA President, Christoph Wanner, deliver the Presidential Address. Wanner placed emphasis on the four late-breaking clinical trial sessions offered in this year’s programme, which is more than ever before. With hope for the future, he noted that there are many news therapeutics on the horizon to be investigated. However, he stressed that in order to carry the success of renal medicine ahead, these therapeutics and patients with kidney disease need to be given the chance to be included in clinical studies. Noting that whilst science is global, implementation is local, as the field strives to bring medications to those who need them; Wanner called on healthcare providers, authorities, and players in Europe to action, to evaluate the four foundational therapies that can help prevent patients from progressing to dialysis.
Spotlighting clinical science, education, and the transfer of knowledge to patients, as the main goals of ERA, Wanner expressed his hope to see this become a reality in the future, before moving on to present this year’s awards and diplomas. Albert Ong,
Chair of the Scientific Committee, was called to the stage to receive a diploma in honour of his service to delivering the 2024 ERA Congress programme.
Subsequently, Wanner presented the 2024 ERA awards. These included the award for outstanding clinical contributions to nephrology, presented to Jack Wetzels, Radboud University, Nijmegen, the Netherlands; the award for outstanding basic science contributions to nephrology, bestowed to Ariela Benigni, Mario Negri Institute, Bergamo, Italy; and the award for research excellence in nephrology, granted to Kerstin Amann, University of Erlangen, Germany. Alongside these, two new awards for outstanding contribution to the society and excellence in the field of sustainable nephrology were presented to Mehmet Sükrü Sever, Istanbul University, School of Medicine, Türkiye; and Giorgina Piccoli, Centre Hospitalier Le Mans, Torino, Italy, respectively.
Wanner also presented awards to acknowledge young investigators who stimulate the dialogue between research and education. Jeroen de Baaji, Radboud University Medical Centre, Nijmegen, the Netherlands, received the Rosanna Gusmano Award for Young Investigators in basic science; the Eberhard Ritz Award for Young Investigators in clinical science was awarded to Andreas Kronbichler, University Hospital Innsbruck, Austria; and the Stanley Shaldon Award for Young Investigators in translational science was awarded to both Elisabet Van Loon and Jasper Callemeyn, University Hospital Leuven, Belgium.
Following the award presentations, the Welcome Ceremony concluded with a performance by the Super Trouper ABBAshow, to celebrate the 50-year anniversary since winning the Eurovision Song Contest.
EMJ were thrilled to be part of the 2024 Congress, and look forward to attending the 2025 ERA Congress, which will take place in Vienna, Austria. Until then, read on to enjoy highlights presented at this year’s Congress.
47
2,200
7,448
main symposia abstracts from 82 countries delegates
Semaglutide Reduces Major Kidney Events in Patients with Type 2 Diabetes
RESEARCH presented at the 61st ERA Congress by Vlado Perkovic, University of New South Wales, The George Institute, and Royal North Shore Hospital, Sydney, Australia, has shown the potential of semaglutide, a glucagon-like peptide-1 (GLP-1) receptor agonist, in improving patient outcomes.
Results showed that patients receiving semaglutide experienced a
24 in the risk of composite primary endpoint %
Findings demonstrated that semaglutide can significantly lower the risk of major kidney disease events, cardiovascular outcomes, and all-cause mortality in patients with Type 2 diabetes and chronic kidney disease (CKD).
The FLOW study (Evaluate Renal Function with Semaglutide Once Weekly) investigated how semaglutide can potentially benefit patients with Type 2 diabetes and CKD. The randomised, double-blind, placebocontrolled trial involved 3,533 patients over a median follow-up period of 3.4 years. Patients were randomly assigned to receive either a weekly subcutaneous injection of semaglutide at 1.0 mg or a placebo.
Results showed that patients receiving semaglutide experienced a 24% reduction in the risk of composite primary endpoint, which included major kidney outcomes and death, resulting from cardiovascular and kidney causes, compared to placebo patients. The reduction risk was
consistent across both cardiovascular and kidney-specific related death outcomes. Semaglutide also improved secondary endpoints; the total estimated glomerular filtration rate slope was 1.16 mL/min/1.73 m2/year slower in the semaglutide group, indicating a slower decline in kidney function. Additionally, there was an 18% reduction in the risk of major cardiovascular events and a 20% reduction in all-cause mortality among patients given semaglutide.
This study’s findings highlight the potential clinical implications of semaglutide, which not only reduces the risk of major kidney and cardiovascular events, but also significantly lowers the risk of all-cause mortality. This substantially highlights the potential of semaglutide to transform treatment strategies for highrisk patients. The promising results of the FLOW trial show semaglutide as a crucial therapeutic option, potentially reshaping the management of kidney and cardiovascular health in patients with Type 2 diabetes.
New Technique Detects Novel Biomarkers for Kidney Diseases with Nephrotic Syndrome
RESEARCHERS discovered that anti-nephrin autoantibodies serve as a reliable biomarker for tracking disease progression in nephrotic syndrome, and presented their findings at the 61st ERA Congress.
Findings showed these autoantibodies were present in 69% of adults with MCD and 90% of children with INS who had not been treated with immunosuppressive drugs
Nephrotic syndrome is an immune-mediated podocytopathy, leading to protein leakage into the urine and elevated proteinuria. Kidney diseases such as minimal change disease (MCD), primary focal segmental glomerulosclerosis, and membranous nephropathy (MN) are linked to the manifestation of nephrotic syndrome. Diagnosis of idiopathic nephrotic syndrome (INS) is often made in children with MCD and focal segmental glomerulosclerosis. Diagnosing these conditions has traditionally been challenging because of overlapping histological features and the hesitance to conduct invasive biopsies, especially in children. The identification of novel nephrotic syndrome biomarkers paves the way for potential personalised treatment approaches.
A multicentre study conducted across Europe and the USA analysed anti-nephrin autoantibodies in 539 patients with glomerular diseases, introducing a novel technique combining immunoprecipitation with enzyme-linked immunosorbent assay to detect anti-nephrin autoantibodies reliably. Findings showed these autoantibodies were present in 69% of adults with MCD and 90% of children with INS who had not been treated with immunosuppressive drugs. The levels of these autoantibodies correlated with disease activity, suggesting their potential
as a biomarker for monitoring disease progression. These antibodies were rarely observed in other kidney diseases studied. Moreover, the research group created an experimental mouse model through active immunisation with recombinant mouse nephrin, which induced a condition similar to MCD. This led to nephrin phosphorylation and significant changes in cell structure, indicating that antibodies targeting nephrin contribute to podocyte malfunction and nephrotic syndrome. Remarkably, this model induced rapid disease manifestation with a single immunisation, even at low antibody concentrations.
Co-lead author of the study, Nicola M. Tomas, University Medical Center HamburgEppendorf, Germany, commented: “The identification of anti-nephrin autoantibodies as a reliable biomarker, combined with our hybrid immunoprecipitation technique, enhances our diagnostic capabilities and opens new avenues for closely monitoring disease progression in kidney disorders with nephrotic syndrome.” Tobias B. Huber, University Medical Center HamburgEppendorf, also a co-lead author of the study, concluded: “By providing insights into underlying mechanisms, these findings lay the groundwork for personalized interventions and pave the way for a new era of precision medicine for these complex conditions.”
Iptacopan Delivers New Hope for C3 Glomerulopathy
IPTACOPAN significantly and meaningfully reduced proteinuria in patients with C3 glomerulopathy (C3G) at 6 months, according to results from the APPEAR-C3G study, presented at the ERA Congress 2024.
C3G is an ultra-rare and severe proliferative glomerulonephritis, characterised by the dysregulation of the alternative complement pathway (AP). Iptacopan, a proximal complement inhibitor, selectively targets Factor B, thereby inhibiting the AP. The APPEAR-C3G Phase III study was designed to assess the efficacy, safety, and tolerability of iptacopan in comparison to placebo for patients with C3G.
APPEAR-C3G was a multicentre, randomised, double-blind, parallelgroup, placebo-controlled, pivotal trial. It included 74 adult patients with biopsyconfirmed C3G, reduced serum C3 levels (<77 mg/dL), urinary protein-to-creatinine ratio (UPCR) of ≥1.0 g/g, and estimated glomerular filtration rate (eGFR) of ≥30 mL/min/1.73 m². All participants received the maximum tolerated dose of reninangiotensin-aldosterone system blockade and vaccinations against encapsulated bacteria before randomisation. The study involved a screening period of up to 90 days, a 6-month randomised double-blind treatment phase (iptacopan 200 mg two times a day versus placebo), and a 6-month open-label iptacopan treatment phase. Historical eGFR data from 2 years prior to screening were used in pre-specified exploratory statistical analyses. The primary objective was to demonstrate the
superiority of iptacopan over placebo in reducing proteinuria, measured by UPCR, after 6 months.
Out of 132 screened patients, 74 were randomised (1:1) to receive either iptacopan (n=38) or placebo (n=36). At 6 months, iptacopan showed a significant reduction in 24-hour UPCR, compared to placebo. Patients on iptacopan had a seven-fold increase in the odds of achieving the composite endpoint of ≥50% proteinuria reduction and stable eGFR. There was an improvement in eGFR (+2.2 mL/min/1.73 m²; nominal 1-sided p=0.1945) with iptacopan, as well as a reduction in total histologic disease activity score. Iptacopan significantly increased serum C3 (185%), and decreased AP activity (37.3%), plasma sC5b-9 (65.1%), and urinary sC5b9/creatine (77.3%). It exhibited a favourable safety profile with no new safety signals, no deaths, and minimal serious adverse events. One serious pneumococcal infection, likely related to iptacopan, was successfully treated with antibiotics.
Results from the APPEAR-C3G trial demonstrated that the use of iptacopan significantly, meaningfully, and safely reduces UPCR and proteinuria in patients with C3G, with a positive trend in eGFR improvement.
It exhibited a favourable safety profile with no new safety signals, no deaths, and minimal serious adverse events
Atrasentan Significantly Reduces Proteinuria Associated with IgA Nephropathy
RESULTS
from ALIGN, an ongoing, Phase III clinical trial, demonstrate that atrasentan, a selective endothelin A (ETA) receptor antagonist, reduces proteinuria in patients with IgA nephropathy (IgAN) at high risk of kidney function loss.
The findings were presented at the 61st ERA Congress, which took place in Stockholm, Sweden, between 23rd–26th May 2024.
Hiddo J.L. Heerspink, University Medical Center Groningen, the Netherlands, and colleagues, investigated the efficacy and safety of atrasentan, including its impact on proteinuria, kidney inflammation, and fibrosis. The trial consisted of 340 patients with biopsy-proven IgAN, with proteinuria of at least 1 g/day. For the primary analysis, 270 patients were randomised to receive either atrasentan 0.75 mg or placebo daily for 132 weeks, alongside their standard medication routine. The researchers evaluated changes in proteinuria by measuring the urine protein to creatinine ratio (UPCR) from 24-hour urine collections, comparing baseline levels to those at Week 36. UPCR reductions in atrasentantreated patients were seen as early as the first 6 weeks of treatment, and at Week 36 patients treated with atrasentan experienced a 36.1% greater reduction in the mean percentage change in UPCR from baseline, compared to those who received placebo (p<0.0001).
Additionally, the researchers investigated the safety of atrasentan in this patient
cohort. There were significantly more instances of fluid retention (11.2% versus 8.2%), anaemia (8.3% versus 2.4%), and hypotension (5.9% versus 4.1%) in patients receiving atrasentan, compared to placebo. However, the number of moderate, severe, and serious treatment-emergent adverse events were similar between those receiving atrasentan and those with placebo.
The final analysis of ALIGN will elucidate the effect of atrasentan on glomerular filtration rates
The interim results of ALIGN have demonstrated that atrasentan significantly reduced proteinuria in patients with IgAN, without an increase in moderate, severe, or serious treatment-emergent adverse events. Additionally, in a future report, the final analysis of ALIGN will elucidate the effect of atrasentan on glomerular filtration rates. The researchers will also report the results of atrasentan usage in patients also receiving sodium-glucose transport protein 2 inhibitor. Nevertheless, the current results indicate that atrasentan is a safe and effective treatment for proteinuria associated with IgAN.
BMI Impacts Mortality Risk Differently in Dialysis Patients
RESEARCH at the 61st ERA Congress investigated the association between the different effects of BMI on all-cause mortality in patients with diabetes who are undergoing different types of dialysis: maintenance haemodialysis (HD) and peritoneal dialysis (PD).
This suggests that patients on HD with high BMIs are not at high risk of mortality
The study used data from the Swedish Renal Registry (SRR), which included 3,235 patients who are diabetic and on dialysis. Of those, 2,452 patients were on HD and 783 were on PD. The patients were divided into six groups based on BMI categories, defined by the World Health Organization (WHO). The follow-up period was 3.9±3.5 years, and patients who switched dialysis types during the study were excluded.
Results showed that patients on HD with a low BMI of ≤18.5 had a significantly higher risk of all-cause mortality compared to the reference group (18.5<BMI≤25.0 kg/m2), with a hazard ratio (HR) of 1.94. Meanwhile, patients on HD with high BMIs of 25.1–30.0 kg/m² (HR: 0.84; classed as overweight), 30.1–35.0 kg/m² (HR: 0.66; Class 1 obesity), and 35.1-40.0 kg/m² (HR: 0.65; Class 2 obesity) had a lower risk of mortality compared to the reference group. This suggests that patients on HD with high BMIs are not at high risk of mortality. However, patients on PD have shown no significant association between BMI and allcause mortality across all BMI categories. This indicates that BMI may not be a critical factor in predicting mortality risks for patients on PD.
The study concluded that patients with diabetes who are overweight and undergoing maintenance HD face an increased risk of all-cause mortality. Patients who are overweight or have Class 1 or Class 2 obesity showed a significant link to better survival rates. However, in patients who are diabetic and on PD, BMI did not significantly influence mortality risk. These findings highlight the importance of keeping different dialysis types under consideration when evaluating the impact of BMI on survival outcomes in patients who are diabetic.
IL-6 Inhibition in Patients with Cardiovascular Disease and Diabetes
INFLAMMATORY biomarkers associated with cardiovascular events and diabetes are significantly reduced with clazakizumab, according to research presented at the 2024 ERA Congress.
Glenn Chertow, Stanford University School of Medicine, USA, and colleagues, presented the findings of Phase IIb of the POSIBIL6ESKD trial, which assessed the impact of IL-6 inhibition with clazakizumab in patients with cardiovascular disease or diabetes on dialysis.
In the trial, 127 patients received a low, medium, or high dose of clazakizumab or placebo every 4 weeks for up to six doses. At Week 12, the geometric mean ratio to baseline serum high-sensitivity C-reactive protein (hs-CRP) concentration was compared between groups.
It was found that treatment with clazakizumab significantly reduced hsCRP at Week 12 in the low, medium, and high dose groups, compared to placebo (decreased by 89%, 92%, and 93%, respectively; p<0.0001). Whilst no patients in the placebo group achieved normalisation of hs-CRP (<2.0 mg/L), it was achieved in 79.2%, 82.1%, and 79.3% in the low, medium,
and high dose groups, respectively. The results demonstrated that clazakizumab caused significant reductions in the following downstream IL-6 biomarkers: fibrinogen, serum amyloid A, secretory phospholipase A2, and lipoprotein(a). Furthermore, there was an increase of at least 0.17 g/dL of mean serum albumin in those treated with clazakizumab. Regarding the safety and tolerability of clazakizumab, there were no cases of sustained Grade 3 or 4 thrombocytopenia or neutropenia.
The results of the POSIBIL6ESKD trial demonstrated that clazakizumab is safe for reducing inflammatory biomarkers in patients with cardiovascular disease or diabetes dialysis. These findings suggest that clazakizumab may reduce the risk of cardiovascular mortality and morbidity associated with IL-6 and its downstream biomarkers in these patients, highlighting its potential as a therapeutic option to improve cardiovascular outcomes in this high-risk population.
Clazakizumab
may reduce the risk of cardiovascular mortality and morbidity associated with IL-6
Pollution's Hidden Toll: Kidney Disease Mortality
AIR pollution has been associated with chronic kidney disease (CKD)-related mortality, according to results from a study by Emanuel Zitt and team, presented at the ERA Congress 2024.
Air pollution has previously been linked to various cause-specific mortalities, yet its impact on CKD-related mortality remains under-researched, particularly within Europe. This study aimed to investigate the relationship between long-term air pollution exposure and CKD-associated mortality using data from Effects of Low-Level Air Pollution: A Study in Europe (ELAPSE).
The results from this study suggest a possible association between air pollution and CKD-related mortality
Data were collected from five populationbased cohorts across four European countries, which were pooled into the ELAPSE cohort. Mortality data were obtained from local registries, identifying CKD-associated deaths, and annual mean exposure levels at home addresses were estimated using Europe-wide hybrid land use regression models for nitrogen dioxide (NO2), black carbon (BC), ozone (O3), particulate matter ≤2.5µm (PM2.5), and several elemental constituents of PM2.5 with a spatial resolution of 100 m2. Cox regression models adjusted for age (time-axis), cohort and sex (strata), calendar year of recruitment, smoking status, marital status, employment status,
and neighbourhood mean income were employed to analyse the data.
Over a mean follow-up period of 20.4 years, 313 out of the 289,564 included individuals died from CKD. Positive associations were observed for PM2.5 (hazard ratio [HR]: 1.31; 95% CI: 1.03–1.66; per 5 µg/m3 increase), BC (HR: 1.26; 95% CI: 1.03–1.53; per 0.5x10−5/m), and NO2 (HR: 1.13; 95% CI: 0.93–1.38; per 10 µg/ m3). Conversely, O3 showed a negative association (HR: 0.71; 95% CI: 0.54–0.93; per 10 µg/m3). These results remained robust after additional adjustments for smoking intensity and duration, BMI, education, and residential greenness; but were sensitive to cohort selection, with the large Austrian cohort contributing 226 cases. Elemental constituents such as copper, iron, potassium, nickel, sulfur, and zinc, associated with various PM2.5 sources (traffic, industry, biomass and oil burning, and long-range transport), were also linked to CKD-related mortality.
The results from this study suggest a possible association between air pollution and CKD-related mortality. This indicates that improving air quality may benefit renal health, highlighting the importance of air pollution control measures as health measures.
Prednisolone Dosage Comparison: Remission and Safety
MINIMAL change disease (MCD) is typically treated with high-dose prednisolone, and these have notable side effects.
with similar rates between the two groups (p=0.502) % The overall remission rate was
Observations suggest that active vitamin D might stabilise the glomerular filtration barrier, reducing albuminuria and benefiting patients with MCD. Findings from a trial that evaluated whether combining lower-dose prednisolone with alfacalcidol would be as effective as high-dose prednisolone in achieving remission and time to remission in patients with MCD, potentially with fewer adverse effects, were presented at the 61st ERA Congress.
In a Danish, multicentre, prospective, open-label, randomised controlled trial, adults with confirmed MCD and nephrotic syndrome were enrolled. Patients were randomised 1:1 to receive either prednisolone 1 mg/kg/day or prednisolone 0.5 mg/kg/day with alfacalcidol 0.5 μg daily. Doses remained the same for 4–16 weeks if remission was not achieved. Remission denotes the urine albumin-creatinine ratio <300 mg/g in two samples. Upon remission, prednisolone was tapered over 25 weeks. Patients were followed for up to a year post-remission. Primary endpoints were time to remission and remission rate, while secondary endpoints included adverse events. The mean follow-up was 40.8 weeks.
A total of 70 patients were randomised equally into two treatment groups, out
of which three were excluded due to diagnosis revision or protocol violation but were included in the intention-to-treat analyses. Baseline characteristics were similar. The cumulative prednisolone dose until remission was significantly lower in the lower-dose prednisolone/alfacalcidol group (1,413 mg versus 2,240 mg in the higher dose group; p=0.002). The overall remission rate was 86%, with similar rates between the two groups (p=0.502). Median time to remission was also comparable (23 days [interquartile range: 12–43] for high-dose prednisolone versus 25 days [interquartile range: 15–35] for lower-dose prednisolone/alfacalcidol; p=0.430). Results were consistent even after excluding the three patients. Severe adverse events were higher in the high-dose prednisolone group compared to the lower-dose prednisolone/alfacalcidol group (10 versus 6, respectively). The most common severe adverse events were infections, with four cases, all in the high-dose prednisolone group.
Combining prednisolone 0.5 mg/kg/day with alfacalcidol showed similar effectiveness to prednisolone 1 mg/kg/day in achieving remission and time to remission in patients with MCD. Severe adverse events were more frequent with high-dose prednisolone.
Incidence of Post-operative Acute Kidney Injury in Males Compared to Females
ACUTE kidney injury (AKI) impacts approximately 6–8% of patients undergoing general elective surgeries, significantly raising the risk of mortality by three-fold.
Additionally, AKI increases the likelihood of developing chronic kidney disease and end-stage renal disease by eight- and three-fold, respectively. It was previously hypothesised that females were at a higher risk for postoperative AKI; however, recent research presented at ERA Congress 2024 showed that AKI occurs more frequently in hospitalised males than females (odds ratio: 2.2). Moreover, females appear to have a protective advantage against AKI until menopause, suggesting that male sex is a risk factor for AKI. Consequently, the researchers hypothesised that males would have a higher incidence of postoperative AKI than females following radical colorectal surgery. The primary objective of the study was to examine and compare the incidence of postoperative AKI in males and females undergoing radical colorectal surgery.
Researchers used the Cancer and Anesthesia: Survival After Radical Surgery (CAN) study database to conduct a post hoc analysis. Termed the Propofol or Sevoflurane Anesthesia in Colon Cancer (PROSACC) study, it aimed to analyse postoperative AKI incidence. The CAN study was a randomised, multicentre study comprising patients with cancer receiving radical surgery at hospitals in China, Croatia, Poland, and Sweden. Patients enrolled in the study underwent colorectal
surgery, and 3,254 patients were included in the analysis. The study's primary outcome was AKI incidence, which was determined by measuring changes in plasma creatinine, while the secondary outcome was gender association with AKI. The secondary outcome was statistically analysed using Pearson’s chi-square test.
Of the 3,254 patients, 2,741 had their postoperative plasma creatinine levels recorded on postoperative Days 1–3, while 986 patients had their creatinine values measured on Days 4–10. Results revealed that, from Days 1–3, 193 patients developed AKI, of which 6% were female and 8% were male (p=0.190); whereas on Days 4–10, 87 patients developed AKI, of which 6% were female and 11% were male (p=0.004). Moreover, results demonstrated that female sex is associated with a 60% decrease in the odds of AKI.
These findings prompted the authors to conclude that at timepoint 4–10 days following radical colorectal surgery, the incidence of AKI is twice as high in males compared to females. Females in this study had higher preoperative risk factors; therefore, the results align with the hypothesis that male sex is a risk factor for postoperative AKI.
Moreover, females appear to have a protective advantage against AKI until menopause, suggesting that male sex is a risk factor for AKI
Semaglutide Proves Promising in Protecting Kidney Function in Patients with Cardiovascular Disease and Obesity
DATA from the SELECT trial (Semaglutide Effects on Heart Disease and Stroke in Patients Overweight or Obesity), was presented at the 61st ERA Congress by
Helen M Colhoun, Institute of Genetics and Cancer, Edinburgh, UK.
The results revealed that semaglutide significantly reduced major kidney-related complication risk in individuals who are overweight or obese without diabetes.
The multicentre randomised, double-blind, placebo-controlled trial aimed to investigate the potential of semaglutide in combatting renal function decline in 17,604 individuals who were overweight or obese (BMI ≥27 kg/m2) with established cardiovascular disease (prior myocardial infarction, prior stroke, or symptomatic peripheral arterial disease), but without diabetes. Patients were initiated on 0.24 mg and escalated up to the maintenance dose of 2.4 mg by Week 16. The median follow-up was 182 weeks.
Semaglutide significantly reduced major kidney-related complication risk in individuals who are overweight or obese
The results showed that patients receiving subcutaneous injections of semaglutide at a dose of 2.4 mg once a week experienced 22% fewer adverse kidney-related events (defined using a five-component composite kidney endpoint) compared to individuals in the placebo arm. The five-component composite score comprised: death resulting from kidney causes, initiation of chronic kidney replacement therapy (dialysis or transplantation), onset of a persistent
estimated glomerular filtration rate (eGFR) <15mL/min/1.73m², persistent ≥50% reduction in eGFR compared to baseline, and onset of persistent macroalbuminuria.
At 104 weeks, the investigators examined the change in eGFR and urinary albumincreatinine ratio (UACR) associated with treatment. This revealed that semaglutide recipients showed a significantly lesser decline in eGFR, especially in participants with baseline eGFR below 60 mL/ min/1.73 m², indicating better kidney function preservation. However, among semaglutide-treated patients, there was also a substantial decrease in UACR; with reductions of 8.1% in those with normal albumin levels, 27.2% in those with microalbuminuria, and 31.4% in those with macroalbuminuria at baseline compared to placebo.
The study results suggest that semaglutide provides a renal benefit in individuals without diabetes who are overweight or obese, with a 22% reduction in the fivecomponent composite kidney endpoint achieved in those randomised to 2.4 mg of subcutaneous semaglutide once per week. The observed effects on eGFR and UACR suggest enhanced management of kidney complications, and these benefits were most notable in those with an eGFR <60 mL/min/1.73 m² and albuminuria, respectively.
Advancements in Glomerulonephritis Treatment: The Impact of Recent Clinical Trials
ELENI Frangou, Limassol General Hospital, Cyprus; and Andreas Kronbichler, Medical University of Innsbruck, Austria, chaired the first symposium of the 61st European Renal Association (ERA) Annual Congress held in Stockholm, Sweden, between the 23th–26th of May. This session evaluated recent clinical trials in glomerulonephritis, from the rapid expansion of clinical trials for IgA nephropathy (IgAN) to the potential of complement and plasma cells as therapeutic targets in membranous nephropathy (MN).
NEW CLINICAL TRIALS IN IgA NEPHROPATHY
IgAN is a progressive, immune complexmediated disease, and the most common primary glomerulonephritis, representing the leading cause of chronic kidney and end-stage renal disease. The mechanism of IgAN involves the formation and deposition of circulating IgA-immune complexes in the glomeruli, triggering inflammation scarring, nephron loss, and ultimately kidney failure.
Johnathon Barratt, University of Leicester, UK, commenced the session by delivering a talk on the transformative progress of clinical trials for IgAN. For two-thirds of Barratt’s career, the clinical trial landscape for IgAN resembled a desolate desert, with patients relying on renin–angiotensin–aldosterone system inhibition (RAAS-i) and lifestyle modifications, inevitably destined for dialysis. However, over the past decade, this stagnation has given way to an explosion in new clinical trial activities. Barratt attributes this shift to several critical factors, including regulatory changes, enhanced understanding of disease pathogenesis, and evolving clinical guidelines.
REGULATORY CHANGES AND CLINICAL GUIDELINES
Drug development in IgAN had been largely static for decades due to the lack of validated measurements for clinical outcomes in large-scale, long-term clinical trials. A pivotal moment in IgAN research was the publication of a study that established proteinuria reduction as a surrogate endpoint for clinical endpoints in IgAN.1 This triggered a re-evaluation by drug regulators of how drug efficacy is assessed in rare kidney diseases. Barratt highlighted the collaboration between academic nephrologists and industry partners, exemplified by the Kidney Health Initiative: a partnership between the American Society of Nephrology (ASN) and the U.S Food and Drug Administration (FDA). The Kidney Health Initiative endorsed the use of early proteinuria changes, observable around 9 months, as a recognisable and provable endpoint for primary glomerular diseases, a criterion now accepted in both the USA and Europe.
This regulatory framework has reshaped clinical trials, enabling the pharmaceutical industry to invest in IgAN treatments confidently. Trials now typically involve
GLOMERULAR INFLAMMATION AND CHRONIC KIDNEY DISEASE CONSEQUENCES
Barratt detailed the strategies for mitigating glomerular inflammation, a key factor in IgAN progression. While systemic glucocorticosteroids are effective antiinflammatories, their significant side effects limit their long-term use. Complement inhibition has emerged as a promising alternative. Trials targeting components of the complement system, such as factor B, D, and C5, have shown potential in reducing proteinuria and inflammation, with drugs like ravulizumab demonstrating significant efficacy.
The average glomerular filtration rate when IgAN diagnosis is made is between 50–60 mL/min, which informs nephrologists that close to half of a patient’s nephrons have been lost. Therefore, when treating IgAN, it is crucial to address maladaptive downstream responses of nephron loss, such as systemic hypertension, glomerular hyperfiltration, and proteinuria, which can contribute to segmental scarring. Managing the downstream consequences of IgAN, particularly in chronic kidney disease,
has seen advancements. New therapies, including sodium-glucose cotransporter 2 inhibitors and endothelin receptor antagonists, have shown effectiveness in preserving kidney function. The PROTECT trial, for example, demonstrated that sparsentan, an oral dual endothelin angiotensin II receptor antagonist, significantly slows kidney function decline.2 Sparsentan received accelerated approval from the FDA in 2023 for proteinuria reduction in high-risk patients with IgAN, with continued approval hinging on sparsentan delaying long-term kidney function decline.
FUTURE PROSPECTS
Barratt stated that the future of IgAN treatment looks promising, with several new therapies receiving regulatory approval. Nefecon, sparsentan, and sodium-glucose cotransporter 2 inhibitors have been approved by the European Medicines Agency (EMA), with more treatments likely to follow. The global nephrology community’s concerted effort in recruiting patients from every continent for IgAN trials has been instrumental in this progress, with
Europe playing a particularly crucial role. As Barratt aptly concluded, the era of passive management of IgAN is over, heralding a new dawn of proactive and innovative treatment strategies.
UNDERSTANDING THE MEMBRANOUS NEPHROPATHY DISEASE MECHANISMS
Nicola M. Tomas, University Medical Center Hamburg-Eppendorf, Germany, provided an in-depth exploration of the pathogenesis and emerging treatments for membranous nephropathy (MN). Tomas’ talk emphasised both the complex role of the complement system in MN, and the promising strides in plasma cell-targeted therapies.
However, to date there are no randomised clinical trials for complement in MN, but that is not the end of the story
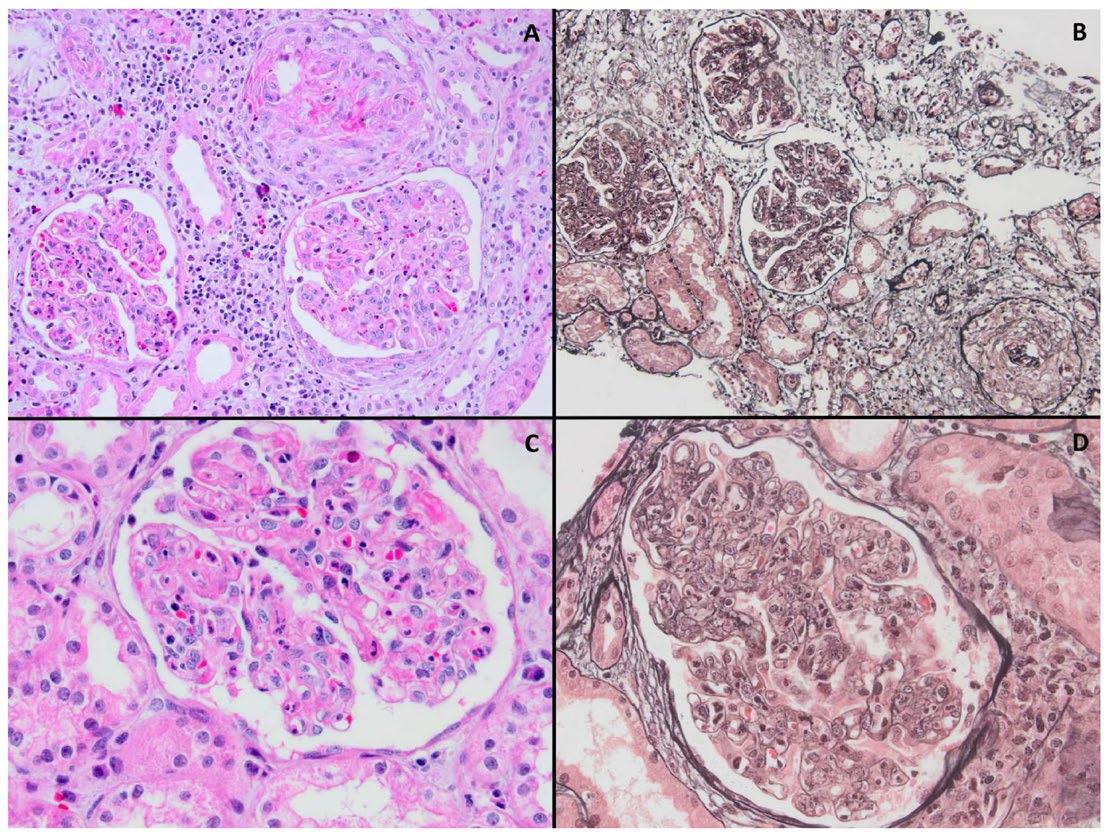
MN is an antibody-mediated autoimmune disease, characterised by the thickening of the glomerular filtration barrier and the deposition of IgG and complement components like C3. Tomas detailed how these histological features, observable through both light and electron microscopy, indicate that podocytes are the primary targets in the disease. MN represents the most common cause of nephrotic syndrome; in most patients, there is no identified underlying cause of MN. Immunofluorescence has detected the granular deposition of IgG autoantibodies and complement components, such as the membrane attack complex, demonstrating that the antibody and complement system play a role in MN pathogenesis.3 The identification of phospholipase A2 receptor 1 (PLA2R) as a target antigen in 2009 marked a breakthrough, followed by the discovery of other antigens implicated in MN.4 Antibodies targeting thrombospondin Type 1 domain-containing 7A and PLA2R podocyte antigens account for 75% of MN cases.3 For these patients, it is known that the autoantibodies are directly pathogenic;
binding to podocytes, inducing complement, triggering disturbance of podocyte structure, and leading to proteinuria.
Therefore, the logical progression is the therapeutic target of the complement system as the final effector mechanism contributing to podocyte damage and target of plasma cells, to reduce autoantibody production. However, to date there are no randomised clinical trials for complement in MN, but that is not the end of the story.
THE ROLE OF THE COMPLEMENT IN MEMBRANOUS NEPHROPATHY
Tomas explained the involvement of the complement system in MN, which is a cascade activated via three pathways (alternative, classical, and lectin). Renal biopsies from patients with MN identified components from all three complement pathways, demonstrating the significance of complement in disease progression. Research at University Medical Center Hamburg revealed strong C1Q deposition in patients from proximity ligation assays, pointing to the classical pathway’s significant role.3 Tomas acknowledged that this was surprising, given that most antibodies against PLA2R1 and thrombospondin Type 1 domain-containing 7A are of the IgG4 subclass, which does not activate the classical pathway. However, the presence of IgG1, IgG2, and IgG3 subclasses, which can bind C1Q, was found in patients, indicating a complex interplay in complement activation.3
B-CELL AND PLASMA CELL TARGETING
Tomas also covered the critical role of B-cells and plasma cells in MN. Plasmablasts and plasma cells are the main source of antibodies, and are typically negative for the cell surface marker CD20, which is currently the focus of B-cell targeted treatments on the market. Tomas reviewed several key clinical trials, including the GEMRITUX and MENTOR trials, which demonstrated the efficacy of rituximab in achieving significant remission
rates compared to supportive care and cyclosporine + glucocorticosteroids.5,6 Despite these advances, 20–40% of patients remain refractory to B-cell targeting, possibly due to the persistence of long-lived plasma cells in the bone marrow escaping treatment, and persisting as drivers of autoimmunity by producing PLA2R autoantibodies. Hence, a potential solution according to Tomas may be the targeting of plasma cells.
However, the presence of IgG1, IgG2, and IgG3 subclasses, which can bind C1Q, was found in patients, indicating a complex interplay in complement activation
Currently the only plasma cell targeting therapy to have preliminary clinical trial data is an anti-CD38 monoclonal antibody, called felzartamab. Data from the Phase 1b/2a M-PLACE felzartamab clinical trial was presented at ASN Kidney Week 2023.7 Two cohorts of patients received nine infusions over 5 months, with an observation period of 12 months. The first cohort was composed of newly diagnosed or relapsed patients, while the second cohort included refractory patients. Early and significant reductions in anti-PLA2R antibodies were observed with 74% of patients, experiencing >50% decrease in anti-PLA2R antibodies.7 Clinically, 47% of patients in cohort one, and 18% of patients in cohort two achieved partial remission.
References
1. Inker LA et al. Early change in urine protein as a surrogate end point in studies of IgA nephropathy: an individual-patient meta-analysis. AJKD. 2016;68(3):392-401.
2. Heerspink HJ et al. Sparsentan in patients with IgA nephropathy: a prespecified interim analysis from a randomised, double-blind, activecontrolled clinical trial. Lancet. 2023;401(10388):1584-94.
3. Seifert L et al. The classical pathway triggers pathogenic complement activation in membranous nephropathy. Nat Comm. 2023;14(1):473.
4. Beck Jr LH et al. M-type phospholipase A2 receptor as target
However, there were no complete remissions reported in the study, which Tomas noted may be due to the relatively short observation period.7 Tomas stressed that the data are promising and demonstrate the potential of plasma cell-targeted therapies.
Tomas concluded by explaining that, although there is mechanistic evidence for a pathogenic role of the complement system in MN, clinical trials seem to be failing. The only complement-targeted clinical trials (RENEW and ‘iptacopan versus rituximab’) have been terminated, and the narsoplimab anti-mannan-binding lectinassociated serine protease-2 antibody trial has an unknown status.8,9,10 However, indirect depletion of antibody-secreting cells has become the mainstay of treatment in membranous nephropathy, though formally off-label in most parts of the world. Moreover, the initiation of the NewPLACE and MONET trials on felzartamab means we may expect data on plasma cell-targeted therapies in the near future.
Change colours to TA area
CONCLUSION
The talks by Barratt and Tomas highlighted a promising future for glomerulonephritis treatment. Advancements in IgAN and MN clinical trials, particularly in targeted therapies and regulatory frameworks, herald a new era of effective disease management, offering improved outcomes for patients previously left with few treatment options.
antigen in idiopathic membranous nephropathy. N Engl J Med. 2009;361(1):11-21.
5. Dahan K et al. Rituximab for severe membranous nephropathy: a 6-month trial with extended follow-up. J Am Soc Nephrol. 2017;28(1):348-58.
6. Fervenza FC et al. Rituximab or cyclosporine in the treatment of membranous nephropathy. N Engl J Med. 2019;381(1):36-46.
7. Rovin BH et al. Safety and efficacy of Felzartamab in primary membranous nephropathy (PMN): final analysis of the M-PLACE study. Abstract 1402, ASN Kidney Week, 2-5 November 2023.
8. BioCryst Pauses Enrollment in BCX9930 Clinical Trials. Available at:
https://ir.biocryst.com/news-releases/ news-release-details/biocryst-pausesenrollment-bcx9930-clinical-trials. Last accessed: 17 June 2024.
9. Study to Evaluate the Safety, Tolerability of BCX9930 in Participants With Either Complement 3 Glomerulopathy (C3G), Immunoglobulin A Nephropathy (IgAN), or Primary Membranous Nephropathy (PMN) (RENEW). NCT05162066. https://clinicaltrials.gov/study/ NCT05162066.
10. Elhadad S et al. MASP2 inhibition by narsoplimab suppresses endotheliopathies characteristic of transplant-associated thrombotic microangiopathy: in vitro and ex vivo evidence. Clinical and Experimental Immunology. 2023;213(2):252-64.
THE 61st European Renal Association (ERA) Congress took place in Stockholm, Sweden, from the 23rd–26th of May 2024. In a multidisciplinary session chaired by Mustafa Arici, Hacettepe University, Ankara, Türkiye; and Olga Barafa, University Hospital of Ioannina, Epirus, Greece, three experts discussed the crucial relationship between kidney function and blood pressure, providing recommendations for clinical practice.
CHRONIC KIDNEY DISEASE: CONTROLLING HYPERTENSION
Liffert Vogt, University of Amsterdam, the Netherlands, opened the session by emphasising the importance of blood pressure (BP) management in patients with chronic kidney disease (CKD), as outlined by the Kidney Disease, Improving Global Outcomes (KDIGO) 2024 clinical practice guidelines, which set an ambitious target for systolic BP <120 mmHg. While awareness of high BP in CKD is increasing, the proportion of patients with CKD who have their BP under control remains under 50%. Vogt brought the audience’s attention to a recent trial conducted in Korea that found that greater adherence to systolic BP control within the target range was associated with a lower risk of adverse kidney events.1
New drugs for CKD, such as dapagliflozin, a sodium-glucose co-transporter 2 (SGLT2) inhibitor, are improving renal function, as well as lowering patient BP (average of 2.9 mmHg).2 However, despite a better prognosis, patient BP still remains above the desired target. Vogt added that, across several recent studies, thiazide diuretics have been shown to be effective treatment approaches in patients with CKD, reducing systolic BP by an average of 14 mmHg, which is more than observed with dapagliflozin. As an add-on to
traditional treatments for CKD such as angiotensin-converting enzyme inhibitors and angiotensin receptor blockers, thiazide diuretics like chlorthalidone, and dietary sodium restriction (<100 mmoL/d), remain powerful options to reduce BP, in addition to lowering proteinuria and estimated glomerular filtration rate. While their effect on the long-term risk of kidney events is not as well-studied as SGLT2 antagonists or selective mineralocorticoid receptor antagonists, Vogt urged the audience to not neglect diuretics and sodium restriction as therapeutic options for patients with CKD.
Vogt then introduced results from an unpublished survey, conducted among Dutch nephrologists, where one-third of patients were reported to have a BP exceeding the recommended target, and almost half did not have an albumin-tocreatinine ratio on target. This was due to a suboptimal dose of renin-angiotensinaldosterone system inhibitors (RAASi), or simply a lack of RAASi use. Expanding on the true burden of CKD globally, Vogt highlighted that two out of three patients with CKD are identified based on lab values, but do not have a corresponding CKD diagnosis, leading to only 60% of patients with CKD being prescribed a RAASi. Furthermore, commenting on recent CKD patient data in the UK, he explained that, in the real-world CKD population, only
0.9%, 2.2%, and 8.0% of patients would have actually been eligible for the three landmark SGLT2-inhibitor trials.3 “What is the validity of these trials if the daily practice is completely different?” questioned Vogt. He attributed the main reason for this ineligibility to a lack of RAASi use.
patients with CKD are identified based on lab values, but do not have a corresponding CKD diagnosis
These data have crucial implications for clinical practice. Better screening strategies for CKD are needed, implementation of RAASi needs to be improved, and a greater focus should be placed on meeting the systolic BP target of <120–130 mmHg. Vogt ended his talk with perhaps a controversial approach to CKD treatment, asking whether patients with CKD will really be in need of newer classes of renoprotective agents once RAASi are adequately prescribed, and BP is controlled. “More pills does not induce more adherence,” he concluded.
MALIGNANT HYPERTENSION: LESSONS LEARNT
Jean-Michel Halimi, University of Tours, France, stressed that ‘malignant hypertension’ (MH) remains a prevalent clinical issue in 2024, despite huge advances in the development of hypertensive drugs. Discussing results from his recent study, 7,769 patients were found to have hypertensive encephalopathy (HE), of which 25% died within 3 years.4 Risk of adverse
outcomes, including heart failure, ischaemic stroke, haemorrhagic stroke, cognitive impairment, and vascular dementia, among others, were all significantly higher in patients with HE compared to those without HE. “These are people who live in France, where there is no financial barrier to medical care,” stressed Halimi. “We shouldn’t have this issue, but this is what we have.”
Halimi then spoke about thrombotic microangiopathy (TMA), which was recently shown to be part of the pathophysiology of MH. The definition of MH has expanded from elevated BP and papilledema to ‘targetorgan damage’, including posterior reversible encephalopathy syndrome, retinopathy, acute kidney injury, TMA, and heart failure. He added that, in MH, the kidney exhibits dysregulated levels of complement, with elevated C5-b9, C3a, and C5a; and pathogenic variants of complement factors B and H.5
Furthermore, in a study of young patients with MH, only 7% had normal renal function at 3 years, 25% required chronic dialysis, and 52% had severe isolated nephrosclerosis.6 Level of internal fibrosis was a crucial prognostic factor significantly associated with renal prognosis. Halimi added that, where possible, a kidney biopsy may be warranted in patients with MH.
Finally, Halimi emphasised the urgent need for new data to examine the relationship between MH and TMA. The first prospective, multicentric cohort on MH is now underway,7 including patients with blood pressure >180/110 leading to acute damage of three target organs (heart, brain, kidney). As of May 2024, 512 patients have been recruited.
Where possible, a kidney biopsy may be warranted in patients with MH
A NOVEL TREATMENT APPROACH FOR HYPERTENSION
Kouichi Tamura, Yokohama City University, Japan, introduced a potential therapeutic option for treating hypertensioncardiovascular-kidney comorbidity. He explained that chronic overactivation of the angiotensin II receptor type 1 (AT1R) signalling system is a key challenge to overcome to achieve the healthy longevity required in an ageing society. Sustained activation of AT1R signalling leads to oxidative stress and inflammation, and subsequently a shortened life expectancy. AT1R-associated protein (ATRAP) has been identified as a specific binding protein to the C-domain of AT1R. In normal kidney cells, ATRAP is abundantly distributed in tubular epithelial cells along nephron segments. However, kidney tubule ATRAP expression decreases as renal function declines in CKD. In visceral adipose tissue, ATRAP expression also tends to be decreased in human metabolic disorders such as hypertension, Type 2 diabetes, and obesity.
Tamura explained that the current hypothesis, supported by two decades of research, is that ATRAP may exert a “functionally selective inhibition on pathological, detrimental AT1R signalling.” In transgenic mice with cardiac-specific ATRAP, cardiac hypertrophy provoked by AT1R-induced hypertension was suppressed; and adipocyte-specific ATRAP enhancement
References
1. Park et al. Findings from the KNOWCKD Study indicate that higher systolic blood pressure time in target range is associated with a lower risk of chronic kidney disease progression. Kidney Int. 2024;105-835.
2. Heerspink HJ et al. Dapagliflozin in patients with chronic kidney disease. Am Heart J. 2024;270:125-35.
suppressed visceral fat accumulation and body weight gain in mice on a high-fat diet. Furthermore, ATRAP-knockout mice exhibited exacerbation of hypertension and an increase in kidney TNF-α expression in a remnant kidney-CKD model.
Tamura provided some interesting insights into the potential avenues for implementation of ATRAP enhancement: inhibitors against microRNA-125 can increase ATRAP expression and suppress the pathological overactivation of AT1R, thus achieving organprotective effects against hypertension and other kidney diseases. He emphasised that ATRAP is an attractive therapeutic target to tackle the comorbidities associated with an ageing population.
CONCLUSION
This comprehensive session highlighted the ongoing challenges and advances in managing hypertension and kidney disease, with speakers advocating for integrated, evidence-based strategies to enhance patient outcomes. There is a critical need to address treatment gaps in kidney disease, and BP control remains a crucial target in clinical practice. Improved screening strategies and patient adherence to medication remain a priority to reduce hypertension-related complications, morbidity, and mortality.
In the real-world CKD population, only 0.9%, 2.2%, and 8.0% of patients would have actually been eligible for the three landmark SGLT2-inhibitor trials
3. Forbes AK et al. Implementation of chronic kidney disease guidelines for sodium-glucose co-transporter-2 inhibitor use in primary care in the UK: a cross-sectional study. EClinicalMedicine. 2024;68:102426.
4. Halimi JM et al. Characteristics and prognosis of patients with hypertensive encephalopathy: a French nationwide cohort study. Hypertension. 2023;80(8):1716-27.
5. Zhang Y et al. Association between thrombotic microangiopathy and activated alternative complement
pathway in malignant nephrosclerosis. Nephrol Dial Transplant. 2020;DOI:10.1093/ndt/gfaa280.
6. Bureau C et al. Nephrosclerosis in young patients with malignant hypertension. Nephrol Dial Transplant. 2023;38(8):1848-56.
7. A new breath for malignant hypertension: implementation of the HAMA cohort (HAMA). NCT03755726. https://classic.clinicaltrials.gov/ct2/ show/NCT03755726.
Immunoglobulin
A
Nephropathy:
Population
Characteristics, Humanistic Burden, and Kidney Outcomes According to Albuminuria
These presentations took place virtually at the 61st ERA Congress, held on May 23rd−26th, 2024, Stockholm Sweden
Speakers: Philipp Csomor,1 Justyna Szklarzewicz,2 Anne-Laure Faucon 3,4
1. CSL Vifor, Glattbrugg, Switzerland
2. University Hospitals of Leicester NHS Trust, UK
3. Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden
4. Department of Clinical Epidemiology, Centre for Epidemiology and Population Health, Paris-Saclay University, France
Disclosure: Csomor is an employee of CSL Vifor. Szklarzewicz received consultancy fees from Travere Therapeutics, Inc. Faucon received funding from CSL Vifor.
Acknowledgements: Writing assistance was provided by Eleanor Roberts, Beeline Science Communications Ltd, London, UK.
Disclaimer The opinions expressed in this article are not necessarily those of CSL Vifor.
Publication of this feature was supported and reviewed by CSL Vifor.
Session Summary
The glomerular disease IgA nephropathy (IgAN) predominately arises in young adults and can progress to chronic kidney disease (CKD) and, ultimately, kidney failure or death. While there are guidelines for treating IgAN, there are still unanswered questions around the condition, including when patients are referred for specialist care, what their health-related quality of life (HRQoL) is, and what other factors may be involved in progression to CKD. These questions were investigated, and findings shown, in three posters presented at the 61st European Renal Association (ERA) Congress in Stockholm, Sweden. The first poster, which surveyed Europebased physicians who treated at least 50 patients with Stage 1−4 CKD, found that nearly a third of patients were referred to them later than they should have been, given their IgAN symptoms. The survey also revealed that, while over three-quarters of patients were in CKD Stage 3 or above, the majority of physicians (98%) rated a patient’s overall health as good or excellent. In the second poster, both patients and
PHARMA PARTNERSHIP
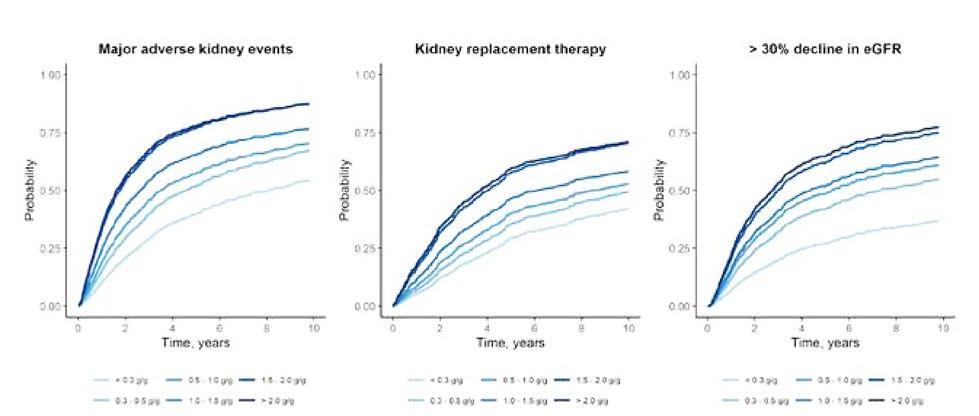
their care-partners (predominantly from Spain and Germany) were surveyed with regard to the humanistic burden of IgAN. In this preliminary analysis of a wider survey, both participant cohorts had a lower HRQoL than a general European population, along with reporting negative work-related impacts of IgAN, and 31% of patients had moderate−severe scores for anxiety and depression. In the third poster, which accompanied an oral presentation, albuminuria was investigated as a factor that may be useful to help ascertain progression and guide IgAN treatment. Utilising data from the Swedish Renal Registry, the authors found that the probability of CKD progression was impacted by albuminuria level, even in cases where this was only slightly above normal. Decreases in albuminuria lowered the hazard ratio for CKD progression. Taken together, these studies show the need to diagnose and treat patients with IgAN on an individualised basis, address both patient and care-partner HRQoL, and consider even those with low-grade albuminuria as at risk of progression.
Introduction
IgAN is an immune-complex mediated glomerular disease with an incidence rate of 0.03−10.5/100,000 persons/year.1-3 Although rare, IgAN is the primary cause of glomerulonephritis and is associated with an increased risk of all-cause mortality and a reduction in life expectancy due to kidney failure.4-6 Signs and symptoms of IgAN can vary, but proteinuria is always present. Progression may be slow to rapid, sometimes necessitating aggressive treatment. Patients with IgAN may experience pain and fatigue, along with associated anxiety and depression, all of which can impact their HRQoL.4,7-9 According to 2021 Kidney Disease: Improving Global Outcomes (KDIGO) guidelines, treatment options for IgAN include the highest tolerated dose of a renin-angiotensin-aldosterone system inhibitor (RAASi), immunosuppressant therapy (where suitable), and supportive care, such as cardiovascular, blood pressure, and lifestyle management.10
Three posters presented at the 61st ERA Congress in Stockholm set out to address some of the questions that remain about how to best assess an individual patient needs and optimise treatment in those with IgAN. The first, led by Philipp Csomor, utilised real-world data to examine patient characteristics. The second, led by Justyna Szklarzewicz, discussed data from a survey regarding HRQoL of both patients with IgAN and their care-partners. Lastly, Anne-Laure
Faucon gave an oral presentation of her group’s investigation into kidney outcomes in patients with IgAN in relationship to albuminuria levels.
Analysis of the Characteristics of Patients with IgA Nephropathy Using Real- World Data from Five European Countries
Philipp Csomor
The first poster11 reported on patient characteristics associated with IgAN through the use of a physician questionnaire and patient chart audit that took place between December 21, 2022–February 6, 2023. The authors proposed that understanding such aspects could help best implement effective, individualised treatment regimens.
The 261 participating physicians were from France, Germany, Spain, Italy, and the UK. Physician inclusion requirements were that they had been in practice between 2−40 years, that they spent more than 40% of their time in a clinical setting, and that they had at least 50 patients with stage 1–4 CKD, with at least four patients who were not on dialysis. Patient chart inclusion requirements were that they had an IgAN diagnosis, were at least 12 years old, were not on dialysis, had an estimated glomerular filtration rate (eGFR) ≥15 mL/min/1.73 m2 ,
and had seen a participating physician within 6 months of the survey date.
Data was collected on 473 patients who were predominantly male (71%) and Caucasian (78%). Of note though, globally, IgAN is most prevalent in people of Asian descent, potentially due to an increased number of risk-associated alleles.12 Agewise, 2% of patients were <18 years old, 16% were aged between 18–30 years, 38% were 31–49 years, 28% were 50–64 years, and 16% were ≥65 years old. This highlights previous findings that IgAN is predominantly a condition that arises in young to middle-aged adults whose lives may be drastically reduced without proper medical management.7
Twenty-two percent of patients had been referred to their current physician within the past year. This was predominantly by a primary care physician (70%), with 9% referred by another nephrologist, of which almost onethird were referred for specialised care. According to the participating physicians, while 17% of patients were referred early and 54% at an appropriate time, around 26% of patients were referred to them late, and 4% extremely late. Contributing factors to this were reported to be that “the patient remained asymptomatic for a long time,” that there was a “lack of engagement from the patient,” and that “the patient had no regularly scheduled doctor appointments.” Specifically for children, but also applicable to adult patients, KDIGO guidelines recommend that, regardless of whether the disease is active or inactive, patients should be continually followed up, “as they can relapse, even after many years.”10
Patients were divided between those with CKD Stages 1 or 2 (24%), Stages 3a or 3b (57%), or Stage 4 (19%). As can be seen from Figure 1, at their most recent visit, a physician’s perception of IgAN severity mostly mapped to CKD stage, with, for example, a much higher percentage with CKD4 being perceived as having severe IgAN, patients in CDK3 being rated as mostly moderate for IgAN, and those with CKD1 having mostly mild IgAN.
However, CKD stage and IgAN severity ratings were not always concordant. For example, 16% with CKD1 were perceived by their physician as having IgAN that was moderate or severe, and 14% with CKD4 were perceived as having mild IgAN.
KDIGO guidelines define high risk of IgAN progression as having proteinuria >0.75−1.00 g/day despite ≥90 days’ optimised supportive care.10 In this current survey, 71% of patients had proteinuria >0.5 g/day, and 46% had proteinuria >1.0 g/ day (8% had no values available), indicating that many were at risk of progression. Further, while nephrotic syndrome (urine protein >3.5 g/day and low serum albumin) is typically rare in patients with IgAN,10 in this survey, 8% were diagnosed with this condition by a nephrologist.
Most patients (92%) were taking a RAASi, with, on average, patients being prescribed five medications. This number increased in patients ≥50 years old. However, 54% of physicians reported a degree of dissatisfaction with their patients’ response to treatment, although satisfaction levels varied between individual treatment options. This may partly be due to the finding that only two-thirds of physicians felt their patients completely adhered to their treatment regimen.
Fatigue (59%), haematuria (41%), and weight gain (41%) were the IgAN symptoms of mild-to-severe intensity reported with the greatest frequency. Comorbid conditions were common, with 54% of patients having hypertension, 22% hyperlipidaemia, 17% obesity, 15% Type 2 diabetes, and 7% peripheral oedema. These figures reflect findings in larger IgAN studies.7
Despite all these findings, one of the key unexpected results in this study was that physicians rated their patient’s overall health as predominantly excellent (56%) or good (42%), with only 2% rating it as poor. The authors discussed how this revealed a “potential gap in physicians’ perceptions of a patient’s health and their risk of progression to kidney failure.”
CKD1 (n=13)*
CKD2 (n=102)
CKD3a (n=126)
CKD3b (n=144)
CKD4 (n=88)
*Small number of participants. CKD: chronic kidney disease.
Taken together, the authors concluded that the findings of this survey indicate “an unmet need for early diagnosis and treatment of IgAN to ensure that patients receive appropriate, individualised care.”
Humanistic Burden of Immunoglobulin A Nephropathy and Focal Segmental Glomerulosclerosis on Patients and Care-Partners (HONUS): Results for Europe
Justyna Szklarzewicz
The second poster13 reported the burden of Ig A nephropathy and focal segmental glomerulosclerosis on patients and carepartners. Proteinuric kidney disease is associated with both clinical and economic burdens, including high healthcare costs.14 To better understand both patient and care-partner burdens associated with IgAN, an ongoing multi-national, crosssectional survey, ‘Humanistic burden of rare nephrotic diseases: understanding of the impact of focal segmental glomerulosclerosis and IgAN on patients
and care-partners study (HONUS)’, is taking place across Europe and the USA.
In this poster, preliminary results presented included patients with a physician-provided diagnosis of IgAN (confirmed by renal biopsy). Patients were aged ≥18 years and were from Spain (n=16), Germany (n=8), France (n=1), and the UK (n=1). They participated in HONUS from January–October 2023. Participants were excluded if they were participating in a kidney disease clinical trial that included potential active treatment at time of enrolment, or had a history of malignancy, co-existing glomerular disease, or secondary IgAN. While patients with focal segmental glomerulosclerosis were also included in this poster, numbers were low, so the authors focus only on IgAN here.
Presented data included 26 patients with a mean age 42.2 years (standard deviation [SD]: 11.6); 61.5% of which were female. The mean time from diagnosis was 9.6 (SD: 8.6) years. Patients were fairly evenly distributed across CKD stages, ranging from Stages 1−2 (13.0%), 3−4 (26.9%), and 5 with dialysis (15.4%). Additionally, 26.9% were transplant recipients, and 7.7% had unknown status. Also surveyed were 22 care-partners with a
Figure 1: Physicians’ perception of IgA nephropathy severity by chronic kidney disease stage at most recent visit.
mean age of 46.6 years (SD: 9.5). Of these, 59.1% were male and 81.8% were the patient’s life partner.
As previously mentioned, IgAN typically starts in young to mid-adulthood so it encompasses a period of life that greatly includes personal and professional development.7 As such, assessing aspects that may impact these factors is vital. Data from this study showed that patients with IgAN experienced impaired HRQoL in several domains. In general, in European populations, mean 12-Item Short Form Survey15 physical component scores (PCS) and mental component scores (MCS) are on average 50.0 for each score.16 Here, mean PCS was 47.3 (SD: 11.6) (median: 51.6) and mean MCS was 43.2 (SD: 10.9) (median: 44.6), indicating a negative impact on overall HRQoL in comparison to the general European population. For care-partners, figures were 53.3 (SD: 8.8) (median: 55.9) for PCS and 47.9 (SD: 10.8) (median: 50.9) for MCS, indicating a potential impact on mental health aspects of HRQoL. These
GAD-7
Minimal (0–4)
Mild (5–9)
Moderate (10–14)
Severe (15–21)
results were similar to those of the 96 USA adult patients with IgAN and their carepartners also taking part in the HONUS study. In the USA patients, mean PCS and MCS scores were 46.8 (SD: 7.9) and 41.9 (SD: 9.1), respectively, with respective carepartner scores of 50.8 (SD: 7.1) for PCS, and 43.8 (SD 10.2) for MCS.17 Taken together, these confirm previous findings about the impact of IgAN on HRQoL.8
Use of the Generalized Anxiety Disorder Assessment-7 measure18 showed that 30.8% of patients and 9.2% of care-partners had moderate-to-severe anxiety scores (Figure 2). In the USA component of the HONUS study, while a similar 29.1% of patients had moderate-to-severe anxiety scores, moderate anxiety scores were seen to be higher in 13.5% of care-partners (no severe scores).17 This is an important aspect of IgAN to address, as a recent, global, longitudinal survey found that anxiety scores may change little over time in patients with primary glomerular diseases, including IgAN.19
Patients with IgAN (n=26) Care-givers (n=22)
GAD-7
Minimal (0–4)
Mild (5–9)
Moderate (10–14)
Severe (15–21)
PHQ-9
Minimal (0–4)
Mild (5–9)
Moderate (10–14)
Moderately severe (15–19)
Severe (20–27)
GAD-7: generalised anxiety disorder assessment-7; IgAN: IgA
PHQ-9
Minimal (0–4)
Mild (5–9)
Moderate (10–14)
Moderately severe (15–19)
Severe (20–27)
Figure 2: Anxiety and depression scores in patients with IgA nephropathy and their care-partners: results for Europe.
Depression scores in this analysis, assessed using the Patient Health Questionnaire-9,20 were moderate-to-severe for 30.8% of patients and 13.8% of care-partners. A higher percentage of both patients (54.1%, of which 51.0% were moderate) and caregivers (40.6%) had moderate-to-severe depression scores in the USA analysis.15 Compared to healthy controls, previous studies have also found higher depression scores in people with glomerular diseases including IgAN.8
Among the 69.2% of patients with IgAN who were employed, findings from the work productivity and activity impairment survey21 showed that over a 7-day period, mean percentage for impairment while working (presenteeism) was 17.7%, with mean percentage for work time missed (absenteeism) being 13.3%. Percentages of activity impairment and overall work impairment for IgAN-related reasons were 27.3% and 17.7%, respectively. In the USA HONUS study, presenteeism percentage was higher, at 25.4%, with absenteeism slightly lower, at 8.2%. For IgAN-related reasons, both activity impairment (34.0%) and overall work impairment (29.8%) were rated as higher.17
For the 86.4% employed IgAN care-partners, mean percent presenteeism was 9.3% and absenteeism was 14.2%. IgAN-related activity impairment was 18.6%, and overall work impairment due to IgAN-related reasons was 9.9%. Corresponding USA figures were mostly higher for care-partners, with 24.7% for presenteeism, 28.8% for activity impairment, and 29.9% for overall work impairment. Absenteeism was lower, at 8.8%.17 Together with the patient figures, these highlight the large burden that IgAN can have on the impacted patient and caregiver’s work and career.
The authors concluded that, at least in these European countries, having IgAN, as well as caring for someone with IgAN, impaired HRQoL, and was associated with anxiety, depression, and impaired productivity. However, the authors noted that scores may have been influenced by the COVID-19 pandemic.
Albuminuria and Subsequent Risk of Kidney Events in Patients With IgA Nephropathy: A Nationwide Cohort Study
Anne-Laure Faucon
The third poster22 discussed albuminuria and the risk of kidney events in patients with IgA nephropathy. Proteinuria levels are one of the main factors KDIGO guidelines use for medical management of IgAN.10 However, some patients with below-target proteinuria can still progress to CKD.6,24 Albuminuria specifically may play a role in IgAN progression, with one meta-analysis of a general population with CKD showing that increase in urinary albumin-tocreatinine ratio (uACR) was associated with progression to end-stage kidney disease.25 With this in mind, this study aimed to “evaluate the risk of CKD progression across the spectrum of uACR.”
This poster, presented orally by Faucon, detailed findings from a cohort of 1,269 patients from the Swedish Renal Registry (taken from 2006–2021) with biopsyproven, primary IgAN. They comprised 74% men, were a median of 53 years old, and had a mean eGFR of 33 mL/ min/1.73 m². Despite the KDIGO guidelines recommendation to treat all patients with IgAN with a RAASi,10 one-fifth were not prescribed such treatment.
“In the first part of the study, we analysed the impact of baseline albuminuria on the risk of CKD progression,” explained Faucon. In these patients, baseline median uACR was 0.7 g/g, with 38% having a uACR >1.0 g/g. Over a median follow-up of 5.5 years, 517 kidney replacement therapy events occurred, 528 patients had an eGFR decline >30%, and there were 667 major adverse kidney events (MAKE, a composite score). According to Faucon, as seen in Figure 3, there was “a strong and incremental association between the level of albuminuria and the risk of CKD progression.” It was of note that substantial CKD progression risk was not just in patients with high albuminuria levels, but also in patients with uACR 0.3−1.0 g/g. “This population,” noted Faucon, “is currently considered at a low risk [for progression].”
In the second part of this study, the authors analysed the impact of 1-year change in uACR in 785 patients who had repeat uACR measurements. Compared to patients with a stable uACR, a 2-fold uACR increase led to hazard ratios (HR) of 1.75 (95% CI: 1.31−2.33) for MAKE, 2.56 (95% CI: 1.79−3.65) for kidney replacement therapy, and 1.18 (95% CI: 0.87−1.60) for >30% decline in eGFR.
Conversely, where uACR had a 2-fold decrease, respective HRs were 0.47 (95% CI: 0.36−0.62), 0.49 (95% CI: 0.36−0.68), and 0.49 (95% CI: 0.37−0.65). The latter HR is particularly important as, according to KDIGO guidelines, >30% decline in albuminuria levels is ‘predictive of protection from progression to kidney failure’.10
“Regardless of baseline uACR,” emphasised Faucon, “any reduction in albuminuria was associated with better kidney outcome.” Combined with indications of poorer kidney outcomes even with microalbuminuria, Faucon
concluded that “this study suggests that we should optimise clinical and pharmaceutical management in patients with IgAN to decrease albuminuria and delay the risk of CKD progression.”
Conclusion
Taken together, these findings suggest that patients with IgAN should be diagnosed and treated early, with albuminuria taken into account, as substantial CKD progression risk can be observed even in patients with uACR <1.0 g/g. This will help provide individualised, monitored treatment regimens that can negate or slow progress to aberrant kidney outcomes. HRQoL is also a factor that needs to be addressed for patients with IgAN, as well as for their care-partners, as the burden can be considerable.
Figure 3: Probability of experiencing major adverse kidney events, kidney replacement therapy, and a >30% decline in estimated glomerular filtration rate over time, according to urinary albumin-to-creatinine ratio.
Time, years
eGFR: estimated glomerular filtration rate.
References
1. Nair R, Walker PD. Is IgA nephropathy the commonest primary glomerulopathy among young adults in the USA? Kidney Int. 2006;69(8):1455-8.
>30% Decline in eGFR
2. McGrogan A et al. The incidence of primary glomerulonephritis worldwide: a systematic review of the literature. Nephrol Dial Transplant. 2011;26(2):414-30.
3. Zaidi O et al. Review on epidemiology, disease burden, and treatment patterns of IgA nephropathy in select APAC countries. BMC Nephrol. 2024;25(1):136.
4. Jarrick S et al. Mortality in IgA nephropathy: a nationwide populationbased cohort study. J Am Soc Nephrol. 2019;30(5):866-76.
5. Barratt J et al. Natural history of IgA nephropathy: analysis of a UK national RaDaR IgA nephropathy cohort. PO1577. J Am Soc Nephrol. 2021;32:S494.
6. Pitcher D et al. Long-term outcomes in IgA nephropathy. Clin J Am Soc Nephrol. 2023;18(6):727-38.
7. Lai KN et al. IgA nephropathy. Nat Rev Dis Primers. 2016;2:16001.
8. Kwon CS et al. A systematic literature review of the epidemiology, healthrelated quality of life impact, and economic burden of immunoglobulin a nephropathy. J Health Econ Outcomes Res. 2021;8(2):36-45.
9. Goh ZS, Griva K. Anxiety and depression in patients with endstage renal disease: impact and management challenges - a narrative review. Int J Nephrol Renovasc Dis. 2018;11:93-102.
10. KDIGO 2021 clinical practice guideline for the management of glomerular diseases. Kidney Int. 2021;100(4s):S1276.
11. Csomor P et al. Analysis of the characteristics of IgA nephropathy patients using real-world data from five European countries. Abstract 1993. Nephrology Dialysis Transplantation. 2024;39(Supplement 1):gfae069-1318.
12. Kiryluk K et al. Discovery of new risk loci for IgA nephropathy implicates genes involved in immunity against intestinal pathogens. Nat Genet. 2014;46(11):1187-96.
13. Bensink M, Szklarzewicz J. Humanistic Burden of Immunoglobulin A Nephropathy and Focal Segmental Glomerulosclerosis on Patients and Care-Partners (HONUS): results for Europe. Abstract 366. Nephrology Dialysis Transplantation. 2024;39(Supplement 1):gfae0691343.
14. Bensink ME, Goldschmidt D. Kidney failure attributed to focal segmental glomerulosclerosis: A USRDS retrospective cohort study of epidemiology, treatment modalities, and economic burden. Kidney Med. 2023;6:100760.
15. Kosinski JEW et al, “User's manual for the SF-12v2 health survey with a supplement documenting the SF-12 health survey,” (2007), QualityMetric Incorporated, Lincoln, RI.
16. Gandek B et al. Cross-validation of item selection and scoring for the SF-12 health survey in nine countries: results from the IQOLA Project. International quality of life assessment. J Clin Epidemiol. 1998;51(11):1171-8.
17. Szklarzewicz J, Bensink ME. Humanistic burden of rare kidney diseases: understanding the impact of IgAN and FSGS on patients and care-partners study (HONUS): A US IgAN results update. Abstract 5300.
18. Spitzer RL et al. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092-7.
19. Murphy SL et al. Longitudinal changes in health-related quality of life in primary glomerular disease: results from the CureGN study. Kidney Int Rep. 2020;5(10):1679-1689.
20. Kroenke K, Spitzer RL. The PHQ9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-13.
21. Reilly MC, Zbrozek AS. The validity and reproducibility of a work productivity and activity impairement instrument. Pharmacoeconomics. 1993;4:353-65.
22. Faucon AL et al. Albuminuria and subsequent risk of kidney events in patients with IgA nephropathy: a nationwide cohort study. Abstract 1444. Nephrol Dial Transplant. 2024;39(Supplement 1):gfae0690406.
23. El Karoui K et al. Treatment of IgA nephropathy: a rapidly evolving field. JASN. 2023;00:1-14.
24. Coresh J et al. Change in albuminuria and subsequent risk of end-stage kidney disease: an individual participant-level consortium metaanalysis of observational studies. Lancet Diabetes Endocrinol. 2019;7(2):115-27.
Abstract Reviews
Sharing insights presented at the European Renal Association (ERA) 2024 Annual Meeting, the following abstract reviews spotlight exciting new developments in the field.
Widespread use of SLGT2 inhibitors (SGLT2i) is likely given recent recommendations for their use in chronic kidney disease and heart failure in addition to their original indication of Type 2 diabetes. Patients with these conditions are likely to be prescribed more than five regular medications, a threshold generally considered to represent polypharmacy. The team performed a computational drug repurposing screen to identify other licensed drugs capable of binding at or near the SGLT2i active site, aiming to identify compounds that could either compete with SGLT2i or also inhibit sodium and glucose transport.
METHODS
The British National Formulary (BnF) listed compounds were obtained from
the National Center for Biotechnology Information (NCBI) PubChem. D-I-TASSER (The Yang Zhang Lab, Ann Arbor, Michigan USA) was used to generate monomeric structural models, and MODELLER (Andrej Sali Lab, San Francisco, California, USA) was used to incorporate MAP-17 and empaglifozin from a reference structure (PDB 7VSI). CHARM-GUI (Lehigh University, Bethlehem, Pennsylvania, USA) was used to insert the protein into a membrane. The centroid of a 5 nanosecond GROMACS molecular dynamics equilibration was used for docking studies using PLANTS (University of Konstanz, Germany).
A bespoke tool was used to identify compounds interacting with key protein residues. CHARM-GUI and the bespoke software were used to prepare membranebound systems to run in GROMACS (University of Groningen, the Netherlands) using the graphics processing unit in Google Colab (Mountain View, California, USA). Ten nanosecond simulations were undertaken (300 Kelvin and 1 bar) to discriminate between binding and non-binding events.
RESULTS
A structural model of membrane-bound SGLT2-MAP17 complex was obtained in the inward open conformation associated with SGLT2i binding. This model was in close agreement with published structures. Empaglifozin, dapaglifozin, canaglifozin, and ertuglifozin all featured in the top 1% of docked compounds in the repurposing screen. Thirteen additional compounds
were identified for investigation by molecular dynamics. Stable proteinligand interactions were identified for all these compounds, including ceftriaxone, tobramycin, clindamycin, fluvastatin, atorvastatin, and ticagrelor.
It is unclear if the stable ligand interactions identified here would result in the inhibition of sodium and glucose transport, or if the interactions might provide competitive inhibition for SGLT2i compounds currently used. The compounds identified have no documented interactions with SGLT2i; nor do they result in adverse effects
suggesting inhibition of the protein. The main limitations of this study are the consideration of only the protein-ligand interactions and not wider pharmacokinetic or pharmacodynamic factors.
CONCLUSION
Plausible interactions between SGLT2 and medicine likely to be prescribed concomitantly, such as antiplatelet agents, statins, and antibiotics have been identified and warrant further investigation.
Influence of Potassium Intake on the Renoprotective Response to Sodium Restriction and Hydrochlorothiazide in Patients with Diabetic Nephropathy
Authors: *Caspar van Lieshout,1 Liffert Vogt,2 Arjan Kwakernaak,1 Marc Hemmelder,3 Goos Laverman,4 Gerjan Navis,1 Martin de Borst1
1. Department of Internal Medicine, Division of Nephrology, University Medical Center Groningen, the Netherlands
2. Department of Internal Medicine, Division of Nephrology, Amsterdam University Medical Centre, the Netherlands
3. Department of Internal Medicine, Division of Nephrology, Maastricht University Medical Centre, the Netherlands
4. Department of Internal Medicine/ Nephrology, Ziekenhuisgroep Twente, Almelo, the Netherlands
*Correspondence to c.j.van.lieshout@umcg.nl
Disclosure: Vogt received consulting fees from AstraZeneca, Bayer, Boehringer Ingelheim, CSL Vifor, and Sanofi Genzyme through payments to the institution. Laverman received grants from Sanofi, AstraZeneca, Boehringer Ingelheim, Abbott, and the Pioneers in Healthcare grant, recieved through payments to the institution; consulting fees from Medtronic, Roche, Sanofi, Novo Nordisk, AstraZeneca, and Boehringer Ingelheim; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Sanofi and Boehringer Ingelheim; travel support for attending meetings from Sanofi; and is a
member of the International Diabetes Advisory Board. Navis is a member of the Health Council of the Netherlands, a member of the Prevention Advisory Board of the Ministry of Health, and Chair of the Health Council’s Advisory Committee on Climate Change and Health. Borst has received a research grant from CSL Vifor through payments to the institution; and consulting fees from CSL Vifor through payments to the institution.
Salt restriction and hydrochlorothiazide (HCT) are known to increase the antihypertensive and antiproteinuric effects of renin-angiotensinaldosterone-system inhibitors (RAASi) in chronic kidney disease.1-4 Additionally, potassium intake affects blood pressure (BP) and albuminuria.5-7 This effect is
likely mediated through potassium’s inhibitory effect on the sodium-chloridecotransporter, increasing natriuresis.8 However, the influence of potassium intake in response to sodium restriction and HCT during RAASi treatment in patients with diabetic nephropathy is unknown.
METHODS
To investigate this matter, the authors performed a post-hoc analysis of a randomised, double-blind, placebocontrolled cross-over trial (n=43).1 The trial investigated the separate and combined effects of low sodium (LS; aim 50 mmol Na+/d) and HCT (50 mg/d) on BP and albuminuria during standardised angiotensin-converting enzyme inhibition (ACEi; lisinopril 40 mg/d) in patients with diabetic nephropathy. Each treatment
period (normal sodium [NS]; LS; NS+HCT; LS+HCT) lasted 6 weeks. The authors categorised participants as above or below the median baseline 24-hour urinary potassium excretion (UKV), stratifying by sex, as a proxy for potassium intake. BP and albuminuria outcomes were defined as a percentage reduction from baseline systolic BP (SBP) and urinary albumin-creatinine ratio (ACR). Within both subgroups, the effects of the interventions were compared to baseline using repeated measures ANOVA (SBP) or paired Wilcoxon rank-sum analysis (log-transformed ACR). Post-hoc between-group comparisons were performed with Bonferroni testing.
RESULTS
A total of 43 patients (six female; mean age 64.9±1.4 years) had baseline UKV data
Figure 1: Violin plot showing the relative change from baseline albumin-creatinine ratio at each study period, for the low and high potassium excretion subgroups.
ACR = Albumin-creatinin-ratio; SR = Sodium restriction; HCT = Hydrochlorothiazide
The high potassium group showed a significant reduction in ACR at LS (p=0.011), HCT (p<0.0001), and their combination (p<0.0001). For the low potassium group, ACR was only significantly reduced from baseline at combined LS+HCT (p=0.034).
available and were included in this analysis. Complete ACR data was available for 33 patients. The mean estimated glomerular filtration rate was 65.2 (±3.9), mean SBP was 146.6±2.4 mmHg, and median albuminuria was 648.6 (251.2–1883.0) mg/24h. Median UKV in the high and low potassium groups was 94 (interquartile range: 90–111) and 64 (49–71) mmol/24u, respectively (p<0.0001). Baseline SBP, ACR, age, and the estimated glomerular filtration rate did not differ significantly between the groups. Although baseline sodium excretion was higher in the high potassium group (mean 191 versus 260 mmol/d; p=0.002), the percentual reduction in sodium excretion at LS was comparable between groups.
LS significantly reduced ACR in the high potassium group (p=0.011), whereas ACR reduction on LS was not significant in the low potassium group (p=0.058; Figure 1). HCT added to ACEi therapy without salt restriction reduced ACR significantly in the high potassium group (p<0.0001), but not in the low potassium group (p=0.2110).
Combining LS and HCT reduced ACR in both high (p<0.0001) and low potassium (p=0.034) groups. When comparing the subgroups, the high potassium group showed a significantly larger ACR reduction (p=0.010) during HCT therapy, and a trend towards a larger reduction with HCT+LS (p=0.050). The effect of LS alone was similar between high and low potassium groups (p=0.485).
Regarding BP, there was a significant reduction in SBP from baseline during LS in the low potassium group (p=0.003), but not in the high potassium group (p=0.208). In both groups, all further treatment conditions significantly lowered SBP from baseline.
Post-hoc analysis showed no significant differences in SBP reduction between high and low potassium groups, although there was a trend towards larger SBP reduction in the low potassium group during LS (p=0.070).
CONCLUSION
The authors found that higher baseline potassium excretion was associated with stronger albuminuria-reducing effects of salt restriction and HCT in patients with diabetic nephropathy on background ACEi therapy. These effects were not mediated by similar effects on BP.
References
1. Kwakernaak AJ et al. Effects of sodium restriction and hydrochlorothiazide on RAAS blockade efficacy in diabetic nephropathy: a randomised clinical trial. Lancet Diabetes Endocrinol. 2014;2(5):385-95.
2. Vogt L et al. Effects of dietary sodium and hydrochlorothiazide on the antiproteinuric efficacy of losartan. J Am Soc Nephrol. 2008;19(5):9991007.
3. Fujisaki K et al. Impact of combined losartan/ hydrochlorothiazide on proteinuria in patients with chronic kidney disease and hypertension. Hypertens Res. 2014;37(11):993-8.
4. De Borst M, Navis G. Sodium intake, RAASblockade and progressive renal disease. Pharmacol Res. 2016;107:344-51.
5. Aburto NJ et al. Effect of increased potassium intake on cardiovascular risk factors and disease: systematic review and meta-analyses. BMJ. 2013;346:f1378.
6. Mente A et al. Association of urinary sodium and potassium excretion with blood pressure. N Engl J Med. 2014;371:601-11.
7. Smyth A et al. The relationship between estimated sodium and potassium excretion and subsequent renal outcomes. Kidney Int. 2014;86:1205-12.
8. Wei K et al. Dietary potassium and the kidney: lifesaving physiology. Clin Kidney J. 2020;13(6):952-68.
Interaction of General Obesity and Abdominal Obesity, and Frailty in Patients with Chronic Kidney Disease
Authors: Changyuan Yang,1,2 Fuhua Lu,1
*Guobin Su1,3
1. State Key Laboratory of Traditional Chinese Medicine Syndrome, The Second Affiliated Hospital of Guangzhou University of Chinese Medicine, China
2. University Medical Center Groningen, University of Groningen, Groningen, the Netherlands
3. Karolinska Institutet, Stockholm, Sweden *Correspondence to guobin.su@ki.se
Disclosure: The authors declared no conflicts of interest.
Acknowledgements: The authors thank the participants of the NHANES study.
Chronic kidney disease (CKD) has become a major public health problem, affecting over 9.1% of adults globally.1,2 Frailty is marked by increased vulnerability to stressors due to a decline in physiological reserves and functioning across multiple organ systems.3 General and abdominal obesity are prevalent, with established associations to frailty in the elderly.4 However, few studies investigated these associations in patients with CKD, yielding inconsistent results.5,6
MATERIALS AND METHODS
This cross-sectional study analysed data from the National Health and Nutrition Examination Survey (NHANES, 2003–2018). Frailty was evaluated by the 36-item frailty index. General obesity was defined as BMI above 30 kg/m2; abdominal obesity was identified if waist circumference (WC) reached 102 cm in males and 88 cm in females. The association of general and abdominal obesity with frailty were
analysed using weighted multivariate logistic regression and restricted cubic splines. The interaction of general and abdominal obesity with frailty was examined.
RESULTS
Out of 80,312 participants, 5,604 adult patients (median age: 71 years; 42% males) with CKD were included in this analysis, with a median estimated glomerular filtration rate of 57.3 mL/min/1.73 m2
The prevalence of general obesity was 43.3%, while abdominal obesity was observed in 71.5% of the population.
Twenty-one percent were frail with general obesity, and 32% were frail with abdominal obesity. Overall, the prevalence of frailty tended to increase with age, whereas the prevalence of general and abdominal obesity tended to decrease with age.
Neither general nor abdominal obesity was associated with frailty. However, there was an interaction between general and abdominal obesity, and frailty. Compared to individuals with normal BMI and WC, those with both general and abdominal obesity, rather than only one, exhibited significantly increased odds of frailty (odds ratio [OR]: 1.53; 95% CI: 1.20–1.95). General obesity was associated with being frail only when patients with CKD had abdominal obesity (OR: 1.59; 95% CI: 1.08–2.36). When treating WC as a continuous variable, a considerable association of WC (for every 5 cm increase) and frailty was observed even after adjusting for BMI in fully adjusted model 3 (OR: 1.09; 95% CI: 1.02–1.17; P=0.01).
By employing the restricted cubic splines model, the authors observed an approximately linear relationship between WC and frailty. Further subgroup analysis based on sex identified threshold values for WC to prevent frailty at 122 cm for males and 103 cm for females, respectively.
CONCLUSIONS
The considerable prevalence of frailty and its potential link to adverse outcomes underscore the significance of understanding the factors contributing to frailty within this specific population. There may be an interaction between general and abdominal obesity, and frailty in patients with CKD. Interventions aimed at preventing frailty should consider both aspects.
References
1. Kalantar-Zadeh K et al. Chronic kidney disease. Lancet. 2021;398(10302):786-802.
2. Matsushita K et al. Epidemiology and risk of cardiovascular disease in populations with chronic kidney disease. Nat Rev Nephrol. 2022;18(11):696707.
3. Evans NR et al. Frailty and cerebrovascular disease: concepts and clinical implications for stroke medicine. Int J Stroke. 2022;17(3):251-9.
4. Yuan L, Chang M, Wang J. Abdominal obesity, body mass index and the risk of frailty in communitydwelling older adults: a systematic review and meta-analysis. Age Ageing. 2021;50(4):1118-28.
5. Li BH et al. The prevalence and influencing factors of frailty in patients with chronic kidney disease: a systematic review and meta-analysis. Int Urol Nephrol. 2023; 56(2):767-79.
6. Yang C et al. Prevalence and associated factors of frailty in patients with chronic kidney disease: a cross-sectional analysis of PEAKING study. Int Urol Nephrol. 2023;56(2):751-58.
Continuous Blood Pressure Monitoring with a Finger Cuff is Unsuitable for Intradialytic Blood Pressure
Monitoring
Authors: Sabrine Chaara,1,2 Paul Rootjes,1-3
Gertrude Wijngaarden,1,2 Menso Nubé,1,2 Camiel de Roij van Zuijdewijn,1,2,4 *Muriel Grooteman1,2
1. Department of Nephrology, Amsterdam University Medical Center, the Netherlands
2. Amsterdam Cardiovasular Sciences, Diabetes & Metabolism, Amsterdam, the Netherlands
3. Gelre ziekenhuizen, Apeldoorn, the Netherlands
4. Spaarne Gasthuis, Hoofddorp, the Netherlands
*Correspondence to mpc.grooteman@amsterdamumc.nl
Disclosure: All authors declared unrestricted grants received by the Amsterdam University Medical Center from Niercentrum aan de Amstel and B.Braun Avitum AG. Grooteman received payment to Amsterdam University Medical Center from Baxter and Fresenius Medical Care Deutschland GmbH, support to attend a meeting from Fresenius Medical Care Deutschland GmbH, and royalties or licenses from Wolters Kluwer. Chaara, Rootjes, Wijngaarden, Nubé, and Zuijdewijn declared no other conflicts of interest.
Intradialytic hypotension (IDH) is the most common complication of haemodialysis (HD). A purely nadir-based definition of IDH (nadir systolic blood pressure [SBP] of <90 mmHg or <100 mmHg, depending on the pre-dialysis SBP) was most strongly associated with mortality; whereas, definitions consisting of symptoms, as outlined in current guidelines, were not.1 The research team recently showed that the vast majority of IDH episodes (98%) are asymptomatic.2 Furthermore, in clinical practice, blood pressure (BP) is routinely measured twice per hour, while additional readings are only performed when symptoms arise. Hence, it is conceivable that the true incidence of IDH might be severely underestimated with the current routine BP-monitoring regimen.
AIMS
As intradialytic BP-drops may induce injury of vital organs, the primary goal is to assess the occurrence of IDH when BP is monitored continuously using a finger cuff (FC).
Yet, first, it appeared essential to validate intradialytic BP measurements using an FC by assessing the level of agreement with the standard oscillometric brachial arterial pressure (oBAP).
METHODS
Forty patients with HD were cross-over randomised to four dialysis modalities, each for 2 weeks: standard HD, cool HD, low-volume haemodiafiltration, and highvolume HDF. BP was measured every 15 minutes with an oBAP, and also every 20 seconds with a non-invasive FC device (ClearSight, Edwards Lifesciences, Irvine). For validation, the same arm sequential BP measurement method was applied. Paired BP measurements were compared with the Bland-Altman method. Bias was defined as the mean difference (MD) between oBAP and FC (oBAP minus FC), and 95% limits of agreement as the MD ±1.96 standard deviation The IDH analysis was restricted to FC measurements with an acceptable level of agreement, defined as a MD of ≤10 mmHg,3 and their corresponding 15-minute interval.
RESULTS
Seventy-five percent of participants were male, the mean age was 69.7 (±13.5 years), and median dialysis vintage was 3.0 years (interquartile range: 1.0–5.8). Diabetes mellitus and cardiovascular disease were present in 48% and 73% of participants, respectively. In 144 dialysis sessions, 33.4% of the FC measurements were missing, of which 43.8% were unexplained.
Validation
The Bland-Altman analysis of 1,221 paired BP measurements revealed a mean bias ± limits of agreement of 13±45 mmHg for SBP and 13±26 mmHg for diastolic BP.
IDH analysis
Twenty-seven percent of the paired BP measurements exhibited acceptable accuracy, resulting in the inclusion of 17,940 FC and 412 oBAP measurements. The FC detected 439 IDH episodes that had a median duration of 40 seconds (two measurements), with 1,703 out of 17,840 measurements meeting the IDH criteria. In contrast, during the same period, only 20 IDH episodes (of 412 measurements) were detected by the oBAP method.
CONCLUSIONS
Continuous BP-monitoring revealed an IDH occurrence which was ±22 times higher than 15-minute interval BP measurements, indicating that the majority of IDH episodes are missed with the current routine regimen.
As the FC showed poor accuracy and precision compared to the oBAP method, this method is, in fact, inappropriate for intradialytic BP-monitoring in patients undergoing HD.
References
1. Flythe JE et al. Association of morality risk with various definitions of intradialytic hypotension. J Am Soc Nephrol. 2015;26(3):724-34
2. Chaara S et al. No relation between intradialytic hypotension and physical adverse symptoms. ERA24, 23-26 May 2024.
3. Stergiou GS et al. A universal standard for the validation of blood pressure measuring devices: Association for the Advancement of Medical Instrumentation/European Society of Hypertension/ International Organization for Standardization (AAMI/ESH/ISO) Collaboration Statement. J Hypertens. 2018;36(3):472-8.
Impact and Interest of Implementing the EKFC Formula over CKD-EPI for Estimating
Glomerular Filtration Rate in Automated
Estimated Glomerular Filtration Rate
Reporting Within Laboratory Practice
Authors: *Laurence Derain Dubourg,1,2,3 Sandrine Lemoine,1,2,4 Pierre Letourneau,1 Lara Cabezas,1 Aurelie De Mul,1,2,5 Laurence Chardon6
1. Service de Néphrologie, Dialyse, Hypertension et Exploration Fonctionnelle Rénale, Centre de Référence des Maladies Rénales Rares MAREGE, filière maladies rares ORKID, Hôpital E. Herriot, Hospices Civils de Lyon, France
2. Faculté de Médecine Lyon Est, Université de Lyon, France
3. CNRS UMR 5305, University of Lyon 1, France
4. INSERM CARMEN 1060 IRIS Team, Lyon, France
5. INSERM1033, Lyon, France
6. Service de Biochimie et Biologie Moléculaire, Laboratoire de Biologie Médicale Multi-Sites (LBMMS), Hospices Civils de Lyon, Bron, France
*Correspondence to laurence.derain@chu-lyon.fr
Disclosure: Derain has received support for attending meetings and/or travel from Boehringer Ingelheim in 2023 for the SFNDT Congress held in Liège, Belgium. The other authors have declared no conflicts of interest.
The automatic reporting of estimated glomerular filtration rate (eGFR) for all creatinine (Pcr) determination is mandatory, and the CKD-EPI 2009 formula1 is considered the most accurate. However, CKD-EPI is inadequate in young adults and is debated in the elderly. The EuropeanKidney-Function-Consortium (EKFC) equation2 provides continuous eGFR
from 2-year-olds to elderly. The authors’ objective was to assess the impact of using the EKFC compared to CKD-EPI.
METHODS
The authors retrieved data from the laboratory database, including gender, age, and Pcr for all patients over 18 years in November 2023. eGFR was calculated using the CKD-EPI and the EKFC. Results were expressed as the mean bias between EKFC and CKD-EPI (as reference) according to age groups.
RESULTS
A total of 10,066 patients (50.5% females; mean age 56.0±21.2 years [18.0–106.7]) underwent Pcr determination (mean 84.7±72.3 µmol/L) with 1,706 (16.9%) and 405 (4.0%) having a GFR <60 or <30 mL/ min/1.73 m2, respectively. Bias EKFC-CKDEPI was small (-3.3±3.1 mL/min/1.73 m2) in the 40–70 years group, whereas it was increased both in young adults and elderly (-16.4±5.1, -6.2±4.6, and -6.9±3.6 mL/ min/1.73 m2 in the 18–25, 25–40, and >70 years groups, respectively). The proportion of misclassified patients with GFR <60 mL/ min/1.73 m2 is small, except in the elderly (9.3%) when CKD-EPI is considered less accurate.
CONCLUSION
The use of EKFC in laboratories to estimate eGFR offers continuous GFR estimation from 2-year-olds to the elderly, and could be an alternative to CKD-EPI.
The automatic reporting of eGFR with EKFC by laboratories could allow for an earlier diagnosis of CKD, and initiation of nephroprotection in young adults and the elderly.
References
1. Levey AS et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150:604-12.
2. Pottel H et al. Development and validation of a modified full age spectrum creatinine-based equation to estimate glomerular filtration rate: a cross-sectional analysis of pooled data. Ann Intern Med. 2021;174:183-91
Congress Interviews
The following interviews delve into the latest developments showcased at the 2024 European Renal Association (ERA) Congress held in Stockholm, Sweden from 23th–26th of May. We spoke with Local Congress President Peter Stenvinkel, Karolinska University Hospital and Karolinska Institutet, who shared with us changes to the ERA scientific programme and the ERA’s vision for the future. Discussions with young investigator awardees Jeroen de Baaij, Jasper Callemeyn, and Elisabet Van Loon provided us insights into their exceptional careers in research and clinical practice.
Featuring: Peter Stenvinkel, Jeroen de Baaij, Jasper Callemeyn, and Elisabet Van Loon
Peter
Stenvinkel
Professor of Nephrology, Karolinska University Hospital and Karolinska Institutet, Stockholm, Sweden
In 2020, Stanford University recognised you as the world’s 13th most influential nephrologist. Following your initial medical training, what led you to pursue a career in nephrology?
To be honest, it was the only place I got a job. But when I started to work in nephrology, I found it to be very diverse, with so many different aspects to it. It’s not just the kidneys; it’s also the heart, brain, gut, skeleton, and the immune system. The diversity was the reason why I wanted to continue working in the field.
Q2 As local congress President for the European Renal Association (ERA), how have you helped shape the 2024 programme and what are the most significant changes compared to the 2023 Congress?
I was part of the Organising Committee, and I think my part
of the programme was to bring in some aspects of solutions that we can get from nature. We had a special session that discussed what we can learn from tigers and the Burmese python, how to generate water from fat, and lessons from the animal kingdom. Of course, we also had the plenary lecture by Barbara NattersonHorowitz, University of California, Los Angeles, USA, an expert on natural solutions that we can help bring to medicine. I've been interested in this area for many years, and we are going to start a post-ERA meeting where we, the clinicians, and basic researchers, meet psychologists, veterinarians, and biologists to brainstorm about solutions from nature, and how we can bring that in to benefit humans.
I just published a popular science book about nature's intelligence, discussing all these aspects. If we want to find solutions for what's happening now on our
planet regarding changes in the environment, we need to combine human intelligence with AI and nature's intelligence, because there are many answers out in nature.
We are also launching a digital game at ERA 2024. Over 2.5 years, we have developed a new game in which health professionals can learn how planetary health works and connect the dots to learn how they best can change their prescription patterns, eating habits, and lifestyle to promote better planetary health.
Q3
What does the 61st ERA Congress’s overarching theme, ‘Rethinking Kidney Health and Transforming Kidney Care’, mean directly for nephrologists and indirectly for patients?
We need to include patients in everything we do, and I think that this is done more and more now. They are the persons we
should work for, and so, rethinking kidney disease applies to both nephrologists and patients. Is this theme aimed at more of a preventative approach, as opposed to an approach of treating when sick?
Yes, preferably, we should have preventive strategies, and I think the key areas are lifestyle habits. We need to live a more sustainable life and we need to change our eating habits. Of course, we also need to be more active and not as sedentary. It's a growing concern among many of our children now in Europe and the USA, as they eat a lot of ultra-processed food, and they are not active enough. Transforming kidney care can be seen as more of a spotlight on some of the elements that physicians may not have focused on as much traditionally.
We need to live a more sustainable life and we need to change our eating habits
Q4
One of the ERA’s goals is to “educate the community about risk factors for kidney disease, lifestyle changes, and the importance of regular health checks” and to “promote healthy lifestyles." What steps is the organisation taking to achieve this?
We have a number of lectures on that. We had a tent in Central Stockholm, where dietitians, nurses, and some doctors were in attendance to educate the general public about the importance of kidney health. They discussed dietary habits and measured blood pressure. I think we make need to make the public aware of how common chronic kidney disease is, and that it is possible to do something about it if it's recognised early.
Q5 What new technologies and innovations being presented at the ERA 2024 Congress do you believe have the potential to significantly impact the field of nephrology in coming years?
AI is here to stay, and we really need to take advantage of the opportunities that this brings. I think kidney disease, and the science, will be much improved by AI.
Do you see a main area where you think it will take off initially?
Yes. In large studies with lots of data, help with processing data and spotting the patterns we can’t
see ourselves will be valuable. We really need the help that AI can offer, because it's a little beyond human intelligence.
Q6
In the recently published review you co-authored, entitled ‘Food as medicine: targeting the uraemic phenotype in chronic kidney disease’, what are the key messages for healthcare professionals?
Food contains a lot of bioactive nutrients. Some, there are way too many of, and some far too little of. In this paper, we discussed what we should eat less of and of course, red meat and ultraprocessed foods are not good for our health or that of the planet. Following plant-based diets gives the opportunity to not only benefit our health, but also planetary health and the environment. So, here we have a win–win situation. If we can change the dietary habits and how we eat food, it will be an opportunity to benefit both our health and the environment.
Do you think it’s going to be quite a difficult mission to challenge people's views around diets?
Yes. We will make an attempt at the Presidential dinner. It will not be an ordinary dinner, because we will test a menu that has been designed by one of Sweden's top chefs, together with the World Wildlife Foundation (WWF), called The One planetary health plate. That plate has only taken 0.5 kg of CO2 to produce, compared to the usual 5 kg, or 10 times more if you
Motivating students is the most interesting part of working as a clinical doctor and researcher
have dinner with red meat in it. We await seeing how the guests will like this plant-based dinner with very, very low CO2 emissions and fingerprint.
Q7 You currently have more than 625 original publications and reviews to your name for your research in nephrology. What do you believe to be the current gaps in literature and what topics merit greater attention?
For transplantation, we know that the outcome has been much better. But after 10–20 years, the grafts start to work less and less well. We need ways to postpone this loss of transplant function. For this, we have the combination of lifestyle habits and maybe new drugs that target complement. This is a hot topic in nephrology. Of course, patients on dialysis have a very high mortality rate, and we need to find ways to postpone progression of kidney disease, so that less patients go on to dialysis. We are thrilled by the new drugs, the sodium glucose cotransporter 2 inhibitors and glucagon-like peptide-1 receptor agonists.
Have transplant populations been included in those trials?
That's the problem. Now we need to find out if we can use these drugs that do so much good in the patients with chronic kidney disease, and see if we can use the same drugs for patients that are transplanted. I think we can, but we need to test that. The optimisation of kidney donors and donor-recipient matching is also very important.
Q8
You have received the Karolina Price award, the Vizenca award, and the Addis Gold medal for your research, but what has been the proudest achievement of your career?
My proudest achievement would be being a lecturer for students and finding out that they are interested in nephrology, asking questions, and starting to think about how they can improve for patients and their future career. I think motivating students is the most interesting part of working as a clinical doctor and researcher. This also involves trying to make them aware of the environmental situation, as working to lessen the CO2 footprint and eat more sustainably is something that will take up quite a large part of their careers.
AI is here to stay, and we really need to take advantage of the opportunities that this brings
Jeroen de Baaij
Associate Professor in Kidney Physiology, Radboud University Medical Center, Nijmegen,
the Netherlands
I'm even more interested in understanding the mechanisms within the kidney, and how it is regulated
Q1 Congratulations on receiving the prestigious ERA Rosanna Gusmano Award for Young Investigators in Basic Science at the 61st European Renal Association (ERA) Congress. What work led to this and what does receipt of this award mean to you?
First, it means a lot that the ERA has awarded the work I have accomplished in the last 10–15 years. It is special and a real award for the team. In the last 10 years, we have been working mainly on identifying new genetic causes for salt and magnesium-wasting disorders in the kidney. These patients have low serum magnesium or potassium levels, which typically runs in the family. This may result in multiple complaints, in the case of magnesium disorders, we often see seizures and muscle cramps. Although, for many of these diseases, we already know the cause, my work mainly focuses on the patient families where we could not find the cause. In the last 10 years, we have identified five or six new genes responsible for these disorders. This is the main achievement that led to this award.
Q2 You are now an Associate Professor in Renal Physiology. What ignited your interest in kidney physiology, and more specifically the genetic and regulatory pathways involved in renal salt and mineral reabsorption?
The kidney is a fascinating organ. To know the number of different processes and regulations taking place in the kidney and the
amount of work that the kidney does daily to filter our blood and create urine is really fascinating. More specifically, if I look at my work and the disorders that we work on, we work towards finding these genetic causes that not only gives an answer to the families regarding the origin of their diseases, but it also teaches us a lot about how the kidney works. As a basic scientist, I'm even more interested in understanding the mechanisms within the kidney, and how it is regulated. Especially from rare diseases, we learn a lot because these patients don't have multiple pathways that are disturbed, they have only one genetic mutation which informs us about how this specific pathway regulates ion transport in the kidney.
Sometimes people ask me "Why do you work on a disease where maybe in the whole of Europe only 50 people are affected?" It teaches us a lot, not only about the 50 patients but about the function of the kidney. We can often translate what we find in these rare patients to much bigger patient groups. For instance, with magnesium disorders, we have these very rare families with one mutation; however, in diabetes, we know that patients lose a significant amount of magnesium in urine, so the same mechanism is affected. By addressing the rare disorders, we can impact millions of people all over Europe.
Q3
Your mission is to decipher the pathophysiological mechanisms of magnesium disorders, including the role of magnesium in chronic kidney disease. Where should future research focus to further improve our understanding of this?
We need improved disease models to get a better understanding of kidney disease. One big limitation of basic science in the kidney is that we don't have good cell models for many of the cells in the kidney. Therefore, the generation of kidney organoid models is an exciting development. If we can get these kidney organoid models into the right differentiation pathways, it allow researchers to generate patient-specific models. If we can take cells from the patient and generate a model in the lab that is specific to the patient and the patient's mutation, it would allow researchers to look at personalised treatments for the specific patient.
Q4
“Personalised drug screening to identify therapeutics that fit the needs of individual patients” is part of your vision for the treatment of rare diseases, but how far are we from this for rare kidney diseases?
My research aims to get personalised drug screening by generating personalised disease models, testing which drug would work in the lab, and then eventually translating this to patients. This can allow us to test drugs that have already been approved. It is, of course, much more challenging to generate new drugs; however, we can repurpose drugs that are already out there for other diseases. Repurposing drugs using the new models that we are generating is quite close, we see examples right now in certain diseases where these organoid models are being used for drug screenings. Together with my colleague Tom Nijenhuis in the Radboud University, we aim to repurpose drugs in cell and animal
models and perform clinical trials for single patients. In an-of-one trial, you can test multiple drugs to develop personalised treatment. However, it is still very much in a research setting and we should see how we can translate this for a much larger population.
Q5 Have you experienced any challenges in translating your research into clinical studies?
The work we have discussed, where I focus on genetic disorders, has mainly been translated into diagnostics. We have better diagnostic genetic panels where these genes have been included, and now, worldwide, patients are being identified with new mutations in the genes that my group identified. This part of the translation is happening right now, but finding therapies remains a big challenge, requiring significant funding and a lot more work to therapeutically target these
pathways. However, it is going much better for other parts of my research, I am also looking at magnesium and other effects on vascular calcification in chronic kidney disease. These patients have mineral reserves with high phosphate calcium levels and form calcifications. We have demonstrated in our cell models that magnesium can prevent this. Currently, clinical trials are being performed with other groups utilising magnesium supplements to see if we can treat patients with this knowledge.
My research aims to get personalised drug screening by generating personalised disease models
Q6 Are there any repurposed medications or therapies right now that are having an impact on patients with rare kidney disorders, particularly magnesium disorders?
Several reports showed that the repurposing of SGLT-2 inhibitors, originally a diabetes drug, is being used more widely for patients with chronic kidney disease. SGLT-2 inhibitors have improved magnesium levels in some patients with rare kidney magnesium disorders. Together with colleagues from Rotterdam and Amsterdam, we are trying to perform small-scale clinical trials with patients with genetic hypomagnesaemia.
Q7 'Hypomagnesaemia with varying degrees of extrarenal symptoms as a consequence of heterozygous CNNM2 variants' is a recent publication you co-authored. What are the key messages from this article for clinicians?
We often see that new genes are being identified in patients at a very young age. However, it is essential to not only identify the gene but also to do the follow-up. We must keep following up with these patients to get a better view of the development of the disease at later ages. Only by studying much larger patient groups can we generate a good phenotypic description, which will help clinicians identify suitable patients in the future and think about genetic screening in patients where the phenotype aligns but with no apparent family history. This paper looked at a group of patients with CNNM2 mutations. This gene was identified 10 years ago, and we now have, I think, a decent core population in Europe. In this paper, we describe 10 patients, but we had another cohort about a few years ago, and in this paper, we tried to show the evolving phenotype in these patients. For the CNNM2 variants, we have an extensive discussion on whether obesity is part of the phenotype or not, and recent studies show that it is more common but not present in all patients. We also discussed seizures in patients with hypomagnesaemia having CNNM2 variants. So, we tried to get a better view of the phenotype of patients with CNNM2 mutations.
Q8 Do you believe that, with genetic screening programmes, the follow-up and characterisation of the patient's phenotype is often neglected?
Often, these mutations are identified in paediatric populations. However, for many diseases, some of the phenotypes may only develop later in life, and cohorts of patients with rare diseases may be in their 40s, 50s, or 60s. These studies are not often published because following
up on these patients for a long time is challenging. However, it is important because one of the questions I always get when I speak to patients with rare kidney disease is, "What can I expect in the next 10, 20, 30 years? What should I do now to improve my phenotype in the future?”
Therefore, I think it's important to follow up with patients later in life, especially patients who have a mutation identified in childhood.
Q9
'Team science' is something you talk about within your own research group, and supporting early career researchers and clinical scientists. What does this look like within your own research group?
'Team science' is a fascinating development because right now, patients with rare diseases are all over Europe; only by working together with people from all over Europe, using different technical and biological expertise, can we solve all the important issues for these patients. To develop treatment for these patients, one might need expertise in therapy, design and model development, which is not possible alone. Only by working in a big team can we solve all these issues, and it's more fun if you work together and get input from
diverse backgrounds. I always try to connect the people within my group as well as with groups outside of my lab through lab visits or regular meetings.
Q10
In terms of your mission and vision, what’s next for your research team?
In the last few years, my team has focused on identifying the genetic causes of rare kidney diseases. Fortunately, with the advances in genetic techniques, more and more patients now receive a genetic diagnosis. In the near future, we will reach the point where most of the genes have been found. The next step is to provide therapy for these patients. Moreover, for many rare kidney diseases, currently, there is no therapy that targets the cause of their disease. There is a lack of gene therapies that target the pathways which are disturbed in the kidneys of these patients. This relies not only on gene therapy, it also includes drug repurposing. From this diagnostic question to a more treatment perspective, it is important for the team to step up now. This is quite a challenge because it requires a new way of thinking and working.
It teaches us a lot, not only about the 50 patients but about the function of the kidney. We can often translate what we find in these rare patients to much bigger patient groups
Jasper Callemeyn Nephrology Fellow and PhysicianScientist, University Hospitals
Q1 Congratulations on receiving a prestigious European Renal Association (ERA) Stanley Sheldon Award for Young Investigators in Translational Science at the 61st ERA Congress. What work led to this, and what does receipt of this award mean to you?
It is an absolute honour to receive this prestigious award. I was awarded this prize for my work studying the role of the innate immune system in rejection after kidney transplantation. I consider this award not merely as a celebration of my work alone, but as the recognition of a group effort in which many people supported me.
Rejection after kidney transplantation is a complex and multifaceted problem
Q2
When did you realise that you wanted to specialise in transplantation nephrology, and how did you come to start your academic research in transplant rejection?
As a resident of Internal Medicine, I was confronted with the impact that end-stage kidney disease has on patients and how life-changing the gift of a kidney transplantation can be. However, survival of kidney allografts after transplantation is often suboptimal, and many cases of premature graft failure can be attributed to rejection. I decided to pursue a career in kidney transplantation with the intention to improve the care for kidney transplant recipients and
to increase our understanding of transplant immunology.
Q3 You presented during the Young Awardees symposium at ERA 2024. What are the key take-home messages from this presentation?
In my presentation, I highlighted that rejection after kidney transplantation is a complex and multifaceted problem. I argued that acknowledging this complexity will improve the care for our patients. In addition, evidence is accumulating on the role of the innate immune system in allorecognition, which may lead to new treatment options and improved outcomes.
Q4 What do you think are the biggest gaps in our understanding of immunemediated transplant rejection that research should focus on addressing to improve patient outcomes?
We highlighted the role of several key players that were hitherto insufficiently acknowledged, such as natural killer cells and other components of the innate immune system. To translate these findings to clinical implementation, we should now aim to further explore the importance and interactions of these mechanisms in larger validation cohorts. This will also require the early involvement of companies, regulatory agencies, and patient organisations.
Q5 Other than receiving your award, what are your key highlights from ERA 2024?
I was impressed by the high quality of many of this year’s sessions. In particular, the late-breaking sessions were a testimony to the revolution that nephrology is currently experiencing. In my area of expertise, the positive results from the trial investigating felzartamab for the treatment of antibodymediated rejection were very promising. If future larger trials confirm this effect, we are truly at a turning point in the care for our patients with antibody-mediated rejection.
Q6 In the recently published article, you co-authored 'Revisiting the changes in the Banff classification for antibodymediated rejection after kidney transplantation.' What was the key message you were trying to deliver?
In this article, we investigated the evolution of the international
Banff classification for allograft pathology, which is used to classify rejection. We demonstrated that the 2017 version of this classification took a step in the wrong direction by no longer acknowledging cases in which the picture of antibodymediated rejection was unclear. This data, together with the work of many other groups, has led to a revision of the Banff 2022 classification, which now incorporates two new phenotypes in the spectrum of microvascular inflammation.
Q7 With the success you’ve had so far, what advice would you give to early-career physicians looking to embark on their research journey?
Find yourself a mentor who can provide you with a nurturing environment to grow in. Dare to question dogma, take the time to step back and think broadly about your subject matter. Follow your data and open yourself up for unexpected turns. Serendipity may lead you to the most profound insights.
Serendipity may lead you to the most profound insights
Elisabet Van Loon Nephrology resident, University Hospitals Leuven, Belgium
Q1 Congratulations on receiving a prestigious European Renal Association (ERA) Stanley Shaldon Award for Young Investigators in Translational Science at the 61st ERA Congress. What work led to this, and what does receipt of this award mean to you?
Connects nephrologists from across Europe and the world, increasing opportunities for collaboration and exchanging new ideas
Thank you, it is an immense honour to receive this award. It recognises the research that my team and I have conducted over the past few years, mainly during my PhD. My research focused on uncovering non-invasive signatures of the pathology of renal allografts, with an important focus on taking the field of noninvasive biomarkers of rejection after renal transplantation further towards clinical implementation.
Q2
How much of an impact do you believe the ERA Congress has, both directly on nephrologists and indirectly on patients?
I think the impact of the congress cannot be underestimated. Very important new trials were presented that have a direct impact on clinical practice, and therefore a very direct potential to improve patient care. It also connects nephrologists from across Europe and the world, increasing opportunities for collaboration and exchanging new ideas to advance the field.
Q3 Was there a particular event or person that encouraged you to pursue a career in nephrology, specifically in kidney transplantation research?
As a medical student, I had an early fascination with nephrology and kidney transplantation. During a clinical rotation, I met my mentor Maarten Naesens who encouraged and inspired me to pursue a PhD in renal transplantation. His help and encouragement during the 4 years of my PhD were unwavering and
Through the lens of omics technologies, we uncover hidden signatures in the molecular landscape
made these years a wonderful time in which I learned a lot that I continue to look back on.
Q4 Your main research focus is on the development and clinical use of non-invasive diagnostic biomarkers of rejection, and the integration of these biomarkers into the risk assessment pipeline for renal transplantation management. How far are we from biomarkers being commonly used in the risk assessment pipeline, and what more needs to be done?
Many biomarkers for rejection have been proposed in the literature, but unfortunately, the essential steps to make them suitable for clinical application were often missing. External validation in independent cohorts with real-world disease prevalence is one such essential step. In recent years, some biomarkers have been validated and shown to have great potential for clinical practice, such as urinary chemokines and donor-derived cell-free DNA. Further steps towards clinical implementation include randomised trials and technical optimisation of tests, as well as approval by authorities and reimbursement.
Q5
In the recently published article you co-authored, entitled ‘The Clinical Relevance of the Infiltrating Immune Cell Composition in Kidney Transplant Rejection’, what was the key message you were trying to deliver, and what does it mean for physicians?
Although convenient from a clinical and ontological point of view, the dichotomy between T cell-mediated rejection and antibody-mediated rejection does not fully reflect immunopathological reality. The relationship between the rejection phenotypes defined by Banff and the types of infiltrating immune cells is currently not well mapped. We studied the infiltrating immune cell types to improve the diagnostic classification by including more causal information and enabling the development of targeted therapies. We found that the total estimated immune cell composition of kidney grafts was poorly related to the main rejection categories defined by Banff and contributed to the evaluation of rejection severity. Intragraft CD8temra cells were associated with graft failure and could be a potential new therapeutic target.
Q6
How have you seen the advent of new technologies significantly impact the field of kidney transplantation in recent years?
Through the lens of omics technologies, we uncover hidden signatures in the molecular landscape, paving the way for accurate prognostics and timely interventions. This enables us to move further towards personalised treatment tailored to the individual. Targeted therapies, such as newer immunotherapies, create a formidable ally in our fight against kidney disease. Furthermore, artificial intelligence is helping us unlock insights from big data that can advance clinical practice.
Q7
In 2023, you were awarded the L(euvense) da Vinci Prize ESOT Leonardo Da Vinci Transplant Research Innovation Award. What has been your proudest achievement since receiving these awards?
For the last 2 years, I have been completing my fellowship, so I have mainly focused on clinical work. I have gained a lot of clinical experience and knowledge, and I am proud to finally graduate as a nephrologist this summer.
Is Lack of Consensus on the Management of Chronic Active Antibody-Mediated Rejection Harming Renal Transplant Recipients?
Author: *Lionel Rostaing1
1. Service de Néphrologie, Hémodialyse, Aphérèses et Transplantation rénale, CHU Grenoble Alpes, France *Correspondence to lrostaing@chu-grenoble.fr
Disclosure: The author has declared no conflicts of interest.
RESEARCH INDICATES THAT VALUABLE DIAGNOSTIC PROTOCOLS AND TREATMENTS ARE NOT BEING LEVERAGED WITHIN THE MANAGEMENT OF CHRONIC ACTIVE ANTIBODY-MEDIATED REJECTION
In 2022, over 92,000 kidney transplants were performed globally.1 With advancements in transplant science, 1-year graft survival rates have reached 94.3% for deceased donor kidney transplant recipients, and 97.8% for living recipients. However, 5-year graft survival remains at 76.3% and 86.5%.2
Antibody-mediated rejection (AMR) is one of the most common causes of immunerelated allograft rejection.3 Chronic active AMR (CABMR) typically develops 6–12 months post-transplant; 76% of kidney transplant recipients with CABMR experience graft loss 1.9 years after diagnosis.4 Despite these alarming figures, consensus guidelines on the management of post-transplant patients have not been updated with advancements in testing
and protocol biopsies, and there is currently no consensus in Europe on CABMR management.5
Given this lack of consensus, what does the clinical landscape look like for patients with CABMR? By conducting an online survey with European nephrologists, transplant nephrologists, and transplant surgeons (N=52) with 3–30 years of experience, the author sought to identify the common practices in the post-transplant monitoring of patients receiving a renal allograft 1 year post-transplant. The survey comprised 58 multiple choice and open-ended questions, which were informed by epidemiological data on AMR, current treatment options, and the personal experiences of the developers. Questions related to respondent demographics, patient caseloads, posttransplant routine screening, and CABMR treatment. Insights from the survey reveal some key barriers to the optimal care of renal transplant recipients.5
VALUABLE DIAGNOSTIC PROTOCOLS ARE NOT BEING USED
Most surveyed physicians restrict posttransplant surveillance to assessing measures of kidney graft function. In the first year following transplant, 88% assess creatinine, and 79% assess proteinuria every 1–3 months. All physicians assess creatinine and proteinuria every 1–6 months.5 However, solely relying on these measures may be suboptimal; research indicates that many CABMR episodes manifest as subclinical changes to the allograft, which do not impact on earlystage creatinine or proteinuria.6
CABMR is characterised by donor-specific antibodies (DSA) in the host binding to human leukocyte antigens within the kidney allograft, leading to complementmediated tissue damage. According to the literature, de novo DSA assays can help monitor alloimmunity risk.7 Yet, the lack of DSA testing guidance has created confusion regarding its applicability, as was substantiated by the author’s survey: 81% of physicians assess de novo DSA in presensitised patients at least once per year, while 67% do so in patients who are not pre-sensitised.5
As demonstrated in the literature, protocol biopsies remain the only definitive CABMR and subclinical rejection diagnostic method.6 Yet, only 27% of survey respondents perform surveillance biopsies routinely 6–12 months post-transplant.5
More recently, a single-centre study comprising two independent cohorts, revealed donor-derived cell-free DNA in peripheral blood as a biomarker of AMR, although its diagnostic value remains unclear.8 Only 13% of surveyed physicians report using cell-free DNA testing in a small portion of patients.5
CHRONIC ACTIVE ANTIBODYMEDIATED REJECTION TREATMENT IS LIMITED TO IMMUNOSUPPRESSION
Immunosuppressants are the primary treatment for CABMR, with all surveyed physicians using mycophenolate mofetil and tacrolimus, and 94% using glucocorticoids.5 More than half (52%) of patients do not receive additional treatments, primarily due to disease severity (67%), and lack of evidence regarding other treatments (61%). Although 33% of physicians believe immunosuppression is sufficient, only 57% of patients achieve adequate disease control without additional treatment modalities.5
Besides maintenance immunosuppression, according to the author’s survey, intravenous immunoglobulins (71%), steroid pulse (71%), and apheresis (62%) are the most commonly used treatments.5 As supported by a review, several biologics have been under investigation for the treatment of CABMR, including the monoclonal antibodies rituximab and eculizumab, and the recombinant monoclonal antibody tocilizumab.9 However, only 50% of survey respondents prescribe rituximab, 31% tocilizumab, and 4% eculizumab, respectively;5 this is a hesitancy that could stem from the need for further efficacy and safety support.5 Rituximab, for example, is associated with an elevated risk of pneumonia, bronchiectasis, and pulmonary fibrosis.10
THE WAY FORWARD
For patients with end-stage renal disease, kidney transplantation offers significantly improved quality of life compared with maintenance haemodialysis.11 Unfortunately, advancements enabling the transplantation of highly sensitised patients with or without preformed DSA(s) are being held back by significant variations in CABMR surveillance and management across Europe. Expert consensus is the critical next step to reducing the burden of transplant rejection.
References
1. Statista. Estimated number of worldwide kidney transplants in 2021, by region. 2023. Available at: https:// www.statista.com/statistics/398657/ kidney-transplants-by-world-region/. Last accessed: 20 November 2023.
2. Poggio ED et al. Long-term kidney transplant graft survival - making progress when most needed. Am J Transplant. 2021;21(8):2824-32.
3. Sellarés J et al. Understanding the causes of kidney transplant failure: the dominant role of antibody-mediated rejection and nonadherence. Am J Transplant. 2012;12(2):388-99.
4. Redfield RR et al. Current outcomes of chronic active antibody mediated
rejection – a large single center retrospective review using the updated BANFF 2013 criteria. Hum Immunol. 2016;77(4):346-52.
5. Rostaing LPE et al. Post-transplant surveillance and management of chronic active antibody-mediated rejection in renal transplant patients in Europe. Transpl Int. 2023;17(36):11381.
6. Terrec F et al. Protocol biopsies on de novo renal-transplants at 3 months after surgery: impact on 5-year transplant survival. J Clin Med. 2021;10(16):3635.
7. Zhang R. Donor-specific antibodies in kidney transplant recipients. Clin J Am Soc Nephrol. 2018;13(1):182-92.
8. Mayer KA et al. Diagnostic value of donor-derived cell-free DNA to
9. van Vugt LK et al. Investigational drugs for the treatment of kidney transplant rejection. Expert Opin Investig Drugs. 2022;31(10):1087-100.
10. Ayyad M et al. Rituximab-induced immune dysregulation leading to organizing pneumonia, bronchiectasis, and pulmonary fibrosis. Cureus. 2023;15(2):e34798.
11. Attiq H et al. Health related quality of life among ESRD patients on hemodialysis and kidney transplant recipients: a comparative study. EJMED. 2023;5(1):44-8.
Immune complex-mediated membranoproliferative glomerulonephritis (iMPGN) can develop in association with autoimmune diseases such as primary biliary cholangitis (PBC), a chronic cholestatic liver disease characterised by destruction of the small and mediumsized bile ducts. Although the pathogenesis cannot be clearly defined, iMPGN and PBC overlap through the activation of innate and adaptive immune cells and the production of proinflammatory mediators. In this report, the authors present a case in which iMPGN and PBC were diagnosed simultaneously.
Key Points
1. The aim of the treatment of membranoproliferative glomerulonephritis due to secondary causes is to treat the underlying primary cause; for which renal support treatment is also essential. Immune complex-mediated membranoproliferative glomerulonephritis (iMPGN) secondary to primary biliary cholangitis (PBC), an autoimmune disease, is a very rare condition and its treatment is that of the secondary cause, PBC.
2. This is a very rare case report describing the association between iMPGN and PBC responding to ursodeoxycholic acid and non-immunosuppressive supportive therapy.
3. Every patient with iMPGN should be investigated for secondary aetiologies, and it should be kept in mind that, with appropriate treatment, iMPGN can be treated without the need for immunosuppressive therapy.
INTRODUCTION
Membranoproliferative glomerulonephritis (MPGN) is a glomerular disease characterised by mesangial expansion, endocapillary proliferation, and double contours of the glomerular basement membrane on light microscopy; by complement deposition with or without immune complex deposits on immunofluorescence; and by electrondense deposits in the mesangium, subendothelium, or subepithelium on electron microscopy. Depending on the pathogenesis, MPGN is divided into complement-mediated MPGN and immune complex-mediated MPGN (iMPGN). iMPGN may develop secondary to chronic infections such as hepatitis B virus, hepatitis C virus, and monoclonal gammopathies, or in association with autoimmune diseases such as systemic lupus erythematosus, rheumatoid arthritis, or primary biliary cholangitis (PBC). Immune complexes, formed by the binding of antigens to antibodies in the bloodstream or in situ, can activate complement pathways, induce inflammatory cytokines, recruit leukocytes, and cause tissue damage.1
PBC is a chronic liver disease that mainly affects middle-aged females and is prevalent worldwide. The unclear aetiopathogenesis is thought to be due to a complex interaction between genetic factors such as HLA-DR8, and environmental factors such as microbial infections. The main histopathologic feature of PBC is chronic, non-suppurative destructive cholangitis leading to progressive loss of intrahepatic bile ducts and cholestasis. The most common symptoms are fatigue and pruritus. Other symptoms include jaundice, xanthomas, osteoporosis, portal hypertension, and hepatic encephalopathy.2 The association between MPGN and PBC is rare and has only been described in a few case reports.3,4 Here the authors present a case diagnosed with iMPGN and PBC, with parallel clinical courses of liver and kidney disease.
CASE PRESENTATION
A 43-year-old female patient with no medical history presented with complaints of fatigue, itching, jaundice, and oedema. She was not taking any medication. There was no family history of autoimmune diseases. The patient was referred to the nephrology department because of a serum creatinine level of 3.13 mg/dL (reference value: 0.5–0.9 mg/ dL) and macrohematuria. The baseline creatinine value was not known. The daily urinary protein excretion rate was 10,400 mg/day (reference value: 80–150 mg/day).
Viral (hepatitis B, hepatitis C, Epstein–Barr virus, HIV, rubella virus, rubeola virus, varicella, cytomegalovirus, and herpesvirus) and autoimmune markers (including rheumatoid factor, antiphospholipid IgM and IgG, the extractable nuclear antigen panel, anti-liver kidney microsomal, anti-double stranded DNA, antineutrophil cytoplasmic antibodies, antiglomerular basement membrane, and anti-smooth muscle) were all negative. Protein electrophoresis for monoclonal gammopathy of renal significance (MGRS) did not reveal any evidence of monoclonal gammopathy or light chain disease. Serum C3 level was 0.16 g/L (normal range: 0.79–1.52 g/L), and C4 level was 0.27 g/L (normal range: 0.16–0.38 g/L). An infectious process could not be detected by acute phase reactants, culture examinations, and imaging studies. Ultrasound-guided percutaneous renal biopsy revealed iMPGN with diffuse endocapillary and focal extracapillary proliferation. Fibrinoid necrosis was present, and neutrophils were noted to be a significant component of the endocapillary hypercellularity, resulting in an exudative picture. Double contours were identified along the glomerular basement membrane. Immunofluorescence staining showed diffuse global distribution of 3+ finecoarse granular IgG and IgA deposits in the mesangium and along the peripheral capillary loops (Figure 1). Κ and λ were both positive; C3, IgM, and C1q were negative. Parallel studies revealed elevated levels of transaminases, alkaline phosphatase, IgM, and IgG. Itching was of great concern.
The anti-mitochondrial antibody (AMA) and anti-nuclear antibody test were positive, >1/320 and +4 positive, respectively, and the patient was diagnosed with PBC (Table 1). The patient was thought to have developed iMPGN secondary to PBC.
Supportive treatments for nephrotic syndrome parameters, low-salt diet, ramipril 10 mg/day, and ursodeoxycholic acid (UDCA) 13 mg/kg/day were started. Outpatient follow-up was initiated. Gradually, liver enzymes, serum creatinine, and proteinuria decreased (Table 1).
Figure 1: Immunofluorescence staining showing diffuse global distribution of 3+ fine-coarse granular IgG and IgA deposits in the mesangium and along the peripheral capillary loops.
Diffuse endocapillary and focal extracapillary proliferation can be discerned at medium power magnification (A: hematoxylin-eosin, B: Jones methamine silver stain). Note the presence of fibrinoid necrosis (A) and an abundance of neutrophils (C). Wide-spread double contours of the glomerular basement membrane, a so-called tram-tracking appearance, can be discerned at high power magnification (D: jones methamine silver stain).
Table 1: Laboratory results at the time of admission and at the 3rd-month follow-up visit.
DISCUSSION
In MPGN associated with autoimmune diseases, immune complexes can accumulate in the subendothelial or mesangial spaces of the glomerulus and cause glomerular damage and inflammation.4 Several hypotheses can be proposed for the development of MPGN during the course of PBC. Immune complexes containing AMAs or other autoantibodies may accumulate
in the glomeruli and cause inflammation and damage.5 In addition, complement activation triggered by antigen-antibody complexes may lead to the formation of membrane attack complexes that damage the endothelium.6 Bile acids or other components of bile may facilitate the deposition of immune complexes by altering the permeability and charge of the glomerular basement membrane.7 Finally, bile epithelial cells, which are the target of autoimmune attacks in PBC, may damage
the kidney with proinflammatory cytokines and chemokines, which may have endocrine as well as paracrine effects.8
In the management of MPGN due to secondary causes, treatment of the underlying primary cause and renal supportive therapy are essential. In the case presented here, the iMPGN has been thought to have developed secondary to PBC. Until the test results were available, attempts were made to control the complications of nephrotic syndrome and acute renal failure with supportive measures. When the diagnosis of PBC was confirmed, treatment with UDCA was started to improve bile flow and reduce oxidative stress.9 In the following period, renal function tests improved significantly under antiproteinuric therapy with ramipril 10 mg/day (maximum dose) and a lowsalt diet. Immunosuppressive therapy was not considered necessary due to the improvement in renal function following the renoprotective therapy. UDCA can reduce the formation of immune complexes by inhibiting the production of proinflammatory cytokines and chemokines, reducing the activation and proliferation of T cells, inducing regulatory T cells, and modulating B cell function. In addition, UDCA can reduce the damage caused by immune complexes by inhibiting complement activation and leukocyte uptake.10
In the literature, the authors found only two cases in which the two diseases were associated with each other. In a case published by Koike et al.,3 a 49-year-old male patient with PBC and Sjoegren’s syndrome was diagnosed with a Type 3 MPGN-like lesion secondary to proteinuria, which was treated with prednisolone and supportive measures.3 In another study by Zand et al.4 on patients with MPGN having autoimmune diseases, a 57-year-old female patient with undifferentiated connective tissue disease and PBC was treated with azathioprine/prednisone in combination with supportive therapy.4 During follow-up, both patients were not on dialysis, as was the case with the authors’ patient. The patient’s first hospitalisation was when the authors took up the case.
For this reason, the baseline creatinine level could not be determined. The patient’s most serious complaint was itching but no infection was found in her medical history. No infectious processes were detected by acute phase reactants, culture examinations, and imaging studies. There was no C3, IgM, or C1q deposition on immunofluorescent microscopy. Lupus or IgA nephropathy were ruled out due to the presence of double contours. The authors suspected it to be glomerulonephritis with a membranoproliferative pattern of injury and IgG and IgA deposition, not only in the mesangium but also along the glomerular capillary walls. Morphologically, both post-infectious and infection-related glomerulonephritis would enter the differential diagnosis. When the results of histopathologic analysis were available, the evaluations were revisited as postinfectious glomerulonephritis was included in the differential diagnosis. However, no evidence of infection was found. When a detailed analysis revealed AMA positivity associated with pruritus, the patient was referred to gastroenterology. The progress in clinical and laboratory values was taken as an indication of a decrease in liver inflammation as a liver biopsy was not performed. After UDCA treatment, both pruritus and renal function tests improved. On the other hand, it was predicted that the immune system modulated by this specific treatment could reduce the formation of immune complexes and their accumulation in the kidneys.9,10 According to the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines, the indication for immunosuppressive treatment in primary MPGN is the presence of proteinuria at a nephrotic level. In this case, it is not a primary MPGN. With the treatment of the underlying pathology, the nephrological examinations began to improve, the serum creatinine level decreased, and the proteinuria decreased to 1,400 mg. In this case, it was decided to continue non-immunosuppressive supportive treatment. The patient was not treated with steroids or other immunosuppressive drugs in both the nephrology or gastroenterology department.
Therefore, the authors controlled secondary iMPGN associated with PBC with UDCA, which is used in the treatment of PBC, by prioritising liver inflammation. The authors knew that secondary MPGN can occur in
References
1. Sethi S, Fervenza FC. Membranoproliferative glomerulonephritis – a new look at an old entity. N Engl J Med. 2012;366(12):1119-31.
2. Hirschfield GM et al. Primary biliary cirrhosis associated with HLA, IL12A, and IL12RB2 variants. N Engl J Med. 2009;11;360(24):2544-55.
3. Koike K et al. A case of glomerulopathy showing podocytic infolding in association with Sjögren’s syndrome and primary biliary cirrhosis. Clin Exp Nephrol. 2008;12:489-93.
the context of autoimmune diseases, but cases like this are very rare. Every patient with iMPGN should be investigated for secondary aetiologies.
4. Zand L et al. Membranoproliferative glomerulonephritis associated with autoimmune diseases. J Nephrol. 2014;27(2):165-71.
5. Rennke H. Secondary membranoproliferative glomerulonephritis. Kidney Int 1995;47:643–56.
7. Li M et al. Mechanisms of bile acid mediated inflammation in the liver. Mol Aspects Med. 2017;56:45-53.
8. Ronca V et al. Immune system and cholangiocytes: a puzzling affair in primary biliary cholangitis. J Leukoc Biol. 2020;108(2):659-71.
9. Lindor KD et al. Primary biliary cholangitis: 2018 practice guidance from the American Association for the Study of Liver Diseases. Hepatology. 2019;69(1):394-419.
10. Yu K et al. Decreased infiltration of CD4+ Th1 cells indicates a good response to ursodeoxycholic acid (UDCA) in primary biliary cholangitis. Pathol Res Pract. 2021;217:153291.
Accessibility and Affordability Issues for Renal Replacement Therapy Remain Challenges
in Resource-Limited Healthcare Settings: A Case Report and Critique of Literature for Chronic Kidney and End-Stage Renal Disease
Author: *Janvier Nzayikorera1
1. Non-affiliated independent researcher *Correspondence to agneaujesus@gmail.com*
Disclosure: The author has declared no conflicts of interest.
Chronic kidney disease (CKD) continues to be a global public health problem. Globally, the prevalence of CKD is approximately 8–16% in the general population. Most patients with CKD advance to kidney failure and require dialysis or kidney transplantation. Screening for CKD, diagnosing CKD, treating CKD and its consequences to stop its progression, and renal replacement therapy (RRT) are all parts of comprehensive CKD care. A 28-year-old male presented with complaints of awareness of his heart beating, abdomen and lower limb swelling, and generalised body weakness for 2 days. His blood pressure was 222/147 mmHg on admission day. Six days post-admission, he displayed violent chest pain and dyspnoea, along with profound generalised body swelling. Laboratory studies revealed creatinine of 22.49 mg/dL (0.6–1.1), urea of 236.5 mg/dL (10.0–50), albumin of 2.15 mg/dL (3.8–5.1), potassium of 7.19 mmol/L (3.5–5.5), and haemoglobin of 6.2 g/dL (8.0–17.0). The diagnoses of uremic pericarditis, pulmonary oedema, hyperkalaemia, hypertensive emergency, and normochromic anaemia secondary to end-stage renal diseases were made. He qualified for the RRT. CKD is a serious, non-communicable disease that is commonly encountered in clinical practice in both developed and developing countries and needs the utmost attention. RRT is crucial for comprehensive CKD management; however, in resource-limited healthcare settings, RRT is non-accessible and non-affordable. The lack of RRT marks the mistreatment of patients with renal diseases by the global healthcare system. The author calls for designing new strategies that aim to ensure equitable accessibility and affordability for RRT globally.
Key Points
1. This manuscript aimed to shed attention on chronic kidney disease (CKD) as one of the most devastating non-communicable illnesses, which is regrettably overlooked in healthcare settings with inadequate resources.
2. Approximately 8–16% of the general population worldwide has CKD. Comprehensive CKD care includes screening for CKD, diagnosing CKD, treating CKD and its implications, halting its progression, and providing renal replacement therapy.
3. The worldwide healthcare system mistreats patients with renal disorders because it denies them access to renal replacement therapy when necessary. To guarantee accessibility and affordability for all patients who require it, new, robust, and transformational strategies are required on a global scale. Further, comprehensive CKD care strategies are required to fully combat all impacts of chronic renal disease.
INTRODUCTION
Kidneys are a vital pair of bean-shaped organs situated in the retroperitoneal space and positioned on either side of the vertebral column at the level of the inferior thoracic and superior lumbar vertebrae. The estimated weight of each adult human kidney is 120–170 g. The dimensions of each human’s kidneys are 12x6x3 cm. The normal functioning of kidneys leads to accurate body fluid composition, such as red blood cell mass; proper excretion of waste products from the metabolism of endogenous substances such as urea and xenobiotic substances; accurate regulation of electrolyte metabolism, such as calcium and phosphate balance; and the synthesising and secretion of hormones, such as erythropoietin. To perform these functions, human kidneys must receive an adequate blood supply, have intact innervation, and have normal and adequate nephrons. Chronic kidney disease (CKD) is one of the most common medical conditions that disturbs the integrity and functional capacities of humans’ kidneys. CKD refers to “structural or functional abnormalities of the kidneys for >3 months, as indicated either by kidney damage with or without decreased glomerular filtration rate (GFR), as defined by pathologic abnormalities markers of kidney damage, such as abnormalities in the composition of the blood or urine or abnormalities in imaging tests.”1,2 Moreover, CKD is also evident when 'GFR<60 mL/min/1.73 m2, with or without kidney damage or albuminuria ≥30 mg
per 24 hours' for >3 months.2-4 According to worldwide kidney data, in 2019, 850 million people had kidney illnesses, of which 843.6 million had CKD.5 Globally, non-communicable diseases continue to increase, and they are among the prominent factors leading to CKD and its increased mortality and morbidity.3,4 For instance, the incidence of end-stage renal disease (ESRD) has been reported to be about 44.8% amongst patients with diabetes; 27.4% among patients with hypertensive and large vessel disease; 7.7% for patients with glomerulonephritis; 3.4% for patients with interstitial nephritis and pyelonephritis; 3.1% for patients with cystic, hereditary, and congenital diseases; 2.4% for patients with tumours and neoplasia; 2.2% for patients with secondary glomerulonephritis and vasculitis; approximately 4.9% for patients with miscellaneous conditions (such as those with HIV/AIDS); and for about 7.5%, the causes are unknown.6
The advancement of medical technologies has improved the diagnosis, prevention, and treatment of CKD. In the 1940s, dialysis technology was available.7 In 1954, the kidney was the first human organ to be transplanted.8 However, all these lifesaving, innovative medical technologies came with many ethical dilemmas related to the distribution of scarce resources.9 For many decades, the non-accessibility and non-affordability of renal replacement therapy (RRT) have been serious medical challenges.3,10,11 In fact, in resource-limited healthcare settings, the situation is still
worse because the majority of patients with kidney diseases who need RRT are not able to access such therapy promptly, and many are not able to afford its payment.12 Here, a 28-year-old male who was diagnosed with ESRD complicated with uremic pericarditis, pulmonary oedema, hyperkalaemia, hypertensive emergency, and normochromic anaemia is reported. He qualified for RRT; however, due to inadequate resources and poor socioeconomic status, RRT was not provided to him.
CASE PRESENTATION
A 28-year-old male presented with complaints of awareness of his heart beating, swelling of the abdomen, swelling of the lower limbs, and generalised body weakness for 2 days. Four months prior to presentation, he was diagnosed with acute glomerulonephritis and severe hypertension. Moreover, 1 month prior, he developed painful abdominal swelling, awareness of his heart beating, dizziness, generalised body weakness, and swelling of the lower limbs, for which he visited a nearby clinic, which treated him and possibly improved him.
A pertinent physical examination revealed a fairly well-looking male who was afebrile. However, he had a moonface appearance, conjunctiva pallor, a distended abdomen, a blood pressure (BP) of 222/147 mmHg, a pulse rate of 101 beats per minute, and a respiratory rate of 19 cycles per minute. Treatment interventions included medications such as intravenous (IV) lasix 40 mg once a day (OD), tablets of nifedipine 40 mg twice per day (BID), tablets of captopril 25 mg OD, and tablets of spironolactone 50 mg OD. Two days following admission, his BP remained high. However, the treatment plan was adjusted by replacing tablets of captopril 25 mg OD with tablets of lisinopril 20 mg OD for 1 month. Tablets of bisoprolol 5 mg OD for 1 month were added. Tablets of nifedipine, spironolactone, IV lasix, and metolazone, as well as oxygen therapy (2 L of O2), were continued.
Despite this treatment plan and the institution of those medications, the patient’s condition did not improve, as evidenced by a constantly raised BP in the range of 160/100 mmHg–230/140 mmHg, and visible difficulty breathing despite being on oxygen therapy. On 26 July, 2023, the patient displayed violent chest pain, dyspnoea, profound generalised body swelling, and body weakness. The chest pain was sharp in nature, and exacerbated by lying down in the supine position and turning his body while in the supine position. Leaning forward could relieve his pain. Physical examination revealed obvious facial swelling, abdominal swelling, bilateral non-pitting oedema, BP of 189/110 mmHg, pulse rate of 105/min, and oxygen saturation of 92–94% on an oxygen mask with no reservoir at a flow rate of 5 L/min. Despite being on oxygen, he had severe respiratory distress and a tachypnoeic status of 43 cycle per minutes. Auscultation of the lungs revealed diffuse crackles on the left and right lung. He had a heart murmur of 7th intensity that was heard without a stethoscope.
His emergent laboratory studies included a complete blood count and differential, liver function test, renal function test, serum electrolyte, and urinalysis (Table 1). Low haemoglobin levels (6.2 g/dL) prompted the transfusion of two units of packed red blood cells. With the diagnoses of uremic pericarditis, pulmonary oedema, hyperkalaemia, hypertensive emergency, and normochromic anaemia secondary to ESRD, the standard treatment plans were to offer him renal RRT. However, due to resource limitations, the patient continued to struggle. His conditions were only managed symptomatically with IV furosemide 120 mg BID, tablets of metolazone 10 mg OD, IV calcium gluconate 10%/10 mL/over 10 min bolus, and IV Actrapid 10 units in 30 mL of 50% dextrose. Nebulisation with salbutamol 5 mL every 6 hours, kayexalate 30 g orally four times a day, morphine 5 mg orally (5 mL every 8 hours), bisacodyl 10 mg tablets at night for 5 days, capsules of cudo forte (one capsule OD for 1 month), omeprazole, and continuation of oxygen therapy were
Table 1: Renal function test, liver function test, complete blood count and differential, serum electrolyte, and urinalysis.
Results of Renal Function Test
Results of Complete Blood Count and Differential
Table 1: Continued.
Results of Urinalysis
Leukocyte, Nitrite, RBC, Glucose, Bilirubin, pus cell Nil
ASAT/SGOT: aspartate aminotransferase/serum glutamic-oxaloacetic transaminase; ALT/SGPT: alanine transaminase/ serum glutamic pyruvic transaminase; Cl-: chlorine ion; FL: femtolitre; Gamma-GT: gamma-glutamyl transferase; IFCC: International Federation of Clinical Chemistry; K+: potassium ions; N/A: not applicable; Na+: sodium ion; MCHC: Mean corpuscular haemoglobin concentration; MCV: mean corpuscular volume; Pg: picograms.
prescribed. Frequent monitoring of his vital signs revealed a persistently high BP of >160 mmHg. Moreover, frequent serum electrolytes continued to reveal a high potassium concentration >5.5 mmol/dL. On 1 August, 2023, the patient reported marked improvement, and on 3 August, 2023, he voluntarily requested discharge. However, his BP remained high (180/110 mmHg), and his potassium levels also remained above 7 mmol/dL. However, these findings did not correlate with a visible improvement picture. The patient was discharged on oral antihypertensive medications with an appointment for a 2-week follow-up.
DISCUSSION
This case report highlights CKD as one of the most serious non-communicable diseases. However, it is still a neglected condition in resource-limited healthcare settings.13 Populations at risk for developing CKD include people with previous comorbidities such as diabetes, hypertension, or any renal disease.14 Suboptimal control of these conditions and ineffective and non-efficient policies for tackling non-communicable diseases, including CKD, especially in developing countries, increase the mortality and morbidity associated with CKD.15
For clinical and epidemiological purposes, three variables are crucial criteria to ascertain the burden and choose appropriate management approaches for CKD. These include the presence of CKD for ≥3 months, the irreversibility of kidney damage, and the reduction of GFR. CKD denotes the progressive and irreversible loss of kidney function.1 Both acute and chronic conditions can provoke nephron loss, which may result in chronic renal insufficiency, chronic kidney diseases, and eventually ESRD and death, as shown in Figure 1. Elevated serum creatinine, proteinuria, and a decline in the GFR may signify the continuum of CKD.16 Continuous loss of the kidneys’ nephrons is the hallmark mechanism leading to the development of CKD. Human kidneys have around 1 million nephrons. The GFR in each kidney is about 120 mL/min. Thus, the single nephron glomerular filtration rate is about 60 nanolitres per minute. Any conditions leading to the loss of nephrons provoke compensatory mechanisms to take place in undamaged and less damaged nephrons, which results in hypertrophy of nephrons. In intact nephrons, single nephron glomerular filtration rate tends to increase; thus, theoretically, GFR is maintained at normal. Such adaptation is possible because of humeral and hormonal changes. The continuous damage to kidney nephrons leads to a
reduction in GFR. According to Kidney Disease: Improving Global Outcomes (KDIGO) working group, a GFR of >90 mL/min (1.73 m2) may indicate normal kidney functions; a GFR of 60–89 may indicate mildly decreased kidney functions or chronic renal insufficiency; a GFR of 45–59 may mark mildly to moderately decreased kidney functions; a GFR of 30–44 may indicate moderately to severely decreased kidney functions; a GFR of 15–29 may designate severely decreased kidney functions; and a GFR of <15 may confirm a kidney failure.3 The whole loss of the kidney’s function indicates ESRD.
Clinical manifestations of CKD vary and depend on the extent of kidney
Examples of Comorbidities That May Cause or Exacerbate Nephron
Diabetes (the more common cause of CKD)
Hypertensive and large vessel disease
Glomerulonephritis
Interstitial Nephritis and Pyelonephritis
Cystic, Hereditary, and Congenital diseases
Tumors and Neoplastic Conditions
damage. Accumulation of waste products, deficiencies of some crucial body chemicals, and the development of complications lead to the apparent appearance of various signs and symptoms that would aid in the diagnosis of CKD and, in fact, the status of its progression.6 Uremic syndrome affects multiple human body systems.17 The presence of uremic symptoms may indicate ESRD. The physician treating the patient with CKD must be able to recognise all conditions that require emergent attention to avoid adverse outcomes. Hyperkalaemia, pulmonary oedema, and acute pericarditis are dangerous complications of CKD that were diagnosed in this patient. He needed emergent or urgent dialysis to prevent cardiac arrest and other
Acute and Chronic Diseases Causing Loss of Nephrons
Chronic Renal Insufficiency Non Progressive Course
Early Recognition and Early initiation of the Appropriate Treatment for CKD
Exogenous Stress
(E.g: Gastro Intestinal Tract Bleeding)
Normal Renal Functions
Chronic Kidney Disease
Continuing Renal Nephrons Loss
Loss
Figure 1: Stepwise progression of chronic kidney disease and possible outcomes.
catastrophic outcomes, but because of resource limitations, dialysis was not offered to him. The differential diagnosis of pericarditis includes pneumonitis and pleuritis. Respiratory distress and pulmonary oedema are common for CKD patients; these are commonly seen in patients with CKD who develop ESRD.17 This patient had respiratory distress, which signified acid-base metabolic disturbances. Arterial blood gas tests would help to ascertain the presence of such disturbances; however, the laboratory setting in which this patient was treated was not equipped for doing such tests.
Serum concentrations of creatinine and blood urea nitrogen (BUN) can be used to predict the development of uremic syndrome and to diagnose impaired renal function. The normal range of BUN is 5–20 mg/dL, while the normal range of serum creatinine is 0.9–1.3 mg/dL (adult males) and 0.6–1.1 mg/dL (adult females).18-20
Serum creatinine is a more specific and sensitive indicator of kidney disease than BUN. However, in chronic renal disease, both BUN and creatinine are relevant to evaluating renal problems because the BUN-to-creatinine ratio provides greater information. The normal range of the BUN-to-creatinine ratio is 10:1–20:1. It is unusual to develop uremic syndrome if the BUN is <60 mg/dL and the serum creatinine level is 8 mg/dL. However, the likelihood of the occurrence of uremic syndrome is high when the BUN level is >100 mg/dL or the serum creatinine level is >12 mg/dL. This patient had a creatinine concentration of 22.49 mg/dL (0.9–1.3) and a BUN concentration of 236.5 mg/dL, which correlated with his uremic syndrome manifestations and complications. Having had pericarditis means that the accumulation of toxic substances (urea) responsible for uremic syndrome is chronic. The pain associated with pericarditis is exacerbated by lying flat and breathing, but such pain is relieved by sitting upright and leaning forward. Fibrosis that occurs as a result of inflammatory healing is responsible for such manifestations. The formation of fibrosis takes a long time. Thus, the occurrence of uremic pericarditis
may firmly connote the chronicity of CKD in this patient.
Albumin consists of about 55–60% of the measured serum proteins.21 Albumin is the main performer in maintaining normal oncotic pressure within the human body. Oncotic pressure is one of the determinants that maintain Starling’s forces. Oncotic pressure plays a role in sucking fluid from interstitial space back to the bloodstream. Albumin loss in patients with CKD leads to hypoalbuminemia, and eventually, an overwhelming accumulation of fluid within the interstitial body compartment. This patient had low serum albumin concentrations (2.15 mg/dL), which explained his generalised body swelling and the presence of pulmonary oedema. Likely, inflammation was the cause of hypoalbuminemia in this patient. Having had a past medical history of acute glomerulonephritis connotes this claim. He would have benefited from a vasculitis workup and urine sediment exam; however, these investigations were not done. Inflammatory status increases vascular permeability and the escape of serum albumin from the vascular compartment, causing expansion of the interstitial space and the increase of distribution volume of albumin.22 He had non-pitting oedema, which would confirm the possibility of albumin accumulation in his interstitial fluid compartment secondary to inflammation because proteins have a higher density than water. Atherosclerotic lesions, vascular calcification, vascular senescence, myocardial fibrosis, and calcification of the heart valves are all outcomes of the systemic, chronic proinflammatory condition that CKD generates.4 Cardiovascular events pose a significant danger to patients with CKD.23-25 In patients with CKD Stage 4–5, cardiovascular events account for almost half of the cases. Studies have shown that patients with ESRD (Stage 5) and advanced CKD (Stage 4) have cardiovascular mortality rates of approximately 40–50%, while controls with normal kidney function have cardiovascular mortality rates of 26%.4,25
This patient had severe respiratory distress, tachypnoeic status, bilateral diffuse lung crackles, and a heart murmur of 7th intensity, confirming cardiovascular events. All drugs used to treat inflammatory conditions can be dangerous bombs that destroy human kidneys. Apart from the recommendation that these drugs should be stopped for patients with CKD, all available guidelines for managing patients with CKD have not addressed how to treat inflammatory conditions in these patients. Further studies are required to investigate what works and what does not work to alter the chronic proinflammatory conditions that CKD generates.
This patient had serum potassium of 7.19 mmol/L (3.5–5.5), which indicated severe hyperkalaemia. Hyperkalaemia in CKD may indicate the chronicity of CKD and the extreme loss of nephrons. Potassium excretion depends on renal tubular secretion. Aldosterone and distal tubular fluid flow rate are major determinants of potassium excretion. Healthy kidneys’ nephrons excrete about 90–95% of ingested potassium, and the rest (5%) is excreted via the stool. An increase in aldosterone levels and increased fluid flow in the distal tubules are important adaptation mechanisms that support patients with CKD in continuing to excrete potassium from the human body. However, profound loss of human kidney nephrons and reduction of GFR to less than 10 mL/L leads to the accumulation of potassium. Hyperkalaemia may be due to the redistribution of potassium between the intracellular and extracellular compartments. A decline in GFR to <5 mL/min provokes the excretion of about 20–50% of potassium ions in the stool. This fact may justify the use of bisacodyl as an enhancer of potassium excretion in conjunction with enhanced stool excretions. However, currently, there are no well-published randomised studies that have investigated the effectiveness and safety of bisacodyl in regards to treating hyperkalaemia in patients with ESRD. Moreover, measuring stool potassium concentration may be a good and easy diagnostic test for detecting CKD progression; however, studies regarding this claim have not been done.
Commonly, patients with CKD develop normochromic anaemia due to the inadequate formation of erythropoietin. Anaemia increases the morbidity and mortality associated with CKD.26,27 Erythropoietin is a hormone formed in the kidneys. Its function is to ensure red blood cell maturation in the bone marrow.26 This patient had a haemoglobin level of 6.2 g/ dL (8.0–17.0) and a mean corpuscular volume of 89.9 FL (86.0–110.0). Having had generalised body weakness would also correlate with the findings of normochromic anaemia. Researchers have discovered erythropoietin-stimulating agents and have made them the standard treatment for anaemia in patients with CKD.28 Epoetin alfa 50 200 U/kg/week by subcutaneous IV 2–3/week or darbepoetin alfa 20–40 mg delivered subcutaneously weekly have been approved for the symptoms control associated with anaemia of CKD.29 This patient required these medications; however, they were unavailable. Thus, the transfusion of packed blood cells was an option for controlling his anaemia. This practice somehow contrasts the KDIGO recommendation statements on red cell transfusion to treat anaemia in CKD, which state that, if possible, red cell transfusions should be avoided to minimise the general risks related to their use.30
Comprehensive management for CKD encompasses screening for CKD, diagnosis of CKD, treating CKD and its complications to prevent CKD development and progression, and RRT.3,6,29,31 All patients with comorbidities known to eventually complicate CKD should be routinely screened. Early recognition of CKD via screening can promote the early initiation of appropriate treatment.32 There is a higher likelihood of a non-progressive CKD course in such a case. Thus, this patient would have benefited from CKD screening services because he had a past medical history of acute glomerulonephritis and severe hypertension. In fact, affirming CKD diagnosis without prior 3-month laboratory findings of this patient is anecdotal. Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers are crucial for preventing CKD progression because of their effects on
reducing long-term remodelling of the nephrons of patients with CKD.29 However, they are contraindicated in ESRD due to the risk of causing hyperkalaemia. From 21–25 July, 2023, among the prescribed medications for this patient were aptopril 25 mg OD and Lisinopril 20 mg OD. Due to a lack of meticulous CKD screening services, on admission day, the diagnosis of ESRD was not made for this patient. It is not clear whether the prescribed oral angiotensin-converting enzyme inhibitors were the cause of the violent deterioration (specifically, hyperkalaemic state) in this patient. The appropriate time for which the diagnosis of CKD would have been made for this patient is also not clear. His high BP of 222/147 mmHg and some features of vital end organ damage indicated a hypertensive emergency that needed meticulous management with appropriate IV antihypertensive medications. IV Lasix was given to this patient, but it was not enough; other intravenous antihypertensive medications would have been given to him if they were available. About 5–10% of adult patients with elevated BP have secondary hypertension.33 Attention should be paid to identifying the cause of secondary hypertension, as most causes of secondary hypertension are potentially correctable. Over 90% of people with severe renal disease have hypertension.15 This patient had resistant hypertension, pointing to secondary hypertension with BP in the range of 160/100–230/140 mmHg. Because he had a moon-face appearance, secondary work-up for hypertension should have been performed, but it was not done due to resource limitations. Studies and experts have emphasised that patients with CKD who develop hypertension and are treated with more than four antihypertensive medications without improvement should be referred to a nephrologist.16 For this patient, more than four antihypertensive medications were used, but his BP remained high from the day of admission until the day of discharge. No referral to a nephrologist was made because of resource limitations and poor socioeconomic status. Thus, comprehensive CKD management was interrupted.
Regarding the management of patients with CKD, it is good medical practice to institute RRT before the onset of uremic syndrome. However, this fact is profoundly and ethically violated due to the nonaccessibility and non-affordability of RRT, especially in resource-constrained healthcare settings. RRT may be accomplished via kidney transplantation or dialysis. Kidney transplantation is the most sustainable and preferable approach. Dialysis can be accomplished either by haemodialysis or peritoneal dialysis. In 2019, the International Society of Nephrology (ISN) developed the framework to guide the establishment or expansion of chronic dialysis programmes in low-resource settings as part of the ISN’s work with the World Health Organization (WHO).34 However, these services are still not comprehensively and equitably available for the patients who need them, especially in developing nations.35-37 Further actions are urgently needed to ensure the proper management of patients with CKD as one of their fundamental human rights. For CKD patients, the criteria for dialysis include GFR <10 mL/min/1.73 m2, creatinine clearance <15 mL/min, chromium >1,000 mmol/L (>11.3 mg/dL), urea >30 mmol/L (>83 mg/ dL), albumin <35 g/L (<3.5 g/dL]), uraemic symptoms, and any acute indications.29 This patient had all these; thus, he qualified for emergency RRT. However, because of resource-limited healthcare settings, RRT was not provided to him. A renal transplant would have been the most profitable therapy for him. The availability of dialysis services would also increase his survival chances. Peritoneal dialysis would be the preferred dialysis approach because of the resource-limited healthcare setting,38 and because peritoneal dialysis has numerous advantages over haemodialysis. Among those advantages are the short time spent in dialysis units, the fact it does not necessitate strict dietary limitations compared to haemodialysis, the rehabilitation rates are better than those detected in haemodialysis, it gives the opportunity to return to full-time employment for most patients, and it also ensures that residual renal function is maintained for a longer period (e.g., 1–2 years), hence improving morbidity and
mortality.6,38,39 He was discharged with fairly good improvement, but predictably, in the near future, he will be admitted with similar complaints. In fact, his prognosis will likely remain very poor without RRT.
CONCLUSION
The main purpose of this manuscript has been to highlight CKD as one of the most serious non-communicable diseases that is unfortunately still neglected in resource-limited healthcare settings, using the case of a 28-year-old male with CKD who developed ESRD. He qualified for RRT; however, RRT was not provided to him due to its non-accessibility, non-affordability, and resource-limited healthcare settings. Renal diseases, including CKD, are commonly encountered in clinical practice in both developed and developing countries. The lack of RRT
References
1. National Kidney Foundation (NKF). K/ DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification and stratification. Am J Kidney Dis. 2002;39(2 Suppl 1):S1-226.
2. Chen K et al. Chronic kidney disease diagnosis and management. JAMA. 2019;322(13):1294-304
3. International Society of Nephrology (ISN). KDIGO 2012 Clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3(1):1-150.
4. Jankowski J et al. Cardiovascular disease in chronic kidney disease: pathophysiological insights and therapeutic options. Circulation. 2021;143(11):1157-72.
5. Jager KJ et al. A single number for advocacy and communicationworldwide more than 850 million individuals have kidney diseases. Kidney Int. 2019;96(5):1048-50.
6. Andreoli TE et al. Andreoli and Carpenter's Cecil Essentials of Medicine (2010) 8th edition, Elsevier Health Sciences.
7. Gabriel R, “History of dialysis and transplantation”, History of dialysis and transplantation. A Patient’s Guide to Dial Transplant (1987), Dordrecht: Springer, pp.153-9.
8. Tantisattamo E et al. History of kidney transplantation: a journey of
marks the mistreatment of patients with renal diseases by the global healthcare system. The author calls for designing new strategies that aim to ensure equitable accessibility and affordability for RRT globally. One of these strategies should be to deal with companies that manufacture and sell the machines, such as dialysis machines and other equipment and substances used for RRT, to ensure cost-effectiveness and their availability in developing countries where resourcelimited healthcare is profoundly common.
Ethical Consideration
After explaining the purpose and potential advantages of publishing this case to the patient and his parents, they gave their consent. They received guarantees that neither their names nor the publication’s intended audience would be revealed.
progression and evolution for success. J Nephrol. 2022;35(7):1783-6.
9. Nzayikorera A et al. Healthcare bioethics: a vital branch of bioethics and a new possible pillar for modern healthcare systems strengthening worldwide. J Community Med Heal Solut. 2023;4(2):63-75.
10. Niang A et al. Hemodialysis versus peritoneal dialysis in resource-limited settings. Curr Opin Nephrol Hypertens. 2018;27(6):463-71.
11. White SL et al. How can we achieve global equity in provision of renal replacement therapy? Bull World Health Organ. 2008;86(3):229-37.
12. Luyckx VA. Ethical challenges relating to provision of sustainable renal care in resource limited settings - focus on sub-saharan Africa. 2019. Dissertation. University of Zurich.
13. Pais P, Iyengar A. Global perspective kidney care for all: addressing the gaps in an imperfect world - a global perspective on improving access to kidney care in low-resource settings. Kidney360. 2023;4(7):982–6.
14. Kidney Health Australia. CKD Management in Primary Care handbook. 2020. Available at: https:// kidney.org.au/health-professionals/ ckd-management-handbook. Last accessed: 13 September 2023.
15. Crews DC et al. Burden, access and disparities in kidney disease. Clin
17. Widiastuti et al. The correlation between disease stage and pulmonary edema sssessed with chest x-ray in chronic kidney disease patients. Imaging Med. 2021;13(1):1-6.
18. Hosten AO, “BUN and Creatinine,” (Walker HK et al), Clinical Methods: The History, Physical, and Laboratory Examinations (1990) 3rd edition, Boston: Butterworths.
19. Nayak SB, “Laboratory Values,” Essentials Biochem (For Med Students) (2013) 2nd edition, Jaypee Brothers Medical Publishers: New Delhi, 389-94.
20. American Board of Internal Medicine (ABIM). Laboratory Test Reference Ranges from January 2024. 2024. Available at: https://www.abim.org/ Media/bfijryql/laboratory-referenceranges.pdf. Last accessed: 11 June 2024.
21. Nicholson JP et al. The role of albumin in critical illness. Br J Anaesth. 2000;85(4):599-610.
22. Soeters PB et al. Hypoalbuminemia: pathogenesis and clinical significance. 2019;43(2):181-93.
23. United States Renal Data System (USRDS). Cardiovascular disease in patients with CKD. 2021. Available
at: https://usrds-adr.niddk.nih. gov/2020/chronic-kidney-disease/4cardiovascular-disease-in-patientswith-ckd Last accessed: 5 March 2024.
24. Foley RN. Clinical epidemiology of cardiovascular disease in chronic kidney disease. J Ren Care. 2010;36(Suppl 1):4-8.
25. Thompson S et al. Cause of death in patients with reduced kidney function. J Am Soc Nephrol. 2015;26(10):2504-11.
26. International Society of Nephrology (ISN). KDIGO clinical practice guideline for anemia in chronic kidney disease. Kidney Int Suppl. 2012;2(4):1-335.
27. Fishbane A, Brunton S. Improving detection and management of anemia in CKD. J Fam Pract. 2022;71(6 Suppl):S23-8.
28. Hayat A et al. Erythropoietin stimulating agents in the management of anemia of chronic kidney disease. Patient Prefer Adherence. 2008;2:195-200.
29. Hui D. Approach to Internal Medicine (2011) 3rd edition, Houston: Springer, 95.
30. Moist LM et al. Canadian Society of Nephrology commentary on the 2012 KDIGO clinical practice guideline for anemia in CKD. AM J Kidney Dis. 2013;62(5):860-73.
31. Kalyesubula R et al. Screening for kidney disease in low- and middleincome countries. Semin Nephrol. 2022;42(5):151315.
32. International Society of Nephrology (ISN), Kidney Disease Improving Global Outcomes (KDIGO). CKD early identification & intervention toolkit. ISN-KDIGO early screening booklet. 2021. Available at: https://kdigo.org/ wp-content/uploads/2019/01/ISN_ KDIGO_EarlyScreeningBooklet_WEB. pdf. Last accessed: 5 March 2024.
33. Viera AJ, Neutze DM. Diagnosis of secondary hypertension: an agebased approach. Am Fam Physician. 2010;82(12):1471-8.
34. International Society of Nephrology (ISN). The ISN framework for developing dialysis programs in lowresource settings. 2021. Available at: https://www.theisn.org/wp-content/
uploads/2021/03/ISN-FrameworkDialysis-Report-HIRES.pdf Last accessed: 5 March 2024.
35. Obrador GT et al. The challenge of providing renal replacement therapy in developing countries: the Latin American perspective. Am J Kidney Dis. 2016;67(3):499-506.
36. Teerawattananon Y et al. To include or not include: renal dialysis policy in the era of universal health coverage. BMJ. 2020;268:m28.
37. Skinner DL et al. Renal replacement therapy in intensive care units in KwaZulu-Natal Province, South Africa. 2021;37(1):10.7196/SAJCC.2021. v37i1.454
38. Niang A et al. Hemodialysis versus peritoneal dialysis in resource-limited settings. Curr Opin Nephrol Hypertens. 2018;27:463-71.
39. Chironda AG et al. Renal replacement therapy (RRT) in Rwanda: benefits, challenges and recommendations. Rwanda Med J. 2019;76(3):1-6.
End-Stage Renal Disease and Neurological Connection
Authors: *Raj Kamal Choudhary,1 Amrendra Kumar Singh,1 Ravi Raman,2 Anjum Perwaz1
1. Jawaharlal Nehru Medical College and Hospital, Bhagalpur, India
2. Patna Medical College and Hospital, India
*Correspondence to akschinku@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Due to the incapacitating nature of end-stage renal disease, people on dialysis frequently acquire undetected psychopathological disorders. This may affect the effectiveness of treatment for a chronic disease. Dialysis is a therapy for kidney failure, but not a cure. As a result of the treatment plan and other restrictions, the patient is forced to make several significant modifications to their daily routines and activities, which in turn has an impact on their ability to socialise and mentally operate. There is a high rate of morbidity and mortality in individuals with renal failure due to neurological complications. Dialysis may not be effective in treating many of the neurological effects of uraemia, such as uraemic encephalopathy, atherosclerosis, neuropathy, and myopathy, despite ongoing improvements in therapy. Brain networks are destroyed in patients on haemodialysis with end-stage renal disease.
Key Points
1. Patients with end-stage renal disease accumulate blood urea and experience nitrogen and electrolyte imbalances due to decreased renal excretion, leading to neurological complications.
2. The Indian healthcare sector has inadequate dialysis facilities, which reduces the frequency of dialysis. This further aggravates neurological complications.
3. Uncontrolled diabetes and uncontrolled hypertension are significant contributors to renal disease. Hence, early and aggressive treatment of hypertension and diabetes can lead to improved patient outcomes for end-stage renal disease.
INTRODUCTION
The complete loss of kidney function characterises the last stage of chronic kidney disease (CKD), known as endstage renal disease (ESRD). Patients with ESRD often struggle with cognitive impairment. Disabilities in many areas of cognition, such as attention, memory, and planning, may lead to longer treatment times, higher healthcare costs, more frequent hospitalisations, and longer overall hospital stays. Understanding the neural processes at play in ESRD may become possible with increased awareness of the cognitive impairments that accompany the disease, and this in turn may pave the way for preventative measures that might lessen the severity of the condition. ESRD is a devastating health problem with a dismal outlook that affects people all over the world. A recent study found that the incidence of ESRD requiring dialysis treatment was greatest among the Taiwanese population.1 In the study, people with ESRD had cerebral signs in addition to systemic issues.
Imaging is a vital tool for detecting structural and functional brain disorders in patients with ESRD. Brain volume loss, deep white matter volume loss, a high prevalence of subcortical white matter lesions, and an elevated stroke incidence have all been documented in patients with ESRD in studies of conventional MRI and CT scans with visual assessment and manual measurements of structures of interests.2,3 Patients with CKD (Stage 4–5) without clinical sign of uremic encephalopathy exhibit MRI spectroscopyobserved metabolic abnormalities in the parieto-occipital white matter, occipital grey matter, basal ganglia, and pons (magnetic resonance spectroscopy). Studies utilising positron emission tomography have shown impaired oxygen and glucose metabolism in the brains of individuals with ESRD, with the effects being most severe in the bilateral prefrontal cortices. Traditional MRI and CT, which rely on subjective visual evaluation and manual measurements of structures of interest, are insensitive to the early and tiny lesions, whereas single-voxel magnetic resonance spectroscopy has a limited
spatial resolution and exposes the patient to radiation.3
Using resting-state functional MRI (rsfMRI), subjects may record their own brain’s normal fluctuations in activity while at rest in the scanner. Low-frequency (0.01–0.80 Hz) fluctuations in the blood-oxygen-leveldependent signals are connected with spontaneous brain activity and may have physiological implications during the resting state. Recent studies using rs-fMRI and the regional homogeneity analysis method have demonstrated that patients with ESRD had reduced regional homogeneity in various areas of the bilateral frontal, parietal, and temporal lobes.4 Further, they found a decline in default-mode network (DMN) regional homogeneity,5 which suggests that frontal and parietal lobes may be trait-related in patients with ESRD with mild nephroencephalopathy. MRIs that provide regional grey matter volume at the voxel scale may be evaluated using a method called voxel-based morphometry, which is both spatially specific and objective. This technique has shown positive results in the treatment of individuals with a variety of conditions, including healthy ageing, schizophrenia, dementia, mild cognitive impairment, addiction, and hepatic encephalopathy. Functional integrity alterations in patients with ESRD may be connected to these morphometric abnormalities, which include significant cerebral atrophy, most notably bilaterally in the caudate nuclei, and diffusely decreased grey matter volume, with higher decreases in the presence of encephalopathy. However, there has been no investigation into how this damaged grey matter could affect function. When voxelbased morphometry is used in tandem with rs-fMRI, scientists may examine both structural and functional brain problems simultaneously. This strategy may prove to be rather effective in learning more about the neurobiological mechanisms at play in patients with ESRD.6
AIMS AND OBJECTIVE
This study aims to find out what different types of neurological complications,
fatigue, oxidative stress, cardiovascular complications, infections, neoplasm, and hypertension are seen in patients with ESRD admitted at the authors’ institute to facilitate treatment that is more beneficial.
FACTORS CONTRIBUTING TO FATIGUE IN END-STAGE RENAL DISEASE
Patients with ESRD often experience extreme fatigue, a medical condition that may have serious consequences for their overall health. Exhaustion may be caused by several different things, such as uraemia, anaemia, malnutrition, inflammation, comorbidities, and a lack of physical activity. Socio-demographic factors such as education and social networks can also contribute. Issues with mental health and behaviour were cited, including insomnia, anxiety, depression, stress, and substance addiction. Symptoms of dialysis include fatigue after treatment, dialysis method, treatment efficacy, and treatment frequency.7
ESRD may affect not only the patient, but also their loved ones. Parental roles might shift as a result of a number of changes within the family dynamic. If a patient with ESRD who is also a parent is unable to fulfil their duty, they may experience a deterioration in self-esteem or self-image. Finally, having a parent who is chronically ill is likely to affect the family’s efficiency and their sense of identity. A person with ESRD may feel like they are failing themselves or others when they do not meet their own or others’ expectations. Systems theory suggests that as parents’ roles change, they may feel a decline in self-esteem that might affect their marriage and family life.8
OXIDATIVE STRESS AND END-STAGE RENAL DISEASE
Due to an unfavourable ratio of antioxidant defence to reactive oxygen species production, oxidative stress develops. Antioxidant insufficiency is common in those with ESRD. At the same time, ageing, diabetes, cardiovascular disease,
inflammation, and the bio-incompatibility of dialysis membranes all contribute to a rise in oxidant activity. Patient outcomes are increasingly at risk from oxidative stress.8
PSYCHOTHERAPEUTIC CHARACTERISTICS IN END-STAGE RENAL DISEASE
Patients on dialysis have benefitted from psychological therapy. The therapy’s ends would shift depending on the individual’s history and current mental state. Individual or group treatment sessions were conducted. There have been several studies done in India that have shown the efficacy of psychotherapy in treating a wide range of persistent medical issues; however, there is a lack of research on ESRD.9 Many psychotherapies and strategies are utilised to alleviate the psychological difficulties in ESRD, including cognitive behavioural therapy.10 This has shown to be useful in the treatment of clinical depression and anxiety in patients with long-term health problems. Behaviour modification and counselling are also used to bring about desired alterations in one’s health-related ways of living.
Similarly, psycho-education is a widespread kind of intervention used in hospitals for a variety of medical disorders. Brief sessions would focus on the most pressing emotional, social, economic, and physical concerns related to the disease. Dependent upon the nature of the issue at hand, family members or others considered important may also be invited to participate in the sessions. It is also common practice for counsellors to address the most frequently mentioned or observed psychological concerns while treating a patient. Adherence, quality of life, morbidity, and death are all predictably affected by psychological therapies in patients with ESRD.11
MECHANISM OF CEREBRAL DISEASES IN PATIENTS WITH ENDSTAGE RENAL DISEASE PATIENTS
There is a complicated relationship between the kidneys and the brain, known as the
‘kidney–brain axis’, which contributes to the high incidence of brain abnormalities in patients with ESRD.12 Similarities in the anatomical and vasoregulatory structures of the brain and kidneys suggest that these two forms of vascular disease may have the same pathogenesis.12 Brain MRI studies have demonstrated structural abnormalities in patients with ESRD.13 Compared to healthy adults of the same age, patients with ESRD had a higher prevalence of white matter lesions, silent infarcts, brain atrophy, and axonal demyelination. In order to better understand the functional impairments of brain networks in patients with ESRD, rsfMRI has recently emerged as a promising approach.
Based on the blood-oxygen-leveldependent principle, rs-fMRI data may be analysed to uncover temporal synchronisations between distant brain areas, commonly known as functional connectivity.14 Depending on the method of analysis, functional connectivity alterations in patients with ESRD may exhibit a wide range of complexity. DMN connectivity impairment in the posterior cingulate cortex, precuneus, and medial prefrontal cortex, or decreased activity in a diffuse pattern across bilateral frontal, parietal, and temporal lobes were found in rs-fMRI studies of patients with ESRD before dialysis was mentioned. In the years thereafter, researchers have identified a handful of symptoms that contribute to decreased connectivity in patients with ESRD. Patients undergoing haemodialysis (HD), a procedure that necessitates the use of complex cognitive behaviour planning, have been demonstrated to have reduced connectivity in the anterior cingulate cortex. Evaluating global functional connectivity revealed abnormal intrinsic dysconnectivity in salience network regions spanning the contralateral insula and dorsal anterior cingulate cortex in patients with ESRD undergoing HD. However, the majority of the aforementioned ESRD studies only included individuals undergoing HD, who had mildto-moderate cognitive impairment.15
URAEMIC TOXINS AND NEUROLOGICAL DISEASE
Uraemic CKD is characterised by the retention of potentially harmful solutes such as urea, creatinine, parathyroid hormone, myoinositol, and 2-microglobulin. The notion that one or more of these retained toxins influence neurological dysfunction in CKD has been the subject of several studies examining the pathophysiology of neurological disease in CKD.16 Clinical symptoms and nerve conduction parameters improved rapidly following kidney transplantation, often within days of surgery, and were demonstrated to be inversely related to the severity of renal impairment. The rapidity with which these changes take place suggests that toxinmediated inhibition of neuronal transmission plays a substantial role in the neurological dysfunction seen in CKD.
CENTRAL NERVOUS SYSTEM COMPLICATIONS
Encephalopathy
Renal failure often leads to encephalopathy, which may be caused by a wide range of conditions such as uraemia, thiamine deficiency, dialysis, transplant rejection, hypertension, fluid and electrolyte imbalances, and pharmaceutical toxicity. Confusion, disorientation, and finally coma and delirium, are typical symptoms of encephalopathy. Seizures, chorea, asterixis, multifocal myoclonus, and tremors are among the symptoms that accompany this disorder. These signals shift on a daily, and sometimes an hourly basis.17
Dementia
Patients with renal failure are at an increased risk of developing dementia. It is expected that 4.2% of elderly dialysis users will develop dementia, most often multi-infarct dementia. It is anticipated that 3.7% of this cohort will get multi-infarct dementia, making it 7.4 times more common than in the overall older population. The unfavourable profile for cerebrovascular disease in these individuals explains this.
Depression and delirium are also prevalent issues in renal failure, but they should be treated differently. Dialysis dementia and progressive multifocal leukoencephalopathy are two examples of subacute and rapidly progressing forms of dementia. Patients with chronic renal failure often have cerebral atrophy, and this is the case even in those without overt mental or emotional deterioration. On the other hand, intellectual deficiencies are often revealed via the use of psychometric testing.18 Possible causes of the shrinkage include atherosclerotic brain damage, arterial hypertension, and endogenous uremic toxins.
Cerebrovascular Disease
Patients with renal failure are at increased risk for developing cerebrovascular disease, a primary cause of mortality in this patient group. This population is at a higher risk for developing atherosclerosis and having an ischaemic stroke. However, the possibility of experiencing haemorrhagic complications is elevated by a number of risk factors. Ischaemic stroke due to renal failure is most often caused by atherosclerosis, thromboembolic disease, and intradialytic hypotension.19 Atherosclerosis is more prevalent and more distantly situated in individuals with chronic renal failure than in the general population. Traditional atherogenic risk factors, such as male sex, age, diabetes, hypertension, dyslipidaemia, and smoking, and variables specific to renal failure and its treatment certainly contribute to this. Renal failure has been linked to or may be related to hyperhomocysteinaemia, problems in calcium-phosphate metabolism, a buildup of guanidino chemicals, and oxidative and carbonyl stress.
Osmotic Myelinolysis
Individuals with renal failure often have osmotic myelinolysis in the central basis pontis, while it may also occur in the midbrain, thalamus, basal nuclei, and cerebellum. Central pontine myelinolysis is characterised by acute progressive quadriparesis, speech and swallowing problems, altered states of consciousness, and other neurological symptoms. When the demyelination spreads to the
middle of the brain, it paralyses both the horizontal and vertical movements of the eye muscles. When the cerebellum or the basal nuclei are damaged, the result might be either Parkinson’s disease or ataxia.20 Hyperintense demyelination patches are seen on T2-weighted MRI scans. In many cases, death is inevitable, and even for those who do make it through, full recovery may take months. Only comfort measures are taken. Considering the unproven pathophysiology, it is prudent to treat chronic hyponatraemia gradually while avoiding hypernatraemia.
Movement Disorders and Restless Legs Syndrome
Renally compromised patients may have trouble moving because of encephalopathy, medicine, or anatomical abnormalities. Involuntary motions come in several forms in metabolic encephalopathy. Clinically, asterixis, also known as ‘flapping tremor’, consists of multifocal action-induced jerks that, in extreme situations, might pass for drop attacks and are likely produced by an abrupt loss of tonus originating in the cortical region. Myoclonus is characterised by sudden, involuntary, and often painful muscular spasms. These cramps vary in frequency and intensity and are followed by brief periods of calm. Myoclonus of action may arise on its own in uraemia, and the condition responds well to benzodiazepines when it does. It has been hypothesised that uremic myoclonus results from a water-electrolyte imbalance, which in turn causes microcirculatory and degenerative alterations in the lower brainstem reticular formation.21 The uremic ‘twitch-convulsive’ syndrome is characterised by severe asterixis and myoclonic jerks, along with fasciculations, muscular twitches, and seizures; it is a common movement condition in uremic encephalopathy. The malfunctioning of the basal ganglia due to thiamine shortage is regarded to be the final cause of chorea.
Opportunistic Infections
Early diagnosis may be challenging since the conventional indications of infection are muted in immunosuppressed
individuals, and they are also more likely to get infections from rare and unusual opportunistic pathogens. Treatment of the infection with antibiotics and reducing dosage of immunosuppressants needs to be begun quickly. Acute, subacute, and chronic forms of neurological infections including meningitis, encephalitis, myelitis, and brain abscess are common in patients with renal failure. Many different types of bacteria may cause opportunistic infections; some well-known examples include Nocardia asteroides, Mycobacterium tuberculosis, and Listeria monocytogenes Aspergillus fumigatus, Candida albicans, Pneumocystis carinii, Histoplasma capsulatum, Mucor spp., Paracoccidioides, and Cryptococcus neoformans are all examples of common fungi.22 Reactivation of latent viruses is very uncommon; however, it may happen with herpes simplex virus, cytomegalovirus, and JC polyomavirus. Cytomegalovirus infection is the most common opportunistic infection after kidney donation. Invasive types may cause meningitis, encephalitis, myelitis, and nerve root involvement, but often cause no symptoms at all. Progressive multifocal leukoencephalopathy is caused by JC polyomavirus reactivation and infection of oligodendrocytes. Symptoms include a fast deterioration into a vegetative state, as well as dementia, ataxia, visual abnormalities, and other focal neurologic impairments. Currently, there is no proven therapy regimen, and all others are in the early stages of development. Infections caused by the metazoan Strongyloides stercoralis and the protozoan Trypanosoma cruzi have both been identified.
Neoplasms
Immunosuppressed patients with renal failure are more likely to get opportunistic infections and develop de novo malignancies. Patients with ESRD have been observed to develop malignant meningioma and primary central nervous system lymphoma. Lymph proliferative illness is more common in those who have had kidney transplants and subsequently underwent immunosuppressive medication. The Epstein-Barr virus is present in the majority of lymph proliferative diseases that develop after a transplant. There
is a high mortality rate associated with this illness, which affects 1–2% of renal transplant recipients. The localisation of post-transplant lymphoproliferative disease has evolved over time in response to modifications in immunosuppressive protocols. Before cyclosporine was used, the illness most often manifested itself in the central nervous system.23
The introduction of cyclosporine increased the frequency of presentations in the thorax and abdomen. There is not yet an accepted treatment standard for posttransplant lymphoproliferative disease. Allograft rejection is more common when immunosuppressant dosages are decreased or stopped altogether. Radiation treatment is often used to treat disorders of the brain and spinal cord. Combinations of acyclovir with surgery, chemotherapeutic drugs, and monoclonal anti-lymphoma immunotherapy have shown to be effective.
Intracranial Hypotension
Patients with orthostatic headache, especially those with associated neck stiffness, nausea, visual problems, dizziness, hearing loss, or abducens nerve palsy, should be evaluated for intracranial hypotension. Early detection is crucial for successful treatment of subdural hematoma with bed rest, increased fluid intake, and steroids. Imaging evidence of brain descent is common, as is diffuse pachymeningeal gadolinium enhancement on MRI of the head. The absence of activity across the cerebral convexities is evident on radioisotope cisternography, even after 24 or 48 hours, and the degree of the leak is occasionally disclosed in these cases. The pressure of the spinal fluid may establish a diagnosis. The disease may arise on its own, as a result of a cerebrospinal fluid leak, or, less often, in cases of dehydration and uraemia.24
Intracranial Hypertension
There are a number of potential triggers for intracranial hypertension in patients with chronic renal failure, including but not limited to idiopathic causes, secondary causes (such as dialysis or steroid use),
and intracranial abnormalities (such as neoplasm, infection, or cerebrovascular disease). Diagnosis of pseudotumor cerebri, also known as idiopathic intracranial hypertension, is made when patients present with symptoms related to excessive intracranial pressure despite normal neuroimaging findings (excluding any nonspecific evidence of raised intracranial pressure). Increased pressure may appear clinically as headache, transient vision impairment, and diplopia due to unilateral or bilateral sixth nerve palsy. Examples of non-specific symptoms include dizziness, nausea, vomiting, and tinnitus. The increasing pressure within the skull affects the optic nerves, leading to papilledema and progressive optic atrophy, which in turn causes a narrowing of the visual field, a loss of colour vision, and eventually blindness. To prevent vision loss due to increased intracranial pressure, the treatment goal is to manage the underlying renal sickness and, if possible, to use acetazolamide, furosemide, or corticosteroids. Fenestration of the optic nerve sheath, lumboperitoneal, ventriculoperitoneal, or ventriculoatrial shunting surgery may be necessary in individuals whose vision continues to deteriorate after maximum medicinal treatment.25
NERVOUS SYSTEM COMPLICATIONS
Mononeuropathy
In uraemia, the nerves in the limbs are more susceptible to compression and local ischaemia. The ulnar, median, and femoral nerves are the ones often affected by this disorder. It is possible for the ulnar nerve in the wrist to be damaged by uraemic tumoral calcinosis, which may manifest in Guyon’s canal. Motor dysfunction with paresis of intrinsic hand muscles, sensory loss in the hypothenar eminence, the little finger, and the lateral region of the ring finger, or a combination of these, are all possible outcomes. Electromyography and nerve conduction studies may verify the site of entrapment and provide evidence of the disease’s severity. If anti-inflammatory medicines, tricyclic antidepressants,
anticonvulsants, and splinting don’t help, or if motor deficits develop, neurolysis surgery may be the next best option.26
Polyneuropathy
Uremic polyneuropathy affects the nerves throughout the body, including the motor, sensory, autonomic, and cranial nerves, and affects around 60% of people with chronic renal failure.27 The condition manifests itself clinically as asymmetrical distal sensory loss across all modalities, with a greater emphasis on the lower limbs, and a male predilection for reasons that are not fully understood. Most peripheral nervous system injuries can be prevented if the glomerular filtration rate is approximately greater than 12 mL/min. Below this threshold (approximately 6 mL/ min), abnormalities in nerve conduction tests and clinical signs of peripheral nerve injury become apparent. The inability to feel vibrations as strongly and a general reduction in temperature sensitivity are early warning signs. There is a widespread presence of contrasting sensations of heat, cold, pain, and tingling. Areflexia, restless legs, muscle weakness, cramping, and atrophy, and increasing hypesthesia to pinprick or touch are all possible late-stage symptoms. In most situations, neuropathy develops over the course of several months. Common side effects of renal failure and dialysis include itchy skin. There is a dearth of understanding about its origin. Autonomic neuropathy has been linked to a wide range of symptoms, including intravascular and orthostatic low blood pressure, incontinence, diarrhoea, constipation, oesophageal dysfunction, hyperhydrosis, and impotence. A battery of cardiovascular autonomic testing should include measurements of heart rate variability while resting flat, breathing deeply, and doing the Valsalva manoeuvre.27
Myopathy
Uraemic myopathy is a disease often seen in patients with ESRD but its exact nature is still up for discussion. Individuals with chronic renal failure may present with a range of musculoskeletal abnormalities, including both functional
and anatomical alterations, due to their uraemic illness. Uraemic myopathy is a common complication in patients with a glomerular filtration rate of <25 mL/ min, and it often increases in parallel with the patient’s diminishing renal function. Dialysis patients as a whole make up an estimated 50% of cases.28 It causes fatigue quickly, and weakness in the upper and upper-mid body. Electromyography and muscle enzyme tests, as well as a physical examination, all come up negative. Atrophy of the fibres, most often the Type II fibres, may be seen on a muscle biopsy rarely. As uraemic myopathy progresses, it may lead to cardiomyopathy. As there is currently no cure for uraemic myopathy, it is crucial to avoid it with regular dialysis treatments, ideally with high-flux membranes.29 In addition, recombinant human erythropoietin for the treatment of renal anaemia and aerobic exercise training for the prevention of secondary hyperparathyroidism, as well as dietary adjustments, may be required. Supplemental l-carnitine has had mixed reviews in the scientific literature.30 Certain subsets of dialysis patients might see significant improvement after taking supplements. Within 2 months of a successful kidney transplant, patients have a dramatic decrease in their complaints, while their physical functioning is not totally restored.
References
1. Chen HJ et al. The impact of hemodialysis on cognitive dysfunction in patients with end-stage renal disease: a resting-state functional MRI study. Metab Brain Dis. 2015;30:124756.
2. Chen HJ et al. Re-establishing brain networks in patients with ESRD after successful kidney transplantation. Clin J Am Soc Nephrol. 2018;13(1):109-17.
3. Chou MC et al. Widespread white matter alterations in patients with end-stage renal disease: a voxelwise diffusion tensor imaging study. Am J Neuroradiol. 2013;34:1945-51.
4. Deng J et al. ImageNet: A large scale hierarchical image database. 2009 IEEE Computer Society Conference on Computer Vision and Pattern Recognition (CVPR), 20-25 June, 2009.
5. Drew DA et al. Anatomic brain disease
CONCLUSION
The number of people who are diagnosed with ESRD is rising rapidly over the globe. Many people on chronic dialysis struggle with exhaustion, which negatively impacts their quality of life. Combating weariness is in the eyes of some patients, and it is just as crucial as staying alive. Struggles exist in reducing the weariness experienced by the dialysis population, despite its critical importance. There is a high rate of morbidity and mortality in individuals with renal failure due to neurological complications. Despite the ongoing advancements in therapy, many of the neurological effects of uraemia do not improve with dialysis, and in some cases, dialysis or kidney transplantation might even make symptoms worse. In order to provide patients with renal failure the best care possible, both neurologists and nephrologists need to be aware of the possibility of neurologic disorders. Working together across disciplines is crucial for effective disease prevention, early detection, and treatment. Functional connection was disrupted in some ways in patients with ESRD using peritoneal dialysis. The most noticeable changes were made to the DMN and salience networks, which both saw reduced and increased connection.
in hemodialysis patients: a crosssectional study. Am J Kidney Dis. 2013;61:271-8.
6. Gusnard DA et al. Medial prefrontal cortex and self-referential mental activity: relation to a default mode of brain function. Proc Natl Acad Sci USA. 2001;98:4259-64.
7. Li S et al. Abnormal degree centrality in neurologically asymptomatic patients with end-stage renal disease: a resting-state fMRI study. Clin Neurophysiol. 2016;127:602-9.
8. Liang X et al. Altered pattern of spontaneous brain activity in the patients with end-stage renal disease: a resting-state functional MRI study with regional homogeneity analysis. PLoS One. 2013;8:e71507.
9. Alradaydeh MF, Khalil AA. The association of spiritual well-being and depression among patients receiving hemodialysis. PPC. 2018;54(3):341-7.
10. Ni L et al. Aberrant default-mode functional connectivity in patients with end-stage renal disease: a restingstate functional MR imaging study. Radiology. 2014;271:543-52.
11. Park BS et al. Differences of connectivity between ESRD patients with PD and HD. Brain Behav. 2020;10:e01708.
12. Dobre M et al. Serum bicarbonate concentration and cognitive function in hypertensive adults. Clin J Am Soc Nephrol. 2018;13(4):596-603.
13. Post JB et al. Cognitive profile of chronic kidney disease and hemodialysis patients without dementia. Nephron Clin Pract. 2010;116(3):c247-55.
14. Makin SD et al. Cerebral small vessel disease and renal function: systemic review and meta-analysis. Cerebrovascular Dis. 2015;39(1):3952.
15. Shi Y et al. Altered functional connectivity density in the brains of hemodialysis end-stage renal disease patients: An in vivo restingstate functional MRI study. PLoS One. 2019;14(12):e0227123.
16. Chen TK et al. Chronic kidney disease diagnosis and management: a review. JAMA. 2019;322(13):1294-304.
17. Vanholder R. Review on uremic toxins: classification, concentration, and interindividual variability. Kidney Int. 2020;98(5):1354. Corrected and republished from: Kidney Int. 2003;63(5):1934-43.
18. Son SJ et al. Effect of hypertension on the resting-state functional connectivity in patients with Alzheimer's disease (AD). Arch Gerontol Geriatr. 2015;60:210-6.
19. Toyoda K et al. Stroke and cerebrovascular diseases in patients with chronic kidney disease. Lancet
Neurol. 2014;13(8):823-33.
20. Moritz ML, Ayus JC. The pathophysiology and treatment of hyponatraemic encephalopathy: an update. Nephrol Dial Transplant. 2003;18(12):2486-91.
21. Wu HH et al. Family aggregation and heritability of esrd in taiwan: a population-based study. Am J Kidney Dis. 2017;70(5):619-26.
22. Bröcker V et al. BK virus nephropathy after kidney transplant. Pathologe. 2011;32(5):399-405. (In German).
23. Haase VH. Hypoxia-inducible factors in the kidney. Am J Physiol Renal Physiol. 2006;291(2):F271-81.
25. Johnston I, Paterson A. Benign intracranial hypertension. II. CSF pressure and circulation. Brain.
1974;97(2):301-12.
26. Arnold J et al. Modulation of stroke risk in chronic kidney disease. Clin Kidney J. 2016; 9(1):29-38.
27. Kiernan MC, Bostock H. Effect of membrane polarization and ischaemia on the excitability properties of human motor axons. Brain. 2000;123(12):2542-51.
28. Couser WG et al. The contribution of chronic kidney disease to the global burden of major noncommunicable diseases. Kidney Int. 2011;80(12):125870.
29. Stenvinkel P, Alvestrand A. Inflammation in end-stage renal disease: sources, consequences, and therapy. Semin Dial. 2002;15(5):32937.
30. Roshanravan B et al. CKD and muscle mitrochondrial energetics. Am J Kidney Dis. 2016;68(4):658-9.