Shafi Ahmed dives into the world of virtual reality, holograms, and the medical metaverse
Editor's Pick:
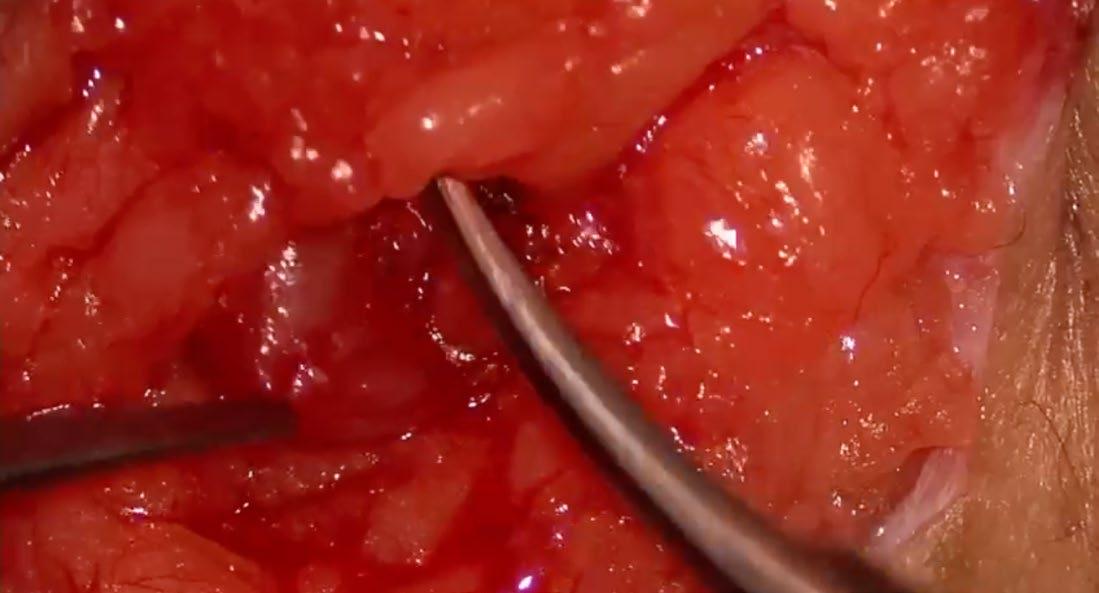
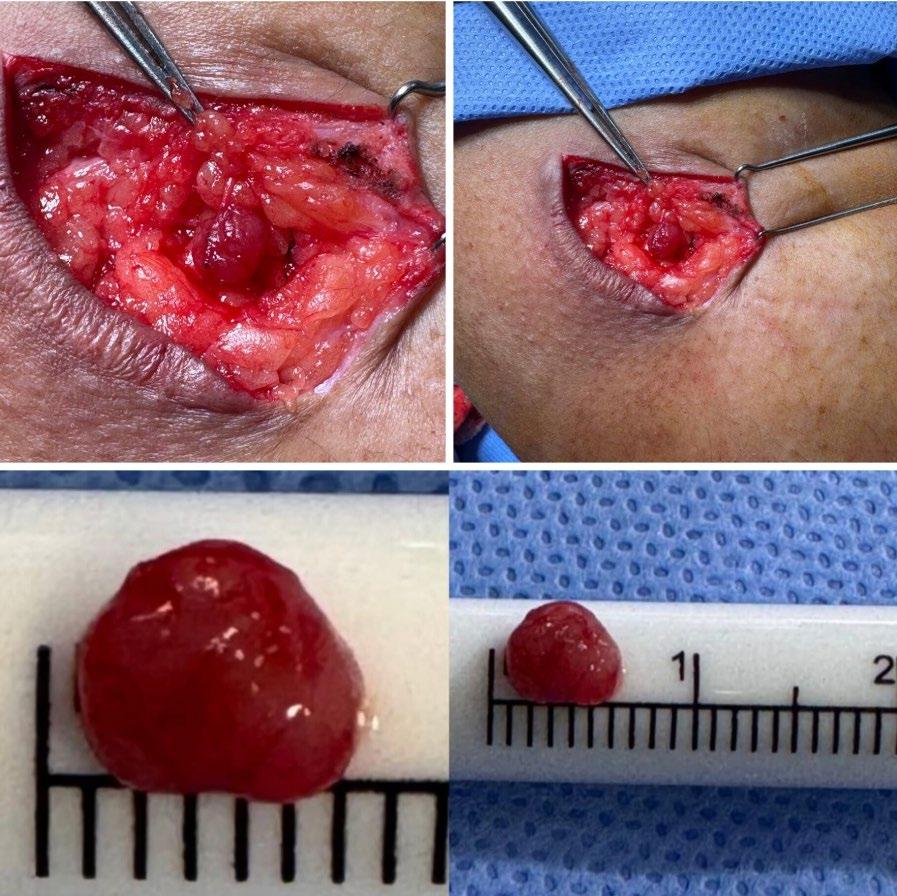
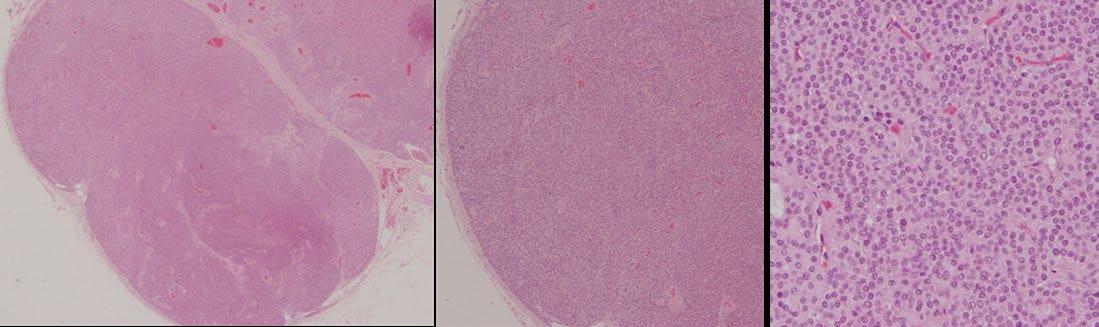
Diagnostic and Surgical Challenges in Extradigital Glomus Tumour: A Case Report
Editor's Pick
52 Editor's Pick: Diagnostic and Surgical Challenges in Extradigital Glomus Tumour: A Case Report
Rani et al. Articles
60 Exploring Bioinformatics-Driven Approaches for Enhanced Diagnosis of Chlamydia trachomatis Infections: Analysis of Target Proteins
Oladipo et al.
73 Exosomes: A Brief Review of Biology and Medical Applications
Sanyal and Banerjee
82 Regenerative Medicine in Orthopaedic Surgery: Pioneering Advances and Their Applications
Islam et al.
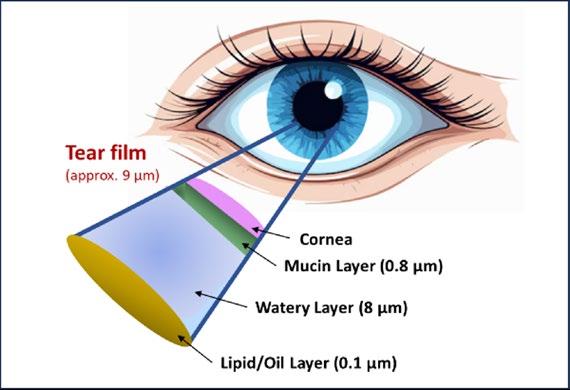
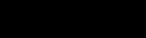
95 Emerging Smart Contact Lens Technology for Wearable Biosensors and Drug Delivery: Biomarkers in Tears
Psoma and Ndege
"The conference addressed how to bring innovation to life for a smarter, integrated NHS system"
Editorial Board
Editor-in-Chief
Dr. Masood Nazir
Medical Director Integrated Care and Chief Clinical Information Officer, NHS Birmingham & Solihull, UK
Dr Masood Nazir is a renowned healthcare leader specialising in digital health transformation, clinical informatics, and integrated care systems. With over 25 years of experience in the NHS, he has been instrumental in driving national initiatives, including the Patient Online Programme, revolutionising digital access for millions of patients across the UK. As Medical Director of Integrated Care for NHS Birmingham & Solihull, Dr Nazir drives the integration of digital pathways to foster innovation, improve patient care, and transform healthcare systems.
Dr. Rozelle Kane
Cambridgeshire & Peterborough
ICS; University of Cambridge, UK
Dr. Kinan Muhammed
Great Western Hospitals NHS Foundation Trust, UK
Maj Dr. Hannah Sophia
Ministry of Defence; University of Central Lancashire, UK
Dr. Rachel Thomas
Priory Hospital, UK
Dr. Nicholas Fuggle
University of Southampton; Alan Turing Institute, UK
Dr. Nick Guldemond
Erasmus University Rotterdam, Netherlands; First Moscow State Medical University, Russia
Prof. Christian Jürgens
BG Hospital Hamburg, Germany
Dr. Vandita Kakkar
Panjab University, India
Dr. Noedir Stolf
University of Sao Paulo Medical School, Brazil
Dr. Axel Sylvan myrecovery, UK
Dr. Olusola Michael Adeleke
King's College London; UCL Queen Square Institute of Neurology, UK
Prof. Dolores Cahill
University College Dublin, Ireland
Aims and Scope
EMJ Innovations is an open-access, peer-reviewed eJournal published annually, which covers new solutions and improvements in medicine in the form of new methods, products, and technologies for healthcare. The journal is aimed at healthcare professionals and presents the key technological advances in medicine alongside the most cutting-edge clinical research.
EMJ Innovations covers key congresses in health technology and innovation and also publishes peer-reviewed research papers, review articles, and case reports in the field. In addition, the journal welcomes the submission of features and opinion pieces intended to create a discussion around key topics in the field and broaden readers’ professional interests. The journal is managed by a dedicated editorial team that adheres to a rigorous double-blind peer-review process, maintains high standards of copy editing, and ensures timely publication.
Further details on coverage can be found here: www.emjreviews.com
Editorial Expertise
EMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors who are recognised authorities in their respective fields.
• Peer review, which is conducted by expert reviewers who are invited by the Editorial team and appointed based on their knowledge of a specific topic.
• An experienced team of editors and technical editors.
Peer Review
On submission, all articles are assessed by the editorial team to determine their suitability for the journal and appropriateness for peer review.
Editorial staff, following consultation with either a member of the Editorial Board or the author(s) if necessary, identify three appropriate reviewers, who are selected based on their specialist knowledge in the relevant area.
All peer review is double blind. Following review, papers are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected.
Editorial staff have final discretion over any proposed amendments.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects. We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial.assistant@emjreviews.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in EMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
EMJ is distributed through controlled circulation to healthcare professionals in the relevant fields across Europe.
Indexing and Availability
EMJ is indexed on DOAJ, the Royal Society of Medicine, and Google Scholar®; selected articles are indexed in PubMed Central®
EMJ is available through the websites of our leading partners and collaborating societies. EMJ journals are all available via our website: www.emjreviews.com
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
This Publication Launch Date: 2017 Frequency: Annually Online ISSN: 2513-8634
All information obtained by EMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, EMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. EMJ is completely independent of the review event (GIANT 2024) and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever. The cover photo is of London, UK, the location of GIANT 2024.
Katrina Thornber, Katie Wright, Aleksandra Zurowska
Creative Director
Tim Uden
Design Manager
Stacey Rivers
Designers
Owen Silcox, Fabio van Paris
Junior Designers
Dillon Benn Grove, Shanjok Gurung
Senior Performance & Insight Lead
Darren Brace
Marketing Director
Kristina Mestsaninova
Chief Content Officer
Justin Levett
Chief Commercial Officer
Dan Healy
Founder and Chief Executive Officer
Spencer Gore
Welcome
Welcome to the 2025 issue of EMJ Innovations! It is a great privilege to publish another issue showcasing key topics and advancements in medical technology.
Last year witnessed an array of medical innovations; however, what stood out is a first-in-human Phase I clinical trial from September 2024 that assessed the potential of stem-cellderived islets as a treatment for Type 1 diabetes in a female patient.1 The results were nothing short of astonishing: following the transplant of her own reprogrammed stem cells, the patient was able to produce her own insulin, achieving sustained insulin independence within 75 days and maintaining long-term glycaemic control.
This landmark study paves the way for large-scale clinical trials that could bebefit millions of people. While proving efficacy in larger populations is key for wide reach, access remains crucial as well, considering the often-prohibitive costs involved in stem cell therapies. We must strive to ensure that the topic of accessibility to groundbreaking treatments remains high on the agenda when it comes to policy discussions.
This journal aims to bring you a taste of what’s on the horizon for medical innovations. I would like to take this opportunity to thank our reviewers, contributors, and our amazing Editorial Board, including our newly appointed Editor in Chief, for bringing together a great issue! I hope you enjoy reading this and I look forward to receiving news of more innovations.
Reference 1. Wang S et al. Transplantation of chemically induced pluripotent stem-cellderived islets under abdominal anterior rectus sheath in a type 1 diabetes patient. Cell. 2024;187(22):6152-64.e18.
Editorial enquiries: editor@emjreviews.com
Sales opportunities: salesadmin@emjreviews.com
Permissions and copyright: accountsreceivable@emjreviews.com
Evgenia Koutsouki Editor
Reprints: info@emjreviews.com Media enquiries: marketing@emjreviews.com
Foreword
Dear Colleagues,
Welcome to the latest issue of EMJ Innovations. It is with great pleasure that I introduce this edition, which captures the pulse of groundbreaking advancements in healthcare and technology from around the globe.
Following the remarkable Global Innovation and New Technology (GIANT) Health Event held in London, UK, on the 9th–10th December 2024, we are thrilled to share exclusive coverage of this transformative event. I have long admired the incredible contributions of Shafi Ahmed, GIANT Health Chairman, to the world of healthcare innovation, and it is an honour to feature his insights in our 2025 issue through an engaging interview. His vision and thought leadership continue to inspire the next generation of innovators.
This issue celebrates the intersection of science, technology, and clinical practice through an array of peer-reviewed articles showcasing the latest advancements across diverse fields. Discover the promise of regenerative medicine in orthopaedic surgery, the potential of smart contact lens technology, and how bioinformatics is unlocking new frontiers in diagnosing diseases. To highlight the year’s most significant contributions to healthcare, we have also curated a collection of highly commended abstracts from 2024, spanning several therapeutic areas.
In addition to these cutting-edge insights, this issue features exclusive interviews with pioneers in the field. David Resühr and Andrea Pfeifer discuss their visionary work in 3D printing, advanced ultrasound techniques, and personalised immunotherapy for neurodegenerative diseases. Plus, we explore the exciting potential of electronic noses through an engaging infographic, showcasing how this technology could revolutionise the way we diagnose, monitor, and treat diseases.
This issue celebrates the intersection of science, technology, and clinical practice
None of this would have been possible without the incredible contributions of our authors, Editorial Board, peer reviewers, and interviewees. Their dedication continues to drive the spirit of innovation that defines EMJ Innovations.
Thank you for joining us on this journey to explore the cutting edge of medicine and technology. I hope you find this issue as inspiring and thought-provoking as I do.
Dr Masood Nazir Medical Director Integrated Care and Chief Clinical Information Officer, NHS Birmingham & Solihull, UK
GIANT 2024
The event showcased six distinct ‘shows within the festival’, providing a platform for world-class speakers, cutting-edge start-ups, and immersive presentations
Review of the Global Innovation and New Technology (GIANT) Health
THE RAPID growth of healthcare innovation over the past year has driven transformative changes within the NHS and other government agencies. At the forefront of this movement is Global Innovation and New Technology (GIANT) Health, the UK’s largest community of over 345,000 NHS leaders, clinicians, and health-tech innovators. In December last year, experts came together to discuss and champion the latest innovations in healthcare.
This year, the event showcased six distinct ‘shows within the festival’, providing a platform for world-class speakers, cutting-edge start-ups, and immersive presentations. With a unified vision to drive innovation within the NHS and support health-tech entrepreneurs, attendees and speakers came together to explore solutions that are shaping the future of healthcare.
Beginning on 9th December, the 'National ICS Innovation Congress’ offered an opportunity for networking with, and learning from, leaders of the UK’s new integrated care boards: experts who are leading the dramatic and profound changes across the NHS. The conference addressed how to bring innovation to life for a smarter, integrated NHS system, and strategies to ensure digital solutions deliver long-term benefits in healthcare. Additionally, panel discussions examined how community-centred technology could improve disease management and ease the strain on secondary care.
The ‘Future Hospital Show’ brought together healthcare leaders, clinicians, administrators, and innovators to explore the transformative shift from analogue to digital healthcare. The event emphasised the transition of care from hospitals into the community, also termed ‘hospital to HOUSEpital’, and the urgent need to redefine healthcare, particularly in reducing outpatient waiting times and administrative tasks, with workshops such as ‘Empowering NHS Doctors: Harnessing AI and Digital Tools for Enhanced Healthcare’. Additionally, experts behind the NHS App came together to highlight both its potential for reshaping patient engagement and secondary care, and its current limitations.
The ‘Innovation, Investment and Impact Show’ gave promising healthtech startups and investors the opportunity to connect, explore industry trends, and learn how to navigate the investment landscape within healthcare. The event reinforced the importance of collaboration in driving forward healthcare innovations and ensuring their successful transition into impactful solutions.
On 10th December, ‘The Women’s Health Technology Show’ was an empowering and thought-provoking event led by experts and innovators in new technologies and strategies to improve detection, diagnosis, and management of women’s health conditions. A key theme was the use of Women’s Health Hubs and AI to address disparities in healthcare, as well as the unique health challenges faced by women.
The transformative role of AI in healthcare was explored in greater detail during ‘The NHS National AI Conference’, in which leaders and stakeholders from integrated care systems, integrated care boards, and senior NHS officials discussed the practical applications of AI in real-world settings. The event not only celebrated the advances in AI but also addressed the challenges and ethical considerations. For example, the
panel discussion ‘The Human Equation vs. the Algorithm: Shaping a Future of Care in the Smart Hospital’ examined the evolution of the smart hospital, and the careful balance between human decision-making and machine learning algorithms.
The exciting and inspiring GIANT Health Event 2024 culminated with the ‘Champions of Innovation Conference’, a dynamic event that showcased groundbreaking technologies and strategies to revolutionise healthcare.
Throughout the 2-day event, speakers and attendees engaged in keynotes, panel discussions, and networking opportunities that emphasised the importance of collaboration in developing innovations within the NHS to ensure a more resilient, efficient, and patient-focused healthcare system.
SUCCESSFUL integration of AI and machine learning into the NHS depends on the implementation of practical education, at varying levels of intensity, across the entire NHS workforce, medical school students, and the general public. During the NHS National AI Conference on 10th December, ‘Beyond Implementation: Building Healthcare's AI-Fluent Workforce’, experts discussed the current and future innovative approaches being implemented to improve AI literacy, develop educational AI curricula, and enhance confidence and trust in AI-implemented healthcare systems.
A LACK OF AI LITERACY
Keith Grimes, Digital Health & Innovation Consultant, Curistica Ltd, UK, began the session by warning that healthcare professionals may be using AI models, such as ChatGPT (OpenAI, San Francisco, California, USA), without having had the adequate training to ensure it is being used safely, responsibly, and equitably. “It is estimated that one in five GPs use ChatGPT, but actually, one in five GPs haven’t had the adequate training,” Grimes explained. He also highlighted the publication of the European Union’s Artificial Intelligence Act in July 2024, and how non-compliance with the legal framework for the regulation of AI systems will be met with a maximum financial penalty of up to 35 million EUR.1
This lead to an in-depth discussion on building an “AI-fluent workforce” in the UK, featuring Alex Aubrey, Clinical Lead for AI at Health Education and Improvement Wales, UK, and Nick Fuggle, co-organiser of the Clinical AI Interest Group at the Alan Turing Institute, London, UK.
Aubrey is responsible for mapping the landscape of AI literacy within the healthcare and social care workforce in Wales, and Fuggle is working on scoping a clinical AI curriculum and potentially
a broader healthcare AI curriculum for everyone working in the NHS. Together, they proposed the key steps needed to ensure that current healthcare professionals, the future workforce, patients, and the general public develop a sufficient understanding of AI: what it is, how to use it effectively, and when its application is appropriate.
Aubrey began by emphasising that improving AI literacy requires hands-on experience, noting: “You have to use it enough to start making mistakes that are very low risk”. This approach, he explained, helps individuals recognise that while AI can be beneficial, it can also make mistakes and is not always appropriate to use. He highlighted the importance of combining formal education pathways with safe, playful experimentation, enabling users to better understand AI’s practical applications and limitations.
A NATIONAL AI CURRICULUM
Fuggle outlined the three main areas to consider in an AI curriculum: who is the target audience for the curriculum, what will be the core components, and how will these educational frameworks be implemented.
Who Should be Taught?
Fuggle raised the question of who the curriculum will be directed at. Will it target medical students, postgraduate medics, those in continuing medical education, everyone working in healthcare, or the entire NHS workforce?
Aubrey explained that medical schools are already taking steps to include AI in their educational frameworks. For example, from next year, Cardiff University, UK, will introduce mandatory AI workshops and training for medical students. Regarding the entire NHS workforce, Fuggle admitted that he has shifted his perspective from thinking everyone in the NHS needs a deep understanding of AI, to thinking that everyone should be aware of it, and have access to education if needed in their specific job role.
Medical schools are already taking steps to include AI in their educational frameworks
Core Components of the Curriculum
The discussion then turned to the curriculum’s content, with Fuggle emphasising the importance of defining a curriculum that is flexible enough to adapt to the rapid developments in AI. “I think it’s really difficult to tell people what they’re
going to need if they qualify in 2 years, but I think that the one thing we probably would agree on is we need to give people the foundational tools to equip them so that they can ask the right questions and understand that basic literacy.”
Fuggle suggested including background knowledge, such as the theory behind machine learning and key terminology. For medical students, he proposed that ethics must play a central role, alongside legal and regulatory considerations. Additionally, training on the implementation in clinical practice is crucial, with training on how to explain to patients how these tools are being used and how they’re influencing their care, to ensure patients can fully consent to the use of AI in their care.
Aubrey also brought to attention the issue surrounding differing definitions within AI terminology. He explained that confusion arises quickly when everyone operates with slightly different terminology, so he relies on the NHS AI Lab dictionary to ensure a consistent and standardised language when discussing AI.
Another issue he highlighted was the hesitation to let students use AI. He proposed that when students use AI to enhance their learning, they can find answers to basic questions quickly, and therefore, have more time to explore more complex topics and apply their knowledge to real-world settings.
Strategies for Rolling Out the Curriculum
Finally, the panel discussed how the AI curriculum may be delivered, with emphasis on key drivers within the government and other stakeholders, with the introduction of leadership training for AI. Fuggle highlighted initiatives such as AI champions, leaders within medical schools who are expected to play a pivotal role in driving these efforts and fulfilling some of the goals discussed.
Aubrey dove into an initiative he has been working on, though still a work in progress, it’s anticipated to be ready for rollout to staff by 2025 or 2026. The concept is “using AI to learn AI”. He explained that creating educational material for the entire NHS workforce, from nurses to surgeons, physiotherapists, opticians, pharmacists, administrative staff, and many more, would
References
1. EUR-Lex. Document 32024R1689. Regulation (EU) 2024/1689 of the European Parliament and of the Council of 13 June 2024
“take a lifetime”. Instead, they decided to leverage AI, specifically a large language model, to develop training tailored to different job roles. Based on a user’s specific role, the AI model can highlight basic applications relevant to their field, then delve into potential challenges, risks, and biases that need to be considered. The plan is to ensure reliable data sources, aiming to minimise the risk of AI “hallucinations” and inaccurate information. He noted that the potential risks of this application are relatively low, with guardrails being put in place. He concluded by highlighting the importance of transitioning from a mindset of risk avoidance to one of risk management. This shift, he stressed, is essential for the successful implementation of AI within the NHS, with the ultimate goal of ensuring that the benefits of such initiatives outweigh the potential risks.
laying down harmonised rules on artificial intelligence and amending Regulations (EC) No 300/2008, (EU) No 167/2013, (EU) No 168/2013, (EU) 2018/858, (EU) 2018/1139 and (EU) 2019/2144 and Directives 2014/90/
EU, (EU) 2016/797 and (EU) 2020/1828 (Artificial Intelligence Act) (Text with EEA relevance). Available at: https:// eur-lex.europa.eu/legal-content/ EN/TXT/?uri=OJ:L_202401689. Last accessed: 20 January 2025.
Breaking the Silence: Tackling Stigma Around Pelvic Floor Dysfunction
PELVIC floor dysfunction can have debilitating and devastating consequences on the health and well-being of women, yet these issues are often under-researched and not discussed openly in wider society. This has led to stigma for people experiencing symptoms, as well as increased barriers to treatment. At the Global Innovation and New Technology (GIANT) Health Event 2024, hosted in London, UK, an expert panel explored the role of technology and digital health in addressing this issue, as well as the innovative Women’s Health Hub concept gaining traction in the UK.
THE UNSPOKEN REALITY
To highlight the importance of raising awareness around how common postnatal pelvic floor symptoms are, Janet Barter, President of the Faculty of Sexual and Reproductive Health and Clinical Lead at Tower Hamlets Women’s Health Hub, UK, recalled to the audience a story from when she was a new general practitioner (GP) many years ago. While conducting a home visit, she was accidentally sent to the incorrect doorstep of a woman with the same name. However, what began as an administrative error turned out to be a blessing in disguise as the woman confided in Barter that she had avoided leaving her house for the past 12 years due to incontinence. This had completely impacted her and her children’s social lives, but she had been too embarrassed to go and talk to someone about it.
“We see it day to day,” explained Imogen Pallister, Highly Specialist Physiotherapist, Pelvic Health Team Lead, Barts Health NHS Trust, UK. “Patients coming through that don't socialise anymore with their friends, they can't speak about it with their families, they end up a lot more housebound. It results in the breakdown of marriages and relationship issues.”
About 25% of people who are postnatal will have symptoms, which may include prolapse, incontinence, bowel or bladder pain, or sexual pain and discomfort, highlighted Sunita Sharma, Chelsea and Westminster Hospital, London, UK. “So, the consequences are huge, but there are barriers in accessing care. There's a stigma on raising concern about their symptoms.”
This stigma causes women to not seek care at the time of symptom appearance, but instead to wait and avoid speaking up due to shame or embarrassment. “I am patient-focused and see lots of these conditions coming in that haven't been addressed properly, that get normalised in society, and then, unfortunately, end up coming into my clinics with a much, much bigger problem,” Pallister said.
This not only reduces the patients quality of life but also leads to a worsening of symptoms, creating more complications and thus more costly issues to fix. “These are huge drains on the National Health Service (NHS) because we then get these patients at a much later stage with vastly different problems and needing a lot more intervention down the line,” Pallister continued.
“We need to start with raising the awareness of our patients that we do see about what can happen, what we can expect, but actually also what services are out there, and what can be done to stop this from becoming a 15-year-old history of urinary incontinence because they had children.”
WHY ARE WE HERE?
The systemic neglect of women’s health has deep roots in sexism and racism within biomedical research, explained Rehan Khan, Consultant in Obstetrics and Gynaecology, Royal London Hospital, UK. Historically, studies have been based on male physiology, with women’s health considered an afterthought. Even now, research in this field remains underfunded and understudied, he explained.
This has in turn led to a lack of awareness and education about issues that primarily affect women. “We know that we've got antenatal education classes that have been around forever, and a lot of this focuses on ‘This is what's happening to the baby. This is what we do. This is how we change nappy.’
But, actually, nobody really discusses with them how you actually give birth, what can happen when you do give birth, and what you do afterwards,” Pallister said.
This has led to cases like that of Barter’s accidental patient from many years ago: women who feel shame about their lifeimpacting post-partum symptoms but do not have the knowledge of how common they actually are or the possible treatment options for them.
THE WOMEN’S HEALTH HUBS
Enter the Women’s Health Hubs: an innovative, patient-centred community service designed to bridge these gaps in care. These hubs aim to provide holistic support by integrating primary, secondary, and community healthcare services, a “single point of access”, explained the panel’s Chairperson, Ishi Bains, NHS GP and Regional Primary Care Clinical Lead for Gynaecology, UK.
These hubs are popping up around the country, including in Hackney, where they operate within GP practices. However, this
is not a one-size-fits-all model, with its inclusion differentiated to meet the individualised needs of those patients in different areas. “The bigger picture is really that Women's Health Hub is a concept. It's about improving care in a collaborative, holistic way,” Bains said.
The success of Women’s Health Hubs depends on addressing several systemic barriers, including access, education, shared language, and economic impact.
Ensuring Equitable Access
Technology is a cornerstone of the Hub model, offering scalable solutions to reduce inequalities. Digital platforms can provide multilingual resources, virtual consultations, and online support groups. For many women, particularly those with sexual pain or trauma, discussing sensitive issues from the privacy of their homes may feel safer.
“You would think that most women wouldn’t want to talk in a group about their sexual progress, their sexual pain, their fear, their stigma, their anxieties, but actually it's about understanding that you're not alone,” Barter explained. “This is what they tell us, that the biggest value is understanding that they're not the only one.”
Designing with the Community in Mind
Khan underscored the importance of co-designing these solutions with the communities they serve: “The thing is, if you don't co-design it with the communities who are going to use the technology, you could fall into a trap that is hundreds of years old. This is what happened with biomedical research.”
This includes ensuring that information is available in multiple languages and communication types. “It's got to be there for people who don't find accessing information digitally easy. It's got to be there for people who don't speak English. It's got to be there for people who have other communication problems. They might be deaf, for example,” Barter explained. “The whole point of Women's Health Hubs is to reduce inequalities, and we're partway there, but we're not there yet.”
The bigger picture is really that Women's Health Hub is a concept. It's about improving care in a collaborative, holistic way
Creating Sustainable Solutions
However, digital solutions alone are not enough. They must be sustainable, accessible, and integrated with inperson care. “You can't overpromise and underdeliver; if you're going to do it, it's got to work, and it's also got to be sustainable. The history of women's health is you get champions, we get very excited to do lots of amazing stuff, and then move on, and it all dies away. So, whatever we do has to be sustainable,” Barter said.
DOING IT DIFFERENTLY
For the first time, women’s health is a national priority in the UK. The Women’s Health Hubs represent a push for collaboration, innovation, and patient-centred care.
“This is not about childbirth on its own, and it's not about the postpartum period,” Khan said. “These problems are lifelong, and events that happen during 15 minutes of pushing will affect the next 50 years of your life.”
This model offers a blueprint for systemic change, combining early intervention, education, and technological innovation. By mapping the patient journey and streamlining care, these hubs have the potential to transform lives.
For Barter, it all comes back to the definition of madness, “where you keep on doing the same thing and expecting something different to happen. If we want something different to happen, then we need to do something differently.”
These problems are lifelong, and events that happen during 15 minutes of pushing will affect the next 50 years of your life
The following highlights showcase the most pivotal, innovative research published across multiple therapeutic areas in medicine in 2024. The selected abstracts mark key advancements in healthcare and highlight future avenues for medical innovation.
Researchers adapted commercially available, disposable strips, similar to those used for glucose testing, to detect breast cancer biomarkers HER2 and CA15-3
A Wearable Solution for Voice Disorders: Soft Magnetoelastic Technology
VOICE disorders, often caused by pathological vocal fold conditions or recovery from laryngeal cancer surgeries, are prevalent sources of dysphonia.1 These disorders impair voice quality, pitch, and loudness, significantly impacting patients’ quality of life.
In order to address this issue, a research team based in California, USA, introduced a self-powered, wearable sensing-actuation system based on soft magnetoelasticity that enables assisted speaking without relying on vocal fold vibrations.
This device has been designed to be lightweight (approximately 7.2 g) and skin-like, with a modulus of 7.83×10⁵ Pa, stability against perspiration, and a maximum stretchability of 164%. Its sensing component captures extrinsic laryngeal muscle movements and converts them into high-fidelity electrical signals. These signals are analysed using machine learning algorithms to achieve a speech recognition accuracy of 94.68%. The system’s actuation component translates these electrical signals into voice signals, bypassing the vocal folds entirely. This non-invasive device holds the potential to restore normal voice function, significantly improving the quality of life for individuals with dysfunctional vocal folds.
Voice is integral to human communication, serving as a medium for expression, emotion, and connection. Disorders affecting the vocal fold, the primary voice-generating organs, severely disrupt social interaction and community integration. Voice disorders, including vocal fold polyps, paralysis, nodules, keratosis, and adductor spasmodic dysphonia, affect 29.9% of people at some point in their lives. Additionally, 7.0% of individuals experience ongoing voice problems, and 7.2% of employed individuals report work absences due to these issues. Laryngeal surgeries, often necessary for
cancer treatment, can exacerbate these challenges, requiring lengthy recovery periods and absolute voice rest lasting months.
The research team highlighted that existing solutions, such as electrolarynx devices, “talk boxes”, or trachea-oesophageal puncture procedures, can be invasive, inconvenient, or uncomfortable. Voice therapy and surgical interventions, while effective, demand prolonged recovery times, ranging from 3 months to a year. These limitations underscore the urgent need for wearable, non-invasive medical devices to assist patients in communicating during treatment and recovery.
This novel magnetoelastic wearable system represents a transformative approach. By enabling speech without vocal fold involvement, it offers a comfortable, efficient, and practical alternative to traditional solutions. With its potential to restore communication, researchers note that this technology addresses a critical need in healthcare today, empowering patients to navigate recovery with confidence and dignity.
of individuals experience ongoing voice problems 7.0 % 7.2 of employed individuals report work absences due to these issues %
Revolutionary Bioink Paves Way for Advanced Lung Engineering
3D-PRINTING has become a powerful tool in personalised medicine, allowing for the creation of tailored tissue-engineering constructs at lower costs.2 However, one major limitation has been the lack of diverse and functional biopolymeric hydrogels for bioinks, which restricts the range of applications in regenerative medicine. A new composite bioink could change this landscape.
This study introduced a bioink combining methacrylated mucin (MuMA), a photocross-linkable derivative of mucin, with hyaluronic acid (HA). Mucin, known for its role in mucus and its hydrogel properties, has been underutilised in bioink applications. However, its unique features offer great promise. HA, a vital component of the extracellular matrix, enhances the ink's viscosity and printability while also being mucoadhesive, further improving the bioink’s functionality.
The bioink is stabilised by photo-crosslinking with 405 nm light, which ensures cell protection during the printing process without compromising cell viability. Rheological tests showed that the ink exhibits shear-thinning behaviour, which improves its handling during printing and further aids in protecting cells. Additionally, the presence of HA enhances the viscosity of the MuMA-based bioink.
Printed scaffolds demonstrated a porous structure, which is crucial for nutrient transport and cellular migration. After 4 weeks in phosphate-buffered saline, the scaffolds maintained 70% of their original mass, indicating strong stability. Biocompatibility assessments using lung epithelial cells (L-132) confirmed cell attachment and growth, suggesting that this bioink is particularly suited for lung tissue engineering.
The versatility of this bioink opens up promising possibilities not only in lung tissue engineering but also in a wide array of biomedical applications. This advancement represents a significant step forward in the use of 3D bioprinting for patient-specific treatments, enhancing the potential for future regenerative therapies.
Gene Therapy Shows Promise in Treating Congenital Deafness
A RECENT clinical trial has brought promising results for children suffering from autosomal recessive deafness 9, a form of congenital deafness caused by mutations in the OTOF gene leading to severe-to-complete, bilateral hearing loss.3 Currently, no pharmacological treatment exists for congenital deafness, making this trial a significant step forward.
Five of the six children exhibited hearing recovery, with average auditory brainstem response thresholds improving by 40–57 dB.
The trial, which took place between October 2022–June 2023, involved six children aged 1–18 years with confirmed OTOF mutations and severe hearing loss. Researchers administered a single injection of adeno-associated virus (AAV1) carrying the human OTOF gene (AAV1-hOTOF) directly into the cochlea via the round window. The goal was to assess the therapy’s safety and efficacy, with a primary focus on any dose-limiting toxicity occurring within 6 weeks.
The trial was conducted at a single
The results demonstrated significant improvements in auditory function. Five of the six children exhibited hearing recovery, with average auditory brainstem response (ABR) thresholds improving by 40–57 dB. The child receiving the lowest dose (9×1011 vector genomes) showed the most dramatic improvement, with ABR thresholds improving from over 95 dB at baseline to 45 dB at 26 weeks. Those receiving higher doses saw similar gains in ABR thresholds.
Importantly, speech perception was
Saliva-Based Test Could Revolutionise Early Breast Cancer Detection
BREAST cancer remains one of the most prevalent cancers among women, reinforcing the urgent need for more effective and accessible detection methods.4 A groundbreaking study is offering a promising solution by utilising salivary biomarkers for the noninvasive detection of breast cancer, paving the way for a faster, more efficient screening process.
In this innovative approach, researchers adapted commercially available, disposable strips, similar to those used for glucose testing, to detect breast cancer biomarkers HER2 and CA15-3, which are known to play a critical role in the progression of breast cancer. The new test demonstrated remarkable sensitivity, with fg/mL. This is significantly more sensitive than traditional ELISA, which typically detects levels in the
The testing mechanism is based on a synchronised double-pulse method that applies a series of 10 rapid voltage pulses to a sensing strip electrode. This process amplifies the detected signal, providing highly accurate results. The sensor’s sensitivity levels were found to be approximately 70/dec for HER2 and 30/dec for CA15-3, indicating the test's robustness in detecting even minute concentrations of biomarkers.
One of the most compelling advantages of this technique is its speed and minimal sample requirement. Testing takes less than 15 milliseconds and requires only 3 µL of saliva, making it a highly efficient and userfriendly option. The simplicity of the test and its potential for widespread use could dramatically improve early breast cancer detection, particularly for those with limited access to traditional screening methods.
Researchers adapted commercially available, disposable strips, similar to those used for glucose testing, to detect breast cancer biomarkers HER2 and CA15-3
New EV-GLYPH Assay Identifies Early Malignant Development in Lung Cancer
A NEW diagnostic tool, the EV-GLYPH assay, has demonstrated potential for non-invasive detection of early-stage lung cancer by analysing glycan patterns on small extracellular vesicles (sEV) released by cancer cells.5
The EV-GLYPH assay combines a microfluidic platform with surfaceenhanced Raman scattering to profile sEV glycosylation. These glycans, reflective of their tumour cell origins, provide critical insights into cancer initiation, progression, and resistance to treatment.
In the clinical study, which consisted of 40 patients, the EV-GLYPH assay successfully distinguished between early-stage malignant lung nodules and benign lung nodules. This represents a significant step forward as current technologies struggle to analyse the trace amounts of tumour-derived sEVs in circulation. The lead researchers noted that this is the first successful identification of distinct sEV glycan signatures between normal and cancerous lung cells, opening new doors for early detection and improved patient outcomes.
In the clinical study, which consisted of 40 patients, the EV-GLYPH assay successfully distinguished between early-stage malignant lung nodules and benign lung nodules.
Glycosylation, a common post-translational modification of proteins, regulates many fundamental biological processes under normal and pathological conditions and is often altered in cancer, promoting tumour proliferation, invasion, and metastasis. By focusing on glycan patterns, the EV-GLYPH assay provides a minimally invasive method to monitor lung cancer progression and potentially guide therapeutic decisions. The success of this assay could transform cancer diagnostics, providing clinicians with a powerful new tool to detect lung cancer in its early stages, when treatment is most effective.
A NOVEL tool, the Platelet Reactivity ExpreSsion Score (PRESS), has shown promise in identifying individuals with hyperreactive platelets and an increased risk of cardiovascular events.6 The development of this tool opens the possibility for a personalised approach to antithrombotic therapy for cardiovascular risk reduction.
Platelets play a central role in atherothrombosis, yet methods to identify individuals with heightened platelet reactivity are limited. Recent research aimed to explore the relationship between hyperreactive platelets and cardiovascular events, introducing PRESS as an innovative tool for this purpose. The research focused on patients with peripheral artery disease (PAD), a condition associated with high cardiovascular risk, and incorporated platelet aggregation tests and RNA sequencing to develop PRESS. This tool was evaluated for its ability to predict platelet hyperreactivity and associated cardiovascular events in both clinical and healthy populations.
Platelet aggregation responses to 0.4 µM epinephrine were analysed in patients with PAD. Those with hyperreactive platelets (>60% aggregation) experienced a significantly higher incidence of the 30-day primary cardiovascular endpoint (37.2%) compared to non-hyperreactive individuals (15.3%), with an adjusted hazard ratio of
2.76 (95% CI: 1.5–5.1; p=0.002). PRESS demonstrated strong predictive ability in cross-validation within the PAD cohort (area under the curve: 0.81; 95% CI: 0.68–0.94; n=84) and in an independent healthy cohort (area under the curve: 0.77; 95% CI: 0.75–0.79; n=35). Additionally, patients with PAD with PRESS scores above the median showed a higher risk of future cardiovascular events (adjusted hazard ratio: 1.90; 95% CI: 1.07–3.36; p=0.027; n=29).
The findings highlight PRESS as a valuable tool for identifying platelet hyperreactivity and cardiovascular risk, with significant implications for clinical practice. By enabling personalised risk assessment, PRESS offers the potential to tailor antithrombotic therapies to individual patient profiles, optimising outcomes and reducing adverse events. Future integration of PRESS into routine cardiovascular risk assessments could transform patient care by enhancing prevention strategies and improving treatment precision.
The development of this tool opens the possibility for a personalised approach to antithrombotic therapy for cardiovascular risk reduction
Revolutionising Gynaecologic Surgery: Transvaginal Hysterectomy with Single-Port Robot
THE FIRST transvaginal Natural Orifice Transluminal Endoscopic Surgery (NOTES) hysterectomy was performed on 11 November 2023, at Baylor College of Medicine, Texas, USA. report demonstrated the feasibility and success of the new da Vinci single port (SP) robotic system for transvaginal NOTES hysterectomy, highlighting a key advancement in the field of gynaecologic surgery.
Whilst transvaginal NOTES has gained popularity since its inception in 2012, challenges in suturing, dissection, and triangulation of traditional NOTES have limited its application for vaginal procedures. Nevertheless, the author has successfully performed over 300 transvaginal NOTES using the robotic da Vinci Xi system for hysterectomy, myomectomy, sacrocolpopexy, and all stages of endometriosis surgeries. The latest advancement, however, is the new da Vinci SP platform, specifically designed for single-port surgery, with robotic elbows that enable "wristed" movements. And on 11 November 2023, the first instance of transvaginal NOTES for gynaecologic procedures with this new advanced platform was reported.
The case report details the 10 steps taken to complete the procedure: patient position (dorsal lithotomy), temporary ureteral stent, transvaginal surgery, port placement
and trocar locations, transvaginal robotic SP docking, robotic hysterectomy, ovarian suspension, abdominal wall omental adhesiolysis, undocking and specimen removal, and vaginal cuff closure. Of note, after the completion of the hysterectomy, the specimen is displaced into the lower abdomen, giving the surgeon a unique opportunity to survey the entire abdominal cavity, enabling additional procedures to be carried out on the robotic platform, such as oophoropexy to the respective lateral pelvic sidewall.
Following the successful procedure, the patient was discharged on the same day. Whilst no significant issues arose during the post-operative course, pathology results revealed adenomyosis and endometriosis after the comprehensive surgery. The feasibility and safety seen in this case report warrant validation from further studies with larger sample sizes before employment of this advanced platform.
3D-Printed Sweat Monitor Redefines Real-Time Health Tracking
A NEW wearable health monitor, fabricated using advanced 3D printing and nanotechnology, is set to transform noninvasive health monitoring by providing real-time insights into an individual’s physiological state through sweat analysis.8
The health monitor integrates microfluidic channels and single-atom catalyst-based bioassays to measure sweat rate and key biomarkers, including glucose, lactate, and uric acid concentrations. Developed through a unique one-step continuous manufacturing process, the health monitor addresses longstanding issues of contamination and evaporation seen in traditional sweat sampling methods.
Using direct ink writing, researchers created self-supporting microfluidic structures capable of harvesting sweat directly from the skin without the need for sacrificial materials, addressing the contamination and sweat evaporation issues associated with traditional sampling methods. A pick-and-place strategy integrated bioassays into the device during fabrication, significantly improving manufacturing efficiency. The incorporation of single-atom catalysts enhances the sensitivity and accuracy of colorimetric bioassays, enabling precise measurements.
In a feasibility study conducted on human participants, the device demonstrated its reliability and functionality, delivering quantitative, in situ results during physical exercise. The ability to continuously monitor biomarkers such as glucose and lactate offers potential applications for managing chronic diseases.
This device promises to usher in a new era of accessible, real-time health data, enabling individuals and healthcare professionals to make informed decisions about their well-being.
Gene Editing Shows Promise for Hereditary Angioedema Attack Reduction
HEREDITARY angioedema (HAE) is a rare genetic disorder that leads to severe and unpredictable swelling attacks, which can be lifethreatening, particularly when affecting the airway.9 The condition, driven by dysregulation of the contact activation pathway, increases the production of bradykinin, causing elevated vascular permeability and subsequent swelling.
Current treatments primarily aim to reduce bradykinin levels through plasma kallikrein inhibitors, but these therapies often require lifelong administration and do not always prevent attacks. NTLA-2002 is an in vivo gene-editing therapy based on CRISPRassociated protein 9 (Cas9) technology, designed to provide long-term control of HAE with a single treatment. It targets the KLKB1 gene, which encodes plasma prekallikrein, the precursor to plasma kallikrein, and seeks to permanently reduce plasma kallikrein levels by editing the KLKB1 gene in the liver.
In the Phase I portion of a combined Phase I–II trial, NTLA-2002 was administered as a single dose at 25 mg, 50 mg, or 75 mg to 10 adult patients with HAE. The primary goal of the trial was to assess the safety and side-effect profile of NTLA2002, while secondary and exploratory endpoints focused on pharmacokinetics, pharmacodynamics, and clinical efficacy, particularly in terms of investigatorconfirmed angioedema attacks.
The most common adverse events reported were infusion-related reactions and fatigue; however, there were no dose-limiting toxic effects, serious adverse events, or clinically significant laboratory findings. Dose-dependent reductions in plasma kallikrein levels were observed across all dose groups, with a reduction of 67% in the 25 mg group, 84% in the 50 mg group, and 95% in the 75 mg group. Similarly, the
number of angioedema attacks per month showed significant reductions, including 91% in the 2 mg group, 97% in the 50 mg group, and 80% in the 75 mg group.
Across all dose groups, the mean reduction in angioedema attacks was 95%, demonstrating the consistent efficacy of NTLA-2002 in reducing both plasma kallikrein levels and attack frequency.
These results indicate that NTLA-2002 holds promise as a one-time, durable treatment option for HAE, potentially offering long-term control without the need for lifelong administration of conventional therapies. However, further studies with larger sample sizes and longer follow-up will be necessary to confirm these findings and better understand the long-term safety and efficacy of NTLA-2002.
The number of angioedema attacks per month showed significant reductions including 91% in the 2 mg group, 97% in the 50 mg group, and 80% in the 75 mg group.
Automation
in Custom Ocular Prosthesis Manufacturing: A Clinical Leap Forward
A FULLY automated digital process for designing and manufacturing custom ocular prostheses has been developed, offering significant improvements in efficiency, reproducibility, and accessibility compared to traditional methods.10
These traditional techniques often result in variable outcomes and extended wait times for patients
Millions of people require ocular prostheses due to eye loss or congenital conditions, with current manufacturing processes reliant on skilled ocularists engaging in time-intensive manual methods. These traditional techniques often result in variable outcomes and extended wait times for patients. While additive manufacturing holds potential, existing approaches remain partially manual, requiring substantial expertise. To address these limitations, researchers have created an automated end-to-end digital workflow that incorporates advanced imaging and 3D printing technologies to streamline prosthesis production.
The process begins with imaging the patient's eye socket using anterior segment optical coherence tomography (AS-OCT). A statistical shape model predicts the optimal prosthesis shape, even when surface data are incomplete. A colour-characterised image of the healthy eye is used to replicate its appearance on the prosthesis. The design is then produced using a multimaterial, full-colour 3D printer and undergoes post-processing to ensure compliance with regulatory standards. In a study involving 10 clinical patients, the new process used five times less labour time than traditional methods.
Furthermore, the process delivered consistent, high-quality prostheses with superior reproducibility.
This innovation holds transformative potential for clinical practice, reducing patient wait times and improving accessibility to high-quality prostheses. By minimising dependence on skilled labour, the approach could alleviate bottlenecks in service delivery while maintaining or improving aesthetic outcomes. Future developments may focus on enhancing material properties, refining procedural workflows, and expanding applications to other prosthetic types. With broader adoption,
References
1. Che Z et al. Speaking without vocal folds using a machine-learningassisted wearable sensing-actuation system. Nat Comms. 2024;15(1):1873.
2. Sasikumar SC et al. 3D bioprinting with visible light cross-linkable mucinhyaluronic acid composite bioink for lung tissue engineering. ACS Appl Bio Mater. 2024;7(8):5411-22.
3. Lv J et al. AAV1-hOTOF gene therapy for autosomal recessive deafness 9: a single-arm trial. Lancet. 2024;403(10441):2317-25.
4. Wan HH et al. High sensitivity salivabased biosensor in detection of breast cancer biomarkers: HER2 and CA15-3.
J Vac Sci Technol B Nanotechnol Microelectron. 2024;42(2):023202.
5. Zhou Q et al. Glycan profiling in small extracellular vesicles with a SERS microfluidic biosensor identifies early malignant development in lung cancer. Adv Sci. 2024;DOI:10.1002/ advs.202401818.
6. Berger JS et al. A Platelet Reactivity ExpreSsion Score derived from patients with peripheral artery disease predicts cardiovascular risk. Nat Commun. 2024;15(1):6902.
7. Guan X et al. Pioneering case: robotic single port (SP) transvaginal NOTES (RSP-vNOTES) for hysterectomy in ten steps. Intelligent Surgery. 2024;1;7:1-6.
8. Chen C et al. 3D-printed flexible microfluidic health monitor for in situ sweat analysis and biomarker detection. ACS Sensors. 2024;9(6):3212-23.
9. Longhurst HJ et al. CRISPR-Cas9 in vivo gene editing of KLKB1 for hereditary angioedema. N Engl J Med. 2024;390(5):432-41.
10. Reinhard J et al. Automatic data-driven design and 3D printing of custom ocular prostheses. Nat Commun. 2024;15:1360.
Congress Interview
Shafi Ahmed, a world-renowned surgeon, futurist, innovator, professor, and Nobel Peace Prize nominee, shares exclusive insights from the Global Innovation and New Technology (GIANT) Health Event 2024 on the future of healthcare. He dives into the world of virtual reality, holograms, and the medical metaverse, and highlights cuttingedge projects that inspire change and redefine what is possible in modern medicine.
Shafi Ahmed Chief Executive Officer, Medical XR, London, UK
The outcomes focus on three shifts: transition from analogue to digital, from hospital to community care, and from treatment to prevention
You mentioned that this is the 8th GIANT Health event, and that for the first time in 32 years as a practicing doctor you’re hopeful that current reforms will lead to a change in healthcare. What sparked your optimism this year particularly, and how is that reflected in how the GIANT Health event has evolved over the past 8 years?
When evaluating the government’s approach, their open admission that the NHS is in crisis is a significant step forward. Recognising that the system is fundamentally broken marks a shift from previous tendencies to downplay issues as minor challenges. Such honesty is crucial for meaningful progress. They acknowledged that our submissions around care, waiting lists, and outcomes won't be a quick turnaround, but instead a long-term plan. The outcomes focus on three shifts: transition from analogue to digital, from hospital to community care, and from treatment to prevention; these are aspirations that we've been talking about for a long time.
These are concepts that have been discussed extensively. Additionally, investment, innovation, and a new way of thinking are essential to driving the transformation.
People are now collaborating to define what change could look like, adjusting targets and improving access to care. On balance, there seems to be a genuine willingness to face the challenges of the shortage of the global workforce, the volume of patients on the waiting list, and the millions of patients awaiting elective surgeries. The approach feels more collective, with a focus on solving these problems together, which is why I find it particularly interesting. From a policy perspective, that’s one side of the story. The other side is the progress in technology. We brought a lot of technological innovation into clinical practice during COVID-19; however, we then paused to reassess and reevaluate the state of healthcare. We went very fast, very rapidly, as a necessity, as a means to an end. But now we're saying: ‘Let's just slow down.’ We are exploring how advanced and exponential
technologies, such as AI, large language models, and others, can support infrastructure improvements, enhance automation, and boost efficiency. These tools also have the potential to reduce waste and improve the clinical experience and potentially outcomes for patients.
Q2 Virtual reality and augmented reality have been central to your work, for example with your company Medical XR, and from using Google Glass and Snapchat Spectacles (Snap Inc., Santa Monica, California, USA) for live operations. How do you see these technologies evolving, and what breakthroughs do you anticipate next?
In the last 10 years, what we've seen is the explosion of what I call 'exponential technologies'. It’s as though we’ve established a new framework and language for innovation in healthcare. Technologies such as AI, deep machine learning, virtual reality, the metaverse, nanotechnology, wearables, sensors, and big data have been emerging for some time. While many of these technologies aren’t entirely new, we’re now seeing their practical
applications and traction within the healthcare sector. Before, they were just words that often felt like science fiction. The most dramatic shift over the last two years has been in the adoption of large language models, and these tools have rapidly transformed perceptions and use cases for AI in healthcare. Not long ago, AI was seen as intimidating or unclear, something many were hesitant to engage with. Today, it has become a part of everyday workflows, with tools like ChatGPT (OpenAI, San Francisco, California, USA) being widely accessible and integrated into daily practices. What once seemed inaccessible has now become accessible, and that's the change.
Q3
You’ve been named the world’s first Chief Medical Metaverse Officer for Aimedis (Steyl, Netherlands). What role do you see the metaverse playing in the future of healthcare, and how do you envision its impact on medical training?
These virtual worlds allow users to access lectures, learn anatomy, and undergo potential therapies
In terms of the metaverse, Aimedis, where I am serving as the world’s first Chief Medical Metaverse Officer, is a company that has been developing the world’s first health metaverse built on Web3 technology. Currently, we operate within Web2, a centralised platform where data is captured but owned by other companies. People are talking about shifting to the next version of the web, the 3D internet called the Web3. So that's the next version where we're going to be. Aimedis is focusing on building this 3D internet, integrating blockchain, AI, NFTs, tokens, avatars, holograms, and deep machine learning into the metaverse. It’s not just about virtual reality; it encompasses immersive, interactive experiences accessible through a web client or browser, avoiding the barriers posed by VR headsets, because how many people have a VR headset? So, that's what we are building.
We launched the first worlds to the public a few months ago. We built Australia, the United Arab Emirates, Japan, and Switzerland, and we launched those worlds. These virtual worlds allow users to access lectures, learn anatomy, and undergo potential therapies, among other experiences. There's a whole new world that you could access healthcare and medical education. You can navigate this space through personal avatars, interacting with other people also as avatars or AI agents. The entire platform is powered by AI, creating an immersive, virtual environment. On the one side, we have faceto-face and physical contact, which is essential to healthcare. This is still vitally important and essential for patients. It's not going away. It's fundamental to who we are. For example, meeting a patient in clinics face to face is important, especially in situations like cancer diagnoses or breaking bad news, where empathy and personal connection are crucial. On the other hand, we now have these online platforms, telemedicine, the EPA, telephone calls, online Doctor services. The metaverse democratises healthcare by providing access anytime, anywhere. It offers experiences tailored to individual needs, balancing face-to-face interactions with online and virtual options. While face-to-face care is essential, expensive, and timeconsuming, online and metaverse solutions offer more accessible alternatives. The next generation, Generation Z and Alpha, being digitally savvy, will benefit from these options, making healthcare more adaptable and increasing availability.
Globally, the healthcare workforce faces significant shortages. The NHS has 10% of vacancies, with 120,000 staff shortages
and a waiting list of 7–8 million. We have got to think of ways to craft a healthcare system that's more accessible. Are these the ideas that we can use? We have to figure out where it sits, where each of those will give the right kind of support and access for patients. That is for us to figure it out.
Are you hoping to develop Metaverse worlds for specific patient populations?
We've already conducted a number of consultations in the metaverse as avatars, which we've published. While we believe patients aren’t yet fully ready for these technologies, the barrier to adoption isn’t the patients, it’s often the clinicians and healthcare systems.
For example, when COVID-19 struck in 2020, we told our patients that we had to move to remote service, and we introduced remote appointments via telephone or telemedicine platforms. The patients didn’t resist. They adapted immediately, asking how they could make it work and support us. Their willingness to embrace change was remarkable. This taught us that we’ve been underestimating our patients’ ability to adapt. It meant to me that we underestimate our patients. Telemedicine has been around for 25 years, yet it wasn’t widely implemented until COVID-19 forced the shift. The resistance didn’t come from patients, it came from us as clinicians and healthcare systems. The needs change, so we are forced to adapt. Patients are ready as long as we've given the framework, as long as we support them through safety, governance, and communicating with them.
Q4 Yesterday, there was a lot of discussion about the ‘future hospital’. You mentioned that you’ve visited 61 countries, and recently went to Rwanda. What have you learnt from healthcare systems worldwide that we should implement into our own hospital system?
I've been very fortunate to have visited many countries. What you learn is that each healthcare system has to manage a different population with different healthcare needs. Some regions, like parts of Africa, have more communicable diseases. Many will have less resources, less infrastructure, fewer doctors, etc. Therefore, each system has to be made or set up in consideration with their own constraints and healthcare needs. That's the first thing. When I was in Africa speaking to various hospitals or leaders, I advised them not to look at the West for solutions, as these systems are far from perfect. As I’ve mentioned before, many of these systems are struggling themselves. Let's look at the GDP; the UK spends 9.6% of its GDP on health, which is 160 billion pounds, for a population of around 70 million, while the USA spends almost 20% of their GDP, which is trillions of dollars.
Healthcare costs are rising every year, driven by an ageing population, the increasing prevalence of chronic diseases, and the introduction of new drugs and therapies. With the costs always going up, we can't possibly put more money into healthcare
systems, we need to have smarter solutions. This means keeping people at home and keeping people empowered by their own data, with personalised, precision, and remote care. This means using the same resources in a smarter fashion, given the constraints of what we have in a healthcare location. So, countries with lower GDP can outmanoeuvre other healthcare systems by thinking differently. They don’t need to replicate existing models like those in the UK or other developed nations. Of course, universal health coverage is amazing for the UK, and it's something which I'm very proud of. But do we do everything well? We don't. By being agile, flexible, and willing to disrupt traditional approaches, these countries can reimagine and reinvent their healthcare systems. They can explore innovative models of care like the shifts currently happening within the NHS, and adopt low-cost, hightech solutions to make healthcare more accessible. Healthcare systems need to, and can, develop by not replicating our systems.
Q5What would you say to someone from the general public who doesn't know much about AI and is concerned about the cost of these high-tech solutions?
We shouldn't be scared of technology, specifically AI. People often worry that AI might replace doctors, but that’s not the case. Instead, think of AI as a tool that enhances the doctor’s role, making them more efficient and effective, enabling them to spend
more time with patients and, perhaps, making doctors more human. AI can take over repetitive, time-consuming tasks such as drafting clinic letters, managing bookings, and updating health records. These processes can run seamlessly in the background, allowing doctors to focus on direct patient care, which is ultimately what patients want. Safety and governance should remain firmly in place to ensure that AI is deployed responsibly and always in the best interest of the patient, improving both their experience and outcomes.
As for concerns about costs, it’s true that healthcare is expensive. We have to make it more cost-effective. I think these technologies can drive innovation, not just in technology itself but in changing practices, outcomes, and experiences. The idea is that these kinds of technologies will help us. They will be more cost-effective, allow us to see more people, more patients can be treated, and would involve less wastage. For example, AI could reduce inefficiencies like missed appointments, which currently cost the NHS billions of pounds annually. By improving communication and streamlining processes, AI can prevent wasted resources and make systems more efficient. Ultimately, adopting smarter technologies can save money and allow health systems to allocate those savings toward critical areas such as cancer care or cutting-edge innovations. It's just being smart and repurposing the same budget in a way that helps more people.
Think of AI as a tool that enhances the doctor’s role, making them more efficient and effective, enabling them to spend more time with patients
Q6
Can you also share more about your humanitarian work, having been nominated for the Nobel Peace Prize for your work in many countries and war zones?
One of my main passions is global access, ensuring anyone has access to healthcare or education. That has driven me throughout my entire career. I worked in Gaza and the West Bank for 10 years building their cancer capacity for surgical training. I've been on many missions over the course of the last 10 years, and through a programme I established with Medical Aid for Palestinians we treated thousands of patients, performed surgeries, and delivered training across multiple hospitals. My work has focused on global education and training, leveraging innovative technologies like virtual reality, holograms, and avatar-based systems to overcome the physical and geopolitical barriers created by conflict. By connecting people and bridging these divides, we’ve made significant strides in accessibility.
One of my TED talks, ‘Connecting a Billion Minds’, encapsulates this philosophy: making healthcare and education accessible by sharing knowledge and experiences on a global scale. For example, by using tools like Google Glass (Mountain View, California, USA), virtual reality, and Snapchat, we’ve been able to teach one part of the world while simultaneously reaching tens of thousands in another.
In Gaza, this approach not only improved healthcare capacity but also reimagined the model of care delivery, making it more accessible and effective. The impact of this work has been humbling. It’s an honour to see how many people it has reached and to be recognised for it. My focus remains on continuing this mission, to rebuild and strengthen healthcare systems in these regions. That commitment is what drives me forward.
Q7Can you tell us about any upcoming, exciting projects you're working on?
I’m particularly excited about my role with Quadrivia AI (London, UK), a company that launched just a few weeks ago. Ali Parsa, the Founder of Quadrivia AI, approached me about 6 months ago to chair the clinical board, and it’s been an incredible journey. Quadrivia AI has developed a remarkably advanced AI solution that is designed to act as an AI agent and has the potential to revolutionise clinical pathways and the entire patient journey. It’s the first customisable and controllable AI Agent for clinicians. Being at the forefront of AI, Ali Parsa’s and his team are building solutions of how AI could be successful in improving the workforce shortage and enhancing the experience of patients and clinicians. It is very exciting.
Interviews
Two individuals at the forefront of innovation in medicine are Andrea Pfeifer, who is leading the way in active immunotherapy for Alzheimer’s disease, and David Resühr, the brain behind several 3D-printed inventions that are transforming medical practice. They discuss their extensive clinical and research careers, and highlight advances in the field of medicine that will transform healthcare as we know it.
Featuring: Andrea Pfeifer & David Resühr
Andrea Pfeifer Chief Executive Officer, AC Immune SA, Lausanne, Switzerland
You began your career with a PhD in Toxicology Cancer Research and later pursued post-doctoral work in Molecular Carcinogenesis, before joining the food and beverage company Nestlé as Head of the Research Centre. How did you transition from a purely scientific background into the business world?
It was a pivotal time when people found out that not all cancers are the same, but that each cancer is different and has a different cause
I am a dedicated scientist, and this journey began early on. When I was 6 years old, I told my parents I wanted to become a scientist, not fully knowing what I was talking about, but nothing changed my determination to actually execute this. And so, I started my career in cancer research, motivated by a family connection and a desire to find a cure for certain cancers, especially the ones still missing a cure.
I became involved in looking at precision medicine in cancer when I joined the National Cancer Institute (NCI). It was a pivotal time when people found out that not all cancers are the same, but that each cancer is different and has a different cause. Identifying
the molecular basis of a cancer allows for the use of precision medicine. I remember the HER2 team, which developed the first breast cancer therapy for women using this new principle of targeting specific mutations in these cancers. In the Phase II study, women with a particular mutation were selected for the study, and the results were highly positive. This was the beginning of modern molecular-based carcinogenic cancer research, teaching me that you really have to get to the root cause of the disease and recognise that each person requires a different approach with precision medicine.
This experience influenced the development of our company, AC Immune. When clinical trials in Alzheimer's disease came back negative, I realised that we had to take the same approach as in cancer, look into the patients, and see what the underlying causes are. However, in Alzheimer's disease, the focus shifts from DNA to proteins, and identifying these is key. This is why, at AC
Immune, there is always a parallel development of diagnostics and therapies around the same target.
The impact of my cancer research had a significant impact on the company, and on the field for that matter. My transition to Nestlé came from an interesting opportunity, which was to establish Life Sciences in Nestlé. Nestlé had basically no presence in this area, and I was able to run bioscience, plant science, and microbiology. I could really bring life sciences into the food industry, which I thought was a very interesting aspect. My time at Nestlé was wonderful, I learned so much, but I was really missing the hardcore science. I felt that my scientific experience, combined with my managerial and leadership skills, could probably do something good in the startup scene, a scene where there basically wasn't a single woman in Switzerland at the time.
When approached by the scientific founders of AC Immune, I was fascinated by the technology. I thought, ‘This is something I should be doing.’ We started
from zero, no business plan, no product, no money, and brought it to where we are today, one of the leaders in neuroscience. It was quite a journey. It was very difficult in neuroscience, unlike with cancer where you can measure the mutated DNA, and you know exactly what possible drug you are looking for. Whereas, in neuroscience, there was no way to look into the brain, we couldn't actually do precision medicine. We were pioneers in developing tracers for tau, alpha synuclein, and TDP-43, enabling us to look into the brain of living patients for the first time. Now, we can perform precision medicine in neuroscience. Alzheimer's disease involves four key proteins: amyloid beta, which forms plaques; tau, which aggregates as tangles and TDP-43, also found in amyotrophic lateral sclerosis (ALS); and alphasynuclein, the Lewy body present in Parkinson’s disease. Each patient has different amounts of these proteins. So, if you want to treat beyond the 30% benefit that we see today, you have to treat the patient according to the underlying pathology. It’s simple but complicated at the same time,
and it was difficult to do at the start, because we just didn't have the tools.
Q2
As the head of Nestlé Global Research, you applied your expertise in molecular diagnostics to the food industry. Can you tell us about the process and significance of your team sequencing the genome of Bifidobacterium, which contributed to the creation of the first probiotic yoghurt?
We launched one of the first products involving the microbiome, which we called probiotics at the time. By the way, if you ask me what the future of the company will be, it's definitely in the microbiome, because my heart is still with it. It has a huge impact, even on brain diseases. There are now copious amounts of clinical data coming out that show that you can inhibit inflammation, prevent osteoporosis, enhance iron uptake, and normalise all gastrointestinal functions. I actually take probiotics now myself, and I can assure you it works, I feel so much better!
What is particularly new is the direct link between the microbiome and the brain. By eliminating bad bacteria in the intestine that produce proteins that go into the brain, you can inhibit conditions like Parkinson's disease, as shown in several ongoing clinical studies. What people always forget, and this is a very important aspect of Alzheimer's disease, is that there is a big lifestyle component. For example, the Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER) is an important study demonstrating that proper lifestyle choices like exercise, eating properly, and maintaining a healthy weight, can reduce the risk of dementia by 40%. And if you combine this with the microbiome, I think you will have much bigger effects.
While we hope a vaccine to prevent Alzheimer's disease will be available soon, there are other preventative measures people can take. I want to just encourage everyone reading this article, that yes, medication is being developed, yes, diagnostics are becoming available, but there are things that you can already do today.
Q3In 2003, you cofounded AC Immune, a biopharmaceutical company focused on advancing research in Alzheimer’s disease. What inspired you to concentrate on neurodegenerative diseases, and what are the primary goals that AC Immune aims to achieve?
I can sum it up in one sentence: our goal is to prevent Alzheimer's disease worldwide. This is partly a dream, but it's also a matter of determination, because, as you know, we are working on vaccines. Today, thanks to improved diagnostics, in the clinical research setting, we can identify people at risk of Alzheimer's disease up to 20 years before symptoms occur. This provides an opportunity to make lifestyle changes and, potentially, also get a vaccine. If this vaccine, or what we call active immunotherapy, can actually prevent these proteins from aggregating in the brain, accumulating, and killing the neurons, then we can truly speak about prevention. In neurology, prevention is even more important because, unlike other tissues, neurons cannot be replaced once they’re damaged by plaques or tangles. The brain doesn’t
regenerate in this way, so once the neurons are lost, they’re gone for good. This is why it’s essential to intervene at the preclinical stage, presymptomatic stage. To identify the people at risk and give them active immunotherapy.
Our ultimate goal is to have an active immunotherapy available by 2030 to eliminate this disease from the world.
Q4
As the CEO of AC Immune, how has the company evolved under your leadership, and what are the most significant contributions it has made to Alzheimer’s disease research and treatment?
I think there are two components: one is how the company evolved, and the other is how the field evolved. One of the major changes since we started the company is that diagnostics have become available. In particular, over the last 2 years, blood biomarkers are no longer just a dream. You can actually get your blood tested for risk factors, like you do for cholesterol. The idea of having an active immunotherapy, eventually, like you take statins, is becoming a reality. Our company has made
major contributions to the imaging field by making these biomarkers available. We now understand that early treatment is crucial because you cannot reverse damage to dead neurons. Currently, we treat conditions much too late. Today, we understand that inhibiting plaque formation is one way to at least delay the disease, but we have to go one step further. Our goal should be prevention so that we can keep the brain intact.
In a way, our company evolved alongside the field, and we’ve made major contributions to diagnostics and active immunotherapy. We were pioneers in many respects, despite having faced setbacks. One thing I'm particularly proud of is that, despite the challenges, including the difficult situation that the biotech industry is in right now, we have shown constant growth and have never laid off any employees. We are a very conservative company. So, despite being in a very challenging field and facing setbacks, both within the field and for AC Immune, we have continued to develop and advance the science. When it comes to active immunotherapy, we are leaders today.
The Alzheimer’s Prevention Initiative (API) study was the first prevention study in the world at the time. We didn’t have biomarkers back then, so the only way to conduct a prevention study was to use a genetic population. This was done with a Colombian population, and unfortunately, the study was slightly underpowered, but it showed positive trends across all biomarkers. We started this study in 2013, and it wasn’t until 2019 that imaging agents became available, showing just how far ahead we are. Last year, we announced the first prevention study in Alzheimer's disease with an anti-tau vaccine. This represents the second phase, where we can identify people who have the pathology but not yet the disease. We’re working with presymptomatic individuals, which is called secondary prevention. Unlike our first study, this is not based on genetics.
So, we conducted the first API study and are now doing the first prevention study with active immunotherapy. Another study we have undertaken is a Phase II study of an active immunotherapy against amyloid plaques.
Additionally, we have an ongoing study on anti-alpha-synuclein targeting against Parkinson’s disease. It's an active Parkinson’s immunotherapy. All of this runs in parallel with our diagnostic tools, such as imaging agents, which will enable us to identify patients, monitor clinical responses, and more. We also have a preclinical pipeline, but I think the three active immunotherapies, combined with our clinical imaging agents, are our most significant contributions to the field.
Q5 How do you envision the field, and AC Immune, evolving?
Based on where we are today, I really believe that precision medicine has become a reality. This means that you’ll soon be able to visit a normal doctor and have your amyloid beta or phospho-tau levels measured, and potentially gain access to preventive therapy. I expect this to become a reality in the next 5–10 years. I’ve also mentioned that Alzheimer’s disease is a disease of at least four different targets, so I think that combination therapy is essential.
One aspect that is certainly adding to the whole story is inflammation. We know that inflammation plays a role in all different neurodegenerative diseases, including Alzheimer's disease, Parkinson's disease, and multiple sclerosis. Therefore, I think managing inflammation will likely be a major factor in combination therapy. Lastly, nutrition, including the impact of the microbiome, could also make an impact alongside these therapies.
Q6
You are a member of the CEO Initiative (CEOi) on Alzheimer's disease. Could you share the key findings from the recently published paper, ‘The global CEO initiative on Alzheimer’s disease performance recommendations for bloodbased biomarker tests’?
The CEO Initiative stems from my long-time collaboration with George Vradenburg, who is a major figure in the USA and in Alzheimer’s disease research. After his mother-in-law died of Alzheimer’s disease, he and his wife decided to take action, leading to the creation of UsAgainstAlzheimer's. I chose to represent the European side of this effort, helping to establish a global initiative that brings together major leaders. It's not just CEOs of companies, but regulatory leaders, the FDA, the FDA commissioner, the European Medicines Agency (EMA), and medical commissioners. The idea is to bring them all together, but in a relaxed situation where we really can discuss the issues, such as how we can advance the field, or why existing treatments aren’t sufficient. Many governments and European communities are represented, making it a platform to discuss what needs to happen globally in our field.
The initiative started in Berlin, but I felt Lausanne was an ideal location, and now everyone is happy to gather in Lausanne once a year. This year marks Lausanne 11. One significant topic has been blood biomarkers, where our group of experts worked together to define what these biomarkers need to fulfil in order to be accepted as a primary or secondary diagnostic. For instance, they defined that, as a primary diagnostic, a biomarker should have 90% sensitivity and 85% specificity, among other criteria. This serves as a guideline for developing new biomarkers and also as a foundation for advising the FDA and EMA on how to use such biomarkers in practice.
This year, we’ll have the opportunity to speak with the head of the EMA, who will be attending Lausanne 11. This offers a chance to potentially influence changes in Europe, especially regarding drugs that have been approved but are not yet fully meeting our expectations. It's a first step, and we need to make sure that they become available for people.
Q7
Looking ahead, how do you envision the landscape of Alzheimer’s disease biomarker tests evolving?
We conduct a lot of validation tests for these biomarkers. In particular, for phospho-tau 217, the sensitivity and specificity are both above 90%, depending on the specific test. I think that, soon, people will be able to go to a doctor and get one of these blood tests done and we canm identify those at risk. At Lausanne 11, we will also be discussing the use of active immunotherapy and what needs to be done to make it globally available. This is a subject we must address now because it's a lengthy process to engage
with governments and secure all the necessary manufacturing and distribution support.
The goal is to have therapies that can be administered before symptoms begin, as long as they are safe and effective. This is really the direction the field is moving toward, with a strong focus on prevention. We call it ‘precision prevention’, because while we aim for prevention, we want to do so using a precise, biomarker-based approach.
Q8
You have received numerous accolades, including the BioAlps Prize 2013, being named one of the top 10 women in biotech by Fierce Biotech, and one of the 300 most influential personalities in Switzerland. What advice do you have for young women hoping to start a career in biotechnology and medicine?
I consider this an achievement of AC Immune, that we are one of the few Swiss companies that has women on every level. I mean, some of the top scientists are women including both the CSO and the CMO. When we started the company, we had no money, we had nobody. We developed all of these very talented women in AC Immune, and today they are some of the world leaders in Alzheimer's disease research, running plenary sessions of 4,000 people. I'm very proud of it. And something I’m equally concerned about is how we can enhance the participation of young women. How can we stimulate and motivate young women to do this hard job?
When I received the Swiss Economic Forum Prize in 2021, I dedicated the prize to young women, to try and encourage them to take this as an example and go for it. I think this part is
very important, to show that it can be done, and that we're doing it with a lot of success. But it's not enough, a lot more needs to be done. In many meetings, I'm still in the only female CEO, it still happens to me. I never really wanted to have this sort of role, I never did in Nestlé, but you automatically get it whether you want it or not. Actually, to some of my young leaders here, I said to be aware that this is pretty hard work. So, I think giving a real example and encouraging them, and providing them with an environment, allows this to happen. When I'm asked, what should we do? I answer that they should believe in themselves. They should believe that they can do it, that they can do an equally good job, maybe even a better job, and that we need them. We need their contribution. We need their experience, but also their social contribution, their sensitivity in business, and we need their input. It's a pleasure for me to see how it can happen. But are we there? Not at all.
Q9You have over 200 papers and abstracts published in leading scientific journals. Other than Alzheimer’s disease, do you have plans to focus on other areas of medicine in the future?
The microbiome is a big one. It’s very high on my list. Another one is to use precision medicine. Precision medicine, of course, applies to many areas of medicine. So, that's certainly one of the aspects I will always keep in mind. Developing women for business is another aspect, it's not a scientific paper, but it's a personal objective. Regarding ALS you will certainly see some activities from AC Immune, because of our imaging agent. Until very recently, diagnosing ALS could take up to 2 years. Having an imaging agent that can identify the relevant protein, which is, in this case, TDP-43 in the brain, is super important.
Last, but not least, there is a certain cross-reactivity of inflammation that is a part of all neurodegenerative diseases. Inflammation is also a significant factor in obesity, so some of the pathways and therapies that work for neurodegenerative diseases might also work in obesity. We are currently investigating one of these compounds. While I would hate for AC Immune to be overly credited for obesity, it is a possibility.
The goal is to have therapies that can be administered before symptoms begin, as long as they are safe and effective
David Resühr
Associate Professor, Department of Cell, Developmental & Integrative Biology; Assistant Professor, Department of Medical Education,
University of Alabama at Birmingham, USA
To form a mental 3D image of the body and the underlying anatomy is not that easy, specifically with the heart
Q1You have been at the forefront of integrating 3D printing into medical education, such as the ‘3D-Printed Forearm Trainer’, and the ‘3D‐Printed Human Heart’. How can 3D-printed anatomical models enhance the learning experience for students, and address gaps in medical training?
Starting off with the 3D‐printed human heart, what triggered it was that it's really hard to imagine the heart in its t3D projections. The heart has two atria and two ventricles, positioned in a specific way within the body and chest, making it difficult to imagine how it sits and where each chamber is located. For anatomy in general, to be able to form a mental 3D image of the body and the underlying anatomy is not that easy, specifically with the heart.
I teach ultrasound, and I got into this around 8 years ago. Together with some colleagues in emergency medicine, we developed a ‘special topics’ course. A basic heart ultrasound is a very important part of point-of-care ultrasound and for the Focused Assessment with Sonography in Trauma (FAST) exam. However, it is difficult to imagine the plane that you are intersecting the heart because when you place the ultrasound probe on someone's chest, you see a greyscale image, 256 shades of grey, which you then have to interpret. I asked myself: ‘How can I teach it better to help students understand something like the parasternal long axis view? How do I teach it?’ So, I thought: ‘Well, we’ve got a 3D printer.’
I went online, and I found the model of the heart on the National Institute of Health (NIH) database, and we 3D-printed a scaled-down model of it. For the first prototype, I simply cut it into two halves with a saw so it could be opened up, and I thought: ‘Wow, that’s not bad.’
Then I had to teach myself how to use the 3D editing software, which was a steep learning curve. I learnt how to use the editing software to make the slices in the software to print out two different halves, so it was possible to print the parts of the heart in a way that would mimic the projection that you see on the ultrasound screen. So, when you hold the model of the heart, you can open it up. I also put magnets in between, so you can just click it apart and easily show the students the left ventricle and the left atrium, the right ventricle and the right atrium, and then you can put it back together. This allowed me to explain to students that by turning the ultrasound probe 90 degrees, they are now intersecting the heart with a beam perpendicular to the previous plane. So, having that side by side when you are teaching ultrasound on standardised patients, for instance, helps a lot. The students who've been able to use the 3D-printed hearts have really enjoyed it and have said that it is much easier to learn. For neuroscience, we 3D-printed smaller, scaled-down versions of the brain, or a hemisected brain, which you can then colour yourself, and this is really useful.
Q2
What initially drew you to the field of anatomical sciences, and what sparked your particular focus on ultrasound technology and 3D printing in medical education?
The first person to get a 3D printer in my department was a colleague of mine, Dr Barger, and he got the 3D printer for a different project. Once he completed that work, he kindly allowed me to use the printer. In the anatomy lab, we have anatomical donors, they are very valuable, and we dissect them. While we do have some anatomical models, these tend to be quite expensive. Even a skeleton model of a hand or foot can range from dozens of dollars to hundreds, depending on how complex they are. So, I thought we must be able to create something cheaper, like print them ourselves. Over the past 10 years, the database for readily printable 3D models of medical education-relevant structures has grown tremendously. It is possible to make a 3D model from a CT scan of an abnormally formed heart, for instance, and that's really useful for surgical planning,
allowing surgeons to evaluate the feasibility of their approach before performing the operation.
The heart was one of the first 3D-printed projects I worked on a couple of years ago. We also did a 3D-printed finger. First, we 3D-printed the inside skeleton, then I made an alginate mould using my own finger to form the outer shape of the model. We then used ballistic gelatin around the 3D-printed bone pieces. We added some tendons made out of a monofilament line, and we used this model to practice joint injections. That sparked the idea to make trainers, also known as phantoms, that will help aspiring physicians and people who are already physicians and residents to learn procedures fast, and provide better and safer patient care with less negative outcomes.
Q3Can you tell us about some of the projects you’ve worked on over the years?
We wanted to print a forearm with the cubital fossa, a region with a big vein, so students could practice drawing blood. However, there was
no mould for 3D printing the whole forearm, so one of my ingenious students came up with the idea to 3D-print it so they could practice drawing blood from patients.
I bought a 3D scanner and scanned the forearm of my student. We used ballistic gelatin; this can either be synthetic, which is oil-based, or organic, made from real gelatin, which means it will go bad, but it's very cheap. It has a similar density to body tissue, so it's very useful. We filled the mould with ballistic gelatin and put in latex tubes that were connected in a way to match the standard branching pattern of the vessels in the forearm. We then filled the vessels with water that had either blue or red food colouring. Of course, we do not believe that arterial blood is red and venous blood is blue, but it’s just useful to help reinforce the concept effectively.
We also 3D-printed a model of the brachial plexus in the axilla, a complex network of nerves. It’s essential to learn where they go, what spinal levels the different nerves are derived from, what the signs and symptoms are if you
have lesions in the articular nerve, etc. So, we printed it and put little magnets in between the different branches, allowing the branches to be detached and rearranged. We also made it possible to colour-code the branches to indicate which spinal level they come from. It's like a big puzzle. I think it's much easier for people who are multi-modal learners, which I believe a lot of people are; it's helpful to be able to hold a model and study with that.
We also did a 3D-printed knee, embedded in ballistics gelatin, and practiced ultrasound-guided injections into the knee and ultrasound-guided aspiration of fluid out of the knee. I have to give credit to all my students who work with me, because they have great ideas, and they are right there at the forefront of learning and innovation. I'm just the fortunate one who can try and harvest the glory.
Q4Are there any new materials you’ve come across that are even closer to mimicking human tissue?
We’ve experimented with all sorts of unconventional ideas. For the ‘Special Topics’ course, which is a week-long boot camp, I've embedded pork butts. We've placed the tip of a 9 mm handgun bullet into a pork butt. When we scanned it, the muscle striations were clearly visible and closely resembled human muscle. You could even see the projectile lodged within the tissue, and gunshot wounds are a common issue faced by physicians in Birmingham, Alabama, USA.
The possibilities with ultrasound gel or with ballistics gel are pretty vast. Ballistics gel is similar to human body tissue. It is non-toxic and very easy to prepare. You
dissolve the powder in water, boil it, add some deformer, and cast it. It is like making jelly, only that jelly tastes much better.
We also have an oil-based gel that melts at a much higher temperature. For that, I use a crock pot to melt blocks of gels, as it remains stable at room temperature and only melts at temperatures exceeding 100 °C. This makes the gel gooey and sticky, which then can be poured into different shapes. Its main advantage is its longevity; it doesn’t spoil. However, it comes with two significant drawbacks: its high cost, around 50 USD per pound, and its higher melting temperature. So, you have to be a little cautious if you're embedding something. Care is needed to let the gel cool sufficiently, otherwise they might melt.
Some people add antimicrobials that dissolve well to organic gelatin to prevent it from spoiling. But I like the idea of not working with toxic substances. When I make phantoms from the organic gel, I don't add any preservatives to it. I would be a hypocrite to get my biweekly agriculture box, which is all organic and green, and then put formaldehyde in everything. Instead, when we're done with our session, we can either re-melt and then re-use them, or we can toss them.
Q5How do you see the integration of ultrasound in the medical curriculum evolving over the next few years, and what innovations do you think will drive this field forward?
It is incredible how much technology has advanced. One thing that I think is great is that technology is becoming much more affordable. One of the caveats of ultrasound is that the
It is possible to make a 3D model from a CT scan of an abnormally formed heart, and that's really useful for surgical planning
machines can be very expensive, but now you can get a handheld device for about 2,000 USD, or sometimes even less. That brings them into the reach of medical education, and not just for the people who are privileged enough or have a grant at university. These handheld devices can even connect to your phone. So, if you are a physician doing rounds in the hospital, you could have your ultrasound probe in one pocket of your lab coat and use it for bedside scanning on the spot. I have a wireless one; on one side, it has a probe that you can use for superficial scanning, you can use that for vascular access, and on the other end, it has a transducer that can scan deeper, like the heart, liver, and kidneys. These models are a bit more expensive, but they’re still far more practical than the massive machines that used to take up an entire room.
Technology is advancing with machine learning and AI. Several companies are working on using machine learning algorithms to interpret the ultrasound images. It's great because it means you could scan someone with an ultrasound probe, and even if you’re not an expert, the system could help you identify what you’re looking at. Since these algorithms are powered by vast databases, it will be able to compare the picture that you have with 1,000s of images in a database and tell you if the image is similar to a normal one, or if it is similar to a pathological one, and what type of pathology it is. It would be used as a diagnostic tool. It's really amazing how we're going to be able to use machine learning to help interpret ultrasound images and use it in general for training.
In rural settings, having a portable ultrasound means that the patients don't have to
travel far. With these devices, you can perform exams on the spot, potentially sparing patients unnecessary procedures and significantly reducing costs. Furthermore, with machine learning, or even with telemedicine, you can do these scans even if you're not an expert. Usually, to become a trained stenographer here in the USA, you have to go to sonography school, which takes at least 2 years, and then you have to specialise, which takes even more time. Instead, someone could use the technology that's built into the portable ultrasound device to interpret the image. If further clarification is needed, the images can be wirelessly transmitted to a remote expert for assistance.
Q6Looking ahead, are there any upcoming projects or research initiatives that you are particularly excited about?
A former student of mine, now in her OB-GYN residency in New Orleans, Ochsner, USA, identified a challenge in locating the cervix. As a man, I didn’t realise the complexity of it. I thought, as an anatomist, it was simply straight ahead at the end, but it’s actually not that straightforward. The cervix can be positioned in different ways, it might be angled in various directions, making it difficult for physicians performing procedures like pap smears. So, she and I actually made a model for pap smears. The model consists of the external female genitalia, with the introitus, the vaginal canal, and up to the cervix. We designed it so the cervix could be placed in different positions. This allows clinicians to practice using a speculum and accurately locating the cervix before performing the procedure. Because for a patient, it's a very uncomfortable procedure. When
the physician is less experienced, practicing with a 3D-printed model could really help minimise the trial and error of locating the cervix, ultimately improving patient comfort and outcomes with better-trained clinicians.
Practicing with a 3D-printed model could really help minimise the trial and error of locating the cervix, ultimately improving patient comfort and outcomes
Adverse Events During Transitions of Care from the Emergency Department to the Inpatient Setting
Author: *Dennis Tsilimingras1
1. Department of Family Medicine and Public Health Sciences, Wayne State University School of Medicine, Detroit, Michigan, USA *Correspondence to dtsilimi@med.wayne.edu
Disclosure: The author declares no conflict of interest.
Medical and public health professionals are acutely aware of the significant public health concerns posed by adverse events (AE) during transitions of care.1 AEs are injuries caused by medical care and not injuries caused by the underlying disease of patients. These injuries result during care transitions from several factors, such as incomplete communication transfers between clinicians and patients who are not adequately prepared during their physician visits, and clinicians who assume responsibility for patient care during the continuum of care.2,3 The consequences of these AEs can be severe, leading to increased morbidity, healthcare utilisation, functional decline, poor patient experiences, and heightened caregiver burden.4
DISCONTINUITIES IN CARE
The causes of AEs during transitions of care often trace back to discontinuities in care.2 These gaps in care emerge with complex healthcare systems that involve multiple professionals.5 The interrelationship of healthcare activities and the intricacy within these systems amplify the risk for error, especially when several and
expedient handoffs become a necessity.6 These issues are pervasive across the care continuum, manifesting between inpatient and outpatient pharmacies, during physician discharge summaries, cross-coverage signouts, discharge planning, and follow-up for abnormal laboratory test results.7,8
ADVERSE EVENTS DURING TRANSITIONS OF CARE
Studies conducted in North America have investigated AEs in patients discharged from the internal medicine service of hospitals in urban areas with strong academic affiliations,9,10 and patients discharged from an internal medicine service run by hospital physicians of a community hospital.4 These studies have found an AE rate of 19–28%4,9,10 in patients with about 33% of the AEs classified as being preventable (meaning that an injury may have the potential of being prevented if the error or system design flaw had not taken place), and about 33% classified as being ameliorable (meaning that an injury whose seriousness or length of time could have been potentially decreased if the clinician had followed different actions or procedures).4,9,10 Within 4 weeks after hospital discharge, approximately 9–21% of subjects had an unscheduled visit to a
physician’s office, 11–33% of subjects visited the emergency department (ED), and 17–24% were readmitted to the hospital.4,9,10 Adverse drug events (ADE) were the most common type of transition of care AEs, accounting for 66–72%. Other AEs included medical procedures (7–17%); therapeutic errors, e.g., during the medication delivery process (4–16%); management errors (14%); hospitalacquired infections (1–11%); and diagnostic errors (3–6%).4,9,10 Approximately 66% of subjects had symptoms resulting from an AE for over a week, while about 33% of subjects experienced a life-threatening injury, and 3% of subjects died from the injury.4,9,10 After a patient is discharged from the ED to home, the incidence rate of AEs is approximately 6%.11 These AEs frequently include diagnostic errors (25.0–28.3%), management errors (29–30.2%), and ADEs (20.8%).11 The majority of ED-originated AEs are preventable (56.6–71.0%) and serious.11 Other studies have reported similar preventability of ED AEs ranging from 36–71%, and found that the majority of AEs were related to ADEs and diagnostic errors.12
AEs occurring during the transition from the ED to the inpatient setting are less explored. A European study examined AEs during this transition of care, focusing solely on diagnostic errors, reporting an incidence rate of over 12%.13 Additionally, a recent study from the USA focused on all types of AEs and found that the incidence rate of AEs is over 22%, with ADEs (42%) identified as the most common AE, followed by management (38%), and diagnostic errors (21%).14 From these AEs, 75% were considered preventable and 33% considered serious in severity. Patients with a considerable length of time in the ED had an increased risk for an AE.14 An example of an AE from the ED to the inpatient setting includes a patient receiving an antibiotic in the ED and experiencing diarrhoea after transfer to the inpatient setting. The patient had prior documentation of experiencing diarrhoea with this particular antibiotic from a previous admission; therefore, the AE was judged to be preventable. If prior documentation did not exist, the AE would have been non-preventable.
UNIQUE CONTRIBUTORS TO ADVERSE EVENTS FROM THE EMERGENCY DEPARTMENT TO THE INPATIENT SETTING
There may be unique contributors to discontinuities and AEs from the ED to the hospital wards, including: 1) overcrowding in the ED places clinicians under intense pressure to move patients to hospital wards, and this pressure may result in deficient diagnostic examinations and may lead to sending patients to the wrong service;15 2) shift changes are critical in the ED and clinicians receiving patients from their colleagues who left for the day may be unfamiliar with and have to send these patients for care to inpatient clinicians (inadequate intra-ED transitions);15 3) clinicians may have less time to understand a patient’s diagnostic examinations when they have to see a large volume of patients in the ED;15 4) concerns among the ED clinicians who wish to decrease a patient’s boarding time and inpatient clinicians who wish to reserve their right to decide if a patient should be admitted to their service and the right to block a patient’s admission or redirect to a different service; 5) ED and inpatient clinicians with various levels of training and backgrounds; 6) patient information that is transferred lacks standardisation; and 7) boarding issues regarding who is in charge of a patient’s care, a patient’s physical proximity with the inpatient care team, and miscommunication between the ED nurse and inpatient care team may lead to delays in a patient’s treatment plan and increase the risk for the occurrence of medical errors.16 As a result, these discontinuities may lead to mis-triage,15 deficient information being transferred,15 unexpected outcomes such as pending test results from the ED coming back positive in the inpatient setting,16 the deterioration of a patient’s condition during the transition from the ED to the inpatient setting,15 and insufficient care when a patient is boarding in the ED.15
STANDARDISED COMMUNICATION TOOLS TO IMPROVE INFORMATION TRANSFER FROM THE EMERGENCY DEPARTMENT TO THE INPATIENT SETTING
Poor communication between clinicians has been linked to patient hand-offs that may result in any healthcare setting. For example, hand-offs may occur when the ED physician signs off patients to the hospitalist physician without a standardised hand-off tool. These hand-offs are responsible for 80% of medical errors and two-thirds of sentinel events (unplanned events causing death, serious physical injury, psychological harm, or related risks).17 Thus, utilising a standardised communication tool to improve information from the ED to the inpatient setting is essential. A recently developed communication tool includes IPASS (Illness Severity, Patient Summary, Actions List, Situation Awareness and Contingency, and Synthesis by the Receiver) and is responsible for an estimated 23% reduction in medical errors and a 30% reduction in preventable adverse events.18
Additional communication tools include SBAR (Situation, Background, Assessment, and Recommendation) that has been utilised both intraprofessionally and interprofessionally.19 Interprofessional communication among physicians, nurses, pharmacists, and social workers, to name a few, is considered vital in the delivery of optimal care and has evolved from the patient safety movement. The benefit of SBAR is that it may be utilised across several disciplines, requiring clinicians to provide all relevant information by increasing understanding and awareness of the situation.20 This tool has been shown to increase patient safety and is regarded as best practice for communicating critical information among clinicians.21 Thus, both communication tools mentioned above may be adopted to improve information transfer between the ED and hospitalist physicians.
INTERVENTIONS TO REDUCE ADVERSE EVENTS FROM THE EMERGENCY DEPARTMENT TO THE INPATIENT SETTING
To address these challenges, specific interventions are proposed for the transition from the ED to the inpatient setting. Trained pharmacist interventions that included medication reconciliation, inpatient pharmacist counselling, low-literacy adherence aids, and tailored telephone follow-up after hospital discharge have been proven effective in reducing AEs during transitions of care, especially from the hospital to home.22 Patients benefit from a tailored intervention that will increase their knowledge of the medications they have been prescribed.23 Patients with low literacy benefit significantly from educational interventions that are provided by pharmacists.24 A pharmacist follow-up within 72 hours after hospital discharge has been proven effective in capturing problems such as filling prescriptions, side effects, and a patient’s understanding of the regimen.25 Similar interventions may benefit patients in reducing AEs from the ED to the inpatient setting. Although a pharmacist intervention may require additional resources and costs for implementation in a healthcare setting, the benefit for patients may be tremendous in reducing the likelihood of an AE and a potential ED visit and/or hospital readmission.
Machine learning has the potential benefits of predicting AEs in patients during transitions of care. A recent study utilised a machine learning intervention to accurately identify patients with acute coronary syndrome.26 This machine learning approach was feasible and effective and may be useful in guiding clinical decision-making during transitions of care.
AI also has enormous potential in the prediction and early detection of ADEs in particular. A systematic review found that the majority of studies developed predictive algorithms and utilised a wide range of AI approaches that were focused on ADEs.27 This review indicated that additional studies of specific models are needed to find the most successful AI methods to detect ADEs.
For example, the performance of AI-based algorithms may be improved by integrating unstructured clinical notes into electronic health record data.27 Thus, AI is a promising approach to reducing the frequency of ADEs.
References
1. Tsilimingras D, Bates DW. Addressing post-discharge adverse events: a neglected area. Jt Comm J Qual Patient Saf. 2008;34(2):8597.
2. Kohn LT et al. (eds.), To Err is Human: Building a safer Health System (1999), Washington DC: National Academy Press.
3. Hamel MB et al. The growth of hospitalists and the changing face of primary care. N Engl J Med. 2009;360:1141-3.
4. Tsilimingras D et al. Post-discharge adverse events among urban and rural patients of an urban community hospital: a prospective cohort study. J Gen Intern Med. 2015;30(8):1164-71.
5. Sharma G et al. Continuity of outpatient and inpatient care by primary care physicians for hospitalized older adults. JAMA. 2009;301(16):1671-80.
6. Schiff G, Rucker T. Beyond structureprocess-outcome: Donabedian’s seven pillars and eleven buttresses on quality. Jt Comm J Qual Improv. 2001;27(3):169-74.
7. Harlan G et al. Pediatric hospitalists and primary care providers: a communication needs assessment. J Hosp Med. 2009;4(3):187-93.
8. Boohaker EA et al. Patient notification and follow-up of abnormal test results. A physician survery. Arch Intern Med. 1996;156(3):327-31.
9. Forster AJ et al. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161-7.
10. Forster AJ et al. Adverse events among medical patients after
CONCLUSION
In summary, AEs during transitions of care from the ED to the inpatient setting represent a significant public health concern, often stemming from discontinuities in complex healthcare systems. To mitigate these issues, targeted communication tools and interventions involving pharmacists, machine learning, and AI can be implemented. These measures aim to improve patient safety and reduce AEs.
discharge from hospital. CMAJ. 2004;170(3):345-9.
11. Forster AJ et al. Adverse events following an emergency department visit. Qual Saf Health Care. 2007;16(1):17-22.
12. Stang AS et al. Adverse events related to emergency department care: a systemic review. PLoS One. 2013;8(9):e74214.
13. Hautz WE et al. Diagnostic error increases mortality and length of hospital stay in patients presenting through the emergency room. Scand J Trauma Resusc Emerg Med. 2019;27(1):54.
14. Tsilimingras D et al. Adverse events in patients transitioning from the emergency department to the inpatient setting. J Patient Saf. 2024;20(8):564-70.
15. Guttmann A et al. Association between waiting times and short-term mortality and hospital admission after departure from emergency department: population based cohort study from Ontario, Canada. BMJ. 2011;342:d2983.
16. Boudi Z et al. Association between boarding in the emergency department and in-hospital mortality: a systematic review. PLoS One. 2020;15(4):e0231253.
17. Agency for Healthcare Research and Quality (AHRQ). Handoffs. Available at: https://psnet.ahrq.gov/primer/handoffs. Last accessed: 17 December 2024.
18. Starmer AJ et al. I-PASS, a mnemonic to standardize verbal handoffs. Pediatrics. 2012;129(2):201-4.
19. von Dossow V, Zwissler B. Recommendations of the German association of anesthesiology and
intensive care medicine (dgai) on structured patient handover in the perioperative setting: The SBAR concept. Anaesthesist 2016;65(Suppl 1):1-4.
20. Powell SK. SBAR-it's not just another communication tool. Prof Case Manag. 2007;12(4):195-6.
21. Dunsford J. Structured communication: improving patient safety with SBAR. Nurs Womens Health. 2009;13:384-90.
22. Schnipper JL et al. Rationale and design of the pharmacist intervention for low literacy in cardiovascular disease (PILL-CVD) study. Circ Cardiovasc Qual Outcomes. 2010;3(2):212-9.
23. Krueger KP et al. Improving adherence and persistence: a review and assessment of interventions and description of steps toward a national adherence initiative. J Am Pharm Assoc. 2003;43(6):668-78.
24. Rothman RL et al. Influence of patient literacy on the effectiveness of a primary care-based diabetes disease management program. JAMA. 2004;292(14):1711-6.
25. Dudas V et al. The impact of follow-up telephone calls to patients after hospitalization. Am J Med. 2001;111(9B):26S-30S.
26. D’Ascenzo F et al. Machine learningbased prediction of adverse events following an acute coronary syndrome (PRAISE): a modelling study of pooled datasets. Lancet. 2021;397(10270):199-207.
27. Syrowatka A et al. Key use cases for artificial intelligence to reduce the frequency of adverse drug events: a scoping review. Lancet Digit Health. 2022;4(2):e137-48.
Diagnostic and Surgical Challenges in Extradigital Glomus Tumour: A Case Report
Editor's Pick
This case report exemplifies the art and science of medicine, combining clinical intuition, patient-centred care, and collaborative expertise to solve complex diagnostic puzzles. Over the years, I have come to appreciate the invaluable synergy between listening carefully to patients, gathering a detailed clinical history, and leveraging the collective experience of colleagues. This report highlights how precise diagnostic tools like MRI, when guided by thoughtful collaboration and attention to detail, can transform patient outcomes, even in the most atypical and challenging cases. It is a testament to the power of teamwork and the pursuit of excellence in healthcare.
Glomus tumours are benign neoplasms with classical presentations of cold intolerance, severe pain, and tenderness, primarily in subungual locations. However, these hallmark symptoms may not always manifest in extradigital sites, complicating the diagnostic process. This case report presents a patient with a 7-year history of debilitating pain due to a glomus tumour located in the right upper arm. Key clinical findings included persistent, unexplained pain without classic glomus symptoms. This case report highlights the importance of recognising atypical presentations of glomus tumours and the pivotal role of MRI in diagnosis. Optimal diagnostic outcomes are achieved when MRI is performed with a well-informed clinical background and close coordination between the patient, surgeon, and radiologist. Precise anatomical localisation, achieved through careful site marking, along with a reduced field of view in imaging, enhances lesion detection and further aids in minimising intraoperative challenges. This approach ensures more accurate diagnoses and improves surgical outcomes in cases where classical symptoms are absent.
Key Points
1. A brief introduction to atypical presentations of the glomus tumour and the importance of identifying them as classical symptoms may be absent, making its diagnosis clinically challenging.
2. Explores strategies to enhance MRI outcomes, emphasising the importance of detailed clinical background and close collaboration between the patient, surgeon, and radiologist to achieve greater diagnostic precision.
3. Emphasises the significance of precise site marking, the correlation between field of view and resolution, and their roles in reducing intraoperative challenges while optimising surgical outcomes.
INTRODUCTION
Glomus tumours are uncommon, benign neoplasms originating from the glomus body, predominantly affecting adults between 20–40 years of age.1 Clinically, they often manifest as small, bluish, or reddish lesions, typically located in the subungual region of the distal extremities.1 Though glomus tumours are diagnosed clinically and confirmed through histopathological studies, due to the atypical and non-specific nature of their presentation, preoperative MRI imaging is instrumental in the diagnosis of extradigital glomus tumours.2,3 Surgical excision remains the gold standard for treatment, consistently yielding excellent functional and cosmetic outcomes and immediate pain relief.4 Following the Surgical CAse REport (SCARE) guidelines,5 the authors present a case involving a patient with a 7-year history of a painful lesion on his right upper arm. Despite undergoing 14 prior MRI scans, the definitive diagnosis was achieved with the 15th MRI, which ultimately led to the resolution of his pain.
PATIENT INFORMATION
The patient, a 42-year-old pharmacist of Indian ethnicity, presented with debilitating pain in his right upper arm, which had been present since 2017. He reported that the pain significantly restricted his daily activities and adversely affected his quality of life, including preventing him from lifting his young child. He was a non-smoker and had been using over-thecounter analgesics, in addition to multiple prescription pain medications, including
gabapentin. Approximately 1 year prior, he was also prescribed antidepressants, which he took for 3–4 months. Before his presentation at our hospital, he sought medical help on three different continents, underwent 25 CT scans and 14 MRI scans, experienced a failed surgical attempt to excise the unidentified lesion, and was prescribed strong analgesics, all without significant relief. In 2024, the patient presented to the authors' neurosurgery department, where a provisional diagnosis of neuroma was made. He was subsequently referred to the plastic surgery department.
CLINICAL FINDINGS AND DIAGNOSTIC ASSESSMENTS
The patient had no significant past medical history and no known allergies. The only notable symptoms were severe pain and tenderness at the antero-medial side of the right upper arm. On physical examination, he was alert, orientated, and vitally stable. Tenderness and a surgical scar from the previous procedure were noted in the right upper arm. Love’s test was elicited by pinpoint localisation of tenderness.6
Examination of the remaining organ systems showed no abnormalities. Laboratory investigations were within normal limits, including complete blood count, C-reactive protein, liver function test, renal function test, lipid profile, and blood glucose. An MRI with contrast and Doppler ultrasound were performed. The clinical scar site was localised, and a skin marker (pumpkin seed oil, in this case) was placed at imaging time.
A well-defined, solid enhancing nodule in the subcutaneous plane in the right proximal arm was noted. The nodule was located at the site of the clinical skin scar, 3.2 mm deep to the skin surface. The nodular lesion measured 6.2×4.2 mm in size (Figure 1). It had smooth margins with signal intensity on T1-weighted sequence and intermediate signal on T2-weighted sequence. The postcontrast study demonstrated intense homogeneous enhancement in the lesion. The perilesional planes were smooth and well preserved. No deeper extension into the muscular plane and no prominent arterial feeder vessels were seen close to the mass.
THERAPEUTIC INTERVENTION
Following the establishment of a working diagnosis and radiological localisation in reference to the previous scar and depth from the skin surface, microscopic excision of the tumour was promptly undertaken (Video 1). The microscopic excision was performed under 5x magnification with an incision made at the previous scar site, guided by the marker placed during MRI. The lesion was located and confirmed to match the MRI findings. Excision and haemostasis were achieved, followed by layered closure. The
Figure 1: MR Angiograph.
MRI with contrast showing the nodular lesion measuring 6.2×4.2 mm in size and no prominent arterial vessels.
Video 1: Intraoperative glomus tumour measuring about 0.5 cm. Unlike the MRI finding, it was highly vascular.
Video 2: Due to the absence of a tourniquet, the intraoperative glomus tumour was indistinguishable from the surrounding adipose tissue, identified due to the size marking, findings of the MRI, and vascularity.
excised mass was non-encapsulated and measured approximately 6×4 mm (Figure 2). The absence of a tourniquet caused the surrounding fat to appear similar to the lesion, complicating identification (Video 2). It was, however, distinguished by its firmer consistency. Contrary to MRI findings, converging vessels were observed intraoperatively, giving the tumour a denser colour, visible under an operative microscope.
The excised lesion was then sent for histopathological examination to confirm the diagnosis. Gross examination revealed a single, grey-brown irregular nodular mucosa-covered soft tissue, measuring 0.4×0.3×0.2 cm. Haematoxylin and eosin (H&E) staining demonstrated a well-circumscribed vascular tumour, characterised by capillary-sized vessels lined by endothelial cells, surrounded by glomus cells arranged in nests, sheets, and trabeculae within a myxoid stroma (Figure 3). The cells were polygonal, with moderate cytoplasm, indistinct borders, and rounded nuclei with amphophilic to eosinophilic cytoplasm. The chromatin appeared homogeneous and bland, with inconspicuous nucleoli and no detectable mitotic activity. These histopathological findings confirmed the diagnosis of a benign glomus tumour.
FOLLOW-UPS AND OUTCOME
Postoperatively, the patient experienced mild soreness at the incision site, which diminished over the next few days. Sutures were removed on the 8th postoperative day, and the patient was completely symptom-free by 2 weeks. He was followed up in the outpatient department for 6 months, during which his symptoms did not recur, and he was able to resume sports activities. A duplex ultrasound scan was performed to assess for any anomalous vascular patterns at the surgical site, confirming normal findings.
PATIENT PERSPECTIVE
Chronic pain can disrupt a patient’s social interactions, limiting their ability to engage with their social circles and family. Almost half of those with chronic pain have experienced reduced contact with their family due to their symptoms.7 This patient experienced intense pain for almost 7 years, where even the slightest touch would provoke extreme discomfort. In the quest to cease his pain, he relentlessly sought medical care, was put on strong analgesia, and underwent serial CT and MRI scans. The pain greatly restricted his daily activities, preventing him from even lifting his young child. The surgery resolved the pain completely and helped the patient return to a normal life.
DISCUSSION
Glomus tumours, first described in 1812, are benign neoplasms comprising approximately 1% of all hand tumours and around 2% of soft tissue tumours.8,9 Also referred to as glomangioma, glomangiomyoma, and glomangiomatosis, these tumours commonly arise in the distal phalanx, particularly in the subungual regions, due to the aberrant functioning of the glomus body.10 The glomus body, an arteriovenous anastomosis primarily located in the fingers and toes, is responsible for thermoregulation. The classic clinical presentation of glomus tumours includes a triad of cold intolerance, severe paroxysmal pain, and tenderness; however, these symptoms are less pronounced in extradigital cases.8 Extradigital glomus tumours can occur anywhere, including the wrist, forearm, elbow, shoulder, thigh, cheek, earlobe, foot, nose, and trachea.11 The diagnosis is primarily clinical and is confirmed through histopathological examination of the tumour. In the case of atypical presentations, the average duration of symptoms exceeds 7 years, with many patients having undergone prior evaluations where their conditions were misdiagnosed.11 However, MRI can help reach a diagnosis. The recurrence rate of glomus tumour is about 4–15% of cases with bone involvement on radiograph present in a few cases.12,13
Figure 2: Intraoperative lesion, indistinguishable from the surrounding adipose cells with converging vascular supply (A and B), and post-excision glomus tumour measuring 6 mm in diameter (C and D).
3: Hematoxylin and eosin staining.
A) Original magnification x40. Well-circumscribed vascular tumour. B) Original magnification x100. Capillary-sized vessels lined by endothelial cells surrounded by glomus cells forming nests, sheets, and trabeculae in a myxoid s troma. C) Original magnification x400. Nests and sheets of equally spaced polygonal cells with moderate cytoplasm. Cell borders are identifiable.
Figure
The efficacy of diagnostic tests for glomus tumours can be significantly enhanced by implementing a targeted scanning protocol that is informed by a thorough clinical background. When clinical suspicion is high, targeted MRI protocols tailored to the suspected anatomical region can greatly improve the detection and characterisation of these lesions. Such protocols may include high-resolution imaging with specific sequences that highlight the vascular nature of glomus tumours and marking the clinical site of suspicion. Therefore, this protocol may facilitate a more accurate diagnosis. This approach underscores the importance of integrating detailed clinical information with advanced imaging techniques to optimise diagnostic accuracy and treatment outcomes.
In the context of MRI for diagnosing glomus tumours, the relationship between the field of view and resolution is a critical factor that influences diagnostic efficacy. The field of view refers to the extent of the anatomical area captured in the MRI image, while resolution refers to the level of detail that the image can reveal. As the field of view increases, the resolution typically decreases, and conversely, a smaller field of view allows for higher-resolution imaging. The authors selected a relatively smaller field of view in conjunction with a high-resolution MRI. The sensitivity and specificity of the scan were enhanced, therefore, leading to a diagnosis of a glomus tumour, which tormented the patient for almost a decade.
Additionally, the tumour’s location further challenged the surgical excision. Tourniquets are routinely employed to create a bloodless surgical field by temporarily restricting blood flow. This reduces intraoperative bleeding and allows for clearer visibility of anatomical structures and distinguishing highly vascular
References
1. El mas L et al. Extradigital glomus tumor of the arm. Dermatol Surg. 2022;48(10):1119-20.
tissues from those with lower vascularity.14 Though a tourniquet could not be applied, the presence of a provisional diagnosis, anatomical reference from the previous scar, radiological localisation, and the presence of converging vessels that were not detected by the MRI ensured successful identification of the tumour intraoperatively.
Furthermore, close coordination between the patient, the treating surgeon, and the radiologist ensured that the diagnostic process was tailored to the patient’s clinical presentation and needs. This dialogue helped in confirming the diagnosis and formulating an effective treatment plan. When the patient is actively involved and informed throughout this process, it also enhances compliance with diagnostic and therapeutic recommendations, ultimately improving patient outcomes. Thus, close coordination among all parties not only improves the accuracy of the diagnostic tests but also ensures a patient-centred approach to care and the success of surgery.
CONCLUSION
Glomus tumours can present significant diagnostic challenges. While MRI is not inherently specific for glomus tumours, its diagnostic sensitivity can be markedly improved by using high-resolution imaging, precisely marking the site of interest, thereby reducing the field of view. Surgical resection of these tumours can be complex; however, incorporating a differential diagnosis and accurate anatomical site marking can facilitate the process. Effective communication between the patient, physician, and radiologist is crucial. This integrated approach improves diagnostic accuracy, especially in cases involving extradigital presentations.
2. Ham KW et al. Glomus tumors: symptom variations and magnetic resonance imaging for diagnosis. Arch Plast Surg. 2013;40(4):392-6.
3. Theumann NH et al. Recurrent glomus tumors of fingertips: MR imaging evaluation. Radiology. 2002;223(1):143-51.
4. Temiz G et al. Extradigital glomus tumor revisited: painful subcutaneous nodules located in various parts of the body. Indian J Dermatol. 2016;61(1):118.
5. Sohrabi C et al. The SCARE 2023 guideline: updating consensus Surgical CAse REport (SCARE) guidelines. Int J Surg. 2023;109(5):1136-40.
6. AI-Qattan MM et al. Magnetic resonance imaging in the diagnosis of glomus tumours of the hand. J Hand Surg Br. 2005;30(5):535-40.
7. Duenas M et al. A review of chronic pain impact on patients, their social environment and the health care system. J Pain Res. 2016;9:457-67.
8. AINuaim B et al. Diagnosis of glomus tumor of the elbow: a case report. Int J Surg Case Rep. 2022;90:106709.
9. AI-Janabi MH et al. Extradigital glomus tumor: a rare case report. Int J Surg Case Rep. 2024;116:109466.
10. Obeidin F, Alexiev BA. Glomus tumor. Available at: https://www.pathologyoutlines. com/topic/softtissueglomus.html. Last accessed: 13 September 2024.
11. Schiefer TK et al. Extradigital glomus tumors: a 20-year experience. Mayo Clin Proc. 2006;81(10):1337-44.
12. Patel J et al. Reappearance of a glomus tumor of the finger after nine years- a rare case report and literature review. J Orthop. 2022;1(1):38-41.
13. Vilardo G et al. Epidemiological analysis of glomus tumors of the hand and association with recurrence rate. Thieme. 2022;50(01):e27-33.
14. Gallagher M et al. Tourniquet use in hand surgery - is it time to re-inflate the evidence? J Plast Reconstr Aesthet Surg. 2020;74(3):608-20.
Exploring Bioinformatics-Driven Approaches for Enhanced Diagnosis of Chlamydia trachomatis Infections: Analysis of Target Proteins
Authors: Elijah Kolawole Oladipo,1,2 *Jerry Ayobami Oluwasegun,2 Mercy Hokah Kibathi,3 Ezinne Janefrances Nwonu,4 Simon Achi Omerigwe,5,6 Simeon Kayowa Olatunde,7,8 Daniel Funsho Akinyemi,9 Ruth Foluke Aminu,10 Muhammad Awwal Hussaini,11 Michael Asebake Ockiya,12 Ahmad Mansur Liadi,13,14 Opeyemi Olayinka Osikoya,13 Eniola Olaitan Kolawole,15 Oluwaseun Adeola Obideyi,4 Taye Olusola Bello,16 Niraj Nivas Tadasare17
1. Department of Microbiology, Laboratory of Molecular Biology, Immunology and Bioinformatics, Adeleke University, Osun State, Nigeria
2. Genomics Unit, Helix Biogen Institute, Ogbomosho, Nigeria
3. Biomedical Sciences and Technology, The Technical University of Kenya, Nairobi, Kenya
4. Medical Biotechnology Department, National Biotechnology Development Agency, Abuja, Nigeria
5. Department of Biomedical Engineering, University of Strathclyde Glasgow, UK
6. Department of Engineering, School of STEM Stanmore College, UK
7. School of Nursing, Faculty of Medicine, Health and Social Care, Canterbury Christ Church University, Kent, UK
8. Department of Pathology, William Harvey Hospital, East Kent Hospital University NHS Foundation Trust, East Kent, UK
9. Department of Biotechnology Federal University of Technology, Akure, Nigeria
10. Department of Medical Microbiology, Kogi State University Anyigba, Nigeria
11. Department of Medical Microbiology, Federal Medical Centre Bida, Nigeria
12. Department of Animal Science, Niger Delta University, Bayelsa State, Nigeria
13. Department of Microbiology, Federal University Dutsin-Ma, Katsina State, Nigeria
14. Department of Medical Microbiology (Virology), College of Medicine University of Lagos (CMUL), Nigeria
15. Department of Biological Sciences
Taraba State University, Jalingo, Nigeria
16. Department of Public Health, Far Eastern Federal University, Vladivostok, Russia
17. National Center for Cell Science, Pune, India
*Correspondence to jerryoluwasegun3@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Chlamydia trachomatis, a major cause of sexually transmitted infection, poses a range of symptoms including genital discharge, pain during urination, and abdominal pains in women, and can lead to serious health complications such as pelvic inflammatory diseases, infertility, and ectopic pregnancy if left untreated. The need for rapid and accurate detection is imperative so prompt treatment and control of the disease can be achieved. This study conducted an immunoinformatic analysis of proteins of Chlamydia trachomatis (incA, hctA, ompA, omcB, rpoB, and HSP60) for the development of a lateral flow assay-based diagnostic test. Detailed in silico evaluation of selected proteins from publicly available genomic databases was conducted to evaluate their suitability as targets for lateral flow assay-based detection. The series of tests included antigenicity, toxicity, solubility, physicochemical characteristics and molecular docking of the derived constructs, and protein sequence. Chimeric construct was derived from the prediction of linear B cell epitopes, helper T cell major histocompatibility complex II binding epitopes, and IL4 and IL10 inducers using bioinformatic tools at standard thresholds. With a Ramachandra’s score of 95.4% and Z-score of -5.1, results indicate that the construct efficacy is high in potential to provide extreme specificity and sensitivity for the detection of Chlamydia trachomatis in clinical samples as compared to traditional culture-based methods using nucleic acid amplification, hereby providing a quicker and more accurate diagnostic tool for Chlamydia trachomatis infection. Findings offer valuable data for the development of a rapid and reliable diagnostic point-of-care test kit for Chlamydia trachomatis that allows for drastic reduction in clinical wait time and treatment.
Key Points
1. Chlamydiosis, caused by Chlamydia trachomatis, is a highly prevalent sexually transmitted infection with severe reproductive health implications, especially for asymptomatic women who often remain undiagnosed. The urgent need for rapid and accurate diagnostic methods is emphasised by the high incidence rates in regions like SubSaharan Africa.
2. This study presents an innovative bioinformatics-driven approach aimed at enhancing the diagnosis of Chlamydia trachomatis infections. Through the analysis of target proteins, the research explores the development of a lateral flow assay kit designed for more efficient and accessible detection.
3. Bioinformatics plays a crucial role in bridging the gap between pathogen genomics and practical clinical diagnostics, offering a pathway to more precise and effective healthcare. The designed chimeric construct demonstrated promising antigenic properties, stability, and non-allergenicity, making it a strong candidate for the development of an affordable and rapid diagnostic tool, potentially transforming the landscape of chlamydia screening and control.
INTRODUCTION
Chlamydiosis is one of the most prevalent sexually transmitted illnesses globally caused by the bacteria Chlamydia trachomatis 1,2 Nineteen serovars of Chlamydia trachomatis, categorised based on ompA genotyping, are linked to the bacterium.3 The World Health Organization (WHO) projected about 129 million new cases of Chlamydia trachomatis cases in 2020,1,4,5 with Sub-Saharan Africa having
the highest incidence with over 10 million new cases reported each year.5 Chlamydia trachomatis is common among reproductive aged women, with a pooled prevalence of infection of 7.8% in Sub-Saharan Africa.6 Sexually transmitted infections with chlamydial lead to serious health issues, financial difficulties, and social concerns thus, the amount of morbidity linked to a sexually transmitted chlamydial infection is huge worldwide.3 A significant concern is that most women infected with Chlamydia
trachomatis are asymptomatic and do not seek medical attention.3 Untreated cases can lead to major consequences for women’s reproductive health, such as pelvic inflammatory disease, tubal factor infertility, and ectopic pregnancy, and a higher chance of contracting other sexually transmitted illnesses.7 Thus, there is a need for rapid and accurate detection to aid prompt treatment and control of the disease. Early screening and diagnosis remain the most important preventive measures.1 The most sensitive assays, nucleic acid amplification tests, are thought to be the best technique for CT detection because of their cell culture-like specificity.8,9 Despite the overall accuracy, these systems have several shortcomings, such as limited turnaround times, high costs, labour-intensive tasks, and the need for sophisticated equipment and highly skilled personnel. Thus, this study aimed to explore more bioinformatics-driven approaches for the enhanced diagnosis of Chlamydia trachomatis infections through analysis of target proteins.
METHODOLOGY
Protein Sequence Retrieval
Seven Chlamydia trachomatis protein sequences (incA, OmpA, hct A, ropB, OmcB, HSP60, HSP61) were downloaded in FASTA file formats from the National Center for Biotechnology Information (NCBI) Protein database (2004), and their accession numbers were recorded.
Antigenicity Prediction
The protein sequences were analysed using VaxiJen v2.0 (The Jenner Institute, Oxford, UK) web server to determine the antigenic and non-antigenic sequences, with the default threshold setting of 0.4 and bacteria selected as the target organism.10 Antigenicity scores of above 0.4 indicate that the peptide is a potential vaccine candidate.11
The antigenicity prediction was performed to ensure the sensitivity of the lateral flow kit being designed.
Prediction of Membrane Topology
The selected antigenic protein sequences were analysed using TMHMM-2.0 (DTU Health Tech, Lyngby, Denmark) for membrane topology prediction.12 Only the outer cell membrane proteins were selected for further analysis.
Linear B Cell Epitope Prediction
B cell epitopes were predicted using the SVMTriP tool (University of Nebraska, Lincoln, Nebraska),13 Immune Epitope Database (IEDB, Maryland, USA),14 and Bepipred Linear Epitope Prediction 2.0 (DTU Health Tech).15 These web servers use algorithms such as Random Forest Regression algorithm15 and Support Vector Machine (SVM)13 to predict antigenic B cell epitopes. Probable epitopes should have scores above the threshold of 0.5 and lengths between 9 and 20 amino acids in order to be chosen for further tests.
Prediction Test for Helper T Cell Major Histocompatibility Complex II Binding Epitopes
The binding of the helper T cell epitopes to major histocompatibility complex (MHC) II alleles were predicted with the aid of the MHC II binding prediction tool on the IEDB Analysis Resource server (Maryland, USA).14 IEDB recommended 2.22 was the selected prediction method. The seven-allele human leukocyte antigen (HLA) reference and peptide length of 15 were chosen. The MHC II reference alleles comprise HLA-DRB1*03:01, HLA-DRB1*07:01, HLA-DRB1*15:01, HLA-DRB3*01:01, HLADRB3*02:02, HLA-DRB4*01:01, and HLADRB5*01:01. The adjusted rank values were used to sort the peptides and those with a score ≤2.0 were selected as good binders.
Prediction of IL4 and IL10 Inducers
The final construct sequence was analysed to determine its ability to stimulate immune responses, toxicity, and allergenicity. Vaxijen was used to evaluate the physical-chemical properties and predict the ability of the construct sequence to induce immune responses using the method of automatic cross-variance. IL-4Pred and IL-10Pred web
servers (Indian Institute Of Technology Delhi, New Delhi, India) were used to assess the ability of the helper T Cell MHC II binding epitopes to induce IL-4 and IL-10 production, respectively.16,17
Construction of the Chimeric Protein
The construct was designed using the epitopes that passed all the analyses described above. The construct comprised AAY sequence for MHC I epitopes merged with GPGPG for MHC II as peptide linker sequences, and KK for B cells epitopes which help in protein folding and its stability.
Solubility and Physicochemical
Characteristics
Protein solubility prediction is essential to understand diverse types of biological processes and to explore the impact of different factors (ionic strength, temperature, PH of medium, and electrostatic repulsion) on the productivity of proteins. It also plays an important role in disease analysis and drug development processes.18,19 Solubility index was evaluated using Protein-Sol web tool (The University of Manchester, UK),19 according to the data on Escherichia coli expression to ensure the production of a soluble, folded, and active protein that can be easily extracted from the system. Protein sequence in FASTA format was submitted for solubility determination. Physicochemical characteristics of the chimeric build were determined using ProtParam tool on ExPASy web server (Swiss Institute of Bioinformatics, Lausanne, Switzerland).20 This included the physicochemical properties predicted including aliphatic index, molecular weight, theoretical pI, amino acid and atomic composition, extinction coefficient, estimated half-life, instability index, and grand average of hydropathicity (GRAVY).
Reverse Translation
The chimeric construct in protein format was reverse translated to its nucleotide sequence in order to determine the codon usage index and codon adaptability. This was done with the aid of the EMBOSS
Backtranseq tool (EMBL European Bioinformatics Institute, Hixton, UK).21 Amino acid linkers were used to link the chimeric construct to obtain the nucleotide sequence. The EMBOSS Backtranseq tools was then used to reverse translate the protein sequence to its DNA sequence in FASTA format. EMBOSS Backtranseq reads a protein sequence and writes the nucleic acid sequence it is most likely to have come from depending on the codon table selected. In this study E. coli K12 was selected because the reverse translated sequence the Codon Adaptation Index (CAI) will be examined.
Codon Optimisation and Computational Cloning of the Construct
Codon optimisation was achieved using CAI calculator web server by Puigbò P et al.22 CAI calculations and guaninecytosine percentage were the basis for the codon adaptation sequences analysed. Computational cloning of the optimised epitope sequences were conducted by inserting them into E. coli_pET-24 a(+) vector for expression using the SnapGene version 6.2.1 (Boston, Massachusetts, USA).23 E. coli has been an ideal expression host for large production of recombinant proteins and has been used in the production of inexpensive rapid diagnostic tests.24 The constructs were inserted into the cloning vector and the insertion and restrictions on site were selected and cloned (5,968 bp).
Predicting the Secondary Structure and Tertiary Structure
The structural features of proteins determine a wide range of functions: from binding specificity and conferring mechanical stability, to catalysis of biochemical reactions, transport, and signal transduction.25 In silco pipelines determining functional characteristics of proteins starting from protein sequences benefit heavily from the addition of structural information.26 Protein stability is paramount for ensuring the efficacy and safety of native conformation, preserving their biological activity during manufacturing, storage, and administration.
The protein modelling web server SOPMA by Geourjon C and Deléage G27 was used to predict the secondary structure of the chimeric construct by evaluating the repeated order of the adjacent amino acid residues in the polypeptide chain. The 3D structure of the amino acid sequence was assessed with ColabFold web tool by Mirdita M et al.28 Five different models were generated and the rank with the least error (blue) was picked with a very high confidence level (>90) and structural quality.
Validation and Ramachandran Plot and Molecular Docking
The quality of the 3D structure was enhanced by using GalaxyWeb Server (Galux Inc. and Seoul National University, South Korea) a server that predicts protein structure from sequence by template-based modelling as well as refines loop or terminus regions by ab initio modelling.29 The Z scores of the refined structure were obtained using the ProSA-web tool by Wiederstein M and Sippl MJ,30 a widely used tool to check 3D models of protein structures for potential errors. Ramachandran plot was derived using the PROCHECK through UCLA-DOE LAB- SAVES V6.0 (the University of California, Los Angeles, USA) for the evaluation of the tertiary structure.31,32 The interaction between the small molecules and protein of the construct at the atomic level was demonstrated using molecular docking. Several molecular docking web servers were proposed; however, a welldeveloped and widely used protein-protein and protein-RNA/DNA docking server was selected for the lateral flow design. The HDOCK server by Huang SY and Zou X33 provides a visualisation function whereby users can interactively view the generated docking results. A more negative docking score implies a more possible binding model and roughly, when the confidence score is above 0.5 to 0.7, the two peptides would be possible to bind better. However, when the confidence score is below 0.5, vice versa.34
RESULTS
Retrieval of Sequences
Using specific accession numbers (ABY76794.1, ABY76793.1, WP 009873136.1, WP 009873002.1, WP 015505969.1, WP 013984953.1, QBP33401.1, ABV55512.1, and AAS19616.1), nine protein sequences from Chlamydia trachomatis were retrieved from the NCBI Protein Database in FASTA format.
Antigenicity of the Retrieved Protein Sequences
The score obtained from the prediction of antigenicity of protein sequences using the VaxiJen server predicts the antigenic and non-antigenic amino acid sequences at a threshold of 0.4 based on physicochemical characteristics. Sequences with a score above 0.4 were considered antigenic. All retrieved sequences passed the VaxiJen antigenicity test at a threshold of 0.4, indicating their potential as antigenic targets, which is an essential factor that influences the introduction and effectiveness of the immunological responses.35 Lower thresholds might increase false positives, while higher thresholds might miss potential antigens. The value has been adopted by many studies and databases, ensuring consistency and comparability across different research works.36
Membrane Topology
All sequences qualified as membrane proteins based on TMHMM-2.0 analysis, confirming their potential as targets for immune response. The position of each sequence was accessed to evaluate their location and, according to the result, all selected sequence were extracellular, suggesting the quicker immunological response and detection.37,38
Linear B Cell Epitope Prediction
The retrieved protein sequences were further evaluated for B cell epitopes using SVMTriP and the prediction tools on the IEDB online server. B cell epitopes with scores above 0.5 and lengths between
16–20 amino acids were selected. Nonallergenic epitopes were confirmed using AllerTOP v. 2.0 (Medical University of Sofia, Bulgaria). Only non-allergenic epitopes were chosen.
HTL Epitope Prediction
To select the ideal HTL epitopes from Chlamydia trachomatis proteins, the IEDB tool known as ‘MHC-II Binding Predictions’ was used and this tool generates a “Percentile rank” for each probable peptide.39 The strong binders with a score of ≤2.0 were selected. After testing the HTL epitopes for IL4 and IL10-inducing capability, nine IL4 and eight IL10-inducing peptides were selected for their strong binding affinity (score ≤2.0) and potential to enhance immune response.
Chimeric Construct, Physicochemical Properties of the Chimeric Construct
The chimeric construct, comprising nine B cell epitopes, nine IL4 inducers, and eight IL10 inducers, was designed using specific linkers (KK, GPGPG, and GPGPG) to ensure proper folding and stability. Physicochemical properties were analysed using Protein-Sol and Expasy ProtParam tools, confirming its
solubility, antigenicity, and stability (Table 1). The average length of amino acid is 328 with a theoretical pI of 8.53. The structure had a molecular weight of 33.492 KDa; a solubility of 0.625, indicating it is a soluble protein; and an aliphatic index of 60.09, indicating thermostability. Instability index of 35.97 classifying the protein as stable, instability index of ≥40 is considered unstable. Thus, the primary construct is nonallergenic, antigenic, and stable in a variety of temperatures.
The construct’s potential efficacy and safety in therapeutic applications is highlighted by the clinical significance of its high antigenicity and non-allergenicity. Strong and targeted immune responses are influenced by high antigenicity.40 The construct’s non-allergenicity ensures safety, lowers the possibility of negative reactions, and boosts patient compliance, making it appropriate for a variety of people, including those with hypersensitivities. All of these characteristics highlight the construct’s potential as a viable option for clinical application, addressing safety and efficacy issues that are essential for effective therapeutic and preventive measures.41
*Antigenicity was determined using VaxiJen with a threshold of 0.4.
†Allergenicity was assessed using AllerTOP v. 2.0.
ǂSolubility was evaluated using Protein-Sol, with values above 0.5 considered soluble.
§An instability index below 40 indicates a stable protein.
Table 1: Physicochemical properties of the primary construct.
Reverse Translation and Codon Optimisation
The guanine-cytosine sequences were optimised after reverse translating the primary construct’s protein sequence into nucleotides in E. coli K12 expression systems. The reverse translation and codon optimisation results yielded a guaninecytosine content of 61.9% with a CAI score of 0.703, indicating the constructs’ stability and excellent possibility of expression in the E. coli K12 expression system. Hence, the construct is stable in designing the lateral flow kit for diagnosis.
Computational Cloning
The team performed computational cloning to assess the capacity of the cloning and expression of the primary construct in an appropriate vector system. They modified the codon of their peptide using the E. coli K12 expression system’s codon usage method in the SnapGene tool and cloned it in pET-24 a (+). The pET-24a (+) vector is used for high-level expression of the primary construct in E. coli, facilitated by the T7 promoter and kanamycin selection marker. The highlighted restriction sites indicate the cloning strategy employed regions that were replaced were PaeR71(158) - BamHI (198) and BamHI (198) - PaeR71(158). The fragments were cut at HindIII (65) – BsrBI (376) and BsrBI (376)-HindIII (65) (Figure 1). Computational cloning in the pET-24a(+) vector confirmed the successful insertion and expression potential of the primary construct.
Secondary Structure and Tertiary Structure Prediction
The authors predicted the secondary structure of the lateral flow assay construct using the SOPMA server, which explained the distributions with 19.82% alpha helix, 19.51% extended strands, 5.18% beta turns, and 55.49% random coil. Secondary structure prediction revealed a high percentage of random coils and extended strands, indicating the potential for forming antigenic epitopes. Tertiary structure analysis using ColabFold confirmed the structural integrity. Collabfold analysis of the tertiary structure of the lateral
flow assay constructed revealed that the predicted local distance difference test is less than 50 and the template modelling score is less than 0.02.
Protein Structure Analysis ProSA-web, and Validation
ProSA-web estimated and verified the whole quality of the basic 3D model and analysed the refined protein structure for errors. ProSA-web analysis validated the 3D model with a Z-score of -5.1, confirming the model’s accuracy and precision (Figure 2).
Ramachandran plot for the validation of the refined tertiary structure was generated through SAVES v6.0 via PROCHECK. The Ramachandran plot showed 95.4% of amino acids in favourable regions indicating that the stereochemical quality of protein structures by plotting the phi (ϕ) and psi (ψ) dihedral angles of each amino acid residues in the peptide,42 making the construct’s suitability for lateral flow test design. The results further indicated that 3.8% of the amino acids were in the allowable region and 0.8% plotted in the disallowed region, the permitted and prohibited regions of dihedral angles (ϕ and ψ) for amino acid residues, is used to verify the tertiary structure of a protein. It is generally agreed upon that a minimum of 95.4% of residues must lie inside the preferred zones.43 Furthermore, 95.4% threshold is based on statistical analysis of known protein structures and is widely accepted in structural biology as a marker of goodquality models.44
Molecular Docking
The HDOCK server predicts a low sequence ID (14.6%) and a medium TM score (0.66576) for the receptor. The ligand score and Max Sub are 0.333 and 0.053, respectively. Molecular docking using the HDOCK server identified Model 1 with a confidence score of 0.9093 and a docking score of -265.28, suggesting strong binding affinity and stability.
Figure 1: Cloning strategy for the primary construct into the pET-24a (+) expression vector.
The diagram shows the positions of various restriction sites and key features of the vector, including the T7 promoter, lac operator, and kanamycin resistance gene. Restriction sites used for cloning (PaeR71 and BamHI).
2: A) Overall 3D model quality and B) local 3D model quality.
Number of Residues
Knowlegde-Based Energy
Sequence Position
Protein structure analysis by ProSA-web. A) The overall 3D model quality is assessed by the Z-score, which compares the model to known structures determined by X-ray and NMR. A Z-score within the range of native proteins indicates a reliable model. B) The local 3D model quality is assessed by the knowledge-based energy profile, with values below 0 indicating energetically favourable and likely correct regions of the protein. The X-axis represents the sequence position (residues 1 to 328), and the Y-axis represents the knowledge-based energy. the Y-axis represents the knowledge-based energy.
Figure
DISCUSSION
Lateral flow test kits are essential tools for rapid and point-of-care diagnostics, relying on the sensitivity, specificity, accuracy, and reliability of their primary, secondary, and tertiary constructs to detect target analytes. From the results, it is established that our primary constructs demonstrate high antigenicity (0.9136), non-allergenicity, and good solubility (0.634), aligning with the report that high-quality monoclonal antibodies enhance test sensitivity and specificity, leading to better diagnostics accuracy.45 The construct’s instability index (35.97) classifies it as stable, with an aliphatic index of 60.09 and a GRAVY score of -0.456, confirming its robustness under various environmental conditions.
The SOPMA analysis of the secondary constructs revealed a favourable distribution of alpha helices (19.82), extended strands (19.51%), beta turns (5.18%), and random coils (55.49%), supporting the protein’s stability and binding potential, consistent with previous studies on protein structure and stability.27,46 Also, supported by Posthuma-Trumpie et al.,47 which highlighted the importance of selecting appropriate secondary constructs, as they affect the sensitivity and specificity of the test.
According to a study by Linares et al.,48 the inclusion of a control line in a lateral flow test kit improves the test’s accuracy and reliability. The tertiary construct, validated by AlphaFold prediction and refined to a 73.5% quality factor, meets these standards. The control lines of the tertiary construct analysis are included to monitor the assay’s performance and reduce the risk of false-positive or false-negative results. Comparing the study by Linares et al.48 to this tertiary construct test analysis, the model 5 ranked 1 from AlphaFold prediction based on post translational modulation score and predicted local distance difference test per-residue confidence level. The predicted local distance difference test was 28.8 and the low post translational modulation was 0.186, this was further refined to meet a 73.5% quality factor. Protein structure analysis and
Ramachandran’s plot shows the allowed conformations of amino acid residues in the protein backbone. It is evident that the conformation of the polypeptides and proteins with the standard four regions of the plot correspond to the different secondary structures of proteins: alpha helices, beta sheets, turns, and random coil. Ramachandran et al.,49 established that allowed conformations of amino acid residues in each of these regions are determined by the steric interactions between the atoms in the backbone and the side chains of neighbouring residues which shows that certain combinations of ϕ and ψ angles are sterically unfavourable and thus energetically disfavoured, while others are allowed and energetically favourable. With plot statistics showing 95.4% favoured region, 3.8% allowed region, and 0.8% disallowed region of the total of 328 residues, the conformity to the alpha helix region of the plot characterised by a tight cluster of points around the ϕ=-60° and ψ=-45° angles, hence an ideal helical conformation. The beta sheet region, on the other hand, is characterised by two clusters of points around the ϕ=-120° and ψ=120°, and ϕ=120° and ψ=-120° angles; this shows the two possible orientations of the beta strand.32
SOPMA predictions indicate a stable folding pattern with significant alpha helices and random coils, consistent with previous studies on protein structure and stability.27,46,50 Similarly, Yan et al.,50 used SOPMA to predict the secondary structure of a protein called SARS-CoV-2 Nsp15 and identified potential drug targets for the treatment of COVID-19. Having Alpha helix (Hh) at 19.82%, Extended strand (Ee) at 19.51%, Beta turn (Tt) at 5.18%, Random coil (Cc) at 55.49%, inferring the protein’s overall folding pattern and potential stability as okay. SOPMA reveals a similarity threshold at 8 and having 4 numbers of states suggesting that the protein is involved in binding to other molecules or participating in signalling pathways that require a rigid, stable structure.27,50 The Z-score and residue score obtained further validated the constructed protein structure analysis to ensure the quality and accuracy of our protein model.
The ProSA-web tool was used for this validation due to its wide acceptability and ability to evaluate protein structures.51 A high positive Z-score indicates that the structure is significantly more stable than random structures.52 With a Z-score of -5.1 across the X-ray and NMR regions as shown in Figure 2, which is significantly lower than the expected value for a random protein of similar size and composition. On further examination, the residue score plot generated by ProSA-web. The plot indicates that several residues in the protein structure have low negative residue scores, indicating suitability.
A fundamental physicochemical property of this construct is its stability. Stability refers to the protein’s ability to maintain its 3D structure and function under various environmental stresses, including temperature, humidity, and light.53 The construct exhibits strong physicochemical stability, evident from its low instability index (35.97), favourable aliphatic index (60.09), and GRAVY score (-0.456).53 This stability suggests its robustness under diverse environmental conditions, potentially making it suitable for applications requiring long-term storage or use in harsh environments.
Solubility is another crucial property for pharmaceuticals, as it directly affects bioavailability and drug efficacy.54 The predicted high scaled solubility (0.634) of the construct indicates good bio accessibility, suggesting its potential for efficient absorption into the bloodstream upon administration.54 This is a critical factor for maximising drug efficacy.
In the context of lateral flow test development, molecular docking simulations played a key role. The team achieved strong binding affinity and specificity by modelling the interaction between the antigen and this protein construct, as evidenced by the TM score of 0.66576. This score indicates good model quality and comprehensive coverage of both the antigen binding site (receptor, 0.996) and the protein construct itself (ligand, 0.085). This can be particularly useful when designing synthetic protein constructs for use in lateral flow tests.55
With the homology model and TM score of 0.66576, it is established that the binding affinity and specificity of the receptor and ligand molecules are on the correct and medium spectrum exhibiting good coverage by both receptor (0.996) and ligand (0.085). This optimised construct design, facilitated by molecular docking, is essential for achieving the high sensitivity and specificity required for effective lateral flow test performance. This approach aligns well with established methodologies in lateral flow test development, where molecular docking is a valuable tool for optimising antigenantibody interactions.55,56
CONCLUSION
This study demonstrated that the designed lateral flow test kit is highly effective and viable for the early detection of Chlamydia trachomatis, which can be deployed as a stand-alone or used as combinational therapeutic with the gold standards (nucleic acid amplification tests not excluding strand displacement amplification, PCR, and transcription-mediated amplification) for the rapid testing of Chlamydia trachomatis The kit as detailed in our research provides public health the accessibility for rapid and widespread screening, facilitating potential increase in test rates thereby controlling spread with reduction in longterm complications.
The development of this lateral flow test kit represents a significant advancement in infectious disease diagnostics considering the speed and convenience, cost effectiveness, and portability supporting the privilege for onsite testing including remote and underserved areas where laboratory facilities are not available.
Future research should reflect opportunities with immunoinformatics where expanded use through broader applications of molecular test kits becoming the norm for major diagnostics, providing global health impact the use of scalable deployment and policy integration enhancing overall disease surveillance and control not just for chlamydia but for other pathogens.
References
1. Rodrigues R et al. Chlamydia trachomatis as a current health problem: challenges and opportunities. Diagnostics (Basel). 2022;12(8):1795.
2. Ljubin-Sternak S, Meštrović T. Chlamydia trachomatis and genital mycoplasmas: pathogens with an impact on human reproductive health. J Pathog. 2014;2014:183167.
3. Witkin SS et al. Chlamydia trachomatis: the persistent pathogen. Clin Vaccine Immunol. 2017;24(10):e00203-17.
4. WHO Global Health Observatory Indicator Details. STI: Incident cases of chlamydia in 15-49 year olds (in thousands). Available at: https://www. who.int/data/gho/data/indicators/ indicator-details/GHO/incident-casesof-chlamydia-in-individuals-(inmillions). Last accessed: 2 July 2024.
5. World Health Organisation. Chlamydia, gonorrhoea, trichomoniasis and syphilis: global prevalence and incidence estimates, 2016. 2019. Available at: https://www.who. int/publications/i/item/chlamydiagonorrhoea-trichomoniasis-andsyphilis-global-prevalence-andincidence-estimates-2016. Last accessed: 2 July 2024.
6. Hussen S et al. Prevalence of Chlamydia trachomatis infection among reproductive age women in sub Saharan Africa: a systematic review and meta-analysis. BMC Infect Dis. 2018;18(1):596.
7. Betha K et al. Prevalence of Chlamydia trachomatis among childbearing age women in India: a systematic review. Infect Dis Obstet Gynecol. 2016;2016:8561645.
8. Meyer T. Diagnostic procedures to detect Chlamydia trachomatis infections. Microorganisms. 2016;4(3):25.
9. Puolakkainen M. Laboratory diagnosis of persistent human chlamydial infection. Front Cell Infect Microbiol. 2013;3:99.
10. Doytchinova IA, Flower DR. VaxiJen: a server for prediction of protective antigens, tumour antigens and subunit vaccines. BMC Bioinformatics. 2007;8:4.
11. Salod Z, Mahomed O. Mapping potential vaccine candidates predicted by Vaxijen for different viral pathogens between 2017-2021-a scoping review. Vaccines (Basel). 2022;10(11):1785.
12. Krogh A et al. Predicting transmembrane protein topology with a hidden Markov model: application to complete genomes. J Mol Biol. 2001;305(3):567-80.
13. Yao B et al. SVMTriP: a method to predict antigenic epitopes using support vector machine to integrate tri-peptide similarity and propensity. PLoS One. 2012;7(9):e45152.
14. Vita R et al. The Immune Epitope Database (IEDB): 2018 update. Nucleic Acids Res. 2019;47(D1):D339-43.
15. Jespersen MC et al. BepiPred-2.0: improving sequence-based B-cell epitope prediction using conformational epitopes. Nucleic Acids Res. 2017;45(W1):W24-9.
16. Dhanda SK et al. Prediction of IL4 inducing peptides. Clin Dev Immunol. 2013;2013:263952.
17. Nagpal G et al. Computer-aided designing of immunosuppressive peptides based on IL-10 inducing potential. Sci Rep. 2017;7:42851.
18. Mehmood F et al. RPPSP: a robust and precise protein solubility predictor by utilizing novel protein sequence encoder. IEEE Access. 2023;11:59397416.
19. Hebditch M et al. Protein–Sol: a web tool for predicting protein solubility from sequence. Bioinformatics. 2017;33(19):3098-100.
20. Medha N et al. Prediction and identification of T cell epitopes of COVID-19 with balanced cytokine response for the development of peptide based vaccines. In Silico Pharmacol. 2021;9(1):40.
21. Madeira F et al. Search and sequence analysis tools services from EMBLEBI in 2022. Nucleic Acids Res. 2022;50(W1):W276-9.
22. Puigbò P et al. CAIcal: a combined set of tools to assess codon usage adaptation. Biol Direct. 2008;3:38.
23. Dey J et al. Molecular characterization and designing of a novel multiepitope vaccine construct against Pseudomonas aeruginosa. Int J Pept Res Ther. 2022;28(2):49.
24. Huleani S et al. Escherichia coli as an antibody expression host for the production of diagnostic proteins: significance and expression. Crit Rev Biotechnol. 2022;42(5):756-73.
25. Gligorijević V et al. Structure-based protein function prediction using graph convolutional networks. Nat Commun. 2021;12(1):3168.
26. Chen J et al. In silico protein function prediction: the rise of machine learning-based approaches. Med Rev (2021). 2023;3(6):487-510.
27. Geourjon C, Deléage G. SOPMA: significant improvements in protein secondary structure prediction by
consensus prediction from multiple alignments. Comput Appl Biosci. 1995;11(6):681-4.
28. Mirdita M et al. ColabFold: making protein folding accessible to all. Nat Methods. 2022;19(6):679-82.
29. Ko J et al. GalaxyWEB server for protein structure prediction and refinement. Nucleic Acids Res. 2012;40(Web Server issue):W294-7.
30. Wiederstein M, Sippl MJ. ProSAweb: interactive web service for the recognition of errors in threedimensional structures of proteins. Nucleic Acids Res. 2007;35(Web Server issue):W407-10.
31. Laskowski RA et al. PROCHECK: a program to check the stereochemical quality of protein structures. Journal of Applied Crystallography. 1993;1;26(2):283-91.
32. Laskowski RA et al. AQUA and PROCHECK-NMR: programs for checking the quality of protein structures solved by NMR. J Biomol NMR. 1996;8(4):477-86.
33. Huang SY, Zou X. A knowledge-based scoring function for protein-RNA interactions derived from a statistical mechanics-based iterative method. Nucleic Acids Res. 2014;42(7):e55.
34. Yan Y et al. The HDOCK server for integrated protein-protein docking. Nat Protoc. 2020;15(5):1829-52.
35. Meraviglia-Crivelli D et al. Therapeutic strategies to enhance tumor antigenicity: making the tumor detectable by the immune system. Biomedicines. 2022;10(8):1842.
36. Sahu TK et al. A comparative analysis of amino acid encoding schemes for the prediction of flexible length linear B-cell epitopes. Brief Bioinform. 2022;23(5):bbac356.
37. Oladipo EK et al. Bioinformatics analysis of structural protein to approach a vaccine candidate against Vibrio cholerae infection. Immunogenetics. 2023;75(2):99-114.
38. Oladipo EK et al. Immunoinformatics aided design of a peptide‐based kit for detecting Escherichia coli O157:H7 from food sources. Journal of Food Safety. 2023;14;43(5).
39. Srivastava S et al. Structural basis for designing multiepitope vaccines against COVID-19 infection: in silico vaccine design and validation. JMIR Bioinform Biotechnol. 2020;1(1):e19371.
40. Ras-Carmona A et al. Prediction of B cell epitopes in proteins using a novel sequence similarity-based method. Sci Rep. 2022;12(1):13739.
41. Sanchez-Trincado JL et al. Fundamentals and methods for T- and B-cell epitope prediction. J Immunol Res. 2017;2017:2680160.
42. Hollingsworth SA, Karplus PA. A fresh look at the Ramachandran plot and the occurrence of standard structures in proteins. Biomol Concepts. 2010;1(34):271-83.
43. Rosenberg AA et al. An amino-domino model described by a cross-peptidebond Ramachandran plot defines amino acid pairs as local structural units. Proc Natl Acad Sci USA. 2023;120(44):e2301064120.
44. Park SW et al. Revisiting the Ramachandran plot based on statistical analysis of static and dynamic characteristics of protein structures. J Struct Biol. 2023;215(1):107939.
45. Deeks JJ et al. Antibody tests for identification of current and past infection with SARS-CoV-2. Cochrane Database Syst Rev. 2020;6(6):CD013652.
46. Yan R et al. Structural basis for the recognition of SARS-CoV-2 by full-length human ACE2. Science. 2020;367(6485):1444-8.
47. Posthuma-Trumpie GA et al. Lateral flow (immuno)assay: its strengths, weaknesses, opportunities and threats. A literature survey. Anal Bioanal Chem. 2009;393(2):569-82.
48. Linares M et al. Panbio antigen rapid test is reliable to diagnose SARSCoV-2 infection in the first 7 days after the onset of symptoms. J Clin Virol. 2020;133:104659.
49. Ramachandran GN et al. Stereochemistry of polypeptide chain configurations. J Mol Biol. 1963;7:95-9.
50. Combet C et al. NPS@: network protein sequence analysis. Trends Biochem Sci. 2000;25(3):147-50.
51. Wiederstein M, Sippl MJ. ProSAweb: interactive web service for the recognition of errors in threedimensional structures of proteins. Nucleic Acids Res. 2007;35(Web Server issue):W407-10.
52. Sippl MJ. Recognition of errors in three-dimensional structures of proteins. Proteins. 1993;17(4):355-62.
53. Salatin S et al. Biological stability of peptides/proteins therapeutic agents. Int J Pept Res Ther. 2023;29(5).
54. Alshamrani M et al. Technologies for solubility, dissolution and permeation enhancement of natural compounds. Pharmaceuticals (Basel). 2022;15(6):653.
55. Meng XY et al. Molecular docking: a powerful approach for structure-based drug discovery. Curr Comput Aided Drug Des. 2011;7(2):146-57.
56. Mao M et al. Design and optimizing gold nanoparticle-cDNA nanoprobes for aptamer-based lateral flow assay: application to rapid detection of acetamiprid. Biosens Bioelectron. 2022;207:114114.
Exosomes: A Brief Review of Biology and Medical Applications
Authors: Katha Sanyal,1 *Abhijit G. Banerjee1
1. Genomic Biomedicine Research and Incubation, Durg, India *Correspondence to abhijitb@cgbmri.co.in
Disclosure: The authors have declared no conflicts of interest.
Extracellular vesicles (EV) are subcellular components derived from a cell that are essential mediators of intercellular communication. Exosomes are a type of extracellular vesicle secreted by the cell. Exosomes have immense therapeutic significance and benefits in a variety of medical applications, including medication nanodelivery, cell and gene therapy, immunological response, biomarker therapy, and anticancer vaccination.
Methods for isolating exosomes, including ultracentrifugation, size-based isolation, immune-affinity capture-based approaches, precipitation, and microfluidic methods, are described in this brief review. Additionally, studies that demonstrate the diverse potential of exosomes as agents in diagnosis and natural agent therapeutics are briefly discussed.
The potential of exosomes extends to anticancer vaccines, with evidence supporting their role in inducing potent antitumor immune responses. Despite advancements, further research is needed to unlock the full diagnostic and therapeutic capabilities of exosomes. In summary, this concise review highlights the multifaceted nature of exosomes, showcasing their crucial role in intercellular communication and their diverse applications in biomedicine.
Key Points
1. Avoiding immune responses to delivery vehicles during delivery of natural and biologic drugs is of paramount importance, unlike the delivery of their synthetic counterparts.
2. This article summarises the potential of extracellular vesicles, including exosomes, as natural cellular 'couriers' of biological information.
3. Affordable and accessible sources of extracellular vesicles vary in the biological world, and may be modified according to the needs of its application, for example with genetically engineered donor cells.
INTRODUCTION
Intercellular communication, whether through direct cell–cell interactions or the transfer of secreted chemicals, is critical for the survival of multicellular organisms. The physiologic processes of the human body are regulated by three distinct organ systems: the neurological system, the immune system, and the endocrine system.1
Cell–cell interaction is important because it:
a) regulates the metabolism and other functions of the tissue's constituent cells;
b) serves as a communication channel that enables the coordination of cellular differentiation and proliferation in both embryonic and adult tissues; and
c) functions as a component of cellular recognition.
Cells spontaneously release endosomal and plasma membrane-originated vesicles, which are called extracellular vesicles (EV). EVs are made up of a fluid core surrounded by a lipid bilayer. Compared to its origin i.e., the donor cell membrane, the lipid bilayer of EVs is more rigid because it is primarily enriched by desaturated lipids such as gangliosides and sphingomyelin.2 These vesicles usually contain heat shock proteins, cytoskeletal proteins, and cytosolic DNA from secreting cells in abundance.3
Transmembrane proteins, integrins, and glycoproteins involved in vesicle trafficking cover the EV.4 EVs have a significant function in cell–cell communication by transporting membrane and cytosolic proteins, lipids, and RNA molecules between cells. Additionally, they contribute to synaptic transmission and hormone release through vesicular exocytosis.
These vesicles are commonly known by various names such as macrovesicles,
ectosomes, shedding vesicles, or microparticles.5-7 The term "exosome" was originally coined for vesicles with a diameter ranging from 30–100 nm, which are ‘exfoliated’ by various cultured cells or their natural tissues.8 Subsequently, it was discovered that exosomes are also secreted into circulation by B lymphocytes and dendritic cells using a similar mechanism through cellular membrane fusion of micro-vesicular bodies (MVB) to be released outside cell (Figure 1).9,10
Exosomes, minute extracellular vesicles essential for intercellular communication, undergo a sophisticated biogenesis predominantly within the endosomal system. The process initiates with inward budding of the plasma membrane, forming early endosomes, which subsequently mature into MVBs through endosomal membrane invagination. Within MVBs, intraluminal vesicles form via the inward budding of the limiting membrane. This intricate process relies on the orchestrated action of various proteins, including endosomal sorting complex required for transport (ESCRT) machinery, lipidmodifying enzymes, and tetraspanins. Upon fusion of MVBs with the plasma membrane, intraluminal vesicles are released into the extracellular space as exosomes. Cargo sorting into exosomes is meticulously regulated and encompasses proteins, lipids, nucleic acids, and metabolites, mirroring the parent cell's physiological state. The biogenesis of exosomes is pivotal in numerous biological processes, such as immune modulation, cancer advancement, and neuronal signalling, underscoring the imperative to comprehend its molecular intricacies.3,4,11
CHARACTERISTICS OF EXOSOMES
Characteristics of the exosomes can be seen in Table 1 12
The cellular origin and physiological state of the cell
A major sorting of lipidic molecules from the parental cells
Multi-vesicular bodies fusion with plasma membrane of the donor cell
Constitutive or inducible, depending on the cell type of origin
Electron microscopy, western blot for exosome enriched biomarkers
Ultracentrifugation at (100,000–120,000 ×g), filtration, density gradient, microfluidics, immunoprecipitation, immune affinity capture, and precipitation methods
Exosomes are small membrane vesicles released into the extracellular environment by various cell types. These vesicles can be isolated using the following methods:
Ultracentrifugation-Based Isolation Techniques
Centrifugation is a technique that employs centrifugal force to segregate mixed substances by exploiting the behaviour of particles in a centrifugal environment and their intrinsic properties such as mass, shape, and density. In the isolation of exosomes, a sequence of centrifugation cycles with varying forces and durations is utilised to separate them from other constituents in the sample based on differences in density and size.13
Ultracentrifugation typically employs forces ranging from approximately 100,000–120,000 ×g, for this purpose.14,15 Initially, a purification step is conducted to eliminate large bioparticles, and the sample is treated with protease inhibitors to safeguard exosomal proteins. Throughout the isolation process, supernatants are harvested intermittently, and either the supernatant or the pellet is resuspended, contingent upon the applied centrifugal force. Sequential centrifugation steps with escalating force are subsequently executed.16 Ultimately, the isolated exosomes are resuspended and stored at -80 °C until further examination. This method is alternatively known as the pelleting method or simple ultracentrifugation method. Ultrafiltration is thus a commonly utilised method for the isolation of exosomes based on size and/ or molecular weight. The process separates suspended particles or polymers mainly according to their mass.
Exosome Isolation on the Basis of Size
Exosomes are first isolated through a series of filtration steps from cell culture supernatants. A standard 100 nm membrane filter is used to eliminate significant amounts of cell debris and floating cells,
allowing flexible components larger than 100 nm to pass while removing rigid ones. Subsequently, tangential flow filtration employing hollow fibres with a 500 kDa molecular weight cutoff is applied to the filtrate, concentrating the retained material, followed by diafiltration to further purify the sample. A 100 nm track-and-echo filter is then utilised in the third step. Rinse cycles are incorporated after each phase to optimise exosome recovery, with continuous monitoring and maintenance of transmembrane pressure during the second and third filtration processes. Confirmation of exosome-associated proteins is achieved through mass spectrometry, alongside electron microscopy validating the vesicle morphology. The method's gentle manipulation ensures high-purity exosome extraction while preserving functional integrity.17,18
Size exclusion chromatography is another technique employed for isolating exosomes based on size by utilising a porous stationary phase to separate macromolecules and particulate debris according to their size. Late elution occurs when components in the sample with small hydrodynamic radii can flow through the pores, while exosomes and other substances with larger hydrodynamic radii are hindered from passing through.19,20
Immunoaffinity Capture-Based Techniques
ELISA is a technique for analysing the antigen and antibody present in a given sample.21 The abundance of proteins and receptors on the exosome membrane creates an attractive opportunity for the development of precise isolation methods. These techniques hinge on immuneaffinitive interactions between these membrane proteins (antigens) and their corresponding antibodies. Both qualitative and quantitative methods can gauge the levels of antigens and antibodies. Ideally, exosome biomarkers suitable for immunebased isolation should be firmly anchored to the membrane, lacking soluble forms, and either exclusively expressed or highly concentrated on the exosome surface from
specific biological origins.22 ELISA outcomes, commonly represented as absorbance values, facilitate swift comparisons of known exosome surface biomarker expressions, thus offering immediate insights into exosome yield and specificity.23
Exosome Precipitation
Exosomes may undergo different degrees of solubility or dispersion, leading them to separate from biological fluids. Waterexcluding polymers like polyethylene glycol (PEG) are employed for this purpose. These polymers bind water molecules, thus prompting less soluble components to precipitate out of the solution.24 Typically, solutions for precipitation containing PEG with a molecular weight of 8000 Da are mixed with samples and incubated. The resulting precipitate containing exosomes is then isolated through low-speed centrifugation or filtration after overnight incubation at 4 °C.25 This method of exosome precipitation is straightforward and does not require specialised equipment. With current technologies, it can be easily integrated into clinical settings and is adaptable for processing large sample volumes.26
Microfluidics-Based Isolation Techniques
This leverages both the physical and biochemical properties of exosomes at the microscale, benefiting from rapid advancements in microfabrication technology. These advancements offer a distinct opportunity to create microfluidic devices capable of efficiently extracting exosomes. These devices employ innovative sorting methods, including auditory, electrophoretic, and electromagnetic manipulations, alongside traditional techniques like size, density, and immunoaffinity. Such devices are expected to significantly reduce sample volume, reagent usage, and isolation duration.27,28 Additionally, this technique allows for precise dynamic control over analyte concentrations during sample processing and analysis.29 Furthermore, it enables manipulation of small sample volumes while maintaining highthroughput capabilities.
APPLICATIONS OF EXOSOMES
Drug Delivery Using Exosomes
Exosomes possess a remarkable capacity to transport beneficial cargo to diseased cells, making them highly promising therapeutic delivery systems on both theoretical and practical fronts. Their small size has been proven to be advantageous for delivering drugs to cancerous cells and neurons. Exosomes can be engineered to carry various therapeutic payloads, such as chemotherapeutic drugs, immunological modulators, antisense oligonucleotides, short interfering RNAs (siRNA), and other agents. They can be sourced from a variety of origins including cow milk, macrophages, dendritic cells, and bone marrow.
For example, exosomes derived from RAW264.7 macrophages have been utilised to transport molecules targeting lung and breast cancer, as well as demonstrating effectiveness in treating Parkinson's disease due to their high catalase concentration.30 Additionally, dendritic cells derived from the bone marrow of C57BL/6 mice offer reduced immunogenicity and have been employed to deliver siRNA to the brain in mice.31 Furthermore, exosomes from human bone marrow mesenchymal stem cells have been investigated for their ability to deliver functional anti-miR-9 antibodies to glioblastoma multiforme cells, serving as mediators of communication between mesenchymal stem cells and glioblastoma cells in the brain.32
The authors have compiled the resources used to isolate exosomes previously, and their prospective use as a medication delivery method (Table 2).31-34
All these studies show the potential of exosomes for use in the delivery of drugs and biologics. Small molecule medication loading is quite effective; however, loading DNA/siRNA still has room for improvement.
Immune Response
The exosome content has been found to be extremely disease-specific and includes information about cancer, viral infections, and neurodegenerative illnesses, including Alzheimer's and prion diseases. However, in recent experiments, engineered exosomes have been shown to play a role in both innate and adaptive immune responses. This finding supports their potential for use in the development of immunotherapies. The transfer and arrangement of antigenic peptides are responsible for the function of exosomes. The delivery of DNA that activates cyclic GMP-AMP synthase stimulator of interferon gene signalling to recipient cells occurs through an innate immune pathway. In this pathway, the detection of cytosolic DNA initiates the expression of inflammatory genes and triggers a Type I interferon response. This in turn may lead to exosomal miRNAmediated gene expression regulation as well as the stimulation of a variety of signalling pathways by surface ligands.35
Exosomes play a role in preventing placental infection by delivering exosomal miRNAs, specifically the chromosome-19 miRNA cluster (C19MC), from specialised placental cells known as trophoblasts to cells outside the placenta. This mechanism helps safeguard the placenta against viruses like poliovirus, human cytomegalovirus, and herpes simplex virus-1.36
Exosomes present in breast milk play a crucial role in promoting post-natal growth and overall health. These exosomes contain
immune-related miRNAs and have been shown to enhance the ex vivo generation of peripheral blood-derived T-regulatory cells. This function potentially aids in regulating immunological tolerance.37
Exosomes play a vital role in promoting viral infection. They disseminate viral components and promote their survival. For this reason, it is possible to deliver vectors containing genes of interest to target cells. Adeno-associated virus exosomes have been shown to effectively transfer genes to the immune system.38 This finding suggested that exogenous administration and endogenous exosomal secretion may trigger immunological responses in a context- and dose-dependent manner.
Exosomes as a Biomarker Source
Exosomes serve as a valuable source of biomarkers due to their critical role in facilitating cell–cell communication. They achieve this by directly interacting with surface ligands and transporting their contents between cells.39
Exosomes play a crucial role in transferring cellular mRNAs and microRNAs among cells.40 The analysis of the horizontal transfer of genetic information may help to investigate cancer recurrence and monitor responses to a certain therapy. The major advantage of using exosomes as biomarkers is that they eliminate the need for invasive methods. Moreover, these methods have been successfully used to detect ovarian, lung, and pancreatic
Table 2: Biological origins and function of exosomes.
cancers from liquid biopsies.41 Exosomes can remain stable and highly specific to target cells even after undergoing adverse conditions, such as numerous freeze‒thaw cycles and changes in pH.42
Even though exosomes and their components are used as biomarkers, these molecules cannot be used to quantify the severity of the disease. However, in the future, further research could identify exosomes as potential diagnostic, prognostic, and therapeutic delivery tools.
Potential Anticancer Vaccines
Understanding the mechanisms underlying antitumor immunity induced by exosomebased dendritic cell (DC) vaccines is crucial for determining the suitability of exosomes as tumour antigens in DC vaccine-based immunotherapy. Current research suggests that exosomes may indeed serve as optimal antigens for DC vaccines.43
DCs being the most effective antigenpresenting cells release numerous exosomes with potent anticancer properties. Exosomes derived from dendritic cells have been shown to induce activation in both CD4+ and CD8+ T cells containing key chaperones like major histocompatibility complex (MHC) I, MHC II, CD86, and HSP70-90.16,44 The transmission of exosomal peptide MHC I to CD8+ T cells is facilitated by the co-stimulation of released IL-2 and exosomal CD80. This process promotes CD8+ T cell proliferation, leading to a more robust antitumor immune response in vivo 45 Several studies have confirmed the activation of CD8+ and CD4+ T cells by exosomes derived from dendritic cells and the initiation of an in vivo antitumor immune response through exosomal CD80 and endogenous IL-2.46
CONCLUSION
Intercellular communication is pivotal for the coordination of physiological processes in multicellular organisms with neurological, immunological, and endocrine systems playing key roles. EVs emerged as crucial mediators in this communication network. Exosomes released by various cells exhibit unique characteristics, including a lipid bilayer enriched with specific and encapsulated cytosolic components for targeting specific tissues and their microenvironment.
Techniques based on size, molecular weight, immunoaffinity capture, ultracentrifugation, precipitation, and microfluidic approaches are employed for exosome isolation. These provide varying degrees of purity and efficiency, facilitating the exploration of exosomes for diverse applications. Exosomes, therefore, possess great promise in drug delivery, acting as carriers for therapeutic payloads such as chemotherapeutic drugs, RNAs, and immunomodulators. Their involvement in immune responses, both innate and adaptive, positions them as potential therapeutic tools. Additionally, exosomes serve as a source of biomarkers, enabling non-invasive detection of diseases, including cancer, and offering stability under adverse conditions.
The potential for exosomes as anticancer vaccines is a growing area of interest with studies demonstrating their ability to induce antitumor immune responses. While current research highlights their diagnostic and therapeutic potential, further investigations are warranted to fully comprehend the extent of their applications and their role in immunotherapy. In summary, exosomes present a multifaceted and promising avenue for advancing the understanding of intercellular communication and developing innovative biomedical applications in the future.
References
1. Buddingh BC et al. Intercellular communication between artificial cells by allosteric amplification of a molecular signal. Nat Commun. 2020;11(1):1652.
2. Laulagnier K et al. Mast cell- and dendritic cell-derived exosomes display a specific lipid composition and an unusual membrane organization. Biochem J. 2004;380(Pt 1):161-71.
3. Yáñez-Mó M et al. Biological properties of extracellular vesicles and their physiological functions. J Extracell Vesicles. 2015;4:27066.
5. Tran H et al. Facilitation of mRNA deadenylation and decay by the exosome-bound, DExH protein RHAU. Mol Cell. 2004;13(1):101-11.
6. Cocucci E et al. Shedding microvesicles: artefacts no more. Trends Cell Biol. 2009;19(2):43-51.
7. György B et al. Membrane vesicles, current state-of-the-art: emerging role of extracellular vesicles. Cell Mol Life Sci. 2011;68(16):2667-88.
8. Trams EG et al. Exfoliation of membrane ecto-enzymes in the form of micro-vesicles. Biochim Biophys Acta. 1981;645(1):63-70.
9. Raposo G et al. B lymphocytes secrete antigen-presenting vesicles. J Exp Med. 1996;183(3):1161-72.
10. Zitvogel L et al. Eradication of established murine tumors using a novel cell-free vaccine: dendritic cell-derived exosomes. Nat Med. 1998;4(5):594-600.
11. Colombo M et al. Biogenesis, secretion, and intercellular interactions of exosomes and other extracellular vesicles. Annu Rev Cell Dev Biol. 2014;30:255-89.
12. Li P et al. Progress in Exosome Isolation Techniques. Theranostics. 2017;7(3):789-804.
13. Zarovni N et al. Integrated isolation and quantitative analysis of exosome shuttled proteins and nucleic acids using immunocapture approaches. Methods. 2015;87:46-58.
14. Rechavi O et al. Cell contactdependent acquisition of cellular and viral nonautonomously encoded small RNAs. Genes Dev. 2009;23(16):1971-9.
15. Yamashita T et al. Effect of exosome isolation methods on physicochemical properties of exosomes and clearance of exosomes from the blood circulation. Eur J Pharm Biopharm. 2016;98:1-8.
16. Viaud S et al. Dendritic cell-derived exosomes for cancer immunotherapy: what's next? Cancer Res. 2010;70:1281-5.
17. Escudier B et al. Vaccination of metastatic melanoma patients with autologous dendritic cell (DC) derived exosomes: results of the first phase I clinical trial. J Transl Med. 2005;3(1):10.
18. Morse MA et al. A phase I study of dexosome immunotherapy in patients with advanced non-small cell lung cancer. J Transl Med. 2005;3(1):9.
19. Feng Y et al. Ischemic preconditioning potentiates the protective effect of stem cells through secretion of exosomes by targeting Mecp2 via miR22. PloS ONE. 2014;9(2):e88685.
20. Lai RC et al. Exosome secreted by MSC reduces myocardial ischemia/ reperfusion injury. Stem Cell Res. 2010;4(3):214-22.
21. Alhajj M, Farhana A, Enzyme Linked Immunosorbent Assay [Internet](2022) Treasure Island: StatPearls Publishing. Available at: https://www.ncbi.nlm. nih.gov/books/NBK555922/. Last accessed: November 2023
22. Doyle LM, Wang MZ. Overview of extracellular vesicles, their origin, composition, purpose, and methods for exosome isolation and analysis. Cells. 2019;8(7):727.
23. Logozzi M et al. Immunocapturebased ELISA to characterize and quantify exosomes in both cell culture supernatants and body fluids. Methods Enzymol. 2020;645:155-80.
24. Zeringer E et al. Strategies for isolation of exosomes. Cold Spring Harb Protoc. 2015;2015(4):319-23.
25. Kim D et al. Chromatographically isolated CD63+CD81+ extracellular vesicles from mesenchymal stromal cells rescue cognitive impairments after TBI. Proc Natl Acad Sci USA. 2016;113(1):170-5.
26. Batrakova EV, Kim MS. Using exosomes, naturally-equipped nanocarriers, for drug delivery. J Control Release. 2015;219:396-405.
27. Lee K et al. Acoustic purification of extracellular microvesicles. ACS Nano. 2015;9:2321-7.
28. Davies RT et al. Microfluidic filtration system to isolate extracellular vesicles from blood. Lab Chip. 2012;12(24):5202-10.
29. Baker S et al. Extracellular vesicles containing P301L mutant tau accelerate pathological tau phosphorylation and oligomer formation but do not seed mature neurofibrillary tangles in ALZ17 mice. J. Alzheimers Dis. 2016;54(3):1207-17.
30. Inamdar S et al. Emerging applications of exosomes in cancer therapeutics and diagnostics. Bioeng Transl Med. 2017;2(1):70-80.
31. Alvarez-Erviti L et al. Delivery of siRNA to the mouse brain by systemic injection of targeted exosomes. Nat Biotechnol. 2011;29(4):341-5.
32. Munoz JL et al. Delivery of functional anti-miR-9 by mesenchymal stem cell-derived exosomes to glioblastoma multiforme cells conferred chemosensitivity. Mol Ther Nucleic Acids. 2013;2(10): e126.
33. Munagala R et al. Bovine milk-derived exosomes for drug delivery. Cancer Lett. 2016;371(1):48-61.
34. Haney MJ et al. Exosomes as drug delivery vehicles for Parkinson's disease therapy. J Control Release. 2015;207:18-30. Erratum in: J Control Release. 2021;339:232-4.
35. Kalluri R, LeBleu VS. The biology, function, and biomedical applications of exosomes. Science. 2020;367(6478):eaau6977.
36. Delorme-Axford E et al. Human placental trophoblasts confer viral resistance to recipient cells. Proc Natl Acad Sci U S A. 2013;110(29):12048-53.
37. Admyre C et al. Exosomes with immune modulatory features are present in human breast milk. J Immunol. 2007;179(3):1969-78.
38. Breuer CB et al. In vivo engineering of lymphocytes after systemic exosome associated AAV delivery. Sci Rep. 2020;10(1):4544.
39. Barry OP et al. Modulation of monocyte-endothelial cell interactions by platelet microparticles. J Clin Invest. 1998;102(1):136-44.
40. Valenti R et al. Human tumorreleased microvesicles promote the differentiation of myeloid cells with transforming growth factor-b–mediated suppressive activity on T lymphocytes. Cancer Res. 2006;66(18):9290-8.
41. Rabinowits G et al. Exosomal MicroRNA: a diagnostic marker for lung cancer. Clin Lung Cancer. 2009;10(1):42-6.
42. Que R et al. Analysis of serum exosomal micro-RNAs and clinicopathologic features of patients with pancreatic adenocarcinoma. World J Surg Onc. 2013;11:219.
43. Lindenbergh MFS et al. Dendritic cells release exosomes together with phagocytosed pathogen; potential implications for the role of exosomes in antigen presentation. J Extracell Vesicles. 2020;9(1):1798606.
44. Chaput N et al. Exosome-based immunotherapy. Cancer Immunol Immunother. 2004;53:234-9.
45. Hao S et al. Novel exosome-targeted CD4+ T cell vaccine counteracting CD4+25+ regulatory T cell-mediated immune suppression and stimulating efficient central memory CD8+ CTL responses. J Immunol. 2007;179:2731-40.
46. Wang L et al. Exosomal pMHC-I complex targets T cell-based vaccine to directly stimulate CTL responses leading to antitumor immunity in transgenic FVBneuN and HLA-A2/HER2 mice and eradicating trastuzumab-resistant tumor in athymic nude mice. Breast Cancer Res Treat. 2013;140(2):273-84.
Regenerative Medicine in Orthopaedic Surgery: Pioneering Advances and Their Applications
Regenerative medicine has significantly impacted orthopaedic surgery by introducing biological therapies aimed at repairing, restoring, or replacing damaged musculoskeletal tissues. Recent advancements in stem cell therapies, platelet-rich plasma (PRP), and tissue engineering have paved the way for improved treatments for cartilage, bone, tendon, and ligament injuries. Mesenchymal stem cells (MSC) and induced pluripotent stem cells (iPSC) are gaining attention for their ability to regenerate tissues, while PRP shows promise in accelerating tendon and cartilage healing. Innovations in cartilage regeneration, including autologous chondrocyte implantation and biomimetic scaffolds, address the limitations of self-repair, and bone regeneration is being enhanced through growth factors like bone morphogenetic proteins (BMP) and synthetic grafts. In tendon and ligament repair, biological augmentation with scaffolds and growth factors is emerging as a novel approach. Moreover, regenerative approaches are making strides in spinal surgery and joint preservation, particularly in osteoarthritis treatment. However, challenges such as regulatory hurdles, cost, and the need for further clinical evidence remain. As the field progresses, the integration of cutting-edge techniques like 3D printing and gene therapy could further revolutionise orthopaedic regenerative medicine.
Key Points
1. Orthopaedic injuries and degenerative conditions, such as osteoarthritis, tendon damage, and cartilage damage are common, and often lead to reduced mobility, chronic pain, and long-term disability. While traditional surgical treatments can involve prolonged recovery times, risk of complications, and incomplete healing, regenerative medicine holds great potential.
2. This review highlights recent advancements in regenerative medicine within orthopaedic surgery, focusing on key areas such as stem cell therapies, platelet-rich plasma, cartilage and bone regeneration, tendon and ligament repair, and the use of biologics in spinal procedures.
3. Regenerative medicine is transforming the future of orthopaedic surgery by offering less invasive, biologically driven treatments that promote long-term tissue healing. While challenges remain, the continued research into stem cells, biomaterials, and tissue engineering is poised to improve patient recovery and revolutionise musculoskeletal care.
INTRODUCTION
Regenerative medicine is a rapidly growing field within orthopaedic surgery, focusing on harnessing the body’s natural healing mechanisms to repair and regenerate musculoskeletal tissues. The rapid growth of orthopaedic injuries and degenerative diseases such as osteoarthritis makes conventional approaches, which frequently end with an invasive surgery or prosthetic implant, limited in temporary relief or in restoring the original function of the musculoskeletal tissues. The regenerative therapies like stem cells, biomaterials, and growth factors have emerged as a new hope to tackle these challenges. These therapies aim to not only treat symptoms but also promote long-term healing by stimulating tissue regeneration. This article examines the latest advancements in regenerative medicine and their applications in orthopaedic surgery, highlighting key advances and future directions.
ORTHOPAEDIC STEM CELL THERAPIES
Stem cell therapies have emerged as a breakthrough in orthopaedic surgery by providing various innovative solutions for musculoskeletal disorders. Because of their capacity to differentiate into multiple cell lineages, stem cells possess regenerative properties and are therefore considered a fundamental platform for regenerative medicine within the field of orthopaedics. Mesenchymal stem cells (MSC), induced pluripotent stem cells (iPSC), and allogeneic stem cells are among the most studied sources of stem cells for therapeutic applications in orthopaedics.
Mesenchymal Stem Cells
MSCs are commonly harvested from bone marrow (BM-MSC) or adipose tissue
(ADSC), widely used for cartilage and bone regeneration. The harvested tissue is processed in a lab to isolate the MSCs and grown in culture to the required number of cells for use.1 The MSCs are injected directly into the injured or degenerated area, such as a joint cartilage repair or bone fracture healing. This procedure is typically done under ultrasound or imaging guidance for precise delivery. According to recent research, MSCs can improve osteoarthritis, tendon injuries, and bone abnormalities. MSCs have demonstrated great promise in the treatment of bone deformities and other orthopaedic disorders. These cells can be produced from a variety of sources, including bone marrow, adipose tissue, and umbilical cord. According to research, MSCs can improve tissue regeneration by secreting bioactive substances that promote healing and reduce inflammation and by their differentiation abilities.2,3 For instance, studies have demonstrated that MSCs can be effectively harvested from the forearm and utilised in hand surgeries to address conditions like scaphoid nonunion and osteoarthritis.4 Furthermore, the regenerative capacity of umbilical cord-derived MSCs has been emphasised; these cells offer a non-invasive cell therapy source that can enhance patient outcomes in orthopaedic surgery.3
The deeper understanding of stem cell function and differentiation mechanisms has been a significant advancement. For example, studies have shown that Wnt signalling pathways are essential for coordinating MSC identification and function during skeletal regeneration.5 This makes it possible to specifically manipulate stem cell behaviour to boost bone repairing procedures. Furthermore, the identification of specific markers, such as Emilin2, has been linked to the accumulation of MSCs at bone regeneration sites, providing new therapeutic targeting options.6
Induced Pluripotent Stem Cells
iPSCs are reprogrammed from adult cells and offer the potential for patient-specific therapies. They can be programmed to become osteocytes (bones), chondrocytes (cartilage), myocytes (muscle), or other relevant cells for orthopaedic applications. They are generated from the patient’s somatic cells, typically taken from skin or blood samples. These cells are reprogrammed to a pluripotent state similar to embryonic stem cells by a genetic reprogramming process. This involves introducing transcription factors such as Oct-4, SOX2, KLF4, and c-MYC into the somatic cells, turning them into iPSCs.
Research on iPSCs for joint and bone regeneration is encouraging, offering another cutting-edge direction in orthopaedic regenerative medicine, even though it has not been widely used clinically yet. Transplanted from somatic cells, iPSCs can develop into any type of cell, including those required for musculoskeletal repair.7,8 Their use in regenerative therapies is particularly advantageous as they can be derived from the patient’s own cells, thus minimising the immune rejection risks.9 Recent studies have explored the potential of iPSCs in generating functional tissues for musculoskeletal regeneration, demonstrating their versatility and effectiveness in preclinical models.10 Furthermore, the effectiveness of producing specific cell types from iPSCs has increased due to developments in differentiation methods, which is crucial for targeted therapy in orthopaedic applications.11
Allogeneic Stem Cells
Donor stem cells are being explored for large-scale use in treating conditions like degenerative joint diseases and spinal cord injuries. The harvested stem cells are processed, purified, and cryopreserved (frozen) for future use, offering a readily available source for transplantation compared to autologous cells from the patients, especially when patient conditions or previous surgeries may limit the availability of autologous sources.7 However, their use raises concerns regarding immunogenicity and the need for
immunosuppression, which can complicate treatment protocols.9 Therefore, ongoing research is focused on optimising the use of allogeneic stem cells with these challenges to overcome.
APPLICATION OF PLATELET-RICH PLASMA
Platelet-rich plasma (PRP) therapy uses a patient’s blood, concentrated with platelets and growth factors, to accelerate healing in injured tissues. The therapy has emerged as a promising treatment modality in orthopaedics, particularly for tendon and ligament injuries, cartilage repair, and post-surgical recovery. PRP is characterised by a high concentration of platelets and growth factors, which are critical for tissue healing and regeneration process. PRP’s capacity to promote angiogenesis, cellular proliferation, and the healing process in general by releasing different growth factors, including PDGF, VEGF, and TGF-β, makes it highly effective.12,13
Each of these growth factors play a distinct role in PRP applications. VEGF mainly functions as an angiogenesis promoter, stimulating new blood vessel development through enhanced endothelial cell movement and growth, which plays a vital role in supplying nutrients and oxygen to healing tissues.14,15 They also modulate the immune response by causing a transition from inflammatory state environment of macrophages (M1) to repairing macrophages (M2). PDGF functions as a powerful growth factor that drives mesenchymal cell division, boosts extracellular matrix (ECM) synthesis, and facilitates cellular migration, which contributes to tissue reconstruction and healing process.16-18 These growth factors stimulate fibroblast proliferation and collagen synthesis, which is critical for supplying nutrients and oxygen to initiate wound healing. By enhancing the deposition of proteins such as collagen and elastin, PRP promotes remodelling of the ECM and ensures the tissue restoration and their functions. TGF-β regulates key cellular activities including, differentiation and ECM production; it exhibits a dual effect on tissue regeneration and fibrosis, depending on specific cellular concentration and environment.19,20
Tendon and Ligament Injuries
PRP is commonly used to treat chronic conditions like tennis elbow, Achilles tendinopathy, and anterior cruciate ligament (ACL) injuries. PRP encourages the regeneration of tendons and ligaments, which aids in their repair. Studies show that platelet-rich plasma (PRP) can enhance recovery from injuries, including rotator cuff tears and Achilles tendon tears. For example, a study showed that PRP injections improved pain scores and shortened recovery periods for individuals having arthroscopic surgery to repair damaged rotator cuffs.21,22 Additionally, PRP has been found to augment tendon healing by reducing scar tissue formation, which is a common complication in traditional surgical interventions.22 However, the clinical effectiveness of PRP may vary, with some studies reporting mixed results regarding its benefits in ligament and tendon repair.23,24
Cartilage Repair
PRP injections have the potential to help heal cartilage, as well as relieve pain and inflammation in osteoarthritis patients by stimulating cartilage regeneration. They contain growth factors such as TGF-β, IGF1, PDGF, BMPs, and fibroblast growth factor (FGF), which can promote chondrocyte proliferation and improve the synthesis of ECM components critical for cartilage regeneration. Studies have indicated that the application of PRP in conjunction with other treatments, such as bone grafts or scaffolds, can lead to significant improvements in cartilage repair. 25,26 The use of PRP in osteoarthritis management has also been explored; according to findings, it may aid in relieving symptoms and enhance joint function by enhancing tissue regeneration.13,26
Post-Surgical Recovery
PRP is used in conjunction with surgical interventions to enhance post-surgical recovery and tissue healing after procedures like rotator cuff repairs and knee surgeries. The application of PRP in surgical settings has also shown to reduce inflammation, lead to quicker recoveries, and improved surgical wound healing. For
example, PRP has been utilised effectively in dental and oral surgeries, where it has shown quicker wound healing and reduced post-surgery complications.27,28 The autologous nature of PRP also minimises the risk of adverse reactions, making it a safe option for enhancing recovery across various surgeries.29 PRP therapy is a biologically active method that stimulates the body’s healing mechanisms. Its use in cartilage repair, tendon and ligament injuries, and post-surgical healing highlights its potentials and advantages.
CARTILAGE REGENERATION METHODS
Cartilage regeneration in orthopaedic surgery remains significantly challenging due to the limited intrinsic healing capacity of cartilage tissue. Recent developments in regenerative medicine have mainly focused on implementing approaches such as autologous chondrocyte implantation (ACI) and the development of scaffolds and biomaterials that improve cartilage healing.
Autologous Chondrocyte Implantation
ACI is a well-established surgical procedure used for cartilage regeneration in the treatment of cartilage defects in the knee, particularly on the femoral condyle and trochlea. It involves harvesting a patient’s own cartilage cells, culturing them in vitro, and reimplanting them into the damaged joint. The procedure involves a small piece of periosteum tissue which covers the bone, or a synthetic membrane placed over the defect and sutured in place. The cultured chondrocytes are then injected below the periosteal flap or membrane into the defect. This membrane helps contain the chondrocytes and integrates them into the tissue. ACI promotes the growth of hyalinelike cartilage, and like the native cartilage it is more durable than fibrocartilage formed through other procedures.30,31
Recently, this method has evolved into more sophisticated approaches such as matrix-associated autologous chondrocyte implantation (MACI), which also combines chondrocytes with biomimetic scaffolds
to improve integration and support the regeneration process.32,33 In order to promote cellular adhesion and growth, scaffolds are used to mimic the natural ECM and to provide a structural framework for cell attachment.32,34 Recent studies have shown that the incorporation of stem cells and growth factors into these scaffolds can significantly enhance the regenerative potential of the implanted cells, which improved cartilage repair.34,35
Scaffolds and Biomaterials
Scaffold materials can be natural (collagen, hyaluronic acid, chitosan, and alginate), synthetic (polylactic acid [PLA], polyglycolic acid [PGA], and polycaprolactone [PCL])' or hybrid scaffolds (a combination of natural and synthetic). In cartilage regeneration, scaffolds can be made from natural or synthetic materials and are often combined with chondrocytes, stem cells, or growth factors to enhance cartilage repair. Recent innovations include biomimetic scaffolds, which mimic the structure and properties of natural cartilage, enhancing cellular adhesion and growth. These are often combined with growth factors or stem cells to promote regeneration.
Biomimetic scaffolds designed to replicate the mechanical and biochemical properties of natural cartilage have shown promise in enhancing the regeneration process.32,36 For instance, oriented scaffolds have been shown to regulate hyaline cartilage regeneration, which is crucial in restoring the joint’s functional characteristics.35 The integration of growth factors such as TGF-β and BMPs into these scaffolds has shown to promote chondrogenesis in combination, hence improving the quality of the regenerated cartilage.34,37
Several investigations emphasised the role of mechanical loading and bioreactor systems in optimising the conditions for cartilage regeneration. It was also demonstrated that mechanical stimulation promotes chondrocyte differentiation and proliferation. This approach shows that the mechanical environment plays a vital role in cartilage tissue regeneration.38 These strategies not only aim to restore
the structural integrity of cartilage but also seek to enhance its functional properties, ultimately improving patient outcomes in joint repair.
BONE REGENERATION METHODS
The use of regenerative medicine in bone healing has seen promising developments, especially with techniques like the use of BMPs, synthetic bone grafts and bioceramics, and 3D printing technologies. Each of these methods contributes uniquely to enhancing bone healing and regeneration.
Bone Morphogenetic Proteins
BMPs are a group of growth factors that stimulate bone formation and repair. They stimulate the recruitment of MSCs to injured bones and signal them to differentiate into osteoblasts to initiate bone formation. Their osteoinductive nature triggers bone-forming cells to make new bone tissue, making them valuable in natural bone healing and clinical bone regeneration process, such as in spinal fusion surgeries or healing large bone fractures.
BMP-2 in particular has gained prominence for its osteoinductive properties, shown to induce differentiation of MSCs into osteoblasts, thereby promoting bone regeneration.39-41 Clinical applications of BMP-2 have shown improved fusion rates in spinal surgeries compared to traditional iliac crest bone grafts, reducing the need for additional surgeries.39,42 However, adverse effects like inflammation and heterotopic ossification have been reported. Therefore, careful optimisation of these delivery methods is required.43,44
Synthetic Bone Grafts and Bioceramics
Materials like calcium phosphate, hydroxyapatite, and bioactive glass are employed to mimic the natural bone matrix. These materials support bone cell proliferation and are often used alongside biological agents like BMPs or MSCs. They are vital substitutes for autologous bone grafts, which are limited by availability and donor site morbidity. Materials like
hydroxyapatite and calcium phosphate are made to mimic the natural bone matrix, acting as a scaffold to promote the integration and proliferation of bone cells.45,46 These materials can be combined with BMPs to enhance their osteogenic potential, creating a synergistic effect that promotes more effective bone healing.47 The incorporation of bioceramics with growth factors has significantly improved outcomes in cases of large bone defects and non-unions.47
3D Printing and Tissue Engineering
3D printing technologies are being used to create patient-specific scaffolds for bone regeneration that are tailored to patients' needs. These scaffolds can be engineered to include BMPs or MSCs to increase their efficacy in bone regeneration.48 The ability to produce customised scaffolds through 3D printing facilitates better integration with the host tissue and improves the overall success rate of bone healing procedures. Research indicates that 3D-printed scaffolds can outperform traditional graft materials in terms of osteogenic activity and structural support.48
The integration of BMPs, synthetic grafts, and advanced 3D printing technologies is transforming orthopaedic surgery. While BMPs provide critical biological signals for bone healing, synthetic materials and 3D-printed scaffolds enhance the mechanical and structural aspects of bone repair. Further research and clinical trials are essential in these technologies to address any potential complications.
APPROACHES IN TENDON AND LIGAMENT REPAIR
Tendon and ligament injuries are also prevalent in both sports and trauma, leading to significant challenges in orthopaedic surgery. Recent advancements in regenerative medicine have introduced innovative therapies aimed at enhancing the healing process of these injuries. The most important approaches to tendon and ligament repair are biological augmentation, growth factor therapy, and cell-based therapies.
Biological Augmentation
Scaffolds made from biological materials like collagen or synthetic polymers are used to enhance the repair of tendons and ligaments. They provide a structural framework that can facilitate cellular attachment and proliferation, which is essential for effective healing. ECM scaffolds, when sterilised appropriately, do not impair ligament healing and can support the formation of a fibrovascular scar, which is crucial for recovery.49 Additionally, the use of collagen-based compounds was demonstrated to enhance the morphofunctional properties of tenocytes, which suggests they can improve the healing for tendon injuries.50
Growth Factor Therapy
Growth factor therapy, particularly for tendon and ligament repair, can enhance the biological healing process. TGF-β and vascular endothelial growth factor (VEGF) are also being used to stimulate tendon regeneration. To stimulate tendon regeneration, they utilise specific proteins to play critical roles in the processes of proliferation and differentiation. TGF-β has been noted for its ability to modulate tenocyte activity and accelerate collagen synthesis, which is vital for tendon repair.51 The application of PRP, which is rich in growth factors like PDGF and TGF-β, has been shown to promote the differentiation of tendon stem cells into active tenocytes, which accelerated the healing process.52 Many studies have proved that PRP can significantly improve tendon healing by increasing tenocyte proliferation and collagen production.53,54
Cell-Based Therapies
Use of MSCs and tenocytes in cell therapies can improve healing outcomes and reducing re-injury rates in tendinopathies and ligament reconstructions. MSCs have the potential to differentiate into tenocytes and aid in the tendon repair process. Different approaches in combination with cell therapies have been introduced in studies to improve outcomes. For example, the combination of tendonderived stem cells (TDSC) with PRP has been shown to enhance tendon healing,
thus emerging as a preferable option in cell therapy.51,54 Tenocytes also play a crucial role in the healing process by secreting ECM components and signalling molecules that recruit other cells to the injury site.55 The intrinsic healing capacity of tenocytes makes them essential for the regeneration of the tendon matrix and the overall repair process.56
USE OF BIOLOGICS IN SPINAL SURGERY
Regenerative approaches in spinal surgeries, particularly in intervertebral disc repair and spinal fusion, have gained significant attention due to their potential to enhance recovery outcomes and less invasive procedures. Recent studies have focused on using biologics, including stem cells, growth factors, and injectable hydrogels.
Intervertebral Disc Repair
The application of stem cells and growth factors represents a promising approach for the repair and function restoration of degenerated intervertebral discs. Research indicates that bone marrow MSCs have better efficacy in repairing the annulus fibrosus of intervertebral discs. A study demonstrated that transplantation of bone marrow MSCs significantly improved collagen type II levels in the repaired tissue.57 Another study shows that the use of TGF-β suppresses inflammation and promotes chondrogenesis in intervertebral disc cells, which aids in disc function restoration.58
Injectable hydrogels, which provide a scaffold for cell growth and nutrient diffusion, are also being explored. These hydrogels can also be loaded with growth factors and stem cells, creating a conducive environment for tissue regeneration. A recent study shows the potential of chitosan hydrogels combined with decellularised nucleus pulposus matrix and growth factor microspheres to prevent intervertebral disc degeneration.59 This approach helps cell viability and enhances the capacity of the injected cells to regenerate.59
Exosomes, types of extracellular vesicles derived from stem cells, have also
emerged recently as a novel therapy. They supply target cells with bioactive molecules that improve tissue repair and cell communication. Stem cell-derived exosomes have also improved ECM formation and nucleus pulposus cell proliferation to help intervertebral disc degeneration.60,61 This cell-free approach can be a less invasive option for traditional stem cell therapies.
Spinal Fusion
BMPs and other biologics are being used to enhance bone fusion in spinal surgeries, which can reduce the use of autografts and invasive methods. BMPs play a critical role in enhancing bone fusion rates. They have been widely used in clinical practice for their capacity to stimulate osteogenesis and reduce autograft reliance, which can lead to donor site morbidity.62 The incorporation of BMPs into spinal fusion procedures has shown surgical outcomes and less complications.62
Use of PRP in spinal fusion with high concentration of growth factors was also investigated for its potential to enhance healing in spinal fusion surgeries. Studies suggest that PRP can improve bone healing, provide faster recovery, and enhance the fusion process.63,64 However, application methods for PRP remain challenging and subjects of further research. The integration of biologics in spinal surgery, particularly with stem cells, growth factors, and innovative scaffold technologies, holds promise for improving patient outcomes.
METHODS IN JOINT PRESERVATION AND OSTEOARTHRITIS
Joint preservation methods have become attractive alternatives to traditional surgical procedures for maintaining joint function and avoiding total knee replacements, as understanding of osteoarthritis (OA) developed. The most used approaches in current research are gene therapy, stem cell and platelet injections, and microfracture and drilling.
Microfracture and Drilling
Microfracture and drilling involve creating small fractures in the subchondral bone to stimulate the repair of articular cartilage. Recent studies indicate that these methods can perform better by integrating cellbased therapies and scaffolds, which improve the quality of the repaired cartilage.65,66 For instance, combining core decompression with new adjuvant therapies can lead to better postoperative outcomes, and development of these techniques is crucial for effective joint preservation.65 The incorporation of scaffolds can provide a supportive environment for chondrocyte proliferation and differentiation, potentially leading to more robust cartilage repair.66
Stem Cell and Platelet-Rich Plasma Injections
The combination of stem cell therapy and PRP injections has shown better results in the progression of OA and cartilage repair compared to conventional treatments in recent studies. A clinical trial demonstrated that patients receiving PRP combined with arthroscopic debridement provided better results than using PRP alone.67 Another study showed significant improvement in joint conditions by using the combination of stem cells with PRP.68 The ability of MSCs to transform into cartilage-forming cells, as well as their anti-inflammatory nature and regenerative properties, make them attractive options to address the underlying pathophysiology of OA.69
Gene Therapy
Gene therapy is an innovative approach in the treatment of OA, particularly in targeting inflammatory pathways. Although this is currently experimental, gene therapies that are able to inhibit pro-inflammatory cytokines such as IL-1 and TNF-α show promise in modifying the disease. Recent studies have indicated that targeting inflammatory mediators can reduce cartilage degradation and improve joint function.70 Gene therapy may alter the inflammation in OA and provide a multifaceted approach to treatment.
Joint preservation strategies for OA, including microfracture and drilling, stem cell and PRP injections, and gene therapy, represent huge developments in OA treatment. By focusing on the preservation and restoration of joint function, these techniques aim to relieve symptoms and address the underlying causes of OA. Further research and clinical trials will be essential to establish their long-term safety and efficacy.
DISCUSSION
Regenerative medicine in orthopaedic surgery has made significant advances in recent years; however, many challenges remain for widespread adoption and efficacy. Numerous studies have shown improvements in the application of regenerative therapies. The review of these studies points out several challenges yet to overcome. The long-term efficacy and safety of these therapies are critical to consider. These studies also need to consider demographic factors such as age, race, and sex in patient groups receiving therapies, as the outcomes may vary depending on an individual’s immune system. These therapies require critical analysis of the methodologies employed.
The long-term safety and efficacy of regenerative techniques like PRP remain critical areas of investigation due to mixed outcomes and challenges with existing therapies. Reports on PRP use in orthopaedics showed variable results, with some studies showing benefits like pain reduction and functional improvement, but the evidence base remains limited. Despite its growing clinical use, there is a significant lack of high-quality prospective randomised studies to confirm longterm efficacy and safety.71 The American Academy of Orthopaedic Surgeons (AAOS) highlights the need for rigorous biological characterisation of PRP preparations, as standardisation is essential for reliable treatment protocols. Variability in PRP preparation methods contributes to inconsistent outcomes, making it difficult to assess the therapy’s long-term effectiveness.72 The heterogeneity in PRP
preparation techniques results in variable concentrations of bioactive molecules which can impact efficacy.
Stem cell therapies offer a cellular component that directly participates in tissue regeneration compared to PRP, which primarily focuses on growth factor-mediated effects. However, the safety profiles of MSC therapies raises concerns, including risks of tumour formation and immune reactions to allogeneic MSCs.73 A systematic review of umbilical cord-derived Wharton’s Jelly as an MSC source also shows the lack of robust clinical data on safety and efficacy.74 Patient responses to therapies like PRP and MSCs are highly variable, with documented risks such as infection and adverse reactions to injected materials.71,72 Large-scale, randomised trials are essential to establish the long-term safety and efficacy of MSCs and other regenerative treatments.75,76 The current lack of robust evidence limits the ability of orthopaedic surgeons to confidently recommend these therapies for widespread clinical use.77
ACI has been recognised as an effective treatment for full-depth chondral defects, particularly in the knee. Long-term studies show that ACI can provide lasting clinical improvement, but its success depends on factors like patient age and activity level, with younger patients often requiring more durable solutions. Challenges with ACI include the risk of chondrocyte dedifferentiation during in vitro expansion, which may affect cartilage quality.78 The procedure is complex, requiring skilled surgery and careful patient selection to achieve the best outcomes.79 Biomimetic scaffolds, made from materials like collagen and hydroxyapatite, have shown promise in enhancing cartilage repair by supporting cell attachment and growth. While these scaffolds can aid osteochondral regeneration, their longterm effectiveness is unclear, as studies report mixed outcomes and highlight the need for further research. Additionally, BMPs have shown potential in promoting bone healing and cartilage regeneration, but their role in improving ACI outcomes still needs to be fully explored. Some studies of BMPs observed potential
complications, including ectopic bone formation and inflammatory responses, which requires careful consideration for long-term results. Application of iPSCs offer a promising approach for generating chondrocytes for cartilage repair, but their long-term safety and efficacy remain uncertain. Concerns include the potential for tumour formation and the stability of differentiated cells.73 Since iPSCs can be derived from a patient’s own cells, they reduce the risk of immune rejection.
A critical analysis of the methodologies employed in the studies reveals several limitations that warrant consideration. One key issue is the lack of standardised protocols for PRP preparation, which contributes to variability in treatment outcomes. The study of Gholami et al.80 highlighted that variations in PRP preparation methods, such as single versus double spinning techniques, differences in platelet concentrations, and the inclusion of coagulants, can significantly influence treatment efficacy. Similarly, Zavarro et al.71 emphasised the importance of thorough biological characterisation of PRP, recommending adherence to guidelines like the Minimum Information for Studies Evaluating Biologics in Orthopaedics (MIBO) to enhance the reliability of study findings. The absence of such standardisation across various studies complicates the interpretation of results and limits the ability to draw definitive conclusions regarding the effectiveness of PRP in orthopaedic applications.
Demographic factors significantly influence the applicability of findings from PRP studies. Many trials focus on specific groups, such as professional athletes, which may not represent the broader population undergoing orthopaedic procedures. For instance, Bubnov et al.81 studied ultrasoundguided PRP injections in professional athletes, but these results may not be applicable to older adults or individuals with comorbidities. Some studies have relatively small sample sizes, raising concerns about the statistical validity and robustness of their conclusions. Growth factors in PRP, such as PDGF and VEGF, interact in complex ways to enhance healing in injuries
and surgeries. These effects can vary widely due to the multidimensional nature of their activity.19,82 The variability in outcomes, combined with limited demographic diversity and small sample sizes, challenges the ability to generalise PRP therapies across diverse patient populations.
Many research studies exhibit methodological limitations, particularly regarding follow-up duration and the outcome measures employed. Several investigations focused on short-term outcomes, which may not accurately reflect the long-term benefits or risks of PRP interventions. Murrell et al.83 emphasise that the existing evidence often lacks comprehensive long-term follow-up data, which is crucial for assessing the sustained efficacy of these treatments. Additionally, the reliance on subjective outcome measures, such as patientreported pain scores, introduces potential bias and variability in evaluating treatment success. As noted by Jacobs et al.84 adopting a more standardised approach to outcome measurement is essential to compare across studies and improving the overall quality of evidence. Addressing these methodological limitations must be considered to enhance the validity and applicability of research findings.
The regulatory and approval processes for emerging regenerative therapies, especially involving biological products like stem cell therapies and gene therapies, can be very lengthy and complex. They require extensive data on safety and efficacy for approval, which can cause delays in the process.85.86 The need for alignment between regulatory processes and reimbursement strategies is critical, and regulatory bodies must facilitate the integration of these therapies into clinical practice. To overcome these hurdles in the process, regulatory bodies can apply pathways to allow conditional approvals based on early, promising clinical data while also gathering long-term evidence. Establishing clear, specific guidelines tailored to regenerative therapies can reduce hurdles and ensure quicker development of therapies. Collaboration between regulators, academic researchers,
and industry stakeholders can create standardised protocols for safety, efficacy, and manufacturing processes. Accelerating the use of real-world evidence and advanced analytics can support market surveillance, enhancing trust without delaying approvals. Use of advanced analytics with real-world evidence can expedite market surveillance while maintaining timely approvals.
Cost and accessibility also pose substantial barriers to the implementation of regenerative medicine in orthopaedic surgery. The high costs of cell-based therapies and other advanced treatments limit their availability to all patients equally.86 The cost of these therapies may discourage patients and healthcare professionals from seeking them, which would limit access to potentially life-changing treatments.87
In the near future, advancements in tissue engineering, gene editing technologies such as clustered regularly interspaced short palindromic repeats (CRISPR), and 3D bioprinting may provide more personalised and effective regenerative medicine solutions.3,86 These innovations could lead to the development of tailored treatments that not only enhance the regenerative capacity of tissues but also significantly improve patient outcomes. The integration of biological, synthetic, and mechanical solutions in orthopaedic surgery is anticipated to restore function and provide better quality of life for patients with musculoskeletal conditions.83 In order to overcome current challenges and achieve the full potential of regenerative medicine, orthopaedic surgery, continued research, and stakeholder collaboration are essential.
CONCLUSION
Recent advances in stem cell therapies for orthopaedic surgery have involved deeper insights into stem cell biology, improved biomaterials, and innovative delivery methods. The integration of these advances with PRP injections has enhanced treatment outcomes due to better tissue healing and regeneration. Recent literature highlights the efficacy of umbilical cord-
derived Wharton’s jelly and other MSCs, which have emerged as promising sources for regenerative applications due to their regenerative capabilities.3,88,89 The application of orthobiologics uses a range of biologically derived materials, offering tailored solutions for bone, ligament, tendon, and cartilage healing.90,91 Innovative technologies like AI and 3D printing further enhance the precision and effectiveness of regenerative methods in orthopaedic surgery, allowing for more personalised approaches and improved outcomes.92-94
Regenerative medicine is reshaping the landscape of orthopaedic surgery by introducing innovative, biologically driven therapies that aim to repair and regenerate damaged tissues rather than merely treating symptoms. Advances in stem cell therapies, PRP, growth factors, and tissue engineering are paving the way for more effective and less invasive treatments for conditions like osteoarthritis, tendon injuries, and bone defects. While challenges related to regulatory approval, cost, and long-term clinical efficacy remain, ongoing research and technological innovations are becoming more refined, offering hope for better overall patient outcomes, with shorter
References
1. Ezquerra S et al. Functional properties of human-derived mesenchymal stem cell spheroids: a meta-analysis and systematic review. Stem Cells Int. 2021;2021:8825332.
2. Akpancar S et al. The current perspectives of stem cell therapy in orthopedic surgery. Arch Trauma Res. 2016;5(4):e37976.
3. Main B et al. Umbilical cord-derived Wharton's jelly for regenerative medicine applications: a systematic review. Pharmaceuticals (Basel). 2021;14(11):1090.
4. Tawonsawatruk T et al. Feasibility of bone marrow mesenchymal stem cells harvesting from forearm bone. Heliyon. 2021;7(7):e07639.
5. Matsushita Y et al. A wnt-mediated transformation of the bone marrow stromal cell identity orchestrates skeletal regeneration. Nat Commun. 2020;11(1):332.
6. Qing Y et al. Emilin2 marks the target region for mesenchymal cell accumulation in bone regeneration.
recovery times and improved quality of life for patients with musculoskeletal conditions.
In the near future, orthobiologics may be employed as intermediate care, placed between surgery and conservative therapies like steroid injection. Clinicians could even witness a complete change in how joint replacement is performed by shifting from ceramic and metal replacements to biological regeneration. In the future, biologic injection may be used as a preventative measure for degenerative joint conditions. While challenges in storing and rapidly growing stem cells for grafting remain, the transformative potential of regenerative medicine is exciting. It could expand the landscape of minimally invasive treatment and potentially even cure conditions that cannot be cured with current treatment options. However, the size and consistency of recent studies is still a hurdle. While enough evidence exists to support regenerative medicine techniques in specific conditions such as osteoarthritis and tendinopathy, broader evidence-based studies will be required before these treatments can be accepted as standard practice in wider clinical settings.
Inflamm Regen. 2024;44(1):27.
7. Li C et al. An urgent demand for novel, safe cell sources for musculoskeletal regeneration. Med One. 2018;DOI:10.20900/mo.20180010.
8. Jevons L et al. Augmentation of musculoskeletal regeneration: role for pluripotent stem cells. 2018;13(2):189206.
9. Lan T et al. Induced pluripotent stem cells can effectively differentiate into multiple functional lymphocyte lineages in vivo with negligible bias. Stem Cells Dev. 2016;25(6):462-71.
10. Sanjurjo‐Rodríguez, C et al. Versatility of induced pluripotent stem cells (ipscs) for improving the knowledge on musculoskeletal diseases. Int J Mol Sci. 2020;21(17):6124.
11. Swartz E et al. A novel protocol for directed differentiation of c9orf72associated human induced pluripotent stem cells into contractile skeletal myotubes. Stem Cells Transl Med. 2016;5(11):1461-72.
12. Verma R et al. Factors affecting the quantity and quality of platelet-rich
plasma and platelet-derived growth factor-bb: an observational study. 2021;04:67-70.
13. Everts P et al. Platelet-rich plasma: new performance understandings and therapeutic considerations in 2020. Int J Mol Sci. 2020;21(20):7794.
14. Melnikov DV et al. Effect of cryoprocessing on platelet-rich autoplasma preparations. Sovrem Tekhnologii Med. 2021;12(6):54-60.
15. Zhang J et al. Hgf mediates the antiinflammatory effects of prp on injured tendons. PLoS One. 2013;8(6):e67303.
16. Efendieva Z et al. Hysteroscopic injections of autologous endometrial cells and platelet-rich plasma in patients with thin endometrium: a pilot randomized study. Sci Rep. 2023;13(1):945.
17. Sarban S et al. The positive impact of platelet-derived growth factor on the repair of full-thickness defects of articular cartilage. Eklem Hastalik Cerrahisi. 2019;30(2):91-6.
18. Beitia M et al. Action of platelet-rich plasma on in vitro cellular bioactivity:
more than platelets. Int J Mol Sci. 2023;24(6):5367.
19. Chellini F et al. Platelet-rich plasma prevents in vitro transforming growth factor-β1-induced fibroblast to myofibroblast transition: involvement of vascular endothelial growth factor (vegf)-a/vegf receptor-1-mediated signaling†. Cells. 2018;7(9):142.
20. Kelc R et al. Platelet-rich plasma, especially when combined with a TGF-β inhibitor promotes proliferation, viability and myogenic differentiation of myoblasts in vitro. PLoS One. 2015;10(2):e0117302.
21. Cai Y et al. Sodium hyaluronate and platelet-rich plasma for partialthickness rotator cuff tears. Med Sci Sports Exerc. 2019;51(2):227-33.
22. Tan Y et al. Augmenting tendon and ligament repair with platelet-rich plasma (PRP). Muscles Ligaments Tendons J. 2013;3(3):139-49.
23. Centeno C et al. Safety and complications reporting on the reimplantation of culture-expanded mesenchymal stem cells using autologous platelet lysate technique. Curr Stem Cell Res Ther. 2010;5(1):8193.
24. O’Dowd A. Update on the use of platelet-rich plasma injections in the management of musculoskeletal injuries: a systematic review of studies from 2014 to 2021. Orthop J Sports Med. 2022;10(12):23259671221140888.
25. Chen T et al. Biological effects and molecular mechanisms of plateletrich plasma on periodontal bone regeneration. Trends J Sci Res. 2022;1(1):16-26.
26. Anitua E et al. Platelet-rich plasma to improve the bio-functionality of biomaterials. BioDrugs. 2013;27(2):97111.
27. Albanese A et al. Platelet-rich plasma (prp) in dental and oral surgery: from the wound healing to bone regeneration. Immun Ageing. 2013;10(1):23.
28. Fernandez-Moure J et al. Plateletrich plasma: a biomimetic approach to enhancement of surgical wound healing. J Surg Res. 2017;207:33-44.
29. Pavlović V et al. Platelet rich plasma: a short overview of certain bioactive components. Open Med (Wars). 2016;11(1):242-7.
30. Mithoefer K et al. Clinical efficacy of the microfracture technique for articular cartilage repair in the knee: an evidence-based systematic analysis. Am J Sports Med. 2009;37(10):2053-63.
31. Harris JD et al. Autologous
chondrocyte implantation: a systematic review. J Bone Joint Surg Am. 2010;92(12):2220-33.
32. Deng Y et al. 4D printed shape memory polyurethane-based composite for bionic cartilage scaffolds. ACS Appl Polym Mater. 2023;5(2):1283-92.
33. Bhattacharya R et al. Novel decellularized animal conchal cartilage graft for application in human patient. J Tissue Eng Regen Med. 2019;13(1):46-57.
34. Huang Y et al. Synergistic interaction of htgf-β3 with hbmp-6 promotes articular cartilage formation in chitosan scaffolds with hadscs: implications for regenerative medicine. BMC Biotechnol. 2020;20(1):48.
35. Guo W et al. Mesenchymal stem cells in oriented plga/acecm composite scaffolds enhance structure-specific regeneration of hyaline cartilage in a rabbit model. Stem Cells Int. 2018;2018:6542198.
36. Camarero‐Espinosa S et al. Articular cartilage: from formation to tissue engineering. Biomater Sci. 2016;4(5):734-67.
37. Eldridge S et al. Agrin induces longterm osteochondral regeneration by supporting repair morphogenesis. Sci Transl Med. 2020;12(559):eaax9086.
38. Song J et al. Erk5 transmits shear force stimulation signals of chondrocyte cultured in an optimized in vitro shear force model. 2021;DOI:10.21203/rs.3.rs-208682/v1.
39. Wu Z et al. Bone morphogenetic protein‐2 against iliac crest bone graft for the posterolateral fusion of the lumbar spine: a meta‐analysis. Int J Clin Pract. 2021;75(4):e13911.
40. Lykissas M, Gkiatas I. Use of recombinant human bone morphogenetic protein-2 in spine surgery. World J Orthop. 2017;8(7):531-5.
41. Behr B et al. A comparative analysis of the osteogenic effects of BMP-2, FGF-2, and VEGFA in a calvarial defect model. Tissue Eng Part A. 2012;18(910):1079-86.
42. Hsu W et al. Improving the clinical evidence of bone graft substitute technology in lumbar spine surgery. Global Spine J. 2012;2(4):239-48.
43. Durham E et al. Optimizing bone wound healing using bmp2 with absorbable collagen sponge and talymed nanofiber scaffold. J Transl Med. 2018;16(1):321.
44. Baron E et al. Postoperative cyst associated with bone morphogenetic protein use in posterior and transforaminal lumbar interbody fusion
managed conservatively: report of two cases. Cureus. 2016;8(2):e485.
45. Agrawal V et al. A review on carrier systems for bone morphogenetic protein‐2. J Biomed Mater Res B Appl Biomater. 2017;105(4):904-25.
46. Chen C et al. Enhanced osteoinductivity of demineralized bone matrix with noggin suppression in polymer matrix. Adv Biol (Weinh). 2021;5(1):e202000135.
47. Sharmin F et al. Large scale segmental bone defect healing through the combined delivery of vegf and bmp‐2 from biofunctionalized cortical allografts. J Biomed Mater Res B Appl Biomater. 2019;107(4):1002-10.
48. Park S et al. Three‐dimensionally printed polycaprolactone/beta‐tricalcium phosphate scaffold was more effective as an rhbmp‐2 carrier for new bone formation than polycaprolactone alone. J Biomed Mater Res A. 2021;109(6):840-8.
49. Proffen B et al. Electron beam sterilization does not have a detrimental effect on the ability of extracellular matrix scaffolds to support in vivo ligament healing. J Orthop Res. 2015;33(7):1015-23.
50. Randelli F et al. Effect of a collagen-based compound on morpho-functional properties of cultured human tenocytes. Cells. 2018;7(12):246.
51. Wang J, Nirmala X. Application of tendon stem/progenitor cells and platelet-rich plasma to treat tendon injuries. Oper Tech Orthop. 2016;26(2):68-72.
52. Zhang J, Wang J. Platelet-rich plasma releasate promotes differentiation of tendon stem cells into active tenocytes. Am J Sports Med. 2010;38(12):2477-2486.
53. Chen L et al. Tendon derived stem cells promote platelet-rich plasma healing in collagenase-induced rat achilles tendinopathy. Cell Physiol Biochem. 2014;34(6):2153-68.
54. Chen L et al. Synergy of tendon stem cells and platelet-rich plasma in tendon healing. J Orthop Res. 2011;30(6):991-7.
55. Jackson J et al. In vitro analysis of the effect of flightless I on murine tenocyte cellular functions. J Orthop Surg Res. 2020;15(1):1-10.
56. Liu M et al. Role of pulsed electromagnetic fields (PEMF) on tenocytes and myoblasts-potential application for treating rotator cuff tears. J Orthop Res. 2017;35(5):95664.
57. Li X et al. Experimental application of bone marrow mesenchymal stem
cells for the repair of intervertebral disc annulus fibrosus. Med Sci Monit. 2016;22:4426-30.
58. Yang H et al. TGF-βl suppresses inflammation in cell therapy for intervertebral disc degeneration. Sci Rep. 2015;5:13254.
59. Ma T et al. Decellularized nucleus pulposus matrix/chitosan hybrid hydrogel combined with nucleus pulposus stem cells and GDF5-loaded microspheres for intervertebral disc degeneration prevention. Mol Med. 2024;30(1):7.
60. Zhu G et al. Exosomal MATN3 of urine‐derived stem cells ameliorates intervertebral disc degeneration by antisenescence effects and promotes npc proliferation and ecm synthesis by activating TGF-β. Oxid Med Cell Longev. 2021;2021:5542241.
61. Liang W et al. Mechanism of action of mesenchymal stem cell-derived exosomes in the intervertebral disc degeneration treatment and bone repair and regeneration. Front Cell Dev Biol. 2022;9:833840.
62. Beiranvand S, Hasanzadeh-Kiabi F. Application of bone morphogenetic protein in spinal fusion surgery. IntechOpen. 2022;DOI:10.5772/ intechopen.96883.
63. Wang R et al. Efficacy of plateletrich plasma containing xenogenic adipose tissue-derived stromal cells on restoring intervertebral disc degeneration: a preclinical study in a rabbit model. Pain Res Manag. 2019;2019:6372356.
64. Wang S et al. Is exclusion of leukocytes from platelet-rich plasma (PRP) a better choice for early intervertebral disc regeneration? Stem Cell Res Ther. 2018;9(1):199.
65. Wu T et al. Systematic analysis of hip-preserving treatment for early osteonecrosis of the femoral head from the perspective of bibliometrics (2010–2023). J Orthop Surg Res. 2023;18(1):959.
66. Obeid B. Orthopedic joint preservation: a comprehensive review. Adv Surg Sci. 2024;12(1):11-22.
67. Chen B et al. Clinical comparative trial of arthroscopic debridement combined with PRP therapy versus pure PRP therapy for knee joint: a clinical comparative trial. Research Square [Preprint]. 2024;DOI:10.21203/ rs.3.rs-4085752/v1.
68. Vinski D. Combination of stem cell & PRP therapy in healthy aging for osteoarthritis. J World Sci. 2024;3(2):142-54.
69. Wang D. Cell membrane vesicles derived from hBMSCs and hUVECs enhance bone regeneration. Bone Res. 2024;12(1):23.
70. Fu L et al. Up-regulation of foxd1 by yap alleviates senescence and osteoarthritis. PLoS Biol. 2019;17(4):e3000201.
71. Zavarro A et al. The top 100 most cited articles on platelet-rich plasma use in regenerative medicine-a bibliometric analysis-from the ESSKA orthobiologic initiative. Bioengineering (Basel). 2022;9(10):580.
72. Acosta-Olivo C et al. Investigation of the association between the acute ankle injury caused by fall from own height and body mass index. J Foot Ankle Surg. 2019;58(2):288-90.
73. Wyles CC et al. Mesenchymal stem cell therapy for osteoarthritis: current perspectives. Stem Cells Cloning. 2015;8:117-24.
74. Main BJ et al. Umbilical cord-derived wharton’s jelly for regenerative medicine applications in orthopedic surgery: a systematic review protocol. J Orthop Surg Res. 2020;15(1):527.
75. Dias I et al. Mesenchymal stem cell studies in the goat model for biomedical research-a review of the scientific literature. Biology (Basel). 2022;11(9):1276.
76. Berebichez-Fridman R et al. The holy grail of orthopedic surgery: mesenchymal stem cells—their current uses and potential applications. Stem Cells Int. 2017;2017:2638305.
77. Dulić O et al. In step with contemporary trends-stem-celltherapy as a key driver of regenerative orthopedics at the clinical center of vojvodina - preliminary data for the treatment of knee osteoarthritis and osteochondral lesions. Med Pregl. 2016;69(suppl 1):77-84.
78. Teixeira L et al. High throughput generated micro-aggregates of chondrocytes stimulate cartilage formation in vitro and in vivo. Eur Cell Mater. 2012;23:387-99.
79. Vonk L et al. Role of matrix-associated autologous chondrocyte implantation with spheroids in the treatment of large chondral defects in the knee: a systematic review. Int J Mol Sci. 2021;22(13):7149.
80. Gholami M et al. A systematic review and meta-analysis of the application of platelet rich plasma in sports medicine. Electron Physician. 2016;8(5):2325-32.
81. Bubnov R et al. Ultrasound guided injections of platelets rich plasma for muscle injury in professional athletes.
comparative study. Med Ultrason. 2013;15(2):101-5.
82. Oudelaar B et al. Concentrations of blood components in commercial platelet-rich plasma separation systems: a review of the literature. Am J Sports Med. 2019;47(2):479-87.
83. Murrell W et al. Regenerative treatments to enhance orthopedic surgical outcome. PM R. 2015;7(4 Suppl):S41-52.
84. Jacobs A et al. Current state of platelet-rich plasma in the treatment of rheumatic disease: a retrospective review of the literature. Curr Rheumatol Rev. 2023;19(4):400-7.
85. Davies B et al. A quantitative, multinational and multi-stakeholder assessment of barriers to the adoption of cell therapies. J Tissue Eng. 2017;8:2041731417724413.
86. Sabesan V et al. Regenerative medicine: what can it do for me?. Int J Complement Altern Med. 2020;13(6):244-50.
87. Husted R et al. Perceived facilitators and barriers among physical therapists and orthopedic surgeons to preoperative home-based exercise with one exercise-only in patients with severe knee osteoarthritis: a qualitative interview study nested in the quadx-1 trial. medRxiv. 2020;DOI:1 0.1101/2020.01.22.20018416.
88. Liang W et al. Current advancements in therapeutic approaches in orthopedic surgery: a review of recent trends. Front Bioeng Biotechnol. 2024;12:1328997.
89. Gupta A et al. Umbilical cord-derived wharton’s jelly for regenerative medicine applications. J Orthop Surg Res. 2020;15(1):49.
90. Sezgin EA, Atik OŞ. Are orthobiologics the next chapter in clinical orthopedics? A literature review. Eklem Hastalik Cerrahisi. 2018;29(2):110-6.
91. Barr S et al. Developmental perspective on regenerative medicine: an update. Sci Insights. 2019;2:1-7.
92. Jeyaraman M et al. Leveraging artificial intelligence and machine learning in regenerative orthopedics: a paradigm shift in patient care. Cureus. 2023;15(11):e49756.
93. Jain M et al. Impact of 3D printing on orthopedic surgery in India: has the technology really arrived. J Orthop Case Rep. 2024;14(6):1-3.
94. Nosrati H, Nosrati M. Artificial intelligence in regenerative medicine: applications and implications. Biomimetics (Basel). 2023;8(5):442.
Emerging Smart Contact Lens Technology for Wearable Biosensors and Drug Delivery:
Biomarkers in Tears
Authors: *Sotiria D. Psoma,1 Geoffrey Ndege1
1. The Open University, STEM, School of Engineering & Innovation, Walton Hall, Milton Keynes, UK *Correspondence to sotiria.psoma@open.ac.uk
Disclosure: The authors have declared no conflicts of interest.
There is a growing need for personalised medicine to manage and prevent diseases, as well as to monitor patient health continuously, even outside the hospital setting. Biosensor devices hold a huge potential in addressing this need and can aid in decentralising healthcare by offering faster disease diagnosis and prognosis. Integrating biosensors with wearables such as contact lenses has widened their scope of application and addresses some key challenges associated with other techniques, such as invasive monitoring and the need for bulky equipment. Indeed, traditional approaches tend to be invasive, such as those used for diabetes management that require regular finger pricks to obtain a blood sample to monitor glucose. In contrast, smart contact lenses use tears, which are naturally and regularly replenished. Tears are rich in biomarkers such as proteins and electrolytes, and variations in their concentration can be monitored non-invasively to offer valuable information related to the onset or progression of disease. In addition, intraocular pressure monitoring for glaucoma has been achieved using contact lenses utilising nanomaterials and microfluidics technology. With these promising successes, current researchers seek to address neurodegenerative diseases and cancer diagnosis and prognosis using contact lenses. Contact lenses can also be used as ocular drug delivery systems as they possess 10 times more drug bioavailability advantage than topical administration. By combining contact lenses with a sensing platform, a power source, an antenna, a data transmitter, and a display, smart contact lenses have become more than vision collection devices. Although considerable challenges remain to be tackled because we are still at the initial stages of this technological advancement, the number of diseases and drugs that could potentially be sensed and delivered, respectively, seems vast.
Key Points
1. Utilisation of smart contact lenses (SCL) for wearable biosensors and drug delivery can have a significant impact on personalised medicine. This paper reviews the current progress and uses of SCLs in healthcare, in combination with their challenges such as the need for non-invasive, continuous monitoring, and efficient drug delivery, potentially transforming disease management and prevention.
2. This review describes the technological innovations in the field of SCLs. The biomarkers that are present in tears and particular diagnostic, therapeutic, and prognostic applications are explained. The challenges and limitations that need to be addressed for the realisation of the full potential of SCLs in wearable biosensors and drug delivery are outlined.
3. There have been promising developments and technological innovations that reveal the strong potential of SCLs for medical applications. Overcoming the existing challenges could transform healthcare by decentralising it, making it more accessible and efficient towards precision medicine.
INTRODUCTION
The global market of contact lenses (CL) has been significantly growing in recent years. Contact lenses are worn for vision correction or cosmetic reasons, making them ideal candidates for non-invasive applications in monitoring biomarkers in tears for the diagnosis of ocular and neurodegenerative diseases.1 CLs have also been used in the medical field for drug delivery in disease treatment, besides other non-medical applications such as eye tracking during virtual reality gaming and as displays for augmented reality.2 CLs are placed on the eye’s surface in close contact with ocular fluids like tears, aqueous, and vitreous humour rich in biochemical analytes.3 The tear film provides the eye
antibacterial properties, oxygen transfer, corneal lubrication and protection, nutrition, and washes debris out. It consists of three layers: the lipid, watery, and mucin (Figure 1). Comparative studies between analyte concentrations in tears and blood have been carried out during the last decade, with the results indicating a positive correlation.4 Analytes in tears such as glucose, lactate, urea, and primary ions of electrolytes Na+, Ca2+, K+, Mg2+, and Cl- have shown a correlation with the equivalent blood levels.4 Moreover, over 50 different proteins have been detected in tears and continue to be investigated as possible biomarkers for additional disease diagnostics such as cancers and renal functioning.5
Figure 1: Structure of the tear film.
A contact lens is a thin, curved layer made from a transparent or slightly tinted soft or rigid material worn in direct contact with the cornea. CLs are classified according to the materials used and are either soft, rigid, or hybrid. Soft materials used include hydroxyethyl methacrylate (HEMA), polyacrylamide, polyethylene terephthalate, and polyvinyl alcohol;1 rigid materials are polymers like polymethyl methacrylate;
whereas hybrid CLs are a combination of soft and rigid materials as illustrated in Figure 2 Integration of microcircuits, microsensors, and other technologies like microfluidics, data transmission, micropower supply systems, and display circuits with a contact lens has led to the development of 'smart contact lenses' (SCL). Poly-HEMA hydrogels or silicones are the most popular materials used in SCLs for biomedical applications.6
The proximity of contact lenses within the tear film offers some advantages for real-time monitoring applications. This is made possible because of the continuous replenishing of tears, which contains a wealth of information about our health. CLs offer a minimally invasive option for disease monitoring compared to other options like finger pricking for blood samples.7 Alternative sources of analytes include sweat, saliva, and interstitial fluid (ISF); however, cross-contamination, for
instance, in the mouth may compromise the accuracy of the results for saliva.8
Skin irritation for smart patches in ISF applications has also been reported, pushing the frontiers of research towards tear-based biosensing.9, 10
Advances in materials science have enabled the use of nanomaterials in biosensing to detect changes at the nanoscale level and develop miniaturised transducers. These innovations may help overcome
Figure 2: Recent innovations in contact lenses in terms of materials and technology employed.
the analytical challenges of detecting low concentrations of certain molecules in tears in the future.11,12
BIOMARKERS IN TEARS
Biomarkers play a critical role in disease diagnosis, prognosis, and prediction of response to therapy. They offer essential insights into disease progression and can inform on appropriate therapeutic approaches. For a long time, biomarkers have been explored invasively through blood sample collections, although recently, tears have received attention as an alternative biomarker source. The two techniques widely used in tear sample collection are Schirmer strips and capillary tubes. The results have indicated that the concentration and composition of biomarkers often depend on the sample collection method, the tear type, and the post-processing handling procedures.13 Nonetheless, new biomarkers have been discovered for diagnostics beyond ophthalmic conditions to include neurodegenerative diseases like Parkinson’s disease, Down’s syndrome, Alzheimer’s, and dementia.14,15
Some key biomarkers that have been measured by electrochemical biosensors include glucose for diabetes, creatinine for renal function, dopamine for glaucoma, lactoferrin for keratoconus, and cortisol for neurological diseases.16 Electrochemicalbased transduction techniques are preferred for tear-based diagnostics9 as optical methods are hard to accurately quantify the concentration other than being an indicator that an analyte is present above a certain threshold.7 Tears can also be used for cancer diagnosis. Some examples of potential tear-based biomarkers include lacryglobin for colon, lung, prostate, and ovarian cancer; cystatin SA, miR-21, and miR-200c for breast cancer; and lactoferrin and cystatin C for eye tumours.17 Further investigations continue to be undertaken to identify more selective and specific biomarkers for diagnosis and early detection of other human diseases.
DIAGNOSTIC APPLICATIONS
Disease diagnosis is very important in healthcare as it provides information on the patient’s condition and informs on decisions taken to manage it. Diagnosis has always been carried out in centralised labs in hospitals and often requires complex sample preparation procedures and bulky equipment. Biosensors have enabled faster and highly sensitive alternatives. SCLs have been and continue to be investigated as potential commercial products for disease diagnosis and as drug delivery microsystems.
Diabetes
One of the diseases that has received a lot of diagnostic attention in using SCL sensing is diabetes. Increased glycaemic levels in the blood due to uncontrolled glucose metabolism results in diabetes and increases the risk of cardiovascular disease development. Other associated conditions such as diabetic retinopathy, diabetic nephropathy, and diabetic neuropathy can develop, potentially leading to lifethreatening consequences.18 This has necessitated point-of-care and self-testing glucose monitoring for effective diabetes management. A downside of blood glucose monitors is the need for a finger prick to obtain a blood sample.18
In 2014, Google (Mountain View, California, USA), in partnership with Novartis (Basel, Switzerland), started testing SCLs that were built to measure glucose levels in tears for potential use in diabetes management.19 However, the project was halted in November 2018. The developed prototype had an electrochemical sensing component, a power supply, an antenna, and a lightemitting diode encapsulated between two lens materials.5 Besides miniaturisation challenges, there have been concerns about the real-time correlation of glucose levels in tears compared to glucose levels in blood due to lag time in tear measurements, and this was the primary reason for the Google Lens project halt. However, after compensation for the lag time, a positive correlation was observed, indicating
the possibility of still using SCLs for the diagnosis and monitoring of diabetes and insulin intervention.20,21
Electrochemical transduction has been the most used technique in SCLs for glucose monitoring using enzymes such as glucose oxidase and glucose dehydrogenase, and lactate oxidase for lactate.22 Concentrations of glucose in the range of 0.01–20 mM have been reported in the literature.23 Optical methods based on nanoparticles embedded in contact lenses have also been explored, with reported linear regression values in the range of 0.1–0.6 mM.18
Glaucoma
Glaucoma is an irreversible eye disorder that results from increased intraocular pressure (IOP), which affects the optic nerve and can lead to loss of vision.24 IOP is the equilibrium between the production and outflow of aqueous humour. There are two types of glaucoma, with openangle glaucoma being the most common condition, and it results from an ineffective drainage angle in the eye hampering the outflow of aqueous humour.24 This leads to progressive elevation of IOP, which can lead to destruction of the optic nerve. The angle-closure glaucoma is not common but is often abrupt and severe and requires immediate medical attention. It occurs when the drainage angle of the eye gets blocked, leading to a sudden surge in IOP.24
Clinical IOP measurements use the Goldmann applanation tonometer, which is somewhat invasive since the device comes into close interaction with the cornea, requires an anaesthetic application, and needs to be handled by a trained professional.25 Advances in technologies such as microfluidics and biosensors are changing IOP sensing using contact lenses and can offer a continuous measurement application that promises a better understanding, taking into account that IOP varies throughout the day and depends on activity levels. The changes in the volume of liquid in microfluidic channels induced by pressure changes in the eye are monitored as an indicator of IOP.12 Compression on a holding chamber with liquid pushes the
liquid into the microfluidic channel where the volume reading is taken using an external image processor such as a digital or smartphone camera.6
Further advances using nanomaterials to monitor IOP have been reported. In 2021, a prototype SCL was developed using a transparent silver nanowire strain sensor with wireless power and communication capability.26 In vivo trials of the SCL on living rabbit eyes, validated by tonometer readings, indicated the feasibility of use in monitoring IOP of patients with glaucoma.26 Sensimed AG developed the SENSIMED Triggerfish® (Sensimed, Etagnières, Switzerland) SCL for IOP monitoring and glaucoma treatment. It is one of the companies that have received FDA approval for its SCL to be commercially used in vivo for IOP measurements,27 demonstrating viability in wider applications.
Stress
Human cortisol is a steroid hormone produced by the adrenal glands that has received significant attention as a biomarker for stress. It is excessively secreted as a response to stress and is associated with depression and anxiety.24 Immunoassay and chromatographic approaches that are used in cortisol monitoring require bulky equipment. This has necessitated the development of wearables such as soft SCLs for real-time monitoring of cortisol in tears. A SCL with a cortisol sensor, microcircuits, antenna, and capacitors was developed using a graphene-effect transistor to produce a measurable electrical signal and achieved a limit of detection of 10 pg/mL.27 Cortisol concentration in tears is about 82.76 ng/mL and increases as stress levels rise.27 Despite higher levels in blood, serum, and urine, tears offer the advantage of continuous monitoring and non-invasiveness. Electrochemical methods have shown potential in cortisol sensing with antibodies, enzymes, and molecular imprinted polymers (MIP) used as receptors, and attempts have been made for their integration into wearables like CLs.28 However, most of these explorations have been focused on human sweat and saliva among the less
invasive options regardless of the enormous potential of CLs.28-30
For instance, a sensing system using photonic hydrogel was developed exploiting MIP and antibody–antigen competitive binding and tested with sweat, while another was based on a fluorophore and aptamer competitive assay to detect cortisol.31 These principles can potentially be explored in SCLs for cortisol detection and monitoring.31,32 Given that long-term exposure to stress can trigger anxiety, depression, and cardiovascular diseases, and potentially lead to drug and substance abuse,33 monitoring and studying stress is very important. Biosensing using SCLs offers a platform for achieving this endeavour as prognostic and diagnostic tools.33
THERAPEUTIC APPLICATIONS
SCLs have been used in glucose monitoring but have also been explored for drug delivery in treating diabetic retinopathy, which is responsible for most adult blindness.1 Current treatment methods for diabetic retinopathy are highly invasive, and they either involve laser irradiation, eye injection, or surgery.16,21 However, SCLs have demonstrated the ability to release embedded therapeutic drugs at the trigger of diabetic retinopathy symptoms.6 Current research explores the possibilities of expanding the number of drugs that can be administered using SCLs. For instance, metformin used for the treatment of diabetes is commercialised as an oral drug, but ocular administration with the use of SCLs is considered for its delivery.34
CLs can also be used as drug delivery channels in the management of other ocular diseases. Most of these diseases require topical administration, with eye drops being the most common way to deliver drugs through the cornea, although ocular barriers limit the drug bioavailability to less than 5% because of the short residence time in the tear film.35 CLs entrap the medication during polymerisation or by soaking the soft lens hydrogels in the drug, and this approach increases the drug bioavailability to about 50%.35 Johnson & Johnson’s drug
delivery Acuvue Theravision CL (Johnson & Johnson, New Brunswick, New Jersey, USA) received FDA approval in 2021 as a daily disposable lens for delivery of H1antihistamine for the prevention of itch in the eyes due to allergies.35
In other cases, CLs have been explored in the treatment of dry eye disease (DED). DED is the most common ocular disease, which occurs when there is insufficient lubrication of the eyes and causes damage to the eye tissues, which may lead to loss of vision.36 CLs loaded with cyclosporin A for the treatment of DED have shown impressive outcomes, stretching the possibilities of integrating SCLs with therapeutics.36 Perhaps more drug delivery using CLs in the treatment of DED will be investigated in the future, given most of the studies are at the clinical trial stage. However, the first treatment of DED is the application of artificial tears to increase the wettability of the eyes, and hydrogel CLs, have shown potential application in the hydration of dry eyes by altering the viscosity of the hydrating solution and entrapping it in the CL to increase retention time on the surface of the eye.36,37
PROGNOSTIC APPLICATIONS
Prognosis is the likelihood of a certain condition’s occurrence or disease progression following its detection or onset. Often, prognostic models are used to utilise multivariable characteristics of individuals to help clinicians make informed decisions on the treatment course for patients. However, one profound challenge is prognostic uncertainty, where there is inadequate data or history about a patient and a lack of model validation.38 Smart biosensing CLs in real-time healthcare applications collect crucial data during diagnosis and monitoring of disease progression, which is important for prognosis and development of prognostic models. The data collected can be utilised in potential prognostic applications as seen in Figure 3.
Lately, healthcare management approaches have changed from reactive to predictive, preventive, and personalised, triggering
DED: dry eye disease; IOP: intraocular pressure.
the need for cost-effective devices and non-invasive biomaterials with minimal patient risks of complications. Traditional analytical techniques such as ELISA, mass spectroscopy, and electrophoresis assays require bulky equipment installed centrally and are time-consuming, often requiring invasive sample collection and extensive sample preparation procedures.39 Contact lenses and tears bypass most of the challenges posed by traditional approaches and provide an avenue for reliable options of prognosis outside the hospital environment. Clinical efforts have been made to identify and systematically categorise patients sharing the same risk of disease, such as cardiovascular disease, as a strategy formulation for preventive and predictive care.40 Identification of biomarkers for such diseases in tears can aid in the development of SCLs for data collection and monitoring in preventive care.
At present, some protein biomarkers like albumin can function as non-specific biomarkers, yet they offer insights into one’s ocular integrity. When high serum
albumin is detected in tears, it is an indicator of plasma leakage and denotes issues with vascular permeability.41 Although the available data concerning albumin in tears is poorly understood, it has been demonstrated that wounded eyes and those with ocular disorders exhibit higher albumin levels.41 Monitoring tear albumin can thus provide information that can help understand its role, help in assessing the general ocular health of an individual, and trigger some specific disease diagnosis.42 In DED prognosis, contact lenses could be used to monitor tear levels in the eyes as a pointer to the disease’s commencement or progression.
CHALLENGES AND LIMITATIONS
Despite the tremendous efforts to accelerate the adoption of SCLs in diagnosis, prognosis, and drug delivery in healthcare, there are still several hurdles that need to be overcome before SCLs can be fully commercialised. The challenges associated with SCLs largely touch on
Figure 3: Medical applications based on contact lenses.
the engineering materials and effective usability aspects. In terms of size, SCLs present miniaturisation challenges given the integration requirements of the wireless communication, power source, antenna, and sensing platform in such a small size as a contact lens.43 In addition, SCLs operate in the tear environment, which is everevolving and is posed with biochemical changes that may affect the attainment of clinical-grade results.44 Safety evaluation of SCLs for clinical application is lengthy, costly, and challenging given that they come into contact with the human mucosal membrane of the eye. They require animal and cytotoxicity tests, irritation, sensitivity, and implantation effect studies, which limits laboratory to commercialisation translation. Shelf life and technology limitations are other challenges that need to be overcome to achieve more clinical applications.45
The eye architecture presents design challenges whereby the SCL needs to be lightweight, maintain its transparency to serve its function, be comfortable and aesthetic to the wearer, discreet and unnoticeable to others, and limit any risks that may arise from contaminations.1 High transparency is crucial for daily use of the SCL, and a transparency rate of over 91% should be achieved, allowing for clear, natural, and unobstructed vision.46 In addition, this contributes to the integration of multiple biosensors without compromising the primary function of the contact lens, which is the provision of clear vision.1 Therefore, material selection is highly important for ensuring inherent high transparency and ensuring that the SCL does not obstruct vision; such materials are graphene and metal nanowires, and ultrathin film technology is widely used.1,47 In continuous applications, energy efficiency is paramount because the data transmission at regular intervals, the transduction mechanism that senses the biomarker-analyte interaction, and the data processing, require a lot of energy. Biofouling, which is the accumulation of foreign molecules on the surface of the sensing platform due to nonspecific binding, affects the reliability of the sensor.46 Sensor selectivity towards the
analyte is another issue that must be addressed because of interference from other similar biological molecules.8
Biomarker concentration in tears poses detection challenges. Some biomarkers are present in minute concentrations and require highly sensitive and effective detection techniques. Some biomarkers have been fronted for multiple disease detection, which makes it difficult to assign them to a specific diagnosis.48 In therapeutics, challenges have been observed with the quick release of drugs from contact lenses, and in methods that use MIPs, the stiff cross-linking of the monomer chains affects the drug release.35 Also, the effects of drug encapsulation on the contact lens on properties such as oxygen permeability and wettability need to be understood.
Finally, a thorough and multidisciplinary investigation is required regarding the importance of future longitudinal studies to assess the effectiveness of SCLs in real-world biosensors and drug delivery applications.49 Some of these challenges include biosensor’s stability and function over extended periods of wearing, avoidance of interference from other substances in tears, long-term biocompatibility of the used materials, and the integration of the biosensor into the contact lens should not compromise its transparency, flexibility, and comfort.24,49 Advanced micro-manufacturing techniques, a reliable power source without adding bulk or weight to the contact lens, and practical and user-friendly methods for reading the data are essential, including wireless communication technologies that can transmit data to external devices without causing discomfort or inconvenience to the wearer.49
PROSPECTS AND INNOVATIONS
The global market for SCLs was valued at 115 million USD in 2018, and is projected to reach 1,603.4 million USD by 2026, with a significant compound annual growth rate of 38.9%.24 Many opportunities are presented
by the emerging concept of SCLs, especially in diagnosing and monitoring different diseases. There is a need for the integration of multiple sensing platforms in one contact lens. For example, SCLs can be developed for both glycaemic control and IOP measurement.3 Initial human trials of glucose monitoring with SCLs have reported results that correlate glucose concentration in blood and tears, but they need further investigation.20 Other aspects that need exploration include therapeutic integration into SCLs, whereby, besides monitoring the variation in biomarker concentration, the drugs encapsulated in the lens can be automatically triggered and released for treatment of ocular diseases.
In terms of therapeutic applications, some ocular drugs that are poorly absorbed through the ocular membranes can be formulated into nanomicelles and nanosuspensions that can be delivered using CLs. By integrating smart sensing, these drugs can be dispersed when required by utilising, for instance, pH or analyte concentration changes.50
More research needs to be undertaken to identify and validate specific biomarkers in tears that can be used in the diagnosis of different diseases. Catecholamines can be studied for the diagnosis of stress and neurodegenerative diseases,51 and more biomarkers need to be identified for the detection of the different types of cancers. This can potentially enable the development of SCLs for those applications. Nanomaterials have also opened a new arena to address the challenges of biomarker concentrations in tears. By using nanomaterials together with other biological analytes, the sensitivity and selectivity of the sensor can be improved, making it possible for measuring concentration in the nano and picomolar ranges.52 To address the challenge of energy supply, effective wireless charging
References
1. Elsherif M et al. Wearable smart contact lenses for continual glucose monitoring: a review. Front Med (Lausanne). 2022;9:858784.
of SCLs can become feasible through wireless powering using radio frequencies in a 3D range or energy harvesting from the human body.24,43,53
CONCLUSION
SCLs have become an integral part of wearable devices, thus revolutionising disease diagnosis, prognosis, and therapeutics. As progress is being made in technological developments, so are advancements with smart wearables, including SCLs, thus addressing some current challenges with energy, miniaturisation, design, and fabrications. Research in microfluidics, materials, and pathology is opening room for the identification of more biomarkers in tears, widening the scope of diseases that can be diagnosed, and providing subsequent alternatives for drug delivery in ocular applications. In addition, adverse effects of SCLs should be significantly considered based on immunological, physiological, and mechanical factors, particularly during the selection of the materials. The innovation potential in SCLs is immense, especially in point-of-care diagnostics, personalised, and preventive healthcare management, and supporting the move towards attaining the highest level of healthcare quality. Nevertheless, we are still in the early stages of these innovations, and many challenges must be overcome before the adoption of SCLs as part of clinical techniques for quick and non-invasive diagnosis. Heightened focus should be aimed at bridging the gap between the laboratory, clinical trials, and commercially viable products for clinical applications. Overall, SCLs and wearable devices hasten the benefits that can be harnessed from the successful deployment of SCLs in not just vision correction and aesthetics but also important sensing platforms in healthcare management.
2. Xia Y et al. State-of-the-art in smart contact lenses for human machine interaction. IEEE Transactions on Human-Machine Systems. 2021;53(1):87-200.
3. Seo H et al. Smart contact lenses as wearable ophthalmic devices for disease monitoring and health management. Chem Rev. 2023;123(19):11488-558.
4. Li MS et al. Current and future perspectives on microfluidic tear analytic services. ACS Sens.
2022;7(5):1300-14.
5. de Souza GA et al. Identification of 491 proteins in the tear fluid proteome reveals a large number of proteases and protease inhibitors. Genome Biol. 2006;7(8):R72.
6. Ma X et al. Smart contact lenses for biosensing applications. Adv Intell Syst. 2021; 3(5):2000263.
7. Phan C-M. Contact lens biosensors: can we sense our tears? Contact Lens Update. 2020. Available at: https:// contactlensupdate.com/2020/02/06/ contact-lens-biosensors-can-wesense-our-tears/. Last accessed: 10 October 2024.
8. Kim J et al. Wearable biosensors for healthcare monitoring. Nat Biotechnol. 2019;37(4):389-406.
9. Tseng RC et al. Contact-lens biosensors. Sensors (Basel). 2018;18(8):2651.
10. Lin Y et al. Wearable biosensors for body computing. Adv Funct Mater. 2020;31(39):2008087.
11. Barmada A, Shippy SA. Tear analysis as the next routine body fluid test. Eye (London). 2020;34(10):1731-33.
12. Kumari M et al. Microfluidics-based nanobiosensors for healthcare monitoring. Mol Biotechnol. 2024;66(3):378-401.
13. Nättinen J et al. comparison of capillary and schirmer strip tear fluid sampling methods using SWATH-MS proteomics approach. Transl Vis Sci Technol. 2020;13:9(3):16.
14. You J et al. Tear fluid protein biomarkers. Adv in Clin Chem. 2013;62:151-196.
15. Bachhuber F et al. Diagnostic biomarkers in tear fluid: from sampling to preanalytical processing. Sci Rep. 2021;11(1):10064.
16. Liu H et al. Electrochemical sensing in contact lenses. Electroanalysis. 2022;34:227-36.
17. Nandi SK et al. Identification of tear-based protein and non-protein biomarkers: Its application in diagnosis of human diseases using biosensors. Int J Biol Macromol. 2021;193(Pt A):838-46.
18. Jeon H-J et al. Optical assessment of tear glucose by smart biosensor based on nanoparticle embedded contact lens. Nano Lett. 2021;21(20):8933-40.
19. Senior M. Novartis signs up for Google smart lens. Nat Biotechnol. 2014;32(9):856.
20. Park W et al. In-depth correlation analysis between tear glucose and blood glucose using a wireless smart contact lens. Nat Comm. 2024;15(1):2828.
21. Elsherif M et al. Wearable contact lens biosensors for continuous glucose monitoring using smartphones. ACS Nano. 2018;12(6):5452-62.
22. Kim J et al. Recent advances in smart contact lenses. Adv Mater Technol. 2020;5(1): 1900728.
23. Pankratov D et al. Tear based bioelectronics. Electroanalysis. 2016;28(6):1250-66.
24. Kazanskiy NL et al. Smart contact lenses - a step towards non-invasive continuous eye health monitoring. Biosensors (Basel). 2023;13(10):933.
25. Hosseinian H et al. A meta-analysis of wearable contact lenses for medical applications: role of electrospun fiber for drug delivery. Polymers (Basel). 2022;14(1):185.
26. Kim TY et al. Smart contact lenses with a transparent silver nanowire strain sensor for continuous intraocular pressure monitoring. ACS Appl Bio Mater. 2021;4(5):4532-41.
27. Ku M et al. Smart, soft contact lens for wireless immunosensing of cortisol. Sci Adv. 2020;6(28):eabb2891.
28. Cardinell BA et al. Toward a labelfree electrochemical impedance immunosensor design for quantifying cortisol in tears. Crit Rev Biomed Eng. 2019;47(3):207-215.
29. Sekar M et al. Review - towards wearable sensor platforms for the electrochemical detection of cortisol. J Electrochem Soc. 2020;167(6):67508.
30. Zea MB et al. Electrochemical sensors for cortisol detections: almost there. TrAC Trends Anal Chem. 2020;132:116058.
31. Semwal V et al. Study on cortisol sensing principle based on fluorophore and aptamer competitive assay on polymer optical fiber. Photonics. 2023;10(7):840.
32. Qin J et al. Photonic hydrogel sensing system for wearable and noninvasive cortisol monitoring. ACS Appl Polym Mater. 2023;5(9):7079-89.
33. Weber CJ et al. Advances in electrochemical biosensor design for the detection of the stress biomarker cortisol. Anal Bioanal Chem. 2024;416(1):87-106.
34. Keum DH et al. Wireless smart contact lens for diabetic diagnosis and therapy. Sci Adv. 2020;6(17):eaba 3252.
35. Wen X et al. Innovative advancement of contact lenses for noninvasive diagnosis and therapy: a mini review. MedComm - Biomater Appl. 2023;2(2):e40.
36. Mondal H et al. A review on dry eye disease treatment: recent progress,
diagnostics, and future perspectives. Pharmaceutics. 2023;15(3):990.
37. Li Q et al. Recent advances in hydrogels for the diagnosis and treatment of dry eye disease. Gels. 2022;8(12):816.
38. Dijkland SA et al. Validation of prognostic models: challenges and opportunities. J Emerg Crit Care Med. 2018;2:91.
39. Zhan X et al. Mass spectrometry analysis of human tear fluid biomarkers specific for ocular and systemic diseases in the context of 3P medicine. EPMA J. 2021;12(4):449-75.
40. Bongaerts V et al. From reactive to proactive preventive cardiovascular risk management in primary care: a feasibility study. European J Prev Cardiol. 2024;31(Suppl 1).
41. Runstrom G. Albumin in tears. PhD Thesis. Aston University. 2013. Available at: https://research.aston. ac.uk/en/studentTheses/albumin-intears. Last accessed: 11 October 2024.
42. Shimmura S et al. Albumin as a tear supplement in the treatment of severe dry eye. Br J Ophthalmol. 2003;87(10):1279-83.
43. Mirzajani H et al. Powering smart contact lenses for continuous health monitoring: recent advancements and future challenges. Biosens Bioelectron. 2022;197:113761.
44. Ray TR et al. Bio-integrated wearable systems: a comprehensive review. Chem Rev. 2019;119(8):5461–533.
45. Zhu Y et al. Lab-on-a-contact lens: recent advances and future opportunities in diagnostics and therapeutics. Adv Mater. 2022;34(24):e2108389.
46. Kim J et al. Wearable smart sensor systems integrated on soft contact lenses for wireless ocular diagnostics. Nat Comm. 2017;8(1):14997.
47. Guo S et al. Integrated contact lens sensor system based on multifunctional ultrathin MoS2 transistors. Matter. 2021;4(3):969-85.
48. von Thun und Hohenstein-Blaul N et al. Tears as a source of biomarkers for ocular and systemic diseases. Exp Eye Res. 2013;117:126-37.
49. Abdulamier AA et al. Advancements and applications of smart contact lenses: a comprehensive review. Results Eng. 2024;24:103268.
50. Zhao L et al. Therapeutic applications of contact lens-based drug delivery systems in ophthalmic diseases. Drug Deliv. 2023;30(1):2219419.
51. Kim AJ et al. Catecholamines: influence on healthy aging and the progression of neurodegenerative
diseases. Neurosci Biobehav Rev. 2024;162:105733.
52. Jino Affrald R. Nanotechnology in smart contact lenses: highlights
on sensor technologies and future prospects. Current Nanomater. 2023;8(4):361-73.
53. Sobianin I et al. Recent advances in
energy harvesting from the human body for biomedical applications. Energies. 2022;15(21):7959.
FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM