126 Platelet-Rich Plasma Applications, The Past 5 Years: A Review Article
Buontempo et al.
138 Mycosis Fungoides Palmaris et Plantaris Progressing to Complete Early-Stage Disease Improved with Phototherapy
Resuello at al.
Editorial Board
Editor-in-Chief
Dr Simone Ribero
Editorial Board
Prof Francesca Farnetani
Dr Hassan Galadari
University of Turin, Italy
University of Modena and Reggio Emilia, Italy
United Arab Emirates University, United Arab Emirates
Dr Jaishree Sharad Skinfinti Aesthetic Skin and Laser Clinic, India
Prof Alin Laurentiu Tatu
Dr Jennifer Cather
Dr Michael Gold
Dunărea de Jos University of Galati, Romania
Modern Research Associates, USA
Gold Skin Care Center, USA
Dr Vishalakshi Viswanath Rajiv Gandhi Medical College, India
Prof Des Tobin
Dr Richard Warren
University of Bradford, UK
University of Manchester, UK
Aims and Scope
EMJ is an online only, peer-reviewed, open access general journal, targeted towards readers in the medical sciences. We aim to make all our articles accessible to readers from any medical discipline.
EMJ allows healthcare professionals to stay abreast of key advances and opinions across Europe.
EMJ aims to support healthcare professionals in continuously developing their knowledge, effectiveness, and productivity. The editorial policy is designed to encourage discussion among this peer group.
EMJ is published quarterly and comprises review articles, case reports, practice guides, theoretical discussions, and original research.
EMJ also publishes 18 therapeutic area journals, which provide concise coverage of salient developments at the leading European congresses. These are published annually, approximately 6 weeks after the relevant congress. Further details can be found on our website: www.emjreviews.com
Editorial Expertise
EMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors are recognised authorities from their respective fields.
• Peer review, which is conducted by EMJ’s Peer Review Panel as well as other experts appointed due to their knowledge of a specific topic.
• An experienced team of editors and technical editors.
Peer Review
On submission, all articles are assessed by the editorial team to determine their suitability for the journal and appropriateness for peer review.
Editorial staff, following consultation with either a member of the Editorial Board or the author(s) if necessary, identify three appropriate reviewers, who are selected based on their specialist knowledge in the relevant area.
All peer review is double blind. Following review, papers are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected.
Editorial staff have final discretion over any proposed amendments.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects.
We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial.assistant@emjreviews.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in EMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
EMJ is distributed through controlled circulation to healthcare professionals in the relevant fields across Europe.
Indexing and Availability
EMJ is indexed on DOAJ, the Royal Society of Medicine, and Google Scholar®; selected articles are indexed in PubMed Central®.
EMJ is available through the websites of our leading partners and collaborating societies.
EMJ journals are all available via our website: www.emjreviews.com
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
This Publication
ISSN 2054-6211
EMJ Dermatology is published once a year. For subscription details please visit: www.emjreviews.com
All information obtained by EMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, EMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. EMJ is completely independent of the review event (EADV 2023) and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever.
Antoniou, Abigail Craig, Ada Enesco, Evan Kimber, Darcy Richards
Design Manager
Stacey Rivers
Senior Designer
Roy Ikoroha
Designer Steven Paul
Junior Designers
Dillon Benn Grove, Shanjok Gurung
Head of Sales
Robert Hancox
Senior Project Manager
Kelly Byrne
Chief Content Officer
Justin Levett
Chief Operating Officer
Dan Scott
Chief Commercial Officer
Dan Healy
Founder and Chief Executive Officer
Spencer Gore
Dear Readers,
Evgenia Koutsouki Editor
Welcome to the 2023 issue of EMJ Dermatology, bringing you all the latest updates from the European Academy of Dermatology and Venereology (EADV) Congress in Berlin, Germany. This year’s congress was characterised by a focus on climate change, in the context of healthcare and dermatology specifically. This issue covers key highlights from the congress, which include a study on the perceptions around females with acne, and data on the impact of sleep disturbances on skin health.
We are delighted to present interviews with key experts in the field, who provide insights into their careers, and discuss the themes of the EADV Congress, sociocultural dermatology, and dermato-oncology. As always, we have chosen to dive deeper into two sessions from the EADV Congress, which focus on atopic dermatitis and hair disorders.
Among the plethora of our peer-reviewed articles, you will be able to read the Editor’s pick, a review of diagnostic evaluation of hair loss, discussing history evaluation and diagnostic workup for these conditions. Other articles include a case report of systemic sclerosis manifesting post-radiotherapy, and a review of recent updates on platelet-rich plasma applications.
I would like to extend my thanks to our Editorial Board, who have offered invaluable support in selecting the articles for this issue, our contributors who have provided highly engaging content, and the peer reviewers who have elevated the quality through their insightful comments. Until next year’s issue, I do hope you enjoy our ongoing stream of content!
Contact us
Editorial enquiries: editor@emjreviews.com
Sales opportunities: salesadmin@emjreviews.com
Permissions and copyright: accountsreceivable@emjreviews.com
Reprints: info@emjreviews.com Media enquiries: marketing@emjreviews.com
Foreword
Dear Colleagues,
Welcome to our latest issue of EMJ Dermatology, featuring a range of peer-reviewed articles and interviews with field experts and European Academy of Dermatology and Venereology (EADV) board members. Also included is our review of the EADV Congress 2023, held in Berlin, Germany, from 11th–14th October. The review offers a detailed overview of the most significant highlights and content presented throughout the congress.
EMJ had the pleasure of speaking to various field experts, namely Christopher Griffiths, OBE, who shared valuable perspectives on promising advances within the fields of inflammaging and psoriasis. Furthermore, Edel O’Toole shed light on the transformative potential of biologics in various types of ichthyosis. Interviews with several EADV board members, including Thrasivoulos Tzellos, Shyam Verma, Robert Hunger, Jan-Christoph Simon, and Margarida Gonçalo, provided fantastic insight into the aims of EADV, and how the annual congress provides a platform for researchers, clinicians, and industry professionals to exchange knowledge, network, and present their latest research findings.
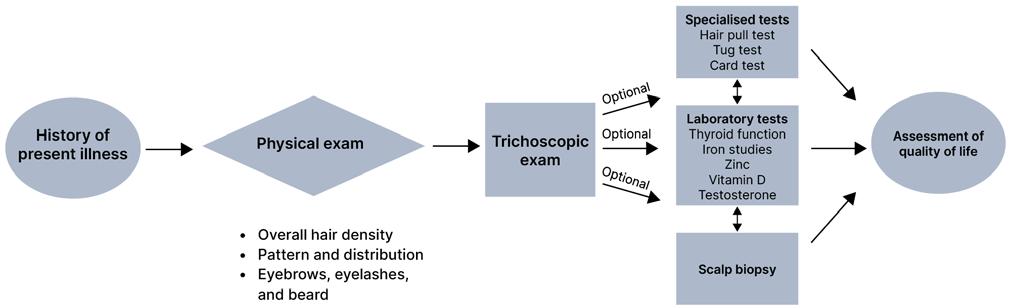
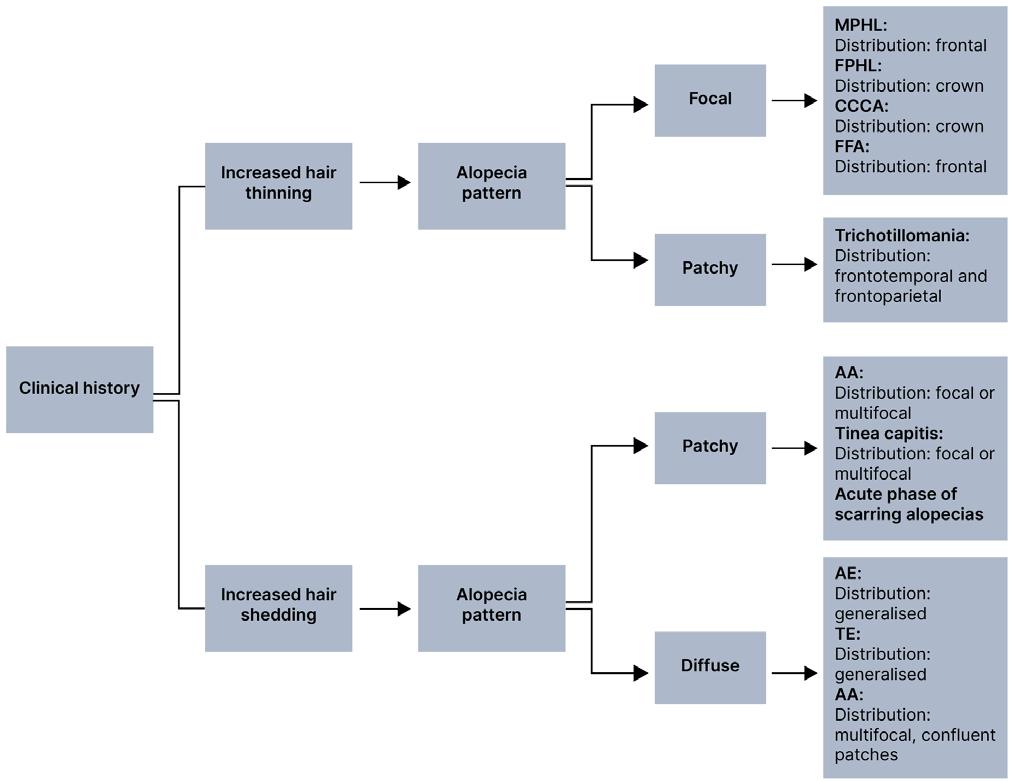
Our articles cover a diverse range of topics. Resuello et al. describe the case of a female presenting with mycosis fungoides, which was improved by full body narrowband ultraviolet B phototherapy, combined with a psoralen ultraviolet A soak for the hands and feet. Kogan et al. provide insight into the interaction between COVID-19 and cosmetic skin-fillers. Nimbark et al. offer an insightful case-report of systemic sclerosis manifesting following radiotherapy. Yacomotti et al. also present a case report, permitting the exploration of reconstructive treatment following Parry–Romberg syndrome. Minta et al. provide a systematic approach for dermatologists to use in order to accurately diagnose hair loss disorders, including clinical examination, laboratory evaluation, and specialised tests. Finally, Buontempo et al. provide an overview of platelet rich plasma's applications and evidence over the past 5 years in randomised controlled trials.
I would like to express my gratitude to all those who have made valuable contributions to this issue of EMJ Dermatology. I hope you enjoy reading, and find it insightful.
Dr Michael Gold Gold Skin Care Center, USA
EADV 2023
Review of the European Academy of Dermatology and Venereology (EADV) Congress 2023
BERLIN, Germany, was the setting for the 2023 European Academy of Dermatology and Venereology (EADV) Congress. With over 15,500 attendees, 600 speakers, and 180 sessions, the congress provided an incredible opportunity for the discussion of the latest technologies, treatments, and products in the dermatology and venereology field. EADV President, Martin Röcken, Eberhard Karl University of Tübingen, Germany, had the “tremendous pleasure” of opening this year’s congress, and he extended his sincere gratitude to the speakers and organising committee for providing a fantastic environment for networking.
Julia Welzel, University Hospital Augsburg, Germany, and President of the German Dermatological Society (DDG), warmly welcomed attendees to the congress. She outlined that in Germany, there are 6,300 active dermatologists working in 108 clinics. Of these, over 4,000 are DDG members, responsible for representing dermatology in political matters of healthcare, research, and teaching. Welzel stated that the beautiful field of dermatology faces great challenges; the incredible breadth of the field must be maintained, and dermatologists are compelled to inspire the brightest young talent through excellent teaching. Both are challenges the DDG actively tackles through supporting young colleagues, and promoting digital dermatology.
Welzel also encouraged participants to explore Berlin’s rich history. Specifically, the Tränenpalast, or Palace of Tears, which offers insight into how both sides of Berlin were able to establish contact under extremely challenging conditions. Berlin Underworld, a series of underground bunkers from the Cold War, and the Brandenburg Gate offer further historical context, with the hope that attendees can relate to Kennedy’s famous words “Ich bin ein Berliner” after visiting these significant landmarks.
The rest of the opening ceremony centred around climate change, its widespread impacts on humanity, and, more specifically, on healthcare. Bernd Scherer, Director of the House of World Cultures, Berlin, Germany, delivered a fascinating presentation entitled ‘The Anthropocene, A New Earth Epoch’. He began by highlighting the exponential increase in global temperatures in the last 50 years, the melting of ice in the Arctic, the death of coral reefs, and deforestation. Together, these factors result in mass migration. This poses a large question regarding the cause of climate change, with scientists analysing both socioeconomic and earth system trends indicative of a new Earth epoch. When considering each of these factors individually, for example, world population, primary energy use, water use, methane levels, surface temperature, and tropical forest loss,
each graph follows the same pattern: a period of slight increase, followed by exponential growth. Each of these increases were induced by humans, and ultimately resulted in the generation of a new epoch.
Technology and capitalist production have allowed humans to use more energy in the last 7 years than the previous 11,000 years. In addition to this, humans have single handily produced a ‘Technosphere’, weighing more than all of the biomass on Earth. It is, therefore, clear to see how humans have transformed the entire planetary system. Scherer concluded by highlighting the statistic that in 1970, the resources on planet Earth were sufficient for its population. In 2004, population growth and increasing consumption meant that 1.50 planets were required to provide sufficient resources, which rose again to 1.75 in 2019. We are, therefore, consuming this planet at an alarming rate, to the detriment of all other species.
The final talk, delivered by Diarmid CampbellLendrum, World Health Organization (WHO), Geneva, Switzerland, specifically focused on climate change in the context of healthcare. Re-emphasising the reality of climate change, and the exponential increase in temperature, disparities in the impact globally were attributed to variations in vulnerability. Unlike viruses, such as COVID-19, climate change cannot be isolated and controlled by public health measures; instead, it affects every aspect of healthcare. More recently, the impact on mental health, particularly in young people, has been a large focus for the WHO, with 45% of young people reporting that climate change has a
negative impact on their daily functioning. Campbell-Lendrum recently co-authored a paper called ‘Climate change and health: three grand challenges’, which summarised a diverse range of connections between climate change and health. The three grand challenges refer to strengthening the climate resilience and environmental stability of health systems and facilities; addressing the wide range of health impacts of climate change; and promoting the health co-benefits of climate change mitigation in other sectors. If tackled correctly, CampbellLendrum believes this could save “millions of lives.” Solutions to climate change exist across all sectors, with the largest carbon reduction possible through renewable energy, followed by agriculture. Many of these methods are already cost-saving. However, with the inclusion of global health gains as a factor, several of these solutions become more compelling. CampbellLendrum concluded by encouraging healthcare professionals to become more actively involved in the conversation surrounding climate change, specifically supporting movements such as the Fossil Fuel Non-Proliferation Treaty.
EMJ had the pleasure of participating in this congress, and looks forward to next year’s congress, held in Amsterdam, the Netherlands. The current issue of EMJ Dermatology offers summaries of the most compelling research presented during EADV 2023, alongside feature articles delving into hair disorders and atopic dermatitis. Engaging interviews with field experts are also included, featuring five EADV board members. We invite you to continue reading for more in-depth insights from this year’s congress. ●
New Study Links Microbial Dysbiosis
and Darier’s Disease
FOR the first time, cutaneous microbiome dysbiosis and its consequences in Darier’s Disease (DD) has been investigated in a study presented at the EADV Congress 2023 in Berlin, Germany. DD, also known as keratosis follicularis, is a rare genodermatosis, caused by a mutation in the ATPA2 gene, and resulting in disrupted calcium signalling and loss of keratinocyte adhesion. DD is characterised by recurrent episodes of inflammation and skin infections that are associated with malodour. This led Amar and colleagues at the Technical University of Munich, Germany, to investigate whether microbial dysbiosis could play a role in the characterisation of DD.
The study collected 1,115 swabs from 14 patients, as well as healthy volunteers who they had been matched with. Swabs were then analysed using 16S ribotyping. Microbiome changes were assessed in relation to DD malodour.
"The study collected 1,115 swabs from 14 patients, as well as healthy volunteers who they had been matched with."
Lastly, inflammation and dysbiosis signatures were explored in DD skin transcriptomes.
The obtained results revealed a diseasespecific microbiome that was characterised by a loss of microbial diversity and potentially beneficial commensals.
DD lesions were dominated by inflammation associated microbes, including Staphylococcus aureus and Staphylococcus warneri, that correlated strongly with disease severity. Dysbiosis was also characterised by expansion of taxa of the Corynebacteria, Staphylococci, and Streptococci genera. These genera also had strong associations with intensity of malodour. Analysis of transcriptomes indicated upregulation of epidermal repair, inflammatory, and immune defence pathways, suggesting an immune response to the dysbiotic microbiome. A skin barrier impairment was indicated by downregulation of barrier genes such as CLDN4 and CDH4
Findings of the study outline further potential biomarkers and intervention targets, as well as highlighting the role of cutaneous dysbiosis in DD inflammation. ●
Non-melanoma Skin Cancer Kills More People than Melanoma
FINDINGS from a new study presented at the EADV Congress 2023 in Berlin, Germany, on 11th October, show that non-melanoma skin cancer (NMSC) leads to a higher number of deaths globally than melanoma, a more serious form of skin cancer. Researchers added that NMSC is underreported, and that the impact of the disease may therefore be higher than previously estimated.
Thierry Passeron, University Hospital of Nice, France, and colleagues carried out research using the World Health Organization (WHO) International Agency for Research on Cancer (IARC) to examine the overall burden of skin cancers. They found that, although NMSC is less likely to result in death than melanoma skin cancer, it is far more prevalent. NMSC accounted for 78% of all skin cancer cases (1.2 million reported cases) in 2020, leading to over 63,700 fatalities, compared with the 57,000 deaths caused by melanoma (324,635 reported cases) in the same year. The researchers added that, “as alarming as these figures are, they may, in fact, be underestimated. NMSC is often underreported in cancer registries, making it challenging to understand the true burden.”
"NMSC
is often underreported in cancer registries, making it challenging to understand the true burden."
Additionally, the team was able to identify the specific population groups who were more at risk of developing skin cancers, including people who work outside, organ transplant recipients, and those with the hereditary skin condition xeroderma pigmentosum. A higher incidence of skin cancer was found in fair-skinned and elderly populations in the USA, Germany, UK, France, Australia, and Italy; however, countries with a high proportion of dark phenotypes were not immune to skin cancer-related fatality either.
The authors concluded that spreading awareness that melanoma is not the only potentially fatal skin cancer is vital, and that effective strategies are needed to reduce the fatalities associated with all skin cancers, tailored to at-risk populations. They add that it is important to note that those with melanin-rich skin are also at risk of dying from NMSC, and more interventions are needed to stop progression of the disease as early as possible. ●
The Burden of Female Adult Acne
ACNE, especially in adult females, significantly impacts the way individuals are perceived, according to data presented at the EADV Congress 2023. The last decade has seen a worldwide increase in acne among females. This condition has been associated with serious consequences, such as low self-esteem, psychological impact, social isolation, and depression, due to the perception of pejorative physical characteristics. Marek Jankowski, Nicolaus Copernicus University, Toruń, Poland, assessed how different anatomical variants of acne affected natural gaze patterns and social perception.
Eye movements of 245 participants were tracked while they viewed images of females with neutral and emotional faces with clear skin, and clinically relevant anatomical variants of acne. Participants had to rate for acne-related visual disturbance and valence intensity. A further 205 participants were asked to rate personality traits of the individuals through an online survey.
Results showed that faces with acne were perceived as significantly less attractive (difference: 1.1593; 95% confidence interval [CI]: 1.0191–1.2995), less trustworthy (difference: 0.3549; 95% CI: 0.2260–0.4838), less confident (difference: 0.9573; 95% CI: 0.7853–1.1293), less successful (difference: 0.6220; 95% CI: 0.4994–0.7445), and less dominant (difference: 0.9086; 95% CI: 0.7495–1.0675). The team noted that female acne around the U-zone, including the jawline, mouth, and chin, was considered the most visually disturbing, and received the lowest attractiveness score. Participants also rated happy female faces with acne as less happy than clear-skin faces.
"Participants also rated happy female faces with acne as less happy than clear-skin faces."
Lead author Jankowski stated that he has consistently seen more social challenges in adult female acne compared with adolescent acne, which was confirmed by the study.
Surprisingly, generalised acne, covering a larger area with more lesions, was associated with higher positive ratings than acne in the U-zone.
“Treatment needs to focus on improving the quality of life of patients, not just reducing the surface area impacted by the acne. Unfortunately, this is not currently a goal when treating acne, with therapeutic guidelines still advocating for certain treatment modalities based on the number of lesions, irrespective of their location. Unsurprisingly, acne severity scores do not correlate with quality of life scores in patients with acne,” said Jankowski. ●
Improvements in Skin Cancer Detection Using Artificial Intelligence
NEW research presented at the EADV Congress 2023, in Berlin, Germany, on 12th October, indicates that skin cancer detection by artificial intelligence (AI) has improved rapidly. Researchers Kashini Andrew and Irshad Zaki, University Hospitals, Birmingham NHS Foundation Trust, UK, found that latest AI software can reach 100% detection rate for melanoma.
The study involved 22,356 patients with suspected skin cancers over the course of 2 and a half years. The third version of the AI was used to assess the patients for skin cancer. This new software used was able to identify 59 out of 59 (100%) cases of melanoma, the most serious form of skin cancer, as well as 189 out of 190 (99.5%) of all skin cancers, and 541 out of 585 (92.5%) of pre-cancerous lesions. This marks a significant improvement from the original version of the software, tested in 2021, which detected only 85.9% of melanoma, 83.8% of all skin cancers, and 54.1% of pre-cancerous lesions.
Andrew and Zaki noted that their findings are encouraging for the future of cancer detection using AI, commenting:
“The latest version of the software has saved over 1,000 face-to-face consultations in the secondary care setting between April 2022 and January 2023, freeing up more time for patients that need urgent attention”. They add, however, that AI should not be used as a standalone tool for detection without the support of a consultant dermatologist. This need to have appropriate clinical oversight of the AI was demonstrated when one case of base cell carcinoma was missed, out of 190, and later picked up on by a dermatologist ‘safety net’.
"The latest version of the software has saved over 1,000 face-to-face consultations in the secondary care setting."
“Further research with appropriate clinical oversight may allow the deployment of AI as a triage tool,” added Andrew. “However, any pathway must demonstrate cost-effectiveness, and AI is currently not a standalone tool in dermatology. Our data shows the great promise of AI in future provision of healthcare." ●
Skin Diseases Linked to Sleep Disturbances
NEARLY half of patients with skin diseases experience sleep disturbances (42%) and reduced productivity at work (49%), suggests data from the ALL PROJECT, presented at the EADV Congress 2023. These disturbances had broad implications on patients’ quality of life.
“Our study is the first to uncover the profound impact of sleep disturbances on the physical functioning of patients with skin disease, and these findings underscore the critical need for early detection and effective management of sleep disturbances,” stated lead author Charles Taieb, European Market Maintenance Assessment (EMMA), Fontenaysous-Bois, France.
"These findings underscore the critical need for early detection and effective management of sleep disturbances."
Sleep disturbances were mainly caused by burning sensation or tingling (17%) and itching (60%). Patients also reported experiencing a feeling of fatigue as soon as they woke up more frequently than patients who do not have a skin disease (81% versus 64%), as well as tingling sensations in the eyes (58% versus 41%), drowsiness during the day (83% versus 71%), and repeated yawning (72% versus 58%). The authors encouraged healthcare providers to ask patients with skin conditions about sleep disturbance during examinations in order to better understand how skin diseases impact their lives.
The ALL PROJECT further analysed the impact of hidradenitis suppurativa, a condition that causes painful skin abscesses and scarring, and is difficult to manage. Data showed that 77% of patients with this condition feel stigmatised due to their disease, and 58% have experienced rejection from others. A further 57% reported others avoided touching them or approaching them (54%). These experiences heavily impacted patients’ self-perception, relationships, and daily lives, leading them to avoid taking selfies and
control their appearance when passing in front of a mirror.
Author Bruno Halioua, a dermatologist in Paris, France stated: “The study highlights the need for immediate action, including public education efforts to increase understanding and improved access to tailored healthcare and support services for patients with hidradenitis suppurativa.” They hope the results will encourage a more inclusive society, improving treatment adherence and reducing patient burden. ●
Prolonged Use of Ruxolitinib Cream in Vitiligo Treatment
RESEARCH regarding the efficacy of the prolonged use of ruxolitinib cream for the treatment of vitiligo in patients with limited, or no, initial response at the 6-month marker has been presented at the EADV Congress 2023. Vitiligo, which is characterised by the destruction of melanocyte cells, is a chronic autoimmune disease that leads to the depigmentation of the skin. To date, limited studies have examined the efficacy of longterm topical treatment in the disease.
Albert Wolkerstorfer, Amsterdam University Medical Center (UMC), the Netherlands, and colleagues from Canada, Germany, the USA, Poland, and France, led two randomised, doubleblinded, and vehicle-controlled Phase III studies in a cohort of adults and adolescents aged over 12 years, with non-segmental vitiligo. Patients were randomised 2:1 to apply 1.5% ruxolitinib cream twice-daily, or vehicle for a 24-week period. All patients were then able to apply 1.5% ruxolitinib cream up to Week 52 of the study.
The TRuE-V1 and TRuE-V2 studies demonstrated that the application of ruxolitinib cream resulted in improvements in the repigmentation of skin, which were stastically superior, and well tolerated at Week 24. Between the open-label period (Weeks 24–52) and long-term extension period of TRuE-V (Weeks 52–104), further
improvements in the repigmentation of facial and body skin were observed in patients who continued ruxolitinib treatment, according to Vitiligo Area Scoring Index (VASI) responses. Those patients who did not achieve a ≥90% improvement in their VASI scores by Week 52 continued to apply the cream for a further 52 weeks.
"The application of ruxolitinib cream resulted in improvements in the repigmentation of skin."
In the group who observed no facial repigmentation at Week 24, improvements in VASI scores at Weeks 52 and 104 were observed in 49 out of 63 (77.8%) and 34 out of 35 (97.1%), respectively. In both groups, 39 out of 71 patients achieved ≥75% improvement from baseline in VASI score at Week 104.
The research team reports that both of these studies highlight the significance of prolonged treatment for patients with vitiligo, even when no, or minimal, repigmentation has been reached following 6 months of treatment. ●
IL-23 p19 Inhibitors Versus Other Biologics in Psoriasis
IL-23 p19 inhibitors have the highest drug survival, according to research presented at the EADV Congress 2023. Zenas Yiu, Division of Musculoskeletal and Dermatological Sciences, University of Manchester, UK, and colleagues compared the drug survival of guselkumab and risankizumab, two IL-23 p19 inhibitors, with other biologics for psoriasis.
Using the data collected from the British Association of Dermatologists Biologic and Immunomodulators Register (BADBIR) from November 2007–June 2023, the researchers measured discontinuation due to adverse effects or ineffectiveness after exposure to specific biologics. The study included 11,877 patients with 19,034 treatment courses, with a median followup of 2.3 years. A total of 6,815 patients were exposed to adalimumab, 5,639 to ustekinumab, 3,051 to secukinumab, 1,072 to ixekizumab, and 367 to brodalumab, while 1,258 were exposed to guselkumab and 832 to risankizumab.
Results show that patients treated with the IL-23 p19 inhibitors had the highest drug
"Researchers
survival, while adalimumab had a lower survival compared for effectiveness with ustekinumab. While secukinumab, ixekizumab, and brodalumab had a similar drug survival earlier when compared with ustekinumab, they had lower drug survival during follow-up.
At 1 year, the unadjusted survival functions for safety were 0.91 for adalimumab, ixekizumab, and brodalumab; 0.94 for ustekinumab; and 0.93 for secukinumab. After the same amount of time, these safety survival functions were 0.95 for guselkumab and 0.97 for risankizumab.
This study included the largest cohort of patients with psoriasis on IL-23 p19 inhibitors. It shows that guselkumab and risankizumab had the highest drug survival in regard to safety and effectiveness, and their drug survival was similar. The researchers believe that dermatologists should take these findings into consideration when treating patients with psoriasis who value treatment effect longevity, and who are due to start biologic therapy. ●
measured discontinuation due to adverse effects or ineffectiveness after exposure to specific biologics."
AN INFORMATIVE session exploring the pathogenesis and diagnosis of atopic dermatitis (AD) was presented on 12th October at the European Academy of Dermatology and Venereology (EADV) Congress 2023. The session was chaired by Patrick Brunner, Icahn School of Medicine at Mount Sinai, New York, USA, and Kilian Eyerich, University of Freiburg, Germany, who delved into how to identify the disease, who is affected by it, and how it may often be mistaken for other skin conditions.
IMMUNOPATHOGENESIS AND DISEASE STRATIFICATION
Eyerich began his presentation by explaining that although the four primary factors in the pathogenesis of atopic dermatitis (AD) are understood (these are exaggerated Type 2 immunity, microbiome alterations, an impaired epidermal barrier, and neuroimmunology), the extent to which the leading factor of AD pathogenesis can be identified in an individual patient is still under discussion. Type 2 immunity is dominant throughout each stage of AD, including lichenified and chronic lesions, with Type 2 immune cells driving the disease, despite discussions of a switch to other T helper cell subsets in the past. Despite its current popularity in dermatology, microbiome research has not seen any significant developments since 2012, and it is still uncertain whether microbial decolonisation is the first step in developing AD. An impaired epidermal barrier, caused by filaggrins and other genetic factors, as well as the neuro-immune axis, are also potential factors which drive inflammation and epiphenomena.
Recent research has increasingly focused on whether there are meaningful endotypes of AD, and how to identify them.
"Recent
Eyerich presented several cases involving patients who suffered an exacerbation of their AD when exposed to pollen in a pollen exposure chamber, their skin showing clear signs of inflammation. This research then allowed dermatologists to ask the question of whether they could apply systemic immunotherapy in order to eventually ‘switch off’ the inflammatory activity of AD. In order to identify meaningful endotypes of AD that may be improved using immunotherapy, two approaches are primarily taken: clustering based on meaningful outcomes and hypothesisfree clustering. The first involves the risk factors predicting the development of comorbidities, and Eyerich gave the example of filaggrin mutations and IgE in the pollen allergy cases. Further analysis on the roles of ethnicity and age in AD development demonstrated that there may indeed be ethnic differences in AD; however, the clinical significance of this is still unknown. The second approach, hypothesis-free clustering, involves taking AD datasets and attempting to identify different endotypes based on machines and clustering. Studies suggest that the integration of clinical, phenotypic, and molecular data over time may result in the ability to identify endotypes of AD, concluded Eyerich, adding that “the methods are in place; what we need are the datasets.”
research has increasingly focused on whether there are meaningful endotypes of AD, and how to identify them."
ATYPICAL MANIFESTATIONS AND DIFFERENTIAL DIAGNOSIS
The atopic march, a concept detailing the ways in which an individual would have AD or another skin disease early in life, and as a result of sensitisation via the skin would go on to develop food allergy, followed later by asthma and rhinitis, is now known to be outdated and inaccurate, explained Brunner. The concept is now better described as an atopic clustering, where an individual can move from one disease to the other, and can have a propensity to develop certain comorbidities; however, this is not the case with the former sequence of events. AD can be classified into high serum IgE and normal serum IgE, with the former being easier to diagnose with atopic comorbidities.
There is a wide range of differential diagnoses that can appear at the same time as AD, or alternatively can mimic the condition, as discussed in the session. AD is identified by a strong Type 2 immune activation across all populations that have been analysed, Brunner reiterated, which is what distinguishes it from other diseases. Additionally, the reaction of a patient to dupilumab, a targeted treatment known to block Type 2 inflammation, is an indicator of AD. Those who do not respond to the treatment likely have a different disease with similar symptoms. Other diseases associated with AD discussed included chronic nodular prurigo, which is difficult to diagnose and often appears to be unrelated to AD; however, it does
respond to dupilumab. Mycosis fungoides, a form of cutaneous T cell lymphoma, and a common differential diagnosis of AD, was also explored, due to its symptoms appearing highly similar, not only to AD but to other skin conditions, such as vitiligo.
ATOPIC DERMATITIS IN CHILDREN VERSUS ADULTS
The increasing number of cases of lifetime or adult-onset AD in developed countries suggests that AD is not a paediatric disease, but a lifelong illness with different phenotypic expressions, according to Pedro Mendes-Bastos, Hospital CUF Descobertas, Lisbon, Portugal. This calls for further study into the differences between paediatric and adult AD, and their differential diagnoses. Mendes-Bastos described a 2015 study where peripheral blood cytometry was used to analyse adults and children with AD, compared with healthy controls. The results demonstrated that paediatric patients with AD had a T helper 1/T helper 2 imbalance, with decreased T helper 1 cytokine production, whereas adults with AD had higher levels of IL-22 and IL-17A cytokines in T cells. This study shows the ways in which the different types of AD might present.
However, it was noted that age of onset is potentially a more valuable metric to use when analysing AD cases, as opposed to the age of the patient.
"There is a wide range of differential diagnoses that can appear at the same time as AD, or alternatively can mimic the condition."
Research has shown that there are different characteristics and comorbidities associated with adult-onset AD compared with paediatriconset AD, which may further our understanding of increasing AD incidences in adults. This would allow dermatologists to categorise the types of AD into two distinct endophenotypes. MendesBastos concluded his section of this session with a call for further research into the differences between adult-onset and paediatric-onset AD.
HEAD AND NECK ATOPIC DERMATITIS
Presented by Giovanni Damiani, University of Milan, Italy, and Case Western Reserve University, Cleveland, Ohio, USA, the final presentation focused on dupilumab-resistant head and neck AD, as well as head and neck AD, which flares during therapy. Damiani reported that only one in four patients react positively to dupilumab, a number that could be improved by switching to JAK inhibitors, such as abrocitinib or upadacitinib, which have the ability to turn down Type 1 and Type 2 cytokines. There are several factors that must be considered when switching the treatment for people with head and neck AD.
Several conditions appear clinically similar to head and neck AD, such as dupilumab-associated red face, dupilumab-driven photosensitivity, and allergic dermatitis. Damiani analysed each of these, looking into the ways in which head and neck AD is linked to each, and how dupilumab treatment triggers reactions in each disease. He concluded his talk by explaining the ways in which, in some of these conditions, microorganisms may form a robust biofilm that is resistant to antifungals and antimicrobials. A deeper analysis into the subject may develop these ideas and allow us to better understand the reasons for which AD may often be dupilumabresistant, and how this may be combatted.
The session ended with questions from the audience and from fellow speakers. This session highlighted the various developments within the field of AD, underlining the complexity of the disease along with its similarity and connections to several other skin conditions. Even though understanding of diagnosis and treatment has come a long way, more research is needed into the differences between endophenotypes of AD in order to treat its various forms more efficiently. ●
AN ENGAGING session at the European Academy of Dermatology and Venereology (EADV) Congress, which took place from 11th–14th October 2023, dove into a selection of hair disorders. Chaired by Ulrike Blume-Peytavi, Charité – Universitätsmedizin Berlin, Germany, and Sergio Vaño-Galván, Ramón y Cajal Hospital, Grupo Pedro Jaén Clinic, Madrid, Spain, the session offered an overview of the diagnosis and treatment of alopecia.
EVALUATING ALOPECIA
Jerry Shapiro, New York University (NYU) Langone Health, USA, presented on evaluating and diagnosing scarring alopecia. Contrary to non-scarring alopecias, where hair follicles are preserved and hair loss is potentially reversible, Shapiro explained that in the case of scarring alopecia, the hair follicles are destroyed, and hair loss is most likely permanent. This is considered a trichologic emergency, and it is imperative to commence treatment as soon as possible in order to save hair follicles. To determine the appropriate course of action, Shapiro encouraged the following approach to evaluating alopecia. The first step is to obtain a thorough clinical history, including the history of hair product use, followed by observation of the scalp with the naked eye. Shapiro then recommended performing a hair pull test to assess shedding, followed by a card test to assess regrowth. Finally, the use of a dermatoscope would provide a closer look at the scalp to check for follicular ostia, erythema, hypo- or hyperpigmentation, atrophy, hyperkeratosis, or telangiectasias.
LYMPHOCYTIC ALOPECIA
Scarring alopecias are classified into three categories. The first, lymphocytic alopecia, includes frontal fibrosing alopecia (FFA). This form of disease is usually seen in older adults, and is more common in females, although it is increasingly seen in males, explained Shapiro. The onset of disease is usually gradual, and it is rarely associated with an itch, burn, or pain. Hair shedding is variable, a pull test is positive on the edges of affected areas during active phases, and the card test shows no regrowth. It is frequently associated with alopecia of the eyebrows and band-like cicatricial alopecia involving the frontal hairline. On trichoscopy, this form presents loss of follicular ostia, perifollicular hyperkeratosis, perifollicular erythema and inflammation, and pili torti.
"In the case of scarring alopecia, the hair follicles are destroyed, and hair loss is most likely permanent."
Blume-Peytavi started by providing an overview of the management of FFA. She explained that this progressive hair loss, observed worldwide, is usually seen in post-menopausal females, but a minority of pre-menopausal females or males can be affected. It is a psychologically debilitating condition that lacks evidence for safety and efficacy of treatment; however, research around FFA is increasing. Blume-Peytavi explained that while the aetiology of FFA is unclear, a few known causes are used as pillars for therapeutic approaches. In patients with
FFA, you can see characteristic perifollicular, lymphocytic inflammatory reaction around the bulge area, where stem cells are located. The destruction of these leads to scarring alopecia, as confirmed by recent research. The therapeutic approach for this is immune suppression or immune modulation, through corticosteroids, hydroxychloroquine, or calcineurin inhibitors. Blume-Peytavi further explained that immune activation is observed in FFA. It may, therefore, be possible that T helper 1-JAK-signal transducer and activator of transcriptionmediated follicular damage and fibrosis result in FFA. Targeting this pathway early in the disease, with JAK inhibition, may prevent the progression of the disease. Other possible causes of FFA include genetic susceptibility, as a xenobioticprocessing enzyme genetic defect has been identified; a hormonal link; and cosmetic products and ultraviolet screens, although this is an issue of controversy.
First-line treatment for FFA consists of topical corticosteroids in an emulsion, solution, or foam; triamcinolone injections in the active rim; and a topical calcineurin inhibitor. As second-line treatment, doxycycline, hydroxychloroquine, oral corticosteroids, and finasteride may be used; and in third-line, mycophenolate mofetil, although this is associated with long-term side effects. Blume-Peytavi also suggested surgery, cosmetic camouflage, and psychologic counselling to further support patients. She stressed the importance of regular followup to assess the effect of treatment, using the Frontal Fibrosing Alopecia Severity Index (FFASI), serial photography, serial measurement of the frontal hairline, and trichoscopy or videotrichoscopy. She concluded that more research is urgently needed to better understand the pathogenesis of the condition, develop preventive or targeted approaches, and evaluate the efficacy of therapies.
"Blume-Peytavi also suggested surgery, cosmetic camouflage, and psychologic counselling to further support patients."
The second form of lymphocytic alopecia introduced by Shapiro, lichen planopilaris, manifests in adults, and has a gradual onset. Variable shedding is associated with itching, pain, and burning, with a positive pull test and no regrowth on the card test. It presents with bare patches or diffuse thinning, often starting at the vertex, and is associated with perifollicular erythema and scaling. Key features of this disease on trichoscopy include loss of follicular ostia, perifollicular scaling, and pigment incontinence in patients with darker skin.
Thirdly, Shapiro introduced chronic cutaneous lupus erythematosus, which affects young or middle-aged adults, and is more common in females. The onset can be either gradual or abrupt, with variable hair shedding, as well as itching, burning, and pain. This condition leads to positive pull test for anagen hairs, and no regrowth on the card test. It manifests through well-circumscribed round or oval plaques, scaly erythematous plaques, changes within the alopecic patch, follicular plugging, telangiectasia, atrophy, and dyspigmentation. Further examination through trichoscopy shows thick arborising vessels, peripilar erythema, keratotic plugs, large yellow dots, and follicular red dots.
The final form of lymphocytic alopecia presented by Shapiro, central centrifugal cicatricial alopecia, is usually found in young adults, and is more common in females of Afro-Caribbean descent. In this case, onset is gradually progressive, with itching, burning, and pain, as well as variable hair shedding. Again, the pull test is positive for anagen hairs, and the card test shows no regrowth. Appearance of this form is symmetric, with centrifugal scarring without overt inflammation, and the scalp may be soft on palpation. Key features on trichoscopy include peripilar white or grey halo around emerging hair, white patches of follicular scarring that interrupt regular honeycomb pigmented network, and lack of follicular ostia.
NEUTROPHILIC ALOPECIA
The second category of scarring alopecia, neutrophilic alopecia, includes folliculitis decalvans and dissecting cellulitis, explained Shapiro.
Folliculitis decalvans is usually found in young or middle-aged adults, and is more common in males. It manifests through a gradually progressive onset, with itching, burning, pain, variable hair shedding, a pull test positive for anagen hairs, and no regrowth on the card test. It predominantly involves the vertex and occipital scalp, with crusting and pustule formation, as well as tufted folliculitis. On trichoscopy, this form manifests as significant polytrichia, peripilar white-yellow scale, peripilar hyperplasia, white and milky-red areas, and lack of follicular ostia.
Finally, dissecting cellulitis is most common in young adults, and likely in males of African descent. Onset of this disease is gradual, leading to variable hair shedding and pain. This type is associated with a positive pull test for anagen hairs, and no regrowth on the card test. It most commonly affects the vertex of the back of the scalp, and leads to formation of firm or fluctuant nodules, pustules, and crusting, and possibly purulent drainage from sinuses. Shapiro noted that the cysts associated with this condition can be painful, and recommended draining these in order to alleviate the pressure. On trichoscopy, you can note marked erythema, follicular pustules, and cutaneous cleft with multiple emerging hairs.
MIXED FORM ALOPECIA
The final category, mixed form alopecia, is not as common, explained Shapiro, and includes folliculitis keloidalis, folliculitis necrotica, and erosive pustular dermatosis.
CONCLUSIONS
Shapiro concluded by stressing the importance of early diagnosis and treatment of alopecia as, in some forms of scarring alopecia, such as chronic cutaneous lupus erythematosus and dissecting cellulitis, hair follicles could be saved if treated before stem cells are destroyed. ●
Bimekizumab 3-Year
Efficacy in Patients with Moderate-to-Severe Plaque Psoriasis: Response Maintenance, Re-treatment, and Effect on High-Impact Areas
Posters presented at the 32nd European Academy of Dermatology and Venereology (EADV) Congress, held in Berlin, Germany, on the 11th–14th October 2023
Presenters: Diamant Thaçi,1 Joseph F. Merola,2 Antonio Costanzo3
1. Institute and Comprehensive Center for Inflammation Medicine, University of Lübeck, Germany
2. Harvard Medical School, Brigham and Women’s Hospital, Boston, Massachusetts, USA
3. Dermatology, Humanitas Clinical and Research Centre, Scientific Institute for Research, Hospitalization and Healthcare (IRCCS), Milan, Italy
Disclosure: Thaçi has served as an investigator and/or consultant/ advisor for AbbVie, Almirall, Amgen, Boehringer Ingelheim, Bristol Myers Squibb (BMS), Celltrion, Eli Lilly, Galapagos, Galderma, Janssen, Kyowa Kirin, LEO Pharma, Novartis, Pfizer, Regeneron, Samsung, Sandoz, Sanofi, Target-Solution, and UCB Pharma; and received grants from AbbVie, LEO Pharma, and Novartis. Merola has been a consultant and/or investigator for AbbVie, Amgen, Biogen, BMS, Dermavant, Eli Lilly, Janssen, LEO Pharma, Pfizer, Novartis, Regeneron, Sanofi, Sun Pharma, and UCB Pharma. Costanzo has been an investigator and/or speaker and/or advisor for AbbVie, Almirall, Amgen, Boehringer Ingelheim, Celgene, Eli Lilly, Galderma, Janssen, LEO Pharma, Novartis, Pfizer, Regeneron, Sandoz, Sanofi, and UCB Pharma.
Acknowledgements: Writing assistance was provided by Eleanor Roberts, Beeline Science Communications Ltd, London, UK.
Support: The publication of this article was fully funded by UCB Pharma.
Disclaimer: The opinions expressed in this article belong solely to the named presenters.
Keywords: High impact areas, IL-17 cytokines, maintenance, monoclonal antibody, Psoriasis Area and Severity Index (PASI), quality of life.
Bimekizumab is a monoclonal IgG1 antibody that selectively inhibits IL-17F in addition to IL-17A, both members of the IL-17 family of proinflammatory cytokines. Bimekizumab provides rapid and long-term response in patients with moderate-tosevere plaque psoriasis. At the European Academy of Dermatology and Venereology (EADV) 2023 Congress, three posters were presented reporting 3-year results from the Phase III/IIIb clinical trials of bimekizumab in plaque psoriasis.
The first poster focused on the subgroup of patients in a pooled analysis who achieved a 90% or 100% improvement from baseline Psoriasis Area and Severity Index (PASI 90/100) or Investigator’s Global Assessment (IGA) of 0 or 1 (IGA 0/1) at Week 16, and showed that these responses could be maintained through to 3 years of treatment. The second poster focused on another subgroup of patients in the pooled analysis, who had scalp, nail, or palmoplantar involvement at baseline, and reported the proportion of patients achieving clearance in these high-impact areas over 3 years. High levels of complete scalp and palmoplantar clearance were shown after 16 weeks, which were sustained through to Year 3. Levels of complete nail clearance increased through the end of Year 1, reflective of the longer time required for nail growth, and were then sustained to the end of Year 3. The third poster presented data from the BE READY randomised withdrawal trial. The analysis focused on patients achieving PASI 90 at Week 16, who were then re-randomised to placebo. Around one-third of these patients retained PASI 75 until Week 56. For the two-thirds of patients who dropped below this level, restarting bimekizumab 320 mg every 4 weeks as ‘escape’ treatment led the majority to return to PASI 90 after 12 weeks. Both groups of patients could enter the subsequent open-label extension, and high responses were sustained through 3 years, showing that treatment interruption did not meaningfully impact long-term disease control.
The results presented in these posters show that high levels of response can be achieved with bimekizumab through 3 years of treatment. Initial responses were well-maintained; patients with scalp, nail, or palmoplantar involvement showed clearance in these high-impact areas; and long-term response was not affected by withdrawal and re-treatment.
Introduction
Psoriasis symptoms can be not only uncomfortable, irritating, and painful, but can also impact several aspects of a patients’ daily life, such as work, social activities, and clothing choice, especially when they affect areas such as the scalp, palm, nails, and soles. Furthermore, depression, anxiety, stress, insomnia, and substance abuse have all been found to be higher in people with psoriasis compared with people without a skin condition.1-3 Factors important to patients when discussing treatment options include overall symptom relief, rapid symptom relief, achieving and maintaining clear skin, effectiveness in ‘high-impact’ areas (such as the nails, scalp, palms, and soles), and
the occurrence of side effects.3 As psoriasis is a chronic disease, and loss of response is observed with some therapies over time, 4 studying long-term efficacy of new treatments is important. These findings highlight the need for long-term, safe, and effective treatments for control of psoriasis symptoms, that can lead to a better quality of life. Furthermore, patients with moderate-to-severe plaque psoriasis may report interruptions in biologic treatment. It is thus important to understand how long responses can be maintained after treatment withdrawal, and whether responses can be recaptured and maintained upon re-treatment.
Phase
III/IIIb
Trials of Bimekizumab in Moderate-to-Severe Plaque Psoriasis
Psoriasis is an autoimmune disease that occurs due to aberrant interactions between epidermal keratinocytes and immune system cells. Such interactions include overexpression by a number of innate and adaptive immune system cells, most prominently T helper 17 lymphocytes, of the proinflammatory cytokines IL-17A and IL-17F. These cytokines can stimulate production of inflammatory mediators and subsequent keratinocyte proliferation, leading to the thick, scaly, erythematous plaques indicative of psoriasis.5-7
As the expression patterns of these cytokines differ,8 targeting both in people with psoriasis may be advantageous. Indeed, dual and selective inhibition of IL-17A and IL-17F by the monoclonal IgG1 antibody bimekizumab9 may lead to more complete suppression of inflammatory responses associated with psoriasis than inhibition of IL-17A alone.10 Bimekizumab is typically administered subcutaneously to adults with plaque psoriasis at a dose of 320 mg, given every 4 weeks for the first 16 weeks, then every 8 weeks.11
In Phase III/IIIb clinical trials in patients with moderate-to-severe plaque psoriasis, bimekizumab use led to rapid and superior efficacy compared with placebo12,13 and with the monoclonal antibodies ustekinumab,12 adalimumab,14 and secukinumab.15 Studies have also shown long-term durability of bimekizumab response. The most common treatmentemergent adverse events in patients treated with bimekizumab were nasopharyngitis, oral candidiasis, and upper respiratory tract infection. These were predominantly mild or moderate. Discontinuation due to adverse events was Iow.12-16
These clinical trials include three large Phase III studies: BE VIVID,12 BE READY,13 and BE SURE,14 and one Phase IIIb study: BE RADIANT.15 For the bimekizumab arms, 320 mg was administered Q4W until Week 16 in all trials. At this point in each study, except BE VIVID, a subset of the Q4W group were switched to 8-weekly dosing (Q8W) throughout the maintenance period. Maintenance period end from baseline was 48 weeks from baseline in BE RADIANT, 52 weeks in BE VIVID and BE SURE, and 56 weeks in BE READY.12-15
At the end of BE VIVID, BE READY, and BE SURE, eligible patients receiving bimekizumab could enter an OLE trial named BE BRIGHT.16 BE RADIANT had an OLE period included.15 Patients in the Phase III studies received treatment for up to 4 years (to OLE Week 144), and those in BE RADIANT for up to 3 years (Week 144/OLE Week 96).15,16 For the OLE stages, all patients receiving bimekizumab with PASI <90 at the end of the maintenance period were initially administered a BKZ Q4W regimen. Patients achieving PASI ≥90 at the beginning of the OLE period who were on a BKZ Q4W regimen at the end of the first year were randomised 1:1 in BE RADIANT and 4:1 in BE BRIGHT to Q4W or Q8W.15 Patients achieving PASI ≥90 at the beginning of the OLE period who were on a BKZ Q8W regimen at the end of the first year remained on this dose.15,16 In BE BRIGHT, at OLE Week 24, patients achieving PASI ≥90 could be switched to Q8W by the investigator, with the remainders reassigned to BKZ Q8W from OLE Week 48 or later.16 In BE RADIANT, all patients were switched to BKZ Q8W from OLE Week 16 (Week 64) or later.15
Throughout these trials, the main assessment tool was the PASI, which ranks degree of severity and percentage of surface involved for a total PASI score of 0−72.17 In these trials, response was defined as percentage reduction in score, e.g., PASI 90 denotes a ≥90% reduction in PASI score. Also used in these studies was the Investigator’s Global Assessment (IGA), which rates psoriasis from 0 (clear) to 4 (severe psoriasis). Response was defined as achieving a score of 0 or 1 (almost clear), with a two-point or bigger improvement from baseline.12-16
Long-Term Response Maintenance in Bimekizumab Week 16 Responders
Diamant Thaçi
Response to some psoriasis therapies may wane over time.4 As such, it is important to examine the long-term effects of a psoriasis treatment. A poster presented at the EADV Congress 2023 by Diamant Thaçi, Institute and Comprehensive Center for Inflammation Medicine, University of Lübeck, Germany, included pooled data from the 1,362 participants in the bimekizumab Phase III/IIIb trials who were initially randomised to BKZ Q4W. Data were reported for the
combined dosing groups (BKZ Total) and for patients who received a BKZ Q4W/Q8W/Q8W (initial/maintenance/OLE) regimen,18 which is consistent with the approved dosing regimen of bimekizumab for psoriasis.11,19 Maintenance of PASI 90, PASI 100, and IGA 0/1 responses from baseline through Year 3 (Week 144/OLE Week 96) were reported in Week 16 PASI 90, PASI 100, and IGA 0/1 responders, respectively. Data were reported using modified non-responder imputation,20 where patients who discontinued due to lack of efficacy or treatment-related adverse events were considered non-responders at subsequent timepoints, with other missing data imputed using multiple imputation methodology.18
Baseline characteristics of all pooled participants who achieved PASI 90 (n=995), PASI 100 (n=719), or IGA 0/1 (n=985) at Week 16, and later entered the OLE phase were similar. Mean ages were approximately 45 years, about 70% were male, 88% were White, and mean psoriasis duration was around 18.2 years. Similarly, approximately 78% in each group received prior systemic therapy, and around 39% received prior biologic therapy. Baseline PASI mean scores were all about 21, with percentages for IGA 3/4 around 66/34%.18
As can be seen in Figure 1, of the 1,362 patients randomised to receive BKZ Q4W over the initial treatment period, at Week 16 86.9% achieved PASI 90, 62.4% achieved PASI 100, and 86.9% achieved IGA 0/1.18 For the BKZ Total group, analysis at Week 48, the last common timepoint for assessment across the trials before OLE entry, found that 96.0%, 88.7%, and 95.8% of Week 16 PASI 90, PASI 100, and IGA 0/1 responders, respectively, maintained their responses.
During the OLE period, marginal decreases were seen in the proportion of patients who maintained PASI 90 and IGA 0/1, with >90% of the BKZ Total group and >95% of patients who received BKZ Q4W/Q8W/Q8W maintaining PASI 90 and/or IGA 0/1 to Week 144. PASI 100 in Week 16 PASI 100 responders was maintained in 78.0% of patients at Week 144. Across all timepoints, level of response was similar in patients who received the BKZ Q4W/Q8W/Q8W dosing regimen compared to the BKZ Total group (Figure 1).18
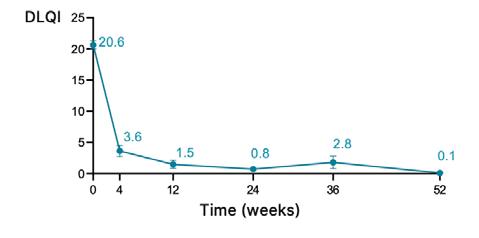
Also reported in this poster were Dermatology Life Quality Index (DLQI)21 0/1 responses in Week
16 PASI 100 responders. The DLQI is a 10-item questionnaire where patients rate how psoriasis has affected several domains over the last week, including skin symptoms; treatment efficacy; and social, work, and relationship activities. DLQI score ranges from 0−30, with a score of 0/1 denoting ‘no effect on a patient’s life’.12-16,21,22
For the Week 16 PASI 100 responders, DLQI mean±standard deviation (SD) baseline score was 10.7±6.4, representing a ‘moderate’ to ‘very large’ effect on a patient’s life.22 Figure 1D shows that among Week 16 PASI 100 responders, 62.4% reported DLQI 0/1 scores at this timepoint. This rose to 89.1% by Week 48, a level maintained through Week 144. Response rates were very similar regardless of dosing regimen.18
Also reported in this poster was that in this Week 16 responder cohort, study discontinuation due to loss of efficacy and adverse events during the maintenance period was 8 out of 1,102 (0.7%) and during the OLE period was 77 out of 1,102 (7.0%).
The authors concluded that “pooled data from five trials found that, among Week 16 responders, high clinical responses were maintained through 3 years of bimekizumab 320 mg treatment.”18
Long-Term Bimekizumab Efficacy in High-Impact Areas
Joseph F. Merola
‘High-impact’ areas for people with psoriasis include the scalp, hands (including the palms and nails), and the soles of the feet.3 Psoriatic lesions in these areas are associated with both treatment challenges and reduced healthrelated quality of life.23 Building on a previous presentation of 2-year bimekizumab efficacy in these 'high-impact' areas,24 Joseph F. Merola, Harvard Medical School, Brigham and Women’s Hospital, Boston, Massachusetts, USA, presented a poster that reported responses in high-impact areas over 3 years (144 weeks) for bimekizumab-randomised patients pooled across all the Phase III/IIIb trials described above.25
For this analysis, scalp IGA and palmoplantar IGA (pp-IGA) were assessed and rated from 0 (clear) to 4 (severe). For nails, the modified Nail
Figure 1: Maintenance in Week 16 bimekizumab-treated responders who entered the BE BRIGHT or BE RADIANT open-label extensions (modified non-responder imputation) of PASI 90 in Week 16 PASI 90 responders (A), PASI 100 in Week 16 PASI 100 responders (B), IGA 0/1 in Week 16 IGA/01 responders (C), and DLQI 0/1 in Week 16 PASI 100 responders (D).18
Week 16 PASI 90 response rate in BKZ-randomised patients (N=1,362)
treatment
BKZ 320 mg Q4W (NRI; initial treatment period)
0 16 Week
24 32
Week 16 PASI 100 response rate in BKZ-randomised patients (N=1,362)
Week 16 IGA 0/1 response rate in BKZ-randomised patients (N=1,362)
BKZ 320 mg Q4W (NRI; initial treatment period)
0 16 Week
24 32 BKZ Total (mNRI; N=985)
Week
Week 16 responses are reported for all BKZ-randomised patients; response rates from Week 16 up to Week 144 are reported among patients randomised to BKZ at the start of BE SURE, BE READY, BE VIVID, and BE RADIANT achieved a PASI 90, PASI 100, or IGA 0/1 response at Week 16, and entered the relevant OLE. To pool data across all four studies, Week 52 and 56 data from the feeder studies were not included; timepoints after Week 48 are from the BE BRIGHT/BE RADIANT OLEs. DLQI responses are at visits common to BE SURE, BE READY, and BE RADIANT. Data were reported using mNRI, where patients who discontinued due to lack of efficacy or treatment-related adverse events were considered non-responders at subsequent timepoints.
BKZ: bimekizumab; DLQI: Dermatology Life Quality Index; IGA: Investigator’s Global Assessment; mNRI: modified non-responder imputation; NRI: non-responder imputation; OLE: open-label extension; PASI: Psoriasis Area and Severity Index; PASI 90/100: ≥90%/100% improvement from baseline in Psoriasis Area and Severity Index; Q4W: every 4 weeks; Q8W: every 8 weeks.
Psoriasis Severity Index (mNAPSI) was used, where each nail was scored 0–13 (maximum total score for hands: 130) in regard to onycholysis/ oil drop dyschromia, nail plate crumbling, pitting, splinter haemorrhages, leukonychia, red spots in lunula, and nail bed hyperkeratosis. Patients with baseline scalp IGA or pp-IGA ≥3 or mNAPSI score >10 were included in the high-impact areas analysis. Proportions of patients who achieved complete regional clearance (0 scores) are reported through Year 3 (study Week 144/ OLE Week 96). As above, data are reported using modified non-responder imputation.25
Baseline characteristics were similar for patients with scalp IGA ≥3 (n=821), pp-IGA ≥3 (n=193), and mNAPSI >10 (n=377), regarding mean age (around 45 years) and race (around 85% White), but differed in regard to gender (69.3%, 74.6%, and 83.8% male, respectively). The groups had a similar duration of psoriasis (around 18 years) and any prior biologic therapy (around 37%), but differed slightly in regard to receiving any prior systemic therapy (77.3%, 84.5%, and 78.8%, respectively).25
Mean±SD baseline PASI scores were all around 22 for patients with scalp IGA ≥3, pp-IGA ≥3, and mNAPSI >10, with mean DLQI scores around 11. Respective weight of respective IGA 3/4 scores were slightly different, being 64.2/35.8%, 56.5/43.0%, and 56.2/43.2%. Baseline scores were also provided in regard to each score across each category. While mean±SD scalp IGA scores for patients with scalp IGA ≥3, ppIGA ≥3, and mNAPSI >10 were similar (around 3.0), respective mean±SD mNAPSI scores were slightly different, at 11.6±17.8, 21.9±28.0, and 31.0±20.5, as were respective mean pp-IGA scores: 0.9±1.3, 3.2±0.4, and 1.3±1.4.25
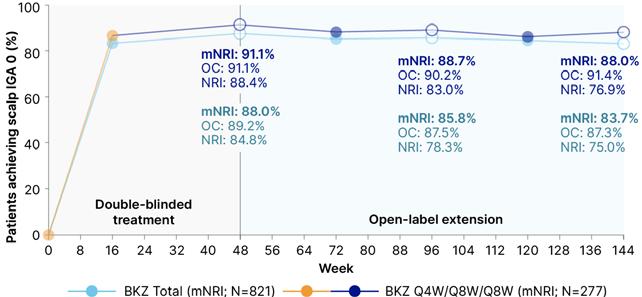
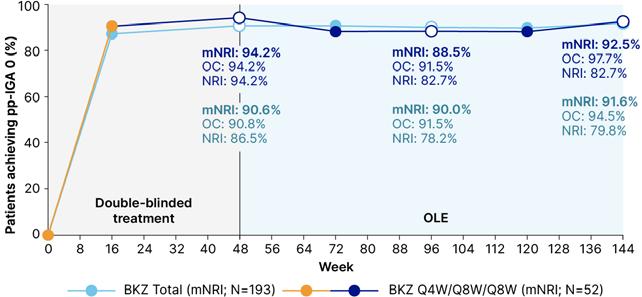
In this poster, scores were reported at Weeks 48, 96, and 144. As Figure 2 shows, for scalp IGA and pp-IGA, complete clearance was high at Week 16. At Week 48, respective percentages of complete clearance were 88.0% and 90.6%. Similar percentages, of 83.7% and 91.6%, respectively, were shown at Week 144. Reflective of nail growth time, at Week 16, around 20–30% of people with baseline mNAPSI >10 achieved clearance at this timepoint. By Week 48, nail clearance was seen in 64.4% of patients, increasing to 69.5% by Week 144. For all assessments, response to bimekizumab in
high impact areas was similar across the 3 years, regardless of dosing regimen (Figure 2).25
The authors concluded that “over 3 years, high percentages of patients treated with bimekizumab achieved complete clearance of scalp, palmoplantar, and nail psoriasis, regardless of dosing regimen.”25
Bimekizumab Response Through 3 Years in Patients Who Stopped and Then Restarted Treatment
Antonio Costanzo
For a variety of reasons, patients treated with biologics may have therapy interruptions. Another poster presented at the EADV Congress 2023, by Antonio Costanzo, Dermatology, Humanitas Clinical and Research Centre, Scientific Institute for Research, Hospitalization and Healthcare (IRCCS), Rozzano, Milan, Italy, reported data from patients who received bimekizumab in the initial treatment period in the BE READY trial, then continued into BE BRIGHT.13,16,26 In BE READY, patients who were Week 16 PASI 90 responders were re-randomised at Week 16 to receive maintenance treatment with BKZ Q4W or Q8W (not reported here), or to placebo (n=105) over Weeks 16–56. Previous analysis of the placebo cohort found that the median time to loss of PASI 90 was 28 weeks from last bimekizumab dose,27 with median time to loss of PASI 75 (considered to be a relapse) being 32 weeks.13
This poster reported long-term outcomes in patients from the withdrawal cohort who received bimekizumab in the BE BRIGHT OLE. A total of 33 patients maintained a response at PASI ≥75 throughout the withdrawal period (the Weeks 16–56 placebo group), and only resumed treatment with BKZ Q4W from Week 56. A total of 66 patients relapsed to PASI <75 during the withdrawal period, and were entered into a 12 week escape arm (BKZ Q4W) before entering the OLE. These patients either received BKZ Q4W (n=54) or Q8W (n=12) on entering the OLE according to PASI response, as described above. At Week 80, those in Q4W achieving PASI 90 were switched to Q8W, at the investigator’s discretion, with all switched from Week 104 or later.26
Figure 2: Complete clearance over 3 years (modified non-responder imputation, non-responder imputation, and observed case) of scalp psoriasis (scalp IGA 0) in patients with baseline scalp IGA ≥3 (A), palmoplantar psoriasis (pp-IGA 0) in patients with baseline pp-IGA ≥3 (B), and nail psoriasis (mNAPSI 0) in patients with baseline mNAPSI >10 (C).24
BKZ Total patients received BKZ 320 mg Q4W to Week 16, then either Q4W or Q8W in the maintenance period and OLE. BKZ Q4W/Q8W/Q8W patients received BKZ 320 mg Q4W to Week 16, then BKZ Q8W throughout the maintenance period, and on OLE entry. As no scalp, palmoplantar, or nail outcomes were collected at Week 48 in BE VIVID, Week 52 data were included at the Week 48 timepoint. To pool data across all four studies, Week 52/56 data from the feeder studies were not included; timepoints after Week 48 are from the BE BRIGHT/BE RADIANT OLEs. For mNRI analyses, patients who discontinued due to lack of efficacy or treatment-related adverse events were considered non-responders at subsequent timepoints.
BKZ: bimekizumab; IGA: Investigator’s Global Assessment; mNAPSI: modified Nail Psoriasis Severity Index; mNRI: modified non-responder imputation; NRI: non-responder imputation; OC: observed case; OLE: openlabel extension; pp: palmoplantar; Q4W: every 4 weeks; Q8W: every 8 weeks.
Figure 3: Achievement of PASI 90 and PASI 100 over 3 years in patients re-treated with bimekizumab in the Escape group (observed case).25
*Data reported from BE BRIGHT OLE are pooled for patients who received BKZ 320 mg Q4W and Q8W; †patients in the Escape group had their OLE Week 0 study assessments at the end of the 12-week escape arm, having achieved PASI 50 at the end of the 12 weeks; 65 out of 66 patients had a PASI measurement recorded at Escape Week 12/OLE Week 0, as one patient missed this visit.
BKZ: bimekizumab; OC: observed case; OLE: open-label extension; PASI: Psoriasis Area and Severity Index; PASI 90/100: ≥90%/100% improvement from baseline in PASI; PBO: placebo; Q4W: every 4 weeks; Q8W: every 8 weeks.
The 66 patients in the Escape group were slightly older (mean±SD: 43.2±11.8 years) than the 33 patients who remained in the placebo group over Weeks 16–56 (n=33; 41.2±10.7 years), slightly more were male (75.8% versus 66.7%), and a slightly lower percentage were White (89.4% versus 97.0%). Disease duration was longer in the group of patients who relapsed and entered the escape arm versus the patients who maintained PASI 75 (mean±SD: 20.6±13.0 versus 14.6±8.3 years), PASI was slightly higher (19.7±7.5 versus 18.2±4.8), and percentages of IGA 3/4 were slightly different (68.2/31.8% versus 72.7/27.3%). Much higher percentages of the Escape group had received any prior systemic therapy (81.8% versus 57.6%) or prior biologic therapy (50.0% versus 18.2%), compared with the placebo group.26
As shown in Figure 3, for the Escape group, 59 out of 65 (90.8%) regained PASI 90, and 41 out
of 65 (63.1%) achieved PASI 100 at Escape Week 12 (OLE Week 0) following bimekizumab retreatment (one patient missed the Escape Week 12 visit). By OLE Week 96, PASI 90 was achieved in 55 out of 59 (93.2%) patients, and PASI 100 in 46 out of 59 (78.0%) patients. Of the patients who continued in the placebo arm until Week 56, 17 out of 33 (51.5%) maintained PASI 90, and 11 out of 33 (33.3%) achieved PASI 100. Results for this placebo group greatly improved following retreatment with bimekizumab, up to OLE Week 96, with 27 out of 28 (96.4%) achieving PASI 90, and 24 out of 28 (85.7%) achieving PASI 100.26
These results, the authors concluded, “indicated that stopping bimekizumab for up to 40 weeks and restarting did not meaningfully impact longterm disease control.”26
Conclusion
These studies show that high levels of response can be achieved with bimekizumab through 3 years of treatment. Initial responses were
References
1. Hepat A et al. Psychological wellbeing of adult psoriasis patients: a narrative review. Cureus. 2023;15(4):e37702.
2. Soliman MM. Depressive, anxiety, stress, and insomnia symptoms in patients with psoriasis: a crosssectional study. Postepy Dermatol Alergol. 2021;38(3):510-9.
3. Gorelick J et al. Understanding treatment preferences in patients with moderate to severe plaque psoriasis in the USA: results from a cross-sectional patient survey. Dermatol Ther (Heidelb). 2019;9(4):785-97.
4. Warren RB et al. Differential drug survival of biologic therapies for the treatment of psoriasis: a prospective observational cohort study from the British Association of Dermatologists Biologic Interventions Register (BADBIR). J Invest Dermatol. 2015;135(11):2632-40.
5. Fitch E et al. Pathophysiology of psoriasis: recent advances on IL-23 and Th17 cytokines. Curr Rheumatol Rep. 2007;9(6):461-7.
6. Sánchez-Rodríguez G, Puig L. Pathogenic Role of IL-17 and therapeutic targeting of IL17F in psoriatic arthritis and spondyloarthropathies. Int J Mol Sci. 2023;24(12):10305.
7. Johansen C et al. Characterization of the interleukin-17 isoforms and receptors in lesional psoriatic skin. Br J Dermatol. 2009;160(2):319-24.
8. van Baarsen LG et al. Heterogeneous expression pattern of interleukin 17A (IL-17A), IL-17F and their receptors in synovium of rheumatoid arthritis, psoriatic arthritis and osteoarthritis: possible explanation for nonresponse to anti-IL-17 therapy? Arthritis Res Ther. 2014;16(4):426.
9. Adams R et al. Bimekizumab, a novel humanized IgG1 antibody that neutralizes both IL-17A and IL17F. Front Immunol. 2020;11:1894.
10. Glatt S et al. Dual IL-17A and IL-17F neutralisation by bimekizumab in psoriatic arthritis: evidence from preclinical experiments and a randomised placebo-controlled clinical trial that IL-17F contributes
well-maintained; patients with scalp, nail, or palmoplantar involvement showed clearance in these high-impact areas, and long-term response was not affected by treatment interruption.
to human chronic tissue inflammation. Ann Rheum Dis. 2018;77(4):523-32.
11. European Medicines Agency (EMA). Bimekizumab summary of product characteristics. Available at: https://www.ema.europa.eu/en/ documents/product-information/ bimzelx-epar-product-information_ en.pdf. Last accessed: 24 October 2023.
12. Reich K et al. Bimekizumab versus ustekinumab for the treatment of moderate to severe plaque psoriasis (BE VIVID): efficacy and safety from a 52-week, multicentre, double-blind, active comparator and placebo controlled phase 3 trial. Lancet. 2021;397(10273):48798.
13. Gordon KB et al. Bimekizumab efficacy and safety in moderate to severe plaque psoriasis (BE READY): a multicentre, doubleblind, placebo-controlled, randomised withdrawal phase 3 trial. Lancet. 2021;397(10273):47586.
14. Warren RB et al. Bimekizumab versus adalimumab in plaque psoriasis. N Engl J Med. 2021;385(2):130-41.
15. Reich K et al. Bimekizumab versus secukinumab in plaque psoriasis. N Engl J Med. 2021;385(2):142-52.
16. Strober B et al. Bimekizumab maintenance of response through 3 years in patients with moderateto-severe plaque psoriasis: results from the BE BRIGHT open-label extension trial. Br J Dermatol. 2023;188(6):749-59.
17. Fredriksson T, Pettersson U. Severe psoriasis--oral therapy with a new retinoid. Dermatologica. 1978;157(4):238-44.
18. Thaçi D et al. Bimekizumab 3-year maintenance of response in Week 16 responders with moderate to severe plaque psoriasis: results from five phase 3/3b trials. Poster P2540. European Academy of Dermatology and Venerology (EADV) Congress, 11-14 October, 2023.
19. UCB, Inc. Bimzelx. Highlights of prescribing information. Available at: https://www.accessdata. fda.gov/drugsatfda_docs/
label/2023/761151s000lbl.pdf. Last accessed: 5 November 2023.
20. Chen J et al. A hybrid approach of handling missing data under different missing data mechanisms: VISIBLE 1 and VARSITY trials for ulcerative colitis. Contemp Clin Trials. 2021;100:106226.
21. Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI)--a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19(3):210-6.
22. Hongbo Y et al. Translating the science of quality of life into practice: what do dermatology life quality index scores mean? J Invest Dermatol. 2005;125(4):659-64.
23. Merola JF et al. Underdiagnosed and undertreated psoriasis: nuances of treating psoriasis affecting the scalp, face, intertriginous areas, genitals, hands, feet, and nails. Dermatol Ther. 2018;31(3):e12589.
24. Merola JF et al. Bimekizumab efficacy in high-impact areas for patients with moderate to severe plaque psoriasis: pooled results through two years from the BE SURE and BE RADIANT phase 3 trials. Poster P1467. European Academy of Dermatology and Venereology (EADV) Congress, 1-10 September, 2022.
25. Merola JF et al. Bimekizumab 3-year efficacy in high-impact areas in moderate to severe plaque psoriasis: pooled results from five phase 3/3b trials. Poster P2547. European Academy of Dermatology and Venereology (EADV) Congress, 11-14 October, 2023.
26. Costanzo A et al. Bimekizumab response through 3 years in patients with plaque psoriasis who stopped and re-started treatment. Poster P2511. European Academy of Dermatology and Venereology (EAVD) Congress, 11–14 October, 2023.
27. Blauvelt A. Bimekizumab efficacy in patients with moderate to severe plaque psoriasis during the randomized withdrawal and retreatment phase of BE READY, a phase 3 trial. Poster 27380. American Academy of Dermatology (AAD) Congress, 5-8 August, 2021.
Secukinumab for Patients with Moderate-toSevere Hidradenitis Suppurativa: Post Hoc
Analyses of Efficacy Endpoints, Draining Tunnels, Skin Pain, and Work Productivity
These poster and oral presentations took place between 11th–14th October 2023, as part of the 32nd European Academy of Dermatology and Venereology (EADV) Congress held in Berlin, Germany
Presenters:
Disclosure:
Christos Zouboulis,1,2 Alexa B. Kimball,3 Falk G. Bechara,4 John R. Ingram,5 Robert Sabat6
1. European Hidradenitis Suppurativa Foundation (EHSF), Dessau, Germany
2. Departments of Dermatology, Venereology, Allergology and Immunology, Städtisches Klinikum Dessau, Brandenburg Medical School Theodor Fontane (MHB) and Faculty of Health Sciences, Brandenburg, Germany
3. Department of Dermatology, Beth Israel Deaconess Medical Center (BIDMC), Harvard Medical School, Boston, Massachusetts, USA
4. Department of Dermatology, Venereology and Allergology, Ruhr-University Bochum, Germany
5. Department of Dermatology and Academic Wound Healing, Division of Infection and Immunity, Cardiff University, UK
6. Psoriasis Research and Treatment Centre, Department of Dermatology, Venereology and Allergology and Institute of Medical Immunology, Charité – Universitätsmedizin Berlin, Germany
Zouboulis is a consultant and participant in advisory boards for Almirall, Boehringer Ingelheim, Incyte, InflaRx, Janssen, Novartis, Sanofi, UCB, and Viatris. Kimbal has received grants from Abbvie, Anapyts Bio, Aristea, Bristol Myers Squibb (BMS), ChemoCentryx, Eli Lilly, Incyte, Janssen, Moonlake, Novartis, Pfizer, UCB, and Sonoma Bio; received fellowship funding from Abbvie and Janssen; received royalties or licenses from BIDMC; received consulting fees from Abbvie, Alumis, Bayer, BMS, Boehringer Ingelheim, Eli Lilly, FIDE, Novartis, Moonlake, Janssen, Pfizer, Priovant, Sonoma Bio, Sanofi UCB, and Ventyx; serves on advisory boards for Target RWE; serves as an advisory council member to the NIH Director; holds stock in Ventyx; and has served on the board of directors of Almirall. Bechara has received honoraria for participation in advisory boards, in clinical trials, and/or as a speaker for AbbVie, AbbVie Deutschland, Boehringer Ingelheim, Incyte, MoonLake Immunotherapeutics, Novartis, Celltrion, Mölnlycke Health Care, UCB, and Janssen-Cilag. Ingram is a consultant for AbbVie, Boehringer Ingelheim, ChemoCentryx, Citryll, Novartis, UCB, and UNION Therapeutics; has served on advisory boards for Insmed and Kymera Therapeutics; is co-copyright holder of HiSQOL, Investigator Global Assessment, and Patient Global Assessment instruments for HS; and his department receives income from copyright of the Dermatology Life Quality Instrument (DLQI) and related instruments.
Sabat has received research grants, scientific awards, or honoraria for participation in advisory boards, clinical trials, or as speaker for one or more of the following: AbbVie, AbbVie Deutschland, Almirall, Amgen, Bayer Schering, Boehringer Ingelheim Pharma, Celgene, Celgene International II Sàrl, Charité Research Organisation, CSL Behring, Dr. Willmar Schwabe, FLEXOPHARM, ICON plc, Incyte, Janssen-Cilag, La Roche-Posay Laboratoire Dermatologique, MoonLake Immunotherapeutics, Novartis, Parexel International, Rheinischen Friedrich-Wilhelms-Universität Bonn, Sanofi–Aventis Deutschland, TFS, and UCB Biopharma
Acknowledgements: Writing assistance was provided by Julia Duffey, Manifold Medical Communications, Matlock, UK.
Support: The publication of this article was funded by Novartis Pharma AG, Basel, Switzerland.
Keywords: Hidradenitis suppurativa (HS), Phase III, post hoc analysis, secukinumab, SUNRISE, SUNSHINE.
Hidradenitis suppurativa (HS) is a chronic, recurrent follicular skin disease characterised by deep and painful dermal inflammatory nodules, abscesses, and draining tunnels. HS is one of the dermatological diseases with the greatest unmet medical need. Post hoc analyses from two identically designed Phase III trials of secukinumab in patients with moderate-to-severe HS (SUNSHINE and SUNRISE) were featured in multiple poster and oral presentations at the 32nd annual European Academy of Dermatology and Venereology (EADV) Congress in Berlin, Germany.
The SUNSHINE and SUNRISE studies represent the largest Phase III trials conducted in HS to date. In these studies, secukinumab demonstrated sustained efficacy with a favourable safety profile, with both trials meeting the primary endpoint. The analyses presented at the EADV Congress were conducted to assess concordance between efficacy endpoints (55% reduction in Hidradenitis Suppurativa Severity Scoring System [IHS4-55] response and Hidradenitis Suppurativa Clinical Response [HiSCR]); the impact of secukinumab on HiSCR 75, HiSCR 90, and HiSCR 100 endpoints; and the effect of secukinumab on draining tunnels and HS-related pain, as well as work productivity and activity impairment (WPAI). Strong concordance between IHS4-55 and HiSCR was found, and IHS4-55 was considered to be a suitable efficacy outcome for HS.
Secukinumab also provided clinically meaningful improvements compared with placebo, as determined by HiSCR 75, HiSCR 90, and HiSCR 100 endpoints by Week 16. These effects were sustained through Week 52. Furthermore, at Week 16, >80% of patients treated with secukinumab experienced no increase in the number of draining tunnels from baseline. Secukinumab also improved HS-related skin pain, and reduced the use of pain medication compared with placebo. Finally, treatment with secukinumab had a beneficial and sustained effect on presenteeism, absenteeism, and general work impairment due to HS. These data, taken together, indicate that secukinumab provides sustained disease control, sustained reduction in pain, and sustained improvement in WPAI and occupational performance up to Week 52.
Concordance Between IHS4-55 Response and HiSCR: A Post Hoc Analysis of the SUNSHINE and SUNRISE Phase III Randomised Trials of Secukinumab in Patients with Moderate-to-Severe Hidradenitis Suppurativa
Due to the clinical heterogenicity of HS, assessment of disease severity is complex, and over 20 different outcome measures have been developed.1,2 HiSCR is a well-recognised dichotomous score currently used in HS clinical trials to assess treatment effects, and assesses morbidity improvement, or lack of, between two time points.1-3 Response is classified as at least a 50% reduction from baseline in the abscesses and inflammatory nodules count, with no increase in abscesses or draining fistulae count.4,5 This endpoint cannot be applied to patients who have fewer than three inflammatory lesions, or >20 draining fistulae.2 HiSCR 75, 90, and 100 represent a ≥75%, ≥90%, and 100% decrease in abscess and inflammatory nodule count, respectively, versus baseline.
A further tool used as a secondary outcome measure in HS clinical trials is the IHS4, which provides a continuous severity score by assigning different weights to different lesion types.1,6 IHS4 disease severity bands classify HS into mild, moderate, or severe disease.1 IHS4 also allows quantification of draining tunnels in a validated manner.1,6 However, the need for dichotomous outcomes in clinical trials led to the development and validation of IHS4-55, a binary version of IHS4, based on a 55% decrease in the total score between two time points.7 Although IHS4-55 has been validated, the concordance between dichotomous outcomes and patientreported outcomes has not yet been evaluated.7
Secukinumab is a monoclonal antibody that selectively neutralises IL-17A, and has been evaluated in the identically designed SUNSHINE and SUNRISE pivotal Phase III trials for the treatment of patients with moderate-tosevere HS.4 Both studies were randomised, double-blind, multicentre, clinical trials that assessed the efficacy and tolerability of secukinumab. Patients were randomised 1:1:1 to one of two subcutaneous secukinumab dosing regimens (300 mg every 2 weeks [SECQ2W] or every 4 weeks [SECQ4W]) for
52 weeks, or to placebo for 16 weeks. At Week 16, patients enrolled into the placebo group were subsequently randomised 1:1 to either SECQ2W or SECQ4W.4 Key inclusion criteria included at least five inflammatory lesions affecting at least two distinct anatomical areas at baseline, and diagnosis of HS ≥1 year prior to enrolment.4 Patients in the antibiotic stratum were permitted to enter the study on stable treatment with selected antibiotics. Individuals with a total fistulae count ≥20 at baseline, active inflammatory disease, or previous exposure to secukinumab or other IL-17(A)-biologics were excluded.4
Secukinumab has previously demonstrated sustained efficacy with a favourable safety profile in patients with moderate-to-severe HS in the SUNSHINE and SUNRISE trials, with both studies meeting the primary endpoint.4 A post hoc analysis was conducted to determine if IHS4-55 response was concordant with HiSCR and Dermatology Life Quality Index (DLQI) response. A DLQI response was defined as a decrease of ≥5 points from baseline. Concordance was defined as the proportion of patients whose responses for the two assessed parameters were consistent during a specific visit. Concordance at Week 16 and 52 was assessed between the following parameters: IHS4-55 and HiSCR response; IHS4-55 and DLQI response; and HiSCR and DLQI response.
A total of 1,084 patients were included in the assessment of concordance between IHS4-55 and HiSCR, and 905 patients were included in the IHS4-55 and DLQI, and HiSCR and DLQI concordance assessments.
Strong concordance between IHS4-55 and HiSCR response at Week 16 and Week 52 (≥85.7% in pooled analysis and by trial) was observed in all treatment arms. Moderate concordance between IHS4-55 and DLQI responses (57.1% to 66.2%), and between HiSCR and DLQI responses (54.6% to 71.4%) in all treatment arms was reported. These data indicate that IHS4-55 is a suitable efficacy outcome for HS, either on its own or in addition to HiSCR.
Effects of Secukinumab on HiSCR 75, HiSCR 90, and HiSCR 100 Endpoints in Patients with Moderate-to-Severe Hidradenitis Suppurativa: A Post Hoc Analysis of the SUNSHINE and SUNRISE Phase III Trials
While HiSCR is a commonly used endpoint, it has previously demonstrated high placebo response rates.8,9 In order to minimise these rates, higher threshold efficacy endpoints have been proposed.
A post hoc analysis was performed to assess the treatment effects of secukinumab on HiSCR 75, HiSCR 90, and HiSCR 100 endpoints in 1,084 patients enrolled in the SUNSHINE and SUNRISE trials (as described above).4 Results from Week 0–16 were based on multiple imputation data, and results from Week 16–52 were based on observed data. The sustainability of response was evaluated by investigating the proportion of patients who achieved HiSCR 75, HiSCR 90, and HiSCR 100 up to Week 52.
A numerically greater proportion of patients treated with secukinumab achieved HiSCR 75, HiSCR 90, and HiSCR 100 versus placebo at Week 16 in both trials. Response rates for the higher threshold efficacy endpoints seen at Week 16 were sustained, with a trend for improvement
to Week 52, in both secukinumab treatment groups.
The majority of patients who achieved an HiSCR 75 at Week 16 maintained this response at Week 52. In SUNSHINE, 62.9% of patients receiving SECQ2W and 70.0% of patients in the SECQ4W group achieved HiSCR 75 at both Weeks 16 and 52. In SUNRISE, 71.4% and 64.4% of patients in the SECQ2W and SECQ4W achieved these endpoints, respectively. Furthermore, patients in the secukinumab group had higher HiSCR 90 and HiSCR 100 response rates versus placebo at Week 16, which were sustained to Week 52.
Treatment continuation was associated with improvement in HiSCR over time, as the majority of patients in the SECQ2W and SECQ4W arms who achieved HiSCR at Week 16 showed improvement to HiSCR 75 at Week 52. In SUNSHINE, 62.1% of patients receiving SECQ2W and 65.4% of patients in the SECQ4W group achieved a HiSCR 75 at Week 52 after achieving an HiSCR at Week 16. For patients participating in SUNRISE, 62.3% and 58.5% of patients receiving SECQ2W and SECQ4W achieved an HiSCR 75 at Week 52 after HiSCR at Week 16, respectively. Additionally, 35% and >25% of patients in the SECQ2W and SECQ4W arms who achieved HiSCR 75 at Week 16 showed improvements to HiSCR 90 and HiSCR 100 at Week 52 (Table 1).
Table 1: Hidradenitis Suppurativa Clinical Response 75, 90, and 100 responses at Week 52 in patients receiving secukinumab who achieved Hidradenitis Suppurativa Clinical Response 75 at Week 16 (post hoc analysis).
This investigation found that secukinumab provided clinically meaningful improvements compared with placebo in high threshold efficacy endpoints in both the SUNSHINE and SUNRISE trials,4 which were sustained through to Week 52. Long-term durability was demonstrated by the fact that >60% of patients receiving secukinumab who achieved HiSCR 75 at Week 16 maintained HiSCR 75 at Week 52 (Table 1), while approximately 60% of patients treated with secukinumab who achieved HiSCR at Week 16 further improved to HiSCR 75 at Week 52. These sustained improvements in HiSCR highlight the long-term benefits of secukinumab in patients with moderate-to-severe HS.
Effect Of Secukinumab on Draining
Tunnels in Patients with Moderate-toSevere Hidradenitis Suppurativa: Post Hoc Analysis of the SUNSHINE And SUNRISE Phase III Randomised Trials
The clinical presentation of HS can vary, with a wide range of inflammatory and non‐inflammatory lesions, including nodules, abscesses, draining tunnels, open pseudocomedones, scars, and ulceration.10 Draining tunnels in patients with HS cause considerable pain, and have a large negative impact on quality of life. Furthermore, they are associated with greater disease severity, irreversible tissue damage, and are predictors of poor response to therapy.11-14
A post hoc analysis of pooled data from the SUNSHINE and SUNRISE trials was conducted to assess the effect of up to 52 weeks of secukinumab treatment on draining tunnels.4 The exploratory endpoints assessed were mean change from baseline to Week 52 in the number of draining tunnels in patients with at least one draining tunnel at baseline, and the proportion of patients reporting no increase in draining tunnels from baseline to Week 52, in all patients and those with at least one draining tunnel at baseline.
All analyses were performed on pooled data from 1,084 patients in both trials, and are reported as observed. The mean±standard deviation (SD) number of draining tunnels at baseline was similar between treatment groups (SECQ2W:
2.90±3.51; SECQ4W: 2.50±3.51; placebo: 2.50±3.19). The majority of enrolled patients had at least one draining tunnel at baseline (Q2W: 66.2%; Q4W: 60.6%; placebo: 62.5%).
A numerically greater mean decrease from baseline in draining tunnels was reported in patients receiving secukinumab versus placebo at Week 16 (Figure 1), with the decrease sustained through to Week 52.
Furthermore, a numerically greater proportion of patients treated with secukinumab versus placebo experienced no increase in the number of draining tunnels from baseline to Week 16 (SECQ2W: 84.5%; SECQ4W: 80.9%; placebo: 75.5%). This effect was sustained through to Week 52, with 80.7% of SECQ2W and 80.9% of SECQ4W patients experiencing no increase in draining tunnels between Week 16 and Week 52 (data not reported for placebo).
When assessing patients with at least one draining tunnel at baseline, a greater proportion of patients in the secukinumab groups versus placebo experienced no increase in the number of draining tunnels at Week 16 (SECQ2W: 82.9%; SECQ4W: 78.2%; placebo: 71.2%). This effect was sustained until Week 52 (SECQ2W: 80.7%; SECQ4W: 82.6%; placebo data not reported).
This analysis demonstrates the sustained effectiveness of secukinumab in reducing the number of draining tunnels in patients with moderate-to-severe HS. Moreover, >80% of patients treated with secukinumab experienced no increase in the number of draining tunnels from baseline to Week 52. These findings are of clinical relevance, as skin tunnel formation is associated with HS disease progression, and irreversible tissue damage.13,14
Secukinumab Provides Sustained Improvements in Pain in Patients with Moderate-to-Severe Hidradenitis
Suppurativa: A Post Hoc Analysis of the SUNSHINE and SUNRISE Phase III Trials
Disease-related pain is one of the most detrimental symptoms for patients with HS.16 The effects of secukinumab on worst HS-related pain in patients with moderate-to-severe HS, using
Figure 1: Mean change in draining tunnels over time up to Week 52 in patients with ≥1 draining tunnel at baseline (post hoc analysis).
Mean change from baseline in draining tunnel s
SECQ2W (N=239)
SECQ4W (N=218) Placebo (N=227)
Figure adapted from Bechara et al. EADV 2023.
Data are presented as observed. At Week 16, patients randomised to placebo were switched to receive SECQ2W or SECQ4W up to Week 52. Only patients on continuous secukinumab treatment for 52 weeks are represented in the graph beyond Week 16.
SECQ2W: secukinumab 300 mg every 2 weeks; SECQ4W: secukinumab 300 mg every 4 weeks.
data from the SUNSHINE and SUNRISE trials, was evaluated in a post hoc analysis.4 Worst skin pain in the 24 hours prior to the visit (daily up to Week 16, and weekly thereafter) was assessed via the patient’s global assessment of skin pain on a continuous Numeric Rating Scale (NRS; 0–10 scale). Categories of worst HS-related skin pain were as follows: NRS=0 (no pain); NRS >0–≤6; NRS >6–≤8; and NRS >8 (severe pain). A mixed-effects model for repeated measures was used to assess the change in NRS scores from baseline to Week 16. The proportion of patients who reported the use of pain medication for HS was also evaluated at 28-day intervals up to Week 16. The achievement of a DLQI response by pain categories at Week 16 was the predefined exploratory endpoint.
Overall, 1,084 patients from the SUNSHINE and SUNRISE trials were included in this analysis.4 The mean NRS±SD pain score at baseline was 5.3±2.5, 5.1±2.5, and 5.2±2.5 in the SECQ2W, SECQ4W, and placebo groups, respectively.
This study found a numerically greater mean reduction from baseline in pain among patients treated with both secukinumab doses compared with the placebo group. At Week 16, the greatest reduction in NRS was seen among SECQ2W patients compared with SECQ4W or placebo (SECQ2W: -1.4±2.2; SECQ4W: -1.1±2.0; placebo: -0.5±2.1). Improvements were sustained through to Week 52, with a change from baseline in NRS of -1.8±2.6 for SECQ2W and -1.5±2.7 for SECQ4W. Patients who switched from placebo to secukinumab also experienced a reduction in skin pain from Week 16 to Week 52 (change in NRS: placebo to SECQ2W: -1.7±2.8; placebo to SECQ4W: -1.6±2.5).
The adjusted mean change from baseline in NRS at Week 16 was -1.3, -1.1, and -0.5 in patients receiving SECQ2W, SECQ4W, and placebo, respectively. The estimated treatment differences between secukinumab and placebo in the change from baseline in NRS score at Week 16 were -0.74 (95% confidence interval: -1.06, -0.42) for SECQ2W and -0.56 (95% confidence interval: -0.88, -0.23) for SECQ4W.
This analysis also evaluated the improvement in pain severity between baseline and Week 52. A small proportion of patients who received SECQ2W with an NRS of >6–≤8 and an NRS of >8 at baseline reported an NRS=0 (baseline NRS: >6–≤8, 8.3%; NRS: >8, 8.6%). Additionally, 63.3% of patients with NRS of >6–≤8, and 45.7% of patients with NRS of >8 at baseline, reported an NRS of >0–≤6 at Week 52. For those patients in the SECQ4W group with an NRS of >6–≤8 or NRS of >8 at baseline, 13.6% and 0.0% had an NRS=0, and 67.8% and 46.4% had an NRS of >0–≤6, respectively.
Use of any pain medication was reduced from 42.7% at baseline to 25.7% at Week 16 for SECQ2W patients, and from 36.7% to 19.9% for SECQ4W patients (Figure 2). For patients in the placebo group, the reported use of pain medication was lower at Week 16 (28.9%) compared with baseline (38.6%). A greater proportion of DLQI responders was observed in the lower pain categories at Week 16 (NRS=0: 70.6%; NRS: >0–≤6, 44.2%; NRS: >6–≤8, 28.1%; NRS: >8, 13.5%).
This analysis showed that secukinumab improved HS-related skin pain at Week 16 compared with placebo, with a trend for further improvement through to Week 52. These data demonstrate that patients receiving secukinumab experienced a reduction both in pain and in use of pain medication over time, with improved quality of life.
Impact of Secukinumab on Hidradenitis
Suppurativa-Related Work Productivity and Activity Impairment: A Post Hoc Analysis of the SUNSHINE and SUNRISE Phase III Trials
HS exerts a substantial negative impact on patient’s quality of life, and is associated with a considerable decrease in an individual’s work ability and productivity, both of which result in a large socioeconomic burden.10,18-22 The impact of secukinumab on WPAI in patients with HS is unknown. Work productivity loss, presenteeism, and absenteeism in employed individuals, and
Figure 2: Frequency of pain medication use in patients enrolled in the SUNSHINE and SUNRISE trials (pooled) from baseline to Week 16 (post hoc analysis).
Pain medication
Figure adapted from Ingram et al. EADV 2023.
Percentage (n/N) are presented, where N represented the number of patients in the group, and n represents the number of patients who used pain medication for HS.
HS: hidradenitis suppurativa; SECQ2W: secukinumab 300 mg every 2 weeks; SECQ4W: secukinumab 300 mg every 4 weeks.
activity impairment in all patients, was evaluated using the WPAI specific-health problem questionnaire at six time points (baseline, and Weeks 2, 16, 28, 44, and 52) in a post hoc analysis of the SUNSHINE and SUNRISE Phase III trials.4 The proportion of patients achieving a ≥20% improvement in work productivity loss and activity impairment was considered to represent a minimal clinically important difference.22 HiSCR and DLQI response (≥5-point improvement in total score compared with baseline) was measured as a correlative analysis with WPAI parameters.
This investigation included 972 patients who completed the WPAI-specific-health problem questionnaire at baseline. The majority of patients were employed (64.6%) and had Hurley Stage II (59.6%) or Stage III (36.6%), with a mean±SD abscess and inflammatory nodule count of 13.1±8.9, mean±SD time since HS symptom onset of 13.0±9.6 years, and a mean±SD time since HS diagnosis of 7.2±7.3 years. Patients reported a substantial mean work productivity loss of 40.2%, and a substantial mean activity impairment of 45.0% at baseline.
At Week 16, compared with placebo, patients in both secukinumab treatment groups had a mean absolute change from baseline improvement in work productivity loss (SECQ2W: -11.7%; SECQ4W: -8.7%; placebo: -1.0%), activity impairment (SECQ2W: -14.0%; SECQ4W: -10.0%; placebo: -3.6%), presenteeism (SECQ2W: -11.9%; SECQ4W: -9.1%; placebo: -1.6%), and absenteeism (SECQ2W: -5.9%; SECQ4W: -1.1%; placebo: 0.1%).
References
1. van Straalen K et al. New treatments and new assessment instruments for hidradenitis suppurativa. Exp Dermatol. 2022;31(Suppl 1):33-9.
2. Daoud M et al. Overview and comparison of the clinical scores in hidradenitis suppurativa: a real-life clinical data. Front Med (Lausanne). 2023;10:1145152.
3. Kimball A et al. Assessing the validity, responsiveness and meaningfulness of the Hidradenitis Suppurativa Clinical Response (HiSCR) as the clinical endpoint for hidradenitis suppurativa treatment.
In general, responses with secukinumab treatment were sustained through to Week 52, with a trend for improvement over time. Additionally, patients who switched from placebo to secukinumab at Week 16 commonly exhibited an improvement in all WPAI outcomes through to Week 52.
A greater proportion of patients in either secukinumab group achieved a ≥20% improvement in work productivity loss (SECQ2W: 62.7%; SECQ4W: 48.0%; placebo: 41.8%) and activity impairment (SECQ2W: 62.9%; SECQ4W: 54.1%; placebo: 46.7%) versus placebo at Week 16. Patients receiving secukinumab improved the response at Week 52 for work productivity loss (SECQ2W: 71.1%; SECQ4W: 60.3%) and activity impairment (SECQ2W: 71.1%; SECQ4W: 63.7%), including patients who switched from placebo to secukinumab.
Patients treated with secukinumab who achieved an HiSCR and DLQI response at Week 16 and Week 52 had numerically higher WPAI improvements in all parameters, compared with patients not achieving these endpoints. However, improvements were still observed in patients not achieving HiSCR or a DLQI response, indicating that secukinumab may have an impact on work productivity in the context of minimal other clinical responses.
The authors concluded that in patients with moderate-to-severe HS, secukinumab has a beneficial effect on WPAI, with the improvement being sustained through to Week 52. Thus, secukinumab reduces the negative impact that HS has on employment and work productivity.
Br J Dermatol. 2014;171(6):143442.
4. Kimball A et al. Secukinumab in moderate-to-severe hidradenitis suppurativa (SUNSHINE and SUNRISE): week 16 and week 52 results of two identical, multicentre, randomised, placebo-controlled, doubleblind phase 3 trials. Lancet. 2023;401(10378):747-61.
5. Kimball A et al. Two Phase 3 trials of adalimumab for hidradenitis suppurativa. N Engl J Med. 2016;375(5):422-34.
6. Zouboulis C et al. Development and validation of the International
Hidradenitis Suppurativa Severity Score System (IHS4), a novel dynamic scoring system to assess HS severity. Br J Dermatol. 2017;177(5):1401-9.
7. Tzellos T et al. Development and validation of IHS4-55, an IHS4 dichotomous outcome to assess treatment effect for hidradenitis suppurativa. J Eur Acad Dermatol Venereol. 2023;37(2):395-401.
8. Kimball A. High placebo rates in clinical trials: is the problem scoring systems or drug efficacy? J Am Acad Dermatol. 2020;83(6):e431.
9. Frew J et al. Quantifying the natural variation in lesion counts over time in untreated hidradenitis suppurativa: Implications for outcome measures and trial design. JAAD Int. 2020;(2):208-21.
10. Sabat R et al. Hidradenitis suppurativa. Nat Rev Dis Primers. 2020;6(1):18.
11. Ofenloch R. Health-related quality of life in hidradenitis suppurativa. Br J Dermatol. 2017;176(4):861-2.
12. Vanlaerhoven A et al. Hurley III hidradenitis suppurativa has an aggressive disease course. Dermatology. 2018;234(5-6):2323.
13. Navrazhina K et al. Epithelialized tunnels are a source of inflammation in hidradenitis suppurativa. J Allergy Clin Immunol. 2021;147(6):2213-24.
14. Scholl L et al. Surgical treatment of sinus tracts and fistulas in perianal hidradenitis suppurativa. J Cutan Med Surg. 2018;22(2):239-41.
15. Bechara FG et al. Effect of secukinumab on draining tunnels in patients with moderate to severe hidradenitis suppurativa: post hoc analysis of the sunshine and sunrise phase 3 randomised trials. Oral Presentation FC03.05. EADV Congress, 11–14 October, 2023.
16. Dufour D et al. Hidradenitis suppurativa: a common and burdensome, yet underrecognised, inflammatory skin disease. Postgrad Med J. 2014;90(1062):216-21.
17. Ingram JR et al. Secukinumab provides sustained improvements in pain in patients with moderate to severe hidradenitis suppurativa: a post hoc analysis of the SUNSHINE and SUNRISE phase 3 trials. Poster P0045. EADV Congress, 11–14 October, 2023.
18. Montero-Vilchez T et al. The burden of hidradenitis suppurativa signs and symptoms in quality of life: systematic review and metaanalysis. Int J Environ Res Public Health. 2021;18(13):6709.
19. Schneider-Burrus S et al. Features associated with quality of life impairment in hidradenitis suppurativa patients. Front Med (Lausanne). 2021;8:676241.
20. Schneider-Burrus S et al. The impact of hidradenitis suppurativa on professional life. Br J Dermatol. 2023;188(1):122-30.
21. Yao Y et al. Work productivity and activity impairment in patients with hidradenitis suppurativa: a crosssectional study. Int J Dermatol. 2020;59(3):333-40.
22. Gáspár K et al. Resource utilization, work productivity and costs in patients with hidradenitis suppurativa: a cost-of-illness study. Expert Rev Pharmacoecon Outcomes Res. 2022;22(3):399408.
23. Wu J et al. Minimal clinically important difference (MCID) for work productivity and activity impairment (WPAI) questionnaire in psoriasis patients. J Eur Acad Dermatol Venereol. 2019;33(2):318-24.
Efficacy and Safety of Upadacitinib in a Phase II
Randomised, Double-Blind, Dose-Ranging Study of Adults with Extensive Non-segmental Vitiligo
This article reviews an oral poster presentation delivered on 12th October 2023 at the European Academy of Dermatology and Venereology (EADV) Congress in Berlin, Germany
Presenter: Thierry Passeron1,2
Speakers:
1. Department of Dermatology, Centre Hospitalier Universitaire de Nice (CHU de Nice), Côte d’Azur University, France
2. INSERM U1065, Centre Méditerranéen de Médecine Moléculaire (C3M), Côte d’Azur University, Nice, France
Disclosure: Passeron is a consultant for AbbVie, Almirall, Amgen, Bristol Myers Squibb (BMS), Calypso Biotech, Galderma, Incyte, Janssen Pharmaceuticals, Eli Lilly, Novartis, Pfizer, Roivant Sciences, UCB, and VYNE Therapeutics; has received grants and/or honoraria from AbbVie, ACM Pharma, Almirall, Amgen, Astellas Pharma, BMS, Calypso Biotech, Celgene, Galderma, Genzyme/Sanofi, GlaxoSmithKline (GSK), Incyte, Janssen Pharmaceuticals, LEO Pharma, Eli Lilly, Novartis, Pfizer, Roivant Sciences, Sun Pharmaceutical Industries, UCB, and VYNE Therapeutics; is the cofounder of Yukin Therapeutics; and has patents on Wnt agonists or GSK3b antagonist for repigmentation of vitiligo and on the use of CXCR3B blockers in vitiligo.
Acknowledgements: Khaled Ezzedine, Iltefat Hamzavi, Nanja van Geel, Bethanee J. Schlosser, Xiaofei Hu, Xiaohong Huang, David Rosmarin, John E. Harris, Heidi S. Camp, and Amit G. Pandya were co-authors of the oral presentation. Medical writing assistance was provided by Hannah Moir, EMJ, London, UK.
Disclaimer: AbbVie participated in the study design, research, analysis, data collection, and interpretation of data, as well as review and approval of the oral presentation. All authors had access to relevant study data. No honoraria or payments were made for authorship. The use of upadacitinib in vitiligo is not approved, and its safety and efficacy in vitiligo have not been evaluated by regulatory authorities. Prescribing information for RINVOQ (upadacitinib) can be found here (last accessed: 20 October 2023).
Support: The study and publication of this article were funded by AbbVie.
Keywords: Facial Vitiligo Area Scoring Index (F-VASI), non-segmental vitiligo (NSV), Total Vitiligo Area Scoring Index (T-VASI), upadacitinib, vitiligo.
Vitiligo is an autoimmune skin disorder characterised by acquired distinct white patches of the skin. Currently, limited treatment options are available for vitiligo, and there are no approved systemic therapies.
At the European Academy of Dermatology and Venereology (EADV) Congress in Berlin, Germany, 11th–14th October 2023, Thierry Passeron, Professor and Chair of Dermatology at the Côte d’Azur University, Nice, France, and Head of the Laboratory INSERM U1065 Team 12, Centre Méditerranéen de Médecine Moléculaire (C3M), Côte d’Azur University, Nice, France, presented an oral presentation summarising data from a Phase IIb study of upadacitinib, an oral selective JAK inhibitor, in patients with non-segmental vitiligo (NSV), during the ‘Free Communications II’ session.
Passeron gave an overview of the multicentre, randomised, double-blind, placebocontrolled, dose-ranging study that evaluated the efficacy and safety of upadacitinib in adults with NSV. This article focuses on the clinical efficacy endpoints and the safety profile outcomes presented at the EADV congress. Overall, the study demonstrated the clinical efficacy of upadacitinib at 24 weeks at different doses versus placebo, with improvements in repigmentation over time, up to Week 52, with a favourable safety profile.
Introduction
Vitiligo is an autoimmune skin disorder that causes depigmentation of the skin and/or leukotrichia of the hair, resulting from the loss of melanocytes.1 The global prevalence of vitiligo ranges from 0.5–2.0%, with more than 75% of patients exhibiting NSV, where vitiligo patches are distributed on both sides of the body.2,3
JAK inhibition is a mode of action of interest in vitiligo, as it disrupts the process of immunemediated melanocyte apoptosis.1 Upadacitinib, an oral selective JAK inhibitor, is currently approved for various immune-mediated inflammatory diseases, including rheumatoid arthritis; atopic dermatitis; psoriatic arthritis; axial spondyloarthritis, including ankylosing spondylitis; ulcerative colitis; and Crohn’s disease.4
Study Design Evaluating Upadacitinib in Non-segmental Vitiligo
In this multicentre, randomised, double-blind, placebo-controlled, dose-ranging study, eligible patients were adults aged 18–65 years with a clinical diagnosis of NSV, baseline Facial Vitiligo Area Scoring Index (F-VASI) of ≥0.5, Total Vitiligo
Area Scoring Index (T-VASI) of ≥5, and with no prior use of topical or systemic JAK inhibitors.5
A total of 185 patients were enrolled and randomly assigned to receive a placebo, or upadacitinib at either 6 mg (UPA6), 11 mg (UPA11), or 22 mg (UPA22), once daily for 24 weeks in the placebocontrolled period (referred to as period one; Figure 1).5 During the blinded extension period, patients who had received upadacitinib during period one continued with their respective regimens, while patients who previously received placebo were switched to receive upadacitinib once daily, at either 11 mg or 22 mg, for up to 52 weeks.5
The treatment groups were comprised of patients with a mean age between 45–48 years, consisting of 71.1–78.6% White, 2.4–9.5% Black, 13.3–15.9% Asian, and 0.0–8.9% from ‘other’ or ’multiple’ races, including Indigenous American or Alaska Native, Native Hawaiian, or Pacific Islander. Passeron reported that patients across all treatment groups had a baseline T-VASI of 21.0–22.3, F-VASI of 1.0–1.2, and 67.3–74.4% reported active vitiligo.
The primary endpoint was percent change from baseline in F-VASI at Week 24, with key secondary endpoints including ≥50% and ≥75% reduction from baseline in F-VASI (F-VASI 50 and
Figure 1: Study design of the Phase IIb, multicentre, randomised, double-blind, placebo-controlled, dose-ranging study.5
F-VASI 75), change from baseline in T-VASI, and ≥50% reduction from baseline in T-VASI (T-VASI 50) at Week 24. These endpoints were followed through the extension period, during which 89.2% (n=165 out of 185) of patients continued, with interim data through Week 52 reported herein.
Efficacy and Safety of Upadacitinib in Non-segmental Vitiligo
Upadacitinib achieved the primary endpoint of percent change from baseline in F-VASI at Week 24, with improvements in both UPA11 (-35.6%) and UPA22 (-34.0%) versus placebo (-14.4%; p≤0.01 and p≤0.05, respectively; using a mixedeffects model for repeated measures).
Patients achieved greater response rates for F-VASI 50 and F-VASI 75 with UPA11 (38.3% and 19.1%, respectively) and UPA22 (39.5% and 14.0%, respectively), compared with placebo (10.9% and 2.2%, respectively; nominal p≤0.05 for both doses and endpoints, based on non-responder imputation with multiple imputation analysis).
Additionally, response rates for T-VASI 50 were greater with UPA22 (11.6%) compared with placebo (2.2%; nominal p≤0.05) at Week 24.
Extension Period Outcomes
Through Week 52 as Observed
Based on as observed analysis, patients treated with upadacitinib continued to show a reduction in F-VASI and T-VASI through Week 52. Percent change from baseline in F-VASI at Week 52 for UPA6, UPA11, and UPA22 was -53.7%, -60.7%, and -69.8%, respectively. Patients who transitioned from placebo to UPA11 or UPA22 also demonstrated a continued reduction in F-VASI (-51.7% and -57.5%, respectively). The proportion of patients achieving F-VASI 50 was 47.8%, 63.6%, and 82.4% with UPA6, UPA11, and UPA22, respectively. Furthermore, approximately 50% of patients achieved F-VASI 75 with 39.1%, 54.5%, and 41.2% of patients at these respective doses.
Passeron also noted improvements in T-VASI through Week 52 (Figure 2), with nearly a 50% reduction observed in UPA22. Patients who transitioned from placebo to UPA11 or UPA22 at
Figure 2: Percent change from baseline in Total Vitiligo Area Scoring Index* through Week 52 over time, as observed.6
*Values are least squares mean (95% CIs), based on ANCOVA using as observed data. Patients who received a placebo in period one were switched to UPA11 or UPA22 in the extension period, in a blinded fashion, per pre-specified randomisation. Data cut-off date of 13 January 2023.
Week 24 also demonstrated reductions in T-VASI (-34.9% and -32.8%, respectively). T-VASI 50 responses were observed in 34.8%, 45.5%, and 41.2% of patients treated with UPA6, UPA11, and UPA22, respectively.
Safety Profile of Upadacitinib in Non-segmental Vitiligo
Treatment-emergent adverse events were generally similar between upadacitinib and placebo during period one, with the most commonly reported being COVID-19, acne, headache, and nasopharyngitis. Study drug discontinuation due to treatment-emergent adverse events was greater in UPA22 than in other groups. One adjudicated event of non-fatal ischaemic stroke was reported with UPA11 during the extension period, but there were no other adjudicated events, such as
venous thromboembolism or gastrointestinal perforation. There was no reported active tuberculosis, or malignancy.
Conclusion
In this Phase II study of adults with NSV, treatment with upadacitinib for 24 weeks resulted in greater improvements versus placebo in clinical outcomes. Observed clinical efficacy continued to improve through Week 52 with upadacitinib treatment. Upadacitinib was generally well tolerated, with no new safety signals identified beyond the known safety profile for upadacitinib. Assessment of upadacitinib as a potential treatment for vitiligo will continue in Phase III trials.
References
1. Qi F et al. Janus kinase inhibitors in the treatment of vitiligo: a review. Front Immunol. 2021;12:790125.
2. Krüger C, Schallreuter KU. A review of the worldwide prevalence of vitiligo in children/adolescents and adults. Int J Dermatol. 2012;51(10):1206-12.
3. Gandhi K et al. Prevalence of vitiligo among adults in the United States. JAMA Dermatol. 2022;158(1):43-50.
4. AbbVie. RINVOQ. Summary of product characteristics. 2019. Available at: https://www.ema. europa.eu/en/documents/productinformation/rinvoq-epar-productinformation_en.pdf. Last accessed: 20 October 2023.
5. AbbVie. Study to evaluate adverse events and change in disease activity with oral tablets of upadacitinib in adult participants with non-segmental vitiligo. NCT04927975.
6. Passeron T et al. Efficacy and safety of upadacitinib in a phase 2 randomized, double-blind, dose-ranging study of adults with extensive non-segmental vitiligo. Abstract FC02.8. European Academy of Dermatology and Venereology (EADV) Congress, 12 October, 2023.
Abstract Reviews
Spotlighting the latest research in the field of dermatology from abstracts presented at the European Academy for Dermatology and Venereology (EADV) Congress 2023.
Efficacy and Improvement of Qualify of Life in Patients Treated with Brodalumab in Real Clinical Practice:
A Case Series of 31 Patients
Authors: *Nerea Mohino-Farré,1 Josep Pujol-Montcusí,1 Anna Sánchez-Puigdollers,1 Mar Cordellat-Martínez,1 Jose David Cánovas-García,1 Clara Martín-Callizo,1 Laia Pastor-Jané,1 Miquel Just-Sarobé1
1. Department of Dermatology, University Hospital Joan XXIII of Tarragona, Spain *Correspondence to nmohino.hj23.ics@gencat.cat
Disclosure: The authors have declared no conflicts of interest.
Keywords: Brodalumab, case series, moderate-tosevere psoriasis, psoriasis.
Psoriasis is a chronic inflammatory skin disorder with systemic implications, and a range of comorbidities, including psoriatic arthritis, cardiovascular disease, and obesity.1 Advances in our understanding of its pathogenesis have led to the development of highly effective therapies that target the IL-23/T helper 17 pathway.2
Patients with moderate-to-severe plaque psoriasis often require systemic treatments, such as biologics. Brodalumab, a fully human recombinant monoclonal antibody of the IgG2 type, binds strongly to IL-17 receptor A,3 effectively inhibiting pro-inflammatory cytokines like IL-17A, IL-17F, IL-17A/F, IL-17C, and IL17E. This mechanism of action helps alleviate inflammation and associated clinical symptoms in patients with psoriasis. The primary objectives of this analysis were to assess the efficacy and safety of brodalumab at the University Hospital Joan XXIII of Tarragona, Spain, and compare these findings with those from clinical trials.4
MATERIALS AND METHODS
The study included 31 patients with moderateto-severe plaque psoriasis who had received treatment with brodalumab for at least 36 weeks, with a maximum follow-up of 52 weeks. Efficacy and quality of life were evaluated using Psoriasis Area and Severity Index (PASI) and Dermatology Life Quality Index (DLQI) scores at Weeks 4, 12, 24, 36, and 52. Of the patients, 83.9% (n=25) had previously received only one biological therapy.
RESULTS
A rapid improvement in PASI scores was observed (Figure 1A), with a 66% reduction from baseline at Week 4, and 90% at Week 12. By Week 12, 84%, 68%, and 58% of patients achieved PASI 75, 90, and 100, respectively. This improvement was sustained until Week 52. Quality of life also improved rapidly (Figure 1B). A DLQI score reduction of 82% was noted at 4 weeks, reaching 93% at Week 12, and maintaining this improvement until Week 52. Six patients discontinued treatment due to lack of efficacy,
Figure 1: Evolution of efficacy and quality of life (using Psoriasis Area and Severity Index and Dermatology Life Quality Index scores) over time.
A) Rapid improvement in PASI: PASI score evolution over time, measured in weeks.
B) Rapid improvement in quality of life: DLQI score evolution over time, measured in weeks.
C) Utility in different patient cohorts: PASI score evolution over time, measured in weeks, in patients with BMI <30 kg/m2 and BMI >30 kg/m2
DLQI: Dermatology Life Quality Index; PASI: Psoriasis Area and Severity Index.
three achieved disease remission at Week 36, and one stopped treatment due to the appearance of joint involvement. Efficacy data, as assessed by PASI scores, were analysed based on BMI and the number of prior treatments received before starting brodalumab (Figure 1C). No significant differences were observed in terms of efficacy or rapid response among different BMI or previous treatment line groups.
CONCLUSION
In this case series, brodalumab demonstrated high effectiveness and a rapid onset of action, with a 90% reduction in baseline PASI scores by Week 12. These results are consistent with those observed in the AMAGINE-2 and AMAGINE-3 clinical trials.4 Concurrent improvements in quality of life were also evident. Notably, in this case series, most patients had obesity, suggesting that brodalumab is an effective treatment option
regardless of BMI. Regarding the number of previous treatment lines, no definitive conclusions on efficacy could be drawn, given that most patients had only received one prior treatment. Importantly, there was only one discontinuation due to adverse effects, indicating a favourable safety profile. ●
References
1. Goff KL et al. The global burden of psoriatic skin disease. Br J Dermatol. 2015;172(6):1665-8.
2. Ghoreschi K et al. Therapeutics targeting the IL-23 and IL17 pathway in psoriasis. Lancet. 2021;397(10275):754-66.
3. European Medicines Agency (EMA). Kyntheum summary of product characteristics. 2023. Available at: https:// www.ema.europa.eu/en/medicines/human/EPAR/ kyntheum. Last accessed: 6 October 2023.
4. Lebwohl M et al. Phase 3 studies comparing brodalumab with ustekinumab in psoriasis. N Engl J Med. 2015;373(14):1318-28.
Clinical Presentation and Diagnostic Features of Onychomatricoma: A Case Report
Authors: Mircea Negruțiu,1 *Sorina Danescu,1 Adrian Baican1
1. Department of Dermatology, Iuliu Hatieganu University of Medicine and Pharmacy, Cluj-Napoca, Romania
*Correspondence to sorina.danescu@umfcluj.ro
Disclosure: The authors have declared no conflicts of interest. The patient's informed consent was obtained.
Onychomatricoma is an infrequent, benign fibroepithelial tumour originating from the nail matrix. While the exact cause of onychomatricoma remains uncertain, the tumour has been associated with trauma and onychomycosis. The thumb, particularly on the dominant hand, is commonly affected.1
A single, painless subungual mass in an adult patient who also has onychodystrophy, splinter haemorrhages, and a yellowed nail is the typical clinical presentation.2 Characteristic MRI findings include the nail plate’s proximal section having
a Y-shape, along with transverse perforations.3 The following dermatoscopic aspects are encountered: multiple cavities, parallel white lines, parallel lesion edges, splinter haemorrhages, dark dots, nail pitting, and thickening of the free edge. The ultrasonographic appearance is of a hypoechoic tumour that affects the nail matrix, with hyperechoic areas corresponding to the finger-like projections.4
Histopathological examination reveals a biphasic growth pattern. The superficial tumour appearance is of multiple digitised projections, with a fibrous core and a thin epithelial covering. The base of the tumour is composed of epithelium with ‘V-shaped’ keratinous zones, similar to the normal nail matrix. The standard recommendation for treatment and recurrence prevention is complete excision, which includes the normal nail matrix close to the lesion.5
This report aims to describe the clinical, dermatoscopic, and sonographic features of a case involving onychomatricoma.
MATERIALS AND METHODS
The authors present the case of a 58-year-old male who presented with a 2-year history of gradual nail dystrophy, and painless symptoms on his right index finger. Initially misdiagnosed as a wart, the patient had received cryotherapy treatment without improvement. Physical examination revealed asymmetrical, longitudinal, thick yellow bands, and over-curvature of the nail plate in the right index finger. There was no history of nail trauma or personal/family history of
Figure 1: Clinical, dermoscopic, and ultrasound findings.
skin cancer or dermatological disorders. The nail was assessed using dermatoscopy and skin ultrasound.
RESULTS
Dermoscopy revealed perforations in the distal portion of the nail plate, along with white longitudinal grooves. Ultrasound imaging (longitudinal view) demonstrated a hypoechogenic tumour affecting the nail matrix, finger-like projections represented by hyperechogenic areas, and reduced blood flow (Figure 1).
CONCLUSION
The diagnosis of onychomatricoma is frequently delayed, as patients often delay seeking medical attention due to the tumour’s slow growth, and lack of pain in most cases.6
Lichen Sclerosus in Prepubertal Males: Breaking the Paradigm
Authors: *Alessia Paganelli,1,2 Paolo Viscardo Fabbri,3 Filippo Ghidini,4 Laura Bigi,1 Claudia Lasagni,1 Pier Luca Ceccarelli3
1. Section of Dermatology, Rare Diseases Outpatient Clinic, Modena University Hospital, Italy
2. IRCCS-Arcispedale Santa Maria Nuova, Reggio Emilia, Italy
3. Department of Anatomic Pathology, Modena University Hospital, Italy
4. Department of Pediatric Surgery, Modena University Hospital, Italy
*Correspondence to alessia.paganelli@ausl.re.it
Disclosure: The authors have declared no conflicts of interest.
Moreover, the unfamiliarity of dermatologists with the clinical features of onychomatricoma contributes to under-recognition of this uncommon nail matrix tumour. Therefore, this report presents a typical case of onychomatricoma, to aid dermatologists in recognising its clinical features, and promoting early detection of this rare condition. ●
References
1. Cinotti E et al. Imaging technique for the diagnosis of onychomatricoma. J Eur Acad Dermatol Venereol. 2018;32(11):1874-8.
2. Hinchcliff KM, Pereira C. Subungual tumors: an algorithmic approach. J Hand Surg Am. 2019;44(7):588-98.
3. Willard KJ et al. Benign subungual tumors. J Hand Surg Am. 2012;37(6):1276-86.
4. Ocampo-Garza J et al. Pigmented onychomatricoma: four cases. Australas J Dermatol. 2018;59(1):e66-9.
5. Gaertner EM et al. Onychomatricoma: case report of an unusual subungual tumor with literature review. J Cutan Pathol. 2009;36(Suppl 1):66-9.
6. Durrant MN et al. Onychomatricoma: a case report with literature review. Foot Ankle Spec. 2012;5(1):41-4.
BACKGROUND AND AIMS
Lichen sclerosus (LS) is a chronic inflammatory condition primarily affecting the genital area, characterised by hypopigmented skin patches, itching, and pain.1 In some cases, LS can also lead to complications like urinary or sexual dysfunction and, more rarely, squamous cell carcinomas arising in areas of chronic inflammation.2,3 Possible risk factors include a family history of LS, metabolic syndrome, and autoimmune disorders. The diagnosis is typically clinical, but histological confirmation may be necessary. Treatment options include emollients, topical corticosteroids, and systemic immunosuppression for severe cases. Traditionally, LS has been considered to be rare, and more common in females, with peak incidence in prepubertal and late adulthood.4 However, recent evidence suggests it may be an underdiagnosed condition, especially in males and children.5,6
This study aims to examine the impact of LS on male paediatric patients by reviewing cases from a tertiary referral centre over the past decade.
Table 1: Patient characteristics.
Results are indicated either as absolute counts (n) and percentages (%).
For parameters other than sex, percentages are calculated on the total of male subjects (n=187). Topical therapy is here not stratified for the type of LS localisation (for details, see main text).
A total of 194 patients aged 18 or under were histologically diagnosed with LS at the authors’ centre, the Modena University Hospital in Italy. Of these, 193 were males. Six patients lacked follow-up data, and were therefore excluded from the study. Mean follow-up duration was 1.9 years. The most frequently affected areas were the foreskin, external urethral orifice, and glans penis, with no perianal or perineal involvement. For clinical characteristics, see Table 1.
RESULTS
Approximately 90% of patients had phimosis as their only symptom, and circumcision led to complete remission in most cases, without the need for adjunctive topical treatments. Active LS in the glans area was observed in 6.4% of cases. Significant external urethral orifice stenosis
requiring urological intervention was present in 4.2% of cases, with most not requiring prolonged steroid therapy.
CONCLUSION
The study challenges the traditional view of LS as primarily affecting post-menopausal females, and suggests a higher prevalence in male children.7,8 However, the study acknowledges some limitations, including the lack of systematic histological analysis of foreskin specimens after circumcision. This suggests that LS incidence in the paediatric population may still be underestimated, and routine histological examination of foreskin may be necessary for a more accurate assessment.9
Surgery, such as circumcision and meatal stricture treatment, appears to be an effective first-choice option, eliminating the need for chronic corticosteroid therapy.10 The availability
of curative strategies raises questions about whether LS should still be considered a chronic condition, potentially impacting patient care and healthcare systems. However, longer-term follow-up and larger studies are needed to confirm these findings. ●
References
1. Powell J, Wojnarowska F. Lichen sclerosus. Lancet. 1999;353:1777-83.
2. Ju T et al. Evaluation of risk in chronic cutaneous inflammatory conditions for malignant transformation. J Eur Acad Dermatol Venereol. 2023;37(2):231-42.
3. Pope R et al. Lichen sclerosus and sexual dysfunction: a systematic review and meta-analysis. J Sex Med. 2022;19(11):1616-24.
4. Virgili A et al.; GLS Italian Study Group. Gender differences in genital lichen sclerosus: data from a multicenter Italian study on 729 consecutive cases.
The Safety Profile of Biological Agents in Patients with Psoriasis and HIV: A Systematic Review
Authors: *Niyaz Mostafa,1 Kevin Phan2
1. Royal Prince Alfred Hospital, Sydney, Australia
2. Department of Dermatology, Westmead Hospital, Sydney, Australia
*Correspondence to nmostafa.research@gmail.com
Disclosure: There are no conflicts of interests or disclosures.
Psoriasis is a chronic, immune-mediated inflammatory skin disorder that is characterised by the presence of well-circumscribed scaly red plaques.1 The disease can be separated
G Ital Dermatol Venereol. 2020;155(2):155-60.
5. Celis S et al. Balanitis xerotica obliterans in children and adolescents: a literature review and clinical series. J Pediatr Urol. 2014;10(1):34-9.
6. Angotti R et al. Lichen sclerosus in pediatric age: a new disease or unknown pathology? Experience of single centre and state of art in literature. Pediatr Med Chir. 2022;44(1).
7. Aziz Filho AM et al. Frequency of lichen sclerosus in children presenting with phimosis: a systematic histological study. J Pediatr Urol. 2022;18:529.e1-529.e6.
8. Ghidini F et al. Could a careful clinical examination distinguish physiologic phimosis from balanitis xerotica obliterans in children? Eur J Pediatr. 2021;180(2):591-5.
9. Czajkowski M et al. Lichen sclerosus and phimosis - discrepancies between clinical and pathological diagnosis and its consequences. Urology. 2021; 148:274-9.
10. Morrel B et al. Penile lichen sclerosus, circumcision and sequelae, what are the questions? Transl Androl Urol. 2022;11(7):910-3.
into mild, moderate, and severe, and is usually categorised by percentage of skin affected; involvement of high-risk areas, such as the groin; and resistance to conventional treatments. Biological agents are typically reserved for severe psoriasis that has failed other therapies, due to the cost and adverse effects associated due to immunosuppressing attributes. HIV is a disease that attacks the immune system progressively, increasing the risk of opportunistic infections and malignancies. Patients with HIV and severe psoriasis who require biological agents are thus thought to be at increased risk of adverse events.2 The authors conducted a systematic review to determine the safety profile of biological agents in patients with HIV and psoriasis.
MATERIALS AND METHODS
A systematic review of existing studies was performed. Eligible studies reported patients with a diagnosis of both psoriasis and HIV being treated with biological agents.
RESULTS
A total of 43 studies were identified from systematic database searches after applying inclusion and exclusion criteria, which totalled 93
patients. In the authors’ pooled cohort, adverse events were reported in 14% (13 out of 93) of patients. The different categories of biological agents being used were IL-17, IL-23, and anti-TNF agents. The pooled proportion of adverse events in each group were 30% (3 out of 10), 3% (1 out of 30), and 13% (6 out of 45), respectively.
CONCLUSION
The evidence examining the safety profile of biological agents in patients with HIV and
psoriasis is very limited. The data is promising, however, revealing the safety of biologic use, and further prospective studies with larger cohorts are required to reaffirm the findings in the present review. ●
References
1. Rendon A, Schäkel K. Psoriasis pathogenesis and treatment. Int J Mol Sci. 201923;20(6):1475.
2. Myers B et al. Biologic treatment of 4 HIV-positive patients: a case series and literature review. J Psoriasis Psoriatic Arthritis. 2021;6(1):19-26.
Congress Interviews
EMJ is delighted to introduce Thrasivoulos Tzellos, Shyam Verma, Robert Hunger, Margarida Gonçalo, and JanChristoph Simon, thought leaders in dermatology who delve into their illustrious careers and ground-breaking research, providing insight into their work with the European Academy of Dermatology and Venereology (EADV).
Thrasyvoulos Tzellos
Head Physician of Dermatology-Venereology, Department of Dermatology, Nordland Hospital Trust, Bodø, Norway; Board Representative to the Executive Committee of the European Academy of Dermatology and Venereology (EADV)
What led to you pursue a career in dermatology research following your medical degree?
I was always interested in research. Right after my medical degree in 2004 I went to a MSc course regarding research and I was lucky enough to come in contact with well-known dermatologists in the research field through the European Academy of Dermatology and Venereology (EADV), like Christos Zouboulis, who were eager to guide me. Soon I understood that dermatological research is a fascinating field with a lot of development and real opportunities to produce evidence that can help patients. The role of the EADV is crucial in facilitating young scientists/dermatologists to come in contact with research networks. Thankfully, the EADV has already organised important and critical structures to achieve this. EADV Task Forces is the best way to join research networks with regular meetings during EADV congresses, and the EADV School organises courses for research techniques. Furthermore, EADV Scholarships can really
boost young scientists’ careers with a research interest. My personal experience is that my career was hugely facilitated by participating in EADV.
Q2
Your main research interests are hidradenitis suppurativa (HS), skin aging, skin carcinogenesis, and atopic dermatitis. What are the most exciting recent advances within these fields?
I feel that for all these fields the exciting advances are the extensive pipeline and the new drugs that will facilitate better treatment and personalised medicine. The more treatments we have for such diseases, the better for our patients. The introduction and development of immunotherapy for atopic dermatitis, HS, and skin cancer was a critical point that really positively changed and will continue to improve the quality of life of patients and most importantly increase survival. The interest of drug companies for these diseases and the large pipeline is only good news for
our patients. New drugs coming means more options and the achievement of personalised medicine. We hope that the future for these diseases will be like psoriasis. It is difficult nowadays to find patients with psoriasis who will not respond to any of the available treatments.
"New drugs coming means more options and the achievement of personalised medicine."
Q3 How does your involvement as a serving member on the board of the European Hidradenitis Suppurativa Foundation (EHSF) contribute to increased awareness of the condition?
HS is indeed a chronic inflammatory skin disease that still has a diagnosis delay of more than 7 years and increasing awareness is critical. I feel that all members of EHSF are well aware of the fact that this is a critical problem and we try to increase awareness by bringing patient organisations to the front, promoting the evidence, and organising sessions and courses both in the EHSF and the EADV. EADV’s help and role is crucial in this. The EADV Task Force for HS brings together experts from the entire world in an effort to maximise potential and awareness, and the EADV School regularly organises HS courses, both for residents and specialists, in an effort to bring knowledge and awareness. HS patient groups always have a place in EADV congresses, and at each EADV congress the EHSF organises a subspecialty meeting.
Q4 How much of an impact do you believe the EADV congress has, both directly on dermatologists and indirectly on patients?
I know from personal experience that the EADV congress and the EADV in general can have a huge positive impact, both for the development and evolution of dermatologists and for patients. The EADV congress is the arena where dermatologists can hear the latest developments, participate in EADV Task Forces, come in contact with patient organisations, and
participate in a big network of scientists from all over the world. The EADV, being one of the leading societies of dermatology worldwide, has a crucial role to play in increasing awareness; building bridges between European Union (EU) regulators, dermatological organisations, patient organisations, and all other important stakeholders; and promoting practical recommendations and new evidence. For all these reasons, the EADV has the unique role and responsibility to continue working on this path towards improving patients’ lives.
Q5 What changes have you brought into effect whilst serving as Representative of the Board on the EADV executive committee?
I started my role as Representative of the Board on the EADV Executive Committee just a few months ago, in January 2023. My goal is to further facilitate good communication between these two groups. I also have a personal interest and expertise to facilitate the development of EADV evidence-based, practical recommendations for many skin diseases, which is very important both for dermatologists and patients. Finding the best evidence, and evaluating and transforming this into easy to understand recommendations for patients, can have a significant positive impact in promoting awareness and facilitating correct diagnosis, treatment, and follow up. There are many questions that are waiting for an evidencebased reply, and the role of the EADV in this is very important. I feel that I can contribute to this effort.
Q6
What are the main focusses of EADV23 and how do they differ from last year’s congress?
I think that EADV23 will not differ much from EADV22 when it comes to sessions and focuses. The EADV Scientific Committee always organises sessions that cover all important aspects, from chronic inflammatory skin diseases and skin cancer to quality of life. The main focus is always clinically relevant sessions that can facilitate better treatment for patients.
Q7
Which sessions are you most looking forward to at EADV23 and why?
I have to say atopic dermatitis and HS. Both are diseases with high unmet needs for our patients and the pipeline and developments are exciting. EADV congress is the arena used by all scientists involved to present new evidence and breakthrough results. For HS, I am looking forward to hear the new evidence for emerging treatments, the Phase 2 and 3 clinical trials results, and the important developments for new improved clinical outcomes such as IHS4-55, as well as quality of life outcomes.
Q8 Are there any innovations on the horizon for the field of dermatology that you think are particularly noteworthy?
I feel that with all these new drugs and the extensive pipeline, personalised medicine will become important in the future. The mRNAbased vaccines for COVID-19 helped researchers find a way to use experimental immunotherapy, so it seems the door is now unlocked. Another innovation will be the use of genes, viruses, and cells for skin treatment. The COVID-19 era also facilitated the quick development of telemedicine in dermatology and I think that this will be an important part of the future. Lastly, artificial skin and 3D printing, along with tissue regeneration, are fields that have a lot to offer in the future of dermatology. ●
"There are many questions that are waiting for an evidence-based reply, and the role of the EADV in this is very important."
Q1
Shyam Verma
Nirvana Skin Clinic, Vadodara, India; International Board Member of the European Academy of Dermatology and Venereology (EADV)
What sparked your interest in sociocultural dermatology, and how widespread is the understanding of this in the dermatology community and beyond?
Travel is the ultimate eye opener, and so is personal interaction with people from across the globe. One gets to appreciate nuances by comparing the practice of dermatology in a given region from colleagues working in different countries. Curiosity is a great driver for appreciating nuances, and one needs to be outgoing to ask to be educated. I have been lucky in meeting like-minded people who are equally curious, and go out of their way to try and understand the differences in the way we practice dermatology.
"Mycology is a relatively small field. Dermatophytosis forms an even smaller part of mycology."
Q2 You are a prominent researcher within the field of superficial dermatophytosis, especially topical steroid abuse. How important is research in this field?
Mycology is a relatively small field. Dermatophytosis forms an even smaller part of mycology, and, therefore, there are not too many who can claim an active interest in that field. However, the current shift in the epidemiology of dermatophytosis in India in the past decade or so, along with the accompanying curious clinical changes, have been remarkable in countries like India and its neighbours, like Nepal, Bangladesh, Sri Lanka, etc. We have been writing
about the differences in the current scenario of dermatophytosis, and we were able to record several interesting features in the process. We then got a chance to form a group of interested people from across India who were keen on delving deeper into the current scenario of dermatophytosis, and who sent skin scrapings of their patients to a research laboratory in Mölbis, Germany, with a special interest in doing specialised genetic testing like PCR and DNA sequencing. Pietro Nenoff, labopartMedical laboratories, Laboratory Leipzig-Mölbis, Germany, from that laboratory, and his colleague Silke Uhrlaß, have been spearheading research in this area, and their reference laboratory has been providing free investigations for institutions from countries with a high prevalence of dermatophytosis. In fact, the Indian Association of Dermatology, Venereology and Leprology (IADVL) has helped centres in Bangladesh and Nepal to get their samples tested. A striking similarity in the pathogenic species has been found in samples from India and other neighbouring countries. All the countries, including India, also share a common problem of easy availability of fixed dose combination creams (cocktail creams) containing antifungal, antibacterial, and potent steroids, such as clobetasol propionate and betamethasone dipropionate, which are used as first-line in treating patients with dermatophytosis. Ethical issues make it difficult to study the exact role of these combination creams in this new variant of dermatophytosis, i.e., trichophyton mentagrophytes genotype VIII, which is now assigned a new species, Trichophyton indotineae. Currently, efforts are underway to identify the species from various South Asian, and even Middle Eastern countries like the
United Arab Emirates. This curious phenomenon has sparked off an interest from the Centers for Disease Control and Prevention (CDC) in this phenomenon, and they have been helping us in conducting whole genome sequencing, which has shown clonal spread in multidrug resistant dermatophytosis in these populations. Terbinafine resistance and now multidrug resistance have been documented in populations in these countries. The phenomenon is becoming a public health concern, especially now some strains are showing resistance to drugs such as itraconazole, which remains our only hope in this dismal scenario. Researchers from Delhi, India, and Switzerland are now also looking at various genetic factors that may be responsible for the curious resistance patterns. The picture should become clearer with further research.
Q3
How is the European Academy of Dermatology and Venereology (EADV) positively impacting the treatment landscape of skin related diseases for patients and healthcare professionals?
The EADV has become the second largest association of dermatologists globally, after the American Academy of Dermatology (AAD), in terms of inclusivity. It has members from over 90 countries and has robust activities for interested members. One of the best resources made available for members is the
monthly journal that they publish, which has a constantly growing impact factor, making it one of the top dermatology journals globally. There is now also an open access journal made available by the EADV, which increases the reach to people from all over the globe. The EADV also runs various courses, master classes, workshops, etc. on an annual basis for interested members; these are not limited to the conferences and run throughout the year. Details are available on the website. I will take this opportunity to encourage all those who are reading this interview to become a member of the EADV, and take advantage of all the facilities available through its membership. The EADV activities comprise of yearlong programmes that facilitate learning and updates for everyone irrespective of age or experience.
Q4
As one of the two International Board Members of the EADV, how do you approach your role?
Currently, the focus is on trying to get back regular members that we lost during the COVID-19 years. We are trying to get old members to once again pay and join. We are also trying to have more interactive teaching learning platforms.
"We have, accordingly, suggested a name change from immunocompromised districts to immunodysregulated districts."
Q5
You are due to co-chair a session entitled ‘IADVL - Indian Association of Dermatologists, Venereologists & Leprologists’ at the EADV Congress 2023. What valuable insights or knowledge can healthcare professionals expect to gain from attending this session?
These are sister society meetings that the EADV organises each year, with large national societies whose members come and attend the congress in large numbers. Such societies are given a slot to run their own full- or half-day meeting. Members from that country give talks in areas of their own expertise. Our session will focus on several talks on various dermatoses in skin of colour. There will be about 15 talks in the session on the 11th of October 2023.
Q6 Which sessions do you highly recommended for all participants to attend at the EADV Congress 2023?
There are certain areas in dermatology, such as psoriasis, atopic dermatitis, skin malignancies, etc., where new molecules, and revisiting of old molecules, for their treatment are always discussed. I think those are very important topics because the latest trends and opinions are discussed by dedicated researchers from across the globe. In addition, sessions on hair and nail disorders, paediatric dermatology, itch, and inflammatory and infectious diseases are always interesting as they are very relevant in day-today practice, and implementing newer views put forward by experts is very helpful in individual practice.
Q7 What were the main conclusions of your most recent publication, entitled ‘Secondary dermatoses over scars and striae—A phenomenon replete with miscellaneous terms indicating dysregulated immunity’?
We feel that so many terms that occupy space in dermatology lexicon, such as isotopic response, isomorphic response, reverse of these phenomena, etc., create confusion. In addition, the concept of the so called
‘immunocompromised districts’ in dermatology is a term that can cause confusion, as the name indicates compromised immunity locally, which is not truly the case. Rather, it is altered immunity that we see in such areas such as scars and striae. Therefore, there is dysregulated immunity in such areas and not compromised immunity. We have, accordingly, suggested a name change from immunocompromised districts to immunodysregulated districts as an umbrella term.
Q8
To date, what achievements are you most proud of in your career?
I do not know if I can pick the ‘proudest’ achievement, but would consider a few milestones in my career as some of the proudest moments personally. Those include the fact that I have delivered over 200 talks in over 30 countries, and have held senior executive positions, such as Director and Vice President of the International Society of Dermatology (ISD) for four terms. I am currently serving my second consecutive term as an elected International Board member of the EADV. These appointments have enabled me to work closely with other high ranking dermatologists from all over the world and have helped develop a very international outlook. I especially take pride in the fact that I am one of the few, if not the only dermatologist on the Indian subcontinent and probably Asia to have held honorary teaching appointments as Clinical Assistant Professor at the department of dermatology in Penn State University, Pennsylvania, USA, for 4 years in the early 2000s, and continue to hold a similar position at The State University of New York, New York, USA. I have held the position of Clinical Associate Professor in the department of dermatology in the University of Virginia, Charlottesvile, USA, for 14 years and had the same appointment in the department of dermatology in Perelman School of Medicine, University of Pennsylvania, Philadelphia, USA. I am happy to say that I have been promoted to the rank of Adjunct Professor of Dermatology a few months ago, which is indeed an honour considering the reputation of the department as a top ranking one in the entire USA. ●
Robert Hunger
Associate Professor of Dermatology, Department of Dermatology, University Hospital
Inselspital Bern, University of Bern, Switzerland; Board of Directors of the European Academy of Dermatology and Venereology (EADV)
Q1 What led you to a career in dermatology and more specifically dermato-oncology?
One of my main interests since medical school was the immune system. So, after graduating, I started my scientific career in immunopathology on a project about autoimmune tissue destruction in the context of an MD-PhD programme. After finishing my MD-PhD degree I started my career in dermatology as a resident in the Department of Dermatology at the University of Bern, Switzerland. There I could extend my scientific studies in immunology on skin diseases. The main topic was the analysis of lymph cells in the lymph fluid draining human skin in various different inflammatory skin diseases. In addition to this work, I also started my scientific career in skin cancer by taking part in vaccine trials for patients with melanoma. For our patients with melanoma, we also began to collect epidemiological data together with other specialities involved in treatment of melanoma. Over the years, we could generate a huge amount of new data about the outcome of our patients with melanoma.
Q2 Are there any ongoing project you are excited about at the Department of Dermatology, University Hospital of Bern, Switzerland?
One of my key interest is still hidradenitis suppurativa. Although this disease has a prevalence rate of 1%, and is not rare, the
interest in this disease is still very poor. One part of the work at our clinic is collecting more epidemiologic data on this disease. However, for me, the most exciting part in this disease is the analysis on the pathogenesis. There are multiple new methods to analyse the steps leading to this debilitating disease, especially in the field of molecular biology. So, at the moment, we have planned a whole set of new experiments to get more insight into the steps leading to this often debilitating disease.
Q3
How crucial is the European Academy of Dermatology and Venereology (EADV) Congress to the education of healthcare professionals, providing them with the latest scientific advances and research?
The EADV Congress is certainly one of the most important meetings in the field of dermatology. It is a huge assembly of more than 10,000 specialists, with several parallel sessions covering almost all aspects of dermatology. It is, therefore, important for science, education, and also for positioning dermatology in medicine and society. At the moment, dermatology is a rapidly evolving field with many new developments, especially in the treatment of inflammatory and neoplastic skin diseases.
"The EADV plays an important role in positioning the field of dermatology in Europe."
Q4 As the chair for the upcoming discussion on hidradenitis suppurativa at EADV, what do you expect to be the main topics addressed during the session?
Hidradenitis suppurativa is one of the neglected disease in dermatology. However, the EADV is very active in promoting knowledge about this very often severe disease. In the session presented on Thursday 12th October, we will discuss pathogenetic aspects of this disease, comorbidities, and also the rare paediatric form of the disease. In the second part of this session, surgical procedures and new systemic treatments are discussed. On Friday 13th, there is another session on the topic of hidradenitis suppurativa. This is not as much as we will hear about psoriasis or atopic dermatitis, but hidradenitis suppurativa has now reached quite an important position in the EADV Congress.
Q5 What sessions are you most looking forward to at EADV23?
There are plenty of very interesting sessions during this congress. The hidradenitis suppurativa sessions are certainly very interesting, as there are important new data on the effect of new systemic compounds in the treatment of the disease. Here, I want to especially mention the new biologics: IL-17 blockers and IL-36 receptor blockage. Now, JAK inhibitors are tested in hidradenitis suppurativa. So, I am very curious about new data in this field. Besides hidradenitis suppurativa, we will also have multiple new data in psoriasis, atopic eczema, and skin cancer.
Q6
How have you seen EADV impact the field of dermatology since your appointment on the board of directors in 2018?
Dermatology is a rapidly evolving field in medicine and science. The EADV plays an important role in positioning the field of dermatology in Europe, and the EADV has promoted some very important initiatives, such as burden of disease, skin cancer protection, etc. However, the most important event EADV organises is certainly the annual congress. It brings a huge amount of dermatologists, not only from Europe but from the whole world, together to exchange knowledge about skin disease. Another important activity is the Journal of the European Academy of Dermatology and Venereology; the quality and importance of this journal has tremendously increased over the past years. The EADV is also very active in organising online courses, hands on courses, etc.
Q7 What is the most exciting breakthrough or piece of research in the field of dermatology that stands out as particularly exciting in the last 12 months?
For me, the introduction of IL-17 blockades, such as secukinumab and bimekizumab, are important new therapeutic options for hidradenitis
suppurativa. But if we look at dermatology in general, the most important breakthrough is the introduction of the JAK inhibitors. These drugs will certainly change the therapy of most inflammatory skin diseases. Also, in the field of skin cancer there are important new developments, especially the introduction of immune therapy, not only for melanoma, but also for locally advanced or metastatic basal cell carcinoma and squamous cell carcinomas.
"It
is a huge challenge to help these patients to cope with this disease."
Q8
With over 100 publications to your name, which areas do feel warrant further investigation?
My main interest is still hidradenitis suppurativa. It is a huge challenge to help these patients to cope with this disease, and especially to find new therapeutic options that may heal or at least suppress the activity of this disease. My main interest here is the analysis of the pathogenetic steps leading to this disease. By analysing the pathogenesis, we hope to find better therapeutic strategies. But we have also new projects in the field of immunology of melanoma. So, I am still involved in the research on skin diseases. ●
Q1
Citation:
Margarida Gonçalo
Senior Dermatologist and Head of the Department of Dermatology at the University Hospital of Coimbra, Portugal; Professor of Dermatology at the University of Coimbra, Portugal; Member of Executive Committee of the European Academy of Dermatology and Venereology (EADV)
What led you to pursue a career in dermatology? Was there a specific person who, or experience that, was particularly influential?
I must admit that as a medical student, dermatology was not my main focus, even though I was acquainted with dermatology, as my mother was a Dermatologist, and I used to help her with the translation of scientific papers. After graduating as a medical doctor, I was mostly interested in Immunology and immunemediated diseases in internal medicine. But as a researcher at the Faculty of Medicine of the University of Coimbra, Portugal, I found it difficult to do both research and a complex residency in internal medicine. Then Dermatology came as a better choice and, as I had a good qualification after the exam for choosing a specialty, I could choose dermatology.
Q2 Alongside your clinical work and research, you have a keen interest in medical education, and were recently appointed as Head of the Dermatology Department, University Hospital, Coimbra, Portugal. What inspired you to follow an academic career path?
I always liked both research and teaching, so it was natural that, after several years of clinical and basic research in immunology and dermatology, I would start an academic career. After some time, mostly dedicated to the clinical
assistance of patients and clinical studies, I began more involved in basic research combining immunology and dermatology. I prepared my PhD thesis on the mechanisms of delayed immunemediated drug eruptions. After I got my PhD degree, I proceeded with aggregation in immunemediated chronic urticaria.
At the Department of Dermatology, where I was a Senior Consultant in Dermatology for many years, I felt I had the capacity and recognition of my fellows to apply for being the Head of the department after the previous Head retired. I wanted to try to improve the organisation of the department to accomplish a better job as a dermatological clinic in assisting patients, especially the more severe cases, and also to participate more actively in local and multicentre clinical trials and clinical research projects.
Q3 With over 365 publications to your name, which areas of dermatology research do you believe require more attention?
Mostly, I have been involved in areas related to immune-mediated skin diseases, often with multi-organ involvement, such as atopic dermatitis, chronic urticaria, adverse drug reactions, allergic contact dermatitis, and autoimmune skin diseases, like lupus erythematosus and dermatomyositis. I believe these are areas where dermatology can give an important contribution to the understanding of the pathomechanisms of skin and systemic
diseases and their treatment. This is, for instance, the case of lupus erythematosus and dermatomyositis, where understanding skin disease can contribute to a correct and earlier diagnosis, therefore improving prognosis and treatment.
Q4 How successful do you believe the European Academy of Dermatology and Venereology (EADV) congresses are in providing a platform for researchers, clinicians, and industry professionals to exchange knowledge, network, and present their latest research findings?
The EADV congresses are a good setting for different purposes. For younger dermatologists, these congresses are the best place to learn from scientific presentations that can inspire them to improve their knowledge to treat patients, or begin a new career in dermatological research.
For more experienced physicians, apart from improving their scientific knowledge, EADV congresses can be a wonderful setting for networking, meeting friends, discussing scientific and other business, meeting with the international pharmaceutical industry, and getting acquainted with drugs and products that are not yet available in their own country.
Q5 What do you believe to be the primary focus of your role as Representative of the Board on the EADV Executive Committee?
The Board Representative at the Executive Committee contributes to the functioning of the Executive Committee, collaborating with their decisions, and acts as a bridge between the Executive Committee and the Board members.
Q6 You are due to chair a session on cutaneous lupus erythematosus at EADV23. What do you expect to be the key themes discussed?
We will be presenting the latest news on lupus erythematosus. We will deal with the clinical presentations of cutaneous lupus erythematosus,
"For younger dermatologists, these congresses are the best place to learn from scientific presentations."
both the more typical and others that are less typical, but that are important in order to recognise the disease earlier, and to improve diagnosis and prognosis. We will also discuss the latest news on the disease’s pathophysiology and its cutaneous manifestations, which are very important in understanding the new treatments that, we hope, will finally be available to treat these patients efficiently and safely.
Q7
What were the main conclusions drawn in your recent publication, entitled ‘Shedding a light on the importance of photopatch testing: a 12-year experience in a dermatology unit’?
One of the areas of adverse drug reactions we have been interested in is drug photosensitivity, which can be diagnosed by photopatch testing in some cases. Therefore, it is important to have regular reviews on photopatch testing results to understand the most frequent causes of photoallergy, and to alert the doctors, the public, and authorities about the need to avoid these products, or at least be alert to the possibility of this adverse effect.
Q8
Are there any recent advances within the field of dermatology that you are particularly excited by?
The new drugs that have very specific targets, such as cytokines and cell receptors, and are changing the treatment of dermatologic disorders like chronic urticaria, psoriasis, atopic dermatitis, lupus erythematosus, chronic prurigo, hidradenitis suppurativa, and oncologic diseases. Nowadays, the exciting studies in dermatology are opening fields of research for systemic diseases that may share similar pathomechanisms, and can benefit from similar therapies, namely in rheumatology, inflammatory bowel diseases, or allergic diseases.
"It is important to have regular reviews on photopatch testing results to understand the most frequent causes of photoallergy."
Q9Are there any recent advances within the field of dermatology that you are particularly excited by?
The new drugs that have very specific targets, such as cytokines and cell receptors, and are changing the treatment of dermatologic disorders like psoriasis, atopic dermatitis, lupus
erythematosus, chronic prurigo, hidradenitis suppurativa, and oncologic diseases. Now, the exciting studies in dermatology are opening fields of research for systems that could share pathomechanisms, or can co-exist with cutaneous manifestations. This is a really exciting time for dermatology. ●
Jan-Christoph Simon
Professor and Chairman, Department of Dermatology, Venereology and Allergology, and Medical-Scientific Head, Department of Internal Medicine, Neurology and Dermatology, University Hospital Leipzig, Germany; Board Member for the European Academy of Dermatology and Venereology (EADV)
Q1 Following your medical training, what inspired you to pursue a career in dermatology?
I was attracted to dermatology while at medical school. I did part of my medical training at Glasgow University, UK, and there a very inspiring dermatologist, Rona McKie, really got me interested. Back in Germany, I did a very extensive MD thesis on the immunology of melanoma in the laboratories of the Max Planck Institute of Immunology, Freiburg. Finally, two mentors really got me hooked: the Chair of the Department of Dermatology in Freiburg, Germany, Erwin Schöpf, and Paul Bergstressser, Chair of Dermatology in Dallas, Texas, USA, where I did my postdoctoral fellowship in immunodermatology.
Q2 With over 340 publications to your name, which areas of dermatology research do you think warrant greater attention?
What warrants greater attention is the effect of nutrition on both skin health and skin disease.
Q3 You recently co-authored a review entitled ‘Developments and perspectives in allergology’. Which key messages were you trying to convey?
First of all, I conveyed the message that dermatology has an important impact on allergology. Then of course, the most recent
advances in allergology: molecular diagnosis that helps us to characterise the allergic response and give a risk assessment of an individual patient in much more detail, which is true personalised medicine. And then, of course, we are in the area of biologicals, where we can intervene very specifically in inflammatory circuits in allergy by using specific monoclonal antibodies or small molecules.
Q4 What are the main responsibilities associated with your role as a board member for the European Academy of Dermatology and Venereology (EADV)?
I joined the EADV very early, because I really liked the idea of a European spirit in dermatology. This also reflects my personal life; part of my high school time was spent in England, and part of my medical school study in Scotland. Now, I serve as an EADV board member. Together with my colleague, Klaus Strömer, we are ambassadors for Germany. In addition, I have also been newly elected to the Honours and Awards Committee, which is highly rewarding, because we give stipends and scholarships to young dermatologists from all over the world. In sum, I really liked the EADV. It is a very nice family of highly professional dermatologists from all over Europe and if they want me to, I am prepared to take even more responsibilities.
Q5
What are the main focuses of EADV23, and how do they differ from last year’s congress?
Being German, I am of course proud that that we are hosting this year’s meeting in our capital Berlin, and I invite all of our colleagues and friends from all over Europe, and the world, to come and join us there. The international Scientific Committee headed by Michel Gillet from Switzerland has put together a spectacular programme. Never before have there been so many therapeutic advances coming into dermatology and we are proud to give an overview of these innovations in Berlin, and also to put everything in a global context. The other thing which we have learned from the past 3 years of the COVID-19 pandemic is the challenges of infections, and dermatology is well prepared to meet that challenge.
Q6
You are due to present a session entitled ‘Nutrition and dermatology’ at EADV23. What will be the key takeaways?
I am going to give an overview of what is known about the nutritional effect on skin health and disease. In addition, I will present our most recent research: we have studied how certain components of our nutrition affect skin inflammation in psoriasis and how simple dietary measures can really help as an adjunct treatment to existing medical treatments of psoriasis.
Q7
What has been your proudest achievement since being appointed as Medical Scientific Director of the Department of Internal Medicine, Neurology and Dermatology at the University Hospital Leipzig?
I have been elected and re-elected to do this for the past 12 years; it is something that comes on top of my job as Professor and Chair of the Department of Dermatology in Leipzig, which is one of the larger departments in Germany. Looking back at the last 3 years, I am proud of how we managed COVID-19 here in Leipzig. In addition, in the last 12 years the respect and acceptance of dermatology as an important player in the concert of the other medical specialties grew steadily to a very high degree.
Q8
Which sessions should not be missed at EADV23?
First of all, I would encourage everyone reading this interview to look at EADV23’s vast programme, which covers all facets of modern dermatology and venereology; there will be something for every taste and interest. We also have a focus on dermatological aesthetics on Saturday and Sunday. Personally I never miss the plenaries, the controversies, or the hot topics, selected by the EADV President, Martin Röcken. Moreover, the EADV is a family, so I never miss the opening of the congress, and the social gathering. In Berlin the German Academy of Dermatology will present itself and invite our guests to a special evening, and we would, of course, be happy if you would pop by.
In sum, the EADV is going to try its very best to make this 2023 meeting a memorable experience for all of our guests from around the world. ●
A New Landmark for Wellbeing in Psoriasis: The POSITIVE Study
1. Institute for Health Services Research in Dermatology and Nursing (IVDP), University Medical Center HamburgEppendorf, Germany
2. Psoriasis Center, Department of Dermatology, University Medical Center Schleswig-Holstein, Kiel, Germany
Disclosure:
Augustin has served as consultant, or has been a paid speaker, for clinical trials sponsored by companies that manufacture drugs used for the treatment of psoriasis, including AbbVie, Almirall, Amgen, Biogen, Boehringer Ingelheim, Celgene, Centocor, Eli Lilly, GlaxoSmithKline (GSK), Janssen, LEO Pharma, Medac, Merck, MSD, Novartis, Pfizer, UCB, and XenoPort. Mrowietz has been an adviser and/or has received speaker honoraria and/or has received grants and/or participated in clinical trials for the following companies: AbbVie, Aditxt, Almirall, Amgen, Aristea Therapeutics, Biogen, Boehringer Ingelheim, Bristol Myers Squibb, Dr. Reddy’s Laboratories, Eli Lilly, Formycon, GSK, Immunic Therapeutics, Janssen, LEO Pharma, Novartis, PhiStone, Sanofi-Aventis, UCB, and UNION Therapeutics.
Acknowledgements: Medical writing assistance was provided by Jennifer Taylor, London, UK.
Disclaimer: The opinions expressed in this article belong solely to the named interviewees.
Support: The publication of this article was funded by Almirall.
Keywords:
Biologics, IL-23p19 inhibitor, psoriasis, tildrakizumab, wellbeing, 5-item World Health Organization Well-Being Index (WHO-5).
Psoriatic disease is a chronic condition that affects both physical and psychological health. Some patients experience stigmatisation, as well as social and professional limitations. The detrimental impacts of the condition can be summarised under the overall umbrella of wellbeing, with evidence accumulating that psoriasis impacts the wellbeing of both patients and their families. Patients with psoriasis have traditionally been evaluated using the Psoriasis Area Severity Index (PASI), which assesses disease severity, and the Dermatology Life Quality Index (DLQI), which examines quality of life. Both of these measures fail to adequately evaluate wellbeing.
In these interviews with EMJ, Matthias Augustin, Director of the Institute for Health Services Research in Dermatology and Nursing (IVDP), University Medical Center Hamburg-Eppendorf, Germany; and Ulrich Mrowietz, Psoriasis Center, Department of Dermatology, University Medical Center Schleswig-Holstein, Kiel, Germany describe the landmark POSITIVE study, the relevance of looking beyond
skin lesions and including measures of wellbeing in clinical practice, and how the 5-item World Health Organization Well-Being Index (WHO-5) can be used to assess wellbeing in patients with psoriasis. They discuss POSITIVE, the first clinical study in dermatology to use patient-reported wellbeing, assessed using the WHO-5, as a primary endpoint to estimate the impact of the IL-23p19 inhibitor, tildrakizumab, on overall wellbeing in a real-world setting. The POSITIVE study is a new landmark for psoriasis management, and demonstrated that treatment with tildrakizumab was associated with improvements in disease severity, and increased wellbeing of patients, recovering back to normal population levels. This is the first time that a biologic treatment for psoriasis has shown these results. The interviewees concluded that wellbeing assessments should be incorporated into daily clinical practice to evaluate treatment response, and provide patients with more holistic management.
INTRODUCTION
Psoriatic disease is a chronic, inflammatory immune condition affecting more than 40 million individuals worldwide.1 In addition to the physical disability associated with the disease, there is increasing evidence demonstrating that it impacts the wellbeing of patients and their families.2-4 New data show how evaluation of patient and family wellbeing could be improved, providing dermatologists with a tool to more comprehensively assess the impact of treatment.5
THE EFFECTS OF PSORIASIS ON WELLBEING
Matthias Augustin
Augustin described the effects of psoriasis on wellbeing, current methods of assessment, how measurement might be improved, and the impact this could have on daily clinical practice.
What Does the Literature Tell Us About How Psoriasis Affects the Wellbeing of Patients and Families?
Psoriasis has a negative impact on the lives of patients, their families, and other people in their social environment.2-4,6 For patients, psoriasis impacts physical appearance, and causes itching and pain.7 However, the effects of the condition are far-reaching, with eight in 10 patients experiencing stigmatisation, as well as social and professional limitations.8 These detrimental impacts can be summarised under
the umbrella of wellbeing,6,9 which is a construct that encompasses all areas of life that may be impaired due to the skin disease.
What Do Patients Tell You About Their Wellbeing?
It is multifaceted, and it takes time to understand the full picture of the burden of disease, particularly since some patients do not communicate their problems, and withdraw from life. I have seen many patients who have not received effective treatment, and who have stopped social contact with others. They do not go to the theatre or the swimming pool, and they do not participate in sports because they do not want to experience others staring at them. Some weeks ago, I saw a patient who had been banned from a public sauna because of his skin condition, even though he emphasised that it was not contagious, and therefore no risk to others. This negative treatment happens throughout life, including bullying in children, and stigmatisation at work. I had a patient working in a bank who told me that customers did not want to take money from him because they thought the lesions on his hands were contagious.
Most patients who come to me have lived with their disease for decades. They start with the hope, mostly in adolescence, that they will be cured. Over time there is disillusionment, and sometimes fear that the condition may continue throughout their life. Thus, the long-term course of the disease, and the omnipresence of the feeling on the skin, contributes to their loss of wellbeing.
Is the Psychological and Social Impact of the Condition
Generally Underestimated by Healthcare Professionals?
Yes, for some it is surely underestimated, and many do not take the time to ask about this.9 When the skin shows lesions and is inflamed, the reflex of a dermatologist is to address the lesions. Of course, this is one of the tasks, but it is very mechanistic, and there is a lot under the surface that may be even more relevant than the visible skin lesions. It is this aspect that many dermatologists fail to explore on an individual patient level. For patients, this is another negative pressure if they are not permitted to talk about what is burdensome to them. They need relief from the emotional pressure.
What
Are the Standard Methods of Psoriasis Assessment in Clinical Practice? Do They Adequately Evaluate Wellbeing?
In clinical practice, psoriasis is typically assessed using the PASI, the Physician Global Assessment (PGA), and the DLQI.10 The PASI and PGA evaluate disease severity, while the DLQI has been used to measure symptoms and their impact on quality of life.6,10
It is clear that we need to measure both the objective phenotype of the disease and the subjective perception of the patient, because one doesn’t replace the other, and they don’t even correlate closely.11 The PASI, for example, has been used for decades as an objective assessment of clinical severity.12 It is also used in most clinical trials, and has become a reference method.12 As for subjective burden, the DLQI is a pragmatic and validated tool,13 and has been widely used in research. However, the DLQI has several shortcomings. One is that it only provides a snapshot of 10 items relating to quality of life,14 without capturing the full spectrum of patient-relevant considerations. Second, the DLQI combines different elements into one question (for example, problems with a partner, close friends, and relatives), making it difficult to interpret the answer.14 Third, the structure of the instrument will lead some patients to respond that a particular question is “not relevant” to them.15,16 For example, there are questions about the impact of the skin condition on sexual life and on work. Patients who do not work or do
not have a partner because of their disease typically answer “not relevant,” and receive a score of 0. The DLQI, therefore, underestimates disease severity, and the extent of quality of life lost.15,16 The result is that we need an additional assessment that captures wellbeing.
Why
Is the World Health Organization’s Statement on Wellbeing, “Health Is a State of Complete Physical, Mental, and Social Wellbeing and Not Merely the Absence of Disease or Infirmity,” Important for
Patients
with
Psoriasis?
The ambition [of this statement]17 is to normalise patient’s lives, and not just alleviate their symptoms. For patients with psoriasis, one target of treatment is to eliminate the skin lesions. However, we also need to address the psychosocial burden of the disease, including the cumulative life course impairment, which comes from missing things in life. Some people have an accumulation of burden which may seem irreversible, even if the lesions are clear.
What Is the Added Value of the 5-item World Health Organization Well-Being Index Questionnaire for Assessing Wellbeing?
The WHO-518,19 has three main advantages over the DLQI and other assessment tools. One is the positive wording of the items, which focus on achieving goals, rather than on reducing burden. For example, feeling cheerful, calm and relaxed, active and vigorous, and fresh and rested, as well as having a life filled with interesting things. When I started using the WHO-5, some patients smiled and laughed at the questions, which they found more inspiring than typical assessments about burden.
A second advantage is that the WHO-5 is a generic instrument that applies to all individuals, and all diseases. It, therefore, evaluates wellbeing in the context of comorbidities, which is important for holistic treatment. This is particularly relevant in psoriasis, which is associated with increased risks of diabetes, cardiovascular disease, mood disorders, obesity, and many other conditions.20
Thirdly, the WHO-5 is very sensitive, and superior to DLQI, in detecting early signals of
deterioration due to disease.21 This provides an indication to start treatment, improve treatment, or even change treatment.
Why Is Wellbeing Becoming a New Endpoint in Clinical Studies?
Wellbeing is the ultimate goal of treatment for all patients.6 This is the most succinct way of stating what we want to achieve. Of course, there are diseases that are life-threatening, and we want to save lives, but even then, it is not just about saving lives. It needs to be associated with a liveable life. In patients with chronic inflammatory skin diseases, wellbeing is undoubtedly the key goal,6 as well as an assessment aim of the World Health Organization (WHO)17 and national health programmes.10 We, therefore, need further clinical studies to investigate whether new therapies are successful in achieving this aim.
How Might Wellbeing Assessment be Incorporated into Daily Clinical Practice?
The WHO-5 questionnaire is not difficult to adopt; it is a short and intuitive questionnaire, and patients understand how to complete it. However, any outcomes tool needs to have an impact on decision-making. I see the impact of the WHO-5 first of all in its use as a screening tool for psychosocial burden. The WHO-5 total score ranges from 0–100, where 0=absence of wellbeing and 100=maximal wellbeing, with a difference of 10 points being considered the threshold for a clinically relevant change.18 A cutoff of ≤50 is used when screening for depressive symptoms, with ≤28 suggesting moderate-tosevere depressive symptoms.18 In our clinical practice, if a patient has a WHO-5 score of <40, then we know that we need to do something more than just prescribe a drug against psoriasis. The patient may benefit from psychological therapy, for example. It may even be that the losses of wellbeing are independent of the skin condition, and are instead due to other severe diseases or financial difficulties, but this also impacts the skin disease, and so we need to know.
A second use for the questionnaire is that when we see no gain in wellbeing according to the WHO-5, then at some point we need to change treatment. In my clinical practice, we have set
this point at 4 months. If there is no improvement in wellbeing after 4 months of taking a particular medication, then we discuss treatment change. Thus, information on wellbeing is more than just a ‘nice to have’; it should also have a real impact on decisions about treatment and management.
ASSESSMENT OF WELLBEING IN THE POSITIVE STUDY
Ulrich Mrowietz
Mrowietz discussed the first clinical study in dermatology to use patient-reported wellbeing (as assessed by the WHO-5) as a primary endpoint to estimate the impact of the IL23p19 inhibitor, tildrakizumab, in a real-world setting. POSITIVE is an ongoing 24-month, Phase IV observational multinational study in adult patients with moderate-to-severe plaque psoriasis treated with tildrakizumab.6
What Was Innovative About the POSITIVE Study?
There are several aspects of the POSITIVE study that are innovative. Indeed, we tend to call this a groundbreaking study because we have implemented a completely different way of assessing the benefit of a treatment for patients. In virtually all studies that have been performed so far, measures of psoriasis disease severity, such as the PASI and PGA, have been used as a primary endpoint. In some cases, these measures were used together with a non-psoriasis-specific patient-reported outcome, such as the DLQI, as a co-primary endpoint. The aim of this type of study is to assess the efficacy and safety of a given drug in a patient population. However, we think that this does not adequately capture the patient’s perspective.
Our assessment in the POSITIVE study reflects an initiative introduced in 2007 by the WHO, called ‘people-centred healthcare’.22 This initiative states that “the essence of people-centred health care and health systems involves a balanced consideration of the values, needs, expectations, preferences, capacities, and health and wellbeing of all the constituents and stakeholders, and encompasses the ill and those who are well. Transforming the current health care system towards a people-centred
orientation requires comprehensive and positive changes spanning four key policy and action domains: individuals, families, and communities; health practitioners; health care organisations; and health systems.”23
A key element of this initiative is that we should no longer ask patients, “What is the matter with you?”, but should ask, “What matters to you?” I always mention this when I give presentations about rethinking psoriatic disease, because this puts the patient at the centre again. The WHO5 questionnaire was introduced to assess the overarching principle of wellbeing.19 In general medicine, the WHO-5 questionnaire has primarily been used in psychiatry and in diabetology.18 In our research, we have previously shown that the WHO-5 is more effective than the DLQI at assessing wellbeing in patients with psoriasis.21 So, the most important novel aspect of POSITIVE is that it was the first clinical study in dermatology to use patient-reported wellbeing as the primary endpoint in the context of a global, people-centred healthcare approach.6
A second innovative aspect of POSITIVE was that we wanted to encompass the entire environment of the patient. That includes partners and family, as well as treating physicians. In the study, we used the FamilyPso questionnaire to assess the burden that the disease of a partner brings to family members.24 The questionnaire has 15 items divided into five domains: perceived strain by social reactions to the partner’s psoriasis; strain caused by cleaning; acute emotional strain attributed directly to the psoriasis; restrictions of social life; and general emotional strain. The items are scaled in a five-point Likert format: 0=not true; 1=somewhat true; 2=moderately true; 3=quite true; and 4=very true, with the supplementary option of “does not apply to me.” The Physician’s Satisfaction Questionnaire (PSQ), which was created for this study based on the compassion subscale of the Professional Quality of Life (ProQOL) questionnaire, was used to evaluate the long-term benefit of tildrakizumab on physician satisfaction with treatment.6,25
What Are the Latest Findings of the POSITIVE Study?
An interim 28-week analysis of the POSITIVE study was presented for the first time at the 32nd European Academy of Dermatology and
Venereology (EADV) conference in October 2023 in Berlin, Germany.5 The objective of this study is to assess the effectiveness of tildrakizumab on the overall wellbeing of patients with moderateto-severe psoriasis treated with tildrakizumab in routine care. A total of 263 patients were enrolled in Austria, Belgium, France, Germany, Italy, Spain, Switzerland, the Netherlands, and the UK. The mean age was 46.3 years, 65.8% were male, the mean BMI was 28.2 kg/m2, and 34.2% were current smokers. At baseline, the mean WHO-5 score was 53.9. To put this into context, the mean WHO-5 score was 63.9 in the general population of the countries participating in the POSITIVE study, 52.2 among females with breast cancer, and 56.0 in patients with Type 2 diabetes.
The mean WHO-5 score significantly increased from 53.9 at baseline to 67.1 at Week 16 (p<0.001; mean change from baseline of 12.4), and to 67.3 at Week 28 (p<0.001; mean change from baseline of 12.7).5 At baseline, 41.2% of patients had a WHO-5 score ≤50 (17.6% of patients ≤28), decreasing to 20.2% (5.2% of patients ≤28) and 20.6% (5.7% of patients ≤28) at Week 16 and Week 28, respectively. After just 16 weeks of treatment with tildrakizumab, wellbeing scores had significantly increased compared with baseline, and were similar to the general population. This benefit was maintained up to Week 28.
The improvement in wellbeing occurred in parallel with improvements in disease severity. Mean PASI score decreased from 13.4 at baseline to 1.6 after 28 weeks of treatment with tildrakizumab (p<0.001), a mean change from baseline of −11.6 (Figure 1).26 At Week 28, 92.6%, 85.1%, and 55.3% of patients achieved PASI ≤5, PASI ≤3, and PASI ≤1 responses, respectively. Taken together, we see the benefit of tildrakizumab to patients not only through the WHO-5 score, but also through the somatic PASI score, which indicates that a high proportion of patients are virtually clear of skin lesions after 28 weeks of treatment. Furthermore, no new safety signals were observed, and 28-week interim safety data, also presented at the EADV conference,27 was consistent with previous studies.28,29
At the conference, 28-week interim data on the impact of psoriasis on the wellbeing of partners of patients included in the POSITIVE study were
Figure 1: Absolute PASI score up to week 28.26
*Mean change from baseline (p<0.001). PASI range: 0–72, no disease to maximal disease.
PASI: Psoriasis Area Severity Index.
also presented.30 The wellbeing of partners was assessed using the FamilyPso questionnaire. Of 263 patients included in the study, 162 (61.6%) had a partner. The questionnaire was completed by 113 partners at baseline, and 64 partners after 28 weeks of patient treatment with tildrakizumab. The mean total FamilyPso score decreased from 1.3 at baseline to 0.8 at week 28 (p<0.001), with a mean change from baseline of −0.4. The mean FamilyPso scores for each domain at baseline and Week 28, respectively, were 1.1 and 0.7 for “perceived strain by social reactions to the partner’s psoriasis,” 1.4 and 1.0 for “strain caused by cleaning,” 1.2 and 0.7 for “acute emotional strain attributed directly to the psoriasis,” 0.9 and 0.4 for “restrictions of social life,” and 1.9 and 1.3 for “general emotional strain.”
Why Are the Findings of the POSITIVE Study Important?
The POSITIVE study is a new landmark for wellbeing in psoriasis. The study demonstrated that treatment with tildrakizumab was associated not only with improvements in disease severity, but also with improvements in the wellbeing of both patients and their partners. This is the first time that a biologic treatment for psoriasis has shown these results.
What Would You Like to See Happen in Future as a Result of the POSITIVE Study?
We think that it is more appropriate to use a patient-centric endpoint, such as the WHO-5, as well as the term wellbeing, instead of simply measuring PASI, PGA, and DLQI. Otherwise, we miss what the disease, and the treatment of the disease, really mean to patients and families.
There is a need to spread the knowledge that psoriasis can be managed by assessing lesion severity (for example, with PGA or PASI), as well as assessing wellbeing with the WHO-5. After a period of treatment, the assessments should be repeated to see if there is improvement. Our ultimate goal is for patients and their partners to be happy. In the scenario of shared decisionmaking, where patients are informed about the disease and potential treatments, we could also include input from the partner of the patient. The investigators of the POSITIVE study hope to communicate our ambitions for wellbeing assessment on a global scale, by embedding the concept into a renewed WHO global report on psoriasis.31
CONCLUSION
Psoriasis has wide-ranging physical and psychological effects on patients and their families. Current assessment methods fail to adequately evaluate the full impact of the disease. The WHO-5 questionnaire is a practical measure for examining patient wellbeing in
References
1. Damiani G et al. The global, regional, and national burden of psoriasis: results and insights from the Global Burden of Disease 2019 study. Front Med (Lausanne). 2021;8:743180.
2. Lewis-Beck C et al. Analysis of the relationship between psoriasis symptom severity and quality of life, work productivity, and activity impairment among patients with moderate-to-severe psoriasis using structural equation modeling. Patient Prefer Adherence. 2013:7:199-205.
3. Bhosle MJ et al. Quality of life in patients with psoriasis. Health Qual Life Outcomes. 2006;4:35.
4. Eghlileb AM et al. Psoriasis has a major secondary impact on the lives of family members and partners. Br J Dermatol. 2007;156(6):1245-50.
5. Sommer R et al. Patient-reported well-being using tildrakizumab in a real-world setting: 28-week interim data of the phase IV POSITIVE study. Abstract 3490. 32nd EADV Congress, 11-14 October, 2023.
6. Augustin M et al. Patient-reported well-being in value-based care using tildrakizumab in a realworld setting: protocol of a multinational, phase IV, 1-cohort prospective observational study (the POSITIVE study). BMJ Open. 2023;13(2):e060536.
7. Mrowietz U, Reich K. Psoriasisnew insights into pathogenesis and treatment. Dtsch Arztebl Int. 2009;106(1-2):11-9.
8. Zhang H et al. Stigmatization in patients with psoriasis: a mini review. Front Immunol. 2021;12:715839.
9. Prignano F et al. Sharing patient and clinician experiences of moderate-to-severe psoriasis: a nationwide Italian survey and expert opinion to explore barriers impacting upon patient wellbeing. J Clin Med 2022;11(10):2801.
clinical trials, and in clinical practice. The POSITIVE study demonstrated that tildrakizumab, was associated with improvements in disease severity, and with increased wellbeing in patients and their partners. Incorporating wellbeing assessment into daily clinical practice would lead to more holistic management of patients with psoriasis.
10. National Institute for Health and Care Excellence (NICE). Psoriasis: assessment and management. 2012. Available at: https:// www.ncbi.nlm.nih.gov/books/ NBK553610/pdf/Bookshelf_ NBK553610.pdf. Last accessed: 12 October 2023.
11. Yang J et al. Psoriatic foot involvement is the most significant contributor to the inconsistency between PASI and DLQI: a retrospective study from China. Clin Cosmet Investig Dermatol. 2023:16:443-51.
12. Spuls PI et al. How good are clinical severity and outcome measures for psoriasis?: Quantitative evaluation in a systematic review. J Invest Dermatol. 2010;130(4):933-43.
13. Liluashvili S, Kituashvili T. Dermatology Life Quality Index and disease coping strategies in psoriasis patients. Postepy Dermatol Alergol. 2019;36(4):41924.
14. Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI) - a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19(3):210-6.
15. Langebruch A et al. Does the Dermatology Life Quality Index (DLQI) underestimate the diseasespecific burden of psoriasis patients? J Eur Acad Dermatol Venereol. 2019;33(1):123-7.
16. Barbieri JS, Gelfand JM. Influence of “not relevant” responses on the Dermatology Life Quality Index (DLQI) for patients with psoriasis in the United States. JAMA Dermatol. 2019;155(6):743-5.
17. World Health Organization (WHO). Constitution. 1948. Available at: https://www.who.int/about/ governance/constitution. Last accessed: 12 October 2023.
18. Topp CW et al. The WHO-5 WellBeing Index: a systematic review of the literature. Psychother Psychosom. 2015;84(3):167-76.
20. Bu J et al. Epidemiology of psoriasis and comorbid diseases: a narrative review. Front Immunol. 2022;13:880201
21. Sommer R et al. Measuring wellbeing in psoriasis: psychometric properties of the WHO-5 questionnaire. J Eur Acad Dermatol Venereol. 2022;36(12):e986-7.
22. World Health Organization (WHO). People-centred health care: a policy framework. 2007. Available at: https://iris.who. int/bitstream/handle/10665 /206971/9789290613176_eng. pdf?sequence=1. Last accessed: 13 October 2023.
23. World Health Organization (WHO). People at the centre of health care: harmonizing mind and body, people and systems. 2007. Available at: https://iris. who.int/bitstream/handle/10665 /206969/9789290613169_eng. pdf?sequence=1&isAllowed=y. Last accessed: 13 October 2023.
24. Mrowietz U et al. FamilyPso - a new questionnaire to assess the impact of psoriasis on partners and family of patients. J Eur Acad Dermatol Venereol. 2017;31(1):12734.
25. NovoPsych. The Professional Quality of Life Scale. 2021. Available at: https://novopsych. com.au/assessments/clinicianself-assessment/the-professionalquality-of-life-scale-5-proqol/. Last accessed: 13 October 2023.
26. Augustin M et al. Real-world effectiveness, quality of life, and treatment satisfaction with tildrakizumab in patients with moderate-to-severe psoriasis: 28-week interim data of the phase IV POSITIVE study. Abstract 3492. 32nd EADV Congress, 11-14
19. World Health Organization (WHO). Wellbeing measures in primary health care/the Depcare Project. 1998. Available at: https://iris.who.int/bitstream/ handle/10665/349766/WHOEURO-1998-4234-43993-62027eng.pdf?sequence=1&isAllowed=y. Last accessed: 13 October 2023.
October, 2023.
27. Mrowietz U et al. Real-world safety of tildrakizumab in patients with moderate-to-severe psoriasis: 28-week interim data of the phase IV POSITIVE study. Abstract 3491. 32nd EADV Congress, 11-14 October, 2023.
28. Thaçi D et al. Five-year efficacy and safety of tildrakizumab in patients with moderate-tosevere psoriasis who respond at
week 28: pooled analyses of two randomized phase III clinical trials (reSURFACE 1 and reSURFACE 2). Br J Dermatol. 2021;185(2):32334.
29. Tsianakas A et al. Real-world effectiveness and safety of tildrakizumab in long-term treatment of plaque psoriasis: results from the non-interventional, prospective, multicentre study TILOT. J Eur Acad Dermatol Venereol. 2023;37(1):85-92.
30. Mrowietz U et al. Impact of patient psoriasis on partner well-being in a real-world setting: 28-week interim data of the phase IV POSITIVE study. Abstract 3489. 32nd EADV Congress, 11-14 October, 2023.
31. World Health Organization (WHO). Global report on psoriasis. 2016. Available at: https:// www.who.int/publications/i/ item/9789241565189. Last accessed: 13 October 2023.
Q1
Interviews
The EMJ team had the pleasure of speaking to Christopher Griffiths, who detailed his efforts in revolutionising the treatment of psoriasis and inflammaging, and Edel O’Toole, who shared their dedication to the field of rare skin diseases.
Christopher Griffiths
Emeritus Professor of Dermatology, University of Manchester, UK; Adjunct Professor, King’s College London, UK; Consultant Dermatologist, King’s College Hospital, London, UK
What led you to pursue a career in dermatology? Was there a specific person or experience that was particularly influential?
There were actually two reasons. When I was about 4 years old, I was given a bird book by my parents and I memorised every bird in the book as a party trick. Not only did I become interested in birdwatching when I was very young, but I was also good at art. So, I had an artistic view of the world and I was good at pattern recognition. When I was in medical school, at St Thomas's Hospital Medical School in London, UK, I went into my first dermatology clinic and I found this relatively straightforward. I was able to recognise the difference between psoriasis and eczema while my medical student colleagues were less assured. I am sure the ability to recognise patterns led me into dermatology and I then realised that this was going to be the specialty for me. I could also see that there were academic opportunities, as well as a nice mix of medicine
and surgery. When people ask if I would do the same again, I say yes, I would go to medical school, do dermatology, and be an academic, which is, I believe, a pretty strong endorsement.
Q2
You have since published over 770 PubMed cited articles. What do you believe are the current gaps in dermatology research?
The big gaps in research are in inflammatory skin disease, which we are still looking to prevent or even cure. It is interesting that we can prevent and cure skin cancers and infections, but inflammatory skin disease (including acne), which affects a lot of people, cannot be prevented or cured yet. A cure needs to be found for these diseases, meaning that you can treat it, and stop treatment without the disease returning. It is not enough if one is still required to continue the medicine to keep the disease in remission; this is the same principle as other
inflammatory diseases such as Crohn’s disease and rheumatoid arthritis.
Q3
You co-founded the International Psoriasis Council and have focused much of your research on this topic. What would you say are the most common misconceptions of this condition?
I do a lot of work around educating the general public about psoriasis, to encourage involvement and engagement, because the stress and psychological detriment that psoriasis causes people is often life ruining. Historically, people with psoriasis were viewed as having leprosy and they were stigmatised because of that. The first person to differentiate leprosy from psoriasis was a one of the founders of British dermatology, Robert Willan, in 1803. But here we are over 200 years on and people are still stigmatised because they have psoriasis. The general public view people with skin conditions as having something contagious, and I can relate many, many stories of people who have not been able to pursue the career they wanted because of this. They feel inhibited to interact with the general public because they are treated as though they have a contagious skin condition. They cannot go to the local swimming pool, they cannot wear a short
sleeved shirt, shorts, or a skirt in summer. Thus, that is the biggest misconception, the stigma due to concern that it is contagious or that the person is not clean.
Q4 Are there any particularly promising advances within the field of psoriasis research that you see impacting practice in the near future?
I have been lucky enough to be involved with all the advances over the last 40 years, ever since working with Lionel Fry at Saint Mary's Hospital in London, UK. When I started as a trainee dermatologist, I was part of the team that showed psoriasis to be an immune-mediated disease, which it was not thought to be until that time. We also performed one of the first studies to show that ciclosporin was highly effective for psoriasis, and that started the idea of targeting the immune system and components of the immune system for treatment of the disease.
"The stress and psychological detriment that psoriasis causes people is often life ruining."
I beleive we set the groundwork for what then became the biologic targeted therapies for psoriasis many years later; we now have 11biologics of, and they have proven to be highly effective and remarkably safe. These treatments have transformed many people's lives for the better -without a doubt the biggest change in dermatological practice I have seen. The number of people that have to be admitted to hospital with severe psoriasis has diminished hugely, and many dermatology departments do not actually need hospital beds anymore because of that.
The newer drugs under development for psoriasis are not new cytokine targets, they are just different ways of targeting the same cytokines such as IL-17, as well as the new small molecules that have recently been approved in Europe, and are taken orally rather than being injected. Deucravacitinib, which targets tyrosine kinase 2, looks very promising. Advanced therapeutics, particularly cell-based therapies, may help in managing or even curing these conditions.
Q5
Across all clinical disciplines there is a focus on personalised medicine. Do you think this is a possibility for conditions like psoriasis and eczema?
I have thought this for many years, which is why a group of us put together a successful application to the Medical Research Council (MRC) in the UK 12 years ago. It is an industryacademic collaboration called ‘PSORT (Psoriasis: Stratification to Optimise Relevant Therapy), it is very much based around a stratified, personalised approach, initially on biologics. We have made a lot of progress with clinical, genetic, and immune biomarkers, as well as an algorithm to predict and reproducibly stratify patients with psoriasis in their response to therapy. We do not have a biomarker yet, but we have a lot of data that could help create a more targeted rather than a trial and error approach to prescribing for this disease. I am a big fan of not just personalised medicine, but also so-called P4 medicine, which is personalised, predictive, preventive, and participatory. It is more of a holistic approach to getting people onto the right treatment for them. It is about the person rather than the disease.
Q6
In the recently published review you co-authored, entitled ‘Inflammaging and the skin’, what was the key message you were trying to deliver?
The other big area of research that I developed over the last 30 years is around skin aging. When I was at the University of Michigan, we published the first work to show that topical retinoids could repair photo-aged skin and we became interested in the underlying mechanisms of photo-aging, which is sun damage. That is what causes most of the features of aging, such as brown spots and wrinkles, rather than just an intrinsic chronological aging. We set up a big research programme to understand mechanisms behind aging, and helped develop the ‘No7’ range for Protect & Perfect, which changed the landscape as to how people think about the science that underpins skin aging therapy. As we move into the more difficult to study chronological and intrinsic aging, it seems there is an inflammatory infiltrate in aging skin, leading to the question of how we can prevent that inflammation. It is like a chicken or egg situation: is the inflammation a result of damage or is it actually contributing to the damage. I think it is probably contributory and one might by targeting this be able to reduce or slow down the aging process.
Q8Can you talk more about the research with Boots and the publicity that followed?
It was a really surprising time actually, because they broadcast it on a Tuesday evening, on the BBC Horizon programme, and I was phoned up 2 days later by a journalist I know at The Times of London, who I talked to about psoriasis previously. She said she wanted to talk to me about the work I did with Boots. I asked why she wanted to do that, and she said: “You may not know this, but you are front-page news in the Daily Mail today, they’ve been reporting about people that are selling out this specific face cream.” I think 50,000 units of this specific face cream were selling a day, compared to what used to be 10,000 units a week. People were queuing around the block to get it, they were limiting the number of samples to three, and people were buying them to resell on eBay up to three times the price. They had to shut down and re-tool the
whole production line, and 15 years on, it is still the number one seller in the UK.
Q9 What leadership skills did you gain during your role as President of the British Association of Dermatologists (BAD)?
I have been lucky enough to be president and chair of a few organisations. It is so important that people who go into those positions receive some training, which is why we set up the Future Leaders Academy for early career researchers in dermatology, across Europe. Then, 4 years ago, we set up a leadership and mentoring training course to give these people the tools they need to be effective leaders. I have three things to say about leadership, with the first one being the importance of being equitable. Everyone in the team, however junior, has something important to say, and you need to listen to what people tell you. Second, you need to be flexible, which is key and may hamper research if not recognised; some people are too fixed on a hypothesis, but it is important to be flexible and to seize opportunities when they come along. Third, a leader should be optimistic, because if the leader is not optimistic, you have a problem. You need someone who sees the big picture.
Q10
You have been awarded an OBE, you have chaired many international societies and councils, and have founded a skin care brand. To date what achievement are you most proud of?
Firstly, I am very proud of the work we have done with psoriasis over the years. From the very inception of immune-mediated drugs, to where we are now, it has been a privilege to be involved with that. In the last few years, I have also become very involved in global health, setting up skin clinics in refugee camps. After visiting dermatology departments in Myanmar about 4 years ago with my colleague Dr Su Lwin we felt that despite there being some talented dermatologists in Myanmar they did not have
"Everyone in the team, however junior, has something important to say."
the resources to really make a difference. This motivated us to set up a charity - the Burma Skincare Initiative (BSI) – in 2019, which had made huge progress until Covid came along, and then a military coup in the country in February 2021. But despite the military coup, which has been catastrophically awful for the people in the country, we have been able to maintain our mission, which is promoting excellence of skincare for the people of Myanmar. It is when one does work like this, that one realises how lucky we are with the National Health Service (NHS) in the UK, which is often taken for granted.
Q11Overall,
what advice would you give to clinicians working with patients with psoriasis, specifically regarding how to improve their practice?
The advice I would give is to treat every patient as an individual with different requirements for treatment, which goes back to that personalised approach. It is the art of medicine, which tends to be forgotten. Patients do not just want someone who knows all the science; they want someone who has got their back, cares about them, and knows them.
Q12Do
you have anything to add?
Going back to the first question, I have always been fascinated by art and as I have gone around the world and talked to people, I noticed a lot of dermatologists are interested in art. I do not think the reasons I went into dermatology are unique, so we set up a course for our trainee dermatologists in Manchester few years ago. Working with the Salford Art Gallery, we employed an art historian to teach about art appreciation and visual literacy, how to look at a painting, and how to describe what you one observes. The trainees that registered on the six week course ended up being better diagnosticians. I along with two colleagues, Dr Helen Young and DrSarah Walsh, organise an annual course at the Tate Gallery and Courtauld Institute in London to teach European dermatologists how to look at a painting in the same way as looking at someone with a skin disease, and how to describe it. ●
Q1
Edel O’Toole
Professor of Molecular Dermatology and Co-director of HARP Clinical PhD programme, Blizard Institute, Queen Mary University of London; Emeritus Centre Lead, Centre for Cell Biology and Cutaneous Research, London; Consultant Dermatologist at the Royal London Hospital, Barts Health NHS Trust, London, UK
After completing your medical degree, what inspired you to complete a PhD on keratinocyte biology?
I was always interested in biology and science. As a child, I loved identifying wild flowers and this is not all that dissimilar to dermatology, where we look and make a diagnosis. When I first started in dermatology, I could see that there were lots of opportunities for research in the field. I decided to go to the USA from Ireland because of the encouragement of Rosemarie Watson, and I was fortunate to land in the laboratory of David Woodley, who nurtured my interest in keratinocyte biology and specifically extracellular matrix.
"There are at least 2,000 skin disorders and there is still a lot to be learned about many of these disorders at a molecular level."
Q2 With over 131 publications to your name, which areas of dermatology research do you believe require the most attention?
Single cell and spatial transcriptomics are leading to high impact publications in the field of dermatology, but understanding the biology of all the lists of annotated genes is important. There are at least 2,000 skin disorders and there is still a lot to be learned about many of these disorders
"There are still lots of discoveries to be made and we badly need more people who can bridge the gap between the clinic and the laboratory."
at a molecular level. There are many rare and common disorders that we can learn a lot more about. Artificial intelligence will likely help with pruning ‘big data’ in the future.
Q3
What are the most significant changes you have seen in the management of rare skin diseases during your time working in the field?
In the last 5 years there is much more hope that there will be effective treatments and pharmaceutical companies are showing interest in rare skin diseases. Some of the major advances have been in the field of epidermolysis bullosa (EB). This includes the landmark paper by Hirsch et al.,1 who used LAMB3 cDNA transduced corrected autologous transgenic keratinocyte cultures to regenerate the entire epidermis in a child with a homozygous mutation in LAMB3, causing junctional epidermolysis bullosa. In another type of EB, recessive dystrophic EB (RDEB) caused by mutations in Type VII collagen (COL7A1), Peter Marinkovich, from Stanford, California, USA, working with Krystal Biotech (Pittsburgh, Pennsylvania, USA), have used topical herpes simplex virus type
1-based gene therapy (Beremagene geperpavec) to deliver COL7A1 and restore Type VII collagen expression.2 There are now also trials of topical sirolimus (rapamycin) and TRPV3 antagonists in pachyonychia congenita, a rare disorder causing painful, disabling plantar calluses. I do a lot of work with Pachyonychia Project, an amazing support group for patients with pachyonychia congenita, and the patients are really enthusiastic about participating in clinical studies.
Q4
As chairman of the Medical Advisory Board of the Ichthyosis Support Group, could you share some of the recent advances in this field that excite you the most?
We are learning a lot more about ichthyosis and in particular about cytokines that are expressed in severe ichthyosis skin. This is leading to repurposing of biologics such as ustekinumab and dupilumab in various types of ichthyosis. We still need to learn more about how biologics affect the skin barrier in ichthyosis, so we need to do more clinical trials. We also know a lot more about the genetic basis of ichthyosis. For example, there are now >14 genes known
to cause non-syndromic autosomal recessive congenital ichthyosis. If necessary, we now can obtain a genetic diagnosis fairly quickly in 80% of patients with ichthyosis. The National Health Service (NHS) in the UK is now offering genome sequencing for unwell neonates, which will include severe ichthyosis and other severe rare genetic disorders.
Q5
What are you most proud of from your time on the European Society for Dermatological Research (ESDR) board from 2018–2022 and specifically as Chair of the Diversity Taskforce?
It was an interesting period as we did not have an ESDR meeting in 2020 and the meeting was virtual in 2021. I co-organised the COVID-19 symposium with Curdin Conrad and invited Michael Ryan, Executive Director of the World Health Organization (WHO) Health Emergencies Programme, who led the operational response to the COVID-19 pandemic worldwide, to join the symposium for a Question and Answer session. He accepted, which was fabulous (he was in my class in medical school). As chair of the Diversity Taskforce, I helped organise Global Health Awards for young dermatology trainees and scientists to attend the ESDR from East Africa and Burma in 2019, and subsequently Tunisia, Egypt, South Africa, and Thailand in 2022. I hosted a round table event around ancestral diversity and from that we came up with a plan going forward to try and make the ESDR more inclusive. There has been progress but we always need to do better.
Q6 What are the greatest challenges you have faced in both your research and clinical career? How did you overcome these?
Being a clinician scientist is like being on an intermittent roller coaster. There are moments of great joy, such as when a student does really well in their PhD viva, my favourite paper gets accepted in a great journal, a grant gets accepted, or research in the lab shows a truly unexpected finding. On the other hand, there are also less joyous and frustrating moments, when
a grant or paper gets rejected, the keratinocytes stop growing, or some infection occurs and work comes to a standstill.
I think it is important if you are doing basic science research that the week is compartmentalised. Time should be allocated for clinic and at a set time you should go back to the laboratory environment; so in effect time management. I think building resilience is also important as a clinical academic, so one can cope with the frustrating moments. It also important to have a trusted mentor whom you can bounce ideas off. The mentor may just say what you were thinking but the reassurance is always good.
In my clinical career, the increase in computer work, general bureaucracy, and regulation of doctors has been irritating. My main focus in the clinical aspect of my career is getting the patients better and I try to put those things to the back of my mind.
Q7 What advice would you give to young clinicians entering the field of dermatology?
Be curious; do not take anything for granted; believe the data; believe what you see, both in clinic and in the laboratory; and find an enthusiastic mentor. If you want to do research, which I hope you do, there are still lots of discoveries to be made and we badly need more people who can bridge the gap between the clinic and the laboratory. Get the best laboratory training possible, which will set you up for a clinician scientist career. ●
References
1. Hirsch T et al. Regeneration of the entire human epidermis using transgenic stem cells. Nature. 2017;551(7680):327-32.
2. Guide SV et al. Trial of Beremagene Geperpavec (B-VEC) for Dystrophic Epidermolysis Bullosa. N Engl J Med. 2022;387(24):2211-9.
Skin Barrier Dysfunction and Increased Risk of Allergen Sensitization May Impact Atopic March in Atopic Dermatitis (AD)1-4
The dysfunctional skin barrier may allow transcutaneous entry of allergens and subsequent potential sensitization1
Skin barrier dysfunction in Atopic Dermatitis increases the risk of allergen sensitization, dysbiosis, infection, and other type 2 inflammatory diseases1-3 Allergen-specific
Skin dysbiosis and increased risk of infections3
• Decreased microbial diversity • Colonization with S. aureus
Increased
Atopic dermatitis can follow multiple trajectories from
The Evolving
Understanding of Prurigo Nodularis (PN) Has Implications for Patient Management
Prurigo Nodularis is a heterogenous, chronic inflammatory, pruritic disease with unique and varied patient characteristics, burden and clinical manifestations1-6
PN patients may differ in their:1-3
Disease Etiology
e.g., primary, idiopathic, neurological
Treatment History
e.g., topicals, gabapentinoids
Lesion Size and Number
A few mm to 2–3 cm, numbers can vary from a few to hundreds
Comorbidities
e.g., atopic, liver and kidney diseases
Nodular is the most common manifestation, but any skin type can present with any variation
Continuous scratching in PN leads to neuroimmune dysregulation and type 2 inflammation, resulting in increased neuronal signaling, further pruritus, skin fibrosis and nodule formation7-9
neuronal
and inflammation
Diagnostic Evaluation of Hair Loss: A Narrative Review
Editor's Pick
Alopecia affects the quality of life of patients, which underscores the importance of dermatologist readiness to evaluate this common chief complaint. This review by Minta et al. provides a systematic approach to hair loss evaluation, encompassing the physical examination, history evaluation, diagnostic workup, and quality of life tools. Overall, the findings outlined in this article aim to aid in the accurate diagnosis of hair loss disorders, while highlighting the importance of standardised quality of life tools in increasing awareness, which may foster earlier referral to dermatology.
1. Ohio State University College of Medicine, Columbus, USA
2. Department of Dermatology, Ohio State University Wexner Medical Center, Columbus, USA
*Correspondence to Brittany.Dulmage@osumc.edu
Disclosure: Minta is supported by the Pelotonia Scholars Program. Dulmage is supported by a Dermatology Foundation Career Development Award. The authors have declared no conflicts of interest. Minta and Rose contributed conception and design of the work. All authors contributed to drafting and revising the work. All authors critically reviewed the manuscript and approved the final version for submission.
The psychosocial impact of alopecia on the quality of life of patients underscores the importance of dermatologist readiness to evaluate this common chief complaint. When evaluating a patient presenting with new-onset hair loss, the differential diagnosis may be broad, encompassing many subtypes of hair loss. Each type of scarring or non-scarring alopecia presents with its own unique aetiology, epidemiology, clinical presentation, trichoscopic findings, and laboratory studies. Further, accurate diagnosis is needed to determine appropriate therapeutic management. This review provides a systematic approach for dermatologists to use in order to accurately diagnose hair loss disorders, including clinical examination, laboratory evaluation, and specialised tests.
Key Points
1. Patients who experience hair loss commonly report embarrassment, changes to social and leisure activities, and a lower ability to engage in work and education. The psychosocial impact of hair loss on the quality of life of patients underscores the importance of dermatologist readiness to evaluate this common chief complaint.
2. When evaluating a patient presenting with new-onset hair loss, the differential diagnosis may be broad. Each type of scarring or non-scarring alopecia presents with its own unique aetiology, epidemiology, trichoscopic findings, and potential management tools. This review provides a systematic approach for dermatologists to use to diagnose hair loss disorders, including clinical examination, laboratory evaluation, and specialised tests.
3. To successfully diagnose and treat patients with hair loss, evaluation begins with a thorough history and physical examination. Pertinent history includes evaluation of alopecia onset and duration, as well as a review of the patient’s medication, infection, and family history. Physical examination should be used to assess the overall hair density, and the pattern and distribution of hair loss.
INTRODUCTION
Hair thinning and hair shedding are complaints commonly encountered in clinical practice. Evaluating a patient with alopecia requires knowledge of the various aetiologies of hair loss, which may be bolstered by understanding the hair follicle cycle. The three main phases of the hair follicle cycle include: anagen or growth phase; catagen or involution phase; and telogen or resting phase, where the duration of anagen determines the hair length.1,2 This article aims to provide clinicians with a systematic approach to hair loss evaluation, including clinical examination, laboratory evaluation, and specialised tests (Figure 1). Clinical and trichoscopic characteristics of non-scarring (Table 1) and scarring alopecias (Table 2) are summarised. To successfully diagnosis and treat patients with hair loss, evaluation begins with a thorough history and physical examaniation.1-3
PHYSICAL EXAM: GLOBAL ASSESSMENT
Overall Hair Density
When inspecting the scalp, it is important to assess the overall density of hair. To evaluate hair density, isolate serial sagittal parts of the hair using your finger or a cotton swab. Start at the frontal hairline to the crown and then move to the occiput and then to the crown.
A visible scalp indicates at least a 50% reduction in hair density compared to normal.2 Hair density may help to differentiate between telogen effluvium (TE) and anagen effluvium (AE). In TE, approximately 20–50% of hair is lost, whereas 80–90% of hair is lost in AE.4
Pattern and Distribution of Hair Loss
Physical examination should be used to determine the pattern and distribution of hair loss. Notable patterns of hair loss include diffuse, focal, patchy, or complete alopecia. In patients presenting with diffuse hair loss, pertinent history may include increased hair shedding or hair thinning (Figure 2). Gradual and progressive hair thinning is classically reported in patterned hair loss (PHL). Conversely, abrupt hair loss is more typical of TE, alopecia areata (AA), and AE. TE typically occurs 3–6 months after a triggering event, such as systemic disease, pregnancy, psychosocial stress, infection (e.g., COVID-19) or change of medication.2,3 If a patient presents with more localised hair loss, this is suggestive of early stages of PHL, frontal fibrosing alopecia (FFA), central centrifugal cicatricial alopecia (CCCA), AA, trichotillomania, and tinea capitis. The distribution of these patches may be frontal, crown, or random. Frontal predominance is highly associated with male PHL and FFA. A crown distribution is associated with female PHL and CCCA. Randomly distributed hair loss can suggest AA; scarring alopecias, such as lichen planopilaris (LPP) or discoid lupus
Figure 1: Approach to a patient of hair loss.
erythematosus; trichotillomania; or tinea capitis. Importantly, more than one pattern and distribution of hair loss can co-exist, which may complicate diagnosis and assessment.2,4
Additionally, hair shaft disorders with increased fragility are typically patchy but can also present with a generalised pattern. Notably, the pattern of AA is variable. At onset, patients with AA may report one or more round patches of alopecia; however, diffuse hair thinning and total alopecia can also be seen.2,4
Involvement of Eyebrows or Eyelashes or Facial and or Body Hair
In addition to the scalp, it is important to assess facial and body hair. AA, FFA, trichotillomania, tinea, and congenital hair shaft disorders may involve the eyebrows and eyelashes.3,5 AA can also involve the beard and facial hair, and generalised total body hair loss can be seen in AA universalis. Pubic region hair loss is a common area of trichotillomania involvement. Body and facial hair loss in AE are dependent on the chemotherapeutic agent, dose, and duration of treatment.3,6 Graham–Little–Piccardi–Lassueur syndrome, a subset of LPP, is associated with non-scarring hair loss of the axilla and groin. If eyebrows and eyelashes are not affected this may suggest PHL or TE.2
Secondary Changes on the Scalp
Generally, perifollicular or widespread secondary changes reflect inflammation of the scalp, which is more typical of infectious hair loss (e.g., tinea capitis) or scarring alopecia. Common secondary changes on the scalp include scales or flakes, erythema, pustules, and/or crusts. Pustules or crusts are common in folliculitis decalvans and tinea capitis. Additionally, folliculitis decalvans and LPP may present with perifollicular scaling. In advanced CCCA, patients can have perifollicular and interfollicular scales with perifollicular erythema.2, Widespread adherent scaling can be seen in tinea capitis, often resembling generalised dandruff.5 Erythema is seen in LPP, FFA, CCCA, folliculitis decalvans, and dissecting cellulitis.
HISTORY EVALUATION
Onset and Duration
Hair loss duration and age of onset provide important diagnostic clues. In acute TE, hair loss usually lasts for less than 6 months.1,3,4 Conversely, PHL and hair shaft disorders with hair fragility tend to be chronic with a longer duration.2 Additionally, hair disorders may have preferential onset during different stages of life. For children, the most common hair loss disorders are AA and tinea capitis.8 Traction alopecia can begin in childhood, but has the highest prevalence in young adult feamles.2 Trichotillomania typically presents in prepubertal or young adults.2, 7
Table 1: Clinical characteristics and trichoscopic features of non-cicatricial alopecia.
Non-scarring alopecia Clinical characteristics
Anagen effluvium
Presentation:
• Pathogenic noxae include cytotoxic drugs, arsenic mercury
• Pull test positive
TE
Presentation:
• Hair shedding within 3-6 months of trigger event
• Pull test positive
Epidemiology:
• Post-pubertal age of onset
Presentation:
• Progressive hair thinning
• Frontal, temporal, and vertex hair loss
AA Epidemiology:
• 10 and 25 years
Presentation:
• Focal round patches, ophiasis/ sisaipho pattern, or diffuse scalp involvement may have facial or body hair loss
• Pull test positive
Trichotillomania Epidemiology:
• Prepubertal to young adulthood age
• Prevalence of approximately 0.5–2.0%
Presentation:
• Irregularly shaped patch with hairs of varying lengths
LAHS Epidemiology:
• Age 2–6 years
Presentation:
• Female blonde child with history of not-growing or easily shedding hair
Traction alopecia Epidemiology:
• African-American females
Presentation:
• Frontal and temporoparietal areas are most frequently affected
Common trichoscopic features
• Exclamation point hairs
• Black dots
• No specific trichoscopic finding
• Miniaturised follicles with variation in size of hair follicles
• Reduced hair thickness
• Features most notable in classically involved pattern areas
In females, PHL and FFA peaks after menopause, though PHL may present any time after puberty.2 Further, it is important to enquire about history of hair regrowth in the affected area to differentiate between scarring versus non-scarring alopecia which may provide insight into prognosis.2
Medication History
To exclude drug-induced alopecia, a thorough medication history, with increased focus on medications initiated 3–6 months prior to the
onset of hair loss should be reviewed. Druginduced alopecia is typically diffuse and nonscarring.2 AE is sudden loss of up to 90% of hair following administration of antineoplastic medication or radiation.2 Medications commonly associated with drug-induced TE include psychiatric medications (e.g., mood stabilisers and antidepressants), anticoagulants (e.g., warfarin and enoxaparin), antithyroid, β-blockers, and retinoids.2,3 Cessation of long-term oestrogen-containing oral contraceptives has also been associated with TE (Table 3).2
2: Pattern and distribution of hair loss.*
*More than one pattern and distribution of hair loss can co-exist.
Family history should be established in all patients, with special attention to hair loss disorders and other related conditions. AA frequently has a positive family history of other autoimmune disease, including vitiligo, pernicious anaemia, Hashimoto’s thyroiditis, and Type 1 diabetes.2,3 PHL, AA, and congenital hair shaft disorders typically have a positive family history of the same hair loss disorder.1,2 If PHL is suspected, it is important to ask about family history of frontal scalp hair thinning, as previous studies have reported that hereditary factors may predispose up to 80% of male PHL.4 If a child presents with alopecia, family history of childhood hair loss may suggest a hereditary shaft disorder.9
Infection History
Alopecia may be caused by scalp or systemic infections (Table 4). Bacterial or fungal infections that can enter the hair follicles or skin of the scalp and induce alopecia include tinea capitis, yeast (e.g., Candida and Malassezia), and Staphylococcus aureus. Clinically, tinea capitis may present with well-demarcated patchy alopecia with seborrheic-like scale.10 Pityriasis capitis secondary to Malassezia infection may result in chronic itch and inflammation which can exacerbate androgenetic alopecia (AGA) or induce TE.11 Systemic infections that can cause hair loss include secondary syphilis and COVID-19. Syphilitic alopecia can present in a diffuse form, resembling TE, or in a moth-eaten
Figure
Table 3: Scalp and systemic infections that can cause alopecia.
Alopecia onset
Pharmacologic agents
Drug-induced anagen effluvium
Hair loss begins approximately 4–5 weeks after drug administration, most commonly due to cytotoxic agents
form resembling a variety of other focal alopecias (i.e., AA, trichotillomania, LPP, or tinea capitis).12,13
During the COVID-19 pandemic, increasing numbers of patients were referred to dermatology with hair complaints.14 Therefore, dermatologists should be aware that COVID-19 infection can induce new-onset alopecia or exacerbate
Drug-induced telogen effluvium
Hair loss onset 2-4 months after initiation of drug
Anticoagulants:
• Heparin
• Warfarin
Antihypertensives:
• β-blockers
• ACE inhibitors
• Diuretics
Hormones:
• Oral contraceptive pills
• Hormone replacement therapy
Antipsychotics:
• Lithium
• Risperidone
Topoisomerase inhibitors:
• Etoposide
• Irinotecan
Antithyroid drugs:
• Carbimazole
• Propylthiouracil
DMARDs:
• Methotrexate
• Leflunomide
• Biologics
Retinoids:
• Isotretinoin
• Aciretin
pre-existing hair loss.14 Mechanistically, newonset diffuse, reversible hair loss (i.e., TE) can be triggered by viral mediated cytokine-storms.15 Additionally, AGA is a risk factor for severe infection due to androgen-mediated upregulation of the COVID-19 transmembrane receptor, which can exacerbate pre-existing patterned hair loss.16
Hair Care Practices
Physical and chemical factors have been shown to play a significant role in hair loss, thus current and past hair care practices should be evaluated.2
Repeated tension on hair, such as tight ponytails or buns, wearing turbans, and using hair extensions can cause traction alopecia.2
Excessive use of chemical hair treatment and excesses brushing can cause hair shaft disorders with increased fragility.2
Special Considerations for Females
Physiologic or iatrogenic changes in serum oestrogen should be considered in the evaluation of female patients with alopecia.
Pregnancy
Physiologic elevations of circulating oestrogen that occurs during pregnancy increases the number of hair follicles in the prolonged anagen phase, resulting in increased hair growth.17,18
Approximately 3–6 months after delivery, dramatic drops in hormone levels cause follicles to return to the telogen phase, resulting in excessive hair shedding known as postpartum TE.18,19 In patients without nutritional deficiencies or other systemic conditions, hair should return to baseline approximately 9–15 months after delivery.18, For patients reporting diffuse hair loss that persists for longer than 1–2 years postpartum, further investigation is warranted to evaluate for aetiologies of more chronic hair loss.18
Table 4: Pharmacologic agents that may cause drug-induced alopecia.
Infection-associated alopecia Alopecia diagnosis
Scalp infection
Dermatophyte infection
Tinea capitis
Malassezia infection
Systemic infections
COVID-19
Secondary syphilis
Pityriasis capitis
TE
Androgenetic alopecia
Syphilitic alopecia
Presentation
• Fine scaling with single or multiple patches of welldemarcated alopecia
• Broken off hairs (‘black dots’) at scalp surface
• Itchy, reddish-brown patches
• White or yellowish scales in the hair
Diffuse hair loss
Frontal, temporal and vertex hair loss
Diffuse hair loss or 'moth-eaten’/ patchy hair loss
Decreased oestrogen secondary to menopause often results in changes in hair quality and structure, with hair becoming thinner and drier, and patients often report hair loss.20,21 Additionally, female PHL commonly presents in
menopause, with weakening of the hair shaft and a wider part due to reduced hair density.21,22
Compared with females who are pre-menopausal, there is an increase in frequency of male pattern changes in females
who are post-menopausal, with patients presenting with a receding hairline and thinning on the vertex scalp.22,23 FFA also presents in the peri-menopausal and post-menopausal state, but usually manifests as receding hair line localised to the frontal and frontotemporal region.1,9
Hormone Replacement Therapy
Hormone replacement therapy (HRT) is often prescribed to females who are post-menopausal to reduce vasomotor symptoms, such as hot flashes and vaginal atrophy.24 HRT most commonly uses combination therapy of oestrogen and progestin. It remains unclear if HRT worsens or improves hair loss, as oestrogens prolong the anagen phase in contrast to the androgenic effect of progestins.24 For patients taking HRT, clinicians should enquire their specific formulation as modifications in the proportion of androgenic progestins may improve alopecia.24
Special Considerations:
Exogenous Testosterone
Testosterone disrupts the hair follicle cycle by shortening the anagen phase and reducing hair follicle diameter.22,23 For patients on exogenous testosterone, the increase in circulating testosterone may cause new onset male PHL.23 For transgender patients receiving hormone therapy, exogenous testosterone was found to be associated with male PHL and hirsutism.25
DIAGNOSTIC WORKUP
Laboratory Tests
In patients who present with new hair loss, it is common for preliminary laboratory tests to be obtained. Laboratory studies, such as complete blood counts, ferritin, thyroid, and vitamin D levels, can aid in understanding the aetiology of alopecia. However, the need for initial laboratory testing in the diagnostic workup of hair loss lacks consensus in the literature.26,27
Thyroid function tests
Alterations in the levels of thyroid hormones may function as a trigger TE. A study that included 1,232 patients with various types of alopecia found that patients aged 21–40 were most likely to have abnormal thyroid levels.28
Further, this study recommended that all patients presenting with new-onset alopecia be screened for thyroid abnormalities.28
Iron studies
The relationship between iron levels and alopecia is widely debated. Kantor et al.29 found that females under the age of 40 with female pattern hair loss and concurrent TE had lower levels of ferritin. However, Olsen et al.30 reported no significant difference in iron deficiency in hair loss patients compared with the control group. Furthermore, Sinclair31 found that iron supplementation did not improve alopecia.
Zinc
Patients with known zinc deficiency often experience alopecia, with regrowth occurring once supplementation is started.32,33 A systematic review found that 67% of patients with AA had decreased levels of zinc compared with those without hair loss.34 To date, however, there are no agreed upon recommendations for zinc supplementation in patients experiencing hair loss.34
Vitamin D
Studies have shown that females who experience female pattern hair loss are more likely to have low concentrations of serum vitamin D levels.35,36 Though the role of vitamin D in the hair growth cycle is known, the potential for vitamin D supplementation as treatment for hair loss is understudied.35
Others
When examining females with a history of infertility, hirsutism, or severe cystic acne, additional laboratory studies, such testosterone and prolactin levels should be considered.37 An English study found that up to 67% of females presenting with female pattern hair loss had polycystic ovary syndrome.37
Trichoscopy
Magnified assessment of hair characteristics can be performed with trichoscopy (Table 5). Trichoscopic evaluation should be used to assess the hair shaft, hair follicle openings (i.e., the follicular ostia), and perifollicular epidermis. Follicular ostia examination differentiates between scarring and non-scarring alopecia,
Type of alopecia Trichoscopy image
Normal scalp
Trichoscopy findings
• Consistent diameter of hair throughout
• Hair follicle containing 2–3 hairs
• Blue circle showing exclamation point hairs AGA
• Only one hair per follicle
• Variation in hair shaft diameter
• Blue circle showing both preservation of the honeycomb network and pinpoint white dots with an irregular distribution
• Yellow circle showing peripilar grey-white halos
where a lack of follicular ostia suggests scarring alopecia (e.g., FFA; Table 1). Scarring alopecia can also present with white dots, which indicate fibrosis, and may be seen in CCCA or inactive end-stage LPP (Table 2). Other differentiating follicular ostia trichoscopic features include black and yellow dots. Black dots indicate broken hairs at the level of the scalp, which commonly suggests AA, tinea capitis, and toxic-induced AE. Sebum or keratonic material on trichoscopic evaluation presents as yellow dots, which may suggest PHL or AA.2,7
Hair shaft defects should be suspected in a patient who reports a change in hair texture, appearance, manageability, and/or growth.8 On trichoscopy, the hair shaft should be evaluated for calibre and shape. The most notable feature of PHL is frontal predominant hair shaft thickness heterogeneity and increased number of miniaturised hair. Other hair shaft abnormalities that may be observed include exclamation mark hairs (AA, trichotillomania, and AE), comma or corkscrew hairs (tinea capitis), and coiled or flame hairs (trichotillomania).9,38
Table 5: Trichoscopic images of common hair loss disorders.
AA
CCCA
Specialised Tests
Hair pull test
The hair pull test is a non-invasive clinical exam that can be used to assess the presence of active hair loss. To perform the test, the clinician holds a hair bundle of approximately 30–40 hairs between the thumb and the index finger and gently pulls along the hair shaft from the scalp toward the hair ends. The test is considered positive if more than 10% of the hairs in each bundle are removed from the scalp area (i.e., unbroken hairs). A positive hair pull test at >1 scalp region (i.e., occipital, two parietal, and vertex) suggests TE or AE. 39,40
Tug test
The tug test, which is used to determine hair fragility, is a key component of hair shaft defect evaluations. To perform this non-invasive clinical exam, a hair bundle should be held in the middle of hair shaft while pulling on the end of the hair shaft. The tug test is considered positive if breakage of the hair shaft occurs, which indicates fragile hair and hair shaft abnormalities.1,8
Card test
To differentiate newly growing hairs from broken hairs, the card test may be used. To perform the card test, a card that contrasts in colour from the patient’s hair should be placed on the scalp against hair shafts in the affected area. Tapered ends indicate newly growing hairs and blunt ends indicate broken hairs.1,40
Scalp biopsy
Scalp biopsies are the gold standard for diagnosing cicatricial alopecia and can assist in the diagnosis of undifferentiated non-scarring alopecia.1,2 Ideally, an active area of the scalp with persistent hair fibres should be biopsied, and completely bald areas should be avoided.2
QUALITY OF LIFE TOOLS
To better characterise how hair loss affects the lives of patients, several standardised tests have been created for clinicians to administer to patients.41-44 Here, the authors highlight two studies that are most commonly used in clinical settings.
Hairdex Index
The Hairdex Index is a questionnaire that consists of 48 questions broken into five sections. Each of the 48 questions is selfgraded on a scale of 0–4, with a score of 4 being the most severe change to a patient’s baseline quality of life.45 The five sections include symptoms, functioning, emotions, selfconfidence, and stigmatisation. A 2021 study including 192 patients with AGA found that higher scores on the Hairdex were positively correlated with a diagnosis of anxiety and depression.46
Dermatology Life Quality Index
The Dermatology Life Quality Index (DLQI) consists of 10 questions, self-rated on a scale of 0–3.47 Though not specific to hair loss disorders, the DLQI has been validated in patients with AGA and AA. A study including 178 patients with AGA or AA found that patients were most like to report embarrassment, changes to social and leisure activities, and a lower ability to engage in working or studying.48
CONCLUSION
The psychosocial impact of hair loss on the quality of life of patients underscores the importance of dermatologist readiness to evaluate this common chief complaint. This review provides a systematic approach for dermatologists to use in order to accurately diagnose hair loss disorders.
When evaluating a patient presenting with new onset hair loss, the differential diagnosis may be broad, encompassing many subtypes of hair loss. Each type of scarring or non-scarring alopecia presents with its own unique aetiology, epidemiology, clinical presentation, trichoscopic findings, laboratory studies, and potential management tools. Furthermore, standardised quality of life tools for hair loss may increase awareness of the clinical significance of alopecia, which may foster earlier referral to dermatology and the development of innovative therapeutic treatment.
References
1. Jackson AJ, Price VH. How to diagnose hair loss. Dermatol Clin. 2013;31(1):21-8.
2. Mubki T et al. Evaluation and diagnosis of the hair loss patient: part I. History and clinical examination. J Am Acad Dermatol. 2014;71(3):415.e1-5.
3. Park A et al. Hair biology: growth and pigmentation. Facial Plast Surg Clin North Am. 2018;26(4):415-24.
4. Kanwar AJ, Narang T. Anagen effluvium. Indian J Dermatol Venereol Leprol. 2013;79(5): 604-12.
5. Alessandrini A et al. Common causes of hair loss - clinical manifestations, trichoscopy and therapy. J Eur Acad Dermatol Venereol. 2021;35(3):629-40.
6. Leung AKC et al. Tinea capitis: an updated review. Recent Pat Inflamm Allergy Drug Discov. 2020;14(1): 58-68.
7. Nguyen B et al. Eyebrow and eyelash alopecia: a clinical review. Am J Clin Dermatol. 2023;24(1): 55-67.
8. Singh S, Muthuvel K. Practical approach to hair loss diagnosis. Indian J Plast Surg. 2021 27;54(4):399-403.
9. Bhat YJ et al. Hair shaft disorders in children - an update. Indian Dermatol Online J. 2023;14(2): 163-71.
10. Gupta AK, Summerbell RC. Tinea capitis. Med Mycol. 2000;38(4):255-87.
11. Huang J et al. Investigation on microecology of hair root fungi in androgenetic alopecia patients. Mycopathologia. 2019;184(4): 505-15.
12. Tognetti L et al. Syphilitic alopecia: uncommon trichoscopic findings. Dermatol Pract Concept. 2017;7(3):55-9.
13. Bomfim ICC et al. Dermatoscopic findings of syphilitic alopecia. An Bras Dermatol. 2020;95(4):518-20.
14. Bostan E, Cakir A. The effect of Covid-19 on the hair diseases observed in health care providers: analysis of 513 participants. Dermatol Pract Concept. 20231;13(1):e2023036.
15. Iancu GM et al. SARS-CoV-2 infection—a trigger factor for telogen effluvium: review of the literature with a case-based
guidance for clinical evaluation. Life. 2023; 13(7):1576.
16. Morravei H et al. Androgenetic alopecia and COVID-19: a review of the hypothetical role of androgens. Dermatol Ther. 2021;34(4):e15004.
17. Gizlenti S, Ekmekci TR. The changes in the hair cycle during gestation and the post-partum period. J Eur Acad Dermatol Venereol. 2014;28(7):878-81.
18. Anzelc M, Bechtel M. Considerations for cutaneous physiologic changes of pregnancy that fail to resolve postpartum. Int J Dermatol. 2023;62(2):190-6.
19. Eastham JH. Postpartum alopecia. Ann Pharmacother. 2001;35(2): 255-8.
20. Zouboulis C et al. Skin, hair and beyond: the impact of menopause. Climacteric. 2022;25(5):434-42.
21. Kamp E et al. Menopause, skin and common dermatoses. Part 1: hair disorders. Clin Exp Dermatol. 2022;47(12):2110-6.
22. Trüeb RM. Aging of hair. J Cosmet Dermatol. 2005;4(2):60-72.
23. Asfour L et al. Male androgenetic alopecia. 2023. Available at: https://www.endotext.org/ section/male/. Last accessed: 14 September 2023.
24. Desai K et al. Understanding hormonal therapies: overview for the dermatologist focused on hair. Dermatology. 2021;237(5):786-91.
25. Gao Y et al. Understanding and addressing hair disorders in transgender individuals. Am J Clin Dermatol. 2018;19(4):517-27.
26. Shapiro J. Clinical practice. Hair loss in women. N Engl J Med. 2007;357(16):1620-30
27. Gür Aksoy G. Diffuse alopecia; nutritional factors and supplements. Turkderm-Turk Arch Dermatol Venerol. 2014;48(Suppl 1):45-7.
28. Vincent M, Yogiraj K. A descriptive study of alopecia patterns and their relation to thyroid dysfunction. Int J Trichology. 2013;5(1):57-60.
29. Kantor J et al. Decreased serum ferritin is associated with alopecia in women. J Invest Dermatol. 2003;121:985-8.
30. Olsen EA et al. Iron deficiency in female pattern hair loss, chronic telogen effluvium, and control groups. J Am Acad Dermatol. 2010;63:991-9.
31. Sinclair R. There is no clear association between low serum ferritin and chronic diffuse telogen hair loss. Br J Dermatol. 2002;147:982-4.
32. Goskowicz M, Eichenfield LF. Cutaneous findings of nutritional deficiencies in children. Curr Opin Pediatr. 1993;5(4):441-5.
33. Alhaj E et al. Diffuse alopecia in a child due to dietary zinc deficiency. Skinmed. 2007;6(4):199-200.
34. Thompson JM et al. The role of micronutrients in alopecia areata: a review. Am J Clin Dermatol. 2017;18(5):663-79.
35. Banihashemi M et al. Serum vitamin D3 level in patients with female pattern hair loss. J Trichology. 2016;8(3):116-20.
36. Rasheed H et al. Serum ferritin and vitamin d in female hair loss: do they play a role? Skin Pharmacol Physiol. 2013;26:101-7.
37. Lee AT, Zane LT. Dermatologic manifestations of polycystic ovary syndrome. Am J Clin Dermatol. 2007;8:201-19.
38. Rudnicka L et al. Hair shafts in trichoscopy: clues for diagnosis of hair and scalp diseases. Dermatol Clin. 2013;31(4):695-708
39. McDonald KA et al. Hair pull test: evidence-based update and revision of guidelines. J Am Acad Dermatol. 2017;76(3):472-7.
40. Mirmirani P et al. A practical, algorithmic approach to diagnosing hair shaft disorders. Int J Dermatol. 2011;50(1):1-12.
41. Nichol MB et al. The application of multiple quality-of-life instruments in individuals with mild-to-moderate psoriasis. Pharmacoeconomics. 1996;10(6):644-53.
42. Williamson D et al. The effect of hair loss on quality of life. J Eur Acad Dermatol Venereol. 2001;15(2):137-9.
43. Dolte K et al. Development of a health-related quality of life questionnaire for women with androgenetic alopecia. Clin Exp Dermatol. 2000;25(8):637-42.
44. Reid EE et al. Clinical severity does not reliably predict quality of life in women with alopecia areata, telogen effluvium, or androgenic alopecia. J Am Acad Dermatol. 2012;66(3):e97-102.
45. Fischer T, Schmidt S et al. [Hairdex: a tool for evaluation of disease-specific quality of life in patients with hair diseases]. Hautarzt. 2001;52(3):219-27. (In German).
46. Yu L et al. Evaluation of anxiety and depression in patients with androgenetic alopecia in Shanghai: a cross-sectional study. Dermatologic Therapy. 2023;DOI:10.1155/2023/5140620.
47. Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI): a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19(3):210-6.
48. Zhang M, Zhang N. Quality of life assessment in patients with alopecia areata and androgenetic alopecia in the People’s Republic of China. Patient Prefer Adherence. 2017;11:151-5.
Systemic Sclerosis Manifesting Post-Radiotherapy:
A Case Report
Authors: *Devanshi Nimbark,1 Hita H. Mehta,
1 Manal D. Dave1
Department of Dermatology, Venereology and Leprosy, Government Medical College, Sir Takhtasinhji Hospital, Bhavnagar, India
*Correspondence to devanshinimbark38@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Morphoea is a chronic inflammatory disease of the skin and underlying tissues, characterised by fibrosis of the skin and subcutaneous tissue without systemic involvement. Radiation-induced morphoea is a rare, often unrecognised, chronically progressive form of radiation-associated localised scleroderma of the skin, infrequently progressing to systemic scleroderma. Systemic scleroderma is characterised by widespread tissue fibrosis along with systemic features, leading to an increased risk of malignancy compared to the general population. The authors present the case of a 67-year-old female, a previously diagnosed case of psoriasis developing squamous cell carcinoma on the ring finger with axillary nodal metastasis, who underwent radiotherapy, and subsequently developed symptoms of systemic sclerosis. This case is unique, as there are nominal reports on generalised morphoea converting to systemic sclerosis post-radiotherapy, along with exaggerated thickening of the skin over the side of radiotherapy. Thus, the authors report this rare side effect of radiotherapy. Treating physicians should always be vigilant in identifying these side effects after radiotherapy to prevent long-term sequelae of the disease, and minimise their impact on the patient’s quality of life.
Key Points
1. The article highlights the crucial role of vigilance in diagnosing rare conditions that may arise following radiotherapy in patients with cancer, to detect any post-irradiation complications and worsening of connective tissue disorders such as systemic sclerosis (SSc).
2. The article reports on a rare case of SSc that occurred after radiotherapy. This case is distinctive as it presented a diagnostic dilemma between post-irradiation morphoea and SSc, initially due to the absence of systemic complaints, and later on, increased cutaneous involvement with systemic symptoms. This dilemma suggested the possibility of de novo SSc secondary to radiotherapy, or the conversion of radiation-induced morphoea to SSc.
3. The key message to take away is to consider SSc and post-radiation morphoea as potential differential diagnoses in patients who present with cutaneous side effects of radiation. Dermatologists should make a timely diagnosis to start treatment early, and prevent the progression of the disease.
INTRODUCTION
Morphoea causes skin and subcutaneous tissue fibrosis, and can sometimes involve the fascia, muscle, or bone. Sclerosis usually begins as an erythematous or violaceous plaque or patch that becomes indurated. The absence of internal organ involvement, sclerodactyly, nail fold capillary changes, and Raynaud's phenomenon distinguishes morphoea from systemic sclerosis (SSc).1 The exact cause of morphoea is unknown. Several triggers have been identified, including traumatic injury, infection, chemicals, and radiation exposure. Unlike idiopathic morphoea, which has a reported incidence rate of 2.7 per 100,000 persons, the incidence of postirradiation morphoea is estimated to be as high as one in 500 patients.1 Patients who receive focal radiotherapy are more likely to develop morphoea; most of these have lesions restricted to the radiation field and nearby tissue.1 A study conducted at Johns Hopkins University, Baltimore, Maryland, USA, and Pittsburgh University, Pennsylvania, USA, to see the impact of radiation therapy in patients with breast cancer with systemic scleroderma, concluded that local tissue fibrosis is not inevitable in SSc, occurring in 50% of cases without any evidence of lung or generalised skin fibrosis flare.2
Psoriasis, a chronic inflammatory disorder, also increases the risk of developing non-melanoma skin cancer, especially in patients treated with psolaren and ultraviolet light A, methotrexate, or biologicals.
The authors’ case is unusual as, secondary to radiotherapy given for squamous cell carcinoma (SCC) with axillary nodal metastasis, the patient developed localised morphoea that progressed to generalised morphoea, also affecting radiation-unexposed sites, and later on also developed systemic manifestations of SSc within 24 months of radiotherapy.
CASE REPORT
A 67-year-old female, a previously diagnosed case of psoriasis for the last 8 years, was being treated with methotrexate 10 mg/week. The patient was non-compliant, with exacerbation of psoriasis during winter. In July 2019, they presented with a raised lesion, having central depression on the right hand's lateral aspect of the ring finger. The patient was further advised for an MRI of the hand, which was suggestive of an altered signal intensity lesion, necessitating further evaluation to rule out cancer.
Ultrasonography of the axilla was performed pre-operatively to evaluate nodal metastasis, revealing the presence of pathological lymph nodes (approximately 23 mm in short axis with cortical thickness of 7 mm, and loss of fatty hila, which were suggestive of malignant node by size and morphologic criteria).
Disarticulation of the ring finger along with axillary lymph node dissection was done, as the excisional biopsy from the finger revealed SCC with perineural invasion. One of the nine lymph nodes sampled was positive for metastasis. The patient's case was discussed by a multidisciplinary tumour board, and adjuvant radiotherapy was planned in September 2019. Over the course of 5 weeks, the right axillae, supra, and infraclavicular fossa were irradiated with a dose of 50.4 Gy/28 fractions at 1.8 Gy/fraction. During ongoing sessions of radiotherapy, the patient developed an acute skin radiation reaction of Grade 2, which eventually subsided. The last dose of radiation was given in October 2019. Thereafter, the patient was asymptomatic for 1 year, after which they developed itching over the skin lesion, and presented to the authors’ outpatient department with a complaint of itching on the indurated plaque that developed over the trunk after almost 1 year of undergoing radiotherapy.
Cutaneous examination revealed well-defined, hyperpigmented, indurated plaque covering twothirds of the back, involving the medial region
of both breasts near the sternum, sparing the nipple-areolar complex, and extending to the upper abdomen, with depigmentation over the accessible sites due to severe itching (Figure 1A and 1B).
The skin biopsy from the back revealed morphoea. The antinuclear antibody (ANA) titre was 1:320. Additional testing for ANA subtypes was negative for anti-topoisomerase antibodies, anti-Smith antibodies, anticentromere antibodies, anti-double-stranded DNA antibodies, anti-Sjögren's-syndromerelated antigen A autoantibodies, anti-Sjögren's antibodies, and anti-U1 ribonucleoprotein (RNP). The patient was started on 10 mg methylprednisolone daily and topical 0.1%
tacrolimus ointment, and was again lost to follow-up for the next 6 months.
During the 6 months, the patient developed Raynaud's phenomenon, gastroesophageal reflux disease, exertional dyspnoea, and complained of difficulty in standing up after sitting, combing their hair, and buttoning their shirt.
Cutaneous examination this time revealed increased skin involvement compared to the initial presentation (Figures 1C and 1D), marked sclerodactyly on the right hand as compared to the left (Figure 2A), a beaked nose, a masked face, and a purse-string mouth (Figure 2B).
A) Well-defined, hyperpigmented indurated plaque with depigmented excoriations over the back. B) Well-defined, hyperpigmented patch over the sternum, also involving the medial areas of the breast and sparing the nipple-areolar complex. C) Increased area of involvement over the back compared with A. D) Reduction in the bulkiness of the breast secondary to increased induration.
Figure 1: Clinical images comparing the area of involvement in both visits.
The modified Rodnan skin score score was 32, and the European League Against Rheumatism (EULAR) score was 18.
Further investigations revealed: haemoglobin: 8 mg/dL; total leukocyte count: 9,830; platelet count: 455,000; serum glutamic pyruvic transferase: 11; creatinine: 0.7; urine routine microscopy: no abnormality detected; erythrocyte sedimentation rate: 47; C-reactive protein: 15.40; pulmonary function test: normal; and ECG: left bundle branch block. Dermoscopy revealed a white structureless area with erythema, accentuated pigment network, and loss of appendages (Figures 2C and 2D).
Histopathology showed thinning and effacement of rete ridges and basal layer hyperpigmentation, along with the presence of periappendageal and perifollicular lymphocytic infiltrates. Dermis displayed thickening and hyalinisation of collagen (Figure 3A and 3B). Nail fold capillaroscopy showed tortuous, regressing capillaries and avascular areas suggestive of SSc (Figures 3C and 3D). A past episode of chronic plaque psoriasis showed multiple welldefined erythematous plaques with scaling over extensors (Figure 4).
ANA profile was repeated and the U1 RNP antibody was mildly positive (1.14 units), with negative
involvement and dermoscopic examination from the site of biopsy.
A) Sclerodactyly markedly visible on the right hand with a scar of amputation. B) Shiny, wrinkle-free, masklike facies with a beaked nose and purse string mouth. C) Polarised dermoscopy from the back. White structureless area (green arrow) with faint erythema loss of appendages (orange arrow), and accentuated pigmentary network (black arrow). D) Non-polarised dermoscopy. Faint erythema (black arrow), and white structureless area (star).
Figure 2: Facial
double-stranded DNA antibodies, anti-nucleosome antibodies, anti-histone antibodies, anti-Sjögren'ssyndrome-related antigen A autoantibodies, anti-Sjögren's antibodies, Scl-70 antibodies, Mi-2 antibodies, anti-Ku antibodies, anti-centromere antibodies, and anti-PM-Scl antibodies.
The patient was referred to a rheumatologist for combined treatment, and was prescribed methotrexate 10 mg/week, mycophenolate mofetil 360 mg twice daily, and prednisolone 5 mg once daily. As the patient developed severe gastric intolerance to mycophenolate mofetil, they were very non-compliant on further visits.
As per the chronology, the patient was diagnosed with generalised morphoea postradiotherapy during their first visit, as there were no systemic manifestations, and the lesion was not limited to the site of radiation. After a further 6 months, there was development of systemic symptoms, putting the authors’ diagnosis of generalised morphoea in dilemma; further, the diagnosis was kept as SSc with anti-U1 RNP positive antibody. The cause of SSc manifesting in the later age after radiotherapy was a matter of concern, whether it is a presentation of de novo SSc, or radiotherapy unmasked the antigens already present in the body.
A) Scanner view in 10x magnification showing thinning and effacement of rete ridges with basal layer hyperpigmentation, perifollicular and periappendageal infiltrate consisting of lymphocytes and plasma cells.
B) 40x magnification of the dermis showing thickening and hyalinisation of collagen with loss of epidermal appendages. C) Dilated capillaries (red arrow), bushy capillaries (blue arrow), meandering (green arrow), and micro-haemorrhage (yellow arrow). D) Receding capillaries (black arrow) with avascular zones (green star).
Figure 3: Histopathologic image and nail fold capillaroscopy.
A
C B
D
Figure 4: Well-defined erythematous plaques with scaling over extensors.
DISCUSSION
Radiation-induced dermatologic manifestations are prevalent, with up to 90% of patients experiencing a local skin reaction. Within the first 2 months of exposure, the earliest changes are consistent with localised irritation and drying of the skin due to inflammatory cytokines. Fibrosis, telangiectasias, and skin necrosis are late effects, defined as 2 months–decades after the last radiation exposure.1 Post-irradiation morphoea would be classified as circumscribed morphoea with lesions confined to the radiated field and surrounding tissue, the majority described in breast cancer patients.
Bleasel et al.3 and Davis et al.4 each report a morphoea frequency of 1:500 per year in irradiated patients with breast cancer, and an incidence of 2.7:100,000 per year in nonirradiated individuals. The incidence differential strongly suggests that radiotherapy is a risk factor. However, only 81 instances of radiationinduced morphoea have been documented in scientific literature since 1989.5 In rare instances, the effects of radiation can extend beyond the irradiated area or even become generalised, defined as four or more indurated plaques on more than two of seven anatomic sites.5,6 Patients with generalised morphoea are more likely to have positive serology for autoantibodies, especially ANA.7
Histological evaluation is essential for differentiating diseases such as chronic radiation dermatitis, cancer recurrence, radiation recall dermatitis, newly-developed carcinoma, and cellulitis.8 In the burnout phase of early lesions, inflammation and infiltration predominate, whereas, in the sclerotising phase of late lesions, extensive fibrosis (thickened collagen fibres) predominates.8 Post-irradiation fibrosis only occurs within the irradiated field during the first 3 months of radiation, whereas radiation-induced morphoea can spread to other tissues.8
It has been proposed that radiation exposure may activate clonal fibroblasts in post-irradiation morphoea, leading to an increase in cytokine production, including that of transforming growth factor β.1 This cytokine has been connected to the pathophysiology of both localised and diffuse scleroderma.1 The increased cytokine response is thought to boost the production of glycosaminoglycans, collagen, and extracellular matrix proteins.1
Given the risk of radiation-induced fibrosis in the skin, lungs, and other organs, scleroderma is regarded as a relative contraindication for radiation therapy. As observed in this case, there are other case reports and case series suggesting that patients with scleroderma may develop exaggerated fibrosis, and it is commonly feared that radiation therapy could trigger a flare-up of systemic rheumatic disease.2
During the initial visit, the patient had plaque only limited over the trunk and absence of systemic complaints, so the diagnosis after the histological examination was kept as radiationinduced morphoea.
On the next visit, after 6 months, the patient had developed the systemic manifestation of SSc, along with typical facies and positive anti-U1 RNP antibody after almost 1.5 years of radiotherapy. Thus, the diagnosis kept by the authors was now questionable. The conundrum occurred between the diagnosis of de novo manifestation of SSc post-radiotherapy, an unmasking of underlying SSc secondary to radiation, and conversion of radiation-induced morphoea to SSc, as the patient had no symptoms or signs of localised or systemic scleroderma before the occurrence of SCC and subsequent radiotherapy.
References
1. Kushi J, Csuka ME. Generalized morphea after breast cancer radiation therapy. Case Rep Rheumatol. 2011;2011:951948.
2. Shah DJ et al. Impact of radiation therapy on scleroderma and cancer outcomes in scleroderma patients with breast cancer. Arthritis Care Res (Hoboken). 2018;70(10):1517-24.
3. Bleasel NR et al. Radiation‐induced localized scleroderma in breast cancer patients. Australas J Dermatol. 1999;40(2):99-102.
Radiation-induced morphoea, conversion of localised scleroderma to systemic scleroderma,9 and de novo SSc post-radiation10 are infrequently described, severe, and unpredictable late side effects, with a wide range of onset times. As soon as histological confirmation is obtained, local and systemic therapy must be started to slow the progression of fibrosis and atrophy, and enhance the patient's quality of life.
Based on the authors’ extensive evaluation and literature search, there are nominal reports in the present literature on the conversion of radiation-induced morphoea to SSc postradiotherapy. Thus, by disclosing this unusual case, the authors want physicians to always raise suspicion and keep track of patient’s symptoms to avoid complications of the disease and manage it at the earliest.
4. Davis DA et al. Localized scleroderma in breast cancer patients treated with supervoltage external beam radiation: radiation port scleroderma. J Am Acad Dermatol. 1996;35(6):923-7.
5. Partl R et al. Radiation-induced morphea—a rare but severe late effect of adjuvant breast irradiation: case report and review of the literature. Strahlenther Onkol. 2018;194(11):1060-5.
7. Marzano AV et al. Localized scleroderma in adults and children.
Clinical and laboratory investigations on 239 cases. Eur J Dermatol. 2003;13(2):171-6.
8. Spalek M et al. Radiation‐induced morphea–a literature review. J Eur Acad Dermatol Venereol. 2015;29(2):197-202.
9. Giuggioli D et al. From localized scleroderma to systemic sclerosis: coexistence or possible evolution. Dermatol Res Pract. 2018;2018:1284687.
10. Darras-Joly C et al. De novo systemic sclerosis after radiotherapy: a report of 3 cases. J Rheumatol. 1999;26(10):2265-7.
COVID-19
and Cosmetic Collagen-Filler Injection-Associated Dermatopathy: A Case Report
Authors:
Disclosure:
*E.A. Kogan,1 A. Das,2 T.A. Demura,1 A.Y. Koroleva,3
Y.A. Yutskovskaya4
1. Institute of Clinical Morphology and Digital Pathology, I.M. Sechenov First Moscow State Medical University, Moscow, Russian Federation
2. N.V. Sklifosovsky Institute of Clinical Medicine, I.M. Sechenov First Moscow State Medical University, Moscow, Russian Federation
3. Center for the Treatment of Complications of Professor Yutskovskaya's Clinic, Moscow, Russian Federation
4. Dermatovenerology and Cosmetology Department, Pacific State Medical University of Health, Moscow, Russian Federation
*Correspondence to koganevg@gmail.com
The authors have declared no conflicts of interest. Written consent was obtained from the patient and this study was approved by the concerned ethical committee.
Received: 19.04.23
Accepted: 26.05.23
Keywords:
Accumulation of nuclear capsid and spike proteins in tissues, case report, COVID-19, cosmetic collagen skin filler, vasculitis.
COVID-19 and cosmetic skin-fillers are two prevalent topics of today’s medicine, yet their interaction is not sufficiently studied. This article is based on a clinicomorphological case where the patient, a 37-year-old female, visited the clinic with complaints of painless palpable subcutaneous pathologic nodular lesions at the site of collagen cosmetic filler injection after severe acute respiratory syndrome coronavirus 2 infection. In order to verify the pathological processes of the lesions, punch biopsy of the affected skin was taken, and histological, histochemical, and immunohistochemical studies were conducted. Atrophy, acanthosis, parakeratosis with vacuolisation of nuclei of the epidermis; sclerosis and abnormal deposition of collagen fibres in the subepithelial layer of dermis; and vasculitis with endothelial hypertrophy and lymphoid perivascular infiltration (CD3 lymphocytes and CD68 macrophages) were found. Spike and nuclear capsid proteins of severe acute respiratory syndrome coronavirus 2 were localised in cells of perivascular inflammatory infiltrates, endothelial cells, and epithelium of glands and epidermis of the skin. The association between the dermatopathy in COVID-19 virus infection and cosmetic fillers were established. The authors discuss and hypothesise possible autoimmune processes that lead to autoimmune vasculitis.
Key Points
1. This article is based on a clinico-morphological case where the patient visited the clinic with complaints of pathologic formations at the site of collagen cosmetic filler injection after severe acute respiratory syndrome coronavirus 2 infection.
2. The patient was a 37-year-old female, who sought medical help for the complaints of painless palpable lesions in the cheek area, localised subcutaneously, persisting without dynamics. These blemishes were localised in the areas where, about 3 months prior, they had opted to inject collagen fillers for cosmetic purposes.
3. To verify the pathological processes of the lesions, punch biopsy of the affected skin was taken, and histological, histochemical, and immunohistochemical studies were conducted. The results and the implications of the findings are discussed in this article.
INTRODUCTION
The COVID-19 pandemic originated as a pneumonia outbreak in Wuhan, Hubei, China, in December 2019.1,2 By the 21st of October 2022, at least 623,893,894 people were affected, and 6,553,936 deaths were reported due to COVID-19, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).3 Not only does COVID-19 affect the lungs, myocardium, kidneys, and central nervous system, but pathological changes have also been described in the skin.4-7 Singh et al.4 have described the prevalent occurrence of maculopapular lesions, urticarial lesions, and chilblain-like lesions (COVID toes) in COVID-19, while the other clinical manifestations of COVID-19 are vesicular lesions, petechiae, livedoid eruptions, and multisystem inflammatory syndrome in children with lesser degrees of occurrence.4,8,9
The use of dermal fillers, especially collagen fillers, for cosmetic purposes has been shown to be one of the most popular non-surgical cosmetic procedures in different populations of the world.10-13 The tissue changes after treatment with a dermal filler include increased collagen fibres expression with minimal angiogenesis, without changes in the epidermis and hypodermis.14,15 Increased incidences of acute inflammation relating to injectable collagen and hyaluronic acid fillers have been reported during the COVID-19 pandemic.16-20 Kato et al.16 have observed an association between COVID-19 and increased cases of acute inflammatory reaction in patients using collagen and hyaluronic acid dermal fillers for cosmetic purposes, and
have hypothesised three probable causes of such correlation: rapid change in lifestyle, T helper 2 system activation due to stress, and immunologic reactions due to frequent exposure to cosmetic skin filler injection. Clinical manifestation of delayed inflammatory reaction to cosmetic dermal fillers have been observed and discussed.16,21 Still, pre-existing information on the interaction between cosmetic collagen skin fillers and COVID-19 is quite insufficient. Hence, studying the interaction between these two prevalent situations of today’s medicine, the COVID-19 pandemic and the use of cosmetic skin fillers, is necessary. This article is based on a clinico-morphological case where the patient visited the clinic with complaints of pathologic skin formations at the site of collagen cosmetic filler injection after SARS-CoV-2 infection. Written consent was obtained from the patient and this study was approved by the concerned ethical committee.
PATIENT INFORMATION
A 37-year-old female presented with complaints of painless nodular lesions in skin of their cheeks after about 8 weeks of first noticing them. The complaints were the appearance of painless palpable subcutaneous nodular lesions in the cheek area. These blemishes were located in the skin area where the patient had opted to inject collagen fillers for cosmetic purposes.22,23 These complaints were first observed 1 week after the patient tested positive for COVID-19. The statement provided by the clinic states that in the 12 calendar months
preceding the presentation of lesions, the following drugs were injected into soft tissues of the face: a preparation based on hyaluronic acid (biorevitalizant) and based on polylactic acid, and preparations based on collagen and placental preparations. Procedures of botulinum toxin therapy and photodynamic therapy were also performed. According to the patient, the most recent and significant intervention was made a few weeks prior to testing positive for COVID-19. The intervention included mechanical cleansing followed by a meso-therapeutic administration of the injectable drug PDRN 6® (Cytolyfe, Austin, Texas, USA). The drug is composed of 2% polynucleotides (DNA) and 0.3% hyaluronic acid, which is unstabilised, with a molecular weight of 1.1. Dosages and administration regimens/schemes are unknown (Figure 1).
Upon clinical examination, status localis was noted as skin of normal physiological colouration, and lesions located in the lower third of the face and represented by tumourlike formations with clear boundaries and dense texture. Lesion foci of different diameters were localised in subdermal level. On the right side of the face in the region of the lower third, a single small papular inflammatory element was present (Figure 2A and 2B).
Ultrasound of soft tissues of the face revealed multiple palpable hypoechoic nodular lesions with clear even contours in the subcutaneous fat anterior to the zygomatic bones, caudally along the contour of the face. These formations were irregular in shape, diffusely heterogeneous, and were merging with each other. Intra- and peri-nodular vessels ranged from 1.40x0.90 mm to 16.00x3.15 mm in size. In some formations, single vessels were visualised.
The echogenicity of the subcutaneous fat was diffusely increased, and blood flow was detected to be unevenly enhanced (Figure 2C). The main clinical diagnosis was post-injection granuloma of the skin and subcutaneous tissue caused by a foreign body. Localised oedema was the complication of the main diagnosis. It was histologically established that vasculitis was limited to the skin. Concomitant diagnosis was noted as acne, the papulo-pustular form, of mild severity.
A joint consultation with an allergist, an immunologist, and a general practitioner was held. It was recommended to examine and exclude vasculitis, since clinical signs of lymphocytic infiltration were observed. After additional laboratory diagnostics, there were no pathological changes found in general blood analysis or biochemical blood analysis; both tests were performed 9 weeks after being tested positive for COVID-19. Non-specific hypoallergenic diet was prescribed with the prescription of a tablet of Longidaza® 3000 (Petrovax, Moscow, Russian Federation) once per day and at night for 10 days, and one Trental® (Sanofi, Bridgewater, New Jersey, USA) 0.1 g tablet, three times daily after meals.
Following further examinations were recommended by the specialists: cyclic citrullinated peptide antibody test, antinuclear antibodies, antistreptolysin-O, and C-reactive protein to exclude an autoimmune component of rheumatoid arthritis and systemic vasculitis. Within 2 weeks of commencement of treatment, weakly pronounced positive changes were noticed in the form of a slight decrease in the size of the formations.
Figure 1: Anamnesis of the patient.
2: Clinical and radiological images on the day of presentation.
A B
A) and B) Clinical pictures of nodular lesions on the day of presentation. C) Ultrasound image. Multiple hypoechoic nodular lesions, with clear contours in subcutaneous fat.
Figure
Figure 3: Microscopical images.
Figure 3 continued.
G H
A) Sclerosis and vasculitis with endothelial hypertrophy and lymphoid perivascular infiltration in the derma, H&E (magnification 400X).
B) CD45 positive lymphocytes in dermal perivascular inflammatory infiltrate (Clone 4KB5, Dako, Agilent, Santa Clara, California, USA). Immunoperoxidase reaction with DAB. (magnification 600X).
C) CD3 positive lymphocytes in dermal perivascular inflammatory infiltrate indicating autoimmune reactions (Clone MRQ-39, Cell Marque, Merck KGaA, Darmstadt, Germany). Immunoperoxidase reaction with DAB (magnification 600X).
D) CD3 positive lymphocytes in dermal perivascular inflammatory infiltrate indicating autoimmune reactions (Clone MRQ-39, Cell Marque). Immunoperoxidase reaction with DAB (magnification 600X).
E) Nuclear capsids of the SARS-CoV-2 virus in endothelial cells and cells of perivascular inflammatory infiltrate (SARS-CoV-2 nucleocapsid rabbit antibody, GeneTex Inc., Irvine, California, USA). Immunoperoxidase reaction with DAB. (magnification 600X).
F) Spike proteins of the SARS-CoV-2 virus in endothelial cells and cells of perivascular inflammatory infiltrate. (SARS-CoV-2 spike rabbit antibody, GeneTex Inc.). Immunoperoxidase reaction with DAB (magnification 600X).
G) Collagen-I deposition in the subepithelial layer of derma (Clone 3G3, Santa Cruz Biotechnology, Dallas, Texas, USA). Immunoperoxidase reaction with DAB (magnification 200X).
H) Collagen-III deposition in the subepithelial layer of derma (Clone B-4, Santa Cruz Biotechnology). Immunoperoxidase reaction with DAB (magnification 200X).
DAB: 3,3′-diaminobenzidine; H&E: haematoxylin and eosin staining; SARS-CoV-2: severe acute respiratory syndrome coronavirus 2.
In order to verify the pathological processes of the lesions, punch biopsy of the affected skin was taken. The harvested skin sample was fixed in 10% formalin solution. Paraffin sections were prepared for histological, histochemical, and immunohistochemical studies.24
For histopathological study, the paraffin sections were stained with haematoxylin-eosin and Van Gieson’s staining.25 Other sets of paraffin sections were assigned for the characterisation of the histochemical markers: CD45 (Clone 4KB5, Dako, Agilent, Santa Clara, California,
USA), CD3 (Clone MRQ-39, Cell Marque, Merck KGaA, Darmstadt, Germany), and CD68 (Clone Kp1 C, Dako).26,27 The expression of collagen-I (Clone 3G3, Santa Cruz Biotechnology, Dallas, Texas, USA), and collagen-III (Clone B-4, Santa Cruz Biotechnology) fibres were evaluated histochemically, and the tissue was examined for the presence of COVID-19 spike proteins (SARS-CoV-2 spike rabbit antibody, GeneTex Inc., Irvine, California, USA) and COVID-19 nuclear capsid (SARS-CoV-2 nucleocapsid rabbit antibody, GeneTex Inc.).28 Negative and positive controls were used.
Histological examination of the skin includes changes in epidermis and dermis. Atrophy, parakeratosis with vacuolisation of nuclei of the epidermis, and acanthosis were detected. Sclerosis and abnormal deposition of collagen fibres in the subepithelial layer of dermis were seen. Vasculitis with endothelial hypertrophy and lymphoid perivascular infiltration were found (Figure 3A).
Immunohistochemical examination revealed dermal accumulation of collagen-I and collagenIII, with predominance of the former. Inflammatory infiltrates showed the presence of CD45 lymphocytes. CD3 lymphocytes were more than 10 cells in 1 mm of the slide, and CD68 macrophages were recorded as 20 cells in 1 mm of the slide.
Proteins of the COVID-19 virus, both spike protein and nuclear capsid protein, were localised in cells of perivascular inflammatory infiltrates, and in endothelial cells of vessels, as well as in the glands of the skin. In epidermis, cells with nuclear vacuolisation were detected to be positive for proteins of COVID-19 (Figure 3B–H).
There were no data confirming a systemic autoimmune process in the patient. The anamnesis, according to the patient, the moment of high COVID-19 viral load coincided with the moment in time of mechanical cleaning of the face, and the administration of Cytolyfe PDRN 6.
DISCUSSION
The detection of COVID-19 spike proteins and COVID-19 nuclear capsid in the cells of perivascular inflammatory infiltrates in the endothelial cells and in the glands of the skin is an indication of some correlation between the COVID-19 and the skin lesions formed. This correlation can be due to either the direct effect of SARS-CoV-2 virus, or indirect effect.
The authors propose the direct effect, as the dermatopathy in this case was an immediate result of COVID-19 disease development in the patient. Earlier in the COVID-19 pandemic, the virus has been directly related with perivascular and perieccrine sweat gland lymphocytic. Predominantly CD3/CD4+ inflammation was observed in patients
who had complaints with acral chilblain-like lesions and suspected SARS-CoV-2.29-36 There is substantial data about direct causation of Type III and Type IV hypersensitivities, vasculitis, and endotheliopathy after COVID-19 disease development.5,37-43 Formation of lesions can be due to some autoimmune reactions.44-50 Antiphospholipid autoantibodies were found in approximately half of the patients who were critically ill due to COVID-19 infection in two different studies.51-54 However, it must be noted that there were no data confirming a systemic autoimmune process in the patient.
Since the complaints were limited only the areas of prior administration with injections of the collagen skin filler, and the unnatural accumulation of collagen-III fibres was found in the intercellular matrix in the biopsy slide, the hypothesis that the injected collagen skin filler made the skin tissue more susceptible to such pathological processes can be made.55-57 The previously mentioned indirect effect can be due to such increased susceptibility of the skin tissue. Kato et al.16 have observed an association between COVID-19 and increased cases of acute inflammatory reaction in patients using the collagen and hyaluronic acid dermal fillers for cosmetic purposes, and have hypothesised three probable causes of such corelation: rapid change in lifestyle, T helper 2 system activation due to stress, and immunologic reactions due to frequent exposure to cosmetic skin filler injection. Clinical manifestation of delayed inflammatory reaction and hypersensitivity to cosmetic dermal fillers have been observed and discussed.16,21,55 Munavalli et al.58 also reported the significant increase of instances of acute inflammatory reaction after use of dermal filler in patients with a background of COVID-19. There have also been reports of delayed-type hypersensitivity reaction to nonhyaluronic acid polycaprolactone dermal filler following COVID-19 vaccination.17,59
CONCLUSION
The results of histological, histochemical, and immunohistochemical analysis of the punch biopsy, when viewed in parallel to the localisation of the lesion and patient’s anamnesis, have established that this dermatopathy is correlated both to COVID-19 infection and cosmetic collagen skin filler injection.
Though there are not enough scientific works to explain this dermatopathy completely, the two proposed explanations in this article, direct and
References
1. Wu F et al. A new coronavirus associated with human respiratory disease in China. Nature. 2020;579(7798):265-9.
2. Zhou P et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020;579(7798):270-3.
3. World Health Organization (WHO). WHO coronavirus (COVID-19) dashboard. Available at: https:// covid19.who.int/. Last accessed: 21 October 2022.
4. Singh H et al. Cutaneous manifestations of COVID-19: a systematic review. Adv Wound Care (New Rochelle). 2021;10(2):51-80.
5. Nakashima C et al. Cutaneous manifestations of COVID-19 and COVID-19 vaccination. J Dermatol. 2023;50(3):280-9.
6. Drenovska et al. Covid-19 pandemic and the skin. Int J Dermatol. 2020;59(11):1312-9.
7. Sachdeva M et al. Cutaneous manifestations of COVID-19: Report of three cases and a review of literature. J Dermatol Sci. 2020;98(2):75-81.
8. Wargo JJ et al. Coronavirus (COVID-19) infection-induced chilblains: a brisk perieccrine inflammatory response. Am J Dermatopathol. 2021;43(2):144-5.
9. Nirenberg MS et al. Histopathology of persistent long COVID toe: a case report. J Cutan Pathol. 2022;49(9):791-4.
10. Sandoval LF et al. Trends in the use of neurotoxins and dermal fillers by US physicians. J Clin Aesthet Dermatol. 2014;7(9):14-9.
11. Park J et al. Analysis of issues and trends in cosmetic plastic procedures using tweets from Twitters. Public Health Affairs. 2017;1(1):129-43.
12. Alharethy SE. Trends and demographic characteristics of Saudi cosmetic surgery patients. Saudi Med J. 2017;38(7):738-41.
13. Hopkins ZH et al. Influence of social media on cosmetic procedure interest. J Clin Aesthet Dermatol. 2020:13(1):28-31.
indirect effects with development of autoimmune reactions, can each be supported to some extent by the pre-existing literature.
14. Yutskovskaya YA, Kogan EA. [Randomized split-face histomorphological study comparing calcium hydroxyapatite volumizer and hyaluronic acid dermal filler]. 2016 Available at: https://cyberleninka.ru/ article/n/randomizirovannoegistomorfologicheskoeissledovanie-po-tipu-split-facepo-sravneniyu-volyumayzera-naosnove-gidroksiapatita-kaltsiya/ viewer. Last accessed: 23 December 2022. (In Russian).
15. Ciccone V et. Comparison of the effect of two hyaluronic acid preparations on fibroblast and endothelial cell functions related to angiogenesis. Cells. 2019;8(12):1479.
16. Kato K et al. Increase in the incidence of acute inflammatory reactions to injectable fillers during COVID-19 era. J Cosmet Dermatol. 2022;21(5):1816-21.
17. Kalantari Y et al. First reported case of delayed-type hypersensitivity reaction to nonhyaluronic acid polycaprolactone dermal filler following COVID-19 vaccination: a case report and a review of the literature. Clin Case Rep. 2022;10(2):e05343.
18. Rowland-Warmann MJ. Hypersensitivity reaction to hyaluronic acid dermal filler following novel coronavirus infection – a case report. J Cosmet Dermatol. 2021;20(5):1557-62.
19. Shome D et al. Delayed hypersensitivity reaction to hyaluronic acid dermal filler post‐COVID‐19 viral infection. J Cosmet Dermatol. 2021;20(5):1549-50.
20. Michel JC et al. Are delayed dermal filler granulomas more common since COVID-19? J Oral Maxillofac Surg. 2023;81(1):42-8.
21. Wang C et al. Hypersensitivity caused by cosmetic injection: systematic review and case report. Aesthetic Plast Surg. 2021:45(1):263-72.
22. Cassuto et al. An overview of soft tissue fillers for cosmetic dermatology: from filling to regenerative medicine. Clin Cosmet Investig Dermatol. 2021; 14:1857-66.
23. Sionkowska A et al. Collagen based materials in cosmetic applications:
a review. Materials (Basel). 2020;13(19):4217.
24. Canene-Adams K. Preparation of formalin-fixed paraffin-embedded tissue for immunohistochemistry. Methods Enzymol. 2013;533: 225-33.
25. Kazlouskaya V et al. The utility of elastic Verhoeff-Van Gieson staining in dermatopathology. J Cutan Pathol. 2013;40(2):211-25.
26. Cohen MC. Leukocyte and stromal cell molecules. Shock. 2007;28(4):498.
27. Bitter M, Dongen J, “Human leukocyte markers and the CD nomenclature,” Lefkovits I (ed.) Immunology Methods Manual: The Comprehensive Sourcebook of Techniques (1997) San Diego: Academic Press, pp.2439-65.
28. Hong J et al. Rabbit monoclonal antibody specifically recognizing a linear epitope in the RBD of SARSCoV-2 spike protein. Vaccines (Basel). 2021;9(8):829.
29. Kanitakis J et al. Chilblain-like acral lesions during the COVID-19 pandemic (“COVID toes”): histologic, immunofluorescence, and immunohistochemical study of 17 cases. J Am Acad Dermatol. 2020;83(3):870-5.
30. Piccolo V et al. Chilblain‐like lesions during COVID‐19 epidemic: a preliminary study on 63 patients. J Eur Acad Dermatol Venereol. 2020;34(7):e291-3.
31. Bassi A et al. Chilblain-like lesions during COVID-19 pandemic: the state of the art. Life (Basel). 2021;11(1):23
32. Landa N et al. Chilblain‐like lesions on feet and hands during the COVID‐19 Pandemic. Int J Dermatol. 2020;59(6):739-43.
33. Colonna C et al. Chilblain-like lesions in children following suspected COVID-19 infection. Pediatr Dermatol. 2020;37:437-40.
34. Garcia-Lara G et al. Chilblain-like lesions in pediatrics dermatological outpatients during the COVID-19 outbreak. Dermatol Ther. 2020;33(5):e13516.
35. Hubiche T et al. Clinical, laboratory, and interferon-alpha response characteristics of patients with
chilblain-like lesions during the COVID-19 pandemic. JAMA Dermatol. 2021;157(2):202-6.
36. López-Robles J et al. Chilblain‐like lesions: a case series of 41 patients during the COVID‐19 pandemic. Clin Exp Dermatol. 2020;45(7): 891-2.
37. McGonagle D et al. COVID-19 vasculitis and novel vasculitis mimics. Lancet Rheumatol. 2021;3(3):e224-33.
38. Iba T et al. The coagulopathy, endotheliopathy, and vasculitis of COVID-19. Inflamm Res. 2020;69(12):1181-9.
39. Goshua G et al. Endotheliopathy in COVID-19-associated coagulopathy: evidence from a single-centre, cross-sectional study. Lancet Haematol. 2020;7(8):e575-82.
40. Roncati L et al. Type 3 hypersensitivity in COVID-19 vasculitis. Clin Immunol. 2020;217:108487
41. Mahdi BM. COVID-19 type III hypersensitivity reaction. Med Hypotheses. 2020;140:109763.
42. Rhodes RH et al. Acute endotheliitis (type 3 hypersensitivity vasculitis) in ten COVID-19 autopsy brains. medRxiv. 2021;DOI:10.1101/2021.01. 16.21249632.
43. Pine AB et al. Circulating markers of angiogenesis and endotheliopathy in COVID-19. Pulm Circ.
2020;10(4):2045894020966547.
44. Joly P; French study Group on auto immune bullous skin diseases, and the French network of rare diseases in Dermatology (FIMARAD). Incidence and severity of COVID-19 in patients with autoimmune blistering skin diseases: a nationwide study. J Am Acad Dermatol. 2022;86(2):494-7.
45. Drenovska et al. Impact of COVID-19 on autoimmune blistering diseases. Clin Dermatol. 2021;39(3):359-68.
46. Novelli L et al. The JANUS of chronic inflammatory and autoimmune diseases onset during COVID-19 - a systematic review of the literature. J Autoimmun. 2021;117:102592.
47. Gracia-Ramos AE et al. New onset of autoimmune diseases following COVID-19 diagnosis. Cells. 2021;10(12):3592.
48. Gao Z-W et al. Autoantibodies in COVID-19: frequency and function. Autoimmun Rev. 2021;20(3):102754.
49. Wang EY et al. Diverse functional autoantibodies in patients with COVID-19. Nature. 2021;595(7866):283-8.
50. Yazdanpanah N, Rezaei N. Autoimmune complications of COVID-19. J Med Virol. 2022;94(1):54-62.
51. Xiao M et al. Antiphospholipid antibodies in critically ill patients with COVID-19. Arthritis Rheumatol.
2020;72(12):1998-2004.
52. Zuo Y et al. Prothrombotic autoantibodies in serum from patients hospitalized with COVID-19. Sci Transl Med. 2020;12(570):eabd3876.
53. Connell NT et al. Coagulopathy of COVID-19 and antiphospholipid antibodies. J Thromb Haemost. 2020;18(9):E1-2.
54. Arcani R et al. “True” antiphospholipid syndrome in COVID-19: contribution of the follow-up of antiphospholipid autoantibodies. Semin Thromb Hemost. 2023;49(1):97-102.
Introduction: Parry–Romberg syndrome (PRS) is a rare neurocutaneous condition that can affect the skin, subcutaneous fat, muscle, and bone on one side of the face. PRS presents with progressive but self-limiting facial haemiatrophy, and its severity ranges from barely noticeable asymmetry to severe disfigurement. The authors describe a 35-year-old male with right facial haemiatrophy. The patient presented in a stable condition at the initial consultation.
Objectives: Adipose tissue autografts were the most used tool to treat many congenital or acquired facial deformities. The authors proposed using cross-linked hyaluronic acid (HA) fillers over those traditionally used to correct facial deformities due to PRS.
Discussion: PRS is usually self-limiting, with the maximal progression of the disease 2–5 years after onset. There is no specific cure for PRS at present. After 7 years of progression from the onset, this patient entered a stable phase. Reconstructive treatment was then indicated, since there were no further signs of atrophy. Since adipose tissue autografts require complicated surgical skills, which take a lot of time
and cost, the authors report a case of PRS augmented by HA filler in a 35-yearold male patient to suggest that HA filler could be a safe and simple alternative to surgical treatment. The authors conclude that HA fillers are a safe tool for treating facial deformities in patients with PRS.
Key Points
1. Hyaluronic acid (HA) fillers can be used for non-cosmetic purposes. HA fillers can be used to reconstruct facial features that have been altered due to congenital abnormalities. For instance, in patients with facial deformities resulting from conditions like Parry–Romberg syndrome, HA fillers can be injected to restore facial symmetry.
2. HA fillers are designed to imitate the densities of the tissues where they will be injected, providing a natural-looking result, with the possibility of being removed with hyaluronidase, an enzyme that can dissolve HA if any complications arise, or if a patient is not satisfied with the results.
3. Extensive anatomical knowledge, including vascular, tissue, and nerve anatomy, is crucial for safe and effective injection of HA fillers. It reduces the risk of complications and help achieving satisfactory results.
INTRODUCTION
First described by Parry in 1825 and Romberg in 1846, this variety of craniofacial findings was labelled as progressive haemifacial atrophy by Eulenberg in 1871. Other names used to describe this disorder include Parry–Romberg syndrome (PRS), idiopathic haemifacial atrophy, progressive facial haemiatrophy, and Romberg’s syndrome. Evidence of the disease dates back to Ancient Egypt, with mummies presenting craniofacial dysmorphism consistent with progressive haemifacial atrophy.1-3
PRS is a rare disease that leads to severe disfigurement after years of progressive haemifacial atrophy, with an estimated prevalence of 1 out of 700,000 people. It affects three times more females than males.4,5 Most patients have initial manifestations in the first two decades of life; however, late presentations are also described.3,6-8
A Mayo Clinic study of 54 patients showed an average age of onset of the disease of 13.6 years with a median of 10.5 years and a range of 0.3–75.0 years. These findings have been corroborated by other large reports.9-12 After the initial presentation, the disorder usually progresses over a 2–10-year self-limited
period before spontaneous stabilisation.13-15 PRS can be categorised as mild, moderate, or severe.16 Mild disease is described as skin and subcutaneous tissue atrophy. Skin and soft tissue involvement manifest on the face, caudal to the forehead. Atrophy begins superficially, although the epidermis is minimally affected. Atrophy may progress to involve fascia, muscle, cartilage, and bone. Mandibular atrophy may be seen in severe cases.3
The pathogenesis of PRS remains unknown, but trauma, autoimmunity, infection, and autonomic dysregulation have all been suggested.17-19 Neurologically-based theories suggest that PRS may result from disordered developmental migration of neural crest cells, neurotrophic viral infection, trigeminal peripheral neuritis,16,20 or peripheral sympathetic nervous system dysfunction after traumatic disruption of the cervical plexus or sympathetic thoracic trunk.21 Systemic associations of PRS are variable, but neurological manifestations of seizures and headaches are common.3
The diagnosis is made on a clinical basis, but can be supported by imaging and skin biopsy. In some cases, the first symptom represents morphoea en coup de sabre, a unilateral frontal or frontoparietal impression of skin and
underlying tissues, with scarring of the dermis.22 Children with morphoea en coup de sabre and PRS present with neuroimaging findings.23,24 PRS has a significant impact on social and life functioning.
The major aesthetic goal of treatment for patients with PRS is the restoration of facial contour and symmetry. Reconstruction often begins with autologous or synthetic fillers, and continues with surgery when indicated for the extent of tissue involvement. Injectable calcium hydroxyapatite, poly-L-lactic acid, silicone, and polyethylene have been used to correct mild or moderate soft tissue atrophy successfully. This paper aims to present the authors’ experience using reticulated hyaluronic acid (HA) fillers for facial augmentation.
CASE REPORT
The authors present a 35-year-old male with right haemifacial atrophy involving the right temporomalar area pre-auricular area extending
to the right side of the jaw, sparing the mouth. The other side of the face appeared intact. Figure 1 shows pre-procedure photographs.
The onset has been estimated at the age of 20, demonstrating gradual progression over the years, leading to considerable wasting of the right side of the face. The patient reported the lesion to have been stable in appearance for the last 8 years.
The psychological distress caused by this condition affected the patient’s quality of life, limiting their inner circle to their closest contacts, and working only virtually. The patient came to the authors’ clinic to seek reconstructive treatment.
A diagnosis of PRS was made based on the clinical picture. Since the lesion had been stable at the consultation time, the authors planned treatment with HA fillers. HA is a good option for many pathologies presenting with unsightly anatomical alterations.25
Figure 1: Pre-procedure photographs.
The treatment was carried out in four sessions. Initially, the authors focused on the recovery of the structure, and then on the refinement and details. Treatment consisted of 12 syringes of cross-linked HA of different concentrations (17.5 and 20 mg/mL).
27G and 30 G needles and 22 G cannulas were used because they are safer.26 The skin was cleaned with alcoholic chlorhexidine because it is an antiseptic with excellent coverage and a low rate of adverse effects.27 Figure 2 shows post-procedure photographs.
DISCUSSION
PRS is mainly a clinical diagnosis, since no established diagnostic criteria exist. A complete history of the disease, a detailed physical examination, consideration of possible differential diagnoses, and complementary studies are required.28 PRS should be suspected in cases of unilateral generalised soft tissue atrophy with thin skin that is not preceded by inflammation or induration.28
PRS affects the dermatomes of one or more branches of the trigeminal nerve, leading to a progressive shrinking and deformation of one side of the face. PRS results in unilateral facial atrophy and deviation of the mouth and nose to the affected side, compromising the aesthetics and the functionality of the face.21
Guerrerosantos et al.29 classified PRS into four types: Types 1 and 2 involve a decrease in facial soft tissue, while Types 3 and 4 present soft tissue thinning, as well as bone and cartilage atrophy. Type 1 is the mildest form and Type 4 is the most severe.30
Histopathological examination of skin affected with PRS usually reveals atrophy of the epidermis, dermis, subcutaneous tissue, skin appendages, vessels, and/or hair follicles,19 and skin fibrosis with collagen fiber thickening and skin oedema.31,32 Inflammation in the form of lymphocytic infiltrates may be present. Degenerative alterations of the vascular endothelium have been identified in electron microscopy.19
Figure 2: Immediate post-procedure photographs.
Although the pathophysiology of this disease is not well known, trauma, infections, cranial vascular malformations, immune-mediated processes, neurological alterations in fat metabolism, and sympathetic dysfunction are considered possible origins of PRS.21 PRS has not only been associated with autoimmune diseases, congenital diseases, and pregnancy, but has also been related to neurological, ophthalmological, cardiac, rheumatological, infectious, endocrine, maxillofacial, and orthodontic manifestations.28
There is numerous treatment available for PRS, from medical treatments to surgical techniques. However, medical treatments are effective only in the progressive phase, and do not address facial deformities. Topical treatments include steroids and calcipotriol plus psoralen (with ultraviolet A). Systemic drugs are oral steroids, methotrexate, D-penicillamine, tetracyclines, and antimalarials (hydroxychloroquine or chloroquine).24 However, the authors’ literature review highlighted that most of the drugs used correspond to a series of cases and small non-randomised trials.33-36
Reconstruction often begins with autologous or synthetic fillers. The use of permanent fillers, semi-permanent fillers, and resorbable fillers has been described. For surgical reconstruction, autologous fat transplantation or surgical flap may be indicated.24,37-40
Autologous fat transplantation has several benefits compared with flap-based procedures, including a reduction in donor site morbidity, operative time, and lower incidence of complications. However, it can result in incision scars in the donor areas, overcorrection, and irregularities.37 In addition, in patients with PRS, 'take fat' (reabsorption of injected fat) is described in a greater proportion than in the general population, which makes a greater number of surgical interventions necessary.41 Long-term results of fat grafting are often disappointing because of the unpredictable rate of reabsorption. Chang et al.42 associated lipotransfer with stromal vascular fraction, proving that it is effective and safe for the treatment of PRS, as it is able to improve the survival of grafts in the face without major complications.
In cases of severe bony abnormality, surgical flaps are indicated. Surgical flaps include free
vascularised flaps43,44 and local pedunculated flaps.45 Other therapeutic possibilities are bone and cartilage grafts, which are used in advanced stages of the syndrome where these structures are affected, and also dermo-fat grafts obtained from the inguinal area.29
There are also treatments described where porous polyethylene implants are associated in the malar region as a complementary treatment to lipotransfer,46 and others where the placement of Integra® Dermal Regeneration Template (Integra LifeSciences, Princeton, New Jersey, USA), a bilaminar dermal regeneration template with an upper layer of silicone sheet that imitates the epidermis, was associated with platelet-rich plasma.47 Surgery generally requires a longer recovery time and risk of complications, such as flap failure.48
Several cases of PRS treated by semi-permanent and permanent fillers have been reported, including calcium hydroxyapatite (CaHA).49 The use of permanent fillers like Poly(methyl methacrylate) has also been described,50 and polyacrylamide hydrogel (PAAG) filler.51 In the case of CaHA and polyacrylamide, the goal is to provide immediate volume and support while stimulating dermal fibroblasts.52 CaHA has a good volumising effect due to collagen stimulation. PAAG filler is composed of 97.5% water and 2.5% cross-linked PAAG. Like CaHA, PAAG induces the formation of connective tissue.51 It has a longer-lasting effect than HA. However, neither of these products can be reversed in the event of inadvertent nerve compression or intravascular injection. Rees et al.53 reported excellent results with liquid silicone. However, over the years, several complications were described using this material, such as chronic cellulitis, nodules, foreign body reaction, and product migration, which were not related to the technique and, in most cases, were impossible to reverse.54
HA has also been used to correct atrophy in PRS patients.48,55-58 HA is a non-permanent, resorbable filler, and has replaced other standard filler materials.59 HA has an identical chemical composition in all species and tissues.60 Therefore, it has a less antigenic effect and less frequency of hypersensitivity reactions than products of animal origin.61
HA treatment carries advantages over a fat transfer since it can be performed in stages, avoiding overcorrections seen with lipotransfer.37 In addition, in the event of an inadvertent intraarterial injection, hyaluronidase can reverse this infrequent complication.62-64
The authors proposed a combined technique to treat the temporal fossa using a 27 Gx1/2 needle for deep injections and a 22 G cannula for a superficial plane. The authors prioritised injections in the supra-periosteal plane in the so-called ‘swift point’,65-68 with volumising products of 20 mg/mL of HA. Veins and arteries run in a deep plane in the temporal fossa, so the authors decided to use a 22 G blunt cannula in the subcutaneous plane with a fan technique. The cannula always runs superficially, remembering that in the first fascia the anterior or frontal branch of the superficial temporal artery is found.69 The authors opted for a 17.5 mg/mL HA filler for superficial injections since it is easier to accommodate in such a shallow plane, where any imperfections are visible.
At the level of the lateral malar region, close to the temporomandibular joint, a 20 mg/mL HA filler with a 27 Gx1/2 needle was used with a bolus technique in a subperiosteal plane. The results were then optimised with a 17.5 mg/mL product of HA, using a 22 G cannula and a fan technique under the superficial musculoaponeurotic system.70
When injecting the preauricular or parotid region, the authors opted for 17.5 mg/mL HA products and a 22 G cannula, with a fan technique and in the hypodermic plane. This region presents the difficulty of massaging and accommodating the filling if necessary since in depth hard structures are lacking, being positioned on the parotid gland.71-73
For the region corresponding to the submalar triangle, the authors chose 20 mg/mL HA products and a 22 G blunt cannula.
References
1. Tollefson MM, Witman PM. En coup de sabre morphea and Parry-Romberg syndrome: a retrospective review of 54 patients. J Am Acad Dermatol. 2007;56(2):257-63.
The technique used was the fan in the hypodermic plane, with subsequent massage of the treated area, inserting a finger inside the patient’s mouth.74,75
It was also necessary to approach the right mental region. For this, the authors used 20 mg/mL products, initially approaching the supra-periosteal plane with a 27 G needle76 and then the hypodermic plane with a 22 G blunt cannula. It must be remembered that the submental artery runs along the mandibular border in a deep plane, and in the case of intravascular injection, it can generate necrosis of the middle of the tongue.77
CONCLUSIONS
The authors report a case of PRS augmented by HA filler in a 35-year-old male patient to suggest that HA filler could be a safe, simple, alternative to surgical treatment.
The authors opted for cross-linked HA for its longer duration, various densities, and reversibility potential in an inadvertent intravascular injection. HA can be successfully used as a non-surgical alternative to correct facial deformities. It is an effective technique leading to cosmetically acceptable results. It is a reversible and relatively simple technique.
For all of the above, the authors concluded that HA filler would be the safest and easiest way to the correct mild to moderate atrophy in patients with PRS. Although they concluded that HA fillers are a safe tool for treating facial deformities in patients with PRS, they emphasise the importance of in-depth knowledge of facial anatomy for safer aesthetic injections, and to manage possible complications. It must not be forgotten that intravascular of the temporal fossa can lead to skin necrosis or blindness.
2. Appenzeller O et al. Neurology in ancient faces. J Neurol Neurosurg Psychiatry. 2001;70(4):524-9.
3. Appenzeller S et al. Neuroimaging findings in scleroderma en coup de sabre. Neurology. 2004;62(9):1585-9.
4. Peterson LS et al. The epidemiology of morphea (localized scleroderma) in Olmsted County 1960-1993. J Rheumatol. 1997;24(1):73-80.
5. Chiu YE et al. A significant proportion of children with
morphea en coup de sabre and Parry-Romberg syndrome have neuroimaging findings. Pediatr Dermatol. 2012;29(6):738-48.
7. Sommer A et al. Clinical and serological characteristics of progressive facial hemiatrophy: a case series of 12 patients. J Am Acad Dermatol. 2006;54(2): 227-33.
8. Archambault LAS, Fromm NK. Progressive facial hemiatrophy: report of three cases. Arch NeurPsych. 1932;27(3):529-84.
9. Fea AM et al. Parry Romberg syndrome with a wide range of ocular manifestations: a case report. BMC Ophthalmol. 2015;15:119.
10. Stone J. Parry-Romberg syndrome: a global survey of 205 patients using the Internet. Neurology. 2003;61(5):674-6.
11. Orozco-Covarrubias L et al. Scleroderma ‘en coup de sabre’ and progressive facial hemiatrophy. Is it possible to differentiate them? J Eur Acad Dermatol Venereol. 2002;16(4):361-6.
12. Blaszczyk M et al. Progressive facial hemiatrophy: central nervous system involvement and relationship with scleroderma en coup de sabre. J Rheumatol. 2003;30(9):1997-2004.
13. Buonaccorsi S et al. ParryRomberg syndrome. J Craniofac Surg. 2005;16(6):1132-5.
14. Roddi R et al. Progressive hemifacial atrophy: historical review and actual features related to a new classification of facial hypoplasia and atrophy. Eur J Plast Surg. 1994;17(4):178-83.
15. Duymaz A et al. Parry-Romberg syndrome: facial atrophy and its relationship with other regions of the body. Ann Plast Surg. 2009;63(4):457-61.
16. Vaienti L et al. Parascapular free flap and fat grafts: combined surgical methods in morphological restoration of hemifacial progressive atrophy. Plast Reconstr Surg. 2005;116(3): 699-711.
17. Bucher F et al. Ophthalmological manifestations of Parry-Romberg syndrome. Surv Ophthalmol. 2016;61(6):693-701.
18. Garcia-de la Torre I et al. Autoantibodies in Parry-Romberg syndrome: a serologic study of 14 patients. J Rheumatol. 1995;22(1):73-7.
19. Pensler JM et al. Clinical and ultrastructural studies of Romberg’s hemifacial atrophy. Plast Reconstr Surg. 1990;85(5):669-74.
20. Pichiecchio A et al. Parry-Romberg syndrome with migraine and intracranial aneurysm. Neurology. 2002;59(4):606-8.
21. El-Kehdy J et al. A review of ParryRomberg syndrome. J Am Acad Dermatol. 2012;67(4):769-84.
22. Van der Cruyssen F et al. Parry Romberg syndrome: a long-term retrospective cohort study of 10 patients. Oral and Maxillofacial Surgery Cases. 2018;4(3):73-83.
23. Holland KE et al. Linear scleroderma en coup de sabre with associated neurologic abnormalities. Pediatrics. 2006;117(1):e132-6.
24. Tolkachjov SN et al. Progressive hemifacial atrophy: a review. Orphanet J Rare Dis. 2015;10:39.
25. Muszalski DA, Yacomotti LM. Treatment with hyaluronic acid injections in a patient with craniosynostosis. EMJ Dermatol. 2022;DOI:10.33590/ emjdermatol/21-00118.
26. Ugradar S, Hoenig J. Measurement of the force required by blunttipped microcannulas to perforate the facial artery. Ophthalmic Plast Reconstr Surg. 2019;35(5):444-6.
27. Bertarini F, Muszalski D. Antisépticos en procedimientos invasivos estéticos y no estéticos. 2020. Available from: https://piel-l. org/blog/48011. Last accessed: 1 January 2022.
29. Guerrerosantos J et al. Classification and treatment of facial tissue atrophy in ParryRomberg disease. Aesthetic Plast Surg. 2007;31(5):424-34.
30. Aydın H et al. Parry-Romberg syndrome. Physical, clinical, and imaging features. Neurosciences (Riyadh). 2015;20(4):368-71.
31. Bergler-Czop B et al. Scleroderma linearis: hemiatrophia faciei progressiva (Parry-Romberg syndrom) without any changes in CNS and linear scleroderma “en coup de sabre” with CNS tumor. BMC Neurol. 2009;9:39.
32. Cory RC et al. Clinical and radiologic findings in progressive facial hemiatrophy (ParryRomberg syndrome). AJNR Am J Neuroradiol. 1997;18(4):751-7.
33. Uziel Y et al. Methotrexate and corticosteroid therapy for pediatric localized scleroderma. J Pediatr. 2000;136(1):91-5.
34. Zulian F et al.; Juvenile Scleroderma Working Group of the Pediatric Rheumatology European Society (PRES). Juvenile localized scleroderma: clinical and epidemiological features in 750 children. An international study. Rheumatology (Oxford). 2006;45(5):614-20.
35. Falanga V, Medsger TA Jr. D-penicillamine in the treatment of localized scleroderma. Arch Dermatol. 1990;126(5):609-12.
36. Kreuter A et al. Pulsed high-dose corticosteroids combined with low-dose methotrexate in severe localized scleroderma. Arch Dermatol. 2005;141(7):847-52.
37. Aloua R et al. Lipofilling as an aesthetic restorative technique for the facial hemiatrophy of ParryRomberg syndrome: an analysis of 27 cases. Int J Surg Case Rep. 2021;79:138-41.
38. Kasielska-Trojan A et al. Autologous fat transfer for facial recontouring in Parry-Romberg syndrome. J Cosmet Dermatol. 2020;19(3):585-9.
39. Xie Y et al. Correction of hemifacial atrophy with autologous fat transplantation. Ann Plast Surg. 2007;59(6):645-53.
40. de Alencar JCG. Autologous fat transplantation for the treatment of progressive hemifacial atrophy (Parry-Romberg syndrome: case report and review of medical literatute). An Bras Dermatol. 2011;86(4 Suppl 1):S85-8.
41. Slack GC et al. Parry-Romberg reconstruction: beneficial results despite poorer fat take. Ann Plast Surg. 2014;73(3):307-10.
42. Chang Q et al. Quantitative volumetric analysis of progressive hemifacial atrophy corrected using stromal vascular fractionsupplemented autologous fat grafts. Dermatol Surg. 2013;39(10):1465-73.
43. Iñigo F, Fernández M. Tratamiento estético de la enfermedad de Romberg: experiencia con 78 casos. Cirugía Plástica. 2001;11(2):67-75.
44. Agostini T et al. Esthetic restoration in progressive hemifacial atrophy (Romberg disease): structural fat grafting versus local/free flaps. J Craniofac Surg. 2014;25(3):783-7.
45. Sabapathy SR et al. Romberg’s disease: modified Washio flap for facial contour reconstruction. Plast Reconstr Surg. 2001;108(3):705-8.
46. Ozturk S et al. Treatment of ‘en coup de sabre’ deformity with porous polyethylene implant. J Craniofac Surg. 2006;17(4): 696-701.
47. Ortega VG, Sastoque D. New and successful technique for the management of Parry-Romberg syndrome’s soft tissue atrophy. J Craniofac Surg. 2015;26(6): e507-10.
48. Jo M et al. Parry-Romberg syndrome augmented by hyaluronic acid filler. Ann Dermatol. 2018;30(6):704-7.
49. Cox SE, Soderberg JM. Idiopathic hemifacial atrophy treated with serial injections of calcium hydroxylapatite. Dermatol Surg. 2010;36(4):542-5.
50. de Vasconcelos Carvalho M et al. Association of aesthetic and orthodontic treatment in ParryRomberg syndrome. J Craniofac Surg. 2010;21(2):436-9.
51. Al-Niaimi F et al. Idiopathic hemifacial atrophy treated with permanent polyacrylamide subdermal filler. Dermatol Surg. 2012;38(1):143-5.
52. Berlin AL et al. Calcium hydroxylapatite filler for facial rejuvenation: a histologic and immunohistochemical analysis. Dermatol Surg. 2008;34 (Suppl 1):S64-7.
53. Rees TD et al. Silicone fluid injections fro facial atrophy. A tenyear study. Plast Reconstr Surg. 1973;52(2):118-27.
54. Rapaport MJ et al. Injectable silicone: cause of facial nodules, cellulitis, ulceration, and migration. Aesthetic Plast Surg. 1996;20(3):267-76.
55. Watchmaker J et al. A case of bilateral Parry-Romberg syndrome successfully treated with hyaluronic acid filler augmentation. J Cosmet Dermatol. 2019;18(5):1261-3.
56. Myung Y, Lee YH, Chang H. Surgical correction of progressive hemifacial atrophy with onlay bone graft combined with soft tissue augmentation. J Craniofac Surg. 2012;23(6):1841-4.
57. Malhotra R. Deep orbital sub-Q restylane (nonanimal stabilized hyaluronic acid) for orbital volume enhancement in sighted and anophthalmic orbits. Arch Ophthalmol. 2007;125(12):1623-9.
58. Feldman I et al. Deep orbital sub-Q hyaluronic acid filler injection for enophthalmic sighted eyes in Parry-Romberg syndrome. Ophthalmic Plast Reconstr Surg. 2018;34(5):449-51.
59. Park S et al. Investigation of the degradation-retarding effect caused by the low swelling capacity of a novel hyaluronic acid filler developed by solid-phase crosslinking technology. Ann Dermatol. 2014;26(3):357-62.
60. Verpaele A, Strand A. Restylane SubQ, a non-animal stabilized hyaluronic acid gel for soft tissue augmentation of the mid- and lower face. Aesthet Surg J. 2006;26(Suppl 1):S10-7.
61. Bugge H et al. Hyaluronic acid treatment of facial fat atrophy in HIV-positive patients. HIV Med. 2007;8(8):475-82.
62. DeLorenzi C. Complications of injectable fillers, part 2: vascular complications. Aesthet Surg J. 2014 ;34(4):584-600.
63. Cavallini M et al. The role of hyaluronidase in the treatment of complications from hyaluronic acid dermal fillers. Aesthet Surg J. 2013;33(8):1167-74.
64. Jung H. Hyaluronidase: an overview of its properties, applications, and side effects. Arch Plast Surg. 2020;47(4):297-300.
65. Sykes JM et al. Upper face: clinical anatomy and regional approaches with injectable fillers. Plast Reconstr Surg. 2015;136(Suppl 6):204S-18S.
66. Carruthers J et al. Suggested injection zone for soft tissue fillers in the temple? Dermatol Surg. 2017;43(5):756.
67. Lamb JP et al. Abstract: threedimensional CT validation of supraperiosteal temple volumization with hyaluronic acid
68. Almeida ART et al. Hyaluronic acid in the rejuvenation of the upper third of the face: review and update. Part 2: temporal and supraorbital regions. Surg Cosmet Dermatol. 2017;DOI:10.5935/ SCD1984-8773.20179201.
69. Cotofana S et al. The six different injection techniques for the temple relevant for soft tissue filler augmentation procedures - clinical anatomy and danger zones. J Cosmet Dermatol. 2020;19(7):1570-9.
70. de Maio M. Correction to: MD Codes™: a methodological approach to facial aesthetic treatment with injectable hyaluronic acid fillers. Aesthetic Plast Surg. 2021;45(2):838-43.
71. Corduff N. The 12-point revitalization guide to pan-facial application of injectable fillers in older women. J Clin Aesthet Dermatol. 2018;11(8):35-40.
72. Kapoor KM et al. Consensus recommendations for treatment strategies in indians using botulinum toxin and hyaluronic acid fillers. Plast Reconstr Surg Glob Open. 2017;5(12):e1574.
73. Kim HJ et al., “Clinical anatomy of the midface for filler injection,” Kim HJ et al. (eds) Clinical Anatomy of the Face for Filler and Botulinum Toxin Injection. (2016) Singapore: Springer Singapore, pp.119-51.
74. Tobias GW, BWJ. The submalar triangle: its anatomy and clinical significance. Facial Plast Surg Clin North Am. 1994;2(3):255-64.
75. de Maio M, Rzany B, “The most common indications,” de Maio M, Rzany B (eds.) Injectable Fillers in Aesthetic Medicine. (2014) Heidelberg: Springer Berlin, pp.69-133.
76. Braz A et al. Lower face: clinical anatomy and regional approaches with injectable fillers. Plast Reconstr Surg. 2015;136(Suppl 5):235S-57S.
77. Wang Q et al. Vascular complications after chin augmentation using hyaluronic acid. Aesthetic Plast Surg. 2018;42(2):553-9.
EMJ Podcasts
The EMJ Podcast aims to provoke conversations around the latest trends and innovations in healthcare, provide engaging and educational content for healthcare professionals, and hosts conversations with physician entrepreneur, Jonathan Sackier.
Listen today
www.emjreviews.com
Platelet-Rich Plasma Applications, The Past 5 Years: A Review Article
Authors: Michael G. Buontempo,1 Lina Alhanshali,2 Jerry Shapiro,3 Kristen Lo Sicco,3 *Michael S Garshick4
1. Department of Dermatology, Hackensack Meridian School of Medicine, Nutley, New Jersey, USA
2. Department of Dermatology, State University of New York System (SUNY) Downstate College of Medicine, USA
3. The Ronald O. Perelman Department of Dermatology, New York University (NYU) Grossman School of Medicine, USA
4. Department of Medicine, Center for the Prevention of Cardiovascular Disease and Leon H. Charney Division of Cardiology, New York University (NYU) School of Medicine, USA
*Correspondence to michael.garshick@nyumc.org
Disclosure: Buontempo and Alhanshali have no conflicts of interest to disclose. Shapiro is a consultant for Aclaris Therapeutics, Incyte, and Replicel Life Sciences; has been an investigator for Regen Lab; and is an investigator for Pfizer. Lo Sicco has been an investigator for Regen Lab; is an investigator for Pfizer; and is a consultant for Pfizer and Aquis. Garshick is a consultant for Kiniksa Pharmaceuticals and Horizon Therapeutics.
Received: 22.06.23
Accepted: 22.09.23
Keywords:
Clinical use of platelet-rich plasma, dermatology, global market of platelet-rich plasma, growth factors, inflammation, orthopaedics, platelet-rich plasma (PRP), randomised controlled trials (RCT), regenerative medicine, wound healing.
Platelet-rich plasma (PRP) is autologous plasma with a platelet concentration that is on average five times greater than baseline, and has been extensively investigated for its potential applications across various medical fields, including orthopaedics, dermatology, wound healing, maxillofacial surgery, and others. This review article aims to provide an overview of PRP's applications and evidence over the past 5 years in randomised controlled trials. Many studies demonstrate PRP's effectiveness in reducing pain and improving functional outcomes, while others report no significant differences compared to alternative treatments or placebo. Across various studies, several key limitations exist, such as small sample sizes, short follow-up durations, and lack of standardisation in PRP preparation methods, highlighting the need for research to further establish PRP's effectiveness in these clinical applications. The article also discusses the different classification systems for PRP, and underscores the importance of understanding the components that influence clinical outcomes, as well as noting the growth of PRP in the marketplace. Overall, while studies exist demonstrating the clinical utility of PRP, standardised reporting is required to determine its full potential, as well as optimal preparation and administration strategies.
Key Points
1. This manuscript provides an overview of randomised controlled trials on the therapeutic potential of platelet-rich plasma (PRP) in various medical fields, such as orthopaedics, dermatology, and maxillofacial surgery. Here, the authors reveal PRP’s varying effectiveness in reducing pain, improving functional outcomes, and contributing to tissue regeneration, underlining its growing prominence in the medical marketplace.
2. This review underscores the prevailing challenges in PRP research, including small sample sizes, short follow-up durations, and a lack of standardisation in preparation methods. The manuscript emphasises the need for accurate documentation of PRP preparation aspects, such as growth factor levels, to facilitate cross-study comparisons, and address the heterogeneity in PRP preparation and administration strategies, which currently hinder the comparability of PRP’s efficacy among different studies.
3. There is a need for further research to establish and normalise standardised reporting, optimal preparation, and administration strategies for PRP. Given the substantial growth of the PRP global market, and its increasing usage, the authors call for blinded randomised controlled trials, and robust characterisation of PRP’s constituents to fully assess its efficacy, and to inform clinicians on its optimal utilisation for diverse medical applications.
INTRODUCTION
Platelets, small anucleate cells derived from megakaryocyte fragments that play a central role in forming blood clots during vascular and tissue injury to maintain homeostasis.1 These cells harbour three types of granules: dense, α, and lysosomal granules. Specifically, the α granules are repositories of a host of bioactive factors, such as growth factors, cytokines, chemokines, cell adhesion molecules, and proteins.1,2
Platelet-rich plasma (PRP), a concentrate of these bioactive constituents, is essentially a cocktail of growth factors, cytokines, and other molecules. PRP’s therapeutic potential has been progressively explored across multiple medical specialties, including musculoskeletal, dermatology, chronic wound healing, and maxillofacial surgery, among others (Table 1).
The clinical utility of PRP dates to the 1970s, and its use has since pervaded several fields, such as orthopaedics/musculoskeletal, dermatology, chronic wound healing, maxillofacial surgery, ophthalmology, urology, and others (Figure 1). This prevalence of PRP applications has also driven a robust growth in its global market, valued at 627.9 million USD in 2022, with a projected annual growth rate of 15.1% compounded yearly from 2023–2030.9
PRP is obtained through a centrifugation process that separates whole blood into distinct layers, comprising of erythrocytes at the bottom, the buffy coat in the middle, and plasma at the top (Figure 2).10 The buffy coat layer, rich in platelets and leukocytes, is not uniform, and can be stratified into sub-layers containing different cell types and platelet concentrations. Closer to the erythrocyte layer, there is typically a high concentration of neutrophils and other granulocytes, alongside a moderate number of platelets. As you ascend towards the upper portion of the buffy coat layer, closer to the plasma, platelet concentration tends to increase, while an increase in mononuclear cells, such as lymphocytes and monocytes, is observed.
A standardised nomenclature system, such as Dohan Ehrenfest’s shorthand naming convention, categorises different types of PRP, primarily based on the depth of buffy coat collection (Figure 2).
The therapeutic efficacy of PRP, especially in tissue regeneration, is often tied to the release of its growth factors and other bioactive molecules. To achieve an immediate release of these factors, PRP can be activated. This is typically achieved through the addition of exogenous coagulation factors, such as thrombin or calcium chloride.11,12 This release, when induced externally by such coagulants, can span from minutes to days. Alternatively, a ‘physiologic activation’
Table 1: Breakdown of frequently cited growth factors and their functions in each major field of plateletrich plasma use.
Stimulate hair follicle stem cells and fibroblasts, promoting hair growth, enhancing skin elasticity and collagen content. Also implicated in the treatment of androgenic alopecia, inflammatory nail diseases, psoriasis, photoageing, melasma, vitiligo, nonhealing wounds, and acne scars.6,7
Accelerates wound healing through granulation, angiogenesis, and re-epithelialisation.6
Improves bone formation and regeneration in dental surgery; reduces post-operative discomfort and complications.6,8
Enhances erectile function via cavernous nerve regeneration and angiogenesis.6
method can be employed. In this method, PRP, when injected, undergoes natural activation, leading to a more prolonged, steady release of platelet factors over 1–2 weeks.11,12 It is worth noting that the choice of activation process can influence the therapeutic potential of PRP. External activation provides an immediate high concentration of growth factors, which might be beneficial in scenarios where a rapid tissue response is desired. In contrast, the slower physiologic activation might be more suitable for sustained release applications. Notwithstanding the widespread use of PRP, its preparation protocols and standardisation to attain a consistent optimal platelet yield remain a matter of discussion.
While a comprehensive understanding of the crucial elements that drive the benefits of PRP in various fields often remains elusive in literature, attempts are frequently made to conjecture the contributing factors to the benefits observed with PRP use. Within orthopaedics, for instance, it is postulated that growth factors stimulate chondrocyte activity, extracellular matrix synthesis, and cartilage repair, and alleviate inflammation.3-7 These growth factors typically form the basis of PRP’s reported benefits across numerous fields (Table 1). However, a consistent depiction of this foundational role in literature is often complicated, due to the lack of formal growth factor analyses in studies demonstrating benefits with PRP use.
*Unspecified areas in “Unspecified” category include: pain management and rehabilitation (n=2), rheumatology (n=1), diagnostic medicine (n=1), and neurology (n=1).
Data collected from a PubMed Medical Subject Heading “Platelet-Rich Plasma” search over the last 5 years, including only randomised controlled trials, and updated on 11th January 2023.
Given the intricate nature of PRP’s constituents, preparation methods, and wide-ranging applications in various medical fields, this review aims to collate and analyse current findings on PRP’s therapeutic utility, while identifying gaps in the literature regarding standardisation, growth factor analyses, and efficacy reports. By synthesising domain-specific data and outcomes, the authors hope to shed light on the mechanisms underlying PRP’s therapeutic benefits, and underscore areas requiring rigorous scientific investigation.
METHODS
The review of the literature was conducted following a structured approach to ensure the inclusion of all relevant studies and data
regarding the clinical use of PRP across diverse medical fields. Emphasis was laid on the most frequent use cases and documented effectiveness. The search, initiated on 11th January 2023, focused on randomised controlled trials (RCT) from the past 5 years. The electronic database PubMed was utilised, employing the Medical Subject Heading term “Platelet-Rich Plasma” to yield 402 pertinent articles.
Post-retrieval, abstracts of the identified articles were examined for relevance, followed by a detailed review of the full-text versions. Studies were then stratified into distinct thematic groups based on their outcomes, enabling a comprehensive summary of each field. Further, each study was critically assessed for limitations, contributing to the formation of summary groups.
Figure 1: Breakdown of randomised controlled trials on PubMed over the past 5 years using platelet-rich plasma (n=402).
Long high spin speed (buffy coat-based/entire BC) - higher WBC - 3–8xbaseline (platelets; L-PRP)
Double spin - high platelet concentration >5x - low neutrophils - low RBC - can concentrate monocyte/macrophage/lymphocytes (P-PRP)
Platelet-rich fibrin (P-PRF or L-PRF)
Top half: Whole blood, pre- and post-centrifugation, with separated layers and buffy coat layers labelled.
Bottom half: Collection methods of PRP as they pertain to the Dohan Ehrenfest shorthand naming convention of PRP. Superficial buffy coat collection (red box) as it pertains to P-PRP and P-PRF, and entire buffy-coat collection (purple box) as it pertains to L-PRP and L-PRF production.
BC: buffy coat; L-PRF: leukocyte- and platelet-rich fibrin; L-PRP: leukocyte- and platelet-rich plasma; P-PRF: pure platelet-rich fibrin; PRP: platelet-rich plasma; P-PRP: pure platelet-rich plasma; RBC: red blood cell; WBC: white blood cell.
Figure created with BioRender.com.
The most extensive and representative studies from each summary group were selected, ensuring a balanced depiction of both the outcomes and limitations within each field of PRP use. This approach aimed to create an inclusive, yet concise, review that encapsulates the breadth of PRP’s clinical application and efficacy.
MUSCULOSKELETAL (n=133)
Knee Osteoarthritis
Studies on PRP’s efficacy in treating knee osteoarthritis (KOA) compared versus placebo with normal saline, or against widely accepted treatments, such as injections of hyaluronic acid (HA) or corticosteroids, have reported mixed results.13,14
An RCT aimed to compare the clinical outcomes of intra-articular injection of PRP and high molecular weight HA in treating KOA. In this study 200 patients with symptomatic KOA (Kellgren–Lawrence Grade 2 or 3) received three blinded intra-articular injections, at 2-week intervals, of either PRP or HA. Clinical evaluations employed metrics like the International Knee Documentation Committee (IKDC) subjective score, Visual Analogue Scale (VAS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) total score, and the re-injection rate over a 36-month follow-up period. By the final evaluation, 189 patients remained in the study.
PRP and HA injections both effectively improved knee symptoms and functional status, with results stable up to 18 months post-injection without any re-injections. Beyond the 18-month period, the PRP group showed a decrease in mean vasscores, reflecting a sustained reduction in pain. Simultaneously, the IKDC subjective scores improved, indicating enhanced knee function over time. WOMAC total scores also decreased over the study period, suggesting overall amelioration in pain, stiffness, and physical function. In contrast, the HA group demonstrated initial improvement followed by a gradual decline in IKDC subjective scores, suggesting a deterioration in knee function. The VAS scores for this group also fluctuated, ultimately increasing, and indicating worsening pain symptoms.
The re-injection rate was notably lower in the PRP group during the 24–36-month follow-up period, highlighting PRP treatment’s longerlasting effect. Despite the higher incidence of short-term post-injection pain in the PRP group, no major complications were associated with either injection type.
In contrast, another study found the benefits of PRP were more aligned with HA.15,16 Specifically, in a double-blind study involving 192 patients observed over an average of 64.3 months (standard deviation [SD]: 7.8 months), both PRP and HA, administered via three weekly injections, led to comparable improvements in IKDC subjective scores, with significant advancements from baseline for both treatments. The only notable difference was a reduced reintervention rate in the PRP group at 24 months (22.6% versus 37.1%; p=0.036).15
Temporomandibular Joint Osteoarthritis
Within the realm of temporomandibular joint osteoarthritis (TMJ-OA) treatments, an RCT delved into the benefits of intra-articular platelet-rich fibrin (PRF) injections following arthrocentesis. Notably, PRF, produced sans anticoagulants, allows a fibrin clot formation during centrifugation, serving as a cellular migration scaffold, and promoting tissue healing. In a study population of 36 patients, equally divided into a PRF group and a control group, the PRF cohort exhibited marked improvements in jaw movement metrics through the 6th month post-treatment, and these positive outcomes persisted until the 12th month. In contrast, the control group, which only underwent arthrocentesis, demonstrated an initial postoperative uptick in jaw movement measurements, but this trend reversed between the 6th and 12th month. Nevertheless, pain levels notably declined in the control group (p<0.001). The overarching inference drawn was the superiority of PRF injections after arthrocentesis over the latter in isolation, in terms of pain alleviation and bolstered functional jaw motions. 17
Shifting focus to a clinical and radiological study conducted in 2019, the impact of PRP, HA, and corticosteroids on TMJ-OA was explored. The research encompassed 31 patients experiencing lateral pain, and 43 patients with posterior pain, grouped into three cohorts: PRP (Group 1), HA
(Group 2), and corticosteroids (Group 3). The findings illuminated that PRP intra-articular injections were notably superior in alleviating TMJ palpation pain when juxtaposed with HA and corticosteroids, as gauged through the VAS scores at varied post-treatment intervals.18
In a more recent RCT from 2022, researchers scrutinised the potency of PRP, HA, and a hybrid of both, succeeding arthrocentesis in 30 patients with TMJ-OA. The outcomes showcased a prominent pain diminution across all cohorts 6 months post-treatment, with the blend of PRP and HA emerging as the most efficacious (p<0.001). Furthermore, parameters such as the maximum mouth opening and both lateral and protrusive mandibular movements witnessed a commendable surge in all tested groups, with the zenith observed in the combined treatment cohort.19
Rotator Cuff Injuries
Research into rotator cuff injuries has elucidated PRP’s potential role. A double-blind RCT assessed PRP versus sodium hyaluronate, either standalone or combined. Using metrics such as the Constant score and the American Shoulder and Elbow Surgeons (ASES) Shoulder Score, results indicated a combined sodium hyaluronate and PRP treatment to be especially beneficial for specific rotator cuff injuries.20
Another RCT compared corticosteroid injections to PRP. While corticosteroids provided initial relief, PRP shone in long-term benefits, demonstrating its potential for sustained recovery in rotator cuff injuries.21
A similar double-blind RCT juxtaposed PRP and corticosteroid injections. The results illuminated that 3 months post-injection, the PRP group manifested noticeable improvements in VAS, ASES, and Western Ontario Rotator Cuff Index scores, though these differences were not significant at the 6-week or 12-month intervals.22
One study evaluated the effectiveness of collagen with PRP, PRP alone, and collagen alone in treating partial-thickness rotator cuff injuries. Utilising a numeric rating scale, QuickDash, and EQ-5D-5L questionnaires for assessment, they found no significant differences between the groups. However, a trend towards improvement
was observed in the combined collagen and PRP group and PRP alone group between the 12th and 24th week follow-ups.23
In summary, the realm of musculoskeletal applications has seen varied PRP outcomes. While certain studies emphasise its potential in pain mitigation and functional improvement, such as in TMJ-OA cases,17-19 others present ambiguous results.13-18,24,25 The discrepancies in outcomes can be attributed to variations in sample sizes, follow-up durations, and PRP preparation methods, highlighting the necessity for more meticulous research in the field.
MAXILLOFACIAL SURGERY (n=89)
The effectiveness of PRP and PRF in maxillofacial surgery has been the focus of various studies, yielding mixed results. Some studies demonstrated the benefits of PRP and PRF in surgical outcomes, such as reduced scar width; improved patient satisfaction and quality of life;26 enhanced recovery of neurosensory disturbances following sagittal split osteotomy (SSO);27 and increased tooth movement rate with injectable PRF, potentially shortening orthodontic treatment.28 PRP is also shown to improve pain alleviation and mouth opening in patients with temporomandibular joint derangement,29 while PRF has shown potential in reducing palatal wound dehiscence in relocation pharyngoplasty for patients with obstructive sleep apnoea.30
In a study of 21 patients with bilateral SSO (15 females, 6 males; average age: 25.48±5.16 years), PRF was evaluated for its potential to hasten recovery from paraesthesia postoperatively. The study analysed the TwoPoint Discrimination (TPD) value, brushstroke direction, and self-reported paraesthesia via the VAS. PRF treatment resulted in a significant reduction in TPD values at both 6- and 12-months post-operation compared with the control group (p=0.001). Similarly, a significant increase in correct brushstroke direction reporting was observed in the treatment group at both timepoints (p=0.001). Moreover, VAS paraesthesia scores were significantly lower in the PRF group at both 6 and 12 months (p=0.001). The results suggest that PRF may expedite paraesthesia recovery after SSO.
At 6 months post-surgery, Group 1 (treatment) showed a mean TPD value of 6.33±0.66 mm, while Group 2 (control) were at 7.29±0.72 mm, with the difference being statistically significant (p=0.001). Similarly, at 12 months, the treatment group’s mean TPD value was lower than the control’s (4.71±0.78 mm versus 6.19±0.75 mm; p=0.001). In the brush directional stroke test, significantly more patients in the treatment group were able to report the correct direction at both 6- and 12-months post-surgery (81.0% versus 28.6% and 100.0% versus 71.4%, respectively; p=0.001). Finally, the self-reported paraesthesia VAS score was also significantly lower in the treatment group at both timepoints (5.62±0.59 versus 7.00±0.70 at 6 months, and 3.52±0.68 versus 4.95±0.59 at 12 months, respectively; p=0.001). These findings indicate that PRF application may enhance the recovery of paraesthesia following SSO.27
Furthermore, PRF has been found to be effective in promoting bone regeneration around immediate dental implants, with primary stability measured between 30 and 60 on the Implant Stability Quotient (IQS) scale,31 and preventing post-operative relapse after Le Fort I osteotomy.32 A combination of bone marrow aspirate concentrate and PRF has been suggested to result in more mature bone formation,33 and PRF alone could enhance the stability of dental implants in the posterior maxilla during the healing period.34
In contrast, other studies found no significant benefits of PRP and PRF in certain applications. For example, PRP showed no healing effects on alveolar defects after rapid maxillary expansion,35 and liquid PRF did not significantly affect implant surface osseointegration.36 Despite some positive findings, many of these studies had limitations, such as small sample sizes and lack of blinding. Therefore, further research is needed to confirm the conclusions, and better understand the role of PRP and PRF in maxillofacial surgery.
WOUND HEALING (n=87)
Chronic wounds do not progress through the normal phases of healing, and can be classified as vascular, diabetic, or pressure ulcers.37 Their prevalence in the USA has created an
economic burden on the healthcare system.38 The treatment of chronic wounds is summarised by TIME: Tissue debridement, Infection control, Moisture balance, and Edges of the wound.37 Further management involves treatment and control of the underlying disease.37
PRP has emerged as a promising adjuvant for the treatment of chronic wounds. The α granules of platelets contain growth factors, including transforming growth factor (TGF-β1, TGF-β2), granulocyte colony-stimulating factor, TNF-α, platelet-derived growth factors, platelet-derived angiogenesis factor, keratinocyte growth factor, hepatocyte growth factor, and insulin-like growth factor, which are released upon platelet activation.39 Growth factors play a vital role in the wound healing process.
The effectiveness of PRP therapy on the management of chronic wounds has been evaluated on various types of chronic wounds, as well as on different end outcomes in regard to wound healing.40-42 Commonly used end outcomes include the size of the wound, time to complete closure of the wound, hospitalisations, and infections. Most of the studies found PRP provided a benefit in at least one end outcome. A double blind RCT aimed to assess the efficacy of platelet gel compared to hydrogel in the treatment of non-healing chronic lower leg ulcers of different aetiologies.43 Thirty patients were treated with platelet gel, and 30 with hydrogel once a week for 3 consecutive weeks, with a last examination 6 months after treatment. They found that after 6 months of treatment, the mean wound area of the experimental group treated with platelet gel decreased to 35.01% (SD: 53.69). The control group (treated with hydrogel) had the wound area decrease to 89.95% (SD: 71.82). Overall, the treatment with platelet gel was statistically significantly more efficacious than hydrogel (p<0.05). Another study analysed diabetic foot ulcers treated with PRP, and reported a higher healing rate than patients treated with conventional dressing.44 One study by Gupta et al.41 found diabetic foot ulcers treated with PRP did not have a better or faster healing than conventional treatment. In the study, patients randomised to receive normal saline dressing had an 81.72±17.2% mean±SD percentage reduction in healing area at 6 weeks compared to 85.98±13.42% in the study group (p=0.29). A limitation of some of these studies
include testing on chronic wounds of various aetiologies, which may have influenced the results. Overall, as platelets contain growth factors that play a significant role in wound healing, the use of PRP demonstrates success in improving end outcomes of the wound healing process; however, further studies are necessary to further establish this effect.
DERMATOLOGY (n=46)
PRP has been effective in several dermatologic diseases, including alopecia, melasma, scars, and vitiligo.45-47 The biggest use has been on patients suffering from androgenetic alopecia (AGA).48,49 Specifically, over the past 5 years, 21 RCTs attempted to assess the efficacy and safety of PRP for the treatment of AGA. Many studies found PRP to be beneficial; however, there are key limitations. A split-scalp study enrolled 35 patients with AGA to assess the effects of PRP on hair growth and thickness. Two 7.6 cmx7.6 cm squares were tattooed on the scalp of participants, who were randomly assigned to PRP or saline injections of three monthly treatment sessions, and an evaluation 3 months after the final treatment session. The PRP treated areas exhibited a mean density increase of approximately 20 hairs/cm2 (p<0.05).50 The placebo side showed a mean density increase of approximately 15 hairs (<0.05). The authors attribute the increase in hair density in the placebo side to the possibility of growth factors diffusing from the PRP-treated areas, therefore leading to an improvement in both the control and PRP-treated sides of the scalp. Additionally, the process of injecting needles into the scalp can lead to the immobilisation of growth factors, which can contribute to improved hair growth. These factors make difficult an effective assessment of the efficacy of PRP in splitscalp studies.
PRP has demonstrated efficacy in vitiligo treatment. There have been five RCTs published in the last 5 years on the use of PRP for the treatment of vitiligo. Four of these studies assessed the efficacy of PRP in addition to laser therapy. All but one found that PRP can be an effective adjunct for treating vitiligo. One study explored the efficacy of PRP versus combined fractional CO2 laser with PRP in the treatment of non-segmental vitiligo. The study enrolled
36 participants who were treated with PRP, fractional CO2, combined PRP, and fractional CO2; and a fourth control group. The study demonstrated that PRP alone provided the best results, followed by PRP with CO2, and then fractional CO2 alone.51 Specifically, the mean surface area reduction of the PRP treated area was 57.01+/-29.67, for the CO2 and PRP, a mean reduction of 54.22+/-37.08 was observed and for Co2 alone, a reduction of 38.08+/-40.32. A study aimed to assess whether the addition of PRP to monochromatic excimer light (MEL) therapy would provide additional benefit in the treatment of localised stable vitiligo. The study enrolled 36 patients with at least two more or less symmetrical patches of localised and stable vitiligo. For each participant, each vitiligo patch was randomly assigned to receive either MEL therapy combined with PRP injections (Group A), or MEL therapy alone (Group B). Group A received MEL therapy twice weekly, with biweekly intradermal PRP. Group B received MEL therapy twice weekly for a 4-month maximum, or until complete repigmentation. The study found that PRP combined with MEL therapy did not benefit the treatment of localised vitiligo.52 PRP has also been utilised in the treatment of melasma. In a split-face trial, the side treated with PRP showed significant improvement after treatment for 6 weeks.53 Other studies tested PRP with hydroquinone or tranexamic acid for melasma, and showed an improvement when PRP was added as an adjuvant.54
OTHER (n=47)
Primarily documented in the realm of regenerative medicine, PRP formulations have been utilised in diverse medical disciplines, including gynaecology and urology.55,56 Notably, PRP’s wound healing attributes can offer significant benefits following a Caesarean section procedure. In a comprehensive study exploring the potential gynaecologic utility of PRP, a cohort of 200 females undergoing Caesarean section were randomly assigned to two groups.55,56 One group received PRP injections after the surgery, and the control group received standard care. The PRP group demonstrated a greater reduction in the REEDA (redness, oedema, ecchymosis, discharge, and approximation) score on Days 1 and 7 after surgery, and continued to show greater improvement until 6 months. The
Vancouver classification and the VAS were also significantly lower in the PRP group.
PRP has also been investigated as a possible treatment for erectile dysfunction (ED). In 2021, the first double-blind, randomised, placebocontrolled clinical trial assessing the use of PRP for ED treatment was performed.57 Poulious et al. randomly assigned 60 males with ED to either 10 mL of PRP injections or 10 mL of normal saline injections in two sessions, with a 1-month interval in between. At 6 months, the minimally clinically important difference was achieved by 69% of patients in the PRP group, compared to 27% in the placebo group (p<0.001). Between the two groups, the risk difference was 42% (95% confidence interval: 18–66).
CONCLUSION
As summarised, PRP has been explored as a potential therapeutic intervention in a variety of medical fields, yielding variable results. Its utilisation in musculoskeletal, maxillofacial surgery, wound healing, dermatology, and other fields such as gynaecology and urology have demonstrated potential benefits in certain cases, while in others, no significant distinctions have been observed compared with alternative treatments or placebo.
The existing body of literature faces substantial limitations. These encompass issues such as small sample sizes, short follow-up durations, and lack of standard protocols for PRP preparation, which collectively hinder the comparability of PRP’s efficacy among different studies. The variability in measured end outcomes, as well as a great heterogeneity in PRP preparation and administration strategies, adds to the complexity. For instance, the platelet counts in PRP can vary greatly depending on the chosen preparation technique, potentially influencing study outcomes.1 Unfortunately, the current literature often fails to adequately document these nuanced distinctions, impeding the ability to conduct accurate cross-study comparisons.
This situation has led to the proposal of numerous classification systems, with two prominent classification systems, the Scientific and Standardization Committee (SSC) of
the International Society on Thrombosis and Haemostasis, Inc. (ISTH) and Khan et al., aiming to address the challenges of inconsistent reporting methods and lack of understanding of PRP components influencing clinical outcomes.12 However, many studies still fail to report aspects of PRP preparation, such as growth factor levels, hampering classification efforts.
Moreover, while the global market for PRP was valued at 627.9 million USD in 2022,59 a robust characterisation and understanding of PRP’s constituents remain an ongoing debate within the scientific community. Blinded RCTs with objective outcome measurements are necessary to fully assess the efficacy of PRP. Further research into different preparation techniques, the best PRP administration strategies, and intervals between injections is vital.
A study analysing trends in PRP usage and costs of injections in orthopaedic surgery demonstrated usage significantly increased between 2010–2019.12,58 The average cost of a PRP injection clustered around 1,000 USD.58 In 2022, the global market for PRP was valued at 627.9 million USD, and the expected compound annual growth rate from 2023–2030 is 15.1%.9 Medicare offers reimbursement for PRP injections when they are performed for patients with chronic, non-healing diabetic, pressure, and/or venous wounds enrolled in an approved clinical research study.59 A study analysing Medicare billing for PRP reports annual charges to Medicare increased from 500,000 USD in 2010 to more than 2 million USD in 2014, a 400% increase.60 These studies demonstrate the growing popularity of PRP in the medical settings. As such, an increase in research to further establish its efficacy, safety, and the best administration and assessment strategies is necessary.
As a growing interest in PRP is evident across diverse medical fields, the implications of the authors’ findings are profound. PRP, while showcasing potential benefits in musculoskeletal, maxillofacial surgery, dermatology, and other specialisations, has yet to prove its unequivocal superiority in all scenarios. Looking ahead, as the field of regenerative medicine continues to evolve, the onus is on the scientific community to devise standardised protocols for PRP preparation, classification, and reporting.
Achieving this uniformity will allow for a more clear insight into PRP’s therapeutic viability, and spotlight clinical scenarios where it can be most beneficial. The roadmap for future research should prioritise surmounting these challenges, refining PRP formulations, and discerning the most efficacious PRP components for diverse clinical applications. Embracing these strategic shifts will be pivotal in realising the full therapeutic potential of PRP.
References
1. Mathew J et al. Physiology, Blood Plasma [Internet] (2022) Treasure Island: Statpearls. Available at: https://www.ncbi.nlm.nih. gov/books/NBK531504/. Last accessed: 19 June 2023.
2. Kaushik A, Kumaran MS. Plateletrich plasma: the journey so far! Indian Dermatol Online J. 2020;11(5):685-92.
3. Pötter N et al. Evaluation of the influence of platelet-rich plasma (PRP), platelet lysate (PL) and mechanical loading on chondrogenesis in vitro. Sci Rep. 2021;11(1):20188.
4. Wang H et al. Application of platelet-rich plasma in spinal surgery. Front Endocrinol (Lausanne). 2023;14:1138255.
5. Sneed D, Wong C. Platelet-rich plasma injections as a treatment for Achilles tendinopathy and plantar fasciitis in athletes. 2023;DOI:10.1002/pmrj.12965.
6. Everts P et al. Platelet-rich plasma: new performance understandings and therapeutic considerations in 2020. Int J Mol Sci. 2020;21(20):7794.
7. Pixley JN et al. A comprehensive review of platelet-rich plasma for the treatment of dermatologic disorders. J Dermatolog Treat. 2023;34(1):2142035.
8. Egierska D et al. Platelet-rich plasma and platelet-rich fibrin in oral surgery: a narrative review. Dent Med Probl. 2023;60(1):17786.
9. Grand View Research. Platelet rich plasma market size & trends. 2023. Available at: https://www. grandviewresearch.com/industryanalysis/platelet-rich-plasma-prpmarket. Last accessed: 19 June 2023.
10. Cavallo C et al. Platelet-rich plasma: the choice of activation method affects the release of bioactive molecules. Biomed Res Int. 2016;2016:6591717.
11. Miranda M et al. Treatment of oral mucositis using platelet-richfibrin: a retrospective study on oncological patients. J Craniofac
Surg. 2023;34(5):1527-9.
12. Gupta V et al. Comparison of platelet-rich plasma prepared using two methods: manual double spin method versus a commercially available automated device. Indian Dermatol Online J. 2020;11(4):5759.
13. Park YB et al. Clinical efficacy of platelet-rich plasma injection and its association with growth factors in the treatment of mild to moderate knee osteoarthritis: a randomized double-blind controlled clinical trial as compared with hyaluronic acid. Am J Sports Med. 2021;49(2):487-96.
14. Sdeek M et al. Intra-articular injection of platelet rich plasma versus hyaluronic acid for moderate knee osteoarthritis. A prospective, double-blind randomized controlled trial on 189 patients with follow-up for three years. Acta Orthop Belg. 2021;87(4):729-34.
15. Di Martino A et al. Platelet-rich plasma versus hyaluronic acid injections for the treatment of knee osteoarthritis: results at 5 years of a double-blind, randomized controlled trial. Am J Sports Med. 2019;47(2):347-54.
16. Lewis E et al. The effectiveness of leucocyte-poor platelet-rich plasma injections on symptomatic early osteoarthritis of the knee: the PEAK randomized controlled trial. Bone Joint J. 2022;104-B(6):66371.
17. Işık G et al. Injectable plateletrich fibrin as treatment for temporomandibular joint osteoarthritis: a randomized controlled clinical trial. J Craniomaxillofac Surg. 2022;50(7):576-82.
18. Gokçe Kutuk S et al. Clinical and radiological comparison of effects of platelet-rich plasma, hyaluronic acid, and corticosteroid injections on temporomandibular joint osteoarthritis. J Craniofac Surg. 2019;30(4):1144-8.
19. Asadpour N et al. Combined platelet-rich plasma and hyaluronic acid can reduce pain in patients undergoing arthrocentesis for temporomandibular joint osteoarthritis. J Oral Maxillofac Surg. 2022;80(9):1474-85.
20. Cai YU et al. Sodium hyaluronate and platelet-rich plasma for partial-thickness rotator cuff tears. Med Sci Sports Exerc. 2019;51(2):227-33.
21. Sari A, Eroglu A. Comparison of ultrasound-guided plateletrich plasma, prolotherapy, and corticosteroid injections in rotator cuff lesions. J Back Musculoskelet Rehabil. 2020;33(3):387-96.
22. Kwong CA et al. Platelet-rich plasma in patients with partialthickness rotator cuff tears or tendinopathy leads to significantly improved short-term pain relief and function compared with corticosteroid injection: a doubleblind randomized controlled trial. Arthroscopy. 2021;37(2):510-7.
23. Godek P et al. Collagen and platelet-rich plasma in partialthickness rotator cuff injuries. Friends or only indifferent neighbours? Randomised controlled trial. BMC Musculoskelet Disord. 2022;23(1):1109.
24. Paget LDA et al. Effect of plateletrich plasma injections vs placebo on ankle symptoms and function in patients with ankle osteoarthritis: a randomized clinical trial. JAMA. 2021;326(16):1595-605.
25. Kirschner JS et al. Efficacy of ultrasound-guided glenohumeral joint injections of leukocytepoor platelet-rich plasma versus hyaluronic acid in the treatment of glenohumeral osteoarthritis: a randomized, double-blind controlled trial. Clin J Sport Med. 2022;32(6):558-66.
26. Menchisheva Y et al. Plateletrich plasma improves esthetic postoperative outcomes of maxillofacial surgical procedures. Acta Chir Plast. 2021;63(3):118-26.
27. Tabrizi R et al. Can platelet-rich fibrin accelerate neurosensory recovery following sagittal split osteotomy? A double-blind, split-mouth, randomized clinical trial. Int J Oral Maxillofac Surg. 2018;47(8):1011-4.
28. Karakasli K, Erdur EA. The effect
of platelet-rich fibrin (PRF) on maxillary incisor retraction rate. Angle Orthod. 2021;91(2):213-9.
29. Dasukil S et al. Intra-articular injection of hyaluronic acid versus platelet-rich plasma following single puncture arthrocentesis for the management of internal derangement of TMJ: a doubleblinded randomised controlled trial. J Craniomaxillofac Surg. 2022;50(11):825-30.
30. Elkahwagi M et al. Role of autologous platelet-rich fibrin in relocation pharyngoplasty for obstructive sleep apnoea. Int J Oral Maxillofac Surg. 2020;49(2):200-6.
31. Diana C et al. Does plateletrich fibrin have a role in osseointegration of immediate implants? A randomized, singleblind, controlled clinical trial. Int J Oral Maxillofac Surg. 2018;47(9):1178-88.
32. Tabrizi R et al. Does plateletrich fibrin increase stability of the maxilla following Le Fort I osteotomy? A single-blind clinical trial study. J Craniomaxillofac Surg. Jun 2020;48(6):531-5.
33. Fontes Martins LC et al. Bone marrow aspirate concentrate and platelet-rich fibrin in fresh extraction sockets: a histomorphometric and immunohistochemical study in humans. J Craniomaxillofac Surg. 2021;49(2):104-9.
34. Tabrizi R et al. Does platelet-rich fibrin increase the stability of implants in the posterior of the maxilla? A split-mouth randomized clinical trial. Int J Oral Maxillofac Surg. 2018;47(5):672-5.
35. Alomari EB, Sultan K. Efficacy of injectable platelet-rich plasma in reducing alveolar bone resorption following rapid maxillary expansion: a cone-beam computed tomography assessment in a randomized split-mouth controlled trial. Angle Orthod. 2019;89(5):705-12.
36. de Oliveira Fernandes GV et al. Liquid platelet-rich fibrin coating implant surface to enhance osseointegration: a doubleblinded, randomized split-mouth trial with 1-year follow-up. Int J Oral Maxillofac Implants. 2022;37(1):159-70.
37. Nagle SM et al. Wound Assessment [Internet] (2022) Treasure Island: Statpearls. Available at: https://www.ncbi.nlm. nih.gov/books/NBK482198/. Last accessed: 19 June 2023.
38. Järbrink K et al. The humanistic and economic burden of chronic wounds: a protocol for a systematic review. Syst Rev. 2017;6(1):15.
39. Pavlovic V et al. Platelet rich plasma: a short overview of certain bioactive components. Open Med (Wars). 2016;11(1):242-7.
40. Tsai HC et al. Use of plateletrich plasma and platelet-derived patches to treat chronic wounds. J Wound Care. 2019;28(1):15-21.
41. Gupta A et al. Efficacy of intralesional platelet-rich plasma in diabetic foot ulcer. J Am Podiatr Med Assoc. 2021;111(3):Article_7.
42. Uçar O, Çelik S. Comparison of platelet-rich plasma gel in the care of the pressure ulcers with the dressing with serum physiology in terms of healing process and dressing costs. Int Wound J. 2020;17(3):831-41.
43. Semenič D et al. Regeneration of chronic wounds with allogeneic platelet gel versus hydrogel treatment: a prospective study. Acta Clin Croat. 2018;57(3):43442.
44. Hossam EM et al. Autologous platelet rich plasma promotes the healing of non-ischemic diabetic foot ulcers. A randomized controlled trial. Ann Vasc Surg. 2022;82:165-71.
45. Ibrahim ZA et al. Therapeutic effect of microneedling and autologous platelet-rich plasma in the treatment of atrophic scars: a randomized study. J Cosmet Dermatol. 2017;16(3):388-99.
46. Min S et al. Combination of platelet rich plasma in fractional carbon dioxide laser treatment increased clinical efficacy of for acne scar by enhancement of collagen production and modulation of laser-induced inflammation. Lasers Surg Med. 2018;50(4):302-10.
47. Khattab FM et al. Evaluation of combined excimer laser and platelet-rich plasma for the treatment of nonsegmental vitiligo: a prospective comparative study. J Cosmet Dermatol. 2020;19(4):86977.
48. Tawfik AA, Osman MAR. The effect of autologous activated plateletrich plasma injection on female pattern hair loss: a randomized placebo-controlled study. J Cosmet Dermatol. 2018;17(1):4753.
49. Ramadan WM et al. Evaluation of adding platelet-rich plasma to combined medical therapy in
50. Shapiro J et al. Evaluation of platelet-rich plasma as a treatment for androgenetic alopecia: a randomized controlled trial. J Am Acad Dermatol. 2020;83(5):1298303.
51. Kadry M et al. Platelet-rich plasma versus combined fractional carbon dioxide laser with platelet-rich plasma in the treatment of vitiligo: a comparative study. Clin Cosmet Investig Dermatol. 2018;11:551-9.
52. Elsaadany AE et al. Comparison between 308-nm excimer light alone versus 308-nm excimer light and platelet-rich plasma in the treatment for localized vitiligo. J Cosmet Dermatol. 2022;21(7):2826-31.
53. Sirithanabadeekul P et al. Plateletrich plasma treatment for melasma: a pilot study. J Cosmet Dermatol. 2020;19(6):1321-7.
54. Gamea MM et al. Comparative study between topical tranexamic acid alone versus its combination with autologous platelet rich plasma for treatment of melasma. 2022;33(2):798-804.
55. Elkhouly NI et al. Does autologous platelet-rich plasma improve wound healing and pain perception after Cesarean section in high-risk patients? Gynecol Obstet Invest. 2021;86(4):336-42.
56. Albanese A et al. Platelet-rich plasma (PRP) in dental and oral surgery: from the wound healing to bone regeneration. Immun Ageing. 2013;10(1):23.
57. Poulios E et al. Platelet-rich plasma (PRP) improves erectile function: a double-blind, randomized, placebo-controlled clinical trial. J Sex Med. 2021;18(5):926-35.
58. Magruder ML et al. Trends in utilization, demographics, and costs of platelet-rich plasma injections: a ten-year nationwide investigation. Phys Sportsmed. 2023:1-9.
59. Centers for Medicare & Medicaid Services (CMS). Autologous platelet-rich plasma. Available at: https://www.cms.gov/ Medicare/Coverage/Coveragewith-Evidence-Development/ Autologous-Platelet-rich-Plasma. Last accessed: 19 June 2023.
60. Werner BC et al. An analysis of current treatment trends in platelet-rich plasma therapy in the medicare database. Orthop J Sports Med. 2020;8(2):2325967119900811.
Mycosis Fungoides Palmaris et Plantaris
Progressing to Complete Early-Stage Disease
Improved with Phototherapy
Authors:
*Tina Elaine M. Resuello,1 Jacqueline Michelle D. Melendres,1 Mary Elizabeth S. Danga,1 Patricia Anne T. Tinio1
1. Department of Dermatology, Rizal Medical Center, Pasig, the Philippines
*Correspondence to tinaelainer@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Acknowledgements: The authors extend their sincere gratitude to Maria Isabel Beatriz Puno-Gomez and Alejandro E. Arevalo for their invaluable contributions to this case report. Their expertise in meticulously examining the biopsy slides and formulating the diagnosis played a pivotal role in the comprehensive understanding of the presented case.
Received: 28.11.22
Accepted: 07.08.23
Keywords: Case report, mycosis fungoides, mycosis fungoides palmaris et plantaris, phototherapy, skin cancer.
Mycosis fungoides is the most common form of cutaneous T cell lymphoma. In this article, the authors describe a case of a 53-year-old female who presented with multiple pruritic, slightly erythematous and hyperpigmented, variably shaped macules, and patches and plaques, with scaling on the bilateral hands and feet. The lesions resembled various benign inflammatory dermatoses, such as contact dermatitis and superficial dermatophytosis, and were treated as such until hyperpigmented, variably shaped macules and patches appeared on the legs and with a bathing trunk distribution. Histopathologic and immunohistochemical findings were consistent with early mycosis fungoides. The patient has improved with full body narrowband ultraviolet B phototherapy, combined with a psoralen ultraviolet A soak for the hands and feet. This case highlights the importance for physicians to recognise that mycosis fungoides may occur with different presentations, and may not present in its classic form. The patient’s quality of life may be improved with early diagnosis.
Key Points
1. Diagnosing early mycosis fungoides relies on clinicopathologic correlation. Multiple skin biopsies examining histology, immunohistochemistry, and T cell receptor monoclonal rearrangement, if feasible, alongside thorough correlation of clinical and pathological data, are crucial for accurate detection of signs of mycosis fungoides.
2. Detecting mycosis fungoides necessitates a robust clinical suspicion of cutaneous T cell lymphoma. This is especially crucial when dealing with chronic, unyielding inflammatory skin disorders that do not respond to treatment.
3. In cases of early-stage disease, it is prudent to give due consideration to the implementation of safer treatments like topical medications and phototherapy. These options can contribute significantly to the management and care process.
INTRODUCTION
Mycosis fungoides is the most common form of cutaneous T cell lymphoma, which is a heterogenous group of non-Hodgkin lymphomas.1 Classic early mycosis fungoides typically begins as persistent and/or slowly progressive scaly pink or red patches on the hands, chest, abdomen, upper thighs, or buttocks.2,3 The lesions are often pruritic and may cause impairment of the quality of life.3 On histology, superficial lymphoid infiltrate are present with characteristic epidermotropism, without spongiosis and lymphoid atypia.4 Immunophenotypically, the cells are characterised by epidermotropic peripheral T lymphocytes, whose phenotype is (cluster of differentiation) CD2+, CD3+, CD4+, CD5+, CD8-, CD45RO+, CD20+, and CD30-, with few exceptions.5 The case of a 53-year-old Filipino female, who developed the classic variant of early mycosis fungoides after a few months with CD8+ mycosis palmaris et plantaris, is described in this report.
CASE REPORT
A 53-year-old Filipino female presented with a 10-month history of extremely pruritic patches on the plantar aspect of both feet, which later involved the palmar aspect of both hands. They were seen and managed by several dermatologists, and were treated as having xerosis cutis, dermatophytosis, and hand and feet dermatitis. Despite trials of various medications, such as topical and oral steroids, topical antifungal medications, and emollients, and in absence of any clear trigger, the lesions did not resolve. However, no initial histopathologic examination was performed.
The lack of improvement of symptoms; the evolution into erythematous scaly plaques; and the appearance of non-pruritic, nonpainful brownish macules and patches over the bilateral legs, which progressed to involve the lower abdomen and buttocks in a bathing trunk distribution 6 months later, prompted consultation at the authors’ institution. Review of systems revealed absence of lymphadenopathy, significant weight loss or gain, and presence of hair thinning but without alopecia. The past medical, family medical, and personal and social history were unremarkable. Cutaneous examination revealed multiple, well- and ill-defined, slightly erythematous and hyperpigmented, variably shaped macules, patches and plaques, with scaling on the bilateral hands and feet, legs and bathing trunk distribution (Figure 1). No lymphadenopathies were observed on palpation.
KOH test and syphilis test were requested; both revealed negative results. A biopsy was performed on the palm and the lower back, which showed orthokeratosis with parakeratosis, epidermal hyperplasia with scant spongiosis, superficial perivascular infiltrates of lymphocytes, few eosinophils, and focal lichenoid interface dermatitis/basal vacuolar change. Atypical lymphocytes infiltrated up into the epithelial layers (epidermotropism) in single units or small clusters. Tissue cells showed positive staining for CD3, CD4, and CD8. The ratio of CD4- to CD8-positive cells was about 3:1. CD7, another marker for T cells, appeared to be intact, but with downregulation compared with CD4 (Figure 2). The cells of interest were negative for CD20 and CD30. Blood count demonstrated mild anaemia and lymphocytopenia. On peripheral blood smear, slightly hypochromic erythrocytes with anisopoikilocytosis and adequate platelet count were observed. No abnormal white
1: Mycosis fungoides palmaris et plantaris progressing to complete classic mycosis fungoides.
Pre-treatment
Post-treatment
blood cells were seen. PET–CT scan results showed low-grade metabolic activity in multiple nodes, which were regarded as reactive or inflammatory without hypermetabolic gross soft tissue masses or evident cutaneous thickening in the extremities and body wall. T cell receptor clonal analysis was not conducted in this case because the morphological evaluation with immunostaining profiling was diagnostic.
Full body narrowband-ultraviolet B (NB-UVB) phototherapy was initiated at 300 mJ/cm2, and increased by 10% increments per session, 2–3 times a week. Eventually, the authors decided to combine treatment with a psoralen ultraviolet A (PUVA) soak for the hands and feet, starting at 0.5 J/cm2, and increasing by 0.5 J per session.
In addition, topical clobetasol lotion 0.05% was applied twice daily continuously for 3 months, and loratadine 10 mg/tab was given as needed for the pruritus once a day. Marked decrease in the number of hyperpigmented macules and patches was noted after 18 sessions with NBUVB phototherapy. With use of the PUVA soak, >90% of the lesions on the palms and soles have resolved. However, after 18 sessions of the PUVA soak, the patient experienced increased pruritus in these areas, which prompted the authors to adapt the panel NB-UVB for the hands and feet (Figure 1). The patient is currently undergoing maintenance phase dosing for the body, with almost complete resolution of lesions and residual hyperpigmented patches seen, as well as on the acral areas with almost complete
Clinical images of hands, feet, and back at diagnosis, and after 18 sessions of full body NB-UVB phototherapy, PUVA soak of the hands and feet, and 2 months of topical clobetasol.
NB-UVB: narrowband-ultraviolet B; PUVA: psoralen ultraviolet A.
Figure
2: Histopathology and immunostaining profiles of mycosis fungoides palmaris et plantaris progressing to full-blown classic mycosis fungoides.
A) An infiltrate of the atypical lymphocytes in the upper dermis (H&E, 20x1). B–D) Positive CD3 and CD4 atypical lymphocytes. D and E) Reduced CD8 and CD7 expression in atypical lymphocytes.
CD: cluster of differentiation; H&E: haematoxylin and eosin.
clearance. The authors plan to further decrease the frequency of visits to once a week to complete 6 months.
DISCUSSION
Mycosis fungoides is the most common type of cutaneous T cell lymphomas, which represents almost 50% of all cases.6 It is characterised by malignant proliferation of CD4+ T cells, with epidermotropism in the skin. The disease is more commonly seen in individuals in their mid-50s, increasing its incidence significantly with age, and demonstrating a four-fold in incidence in patients over 70 years.7 The diagnostic algorithm
for the diagnosis of early mycosis is based on a point-based algorithm proposed by the International Society for Cutaneous Lymphoma (ISCL) and the European Organization of Research and Treatment of Cancer (EORTC). The diagnosis is made when a total of four points or more is determined.4
Among these criteria, clinical presentation is one of the significant factors in the diagnosis of early mycosis fungoides. About 70–75% of patients with mycosis fungoides present the classic form of the disease, characterised by commonly pruritic, well-demarcated, erythematous patches and/or plaques with variability in the size, shape, and colour, and occasional poikiloderma.
Figure
CD7
CD8
CD4
CD3 H&E
back palm
The lesions are usually large in size, around >5 cm, and have predilection to non-sun-exposed areas, such as the buttock, flanks, inner thighs, and inner arms. The fixed character of the lesions or the waxing and waning of the skin lesions over months, or even years, should incline the clinician on a diagnosis of mycosis fungoides.4
Lebas et al.8 described the mimicker and variants of mycosis fungoides, including hyperkeratotic, hypopigmented mycosis fungoides associated with follicular mucinosis, granulomatous slack skin, pagetoid reticulosis, interstitial mycosis fungoides, poikilodermatous, anetodermic, and invisible types. Interestingly, the authors’ case initially presented as mycosis fungoides palmaris et plantaris before it progressed into a full-blown, early disease. This exceedingly rare variant is more predominant in males. The lesions occur in the palms and soles, and can present variably as annular, erythematous to hyperpigmented patches and plaques,9 tumours, pustules, verrucous changes, ulceration, and nail dystrophy.10,11 It has an indolent course, remaining confined to the area of initial involvement with limited spread, which is paradoxical in the authors’ case, wherein lesions progressed to the classic type of mycosis fungoides. Dermatophyte infections, eczema, palmoplantar psoriasis, or secondary syphilis should always be ruled out in the diagnosis.9 Histopathologically, mycosis fungoides palmaris et plantaris may have spongiotic dermatitis, making a correct diagnosis difficult in some cases. Thus, immunophenotyping and T cell clonality must be performed to confirm the diagnosis. CD8+ aggressive epidermotropic T cell lymphoma has been associated with metastatic involvement of distal anatomic sites and poor prognosis.12 The authors’ patient presented with a rare case of CD8+ cytotoxic T cell lymphoma, without peripheral blood involvement, and good response to treatment.
Early mycosis fungoides has an indolent course, and thus, safer treatment options should always be considered. In patients with patch/
References
1. Akinbami AA et al. Mycosis fungoides: case report and literature review. Clin Med Insights Case Rep. 2014;7:95-8.
plaque stage mycosis fungoides and mycosis fungoides palmaris et plantaris, the primary goal is to improve symptoms and quality of life while avoiding treatment-related toxicity because of its excellent prognosis.7 This involved either expectant management through watchful waiting, or the utilisation of skin-directed therapies.7,13 Current skin-directed treatment options for early mycosis fungoides include topical corticosteroids, topical chemotherapy (i.e., nitrogen mustard), topical retinoids (i.e., bexarotene or tazarotene), topical imiquimoid,14 phototherapy, local radiation therapy, and total skin electron irradiation for patients with severe skin symptoms.15 Phototherapy is an important treatment modality that may be used alone, or in conjunction with topical therapies. The reported complete response rates, defined as >90–95% clearance, for early stage mycosis fungoides (Stage IA–IIA) for NB-UVB ranged from 54–90%, while the complete response rate was reported as 65–85% PUVA.16 In a systematic review and meta-analysis by Phan et al.17 comparing the efficacy of NB-UVB with PUVA, they concluded that NB-UVB, due to its safety profile, is a viable alternative to PUVA for treatment of early-stage mycosis fungoides.
CONCLUSION
Mycosis fungoides is an exceedingly uncommon skin condition with a variety of clinical manifestations, making its diagnosis still challenging without the adjunct of immunohistochemical staining and T cell receptor gene rearrangement. Thus, clinicopathologic correlation is the best way of diagnosis. The authors highlighted the importance of high clinical suspicion for cutaneous T cell lymphoma in patients with chronic unremitting inflammatory dermatoses that are recalcitrant to treatment. Phototherapy alone, or in conjunction with topical therapies, is both a viable and safe treatment option for the management of early-stage mycosis fungoides.
2. Parida DK, Barik SK. Surviving with mycosis fungoides for twenty years: an autobiographical case report. Cureus. 2021;13(12):e20699.
3. Qiang J et al. Atypical mycosis fungoides: a case report. JAAD. 2015;72(5, Suppl 1):AB156.
4. Miyagaki T. Diagnosis of early mycosis fungoides. Diagnostics (Basel). 2021;11(9):1721.
5. Zarami BA. Mycosis fungoides: a report of two cases. Int J Case Rep Images. 2018;9:100895Z01BZ2018.
6. Ozgur T et al. Histopathologic evaluation of parapsoriasis from the perspective of NB-UVB/PUVA therapy on the outcome and recurrence of the disease. Indian J Dermatol. 2021;66(1):96-8.
7. Wilcox RA. Cutaneous T‐cell lymphoma: 2016 update on diagnosis, risk‐stratification, and management. Am J Hematol. 2016;91(1):151-65.
8. Lebas E et al. A comprehensive update of the atypical, rare and mimicking presentations of mycosis fungoides. Dermatology Ther (Heidelb). 2021;11(6):1931-51.
9. Altınışık DD et al. Atypical variants of mycosis fungoides. J Turk Acad Dermatol. 2021;15(2):30-3.
10. Ahn CS et al. Mycosis fungoides: an updated review of clinicopathologic variants. Am J Dermatopathol. 2014;36(12):93348.
11. Beiser I et al. Mycosis fungoides palmaris et plantaris on the plantar aspect of the foot: a case report. Am J Case Rep. 2020;21:e923361.
12. Yumeen S et al. CD8+ mycosis fungoides palmaris et plantaris with peripheral blood involvement. JAAD Case Rep. 2020;6(5):434-7.
13. Hristov AC et al. Mycosis fungoides and Sézary syndrome: 2019 update on diagnosis, risk‐stratification, and management. Am J Hematol. 2019;94(9):102741.
14. Wennberg E et al. Topical treatments for early-stage mycosis fungoides using grading recommendations assessment,
development and evaluation (GRADE) criteria: a systematic review. JAAD Int. 2021;3:26-41.
15. Mazzeo E et al. The current management of mycosis fungoides and Sézary syndrome and the role of radiotherapy: principles and indications. Rep Pract Oncol Radiother. 2014;19(2):77-91.
16. Olsen EA et al. Guidelines for phototherapy of mycosis fungoides and Sézary syndrome: a consensus statement of the United States Cutaneous Lymphoma Consortium. J Am Acad Dermatol. 2016;74(1):27-58.
17. Phan K et al. Comparison of narrowband UV-B with psoralen–UV-A phototherapy for patients with early-stage mycosis fungoides: a systematic review and meta-analysis. JAMA Dermatol. 2019;155(3):335-41.