Lis Neubeck, Melanie Gunawardene, and 2024 ESC President Thomas Lüscher share their insights
Clinical Conundrum: Lifetime Management of Aortic Stenosis in Young Patients Editor's Pick:
04 Editorial Board
07 Welcome 09 Foreword
Congress Review
10 Review of the European Society of Cardiology (ESC)
Congress 2024, 30th August–2nd September 2024
Congress Features
26 New Directions in the Management of Atrial Fibrillation
Katrina Thornber
31 Artificial Intelligence and Digital Biomarkers: A Revolution in Cardiovascular Diagnostics
Katie Wright
Abstract Reviews
36 The Fate of Coronary Artery Bypass Grafting in the Elderly: Treat and Forget
Gastino et al.
38 Machine Learning and Traditional Analysis of the Interaction Between Cardiovascular Diseases and Haematological Malignancies
Caller et al.
40 Ablation of Tachyarrhythmias with Zero Fluoroscopy Technique in Patients Under 18 Years of Age: 4-Year Follow-Up
Chavez-Gutierrez et al.
42 Abstract Highlights
Congress Interviews
50 Melanie Gunawardene
54 Lis Neubeck
57 Thomas Lüscher
Interviews
61 Advancing the Understanding of Hypertrophic Cardiomyopathy Towards Improved Patient Outcomes: Interview with Two Key Opinion Leaders
69 David L. Fischman
72 Saraschandra Vallabhajosyula Articles
76 Editor's Pick: Clinical Conundrum: Lifetime Management of Aortic Stenosis in Young Patients
Kipshidze et al.
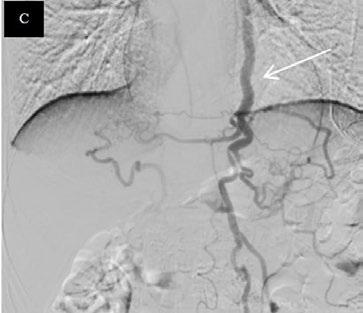
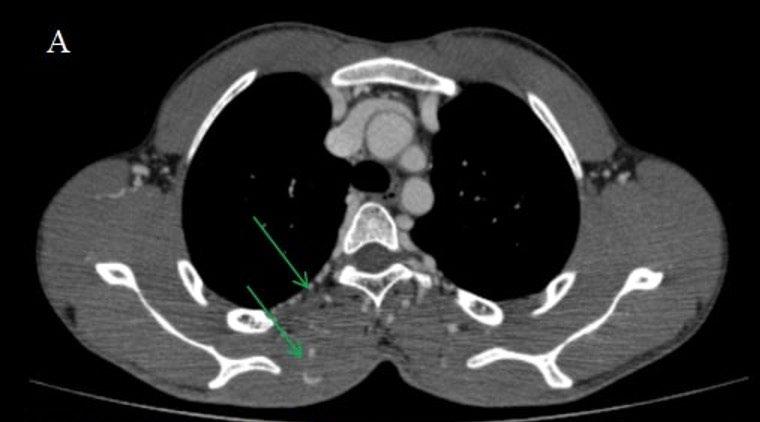
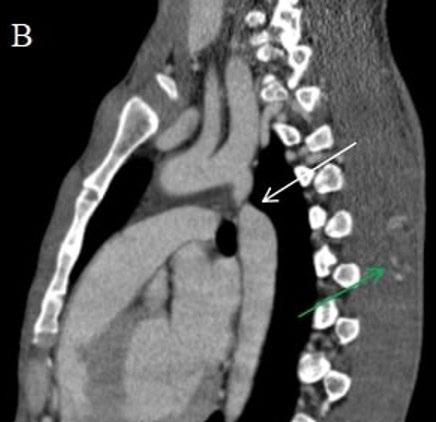
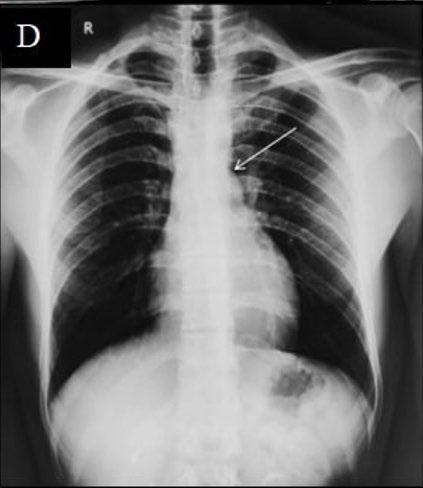
83 Coarctation of Aorta Masquerading as a Spinal Arteriovenous Malformation: A Case Report
Badhe et al.
90 Prevalence, Clinical Aspects, and Risk Factors of Aortic Stenosis Among Haemodialysis Patients Attending Nephrology Centre of Benghazi
Ezwaie et al.
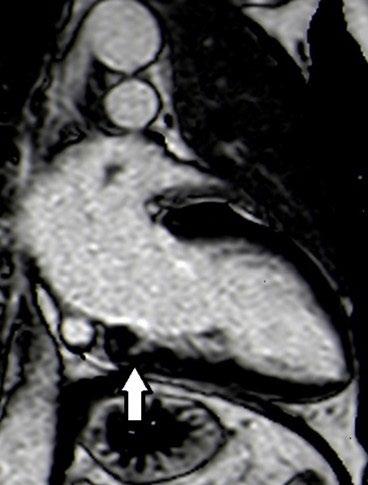
98 Myocardial Crypts and Ventricular Fibrillation: Two Case Reports
Di Spigno et al.
106 Depressive Symptoms and Left Ventricular Diastolic Dysfunction Among Men and Women with HIV
Martinez et al.
"We have now reached a point where cardiac disease treatment can be individualised"
Editorial Board
Editor-in-Chief
Prof Çetin Erol
İbn-i Sina Hospital, Ankara University, Ankara, Türkiye
Professor Cetin Erol specialised in internal medicine and cardiology at Ankara University School of Medicine and subsequently became head of the Cardiology Department, where he continues to serve as an Emeritus Professor. Additionally, Erol is currently the Governor of the Istanbul Consortium Chapter of the American College of Cardiology. His primary research domains are echocardiography, hypertension, and invasive cardiology.
Larner College of Medicine's University of Vermont, USA
Dr Constantine E. Kosmas
Lipid Clinic, National and Kapodistrian University of Athens, Greece
Dr Nicholas Kipshidze
New York Cardiovascular Research, USA
Dr Ronald J. Krone
Washington University School of Medicine, Missouri, USA
Dr Carl J. Lavie
The University of Queensland School of Medicine, Australia
Dr Carl J. Pepine
University of Florida, USA
Prof Denilson Campos de Albuquerque
Pedro Ernesto University Hospital, Brazil
Dr Sazzli Kasim
Universiti Teknologi MARA, Malaysia
Prof Khai Pham Gia
Bach Mai Hospital, Vietnam
Dr Sanjog Kalra
University of Toronto, Canada
Dr Amandeep Goyal
University of Kansas Medical Center, USA
Prof Dr Rainer Wessely
University of Technology Munich and Fresenius, University of Applied Sciences, Germany
Prof Stephen Lee
University of Hong Kong, Hong Kong
Aims and Scope
EMJ Cardiology is an open-access, peer-reviewed eJournal, committed to helping elevate the quality of healthcare in cardiology and to contribute in advancing the development of this field by informing healthcare professionals on all aspects of cardiovascular disease.
The journal is published annually, six weeks after the European Society of Cardiology (ESC) Congress, and features highlights from this congress, alongside interviews with experts in the field, reviews of abstracts presented at the congress, as well as in-depth features on congress sessions. The journal also covers advances within the clinical and pharmaceutical arenas by publishing sponsored content from congress symposia, which is of high educational value for healthcare professionals. This content undergoes rigorous quality control checks by independent experts and the in-house editorial team.
EMJ Cardiology also publishes peer-reviewed research papers, review articles, and case reports in the field. In addition, the journal welcomes the submission of features and opinion pieces intended to create a discussion around key topics in the field and broaden readers’ professional interests. EMJ Cardiology is managed by a dedicated editorial team that adheres to a rigorous double-blind peer-review process, maintains high standards of copy editing, and ensures timely publication.
EMJ Cardiology endeavours to increase knowledge, stimulate discussion, and contribute to a better understanding of cardiology. Our focus is on research that is relevant to all healthcare professionals. We do not publish veterinary science papers or laboratory studies not linked to patient outcomes. We have a particular interest in topical studies that advance knowledge and inform of coming trends affecting clinical practice in cardiology.
Further details on coverage can be found here: www.emjreviews.com
Editorial Expertise EMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors who are recognised authorities in their respective fields.
• Peer review, which is conducted by expert reviewers who are invited by the Editorial team and appointed based on their knowledge of a specific topic.
• An experienced team of editors and technical editors.
• A team of internal and independent medical writers.
Peer Review
On submission, all articles are assessed by the editorial team to determine their suitability for the journal and appropriateness for peer review.
Editorial staff, following consultation with a member of the Editorial Board if necessary, identify three appropriate reviewers, who are selected based on their specialist knowledge in the relevant area.
All peer review is double blind. Following review, papers are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected.
Editorial staff have final discretion over any proposed amendments.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects. We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial.assistant@emjreviews.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in EMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
EMJ is distributed through controlled circulation to healthcare professionals in the relevant fields globally.
Indexing and Availability
EMJ is indexed on DOAJ, the Royal Society of Medicine, and Google Scholar®.
EMJ is available through the websites of our leading partners and collaborating societies. EMJ journals are all available via our website: www.emjreviews.com
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
This Publication Launch Date: 2013 Frequency: Yearly Online ISSN: 2054-3174
All information obtained by EMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, EMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. EMJ is completely independent of the review event (ESC 2024) and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever. The cover photo is of London, UK the location of ESC 2024.
Ultrasound Renal Denervation (uRDN) as a treatment option for hypertension, alongside lifestyle changes and medication.1
ACHIEVE Study mean o ce systolic blood pressure through 8 years 3 (n=27)
RADIANCE™ RCTs combined results mean o ce systolic blood pressure at 2 months 2 (n=293)
Editor
Evgenia Koutsouki
Editorial Manager
Darcy Richards
Copy Editors
Noémie Fouarge, Katheeja Imani, Jenna Lorge
Editorial Co-ordinators
Victoria Antoniou, Abigail Craig
Editorial Assistants, Helena Bradbury, Ada Enesco, Katrina Thornber, Katie Wright, Aleksandra Zurowska
Creative Director
Tim Uden
Design Manager
Stacey Rivers
Senior Designer
Steven Paul
Designers
Owen Silcox, Fabio van Paris
Junior Designers
Dillon Benn Grove, Shanjok Gurung
Senior Performance & Insight Lead
Darren Brace
Marketing Director
Kristina Mestsaninova
Chief Content Officer
Justin Levett
Chief Commercial Officer
Dan Healy
Founder and Chief
Executive Officer
Spencer Gore
Welcome
Dear Readers,
It is a great pleasure to introduce this issue, which brings you key highlights from the European Society of Cardiology (ESC) Congress 2024, hosted in London, UK. The proximity of this Congress gave the EMJ team a unique opportunity to be in the midst of the most significant advances in the field.
This year saw a wealth of groundbreaking research and pivotal guideline updates, incorporating patient perspectives, marking a shift towards more patient-centred care. Within these pages we bring you the major developments from this event.
Our team had the privilege of conducting in-depth interviews with experts in cardiology, exploring key areas, including cardiac catheterisation, cardiogenic shock, and atrial fibrillation.
Our peer reviewed content spans diverse topics, from aortic stenosis in young patients and the challenges around managing this population, to a study on the association between depressive symptoms and echocardiographic indices of left ventricular diastolic dysfunction in people living with and without HIV.
I would like to take this opportunity to thank our reviewers, Editorial Board, and our esteemed contributors for bringing this high-quality issue together. Until next year’s issue, I invite you to engage with this content. I look forward to receiving your submitted articles and feedback, which is crucial to our ongoing vision of elevating the quality of healthcare.
Editorial enquiries: editor@emjreviews.com
Sales opportunities: salesadmin@emjreviews.com
Permissions and copyright: accountsreceivable@emjreviews.com
Evgenia Koutsouki Editor
Reprints: info@emjreviews.com Media enquiries: marketing@emjreviews.com
Foreword
It is my pleasure to welcome you to the latest issue of EMJ Cardiology, featuring a range of peer-reviewed articles and interviews with experts in cardiology. Plus, find a comprehensive review of the European Society of Cardiology (ESC) Congress 2024, with coverage of the most significant content from the event, coupled with impactful abstracts and features.
In this issue, you will find the latest research on ablation therapies, novel risk assessment strategies, and the use of AI and digital biomarkers for personalised cardiovascular healthcare. Additionally, this issue features an insightful interview with the new ESC President, Thomas Lüscher, who reveals what we can expect from the ESC in the coming years, as well as the impact the ESC hopes to have on global cardiovascular medicine. I think that the new ESC Clinical Practice Guidelines are particularly important. These guidelines incorporate the latest research on the management of atrial fibrillation, elevated blood pressure and hypertension (now defined as separate parameters), chronic coronary syndromes, and peripheral arterial and aortic diseases.
The EMJ team have had the pleasure of speaking with several other experts in cardiology, with specialties ranging from cardiogenic shock to atrial fibrillation, and more. We have selected five peer-reviewed articles for inclusion in this issue, which cover various topics in cardiology. This includes a feature delving into the ongoing debate about managing aortic stenosis in younger patients, a study on the prevalence of aortic stenosis in patients undergoing haemodialysis, and research on left ventricular diastolic dysfunction in adults with HIV.
The latest research on ablation therapies, novel risk assessment strategies, and the use of AI and digital biomarkers
I would like to thank all the authors, Editorial Board, peer reviewers, and interviewees for their invaluable contributions to this edition of EMJ Cardiology Çetin Erol İbn-i Sina Hospital, Ankara University, Türkiye
ESC 2024
We have now reached a point where cardiac disease treatment can be individualised
Review of the European Society of Cardiology (ESC) Congress
PERSONALISING cardiovascular care was the central theme at the European Society of Cardiology (ESC) Congress 2024, which took place in London, UK, between 30th August–2nd September. Home to the largest cardiac centre in Europe, London provided the perfect setting for the cardiology community to gather and explore cutting-edge updates in the field.
The Welcome Address was delivered by ESC President Franz Weidinger, who proudly emphasised how the event brings together the greatest minds in cardiovascular science and medicine. Before inviting John McMurray, Chair of the ESC Congress Programme Committee, to the stage, Weidinger highlighted that this year, there were representatives from 106 cardiac societies from around the world, with attendees from over 163 countries.
With over 1,200 sessions included in the comprehensive programme, McMurray explored the programme highlights with the audience. He noted that we have now reached a point where cardiac disease treatment can be individualised. To reflect this, several sessions within the programme were dedicated to individualised cardiac care. McMurray also spotlighted four new guidelines sessions covering the management of: elevated blood pressure and hypertension, chronic coronary syndromes, atrial fibrillation, and peripheral arterial and aortic diseases.
McMurray also drew attention to 12 Hot Line sessions that comprised of late-
breaking clinical trials, including 38 new, large randomised controlled trials and 11 ‘Ask the trialists’ sessions. The audience were signposted to the 26 late-breaking science sessions covering 162 clinical trial updates, smaller trials, clinic studies, registries, cohort/epidemiological studies, and basic science.
The 2024 programme included a new obesity track in recognition of this increasing global health concern. Digital health was also recognised as a key topic, with the Congress dedicating a special stage to digital health transformation and implementation within the field. McMurray also stressed the importance of recognising patient perspectives, noting several sessions committed to understanding patient experiences within the programme. In terms of research, this year’s Congress received 8,620 abstract submissions from 117 countries, of which 4,451 were accepted. The programme itself included 130 oral abstract sessions, 400 moderated ePoster sessions, 86 clinical case sessions, and 11 award sessions in total.
The opening ceremony saw several experts receive awards. Weidinger presented the ESC gold medals to “three extraordinary individuals who have made outstanding lifetime contributions to cardiology,” whose work has helped inspire and pave the way for others. The recipients of these awards were Milton Packer, Baylor University Medical Center, Dallas, Texas, USA; Peter J. Schwarz, IRCCS Italian Auxological Institute, Milan, Italy; and Karin Sipido, KU Leuven, Belgium, for their work in heart failure, long QT syndrome, and basic and translational research, respectively.
Following this, President’s Awards were bestowed to Eva Prescott, Bispebjerg University Hospital, Copenhagen, Denmark, and Chair of the Clinical Practice Guidelines of the ESC; and Hector Bueno, National Centre for Cardiovascular Research (CNIC), Madrid, Spain, for their exceptional voluntary work in going above and beyond for the ESC, and their mission to reduce the burden of cardiovascular disease. Weidinger also congratulated the 750 newly elected fellows of the ESC, commenting: “Your expertise and experience are invaluable to bringing up the next generation of outstanding minds in our field.”
During the Presidential Address, Weidinger emphasised the impact of heart disease, stating: “Every day, together, we fight the world’s number one killer, cardiovascular disease.” Whilst progress has been made, with a decline in cardiovascular disease mortality, improved control of modifiable risk factors, and better outcomes for many disease domains, he noted that many challenges remain. Moreover, new risk factors influencing cardiovascular health outcomes that result in cardiovascular disease disparities based on income, education, and geography present additional challenges. He emphasised that these risk factors are strongly related to the alarming global rise in diabetes and obesity. In addition, air and noise pollution, climate change, physical inactivity, poor nutrition, and an ageing population contribute to a picture of risk that is not amenable by medical therapy alone.
When considering how this may be approached, Weidinger commented: “This clearly calls for a more holistic, crosssectoral, societal approach.” He reflected on how the ESC has been an advocate for a European policy and regulatory environment favourable to improving cardiovascular health. He explained that the ESC has also focused on supporting member states with
their national health policies, discussing that European and national cardiovascular health plans are vital in helping to pave the way for a further decrease in cardiovascular disease within Europe and around the world. “We must keep working to make this a reality,” Weidinger stated.
The ceremony concluded by discussing advances in technology, which are already transforming medical practice, delivery of care, and scientific research. If these advances are effectively combined with evidence-based medicine, Weidinger stressed that there is a potential in the future to fundamentally change scientific research and patient management to deliver the right treatment to the right patient at the right time, which is why the theme of personalised care was chosen for 2024.
Whilst he noted the potential for combining genomics, transcriptomics, proteomics, and metabolomics with AI and digital technologies to help understand the complex mechanisms underlying cardiovascular disease and develop personalised biomarkers, he warned that addressing the pros and cons of AI will be of paramount importance to minimise potential risks to the health, safety, and rights of patients.
Noting that we are living in challenging times, Weidinger poignantly stated: “These are times in need of deliberate, resolute action, standing together while advancing our mission through collaboration and mutual support.” He emphasised that the collective strength of the cardiology community comes from the attendee’s individual passion and commitment to the field, and closed by imploring delegates to enjoy the Congress and carry the inspiration of the moment into the days and years ahead.
EMJ was delighted to attend the 2024 ESC Congress, and looks forward to next year’s event, which will take place in Madrid, Spain. Until then, read on to enjoy highlights presented during this year’s Congress.
Addressing the pros and cons of AI will be of paramount importance to minimise potential risks to the health, safety, and rights of patients
Is Fasting Necessary for Cardiac Catheterisation Laboratory Procedures?
FASTING before cardiac catheterisation procedures requiring conscious sedation does not reduce the risk of complications, according to latebreaking research presented at the ESC Congress 2024.
Patients who had been referred for coronary angiography, coronary intervention, or cardiac implantable electronic devicerelated procedures were recruited into the SCOFF trial. This was a randomised, prospective open-label, blinded endpoint design trial that assessed the noninferiority of not fasting prior to cardiac catheterisation laboratory procedures requiring conscious sedation. In total, 716 patients were recruited from six sites in New South Wales, Australia. The mean age was 69 years, and 35% of participants were female. Patients in the fasting group received no solid food for 6 hours and no clear liquids for 2 hours before the procedure, whereas participants in the no-fasting group were encouraged to have regular meals as normal.
Occurrences of hypotension, aspiration pneumonia, hyperglycaemia, and hypoglycaemia were assessed as a composite outcome using a Bayesian approach. The analysis revealed that the composite outcome occurred in 19.1% of patients in the fasting group, compared to 12.0% in the no-fasting group. In an intention-to-treat analysis, the no-fasting group had 5.2% fewer primary outcome events compared to the fasting group (95% CI: -9.6 to -0.9). With a non-inferiority margin of 3%, no fasting was proven to not be inferior to fasting since the upper confidence limit (-0.9%) was lower than 3%.
This finding was accompanied by a likelihood of >99.5% that no-fasting is not worse than fasting. Moreover, the results
These findings suggest a potential adjustment to the fasting requirements outlined in clinical guidelines
revealed a 99.1% likelihood that no-fasting is actually superior to fasting. Additionally, the absolute risk difference between the two groups was 7.1% in favour of nofasting, with a number needed to treat 14.1 to prevent one primary outcome event in the no-fasting group. The research also demonstrated that post-procedure patient satisfaction was greater in the no-fasting group, assessed using a questionnaire where a lower score indicates greater satisfaction (11 versus 15 points; 95% CI: 3.36–4.67; Bayes factor ≥100).
However, there were no significant differences between groups in contrast-
induced nephropathy, new intensive care admissions post-procedure, new ventilation requirements post-procedure, new intensive care unit admissions, 30-day readmissions, 30-day mortality, 30-day pneumonia, or pre-procedure patient satisfaction.
Overall, the results of the SCOFF trial suggest that fasting is not necessary for patients undergoing conscious sedation for cardiac catheterisation laboratory procedures, as there is not an increased risk of complications, and patient satisfaction is higher. These findings suggest a potential adjustment to the fasting requirements outlined in clinical guidelines.
Transcatheter Versus Surgical Aortic Valve Replacement in Women with Severe Aortic Stenosis
A NOVEL study focused specifically on women, the RHEIA trial, presented at the ESC Congress 2024, demonstrated the superiority of transcatheter aortic valve implantation (TAVI) over surgical aortic valve replacement in treating severe aortic stenosis.
Historically, most data comparing TAVI and surgical valve replacement have been derived from subgroup analyses of larger trials, often leaving questions about gender-specific outcomes. To address this gap, the RHEIA trial was designed as a dedicated, randomised study to compare the safety and efficacy of TAVI versus surgical replacement in women with severe symptomatic aortic stenosis.
The trial enrolled 443 women from 48 sites across 12 European countries, with a mean age of 73 years. Participants were randomised to undergo either TAVI with a third-generation balloon-expandable system, or surgical aortic valve replacement, with a follow-up period of 1 year. The primary composite endpoint was a combination of allcause mortality, stroke, and rehospitalisation due to valve- or procedure-related symptoms or worsening heart failure.
Results showed that the incidence of the primary composite endpoint was significantly lower in the TAVI group (8.9%) compared to the surgical group (15.6%). This reduction was largely driven by fewer rehospitalisations for valve-related issues or heart failure in the TAVI group (4.8% versus 11.4%). Additionally, TAVI was associated with a lower incidence of new-onset atrial fibrillation (3.3% versus 28.8%) and a shorter median hospital stay (4 days versus 9 days).
However, TAVI did have higher rates of new permanent pacemaker implantation (8.8% versus 2.9%) and mild paravalvular aortic regurgitation (15.5% versus 2.4%) at 1 year. Despite these drawbacks, the overall findings suggest that TAVI, particularly with balloonexpandable devices, could be the preferred treatment for women with severe aortic stenosis. TAVI treatment could also reduce healthcare resource utilisation by lowering the number of hospitalisations.
No Benefit to Continuing Oral Anticoagulants with Transcatheter Aortic Valve Implantation
IN PATIENTS undergoing transcatheter aortic valve implantation (TAVI), it is not necessary to continue oral anticoagulants (OAC), as demonstrated in the POPular PAUSE TAVI trial presented at the ESC Congress 2024.
It is not well understood if OACs should be interrupted in patients undergoing TAVI, especially for those with a long-term indication, such as atrial fibrillation, or in patients who are elderly and have other health conditions. Therefore, researchers conducted the POPular PAUSE TAVI, an open-label, investigatorinitiated, non-inferiority trial in patients on OAC with planned TAVI, to investigate if continuing OACs is necessary in these patients.
In total, 858 patients from 22 European sites were randomised in a 1:1 ratio to continue OAC or to stop OAC at least 48 hours before TAVI (mean age: 81 years; 34.5% female). The mean CHA2DS2-VASC score was 4.5, indicating moderate-to-high risk of stroke in the cohort. Over 80% of patients were taking direct oral anticoagulants (81.9%), and the rest were taking vitamin K antagonists (18.1%).
The primary composite endpoint, which included cardiovascular mortality, stroke of any cause, myocardial infarction, major vascular complications, and major bleeding within 30 days after TAVI, occurred in 16.5% of patients in the continued OAC group. Similarly, these events occurred in 14.8% of patients in the
interrupted OAC group (risk difference: 1.7%; 95% CI: -3.1–6.6; P=0.18 for non-inferiority). The non-inferiority margin of 4% was not met, indicating that continuing OACs was not inferior to interrupting OACs in these patients, and there was no difference in thromboembolic events with continued versus interrupted OACs (8.8% versus 8.2%; risk difference: 0.6; 95% CI: -3.1–4.4). However, bleeding occurred in 31.1% of patients who continued OACs, compared to 21.3% in the interrupted group (risk difference: 9.8; 95% CI: 3.9–15.6).
The results of the study demonstrate that continuation of OACs does not decrease the risk of thromboembolic events, such as stroke, but does increase the risk of bleeding. These findings highlight the need to determine the optimal periprocedural anticoagulation strategy for patients undergoing TAVI. Additionally, patients at high risk for thromboembolism were excluded from the study, suggesting that future research should focus on this population to better understand the risks and benefits in these individuals.
It is not well understood if OACs should be interrupted in patients undergoing TAVI
Stents Outperform Balloon Angioplasty in Coronary Disease Treatment
A NEW trial, REC-CAGEFREE I, presented at the ESC Congress 2024, has confirmed that drug-eluting stents (DES) remain the most effective treatment for patients undergoing percutaneous coronary intervention (PCI) with previously untreated non-complex coronary artery disease, surpassing the effectiveness of the novel paclitaxelcoated balloon angioplasty (DCB).
As millions of people undergo PCI annually, the original goal of the trial was to reduce the rates of multiple cardiac events. Traditional PCI involves inflating a balloon inside the narrowed artery to restore blood flow, followed by DES implantation to prevent re-narrowing of the vessel. Although PCI with DES is highly effective, around 2% of patients experience restenosis annually, prompting exploration of alternatives like DCB.
The trial cohort comprised 2,272 adult patients from 43 sites in China between February 2021–May 2022, with an average age of 61 years. Participants were assigned to one of two treatment groups in a 1:1 ratio, either receiving DCB, with the option of rescue stenting, or DES.
Of the 1,133 participants who underwent treatment with DCB, 9% had to have a rescue DES due to unsatisfactory results. The study showed a combined 2-year rate of cardiac death, myocardial infarction, and revascularisation was 6.4% for DCB and 3.4% for DES, with DCB showing a higher risk of revascularisation (3.1% versus 1.2%).
Additionally, the findings highlighted a
discrepancy in outcomes based on vessel diameter, showing a higher incidence of repeat revascularisation in the DCB group, particularly in patients with larger arteries. In small vessel disease (≤3.0 mm), DCB performed similarly to DES; however, in larger vessels (>3.0 mm), DES was superior.
While prior studies have suggested DCBs could be effective in small vessel disease, this trial suggests their efficacy is limited to specific contexts.
DES remains the most effective treatment for patients undergoing PCI
The study's lead author, Ling Tao, Xijing Hospital, Shaanxi, China, stated that the "leave nothing behind" strategy using DCBs was unsuccessful. Based on the findings, DES implantation should remain the standard treatment for patients with noncomplex coronary artery disease, offering the best balance of safety and efficacy.
Cryoballoon Versus Radiofrequency Ablation: Comparing Speed and Success
GROUNDBREAKING findings from the CRABL-HF trial comparing the efficacy of cryoballoon (CB) ablation to radiofrequency (RF) ablation in treating patients with atrial fibrillation (AF) and heart failure with reduced ejection fraction (HFrEF) were presented at the ESC Congress 2024.
CB ablation was equally effective at reducing AF and atrial tachycardia recurrences compared to RF ablation
The study showed that, at 1-year followup, CB ablation was equally effective at reducing AF and atrial tachycardia recurrences compared to RF ablation. CB ablation also had the added benefit of shorter procedure times and less fluid usage, suggesting a lower risk of worsening heart failure.
AF, affecting over 37 million globally, often coexists with heart failure, and HFrEF affects around 60% of patients with heart failure. The presence of AF increases the risk of stroke, hospitalisation, and death. RF ablation is the most commonly used method. It uses heat to destroy heart tissue, but it is technically complex and requires longer procedure times. CB ablation, by contrast, uses cold temperatures to target problematic tissue, simplifying the procedure and shortening the time.
The study’s lead investigator emphasised the need to compare RF and CF to help guide clinical decision-making for these ablation procedures.
The CRABL-HF trial was conducted across five sites in Japan and included 110 patients with HFrEF and AF aged 20–85 (79% male; median age: 69 years). Patients were evenly randomised between the two ablation techniques (55 in each), and
AF episodes were monitored for 1 year using cardiac implantable devices or daily ambulatory electrocardiographs.
Both CB and RF ablation showed similar results, with 21.8% of patients in the RF group and 22.2% in the CB group experiencing atrial tachyarrhythmias lasting 30 seconds or more. Importantly, CB ablation procedures were significantly shorter (median: 101 versus 165 minutes), with reduced fluid volumes used without increasing left atrial pulse pressure, potentially reducing heart failure risks.
Heart function improved in both groups, with significant increases in left ventricular ejection fraction and decreases in left atrial volume index. Safety profiles were comparable, with only one procedurerelated complication in each group and no procedure-related deaths. Quality of life, measured by the Atrial Fibrillation Effect on Quality of Life questionnaire (AFEQT), improved similarly in both groups after ablation, demonstrating the efficacy of both treatments.
In conclusion, CB ablation proved to be a faster, simplified alternative to RF ablation, with similar clinical outcomes, suggesting it is a viable option for treating AF in patients with HFrEF.
Complete Revascularisation in Older Patients with STElevation Myocardial Infarction
NOVEL research presented at the ESC Congress 2024 confirmed that complete coronary revascularisation significantly reduces cardiovascular events in older patients with myocardial infarction and multivessel disease compared to culprit-only revascularisation.
The findings, based on data collected in seven different clinical trials, suggest that treating both culprit and non-culprit lesions improves outcomes, particularly within the first 4 years following a heart attack.
The EARTH-STEMI study focused on patients aged ≥75 years who had experienced ST-segment elevation myocardial infarction (STEMI). While complete revascularisation has been the standard treatment for patients with STEMI and multivessel disease, its application in older patients has remained underused. This study aimed to address this knowledge gap, and provide insights into its efficacy in this age group.
The meta-analysis pooled data from 1,733 patients across seven major trials, including COMPLETE, FIRE, FULL REVASC, and DANAMI-3–PRIMULTI, among others. Of these, 816 patients received complete revascularisation, while 917 underwent culprit-only revascularisation. The study found that complete revascularisation was associated with a 22% reduction in the risk of death, myocardial infarction, and ischaemia-driven revascularisation over 4 years compared to culprit-only procedures.
At the longest follow-up period, complete revascularisation also resulted in a 24% reduction in the risk of cardiovascular death or myocardial infarction. However, the team found no significant differences in all-cause mortality, cardiovascular death, or non-cardiovascular death between the two groups.
Further data will be required in order to assess the long-term benefits beyond 4 years
The safety profiles of both approaches were similar, with no significant differences in adverse outcomes such as stroke, stent thrombosis, major bleeding, or acute kidney injury.
These findings support the use of complete revascularisation in older patients; however the lead author noted that further data will be required in order to assess the long-term benefits beyond 4 years. Future updates from the ongoing FIRE trial are expected to provide some necessary additional insights.
No Advantage to ‘No-Touch’ Vein Harvesting
CORONARY artery bypass grafting (CABG) is a common treatment for ischaemic heart disease, but vein graft failure occurs in up to 50% of patients within 10 years.
The ‘no-touch’ technique, where the saphenous vein is harvested with surrounding tissue, was hypothesised to reduce graft failure compared to the conventional method, where the vein is stripped of surrounding tissue.
The SWEDEGRAFT trial aimed to evaluate whether the ‘no-touch’ technique improved outcomes in patients undergoing CABG, with results presented at the ESC Congress 2024. The randomised study included 902 patients from Sweden and Denmark undergoing first-time, non-emergent CABG with at least one saphenous vein graft.
Participants were randomly assigned to either the ‘no-touch’ or conventional harvesting technique in a 1:1 ratio. The primary endpoint was graft failure within 2 years, defined by graft occlusion, stenosis, or death. Secondary endpoints included
major adverse cardiovascular events and post-operative leg wound complications.
The trial found no significant difference in graft failure between the ‘no-touch’ (19.8%) and conventional (24.0%) groups (P=0.15). MACE incidence was similar between groups (12.6% versus 9.9%; P=0.195).
However, leg wound complications were significantly higher in the ‘no-touch’ group at both 3 months (24.7% versus 13.8%) and 2 years (49.6% versus 25.2%).
The study concluded that the ‘no-touch’ technique did not reduce graft failure or improve clinical outcomes compared to the conventional method and was associated with more leg wound complications. These findings do not support the routine use of the ‘no-touch’ technique in CABG, and future guidelines should consider these results.
Beta-Blockers After Myocardial Infarction:
Is it Best to Continue or Pause?
DISCONTINUING beta-blockers showed no cardiovascular safety advantages over continued use in patients with a history of myocardial infarction (MI), nor did it improve their quality of life (QoL), according to a late-breaking research presented at the ESC Congress 2024.
Advances in MI management and findings from observational studies have led doctors to question the need for continuing beta-blockers beyond a year after MI, as unnecessary treatment may cause side effects. Johanne Silvain, Sorbonne University, Paris, France, and colleagues conducted the ABYSS trial to provide definitive randomised data comparing beta-blocker interruption with continuation in terms of cardiovascular events and QoL. However, they were not able to demonstrate safety preservation in clinical outcomes or any improvement in QoL following betablocker discontinuation.
The ACTION Group conducted an openlabel, non-inferiority, randomised ABYSS trial, involving patients with a history of MI who were on long-term beta-blockers, had a left ventricular ejection fraction of at least 40%, and had no cardiovascular events in the past 6 months. Participants were randomly assigned (1:1) to either discontinue or continue beta-blocker
therapy. The primary endpoint was a mixture of death, non-fatal MI, non-fatal stroke, or cardiovascular hospitalisation at the longest follow-up (minimum 1 year), based on non-inferiority analysis.
Advances in MI management and findings from observational studies have led doctors to question the need for continuing beta-blockers beyond a year after MI
The secondary endpoint assessed changes in QoL using the European QoL-5 Dimensions questionnaire.
A total of 3,698 patients were randomised from 49 sites in France (mean age: 64 years; 17% female). The median time between the last MI and randomisation was 2.9 years (interquartile range: 1.2–6.4 years). Over a median follow-up of 3 years,
Patients were randomised 3,698
Sites in France
(years)
beta-blocker discontinuation was not shown to be non-inferior to continuation. In the interruption group, primary outcome events occurred in 23.8% of patients, and in the continuation group, primary outcome events occurred in 21.1% (risk difference: 2.8 percentage points; 95% CI: <0.1–5.5), with a hazard ratio of 1.16 (95% CI: 1.01–1.33; P=0.44 for non-inferiority).
In the interruption group, 4.1% of patients died compared to 4.0% in the continuation group, while MI occurred in 2.5% and 2.4%, respectively. Cardiovascular-related hospitalisations were higher in the interruption group (18.9%) than in the continuation group (16.6%). Beta-blocker discontinuation also led to increased systolic and diastolic blood pressure and heart rate at 6 months and during follow-up. No improvement in QoL was observed.
Silvain discouraged stopping chronic beta-blocker treatment in patients post-MI considering the differences in cardiovascular hospitalisations between both groups, negative effects on blood pressure, and no QoL improvements, thereby highlighting the need for further research from ongoing trials.
NEW evidence highlights the significant benefits of transcatheter edgeto-edge repair (T-TEER) in treating secondary tricuspid regurgitation (TR), according to recent findings presented at the ESC Congress 2024.
Secondary TR, where the tricuspid valve fails to close properly, can severely impact patients' quality of life by causing symptoms like fatigue, fluid retention in the abdomen and lower limbs, and impairments in kidney and liver function.
The Tri.fr trial, led by Erwan Donal from the Hospital of Rennes, France, was designed to evaluate the efficacy of T-TEER combined with optimal medical therapy in patients with symptomatic, severe secondary TR. The trial aimed to determine whether T-TEER could offer a new treatment option to patients who were not eligible for surgical intervention due to associated risks.
This open-label, randomised trial involved 300 patients across 24 centres in France and Belgium (mean age: 78 years; 54% female), of whom 40% had been hospitalised for heart failure within 1 year before enrolment, and 15% had a cardiac implantable electronic device.
Participants were randomly assigned to receive either T-TEER alongside optimal medical therapy, or medical therapy alone. The primary endpoint of the trial was the Packer composite score, which combined New York Heart Association (NYHA) class, patient global assessment (PGA), and major cardiovascular events.
Results showed that the T-TEER group had a significantly higher rate of improvement in the composite endpoint compared to the control group (74.1% versus 40.6%).
After 1 year, the severity of TR was markedly reduced in the T-TEER group, with a significant improvement in TR grades. Additionally, there were lower rates of hospitalisation and death in the T-TEER group, though these outcomes were not the primary focus of the trial. Quality of life, measured by the Kansas City Cardiomyopathy Questionnaire (KCCQ) score, significantly improved in the T-TEER group compared to the control group (69.9 versus 55.4).
T-TEER group had a significantly higher rate of improvement in the composite endpoint compared to the control group
The Tri.fr trial highlights the potential of T-TEER as an effective treatment for secondary TR, offering substantial improvements in both clinical outcomes and patient-reported quality of life. T-TEER, when combined with rigorous medical management, could be a promising option for patients with severe secondary TR.
Trial Explores Invasive Treatment for Older Patients with Myocardial Infarction
A NEW study presented at the ESC Congress 2024 found that an invasive strategy did not significantly reduce the combined risk of cardiovascular-related death or non-fatal myocardial infarction (MI) compared to a conservative approach.
The SENIOR-RITA trial is the largest study to date in older patients with a non-STelevation myocardial infarction (NSTEMI). The trial found that invasive strategies have no significant effect on cardiovascular death or non-fatal MI risks. However, it did result in fewer non-fatal MIs and subsequent revascularisation procedures, according to findings presented at ESC.
Older patients with NSTEMI are often treated conservatively due to concerns about procedural risks, despite guidelines recommending invasive strategies for highrisk patients. The SENIOR-RITA trial aimed to determine whether an invasive strategy combined with optimal medical therapy would outperform medical therapy alone in reducing cardiovascular death or non-fatal MI in patients aged ≥75 years.
The trial included nearly 1,520 patients from 48 National Health Service (NHS) sites in England and Scotland, with an average age of 82.4 years. The participants were randomly assigned to receive either optimal medical therapy alone or to receive an invasive strategy, including coronary angiography and potential revascularisation. The primary endpoint was the combined risk of cardiovascular death or non-fatal MI, with secondary outcomes including revascularisation rates and bleeding complications.
After a median follow-up of 4.1 years, there was no significant difference in the primary endpoint between the invasive and conservative strategy groups (25.6% versus 26.3%). However, the invasive strategy group saw a reduction in non-fatal MIs (11.7% versus 15.0%) and required fewer revascularisation procedures (3.9% versus 13.7%) compared to the conservative group.
The study authors emphasised that the results suggest invasive strategies do not reduce the overall combined risk of cardiovascular death or non-fatal MI, but it they do have some benefits, particularly in reducing recurrent MIs and the need for additional procedures.
The authors also noted that the invasive approach was generally safe, and that age should not be a barrier to individualised care, including access to angiography and interventions.
New Directions in the Management of Atrial Fibrillation
Authors: Katrina Thornber, EMJ, London, UK
Citation: EMJ Cardiol. 2024;12[1]:26-30.
https://doi.org/10.33590/emjcardiol/DPSU4455.
MANAGEMENT of atrial fibrillation (AF) was a prevalent topic at this year's European Society of Cardiology (ESC) Congress 2024. With an ever-growing rate of patients needing ablation therapy and new treatment strategies on the rise, a streamlined treatment approach is yet to be defined. Researchers came together to present timely late-breaking research and its clinical implications, but more importantly, to discuss what questions remain unanswered regarding the management of this condition.
THE EVOLVING LANDSCAPE OF RISK FACTORS
Gregory Lip, University of Liverpool, UK, opened the session by emphasising the need for a more comprehensive and integrated approach to risk assessment and management of AF, following recent findings.
In recent years, there has been a push for a streamlined approach to AF management and risk assessment, with an emphasis on the following three parameters: stroke prevention, managing symptoms with rate and rhythm control, and identification of cardiovascular risk factors and associated comorbidities. These ‘three pillars’ have been consistently featured in recent AF guidelines, albeit with slight variations. For example, the 2020 ESC guidelines incorporated the ABC pathway (‘Avoid stroke’, ‘Better symptom management’, ‘Cardiovascular risk factor and comorbidity management’). The mAFA trial demonstrated the efficacy of a telehealth intervention based on the ABC pathway, with adherence rates above 70% and persistence over 90%, compared to standard care.1 Furthermore, the MIRACLEAF trial, which employed both in-person
and telehealth-based care using the ABC pathway, showed significant reductions in adverse outcomes.2 Specifically, the risk of mortality was 50% lower, the risk of stroke was 36% lower, and risk of hospitalisation was 31% lower in the intervention group.2 Lip noted that the outcomes achieved with an integrated care approach could ease the substantial healthcare burden associated with AF.
However, Lip also stressed that, whilst recent guidelines do feature the ‘three pillars’, they lack consideration of certain risk factors which have become more significant in recent years. For example, the impact of sex in AF-related stroke risk has shifted. Previous research demonstrated that female patients with AF have a 20–40% higher risk of ischaemic stroke.3 Lip explained that recent data indicate that the difference between males and females has diminished significantly, likely due to improved awareness and preventive measures for female patients.4 However, Lip did admit that this trend has been primarily observed in Swedish and Danish cohorts, so it may not be universally applicable, highlighting the need to regularly update risk stratification.
Lip also noted that current risk assessment strategies have not incorporated recent evidence that demonstrated the impact of environmental factors on AF. Lip emphasised the significance of this omission, as recent research has revealed that air pollution has a greater impact on AF onset in both female patients and those over 65 years, and is more likely to cause AF complications in younger, female patients.5 Overall, Lip stressed that using a simple care pathway, such as the ABC pathway, but in a holistic or integrated care manner, will improve the management, and therefore outcomes, of patients with AF. Lip stressed that new guidelines need to integrate emerging findings with traditional risk factors, such as the impact of air pollution. AF management, he concluded, is not a one-size-fits-all approach; it must be holistic and adaptable to reflect the dynamic nature of AF itself.
AF management is not a onesize-fits-all approach; it must be holistic and adaptable to reflect the dynamic nature of AF itself
AF BURDEN OR AF RECURRENCE?
Carina Blomstrom-Lundqvist, Orebro University Hospital, Sweden, proposed that AF burden, not AF recurrence, should be the endpoint in all AF ablation trials.
Blomstrom-Lundqvist began by explaining that, historically, AF recurrence, defined as the time to the first AF episode (with a threshold of 30 seconds), has been the ‘gold standard’ endpoint in AF trials. Because this metric has been so widely used, it allows for comparisons across many studies. However, there has been a recent shift towards AF burden as a more suitable measure, and Blomstrom-Lundqvist thoroughly discussed the reasons for this, comparing studies using these two metrics. Specifically, the CIRCA-DOSE trial reported a 53% 1-year efficacy with the traditional ‘time to first AF recurrence’ endpoint, versus a much higher 98% efficacy when AF burden reduction was measured.6 This demonstrates that AF burden correlates better with clinically relevant outcomes, whereas AF recurrence underestimates the true impact of ablation.
Lip supported the move toward AF burden as a more meaningful endpoint, and highlighted the limitations of the 30-second threshold, noting that a 29-second AF episode does not necessarily indicate low risk. AF burden, which captures the total time a patient spends in AF, is more comprehensive, and reflects the fluctuating nature of AF and its associated comorbidities.
Unlike AF recurrence, AF burden is closely linked to hard clinical outcomes. A recent study showed that AF burden had a greater effect on quality of life than either AF duration or the number of episodes.7 Furthermore, recent data indicate that AF burden is associated with mortality among patients with cardiac implantable electronic devices, with the greatest risk of mortality found when weekly AF progression exceeded 24 hours.8,9 AF burden is also a stronger predictor of ischaemic stroke in patients with paroxysmal AF, as demonstrated by the KP-RHYTHM Study.10
Currently, the 2024 AF ablation consensus document strongly advises that AF burden be reported as the primary endpoint in AF ablation trials.11
While the 30-second threshold remains in place to maintain continuity with previous research, this approach is increasingly seen as inadequate. Continuous AF burden measurements showed a more significant correlation with stroke risk than binary thresholds like AF recurrence, highlighting its direct effect on clinical outcomes.
Blomstrom-Lundqvist acknowledged that more research is needed to determine the most reliable way to measure AF burden, particularly when aiming to improve survival. Should continuous monitoring be employed? Should ablation be repeated if AF burden exceeds a certain threshold, such as 50%? These are questions that remain unanswered.
EMERGING TRENDS: PULSED FIELD ABLATION
Pulsed field ablation (PFA), a non-thermal procedure that uses high-voltage electrical pulses, is an emerging technology for the treatment of cardiac arrhythmias, and therefore the centre of many conversations on AF management. Indeed, Tom De Potter, Cardiovascular Research Center, Aalst, Belgium, joked about the current buzz around PFA, saying, “Another talk on PFA... seriously?” highlighting the increasing popularity of this modality. De Potter began his presentation by revealing that he had changed the title of his talk from “Should PFA replace radiofrequency (RF) or cryoballoon?” to “PFA will replace RF or cryoballoon.” He explained that debating whether it should replace these techniques is too philosophical, as there are currently not enough data for that discussion.
He explained that PFA is an AF ablation modality that works by damaging cell membranes using direct current. It is also called non-thermal ablation or voltagemediated, tissue-selective ablation. De Potter noted that whilst tissue-selectivity is true in theory, it is not always perfect in practice. However, early clinical data have shown that PFA can spare vital structures such as oesophageal and phrenic nerves, which partly explains the enthusiasm for this modality.
Early clinical data have shown that PFA can spare vital structures such as oesophageal and phrenic nerves
Whilst there aren’t much data on this newer technology, De Potter highlighted recent studies that show that PFA is a straightforward and safe modality. For instance, the 5S study demonstrated that PFA has a shallow learning curve, in terms of both procedure time and ablation time, regardless of the operator’s experience.12 The study also showed that complication rates with PFA seem to lack the collateral damage seen with other ablation modalities.
On the other hand, De Potter did acknowledge concerns surrounding PFA, such as its potential link to silent cerebral injury, haemolysis, and coronary spasms, and the potential long-term effects on the autonomic nervous system. “The appeal of PFA is easy to understand,” he said, “but it’s not without its own challenges.” However, he explained that the issue of silent cerebral injury in particular, appears to be a result of the ‘platform phenomenon’, meaning it is related more to procedural factors, such as fluid management and embolism avoidance, than to the thermal energy itself.
Although the data on PFA are limited, he referenced a randomised study comparing PFA to conventional thermal ablation for paroxysmal AF.13 The study revealed that PFA was non-inferior to conventional
ablation, and was associated with a low overall incidence of adverse events. He did note one mortality in the PFA cohort due to cardiac tamponade, but explained that, again, this is likely due to the ‘platform phenomenon’ rather than an inherent PFA energy-specific issue.
Recently, a real-world study was published which demonstrated the safety of PFA in over 17,000 patients with AF.14 The published results provide support for the ‘platform theory’, as the rate of tamponade decreased with operator experience, suggesting that with better training, procedural risks decrease, even as the energy source remains unchanged.
De Potter expanded on the growing popularity, explaining that whilst there is an increase in the number of ablation procedures worldwide, most electrophysiology centres do not fulfil the recommended requirements for ablation treatment, and the number of centres has not increased to meet the growing demand. This may thus explain the push for PFA in clinical practice, he proposed.
He argued that, whilst there are compelling arguments in favour of PFA, not all of them are entirely clinical. De Potter emphasised the importance of acknowledging the influence of industry in the drive for implementing PFA as an approach to AF management, especially as the demand for PVI and AF ablation continues to grow.
References
1. Guo Y et al. Mobile health technology to improve care for patients with atrial fibrillation. J Am Coll Cardiol. 2020;75(13):1523-34.
2. M Li et al. MIRACLE-AF - A novel model of integrated care of older patients with atrial fibrillation in rural China. ESC Congress 2024. 1 September 2024.
3. B Corica et al. Sex as a risk factor for atrial fibrillation-related stroke. Thromb Haemost 2024; 124(4):281-85.
4. Teppo K et al. Ischaemic stroke in women with atrial fibrillation: temporal trends and clinical implications. Eur Heart J. 2024;45(20):1819-27.
5. Zhang J et al. Associations of ambient air pollution with incidence and dynamic progression of atrial fibrillation. Sci Total Environ. 2024;951:175710.
6. Andrade JG et al. Cryoballoon or
radiofrequency ablation for atrial fibrillation assessed by continuous monitoring: a randomized clinical trial. Circulation. 2019;140(22):1779-88.
7. Jansson V et al. Atrial fibrillation burden, episode duration and frequency in relation to quality of life in patients with implantable cardiac monitor. IJC Heart Vasculature. 2021;34:100791.
8. Peigh G et al. Association of atrial fibrillation burden and mortality among patients with cardiac implantable electronic devices. Circulation. 2024;150(5):350-61.
9. Piccini JP et al. Atrial fibrillation burden, progression, and the risk of death: a case-crossover analysis in patients with cardiac implantable electronic devices. Europace. 2019;21(3):404-13.
10. Go AS et al. Association of burden of atrial fibrillation with risk of ischemic stroke in adults with paroxysmal atrial
fibrillation: the KP-RHYTHM study. JAMA Cardiol. 2018;3(7):601-8.
11. Tzeis S et al. 2024 European Heart Rhythm Association/Heart Rhythm Society/Asia Pacific Heart Rhythm Society/Latin American Heart Rhythm Society expert consensus statement on catheter and surgical ablation of atrial fibrillation. Europace. 2024;26(4):euae043.
12. Schmidt B et al. 5S Study: safe and simple single shot pulmonary vein isolation with pulsed field ablation using sedation. Circ Arrhythm Electrophysiol. 2022;15(6):e010817.
13. Reddy VY et al. Pulsed field or conventional thermal ablation for paroxysmal atrial fibrillation. NEJM. 2023;389:1660-71.
14. Ekanem E et al. Safety of pulsed field ablation in more than 17,000 patients with atrial fibrillation in the MANIFEST-17K study. Nat Med. 2024;30(7):2020-9.
Artificial Intelligence and Digital Biomarkers: A Revolution in Cardiovascular Diagnostics
THIS YEAR, the European Society of Cardiology (ESC) Congress 2024, which took place in London, UK, between 30th August–2nd September, hosted an insightful symposium entitled ‘Artificial intelligence unleashed on digital biomarkers: a new era in personalised cardiovascular healthcare’. The session explored the applications of AI in cardiac diagnostics, highlighting its potential to positively impact patient care. The speakers covered key topics, including how vascular retinal imaging could predict cardiovascular risk and whether speech analysis could aid in the detection of acute decompensated heart failure.
RETINAL IMAGING FOR CARDIOVASCULAR RISK ASSESSMENT
Sungha Park, Yonsei University, Seoul, Republic of Korea, presented a compelling case for the use of retinal imaging in cardiovascular risk assessment. He highlighted the strong correlation between the media-to-lumen ratio of small arteries and retinal arterioles, noting that retinal arterial narrowing may reflect broader arterial diseases, including those in the kidneys and brain.1 Retinal arterial remodelling, indicative of systemic changes in small arteries, is associated with adverse cardiovascular complications.2 Typical signs of arterial damage in the retina, such as microhaemorrhages and microaneurysms, are also linked to cardiovascular disease.3
Despite the clinical significance of these findings, there is often a lack of consensus among ophthalmologists regarding the diagnosis of retinal abnormalities, as interpretation can be subjective. AI technology has already demonstrated high accuracy in diagnosing ocular diseases like diabetic retinopathy and glaucoma, as well as measuring vascular dimensions. A 2018 study showed that AI could predict cardiovascular risk factors, such as age,
gender, and smoking, from retinal fundus photographs with remarkable accuracy.4
Park’s team explored whether deep learning-based analysis of retinal images could predict coronary artery calcium (CAC), a known cardiovascular risk marker.5 Using a large dataset of 28,000 retinal images from multiple health centres and the UK Biobank, they trained a deep learning model that successfully predicted the presence of CAC.
Retinal arterial remodelling, indicative of systemic changes in small arteries, is associated with adverse cardiovascular complications
The model showed a correlation between higher scores and risk factors, such as age, male sex, hypertension, and diabetes. This deep learning model, named Reti-CVD, showed promise in stratifying cardiovascular risk and performed comparably to traditional risk models like Pooled Cohort Equations (PCE) and QRISK®3 (ClinRisk, UK).
Further studies6 validated the association between retinal arterial changes and cardiovascular disease, leading to the approval of the deep learning fundoscopic model by the Ministry of Food and Drug Safety of the Republic of Korea in 2023 for clinical use. The system offers advantages, such as minimal space requirements, low radiation exposure, and quick results within 5 minutes, making it suitable for use in the clinic. Although more validation is needed, early results suggest that this AI-based approach could be a valuable, cost-effective alternative to traditional cardiovascular risk assessments, especially in cases where access to more expensive and time-consuming diagnostic tools like CT scans is limited.
Given small vessel remodelling in the retina is a marker of both systemic organ damage and adverse cardiovascular outcomes, using deep learning systems to visualise the retina’s microvasculature can provide more precise cardiovascular risk stratification, particularly for individuals in borderline to intermediate risk categories.
CAN SPEECH ANALYSIS DETECT HEART FAILURE?
Abhinav Sharma, McGill University Health Centre, Montréal, Canada, introduced the evolving use of voice analysis to detect acute decompensated heart failure.
He highlighted the increasing integration of mobile applications in healthcare due to lower costs and higher mobile phone penetration. In heart failure, while symptoms like dyspnoea and fatigue are well-known, the impact of speech changes due to fluid overload is less explored. Sharma and his team initially studied voice detection using chatbots during the COVID-19 pandemic and found high accuracy in symptom detection. However, they have now moved to more advanced AI-based speech analysis.7
Speech analysis in patients with heart failure focuses on how pulmonary oedema affects vocal folds, altering speech characteristics like jitter and shimmer, which are detectable through both time and frequency domain analysis. Early studies showed that volume changes from fluid retention affected speech, with one trial noting that phonation threshold pressure rose in response to diuretics.8 Other studies used acoustic analysis of patients’ speech to detect creakiness, a feature that correlated with changes in body weight.9
Recent research that focused on developing vocal biomarkers from large datasets, analysing various speech features to predict heart failure risk, and, although the results showed some promise, the accuracy was moderate.10 Further studies, including a trial in 2022 that analysed speech in multiple languages,
reinforced the concept that volume status affects the voice, demonstrating detectable changes between “wet, congested, and dry,” decongested states.11
Sharma emphasised the shift from invasive monitoring like CardioMEMS to non-invasive, cost-effective methods like mobile apps that can frequently monitor patients with heart failure. Despite the promise of such technology, challenges remain, such as privacy concerns, potential false positives due to ambient noise, and increased administrative burden. Ultimately, the success of voice-based monitoring will depend on whether it can significantly impact patient management and outcomes.
Future directions could include simplifying voice biomarkers and addressing privacy and cybersecurity concerns, while the long-term goal is to ensure that these technologies improve heart failure management by offering meaningful insights and care alterations.
DIGITAL BIOMARKERS FOR PATIENT STRATIFICATION
Florian Wenzl, University of Zurich, Switzerland, emphasised that, although AI is still evolving, it is becoming a crucial tool in predicting outcomes and aiding decisionmaking in clinical settings. AI’s role in risk stratification spans various areas, such as analysing clinical data, biomarkers, imaging, and wearable device data, to predict patient outcomes and improve treatment strategies.12
Wenzl discussed current applications, focusing on patients with non-ST segment elevation acute coronary syndrome (NSTE-ACS) and post-percutaneous coronary intervention. The development of the GRACE 3.0 score, a new AI-driven tool for risk stratification in patients with NSTE-ACS, was also highlighted, given that this score, which has been validated using large datasets, outperformed previous versions by accounting for sex-specific differences in risk factors.13 The GRACE 3.0 score has shown an improved ability to predict risk, particularly in low-to-intermediate risk patients who may benefit from early invasive treatment and is now available as an online calculator to assist clinicians.14
In a broader context, Wenzl pointed to future AI applications in medicine, particularly in integrating diverse data sources ranging from biometric data to wearable technology. In his concluding remarks, he underscored the immense potential of AI in medicine, while also noting the importance of rigorous external validation to ensure reliability and accuracy in clinical practice.
MANAGING ARRHYTHMIA WITH ARTIFICIAL INTELLIGENCE
Renate B. Schnabel, University Heart and Vascular Centre in Hamburg, Germany, provided an update on AI-based strategies for diagnosing and treating arrhythmias. Although advancements are continuously being made, AI and machine learning are already enhancing arrhythmia management, particularly in electrocardiogram (ECG) analysis, where deep learning algorithms help detect patterns and signatures in heart rhythms. AI is also being applied in virtual heart simulations, cardiac imaging, and robotics, while advances in telecommunication support AI-powered atrial fibrillation (AF) screening, Schnabel explained.
Schnabel highlighted the potential of combining big data from electronic health records and other sources to build predictive models for AF. She discussed the use of AI to identify individuals at high risk of AF, investigated in a recent study, although low patient engagement in this limited its effectiveness.15 However, among those who participated, AI screening nearly doubled AF detection rates. AI applications in smartphone-based pulse detection, or photoplethysmography, have shown strong correlations with ECG data, improving arrhythmia management, particularly in post-ablation monitoring of patients with AF.
AI’s role in analysing biomarkers to predict AF and its adverse outcomes has been explored by her team, who used machine
learning to analyse biomarkers and clinical risk factors in a large cohort study.16 The results showed that AI-based predictions, including those involving the heart failure marker, NT-proBNP, were comparable to traditional statistical methods, confirming the validity of these AI models. Further research has demonstrated that AI could predict AF and other cardiovascular conditions using ECG data, even outperforming some conventional methods in identifying high-risk individuals for AF during monitoring.17
Schnabel stressed the importance of understanding how AI algorithms make decisions, advocating for methods like attention maps and deep learning models that can help clinicians interpret AI predictions. She noted that the future of arrhythmia care will likely involve combining data from multiple sources, such as ECG, MRI, and simulations with AI to improve diagnostics, treatment, and risk prediction. However, she also highlighted the necessity for trustworthiness, reliability, and clinical validation to ensure AI’s safe and effective implementation in cardiology.
CONCLUSION
As the symposium closed, a discussion raised a crucial issue regarding the interoperability of data and technologies in the medical field, particularly for improving risk prediction in AI-driven medicine. Given the industry is still in its early stages, only a tiny fraction of the vast amount of data collected daily from hospitals, wearables, and even public sources is being utilised in AI projects. The experts emphasised that it remains unclear which types of data will ultimately lead to the most accurate predictions, underscoring the need to integrate more diverse sources of information and the session concluded with optimism about the future of AI in cardiovascular medicine, emphasising the importance of ongoing collaboration and discussion on these emerging technologies.
References
1. Rizzoni D et al. Relationship between media-to-lumen ratio of subcutaneous small arteries and wall-to-lumen ratio of retinal arterioles evaluated noninvasively by scanning laser Doppler flowmetry. J Hypertens. 2012;30(6):1169-75.
2. Wong TY, McIntosh R. Hypertensive retinopathy signs as risk indicators of cardiovascular morbidity and mortality. Br Med Bull. 2005;73-4:57-70.
3. Van den Born BJ et al. alue of routine funduscopy in patients with hypertension: systematic review. BMI. 2005;331(7508):73
4. Poplin R et al. Prediction of cardiovascular risk factors from retinal fundus photographs via deep learning. Nat Biomed Eng. 2018;2(3):158-64.
5. Rim TH et al. Deep-learning-based cardiovascular risk stratification using coronary artery calcium scores predicted from retinal photographs. Lancet Digit Health. 2021;3(5):e30616.
6. Yi JK et al. Cardiovascular disease risk assessment using a deep-learningbased retinal biomarker: a comparison with existing risk scores. Eur Heart J Digit Health. 2023;4(3):236-44.
7. Sharma A et al. Voice-assisted artificial intelligence-enabled screening for severe acute respiratory syndrome coronavirus 2 exposure in cardiovascular clinics: primary results of the VOICE-COVID-19-II randomized trial. J Card Fail. 2023;29(10):1456-60.
8. Murton OM et al. Acoustic voice and speech biomarkers of treatment status during hospitalization for acute decompensated heart failure. Appl Sci (Basel). 2023;13(3):1827.
9. Murton OM, Hillman RE, Mehta DD, et al. Acoustic speech analysis of patients with decompensated heart failure: A pilot study. J Acoust Soc Am. 2017;142(4):EL401.
10. Maor E et al. vocal biomarker is associated with hospitalization and mortality among heart failure patients. J Am Heart Assoc. 2020;9(7):e013359.
11. Amir O et al. Remote speech analysis in the evaluation of hospitalized patients with acute decompensated heart failure. JACC Heart Fail. 2022;10(1):41-9.
12. Lüscher TF et al. Artificial intelligence in cardiovascular medicine: clinical applications. Eur Heart J. 2024;DOI:10.1093/eurheartj/ehae465.
13. Wenzl FA et al. Sex-specific evaluation and redevelopment of the GRACE score in non-ST-segment elevation acute coronary syndromes in populations from the UK and Switzerland: a multinational analysis with external cohort validation. Lancet. 2022;400(10354):744-56.
14. Wenzl FA, Lüscher TF. Application of a sex-specific GRACE score in practice - authors' reply. Lancet. 2023;401(10370):23.
15. Hill NR et al. Identification of undiagnosed atrial fibrillation using a machine learning risk-prediction algorithm and diagnostic testing (PULsE-AI) in primary care: a multicentre randomized controlled trial in England. Eur Heart J Digit Health. 2022;3(2):195-204.
16. Neyazi M et al. Deep learning-based NT-proBNP prediction from the ECG for risk assessment in the community. Clin Chem Lab Med. 2023;62(4):74052.
17. Noseworthy PA et al. Artificial intelligence-guided screening for atrial fibrillation using electrocardiogram during sinus rhythm: a prospective non-randomised interventional trial. Lancet. 2022;400(10359):1206-12.
Abstract Reviews
Sharing insights from the European Society of Cardiology (ESC) Congress 2024, the following abstract reviews spotlight exciting new developments in the field.
The Fate of Coronary Artery Bypass Grafting in the Elderly: Treat and Forget
Coronary artery bypass grafting (CABG) is a treatment option offered to a growing population of octogenarians, considering the constant rise in life expectancy.1 The dark side of surgical myocardial revascularisation for octogenarians is the lack of information on follow-up and comparability of mid-term outcomes with younger patients,2 as well as the benefits of tertiary prevention (mid-term
management of coronary artery disease after CABG).3 Hence, the purpose of this study is to evaluate the 10-year outcomes of octogenarian patients after isolated CABG included in an Italian nationwide prospective registry.4
METHODS
The PRIORITY project was designed to evaluate the long-term outcomes of two large prospective multicentre cohort studies on isolated CABG.5 Patients younger and older than 80 years were identified. The primary endpoints were all-cause mortality and the overall rate of major adverse cardiac and cerebrovascular events (MACCE) at 10 years. Secondary outcomes included the individual components of MACCE. Baseline differences between the study groups were balanced with propensity score matching and inverse probability of treatment weight (IPTW).6 Time to events was analysed using Cox regression and competing risk analysis.7
RESULTS
The cohort consisted of 10,989 patients who underwent isolated CABG with complete baseline clinical characteristics, operative data, and administrative followup. Of the patients, 872 (7.9%). The median follow-up time was 7.9 years. As expected, octogenarians showed poorer 10-year survival (hazard ratio [HR]: 3.09; 95% CI: 2.93–3.25; p<0.001) and MACCE (HR: 2.13; 95% CI: 2.04–2.22; p<0.001). Interestingly,
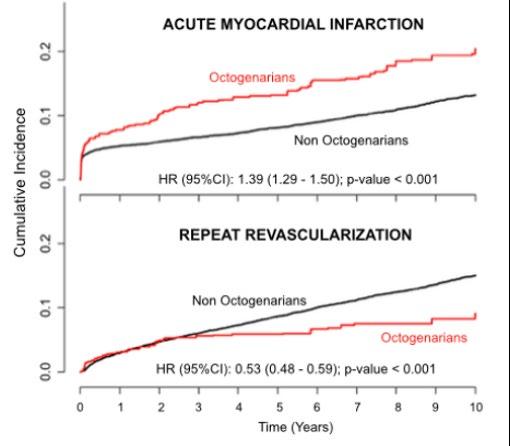
although experiencing a higher cumulative incidence of myocardial infarction (MI) at 10 years (HR: 1.39; 95% CI: 1.29–1.50; p<0.001), octogenarians underwent a reduced incidence of 10-year myocardial
revascularisation (HR: 0.53; 95% CI 0.48–0.59; p<0.001), corroborating the hypothesis of undertreatment for the elderly (Figure 1).
Figure 1: Inverse probability of treatment weight cumulative incidence of acute myocardial infarction and repeat revascularisation at 10 years.
Cumulative incidence
Acute myocardial infraction
Octogenarians
Non-octogenarians
HR (95% CI): 1.39 (1.29–1.50); p-value<0.001
Repeat revascularisation
Non-octogenarians
Octogenarians
HR (95% CI): 0.53 (0.48–0.59); p-value<0.001
Time (years)
HR: hazard ratio.
CONCLUSION
The main finding of this study was the opposite effect of advanced age on acute MI and repeat revascularisation. Indeed, apart from the expected worse survival and MACCE, the higher incidence of acute MI in octogenarians is not concordant with repeat revascularisation, which is significantly more represented in younger patients. It suggests a tendency for conservative approaches by managing the patient’s signs and symptoms with medical therapy alone.8 This result opens a debate on the choice of treating the elderly with CABG without guaranteeing clinical assistance comparable to younger patients.9 Clinicians should make meticulous considerations of the risks and benefits for each treatment option considering the personalised nature of cardiovascular medicine and surgery.
References
1. Ralapanawa U, Sivakanesan R. Epidemiology and the magnitude of coronary artery disease and acute coronary syndrome: a narrative review. J Epidemiol Glob Health. 2021;(2):169-77.
2. Kirov H et al. Comparing outcomes between coronary artery bypass grafting and percutaneous coronary intervention in octogenarians with left main or multivessel disease. Sci Rep. 2023;13(1):22323.
3. Schwann TA et al. Bilateral internal thoracic artery versus radial artery multi-arterial bypass grafting: a report from the STS database. Eur J Cardiothorac Surg. 2019;56(5):926-34.
4. Barili F et al. Lo studio PRIORITY - predicting long term outcomes after isolated coronary artery bypass surgery. G Ital Cardiol. 2021;22(4):327-31.
5. Seccareccia F et al. The Italian CABG outcome study: short-term outcomes in patients with coronary artery bypass graft surgery. Eur J Cardiothorac Surg. 2006;29(1):56-62.
6. Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46(3):399-424.
7. Barili F et al. An original model to predict intensive care unit length-of stay after cardiac surgery in a competing risk framework. Int J Cardiol. 2013;168(1):219-25.
8. Tarakji KG et al. Temporal onset, risk factors, and outcomes associated with stroke after coronary artery bypass grafting. JAMA. 2011;305(4);381-90.
9. Berezhnoi K et al. Effects of complete revascularization on long-term treatment outcomes in patients with multivessel coronary artery disease over 80 years of age admitted for acute coronary syndrome. Cardiovasc Diagn Ther. 2019;9(4):301-9.
Machine Learning and Traditional Analysis of the Interaction Between Cardiovascular Diseases and Haematological Malignancies
Authors: Tal Caller,1 Alexander Fardman,3 Efrat Sharon,1 Nili Naftali-Shani,1,2 Jonathan Leor,1 Elad Maor,3 *Tomer Itkin1,2
1. Neufeld and Tamman Cardiovascular Research Institute, The Olga & Lev Leviev Cardiothoracic and Vessels Center, Sheba Medical Center, Faculty of Medical and Health Sciences, Tel Aviv University, Israel
2. Sagol Center for Regenerative Medicine, Department of Pathology, Faculty of Medical and Health Sciences, Tel Aviv University, Israel
3. Department of Cardiology, The Olga & Lev Leviev Cardiothoracic and Vessels Center, Sheba Medical Center, Ramat Gan, Israel *Correspondence to tomitkin@tauex.tau.ac.il
Disclosure: The authors declare no conflicts of interest.
Keywords: Cancer risk factors, cardiovascular disorders, haematological malignancies, reverse cardio-oncology.
Cardiovascular disorders (CVD) and clonal haematopoiesis of indeterminate potential, the very early state with developmental potential of haematological malignancies, exhibit reciprocal interactions.1,2 While the presence of clonal haematopoiesis of indeterminate potential confers a risk for heart failure, it is unclear if CVDs are associated with elevated risk in development of haematological malignancies.
MATERIALS AND METHODS
In the authors' preliminary study, to determine the association between CVDs
and the risk for haematological cancer, they evaluated 27,231 adults. These individuals, who participated in a preventive healthcare screening programme between 2000–2018, were free of CVD and cancer at baseline. Each participant underwent a complete physical evaluation, blood test, and exercise stress test at baseline. CVD was defined as ischaemic heart disease, stroke, atrial fibrillation, or hypertension. Machine learning and traditional survival analyses were applied to evaluate the association between CVD and haematological cancer. For machine learning, the team used the random forest method using Curat package in r, and incorporated all continuous variables gathered into the model (70% training, 30% test). For survival analysis, they first matched each patient with CVD to a control patient by propensity scores to balance for age, sex, smoking, diabetes, renal function, BMI, and length of follow-up. Then, patients with and without CVD were compared using Cox proportional hazard regression.
RESULTS
Using machine learning, they found that the strongest features associated with haematological cancer in the cohort were low estimated glomerular filtration rate, age, high atherosclerosis cardiovascular disease score, and BMI. Of note, systolic and diastolic blood pressure were also strongly associated with haematological cancer. Next, the team successfully matched 5,500 patients with CVD to controls with a median follow-up of 9.2 years (interquartile range: 5–15 years). During follow-up, 1,380 individuals developed cancer. Of them, 186 individuals developed haematological cancer.
They used Cox proportional hazard regression and the Kaplan Mayer method to determine the risk and hazard ratio of developing haematological cancer. Compared with subjects without CVD, patients with CVD were 91% more likely to develop cancer during follow-up, and 62% more likely to develop haematological
cancer (hazard ratio: 1.61; 95% CI: 1.21–2.16). Moreover, the 10-year risk of developing haematological cancer was 1.9% for patients with CVD and 1.0% for individuals without CVD. Notably, the increased incidence of haematological cancers included 38% increase in cases of leukaemia but only 11% increase in cases of lymphoma.
Figure 1: Illustration of hypothetical model for the flow of events by which cardiovascular diseases augment development of haematological malignancies.
The model is based on recent findings and the authors' results, demonstrating that CVDs are a risk factor for development of haematological malignancies. In the course of CVD pathogenesis, as part of the heart repair efforts cardiac cells alter their secretome and release factors, that are potentially tissue-transformative, into the blood. Upon arrival to the bone marrow, these factors modify cells in the microenvironment in a way that is potentially supportive for development of haematological malignancies from haematopoietic cells in a pre-tumorigenic state. This figure was generated using Biorender.com.
CVD: cardiovascular disease.
CONCLUSION
Herein, by applying machine learning and traditional analysis, the authors show that CVD risk and CVDs are associated with increased incidence of haematological cancer. Their previous study demonstrated, in murine models, that CVDs promote existing solid tumour growth via release of blood-carried factors.3 It was shown in murine models that CVDs modulate the
bone marrow microenvironment, affecting haematopoietic developmental lineage trajectories.4,5 Thus, they hypothesise a model in which CVDs modulate the human bone marrow microenvironment via secretion of blood-carrying factors. Transformed marrow microenvironment may display plasticity properties that can potentially augment accelerated development of haematological malignancy from a pretumorigenic state (Figure 1).
Currently, basic research studies are conducted to confirm this hypothesis. Deciphering the action mechanisms between CVDs and haematological malignancies
References
1. Fuster JJ et al. Clonal hematopoiesis associated with TET2 deficiency accelerates atherosclerosis development in mice. Science. 2017;355(6327):842-7.
2. Jaiswal S et al. Age-related clonal hematopoiesis associated with adverse outcomes. N Engl J Med. 2014;371(26): 2488-98.
could lead to therapeutic advances in cardiovascular and cancer treatment and may ultimately improve patient outcomes.
3. Caller T et al. Small extracellular vesicles from infarcted and failing heart accelerate tumor growth. Circulation. 2024;149(22):1729-48.
4. Courties G et al. Ischemic stroke activates hematopoietic bone marrow stem cells. Circ Res. 2015;116(3):407-17.
5. Itkin T, Rafii S. Cardiovascular diseases disrupt the bone-marrow niche. Nature. 2022;601(7894):515-7.
Ablation of Tachyarrhythmias with Zero Fluoroscopy Technique in Patients Under 18 Years of Age: 4-Year Follow-Up
Authors: *Carlos A. Chavez-Gutierrez,1,2 Maria F. Valdez-Perales,2 Vitelio A. Mariona-Montero,1,2 Sara I. Garcia Garcia,2 Rafael Garcia-Leon1,3
1. Department of Cardiac Electrophysiology, Mexican Institute of Social Security (IMSS) National Medical Center of the West Pediatric Hospital, Guadalajara, Mexico
2. Department of Cardiology Pediatric, Mexican Institute of Social Security (IMSS) National Medical Center of the West Pediatric Hospital, Guadalajara, Mexico
3. Cardiology Workshop, Cardiosurgery, Mexican Institute of Social Security (IMSS) National Medical Center of the West Pediatric Hospital, Guadalajara, Mexico
*Correspondence to carloschavezep@gmail.com
Disclosure: The authors have declared no conflicts of interest.
In the general preschool paediatric population, arrhythmias occur in 5% of individuals, with an increased incidence in adolescence.1 Treatment of rapid arrhythmias or tachyarrhythmias may include ablation of the cardiac structures.2,3
Catheter ablation is the possibility of producing an injury to the endocardium by administering energy through the catheter in a limited and controlled way to those parts of the cardiac tissue where tachycardias are initiated and/or maintained. It is performed through a catheter connected to an energy source, which is introduced through arterial or venous lines to the chambers of the heart.4 In recent years, different technological innovations have emerged, aimed at better understanding and identifying the substrate of arrhythmia, thus facilitating catheter navigation and reducing the need for fluoroscopy.5
OBJECTIVE
To describe the clinical characteristics of paediatric patients undergoing ablation with zero fluoroscopy in a paediatric hospital of the National Medical Center of the West (CMNO), Guadalajara, Mexico.
MATERIAL AND METHODS
In this descriptive and retrospective study, the clinical characteristics of 42 patients who were taken to arrhythmia ablation by zero fluoroscopy technique at the CMNO Mexican Institute of Social Security (IMSS)
paediatric hospital over 4 years, from June 2019–May 2023, were analysed.
RESULTS
This study included a total of 42 patients (55% male), with a median age of 13 years (range: 4–17 years), and a median weight of 49 kg (standard deviation: ±19.5 kg). Of the arrhythmias treated, supraventricular tachycardia accounted for 97.6% of cases and ventricular arrhythmias for 2.4%.
Of the supraventricular tachycardias, atrioventricular reentrant tachycardia accounted for 68.35%. There were 25 cases of Wolff-Parkinson-White syndrome, in which 28% (seven) were of the right lateral location, 24% (six) were right posteroseptal, 20% (five) left lateral, 12% (three) right anterolateral, 8% (two) right posterolateral, 4% (one) left posterolateral, and 4% (one) right oblique. Structural heart disease was present in 31% of the cases, the most frequent being Ebstein’s anomaly (41.7%).
The immediate success rate was 97.3%, with recurrence in the first 3 months of follow-up (5.4%). A Kaplan-Meier curve was performed, showing a success rate of 77.3% at 12 months of follow-up. No statistical significance was found in patients with congenital heart disease and recurrence, p=0.698, and with Fisher’s exact test, p=0.530.
CONCLUSION
Ablation of cardiac arrhythmias in children under 18 years of age without the use of fluoroscopy is an effective procedure, obtaining an immediate success rate of 97.3% in patients; 77.3% of patients are free of recurrence 1 year after treatment. There was no statistical significance for patients with congenital heart disease who might have recurrence.
References
1. Smith G, Clark JM. Elimination of fluoroscopy use in a pediatric electrophysiology laboratory utilizing three-dimensional mapping. Pacing Clin Electrophysiol. 2007;30(4):510-8.
2. Singh HR. ALARA in pediatric electrophysiology laboratory. Children (Basel). 2022;9(6):866.
3. Sommer P et al. Safety profile of near-zero fluoroscopy atrial fibrillation ablation with nonfluoroscopic catheter visualization: experience from 1000 consecutive procedures. Europace. 2018;20(12):1952-8.
4. Ergul Y et al. Electroanatomic mapping-guided catheter ablation of supraventricular tachycardia in children with ebstein's anomaly. Pediatr Cardiol. 2018;39(7):1445-52. [Epub ahead of print].
5. Pereira-López GI et al. Safety and effectiveness of radiofrequency ablation in pediatric patients. Fifteen years experience. REC: CardioClinics. 2021;56(3):190-6.
The following highlights showcase groundbreaking research in cardiology, spotlighting key abstracts presented at the European Society of Cardiology (ESC) Congress 2024. From the impact of air pollution and ultra-processed foods on cardiovascular outcomes, to the development of novel risk strategies, the selected highlights provide an overview of the latest advancements in the field.
Organ Perfusion Pressure as a Predictor of Cardiogenic Shock Mortality
RISK of in-hospital all-cause death is lower in patients with a higher organ perfusion pressure (OPP) when hospitalised for cardiogenic shock, according to a recent study conducted in Italy and presented at the ESC Congress 2024.
Cardiogenic shock has a high mortality rate and management of this condition remains a challenge. Therefore, developing a comprehensive risk assessment strategy for patients with cardiogenic shock is crucial to improving outcomes.
Cardiogenic shock has a high mortality rate and management of this condition remains a challenge
characteristic curve analysis (specificity 66.4%; sensitivity 53.8%; area under the curve: 0.61). An OPP greater than 59.5 mmHg was a significant predictor of reduced in-hospital all-cause mortality in patients with cardiogenic shock related to acutely decompensated heart failure (HR: 0.315; 95% CI: 0.151–0.660; p=0.002), but not in patients with cardiogenic shock related to acute myocardial infarction (HR: 0.628; 95% CI: 0.392–1.007; p=0.054). Higher OPP remained a significant predictor of in-hospital all-cause death after multivariable adjustment for significant clinical data, including age and Sequential Organ Failure Assessment score (HR: 0.984; 95% CI: 0.972–0.996; p=0.010).
Researchers evaluated the use of OPP as a predictor of outcomes in cardiogenic shock. The trial consisted of 316 patients with cardiogenic shock enrolled in the multicentre Altshock-2 registry. The mean age was 64 years and 20% of participants were female. OPP was calculated as mean arterial pressure minus central venous pressure. Among the cohort, the mean left ventricular ejection fraction: 24±10%, the mean arterial pressure was 71±16 mmHg; and the mean central venous pressure was 12±6 mmHg. Based on the calculation previously mentioned, mean OPP was 59.1±17.3 mmHg.
Whilst in-hospital all-cause death occurred in 37% patients, a univariable analysis revealed that higher OPP was significantly associated with a reduced risk of in-hospital all-cause mortality, both when analysed as a continuous variable (hazard ratio [HR]: 0.981 per mmHg; 95% CI: 0.969–0.993; p=0.003) and when dichotomised (HR: 0.522; 95% CI: 0.354–0.770; p=0.001) based on the optimal cut-off value of 59.5 mmHg identified through receiver operating
It was also determined that higher OPP was significantly associated with improved long-term overall survival (p<0.001).
Furthermore, higher OPP was not associated with worsening renal function 24 hours after the onset of cardiogenic shock, in-hospital length of stay, or the composite outcome of left ventricular assist device implantation or heart transplantation.
These findings highlight the importance of monitoring OPP, as it may serve as a valuable prognostic marker for improving long-term survival in patients with cardiogenic shock.
SGLT2 Inhibitors Reduce Ventricular Arrhythmias in Patients with Heart Failure
SODIUM-GLUCOSE cotransporter Type 2 inhibitors (SGLT2i) are a class of drugs primarily used to treat diabetes but have also demonstrated beneficial effects in heart failure patients; however, their impact on heart rhythm disorders, particularly atrial arrhythmias (AA) and ventricular arrhythmias (VA), remains unclear.
An abstract presented at the 2024 ESC Congress has detailed a retrospective multicentre study conducted by Carlos Minguito-Carazo, University Hospital of León, Spain, and colleagues. This study aimed to explore the effects of SGLT2i initiation on arrhythmic events in patients with heart failure with implantable cardiac defibrillators (ICD). The study analysed data from patients treated between 2015–2020, comparing arrhythmia occurrences 1 year before and 1 year after starting SGLT2i therapy.
A total of 195 patients, with a median age of 66.8 years and 18.5% being women, were included. These patients either had an ICD or a combined cardiac resynchronisation therapy device. The analysis focused on the prevalence of VAs, which include dangerous conditions like sustained ventricular tachycardia and ventricular fibrillation. Non-sustained ventricular tachycardia was also considered, though it is less clinically significant. AAs, specifically atrial fibrillation, were also monitored.
The study found a significant reduction in VA after the introduction of SGLT2i therapy
The study found a significant reduction in VA after the introduction of SGLT2i therapy. The percentage of patients experiencing any VA dropped from 52.3% to 30.3%. More clinically relevant arrhythmias, excluding non-sustained ventricular tachycardia, also significantly decreased from 21.5% to 8.7%.
Additionally, the number of arrhythmic episodes per patient declined, indicating a protective effect of SGLT2i against VAs.
Percentage of patients experiencing any VA dropped from
Arrhythmias, excluding non-sustained ventricular tachycardia, also significantly decreased from 52.3 % to 30.3 % 21.5 % to 8.7 %
However, this positive effect did not extend to AAs, the incidence of atrial fibrillation and its burden remained largely unchanged, with no statistically significant differences observed. While SGLT2i treatment appears to offer protection against life-threatening VAs, its effect on atrial rhythm disturbances remains limited. Nonetheless, this study highlights the potential of SGLT2i to reduce the incidence of dangerous VAs in patients with heart failure with ICDs, though their impact on AAs requires further investigation.
Noise Exposure Linked to Poorer 1-Year Survival After Myocardial Infraction
A LINK between environmental noise exposure and risk of myocardial infraction (MI) has been shown in a study presented at the ESC Congress 2024.
The observational, longitudinal study collected data from a French observatory (RICO) between 2004–2009. It aimed to investigate the association between environmental noise exposure and with prognosis after a MI and analyse the relationship between residential environmental noise exposure and 1-year prognosis after MI, with the outcome being defined by major adverse cardiovascular events (MACE).
Medical data was collected from 864 patients hospitalised for an acute MI and registered in the database between 1 January 2004, and 31 December 2008. Participants who survived at least 28 days post-MI were followed for 1 year to assess the incidence of MACE, which included cardiac death, re-hospitalisation for heart failure, recurrent MI, emergency revascularisation, stroke, and angina.
Environmental noise levels were measured both daily (LAeq,24h) and at night (Lnight), and the annual averages were considered for analysis. The study also accounted for exposure to outdoor air pollutants, specifically nitrogen dioxide (NO2) and particulate matter (PM10), within the 30 days preceding a MACE.
Results showed that 29% of the patients experienced a MACE during the 1-year follow-up, with cardiac death being the most frequent outcome, occurring in 32% of these cases. One of the key findings was that for every 10 dB(A) increase in Lnight, the hazard ratio for MACE increased by 25%, even after adjusting for air pollutants and other confounding factors. This association was particularly pronounced among older patients and varied by gender.
The study authors noted that this is the first time that a significant link was revealed between nighttime noise exposure and
For every 10 dB(A) increase in Lnight, the hazard ratio for MACE increased by 25 %
1-year survival prognosis after a first MI. They also emphasised that if confirmed by larger, prospective studied, these results could lead to new environment-based secondary prevention strategies for patients recovering from MI.
The study’s lead author and researcher Mirabelle Plomb, University of Besancon, France, concluded that the findings highlight the need for consideration on environmental noise as a serious factor in the recovery of patients with heart attack. Reducing noise pollution, especially at night, might be a vital step in improving outcomes for these patients.
Arterial Stiffness Predicts Cardiovascular Events in Post-Heart Attack Patients
A STUDY presented at the ESC Congress 2024 revealed that arterial stiffness, measured by pulse wave velocity (PWV) and augmentation index (Aix), is a strong predictor of major adverse cardiovascular events (MACE) in patients that have suffered a heart attack.
Patients with elevated arterial stiffness were found to have a significantly lower event-free survival rate
The study followed 114 post-infarct patients (89 male with an average age of 62.5 years) over a median period of 16.2 years and aimed to evaluate the prognostic relevance of PWV and Aix. Both measures of arterial stiffness were calculated using the oscillometric based pulse wave analysis method (Arteriograph), which sought to determine the optimal PWV and Aix cut-off values for predicting MACE. This included outcomes such as all-cause death, non-fatal heart attack, ischaemic stroke, hospitalisation for heart failure, and coronary revascularisation.
The results revealed a significant correlation between PWV and Aix values, with 140 MACE events occurring in the 16.2 years of follow-up period. The study established optimised cut-off values for predicting MACE: PWV at 9.83 m/s and Aix at 34.8%.
Patients with elevated arterial stiffness, were found to have a significantly lower event-free survival rate as indicated by higher PWV and Aix values, which was demonstrated by a Kaplan-Meier analysis. A multivariate cox regression analysis confirmed PWV and Aix as an independent predictor of MACE.
The findings emphasise the importance of measuring arterial stiffness in post-heart attack patients to improve individual risk stratification. Elevated PWV, in particular, emerged as a key marker for predicting future adverse cardiovascular events, highlighting its clinical relevance in managing very high-risk cardiovascular patients.
Ultra-Processed Foods Linked to Cardiometabolic Multimorbidity Risk
A 20-YEAR observational study conducted in Attica, Greece, presented at the ESC Congress 2024 has found a significant association between the consumption of ultra-processed foods (UPF) and an increased risk of cardiometabolic multimorbidity, defined as the co-occurrence of Type 2 diabetes and cardiovascular disease (CVD).
Researchers sought to explore the effects of UPF intake on cardiometabolic health in the Mediterranean region, where traditional diets are often considered protective. The study recruited 3,042 men and women free of cardiovascular disease between 2001–2002. Participants' diets were assessed using a validated food frequency questionnaire, with UPF intake categorised using the NOVA classification system. UPFs were further classified into subgroups, including bread and cereals, sweets and desserts, artificially sweetened beverages, spreads and sauces, processed meats, and savoury snacks.
cases of cardiometabolic multimorbidity were recorded in total over the 20-year period
Over the 20-year period, a total of 231 cases of cardiometabolic multimorbidity were recorded. Participants reported a median UPF consumption of 26.6 servings per week, contributing approximately 40% of their total daily energy intake.
The findings revealed a clear doseresponse relationship between UPF consumption and cardiometabolic multimorbidity. As UPF intake increased, so did the risk of developing both diabetes and CVD. Individuals in the highest tertile of UPF consumption (44.7 servings per week) had a 14.7% incidence of multimorbidity, compared to 9.5% in the lowest tertile (11.8 servings per week). After adjusting for various factors, each standard deviation increase in UPF consumption was associated with a 26% higher risk of multimorbidity (odds ratio [OR]: 1.26; 95% CI: 1.17–1.85).
Notably, specific subgroups of UPFs had varying effects. Consumption of artificially sweetened beverages (OR: 1.06; 95% CI: 1.02–1.13) and spreads and sauces (OR: 1.06; 95% CI: 1.02–1.13) was linked to a higher risk of multimorbidity, while an inverse association was found for breads and cereals (OR: 0.95; 95% CI: 0.92–0.98).
The researchers emphasised the need to re-evaluate the impact of foods based on their nutritional roles rather than solely their processing levels, particularly within specific cultural and dietary contexts.
Assessing Albumin-Bilirubin Score in Patients with Chronic Heart Failure
LIVER dysfunction, one of the most common comorbidities, is known to be associated with worse clinical outcomes in patients with chronic heart failure (CHF).
The albumin-bilirubin (ALBI) score was recently developed in order to assess liver function in an effective and convenient way; however, the prognostic significance of this score is yet to be clarified. Recent research presented at the ESC Congress 2024 aimed to shed light on the significance, hoping to improve assessment of liver function for clinicians in the future.
In order to investigate the clinical significance of the ALBI score on outcome prediction in patients with CHF, the Japanbased team examined 1,567 symptomatic CHF patients (median age: 74; interquartile range [IQR]: 64–82 years; mean left ventricular ejection fraction: 49±15.9%; median N-terminal pro-brain natriuretic peptide: 801 [IQR: 372–1,820] pg/mL) in a multicentre registry with 27 Japanese sites between January–December 2023. ALBI scores were calculated, and patients were divided into three groups according to the ALBI grade: ALBI score ≤-2.60 (Grade 1; n=691), ALBI score >-2.60 and ≤-1.39 (Grade 2; n=864), ALBI score >-1.39 (Grade 3; n=12). The team’s primary outcome of interest was a composite of all-cause death and hospitalisation due to worsening heart failure.
The researchers found that during a median follow-up period of 537 (IQR: 285–701) days, the primary outcome occurred in 267 patients (17%). Higher ALBI scores were significantly related to increased incidence of the primary outcome (P for trend <0.001). Multivariable Cox regressions showed that a higher ALBI score was independently associated with higher risk of the primary outcome (hazard ratio: 2.8; 95% CI: 2.08–3.77; P<0.001), including after adjustment for the Meta‐Analysis Global Group in Chronic (MAGGIC) heart failure risk score as an established risk prediction
The team’s primary outcome was a composite of all-cause death and hospitalisation due to worsening heart failure
model, N-terminal pro-brain natriuretic peptide, aspartate aminotransferase, and platelet counts. Addition of the ALBI score to the MAGGIC score significantly increased c-index from 0.70 (95% CI: 0.66–0.74) to 0.73 (95% CI: 0.69–0.76) (P<0.001). The net reclassification improvement afforded by the ALBI score was 26% for the primary outcome (P<0.001).
The team concluded that liver dysfunction assessed by the ALBI score was independently associated with worse clinical outcomes in CHF. Additionally, using this score in tandem with the existing risk prediction models increased the ability to predict outcomes. This research highlights the potential of the ALBI score in clinical practice when assessing patients with CHF.
Novel Risk Score Predicts Mortality in Patients with Heart Failure
FRAILTY or congestion in patients with heart failure (HF) is strongly associated with clinical outcomes. This research, presented at the ESC Congress 2024, aimed to develop a risk prediction model for all-cause mortality in heart failure patients with preserved ejection fraction (HFpEF) by incorporating frailty and congestion assessments. These assessments are often overlooked in current models.
The researchers analysed data from 1,212 patients (81±9 years; 55% female) enrolled in the PURSUIT-HFpEF study, a multicentre registry tracking in patients with HFpEF hospitalised for acute decompensation. Clinical Frailty Scale (CFS), blood test results, and estimated plasma volume status (ePVS), which was calculated using the Duarte formula, were evaluated. Patients were followed for a median of 713 days to record all-cause mortality.
The cohort was split into derivation and validation groups at a 2:1 ratio. A stepwise model selection based on the Bayesian Information Criterion (BIC) was applied to 51 clinical parameters, including CFS and ePVS, to identify independent predictors of mortality. The resulting model, which incorporated age, sex, CFS, NT-proBNP, and ePVS, was tested for accuracy using time-dependent receiver operating characteristic curves.
During follow-up, all-cause death was observed in 315 patients (25.9%). Age, sex, CFS, NT-proBNP, and ePVS were selected as independent predictors of all-cause death. The risk model performed well, with an area under the curve of 0.79 in the derivation cohort and 0.70 in the validation cohort for predicting 1-year mortality. A risk score cut-off value of 6 provided 74.9% sensitivity and 74.4% specificity.
In conclusion, the novel model incorporating frailty (CFS) and congestion (ePVS) effectively predicted mortality in patients with HFpEF and could be a useful tool for risk stratification in clinical practice.
The novel model incorporating frailty (CFS) and congestion (ePVS) effectively predicted mortality
A risk score cut-off value of 6 provided
74.9 % sensitivity and
74.4 % specificity.
Congress Interviews
Experts in cardiology discuss advancements in the field, highlights from the European Society of Cardiology (ESC) 2024 Congress, and more. Conversations are centred around current topics: management of atrial fibrillation, digital cardiology, and acute coronary syndromes. Plus, the new ESC President, Thomas Lüscher, reveals what you can expect from the ESC in the coming years.
Featuring: Melanie Gunawardene, Lis Neubeck, and Thomas Lüscher.
Following your medical training, what inspired you to pursue a career in clinical electrophysiology, with a particular focus on atrial fibrillation (AF)?
It really came down to the people who inspired me and who I met along the way. I was a very young student when I started doing my thesis as part of cardiology, and I had really great mentors and people around me who were passionate, supportive, engaging, and thought-provoking. That really fuelled and motivated me to become a person like them. That was around the time I was already starting to do some clinical research on AF. I stayed with the medical group after finishing my thesis and continued to work with them on a few more studies. Then I went on to work at a university hospital, where I worked on my first project on AF, and one thing led to another. I just kept going from there and never changed from that field. I was hooked from very early on.
Q2
During the recent 'Great Debates' session at European Society of Cardiology (ESC) Congress 2024, you presented on ‘Persistent atrial fibrillation: Ablation First vs. Antiarrhythmic Medication’. Could you summarise the key takeaway from your discussion?
I was pleased to present a commentary and also listen to strong arguments from both sides. I think what it comes down to is that we have good rhythm control strategies in place for AF. The question is: do they also apply for persistent AF? Of course, when we have patients who are highly symptomatic or suffering from heart failure, we know that we need to apply rhythm control strategies. AF ablation is superior in terms of AF burden reduction, symptom relief, quality of life, and hospitalisations. Also, it doesn’t have the complication rate you might expect, even though it’s an invasive procedure. That aside, prescribing antiarrhythmic
Melanie Gunawardene
drugs can be difficult because they’re not very effective. Clinical trials show that they are much less effective compared to catheter ablation, but then everybody says ablation is invasive and has complications. However, drugs also have complications, which are not small and can’t be ignored. So, many patients aren’t able to take these drugs. There has just been a study that looked at patients with new-onset AF, and of those that received antiarrhythmic drugs, they had a two-fold increase in syncope and a five-fold increased risk of pacemaker implantation. This really shows that antiarrhythmic drugs are associated with poor outcomes and can cause harm to our patients. So why should we use them if they’re not effective? However, we still lack clear evidence that firstline ablation is superior for persistent AF over antiarrhythmic drugs.
We should apply effective therapies earlier and find patients before symptoms become persistent. Usually,
there’s a natural course of the disease that starts with paroxysmal episodes, which progress and become persistent. But some patients present with all types of symptoms the first time they’re diagnosed. It would be best to get them as soon as possible to start treatment. To gain more answers to this topic, we are currently conducting a multicentre, randomized trial in Germany in which we investigate immediate catheter ablation with the cryoballoon versus antiarrhythmic drugs in patients presenting with new-onset AF to the emergency department (EMERGE-Cryo study).
Q3
Reflecting on the past year, what would you identify as the most significant breakthrough or piece of research in the management of AF?
I think in the past year, what has really changed was the CASTLE-HTx study by Christian Sohns from Germany. The study randomised patients with AF and heart failure, and
those patients with heart failure were being evaluated for heart transplantation. So, you could say it was a novel, sicker cohort with advanced stages of heart failure. They randomised those patients to ablation or antiarrhythmic drugs, and what they found is that catheter ablation prevented death, heart transplantation, and implantation of left ventricular assist devices and was superior to antiarrhythmic drugs. Yesterday, they presented the 2-year outcome of the study, and it showed that the benefit continued. Before this study, we were all reluctant and unsure if we should subject these very sick patients to ablation because we thought AF was just a part of that very progressed disease and late-stage heart failure. But we were shown that even in the sickest patients, if we treat them and maintain sinus rhythm, we can save those patients. I think it is really important that sinus rhythm is a pillar of heart failure treatment. This is something we have to transfer to all cardiologists
out there. For me, this was the most interesting research presented at the ESC Congress this year.
I think it is really important that sinus rhythm is a pillar of heart failure treatment
Q4 What were the main conclusions drawn in your recent publication, entitled ‘Contemporary catheter ablation of complex atrial tachycardias after prior atrial fibrillation ablation: pulsed field vs. radiofrequency current energy ablation guided by high-density mapping’?
The study aims to answer the question of, when patients come back with the recurrence of atrial tachycardia and often have a complex substrate, do we need to apply a new energy source? Pulsed field ablation gives us a new technology, and preclinical studies have shown that lesions can be created with pulsed ablation in scarred or prior ablated myocardium. It’s more homogeneous and goes through fibrosis, whereas radiofrequency might not do that. So, we thought we would compare both energy sources in the study. However, we found that it was not better in the 1-year outcome. We had high rates of AF termination, but we did not achieve the outcome we thought we would. The conventional approach was better. This might be due to the type of catheter we
used and the energy delivery itself. But I’m still hopeful that with different catheter designs, we can achieve those transmural effects and better outcomes in these patients.
Q5
In an upcoming session at ESC, you will discuss ‘Weight Reduction to Improve Outcomes After Atrial Fibrillation Ablation in Patients with Obesity’. With obesity being a major theme at this year's Congress, how do you see the topic of obesity shaping emerging therapeutic options and the future of cardiovascular care?
This is a very important issue. Yesterday, the new guidelines for AF were published, and there is a new acronym called AFCARE, which includes comorbidities. We know that we want to achieve sinus rhythm for our patients, but there are some comorbidities that interfere and lead to AF occurrence. What we know is that weight reduction itself, even if we don’t apply any other therapy, reverses and reduces AF.
So, just by making lifestyle changes, we can reach a goal that allows us to maybe even avoid invasive therapy that otherwise could cause complications. And if those patients undergo AF ablation, outcomes are much better if they achieve and maintain weight loss. So, just by losing weight and exercising, you can do a whole lot. And I’m not talking about mild effects, but very significant ones. This topic is very important in cardiovascular medicine, not just for AF but also because weight reduction influences all cardiovascular diseases, and we can prevent them from occurring or help patients who already have these diseases.
Regarding emerging therapeutic options, while weight reduction is a great thing, it absolutely depends on patient compliance and motivation. Sometimes it is difficult for a patient to actually do, and it’s hard to explain clinical data to a person who comes into your practice, to understand what matters to them without scaring them away.
Q6
What we know is that weight reduction itself, even if we don’t apply
any
other therapy, reverses and reduces AF
Personalised medicine is another central theme at this year’s Congress. How do you envision the role of personalised medicine evolving in cardiology, particularly in the management of AF?
I think it’s something we cannot avoid in personalised medicine because we do studies where we randomise patients and look for an outcome, but it’s
never about an individual person, it’s always a cohort of patients. However, within that cohort, people have different baseline characteristics. We have more and more information before a procedure: electrocardiograms, echocardiograms, and clinical history, and it’s very hard to put this all together. This is also where I see AI being helpful. It can give us a better understanding by putting all this information on different levels together, especially for patients who are limited in our success for rhythm control. We need better strategies to achieve
better efficacy, so this could be a way forward to create personalised approaches.
Q7
Which sessions would you highly recommend for all participants to attend at the ESC Congress 2024?
Definitely the guideline sessions, as I think it is very important for physicians to know the current guidelines in Europe, and the highlight sessions because we also need to know what’s new, what’s happening, and where the field is headed.
Lis Neubeck
Professor of Nursing and Head of Cardiovascular Health, School of Health and Social Care, Edinburgh Napier University, UK
How can we predict and appropriately use the technology for the right person at the right time?
Can you share how your career evolved from starting as a cardiac nurse to becoming the Past President of the Association of Cardiovascular Nurses and Allied Professionals (ACNAP) of the European Society of Cardiology (ESC)?
I think it's a long journey, but being a volunteer for the ESC has been an incredibly important part of my career development, and I'm very grateful for the opportunities that working within the ESC has given me. I started as part of the programme committee for the annual Congress that ACNAP runs and then moved on to becoming the secretary-treasurer, and then the journey of 6 years of being President, Elect President, and now past President. But I continue in my role as ESC Patient Forum Lead. I will continue to be engaged with the ESC, and I recommend it to all of my nursing colleagues to be part of this really important organisation. It's a great opportunity to connect with your networks across Europe and to make lifelong friends.
Q2
Your research delves into innovative approaches for secondary prevention of cardiovascular disease. Could you share some of the most promising advancements in this area and their potential impact on patient care?
I've been interested in alternative models to secondary prevention for a very long time. I'm very aware that not everybody gets access to cardiac rehabilitation, so I've
been looking at digital models. My PhD was about increasing access to cardiac rehab, and we've been talking about the role of technology in supporting patients for a long time, but really it took off during the COVID-19 pandemic. We saw a change in the way people approached this. Rather than being a little bit of a fringe offering, it became a mainstream offer to offer people alternatives in digital health. I think now we've reached a time where we also need to consider the implications of AI large language models. How can we predict and appropriately use the technology for the right person at the right time? I'm really excited to see how that evolves over the coming years.
Q3 The Congress spotlight this year was personalised care, so I imagine you've seen a lot of that in the sessions you've attended.
I have, yes, and because I'm ESC Patient Form Lead, I've been engaged with the patients throughout the entire Congress. We have them involved in around 24 sessions. They've been a part of all of the new guidelines that have been released, and we're very focused and very keen to ensure that there's a golden thread of that patient voice woven throughout the whole of the ESC so that we can ensure that we prepare information, guidelines, and scientific documents that focus on patient centred care with this idea of tailoring it to the individual and recognising the individual needs within cardiovascular care.
Q4 As the ESC Patient Forum Lead, what are the primary goals of this initiative, and how can the ESC leverage the Patient Forum to drive healthcare policy changes at both national and EU levels?
Yes, absolutely. I mentioned the patient’s voice as the golden thread earlier. In that respect, we're inward facing into the ESC, trying to make sure that this idea of patient-centredness underpins everything we do. The ESC has made it its strategic goal to focus on person-centred care, looking at how patients can be engaged in a range of activities.
The ESC has made it its strategic goal to focus on personcentred care
But I think we've also been involved in advocacy activities. We recently attended an advocacy meeting where patients presented their stories, and sometimes that story, that key message, reaches out more to the hearts of politicians than all the statistics and facts we can bring. So, I think having the patients involved is absolutely critical in raising awareness about the elements of cardiovascular disease that we still need to tackle.
Q5 Do you think the awareness of cardiovascular disease has increased over the past few years, since COVID-19?
I'd love to say yes. I'm particularly interested in women's health, and I know that women do not think cardiovascular disease is likely going to cause them long-term problems. So, if you ask women what they fear, they fear breast cancer, but actually, they have a much lower chance of developing breast cancer than cardiovascular disease. For me, I think there's still some communication work to be done about the risk of cardiovascular disease, and I hope that we will be able to do that through the patient form, the ESC, and our advocacy work.
Q6 What emerging trends in cardiac nursing are you currently most excited about?
I think I have to say digital health because I think that's a key component, but I think we need to recognise more about the interdisciplinary team working together. We shouldn't work in silos, not just within cardiovascular care. We should be working across the spectrum of conditions that affect patients. Most patients are multimorbid, so we need to work together. We need to break down some of those barriers, and we need to provide training and education on how to incorporate digital tools, including AI, into our nursing development programmes. For me, I think that is really
a key challenge for us as educators because some of us have not had the education in this space.
We've learnt on the job, but we potentially could also do with upskilling. Certainly, there are many people who are frightened of the way technology might potentially replace them, but I don't see that happening. I think there's more than enough work to go around and share. We have developed a core curriculum for cardiovascular nurses and allied professionals, which is an introductory level curriculum that aims to bring everybody across Europe up to a standard, but we would like to develop advanced curricula, and I see the role of nurses and allied professionals really evolving, and us having more opportunity to lead and develop these changes.
Q7 What are your future aspirations, both in your research and in your roles within professional organisations like the ESC and ACNAP?
I guess within ACNAP, I will continue to work on next year's programme. I'm leading other projects for ACNAP, including a handbook on cardiovascular nursing and allied professionals, which will complement the curriculum. We're developing certification programmes and exams. I think there are a lot of opportunities for me, ongoing within ACNAP, and for people who are coming along behind me, or leading the way in new and different
pathways. I also think there is more opportunity to bring that patient voice. I think ACNAP probably has a very strong opportunity to raise awareness of the patient's voice. We will be appointing a patient to our board for the first time within the ACNAP. So ACNAP will be having a patient voice, and I would like to see that replicated in other associations.
We need to grow the patient forum because the busier we become, the more opportunities there are for us to do more, and the more the ESC becomes aware of the value of that voice, the more demand there is for us to be engaged in everything. So, I think there are a lot of opportunities. There are always challenges, but I'm excited about those because I think it gives us a chance to try to make a change. And because I've
now been engaged with the ESC for probably about 16 or 17 years, I've seen a huge change over time, and I hope that change will continue, and I'll be able to look back, maybe in 10 or 15 years, when I'm thinking about retiring, to say we can see a difference.
Q8
What are some of the most anticipated sessions or highlights featured in this year’s Congress?
I'm very excited about the new guidelines presented at Congress, which are always incredibly important and exciting. I'm also really pleased to see the emphasis on patientcentredness coming out in the guidelines; that is always a highlight. I do think our digital offering is becoming greater and greater, and I will be participating in a session on
chatbots and how we could use them more effectively. I think the opportunities are endless here, and I hope we can move in a way that is commensurate with the speed at which technology is advancing because that's always a challenge in research. So is the question: how do we evaluate something? By the time we get the funding and we go ahead and try to develop it, it's already outmoded, so we need to think in a more agile way about how we evaluate technology.
I think some of these things are just unbelievably exciting. Large language models, AI–the potential is absolutely enormous, and I'm really excited to see many of the presentations that will be available online for people to watch back. I think it's a wonderful Congress for those opportunities.
Thomas Lüscher
Director
of Research,
Education, and Development and Consulting Cardiologist, Royal Brompton & Harefield Hospital Trust, UK; Professor of Cardiology, King’s College London, UK; President, European Society of Cardiology (ESC)
Congratulations on your recent election as President of the European Society of Cardiology (ESC). What are your main priorities for the organisation during your term, and how do you plan to address key issues facing European and global cardiology?
The strategy that is most important to me is digital cardiology, involving, of course, digital health in general, but in particular artificial intelligence and machine learning (AI/ML). I am convinced that this will markedly change our field, and medicine at large. I just wrote a review article covering this field;1 AI/ML has a lot of potential in imaging, pathology, biopsies, face and voice recognition for diagnosis, and algorithms for diagnosis and risk prediction as a basis for personalised medicine. This is certainly one aspect, but another priority is that we want to be more transparent about the society. We will have an induction day where all the newly elected volunteers will come to the European Heart House to learn about the governance, legal, and budgetary aspects of the organisation and get to know the staff. We have more than 230 employees, so our volunteers have to understand who does what. Further, they will learn what they can do in a specific position and decide when they have to refer to the leadership in their projects. Moreover, it is essential to understand the finances and budgeting of the society. Finally, we also want to
include more societies that are a bit at the periphery of the ESC, such as Northern Africa and Middle Eastern National Cardiac Societies, as well as those of the East and Eurasia. Indeed, we would like to include them more in the future and hear what their needs and expectations are. Of note, we are a global society, we have 58 national cardiac societies and 47 affiliated cardiac societies. At our recent Annual Congress in London at the end of August, we had participants from over 80 countries. So, this is a very important strategy, to be global, not just with the journals that have already succeeded a lot at this, but with the Congress and our interactions with these parts of the world.
Q2
With such a strong focus on AI and machine learning, are there areas within cardiology where you think AI might not be as effective?
Well, it's a neuronal network, and our brain is also a neural network. At the moment, AI is very good in terms of remembering everything because the data storage is much bigger than our brain, it can combine things very well, and it has enormous statistical and mathematical skills. Interestingly, AI systems could even learn empathy. The mirror neurons that were discovered about 30 years ago by neuroscientists in Parma, Italy, are the basis of empathy and, in principle, you could program a neuronal network accordingly as well, at least seems possible.
Whether it can actually produce new ideas is, of course, a big question, maybe not. Manual skills are still very important in medicine. Robotics are not that advanced at the moment, maybe in another decade or two they will be comparable to current operators, but we’re still a bit better at manual skills, ideas, and creativity. However, for any algorithm, we have to assure that they are developed on a huge database, on good, solid data, and verified independently, ideally in another country or another area, so that we're sure that it is good for use in medicine.
Q3You have a broad clinical and research scope in prevention, coronary heart disease, heart failure, vascular disease, and percutaneous interventions, with over 840 original research articles and more than 200 reviews and book chapters. Over the years, how has your focus shifted, and what areas of research interest you most currently?
I started in basic science with endothelial biology, which at the time was a very, very hot topic and only pursued by a handful of scientists in the world. More recently, due to my professional activity as an interventional cardiologist, I have been interested in acute coronary syndromes. Currently, we work a lot on acute coronary syndromes, not only on how to better diagnose them but also on how to predict outcomes.
In particular, cardiogenic shock is a huge unmet medical need.
Cardiogenic shock is a huge unmet medical need
We have discovered a new pathway that possibly could lend itself to a trial, which we're currently discussing. I am also looking at inflammation as a cause of plaque instability and rupture. Thanks to my current job in the UK, I have access to these huge registries that are quite unique. They're not perfect, but they're huge. Even though the data set is sometimes a little bit like a Swiss cheese, it still has very important scientific power because of its size. Usually, we look at registries with more than a million patients and analyse part of them, and so that is a very, very exciting new field. I created a large biobank in Switzerland of patients with acute coronary syndromes, and there we have discovered a couple of new markers, some of which are potentially involved in the disease process itself, and potentially also targets for new therapeutic strategies. Another topic that I'm very interested in is resilience. It is interesting that even if you smoke, if you have a high low-density lipoprotein, or a high blood pressure, it is not certain that you will get cancer, an infarction,
or a stroke. In fact, it's usually only half of those who have the risk factor. So, the interesting question is, why are some protected from the untoward effects, let's say of low-density lipoprotein cholesterol?
We have looked at blood vessels that are resilient to atherosclerosis because it affects mainly the coronary arteries and the periphery arteries, but the mammary artery that runs in the inside of the chest wall is completely protected. We have sequenced this mammary artery and compared it to the coronary artery and are now pursuing pathways and factors in arteries that differ in patients who are protected from atherosclerosis despite the presence of risk factors. I think that's sort of the backside of the coin.
Q4
The Zurich Heart House, which you founded, is a major centre for cardiology research and education in Europe. How has the foundation's work influenced the broader cardiology community, and what future initiatives have been planned?
Actually, I founded the Zurich Heart House 30 years ago this year. We trained more than 150 research fellows from around the world, and about 30 of those now have academic positions in other institutions, professorships, chairs, or are leading cardiology departments in regional hospitals. We're very proud that we have been able to foster the careers of many promising
young cardiologists. But not just cardiologists, we also trained ophthalmologists, because the blood vessels in the eye were of interest; nephrologists; and even one gynaecologist, and that's a major achievement. Our education centre did a lot of post-graduate courses, and we have trained more than 300 young cardiologists in heart failure management through our post-graduate courses, who are now leading many heart failure units around the world. Of course, we continue to train and support, not in large congresses like the ESC, but in smaller, focused master courses. We train physicians in different countries. We have done that in Georgia, Romania, Mexico, Portugal, and India, and it's really quite enchanting to meet these people and to make them happy that they have learnt something. My motivation for fostering young cardiologists is because you cannot win without young people. You need bright young people around you, and so this is my advice to any young person: together, you can advance the field This is really fulfilling. Humans don't work for money alone, they work also to have fun, and to have the sense of doing something important in their lives. At the end of your career, it’s
more important what came out of your collaborations, and how much you could foster the careers of others than to publish another paper under your name.
Q5You first attended the ESC Congress in 1988. Over the years, how has the ESC evolved, and how do you see the ESC continuing to adapt and lead in the future?
Well, it's a fantastic story. I have written an article about this, it's called ‘From a club of friends to an institution: past successes and future challenges for the European Society of Cardiology’.2 They founded the ESC 74 years ago, so next year we will have the 75th anniversary. It’s a privilege for me to celebrate that. The first Congress was led by John Parkinson, who described the Wolff–Parkinson–White syndrome, an inherited arrhythmia disorder. At the time, it was a small congress, and then they decided to do it every year. Initially, all the sceptics said that this would be crazy, but the annual congress became more and more successful. Then, in 1980, they started their own journal, and this has become, over the years, the number one journal in cardiovascular medicine. Then, they realised that
they needed staff and a house to accommodate these collaborators, and so in Sophia Antipolis, France, they built the European Heart House. This has grown a lot, from a few dozen employees to currently 230 employees who cover different aspects of our activities, whether it’s the journals, guidelines, education programmes, or the development of projects, which are financed by the congresses (currently 10 in number), the income from the 17 ESC journals, other activities, and also in collaboration with industry. We started an advocacy office at the European level, and we certainly hope that this will eventually lead us to the possibility of having a cardiovascular health plan supported by the EU to foster research and other aspects of cardiovascular medicine. Then the journal family grew, and we now have 17 journals, covering the entire cardiovascular field. We started a textbook on cardiovascular medicine, which will now be in its fourth edition. We’ve designed it, and then we'll also have a cut-down version for the young cardiologists who want to pass the ESC European Exam in Core Cardiology. We have close to 1,000 young colleagues who try
We would like to involve, as I mentioned earlier, more countries that need support in education and guidelines in their own cardiovascular health care systems
to pass this exam every year. The ESC also wants to be more of a global player. This was achieved for the journals since I took over the ESC European Heart Journal in 2009, and the Congress is now global, but we would like to involve, as I mentioned earlier, more countries that need support in education and guidelines in their own cardiovascular health care systems.
Q6 Are there specific strategies or collaborations you're looking to implement to ensure this collaboration with other countries?
First of all, we have large registries. One of them is called EuroHeart Registry, where the idea is to have ongoing registries, starting now, in the UK, Scandinavia, the Baltic states, places that already have registries that can be used to get continuous and representative insight on what's going on in clinical practice. We’ve expanded it to Romania, Hungary, and Portugal, where there are existing registries in some areas. The vision is that
eventually, we can cover all of the ESC member states, and then we will have the ability to nest pragmatic trials into this running registry. So, this has to grow over time. It's expensive, and we need support from the EU, our industry partners, and foundations to provide continuous insight into the quality of care, and to provide the opportunity to test new interventions in terms of what they can achieve in the European cardiovascular community.
Q7 Reflecting on this year's ESC Congress, what do you consider to be the most significant piece of research or the most impactful discussion?
Well, the problem was, of course, that I had so many meetings, so I was not able to listen to everything that I wanted to. But what is worth mentioning is that we had 12 hotline sessions, each of them with four to five presentations. So, more than 50 hotlines in total, many of which were published. So, it
was extremely successful in providing the newest information to the audience. There were also a lot of good educational sessions for practicing clinicians. And, not to forget, the awards ceremony for young cardiologists across 11 different topics, ranging from imaging to intervention, from prevention to heart failure, and alike. This was very exciting for them, their colleagues, and their families.
Q8 What are some of the most valuable lessons you’ve learned from your extensive career in cardiology that you believe will guide your presidency at the ESC?
Well, working in the ESC is a fantastic experience. You meet the smartest and brightest people in your community, it’s extremely stimulating, and we learn from each other. When fantastic brains are assembled in these committees, on the board, and so forth, it is really a very exciting experience.
References
1. Lüscher TF et al. Artificial intelligence in cardiovascular medicine: clinical applications. Eur Heart J. 2024;DOI:10.1093/ eurheartj/ehae465.
2. Lüscher TF. From a club of friends to an institution: past successes and future challenges for the European Society of Cardiology. Eur Heart J. 2024:ehae505. (Epub ahead of print)
Advancing the Understanding of Hypertrophic Cardiomyopathy Towards Improved Patient Outcomes: Interview with Two Key Opinion Leaders
Interviewees:
Gerald Carr-White,1 Michelle Michels2
1. Deputy Medical Director of the Cardiovascular, Respiratory and Critical Care Unit, Guy’s and St Thomas’ NHS Foundation Trust, London, UK
2. Head of the Center of Expertise for Inherited Cardiovascular Disease, Erasmus University Medical Centre, Rotterdam, the Netherlands
Disclosure: Carr-White has no disclosures. Michels has received a research grant from Bristol Myers Squibb; and consultancy and speaker fees from Bristol Myers Squibb, Cytokinetics, and Alnylam.
Acknowledgements: Medical writing assistance was provided by Juliet George, Chester, UK.
Disclaimer: The content of the article was authored independently and does not reflect the opinions of Cytokinetics.
Support: The publication of this article was supported by an educational grant from Cytokinetics.
Interview Summary
Hypertrophic cardiomyopathy (HCM) is an inherited disorder that may cause disabling and potentially life-threatening symptoms related to thickening of the left ventricular wall. The impact of pathophysiological research on the treatment of HCM was central to the discussions with Gerald Carr-White, Deputy Medical Director of the Cardiovascular, Respiratory and Critical Care Unit at Guy’s and St Thomas’ NHS Foundation Trust, London, UK; and Michelle Michels, Head of the Center of Expertise for Inherited Cardiovascular Disease at the Erasmus University Medical Centre, Rotterdam, the Netherlands, during interviews conducted for the European Medical Journal (EMJ) in May and August 2024. The experts provided an overview of current options for the symptomatic treatment of HCM, including the advent of targeted therapies, cardiac myosin inhibitors (CMI), for the obstructive form of the condition. They explored the advantages and limitations of current therapies and shared their informed opinions on how precision medicine and genetic therapies have the potential to transform patient care. While highlighting the treatment of non-obstructive disease as a significant unmet need, Carr-White and Michels expressed optimism for the future of HCM treatment, driven by an understanding of the underlying pathophysiology and guided by increasing clinical and real-world evidence.
INTRODUCTION
HCM is an inherited heart condition characterised by a thickening of the left ventricular wall that may be obstructive (oHCM) or non-obstructive (nHCM) to blood flow from the heart. The effects of HCM can range from mild or even asymptomatic, to severely disabling with risk of sudden cardiac death (SCD). However, until recently, pharmacological treatment of HCM was based solely on existing therapies for controlling arrhythmia and blood pressure, such as beta blockers and calcium channel blockers. In this interview article, cardiology specialists, Michelle Michels and Gerald Carr-White, share their views on how advances in pathophysiological research have led to targeted pharmacotherapies developed specifically for HCM, shaping the future of patient care.
Michels provided an overview of the condition: “HCM is characterised by left ventricular hypertrophy that is not explained by known loading conditions such as hypertension or aortic valve disease. In adults, HCM is defined by an increased wall thickness of ≥15 mm, and most patients will have some kind of obstruction [denoted by] a pressure gradient in the left ventricular outflow tract (LVOT) of ≥30 mmHg.” Both experts emphasised the importance of actively searching for an obstruction by performing a Valsalva manoeuvre and/or exercise during the assessment. “If you use provocation during your echocardiography, about 75% of patients will have some form of obstruction,” Michels noted, with the remaining patients designated as having nHCM.
Discussing the aetiology of HCM, Michels explained, “We’re able to identify likely pathogenic or pathogenic gene variants in about half the patients, and most of these are in the sarcomere (the smallest contractile unit of the heart). However, there are also cases of HCM without an identified gene variant.” Carr-White concurred, stating, “Our genetic understanding is changing. Quite a lot of patients with HCM have a monogenic ‘spelling mistake’ in one of the genes that tend to pass through families in an autosomal dominant pattern;
but we’re also starting to see some cases without the common HCM genes, so it could be more of a polygenic inheritance with several different genes interacting with environmental factors.”
Carr-White also noted that HCM is also more common than generally realised: “Most people with HCM probably remain undiagnosed, but we think about one in 300 or 400 people have HCM.” Michels added, “If you also take into account the prevalence of unaffected gene carriers, so those who carry a likely pathogenic or pathogenic gene but without hypertrophy, it might be as high as one in 200 people.”1
Presentation: The Symptoms and Impact of HCM
Although HCM has considerable clinical heterogeneity, core symptoms were described as breathlessness, palpitations, and/or dizziness on exertion, which may be accompanied by chest pain. There is also an association with cardiac arrest and SCD; however, the experts emphasised that SCD was rare as the first presentation of HCM. At the other end of the scale, Michels also pointed out that HCM can be asymptomatic and so may be diagnosed incidentally during a physical examination, electrocardiogram, or family screening.
Regarding the impact on daily life, CarrWhite explained, “It’s quite a spectrum, but there’s a reasonably large group (probably about 20% of patients, more often those with oHCM), who can have quite disabling symptoms with very marked chest pain, dizziness, breathlessness, and syncope at times. However, there are very effective treatments for symptomatic LVOT obstruction (as summarised below). With the armoury of treatments currently available, you can hope to significantly improve patients’ symptomology in the vast majority of cases.”
Pathophysiology of HCM
A more detailed understanding of the pathophysiology underlying HCM has, in recent years, been pivotal in directing the development of treatments specifically for HCM. Carr-White summarised: “In most monogenic HCM disorders, you see ‘spelling mistakes’ in the genes for proteins that sit within the cardiac myocyte, particularly within the sarcomere. Most of these genetic changes affect the myosin–actin cross bridges and the contractility of how the cell beats. This creates overactivation, as you often get more of these cross bridges, and so more contractile function at the cellular level. Over time, this leads to hypertrophy of the muscle and fibrosis. This myocyte disarray is one of the characteristic features observed under the microscope.” Michels emphasised, “What is very important in HCM is that the heart muscle becomes stiffer, so its ability to relax is also hampered by the increased number of cross-bridges.”
According to Carr-White, the impact of these pathophysiological insights has been significant: “Understanding the pathophysiology of HCM has helped to develop a group of directly acting myosin inhibitors, which target the actual pathophysiology underlying HCM. I think that’s been a great advance.” Michels agreed, “This knowledge has led to new insights and new therapies, and is altering the treatment options for patients with HCM.”
Symptomatic Treatment Strategies
The experts went on to describe the rapidly evolving treatment landscape for HCM. Carr-White commented, “The first thing to do is improve the patient’s symptoms, considering medications or, if necessary, more invasive therapies.” Michels recommended a recent review by Hutt and Desai2 as an excellent summary of current medical treatment strategies, and Carr-White highlighted the 2023 European Society of Cardiology (ESC) cardiomyopathy guidelines as a valuable new resource,3 being the first European guidance on the
overall management of cardiomyopathies (a specific guideline for HCM had been published a decade earlier in 2014).4 The USA Guideline for the management of HCM was also revised in 2024.5
The experts described the European and USA guidelines as similar in terms of recommendations for the symptomatic treatment of HCM. After general measures such as weight loss, the avoidance of dehydration, and reducing excess alcohol consumption, both guidelines recommend either beta blockers or calcium channel blockers (verapamil, diltiazem) as first-line treatments for obstructive disease.3,5 If patients are unable to tolerate these firstline therapies, have contraindications, or don’t respond, the European guidelines recommend adding disopyramide (a sodium channel blocker) or mavacamten (a cardiac myosin inhibitor [CMI], in adults only; Figure 1). If this also fails, then alcohol septal ablation or surgical myectomy are further options.3 “The only slight difference in the USA guidelines is their second-line puts septal ablation, mavacamten, and disopyramide all in parallel,”5 said CarrWhite. Michel described CMIs as the ‘new kids on the block’, recommended by both the European and USA guidelines for the treatment of oHCM: “Now we have CMIs as the next step if the first-line medical treatment fails, whereas previously the next step would have been septal reduction therapy. This makes a huge difference for patients.”
Regarding non-obstructive disease, CarrWhite commented, “Treating patients with nHCM tends to be more difficult. [The advice is] to try calcium antagonists, beta blockers, sometimes low-dose diuretics, and occasionally a small dose of nitrates.” Clinical studies of the CMIs for nHCM are currently ongoing.6,7 Overall, the USA guidelines describe symptomatic nHCM as “a diagnostic and therapeutic challenge” due to differences in disease onset, severity, and risk of adverse outcomes.5
First-Line Pharmacotherapies: Beta Blockers and Calcium Channel Blockers
Current first-line therapies for HCM have
Symptoms
Beta-blockers (Class I)
Beta-blockers or verapamil may be considered (Class IIb)
Still symptomatic or intolerant/ contraindication to beta-blockers
Still symptomatic
Still symptomatic
been the foundation of care for many decades, developed in what Michels described as “a different era” in terms of clinical study.8 The experts emphasised the value of extensive real-world clinical experience with these drugs, while also noting the limited number of supportive pathophysiological or clinical studies specific to HCM.
Referring to obstructive disease, Carr-White commented, “In day-to-day practice, we’ve all used beta blockers for decades, and treatment definitely does improve patients’ symptoms. However, in terms of scientific evidence, there are very few good clinical trials in HCM. There are some trials showing that beta blockers reduce the outflow tract gradients, but these are quite small (certainly nothing along the lines of the CMI
trials we’ve seen recently).” Michels added, “We believe the mechanism of action is that diastolic pressure is reduced and left ventricular filling is improved. Small clinical trials, including, most recently, a placebocontrolled, 2-week study of metoprolol,9 observational cohort trials, and clinical experience have led to beta blockers becoming the first line of treatment in oHCM. Beta blockers followed by calcium channel blockers, which have also been tested in small groups of patients, have been used for a long time in HCM, and in general are readily available and quite easy to use.”
Regarding safety, Carr-White described beta-blockers and calcium channel blockers as having a generally favourable profile, established over decades of use in various
Figure 1: Flow chart on the management of left ventricular outflow tract obstruction (European guidelines).3
LVOTO: left ventricular outflow tract obstruction; N: no; Y: yes.
Septal reduction therapies (Class I)
Diltiazem (Class I) Mavacamten (Class IIa)
Verapamil (Class I) Disopyramide (Class I)
cardiological conditions: “I think they’re safe drugs, and most people tolerate them reasonably well. However, quite a few people struggle with beta blockers; they often get cold extremities, fatigue, erectile problems, and poor sleep.” Michels expanded on this point, explaining that beta blockers are unsuitable for patients with bradycardia, low blood pressure, or certain pulmonary diseases, due to their slowing effect on the heart. A specific caution was also raised about the risk of pulmonary oedema with calcium channel blockers in patients with high LVOT gradients.
Second-Line Pharmacotherapies: Disopyramide
The addition of disopyramide is a treatment option for oHCM in patients who do not respond to or tolerate first-line therapies.3,5 Michels described it as “a negative inotropic drug without a vasodilator effect, which can be very helpful in oHCM. However, there are important side effects, especially anticholinergic ones, and it can’t be combined with other drugs that also prolong the QT interval. It can also be a problem for patients with glaucoma or males with prostatism.” Based on their clinical experience, both experts also highlighted difficulties with drug availability. “Certainly, in the UK, it is hard to get hold of disopyramide, so the vast majority of physicians would consider mavacamten [as their second-line therapy],” said Carr-White.
The arrival of targeted therapies in the form of CMIs has been a notable development for the treatment of oHCM.10 The CMIs mavacamten and aficamten reversibly bind to cardiac myosin ATPase at two distinct allosteric sites, inhibiting its activity and thereby reducing actin–myosin cross-bridge formation.6,11 Carr-White explained, “We’re very excited by these new drugs. They target the actual pathophysiology underlying HCM: the hyper-contractility due to the increased number of actin–myosin bridges.” Michels shared this enthusiasm: “We know that mavacamten binds specifically to the myosin head.12 It’s a very small molecule,
and it reduces the number of cross-bridges to the level seen in those without HCM.6,12 These are impressive data. It’s working on the known changes in the sarcomere.”
Currently, mavacamten is the only CMI approved in the USA and Europe,13-15 with aficamten likely to be the next-in-class.3,5 Michels summarised, “There are three important Phase III trials: the EXPLORERHCM trial and the VALOR-HCM trial,16-18 both double-blind, placebo-controlled trials of mavacamten in oHCM, and both very positive in the primary and secondary endpoints [of improved exercise capacity, LVOT obstruction, New York Heart Association [NYHA] functional class, and health status]. Then, this year, we had the results of the SEQUOIA-HCM trial of aficamten in patients with symptomatic oHCM,19 which was also double-blind and placebo-controlled, and demonstrated very good efficacy (reaching primary and all secondary endpoints), as well as safety. This is a great difference compared to the other drugs that we use in HCM, because these are really large, placebo-controlled randomised trials, something we haven’t seen before.” Carr-White reinforced this point: “The trials have shown very clearly that CMIs reduce LVOT obstruction, and the associated symptoms, considerably.”
Regarding safety, Carr-White observed, “The side-effect profile seems favourable based on the limited number of patients we’ve treated, as well as the trial data and real-world data, particularly in the USA. The only thing to watch for is the small risk of worsening left ventricular dysfunction.” Michels continued, “Because they influence systolic function, these drugs are only suitable for patients who still have a preserved ejection fraction (although most patients with oHCM do have a high ejection fraction). Also, mavacamten can’t be used in females of childbearing age who are not using effective contraception due to its potential effect on the fetus.13,14 There are drug–drug interactions, though in my experience we have always been able to adjust the background medication.”
In terms of practicalities, both experts highlighted frequent echocardiographic
monitoring for left ventricular dysfunction as a current limitation of using the approved therapy, mavacamten. “In order to use mavacamten, there’s a very strict protocol to follow, including many echocardiograms.13,14 This puts a burden on healthcare resources,” said Michels, and Carr-White agreed, “I hope as we gain greater experience, we may be able to find a more personalised way to monitor for left ventricular dysfunction.”
Overall, the experts’ opinion on the prospects for these new targeted therapies in HCM was strongly positive. “They’re a very exciting treatment, and I think they will be used more and more,” said CarrWhite. “We’re entering the era of precision medicine for HCM. If you look at the trials, the real-world data, and also our own experience, the majority of patients really improve,” observed Michels.
UNMET NEEDS AND FUTURE PERSPECTIVES
Treatment Developments
As described above, the advent of targeted therapies may frame an encouraging future for the medical management of HCM. Both experts noted the anticipated arrival of aficamten as the next-in-class CMI, based on positive Phase III clinical data from the SEQUOIA-HCM trial.19 Within the same CMI class, mavacamten and aficamten exhibit overlapping but distinct profiles.11 “A notable difference is that aficamten has a shorter half-life [than mavacamten], which makes it a little easier to dose in patients,” said Michels. “Also, mavacamten is metabolised through cytochrome P450, which is why you see drug–drug interactions that you don’t see with aficamten. These are two important differences, just in pharmacokinetics.” In addition, Michels expressed interest in the ongoing Phase III MAPLE-HCM study (NCT05767346) which compares aficamten head-to-head with the beta blocker, metoprolol, in patients with symptomatic oHCM.20 This investigation is particularly significant, as the lack of a head-to-head comparison has, to date, prevented the recommendation of CMIs as
a first-line therapy, according to the European guidelines.3
Michels also highlighted recent research into metabolic and gene therapies: “There have been developments in metabolic therapy, including a Phase II trial with ninerafaxstat in non-obstructive disease, but we have to wait for the Phase III trial.21 Gene therapy is also being studied. It’s only in Phase I, but I think it could be very promising.” Carr-White added that the USA Cleveland Clinic had enrolled the first patient in the Phase Ib gene therapy (MyPeak-1) trial for nHCM,22 and stated, “I think that gene-modifying replacement therapy is going to really expand over the next 5 years, and that will be very exciting.”
Unmet Needs
Michels and Carr-White discussed what they viewed as the key unmet needs for the symptomatic treatment of HCM, highlighting the development of therapies for nHCM as a priority. “We have seen a lot of recent developments in patients with oHCM but a quarter of patients have nHCM, and currently, we don’t have any specific therapy for this group, who can be severely symptomatic. So, it’s good that CMIs, mavacamten and aficamten, are currently being studied in Phase III trials for nHCM (ACACIA-HCM [NCT06081894]; ODYSSEYHCM [NCT05582395]),6,7,23,24 said Michels, who also spoke about the need for realworld evidence to further guide the use of CMIs: “Mavacamten has been available here in the Netherlands for just 5 months, so we need real-world data on both the efficacy and safety of the drug. This might help to reduce the number of echocardiograms. It would also be helpful to be able to predict which patients won’t respond to the treatment. That’s very important in precision medicine. There is also an unmet need for treating HCM with a reduced ejection fraction, as CMIs cannot be used in these patients.”
Carr-White outlined further unmet needs in patient management: “The biggest problem in the UK is the increasing number of patients as we improve diagnosis and screening. It’s not uncommon for patients
with HCM, a potentially lethal condition, to wait 12 months or longer to be seen. Therefore, I think that the priority here is to develop functional ‘hub and spoke’ networks, and free up space within the system to fast-track those who need treatment the most: the symptomatic and high-risk patients.” Carr-White also addressed the urgent need to improve psychological services for patients with HCM: “They are often a quite vulnerable group, particularly when worried about the risk of sudden death and passing the condition on to their children. Cardiologists tend to focus on the cardiac side of things, whereas genetics nurses or counsellors may be better at addressing psychological concerns. Also, if a physician has limited experience with HCM, it’s important to embed them within a wider team and direct them to think about three aspects: treating symptoms (highlighting new treatments); assessing the risk of sudden death (annually); and genetic testing the wider family.”
Future Perspectives
Looking to the future, the experts emphasised the importance of further elucidating the cardiac pathophysiology in HCM. Carr-White predicted, “It will be an iterative process, getting more precise, targeted molecules as we gain a greater understanding of the pathophysiology. Also, going forward, we hope that because [a drug] targets the underlying pathophysiology, it may be able to target the natural progression of the condition.” Michels agreed, “Is it beneficial to treat earlier? Do you only treat symptoms, or do you also treat to prevent problems from happening in the future?”
Carr-White speculated, “We may get more personalised medicine with different approaches to particular genes,” and Michels noted that, “the CMIs were developed based on HCM caused by a specific underlying gene variant. However, in the clinical trials, we give them to every patient with the oHCM phenotype, and
both groups respond. So that’s intriguing.” Michels also highlighted the importance of being able to predict how the phenotype will develop for likely pathogenic or pathogenic gene carriers but noted the difficulty of this process: “There’s extreme clinical heterogeneity, even among patients carrying the same background gene, so I think it’s important to look also at ‘second hits’; for example, obesity and hypertension. I think that’s vital for the patients. It’s also critical to phenotype your patients well, because phenocopies like cardiac amyloidosis or Fabry’s disease have their own specific treatments. That’s the flip side of the coin [of precision medicine].”
Looking ahead to future clinical study programmes, Carr-White suggested, “We need to look at harder outcomes such as SCD and prognosis, which we’ve never really examined in HCM. This will involve multicentre trials, or large registries, across Europe, or Europe and the USA. I think that’s the next level of research, which will be very exciting but will come with quite a few challenges.”
CONCLUSIONS
Overall, the experts were highly optimistic about the future of treatment for HCM, with further developments expected in targeted treatments based on pathophysiological and genetic findings, and a greater volume of robust clinical data and real-world evidence. Carr-White commented, “Drugs are coming through the system that will target slightly different parts of the sarcomere, and numerous different genetic therapies are also being trialled. I think that combination of approaches will give us plenty of opportunities.” “I see many patients with HCM,” said Michels, “and most are really excited about these new developments. I think the landmark change of the CMIs is really promising. It’s very good that most patients do improve, and I believe it’s important, when you see patients, to stay motivated to try and improve their lives. I think the future looks bright for HCM.”
References
1. Massera D et al. How common is hypertrophic cardiomyopathy… really?: disease prevalence revisited 27 years after CARDIA. Int J Cardiol. 2023;382:64-7.
2. Hutt E, Desai MY. Medical treatment strategies for hypertrophic cardiomyopathy. Am J Cardiol. 2024;212S:S33-41.
3. Arbelo E et al; ESC Scientific Document Group. 2023 ESC Guidelines for the management of cardiomyopathies. Eur Heart J. 2023;44(37):3503-626.
4. Elliott PM et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: the Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur Heart J. 2014;35(39):2733-79.
5. Ommen SR et al. 2024 AHA/ACC/ AMSSM/HRS/PACES/SCMR guideline for the management of hypertrophic cardiomyopathy: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2024;149(23):e1239-311.
6. Braunwald E et al. Mavacamten: a first-in-class myosin inhibitor for obstructive hypertrophic cardiomyopathy. Eur Heart J. 2023;44(44):4622-33.
7. Cytokinetics®. Cytokinetics announces start of ACACIA-HCM, a pivotal phase 3 clinical trial of aficamten in patients with symptomatic non-obstructive hypertrophic cardiomyopathy in patients with symptomatic non-obstructive hypertrophic cardiomyopathy. 2023. https:// ir.cytokinetics.com/news-releases/ news-release-details/cytokineticsannounces-start-acacia-hcm-pivotalphase-3-clinical. Last accessed: 5 September 2024.
8. Cohen LS, Braunwald E. Amelioration of angina pectoris in idiopathic hypertrophic subaortic stenosis with
9. Dybro AM et al. Randomized trial of metoprolol in patients with obstructive hypertrophic cardiomyopathy. J Am Coll Cardiol. 2021;78(25):2505-17.
10. Masri A, Olivotto I. Cardiac myosin inhibitors as a novel treatment option for obstructive hypertrophic cardiomyopathy: addressing the core of the matter. J Am Heart Assoc. 2022;11(9):e024656.
11. Hartman JJ et al. Aficamten is a smallmolecule cardiac myosin inhibitor designed to treat hypertrophic cardiomyopathy. Nat Cardiovasc Res. 2024:1003-16.
12. Kawas RF et al. A small-molecule modulator of cardiac myosin acts on multiple stages of the myosin chemomechanical cycle. J Biol Chem. 2017;292(40):16571-7.
13. Bristol Myers Squibb. Camzyos® prescribing information. 2024. Available at: https://packageinserts. bms.com/pi/pi_camzyos.pdf. Last accessed: 9 September 2024.
14. Bristol Myers Squibb. Camzyos® summary of product characteristics. 2024. Available at: https://www.ema. europa.eu/en/documents/productinformation/camzyos-epar-productinformation_en.pdf. Last accessed: 10 September 2024.
15. Yacoub MS et al. A systematic review and meta-analysis of the efficacy and safety of mavacamten therapy in international cohort of 524 patients with hypertrophic cardiomyopathy. Heart Fail Rev. 2024;29(2):479-96.
16. Olivotto I et al. Mavacamten for treatment of symptomatic obstructive hypertrophic cardiomyopathy (EXPLORER-HCM): a randomised, double-blind, placebocontrolled, phase 3 trial. Lancet. 2020;396(10253):759-69.
17. Spertus JA et al. Mavacamten for treatment of symptomatic obstructive hypertrophic cardiomyopathy (EXPLORER-HCM): health status
analysis of a randomised, doubleblind, placebo-controlled, phase 3 trial. Lancet. 2021;397(10293):246775.
18. Desai MY et al. Mavacamten in patients with hypertrophic cardiomyopathy referred for septal reduction: week 56 results from the VALOR-HCM randomized clinical trial. JAMA Cardiol. 2023;8(10):968-77.
19. Maron MS et al; SEQUOIA-HCM Investigators. Aficamten for symptomatic obstructive hypertrophic cardiomyopathy. N Engl J Med. 2024;390(20):1849-61.
20. Cytokinetics®. Cytokinetics announces start of MAPLE-HCM, a phase 3 clinical trial of aficamten compared to metoprolol in patients with symptomatic obstructive hypertrophic cardiomyopathy. 2023. Available at: https://ir.cytokinetics.com/newsreleases/news-release-details/ cytokinetics-announces-start-maplehcm-phase-3-clinical-trial. Last accessed: 4 September 2024.
21. Maron M et al. Safety and efficacy of metabolic modulation with ninerafaxstat in patients with nonobstructive hypertrophic cardiomyopathy. JACC. 2024;83(21):2037-48.
22. Haroldson J et al. MyPeak-1: a phase 1b study to evaluate safety and efficacy of TN-201, an adenoassociated virus serotype 9 (AAV9) investigational gene therapy, in adults with MYBPC3-associated hypertrophic cardiomyopathy (HCM). J Cardiac Failure. 2024;30(Suppl 1):S5.
23. Masri A et al; REDWOOD-HCM Investigators. efficacy and safety of aficamten in symptomatic nonobstructive hypertrophic cardiomyopathy: results from the REDWOOD-HCM trial, cohort 4. J Card Fail. 2024;DOI: 10.1016/j. cardfail.2024.02.020.
24. Ho CY et al. Evaluation of mavacamten in symptomatic patients with nonobstructive hypertrophic cardiomyopathy. J Am Coll Cardiol. 2020;75(21):2649-60.
Deputy Medical Director of the Cardiovascular, Respiratory and Critical Care Unit, Guy’s and St Thomas’ NHS Foundation Trust, London.
Michelle Michels
Head of the Centre of Expertise for Inherited Cardiovascular Disease, Erasmus University Medical Centre, Rotterdam, the Netherlands.
Interviews
Two experts in cardiology, David L. Fischman and Saraschandra Vallabhajosyula, discuss their extensive clinical and research careers, and highlight advances in the field. The topics covered include cardiac catheterisation, cardiogenic shock, and challenges within the field of percutaneous coronary interventions.
Featuring: David L. Fischman and Saraschandra Vallabhajosyula
David L. Fischman Co-Director, Cardiac Catheterisation Laboratory, Thomas Jefferson Hospital, Philadelphia,
With over 20 years of experience as a cardiologist, what initially sparked your interest in the field, and continues to motivate you at present?
Q2
Every student I teach, every study I participate in, or paper I write, is done with the patient in mind
A seventh grade English class project prompted me to read a book entitled ‘The Making of a Surgeon’ by William Nolen. In this biographical account, Nolen related his transformation from a medical student to surgeon, having passed through the storied walls of Bellevue Hospital, New York, USA, for his surgical residency. Although I did not become a surgeon, the tale of his experience impacted me such that I wanted to pursue a career in medicine. I was particularly taken by the relationship he developed with his patients, which has been the foundation of my career. Every student I teach, every study I participate in, or paper I write, is done with the patient in mind. I hope that my work will have an impact on the patient. This question prompts me now to go back and read this book again, to see how it motivated me then, and how it relates to my 30+ years in practice.
In 2021 you authored the article, ‘Cardiotwitter: New Virtual Tools to Advance Skillsets in Interventional Cardiology’. What motivated you to write this article, and ultimately grow your own online presence? How does social media impact the field of interventional cardiology in your opinion?
In 2018, I took to social media, Twitter (now ‘X’), to be specific. I did this with the thought that I would use this to educate my patients. I shortly learned that my tweets were reaching the medical community, and less the patient. From there, it took off. It was a means to share cases, ideas, and treatment strategies with colleagues across the globe, prompting me to share this with the cardiology community with the publication of this paper. Social media has made the world a smaller place. I have made friends from across the globe. When you cannot attend every cardiology meeting, it is nice to know that a Twitter colleague will keep you updated as new advances are being discussed, and for this reason, social media remains invaluable to me as an
interventional cardiologist. Now I am looked at as a ‘Cardiotwitter’ influencer; who would have thought?
Q3 Could you please summarise the key takehome messages for cardiologists from your recent article, ‘InHospital Outcomes of Combined Coronary Revascularization and Transcatheter Aortic Valve Implantation in Inpatient Nationwide Analysis’?
My early career started with research on coronary stents, culminating in the publication of the STRESS trial, which demonstrated the benefits of coronary stenting over balloon angioplasty. This study, of which I was the first author, led to the 1994 U.S. Food and Drug Administration (FDA) approval of coronary stents to prevent restenosis. The concept of a balloon expandable stent was the foundation for the development of trans-catheter aortic valve replacement with a balloonexpandable valve. How do the two fit together? We studied this
in our paper; our analysis showed that combining transcatheter aortic valve implantation and percutaneous coronary intervention (stent placement) during the same hospitalisation is associated with worse outcomes. This paper further highlights my career ethic of patient first, where undergoing transcatheter aortic valve implantation should be individualised and tailored, based on the patient's clinical condition.
Q4 Where can we expect to see your research focus lie in the future?
The cardiac catheterisation (cath) lab has been the centre of my career. It should be no surprise that my future research will be focused around it. 2023 was the hottest year ever recorded, and the USA is a significant contributor to global emissions. The cath lab is not immune from this; it is one of the most intense users of energy in the healthcare sector. Our cath lab recently demonstrated the potential for recycling non-contaminated waste to the extent that, if all
USA cath labs recycled, we could generate a minimum of 1.36 million kg of recyclable waste from percutaneous coronary intervention procedures alone. This is a good starting point. We hope to pursue this concept further by studying means to recycle contaminated, as well as non-contaminated waste, as we seek to develop protocols to be adopted globally. My second focus will be on artificial intelligence (AI). How can we adopt the use of AI in the cath lab? Maybe I will start by asking AI this question.
Q5 As Director of the Interventional Cardiology Fellowship Program, what qualities do you attempt to instil, and believe are integral for the next generation of cardiologists?
I have trained hundreds of cardiology fellows during my years at Thomas Jefferson University Hospital, Philadelphia, Pennsylvania, USA, many of whom have been interventional cardiology fellows. As the Director of the Interventional Cardiology Fellowship, I am
Undergoing transcatheter aortic valve implantation should be individualised and tailored
responsible for the development of the next generation of interventional cardiologists. I take this seriously. As I tell each new class of fellows, it is not just the technical aspect of the training that is important, but everything that comes before and after the cath lab trip. It is a privilege that a patient allows us to care for them, and I remind the fellows that we cannot make light of this. The most important things are knowledge and communication. We must know our patients, and communicate with them. We must be there to alleviate their fears and answer their questions. Everyone is a ‘VIP’.
Q6
You were recently featured on a podcast where you summarised the impact of stress on heart health. Can you provide our readers the key take-home messages from this discussion, and what can be done day-to-day to improve our heart health?
Stress is commonplace, as if dealing with a pandemic was not stressful enough. My comments were simple. The first is to recognise that you are under stress, and by this I am not referring to acute stress, but chronic stress, whether it be work- or homerelated. Can you pinpoint the cause of your stress, and if so, are there ways to eliminate it? Many times, there are no immediate or easy ways to eliminate the stress; in these cases, it is good to have someone to discuss this with, either a family member, friend, or professional. This is particularly important, as too often we pick up bad habits when we are under
stress. These include poor dietary habits, smoking, drinking, and not exercising, to name a few, all of which can be detrimental to our heart health.
Q7
What are the most significant challenges you have seen in the field of cardiology during your time working in this field?
Interventional cardiology has been fraught with many challenges over the past several decades, the most important of which, I think, is making sure that each patient is getting the most appropriate treatment, as clinical trials would support. Two examples come readily to mind, the first of which is coronary stenting. Is this technology being overused? The recent ISCHEMIA trial showed that, in stable patients with ischaemia, an initial invasive therapy did not reduce the risk of an ischaemic cardiovascular event compared with a conservative approach, yet coronary stenting remains commonplace in patients with chronic coronary artery disease. A second example is the use of intracoronary imaging. Despite multiple trials demonstrating that the use of intravascular ultrasound during coronary intervention reduces the need for repeat interventions compared to the use of angiography alone, its use remains infrequent. Examples such as these give us pause to reflect on how to best treat our patients, and importantly challenge us to make sure we are incorporating advanced technologies appropriately into everyday practice.
Saraschandra Vallabhajosyula
Warren Alpert Medical School of Brown University; Lifespan Cardiovascular Institute, Providence, Rhode Island, USA
As one of only 100 physicians in the USA who is a quintuple board-certified physician in interventional cardiology, cardiovascular medicine, critical care medicine, and internal medicine, what inspired you to pursue such an extensive path in medicine, and what motivates you to continue researching?
Acute cardiovascular care is a very interesting field that lies at the intersection of cardiology, critical care medicine, interventional cardiology, advanced heart failure, and cardiac surgery. Physicians working in these fields must work closely with multidisciplinary teams consisting of physicians and non-physicians. Critical care cardiology is a young field, and in combination with either interventional cardiology or heart failure cardiology, it is aiding in developing unique care pathways and perspectives for these patients. Therefore, these considerations were important in shaping my interest in this field.
Q2
The data are rapidly evolving with constant updates to our scientific knowledge and healthcare delivery
You recently coauthored the paper ‘Factors associated with Acute Limb Ischemia in Cardiogenic Shock and downstream Clinical Outcomes: Insights from the Cardiogenic Shock Working Group’. What were the key takeaways, and how might this research advance clinical outcomes for patients with acute limb ischaemia?
The rate of acute limb ischaemia (ALI) was 6% among cardiogenic shock patients. Factors most associated with ALI include peripheral vascular disease and multiple mechanical circulatory
support devices. The downstream ramifications of ALI were dire, with a considerably higher risk of mortality. When we place these devices, we must be thoughtful and meticulous with our technique to improve outcomes for these sick patients.
Q3
As Director of the Cardiac Intensive Care Unit (CICU) at the Rhode Island Hospital, what are you hoping to achieve within this role to ensure the highest quality of care for patients?
We are in very exciting times in the critical care cardiology space. The data are rapidly evolving with constant updates to our scientific knowledge and healthcare delivery. The focus in the CICU should be on processes of care, meticulous prevention of iatrogenic harm, and multidisciplinary management of high-acuity disease states. My hope is that the Brown/Lifespan CICU continues to be at the forefront of strong and dynamic healthcare delivery and serves as the local and national leader for critical care cardiology.
Q4 Your work has highlighted the need for a multi-disciplinary approach to treating patients with cardiogenic shock, and your team has proposed the establishment of a Cardiogenic Shock Team Collaborative. What does this approach entail and how can it improve patient outcomes?
Cardiogenic shock continues to carry a high mortality rate despite contemporary care, with no breakthrough therapies shown to improve survival over the past
few decades. Managing patients with cardiogenic shock remains challenging even in well-resourced settings, and an important subgroup of patients may require cardiac replacement therapy. As a result, the idea of leveraging the collective cognitive and procedural proficiencies of multiple providers in a collaborative, team-based approach to care (the ‘shock team’) has been advocated by professional societies and implemented at select high-volume clinical centres. A slowly maturing evidence base has suggested that cardiogenic shock teams may improve patient outcomes. Although several registries exist that are beginning to inform care, particularly around therapeutic strategies of pharmacologic and mechanical circulatory support, none of these are currently focused on the shock team approach, multispecialty partnership, education, or process improvement. We propose the creation of a Cardiogenic Shock Team Collaborative, akin to the successful Pulmonary Embolism Response Team Consortium, with a goal to promote the sharing of care protocols, educate stakeholders, and discover how process and performance may influence patient outcomes, quality, resource consumption, and costs of care.
Q5 During the Society for Cardiovascular Angiography & Interventions (SCAI) 2024 Scientific Sessions, you gave a talk on the current landscape of mechanical circulatory support devices. How do you foresee the landscape evolving in the future?
We are at a very interesting phase in this field. Mechanical circulatory support (MCS) has been in use for over 50 years, but only last year, the first positive clinical trial was published. There is much enthusiasm for these devices, but this must be tempered with
thoughtful patient selection and meticulous technique. Further, the development of multidisciplinary teams to determine the timing of insertion, escalation, and deescalation of MCS is crucial to ensure the best outcomes for patients.
Cardiogenic shock continues to carry a high mortality rate despite contemporary care
My
proudest achievement in my career is to see my learners and trainees grow and flourish
Q6
You were recently awarded the SCAI's ‘30 in Their 30s’ award for clinical excellence, and for encompassing the qualities expected of future leaders in interventional cardiology. So far in your career, what has been your proudest achievement?
I am very grateful to the SCAI for this kind recognition. Many congratulations to all my colleagues who were also recognised in the same category! My proudest achievement in my career is to see my learners and trainees grow and flourish. I have had the fortune of training many young minds, and I’m very privileged to be in a role to mentor them towards independent practice, either clinically or academically.
Q7
You currently have more than 290 publications to your name for your research in areas including cardiogenic shock, acute myocardial infarction, high-risk percutaneous coronary intervention, mechanical circulatory support, non-cardiac organ failure, septic shock, and circulatory shock. What do you believe are the current gaps in the literature, and where will your research focus lie next?
Despite all the interest in cardiogenic shock and related disease states, the mortality remains very high at 40–50%. This is an important public health issue, and we need to come at it in a multi-pronged approach. Multidisciplinary teams, timely use of MCS, careful evaluation and prevention of end-organ damage, and long-term care for the prevention of re-hospitalisations are crucial.
We provoke conversation around healthcare trends and innovationwe also create engaging educational content for healthcare professionals. Join us for regular conversations with physician & entrepreneur, Jonathan Sackier. Listen Now
Clinical Conundrum: Lifetime Management of Aortic Stenosis in Young Patients
Editor's Pick
For this year’s edition of EMJ Cardiology, my editor’s pick is ‘Clinical Conundrum: Lifetime Management of Aortic Stenosis in Young Patients’ by Kipshidze et al. This feature discusses an important issue in modern healthcare: the long-term outcomes of transcatheter aortic valve replacement (TAVR) in patients under 65. With current guidelines favouring surgical aortic valve replacement, yet more young patients undergoing TAVR; this article addresses a growing area of concern. Kipshidze et al. delves into the complexities of this evolving landscape and highlights the key challenges that remain unresolved.
Prof Çetin Erol
İbn-i Sina Hospital, Ankara University, Turkey
Authors: Nicholas Kipshidze,1 Konstantinos Toutouzas,2 *Nodar Kipshidze,3 George Dengas1
1. Icahn School of Medicine at Mount Sinai, New York, USA
2. National and Kapodistrian University of Athens, Greece
3. Columbia University, New York, USA
*Correspondence to nk2988@caa.columbia.edu
Disclosure: The authors have declared no conflicts of interest.
The management of aortic stenosis (AS) in younger patients presents significant clinical challenges. While transcatheter aortic valve replacement (TAVR) offers a minimally invasive approach with favourable short- and mid-term outcomes, its long-term efficacy in patients under 65 years remains uncertain, particularly given the extended life expectancy of these patients. Current guidelines favour surgical aortic valve replacement for younger individuals due to concerns about the durability of TAVR valves. However, an increasing number of younger patients are opting for TAVR, drawn by its shorter hospital stay and reduced operative complications, revealing a disconnect between clinical practice and established guidelines. This discrepancy underscores the need for alternative strategies. Emerging technologies such as novel implant-free devices, show promise in extending valve life and delaying the need for TAVR. Additionally, ongoing research into pharmaceutical interventions, including RNA-based therapies and anti-calcification drugs, aims to slow the progression of AS. As the field evolves, there is a growing emphasis on developing strategies that balance immediate patient benefits with long-term outcomes, ultimately enhancing the quality of life and survival rates for younger individuals with AS.
This review highlights the necessity of innovative approaches tailored to the unique needs of this population, emphasising the importance of continued research and adaptation of clinical practices.
Key Points
1. Transcatheter aortic valve replacement (TAVR) is increasingly being used for younger, lower-risk patients with longer life expectancies compared to those treated at the start of the TAVR era, making long-term durability data crucial. The implications include concerns regarding lifelong coronary access, valve longevity, and the potential need for repeat TAVR procedures in the future.
2. There is a significant unmet need for innovative non-implant technologies that could delay the need for transcatheter aortic valve implantations in younger patients who are more likely to require multiple valve implants over their lifetime, or even eliminate the need for transcatheter aortic valve implantations in some patients altogether.
3. Future research should focus on valve design and materials that can enhance durability. Additionally, exploring medical therapies that utilise new drugs to slow the progression of valve degeneration and/or developing no-leavebehind technologies that may extend the time to initial operation and improve valve longevity could help address this clinical challenge.
INTRODUCTION
The number of transcatheter aortic valve replacements/implantations (TAVR/TAVI) has nearly equalled that of the number of surgical aortic valve replacements (SAVR) among patients under the age of 65 years with severe isolated aortic stenosis (AS) in the USA.1 The substantial growth in TAVR procedures can be attributed to the growing preference to treat younger patients through minimally invasive means. In fact, growing evidence has demonstrated that patients exhibited superior outcomes during their hospital stay when undergoing TAVI as opposed to SAVR. Furthermore, TAVI was linked to reduced odds of in-hospital death, stroke, acute renal damage, and significant bleeding.2 Although TAVI is recommended for individuals across a spectrum of surgical risk, current guidelines in the USA uphold that SAVR should be the preferred option for patients who are under the age of 65 years or those with a life expectancy of more than 20 years at the time of their valvular intervention.3 Despite guidelines and expert consensus, the trends show a clear deviation from official recommendations, which reveals a gap in the long-term management of younger patients who undergo TAVR.4 The implications encompass concerns regarding lifelong coronary access, the longevity of the valve, and the
possibility of repeat TAVR procedures in the future. Although 5- and 10-year follow-up studies have shown positive results, there is a paucity of long-term evidence on the durability of these valves.5-9
DISCUSSION
While studies assessing the motivations among patients choosing TAVI over SAVR remain sparse, current evidence suggests that patients cite a desire for a minimally invasive procedure with shorter in-hospital stays.10 Nevertheless, it remains the case that a significant number of patients continue to get the discouraging message that they do not meet the age criteria for TAVR. Individuals below the age of 65 years will probably surpass the lifespan of their transcatheter aortic valve (TAV) due to the progressive degradation of the valve tissue, necessitating further replacement. At the same time, untreated AS is associated with a substantially increased mortality risk, regardless of the severity degree.11 Given that TAVR represents a comparatively recent therapeutic alternative, there is currently a dearth of extensive clinical investigations that can substantiate the long-term efficacy of this procedure for younger individuals necessitating numerous valve replacements.
Furthermore, regulatory bodies (under International Organization for Standardization [ISO] standards) dictate that ex vivo durability testing for transcatheter heart valves run for a minimum of 200 million cycles, equivalent to approximately 5 years.12,13 Recently, the SAPIEN 3 THV (Edwards Lifesciences, Irvine, California, USA) was tested up to 1 billion cycles (equivalent to 25 years) and demonstrated promising durability results at the bench side.14 The most extensive data on in vivo durability are derived from the NOTION randomised controlled trials study, which demonstrates favourable durability outcomes for both SAVR and TAVI over an 10-year period.15 As the frequency of TAVI rises among individuals below the age of 65 years, it is important to acknowledge that the average age seen in the NOTION study was 79.1 years. In two randomised controlled trials involving individuals with moderate risk, the average age of the participants surpassed 80 years.5,6 Nevertheless, there remains an association between the age of a patient receiving a surgical replacement of biological valves and the rate of valve failure, with younger patients experiencing a somewhat higher likelihood of accelerated valve deterioration.16
A prudent strategy would involve opting for open-heart surgery while considering ongoing developments in other medical technologies and therapies at the time of the procedure. However, it is important to bear in mind that the performance of redo surgery or transcatheter intervention in older individuals is not without its own inherent risks. Regrettably, the existing medical therapy for AS is presently confined to symptom management and enhancing the patient’s quality of life. At the same time, TAVR treatment delays have been linked to mortality rates of 3.8% and 23.3% at 1 and 6 months, respectively, with the 2019 USA national average being around 7 weeks from intake to treatment.4,17
There is a significant unmet need for innovative non-implant technologies that have the potential to delay the need for TAVI in younger patients who are more likely to require numerous valve implants over the course of their lifespan, or even
eliminate the requirement for TAVI in some patients entirely. It may be advantageous to reconsider the utilisation of balloon aortic valvuloplasty (BAV), a previously overlooked technology, as a temporary measure to significantly extend the effectiveness of BAV treatment until a more definitive approach can be implemented.18,19 The function of BAV, on the other hand, is conditional on the particular clinical situation. Patients who have significant AS and a congenital bicuspid valve may be candidates for this therapy as a definitive treatment option.18,20
New BAV involves the application of highpressure inflations, which may lead to the prominent occurrence of intra-leaflet fractures within calcified nodular deposits. The increased flexibility of valve leaflets may be further enhanced by the process of calcification softening. Accurate balloon sizing by the utilisation of preprocedural transthoracic echocardiography or CT is imperative in order to mitigate the potential risks associated with high-pressure inflations. It should be noted that highpressure inflation has the potential to damage the valve with protrusion into the left ventricle and induce aortic regurgitation. A low-profile (5F) BAV device was designed for trans-radial applications, utilising highpressure inflations. The FIM study for this device is scheduled to commence in the fourth quarter of 2024. The authors’ present research focuses on exploring the application of reinforced (scoring-like) valvulotomy balloons as a viable technique for the treatment of calcified leaflets. These balloons have the potential to alter calcified leaflets by reducing inflated pressure requirements, hence improving safety. Furthermore, it is possible that the utilisation of modified intravascular lithotripsy catheters could potentially offer benefits in the treatment of deteriorated valves.21
There exists the potential for the application of several anti-restenotic drugs, including sirolimus, paclitaxel, dexamethasone, colchicine, antifibrotics, anti-calcification substances, matrix metalloproteinases, and new anti-inflammatory chemicals, to have the potential to be used in BAV coating.22-25 Furthermore, an option for balloon
valvuloplasty is the utilisation of a novel device called Leaflex (Pi-Cardia, Rehovot, Israel) in patients who may be considered too old or feeble for TAVI, or even improve the outcomes of TAVI in patients who have severely calcified aortic valves and bicuspid aortic valves. The Leaflex device is a transfemoral transcatheter tool that employs a pair of mechanical components to assess and score calcification in the aortic valve. The system comprises a patented expander that is inserted into the left ventricular outflow canal, elevating the aortic leaflets to make contact with the frame. Additionally, there are three scoring arms positioned in the aortic root. In essence, the process involves the alteration of leaflet motion through the deliberate exertion of force, which effectively scores the calcification present inside the leaflets while ensuring that the calcium particles do not get embolised. One notable benefit of this approach is the facilitation of enhanced mobility of the valve leaflets, rendering them more flexible and expanding the flow area.26
Beyond surgical intervention, current pharmaceutical therapies are incapable of reversing the stenosis of the aortic valve. In recent times, there has been significant progress in establishing the connections between inflammation and AS, as well as between lipoprotein(a) and PCSK-9.27-29
Multiple research groups, including the author’s, are actively engaged in studying the primary and secondary prevention of AS. Although lipoprotein(a) has been associated with the calcification of the aortic valve, the progression of AS is a gradual process that spans many years. The implementation of clinical studies aimed at preventing or delaying the evolution of AS would likely entail greater time and financial resources compared to trials focused on atherosclerotic cardiovascular disease, which typically observe benefits within a maximum follow-up period of 5 years or less. The CHIANTI study is currently in progress aiming to obtain primary endpoints by the year 2025. In addition, the authors’ research group is currently engaged in the development of therapeutic RNA and/or peptide vaccines aimed at mitigating chronic inflammation, which is recognised as a primary catalyst for the degradation of valve leaflets.30-33
Most recently, there has been promising research on the use of osteopontin to stabilise and slow amorphous calcium phosphate, which is believed to be a primary driver of human aortic valve leaflet calcification.34
The field of focused ultrasound is experiencing rapid advancements, offering a non-invasive therapeutic approach that has promise for enhancing patients’ quality of life and reducing healthcare expenses associated with calcifications on heart valves. Pulsed cavitation-focused ultrasound, also known as histotripsy, is employed to administer mechanical energy to the calcium deposits on the valve at the point of beam convergence. This intervention enhances blood circulation and augments the functionality of the valves in terms of their capacity to open. This procedure bears resemblance to lithotripsy, a medical intervention commonly employed for the treatment of kidney stones. The primary indication is for individuals diagnosed with severe and symptomatic AS.35,36
Returning to surgical interventions, the existing choices for prosthetic valve replacement, including bioprosthetic and mechanical heart valves, are constrained by the occurrence of structural valve degeneration, which necessitates further surgical intervention or the lifelong administration of anticoagulant medications. Over the past decade, many strategies, such as advanced calcium-blocking tissue technology, have been proposed to potentially enhance the durability of valve leaflets and decrease the need for further interventions.37-41 It should be noted that recent research investigating the mechanisms of TAV degeneration demonstrated TAV function can be severely impacted by both non-calcific and calcific mechanisms of tissue degeneration. This study highlights the importance of considering non-calcific factors in TAV degeneration.14 Interestingly, Sato et al.42 provide a histopathological evaluation of one THV that had been explanted 2 months after a TAVR procedure. The THV was severely deteriorated and showed microvessels originating from the animal pericardial tissue used for the bioprosthetic leaflets.
The new growth of blood vessels, known as neovascularisation, indicated a possible reason for the valve’s dysfunction.42
Additionally, a number of novel polymer technologies have been devised with the aim of developing an optimal alternative for polymeric heart valve substitutes, thereby addressing the aforementioned drawbacks.43,44
The utilisation of drug-eluting heart valves in clinical practice remains limited and not yet widespread. Although drug-eluting stents and drug-eluting balloons have been widely used in cardiovascular procedures, the utilisation of drug-eluting technology in heart valves is now being explored and developed. The drug-eluting heart valve concept entails the integration of pharmaceutical substances within the valve structure or coating to mitigate concerns such as calcification, pannus formation, tissue degeneration, or inflammation, which may result in valve dysfunction or failure in the long run. The medicine would seek to mitigate these effects and maybe extend the longevity of the valve. Numerous preclinical investigations are currently being conducted to examine the viability and possible advantages of drug-eluting heart valves. Recently, first-in-human results were reported with nitric oxide coated TAVR.45
Various procedures are now being investigated, encompassing the utilisation of coatings for local drug delivery, tissue engineering methodologies, and gene therapy techniques. There continues to be progress in the realm of TAVR, with the investigation of drug-eluting TAVR valves currently an area of active exploration. The potential advantages associated with drugeluting TAVR would be comparable to those observed with drug-eluting stents or drug-
References
1. Sharma T et al. National trends in TAVR and SAVR for patients with severe isolated aortic stenosis. JACC. 2022;80(21):2054-6.
2. O’Riordan M. TCTMD. National Data Point to Soaring TAVI Rates in Patients Under 65. tctMD. 2024. Available at: https://www.tctmd.com/
eluting balloons. These advantages entail the targeted administration of medication to enhance the long-term efficacy and robustness of the implanted device. The application of drug-eluting technology in TAVR has the potential to mitigate issues associated with valve degeneration, calcification, and inflammation, which can adversely affect the long-term durability and functionality of the prosthetic valve.
The administration of medication directly to the valve has the potential to mitigate or postpone these issues, enhancing the durability of the valve and diminishing the necessity for subsequent procedures. Nevertheless, it is crucial to acknowledge that the advancement and clinical implementation of drug-eluting TAVR is currently in the exploratory phases.
CONCLUSION
With the increasing use of TAVR among persons under the age of 65 years, the optimal care of these patients has received less attention. Furthermore, as life expectancy in most high-income nations has increased since the introduction of these valves, the subject of long-term durability of implantable valves, whether surgical or transcatheter, has become more relevant for a variety of age groups. Future research should look into design and materials that can help these valves last longer. Thus, medical therapy research utilising new medicines to decrease the evolution of valve degeneracy and/or no-leave-behind technologies that may lengthen the time to index operation as well as improve valve longevity may aid in resolving this clinical quandary.
news/national-data-point-soaringtavi-rates-patients-under-65. Last accessed: 1 July 2024.
3. Otto CM et al. 2020 ACC/AHA Guideline for the management of patients with valvular heart disease. JACC. 2021;77(4):e25-197.
4. Goel SS, Reardon MJ. Indication creep in transcatheter aortic valve
implantation-data or desire? JAMA Cardiol. 2023;8(6):519.
5. Leon MB et al. Transcatheter or surgical aortic-valve replacement in intermediate-risk patients. N Engl J Med. 2016;374(17):1609-20.
6. Reardon MJ et al. Surgical or transcatheter aortic-valve replacement in intermediate-risk patients. N Engl J
Med. 2017;376(14):1321-31.
7. Forrest JK et al. 4-Year outcomes of patients with aortic stenosis in the evolut low risk trial. JACC. 2023;82(22):2163-5.
8. Mack MJ et al. Transcatheter aortic-valve replacement in low-risk patients at five years. N Engl J Med. 2023;389(21):1949-60.
9. Hariri EH et al. Role of aortic valve replacement in moderate aortic stenosis: a 10-year outcomes study. Open Heart. 2024;11(1):e002616.
10. Heen AF et al. Patient values and preferences on valve replacement for aortic stenosis: a systematic review. Heart. 2021;107(16):1289-95.
11. Généreux Pet al. The mortality burden of untreated aortic stenosis. JACC. 2023;82(22):2101-9.
12. Lu PC, Liu J shing, Xi B, Li S, Wu J, Hwang NHC, “Accelerated Fatigue Testing of Prosthetic Heart Valves,” Hwang NHC, Woo SLY (eds.), Frontiers in Biomedical Engineering (2003), Boston, Springer, pp.185-96.
13. ISO 5840-3: Cardiovascular implants — Cardiac valve prostheses — Part 3: Heart valve substitutes implanted by transcatheter techniques. 2021. Available at: https://www.iso.org/ standard/67606.html. Last accessed: 1 July 2024.
14. Sathananthan J et al. Long-Term Durability of Transcatheter Heart Valves. JACC Cardiovasc Interv. 2020;13(2):235-49.
15. Thyregod HGH et al. Transcatheter or surgical aortic valve implantation: 10-year outcomes of the NOTION trial. EUR Heart J. 2024;45(13):1116-24.
16. American College of Cardiology. Surgical aortic valve replacement: biologic valves are better even in the young patient. 2015. Available at: https://www.acc.org/latest-incardiology/articles/2015/03/03/09/28/ surgical-aortic-valve-replacementbiologic-valves-are-better-even-inthe-young-patient. Last Accessed: 22 February 2024.
17. Malaisrie SC et al. Mortality while waiting for aortic valve replacement. Ann Thorac Surg. 2014;98(5):1564-71.
19. Hara H et al. Percutaneous balloon aortic valvuloplasty revisited: time for a renaissance? Circulation. 2007;115(12):e334-8.
20. Zhong J et al. Balloon aortic valvuloplasty in the modern era: a review of outcomes, indications, and technical advances. JSCAI. 2023;2(4):101002.
21. Bernava G et al. Lithotripsy of calcified aortic valve leaflets by a novel ultrasound transcatheterbased device. Front Cardiovasc Med. 2022;9:850393.
22. Tulek B at al. Anti-inflammatory and anti-fibrotic effects of sirolimus on bleomycin-induced pulmonary fibrosis in rats. CIM. 2011;34(6):E341.
23. Spargias K et al. Valvuloplasty with a paclitaxel-eluting balloon prevents restenosis in an experimental animal model of aortic stenosis. J Heart Valve Dis. 2014;23(4):484-91.
24. Van Den Branden A at al. New therapeutics targeting arterial media calcification: friend or foe for bone mineralization? Metabolites. 2022;12(4):327.
25. Dayawansa NH et al. Uncoupling the vicious cycle of mechanical stress and inflammation in calcific aortic valve disease. Front Cardiovasc Med. 2022;9:783543.
26. Baumbach Aet al. Non-implant valve repair for calcific aortic stenosis: the Leaflex study. EIJ. 2021;16(16):1366-9.
27. Kronenberg F et al. Lipoprotein(a) in atherosclerotic cardiovascular disease and aortic stenosis: a European Atherosclerosis Society consensus statement. Euro Heart J. 2022;43(39):3925-46.
28. Moncla LHM et al. Calcific aortic valve disease: mechanisms, prevention and treatment. Nat Rev Cardiol. 2023;20(8):546-59.
29. Bergmark BA et al. An exploratory analysis of proprotein convertase subtilisin/kexin type 9 inhibition and aortic stenosis in the FOURIER trial. JAMA Cardiol. 2020;5(6):709.
30. Bonaventura A, Abbate A. Colchicine for cardiovascular prevention: the dawn of a new era has finally come. Eur Heart J. 2023;44(35):3303-4.
31. Johnson TM et al. Aortic stenosis risk in rheumatoid arthritis. JAMA Intern Med. 2023;183(9):973.
32. Iversen P et al. Pre-clinical findings of a novel therapeutic vaccine to limit the progression of cardiovascular disease: atherovaxtm. J Am Coll Cardiol. 2023;81(Suppl 8):2110.
33. Iversen PL et al. A novel therapeutic vaccine targeting the soluble TNFα receptor II to limit the progression of cardiovascular disease:
AtheroVaxTM. Front Cardiovasc Med. 2023;10:1206541.
34. Sivaguru M et al. Osteopontin stabilization and collagen containment slows amorphous calcium phosphate transformation during human aortic valve leaflet calcification. Sci Rep. 2024;14(1):12222.
35. Trifunovic-Zamaklar D et al. Systematic brain magnetic resonance imaging and safety evaluation of non-invasive ultrasound therapy for patients with severe symptomatic aortic valve stenosis. Eur Heart J Cardiovasc Imaging. 2023;24(7):e108-9.
36. Messas E et al. Treatment of severe symptomatic aortic valve stenosis using non-invasive ultrasound therapy: a cohort study. The Lancet. 2023;402(10419):2317-25.
37. Flameng W et al. A randomized assessment of an advanced tissue preservation technology in the juvenile sheep model. JTCVS. 2015;149(1):340-5.
38. Nazif TM et al. Real-World experience with the SAPIEN 3 ultra transcatheter heart valve: a propensitymatched analysis from the United States. Circ Cardiovasc Interv. 2021;14(9):e010543.
39. Pibarot P et al. Structural deterioration of transcatheter versus surgical aortic valve bioprostheses in the PARTNER-2 trial. J Am Coll Cardiol. 2020;76(16):1830-43.
40. Eichinger S et al. Early degeneration caused by cusp tear of first-generation trifecta bioprosthesis. Ann Thorac Surg. 2018;106(6):e297-298.
41. Tchouta L et al. Early failure of the trifecta GT bioprostheses. JTCVS Techniques. 2020;4:106-8.
42. Sato Y et al. Microvessels are normally observed in all pericardial bioprosthetic leaflets. JACC: Cardiovas Interv. 2023;16(20):2572-3.
43. Ge J et al. Preliminary implantation of a novel TAVR device with polymeric leaflets for symptomatic calcific aortic disease. JACC: Case Reports. 2023;17:101901.
44. Singh SK et al. Polymeric prosthetic heart valves: a review of current technologies and future directions. Front Cardiovasc Med. 2023;10:1137827.
45. Yadav, Pradeep. SIEGEL TAVR: A Revolutionary Ultra-Low Profile Aortic Valve Based Upon Rhenium Superalloys (Mirus). Presentation. New York Valves, 6 June, 2024.
Coarctation of Aorta Masquerading as a Spinal Arteriovenous Malformation: A Case Report
Coarctation of the aorta is a congenital disease involving the cardiovascular system. It has a varied presentation and is often under-diagnosed in clinical practice. The authors report a case of an unusual presentation of coarctation of the aorta with a series of events leading to the final diagnosis. A 28-year-old man presented with complaints of backache and pain in both lower limbs with tingling and numbness for 8 months. He was provisionally diagnosed with spinal arteriovenous malformation based on investigations done elsewhere and was referred to the authors’ hospital for further management. On angiography, the transfemoral catheter and guide wire could not be negotiated beyond the descending thoracic aorta distal to the origin of the left subclavian artery. Transradial access demonstrated the coarctation of the aorta. Coarctation presenting as a spinal pathology is rare and has been described only in few of the literatures, so it is important to recognise it. This article also describes the pathophysiology and radiological features of coarctation.
Key Points
1. Coarctation of the aorta is a congenital cardiovascular disease with variable presentations, ranging from asymptomatic cases to acute emergencies, and can mimic other conditions.
2. This case report describes multiple tortuous flow voids in the spine on an MRI, which were initially misdiagnosed elsewhere as a spinal arteriovenous malformation. Later on, the patient underwent a digital subtraction angiography at the authors’ institute, where the patient was diagnosed with coarctation of the aorta. This was also confirmed on a CT aortogram.
3. Coarctation of the aorta can have a multitude of presentations, as illustrated by the authors’ case of a young man who was initially misdiagnosed with spinal arteriovenous malformation elsewhere. Due to its varied and sometimes atypical presentations, early and accurate diagnosis can be achieved with a proper understanding of the pathophysiology and the use of radiological investigations like CT and MRI, which are crucial for surgical planning and follow-up.
INTRODUCTION
Coarctation of the aorta is a congenital disease involving the cardiovascular system.1 The presentation can range from being asymptomatic to acute clinical emergencies. When symptomatic, the patients present with a myriad of symptoms like congestive heart failure in children, neurological deficits, lower limb claudication, hypertensive crisis, and intracranial haemorrhage. Knowing that the disease can present in many forms is important to avoid misdiagnosis. The authors report a case of a young man provisionally diagnosed with spinal arteriovenous malformation and was later found to have coarctation of the aorta. The pathophysiology and the radiological features of coarctation of the aorta have been discussed in this article.
CLINICAL CASE
A 28-year-old man presented with complaints of backache and pain in both lower limbs with tingling and numbness for 8 months. He had no significant medical history in the past. He was investigated with an MRI of the spine in a different hospital. On the MRI, there were multiple tortuous flow voids in the spine (Figure 1).
Based on the history of backache and pain in both lower limbs, along with the findings from the MRI, a provisional diagnosis of spinal arteriovenous malformation was made. Since there was no facility for angiography in that particular hospital, the patient was referred to the authors’ hospital (tertiary care centre) for a spinal digital subtraction angiography. On digital subtraction angiography, the transfemoral catheter and guide wire could not be negotiated beyond the descending thoracic aorta distal to the origin of the left subclavian artery with non-opacification of the arch, suggesting coarctation of the aorta. A transradial access was obtained, and subsequent imaging confirmed the diagnosis. Extensive tortuous collaterals were noted (Figure 2), which were responsible for the tortuous flow voids seen on MRI.
The patient was referred to the Department of Cardiovascular Thoracic Surgery and was advised a CT aortogram, which showed a post-ductal coarctation with multiple intercostal, spinal, scapular, and paravertebral collaterals (Figure 3A, 3B, 3C).
A preoperative chest radiograph showed notching along the inferior aspects of the ribs with a “figure of 3” appearance (preand post-stenotic dilatation leading to the abnormal contour of the left mediastinal border, characteristic of coarctation; Figure 3D, 3E).
A 2D echocardiogram was done, which showed turbulence at the site of coarctation with mild left ventricular hypertrophy.
The patient was offered surgical management in the form of coarctoplasty. However, due to financial constraints, the patient was managed conservatively on an outpatient basis and was lost to follow-up.
DISCUSSION
Coarctation of the aorta is a congenital anomaly of the cardiovascular system. It is a narrowing in the calibre of the aorta most commonly found adjacent to the attachment of the ligamentum arteriosum.1 The ductus arteriosus allows communication between the aorta and the left pulmonary artery, which is an important component of fetal circulation and is obliterated in post-natal life. Postnatally, the ductus forms the ligamentum arteriosum, which is a fibromuscular tissue with varying amounts of ductal tissue extending into the aorta. This leads to the development of coarctation of the aorta and explains the location of the narrowing in relation to the ligamentum arteriosum. Coarctation of the aorta is commonly associated with other congenital heart diseases, the most common being a bicuspid aortic valve. It is also commonly associated with Turner’s syndrome.2 Berry aneurysms are found in the intracranial vasculature in a few patients with coarctation. Coarctation can be preductal (common in children) or postductal (common in adults).2
Sagittal T1 (A) and T2 (B) weighted sequences of the MRI spine show multiple tortuous flow voids in the paraspinal, anterior subarachnoid space, and scapular regions (arrows).
2: Digital subtraction angiography demonstrating coarctation of aorta.
Transradial angiography shows multiple collaterals. Right (A) and left (B) subclavian shoots show multiple dilated and tortuous spinal collaterals (arrow). Left subclavian shoot at the thoracodorsal level (C) shows prominent left internal thoracic artery (arrow).
Figure 1: MRI of the spine.
Figure
A) Contrast enhanced CT scan of the thorax shows multiple collaterals (green arrows) in the intercostal and scapular regions. B) Sagittal section shows post ductal coarctation (white arrow) with scapular collaterals (green arrow). C) 3D reconstructed CT image of the aorta shows severe narrowing (white arrow) in the aorta distal to the origin of the left subclavian artery. Both the internal thoracic arteries are prominent (yellow arrows). D) Frontal chest radiograph shows pre and post stenotic dilatation with “figure of 3” appearance (long arrow). E) There is notching (short arrows) of the inferior aspect of the third to ninth ribs on both sides; magnified.
Due to the narrowing of the descending thoracic aorta, there is hypoperfusion of the visceral organs and the lower extremities. To maintain adequate perfusion, there is a development of collateral circulation through various anastomotic channels. The extent of the collaterals varies depending on the severity of the narrowing. The common sites of collateral formation are the intercostal, scapular, and paraspinal regions, which were seen in the authors’ case in the form of flow voids on the MRI of the spine. The anterior intercostal arteries are a branch of the internal thoracic artery that arises from the subclavian artery. There are 11 paired posterior intercostal arteries, wherein the first two arise from the superior intercostal artery, which is the branch of the costocervical trunk of the subclavian
artery. The rest arise from the descending thoracic aorta. The scapular anastomosis has its supply from the intercostal arteries apart from the branches of the subclavian and axillary arteries. The internal thoracic artery divides into the musculophrenic and superior epigastric arteries. The superior epigastric artery anastomoses with the inferior epigastric artery, which is a branch of the external iliac artery. The anterior spinal artery is a branch of the vertebral arteries that anastomoses with the branches of the descending thoracic aorta. These are the common pathways for rerouting the blood in cases of coarctation.3,4
The presentation of coarctation of the aorta varies from asymptomatic to acute emergencies. Clinical manifestation
Figure 3: CT and radiographic findings in coarctation of aorta.
depends on the severity of the narrowing, the amount of collateral formation, and the presence of associated congenital diseases.2 In neonates, there may be changes in congestive heart failure due to increased afterload. Differential cyanosis or clubbing occurs due to hypoperfusion in the lower extremities. In a newborn, differential cyanosis indicates persistent pulmonary hypertension and left heart anomalies (aortic arch hypoplasia, interrupted arch, critical coarctation, and critical aortic stenosis). Reversed differential cyanosis may be seen in patients with transposition of great arteries and coexistent coarctation.4 In adults, the most common presentation is systemic hypertension. The proposed mechanism is renal hypoperfusion, which leads to the secretion of renin, which causes a rise in blood pressure. Other mechanisms include endothelial dysfunction, reduced arterial compliance, and blunted baroreceptor sensitivity.4 Other patterns of presentation include lower limb claudication, intracranial haemorrhage (due to aneurysmal rupture), backache, and lower limb weakness due to the mass effect of the spinal collaterals.7-9 Clinical examination findings include changes in the body habitus where the lower limbs appear atrophic due to hypoperfusion, radio-femoral delay, and differences in the systolic blood pressures between the upper and lower limbs. On auscultation, there may be a systolic murmur over the scapula.1
Transthoracic echocardiography is used for diagnosis as well as during the follow-up of patients with coarctation. The suprasternal notch acoustic window demonstrates the site of narrowing along with the Dopplerbased gradients. A ‘diastolic run-off’ or ‘tail’ in the descending aorta is characteristic. The left ventricular mass and function can be assessed along with the presence of associated congenital anomalies.10
Radiology plays an important role in the diagnosis as well as management of the coarctation of the aorta. On a plain chest radiograph, there are subtle findings that may provide a hint about the diagnosis. The heart shadow is enlarged. There is prestenotic and poststenotic dilatation of
the aorta resulting in the “figure of 3” sign.2 There is notching of the inferior aspects of the third to ninth ribs on both sides due to the extensive intercostal collaterals (Roesler’s sign). The first two spaces are spared as they arise from the subclavian system and are therefore preductal. The tenth and the eleventh posterior intercostal arteries do not anastomose with the anterior branch of the internal thoracic arteries. Rib notching is commonly bilateral. Unilateral rib notching may be seen if the narrowing is proximal to the origin of the left subclavian artery or if proximal to the origin of the aberrant right subclavian artery.11 CT has evolved to be one of the most important modalities in the diagnosis of coarctation. The properties of CT such as multiplanar reconstructions, the use of maximum intensity projection, and 3D reconstruction provide input on multiple factors such as the severity of coarctation, status of the collateral circulation, and associated other congenital anomalies.12-14 MRI has a promising role given its lack of ionising radiation, superior contrast resolution, and multiplanar imaging.15 MRI angiography can be done either with or without the use of intravenous contrast.16 Time-of-flight angiography can be used in cases where contrast agents are contraindicated in patients. The use of phase contrast imaging can provide the pressure gradient across the stenosis.2,17,18
Catheter angiography, although an invasive procedure, is considered a gold standard for the haemodynamic assessment in coarctation of the aorta.19,20 On angiography, it is possible to gauge the pressure gradient across the stenotic segment.
The differential diagnoses for rib notching on a chest radiograph include pulmonary arteriovenous fistula, neurofibromatosis, superior vena cava obstruction, patients with shunts (Blalock-Taussig), congenital heart diseases (tricuspid atresia, tetralogy of Fallot), etc.21,22 Interrupted aortic arch can be considered as a differential of coarctation, where there is a discontinuity between the arch and the descending thoracic aorta.23 Some consider it to be the most severe spectrum of coarctation. It is not seen in isolation and occurs commonly with other congenital defects such as a
ventricular septal defect or a patent ductus arteriosus.24 Severe atherosclerotic disease can involve the mid-thoracic aorta and can be considered an acquired variant of coarctation.25 Few cases have been reported previously where coarctation has been misdiagnosed initially as spinal vascular malformation.7
The objective of treatment for coarctation of the aorta is to recanalise the stenotic segment by either surgical or endovascular methods. Surgical method includes resection and anastomosis, or the use of bypass grafts. Surgery is preferred in cases of infants with coarctation. The endovascular method involves balloon angioplasty or stenting.26,27
CONCLUSION
Coarctation of the aorta is a common congenital disease affecting infants and young adults. It has a varied presentation and often is under-diagnosed in clinical
References
1. Law MA, Tivakaran VS, Coarctation of the Aorta (2023) Treasure Island: StatPearls. Available at: https://www. ncbi.nlm.nih.gov/books/NBK430913/. Last accessed: 8 August 2023.
2. Karaosmanoglu AD et al. CT and MRI of aortic coarctation: pre- and postsurgical findings. A J Roentgenol. 2015;204(3):W224-33.
3. Donald Kirks et al. Mediastinal collateral arteries: important vessels in coarctation of the aorta. American Journal of Roentgenology. 1986;146:757-62.
4. Agasthi P et al. Management of adults with coarctation of aorta. World J Cardiol. 2020;12(5):167-91.
5. Singh J, Singh A. Differential cyanosis. Am J Med. 2013;126(10):e9.
6. Kenny D et al. Hypertension and coarctation of the aorta: an inevitable consequence of developmental pathophysiology. Hypertens Res. 2011;34(5):543-7.
7. Yalavarthy A et al. Atypical presentation of coarctation of aorta mimicking a spinal vascular malformation. Neuroradiol J. 2011;24(5):787-90.
practice. It is important to understand the pathophysiology behind the presenting symptoms especially when the patient presents with atypical symptoms. With the aid of adequate radiological investigations, it is possible to diagnose coarctation of the aorta early and promptly. CT and MRI help in surgical planning and follow-up imaging.
Patient perspective
"I had these complaints for quite some time (many months) and have been visiting the hospital for the same. I am grateful that finally I know what disease I have although I am surprised that this is a condition I had since my childhood, but never experienced any symptoms till now. I hope the surgery is uneventful and I will be rid of my symptoms."
Informed consent
Written informed consent has been obtained from the patient for drafting this manuscript and for publishing it.
8. LeBlanc FE et al. Neurological complications of aortic coarctation. Can Med Assoc J. 1968;99(7):299303.
9. Benyounes N et al. Subarachnoid hemorrhage revealing aortic coarctation in a young man. Neuroradiology. 2011;53(11):931-2.
10. 8. Raza S et al. Coarctation of the aorta: diagnosis and management. Diagnostics (Basel). 2023;13(13):2189.
11. Gooding CA et al. Fate of rib notching after correction of aortic coarctation. Am J Roentgenol Radium Ther Nucl Med. 1969;106(1):21-3.
12. Nance JW et al. Coarctation of the aorta in adolescents and adults: A review of clinical features and CT imaging. J Cardiovasc Comput Tomogr. 2016;10(1):1-12.
13. Rijo D et al. Coarctation of the aorta in adults: pre and postoperative evaluation with CT angiography. Rev Port Cir Cardiotorac Vasc. 2012;19(3):167-8.
14. Eichhorn J et al. Rings, slings and other vascular abnormalities. Ultrafast computed tomography and magnetic resonance angiography in pediatric cardiology. Z Kardiol. 2004;93(3):201-8.
15. Haramati LB et al. MR imaging and CT of vascular anomalies and connections in patients with congenital heart disease: significance in surgical planning. Radiographics. 2002;22(2):337-49.
16. Fitoz S et al. Contrast-enhanced MR angiography of thoracic vascular malformations in children. Int J Cardiol. 2007;123(1):3-11.
17. Ming Z et al. Diagnosis of congenital obstructive aortic arch anomalies in Chinese children by contrastenhanced magnetic resonance angiography. Journal of Cardiovasc Magn Reson. 2006;8(5):747-53.
18. Hellinger JC et al. Congenital thoracic vascular anomalies: evaluation with state-of-the-art MR imaging and MDCT. Radiol Clin North Am. 2011;49(5):969-96.
19. Miabi Z et al. Comparison of CT angiography and digital subtraction angiography in the diagnosis of aortic coarctation. Pak J Biol Sci. 2011;14(1):74-7.
20. Sharma S et al. Intravenous digital subtraction angiography in the preoperative evaluation of coarctation of the thoracic aorta. Indian Heart J. 1990;42(2):105-8.
21. Kagawa T et al. Rib notching: with reference to its various causes and diagnostic implication of cardiovascular diseases. Jpn Circ J. 1968;32(7):989-94.
22. Rexler CJ et al. Diagnostic implications of rib notching. Am J Roentgenol Radium Ther Nucl Med. 1964;91:1064-74.
23. Jeetoo SD, du Plessis V. Severe coarctation in an adult mimicking
an aortic interruption on computed tomography imaging. Eur J Cardiothorac Surg. 2013;43(1):197.
24. Shirani S, Soleymanzadeh M. Diagnosis of aortic interruption by CT angiography. Pol J Radiol. 2013;78(1):72-4.
25. 23. Thani KB. Coarctation of the thoracic aorta masquerading as bilateral aorto-iliac stenosis. J Cardiol Cases. 2011;4(3):e172-5.
26. Suradi H, Hijazi ZM. Current management of coarctation of the aorta. Glob Cardiol Sci Pract. 2015;2015(4):44.
27. Shih MCP et al. Surgical and endovascular repair of aortic coarctation: normal findings and appearance of complications on CT angiography and MR angiography. Am J Roentgenol. 2006;187(3):W302-12.
Prevalence, Clinical Aspects, and Risk Factors of Aortic Stenosis Among Haemodialysis Patients Attending Nephrology Centre of Benghazi
Authors: *Mohamed O. Ezwaie,1,2 Malak M. Alagoury,2,3 Halima M. Bushiha,2,3 Nada Elhamdi,2,3 Dareen Zugbia2,3
1. Benghazi Medical Center, Department of Medicine, Faculty of Medicine, University of Benghazi, Libya
2. Libyan International Medical University, Benghazi, Libya
3. Member of clinical research group
*Correspondence to mohamed.ezwaie@uob.edu.ly
Disclosure: The authors have declared no conflicts of interest.
Acknowledgements We appreciate the contribution of our cardiologists, namely, Zaki Beltamar, Seham Erhoma, Ajawad Elawami, and Moneer Faitorui, for their commitment to perform weekly sessions of echocardiography during period of our research.
Background: Cardiac valve calcifications (CVC) are common among patients on haemodialysis (HD). The valves most commonly involved are mitral and secondarily aortic valves. In Libya, there is a lack of research in this field. This is the author’s motivation to conduct this study, which has a significant impact on the health status of patients on HD.
Objective: To identify aortic valve calcifications (AVC), prevalence of aortic stenosis (AS) in patients on HD, and to determine clinical aspects and risk factors that may lead to the development of AS.
Patients and Methods: A cross-sectional study was conducted between May–November 2023 of adult patients on chronic HD who had received haemodialysis for more than 1 year. Patients with previous cardiac surgery, a history of endocarditis, or severe anaemia (haemoglobin <7.5 mg/dL) were excluded. A sample of 48 patients were enrolled in the study, with all patients undergoing clinical, biochemical, and a trans-thoracic echocardiographic evaluation.
Results: Patients were aged 31–60 years ±13.2 standard deviation. AS had a prevalence of 6.3%, mitral regurgitation had a prevalence of 33.3%, and CVC was detected in 60.4% of patients on chronic HD, with AVC seen in 52.1% and mitral valve calcification seen in 25%. Patients with AVC were more often females (58.6%). Diabetes was seen in 64.6% of cases, and autosomal polycystic kidney disease was seen in 25%.
The authors found that dyspnoea was the most common symptom (66.7%), followed by palpitations (35.4%) and asymptomatic patients (27.1%). Clinically detected AS was observed in three individuals (6.3%). Surprisingly, patients did not exhibit significant differences in age, duration of dialysis, or comorbidities. However, hyperphosphatemia was detected in 56.25% of patients, and hyperparathyroidism was recorded in 64.50%.
Conclusion: The study has shown that aortic stenosis is the second most common valvular lesion in patients on chronic HD, preceded by mitral valve regurgitation. However, asymptomatic AVC has the highest prevalence among patients on chronic HD. Hyperphosphatemia and hyperparathyroidism are major risk factors that enhance the calcification of cardiac valves.
Value of the Research: Though it is a snapshot study, it addresses an important comorbidity in patients on chronic HD. Namely, prevalence of aortic stenosis, CVCs, and associated risk factors, which had been reported in many regional and global nephrology literature, but the national Libyan literature still lacks such chronic HD patients' data.
Key Points
1. Cardiac valve calcifications are common among patients on haemodialysis. The most commonly involved are mitral and secondarily aortic valves.
2. This cross-sectional study addresses an important comorbidity in patients on chronic haemodialysis, exploring important risk factors contributing to the increased prevalence of these cardiac lesions in this sector of patients.
3. This study is a forward step in Libyan nephrology literature, encouraging more active and long-term research from other institutes in Libya.
INTRODUCTION
Cardiovascular disease is still the leading cause of death in patients on haemodialysis (HD).1 Cardiac valve calcification (CVC) is expected to occur 10–20 years earlier in patients with chronic kidney disease (CKD) than in the general population, and its progression is estimated to be 10 times faster in patients on HD.2,3 Aortic valve calcification (AVC) varies between 44–55% in patients on chronic HD.4 Calcified aortic valve disease results from the deposition of calcium nodules on the aortic valve, lipid/inflammatory mediators, as well as anatomic and genetic mechanisms unique to aortic valves causing endothelial injury, valve thickening, and functional stenosis.5,6,7 This degenerative process is attributed to additional factors in uremic patients, such as uremic milieu with retained toxins, loss of calcification inhibitors that promote intimal and medial vascular calcification, metabolic bone disease, chronic hypertension, and
volume overload, which are also pathogenic factors in such population.8 Aortic stenosis (AS) in patients on HD has a progressive calcific degeneration of valve leaflets, when compared with patients without CKD.9,10
Symptomatic aortic stenosis depends on the severity of valve lesion, and the typical symptoms include dyspnoea and presyncope. However, patients on HD may present with dialysis-related hypotension, dialysis intolerance, peridialysis atrial arrhythmias, and post-dialysis fatigue.11,12
The authors’ research covers the prevalence of aortic stenosis and any associated CVCs in patients on HD attending Benghazi Nephrology Center, linked with clinical aspects of AS, and explores the risk factors that may lead to the development of aortic stenosis in patients on HD.
The main objectives of this study were to determine the prevalence of AS and CVCs in patients on chronic HD, determine the clinical aspect of AS, and identify risk
factors that may lead to the development of AS and CVCs in patients on HD.
PATIENTS AND METHODS
Study Design
This is a cross-sectional (case-series) echocardiography-based prospective study conducted with patients on chronic HD; utilising echocardiography performed by four independent cardiologists.
Sampling
A sample of 48 patients on chronic HD, selected by convenience sampling, was completed between May 2023–November 2023. Patients were subjected to a clinical questionnaire and transthoracic echocardiography on a non-haemodialysis day to determine the presence of CVCs or lesions.
Inclusion and Exclusion Criteria
The inclusion criteria was patients on haemodialysis for >1 year and aged >18 years. Exclusion criteria included previous cardiac valve surgery, history of endocarditis, or patients who were severely anaemic (haemoglobin <7.5 gm/dL) to avoid overlap with ostensible cardiac valve lesion.
Clinical Questioner and Interview
Using a self-structured questionnaire, reported information was collected on name, age, and duration of dialysis. Medical chart reviews were conducted to determine comorbidities such as a history of diabetes, dyslipidaemia, atherosclerotic cardiovascular disease, or any other chronic medical condition. Current symptoms like dyspnoea, palpitation, chest pain, or intermittent claudication were recorded. In addition, general and cardiac examinations were done to evaluate patients at the beginning and end of the study period, patients were then referred to the Centre’s cardiologists on a non-dialysis day to perform transthoracic echocardiography. Relevant laboratory data were recorded, including patients’ haemoglobin, parathyroid
hormone (PTH), calcium, and phosphorus levels over the study period.
Statistical Analysis
Data were recorded, stored, and prepared for analysis. All statistical analyses and data processing were performed using the Statistical Package for Social Sciences (SPSS) version 28 software (IBM, New York, USA). Data presented as mean ± standard deviation (SD) for quantitative variables and summarised as frequencies and percentages for categorical variables. For inferential statistics, variables were analysed by chi-squared test, and a p-value of <0.05 is considered a statistically significant finding.
Ethical Statement
This study has been approved by the Libyan International Medical University ethics research committee (ERC) and was issued an ethical approval code: MDC-2023-00129. All questionnaires were anonymous and unidentified to ensure the confidentiality of the collected information. Respondents have provided written consent to both answer the questions and to participate in the study.
RESULTS
The study recruited 48 patients (20 [41.7%] male and 28 [58.3%] female) on chronic HD. Patients’ age ranged from 31–60 years ±13.2 SD. The majority of patients (n=29, 60.4%) were on chronic HD for 1–5 years, while 10 (20.9%) patients were on chronic HD for more than 10 years patients; the mean duration of HD was 6.48 years ±5.16 SD. The primary causes of endstage renal disease were diabetes (n=31, 64.6%), autosomal dominant polycystic kidney disease (ADPKD; n=12, 25.0%), and unknown CKD (probably chronic glomerulonephritis; n=5, 10.4%). Diabetes is more common in females (n=18, 58.1%) than in males (n=13, 41.9%). While ADPKD is more common in male patients (n=8, 66.7%) than female patients (n=4, 33.3%). This study has shown that hypertension has a high prevalence, being present in 44
patients (91.6%), due to poor compliance with medications.
Exploring dialysis sessions from a clinical point of view, the authors found that dyspnoea is the most common complaint among the cohort of patients, being recorded in 32 patients (66.7%). Palpitation was recorded in 17 patients (35.4%) and chest pain in four patients (8.3%). It is worth mentioning that dyspnoea is more common in males than females (p=0.023), while asymptomatic dialysis sessions are more common in females than males (p=0.024; Table 1). Forty-eight patients were subjected to transthoracic echocardiographic study by independent cardiologists. Aortic valve calcification was detected in 25 patients (52.1%), while AS was detected in three patients (6.3%). Mitral valve calcification was detected in 12 patients (25%), while mitral regurgitation (MR) was detected in 16 patients (33.3%). The details of the echocardiographic findings are depicted in Table 2. When reviewing patients’ available laboratory data profiles during the study period, the authors found that the patient cohort had mean values of serum calcium 9.98±3.31 mg/dL, serum phosphorus 5.18±1.66, intact PTH 863.43±138.20 pg/mL, and haemoglobin 10.49±2.35 g/dL, indicating disturbed mineral bone homeostasis, with no statistically significant gender differences. Meanwhile, vitamin D2 levels were found in a few patient records (n=8, 16.6%), with a marginal mean value of 28.6±5.68 ng/mL (Table 3).
DISCUSSION
Despite advances in HD technology, AS and CVC are considered a high prevalence comorbidity in patients on chronic HD, occurring 4–5 times more commonly and in a shorter time frame than in the general population. They are anticipated to be surrogate markers of future coronary artery disease.13,14 In the UK, it is estimated that 1.5% of the over-55-year-old population has AS.15 Vascular calcification is defined as a form of calcium-phosphate complexes deposition in the vasculature, mainly including intimal calcification, Mönckeberg
medial arterial calcification, and valvular calcification.16 In a recent Kidney Disease: Improving Global Outcomes (KDIGO) 2019 report, the prevalence of aortic valve calcific abnormalities ranged from 28–85%; however, AS (as opposed to aortic calcification) was present in 9.5% of patients with CKD, compared with 3.5% of the general population, with similar patterns for mitral regurgitation (43% versus 24%, respectively).17-19 It is prudent to identify these cardiac lesions in patients on chronic HD.
In this cross-sectional echocardiographybased study, patients’ age ranged from 31–60 years ±13.2 SD. Of the 48 patients, 20 (41.7%) were male and 28 (58.3%) were female. This matter differs from region to region, with males starting chronic HD earlier than females in some countries. In a multicentre study conducted in Serbia from 2014–2019, there had been a relative propensity of males on HD, with male patients making up about twice that of female patients throughout the 5 years investigated.20 Another larger multicentre study, conducted in 12 countries (across Europe, Asia, and the USA), has shown that, in all age groups, more males than females were on haemodialysis (59% versus 41% overall, respectively), with large differences observed between countries. The male-tofemale mortality rate ratio in the general population varied from 1.5–2.6 for age groups <75 years, but in patients on chronic HD the ratio was close to one.21
The majority of patients (n=29, 60.4%) in the authors’ study had a duration of HD between 1–5 years (mean 6.48 years ±5.16 SD), but it was found to not be statistically significant. In a study from Morrocco, a single-centre cross-sectional descriptive and analytical study of 111 adult patients who were on chronic HD for more than 6 months in 2013, the average age of patients was 44 years ±14 SD.22 The average duration of haemodialysis was 146 months ±80 SD, and a univariate analysis showed that haemodialysis duration was associated with the occurrence of CVCs, approaching a marginal level of significance (p=0.09).22 A recent metanalysis in 2023 has shown that older age (odds ratio: 1.09; 95% CI: 1.06–1.12)
and longer duration of dialysis (odds ratio: 1.08; 95% CI: 1.01–1.16) were significantly associated with a higher prevalence of cardiovascular calcifications.23
In the authors’ study, diabetes was the most prevalent comorbidity (64.6%), followed by ADPKD (25%). A Korean epidemiological study covering 2002–2017 showed that diabetes is still the most common aetiology of an incident in patients on HD, steadily increasing from 23.84–47.84% over a 15year study period.24 In a Chinese study published in 2016, patients with diabetes had a higher CVC and coronary artery calcification score, and higher incidence rate of major adverse cardiovascular events.25 It has been shown in the current study that dyspnoea is the most common symptom (66.6%) in patients with moderate-to-severe AS or MR, followed by palpitations (35.4%). However, patients with a milder degree of cardiac valve lesions exhibited tolerance during dialysis sessions, were more commonly asymptomatic (27.0%), and had no record of chest pain manifestation during this study (Table 1).
In a 2021 cohort study conducted in Japan on 35 patients on chronic HD with a median follow-up of 4 years, exercise intolerance in the form of shortness of breath was found in 34%, syncope in 14%, and chest pain in 20% of patients with AS.26 Echocardiographic assessment of the current authors’ cohort of patients showed that AS was observed in 6.25% patients; aortic valve calcification was detected in 52.1% of patients, with modest female predominance (58.6%); MR was detected in 33.3%; and mitral valve calcification occurred at a rate of 25% (Table 2). In a retrospective echocardiography-based study from Singapore including 4,119 patients with severe AS (aortic valve area <1 cm2) from 2000–2018, researchers detected severe CKD in 230 patients (5.5%) and found that females constituted 58.3% of patients (versus 58.3% in this study).27 It also found that severe AS was present is in 34±4% of patients with severe CKD; however, the Singaporean patients were relatively older (80 years ±8 SD), compared to this study cohort of patients (31–60 years ±13.2 SD). Diabetes was recorded in 41.7%,
compared to 64.6% in the current study.27,28
The degree of aortic valve leaflet calcification is a strong predictor of AS development. In a retrospective multicentre study involving 1,507 patients on chronic HD, the median time for progression from one to two or three leaflets calcification was 3–4 years.29 The adjusted hazard ratios (95% CI) of two- and three-leaflet calcified were 2.12 (1.49–3.00) and 4.43 (3.01–6.52), respectively, compared to one-leaflet calcification.29 When exploring potential risk factors for CVCs, the authors found that most of their patients (n=37, 77.1%) were normo-calcemic (mean 9.98±3.3 SD; P=0.092), and 27 patients (56%) had serum phosphorus levels of >4.5 mg/dL, being hyperphosphatemia (mean 5.18 ±1.66 SD; p=0.558); a result that has been confirmed in several studies. In Libyan literature, the prevalence of hyperphosphatemia in patients on chronic HD was found to be 68%.30 A retrospective study in Japan, conducted over 10 years and including 441 patients on chronic HD, found a significant correlation between high phosphate levels and the occurrence of AS, and mandates annual echocardiographic screening for these patients.31,32 However, the prevalence of secondary hyperparathyroidism has been studied in the Libyan dialysis population, with prevalence ranging from 17.0–27.1%.30,33 In this study, the authors found that serum intact PTH was high (>200 pg/ mL [mean 863.43 ±138.20 SD; p=0.29]) in 31 patients (64.5%), which defines a high prevalence of a state of secondary hyperparathyroidism in the patient cohort (Table 3).34 The lack of statistical significance of these biochemical findings is attributed to a smaller sample size.
Gender differences contribute as risk factors for AS in patients on chronic HD, with male patients being more prone to accelerated cardiac valves and coronary calcifications, and it is predicted that testosterone probably plays a role in accelerated calcifications.35 In this study; the female-to-male ratio was 1.3:1, which is a marginal finding. Furthermore, no racial differences exist in the study, since all patients are native Libyans. However,
X2: Chi-square test.
Table 2: Echocardiograph findings in patients on chronic haemodialysis and their impact on cardiac valves.
several reports show racial differences do exist. In comparison to Black patients, White patients with advanced CKD may have a more rapid progression of AS.36,37 Though it is beyond the authors’ current research, it is worth mentioning that CVCs were more frequently found in haemodialysis compared to peritoneal dialysis patients.38
The preservation of residual renal function, and less shear stress on valve leaflets in peritoneal dialysis patients, might be making the difference compared to patients on haemodialysis. Furthermore, peritoneal dialysis patients may have a greater timeaveraged exposure to phosphate clearance than haemodialysis.39
Table 3: Laboratory data available during the study period.
iPTH: intact parathyroid hormone; No: number; SD: standard deviation.
CONCLUSION
The prevalence of AS is high (6.3%) in this cohort of Libyan patients on HD. The prevalence of CVC among patients on HD was observed in 60.4%, aortic valve calcification in 52.1%, mitral valve calcification in 25%, and mitral regurgitation was recorded in 33.3% of patients. The authors observed that the majority of patients had a duration of 1–5 years on chronic HD therapy, stating that the cardiac calcification process had already started during their CKD stages. Dyspnoea was the most common symptom in patients with AS. On the other hand, it was found that gender difference is marginal. A majority of patients
References
1. Ureña-Torres P et al. Valvular heart disease and calcification in CKD: more common than appreciated. Nephrol Dial Transplant. 2020;35(12):2046-53.
2. Gansevoort RT et al. Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms, and prevention. Lancet. 2013;382(9889):339-52.
3. Brandenburg VM et al. Valvular calcification in chronic kidney disease. Adv Chronic Kidney Dis. 2019;26(6):464-71.
4. Kim D et al. Effect of end-stage renal disease on rate of progression of aortic stenosis. Am J Cardiol. 2016;117(12):1972-7.
in the study had high phosphorus and intact parathyroid levels, though this was not statistically significant, probably due smaller sample size. Age and duration of dialysis were not found to be significant risk factors.
RECOMMENDATIONS
The authors suggest an echocardiography screening programme for AS in highrisk individuals, such as middle and old-age patients on chronic HD.40 They also recommend having strict control of hyperphosphatemia and secondary hyperparathyroidism in patients on chronic HD.
5. Chao CT et al. Risk factors associated with altered circulating micro RNA -125b and their influences on uremic vascular calcification among patients with end-stage renal disease. J Am Heart Assoc. 2019;8(2):e010805.
6. London GM et al. Calcification of the aortic valve in the dialyzed patient. J Am Soc Nephrol. 2000;11(4):778-83.
7. Tanase DM et al. Contribution of oxidative stress (OS) in calcific aortic valve disease (CAVD): from pathophysiology to therapeutic targets. Cells. 2022;11(17):2663.
8. O'Brien KD. Pathogenesis of calcific aortic valve disease: a disease process comes of age (and a good deal more). Arterioscler Thromb Vasc Biol. 2006;26(8):1721-8.
9. Ren SC et al. Vascular calcification in chronic kidney disease: an update and perspective. Aging Dis. 2022;13(3):673-97.
10. Petrović D et al. Risk factors for aortic valve calcification in patients on regular hemodialysis. Int J Artif Organs. 2009;32(3):173-9.
11. Ngiam N et al. Clinical profile and outcomes in patients with moderate to severe aortic stenosis with or without concomitant chronic kidney disease. Singapore Med J. 2023;DOI:10.4103/ singaporemedj.
12. Mentias A et al. Management of aortic stenosis in patients with end-stage renal disease on hemodialysis. Circ Cardiovasc Interv. 2020;13(8):e009252.
13. Kawase Y et al. Severe aortic stenosis in dialysis patients. J Am Heart Assoc.
2017;6(7):e004961.
14. Herzog C. Kidney disease in cardiology. Nephrol Dial Transplant. 2008;23(1):426.
15. Strange GA et al. Uncovering the treatable burden of severe aortic stenosis in the UK. Open Heart. 2022;9(1):e001783.
16. Phadwal K et al. Autophagy as a novel therapeutic target in vascular calcification. Pharmacol Ther. 2020;206:107430.
17. Yusuf Selcoki et al. Cardiac valve calcifications and predictive parameters in hemodialysis patients. CEJMed. 2007;2(3):304-12.
18. Marwick TH et al. Chronic kidney disease and valvular heart disease: conclusions from a kidney disease: improving global outcomes (KDIGO) controversies conference. Kidney Int. 2019;96(4):836-49.
19. Rattazzi M et al. Aortic valve calcification in chronic kidney disease. Nephrol Dial Transplant. 2013;28(12):2968-76.
20. Djukanović L et al. Gender-specific differences in hemodialysis patients: a multicenter longitudinal study from Serbia. Int Urol Nephrol. 2022;54(12):3233-42.
21. Hecking M et al. Sex-specific differences in hemodialysis prevalence and practices and the male-to-female mortality rate: the dialysis outcomes and practice patterns study (DOPPS). PLOS Medicine. 2014;11(10):e1001750.
22. Faqih SA et al. Valvular calcifications in a patient on hemodialysis in Morocco. Pan Afr Med J. 2016;24:115.
23. Zhang J et al. Associated factors of cardiac valve calcification and its prognostic effects among patients with chronic kidney disease: a systematic
review and meta-analysis. Front Cardiovasc Med. 2023;10:1120634.
24. Choi HS, et al. Trends in the incidence and prevalence of end stage renal disease with hemodialysis in entire Korean population a nationwide population-based study. Medicine (Baltimore). 2021;100(13):e25293.
25. Zhu L et al. Comparison of coronary plaque, coronary artery calcification and major adverse cardiac events in Chinese outpatients with and without type 2 diabetes. Springerplus. 2016;5(1):1678.
26. Horiguchi Y et al. Prognosis of hemodialysis patients with progressive aortic stenosis: a prospective cohort study. Ren Replace Ther. 2021;7(1):48.
27. Bohbot Y et al. Severe aortic stenosis and chronic kidney disease: outcomes and impact of aortic valve replacement. J Am Heart Assoc. 2020;9(19):e017190.
28. Sayarlioglu H et al. Prevalence and risk factors of valvular calcification in hemodialysis patients. Iran J Kidney Dis. 2013;7(2):129-34.
29. Kurasawa S et al. Number of calcified aortic valve leaflets: natural history and prognostic value in patients undergoing hemodialysis. Eur Heart J Cardiovasc Imaging. 2023;24(7):909-20.
30. Ezwaie MO et al. Prevalence and morbidity of severe hyperparathyroidism in the haemodialysis population. Jamahiriya Med J. 2009;9:276-80.
31. Torigoe M et al. association between serum phosphate levels and the development of aortic stenosis in patients undergoing hemodialysis. J Clin Med. 2021;10(19):4385.
32. Dejan P et al. Hyperphosphatemia: the risk factor for adverse outcome in maintenance hemodialysis patients. J
Med Biochem. 2012;31(3):239-45.
33. Buargub MA et al. Prevalence and pattern of renal osteodystrophy in chronic haemodialysis patients: a cross sectional study of 103 patients. Saudi J Kidney Dis Transpl. 2006;17(3):401-7.
34. Oxlund CS et al. Progressive valvular calcifications with critical aortic stenosis in a 25-year-old woman with end-stage renal disease on haemodialysis: a case report. Eur Heart J Case Rep. 2021;5(7):ytab061.
35. Aurigemma C et al. Heart valve disease gender difference in the era of transcatheter treatment. Heart Vessels Transplant. 2023;DOI:10.24969/ hvt.2022.375.
36. Perkovic V et al. Accelerated progression of calcific aortic stenosis in dialysis patients. Nephron Clin Pract. 2003;94(2):c40-5.
37. Husain A et al. Progression in the severity of aortic stenosis according to race among those with advanced chronic kidney disease. Cardiovasc Diagn Ther. 2020;10(1):24-30.
38. Rroji M et al. Is residual renal function and better phosphate control in peritoneal dialysis an answer for the lower prevalence of valve calcification compared to hemodialysis patients? Int Urol Nephrol. 2014;46(1):175-82.
39. Evenepoel P et al. Phosphorus metabolism in peritoneal dialysisand haemodialysis-treated patients. Nephrol Dial Transplant. 2016;31(9):1508-14.
40. Bae JY et al. A call to consider an aortic stenosis screening program. Trends Cardiovasc Med. 2024;34(5):297-301.
Myocardial Crypts and Ventricular Fibrillation: Two Case Reports
Authors: *Francesco Di Spigno,1 Andrea Caraffini,2 Eleonora Canu,2 Nicola De Santis,2 Daniela Aschier1
1. Cardiology Department Guglielmo Da Saliceto Hospital, Piacenza, Italy
2. Department of Clinical and Experimental Medicine, University of Parma, Italy
*Correspondence to Francesco.dispigno@yahoo.com
Disclosure: The authors have declared no conflicts of interest.
Left ventricular myocardial crypts are defined as invaginations traversing >50% of the myocardial wall, with an incidence of 9.1% in the general population. Several studies have suggested that these morphological findings could be a marker of myocardial disease. The authors present two cases of cardiac arrest (CA) due to ventricular fibrillation (VF) and incidental findings on cardiac magnetic resonance (CMR) of myocardial crypts, discuss the diagnosis, the possible correlation with hypertrophic cardiomyopathy, and hypothesise the significance of this entity.
Case Presentation
Case 1 discusses a 58-year-old male affected by arterial hypertension, with a family history of hypertrophic cardiomyopathy (HCM), who presented to the emergency department for a CA due to VF. The 12-lead electrocardiogram was negative for ST-elevation myocardial infarction, Bragada’s pattern, or QT time elongation. Blood gas analysis showed no ionic abnormalities and no hypoxia. Coronary arteries were free from stenosing atheromatous lesions at coronary angiography. CMR showed isolated left ventricular crypt with mild hypertrophy of myocardial wall, preserved ejection fraction, no hyperintensity in the short tau inversion recovery sequences compatible with oedema, and no sign of fibro-adipose tissue substitution at postcontrast sequences. An implantable defibrillator for secondary prevention was implanted and genetic testing was carried out for HCM.
Case 2 discusses a 59-year-old Peruvian male, with a family history of cardiovascular diseases, who suffered from CA due to VF while under elective ear surgical intervention. A defibrillation with a single DC shock was sufficient to restore sinus rhythm. The 12 lead electrocardiogram was negative for ST-elevation myocardial infarction, Bragada’s pattern, or QT time elongation. Transthoracic echocardiography showed mild ventricular hypertrophy and normal global and regional biventricular kinetics (60%), along with mild mitral regurgitation. Coronary arteries were free from stenosing atheromatous lesions at coronary angiography. At CMR, an isolated left ventricular crypt in the inferior basal wall with an extension of 7 mm LL was detected; there wasn’t hyperintensity in the short tau inversion recovery sequences
compatible with oedema and no sign of fibro-adipose tissue substitution at postcontrast sequences was seen. The authors performed genetics testing for HCM, still ongoing. An implantable defibrillator for secondary prevention was implanted.
Discussion
These cases suggest that the presence of crypt could be a marker of myocardial disease. This should warrant clinical follow-up prior to the potential development of left ventricular hypertrophy and the occurrence of serious cardiovascular events, such as heart failure or death. With the evolution of new imaging techniques such as CMR and CT, the detection of these myocardial defects is more accurate. Genetic testing is useful to identify carriers of pathological mutation of HCM that need close follow-up.
Key Points
1. Myocardial crypts, defined as invaginations of the myocardial wall, are often considered markers of myocardial disease. In particular, they are associated with hypertrophic cardiomyopathy.
2. The authors present a case series of two patients who underwent resuscitated cardiac arrest without any explainable cause, and in whom myocardial crypts were found during heart MRI.
3. Myocardial crypts are frequent findings during autopsy or imaging studies but there is a lack of understanding of their prognostic significance in terms of cardiovascular risk or myocardial pathology. Future studies and observations using cardiac MRI will shed light on this topic.
INTRODUCTION
Left ventricular myocardial crypts are rare structural abnormalities and are defined as invaginations traversing major than a half of the myocardial wall, and are generally situated at the basal or mid-inferior portion of the septum or at the apical and in the medium segments of the ventricular wall.1-3 In a large study on the general population undergoing cardiac computed tomography, the incidence of crypts was 9.1%, comparable with previous studies on CMR investigation. This shows that crypts are not associated with major adverse cardiovascular events in an intermediateterm period of observation.4-5 Due to the increasing use of advanced imaging, they were found to be more frequently incidental findings than previously thought.5 It’s important to discriminate left ventricular (LV) crypts from similar isolated non-compaction cardiomyopathy, and myocardial diverticula. While crypts are present predominantly at the basal or mid-inferior portion of the septum and penetrate the myocardium perpendicular to the endocardial border, non-compaction is
predominantly seen in the apex and midventricular wall portion of LV and it’s a noncompacted stratum of myocardial muscle oriented parallel to another layer of compact myocardium.6-7
On the other hand, ventricular diverticula are described as congenital abnormalities, characterised by an extroflection of the myocardial muscle across the entire wall. Crypts and diverticula contract themselves simultaneously with systole, but the diverticula have a narrow attachment collar and extend widely beyond the walls of the ventricle and the external myocardial margin.6-8 The genesis or the process of the remodelling of myocardial crypts during life is unclear as there aren’t studies of imaging that document the evolution of these myocardial anomalies from childhood to adult life.
Their formation probably takes place during embryological modification of the myocardium, related to a failure of reabsorption of the trabeculated area of the myocardial ventricular wall.9 This is probably due to altered contractility properties of
embryonic myocytes, which cause an unusual mechanical tension towards the insertion points, pulling apart the myocardial fibres and generating the crypts.10 Near crypts are usually seen in myocyte disarray, supporting the concept of disruption of normal myocyte disposition as a morphological substrate for crypt genesis.11
While CMR imaging is the gold standard diagnostic technique to detect myocardial abnormalities, transthoracic echocardiography (TE) can be an initial diagnostic instrument that may reveal some abnormalities or suspects that can guide further investigation.12-13 CMR imaging is better than standard 2D echocardiography in evaluating myocardial wall hypertrophy. Above all, in LV apical and anterolateral portions, it allows for a view of myocardial crypts and papillary muscle abnormalities, subclinical abnormal clues in patients with myocardial myofibrils gene mutations.14-16 Some studies highlighted that atypical presentation of HCM is more frequent than what was known.17-19 A particular entity is represented by focal segmental hypertrophy, a variant that sometimes involves only one or two myocardial segments, often with a non-contiguous pattern. In patients with HCM, it is noted that focal segmental LV hypertrophy is limited to the anterolateral free wall, posterior septum, or apex in 12% of cases.17-19
A lot of studies tried to show the correlation between findings of myocardial crypts or cleft and HCM, hypothesising that they could be a pre-phenotypic sign of that disease.20-22 A better understanding of these findings is essential. This has also been mentioned in the 2014 European Society of Cardiology (ESC) guidelines of hypertrophy cardiomyopathy, cited as a finding to pay attention to in patients who are suspected to have cardiomyopathy.14
Related to these recommendations the authors present two cases of patients who had a cardiac arrest (CA) due to ventricular fibrillation (VF), resuscitated promptly with direct current (DC) shock.
In both cases, the authors followed the current evidence and guidelines on
the management of CA to identify the underlying aetiology, and to choose the best therapeutic strategy for the patient.23
CASE PRESENTATION
Patient 1
A 58-year-old Italian male affected by arterial hypertension, with a family history of HCM and without any previous cardiovascular history or significant comorbidities, presented to the emergency department after CA while doing sport. A single defibrillation with DC shock on VF was performed outside the hospital. On admission, a 12-lead electrocardiogram (ECG) was negative for ST elevation myocardial infarction (STEMI), any Bragada’s pattern, or QT time elongation.24-25 The ECG tracing was not suggestive of HCM or arrhythmogenic dysplasia of the right ventricle or LV hypertrophy.26
Blood gas analysis showed no ionic abnormalities (K+ 3.8 mmol/L with a normal value of 3.6–5.2 mmol/L) or signs of hypoxia. Coronary angiography showed coronary arteries free from stenosing atheromatous lesions.
During hospitalisation, the patient was subjected to a flecainide test to exclude a possible implication of underlying Bragada’s syndrome, and the results for Bragada’s ECG pattern were negative.27 Moreover, the authors performed TE with contrast (sulphur hexafluoride) to obtain the best definition of the LV kinetics, with a supplementary analysis with speckle tracking, which showed mild hypertrophy (maximal diameter of 12 mm at basal septum), normal biventricular kinesis (ejection fraction 60%) and volumes, and excluded abnormalities of valvular apparatus. An isolated distal anterior myocardial crypt was found.
CMR was performed because of the last finding and an isolated LV crypt in the midapical site of the septum with an extension of 9x6 mm antero-posterior (AP) x laterolateral (LL) was detected (Figure 1); at that level, the ventricular wall was focally thinned. The papillary muscles appeared
apicalised and bifid. STIR sequences didn’t highlight any compatible feature with oedema and no sign of fibro-adipose tissue substitution at postcontrast sequences was seen. During the observation, in the authors’ department at the ECG telemetry, no ventricular or supraventricular arrhythmias were detected, so the administration of anti-arrhythmic drugs was not required.
After the exclusion of the primary cause of CA, and considering the clinical suspicion based on instrumental findings, the patient underwent implantable cardioverter defibrillator (ICD) implantation for secondary prevention. Based on clinical suspicion of HCM, genetic testing was carried out for the patient.
Patient 2
A 59-year-old Peruvian male, with cardiovascular risk factors, a family history of cardiovascular diseases, and no previous cardiovascular events or significant comorbidities, suffered from CA due to VF while under elective ear surgical intervention and was treated by single defibrillation with DC shock, restoring sinus rhythm.
The 12-lead ECG excluded STEMI, Bragada’s pattern, or QT time elongation.24,25 The
ECG pattern was not suggestive of HCM or arrhythmogenic dysplasia of the right ventricle, and there were no signs of LV hypertrophy found in ECG.26
No other reversible causes were identified, and no ion abnormalities at blood gas analysis, or other laboratories blood alteration.
TE showed mild ventricular hypertrophy (maximal diameter of 12 mm at basal septum), normal global and regional biventricular kinetics (left ventricular ejection fraction 60%), along with mild mitral regurgitation but without valve prolapse.28
Coronary arteries were free from stenosing atheromatous lesions at coronary angiography and the Flecainide challenge test was negative for Bragada’s ECG pattern.27
A CMR was performed to further characterise this finding, which showed an isolated LV crypt in the inferior basal wall with an extension of 7 mm LL (Figure 2); STIR sequences didn’t highlight any compatible feature with oedema or signs of fibro-adipose tissue substitution at postcontrast sequences. During the observation, in the authors’ department
Figure 1: Four-chamber phase-sensitive inversion recovery sequence showed left ventricular crypt in the mid-apical site of the septum (dimension of 9x6 mm antero-posterior x latero-lateral).
Figure 2: Two-chamber phase-sensitive inversion recovery sequence showed left ventricular crypt in the inferior basal wall (dimension of 7 mm latero-lateral).
at the ECG telemetry, no ventricular or supraventricular arrhythmias were detected. The subsequent clinical course was regular.
Like the previous case, the patient was first implanted with an intravenous unicameral ICD for secondary prevention and genetic testing for HCM was carried out.
DISCUSSION
HCM is the most frequent genetic cardiovascular disease.16 According to the ESC guidelines, HCM it is a pathological condition that occurs when myocardial thickness in any myocardial segment is ≥15 mm, with not explained by conditions of increased post-load. In case of minor wall thickness (13–14 mm), further evaluation including family history for syncope, sudden death, genetic tests, and ECG suggestive pattern is required.14 HCM exhibits the classic characteristics of a monogenic disorder that follows an autosomal dominant mode of inheritance. Changes in more than a dozen genes that code for proteins associated with the sarcomere are responsible for the development of HCM. The genes MYH7 and MYBPC3 are the most frequently occurring, accounting for around half of all patients with familial
HCM. Meanwhile, TNNT2, TNNI3, and TPM1 mutations are relatively rare, contributing to less than 10% of HCM cases. Additionally, ACTC1, MYL2, MYL3, and CSRP3 mutations are also established causes of HCM, although they are uncommon. There is strong evidence for the role of these nine genes in HCM.
Other genes mutations have also been linked to HCM, but they are typically found in sporadic cases and small families.29 HCM is also characterised by multiple phenotypic and genotypic heterogeneity.17 The clinical presentation of HCM is variable and while several patients with HCM are asymptomatic, others may present even with sudden cardiac death (SCD) as their first clinical symptom, most commonly because of ventricular arrhythmias.8,16 In these cases, the authors present two males with CA, without any reversible or secondary identifiable cause like systemic inflammatory disease or toxic cause, with CMR finding of myocardial crypt; the first located in the mid-apical site of the septum, the last one in the inferior basal wall. Both cases didn’t show a frank hypertrophy phenotype according to the definition of HCM, but the clinical presentation along with mild hypertrophy of the basal septum
(12 and 13 mm) and crypt finding led the authors to hypothesise a correlation between myocardial crypts and initial stage of HCM. In both these cases, global cardiac mass was within the normal range. Indeed, the correlation between LV mass and maximal wall thickness was not very strong, and in patients with asymmetric HCM, especially when only a small portion of the LV is affected, LV mass can still be within the normal range.14
Prior studies and cases have suggested that myocardial crypts may serve as precursor events or indicators of HCM in individuals who do not exhibit clear manifestations of the condition.30 In a limited investigation, the identification of two or more hidden chambers on CMR provided a 100% accurate indication in predicting the presence of HCM mutation carriers.31
In 2014 a study was conducted with MRI, where the relationships between the positive genotype for HCM mutations and the heart MRI images of phenotypically negative patients were investigated.21 In this paper, the author demonstrates that myocardial crypts and anterior mitral valve leaflet elongation are the two parameters that most strongly associate with the presence of sarcomere gene mutations. Observations also suggest that MYBPC3 mutation carriers have a two-fold prevalence of crypts and less LV systolic cavity reduction compared with the other combined mutations.21
It is widely understood that, among individuals with HCM, the most prevalent cause of death is SCD resulting from VF or ventricular tachycardia (VT). This unfortunate outcome often impacts young individuals who present frequently without symptoms.32 With these two case reports the authors suspected an association between the finding of crypts in an apparent healthy heart with CA.
The possible causes of ventricular arrhythmias in HCM include intraventricular conduction dispersion, which is caused by varying sizes of cardiomyocytes; the presence of fibrosis and disarray, which provide alternative conduction pathways
that promote re-entry; and disruptions in intercalated discs that disrupt the smooth transmission of action potentials between cardiomyocytes, leading to arrhythmias.33-35 It’s difficult to demonstrate that these mechanisms could be present in a structural and functionally normal heart, only with a mutation of HCM present and not that of Frank’s disease. The infrequency of these discoveries in patients with a history of CA can be attributed to the low survival rate in these individuals.36 A previous study has reported evidence of myocardial invagination in the autopsy of a young man’s death of CA with asymmetrical ventricular hypertrophy.37-38
At present, there are no case reports describing a clear link in the literature between the finding of myocardial crypts and increased susceptibility to the onset of ventricular arrhythmias or SCD.
An active search for structural changes in imaging, collection of databases with this information, and ideally an anatomopathological finding in the future will be able to help in giving a more specific prognostic role to myocardial crypts.
Against these suspicions, in 2021 a major study on this topic was published that demonstrated that myocardial crypts are commonly found among the general population and do not show any connection with significant adverse cardiovascular events in the medium term.4 However, there is an error; the limitations of the study can’t rule out the current author's doubts. The population of this study was composed completely of Danish people, but there are some studies that demonstrate differences in mortality and incidence between racial groups for HCM.39
Further pathological investigations are required on heart tissue with HCM and various underlying causes, as well as normal hearts, to deepen knowledge of this entity. The role of myocardial anomalies in the risk of experiencing fatal arrhythmic events will become clearer in the future through further research, enhanced survival rates for CA, and the easier availability of advanced imaging techniques such as
CMR and cardiac CT. Another crucial point in most cases is the reduced availability of genetic testing, with extremely long times to obtain results. Improvement in this aspect could guarantee major information on the association between certain types of mutation and phenotypical patterns in vivo, or the risk of sudden death.40-42
Furthermore, it would be reasonable to conduct a multicentre prospective registry involving a substantial patient population who underwent CMR imaging, to monitor clinical outcomes continuously. This registry, like the EuroCMR registry, could offer valuable insights into the possible clinical significance of crypts, specifically concerning HCM.15
According to literature data, the occurrence of ventricular arrhythmias and syncope is thought to be very rare in pre-LVH mutation carriers, and current risk stratification strategies and guidance do not include these individuals.4
References
1. Petryka J et al. Prevalence of inferobasal myocardial crypts among patients referred for cardiovascular magnetic resonance. Circ Cardiovasc Imaging 2014;7(2):259-64.
2. Johansson B et al. Clefts can be seen in the basal inferior wall of the left ventricle and the interventricular septum in healthy volunteers as well as patients by cardiovascular magnetic resonance. J Am Coll Cardiol. 2007;50(13):1294-5.
3. Basso C et al. Myocardial clefts, crypts, or crevices. Circ Cardiovasc Imaging. 2014;7(2):217-9.
4. Sigvardsen PE et al. Left ventricular myocardial crypts: morphological patterns and prognostic implications. Eur Heart J Cardiovasc Imaging. 2021;22(1):75-81.
5. Child N et al. Prevalence of myocardial crypts in a large retrospective cohort study by cardiovascular magnetic resonance. J Cardiovasc Magn Reason. 2014;16(1):66
6. Brouwer WP et al. Multiple myocardial crypts on modified long-axis view are a specific finding in pre-hypertrophic HCM mutation carriers. Eur Heart J Cardiovasc. 2012;13(4):292-7.
7. Jenni R. Echocardiographic and pathoanatomical characteristics of
CONCLUSION
In conclusion, the authors’ case studies highlight important cardiovascular consequences that could be associated to left myocardial crypt, in the absence of other pathological finding at second level diagnostic tool. The occurrence of VF and VT increases the risk of SCD, especially when it happens in extra-hospital conditions, and when an external cardiac defibrillator isn’t available. Early identification of these patients could be essential to manage the early stages of HCM and prevent malignant arrhythmias or SCD. The implantation of ICD is highly effective in terminating VF and VT, indicating that these devices have a role in the primary and secondary prevention of malignant arrhythmias. Genetic testing and genetic counselling are useful to identify carriers of pathological mutation of HCM that need close clinical and instrumental follow-up in good clinical practice.45
isolated left ventricular non-compaction: a step towards classification as a distinct cardiomyopathy. Heart. 2001;86(6):666-71.
8. Almeida PC et al. Role of cardiac magnetic resonance in the diagnosis of infiltrative, hypertrophic, and arrhythmogenic cardiomyopathies. Front Biosci (Schol Ed). 2022;14(1):7.
9. Captur G et al. The embryological basis of subclinical hypertrophic cardiomyopathy. Sci Rep. 2016;6:27714.
10. Cresti A et al. Multimodality imaging and clinical significance of congenital ventricular outpouchings: recesses, diverticula, aneurysms, clefts, and crypts. J Cardiovasc Echogr. 2018;28(1):9-17.
11. Kuribayashi T, Roberts WC. Myocardial disarray at junction of ventricular septum and left and right ventricular free walls in hypertrophic cardiomyopathy. Am J Cardiol. 1992;70(15):1333-40.
12. Pavasini R et al. The use of multimodality imaging for the diagnosis of myocardial outpouchings and invaginations: a systematic review. Life (Basel). 2023;13(3):650.
13. Høyland K et al. Echocardiographic features of left ventricular recess, cleft, diverticulum, and aneurysm: a
14. Elliott PM et al.; Task Force Members. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: the task force for the diagnosis and management of hypertrophic cardiomyopathy of the European society of cardiology (ESC). Eur Heart J. 2014;35(39):2733–79.
15. Brouwer WP et al. Multiple myocardial crypts on modified long-axis view are a specific finding in pre-hypertrophic HCM mutation carriers. Eur Heart J Cardiovasc Imaging. 2012;13(4):292-7.
16. Germans T et al. Structural abnormalities of the inferoseptal left ventricular wall detected by cardiac magnetic resonance imaging in carriers of hypertrophic cardiomyopathy mutations. J Am Coll Cardiol. 2006;48(12):2518-23.
17. To AC et al. Cardiac magnetic resonance in hypertrophic cardiomyopathy. JACC Cardiovasc Imaging. 2011;4:1123-37.
18. Olivotto I et al. Myofilament protein gene mutation screening and outcome of patients with hypertrophic cardiomyopathy. Mayo Clin Proc. 2008;83(6):630-8.
19. Rickers C et al. Utility of cardiac magnetic resonance imaging in the diagnosis of hypertrophic cardiomyopathy. Circ. 2005;112:85561.
20. Maron MS et al. Prevalence and clinical profile of myocardial crypts in hypertrophic cardiomyopathy. Circ Cardiovasc Imaging. 2012;5(4):441-7.
21. Captur G et al. Prediction of sarcomere mutations in subclinical hypertrophic cardiomyopathy. Circ Cardiovasc Imaging. 2014;7:863-71.
22. Moon JC, McKenna WJ. Myocardial crypts: a prephenotypic marker of hypertrophic cardiomyopathy? Circ Cardiovasc Imaging. 2012;5(4):431-2.
23. Katja Zeppenfeld et al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J. 2022;43(40):39974126,
24. Rautaharju PM et al. AHA/ACCF/ HRS recommendations for the standardization and interpretation of the electrocardiogram: part IV: the ST segment, T and U waves, and the QT interval: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Endorsed by the International Society for Computerized Electrocardiology. J Am Coll Cardiol. 2009;53(11):982-91.
25. Luna ABD et al. Current electrocardiographic criteria for diagnosis of Brugada pattern: a consensus report. J Electrocardiol. 2012;45(5):433-42.
26. Peguero J et al. Electrocardiographic criteria for the diagnosis of left ventricular hypertrophy. J Am Coll Cardiol. 2017,69(13):1694-703.
27. Obeyesekere MN et al. How to perform and interpret provocative testing for the diagnosis of Brugada syndrome, long-QT syndrome, and catecholaminergic polymorphic ventricular tachycardia. Circ Arrhythm Electrophysiol. 2011;4(6):958-64.
28. Marian AJ, Braunwald E. Hypertrophic cardiomyopathy: genetics, pathogenesis, clinical manifestations, diagnosis, and therapy. Circ Res. 2017;121(7):749-70.
29. Muthukumar L et al. Association between malignant mitral valve prolapse and sudden cardiac death: a review. JAMA Cardiol. 2020;5(9):105361.
30. Rowin EJ, Maron MS. Myocardial crypts in hypertrophic cardiomyopathy: the new gang in town. Eur Heart J Cardiovasc. Imaging. 2012,13(4):281-3.
31. Wessel P. Brouwer et al. Multiple myocardial crypts on modified longaxis view are a specific finding in prehypertrophic HCM mutation carriers. Eur Heart J Cardiovasc Imaging. 2012;13(4):292-7.
32. Maron BJ et al. Epidemiology of hypertrophic cardiomyopathy-related death: revisited in a large non-referralbased patient population. Circ. 2000;102(8):858-64
33. Saumarez RC et al. Ventricular fibrillation in hypertrophic cardiomyopathy is associated with increased fractionation of paced right ventricular electrograms. Circ. 1992;86(2):467-74.
34. Saumarez RC et al. The significance of paced electrogram fractionation in hypertrophic cardiomyopathy. A prospective study. Circ. 1995;1(11):2762-8.
35. O'Mahony C et al. Sudden cardiac death in hypertrophic cardiomyopathy. Circ Arrhythm Electrophysiol.
2013;6(2):443-51.
36. Sawyer KN et al. Sudden cardiac arrest survivorship: a scientific statement from the American Heart Association. Circ. 2020;141(12):e654-85.
37. Teare D. Asymmetrical hypertrophy of the heart in young adults. Br Heart J. 1958;20(1):1-8.
38. Afonso L et al. Myocardial cleft, crypt, diverticulum, or aneurysm? Does it really matter? Clin Cardiol. 2009;32(8):e48-51.
39. Minhas AMK et al. Demographic and regional trends of hypertrophic cardiomyopathy-related mortality in the United States, 1999 to 2019. Circ Heart Fail. 2022;15(9):e009292.
40. Ingles J et al. Application of genetic testing in hypertrophic cardiomyopathy for preclinical disease detection. Circ Cardiovasc Genet. 2015;8(6):852-9.
41. McNally E, Dellefave L. Sarcomere mutations in cardiogenesis and ventricular noncompaction. Trends Cardiovasc. Med 2009;19(1):17-21.
42. Bonaventura J et al. Genetic testing in patients with hypertrophic cardiomyopathy. Int J Mol Sci. 2021;22(19):10401.
43. Fonseca Ferreira M et al. Pre-left ventricular hypertrophy stage in hypertrophic cardiomyopathy – is really benign? Presentation 2. ESC, 27-30 August 2021.
44. Maron, B J et al. Efficacy of implantable cardioverter-defibrillators for the prevention of sudden death in patients with hypertrophic cardiomyopathy. N Engl J Med. 2000;342(6):365-73.
45. Girolami F et al. Genetic testing and counselling in hypertrophic cardiomyopathy: frequently asked questions. J Clin Med. 2023;12(7):2489.
Depressive Symptoms and Left Ventricular Diastolic Dysfunction Among Men and Women with HIV
Authors: Claudia Martinez,1 Nel Jason Haw,2 Violeta J. Rodriguez,3 Jorge R. Kizer,4,5 Wendy S. Post,2 Katherine C. Wu,6 Joao A. C. Lima,6 Jenni M. Wise,7 Maria L. Alcaide,1 Michael Plankey,8 Deborah Konkle-Parker,9 Sofia Kozlova,1 Margaret A. Fischl,10 Adaora A. Adimora,11 Matthew Budoff,12 Yasmeen Golzar,13 Jason Lazar,14 Frank J Palella,15 Carlos J. Rodriguez,16 Andrea M. Weinstein,17 Gina Wingood,18 Amanda Blair Spence,8 Heather McKay,2 *Deborah L. Jones19
1. University of Miami Miller School of Medicine, Florida, USA
2. Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Johns Hopkins University, Baltimore, Maryland, USA
3. University of Illinois Urbana-Champaign, USA
4. San Francisco Veterans Affairs Health Care System, California, USA
5. Department of Medicine, Epidemiology and Biostatistics, University of California, San Francisco, USA
6. Department of Medicine, Division of Cardiology, Johns Hopkins University, Baltimore, Maryland, USA
7. Department of Family, Community, and Health Systems, School of Nursing, University of Alabama at Birmingham, Alabama, USA
8. Department of Medicine, Division of Infectious Disease, Georgetown University Medical Center, Washington, D.C., USA
9. University of Mississippi Medical Center, Schools of Nursing, Medicine and Population Health, Jackson, Mississippi, USA
10. AIDS Clinical Research Unit, University of Miami Miller School of Medicine, Florida, USA
11. Department of Epidemiology, Division of Infectious Diseases, School of Medicine, University of North Carolina at Chapel Hill, North Carolina, USA
12. Lundquist Institute at Harbor-UCLA, UCLA David Geffen School of Medicine, Los Angeles, California, USA
13. Cook County Health, Chicago, Illinois, USA
14. State University of New York Downstate Medical Center, Brooklyn, USA
15. Northwestern University Feinberg School of Medicine, Chicago, Illinois, USA
16. Albert Einstein College of Medicine, Bronx, New York, USA
17. Department of Psychiatry, School of Medicine, University of Pittsburgh, Pennsylvania, USA
18. Columbia University, New York, USA
19. Department of Psychiatry and Behavioral Sciences, University of Miami Miller School of Medicine, Florida, USA
*Correspondence to d.jones3@med.miami.edu
Disclosure:
The MACS/WIHS Combined Cohort Study (MWCCS) was sponsored by the National Institutes of Health (NIH). Kizer has declared stock ownership in Abbvie, Abbott, Bristol Myers Squibb, Johnson & Johnson, Medtronic, Merck, and Pfizer. All other authors have declared no conflicts of interest.
Acknowledgements: Data in this manuscript were collected by the MACS/WIHS Combined Cohort Study (MWCCS). The contents of this publication are solely the responsibility of the authors and do not represent the official views of the National Institutes of Health (NIH). MWCCS (Principal Investigators): Atlanta CRS (Ighovwerha Ofotokun, Anandi Sheth, and Gina Wingood), U01-HL146241; Baltimore CRS (Todd Brown and Joseph Margolick), U01-HL146201; Bronx CRS (Kathryn Anastos, David Hanna, and Anjali Sharma), U01-HL146204; Brooklyn CRS (Deborah Gustafson and Tracey Wilson), U01-HL146202; Data Analysis and Coordination Center (Gypsyamber D’Souza, Stephen Gange and Elizabeth Topper), U01-HL146193; Chicago-Cook County CRS (Mardge Cohen and Audrey French), U01-HL146245; Chicago-Northwestern CRS (Steven Wolinsky, Frank Palella, and Valentina Stosor), U01-HL146240; Northern California CRS (Bradley Aouizerat, Jennifer Price, and Phyllis Tien), U01-HL146242; Los Angeles CRS (Roger Detels and Matthew Mimiaga), U01HL146333; Metropolitan Washington CRS (Seble Kassaye and Daniel Merenstein), U01-HL146205; Miami CRS (Maria Alcaide, Margaret Fischl, and Deborah Jones), U01-HL146203; Pittsburgh CRS (Jeremy Martinson and Charles Rinaldo), U01HL146208; UAB-MS CRS (Mirjam-Colette Kempf, Jodie Dionne-Odom, Deborah Konkle-Parker, and James B. Brock), U01-HL146192; UNC CRS (Adaora Adimora and Michelle Floris-Moore), U01-HL146194. The MWCCS is funded primarily by the National Heart, Lung, and Blood Institute (NHLBI), with additional co-funding
from the Eunice Kennedy Shriver National Institute Of Child Health & Human Development (NICHD), National Institute On Aging (NIA), National Institute Of Dental & Craniofacial Research (NIDCR), National Institute Of Allergy And Infectious Diseases (NIAID), National Institute Of Neurological Disorders And Stroke (NINDS), National Institute Of Mental Health (NIMH), National Institute On Drug Abuse (NIDA), National Institute Of Nursing Research (NINR), National Cancer Institute (NCI), National Institute on Alcohol Abuse and Alcoholism (NIAAA), National Institute on Deafness and Other Communication Disorders (NIDCD), National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), National Institute on Minority Health and Health Disparities (NIMHD), and in coordination and alignment with the research priorities of the National Institutes of Health, Office of AIDS Research (OAR). MWCCS data collection is also supported by UL1TR000004 (UCSF CTSA), UL1-TR003098 (JHU ICTR), UL1-TR001881 (UCLA CTSI), P30-AI-050409 (Atlanta CFAR), P30-AI-073961 (Miami CFAR), P30-AI-050410 (UNC CFAR), P30-AI-027767 (UAB CFAR), P30-MH-116867 (Miami CHARM), UL1TR001409 (DC CTSA), KL2-TR001432 (DC CTSA), and TL1-TR001431 (DC CTSA). The authors gratefully acknowledge the contributions of the study participants and dedication of the staff at the MWCCS sites.
Received: 06.11.23
Accepted: 23.06.24
Keywords: Depressive symptoms, HIV, left ventricular diastolic dysfunction.
Erratum: This article was first published on 29.08.2024. Since then, an erratum was made. The erratum can be seen here
Abstract
Background and Aim: The prevalence of depressive symptoms and major depressive disorder is high among adults living with HIV. Depressive symptoms are associated with increased cardiovascular disease risk. This study examined the association between depressive symptoms and echocardiographic indices of left ventricular diastolic dysfunction (LVDD) among men and women living with and without HIV.
Methods: Cross-sectional analysis included individuals in the Multicenter AIDS Cohort Study (MACS) and Women’s Interagency HIV Study (WIHS) who participated in transthoracic echocardiogram substudies and completed measures of depressive symptoms at the same visit as, or up to 6 months prior to, the transthoracic echocardiogram visit. Participants had helper T cells (CD4) >350 cells/mm3 and HIV RNA viral load <499 copies/mL. The presence of LVDD was defined according to the Characterizing Heart Function on Antiretroviral Therapy (CHART) criteria. Secondary outcomes were continuous values of each component of the CHART criteria: left ventricular ejection fraction >50%, septal e’ velocity, lateral e’ velocity, left atrial volume index, left ventricular mass index, and relative wall thickness. Logistic and linear regression were used to adjust for sociodemographic, behavioural, cardiometabolic, and HIVrelated factors.
Results: Among 874 men (51% with HIV) and 1,191 women (76% with HIV), in whom the overall prevalence of LVDD was 22.5% and depressive symptoms 30.8%, depressive symptoms were not significantly associated with LVDD. The associations between individual LVDD components and depression were in the small to medium range, though generally not significant.
Conclusion: Findings warrant further research regarding the association between LVDD and depressive symptoms in the era of combination antiretroviral therapy.
Key Points
1. Major depressive disorder and cardiovascular disease are common in patients living with HIV, yet the association between mental health and heart structure changes is not well known.
2. This study examined the relationships between symptoms of depression and diastolic dysfunction by echocardiogram in two well-characterised, longstanding prospective cohorts of men and women living with and without HIV in the USA.
3. Depressive symptoms differed by gender, and when compared by HIV status, men living with HIV had more depressive symptoms. However, depressive symptoms were not associated with diastolic dysfunction in this study.
INTRODUCTION
The prevalence of both major depressive disorder and cardiovascular disease (CVD) is higher among persons living with HIV (PWH) when compared to the general population.1,2 Evidence suggests that both depression and HIV are associated with increased risk for CVD. Studies in the Women’s Interagency HIV Study (WIHS) and Multicenter AIDS Cohort Study (MACS) indicate that among PWH, 47% of women and 26% of men reported high levels of depressive symptoms,3-6 as well as high rates of heart failure.7,8 Depressive symptoms and major depressive disorder (MDD) can potentially increase the risk for CVD in the context of HIV, as both HIV and depression have been independently associated with CVD including heart failure (HF). 9 MDD has been associated with a 30% increase in the risk of myocardial infarction (MI) among PWH after adjusting for traditional CVD risk factors.10 It is unclear whether depressive symptoms impact CVD risk through the intensity and duration of depression.
While previous studies have documented some associations between HIV and changes in heart structure and function, including heart failure among men and women living with HIV, 11-13 and in relation to antiretroviral medications,13 there is limited data examining heart failure precursor specific knowledge among PWH in relation to depressive symptoms, which limits HIVspecific insights into CVD prevention and treatment.12,15 To address this gap, this study utilised data from two large prospective, multicentre cohort studies of men and women with and without HIV infection
in the USA, the MACS and the WIHS, to investigate cross-sectional relationships between symptoms of depression and left ventricular diastolic disfunction (LVDD). In addition, this study evaluated the potential modification of these relationships by HIV status and sex, and associations between LVDD and depression among those living with HIV.
METHODS
Study Participants
This study used data collected from substudies conducted within two longstanding prospective cohort studies of the natural and treated histories of HIV-1 infection: the MACS and the WIHS (subsequently combined into the MACS/ WIHS Combined Cohort Study [MWCCS] in 2019). The MACS was a multicenter study, established in 1984, among men with or at risk for HIV infection, conducted at four sites within the USA: Baltimore, Maryland/ Washington, D.C.; Chicago, Illinois; Pittsburgh, Pennsylvania/Columbus, Ohio; and Los Angeles, California. 16,17 The WIHS was a multicentre study of women living with and without HIV that collected data from 10 sites throughout the USA starting in 1994: Bronx, New York; Brooklyn, New York; Washington, D.C.; Chicago, Illinois; San Francisco, California; Chapel Hill, North Carolina; Miami, Florida; Birmingham, Alabama; Jackson, Mississippi; and Atlanta, Georgia.18 Data collection instruments for each are available online on the MWCCS website.19 All sites obtained approval from their institutional review boards, and all
participants provided written informed consent.
Data for the present study were obtained from transthoracic echocardiogram (TTE) sub-studies conducted within each cohort. Briefly, 1,195 participants in the MACS completed a TTE from 2017–2019, and 1,654 participants in the WIHS completed a TTE visit from 2014–2019.20 Details of the echocardiographic assessments have been described previously.12,20 Both studies included sonographer training and certification, standardised imaging protocols, and centralised imaging interpretation. Data available by 1 August 2022 were used in this analysis.
Participants were included in the present study if they completed a depression questionnaire at the same visit as, or up to 6 months prior to, the TTE visit. They were excluded if they were pregnant (due to physiologic changes during pregnancy), had HIV RNA viral load (VL) >499 copies/ mL, a CD4+ T lymphocytes (CD4) cell count <350 cells/mm3 closest to the TTE visit, a personal or family history of CVD up to 2.5 years prior to the TTE visit, or systolic dysfunction (defined as having left ventricular ejection fraction <50%) at the TTE, or if diastolic dysfunction could not be calculated because of at least one key missing measurement in the component variables. Finally, they were excluded if they had missing data in any one of the key covariates in the main analysis, resulting in a reduction of 3.6% of the total sample after all other exclusions were applied (Supplementary Figure 1).
Measurement of ze Symptoms
Depressive symptoms were assessed using Center for Epidemiologic Studies Depression Scale (CES-D) scores and self-reported antidepressant medication use, assessed on the same visit as, or up to 6 months prior to, the TTE visit.21 The CES-D questionnaire contains 20 items on the frequency of selfreported depression symptoms, scored on a scale of 0 (rarely or none of the time) to 3 (most of the time). The final scale ranges from 0– 60, with higher scores indicating greater severity of depressive symptoms. A
threshold of 16 was considered suggestive of depressive symptomatology, with the presence of depressive symptoms defined as either a CES-D score of ≥16 or selfreported use of antidepressant medication. A score of >20 was also considered to improve sensitivity and specificity in the context of HIV infection.22
Outcomes of Interest
The primary outcome of interest was the presence of LVDD, which was calculated using the criteria defined by the Characterizing Heart Function on Antiretroviral Therapy (CHART) Study.9,11 These criteria include: left ventricular (LV) ejection fraction ≥50%; evidence of impaired LV relaxation, defined as having either septal e’ velocity <7 cm/s or lateral e’ velocity <10 cm/s; evidence of chronically elevated LV filling pressure, defined as having left atrial volume index >28 mL/m2; LV hypertrophy, defined as having LV mass index >95g/m2 in women or >115 g/m2 in men; or concentric LV remodelling, defined as having relative wall thickness >0.42. Secondary outcomes of interest were the continuous values of each individual component used in the CHART criteria.9,11
Statistical Analyses
Descriptive analyses were conducted to assess the distributions (frequencies and proportions) of characteristics on or at the visit closest to the TTE visit, stratified by HIV serostatus and cohort. Regression analyses were used to evaluate the relationships between depressive symptoms with the presence of LVDD (logistic regression) and its individual components (linear regression). All logistic and linear regression models were run separately by cohort, which stratifies the analyses by sex assigned at birth and accounts for potential differences in the study populations and outcome ascertainment. For all outcomes, separately nested models were developed to serially adjust for sociodemographic, behavioural, traditional CVD, and HIV-related risk factors. Model 1 accounted for age (modelled as a natural spline term with two knots), selfreported race/ethnicity (White, Black, other), study site, smoking status (never, former,
current), alcohol consumption (none, <14 drinks/week, ≥14 drinks/week), use of recreational drugs (poppers, crack, cocaine, uppers, injectable drugs, or other) since last visit, and HIV serostatus. Model 2 accounted for all variables in Model 1 as well as traditional CVD risk factors: BMI (weight [kg]/ height [m]2, modelled as a natural spline term with two knots), hypertension (categorised as no hypertension [<140/90 mmHg] and no use of antihypertensive medications, controlled [<140/90 mmHg] and use of antihypertensive medication, or uncontrolled with or without medication [>140/90 mmHg]), diabetes (defined as present if ever self-reported anti-diabetic medication, fasting glucose ≥126 mg/dL, HbA1C≥6.5%, or self-reported diabetes [WIHS]; or current HbA1C ≥6.5%, fasting glucose ≥126 mg/ dL, or diagnosed with diabetes and selfreported use of medications [MACS]), and treated or untreated hepatitis C virus (HCV) status at visit. Model 3 restricted each sample to those living with HIV, and further adjusted for undetectable viral load (defined as below the ratio of detection of the HIV RNA test used, which was 20 copies/mL), current CD4 cell count, nadir CD4 cell count, current use of cART, and history of clinical AIDS. Interaction terms assessed whether associations between depressive symptoms and LVDD and the continuous components of LVDD varied by HIV serostatus and cohort.
Since the prevalence of LVDD in the sample is relatively high (approximately 24%), modified Poisson regression with robust variance estimation was conducted in sensitivity analyses to assess potential overestimation of odds ratios (OR). Statistical significance was determined by a two-sided p<0.05. Analyses were conducted using Stata 17 (StataCorp, College Station, Texas, USA).
RESULTS
Descriptive Statistics
This study was comprised of 874 men (n=433 living with HIV) and 1,191 women (n=783 living with HIV), an average 54 years old (Table 1 and 2). One-third (32.6%) identified as White, 49.2% as Black, and
18.2% as other. One-third (33.1%) of participants were never smokers, whereas 30.3% were current smokers. Women were more likely to smoke compared to men (37.1% versus 21.1%). More than one-third (38.4%) reported no alcohol use since their last visit; alcohol use, defined as <14 drinks a week, was more frequent in women than in men (51.0% versus 21.1%). Overall, 18.3% had prevalent diabetes mellitus, including 13.8% of those in the MACS and 21.5% in the WIHS. Women were more likely to have HCV at the study visit compared to men (16.6% versus 4.9%). Men were more likely to report recreational drug use than women (30.5% versus 26.6%). Recreational drug use was higher among women living without HIV compared to those living with HIV (33.6% versus 23.0%). There were no notable differences by HIV serostatus or by cohort in the prevalence of hypertension. Men were more likely to have depressive symptoms than women (34.9% versus 27.9%). Among men, symptoms were higher among those living with HIV compared to those without HIV (39.7% versus 30.2%), but not in women (WIHS).
Adjusted Associations of Depressive Symptoms with Left Ventricular Diastolic Dysfunction and its Components
After adjustment for sociodemographic characteristics and CVD risk factors, depressive symptoms were not statistically significantly associated with LVDD in the MACS (OR: 0.94; 95% CI: 0.64, 1.37) or the WIHS (OR: 0.83; 95% CI: 0.57, 1.17) (Table 1 and 2). Associations between depressive symptoms and each of the individual components of LVDD by cohort and HIV serostatus were not statistically significant (Table 1 and 2). Among the MACS, the presence of depressive symptoms was associated with greater LV mass (β: 1.94, p=0.30) among men living with HIV and with lower LV mass (β: -3.8, p=0.06) among men not living with HIV. Despite these contrasting trends, the interaction by HIV was not statistically significant. Despite these overall differences, the interactions between HIV serostatus and cohort were not statistically significant. Poisson models showed a similar pattern of results.
Table 1: Study population characteristics, by cohort and HIV serostatus.
Depressive
(IQR)
Table 1 continued.
Viral load, median (IQR) among those with viral load >20 copies/mL
Nadir CD4+ T cell count (cells/mm3), median (IQR)
Current CD4+ T cell count (cells/mm3),
HAART, n (%)
Cumulative years of HAART use, median (IQR)
Table 1 continued.
Cumulative years of NRTI use, median (IQR)
(6.5, 19.9) N/A NNRTI use, n (%)
Cumulative years of NNRTI use, median (IQR)
Cumulative years of PI use, median (IQR)
History of AIDS, n (%)
*Uncontrolled hypertension defined as having a systolic blood pressure >140 mmHg or diastolic blood pressure >90 mmHg. Controlled hypertension defined as having a systolic blood pressure <140 mmHg and diastolic blood pressure <90 mmHg and taking anti-hypertensive medication. No hypertension defined as having a systolic blood pressure <140 mmHg and diastolic blood pressure <90 mmHg and not taking anti-hypertensive medication.
†For MACS, diabetes mellitus defined as glycosylated haemoglobin ≥6.5% or fasting blood glucose ≥126 mg/dL (or diagnosed with diabetes and use of diabetes mellitus medications).
‡Poppers and uppers specified as separate drugs in MACS, while in WIHS, this is included with other drug use.
CD4: cluster of differentiation 4; CESD: Center for Epidemiologic Studies - Depression scale; HAART: highly active antiretroviral therapy; HIV+: HIV positive; HIV-: HIV negative; IQR: interquartile range; MACS: Multicenter AIDS Cohort Study; n (%): number of individuals and percentage of sample; NRTI: nucleoside reverse transcriptase inhibitor; NNRTI: non-nucleoside reverse transcriptase inhibitor; PI: protease inhibitor; TTE: transthoracic echocardiogram; WIHS: Women’s Interagency HIV Study.
Table 2: Study population characteristics, by cohort and HIV serostatus.
Table 2 continued.
load, median (IQR) among those with viral load >20 copies/mL
Nadir CD4+ T cell count (cells/mm3), median (IQR)
Table 2 continued.
use, n (%)
Cumulative years of NNRTI use, median (IQR)
of AIDS, n (%)
*Uncontrolled hypertension defined as having a systolic blood pressure >140 mmHg or diastolic blood pressure >90 mmHg. Controlled hypertension defined as having a systolic blood pressure <140 mmHg and diastolic blood pressure <90 mmHg and taking anti-hypertensive medication. No hypertension defined as having a systolic blood pressure <140 mmHg and diastolic blood pressure <90 mmHg and not taking anti-hypertensive medication.
†For MACS, diabetes mellitus defined as glycosylated haemoglobin ≥6.5% or fasting blood glucose ≥126 mg/dL (or diagnosed with diabetes and use of diabetes mellitus medications).
‡Poppers and uppers specified as separate drugs in MACS, while in WIHS, this is included with other drug use.
CD4: cluster of differentiation 4; CESD: Center for Epidemiologic Studies - Depression scale; HAART: highly active antiretroviral therapy; HIV+: HIV positive; HIV-: HIV negative; IQR: interquartile range; MACS: Multicenter AIDS Cohort Study; n (%): number of individuals and percentage of sample; NRTI: nucleoside reverse transcriptase inhibitor; NNRTI: non-nucleoside reverse transcriptase inhibitor; PI: protease inhibitor; TTE: transthoracic echocardiogram; WIHS: Women’s Interagency HIV Study.
Table 3: Adjusted associations between depressive symptoms and indices of subclinical left ventricular dysfunction, by cohort and HIV status.
Multicenter AIDS Cohort Study (MACS)
Women’s Interagency HIV Study (WIHS)
Left
Table 3 continued.
Left ventricular ejection fraction (%)
Septal e’ velocity (cm/s)
β (95% CI)
Lateral e’ velocity (cm/s)
β (95% CI)
Left atrial volume, indexed (mL/m2)
β (95% CI) 0.00 (-0.96, 0.96)
Left ventricular mass, indexed (g/m2)
β (95% CI)
p-value 0.65 0.30 0.06 N/A 0.14 0.19 0.70 N/A N/A
Table 3 continued.
Relative wall thickness
β (95% CI) -0.0041 (-0.0129, 0.0046)
(-0.0148, 0.0100)
(-0.0180, 0.0076)
(-0.0015, 0.0148)
(-0.0013, 0.0173)
(-0.0124, 0.0193)
Final models were adjusted for race, site, smoking status, alcohol use since last visit, use of any recreational drug, HIV status, age at visit, body mass index at visit, hypertension status at visit, diabetes status at visit, and Hepatitis C status at visit. The analysis for the left ventricular diastolic dysfunction outcome excludes the 45 participants with left ventricular systolic dysfunction.
CHART: Characterizing Heart Function on Antiretroviral Therapy Study; OR: odds ratio.
Among participants living with HIV, associations between depressive symptoms and LVDD showed a similar pattern. Among both men and women living with HIV, depressive symptoms were associated with greater LV mass compared to those without depressive symptoms (β: 2.16 [95% CI:-1.51, 5.84] and 1.68 [95% CI: -0.77, 4.14]), although neither reached statistical significance at the 0.05 level. Using a cutoff of 20 on the CES-D scale instead of 16 resulted in similar findings for those living with HIV.
Among PWH, HIV clinical characteristics and LVDD were not statistically significantly associated except for nadir CD4+ T cell count among women (Table 3), though this was a small positive effect.
DISCUSSION
This study examined the relationships between symptoms of depression and LVDD in two well-characterised, longstanding prospective cohorts of men and women living with and without HIV in the USA.
Despite differences in sociodemographics and CVD risk factors among men and women in this study, no statistically significant differences were found by HIV serostatus status or by sex at birth in observed associations between depressive symptoms and the likelihood of LVDD, or with the individual components of the CHART criteria for LVDD.11 Findings suggest that while LVDD is prevalent among men and women with depressive symptoms, when controlling for sociodemographics, health, and other HIV related factors, depressive symptoms do not appear to be associated with LVDD.
In contrast with the current study, results from smaller previous studies identified that LVDD was correlated with major depressive symptoms23,24 in people living with and without HIV.25-27 This could be explained by the fact that the MACS and WIHS are longlived cohorts in which most participants were well controlled, had been receiving antiretroviral therapy (ART), and who had documented depressive symptoms prior to the echocardiogram. As such, this sample included mostly persons who were on ART
and/or had a high degree of virologic control but did not distinguish between depressive symptoms and MDD. In addition, previous reports did not compare heart function by HIV serostatus and by sex assigned at birth. This study comprises an important and novel contribution to the literature by evaluating associations between depressive symptoms and LVDD among participants by sex at birth and HIV serostatus. This analysis did not account for prior depressive symptoms or for the cumulative effect of depressive symptoms. Future research should consider examining these associations using measures of depressive symptoms that account for potential intensity and cumulative effects. Furthermore, in this study, there was a conflicting finding about ART status and LVDD between the cohorts. Specifically, the association between ART and LVDD was considerably negative among men (OR: 0.55) versus positive among women (OR: 2.45). As it appears that such a result has not been reported in the literature before, this finding warrants further research and examination to evaluate similar directionality in other groups. Finally, the use of newer ART now available (e.g., integrase strand transfer inhibitor-based regimens) should be evaluated in the future; this sample did not allow for further exploration of different types of ART, which may have a differential role on cardiac function.
Limitations of this study include that the data collected from this study was at a time when they were two different cohorts; therefore, the data was analysed for each of the cohorts. There were unique intrinsic differences in the cohorts including ethnicity and background differences. WIHS participants who were women were predominantly Black women from low socioeconomic backgrounds, many of whom were from the Southern USA (Alabama, Mississippi, Georgia, North Carolina, and Florida), where Medicaid expansion has not been adopted.28 Moreover, WIHS participants had fewer financial and medical resources than MACS participants, who were generally of higher income, higher education, not residing in the South, and predominantly White. Overall, MACS participants as a group were less subject to issues of systemic racism;
these differences may have obscured results in the primary analyses and limited the generalisability of these findings. As such, these comparisons between cohorts (and therefore, comparisons by sex) may be biased by these broader cohort differences. Hence, there are many potential variables that can affect these findings. However, moving forward, the cohorts have unified, and the data is being harmonised, and each site will have both men and women enrolled in the MWCCS. Further research is needed to disentangle these relationships. Given the cross-sectional nature of this study design, inferences about causality cannot be made, and the potential for residual confounding and spurious associations remains despite adjustment for multiple covariates. A longitudinal study could offer more statistical power and enable the examination of the temporality of depressive symptoms and CVD outcomes, and vice versa.
This study has important strengths. A primary strength is the study population, which was drawn from two well-established ethnically and socially diverse cohorts; among whom over half were women. These longstanding cohorts utilised standardised data collection and intensively trained TTE testing, with centralised analyses, minimising potential information bias due to measurement error. Moreover, data from the ART era facilitates the understanding of depressive symptoms and subclinical heart structure and function in the context of virally suppressed HIV. Additionally, the inclusion of people living without HIV with otherwise similar risk phenotypes improved adjustment for potential confounders that may be associated with depression and alter cardiac structure and function.
CONCLUSION
In summary, this study examined the presence of depressive symptoms and TTE indices of LVDD among men and women both living with and without HIV. Depressive symptoms differed by gender and when compared by HIV status, men living with HIV had more depressive symptoms. However, the presence of depressive symptoms was
not associated with LVDD. Longitudinal analysis could offer more statistical power and enable evaluation of the intensity and temporality of depressive symptoms and CVD outcomes, particularly in the context of
1. Polanka BM et al. Examining depression as a risk factor for cardiovascular disease in people with HIV: a systematic review. Ann Behav Med. 2023;57(1):1-25.
2. Pieper AA, Treisman GJ. Depression, mania, and schizophrenia in HIVinfected patients. 2021. https://pro. uptodatefree.ir/Show/4864. Last accessed: 31 October 2023.
3. Park KS et al. Associations of depression and anxiety with cardiovascular risk among people living with HIV/AIDS in Korea. Epidemiol Health. 2021;43:e2021002.
4. Celano CM et al. Depression and anxiety in heart failure: a review. Harv Rev Psychiatry. 2018;26(4):175-84.
5. Levy ME et al. Depression and psychosocial stress are associated with subclinical carotid atherosclerosis among women living with HIV. J Am Heart Assoc. 2020;9(13):e016425.
6. Irwin MR et al. Increased risk of depression in non-depressed HIV infected men with sleep disturbance: prospective findings from the Multicenter AIDS Cohort Study. EBioMedicine. 2018;36:454-60.
7. Sbolli M et al. Depression and heart failure: the lonely comorbidity. Eur J Heart Fail. 2020;22(11):2007-17.
8. Feinstein MJ et al. Adjudicated heart failure in HIV‐infected and uninfected men and women. J Am Heart Assoc. 2018;7(21):e009985.
9. Schwartz RM et al. Chronic depressive symptoms and Framingham coronary risk in HIV-infected and HIV-uninfected women. AIDS Care. 2012;24(3):394403.
10. Khambaty T et al. Association between depressive disorders and incident acute myocardial infarction in human immunodeficiency virus–infected adults: Veterans Aging Cohort Study. JAMA Cardiol. 2016;1(8):929-37.
HIV infection, in which current CVD clinical risk prediction tools remain suboptimal.
11. Butler J et al. Diastolic dysfunction in individuals with human immunodeficiency virus infection: literature review, rationale and design of the Characterizing Heart Function on Antiretroviral Therapy (CHART) Study. J Card Fail. 2018;24(4):255-65.
12. de Vasconcellos HD et al. Associations between HIV serostatus and cardiac structure and function evaluated by 2‐dimensional echocardiography in the Multicenter AIDS Cohort Study. J Am Heart Assoc. 2021;10(7):e019709.
13. Nazari I, Feinstein MJ. Evolving mechanisms and presentations of cardiovascular disease in people with HIV: implications for management. Clin Microbiol Rev. 2024;37(1):e0009822.
14. Jachymek M et al. Unveiling the heart of the matter: echocardiographic insights into diastolic function and left ventricular and atrial changes in HIV patients with controlled viremia. J Clin Med. 2024;13(2):463.
15. Silverberg MJ et al. Initial antiretroviral therapy regimen and risk of heart failure. AIDS. 2023;38(4):547-56.
16. D’Souza G et al. Characteristics of the MACS/WIHS combined cohort study: opportunities research on aging with HIV in the longest US observational study of HIV. Am J Epidemiol. 2021;190(8):1457-75.
17. Kaslow RA et al. The Multicenter AIDS Cohort Study: rationale, organization, and selected characteristics of the participants. Am J Epidemiol. 1987;126(2):310-8.
18. Adimora AA et al. Cohort profile: the women’s interagency HIV study (WIHS). Int J Epidemoil. 2018;47(2):393-94i.
19. MACS/WIHS Combined Cohort Study (MWCCS). Data collection. https:// statepi.jhsph.edu/mwccs/datacollection-forms/. Last accessed: 31 October 2023.
20. Shitole SG et al. HIV and cardiac endorgan damage in women: findings from
an echocardiographic study across the United States. Clin Infect Dis. 2023;76(2):210-9.
21. Radloff LS. The CES-D Scale: a selfreport depression scale for research in the general population. Appl Psychol Meas.1977;1(3):385-401.
22. Vilagut G et al. Screening for depression in the general population with the Center for Epidemiologic Studies Depression (CES-D): a systematic review with meta-analysis. PLoS One. 2016;11(5):e0155431.
23. Bagherian-Sararoudi R et al. Relationship between left ventricular ejection fraction and depression following myocardial infarction: an original article. ARYA Atheroscler. 2013;9(1):16-21.
24. van Melle JP et al. Relationship between left ventricular dysfunction and depression following myocardial infarction: data from the MIND-IT. Eur Heart J. 2005;26(24):2650-6.
25. Hsue PY et al. Impact of HIV infection on diastolic function and left ventricular mass. Circ Heart Fail. 2010;3(1):132-9.
26. Cardoso JS et al. Left ventricular dysfunction in human immunodeficiency virus (HIV)-infected. Int J Cardiol. 1998;63(1):37-45.
27. Castro Sd et al. Frequency of development of acute global left ventricular dysfunction in human immunodeficiency virus infection. J Am Coll Cardiol. 1994;24(4):1018-24.
28. Foundation KF. Status of state action on the medicaid expansion decision. 2022. https://www.kff.org/healthreform/state-indicator/state-activityaround-expanding-medicaid-underthe-affordable-care-act/?currentTime frame=0&sortModel=%7B%22colId%2 2:%22Location%22,%22sort%22:%22asc%22%7D. Last accessed: 31 October 2023.
FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM