

Volume 11.1 October 2023 emjreviews.com
4 Editorial Board 7 Welcome 9 Foreword Congress Review 10 Review of the European Society of Cardiology (ESC) Congress 2023, 25th–28th August 2023 Congress Features 20 2023 European Society of Cardiology Guidelines for the Management of Cardiovascular Disease in Patients with Diabetes Robin Stannard 24 Artificial Intelligence and Heart Failure Evan Kimber Abstract Reviews 27 Temporal Trends in Neurologically Intact Survival After Paediatric Out-of-Hospital Cardiac Arrest: A Nationwide Population-Based Observational Study in Japan Goto and Funada 28 Sex-Based Differences in Short-Term Survival Following Out-of Hospital Cardiac Arrest Zylyftari et al. 31 Adult Survivors of Childhood Cancer Have Significant Levels of Impaired Cardiorespiratory Fitness, Inflammatory Markers, and Poor Quality of Life Outcomes McCune et al. 33 Abstract Highlights Contents 2 T Area ● Month 2023 ● Creative Commons Attribution-Non Commercial 4.0 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0
Congress Interviews 41 Nina Ajmone Marsan 44 Blanche Cupido Interviews 48 Andrew Mitchell 52 Hannah Gower Infographic 56 Introducing Mavacamten for the Treatment of NYHA Class II and III Symptomatic Obstructive HCM in Adult Patients Feature 58 The Impact of Guideline-Directed Medical Therapy Adherence on Cardiovascular Outcomes: A Critique of Recent Trials Han Naung Tun Articles 61 Editor's Pick: Obstructive Sleep Apnoea as an Exacerbator of Vasospastic Angina Michael et al. 66 Characterisation of Patients with Acute Coronary Syndrome: A 10-Year Experience Dzebu et al. 75 Risk Factors and Patterns of Myocardial Injury in Patients with COVID-19: A Single-Centre Cohort Study Javed et al. 87 PCSK9 Targeting in the Management of Hypercholesterolaemia Kosmas et al. Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 3 reative
Editorial Board
Editor-in-Chief
Prof Dr Çetin Erol İbn-i Sina Hospital, Ankara University, Türkiye
Editorial Board
Dr Pierfrancesco Agostoni Ziekenhuis Netwerk Antwerpen (ZNA) Middelheim, Antwerp, Belgium
Prof Denilson Campos de Albuquerque
Dr Andy Wai Kwong Chan
Dr Sazzli Kasim
Dr Ronald J. Krone
Pedro Ernesto University Hospital, Rio de Janeiro, Brazil
Andy Wai Kwong Chan Heart Centre, Hong Kong
Universiti Teknologi MARA, Selangor, Malaysia
Washington University School of Medicine, St. Louis, Missouri, USA
Prof Dr Uwe Nixdorff European Prevention Center Joint with Medical Center Düsseldorf (Grand Arc), Germany
Dr Sanjog Kalra
Albert Einstein Health Network, Philadelphia, Pennsylvania, USA
Dr Constantine Kosmas Cardiology Unlimited PC, New York City, USA
Dr Nicholas Kipshidze New York Cardiovascular Research, New York City, USA
Dr Christian Bär
Dr Carl J. Lavie
Prof Stephen Lee
Dr Carl J. Pepine
Prof Khai Pham Gia
Dr Amandeep Goyal
Prof Dr Rainer Wessely
Dr Han Naung Tun
Hannover Medical School, Germany
The University of Queensland School of Medicine, New Orleans, Louisiana, USA
University of Hong Kong, Pokfulam, Hong Kong
University of Florida, Gainesville, USA
Bach Mai Hospital, Vietnam
Marietta Memorial Hospital, Ohio, USA
University of Technology Munich and Fresenius
University of Applied Sciences, Cologne, Germany
Larner College of Medicine's University of Vermont, Burlington, USA
4 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0
Aims and Scope
EMJ is an online only, peer-reviewed, open access general journal, targeted towards readers in the medical sciences. We aim to make all our articles accessible to readers from any medical discipline.
EMJ allows healthcare professionals to stay abreast of key advances and opinions across Europe.
EMJ aims to support healthcare professionals in continuously developing their knowledge, effectiveness, and productivity. The editorial policy is designed to encourage discussion among this peer group.
EMJ is published quarterly and comprises review articles, case reports, practice guides, theoretical discussions, and original research.
EMJ also publishes 18 therapeutic area journals, which provide concise coverage of salient developments at the leading European congresses. These are published annually, approximately 6 weeks after the relevant congress. Further details can be found on our website: www.emjreviews.com
Editorial Expertise
EMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors are recognised authorities from their respective fields.
• Peer review, which is conducted by EMJ’s Peer Review Panel as well as other experts appointed due to their knowledge of a specific topic.
• An experienced team of editors and technical editors.
Peer Review
On submission, all articles are assessed by the editorial team to determine their suitability for the journal and appropriateness for peer review.
Editorial staff, following consultation with either a member of the Editorial Board or the author(s) if necessary, identify three appropriate reviewers, who are selected based on their specialist knowledge in the relevant area.
All peer review is double blind.
Following review, papers are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected.
Editorial staff have final discretion over any proposed amendments.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects.
We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial.assistant@emjreviews.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in EMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
EMJ is distributed through controlled circulation to healthcare professionals in the relevant fields across Europe.
Indexing and Availability
EMJ is indexed on DOAJ, the Royal Society of Medicine, and Google Scholar®; selected articles are indexed in PubMed Central®.
EMJ is available through the websites of our leading partners and collaborating societies.
EMJ journals are all available via our website: www.emjreviews.com
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
This Publication
ISSN 2054-3174
EMJ Cardiology is published once a year. For subscription details please visit: www.emjreviews.com
All information obtained by EMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, EMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. EMJ is completely independent of the review event (ESC 2023) and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever.
Front cover and contents photograph: Amsterdam, Netherlands home of the ESC 2023 © Alexi Tauzin / stock. adobe.com
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 5

EMJ Podcasts The EMJ Podcast aims to provoke conversations around the latest trends and innovations in healthcare, provide engaging and educational content for healthcare professionals, and hosts conversations with physician entrepreneur, Jonathan Sackier. Listen today www.emjreviews.com
Editor
Evgenia Koutsouki
Editorial Manager

Anaya Malik
Copy Editors
Noémie Fouarge
Kirsty Hewitt, Jaki Smith
Editorial Co-ordinator

Natasha Meunier-McVey
Editorial Assistants
Victoria Antoniou, Abigail
Craig, Evan Kimber, Jivitesh
Newoor, Darcy Richards
Head of Publishing Operations
Tian Mullarkey
Design Manager
Stacey Rivers
Senior Designer
Roy Ikoroha
Designers
Steven Paul
Junior Designers
Dillon Benn Grove, Shanjok Gurung
Head of Sales
Robert Hancox
Business Unit Leader
Billy Nicholson
Director of Performance
Keith Moule
Chief Operating Officer
Dan Scott
Chief Commercial Officer
Dan Healy
Founder and Chief Executive Officer
Spencer Gore
Welcome letter
Evgenia Koutsouki Editor

Dear Readers,
Welcome to the 2023 issue of EMJ Cardiology, which brings insights from the European Society of Cardiology (ESC) Congress. Key highlights from the congress, which this year took place in Amsterdam, the Netherlands, include a study demonstrating how crucial patient awareness of heart attack symptoms is in reducing the chance of hospital death, highlighting the importance of patient education. Among the late-breaking studies was one demonstrating that atrial fibrillation ablation is associated with improved outcomes when compared to medical therapy in patients with end-stage heart failure.
For this issue we are very proud to have interviewed Nina Ajmone Marsan, an expert in non-invasive cardiovascular imaging, who discusses key findings from her research; and Blanche Cupido, a specialist in adult congenital heart disease.
The article on the recent ISCHEMIA trial opens up a great discussion on the importance of adhering to guideline-directed medical therapy when it comes to trial design and execution. Our issue also features, among other articles, an interesting case report on obstructive sleep apnoea as an exacerbator of vasospastic angina, which leads to possibilities of enhanced management in patients with treatmentresistant angina.
I would like to take this opportunity to thank the EMJ team, our Editorial Board, peer reviewers, and all the contributors who made this journal a collection of great content of outstanding quality. We look forward to receiving your feedback and contributions over the next year, and I hope you enjoy this issue!
Contact us
Editorial enquiries: editor@emjreviews.com
Sales opportunities: salesadmin@emjreviews.com
Permissions and copyright: accountsreceivable@emjreviews.com
Reprints: info@emjreviews.com
Media enquiries: marketing@emjreviews.com
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 7

Stay up to date with new advancements across European healthcare Visit EMJ for our comprehensive collection of peerreviewed research articles, latest interviews, and features across a range of therapeutic disciplines. Visit EMJ www.emjreviews.com
Foreword

Dear Colleagues,
Welcome to our latest issue of EMJ Cardiology, featuring enlightening interviews with field experts, an assortment of peer-reviewed articles, and a review of European Society of Cardiology (ESC) Congress 2023, held in Amsterdam, the Netherlands, from 25th–28th August.
This issue contains a wide array of articles exploring diverse subjects. A standout contribution by Dzebu et al. delves into percutaneous coronary intervention for acute coronary syndrome, and illuminates the prevalence of risk factors like hypertension and the efficacy of radial access. Javed et al. present an insightful study exploring the connection between COVID-19 and myocardial injury. An illuminating review article by Kosmas et al. takes a comprehensive view of proprotein convertase subtilisin/kexin type 9 inhibition as a promising strategy in managing hypercholesterolemia.
My Editor’s Pick is a fascinating case report, where the authors present a compelling case of a 47-year-old female with vasospastic angina who experienced persistent symptoms despite conventional treatments. The discovery
of severe obstructive sleep apnoea led to a transformative intervention with continuous positive airway pressure, resulting in remarkable symptom improvement. This study underscores the intricate interplay between obstructive sleep apnoea and vasospastic angina, shedding light on a potential avenue for enhanced management in patients with treatment-resistant angina.
The EMJ team had the pleasure of interviewing prominent field experts. Nina Marsan sheds light on their journey to specialise in valvular heart disease and cardiomyopathies, and as a speaker at ESC 2023. Andrew Mitchell details their efforts in revolutionising health data management using advanced technology. Hannah Gower shares their dedication to junior doctor support and advancements in heart failure management.
I extend my heartfelt gratitude to all the individuals who have offered their expertise and dedication to this EMJ Cardiology issue. I trust that our valued readers will take great pleasure from immersing themselves in the content, and I hope it leads to a more profound comprehension of the dynamic and evolving field of cardiology.
 Çetin Erol
Çetin Erol
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 9
Ankara University, Türkiye
ESC 2023
Review of the European Society of Cardiology (ESC) Congress 2023
Location: Amsterdam, the Netherlands
Date: 25th–28th August 2023
Citation:
EMJ Cardiol. 2023;11[1]:10-19. DOI/10.33590/emjcardiol/10309813. https://doi.org/10.33590/emjcardiol/10309813.
The European Society of Cardiology (ESC) inaugural session unfolded against the backdrop of Amsterdam, the Netherlands, between 25th–28th August 2023. The President of the ESC, Franz Weidinger, Vienna Medical University, Austria, declared that the mission of this year’s congress is to join forces to protect the heart. They highlighted the remarkable strides taken by cardiovascular medicine over the past few decades, which have enhanced and extended lives through pioneering achievements. From managing myocardial infarctions and controlling risk factors to treating valvular heart conditions and quelling life-threatening arrhythmias, the journey has been inspiring.
Extending a warm welcome to all attendees of the ESC Congress 2023, Weidinger emphasised to the audience that, as the collective consolidate their strengths, embrace learning, and engage in fruitful exchanges, the congress is dedicated to nurturing and cultivating the fundamental unity intrinsic to the cardiovascular community.
Thanks to an exceptional programme crafted by a dedicated team of experts, the ESC Congress 2023 featured a multitude of remarkable sessions. The Chair of the Congress Programme Committee, John McMurray, University of Glasgow, UK, was invited to share their reflections and personal highlights from the ESC Congress 2023. McMurray extended a warm welcome to the 30,000 participants, and expressed gratitude to the over 60 members of the ESC Congress Programme Committee, as well as the ESC staff, who have diligently worked throughout the past year to curate an outstanding
programme. They also expressed appreciation to the individuals who submitted their original research, including over 3,000 presenters from 86 countries, showcasing more than 3,700 abstracts and clinical cases.
This year’s congress takes centre stage, with a spotlight on heart failure, a theme that weaves through the intricate challenges managed and experienced by all cardiologists. This theme courses through the programme, notably echoed by a dedicated update on the 2021 heart failure guidelines introduced at the congress. Echoing the heartbeat of progress, the congress presented four new ESC guidelines, one for every day of the event, encompassing acute coronary syndromes, endocarditis, cardiomyopathies, and cardiovascular disease in diabetes. Spanning 16 sessions, attendees actively engaged with guideline task forces, posing questions and forging valuable insights.
Another congress highlight included the riveting hot line sessions, which included nine in total, along with an additional 17 sessions unveiling late-breaking science. This platform showcased a staggering 115 clinical trials, trial updates, and registries, offering a robust exploration of topics such as acute coronary syndromes, coronary interventions, acute and chronic heart failure, and atrial fibrillation. The digital health hub stood out as a noteworthy component of the congress, featuring an assembly of 37 sessions delving into the profound implications of this vital technology across various subspecialties.
Congress Review ● ESC 2023 10 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0

ESC 2023 ● Congress Review Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 11
McMurray enthusiastically affirmed that the programme is both exciting and comprehensive, delivering the latest updates spanning the entire spectrum of cardiology.
Weidinger took the honour of introducing 603 new fellows from 74 countries to the ESC community. This marked a profoundly significant milestone in their careers, signifying recognition of their exceptional dedication, expertise, and notable contributions to the field of cardiovascular science. This year’s recipients of the ESC President Awards were Gunnar Olson, Vastra Frolunda, Sweden; Chris Plummer, Newcastle Upon Tyne Hospitals, UK; and Maria Ximeris, Greece.
The board bestows Gold Medals in recognition of an individual’s lifelong scientific contributions. This year, three distinguished individuals were honoured with the Gold Medal: Bertram Pitt, University of Michigan, Ann Arbor, USA; Silvia Priori, IRCCS Fondazione Salvatore Maugeri, Pavia, Italy; and Arthur Wilde, Amsterdam University Medical Centres (UMC), the Netherlands.
confront, as well as the opportunities and actions that will empower us to address them effectively.
These six scenarios encompass: the ageing population and multimorbidity, including the challenges posed by demographic changes; the future of cardiology, including the role of precision medicine through progressively refined diagnostic and therapeutic options; cardiologists of the future, including the subspecialisation that shapes the profiles of future cardiologists; digital health, including the significant role of digital tools, artificial intelligence, and big data analytics in shaping medicine and research; patient-centred healthcare; and societal changes, exploring topics such as climate change and environmental sustainability, inclusivity and diversity, and freedom from bias and undue influence. These scenarios act as strategic guides to enable the ESC to navigate a dynamic future while prioritising excellence, inclusivity, and innovative approaches.
As the scientific programme unfolded, the envisioned future scenarios truly came to life. Sessions explored captivating topics such as artificial intelligence, machine learning, advanced digital diagnostics, innovative approaches to public health and health economics, genetic testing, remote patient care, and much more.
A special ESC Gold Medal Award was presented to Isabel Bardinet, Sophia-Antipolis, France, in recognition of their unwavering commitment to the ESC, valuable guidance, advice, and boundless energy that have benefited numerous individuals. This award served as a tribute to their exceptional 14-year tenure as Chief Executive Officer of the ESC.
The ESC has developed its strategic plan for the period of 2023–2028, yielding a remarkable asset that will dynamically guide their ongoing journey within an ever-evolving landscape. This collective effort aimed to identify future trends that will impact cardiovascular science, healthcare provisioning, the society at large, and the operating environment of the ESC. From these identified trends, they embarked on a democratic selection process to formulate future scenarios that depict the major challenges the ESC will
EMJ had the pleasure of participating in this congress and is eagerly anticipating the next edition, scheduled to be held from 30th August–2nd September 2024, in London, UK. The current issue of EMJ Cardiology offers succinct summaries of pertinent press releases and abstracts presented at the ESC Congress 2023, accompanied by informative features that delve into the latest ESC guidelines and the role of artificial intelligence in heart failure. This issue also includes engaging interviews with experts in the field. We invite you to continue reading for more in-depth insights from this year’s congress. ●
Congress Review ● ESC 2023 12 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0
"The board bestows Gold Medals in recognition of an individual's lifelong scientific contributions."
"These scenarios act as strategic guides to enable the ESC to navigate a dynamic future."
Awareness of Heart Attack Symptoms Reduces Chance of Death
HEART attack symptoms can include dizziness, cold sweats, loss of consciousness, nausea, and chest pain radiating to the arms, jaw, and neck. Fast treatment is crucial to a full recovery. Research presented at the ESC Congress 2023 investigated the association between symptom recognition, time to treatment, and clinical outcomes.
Data from the Korean Registry of Acute Myocardial Infarction for Regional Cardiocerebrovascular Centers (KRAMI-RCC), a registry of patients having experienced myocardial infarction in South Korea, were analysed. Nurses asked survivors of myocardial infarction whether they were aware of symptoms such as chest pain; shortness of breath; cold sweats; radiating pain to the jaw, shoulder, or arm; dizziness, vertigo, light-headedness, or loss of consciousness; and stomach ache. Patients who could identify at least one symptom were classified as ‘recognised symptoms’; otherwise they were classified as ‘did not recognise symptoms’. The researchers then compared patient characteristics, time to life-saving treatment, and survival between the two groups.
Overall, 11,894 patients who had experienced myocardial infarction were included, of whom
10,623 (90.4%) had a first-time event and 1,136 (9.6%) had a repeat event. In total, 52.3% of patients recognised the symptoms of myocardial infarction. Considering each symptom separately,
92.9% could identify chest pain as a symptom of myocardial infarction, 32.1% recognised shortness of breath, and 31.4% recognised cold sweats. Furthermore, just over one in four recognised radiating pain (27.4%), while only 7.5% identified vertigo/light-headedness/loss of consciousness, and 1.3% recognised stomach ache. Regarding demographic data, males were more likely to recognise symptoms than females. Younger patients with a higher education level, and living with a spouse, were also more likely to identify symptoms. Finally, patients who recognised symptoms had a lower in-hospital mortality rate (1.5%) compared with those who did not (6.7%).
Kyehwan Kim, Gyeongsang National University Hospital, Jinju, South Korea, summarised: “The findings indicate that education is needed for the general public and heart attack survivors on the symptoms that should trigger calling an ambulance. In our study, patients who knew the symptoms of a heart attack were more likely to receive treatment quickly and subsequently survive. Women, older patients, those with a low level of education, and people living alone may particularly benefit from learning the symptoms to look out for.” ●

ESC 2023 ● Congress Review Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 13
"92.9% could identify chest pain as a symptom of myocardial infarction."
Exercise Capacity Inversely Correlated with Atrial Fibrillation Incidence
EXAMINING the relationship between exercise performance and risk of atrial fibrillation (AF), as well as any subsequent comorbidities, regular physical activity has been found to help reduce inflammation and improve heart function. This research was presented at the ESC Congress 2023. AF is the most common heart rhythm disorder, affecting more than 40 million people worldwide. It is estimated that one in three Europeans will develop AF during their lifetime.
a steeper grade in successive 3-minute stages. Fitness was calculated according to the rate of energy expenditure achieved, expressed in metabolic equivalents (MET).
This retrospective study involved 19,680 patients between 2003–2012, without previous diagnosis of AF, who were referred to exercise treadmill testing. Baseline characteristics and exercise parameters during testing were available in all enrolled subjects. Multivariable Cox proportional hazard models were used to identify independent associations between exercise performance and risk of new-onset AF, risk of ischaemic stroke, and major adverse cardiovascular events (MACE). Cubic spline regression models assessed the risk of new-onset AF across fitness levels. This analysis included 15,450 of the individuals, with average age of 55 years and 59% male. Fitness was assessed using Bruce protocol, asking participants to walk faster and at
At a median follow-up duration of 137 months, 515 new-onset AF cases were discovered in this dataset. There was an 8% lower risk of AF incidence (hazard ratio [HR]: 0.92; 95% confidence interval [CI]: 0.88–0.97), a 12% lower risk of ischaemic stroke incidence (HR: 0.88; 95% CI: 0.83–0.94), and a 14% lower risk of MACE (HR: 0.86; 95% CI: 0.84–0.88) for every one peak achieved METs increase in the exercise treadmill testing after adjusting confounding factors. In further analysis, the peak achieved METs during exercise were significantly associated with risk of new-onset AF across various subgroups, including age, sex, BMI, and underlying diseases. The researchers found significant interactions in age (p=0.0047) and presence of chronotropic incompetence (p=0.0212) subgroups.
The researchers were therefore able to conclude that exercise capacity is inversely correlated with AF incidence across fitness level, and a better exercise performance indicates a lower AF incidence, ischaemic stroke incidence, and MACE. Regular physical activity may help to reduce inflammation and improve heart function, preventing development of AF. This study reinforces the attitudes of clinicians in their recommendations and behaviour when diagnosing or treating patients for AF. ●

14 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0
Congress Review ● ESC 2023
"It is estimated that one in three Europeans will develop AF during their lifetime."
Aspirin Reduces Recurrent Myocardial Infarction, Stroke, and Death Risk

FOLLOWING diagnosis of a first myocardial infarction (MI), patients not concordant with longterm aspirin therapy for secondary prevention were found to have an increased risk of recurrent MI, stroke, and death, compared with patients concordant with treatment, according to research presented at the ESC Congress 2023.
A research team, led by Anna Meta Kristensen, Department of Cardiology, Copenhagen University Hospital – Bispebjerg, Denmark, and Frederiksberg, Denmark, analysed data from Dutch nationwide registries to evaluate the risks associated with discontinuing long-term aspirin following a first MI diagnosis compared with continued aspirin use.
The study enrolled 40,114 patients aged ≥40 years who were diagnosed with their first MI, treated with coronary stenting between 2004–2017, and were concordant with aspirin therapy during the first year following diagnosis. Patients were excluded if they had a stroke or recurrent MI within the first year or were taking anticoagulants.
The authors looked at concordance, measured as the proportion of days individuals had their medication in the preceding 2 years, with aspirin treatment at 2, 4, 6, and 8 years post-initial MI diagnosis. Those who took aspirin as prescribed >80% of the time were classified as adherent and those who took their aspirin ≤80% of the time were deemed non-adherent. Patients were excluded at each 2-year time point if they experienced recurrent MI, stroke, death, or had commenced P2Y12 inhibitors or anticoagulants.
Aspirin concordance was found to decrease over time, with 90% concordance at 2 years, 84% at 4 years, 82% at 6 years, and 81% at 8 years. To determine the absolute and relative risks of recurrent MI, stroke, or death at each of the 2-year time points, multivariable logistic regression was performed to account for age, sex, diabetes, hypertension, hypercholesterolaemia, cancer, chronic kidney disease, chronic obstructive pulmonary disease, peptic ulcer, and former bleeding.
This revealed that at 2, 4, 6, and 8 years, those non-adherent with aspirin were, respectively, 29%, 40%, 31%, and 20% more likely to experience recurrent MI, stroke, or death than their adherent counterparts.
The study focused on patients with a first MI treated with coronary stenting, not taking any other anti-thrombotic medication; therefore, the authors reported that their findings cannot be generalised to all patients with an MI. They also highlighted that given their use of registry data, information regarding the reasons for non-adherence were not available, and further suggested that the results represent an association, not causality.
In conclusion, Kristensen stated: “We recommend that all patients who have had a heart attack stay adherent to their aspirin, in accordance with guidelines until randomised controlled trials have proven otherwise, and clinical guidelines have been changed.” ●
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 15
ESC 2023 ● Congress Review
"Patients were excluded if they had a stroke or recurrent MI within the first year or were taking anticoagulants."
Ablation of Atrial Fibrillation Enhances Results in End-Stage Heart Failure
LATE-BREAKING research presented at the ESC Congress 2023 indicated that atrial fibrillation (AF) ablation is associated with reduced occurrences of death, urgent heart transplantation, or left ventricular assist device (LVAD) implantation, when compared with medical therapy in patients with end-stage heart failure.
Patients with end-stage heart failure eligible for heart transplantation have often been overlooked in significant clinical trials. Hence, they are left without specific recommendations or concrete evidence regarding the best approach to managing AF alongside advanced heart failure. This situation has led to uncertainty in applying existing guidelines to this group, and numerous novel advances in heart failure therapy are withheld in clinical practice for these individuals.
In the CASTLE-HTx trial, the objective was to assess whether AF ablation outperforms medical therapy in terms of reducing mortality and the necessity for immediate heart transplantation or LVAD implantation.
The trial included individuals experiencing symptomatic AF along with end-stage heart failure, who were eligible for heart transplantation as per the guidelines from the ESC and the International Society for Heart and Lung Transplantation (ISHLT).

Patients were assigned randomly in a 1:1 ratio to either undergo initial catheter ablation or receive medical therapy for the management of AF (either rate control or rhythm control). In both groups, patients were administered heart failure therapy following established guidelines. The primary outcome measure encompassed a combination of all-cause mortality, aggravation of heart failure necessitating urgent heart transplantation, or the insertion of an LVAD.
The study involved 194 participants, with an average age of 64 years, and females constituting 19% of the group. The study was halted for efficacy by the Data Safety Monitoring Board 1 year after the randomisation process was concluded. Regarding the primary outcome, it was observed in eight (8.2%) patients in the ablation group and 29 (29.9%) patients in the medical therapy group, resulting in a hazard ratio of 0.24 (95% confidence interval: 0.11–0.52; p<0.001).
The authors emphasised that between AF ablation and medical therapy for patients with end-stage heart failure, ablation demonstrated lower occurrences of death, the need for urgent heart transplantation, or LVAD implantation. Additionally, it led to a decrease in AF burden and an improvement in left ventricular ejection fraction. Notably, listing for transplantation should not be delayed due to extended waiting times and the elevated mortality rate among those on the transplant waiting list. ●
16 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Congress Review ● ESC 2023
"The trial included individuals experiencing symptomatic AF along with end-stage heart failure."
Bystander Defibrillation's Crucial Role in Cardiac Arrest Survival

ALTHOUGH previous studies have investigated the best location for automated external defibrillators, there is limited evidence regarding the potential impact of ambulance response times on their placement. Hence, Mathias Hindborg, Nordsjællands Hospital, Hillerød, Denmark, and colleagues investigated the relationship between automated external defibrillator use and survival rates in relation to ambulance response times.
Data from the Danish Cardiac Arrest Registry were utilised to examine out-of-hospital cardiac arrests that occurred from 2016–2020. Information on age, sex, location, bystander defibrillation and cardiopulmonary resuscitation (CPR), ambulance response time, and survival at 30 days after the cardiac arrest was collected. The study specifically focused on adults who experienced a witnessed cardiac arrest, received CPR from a bystander, and had an ambulance arrive within 25 minutes or less.
The research team conducted a comparative analysis of the likelihood of survival in patients who underwent defibrillation from a bystander before the arrival of an ambulance as opposed to those who did not. The variance was assessed over the course of eight distinct intervals of ambulance response time. The statistical analyses were controlled for numerous factors that could potentially impact the association, including age, sex, site of arrest (public or private), and other medical conditions, namely a history of heart attack or stroke.
The study included a cohort of 7,471 mature individuals who underwent a cardiac arrest outside of a hospital, where a bystander was present and performed CPR before the arrival of the ambulance. Among them, 14.7% (1,098 out of 7,471) were given bystander defibrillation before the ambulance’s arrival, while 85.3% (6,373 out of 7,471) were not. The results indicated that 44.5% (489 out of 1,098) of those who received bystander defibrillation survived for 30 days, whereas only 18.8% (1,200 out of 6,373) did so in the absence of bystander defibrillation.
Patients who received bystander defibrillation demonstrated higher survival rates than those who did not, for all ambulance arrival time intervals except for 0–2 minutes, where the increase in survival did not reach statistical significance. Bystander defibrillation was found to increase the likelihood of survival by 37% when ambulance arrival time was between 2–4 minutes, 55% for arrival in 4–6 minutes, and nearly two-fold for the remaining intervals studied, with relative risks of 2.23 for 6–8 minutes, 1.99 for 8–10 minutes, 1.89 for 10–12 minutes, 1.86 for 12–15 minutes, and 1.98 for 15–25 minutes, compared with no defibrillation.
The results showcase the added benefit of bystander defibrillation on survival; therefore, the authors recommend that when resources are limited, defibrillators should be located in areas where ambulance response times are likely to be more than 6 minutes. ●
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 17 ESC 2023 ● Congress Review
"Data from the Danish Cardiac Arrest Registry were utilised to examine out-of-hospital cardiac arrests."
Neighbourhood Impact on Heart Health and Longevity

RECENT research highlights the importance of an individual’s surroundings and its impact on heart health and longevity. The research team utilised data from the PURE-China study to investigate the association between neighbourhood characteristics, cardiovascular disease (CVD), and death. A total of 35,730 adults aged 35–70 years from 115 communities (70 urban and 45 rural) in 12 provinces of China between 2005–2009 were included.
Trained researchers conducted in-person interviews to gather baseline information concerning the neighbourhood environment using the Neighbourhood Environment Walkability Scale (NEWS). The questionnaire contained eight subscales, and the scores for each subscale were tallied to obtain a total NEWS score. High scores corresponded to positive perceptions about the community.
The participants were followed up for all-cause death, death due to CVD, major CVD events, myocardial infarction, stroke, and heart failure. The primary objective was to determine the combined incidence of major cardiovascular disease events and all-cause mortality.
Mengya Li, National Centre for Cardiovascular Diseases, Beijing, China, and colleagues examined the correlations between every subscale and the overall score, along with the health results, by adjusting for factors that could influence the relationships, including age, sex, BMI, education, household income, and marital status, among other aspects.
During a median follow-up of 11.7 years, there were a total of 2,034 deaths related to all causes.
Out of these, 765 were attributed to CVD, whereas 3,042 were deemed major CVD events. An elevated score in the neighbourhood environment was associated with a 6% decrease in the possibility of experiencing the primary outcome of major CVD events and all-cause mortality, a 12% lower chance of succumbing to death during the follow-up period, and a 10% reduction in the risk of fatality due to CVD.
The safety from crime subscale exhibited the strongest correlation with health outcomes. An increase in the score for neighbourhood safety was linked with a decrease of 9% in the risk of death during follow-up, a 10% reduction in the risk of CVD-related death, a 3% decrease in the possibility of major CVDs, a 6% decrease in the risk of myocardial infarction, and a 10% decrease in the likelihood of heart failure.
A high score on all subscales was associated with a decrease in the risk of all-cause death during follow-up, with the risk ranging from 2–9% lower. Furthermore, a high score on the subscale for walking time to amenities was also linked with a 1% reduction in the risk of CVDrelated death, major CVDs, and heart attack.
The authors stated that the findings may be implemented by policymakers to address and alleviate the detrimental impact of unfavourablecommunity conditions on overall health. ●
18 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Congress Review ● ESC 2023
"The safety from crime subscale exhibited the strongest correlation with health outcomes."
Maintaining Dual Antiplatelet Therapy as Standard Following Stent Implantation
RECENT research presented at the ESC Congress 2023 revealed that prasugrel monotherapy following percutaneous coronary intervention (PCI) with drug-eluting stents is not superior to dual-antiplatelet therapy (DAPT) in terms of major bleeding. However, it is deemed non-inferior for cardiovascular events in patients with acute coronary syndrome (ACS) or high bleeding risk (HBR).
The ESC guidelines recommend 6 months of DAPT for HBR patients with ACS, and 12 months of DAPT for patients with ACS who are not at HBR following PCI. For patients without ACS, a shorter duration of 1–3 months of DAPT is advised for those with HBR after PCI.
The STOPDAPT-3 trial investigated the effectiveness and safety of using aspirin-free prasugrel monotherapy in comparison to a 1-month DAPT involving aspirin and prasugrel for patients with ACS or HBR who underwent PCI with cobalt-chromium everolimus-eluting stents. Between January 2021–April 2023, the study enrolled 6,002 patients with ACS or HBR from 72 medical centres in Japan.
At the 1-month mark, the no-aspirin approach did not show superiority over DAPT concerning the primary bleeding endpoint (4.47% versus 4.71%; hazard ratio: 0.95; 95% confidence interval: 0.75–1.20; p for superiority=0.66). However, the no-aspirin strategy demonstrated non-inferiority to DAPT with a relative 50% margin concerning the primary cardiovascular endpoint (4.12% versus 3.69%; hazard ratio: 1.12; 95% confidence interval: 0.87-1.45; p for non-inferiority=0.01).
There were no notable differences in the incidence of all-cause death (2.28% versus 2.11% in the no-aspirin and DAPT groups, respectively). The major secondary endpoint occurred in 7.14% of patients in the no-aspirin group and 7.38% of patients in the DAPT group, with no significant difference, indicating a similar effect on overall clinical benefit for both groups.
The no-aspirin group exhibited a higher rate of any coronary revascularisation (1.15% versus 0.57%) and definite or probable stent thrombosis (0.71% versus 0.44%), compared with the DAPT group. However, there was no difference in definite stent thrombosis between the two groups (0.47% versus 0.37%). In a subgroup analysis categorised by ACS and non-ACS, the increased risk of cardiovascular events in the no-aspirin group compared with the DAPT group was observed in patients with ACS but not in those without ACS.
The authors concluded that while the aspirinfree strategy, when compared with the DAPT strategy, did not lead to a reduction in major bleeding within the first month following PCI, it was non-inferior concerning the co-primary cardiovascular endpoint, with a relative margin of 50%. This suggests that using aspirin for a limited period of 1 month after PCI as part of DAPT might have offered protection to vulnerable coronary lesions, especially in patients with ACS, without a significant increase in major bleeding. Therefore, they stated the standard strategy for PCI should continue to be DAPT, even in the era of new-generation drug-eluting stents. ●

Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 19 ESC 2023 ● Congress Review
"The STOPDAPT-3 trial investigated the effectiveness and safety of using aspirin-free prasugrel monotherapy."
2023 European Society of Cardiology (ESC) Guidelines for the Management of Cardiovascular Disease in Patients with Diabetes
Authors: Robin Stannard, EMJ, London, UK
Citation:
EMJ Cardiol. 2023;11[1]:20-23. DOI/10.33590/ emjcardiol/10301135.
https://doi.org/10.33590/emjcardiol/10301135.
The 2023 update of the European Society of Cardiology (ESC) guidelines for the management of cardiovascular disease (CVD) in patients with diabetes was presented in a symposium session at the ESC Congress 2023, held in Amsterdam, the Netherlands, from the 25th–28th of August. The updates redefined the 2019 guidelines, acknowledging recent findings from cardiovascular outcome trials (CVOT) on the safety and efficacy of glucose-lowering medications to provide practice-changing recommendations. The session also introduced a novel tool in predicting CVD risk, SCORE2-Diabetes, an innovative model that accounts for conventional and diabetes-related risk factors, stratified by geographical location.
INTRODUCTION
Patients with diabetes have an increased risk of CVD. The presence of two comorbidities, diabetes and CVD, can have a major impact on patient prognosis, and affect treatment strategy. Diabetes diagnosis can result in an increased risk of developing chronic kidney disease which, in turn, can impact prognosis and act as a driver of CVD. Nikolaus Marx, University Hospital Aachen, Germany, and symposium Co-Chair, highlighted the importance of identifying individuals with these comorbidities through screening, an essential aspect of the new guidelines. Due to the high levels of undetected diabetes in patients with CVD, it is recommended that all patients with CVD be screened for diabetes using fasting glucose and/or HbA1c, tools that are readily available to cardiologists. In turn, patients with diabetes must also be screened for CVD and the presence of kidney disease through assessing estimated glomerular filtration rate, defined by Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI), and urine albumin creatinine ratio, assessing albuminuria in the spot urine.
The 2023 guidelines also focus on the management of CVD in patients with Type 2 diabetes (T2D), focusing on clinical approaches and key recommendations. Special attention is given to the proven cardiovascular (CV) benefit of, and safety of, glucose-lowering medications. The experts also highlight the importance of identifying and effectively treating heart failure (HF) in patients with diabetes, to reduce HFrelated hospitalisation and all-cause mortality.
PREDICTING CARDIOVASCULAR RISK WITH SCORE2-DIABETES
The first presenter, Emanuele Di Angelantonio, University of Cambridge, UK, focused their discussion on the novel CV risk assessment tool for patients with diabetes, SCORE2-Diabetes. Patients with diabetes have an average twofold increase in developing CVD, including
20 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Congress Feature ● ESC 2023
"The presence of two comorbidities, diabetes and CVD, can have a major impact on patient prognosis."
coronary heart disease, stroke, and other CV events. Diabetes is also associated with multiple CVD risk factors, such as dyslipidaemia and hypertension, each of which mediates an increased risk of disease. Di Angelantonio highlighted that this increased risk is directly reflected in years of life lost by both males and females with T2D, who have a reduced life expectancy of approximately 6 years.
Over recent years, a special emphasis has been placed on developing diabetes-specific CV risk prediction models that can identify those most at risk, as well as those who would benefit most from intervention. Models developed so far have combined conventional risk factors, including age, sex, and lifestyle factors, and diabetes-specific factors, such as HbA1c, diabetes duration, and target organ damage (TOD). Current models include ADVANCE, which can predict 4-year CV risk; UKPDS, which predicts CVD risk in the UK; and DIAL, which can predict lifetime risk. Di Angelantonio highlighted that, although useful, these tools have many limitations, including a basis on older patient cohorts and a lack of geographical calibration.

For the presentation of the novel 2023 ESC Guidelines, the Society developed a new risk prediction tool, SCORE2-Diabetes. SCORE2Diabetes was developed and tested in external cohorts, and has extended features above previously used predictions tools. The SCORE2Diabetes prediction model was calibrated to different regions in Europe, based on their associated level of risk.
Different regions of Europe are classified as low, moderate, high, and very high risk. Di Angelantonio presented an example of a model patient with a specific risk profile, and demonstrated how, by using the SCORE2Diabetes system, CVD can be predicted according to the region of Europe where they reside. SCORE2-Diabetes can estimate 10year CVD risk for patients with T2D, and can discriminate risk based on both conventional risk factors and those related to T2D. Concluding the presentation, Di Angelantonio underlined that the new guidelines recommend that for patients with atherosclerotic CVD (ASCVD) or severe TOD, SCORE2-Diabetes should always be used to classify patients into either low, moderate, or high-risk categories.
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 21 ESC 2023 ● Congress Feature
"SCORE2-Diabetes was developed and tested in external cohorts, and has extended features above previously used predictions tools."
GLUCOSE-LOWERING MEDICATIONS FOR THE REDUCTION OF ATHEROSCLEROTIC CARDIOVASCULAR DISEASE RISK
The second presentation delved into guideline updates surrounding the recommended indications for first- and second-line glucoselowering medications. Darren Keith McGuire, University of Texas Southwestern Medical Center, Dallas, USA, presented a series of updates on the 2019 guidelines, changed due to the results of meta-analysis and CVOT. McGuire highlighted the importance of the different recommendations for patients with or without ASCVD and TOD, and drew special attention to the totality of evidence now supporting the proven CV benefit and safety of glucose-lowering medications.
First-line recommendations for reducing CV risk independent of glucose control is treatment using both GLP-1 receptor agonists (RA) and SGLT2 inhibitors. This is an update from previous guidelines, which encouraged the use of GLP-1 RA and/or SGLT2 inhibitors. This change is based on the clinical indications for simultaneous use and meta-analysis of CVOTs with GLP-1 RA. Data presented demonstrated a 15% fatal risk reduction for CV death, a 12% fatal risk reduction for non-fatal or fatal myocardial infarction, and what McGuire described as a “robust” observation of 19% fatal risk reduction for stroke. Additional stratification of these results revealed a significant improvement in patients with established ASCVD compared to patients without. SGLT2 inhibitors showed less consistency in efficacy, but still maintained a statistically significant decrease in CV death, myocardial infarction, and stroke. When stratified by the presence or absence of ASCVD, there was an 11% relative risk reduction for those with ASCVD, and no demonstrated benefit for those without.
McGuire concluded that the ESC updated recommendations were that both classes of drug had the same indications, with proven efficacy and proven CV benefit for those with T2D.
McGuire then spoke about second-line medications, explaining that the broad clinical consensus is the use of a glucose-lowering agent with suggested CV benefits, such as metformin or pioglitazone. Meta-analysis of the CV effects demonstrated safety and plausible CVD efficacy of metformin; however, it did not conclusively
show CVD efficacy. Analysis of pioglitazone demonstrated nominal significance; however, this again demonstrated no conclusive CVD efficacy, though data did support a 17% risk reduction in CVD death. McGuire also acknowledged the concern about HF, with meta-analysis data for pioglitazone showing a 32% statistically significant risk of heart failure; however, they highlighted that this represented a very small absolute risk difference of approximately 0.4%. McGuire additionally underlined that most of this additional risk appeared to be driven by plasma volume expansion, and therefore that the risks should be manageable.
Summarising the updated recommendations in the guidelines, McGuire explained that for patients with T2D, without ASCVD or severe TOD, but with a calculated 10-year CVD risk ≥10%, treatment with an SGLT2 inhibitor or GLP1 RA should be considered to reduce CV risk. Additionally, patients with T2D, without ASCVD or severe TOD, and with a SCORE2-Diabetes of high to very high risk, metformin and/or an SGLT2 inhibitor and/or GLP-1 RA is recommended. Finally, for patients with ASCVD, SGLT2 inhibitors and GLP-1RA are recommended.
HEART FAILURE AND DIABETES
Patients with T2D have a higher incidence of HF compared to controls, resulting in an accelerated time to first cardiac event. It is therefore essential that patients with T2D undergo regular systematic screening for HF symptoms at every clinical encounter, explained Katharina Schütt, University Hospital Aachen. The 2023 guidelines provide clear recommendations on how to screen and diagnose HF in patients with T2D, according to the HF guidelines. Patients are at high risk, and therefore a systematic survey is recommended at each clinical encounter. If HF is suspected due to symptoms or abnormal ECG, the ESC recommends physicians measure B-type natriuretic peptide or N-terminal-pro B-type natriuretic peptide. In addition to this, the diagnostic tests recommended in patients with suspected HF include 12 lead ECG; transthoracic echocardiography; chest radiography (X-ray); and routine blood tests for comorbidities, such as full blood count, urea, creatine, electrolytes, thyroid function, lipids, and iron status.
22 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Congress Feature ● ECR 2023
If these tests are negative, then the guidelines recommend regular repetition. However, if they are positive, HF is defined through left ventricular (LV) measurements, in accordance with HF guidelines.

Schütt then discussed updates to the guidelines surrounding the treatment of HF in patients with T2D. All patients with HF and T2D are recommended SGLT2 inhibitors to reduce HF-related outcomes, such as CV death and HF hospitalisation. This is recommended irrespective of left ventricle ejection fraction, and independent of HbA1c and concomitant glucose-lowering medication. For all patients with HF with reduced ejection fraction (HFrEF; New York Heart Association [NYHA] Class II–IV) and T2D, the SGLT2 inhibitors dapagliflozin, empagliflozin, or sotagliflozin are recommended to reduce the risk of hospitalisation. This recommendation is based on evidence from the DAPA-HF, EMPEROR-Reduced, and SOLOIST-WHF trials, where the three SGLT2 inhibitors demonstrated significantly reduced total CV death and HF hospitalisation. In addition to this, regardless of the presence or absence of T2D, the three SGLT2 inhibitors are recommended in all patients with HFrEF.
Concluding their presentation, Schütt touched on novel recommendations in the 2023 guidelines regarding the initiation and up-titration of HFrEF medications, based on the findings of the STRONG-HR trial, which included patients on a higher dose than standard care. The trial allowed for a defined dose prior to discharge, with subsequent frequent follow-up visits in the first 6 weeks following an HF hospitalisation. This resulted in a significant reduction in 100-day re-admission for HF and all-cause death. ESC guidelines recommend this strategy to reduce readmission and all-cause mortality.
CONCLUSION
The 2023 updated guidelines provided a clear overview of changing recommended practices surrounding the screening, diagnosis, and management of patients with diabetes, who are at risk of CVD. Marx also highlighted a series of additional updates to the guidelines that were not covered in the symposium, including CV risk reduction in patients with diabetes; management of coronary artery disease and diabetes; arrhythmias; T1D and CVD; and person-centred care.
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 23 ECR 2023 ● Congress Feature
Artificial Intelligence and Heart Failure
Authors: Evan Kimber, EMJ, London, UK
Citation:
EMJ Cardiol. 2023;11[1]:24-26. DOI/10.33590/ emjcardiol/10303109.
https://doi.org/10.33590/emjcardiol/10303109.
ADOPTING a forward-thinking mindset, Olav Wendelboe Nielsen, Copenhagen University Hospital, Denmark, and Robyn Anne Clark, Flinders University, Adelaide, Australia, welcomed delegates to a futuristic session, focusing on the increasing role that artificial intelligence (AI) is playing in the cardiology specialty. This symposium was one of the highlights from the European Society of Cardiology (ESC) Congress 2023, which took place in Amsterdam, the Netherlands, between 25th–28th August.
SCREENING FOR CARDIAC DYSFUNCTION
To emphasise the importance of this topic, Oguz Akbilgic, Wake Forest School of Medicine, Winston-Salem, North Carolina, USA, stated that cardiovascular disease is the leading cause of death worldwide. Advances in treating other diseases have led to a higher risk of death from cardiovascular sources in older patients, with ischaemic heart disease alone being responsible for 16% of all deaths. Akbilgic continued by focusing on screening, and more specifically, targeting the asymptomatic patients early enough in the cardiovascular disease process, which develops in severity over time. Akbilgic highlighted the lack of population screening at present, bringing to attention the high treatment and hospitalisation costs associated with beginning intervention when symptoms arrive, persist, and worsen. Talking about the healthcare system in the USA, Akbilgic stated: “We have spent a lot of money treating heart failure, but not a lot preventing it.”
with ECG. The methodological approaches to applying this involve machine learning, feature engineering, and deep learning being employed to build on a conventional electrocardiography, with initiatives such as decision trees and symbolic pattern recognition. The goal of the research, which Akbilgic is involved in, is to screen large patient populations at the asymptomatic stage, identifying those at risk and in early stages of the disease. Akbilgic gave a quick run-through of the ECG-AIR app, which is a pioneer remote AI platform that enables retrieval and analysis of digital smartwatch electrocardiography for cardiovascular disease detection and prediction, and presents a first-look at the future of this field. Akbilgic acknowledged some of the minor teething points, as well as the next steps in this research, and finished by listing the opportunities electrocardiographic AI provides as a lowcost, accessible, and remote initiative, with the ability to assist with timely risk detection for cardiovascular disease.
ARTIFICIAL INTELLIGENCEENHANCED IMAGING FOR DIAGNOSIS AND MONITORING
Discussing electrocardiographic AI, Akbilgic spoke about the remote applications, growing literature support, and ease in combining AI
Sandy Engelhardt, University Hospital Heidelberg, Germany, delivered an insightful segment informing on how AI can be utilised to create knowledge from image data and support
24 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Congress Feature ● ECR 2023
"We have spent a lot of money treating heart failure, but not a lot preventing it."
targeted therapies, building on important measures such as ejection fraction. Engelhardt presented a novel approach that estimates cardiac motion, using MRI to identify and label contractile and relaxative motions, and an algorithm that identifies five different phases in the cardiac cycle. This algorithm employs selfsupervised motion modelling estimates, and uses vector fields between timestamps to classify motion patterns and detect cardiac phases based on these rather than blood pool volumes.
onto a larger scale and into multiple centres. In order to take this work further, and allow the algorithm to develop, a federated learning infrastructure is being rolled out. The words “the data stays, but the algorithm travels,” nicely summarise this initiative, as it aims to scale up the research but preserve privacy with crossinstitutional co-operation.
IMPROVING OUTCOMES
Comparing this self-supervised approach with segmentation-based methods, Engelhardt praised the accuracy and drew attention to areas where AI-enhanced imaging outperformed the traditional technique. “This gives us, from a technical point of view, a lot of confidence in the motion curves we estimate,” was Engelhardt’s summary of the findings they presented.
Engelhardt went on to demonstrate the direct usefulness of this method for clinicians in estimating characteristic curves for different pathologies, such as myocardial infarction or abnormal right ventricle, and in allowing comparison of these against healthy subjects.

Engelhardt concluded by spotlighting the requirement of reproducible data and expansion
Delivering their part of this fascinating symposium, discussing the lens of a cardiologist who is an expert in heart failure and not computational science, Harriette Van Spall, McMaster University, Hamilton, Canada, addressed the audience on the applications of AI in analysing the clinical outcomes of heart failure. Van Spall focused on machine learning algorithms, noting the separation between supervised and unsupervised machine learning brackets when identifying patterns and relationships, utilising either labelled or unlabelled datasets.
Detailing positive applications, Van Spall explained how machine learning allows for early diagnoses of left ventricle dysfunction, guides the interpretation of diagnostic data, and helps with classification of phenotypes, as well as aiding the labelling of disease stage and severity. Moreover, machine learning is useful in predicting
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 25 ECR 2023 ● Congress Feature
"The words “the data stays, but the algorithm travels,” nicely summarise this initiative."
clinical events, and according to Van Spall, unlocks several possibilities for tailoring care in precision medicine to specific groups of patients. There are also numerous benefits for drug development and the enrichment of clinical trials, such as facilitating more precise populations who are less likely to experience adverse events via methods of remote recruitment. Van Spall underscored this exciting section nicely, by stating: “AI provides the potential for powerful answers, and ways in which we can analyse complex data.”
Drawing attention to limitations in this field, Van Spall addressed the absence of actionable solutions involving the use of AI in heart failure. They highlighted how helpful these mechanisms are in communicating outcomes and risks to patients, but what remains unknown is which therapies will improve these outcomes. Furthermore, data privacy and cloud computing offer challenges to the future of this branch of medicine, not to mention the lack of prospective studies. However, there are numerous possibilities that AI offers for drug development, in particular facilitating production, efficiency, implementation through clinical trial monitoring, and automated manufacturing. Van Spall concluded by comparing knowledge gaps with the great potential AI offers the field of heart failure.
FROM SCREENING TO TREATMENT

Muthiah Vaduganathan, Brigham and Women’s Hospital, Harvard Medical School, Boston, USA, urged clinicians to think critically about the ways in which they can implement AI into their decision-making, in order to improve efficiency in their own practice. One important question that arose during this session was: “Where does the use of AI fit in the new published guidelines?” Clark encouraged attendees to “go and make some noise” in order to address this uncertainty.
Bringing home all the aspects mentioned, the importance of asking the right questions of AI and enhancing the human aspects involved were emphasised. As we step into a new age that incorporates AI in cardiology, selecting the right model to deploy, whether this is applied to diagnosis or treatment, and understanding the overlap between these new methods and traditional statistical modelling is more important than ever before. ●
26 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Congress Feature ● ECR 2023
"AI provides the potential for powerful answers, and ways in which we can analyse complex data."
Abstract Reviews
Unveiling the latest key findings in the field of cardiology from novel abstracts presented at the European Society of Cardiology (ESC) Congress 2023.
Temporal Trends in Neurologically Intact Survival After Paediatric Out-of-Hospital Cardiac Arrest: A Nationwide Population-Based Observational Study in Japan
Authors: *Yoshikazu Goto,1 Akira Funada2
1. Emergency and Disaster Medicine, Kanazawa University Graduate School of Medicine, Japan
2. Cardiology, Saiseikai Senri Hospital, Suita, Japan *Correspondence to gotoyosh@med.kanazawa-u.ac.jp
Disclosure: The authors have declared no conflicts of interest.
Acknowledgements: The authors would like to thank the Fire and Disaster Management Agency (FDMA) for maintaining the database.
Keywords: Cardiac arrest, children, outcome, out-ofhospital, resuscitation, trends.
Citation: EMJ Cardiol. 2023;11[1]:27-28. DOI/10.33590/emjcardiol/10305670. https://doi.org/10.33590/emjcardiol/10305670.
BACKGROUND AND AIMS
Out-of-hospital cardiac arrest (OHCA) in children is associated with poor outcomes. However, the temporal trends in survival, especially neurologically intact survival in paediatric patients with OHCA, remain unclear.1-4 The aim of this study was to examine temporal trends in neurologically intact survival in paediatric patients with OHCA for over 16 years.
MATERIALS AND METHODS
The authors reviewed the data of 27,202 children (aged <18 years) who experienced OHCA and were treated by emergency medical service providers. Data were obtained from the All-Japan Utstein Registry from January 2005–December 2020. The authors analysed the temporal trends in the 1-month neurologically intact survival (Cerebral Performance Category [CPC] Scale 1 or 2) rate over time. Subgroup analyses for outcomes were performed by type of bystander cardiopulmonary resuscitation (CPR), dispatcherassisted CPR, age group (infant [<1 year], child [1–11 years], adolescent [12–17 years]), witnessed status, and cause of arrest. The primary endpoint was the 1-month neurologically intact survival.
RESULTS
The frequency of bystander CPR significantly increased from 50.0% in 2005 to 63.1% in 2020, and the frequency of dispatcher-assisted chest compression-only CPR significantly increased from 7.7% to 40.6% (both p for trend <0.0001). The rate of initial shockable rhythm significantly decreased from 5.0% to 3.4% (p for trend <0.0001). The multivariate logistic regression model showed that calendar year, age, witnessed arrest, presence of bystander CPR, initial shockable rhythm, and non-cardiac causes were associated with increased odds of CPC 1–2. The overall crude rates of 1-month CPC 1–2 significantly increased from 4.9% in 2005 to 11.0% in 2020 (p for trend <0.0001).
In patients who received standard CPR with rescue breathing and chest compression CPR, the 1-month CPC 1–2 rate significantly increased from 8.0% to 24.2% and 4.7% to 10.8% (p for trend <0.0001), respectively. The rate of CPC 1–2 in patients who underwent dispatcher-assisted CPR also increased from 4.4% to 9.2% (p for trend <0.0001). With regards to patient age
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 27 Abstract ● ECR 2023
groups, the rate of 1-month CPC 1–2 significantly increased from 2.4% in 2005 to 7.5% in 2020 for infants, 6.0% to 14.8% for children, and 6.5% to 11.4% for adolescents (p for all trends <0.0001). For witnessed arrest, the rate of 1-month CPC 1–2 significantly increased from 9.9% to 24.9% for witnessed arrest, and 2.7% to 3.1% for unwitnessed arrest. The rate of 1-month CPC 1–2 significantly increased from 4.9% to 13.8% for presumed cardiac causes, and 5.0% to 9.6% for non-cardiac causes.
CONCLUSION
The 1-month neurologically intact survival rate significantly increased from 2005 to 2020 for paediatric patients with OHCA in Japan, regardless of bystander CPR type, age, witnessed status, and cause of arrest. A frequency of
Sex-Based Differences in Short-Term Survival Following Out-ofHospital Cardiac Arrest
Authors: *Nertila Zylyftari,1,2,3 Filip Gnesin,2 Amalie Lykkemark Møller,4,5 Elisabeth Helen Anna Mills,6,7 Sidsel G. Møller,8 Britta Jensen,9 Kristian Bundgaard Ringgren,6,10 Frederik Folke,1,8,11 Gunnar Gislason,1,11,12 Christian Torp Pedersen,2,4,6 Christina Ji-Young Lee1,2
1. Department of Cardiology, Herlev and Gentofte Hospital, Copenhagen University Hospital, Denmark
2. Department of Cardiology, Nordsjællands Hospital, Hillerød, Denmark
3. Department of Cardiology, Slagelse Hospital, Denmark
4. Department of Public Health, University of Copenhagen, Denmark
5. Cancer Surveillance and Pharmacoepidemiology, Danish Cancer Society Research Center, Danish Cancer Society, Copenhagen, Denmark
6. Department of Cardiology, Aalborg University Hospital, Denmark
7. Department of Clinical Medicine, Aalborg University, Denmark
8. Copenhagen Emergency Medical Services, Denmark
9. Public Health and Epidemiology, Department
dispatcher-assisted chest compression-only CPR rate increase of almost five-fold over time was associated with a two-fold increase in the overall 1-month CPC 1–2 rate over time. ●
References
1. Goto Y et al. Temporal trends in neurologically intact survival after paediatric bystander-witnessed out-ofhospital cardiac arrest: a nationwide population-based observational study. Resusc Plus. 2021;6:100104.
2. Albrecht M et al. Association between shockable rhythms and long-term outcome after pediatric out-of-hospital cardiac arrest in Rotterdam, the Netherlands: an 18-year observational study. Resuscitation. 2021;166:110-20.
3. Nehme Z et al. Trends in the incidence and outcome of paediatric out-of-hospital cardiac arrest: a 17-year observational study. Resuscitation. 2018;128:43-50.
4. Fink EL et al.; Resuscitation Outcomes Consortium. Unchanged pediatric out-of-hospital cardiac arrest incidence and survival rates with regional variation in North America. Resuscitation. 2016;107:121-8.
of Health Science and Technology, Aalborg University, Denmark
10. Department of Anaesthesiology and Intensive Care, North Denmark Regional Hospital, Denmark
11. Department of Clinical Medicine, University of Copenhagen, Denmark
12. The Danish Heart Foundation, Copenhagen, Denmark
*Correspondence to nertila.zylyftari.01@regionh.dk
Disclosure: Zylyftari has received support from European Union's Horizon 2020 research and innovation programme under acronym ESCAPE-NET, registered under grant agreement No 733381, and the COST Action PARQ (grant agreement no. CA19137), supported by European Cooperation in Science and Technology (COST), and Helsefonden. Gnesin has received a grant from the Danish Cardiovascular Academy (Danish Heart Foundation and Novo Nordisk Foundation). Møller reports employment by Novo Nordisk A/S; and reports no disclosures relevant to the manuscript. Torp Pedersen has received a grant for epidemiological study from Novo Nordisk, and a grant for randomised study from Bayer. Lykkemark Møller, Mills, Jensen, Bundgaard Ringgren, Folke, Gislason, and Lee declare no conflicts of interest.
Acknowledgements: The authors would like to thank TrygFonden, which supports the Danish Cardiac Arrest Registry, and Emergency Medical Services personnel, who filled out the case report for each out-of-hospital cardiac arrest for the Danish Cardiac Arrest Registry.
Keywords: Out-of-hospital cardiac arrest (OHCA), sex, 30-day survival.
28 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Abstract ● ECR 2023
Citation: EMJ Cardiol. 2023;11[1]:28-30. DOI/10.33590/emjcardiol/10309244. https://doi.org/10.33590/emjcardiol/10309244.
BACKGROUND AND AIMS
Out-of-hospital cardiac arrest (OHCA) is the most common cause of cardiac-related death, and continues to be a public health burden with poor survival.1-3 Cardiovascular disease is the leading cause of death among females, who are known to have a different presentation compared to males.4 Although sex differences in cardiovascular diseases are well described, they have not been completely understood in survival after OHCA.
Therefore, the aim of this study was to examine sex differences in patient characteristics and the 30-day survival in patients with OHCA during 20 years of follow-up.
MATERIALS AND METHODS
The authors conducted an observational and register-based study, using nationwide Danish register data. All residents in Denmark have a unique person identification number, which enabled the authors to crosslink data from different registers on an individual level. From the Danish Cardiac Arrest Registry, they identified all patients with OHCA between 2001–2020, who were aged between 18–100 years, with a presumed cardiac cause of OHCA, which was not witnessed by emergency medical services during their arrest. Baseline characteristics were expressed as medians (quartile 1–3) or frequencies (percentages), and temporal trend analyses of 30-day survival were performed according to sex.
RESULTS
Between 2001–2020, a total of 50,270 patients with OHCA were included, 17,179 of whom were female (34%). Compared to males, females were older, with a median age of 76 years (quartile 1–3: 66–84), and were more likely to have a low socioeconomic status. Females had a higher burden of chronic obstructive pulmonary disease (19% versus 14%; p<0.001),
and psychiatric disease (13% versus 8%; p<0.001). By comparison, males had more ischaemic heart disease (24% versus 17%; p<0.001) and diabetes (17% versus 14%; p<0.001).
Looking at medication use 180 days before OHCA, females had more prescriptions of antibiotics (48% versus 35%; p<0.001), steroids (18% versus 13%; p<0.001), and QT-prolonging drugs (17% versus 11%; p<0.001). Males had more prescriptions of anticoagulant drugs (17% versus 13%; p<0.001) and statins (32% versus 25%; p<0.001).
Related to cardiac arrest-related factors, OHCA experienced by females were more often in a private home (83% versus 74%; p<0.001), were less likely to be witnessed by a bystander (48% versus 53%; p<0.001), and were less likely to have shockable heart rhythm by emergency medical services arrival (14% versus 28%; p<0.001). No sex differences were observed for receiving cardiopulmonary resuscitation.
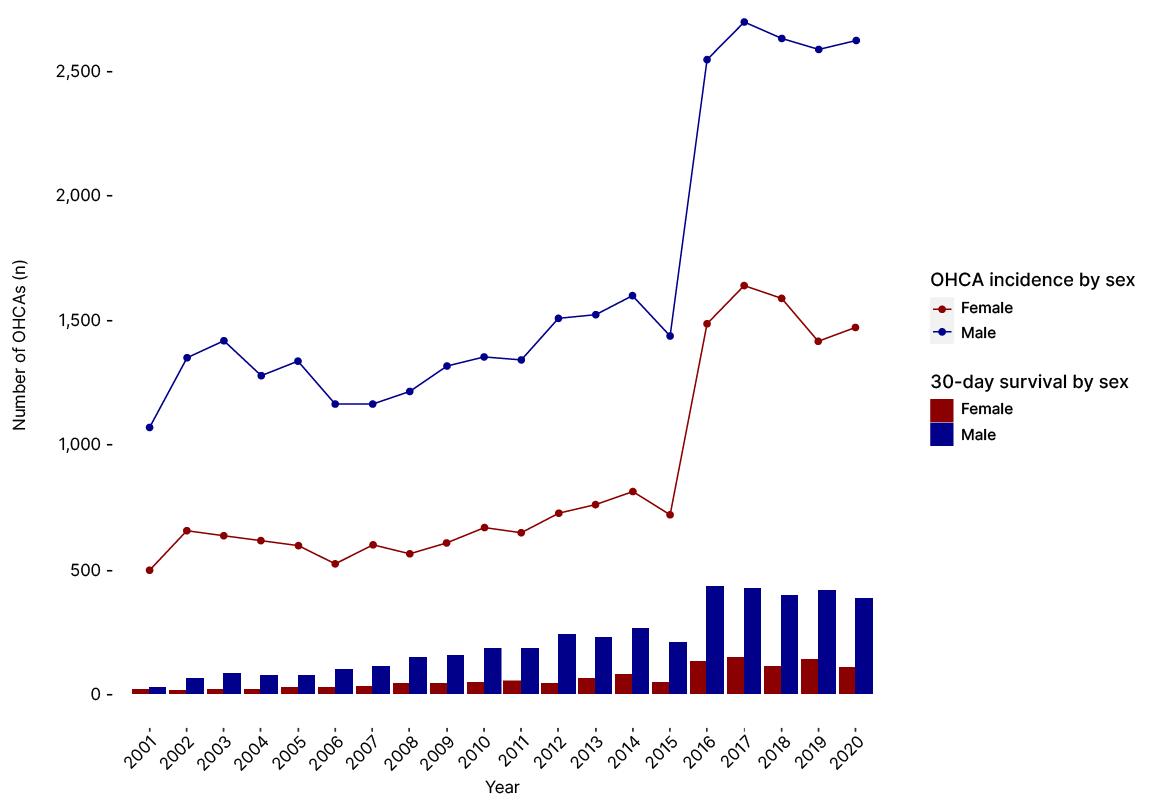
In analysis of the temporal trend of OHCA incidence and 30-day survival by sex during 2001–2020, an increase in 30-day survival for both sexes was observed (Figure 1). However, females had lower 30-day survival compared to males throughout the period of study. The average 30-day survival by sex during 2001–2010 versus 2011–2020 was 5% versus 8% for females, and 8% versus 15% for males, respectively.
CONCLUSION
Females had poorer prognostic patient characteristics and cardiac arrest-related factors compared to males. Although 30-day survival improved in both sexes during the period 2001–2020, females had lower 30-day survival compared to males. Further research is warranted to understand sex differences of patients with OHCA, in order to improve survival rates among females. ●
References
1. Gräsner J-T et al. Survival after out-of-hospital cardiac arrest in Europe - results of the EuReCa TWO study. Resuscitation. 2020;148:218-26.
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 29 Abstract ● ECR 2023
OHCA: out-of-hospital cardiac arrest.
2. Berdowski J et al. Global incidences of out-of-hospital cardiac arrest and survival rates: systematic review of 67 prospective studies. Resuscitation. 2010;81(11):1479-87.
3. Gräsner J-T et al. European Resuscitation Council Guidelines 2021: epidemiology of cardiac arrest in
Europe. Resuscitation. 2021;161:61-79.
4. Vogel B et al. The Lancet women and cardiovascular disease Commission: reducing the global burden by 2030. Lancet. 2021;397(10292):2385-438.
30 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Abstract ● ECR 2023
Figure 1: Temporal trend of out-of-hospital cardiac arrest incidence and 30-day survival by sex during 2001–2020.
Adult Survivors
of Childhood Cancer
Have Significant Levels of Impaired Cardiorespiratory Fitness, Inflammatory Markers, and Poor Quality of Life Outcomes
Authors: C. McCune.1,2 C. Watson,2 M. Harbinson,1,2 A. McCarthy,3 R. Johnston,3 L. Dixon1,2
1. Department of Cardiology, Belfast Health and Social Care Trust, UK
2. Wellcome-Wolfson Institute of Experimental Medicine, Queen's University Belfast, UK
3. Royal Belfast Hospital for Sick Children, UK
*Correspondence to cmccune02@qub.ac.uk
Disclosure: The authors have declared no conflicts of interest.
Keywords: Anthracycline, cardio-oncology, survivors of childhood cancer.
Citation: EMJ Cardiol. 2023;11[1]:31-32.
DOI/10.33590/emjcardiol/10306774. https://doi.org/10.33590/emjcardiol/10306774.
BACKGROUND AND AIMS
Almost two-thirds of the 35,000 children diagnosed with cancer in Europe each year are treated with anthracycline chemotherapy.1 Despite improved survival rates, this therapy is responsible for symptomatic heart failure in up to 10% of patients decades after treatment.2 Furthermore, emerging evidence suggests that the late effects of the drug extend beyond systolic impairment.3,4
MATERIALS AND METHODS
Queen’s University Belfast, UK, conducted a study of 86 adult survivors of childhood cancer who were treated with over 100 mg/ m2 doxorubicin equivalent. Each participant completed a 36-Item Short Form Health Survey
(SF36) questionnaire to assess quality of life compared with Irish normative data.5,6 A 6-minute walk test (6MWT) was performed, and per cent predicted values were calculated, adjusted for age, sex, weight, and height.7,8 Cardiac biomarker analysis (wide-range C-reactive protein [wrCRP], N-terminal prohormone of brain natriuretic peptide, and troponin T), and cardiac imaging with echocardiography and MRI were performed.
Of the 86 survivors of childhood cancer studied, 55% were male, with an average age of 28 years (range: 18–53 years). The average anthracycline dose administered was 270 mg/m2 (108–705 mg/m2).
Echocardiography demonstrated that 16% had an ejection fraction of <53%, and 29% had a global longitudinal strain of <-18%. A noteworthy 70% of these survivors achieved the National Health Service (NHS) exercise benchmarks.9
Cardiorespiratory fitness, as measured by 6MWT, was below the lower limit of normal (<80% predicted) in 40% (34) of patients. In terms of quality of life, survivors of childhood cancer consistently underperformed against the standard, especially in general health (abnormal in 20% of participants), mental health (16%), and physical functioning (13%). Wide range C-reactive protein fell within the low cardiovascular risk category (<1 mg/L) in 31 patients, medium risk (1–3 mg/L) in 27 patients, and high risk (>3 mg/L) in 28 of the 86 patients.10
RESULTS
Outcomes varied by exercise habit. Inactive survivors of childhood cancer displayed abnormal wrCRP levels (p=0.002), underperformed in the 6MWT (p=0.002), and showed diminished indexed stroke volumes in MRI results (p=0.015) compared with participants who undertook regular exercise. A positive relationship was observed between the amount of exercise (measured in minutes per week) and improved 6MWT, fractional shortening, and septal E/e’ (all p<0.05). Those engaging in intense physical activity exhibited improved outcomes in 6MWT and quality of life metrics, as well as reduced frailty, wrCRP, N-terminal prohormone of brain natriuretic peptide, and global longitudinal strain (all p<0.05).
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 31 Abstract ● ECR 2023
CONCLUSION
In conclusion, anthracycline chemotherapy treatment for childhood cancer is associated with abnormal cardiac imaging, but also an increased prevalence of impaired cardiorespiratory fitness, inflammation, and impaired quality of life in every domain. It remains uncertain whether sedentary behaviour results from cardiotoxicity, or if exercise counteracts its effects. This field warrants further exploration. ●
References
1. Vassal G et al.; ENCCA Long-term Sustainability (LTS) Working Group. The SIOPE strategic plan: a European cancer plan for children and adolescents. 2015. Available at: https://discovery.ucl.ac.uk/id/eprint/1529282/1/ Vassal_SIOPE%20strategic%20plan%20PUBLISHED%20 REPORT.pdf. Last accessed: 22 August 2023.
2. Lieke Feijen EAM et al.; DCOG-LATER Study Group. Risk and temporal changes of heart failure among 5-year childhood cancer survivors: a DCOG-LATER study. J Am Heart Assoc. 2019;8(1):e009122.
3. Lipshultz SE et al. Cardiovascular disease in adult survivors of childhood cancer. Annu Rev Med. 2015;66:161-76.
4. Foulkes SJ et al. Exercise for the prevention of anthracycline-induced functional disability and cardiac dysfunction: the BREXIT study. Circulation. 2023;147(7):532-45.
5. Blake C et al. The Short Form 36 (SF-36) Health Survey: normative data for the Irish population. Ir J Med Sci. 2000;169(3):195-200.
6. Rand Corporation. 36-Item Short Form Survey from the RAND Medical Outcomes Study. Available at: https:// www.rand.org/health-care/surveys_tools/mos/36-itemshort-form.html. Last accessed: 22 August 2023..
7. American Thoracic Society (ATS). ATS statement: guidelines for the six-minute walk test. 2002. Available at: https://www.atsjournals.org/doi/epdf/10.1164/ ajrccm.166.1.at1102?role=tab. Last accessed: 22 August 2023.
8. Enright PL. The six-minute walk test. Respir Care. 2003;48(8):783-5.
9. National Health Service (NHS). Physical activity guidelines for adults aged 19 to 64. Available at: https:// www.nhs.uk/live-well/exercise/exercise-guidelines/ physical-activity-guidelines-for-adults-aged-19-to-64/. Last accessed: 22 August 2023.
10. Ridker PM. C-reactive protein, inflammation, and cardiovascular disease. Tex Heart Inst J. 2005;32(3):384-6.
32 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Abstract ● ECR 2023
Abstract Highlights
The following selected highlights showcase intriguing and relevant abstracts presented at the European Society of Cardiology (ESC) Congress 2023, which were centred around congenital heart disease.
Citation: EMJ Cardiol. 2023;11[1]:33-40. DOI/10.33590/emjcardiol/10300489. https://doi.org/10.33590/emjcardiol/10300489.

Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 33 ESC 2023 ● Abstract Highlights
Novel Insights on Right Ventricular Adaptation to Systolic Flow
MYOCARDIAL work (MW) represents an innovative methodology that integrates global longitudinal analysis with non-invasive assessment of ventricular pressure, enabling a comprehensive evaluation of ventricular performance. While this approach has been applied to the subpulmonary right ventricle (spRV), its application to the systemic right ventricle (sRV) remains unexplored.
The researchers extracted MW indexes from ventricular pressure-strain loops in a cohort of 48 patients with sRV. This cohort comprised of 32 individuals with transposition of the great arteries following atrial switch repair, and 16 with congenitally corrected transposition of the great arteries. The mean age of this group was 38.5±10 years, and it consisted of 56% males. Additionally, a control group of 20 healthy volunteers with spRV was included for comparative purposes.
Echocardiographic parameters and analysis of global longitudinal strain (GLS) revealed compromised systolic function in the sRV group. This included findings such as Tricuspid Annular Plane Systolic Excursion (TAPSE), measuring 12.3±3 mm, an S wave of 6.9±2 cm/s, fractional area change at 29.0% (23–35), GLS at -13.4±3.0%, RV septum GLS at -12.0±4.0%, and RV free-wall GLS at -14.8±4.0%.
The MW indexes were found to be below the normal reference values typically reported for the left ventricle. This included the global work index (GWI), measuring 1,056±331 mmHg% and the global constructive work (GCW) at 1490±269 mmHg%. On the other hand, global wasted work (GWW) and global work efficiency (GWE) showed
mild increases at 245.5±162.0 mmHg% and 87.0±9.0%, respectively.
The researchers observed that the sRV free-wall contributed more significantly to global performance compared to the septum. Specifically, GWI for the septum was 879±318 mmHg%, while for the free-wall, it was 1,241±412 mmHg% (p<0.0001). Similarly, GCW for the septum was 1,348±287 mmHg%; whereas for the free-wall, it was 1,626±377 mmHg% (p<0.0001). Interestingly, the analysis of segmental pressurestrain loops revealed higher wasted work values in dyssynchronous segments.
In comparison to spRV, MW indexes of performance were notably higher in sRV (spRV GWI: 349.3±99.0 mmHg%; p<0.0001, and spRV GCW: 451.1±104.0 mmHg%; p<0.0001). This difference likely signified the adaptation of the sRV to increased afterload. However, in response to chronic exposure to systemic pressure, there was a significant increase in both GWW and GWE in sRV compared with spRV (spRV GWW: 43.1±22.0 mmHg%; p<0.0001, and spRV GWE: 92.4±4.0; p=0.0005).
The authors concluded that evaluating MW in sRV patients is feasible, as it can offer valuable insights into ventricular global as well as segmental performance and efficiency; the findings are indicative of the sRV's adaptation to systemic loading. ●
34 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Abstract Highlights ● ESC 2023
"Global wasted work (GWW) and global work efficiency (GWE) showed mild increases."
Non-invasive Pressure Flow Plots in Patients of Fontan
IN PATIENTS who have had the Fontan procedure, the slope of pulmonary artery pressures, measured invasively, plotted against cardiac output (CO) during exercise has prognostic significance. A research team, led by Aleksandra Cieplucha, Katholieke Universiteit (KU) Leuven, Belgium, proposed a methodology to calculate peripheral venous pressure (PVP)/CO slopes in a non-invasive way, utilising echocardiography combined with cardiopulmonary exercise testing (CPET), and simultaneous peripheral venous pressure measurements. Overall, the team aimed to assess PVP/CO slopes and their relationship with peak O2 consumption in patients.

Adult patients post-Fontan procedure who attended the outpatient clinic at KU Leuven were included in the study. All included patients underwent CPET-echo-PVP, where the peripheral intravenous line connected to the pressure transducer was zeroed at the mid-axillary level. Bloodwork was performed with the PVP/CO slope, calculated as a linear approximation using linear regression analysis from pressure-flow plots. Finally, univariable regression analysis was performed, permitting the identification of potential determinants of PVP/CO slope.
Overall, 20 patients (mean age 30.5±10.4; 11 [55%] females; and 15 dominant left ventricle [75%]) were included in the study with a N-terminal pro B-type natriuretic peptide of 297±235 pg/mL. Each participant performed staged exercise tests, achieving a workload of 102±30 Watts with a peak O2 consumption of 19.2±3.8 mL/kg/min. CO, heart rate, and PVP all increased during exercise. Furthermore, stroke volume index increased from baseline to peak exercise in nine patients (45%). The average PVP/CO slope was 2.21±1.53 mmHg/L/min, with the value exceeding 3 mmHg/L/min in five (25%) patients. The researchers also identified potential determinants of PVP/CO slope, including peak O2 consumption, peak workload during exercise; N-terminal pro B-type natriuretic peptide, New York Heart Association (NYHA) Functional Classification; and rest-to-peak change in tissue-Doppler e’ of the lateral wall of dominant ventricle.
To conclude, CPET-echo-PVP could be a reliable method in identifying determinants of exercise limitation in patients who have had the Fontan procedure. The PVP/CO slope, reflecting total pulmonary resistance, is related to peak O2 consumption, diastolic function, and heart rate reserve. The authors suggest that as it reflects hydraulic load to the systemic venous system, it may be an important target in patients. ●
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 35 ESC 2023 ● Abstract Highlights
"The team aimed to assess PVP/CO slopes and their relationship with peak O2 consumption in patients."
Systemic Right Ventricle: Echocardiographic Variables Associated with Mortality
IMPAIRED subpulmonary left ventricle (LV) function in adult patients with a systemic right ventricle (sRV) is associated with heart or heartlung transplantation and mortality, according to an abstract presented at the ESC Congress 2023, which took place in Amsterdam, the Netherlands, between 25th–28th August.

Authors from the Royal Brompton and Harefield Hospitals, London, UK, reviewed data from 120 adult patients with an sRV who had echocardiography performed between 2011–2019, to evaluate the correlation and relative prognostic power of subpulmonary LV function in this cohort. Of patients included, 60.0% were male, the average age was 43.5±12.1 years, 37.5% had congenitally corrected transposition of the great arteries, 66.4% were receiving ≥1 heart failure therapy, and 79.0% had heart failure classified as New York Heart Association (NYHA) Functional Class I/II. The study endpoints were transplantation or death, and the median followup duration was 4.9 years.
Subpulmonary LV function was determined using 4-chamber global longitudinal strain (GLS), fractional area change (FAC), and free-wall longitudinal strain (FWLS). Linear regression and Cox regression were used to assess the correlation between the subpulmonary LV function echocardiographic variables and the association between these variables and transplantation or mortality, respectively.
The analysis identified that 52.5% displayed, at a minimum, moderate systolic sRV dysfunction at baseline (median SRV FAC: 27.0%) and 81.7% of all patients had visually preserved subpulmonary LV function (LV FAC: 47.0%). Median values for GLS and LV FWLS were -15.2% and -19.9%, respectively. The correlation between LV FAC and GLS was noted to be weak (r=0.25).
Out of the 120 patients enrolled in the study, three patients underwent either a heart or heartlung transplant, and 24 patients died. Whilst LV FWLS was not found to be a predictor of transplantation or death, univariable Cox analysis revealed that GLS and LV FAC were predictors (/5%; hazard ratio: 1.60; 95% confidence interval: 1.10–2.31; p=0.0100; and /5%; hazard ratio: 0.55; 95% confidence interval: 0.47–0.65; p<0.0001), respectively. However, LV GLS was not found to be a predictor on bivariable analysis. Despite this, the authors suggested that LV FAC and GLS should be included as part of a comprehensive echocardiographic assessment, highlighting that LV FACS has better prognostic value in this patient cohort.
The team concluded that in adults with an sRV, impaired subpulmonary LV systolic function was strongly associated with death and heart or heart and lung transplantation. ●
36 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0
Abstract Highlights ● ESC 2023
"In adults with an sRV, impaired subpulmonary LV systolic function was strongly associated with death."
Value of Left Ventricular Strain-Volume Loops as Biomarkers

SIGNIFICANT characteristics of left ventricular (LV) strain-volume (SV) loops have been observed between patients with bicuspid aortic valve (BAV) and healthy controls. This evidence is compelling for its potential in providing new insights in cardiac haemodynamics and in detecting LV remodelling at an early stage, as well as being a promising new prognostic marker. The current research is sourced from an abstract presented at the ESC Congress 2023, which took place in Amsterdam, the Netherlands, between 25th–28th August.
Patients with BAV were compared with healthy controls, grouped based on age and sex, and apical two, three, and four chamber views were used to measure LV global longitudinal strain and volume, in order to construct SV-loops. Univariable Cox regression was employed to assess the composite endpoint of all-cause mortality, heart failure, and supraventricular and ventricular arrhythmias. A total of 113 patients were included, with mean age of 32 years, and 40% female. Median aortic jet velocity was 2.3 m/s and 21 patients (19%) experienced moderate aortic regulation. Sslope was significantly lower
in patients with BAV (0.21% /mL [interquartile range (IQR): 0.17-0.28] versus 0.27% /mL [IQR: 0.24–0.34]; p<0.001), as was ESlope (0.19% /mL [IQR: 0.12–0.25] versus 0.29% /mL [IQR: 0.21–0.43]; p<0.001). Greater uncoupling was seen in patients with BAV for both early (0.48±1.29 versus 0.05±1.21; p=0.018) and late diastolic (0.66±1.02 versus -0.07±1.07; p<0.001).
In a median follow-up period of 9.9 years, 17 patients experienced a primary endpoint. Echocardiographic parameters associated with the primary endpoint were early diastolic uncoupling (hazard ratio [HR]: 1.82; p=0.009), E/e’ ratio (HR: 1.29; p<0.001), ESslope (HR: 0.55; p=0.030), and LV end-systolic volume (HR: 1.05; p=0.030).
The researchers showed support for the capabilities of this technique, through the significant differences in SV-loop characteristics observed between patients with BAV and healthy controls in this investigation. SV-loops as biomarkers are presented as valuable tools for cardiologists, and clinicians can expect to see more research emerge on this topic soon, as this work translates into practice. ●
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 37 ESC 2023 ● Abstract Highlights
"The researchers showed support for the capabilities of this technique, through the significant differences in SV-loop characteristics observed."
Haemodynamic Consequences of High Risk Anatomical Features
RESEARCHERS from the Netherlands presented key results from their study in patients with anomalous aortic origin of a coronary artery (AAOCA) at the ESC Congress 2023. The study aimed to evaluate the haemodynamic consequences of the high-risk anatomical features in AAOCA through fractional flow reserve (FFR), a technique that assesses further risk stratification of myocardial ischaemia and sudden cardiac death.

The prospective cohort study took place in a tertiary AAOCA referral centre, and included patients with the condition who had undergone diagnostic work-up according to the MuSCAT trial. This spanned from July 2020–January 2023, and included 30 patients (57% female), with a mean age of 48.7±15.3 years at the time of AAOCA diagnosis. Researchers detailed that CT angiography (CTA) of the intraluminal space, and orifice geometry using intravascular ultrasound were applied to assess the presence and length of the intramural segment.
Results showed that 90% of patients presented with an anomalous aortic origin of the right coronary artery. FFR adenosine levels, measured in all patients, reflected significant correlations to the following: hypoplasia of the proximal segment on CTA (R=0.400; p=0.029); the inter-luminal space at 2 mm from the ostium on CTA (R=0.517; p=0.003); the length of the intramural course on CTA (R=0.500; p=0.005); the orifice shape on intravascular ultrasound (IVUS; R=0.460; p=0.011); and the minimal lumen area on IVUS (R=0.371; p=0.044).
The researchers concluded that FFR was significantly reduced in high-risk anatomical features of increased hypoplasia of the proximal segment on CTA, lower inter-luminal space at 2 mm from the ostium on CTA, longer intramural course on CTA, increased slit-like orifice shape on IVUS, and lower minimal lumen area on IVUS, which all appear as haemodynamically relevant in the pathophysiology of AAOCA. ●
38 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0
Abstract Highlights ● ESC 2023
"Results showed that 90% of patients presented with an anomalous aortic origin of the right coronary artery."
Non-Cardiac Surgery Risk Stratification in Adult Congenital Heart Disease

ADULTS with congenital heart disease (ACHD) often undergo multiple surgeries throughout their lives. Data regarding the specific risk of non-cardiac surgery and the subsequent impact of this on the severity of ACHD outcome are limited. A research team, led by Alicia Jeanette Fischer, University of Münster, Germany, aimed to assess frequency and outcome of non-cardiac surgery and to identify patients with ACHD specifically at risk.
All ACHD cases admitted for non-cardiac surgery between 2011–2018 in Germany were included in the study. Non-cardiac surgery was categorised as either low, medium, or high risk based on a risk score validated for patients without congenital heart disease. Demographic data as well as medical data regarding diagnoses, in-hospital complications, and mortality were analysed, with the primary endpoints investigated being major adverse cardiovascular events, major infection, major bleeding, thromboembolism, and in-hospital death. Outcomes in the ACHD cohort were compared to those of a propensity score matched cohort of non-ACDH.
Overall, 13,041 ACHD were included in the analysis, with 72%, 21%, and 7% categorised as having simple, moderate, and complex heart defects, respectively. Low-risk surgery was performed for 23.0% of simple ACHD cases, while intermediate and high-risk surgery was performed for 31.1% and 45.0%, respectively.
In the medium complexity ACHD cohort, 35.8% received low-risk, 42.3% intermediate-risk, and 21.8% high-risk surgery. Finally, regarding complex ACHD, 42.4% underwent low-risk, 41.2% intermediate-risk, and 16.4% high-risk surgery. Simple ACHD cases more frequently presented with typical cardiovascular risk factors, such as dyslipidaemia, diabetes, and arterial hypertension, compared with other categories of ACHD severity at the time of non-cardiac surgery (p<0.001 for all). Compared with a propensity score matched cohort, patients with congenital heart disease more frequently met the endpoints, depending on complexity of the disease and pre-defined risk of surgery. Following adjustment on multivariable logistic regression analysis, moderate and severe complexity was associated with adverse outcomes. Specifically, risk for death was increased in moderately complex (odds ratio: 1.44; 95% confidence interval: 1.15–1.81; p=0.001) and severely complex ACHD (odds ratio: 2.28; 95% confidence interval: 1.63–3.20; p<0.001)
when compared with a non-ACHD cohort. Finally, compared to low-risk surgeries, mid- and highrisk surgeries increased the risk of death, yielding odds ratios of 7.66 and 8.03, respectively.
To conclude, ACHD are at increased risk of adverse outcomes when undergoing non-cardiac surgery. This risk increases with the complexity of disease and surgical risk classifications were also associated with a much higher adverse outcome in patients undergoing high-risk procedures. ●
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 39 ESC 2023 ● Abstract Highlights
"All ACHD cases admitted for non-cardiac surgery between 2011–2018 in Germany were included in the study."
Predicting Low-Density Lipoprotein-Lowering Drug Impact on Congenital Heart Disease Risk
WITH the emergence of novel long-lasting lowdensity lipoprotein cholesterol (LDL) lowering therapies, such as silencing RNA treatments, which maintain clinical effects for up to 6 months post-administration, there is a significant likelihood that females of childbearing age could become pregnant during the drug's active period. In cases where clinical data is lacking, the Mendelian randomisation (MR) paradigm can be employed to forecast the impact of drug target perturbation using genetic data.
The research team sought to employ genetic data for the purpose of assessing the potential impact of LDL reduction through various drug targets, such as statins, ezetimibe, and proprotein convertase subtilisin/kexin type 9 (PCSK9) on congenital heart disease. They extracted uncorrelated genome-wide significant variants (p<5x10-8) related to LDL levels, along with their association estimates, both in the overall dataset and within the HMGCR, NPC1L1, and PCSK9 gene regions (with a margin of +/- 10 kB).
The data were sourced from genome-wide association studies summary data from the UK Biobank, encompassing 469,897 individuals. Furthermore, gene-outcome association data were obtained from genome-wide association studies results derived from FinnGen 8th Release, involving 342,499 individuals, focusing on various congenital heart conditions including conotruncal defects; congenital malformations of the great arteries; septal defects; congenital diseases of the aortic or mitral valves; and the vertebral, anorectal, cardiovascular, tracheo-oesophageal, renal, and limb anomaly (VACTERL) association. To analyse the impact of drug targets on these conditions, a drug-target MR analysis was conducted using the inverse-variance weighted MR approach.
Genetically-proxied LDL reduction through PCSK9 was linked to increased odds of VACTERL association (odds ratio [OR]: 1.70; 95% confidence interval [CI]: 1.25–2.32; p<0.001), conotruncal defects (OR: 3.97; 95% CI: 1.37–11.53; p=0.011), and overall congenital heart disease of any type (OR: 1.49; 95% CI: 1.08–2.05; p=0.015).
On the other hand, genetically-proxied LDL lowering via HMGCR was associated with higher odds of congenital malformations involving the great arteries (OR: 5.85; 95% CI: 1.07–31.84; p=0.041). However, it is important to note that genetically driven LDL reduction through NPC1L1 drug targets did not reveal significant differences in the risk of congenital heart disease, albeit the statistical power for these analyses was somewhat limited.
These findings provide genetic evidence indicating that the utilisation of LDL-lowering medications during pregnancy might have the potential to influence the risk of congenital heart disease. The authors emphasise that these results are specifically relevant to medications capable of crossing the placental barrier and directly affecting foetal LDL metabolism. They affirm the findings should not be extended to deduce the indirect consequences of lowering maternal LDL.
These outcomes underscore the significance of exercising caution when contemplating statin use during pregnancy. Additionally, they propose that long-lasting PCSK9-inhibiting agents, like monoclonal antibodies and silencing RNA therapies, which possess the ability to traverse the placental barrier, should be employed with great care by females who are planning to conceive. ●
40 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0
Abstract Highlights ● ESC 2023
"A drug-target MR analysis was conducted using the inverse-variance weighted MR approach."
Congress Interviews
Nina Ajmone Marsan delved into the importance of cardiovascular imaging and the role of artificial intelligence in advancing cardiology. Blanche Cupido discussed their inspiration for specialising in adult congenital heart disease and spotlighted their contributions to cardiovascular research.

Citation: EMJ Cardiol. 2023; DOI/10.33590/emjcardiol/10305570. https://doi.org/10.33590/emjcardiol/10305570.
Q1How did you become a cardiologist specialising in non-invasive cardiac imaging, and specifically focusing on valvular heart disease and cardiomyopathies?
During my training in Cardiology, I quickly developed a passion for imaging, as it provides every cardiologist the tool to meticulously track the patient's journey, from preventive measures and accurate diagnoses, to continuous monitoring and appropriate treatment. In every cardiovascular disease, imaging serves as the eyes to comprehend clinical pathophysiology, and plays a crucial role in effectively managing cardiovascular conditions. I further focused my interest and expertise particularly on valvular heart disease and cardiomyopathies; as recently as 20 years ago, not much was known about their pathophysiological mechanisms, and treatments were limited. As a result, there were significant opportunities for further research in these fields, which have indeed taken remarkable strides forward in the last decade.
Q2You have authored over 500 international publications on noninvasive cardiovascular imaging. Could you briefly highlight any significant findings from your published work? Also, what do you believe to be the current gaps in literature?
Through my research in the field of non-invasive cardiovascular imaging, I have always striven to go beyond the mere technical aspects of the different imaging modalities. While optimising the performance of these imaging techniques is undeniably crucial, I believe that demonstrating their clinical value, in terms of their significant impact on patient management and outcomes, is essential. The publications of my research group have therefore focused on the role of cardiovascular imaging in improving diagnosis and risk stratification of various cardiovascular diseases, mainly highlighting how imaging can help the treating physicians in decision-making, particularly related to treatment options. In the field of cardiovascular imaging, as well as across
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 41 ESC 2023 ● Interview
Nina Ajmone Marsan
Associate Professor, Leiden University Medical Center, the Netherlands
Featuring: Nina Ajmone Marsan and Blanche Cupido
various other fields of cardiology, current and future research should try to transition towards precision medicine. This transition should aim to identify the highly distinctive phenotype that sets apart each patient within a specific diagnosis, ultimately resulting in an individualised approach to both management and treatment. I believe this shift in paradigm to hold significant importance, not only for early diagnosis and the prevention of disease progression, but also notably for tailoring customised treatment strategies.
Q3
Are there any innovations on the horizon in the field of cardiovascular imaging that you think are particularly noteworthy?
In the field of cardiovascular imaging, as well as in other fields of cardiology and medicine in general, we are at the forefront of a new era defined by the integration of artificial intelligence (AI). I often refer to this phase as the "next industrial revolution," which is characterised by the remarkable strides AI is making in redefining our practices. Personally, I embrace and actively drive technological advancements, including the integration of AI into our clinical practices. I believe that this integration will help us in achieving the personalised and precise medicine approach I mentioned earlier. It offers completely novel and exciting possibilities, specifically in cardiovascular imaging. However, it requires new, specialised skills, even from those already established as experts in the field, of which I admittedly still lack many. This requires an understanding of the entire spectrum of applications, identifying the boundaries for utilisation, and redefining the roles of imagers and physicians at large.
into play. The overarching goal was to pinpoint the first signs of the disease to improve early diagnosis and, more importantly, to identify new potential targets for medical treatments, which we currently lack. I have learnt, and am still learning, a lot from this project, which has changed aspects of my daily clinical practice; for example, I now routinely inquire about family history in cases of valvular heart disease, and carry out screenings of family members. This project has changed and redirected my clinical research. Through the use of imaging, we are currently trying to visualise the pathophysiological processes of valvular heart disease more in detail, in order to monitor them for progression over time, and make well-timed therapeutic decisions.
Q5At the European Society of Cardiology (ESC) Congress 2023, you were a speaker, and chaired several sessions. One in particular focused on ‘Novel approaches to patients with symptomatic tricuspid regurgitation’. What are some of the most promising imaging modalities or approaches for this specific valve disease?
Q4
With the rapid advancements in technology, along with the increasing understanding of the genetic and molecular basis of valvular heart disease, how do you envision the future in terms of diagnosis and personalised treatment strategies for patients?
Several years ago, I started a new translational research endeavour, with the aim of unravelling the pathophysiological mechanisms behind degenerative valvular heart disease, from the genetic base (primarily inflammatory) that come
Tricuspid regurgitation is currently the target of numerous new transcatheter treatments. Therefore, this valvular heart disease has gained renewed attention, and requires sophisticated imaging for the pre-procedural assessment and planning, for the intra-procedural guidance, and for follow-up analysis. The complex anatomy and function of the tricuspid valve apparatus, encompassing the right ventricle and the right atrium, should be properly assessed with a multi-modality approach, including 3D echocardiography (trans-thoracic, trans-oesophageal, intracardiac), computed tomography, and MRI. Dedicated software and specific protocols for the tricuspid valve have been developed for each of these imaging techniques, and they are the focus of current clinical research. Several highly intriguing simulation tools have also been developed for specific transcatheter procedures related to tricuspid regurgitation. Even for expert imagers, there is great excitement, and new challenges when dealing with patients suffering from tricuspid regurgitation. During the ESC Congress 2023, there were indeed several sessions and interesting discussions dedicated to this topic.
42 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Interview ● ESC 2023
Q6As a specialist involved in guiding percutaneous procedures for structural heart disease, what are your thoughts on the future integration of imaging modalities into these procedures?
The role of the interventional imager in transcatheter procedures for valvular heart disease has transformed into that of a multidisciplinary collaborator, seamlessly integrating diverse imaging techniques to enhance precision, safety, and the overall success of these complex cardiovascular interventions. During these sophisticated procedures, echocardiography, in addition to fluoroscopic guidance, offers realtime, anatomically accurate visualisation of the cardiac structure. Both CT and MRI contribute by delivering pre-procedural roadmaps, helping to anticipate challenges, and tailor the approach to the patient's unique anatomy. The potential of integrating this complementary information in real-time is of crucial value, and has already been explored for fluoroscopy, 3D echocardiography, and CT, yielding very promising results. I expect significant advancements in the development of these applications in the near future. As technology continues to evolve, these integrative approaches will undoubtedly contribute to achieving unprecedented levels of procedural precision and patient outcomes.
Q7What led you to become a board member for the European Association of Cardiovascular Imaging (EACVI)? As the past Chair of the EACVI Education Committee of EACVI, what initiatives have you undertaken to promote education and training in the field of cardiovascular imaging?
EACVI is currently the leading community for cardiovascular imaging, promoting the use of multi-modality imaging at the highest standard, across cardiology and relevant medical specialities. Being involved in the EACVI programmes, and particularly as active board member, has been therefore very important to me. I believe that it is through such an association that we can ultimately achieve the goal of spreading excellence in cardiovascular imaging at all levels. During my tenure as the Chair of the Education
Committee 2020–2022, my primary focus was on developing educational programmes specifically tailored for “non-imagers”. These programmes were designed for general cardiologists and allied professionals, including anaesthesiologists and sonographers. Moreover, a unique dimension was introduced through the expansion of education to include patients themselves. The main objective was to create more awareness and provide the knowledge and competencies on the crucial role of imaging from diagnosis, management, and follow-up of patients to a broader community, uniting overall professionals dedicated to cardiovascular health. In parallel, I also promoted specific courses and training in advanced cardiovascular imaging. For example, I emphasised the importance of programmes for interventional imagers, a role I previously highlighted as a new and crucial presence within the field of percutaneous treatments for structural heart disease, demanding highly specialised skills.
Q8Given your involvement in the supervision of PhD students, and leading a research team, which do you think are the most important leadership skills, and how did you develop them?
Supervising PhD students is by far the most enriching role for me. I believe it transcends academic instructions and mere leadership; it encompasses mentorship, knowledge cultivation, legacy creation, and global collaboration. As a mentor, guiding these talented colleagues extends beyond imparting technical expertise; it involves nurturing their growth as independent researchers, critical thinkers, and effective communicators. Mentorship also fosters a lasting legacy, as the impact of your guidance reverberates through your students' contributions to academia and society. As they embark on their own research paths, they carry forward the insights, methodologies, and values instilled during their mentorship journey. Furthermore, supervising PhD students offers an opportunity to exchange ideas and expertise beyond national borders, leading to the development of an international network, and enriching the academic landscape. ●
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 43 ESC 2023 ● Interview
"The role of the interventional imager in transcatheter procedures for valvular heart disease has transformed into that of a multidisciplinary collaborator."
Blanche Cupido Consultant
Adult Cardiologist, Groote Schuur Hospital, Cape Town, South Africa; University of Cape Town (UCT) Private Academic Hospital, South Africa
Citation: EMJ Cardiol. 2023; DOI/10.33590/emjcardiol/10309169. https://doi.org/10.33590/emjcardiol/10309169.
Q1As a senior clinical cardiologist, can you tell us about what inspired you to specialise in adult congenital heart disease?
I have worked in the public healthcare sector in South Africa since 2001, when I obtained an undergraduate degree from the University of Cape Town (UCT). South Africa is a diverse country and is, regrettably, also known as the most unequal country in terms of income distribution globally (Gini score of inequality 63 in 2021). Although we provide excellent care to those who can afford it, many of our patients lack access to even basic primary level healthcare. During my time as a junior doctor, working in rural Northern KwaZulu-Natal, one of the poorest provinces in South Africa, I witnessed firsthand the effects of the fragmented health service, and subsequently made a commitment to improving healthcare to those with meagre financial ability.

After completing my subspecialisation in cardiology in 2013, I encountered several patients with congenital heart disease (CHD), presenting either with complicated pregnancies or clinical emergencies (heart failure and arrhythmias). I recall a 24-year-old female patient, presenting in pregnancy at 26 weeks gestation, with heart failure and profound cyanosis. The patient was known with an atrioventricular septal defect, banded in infancy. Their family moved to a rural area, and they were subsequently lost to follow-up, thus never receiving definitive corrective surgery. The patient presented after a care gap of over 22 years with severe pulmonary stenosis, due to the pulmonary artery band (gradient 120 mmHg)!
Another patient presented at 36 weeks gestation, with a dilated aortic root of 6 cm, and severe aortic incompetence due to a bicuspid aortic valve (de novo diagnosis). Upon attempting to seek clinical help in the management of these complex patients, it became clear that there was a distinct deficiency in expertise in complex adult CHD (ACHD) in South Africa, sparking my desire to improve my own knowledge pertaining to these disorders. I had the opportunity to train as an ACHD Fellow with Kate English at Leeds General Infirmary, UK. Not only did I gain experience in the management of patients with ACHD, but learnt a great deal around systems and service delivery in this field. My relationship and collaboration with this amazing clinical unit has continued.
Q2In 2017, you established a dedicated ACHD-specialist driven ACHD unit in Cape Town, the first of its kind in Sub-Saharan Africa. Could you please elaborate on the significance of establishing this unit? What were the challenges you faced and had to overcome in the process?
There are several other clinics where adult patients with CHD are being seen, and where important and much needed work is being done diligently. My aim, however, was to establish an ACHD-specialist-led referral centre, where complex adult patients with CHD could be assessed and offered a complete range of clinical services, on par with similar centres of excellence abroad. Starting a service from scratch posed many challenges. There was little awareness or recognition for the need of such a service, both from our local institution
44 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Interview ● ESC 2023
and the regional and national healthcare sector. In 2013, prior to my training, we noted that within the existing cardiac clinic services, we had around 40–50 patients with CHD, despite children’s surgery having started in the 1960s, and continuing at a rate of 350–400 surgeries per annum at the children’s hospital. These patients, once overaged for the children’s hospital, were often lost to follow-up, as no adequate CHD services existed in the adult cardiology framework. Many patients remained under the care of their paediatrician, though these visits were often erratic. When admissions for emergencies were required, overage patients could only be admitted to adult hospitals, where none of the clinicians knew them or the complexity of their disease, or were not necessarily trained adequately to deal with it.
Initially, I utilised existing clinic space and time to create this specialised clinic; no additional hospital resources were required. It started as a fortnightly service, alternating with the general cardiac clinic. Most referrals came from the overaged population at the local children’s hospital. The first task was to build a service on the adult cardiology side, in parallel with a new established transition clinic at the children’s hospital. Over a period of 3 years, most overaged patients transitioned successfully to the adult congenital clinic. Currently, we transfer patients around age 15.
The service has allowed for continuity of care and the effective reduction of care gaps. We collaborate extensively with our paediatric colleagues, and have established a multidisciplinary team, including advanced imaging (MRI and CT), cardiopulmonary exercise testing, pulmonology, obstetrics, cardiothoracic surgery, and advanced heart failure and transplantation services. For further expansion of the service, buy-in from institutional and governmental structures will be required. This is an ongoing challenge, given the competing health priorities in developing countries, where the burden of communicable and other non-communicable diseases, maternal and perinatal health, and injury-related disease is overwhelming, thus making ACHD a low priority to funders. Further challenges relate to training and increasing the number of clinically trained ACHD specialists.
Q3As the Regional Ambassador for Africa within the International Society of Adult Congenital Heart Disease (ISACHD), what initiatives do you have in place to promote awareness and improve care for patients with adult congenital heart disease?
My role as the Secretary, and Regional Ambassador for Africa, within the ISACHD is relatively new. As an organisation, we promote awareness of ACHD, and are involved with global educational programmes. The website provides links to useful information, as well as a forum where complex cases are discussed.1 The aim is to encourage collaboration and discussion around topics from diverse clinical settings. I am actively promoting the incorporation of more teaching time in the adult cardiology curriculum, including topics pertaining to ACHD in congress and Fellows Courses, and to upskill general cardiologists in the management of ACHD emergencies, whilst establishing robust referral pathways. The interest remains largely from paediatric cardiology at this point, but there is a growing recognition of the complexities of patients with ACHD in general adult cardiology.
Q4You are the Chair of the Education Committee for the SA Heart®. How do they enhance public awareness, guidelines, fellowship, research, training, and teaching in cardiovascular healthcare delivery?
The Education Committee of SA Heart® coordinates various educational activities aimed at cardiovascular practitioners in South Africa, with a local reach to Sub-Saharan Africa as well. The Committee comprises a member from each of the special interest groups: interventional cardiology, electrophysiology, basic sciences, lipidology, allied professionals (e.g., nurses, cardiac physiologists, radiographers), paediatric cardiology, and cardiac imaging. The special interest groups are responsible for the development and promotion of educational webinars, in-person academic meetings, and conferences, that are then endorsed by the Education Committee. An annual Cardiology
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 45 ESC 2023 ● Interview
"I am actively promoting the incorporation of more teaching time in the adult cardiology curriculum."
Fellows Examination Preparation course is aimed at preparing cardiology trainees for their final cardiology certification examination. This involves a 3-day programme, summarising basic concepts and the latest up-to-date information, presented by local thought-leaders. The last day of the course entails a mock-examination, similar to the final objective structured clinical and oral examination that they will do as part of their certification. The committee is also responsible for the endorsements of academic meetings, allocation of travel and research grants, and contributes to the academic programme development of the Scientific Committee of the SA Heart® Congress.
The current engagement with the public is through bi-weekly educational posts distributed through our various social media platforms (Facebook, Instagram, LinkedIn, and X (formerly Twitter); search ‘South African Heart Association’).
A novel role, which I instituted during my tenure as SA Heart® President, was a platform for academic training unit heads of department to meet 2–3 times annually, to discuss issues pertaining to training posts, the examination processes, and other issues related to the development of the discipline, and the training of Fellows in South Africa. All training in cardiovascular care occurs at the eight academic training centres, so this this allows for uniformity to be created, at least in principle for now, thus hopefully strengthening the voice of clinicians and training institutions when dealing with training bodies and government.
Q5You have recently published a paper focusing on the management of rheumatic heart disease in pregnancy. What are the major take-home messages from that article?
Rheumatic heart disease remains a leading cause of mortality and morbidity in female patients who are pregnant in low- and middleincome countries. There is also a rise in these pathologies in high-income countries due to immigration. The article2 provides a step-wise, evidence-based approach to the clinical and diagnostic assessment of rheumatic heart disease, looking at four major steps: maintaining a high index of suspicion; preconception
counselling and risk stratification; the lesionspecific management and intervention, especially pertaining to mitral stenosis, the most dominant and severe of these lesions; and the peripartum and post-partum period.
Q6 During the European Society of Cardiology (ESC) Congress in 2022, you presented on the topic of how to overcome diagnostic challenges in endocarditis. Could you share the take-home message from this presentation?
Although infective endocarditis in pregnancy is rare, it carries a very high mortality (+/- 11%) and morbidity. There are many clinical diagnostic challenges; the symptoms may be relatively non-specific; and there is also an overlap with some symptoms of pregnancy. Cardiac imaging, too, may be more difficult than usual. In terms of antibiotic therapies, these are largely similar, but be cognisant of the teratogenic profile of the drugs. Always maintain a multidisciplinary approach with these rare but difficult cases.
Q7Were there any outstanding sessions from the ESC Congress 2022 that come to mind?
The standout for me was the INVICTUS trial, which compared the direct oral anticoagulant rivaroxaban with the vitamin K antagonist (VKA) warfarin, in patients with echocardiographic proven rheumatic heart disease and atrial fibrillation. Twenty-four countries in Africa and South America participated. A total of 4,565 patients were randomised to either rivaroxaban 20 mg daily, or adjusted dose VKA. Median follow-up was 3.1 years. The primary outcome was a composite of stroke, systemic embolism, myocardial infarction, or death from vascular or unknown causes. This outcome occurred at 8.26% per year in the rivaroxaban group, compared with 6.46% in the VKA group (statistically more events in the rivaroxaban arm), concluding that in patients with rheumatic heart disease and atrial fibrillation, warfarin reduced cardiovascular events and mortality without increasing major bleeding when compared with rivaroxaban, and should thus be the standard of care for this patient group.
46 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Interview ● ESC 2023
Q8Are there any exciting innovations on the horizon for the management of adult congenital heart disease, valvular heart disease?

In our clinical context, we are increasingly using percutaneous pulmonary valve implants for patients with Tetralogy of Fallot with late residual pulmonary incompetence. We are also only now introducing MitraClip to South Africa for degenerative or secondary mitral regurgitation in patients who are too high-risk for surgical options. This is an exciting development for us. The two national centres that will be involved in the first implants are Groote Schuur Hospital, which is where I work, and Tygerberg Hospital, both in Cape Town, South Africa.
Q9As a specialist in a relatively rare and complex field, how do you approach patient care, considering the unique challenges faced by patients with ACHD, and the importance of individualised treatment plans?
The biggest challenge I face is the sheer volume of patients. For those patients who do get to our clinic, each patient is clinically evaluated, the residual lesions assessed by cardiac imaging (at least echocardiography; more advanced imaging is reserved for specific clinical indications), and a functional status assessed. We have intermittent support in terms of genetics and psychiatry
input, though this is an area we need to expand on. Furthermore, we are struggling to establish a cohort of specialist nurses for this area, which, as you well know, is an essential component to a service.
Q10
What are some points of emphasis you incorporate into practice to be the best cardiologist you can be, particularly in the field of ACHD?
Give your best for each patient. Try to, within your ability and influence, provide the best and most holistic clinical care. Be intentional about educating your patients about their disease, allowing for realistic expectations, and forming a partnership in their management strategy. ●
References
1. International Society for Adult Congenital Heart Disease (ISACHD). Welcome to the International Society for Adult Congenital Heart Disease. Available at: https://www. isachd.org/. Last accessed: 1 September 203.
2. Cupido B et al. Managing rheumatic heart disease in pregnancy: a practical evidence-based multidisciplinary approach. Can J Cardiol. 2021;37(12):2045-55.
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 47 ESC 2023 ● Interview
Interviews
Andrew Mitchell
Consultant Cardiologist at Jersey, General Hospital, Saint Helier, Jersey; Honorary Consultant Cardiologist at Oxford University Hospitals NHS Foundation Trust, UK

Citation: EMJ Cardiol. 2023; DOI/10.33590/emjcardiol/10300800. https://doi.org/10.33590/emjcardiol/10300800.
Q1Please could you outline the primary duties you undertook while serving as Chief Clinical Information Officer for the Island of Jersey?
As well as being a full-time Cardiologist in Jersey and Honorary Cardiologist in Oxford, UK, I was appointed as Chief Clinical Information Officer for the Island of Jersey in Summer 2019. My mission was to set out a programme of work to transform the way that health data were stored, shared, and managed on Jersey. We developed a vision to create one of the most technologically advanced digital health systems in Europe, an ambitious target but potentially an achievable one. Jersey has some of the fastest internet connections in the planet, with fibre network to every habitable building as well as a connected mobile telecommunication services. We are also rated as one of the most advanced and regulated finance centres in the world, so we have a group of professionals who have a vested interest in accessing high quality, secure patient data. Alongside this, Jersey is the perfect place to test and innovate new digital health

solutions. Our team has a dedicated digital health research laboratory called The Allan Lab, which is regularly approached by novel start-ups as well as established technology companies, looking to gain proof of concept and early-stage development data and funding. Many of these technologies have since been incorporated early into our clinical practice in Jersey.
Our programme of work changed with the onset of the COVID-19 pandemic. We accelerated some technology components and delivered new ways of remote working for our clinicians. We had to develop ways to communicate COVID-19 tests to and from the UK using multiple providers, wrote our own Jersey COVID-19 Alert application, and used digital health technologies to become one of the only paperless Nightingale hospitals in the British Isles.
As we exit the pandemic, we have a new hospital being designed for Jersey over the coming years, so we have an amazing opportunity to incorporate and integrate some of the most innovative health technologies.
48 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Interview
The EMJ team had the pleasure of speaking to Andrew Mitchell, who detailed the efforts being made to revolutionise health data management using advanced technology, and Hannah Gower, who shared information on junior doctor support and advancements in heart failure management.
Meanwhile The Allan Lab, led by director Austin Gibbs and supported by innovation fellow Chris Brown, continues to work in the field of immersive health technologies, ECG signal improvement, and is currently focusing on integrating clinical artificial intelligence (AI) solutions into our clinical practice.
Q2Please could you explain the rationale and background of the Heart for Life programme, which you set up in Jersey in 2010 with your wife, Claire Mitchell?

Every week in the UK, at least 12 young children and adults die from sudden cardiac death. Many of these people had no idea that there was potentially something wrong with them. Heart screening using simple techniques such as a 12 lead ECG and an echocardiogram can pick up many of the cardiac abnormalities that increase the risk of death. As many of the conditions are hereditary, such as hypertrophic cardiomyopathy and long QT syndrome, cascade screening of first-degree relatives picks up even more cases allowing targeted interventions in those at highest risk.
In 2010 Claire and I launched Heart for Life to provide Islanders access to high quality heart screening. The website allows users to choose the package of heart tests that they want, as well as providing information about some of the common and less common heart conditions. We then set up and published a community heart screening research project to see if we could change the screening model and take our
equipment to the students rather than bringing them to a clinic. We have subsequently been involved in screening the Jersey’s top football, rugby, and cricket teams. The service is currently provided as a user-pays model, but we have an aim to fund raise and develop a business model that allows us to provide heart screening free for all Islanders.
Q3You have helped establish several charities in Jersey. Please could you describe the notable projects undertaken by these organisations and summarise their greatest achievements to date?
One of the biggest challenges I faced on moving to Jersey was accessing rapid government funding to appoint our Heart Team. Over the last decade, I have raised over 1.5 million GBP of charitable monies, which has allowed us to build the Jersey Heart Team and secure agreement for permanent government funding. Fundraising is hard and time-consuming but also emotionally rewarding. To support this work, and to develop new initiatives in Jersey, I helped establish the Jersey Heart Support Group in 2011. One of our first projects was to fund the provision of an automated external defibrillator to all schools in Jersey, making Jersey a place with one of the highest numbers of automated external defibrillators per capita in the British Isles.
Alongside this, I became a committee member of the new Jersey branch of the British Heart Foundation (BHF). We organised annual fundraising events including Heart Hero awards and
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 49 Interview
generated considerable monies for the charity. Our work in Jersey was recognised by the BHF in 2016 at an awards ceremony at the Houses of Parliament in London, UK.
I am currently working on a new and larger charitable project which is called the Jersey Research Foundation. This charity is designed to stimulate the concepts of research, innovation, questioning and entrepreneurship in Islanders. Grants will be offered to individuals across all industry in Jersey, including health, with the expectation that this will create new businesses and research opportunities in the Island.
Q4You lead the Jersey Heart Team, which was selected as a ‘Syncope Pioneer’ by Syncope Trust and Reflex Anoxic Seizures (STARS) in 2021. Please highlight the work that resulted in this achievement.
Blackouts (syncope) are a common cause of hospital admission and as many as half the population will pass out in their life. This can often lead to hospital admission and investigations, which can be time-consuming and often unrewarding. We appointed a specialist nurse Kelly-Anne Kinsella to set up a dedicated Transient Loss of Consciousness Clinic (TLoC) to see and assess patients within a few days of presentation to hospital. We also trained up one of our clinical physiologists to implant loop recorders, increasing access to this valuable procedure. This reduced hospital admissions and bed stays as well as leading to more appropriate use of investigations and a more rapid clinical diagnosis. For this work, the team were included in the 2021 Syncope Pioneers report and Jersey General Hospital became recognised internationally as a centre of excellence.
and North America and tailor our services to provide a unique way of managing heart (and other) conditions. In addition, we established a fellowship training programme attracting doctors who want to train in cardiology to get a year of high intensity clinical experience and teaching, launching them into successful UK cardiology rotations. Consequently, the Jersey Heart Team has been awarded numerous local and national awards for its innovative approach to healthcare management and training. Perhaps the most prestigious of these were to be shortlisted to the top four cardiology units in the 2016 Cardiology Team of the Year by the British Medical Journal. In addition, arrhythmia nurse specialist Angela Hall was selected by the Royal College of Nursing as Nurse of the Year in 2018. An amazing achievement when you consider there are over 700,000 nurses working across the British Isles. Personally, my work has been recognised by other organisations including the Arrhythmia Alliance, the Government of Jersey as well as the Institute of Directors, receiving a highly commended award in 2015 as UK Public Sector Director of the Year.
Q6Could you provide an overview of your 2017 EMJ Cardiology article, entitled ‘Ectopic Beats: How Many Count?’
Q5
In addition to being recognised as an international centre of excellence by STARS, the Jersey Heart Team has been shortlisted for several other prestigious national awards. Please could you tell us about these?
Jersey is a wonderful place to innovate and develop new health services. As Jersey is not part of the English National Health Service (NHS), we can extract components of healthcare guidelines from the UK, Europe,
Ectopic beats are extra heat beats which usually come from the top (atrium) or the bottom (ventricle) of the heart. They are incredibly common, and most people will have a handful each day. In some people, however, ectopic beats can be associated with heart symptoms such as palpitation, as well as being linked with underlying heart conditions such as heart failure. For this reason, many patients seek medical advice when they notice an abnormal heart rhythm, or if they are alerted to it by a medical device such as a smart watch or a blood pressure machine. Our article reviews the current literature on ectopic beats and provides the treating physician with an understanding of when they should be deemed significant and when treatment may be appropriate.
50 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Interview
"We established a fellowship training programme attracting doctors who want to train in cardiology."
Q7How important do you believe digital health interventions are for the prevention of cardiovascular disease?
Further, how can associations such as the European Society of Cardiology (ESC) and American College of Cardiology (ACC) ensure that digital healthcare remains a key priority for the cardiology community?

Most European healthcare services are established to look after people when they are ill or need an operation, but with current growth and demand, systems struggle to get adequate health staff and resource to deliver this efficiently. Digital health technologies are the enabler for a modern health service and will help move the focus away from care to prevention. One of the terms I use is that we need to start to ’dedoctorfy medicine’. We should give the patient access and control over their health data, as well as the digital tools and knowledge to monitor their own health condition so that they are less reliant on health staff. We can then move away from the current position where a patient asks the doctor what is wrong, to a point where the patient has a deep understanding of their health conditions as well as treatment options. By enabling these types of technologies patients can ‘take charge’ of their own health management. They can also start to access health care globally rather than locally, creating opportunities for health professionals in other countries as well as increasing capacity in the local network.
Coronary heart disease remains one of the leading causes of death yet many heart attacks are preventable. Digital machine learning technologies such as the assessment of fat-attenuation index in heart scans by Caristo Diagnostics (Oxford, UK) and AI technologies for assessing echocardiograms by Ultromics (Oxford,
UK), offer an insight into how cloud-based software can, as a service, help to accurately predict patient’s risk and allow early risk reducing interventions. Novel AI systems such as from Google (Menlo Park, California, USA) and the ChatGPT service from OpenAPI (San Francisco, California, USA) are just the start of new augmented intelligence support systems.
Q8Please could you share the key take-home messages from your 2020 EMJ Innovations article, entitled ‘The Era of Immersive Health Technology’?
Immersive health technologies are revolutionising the delivery of healthcare, therapeutic techniques, rapid knowledge access, and research. Our review paper summarises some of the current developments and describes the four main types of immersive health technology: augmented reality, virtual reality (VR), machine learning, and AI. VR systems are quickly developing and in clinical practice we now routinely offer clinical VR to patients undergoing invasive or uncomfortable procedures such as pacemaker implantation or pericardiocentesis. VR also offers great potential to improve the training of healthcare professionals through reality-simulation training, now available in a multi-user environment. In the paper, we described examples of the use of other immersive technologies in healthcare, their opportunities and pitfalls, and how the use of these technologies could be improved further in the future are highlighted. Systems such as AI and machine learning are providing clinicians with clinical support services, which are augmenting the knowledge based of health workers and, with the speed of development, it is probably one of the most exciting times to be involved in healthcare. ●
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 51 Interview
Hannah Gower Cardiology and Internal Medicine Speciality Registrar, Royal Cornwall Hospitals NHS Trust, UK

Citation: EMJ Cardiol. 2023; DOI/10.33590/emjcardiol/10306448. https://doi.org/10.33590/emjcardiol/10306448.
Q1You were one of three trainees from your National Health Service (NHS) Trust to have received one of the prestigious regional awards for the 2022 Medical Awards for Training Achievements (MAFTA). Could you tell us a bit more about this? Why did you receive the School of Medicine Trainee of the Year?
It is an award that recognises the contributions of southwest training doctors to regional education and training opportunities. It was awarded to me based on nominations for contributions to supporting junior doctors and my other colleagues. There is often not much you can control within the leviathan machine that is the NHS, but we can control how we interact with each other and our patients. As a Cardiology and Medical Registrar, I am in this unique position where I can be the link between our consultant body of two major inpatient specialties with the junior team. I try to focus my attention on supporting my fellow junior doctors and the wider team, both mentoring and educating where I can, to foster a sense of camaraderie and team spirit in the face of many systematic challenges.
I am keen on teaching, and I contribute to our local hospital and medical school teaching programmes, with the hope of making cardiology more accessible. I think cardiology can be a topic that people often fear, especially in the acute setting. I want to reassure trainees and inspire them to see that cardiology is truly fascinating with such a wide scope of focus for all interests.
Q2In 2021, you published a case report entitled ‘A Rare Finding: A Left Atrial Cavernous Haemangioma’. How could this report help inform other clinicians when they encounter similar cases?
Whenever we put forward case reports to be published, it is often to demonstrate a nuanced case where there is often lack of guidance on how to manage the unique scenario, due to the nature of their infrequency. It enables clinicians to consider how the authors manage the situation and consider modelling any future similar scenarios on their approach or alternatively, build upon the strategy and offer an alternative option.
Q3You started as a Clinical Fellow in cardiology for the Royal Devon and Exeter NHS Foundation Trust, UK, and are now a Cardiology Registrar at the Royal Cornwall Hospitals NHS Trust. What do you consider to have been the most significant advances in clinical cardiology and cardiovascular pharmacotherapy during these periods?
As a hopeful future Heart Failure Consultant, the big difference I have seen is the introduction of sodium-glucose co-transporter-2 inhibitors and the impact of the REVIVED-BCIS2 trial. These are two key things that, even in my short junior cardiology career, I have seen change how we practice management of heart failure day-today. I will be most interested to see how this impacts our use of devices in heart failure with reduced ejection fraction, especially cardiac resynchronisation therapy. It is an exciting place to know that there are potential major changes in the near future for heart failure management.
52 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Interview
Q4What do you consider to be the major unmet needs in cardiovascular medicine? How might these be addressed going forwards?
In the Southwest Peninsula, we do not just have an older population but also a frail, older population. One area that we could benefit from is a direct connection between the care of elderly/ frailty services with our cardiology services. We often run parallel models of care next to each other; however, the patient care can be quite binary: they are either with the cardiology team or they are in the care of elderly team. In the future, I would really hope that we can start to merge our services, and maybe even see joint clinics and the inclusion of care of elderly specialities in our multidisciplinary team meetings.

That is where I think the needs are unmet currently, but I am optimistic that they will be addressed, especially in the next coming generations of Cardiology Registrars, who also will be dual trained with a general internal medicine Certificate of Completion of Training alongside their cardiology Certificate of Completion of Training.
Q5As you have mentioned, you have published a case report and are in the process of submitting another. What other interesting cases have you encountered as a Cardiologist? What are the key learnings that you have taken away from these situations and how have you applied them in your daily practice?
I find anything that' is new, or anything that can change your day-to-day practice, interesting. I read an intriguing recent case report about neurogenic pulmonary oedema in the absence of heart failure, with normal albumin and normal renal function, which I thought was fascinating. It was not something I had ever heard of before, and never had even considered as a potential cause of pulmonary oedema. Therefore, it just widens your differentials when you consider these patients presenting in front of you. That is probably a rare case, as you report the rarest and the most unusual ones.
A great thing about case reports is that they are a great opportunity for junior or new team members to write up cases while being supported by more senior clinicians. The ‘cycle of case report life’ in a way, where now I am mentoring a medical student and foundation doctor with their submissions.
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 53 Interview
"One area that we could benefit from is a direct connection between the care of elderly/frailty services with our cardiology services."
Q6
Digital health was a recurring theme across a lot of the content presented at the European Society of Cardiology (ESC), and digital health in cardiology quite a big topic at the moment. How important do you believe digital health interventions are in the prevention of cardiovascular disease? Is something that you are involved with at your NHS Trust?
Whilst I am not aware of anything in Cornwall at the moment, I do believe, particularly as I quite like technology, that digital health has a huge role to play. I would be cautious, though, because traditionally technology can gather a lot of data but not necessarily a lot of information that is valuable, particularly when we want to reassure patients. Sometimes, I can be almost paradoxically unhelpful, particularly in patients with heart rate monitors where you are trying to reassure them that the data collected does not necessarily reflect pathology.
In addition to that, we must have an awareness that technology is expensive. If we are not supplying it on the NHS, we could create a tier system where less fortunate individuals are not able to access the same opportunities as those who can afford it.
Q7Between 2021 and 2022, you published several papers as a member of the RECOVERY Collaborative Group. Could you tell us a bit more about the findings and wider relevance of the group and the research conducted by it?
I was a contributor, like many junior doctors, medical students, and nurses across the NHS. I think that anyone who was working amongst inpatients with COVID-19 had a role in contributing to the RECOVERY trial, but this was mostly when I was based on the COVID-19 wards.
The RECOVERY trial was a widespread national programme with multicentre contributors. It originally stemmed from thinking about the first wave. We had this new condition that no-one knew how to treat. A paper from a group in China was initially published, which was one of a kind. Interestingly, they commented a lot about acute coronary syndrome and the cardiovascular complications. It then evolved, and we began to understand that there were a lot more renal
and cardiovascular complications. Though, interestingly, that has evolved further. Now you are seeing a lot of COVID-19 myocarditis and COVID-19-related heart failure.
It was really exciting in many ways because you had this novel condition that no-one knew how to manage, and you felt very much at the forefront. However, that was also quite terrifying because you could not use your previous understanding of viral conditions in this circumstance. It was great to be part of such a wide scale project. Many of us were collaborators and it was a real opportunity to understand research, something that I had never really done before as an undergraduate. Even being a small part of that was a good first step into the world of research.
Q8 What advice would you give to medical students and trainees who may be considering a career in cardiology?
Do not feel overwhelmed by the eagerness and success of others. I think cardiology can attract very high flying, very capable, and very articulate type A personalities. For some people who do not identify with that cohort, they might feel that this is not for them. In other centres that could be the culture, but that is why I love the southwest because we have a range of characters and personalities. You can be the surfer who wants to have a good work–life balance and be a Cardiologist and just as easily be a multipublished, leader in your field, head of the British Heart Rhythm Society (BHRS).
We also need to emphasise to students and junior colleagues, as my supervisor often stated to me: “It is a marathon, not a sprint.” It is a craft that takes a considerable length of time to develop and while the annual review of competency progression, exams, and courses are all stepping stones to the next phase, it is also okay to take some time off the training treadmill and broaden your experiences and understanding. I did that when I undertook a clinical fellow in cardiology.
54 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Interview
"The RECOVERY trial was a widespread national programme with multicentre contributors."
At the beginning of that post, I would have never thought that cardiology would be the career for me, and now I cannot think how else I would spend my working time.
Just by the very nature of the NHS, it has evolved, grown, and exceeded its capacity, and I feel like it needs a reshape and some reorganisation.
Q9
When you finished medical school, did you get a choice of which NHS Trusts you were going to, or did you just get posted to Cornwall?

UK graduates apply for foundation programme posts, which is the next stop in medical training following undergraduate degree. They are compared to one another through a central system. Graduates then can rank their desired posts and locations, with those highest ranking having first choice.
I am from Devon, UK, originally, which is just one county east from Cornwall, and I studied in Glasgow, UK. While I absolutely adored Scotland, it is an amazing country and excellent place to learn and train, family is vital to me, so I came back to the southwest to spend more time with them following completion of the foundation programme to take up a Core Medical Trainee post in Exeter, UK.
Q10Where
do you see your attention and focus in the coming years?
If given the opportunity, I would very much like to see the management, recruitment, and welfare of junior doctors improved.
We need more nurse, doctor, and physiologist managers who understand the challenges faced on the shop floor. I think that the COVID-19, with the rapid development of remote working, has widened the communication barrier between front-line staff and management. I think that any attempts to narrow that gap of experiences between the various stakeholders in the NHS is key. I am sure there are a number of patients who are also frustrated with the system and feel they are left unheard for the same systematic issues that face staff. I am undertaking a full-time Master’s degree in health care leadership and management at the University of Exeter, UK, later this year, hopefully to further my understanding of NHS management and to equip myself with the skills to take on some of these challenges in the future.
I also feel the same for heart failure. I would love to see a heart failure ward run by specialist heart failure nurses, with a provision of co-care through elderly and cardiologist multidisciplinary teams. In heart failure care, if you are not on a cardiology ward, you do not do as well and you have longer hospital stays. I see that as a perfect opportunity for a really merged multidisciplinary team approach. A combination of those two would be brilliant. However, I am still quite a junior registrar, maybe that is a question to ask me again after several years as a Consultant. ●
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 55 Interview
Introducing Mavacamten for the Treatment of and III Symptomatic Obstructive HCM in Adult
Obstructive HCM Represents a Chronic and Progressive Disease, Posing Challenges in Both Diagnosis and Treatment
HCM is characterised by LV hypertrophy that cannot be explained by another cardiac or systemic disease.
Variable disease presentation and non-specific symptoms can make diagnosis difficult.
Mavacamten is a First-in-Class Therapy Pioneering Therapeutic Approach, Addresses Fundamental Pathophysiology of Obstructive Mavacamten significantly improved symptom control and exercise capacity (pVO2) versus placebo
Percentage of patients achieving primary composite
Treatment difference: 19%; 95% CI: 8.67–30.13; p=0.0005
Current pharmacologic therapies, β-blockers, and calcium channel blockers address symptoms, but may not alter natural history of HCM.
SRTs are complex, invasive procedures with significant risks. Following SRT, up to 30% of patients still require treatment for symptoms.
There is an unmet need for an approved non-invasive treatment that targets obstructive HCM.
Most commonly reported adverse reactions with mavacamten:
Cardiac disorders: Respiratory, thoracic, and mediastinal disorders:
Proportion of patients (%)
No patients discontinued treatment permanently due to a LVEF <50%.
Mavacamten reduces LVEF and may cause heart failure due to systolic dysfunction defined as symptomatic LVEF <50% Patients with a serious intercurrent illness, such as infection or arrhythmia (including atrial fibrillation or other uncontrolled tachyarrhythmia), or those undergoing major cardiac surgery, may be at greater risk of systolic dysfunction and progress to heart failure.
blocker (n=45/123) +/- blocker (n=22/128)
*92% and placebo remained †Primary defined increase class mL/kg/min worsening
Mavacamten significantly reduced the proportion proceeded or remained guideline-eligible for SRT
Treatment di erence: 59% 95% CI: 44–74; p<0.0001
Placebo No for Guideline-eligible, proceeded
SRT eligibility at Week 16* 82% 77% 18%
Mavacamten maximally tolerated background therapy (n=56)
References
23%
Placebo + maximally tolerated background therapy (n=56)
*In the patients prior to patients for SRT In the chose or at Week remained after 16 taking evaluable, meeting
1. Ho CY et al. Genotype and lifetime burden of disease in hypertrophic cardiomyopathy:
2. Olivotto I et al. Patterns of disease progression in hypertrophic cardiomyopathy:
3. Argulian E et al. Misconceptions and facts about hypertrophic cardiomyopathy.
4. Elliott PM et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic European Society of Cardiology (ESC). Eur Heart J. 2014;35(39):2733-79.
5. Ommen SR et al. 2020 AHA/ACC guideline for the diagnosis and treatment Association Joint Committee on Clinical Practice Guidelines. Circulation.
6. Maron BJ et al. Management of hypertrophic cardiomyopathy: JACC state-of-the-art
7. Desai MY et al. Myosin inhibition in patients with obstructive hypertrophic
8. European Medicines Agency (EMA). CAMZYOS Summary of Product Characteristics. https://www.ema.europa.eu/en/documents/product-information/camzyos-epar-product-information_en.pdf.
The Safety Profile of Mavacamten is Comparable Between the EXPLORER-HCM and VALOR-HCM Trials
37% 17%
100 80 60 40 20 0 Percentage Mavacamten
+/-
100 80 60 40 20 0
Dizziness
Systolic dysfunction* (5%) (12%) (5%) (17%)
Nervous system disorders:
Syncope
Dyspnoea
patients
~4x guideline-eligible
primary endpoint
2020;142(25):e558-631.
NYHA Class II Patients
Therapy and as a Addresses the Obstructive HCM
control (NYHA class)
endpoint at Week 30*
Twice as many patients achieved the primary composite endpoint vs. placebo
of patients in the mavacamten placebo treatment arms also remained on background therapy. †Primary composite endpoint defined as a ≥1.5 mL/kg/min increase in pVO2 and ≥1 NYHA reduction, or a ≥3.0 mL/kg/min increase in pVO2 and no worsening in NYHA class.
proportion of patients who SRT vs placebo
No longer guideline-eligible for SRT
Guideline-eligible, or proceeded with SRT
~4x more patients were no longer guideline-eligible for SRT
the mavacamten group, two patients chose to proceed with SRT to or at Week 16, and eight patients remained guideline-eligible SRT after 16 weeks of treatment. placebo group, two patients chose to proceed with SRT prior to Week 16, and 39 patients remained guideline-eligible for SRT 16 weeks. In two patients taking placebo, SRT status was not evaluable, and was imputed as meeting the primary endpoint.
The publication of this infographic was supported by Myokardia and Bristol Myers Squibb.
EMJ Cardiol. 2023; DOI/10.33590/emjcardiol/10303519. https://doi.org/10.33590/emjcardiol/10303519.
Once-Daily Mavacamten O ers Individualised and Personalised Dosing to Achieve the Optimal Response
Week 4* Week 8* Week 12* Week 12 + every 12 weeks
5 mg QD; initiate only if LVEF ≥55% ≥20 mmHg ≥20 mmHg
LVEF ≥55%, and Valsalva LVOT gradient ≥30 mmHG
<20 mmHg
1.
dose (treatment not paused) <20 mmHg ≥20 mmHg ≥20 mmHg ≥20 mmHg ≥20 mmHg
Maintain on the current dose and follow-up 12 weeks later
Up-titration to next higher daily (mg) dose level:
• 2.5 mg→ 5 mg; 5 mg→ 10 mg; 10 mg→ 15 mg
Futher up-titration is allowed after 12 weeks of treatment on the current dose level if LVEF ≥55%.
See current dose (treatment not paused)
Dosing for patients with CYP2C19 intermediate, normal, rapid, and ultra-rapid metaboliser phenotypes The incidence of patients with CYP2C19 intermediate, normal, rapid, and ultra-rapid metaboliser phenotypes ranges from approximately 98% in Caucasians to 82% in Asian populations
• The starting dose for patients with a CYP2C19 poor metaboliser phenotype is one 2.5-mg capsule orally, once daily.
• If treatment is initiated before CYP2C19 phenotype is determined, you should follow dosing instructions for CYP2C19 poor metaboliser phenotype until phenotype is determined.
Mavacamten is available in 2.5 mg, 5 mg, 10 mg, and 15 mg
Prescribed doses should be taken in a single capsule
Treatment should be taken once daily at the same time each day, with or without food
cardiomyopathy: insights from the Sarcomeric Human Cardiomyopathy Registry (SHaRe). Circulation. 2018;138(14):1387-98. cardiomyopathy: an individualized approach to clinical staging. Circ Heart Fail. 2012;5(4):535-46. cardiomyopathy. Am J Med. 2016;129(2):148-52. hypertrophic cardiomyo-pathy: the Task Force for the Diagnosis and Management of Hypertrophic cardiomyopathy of the treatment of patients with hypertrophic cardiomyopathy: a report of the American College of Cardiology/American Heart 2020;142(25):e558-631.
state-of-the-art review. J Am Coll Cardiol. 2022;79(4):390-414. cardiomyopathy referred for septal reduction therapy. J Am Coll Cardiol. 2022;80(2):95-108. Characteristics. 2023. Available at: https://www.ema.europa.eu/en/documents/product-information/camzyos-epar-product-information_en.pdf.
2.
Recheck clinical status, Valsalva LVOT gradient, and LVEF at Week 4 after dose increase, and maintain the current dose for the next 8 weeks unless LVEF <50%
Recheck at Week 4
Futher up-titration is allowed after 12 weeks of treatment on the current dose level if LVEF ≥55%.
Recheck at Week 4
Patients with a CYP2C19 poor metaboliser phenotype: maximum dose is 5mg. If titrating from 2.5 mg to 5 mg, follow-up 4 and 8 weeks later.
Key
CI: confidence interval; CYP2C19: cytochrome P450 2C19; HCM: hypertrophic cardiomyopathy; LV: left ventricular; LVEF: left ventricular ejection function; LVOT: left ventricular outflow tract; NYHA: New York Heart Association; QD: once daily; SRT: septal therapies.
Last accessed: 15 August
2023.
Current
• Maximum dose for patients with CYP2C19 poor metaboliser phenotype is 5 mg. <20 mmHg LVEF <50% Decrease to 2.5 mg QD Maintain at 5 mg QD
1. Restart on 2.5 mg QD if LVEF ≥50%
2. Recheck clinical status, Valsalva LVOT gradient, and LVEF in 4 weeks, and maintain the current dose for the next 8 weeks unless LVEF <50%
LVEF 50–55%, regardless of Valsalva LVOT gradient or LVEF >55% and Valsalva LVOT gradient <30 mmHG
3. 4.
Confirm patient eligibility based on Summary of Product Characteristics before initiating treatment. The potential for drug interactions should be considered according to the Summary of Product Characteristics prior to initiation with mavacamten and throughout continued treatment.
Therapeutic Indication:
Mavacamten is indicated for the treatment of symptomatic (New York Heart Association, NYHA, class II-III) obstructive hypertrophic cardiomyopathy (oHCM) in adult patients.
The Impact of Guideline-Directed Medical Therapy Adherence on Cardiovascular Outcomes: A Critique of Recent Trials
Authors: *Han Naung Tun1
Larner College of Medicine, University of Medicine, Burlington, Vermont, USA *Correspondence to annasxhan@gmail.com
Disclosure: Tun has declared no conflicts of interest.
Received: 12.06.23
Accepted: 09.08.23
Keywords: Evidence gaps, guideline-directed medical therapy (GDMT), ISCHEMIA trial, medication optimisation.
Citation: EMJ Cardiol. 2023;11[1]:58-60. DOI/10.33590/emjcardiol/10306358. https://doi.org/10.33590/emjcardiol/10306358.
INTRODUCTION
This review scrutinises the role of guideline-directed medical therapy (GDMT) adherence in some studies and how it influenced cardiovascular outcomes. Furthermore, it explicates the methodology, outcomes, and clinical implications of the ISCHEMIA trial, emphasising the necessity of achieving optimal adherence in clinical practice. Numerous landmark clinical trials in recent years have had profound implications on interventional practice in cardiovascular medicine. Among these, the COAPT and ORBITA trials warrant mention. A consistent element in such investigations is the implementation of GDMT, a key factor often not given due emphasis while appraising trials with potential practice-changing outcomes.
GUIDELINE-DIRECTED MEDICAL THERAPY
Recent interventional trials, including cardiovascular outcomes assessment of the MitraClip percutaneous therapy for patients with heart failure and functional mitral
regurgitation (COAPT) and percutaneous coronary intervention in stable angina (ORBITA), have demonstrated significant influences on clinical practice. A pivotal feature of such studies is GDMT, which is often neglected in trial evaluations.1,2 The ISCHEMIA trial stands as a watershed study in the field of cardiovascular medicine. Its central focus lay on the outcomes of patients with stable coronary artery disease (CAD) and moderate or severe ischaemia. The pivotal comparison was between an invasive strategy encompassing GDMT with possible revascularisation, and a conservative strategy consisting solely of GDMT.3
The relevance of GDMT in this context cannot be overstated. GDMT refers to a therapeutic approach that utilises established medications and lifestyle interventions in accordance with medical guidelines. It typically includes antiplatelet drugs, statins, angiotensin-converting enzyme inhibitors, β-blockers, and lifestyle changes, such as regular exercise, dietary modifications, and smoking cessation. In the ISCHEMIA trial, GDMT was administered equally to both intervention groups, highlighting its importance in contemporary cardiovascular care.3
58 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Feature
The ISCHEMIA trial provided a novel perspective on the role of GDMT in managing patients with ischaemic heart disease. It indicated that, in many instances, an initial conservative strategy using optimal GDMT alone can yield outcomes comparable with those from an initial invasive strategy. This finding was pivotal, as it emphasised the critical role of GDMT in managing ischaemic heart disease, and the potential to achieve substantial patient benefits, even without resorting to invasive interventions.
Historical studies evaluating coronary artery bypass grafting and percutaneous coronary intervention in CAD, such as the MASS-2 trial, were also conducted in the context of GDMT.4 However, the evolution of medical therapy for heart failure and risk factor modification over time has rendered these trials obsolete. Therefore, a more contemporary study, such as the ISCHEMIA trial, becomes the cornerstone of this discussion.
The ISCHEMIA trial implemented a methodology involving enrolling individuals with moderate or severe ischaemia, excluding those with significant left main CAD, or other particular conditions. The trial conducted a pre-specified subanalysis, hypothesising better outcomes for non-adherent patients randomised to an invasive strategy. It utilised a modified four-item Morisky–Green–Levine Adherence Scale to capture medicationtaking behaviour, and a seven-item Seattle Angina Questionnaire (SAQ-7) summary score to assess health status. Subsequent analysis of adherence and outcomes was conducted using Bayesian proportional odds models. The study found that 27.8% of patients were non-adherent at the start. Non-adherence was correlated with worse symptoms and a decline in health status in both trial arms.5 In-depth analysis also suggested a potential benefit from an invasive strategy for these patients.5
Adherence, or the lack thereof, poses a persistent challenge in clinical practice. Although the appeal for selecting an invasive strategy for patients with lower probabilities of medication adherence is tempting, this study demonstrated no apparent benefits in pursuing such an approach. What becomes alarming is the worse outcomes experienced by both adherent and non-adherent groups, emphasising the importance of optimising medical therapy.
However, the ISCHEMIA trial also revealed some critical challenges.3,6,7 For one, adherence to GDMT in real-world settings is often lower than in the context of a clinical trial, which can potentially limit the effectiveness of a GDMTbased approach.3,7
In response to these challenges, the trial underscored the significance of not solely granting patients access to healthcare providers throughout the entire care continuum, but also equipping them with a more profound comprehension of their treatment regimen and its advantages to enhance adherence. The ISCHEMIA trial also laid the foundation for future investigations. It underscores the need for future studies to focus not only on clinical outcomes, but also on patient-oriented outcomes, such as quality of life and costeffectiveness. With an increasing emphasis on value-based healthcare, these considerations are becoming increasingly important.
EVIDENCE GAP AND BARRIERS
The ISCHEMIA trial, while instrumental in refining the management strategy for stable ischaemic heart disease, has left certain evidence gaps, and posed questions that need to be addressed by future research. These questions and gaps pertain to the trial design, execution, and its external validity. The trial’s patient population selection is a notable limitation. Particularly, the exclusion of patients with the most severe form of ischaemia, including those with left main CAD, which raises the question of the trial’s applicability to this high-risk patient group. Another evidence gap emerges in the context of the timing of the invasive strategy. The trial did not directly compare an immediate invasive strategy with a deferred one, which is only undertaken upon the failure of GDMT.
Another significant area where the ISCHEMIA trial falls short is the optimisation of GDMT. The trial underscored the importance of GDMT, but did not delve into the specifics of how it could be tailored for individual patients with CAD. The optimisation of medical therapy, taking into account patient characteristics, tolerance, and response, can significantly impact outcomes, and necessitates more focused research.
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 59 Feature
The ISCHEMIA trial rightly emphasised the importance of medication adherence, but failed to investigate measures to enhance it. A deeper understanding of factors affecting adherence, such as medication cost, regimen complexity, patient education, and socioeconomic factors, is needed.
Quality of life assessment in the trial could also be enhanced. Although the SAQ-7 was used to assess health status, future studies could consider including more objective assessments, such as exercise capacity, hospitalisation rates, and more specific angina measures. Such assessments would provide a more holistic view of the impact of different strategies on patients’ quality of life. Therefore, a better understanding and application of GDMT in real-world settings is crucial.
CONCLUSIONS
The new sub-study of ISCHEMIA opens up new avenues for exploration, especially in regard to quality of life and cost-effectiveness, and raises crucial questions for future trials. It highlights that non-adherence in CAD could significantly contribute to increased morbidity, hospitalisation, and mortality. Consequently, it underscores the imperative to address medication adherence in patients with CAD in both invasive and non-invasive groups, with the aim of reducing hospitalisation, improving clinical outcomes, and reducing healthcare costs. This ISCHEMIA subanalysis highlights that the implementation of a simple GDMT protocol is vital for improving health outcomes, and is practical for real-world settings. It paves the way for future investigations to consider how GDMT optimisation and medication adherence can be incorporated in clinical studies involving invasive strategies.
References
1. Stone GW et al. Transcatheter mitral-valve repair in patients with heart failure. N Engl J Med. 2018;379(24):2307-18.
2. Al-Lamee R et al.; ORBITA investigators. Percutaneous coronary intervention in stable angina (ORBITA): a double-blind, randomised controlled trial. Lancet. 2018;391(10115):31-40. Erratum in: Lancet. 2018;391(10115):30.
3. Riley RF et al. The ongoing national medical staffing crisis: impacts
on care delivery for interventional cardiologists. J Soc Cardiovasc Angiogr Interv. 2022;1(3):100307
4. Hueb W et al. The medicine, angioplasty, or surgery study (MASS-II): a randomized, controlled clinical trial of three therapeutic strategies for multivessel coronary artery disease: one-year results. J Am Coll Cardiol. 2004;43(10):1743-51
5. Garcia RA et al.; ISCHEMIA Research Group. Association of medication adherence with health outcomes in the ISCHEMIA trial. J
Am Coll Cardiol. 2022;80(8): 755-65.
6. Maron DJ et al.; ISCHEMIA Research Group. Initial invasive or conservative strategy for stable coronary disease. N Engl J Med. 2020;382(15):1395-407.
7. Spertus JA et al. Prevalence, predictors, and outcomes of premature discontinuation of thienopyridine therapy after drug-eluting stent placement: results from the PREMIER registry. Circulation. 2006;113(24):2803-9.
FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM
60 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Feature
Obstructive Sleep Apnoea as an Exacerbator of Vasospastic Angina
Editor's Pick
My Editor’s Pick is entitled ‘Obstructive Sleep Apnoea as an Exacerbator of Vasospastic Angina’. In this fascinating case report, the authors present a compelling case of a 47-year-old female with vasospastic angina, who experienced persistent symptoms despite conventional treatments. The discovery of severe obstructive sleep apnoea (OSA) led to a transformative intervention with continuous positive airway pressure, resulting in remarkable symptom improvement. This study underscores the intricate interplay between OSA and vasospastic angina, shedding light on a potential avenue for enhanced management in patients with treatment-resistant angina. The findings prompt further investigation into this intriguing relationship, suggesting the potential benefits of screening and addressing OSA in the context of vasospastic angina management.
Authors:
*Faith Michael,1 Anthony Main,2 Andreas Kumar1,2
1. Northern Ontario School of Medicine University, Sudbury, Canada
2. Department of Cardiology, Health Sciences North, Sudbury, Canada *Correspondence to famichael@nosm.ca

Disclosure: The authors have declared no conflicts of interest. Informed written consent was obtained from the patient.
Received: 23.04.22
Accepted: 18.04.23
Keywords: Obstructive sleep apnoea (OSA), vasospasm, vasospastic angina.
Citation: EMJ Cardiol. 2023; 11[1]:61-65. DOI/10.33590/emjcardiol/10005818. https://doi.org/10.33590/emjcardiol/10005818.
Abstract
Little is known about the association between obstructive sleep apnoea (OSA) and vasospastic angina. The authors report the case of a 47-year-old female with vasospastic angina who had a high symptom burden despite nitroglycerine and a calcium channel blocker. After a sleep study revealed severe OSA, the patient was started on continuous positive airway pressure. Following 8 weeks of continuous positive airway pressure, the patient reported remarkable improvement in their symptoms. This case suggests an under-recognised link between OSA and vasospastic angina. While further clinical research is required, screening and treatment of OSA may be beneficial for patients with treatment refractory vasospastic angina.
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 61 Article
Çetin Erol Ankara University, Türkiye
Key Points
1. Vasospastic angina is an under-recognised cause of chest pain that affects females more commonly than males. Obstructive sleep apnoea (OSA) has been associated with nocturnal angina. However, the possible association between OSA and vasospastic angina is not well understood.
2. The authors report the case of a 47-year-old female with vasospastic angina who experienced debilitating symptoms despite nitroglycerine and a calcium channel blocker. A sleep study revealed severe OSA. They experienced remarkable improvement in their symptoms following the initiation of continuous positive airway pressure therapy.
3. OSA can worsen vasospastic angina via numerous mechanisms, including increased sympathetic tone and endothelial dysfunction. While further research is required, screening for OSA may be beneficial for patients with treatment refractory vasospastic angina.
PRESENTATION
A 47-year-old perimenopausal female had four presentations to the emergency department with acute chest pain syndrome. The chest pain occurred immediately after light physical activity, such as housework or walking two blocks. The pain radiated into their jaw, and was provoked by stress, fatigue, and cold weather. The patient’s medical history included hypertension, dyslipidaemia, a mildly elevated BMI of 27 kg/m2, migraines, and depression. From a reproductive perspective, menarche occurred at age 12 years and they were approaching menopause with increasing cycle irregularity. The patient had two previous pregnancies and was not on oral contraceptives. There was no family history of coronary artery disease. They were a lifelong non-smoker and consumed one alcoholic drink per week. Medications included lansoprazole and duloxetine. They were not on any sedatives or narcotics. The patient responded to nitroglycerine spray in the emergency department, but serial troponins and ECGs were negative. Their symptoms were frequently attributed to anxiety, and they were discharged home.
ASSESSMENT
The patient continued to experience chest pain on a weekly basis, including waking up with angina at night. In fact, the patient reduced their work hours due to the burden of their symptoms. The patient re-presented to the emergency department, where initial vitals included an
elevated blood pressure of 158/96 mmHg, heart rate of 83 beats per minute, and O2 saturation of 99% on room air. Serial troponins were negative and ECG changes were limited to transient T wave inversions in lead V2. Chest X-ray, D-dimer, liver enzymes, lipase, and bilirubin were all within normal limits. The patient was discharged home with an antihypertensive and Cardiology follow-up.
The patient underwent further outpatient investigations as the cause of their chest pain remained unclear. An echocardiogram demonstrated preserved left ventricular function with an ejection fraction of 72% by the Simpson method, no regional wall motion abnormalities, normal right ventricular function, right ventricular systolic pressure of 25 mmHg, no significant valvular disease, and no pericardial effusion. A Holter monitor did not identify any significant abnormalities. Oesophagogastroduodenoscopy was negative and pulmonary function tests were normal.
DIAGNOSIS
The differential was narrowed to coronary artery disease versus uncontrolled hypertension. The patient underwent a coronary angiogram, which only demonstrated a 30–40% left anterior descending coronary artery stenosis (Figure 1). Their antihypertensives were titrated up to achieve a systolic blood pressure of 120–130 mmHg. However, they continued to have chest pain, prompting consideration of atypical causes of chest pain. Ultimately, the
Article
62 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0
clinical presentation, including association of the chest pain with exposure to cold weather and often immediately after exercise, as well as a positive response to nitroglycerine, led to the presumed diagnosis of vasospastic angina.
Standard treatment for vasospastic angina was initiated. The patient responded well to nitroglycerine patches, but use was limited by severe headaches. Therefore, diltiazem was titrated up to 360 mg daily and a nitroglycerine spray was prescribed for use on an as needed basis. While the patient experienced significant improvement, they continued to have symptoms, including nocturnal episodes, and were requiring nitroglycerine spray on a weekly basis.
After endorsing a history of fatigue, frequent headaches, and gasping for air at night, the patient was sent for a sleep study. They completed the Epworth Sleepiness Scale (ESS), which is a self-administered questionnaire to assess daytime sleepiness on a scale of zero to 24, and were found to have an elevated score of 11, consistent with excessive sleepiness.1 Based on the sleep study, the apnoea-hypopnoea index (AHI) was severely elevated at 43.5 events per hour, and the O2 desaturation index was severely
elevated at 60.3 events per hour. The patient was diagnosed with obstructive sleep apnoea (OSA) and started on continuous positive airway pressure (CPAP).
MANAGEMENT
They were reassessed after 8 weeks of CPAP. The AHI was reduced to 3.9 events per hour with CPAP, and they now scored zero on the ESS. The patient endorsed remarkable improvement in their chest pain. They no longer experienced nocturnal angina, which previously occurred at least once per week. The patient also reported less daytime angina, only requiring nitroglycerine spray twice in the previous 8 weeks. Furthermore, the patient endorsed increased exercise capacity, and was able to walk up to 10 km per day without any post-exercise chest pain since starting CPAP therapy.
The authors hypothesise that the patient’s vasospastic angina was exacerbated by underlying OSA. Invasive testing for coronary vasospasm was considered but not performed. The authors’ centre, like many others, does not perform provocative testing due to the high

Article Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 63
Figure 1: Coronary angiogram revealed subclinical coronary artery disease with a 30–40% left anterior descending coronary artery stenosis.
risk of myocardial ischaemia and arrhythmias from uncontrolled, pharmacologically-provoked vasospasm. Unexpectedly, CPAP therapy had a remarkable effect on the patient’s angina burden.
Cardiovascular disease among females is inadequately researched, diagnosed, and treated.2 Vasospastic angina is likely an under-recognised cause of chest pain that affects females more frequently than males.3 OSA has been associated with nocturnal angina.4,5 However, the possible link between OSA and vasospastic angina is not well investigated. Some reports suggest that OSA is more common in those with vasospastic angina.6,7 In fact, Tamura et al.6 found that moderate-tosevere OSA (defined as AHI ≥15 events per hour) was independently associated with vasospastic angina (odds ratio: 9.61, 95% confidence interval: 2.11–43.78; p=0.003). Furthermore, within the context of limited literature, it appears that OSA exacerbates vasospastic angina. Teragawa et al.7 identified a trend towards more anginal attacks in the OSA group (2.9±0.6 per month) compared to the non-OSA group (1.3±0.8 per month; p=0.09). There was also a statistically significant difference in the frequency of intractable vasospastic angina among the OSA group (47%) relative to the non-OSA group (19%; p<0.05).7
There are a number of theories regarding the relationship between OSA and vasospastic angina.
Vasospastic angina involves transient coronary vasoconstriction that can lead to myocardial ischaemia.7 On the other hand, OSA is characterised by recurrent airway obstruction that leads to hypoxia, hypercapnia, and sleep fragmentation.8
OSA has been correlated to higher levels of pro-inflammatory cytokines that augment calcium sensitisation of vascular smooth muscle, predisposing to contraction.6 Additionally, increased sympathetic nervous system activity with arousal from sleep increases the tone of coronary arteries.8,9 Repetitive hypoxaemia, such as in the setting of recurrent airway obstruction, may also lead to the production of reactive O2 species and contribute to endothelial dysfunction.6,9 Finally, in animal models, the process of hypoxia and reoxygenation was associated with higher levels of the vasoconstrictor prostaglandin H2, and rendered bovine coronary arteries less responsive to the vasodilatory effects of nitric oxide.10
There may also be sex-specific mechanisms at play. The prevalence of vasospastic angina has been reported to be higher in females, especially with increasing age.3,11 A lower level of oestrogen in the post-menopausal state has been associated with increased inflammation and sympathetic nervous system activation, both of which would contribute to a favourable environment for vasospasm.12
This case highlights the association between OSA and vasospastic angina. While the authors’ patient experienced some improvement with antianginal therapy, their symptoms still had a significant impact on their quality of life. Unexpectedly, CPAP therapy provided the patient with substantial relief. Vasospastic angina is likely an underdiagnosed cause of chest pain among females. The combination of increased sympathetic tone, reactive O2 species, pro-inflammatory cytokines, and endothelial dysfunction may explain how OSA can worsen vasospastic angina. Providers should consider screening patients with vasospastic angina for symptoms of OSA, as CPAP therapy may improve symptom burden.
References
1. Johns MW. The Epworth Sleepiness Scale (ESS). Available at: http:// www.epworthsleepinessscale. com/. Last accessed: 23 April 2022.
2. Norris CM et al. State of the science in women's cardiovascular disease: a Canadian perspective on the influence of sex and gender. JAHA. 2020;9(4):e015634.
3. Elbadawi A et al. Temporal trends and outcomes of hospitalizations
with Prinzmetal angina: perspectives from a national database. Am J Med. 2019;132(9):1053-61.e1.
4. Philip P, Guilleminault C. Letter to the editor: ST segment abnormality, angina during sleep and obstructive sleep apnea. Sleep. 1993;16(6):558-9.
5. Franklin KA et al. Sleep apnoea and nocturnal angina. Lancet. 1995;345(8957):1085-7.
6. Tamura A et al. Association between coronary spastic angina pectoris and obstructive sleep apnea. J Cardiol. 2010;56(2): 240-4.
7. Teragawa H et al. How is the presence of obstructive sleep apnea associated with vasospastic angina? Circulation. 2018;126 (Suppl 21):A18566.
8. Dempsey JA et al. Pathophysiology of sleep apnea. Physiol Rev. 2010;90(1):47-112.
Article 64 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0
9. Sakakibara M et al. Sleepdisordered breathing is an independent risk factor of aborted sudden cardiac arrest in patients with coronary artery spasm. Circulation. 2012;76(9):2204-10.
10. Zou MH, Bachschmid M. Hypoxiareoxygenation triggers coronary
vasospasm in isolated bovine coronary arteries via tyrosine nitration of prostacyclin synthase. J Exp Med. 1999;190(1):135-9.
11. Kawana A et al.; Japanese Coronary Spasm Association. Gender differences in the clinical characteristics and outcomes of
patients with vasospastic angina. Circulation. 2013;77(5):1267-74.
12. Maas AHEM. Vasospastic angina behaves differently in men and women. Int J Cardiol. 2017;249: 79-80.
FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM
Article Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 65
Characterisation of Patients with Acute Coronary Syndrome: A 10-Year Experience
Authors: *Andrew Sefenu Dzebu,1 Suilbert Rodríguez Blanco,2 Jose Manuel Aguilar Medina2
1. Cardiothoracic Centre, Ho Teaching Hospital, Ho, Ghana
2. Cardiology Service, Hermanos Ameijeiras Hospital, Havana, Cuba *Correspondence to asdzebu@icloud.com
Disclosure: The authors have declared no conflicts of interest.
Received: 23.05.23
Accepted: 26.07.23
Keywords: Acute coronary syndrome, diabetes, hypertension, percutaneous coronary intervention, radial access.
Citation: EMJ Cardiol. 2023;11[1]:66-74. DOI/10.33590/emjcardiol/10300187. https://doi.org/10.33590/emjcardiol/10300187.
Abstract
Introduction: Coronary intervention is a therapeutic method for acute coronary syndrome.
Objectives: Characterise patients with acute coronary syndrome treated by percutaneous coronary intervention.
Method: Analytical, observational, retrospective, and cross-sectional study of 1,469 patients with the diagnosis of acute coronary syndrome, treated with percutaneous coronary intervention at the Hermanos Ameijeiras Hospital, Havana, Cuba, between 2010–2019.
Results: The mean age of the patients was 61.1±10.6 years, 72% were male, and 68.3% had acute coronary syndrome without persistent ST-segment elevation. The commonest risk factor was hypertension (69%). Radial access was used in 75.0% of procedures, and 82.0% had a single occluded epicardial coronary artery (42.4% anterior descending artery, 29.7% right coronary artery). One (63.3%) bare metal stent was implanted in 70.7% of patients, with a 96.0% angiographic success rate. There were complications in 1.1% of cases. Diabetes was significantly associated with the failure of the procedure.
Conclusions: Most of the patients were middle-aged, with hypertension and a diagnosis of non-ST-segment elevation acute coronary syndrome, where the most frequently treated artery is the left anterior descending artery, and the radial artery is the most commonly used vascular access route with an elevated number of successful procedures. The presence of diabetes is significantly associated with the failure of the procedure.
Article 66 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0
Key Points
1. Identifiable and treatable risk factors are significantly prevalent in middle-aged patients with acute coronary syndrome.
2. This was an analytical, observational, retrospective, and cross-sectional study of 1,469 patients with the diagnosis of acute coronary syndrome, treated with percutaneous coronary intervention at the Hermanos Ameijeiras Hospital, Havana, Cuba, between 2010–2019.
3. The presence of diabetes was related to the failure of percutaneous coronary intervention.
INTRODUCTION
Cardiovascular diseases are the leading cause of mortality worldwide. The total prevalence of cardiovascular disease has almost doubled from 271 million in 1990 to 523 million in 2019, and the number of deaths from cardiovascular causes has progressively increased from 12.1 million in 1990 to 18.6 million in 2019.1
In the USA, 697,000 people died in 2020 due to cardiovascular causes; one in five deaths. That is equivalent to one death every 34 seconds. Half of these deaths were due to coronary artery disease (CAD). Each year, 805,000 persons have an acute coronary syndrome (ACS), equivalent to one every 40 seconds.2
Between 2019–2020, 56,993 people died in Cuba from cardiovascular causes, making it the leading cause of mortality in Cuba. Almost half of these deaths were due to ACS. This translates into 12.8 and 12.9 years of potential life lost, respectively. Worldwide, mortality caused by cardiovascular disease continues to increase, making it the third cause of all death in 2019.1,3,4
ACS has a variable clinical expression, such as acute myocardial infarction, unstable angina, and sudden cardiac death. They are mainly a consequence of atherosclerosis of the coronary arteries.#5,6
Many risk factors (RF) have been related to ACS. For preventive purposes, these risk factors are divided into non-modifiable (age, sex, genetics) and modifiable (hypertension, obesity, smoking, diabetes, dyslipidaemia). The presence of certain clinical entities, such as chronic kidney disease, atrial fibrillation, heart failure, and malignancies,
among others, also increases the risk of major adverse cardiovascular events. RFs may not be distributed similarly in all populations; however, they are present in an important proportion of patients with CAD, being an important challenge for different health systems.7-12
Patients with ACS have been classified into ACS with ST-segment elevation (STE-ACS) and ACS without persistent ST-segment elevation (NSTE-ACS), given the importance of the worse prognosis associated with the first group, and the benefit derived from prompt reperfusion.10,13-15
Patients with STE-ACS and NSTE-ACS (very high-risk and high-risk subgroups) have an indication for invasive coronary angiography with the intention of performing percutaneous coronary intervention (PCI), given the proven effectiveness and superiority of resolving the pathological substrate causing coronary occlusion (atherothrombotic in most patients).16
When performing invasive coronary angiography in patients with ACS with an indication for this procedure, the intention is to demonstrate occluded epicardial arteries (responsible for the clinical episode) and proceed to carry out angioplasty with balloon/placement of a stent (in patients who have favourable coronary anatomy) to open the culpable artery, thus reperfusing the segment of myocardium at risk. In a proportion of patients, no epicardial obstructive lesion is demonstrated during coronary angiography, the so-called myocardial infarction with non-occlusive coronary arteries (MINOCA). Coronary lesions not responsible for the current clinical episode can also be identified. The ideal therapeutic approach to these lesions is still the subject of active research.10,17
Article Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 67
Several interventions have demonstrated their therapeutic efficacy and decreased mortality in patients with ACS. These include continuous monitoring of patients in coronary units, fibrinolysis, dual antiplatelet therapy, and early use of β-blockers. The COLCOT study has shown the effectiveness of the anti-inflammatory drug, colchicine, in the prevention of post-ACS major adverse cardiovascular events.18
In the Cuban population, there is a high incidence of CAD, with ACS being a common form of presentation. The use of PCI as an invasive treatment method in this entity is increasing progressively given the improvement of the technique and the advances in the materials used. Knowledge of the factors associated with the success of coronary intervention increases its clinical benefit and helps risk stratification in these cases. The authors found few studies published in the country with a large sample offering statistical strength to the analysis, hence the decision to carry out this study. The aim of this research is to characterise patients with ACS treated by PCI.
METHODS
This was an analytical, observational, retrospective, and cross-sectional study. It was carried out in the Department of Interventional Cardiology, Cardiology Service of the Hermanos Ameijeira Clinical-Surgical Hospital in Havana, Cuba, from 1st January 2010–31st December 2019. The sample was made up of patients who were treated with PCI in the haemodynamics laboratory of the Hermanos Ameijeiras Hospital during the study period. Inclusion criteria included age over 18 years, diagnosis of ACS, and treatment with PCI. Exclusion criteria included patients with an incomplete report of the interventional procedure.
Sample
From a total of 1,502 patients, 33 were excluded due to incomplete documentation of clinical data on the paper records from the archives, which may have occurred due to the stress of workflow at the cathetirisation laboratory. These cases were distributed randomly in the first 7 years of the investigation. The sample was made up of 1,469 consecutive patients who met the inclusion criteria.
Data Collection Techniques
At the institution where the research was carried out, there is a printed form with the demographic and clinical data of the patients treated by PCI, as well as a digital record, in addition to those related to the procedure. This evidence is kept on file, for research purposes only, in the interventional cardiology department. For the current investigation, a duplicate report of patients treated in the context of ACS was obtained. These records match the electronic record data for these patients. The data was collected in a form designed for this purpose and processed with version 20.0 of the SPSS Statistics program (IBM, Armonk, New York, USA).
Ethical Issues
Authorisation was requested from the hospital in order to access patient data. Subsequently, approval from the Research Committee of the institution was obtained. The confidentiality of patient data was respected while clinical records were examined. Only the authors accessed these records, and the Helsinki Declaration was respected.19
Techniques of Processing and Analysis of Data
The collected data was transferred to an Excel (Microsoft, Redmont, Washington, USA) database designed for this purpose. Statistical analysis was carried out with version 20.0 of the SPSS Statistics software package (IBM).
Variables were summarised in absolute numbers and percentages. To analyse the relationship with the qualitative variables, the χ2 test was performed, with correction, and when there were 25% or more expected frequencies lower than five, Fisher’s exact test was used. The results were presented in tables and graphs as applicable, to facilitate their better reading and understanding.
RESULTS
Table 1 shows the distribution of demographic variables, such as age and sex. It was observed that age had a natural distribution (sigmoid) where most patients were between 40–69 years old. There was a clear predominance
68 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Article
of patients of the male sex. Clinical variables, such as the presence of risk factors, and the clinical diagnosis with which they presented to the hospital, can also be observed in this table. Hypertension, smoking, and diabetes represent the most important risk factors in these patients, present in 69.0%, 31.2%, and 23.3% of the sample, respectively. Most of the patients (68%) presented with NSTE-ACS.
The distribution of the angiographic variables is described in Table 2. The left anterior descending artery (LAD) was the most affected artery in ACS, followed by the right coronary artery (RCA). No angiographically significant coronary artery occlusion was identified in 12.9% of patients. The majority of patients (82%) had a culprit lesion in an epicardial artery. A single stent was implanted in 63% of cases, and the most widely used were bare metal stents (BMS; 70%). Three-quarters (75%) of the angioplasties were performed via radial access.
The complication rate was low (1.1%), with death being the most common complication in this study, with 11 patients (0.7%) dying during the study period. Almost all the procedures performed during this period were considered successful (96.1%).
Of the failures, the most common cause was the presence of a fatal complication or technical difficulty in stent implantation that led to the termination of the procedure.
Table 3 shows no statistically significant relationship between the demographic variables (age and sex) and the final assessment of the procedure. The presence of diabetes is related to an unsuccessful final angiographic result of the procedure. The presence of the other risk factors did not significantly affect the final result. In addition, the clinical diagnosis was not statistically significant for the final result either.
Variable Number % Age 18–29 3 0.2 30–39 35 2.4 40–49 157 10.7 50–59 431 29.3 60–69 512 34.9 70–79 281 19.1 >80 50 3.4 Sex Male 1,057 72.0 Female 412 28.0 Presence of risk factors Hypertension 1,014 69.0 Diabetes 342 23.3 Obesity 134 9.1 Smoking 459 31.2 Dyslipidaemia 278 18.8 Clinical diagnosis STE-ACS 466 31.7 NSTE-ACS 1,003 68.3 Source: Percutaneous Coronary Intervention Report. NSTE-ACS: non-ST-elevation acute coronary syndrome;
STE-ACS: ST-elevation acute coronary syndrome.
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 69 Article
Table 1: Distribution of the demographics and clinics variables of the patients.
Source: Percutaneous Coronary Intervention Report.
ACS: acute coronary syndrome; BMS: bare-metal stent; CxA: circumflex artery; DES: drug-eluting stent; LAD: left anterior descending artery; LM: left main artery; NSTE-ACS: non-ST-elevation acute coronary syndrome; RCA: right coronary artery; STE-ACS: ST-elevation acute coronary syndrome.
During PCI to the LAD and RCA, the most frequently treated coronary arteries (49.2% versus 33.6% of successful cases, respectively), there were disproportionately more failures of the procedure in RCA (45.1%) compared with the LAD (35.3%). Of the patients who received stents, 100% of the failures occurred in patients receiving BMS. It should be noted that the majority of patients who did not receive a stent (N=59) includes those who underwent balloon angioplasty, and those in whom the implantation failed. The implantation of one or two stents was significantly related to the success of the procedure. The use of radial access showed a higher success rate as compared with the rest of the access routes studied, although without being significant (p=0.09).
DISCUSSION
The findings of age, sex, and clinical diagnosis of this study coincide with those found by other researchers such as Galappatthy et al.,20 who found an average age of 61.4±11.8 years, with 32.8% presenting with STE-ACS. Montero-Jimeno et al.21 found a predominance of males (51.89%) in patients with ACS, although patients with STE-ACS predominated (54.7%). In their study, Guerra-Frutos et al.22 observed a prevalence of the male sex (65.30%) and the most affected age group was 60–69 years (30.61%).10,20-23
Variable Number (STE-ACS/NSTEACS/ACS) % (STE-ACS/NSTE-ACS/ ACS) Culprit artery (single artery disease) RCA 169/267/436 36.3/26.6/29.7 LM 9/19/28 1.9/1.9/1.9 LAD 239/383/622 51.3/38.2/42.4 CxA 44/149/193 9.4/14.9/13.1 None 5/185/200 1.1 /18.4/12.9 Number of diseased arteries 1 404/803/1,207 86.7/80.1/82.2 2 48/171/219 10.3/17.0/14.9 3 14/29/43 3.0/2.9/2.9 Number of stents implanted 0 19/40/59 4.1/4.0/4.0 1 310/620/930 66.5/61.8/63.3 2 101/242/343 21.7/24.1/23.3 3 27/86/113 5.8/8.6/7.7 ≥4 9/15/24 1.9/1.5/1.7 Type of implanted stent None 19/40/59 4.1/4.0/4.0 BMS 346/692/1,038 74.2/69.0/70.7 DES 101/271/372 21.7/27.0/25.3 Vascular access route Radial 363/744/1,107 77.9/74.2/75.4 Femoral 71/168/239 15.2/16.7/16.3 Others 32/91/123 6.9/9.1/8.4
Table 2: Descriptive statistics of angiographic variables.
70 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Article
Fisher's test was used; p=0.05.
Source: Percutaneous Coronary Intervention Report.
NSTE-ACS: non-ST-elevation acute coronary syndrome; STE-ACS: ST-elevation acute coronary syndrome.
Park et al.24 in their study found that young patients with significant coronary lesions, compared with older patients (>70 years), were mainly male, smokers, and had elevated lipid profiles (total cholesterol, low-density lipoproteincholesterol, and triglycerides), findings similar to the results of this present study. In young patients, no statistical association was observed between hypertension, diabetes, and previous myocardial infarctions. Guerra-Frutos et al.23 and Mohsen et al.25 found hypertension as the most common RF in patients with STE-ACS. Valdés-Martín et al.26 found that the most common RFs in patients younger than 45 years with STE-ACS were tobacco use, hypertension, and dyslipidaemia.
Fonseca-Marrero et al.27 pointed out that tobacco use is an RF related to STE-ACS.23-27
De Lange et al.28 observed that being female, young, and non-diabetic had a high probability of having normal or near-normal coronary arteries at invasive coronary angiography. Ayach et al.,29 in their study on ACS in patients under 35 years of age, found that male sex (91.0%) was a risk factor for NSTE-ACS and having multi-vessel CAD (43.8%). According to Shi et al.,30 early ACS (<55 years in females) predominated, and regression analysis in the same study revealed female sex was an RF for early ACS, as was hypertriglyceridaemia.28-30
Variable Success (%) Failed (%) Total (%) Statistical significance Age 18–29 3 (0.2) 0 (0.0) 3 (0.2) 0.542 30–39 33 (2.3) 2 (3.4) 35 (2.4) 40–49 152 (10.8) 5 (8.6) 157 (10.7) 50–59 420 (29.8) 11 (19.0) 431 (29.3) 60–69 490 (34.7) 22 (37.9) 512 (34.9) 70–79 266 (18.9) 15 (25.9) 281 (19.1) ≥80 47 (3.3) 3 (5.2) 50 (3.4) Sex Male 1,013 (71.8) 44 (75.9) 1,057 (72.0) 0.554 Female 398 (28.3) 14 (24.1) 412 (28.0) Presence of risk factors Hypertension 968 (68.6) 46 (79.3) 1,014 (69.0) 0.110 Diabetes 319 (22.6) 23 (39.7) 342 (23.3) 0.040 Obesity 130 (9.2) 4 (6.9) 134 (9.1) 0.815 Smoking 445 (31.5) 14 (24.1) 459 (31.2) 0.251 Dyslipidaemia 261 (18.5) 15 (25.9) 276 (18.8) 0.170 Clinical diagnosis on presentation STE-ACS 449 (31.8) 17 (29.3) 466 (31.7) 0.774 NSTE-ACS 962 (68.2) 41 (70.7) 1,003 (68.3) Vascular access route Radial 1,070 (75.8) 37 (63.8) 1,107 (75.4) 0.092 Femoral 224 (15.9) 15 (25.9) 239 (16.3) Others 117 (8.3) 6 (10.3) 123 (8.4)
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 71 Article
Table 3: Relationship between demographic, clinical, and vascular access route versus clinical variables.
The most frequently obstructed epicardial coronary artery was the LAD (42%), followed by the RCA (29.7%), unlike what was found by Wang et al.,31 where RCA (44%) was the most frequently obstructed, followed by the LAD (40%). Most (82%) of the patients in this sample had a single angiographically occluded epicardial coronary artery. Patients with ACS with non-obstructive coronary arteries, a subgroup that includes acute MINOCA, represent 12.9%, a figure similar to that found by other authors, in a range of 1–14%. The use of biomarkers in this study was not documented; therefore, myocardial infarction per se cannot be discussed. However, the group of patients with STE-ACS without angiographically significant coronary lesions, 1.1% of the sample, could be part of the subgroup with MINOCA (Table 2). Valdés-Martín et al.26 found that most of their sample had an occluded epicardial coronary artery. In the majority, the LAD (40.4%) and the RCA (28.3%) were the most affected epicardial coronary arteries. No angiographically significant coronary lesions were present in six patients (20.0%) of the 30 patients with STE-ACS in the sample, and PCI (56.6%) was the most widely used revascularisation method in STE-ACS.10,26,31,32
Cid Álvarez et al.33 described the use of drugeluting stents in 92% in Spain as of 2017, while the most used stent in this study is the BMS (70.5%) due to its greater availability in this setting for reasons beyond the scope of this study. The use of the radial access route, which is the default, was practiced in 75% of the sample of this study, slightly lower than what was found in the Spanish registry (1990–2018), with a penetration of 86.4% of the use of the said route. It is expected that the use of radial access during PCI in this centre will increase given its proven superiority, especially in local complications33-39 (Figure 1).
Very few complications were registered during the period of study, including 11 fatalities (0.7%). More fatal complications were documented than non-fatal ones in this study. Being a retrospective study, it is known that there could be an inherent problem of underreporting data for the purpose of a statistical study. The success rate of PCI in ACS in this study was 96%. This could be explained by the participation of well-trained operators, and partially because of the bias present in data collection in a retrospective study.40,41
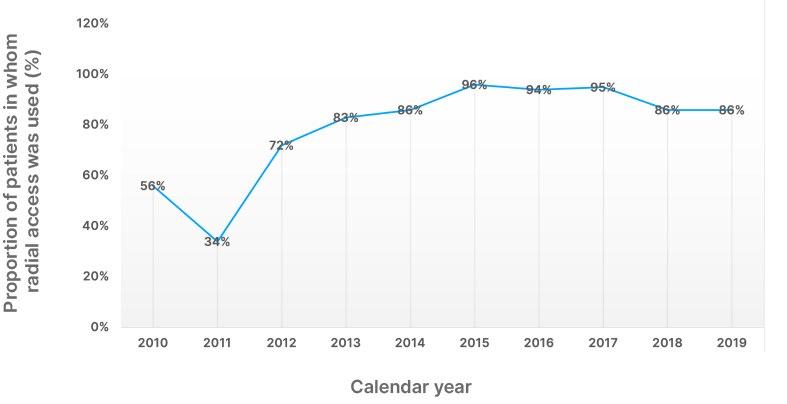 Source: Percutaneous Coronary Intervention Report.
Source: Percutaneous Coronary Intervention Report.
Article 72 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0
Figure 1: Proportion of radial access use in percutaneous coronary intervention for acute coronary syndrome during a 10-year period at the Hermanos Ameijerias Hospital, Havana, Cuba.
In this study, no statistically significant relationship between age, sex, and clinical diagnosis was demonstrated. Failure of the procedure had a statistically significant association (p=0.04) with the presence of diabetes. The superiority of coronary artery bypass graft to PCI in patients with diabetes with multivessel CAD has been demonstrated in chronic coronary syndrome, but not in ACS. The RCA, the second most frequently occluded artery in this study, had disproportionately more failed cases, being a possible explanation for the highly significant relationship calculated. Technically, RCA ostium cannulation can be more difficult than ostium of the left main artery; however, Welty et al.42 found no differences in the success of PCI to the RCA versus the LAD or circumflex artery, unlike the results obtained by Savage et al.,42 who found a significant relationship between PCI to the RCA and failure of the procedure.42-46
The number of stents used in this study paradoxically had a reverse relationship with the success of the procedure, taking into account that complex lesions could require more stents, which translates into a greater risk of complications and/or failure of the procedure. The implantation of increasing numbers of stents is related to in-stent restenosis, an objective beyond the scope of this study. The stents used during the period of this study (mostly BMS) had a wider profile and more difficult manoeuvrability
References
1. Roth GA et al. Global burden of cardiovascular diseases and risk factors, 1990-2019: updated from the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):2982-3021.
2. Centers for Disease Control and Prevention (CDC). Heart disease facts. Available at: https://www.cdc. gov/heartdisease/facts.htm. Last accessed: 2 November 2022.
3. Ministerio de Salud Pública –Republica de Cuba. Anuarios Estadísticos del Ministerio de Salud Pública. 2021. Available at: https:// salud.msp.gob.cu/portfolio/anuarioestadistico/. Last accessed: 8 February 2023.
4. Amini M et al. Trend analysis of cardiovascular disease mortality, incidence, and mortality-toincidence ratio: results from global burden of disease study 2017. BMC Public Health. 2021;21(1):401.
compared to current stents, which may explain the high proportion of failures with BMS stents in this study, making the statistical relationship between the type of stent and the success of the procedure insignificant. Regarding the use of radial access, there is also a positive relationship with the outcome of the procedure, although insignificant.37-41,45
CONCLUSIONS
To conclude, most of the patients were middle-aged, hypertensive, diagnosed with NSTE-ACS, and the most frequently treated artery was the LAD. The vascular access most frequently used was the radial artery and PCIs had a high success rate. The presence of diabetes was significantly associated with the failure of the procedure.
RECOMMENDATIONS
The authors recommend to do further studies, preferably prospective, where all complications (major and minor), including those related to the vascular access route, are collected and actively documented. They further recommend the implementation of preventive and therapeutic strategies to control coronary risk factors in the Cuban population.
5. Kotecha T, Rakhit RD. Acute coronary syndromes. Clin Med (Lond). 2016;16(Suppl 6):s43-8.
6. Singh A et al., Acute Coronary Syndrome [Internet] (2022) Treasure Island: StatPearls. Available at: http://www.ncbi.nlm. nih.gov/pubmed/29083796. Last accessed: 8 July 2023.
7. Collet J-P et al.; ESC Scientific Document Group. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021;42(14):1289-367.
8. Costello BT, Younis GA. Acute coronary syndrome in women: an overview. Tex Heart Inst J. 2020;47(2):128-9.
9. Tan CE, Glantz SA. Association between smoke-free legislation and hospitalizations for cardiac, cerebrovascular, and respiratory diseases. Circulation.
2012;126(18):2177-83.
10. Ibanez B et al.; ESC Scientific Document Group. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with STsegment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119-77.
11. Xu J-J et al. Effects of metabolic syndrome on onset age and longterm outcomes in patients with acute coronary syndrome. World J Emerg Med. 2021;12(1):36-41.
12. León Alvarez JL et al. Circadian blood pressure variability in hypertensive patients with coronary heart disease. JCCI. 2020;3(2): 1-10.
13. Thygesen K et al.; Executive Group on behalf of the Joint European
Article Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 73
Society of Cardiology (ESC)/ American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth universal definition of myocardial infarction (2018). Circulation. 2018;138(20):e618-51.
14. Gulati M et al. 2021 AHA/ACC/ ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: executive summary. J Am Coll Cardiol. 2021;78(22):2218-61.
15. Bayés De Luna A, ECGs for beginners (2014) Hoboken: John Wiley & Sons, Inc.
16. Andersen HR et al.; DANAMI-2 Investigators. A comparison of coronary angioplasty with fibrinolytic therapy in acute myocardial infarction. N Engl J Med. 2003;349(8):733-42.
17. Mehta SR et al.; COMPLETE Trial Steering Committee and Investigators. Complete revascularization with multivessel PCI for myocardial infarction. N Engl J Med. 2019;381(15):1411–21.
18. Bouabdallaoui N et al. Time-totreatment initiation of colchicine and cardiovascular outcomes after myocardial infarction in the Colchicine Cardiovascular Outcomes Trial (COLCOT). Eur Heart J. 2020;41(42):4092-9.
19. Declaration of Helsinki (1964). BMJ. 1996;313(7070):1448-9.
20. Galappatthy P et al. Management, characteristics and outcomes of patients with acute coronary syndrome in Sri Lanka. Heart. 2018;104(17):1424-31.
21. Montero-Jimeno A de J et al. Síndrome coronario agudo en el servicio de emergencias del Hospital Universitario Clínico Quirúrgico Comandante Faustino Pérez Hernández, de Matanzas. Rev Méd Electrón. 2022;44(1): 100-15.
22. Guerra-Frutos LC et al. Caracterización de pacientes con síndrome coronario agudo con elevación del ST en una Unidad de Cuidados Coronarios. 16 de Abril. 2020;59(278):e1007.
23. Dégano IR et al. Epidemiology of acute coronary syndromes in Spain: estimation of the number of cases and trends from 2005 to 2049. Rev Esp Cardiol. 2013;66(6):472-81.
24. Park JS et al. The epidemiological and clinical characteristics of patients admitted for coronary angiography to evaluate ischemic
heart disease. Korean J Intern Med. 2007;22(2):87-92.
25. Mohsen FS et al. Caracterización del síndrome coronario agudo en el Instituto de Cardiología y Cirugía Cardiovascular, 2009-2010. Revista Cubana de Cardiología y Cirugía Cardiovascular. 2012;16(4):397406. (In Spanish).
26. Valdés-Martín A et al. Caracterización del síndrome coronario agudo en adultos menores de 45 años de una institución especializada en la Habana, Cuba, entre 2013 y 2014. Revista Médicas UIS. 2015;28(3):281-90.
27. Fonseca-Marrero CA et al. Factores de riesgo asociados a las variantes clínicas del síndrome coronario agudo. Rev Cubana Med. 2020;60(3):e1364.
28. de Lange TS et al. Clinical characteristics of patients with suspected cardiac chest pain and angiographically normal coronary arteries in a secondary care hospital. Neth Heart J. 2017;25(6):370-5.
29. Ayach B et al. Characteristics of acute coronary syndrome presentation in young patients. J Am Coll Cardiol. 2017;69(11):276.
30. Shi X-J et al. Clinical characteristics of patients with premature acute coronary syndrome and adverse cardiovascular events after PCI. Exp Ther Med. 2019;18(1):793-801.
31. Wang JC et al. Coronary artery spatial distribution of acute myocardial infarction occlusions. Circulation. 2004;110(3):278-84.
32. Ache Y et al. Infarto agudo de miocardio sin lesiones coronarias obstructivas - MINOCA: un enigma para el cardiólogo clínico. Rev Urug Cardiol. 2020;35:36-45.
33. Cid Álvarez AB et al. Registro Español de Hemodinámica y Cardiología Intervencionista. XXVIII Informe Oficial de la Sección de Hemodinámica y Cardiología Intervencionista de la Sociedad Española de Cardiología (1990-2018). Rev Esp Cardiol. 2019;72(12):1043-53.
34. Babapulle MN et al. A hierarchical Bayesian meta-analysis of randomised clinical trials of drug-eluting stents. Lancet. 2004;364(9434):583-91.
35. Valgimigli M et al. Radial versus femoral access in patients with acute coronary syndromes undergoing invasive management: a randomised multicentre trial. Lancet. 2015;385(9986):2465-76.
36. Le May M et al. Safety and efficacy of femoral access vs radial access in ST-segment elevation myocardial infarction. JAMA Cardiol. 2020;5(2):126-34.
37. Romagnoli E et al. Radial versus femoral randomized investigation in ST-segment elevation acute coronary syndrome: the RIFLESTEACS (Radial Versus Femoral Randomized Investigation in ST-Elevation Acute Coronary Syndrome) study. J Am Coll Cardiol. 2012;60(24):2481-9.
38. Sandoval Y et al. Transradial artery access complications. Circ Cardiovasc Interv. 2019;12(11):e007386.
39. Jolly SS et al. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): a randomised, parallel group, multicentre trial. Lancet. 2011;377(9775):1409-20.
40. Tavakol M et al. Risks and complications of coronary angiography: a comprehensive review. Glob J Health Sci. 2011;4(1):65-93.
41. Rodriguez Blanco S et al. Via de acceso transradial. Tecnica y complicaciones. Rev Cuba Cardiol Cir Cardiovasc. 2014;20(4):226-42.
42. Savage MP et al. Clinical and angiographic determinants of primary coronary angioplasty success. M-HEART Investigators. J Am Coll Cardiol. 1991;17(1):22-8.
43. Welty FK et al. Significance of location (anterior versus inferior) and type (Q-wave versus nonQ-wave) of acute myocardial infarction in patients undergoing percutaneous transluminal coronary angioplasty for postinfarction ischemia. Am J Cardiol. 1995;76(7):431-5.
44. Chaitman BR et al. Myocardial infarction and cardiac mortality in the Bypass Angioplasty Revascularization Investigation (BARI) randomized trial. Circulation. 1997;96(7):2162-70.
45. Farkouh ME et al. Strategies for multivessel revascularization in patients with diabetes. N Engl J Med. 2012;367(25):2375-84.
46. Thuijs DJFM et al.; SYNTAX Extended Survival Investigators. Percutaneous coronary intervention versus coronary artery bypass grafting in patients with threevessel or left main coronary artery disease: 10-year follow-up of the multicentre randomised controlled SYNTAX trial. Lancet. 2019;394(10206):1325-34.
74 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Article
Risk Factors and Patterns of Myocardial Injury in Patients with COVID-19: A Single-Centre Cohort Study
Authors: Muhammad Rumman Javed,1 *Tehreem Zahid,2 Nasr-us-Salam Ghulam Akbar,1 Palwasha Alavi,2 Ammar Khalid Choudry,2 Maliha Aziz2
1. Shifa International Hospital, Islamabad, Pakistan
2. Clinical Research Center, Shifa International Hospital, Islamabad, Pakistan *Correspondence to dr.tehreemzahid@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Received: 02.02.23
Accepted: 24.07.23
Keywords: COVID-19, coronavirus disease, myocardial.
Citation: EMJ Cardiol. 2023;11[1]:75-86. DOI/10.33590/emjcardiol/10300480. https://doi.org/10.33590/emjcardiol/10300480.
Abstract
Objective: The primary objective was to compare the risk factors and trends of patients with COVID-19 with and without biochemical evidence of myocardial injury. Secondary objectives were the duration of hospitalisation, admission to an intensive care unit, mode of resuscitation, and use of supplemental O2.
Design, and place and duration of study: This retrospective cohort study was conducted at Shifa International Hospitals, Islamabad, Pakistan. The study was conducted from May 2021–May 2022.
Methodology: 113 patients admitted with a confirmed diagnosis of COVID-19 and troponin-I investigation were included in the study. Patients were divided into two groups: with and without myocardial injury on admission. Demographics, symptoms, diagnostics, vitals, comorbidities, and outcomes were noted. The χ2 exact test for categorical variables and independent t-test for continuous variables were used. All statistical analyses were performed with SPSS Statistics®, version 26.0 (IBM®, Armonk, New York, USA), with 0.05 as a level of significance.
Results: Out of 113 patients, 47 patients (42%) had no myocardial injury on admission. The mean age of the patients was 63 years. Patients with myocardial injury were older, male, and unvaccinated against COVID-19 (p<0.01). No vital signs or presenting symptoms were statistically significant for myocardial injury. A comorbidity of hypertension on admission was suggestive of myocardial damage. Patients with myocardial injury had a higher risk of requiring resuscitation by cardiopulmonary resuscitation or pharmacologic means.
Conclusion: Patients with myocardial injury did not have any impact on the composite of secondary outcomes, such as the duration of hospitalisation, admission to an intensive care unit, and use of supplemental O2.
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 75 Article
Key Points
1. Acute myocardial injury (AMI) occurred in 0.5% of patients who had recovered from COVID-19, based on a large population of more than 20 million patients. Additionally, after COVID-19 recovery, survivors’ risk of AMI increases by almost 93%. Hence, it is pivotal to understand the link between myocardial injury and COVID-19 disease.
2. The authors present a prospective observational cohort study on 113 patients with COVID-19.
3. When treating patients with COVID-19, the increased risk of myocardial injury necessitates a multifaceted strategy, which includes early detection, vigilant monitoring, and specialised therapies. Medical practitioners need to be on the lookout for cardiac involvement in patients with COVID-19, particularly troponin elevation, and take swift action to prevent future consequences.
INTRODUCTION
Coronavirus disease is a respiratory infection caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) coronavirus that has resulted in a worldwide pandemic.1 Coronaviruses are positive-sense, single-stranded RNA viruses with particles of irregular shape, and a crownlike outer covering composed of club-shaped polymers. Its strains have been implicated in respiratory illness in the past, both in rare cases of immunocompromised individuals, and in community-based outbreaks.2,3 Following COVID-19, there has been growing interest in the impact of viruses on the cardiovascular system, even though they have long been implicated in a host of cardiovascular complications, such as myocarditis, acute myocardial infarction, and exacerbation of heart failure.4-6 The spike protein for SARS-CoV-2 is important in its transmission and pathophysiology, particularly in respiratory illness, but it can also infect cardiac tissue by binding to angiotensin-converting enzyme-2 (ACE-2) receptors, causing inflammation and myocardial damage. Animal models and autopsies of the heart have demonstrated SARSCoV-induced damage to the myocardium.7-10
Myocardial infiltration by mononuclear cells and lymphocytes has also been seen in patients with COVID-19.11-13 There are a myriad of cardiovascular complications after COVID-19 infection, such as myocardial injury, acute myocardial infarction, myocarditis, endocardial fibrosis, venous thromboembolism, and arrhythmias cited in the literature.14 These complications are linked to pre-existing comorbidities, such as diabetes; pre-existing
cardiovascular disease; renal disease; pulmonary disease; coagulation abnormalities; and deranged laboratory parameters, such as elevated C-reactive protein (CRP), troponin, and deteriorating left ventricular ejection fraction (EF).15,16
Patients with underlying illnesses are at a greater risk for complications or death; according to early COVID-19 case reports, up to 50% of hospitalised patients have underlying comorbidity. In the largest reported clinical cohort of COVID-19 to date,17 acute cardiac injury, shock, and arrhythmia were observed in 7.2%, 8.7%, and 16.7% of patients, respectively. Cardiac troponin is the recommended biomarker for myocardial necrosis, and it is a key part of diagnosing myocardial infarction.18-20 The creation of more sensitive assays has enhanced our ability to quantify cardiac troponin, with the new generation of high-sensitivity assays capable of detecting cardiac troponin concentrations in the majority of healthy individuals.21 This has allowed us to understand how baseline cardiac troponin levels can serve as prognostic indicators in populations that are at risk of cardiovascular disease, and has opened the door for further research in that domain.22
To this day, information regarding the effects of coronavirus on the myocardium and the mortality related to this is insufficient. It is important to know which patients have a higher chance of developing myocardial damage. This study aims to provide data on patients with COVID-19, with and without myocardial disease, to physicians in order to help tailor patient care.
76 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Article
MATERIALS AND METHODS
This single-centre retrospective study was conducted at Shifa International Hospital, Islamabad, Pakistan, from March 2021–May 2022. Patients were sampled using the consecutive sampling method. All patients 12 years of age and above admitted to the authors’ hospital with a reverse transcriptase-PCR confirmed diagnosis of COVID-19 were included in the study. Patients who did not require admission were excluded from the study. The study was approved by the Institutional Review Board and Ethics Committee of Shifa International Hospital, reference number 352-21.
The authors collected data from 113 subjects using non-electronic and electronic medical record data, including progress reports, graphic charts, laboratory reports, and imaging data. Patients were divided into two groups: with and without myocardial injury on admission, defined as high-sensitivity cardiac troponin I (cTnI) levels >34.4 pg/mL in males, and >15.6 pg/mL in females. Various parameters were reported on a web-based questionnaire. Data collected included age, sex, BMI, presenting symptoms, diagnostics, vitals, and comorbidities. Patients with raised troponin were also asked about ischaemic symptoms, such as jaw pain, chest pain, and shortness of breath. Vaccination against COVID-19 was also noted.
All patients had an extensive work-up done upon admission, which included a complete blood count; liver function tests; renal function tests; serum electrolytes; coagulation profiles, such as activated partial thromboplastin time; and cardiac and inflammatory biomarkers, such as cTnI, CRP, procalcitonin, lactate dehydrogenase (LDH), ferritin, and D-dimers. All patients underwent high-resolution CT (HRCT)/ chest X-ray imaging at admission, and findings were recorded. Any rise in cardiac biomarkers prompted transthoracic echocardiogram and electrocardiogram (ECG). All medications used by the patients were documented, as well as the mode of ventilation, use of supplemental O2, length of stay at the hospital, intensive care unit (ICU) admission, mode of resuscitation, and any other co-interventions.
The primary objective was to compare the risk factors and trends of patients with COVID-19 with and without biochemical evidence of myocardial injury. Secondary outcomes were the duration of hospitalisation, admission to ICU, mode of resuscitation, and use of supplemental O2.
Patient and Public Involvement
The authors clarify that patients were not involved in this research.
Statistical Analysis
Categorical variables are presented as percentages, and continuous variables as mean and standard deviation. Categorical variables are sex, symptoms, comorbidities, mode of confirming the diagnosis, ECG pattern, echocardiographic findings, medication, interventions, mode of resuscitation, ICU stay, lung infiltrates on chest X-ray/CT, prior vaccination against COVID-19, and clinical events during hospitalisation.
Continuous variables are age; weight; height; BMI; vital signs, including lowest blood pressure reading, highest respiratory rate, lowest saturation, and highest pulse recorded; troponin; LDH; ferritin; D-dimer; complete blood count; electrolytes; CRP; creatinine phosphokinase; creatine kinase-myocardial band (CKMB), serum urea; liver function tests; and length of hospital stay. The χ2 exact test for categorical variables and independent t-test for continuous variables were used. All statistical analyses were performed with SPSS® Statistics, version 26.0 (IBM®, Armonk, New York, USA), with 0.05 as a level of significance.
RESULTS
A total of 1,375 patients presented to the authors’ centre with reverse transcriptase PCR-confirmed coronavirus disease, out of which 1,215 were managed on an outpatient basis and were excluded. A total of 160 patients with reverse transcriptase-PCR-confirmed COVID-19 were admitted, out of which 113 patients had a high sensitivity troponin-I test at baseline, and were enrolled in the study. Table 1 shows the baseline characteristics of the patients. Patients were
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 77 Article
divided into two groups: Group A, which included patients without myocardial injury, and Group B, which included patients with myocardial injury on admission. The mean high sensitivity troponin-I was 1115±5625 pg/mL. Out of 113 patients, 47 patients (42%) had no myocardial injury on admission. The mean age of the patients was noted to be 63 years, which was higher for those with myocardial injury compared with those without myocardial injury (67 versus 61; p<0.01). Patients with myocardial injury were older, male, and unvaccinated against COVID-19 (p<0.01). No vital signs were statistically significant for myocardial injury. All 113 patients had a chest X-ray at the time of admission, of which 112 (99.3%) patients had a COVID-19-like picture, and one (0.7%) did not. HRCT was done for 101 individuals, of which 89 (86.4%) patients had a COVID-19-like picture, whereas 12 (11.7%) did not. HRCT could not be performed for two (1.9%) patients.
The patients presented with a host of signs and symptoms. The most common symptom was fever (88%), followed by shortness of breath (81%), cough (69%), and myalgia (56%). Only 2% of the patients were asymptomatic. No symptom was statistically significant for myocardial injury (Figure 1A).
The laboratory differences and baseline characteristics between the two groups, elevated troponin (n=47) and normal troponin (n=66), were compared. Out of all parameters in the authors’ study, a raised CKMB and comorbidity of hypertension were found to be statistically significant for myocardial injury. This is in line with the normal diagnostic approach to myocardial injury, specifically in the case of myocardial infarction.23 The parameters measured include CKMB (IU/L), serum ferritin (µg/L), CRP (mg/L), LDH (units/L), and
white Baseline Group A Group B Characteristics Overall (Normal troponin; n=47) (Elevated troponin; n=66) p Age (years) 63±14 61±14 67±12 0.01 Sex (%) Male Female 31 (56) 24 (44) 47 (71) 19 (29) 21 (45) 26 (55) 0.01 BMI (kg/m2) 29±20 31±26 27±5 0.33 Vaccinated (%) 37 (33) 19 (29) 18 (38) 0.01 Respiratory rate per minute 26±12 27±14 24±6 0.22 Lowest saturation (%) 83±6 82±6 83±7 0.48 Highest pulse per minute 103±15 101±15 105±15 0.22 Highest CKMB (IU/L) 8±24 3±6 16±36 0.04 Hypertension 74 (65) 36 (32) 38 (34) 0.01
CKMB: creatine kinase-myocardial band.
78 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Article
Table 1: Baseline characteristics of both groups.
A) Presenting symptoms of the patients. B) Electrocardiography findings of the patients.
C) Echocardiography findings of the patients.
ECG: electrocardiogram; EF: ejection fraction; LBBB: left bundle branch block; LV: left ventricle; SOB: shortness of breath; RBBB: right bundle branch block.
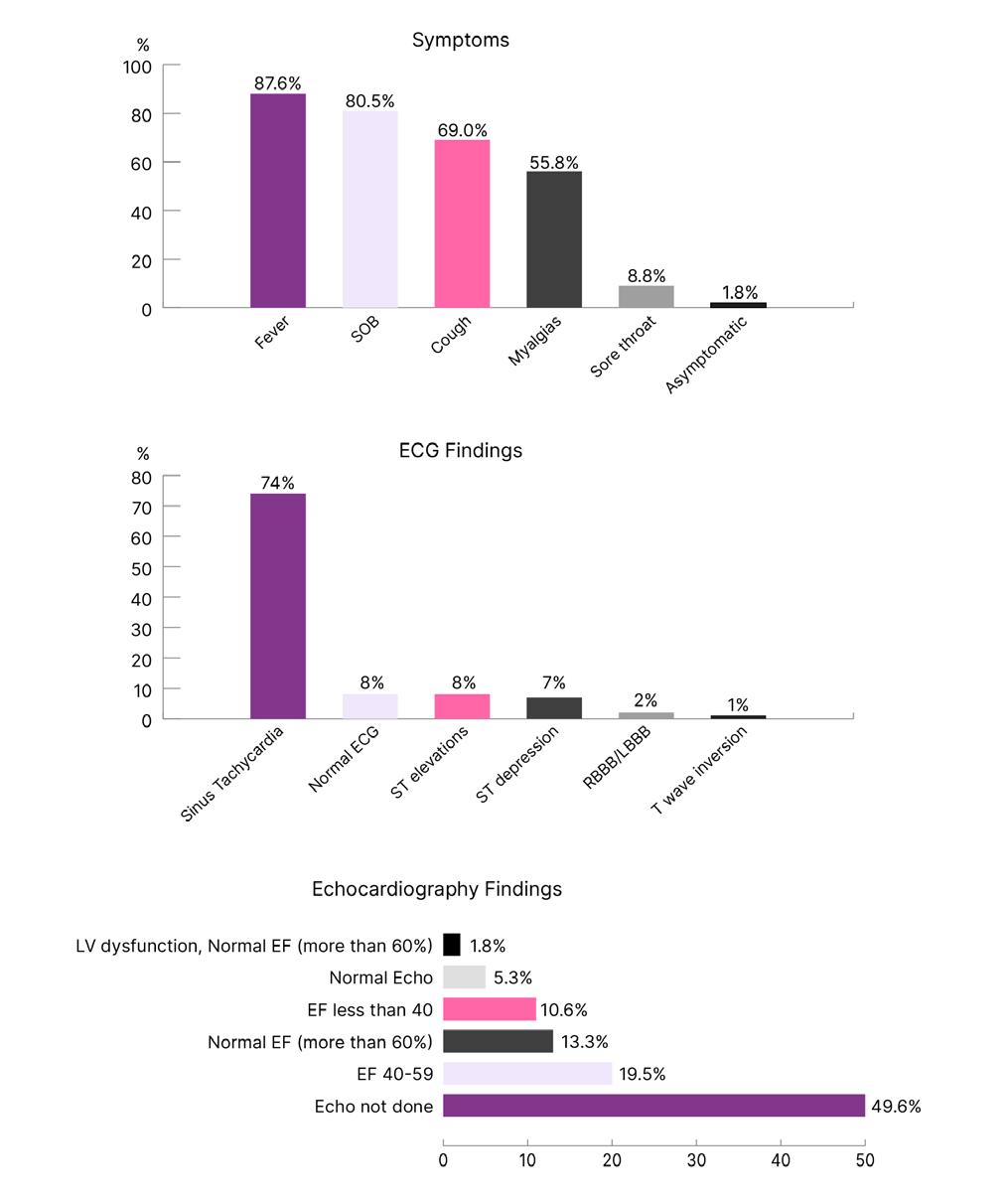
A B C Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 79 Article
Figure 1: Clinical picture of the study population.
blood cell count (109). The mean value and standard deviation of each parameter were obtained for both groups. The p value, which indicated the level of statistical significance between the two groups, was also identified. For CKMB, the mean value for the elevated troponin group (8±24) was higher than the normal troponin group (3±6), with a p value of 0.04, which was considered to be statistically significant at a level of 0.05. The mean value of serum ferritin in the elevated group (1163±1472) was slightly higher than in the normal group (1058±1349), with a p value of 0.99, indicating no statistical significance. In a similar vein, the elevated group's mean CRP (76) was higher than the normal group (57), with a p value of 0.18, indicating no statistical significance. The mean value of LDH in the elevated group (459±251) was lower than in the normal group (686±417), with a p value of 0.59, indicating no statistical significance. Similarly, the mean value of white blood cell count in the elevated group (16938±16848) was lower than in the normal group (15681±3777), with a p value of 0.52, again indicating no statistical significance. In conclusion, the only parameters that showed a statistically significant difference between the two groups were CKMB level and comorbidity of hypertension, with a p value of less than 0.05.
In the authors’ study of 113 patients and their associated comorbidities, 74 (65%) had hypertension, highlighting it as the most common comorbidity. This was followed by 55 (49%) patients with diabetes, 29 (26%) with ischaemic heart disease, 12 (11%) with chronic kidney disease (CKD), nine (8%) with chronic lung disease, seven (6%) with malignancy, and three (3%) with a stroke. Additionally, one patient (1%) each had heart failure and chronic liver disease. Of the 47 patients with elevated troponin levels, 38 (34%) had hypertension, 27 (24%) had diabetes, 14 (12%) had ischaemic heart disease, eight (7%) had CKD, five (4%) had chronic lung disease, three (3%) had malignancy, two (2%) had a stroke, and one (1%) had heart failure. Of the 66 patients with normal troponin levels, 36 (32%) had hypertension, 28 (25%) had diabetes, 15 (13%) had ischaemic heart disease, four (3%) had CKD, four (3%) had chronic lung disease, four (3%) had malignancy, one (1%) had a stroke, and none had heart failure or chronic liver disease. The difference in hypertension between the two groups was significant (p=0.01), while
the difference in CKD approached significance (p=0.06). The differences in other comorbidities were not found to be significant.
Both groups of patients had ECG and echocardiogram done at some point during their hospital stay. The most common finding on the ECG was sinus tachycardia (74%), followed by ST elevation (8%). Eight percent of patients had normal ECG (Figure 1B). Findings on the echocardiography report were stratified according to EF. Most patients (20%) had an EF of 40–59% (Figure 1C).
The length of hospital stay ranged from 4–25 days, with an average of 9 days. Overall, a total of 22 (20%) patients required ICU admission, which was equal for both groups. Mechanical ventilation was used in nine (8%) patients, which was more for patients with myocardial injury, but this value was not statistically significant. A total of 14 patients (12%) developed myocardial infarction, nine patients (8%) developed arrhythmias, and three patients (3%) required revascularisation. One patient (1%) developed non-fatal cardiac arrest, one (1%) patient developed lower limb deep venous thrombosis, one (1%) patient developed arterial thrombus, and one (1%) patient developed acute heart failure. Four patients (3%) required cardiopulmonary resuscitation, and all of these patients had a myocardial injury (p=0.02). Seventeen patients required pharmacologic resuscitation, which was more for patients with myocardial injury. Five patients (4%) died during the hospital stay (Table 2).
DISCUSSION
In late 2019, there was an identification and subsequent dissemination of an unfamiliar infectious pneumonia originating from Wuhan, China. The causative agent in question can be classified as SARS-CoV-2, which is commonly referred to as COVID-19.24 The manifestation of symptoms resulting from COVID-19 infection exhibits disease progression that extends beyond the respiratory system, affecting various organ systems. In a previous report, a patient afflicted with SARS-CoV-2 exhibited left ventricular dysfunction and pericarditis in the absence of any respiratory manifestations.25
80 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Article
*Denotes the values are statistically significant. CPR: cardiopulmonary resuscitation; HsTI: high sensitivity troponin-I;
intensive care unit; PCI: percutaneous coronary intervention.
It is crucial to comprehend the risk factors pertaining to cardiac involvement in COVID-19 infection. Prior studies have indicated a heightened mortality rate in cases where infections are accompanied by cardiac injury.26,27
Acute cardiac injury is a comprehensive phrase that may encompass various cardiovascular conditions. With the accumulation of additional data from a larger patient population, the evidence supporting the correlation between acute cardiac injury and unfavorable outcomes in individuals with COVID-19 is increasingly
robust. According to a meta-analysis conducted on COVID-19 data obtained from peer-reviewed publications, it has been observed that the occurrence of acute cardiac injury in individuals diagnosed with COVID-19 was found to be approximately 15%. Furthermore, the analysis revealed that severe cases of COVID-19 were nearly five times more prone to exhibit acute cardiac injury in comparison to milder cases.28
The medical terminology ‘acute (or chronic) myocardial injury’ is used to describe a situation where the levels of cTnI exceed the upper
Outcomes Overall Elevated troponin (HsTi) Normal troponin (HsTi) p ICU admission 22 (19) 11 (10) 11 (10) 0.37 Myocardial infarction 14 (12) 10 (9) 4 (3) 0.02* Acute heart failure 1 (1) 1 (1) 0 (0) 0.23 Non-fatal cardiac arrest 1 (1) 1 (1) 0 (0) 0.23 Deep venous thrombosis 1 (1) 0 (0) 1 (1) 0.40 Arterial thrombosis 1 (1) 0 (0) 1 (1) 0.40 Arrhythmia 9 (8) 2 (2) 7 (6) 0.22 Mechanical ventilation 9 (8) 6 (5) 3 (3) 0.11 CPR 4 (3) 4 (3) 0 (0) 0.02* Pharmacologic resuscitation 17 (15) 11 (10) 6 (5) 0.04* PCI 3 (3) 1 (1) 2 (2) 0.77 Length of hospital stay (days) 9±4 9±4 11±4 0.68 Mortality 5 (4) 3 (3) 2 (2) 0.39
ICU:
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 81 Article
Table 2: Clinical outcomes between both groups.
reference limit of the 99th percentile. In the broader populace, elevated troponin levels are correlated with an increased propensity for cardiovascular disease and mortality. Nevertheless, after accounting for additional risk factors, it has been observed that troponin I levels exhibit a correlation with mortality associated with cardiovascular disease, whereas troponin T levels demonstrate a correlation with mortality unrelated to cardiovascular disease. In various published studies concerning Chinese patients diagnosed with COVID-19, it has been observed that a notable proportion of study participants, ranging from 8–12%, exhibited elevated levels of cTnI.29-31
Similar to earlier studies of other viral infections, acute cardiac injury in COVID-19 caused by SARS-CoV-2 infection has been primarily defined as an elevation in serum cardiac markers above the 99th percentile upper reference range. The incidence has ranged from about 8–36%. The mortality rate has been significant, over 50% in the initial reports, when using an expansive and comprehensive definition of acute cardiac injury as an elevated high-sensitivity troponin I or troponin T upon admission, or throughout hospitalisation.32-35
CTnI and cardiac troponin T (cTnT) are sarcomeric proteins that are found in the cardiomyocytes, and have a unique aminoacidic protein structure that is distinct from that of skeletal muscle troponins. When myocardial necrosis (i.e., myocardial injury) occurs, the injured cardiomyocytes release the cardiac troponin. The levels of cTnI and cTnT are measured and quantified in the blood plasma to assess for cardiac injury.36,37 Specifically for COVID-19, patients diagnosed with it frequently display acute cardiac injury, which is defined as an increase in the levels of high-sensitivity cTnI or cTnT during their hospital stay, or at the time of admission. The prevalence of this condition varies between 10–35%, depending on the population being studied and the method of measurement.38 Further clarity is still required with regard to the mechanism that culminates in myocardial injury, either singularly or synergistically. The pathological response of the virus itself has been attributed to SARS-CoV-2 adhering to the ACE-2, a membrane-bound protein, to enter respiratory and cardiac cells. Although the affinity for ACE-2 in SARS-CoV-2 is
lower than that shown by SARS-CoV-2, and the former has displayed less associated cardiac pathologies, a comparable pattern is still seen. It was observed that, despite ACE-2 receptors being present on vascular endothelial cells, SARS-CoV-2 activity was not found on them. As a result, other paradigms need to be carefully considered.39-43
Other hypothesised pathways of myocardial injury include a cytokine storm driven by an inappropriate response by Type 1 and Type 2 T helper cells and COVID-19 infection-induced hypoxemia, and respiratory failure, causing damage to the myocardial cells.44 As described in the literature, an increase in viral load leads to a rise in cytokine expression, which fuels the inflammatory response.45 Another study examined 95 autopsies of patients who were SARS-CoV-2-positive, and discovered that the virus targeted endothelial cells more specifically, which they hypothesised could further destroy myocytes through paracrine effects.46 They also discovered that increased transcriptomic changes were seen, which can heighten the immune response and exacerbate proinflammatory gene expression.46 The burden of inflammation and endothelial dysfunction can also drive the pathogenesis of heart failure, particularly in cases of SAR-CoV-2-induced acute myocarditis.47
COVID-19 infection-induced myocarditis has also been described in the literature; however, the pathogenesis is still not understood, especially as some cases of myocarditis exhibit direct myocyte injury and some do not. Various case reports describe acute myocarditis in the setting of COVID-19, and while myocardial involvement is involved in a worse prognosis, such has not been established for isolated myocarditis.48 However, the fatality increases when both acute respiratory distress syndrome and cardiac inflammation are present; thus, the probability of myocarditis should be taken into consideration when making the appropriate diagnosis based on the clinical and laboratory data.49
The authors’ findings were statistically significant for raised CKMB in the elevated troponin group, signifying myocardial injury. This relationship has already been established in the literature, and only serves to reinforce the presence of acute myocardial damage.50
82 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Article
Additionally, Han et al.51 demonstrated that raised venous CKMB levels and cTnI levels in COVID-19 infection are associated with increased severity and case fatality.
Amongst both groups, 74% had sinus tachycardia on ECG, a pattern that has been observed and described before as the most common electrocardiac abnormality seen in COVID-19 infection.52 A similar trend was seen in a study conducted on patients presenting with severe acute respiratory syndrome, where 71.9% of the patients had sinus tachycardia at some point of hospitalisation. Clarity is needed if this is reference to the normal physiological response, or specific to the virus species.53 However, the presence of persistent tachycardia has also been seen in the manifestation of post-acute COVID-19 syndrome, indicating possible lasting cardiovascular effects of the viral infection.54 The phenomenon has been attributed to heart tissue inflammation, particularly myocardial inflammation, which is as widespread as 78% in patients who are post-COVID-19 infection, and causes tachycardia, palpitations, and chest pain in the months following discharge.55,56
In the authors’ study, 8% of patients demonstrated ST-elevations on ECG, 7% had ST depression, and 1% had T-wave inversions, which are in line with the current literature that describes myocardial injury in COVID-19. These ECG patterns have been mostly described in patients with COVID-19 admitted to ICU.57 An additional study revealed that 41% of patients displayed non-specific repolarisation changes, such as ST segment and T-wave abnormalities. This finding was reportedly the result of myocardial injury, and was linked to negative outcomes, such as a greater need for ICU admission, more frequent use of mechanical ventilation support, and higher mortality.58,59 ST-elevations seem to be a rare presentation, as demonstrated by the literature,60,61 but additional clarity is required to distinguish ST-elevation aetiology in COVID-19 infection.
Tavazzi et al. were the first to describe acute myocardial injury due to COVID-19. The patient reported flu-like symptoms, respiratory distress, hypotension, and cardiogenic shock. The patient was treated with venous-arterial extracorporeal membrane oxygenation and mechanical ventilation, and had an uneventful
recovery. Viruses were found in the myocardium, suggesting either a viraemic phase, or the migration of infected macrophages from the lungs into the heart.13
Cardiovascular complications after COVID-19 infection have been sporadically reported in the literature. According to the preliminary results of the LATE-COVID study by Lewek et al.,15 severe cardiovascular complications were observed in 27.5% of inpatients. In comparison to those with mild complications, patients with severe complications had a significantly higher prevalence of diabetes, a decreased EF, higher resting heart rate at admission, and higher levels of CRP and troponin T. Dyspnoea and exercise intolerance were also more frequent in patients with severe complications. These findings were limited to a small cohort of 51 patients, but directed attention toward the possible cardiovascular implications of COVID-19.15
A study by Ferrante et al.62 explored the risk factors for myocardial injury, using a chest CT scan as the screening test. The study included 332 patients, of whom 37% had a myocardial injury, which was lower than the authors’ value of 58.1%. Despite the higher myocardial injury ratio in the authors’ cohort, the authors’ mortality rate was much lower (4.4% versus 20.5%). Ferrante et al.’s62 findings concluded that myocardial injury was independently associated with an increased risk of death. Older age, lower estimated glomerular filtration rate, and lower pressure of O2in blood/fraction of inspired O2 ratio on admission were other independent predictors for both myocardial injury and death. The main risk factors in the authors’ study were old age, male sex, high CKMB on admission, and the comorbidity of hypertension. CKD was found more in patients with myocardial injury in the authors’ study, but the results were not statistically significant.62
Guo et al.34 studied 187 patients with COVID19-associated cardiovascular complications, out of whom 23% died. The mortality, again, was higher than that reported in the authors’ study. The mean age of their cohort was 58.50 years, which was lower than in this study (63.38 years). Subsequently, they had a lower percentage of myocardial injury (27.8%). Overall, 91.2% of the authors’ cohort had pre-existing cardiovascular comorbidities, such as hypertension and
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 83 Article
ischaemic heart disease. This was higher than that reported by Guo et al.,34 who reported 35.3% of patients.
A meta-analysis by Yang et al.63 revealed the most common comorbidity in patients with COVID-19 to be hypertension, which was 21.1% in their study and 65.5% in the authors’ study. The stark difference could be due to the higher rate of hypertension in Southeast Asian populations. Diabetes and ischaemic heart disease were the second and third most common comorbidities in their study, as well as in the authors’; however, the authors’ percentage of comorbidities was higher. This skew in the data could be because more patients with comorbidities prefer admission to the authors’ hospital, as it is privately run.
LIMITATIONS
The authors’ study had a few limitations. Their results were based on a small cohort, which cannot extrapolate findings to a larger population. The authors also did not have data regarding myocardial injury before admission, to rule out previous/chronic myocardial injury, which may confound the results of troponin testing.
Findings from a single-centre study with a limited sample size may not be representative of the broader population or different healthcare settings. These study results might be influenced by confounding factors, such as patient demographics, healthcare practices, and resource availability, which could limit the generalisability of the authors' findings to other regions or healthcare systems.
Differences in laboratory techniques, equipment, or personnel expertise could have introduced measurement bias and affected the reliability and validity of the results.
The determination of secondary outcomes, such as the duration of hospitalisation, admission to ICU, mode of resuscitation, and use of supplemental O2, might have been subjective or influenced by factors, such as healthcare provider preferences or availability of resources. This subjectivity could have introduced bias into the assessment of these outcomes.
The study's duration and timing of data collection might have limited the ability to capture the full spectrum of COVID-19 outcomes. The pandemic was dynamic, and the course of the disease, as well as treatment strategies and guidelines, evolve over time. Therefore, a single-centre study might not capture the latest trends, or provide insights into the long-term outcomes of patients with COVID-19, and this could be a possible temporal limitation of the study.
CONCLUSIONS
Acute myocardial injury, as indicated by troponin elevation, is common in patients with COVID-19, particularly in the elderly with underlying comorbidities. It is associated with increased risk of progressive severe disease, myocardial infarction, need for cardiopulmonary resuscitation, and pharmacologic resuscitation. Addressing the increased risk of myocardial injury in patients with COVID-19 demands a multifaceted approach that encompasses early detection, close monitoring, and tailored interventions. Healthcare professionals should remain vigilant in recognising signs of cardiac involvement in patients with COVID-19, including troponin elevation, and promptly implement appropriate measures to mitigate further complications. Therefore, targeted treatment and preventative strategies are urgently needed for this vulnerable patient group.
References
1. Cleveland Clinic. Coronavirus disease (COVID-19): what is it, symptoms, causes & prevention. Available at: https:// my.clevelandclinic.org/health/ diseases/21214-coronaviruscovid-19. Last accessed: 17 July 2023.
2. Pene F et al. Coronavirus 229E-related pneumonia in immunocompromised patients. Clin Infect Dis. 2003;37(7):929-32.
3. Peiris JS et al. Coronavirus as a possible cause of severe acute respiratory syndrome. Lancet. 2003;361(9366):1319-25.
4. Nguyen JL et al. Seasonal influenza infections and cardiovascular disease mortality. JAMA Cardiol. 2016;1:274.
5. Dec GW Jr et al. Active myocarditis in the spectrum of acute dilated cardiomyopathies. Clinical features, histologic correlates, and clinical outcome. N Engl J Med. 1985;312(14):885-90.
84 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Article
6. Feldman AM, McNamara D. Myocarditis. N Engl J Med. 2000;343(19):1388-98.
7. Oudit GY et al. SARS-coronavirus modulation of myocardial ACE2 expression and inflammation in patients with SARS. Eur J Clin Invest. 2009; 39(7):618-25.
8. Booth CM et al. Clinical features and short-term outcomes of 144 patients with SARS in the greater Toronto area. JAMA. 2003;289(21):2801-9.
9. Farshidfar F et al. Cardiovascular complications of COVID-19. JCI Insight. 2021;6(13):e148980.
10. Hoffmann M et al. A multibasic cleavage site in the spike protein of SARS-CoV-2 is essential for infection of human lung cells. Mol Cell. 2020;78(4):779-84.e5.
11. Zhang P et al. Association of inpatient use of angiotensin converting enzyme inhibitors and angiotensin II receptor blockers with mortality among patients with hypertension hospitalized with COVID-19. Circ Res. 2020;126(12):1671-81.
12. Sala S et al. Acute myocarditis presenting as a reverse TakoTsubo syndrome in a patient with SARS-CoV-2 respiratory infection. Eur Heart J. 2020;41(19):1861-2.
13. Tavazzi G et al. Myocardial localization of coronavirus in COVID-19 cardiogenic shock. Eur J Heart Fail. 2020;22(5):911-5.
14. Long B et al. Cardiovascular complications in COVID-19. Am J Emerg Med. 2020;38(7):1504-7.
15. Lewek J et al. COVID-19, and cardiovascular complicationspreliminary results of the LATECOVID study. Arch Med Sci. 2021;17(3):818-22.
16. Desai AD et al. Long-term complications of COVID-19. Am J Physiol Cell Physiol. 2022;322(1):C1-11.
17. Wang D et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061-9.
18. Thygesen K et al. Third universal definition of myocardial infarction. Eur Heart J. 2012;33(20):2551-67.
19. Lee CC et al. High-sensitivitycardiac troponin for accelerated diagnosis of acute myocardial infarction: a systematic review and meta-analysis. Am J Emerg Med. 2020;38(7):1402-7.
20. Bakshi TK et al. Causes of elevated troponin I with a normal coronary angiogram. Internal Med J. 2002;32(11):520-5.
21. Rubini-Gimenez et al. Rapid rule out of acute myocardial infarction using undetectable levels of highsensitivity cardiac troponin. Int J Cardiol. 2013;168(4):3896-901.
22. Leite L et al. High sensitivity troponins: a potential biomarkers of cardiovascular risk for primary prevention. Front Cardiovasc Med. 2022;30:9:1054959.
23. Apple FS et al. Plasma 99th percentile reference limits for cardiac troponin and creatine kinase MB mass for use with European Society of Cardiology/ American College of Cardiology consensus recommendations. Clin Chem. 2003;49(8):1331-6.
24. Kaye AD et al. Impact of COVID-19 infection on the cardiovascular system: an evidence-based analysis of risk factors and outcomes. Best Pract Res Clin Anaesthesiol. 2021;35(3):437-48.
25. Aghagoli G et al. Cardiac involvement in COVID‐19 patients: risk factors, predictors, and complications: a review. J Card Surg. 2020;35(6):1302-5.
26. Soumya RS et al. Impact of COVID-19 on the cardiovascular system: a review of available reports. Cardiovasc Drugs Ther. 2021;35(3):411-25.
27. Su YB et al. Cardiovascular manifestation and treatment in COVID-19. JChin Med Assoc. 2020;83(8):704-9.
28. Vakhshoori M et al. Acute cardiac injury in COVID-19: a systematic review and meta-analysis. Arch Iran Med. 2020;23(11):801-12.
29. Thygesen K et al. Executive Group on behalf of the Joint European Society of Cardiology (ESC)/ American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) task force for the universal definition of myocardial infarction. Fourth universal definition of myocardial infarction (2018). Circulation. 2018;138(20):e618-51.
30. Welsh P et al. Cardiac troponin T and troponin I in the general population: comparing and contrasting their genetic determinants and associations with outcomes. Circulation. 2019;139(24):2754-64.
31. Lippi G, Plebani M. Laboratory abnormalities in patients with COVID-2019 infection. Clin Chem Lab Med. 2020;58(7):1131-4.
32. Wang D et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061-9.
33. Shi S et al. Association of cardiac injury with mortality in hospitalized patients with COVID-19 in Wuhan, China. JAMA Cardiol. 2020;5(7):802-10.
34. Guo T et al. Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020;5(7):811-8.
35. Lala A et al. Prevalence and impact of myocardial injury in patients hospitalized with COVID-19 infection. J Am Cardiol. 2020;76(5):533-46.
36. Mair J et al. How is cardiac troponin released from injured myocardium? Eur Heart J Acute Cardiovasc Care. 2018;7(6):553560.
37. Marjot J et al. Quantifying the release of biomarkers of myocardial necrosis from cardiac myocytes and intact myocardium. Clin Chem. 2017;63(5):990-6.
38. Cremer PC. SARS-CoV-2 and myocardial injury: few answers, many questions. Cleve Clin J Med. 2020;87(9):521-5.
39. Zheng YY et al. COVID-19 and the cardiovascular system. Nat Rev Cardiol. 2020;17(5):259-60.
40. Xiong TY et al. Coronaviruses and the cardiovascular system: acute and long-term implications. Eur Heart J. 2020;41(19):1798-800.
41. Li W et al. Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature. 2003;426(6965):450-4.
42. Kirtipal N et al. From SARS to SARS-CoV-2, insights on structure, pathogenicity and immunity aspects of pandemic human coronaviruses. Infect Genet Evol. 2020;85:104502.
43. Hui DSC, Zumla A. Severe acute respiratory syndrome: historical, epidemiologic, and clinical features. Infect Dis Clin North Am. 2019;33(4):869-89.
44. Alhogbani T. Acute myocarditis associated with novel Middle East respiratory syndrome coronavirus. Ann Saudi Med. 2016;36(1):78-80.
45. Lindner D et al. Association of cardiac infection with SARSCoV-2 in confirmed COVID-19 autopsy cases. JAMA Cardiol. 2020;5(11):1281-5.
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 85 Article
46. Bräuninger H et al. Cardiac SARSCoV-2 infection is associated with pro-inflammatory transcriptomic alterations within the heart. Cardiovasc Res. 2022;118(2):54255.
47. Inciardi RM et al. Coronavirus 2019 disease (COVID-19), systemic inflammation, and cardiovascular disease. J Am Heart Assoc. 2020;9(16):e017756.
48. Castiello T et al. COVID-19 and myocarditis: a systematic review and overview of current challenges. Heart Fail Rev. 2022;27(1):251-61.
49. Jaiswal V et al. COVID-19 infection and myocarditis: a state-ofthe-art systematic review. J Prim Care Community Health. 2021;12:21501327211056800.
50. Ravkilde J et al. Independent prognostic value of serum creatine kinase isoenzyme MB mass, cardiac troponin T and myosin light chain levels in suspected acute myocardial infarction. Analysis of 28 months of follow-up in 196 patients. J Am Coll Cardiol. 1995;25(3):574-81.
51. Han H et al. Analysis of heart injury laboratory parameters in 273 COVID-19 patients in one hospital in Wuhan, China. J Med Virol. 2020;92(7):819-23.
52. Long B et al. Electrocardiographic manifestations of COVID-19. Am J Emerg Med. 2021;41:96-103.
53. Yu CM et al. Cardiovascular complications of severe acute respiratory syndrome. Postgrad Med J. 2006;82(964):140-4.
54. Ståhlberg M et al. Post-COVID-19 tachycardia syndrome: a distinct phenotype of post-acute COVID-19 syndrome. Am J Med. 2021 Dec;134(12):1451-6.
55. Yong SJ. Long COVID or postCOVID-19 syndrome: putative pathophysiology, risk factors, and treatments. Infectious diseases. 2021;53(10):737-54.
56. Sykes DL et al. Post-COVID-19 symptom burden: what is longcovid and how should we manage it? Lung. 2021;199(2):113-9.
57. Li Y et al. Electrocardiographic characteristics in patients with coronavirus infection: a singlecenter observational study. Ann Noninvasive Electrocardiol. 2020;25(6):e12805.
58. Bertini M et al. Electrocardiographic features of 431 consecutive, critically ill COVID-19 patients: an insight into the mechanisms of cardiac involvement. Europace. 2020;22(12):1848-54.
59. Wang Y et al. Electrocardiogram analysis of patients with different types of COVID-19. Ann Noninvasive Electrocardiol. 2020;25(6):e12806.
60. De Carvalho H et al. Electrocardiographic abnormalities in COVID-19 patients visiting the emergency department: a multicenter retrospective study. BMC Emerg Med. 2021;21(1):141.
61. Zeijlon R et al. The role of admission electrocardiogram in predicting outcome in patients hospitalized for COVID-19. J Electrocardiol. 2022;75:10-8.
62. Ferrante G et al. Risk factors for myocardial injury and death in patients with covid-19: insights from a cohort study with chest computed tomography. CardiovascRes. 2020;116(14):2239-46.
63. Yang J et al. Prevalence of comorbidities and its effects in patients infected with SARSCOV-2: a systematic review and meta-analysis. Int J Infect Dis. 2020;94:91-5.
FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM
86 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0 Article
PCSK9 Targeting in the Management of Hypercholesterolaemia
Authors: Constantine E. Kosmas,1,2 Evangelia J. Papakonstantinou,3 Jacqueline Carreño,4 Rogers Echavarria Uceta,2 Eliscer Guzman,1,2 *Andreas Sourlas5
1. Division of Cardiology, Department of Medicine, Montefiore Medical Center, New York City, USA
2. Cardiology Clinic, Cardiology Unlimited, New York City, USA
3. General Directorate of Public Health and Social Welfare, Attica Region, Athens, Greece
4. Centro Medico Dominicano, New York City, USA
5. Health Centre of Astros, Arkadia, Greece *Correspondence to med3553@edu.med.uoc.gr
Disclosure: The authors have declared no conflicts of interest.
Received: 03.08.23
Accepted: 17.08.23
Keywords: Alirocumab, cardiovascular disease, emerging therapies, evolocumab, hypercholesterolaemia, inclisiran, low-density lipoprotein cholesterol (LDL-C), PCSK9 inhibitors, proprotein convertase subtilisin/kexin type 9 (PCSK9), statins.
Citation: EMJ Cardiol. 2023;11[1]:87-97. DOI/10.33590/emjcardiol/10303462. https://doi.org/10.33590/emjcardiol/10303462.
Abstract
It has long been established that elevated plasma concentrations of low-density lipoprotein cholesterol (LDL-C) are among the prominent contributors leading to the development of atherosclerotic plaques and, ultimately, cardiovascular disease. In the current era of optimal risk factor modification, proprotein convertase subtilisin/ kexin type 9 (PCSK9) targeting has emerged as a potent therapeutic approach in the management of hypercholesterolaemia, addressing several substantial, unmet clinical needs. PCSK9 monoclonal antibodies, evolocumab and alirocumab, as well as inclisiran, which is a small interfering RNA that halts the transcription of PCSK9 mRNA, are being increasingly used in current clinical practice, as they induce intensive LDL-C reductions without any significant safety and tolerability concerns. Based on the success of these agents, the concept of PCSK9 targeting with novel agents with enhanced biological properties, or via different administration routes, has received considerable attention. In this regard, numerous antisense oligonucleotides, peptides, and proteins are currently under evaluation in randomised controlled trials, yielding propitious results up to date; they may enter clinical use in the coming years. Meanwhile, a PCSK9 vaccine, as well as genome editing via clustered regularly interspaced palindromic repeats/Cas9, hold great promise to eradicate LDL-C altogether as a cardiovascular risk factor. This review aims to present and discuss the current clinical and scientific evidence pertaining to the field of medications that exert their biological effect by targeting PCSK9, which are either in use in clinical practice, or are currently being evaluated in pre-clinical or clinical studies, and may prove beneficial in the near future.
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 87 Review
Key Points
1. Proprotein convertase subtilisin/kexin type 9 (PCSK9) monoclonal antibodies and inclisiran have ushered in a new, exciting era of hypercholesterolaemia management, addressing several unmet needs.
2. Unprecedentedly low low-density lipoprotein cholesterol concentrations can be achieved with PCSK9 monoclonal antibodies and inclisiran, without any significant safety and tolerability concerns.
3. PCSK9 targeting with antisense oligonucleotides, as well as various peptides and proteins, are under evaluation in randomised clinical trials, having provided encouraging results.
INTRODUCTION
Cardiovascular disease (CVD) has consistently been the leading cause of disease burden in the world, and the reduction of CVD mortality consists a major public health challenge in most societies.1 Elevated low-density lipoprotein cholesterol (LDL-C) levels in the bloodstream are a well-established causative, modifiable risk factor for atherosclerotic plaque formation. It is estimated that 2.6 million deaths are attributed to raised cholesterol levels worldwide annually; hence, hypercholesterolaemia is rightly considered a silent epidemic by many researchers.2 In view of the above, lipidmodifying therapies are a fundamental pillar in current preventive cardiology practice.
Among the available pharmacologic agents, statins are an effective lipid-modifying therapy that has proved its clinical value over the last decades. Statins have become the mainstay of lipid-lowering therapy. Nevertheless, a significant percentage of patients (7–29%) experience statin-associated muscle symptoms, which, although mild in severity in most patients, are one of the principal reasons for statin non-adherence and/or discontinuation, which inevitably contributes to adverse cardiovascular outcomes.3 Additionally, it has been demonstrated that statins exert a detrimental effect on glycaemic control, resulting in a significant increment of new-onset diabetes.4
The current era of preventive cardiology continues to emphasise the significance of LDL-C goal attainment of each patient, according to the individual risk stratification for CVD. However, cumulative evidence suggests that only a disappointing 20% of very high-risk patients
achieve the recommended risk-defined LDL-C threshold.5 This phenomenon is also observed in patients with familial hypercholesterolaemia, further increasing their already increased CVD risk.6
Another intriguing phenomenon is that many patients remain at a significant residual CVD risk despite LDL-C goal attainment, reinforcing the need for the development of novel lipidmodifying agents.7 In this regard, the addition of proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors in the lipid-lowering armamentarium was monumental, irrevocably changing the scope of lipid-lowering treatment, and closing the gap in optimal LDL-C reduction. This is due to the fact that unprecedentedly low levels of LDL-C can be reached by PCSK9 inhibitors, which also possess a favourable safety and tolerability profile. Therefore, the concept of PCSK9 targeting via different mechanisms or administration routes has garnered considerable attention over the last decade. In this article, the authors will explore the field of medications that exert their biological effect by targeting PCSK9, which are either in use in clinical practice, or are currently being evaluated in pre-clinical or clinical studies.
WHY IS TARGETING THE PROPROTEIN CONVERTASE SUBTILISIN/KEXIN TYPE 9 PATHWAY SUCCESSFUL?
The impetus for the breakthrough discovery of the crucial role of PCSK9 as a pivotal regulator of LDL-C levels was initiated in 2003, when a novel gain-of-function missense mutation in PCSK9 was identified as a cause of familial
Review
88 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0
hypercholesterolaemia and premature CVD.8 Conversely, loss-of-function mutations in PCSK9 were recognised to induce low LDL-C levels, providing substantial protection against CVD to their carriers.9
The mechanism through which PCSK9 exerts its biological effect on LDL-C homeostasis has now been fully elucidated. PCSK9 is a serine protease predominantly derived from hepatocytes and, to a lesser extent, from the small intestine, kidney, pancreas, and immune system. PCSK9 possesses the ability to bind to the low-density lipoprotein receptor (LDL-R), leading to its lysosomal degradation in a non-enzymatic fashion, thus decreasing the availability of LDL-R on the surface of the hepatic cell membrane. As a result, the removal rate of LDL-C from the bloodstream is decreased.10 Therefore, the pharmacological inhibition of PCSK9 function became an attractive treatment strategy to lower circulating LDL-C levels substantially.
Recent evidence suggests that the function of PCSK9 may not be limited to LDL-C metabolism. On the contrary, there are indications that the inflammatory response, platelet aggregation, and thrombosis, as well as neuronal apoptosis, may be mediated to some extent by PCSK9.11 Additionally, there is an indication of a linear association between high circulating PCSK9 levels and adverse cardiovascular outcomes.12
PROPROTEIN CONVERTASE SUBTILISIN/KEXIN TYPE 9 MONOCLONAL ANTIBODIES
The approval of the first PCSK9 inhibitor from the U.S. Food and Drug Administration (FDA) in 2015 came to address several unmet needs in the management of hypercholesterolaemia and, ultimately, CVD. Today, alirocumab and evolocumab have come to represent valuable additions to the lipid-lowering armamentarium used in current clinical practice.
The beneficial properties of PCSK9 inhibitors have been substantiated by numerous studies to date. The most notable studies, which evaluated the impact of PCSK9 inhibitors on cardiovascular outcomes, were the ODYSSEY LONG TERM13 and FOURIER14 trials.
In ODYSSEY LONG TERM, which included 2,341 patients on background statin treatment at the maximum tolerated dose, treatment with alirocumab resulted in a decrement of LDL-C values by 52.4% after 78 weeks. Additionally, alirocumab led to a lower rate of major adverse cardiovascular events, thus providing evidence for the favourable cardiovascular outcomes deriving from PCSK9 inhibitors therapy.13 The above findings were confirmed by the FOURIER trial, which assessed the effect of evolocumab on 27,564 patients who were receiving statin treatment over a median follow-up period of 2.2 years. Treatment with evolocumab led to a significant reduction of the primary endpoint (cardiovascular death, myocardial infarction, stroke, hospitalisation for unstable angina, or coronary revascularisation) by 15%, as well as of the secondary endpoint (cardiovascular death, myocardial infarction, or stroke) by 20%. Additionally, the magnitude of the improved cardiovascular outcomes tended to increase over time.14
An open-label extension study of the FOURIER trial, FOURIER-OLE, which enrolled a total of 6,635 patients, indicated that LDL-C lowering with evolocumab was associated with persistently low rates of adverse events over a median follow-up period of 5 years, and maximum exposure time over 8 years.15 Meanwhile, mounting evidence suggests that PCSK9 inhibitors are a safe therapeutic intervention in patients with diabetes, which do not adversely affect glucose metabolism, as opposed to statins.16
Since the advent of PCSK9 inhibitors, a putative concern was that the very low achieved LDL-C levels may be associated with cognitive deficits or other significant side effects. However, current evidence suggests that attaining low LDL-C levels, even below 15 mg/dL, is safe and well-tolerated, and that cognitive function is not affected in patients receiving PCSK9 inhibitors after 96 weeks of treatment.17-19 Conversely, the robust decrease in circulating LDL-C values led to further improvement of cardiovascular outcomes, indicating that the concept of ‘the lower, the better’ regarding circulating LDL-C levels may be pursued in clinical practice.17 It has been demonstrated that for each 1 mmol/L (38.67 mg/ dL) reduction in circulating LDL-C values induced by statin therapy, a 22% proportional reduction
Review Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 89
in the risk of major vascular events is achieved.20 However, relevant data regarding PCSK9 inhibitors therapy are lacking to date.
The approach of ‘the earlier, the better’ regarding the initiation of LDL-C lowering therapy has gained much attention over the last decade. Numerous studies have shown that the administration of PCSK9 inhibitors in patients with acute coronary syndrome as early as possible leads to improved cardiovascular prognosis; however, it warrants further evaluation by large-scale clinical studies, so that more reliable and concrete conclusions can be drawn.21
The realisation in numerous epidemiological and genetic studies that elevated levels of lipoprotein (a) [Lp(a)] are a causal and independent risk factor for CVD, has led to an intensive investigation into therapeutic strategies targeting Lp(a). Treatment with PCSK9 inhibitors induces reductions of approximately 25–30% in circulating Lp(a), a characteristic of paramount importance, taking into account the shortage of therapeutic interventions for hyperlipoproteinaemia (a) thus far.22 To date, lipoprotein apheresis remains the only therapy approved by the FDA for lowering Lp(a) levels in the USA. The exact mechanism of Lp(a) reduction by PCSK9 inhibitors, as well as their potential role in the management of hyperlipoproteinaemia (a) in clinical practice, remains to be elucidated.
A significant barrier limiting the widespread use of PCSK9 inhibitors that is yet to be overcome is their associated annual cost. The adverse cost-effectiveness of PCSK9 inhibitors, which in many countries is well beyond the highest acceptable willingness-to-pay threshold per quality-adjusted life years, renders them as not affordable for most healthcare systems or private insurance companies.23 Indeed, rates of prescription approval for PCSK9 inhibitor therapy by health insurance companies, even for patients who appeared to meet labelled indications, were extremely low.24 However, a more recent price reduction of 60% from their initial pricing,23 and the expected further reduction in price over time, will eventually allow more patients to receive PCSK9 inhibitors in the foreseeable future.
INCLISIRAN
One of the most exciting advances in biology has been the discovery of small interfering RNAs, mediating their action by selective posttranscriptional gene silencing. The advent of inclisiran, which is a long-acting, short-chain small interfering RNA, was a remarkable feat of drug development that ignited the dawn of a new era of lipid-lowering therapy. In contrast to the PCSK9 monoclonal antibodies, whose site of action lies on an extracellular level, inclisiran acts intracellularly by halting the hepatic synthesis of PCSK9 mRNA.25 Inclisiran is among the five approved small interfering RNA medications by the FDA; it is a drug discovery paradigm for the development of novel drugs.
In the ORION-1 Phase II trial, which was the benchmark for subsequent studies, a single dose of 500 mg inclisiran resulted in a reduction of circulating LDL-C levels by 41.9% at Day 180, whereas the two-dose regimen of 300 mg of inclisiran yielded a decrement of 52.6% in LDL-C levels in the same period. Moreover, inclisiran appeared to have an acceptable safety and tolerability profile, as the incidence of serious adverse events did not differ substantially between treatment and placebo groups.26
The above findings have been replicated in several more recent randomised, controlled trials. The most comprehensive evidence regarding the efficacy of inclisiran has been documented in two Phase III trials, ORION-10 and ORION-11.27 The studies comprised a total of 3,178 patients with elevated LDL-C levels, despite maximumtolerated statin treatment. The follow-up period for both studies was 1.5 years. Administration of 284 mg of inclisiran subcutaneously every 6 months resulted in a 45.8–51.3% decrease in circulating LDL-C levels. Regarding the safety of inclisiran, mild injection site reactions were more common in the inclisiran group.27
Preliminary data on the long-term safety profile of inclisiran were provided by the ORION-3 study, a 4-year open-label extension study of ORION-1.28 The study indicated that the repeated exposure to inclisiran was not associated with the emergence of severe adverse events, and resulted in sustained reductions in LDL-C levels.28 Furthermore, it has been suggested that inclisiran is a safe therapeutic option in patients with mild or moderate hepatic impairment.29
Review 90 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0
Although evolocumab, alirocumab, and inclisiran exhibit similar potency in decreasing circulating LDL-C values, inclisiran offers the advantage of a considerably more convenient dosing regimen, as it is administered at 6-month intervals. This beneficial property of inclisiran has the potential to eradicate medication nonadherence and, consequently, to improve the rates of achievement of LDL-C goals in the foreseeable future.30
Another question to be answered is whether the beneficial characteristics of inclisiran are translated into improved CVD outcomes. Thus, the results of the ORION-4 study, which is the first trial investigating the effects of inclisiran on major adverse cardiovascular events, are eagerly awaited at the second half of 2026.31
A summary of the key clinical trials of PCSK9 monoclonal antibodies and inclisiran is shown in Table 1.
Trial Design
ODYSSEY LONG TERM13
Double-blind, placebo-controlled, parallel-group, multinational, Phase III RCT
Participants
2,341 patients at high CVD risk with LDL-C ≥70 mg/dL, on high-dose or maximum tolerated statin therapy
Intervention Results
Alirocumab for 78 weeks versus placebo
52.4% reduction in LDL-C levels
Lower rates of MACE in the alirocumab group (1.6% versus 3.3%)
FOURIER14 and a prespecified secondary analysis of FOURIER investigating the safety and clinical efficacy of achieving extremely low LDL-C concentrations17
Double-blind, placebo-controlled, multinational, Phase III RCT
27,564 patients with ASCVD and LDL-C ≥70 mg/dL or non-HDL-C ≥100mg/ dL on lipid-lowering therapy
Evolocumab for a median duration of 2.2 years versus placebo
59% reduction in LDL-C levels at 48 weeks
Reduction of the primary end point (cardiovascular death, myocardial infarction, stroke, hospitalisation for unstable angina, or coronary revascularisation) in the evolocumab group (9.8% versus 11.3%)
Decrease of the secondary end point (cardiovascular death, myocardial infarction, or stroke) in the evolocumab group (5.9% versus 7.4%)
Further reductions of LDL-C concentrations, beyond current guidelines, lead to further improvement of cardiovascular prognosis, without safety concerns
Review
Table 1: Summary of key clinical trials of PCSK9 monoclonal antibodies and inclisiran.
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 91
Table 1 continued.
Trial Design Participants
FOURIER-OLE, open-label extension of the FOURIER trial15
Multicenter, openlabel, single-arm Phase III trial
Intervention Results
EBBINGHAUS18
6,635 patients who participated in the FOURIER trial, regardless of the initial treatment allocation
Evolocumab for a median duration of 5 years
Long-term achievement of lower LDL-C levels (<20 mg/ dL) is associated with improved cardiovascular outcomes, with no significant safety concerns
A trial evaluating the effect of alirocumab on neurocognitive function19
ORION-126
Double-blind, placebo-controlled, multicenter, Phase III RCT
Double-blind, placebo-controlled, Phase IV RCT
Double-blind, placebo-controlled, parallel-group, Phase II RCT
1,204 patients with ASCVD, LDL-C ≥70 mg/dL or nonHDL-C ≥100 mg/ dL receiving statin therapy
2,176 patients with high or veryhigh CVD risk on maximally tolerated statin therapy
501 patients with high CVD risk, LDL-C ≥70 mg/dL on maximum tolerated statin therapy
Evolocumab for a median of 19 months versus placebo
No significant difference in cognitive function between evolocumab and placebo groups
Alirocumab for 96 weeks versus placebo
Single or two doses of inclisiran over 180 days versus placebo
No impact on neurocognitive function by alirocumab, using the CANTAB scale
Reduction of LDL-C and PCSK9 levels up to 52.6% and 69.1%, respectively
No significant difference in serious adverse events between the inclisiran and placebo groups (11% versus 8%)
5% of patients receiving inclisiran had injection site reactions
ORION-10 and ORION-1127
Double-blind, placebo-controlled, parallel-group, Phase III RCT
1,561 and 1,617 patients with ASCVD and LDL-C ≥70 mg/ dL
Inclisiran over a period of 540 days versus placebo
45.8–51.3% decrease in LDL-C levels
Reduction of PCSK9 levels by 63.6–69.8%
Similar incidence of adverse events in the inclisiran and placebo groups, although injectionsite reactions were in patients receiving inclisiran (2.6% versus 0.9%; 4.7% versus 0.5%)
Review 92 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0
Trial Design Participants Intervention Results
ORION-328 Open-label, multicenter, longterm extension study of the ORION-1 Phase II trial
382 patients with high CVD risk, LDL-C ≥70 mg/dL on maximum tolerated statin therapy
Inclisiran over a period of 4 years
34.3–53.8% reduction in LDL-C concentrations
62.2–77.8% decrease in PCSK9 levels
No significant safety concerns
ORION-431 Double-blind, placebo-controlled, Phase II RCT
15,000 patients with ASCVD Inclisiran for a planned median duration of about 5 years
Ongoing
Evaluation of inclisiran on MACE
ASCVD: atherosclerotic cardiovascular disease; CANTAB: Cambridge Neuropsychological Test Automated Battery; CVD: cardiovascular disease; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; MACE: major adverse cardiovascular event; PCSK9: proprotein convertase subtilisin/ kexin type 9; RCT: randomised controlled trial.
EMERGING THERAPIES: WHAT IS NEXT?
Although three PCSK9-targeting medications are currently approved, and are extremely valuable in the management of hypercholesterolaemia, the endeavour for the development of novel drugs that target PCSK9 has not yet ceased. On the contrary, several promising therapeutic interventions are under pre-clinical or clinical evaluation.
Antisense Oligonucleotides
Cepadacursen sodium (CiVi 007) and CiVi 008, which is the oral formulation of the subcutaneously administered CiVi 007, are long-acting, third-generation antisense oligonucleotides that inhibit the production of PCSK9 at the level of its synthesis by mRNA.
CiVi 007 has the potential to combine robust LDL-C reduction with convenient dosing and an affordable price. It has completed a Phase I and Phase II trial, but the results have yet to become available.32 CiVi 008, the only oral antisense oligonucleotide in development targeting PCSK9, is now in the pre-clinical
development stage, and the clinical trials are awaited with interest.
Although AZD8233 (ION449), an antisense oligonucleotide targeting PCSK9 gene expression, had provided promising results in a Phase II trial (73% reduction of LDL-C), it was announced that the manufacturing company would halt clinical studies due to lack of goal attainment.32
Peptides and Proteins
Lerodalcibep (LIB003) is a recombinant fusion protein of a PCSK9-binding domain, adnectin, and human serum albumin. Adnectin, the targetbinding protein, attaches to PCSK9; therefore, the interaction with the LDL-R is impeded. In a Phase II clinical trial, the subcutaneous administration of LIB003 every month resulted in an approximately 60% reduction of circulating LDL-C levels over a 36-week dosing period, and had a benign side effect profile.33 The safety and efficacy of LIB003 are currently evaluated in Phase III clinical trials, and the results are awaited at the end of 2023.34
Table 1 continued.
Review
Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 93
CiVi 007 and CiVi 008
• ASO
• Subcutaneously (CiVi 007); orally (CiVi 008)
• Completed Phase II clinical trial
Alirocumab
• Monoclonal antibody
• Subcutaneously every 2 or 4 weeks
Evolocumab
• Monoclonal antibody
• Subcutaneously every 2 or 4 weeks
Inclisiran
• siRNA
• Subcutaneously every 6 months
PCSK9 targeting
LIB003 (Lerodalcidep)
• Recombinant fusion protein
• Subcutaneously every month
• In Phase III clinical trial
MK-0616
• Macrocyclic peptide
• Orally, once daily administration
• Initiation of Phase III clinical trial
NNC0385-0434
• Small molecule peptide
• Orally, once daily administration
• Initiation of Phase II clinical trial
CVI-LM001
• Small molecule
• Orally, once daily administration
• Completed Phase I clinical trial
AT04A
• Vaccine
• One subcutaneous administration
• Completed Phase I clinical trial
ASO: antisense oligonucleotides; CiVi 007: cepadacursen sodium; CiVi 008: oral form of cepadacursen sodium; PCSK9: proprotein convertase subtilisin/kexin type 9; siRNA: small interfering RNA.
MK-0616, an oral macrocyclic peptide inhibitor of PCSK9, might be a revolutionary addition to lipid-lowering therapy. In a Phase IIb clinical trial comprising 381 patients, once-daily administration of MK-0616 resulted in clinically meaningful LDL-C reduction of up to 60.9%. Meanwhile, there was no association with the emergence of adverse events during the 8 weeks of treatment and additional 8 weeks of follow-up.35 Thus, MK-0616 holds the potential to become the first oral PCSK9 inhibitor, and to be a major player in hypercholesterolaemia management. A Phase III trial of MK-0616 is expected to be initiated in the second half of 2023.36
Numerous other drugs that exert their action by targeting PCSK9 are being evaluated in preclinical or early clinical studies. NNC0385-0434 is a small molecule peptide PCSK9 inhibitor administered orally, once-daily. It has a similar structure to LDL-R and inhibits PCSK9 binding to
LDL-R. A Phase II clinical trial of NNC0385-0434 was completed in the first half of 2023, and the results are awaited.32 CVI-LM001 is a first-in-class oral small molecule PCSK9 modulator inhibiting PCSK9 transcription, and degradation of LDL-R mRNA. Preliminary clinical data show that CVI-LM001 reduces the expression level of the PCSK9 gene by 90%, and exhibits good pharmacokinetics.37
The addition of oral PCSK9 targeting agents to the lipid-lowering armamentarium may be particularly useful in patients who are not comfortable with injections, leading to improved treatment compliance, and eventually better cardiovascular prognosis.
Vaccines and Clustered Regularly Interspaced Palindromic Repeats/Cas9
Last but not least, a PCSK9 vaccine, namely AT04A, as well as genome editing via clustered regularly interspaced palindromic repeats/
Figure 1: Therapeutic interventions targeting proprotein convertase subtilisin/kexin type 9.
Review 94 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0
Cas9, hold great promise to transform the treatment landscape for patients with hypercholesterolaemia in the future.38-40
AT04A has completed a Phase I clinical trial providing encouraging results, while the approaches of PCSK9 gene editing are only at the in vivo stage of development.38
Future Hopes: Identification of New Molecular Targets
To date, there is intensive research for the identification of factors that may play a role in the regulation of LDL-C/PCSK9 homeostasis, which could lead to the recognition of novel mechanisms for LDL-C lowering. For instance, annexin A2 has been identified as a natural extrahepatic inhibitor of the PCSK9, while mice that are deficient in the protein denitrosylase S-nitroso-coenzyme A reductase 2 exhibit
marked reductions in serum cholesterol, due to reduced secretion of PCSK9.41,42
Thus, alternative pathways might present exciting opportunities for the development of novel pharmacologic interventions.
An overview of the therapeutic interventions targeting PCSK9 that are currently in use, or are being evaluated in pre-clinical or clinical trials, is shown in Figure 1, and their mechanism of action is shown in Figure 2
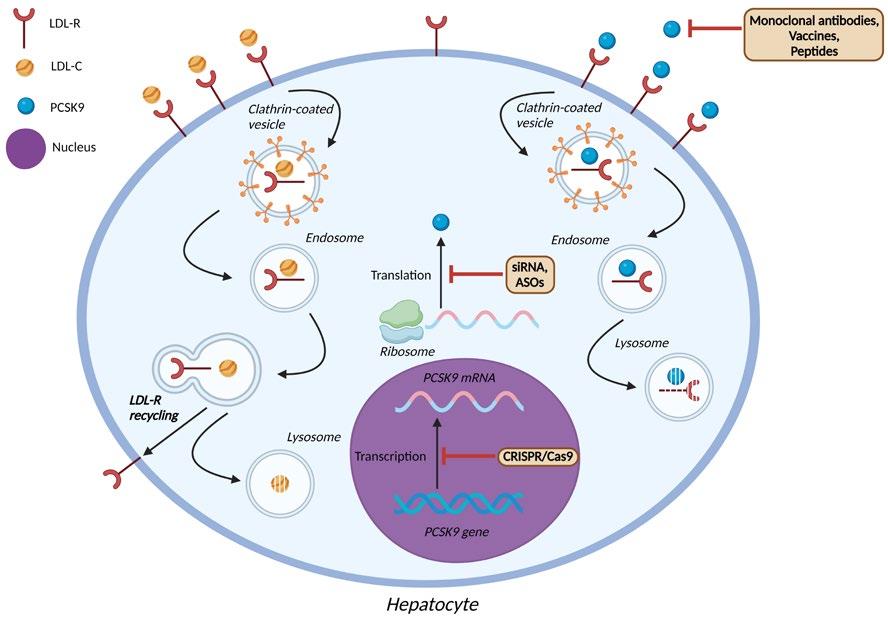
CONCLUSION
Indisputably, the advent of medications that act via the targeting of PCSK9 has ushered in a new, stunning era of preventive cardiology and optimal risk factor modification. PCSK9 monoclonal antibodies and inclisiran, which are currently
ASO: antisense oligonucleotides; LDL-C: low-density lipoprotein cholesterol; LDL-R: low-density lipoprotein receptor; PCSK9: proprotein convertase subtilisin/kexin type 9; siRNA: small interfering RNA.
Figure 2: Mechanism of action of pharmacologic agents targeting proprotein convertase subtilisin/kexin type 9.
Monoclonal antibodies, vaccines, peptides
Review Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 95
in use, have garnered an increasing reputation, capitalising on their potency and efficacy in decreasing both circulating LDL-C values and major adverse cardiovascular events, as well as on their favourable safety and tolerability profile. Novel pharmacological agents with enhanced pharmacokinetic and pharmacodynamic properties are being evaluated in clinical trials, having provided propitious results up to date. However, cardiovascular outcomes studies are eagerly awaited, so as to ascertain whether the marked reduction in LDL-C levels induced by these novel agents are also translated into improved cardiovascular prognosis.
Additionally, large-scale trials evaluating the long-term safety and tolerability of these
References
1. Roth GA et al;. GBD-NHLBI-JACC Global Burden of Cardiovascular Diseases Writing Group. Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):29823021.
2. Mozaffarian D et al.; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics-2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29-322.
3. Stroes ES et al.; European Atherosclerosis Society Consensus Panel. Statin-associated muscle symptoms: impact on statin therapy-European Atherosclerosis Society Consensus Panel statement on assessment, aetiology and management. Eur Heart J. 2015;36(17):1012-22.
4. Kosmas CE et al. Impact of lipidlowering therapy on glycemic control and the risk for new-onset diabetes mellitus. Drugs Context. 2018;7:212562.
5. Fox KM et al. Treatment patterns and low-density lipoprotein cholesterol (LDL-C) goal attainment among patients receiving high- or moderate-intensity statins. Clin Res Cardiol. 2018;107(5):380-8.
6. Iyen B et al. Statin treatment and LDL-cholesterol treatment goal attainment among individuals with familial hypercholesterolaemia in primary care. Open Heart. 2021;8(2):e001817.
therapeutic interventions are awaited with interest. Another question that is yet to be answered is whether these agents would be tolerable in specific categories of patients, such as in those with renal or hepatic impairment, or in females who are pregnant with familial hypercholesterolaemia.
Considering all of the above, the future seems vivid for the medications that target PCSK9, with the optimal goal of eradicating hypercholesterolaemia as a cardiovascular risk factor via pharmacotherapy being closer than ever. Meanwhile, the success story of alirocumab, evolocumab, and, more recently, inclisiran, has paved the way for the development of novel therapies for a number of different diseases.
7. Sampson UK et al. Residual cardiovascular risk despite optimal LDL cholesterol reduction with statins: the evidence, etiology, and therapeutic challenges. Curr Atheroscler Rep. 2012;14(1):1-10.
8. Abifadel M et al. Mutations in PCSK9 cause autosomal dominant hypercholesterolemia. Nat Genet. 2003;34(2):154-6.
9. Cohen J et al. Low LDL cholesterol in individuals of African descent resulting from frequent nonsense mutations in PCSK9. Nat Genet. 2005;37(2):161-5.
10. Xia X-D et al. Regulation of PCSK9 expression and function: mechanisms and therapeutic implications. Front Cardiovasc Med. 2021;8:764038.
11. Liu C et al. PCSK9 inhibition: from current advances to evolving future. Cells. 2022;11(19):2972.
12. Zhou Y et al. Association between circulating proprotein convertase subtilisin/kexin type 9 and major adverse cardiovascular events, stroke, and all-cause mortality: systemic review and metaanalysis. Front Cardiovasc Med. 2021;8:617249.
13. Robinson JG et al.; ODYSSEY LONG TERM Investigators. Efficacy and safety of alirocumab in reducing lipids and cardiovascular events. N Engl J Med. 2015;372(16):1489-99.
14. Sabatine MS et al.; FOURIER Steering Committee and Investigators. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376(18):1713-22.
15. O'Donoghue ML et al. Longterm evolocumab in patients with established atherosclerotic cardiovascular disease. Circulation. 2022;146(15):1109-19.
16. Sabatine MS et al. Cardiovascular safety and efficacy of the PCSK9 inhibitor evolocumab in patients with and without diabetes and the effect of evolocumab on glycaemia and risk of new-onset diabetes: a prespecified analysis of the FOURIER randomised controlled trial. Lancet Diabetes Endocrinol. 2017;5(12):941-50.
17. Giugliano RP et al.; FOURIER Investigators. Clinical efficacy and safety of achieving very low LDLcholesterol concentrations with the PCSK9 inhibitor evolocumab: a prespecified secondary analysis of the FOURIER trial. Lancet. 2017;390(10106):1962-71.
18. Giugliano RP et al. Cognitive function in a randomized trial of evolocumab. N Engl J Med. 2017;377(7):633-43.
19. Janik MJ et al. Alirocumab treatment and neurocognitive function according to the CANTAB scale in patients at increased cardiovascular risk: a prospective, randomized, placebocontrolled study. Atherosclerosis. 2021;331:20-7.
20. Baigent C et al.; Cholesterol Treatment Trialists’ (CTT) Collaboration. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376(9753):1670-81.
Review 96 Cardiology ● October 2023 ● Creative Commons Attribution-Non Commercial 4.0
21. Hao Y et al. Effect of the early application of evolocumab on blood lipid profile and cardiovascular prognosis in patients with extremely high-risk acute coronary syndrome. Int Heart J. 2022;63(4):669-77.
22. Kosmas CE et al. Therapeutic management of hyperlipoproteinemia (a). Drugs Context. 2019;8:212609.
23. Kosmas CE et al. Safety and tolerability of PCSK9 inhibitors: current insights. Clin Pharmacol. 2020;12:191-202.
24. Hess GP et al. Proprotein convertase subtilisin/kexin type 9 inhibitor therapy: payer approvals and rejections, and patient characteristics for successful prescribing. Circulation. 2017;136(23):2210-9.
25. Kosmas CE et al. Inclisiran: a new promising agent in the management of hypercholesterolemia. Diseases. 2018;6(3):63.
26. Ray KK et al. Inclisiran in patients at high cardiovascular risk with elevated LDL cholesterol. N Engl J Med. 2017;376(15):1430-40.
27. Ray KK et al.; ORION-10 and ORION-11 Investigators. Two phase 3 trials of inclisiran in patients with elevated LDL cholesterol. N Engl J Med. 2020;382(16):1507-19.
28. Ray KK et al. Long-term efficacy and safety of inclisiran in patients with high cardiovascular risk and elevated LDL cholesterol (ORION-3): results from the
4-year open-label extension of the ORION-1 trial. Lancet Diabetes Endocrinol. 2023;11(2):109-19.
29. Kallend D et al. Pharmacokinetics and pharmacodynamics of inclisiran, a small interfering RNA therapy, in patients with hepatic impairment. J Clin Lipidol. 2022;16(2):208-19.
30. Kosmas CE et al. Inclisiran for the treatment of cardiovascular disease: a short review on the emerging data and therapeutic potential. Ther Clin Risk Manag. 2020;16:1031-7.
31. University of Oxford. A randomized trial assessing the effects of inclisiran on clinical outcomes among people with cardiovascular disease (ORION-4). NCT03705234. https://clinicaltrials.gov/show/ NCT03705234.
32. Arnold N, Koenig W. PCSK9 inhibitor wars: how does inclisiran fit in with current monoclonal antibody inhibitor therapy? Considerations for patient selection. Curr Cardiol Rep. 2022;24(11):1657-67.
33. Stein A et al. Safety, tolerability and LDL-C reduction with LIB003 a novel anti-PCSK9 recombinant fusion protein: results of openlabel extension phase 2b study. Circulation. 2019;140:A17222.
34. LIB Therapeutics LLC. Study of efficacy and safety of LIB003 in patient with CVD on statins requiring additional LDL-C reduction (LIBerate-CVD). NCT04797247. https://clinicaltrials. gov/show/NCT04797247.
35. Ballantyne CM et al. Phase 2b randomized trial of the oral PCSK9 inhibitor MK-0616. J Am Coll Cardiol. 2023;81(16):1553-64.
36. Merck Sharp & Dohme LLC. A study of MK-0616 (oral PCSK9 inhibitor) in adults with hypercholesterolemia (MK-0616-013). NCT05952856. https://clinicaltrials.gov/show/ NCT05952856.
37. Liu J et al. CVI-LM001, a firstin-class novel oral PCSK9 modulator, lowers plasma Ldl-c and reduces circulating PCSK9 in preclinical animal models and in hyperlipidemic human subjects. Circulation. 2020;142:A12579.
38. Zeitlinger M et al. A phase I study assessing the safety, tolerability, immunogenicity, and low-density lipoprotein cholesterol-lowering activity of immunotherapeutics targeting PCSK9. Eur J Clin Pharmacol. 2021;77(10):1473-84.
39. Musunuru K et al. In vivo CRISPR base editing of PCSK9 durably lowers cholesterol in primates. Nature. 2021;593(7859):429-34.
40. Katzmann JL et al. Gene therapy targeting PCSK9. Metabolites. 2022;12(1):70.
41. Seidah NG et al. Annexin A2 is a natural extrahepatic inhibitor of the PCSK9-induced LDL receptor degradation. PLoS One. 2012;7(7):e41865.
42. Stomberski CT et al. A multienzyme S-nitrosylation cascade regulates cholesterol homeostasis. Cell Rep. 2022;41(4):111538.
FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM
Review Creative Commons Attribution-Non Commercial 4.0 ● October 2023 ● Cardiology 97

Receive our free newsletters and alerts Get the latest updates on all our upcoming journals and receive first-class insights into ground-breaking news and advancements in medicine across multiple therapeutic areas. www.emjreviews.com Join our mailing list
