Stefan Wöhrl, Stefano del Giacco, and new EAACI president Maria Torres
Article:
10 Review of the European Academy of Allergy and Clinical Immunology (EAACI) Congress 2024, 31st May–3rd June 2024
Congress Feature
20 Breakthroughs in Food Allergy Therapy Helena Bradbury Symposium Reviews
26 Transforming Management of Indolent Systemic Mastocytosis With Precision Medicine
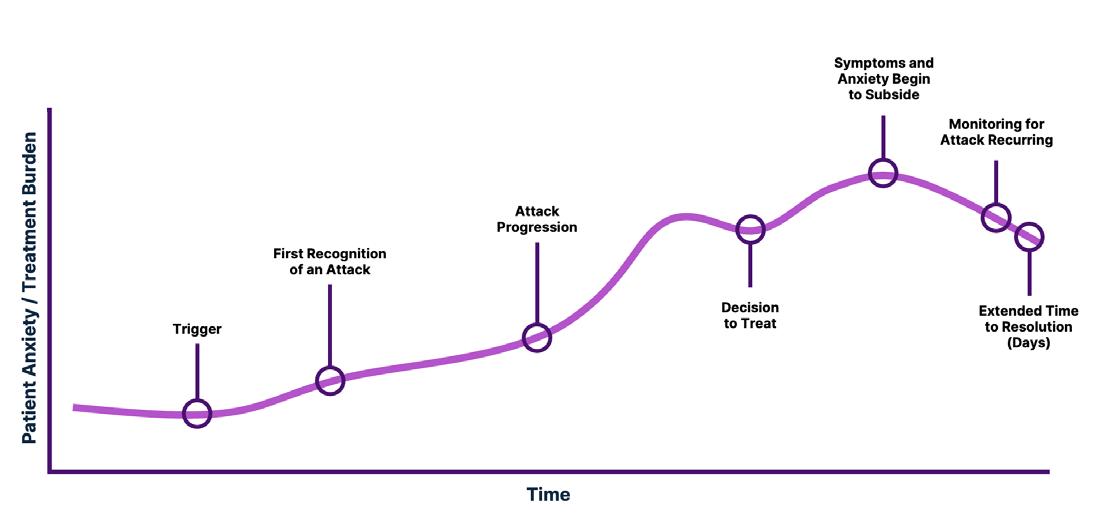
37 Closing Gaps in Hereditary Angioedema Management: Addressing Delays in On-Demand Treatment
Abstract Review
44 Hereditary Angioedema Type I in a 57-Year-Old Woman
Kikvidze and Makharashvili
46 Abstract Highlights Congress Interviews
56 Stefan Wöhrl
60 Stefano del Giacco and Maria Torres Articles
63 Performance Analysis of Non-invasive Biomarkers in the Treatment of Eosinophilic Oesophagitis
Narváez-Fernández and Tomás-Perez
70 Thymoma-Associated Good Syndrome: A Case Report and Literature Review
Muhd Yazid et al.
"EAACI Congress 2024 is a chance for knowledge exchange between colleagues in the field"
Editorial Board
Editor-in-Chief
Prof Jacques Bouchard
La Malbaie Hospital, Qubec, Canada.
Professor Bouchard is a consultant in allergy and respiratory physiology at Hôpital de La Malbaie, and a vice-chair of the Family Physician Airways Group of Canada. With over 30 years of experience, Bouchard founded the Quebec Respiratory Health Education Network, a non-profit organisation that provides training for respiratory healthcare professionals.
Dr Enrico Heffler
Humanitas University, Italy
Prof Igor Kaidashev
Poltava State Medical University, Ukraine
Dr Sarah Karabus
Red Cross War Memorial Children's Hospital, South Africa
Dr Ting Fan Leung
The Chinese University of Hong Kong, Hong Kong
Prof Branimir Nestorovic
University Children's Hospital Belgrade, Serbia
Dr Reynold A Panettieri
Rutgers Institu te for Translational Medicine and Science, USA
Dr Michael Rudenko
London Allergy and Immunology Centre, UK
Dr Stefan Wöhrl
Floridsdorf Allergy Center, Austria
Dr James Woijoo Kim
Family Physician Airway Group of Canada, Canada
Aims and Scope
EMJ Allergy & Immunology is an open-access, peer-reviewed eJournal committed to helping elevate the quality of healthcare for allergic and immunological diseases globally by informing healthcare professionals on all aspects of these conditions.
The journal is published annually, six weeks after the European Academy of Allergy and Clinical Immunology (EAACI) Congress, and features highlights from this congress, alongside interviews with experts in the field, reviews of abstracts presented at the congress, as well as in-depth features on congress sessions. The journal also covers advances within the clinical and pharmaceutical arenas by publishing sponsored content from congress symposia, which is of high educational value for healthcare professionals. This undergoes rigorous quality control checks by independent experts and the in-house editorial team.
EMJ Allergy & Immunology also publishes peer-reviewed research papers, review articles, and case reports in the field. In addition, the journal welcomes the submission of features and opinion pieces intended to create a discussion around key topics in the field and broaden readers’ professional interests.
EMJ Allergy & Immunology is managed by a dedicated editorial team that adheres to a rigorous double-blind peer-review process, maintains high standards of copy editing, and ensures timely publication.
EMJ Allergy and Immunology endeavours to increase knowledge, stimulate discussion, and contribute to a better understanding of the diseases of the immune system.
EMJ Allergy & Immunology focuses on topics that are relevant to healthcare professionals in the field. We do not publish veterinary science papers or laboratory studies that are not linked to patient outcomes. We have a particular interest in topical studies that advance knowledge and inform of coming trends affecting clinical practice in the field.
Further details on coverage can be found here: www.emjreviews.com
Editorial Expertise
EMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors who are recognised authorities in their respective fields.
• Peer review, which is conducted by expert reviewers who are invited by the Editorial team and appointed based on their knowledge of a specific topic.
• An experienced team of editors and technical editors.
Peer Review
On submission, all articles are assessed by the editorial team to determine their suitability for the journal and appropriateness for peer review.
Editorial staff, following consultation with either a member of the Editorial Board or the author(s) if necessary, identify three appropriate reviewers, who are selected based on their specialist knowledge in the relevant area.
All peer review is double blind.
Following review, papers are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected.
Editorial staff have final discretion over any proposed amendments.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects. We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial.assistant@emjreviews.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in EMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
EMJ is distributed through controlled circulation to healthcare professionals in the relevant fields across Europe.
Indexing and Availability
EMJ is indexed on DOAJ, the Royal Society of Medicine, and Google Scholar®; selected articles are indexed in PubMed Central®
EMJ is available through the websites of our leading partners and collaborating societies. EMJ journals are all available via our website: www.emjreviews.com
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
Indexed by: Directory of Open Access Journals (DOAJ) Online ISSN: 2398-9130
All information obtained by EMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, EMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. EMJ is completely independent of the review event (EAACI 2024) and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever. The cover photo is of Valencia, Spain, the location of EAACI 2024.
CoMiSS: A Rich Decade of Science and Clinical Practice
Hear key paediatric experts reflect on 10 years of CoMiSS™, a tool raising awareness of cow’s milk allergy symptoms in infants and young children
The publication of this podcast was funded by Nestlé Health Science
Vandenplas Dr Hannah Moir
Moderator:
Editor
Evgenia Koutsouki
Editorial Manager
Darcy Richards
Copy Editors
Noémie Fouarge, Katheeja Imani, Jenna Lorge
Editorial Co-ordinator
Abigail Craig
Editorial Assistants
Victoria Antoniou, Helena Bradbury, Ada Enesco, Laith Gergi, Katrina Thornber, Aleksandra Zurowska, Katie Wright
Creative Director
Tim Uden
Design Manager
Stacey Rivers
Senior Designers
Roy Ikoroha, Steven Paul
Designer Owen Silcox
Junior Designers
Dillon Benn Grove, Shanjok Gurung
Marketing Director
Kristina Mestsaninova
Chief Content Officer
Justin Levett
Chief Commercial Officer
Dan Healy
Founder and CEO
Spencer Gore
Welcome
Dear Readers,
It is a great pleasure to welcome you once again to this issue of EMJ Allergy and Immunology. This year’s European Academy of Allergy and Clinical Immunology (EAACI) Congress was a truly captivating experience for our team. We had the opportunity to listen to all the key issues in the field with a focus on data science, homing in on how this can facilitate the development of personalised medicine. We have focused on a session of particular interest examining food allergy, the role of anti-IgE and the gut microbiome.
In this issue, you will find insights around key abstracts exploring topics ranging from the benefit of synbiotics in infants with cow’s milk allergy to a test for improving the accuracy of asthma diagnosis, as well as a study showing that reducing the number of common infections experienced in early-life might be a strategy for paediatric asthma primary prevention. Make sure not to miss the interviews with the President and the Secretary General of EAACI, who provide key insights on this year’s themes.
In closing, I would like to express my gratitude to our Editorial Board, contributors, and peer reviewers for working on elevating the quality of this content and having an immensely positive effect on bringing together another great issue. We are looking forward to your rating of our content and your comments, and until our next issue, we anticipate your submitted manuscripts.
Editorial enquiries: editor@emjreviews.com
Sales opportunities: salesadmin@emjreviews.com
Permissions and copyright: accountsreceivable@emjreviews.com
Editor
Reprints: info@emjreviews.com
Media enquiries: marketing@emjreviews.com
Evgenia Koutsouki
Foreword
Welcome to the latest issue of EMJ Allergy & Immunology. Our daily practice in the field of diseases, directly or indirectly affecting allergies, is constantly evolving. We are inundated with information from all sides, the sources of which are often not clearly known. It is therefore important to return to the basis of medicine; that is to say, to rely on data and scientific evidence from clinical experiments and clearly demonstrated therapeutic experiences.
The European Academy of Allergy and Clinical Immunology (EAACI) Congress was held this year in Valencia, Spain, from 31st May–3rd June 2024, with the added availability to use a hybrid platform. The aim was to revolutionise patient care through the power of data science.
The Congress responded well to this objective through plenary sessions, posters, exchanges that included pro and cons sessions, practical workshops, and more, all coordinated efficiently by the organisation. We must also highlight the postgraduate courses, which are always interesting. Once again this year, the interdisciplinary approach was highlighted by targeting the essential collaboration of health professionals at all levels.
The emergence of new technologies and their place has been well presented, especially in relation to the impact that artificial intelligence will have on our ways, not only to consult the published data, but also to establish diagnostic hypotheses as well as treatment. Moreover, the growing presence of broadcast tools, such as online webinars and podcasts, will undoubtedly improve our knowledge.
The aim was to revolutionise patient care through the power of data science
In this issue, you will find a complete report of this Congress, and I hope that, by reading it, your knowledge in the vast field of allergy is enriched. I would like to take this opportunity to thank all the team and everyone who contributed to this publication.
The next EAACI Congress will be held in Glasgow, UK, in June 2025.
Jacques Bouchard Hôpital de la Malbaie and Université Laval, Quebec, Canada
EAACI 2024
EAACI Congress 2024 is a chance for knowledge exchange between colleagues in the field
Review of the European Academy of Allergy and Clinical Immunology (EAACI) Congress 2024 Congress Review
DATA science dominated the discussions at this year’s European Academy of Allergy and Clinical Immunology (EAACI) Congress 2024. More than 8,000 attendees gathered for groundbreaking research and the latest advances in allergy and clinical immunology under the theme ‘Revolutionising Patient Care Through the Power of Data Science’.
The renowned Congress was held at Feria de Valencia, Spain, a highly esteemed convention and exhibition centre known for its modernity and versatility, in a city with rich historical heritage. The main aim of the Congress was to highlight the importance of data science in allergy and clinical immunology, particularly concerning the development of personalised medicine. Revolutionary research on this topic was showcased during the congress against the backdrop of Valencia's beautiful architecture and Mediterranean coast.
Data science is transforming the way we understand and treat allergies
Given the overarching theme of the Congress, it was perfectly fitting that experts in the field were welcomed by a mistress of ceremonies like no other – a computer-animated, AI robot, the self-proclaimed ‘multi-lingual cousin of ChatGPT’. With the audience captivated by the entertaining and impressive start to the Opening Ceremony, EAACI President, Stefano del Giacco, emphasised the importance of data science, AI, and
digital approaches to transform precision medicine, immunotherapy, and healthcare. He noted that data science is transforming the way we understand and treat allergies.
The Vice President of Congresses, Mo Shamji, explained that the EAACI Congress 2024 is a chance for knowledge exchange between colleagues in the field, and offers a unique experience of learning, networking, and experiencing. Attendees had the opportunity to take part in over 150 sessions including cutting-edge abstract presentations, networking events, and practical workshops. In addition to the use of data science for the development of personalised medicine, key topics at this year’s congress were AI, allergen immunotherapy, immune modulators, biologicals, prevention of allergic diseases, novel treatments for allergy and asthma, innovative approaches in clinical trials, 'One Health', and more.
The award presentations commenced with the Clemens von Pirquet Award for Clinical Research, which was presented to Mariana Castells from Harvard Medical School, USA. Following this, the Daniel Bovet Award for Treatment and Prevention was awarded to
Philippe Eigenmann, University Hospitals of Geneva, Switzerland. Emma Guttman-Yassky from the Icahn School of Medicine at Mount Sinar, New York, USA, was then awarded the Paul Ehrlich Award for Experimental Research, and Carmen Vidal from the University of Santiago de Compostela, Spain, was recognised for her work with the Charles Blackley Award for the Promotion of the Speciality.
Each year, EAACI honours excellence in basic and clinical research by awarding the title of EAACI Fellow to members who have made exceptional contributions in their field. These fellows will constitute an elite advisory board, which the Academy will consult upon in the coming years. The EAACI Clinical Fellow was awarded to Santiago Quirce from La Paz University Hospital, Madrid; George Du Toit from King’s College London, UK, and Margitta Worm from Charité, Medical University, Berlin, Germany. To recognise excellence in basic research, the EAACI Research Fellow was awarded to Domingo Barber, University San Pablo, Madrid, Spain, and Liam O’Mahony, University College Cork, Ireland.
Gilles Augusto, from Insel Hospital, Bern, Switzerland, was presented with the Allergy Award, for his paper titled ‘In vitro data suggest that Indian delta variant B.1.617 of SARS-CoV-2 escapes neutralisation by both receptor affinity and immune evasion’, as this was the most cited article in the EAACI Allergy journal between 2022 and 2023.
To wrap up the inspiring Opening Ceremony, del Giacco presented two awards which recognise exceptional young scientists, to promote innovation and breakthroughs in allergy research. Firstly, the prestigious EAACI PhARF 2024 Award to Stefan Schülke from the Paul-Ehrlich-Institut in Langen (Hesse), Germany, for his work on immune modulation with the use of novel therapeutics and adjuvants. Secondly, Urszula Radzikowska from the Swiss Institute of Allergy and Asthma Research was awarded the EAACI AllergoPharma Research Award, for her key publication in the field of immune metabolism.
Read on for more highlights from EAACI 2024, and return next year for our coverage of EAACI Congress 2025 in Glasgow, under the new presidency of María José Torres!
Avocado Allergy: A Hidden Anaphylaxis Trigger
FOOD allergies are a leading cause of anaphylaxis, especially in adults, with seeds and nuts being the most commonly reported triggers, according to a study presented at EAACI 2024.
However, there is only limited information on other foods that can induce anaphylaxis. Avocado allergy, often associated with latex cross-reactivity, is not frequently documented in the literature. Only three allergenic molecules in avocados have been identified, and there has been just one recorded case of anaphylaxis caused by avocados.
This study discussed the case of a 28-yearold previously healthy patient who was admitted to the emergency department due to severe anaphylaxis. This condition included respiratory, cardiovascular, and neurological symptoms, which were triggered by accidental avocado ingestion. The patient required an adrenaline infusion and a 48-hour stay in the intensive care unit.
During the patient's assessment, four previous anaphylactic reactions were identified: three were related to avocado
and one to a particular SARS-CoV-2 vaccine. Allergy testing showed a serum IgE level of less than 40 kU, and a multiplex test did not detect any IgE value greater than 0.10 kU.
No specific allergen was identified, so a two-dimensional immunoblot was conducted using the patient's serum to detect selective IgE antibodies against avocado proteins. Eight proteins have been found to be reactive so far.
This case underscores the seriousness of avocado allergies and the necessity of thoroughly examining patients with a history of anaphylaxis. Some sensitising molecules may still need to be identified, making diagnosis and classification more challenging.
Allergy testing showed a serum IgE level of less than 40 kU, and a multiplex test did not detect any IgE value greater than 0.10 kU
Platelet-Leukocyte Interactions:
New
Mechanisms in Asthma Pathogenesis
RECENT research has indicated the role of free platelets and their complexes with leukocytes in the pathogenesis of allergic asthma. These results were presented at the 2024 EAACI Congress. Platelets have been observed to play significant roles in leukocyte extravasation, tissue remodelling, and lung function, as demonstrated in in vivo models of allergic pulmonary inflammation.
Platelet depletion effectively reduced circulating platelets during the first phase of the experiment, with recovery by
Patients with asthma often present with elevated levels of platelet-leukocyte complexes and experience mild thrombocytopenia upon allergen exposure, accompanied by an increase in plateletderived mediators. These findings suggest localised recruitment and potential interactions of platelets and their progenitor megakaryocytes with surrounding structural cells in the lungs. Both in vivo models and studies involving human patients reveal that platelets are instrumental in the development and exacerbation of allergic airway inflammation, yet their specific contributions remain not fully understood. A recent experimental series was conducted to investigate the role of platelets in the allergic airway inflammation phenotype in vivo and in patients with asthma in response to house dust mites (HDM).
The study utilised female BALB/c mice, treated intranasally with HDM extract or a phosphate-buffered saline control. To examine the effects of platelet depletion, mice were administered a control IgG or a platelet-depleting antibody intravenously prior to HDM or phosphate-buffered saline treatments.
Blood and bronchoalveolar lavage (BAL) samples were collected on specific days to quantify platelets and perform differential leukocyte counts.
Additionally, plasma IgE and BAL interleukin (IL)-4 and IL-13 levels were measured using enzyme-linked immunosorbent assays.
Results indicated that platelet depletion effectively reduced circulating platelets during the first phase of the experiment, with recovery by Day 14. HDM exposure induced significant blood and BAL eosinophilia, which was inhibited in the platelet-depleted group. Moreover, plasma IgE and BAL IL-4 and IL-13 levels were significantly elevated in the HDM group but not in the platelet-depleted mice. Complementing the animal studies, venous blood samples from patients with asthma and control volunteers were analysed using flow cytometry. Patients with asthma exhibited mild thrombocytopenia compared to controls, with higher frequencies of granulocytes and platelet-neutrophil and platelet-eosinophil complexes.
The established asthma model and human case-control studies provide a deeper understanding of platelet involvement in allergic airway inflammation and support further work expanding on platelet involvement. Future research aims to explore potential intervention strategies and candidate mechanisms for asthma treatment, paving the way for novel therapeutic approaches.
Pink Peppercorn: Safe for Patients with Pistachio Allergy Despite High Risk
A CASE study recently presented at EAACI 2024 revealed that pink peppercorn poses low allergenic risk for patients with a severe pistachio allergy, atopic dermatitis, and indolent systemic mastocytosis (ISM).
Tree nut (TN) allergies are among the most common IgE-mediated food allergies, affecting between 0.05–4.90% of the population. TN allergies often cause mild symptoms but can also lead to severe and potentially fatal reactions.
Pistachios, part of the Anacardiaceae family, share allergenic components with cashews, mangoes, and pink peppercorns. The close phylogenetic relationship among these plants results in varying cross-reactivity rates. However, the allergenic potential of pink peppercorns has remained underinvestigation until now.
In this study, a 38-year-old man with atopic dermatitis, coronary heart disease, and obesity experienced a severe anaphylactic reaction after consuming pistachios. He was subsequently referred to an allergy clinic for further evaluation. The allergological work-up included prick-to-prick testing with various Anacardiaceae family members and other cross-reactive allergens. Specific IgE levels were measured when commercially available. An oral food challenge with pink peppercorn was arranged due to its widespread use without mandatory labelling. The patient, who had elevated basal serum tryptase levels (76.8 µg/L), was referred to the Department of Haematology for further evaluation.
Although imaging tests returned normal results, a bone marrow biopsy revealed dense mast cells (approximately 10%) with spindle cell morphology exceeding 25%.
Despite the absence of the KIT816V mutation in peripheral blood and bone marrow, the patient was diagnosed with ISM. The prickto-prick testing results showed positive skin test reactions for pistachio, cashew, and pink peppercorn. Additionally, laboratory tests indicated high sensitisation to pistachio, cashew, and the major cashew allergen ana o 3, with specific IgE levels of 17.1 kUA/L. Specific IgE levels for other allergens tested negative. Despite the patient’s high-risk profile and the unavailability of specific IgE testing for pink peppercorn, an oral food challenge with up to eight peppercorns resulted in no adverse reaction.
In conclusion, the patient can safely consume pink peppercorn, highlighting its low allergenic potential even in high-risk individuals. This case underscores the importance of comprehensive allergological evaluation and patient education regarding cross-reactivity within the Anacardiaceae family. Furthermore, it emphasises the need for food manufacturers to provide adequate labelling to prevent accidental consumption by allergic individuals. The study calls for further research to fully determine the allergenicity of pink peppercorn and ensure the safety of allergic patients.
Tree nut allergies are among the most common IgE-mediated food allergies, affecting between
0.05–4.90% of the population
Molecular Tools in Support of Walnut Oral Immunotherapy
BEATRICE ALUTO,
Institute of Sciences of Food Production-CNR, Grugliasco, Italy, presented findings from a recent study at the 2024 EAACI Congress. This study aimed to investigate the molecular alterations that take place during walnut oral immunotherapy (OIT), to determine how these changes relate to the suppression of basophil activity.
Walnut OIT is designed to help individuals tolerate walnuts, reducing the severity of allergic reactions. Despite its increasing use, the mechanisms behind OIT and its long-term effects are not fully understood. The basophil activation test (BAT) is a key tool for assessing reductions in basophil reactivity during immunotherapy.
Proteins from raw, boiled, and roasted walnuts were extracted and analysed using BAT and LDS-PAGE. The immunoreactive bands were identified using HPLC-HRMS/MS. Patients' sera were periodically tested to monitor changes in specific IgE levels and basophil activity. The study followed 40 patients over 2 years, with serum samples taken every 3 months. The aim was to achieve a maintenance dose of 15 g of walnuts. Progress was monitored monthly using BAT.
In six patients, specific tests were conducted against walnut soluble and insoluble proteins. Immunoblotting revealed prevalent soluble proteins such as globulins, legumins, and vicilins. The analysis also suggested that oil bodies might contain oleosins.
Results showed a trend of IgE reduction after tolerance development, though the decrease was gradual and required longer monitoring. Basophil activity was significantly reduced, aligning with existing literature. Patients demonstrated improved walnut tolerance behaviour over time.
While patients exhibited reduced symptoms and improved walnut tolerance, the reduction in IgE was not immediate. Basophil activity decreased significantly, indicating the effectiveness of OIT. However, long-term monitoring is essential for a comprehensive understanding of OIT's effectiveness. This study highlights the importance of continued BAT analysis alongside OIT to ensure thorough treatment evaluation.
While patients exhibited reduced symptoms and improved walnut tolerance, the reduction in IgE was not immediate
Acquired Angioedema is Secondary to Underlying Diseases
EFFECTIVE management of acquired angioedema (AAE) can be achieved by treating the underlying disease, according to a study from Istanbul University.
of
405 patients 181 (44.69%) 6 (1.48%) had bradykininmediated angioedema, and were diagnosed with AAE with isolated recurrent angioedema,
AAE typically presents without a family history and has a later onset in life. Diagnosis requires measuring C1q levels and detecting autoantibodies to C1-INH. Researchers investigated the characteristics and treatment outcomes of patients with AAE, a rare, bradykinin-mediated recurrent angioedema which often occurs secondary to lymphoproliferative or autoimmune diseases.
This study presented at EAACI 2024 aimed to present the characteristics and treatment responses of patients with AAE who experienced isolated recurrent angioedema for more than 6 weeks between January 2018–January 2024. The demographic and clinical features of the patients with AAE were evaluated. Out of 405 patients with isolated recurrent angioedema, 181 (44.69%) had bradykininmediated angioedema, and six (1.48%) were diagnosed with AAE. The median age of patients with AAE was 48.5 years, with an interquartile range of 32.75–60.50 years, and half of the patients were female. The underlying conditions included lymphoid malignancy in five patients and an autoimmune disease in one patient. All patients with AAE had low C4 levels. C1-INH levels were low in five patients and normal in one; however, the patient with normal C1-INH levels had low C1-INH function. C1q
levels were measured in four patients, with three showing low levels and one normal.
The abdomen was the most commonly affected area in patients with AAE. Treatment for angioedema episodes included icatibant, C1-INH concentrate, or fresh frozen plasma, all of which were effective. During the investigation of a patient, long-term prophylaxis with danazol was required due to frequent attacks, leading to a decrease in attack frequency. Following the treatment of underlying diseases, three patients experienced no recurrence of angioedema, while others had attacks after an initial attack-free period. Post-treatment C4 and C1-INH levels were measured in two patients who remained attack-free after treating the underlying disease, and these levels were within the normal range.
The study highlights the importance of identifying and treating the underlying causes of AAE. Effective management of the underlying disease can lead to significant improvement in angioedema symptoms, and in some cases, complete resolution. The research underscores the need for continued patient monitoring and tailored treatment approaches to manage this rare condition effectively.
Out
Role of Milk Allergy in Childhood Dental Health
DENTAL caries poses a widespread health challenge for children, and milk and dairy products play a pivotal role in maintaining oral and dental health. The impact of cow's milk allergy (CMA) on dental health may be complex, and potentially influenced by changes in dietary patterns.
66 children
56.1% 39.3 months were male with a median age of diagnosed with IgE-mediated CMA, of which
This study presented at EAACI 2024 aims to identify potential risk factors affecting oral health in children with CMA and ascertain whether CMA itself poses a significant risk compared to healthy controls.
The research involved 66 children diagnosed with IgE-mediated CMA, of which 56.1% were male with a median age of 39.3 months. They were compared with 44 healthy controls, of which 61.4% were male with a median age of 42.5 months. Both groups were similar in age, gender distribution, maternal education levels, daily exposure to cariogenic foods, and biochemical markers.
Children with CMA demonstrated significantly reduced intake of lactose, calcium, fluoride, and phosphorus compared to their healthy counterparts (p<0.05) but consumed higher levels of vitamin D and glucose (p<0.05).
Sucrose intake although higher in the control group, did not reach statistical significance (p=0.117). Regarding dental health, the prevalence of early childhood caries, mean number of decayed, missing, and filled teeth (DMFT/DMF) scores for teeth and surfaces, and plaque index were comparable between the CMA and control groups. However, the CMA group exhibited a higher gingival index than the controls (0.8±0.3 versus 0.7±0.4, p=0.030). Exploring predictors of DMFT occurrence among patients with
CMA revealed no significant differences in breastfeeding duration, oral hygiene
practices, PI score, or biochemical markers between those with DMFT≥1 and DMFT: 0 (p>0.05). Notably, maternal education level emerged as a significant factor associated with DMFT≥1 (p=0.002), alongside a higher frequency of daily consumption of cariogenic foods, though this association did not reach statistical significance. Multivariate analysis identified several significant predictors of DMFT occurrence, including maternal education level, asthma diagnosis, serum 25-OH vitamin D levels, and dietary sucrose intake. Particularly, maternal education levels below eight years (odds ratio: 12.432, 95% CI: 1.160–133.261, p=0.037) and serum 25-OH vitamin D levels below 25 µg/L (odds ratio: 9.434, 95% CI: 1.682–53.549, p=0.011) were significantly linked to DMFT occurrence in children with CMA.
The study concludes that CMA itself does not appear to directly influence dental issues during early childhood, the development of early childhood caries in CMA-diagnosed children is associated with inadequate levels of 25-OH vitamin D and lower maternal education. Hence, maintaining effective preventive and therapeutic oral health programmes and monitoring vitamin D levels regularly in children with CMA is crucial.
Pollen Linked to Higher Virus Infection Rates
DURING the COVID-19 pandemic, an intriguing correlation emerged between airborne pollen concentrations and SARS-CoV-2 infection rates, particularly evident during the spring pollen season.
Prior research using a rhinovirus infection model demonstrated that pollen exposure diminishes the Type I and Type III interferon response of nasal epithelial cells, leading to heightened virus production.
Given the increasing prevalence of allergies and the continuous emergence of novel viral pathogens, understanding the implications of co-exposure to mixed bioaerosols, such as respiratory viruses and pollen, is crucial. This study, presented at EAACI 2024, aimed to explore the effects of co-exposure to pollen aerosols and coronaviruses on nasal epithelial cells. Researchers isolated nasal epithelial cells from donors with known atopy status using conchotomic surgery specimens. These cells were expanded and seeded into cell culture inserts, and airlift was performed after 5–7 days. After 4 weeks of culture at the air-liquid interface, the cultures exhibited typical differentiated nasal epithelium characteristics, including tight junctions, mucus production, and cilia formation. Individual exposure models for pollen and virus exposure were established first; subsequently, co-exposure experiments were conducted. Key readouts included cytokine and chemokine levels, and the production of infectious virus particles.
It was found that stimulation with ambrosia pollen significantly increased arlamin levels, and infection with human coronavirus 229E revealed peak infectiousness in nasal epithelial cells after 48 hours. Interestingly, exposure to various pollen types induced a higher pro-inflammatory response in nasal epithelial cells from female donors compared to male donors.
Infection with human coronavirus 229E revealed peak infectiousness in nasal epithelial cells after 48 hours
This study highlighted sex-based differences in pro-inflammatory cytokine production by nasal epithelial cells in response to pollen exposure. Additionally, the cytokine response varied between different stimulants, with pollen extracts inducing distinct cytokine profiles compared to more physiological aerosol exposures. These findings underscore the importance of considering co-exposure scenarios in understanding the immune response dynamics in nasal epithelial cells, which could inform strategies to mitigate the impact of respiratory viruses, especially in individuals with allergies.
KEY experts in allergy and immunology congregated in Valencia, Spain, for the European Academy of Allergy and Clinical Immunology (EAACI) Annual Congress from the 31st May–3rd June 2024. The scientific programme included a compelling session that unveiled the latest breakthroughs in food allergy therapy, including the OUtMATCH and PROTECT trials, and explored the critical role of the microbiome in allergy development.
THE ROLE OF ANTI-IGE IN THE MANAGEMENT OF FOOD ALLERGY
Robert A. Wood, The Johns Hopkins University School of Medicine, Baltimore, Maryland, USA, began by discussing the OUtMATCH (Omalizumab as Monotherapy and as Adjunct Therapy to Multi-Allergen Oral Immunotherapy in Food Allergic Children and Adults) trial, a Phase III trial designed to assess the safety and efficacy of omalizumab for reducing allergic reactions; specifically to peanut, cashew, egg, milk, and walnut.1 As explained by Wood, success in this trial was defined as the ability to consume a single dose of ≥600 mg protein (1,044 mg cumulative) without dose-limiting symptoms for peanut, and ≥1,000 mg protein (2,044 mg cumulative) for cashews, walnuts, egg, milk, hazelnut, and wheat.
Regarding trial design, OUtMATCH spanned three distinct stages, with total enrolment lasting approximately 4 years and 8 months. In the first stage, spanning 16–20 weeks, each participant was randomised to receive biweekly or monthly injections of omalizumab or placebo injection. An oral challenge was then performed, in which participants ingested small quantities of food allergen and researchers closely monitored for any indications of allergic reaction. Following this, some participants (n=60) enrolled in the Open Label Extension, assessing the long-term effects of omalizumab, whilst
the remainder (n=61–225) proceeded to second stage. The second stage, spanning 14–15 months, comprised three components; initially all participants received omalizumab injections, biweekly or monthly, for 8 weeks. The cohort was subsequently divided into two groups, one receiving multi-allergen oral immunotherapy (OIT) and omalizumab for 8 weeks, followed by placebo injections for 44 weeks, and the other group receiving 52 weeks of placebo OIT and omalizumab. Based on results of the prior stages, participants would be recommended allergen-containing diets, and their responses monitored, as part of the final stage.1,2
This is the first medicine ever approved to reduce allergic reactions to multiple foods following an accidental exposure
“This was a unique collaboration between NIAID, CoFAR, and industry,” Wood exclaimed. FDA approval of omalizumab was granted on the 2nd February 2024 for “IgE-mediated food allergy in adult and paediatric patients aged 1 year and older for the reduction of allergic reactions, including anaphylaxis, that may occur with accidental exposure to one or more foods.” Wood praised this result, highlighting that this is the first medicine ever approved to reduce allergic reactions to multiple foods following
an accidental exposure. The OUtMATCH trial marks a significant advancement in the field of allergy and immunology, combatting reactions to a plethora of allergens.
HOW CAN MANIPULATIONS OF THE GUT MICROBIOME INFLUENCE FOOD ALLERGY?
Susan Lynch, University of California San Francisco, USA, next took to the stage, sharing several compelling facts on the microbiome; 95% of our microbiota is located in the gastrointestinal tract, and there are approximately 1.3 times more microbes than human cells in the body. Referencing a 2023 study, 16S rRNA sequencing, coupled with metabolic analysis, revealed significant differences in the infant faecal microbiomes between those who did, and did not, develop
peanut allergies. For instance, infants with a peanut allergy exhibited depletion of Clostridium sensu stricto and elevation of Streptococcus bacterium. Two antiinflammatory short-chain fatty acids, butyrate and isovalerate, are additionally expressed at significantly greater levels in infants who go on to develop peanut allergies, compared to those who do not.3
Correlation does not equal causation; however, so how do we know these metabolic differences drive allergic conditions? To answer this question, Lynch cited a 2019 study from the Department of Pathology and Committee on Immunology, University of Chicago, Illinois, USA.4 Here, Nagler and colleagues took mice raised without a microbiome, known as germ-free mice, and inoculated them with the faeces of those allergic to cow’s milk. Interestingly, results revealed phenotypic features of the
allergy in those inoculated, underscoring the role the microbiome plays in allergy development. Possible factors suspected to influence this process include arachidonic acid, pyruvate, and linoleic acid metabolism. Notably, a significant enrichment of 12,13-diHOME, a lipid product of the linoleic acid metabolism, in the faecal sample of those with an allergy was observed.5
To better understand what caused enrichment of linoleic acid metabolite, Fujimura KE et al.5 performed shotgun metagenomic analysis. Two bacterial species, Bifidobacterium bifidium and Enterococcus faecalis, were found to encode an enzyme responsible for the breakdown of linoleic acid to 12,13-diHOME, known as epoxide hydrolase.5 As highlighted by Lynch, this finding is highly significant as it shows gut microbes directly drive the
production of lipids responsible for allergy development. Further research by Nagler and team identified that as the concentration of 12,13-diHOME lipid increases, the frequency of T regulatory cells decreases, as well as their capacity to secrete the antiinflammatory cytokine IL-10.5
BIOMARKER-DRIVEN APPROACHES TO MODULATE AND EVALUATE NOVEL THERAPEUTICS IN ALLERGIC DISEASES
Mohamed Shamji, Imperial College London, UK, began by summarising the prevalence, clinical symptoms, and management of peanut allergy. Affecting approximately 2% of the Western population, and associated with the highest rates of accidental exposure, peanut allergies are a
prominent global health concern. Current recommended management comprises a combination of strict allergen avoidance and having a pre-loaded adrenaline autoinjector (AAI) readily on hand.
Touching on existing treatments, Shamji spoke of treatments such as omalizumab and peanut sublingual immunotherapy (SLIT). As a sublingual therapy, Peanut SLIT medication is placed under the tongue and has shown promise in treating toddlers who are peanut allergic. Despite these efforts, Shamji stressed the unmet need for novel therapeutic innovations.
Virus-like particles (VLP) are nanoscale structures comprising of viral proteins, but are non-infectious as they lack viral genetic material. As highlighted by Shamji, VLPs offer great therapeutic potential for allergic diseases. A novel VLP platform, for example, was recently developed, based on the cucumber mosaic virus and containing tetanus toxoid universal T cell epitope TT830-843, to enhance T helper cell-dependent IgG responses. This vaccination approach was tested in three scenarios: against IL-5 to treat insect-bite hypersensitivity in horses,6 against IL-31 to treat atopic dermatitis in dogs,7 and notably against Fel d 1 in cats to reduce allergic
symptoms of owners.8 In all cases, there was a clear reduction in immune reactivity as a result.
Within Shamji’s lab, the VLP-Peanut001 was assessed in ex vivo following a successful pre-clinical phase. Exposing T helper 2 (Th2) cells and dendritic cells, in a dosedependent manner, to VLP Peanut resulted in a downregulation of transcription factor GATA3 and inhibition of proliferation of Th2 and Th2a cells. This finding is significant as it demonstrates that VLP Peanut can actively lower immune hyperactivity. VLP Peanut promoted significant proliferation of CD19+ B cells, and exhibited reduced ability to induce FcɛRI and FcɛRII-mediated responses.
Based on the ex vivo trial success, the first-in-human Phase I clinical trial, VLP101 (PROTECT), was subsequently launched. Results revealed that VLP Peanut is welltolerated when given as a skin-prick test, giving hope to a novel therapeutic on the horizon. The trial had two parts. In Part A, healthy adults (n=16) were divided into four groups of four and given increasing doses of VLP Peanut subcutaneously, while peanut-allergic adults (n=6) received increasing concentrations of VLP Peanut via skin prick tests. In the double-blind part, peanut-allergic adults (n=24) were
divided into four groups and treated with escalating subcutaneous doses of VLP
Peanut or a placebo.
References
1. Wood RA et al. Protocol design and synopsis: Omalizumab as monotherapy and as adjunct therapy to multiallergen OIT in children and adults with food allergy (OUtMATCH). J Allergy Clin Immunol Glob. 2022;1(4):225-32.
2. Wood RA et al. Omalizumab for the treatment of multiple food allergies. N Engl J Med. 2024;390:889-99.
3. Chun Y et al. Longitudinal dynamics of the gut microbiome and metabolome in peanut allergy development.
CONCLUSION
Overall, this session presented significant advancements in the management of food allergies, showcasing the evolving landscape of the field, and stressing the potential of both pharmacological and microbiome-targeted therapies to improve patient outcomes.
J Allergy Clinical Immunol. 2023;152(6):1569-80.
4. Feehley T et al. Healthy infants harbor intestinal bacteria that protect against food allergy. Nat Med. 2019;25(3):448-53.
5. Fujimura KE et al. Neonatal gut microbiota associates with childhood multisensitized atopy and T cell differentiation. Nat Med. 2016;22(10):1187-91.
6. Fettelschloss-Gabriel A et al. Treating insect-bite hypersensitivity
in horses with active vaccination against IL-5. J Allergy Clin Immunol. 2018;142(4):1194-205.
7. Bachmann MF et al. Vaccination against IL-31 for the treatment of atopic dermatitis in dogs. J Allergy Clin Immunol. 2018;142(1):279-81.
8. Thoms F et al. Immunization of cats against Fel d 1 results in reduced allergic symptoms of owners. Viruses. 2020;12(3):288.
Transforming Management of Indolent Systemic Mastocytosis With Precision Medicine
This
symposium took place as part of the European Academy of Allergy and Clinical Immunology (EAACI) Congress held in Valencia, Spain, between the 31st May–3rd June 2024
Speakers: Massimo Triggiani,1 Iván Álvarez-Twose,2 Frank Siebenhaar3,4
1. Division of Allergy and Clinical Immunology, University of Salerno, Italy
2. Institute of Mastocytosis Studies of Castilla-La Mancha (CLMast) Virgen del Valle Hospital, Toledo, Spain
3. Institute of Allergology, Charité – Universitätsmedizin Berlin, Germany
4. Fraunhofer ITMP, Immunology and Allergology, Berlin, Germany
Disclosure: Triggiani has received honoraria as a speaker/advisor from Blueprint Medicines, Cogent, and Istituto Gentili. Álvarez-Twose has received research funding and honoraria as a speaker/advisor from Blueprint Medicines and Novartis. Siebenhaar has received research funding and/or honoraria as a speaker/advisor from Allakos, Blueprint Medicines, Celldex, Cogent, Escient, GSK, Granular, Invea, Moxie, Noucor, Novartis, Sanofi/Regeneron, Third Harmonic Bio, and UCB.
Acknowledgements: Medical writing assistance was provided by Nicola Humphry, Nottingham, UK. Thanks are given to the presenters of the sessions summarised in this article.
Disclaimer: Avapritinib is approved by the European Medicines Agency (EMA) for the indication of indolent systemic mastocytosis with moderate-tosevere symptoms inadequately controlled on symptomatic treatment. Not all products or indications of products are approved in certain regions or countries. Please consult your local prescribing information. Any data regarding non-Blueprint Medicines products are based on currently available public information at the time of the symposium. The symposium was not intended for non-healthcare professionals, including nurses.
Keywords: High disease burden, indolent systemic mastocytosis (ISM), precision medicine, KIT D816V mutation, tryptase, urgency to treat.
Support: The publication of this article was funded by Blueprint Medicines Switzerland GmbH, who reviewed the content for medical accuracy. The views and opinions expressed are exclusively those of the speakers.
Meeting Summary
This symposium, held on the first day of the 2024 European Academy of Allergy and Clinical Immunology (EAACI) Congress, aimed to broaden clinicians’ understanding of indolent systemic mastocytosis (ISM) diagnosis, the tools available to help assess the disease burden and severity of symptoms, and the use of symptomatic therapies and novel precision medicines.
Speakers described the hallmark symptoms of ISM as typical skin lesions, anaphylaxis and other mast cell-mediator release symptoms, and bone mass loss. Serum tryptase testing and screening for KIT D816V mutation using high-sensitivity PCR assays were considered key elements of ISM diagnosis, though bone marrow study becomes essential for diagnostic confirmation.
A stepwise approach to symptomatic management was recommended, with the caveat that symptomatic treatments are used off-label for ISM. It was noted that polypharmacy is often required to achieve adequate responses, and that novel therapeutics are needed in patients with inadequately controlled disease, highlighting the remaining unmet need.
Speakers stressed that the success of ISM therapy should be measured primarily by symptom improvement, and that validated tools are needed to assess a broad range of patient-reported symptoms and quality of life. Several current and upcoming tools for this purpose were described.
Clinical trial data of several precision medicines for ISM were described. These included avapritinib, recently authorised by the European Medicines Agency (EMA) for use in adults with ISM with moderate-to-severe symptoms inadequately controlled on symptomatic treatment, and investigational medicines bezuclastinib and elenestinib.
The overall message of the symposium was that, in this era of precision medicine, the emergence of novel targeted treatments brings an opportunity to transform the management of ISM.
INTRODUCTION
Systemic mastocytosis (SM) is a rare myeloid neoplasm characterised by clonal proliferation and accumulation of neoplastic mast cells in various organs.1,2 Activated mast cells release pro-inflammatory mediators, which can result in severe and often unpredictable symptoms, including life-threatening anaphylaxis.2 The indolent form (ISM) is the most common subtype of SM, representing approximately 90% of SM cases.1
Massimo Triggiani, Professor of Internal Medicine at the Division of Allergy and Clinical Immunology, University of Salerno, Italy, explained that mast cells are unique among blood cells in expressing high levels of the KIT receptor at all stages
of maturation.3 In the vast majority (approximately 95%) of SM cases, the primary driver of disease is KIT D816V mutation, which results in increased proliferation and activation of mast cells,1 and this provides an opportunity for targeted treatments.
Over the past few years, major advances have been made in developing precision medicine approaches for ISM, with the emergence of KIT-targeted tyrosine kinase inhibitors (TKI).4-7 To make the best use of these opportunities, Triggiani stressed that a precision medicine approach to therapy needs to begin with accurate diagnosis and the use of patient-reported outcome measures to assess individual patient experience and disease burden.8
PRECISION MEDICINE BEGINS WITH ACCURATE DIAGNOSIS: HALLMARK SYMPTOMS AND DIAGNOSTIC PARAMETERS FOR INDOLENT SYSTEMIC MASTOCYTOSIS
Because mast cells have multiple activating receptors, and release a wide range of proinflammatory and vasoactive mediators,9 patients with ISM can experience a broad spectrum of signs and symptoms (Figure 1).10
Iván Álvarez-Twose, Haematologist at the Institute of Mastocytosis Studies of CastillaLa Mancha (CLMast), Virgen del Valle Hospital, Toledo, Spain, explained that ISM is a highly heterogenous subtype of SM, and this can present a challenge for timely diagnosis. Indeed, the average time from initial symptoms to diagnosis is 6 years.11
Despite the wide range of signs and symptoms, Álvarez-Twose emphasised several hallmark symptoms that are often associated with ISM.
Skin Lesions
These are the most common signs of SM, observed in over 80% of patients.12 Patients with ISM commonly present with typical, small, monomorphic, maculopapular, brown or red skin lesions (mastocytosis in the skin [MIS]).12 The majority of adult patients with MIS will have a systemic involvement, e.g., SM with mast cells present not only in the skin but also in other organs such as the bone marrow (BM), gastrointestinal tract, spleen, or liver.2,12 As a general rule, all adult patients with MIS should undergo a BM aspirate and biopsy to confirm the ISM diagnosis.12 The Fuchs risk score proposed by the European Competence Network on Mastocytosis (ECNM) can be used to predict SM in patients with MIS.13 It includes serum tryptase levels, bone symptoms or osteoporosis, and constitutional or cardiovascular symptoms, with a score >2 being associated with high probability of SM.13
Anaphylaxis and Other Mast CellMediator Release Symptoms
Other patients may present without skin lesions but with different symptoms related to the release of mast cell mediators.13 Mast cell activation (MCA) symptoms are normally acute and systemic, with involvement of ≥2 organ systems, such as the skin, gastrointestinal tract, respiratory system, or cardiovascular system.13-15 MCA can cause a broad spectrum of symptoms, such as diarrhoea, vomiting, flushing, pruritus, hypotension, rhinorrhoea, and shortness of breath, among other manifestations.15 Anaphylaxis is also common (up to half of adult patients) and often severe (approximately 48% of reactions) in SM.14,15 In patients with MCA symptoms but without MIS, the REMA (Red Española de Mastocitosis [Spanish Mastocytosis Network]) score can be used to predict SM with high sensitivity and specificity.16 The REMA score considers sex, serum tryptase levels, pruritis, hives/ angioedema, and presyncope/syncope.16
Bone Mass Loss
Some patients with ISM can present with bone fractures due to osteoporosis.6,17 Osteoporosis is quite common in patients with ISM, it can occur in one-third of patients during the course of the disease, and its prevalence may be underestimated.17 Overall, ISM is diagnosed in 0.5% of patients with osteoporosis, but ISM incidence is 10 times higher in young men with osteoporosis (>5%) and should raise high suspicion of SM in this population.18
KIT D816V mutation leads to constitutive activation of the KIT receptor, and abnormal proliferation and accumulation of mutated mast cells in various organs.3,8 Activated mast cells release various mediators, including tryptase, a highly specific marker for mast cells.8,19 These two biomarkers, KIT D816V mutation and serum tryptase, can be measured in peripheral blood and serve as key elements of SM diagnosis.9 The highsensitivity PCR assays (e.g., droplet digital PCR or allele-specific oligonucleotide PCR) are extremely useful for the detection of KIT D816V mutation in peripheral blood
Figure 1: Clinical signs and symptoms associated with indolent systemic mastocytosis.10
Patients with ISM may experience a spectrum of signs and symptoms
from patients with SM. Next-generation sequencing should not be used for screening of the KIT D816V mutation due to lower sensitivity.20,21 Finally, a complete BM study should be performed to confirm the diagnosis of SM.12
Álvarez-Twose highlighted the value of flow cytometry for the diagnosis of SM, as it can be useful for the identification, enumeration, and characterisation of neoplastic BM mast cells even when they coexist with normal BM mast cells.22
Diagnosis of SM requires one major and one or more minor, or at least three minor criteria from the following:23
Major Criteria
• Multifocal dense infiltrates of mast cells (≥15 mast cells in aggregates) in BM biopsies or extracutaneous organs
Skin
Rash
Flushing
Itching
GI symptoms
Diarrhea
Abdominal Pain
Nausea
Vomiting
Minor Criteria
• ≥25% atypical or spindle-shaped mast cells
• KIT-activating KIT gene mutation (e.g., D816V) in BM biopsies or extracutaneous organs
• Aberrant CD2, CD25, and/or CD30 expression on mast cells
• Baseline tryptase ≥20 ng/mL
Algorithms for the diagnosis of SM are available in the literature and can help to sub-classify SM into six subtypes of the disease, including ISM.9,24 Moreover, Álvarez-Twose shared that the GEMAST app (Euromedice, Educiones Médicas SL Badalona, Spain) has been developed and can be downloaded free of charge, which can help in the identification, diagnosis, classification, and prognostic stratification of patients with SM.
DISEASE BURDEN IN ISM: USING PRO TOOLS TO ASSESS THE INDIVIDUAL PATIENT EXPERIENCE
Frank Siebenhaar, Assistant Professor at the Institute of Allergology, Charité – Universitätsmedizin Berlin, Germany, stressed that around 40% of patients with ISM experience moderate-to-severe mastocytosis-related symptoms, and a similar proportion experience a moderateto-severe quality of life (QoL) impairment, representing a substantial unmet need.25,26
This has a negative impact on a patient’s ability to work; one-third (32%) of patients with non-advanced SM need to reduce their working hours, 14% reported having been on medical disability, and 12% reported that they do not work at all due to their disease (N=98).27 This impact occurs despite patients taking multiple medications to control their symptoms; approximately twothirds (75%) of patients with ISM have taken ≥4 classes of drugs to treat their disease, representing a substantial polypharmacy burden (Blueprint Medicines Corporation, data on file [REF-00686]).
Siebenhaar explained that there are several patient-reported outcome measure tools that can be used to assess disease burden in ISM, covering areas such as symptom burden, QoL impairment, and disease control. These tools can enable clinicians and patients to monitor the disease.
Symptom burden can be assessed using the Mastocytosis Activity Score (MAS), the Mastocytosis Symptom Assessment Form, or the Indolent Systemic Mastocytosis Symptom Assessment Form (ISM-SAF). The MAS assesses nine items across three domains: skin (itching, wheals, and flushing symptoms); gastrointestinal tract (diarrhoea and abdominal pain); and “other” (muscle/joint pain, fatigue, headache, and concentration). Each item scores from 0–4 points by severity, and total points are normalised to a maximum total score of 100.
QoL impairment can be assessed using one of the Mastocytosis Quality of Life questionnaires: MC-QoL or MQLQ. The MCQoL questionnaire assesses 27 items across four domains: symptoms, functioning/social
life, emotions, and skin. Each item scores from 0–4 points by severity, and total points are normalised to a maximum total score of 100.
Another tool has recently been developed to assess disease control in adults with cutaneous mastocytosis or ISM: the Mastocytosis Control Test (MCT; manuscript in preparation). This is a short simple test which assesses five items, each of which can score from 0–4 points. The maximum score is 20 points, and a score of ≥13 reflects a well-controlled disease.
Each of these tools (MAS, MC-QoL, MCT) are available in several different languages, free-of-charge for routine clinical use and non-commercial research.28 The MASTHAVE Mastocytosis App is also being developed as a collaboration between the Global Allergy and Asthma Excellence Network (GA2LEN), MOXIE, and Blueprint Medicines, which will include many of these tools and allow patients to track their SM disease burden in a digital app and share their data with their clinician.
SYMPTOMATIC MANAGEMENT OF ISM: ARE WE DOING ENOUGH?
In SM, greater disease burden (aggressiveness) is associated with more prominent organopathy, whereas lesser disease burden is associated with more prominent mast cell mediator symptoms (such as skin, gastrointestinal, cardiovascular, and neurologic symptoms).29 Consequently, symptoms of mast cell mediator release have been observed in 91% of patients with ISM (N=76).30
Common presenting symptoms of MCA include flushing and pruritis of the skin, dyspnoea and wheezing in the respiratory system, abdominal cramps and diarrhoea in the gastrointestinal system, and hypotension and syncope in the cardiovascular system, as well as anxiety and cognitive impairment.31 In severe cases, anaphylaxis can occur, and this condition has been observed in 22–49% of adults with mastocytosis.31 Anaphylaxis in the general adult population is most likely to
be triggered by food or medication, whereas in patients with SM, Hymenoptera sting (e.g., bees, wasps, or ants) is the most common trigger.32
Álvarez-Twose explained that a stepwise approach to symptomatic management is generally used for ISM in clinical practice, though he stressed that all symptomatic treatments are used off-label.
The basic management for ISM involves prophylactic avoidance of known triggers, and therapy with antihistamines to block the H1 and H2 receptors.9
Additional therapies and measures may be required, such as proton-pump inhibitors or mast-cell stabilisers to manage refractory gastrointestinal symptoms; mast-cell stabilisers, aspirin, or anti-leukotriene to control refractory flushing, tachycardia, or hypotension; UV-light therapy for refractory skin symptoms; or corticosteroids to manage other refractory symptoms.9 In some patients with ISM who experience refractory symptoms, additional specific therapies may be appropriate, such as adrenaline (for anaphylaxis), anti-IgE therapy, and TKIs.9
The adjuvant approaches in ISM include calcium/vitamin D supplements, bisphosphonates, or denosumab to manage osteoporosis; life-long venom immunotherapy to control Hymenoptera venom allergy; and anxiolytics, antidepressants, or psychotherapy to address stress-induced anaphylaxis, depression, or anxiety.33
Overall, a combination of symptomatic treatments rather than a single agent may be needed to achieve adequate control of symptoms.9 There remains an unmet need for patients with inadequately controlled disease despite the use of multiple drugs.2
PRECISION MEDICINE ERA IN ISM: CURRENT AND EMERGING TARGETED TREATMENTS
Over the last few years, several novel precision medicines have been (or are being) developed to target human mast cells.34 These include inhibitors of mastcell mediators or their secretion, such as lirentelimab (a siglec-8 inhibitor), and ibrutinib (a Bruton’s tyrosine kinase [BTK] inhibitor), and agents that deplete mastcell numbers, such as barzolvolimab (a KIT antibody) and the TKIs that target the KIT receptor: avapritinib, bezuclastinib, elenestinib, masitinib, and midostaurin.35
Siebenhaar stressed that symptom improvement is the gold standard by which the success of ISM therapy should be measured, since clinical studies have shown that tryptase levels do not correlate with symptom severity at baseline.6 Therefore, validated tools are needed to assess response to therapy and symptom improvement across a broad range of symptoms.
Avapritinib*
*Avapritinib is authorised by the EMA for use in adult patients with ISM with moderate-to-severe symptoms inadequately controlled on symptomatic treatment (ava EMA SmPC). This medicinal product is subject to additional monitoring.
Avapritinib is a tyrosine kinase inhibitor designed to selectively target the KIT D8161V mutation, the main driver of SM disease.7 It was authorised by the EMA for use in ISM based on results from the PIONEER clinical study (NCT03731260),36 a randomised, double-blind, placebocontrolled trial of avapritinib in adult patients with ISM.7
In PIONEER, the first randomised, doubleblind, placebo-controlled Phase II trial, patients with moderate-to-severe ISM (ISMSAF total symptom score [TSS] >28) were randomised, 2:1 to 25 mg avapritinib oncedaily (n=141) or placebo (n=71), both with best supportive care (BSC).4 The primary endpoint was the mean change in TSS (range 0–110) from baseline to Week 24.
Figure 2: Mean total symptom score absolute change from baseline to 24 weeks, individual Indolent Systemic Mastocytosis Symptom Assessment Form, by treatment group.37
Avapritinib 25 mg QD, 24 weeks, n=131
Avapritinib 25 mg QD, 48 weeks
TSM: total symptom score; QD: once daily.
Placebo, 24 weeks, n=66
Figure 3: Percentage change in mean Mastocytosis Quality of Life questionnaire component score from baseline to Week 24.4,37
https://clinicaltrials.gov/study/NCT03731260) systemic mastocytosis; QD, once daily; SAF, Symptom Assessment Form; SE, standard error; TSS, total symptom score. al. AAAAI 2023; Oral presentation, abstract number: 627; 2. Gianetti MP et al. AAAAI 2024; Poster number: 783. de mastocitosis sistémica indolente (MSI) está aprobada por la EMA pero no está autorizada en España. Avapritinib (AYVAKYT) está comercializado las indicaciones de mastocitosis sistémica avanzada (MS avanzada) y tumores del estroma gastrointestinal (GIST) con mutación PDGFRA
*p≤0.05; BSC, best supportive care; MC-QoL, Mastocytosis Quality of Life questionnaire.
*p≤0.05
BSC: best supportive care; MC-QoL: Mastocytosis Quality of Life questionnaire; QoL: quality of life.
Key secondary endpoints included safety, the proportion of participants achieving ≥30% and ≥50% TSS reduction, and the proportion of participants achieving >50% reduction in serum tryptase, BM mast cell
burden, and blood KIT D816V variant allele fraction (VAF).4 The 5-year open-label extension aims to collect data on long-term efficacy and safety.4
Overall, avapritinib significantly improved ISM symptoms and underlying mast cell burden versus placebo, indicative of disease modification.4 The primary endpoint was met for this trial.4 At Week 24, the mean decrease from baseline in TSS was 15.6 points (95% CI: -18.6 to -12.6) with avapritinib versus 9.2 points (95% CI: -13.1 to -5.2) with placebo (p=0.003).4
Symptom reduction was observed across all domains of the ISM-SAF with avapritinib versus placebo, including abdominal pain, nausea, diarrhoea, skin spots, itching, flushing, fatigue, bone pain, brain fog, headache, and dizziness (Figure 2),37 and symptom improvement with avapritinib was maintained up to Week 48.4 After 24 weeks, patients treated with placebo switched to avapritinib and achieved similar improvement in symptoms at Week 48.4
Avapritinib also showed reductions in all biomarkers of mast cell burden. Over 24 weeks of treatment, 54% of patients treated with avapritinib versus none (p<0.001) in the placebo group achieved >50% reductions in serum tryptase, 53% of patients treated with avapritinib versus 23% (p<0.001) in the placebo group achieved >50% reductions in BM mast cell burden aggregates, and 68% of patients treated with avapritinib versus 6% (p<0.001) of the placebo group achieved >50% reductions in KIT D816V VAF.4 Importantly, at baseline, 62% of patients in the avapritinib group used ≥3 symptomatic treatments, and after 48 weeks of treatment, one-third of patients had decreased their BSC use and 4% were able to completely discontinue BSC, contributing to reduction in polypharmacy.39 During this same period, the QoL of patients treated with avapritinib also improved, with a decrease in the mean MC-QoL total score of 34% (95% CI: -40% to -29%) with avapritinib versus 18% (95% CI: -25% to -11%) with placebo.4 The changes in MCQoL component scores are shown in Figure 3.4 Siebenhaar also noted that avapritinib is the first treatment that can lead to improvement and even resolution of skin lesions in patients with ISM, which can have a big impact on patients’ QoL. After 24 weeks of avapritinib treatment versus placebo, the surface area of skin lesions
reduced by a mean of 37% versus 2% in the most affected skin region, and the colour of the skin lesions lightened in 86% versus 0%, respectively.40
Siebenhaar highlighted the favourable safety profile for avapritinib at 25 mg once daily after 24 weeks of treatment; oedemas (including oedema peripheral, face oedema, and periorbital oedema) were the most common adverse event (AE) in the avapritinib group (with an incidence ≥2 times that of placebo, not thought to be related to underlying ISM), occurring in 8.5%, 7.1%, and 6.4 %, respectively, of patients receiving avapritinib, and 4.2%, 1.4%, and 2.8%, respectively, of patients receiving placebo.4 The majority of AEs were of Grade 1–2 (70% versus 72%, for avapritinib versus placebo, respectively), and the frequency of serious AEs was lower in the avapritinib than the placebo group (5% versus 11%, respectively).4 AEs resulting in treatment discontinuation occurred in just 2% of patients treated with avapritinib and 1% of patients receiving placebo.5 Importantly, no new safety concerns were observed during the longer-term, openlabel evaluation (median follow-up of 18 months), with the most common treatmentrelated AEs consistent with those already reported.41
Precision Medicines in Clinical Development*
*Note that these medicines are not approved for ISM in the European Union (EU).
Bezuclastinib
Bezuclastinib is an investigational, selective KIT D816V TKI currently being assessed in the Summit clinical study (NCT05186753).42 Summit is a randomised, double-blind, placebo-controlled trial in adult patients with non-advanced SM (including ISM and smoldering SM) and inadequate symptom control despite BSC.5 In Part 1b of the study, patients were randomly assigned to 100 mg or 150 mg once daily of bezuclastinib plus BSC (each n=11), or to placebo plus BSC (n=12).43
Over the initial 12 weeks of treatment (data cutoff, 18 December 2023), bezuclastinib 100 mg was associated with significant symptom improvement, with a 41% mean improvement in MAS from baseline to Week 12, compared with a 21% mean improvement for placebo. Half (50%) of patients treated with 100 mg bezuclastinib achieved ≥50% improvement in MAS compared with no placebo patients.43 In addition, patients reported a significant improvement in QoL with MC-QoL total score with bezuclastinib 100 mg versus placebo (-24.9 versus -12.4, p=0.046).43
Bezuclastinib also elicited reductions across markers of mast cell burden.43 Of those patients with baseline tryptase ≥20 ng/mL, nearly all patients treated with bezuclastinib achieved <20 ng/mL (100% on 100 mg, 89% on 150 mg, and 0% on placebo). Among patients with detectable KIT D816V at baseline, ≥50% reduction in KIT D816V VAF was achieved by 100% of patients on 100 mg bezuclastinib, 89% on 150 mg bezuclastinib, and none on placebo). Among patients with evaluable BM, ≥50% reduction in BM mast cells was achieved by 86% of patients on 100 mg bezuclastinib, 78% on 150 mg bezuclastinib, and 40% on placebo.
The early data, after 12 weeks of treatment, show an encouraging safety and tolerability profile for bezuclastinib at 100 mg, with the majority of treatment-related AEs being low grade, no serious AEs and no dose reductions due to AEs.
Elenestinib
Another investigational TKI that selectively targets KIT D816V, elenestinib, is being assessed in the HARBOR clinical study (NCT04910685).44 HARBOR is a randomised, double-blind, placebocontrolled trial in adult patients with ISM
References
1. Bose P, Verstovsek S. Avapritinib for systemic mastocytosis. Expert Rev Hematol. 2021;14(8):687-96.
2. Lee HJ. Recent advances in diagnosis and therapy in systemic mastocytosis. Blood Res. 2023;58(Suppl 1):96-108.
and inadequate symptom control despite BSC.6,44 In Part 1 of the study, patients with a moderate-to-severe symptom score (based on ISM-SAF TSS) were randomly assigned 3:1 to 25 mg, 50 mg, or 100 mg once daily of elenestinib plus BSC (n=10, n=10, and n=9, respectively), or to placebo plus BSC (n=10).6
Over the first 12 weeks of treatment, clinically meaningful symptom improvement was observed for all dose cohorts; mean reduction from baseline in ISM-SAF TSS was 22.2% for placebo, 28.5% for elenestinib 25 mg, 31.8% for elenestinib 50 mg, and 33.6% for elenestinib 100 mg.6,45
Biomarkers of mast-cell burden also improved in a dose-dependent manner. Patients receiving elenestinib at 25 mg, 50 mg, and 100 mg versus placebo showed a mean percent changes from baseline for serum tryptase of 15.4%, -50.9%, and -68.4% versus +3.3%, for KIT D816V VAF of -37.5%, -70.4%, and -77.0% versus -2.5%, and for BM mast cells of -22.6%, -28.1%, and -57.9% versus -20.0%.6,45
After a median duration of treatment of 22 weeks, elenestinib was generally well tolerated at all dose levels. There were no treatment-related serious AEs, or AEs that led to drug discontinuation.45
CONCLUSION
Overall, the emerging precision medicine approaches targeting the primary driver of ISM, KIT D816V mutation, demonstrated encouraging efficacy and favourable safety profiles in patients with ISM, with improvements in symptom severity, mastcell burden and QoL.
3. Katayama N et al. Stage-specific expression of c-kit protein by murine hematopoietic progenitors. Blood. 1993;82(8):2353-60.
4. Gotlib J et al. Avapritinib versus placebo in indolent systemic mastocytosis. NEJM Evid. 2023;2(6):EVIDoa2200339.
5. Modena B et al. Initial results from summit: an on-going, 3-part, multicenter, randomized, double-blind, placebo-controlled phase 2 clinical study of bezuclastinib in adult patients with nonadvanced systemic mastocytosis (nonadvsm). J Allergy Clin Immunol. 2024;153(Suppl 2):AB224.
6. Tashi T et al. Elenestinib, an investigational, next generation KIT D816V inhibitor, reduces mast cell burden, improves symptoms, and has a favorable safety profile in patients with indolent systemic mastocytosis: analysis of the Harbor trial. Blood. 2023;142(Suppl 1):76
7. AYVAKYT® (avapritinib). Summary of Product Characteristics; November 2023. Available at: https://www.ema. europa.eu/en/documents/productinformation/ayvakyt-epar-productinformation_en.pdf. Last accessed: 14 June 2024.
8. Pyatilova P et al. Refined treatment response criteria for indolent systemic mastocytosis proposed by the ECNM-AIM Consortium. J Allergy Clin Immunol Pract. 2022;10(8):2015-24.
9. Valent P et al. Personalized management strategies in mast cell disorders: ECNM-AIM User’s guide for daily clinical practice. J Allergy Clin Immunol Pract. 2022;10(8):1999-2012.
10. Pyatilova P, Siebenhaar F. Measuring symptom severity and quality of life in mastocytosis. Immunol Allergy Clin North Am. 2023;43(4):751-62.
11. Mesa RA et al. Patient-reported outcomes among patients with systemic mastocytosis in routine clinical practice: results of the TouchStone SM Patient Survey. Cancer. 2022;128(20):3691-9.
12. Hartmann K et al. Cutaneous manifestations in patients with mastocytosis: Consensus report of the European Competence Network on Mastocytosis; the American Academy of Allergy, Asthma & Immunology; and the European Academy of Allergology and Clinical Immunology. J Allergy Clin Immunol. 2016;137(1):35-45.
13. Fuchs D et al. Scoring the risk of having systemic mastocytosis in adult patients with mastocytosis in the skin. J Allergy Clin Immunol Pract. 2021;9(4):1705-12.E4.
14. Brockow K et al. Anaphylaxis in patients with mastocytosis: a study on history, clinical features and risk factors in 120 patients. Allergy. 2008;63(2):226-32.
15. Gülen T et al. Selecting the right criteria and proper classification to diagnose mast cell activation syndromes: a critical review. J Allergy Clin Immunol Pract. 2021;9(11):391828.
16. Álvarez-Twose I et al. Validation of the REMA score for predicting mast cellclonality and systemic mastocytosis in patients with systemic mast cell activation symptoms. Int Arch Allergy Immunol. 2012;157(3):275-80.
17. Gaudio A et al. Hematological diseases
and osteoporosis. Int J Mol Sci. 2020;21(10):3538.
18. Gehlen M et al. Osteoporosis caused by systemic mastocytosis: prevalence in a cohort of 8392 patients with osteoporosis. Calcif Tissue Int. 2021;109(6):685-95.
19. Akin C. How to evaluate the patient with a suspected mast cell disorder and how/when to manage symptoms. Hematology Am Soc Hematol Educ Program. 2022;2022(1):55-63.
20. Arock M et al. KIT mutation analysis in mast cell neoplasms: recommendations of the European Competence Network on Mastocytosis. Leukemia. 2015;29(6):1223-32.
21. Hoermann G et al. Standards of genetic testing in the diagnosis and prognostication of systemic mastocytosis in 2022: recommendations of the EU-US Cooperative Group. J Allergy Clin Immunol Pract. 2022;10(8):1953-63.
22. Sánchez-Muñoz L et al. Flow cytometry in mastocytosis: utility as a diagnostic and prognostic tool. Immunol Allergy Clin North Am. 2014;34(2):297-313.
23. Valent P et al. Updated diagnostic criteria and classification of mast cell disorders: a consensus proposal. Hemasphere. 2021;5(11):e646.
24. Beyens M et al. Mastocytosis and related entities: a practical roadmap. Acta Clin Belg. 2023;78(4):325-35.
25. Siebenhaar F et al. Development and validation of the mastocytosis activity score. Allergy. 2018;73(7):1489-96.
26. Siebenhaar F et al. Development and validation of the mastocytosis quality of life questionnaire: MC-QoL. Allergy. 2016;71(6):869-77.
27. Mesa R et al. The Burden of systemic mastocytosis in the EU: evidence from the PRISM patient survey. Poster PCR136. ISPOR Europe, 12-15 November, 2023.
28. MOXIE. 2024. Available from: https:// moxie-gmbh.de/. Last accessed: 21 June 2024.
29. Pardanani A. Systemic mastocytosis in adults: 2023 update on diagnosis, risk stratification and management. Am J Hematol. 2023;98(7):1097-116.
30. Gülen et al. High prevalence of anaphylaxis in patients with systemic mastocytosis - a singlecentre experience. Clin Exp Allergy. 2013;44(1):121-9.
31. Gülen T. Management of mediator symptoms, allergy, and anaphylaxis in mastocytosis. Immunol Allergy Clin North Am. 2023:43(4):681-98.
32. González-de-Olano D, Álvarez-Twose.
Insights in anaphylaxis and clonal mast cell disorders. Front Immunol. 2017;8:792.
33. González-de-Olano D et al. Mast cell activation syndromes and anaphylaxis: Multiple diseases part of the same spectrum. Ann Allergy Asthma Immunol. 2020;124(2):143-5.
34. Lemal R et al. Omalizumab therapy for mast cell-mediator symptoms in patients with ISM, CM, MMAS, and MCAS. J Allergy Clin Immunol Pract. 2019;7(7):2387-95.
35. Kolkhir P et al. Understanding human mast cells: lesson from therapies for allergic and non-allergic diseases. Nat Rev Immunol. 2022;22(5):294-308.
36. Blueprint Medicines Corporation. (PIONEER) Study to evaluate efficacy and safety of avapritinib (blu-285), a selective KIT mutationtargeted tyrosine kinase inhibitor, versus placebo in patients with indolent systemic mastocytosis. NCT03731260. Available at: https:// classic.clinicaltrials.gov/ct2/show/ NCT03731260. Last accessed: 30 May 2024.
37. Gianetti MP et al. Avapritinib decreased symptom burden in patients with indolent systemic mastocytosis in the registrational double-blind, placebo-controlled PIONEER study. J Allergy Clin Immunol. 2024;153(Suppl 2):AB254.
38. Castells M et al. Efficacy and safety of avapritinib in indolent systemic mastocytosis (ism): results from the double-blind placebo-controlled PIONEER Study. Oral presentation 690. AAAAI Annual Meeting, 24-27 February, 2023.
39. Akin C et al. Reductions in polypharmacy for patients with indolent systemic mastocytosis on avapritinib. J Allergy Clin Immunol. 2024;153(Suppl 2):AB225.
40. Maurer M et al. Avapritinib improved skin findings in patients with indolent systemic mastocytosis (ISM) in the registrational, double-blind, placebo controlled PIONEER study. J Allergy Clin Immunol. 2024;151(Suppl 2):AB340.
41. Gianetti MP et al. Avapritinib decreased symptom burden in patients with indolent systemic mastocytosis in the registrational double-blind, placebo-controlled PIONEER study. Poster 783. AAAAI Annual Meeting, 24-27 February, 2023.
42. Cogent Biosciences, Inc. (Summit) A study to evaluate the efficacy and safety of CGT9486 versus placebo in patients with indolent or smoldering systemic mastocytosis. Available at: https://classic.clinicaltrials.gov/ct2/ show/NCT05186753. Last accessed: 30 May 2024.
43. Modena B et al. Initial results from summit: an ongoing, 3-part, multicenter, randomized, double-blind, placebo-controlled phase 2 clinical study of bezuclastinib in adult patients with nonadvanced systemic mastocytosis (NonAdvSM). Poster 694. AAAAI Annual Meeting, 24-27 February, 2023.
44. Blueprint Medicines Corporation. (HARBOR) Study to evaluate efficacy and safety of BLU-263 versus placebo in patients with indolent systemic mastocytosis. Available at: https:// classic.clinicaltrials.gov/ct2/show/ NCT04910685. Last accessed: 30 May 2024.
45. Tashi T et al. Elenestinib, an investigational, next generation KIT D816V inhibitor, reduces mast cell burden, improves symptoms, and has a favorable safety profile in patients with indolent systemic mastocytosis: analysis of the HARBOR trial. Presentation 76. ASH Annual Meeting and Exhibition, 10-14 December, 2023.
FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM
Closing Gaps in Hereditary Angioedema Management: Addressing Delays in On-Demand Treatment
This symposium took place on the 1st of June 2024 as part of the European Academy of Allergy & Clinical Immunology (EAACI) Congress held in Valencia, Spain
Chairperson: Douglas Jones1
Speakers: Thomas Buttgereit,2 Emily Carne,3 Danny Cohn4
1. Rocky Mountain Allergy, Asthma, and Immunology, Layton, Utah, USA
2. Institute of Allergology, Charité – Universitätsmedizin Berlin; Corporate Member of Freie Universität Berlin and HumboldtUniversität zu Berlin, Germany
3. University Hospital of Wales, Cardiff, UK
4. Amsterdam University Medical Center, the Netherlands
Disclosure: Buttgereit is a speaker/advisor for, and/or received research funding from, Aequestive, BioCryst, CSL Behring, GSK, Hexal, KalVista, Medac, Novartis, Pharming, Pharvaris, Roche, Sanofi-Aventis, Swixx BioPharma, and Takeda. Carne is a speaker and consultant for KalVista. Cohn is a speaker and/or consultant for Astria, BioCryst, CSL Behring, Intellia, Ionis Pharmaceuticals Inc, KalVista, Pharming, Pharvaris, and Takeda. Jones is a consultant and speaker for Takeda, Pharming, CSL, Genentech, and KalVista; he is also a consultant for Pharvaris.
Acknowledgements: Medical writing assistance provided by Caroline E. Cross, Reading, UK.
Disclaimer The opinions expressed in this article belong solely to the named speakers.
Support: The symposium and publication of this article was supported by KalVista Pharmaceuticals.
INTRODUCTION
Hereditary angioedema (HAE) is a rare genetic condition characterised by unpredictable episodes of cutaneous or submucosal swelling in different parts of the body, which can be life-threatening when affecting the upper respiratory tract.1
People with HAE are often highly anxious due to the burden of illness and treatment
they face, and this is compounded by the complex decision-making process they face every time they experience the first signs of an attack.
Treatment guidelines recommend that all patients with HAE always carry on-demand treatment, to use if they experience an attack.1 The guidelines also state that all HAE attacks should be treated as soon as possible.1
However, current on-demand treatments are administered parenterally, either intravenously or subcutaneously, and are associated with limitations that make it difficult for patients to follow treatment guidelines. As a result of delayed or nontreatment, patients continue to experience ongoing attack burden that negatively impacts their quality of life.
In this sponsored symposium, Chair Douglas Jones, Rocky Mountain Allergy, Asthma, and Immunology, Layton, Utah, USA, was joined by fellow HAE experts Thomas Buttgereit, Charité – Universitätsmedizin Berlin, Germany; Emily Carne, University Hospital of Wales, Cardiff, UK; and Danny Cohn, Amsterdam University Medical Center, the Netherlands.
Through a series of short presentations, discussions, and audience Q&A, the panel highlighted how better communication between healthcare professionals (HCP) and patients could encourage more patients to carry on-demand treatment all of the time, and treat all attacks early. Panel members also discussed how orally administered on-demand treatments, currently being tested in clinical trials, could help patients to treat attacks more quickly, and easily, and improve quality of life.
CHALLENGES WITH DELAYS IN ON-DEMAND TREATMENT
Douglas Jones
Jones opened the symposium by articulating the decision-making process that someone with HAE would go through if they entered the conference hall and started to experience a slight tingle in their lip or cheek. He described how this would be enough to start them worrying whether they were about to experience an HAE attack. They might be in conversation with a colleague, but at the same time, they would have to decide whether they should excuse themselves to find a private space to administer on-demand treatment, and potentially miss the opening presentation.
This typifies the dilemma everyone with HAE faces day-to-day, and contributes to feelings of anxiety and frustration, Jones explained.
Prompt treatment of HAE attacks is associated with a shorter time to resolution of symptoms and shorter total attack duration, regardless of attack severity.1,2
The current international World Allergy Organization (WAO) and European Academy of Allergy & Clinical Immunology (EAACI) treatment guidelines recommend that attacks are treated as early as possible, and that all patients have sufficient on-demand medication to treat at least two attacks and always carry on-demand medication.1
However, Jones asked: “Are patients following these guidelines?” Studies show that only 36% of patients always carry their on-demand treatment, and travel an average of 3.5 hours from home without their medication.3 Patients can delay up to 3.8 hours before treating attacks with ondemand medicine (KalVista Pharmaceuticals, unpublished data) and more than 40% of attacks remain untreated.4
“Clearly, there is a massive gap between what the guidelines say and what patients actually do,” Jones emphasised, inviting the panel to discuss this further, via a series of specific questions.
Why do patients delay, or forgo, treatment for HAE attacks?
People with HAE prefer to self-administer treatment in a private space. They would rather do so at home, and many do not carry the medication with them when they go out, Buttgereit explained. He added: “Individuals may have issues with the parenteral route of administration of the treatment,” and some experience injection site reactions. Others need help with injections and may have to attend hospital. This can lead to further treatment delays and contributes to the burden of treatment.
In addition, Carne said myths circulate among patients about when to treat attacks. “In the past, patients have been told to ‘wait and see’ and hold off with treatment. As clinicians, we need to dispel those myths.”
Cohn concurred, adding that previous guidelines recommended treating only severe attacks. “It is important that at every clinic visit, we remind patients that, in line with current guidelines, all HAE attacks should be treated as early as possible.”
Carne added that it is important to understand from each patient what their own personal reasons for delaying treatment are. They gave the example of a patient who has a needle phobia and will avoid both hospitals and self-treatment at all costs.
Jones agreed, saying: “In order for patients to trust us, and to trust the recommendations we are giving, we have to listen, so we know where they are and where we can guide them to.”
How do you discuss the benefits of treating attacks early with your patients?
“As nurses, we often have more time with our patients than the physician. We can listen to them and understand their life and the difficulties they face,” Carne said. This knowledge helps to create a shared care environment with collaborative decisionmaking between the healthcare team and the patient.
“It is also very important to help the patient understand that it is not risky to treat early. It is riskier to not treat when you should have done,” Carne emphasised.
Cohn agreed, adding: “Often patients will say, ‘This discomfort in my abdomen could be something else, let’s just wait.” When they finally decide to treat the attack, it has evolved, and the symptoms may be more severe and take longer to resolve. Patients need to be reassured that there are no significant risks or side effects to taking currently licenced drugs.
The panel agreed that patient education is an ongoing process and conversations around when and how to treat attacks
should take place at every clinic visit. Buttgereit highlighted the value of HAE specialist centres: “Here, the whole team, from the nurse to the physician, give the same information.”
What are the key takeaway messages and the call to action for HCPs who care for patients with HAE?
“The sooner the better for treatment,” Cohn reiterated. HAE is a potentially fatal condition. Early treatment allows patients to lead a normal life and do activities as and when they want to.
Buttgereit agreed and added that all HCPs should understand that HAE is a severe disease that affects quality of life and causes significant anxiety to patients. “All physicians should follow the guidelines: ‘Treat early, treat every attack,”1 Buttgereit said.
Jones went on to reiterate that HAE provokes anxiety in patients, because of the burden of disease and the burden of treatment. He described the patients’ attack journey (Figure 1), from trigger to attack progression and treatment.
The unpredictability of attacks and anticipation of on-demand treatment creates anxiety. The life-threatening nature of this condition also creates anxiety. Once triggered, patients often wait before treating an attack, asking themselves questions about the implications of treating or not treating. If the patient self-treats, they need to remain vigilant to check that symptoms subside, and at the same time, watch out for recurrences. Then, the attack itself may take multiple days to resolve (Figure 1).
Treating attacks early can help patients regain some control, explained Jones. “The decision to treat can make the situation more predictable. From that moment, the patient can take control, which helps to reduce anxiety.”
HAE ON-DEMAND TREATMENT CLINICAL TRIAL LANDSCAPE
Danny Cohn
The landscape for on-demand treatment for HAE is changing, explained Cohn. “We are facing a paradigm shift in on-demand treatments for HAE that are easier to administer,” they said. The first C1-inhibitor concentrates to treat HAE attacks were developed more than 40 years ago and until now, all on-demand medications have been administered parenterally. “Now we are seeing new products in clinical trials, including oral drugs to treat angioedema attacks,” Cohn explained. They then outlined recent and ongoing clinical trials of two new oral on-demand medications, deucrictibant and sebetralstat.
Deucrictibant
Deucrictibant targets the bradykinin B2 receptor to inhibit swelling in HAE.5 In a randomised, double-blind, placebocontrolled cross-over Phase II clinical trial, RAPIDe-1 study, 74 patients from 13 countries were enrolled and treated
with study drug or placebo.6 Primary and key secondary endpoints were met.6 HAE symptoms were reduced, and it took less time to relieve symptoms and resolve attacks, compared to placebo.6 There was also a reduction in the use of rescue medication and the drug was well tolerated.6
Sebetralstat
Sebetralstat is an oral plasma kallikrein inhibitor with rapid absorption after ingestion.7 The results of a Phase III randomised, double-blind, placebocontrolled trial of sebetralstat (KONFIDENT) have now been published.7 This was a 3-way cross-over study, with 136 patients from 17 countries randomised. Patients self-treated up to three HAE attacks with either 300 mg sebetralstat, 600 mg sebetralstat, or placebo.7 The trial was event-driven and there were 264 attacks before the trial was finalised.
Primary and secondary end-points were measured using patient-reported outcomes on the seven-point Patient Global Impression of Change (PGI-C) scale, and the five-point Patient Global Impression of
Figure 1: Illustrative impression showing anxiety and on-demand treatment burden during a hereditary angioedema attack.
Severity (PGI-S) scale. The primary endpoint was time to the onset of symptom relief, defined as a rating of ‘a little better’ on the PGI-C scale at two or more consecutive time points within 12 hours after the first administration of the trial agent.7 Secondary endpoints included time to reduction in attack severity and time to complete attack resolution.7 These were defined, respectively, as an improved rating on the PGI-S scale, with ratings ranging from ‘none’ to ‘very severe’, at two or more consecutive time points within 12 hours, and complete attack resolution (a rating of ‘none’ on the PGI-S scale) within 24 hours.7
More than half of patients self-administered the study medication within 1 hour of an attack starting, and a quarter of patients self-administered within 6 minutes.7 The time to beginning of symptom relief was much shorter in both sebetralstat groups (1.6 hours for 300 mg dose and 1.8 hours for 600 mg dose) compared to patients taking the placebo (>6 hours).7 In addition, the observed safety profile of sebetralstat was equivalent to that of placebo.7 In an ongoing open-label extension trial, KONFIDENT-S,8 initial data suggests that the median time from attack recognition to treatment is 9 minutes.8 Cohn finished his presentation by asking colleagues on the panel the following question:
Do you think the barriers to treatment for an oral drug are going to be different for patients when thinking about very early symptoms?
Jones responded by reminding the audience of the scenario of someone with HAE attending this symposium who is faced with a choice between leaving the discussion to find a private space to inject/ infuse medication, or being able to take a pill. “I think having an orally administered treatment changes the dynamic of when and how early to treat, and removes a barrier for patients,” they said.
Carne reiterated that patients already carry a burden of illness; therefore, anything that reduces the burden of treatment is important. “Removing a needle is reducing the burden of treatment,” Carne said.
“Being able to take a tablet means you don’t have to identify yourself as being someone with HAE,” Buttgereit added. Cohn also commented, saying: “It also gives patients more independence. They do not need to rely on HCPs or family members to help them.”
AUDIENCE Q&A
Jones invited questions from the audience, which included the following:
Currently, if we treat prodromal symptoms of an attack, it is off-label treatment. Should we redefine what an HAE attack is?
Carne acknowledged this is an important question and said, “If we are not clear on when to treat, how can we advise our patients?” Cohn’s view is that patients know when an attack is starting, and early signs might be invisible, for example, manifesting as fatigue, or irritability. “We need to define what a prodrome is. Why wait for a fullblown attack when you know the prodrome is going to evolve into an attack?”
It can be a challenge to persuade less experienced colleagues to advise patients to treat early. Do you think an oral medication will help remove a psychological barrier to treat? “Yes,” Carne said. “The threshold for treating with a tablet is going to be lower than for an injection.”
Buttgereit added: “We are trained to believe that intravenous treatment is the fastest way to treat, but now, on the horizon, we have something that is just as quick.” Cohn reminded the audience that it is the type of drug that ensures rapid effect, not the route of administration.
How will guidelines evolve as the paradigm shifts to early treatment of all attacks?
“Treat at the very first sign of anything that may lead to an attack,” Cohn suggested. The threshold to treat should be as low as
possible. Carne added that “patient power” is also key. “We have excellent HAE patient networks around the world and when we see treatments working, the pressure will be on to update the guidelines to reflect that.”
Will these new treatments change your recommendations to patients on taking long-term prophylactics (LTP)?
“That is difficult to predict, but at the moment, no, I don’t think so,” Buttgereit asserted. “The current guidelines recommend that treatment of HAE should be individualised, and all patients should be considered for LTP and carry on-demand treatments. Some patients experience breakthrough attacks despite being on LTP, so it is necessary to always keep on-demand treatment with you,” Buttgereit added. In addition, said Cohn: “Those patients that are otherwise well-controlled with infrequent, mostly mild attacks, may discontinue LTP if an oral on-demand option is available.”
CONCLUSION:
HOW DO WE CLOSE THE COMMUNICATION GAP IN HEREDITARY ANGIOEDEMA MANAGEMENT AND HELP OUR PATIENTS ADDRESS DELAYS IN ON-DEMAND TREATMENT?
The panel’s consensus view was articulated by Jones when he said: “We, as HCPs, need to communicate with patients, educate them, hear them, acknowledge them, help them feel understood. Empower them.”
Jones then summarised the discussions (Figure 2). Patients currently delay and forgo on-demand treatment, and yet we know they can benefit from treating attacks early. Faster time to attack resolution and recovery is important to patients,9 and new oral on-demand medicines are in the pipeline that should help to address this.6,7 All HCPs should ask their patients about the barriers they face to treating all attacks as early as possible; then, reinforce them to treat early, and emphasise the need to carry on-demand treatment at all times.
Figure 2: Summary.
References
1. Maurer M et al. The international WAO/ EAACI guideline for the management of hereditary angioedema. The 2021 revision and update. World Allergy Organ J. 2022;77(7):1961-90.
2. Maurer M et al. Hereditary angioedema attacks resolve faster and are shorter after early icatibant treatment. PLoS One. 2013;8(2):e53773.
3. Geng B et al. Understanding why hereditary angioedema patients often do not carry their on-demand treatment with them. Ann Allergy Asthma Immunol. 2023;131 (5, Suppl 1):S37.
4. Longhurst HJ et al. Real-world outcomes in hereditary angioedema: first experience from the Icatibant
outcome survey in the United Kingdom. Allergy Asthma Clin Immunol. 2018;14:28.
5. Lesage A et al. In vitro pharmacological profile of PHA-022121, a small molecule bradykinin B2 receptor antagonist in clinical development. Int Immunopharmacol. 2022;105:108523.
6. Pharvaris Corporate Presentation. Pioneering science for patient choice. Available at: https://ir.pharvaris.com/ static-files/d6931544-3964-4793bb81-8e123f9507ac. Last accessed: 5 June 2024.
7. Riedl MA et al. Oral sebetralstat for on-demand treatment of hereditary angioedema attacks. N Eng J Med. 2024;DOI:10.1056/NEJMoa231419.
8. Farkas H et al. Sebetralstat as oral
on-demand treatment for hereditary angioedema: interim analysis of the open-label KONFIDENT-S trial. Poster D1.246. EAACI Annual Meeting, 31 May–3 June, 2024.
9. Christiansen S et al. Delayed ondemand treatment of hereditary angioedema attacks: patient perceptions and associated barriers. J Allergy Clin Immunol. 2024;DOI: 10.1016/j.jaci.2023.11.297.
10. Manning M et al. Anxiety associated with on-demand treatment of hae attacks may result in suboptimal attack management. Ann Allergy Asthma Immunol. 2023;131(5, Suppl 1):S42.
11. Ogbogu P et al. Characterizing the negative impact of delayed on-demand treatment of HAE attacks. J Allergy Clin Immunol. 2024;153(2):AB94.
Abstract Review
Read on to learn more about one of the cutting-edge study presented at the European Academy of Allergy & Clinical Immunology (EAACI) 2024 Annual Congress. This abstract reveals the varied symptoms associated with hereditary angioedema, and its diagnostic complexities.
Hereditary Angioedema Type I in a 57-Year-Old Woman
Authors: M. Kikvidze,1,2,3 *N. Makharashvili2,3
1. Academician Nikoloz Kipshidze Central University Clinic, Tbilisi, Georgia
2. Raymann, Tbilisi, Georgia
3. Curatio Clinic, Tbilisi, Georgia
*Correspondence to Nutsamakharashvili.md@gmail.com
Disclosure: The authors have declared no conflicts of interest.
This abstract outlines the case of a 57-yearold Georgian woman referred to an allergist by a gastroenterologist due to a 10-day history of sudden-onset cramping, left lower quadrant abdominal pain, diarrhoea, and weight loss, accompanied by generalised oedema. The patient experienced an increased attack frequency of 20–25 episodes per year, occurring randomly without discernible triggers and typically resolving within 3–5 days. Symptomatic treatment with H1-antihistamines proved ineffective. The patient’s medical history revealed symptom onset at 2 years old, with an unspecified first episode, and at 8 years old she underwent bowel resection for diagnosed bowel obstruction. Significantly,
hereditary angioedema was prevalent in the family, affecting her brother (fatal laryngospasm at 25 years old), grandfather, two uncles, and a cousin.
MATERIALS AND METHODS
For this study, the authors conducted complement studies of C4 protein levels, C1 esterase inhibitor concentration and function, and total IgE level (Table 1).
RESULTS
Consequently, the patient was diagnosed with hereditary angioedema (HAE) Type I (Table 2). Management involved a routine medication regimen of danazol at 200 mg three times a day. The dosage was titrated to the usual maintenance dosage, supplemented by emergency guidelines.
CONCLUSION
This abstract highlights the diagnostic complexities associated with the often non-specific symptoms of hereditary angioedema, underscoring the need for a thorough medical history and meticulous laboratory assessments for precise identification and effective management of this challenging condition.
Key takeaways include that HAE is characterised by recurrent, genetically mediated angioedema associated with increased vascular permeability primarily due to bradykinin; common HAE attack
locations are the face, throat, abdomen, hands, feet, and genitals; and that attacks may be triggered by injury, stress, or even excitement, but may also appear for unknown reasons.
Table 1: Complement studies: C1-INH concentration, C1-INH function, C4, and total IgE.
C1 esterase inhibitor.
Table 2: Classification of the different forms of hereditary angioedema.
The following selected highlights explore several groundbreaking abstracts presented at the European Academy of Allergy & Clinical Immunology (EAACI) Congress 2024. Topics covered include a novel strategy to detect asthma with nanosensors, the impact of pollution on rhinitis, and advancements in treatment of hereditary angioedema.
Benefit of Synbiotics in Infants with Cow’s Milk Allergy
INFANTS with cow’s milk allergy (CMA) who consume an amino acidbased formula with added synbiotics exhibit beneficial changes in their gut microbial composition, reports a study presented at EAACI 2024.
Researchers assessed the impact of amino acid-based formulas with (AAF-S) and without (AAF) synbiotics on faecal shortchain fatty acids (SCFA) and branched SCFA (BCFA) over a period of 12 months.
Researchers assessed the impact of amino acid-based formulas with and without synbiotics
The study analysed faecal samples from children aged ≤13 months, all of whom had IgE-mediated CMA and were participants in the PRESTO study (NTR3725). Samples were collected at the start of the study, and again at 6, 12, 24, and 36 months. All samples were taken at least 60 minutes after feeding. The concentrations of SCFA and BCFA in these samples were measured using gas chromatography, and statistical comparisons between the AAF and AAF-S groups were performed using the Wilcoxon rank sum test.
Out of 169 randomised infants, faecal samples were collected from 161 (95%), with 85 (53%) assigned to the AAF group and 76 (47%) to the AAF-S group. The average age of the infants at baseline was 9.35±2.56 months. After 6 months of consuming the formula, children in the AAF-S group showed significantly lower median faecal propionate concentrations and a lower percentage of propionate relative to the total SCFA (acetate, butyrate, propionate) compared to the AAF group. Additionally, the AAF-S group had lower median faecal concentrations of valerate and BCFAs isobutyrate and
isovalerate. Conversely, the percentage of acetate from the total SCFA was significantly higher in the AAF-S group. No significant differences in faecal butyrate concentrations were observed at 6 months, nor were there differences in SCFA or BCFA at baseline or at 12, 24, and 36 months.
The study concluded that the inclusion of synbiotics in an amino acid-based formula results in faecal microbial metabolite profiles that closely resemble those observed in healthy, exclusively breastfed infants. The observed effects on SCFA and BCFA concentrations were transient, appearing only 6 months after starting AAF-S. This may be due to reduced consumption of AAF-S and increased intake of complementary foods as children grow older.
Novel Breath Test Improves Accuracy of Asthma Diagnosis
RECENT findings presented at EAACI 2024 demonstrate the potential of a novel point-of-care (POC) breath test for asthma diagnosis, utilising deep neural networks (DNN) and nanosensors to provide a non-invasive and accurate diagnostic tool.
The method shows promise for diagnosing paediatric asthma, which could enhance early intervention strategies
Standard asthma diagnosis relies heavily on detailed clinical history and physical examination, processes that can be subjective and inconsistent. To address the need for a more objective diagnostic method, researchers developed a breath test that analyses volatile organic compounds (VOC) in exhaled breath, combined with advanced machine learning techniques.
The study's cohort included 25 individuals, comprising 15 diagnosed with asthma and 10 healthy controls with no history of respiratory disease. Researchers collected end-tidal breath samples and analysed 13 VOC parameters using nanosensors. Principal component analysis was employed to identify key parameters that would inform the algorithm's learning process. The primary component of the diagnostic tool was a 13-layer deep neural network (DNN) model. This model was trained on a dataset of 688 data points, encompassing patient information, VOC biomarkers, and lung function parameters. The comprehensive dataset of a diverse range of parameters facilitated nuanced learning, enabling the DNN to classify respiratory health accurately.
The study's results indicate a high level of accuracy, with the model achieving a 93% accuracy rate and an area under the curve value of 0.95. These findings demonstrate the model's effectiveness in distinguishing between asthmatic and nonasthmatic individuals. Beyond its diagnostic capabilities, this breath analysis approach holds potential for asthma phenotyping and identifying the underlying drivers of inflammation. Researchers noted that the breath test could lead to the development of targeted therapies, including biologic treatments, offering more personalised care for asthma patients. Moreover, the method shows promise for diagnosing paediatric asthma, which could enhance early intervention strategies.
These findings led the authors to conclude that the integration of nanosensor technology with deep learning algorithms represents a significant step forward in asthma diagnosis. Furthermore, the VOC breath test not only improves diagnostic accuracy, but also has the potential to inform more tailored treatment approaches, thereby enhancing patient care and management.
Olfactory Training in Chronic Rhinosinusitis with Nasal Polyps
NOVEL research conducted at The First Affiliated Hospital of Nanchang University, China, has identified key factors that influence olfactory recovery in patients undergoing endoscopic sinus surgery for chronic rhinosinusitis with nasal polyps (CRSwNP).
The research presented at EAACI 2024 highlights the potential benefits of combining glucocorticoid therapy with olfactory training (OT) to improve postoperative outcomes.
The study enrolled 213 patients with CRSwNP who had undergone endoscopic sinus surgery, and divided them into two groups: those who experienced olfactory recovery (99 patients) and those who continued to suffer from olfactory dysfunction (114 patients). The research aimed to develop a predictive model for olfactory recovery using logistic regression and support vector machine approaches.
Within the olfactory dysfunction group, patients were randomly assigned to three treatment subgroups: glucocorticoid therapy alone (GC group, 38 patients), olfactory training alone (OT group, 36 patients), and a combination of both therapies (GCwOT group, 34 patients). Follow-up assessments were conducted at 1, 3, and 6 months post-therapy, evaluating outcomes with various clinical scores, including the Total score for Threshold, Discrimination, and Identification (TDIS).
Results indicated that combination of glucocorticoids and OT significantly
improved olfactory function in patients with eosinophilic CRSwNP (ECRSwNP) and reduced olfactory fluctuations. Notably, in the ECRSwNP group, the GCwOT group showed higher TDIS improvements at 3 and 6 months compared to the GC group. However, there was no significant difference compared to the OT group alone. For patients with non-eosinophilic CRSwNP, the GCwOT group showed better TDIS improvements at 1 month compared to the OT group alone.
The study concluded that age and olfactory cleft scores are critical factors influencing post-operative olfactory recovery. The researchers also emphasised that persistence in olfactory training for 6 months can yield significant improvements, particularly for patients unable to use steroids.
This research underscores the importance of personalised treatment plans for patients with CRSwNP and the potential of combining therapies to enhance recovery outcomes. The use of machine learning in developing prediction models marks a significant advancement in understanding and treating olfactory dysfunction post-surgery.
Combination of glucocorticoids and OT significantly improved olfactory function in patients with eosinophilic CRSwNP
Air Pollution Impacts Respiratory Health in Patients with Rhinitis
AIR pollution has a detrimental impact on respiratory health, particularly in individuals suffering from allergic rhinitis (AR) and non-allergic rhinitis (NAR), according to a recent study presented at EAACI 2024.
The study, conducted at Kirikkale University Faculty of Medicine, Türkiye, included 58 participants to explore the effects of air pollution during both clean (summer) and polluted (winter) seasons (45 patients with rhinitis; 13 healthy controls; age distribution: 30.4+9.4 years). Of individuals with rhinitis, one-third reported dyspnoea, and the other third had completely controlled symptoms. Participants underwent pulmonary function and bronchial provocation tests (BPT), alongside clinical and laboratory evaluations, to measure bronchial airway hypersensitivity, serum oxidant-antioxidant stress levels, and nasal symptoms.
Key findings from the study revealed that during winter, when air pollution levels were higher, the forced expiratory volume in 1 second (FEV1%) decreased across all groups. Notably, the decline was more significant in the NAR group compared to the AR and control groups. In winter, the NAR group experienced a reduction in FEV1% from 93.9±10.4 to 90.6±11.3 (P=0.026) and a decrease in total antioxidant stress levels from 1.6±0.2 to 1.51±0.15 (P=0.041) compared to the
summer. Similarly, FEV1% following BPT was shown to be lower in winter (P=0.020).
Despite the AR group showing a higher rate of positive BPT during polluted periods, the increase was not statistically significant. The study also found a negative correlation between changes in total nasal symptom scores and antioxidant stress indicators (r=0.284; P=0.039), suggesting that worsening nasal symptoms were associated with decreased antioxidant defences.
The research underscores the adverse effects of air pollution on respiratory health, particularly in individuals with rhinitis. This is the first study to evaluate the relationship between AR and NAR phenotypes and bronchial hyper-responsiveness through the oxidant-antioxidant pathways influenced by air pollution. The findings highlight the need for increased awareness and measures to protect vulnerable populations from the harmful effects of polluted air, which deteriorates respiratory function not only in patients with rhinitis, but also healthy individuals.
This is the first study to evaluate the relationship between AR and NAR phenotypes and bronchial hyper-responsiveness through the oxidant-antioxidant pathways
Real-World, Long-Term Effectiveness and Safety of Lanadelumab for Hereditary Angioedema
THE ENABLE study is an ongoing Phase IV, non-interventional, prospective, multicentre investigation evaluating the long-term effectiveness of lanadelumab in patients with hereditary angioedema (HAE) in real-world clinical settings.
Results from this interim analysis were presented at the 2024 EAACI Congress.
This interim analysis covers data from December 11th 2019–April 17th 2023, expanding on previously reported 24-month findings. The study involves patients aged ≥12 years with HAE Type I/II from 18 sites across Austria, Germany, Israel, Italy, Kuwait, Spain, and Switzerland. Participants are monitored for up to 24 or 36 months based on their enrolment date. The primary measure is the incidence rate ratio of HAE attacks post-lanadelumab initiation compared to the baseline period, while safety is assessed through treatmentemergent adverse events (TEAE).
Out of 140 enrolled patients (129 with Type I; 10 with Type II; 1 undifferentiated), 138
received lanadelumab. The mean age was 41 years, with a majority being female (62.3%) and White (97.8%). The mean time from HAE symptom onset to diagnosis was 8.8 years, and the average duration on lanadelumab was 603.6 days. Initially, 97.1% of patients were started on a biweekly dose, with 43.1% reducing to a monthly dose by month 36. The HAE attack rate dropped significantly from 3.70 attacks/month at baseline to 0.35 on treatment, with 65.2% experiencing a ≥90% reduction. Most TEAEs (84.0%) were mild or moderate, and unrelated to lanadelumab. There were no deaths or serious treatment-related TEAEs. The study confirms lanadelumab’s long-term efficacy in reducing HAE attacks, and a safety profile consistent with prior research.
The study involves patients aged ≥12 years with HAE Type I/ II from 18 sites across Austria, Germany, Israel, Italy, Kuwait, Spain, and Switzerland
Early-Life Infections: Risk of Asthma and Adverse Lung Function
REDUCING the number of common infections experienced in earlylife could be a strategy for paediatric asthma primary prevention, according to research presented at EAACI 2024.
Whilst the development of asthma has been linked to infections of the respiratory tract in early-life, details on the subtypes and burden of these infections, and their role in asthma development, are lacking.
Those who experience a higher infection burden (>16) had a significantly increased risk for developing asthma
Researchers from Copenhagen Prospective Studies on Asthma in Childhood (COPSAC), Gentofte, Denmark, used data from the COPSAC2010 birth cohort and generalised estimating equations to evaluate the association between early-life infections and their subtypes, with the risk of asthma in those aged 3–10 years, and lung function at 10 years.
In total, 662 children with prospectively registered daily diary entries of acute otitis media, acute tonsilitis, cold, fever, gastroenteritis, and pneumonia, between the ages of 0–3 years, with a diagnosis of
asthma between the ages of 3–10 years, were included in the study.
The analysis found that, on average, between the ages of 0–3 years, children experienced 16 infections, and those who experience a higher infection burden (>16) had a significantly increased risk for developing asthma between 3–10 years (adjusted odds ratio: 3.61; 95% CI: 2.39–5.45; P<0.001). This was driven by cold, fever episodes, gastroenteritis, and pneumonia (P<0.050), but not by acute otitis media or acute tonsillitis. This association between infections and asthma risk was higher in children with a diagnosis of allergic rhinitis at 6 years of age (P-interaction=0.046). Additionally, the study identified that increased infection burden was associated with reduced lung function and a greater fractional exhaled nitric oxide by the age of 10 years.
From the study findings, the authors concluded that primary prevention of paediatric asthma could include strategies aimed at reducing the burden of early-life infections.
Drug Allergy: Severity and Impact on Quality of Life
NEW data from the BIOGRIAL study were presented at EAACI Congress 2024.
The study set to explore the severity of drug allergy and quality of life (QoL) for the individuals involved.
Utilising data from 18 allergy-referral centres involved in the BIOGRIAL study in Spain, the authors analysed the frequency and severity of immediate allergic reactions to drugs in 337 patients. In total, there were 436 reported reactions, of which 54.1% (n=236) were secondary to nonsteroidal anti-inflammatory drugs (NSAID), 30.2% occurred following β-lactam antibiotic use, and 15.4% occurred as a result of other drug classes.
Reaction severity was graded using the Drug-adapted version of the Food Allergy Severity Score (D-FASS). Severe reactions were defined as Grade 4 (bronchial/laryngeal involvement) and Grade 5 (cardiovascular/neurological involvement). QoL was measured using the drug hypersensitivity questionnaire (DrHy-Q).
The findings revealed that severe reactions secondary to β-lactams were more common than severe reactions resulting from NSAID use. In the β-lactam group, 60.6% of reactions were severe, with 43.2% classified as Grade
5, compared to 38.6% of reactions being severe in the NSAID group, where 19.1% were classified as Grade 5. These differences in severity were significant (P<0.01).
Those with severe drug reactions had a worse QoL, particularly in the fear and insecurity domains
In terms of QoL, 145 individuals with NSAID allergy, 123 with β-lactam allergy, and 59 with other drug allergies completed the DrHy-Q questionnaire. This highlighted that those with severe drug reactions had a worse QoL, particularly in the fear and insecurity domains. Responses to the DrHy-Q questionnaires also revealed that QoL was worse for those with β-lactam allergic reactions than for those with other drug allergies (P=0.03).
The authors concluded that reaction severity is different between those with β-lactam and NSAID allergies, and that irrespective of drug type, those with severe allergic reactions have a worse QoL.
Deucrictibant: A New Therapeutic Option for Hereditary Angioedema
PROMISING results from a recent Phase II study pesented at EAACI 2024 have shown that deucrictibant, a selective antagonist of the bradykinin B2 receptor, may be effective for the treatment of hereditary angioedema (HAE), both as a preventative measure and on-demand.
HAE attacks, which are caused by excess bradykinin activating bradykinin B2 receptors, can significantly impact patients' quality of life. Therefore, these findings offer a valuable new therapeutic option for patients.
The CHAPTER-1 study (NCT05047185) evaluated the efficacy and safety of deucrictibant for long-term prophylaxis of HAE attacks. Conducted in two parts, the study involved 34 participants from Canada, Europe, UK, and USA. In part 1, participants received a double-blinded treatment with either a placebo or one of two doses of deucrictibant (20 mg/day or 40 mg/day) for 12 weeks. In part 2, participants had the option to continue with an open-label treatment of deucrictibant at 40 mg/day.
Health-related quality of life (HRQoL) was a key focus, assessed through the Patient Global Assessment of Change (PGAchange) and the Angioedema Quality of Life questionnaire (AE-QoL). The PGA-change measures overall changes in HRQoL on a five-point scale from ‘much worse’ to ‘much better’. The AE-QoL questionnaire, specifically validated for HAE, evaluates HRQoL across four domains: ‘nutrition’, ‘fatigue/mood’, ‘fear/shame’, and ‘functioning’.
In part 1 of the study, deucrictibant showed significant improvement in HRQoL. At Week 12, 80% of participants on 20 mg/day, and 78% on 40 mg/day reported feeling “much better” in the PGA-change assessment, compared to just 13% in the placebo group. All participants (100%) receiving 40 mg/ day of deucrictibant reported improvement, while 63% of the placebo group reported “no change.” Additionally, the AE-QoL scores showed marked improvements.
Participants on 20 mg/day and 40 mg/day of deucrictibant saw their scores improve by 19.0 and 25.9 points, respectively, compared to an 11.9-point improvement in the placebo group. The domains ‘fear/ shame’ and ‘functioning’ showed the greatest improvement with deucrictibant treatment.
The CHAPTER-1 trial results indicate that prophylactic treatment with oral deucrictibant for 12 weeks can lead to clinically meaningful improvements in the quality of life for individuals with HAE. The significant enhancements in HRQoL measures highlight deucrictibant's potential as an effective long-term treatment option for HAE.
Health-related quality of life was a key focus
Effect of Air Pollution Exposure in Pregnancy on DNA Methylation
MODULATION of the immune system, pulmonary disease exacerbation, and cardiovascular disease are known consequences of exposure to ambient air pollution.
However, the effect of this exposure on health in pregnant persons is sparse. New research presented at EAACI Congress 2024, endeavoured to explore the association between PM2.5 (particulate matter <2.5 μM) and DNA methylation in pregnancy.
When controlling for pregnancy status, 321 differentially methylated CpGs were found to be associated with PM2.5
In a case-control analysis, researchers looked at data from 54 pregnant individuals and 84 age-matched non-pregnant individuals. Using US Environmental Protection Agency data and an individual’s zip code, PM2.5 was calculated. Following extraction of DNA from peripheral blood mononuclear cells, DNA methylation was assessed via a custom asthma and allergy array that targeted functional CpG sites. After quality control and processing, the researchers looked at the relationship between PM2.5 and DNA methylation, pregnancy status, and the interaction between them.
When controlling for pregnancy status, 321 differentially methylated CpGs were found to be associated with PM2.5 levels. While controlling for PM2.5 levels, 17 differentially methylated CpGs were found to be associated with pregnancy. Interaction term for pregnancy and PM2.5 was found to be associated with 107 differentially methylated
CpGs. Moreover, genes located closest to the PM2.5 differentially methylated CpGs were enriched for microRNA pathways.
Overall, these preliminary results highlight associations between PM2.5, DNA methylation, and pregnancy; and indicate that pregnancy status modifies the PM2.5-DNA methylation association. The team concluded that further analysis and epigenetic research is needed to understand the mechanisms that underly microRNA dysregulation in pregnancy.
Congress Interviews
Experts in allergy and immunology discuss advancements in the field, including the use of modern skin tests in allergology and sublingual tablet immunotherapy for paediatric patients. Plus, a joint interview with the current and future presidents of the European Academy of Allergy & Clinical Immunology (EAACI) gives insight into the largest European medical association in the field.
Stefan Wöhrl Professor of Dermatology & Venerology, Medical University of Vienna, Austria
We have to reach out to other specialities to help us because there are simply too many patients to deal with
Your research spans dermatology, venereology, and allergology. What drew you to these areas, and how do they overlap?
In dermatology, the immune system is always an important player. We have a lot of hypersensitive reactions, and that's how I came into contact with allergology, via eczema. Delayed type (Type 4) allergy/ allergic contact eczema was my entrance into the field. Besides allergic contact eczema, eczema turns out to often be mediated by drugs, and the next step for me was to study drug hypersensitivity. Additionally, hymenoptera venom allergy in Austria is managed by dermatologists. Therefore, this was the second branch, taking care of these patients, mainly by allergen-specific immunotherapy with hymenoptera venom. This field also involves the management of anaphylaxis. Thinking about anaphylaxis not only involves IgE-mediated food allergy, but also mastocytosis and mast cell tumours. When I entered
medicine 25 years ago, it was not so clear that we would end up with a connection between mast cell biology, anaphylaxis, and venom. Nowadays, this field has expanded to also comprise various aspects of drug hypersensitivity.
Q2
Are there any particularly exciting sessions at the European Academy of Allergy and Clinical Immunology (EAACI) that you have attended, relating to your specialties?
This is what really has changed a lot. Drug hypersensitivity has always been a niche area of interest, and now we are having plenary sessions on β-lactam hypersensitivity. I think the main driver for us is that the diagnosis is wrong in most cases, and how to get rid of the false label penicillin-allergy. The real driver for this comes from another area of medicine, which is the bacterial resistance to antibiotic drugs. As we have no alternatives, we have to return to penicillin. There are just a few allergists in the world, and then there's 10% of
the population claiming to be, or being labelled as, ‘suffering from penicillin allergy’. So, it is very clear that allergists cannot cope with this alone. We have to reach out to other specialities to help us because there are simply too many patients to deal with. I think from this Congress, this is one of my major conclusions. We have now come to the point where we need to address this in a different way. We have to create simple standard operating procedures that can be understood by general practitioners, and by most specialists in internal medicine who can take the load of patients when there are simply too many.
Q3
Can you provide any insights into the future trends or directions that you think the fields of drug hypersensitivity and molecular allergology will take in the next decade?
I think what we will see in the future is, of course, what we see in many fields of medicine: a lot of new drugs. Biologics have also entered allergy, and the one very old drug, anti-IgE, is now finally used in a different way; for example, to take care of children with severe food allergies, we must not treat the allergy, but control anaphylaxis. Plus, we have modern high-dose sublingual allergen immunotherapy now, which has finally arrived in the paediatric field. So, in paediatric allergology we already have the licence for subcutaneous immunotherapy, but now also for modern sublingual tablet immunotherapy. I think this is another new aspect of this conference, that we have to use what is standard also in other medical specialties. We should prefer evidence-based therapy, and rely on drugs that have proven to be useful in studies, and not what has always been used in the
traditional setting. I think this is also another nice aspect, that now we have new licensed drugs also available for children.
Q4
In your last interview with us in 2018, you said that you felt atopic eczema was a largely overlooked topic within the field. Six years later, does this still hold true?
Six years ago, as a dermatologist, I was always a little bit anxious about what was going to happen with eczema, because psoriasis was exploding; every few months, they had a new drug for psoriasis. Now, finally, we are here for eczema; we have a lot of new drugs. However, in my point of view, we have a problem, and that is the price. Pricing is extremely high. We have a lot of new drugs for the many severe patients on the top of the pyramid, but what about the base? There, we
don't have many new treatments to offer, and that is a little bit of a strange feeling. If you go and listen to the lectures, you have the impression that nearly every patient is treated with a new, expensive biological or JAK-inhibitor drug. However, everybody knows that if we really followed this track, then we would simply crash our entire healthcare systems, because all these new drugs are too expensive. My feeling is that that we got a little bit out of balance; there are these few privileged patients who receive these new medicines, and then there are the many other underprivileged patients, for whatever reason, who don’t manage to get to the point where they can get access to the new medication. This is not very special about allergology. It's a problem with all medicines, that the old drugs are cheap, and the new drugs are innovative and at the same time extremely expensive, leading to disparities in access to treatment. To return to the original question, of course now we have JAK inhibitors for eczema reactions, we have a lot of biologicals, and we have, especially with anti-interleukins, a new way of understanding the pathophysiology of atopic diseases. We don't treat the eczema, we don't treat the rhinitis, we don't treat the asthma; we can treat the underlying allergy, and indirectly, we control all the different aspects of these allergic diseases.
Q5 How does EAACI increase awareness of different aspects of allergy and immunology, and what could they focus on more?
I think the most important thing about EAACI is that it brings together so many different specialties, as allergology and
clinical immunology in every single country are organised in a completely different way. This poses a great difficulty for pharmaceutical companies when they want to develop new drugs. It is difficult to find out whom to address and who is the person responsible in each country to see the right patients for this diagnosis. I think this is one of the great things about EAACI; bringing together these people. In most countries, allergology does not exist as an own specialty but only as a subspeciality, or allergology does not exist at all. Allergology is a small specialty, and although a decent proportion of the population is affected by allergic diseases, allergology is often not seen by healthcare politics. This makes an organisation like EAACI a very important player on political grounds to make allergology visible; it is big enough to make an impact.
Q6 Are there any research areas you feel merit greater attention at next year’s EAACI?
A thing, we haven't addressed until now is molecular allergology. This field is really evolving at high speed, so you never know what comes next. I think what we currently see, if we look at the molecular sensitisation pattern to food and inhalant allergens, is that now we can better understand what the specific molecular allergens are. However, what is still difficult is the sensitisation aspect; measuring specific IgE does not actually mean suffering from an allergy. For every allergy specialist or every clinician who treats patients, this is one of the most important things to understand. You have to find out which of the sensitisations that are detected with allergy tests have actual implications for the patient, and which ones remain
‘silent’, either because they will become an allergy sometime in the future, or were outgrown sometime in the past. Allergy tests are very sensitive, and they still will pick up sensitisations that have lost their meaning for the patient. This is, at the moment, a part of the problem that makes using molecular allergology a little bit complex. We get a lot of information, and we somehow have to filter it, to make it useful for the sake of the better management of the patient. At the moment, this is a lot of work. It remains to be seen how much AI can help us sort through this information in a better way. Currently, I'm a little bit critical about the usefulness of AI, and the reproducibility of AI for solving this puzzle in a better and more clinically relevant way. In my daily clinical practice, more information gathered with the help of molecular allergology from a single patient means to me that I need much more time for the individual patient, at least double or triple the time, than when I compare it with conventional extract-based diagnosis.
Another thing that is very important to me is that, although we have all these new modern tools, skin tests are the major work-horses in allergology: the skin prick test, the intradermal skin test, and also the patch test for late-type hypersensitivity, which is not a major topic at EAACI. We have the problem that these commercially available, standardised skin test substances are disappearing at a dramatic pace. On one hand, in Type 4 (delayed type) allergy, we don't have a replacement at the moment for the patch test, and on the other hand, in Type 1 allergy, the skin tests have one big advantage over in vitro molecular allergology testing. It is ready after 15 minutes, so you can discuss test results with the patient within 15 minutes, and you don't have to wait for laboratory results to come in the next day. After a skin test, the patient doesn't have to come back to the office for another appointment, and this saves a lot of time for the mostly easy cases in times of very limited resources. Let's make sure that we don't lose the skin test substances!
Q7 Lastly, what has been your key takeaway from this year’s Congress?
My key takeaway is that we should try to make it possible to de-label as many patients as possible with this false labelling of ‘penicillin allergy’. We somehow need to find out, for each country and each healthcare system, how we can move along with this. The conventional allergological approach is working well and is getting good results, but it is too time-consuming for the many falsely labelled patients. There are too many patients, and too few allergy specialists. We have to solve this problem by outreaching to other specialities and to general medicine. This is my personal key message.
Maria Torres2
1. President, European Academy of Allergy and Clinical Immunology (EAACI)
2. Secretary General, EAACI
What distinguishes EAACI? We are actually the ones who write the guidelines
As the largest medical association in Europe for allergy and clinical immunology, what distinguishes EAACI from other organisations in the field?
Stefano: Yes, EAACI is the largest organisation in the field of allergy and clinical immunology in the world, and it embraces not only the European national societies, but also international societies. So, it's called ‘European Academy’, but it welcomes groups of allergy scientists, researchers, and clinicians from all over the world. What distinguishes EAACI? We are actually the ones who write the guidelines, the position papers; we have an enormous responsibility, because our task is to tell clinicians what to do in their daily clinical practice. EAACI embraces everyone, from the top scientists in the field to the clinician who is working everyday with patients in the most remote office, in Europe or somewhere else. We are very proud of this, but it is also a very hard task.
Q2
What do you hope to achieve this year at EAACI, and what do you hope all the healthcare professionals present will take from this year’s Congress?
Maria: I think that they will learn that new technologies can be applied to absolutely everything. Not only for science, but also to carry out patient evaluations. Now, we know that there are probably not enough allergists everywhere to be able to diagnose and treat the increased number of patients that we are going to have. So, new technologies, like AI, can help a lot in diagnosing our patients. Even if they are in a remote place, if they
need advice, they will probably be able to contact another office to help with patient diagnosis and treatment. I think that this is the biggest message that we can take from this meeting.
Q3
EAACI 2024 will see an array of fascinating lectures presented by experts from around the globe. Are there any sessions that you are particularly excited about attending this year?
Maria: Well, I come from the field of drug allergy, so I mainly focus on that. There have been so many presentations on how we can diagnose our patients with data only coming from the patient’s clinical history; this will allow quick delabelling and will have a high impact in the health system.
Stefano: Yes, there are many, many fields in which we are very active, and there are excellent lectures and news in many specific fields. However, I think we can stick to the motto of the Congress: revolutionising patient care with AI and technology. So, all the lectures related to the application of AI in daily clinical practice or in research are really valuable: these kind of topics are very popular, but no one actually knows how to apply this into their daily practice. We are trying to understand and to learn; we know so far that there are still limits, that human beings still count a lot. I think that we have moved forward, but we are still not there, even if there are many fascinating insights at the Congress about this.
Stefano del Giacco1 and
Q4 As president, and future president, of EAACI, how do you hope to improve collaboration and knowledge sharing among international experts at the Congress?
Stefano: Well, collaboration is already ongoing. We have several programmes in which we collaborate with other societies. We have our sister societies, we have the national societies (NAS), we have the International Society Council (ISC). We collaborate with many, many stakeholders and societies including regulatory bodies, like the European Medical Association (EMA), and we are active even at the European Parliament. We are part of alliances at the European level and at the international level. We are really trying to uniform the knowledge and the perception of allergies as a serious problem, which sometimes it is not seen as. I think that collaboration is fundamental in this field;
otherwise, this will not fall on the right ears.
Maria: We, as a society, have many different specialties working together. From basic scientists to immunologists, to dermatologists, pure allergists, and nutritionists, we all work together to get the best diagnosis and treatment of allergic diseases. I think that this is a great advantage. We have also learned a lot during the pandemic, which was an opportunity to find new ways of diagnosing our patients, through telemedicine, teleconferences, etc., and this is the focus of this meeting. Now this has come to be with us, we need to get adapted to using it in the future.
Q5
Stefano, how has EAACI evolved during your presidency?
Stefano: First of all, I must say that the best achievement we got under my presidency is that we
came back to normal life, because we were still recovering from the pandemic. Many scientific academies and societies were suffering a lot. We were able to stay stable during the pandemic. Now, I can say that, with this Congress, we are really back to ‘normal life’, with an exceptional number of in-person attendees. This is a great achievement. In terms of evolution, I think that, talking about new technologies, we have created our EAACI Knowledge Hub, which is the place to go for people who want to have online learning in this field, and this is one of our best achievements. We invested a lot, but the results are now coming in, and are fantastic. I would say to someone who seeks education in allergy and clinical immunology that they should go to our Knowledge Hub. And, between many others, seeing smiles on the faces of our members after the dark time of the pandemic, is surely one of the best achievements.
There are probably not enough allergists everywhere to be able to diagnose and treat the increased number of patients
Q6
Maria, as the incoming president, what future developments do you envision for EAACI?
Maria: I hope to be able to continue what Stefano has already done. I think that one of the main tasks is focusing on embracing all of our members, to create a network: a network of specific topics, for example, a network of education, a network of research, and a network of clinical centres. Of course, one of the main points that we have to work hard at is to put the patients at the centre of all our activity.
Q7
What advice would you give to clinicians at the beginning of their careers entering the field of allergy and immunology?
Maria: I can say that the Academy offers a huge opportunity to learn; to learn science, to learn about clinics, to make friends, to meet colleagues, to travel. We have a lot of grants where they can go to learn how to do specific techniques in the best centre in the world. It is also a place where they have fun.
Stefano: Following on from what Maria said; first of all, I fully agree with her, of course. The EAACI junior membership is free until the age of 35 years. So, the first piece of advice I would give is to become an EAACI member. This is a beautiful specialty. As a junior doctor, you have to take care of it. The first years are the best ones to improve your knowledge, and to become a true allergist and clinical immunologist; we offer this possibility at EAACI, as Maria said, with travel grants and lots of educational opportunities. So, I would really say: work hard, follow EAACI, and the results will come together with great memories that you will carry on for life.
Performance Analysis of Non-invasive Biomarkers in the Treatment of Eosinophilic Oesophagitis
Introduction: Eosinophilic oesophagitis (EoE) is an emerging disease of the oesophagus. However, so far there are no fully validated biomarkers for diagnosis and monitoring. Moreover, research focuses on parameters that are not very useful and accessible for routine clinical practice. Thus, endoscopy remains the main method of follow-up in this population.
Methods: The team analysed the levels of total Ig E, absolute eosinophil count (AEC), eosinophil cationic protein, and immunoglobulin G4 in a cohort of 399 adult patients with EoE (without other oesophageal pathologies). After controlling for confounding factors, they compared patients with active EoE and those in remission (responders).
Results: It was observed that, in responders, the AEC was lower (p=0.014). Furthermore, in corticosteroid-controlled patients, total Ig E was lower (p=0.016); while in proton pump inhibitors, responders both absolute (p=0.007) and percentage (p=0.002) eosinophils were lower.
Conclusion: The team considers that AEC is probably the most accessible and useful marker for monitoring treatment response in EoE.
Key Points
1. Effective differentiation between active disease and remission in eosinophilic oesophagitis (EoE) is pivotal for guiding clinical management and enhancing outcomes for affected patients.
2. The study described is a prospective cohort study. In this type of study, the progression of variables (such as total IgE levels, eosinophil count, eosinophil cationic protein, and immuniglobin G4) is compared between patients with active EoE and those in remission over time to gain a better understanding of the disease and its clinical manifestations.
3. Total Ig E levels, eosinophil count, eosinophil cationic protein, and immuniglobin G4 are promising markers to distinguish between active and remission phases of EoE, offering potential for improved clinical monitoring and treatment management.
INTRODUCTION
Eosinophilic oesophagitis (EoE) is an immune-mediated condition affecting the oesophagus, clinically characterised by symptoms of oesophageal dysfunction and histologically marked by predominant eosinophilic inflammation.1 It has been reported to have a prevalence of 34.2 cases per 100,000 person-years, and an overall incidence rate of 4.4 new cases per 100,000 person-years.2 Onset can occur at any age, with a peak in adults aged 30–50 years.1,2 It is currently the most common cause of food bolus impaction in the oesophagus in patients attending the emergency department.1 Although conditions such as rhinitis, asthma, and eczema are more prevalent in this population, atopy has not been demonstrated as a predisposing factor.1,2 Various clinical presentations (phenotypes) and underlying pathogenic mechanisms (endotypes) have been recently described.3 Proton pump inhibitors (PPI), topical corticosteroids (TC), and an empirical diet (ED) can be offered as firstline anti-inflammatory treatments.1 Upper gastrointestinal (GI) endoscopy remains the gold standard for diagnosis and monitoring, involving multiple biopsies that reveal a density of ≥15 eosinophils per high-power field under light microscopy.1-3 Hence, the quest for new non-invasive biomarkers is a significant objective. In this study, the team compared variations in total IgE levels, absolute eosinophil count (AEC), eosinophil cationic protein (ECP), and immunoglobulin G4 (IgG4) values between patients with uncontrolled (active) EoE and those with controlled disease (remission).
MATERIALS AND METHODS
The team conducted a prospective analysis of patients aged 18 years or older who were diagnosed with EoE and treated at the allergy department of Hospital Universitario La Paz in Madrid, Spain. Patients were selected after excluding any concurrent oesophageal pathologies (as confirmed by the gastroenterologist unit). This study received approval from the hospital’s ethics committee under protocol number PI-5401.
Patients with a documented history of atopic comorbidities in remission or under control and who did not require systemic treatments, such as corticosteroids or biologics, were specifically included. Patients with concurrent medical conditions or undergoing treatments that could potentially influence the serum parameters under investigation were excluded from the study.
For the purpose of analysis, the patients were categorised into three groups based on their prescribed treatment regimens: PPIs Group, patients receiving omeprazole at a dosage of 20 mg every 12 hours; TC Group, patients administered fluticasone (Flixonase®) at a dosage of 400 µg every 12 or 24 hours; and ED Group, patients managed with an empirical diet comprising either three or six food groups, in accordance with the team’s clinical practice protocol. These food groups included milk, wheat, and egg, as well as legumes, nuts, and fish/seafood.
They assessed treatment response by performing upper GI endoscopy and collecting multiple biopsies. For patients in the PPIs group, response evaluation occurred at 8 weeks; whereas for those in the TC and ED groups, assessment was conducted at 12 weeks following the initiation of treatment.
All data processing procedures were closely monitored and overseen by our biostatistics department. In the descriptive analysis, we presented the variables as medians and interquartile ranges. They employed the Mann-Whitney test to compare variables, and statistical significance was established at a threshold of p<0.05.
RESULTS
The study included 399 patients. Table 1 consists of the description of the population’s characteristics. The study population was relatively young, with a median age of 33 years (interquartile range 23–42). A majority of the patients were male (74% [n=296]), and 76% of them (n=304/399) had a history of atopy. Furthermore, the majority of patients (78%
[n=272/351]) responded positively to one of the selected treatments. In Table 2, the team conducted a comparison of patients concerning remission histological criteria. It was observed that patients in remission (defined as having <15 eosinophils per high-power field) were generally older at the time of the study (p=0.019) and exhibited lower AEC values (p=0.014). Finally, Table 3 presents the variation in serum parameters based on the treatment received.
DISCUSSION
EoE is a chronic inflammatory disease whose diagnosis and follow-up currently require multiple oesophageal endoscopies.4 The identification of non-invasive, accurate, and reliable biomarkers remains a challenge.5 In this regard, Dellon et al.6 analysed a large panel of serum biomarkers but did not identify useful markers for the treatment of the disease. Reporting of new data on the pathophysiology of the disease has led to the identification of promising markers, although few can differentiate EoE from other atopic diseases.7 In addition, significant oesophageal infiltration of Ig G plasma cells and elevated levels of IgG4 have been identified in these patients, although their contribution to EoE is unclear.8,9 No robust and definitive biomarker for the management of EoE has yet been identified, although many of the data point to AEC and, more recently, ECP.4,5
General data for this study’s population (Table 1) coincide with the characteristics already described in these patients, such as association with multiple atopic comorbidities.4 Table 2 shows that in the responder group, patients were older at the time of the study (p=0.019); older age could improve adherence to treatment. AEC was also lower in responders (median 290 eos.×10E3/µL; p=0.014). While the percentage of eosinophils showed a nonsignificant trend (p=0.06). That difference is probably due to the low AEC. Perhaps in larger studies, this difference will be clearly significant. Thus, the team could propose an AEC value (both absolute and percentage)
at which EoE could be considered controlled or uncontrolled. In this regard, RodríguezSánchez et al.10 reported a significant decrease in eosinophils although they assessed patients treated with diet alone.
Schlag et al.11 reported a decrease in AEC and ECP after treatment with TC. Furthermore, Min et al.12 demonstrated an association between AEC and ECP in the diagnosis of EoE, although only AEC could predict oesophageal eosinophilia after TC treatment. Subsequently, Wechsler et al.13 reported that the combination of AEC, ECP, and other serum parameters was superior in the differential diagnosis of EoE. Doménech Witek et al.14 reported that serial determination of ECP would be useful in the follow-up of EoE, while Cengiz15 reported on the potential of ECP in the diagnosis of EoE. Despite the promising results of ECP,11,14 the team found no differences, probably due to the strict control of potential confounders during patient selection.
When analysing the markers with respect to their response to treatment (Table 3), it was observed that total IgE was significantly lower in patients responding to TC (p=0.016). This finding is interesting considering that the selected population had atopic comorbidities in remission or were fully controlled. This variable has been rarely investigated because IgE does not seem to be involved in the pathophysiology of EoE. Rodríguez-Sánchez et al.10 did not detect changes in total IgE or ECP, probably because their cohort was only treated with diet.
The team observed that AEC and percentage were significantly lower in patients who responded to PPIs (p=0.007 and p=0.002, respectively). Few articles report similar findings, given that most patients received empirical PPIs prior to the diagnosis of EoE. They believe that this type of drug may favour a noninflammatory environment, thus potentially explaining these findings.
Weidlich et al.8 observed higher levels of IgG4 in patients with EoE, although these decreased after treatment with TC. Rizvi et al.9 on the other hand, reported more
Table 1: General characteristics of the population.
frequent positivity of IgG cells among paediatric patients who responded to PPIs. This study reported no significant differences.
CONCLUSION
Consequently, despite the limitations in methodology, the data imply that AEC, particularly in patients treated with PPIs, represents a promising and readily accessible marker for monitoring treatment response in individuals with EoE. Nevertheless, additional studies are required to validate our findings.
Table 3: Comparison of markers by treatment group.
Eos % responders m (IQR)
(3.2–8.2)
% non-responders m (IQR)
(3.6–8.1)
IgG4 responders m (IQR) IgG4 non-responders m (IQR)
1. Lucendo AJ et al. Guidelines on eosinophilic esophagitis: evidence-based statements and recommendations for diagnosis and management in children and adults. United European Gastroenterol J. 2017;5(3):335-58.
2. Navarro P et al. Systematic review with meta-analysis: the growing incidence and prevalence of eosinophilic
oesophagitis in children and adults in population-based studies. Aliment Pharmacol Ther. 2019;49(9):1116-25.
3. Ruffner MA, Cianferoni A. Phenotypes and endotypes in eosinophilic esophagitis. Ann Allergy Asthma Immunol. 2020;124(3):233-9.
4. Grueso-Navarro E et al. Bloodbased biomarkers for eosinophilic esophagitis and concomitant atopic diseases: a look into the potential of
extracellular vesicles. Int J Mol Sci. 2023;24(4):3669.
5. Votto M et al.et al. Non-invasive biomarkers of eosinophilic esophagitis. Acta Biomed. 2021;92(S7):e2021530.
6. Dellon ES et al. Utility of a noninvasive serum biomarker panel for diagnosis and monitoring of eosinophilic esophagitis: a prospective study. Am J Gastroenterol. 2015;110(6):821-7.
7. Hines BT et al. Minimally invasive biomarker studies in eosinophilic esophagitis: A systematic review. Ann Allergy Asthma Immunol. 2018;121(2):218-28.
8. Weidlich S et al. IgG4 is elevated in eosinophilic esophagitis but not in gastroesophageal reflux disease patients. J Clin Gastroenterol. 2020;54(1):43-9.
9. Rizvi SA et al. Esophageal epithelial immunoglobulin G is an important marker for the diagnosis and management of pediatric eosinophilic esophagitis. JGH Open. 2022;6(6):402-7.
10. Rodríguez-Sánchez J et al. Effectiveness of serological markers of eosinophil activity in monitoring eosinophilic esophagitis. Rev Esp Enferm Dig. 2013;105(8):462-7.
11. Schlag C et al. Peripheral blood eosinophils and other noninvasive biomarkers can monitor treatment response in eosinophilic oesophagitis. Aliment Pharmacol Ther. 2015;42(9):1122-30.
12. Min SB et al. Longitudinal evaluation of noninvasive biomarkers for eosinophilic esophagitis. J Clin Gastroenterol. 2017;51(2):127-35.
13. Wechsler JB et al. Noninvasive biomarkers identify eosinophilic esophagitis: a prospective longitudinal study in children. Allergy. 2021;76(12):3755-65.
14. Doménech Witek J et al. Assessing eosinophilic cationic protein as a biomarker for monitoring patients with eosinophilic esophagitis treated with specific exclusion diets. World Allergy Organ J. 2017;10(1):12.
15. Cengiz C. Serum eosinophilic cationic protein is correlated with food impaction and endoscopic severity in eosinophilic esophagitis. Turk J Gastroenterol. 2019;30(4):345-9.
Thymoma-Associated Good Syndrome: A Case Report and Literature Review
Authors: Nurafiqah Farhana Muhd Yazid,1 *Ho Wen Chung,2 Nur Qystina Ahmad Senusi3
1. Faculty of Medicine & Health Sciences, Universiti Sains Islam Malaysia, Nilai, Malaysia
2. Faculty of Medicine & Health Sciences, Universiti Putra Malaysia, Serdang, Malaysia
3. Department of Medicine, Hospital Serdang, Malaysia *Correspondence to wenchung@upm.edu.my
Disclosure: The authors have declared no conflicts of interest. Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Thymoma is often associated with many other autoimmune disorders and clinical conditions. Good syndrome is one of the rare associations between thymoma and immune deficiency that occurs in both males and females in the 4th or 5th decade of life. Patients can present with various invasive encapsulated organisms, and opportunistic viral and fungal infections, due to immune defects. The authors report a case of a 57-year-old male with underlying thymoma and lichen planus which were diagnosed 3 years apart. He presented with atypical pneumonia during the COVID-19 pandemic, and was treated for multiple atypical infections, including cytomegalovirus and Pneumocystis carinii pneumonia. His immunological investigation panel revealed low IgA and IgG levels with normal IgM levels, and an overall deficient total B cell count. His CD4:CD8 ratio was reversed at 0.28. The patient recovered well after Ig replacement therapy once the Good syndrome diagnosis was made. The authors highlight the importance of a high index of clinical suspicion in dealing with this uncommon concomitant occurrence of Good syndrome during the COVID-19 pandemic for a swift and timely diagnosis and management. Immunological investigation panels, including T cell subsets, B cells, and quantitative Ig levels, should be considered routinely in patients with underlying thymoma presenting with opportunistic infections.
Key Points
1. Even during a pandemic, physicians should remain vigilant for rare immunodeficiencies such as Good syndrome, in patients experiencing refractory severe infections.
2. Ig levels should be assessed in patients with thymoma who present with unresolved infections.
3. Intravenous Ig replacement therapy is effective in treating Good syndrome.
INTRODUCTION
Thymoma-associated Good syndrome (GS) is a rare and intriguing clinical entity. It is characterised by the coexistence of thymoma and hypogammaglobulinaemia, leading to immune system dysfunction and invasive infections due to encapsulated bacteria, fungi, and viruses.1 It commonly occurs in both male and female adults in their 40s–60s.2 Many patients with GS also may have lichen planus involvement, which some authors have even included in the clinical features of GS. This is a case of a male patient with underlying thymoma, who was also receiving treatment for lichen planus, and presented during the COVID-19 pandemic with multiple opportunistic infections leading to the diagnosis of GS. He was successfully treated with intravenous (IV) Ig. The authors intend to highlight the diagnostic dilemma of atypical infections that could mimic COVID-19, which reminds us to have a high index of suspicion, and investigate thoroughly when encountering such atypical infections with poor response to antimicrobial treatment, more so in the background of underlying thymoma.
CASE REPORT
The patient is a 57-year-old male with an underlying prolapsed disc and thymoma. He was found to have a thymoma 4 years before presentation, after an incidental finding of widened mediastinum on a chest radiograph, done pre-operatively for a left elbow abscess and cellulitis. A contrastenhanced CT thorax done back then showed a large well-defined solid mass at the right lower anterior mediastinum measuring approximately 8.5×9.0×9.3 cm. A CT-guided biopsy reported thymoma type B2, but he defaulted on the subsequent follow-up. He also had a history of lichen planus involving oral mucosa and bilateral upper and lower limbs since approximately 7 months, and was on oral azathioprine 150 mg daily, as well as multiple courses of oral prednisolone.
He presented to the authors with a 1 month history of shortness of breath, and reduced effort tolerance associated with fever. He was tachypnoeic with Type 1 respiratory failure. The oxygen saturation was 78% on room air. White cell count was raised at 11.1×109 /L (reference range [RR]: 4.5–11.0×109 /L), c-reactive protein was 99.8 mg/dL (RR: 0.3–1.0 mg/dL), and erythrocytes sedimentation rate was 81 mm/h (RR: <15 mm/h). Both serum albumin and globulin levels were low at 29 g/L (RR: 35–50 g/L) and 19 g/L (RR: 23–34 g/L), respectively. The chest radiograph showed consolidation in both lung fields (Figure 1). Urgent CT thorax-abdomen-pelvis showed features of organising pneumonia with thymoma 6.9×4.8×7.6 cm, and no evidence of pulmonary embolism. He was treated for healthcare-associated pneumonia as he was admitted to another hospital for a prolapsed disc just 5 days prior. IV piperacillin/tazobactam was started along with IV dexamethasone due to suspicion of COVID-19 pneumonia. However, he continued to further deteriorate, needing invasive ventilation with PaO2/FiO2 ratio of 300. His nasopharyngeal swab for SARS-CoV-2 PCR was repeatedly negative three times.
He remained critically ill with persistent respiratory failure despite treatment escalation with IV meropenem, and additional IV amphotericin B and oral oseltamivir. Tracheal aspirate for respiratory infection panels was positive for Pneumocystis carinii pneumonia (PCP) DNA, and his serum cytomegalovirus (CMV) PCR was also positive. Serum anti-HIV antibody, hepatitis B surface antigen, and anti-hepatitis C virus antibodies taken were all negative, and the tracheal aspirate for tuberculosis GeneXpert turned out to be negative. IV trimethoprimsulfamethoxazole and IV ganciclovir were initiated. Given the presence of opportunistic infections with low globulin levels, a diagnosis of non-HIV-related secondary immunodeficiency was suspected.
His acetylcholine receptor antibody was found to be positive at 1.29 nmol/L (RR: <0.4 nmol/L). Serum Ig results came back with normal levels of IgM at 1.41 g/L (RR: 0.4–2.3 g/L), and low IgA and IgG at 0.59 g/L (RR: 0.7–4.0 g/L) and 1.03 g/L (RR: 7.0–16.0 g/L), respectively (Table 1). Both complement levels C3 at 0.77 g/L (RR: 0.5–0.9 g/L) and C4 at 0.14 g/L (RR: 0.1–0.4 g/L) were normal. T and B cell panels enumeration showed reduced B cells, Th cells, natural killer cells, and a low CD4:CD8 ratio (Table 2). Diagnosis of GS with subclinical myasthenia gravis (MG) was subsequently made. A cycle of IV Ig 0.4 g/ kg was initiated.
The prolonged intensive care unit stay was also complicated by upper gastrointestinal bleeding, pneumothorax secondary to barotrauma, Acinetobacter modestus, and extended spectrum β-lactamase Klebsiella pneumonia infection. He had undergone oesophagogastroduodenoscopy,
tracheostomy, chest tube insertion, and treatment with high dose IV ampicillin/ sulbactam for his intensive care unit stayrelated complications.
Following the treatment with IV Ig, he was able to be weaned off invasive ventilation to tracheostomy mask O2 10 L/ min supplementation. He then requested a transfer against medical advice to another healthcare facility for rehabilitation.
Although the presentation of this patient is typical of GS, he presented to the hospital during the COVID-19 pandemic. Consequently, he was treated with immunosuppressants such as dexamethasone, and underwent repeated nasopharyngeal swabs for SARS-CoV-2 PCR testing before any suspicion of opportunistic lung infection could be raised, ultimately leading to the diagnosis of GS.
Figure 1: Plain chest radiograph upon admission showing consolidation in both lung fields.
Table 1: Immunoglobulin, complement C3, and C4 level.
Parameters Result
Complement C3 (g/L)
Complement C4 (g/L) 0.14
from de Vries et al.3
DISCUSSION
GS was first reported by Good et al.4 in 1954, describing an association between thymoma and hypogammaglobulinaemia. The incidence of hypogammaglobulinaemia in patients with thymoma was approximately 6–11%. Most cases of GS are adult-onset affecting people from 40–60 years old, with a prevalence of one per 700,000 adults.2 The immunodeficiency may precede thymoma discovery. Some literature reported that the full syndrome is generally established within 6 years of the first presentation, characterised by severe or chronic infections, with or without autoimmune manifestations.1 This is consistent with the authors’ case, where the patient was diagnosed with thymoma 4 years prior, found out to have lichen planus 3 years later, and subsequently presented with severe opportunistic infections leading to the diagnosis of GS.
Clinical Features
The diagnosis of GS is challenging and requires a high index of suspicion in combination with immunological testing. Similar to X-linked agammaglobulinaemia
and common variable immune deficiency (CVID), GS commonly presents with recurrent sinopulmonary infection secondary to encapsulated organisms.1 GS was previously thought to be a subset of CVID with thymoma. However, in contrast with X-linked agammaglobulinaemia and CVID, opportunistic infections caused by CMV, mucocutaneous candidiasis, varicella zoster, human herpesvirus, and P. carinii have also been seen in GS.1 This is consistent with the authors’ case whereby the patient had respiratory failure secondary to PCP, and possibly CMV pneumonia. Apart from respiratory illness (74%), Jansen et al.5 reported that 35% of the studied GS population had gastrointestinal infections, and 21% had skin and soft tissue infections, followed by 15% with urinary tract infections. With regard to causative micro-organisms, bacterial infections account for 80% of the cases, followed by viral (23%) and fungal infections (26%).5
GS has been associated with autoimmune conditions such as pure red cell aplasia (31.3%), MG (27.7%), and lichen planus in 51.2% of patients.6 Relating to this, the authors’ patient was being treated for lichen planus 1 year before the current encounter
Adapted
Table 2: T and B cell panels enumeration.
NK: natural killer; Th: T helper.
and was found to have subclinical MG during admission. The most common form of lichen planus found in those with GS was the erosive type concerning 89% of cases, followed by reticulated plaque and hyperkeratotic plaque in approximately 21% and 11% of cases, respectively.7 In certain cases, LP lesions may be improved or resolved after thymectomy.8
One interesting aspect of this case is that since the patient presented with severe pneumonia during the COVID-19 epidemic, the initial diagnosis of COVID-19 was at the top of the list. Multiple reports have emerged linking the complicity of COVID-19 in patients with GS.9,10 Some also highlighted the diagnostic dilemma in dealing with an immunocompromised patient, and severe pneumonia that could mimic COVID-19
during this period of epidemic. Tehrani et al.11 documented that their patient with CVID was empirically treated for COVID-19 but turned out positive for PCP.
Laboratory Findings
Marked hypogammaglobulinaemia with reduced or absent numbers of circulating B cells is the most prominent immunological finding in GS. A study found that almost 100% of patients with GS have low serum IgG levels, 86% have low IgA, and 92.6% have low IgM levels.6 In the authors’ case, the patient had low IgG and IgA with normal levels of IgM. Other important alterations in the immune profile of GS are the inversion of CD4/CD8 T cell ratio, and reduction of T cell mitogen proliferative responses. Interestingly, opportunistic infections like
CMV infection and PCP can occur in the presence of significantly greater T cell numbers in the GS population.12 This was also seen in the authors’ patient, as his Th CD4 counts were 394 cells x106 /L, slightly lower than the normal range (432–1,976 cells x106 /L). This suggests functional T cell defects that are responsible for the development of these infections. The authors were unable to investigate further on lymphocyte proliferative response and specific antibody response to vaccination, as the patient decided to be discharged against medical advice.
Management and Prognosis
Complete surgical tumour resection with or without post-operative chemotherapy or radiotherapy reduces the risk of local invasion, and alleviates the associated autoimmune conditions. Nonetheless, the immunological irregularities are irreversible by the excision of the thymoma alone.6 This implies that hypogammaglobulinaemia stems from either an autoimmune or immunoregulatory process.13 Ig replacement therapy is used for antibody deficiency to control and prevent severe recurrent infections.
References
1. Tarr PE et al. Infections in patients with immunodeficiency with thymoma (Good syndrome). Report of 5 cases and review of the literature. Medicine (Baltimore). 2001;80(2):123-33.
2. Kabir A et al. Good’s Syndrome: time to move on from reviewing the past. Front Immunol. 2022;12:815710.
3. De Vries E et al. Patientcentred screening for primary immunodeficiency, a multi-stage diagnostic protocol designed for nonimmunologists: 2011 update. Clin Exp Immunol. 2012;167(1):108-19.
4. Good RA et al. Thymic tumour and acquired agammaglobulinemia: a clinical and experimental study of the immune response. Surgery. 1956;40(6):1010-7.
In terms of overall prognosis, median survival for patients with GS is 14 years with a mortality rate of 41%, which largely depends on the severity and type of complications.5 This mortality rate is undeniably higher than in CVID. However, note that the median age of GS diagnosis is much older, at 58 years old, compared to CVID, which is 30 years old for males and 33.5 years old for females.5 This large age gap in the presentation of the two conditions may also contribute to the overall prognosis.
CONCLUSION
Despite the COVID-19 epidemic, one should not only think about COVID-19, especially when the standard treatment does not show improvement. A high index of suspicion is pivotal in diagnosing GS, especially when there is a combination of thymoma and opportunistic infection. Serum IgG, M, and A can be performed routinely in patients with thymoma, with a more extensive study for those with opportunistic infections or other autoimmune associations. Ig replacement therapy is effective in treating immunodeficiency in GS.
5. Jansen A et al. Prognosis of Good syndrome: mortality and morbidity of thymoma associated immunodeficiency in perspective. Clin Immunol. 2016;171:12-7.
6. Shi Y, Wang C. When the Good syndrome goes bad: a systematic literature review. Front Immunol. 2021;12:679556.
7. Gatt PL et al. Oral lichen planus in patients with Good’s syndrome: a literature review. Cureus. 2023;15(2):e35177.
8. Fatrez B et al. Good syndrome associated with lichen planus: a case report and review. Eur J Dermatol. 2020;30(6):756-7.
9. Duarte M et al. A case of severe COVID-19 in a patient with Good’s syndrome. Eur J Case Rep Intern Med. 2021;8(10):002976.
10. Tabarsi P et al. Clinical and genomic evaluations of a persistent fatal SARSCoV-2 infection in a goods syndrome patient: a case report. BMC Infect Dis. 2024;24(1):216.
11. Tehrani S et al. Case report: pneumonia in a patient with combined variable immunodeficiency: COVID-19 or pneumocystis pneumonia? Front Med (Lausanne). 2022;9:814300.
12. Kelleher P, Misbah SA. What is Good’s syndrome? Immunological abnormalities in patients with thymoma. J Clin Pathol. 2003;56(1):126.
13. Agarwal S, Cunningham-Rundles C. Thymoma and immunodeficiency (Good syndrome): a report of 2 unusual cases and review of the literature. 2007. Ann Allergy Asthma Immunol. 2007;98(2):185-90.