Solving The Fertility Riddle: Decipher It or We Will All Be Devoured Feature: Editor’s Pick:
10 Advances in Therapy to Address Proteinuria in Patients with Immunoglobulin A Nephropathy
20 The Power of Real-World Evidence with CORE-VNS
Poster Review
28 Addressing Proteinuria in Patients with Immunoglobulin A Nephropathy Through Concomitant Use of Sparsentan and Sodium-Glucose Cotransporter-2 Inhibitors
Interview
37 Robert Norman Feature
43 Solving The Fertility Riddle: Decipher It or We Will All Be Devoured
Carneiro and Sampaio Articles
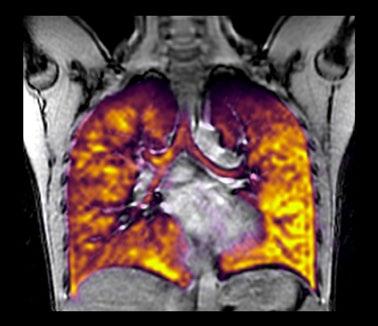
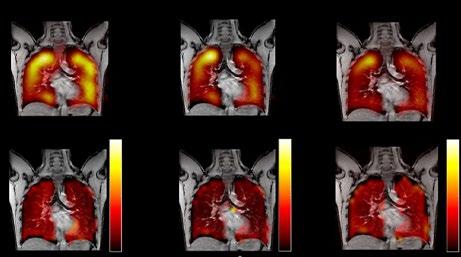
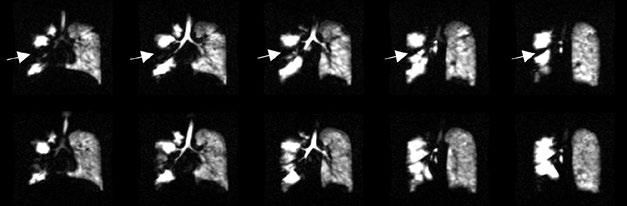
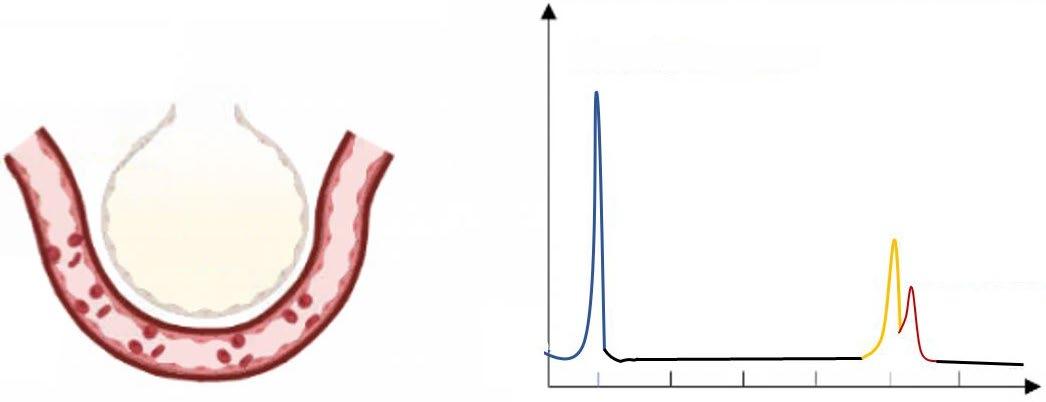
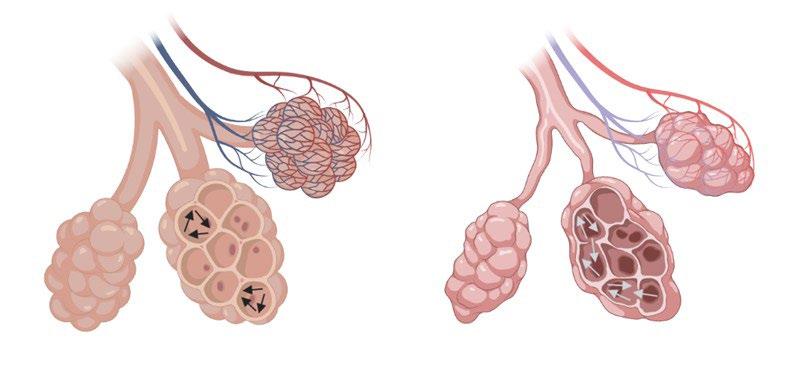
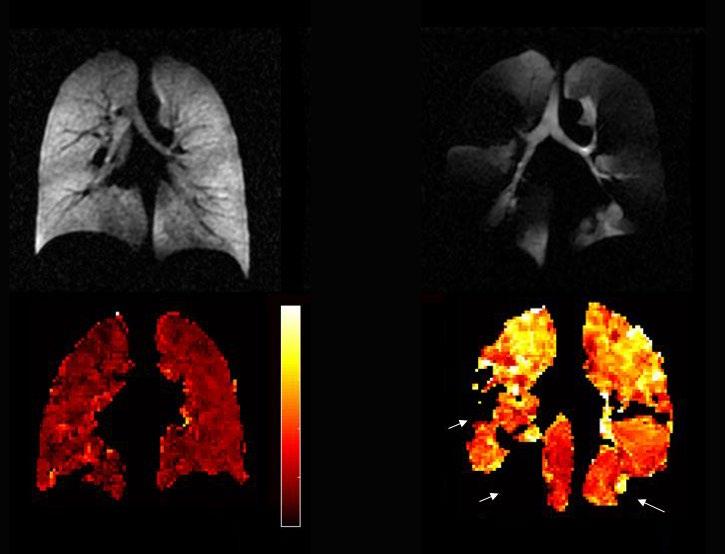
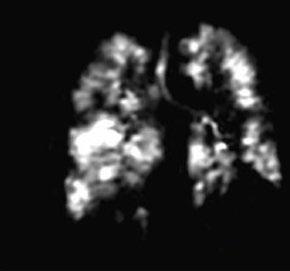
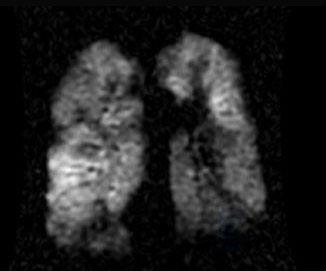
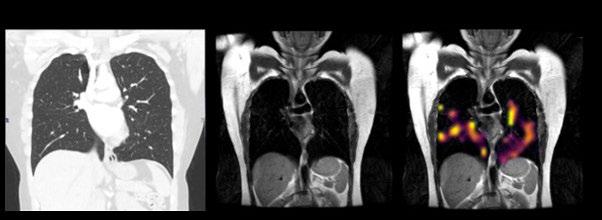
48 Editor's Pick: Clinical Applications of Hyperpolarised Xenon-129 MRI
Ng et al.
62 The Role of IL-5 in Type 2 Inflammatory Diseases
Bagnasco et al.
73 Allergic Reactions to NSAIDs during Febrile States: Case Report and Review of the Literature
Bakiri and Mingomataj
83 Abdominal Cocoon and Recurrent Haemorrhagic Ascites, Unexpected Findings in Endometriosis: A Case Report and Review of Literature
Jamil and Jamil
89 Evaluating Diagnostic Performance of Extrapulmonary Tuberculosis Using Cartridge-Based Nucleic Acid Amplification Test Assay: A Retrospective Cross-Sectional Study at a Tertiary Health Care Setup in India
Kashyap et al.
97 Challenges in Diagnosing Radiographic Axial Spondyloarthritis: A Case Study of a Young Adult in a Secondary-Level General Hospital in Guayaquil, Ecuador
Acuria et al.
102 Knowledge, Attitude, and Preventive Practices on Human Papillomavirus Vaccination Among Mothers of Adolescent Girls in Selected Secondary Schools of Lagos, Nigeria
Akinyemi et al.
113 Adverse Drug Events from First-line Anti-tuberculosis Drugs in a Tertiary Medical Center
Jorge et al.
120 Incidental Idiopathic Left Uncal Herniation: A Case Study and Literature Review
Chan et al.
125 All that Torse is Not an Ovary: Ferreting Torsed Subserosal Fibroid in a Flurry of Fibroids: A Case Report
Moharkar et al.
"Women's health is absolutely fundamental to the health of society"
Editorial Board
Editor-in-Chief
Prof Markus Peck-Radosavljevic
Klinikum Klagenfurt am Wörthersee, Austria
Current Chairman and Head of the Department of Gastroenterology and Hepatology, Endocrinology, Rheumatology and Nephrology at Klinikum Klagenfurt am Wörthersee, with expertise in portal hypertension, hepatocellular carcinoma, and HIV-HCV coinfection.
Prof Ahmad Awada
Jules Bordet Institute, Belgium
Prof Sorin T. Barbu
“Iuliu Hațieganu” University of Medicine and Pharmacy, Romania
Dr Abdullah Erdem Canda
Yildirim Beyazit University, Türkiye
Prof Ian Chikanza
Harley Street Clinic, UK
Prof Lászlo Vécsei
University of Szeged, Hungary
Dr Pierfrancesco Agostoni
St. Antonius Hospital, the Netherlands
Dr Fernando Alfonso
Hospital Universitario de La Princesa, Spain
Dr Emanuele Angelucci
IRCCS Ospedale Policlinico San Martino, Italy
Dr George Anifandis
University of Thessaly, Greece
Dr Riccardo Autorino
Virginia Commonwealth University, USA
Dr Mátyás Benyó University of Debrecen, Hungary
Prof Andrew Bush Imperial College London, UK
Dr Hassan Galadari
United Arab Emirates University, United Arab Emirates
Dr Amir Hamzah Abdul Latiff
Pantai Hospital, Malaysia
Dr Lorenz Räber
Bern University Hospital, Switzerland
Breaking Barriers in Electrophysiology with Dr. Devi Nair
Dr. Devi Nair, a trailblazing electrophysiologist shares how she shaped her path in a male-dominated industry. Her story is one of empowerment, illustrating how she has harnessed her expertise and voice to break barriers and set new standards in the world of cardiology, inspiring the next generation of female leaders in the field.
In this exclusive interview, Dr. Nair reflects on the challenges and milestones in her career, reflects on inspirations to advance electrophysiology, and the impact of her collaboration with Siemens Healthineers.
Scan the QR code to download the interview.
Dr. Devi G Nair, MD, FACC, FHRS
Director of Cardiac Electrophysiology & Research
Jonesboro, Arkansas
Dr. Nair is the Director of a Cardiac Electrophysiology Division in Jonesboro, Arkansas. Her clinical practice focuses on heart rhythm disorders including atrial and ventricular arrhythmias, bradycardia, heart failure and the treatments for these disorders including cardiac ablation, pacemakers, defibrillators, cardiac resynchronization therapy devices, and left atrial appendage occlusion therapy.
Aims and Scope
EMJ, the flagship journal of the EMJ portfolio, is an openaccess, peer-reviewed eJournal, committed to elevating the quality of healthcare globally by publishing high-quality medical content across the 18 clinical areas covered in our portfolio. The journal is published quarterly and showcases the latest developments across these clinical areas.
EMJ publishes peer-reviewed research papers, review articles, and case reports across all therapy areas of the EMJ portfolio. In addition, the journal publishes features and opinion pieces create a discussion around key topics in the field and broaden readers’ professional interests. The journal also features interviews with leading experts in various clinical disciplines.
The journal covers advances within the pharmaceutical arena by publishing sponsored content from congress symposia, which is of high educational value for healthcare professionals. This undergoes rigorous quality control checks by independent experts and the in-house editorial team.
EMJ endeavours to increase knowledge, stimulate discussion, and contribute to the delivery of world-class updates in the clinical realm. We do not publish veterinary science papers or laboratory studies that are not linked to patient outcomes. Further details on coverage can be found here: www.emjreviews.com
Editorial Expertise
EMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors who are recognised authorities in their respective fields.
• Peer review, which is conducted by expert reviewers who are invited by the Editorial team and appointed based on their knowledge of a specific topic.
• An experienced team of editors and technical editors.
• A team of internal and independent medical writers.
Peer Review
Every review article, case report, feature, and research article published in EMJ undergoes peer review by at least two independent experts.
On submission, all manuscripts are assessed and undergo a technical check by the EMJ Editorial staff to determine their suitability for the journal and appropriateness for peer review. Editorial staff identify appropriate reviewers who are selected based on their specialist knowledge in the relevant area. All peer review is double-blind.
Following review, manuscripts are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected. Editorial staff are responsible for ensuring that necessary amendments to the manuscript have been made, with input from our Editorial Board or the original reviewers where necessary. The Editor of EMJ has final discretion over any proposed amendments. Manuscripts authored by members of the Editorial Board are subjected to the same double-blind process. Short opinion pieces are published following internal review and publication is at the discretion of the Editor. Congress-associated content authored by the EMJ Editorial staff undergoes internal quality control checks. Congress-related content sponsored or funded by our industry partners undergoes quality control checks independently. Industry-supported content that falls into any of
the categories that are eligible for peer review, undergoes the same peer review process.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects. We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial.assistant@emjreviews.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in EMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
EMJ is distributed through controlled circulation to healthcare professionals in the relevant fields globally.
Indexing and Availability
EMJ is indexed on DOAJ, the Royal Society of Medicine, and Google Scholar®.
EMJ is available through the websites of our leading partners and collaborating societies.
EMJ journals are all available via our website: www.emjreviews.com
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
All information obtained by EMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, EMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. EMJ is completely independent of any event reviews in this issue and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever. The cover photo is of Radcliffe Science Library Oxford, the location of work for the primary author of Editor's Pick.
It’s time to rethink insomnia. It’s no longer considered just a symptom of other medical conditions but recognised by international-classification systems as an independent condition with underlying causes, which should be managed independently of other co-morbidities.1,2
1. Riemann D, et al. J Sleep Res. 2023;32(6):e14035. 2. Wilson S, et al. J Psychopharmacol. 2019;33(8):923–947. This information is intended for healthcare professionals. This advert has been created and paid for by Idorsia Pharmaceuticals UK Ltd. UK-DA-00660 | October 2024
Editor
Evgenia Koutsouki
Editorial Manager
Darcy Richards
Copy Editors
Noémie Fouarge, Katheeja Imani, Jenna Lorge
Editorial Co-ordinators
Victoria Antoniou, Abigail Craig
Editorial Assistants
Helena Bradbury, Ada Enesco, Katrina Thornber, Katie Wright, Aleksandra Zurowska
Creative Director
Tim Uden
Design Manager
Stacey Rivers
Designers
Owen Silcox, Fabio van Paris
Junior Designers
Dillon Benn Grove, Shanjok Gurung
Senior Performance & Insight Lead
Darren Brace
Marketing Director
Kristina Mestsaninova
Chief Content Officer
Justin Levett
Chief Commercial Officer
Dan Healy
Founder and Chief Executive Officer
Spencer Gore
Welcome
Dear Readers,
I would like to welcome you to the last EMJ issue of 2024, which brings a great array of articles across different clinical disciplines, including respiratory health, microbiology, and rheumatology, among others, with many of these bringing issues of women’s health into the spotlight.
According to a WHO report, a woman dies every 2 minutes across the world due to pregnancy or childbirth.1 It is shocking that in this day and age maternal mortality has gone up in certain regions. We can, and should, do better. Whilst it is positive to see neglected conditions like menopause and endometriosis gaining more attention, there is a lot still to be done to improve maternal health across the world.
As I bring this welcome to a close, I would like to thank you for your ongoing support and acknowledge the immense help provided by our peer reviewers, Editorial Board, and contributors, who continue to produce great content. I hope you enjoy reading this issue, and I wish you a happy holiday season. I look forward to touching base in 2025!
Reference
1. World Health Organization (WHO). A woman dies every two minutes due to pregnancy or childbirth: UN agencies. Available at: https://www.who. int/news/item/23-02-2023-a-woman-dies-every-two-minutes-due-topregnancy-or-childbirth--un-agencies. Last accessed: 2 December 2024.
Editorial enquiries: editor@emjreviews.com
Sales opportunities: salesadmin@emjreviews.com
Permissions and copyright: accountsreceivable@emjreviews.com
Evgenia Koutsouki Editor
Reprints: info@emjreviews.com Media enquiries: marketing@emjreviews.com
HOW CAN WE IMPROVE THE TREATMENT OF ESSENTIAL TREMOR?
Share your clinical insights on essential tremor in two brief surveys to help elevate the standard of patient care. Your expertise matters!
Help us identify key gaps in current treatment, improve understanding, and help provide the best support for those affected by essential tremor.
BE PART OF THE CHANGE
Advances in Therapy to Address Proteinuria in Patients with Immunoglobulin A Nephropathy
This presentation took place at the Nephro Update Europe congress, held on 6th−7th September, 2024, in Vienna, Austria, and virtually.
Latus received relevant speaker fees, travel and congress grants, board participation, educational support, and consultancy fees within the last 3 years from AstraZeneca, Bayer, Boehringer Ingelheim, CSL Vifor, Novartis, Otsuka Alexion, and Stada.
Writing assistance was provided by Eleanor Roberts, Beeline Science Communications Ltd, London, UK.
The opinions expressed in this article are not necessarily those of CSL Vifor.
Support: Publication of this feature was supported and reviewed by CSL Vifor.
Meeting Summary
PARTNERSHIP
As the majority of patients with IgA nephropathy (IgAN) progress to kidney function loss, it is important to treat this primary glomerulonephritis in a way that will prevent or slow such progression. In a presentation delivered at the 2024 Nephro Update Europe congress, Jörg Latus, from Robert-Bosch-Krankenhaus GmbH, Stuttgart, Germany, discussed the relevance of assessing proteinuria levels in patients with IgAN and how this is recognised in the 2024 Kidney Disease Improving Global Outcome (KDIGO) guidelines, currently in draft form. Since the 2021 KDIGO guidelines, therapy choices for IgAN advances have widened and include those specifically developed for IgAN, such as the dual endothelin and angiotensin II receptor antagonist sparsentan and modified-release budesonide (MRB), as well as sodium-glucose cotransporter-2 inhibitors (SGLT2i), which have a broader role in chronic kidney disease treatment. Latus discussed some of the pivotal trials that led to these medications being approved for use in patients with IgAN, along with real-world data for sparsentan. Also discussed were trials for other IgAN pathogenesis-targeting medications, future approval of which is hoped to open the choice of treatments for patients with IgAN at risk of progressive kidney function loss such that more individualised therapy regimens can be provided.
PHARMA
Introduction
Although IgAN is a rare disease, it is a major cause of primary glomerulonephritis,1,2 and an important disease to recognise and control as the majority of patients with IgAN progress to kidney failure in the 20−30 years following diagnosis.3 In a presentation at the Nephro Update Europe congress, Jörg Latus, an expert in the field of kidney diseases, discussed IgAN treatment and highlighted the importance of recognising and controlling proteinuria as a means to mitigate kidney failure progression.4
In Europe, where the population is an estimated 745 million,5 the overall annual incidence of IgAN is 0.76 per 100,000, equating to around 5,662 new cases, with a point prevalence of 2.53 per 10,000, equating to around 188,485 patients. Point prevalence is highest in North-Eastern Europe and lowest in Southern Europe; it is also lower in paediatric and elderly populations.2 However, Latus said, “we all know that IgAN is underdiagnosed as a lot of patients are not biopsied”.
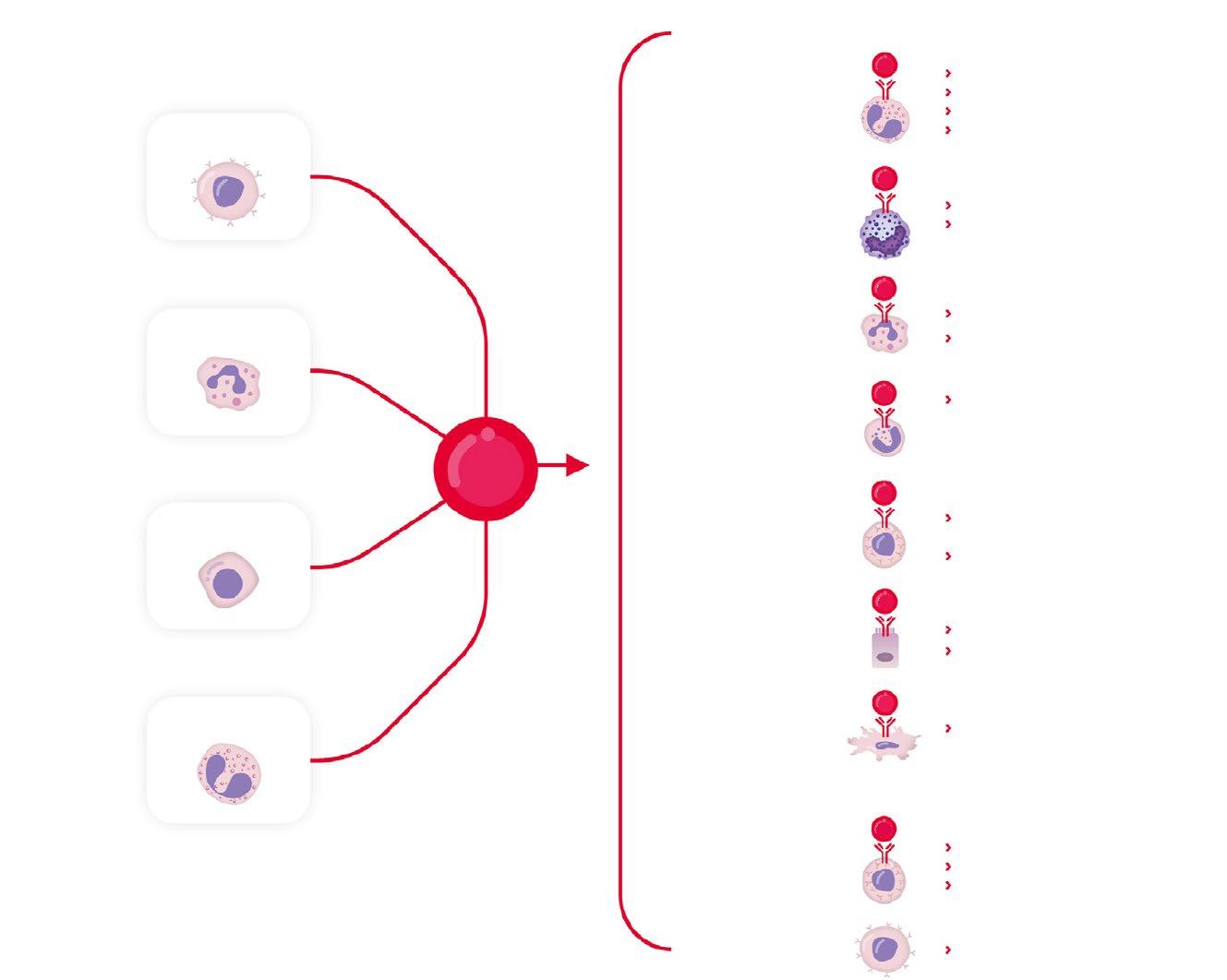
There are multiple factors involved in the pathogenesis of IgAN, as encompassed by the ‘four-hit’ model. Initiation of IgAN, prior to the first hit, occurs when stimulation of mucosal innate immune cells by the gut microbiome leads to increased activation of mucosal IgA-committed B cells via ‘B cell activation factor’ (BAFF) and ‘a proliferationinducing ligand’ (APRIL) signalling. Hit 1 is then an increase in circulating levels of galactose-deficient IgA1 (gd-IgA1), with Hit 2 being the generation of anti-gd-IgA1 autoantibodies. Hit 3 is the formation of immune complexes containing gd-IgA1 and IgA, IgG, and IgM autoantibodies. This is followed by Hit 4, where there is glomerular mesangial deposition of these complexes and activation in mesangial cells of inflammatory and fibrotic pathways, including the complement system.6
According to 2021 KDIGO guidelines, idiopathic IgAN is diagnosed once secondary causes of IgA-dominant glomerulonephritis are ruled out. A kidney biopsy can then be assessed using the MEST-C instrument (mesangial [M] and endocapillary [E]
hypercellularity, segmental sclerosis [S], interstitial fibrosis/tubular atrophy [T], and crescents [C]). The guidelines suggest that progression risk at diagnosis can be estimated using the International IgAN Prediction Tool, which includes estimated glomerular filtration rate (eGFR), blood pressure, age, and proteinuria at biopsy; race; renin-angiotensin system inhibitor (RASi) and immunosuppression use; and individual MEST-C component scores. Use of this tool can help inform discussion with the patient to lead to shared decisions regarding individualised treatment.7 However, observed Latus, it may not routinely be used in practice.
Much of this session discussed both the 20217 and the 2024 updated KDIGO guidelines, which are currently in draft form. It is to be noted that final guideline content may change based on feedback on the draft.8
The Role of Proteinuria in IgA Nephropathy
According to Latus, proteinuria levels are the “strongest prognostic factor for disease progression in IgAN”. Indeed, in clinical trials, proteinuria reduction is often used as a surrogate endpoint for therapy efficacy.9
Recently, the UK National Registry of Rare Kidney Diseases (RaDaR) carried out a study investigating proteinuria in patients with IgAN, including 30 years of data from 2,439 patients. Analysis showed that the median time to proteinuria from registry entry was 4.5 years, and that those with time-averaged proteinuria >0.88 g/g were likely to progress quicker to kidney failure or death compared with patients where this value was <0.88 g/g. Also shown was that an estimated 30% of patients with time-averaged proteinuria of 0.44 to <0.88 g/g, and 20% of patients where this figure was <0.44 g/g, developed kidney failure within 10 years of diagnosis.3 Similarly, a study analysing data from the Toronto Glomerulonephritis Registry (n=542) showed that survival without kidney failure was highest and longest in patients with proteinuria <0.3 g/day, and progression to kidney failure was highest and quickest in those with proteinuria >3.0 g/day.10
Even in patients with proteinuria in the low ranges, eGFR decline can be significant over a number of years.11 In the RaDaR study, for adults <50 years old at diagnosis, it was estimated that an annual change in eGFR of 1 mL/min/1.23 m2 would result in them reaching kidney failure in their expected lifetime. The RaDaR study also found that, although lowering proteinuria levels was associated with reductions in eGFR slope decline, the decline still occurred in patients even if there was no increase in proteinuria or if proteinuria levels decreased.3
Latus said that these studies show that “there is no safe proteinuria level”, overturning beliefs that he reported from colleagues that there is a low risk of kidney progression if proteinuria is <1.0 g/day. This is reflected in the updated 2024 KDIGO guidelines, which state that "a patient with IgAN is at risk of progressive loss of kidney function if they have proteinuria ≥0.5 g/d (or equivalent), while on or off treatment".8
“This is a very important part of the guideline,” said Latus, and stressed how now “the 1.0 g/day should be deleted, and we must talk about 0.5 g/day”.
Treatments Targeting the ‘Four Hits’ of IgA Nephropathy
“In nephrology, we try to preserve kidney function,” explained Latus. This is reflected in the 2024 draft KDIGO guidelines, where the goal in patients with IgAN at risk of progressive kidney function loss “is to reduce the rate of loss of kidney function to <1 mL/min per year for the rest of the patient’s life”.8 However, commented Latus, “this is not that easy to achieve”.
In patients at risk of progressive kidney disease (proteinuria ≥0.5 g/day), management of nephron loss is driven by the need to tackle specific drivers and their response to treatment. This includes addressing IgAN from the perspective of an autoimmune disease and having treatment goals that include reducing pathogenic forms of IgA and IgA immune complex formation. Management also
includes having treatment goals that include maintaining blood pressure control; reducing cardiovascular risk; reducing glomerular hyperfiltration and glomerular inflammation, and the impact of proteinuria on the tubulointerstitium.8
To achieve these goals, multiple drugs may be needed, Latus explained. The highest KDIGO recommendation is for a RASi such as an angiotensin-converting enzyme inhibitor (ACEi) or an angiotensin receptor blocker (ARB).7,8 While, according to Latus, RAS inhibition is “a significant pillar in the treatment of IgAN”, he also discussed a study investigating 96 patients prescribed a RASi, which showed that 3 months’ treatment led to complete proteinuria remission in only 6.3% of patients, with 30.2% showing partial remission and 63.5% having no remission.12
According to 2021 KDIGO guidelines, while glucocorticoids may also be added to therapy, prescribing should encompass individual risk stratification and only be considered in patients where eGFR is ≥30 mL/min/1.73 m2. Glucocorticoids should also be avoided in patients who have diabetes; a body mass index >30 kg/m2; latent infections, such as viral hepatitis or tuberculosis; secondary disease, such as cirrhosis; severe osteoporosis; uncontrolled psychiatric illness; or active peptic ulceration.13 The updated draft KDIGO guidelines also include patients with prediabetes and cataracts in those where glucocorticoids are not recommended.8 In his personal experience though, Latus reported how he treats very few patients with this medication.
Innovative Approaches to IgAN Treatment to Target Proteinuria
The updated KDIGO guidelines include treatments that are now approved for patients with IgAN,8 most notably sparsentan,14 SGLT2i,15 and MRB.16 Latus provided an overview of studies of these medications with regard to their actions on proteinuria.
Sparsentan
Sparsentan is a dual endothelin and angiotensin II receptor antagonist14 that the draft KDIGO guidelines recommend for patients at risk of progressive kidney function loss.8 In the international Phase III PROTECT trial, following discontinuation of maximal RASi, adult participants with 24-hour urine protein excretion (UPE) ≥1.0 g/day received either 400 mg/day sparsentan (n=202) or 300 mg/day of the ARB irbesartan (n=202), following a 2-week titration period where doses were 200 mg/ day and 150 mg/day, respectively. Of note, highlighted Latus, in both groups, almost all participants (approximately 97%) received the full dose of each drug, with those not receiving such doses remaining on the titration period dose. The blinded treatment period was for 110 weeks, after which medication was discontinued. Standard care was then administered for 4 weeks, then participants from either group could take part in an open-label extension period of 400 mg/day sparsentan for 156 weeks.17,18
Mean, respective, baseline characteristics in the sparsentan/irbesartan groups were similar with regard to age (46.6 and 45.4 years) and gender (69% and 71% male), eGFR (56.8 and 57.1 mL/min/1.73 m2), and proteinuria (UPE 1.8 and 1.8 g/day; urine protein–creatinine ratio [UPCR] 1.3 and 1.2 g/g). They were also similar with regard to respective hypertension history (72% and 71%) and blood pressure readings (128.0/81.6 and 129.9/83.2 mmHg); time from kidney biopsy (4.0 and 4.0 years), and ACEi or ARB dose at screening (130 and 125 mg/day). No participant was treated with an SGLT2i.18
For the primary endpoint at 36 weeks, treatment with sparsentan resulted in a rapid, significant, and clinically meaningful greater reduction from baseline in proteinuria (–49.8%) compared with irbesartan (–15.1%). This represents a between-group relative reduction of 41% (least squares mean ratio: 0.59; 95% CI: 0.51, 0.69; p<0.001). In the sparsentan group, 31% had a complete response (UPE <0.3 g/day), compared with 11% in the irbesartan group (relative risk [RR]: 2.5; 95% CI: 1.6, 4.1), with partial response (UPE <1.0 g/day) shown in 78% of the sparsentan group compared with 53%
of the irbesartan group (RR: 1.5; 95% CI: 1.1, 1.9). A post-hoc assessment showed the proportion of patients where UPE was <0.5 g/day to be 51% in the sparsentan group compared with 24% in the irbesartan group (RR: 2.1; 95% CI: 1.5, 2.9).18
This trial also examined changes in eGFR and showed that up to Week 110, a decrease in such was shown in both groups. The total slope (calculated from Day 1 to Week 110) and chronic slope (total slope minus the acute effect, calculated from Week 6–110) were, respectively, –2.9 and –2.7 mL/min/ 1.73 m2 per year in the sparsentan group and –3.9 and –3.8 mL/min/1.73 m2 per year in the irbesartan group. Between-group differences were, respectively, 1.0 mL/ min/1.73 m2 per year (95% CI: –0.03, 1.94; p=0.058) and 1.1 mL/min/1.73 m2 per year (95% CI: 0.1, 2.1; p=0.037).18
These findings, postulated Latus, represented very low eGFR decreases in patients with IgAN. However, although the between-group difference in chronic slope was only 1.1 mL/ min/1.73 m2 per year, Latus discussed how this can be extrapolated to delayed time to kidney failure in the long term. Utilising data from the PROTECT trial alongside findings from studies of other medications for IgAN, Figure 1 illustrates theoretical delayed times to kidney failure. In this scenario, treatment was initiated in a patient who had an eGFR of 57 mL/min per 1.73 m², which was similar to the mean baseline eGFR of patients enrolled into PROTECT. Projecting the slope of eGFR decrease found in the PROTECT study, it was estimated that the patient would reach kidney failure (eGFR <15 mL/min per 1.73 m²) in 15.6 years if taking sparsentan and 11.1 years if taking irbesartan, representing a difference of 4.5 years, and in 7.9 years if on RASi standard of care, representing a difference between this and sparsentan of 7.7 years.18
While, in the PROTECT trial, treatmentemergent adverse events (TEAE) more often present in the sparsentan group included hypotension (13%) and dizziness (15%), compared with, respectively, 4% and 6% in the irbesartan group, Latus reported that sparsentan overall had “a very good safety profile”.18
Figure 1: Theoretical/projected delayed time to kidney failure based on linear extrapolation of estimated glomerular filtration rate slopes.18-23
(PROTECT Clinical Trial)
(PROTECT Clinical Trial)
SoC* (5 prior RCTs)
Mean of observed chronic or total slopes for SoC ACEi/ARB as reported in five other different randomised controlled trials in IgAN, outside of sparsentan development program
Based on linear extrapolation of the eGFR slopes calculated in the PROTECT study and five randomised controlled trials. These data are extrapolated and act under the assumption that eGFR decline is constant and decreases in a linear fashion in the course of the disease, which is not necessarily accurate for real-world, long-term effects. Outcomes may vary on an individual basis. Outcomes presented are not efficacy outcomes and should be validated in the future with long-term data as they become available.
*ACEi and/or ARB.
†Mean of observed chronic or total slopes for SoC, as reported in five IgAN randomised controlled trials.
ACEi: angiotensin-converting enzyme inhibitor; ARB: angiotensin receptor blocker; eGFR: estimated glomerular filtration rate; IgAN: immunoglobulin A nephropathy; RASi: renin-angiotensin system inhibitor; SoC: standard of care.
Sparsentan Use Beyond Clinical Trials
To understand the use of sparsentan in a real-world setting, Latus shared an analysis of real-world data from Stuttgart, Germany, on the use of sparsentan in patients with IgAN with an eGFR >30 mL/min per 1.73 m² and UPCR >0.75 g/g. Results presented included 23 patients with a median age of 38 years, 57% of which were male, with a median time from initial kidney biopsy to sparsentan initiation of 34 months. These patients had a median baseline eGFR of 42 mL/min per 1.73 m², UPCR of 1.5 g/g, and blood pressure value of 130/80 mmHg, with 65% exhibiting arterial hypertension. At baseline, all patients were being treated with a RASi, with 74% on a maximal indicated dose. All had been treated stably with an SGLT2i in the past, and 57% had a history of
glucocorticoid therapy (17% ongoing with MRB at screening).24
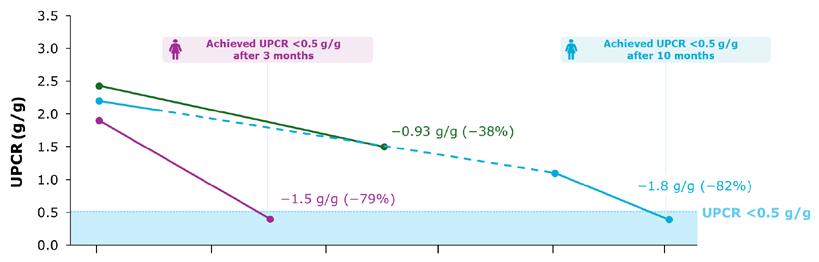
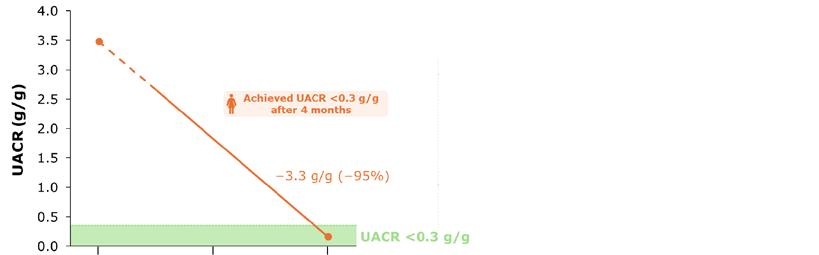
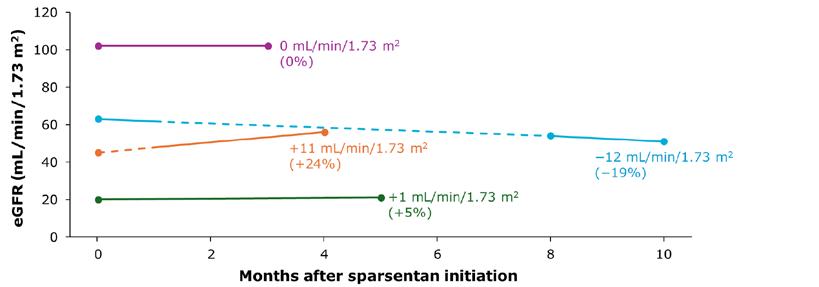
Efficacy results showed a significant decrease in UPCR from baseline at Week 2 (n=20), Week 10 (n=21), Week 14 (n=18), and Week 22 (n=8). Proteinuria reduction was >50% in 87% of participants, >30% in 9%, and ≤30% in 4% of participants. Also shown was that 35% achieved complete proteinuria remission and 52% showed partial remission (Figure 2).24
Sparsentan was generally well tolerated with no evidence of serious adverse events. Hypotension occurred in 8.7% of patients (two cases). One of these patients temporarily ceased treatment for 4 weeks and experienced no hypotension when the treatment was restarted. There were
+7.7 years vs RASi SoC
Number of patients (n=23)
Definition of proteinuria at least once at any time over the course of the treatment period: complete remission is 0.3 g/g, and partial remission is 1.0 g/g if baseline between 0.75−1.0 g/g, then <0.75 g/g.
also reports of dizziness, headache, mild hyperkalaemia, gout, and pruritus, each affecting one patient. No patient had to permanently discontinue sparsentan treatment due to a treatment-related adverse event.24 While preliminary, these results show the utility of sparsentan for proteinuria reduction in a real-world setting.
Sodium-Glucose Cotransporter-2 Inhibitors
Latus also discussed the use of SGLT2is, which are now recommended in the 2024 draft KDIGO guidelines for "patients at risk of progressive kidney function loss".8 A meta-analysis of trials with an SGLT2i showed a relative risk of kidney disease progression of 0.49 (95% CI: 0.32, 0.74). Of note though, Latus said: “Keep in mind that the study population investigated in these trials were an older population with less eGFR compared to the IgAN trials, and that the RAS inhibition was not optimised.”15
To understand the effects of combination therapy, one ongoing trial is investigating 12 weeks of treatment with an SGLT2i added
to sparsentan (after it has been taken for ≥8 weeks), compared with sparsentan alone. This includes around 60 participants from the PROTECT open-label extension period. Another study, SPARTACUS, includes participants on stable SGLT2i and RASi treatment where the RASi was discontinued and sparsentan is introduced for 24 weeks. These studies will evaluate safety and efficacy of this combination.25
Modified-Release Budesonide
Another updated recommendation in the draft 2024 KDIGO guidelines for patients at risk of progressive kidney function loss is a 9-month course of a modifiedrelease formulation of the glucocorticoid budesonide (MRB).8,16 Investigation of this formulation was carried out in the Phase III, randomised, placebo-controlled NefIgArd trial. This included 364 adults with persistent proteinuria ≥1.0 g/day despite optimised treatment. MRB was administered at a dose of 16 mg/day for 9 months, compared to a placebo group also on optimised treatment. Findings included a significant percentage decrease
Figure 2: Remission status and proportion of patients reaching complete/partial remission of proteinuria.24
in UPCR from baseline, which was also significantly different from the placebo group. Continued decreases were shown up to 12 months even though MRB was stopped at 9 months. While there was a subsequent increase in proteinuria 2 years from baseline, levels were similar to those shown at 9 months.23
An increase was shown in eGFR at Month 3 in the MRB group, with a decrease in the placebo group; however, by Month 9, while decreases remained in the placebo group, eGFR was at baseline in the MRB group. At follow-up, 2 years from study start, although eGFR declined in both groups, following a similar slope, the change from baseline in the MRB group was lower than that of the placebo group.23
In this study, discontinuations in the 9-month treatment period due to TEAEs occurred in 17 (9%) patients in the MRB group and three (2%) in the placebo group. The incidences of infections were similar between groups, at rates of 35% in the MRB group and 31% in the placebo group. Latus reported that TEAEs were similar to what he would expect to be associated with glucocorticoid treatment, such as peripheral oedema (17%), hypertension (12%), muscle spasms (12%), and acne (11%). There were no incidences of new-onset diabetes and no treatment-related fatalities.23
Clinical Trials Aimed at IgAN Pathogenesis
Latus highlighted how KDIGO guidelines recommend that patients with proteinuria >1.0 g/day despite at least 3 months’ supportive care should be considered for enrolment in a clinical trial.7,8 One such trial, the international VISIONARY Phase II trial, is investigating the drug sibeprenlimab plus standard care over 12 months, compared to placebo plus standard care.26 This humanised IgG2 monoclonal antibody binds to and neutralises the activity of the B cell regulator APRIL.6 By blocking APRIL, it is hoped to reduce levels of galactosedeficient IgA1 along with associated immune complexes. Patients aged ≥18 years with biopsy-confirmed IgAN (n=155) were randomly assigned on an equal basis
to receive placebo or 2, 4, or 8 mg/kg sibeprenlimab per day. They were stratified at screening according to 24-hour UPCR (≤2.0 versus >2.0 g protein/g creatinine). Results after 12 months showed a dosedependent, "significant linear treatment effect in change from baseline in 24-hour UPCR (p<0.001)". In line with the actions of this drug at the Hit 2 level,6 a dosedependent decrease in serum gd-IgA1 levels, as well as IgG, IgM, and APRIL, over time was shown in all active treatment groups. There was no evidence of a treatment-related adverse toxic effect or of clinically meaningful immunosuppression or infections over the study period.27
The vasoactive peptide endothelin-1 (ET-1) is involved in chronic kidney disease pathogenesis via its action at the endothelin type A receptor (ETA) receptor.28
In the international, randomised, ALIGN Phase III study (n=340), investigation was carried out of the ETA receptor antagonist atrasentan versus placebo in patients with biopsy-proven IgAN and baseline total proteinuria >1.0 g/day despite optimised RASi treatment.29,30 Interim analysis from baseline to Week 36 (n=270) showed that atrasentan administration (0.75 mg/day) led to a 38.1% reduction from baseline in UPCR (median baseline: 1.4 g/g) compared with a 3.1% reduction with placebo (median baseline: 1.4 g/g). Relative reduction in mean percentage change for atrasentan compared with placebo was –36.1% (95% CI: –44.6, –26.4; p<0.001). Reductions in proteinuria with atrasentan were shown at the first assessment at 6 weeks. Atrasentan was generally well-tolerated with a favourable safety profile; TEAEs in the safety set were balanced between the treatment arms.31
The ongoing APPLAUSE-IgAN multicentre, randomised, Phase III trial is investigating iptacopan, a proximal complement inhibitor that binds factor B and inhibits the alternative complement pathway.32,33 The study includes 470 adults with primary IgAN administered 200 mg iptacopan twice daily or a placebo. Interim results at 9 months (n=250) showed reductions from baseline in 24-hour UPCR of 43.8% in the iptacopan group (from median 1.8 g/g at baseline)
compared with 9.0% in the placebo group (from median 1.9 g/g at baseline). Relative percentage reduction was 38.3% (95% CI: 26.0, 48.6; p<0.0001). Iptacopan was well-tolerated and had a favourable safety profile, with the rate of TEAEs leading to discontinuation similar between the treatment arms.34
These studies, Latus said, show promising results and point to future questions regarding tailoring specific treatments to particular patients, taking into account autoimmunity and chronic kidney disease progression.
Finally, Latus discussed the importance of looking at results for the comparator group in clinical trials with regard to between-group differences (Table 1). “When we talk about
treatment effects,” he said, “we always have to keep in mind how the other group was doing.” Understanding this can help guide more individualised treatment choices.
Conclusion
Updated 2024 draft KDIGO guidelines recognise the importance of proteinuria remission and expand recommended treatment choices for patients with IgAN at risk of progressive kidney failure to include sparsentan, an SGLT2i, and MRB.8 This will help provide more tailored therapy to patients on a more individualised basis. With a number of other treatments in trial, a lot more therapies will come in the future, concluded Latus.
Note, the clinical trials presented on this slide have used different study designs. Direct comparisons should not be made, and data should be interpreted with caution. eGFR: estimated glomerular filtration rate.
Table 1: Treatment effects in clinical trials.
References
1. Lai KN et al. IgA nephropathy. Nat Rev Dis Primers. 2016;2:16001.
2. Willey CJ et al. The incidence and prevalence of IgA nephropathy in Europe. Nephrol Dial Transplant. 2023;38(10):2340-9.
3. Pitcher D et al. Long-term outcomes in IgA nephropathy. Clin J Am Soc Nephrol. 2023;18(6):727-38.
4. Latus J. Navigating IgAN treatments: from clinical trials to innovative approaches. Nephro Update Europe, 6-7 September, 2024.
5. Worldometer. Europe Population. Available at: https://www. worldometers.info/world-population/ europe-population/. Last accessed: 4 October 2024.
6. Stamellou E et al. IgA nephropathy. Nat Rev Dis Primers. 2023;9(1):67.
7. Kidney Disease Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group. KDIGO 2021 Clinical practice guideline for the management of glomerular diseases. Kidney Int. 2021;100(4s):S1-276.
8. Kidney Disease Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group. KDIGO 2024 Clinical practice guideline for the management of immunoglobulin A nephropathy (IgAN) and immunoglobulin A vasculitis (IgAV). Public review draft. 2024. Available at: https://kdigo.org/wp-content/ uploads/2024/08/KDIGO-2024-IgANIgAV-Guideline-Public-Review-Draft. pdf. Last accessed: 4 October 2024.
9. Thompson A et al. Proteinuria reduction as a surrogate end point in trials of IgA nephropathy. Clin J Am Soc Nephrol. 2019;14(3):469-81.
10. Reich HN et al. Remission of proteinuria improves prognosis in IgA nephropathy. J Am Soc Nephrol. 2007;18(12):3177-83.
11. Stamellou E et al. Long-term outcomes of patients with IgA nephropathy in the German CKD cohort. Clin Kidney J. 2024;17(8):sfae230.
12. Bagchi S et al. Supportive management of IgA nephropathy with renin-angiotensin blockade, the AIIMS primary IgA nephropathy cohort (APPROACH) study. Kidney Int Rep. 2021;6(6):1661-8.
13. Rovin BH et al. Executive summary of the KDIGO 2021 guideline for the management of glomerular diseases. Kidney Int. 2021;100(4):753-79.
14. European Medicines Agency (EMA). Filspari. Sparsentan. 2024. Available at: https://www.ema.europa.eu/en/ documents/product-information/
filspari-epar-product-information_ en.pdf. Last accessed: 4 October 2024.
15. Nuffield Department of Population Health Renal Studies Group and SGLT2 inhibitor Meta-Analysis CardioRenal Trialists' Consortium. Impact of diabetes on the effects of sodium glucose co-transporter-2 inhibitors on kidney outcomes: collaborative metaanalysis of large placebo-controlled trials. Lancet. 2022;400(10365):1788801.
16. European Medicines Agency (EMA). Kinpeygo. Modified-release budesonide. Available at: https:// www.ema.europa.eu/en/documents/ product-information/kinpeygo-eparproduct-information_en.pdf. Last accessed: 4 October 2024.
17. Heerspink HJL et al. Sparsentan in patients with IgA nephropathy: a prespecified interim analysis from a randomised, double-blind, activecontrolled clinical trial. Lancet. 2023;401(10388):1584-94.
18. Rovin BH et al. Efficacy and safety of sparsentan versus irbesartan in patients with IgA nephropathy (PROTECT): 2-year results from a randomised, active-controlled, phase 3 trial. Lancet. 2023;402(10417): 2077-90.
19. Wheeler DC et al. A pre-specified analysis of the DAPA-CKD trial demonstrates the effects of dapagliflozin on major adverse kidney events in patients with IgA nephropathy. Kidney Int. 2021;100(1):215-24.
20. Manno C et al. Randomized controlled clinical trial of corticosteroids plus ACE-inhibitors with longterm follow-up in proteinuric IgA nephropathy. Nephrol Dial Transplant. 2009;24(12):3694-701.
21. Lv J et al. Effect of oral methylprednisolone on decline in kidney function or kidney failure in patients with IgA nephropathy: the TESTING randomized clinical trial. Jama. 2022;327(19):1888-98.
22. Li PK et al. Hong Kong study using valsartan in IgA nephropathy (HKVIN): a double-blind, randomized, placebocontrolled study. Am J Kidney Dis. 2006;47(5):751-60.
23. Lafayette R et al. Efficacy and safety of a targeted-release formulation of budesonide in patients with primary IgA nephropathy (NefIgArd): 2-year results from a randomised phase 3 trial. Lancet. 2023;9;402(10405):85970.
24. Schanz M et al. First real-world evidence of sparsentan efficacy in patients with IgA nephropathy treated
with SGLT2 inhibitors. Poster 263. Deutsche Gesellschaft für Nephrologie eine jährliche Tagung, 26-29 September, 2024.
25. Ayoub I et al. Sparsentan and sodiumglucose cotransporter-2 inhibitors (SGLT2is) in the PROTECT openlabel extension (OLE) substudy and SPARTACUS: trials in progress. Poster PA-PO902. ASN Kidney Week, 2-5 November, 2023.
26. Otsuka Pharmaceutical Development & Commercialization, Inc. Visionary study: phase 3 trial of sibeprenlimab in immunoglobulin A nephropathy (IgAN). NCT05248646. https://clinicaltrials. gov/study/NCT05248646.
27. Mathur M et al. A phase 2 trial of sibeprenlimab in patients with IgA nephropathy. N Engl J Med. 2024;390(1):20-31.
28. Kohan DE, Barton M. Endothelin and endothelin antagonists in chronic kidney disease. Kidney Int. 2014;86(5):896-904.
29. Chinook Therapeutics, Inc. Atrasentan in patients with IgA nephropathy (ALIGN). NCT04573478. https:// clinicaltrials.gov/study/NCT04573478.
30. Novartis. Novartis investigational atrasentan Phase III study demonstrates clinically meaningful and highly statistically significant proteinuria reduction in patients with IgA nephropathy (IgAN). 2023. Available at: https://www.novartis. com/news/media-releases/novartisinvestigational-atrasentan-phaseiii-study-demonstrates-clinicallymeaningful-and-highly-statisticallysignificant-proteinuria-reduction-patients-iga-nephropathy-igan. Last accessed: 4 October 2024.
31. Heerspink HJL et al. ALIGN phase 3 primary endpoint analysis: atrasentan shows significant reduction in proteinuria in patients with IgA nephropathy. Abstract 109. ERA Congress, 23-26 May, 2024.
32. Novartis Pharmaceuticals. Study of efficacy and safety of LNP023 in primary IgA nephropathy patients (APPLAUSE-IgAN). NCT04578834. https://clinicaltrials.gov/study/ NCT04578834.
33. Novartis. Novartis investigational iptacopan Phase III study demonstrates clinically meaningful and highly statistically significant proteinuria reduction in patients with IgA nephropathy (IgAN). 2023. Available at: https://www.novartis. com/news/media-releases/novartisinvestigational-iptacopan-phaseiii-study-demonstrates-clinicallymeaningful-and-highly-statisticallysignificant-proteinuria-reduction-
patients-iga-nephropathy-igan. Last accessed: 4 October 2024.
34. Perkovic V et al. Efficacy and safety of iptacopan in patients with primary IgA nephropathy: interim analysis results of the Phase 3 APPLAUSE-IgAN study. Abstract 456. ERA Congress, 23-26 May, 2024.
35. Rauen T et al. Intensive supportive care plus immunosuppression in IgA nephropathy. N Engl J Med. 2015;373(23):2225-36.
36. Rauen T et al. After ten years of follow-up, no difference between supportive care plus immunosuppression and supportive
care alone in IgA nephropathy. Kidney Int. 2020;98(4):1044-52.
37. Hou FF et al. Effectiveness of mycophenolate mofetil among patients with progressive IgA nephropathy: a randomized clinical trial. JAMA Netw Open. 2023;6(2):e2254054.
The Power of Real-World Evidence with CORE-VNS
This symposium took place on 7th September 2024 as part of the 15th European Epilepsy Congress held in Rome, Italy, 7th–11th September 2024.
Chairperson: Arjune Sen1
Speakers: Gaia Giannicola,2 Arjune Sen1
1. Consultant Neurologist, John Radcliffe Hospital, Oxford, Professor of Global Epilepsy, University of Oxford, UK
2. Clinical Senior Project Manager and Program Manager, Neuromodulation, LivaNova, Milan, Italy
Disclosure:
Sen is an investigator associated with the CORE-VNS Study, and in that capacity they or their institutions receive compensation from LivaNova for study-related activities. Giannicola is an employee of LivaNova and holds stock options.
Acknowledgements: Writing assistance was provided by Rachel Danks, RSD Medical Communications Ltd, Gloucestershire, UK.
Disclaimer: The opinions expressed in this article belong solely to the named speakers. This is a promotional article funded and reviewed by LivaNova PLC. Safety information for VNS TherapyTM can be found at the end of this article. For full prescribing and important safety information, please see the VNS TherapyTM System Epilepsy Physician’s Manual available at epilepsy.livanova.com/manuals.
Support: The symposium and publication of this article was funded by LivaNova USA, Inc., a wholly-owned subsidiary of LivaNova PLC. The opinions expressed in this article belong solely to the named speakers.
Meeting Summary
This article summarises a LivaNova-sponsored symposium entitled ‘The Power of Real-World Evidence with CORE-VNS’, delivered on 7th September 2024 as part of the 15th European Epilepsy Congress in Rome, Italy. The symposium explored real-world data from CORE-VNS, a global, prospective long-term study of patients receiving adjunctive Vagus Nerve Stimulation (VNS) TherapyTM for drug-resistant epilepsy (DRE), which represents one of the most comprehensive contemporary real-world clinical data sets in DRE. The presentations provided an overview of the strengths, limitations, and executional requirements of large-scale real-world evidence studies in DRE. In addition, the impact of adjunctive VNS Therapy on both seizure and non-seizure outcomes in DRE within the European healthcare setting was explored.
In the symposium, two speakers closely involved in the conduct of the CORE-VNS study discussed insights from the study to date. Gaia Giannicola, Clinical Senior Project Manager and Program Manager for Neuromodulation at LivaNova, Milan, Italy, described the power of real-world data in the context of the CORE-VNS study, while Arjune Sen, Consultant Neurologist at the John Radcliffe Hospital in Oxford and Professor of Global Epilepsy at University of Oxford, UK, chaired the meeting and presented an interim analysis of European patients enrolled in the CORE-VNS study.
Introduction
Epilepsy affects approximately 50 million people around the world, and is associated with a high risk of disability, psychiatric comorbidity, social isolation, and premature death.1 More than one-third of people living with epilepsy continue to experience seizures, despite taking adequate and correctly dosed anti-seizure medications (ASM).2 DRE, defined as the failure of adequate trials of two antiseizure medicine schedules to achieve sustained seizure freedom,1,3 may require additional non-pharmacological interventions such as surgery, dietary therapy, and/or neuromodulatory interventions.1,4
The VNS Therapy system is the most widely available form of neuromodulatory therapy for the treatment of DRE.4,5 Since its initial approval in 1994, the technology behind the VNS Therapy system has evolved, and it is indicated outside the USA for use as an adjunctive therapy in reducing the frequency of seizures in patients whose epileptic disorder is dominated by focal seizures (with or without secondary generalisation) or generalised seizures that are refractory to seizure medications.6 In the USA, the VNS Therapy system is indicated for use as an adjunctive therapy in reducing the frequency of seizures in patients 4 years of age and older with partial onset seizures that are refractory to antiepileptic medications.7
The real-life global experience of people with DRE treated with adjunctive VNS is currently being assessed in the ongoing CORE-VNS Post-Market Study.4,5 This study, which has enrolled more than 800 patients in total, provides the opportunity to analyse a broad set of clinical and healthcare
utilisation endpoints in a large and diverse patient population, enabling extensive subpopulation analysis.
The study design for the CORE-VNS study has been published previously.4 In brief, the CORE-VNS study is an international, multicentre, prospective, observational, allcomers, post-market study enrolling people with DRE either receiving VNS Therapy for the first time or undergoing a VNS Therapy battery change.4 The presentations included at the LivaNova symposium described the design and baseline characteristics of patients participating in CORE-VNS, as well as the results of a recent interim analysis in a European subpopulation of the study.
The Power of Real-World Data: The CORE-VNS Study
Giannicola began her presentation by observing that the CORE-VNS study offers one of the most comprehensive contemporary real-world clinical data sets in DRE. A total of 827 patients consented to be part of this study at 61 sites in 16 countries across five continents, including 262 patients in 23 sites across the USA and Canada, 219 patients in 15 sites in six western European countries, and 346 patients in 23 sites across Asia-Oceania, Latin America, and the Middle East (data on file). Patients were assessed at baseline and then followed at 3, 6, 12, 24, and 36 months after enrolment.4,5
Endpoints analysed in the CORE-VNS study include seizure-associated outcomes comprising traditional measures of clinical benefit such as changes in seizure frequency
and severity, as well as non-seizure outcomes including measures of sleep quality, quality of life, ASM use, and healthcare resource utilisation data. In addition, safety data collected include all deaths, adverse events (AE) related to VNS Therapy, and device deficiencies (data on file).4,5
In order to convey the value of realworld evidence, Giannicola noted that health outcomes in clinical practice are multifactorial, with many contributing elements. She provided data to show that the relative influence of the five major factors impacting health outcomes may be estimated as follows: social circumstances (15–40%), environmental and physical influences (5–20%), behaviour (30–50%), genetics (20–30%), and medical care (10–20%).8 Real-world evidence enhances our understanding of treatment effectiveness, safety, and outcomes in routine clinical practice, beyond the controlled environment of clinical trials. In particular, real-world evidence bridges the gap between clinical research and everyday healthcare, driving more informed, effective, and patientcentred solutions.
As a real-world study, CORE-VNS provides extensive long-term data that can offer valuable insights to guide various stakeholders, including healthcare providers, regulatory bodies, and insurance providers regarding the use of VNS Therapy. In addition, it offers long-term health outcome data associated with the use of different VNS Therapy features (such as Scheduled Programming or AutoStimulation) across a global landscape. Furthermore, the large sample size and broad inclusion criteria allow for broad applicability to everyday clinical practice. This inclusivity also facilitates in-depth subpopulation analyses, including an evaluation of the performance of VNS Therapy in groups that are typically more challenging to recruit for focused research studies.
Giannicola commented that it was only possible to carry out the CORE-VNS study due to the hard work of multiple key players all around the world. At each of the 61 clinical sites, the study teams, study nurses, study coordinators, and
investigators are all jointly responsible for the conduct of the study in accordance with the clinical protocol, good clinical practice, and applicable regulatory requirements. Other key players on the LivaNova side include the clinical data management team, biostatisticians, programming experts, clinical monitors, safety specialists, and the clinical project management team.
CORE-VNS began with the first patient enrolment in 2018. The last patient was initiated in 2021, and the study is now in the close-out phase, with the last patient’s last visit expected by the end of 2024. The study relies on a combination of planning, executing, monitoring and controlling, and communication to ensure that it is delivered efficiently, accurately, and in a timely manner. In addition to standard data management activities, a strong data management strategy was developed in the CORE-VNS study with a focus on the review of seizures based on the 2017 International League Against Epilepsy (ILAE) classification.9 This includes, but is not limited to, the verification of consistent records of seizure frequency and type across visits, as well as consistency in seizure types, epilepsy type, and epilepsy syndromes captured. The data require careful monitoring and controlling through multiple data review cycles, resulting in data review meetings between clinical sites, medical affairs, and clinical affairs. Effective communication is ensured by tight collaboration between clinical sites, the clinical project management team, clinical monitors, statistics and data management experts, and the medical affairs team.
The large scale of the study and the dedication of all players to reach high data quality results is demonstrated by the numbers quoted by Giannicola. For example, more than 25,000 queries and edit checks have been resolved, and 4,052 seizure forms have been reviewed. In total, 3,279 patient follow-up visits have been conducted, 379 monitoring visits have been accommodated, and 252 patients with suspected genetic epilepsy have been reviewed from a clinical and genetic testing point of view by a special working group composed of paediatricians and genetics experts.
Giannicola reported that a total of 819 patients, out of the 827 who consented to be part of the study, met the eligibility criteria. Approximately 40% of the patients were under 18 years of age at implant, and a median of six ASMs had been trialled at baseline (range: 2–20). The median (range) time between epilepsy diagnosis and consent was 10 (0–62.5) years in the first-implant cohort. Cognitive status was impaired in 70.5% of the population, and the most common epilepsy type was focal (47.7%), followed by combined (34.2%) and generalised (16.1%) epilepsy. The aetiology of epilepsy was unknown in 41.2% of patients, with structural aetiology being the most commonly known type (33.3%), followed by genetic (17.0%), infectious (6.2%), immune (1.8%), and metabolic (0.5%) aetiologies. Data were also collected on 252 patients who had undergone genetic testing before baseline. On the basis of this dataset, Giannicola noted that COREVNS is on track to be one of the most comprehensive contemporary real-world clinical datasets available in DRE to date.
Giannicola concluded her presentation by reminding the audience that patients in CORE-VNS are affected by severe DRE and had inadequate seizure control despite a median of six ASMs prior to VNS Therapy. A large cross-functional team active across the globe is continuously monitoring and sampling data quality and entry to ensure highest quality results. Giannicola noted that although real-world evidence cannot substitute for randomised controlled trials (RCT), CORE-VNS provides insights to questions which cannot be answered by prior RCTs with VNS Therapy. The last patient will have their last visit at the end of 2024, upon which the study will be closedout and multiple further analyses will begin.
CORE-VNS: Contemporary VNS Therapy Outcomes of People with Drug-Resistant Epilepsy in Europe
Sen followed Giannicola’s talk on the CORE-VNS study design and baseline characteristics with a presentation of the results of an interim analysis of the
CORE-VNS study conducted among a subset of patients in Europe.
Of 338 patients who signed the informed consent and met the eligibility criteria, 11 did not have a record of VNS implant, leaving a total of 327 patients in the modified safety population (mSAF), a subset of subjects, with a signed informed consent and who met all eligibility criteria, who went through a VNS Therapy implant procedure (successful and unsuccessful). Among patients in the mSAF, 226 had their first implant during the trial, 100 underwent reimplantation, and one patient had an aborted implantation due to an AE. Unless otherwise stated, the analyses below refer to the first-implant population of 226 patients in the mSAF.
Patients included in the 'European' population were recruited in Israel (30%), the UK (27%), Belgium (16%), Italy (9%), the Netherlands (7%), Poland (6%), and Austria (5%). The mean (standard deviation) age at time of informed consent was 27.6 (17.3) years, and 65.4% of patients were aged ≥18 years at informed consent. Overall, 170 of 338 patients (50.3%) were female.
Among patients receiving their first VNS Therapy implant (n=226), the median (range) interval between diagnosis of epilepsy and informed consent was 10.8 (0.5–58) years, which highlights the considerable length of time that patients have to wait to receive VNS therapy. Individuals in this population had received a median (range) of seven (3–16) prior ASMs before being enrolled in the registry, suggesting that this is a highly refractory group. The number of prior ASMs is slightly higher than in the global population, potentially as a result of the greater drug availability. Focal epilepsy was the most common epilepsy type in this group (54%), followed by combined (30%) and generalised (14%) disease. Overall, 41% of first-implanted patients had epilepsy of an unknown aetiology, with 34%, 20%, 4%, and 1% having structural, genetic, infectious, and immune aetiologies, respectively. Just over one-third (36.7%) of first-implanted patients had normal cognitive status, with 18.1% experiencing severe impairment,
25.2% moderate impairment, and 19.9% living with minimal cognitive impairment. This population is therefore truly reflective of real-world clinical practice, unlike RCTs, where the study population may be enriched according to type of epilepsy or cognitive status.
Analysis of seizure frequency among firstimplanted patients in the mSAF population revealed a reduction in seizure frequency at the end of the study compared with baseline for all types of epilepsy (reduction in seizure frequency from baseline at 36 months was 60.2% for all seizures [n=157 at 36 months], 57.8% for focal seizures [n=135 at 36 months], and 74.4% for generalised seizures [n=37 at 36 months]; Figure 1). The reduction in seizure frequency increased with time for all seizure types, with a notable reduction evident early in the study. This is consistent with other neuromodulatory therapies, which show that seizure frequency decreases with increasing duration of neuromodulation, and that the effect on all seizures is observable early after implantation. Sen cautioned that this is
an interim analysis only and does not include 36-month data for all participants; although he noted that the interim analysis does seem to suggest a positive impact on seizures, irrespective of type.
As well as reduction in seizure frequency, there was a reduction in seizure counts over the previous 3 months between baseline (67 seizures; n=224) and 36 months (20 seizures; n=169), with some improvement noticeable by 3 months (37.5 seizures; n=190). This again suggests that VNS Therapy has a positive impact on the number of seizures.
Furthermore, disaggregation of the data reveals a reduction in seizure frequency for focal impaired awareness–motor seizures (median [95% CI] reduction of 67% [50–86.1] at 36 months [n=76] versus baseline), focal to bilateral tonic-clonic seizures (100% [58.3–100] reduction at 36 months [n=35] versus baseline), and generalised tonicclonic seizures (73.2% [10–73.2] reduction at 36 months [n=24] versus baseline),
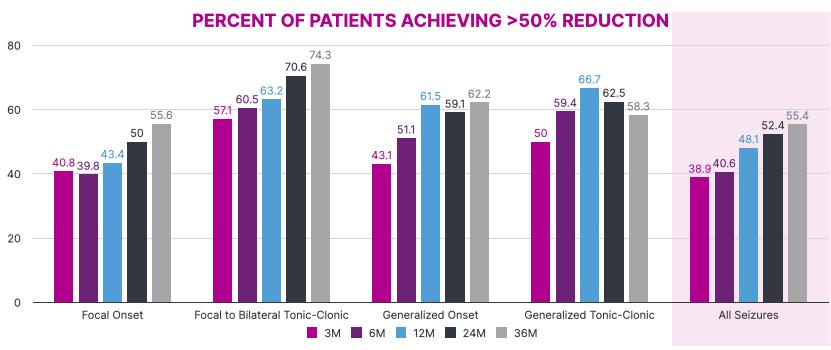
Figure 1: Median percent reduction in seizure frequency (interim data).
PERCENT OF PARTICIPANTS ACHIEVING >50% REDUCTION
although the wide confidence intervals for these datapoints should be noted.
The proportion of patients achieving >50% reduction in seizure rate increased progressively over the 36-month followup for all seizures, focal-onset seizures, focal to bilateral tonic-clonic seizures, generalised onset seizures, and generalised tonic-clonic seizures, notwithstanding the comparatively low number of patients in the 36-month dataset. Sen drew the audience’s attention to the relatively high proportion of patients achieving a greater than 50% reduction in number of seizures (Figure 2).
Of 157 patients for whom 36-month response data were available, 10.2% achieved a 100% seizure-frequency reduction at 36 months, while 33.8% achieved ≥80% improvement, and 21.6% achieved ≥50 to <80% improvement in seizure rate at 36 months.
Because CORE-VNS tracks seizures by their specific type according to 2017 ILAE classification, it is important to assess whether seizure semiology changes in the course of VNS Therapy, resulting in the
reporting of seizure types not reported at baseline. Sen presented an interim analysis showing that reporting of generalised seizure types not reported at baseline is very infrequent and occurs in less than 4% of patients. The picture is different for some focal seizure types. Approximately 20% of patients reported a specific focal seizure type in the course of VNS Therapy, which was not reported at baseline. The reason for this finding is not yet clear, although Sen speculated that it may represent natural seizure evolution of certain epilepsy types and/or VNS-associated changes in focal seizure propagation and therefore severity.
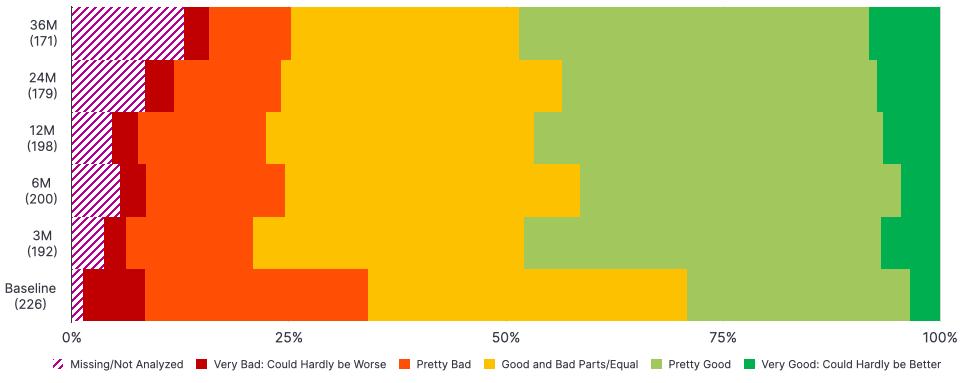
As well as seizure rate and counts, it is also important to consider the quality of life of patients with DRE. The percentage of patients reporting a very good quality of life (“could hardly be better”) appeared to increase between baseline and 36 months, while the percentage of patients with a very poor quality of life (“could hardly be worse”) decreased from baseline to 36 months (Figure 3).
In addition, there appears to be a reduction between baseline and 36 months in the
VNS implant-naïve participants. LivaNova Data on File. M: month.
of
of life (first-implanted patients; percent of patients reporting; interim data).
percentage of patients reporting that the frequency of their seizures has an impact on their quality of life, as well as a reduction in the percentage of patients who report that the difficulty or intensity of their seizures impacts their quality of life, or that their ASM affects their quality of life. Again, Sen noted that these are interim data with further work needed but commented that this might be due to the increasing availability of new treatments for epilepsy that have improved side effect profiles, although he noted that newer treatments can adversely affect mood.
Across the European study, there were 13 AEs that led to study termination. This included 11 serious AEs and six deaths (one suicide, two cases of drowning, one subdural haematoma due to seizurerelated fall, one sudden unexpected death in epilepsy, and one case of propofol infusion syndrome). Explantation of the VNS Therapy device occurred in eight patients. The treatment-emergent AEs (TEAE) recorded were consistent with previous experience of VNS Therapy, with 34.6% of 327 patients experiencing at least one TEAE. Dysphonia and dyspnoea were the most common TEAEs, reported in 11.6%
and 5.8% of patients, respectively. Other TEAEs of interest included neck pain (4.0% of patients), implant site infection (1.8%), cardiac disorders (0.9%), vocal cord paralysis (0.6%), and sudden unexpected death in epilepsy (0.3%).
Sen concluded by reiterating that this presentation represented an interim analysis and that the final results may differ. Other limitations include the fact that CORE-VNS is an open-label registry, and as such is unblinded and has no control arm, while other anti-seizure treatments (for example, ASMs) could be added, withdrawn, or altered during treatment with VNS Therapy. In addition, missing data were not imputed in this interim analysis, so the bias arising from drop-outs and missing data has not been accounted for. Sen noted, however, that these limitations should also potentially be considered as strengths as they demonstrate that the study reflects real clinical practice, with data that may be more applicable to the everyday experience of patients and physicians.
Figure 3: Summary
quality
LivaNova Data on File.
M: month.
Conclusion
CORE-VNS is the largest multicentre global post-market registry of patients diagnosed with DRE and treated with the VNS Therapy system, and provides additional insights into the effects of VNS Therapy that could not be addressed by prior RCTs alone. The CORE-VNS data presented here offer crucial evidence to guide informed treatment decisions for patients with DRE.
More than half of the 338 European patients in CORE-VNS had focal epilepsies, and approximately one-third of patients were children. The majority of European patients included in CORE-VNS were from Israel and the UK. Not all patients have yet undergone
References
1. World Health Organisation (WHO). Epilepsy: a public health imperative. 2019. Available at: https://www.who. int/publications/i/item/epilepsya-public-health-imperative. Last accessed: 24 September 2024.
2. Chen Z et al. Treatment outcomes in patients with newly diagnosed epilepsy treated with established and new antiepileptic drugs: a 30-year longitudinal cohort study. JAMA Neurol. 2018;75(3):279-86.
3. Kwan P et al. Definition of drug resistant epilepsy: consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia. 2010;51(6):1069-77.
the 36-month follow-up visit, with data from 169 of the 226 newly implanted patients available for analysis in this interim dataset. However, this interim analysis demonstrates that seizure frequency (of all seizures) was reduced at the 36-month visit by 60%, with the greatest reduction seen for generalised seizures, which were reduced by 74%. In addition, 55% of patients had experienced more than 50% seizure frequency reduction, and 34% had experienced more than 80% seizure frequency reduction by the 36-month visit. Finally, no unexpected AEs or safety concerns occurred at the point of interim analysis.
4. Sen A et al. Vagus nerve stimulation therapy in people with drug-resistant epilepsy (CORE-VNS): rationale and design of a real-world post-market comprehensive outcomes registry. BMJ Neurol Open. 2021;3(2):e000218.
5. Kwan P et al. Baseline characteristics and predictors for early implantation of vagus nerve stimulation therapy in people with drug-resistant epilepsy: observations from an international prospective outcomes registry (CORE-VNS). Epilepsia Open. 2024;9(5):1837-46.
6. LivaNova. VNS Therapy™ Safety Information. Available at: https://www. livanova.com/epilepsy-vnstherapy/engb/safety-information. Last accessed: 24 September 2024.
7. FDA. Summary of safety and effectiveness data. VNS Therapy System. 2017. Available at: https:// www.accessdata.fda.gov/cdrh_docs/ pdf/p970003s207b.pdf. Last accessed: 10 October 2024.
8. HealthAffairs. Health Policy Brief. 2014. Available at: https://www.healthaffairs. org/do/10.1377/hpb20140821.404487/ full/healthpolicybrief_123.pdf. Last accessed: 24 September 2024.
9. Fisher RS et al. Operational classification of seizure types by the International League Against Epilepsy: position paper of the ILAE Commission for Classification and Terminology. Epilepsia. 2017;58(4):522-30.
Safety Information for VNS TherapyTM
Epilepsy (Non-US)—The VNS Therapy System is indicated for use as an adjunctive therapy in reducing the frequency of seizures in patients whose epileptic disorder is dominated by partial seizures (with or without secondary generalisation) or generalised seizures that are refractory to seizure medications.
Incidence of adverse events following stimulation (>5%) were voice alteration, increased coughing, hoarseness, shortness of breath, sore throat and nausea. Infection is the most common complication of the surgical procedure.
Please see important safety information at epilepsy.livanova.com/ous-safety-information. The complete copy of the VNS Therapy™ System Epilepsy Physician’s Manual available at epilepsy.livanova.com/manuals.
Addressing Proteinuria in Patients with Immunoglobulin A Nephropathy
Through Concomitant Use of Sparsentan and Sodium-Glucose Cotransporter-2 Inhibitors
This presentation took place at the American Society of Nephrology (ASN) Kidney Week Congress, held from 23rd−27th October 2024 in San Diego, California, USA, and virtually.
Presenters: Isabelle Ayoub,1 Laura Kooienga,2 Prasanth Ravipati3
1. Division of Nephrology, Ohio State University Wexner Medical Center, Columbus, USA
2. Colorado Kidney Care, Denver, USA
3. University of Nebraska Medical Center, Omaha, USA
Disclosure: Ayoub reports a contract with George Clinical for being the US national leader on SPARTACUS (payment to their institution for salary support); payment from Travere Therapeutics; payment from Aurinia, Calliditas Therapeutics, HiBio, Otsuka Pharmaceuticals, Sanofi, Travere Therapeutics, Inc., and Vera Therapeutics for participation in advisory board activity; and speaker honorarium from Roche. Kooienga is the principal investigator for sponsor studies from Akebia Therapeutics, AstraZeneca, Boehringer Ingelheim, CARA Therapeutics, Chinook Therapeutics, CSL Behring, Galderma, Omeros, Otsuka, Reata Pharmaceuticals, Sanifit, Travere Therapeutics, and Visterra. Ravipati reports no financial disclosures related to the poster presentation.
Acknowledgements: Medical writing assistance was provided by Eleanor Roberts, Beeline Science Communications, Ltd, UK.
Disclaimer: The opinions expressed in this article are not necessarily those of CSL Vifor.
Keywords: Angiotensin II (Ang II), dual endothelin (ET) Type A receptor (ETAR) and Ang II subtype 1 receptor (AT1R) antagonist (DEARA), endothelin 1 (ET-1), glomerulonephritis, immunoglobulin A nephropathy (IgAN), kidney disease, proteinuria, sodium-glucose cotransporter-2 inhibitor (SGLT2i), sparsentan.
Support: The publication of this article was supported by CSL Vifor.
Meeting Summary
PHARMA PARTNERSHIP
IgA nephropathy (IgAN) can impact life expectancy in those affected, thus efficacious treatment is key. Endothelin 1 (ET-1) and angiotensin II (Ang II) are instrumental in the development of IgAN-associated renal damage. Use of sparsentan, a dual ET Type A receptor (ETAR) and Ang II subtype 1 receptor (AT1R) antagonist (DEARA), can lead to reductions in proteinuria and thereby help to slow kidney function decline in patients with IgAN. Sparsentan is included in the 2024 draft Kidney Disease Improving Global Outcome (KDIGO) guidelines for patients with IgAN at risk of progressive kidney function loss. Additionally, other KDIGO guidelines recommend a sodium-glucose cotransporter-2 inhibitor (SGLT2i) for all adults at risk of chronic kidney disease (CKD) progression as they are associated with reductions in both kidney and cardiac morbidity and mortality risks. If needed, there is the potential to combine these drugs. Studies regarding such use were presented in three posters at the American Society of Nephrology’s (ASN) Kidney Week 2024. The first included updated interim findings from the open label extension (OLE) study of the Phase III PROTECT trial of sparsentan in a subset of participants where an SGLT2i had been added at the investigators' discretion. Here, SGLT2i addition led to further proteinuria reduction. The second poster detailed a prespecified interim analysis of the SPARTACUS trial wherein participants with IgAN receiving an SGLT2i and angiotensinconverting enzyme inhibitor (ACEi)/angiotensin receptor blocker (ARB) treatment were switched to sparsentan plus an SGLT2i. Such a regimen led to proteinuria reduction from baseline. In the final poster, including four patients with IgAN in tertiary care, the concomitant use of sparsentan with an SGLT2i led to proteinuria reduction in the real-world setting regardless of proteinuria levels or kidney function at sparsentan initiation. Taken together, these studies suggest the utility of concomitant use of sparsentan with an SGLT2i in patients at risk of kidney failure progression.
Introduction
IgAN is an immune-complex mediated glomerular disease that typically first occurs in young- to mid-adulthood1,2 and is more common in males.3 Though rare, with an incidence rate of up to 5.7 per 100,000 per year, IgAN is a leading cause of primary glomerulonephritis.2,4 Disease progression in IgAN may be slow in some, but rapid in others.5,6 Symptoms can also vary, ranging from asymptomatic microscopic haematuria to rapid decline in renal function.7,8 Sustained proteinuria strongly predicts kidney function decline, with each incremental g/day >1 g associated with a 10- to 25-fold more rapid rate of decline.9 According to one study, compared with sex and aged-matched controls, IgAN confers a 6-year reduction in life expectancy and a 1.53-fold increased risk in all-cause mortality.8 Another study of adults with
IgAN showed an estimated 20-year survival rate of 0.28 (95% CI: 0.25, 0.31).10 As such, IgAN is an important disease to recognise and control.
IgAN can develop due to an inherited abnormality and/or following a mucosal infection.11,12 The result is increased levels of galactose deficient IgA1 (Gd-IgA1) and subsequent production of Gd-IgA1 antibodies, followed by deposition of Gd-IgA1-containing immune complexes in mesangial cells. Resulting cell activation and proliferation is stimulated by, and in turn stimulates, several mediators including ET-1 and Ang II. ET-1 has a role in vascular tone and glomerular arteriolar regulation, as well as in fluid, sodium, and renin-angiotensinaldosterone system homeostasis.13 Rapid IgAN progression is associated with increased ET-1 renal expression14 and sustained activation of the ETAR is
associated with fibrosis, tubulointerstitial inflammation, and proteinuria in IgAN.15 Ang II can enhance vasoconstriction caused by ET-1 and stimulate renal release of this molecule.16,17 Via the AT1R, Ang II is involved in proteinuria development, as well as tubulointerstitial fibrosis, renal inflammation, and vascular dysfunction in CKDs.17
According to draft 2024 KDIGO guidelines (with note that final guidance may change based on feedback), patients with IgAN at risk of progressive loss of kidney function are those with proteinuria ≥0.5 g/d (or equivalent) with or without treatment. Treatment goals for such patients include reduction ‘in the rate of loss of kidney function to <1 mL/min per year for the rest of the patient’s life.’18 This should be guided by urine protein excretion, which, the guidelines stipulate, ‘should be maintained at <0.5 g/d (or equivalent) and preferably <0.3 g/d (or equivalent).’ 18
Along with lifestyle advice, cardiovascular risk assessment, and blood pressure control, the draft guidelines state that management of IgAN-induced nephron loss should include ‘measures to reduce glomerular hyperfiltration and the impact of proteinuria on the tubulointerstitium.’ Treatment to achieve this goal includes the use of renin-angiotensin system blockade or a DEARA with or without an SGLT2i.18
Sparsentan is a once-daily, oral, novel, non-immunosuppressive, single-molecule, highly selective DEARA that directly targets glomerular injury in the kidney.17,19 It has been shown to have protective, preservative, antifibrotic, and antiinflammatory effects on a variety of kidney structures and mechanisms.20 The Phase III PROTECT trial showed that sparsentan administration led to sustained proteinuria reduction and kidney function preservation in patients with IgAN.21 Sparsentan is fully approved in the USA to ‘slow kidney function decline in adults with primary IgAN who are at risk for disease progression,’22 and has received conditional marketing authorisation in the EU (April 2024) for adults with IgAN with a urine protein-tocreatinine ratio (UPCR) ≥0.75 g/g.23
SGLT2is work to enhance urinary glucose excretion by reducing glucose reabsorption in the kidney proximal convoluted tubule.24 While developed for treatment of Type 2 diabetes, SGLT2is can also reduce albuminuria and slow the rate of estimated glomerular filtration rate (eGFR) decline,25,26 including in non-diabetic patients with CKD-associated proteinuria.27 Subgroup analysis of the ‘Dapagliflozin and Prevention of Adverse Outcomes in CKD’ (DAPA-CKD)28 and the ‘EMPAgliflozin once daily to assess cardio-renal outcomes in patients with chronic KIDNEY disease’ (EMPA-KIDNEY) trials29 showed that SGLT2i administration may be associated with reduced risk of progression to kidney failure in patients with IgAN,28,29 which was 0.49 (95% CI: 0.32, 0.74) in a meta-analysis of these trials.30
With these findings in mind, the combination of sparsentan with an SGLT2i is postulated to provide therapeutic benefits, including kidney protection, for patients with IgAN at high risk of disease progression. At the ASN’s Kidney Week 2024, three posters were presented highlighting the efficacy and safety of the combination of sparsentan and an SGLT2i in clinical trial and real-world settings.
Updated Results from the Ongoing Protect Study Open-label Extension: Adding an SGLT2i to Sparsentan According to Need
In the PROTECT trial double-blind period, patients were randomised to either sparsentan 400 mg/day or irbesartan 300 mg/day for 110 weeks.21 Participants who completed this period could enter the PROTECT OLE. Following a 4-week study drug withdrawal period (during which participants received ACEi/ARB treatment) all participants received sparsentan to a target dose of 400 mg/day, between Weeks 114 and 270. At the investigators' discretion, a concomitant SGLT2i could be initiated at any time during the OLE. Of note, a separate substudy of the PROTECT OLE is being carried out where participants are randomised to receive an SGLT2i, participants in this substudy were excluded from this analysis.31,32
Early clinical data (2023) from 21 participants in the PROTECT OLE showed that adding an SGLT2i to ongoing sparsentan treatment demonstrated a benefit regarding proteinuria reduction and was generally well-tolerated.33 Presented in this current poster were updated data from 61 patients who received at least one dose of a concomitant SGLT2i. The baseline was defined as the OLE visit closest to SGLT2i initiation.32
In this cohort, 70% were male, 70% were White, 21% were Asian, and 3% were Black/African American. They had a mean (standard deviation [SD]) age of 46.2 (11.7) years and median (interquartile range [IQR]) time from start of OLE treatment to SGLT2i initiation of 261.0 (148.0−411.0) days. Of the 61 participants, at SGLT2i initiation, 80% had a history of hypertension and 66% were taking antihypertensive medications, including calcium channel blockers (43%), diuretics (34%), beta-blockers (25%), and alpha-blockers (11%).32
At baseline, median (IQR) UPCR was 1.3 (0.8−2.3) g/g. As shown in Figure 1A, the combination of sparsentan and an SGLT2i led to a reduction in proteinuria at Week 12 that remained at Week 48 (evidenced by percentage change from baseline in UPCR geometric mean).32 Body weight (Figure 1B) and blood pressure (Figure 1C) were relatively stable over the 48 weeks, with slight reductions in eGFR (Figure 1D) over this period.32
The addition of an SGLT2i to sparsentan was generally well-tolerated. Forty-six (75%) participants had a treatmentemergent adverse event (TEAE). TEAEs in ≥5% of patients included hyperkalaemia (11%), COVID-19 (10%), hypertension (7%), and hypotension (7%), as well as CKD, cough, decreased GFR, peripheral oedema, and upper respiratory tract infection (all 5%). Seven participants (11%) had a serious TEAE, including 3% (two participants) with hyperkalaemia, and 2% (one participant each) reporting acute kidney injury, CKD, COVID-19, headache, small intestinal obstruction, spontaneous abortion, and umbilical hernia. No cases of Hy’s law were reported (alanine aminotransaminase or aspartate
aminotransaminase >3x upper limit of normal plus total bilirubin >2x upper limit of normal).32
The authors concluded that data are consistent with an additive benefit on proteinuria reduction with combination therapy of stable sparsentan plus an SGLT2i.32
Prespecified Interim
Analysis of the Phase II
SPARTACUS Trial: Combination of Sparsentan and an SGLT2I
The efficacy and safety of the combination of sparsentan and an SGLT2i is also being explored in the ongoing, exploratory, openlabel, single-arm, multicentre, Phase II SPARTACUS trial. Eligibility criteria include being aged ≥18 years with biopsy-proven IgAN, a urine albumin-to-creatinine ratio (UACR) of ≥0.3 g/g, and an eGFR of ≥25 mL/min/1.73 m2 despite stable use of an SGLT2i and maximum labelled dose of ACEi/ ARB therapy for ≥12 weeks. At baseline, ACEi/ARB use was stopped, and then sparsentan (400 mg/day) was added to the SGLT2i for 24 weeks.34
The primary efficacy endpoint in SPARTACUS is change from baseline in UACR at Week 24. Secondary efficacy endpoints are achievement of UACR of <0.2 g/g, and 30% and 50% reduction in UACR at Week 24, as well as change from baseline in UACR, UPCR, eGFR, and blood pressure at each visit. Changes are analysed with a mixed model repeated measures approach. Safety is also being assessed.34,35
In the poster presented here, data from 20 patients in a prespecified interim analysis at Week 24 were described. Mean (SD) age was 52.9 (15.0) years, weight was 90.9 (22.8) kg, and BMI was 31.4 (5.6) kg/m2 Patients were predominantly male (65%) and were White (55%) or Asian (45%).
Median (IQR) UACR at baseline was 0.84 (0.52−1.26) g/g, with UPCR being 1.45 (1.06−2.40) g/g. Mean (SD) eGFR was 54.8 (20.6) mL/min/1.73 m2, and systolic/diastolic blood pressure was 129.8 (12.5)/78.8 (10.9)
Figure 1: A) Percentage urine protein-to-creatinine ratio change from baseline, B) body weight, C) blood pressure, and D) estimated glomerular filtration rate over 48 weeks.32
Baseline: OLE visit closest to start of SGLT2i medication.
mmHg. Haematuria was present in 50% of participants and glycosuria in 90%.35
As can be seen in Figure 2A, sparsentan plus an SGLT2i led to rapid (at Week 4) and sustained reduction in UACR. The percentage UACR change at Week 24 was −39.5%. At this time point, switching from ACEi/ARB therapy to sparsentan on a background of an SGLT2i allowed patients to reach target response endpoints, as evidenced by 16% of participants with a UACR <0.2 g/g, along with nearly two-thirds having a ≥30% reduction in UACR from baseline and one third having a
≥50% reduction from baseline. EGFR levels were relatively stable (Figure 2B) and there were slight blood pressure decreases (Figure 2C).35
Sparsentan was generally well-tolerated with no unexpected safety signals. Twelve patients (60%) experienced a TEAE, which was deemed sparsentan-related in five participants (25%) and SGLT2i-related in one (5%). TEAEs reported in at least two participants included dizziness, headache, hypertension, hypotension, oedema, peripheral oedema, and osteoarthritis (all occurring in 10% of patients).
Figure 2: Changes in A) urine albumin-to-creatinine ratio, B) estimated glomerular filtration rate, and C) blood pressure at each visit.35
Percentage (95% CI) geometric least-squares mean change from baseline in UACR
Least-squares mean (95% CI) change from baseline in eGFR (mL/min/1.73 m 2 )
Least-squares mean (95% CI) change from baseline in BP (mmHg)
There was one severe TEAE of gout (5%), and three serious AEs of cerebrovascular accident in one patient, and, in the same patient, osteoarthritis and acute kidney injury (which was mild, unrelated to sparsentan or SGLT2i treatment, and resolved after treatment interruption). One TEAE of vertigo led to treatment discontinuation. No participant displayed any abnormal liver function test results.35
Similar to the PROTECT conclusion, the authors here surmised that these findings following the addition of an SGLT2i to stable sparsentan ‘are consistent with an additive benefit on proteinuria reduction’ such that the combination ‘represents an effective treatment with a good safety profile for patients with IgAN.’35
Figure 3: Change in A) urine protein-to-creatinine ratio, B) urine albumin-to-creatinine ratio, and C) estimated glomerular filtration rate following initiation of sparsentan.36
Solid lines indicate sparsentan + SGLT2i combination treatment; dashed line indicates sparsentan administered alone. Values reflect mean (%) change from sparsentan initiation (Month 0) to last follow-up.
Real-World Evidence: A Case Series of Sparsentan in Combination with an SGLT2I
While the above studies show the efficacy and safety of the combination of sparsentan and an SGLT2i in the trial setting, realworld evidence is still limited. The final poster reported data for one male and three female patients who attended a tertiary care centre and were selected by their healthcare provider for inclusion in this
case series. All patients were White with an age range of ~25−65 years and biopsyproven IgAN diagnosed from between 4 months to 11 years before baseline. Prior to receiving the sparsentan/SGLT2i combination, three patients received steroid/ immunosuppressive treatment alone or in combination with a renin-angiotensin system inhibitor. One patient received losartan alone. These treatments were discontinued prior to sparsentan/SGLT2i initiation.36
Figure 3 shows data from when the patients were initiated on sparsentan to the time of analysis. All patients received sparsentan initially at a dose of 200 mg/day, increasing to 400 mg/day after 2 weeks (or closest follow-up visit), as per label instructions. Patients received the SGLT2i dapagliflozin for ~3−5 months. As shown in Figure 3, at the time of analysis, all patients had been receiving both drugs for ~2 months. While three of the four patients were either already receiving dapagliflozin or were initiated on it concurrently with sparsentan, for one, dapagliflozin was initiated ~1 month after sparsentan initiation.36
Figure 3A shows UPCR from baseline for three of the patients, with Figure 3B showing UACR for the fourth. Decreases in these measures of proteinuria from baseline (38−82% change in UPCR and a 95% change in UACR) occurred in all patients regardless of eGFR at initiation (Figure 3C).36
As previously discussed, in the 2024 draft KIDGO guidelines, urine protein excretion should be maintained at preferably <0.3 g/d and at least <0.5 g/d.18 Here, one patient (who received 1 month of sparsentan treatment alone, then the combination for 3 months) achieved UACR 0.16 g/g (Figure 3B), and two patients achieved UPCR of
References
1. Selewski DT et al. CureGN Consortium. Clinical characteristics and treatment patterns of children and adults with IgA nephropathy or IgA vasculitis: findings from the CureGN study. Kidney Int Rep. 2018;3(6):1373-84.
2. Nair R, Walker PD. Is IgA nephropathy the commonest primary glomerulopathy among young adults in the USA? Kidney Int. 2006;69(8):1455-8.
3. O'Shaughnessy MM et al. Glomerular disease frequencies by race, sex and region: results from the International Kidney Biopsy Survey. Nephrol Dial Transplant. 2018;33(4):661-9.
4. McGrogan A et al. The incidence of primary glomerulonephritis worldwide: a systematic review of the literature. Nephrol Dial Transplant. 2011;26(2):414-30.
5. El Karoui K et al. Treatment of IgA nephropathy: a rapidly evolving field. J Am Soc Nephrol. 2024;35(1):103-16.
0.4 g/g, one after 3 months’ combination therapy and one where dapagliflozin was added for 2 months following 8 months’ sparsentan treatment (Figure 3A).36
At sparsentan initiation, all patients had haematuria, which resolved in one patient at follow-up. The sparsentan plus dapagliflozin combination was generally well-tolerated with relatively stable blood pressure.36
The authors concluded that this case series ’supports the safety and effectiveness of sparsentan in combination with the SGLT2i dapagliflozin in patients with IgAN.’ Proteinuria improvements were observed regardless of eGFR or UPCR/UACR at sparsentan initiation. These cases also highlight greater proteinuria improvements achieved with the sparsentan and SGLT2i combination than with previous treatments.36
Conclusion
The findings shown in these three posters highlight how sparsentan in combination with an SGLT2i represents an effective treatment regimen with a well-tolerated safety profile for patients with IgAN at risk of progressive kidney function decline.
6. Kidney Disease: Improving Global Outcomes (KDIGO). Glomerular Diseases Work Group. KDIGO 2021 clinical practice guideline for the management of glomerular diseases. Kidney Int. 2021;100(4S):S1-276.
7. Lai KN et al. IgA nephropathy. Nat Rev Dis Primers. 2016;2:16001.
8. Jarrick S et al. Mortality in IgA nephropathy: a nationwide populationbased cohort study. J Am Soc Nephrol. 2019;30(5):866-76.
9. Reich HN et al. Toronto Glomerulonephritis Registry. Remission of proteinuria improves prognosis in IgA nephropathy. J Am Soc Nephrol. 2007;18(12):3177-83.
10. Pitcher D et al. Long-term outcomes in IgA nephropathy. Clin J Am Soc Nephrol. 2023;18(6):727-38.
11. Kiryluk K et al. Aberrant glycosylation of IgA1 is inherited in both pediatric IgA nephropathy and HenochSchönlein purpura nephritis. Kidney Int. 2011;80(1):79-87.
12. 12. Magistroni R et al. New developments in the genetics, pathogenesis, and therapy of IgA nephropathy. Kidney Int. 2015;88(5):974-89.
13. Jandeleit-Dahm KA, Watson AM. The endothelin system and endothelin receptor antagonists. Curr Opin Nephrol Hypertens. 2012;21(1):66-71.
14. Tycová I et al. Molecular profiling in IgA nephropathy and focal and segmental glomerulosclerosis. Physiol Res. 2018;67(1):93-105.
15. Kohan DE et al. Targeting the endothelin a receptor in IgA nephropathy. Kidney Int Rep. 2023;8(11):2198-210.
16. Lin YJ et al. Angiotensin II enhances endothelin-1-induced vasoconstriction through upregulating endothelin type A receptor. Biochem Biophys Res Commun. 2014;451(2):263-9.
17. Komers R, Plotkin H. Dual inhibition of renin-angiotensin-aldosterone system and endothelin-1 in treatment
of chronic kidney disease. Am J Physiol Regul Integr Comp Physiol. 2016;310(10):R877-84.
18. Kidney Disease Improving Global Outcomes (KDIGO). KDIGO 2024 Clinical practice guideline for the management of immunoglobulin A nephropathy (IgAN) and immunoglobulin A vasculitis (IgAV). Public review draft. 2024. Available at: https://kdigo.org/wp-content/ uploads/2024/08/KDIGO-2024-IgANIgAV-Guideline-Public-Review-Draft. pdf. Last accessed: 15 November 2024.
19. Trachtman H et al. Sparsentan. Dual angiotensin II AT1 receptor blocker and endothelin ETA receptor antagonist, treatment of focal segmental glomerulosclerosis, treatment of IgA nephropathy. Drugs Future. 2020;45(2):79-98.
20. Kohan DE et al. Mechanism of protective actions of sparsentan in the kidney: lessons from studies in models of chronic kidney disease. Clin Sci (Lond). 2024;138(11):645-62.
21. Rovin BH et al., DUPRO steering committee and PROTECT Investigators. Efficacy and safety of sparsentan versus irbesartan in patients with IgA nephropathy (PROTECT): 2-year results from a randomised, activecontrolled, phase III trial. Lancet. 2023;402(10417):2077-90.
22. Travere Therapeutics, Inc. Travere Therapeutics announces full FDA approval of FILSPARI® (sparsentan), the only non-immunosuppressive treatment that significantly slows kidney function decline in IgA Nephropathy. September 5, 2024. Available at: https://ir.travere.com/ node/15251/pdf. Last accessed: 19 November 2024.
23. European Medicines Agency (EMA). Filspari® summary of product characteristics. 2024. Available at: https://www.ema.europa.eu/en/
documents/product-information/ filspari-epar-product-information_ en.pdf. Last accessed: 15 November 2024.
24. Vallon V. The mechanisms and therapeutic potential of SGLT2 inhibitors in diabetes mellitus. Annu Rev Med. 2015;66:255-70.
25. Wanner C et al.. Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med. 2016;375(4):323-34.
26. Mosenzon O et al. Effects of dapagliflozin on development and progression of kidney disease in patients with type 2 diabetes: an analysis from the DECLARE-TIMI 58 randomised trial. Lancet Diabetes Endocrinol. 2019;7(8):606-17.
27. Cherney DZI et al. DIAMOND investigators. Effects of the SGLT2 inhibitor dapagliflozin on proteinuria in non-diabetic patients with chronic kidney disease (DIAMOND): a randomised, double-blind, crossover trial. Lancet Diabetes Endocrinol. 2020;8(7):582-93.
28. Wheeler DC et al. A pre-specified analysis of the DAPA-CKD trial demonstrates the effects of dapagliflozin on major adverse kidney events in patients with IgA nephropathy. Kidney Int. 2021;100(1):215-24.
29. EMPA-KIDNEY Collaborative Group. Impact of primary kidney disease on the effects of empagliflozin in patients with chronic kidney disease: secondary analyses of the EMPA-KIDNEY trial. Lancet Diabetes Endocrinol. 2024;12(1):51-60.
30. Nuffield Department of Population Health Renal Studies Group; SGLT2 inhibitor Meta-Analysis Cardio-Renal Trialists' Consortium. Impact of diabetes on the effects of sodium glucose co-transporter-2 inhibitors on kidney
outcomes: collaborative meta-analysis of large placebo-controlled trials. Lancet. 2022;400(10365):1788-801.
31. Travere Therapeutics, Inc. A study of the effect and safety of sparsentan in the treatment of patients with IgA nephropathy (PROTECT). NCT03762850. Available at: https://clinicaltrials.gov/ study/NCT03762850?term=protect&intr=sparsentan&rank=1. Last accessed 19 November 2024.
32. Kooienga L et al. Concomitant sparsentan (SPAR) and sodium-glucose cotransporter-2 inhibitors (SGLT2is) in patients with IgA nephropathy in the PROTECT open-label extension (OLE). Abstract FR-PO851. ASN Kidney Week, 23-27 October, 2024.
33. Kooienga L et al. Concomitant sparsentan and sodium-glucose cotransporter-2 inhibitors (SGLT2i) in patients with IgA nephropathy (IgAN) in the PROTECT open-label extension (OLE). SA-PO903. J Am Soc Nephrol. 2023;34(11S):979.
34. Travere Therapeutics, Inc. A study to investigate safety and effect of sparsentan in combination with SGLT2 inhibition in participants with IgAN (SPARTACUS). NCT05856760. Available at: https://clinicaltrials.gov/study/ NCT05856760?term=SPARTACUS&intr=sparsentan&rank=1. Last accessed 19 November 2024.
35. Ayoub I et al. Concomitant sparsentan (SPAR) and SGLT2 inhibitors in adults with IgA nephropathy (IgAN) in the ongoing Phase 2 SPARTACUS trial. Abstract FR-PO849. ASN Kidney Week, 23-27 October, 2024.
36. Ravipati P et al. Sparsentan (SPAR) in combination with SGLT2 inhibitors (SGLT2i) in patients with IgA nephropathy (IgAN): a case series. Abstract FR-PO906. ASN Kidney Week, 23-27 October, 2024.
Interview
Ahead of this issue, EMJ spoke to Robert Norman, The University of Adelaide, Australia, an expert in the field of reproductive and women’s health. Having contributed significantly to IVF and reproductive endocrinology research, Norman discusses how healthcare systems could improve the early detection and management of reproductive disorders such as endometriosis, PCOS, and ovarian insufficiency.
Norman Professor for Reproductive and Periconceptual Medicine, The University of Adelaide, Australia
Q1You have contributed significantly to research on polycystic ovary syndrome (PCOS) and are the current Chair of the Australian National PCOS Alliance. How can healthcare systems better manage and support women with PCOS, and where do you think research should be focusing in this field today?
Women's health is absolutely fundamental to the health of society
Looking back to the year 2000, we were very divided across the world in understanding PCOS. The Americans had a different definition from the Europeans, and there was little consideration of what the rest of the world thought about PCOS. Within Australia, the results of a survey, which presented identical cases to internal medicine specialists and gynaecologists, showed that they each had completely different views as to what investigations and treatments should be done. We were very divided internationally.
I was lucky enough to be at the Rotterdam consensus in 2003 where we started to see some green shoots across the Atlantic. I think I was the only nonEuropean, non-American at that meeting. When I came back, I met
up with a person called Helena Teede, a physician endocrinologist who just finished her PhD. She was interested in PCOS, but she didn't know anybody outside of Australia; whereas, I knew everybody internationally! Teede has tremendous gifts in diplomacy, organisation, and raising money, and I was lucky enough to be involved with her. I remember her saying to me: “Rob, we've got to do guidelines for PCOS for Australia; we've got all this evidence that patients are unhappy and doctors don't know what's going on.” So, in 2011, we came up with Australian guidelines, which were evidence based, and published them in the Medical Journal of Australia. We were then invited by the National Institutes of Health (NIH) to a meeting on PCOS, and afterwards, the organisers took us off into a room on our own and said: “You guys know what you're doing. You're the best in the world and we've got to bring about a change.” So, the NIH came on board with our attitude.
We then did the international guidelines in 2018, this involved people from every continent, and, for the first time, we were getting
Robert
unanimity. We've recently updated this and published it last year, and that was with an even wider group of people. So, to come back to your question, how can healthcare systems better manage and support patients with PCOS? I think it's by working together, by basing our decisions on the best evidence available, and getting an international consensus.
Q2
How can healthcare systems improve early detection and management of reproductive disorders such as endometriosis, PCOS, and ovarian insufficiency in women?
Talking mainly about Australia, because that's my experience in this area, I think we are starting to recognise that women's health is absolutely fundamental to the health of society. There's been a tremendous emphasis in Australia on things such as PCOS, endometriosis, pelvic pain, menstrual disorders, and, increasingly, menopause. This all originated because there were a number of support groups that went to prominent politicians and highlighted that there was
a significant lack of funding in these important areas. This was particularly significant for endometriosis, and I think there were about five or six female parliamentarians that raised this, and the government has now put large sums of money into endometriosis research and education. There’s also now a recommendation that medical schools must put aside a mandatory amount of time for teaching about endometriosis, menopause, and PCOS, and there’s a big demand for GPs to have strong education in areas such as menopause. We also have the trades unions who are pushing for menstrual leave, IVF leave, and there's even talk now about taking time off for menopause.
The other thing that we've highlighted is something we call period poverty, and this is where menstrual products are made available free of charge to young girls and to people who can't afford them. There's been a strong message that if you go to the toilet anywhere publicly, there's toilet paper, so why are there not menstrual products?
Thanks to the work of several groups, value-added tax has been taken off all period products.
We've also developed excellent guidelines for endometriosis. We've just produced a premature ovarian insufficiency guideline together with the European Society of Human Reproduction and Embryology (ESHRE), and we have got both an ESHREand an Australian-approved unexplained infertility guideline.
Clinically, there are also many new developments occurring. Endometriosis is usually diagnosed by laparoscopy, which is expensive, and many laparoscopies have to be done to make the diagnosis. However, the government has funded important work investigating non-invasive methods, such as blood tests, to push progress in that area. I think Australia is almost the world leader at the moment in diagnosis using ultrasound methods. This has been coupled with deep learning and AI, so we're hoping that we can move away from laparoscopies completely.
In summary, we've pioneered political advocacy, we've delivered good medical practice, we've had very strong patient support, we’ve developed new diagnostic protocols, and we're trying to get education to medical schools and to all doctors.
Q3Obesity is a growing global health issue. How does obesity specifically affect women’s reproductive health, and what public health strategies would you recommend to address this issue?
Obesity has been a Western disease for a long time, but we now know that it's an international disease affecting many different countries. Thus, it has become an international problem in terms of general health, and particularly, women's health. We've got good evidence from our research that as the rates of obesity go up, rates of PCOS go up. On the other hand, if you're prone to PCOS and you stay at a low weight, you're less likely to get it.
There's also a lot of evidence that natural fertility is affected by obesity for both males and females, and if you do get pregnant, there are many metabolic issues that can occur, such as gestational diabetes. But there's also hypertension, preterm labour, and overall problems with delivery.
Later in life, diabetes mellitus, endometrial cancer, and cardiovascular disease are more common in women who are overweight. So, obesity clearly affects women's reproductive health throughout life, in addition to all the other problems that can affect your general health.
What are we doing about it? Well, one of our recommendations from our PCOS guidelines was to try
and deal with the weight before it occurs. Specifically, weight gain in the teenage years is the big problem. If you can encourage people not to put on too much weight when they're teenagers, they're less likely to get problems later. It's much easier to stop weight gain than just to lose weight. We've been trying to raise awareness among families and the general public about the benefits of maintaining a healthy weight. But one of the problems that we're facing is this issue of the stigma associated with the name obesity. It's almost not correct to use the words obesity and overweight now. We are therefore working through how we use terminology that's not offensive to people, while making sure we can deliver our message. All our programs for women's health deliver lifestyle information, for example, encouraging people to exercise for at least 150 minutes a week and to eat a relatively low-calorie diet that avoids processed foods. We also have medicines that can help with this, including GLP-1 receptor agonists, such as Ozempic (Novo Nordisk, Bagsværd, Denmark), which are having a huge impact, and people are losing large amounts of weight.
Q4Given your pioneering work in infertility and reproductive health, how do you see access to assisted reproductive technologies evolving?
I think we have a couple of trends emerging. One is the difference between rich and poor, which affects the access to fertility investigation and treatment. In the UK, you've got postcode access to IVF, meaning it's very patchy across your country, but it’s also very patchy across the world and the people who probably need IVF the most are the ones who can
least afford it. I originally came from Africa, and I'm aware that the access to IVF is extremely limited there. In Australia, inexpensive access is quite good because the government will fund up to 70% of the cost for any number of IVF cycles.
On the other hand, we're seeing increased complexity associated with assisted reproductive technology. We're using things such as AI, genetic testing, more advanced equipment, and expensive drugs. We're getting better results that way, but it's just pushing up the price and taking it away from a lot of people. So really, what I'm hoping we achieve is for the vast majority of people to receive simpler fertility treatment, and that includes being able to work out who's going to get pregnant by themselves without any help. We've worked with people in Vietnam who have developed a method that doesn't use any drugs at all and matures the eggs in the laboratory. They call that in vitro maturation, and that has a lot of promise.
A problem ahead is that we've got increasing privatisation of fertility, so most countries don't have public services for infertility, and it's a place where you can make a lot of money.
Q5
How do environmental factors like pollution, climate change, and endocrine disruptors impact women’s health, and what preventive measures could be implemented?
The vast amount of infertility that we're seeing in society, and the decreasing fertility rate across the whole world, is primarily a socioeconomic problem. It has to do with money, political systems, social attitudes, etc. As we see the total fertility rate dropping across
the world, the primary focus we should have is to work out how we can make it more economic for people to have children earlier in life. To achieve this, we need to focus on political change, such as childcare and leave after giving birth. That's the only thing that's going to change our total fertility rate. It's not going to be more IVF.
However, we then have the problem of pollution, climate change, and endocrine disruptors, which we can show are very significant in animals. We do think that the results from semen analysis are becoming more concerning in some countries. These are probably the main harbingers of something in the environment affecting fertility, but at the moment it's difficult to clearly identify the role of pollution, climate change, and endocrine disruptors. There are other people who feel more strongly about these issues than I do, and I think what they're concerned about is totally valid. But I do believe if we're going to raise our fertility rates as a society, it's more important to look at the socio-economic factors rather than the pollutants that we've got.
Q6In 2009, you founded the Robinson Research Institute, which now includes 450 researchers focusing on preconception, pregnancy, neonatal care, and paediatrics. What accomplishment related to the institute are you most proud of?
When we founded the Robinson Institute in 2009, we had some very successful groups around The University of Adelaide, Australia, focusing on paediatrics, obstetrics, gynaecology, and epidemiology, but they were all kind of working as if they were private businesses; looking after themselves rather than collaborating. So, the concept of the Robinson Institute was to try and get people to work together, to see outside of their little pool, and to encourage collaboration. Our basic concept was that we wanted to look at what we call parenting before conception. So, before an egg and a sperm get together, how can we optimise the environment biologically, environmentally, socially, and economically. We wanted to maintain this concept from before pregnancy right through to the age of 18 years.
But this was a life course, it was a continuum, it wasn't a bunch of separate groups looking at just one piece of that. We put money into that, and we have had people go on to receive huge grants. For instance, in diabetes, one group is looking at things that predispose us to diabetes at a sperm and egg level, in pregnancy, in early life, and in teenage years.
We also have people who are experts in genetics and molecular biology. We've got others who are really good at doing clinical trials or who are well versed with health systems. We cover the whole spectrum of medicine, from basic laboratory and epidemiology right the way through to health systems and changing the way that society operates.
The vast amount of infertility that we're seeing in society is primarily a socioeconomic problem
I would highlight a couple of successes. We've been very successful at IVF, and at one stage, we would have been in the top three or five units in the world. One of the big prizes in Australia is called the Eureka Prize, and this is for spectacular discoveries. This year, two of our groups won a Eureka Prize, one for AI in endometriosis, and the other one for new ways of treating cystic fibrosis.
The work that struck me most in the area of cerebral palsy was the work of Alastair MacLennan, joint Head of the Australian Collaborative Cerebral Palsy Research Group at the Robinson Research Institute, The University of Adelaide, Australia. MacLennan was an expert on medical–legal issues, and he was constantly in the courts giving information about cerebral palsy when obstetricians were being sued because they had allegedly done the wrong thing during labour. He believed this association wasn’t accurate. We've now discovered that at least 25% of all cases of cerebral palsy are genetic in origin, nothing to do with labour, and nothing to do with the doctor. This is changing the whole medical–legal environment in our country.
Q7Are there any exciting developments on the horizon that will be particularly influential to the future of women’s health?
I think that, increasingly, genetics is going to play a role. My main interest has been infertility and PCOS, and if we could screen a person for various genes, we could identify specific subtypes rather than simply diagnosing a generic condition in a patient. We will then be able to tailor treatment much more appropriately to that person. I think the personalisation of medicine is going to become more and more important, and that will come through genetics, but also through big data. Specifically, we need to assemble big cohorts together to provide very large amounts of information, and then analyse that data.
I think we are also going to see big changes in the way that women's health is managed. The next thing I hope that will happen is that society will start to see that having children is important. Obviously, people who absolutely do not want children can decide not to do that, but the evidence
is that most couples want one child more than they've actually got, and we need to look at how society can make that possible without people losing their careers for example. Currently, I think Western societies are not doing that very well. Our emphases have become far too economic, and we are neglecting to look after people who would like to have children but who don't want to be at a disadvantage.
Also, returning to the use of AI in diagnosing endometriosis as I mentioned earlier, one of our groups, headed by Louise Hull, The University of Adelaide, Australia, is recruiting thousands of women who have pelvic pain and other pelvic problems. They have a free MRI and a free vaginal ultrasound. They're then inputting all the data so that they can develop diagnostic models through deep learning and AI. One would then hope that that would be rolled out to every ultrasound and every radiology department in the country to aid in the diagnosis of endometriosis, PCOS, early endometrial cancer, adenomyosis, and even ovarian cancer.
VNS Therapy™ is an established neuromodulation therapy, indicated for both adult and paediatric patients with focal or generalised seizures, and is well tolerated by most patients without contributing to ASM toxicity.
Reduced seizure burden2,3
Seizure frequency
Seizure severity (SSQ)
Post-ictal recovery
Quality of Life (QoL) Improvements
Find out if VNS Therapy™ is right for your patient
Memory Alertness3,4
Seizure worry5 Reduction of hospitalisations and health related events6 Depressive symptoms7
Incidence of adverse events following stimulation (>5%) were voice alteration, increased coughing, pharyngitis, paresthesia, dyspnea, dyspepsia, and nausea. The most commonly reported complication following the implant procedure is infection. For a full list of side effects, please refer to labelling.
INTENDED USE / INDICATIONS
Epilepsy (Non-US)—The VNS Therapy system is indicated for use as an adjunctive therapy in reducing the frequency of seizures in patients whose epileptic disorder is dominated by focal seizures (with or without secondary generalisation) or generalised seizures that are refractory to anti-seizure medications.
Incidence of adverse events following stimulation (>5%) were voice alteration, increased coughing, pharyngitis, paresthesia, dyspnea, dyspepsia, and nausea. The most commonly reported complication following the implant procedure is infection. For a full list of side effects, please refer to labelling.
Please see important safety information at epilepsy.livanova.com/ous-safety-information. The complete copy of the VNS Therapy™ System Epilepsy Physician’s Manual available at epilepsy.livanova.com/manuals.
MANUFACTURER
LIVANOVA USA, INC.
100 Cyberonics Boulevard
Houston, Texas 77058, USA
Tel: +1 (281) 228-7200 / +1 (800) 332-1375
Fax: +1 (281) 218-9332
www.livanova.com
EC REPRESENTATIVE
LIVANOVA BELGIUM NV Ikaroslaan 83
B-1930 Zaventem, BELGIUM
Tel: +3227209593
Fax: +3227206053
www.vnstherapy.co.uk
Not approved in all geographies. Consult your labelling
Fertility rates have reached the lowest level in recent years all over the world, even in traditionally overpopulated nations such as China and India, with detrimental results in various aspects of our lives, including the economy, politics, environment, and society.1 Infertility, on the other hand, is on the rise and may reach one in every six people worldwide, according to the report released by the WHO in 2023.2 Infertility is defined as the inability to achieve a successful pregnancy after 1 year of unprotected intercourse and may be caused both by male and female factors and, in some instances, by a combination of both. According to the WHO, it is a global problem that affects millions; however, sadly, there is a lack of investment in research and funding, making access to proper treatment a privilege for very few people.2
UNDERSTANDING THE FERTILITY CRISIS
Explanations to the current situation may lie in the changing roles women have attained over the past 70 years, both in the workplace and society.1 Increased access to contraception, education, and the never-
ending battle to narrow the gender gap have contributed to this new scenario in which women have the choice to either postpone pregnancy or decide against motherhood in order to pursue other roles.1 Men, on the other hand, have also experienced relevant challenges such as job instability, and unemployment which adversely affects male fertility.3 Moreover, the decline in sperm parameters has been persistently observed all over the world and has sparked concerns in the medical community and the general public.4 Such a decrease in sperm counts may be related to a number of factors, including hazardous environmental exposures and climate change.5
In fact, family building has changed tremendously in the past years due to a number of factors, including the everincreasing demands on the job market, affecting both men and women, which means young people must invest a great deal of time and effort to find and maintain a job, leaving little time to important aspects of personal life such as finding a suitable partner, building a family, and actually spending time with them. The current unstable post-pandemic world situation with wars and economic uncertainty aggravates the problem.2
In addition, many women are giving up motherhood even in societies where traditional values prevail, and having children is deeply tied to a woman’s societal status.6 Reasons for women being without children are not clear, yet but may reflect a deep cultural and social change in the way women perceive themselves and pursue their goals and dreams, as well as the heavy burden many associate with childcare as there is a dearth of supportive policies for working mothers.7
Women who choose to balance career and motherhood do pay a price called the 'baby penalty' or 'motherhood penalty'. 8,9 In fact, mothers apparently are expected to be less available and devoted to work as they need to care for their children.9 Consequently, these women are left with a Sophie’s choice: their careers or their families. This usually results in reduced opportunities for career advancement as they are forced to work less hours, and some even abandon the labour force for good.10 In some areas, such as medicine, female physicians face huge challenges when it comes to juggling motherhood and the massive demands at work. Thus, quite a few end up either postponing or sacrificing family building so as to progress in their career.8,9
Delaying pregnancy creates another problem as women have a fixed, non-renewable number of oocytes, which results in decreased chances of pregnancy and elevated odds of infertility and miscarriage in their late 30s and early 40s.11 The reasons why the ovaries age so early are not completely understood. Women, however, often seem to be unaware of this and postpone pregnancy, not only to study and build a career but also because of economic instability, the absence of mother- and child-friendly policies at work, as well as the lack of a partner to share childcare responsibilities.11 Moreover, Nobel laureate Claudia Golding has shown motherhood affects women’s paycheques and further deepens the gender gap.7 Therefore, women should be granted support to face these challenges; otherwise, the gender gap will keep growing.
Social oocyte cryopreservation would be the alternative for those deciding to postpone pregnancy; but sadly, it is not available to all. In addition, there remain questions related to the adequate number of oocytes that should be preserved to obtain a live birth, as well as concerns regarding the risks involving pregnancies at later ages and offspring health. Social and ethical implications of freezing eggs, along with cost-effectiveness analysis and the development of public health policies, should also be taken into consideration.12 There is no doubt, however, that women should be properly counselled and educated on ovarian ageing and the real efficacy of current assisted reproduction techniques to obtain a live birth according to female age.
For those facing infertility, life may be even harder as access to modern assisted reproductive technologies (ART) remains a privilege for a few.13 In low- and middleincome countries, the situation may be worse as the costs involved are high, insurance coverage is rarely available, and public ART options are scarce or absent.14 Moreover, the workplace is usually not supportive of those needing to undergo fertility treatments, which entail several doctor’s appointments, ultrasounds, and medical procedures such as IVF, which may compromise their work schedule, thus increasing stress and job resignation.10 Data shows that almost half of the infertile couples may never seek any treatment, and around 25% will forsake it due to emotional stress.15
Although women frequently carry the heaviest burden as far as fertility treatment is concerned, one should not forget that males may account for up to 50% of the causes of infertility. Sadly, care for male reproductive health is often overlooked, receiving little attention in terms of funding and attention in the public fertility health agenda.16 Male age also appears to affect both fertility and the progeny’s health, with increased chances of congenital anomalies as well as autism, schizophrenia, bipolar disorders, and paediatric leukaemia.17
Eliminating the inequities in reproductive healthcare is a herculean task, which fortunately has attracted the attention of
several entities, such as the International Monetary Fund and the World Economic Forum, as well as medical organisations such as the International Federation of Fertility Societies (IFFS), which launched the International Fertility Education Initiative to increase awareness on reproductive health and relevant issues such as ovarian ageing, preconception care, and preventable causes of infertility.18 IFFS has recently launched a global campaign called 'More Joy'19 to increase public awareness and encourage family-building policies. The aim is to involve companies and policymakers to increase the provision of affordable, accessible, and equitable fertility care, as well as provide support at work for those facing fertility treatments. IFFS has also released a consensus report discussing the reduced global fertility rates and its consequences on reproductive health and family-building as the number of children per woman has decreased far below the replacement level.20
Following this lead, the Economist Impact has recently published a report, 'Fertility policy and practice: a Toolkit for Europe',21 which contains essential recommendations to beat the fertility crisis, including the need to develop a long-term plan, place investments in parenthood support and family services, as well as increase research and collaboration in all areas involved, from policymakers to communities and healthcare workers. Furthermore, gender equality at home and in the workplace is a key element in the fertility equation, which should be prioritised so that women can balance work and motherhood if they wish to do so. Although such reports should be praised, the document concentrates only on European countries, leaving out low income regions where fertility diagnosis and treatment are most needed.
Despite major technological advances in assisted reproduction, proper diagnosis and care are not available to anyone who might need it. In low and middle-income countries,
the direct costs of ART make it unaffordable to the majority who need it. Therefore, the implementation of public health policies that prioritise reproductive healthcare is of the utmost importance.14 Everyone should be entitled to decide if and when to build a family. Moreover, when ART is indicated, it should be available; however access to sophisticated ART treatments remains a barrier even in developed countries such as the USA and the UK. In America, almost 19 states have issued laws to increase fertility treatment coverage, but adequate access to care remains limited, mainly for underserved individuals. Thus, the American Society for Reproductive Medicine (ASRM) set up the Diversity, Equity, and Inclusion Taskforce to study and find solutions to reduce the inequities in fertility care.22 The pro-fertility wave has spread to countries such as Sweden and Japan, resulting in interesting family-friendly actions. While the Japanese are developing dating apps to boost marriage rates, Swedish grandparents may now be eligible to receive paid parental leave. Although such initiatives should be praised, there is much more to be done to overcome the fertility crisis.
CONCLUSION
In summary, considering all this evidence together makes it easy to understand why global fertility rates and live births have been dropping since 1950. Reasons to eradicate health inequities in the provision of reproductive care seem crystal clear if we are to respect basic fundamental human rights such as if and when to have a child and build a family. In the mythical Greek Sphynx tale, Oedipus saved the city of Thebes by solving the riddle and was crowned King. There is no doubt the current fertility riddle is more formidable, complex, and challenging, but it must be solved or populational ageing combined with plunging birth rates and increased infertility may create the perfect demographic and economic storm which will spare no one.
References
1. Vollset SE et al. Fertility, mortality, migration, and population scenarios for 195 countries and territories from 2017 to 2100: a forecasting analysis for the Global Burden of Disease Study. Lancet. 2020;396(10258):1285-306.
2. World Health Organization (WHO). Infertility prevalence estimates, 1990–2021. 2023. Availale at: https://iris.who.int/bitstream/hand le/10665/366700/9789240068315eng.pdf?sequence=1. Last accessed: 4 November 2024.
3. Matysiak A, Vignoli D. Family life courses, uncertain futures, and the changing world of work: state-ofthe-art and prospects. Eur J Popul. 2024;40(1):19.
4. Levine H et al. Temporal trends in sperm count: a systematic review and meta-regression analysis of samples collected globally in the 20th and 21st centuries. Hum Reprod Update. 2023;29(2):157-76.
5. Skakkebæk NE et al. Environmental factors in declining human fertility. Nat Rev Endocrinol. 2022;18(3):139-57.
6. Bhambhani, C & Inbanathan, A. Not a mother, yet a woman: exploring experiences of women opting out of motherhood in India. Asian J Women’s Stud. 2018;24(2):159-82.
7. Kim KM et al. Parenthood and paychecks-the gender pay gap in medicine. JAMA. 2024;DOI: 10.1001/jama.2024.22123.
8. Hoffman R et al. Motherhood and medicine: systematic review of the experiences of mothers who are doctors. Med J Aust. 2020;213(7):329-34.
9. Torres AJC et al. The impact of motherhood on women's career progression: a scoping review of evidence-based interventions. Behav Sci (Basel). 2024;14(4):275.
10. Imai Y et al. Risk factors for resignation from work after starting infertility treatment among Japanese women: Japan-Female Employment and Mental health in Assisted reproductive technology (J-FEMA) study. Occup Environ Med. 2020;78(6):426-32.
11. Seifer DB et al. Ovarian Aging and Fertility. JAMA. 2024;DOI:10.1001/ jama.2024.18207.
12. Alteri A et al. Elective egg freezing without medical indications. Acta Obstet Gynecol Scand. 2019;98(5):647-52.
13. Mackay A et al. Inequity of access: scoping the barriers to assisted reproductive technologies. Pharmacy (Basel). 2023;11(1):17.
14. Njagi P et al. Financial costs of assisted reproductive technology for patients in low- and middle-income countries: a systematic review. Hum Reprod Open. 2023;2023(2):hoad007.
15. Domar A et al. Barriers and factors associated with significant delays to initial consultation and treatment for infertile patients and partners of infertile patients. Reprod Biomed
Online. 2021;43(6):1126-36.
16. Esteves SC, Humaidan P. Towards infertility care on equal terms: a prime time for male infertility. Reprod Biomed Online. 2023;47(1):11-14.
17. Kaltsas A et al. Impact of advanced paternal age on fertility and risks of genetic disorders in offspring. Genes (Basel). 2023;14(2):486.
18. Harper JC et al. The international fertility education initiative: research and action to improve fertility awareness. Hum Reprod Open. 2021;2021(4):hoab031.
19. International Federation of Fertility Societies (IFFS). More Joy. Available at/: https://www.iffsreproduction.org/ morejoycampaign/. Last accessed: 4 November 2024.
20. Fauser BCJM et al. Declining global fertility rates and the implications for family planning and family building: an IFFS consensus document based on a narrative review of the literature. Hum Reprod Update. 2024;30(2):153-73.
21. Fertility policy and practice: a Toolkit for Europe. Available at: https://impact.economist.com/ perspectives/health/fertility-policyand-practice-toolkit-europe. Last accessed: 4 November 2024.
22. Mahabamunuge J, Seifer DB. Moving toward narrowing the United States Gap in Assisted Reproductive Technology (ART) racial and ethnic disparities in the next decade. J Clin Med. 2024;13(8):2224.
Clinical Applications of Hyperpolarised Xenon-129 MRI
Editor's Pick
The editor’s pick for this issue is a review article discussing the promise of hyperpolarised xenon MRI, a non-invasive imaging technique used in respiratory medicine to assess lung function, including ventilation and diffusion, without ionising radiation. By making an inert gas visible via MR spectroscopy, it allows for the visualisation and quantification of gas flow and gas exchange disruptions in the lungs. This technique has shown promise in providing reliable measurements of disease severity and assessing progression and treatment response more sensitively than conventional methods. Further multi-centre studies could help to evaluate this exciting innovation’s role in different disease settings.
Authors: *Kher Lik Ng,1,2 James Grist,2 Fergus Gleeson,1,2 Emily Fraser1
1. Oxford University Hospitals NHS Foundation Trust, UK
2. University of Oxford, UK
*Correspondence to kherlikng@nhs.net
Disclosure: The authors have declared no conflicts of interest.
Conventional imaging modalities, the X-ray and CT, are essential diagnostic tools in respiratory medicine, providing qualitative information regarding the pattern and extent of pulmonary pathology. Neither provide information regarding the functional impact of pulmonary diseases and additional investigations are required to assess this. Hyperpolarised xenon-129 MRI (HPX-MRI) is a non-invasive, ionising-free imaging modality that can provide functional measurements of ventilation and diffusion within the lung. The MRI-based technique involves the subject breathing in an inert gas that has been hyperpolarised to make it visible using MR spectroscopy. The gas mirrors the flow of oxygen through the bronchial tree, across the alveolar membrane, and into the pulmonary capillaries, and thus disruptions in the passage of gas due to ventilation and diffusion abnormalities can be visualised and quantified. Functional measurements of ventilation and gas exchange within regional areas of the lung can be obtained. HPX-MRI has the potential to detect early lung disease not yet evident using standard investigations and has been shown to be a sensitive modality to assess treatment responses. The role of HPX-MRI in respiratory medicine has the potential to be wide-reaching, but to date it remains largely a research tool. This review article summarises the current and possible future clinical applications of HPX-MRI in the investigation and management of lung diseases, pitched at a level comprehensible and relevant to the respiratory-focused clinicians.
Key Points
1. Hyperpolarised xenon-129 MRI (HPX-MRI) is a functional imaging technique that provides global and regional measurements of ventilation and gas exchange and can assist in the assessment and management of respiratory diseases.
2. An overview of the technology and clinical applications of HPX-MRI, aimed at respiratory-focused clinicians.
3. HPX-MRI is a functional imaging modality that is safe, quantitative, and reproducible. Clinical studies have highlighted its role in phenotyping respiratory pathology, early-stage disease detection, assessing progression, and therapeutic response to treatment.
INTRODUCTION
The advent of CT has enabled the assessment of different tissue densities of internal organs in 'slices', and thereby transformed the diagnosis and management of many respiratory diseases.1,2 Although CT provides valuable spatially resolved information about lung structure and pathology, correlating radiological findings with functional investigations is necessary to understand the physiological impact of a disease. MRI is capable of producing detailed images of soft tissue structures; however, until recently, its utility for investigating pulmonary conditions has been limited. The development of hyperpolarised gas MRI has enabled functional imaging of the airways and alveoli and provides a reliable measure of gas exchange, improving our understanding of respiratory pathology.3,4 Hyperpolarised gas MRI can identify regional areas of abnormality and directly measure the physiological impact of disease locally and for the whole lung. This review summarises the current and potential applications of hyperpolarised xenon-129 MRI (HPX-MRI) in the investigation and management of respiratory diseases.
Conventional MRI relies on the signal generated from exciting protons to generate images. As the lung parenchyma has a high air content and low proton density, the signal generated from the lung is limited and precludes adequate structural assessment.5 More recently, there have been some advancements in MRI resulting in enhanced visualisation of lung structure using techniques such as ultra-short echo-time and zero echo-
time imaging. These approaches acquire data from the rapidly decaying signal from protons in the lungs, providing improved visualisation of structure in comparison to conventional MRI, but still does not provide visualisation of lung function.6,7
For many lung diseases, high-resolution CT imaging provides a diagnosis, informs the need for treatment, and enables longitudinal monitoring of disease.8 However, traditional imaging does not assess the functional impact of diseases and may poorly differentiate incidental findings from disease in its early stage when it may be reversible or more readily treatable.9 Current pulmonary function testing in clinical practice provides a useful ‘global’ assessment of lung function but lacks the ability to localise areas of lung abnormality. Given the heterogeneity of many pulmonary diseases and the way they progress, assessing regional function may provide important prognostic information. Furthermore, traditional pulmonary function testing is reliant on patient effort and technique and is associated with a degree of inherent variability (up to 15% for gas transfer), and consequently may not always provide reliable measurements.10-12 These limitations highlight the advantage of novel and more sensitive diagnostic techniques that can both detect and assess functional components of lung disease.
Current functional imaging techniques used in clinical practice are planar ventilation/perfusion (V/Q) scintigraphy and single photon emission CT (SPECT) V/Q. These display the
distribution of radiolabelled gas and macroaggregates of albumin during the ventilation (V) and perfusion (Q) phases, respectively.13,14 These planar images provide limited spatial information, which although improved using SPECT, has significantly lower spatial resolution than hyperpolarised gas MRI.15,16 SPECT V/Q enables disease quantification but involves ionising radiation, limiting its use for repeated scanning in patients with chronic disease.14,17
The development of hyperpolarised noble gases, helium-3 (3He) and xenon129 (129Xe), as inhaled contrast agents in pulmonary MRI started in the 1990s.18-21 The inhalation of hyperpolarised xenon129 enables direct visualisation of functioning lung structure as it flows and fills the airways and alveoli, mirroring the passage of oxygen.22 Abnormalities in ventilation due to airway narrowing or bullae formation can be qualitatively and quantitatively measured.15 Defects in the transfer of gas across the alveolar capillary can also be assessed, providing a sensitive measurement of the membrane and pulmonary vasculature integrity.3
HPX-MRI is a state-of-the-art non-invasive, ionising-radiation-free functional imaging modality that is reproducible, quantitative, safe, and involves minimal patient effort.3,4
The potential role of this modality in respiratory medicine is wide-reaching but it remains, to date, largely a research tool. Clinical studies, however, indicate a valuable role in enhanced phenotyping, early-stage disease detection, therapeutic guidance, and improving our understanding of disease mechanisms.23
HYPERPOLARISED XENON-129 MRI
Conventional MRI relies upon the signal provided by protons primarily attached to water and fat molecules. Other atoms visible in an MRI scanner include the inert atmospheric gas, xenon-129, phosphorus-31, and sodium-23/ carbon-13, which are present at very low natural abundance, and so detecting signals from these atoms in vivo is challenging.24 However, using concentrated xenon-129 gas
and a process known as ‘hyperpolarisation’, it is possible to transiently boost its signal by approximately 5–6 orders of magnitude for a limited time.3,24,25 This, in turn, provides enough signal to directly image the spatial distribution and movement of inhaled xenon-129 gas in vivo. Hyperpolarisation is achieved when a gas mixture containing xenon-129 is fed into an optical cell containing Rubidium (Rb) vapour and a laser polarises the Rb atoms. The resulting Rb-129Xe interaction transfers the electron spin polarisation to the xenon-129 nuclei.3 This process is called spin exchange optical pumping.
To image xenon-129, a radiofrequency coil (fitted around the chest) and a broadband radiofrequency amplifier and software (for tuning to the resonance frequency of xenon-129) are required for signal detection.4 These devices are not commonplace in most MRI units and require additional funding to purchase. The scan process involves the patient inhaling up to 1L of xenon-129 from a gas delivery bag and holding their breath for around 10–15 seconds whilst lying in the MRI scanner. Xenon-129 has been evaluated for its safety and tolerability, and major adverse effects have not been reported. Mild side effects are recognised, but are transient and include dizziness, paraesthesia, and euphoria.26-28
The process of hyperpolarisation therefore enables the signal from xenon-129 to be detected within the lungs after it is inhaled by the subject. Airway abnormalities causing ventilation defects, such as bronchial wall narrowing due to asthma, appear as regional signal defects and can be quantified using a gas distribution cluster-map. In this form of static ventilation imaging, measurement of ventilation deficits is represented by the ventilation defect percentage (VDP), defined as the fraction of unventilated lung. This is calculated from the ventilation defect volume divided by thoracic cavity volume, expressed as a percentage (Figure 1A).29,30
Delays in the diffusion of gas across the alveolar-capillary epithelium into red blood cells (RBC) due to structural abnormalities at this interface or the pulmonary vasculature,
can be quantified and assessed using 'dissolved-phase' imaging. After inhalation, xenon-129 diffuses from the alveoli (gasphase) into the alveolar capillary membrane. About 2% of the inhaled xenon-129 then diffuses into the capillary blood stream, where it transiently binds with haemoglobin in RBCs (dissolved-phase).3,31-33 Due to an MRI phenomenon known as ‘chemical shift’, xenon-129 exhibits different resonance frequencies within the three different compartments. Following detection and reconstruction of the MR data, it is possible to assess the ratio of xenon-129 within gas phase, tissue barrier and plasma (TP), and RBC components (Figures 1B and 2A).24,34,35 Typically, 1–2% of the xenon-129 signal originates from xenon-129 dissolved in the lung tissue, and is not exclusively from xenon-129 bound to haemoglobin.
It is also possible to assess the movement of xenon-129 gas within the alveoli using ‘diffusion-weighted imaging’, and from this, obtain information about the integrity of the alveoli.3 Gas movement (referred to here as ‘diffusion’) is mainly limited by the proximity of the surrounding tissue. Therefore, in diseases where there is destruction of the alveolar architecture (e.g. emphysema), gas can move more freely within the remaining enlarged alveolar spaces (Figure 2B). This is represented by apparent diffusion coefficient (ADC) that measures the Brownian motion of xenon-129 within the alveoli, with increased values denoting greater movement of gas due to reduced alveolar integrity.3
CLINICAL APPLICATIONS
Obstructive Airway Diseases Asthma
Assessment of regional ventilation defects, disease
severity and treatment response
Asthma is a chronic disease characterised by airway hyper-responsiveness and inflammation, resulting in increased airways resistance.36 The severity and distribution of the disease can be both visualised and quantified by assessing the
pattern of xenon-129 within the airspaces after inhalation using ventilation maps. Typically, a heterogeneous distribution of gas is observed and ventilation defects (indicated by raised VDP) have been reported, even in cases of well-controlled asthma (Figure 1C).29,30,37-40 Heterogeneity is normally represented by the coefficient of variation, which is calculated as the ratio of the standard deviation to the mean of the xenon-129 signal intensity. In keeping with the typically reversible nature of the disease, Svenningsen et al.29 and Safavi et al.37 found significant improvement in the extent of ventilation defects, alongside a reduction in the coefficient of variation on ventilation maps, following bronchodilator treatment (Figure 1C).
VDP has been found to correlate well with forced expiratory volume in 1 second (FEV1), FEV1/forced vital capacity (FVC) ratio, forced expiratory flow between 25% and 75% of vital capacity, fractional exhaled nitric oxide, and lung clearance index (LCI).30,37-42 LCI is a non-imaging lung function measurement technique commonly used in children unable to undertake spirometry. LCI assesses small airway inhomogeneity by measuring the ventilation distribution of a tracer gas over cycles of tidal breathing, and has been found to be more sensitive at detecting ventilation abnormalities than FEV1 43,44 Following bronchodilator challenge, Safavi et al.37 found an improvement in VDP, but not in LCI, in children with asthma, suggesting the potential capability of HPX-MRI to detect more subtle ventilation inhomogeneity than LCI and greater sensitivity in assessing response to treatment. The VDP may also provide a more accurate measure of disease severity, with Lin et al.42 showing that higher VDP scores correlated well with clinical severity in children, assessed by number of healthcare attendances and use of corticosteroids. Given the sensitivity of HPX-MRI in identifying ventilation defects, it may also provide a more sensitive method of assessing and monitoring treatment response in comparison to conventional lung function tests (LFT). McIntosh et al.45 and Kooner et al.46 reviewed the impact of the novel biologic treatment,
A) HPX-MRI ventilation imaging showing xenon-129 gas distribution (yellow to purple) within the tracheobronchial tree and lung fields in a young healthy control. B) Examples of the gas, TP, and RBC phases (not corrected for coil inhomogeneity) reconstructed into HPX-MRI ratio maps in a healthy volunteer. The gas phase demonstrated distribution of xenon-129 gas within the airways with no evidence of ventilation defects, indicative of normal airway calibre. The TP phase similarly demonstrated distribution of xenon-129 as in the gas phase, indicating normal gas transfer from the airways into the interstitial membrane and plasma. The RBC phase also demonstrated distribution of xenon-129 similar to the TP phase, demonstrating normal gas transfer into the red blood cells from the interstitial membrane and plasma. C) HPX-MRI ventilation images depicting ventilation defects (arrows), which improved following bronchodilator administration. There are other areas of persistent ventilation defects that had not resolved following bronchodilator administration. Original image provided by POLARIS group, University of Sheffield. HPX-MRI: hyperpolarised xenon-129 magnetic resonance imaging; RBC: red blood cell; TP: tissue barrier and plasma.
Figure 1: Example images of hyperpolarised xenon-129 MRI.
Figure 2: Illustrative images showing the movement of xenon gas within the alveolar capillary unit.
Alveoli/Airspace
Chemical/frequency shift (ppm)
A(i) Similar to oxygen, xenon-129 moves into the alveoli during the ventilation phase, before diffusing into the tissue/ alveolar membrane and plasma (blue to yellow). Xenon-129 then binds to the red blood cells (yellow to red). (Created with Biorender.com). A(ii) The chemical/frequency shift represents a change in the resonance frequency of xenon-129, due to alterations in the chemical environment within each compartment. When xenon-129 atoms move between compartments, the xenon-129 signal frequency changes instantaneously, occurring simultaneously with the physical movement of xenon atoms. This figure depicts the distinct frequency shifts of xenon-129 on the xenon-129 spectrum. The colour of each frequency shift in each compartment corresponds with the colour of xenon-129 in each compartment in Panel Figure A(i). B) Schematic description of gas flow (arrows) within the alveoli, with more free-moving gas in emphysematous alveoli due to destruction of alveolar tissue contributing to raised ADC in COPD. (Created with Biorender.com).
ADC: apparent diffusion coefficient; COPD: chronic obstructive pulmonary disease; ppm: parts per million.
benralizumab, which showed improvement in VDP, although not in FEV1 or LCI, as early as 14-days post-treatment.
HPX-MRI also has a potential role in guiding bronchial thermoplasty. Ventilation defects have been shown to correspond to airway narrowing, and Svenningsen et al.47 undertook HPX-MRI on patients with asthma, pre-procedure, to identify the most severely affected airways.47 Investigators found that this image-targeted approach reduced the number of thermoplasty treatments required compared to patients enrolled in the standard non-image guided arm.47,48
Chronic Obstructive Pulmonary Disease
Assessment of regional ventilation defects, integrity of alveolar tissue and lung function
Chronic obstructive pulmonary disease (COPD) is characterised by persistent respiratory symptoms resulting from airflow obstruction secondary to chronic inflammation, and a variable reduction in the integrity of the lung parenchyma due to the presence of emphysema.49 HPX-MRI can be used to quantify ventilation defects through the VDP and provide a measure of the quality of alveolar tissue via diffusion (ADC) measurements (Figure 2B and 3A). In COPD, the VDP and ADC are raised, with regional measurements typically highest in the upper lobes where emphysema is most prevalent.50-55 The ADC correlates with measures of airflow obstruction on LFT, diffusing capacity of the lungs for carbon monoxide (DLco) transfer factor, and quantitative emphysema scores on CT.50,51,5358 Similar to asthma, the VDP correlates well with FEV1 and FEV1/FVC ratio.
HPX-MRI enables the assessment of gas exchange at the alveolar-capillary membrane, providing an additional measure of functional deficit in COPD. Calculating the ratio of xenon-129 in the gas phase (i.e. within the alveoli), TP (representing the alveolar capillary membrane and plasma), and RBC from dissolved-phase imaging can provide sensitive gas transfer measurements. In COPD with emphysema, reductions are typically seen in all ratios:
the TP:Gas (a measure of gas diffusion across the interstitial tissue providing information on tissue density), RBC:Gas (the HPX-MRI counterpart of DLCO, and a measure of gas transfer from alveoli into the RBCs), and RBC:TP (a measure of gas exchange efficiency from interstitial tissue to blood).55,59
HPX-MRI may play a useful role in the early diagnosis of COPD when LFT parameters remain within normal range. Functional alveolar wall thickness can be computed from xenon-129 uptake, and has been shown to be increased in ‘healthy’ smokers with normal lung function compared with healthy non-smokers, thereby detecting the early-stage changes associated with COPD.57,60-62 Using an innovative 3D alveolar gas-exchange model extrapolated from HPX-MRI dissolved-phase imaging data, the functional volume of pulmonary tissue, capillaries, and veins can be measured.63 Unsurprisingly, this is diminished in COPD compared to healthy controls, but interestingly, significant reductions in the functional volume of pulmonary tissue were also noted in patients with only very minimal emphysematous changes on CT. This suggests a potential additional method of assessing asymptomatic early-stage disease.
A further clinical application of HPX-MRI is the potential detection of collateral ventilation in severe COPD. Collateral ventilation refers to the direct flow of air between alveolar structures, bypassing the normal airway route.64 In severe emphysema, where lung volume reduction treatment is being considered, establishing the presence of collateral ventilation between lung lobes is essential to determining the likelihood of procedural success. Traditionally, this is assessed by two modalities: quantitative CT analysis of lung fissure integrity, and through endobronchial catheter occlusion of the lobar airway using the Chartis system® (PulmonX Inc., Redwood City, California, USA).65 Using the Chartis system®, if there is no collateral ventilation, the occluded airway results in lobar lung collapse following the one-way expiration of air. However, in the presence of collateral ventilation, the lung lobe does not deflate
due to the flow of air from adjacent lobar structures. Whilst this method is sensitive, it is invasive, time consuming, and requires technical expertise available only in a limited number of specialist centres. Advances in dynamic HPX-MRI ventilation imaging may provide a more convenient and non-invasive alternative, enabling the measurement and visualisation of collateral ventilation in patients with COPD. This has been evaluated in studies by Marshall et al.66,67 and Chen et al.68 who used 3HeMRI and HPX-MRI, respectively, to assess the presence of collateral ventilation, demonstrated by delayed filling of gas in non-ventilated regions (Figure 3B).
Idiopathic Pulmonary Fibrosis
Assessment of septal wall thickness, lung function, disease severity and prognosis
Idiopathic pulmonary fibrosis (IPF) is a progressive fibroproliferative disease characterised by the progressive accumulation of scar tissue that gradually replaces the normal lung parenchyma.69 Established fibrosis is evident on CT, and disease progression is traditionally assessed through worsening CT findings and a fall in the LFT parameters, such as FVC and DLCO. The role of HPX-MRI has been investigated in several research studies, and findings suggest it may be a more sensitive way of evaluating disease progression and response to treatment.
Unsurprisingly, studies using HPX-MRI dissolved-phase imaging to measure the RBC:TP and RBC:Gas have found the ratios to be consistently lower than in controls, signifying reduced gas transfer due to thickening and fibrosis of the interstitium.70-81 These dissolved-phase parameters strongly correlated with measurements of septal wall thickness and DLCO. However, RBC:TP has the advantage over DLCO in that it is more reproducible (and therefore more accurate) and can directly measure the function of alveolar-capillary membrane regionally.82 It can be measured continuously after inhalation of xenon-129, independent of the patient’s effort. In IPF, the pattern of HPX-MRI abnormalities is typically most marked in the basal and
peripheral lung regions, consistent with the distribution of disease.74,78
Studies comparing histology and CT findings have shown that early fibrotic changes identified histologically may not be evident on CT.83,84 Through the ability of HPX-MRI to probe the lung parenchyma functionally, regional abnormalities in gas transfer can be identified that may be below the resolution of CT.72,85 Hahn et al.72 reported that patients with IPF who have progressive disease demonstrated a reduction in the RBC:TP in normal appearing lung, in comparison to those who did not progress over the study period.72 Comparing visually detected and semi-quantitative assessed lung fibrosis with HPX-MRI parameters, no significant correlation was seen, suggesting that functional HPX-MRI changes may predate radiological fibrosis on CT.77,79
Studies evaluating HPX-MRI dissolvedphase imaging in IPF have found that the uptake of xenon-129 into the interstitial tissue (represented by TP compartment) is raised, demonstrated by an elevated TP:Gas ratio.70,74,76,77,79,81 This indicates that there is a larger tissue volume relative to the alveolar gas volume for xenon-129 to dissolve. The apparent ratio increase can be due to fibrotic tissue formation, as well as a reduction in lung compliance, which reduces the ventilation volume and thereby increases the TP:Gas ratio. Interestingly, this finding has been identified by Qing et al.79 even in patients with normal or mildly impaired pulmonary function tests and radiologically early disease, suggesting that HPX-MRI may pick up early fibrosis, or possibly areas of active fibrogenesis, which theoretically may have a reversible component.79 HPX-MRI may also provide important prognostic information. Rankine et al.80 found that the presence of both abnormal TP and RBC phases inferred an increased risk of mortality and/or the need for lung transplantation.
Long COVID/Post-COVID-19 Syndrome
Assessment of lung function
Post-COVID-19 syndrome, more commonly known as long COVID, has been defined by the National Institute for Health and Care
He ADC ~0.2 cm /s
He ADC ~0.5 cm /s
A) An example of helium-3 MRI ADC maps (HPX-MRI produces similar ADC maps) with corresponding ventilation images in a healthy volunteer and a patient with emphysematous lungs, highlighting higher ADC (bright yellow) in areas of abnormal emphysematous lungs. The patchy voids (arrows) in the ADC map of the patient with emphysematous lungs signify areas of ventilation defect where ADC cannot be quantified. The whole lung mean ADC of approximately 0.5 cm2/s was higher in emphysematous lungs than in healthy lungs (approximately 0.2 cm2/s). Original image provided by POLARIS group, University of Sheffield. B) HPX-MRI images illustrating the dynamic filling of ventilated defects (arrow) in a patient, suggesting the presence of collateral ventilation. C) Chest CT, proton (1H), and RBC:TP HPX-MRI images illustrating the heterogenous pattern of xenon-129 signal and reduced RBC:TP ratio in a patient not hospitalised for COVID-19 infection with unremarkable lung parenchyma on chest CT, months after the initial infection.
ADC: apparent diffusion coefficient; HPX-MRI: hyperpolarised xenon-129 magnetic resonance imaging; RBC: red blood cell; TP: tissue barrier and plasma.
Figure 3: Example images of hyperpolarised helium-3 and xenon-129 MRI.
HPX-MRI (RBC:TP)
Excellence (NICE) guideline as ‘signs and symptoms that develop during or following an infection consistent with COVID-19, which continue for more than 12 weeks and are not explained by an alternative diagnosis’.86 Breathlessness is a particularly common symptom, and conventional investigations are often unremarkable.
Several studies have examined the role of HPX-MRI to investigate breathlessness in previously hospitalised patients with COVID-19. Li et al.87 evaluated patients at baseline and at 1-month follow-up after hospital discharge with COVID-19 pneumonia and identified the presence of ventilation defects on HPX-MRI. These abnormalities were co-located within areas of residual ground glass opacification related to the primary pneumonic process. The ground glass changes on chest CT were also associated with reduced gas transfer and functional septal wall thickening, although interestingly, reduced RBC:TP ratio and raised VDP were also seen within normal areas of lung on CT. This likely indicates the persistence of microstructural damage following radiological resolution. Furthermore, Grist et al.88 showed impaired gas transfer measured by the RBC:TP ratio in 12 patients post-COVID-19, despite a normal or near-normal chest CT 3–6 months following hospital discharge. Matheson et al.89 reported similar findings with significantly reduced RBC:TP ratios 6–12 months after infection in 12 patients posthospitalisation.The presence of persisting functional lung abnormalities following COVID-19 pneumonia severe enough to warrant hospitalisation is not necessarily surprising. Patients not hospitalised for COVID-19 rarely have evidence of a prior pneumonic illness on their chest CT scans, although breathlessness in this group is a common finding. Interestingly, in a small pilot study by Grist et al.88 seven out of 11 non-hospitalised patients from the first wave of the pandemic were found to have significant reductions in RBC:TP ratio and DLCO 3–15 months after their initial infection.
Although the participant numbers within these studies were small and the association with symptoms unclear, it is of note that many of the participants had their
initial infection over 6 months previously, indicating that the abnormalities seen cannot be explained by a transient viral lung injury (Figure 3C).88,89 The pathophysiology underlying these HPX-MRI abnormalities is also unknown, although, the low RBC:TP ratio suggests that the defect lies at the alveolar-capillary membrane due to either alveolar membrane damage and/ or disruption of pulmonary blood flow. A larger multicentre research trial is currently underway to further assess the impact of COVID-19 on lung function using HPX-MRI.90
Other lung conditions
The role of HPX-MRI has also been evaluated in a range of other diseases, including cystic fibrosis (CF), lymphangioleiomyomatosis, and pulmonary hypertension (PH). In each condition, the potential main advantage of HPX-MRI over conventional investigations lies in its ability to detect early abnormalities and identify subtle changes in disease status, both in terms of treatment response and disease progression.
In CF, for example, ventilation abnormalities can be observed through VDP measurements in the absence of lung function changes.91-104 Following antibiotics during CF exacerbation, Rayment et al.105 found a larger improvement in the VDP than either the FEV1 or LCI, suggesting superior sensitivity of the VDP over other measurements. In lymphangioleiomyomatosis, early cystic lung changes have been identified and can be functionally assessed through VDP and ADC measurements when spirometry values are preserved.96,106 In the setting of PH, which is formally diagnosed via right heart catheterisation, the role of HPX-MRI has been evaluated as a noninvasive alternative.107-109 Comparing HPX-MRI parameters to COPD, IPF, and heart failure, PH exhibited unique characteristics with focal reductions in gas transfer (RBC:TP).107 Investigators found that in the absence of lung disease, HPXMRI had good diagnostic accuracy when compared to right heart catheterisation in pre-capillary disease, although, further work looking at its application in a larger cohort and different subtypes of PH is
required.108 HPX-MRI has also been studied in paediatric populations. In this setting, the modality has the advantage over conventional lung function tests due to the ease of performing the technique, as only a single breath hold is required, rather than multiple breathing manoeuvres. Furthermore, HPX-MRI measurements have been found to be highly reproducible, even between centres, making it appealing as a longitudinal tool.101 HPX-MRI has been trialled as an alternative method to detect ventilation abnormalities in children who were unable to perform spirometry following bone marrow and stem cell transplant.95,96,110 In bronchopulmonary dysplasia, a congenital condition characterised by diminished lung tissue due to immature alveoli formation, HPXMRI has been utilised to quantify the extent of functional impairment through the reductions in the TP:Gas ratio.95
References
1. Richmond C. Sir Godfrey Hounsfield. BMJ. 2004;329(7467):687.
2. Robb WL. Perspective on the first 10 years of the CT scanner industry. Academic Radiology. 2003;10(7):756-60.
3. Roos JE et al. Hyperpolarized gas MRI: technique and applications. Magn Reson Imaging Clin N Am. 2015;23(2):217-29.
4. Eddy RL, Parraga G. Pulmonary xenon-129 MRI: new opportunities to unravel enigmas in respiratory medicine. Eur Respir J. 2020;55(2):1901987.
5. Bergin CJ et al. Magnetic resonance imaging of lung parenchyma. J Thorac Imaging. 1993;8(1):12-7.
6. Hatabu H et al. Expanding applications of pulmonary MRI in the clinical evaluation of lung disorders: Fleischner Society Position Paper. Radiology. 2020;297(2):286-301.
7. Guo F et al. Ultra-short echo-time magnetic resonance imaging lung segmentation with under-annotations and domain shift. Med Image Anal. 2021;72:102107.
CONCLUSION
This review has summarised the versatility and potential clinical applications of HPXMRI in the diagnosis and phenotyping of pulmonary diseases. Studies have shown that it can provide reliable measurements of disease severity, assess progression, and monitor treatment response more sensitively than conventional methods. HPX-MRI has the advantage over traditional lung function modalities by providing regional and spatial functional measurements and can detect evidence of preclinical disease. Its utility in pre-procedure assessments, such as lung volume reduction procedures, may negate the need for invasive tests. However, to date, most HPX-MRI studies have involved relatively small patient cohorts, and as a modality, it remains within the research realm. With technological advances, including improved transportability of hyper-polarised xenon-129 gas, larger multi-centre site studies are needed to further evaluate its role in different disease settings and assist in its translation into clinical practice.
8. Lynch DA, Oh AS. High-spatial-resolution CT offers new opportunities for discovery in the lung. Radiology. 2020;297(2):472-3.
9. van Beek EJ, Hoffman EA. Functional imaging: CT and MRI. Clin Chest Med. 2008;29(1):195-216, vii.
10. Hruby J, Butler J. Variability of routine pulmonary function tests. Thorax. 1975;30(5):548-53.
11. Herpel LB et al. Variability of spirometry in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2006;173(10):1106-13.
12. McCormack M. Facing the noise: addressing the endemic variability in DLCO testing. Resp Care. 2012;57(1):17-25.
13. Mirza H, Hasmi MF. Lung ventilation perfusion scan (VQ scan) [Internet] (2023) Treasure Island: StatPearls. Available at: https://www.ncbi.nlm. nih.gov/books/NBK564428/. Last accessed: 17 July 2023.
14. Petersson J et al. Physiological evaluation of a new quantitative SPECT method measuring regional ventilation and perfusion. J Appl Physiol (1985). 2004;96(3):1127-36.
15. Bourhis D et al. V/Q SPECT for the assessment of regional lung function: generation of normal mean and standard deviation 3-D maps. Front Med (Lausanne). 2020;7:143.
16. Benjamin J et al. Comparison of hyperpolarized xenon-129 MR and Tc-99m DTPA aerosol lung ventilation imaging in patients with COPD and asthma. Abstract [Poster session]. Joint ISMRM-ESMRMB, 10-16 May, 2014.
17. Petersson J et al. Physiological imaging of the lung: single-photonemission computed tomography (SPECT). J Appl Physiol (1985). 2007;102(1):468-76.
18. Ebert M et al. Nuclear magnetic resonance imaging with hyperpolarised helium-3. The Lancet. 1996;347(9011):1297-9.
19. MacFall JR et al. Human lung air spaces: potential for MR imaging with hyperpolarized He-3. Radiology. 1996;200(2):553-8.
20. Kauczor HU et al. Imaging of the lungs using 3He MRI: preliminary clinical experience in 18 patients with and without lung disease. J Magn Reson Imaging. 1997;7(3):538-43.
21. Mugler JP et al. MR imaging and spectroscopy using hyperpolarized 129Xe gas: preliminary human results. Magn Reson Med. 1997;37(6):809-15.
22. Gefter WB et al. Pulmonary functional imaging: part 2 – state-of-the-art clinical applications and opportunities for improved patient care. Radiology. 2021;299:524-38.
23. Ohno Y et al. Pulmonary functional imaging: part 1 – state-of-the-art and physiologic underpinnings. Radiology. 2021;299(3):508-23.
24. Dietrich O. Detecting COVID19-related chronic pulmonary injury with 129Xe MRI. Radiology. 2021;301(1):E373-4.
25. Beek EJR et al. Functional MRI of the lung using hyperpolarized 3-helium gas. J Magn Reson Imaging. 2004;20(4):540-54.
26. Driehuys B et al. Chronic obstructive pulmonary disease: safety and tolerability of hyperpolarized 129Xe MR imaging in healthy volunteers and patients. Radiology. 2012; 262(1):279-89.
27. Shukla Y et al. Hyperpolarized 129Xe magnetic resonance imaging: tolerability in healthy volunteers and subjects with pulmonary disease. Acad Radiol. 2012;19(8):941-51.
28. Walkup LL et al. Feasibility, tolerability and safety of pediatric hyperpolarized 129Xe magnetic resonance imaging in healthy volunteers and children with cystic fibrosis. Pediatr Radiol. 2016;46(12):1651-62.
29. Svenningsen S et al. Hyperpolarized (3) He and (129) Xe MRI: differences in asthma before bronchodilation. J Magn Reson Imaging. 2013;38(6):1521-30.
30. Ebner L et al. Hyperpolarized 129Xenon magnetic resonance imaging to quantify regional ventilation differences in mild to moderate asthma: a prospective comparison between semiautomated ventilation defect percentage calculation and pulmonary function tests. Invest Radiol. 2017;52(2):120-7.
31. Miller KW et al. Xenon NMR: chemical shifts of a general anesthetic in common solvents, proteins and membranes. Prc Natl Acad Sci USA. 1981;78(8):4946-9.
32. Swanson SD et al. Distribution and dynamics of laser-polarised 129Xe magnetization in vivo. Magn Reson Med. 1999;42(6):1137-45.
33. Bifone A et al. NMR of laser-polarized xenon in human blood. Proc Natl Acad Sci USA. 1996;93(23):12932-6.
34. Marshall H et al. In vivo methods and application of xenon-129 magnetic resonance. Prog Nucl Magn Reson Spectrosc. 2021;122:42-62.
35. Mugler JP et al. Simultaneous magnetic resonance imaging of ventilation distribution and gas uptake in the human lung using hyperpolarized xenon-129. Proc Natl Acad Sci USA. 2010;107(50):21707-12.
36. British Thoracic Society and Scottish Intercollegiate Guidelines Network. British guideline on the management of asthma: a national clinical guideline. 2019. Available at: https://www.britthoracic.org.uk/quality-improvement/ guidelines/asthma/. Last accessed: 17 July 2023.
37. Safavi S et al. Evaluating postbronchodilator response in wellcontrolled paediatric severe asthma using hyperpolarised HPX-MRI: a pilot study. Respir Med. 2021;180:106368.
38. Mussell GT et al. Xenon ventilation MRI in difficult asthma: initial experience in a clinical setting. ERJ Open Res. 2021;7(3):00785-2020.
39. Svenningsen S et al. Reproducibility of hyperpolarized 129Xe MRI ventilation defect percent in severe asthma to evaluate clinical trial feasibility. Acad Radiol. 2021;28(6):817-26.
40. He M et al. Using Hyperpolarized 129Xe MRI to quantify the pulmonary ventilation distribution. Acad Radiol. 2016;23(12):1521-31.
41. Safavi S et al. Correlation of hyperpolarised Xenon-129 magnetic resonance imaging (HPX-MRI) of the lung with multi-breath washout (MBW) in children with severe asthma. Eur Res J. 2020;56:4339.
42. Lin NY et al. 129Xe MRI as a measure of clinical disease severity for pediatric asthma. J Allergy Clin Immunol. 2021;147(6):2146-53.e1.
43. Davies JC et al. Lung clearance index in CF: a sensitive marker of lung disease severity. Thorax. 2008;63(2):96-7.
44. Foong RE et al. The clinical utility of lung clearance index in early cystic fibrosis lung disease is not impacted by the number of multiple-breath washout trials. ERJ Open Res. 2018;4(1):00094-2017.
45. McIntosh M et al. Response to benralizumab in severe asthma: 129Xe MRI, oscillometry and clinical measurements. Abstract D18 Asthma: Physiological Phenotypes and Treatable Traits. ATS International Conference; 15-20 May, 2020.
46. Kooner HK et al. CT mucus score predicts benralizumab response in severe asthma. Abstract TP120 Asthma: Clinical Studies. ATS International Meeting 14-19 May, 2021.
47. Svenningsen S et al. Bronchial thermoplasty guided by hyperpolarised
gas magnetic resonance imaging in adults with severe asthma: a 1-year pilot randomised trial. ERJ Open Res. 2021;7(3):00268-2021.
48. Hall CS et al. Single-session bronchial thermoplasty guided by 129Xe magnetic resonance imaging. a pilot randomized controlled clinical trial. Am J Respir Crit Care Med. 2020;202(4):524-34.
49. Global Initiative for Chronic Obstructive Lung Disease. 2023 GOLD report. 2023. Available at: https:// goldcopd.org/2023-gold-report-2/. Last accessed: 17 July 2023.
50. Kirby M et al. Hyperpolarized 3He and 129Xe MR imaging in healthy volunteers and patients with chronic obstructive pulmonary disease. Radiology. 2012;265(2):600-10.
51. Kaushik SS et al. Diffusion-weighted hyperpolarized 129Xe MRI in healthy volunteers and subjects with chronic obstructive pulmonary disease. Magn Reson Med. 2011;65(4): 1154-65.
52. Dregely I et al. Hyperpolarized Xenon-129 gas-exchange imaging of lung microstructure: first case studies in subjects with obstructive lung disease. J Magn Reson Imaging. 2011;33(5):1052-62.
53. Tafti S et al. Emphysema index based on hyperpolarized 3He or 129Xe diffusion mri: performance and comparison with quantitative ct and pulmonary function tests. Radiology. 2020;297(1):201-10.
54. Kirby M et al. Pulmonary ventilation visualized using hyperpolarized helium-3 and xenon-129 magnetic resonance imaging: differences in COPD and relationship to emphysema. J Appl Physiol (1985). 2013;114(6):707-15.
55. Qing K et al. Probing changes in lung physiology in COPD using CT, perfusion MRI, and hyperpolarized Xenon-129 MRI. Acad Radiol. 2019;26(3):326-34.
56. Matin TN et al. Chronic obstructive pulmonary disease: lobar analysis with hyperpolarized 129Xe MR imaging. Radiology. 2017;282(3):857-68.
57. Ruppert K et al. Using hyperpolarized Xenon-129 MRI to quantify early-stage lung disease in smokers. Acad Radiol. 2019;26(3):355-66.
58. Doganay O et al. Time-series hyperpolarized xenon-129 MRI of lobar lung ventilation of COPD in comparison to V/Q-SPECT/CT and CT. Eur Radiol. 2019;29(8):4058-67.
59. Myc L et al. Characterisation of gas exchange in COPD with dissolvedphase hyperpolarised xenon-129 MRI. Thorax. 2021;76(2):178-81.
60. Stewart NJ et al. Reproducibility of quantitative indices of lung function
and microstructure from 129 Xe chemical shift saturation recovery (CSSR) MR spectroscopy. Magn Reson Med. 2017;77(6):2107-13.
61. Kern AL et al. Mapping of regional lung microstructural parameters using hyperpolarized 129 Xe dissolvedphase MRI in healthy volunteers and patients with chronic obstructive pulmonary disease. Magn Reson Med. 2019;81(4):2360-73.
62. Kern AL et al. Regional investigation of lung function and microstructure parameters by localized 129 Xe chemical shift saturation recovery and dissolved-phase imaging: a reproducibility study. Magn Reson Med. 2019;81(1):13-24.
63. Doganay O et al. Gas exchange and ventilation imaging of healthy and COPD subjects using hyperpolarized xenon-129 MRI and a 3D alveolar gas-exchange model. Eur Radiol. 2023;33(5):3322-31.
64. Terry PB, Traystman RJ. The clinical significance of collateral ventilation. Ann Am Thorac Soc. 2016;13(12):2251-7.
65. Klooster K et al. An integrative approach of the fissure completeness score and chartis assessment in endobronchial valve treatment for emphysema. Int J Chron Obstruct Pulmon Dis. 2020;15:1325-34.
66. Marshall H et al. Direct visualisation of collateral ventilation in COPD with hyperpolarised gas MRI. Thorax. 2012;67(7):613-17.
67. Marshall H et al. Imaging collateral ventilation in patients with advanced chronic obstructive pulmonary disease: relative sensitivity of 3 He and 129 Xe MRI. J Magn Reson Imaging. 2019;49(4):1195-7.
68. Chen M et al. Delayed ventilation assessment using fast dynamic hyperpolarised Xenon-129 magnetic resonance imaging. Eur Radiol. 2020;30(2):1145-55.
69. National Institute for Health and Care Excellence (NICE). Idiopathic pulmonary fibrosis in adults: diagnosis and management. 2017. Available at: https://www.nice.org. uk/guidance/cg163/resources/ idiopathic-pulmonary-fibrosis-inadults-diagnosis-and-managementpdf-35109690087877. Last accessed: 17 July 2023.
70. Kaushik SS et al. Measuring diffusion limitation with a perfusion-limited gas--hyperpolarized 129Xe gastransfer spectroscopy in patients with idiopathic pulmonary fibrosis. J Appl Physiol (1985). 2014;117(6):577-85.
71. Stewart NJ et al. Experimental validation of the hyperpolarized 129 Xe chemical shift saturation recovery technique in healthy volunteers and
subjects with interstitial lung disease. Magn Reson Med. 2015;74(1):196-207.
72. Hahn AD et al. Hyperpolarized 129Xe MR spectroscopy in the lung shows 1-year reduced function in idiopathic pulmonary fibrosis. Radiology. 2022;305(3):688-96.
73. Weatherley ND et al. Hyperpolarised xenon magnetic resonance spectroscopy for the longitudinal assessment of changes in gas diffusion in IPF. Thorax. 2019;74(5):500-2.
74. Mummy DG et al. Hyperpolarized 129Xe MRI and spectroscopy of gasexchange abnormalities in nonspecific interstitial pneumonia. Radiology. 2021;301(1):211-20.
75. Robertson SH et al. Uncovering a third dissolved-phase 129 Xe resonance in the human lung: quantifying spectroscopic features in healthy subjects and patients with idiopathic pulmonary fibrosis. Magn Reson Med. 2017;78(4):1306-15.
76. Wang Z et al. Quantitative analysis of hyperpolarized 129 Xe gas transfer MRI. Med Phys. 2017;44(6):2415-28.
77. Wang JM et al. Using hyperpolarized 129Xe MRI to quantify regional gas transfer in idiopathic pulmonary fibrosis. Thorax. 2018;73(1):21-8.
78. Collier GJ et al. Dissolved 129 Xe lung MRI with four-echo 3D radial spectroscopic imaging: quantification of regional gas transfer in idiopathic pulmonary fibrosis. Magn Reson Med. 2021;85(5):2622-33.
79. Qing K et al. Hyperpolarized Xenon-129: a new tool to assess pulmonary physiology in patients with pulmonary fibrosis. Biomedicines. 2023;11(6):1533.
80. Rankine LJ et al. 129Xenon gas exchange magnetic resonance imaging as a potential prognostic marker for progression of idiopathic pulmonary fibrosis. Ann Am Thorac Soc. 2020;17(1):121-5.
81. Mata J et al. Evaluation of regional lung function in pulmonary fibrosis with Xenon-129 MRI. Tomography. 2021;7(3):452-65.
82. Mammarappallil JG et al. New developments in imaging idiopathic pulmonary fibrosis with hyperpolarized Xenon magnetic resonance imaging. J Thorac Imaging. 2019;34(2):136-50.
83. Schettino IA et al. Accuracy of high resolution CT in assessing idiopathic pulmonary fibrosis histology by objective morphometric index. Pathol Res Pract. 2002;198(5):347-54.
84. Yagihashi K et al. Radiologicpathologic discordance in biopsyproven usual interstitial pneumonia. Eur Respir J. 2016;47(4):1189-97.
85. Kaushik SS et al. Single-breath clinical imaging of hyperpolarized (129)Xe in the airspaces, barrier, and red blood cells using an interleaved 3D radial 1-point Dixon acquisition. Magn Reson Med. 2016;75(4):1434-43.
86. National Institute for Health and Care Excellence (NICE). NICE, SIGN and RCGP set out further details about the UK guideline on management of the long-term effects of COVID-19. 2020. Available at: https://www.nice.org. uk/news/article/nice-sign-and-rcgpset-out-further-details-about-the-ukguideline-on-management-of-thelong-term-effects-of-covid-19. Last accessed: 20 April 2023.
87. Li H et al. Damaged lung gas exchange function of discharged COVID-19 patients detected by hyperpolarized 129Xe MRI. Sci Adv. 2021;7(1):eabc8180.
88. Grist JT et al. Lung abnormalities depicted with hyperpolarized Xenon MRI in patients with long COVID. Radiology. 2022;305(3):709-17.
89. Matheson AM et al. Persistent (129) Xe MRI pulmonary and CT vascular abnormalities in symptomatic individuals with post-acute COVID-19 syndrome. Radiology. 2022;305(2):466-76.
90. University of Oxford. An investigation to explore the use of a type of MRI scan using an inhaled gas in identifying lung damage associated with long COVID sufferers. ISRCTN14304264. 2022. Available at: https://www.isrctn.com/ ISRCTN14304264. Last accessed: 24 November 2024.
91. Alam FS et al. Intra- and inter-visit repeatability of 129 xenon multiple-breath washout MRI in children with stable cystic fibrosis lung disease. J Magn Reson Imaging. 2023;58(3):936-48.
92. Couch MJ et al. A two-center analysis of hyperpolarized 129Xe lung MRI in stable pediatric cystic fibrosis: potential as a biomarker for multi-site trials. J Cyst Fibros. 2019;18(5): 728-33.
93. Kaireit TF et al. flow volume loop and regional ventilation assessment using phase-resolved functional lung (PREFUL) MRI: comparison with 129 Xenon ventilation MRI and lung function testing. J Magn Reson Imaging. 2021;53(4):1092-105.
94. Shammi UA et al. Comparison of hyperpolarized 3He and 129Xe MR imaging in cystic fibrosis patients. Acad Radiol. 2022;29 (Suppl 2):S82-90.
95. Willmering MM et al. Pediatric 129 Xe gas-transfer MRI-feasibility and applicability. J Magn Reson Imaging. 2022;56(4):1207-19.
96. Roach DJ et al. Hyperpolarized 129Xenon MRI ventilation defect quantification via thresholding and linear binning in multiple pulmonary diseases. Acad Radiol. 2022;29 Suppl 2(Suppl 2):S145-55.
97. Couch MJ et al. Comparison of functional free-breathing pulmonary 1H and hyperpolarized 129Xe magnetic resonance imaging in pediatric cystic fibrosis. Acad Radiol. 2021;28(8):e209-18.
98. Thomen RP et al. Hyperpolarized 129Xe for investigation of mild cystic fibrosis lung disease in pediatric patients. J Cyst Fibros. 2017;16(2):275-82.
99. Kanhere N et al. Correlation of lung clearance index with hyperpolarized 129Xe magnetic resonance imaging in pediatric subjects with cystic fibrosis. Am J Respir Crit Care Med. 2017;196(8):1073-5.
100. Zanette B et al. A 3D stack-of-spirals approach for rapid hyperpolarized 129 Xe ventilation mapping in pediatric cystic fibrosis lung disease. Magn Reson Med. 2023;89(3):1083-91.
101. Marshall H et al. 129 Xe and freebreathing 1 H ventilation MRI in patients with cystic fibrosis: a dualcenter study. J Magn Reson Imaging. 2023;57(6):1908-21.
102. Thomen RP et al. Regional StructureFunction in Cystic Fibrosis Lung Disease Using Hyperpolarized 129Xe and ultrashort echo magnetic resonance imaging. Am J Respir Crit Care Med. 2020;202(2):290-2.
103. Willmering MM et al. Sensitive structural and functional measurements and 1-year pulmonary outcomes in pediatric cystic fibrosis. J Cyst Fibros. 2021;20(3):533-9.
104. Smith LJ et al. The assessment of short and long term changes in lung function in CF using 129Xe MRI. Eur Respir J. 2020;56(6):2000441.
105. Rayment JH et al. Hyperpolarised 129Xe magnetic resonance imaging to monitor treatment response in children with cystic fibrosis. Eur Respir J. 2019;53(5):1802188.
106. Walkup LL et al. Cyst ventilation heterogeneity and alveolar airspace dilation as early disease markers in
lymphangioleiomyomatosis. Ann Am Thorac Soc. 2019;16(8):1008-16.
107. Dahhan T et al. Abnormalities in hyperpolarized (129)Xe magnetic resonance imaging and spectroscopy in two patients with pulmonary vascular disease. Pulm Circ. 2016;6(1):126-31.
108. Bier EA et al. Noninvasive diagnosis of pulmonary hypertension with hyperpolarised 129Xe magnetic resonance imaging and spectroscopy. ERJ Open Res. 2022;8(2):00035-2022.
109. Wang Z et al. Diverse cardiopulmonary diseases are associated with distinct xenon magnetic resonance imaging signatures. Eur Respir J. 2019;54(6):1900831.
110. Walkup LL et al. Xenon-129 MRI detects ventilation deficits in paediatric stem cell transplant patients unable to perform spirometry. Eur Respir J. 2019;53(5):1801779.
The Role of IL-5 in Type 2 Inflammatory Diseases
Authors: Diego Bagnasco,1,2 Alvise Berti,3,4 Gabriele Brembilla,5 Giorgio Walter Canonica,6,7 Giovanna Elisiana Carpagnano,8 Cristiano Caruso,9 Nunzio Crimi,10 Eugenio De Corso,11 Stefano Del Giacco,12 Carlo Lombardi,13 Andrea Matucci,14 Maria Rosaria Mollo,5 Chiara Sartor,5 Gianenrico Senna,15 Gilda Varricchi16,17
1. Respiratory and Allergy Clinic, Policlinico San Martino, Genova, Italy
2. Department of Internal Medicine, University of Genoa, Italy
3. Center for Medical Sciences and Department of Cellular, Computational and Integrative Biology, University of Trento, Italy
4. Unit of Rheumatology, Santa Chiara Regional Hospital, APSS, Trento, Italy
5. GSK Medical Department, Verona, Italy
6. Department of Biomedical Sciences, Humanitas University, Pieve Emanuele, Milan, Italy
7. Personalized Medicine, Asthma and Allergy, Humanitas Clinical and Research Center, IRCCS, Rozzano, Italy
8. Department of Basic Medical Science, Neuroscience and Sense Organs, University of Bari Aldo Moro, Italy
9. UOSD Allergy and Clinical Immunology, Fondazione Policlinico A. Gemelli IRCCS, Catholic University of the Sacred Heart, Rome, Italy
12. Department of Medical Sciences and Public Health, University of Cagliari, Italy
13. Departmental Unit of Allergology-Clinical Immunology & Pneumology, Fondazione Poliambulanza Istituto Ospedaliero, Brescia, Italy
14. Immunoallergology Unit, Careggi University Hospital, Florence, Italy
15. University of Verona, Italy
16. Department of Translational Medical Sciences and Center for Basic and Clinical Immunology Research, University of Naples Federico II, Italy
17. World Allergy Organization (WAO) Center of Excellence (COE), Naples, Italy
Disclosure:
Bagnasco has received speaker’s honoraria and advisory board membership from AstraZeneca, Chiesi, Firma, GSK, Novartis, Menarini, Sanofi, and Zambon. Berti has received funding from GSK for advisory boards and from Medscape for speaker fees. Canonica reports research or clinical trial grants paid to his institution from AstraZeneca, GSK, Menarini, and Sanofi Genzyme; and fees for lectures or advisory board participation from AstraZeneca, CellTrion, Chiesi, Faes Farma, Firma, Genentech, Guidotti-Malesci, GSK, HAL Allergy, Innovacaremd, Menarini, Novartis, OM-Pharma, Red Maple, Sanofi-Aventis, Sanofi-Genzyme, StallergenesGreer, and Uriach Pharma. Caruso has advisory board memberships with GSK and AstraZeneca. De Corso has participated in speaker’s bureaus for AstraZeneca, GSK, Regeneron, and Sanofi Genzyme. Del Giacco has received advisory board and speaker fees from AstraZeneca, Chiesi, GSK, Novartis, Sanofi, Stallergenes, and Takeda, and unrestricted grants to his Institution from AstraZeneca, GSK, Novartis, and Sanofi. Matucci has received speaker’s honoraria and advisory board membership with AstraZeneca, Chiesi, CSL Behring, GSK, Novartis, and Sanofi Genzyme; and research grants from AstraZeneca and Novartis. Senna declares fees for speeches and participation in advisory boards for GSK, Menarini Group, AstraZeneca, Sanofi, and Novartis Specialization School of Allergy and Clinical Immunology. Brembilla, Mollo, and Sartor are employees of, and hold financial equities in GSK. Carpagnano, Crimi, Lombardi, and Varricchi declare advisory board membership with GSK.
Acknowledgements: Medical writing assistance was provided by Eleanor Roberts, Beeline Science Communications, Ltd, UK.
Disclaimer: The views expressed herein are those of the authors and not necessarily the company.
Keywords: Chronic rhinosinusitis with nasal polyps (CRSwNP), eosinophilic granulomatosis with polyangiitis (EGPA), eosinophils, IL-5, severe asthma (SA), targeting therapy.
Support: This article was funded by GSK, which organised the expert meeting where this topic was discussed. PHARMA
PARTNERSHIP
Abstract
Type 2 inflammation is involved in severe asthma (SA), chronic rhinosinusitis with nasal polyps (CRSwNP), and eosinophilic granulomatosis with polyangiitis (EGPA). The pathogenesis of these diseases involves various immune system cells and target tissues, along with numerous cytokines, chemokines, and other inflammatory molecules. The role of eosinophils and the cytokine IL-5 and its receptor (IL-5R) is becoming a significant focus in these diseases, with numerous studies, from in vitro experiments to clinical trials, demonstrating correlations between IL-5 levels with eosinophil numbers and activity in SA, CRSwNP, and EGPA. Eosinophils and IL-5 are involved, both directly and indirectly, in disease initiation and exacerbation, as well as in tissue remodelling and disease progression. An advisory board of experts discussed how understanding the actions of IL-5 within Type 2 inflammation in SA, CRSwNP, and EGPA can highlight the importance of its role in managing patients with these diseases and help identify suitable biomarkers for disease onset, exacerbation, and progression. Therapies targeting eosinophil generation, priming, and activation could lead to more effective disease control and help prevent the tissue damage associated with these conditions, which can be difficult to reverse in chronic cases.
INTRODUCTION
Type 2 immunity involves both adaptive and innate immune responses to pathogens and toxic substances. However, when these mechanisms are upregulated in response to an innocuous allergen or stimulus, a range of Type 2-associated inflammatory diseases can occur. Type 2 inflammation plays a role in triggering and progression of SA, CRSwNP, and EGPA. These diseases affect airway epithelium and show some common features including inflammatory cell trafficking into airway tissues, epithelial barrier disruption, goblet cell hyperplasia, increased mucus production, and tissue remodelling (Figure 1).1,2
One mechanism behind Type 2 inflammation is characterised by the production of IgE by B cells, following their activation by T-helper 2 (Th2) cells (Figure 1).1,2 This mechanism also involves a number of other immune cells and factors that together contribute to development and progression of SA, CRSwNP, and EGPA. Here though, the authors focus on the cytokine IL-5, whose role in such conditions is highlighted by the efficacy of IL-5-targeting therapies.1 While IL-5 is produced by, and has actions on, a number of immune cells, including Th2 cells, mast cells, and Type 2 innate lymphoid cells (ILC2), another focus here will also be on eosinophils (Figure 1).2 This was prompted by a discussion by a board of experts, who highlighted the importance of understanding the impact of IL-5 and
1: The overarching role of IL-5 and eosinophils in severe asthma, chronic rhinosinusitis with nasal polyps, and eosinophilic granulomatosis with polyangiitis.
Severe Asthma: Allergic Eosinophil Airway Inflammation
Severe Asthma: Nonallergic Eosinophil Airway Inflammation
Eosinophils
CRSwNP: chronic rhinosinusitis with nasal polyps; EGPA: eosinophilic granulomatosis with polyangiitis; IL: interleukin; ILC2s: type 2 innate lymphoid cells; NKT: natural killer T; TH2: T-helper 2; TSLP: thymic stromal lymphopoietin.
eosinophils in SA, CRSwNP, and EGPA when managing patients with these diseases.3
EOSINOPHILS AND IL-5 INVOLVEMENT IN TYPE 2 INFLAMMATION
Eosinophils are bone marrow-derived leucocytes found in abundance in SA, CRSwNP, and EGPA, both locally, including in airway epithelium, and remotely (Figure 2).4-6 Even in people without asthma or those who do not smoke, higher blood eosinophil counts (>400 cells/μL) are frequently, although not necessarily, associated with airflow obstruction and lung function decline.7
Eosinophils are major releasers of inflammatory mediators, including IL-5 and other cytokines, chemokines, granule proteins, and lipid mediators (Figure 1).8 The presence of IL-5, along with IL-3 and granulocyte-macrophage colony-stimulating factor (GM-CSF), may also enhance the responsiveness of eosinophils to other stimuli and activation of downstream pathways. This can lead to a ‘hyperresponsive’ phenotype including increased levels of eosinophil degranulation and inflammation.9 As part of this, IL-5 expression can upregulate eosinophil extracellular trap-forming cell death, increasing inflammation and tissue damage.10 In this process, released extrudate includes the granule proteins eosinophil-derived neurotoxin (EDN), eosinophil peroxidase,
Figure
Blood Stream
Fibroblasts
ILC2s
Dendritic cells
TH2 Cells
Naïve T Cells
IL-5
Goblet Cells
NKT Cells
Macrophages
Figure 2: Eosinophil-related disorders according to blood eosinophilia.
Combinations of Single Organ Diseases
Single Organ Disease Systemic Disease (EGPA/HES)
0 Normal Eosinophils 500 cells/μL Eosinophilia 1500 cells/μL Hypereosinophilia
Adapted from Lombardi et al.3 2024 under CC-BY-NC-4.0.
CRSwNP: chronic rhinosinusitis with nasal polyps; EGPA: eosinophilic granulomatosis with polyangiitis; EoE: eosinophilic oesophagitis; HES: hypereosinophilic syndrome.
major basic protein (MBP), and eosinophil cationic protein (ECP). Extrudate can also include chromatic structures (‘DNA traps’ or ‘eosinophil extracellular traps’), cytokines (including IL-5), chemokines, enzymes, and growth factors (Figure 1).8,11
Eosinophils have numerous downstream and bidirectional effects that contribute to the pathogenesis of Type 2 inflammation.8 For example, they can act together with mast cells in allergic reactions, with histamine released from such cells inducing eosinophil chemotaxis (Figure 1),12 and can stimulate lymph node T cells to produce IL-5 following an allergen challenge.13
Eosinophils may also have a direct role on both naïve and memory B cell proliferation, secretion of IgA, IgG, and IgM from B cells, and B cell survival, in peripheral blood and tissues. In vitro studies show that this may occur through direct contact or, to a lesser extent, through contact of B cells with eosinophil-derived soluble factors,
independently from other B cell modulators such as T cell derived cytokines.14
Eosinophil activity is primarily directed by IL-5 through the IL-5Ra subunit. This is specific to IL-5, unlike the beta-subunit, which is also shared by IL-3 and GMCSF.15 IL-5 and IL-5Ra play a significant role in eosinophil growth, maturation, and differentiation in the bone marrow; in eosinophil proliferation, activation, and recruitment throughout the body; and eosinophil survival and mortality.15-17 The IL-5R is also expressed, to a lesser extent, on other immune cells, such as neutrophils, basophils, B cells, and mast cells, as well as on non-immune cells associated with the airway epithelium, including ciliated epithelial cells and lung fibroblasts (Figure 3).16,18-21 This widespread activity is postulated to underpin the sometimes broad effects of IL-5 targeting treatments.1
IL-5-producing immune cells involved in asthma and CRSwNP pathobiology
Evidence in humans
Cell
Basophil
Mast cell Neutrophil
Plasma cell
Airway epithelial cell
Fibroblast
Proliferation and differentiation
Prolonged survival
Recruitment to tissue
Activation/degranulation
Proliferation and differentiation
Activation/degranulation
Cytokine production
Activation
Expresses the IL-5R, although the physiological relevance of this is unknown
Upregulation of genes involved in cell cycle and proliferation
Immunoglobulin production
Impaired epithelial barrier integrity
Activation
Proliferation
Evidence in mice
Proliferation and differentiation
Prolonged survival
Immunoglobulin class switching
Increased CTL production
Adapted from Bachert et al.2 2023
CRSwNP: chronic rhinosinusitis with nasal polyps; CTL: cytotoxic T lymphocyte; IL: interleukin; ILC2: innate lymphoid cell type 2; TH2: T-helper 2 cells.
SEVERE ASTHMA AND CHRONIC RHINOSINUSITIS WITH NASAL POLYPS
CRSwNP and SA are respectively characterised as upper and lower airway diseases. Disruption to the respiratory system can occur due to various inducers, including allergens, and triggers, such as smoking, infections, and pollution. When such inducers and/or triggers are present at the airway epithelium, the ‘alarmins’ IL-25, IL-33, and thymic stromal lymphopoietin signal to eosinophils, ILC2s, dendritic cells, and Th2 cells. These can, in turn, secrete Type 2 cytokines, including IL-5 (Figure 1).1,15
IL-5 and Eosinophils in Severe Asthma
Asthma symptoms can range from mild, episodic wheezing to chronic airway narrowing and life-threatening episodes. These symptoms are caused by the actions of innate and adaptive immune cells, along with epithelial cells, causing airway hyperresponsiveness, inflammation, excessive mucus production, and tissue remodelling.22 Of the approximately 300 million people worldwide with asthma,22 an estimated 5−12% have a chronic, severe form (SA), which in some may be uncontrolled.23 Despite advances in management over the decades, there are globally an estimated 1,000 deaths a day due to asthma.22
Figure 3: IL-5 signalling in different cell types.
At least 84% of adults with SA may have eosinophilic ‘T2-high’ asthma,5 characterised by blood eosinophils ≥150 cells/μL, the presence of tissue eosinophils, IgE >114 kUL-1, and fractional concentration of exhaled nitric oxide (FeNO) >19.5 parts per billion (though of note, precise levels of each may differ between guidelines).1 People with eosinophilic SA are more likely to be female, have adultonset asthma and nasal polyps,5 and have higher levels of blood and sputum eosinophil progenitors, ILC2s, and CD4+ T cells.24
Eosinophilic inflammation in people with asthma is associated with worse lung function and airflow obstruction over time compared to those without such inflammation.25 In vitro studies show that eosinophils from people with asthma can induce smooth muscle cell contraction, potentially contributing to asthma symptoms.26 Typically, people with eosinophilic asthma require high doses of oral steroids to achieve disease control and they may be refractory to inhaled corticosteroids.22 Notably, there is an approximately 1.4-fold increase in the likelihood of ≥2 exacerbations if blood eosinophil count is >400 cells/μL, compared with ≤400 cells/μL, suggesting that levels of these cells could be used to predict asthma exacerbation risk.27 This risk can more comprehensively be calculated by also taking into account FeNO and presence of clinical risks, such as comorbidities or environmental exposure.28
Two distinct subtypes of eosinophils have been identified in vivo with regard to airway diseases: IL-5-dependent inflammatory eosinophils (iEOS) and non-IL-5-dependent tissue-resident eosinophils (rEOS).29-31 In eosinophilic SA (or models of such), iEOS are found in peripheral blood, nasal polyps,30 and the lungs.29 In peripheral blood, iEOS have increased activation markers and in nasal polyps they have increased IL-3R and IL-5R, with the percentage of iEOS correlating with eotaxin-3 expression.30 There is significant correlation between peripheral blood iEOS proportion and asthma severity, exacerbations, and nasal polyp numbers.31 In general, in patients with asthma, the proportion of circulating iEOS to total eosinophil count is significantly higher compared with healthy controls.32 Following a trigger, iEOS can infiltrate the airways from
the blood.29 However, with IL-5 inhibition and gains in asthma control, there is a reduction of iEOS and an increase in rEOS.31
Granular proteins and DNA traps released from eosinophils can increase airway inflammation in SA33 and damage structural cells in the lung.34 These proteins are involved in airway remodelling by modulating fibroblast and smooth muscle cell activity, leading to muscle hyperplasia and hypertrophy.35 Studies on specific granular proteins have shown that MBP levels are significantly elevated in sputum from patients with asthma,36 especially during exacerbations,36 and that eosinophils and MBP are abundant in bronchial tissue in cases of fatal asthma.37 Further, ECP is raised in serum in allergen-provoked asthma.38 With this in mind, granule protein levels could be useful biomarkers for SA exacerbations.
Mucus plugs are present in many patients with asthma, causing airflow obstruction. They can significantly contribute to SA pathology and to fatalities during asthma exacerbations,39,40 so are a critical therapeutic target in SA. There is a correlation between mucus plug development and eosinophil number, IL-5 expression, and eosinophil peroxidase levels. The latter is associated, alongside reactive oxidants, with changes to mucin polymers shown in mucus plugs, with eosinophil granule proteins as a whole associated with increased mucus viscosity. These elements combined also exhibit decreased degradation to usual mucus-eliminating factors such as proteases, and increased contribution to inflammatory mechanisms.39,41 Another marker of eosinophilic inflammation is the formation of ‘Charcot–Leyden crystals’ (CLC) from galectin-10. Combined, CLCs and DNA traps can also form part of mucus plugs42 (Figure 1) where they contribute to airway obstruction impenetrable to bronchodilators.39
Several findings highlight the role of IL-5 in asthma. For example, this cytokine is upregulated in bronchial mucosa following allergen exposure,43 and serum IL-5 levels are higher in people with SA compared to those with mild or no asthma.44 During asthma exacerbations, IL-5 and eotaxin expression can promote eosinophilic
recruitment to airway epithelium, leading to airway hyperresponsiveness.16 Not only during attacks but also in people with stable asthma, IL-5 levels are inversely correlated with apoptotic eosinophil counts.45 In allergic asthma, eosinophil numbers correlate with high levels of IL-5 in sputum, serum, peripheral blood T cell supernatants, and bronchoalveolar lavage fluid (BALF).15,46-48 Increased soluble IL-5Ra is also found in BALF following allergen challenge, indicating eosinophil tissue migration across the epithelium, as the receptor is shed at this point.49 Further, FeNO levels correlate with both airway IL-5 and eosinophils in SA, but not blood eosinophil count, suggesting that assessing systemic versus airway Type 2 inflammation may be more accurate when combining blood eosinophil counts with FeNO measurements.50
Of particular importance are correlations between IL-5 and disease pathogenesis and severity. For example, higher IL-5 expression in BALF is associated with increased asthma symptoms, abnormal airway physiology, and decreased pulmonary function.43,51 IL-5 can also promote eosinophil degranulation, associated with bronchial epithelium injury.16,52 That this cytokine may be involved in decreasing epithelial barrier integrity and tissue damage is evidenced by an in vitro study showing that IL-5 signalling to airway epithelial cells can lead to downregulation of adhesion molecules.20 In vivo, IL-5 expression has also been associated with peri-bronchial smooth muscle layer thickening and peri-bronchial fibrosis in airway remodelling, attributed to eosinophil action.53 One possible downstream mechanism for these findings involves tumour growth factor-β, which is secreted by eosinophils in people with SA54 and can promote myofibroblast transformation, leading to airway remodelling.34 Such remodelling is associated with higher asthma medication use, reduced lung function, and airway hyperresponsiveness.55 These findings are significant because they suggest a role for disease modification through IL5-targeting, glucocorticoid-sparing means. Indeed, blocking IL-5 can lead to a significant decrease in circulating eosinophil levels56,57 and can significantly reduce levels of lung eosinophils in patients with corticosteroidresistant asthma.56
While there is an intimate relationship between eosinophils and IL-5, it is not exclusive. Airway remodelling can occur without eosinophilic inflammation,55 suggesting that other IL-5-expressing cells may play a role in SA pathogenesis. For example, ILC2 numbers are increased in the airways following an allergen challenge,58 and these cells are a source of IL-5 in the lungs of people with asthma (Figure 1 and Figure 3).59 IL-5 can also enhance histamine release from basophils in vitro;60 however, there is an inverse relationship between rate of activated basophils and effectiveness of IL-5-targeting therapy.61 Further, in asthma, elevated synthesis of airway collagen may be driven by IL-5 activation of fibroblasts and IL-5Ra expression in lower airway lung fibroblasts is significantly greater in people with asthma compared with healthy controls.21 This suggests that cells other than eosinophils could also be a target for decreasing SA manifestations.
IL-5 and Eosinophils in Chronic Rhinosinusitis with Nasal Polyps
Global prevalence estimates for CRSwNP are between 1.1−4.4%.62 Symptoms of CRSwNP include not only nasal polyps but also inflamed mucosa, postnasal drip, frontal sinus pain and pressure, and airway impedance.63 Notably, CRSwNP and asthma may be comorbid,62,64 with comorbidity increasing CRSwNP severity,64,65 asthma exacerbation frequency,64,66 and oral corticosteroid use, and decreasing health-related quality of life.62
CRSwNP predominantly arises due to Type 2 inflammation.67 This may drive nasal polyp formation through oedema, plasma protein retention, and fibrin deposition.68 Several findings point to the role of IL-5 in CRSwNP. Similar to SA, in this disease epithelial cell alarmins can lead to ILC2 activation and to IL-5 accumulation and production (Figure 1).10 Such upregulation of IL-5 in nasal polyps69 correlates with CRSwNP severity.17 Higher levels of IL-5 in nasal secretions and nasal polyp tissue are especially shown in people with uncontrolled CRSwNP, compared to those where it is controlled, with higher nasal secretion of IL-5 correlating with a higher number of polyp surgeries.70
Elevated IL-5 levels have also been shown in nasal polyps associated with aspirinexacerbated respiratory disease, alongside high numbers of antibody-secreting cells, including plasma cells and plasmablasts. Increased expression of IL5-Ra in such patients is proposed to have a role in local antibody production and is correlated with disease severity and recurrence of nasal polyposis.71,72 That IL-5Ra might have a role in epithelial-mesenchymal cell transition in CRSwNP is evidenced in an investigation of another disease, pulmonary fibrosis, where the receptor was upregulated in such cells as fibrosis progressed.73 Other IL-5R-expressing cells found elevated in people with CRSwNP include IgG+ B cells, basophils, mast cells, and ILC2s, indicating a potential IL-5-linked role of these cells in disease pathology.6
Similar to airway epithelium in SA, the increased presence of eosinophils and other Type 2 inflammatory cells is shown in polyps in CRSwNP.68 Eosinophil-dominant CRSwNP features include dysosmia, nasal discharge, multiple bilateral polyps, involvement of the ethmoid sinus and accompanying asthma, drug allergies, and aspirin intolerance.74 Eosinophilia is more marked in patients where CRSwNP reappears following surgery, compared to a higher neutrophil number in patients where surgery is more successful.74 IL-5 can promote eosinophilassociated inflammation in CRSwNP,75 and upregulation of leukotrienes in eosinophils, as well as in mast cells and basophils, in CRSwNP is potentially via IL-5/IL-5Ra signalling as inhibition of this receptor subunit in patients with CRSwNP results in downregulation of these inflammatory molecules.19,76 Furthermore, the release of IL-5 from eosinophils can lead to B cell Ig class switching.6
The actions of eosinophils in CRSwNP may lead to collagen deposition, fibroblast activation, epithelial damage, and dysosmia.6,77 These may be due to the release of eosinophil granule proteins. For example, in eosinophil-dominant CRSwNP, ECP levels in nasal secretions correlate with polyp severity and the presence of asthma.78 Additionally, EDN is found at high levels in nasal polyps and serum EDN levels are significantly higher in patients with
eosinophilic CRSwNP compared with other nasal diseases, correlated with disease activity. IL-5 plays a role here with in vitro stimulation of eosinophils with this cytokine leading to EDN production and stimulation of nasal epithelial cells, and EDN presence resulting in changes in genes associated with epithelial-mesenchymal transition.79 CLCs from eosinophils are also abundant in nasal polyps, co-located in areas of eosinophil extracellular trap-forming cell death, and positively correlating with levels of IL-5.42 Levels of CLC-associated galactin-10 also correlate with CRSwNP severity.80 These findings point to a need to more fully understand the relationship between IL-5 and eosinophils in CRSwNP pathology.
IL-5 AND EOSINOPHILS IN EOSINOPHILIC GRANULOMATOSIS WITH POLYANGIITIS
Also being investigated, though to a lesser extent than has been carried out for SA and CRSwNP, is the role of IL-5 in EGPA, another disease that can have Type 2 inflammatory processes feature in its pathogenesis. Known originally as Churg–Struss syndrome, EGPA is characterised by multisystem tissue eosinophilia, which leads to eosinophil-rich granulomatous infiltration, small-vessel necrotising vasculitis, diseaseonset asthma, recurrent rhinitis and sinusitis, and, in some cases, polyposis. Peripheral blood eosinophilia in EGPA can typically be >1,000−1,500 cells/μL, with eosinophil levels correlating with disease activity. EGPA is typically diagnosed in adulthood, with prevalence estimates ranging from 10.7−18.0 per 1,000,000.4,81-84
EGPA can be either antineutrophil cytoplasmic antibody (ANCA)-positive, in around 30−40% of patients who present more often with vasculitic lesions, or ANCAnegative, where eosinophil-related organ infiltration is more prominent.4,81,82 The disease usually progresses through several phases: a prodromal phase dominated by asthma and chronic rhinosinusitis; a phase with increased eosinophil and organ involvement, such as lung infiltrates and cardiomyopathy; and a vasculitic phase, which may include neuropathy,
glomerulonephritis, and palpable purpura. These phases may not occur sequentially and can overlap.4,81,82 Immunosuppressive therapies can be used to block vasculitisassociated inflammation, leading to vasculitis remission, but may not impact other phases and/or may lead to treatment-related damage accrual.85
Eosinophils are one of the primary cell types involved in the pathogenesis of EGPA. Increased presence of these cells may lead to tissue damage in EGPA through the secretion of granule proteins.81 For example, eosinophils may have a direct role in EGPArelated axonal neuropathy and prothrombotic endothelial damage, causing irreversible peripheral nerve damage.86 In patients with EGPA-associated cardiac damage, peripheral eosinophilia is also notably pronounced.82 Eosinophils develop from IL-5R-expressing CD34+ progenitor cells, and IL-5-producing CD34+ cells have been found in peripheral blood and bone marrow samples in people with EGPA. As such, the potential benefits of targeting these early-phase cells to reduce the accumulation of tissue eosinophils in EGPA prior to any damage is an unmet need of the disease.87
At least part of EGPA manifestations are mediated by Th2 cells and their associated cytokines, including IL-5, along with IL-4 and IL-13 (Figure 1).4 Understanding IL-5 involvement in EGPA could provide a valuable biomarker for the disease and enhance understanding of disease activity. Studies indicating a role for IL-5 in EGPA include one showing that T cell primed peripheral blood mononuclear cells from patients with EGPA release significantly more IL-5 than cells from healthy controls.88 Another
References
1. Kolkhir P et al. Type 2 chronic inflammatory diseases: targets, therapies and unmet needs. Nat Rev Drug Discov. 2023;22(9):743-67.
2. Bachert C et al. The unified airway hypothesis: evidence from specific intervention with anti-IL-5 biologic therapy. J Allergy Clin Immunol Pract. 2023;11(9):2630-41.
3. Lombardi C et al. Anti-IL-5 pathway agents in eosinophilic-associated
investigation found that increased plasma IL-5 was correlated with EGPA exacerbation and demonstrated that, during active EGPA, IL-5 expression is elevated in BALF compared to people with inactive EGPA and those with asthma, indicating a role of IL-5 in EGPA activity levels. A significant correlation was also found between IL-5 concentration in BALF and both BALF and blood eosinophil levels, indicating the elevated presence of IL-5 in airways during active EGPA.89 A role for B cells in EGPA pathogenesis has also been suggested4 as IL-5 from Th2 cells acting on B cells leads to elevated ANCA, IgE, and IgG4 production in people with EGPA.82 The role of IL-5 in EGPA is further supported by several studies highlighting the effectiveness of IL-5/ IL-5Ra-targeting medications for this disease.4,81,82
CONCLUSION
Numerous studies highlight the role of IL-5 and eosinophils in Type 2 inflammation occurring in SA, CRSwNP, and EGPA (Figure 1). Eosinophil activation and number is related to disease severity in these diseases, underscoring the potential benefits of inhibiting eosinophil priming and activation, as well as targeting upstream eosinophil generation.90 Current advances in understanding the complexity of the IL-5 pathway across all relevant cells and targets, not just eosinophils, is beneficial for patient phenotyping and management. Such approaches could lead to more effective disease control, prevent tissue damage and remodelling, help manage chronicity, and improve a patient’s overall health-related quality of life.1,3,6,10,15,21,23,45,52,56,67,68,85,89
disorders across the lifespan. Drugs. 2024;84(6):661-84.
4. Greco A et al. Churg-Strauss syndrome. Autoimmun Rev. 2015;14(4):341-8.
5. Heaney LG et al. Eosinophilic and noneosinophilic asthma: an expert consensus framework to characterize phenotypes in a global real-life severe asthma cohort. Chest. 2021;160(3):814-30.
6. Gevaert P et al. The roles of eosinophils and interleukin-5 in the pathophysiology of chronic rhinosinusitis with nasal polyps. Int Forum Allergy Rhinol. 2022;12(11):141323.
7. Hancox RJ et al. Associations between blood eosinophils and decline in lung function among adults with and without asthma. Eur Respir J. 2018;51(4):1702536.
8. Hogan SP et al. Eosinophils: biological properties and role in health and disease. Clin Exp Allergy. 2008;38(5):709-50.
9. Zhu Y, Bertics PJ. Chemoattractantinduced signaling via the Ras-ERK and PI3K-Akt networks, along with leukotriene C4 release, is dependent on the tyrosine kinase lyn in IL-5- and IL-3-primed human blood eosinophils. J Immunol. 2011;186(1):516-26.
10. Bachert C et al. Biologics for chronic rhinosinusitis with nasal polyps. J Allergy Clin Immunol. 2020;145(3):72539.
11. Ueki S et al. Eosinophil extracellular trap cell death-derived DNA traps: their presence in secretions and functional attributes. J Allergy Clin Immunol. 2016;137(1):258-67.
12. Galdiero MR et al. Bidirectional mast cell-eosinophil interactions in inflammatory disorders and cancer. Front Med. 2017;4:103.
13. Shi HZ et al. Endobronchial eosinophils preferentially stimulate T helper cell type 2 responses. Allergy. 2004;59(4):428-35.
14. Wong TW et al. Eosinophils regulate peripheral B cell numbers in both mice and humans. J Immunol. 2014;192(8):3548-58.
15. Pelaia C et al. Interleukin-5 in the pathophysiology of severe asthma. Front Physiol. 2019;10:1514.
16. Kotsimbos AT, Hamid Q. IL-5 and IL-5 receptor in asthma. Mem Inst Oswaldo Cruz. 1997;92(Suppl 2):75-91.
17. Simon HU et al. Direct demonstration of delayed eosinophil apoptosis as a mechanism causing tissue eosinophilia. J Immunol. 1997;158(8):3902-8.
18. Lawrence MG et al. Interleukin-5 receptor alpha (CD125) expression on human blood and lung neutrophils. Ann Allergy Asthma Immunol. 2022;128(1):53-60.
19. Buchheit KM et al. Mepolizumab targets multiple immune cells in aspirinexacerbated respiratory disease. J Allergy Clin Immunol. 2021;148(2):57484.
20. Barretto KT et al. Human airway epithelial cells express a functional IL-5 receptor. Allergy. 2020;75(8):2127-30.
21. Bajbouj K et al. IL-5 receptor expression in lung fibroblasts: potential role in airway remodeling in asthma. Allergy. 2023;78(3):882-5.
22. Global Initiative for Asthma. Global strategy for asthma management and prevention. 2024. Available at: https://ginasthma.org/wp-content/ uploads/2024/05/GINA-2024-StrategyReport-24_05_22_WMS.pdf. Last accessed: 1 November 2024.
23. Calhoun WJ, Chupp GL. The new era of add-on asthma treatments: where do we stand?. Allergy Asthma Clin Immunol. 2022;18(1):42.
24. Smith SG et al. Increased numbers of activated group 2 innate lymphoid cells in the airways of patients with severe asthma and persistent airway eosinophilia. J Allergy Clin Immunol. 2016;137(1):75-86.
25. Azim A et al. Clinical evaluation of type 2 disease status in a real-world population of difficult to manage asthma using historic electronic healthcare records of blood eosinophil counts. Clin Exp Allergy. 2021;51(6):811-20.
26. Janulaityte I et al. Asthmatic eosinophils promote contractility and migration of airway smooth muscle cells and pulmonary fibroblasts in vitro. Cells. 2021;10(6):1389.
27. Price D et al. Predicting frequent asthma exacerbations using blood eosinophil count and other patient data routinely available in clinical practice. J Asthma Allergy. 2016;9:1-12.
28. Couillard S et al. Derivation of a prototype asthma attack risk scale centred on blood eosinophils and exhaled nitric oxide. Thorax. 2022;77(2):199-202.
29. Mesnil C et al. Lung-resident eosinophils represent a distinct regulatory eosinophil subset. J Clin Invest. 2016;126(9):3279-95.
30. Matucci A et al. High proportion of inflammatory CD62Llow eosinophils in blood and nasal polyps of severe asthma patients. Clin Exp Allergy. 2023;53(1):78-87.
31. Vultaggio A et al. Blood CD62L inflammatory eosinophils are related to the severity of asthma and reduced by mepolizumab. Allergy. 2023;78(12):3154-65.
32. Cabrera López C et al. Eosinophil subtypes in adults with asthma and adults with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2023;208(2):155-62.
33. Choi Y et al. Eosinophil extracellular traps activate type 2 innate lymphoid cells through stimulating airway epithelium in severe asthma. Allergy. 2020;75(1):95-103.
34. Siddiqui S et al. Eosinophils and tissue remodeling: relevance to airway disease. J Allergy Clin Immunol. 2023;152(4):841-57.
36. Frigas E et al. Elevated levels of the eosinophil granule major basic protein in the sputum of patients with bronchial asthma. Mayo Clin Proc. 1981;56(6):345-53.
37. Frigas E, Gleich GJ. The eosinophil and the pathophysiology of asthma. J Allergy Clin Immunol. 1986;77(4):527-37.
38. Dahl R et al. Variations of blood eosinophils and eosinophil cationic protein in serum in patients with bronchial asthma. Studies during inhalation challenge test. Allergy. 1978;33(4):211-15.
39. Dunican EM et al. Mucus plugs in patients with asthma linked to eosinophilia and airflow obstruction. J Clin Invest. 2018;128(3):997-1009.
40. Aegerter H, Lambrecht BN. The pathology of asthma: what is obstructing our view?. Annu Rev Pathol. 2023;18:387-409.
41. Arima M et al. Eosinophilic mucus diseases. Allergology International. 2024;73(3):362-74.
42. Persson EK et al. Protein crystallization promotes type 2 immunity and is reversible by antibody treatment. Science. 2019;364(6442):eaaw4295.
43. Robinson D et al. Activation of CD4+ T cells, increased TH2-type cytokine mRNA expression, and eosinophil recruitment in bronchoalveolar lavage after allergen inhalation challenge in patients with atopic asthma. J Allergy Clin Immunol. 1993;92(2):313-24.
44. Motojima S et al. Clinical significance of measuring levels of sputum and serum ECP and serum IL-5 in bronchial asthma. Allergy. 1993;48(Suppl 17):98106.
45. Xu J et al. Apoptotic eosinophils in sputum from asthmatic patients correlate negatively with levels of IL-5 and eotaxin. Respir Med. 2007;101(7):1447-54.
46. Park SW et al. Association of interleukin-5 and eotaxin with acute exacerbation of asthma. Int Arch Allergy Immunol. 2003;131(4):283-90.
47. Walker C et al. Activated T cells and eosinophilia in bronchoalveolar lavages from subjects with asthma correlated with disease severity. J Allergy Clin Immunol. 1991;88(6):935-42.
48. Walker C et al. Allergic and nonallergic asthmatics have distinct patterns of T-cell activation and cytokine production in peripheral blood and bronchoalveolar lavage. Am Rev Respir Dis. 1992;146(1):109-15.
49. Liu LY et al. Decreased expression of membrane IL-5 receptor alpha on human eosinophils: I. Loss of membrane IL-5 receptor alpha on airway eosinophils and increased soluble IL-5 receptor alpha in the airway after allergen challenge. J Immunol. 2002;169(11):6452-8.
50. Couillard S et al. Fractional exhaled nitric oxide nonsuppression identifies corticosteroid-resistant type 2 signaling in severe asthma. Am J Respir Crit Care Med. 2021;204(6):731-4.
51. Hamid Q et al. Expression of mRNA
for interleukin-5 in mucosal bronchial biopsies from asthma. J Clin Invest. 1991;87(5):1541-6.
52. Mould AW et al. The effect of IL-5 and eotaxin expression in the lung on eosinophil trafficking and degranulation and the induction of bronchial hyperreactivity. J Immunol. 2000;164(4):2142-50.
53. Cho JY et al. Inhibition of airway remodeling in IL-5-deficient mice. J Clin Invest. 2004;113(4):551-60.
54. Balzar S et al. Increased TGF-beta2 in severe asthma with eosinophilia. J Allergy Clin Immunol. 2005;115(1):11017.
55. Hsieh A et al. Airway remodeling heterogeneity in asthma and its relationship to disease outcomes. Front Physiol. 2023;14:1113100.
56. Varricchi G et al. Interleukin-5 pathway inhibition in the treatment of eosinophilic respiratory disorders: evidence and unmet needs. Curr Opin Allergy Clin Immunol. 2016;16(2):186200.
57. Caruso C et al. Severe eosinophilic asthma and aspirin-exacerbated respiratory disease associated to eosinophilic gastroenteritis treated with mepolizumab: a case report. Allergy Asthma Clin Immunol. 2020;16:27.
58. Chen R et al. Allergen-induced increases in sputum levels of group 2 innate lymphoid cells in subjects with asthma. Am J Respir Crit Care Med. 2017;196(6):700-12.
59. DeKruyff RH et al. Innate immunity in the lung regulates the development of asthma. Immunol Rev. 2014;260(1):23548.
60. Hirai K et al. Enhancement of human basophil histamine release by interleukin 5. J Exp Med. 1990;172(5):1525-8.
61. Caruso C et al. Basophil activation and serum IL-5 levels as possible monitor biomarkers in severe eosinophilic asthma patients treated with anti-IL-5 drugs. Allergy. 2021;76(5):1569-71.
62. Khan A et al. The GALEN rhinosinusitis cohort: chronic rhinosinusitis with nasal polyps affects health-related quality of life. Rhinology. 2019;57(5):343-51.
63. Schleimer RP. Immunopathogenesis of chronic rhinosinusitis and nasal polyposis. Annu Rev Pathol. 2017;12:331-57.
64. Canonica GW et al. Chronic rhinosinusitis with nasal polyps impact in severe asthma patients: evidences from the Severe Asthma Network Italy (SANI) registry. Respir Med. 2020;166:105947.
65. Stevens WW et al. Clinical characteristics of patients with chronic
rhinosinusitis with nasal polyps, asthma, and aspirin-exacerbated respiratory disease. J Allergy Clin Immunol Pract. 2017;5(4):1061-70.
66. Matucci A et al. Asthma and chronic rhinosinusitis: how similar are they in pathogenesis and treatment responses?. Int J Mol Sci. 2021;22(7):3340.
67. Stevens WW et al. Associations between inflammatory endotypes and clinical presentations in chronic rhinosinusitis. J Allergy Clin Immunol Pract. 2019;7(8):2812-20.e3.
68. Kato A et al. Endotypes of chronic rhinosinusitis: relationships to disease phenotypes, pathogenesis, clinical findings, and treatment approaches. Allergy. 2022;77(3):812-26.
69. Tomassen P et al. Inflammatory endotypes of chronic rhinosinusitis based on cluster analysis of biomarkers. J Allergy Clin Immunol. 2016;137(5):1449-56.
70. De Corso E et al. Correlation between inflammatory biomarkers and disease control in chronic rhinosinusitis with nasal polyps. Int Forum Allergy Rhinol. 2024;14:1195-205.
71. Buchheit KM et al. IL-5Rα marks nasal polyp IgG4- and IgE-expressing cells in aspirin-exacerbated respiratory disease. J Allergy Clin Immunol. 2020;145(6):1574-84.
72. Sohail A et al. Nasal polyp antibodysecreting cells display proliferation signature in aspirin-exacerbated respiratory disease. J Allergy Clin Immunol. 2024;153(2):527-32.
73. Chen S et al. Epithelial IL5RA promotes epithelial-mesenchymal transition in pulmonary fibrosis via Jak2/STAT3 cascade. Pulm Pharmacol Ther. 2024;84:102286.
74. Tokunaga T et al. Novel scoring system and algorithm for classifying chronic rhinosinusitis: the JESREC study. Allergy. 2015;70(8):995-1003.
75. Kato A. Immunopathology of chronic rhinosinusitis. Allergol Int. 2015;64(2):121-30.
76. Pérez-Novo CA et al. Prostaglandin, leukotriene, and lipoxin balance in chronic rhinosinusitis with and without nasal polyposis. J Allergy Clin Immunol. 2005;115(6):1189-96.
77. Takabayashi T, Schleimer RP. Formation of nasal polyps: The roles of innate type 2 inflammation and deposition of fibrin. J Allergy Clin Immunol. 2020;145(3):740-50.
78. Sun DI et al. Clinical significance of eosinophilic cationic protein levels in nasal secretions of patients with nasal polyposis. Eur Arch Otorhinolaryngol. 2009;266(7):981-6.
79. Tsuda T et al. Eosinophil-derived neurotoxin enhances airway remodeling in eosinophilic chronic rhinosinusitis and correlates with disease severity. Int Immunol. 2019;31(1):33-40.
80. Gelardi M et al. Chronic rhinosinusitis with nasal polyposis (CRSwNP): the correlation between expression of galectin-10 and clinical-cytological grading (CCG). Am J Rhinol Allergy. 2022;36(2):229-37.
81. Emmi G et al. Evidence-based guideline for the diagnosis and management of eosinophilic granulomatosis with polyangiitis. Nat Rev Rheumatol. 2023;19(6):378-93.
82. Vaglio A et al. Eosinophilic granulomatosis with polyangiitis (Churg-Strauss): state of the art. Allergy. 2013;68(3):261-73.
83. Grayson PC et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology classification criteria for eosinophilic granulomatosis with polyangiitis. Ann Rheum Dis. 2022;81(3):309-14.
84. Berti A et al. The epidemiology of antineutrophil cytoplasmic autoantibody-associated vasculitis in Olmsted County, Minnesota: a twentyyear US population-based study. Arthritis Rheumatol. 2017;69(12):233850.
85. Pagnoux C, Berti A. Advances in the pharmacotherapeutic management of eosinophilic granulomatosis with polyangiitis. Expert Opin Pharmacother. 2023;24(11):1269-81.
86. Fagni F et al. Eosinophilic granulomatosis with polyangiitis: dissecting the pathophysiology. Front Med (Lausanne). 2021;8:627776.
87. Bossios A et al. IL-5 expression and release from human CD34 cells in vitro; ex vivo evidence from cases of asthma and Churg-Strauss syndrome. Allergy. 2010;65(7):831-9.
88. Hellmich B et al. Proinflammatory cytokines and autoimmunity in Churg‐Strauss syndrome. Ann NY Acad Sci. 2005;1051(1):121-31.
89. Jakiela B et al. Increased production of IL-5 and dominant Th2-type response in airways of Churg-Strauss syndrome patients. Rheumatology. 2012;51(10):1887-93.
90. Fulkerson PC, Rothenberg ME. Targeting eosinophils in allergy, inflammation and beyond. Nat Rev Drug Discov. 2013;12(2):117-29.
NX-IT-IMU-MONO-240001 November 2024
Allergic Reactions to NSAIDs during Febrile States: Case Report and Review of the Literature
Authors: Alketa H. Bakiri,1,2 *Ervin Ç. Mingomataj3
1. Department of Internal Medicine, American Hospital 3, Tirana, Albania
2. Department of Medical Sciences, Albanian University, Tirana, Albania
3. Department of Allergology & Clinical Immunology, "Mother Theresa" School of Medicine, Tirana, Albania
*Correspondence to allergology@gmx.de
Disclosure: The authors have declared no conflicts of interest.
Acknowledgements: Both authors contributed equally to this work.
The high frequency of allergic reactions (AR) to non-steroidal anti-inflammatory drugs (NSAID) has been linked to their extensive usage, resulting in adverse reactions that affect various systems and organs. This literature review, initiated by a case report of an immediate rash following NSAID administration for fever reduction, explores the possible mechanisms that drive such reactions. The results indicate that, in certain instances, NSAIDs can induce ARs specifically in the presence of an inflammatory febrile response following viral infections through a complex interaction of similar mechanisms. This intricate process involves the activation of proallergic-pyrogenic mediators like complement factor C5a, IL-1 β and IL-6, and TNF-α, in addition to the modulation of immune cells through specific signal pathways. Moreover, factors such as compromised skin barrier function in some severe skin ARs, and the activation of memory CD4+ T helper 2 cells by TNF-family molecules, contribute to the emergence of ARs in reaction to NSAID exposure during a febrile condition. This case report underscores the significance of thoroughly reviewing the patient’s medical history to ensure safe treatment. Meanwhile, the transient drug hypersensitivity reactions necessitate further exploration for a comprehensive understanding of the underlying mechanisms.
Key Points
1. Non-steroidal anti-inflammatory drugs can elicit allergic reactions only during febrile events.
2. The literature suggests an infection-related inflammatory response activates proallergic-pyrogenic mediators, such as IL-1β and IL-6, complement factor C5a, and TNF-α.
3. In this case, the immune cell interaction seems to potentiate similar mechanisms, activate memory CD4+ T helper 2 cells, and disturb skin barrier function.
INTRODUCTION
Non-steroidal anti-inflammatory drugs (NSAID) are useful in treating musculoskeletal disorders, headaches, pain, fever, and others.1,2 Fever is a phylogenetically ancient host reaction to invading microorganisms and other noxious stimuli. Endothermic organisms produce febrile temperatures through endogenous heat production at the expenditure of a higher metabolic rate.3 Despite its advantage for host defence, most doctors, nurses, and patients use antipyretics to improve fever and well-being.
The widespread use explains the frequent allergic reactions (AR) to them, ranging from asthma and rhinitis to urticaria and angioedema, various skin eruptions, and anaphylactic shock.1,2 Drug allergy (DA) management represents a physician challenge and persistent distress for the patient. The disease history could establish the diagnosis of NSAID hypersensitivity, because often, skin prick tests with NSAIDs are not successful, and no reliable in vitro tests are available. The only determinative diagnostic test is the oral challenge, while a tolerance test serves us to identify alternative NSAIDs in a hypersensitised patient.1,4 Initiated by a case of repeated immediate NSAID-induced rash episodes when administered for fever release but symptom-free when taken for non-febrile events, the following review aimed to explore the common mechanisms involved in the allergic response to NSAIDs and fever.
A CASE DESCRIPTION
A 39-year-old subject admitted for respiratory febrile infection reported generalised urticarial rash events after intake of antipyretics (acetaminophen, ibuprofen, etc.) only during febrile episodes. The mentioned drug reaction occurred first after extensive combined therapy for chronic tonsillitis (first amoxiclav, then clarithromycin), and then after prolonged treatment for COVID-19 (ceftriaxone, levofloxacin, dexamethasone, etc.). The urticarial reaction occurred within the first hour after NSAID intake, and the emergent
treatment with glucocorticoids resolved them within 5–6 hours without sequels. In more recent episodes, NSAID-related reactions happened before the beginning of any antibiotic therapy. In contrast, the further intake of any antipyretic drug didn’t induce allergic reactions when used for non-febrile events (such as headaches). The subsequent administration of any mentioned antibiotic after these episodes did not represent allergological clinical relevance.
The subject mentioned that previously an allergist considered the disease history impossible or inconsistent, and stated that a negative drug provocation test as a test of choice5,6 always excludes an AR. Being convinced about the presence of DA based on disease history, the authors commented for the patient that a negative result for the drug provocation test will be expected, and this does not necessarily predict an AR lack when NSAID should be used for fever reduction. In such circumstances, they considered aquatic baths at 29–33 °C and parenteral glucocorticoids the most suitable alternative against the fever. Appreciating the avoidance of suspicious drugs as the first choice, they suggested eventual premedication with antihistamines and leukotriene modifiers, and the controlled use of an NSAID only as add-on therapy (to large dose glucocorticoids) under medical surveillance.4,5,7 Cyclooxygenase (COX)2 inhibitors (like rofecoxib) represent an additional therapeutical alternative, as studies in humans or animals conclusively confirm the pivotal role of COX-2 in the febrile response after natural episodes or exposure to pyrogens, respectively.8 However, this alternative may be unsafe since the subject is allergic to acetaminophen, an inhibitor of the inducible COX-2 subtype synthesised in the brain.
Regarding the differential diagnosis, negative serological results for Epstein-Barr virus, human herpesvirus 6, cytomegalovirus, etc., excluded a viral exanthema during the medical treatment of viral infection.6 Additional undetermined agents should be considered as a cause of such reactions. Especially in children, viruses may induce
maculopapular rash or urticaria due to skin infiltration or immunologic response. In antibiotic-related skin eruptions, the culprit drug triggers the reaction after a transient virus-induced immune activation.9
Like in other studies, the skin test with acetaminophen and ibuprofen resulted negative, while basophil activation or lymphocyte transformation tests were unavailable.6,7,10 Further haematological and biochemical investigations did not differentiate between the two types of exanthema. Despite the difficulty distinguishing between infection-induced and drug-induced skin eruption in the acute phase, the outbreak of skin symptoms after the NSAID intake during different febrile infections supported a DA presence, including the cofactorial role of the infective agent in the transient reduction of immune tolerance. The urticaria outbreak before antibiotic exposure reinforced DA diagnosis and excluded the antibiotics' hypersensitivity.
DISCUSSION
Biological Mechanisms of Fever
NSAIDs like acetaminophen and ibuprofen are widely used for antipyretic and analgesic purposes. They reach this effect due to COX inhibition, thereby impairing the ultimate transformation of arachidonic acid to prostaglandins (PG), prostacyclin, and thromboxanes.2 The crucial effect is the inhibition of PGE2, which binds to its receptors on thermoregulatory neurons in the anterior hypothalamus, primarily eliciting fever.11
Several studies demonstrated that febrile PGE2 synthesis implicates different biological factors. Concerning the immune cells, this effect involves lymphocytes, mononuclear phagocytes, or neutrophils that exacerbate the immune response.2,12,13 The experimental inoculation of common pyrogens, bacterial lipopolysaccharide, or polyinosinic:polycytidylic acid (poly I:C), induces an inflammatory response and immediate fever implying IL-1β, IL-6, TNF-α, anaphylatoxic complement factor C5a, granulocyte colony-stimulating factor, and platelet-activating factor.13-15
Another factor in the febrile response is the sympathetic stimulation of β3agonist receptors in immune cells and the central nervous system.13,16
About the enzymes, the PGE2 synthesis needs COX-1 and COX-2, phospholipases A2, or terminal PGE synthases (PGES).14 The ‘inflammatory’ set comprises inducible COX-2 isoforms and microsomal PGES-1. The PGE2 receptors are multiple; one of them, EP3, is likely to be a primary ‘fever receptor’.14
The accelerated PGE synthesis and inflammatory rise of body temperature need the interaction between immune and neuronal factors. The early febrile response can occur through COX-independent mechanisms.11,17,18 In contrast, experimental suppression of some pyrogenic cytokines and sympathetic response can lead to the abrogation of PGE production and lack of febrile reaction.11,12,15,16 Apart from the generalised up-regulation, pyrogenic enzymes and cytokines are also synthesised or transported into certain central nervous structures, such as cerebral ventricles, endothelial and perivascular brain–blood barrier cells, microglia, hypothalamus, and cerebrospinal fluid.11,12,14,15,19 The PGE and other pyrogenic factors in the hypothalamus can activate a specific set of pathways, including the ventromedial preoptic area, which is a key regulatory site for thermoregulation, and the paraventricular nucleus, which produces autonomic and endocrine responses that cause hyperthermia.20-22 The ‘thermostat turn-up’ pathway activates the raphe pallidus, where premotor sympathetic neurons driving thermogenesis in the brown adipose tissue and skin vasoconstriction are located. Further, neuropeptides and peptide hormones modulate inflammatory signalling and thermo-effector pathways involved in fever.14,19-21
In summary, the febrile reaction implies an interaction between immune cells, endothelia, and certain thermoregulatory and effector formations in the central nervous system, which activate different inducible enzymes for the PGE2 synthesis (Table 1). Additional factors on the PGE2 stimulation include some sympathetic fibres
and receptors, and many inflammatory pyrogenic factors like IL-1β, IL-6, TNF-α, or complement fraction C5a, which mediate the thermogenesis and hyperthermia. They act as necessary cofactors in the inflammatory acceleration of PGE2 synthesis due to COX-dependent and -independent mechanisms.
Pyrogenic Factors Implicated in Immuno-Allergic Pathologies
Cytokines are highly inducible, secreted proteins mediating intercellular communication in the nervous and immune systems.17 Besides the infectionrelated events such as febrile reaction, inflammatory pain, or polymorphonuclear cell mobilisation,11,12-14,23-25 some immune-
Table 1: Mechanisms of febrile response.2,11-22
Febrile elicitors
Endogenous pyrogenic factors
PGE2-producing enzymes
PGE2-activated/ PGE2-producing tissues/cells
PGE2 targets
Final effects
mediated components can exacerbate cellular responses and create complex pathways that lead to various clinical manifestations.2,13 So, pyrogenic compounds IL-1, IL-6, C5a, or TNF-α are involved in autoimmune and hypersensitive pathologies.26-31 NSAID-related DAs include drug reaction with eosinophilia and systemic symptoms (DRESS), toxic epidermal necrolysis (TEN), Stevens-Johnson syndrome (SJS), and T cell-mediated, IgE-mediated, and cross-hypersensitivity allergies, often mediated by abovementioned acute phase reactants.7,27,29,32-36
In these cases, the pyrogenic cytokines activate many immune cells and complex processes. Thus, the mast cells (MC) play a crucial role in the baseline inflammatory
processes related to IgE response or COX-1 inhibition after exposure to NSAIDs.37 During degranulation, MCs release preformed and de novo-formed inflammatory mediators like TNF-α or platelet-activating factor, mediating the increase of vascular permeability. In turn, MC activation occurs under the effect of C5a, or other inflammatory cytokines.27,28,38,39 Being produced at the early stage of allergen sensitisation, then TNF-α continues to promote the inflammation cascade in the effector phase of ARs.31 MCs, the most important effector cells in IgE-mediated hypersensitivity reactions, effectively combat bacterial infections by releasing antimicrobial peptides.40 Like the MCs, the cutaneous dendritic cells (DC) play a crucial role in allergen detection and processing, which leads to allergy development. Still, they are also essential in host defence against bacteria by releasing cytokines such as TNF and IL-17.40 Another source of proinflammatory cytokines, such as IL-1β, IL-6, and TNF-α, are alternatively-activated macrophages (M2 macrophages), which, among others, exacerbate the inflammatory response in contact dermatitis.41 The ‘nonceliac wheat sensitivity’ (NCWS) represents a further case for TNF family implication, in which the production of TNF-α by CD45+, CD3+, CD4+, and CD8+ cells, as well as of IL-17 by CD4+ cells in the rectal tissue of nonceliac wheat sensitivity patients significantly overpassed the controls.42 T helper (Th) 2 cells, together with Group 2 innate lymphoid cells (ILC2) drive allergic pathology under the effect of IL-13 and TNF-family cytokine TL1A that co-stimulates T cells through its receptor DR3.43 This receptor is required for ILC2 expansion and function in T cell-dependent and -independent models of allergic disease. In contrast, DR3-deficient ILC2 can still differentiate, expand, and produce IL-13 when stimulated by IL-25 or IL-33, mediating intestinal helminth expulsion.43
Therefore, some pyrogenic cytokines, especially TNF-α, contribute to various hypersensitivity disease development (Table 2). They comprise IgE-mediated, T cellmediated, and some severe cutaneous DAs, also caused by NSAIDs. These pathologies involve a complex interaction mediated
by diverse immune cells and mechanisms, affecting MCs, DCs, M2 macrophages, ILC2 cells, and specific T cell subpopulations.
Pyrogenic Factors, NSAIDs, Viral Infections, and Characteristics of Immuno-Allergic Response
When many people use a drug such as NSAIDs, adverse reactions can occur, conditioned by diverse genetic profiles, including the HLA, viral infections, or other underlying conditions.5,44 Responders can be selective or cross-intolerant, involving IgE or T cell immunologic mechanisms, COX-inhibitory pathway, or other (non)immunologic mechanisms.7 Phenotypically, reactions can be classified as acute generalised exanthematic pustulosis, chronic spontaneous urticaria, contact dermatitis, DRESS, fixed drug eruption, NSAID-exacerbated cutaneous disease, NSAID-exacerbated respiratory disease, NSAID-induced urticaria/angioedema, single NSAID-induced delayed hypersensitivity reaction, single NSAID-induced urticaria, angioedema, or anaphylaxis, SJS, and TEN.
Besides promoting allergic responses,27,28,38, 39,41 certain inflammatory mediators like IL1β, IL-6, TNF-α, etc., may induce pyrogenic effects reaching amplified concentrations and more complex immune cell interactions (Figure 1).13-15,45 Thus, increased levels of TNF-α and IL-6 are observed in patients with COVID-19, especially in the severe group. Given the similarities of clinical features and pathogenesis between TEN and COVID-19, it is proposed that applying TNF-α inhibitor etanercept could attenuate disease progression in severe group COVID-19 patients by suppressing systemic auto-inflammatory responses.46 In the case of TEN, TNF antagonists are considered a controversial therapeutic alternative to large glucocorticoid doses or other immunosuppressors.33,35 The therapeutic use of anti-TNF-antibodies in autoimmune or viral pathologies is debatable because of T helper 2 (Th2) activation,26,30,47 and the amplification of similar immune responses in these cases may explain the induction of DA to NSAIDs during febrile infections.33,35 While the systemic use of NSAIDs or other drugs causes severe DA reactions like SJS
Table 2: Pyrogenic factors and allergic response.26-29,31,35,38-43
or TEN, many etiological factors including herpes simplex virus are suspected in many cases of erythema multiforme minor and a solitary case of DRESS (caused by chikungunya virus).48-50
The compromising of barrier function because of epithelial detachment in TEN and SJS represents an additional factor in the DA development after an infective event.33,35 In such circumstances, the organism may consider the intensified superficial contact with an allergen as exposure to a toxin.51,52 Like in other occasions, the immune response may switch via regulatory IL-10-dependent mechanisms.53,54 In SJS, epithelia-attached HIV leads to a dysregulated response by CD8+ T cells that recognise viral particles and their hyperactivation mimics the drug hypersensitivity reactions.55 Further viral reservoirs and first contact points in the mucosa are resident Langerhans and dermal dendritic cells. Consequent skin cytokine responses and dysregulated lymphoid populations create a crucible for hypersensitivity.56
Meanwhile, experiments in mice have shown that the TNF family costimulatory molecules OX40L/CD252 and CD30L/CD153 promote the reactivity of effector memory CD4+ Th2 cells after allergen exposure (Figure 1).45 In contrast, the blockade of costimulatory molecules induced a tolerogenic state and lack of eosinophilic inflammation. This indicates that several TNF costimulatory interactions may control the memory T cell responses and the severity of inflammatory reactions following (re)exposure to an allergen.45 Maybe, in this reported case, the coincident experience of viral fever and NSAID intake, among others, amplifies the TNF-related inflammatory mechanisms, including the ‘wake-up’ of memory CD4+ Th2 cells that lead to allergic symptoms. In contrast, the NSAID intake in non-febrile conditions does not amplify enough of the responsible mechanisms.
Apart from the crucial role in the immune protection against viral infections, the tissue-resident memory and regulatory T cells, once they cross-recognise the drug antigen, could be activated to attack
surrounding epidermal cells through effectors, resulting in drug-induced tissue damage.57 A murine model of cytomegalovirus infection also manifested the antigen-virus interaction and virusinduced immune tolerance reduction, evidencing an allergic airway sensitisation only when airway infection has been combined with inhaled environmental antigens.58 Viral activation of airway mucosal CD11b+ DCs promoted their uptake and processing, thus, providing an ‘opened door’ for otherwise harmless ambiental agents. The airway re-exposure to the inhaled antigen induced a Th2 cell response, diverse mucosal pathohistological alterations, and amplified mucus secretion and airflow obstruction.58 Such dynamic data agree with the knowledge that, especially in children, most of the skin symptoms presumed as drug allergies are likely viral-induced or because of a drug-virus interaction. Usually, they do not personify a permanent, drugspecific, adaptive immune response (at least) to antibiotics.9,59
A study on mitochondrial oxidative stress shed additional light on the role of inflammatory cytokine IL-1β during NSAID exposure, an important PGindependent pathway that induces gastric mucosal injury. Indomethacin timedependently stimulated the expression of proinflammatory molecules such as intercellular adhesion molecule 1, vascular cell adhesion molecule 1, IL-1β, monocyte chemotactic protein-1, and nuclear translocation of nuclear factor kappa-B (NF-κB) in gastric mucosa, in parallel with the increase of neutrophil infiltration and injury of gastric mucosa in rats.60 Meanwhile, the NF-κB signalling and the inhibition of regulatory TNF receptor 2 in CD4+ T cells aggravated the experimental airway inflammation in mice increasing the expression of cytokines IL-4, IL-5, IL-17, and TNF-α in serum and bronchoalveolar lavage fluid.61 Also, IL-3, IL-5, and GM-CSF could enhance p38 MAPK and NF-κB activity, and induce the expression of adhesion molecules intercellular adhesion molecule 1, CD11b, and CD18 on eosinophils during allergic inflammation.62,63 Inducing allergic exacerbation and eosinophilic inflammation,
viral respiratory infections, and stimulation with poly (I: C) increase the percentage of CD11b+ cells and enhances the secretion of IL-8, with effects mediated via the p38 MAPK and NF-κB signalling pathways.64 In such situations, the additional increase of endogenous TGF-β expression impairs glucocorticoid anti-inflammatory action.63
In contrast to infection and NSAID effects, and despite the mentioned glucocorticoid insensitivity, its large doses suppress the NF-κB (and activator protein-1) signalling pathways, showing an anti-inflammatory effect. The interactions between NF-κB and the glucocorticoid receptor result in differing effects on histone acetylation and deacetylation.65,66 These data suggest that NSAIDs and viral infections activate inflammatory cytokines IL-1β, TNF-α, etc., which, via the p38 MAPK and NF-κB signalling pathways, could lead to allergic exacerbations and relative glucocorticoid insensitivity.
CONCLUSION
In conclusion, the collected data support the concept that, sometimes, NSAIDs may trigger ARs specifically in the presence of an inflammatory febrile response following viral infections, through a complex interplay of similar mechanisms. This mosaic may comprise the simultaneous involvement of proallergic-pyrogenic factors like C5a, IL-1β, IL-6, and especially TNF-α, in addition to the immune cells interaction that modulates the inflammatory response through the p38 MAPK and NF-κB signalling pathways. Additional ‘wake-up’ factors include the compromised barrier function because of epithelial detachment in TEN and SJS, and the possible implication of TNF family molecules that activate memory CD4+ Th2 cells after NSAID exposure during febrile conditions. In this case, an amplified TNF-related interaction may elicit the AR
References
1. Nettis E et al. Update on sensitivity to nonsteroidal anti-inflammatory drugs. Curr Drug Targets Immune Endocr Metabol Disord. 2001;1(3):233-40.
because of the simultaneous infective febrile response and consecutive NSAID intake. In contrast, NSAID administration for nonfebrile conditions, or its avoidance during any febrile infection, does not recruit the immune system to mount the production of cytokines that provoke an acute allergic response.
Therefore, the literature findings (and the authors’ case report) indicate that regulatory and memory lymphocyte subpopulations can modulate the immune response toward allergic processes during inflammatory states (such as febrile viral infections). Maybe this condition, in combination with NSAID exposure, also provokes a (transient) decrease of the excitatory threshold for immune effector cells, thus inducing an AR. So, the infection and fever serve as cofactors for DA.
In this case study, the long COVID-19 and chronic tonsillitis could have contributed to this scenario. Considering the avoidance of responsible drugs as the best decision, the general scientific opinion accepts the use of aquatic baths at 29–33 °C and parenteral glucocorticoids as treatments of choice. Further alternatives are the use of COX-2 inhibitors and premedication with antihistamines or leukotriene modifiers that may help us in the controlled administration of an NSAID (as an add-on therapy to parenteral glucocorticoids). Concerning diagnosis, the drug challenge remains a gold standard test for the DA, but not all that glitter is gold. This case also teaches us that it is crucial to consider medical history thoroughly to ensure safe treatment. Future drug hypersensitivity classifications may incorporate such a fever-dependent ‘on/off’ (fed-on/off) mechanism (alias fever and drug-dependent ‘on/off’ allergic [feddonoffa] response). At the same time, such transient DA reactions need further investigation to understand comprehensively the underlying processes.
3. Schaffner A. [Fever--a useful or noxious symptom that should
be treated]? Ther Umsch. 2006;63(3):185-8. (in German)
4. Altamura Namazy J, Simon RA. Sensitivity to nonsteroidal antiinflammatory drugs. Ann Allergy
Asthma Immunol. 2002;89(6):542-50.
5. Fernandez J, Doña I. Diagnosing and managing patients with drug hypersensitivity. Expert Rev Clin Immunol. 2018;14(1):29-41.
6. Tsabouri S, Atanaskovic-Markovic M. Skin eruptions in children: drug hypersensitivity vs viral exanthema. Pediatr Allergy Immunol. 2021;32(5):824-34.
7. Blanca-Lopez N et al. NSAID-induced reactions: classification, prevalence, impact, and management strategies. J Asthma Allergy. 2019;8(12):217-33.
8. Simmons DL et al. Nonsteroidal antiinflammatory drugs, acetaminophen, cyclooxygenase 2, and fever. Clin Infect Dis. 2000;31(Suppl 5):S211-8.
9. Anci E et al. Viral infections and cutaneous drug-related eruptions. Front Pharmacol. 2021;11:586407.
10. Nomura Y et al. An elevated value on drug-induced lymphocyte stimulation test for immunoglobulin is an immunological abnormality of Kawasaki disease. Int Arch Allergy Immunol. 2010;153(1):102-6.
11. Nilsberth C et al. The role of interleukin-6 in lipopolysaccharideinduced fever by mechanisms independent of prostaglandin E2. Endocrinology 2009;150(4):1850-60.
12. Blatteis CM et al. Cytokines, PGE2 and endotoxic fever: a re-assessment. Prostaglandins Other Lipid Mediat. 2005;76(1-4):1-18.
13. Kawano Y et al. G-CSF-induced sympathetic tone provokes fever and primes anti-mobilizing functions of neutrophils via PGE2. Blood 2017;129(5):587-97.
14. Romanovsky AA et al. Fever and hypothermia in systemic inflammation: recent discoveries and revisions. Front Biosci. 2005;10:2193-216.
15. Davidson J et al. Cytokines and cytokine inducers stimulate prostaglandin E2 entry into the brain. Pflugers Arch. 2001;442(4):526-33.
16. Szentirmai É, Kapás L. Sleep and body temperature in TNFα knockout mice: The effects of sleep deprivation, β3AR stimulation and exogenous TNFα. Brain Behav Immunol. 2019;81:260-71.
17. Hamzic N et al. Immune-induced expression of lipocalin-2 in brain endothelial cells: relationship with interleukin-6, cyclooxygenase-2 and the febrile response. J Neuroendocrinol. 2013;25(3):271-80.
18. Mota CMD, Madden CJ. Neural circuits mediating circulating interleukin1β-evoked fever in the absence of prostaglandin E2 production. Brain Behav Immunol. 2022;103:109-21.
19. Conti B et al. Cytokines and fever. Front Biosci. 2004;1(9):1433-49.
20. Saper CB. Neurobiological basis of fever. Ann N Y Acad Sci. 1998;29(856):90-4.
21. Clénin GE et al. [Ibuprofen-induced, transient ANA- and anti-histonepositive leukocytoclastic vasculitis]. Hautarzt. 2000;51(9):678-81. (in German)
22. Zhang YH et al. Specific roles of cyclooxygenase-1 and cyclooxygenase-2 in lipopolysaccharide-induced fever and Fos expression in rat brain. J Comp Neurol. 2003;463(1):3-12.
23. Mason MJ, van Epps D. Modulation of IL-1, tumor necrosis factor, and C5a-mediated murine neutrophil migration by alpha-melanocytestimulating hormone. J Immunol. 1989;142(5):1646-51.
24. Sayers TJ et al. Effect of cytokines on polymorphonuclear neutrophil infiltration in the mouse. Prostaglandin- and leukotrieneindependent induction of infiltration by IL-1 and tumor necrosis factor. J Immunol. 1988;141(5):1670-7.
25. Vardeh D et al. COX2 in CNS neural cells mediates mechanical inflammatory pain hypersensitivity in mice. J Clin Invest. 2009;119(2):287-94.
26. Kato T et al. Hypersensitivity reaction against influenza vaccine in a patient with rheumatoid arthritis after the initiation of etanercept injections. Mod Rheumatol. 2006;16(5):327-9.
27. Nguyen SMT et al. Mechanisms governing anaphylaxis: inflammatory cells, mediators, endothelial gap junctions, and beyond. Int J Mol Sci. 2021;22(15):7785.
28. Komi DEA et al. Mast cell biology at the molecular level: a comprehensive review. Clin Rev Allergy Immunol. 2020;58(3):342-65.
29. Shiohara T et al. Monitoring the acute response in severe hypersensitivity reactions to drugs. Curr Opin Allergy Clin Immunol. 2015;15(4):294-9.
30. Sylvester MK et al. The interactions between autoinflammation and type 2 immunity: from mechanistic studies to epidemiologic associations. Front Immunol. 2022;24(13):818039.
31. Ahmad S et al. The key role of TNFTNFR2 interactions in modulating allergic inflammation: a review. Front Immunol. 2018;9:9:2572.
32. Bellanti JA. Cytokines and allergic diseases: clinical aspects. Allergy Asthma Proc. 1998;19(6):337-41.
33. Zhang S et al. [Drug-induced toxic epidermal necrolysis with secondary aspergillus fumigatus infection: a case
report]. Beijing Da Xue Xue Bao Yi Xue Ban. 2019;51(5):977-80. (in Chinese)
34. Doña I et al. Progress in understanding hypersensitivity reactions to nonsteroidal anti-inflammatory drugs. Allergy 2020;75(3):561-75.
35. Hasegawa A, Abe R. Recent advances in managing and understanding Stevens-Johnson syndrome and toxic epidermal necrolysis. F1000Res. 2020;9:F1000 Faculty Rev-612.
36. Loh TY, Cohen PR. Ketoprofeninduced photoallergic dermatitis. Indian J Med Res. 2016;144(6):803-6.
37. Edsel M et al. Mast cells in aspirinexacerbated respiratory disease. Curr Allergy Asthma Rep. 2024;24(2):73-80.
38. Zhang Z, Kurashima Y. Two sides of the coin: mast cells as a key regulator of allergy and acute/chronic inflammation. Cells 2021;10(7):1615.
39. Saggini A et al. Allergic inflammation: role of cytokines with special emphasis on IL-4. Int J Immunopathol Pharmacol. 2011;24(2):305-11.
40. Metz M, Maurer M. Innate immunity and allergy in the skin. Curr Opin Immunol. 2009;21(6):687-93.
41. Suzuki K et al. Roles of alternatively activated M2 macrophages in allergic contact dermatitis. Allergol Int. 2017;66(3):392-7.
42. Mansueto P et al. TNF-α, IL-17, and IL-22 production in the rectal mucosa of nonceliac wheat sensitivity patients: role of adaptive immunity. Am J Physiol Gastrointest Liver Physiol. 2020;319(3):G281-8.
43. Meylan F et al. The TNF-family cytokine TL1A promotes allergic immunopathology through group 2 innate lymphoid cells. Mucosal Immunol. 2014;7(4):958-68.
44. Sachs B, Merk HF. [Drug allergies. Clinical aspects, pathophysiology, and treatment of cutaneous manifestations]. Hautarzt. 2005;56(1):8-15. (in German)
45. Gracias DT et al. Combination blockade of OX40L and CD30L inhibits allergen-driven memory TH2 cell reactivity and lung inflammation. J Allergy Clin Immunol. 2021;147(6):2316-29.
46. Chen XY et al. TNFα inhibitor may be effective for severe COVID-19: learning from toxic epidermal necrolysis. Ther Adv Respir Dis. 2020;14:1753466620926800.
47. Benucci M et al. Correlation between atopy and hypersensitivity reactions during therapy with three different TNF-alpha blocking agents in rheumatoid arthritis. Clin Exp Rheumatol. 2009;27(2):333-6.
48. Carrozzo M et al. [Erythema multiforme. A heterogeneous pathologic phenotype]. Minerva Stomatol. 1999;48(5):217-26. (in Italian)
49. Sil A et al. Sulfasalazine-induced drug reaction with eosinophilia and systemic symptoms (DRESS) with concomitant acute chikungunya virus infection: possible role of new viral trigger. BMJ Case Rep. 2021;14(10):e244063.
50. Munshi R, Maurya M. A case report of cefixime, paracetamol, and nimesulide induced toxic epidermal necrolysis in a woman with Dengue infection without any other associated comorbidities. Curr Drug Saf. 2024;19(2):286-90.
51. Mingomataj EÇ, Bakiri AH. Regulator versus effector paradigm: interleukin-10 as an indicator of the switching response. Clin Rev Allergy Immunol. 2016;50:97-113.
52. Bakiri AH, Mingomataj EÇ. Novel insights on interleukin-10 functions: a manipulative tool for the deviation of immune response and disease outcome. Eur Med J (Allergy & Immunology). 2019;4(1):88-94.
53. Mingomataj EÇ, Bakiri A. Barrier integrity damage-elicited allergic response (BIDEAR) syndrome: a proper entity? Int J Clin Med Allergy. 2021;6(1):71-2.
54. Bakiri A, Mingomataj EÇ. The lifestyle and the usefulness of patch tests among elderly male patients; reflections on the role of T helper 2 profile in allergic contact dermatitis. J Clin Exp Immunol. 2023;8(3):599-602.
55. Manenzhe SC et al. Exploring the association between erythema multiforme and HIV infection: some mechanisms and implications. AIDS Res Ther. 2024;21(1):24.
56. Chimbetete T et al. HIV-associated immune dysregulation in the skin: a crucible for exaggerated inflammation and hypersensitivity. J Invest Dermatol. 2023;143(3):362-73.
57. Shiohara T et al. Crucial role of viral reactivation in the development of severe drug eruptions: a comprehensive review. Clin Rev Allergy Immunol. 2015;49(2):192-202.
58. Reddehase MJ. Adverse immunological imprinting by cytomegalovirus sensitizing for allergic airway disease. Med Microbiol Immunol. 2019;208(3-4):469-73.
59. Norton AE et al. Antibiotic allergy in pediatrics. Pediatrics. 2018;141(5):e20172497.
60. Bindu S et al. The nonsteroidal anti-inflammatory drug induces proinflammatory damage in gastric mucosa through NF-κB activation and neutrophil infiltration: anti-inflammatory role of heme
oxygenase-1 against nonsteroidal anti-inflammatory drug. Free Radic Biol Med. 2013;65:456-67.
61. Li XM et al. Impaired TNF/TNFR2 signaling enhances Th2 and Th17 polarization and aggravates allergic airway inflammation. Am J Physiol Lung Cell Mol Physiol. 2017;313(3):L592-601.
62. Wong CK et al. Interleukin-3, -5, and granulocyte-macrophage colonystimulating factor-induced adhesion molecule expression on eosinophils by p38 mitogen-activated protein kinase and nuclear factor-[kappa] B. Am J Respir Cell Mol Biol. 2003;29(1):133-47.
63. Xia YC et al. Glucocorticoid insensitivity in virally infected airway epithelial cells depends on transforming growth factor-β activity. PLoS Pathog. 2017;13(1):e1006138.
64. Månsson A et al. TLR3 in human eosinophils: functional effects and decreased expression during allergic rhinitis. Int Arch Allergy Immunol. 2010;151(2):118-28.
65. Oppong E et al. Molecular mechanisms of glucocorticoid action in mast cells. Mol Cell Endocrinol. 2013;380(12):119-26.
66. Adcock IM et al. Glucocorticoids: effects on gene transcription. Proc Am Thorac Soc. 2004;1(3):247-54.
Abdominal Cocoon and Recurrent Haemorrhagic Ascites, Unexpected Findings in Endometriosis: A Case Report and Review of Literature
Authors: *Rosheen Jamil,1 Maheen Jamil2
1. Mayo Hospital, King Edward Medical University, Lahore, Pakistan
2. Allama Iqbal Medical College, Jinnah Hospital, Lahore, Pakistan *Correspondence to rosheen.jamil.20@gmail.com
Disclosure: The authors have declared no conflict of interest.
Introduction: The presentation of endometriosis as massive haemorrhagic ascites and the presence of concurrent encapsulating sclerosing peritonitis is extremely rare in medical literature. This presentation warrants a strong suspicion for endometriosis especially in a nulliparous, reproductive-age woman.
Case Report: A 22-year-old woman presenting with nonspecific abdominal discomfort, distension, massive ascites, dysmenorrhea, anaemia, and mild weight loss is reported here.
Diagnosis: Based on biopsy results at laparotomy, negative Tuberculosis cultures, a poor response to the anti-tuberculosis therapy, and, finally, an excellent response to combined oral contraceptive pills, endometriosis was confirmed as the diagnosis of exclusion in this case.
Interventions and outcomes: The patient received medical treatment for endometriosis and had an excellent response to treatment.
Methods: The team conducted a thorough literature review on PubMed/MEDLINE, Cochrane, and Science Direct and shortlisted 13 highly relevant articles for the case report. The patient provided informed written consent for the publication of this case report, with no patientidentifying information included in the article. The figures in the case report have not been published elsewhere, so the authors did not require copyright permission.
Conclusion: This is one of the few cases reported in the literature in which endometriosis presented with haemorrhagic ascites and sclerosing peritonitis. Endometriosis should be considered a differential diagnosis in a nulliparous, reproductive-age female who presents with massive recurrent haemorrhagic ascites.
Key Points
1. Overall, 10–15% of all reproductive-age women and 70% of women with chronic pelvic pain have endometriosis. Haemorrhagic ascites as the first presentation of endometriosis is rarely reported.
2. This is a case report describing a young woman with recurrent haemorrhagic ascites and an abdominal cocoon found during laparotomy who was diagnosed with endometriosis after 18 months of anti-tuberculosis treatment.
3. The distinct presentation of endometriosis should be considered in the differential diagnosis of women of reproductive age who present with massive recurrent haemorrhagic ascites.
INTRODUCTION
Endometriosis is defined as the presence of endometrial glands and stroma outside the uterine cavity, which commonly presents with subfertility and chronic pelvic pain in reproductive-age women. It affects roughly 10% of the global reproductive-age women’s population. However, this percentage is significantly higher in women with chronic pelvic pain at about 75% and in those with infertility at about 40%.1 Since Brews described the first case of endometriosis presenting as haemorrhagic ascites (HA) in 1954, less than 100 cases have been documented so far.2
The first presentation of endometriosis as recurrent HA is rare in the literature and warrants strong clinical suspicion, especially in young, nulliparous, reproductive-age women of African descent. The criterion for HA is the presence of more than 10,000 red blood cells per microliter. Furthermore, only six cases have been reported in which women presented with both endometriosisrelated ascites and encapsulating peritonitis, both of which were present in this case. Encapsulating peritonitis, abdominal cocoon, or frozen ascites is characterised by a fibrin membrane that entraps the bowel loops.3
The authors present the case of a 22-year-old woman with massive recurrent haemorrhagic ascites, first diagnosed on an abdominal ultrasound scan for occasional abdominal discomfort, abdominal distension, mild weight loss, and a thin fibrinous membrane encasing the bowel loop on laparotomy. Endometriosis was subsequently confirmed as the
diagnosis of exclusion because of this patient’s excellent response to the combined oestrogen-progesterone oral contraceptive pills. This case provides valuable insights for the consideration of endometriosis as an important differential diagnosis in the evaluation of nulliparous women of childbearing age presenting with massive HA.
CASE PRESENTATION
The case presented here is of a 22-yearold Pakistani woman who presented with abdominal distension, intermittent dull abdominal pain and discomfort, and 8 kg unintentional weight loss in 2 years. Menarche was at age 11 years. She was not sexually active. She had primary dysmenorrhoea but regular menstrual cycles and no history of cyclic pelvic pain. The patient had a past surgical history of an open laparotomy and appendectomy at age 12 years for acute abdominal pain; intra-operatively, a thin fibrinous membrane encasing the bowel loops was found. Based on tuberculous suspicion, histopathology was done then, but no acid-fast bacilli were detected. The surgeon reported no suspicion or findings of endometriosis during this laparotomy.
Apart from past surgical history, there was no significant medical history, and she was not on any regular medication apart from the occasional use of ibuprofen for primary dysmenorrhea. On presentation, physical examination revealed generalised distension but no tenderness. The percussion note was dull, particularly in the lower quadrants.
INVESTIGATIONS
Blood analysis showed microcytic anaemia with a haemoglobin of 11.5 g/dL. An ultrasound scan of the abdomen and pelvis revealed moderate to significant ascites in the pelvis, extending to the right and left paracolic gutters. The uterus and right adnexa were normal; however, there was a haemorrhagic cyst with internal echoes in the left adnexa and the left hydrosalpinx. An ultrasound-guided ascitic tap revealed chocolate-coloured haemorrhagic fluid. Cytological analysis of the ascitic fluid showed numerous red blood cells and some lymphocytes, but there was no evidence of malignant cells. Fluid was exudative with a decreased serum asciticalbumin gradient. Cultures were negative, and no acid-fast bacilli were detected.
Serum tumour markers demonstrated no significant increase in CA-125 levels. CT of the abdomen and pelvis showed moderate to significant loculated ascites, more marked in the pelvis and extending to the right and left paracolic gutters. The decision for exploratory laparotomy was made to obtain tissue biopsy, as an imaging-guided attempt for biopsy was considered difficult due to the loculated nature of ascites and the presence of peritoneal adhesions because of previous laparotomy.
Findings at laparotomy included multiple adhesions, approximately 4 L of haemorrhagic ascites, a thin fibrinous membrane encasing bowel loops, and a normal-appearing uterus and ovaries. Multiple biopsies of the omentum and ovarian lining were obtained. Histopathology revealed many hemosiderin-laden macrophages and benign-appearing mesothelial cells. There was no evidence of malignant cells. Cultures were negative, and acid-fast bacilli were not detected.
TREATMENT
Based on clinical suspicion and the increased burden of disease in the region, peritoneal tuberculosis (TB) was suspected, and empiric treatment of TB was started. The first-line anti-TB therapy
(ATT) regimen continued for 1.5 years. However, after 8 months of ATT initiation, imaging, as shown in Figure 1, confirmed the recurrence of ascites, which was drained. After completing the course of ATT, a follow-up MRI of the pelvis revealed a left-sided large hematosalpinx with left paracolic haemorrhagic fluid. There was a small endometrioma in the left ovary and bilateral haemorrhagic follicles. The uterus was unremarkable.
An alternative diagnosis of endometriosis was considered due to the ineffective response to ATT, the lack of objective proof of TB, and an indication of endometriosis on MRI. The patient was started on continuous oestrogen-progesterone oral contraceptive pills.
OUTCOME AND FOLLOW-UP
The patient responded well to combination oral contraceptive pills (COCP), and imaging showed decreasing trends in intrabdominal fluid collection. The patient reported no active complaints and was asymptomatic. Continuous COCPs were continued for 1 year, and the patient remained amenorrhoeic. Follow-up imaging revealed no evidence of ascites recurrence; the patient discontinued using COCPs for 3 months and began to have regular menstruation again. However, then she started experiencing discomfort and pain in the left lower quadrant. As shown in Figure 2, the abdominal ultrasound confirmed the re-accumulation of fluid in the left paracolic gutter, which measured around 370 mL. She was then placed back on continuous COCP and has reported no active complaints. She is now under periodic surveillance to look for a recurrence of ascites. The patient is not currently planning for a family; however, she was counselled regarding potential fertility and pregnancy complications in the future. She was also counselled on the possibility of IVF and surgery if needed. Other medical or surgical treatment options can also be considered depending on the patient’s preference.
Figure 1: An ultrasound image of the abdomen and pelvis shows a small amount of fluid in the pelvis after laparotomy and the drainage of ascites.
DISCUSSION
Endometriosis is a benign condition in which cells lining the uterus, or endometrium, deposit outside the uterus, causing pain and infertility. Overall, 10–15 % of all reproductive-age women and 70% of those with chronic pelvic pain have endometriosis.4 Endometriosis usually presents with chronic, cyclical pelvic pain, deep dyspareunia, and subfertility; however, recurrent HA as an initial presentation of endometriosis is extremely rare.5
Endometriosis presenting as massive HA is often initially mistaken for peritoneal TB or ovarian or primary peritoneal malignancy as its symptoms of weight loss and decreased appetite often mimic the symptoms in these gynaecological malignancies.6 Additionally, fibroids, Meigs syndrome, benign ovarian tumours, and ovarian hyperstimulation syndrome are among the benign gynaecologic diseases that have been linked to ascites, which makes it challenging to arrive at a final diagnosis.7 In the most
recently published systematic review and meta-analysis, the highest prevalence of HA was noted in nulliparous women of African origin. Abdominal distension, weight loss, abdominal pain, and abnormal uterine bleeding were the most common symptoms. In contrast, pelvic mass was the most common physical finding.8 Due to the unusual presentation, it is often dealt with as a diagnostic dilemma, leading to delayed treatment and adding to the patient’s distress. This case emphasises the need for its early recognition and treatment.
The exact cause of endometriosis is not entirely understood; however, various theories exist to explain its pathophysiology. The most postulated theory is that retrograde menstruation of oestrogensensitive endometrial cells implanting on peritoneal surfaces elicits an inflammatory response accompanied by angiogenesis, adhesions, fibrosis, scarring, and organ distortion, leading to pain and infertility.7 Furthermore, the precise pathophysiology of endometriosis causing HA and
Figure 2: An ultrasound image of the abdomen and pelvis shows re-accumulation of fluid in the left paracolic gutter after completing the course of anti-tuberculosis therapy for 18 months, prompting a change in treatment to combination oral contraceptive pills, considering endometriosis as the primary diagnosis.
encapsulating peritonitis is unknown; however, according to Bernstein, it may be caused by irritation of the peritoneum by free blood released from ruptured endometrioma, which further enhances fibrosis and inflammation.9 Bloody ascites may be the result of enhanced angiogenesis and friable soft tissue erosions on serosal or peritoneal surfaces, causing micro or frank bleeding. Bloody pleural effusions could be another common finding in patients with HA due to endometriosis, and the most likely cause for this is anatomical abnormalities in the diaphragm.10
The presentation of massive haemothorax is almost always in conjunction with massive ascites. Many of them have diaphragmatic and pleural lesions that need to be surgically repaired.11 The gold standard for diagnosing diaphragmatic endometriosis is video laparoscopy; for thoracic endometriosis, it is video-assisted thoracoscopic surgery.12 Endometriosis risk factors include early age at menarche, shorter menstrual length, and taller height; risk factors associated with a lower risk
include smoking, parity, and higher BMI.13
A study by Kaabachi et al.14 showed a statistically significant increase in the expression of IL-37 mRNA in peritoneal fluid in women with endometriosis compared to healthy controls. Moreover, levels of IL-37 mRNA were directly correlated with disease severity.14
Encapsulating sclerosing peritonitis or abdominal cocoon syndrome is defined as a fibro-collagenous membrane surrounding the small bowel or cocoonlike appearance.15 According to a recent systematic review by Magalhães et al.16 on endometriosis-related ascites and encapsulating peritonitis, only six cases of endometriosis-associated encapsulating peritonitis can be found in the literature. The most common primary cause of abdominal cocoon syndrome is idiopathic. However, its secondary causes include endometriosis, peritoneal dialysis, ventriculoperitoneal or peritoneo-venous shunts, liver transplantation, recurrent peritonitis, and familial Mediterranean fever.17 A case report by Yılmaz on a young female patient
on haemodialysis revealed diffuse peritoneal thickening and cocoon formation, with recurrent hemoperitoneum corresponding with her menstrual cycles. Endometriosis was further confirmed on biopsy.18 Both endometriosis and encapsulating peritonitis were present in the authors’ case.
References
1. Gonzalez A et al. Endometriosis presenting as recurrent haemorrhagic ascites: a case report and literature review. Int J Fertil Steril. 2020;14(1):72-5.
2. Gungor T et al. A systematic review: endometriosis presenting with ascites. Arch Gynecol Obstet. 2011;283(3):513-8.
3. Machado NO. Sclerosing encapsulating peritonitis: review. Sultan Qaboos Univ Med J. 2016;16(2):e142-51.
4. Ashkenazi MS et al. The clinical presentation of endometriosis and its association to current surgical staging. Journal of Clinical Medicine. 2023;12(7):2688.
5. Morgan TL et al. Endometriosis presenting with hemorrhagic ascites, severe anemia, and shock. Am J Emerg Med. 2013;31(1):272.e1-3.
6. Ahmed U, Chughtai N. Endometriosis presenting as relapsing haemorrhagic ascites in a South Asian woman: a case report. J Pak Med Assoc. 2024;74(1):165-8.
CONCLUSION
Despite its rarity, this case highlights the importance of the unique presentation of endometriosis that should be considered in the differential diagnosis of women of reproductive age presenting with massive haemorrhagic ascites.19
8. Wang X et al. Endometriosis presenting with recurrent massive hemorrhagic ascites and diagnosed by core needle biopsy: a case report. Medicine (Baltimore). 2019;98(19):e15477.
9. Bernstein JS et al. Massive ascites due to endometriosis. Digest Dis Sci. 1961;6:1-6.
10. Chan-Tiopianco M et al. Clinical presentation and management of endometriosis-related hemorrhagic ascites: a case report and systematic review of the literature. Cureus. 2021;13(6):e15828.
11. Ezemba N et al. Thoracic endometriosis syndrome in Nigeria: a single-centre experience. Interact Cardiovasc Thorac Surg. 2021;32(2):256-62.
12. Patrucco Reyes S et al. A case of hemothorax as manifestation of thoracic endometrial syndrome. J Investig Med High Impact Case Rep. 2021;9:23247096211052191.
13. Parasar P et al. Endometriosis: epidemiology, diagnosis and clinical management. Curr Obstet Gynecol Rep. 2017;6(1):34-41.
14. Kaabachi W et al. Interleukin-37 in endometriosis. Immunol Lett. 2017;185:52-5.
15. Pokharel P et al. Abdominal cocoon syndrome. J Nepal Health Res Counc. 2019;17(2):264-6.
16. Magalhães TF et al. Ascites and encapsulating peritonitis in endometriosis: a systematic review with a case report. Rev Bras Ginecol Obstet. 2018;40(3):147-55.
17. Çolak Ş, Bektaş H. [Abdominal cocoon syndrome: a rare cause of acute abdomen syndrome]. Ulus Travma Acil Cerrahi Derg. 2019;25(6):575-9. (In Turkish)
18. Yılmaz F et al. A case of cyclic hemoperitoneum in a hemodialysis patient: Encapsulated peritoneal sclerosis complicated by endometriosis and fungal peritonitis. Semin Dial. 2021;34(2):176-9.
19. Bignall J et al. Endometriosis: a rare and interesting cause of recurrent haemorrhagic ascites. BMJ Case Rep. 2014;2014:bcr2013010052.
Evaluating Diagnostic Performance of Extrapulmonary Tuberculosis Using Cartridge-Based Nucleic Acid Amplification Test Assay: A Retrospective Cross-Sectional Study at a Tertiary Health Care Setup in India
Background: Extrapulmonary tuberculosis (EPTB) diagnosis is difficult due to its subclinical or nonspecific clinical symptoms, paucibacillary nature, and difficulties in obtaining qualified pathological specimens for Mycobacterium tuberculosis detection. Given the paucibacillary nature of EPTB, and drug resistance as high as 19%, rapid diagnostic methods like Xpert MTB/RIF (Cepheid, Sunnyvale, California, USA) can make a significant clinical impact. In this study, the authors aim to determine the positivity rate of Mycobacterium tuberculosis in EPTB samples by Xpert MTB/RIF or cartridge-based nucleic acid amplification test (CBNAAT) in a tertiary healthcare setup.
Materials and methods: This was a retrospective cross-sectional study where presumptive extrapulmonary cases of any age were considered for inclusion. A total of 688 suspected extrapulmonary samples were analysed by CBNAAT over a period of 7 months.
Result: A total of 25% (170/688) of the cases were reported to be positive, while the combined rate of Error, Invalid, and No result was 8.5% (59/688). Rifampicin resistance was seen in 14 isolates, while four isolates showed indeterminate results.
Conclusion: Varied clinical presentations and the paucibacillary nature of the extrapulmonary samples often lead to the failure of diagnosis by conventional diagnostic tests (smear microscopy and culture). Hence, molecular diagnostic techniques play a crucial role in rapid diagnosis. The present study thus highlights the impact of CBNAAT in the definite diagnosis of extrapulmonary tuberculosis in a tertiary healthcare centre.
Key Points
1. Extrapulmonary tuberculosis (EPTB) poses significant diagnostic challenges due to its diverse clinical presentations. With tuberculosis remaining a major global health concern, timely and accurate diagnosis of EPTB is critical to improving patient outcomes and reducing disease burden.
2. This study evaluates the performance of the cartridge-based nucleic acid amplification test (CBNAAT) assay in diagnosing extrapulmonary tuberculosis across various specimen types in a high-burden tertiary care centre in India.
3. CBNAAT is an effective diagnostic tool for EPTB, providing rapid and reliable results. However, resource constraints and methodological limitations highlight the need for continued refinement and integration with other diagnostic strategies in resource-limited settings.
INTRODUCTION
Tuberculosis (TB) represents a significant global public health issue, ranking as the 13th leading cause of mortality and standing as the second most lethal infectious disease globally, following COVID-19. It poses a significant diagnostic and therapeutic challenge globally. India accounts for around 21% of the TB incidence.1 Mycobacterium tuberculosis (MTB) primarily infiltrates the lungs, giving rise to tuberculous lesions recognised as pulmonary TB. However, there are instances where it may infrequently invade other locations as well. Extrapulmonary tuberculosis (EPTB) is characterised, according to WHO classification criteria, as an infection caused by MTB that impacts tissues and organs outside the pulmonary parenchyma.2 In 2019, extrapulmonary tuberculosis (EPTB) cases constituted 15% of the 7.2 million reported cases of TB worldwide.3 In India, EPTB makes up 10–15% of the total TB cases, mainly affecting the pleura, lymph nodes, gastrointestinal tract, and various other organs, with a notable case mortality rate ranging from 25–50%.4
Individuals with compromised immune systems and young children exhibit an increased prevalence of EPTB.5-7
In resource-limited settings, the primary method for diagnosing TB is still smear microscopy. In highly prevalent bacillary diseases like cavitary TB, its sensitivity is approximately 50%, but it decreases to 10–20% for paucibacillary disease.8-10
Microbiological culture of MTB stands as the gold standard test; however, obtaining
a complete culture result takes a minimum of 10 days in liquid media and up to 8 weeks on solid media.9-11 Additionally, there is an added delay of 3–4 weeks for drug susceptibility testing.12
Diagnosing EPTB proves challenging because of its subclinical or nonspecific clinical symptoms, paucibacillary nature, and the challenges in obtaining adequately qualified pathological specimens for detecting MTB. The delayed diagnosis of EPTB may result in untimely treatment and subsequent severe consequences.
To address the challenges associated with MTB diagnosis, in December 2010, the WHO endorsed the use of cartridge-based nucleic acid amplification test (CBNAAT)/ GeneXpert MTB/RIF1 (Cepheid, Sunnyvale, California, USA) in TB laboratories. India incorporated CBNAAT into its Revised National Tuberculosis Control Program (RNTCP) in 2012.13 The CBNAAT assay employs a closed system based on real-time polymerase chain reaction (PCR), requiring minimal technical expertise for the diagnosis of TB and rifampicin resistance within 2 hours.14 In 2013, WHO updated its policy statement, endorsing the use of Xpert MTB/ RIF instead of conventional microscopy and culture as the initial diagnostic tests for all adults and children suspected of having pulmonary TB. Furthermore, in 2014, WHO recommended CBNAAT over conventional tests (including microscopy, culture, or histopathology) for examining specific non-respiratory specimens (such as lymph nodes and other tissues) from patients suspected of having extrapulmonary TB.15
Considering the paucibacillary nature of EPTB and the prevalence of drug resistance reaching as high as 19%, the implementation of rapid diagnostic methods like Xpert MTB/RIF can have a substantial clinical impact.16,17 In this study, the authors aim to determine the positivity rate of MTB in EPTB samples by Xpert MTB/RIF or CBNAAT in a tertiary health care setup.
METHODS
The research conducted was a retrospective cross-sectional study spanning 7 months, from January–August 2022. A total of 688 suspected extra-pulmonary samples were collected. Presumptive EPTB cases of any age were considered for inclusion. All samples, received in sterile containers, were aseptically collected specimens, typically devoid of other microorganisms (sterile). These specimens included fluids such as spinal, pleural, pericardial, synovial, ascitic, blood, tissues (lymph node, tissue biopsies), fine needle aspirates, and infected specimens (gastric lavage, bronchial washings, pus). In the initial process, samples were concentrated at 3,000 g for 15 minutes, and sediments were then resuspended in 2–5 mL of sterile phosphate buffer saline for another 15 minutes (phosphate-buffered saline).18 Contaminated samples underwent decontamination with N-acetyl-cysteine sodium hydroxide (NALCNaOH) before centrifugation. Biopsy samples were cut into small pieces with a sterile scalpel or blade and homogenised in sterile saline. Fine needle aspirate samples were collected by a pathologist, while other body fluid samples were collected by physicians during patient investigations and sent to the Directly Observed Therapy Centre for microscopic investigation and analysis through the GeneXpert MTB/RIF assay. For the GeneXpert MTB/RIF assay, samples with sufficient volume were treated with sample reagent containing NaOH and isopropanol, following the manufacturer’s instructions.19.20
Sample Size Calculation
This retrospective study utilised the available data or cases within a specified time period (7 months); hence, the total
number of available samples during the defined study period (688 samples) was used as the sample size. All the collected samples were considered for inclusion in the study, provided they met the study’s inclusion criteria and were suitable for analysis. Any specific exclusion criteria or limitations in the data were carefully considered to ensure the integrity and representativeness of the sample.
Ethical Consideration
The retrospective nature of this study utilised existing data collected as part of routine investigation protocol; hence, no formal ethical consent was required/sought. However, adherence to ethical principles was ensured throughout the study, including the protection of patient confidentiality and privacy. All data were handled securely and anonymised to maintain patient anonymity. The study complied with relevant data protection and sought appropriate permissions for data access and use.
Data Management and Statistical Analysis
The data were recorded using the Microsoft Excel (Redmond, Washington, USA) spreadsheet program. Categorical variables were analysed using frequencies and percentages. Graphical representation, including data and bar/pie charts, was employed for appropriate data visualisation.
RESULTS
In this study, a total of 688 suspected extra-pulmonary samples were analysed over a period of 7 months. The age of the patients ranged from 1.5 months to 88 years, with a mean age of 27.49±16.82 years.
A total of 25% (170/688) of the cases were reported to be positive, while the combined rate of Error, Invalid, and No result was 8.5% (59/688). Rifampicin resistance was seen in 14 isolates, while four isolates showed indeterminate results.
Table 1 depicts the comprehensive overall distribution of the specimen types among
the extra-pulmonary samples. A total of 351 pus, 155 cerebrospinal fluid, 56 pleural fluid, 51 ascitic fluid, 14 knee and synovial fluid, 34 tissue biopsy, and 27 lymph node biopsy samples were tested by CBNAAT. Table 2 and Table 3 depict the age and site-wise distribution of positivity of extrapulmonary TB among females and males, respectively.
DISCUSSION
Both developed as well as developing countries have seen an increase in the burden of TB over the past few decades, and a huge proportion of this surge is associated with the HIV epidemic. Disease pattern has evolved with the increased emergence of EPTB and disseminated TB. Drug resistance is a significant issue, especially for people with EPTB and HIV coinfection.21 Diagnosis of EPTB is rather challenging due to the paucibacillary nature of the samples.22 The WHO endorsement of GeneXpert particularly applied to the diagnosis of pulmonary TB because it was created and optimised for testing sputum samples, and the original largescale evaluations were performed on patients with pulmonary TB only. However, evaluations of the GeneXpert assay have more recently been extended to a range
of extrapulmonary samples.23 This study reported an overall positivity rate of 25% by CBNAAT for extrapulmonary samples, indicating a significant burden of MTB infection among suspected EPTB cases. Similar results were observed in a study conducted by Nishal Net al.24 focusing on the diagnostic yield of CBNAAT in the diagnosis of EPTB. In this study, CBNAAT yielded positive results in 30.76% of EPTB cases.24 It is noteworthy that the combined rate of Error, Invalid, and No result was 8.5% (59/688 cases). These results suggest that while the CBNAAT assay is a valuable tool, there are still challenges associated with the accuracy and reliability of the test. Further investigation and quality control measures are necessary to address these limitations and improve the overall performance of the assay. The presence of rifampicin resistance in 14 isolates raises concerns about drug-resistant strains of MTB in the extra-pulmonary setting. This finding highlights the importance of detecting drug resistance early to guide appropriate treatment strategies and prevent the spread of resistant strains.
Table 1 provides a detailed analysis of the performance of the CBNAAT assay and the characteristics of MTB infection across various sample types. Pus samples, which
Table 1: Percentage-wise distribution of the specimen types of extra-pulmonary samples (n=688).
Table 2: Age and site-wise distribution of positivity of extrapulmonary tuberculosis in females (n=170).
CFS: cerebrospinal fluid.
Table 3: Age and site-wise distribution of positivity of extrapulmonary tuberculosis in males (n=170).
CFS: cerebrospinal fluid.
comprised the largest proportion of the specimens (351 samples), exhibited a relatively high positivity rate of 37.6% (132/351 samples). This suggests that pus samples are a valuable source for detecting MTB in extra-pulmonary cases. However, it is important to note that a significant number of samples (26/351) resulted in Error, Invalid, or no DNA findings. This indicates technical challenges or issues related to the quality of the samples or the CBNAAT assay process. Among the ascitic fluid samples (51 samples), the CBNAAT assay detected MTB in only two cases
(3.92%). It is noteworthy that three samples yielded Error, Invalid, or no DNA results. This suggests potential limitations in the sensitivity of the assay for detecting MTB in ascitic fluid, or challenges associated with the collection and processing of these particular samples.
Lymph node biopsy samples (27 samples) demonstrated the highest positivity rate among all specimen types, with 44.44% (12/27 samples) testing positive for MTB, which is in concordance with the findings of another study done on EPTB.24 A study
done by Kumari et al.25 on the correlation of tubercular lymphadenopathy with ZiehlNeelsen staining also had similar findings. In the authors’ study, three samples resulted in Error, Invalid, or no DNA findings, and two samples showed rifampicin resistance for lymph node biopsy. These findings suggest the need for careful interpretation of results and further investigation into assay performance in lymph node biopsy samples. TB lymphadenitis can be difficult to diagnose since it mimics several other infections, including leprosy, sarcoidosis, and fungal infections.21 Diagnosis of TB lymphadenitis relies on fine-needle aspiration cytology, a less invasive technique than excision biopsy.26
For pleural fluid samples (56 samples), the CBNAAT assay showed a positivity rate of 12.5% (7/56 samples). The positivity of pleural TB ranged from 3–25%, as reported in many studies.24 Similar to ascitic fluid samples, a subset of pleural fluid samples (3/56) resulted in Error, Invalid, or no DNA findings. This indicates the need for further investigation to understand the factors influencing assay performance in pleural fluid specimens. All patients with an unidentified pleural effusion should be evaluated for tuberculous pleuritis.
Cerebrospinal fluid (CSF) samples, the second-largest group with 155 samples, exhibited a positivity rate of 9.67% (15/155 samples). Interestingly, 15 CSF samples were associated with Error, Invalid, or no DNA results, suggesting potential challenges or limitations in detecting MTB in CSF samples using the CBNAAT assay. Additionally, three CSF samples yielded indeterminate rifampicin resistance results, indicating the complexity of interpreting assay outcomes in this specimen type. TB meningitis is the most lethal form of meningitis and, if left untreated, almost always results in death. Delaying therapy frequently results in longterm neurological complications.21 The diagnosis of TB meningitis is a challenge owing to the difficulty in obtaining a sufficient volume of CSF sample, especially in cases of paediatric population.21,27 Joint/synovial fluid samples (14 samples) exhibited a lower positivity rate of 7.14% (1/14 samples). Two samples in this category
were reported as Error, Invalid, or no DNA. The relatively low number of positive cases suggests that joint/synovial fluid may not be the primary specimen type for detecting MTB in extra-pulmonary cases. Osteoarticular tuberculosis accounts for around 10–15% of EPTB.28 While infections can occur in any bone or joint, but the spine, hip, and knee account for 70–80% of the infections.21 In the developing world, osteoarticular tuberculosis is a significant issue and one of the leading causes of osteomyelitis.29 Due to deep, inaccessible lesions, detection of osteoarticular TB is challenging.21 Early diagnosis and prompt initiation of antitubercular therapy are essential in these situations because delay results in irreversible joint damage, permanent disability of various degrees, and may also cause kyphosis and neurological complications.21,29
A comparison between Table 2 and Table 3 reveals some interesting patterns. Overall, females had a higher proportion of positive cases in each age group compared to males. The age group of 15–29 years showed the highest positivity rate in both males and females. These findings suggest that certain age groups, particularly adolescents and young adults, may be more susceptible to extrapulmonary TB infection. Among the specimen types, pus samples consistently had the highest positivity rates in both genders and across different age groups. Pus samples appear to be a reliable specimen type for detecting MTB in both males and females. CSF and lymph node biopsy samples also demonstrated significant positivity rates, highlighting their importance in the diagnosis of extrapulmonary TB, especially in paediatric cases. It is important to note that the differences observed between males and females could be influenced by various factors, including differences in immune response, exposure to risk factors, and healthcare-seeking behaviour. Further research is warranted to explore these gender-related differences and their implications for TB diagnosis and management.
Recent advancements in the field of tuberculosis diagnostics have brought
attention to the potential of molecular techniques.30 Notably, studies in the current literature emphasise the growing significance of nucleic acid amplification tests, such as CBNAAT, in the accurate and rapid diagnosis of EPTB. These molecular methods have demonstrated superior sensitivity, particularly in cases with paucibacillary nature, where conventional methods often fall short.31 The findings align with the present study, affirming the efficacy of CBNAAT in enhancing diagnostic capabilities for EPTB.
Moreover, the ongoing research landscape underscores the importance of adopting innovative diagnostic approaches for tuberculosis, given the dynamic nature of the disease and the rising concern of drug resistance. The integration of CBNAAT into routine diagnostic protocols has proven instrumental in addressing these challenges, offering a timely and precise method for detecting both pulmonary and EPTB.30 As the global health community continues to combat the tuberculosis burden, incorporating cutting-edge diagnostic technologies like CBNAAT becomes paramount for achieving accurate diagnoses and initiating prompt therapeutic interventions.
CONCLUSION
In conclusion, this study provides valuable insights into the performance of the CBNAAT assay and the characteristics of MTB infection in different specimen types. It highlights the importance of considering age, gender, and specimen
References
1. Komanapalli SK et al. Role of CBNAAT in diagnosing extra pulmonary tuberculosis in correlation with FNA in a tertiary care center. Int J Res Med Sci. 2018;6(12):4039.
2. Ramirez-Lapausa M et al. Extrapulmonary tuberculosis: an overview. Rev Esp Sanid Penit. 2015;17(1):3-11.
3. World Health Organization (WHO). Global tuberculosis report 2019. 2019. Available at: https://www.
type when diagnosing EPTB. Future efforts should focus on refining diagnostic techniques, ensuring quality control measures, and developing strategies to combat drug resistance in EPTB cases.
Limitations
This study has several limitations. First, as CBNAAT is currently the frontline diagnostic test under the National Tuberculosis Elimination Program (NTEP) in India, the authors did not include a comparison with conventional diagnostic methods for all cases. This is due to both the limited availability of these resources and the high patient volume at their tertiary care centre, which primarily relies on CBNAAT for timely and efficient diagnosis of EPTB.
Second, while CBNAAT provides rapid and specific detection of MTB, it may not detect all forms of EPTB, particularly those with low bacillary load, leading to potential underdiagnosis in paucibacillary cases. Additionally, for patients with CBNAATnegative results, the authors were not able to consistently obtain data on follow-up diagnostic investigations or alternative diagnoses, which limits our ability to fully evaluate diagnostic accuracy in these cases.
Lastly, this study focuses on a single tertiary centre with a high tuberculosis burden, which may limit the generalisability of their findings to settings with differing TB prevalence or diagnostic capabilities. Future studies could benefit from multicentre data and include various diagnostic tools to enable a comprehensive evaluation of diagnostic pathways for EPTB.
who.int/publications/i/item/globaltuberculosis-report-2019. Last accessed: 14 October 2024.
4. Takhar RP. NAAT: A new ray of hope in the early diagnosis of EPTB. Emerg Med (Los Angel). 2016;6(4):328.
5. Solovic I et al. Challenges in diagnosing extrapulmonary tuberculosis in the European Union, 2011. Euro Surveill. 2013;18(12):20432.
6. Peto HM et al. Epidemiology of extrapulmonary tuberculosis in the United States, 1993-2006.
Clin Infect Dis. 2009;49(9):1350-7.
7. Yang Z et al. Identification of risk factors for extrapulmonary tuberculosis. Clin Infect Dis. 2004;38(2):199-205.
8. Houda Ben A et al. Extrapulmonary tuberculosis: update on the epidemiology, risk factors and prevention strategies. Int J Trop Dis. 2018;1(1):206-9.
10. von Groote-Bidlingmaier F et al. The yield of different pleural fluid volumes for mycobacterium tuberculosis culture. Thorax. 2013;68(3):290-1.
11. Pfyffer GE, Wittwer F. Incubation time of mycobacterial cultures: how long is long enough to issue a final negative report to the clinician. J Clin Microbiol. 2012;50(12):4188-9.
12. Satta G et al. Mycobacterium tuberculosis and whole-genome sequencing: how close are we to unleashing its full potential. Clin Microbiol Infect. 2018;24(6):604-9.
13. Mathur RB et al. Role of cartridgebased nucleic acid amplification test to diagnose tuberculosis at tertiary care teaching hospital in Rajasthan, India. Int J Res Med Sci. 2019;7(11):4243.
14. Lawn SD, Nicol MP. Xpert® MTB/ RIF assay: development, evaluation and implementation of a new rapid molecular diagnostic for tuberculosis and rifampicin resistance. Future Microbiology. 2011;6(9):1067-82.
15. World Health Organization. Xpert MTB/RIF implementation manual: technical and operational ‘howto’: practical considerations. 2014. Available at: https://www.who.int/ publications/i/item/9789241506700. Last accessed: 14 October 2024.
16. Swaminathan S et al. Drug resistance among extrapulmonary TB patients: six years’ experience from a supranational reference laboratory. Indian J Med Res. 2015;142(5):568.
17. Sharma SK et al. Drug resistance patterns among extra-pulmonary tuberculosis cases in a tertiary care centre in North India. Int J Tuberc Lung Dis. 2017;21(10):1112-7.
18. Wu X et al. Assessment of the Xpert MTB/RIF Ultra assay on rapid diagnosis of extrapulmonary tuberculosis. Int J Infect Dis. 2019;81:91-6.
19. Metaferia Y et al. Assessment of extrapulmonary tuberculosis using gene Xpert MTB/RIF assay and fluorescent microscopy and its risk factors at Dessie Referral Hospital, Northeast Ethiopia. BioMed Research International. 2018;2018:1-10.
20. Sachdeva K, Shrivastava T. CBNAAT: A boon for early diagnosis of tuberculosis-head and neck. Indian J Otolaryngol Head Neck Surg. 2018;70(4):572-7.
21. Mehta PK et al. Diagnosis of extrapulmonary tuberculosis by PCR. FEMS Immunol Med Microbiol. 2012;66(1):20-36.
22. Jain A. Extra pulmonary tuberculosis: a diagnostic dilemma. Ind J Clin Biochem. 2011;26(3):269-73.
23. Lawn SD, Zumla AI. Diagnosis of extrapulmonary tuberculosis using the Xpert ® MTB/RIF assay. Expert Review of Anti-infective Therapy. 2012;10(6):631-5.
24. Nishal N et al. Diagnostic yield of CBNAAT in the diagnosis of extrapulmonary tuberculosis: a prospective observational study.
Lung India. 2022;39(5):443.
25. Kumari M et al. Rapid Diagnosis of Tubercular Lymphadenopathy by Cartridge-Based Nucleic Acid Amplification Test (CBNAAT) and its correlation with Ziehl-Neelsen staining on fine needle aspiration cytology. 2020;10(7):17-21.
26. Derese Y et al. Comparison of PCR with standard culture of fine needle aspiration samples in the diagnosis of tuberculosis lymphadenitis. J Infect Dev Ctries. 2012;6(1):53-7.
27. Kulkarni SP et al. Evaluation of an in-house-developed PCR for the diagnosis of tuberculous meningitis in Indian children. J Med Microbiol. 2005;54(Pt 4):369-73.
28. Titov AG et al. Use of polymerase chain reaction to diagnose tuberculous arthritis from joint tissues and synovial fluid. Arch Pathol Lab Med. 2004;128(2):205-9.
29. Pandey V et al. The role of polymerase chain reaction in the management of osteoarticular tuberculosis. International Orthopaedics (SICOT). 2009;33(3):801-5.
30. MacLean E et al. Advances in molecular diagnosis of tuberculosis. j Clin Microbiol. 2020;58(10):e01582-19.
31. Kay AW et al. Xpert MTB/RIF Ultra assay for tuberculosis disease and rifampicin resistance in children. Cochrane Database Syst Rev. 2022;9(9):CD013359.
Challenges in Diagnosing Radiographic Axial Spondyloarthritis: A Case Study of a Young Adult in a Secondary-Level General Hospital in Guayaquil, Ecuador
Authors: Lady Wendy Gaibor Acuria,1 *Galo Guillermo Farfán Cano,2 Carla V Moncayo Fernandez,3 Carlos R. Cedeño Cevallos4
1. Maimonides University, Buenos Aires, Argentina
2. Rey Juan Carlos University, Madrid, Spain
3. Catholic University of Santiago of Guayaquil, Ecuador
Radiographic axial spondyloarthritis is a chronic autoimmune disorder primarily affecting the axial skeleton, causing pain, stiffness, and, in advanced cases, structural damage. Its varied clinical presentation complicates diagnosis, particularly in resource-limited settings like secondary-level hospitals in Ecuador. This report details the case of a 34-year-old female initially misdiagnosed with seronegative rheumatoid arthritis and treated with methotrexate, hydroxychloroquine, and corticosteroids. Despite treatment, her symptoms persisted until an MRI, limited by unavailable STIR sequences, confirmed left-sided sacroiliitis. The case was further complicated by idiopathic sudden hearing loss, severe hip involvement, and osteopenia. Cultures were negative, and the diagnosis was ultimately based on clinical criteria and imaging findings. This case highlights the challenges of diagnosing radiographic axial spondyloarthritis in resource-limited settings, and underscores the importance of interdisciplinary evaluation to avoid diagnostic delays and long-term disability.
Key Points
1. Early diagnosis of radiographic axial spondyloarthritis is crucial for comprehensive management and long-term disability prevention, especially in resource-limited settings such as primary and secondary healthcare facilities in Ecuador.
2. Interdisciplinary collaboration and access to advanced imaging techniques, such as MRI with STIR sequences, are essential to avoid diagnostic delays in complex autoimmune diseases.
3. Strengthening local training programmes for healthcare providers on the clinical recognition of axial spondyloarthritis can enhance diagnostic accuracy in emerging economies with limited access to specialised resources.
INTRODUCTION
Radiographic axial spondyloarthritis (r-axSpA), formerly known as ankylosing spondylitis (AS), is a chronic inflammatory disease that primarily affects the sacroiliac joints and axial skeleton. It leads to pain, stiffness, and, over time, structural deformities such as thoracolumbar kyphosis.1 The prevalence of r-axSpA globally ranges from 0.1–1.4%, and the condition is closely associated with the HLA-B27 gene, although environmental and microbial triggers also play a role in its pathogenesis.2,3 Diagnosing r-axSpA in the early stages is crucial to preventing permanent damage; however, this is often delayed, especially in settings with limited access to advanced imaging techniques.
In about 25.8% of cases, extra-articular manifestations such as uveitis, psoriasis, or inflammatory bowel disease accompany axial symptoms.4
The paradoxical occurrence of bone destruction and new bone formation, driven by inflammatory mediators like TNF and IL17A, characterise the disease. In advanced stages, this can lead to the formation of a 'bamboo spine' due to syndesmophytes.5 Early diagnosis and targeted therapy, such as TNF-α and IL-17 inhibitors, are essential to prevent long-term disability.6 However, in secondary-level healthcare settings, especially in developing regions, diagnosis is often delayed due to limited access to specialised tests and imaging techniques.
Although non-HLA genes also contribute to the development of this condition, HLA-B27 is the primary genetic factor.6-8 In r-axSpA, there is a paradoxical occurrence of inflammatory bone destruction and new bone formation at the entheses, leading to the formation of syndesmophytes and, in severe cases, a rigid 'bamboo spine' characteristic of r-axSpA.2,5
Proinflammatory mediators, such as cyclooxygenase (COX), TNF, IL-17A, and JAK, have been validated by clinical observations.5 Effective therapies focus on targeting these mediators, particularly TNF- and IL-17A, which are crucial in
inflammation. The gut microbiome is also important, particularly when weakened mucosal barriers permit microbial invasion and trigger systemic immune responses. Interactions between the gut microbiome, genetic factors, and environmental factors result in diverse clinical presentations of spondyloarthritis (SpA).5
SpA is an umbrella term covering a group of diseases, including psoriatic arthritis, reactive arthritis, and enteropathic arthritis.9 Early diagnosis and targeted therapies, such as TNF-α and IL-17 inhibitors, are crucial to prevent long-term disability.10-14
This report presents the case of a young adult female from Ecuador, initially misdiagnosed with seronegative rheumatoid arthritis (RA) and later diagnosed with r-axSpA. The case underscores the diagnostic difficulties in Ecuador, where healthcare providers often face equipment limitations and a lack of access to specialised tests such as MRI with STIR sequences.
CASE PRESENTATION
A 34-year-old female presented to a secondary-level hospital in Guayaquil, Ecuador, with a 6-month history of joint pain, lower extremity oedema, and episodic hypochromic skin lesions. The lesions were non-specific and did not persist long enough to establish a diagnosis of psoriasis. Initially diagnosed with RA in November 2022, she was treated with prednisone (10 mg daily), methotrexate (12.5 mg weekly), and hydroxychloroquine (200 mg daily). Despite treatment, her symptoms persisted, and her right hip pain worsened, significantly limiting her mobility by March 2023, necessitating the use of a walker. She also reported recurrent episodes of childhood hip pain.
Radiological Findings
Initial X-rays revealed severe bilateral destruction of the femoral heads and chronic hip subluxation (Figure 1). These changes were suggestive of significant
The X-ray shows significant destruction of the femoral heads, indicative of possible inflammatory changes. Arrows highlight areas of concern. MRI and diagnostic reassessment.
inflammatory damage, potentially exacerbated by prolonged corticosteroid use, contributing to avascular necrosis. A DEXA scan, though unavailable, was inferred based on clinical interpretation and osteopenia observed on the X-rays. The radiological findings pointed to a T-score of -2.4 in the L1-L4 vertebrae and the femur, suggesting reduced bone mineral density, which further complicated the case.
In November 2023, an MRI was ordered to confirm sacroiliitis using STIR sequences, but due to equipment malfunction and the limited availability of imaging resources, these sequences were not available. The MRI still revealed unilateral left-sided sacroiliitis, coccygeal erosions, and joint widening (Figure 2). While bilateral sacroiliitis is more common in r-axSpA, this case presented with unilateral involvement, raising the need to consider other differential diagnoses such as psoriatic arthritis or an infectious cause. However, cultures for tuberculosis and bacterial infections returned negative, ruling
out these aetiologies. No biopsy was performed on the sacroiliac joint due to the limitations of the hospital’s resources.
Given the persistence of symptoms, elevated C-reactive protein levels (Table 1), and clinical findings, the diagnosis was primarily based on clinical criteria for r-axSpA, despite the lack of bilateral sacroiliitis and without definitive support from STIR sequences.
Ethical Considerations
Informed consent was obtained from patients to use their clinical information for this study.
DISCUSSION
This case underscores the diagnostic challenges faced in diagnosing r-axSpA in Ecuador, particularly in secondarylevel hospitals with limited resources. The patient’s initial misdiagnosis with
Figure 1: Bilateral anteroposterior hip X-ray.
seronegative RA delayed the correct diagnosis and led to treatment with corticosteroids, which likely contributed to avascular necrosis of the femoral heads. The absence of STIR sequences on the MRI and the unusual presentation of unilateral sacroiliitis added further complexity to the case.
Although the presentation of unilateral sacroiliitis is atypical for r-axSpA, this diagnosis was supported by the exclusion of infectious causes, the patient’s clinical history, and the elevated inflammatory markers. The episodic hypochromic skin lesions were not consistent with psoriatic arthritis, and their transient nature precluded a definitive diagnosis of psoriasis. This case also highlights the importance of recognising the limitations of healthcare settings when interpreting clinical and imaging findings, particularly in regions with restricted access to advanced diagnostics.
The discussion also considered the impact of prolonged corticosteroid use, which may have contributed to avascular necrosis, further complicating the clinical picture. Access to therapies such as TNF-α inhibitors and IL-17 blockers remains limited in these settings,
emphasising the need for healthcare reforms to improve diagnostic and treatment options for patients with spondyloarthropathies.
r-axSpA frequently presents with significant axial skeleton involvement but may also manifest with extra-articular symptoms, such as sudden hearing loss, as seen in this patient.1,2 The presence of severe hip involvement and reduced bone mineral density further complicated the clinical picture.
r-axSpA belongs to the broader category of spondyloarthropathies, which also includes psoriatic arthritis, reactive arthritis, and enteropathic arthritis.9 The association between r-axSpA and the HLA-B27 genotype has been well documented; however, only 24.4% of the disease’s genetic basis is attributable to HLA-B27. 11 In recent studies, novel genetic variants, such as mutations in the RELN gene, have offered additional insights into the pathogenesis of r-axSpA.13
Therapeutic strategies involving TNF-α inhibitors such as infliximab, adalimumab, etanercept, golimumab, and certolizumab are now the gold standard for active disease management.12
Figure 2: Lumbar magnetic resonance imaging.
MRI findings indicate unilateral sacroiliitis and erosive changes, warranting further investigation for differential diagnoses.
Table 1: Relevant laboratory results.
CRP: C-reactive protein.
However, access to these treatments remains limited in secondary-level hospitals in developing regions. The use of MRI in this case was pivotal for diagnosis, as sacroiliitis was not evident in initial radiographs, underscoring the importance of advanced imaging techniques in detecting early-stage r-axSpA.5
Robotic-arm-assisted total hip arthroplasty has been proposed as an option to manage severe hip ankylosis and improve recovery in complex cases.15 Despite recent advances in treatment, public awareness of r-axSpA remains low, leading to delays in diagnosis and poorer outcomes.16
References
1. Shao X et al. Acquired pure red cell aplasia in a patient with ankylosing spondylitis- a case report and literature review. Medicine. 2019;98:16160.
2. Bai LL et al. The CT image changes in ankylosing spondylitis from fracture to andersson lesions: a case report and literature review. Clin Interv Aging. 2020;15:2227-30.
3. Srinivasalu H et al. Recent updates in juvenile spondyloarthritis. Rheum Dis Clin. 2021;47:565-83.
4. Garrido-Cumbrera M et al. The European map of axial spondyloarthritis: capturing the patient perspective—an analysis of 2846 patients across 13 countries. Curr Rheumatol Rep. 2019;21(5):19.
5. UpToDate. Pathogenesis of spondyloarthritis. 2024. Available at: https://www.uptodate.com/contents/ pathogenesis-of-spondyloarthritis.
CONCLUSION
This case illustrates the complexities of diagnosing r-axSpA in resource-limited settings, such as secondary-level hospitals in Ecuador. Limited access to advanced imaging techniques and the potential for misdiagnosis increase the likelihood of delayed recognition of r-axSpA. Early interdisciplinary evaluation, along with improved diagnostic resources, is essential to prevent long-term disability and improve patient outcomes in these settings.
Last accessed: 6 March 2024.
6. Brewerton DA et al. Ankylosing spondylitis and HL-A 27. Lancet. 1973;1(7809):904-7.
7. Schlosstein L et al. High association of an HL-A antigen, W27, with ankylosing spondylitis. N Engl J Med. 1973;288(14):704-6.
8. Reveille JD et al. The prevalence of HLA-B27 in the US: data from the US National Health and Nutrition Examination Survey 2009. Arthritis Rheum. 2012;64(5):1407-11.
9. Walsh JA, Magrey M. Clinical manifestations and diagnosis of axial spondyloarthritis. J Clin Rheumatol. 2021;27:547-60.
10. Rodrigues AC et al. Kidney disease in ankylosing spondylitis: a case series and review of the literature. Braz J Nephrol. 2023;45:36-44.
11. Balaji SM, Balaji P. Complete ankylosis of temporomandibular joint and cervical spine - a case report.
Indian J Dent Res. 2021;32:533-6.
12. Zouris G et al. The use of TNF-α Inhibitors in active ankylosing spondylitis treatment. Cureus. 2024;16(6):e61500.
13. Alenizi D. Adalimumab induced psoriasis in a Crohn’s disease patient: a case report. J Pak Med Assoc. 2024;74:1361-3.
14. Beheshti FS et al. Single-stage bilateral conversion arthroplasty for hip fusion via direct anterior approach in a patient with severe ankylosing spondylitis and kyphoscoliosis: a case report. J Med Case Rep. 2023;17:508.
15. Chai W et al. Use of robotic-arm assisted technique in complex primary total hip arthroplasty. Orthop Surg. 2020;12:686-91.
16. Barajas-Ochoa A et al. Ranking the importance of their own diseases: a positioning analysis in rheumatic patients and their proxies. Rheumatol Clin. 2022;8:429-34.
Knowledge, Attitude, and Preventive Practices on Human Papillomavirus Vaccination
Among Mothers of Adolescent Girls in Selected Secondary Schools of Lagos, Nigeria
Authors: *Akinbowale Akinyemi,1 Adedamola Akintokun,1 Elizabeth Akanbi1
1. Department of Medicine, Faculty of Clinical Sciences, Lagos State University College of Medicine, Lagos, Nigeria *Correspondence to akin.akinyemi81@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Received: 28.05.24
Accepted: 14.11.24
Keywords: Adolescent, attitudes, cross-sectional studies, health knowledge, human papillomavirus (HPV) infections, mothers, practice, uterine cervical cancer, vaccination.
Background and aims: Human papillomavirus (HPV) is a sexually transmitted infection linked to genital, anal, and oral warts, as well as cervical and other cancers. Low- and middle-income countries, such as Nigeria, face heightened HPV-related disease risks. Vaccination is crucial for global burden reduction, especially in these regions. This study assessed the knowledge, attitudes, and preventive practices concerning HPV infection and vaccination among mothers of adolescent girls in Lagos, Nigeria.
Materials and methods: A descriptive cross-sectional study was conducted in Lagos. Using multi-stage sampling, 312 mothers of adolescent girls attending secondary schools were selected. Data was collected through self-administered questionnaires and analysed using SPSS Statistics.
Results: Most respondents were aged 40–49 (53.5%) and married (81.1%). Only 43.9% had heard of HPV, although the majority were aware of cervical cancer. A majority (59.0%) had not heard of HPV vaccines. Most respondents demonstrated poor HPV knowledge (61.9%), though many were willing to vaccinate their daughters if free (69.4%). However, fewer were willing to pay for vaccination (47.7%), and most daughters (85.6%) hadn't been vaccinated. School-based vaccination programmes were the primary source of vaccination information (81.3%). Significant associations were found between respondents' level of education and their HPV knowledge, as well as willingness to vaccinate their daughters (p<0.001, 0.008).
Conclusion: The study reveals significant knowledge gaps among respondents regarding HPV and cervical cancer, indicating poor HPV-related knowledge and practices in Nigeria. To address this, broad awareness programmes, health facility outreach, media campaigns, and improved vaccine accessibility through government support are recommended.
Key Points
1. Low- and middle-income countries like Nigeria bear the greatest burden of human papillomavirus (HPV)-related diseases, such as cervical cancer. Vaccination is a key prevention strategy, and maternal awareness is important for this.
2. A cross-sectional study of Nigerian mothers to assess their knowledge, attitudes, and preventive practices regarding HPV vaccination for adolescent girls.
3. Educating mothers and improving access to HPV vaccines through media campaigns, global health partnerships, and school-based vaccination programmes are ways to increase vaccine uptake and reduce the burden of HPV-related diseases in Nigeria.
INTRODUCTION
Human papillomavirus (HPV) is a sexually transmitted infection of the Papovaviridae family that infects humans, particularly the skin and mucous membrane of the genital, anal, or oral cavities. This infection can lead to warts (papillomas) and a variety of neoplasms, especially cancer of the uterine cervix in women, as well as a significant proportion of anogenital (vulvar, vaginal, penile, and anal) and oropharyngeal cancers.1 Most HPV infections resolve within 12–24 months of infection and do not result in symptoms or illness.2 The majority of people are infected through sexual contact.3 At some point in their lives, most individuals who are sexually active will be infected with HPV, and some may be repeatedly infected. About 90% of infections are cleared eventually, while they persist in the other 10% and put them at an increased risk of developing cancer. Of the 10%, half develop malignancy by the end of the 30th year of persistent high-risk HPV infections.4 HPV is the most common viral infection of the genital tract.5 Over 130 different HPV types have been identified, and they are divided into low- and high-risk categories based on their potential for oncogenesis in the presence of persistent infection.4 Of the several high-risk HPV types, two (16 and 18) are responsible for over 70% of all high-grade cervical pre-cancers.6,7 Among the more benign HPV-associated conditions, genital warts are unambiguously linked to HPV-6 and -11.6 Studies show the global prevalence of HPV infection to be about 11–12%, with the highest rates in sub-Saharan Africa, Eastern Europe, and Latin America.8 In Nigeria, cervical
cancer, primarily caused by HPV, is the most common gynaecological cancer, with over 12,000 new cases annually and over 7,000 deaths each year.9 This contributes to approximately 11% of new cases diagnosed in sub-Saharan Africa.10 Nigeria also ranks fifth among countries with respect to death count from cervical cancer, after India, China, Brazil, and Bangladesh.11 This high burden underscores the critical need for effective HPV vaccination strategies.
Despite these figures, only 3% of 10–20-year-old females in low- and middle-income countries (LMIC) are vaccinated against HPV, compared to 34% in developed countries.12 Previous research in Nigeria shows varying HPV prevalence rates, with one study in the southwest reporting 18.6%,13 and another reporting 36.5% among women attending outpatient clinics in Lagos, Nigeria.14 The significant contribution of high-risk HPV types to overall cases, and the particularly high burden in LMICs that have low vaccination rates, is a cause for concern.15 These statistics reflect a significant public health challenge, particularly in developing countries like Nigeria.
Cervical cancer prevalence has declined in developed countries due to effective screening methods like DNA testing and cytology, which are largely unavailable in developing countries.16 Sub-Saharan countries also have the lowest proportion of screened women among LMICs.17 Vaccination against HPV is therefore a crucial primary prevention strategy and has showed significant reductions in the prevalence of high-risk HPV types, especially among young females.18
Vaccination uptake is influenced by parental knowledge and attitudes, especially mothers,19 yet studies indicate a low level of awareness about HPV and its vaccine among Nigerian women, including university students.20 This gap in knowledge contributes to low vaccination rates and high cervical cancer incidence.
Given that the WHO recommends HPV vaccination for girls aged 9–13 years,21 it is critical to understand the role of mothers, who primarily care for children in this age range, in vaccine uptake. This study seeks to assess the mothers’ knowledge, attitudes, and preventive practices concerning HPV infection and vaccination among adolescent girls in Lagos.
By identifying barriers and facilitators to vaccination, the study hopes to inform targeted interventions that can improve vaccine coverage and lower the burden of HPV-related diseases in this high-risk population, ultimately contributing to a reduction in cervical cancer incidence and mortality.
MATERIALS AND METHODS
Study Design
This is a descriptive cross-sectional study designed to assess the knowledge, attitudes, and preventive practices regarding HPV vaccination among mothers of adolescent girls in selected secondary schools in Lagos.
Setting
This study was carried out in Lagos, with an estimated population of 24.6 million people in 2015, making it the largest city in Africa. Ikeja, which lies at the centre, is the capital of Lagos State. Lagos State has six education districts, and Education District VI is divided into three administrative zones, which are Ikeja, Mushin, and Oshodi/Isolo, with a total of 106 secondary schools.22 Data collection was done in January 2024 in the selected schools. Ethical approval was obtained from the Health Research and Ethics Committee of Lagos State University College of Medicine.
Participants
• Eligibility criteria: participants included in the study were mothers of female secondary school students in the Ikeja Local Government Area aged 9–14 at the time of the study.
• Selection of participants: a multi-stage sampling technique was employed. Two secondary schools were chosen by simple random sampling from the list of secondary schools within Ikeja Local Government Area. One school is located in an urban area with a higher average household income, and it predominantly serves children from middle- to upper-income families. The second school, in a rural area, predominantly serves students from lower-income households. For each selected school, 8 classes were randomly chosen out of 20, and the mothers of all female students in these classes were invited to participate in the survey. Three hundred and twelve mothers accepted the invitation. Informed consent was obtained from all participants, and confidentiality and anonymity were ensured.
Variables
• Outcomes: the main outcomes of interest include knowledge, attitudes, and preventive practices related to HPV vaccination among mothers.
• Exposures: socio-demographic factors (age of respondents, level of education, occupation, marital status, ethnicity, religion), and overall HPV knowledge.
Data Sources/Measurement
• Sources of data: data were collected using a semi-structured, self-administered questionnaire. This questionnaire was pretested and adapted after reviewing existing literature on the subject.
• Methods of assessment: the questionnaire is comprised of four sections: socio-demographic data, knowledge on HPV infection and vaccination, attitude towards HPV vaccination, and HPV prevention practices.
Bias
To reduce courtesy bias, participants were assured of anonymity and confidentiality, ensuring their responses were genuine. Additionally, the questionnaire was refined after conducting a pilot test to minimise recall bias. This ensured that questionnaire items were clear, concise, and easy to interpret. A “don’t know” option was also included for questions where respondents might be unable to recall specific information, allowing them to accurately report their level of knowledge or experience.
Study Size
The calculated sample size for the study was 310 participants, determined using Cochran’s formula for descriptive studies, n=Z2Pq/d2
Where n: sample size, Z: z-score at 95% confidence level, P: prevalence of attribute among the population, q: 1–P, d: desired level of precision (0.05), and P=28% (proportion of population who have knowledge on HPV).23
Quantitative Variables
Quantitative variables were handled in the analyses using descriptive statistics, including frequency tables, means, and standard deviations. Statistical Package for the Social Sciences software
(SPSS Statistics version 26, IBM, Armonk, New York, USA) was utilised for data analysis.
Statistical Methods
The statistical relationship between categorical variables was examined using Chi-square test or Fisher’s exact test, as appropriate. Descriptive statistics were used to summarise the data. Nine questions from the knowledge section of the study questionnaire were scored and used to evaluate the participants’ overall knowledge about HPV infection and vaccination. Thus, respondents were classified based on how many questions were answered correctly, with poor knowledge being equal to a score of 0–3, 4–6 as fair knowledge, and 7–9 as good knowledge.
RESULTS
The socio-demographic data of the respondents is presented in Table 1. Three hundred and twelve mothers were surveyed, they had a mean age of 42.03±6.3, and most (81.1%) of the respondents were married. The knowledge of mothers on HPV infection and vaccination is also depicted in Table 1. Less than half (43.9%) of the respondents had heard about HPV, and the proportion of respondents aware of HPV vaccines (35.6%) was even smaller (Table 1).
Table 1: Socio-demographic data and human papillomavirus knowledge of respondents.
Table 1: Continued.
human papillomavirus.
Table 2: Overall knowledge, attitudes, and practices of respondents regarding human papillomavirus vaccination.
Table 2: Continued.
HPV: human papillomavirus.
Table 2 contains the participants’ overall knowledge about HPV infection and vaccination, which was evaluated by scoring nine questions on HPV knowledge. Therefore, this article classified poor knowledge as having a score of 0–3, 4–6 as fair knowledge, and 7–9 as good knowledge. A significant percentage (61.9%) of respondents demonstrated poor overall knowledge of HPV. The attitudes of mothers towards HPV vaccination and their preventive practices are also presented (Table 2). Only 5.1% (16/312) of the daughters of respondents have been vaccinated. Most of the respondents with vaccinated daughters learned about and arranged for vaccination through schoolbased vaccination programmes (81.3%).
Table 3 shows that there was a statistically significant association between the level of education of respondents and their knowledge of HPV infection and vaccination (p<0.001), and also between occupation and knowledge of HPV infection and vaccination (p<0.001). A statistically significant relationship between respondents with vaccinated daughters and their ethnicity (p=0.042) was also found (Table 3).
DISCUSSION
Public awareness of HPV and vaccinations is crucial to reducing the burden of cervical cancer in Nigeria. Therefore, this study aims to explore the knowledge, attitudes, and preventive practices regarding the virus. In this study, 64.4% of 312 participants surveyed were aware of cervical cancer, but only 43.9% had heard of HPV. This is consistent with findings from a community-based study assessing the HPV knowledge of mothers and their willingness to vaccinate their adolescent daughters in Shomolu, Lagos, that revealed a greater familiarity with cervical cancer compared to HPV.23 Similarly, a study assessing HPV awareness and uptake of cervical cancer screening among mothers of adolescent students in Abakaliki, Ebonyi State, reported only 42.8% awareness of HPV.24 This shows a gap in public knowledge concerning the virus despite a clear high level of awareness about cervical cancer.
Interestingly, 25.6% of participants recognised HPV infection as a risk factor for cervical cancer in this study. This is a slight decrease from the 29.1% awareness found in an earlier study investigating the level of knowledge and acceptability of
Table 3: Factors associated with mothers’ overall knowledge on human papillomavirus, willingness and vaccination status of their daughters.
HPV: human papillomavirus.
Age group (years)
29–39 105(100.0) 19(18.1) 22(21.0) 64(61.0) 0.295
40–49 167(100.0) 31(18.6) 38(22.8) 98(58.7)
HPV vaccination among women attending a gynaecology clinic at the Lagos University Teaching Hospital.25 This suggests that more efforts are needed to raise public awareness regarding HPV’s association with cervical cancer. Notably, respondents in that study and another conducted in Lagos selected mass media as their main source of information.23 The majority (32.1%) of respondents in this article cited health professionals as their singular primary source of information. However, mass media (print, broadcast, and internet) combined to surpass this with 44.5%, emphasising its crucial role in disseminating knowledge about HPV infection and vaccination.
In this study, 35.6% of participants were aware of the HPV vaccine, an almost two-fold increase from the study at a gynaecology clinic in Lagos, where awareness stood at 18.9%.25 This is an encouraging finding, as a study that reviewed the acceptability and readiness for introducing HPV vaccines in subSaharan Africa highlighted that increased knowledge is essential for the successful implementation of a widespread vaccine programme.26 While integrating the HPV vaccine into the National Programme for Immunisation schedule is a welcome development, previous research has shown that culturally appropriate health promotion efforts are necessary to enhance understanding and uptake.27
Encouragingly, 70.6% of mothers in this study who knew about cervical cancer recognised that it could be prevented and that vaccines were beneficial for this. This is similar to findings of a study in Western Nigeria evaluating the factors influencing parental willingness to vaccinate adolescent daughters against cervical cancer, where 62% of participants had the same awareness.28 In addition, 64.9% of the vaccine-aware population agreed that it should be given at a young age before the onset of sexual activity, which is much higher than the 48.1% found in another Lagos study.23 This increase could be due to the greater proportion of respondents with higher education, who likely possess a better understanding of cervical cancer prevention and the importance of early vaccination.
The proportion of respondents willing to have their daughters vaccinated was 25% in this study. A similar study among mothers in Southeast Nigeria reported a significantly larger proportion (84.6%) of mothers desiring vaccination for their daughters.29 Another study among medical and dental students in Benin City, Nigeria, also revealed that the majority had a positive attitude towards vaccination.30 The demographic differences between the participants in these studies may explain this. Among the respondents who expressed hesitation or unwillingness to vaccinate their daughters, the most common reason (30.3%) given was they had not previously considered vaccination.
The majority (69.4%) of the respondents expressed willingness to pursue vaccination if the vaccines were offered free of charge. However, this figure decreased to 47.7% with the option of payment, and this is likely to be similar in other parts of the country. This underscores the impact of vaccine cost on vaccination rates and echoes the findings of studies on HPV vaccination in Nigeria and sub-Saharan Africa, where the cost of the HPV vaccine emerged as a significant barrier.27,29 Global health partnerships between governments, international health organisations, and non-governmental bodies can help make HPV vaccines freely available or heavily subsidised, ensuring accessibility for all socio-economic groups.
This study revealed that only a minority of respondents’ daughters (5.1%) had received the HPV vaccine. A cross-sectional study among female undergraduates in Lagos found that a mere 1.1% of respondents had received the HPV vaccine.31 Similarly, findings among female secondary school students from Benin, Nigeria, show an extremely low vaccination rate (0.5%).32
Interestingly, a significant proportion (81.3%) of mothers with vaccinated daughters in this study reported learning about and facilitating their daughters’ vaccination through school-based programmes. This differs from research conducted in Beijing, China, where most recommendations came from family and friends, and only a few received recommendations from healthcare
professionals.33 This exposes the potential of school-based programmes as an effective avenue to enhance HPV vaccination uptake and improve coverage in developing countries like Nigeria.
This study revealed that over half of the respondents with unvaccinated daughters (50.5%) cited a lack of awareness of where to get the vaccine as the primary reason for non-vaccination. This contrasts with a similar study conducted in Western Kenya among mothers of adolescent girls, where the high cost of vaccines and their nonavailability were reported as the main hindrances.34 In a study among female public school teachers in Mushin, Lagos, a lack of awareness about the vaccine and its benefits was the primary reason cited by most (54.1%) for not vaccinating their children.35 This highlights the urgent need to disseminate information about HPV vaccines and provide accessible vaccination facilities for mothers to take their daughters. Policies and funding should be aimed at making vaccines as accessible to communities as possible, either through primary health care centres or secondary schools.
This study found significant associations between respondents’ level of education and their knowledge of HPV infection and vaccination, as well as between occupation and knowledge of HPV. Among those with tertiary education, over half (51.7%) demonstrated good or fair knowledge of HPV. This study also showed that respondents with professional occupations exhibited greater knowledge than others did. This greater HPV awareness is likely due to increased exposure to information sources during their education and better access to various sources of health information.
Factors such as age group and occupation did not significantly influence mothers’ attitudes towards vaccination. Instead, a statistically significant relationship was observed between respondents’ willingness to vaccinate their daughters and their ethnicity (p=0.017) and level of education (p=0.008). Specifically, a higher proportion of Igbo respondents and those with tertiary education expressed a willingness to
vaccinate their daughters. This aligns with findings from a similar study in Lagos, which reported that mothers with a tertiary level of education had an almost 30-fold increased probability of vaccine acceptance.36 This highlights the pivotal role of increased female education in promoting vaccine acceptance.
Mothers’ education, occupation, and overall knowledge did not influence vaccination practices significantly. Notably, the number of respondents with secondary education who vaccinated their daughters was comparable to those with tertiary education. The lack of a significant difference between these two groups may indicate that awareness of vaccination does not always translate into action, possibly due to financial barriers. However, ethnicity also showed a significant association with vaccination status. These findings may reflect some innate cultural values, such as stronger health-seeking behaviour. The link between ethnicity and positive HPV attitudes and behaviours provides a basis for further research.
One limitation of this study is that there could have been some recall bias among respondents. Questions were pilot-tested, and a “don’t know” option was added to reduce guessing and inaccuracies. Mothers may have also shown some courtesy bias by providing responses they believe are socially acceptable. This was addressed by assuring respondents of anonymity and confidentiality to ensure genuine responses. Future studies may consider incorporating qualitative interviews to look into the reasons behind certain attitudes and practices, as the crosssectional nature of this study limits the ability to establish a causal relationship between the variables examined.
CONCLUSION
Overall, this study highlights significant gaps in knowledge regarding HPV infection and its link to cervical cancer among respondents, as well as inadequate vaccination coverage in the country. It is therefore essential that initiatives focus on increasing HPV awareness, improving access to vaccination services, and prioritising HPV prevention efforts.
References
1. Rajaram S. “Human Papillomavirus Carcinogenesis and Natural History in Cancer Cervix”, Ahuja M et al. (eds.), Precancerous Lesions of Cervix: Prevention, Early Diagnosis and Management (2014) 1st edition, New Delhi: Jaypee Brothers Medical Publishers Pvt. Ltd., pp.1-2.
2. de Sanjosé S et al. The natural history of human papillomavirus infection. Best Pract Res Clin Obstet Gynaecol. 2018;47:2-13.
3. Chesson HW et al. The estimated lifetime probability of acquiring human papillomavirus in the United States. Sex Transm Dis. 2014;41(11):660-4.
4. Zandberg DP et al. The role of human papillomavirus in nongenital cancers. CA Cancer J Clin. 2013;63(1):57-81.
5. Bowden SJ, Kyrgiou M. Human papillomavirus. Obstet Gynaecol Reprod Med. 2020;30(4):109-18.
6. Bosch FX et al. Comprehensive control of human papillomavirus infections and related diseases. Vaccine. 2013;31(Suppl 7):H1-31.
7. Ramakrishnan S et al. Overview of high-risk HPV's 16 and 18 infected cervical cancer: pathogenesis to prevention. Biomed Pharmacother. 2015;70:103-10.
8. Forman D et al. Global burden of human papillomavirus and related diseases. Vaccine. 2012;30 (Suppl 5):F12-23.
9. International Agency for Research on Cancer. Global Cancer Observatory: Cancer Today: population factsheets. 2020. Available at: https://gco.iarc. who.int/media/globocan/factsheets/ populations/566-nigeria-fact-sheet. pdf. Last accessed: 15 May 2022.
10. Bray F, Parkin DM.; African Cancer Registry Network. Cancer in subSaharan Africa in 2020: a review of current estimates of the national burden, data gaps, and future needs. Lancet Oncol. 2022;23(6):719-28.
11. Cervical Cancer-Free Coalition. Cervical cancer global crisis card. 2013. Available at: http://www. cervicalcancerfreecoalition.org/ cervical-cancer-global-crisis-card/. Last accessed: 23 May 2022.
12. Bruni L et al. Global estimates of human papillomavirus vaccination coverage by region and income level: a pooled analysis. Lancet Glob Health. 2016;4(7):e453-63.
13. Nejo YT et al. Prevalence and risk factors for genital human papillomavirus infections among women in Southwest Nigeria. Arch
Basic Appl Med. 2018;6(1):105-12.
14. Okunade KS et al. Prevalence and risk factors for genital high-risk human papillomavirus infection among women attending the outpatient clinics of a university teaching hospital in Lagos, Nigeria. Pan Afr Med J. 2017;28:227.
15. Sung H et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209-49.
16. Poole DN et al. A cross-sectional study to assess HPV knowledge and HPV vaccine acceptability in Mali. PLoS One. 2013;8(2):e56402.
17. Lemp JM et al. Lifetime prevalence of cervical cancer screening in 55 low-and middle-income countries. JAMA. 2020;324(15):1532-42.
18. Oliver SE et al. Prevalence of human papillomavirus among females after vaccine introduction-National Health and Nutrition Examination Survey, United States, 2003-2014. J Infect Dis. 2017;216(5):594-603.
19. Mihretie GN et al. Knowledge and willingness of parents towards child girl HPV vaccination in Debre Tabor Town, Ethiopia: a communitybased cross-sectional study. Reprod Health. 2022;19(1):136.
20. Makwe CC et al. Human papillomavirus (HPV) infection and vaccines: knowledge, attitude and perception among female students at the University of Lagos, Lagos, Nigeria. J Epidemiol Glob Health. 2012;2(4):199206.
21. World Health Organization (WHO). Comprehensive cervical cancer prevention and control - a healthier future for girls and women. 2013. Available at: https://www.who.int/ publications/i/item/9789241505147. Last accessed: 15 May 2022.
22. Lagos State Government. Brief history of Education District VI. 2023. Available at: https://educationdistrict6. lagosstate.gov.ng/. Last accessed: 19 September 2023.
23. Ezenwa BN et al. Mothers’ human papilloma virus knowledge and willingness to vaccinate their adolescent daughters in Lagos, Nigeria. Int J Womens Health. 2013;5:371-7.
24. Azuogu BN et al. Appraisal of willingness to vaccinate daughters with human papilloma virus vaccine and cervical cancer screening uptake among mothers of adolescent students in Abakaliki, Nigeria. Niger J Clin Pract. 2019;22(9):1286-91.
25. Okunade KS et al. Knowledge and acceptability of human papillomavirus
vaccination among women attending the gynaecological outpatient clinics of a university teaching hospital in Lagos, Nigeria. J Trop Med. 2017;2017:8586459.
26. Perlman S et al. Knowledge and awareness of HPV vaccine and acceptability to vaccinate in subSaharan Africa: a systematic review. PLoS One. 2014;9(3):e90912.
27. Amponsah-Dacosta E et al. Health systems constraints and facilitators of human papillomavirus immunization programmes in sub-Saharan Africa: a systematic review. Health Policy Plan. 2020;35(6):701-17.
28. Akinleye HW et al. Parental willingness to vaccinate adolescent daughters against human papilloma virus for cervical cancer prevention in Western Nigeria. Pan Afr Med J. 2020;36:112.
29. Ogochukwu TN et al. Vaccination against human papilloma virus in adolescent girls: mother’s knowledge, attitude, desire and practice in Nigeria. J Infect Dis Preve Med. 2017;5(1):151.
30. Onowhakpor AO et al. Human Papilloma Virus vaccination: knowledge, attitude and uptake among female medical and dental students in a tertiary institution in Benin-City, Nigeria. Journal of Community Medicine and Primary Health Care. 2016;28(2):101-8.
31. Okoka EM et al. Knowledge, attitude, and factors affecting human papilloma virus vaccine uptake among female undergraduate students in public tertiary institutions in Lagos State Nigeria. Int J Med Stud. 2023;11(Suppl 1):S51.
32. Ezeanochie M, Olasimbo P. Awareness and uptake of human papilloma virus vaccines among female secondary school students in Benin City, Nigeria. Afr Health Sci. 2020;20(1):45-50.
33. Liu Y et al. Knowledge, practice and attitude towards HPV vaccination among college students in Beijing, China. Hum Vaccin Immunother. 2020;16(1):116-23.
34. Mabeya H et al. Mothers of adolescent girls and human papilloma virus (HPV) vaccination in Western Kenya. Pan Afr Med J. 2021;38:126.
35. Toye MA et al. Knowledge, perceptions and practice of cervical cancer prevention among female public secondary school teachers in Mushin local government area of Lagos State, Nigeria. Pan Afr Med J. 2017;28:221.
36. Rabiu KA et al. Parental acceptance of human papillomavirus vaccination for adolescent girls in Lagos, Nigeria. J Family Med Prim Care. 2020;9(6):29507.
Adverse Drug Events from First-line Anti-tuberculosis Drugs in a Tertiary Medical Center
Authors: *Marie Joyce Jorge,1 Christian Bernard Esporlas,1 Marie Louise Emille Largoza,1 Rosally Zamora1
1. Department of Internal Medicine, East Avenue Medical Center, Quezon City, Philippines *Correspondence to: mariejoycejorge@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Received: 16.12.23
Accepted: 14.11.24
Keywords: Adverse drug reactions (ADR), directly observed treatment, tertiary medical centre, tuberculosis (TB).
Background: Tuberculosis (TB) has remained one of the top causes of morbidity and mortality in the Philippines since 2018. However, adverse drug reactions (ADR) from first-line anti-tuberculosis medications such as rifampicin, isoniazid, pyrazinamide, and ethambutol cause significant impact on treatment adherence. This study aimed to determine the incidence of ADRs among patients treated with first-line anti-tuberculosis medications at a Philippine Department of Health tertiary medical centre.
Methods: In this retrospective cohort study, rifampicin-susceptible patients undergoing first-line anti-TB treatment enrolled in the Tuberculosis-Directly Observed Treatment Strategy at the East Avenue Medical Centre, Quezon City, Philippines, were included. Pertinent data obtained from chart review included sociodemographic factors, clinical characteristics, duration of treatment prior to the appearance of adverse drug reactions, type of ADRs, TB medication causing the ADR, and treatment outcomes.
Results: A total of 524 patients treated with first-line anti-TB treatment were identified, with 46 (8.78%) noted to have ADRs to the treatment regimen. Most reaction types included mild or localised skin reactions (34.8%), severe skin rash secondary to hypersensitivity (32.6%), and jaundice due to hepatitis (21.7%). Reaction to more than one medication was seen in 89.1% of patients with ADRs, with rifampicin having the highest frequency of ADR (4.3%) among the anti-TB medications.
Conclusion: The incidence of ADRs among patients treated with first-line anti-TB medications at East Avenue Medical Centre in the Tuberculosis-Directly Observed Treatment Strategy is frequent and comparable to other relevant study populations. A larger sample size and exploration of other methodological studies are recommended to further expand on this study.
Key Points
1. According to the WHO, the Philippines ranks fourth among 30 high tuberculosis (TB) burdened countries. Tuberculosis management warrants a prolonged multidrug regimen, thus raising concerns about the impact of adverse drug reactions (ADR) on treatment adherence.
2. This is a retrospective cohort study comprising pertinent data obtained from chart review of rifampicin-susceptible patients enrolled in a tertiary medical centre’s TB Directly Observed Treatment Strategy, dating 2021 and earlier.
3. The prevalence of ADRs among patients undergoing first-line TB treatment is frequent. Active surveillance and timely management of these ADRs must be enforced to reduce their impact on treatment adherence.
INTRODUCTION
Tuberculosis (TB) is caused by the bacteria Mycobacterium tuberculosis, a complex, rod-shaped, non-spore-forming, thin, aerobic bacterium.1 Since 2016, it has caused 6.3 million new cases of TB, 95% of which come from developing countries. One of these is the Philippines.2 Treatment is based on different treatment categories for specific indications, namely for Category I treating Pulmonary TB (PTB), Miliary TB, and Extrapulmonary TB (EPTB), except for central nervous system (CNS), bone, or joint infections; Category Ia treating for CNS, bone, and joint infections; Category II for retreatment of rifampicin (RIF) susceptible PTB and EPTB; and Category IIa for retreatment of RIF susceptible CNS, bones, or joint infections.
The virulence of the tubercle bacilli brought about by its properties of resistance to oxidative stress, intracellular survival in macrophages, and high lipid concentration of its cell wall, proved the need for a prolonged multidrug chemotherapy treatment by a four different drug regimen via RIF, isoniazid (INH), ethambutol (EMB), and pyrazinamide (PZA) for TB. To increase treatment adherence, the WHO has established a treatment control strategy via the Directly Observed Treatment Strategy (DOTS), which employs the commitment of the government to eradicate the disease. Processes such as case detection via sputum smear microscopy, standardised treatment regimen directly of 6–9 months, provision of the drug, and standardised recording and reporting system that allows
assessment of treatment results.2 However, these drugs are known to have caused adverse events.3 Their management poses challenges as they may cause clinicians to shift drugs to second-line treatment options, lead to undertreatment, or impact adherence to medication.4 There are no published data on the prevalence of adverse reactions in the country to date.
This study aimed to determine the incidence, characteristics, significant risk factors, and outcomes of adverse drug reactions (ADR) among patients treated with first-line anti-tuberculosis medications at a Department of Health tertiary medical centre. Significant differences between treatment outcomes of patients with ADRs to a single first-line anti-tuberculosis medication compared to patients with ADRs to more than one first-line anti-tuberculosis medication were also determined. Established data in this study surrounding adverse reactions to anti-TB medications can be beneficial economically to allocate resources in preventing these adverse reactions with regards to optimising the drugs’ pharmacokinetics and pharmacodynamics.
METHODOLOGY
Definition of Terms
ADRs were defined according to the listed ADRs in Table 12 of the DOH National Tuberculosis Program Manual of Procedures, 6th edition.2 Minor ADRs include gastrointestinal tolerance, mild
or localised skin reactions, orange-coloured urine, burning sensation in the feet due to peripheral neuropathy, arthralgia due to hyperuricemia, and flu-like symptoms (fever, muscle pains, inflammation of the respiratory tract). Major ADRs include severe skin rash due to hypersensitivity, jaundice due to hepatitis, impairment of visual acuity and colour vision due to optic neuritis, oliguria, or albuminuria due to renal disorder, psychosis, convulsion, thrombocytopenia, anaemia, and shock.
Research Design
The study employed a retrospective cohort study. The investigators gathered data from the East Avenue Medical Centre TBDOTS department from years earlier than 2021 through chart review until the study population size was met. Data gathering utilised an online data collection form made especially for the study. Only pertinent data for the sociodemographic (sex, age), clinical characteristics (TB case type, TB diagnosis type, TB treatment history, comorbidities), duration of treatment prior to the appearance of ADRs, TB medication causing the ADR, and treatment outcomes were obtained from the charts for review. The diagnosis of ADRs were obtained from the examining physician’s assessment in the reviewed chart. Symptoms such as mild gastrointestinal disturbances, hepatotoxicity, ototoxicity, nephrotoxicity, peripheral neuropathy, and cutaneous ADRs were determined. Patients were selected based on the inclusion and exclusion criteria (Table 1).
Statistical Analysis
SPSS version 27.0 was used for data processing and analysis. Mann-Whitney U test was used to compare non-normal
continuous variables, while Chi-square test was used to compare categorical noncontinuous variables and, in cases where this was not applicable, Fisher’s exact test was used. To determine the factors associated with the presence of ADR, a simple logistic regression was used. P≤0.05 were considered statistically significant.
RESULTS
A total of 524 patients treated with first-line anti-tuberculosis medications were identified (Table 2). From these patients, 46 (8.78%) were identified to have ADRs to the treatment regimen. Sex (M/F) ratio for patients with ADR and without ADR were at 1.875 and 1.795, respectively. Patient age ranges were from 19–85 years, with median age for patients with ADR at 42.5 years and for patients without ADR at 45 years. The majority of cases presented with pulmonary TB, clinically diagnosed TB, and as new treatment cases. More ADR was seen in patients with diabetes as compared to patients with HIV.
The top three reaction types in decreasing order of frequency (Table 3) included mild or localised skin reactions (34.8%), severe skin rash secondary to hypersensitivity (32.6%), and jaundice due to hepatitis (21.7%). Reaction to more than one medication was seen in 89.1% of patients with ADRs. Among the anti-TB medications, rifampicin has the highest frequency of ADR (4.3%). While the majority of outcomes of patients with ADR were classified as treatment completed, the outcome was not statistically significant.
Using simple logistic regression analysis to determine significantly associated variables to the presence of ADR, patients with
Rifampicin susceptible patients undergoing Category 1 treatment before 2021.
Paediatric patients (aged ≤18 years). Patients with multidrug-resistant tuberculosis.
Table 1: Inclusion and exclusion criteria.
Table 2: Sociodemographic
Note: Other comorbidities not specified were not included. IQR: interquartile range; TB: tuberculosis.
extrapulmonary TB have about 2.231 higher odds of having ADR than those that have pulmonary TB. Patients under retreatment have about 0.280 lower odds of having ADR than those treated as new cases. The TB history of a patient was also associated with the presence of ADR and vice-versa.
DISCUSSION
Sociodemographic (sex, age), clinical characteristics (TB case type, TB diagnosis type, TB treatment history, comorbidities), duration of treatment prior to the appearance of ADRs, TB medication causing the ADR, and treatment outcomes were obtained. In this study, among a total of 524 patients on first-line anti-TB medications, 8.78% of patients were noted to have ADRs. The median age for those with ADRs was 42.5 years old, which is younger than the cited age (>60 years old) at risk for developing ADRs.
Of the common adverse drug reactions that were cited, multiple studies have shown that the most frequently observed ADRs included gastrointestinal and hepatobiliary manifestations.5-14 In particular, nausea, vomiting, and epigastric pain were the more commonly cited gastrointestinal manifestations.15 On the contrary, in this study, the most common ADR was found to be skin manifestations, ranging from mild or localised skin reactions (34.8%) to severe skin rash secondary to hypersensitivity (32.6%), followed by jaundice due to hepatitis (21.7%). However, there is a paucity in available related literature detailing why skin manifestations were found to be the most frequent ADR.16
In patients having ADR with anti-TB medications, approximately 20% have symptoms of tingling and burning sensation in the hands and feet. This was most attributed to treatment with isoniazid and, to a lesser degree, with ethambutol.17 In
Table 3: Frequency distribution and incidence of adverse drug reaction types among patients with adverse drug reactions to first-line anti-tuberculosis medications.
a study conducted in Shenzhen, China, optical neuritis also occurred concomitantly with peripheral neuritis, but this was associated with when linezolid was used as treatment for MDR-TB.18 The study employed the Michigan Neuropathy Screening Instrument (MNSI) and serum trough levels for monitoring of linezolid neurotoxicity. This study reported a single patient having self-reported symptoms of a tingling sensation. Data was lacking as to which drug was attributable for the event as this was reported upon intake of a fixed-dose combination drug.
One notable significant finding in this study is that patients with extrapulmonary TB have about 2.231 higher odds of having ADR than those who have pulmonary TB. This result, however, was not consistently reflected in other studies that showed varying
results from the predominance of ADRs in pulmonary TB19, predominance of ADRs in extrapulmonary TB20-22, and no significant difference between the two groups.23
Patients under retreatment have about 0.280 lower odds of having ADR than those treated as new cases. The TB history of a patient was also associated with the presence of ADR and vice-versa.
Among those infected with TB, HIV and diabetes were of particular interest due to their strong association with the disease.24 A state of immune deficiency is observed in these comorbidities due to their defects in bacterial recognition, phagocytic activity, and cellular activation which results in impaired production of chemokines and cytokines to prevent TB infection.25 In patients with diabetes or HIV, oxidative
stress and polypharmacy are believed to increase the risk for ADRs.16, 26
Comparing the present study population proportion to known population proportion from literature, there appears to be a significant difference between it and that of a multiregional study in China in 2013.17 Multicentre studies in Iran in 20147 and New Delhi, India in 202027, and single hospital studies in Kerala, India in 201513, Ghana in 202128, and Pune, India in 20215 were also noted to have significant differences with the study population.
The current study's mean duration of treatment prior to the appearance of ADR is 35 days, with a standard deviation of 27.09 and the duration ranging from 6–90 days. This is found to be statistically longer compared to a single hospital study in Kerala, India in 201513, a multicentre study in Iran in 20147, and a 6-year prospective study in Brazil in 2016.29
In this study, the outcomes of patients who developed ADRs were mostly treatment completed, although the outcome was not statistically significant. Comparing these results to previous studies, there was a noted dissimilarity, as ADRs could be associated both with unfavourable8 and favourable3 outcomes.
CONCLUSION
The study showed the incidence of ADRs, the outcomes, determination of known risk factors, and mean duration of patients taking anti-TB medications enrolled at the East Avenue Medical Centre TB-DOTS clinic as discussed.
Very sparse literature is available in the Philippines that detail the incidence of ADRs among those who are receiving anti-TB treatment and the other factors that may influence it. This study’s data demonstrated a few key differences between the international and local settings, such as the younger median age at risk of developing ADRs (42.5 years old) and which ADRs are more common, notably the skin manifestations as
compared to the gastrointestinal and hepatobiliary manifestations.
There are notable limitations to this study. The applicability of the inferences made from the results may be dampened by the small sample size and that it was only made from data collated from one local tertiary hospital. A larger sample size and employment of other methodological studies are warranted to further expound on this study.
A successful course of TB treatment relies largely on the patient's compliance with the medications. Given the multidrug constitution of the anti-TB regimen, the concomitant comorbidities such as diabetes and HIV, and the overall length of duration of the regimen, the appearance of one or more ADRs may be unavoidable and poses a significant threat to the adherence to anti-TB medications. Awareness and immediate recognition of these ADRs will contribute to better adherence, more bolstered safety monitoring, and aid in promoting the rational use of medicines.
This study also suggested the possible variation of risk factors for ADRs across regions. Although, as mentioned, a larger sample size from a multi-centre study can further establish this.
Exploration of other disease manifestations of tuberculosis, notably on extrapulmonary symptoms, and their association with ADRs is also recommended and warrants further exploration. The paucity of available relevant literature exploring the rationale of higher incidence of ADRs in extrapulmonary TB serves also as a notable limitation and an area for further studies.
Given the strong link between the known risk factor of diabetes in developing ADRs, a longitudinal study may be better suited to further elicit this response.
In the era of globalisation and constant migration of people wherein the threat of disease spread is ever-growing, it is important to tackle possible obstacles such as ADRs to effective treatment of communicable diseases such as tuberculosis to prevent its spread on a global scale.
ETHICAL CONSIDERATIONS
A waiver of consent approved by the East Avenue Medical Centre Institutional Ethics Review Board was obtained for the retrospective chart review. Obtained data from the data collection form were stored
References
1. Loscalzo J et al. (eds.) “Part 5: Infectious Diseases,” Harrison’s Principles of Internal Medicine SelfAssessment and Board Review (2021) 21st edition, New York: McGraw-Hill Education, pp.153-325.
2. Republic of the Philippines Department of Health. National tuberculosis control program manual of procedures 6th edition pocket guide. 2021. Available at: https://ntp.doh.gov.ph/download/ ntp-mop-6th-edition-pocket-guide. Last accessed: 7 April 2022.
3. Choi H et al. Incidence and outcomes of adverse drug reactions to firstline anti-tuberculosis drugs and their effects on the quality of life: a multicenter prospective cohort study. Pharmacoepidemiol Drug Saf. 2022;31(11):1153-63.
4. Tekle B et al. Defaulting from DOTS and its determinants in three districts of Arsi zone in Ethiopia. Int J Tuberc Lung Dis. 2002;6(7):573-9.
5. Gaikwad DR. Adverse drug reactions in patients with first line anti-tuberculosis treatment. Indian J Basic Appl Med Res. 2021;10(4):82-90.
6. Verma R et al. Adverse drug reactions associated with first-line antitubercular drugs in a tertiary care hospital of central India: a study of clinical presentations, causality, and severity. Asian J Pharm Clin Res. 2014;7:140-3.
7. Farazi A et al. Adverse reactions to antituberculosis drugs in Iranian tuberculosis patients. Tuberc Res Treat. 2014; 2014:412893.
8. Castro ATE et al. Incidence and risk factors of major toxicity associated to first-line antituberculosis drugs for latent and active tuberculosis during a period of 10 years. Rev Port Pneumol (2006). 2015;21(3):144-50.
9. Pore SM, Shinde K. Risk factors for drug induced hepatitis with first-line antituberculosis drugs in hospitalized patients of pulmonary tuberculosis. J Postgrad Med. 2014;60(1):90-2.
electronically in a Google Drive (Google, Mountain View, California, USA) subjected to the existing privacy policies of Google in compliance to the Philippine National Guidelines for Health and Health-Related Research (2017) and Philippine Data Privacy Act of 2012.
10. Marra F et al. Adverse drug reactions associated with first-line antituberculosis drug regimens. Int J Tuberc Lung Dis. 2007;11(8):868-75.
11. Yee D et al. Incidence of serious side effects from first-line antituberculosis drugs among patients treated for active tuberculosis. Am J Respir Crit Care Med. 2003;167(11):1472-7.
12. Singh AK, Pant N. Adverse effects of first line antitubercular medicines on patients taking directly observed treatment short course: a hospitalbased study. Int J Med Public Health. 2014;4(4):354-8.
13. Athira B et al. A study on adverse drug reactions to first line antitubercular drugs in DOTS therapy. Int J Pharmacol Clin Sci. 2015;4:7-11.
14. Carroll MW et al. Frequency of adverse reactions to first- and second-line anti-tuberculosis chemotherapy in a Korean cohort. Int J Tuberc Lung Dis. 2012;16(7):961-6.
15. El Hamdouni M et al. Incidence of adverse reactions caused by first-line anti-tuberculosis drugs and treatment outcome of pulmonary tuberculosis patients in Morocco. Infection. 2019;48(1):43-50.
16. Sharma RK et al. Spectrum of cutaneous adverse drug reactions to anti-tubercular drugs and safe therapy after re-challenge - a retrospective study. Indian Dermatol Online J. 2020;11(2):177-81.
17. Lv X et al. Adverse reactions due to directly observed treatment strategy therapy in Chinese tuberculosis patients: a prospective study. PLoS One. 2013;8(6):e65037.
18. Zhang P et al. Linezolid-associated neuropathy in patients with MDR/XDR tuberculosis in Shenzhen, China. Infect Drug Resist. 2022;15:2617-24.
19. Jayapriya B et al. Pattern of adverse drug reactions of antitubercular drugs in tuberculosis patients with comorbidities and risk factors in South Indian government healthcare facilities. Natl J Physiol Pharm
Pharmacol. 2021;11(8):920-4.
20. Michael OS et al. Adverse events to first line anti-tuberculosis drugs in patients co-infected with HIV and tuberculosis. Ann Ib Postgrad Med. 2016;14(1):21-9.
21. Djochie RDA et al. Determinants of adverse reactions to firstline antitubercular medicines: a prospective cohort study. J Pharm Policy Pract. 2023;16(1):70.
22. Yagi M et al. Factors associated with adverse drug reactions or death in very elderly hospitalized patients with pulmonary tuberculosis. Sci Rep. 2023;13(1):6826.
23. Navelkar R et al. Adverse drug reactions to first-line antituberculosis drugs at four DOTS centers in Goa, India. Indian J Health Sci Biomed Res (KLEU). 2023;16(1)115-8.
24. Duarte R et al. Tuberculosis, social determinants and co-morbidities (including HIV). Pulmonology. 2018;24(2):115-9.
25. Ayelign B et al. Immunological impacts of diabetes on the susceptibility of Mycobacterium tuberculosis. J Immunol Res. 2019:2019:6196532.
26. Pooranagangadevi N, Padmapriyadarsini C. Treatment of tuberculosis and the drug interactions associated with HIV-TB co-infection treatment. Front Trop Dis. 2022;3:834013.
27. Imam F et al. Adverse drug reaction prevalence and mechanisms of action of first-line anti-tubercular drugs. Saudi Pharm J. 2020;28(3):316-24.
28. Amalba A, Bugri AA. Assessing the prevalence and effect of adverse drug reactions among patients receiving first line anti-tubercular medicines in the Tamale Teaching Hospital, Ghana. Pan Afr Med J. 2021;38:191.
29. Sant'Anna FM et al. Adverse drug reactions related to treatment of drugsusceptible tuberculosis in Brazil: a prospective cohort study. Front Trop Dis. 2022;2:748310.
Incidental Idiopathic Left Uncal Herniation: A Case Study and Literature Review
1. Department of Neurosurgery, Royal Stoke University Hospital, Stoke-on-Trent, Staffordshire, UK
2. School of Medicine, Keele University, Staffordshire, UK
3. Department of Radiology, Royal Stoke University Hospital, Stoke-on-Trent, Staffordshire, UK
*Correspondence to wengkit.chan@uhnm.nhs.uk
Disclosure: The authors have declared no conflicts of interest.
Acknowledgements: The authors would like to thank the staff at the Neurosurgery Outpatient Clinic, Royal Stoke University Hospital, for their dedication and professionalism in managing the patient.
Background: Idiopathic uncal herniation in patients is a very rare phenomenon, with only two cases documented in the English literature.
Case Report: The authors report a previously fit and well patient in their 60’s who presented with a 12-month history of headaches and vomiting. On clinical examination, there was no focal neurology, and all cranial nerves were intact. MRI revealed an incidental finding of left uncal herniation, which was likely developmental. The patient was discharged from neurosurgery, with a plan for the GP to refer to neurology for the headaches and vomiting.
Discussion: A correct diagnosis of idiopathic brain herniation is important to avoid unnecessary invasive procedures. Herniation should be differentiated from other pathologies, including tumours, encephaloceles, and dural venous sinus thrombosis.
Conclusion: Incidental findings of uncal herniation remain an extreme rarity. Future research is required to guide management and prognostication in this select group of patients.
Key Points
1. Idiopathic uncal herniation remains an extremely rare and poorly researched phenomenon with unclear pathophysiology.
2. Proper identification of idiopathic brain herniation is important to mitigate the need for unnecessary invasive procedures.
3. Incidental findings of uncal herniation should be managed conservatively.
INTRODUCTION
The uncus is a hook-shaped structure located on the most anteromedial aspect of the parahippocampal gyrus, which is part of the medial temporal lobe.1 Functionally, it is a part of the limbic and olfactory systems, and thus plays a putative role in olfaction, emotion, and memory.2
Uncal herniation is a sub-type of transtentorial herniation, characterised by medial and downward displacement of the uncus against the tentorial edge, compressing the midbrain and oculomotor nerve (cranial nerve III).3 This is an acquired, emergent condition that is usually caused by an underlying brain lesion or an expanding mass effect (e.g., traumatic brain injury, subdural haemorrhage, extradural haemorrhage, or intracerebral haemorrhage). Very rarely, uncal herniation may occur with minimal or unrelated symptoms without any discernible aetiology.4
To the best of the authors' knowledge, there are only two reported cases of idiopathic uncal herniation in the current English literature.4,5 Given the extreme rarity and clinical significance, the authors present a case of an incidental finding of idiopathic uncal herniation diagnosed on MRI, with a brief review of the existing literature.
CASE REPORT
A patient in their 60’s presented to the Neurosurgical Outpatient Clinic of the Royal Stoke University Hospital (RSUH), Stoke-on-Trent, Staffordshire, UK, with a 12-month history of pressure in the neck radiating to the front of the head, with associated vomiting. They also reported pressure and pain in their right ear, and had been diagnosed with sensorineural hearing loss and tinnitus by their GP. They were
prescribed a hearing aid, which improved their hearing but not their headaches.
In their background history, the patient was right-hand dominant and had recently retired and lived alone. They had never smoked but consumed alcohol on a social basis. Past medical history included obstructive sleep apnoea (for which they used a continuous positive airway pressure machine), hypothyroidism, hypertension, osteoarthritis, depression, gastrooesophageal reflux disease, and insomnia. Their medications included: simvastatin, extended-release oxycodone, sertraline, omeprazole, levothyroxine, lisinopril, hyoscine, amitriptyline, bisoprolol, and a buprenorphine transdermal patch. They did not have any known drug allergies.
On examination, their Glasgow Coma Scale (GCS) score was 15/15, and their cranial nerves were intact. They exhibited normal tone and power in all four limbs and walked with a normal gait. Their BMI was elevated at 33.1.
An MRI head (Figure 1) demonstrated a left medial temporal lobe herniation across the medial tentorium that was indenting the left cerebral peduncle. Scattered white matter small vessel ischaemic changes were also noted, with no enhancing abnormality or tumour identified. The rest of the imaging appeared unremarkable. Following discussion at the neuroradiology multidisciplinary team meeting, the consensus was that the MRI appearance was in keeping with an incidental left uncal herniation. It was felt that this was likely to be a developmental anomaly, which could not account for their tinnitus and hearing loss. Subsequently, the patient was discharged from neurosurgery, with a recommendation for their GP to refer them to the neurology team for their headaches.
1:
T1-weighted MRI head showing a left medial temporal lobe herniation across the medial tentorium that is indenting the left cerebral peduncle.
A) Gadolinium-enhanced T1-weighted axial and B) coronal MRI head. White matter scattered small vessel ischaemic changes are noted as well, with no enhancing abnormality or tumour identified. Department of Radiology, Royal Stoke University Hospital, Stoke-on-Trent, Staffordshire, UK.
DISCUSSION
First, the authors considered whether the patient’s MRI findings were in keeping with their clinical presentation. Given the chronicity and lack of progression of their symptoms (intermittent, stable, episodic headaches associated with vomiting for almost one year); lack of focal neurological deficits on examination, in particular, no evidence of left-sided cranial third nerve palsy; and lack of other acute intracranial findings on imaging (e.g., mass effect or congenital malformation) that could contribute to herniation, it would be reasonable to label the left uncal herniation observed on imaging as idiopathic in nature, and therefore, likely a developmental anomaly.
Indeed, idiopathic brain herniation is an extremely rare finding, with a prospective study on idiopathic cuneus gyrus herniation showing a prevalence of just
0.73%.6 To date, the authors are aware of only 18 reported cases of idiopathic brain herniation in the English literature, of which, only two have been reported as idiopathic uncal herniation.
Yavarian et al.4 reported the case of a 46-year-old male who presented with a sudden onset right-sided facial nerve palsy, whose MRI revealed an uncal/ parahippocampal gyrus herniation. Similarly, Ram and Sherry5 reported a case of a 40-year-old female with a longstanding history of chronic headaches which were associated with nausea, photophobia, diplopia, and dizziness since the age of 2 years. The patient’s MRI showed bilateral uncal herniation, greater on the right than the left, in the absence of any other intracranial abnormality.5 In both of these cases, there were no known specific triggers or history of head trauma, and detailed neurological examination did not reveal any focal neurological deficits.
Figure
Gadolinium-enhanced
The pathophysiology of idiopathic uncal herniation remains unclear. Some studies propose that localised dural and dural extension defects arising during meningeal embryogenesis may be responsible for focal brain parenchymal herniation.7 Others suggest that a wide tentorial incisura and angle of the tentorium cerebelli in relation to the tentorial incisura are risk factors for developing idiopathic uncal herniation.5 Meanwhile, the occurrence of chronic uncal herniation in the paediatric age group has been attributed to a negative pressure gradient created in the posterior fossa secondary to shunt placement or malfunction, as seen in children with Dandy-Walker syndrome or other large, cystic cavities in communication with the fourth ventricle.8
In recent years, research has supported the direct correlation between elevated BMI, percentage body fat, and raised intracranial pressure (ICP). Indeed, previous studies hypothesised that central obesity leads to raised intra-abdominal pressure, leading to poor venous return from the brain, and subsequently increased ICP.9 This may explain the incidental uncal herniation seen in the authors' patient.9 Another possible cause could be use of the continuous positive airway pressure machine, which decreases systemic venous return by increasing intrathoracic pressure, leading to raised ICP.10 However, in both instances, the authors have not reliably explained why the raised ICP would only be unilateral rather than bilateral. Additionally, the authors do not routinely see uncal herniation in patients presenting with idiopathic intracranial hypertension.
In an acute emergent setting, uncal herniation requires prompt monitoring and reduction of the raised ICP, which may involve temporising medical measures or more definitive surgical decompression techniques.11 However, given its rarity, there is no consensus regarding how to manage incidental findings of brain herniation. For symptomatic uncal herniation, we need to address the underlying cause, such as idiopathic intracranial hypertension, shunt malfunction, or space-occupying lesion.
If the uncal herniation is asymptomatic, adoption of a conservative approach should be considered.
In terms of complications, the authors wonder if chronic brain herniation is a poor prognostic marker. Naidich et al.12 concluded the same in a case series they reported, in which two of the seven paediatric patients diagnosed with chronic transincisural herniation died from further (unspecified) complications at the ages of 3 months and 4.5 years. Certainly, any significant uncal herniation may compress the surrounding vital brain structures. For example, compression of the oculomotor (cranial nerve III) nerve results in an ipsilateral oculomotor nerve palsy, which manifests as a ‘fixed dilated’ pupil and a ‘down and out’ pupil due to paralysis of the superior, inferior, and medial rectus muscles, and the inferior oblique muscle. Compression of the ipsilateral midbrain cerebral peduncle causes contralateral hemiparesis, while compression of the contralateral cerebral peduncle, due to extensive midline shift, causes a false-localising ipsilateral hemiparesis, also known as the Kernohan-Woltman notch phenomenon.13 Compression of the posterior cerebral artery leads to occipital infarction, resulting in homonymous hemianopia, if unilateral, or cortical blindness, if bilateral. Finally, if left untreated, uncal herniation progresses to central herniation, resulting in secondary brainstem haemorrhages (Duret haemorrhages), as well as abnormal respiratory patterns leading to respiratory arrest due to disruption of the ascending respiratory activating system.11
LEARNING OUTCOMES
Firstly, clinicians should recognise idiopathic and chronic uncal herniation to avoid misdiagnosis. Proper identification of idiopathic brain herniation is also important to mitigate the need for unnecessary invasive procedures, such as biopsies and surgeries. For example, the misinterpretation of a parahippocampal herniation as a medial temporal lobe lesion in a 41-year-old man who presented with
right-sided trigeminal neuralgia resulted in unnecessary invasive surgical exploration, including a biopsy which revealed the findings of a normal brain.14
Secondly, idiopathic uncal herniation should remain a diagnosis of exclusion. Therefore, thorough history taking, clinical examination, biochemistry, and basic imaging should be performed to establish a specific cause first. In particular, it is important that clinicians are able to distinguish between herniations and mass lesions. MRI findings of a focal region of soft tissue signal intensity which is isointense compared to the adjacent brain parenchyma, and a lack of signal
References
1. Isolan GR et al. Vascularization of the uncus – anatomical study and clinical implications. Surg Neurol Int. 2021;12:393.
2. Von Der Heide RJ et al. Dissecting the uncinate fasciculus: disorders, controversies and a hypothesis. Brain. 2013;136:1692-707.
3. Munakomi S, Mohan Kumar B. Case report: frontalis sign for early bedside consideration of impending uncal herniation. F1000Res. 2016;5:125.
4. Yavarian Y et al. Herniation of uncus and parahippocampal gyrus: an accidental finding on magnetic resonance imaging of cerebrum. Acta Radiol Short Rep. 2015;4(1):2047981614560077.
5. Ram CP, Sherry R. Nonemergent descending transtentorial temporal lobe herniations – case reports of idiopathic [bilateral uncal] and chronic [unilateral uncal and parahippocampal] herniations with review of literature. J Med Imaging Case Rep. 2020;4(1):4-8.
abnormality or contrast enhancement are useful characteristics in differentiating brain herniations from other pathologic masses.15
In conclusion, idiopathic uncal herniation remains an extremely rare and poorly researched phenomenon. Physicians are frequently compelled to intervene for these patients. Therefore, a thorough history and clinical examination are key to determining if the presenting symptoms are due to the radiological finding. For patients in whom the uncal herniation is an incidental finding, the authors would recommend a conservative approach to avoid unnecessary complications.
6. Maldjian C, Adam R. Prevalence of idiopathic cuneate gyrus herniation based on emergency room CT examinations. Emerg Radiol. 2014;21(4):387-9.
7. Duarte MP et al. Magnetic resonance imaging of idiopathic herniation of the cuneus gyrus. J Neuroimaging. 2007;17(4):353-4.
8. Udayakumaran S et al. Chronic uncal herniation secondary to posterior fossa shunting: case report and literature review. Childs Nerv Syst. 2010;26(2):267-71.
9. Sugerman HJ et al. Increased intraabdominal pressure and cardiac filling pressures in obesity-associated pseudotumor cerebri. Neurology. 1997;49(2):507-11.
10. Yiallourou TI et al. Continuous positive airway pressure alters cranial blood flow and cerebrospinal fluid dynamics at the craniovertebral junction. Interdiscip Neurosurg. 2015;2(3):152-9.
Island: StatPearls. Available at: https://www.ncbi.nlm.nih.gov/books/ NBK537108/. Last accessed: 4 April 2024.
12. Naidich TP et al. Chronic cerebral herniation in shunted DandyWalker malformation. Radiology. 1986;158(2):431-4.
13. Beucler N et al. The KernohanWoltman notch phenomenon : a systematic review of clinical and radiologic presentation, surgical management, and functional prognosis. J Korean Neurosurg Soc. 2022;65(5):652-64.
14. Horowitz M et al. Misinterpretation of parahippocampal herniation for a posterior fossa tumor: imaging and intraoperative findings. J Neuroimaging. 2002;12(1):78-9.
15. Seok HY, Lee DH. Magnetic resonance imaging of idiopathic herniation of the lingual gyrus: a case report. Investig Magn Reson Imaging. 2017;21(3):195-8.
All that Torse is Not an Ovary: Ferreting Torsed Subserosal Fibroid in a Flurry of Fibroids: A Case Report
Adnexal structures that can undergo torsion include the ovary, isolated fallopian tube, both tube and ovary, broad ligament leiomyoma, and pedunculated leiomyoma. Torsion of a subserosal leiomyoma, like ovarian torsion, demands prompt surgical attention to avoid further complications like infection and peritonitis. Here, the authors provide an overview of a 35-year-old patient who was suspected of having an ovarian torsion. On ultrasound, there were multiple intramural and subserosal leiomyomas with normal ovaries. One of the pedunculated subserosal leiomyomas showed altered morphology suspicious for torsion. The diagnosis for leiomyoma torsion was further confirmed on MRI and later correlated with the intraoperative findings.
Key Points
1. Torsion of a subserosal leiomyoma, such as ovarian torsion, demands prompt surgical attention to avoid further complications like infection and peritonitis.
2. This case report highlights the imaging findings of torsed subserosal fibroid amongst other uncomplicated fibroids on ultrasound and MRI, and its correlation with post-operative specimen.
3. Heterogeneity with loss of whorled pattern in a pedunculated subserosal fibroid and presence of normal ovaries favour torsed subserosal leiomyoma on ultrasonogram. On MRI, heterogeneous appearance and non-enhancement, along with bridging vessel and dark fan sign increase the diagnostic confidence.
INTRODUCTION
Leiomyomas or fibroids are the most frequently encountered benign neoplasm of smooth muscle origin in women of reproductive age group.1-3 Pedunculated leiomyoma (a type of subserosal leiomyoma) is uncommon and its torsion is rare, and therefore not commonly diagnosed. Pedunculated subserosal fibroid requires immediate surgical intervention. A delay in diagnosis can lead to unfavourable outcomes like gangrene and peritonitis.1,2
CASE REPORT
A 35-year-old patient came with acute lower abdominal pain predominantly on the left side. Pregnancy test using urine yielded a negative result. Ovarian torsion was
A
suspected, and the patient was referred for an ultrasonography examination.
Ultrasonography of the pelvis showed multiple subserosal and intramural hypoechoic lesions with a whorled appearance suggestive of leiomyomas. There was a large, well-circumscribed heterogeneously hyperechoic lesion in the left adnexa connected to the uterus via a pedicle, suggestive of a pedunculated leiomyoma. Doppler examination showed vascularity in the proximal part of the pedicle, with the absent flow in the distal part. There was patchy arterial flow with absent venous flow in the leiomyoma. Both the ovaries were normal, ruling out ovarian torsion (Figure 1 A–C).
MRI pelvis was performed subsequently to further confirm the ultrasonography
B C
A and B) Ultrasonography images through the left adnexa show well-circumscribed heterogeneously hyperechoic lesion (*) connected to the uterus via a pedicle (white arrow), suggestive of a pedunculated leiomyoma. C and D) Doppler ultrasound images show vascularity in the proximal part of the pedicle with absent flow in distal part. There was patchy arterial flow with a monophasic waveform and absent venous flow in the leiomyoma. E and F) Both the ovaries were normal.
Figure 1: Transabdominal ultrasonography of pelvis on B-mode and colour Doppler.
findings. MRI showed multiple T2 hypointense intramural and subserosal leiomyomas. A pedunculated leiomyoma was seen in the left adnexa, showing a heterogeneous T2 hyperintense signal (Figure 2 A–D). Post-contrast sequences showed non-enhancing areas in the pedunculated leiomyoma with associated diffusion restriction (Figure 3 A–C).
Pre-operative blood parameters revealed mild leukocytosis (white blood cell counts 13,000 /μL) and low haemoglobin levels (-9 gm/dL). The patient was taken up for an emergency open myomectomy in view of urgent exploration of torsed fibroid and the need for fertility preservation. A twisted pedicle of the leiomyoma was observed intraoperatively. The torsed leiomyoma was dark and dusky in appearance as compared to other uncomplicated leiomyomas that were pink on gross morphology (Figure 4 A and B).
DISCUSSION
A woman at reproductive age with lower abdominal pain can present as an acute surgical emergency with obstetric or nonobstetric causes. Obstetric causes include ectopic pregnancy, uterine dehiscence, and abruptio placenta. Non-obstetric causes are ovarian torsion, urinary tract calculi, appendicitis, and leiomyoma degeneration/torsion.3
Patients with uterine leiomyomas are usually asymptomatic, but may sometimes present with dysmenorrhoea, menorrhagia, or infertility. Various possible complications related to leiomyomas are degeneration, urinary retention, uterine prolapse, and torsion.1-4 Pedunculated leiomyoma is uncommon, and its torsion is rare. The risk of torsion is higher when the stalk of the pedunculated subserosal fibroid is slender and elongated.1
A) T2 weighted axial image of the MRI pelvis at a lower level, B) T2 weighted axial image of the MRI pelvis at a higher level , and C/D) T2 weighted coronal and sagittal images of the MRI pelvis show multiple T2 hypointense intramural and subserosal leiomyomas (*). Large subserosal leiomyoma is noted in the right adnexa (white arrow), with a pedunculated leiomyoma in the left adnexa (black arrow) connected to the uterus via pedicle. The pedunculated leiomyoma shows heterogenous T2 hyperintense signal.
Figure 2: MRI pelvis T2W sequence.
Figure 3: MRI pelvis post contrast T1FS, and diffusion weighted with apparent diffusion coefficient map.
A B C
A) Axial post-contrast T1 fat saturated, B) diffusion weighted, and C) apparent diffusion coefficient images show non-enhancing area in the pedunculated fibroid on the left, with corresponding hyperintense signal on diffusion weighted and drop in signal on apparent diffusion coefficient images suggestive of diffusion restriction (white arrows).
Figure 4: Post myomectomy intraoperative specimens.
A B
A) Intraoperative and B) post-myomectomy specimen images show multiple intramural and subserosal leiomyomas of variable sizes. The torsed leiomyoma (yellow arrow) is dark and dusky as compared to other uncomplicated leiomyomas which are pink on gross morphology.
Leiomyoma torsion initially causes venous stasis, congestion, and oedema. There is subsequent arterial compromise that leads to gangrene and haemorrhagic necrosis.1 Since there is an overlap with the imaging findings of fibroid degeneration, most of the time the diagnosis is made intraoperatively by confirming the vascular pedicle that has undergone twisting.1,2,4
On ultrasonography, a normal uterine leiomyoma appears as a hypoechoic solid mass with a whorled pattern and peripheral vascularity. Torsed subserosal fibroid appears heterogeneously hypoechoic to hyperechoic with loss of whorled pattern and absence of vascularity on colour Doppler. The presence of the twisted pedicle differentiates heterogeneity in torsed leiomyoma from degenerative fibroid and leiomyosarcoma. The pedicle often shows a twist with
Ultrasonography
MRI
Clinical presentation
Management
Torsed subserosal fibroid
a resultant abrupt vascular cut-off. Sometimes on colour Doppler, due to congestion, only arterial waveforms are elicited with absent venous flow.1,2
A typical leiomyoma shows a T1 and T2 hypointense signal on MRI. A torsed leiomyoma is heterogeneously hyperintense on T2W imaging and intermediate/ heterogeneous on T1W imaging. It shows a peripheral rim of enhancement (due to oedema and obstructed venous channels) with a central non-enhancing necrotic core. Table 1 differentiates between a torsed subserosal fibroid and an uncomplicated fibroid. There are flow voids between the subserosal leiomyoma and uterus, which is described as the ‘bridging vessel’ sign in the literature.1 This helps to differentiate whether the lesion originates from the uterus or adnexa. Another sign called the
B-mode ultrasound: Heterogeneously hypoechoic or hyperechoic solid mass with loss of whorled pattern
Colour Doppler: Twisted pedicle with abrupt cut off and diminished vascularity in the fibroid
Heterogeneously hyperintense on T2W
Intermediate/heterogenous signal on T1W
Peripheral enhancement with central non-enhancing necrotic area
Bridging vessel sign and dark fan sign increases the diagnostic confidence
Acute abdominal pain
It is a surgical emergency and needs urgent exploration in the form of either myomectomy or hysterectomy.
Gross pathology
Dark and dusky fibroid due to loss of vascularity
Uncomplicated fibroid
B-mode ultrasound: hypoechoic solid mass with whorled pattern
Colour Doppler: Peripheral vascularity
T1 and T2 hypointense lesion with variable enhancement pattern
Commonly asymptomatic
Patient can be managed both conservatively and surgically. Conservative management includes GnRH agonists and SPRM.
Surgical options include open, hysteroscopic or laparoscopic guided myomectomy or hysterectomy.
Table 1: Torsed subserosal fibroid versus uncomplicated fibroid.
‘dark fan sign’ is appreciated in the postcontrast sequence, where the uterus adjacent to the twisted leiomyoma shows poor enhancement.1 An increase in the size of the subserosal fibroid on serial imaging with altered perfusion is another clue in the cross-sectional imaging.4 CT can help in diagnosis by demonstrating a twisted vascular pedicle with non-enhancement of the pedunculated leiomyoma. It also rules out other causes of acute abdomen.5
Management of uterine leiomyoma can be both surgical and conservative. It depends on the patient’s age, symptoms, and desire to preserve the fertility, as well as on surgeon’s experience and technology available in the institution. For an asymptomatic uncomplicated uterine leiomyoma various medications like gonadotrophin-releasing hormone agonists or selective progesterone receptor modulators can be used. Surgical options available are open, hysteroscopic, or laparoscopic guided myomectomy or hysterectomy. Minimally
References
1. Dhillon MS et al. Torsion of a huge subserosal uterine leiomyoma: a challenging case of acute abdomen. SAJR. 2023;27(1):1-5.
2. Chang CT et al. Pedunculated subserosal leiomyoma with torsion, a rare cause of abdominal pain: a case report. Medicine. 2023;102(5): e32838.
invasive/non-invasive procedures for leiomyomas are uterine artery embolisation and high-frequency magnetic resonanceguided focussed ultrasound surgery. Large fibroid (10–12 cm) and multiple fibroids are contraindications to laparoscopic myomectomy. Laparoscopic hysterectomy is preferred in the elderly symptomatic women who do not wish to preserve fertility.6
CONCLUSION
With clinical presentation similar to ovarian torsion, torsion of a leiomyoma, although a rare diagnosis, is an important differential in reproductive age group women with acute lower abdominal pain. The presence of a stalk between the uterus and the leiomyoma with absent vascularity and normal ovaries is key in the diagnosis. Prompt diagnosis and management is essential to avoid ischaemic gangrene, infection, and subsequent peritonitis.
3. Kim HJ et al. Differential diagnosis of uterine leiomyoma torsion mimicking ovarian torsion in a second trimester of pregnancy: a case report. Int J Women's Health. 2022;14:1777-82.
4. Le D et al. Imaging findings of a torsed pedunculated uterine leiomyoma: a case report. Radiol Case Rep. 2020;15(2):144-9.
5. Roy C et al. Acute torsion of uterine leiomyoma: CT features. Abdom Imaging. 2005;30(1):120-3.
6. Donnez J, Dolmans MM. Uterine fibroid management: from the present to the future. Human reproduction update. 2016;22(6):665-86.