New Developments in Clinical Trials for Osteoarthritis
Tom Davenport and Rick Abramson discuss the emerging role of AI in the healthcare space Interviews:
AI in Clinical Neurology: Revolutionising Patient Care and Navigating Ethical Frontiers Congress Feature:
The Importance of Early Recognition, Diagnosis, and Treatment of Friedreich Ataxia
What Happens When People Don’t Bolus for Extended Periods of Time While Using Control-IQ Technology?
▼: Short and Long-Term Disease Control in Moderate-to-Severe AD Through Selective IL-13 Inhibition
Improving Assessment of Steatotic Liver Disease with Noninvasive Ultrasound-based Technique
Editor's Pick: New Developments in Clinical Trials for Osteoarthritis: Are We Closer to Improving Pain Management and Disease Modification?
al.
The Application, Safety, and Recent Developments of Commonly Used Gadolinium-Based Contrast Agents in MRI: A Scoping Review
74 Deep Learning-Based Approaches for Brain Tumour Segmentation and Classification
Baiju et al.
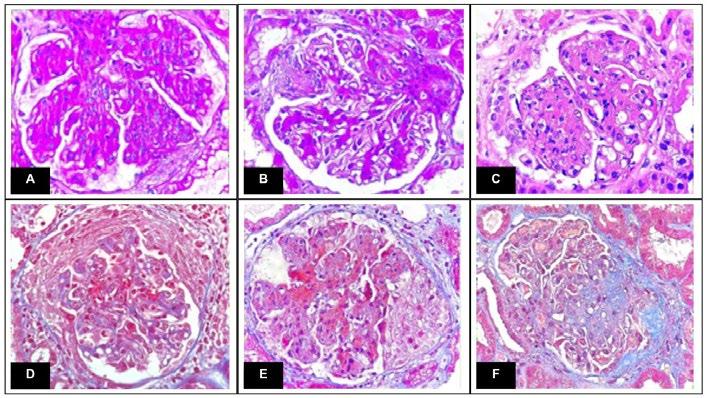
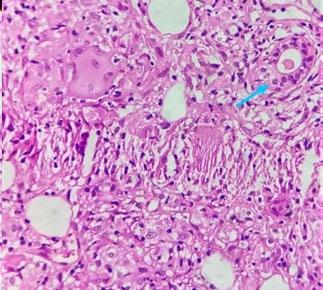
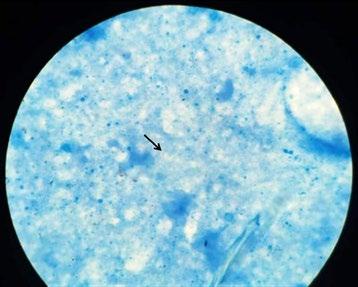
84 Evolution of Proliferative Lupus Nephritis with Focal Extracapillary Proliferation in Latin American Patients with Lupus
Daza et al.
94 Cytokine Profile Associated with COVID-19 Severity and Outcome: A Hospital-Based Study from Kashmir, North India
Farooq et al.
105 Right Lateral Digital Rectal Examination in Men with Suspected Prostate Disease Presenting with Lower Urinary Tract Symptoms
Takure
117 Prevalence of Obstructive Sleep Apnoea in Sleep Referrals and Related Medical Conditions in a Local Chest Unit in Hong Kong
Le et al.
126 Pelvic Atherosclerosis in Women: A Case Report of the Alleviation of Dyspareunia and Vaginal Dryness after Pelvic Artery Revascularisation
Mohan et al.
132 Amlodipine-Induced Gynaecomastia in a Patient with Spinal Cord Injury
Chow and Swarna
138
"We see AI being used in early-detection initiatives
Editorial Board
Editor-in-Chief
Prof Markus Peck-Radosavljevic
Klinikum Klagenfurt am Wörthersee, Austria
Current Chairman and Head of the Department of Gastroenterology and Hepatology, Endocrinology, Rheumatology and Nephrology at Klinikum Klagenfurt am Wörthersee, with expertise in portal hypertension, hepatocellular carcinoma, and HIV-HCV coinfection.
Prof Ahmad Awada
Jules Bordet Institute, Belgium
Prof Sorin T. Barbu
“Iuliu Hațieganu” University of Medicine and Pharmacy, Romania
Dr Abdullah Erdem Canda
Yildirim Beyazit University, Türkiye
Prof Ian Chikanza
Harley Street Clinic, UK
Prof Lászlo Vécsei
University of Szeged, Hungary
Dr Pierfrancesco Agostoni
St. Antonius Hospital, the Netherlands
Dr Fernando Alfonso
Hospital Universitario de La Princesa, Spain
Dr Emanuele Angelucci
IRCCS Ospedale Policlinico San Martino, Italy
Dr George Anifandis University of Thessaly, Greece
Dr Riccardo Autorino
Virginia Commonwealth University, USA
Dr Mátyás Benyó University of Debrecen, Hungary
Prof Andrew Bush Imperial College London, UK
Dr Hassan Galadari
United Arab Emirates University, UAE
Dr Amir Hamzah Abdul Latiff
Pantai Hospital, Malaysia
Dr Lorenz Räber
Bern University Hospital, Switzerland
Aims and Scope
EMJ, the flagship journal of the EMJ portfolio, is an open-access, peer-reviewed eJournal, committed to elevating the quality of healthcare globally by publishing high-quality medical content across the 18 clinical areas covered in our portfolio. The journal is published quarterly and showcases the latest developments across these clinical areas.
EMJ publishes peer-reviewed research papers, review articles, and case reports across all therapy areas of the EMJ portfolio. In addition, the journal publishes features and opinion pieces create a discussion around key topics in the field and broaden readers’ professional interests. The journal also features interviews with leading experts in various clinical disciplines.
The journal covers advances within the pharmaceutical arena by publishing sponsored content from congress symposia, which is of high educational value for healthcare professionals. This undergoes rigorous quality control checks by independent experts and the in-house editorial team.
EMJ endeavours to increase knowledge, stimulate discussion, and contribute to the delivery of world-class updates in the clinical realm. We do not publish veterinary science papers or laboratory studies that are not linked to patient outcomes. Further details on coverage can be found here: www.emjreviews.com
Editorial
Expertise
EMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors who are recognised authorities in their respective fields.
• Peer review, which is conducted by expert reviewers who are invited by the Editorial team and appointed based on their knowledge of a specific topic.
• An experienced team of editors and technical editors.
• A team of internal and independent medical writers.
Peer Review
Every review article, case report, feature, and research article published in EMJ undergoes peer review by at least two independent experts.
On submission, all manuscripts are assessed and undergo a technical check by the EMJ Editorial staff to determine their suitability for the journal and appropriateness for peer review Editorial staff identify appropriate reviewers who are selected based on their specialist knowledge in the relevant area. All peer review is double-blind.
Following review, manuscripts are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected. Editorial staff are responsible for ensuring that necessary amendments to the manuscript have been made, with input from our Editorial Board or the original reviewers where necessary. The Editor of EMJ has final discretion over any proposed amendments. Manuscripts authored by members of the Editorial Board are subjected to the same double-blind process. Short opinion pieces are published following internal review and publication is at the discretion of the Editor. Congress-associated content authored by the EMJ Editorial staff undergoes internal quality control checks. Congress-related content sponsored or funded by our industry partners undergoes quality control checks independently. Industry-supported content that falls into any of the categories that are eligible for peer review, undergoes the same peer review process.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects. We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial.assistant@emjreviews.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in EMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
EMJ is distributed through controlled circulation to healthcare professionals in the relevant fields globally.
Indexing and Availability
EMJ is indexed on DOAJ, the Royal Society of Medicine, and Google Scholar®.
EMJ is available through the websites of our leading partners and collaborating societies.
EMJ journals are all available via our website: www.emjreviews.com
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
All information obtained by EMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, EMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. EMJ is completely independent of any event reviews in this issue and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever. The cover photo is of London, England, the location of work for the primary author of the Editor's Pick.
• Challenges when evaluating treatments for epilepsy
• Why Seizure Freedom can be so H.A.R.D. to achieve
This infographic contains methodologies of analysis, study design, and sources of support for different research reporting of Seizure Freedom presented at the American Epilepsy Society (AES) Annual Meeting 2022.
Data collected from studies/research involving humans presented at AES 2022
Learn why Seizure Freedom is so H.A.R.D. to understand
Editor
Evgenia Koutsouki
Editorial Manager
Darcy Richards
Copy Editors
Noémie Fouarge, Katheeja Imani, Jenna Lorge
Editorial Co-ordinators
Victoria Antoniou, Abigail Craig
Editorial Assistants
Helena Bradbury, Ada Enesco, Katrina Thornber, Katie Wright, Aleksandra Zurowska
Creative Director
Tim Uden
Design Manager
Stacey Rivers
Senior Designer
Steven Paul
Designers
Owen Silcox, Fabio van Paris
Junior Designers
Dillon Benn Grove, Shanjok Gurung
Senior Performance & Insight Lead
Darren Brace
Marketing Director
Kristina Mestsaninova
Chief Content Officer
Justin Levett
Chief Commercial Officer
Dan Healy
Founder and Chief
Executive Officer
Spencer Gore
Welcome
Dear Readers,
It is a great pleasure to welcome you to the Autumn issue of EMJ
In this issue, we hone into the world of AI, with exclusive interviews from two leading experts. Be sure not to miss Rick Abramson’s discussion of the promising applications of AI in early detection initiatives, as well as the challenges of ensuring human oversight and patient safety whilst implementing AI approaches in radiology.
Tom Davenport shares his perspective on AI applications beyond administrative aspects of clinical practice and how it might help make medicine more affordable.
Also check out our great selection of articles, including an interesting study on the cytokine storm during COVID-19 infection, with a particular focus on IL-6, IL-10, vascular endothelial growth factor, and IL-8, and their potential prognostic and predictive significance.
Additionally, for any rheumatologists among you, an insightful narrative review discusses Phase II and III trials for new therapeutic agents in osteoarthritis.
In closing, I would like to thank our peer reviewers, Editorial Board, authors, and interviewees for their invaluable contribution! Stay tuned for our Winter edition, which will discuss key aspects of women’s health. Until then, enjoy reading this issue!
Editorial enquiries: editor@emjreviews.com
Sales opportunities: salesadmin@emjreviews.com
Permissions and copyright: accountsreceivable@emjreviews.com
Evgenia Koutsouki Editor
Reprints: info@emjreviews.com Media enquiries: marketing@emjreviews.com
Foreword
Welcome to the latest issue of EMJ, exploring the emerging role of AI in healthcare, with expert interviews and a range of peer-reviewed articles shedding light on the topic. The articles cover themes such as deep learning-based approaches to analysing and classifying brain tumours, as well as new developments in clinical trials for osteoarthritis.
Our congress feature, covering a session from the 10th European Academy of Neurology (EAN) Annual Congress, held in Helsinki, Finland, from 29th June–2nd July 2024, delves into the ways in which AI could revolutionise patient care in clinical neurology. This feature addresses the ethical implications of AI in medicine, as well as the perspectives of researchers and trainees alike.
In an eye-opening article about the application of AI in brain tumour classification, the authors discuss the various deep learning techniques and approaches that could revolutionise clinical care in neurology. They emphasise the benefits of these methods, which are built to accommodate large amounts of unstructured data, and though they take some time to set up, they provide instant results. The authors are sure to emphasise, however, that AI is a tool designed to aid clinical decision-making, not replace it.
This issue of EMJ also includes fascinating interviews with Tom Davenport and Rick Abramson, leaders in the field of innovation and AI in healthcare. Davenport discusses the ways in which mobile applications have transformed medicine for those who would not otherwise have access to healthcare, as well as the value of humans and machines working in tandem. Abramson gives his own thoughts on the topic, addressing the challenges that need to be addressed in order to advance AI in healthcare, and emphasises the need for healthcare professionals to be more open-minded about human control and the use of AI. Abramson also describes his role as one of the first international teleradiologists and how AI may go on to help with workload challenges amongst healthcare professionals.
This feature addresses the ethical implications of AI in medicine
I would like to extend thanks to all the authors, reviewers, interviewees, and Editorial Board members for their continued dedication and commitment to EMJ. I hope this issue proves to be an insightful and educational read for all healthcare professionals.
Prof Markus Peck-Radosavljevic
Professor of Medicine, Chairman, Department of Gastroenterology and Hepatology, Endocrinology, Rheumatology and Nephrology, Klinikum Klagenfurt am Wörthersee, Klagenfurt, Austria
AI in Clinical Neurology: Revolutionising Patient Care and Navigating Ethical Frontiers
THE transformative effect of AI integration in clinical neurology was a focal point of the 10th European Academy of Neurology (EAN) Annual Congress, held in Helsinki, Finland, from 29th June–2nd July 2024. This topic was explored in depth in a dedicated studio session entitled ‘Revolutionizing Clinical Neurology: The Transformative Impact of AI’, chaired by Raphael Wurm, Medical University of Vienna, Austria, and member of the EAN Resident and Research Fellow Section (RRFS) and Communication Committee. The main goal of the session was to comprehensively explore the ethical implications, challenges, and opportunities that AI presents in reshaping patient care.
THE RESIDENT AND RESEARCH FELLOW SECTION PERSPECTIVE
Wurm opened the session with a presentation focusing on the perspective of neurology trainees and research fellows at the beginning of their careers on navigating the evolving medical landscape marked by the early adoption of AI in clinical practice. Wurm began by asking: “What will AI integration in clinical neurology look like” to AI? ChatGPT 3.5 (OpenAI, San Francisco, California, USA) identified how AI is poised to enhance the analysis of medical data; contribute to personalised treatment options; identify medication contraindications; and improve diagnostic accuracy, particularly in neuroimaging modalities like MRI and CT.
Wurm acknowledged these advancements but highlighted a significant gap in the integration of AI into medical education. He proposed that AI could be leveraged to link healthcare records with training resources, providing immediate access to relevant information for medical students and residents. Furthermore, AI-powered virtual patient interactions could simulate complex clinical scenarios, offering students tailored
educational experiences that develop both technical and soft skills.
Wurm highlighted the patient-facing opportunities of AI in clinical neurology. Start-ups are outpacing public health systems and academia in developing chatbots for diagnosis and triage. In Europe, there are already ten health chatbots that patients are beginning to access, answering questions similarly to healthcare professionals. The first chatbot that can mimic a therapeutic intervention has received Class IIa UKCA medical device certification and has been approved for medical use in the UK.1 The Limbic Access AI chatbot (Limbric, London, UK) is a mental health app that uses machine learning to identify eight common mental health disorders and triage patients seeking psychological support from NHS’s Talking Therapies services.1 Limbic Access is used by 25% of people accessing the National Health Service (NHS) Talking Therapies services and has saved an estimated 30,000 clinical hours.1 Wurm indicated that similar chatbots could be applied in neurology to alleviate symptoms in nonemergency situations when accessing an expert is challenging. However, any
software at the point of contact for patients requires regulation to ensure that the information is accurate and if human intervention is required, it can be quickly identified.
The concluding remarks by Wurm emphasised the unique perspective of young neurologists at the forefront of AI application. There is significant potential to leverage the power of AI to improve medical education and augment the delivery of patient care, addressing tasks potentially overwhelming human capabilities. Similar to how people feel comfortable relying on autopilot when flying, Wurm hopes that we can reach a point where AI in healthcare is readily accepted. Nevertheless, he acknowledged the importance of regulating AI in medical use to ensure accuracy, data privacy, and equitable access in all regions of Europe and the wider globe because, currently, access to these technologies carries a significant cost.
NAVIGATING THE ETHICAL LANDSCAPE: IMPLICATIONS OF AI IN THE REALM OF NEURO-DATA
Marcello Ienca, College of Humanities at École polytechnique fédérale de Lausanne, Switzerland, presented on the ethical implications of AI in clinical neurology. He began by challenging the misconception that ethics is merely a discipline tasked with policing medicine and serving as a
regulatory hurdle. Part of this misconception comes from the primary goal of ethics to prevent harm but fails to consider the other side of the coin, which is the promotion of good. Instead, Ienca framed ethics as a discipline focused on maximising human wellbeing, ensuring that technological innovation is designed and developed with this in mind.
Similar to how people feel comfortable relying on autopilot when flying, Wurm hopes that we can reach a point where AI in healthcare is readily accepted
Epidemiological data indicates that a large proportion of the global population is going to experience at least one neurological disorder in their lifetime. Therefore, Ienca stated that there is a moral obligation to accelerate technological innovation in the context of clinical neurotechnology, leveraging the full power that AI can bring to various domains of scientific enterprise. AI has the potential to improve neuroscience research, provide more accurate diagnoses, provide personalised therapy, and embed AI in neural interfaces. Ienca stressed that we must remove unnecessary obstacles preventing the translation of these technologies and the delivery of muchneeded solutions worldwide.
However, some classical ethical considerations need to be addressed. The first one is privacy. Ienca discussed “neuro privacy,” the risk of revealing sensitive information through retrospective data mining. This can include the identification of digital biomarkers that are predictive of neurological characteristics. For example, AI models can use digital phenotyping and smartphone behaviour to identify dementia. This could potentially be abused by employers or healthcare insurance providers, leading to new forms of discrimination based on neurological features. In addition, in the last 20 years, there has been significant debate regarding brain reading, which is the possibility of extracting privacy-sensitive information from neural data processing. Moreover, this debate has been revamped in recent months with numerous editorials published exploring the topic due to AI and deep learning models proving extremely effective at reconstructing visual and semantic content from neural activity. This reverse inference AI technology is needed clinically because, for example, it can power speech neuroprosthesis to treat disorders like aphasia; but if this technology is abused, it could lead to more significant violations of privacy.
The final point that Ienca focused on was the problem of equitable access; it is essential that AI technology is used in clinical neuroscience in a way that democratises the technology and does not amplify existing inequalities. Ienca posed the issue of AI being used in the neurotech field, not to restore function in people with a disorder, but to augment and enhance human capabilities above normality. This could lead to novel forms of inequality at the cognitive level.
PERSPECTIVES ON THE INTEGRATION OF AI IN NEUROLOGY
Philippe Ryvlin, University Hospital of Lausanne, Switzerland, concluded the session by discussing the current state and future of AI integration in clinical neurology. Ryvlin had the opportunity to participate
in the organisation of the first-of-its-kind international conferences dedicated to AI in epilepsy and neurological disorders hosted in the USA. From these conferences, Ryvlin emphasised that Europe is lagging behind the USA in the development of AI tools and integration into the healthcare system. Europe must acknowledge this divergence and its potential impact on patient care.
Notably, the chatbot's responses were rated significantly higher in quality than physicians.
Physicians 22.1%
Similarly, empathy ratings were higher for the chatbot than for physicians.4
Physicians 4.6%
A key focus of Ryvlin’s presentation explored the advances of AI in diagnostics, stating that the largest impact of AI in clinical practice will be in this field. Already, AI tools are used to detect abnormalities and interpret neuroimaging automatically. Specifically, this has been demonstrated by recent validation of an electroencephalogram (EEG)-based algorithm that can classify EEGs as normal or abnormal. This will help physicians review EEG and neuroimaging faster, reducing the rate of mis-abnormalities. By aiding neurologists in making more accurate diagnoses, less invasive testing will be required, and treatments will be guided more accurately.
Ryvlin discussed a paper published in 2023 by a research group at Google (Mountain View, California, USA) that compared their large language model Med-PaLM against clinicians on several diagnostic tasks.2 The study found that when clinicians and Med-PaLM were tasked with answering medical questions, there was an almost equal performance (Med-PaLM 92.6% verses clinician 92.9%) based on scientific and clinical consensus.2 Although the model
Ryvlin emphasised that Europe is lagging behind the USA in the development of AI tools and integration into the healthcare system. Europe must acknowledge this divergence and its potential impact on patient care
had a higher likelihood of causing potential harm (2.3% compared to clinicians’ 1.3%), Ryvlin suggested that current optimised models might perform even better. He acknowledged the inherent risks but stressed the significant potential benefits of AI in augmenting clinical decision-making.
Ryvlin also referenced a recent publication where an academic group tested ChatGPT4’s accuracy in diagnosing complex clinical cases.3 The study revealed that ChatGPT-4 correctly diagnosed 57% of cases, outperforming 99.8% of expert physicians.3 This finding underscores the potential of AI to enhance diagnostic accuracy significantly. In addition, Ryvlin discussed results from a recent study that compared physician and AI chatbot responses to patient queries on a public social media forum. Participants rated the quality and empathy of responses without knowing the source.4 Notably, the chatbot’s responses were rated significantly higher in quality (78.5%) than physicians (22.1%). Similarly, empathy ratings were higher for the chatbot (45%) than for physicians (4.6%).4 Ryvlin connected this to the potential use of AI in improving the soft skills of medical trainees, suggesting that AI could help identify and enhance empathetic communication. However, Ryvlin cautioned against allowing technology to fully replace human clinicians, highlighting the complexity
References
1. Future Care Capital. Limbic Access is first AI chatbot to receive medical device certification in UK. Available at: https://futurecarecapital.org.uk/latest/ limbic-access-gains-certification-inuk-first/. Last accessed: 29 July 2024.
of integrating AI into healthcare systems to protect individuals’ employment and ensure patient interaction with healthcare professionals.
Concluding his presentation, Ryvlin stressed the transformative potential of AI in clinical neurology, urging the European medical community to develop and adapt its own AI solutions to avoid becoming overly dependent on costly technologies governed by aggressive businesses and non-European entities.
CONCLUSION
The session at EAN 2024 highlighted both the promise and the challenges of integrating AI into clinical neurology. While AI has the potential to revolutionise patient care, enhance diagnostic accuracy, and improve medical education, these benefits must be weighed against the ethical concerns and risks of inequality. The session underscored the importance of developing robust regulatory frameworks to ensure that AI technologies are safe, equitable, and used to augment rather than replace human expertise in neurology. As Europe navigates this complex landscape, it must strive to lead in AI innovation to ensure that these technologies are harnessed for the benefit of all.
2. Singhal K et al. Large language models encode clinical knowledge. Nature. 2023;620(7972):172-80.
3. Eriksen AV et al. Use of GPT-4 to diagnose complex clinical cases. NEJM AI. 2023;1(1):AIp2300031.
4. Ayers JW et al. Comparing physician and artificial intelligence chatbot responses to patient questions posted to a public social media forum. JAMA internal medicine. 2023;183(6):589-96.
Speakers:
The Importance of Early Recognition, Diagnosis, and Treatment of Friedreich Ataxia
This industry-sponsored symposium took place during the European Association of Neurology (EAN) Congress held in Helsinki, Finland, 29 June−2 July, 2024.
Mathieu Anheim,1 Jörg Schulz2
1. Department of Neurology, Movement Disorders Unit, University Hospital of Strasbourg, France
2. Department of Neurology, RWTH Aachen University Hospital, Germany
Disclosure: Anheim declares honoraria from Biogen, Reata Pharmaceuticals, AbbVie, Merz, Orkyn, Linde, Aguettant, Ipsen, Asdia, Ever Pharma, and Teva. Schulz declares honoraria from Merz, Teva, Bayer, UCB, Lilly, Boehringer, GSK, Bial, Novartis, Biogen, and Eisai; research support from Biogen, Eisai, and Lilly; and an advisory/consultant role with Forward Pharma, MSD, Lundbeck, Biogen, Eisai, Novo Nordisk, Roche, Reata, and Lilly.
Acknowledgements: Medical writing assistance was provided by Eleanor Roberts, Beeline Science Communications, Ltd, UK. Patients gave informed, written consent for video recordings and to the use of the video recordings.
Disclaimer The symposium content and views expressed herein are those of the speakers and not necessarily the company. The content is based on the omaveloxolone European Medicines Association (EMA) approved label. This information is intended for healthcare professionals in the EU.
Support: The symposium and publication of this article was supported by Biogen.
Editorial Note: This article was temporarily removed from 27.11.24 to 14.08.25 for review. The review has been completed, and the content remains unchanged from its original publication.
Meeting Summary
At the 2024 European Association of Neurology (EAN) Congress, one satellite symposium discussed the recognition, diagnosis, and treatment of Friedreich ataxia (FA), the most common hereditary ataxia. This condition is characterised by progressive neurodegeneration, multisystem complications, loss of ambulation, and reductions in the ability to carry out activities of daily living (ADL). For many, there is also a premature death. FA is caused by guanine-adenine-adenine triplet (GAA) repeat expansions in the gene FXN. This codes for the protein frataxin, loss of which is associated with impaired
PHARMA PARTNERSHIP
mitochondrial function, increased sensitivity to oxidative stress and reactive oxygen species levels, increased inflammation, and cell death.
Decreased frataxin leads to the symptoms of FA, including increasing spasticity, pain, dysphagia, cardiac problems, speech impairment, pes cavus, and scoliosis. The speakers highlighted how delays in diagnosis can occur when FA is mistaken for other ataxias and they called for the use of genetic and biochemical testing early in the patient pathway. This is best accomplished by prompt referral to specialists in ataxia. Treatment and care for patients with FA, along with their families, require a multidisciplinary approach involving allied healthcare professionals, among other specialists. Effective communication and support amongst such networks is key to providing individualised treatment where a patient’s health and disease progression are regularly monitored and associated conditions are treated appropriately. Currently, the only approved FA-specific drug treatment in the EU and the USA for patients 16 years and older is omaveloxolone. Clinical trials of this drug have shown that it can provide a sustained benefit in slowing disease progression over a 3-year period in patients aged 16 years and older. This benefit is particularly evident when omaveloxolone prescription is not delayed. In the future, other pipeline drugs are expected to add to potential disease-slowing treatments for FA.
Introduction
FA is a complex, autosomal recessive, cerebellar ataxia involving progressive degeneration of central and peripheral nervous systems, including loss of several types of neurons and associated nerves. This presents as effects in cardiac, musculoskeletal, and endocrine systems.1,2 While FA is considered rare, it is the most common hereditary ataxia, accounting for around 50% of all ataxia cases.1 In Caucasian individuals, overall prevalence is generally cited as being 1 in 20,000–50,000.3 However, studies from individual countries indicate that prevalence varies from 0.1 in 100,000 in Finland to 4.7 in 100,000 in Northern Spain, with figures for other European countries falling between these two.4-6
As part of a satellite symposium at EAN 2024, two experts in FA, Mathieu Anheim and Jörg Schulz, discussed the recognition and diagnosis of FA, along with current treatments. The symposium started with video testimonies from people involved in FA. Bart Jan, the father of a 20-yearold with FA, discussed how the biggest challenge was getting a diagnosis and how, for them, “it took us close to 6 years, travelling from doctor to doctor, appointment to appointment”. Stephan
Rouillon, from the French Association for Friedreich Ataxia,7 discussed the importance of patients “finding the right specialists and understanding what can be done to improve their life.” Susan Milman, from Euro-Ataxia,8 emphasised how patients and families “need information about how to live with the condition and how not to let the condition destroy their lives.”
Recognising the Signs and Symptoms of Friedreich Ataxia
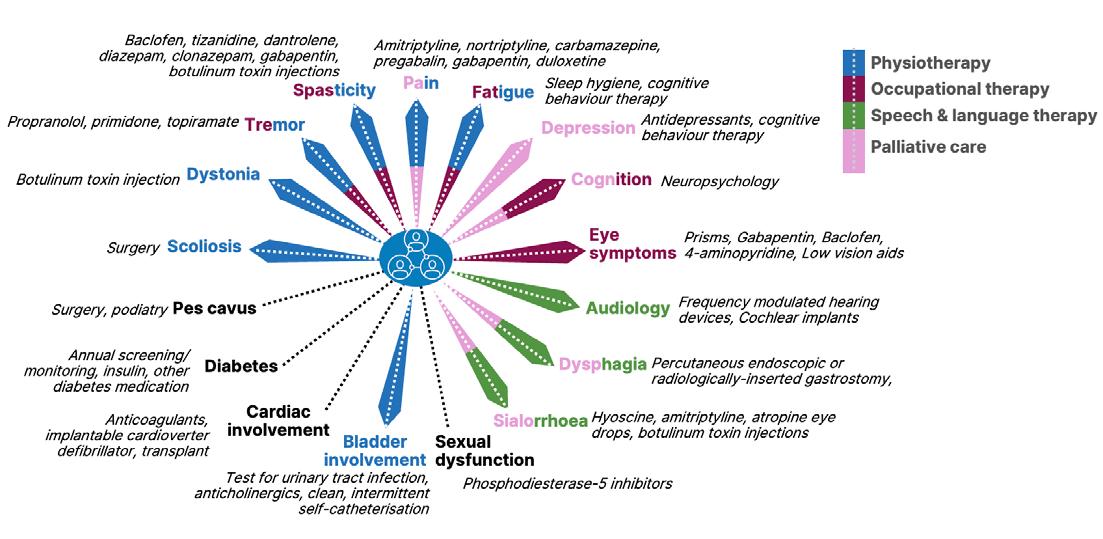
Many key clinical features of FA are classed as neurological.1,2,9,10 Of note, said Anheim, is combined proprioceptive and cerebellar ataxia, the latter of which is associated with slurred speech due to cerebellar dysarthria. There is also the abolition of tendon reflexes and hypopallesthesia due to sensory neuronopathy or ganglionopathy, which can be identified with electroneuromyography. Additionally evident may be bilateral extensor plantar reflexes, flexor spasms, urinary urgency/incontinence, and square wave jerks. In the context of mitochondrial disease, Anheim discussed extraneurological signs of FA. These include hypertrophic cardiomyopathy, scoliosis, pes cavus, diabetes, optic neuropathy, and deafness.1,2,9,10 Many of the symptoms associated with these features are depicted in Figure 1
Partially adapted from de Silva et al.,11 2019
Progression of Friedreich Ataxia
The onset of FA symptoms is typically in childhood, aged 8–14 years (‘typical-onset FA’), though in some it may be earlier (0–7 years, ‘early-onset FA’), or more into adolescence/young adulthood (15–24 years), or even later (>24 years, ‘lateonset FA’). In general, the progression of ambulatory factors of FA is faster in earlyonset FA compared to any other groups.13 While cardiomyopathy and diabetes may occur early in patients with early- and typical-onset FA, these may be at a lower rate or absent in patients with late-onset FA. Additionally, foot deformities due to pes cavus, other cardiovascular issues, and pronounced scoliosis also occur at a much lower rate in patients with late-onset FA.9
Over the years, initial unsteady gait and general clumsiness gradually become difficulty in standing and walking as well as problems with falls. The frequency and intensity of these symptoms increase over time, leading to the need for ambulatory walking aids, and at later stages, seated mobility aids.9,14
Ambulation loss, which is seen as a critical milestone in FA progression,15 usually occurs by the mid-to late-20s in patients with early-onset FA.10 However, FA burden is not just in ambulation, but through functional disabilities. For example, curtailment of the ability to carry out ADLs such as feeding oneself or drinking; marked cerebellar dysarthria leading to difficulties in speaking clearly and being understood; and sight fixation problems due to square wave jerks, among others.6,10,16 In patients with late-onset FA, there is usually a longer disease duration before ADLs are impacted and seated mobility aids are required.17
Overall, prognosis is poor, and the mean age of death is 36.5 (range: 12–87) years.1,18 Primarily, the cause of death in FA is due to cardiac dysfunction, predominantly in the form of arrhythmia or congestive heart failure.18
Figure 1: Friedreich ataxia symptoms and their management.9-12
Genetics of Friedreich Ataxia
In FA, GAA repeat expansions in the gene FXN on chromosome 9 are inherited in an autosomal recessive pattern. Typically, there are between 200 to over 900 GAA units in patients with FA, compared to 7–22 units in non-affected controls. GAA repeat expansion impairs normal expression of the FXN gene, which codes for frataxin, a protein involved in mitochondrial iron homeostasis and biosynthesis of iron-sulphur clusters, impacting their assembly and transfer to mitochondrial components.19,20 Most patients with FA are homozygous for GAA expansion (96%), with a minority being compound heterozygous, where there is GAA expansion on one allele and a point mutation or exon deletion on the other (4%).21,22
Decreased viable FXN expression leads to around 70−95% reduction in frataxin production compared to levels in unaffected people.23 Decreased frataxin levels result in impaired mitochondrial function, increased sensitivity to oxidative stress, and increased levels of reactive oxygen species. This can lead to increased inflammation, and ultimately, cell death.19,21,24
In general, lower frataxin levels correlate with greater disease severity.19,21 In homozygous patients, the amount of frataxin manufactured generally corresponds to the number of GAA repeats on the least-affected allele. That is, there is an inverse correlation between the length of the allele with the shorter GAA expansion and frataxin levels, as well as with age of onset, and disease progression rate. This means that earlier disease onset and faster progression are associated with longer alleles, and those with shorter GAA expansion on this allele typically have later disease onset, sometimes into middle or even older age.17,19,21-25
be searched for with specific molecular analysis as it cannot be found using targeted gene panel or whole exome sequencing. Genetic testing is vital to distinguish FA from other ataxias with sensory neuropathy that may mimic FA. These include abetalipoproteinaemia, due to mutations in the MTP (microsomal triglyceride transfer protein) gene, and ‘ataxia with vitamin E deficiency,’ due to mutations in the alpha-TTP (tocopherol transfer protein) gene. Genetic testing can also distinguish FA from ataxias without peripheral neuropathy, such as Neimann-Pick disease Type C (NPC), due to mutations in the NPC1/2 gene, and from ataxias with sensory and motor neuropathy, such as ataxia telangiectasia (AT), due to mutations in the ATM (AT mutated) gene.26
Anheim also discussed how assessing biomarkers may be useful for distinguishing FA from treatable diseases with symptoms resembling FA. For example, vitamin E is markedly reduced in ‘ataxia with vitamin E deficiency’,27 and is malabsorbed, along with fats and other fat-soluble vitamins, in patients with abetalipoproteinaemia.28 Further, NPC can be distinguished by raised plasma oxysterol levels,29 and ‘ataxia with oculomotor apraxia Type 2’ can be distinguished by raised serum alpha-fetoprotein levels.30 Brain scan investigation in patients with FA may reveal upper cervical cord atrophy but little-to-no cerebellar atrophy.11
Clinical Symptoms
Genetic and Biochemical Testing
Genetic testing should be carried out in all patients displaying any signs of cerebellar ataxia, said Anheim. He discussed how, in his experience, GAA expansion must
Using case studies, Anheim pointed out examples of what can be deduced in a clinical examination. For example, sway should be detected when a patient stands with their feet together (which worsens when their eyes are closed), and hypermetria (overshooting the intended goal) should occur when a patient tries to move their heel down their shin or touch their nose then, sequentially, the examiner’s fingers. Another example was of a patient having difficulties with balance and gait when turning around during a walking test. They also displayed saccadic pursuits on ocular examination, and disappearance of ankle, knee, and extensor plantar reflexes.
Diagnosis of Friedreich Ataxia
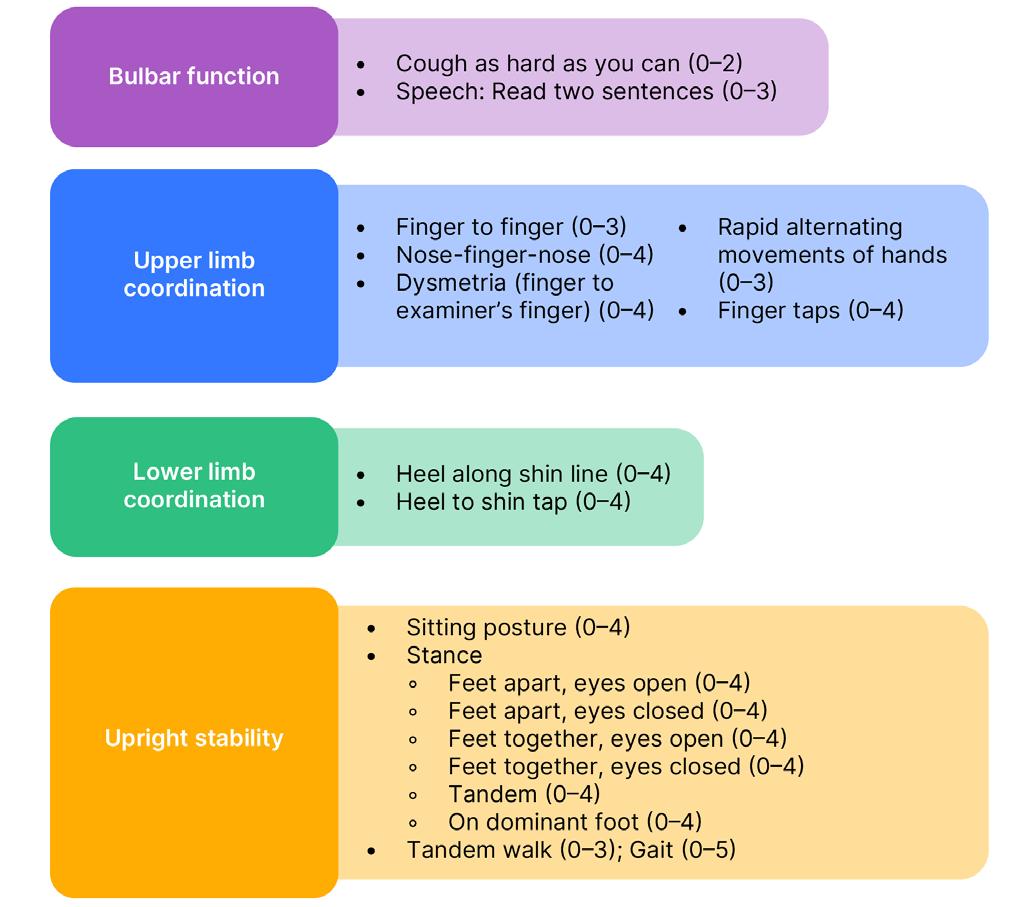
Such symptoms can be assessed and tracked using validated neurological rating scales. The modified FA Rating Scale (mFARS) helps assess neurological deficits in four domains: bulbar function, upper limb coordination, lower limb coordination, and upright stability. Combined scores range from 0−93 (best to worst); more details are shown in Figure 2 31,32 In another case presented by Anheim, a patient with an mFARS score of 58 had lost most of their ambulation ability and was a wheelchair user. On standing, they could only walk with the support of a person and a mobility aid, and they had difficulty coordinating their lower limb movements.
A slightly faster but less FA-specific scoring method is the Scale for the Assessment and Rating of Ataxia (SARA). This can be used to assess stance, gait, limb kinetic function, sitting, and speech. Combined scores range from 0–40 (best to worst).33
Avoiding Diagnostic Delay
As stressed though testimony in the introduction to this symposium, it is important to recognise that many patients and caregivers with FA wait a long time for a diagnosis with the journey including visits to primary then a number of specialist care providers, mis- and missed diagnoses, genetic testing, and involvement of patient organisations along the way.25,34,35 Accordingly, Anheim emphasised that a crucial first step to diagnosis is to swiftly refer the patient to a specialist neurologist/ neuropaediatrician who understands how to diagnose FA and can help put together the best care package for the individual. As prognosis may be poor, and especially for those with early-onset FA, progression can be reasonably rapid, it is vital that patients are diagnosed and have a care plan in place as soon as possible so they can live a more supported and comfortable life.1,16,36
Treatment
FA is a multisystem disorder that needs a multisystem approach with regard to clinical management and care.1,11,16
With this in mind, in 2022, best practice recommendations were developed in collaboration with healthcare professionals, researchers, and patients with FA and their families/caregivers.12 As illustrated in Figure 1, overall, there is a need for physiotherapy, occupational therapy, speech and language therapy, and later in life, palliative care. Treatment should be individualised according to symptoms and needs. For example, surgery may be needed for scoliosis and pes cavus, and muscle relaxants, pain relief, and botulinum toxin injections may be needed for dystonia, tremors, spasticity, pain, eye symptoms, and sialorrhoea. Further, cognitive behaviour therapy may be of use for symptoms such as fatigue and depression, and antidepressants may be prescribed for the latter, as well as, in some cases, for pain.11
Schulz discussed how individualised treatment may be coordinated by a primary care physician or a neurologist, and how allied specialist teams are necessary to help a patient and their family over the course of FA.11,37 A care review should be offered every 6−12 months, wherein a general or specialist ataxia neurologist monitors disease progression and manages comorbidities as needed.
The multidisciplinary team can also provide individualised follow-ups, for example in the realms of diabetes care, cardiomyopathy, scoliosis, and other treatable or manageable symptoms. Vital for the patient and their family is effective, mutually supportive communication among the healthcare professionals providing care.11,37
As discussed previously, deficits in frataxin in FA lead to impaired mitochondrial function and increased oxidative stress and inflammation.19,24 Also seen in the cells of people with FA, and in pre-clinical models, is suppression of levels and activity of the protein nuclear factor erythroid 2-related factor (Nrf2). This is important in patients with FA as impaired Nrf2 signalling correlates with low levels of frataxin expression. Nrf2 can also induce the expression of a
Omaveloxolone
(scores from best [0] to worst in 0.5 increments).31,32
number of cytoprotective proteins involved in supporting mitochondrial function, bioenergetics, and proteostasis, and in inhibiting inflammatory responses and curtailing oxidative stress.38
Usually, Nrf2 levels are kept low due to degradation coordinated by kelch-like ECHassociated protein 1 (Keap1).38 The drug omaveloxolone, a semi-synthetic derivative of oleanolic acid, has been developed to help counter such actions by increasing the availability of Nrf2. Omaveloxolone can bind to Keap1 and inhibit its ability to target Nrf2 for degradation, allowing
Nrf2 to translocate into the nucleus and regulate the transcription of its target gene. Omaveloxolone can also inhibit inflammation directly by inhibiting proinflammatory signalling pathways and reducing the production of proinflammatory mediators,39 and both in vitro and in vivo, it has been shown to restore mitochondrial activity and decrease oxidative stress.40
Omaveloxolone is currently the only drug licenced for the treatment of FA in the EU and USA. It is indicated for patients aged 16 years or older at a dose of 150 mg/day.41 The ’MOXIe’ clinical trial programme for
Adapted from Rummey C et al.31 and Friedreich’s Ataxia Research Alliance32
evaluating omaveloxolone in patients aged 16−40 years included a two-part, Phase II, double-blind, randomised, placebocontrolled trial.42 Part 1 was a dose-ranging study, over 12 weeks, assessing the pharmacodynamics, pharmacokinetics, and safety of omaveloxolone doses from 2.5–300 mg/day versus placebo (n=69).43 Part 2, over 48 weeks, assessed efficacy and safety of 150 mg/day omaveloxolone versus placebo.44
In Part 2, the full analysis set used for primary analysis of efficacy included all patients who had at least one postbaseline measurement but did not include patients with pes cavus due to Part 1 results showing outliers in this group.43 At baseline, most participants were ambulatory with mean ± standard deviation (SD) mFARS scores of 40.9±10.4 for the omaveloxolone group (n=40) and 38.8±11.0 for the placebo group (n=42). In this study, a version of the mFARS was used that included two additional assessments of bulbar function taken from the previous, slightly longer, FARS neurological assessment;31 as such scores ranged from 0−99. Section GAA1 repeat length was slightly higher in the omaveloxolone group (mean ± standard deviation, 739.2±214.9) compared with the placebo group (693.8±277.2).44
Results showed that by Week 48, placebo group participant scores worsened (mean ±standard error of the mean; 0.85±0.64; 95% CI: -0.43, 2.13) while those in the omaveloxolone group improved (-1.55±0.69; 95% CI: −-2.93, −0.18). The difference between them (-2.40±0.96; 95% CI: -4.31, -0.50) was significant (p=0.014).44
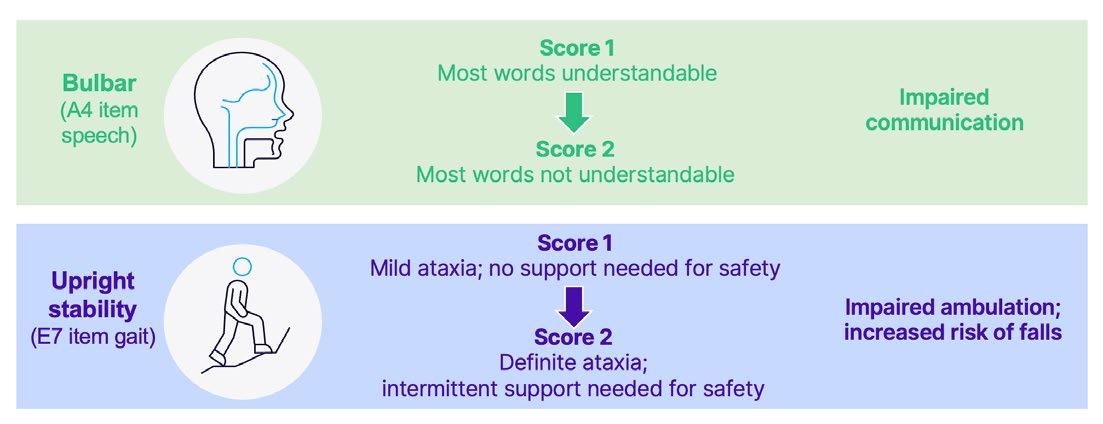
Of the several components of mFARS, omaveloxolone had the greatest effect on upright limb coordination, followed by upright stability scores.44,45 Such differences are relevant as Shulz discussed how a one-point worsening on scores of upright stability can mean a patient going from having mild ataxia, with little need for safety support, to having definite ataxia, with intermittent need for safety support due to impaired ambulation and the risk of falls. Improvements compared to placebo were also shown in bulbar scores.44 A onepoint change here can mean the difference between a patient being able to speak at a mostly understandable level, to one where clear verbal communication is difficult (Figure 3).32
Adapted from Rummey C et al.31 and Friedreich’s Ataxia Research Alliance32 A4: Subscale A, instruction 4 on the mFARS, assessing speech; E7: Subscale E, instruction 7 on the mFARS, assessing gait.
Figure 3: Clinical implications of changes in modified Friedreich’s ataxia rating scale (mFARS) scores.32
Secondary endpoints were analysed using a fixed-sequence hierarchical approach to maintain the familywise overall Type I error rate of 0.05. Using this strategy, numeric, though not statistically significant, improvements were shown in scores of Clinician and Patient Global Impression of Change (PGIC) measures, fall frequency, dexterity, and walking.44 The ‘FA-validated ADL’ (FA-ADL)46 scale showed that omaveloxolone improved scores from baseline and reached nominal statistical significance compared to placebo at Week 48 (p=0.04). Post-hoc analysis of the proportion of patients that improved or worsened in primary and secondary measures at Week 48 showed that a greater proportion of patients in the omaveloxolone group improved, and fewer worsened, on the mFARS, ADL scale, and PGIC measure.44
Overall, omaveloxolone was generally well-tolerated with a serious adverse event (AE) in 6% of the placebo and 10% of the omaveloxolone group. AEs occurring in ≥25% of patients in placebo/omaveloxolone groups, respectively, included headache (25%/37%), alanine aminotransferase (ALT) increase (2%/37%), contusion (37%/33%), nausea (14%/33%), upper respiratory tract infection (29%/28%), and excoriation (23%/26%). Schulz reported that, in general, excess AEs in the omaveloxolone group were limited to the first 12 weeks of treatment, with lower frequencies reported between 12–48 weeks. Discontinuations due to an AE were 4% in the placebo group and 8% in the omaveloxolone group.39,42,44,47,48
In patients treated with omaveloxolone in the MOXIe study, increases above the upper limit of normal (ULN) were observed for ALT or aspartate aminotransferase (AST) (29.4% ≥3x ULN; 15.7% ≥5x ULN) and BNP (13.7% >ULN), with hypercholesterolaemia observed at a rate of 2%. Maximal increase occurred within the first 12 weeks of treatment.41,44,48 This is not unexpected because, as an Nrf2 activator, omaveloxolone has been reported to increase aminotransferase expression, partially due to its pharmacodynamic effects.49
According to prescribing guidelines, ALT, AST, and bilirubin levels should be ascertained prior to omaveloxolone initiation,
then monthly for the first 3 months, then periodically as clinically indicated. Omaveloxolone should be discontinued immediately if ALT or AST increases to >5x ULN or to >3x ULN if accompanied by bilirubin >2x ULN. Liver tests should then be repeated. While for patients with severe hepatic impairment (Child-Pugh Class C), use of omaveloxolone should be avoided, in patients with moderate impairment (ChildPugh Class B), the dose should be 100 mg/day with close monitoring for adverse reactions, with consideration of lowering to 50 mg/day if adverse reactions occur. Increases in low-density lipoprotein and decreases in high-density lipoprotein, as well as decreases in body weight, may also occur and should be monitored and treated according to standard clinical guidelines.41
Open-Label Extension, Follow-on, and Real-World Studies of Omaveloxolone
An ongoing open-label extension (OLE) study is being carried out to assess the long-term safety and tolerability of 150 mg/ day omaveloxolone in qualified patients with FA following the completion of Part 1 or Part 2. Participants who were initially in the placebo group in Part 2 were switched to omaveloxolone during the OLE trial.50,51
Results from the OLE include that after 72 weeks, the notable difference between omaveloxolone and placebo in mFARS change from baseline scores shown in Part 1 and 2 remained, favouring the omaveloxolone-omaveloxolone group (n=40) over the placebo-omaveloxolone group (n=42) (least squares mean difference: -2.91, standard error: ±1.44). While by the end of OLE study mFARS scores had increased above baseline in both groups, it was of note that scores did not rise above extension baseline in the omaveloxolone-omaveloxolone group until Week 120 testing. This, said Schulz, indicated that omaveloxolone had a slowing effect on disease progression. Also discussed by Schulz was that, at the end of Part 2, participants were required to enter a washout period of 4 weeks. During this time, mFARS scores in the omaveloxolone-treated group returned to baseline,51 showing that gains in Part 2 had been due to this drug.
Data from the MOXIe trial was also compared to data from the large, global, multicentre, prospective natural history, longitudinal ‘FA Clinical Outcome Measures Study’ (FA-COMS).52 Omaveloxolone was associated with slower disease progression (55% reduction in mFARS) in treated patients compared to the propensitymatched FA-COMS cohort over a 3-year period. In the primary pooled population (136 patients in each group), by Year 3, patients in the FA-COMS matched set progressed 6.6 points on mFARS, whereas patients treated with omaveloxolone in MOXIe OLE progressed 3.0 points (difference: -3.6; nominal p=0.0001).50
The Future of Friedreich Ataxia Treatment
While omaveloxolone is currently the only therapy approved specifically for FA in the EU and USA, a number of other drugs that may improve mitochondrial function, reduce oxidative stress, or modulate frataxincontrolled metabolic pathways, are in human trials. Schulz noted, however, that such drugs only target the results of frataxin loss in FA. To target frataxin itself, trials are also being carried out for therapies that can act as frataxin replacements, stabilisers, or enhancers; increase FArelated gene expression; or replace or edit FA-related genes.53
References
1. Williams CT, De Jesus O, Friedreich Ataxia [Internet] (2023) Treasure Island: StatPearls. Available at: https://www.ncbi.nlm.nih.gov/books/ NBK563199/. Last accessed: 31 July 2024.
2. Coarelli G et al. The inherited cerebellar ataxias: an update. J Neurol. 2023;270(1):208-22.
3. Vankan P. Prevalence gradients of Friedreich’s ataxia and R1b haplotype in Europe co-localize, suggesting a common Palaeolithic origin in the Franco-Cantabrian ice age refuge. J Neurochem. 2013;126(Suppl 1):11-20.
4. Juvonen V et al. Dissecting the epidemiology of a trinucleotide repeat disease - example of FRDA in Finland. Hum Genet. 2002;110(1):36-40.
5. Polo et al. Hereditary ataxias and paraplegias in Cantabria, Spain. An
Conclusion
As FA is a progressive, often lifeshortening, condition, this symposium highlighted how diagnosis should occur as soon as possible after ataxia presents, via referral to a specialist centre for clinical evaluation and genetic analysis.2,11,25,34,35,54 FA is characterised by multisystem complications16 so treatment and care, as well as family/caregiver support, requires a multidisciplinary approach involving allied healthcare professionals and others.11 Effective communication and support amongst this multidisciplinary team is key to providing individualised treatment where patient progress is regularly monitored and associated conditions treated appropriately.37
Currently, the only FA-specific approved drug treatment in the EU and USA is omaveloxolone.41 This has been shown to provide a sustained benefit over a 3-year period in patients aged 16 years and older including slowing progression of FA symptoms. Such results were particularly apparent when omaveloxolone use was not delayed.43,44,47,50,51, In the near future, other pipeline drugs are being investigated to address disease manifestations of FA.52
epidemiological and clinical study. Brain. 1991;114(Pt 2):855-66.
6. Buesch K, Zhang R. A systematic review of disease prevalence, health-related quality of life, and economic outcomes associated with Friedreich’s Ataxia. Curr Med Res Opin. 2022;38(10):1739-49.
7. Association Francaise Ataxie de Friedreich. Available at: https://www. afaf.asso.fr/. Last accessed: 20 August 2024.
8. Euro Ataxia. Availavle at: https://www. euroataxia.org/. Last accessed: 16 July 2024.
9. Reetz K et al. Nonataxia symptoms in Friedreich Ataxia: report from the Registry of the European Friedreich’s Ataxia Consortium for Translational Studies (EFACTS). Neurology. 2018;91(10):e917-30.
10. Harding A E. Friedreich’s ataxia:
a clinical and genetic study of 90 families with an analysis of early diagnostic criteria and intrafamilial clustering of clinical features. Brain. 1981;104(3):589-620.
11. de Silva R N et al. Diagnosis and management of progressive ataxia in adults. Pract Neurol. 2019;19(3):196207.
12. Corben L A et al. Clinical management guidelines for Friedreich ataxia: best practice in rare diseases. Orphanet J Rare Dis. 2022;17(1):415.
13. Rummey C et al. Natural history of Freidreich ataxia. Heterogeneity of neurologic progression and consequences for clinical trial design. Neurology. 2022;99(14):e1499-e1510.
14. Parkinson M H et al. Clinical features of Friedreich’s ataxia: classical and atypical phenotypes. J Neurochem. 2013;126(Suppl 1):103-17.
15. Rummey C et al. Predictors of loss of ambulation in Friedreich’s ataxia. E Clinical Medicine. 2020;18:100213.
16. Cook A, Giunti P. Friedreich’s ataxia: clinical features, pathogenesis and management. Br Med Bull. 2017;124(1):19-30.
17. Lecocq C et al. Delayed-onset Friedreich’s ataxia revisited. Mov Disord. 2016;31(1):62-9.
18. Tsou A Y et al. Mortality in Friedreich ataxia. J Neurol Sci. 2011;307(1-2):469.
19. Clark E et al. Role of frataxin protein deficiency and metabolic dysfunction in Friedreich ataxia, an autosomal recessive mitochondrial disease. Neuronal Signal. 2018;2(4):Ns20180060.
20. Campuzano V et al. Friedreich’s ataxia: autosomal recessive disease caused by an intronic GAA triplet repeat expansion. Science. 1996;271(5254):1423-7.
21. Campuzano V et al. Frataxin is reduced in Friedreich ataxia patients and is associated with mitochondrial membranes. Hum Mol Genet. 1997;6(11):1771-80.
22. Galea C A et al. Compound heterozygous FXN mutations and clinical outcome in friedreich ataxia. Ann Neurol. 2016;79(3):485-95.
23. Filla et al. The relationship between trinuceotide (GAA) repeat length and clinical features in Friedreich ataxia. Am J Hum Genet. 1996;59(3):554-60.
24. Gomes C M, Santos R. Neurodegeneration in Friedreich’s ataxia: from defective frataxin to oxidative stress. Oxid Med Cell Longev. 2013;2013:487534.
25. Indelicato E et al. Onset features and time to diagnosis in Friedreich’s Ataxia. Orphanet J Rare Dis. 2020;15(1):198.
26. Anheim M et al. The autosomal recessive cerebellar ataxias. N Engl J Med. 2012;366(7):636-46.
27. Schuelke M, Ataxia with Vitamin E Deficiency [Internet] (2005, updated 2023) Seattle: GeneReviews® Available at: https://www.ncbi.nlm.nih. gov/books/NBK1241/. Last accessed: 1 August 2024.
28. Burnett JR et al., Abetalipoproteinemia [Internet] (2018, updated 2022) Seattle: GeneReviews®. Available at: https://www.ncbi.nlm.nih.gov/ books/NBK532447/pdf/Bookshelf_ NBK532447.pdf. Last accessed: 1 August 2024.
29. Reunert J et al. Rapid diagnosis of 83 patients with Niemann Pick Type C disease and related cholesterol transport disorders by cholestantriol
screening. EBioMedicine. 2016;4:170-5.
30. Watanabe M et al. Familial spinocerebellar ataxia with cerebellar atrophy, peripheral neuropathy, and elevated level of serum creatine kinase, gamma-globulin, and alpha-fetoprotein. Ann Neurol. 1998;44(2):265-9.
31. Rummey C et al. Psychometric properties of the Friedreich Ataxia Rating Scale. Neurol Genet. 2019;5(6):371.
32. Friedreich’s Ataxia Research Alliance. Friedreich’s Ataxia Rating Scale (FARS) and Modified FARS (mFARS). 2023. Available at: https://www.curefa.org/ pdf/Instructions-for-administeringthe-mFARS.pdf. Last accessed: 16 July 2024.
33. Schmitz-Hübsch T et al. Scale for the assessment and rating of ataxia: development of a new clinical scale. Neurology. 2006;66(11):1717-20.
34. Giunti P et al. Impact of Friedreich’s Ataxia on health-care resource utilization in the United Kingdom and Germany. Orphanet J Rare Dis. 2013;8:38.
35. Eurodis: Rare Diseases Europe. Patient journey through diagnosis. Available at: https://www.eurordis.org/wp-content/ uploads/2020/07/solverd-infographic. jpeg. Last accessed: 16 July 2024.
36. Patel M et al. Progression of Friedreich ataxia: quantitative characterization over 5 years. Ann Clin Transl Neurol. 2016;3(9):684-94.
37. Ataxia UK. Management of the ataxias towards best clinical practice. Third edition. 2016. Available at: https:// www.ataxia.org.uk/wp-content/ uploads/2020/11/Ataxia_UK_Medical_ Guidelines._Third_Edition._v3m_ Dec_2016_-_updated_Sep_2019.pdf. Last accessed: 16 July 2024.
38. Chiang S et al. Antioxidant defense mechanisms and its dysfunctional regulation in the mitochondrial disease, Friedriech’s ataxia. Free Radic Biol Med. 2020;159:177-88.
39. Probst B L et al. RTA 408, a novel synthetic triterpenoid with broad anticancer and antiinflammatory activity. PLoS One. 2015;10(4):e0122942.
40. Abeti R et al. Novel Nrf2-Inducer prevents mitochondrial defects and oxidative stress in Friedreich’s ataxia models. Front Cell Neurosci. 2018;12:188.
41. Skyclarys (omaveloxolone) prescribing information. Available at: https:// www.skyclarys.com/docs/skyclarys_ us_prescribing_information/. Last accessed: 1 August 2024.
42. Biogen (Reata, a wholly owned subsidiary of Biogen). RTA 408
Capsules in Patients With Friedreich’s Ataxia - MOXIe. NCT02255435. https:// clinicaltrials.gov/show/NCT02255435.
43. Lynch D R et al. Safety, pharmacodynamics, and potential benefit of omaveloxolone in Friedreich ataxia. Ann Clin Transl Neurol. 2019;6(1):15-26.
44. Lynch D R et al. Safety and efficacy of omaveloxolone in Friedreich ataxia (MOXIe study). Ann Neurol. 2021;89(2):212-25.
45. Lynch DR. Correction to safety and efficacy of omaveloxolone in Friedreich ataxia (MOXIe study). Ann Neurol. 2023;94(6):1190.
46. Traschütz A et al. FARS-ADL across ataxias: construct validity, sensitivity to change, and minimal important change. Mov Disord. 2024;39(6):965-74.
47. Subramony SH et al. Assessment of cardiac safety in patients with Friedreich’s Ataxia in the MOXIe trial of omaveloxolone. Poster 124. MDA Clinical & Scientific Conference, Dallas, TX, USA. March 5-8, 2023. Available at: https://www.mdaconference. org/abstract-library/assessmentof-cardiac-safety-in-patients-withfriedreichs-ataxia-in-the-moxie-trialof-omaveloxolone/. Last accessed: 16 July 2024.
48. Lynch D et al. The MOXIe trial of omavelocolone in Friedreich ataxia: Exploring the transient nature of treatment-emergent adverse events (P7-3.016). Neurology. 2024;102(17 Suppl 1) :3490.
49. Lewis J H et al. Effects of bardoxolone methyl on hepatic enzymes in patients with type 2 diabetes mellitus and stage 4 CKD. Clin Transl Sci. 2021;14(1):299309.
50. Lynch D R et al. Propensity matched comparison of omaveloxolone treatment to Friedreich ataxia natural history data. Ann Clin Transl Neurol. 2024;11(1):4-16.
51. Lynch DR et al. Efficacy of omaveloxolone in Friedreich’s ataxia: delayed-start analysis of the MOXIe extension. Mov Disord. 2023;38(2):31320.
52. Friedreich’s Ataxia Research Alliance. FA Clinical Outcome Measures (FA-COMS). NCT03090789. https:// clinicaltrials.gov/show/NCT03090789.
53. Friedreich’s Ataxia Research Alliance. Friedreich’s ataxia treatment pipeline. 2024. Available at: https://www.curefa. org/wp-content/uploads/2024/06/ Pipeline-June-18-2024.pdf. Last accessed: 16 July 2024.
54. Schulz J B et al. Diagnosis and treatment of Friedreich ataxia: a European perspective. Nat Rev Neurol. 2009;5(4):222-34.
What Happens When People Don’t Bolus for Extended Periods of Time While Using Control-IQ Technology?
This poster presentation took place on 22nd June 2024, as part of the American Diabetes Association (ADA) 84th Scientific Sessions held in Orlando, Florida, USA
Presenter: Miranda R. Polin1
1. Tandem Diabetes Care, San Diego, California, USA
Disclosure: Polin is an employee of Tandem Diabetes Care.
Acknowledgements: Miranda R. Polin, Andrew K. Johnson, Laurel H. Messer, Jordan E. Pinsker, and Alexandra Constantin were co-authors of the poster. Medical writing assistance was provided by Hannah Moir, EMJ, London, UK.
Disclaimer: Tandem Diabetes Care participated in the study design, research, analysis, data collection, and interpretation of data, as well as review and approval of the poster. All authors had access to relevant study data. No honoraria or payments were made for authorship. The t:slim X2 insulin pump is intended for the subcutaneous delivery of insulin, at set and variable rates, for the management of diabetes in persons requiring insulin. The pump is indicated for use in persons 6 years of age and greater.
Support: The study and publication of this article were funded by Tandem Diabetes Care.
Meeting Summary
Individuals with diabetes often face challenges in managing diabetes-related tasks such as glucose monitoring, insulin treatment, and maintaining glycaemic control, leading to a psychosocial burden. Integrating new devices and technologies into diabetes care is crucial to improve quality of life.
During the American Diabetes Association (ADA) Scientific Sessions in Orlando, Florida, USA, on 21st–24th June 2024, Miranda R. Polin, Senior Data Analyst at Tandem Diabetes Care in San Diego, California, USA, presented a poster entitled ‘What Happens When People Don’t Bolus for Extended Periods of Time while Using the t:slim X2 with Control-IQ Technology?’ summarising glycaemic data in relation to bolus administration. The study utilised real-world data from users of an automated insulin delivery (AID) system that incorporates continuous glucose monitoring (CGM) and an insulin pump with advanced hybrid closed-loop technology (t:slim X2TM with Control-IQ Technology, Tandem Diabetes Care, San Diego, California, USA) to automate insulin delivery.
Polin provided insight regarding the glycaemic control seen in users of Control-IQ Technology who do not manually bolus for prolonged periods of time. The study demonstrated a higher time-in-range (TIR; 3.9–10.0 mmol/L [70–180 mg/ dL]) on the days they did not bolus, compared with manual bolusing, without increasing the risk of hypoglycaemia. Polin suggested that when using systems such as ControlIQ Technology, even without user given boluses, adequate glycaemic control may be achieved under certain conditions. This opens up the possibility that closed-loop technology can positively impact outcomes even when user behaviours are not consistent.
Introduction
Individuals with diabetes, particularly Type 1, often require intensive insulin therapy.1 Polin highlighted the challenges of diabetes management, including monitoring glucose levels, carbohydrate counting, calculating insulin boluses, and administering multiple daily injections, particularly at mealtimes.1 Moreover, the burden of calculating carbohydrates before meals frequently results in missed boluses.2
Technological advancements such as CGM and AID systems have transformed diabetes care,3 with the ADA recommending such devices to achieve early glycaemic control, particularly in Type 1 diabetes.4 Advanced hybrid closed-loop systems, like the t:slim X2 with Control-IQ Technology, combine CGM with an insulin pump and proprietary algorithm to automate insulin delivery.3
This article reviews a study exploring real-world glycaemic outcomes in users who do not manually administer boluses for prolonged periods of time when using closed-loop Control-IQ technology.
Methods
Real-world data from 291,769 users of the t:slim X2 pump with Control-IQ technology (Figure 1) were obtained from the Tandem Diabetes Care t:connect database between January 2020–December 2023.
Polin explained that the proprietary algorithm aims to prevent hyperglycaemia by predicting CGM levels 30 minutes into the future and pre-emptively increasing basal
insulin delivery when glucose levels are predicted to be >8.9 mmol/L (>160 mg/dL). It also pre-emptively delivers an automatic correction bolus up to once an hour based on predicted glucose levels >10 mmol/L (>180 mg/dL) and attenuated to 60%, aimed at achieving a target of 6.1 mmol/L (110 mg/ dL; Figure 2). The purpose of this automatic correction bolus is to maximise TIR (3.9–10 mmol/L [70–180 mg/dL]) and mitigate hyperglycaemia that can occur for reasons such as when users do not consistently initiate meal boluses.3
Users of Control-IQ technology were included in the analysis if they had used the system for a minimum of 7+ consecutive days without user-initiated bolusing and ≤1 manual bolus per day (referred to as fully closed loop use). Users were categorised into four groups: 7 (1 week), 14 (2 weeks), 30 (1 month), and/or 182 (6 months) consecutive days of fully closed-loop use.
For the individuals who fell into the four categories above, data were analysed including TIR, i.e., the percentage of CGM recordings between 3.9–10 mmol/L (70–180 mg/dL) and time-below-range (<3.9 mmol/L [<70 mg/dL]) on days with fully closed loop use (without bolusing) and compared to days with user-initiated boluses.
Results
The study found approximately one in 10 users (28,790 out of 291,769 users) of Control-IQ technology had sustained periods (7+ days) without bolusing. The database contained 1,728,304 days without boluses, averaging 61 days per user.
Figure 1: Interface of continuous glucose monitoring with Control-IQ technology.
Daily Timeline
Figure 2: Examples of automatic correction boluses reducing hyperglycaemia in the absence of user-given boluses.
CGM Alerts: 9:07 PM - CGM Out of Range.
Event: CGM Alerts: 9:07 PM - CGM Out of Range.
Avg: average; Carbs: carbohydrates; SD: standard deviation; TDI: total daily insulin.
Overall, 27,688 users had periods of 7–13 consecutive days without user-initiated boluses, 11,127 users had periods of 14–29 consecutive days, 3,813 users had periods of 30–181 consecutive days (1–6 months), and 102 users had periods of 182 consecutive days or more (6+ months) without user-initiated boluses.
On days without boluses, median TIR was 62% (interquartile range: 50–74%) in all four groups (Figure 3a), whereas median TIR for days with boluses was 57–60% (interquartile range: 46–70%; Figure 3b). The time-belowrange was less than 0.6% for both days without boluses and days with boluses.
Glucose (mg/dL) Bolus (u)
(u/hr)
Discussion
The study identified that 10% of real-world users of Control-IQ technology have spent 7 days or more without bolusing. Polin reported that the burden of bolusing itself may be a potential reason, though it is not possible to ascertain from these data. Other reasons could include age-related behavioural factors, illness, medications, or changes in circumstances or therapy regimens, including diet control. Another poster presented at the ADA by Fu and colleagues used statistical simulations to demonstrate TIR outcome of 62% with Control-IQ technology when users did not bolus for small-medium carbohydrate meals (≤40 g carbohydrates), which suggests that lower carbohydrate diets may be a good strategy to maximise TIR when not giving boluses.2
One key finding was that glycaemic control in those who do not bolus for extended periods of time have slightly higher TIR (62%) on days when they do not bolus compared to days when they take manual boluses (57%), without an increased risk of hypoglycaemia. The automatic correction bolus is likely useful in counteracting
hyperglycaemia on the days without usergiven boluses and is a unique feature of Control-IQ technology. Further, the automatic correction boluses do not lead to additional hypoglycaemia, which is a theoretical (but not substantiated) concern. It is unclear why days with user-given boluses had a slightly lower TIR, though it is possible that when people have more hyperglycaemia, they are more inclined to give correction boluses to compensate (reverse causation). Regardless, these data indicate that closed-loop systems like Control-IQ technology may be helpful in maximising TIR, for those who do not, or find it difficult to, bolus consistently. The user and healthcare professional can maximise TIR by programming settings that match their behaviour, such as strengthening the correction factor to maximise the automatic correction bolus for those who do not bolus themselves.3 Polin suggested that Control-IQ technology may attenuate hyperglycaemia enough to be acceptable for glycaemic control in a subset of individuals.
Polin stated that such devices enable ease of use, reduce the need for manual input, and improve accessibility for those who
Figure 3: Percentage of time in and below range (3.9–10 mmol/L [70–180 mg/dL]) in Control-IQ technology users who have used the system without boluses for varying periods of time (“days in full closed-loop category”: A) on days with no user-given boluses (fully closed-loop use), compared with B) days with user-given boluses.
A B
struggle with carbohydrate counting and bolusing. Additionally, Polin noted such technologies have the potential to simplify and reduce the burden of diabetes care by making management more accessible, facilitating individuals in becoming more proficient in device use earlier on, rather than transitioning from one pump to another, ultimately freeing up time and improving quality of life.5
Overall, Control-IQ technology and other systems are valuable in reducing the burden of manual input and improving diabetes management for a wider range of individuals, in line with the ADA recommendations that diabetes technology should be offered to everyone.4
References
1. Pauley ME et al. Barriers to uptake of insulin technologies and novel solutions. Med Devices (Auckl). 2021;14:339-54.
2. Fu L et al. 951-P: The t:slim X2 with Control-IQ technology overcomes missed boluses for moderate meals. Diabetes. 2024;73(Suppl 1):951-P.
Conclusion
Findings from this study led the authors to recommend that healthcare professionals consider strategies to simplify diabetes management for those using Control-IQ technology, and not require consistent bolusing behaviour as a prerequisite for starting the system. Healthcare professionals can further maximise glycaemic outcomes by optimising settings such as correction factor, discussing low carbohydrate diets, and reviewing additional medications. This approach may reduce the need for stringent bolus behaviours and ultimately reduce the burden of diabetes.
3. Messer LH, Breton MD. Therapy settings associated with optimal outcomes for t:slim X2 with ControlIQ technology in real-world clinical care. Diabetes Technol Ther. 2023;25(12):877-82.
4. American Diabetes Association (ADA) Professional Practice Committee. Summary of Revisions: Standards of Care in Diabetes—2024. Diabetes Care. 2024;47(Suppl 1):S5-10.
5. Sherr JL et al. Automated insulin delivery: benefits, challenges, and recommendations. A consensus report of the Joint Diabetes Technology Working Group of the European Association for the Study of Diabetes and the American Diabetes Association. Diabetologia. 2023;66(1):3-22 [Epub ahead of print].
Clinical Practice Insights for Hyperpigmentation Treatment
Support: The publication of this article was funded by Beiersdorf AG.
Interview Summary
Hyperpigmentation disorders, a group of common skin conditions characterised by darkened patches due to excess melanin production, affect a significant portion of the global population, with women more frequently impacted than men. They are a leading reason for dermatology visits, particularly among people with skin of colour. Risk factors include genetic predisposition, medication use, and sun exposure, with visible light (VL) playing a significant role. While not physically harmful, the conditions, which include post-inflammatory hyperpigmentation (PIH), melasma, and solar lentigines (age spots) can lead to psychological distress and social stigmatisation. As such, they can have a significant impact on patients' self-esteem and quality of life (QoL).
Hyperpigmentation disorders are challenging to manage. Current treatments include over-the-counter and prescription oral and topical treatments, sunscreen, chemical peels, and laser therapy. However, all these treatments have limitations, and many are associated with side effects and complications, especially in darker skin tones. Hydroquinone, the gold standard of hyperpigmentation management for decades,
for example, can cause erythema, desquamation, and a burning sensation, and longterm use of high-concentration hydroquinone can result in exogenous ochronosis. In addition, chemical peels and laser therapy can trigger both irritation and PIH.
Isobutylamido-thiazolyl-resorcinol (Thiamidol), a tyrosinase inhibitor identified using recombinant human tyrosinase, is a promising addition to traditional treatments. It has shown efficacy in reducing hyperpigmentation with a good safety profile. As such, it has potential to enhance a holistic approach to hyperpigmentation disorder management.
Here, Thierry Passeron, University Hospital of Nice, France; Ncoza Dlova, University of KwaZulu-Natal, Durban, South Africa; and Vasanop Vachiramon, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand, talk about the evolving hyperpigmentation management landscape. They outline the impact, aetiology, pathophysiology, and current treatment approaches for hyperpigmentation disorders. They summarise the evidence base for Thiamidol and, reflecting on their own research and experience, they also explain how and why they are using the ingredient to enhance the management of hyperpigmentation in routine practice.
INTRODUCTION
Pigmentation disorders (PD) are common. A global survey of 48,000 people across 34 countries conducted between December 2022–February 2023 found that as many as 50% of the global population reported suffering from at least one pigmentation disorder. Women, the survey reported, were affected more frequently than men.1
While hypopigmentation refers to lightened areas of skin, hyperpigmentation describes darkened patches or lesions caused by the excess production, distribution, or transport of melanin.2 “Hyperpigmentation is one of the most common causes of dermatology visits, particularly in patients with skin of colour,” said Dlova.
Common hyperpigmentation disorders include PIH, melasma, solar lentigines, and ephelides (freckles).2 These conditions vary in appearance, have varying aetiologies, and their frequency depends on skin type (see Table 1), which is usually defined as per the Fitzpatrick scale of response to ultraviolet (UV) exposure:2
• Fitzpatrick skin Type I: white, very fair skin; red or blonde hair; blue eyes; freckles
• Fitzpatrick skin Type II: white, fair skin; red or blonde hair; blue, hazel, or green eyes
• Fitzpatrick skin Type III: cream white, fair skin; any eye or hair colour
• Fitzpatrick skin Type IV: brown skin (typical of Mediterranean descent)
• Fitzpatrick skin Type V: dark brown skin (typical of Middle Eastern descent)
• Fitzpatrick skin Type VI: black skin
PDs can have a significantly negative impact on QoL.1 Almost a third (28%) of the 48,000 people who responded to the global survey described above reported a Dermatology Life Quality Index (DLQI) score of >10 out of 30, indicating their lives were severely affected by their skin disease, with 44% saying they felt they had to conceal visible areas of affected skin.1 Passeron, who was part of the study team, said that melasma was the hyperpigmentation disorder with the highest impact on QoL. “The impact is highly dependent on culture and background,” he said, explaining that the impact can vary a lot depending on the patient. “It can be stigmatising. People say they feel dirty, and that their friends and family like them less because of the lesions,” he added. Dlova said people living with PIH and melasma often felt frustrated, stressed, or embarrassed. “They do not like having to wear makeup on a daily basis to camouflage melasma,” she said. “Some avoid taking pictures when they are with friends or sharing pictures on social media because
they are very conscious of pigmentation disorders.” Vachiramon said such disorders could be particularly impactful for people in public-facing occupations. “While it is not harmful to your general health, it can lead to a loss of confidence. I have one patient
with melasma who is an actor, and he has to conceal his affected skin. He has to wear make up every day, which is very difficult for him,” he explained.
Table 1: Types of hyperpigmentation disorder and susceptible populations.2
Hyperpigmentation Disorder
PIH
Irregular dark macules or patches
Melasma Well-defined brown or grey macules
Solar Lentigines Clearly defined macules between 1–3 cm. Light yellow to dark brown or variegated in colour
Ephelides Red or tan to light brown, sharply defined macules of 1–2 mm
HYPERPIGMENTATION: RISK FACTORS, AETIOLOGY, AND PATHOPHYSIOLOGY
The leading risk factors for hyperpigmentation disorders are genetic predisposition; medication side effects, such as antibiotics, oral contraceptives, antimalarials, and tricyclic antidepressants; and sun exposure.3 Importantly, blue light, or VL, plays a key role in the development of melasma and PIH by worsening lesions.4
Hyperpigmentation disorders have varying aetiologies and pathophysiologies. In those who are genetically predisposed to PIH, for example, dark patches can develop following skin inflammation or injury.3 Typical triggers of excess melanin production that lead to PIH include burns, wounds, acne, and other inflammatory dermatoses.3 Solar lentigines (age spots) and ephelides develop after sun exposure.2 Melasma, a chronic condition that can last for 10–20 years, with regular relapses during this time,5 has a very complex, multifaceted
Childhood onset after sun exposure in susceptible individuals
Fitzpatrick IV–VI (darker skin types)
Caucasian or Asian skin
Fitzpatrick I or II (lighter skin)
pathophysiology. Traditionally, it was thought to be closely related to pregnancy and oral contraceptives. However, only around 20% of cases start during pregnancy, and the impact of oral contraceptives appears to have only a weak influence on disease evolution,5 said Passeron. Onset is earlier in lighter skin types, and may occur later, sometimes post-menopausal, in Types V and VI.5 “The darker the skin, the later the melasma starts,” Passeron said, adding that vascularisation also plays a role, and there is increasing evidence to show that melanocytes are not the only cells involved in the development and relapse of the condition.5. Fibroblasts and sebocytes, he explained, play a key role. “Pregnancy is far from being the only thing at play here,” he added.
CURRENT TREATMENT
LANDSCAPE AND UNMET NEEDS
Hyperpigmentation treatment “can be a challenge”, said Dlova. “It takes time, and
Fitzpatrick III–VI (darker skin types)
treatment may be ineffective in some individuals. Sometimes there is only partial reduction of the pigmentation; however, patients are looking for complete clearance, and sometimes that is impossible.”
The first step is accurate diagnosis and an understanding of the individual patient, she went on. “You need to know what is causing the pigmentation. Is an underlying disease causing inflammation, and therefore pigmentation? Is it a pigment disorder, like melasma? How deep is the pigmentation? Look at the occupation of the patient and where they live: are they exposed to the sun a lot?” Vachiramon reiterated the patientcentric approach. “When you deal with a person who has this condition, you have to really understand what the exact cause of the hyperpigmentation is, because we approach treatment in different ways,” he said, going on to explain that the appearance of the lesions will guide diagnosis (see Table 1).
In most cases, advising the use of overthe-counter topical treatments, or cosmeceuticals, and protective sunscreen will be the first course of action. All three doctors emphasised the importance of products that block VL as well as UV light. “Sunscreens are used to minimise the pigmentation and enhance the efficacy of other topical creams,” said Dlova. “VL has been shown in the literature to trigger or exacerbate pigmentation in patients,3 so we need to make sure the product has protection against VL, yet most sunscreens do not.” When choosing a sunscreen, then, patients cannot rely solely on sun protection factor (SPF), which is a measure of how well it will protect the skin from UVB rays, said Passeron. “So far, the only way to protect against VL is to use a tinted product e.g., that contains iron oxide,” he said. His recommendation was to use a tinted sunscreen with high UVA and UVB protection, at the equivalent of a teaspoon’s worth on the face. He did, however, recognise the limitations of this approach. “That’s fine if you have an intermediate skin tone, but not if you have very light, Asian, or darker skin,” he said, explaining that appropriately-coloured tinted sunscreens were lacking for these patient groups. Wearing a tinted cosmetic over the top of a high-protection UVA/UVB
product can be a useful solution for some people with darker skin tones. However, the regimen can be time-consuming and burdensome. “People have to do it every day, and reapply during the day,” Passeron added.
Patients also need to be prepared for what lies ahead, particularly in melasma, said both Passeron and Vachiramon. “In the case of melasma, we need to remind people that this is a chronic disease that we cannot cure, and that can last 10–20 years,”5 said Passeron. “We need to really explain the crucial role of predisposing factors, especially sun exposure, in worsening melasma, and we need to tell them that they must apply sunscreen all year round.” Vachiramon added: “You have to tell your patient to be very patient, and that the use of sunscreen is very important for the prevention of future relapses.” While a number of cosmeceuticals are available for melasma, cost can also be an important factor, particularly in underresourced countries, Dlova went on. Many cosmeceuticals are marketed in small packs, which can be impractical for people with larger areas of hyperpigmentation, compounding a lack of affordability, she added. “You need to make sure they can afford the treatment.”
Medical Interventions
When people do not respond, or have an inadequate response, to cosmeceuticals and preventative interventions, dermatologists will tend to consider prescription approaches. There are a number of available treatments, many of which are often used in combination to target the cause of the hyperpigmentation, said Dlova. “We have a whole range of treatments for melasma and PIH. Some work together and have a synergistic effect,” she said. “You cannot only use one treatment. Depending on the pathogenesis of the disease, you have to target multiple pathways,” she went on. “In melasma, for example, you have to target the inflammation and inhibit the tyrosinase (the rate-limiting enzyme of melanin production), and there’s a whole vascular element to it as well. We have to use multiple treatments that target different pathogenic aetiologies.” Triple combination therapy (hydroquinone,
retinoic acid, and corticosteroid) is the recommended treatment for melasma.2 Passeron explained that for melasma, the combination, often called the Kligman’s Trio, would usually be delivered for 3–4 months. The patient would be advised to use cosmetic agents and sunscreen as maintenance therapy for the rest of the year, with annual administration of the combination being advised if necessary. For those who do not respond well to combination therapy, chemical peels, as well as light or laser therapy, may be options.2
Unmet Needs
The range of unmet needs in hyperpigmentation management stretches right the way along the treatment pathway. Passeron pointed to the lack of tinted, VL-protecting sunscreen products that are suitable for people with very light, Asian, or black skin, and Dlova highlighted that in many parts of the world, hyperpigmentation treatments were considered cosmetic, and therefore not covered by health insurance policies.
There are also important safety concerns around triple combination therapy. It has been associated with side effects, including erythema, desquamation, and a burning sensation, and long-term use of highconcentration hydroquinone can result in exogenous ochronosis, which is a blue-black hyperpigmentation.6 Furthermore, the use of hydroquinone has been linked to a potential risk of drug-induced carcinogenesis, leading to the compound being banned as a cosmetic ingredient in Europe.6
Both chemical peels and laser therapy also have their limitations. Passeron said peeling agents should only be advised during the winter months and should be used “with great care” in darker skin tones as they can worsen or trigger PIH.7 In terms of laser therapy, Vachiramon said there was no standard guidance on its use, with clinicians being guided instead by best practice advice. In his practice, he would usually suggest the approach if topical therapies yielded inadequate results after
2–4 months, or in patients who were unhappy to wait for them to take effect. However, it “can make the condition worse”, he said, adding it can remove hyperpigmentation caused by conditions such as melasma and solar lentigines, but leave dark spots of PIH on the skin.8 “This is common, especially among darker-skinned patients,” Vachiramon said.
Enhancing the treatment of hyperpigmentation disorders, then, is a priority for many dermatologists.
OPTIMISING HYPERPIGMENTATION MANAGEMENT WITH THIAMIDOL
Inhibiting the activity of tyrosinase, the rate-limiting enzyme of melanin, has been described as the safest and most effective way to treat hyperpigmentation.9 Despite the safety concerns, hydroquinone has been a mainstay of this approach for decades. Other tyrosinase inhibitors, such as kojic acid and arbutin, have been developed, but, as Passeron pointed out, they have not been compared to hydroquinone in a clinical trial. According to Mann et al.,9 the compounds’ “unsatisfactory efficacy” is largely due to them being tested on the only commercially available active tyrosinase, which is isolated from the mushroom Agaricus bisporus. The differences between the mushroom tyrosinase and mammalian enzyme both in terms of catalytic activities and substrate specificities, are significant.9 Thiamidol, however, is the first tyrosinase inhibitor that has been identified using a recombinant human tyrosinase construct.9
Thiamidol has been shown to be safe and effective in various forms of hyperpigmentation.9,10 Data show it can visibly reduce the appearance of solar lentigines within 4 weeks, with some being indistinguishable from the normal adjacent skin at 12 weeks, for example.9 One study asked women with mild-to-moderate melasma to treat one side of their face with a formulation containing 2% hydroquinone, and the other with a formulation containing Thiamidol.10 At 12 weeks, modified Melasma Area and
Severity Index (MASI) scores significantly improved on both sides, though by a significantly higher margin on the Thiamidoltreated side.10 The study also recorded that 79% of patients improved following treatment with Thiamidol, compared to 61% with hydroquinone.10 During treatment, no patients reported worsening of MASI on the Thiamidol side, while approximately 10% of patients saw worsening on the hydroquinonetreated side.10 Numerous studies have found Thiamidol to be well tolerated,9-11 and it has also been associated with QoL improvements.6,11 Vachiramon said: “I think this is one of the things we have been waiting for. We wanted something that worked very well, with fewer side effects, and I think that is what we get with this ingredient.”
Optimising Triple Therapy
In some studies conducted by independent researchers, Passeron said, Thiamidol has been shown to have similar efficacy as hydroquinone,6 but with a strong tolerance.9-11 As such, it has the potential to enhance existing hyperpigmentation treatment approaches. To investigate this hypothesis, his team carried out a 24-week, double-blind prospective randomised trial, comparing traditional triple therapy (the gold standard of melasma treatment since 1974) to a new trio that replaced hydroquinone with Thiamidol.6
A total of 40 participants living with melasma were randomised to receive either the new trio (0.1% Thiamidol, 0.1% retinoic acid, and 0.1% dexamethasone acetate) or traditional triple therapy (5% hydroquinone, 0.1% retinoic acid, 0.1% dexamethasone acetate). They applied the formulations, which were both prepared in the hospital pharmacy and had an identical appearance, to the whole face except the eye area, every evening for 12 weeks. Subjects in both arms were given the same volume of topical cream, in identical packaging, as well as SPF 50+ topical sunscreens to be applied until Week 24. The primary endpoint was a change in modified MASI (mMASI) score between baseline and Week 12. QoL, as measured by the Melasma Quality of Life scale (MelasQoL) score, was also assessed.
At Week 12, analysis included 20 patients in the traditional triple therapy group and 19 in the new trio group.6
At Week 12, there was an adjusted mean improvement in mMASI score of 63% from baseline in the new trio group. This compared to an improvement of 39% in the traditional triple therapy group. The adjusted mean difference between the groups was -1.49. While this did not reach statistical significance, as Passeron’s paper highlighted, the difference was clinically relevant. The adjusted mean improvement in the MelasQoL score at Week 12 compared with baseline was -12.57. This compared to a change of -6.66 in the traditional triple therapy group. Only the new trio group recorded a statically significant improvement of the MelasQoL.6
Passeron said: “We demonstrated that there was no statistical difference between the traditional trio and the new trio after 3 months. While there was a progressive worsening after cessation, there was no rebound, and this was similar in both groups.” Turning to tolerance, he said there was some irritation in both groups, but added that this was likely linked to the high concentration of retinoic acid.6
Based on these findings, Passeron’s department has removed the traditional trio from practice. Instead, the team is using the new trio, with a reduced 0.05% concentration of retinoic acid to improve tolerance, on the same basis as the traditional trio, i.e., 3 or 4 months a year, during the winter months, with recommendations for continuous use of sunscreen.
Asked why they had made the decision, he said the efficacy was at least as good as traditional triple therapy, but he found the tolerance to be much better. He also pointed to the QoL improvements seen in the study. “I think this really is an advance for the care of melasma,” he added.
The main limitation of Passeron’s study, the authors wrote, was that the majority of participants had lighter skin types. Only three participants had Type V skin, all of
whom were randomised to the traditional trio group, and none had Type VI.6
Managing Hyperpigmentation in Skin of Colour
Hyperpigmentation can be particularly challenging to manage in skin of colour. Many common treatments, including hydroquinone, chemical peels, and laser therapy, can all induce PIH, particularly in Fitzpatrick skin Types IV–VI. 11 A review of trials of Thiamidol in melasma and acnerelated PIH in skin of colour, published in 2024, concluded it was safe, effective, and a “reliable hyperpigmentation management option in this patient group”.11
A total of 234 participants, 232 of whom had skin of colour, took part in the four studies (three randomised controlled trials and one observational real-world study) reviewed in the paper. Of these, 141 had melasma, and 93 had acne-related PIH. All studies demonstrated that Thiamidol effectively reduced hyperpigmentation in both melasma and PIH, without “causing sensitivities which bear the risk of PIH”. One, an observational study of participants with skin Types V and VI, found that the treatment significantly lightened hyperpigmentation in the affected areas, without lightening the surrounding skin. This, wrote the authors, underlined that Thiamidol’s mode of action was gentle, without bleaching properties.11
Dlova, who conducted the observational study included in the review, said she had found the treatment to be especially effective in acne-related PIH. In the study, 32 participants with skin Types V (n=24) and VI (n=5) used the study skincare regimen of three Thiamidol-containing products (day cream SPF 30 and dual serum in the morning, and night cream before bed) every day for 12 weeks. They were asked to refrain from using any other skin products, except cleanser and sunscreen. Clinical grading of efficacy and irritation, as well as patient-reported assessments, were carried out at baseline and Weeks 4, 8, and 12. At 4 weeks, melanin index score of lesions was lower than at baseline (654.1 versus 733.4). At Week 8, researchers recorded a score of 656.7, and at the end of the treatment
period, a score of 632.7. In addition, melanin index only significantly lowered in lesional, not peri-lesional skin, resulting in a more even skin tone, rather than undesired lightening of dark skin tone. Improvements were statistically significant for all points in time when compared to baseline (p<0.001).
Skin evenness, as assessed by the investigator, improved by 13.8% at 4 weeks, 51.7% at 8 weeks, and 89.7% at 12 weeks. In addition, the proportion of participants agreeing with the statement ‘my dark spots appear less pronounced’ was 86.2% at 4 weeks, 89.7% at 8 weeks, and by the end of the study, 100%. In addition, overall tolerability was graded as excellent.12
Based on these and previous efficacy and safety data, Dlova said she now recommends Thiamidol in routine practice, particularly for acne-induced PIH, and explained that she had seen similar results in the clinic as those she observed during the trial.
In melasma, she feels it has potential to be used in combination with other available agents. “Thiamidol inhibits tyrosinase, but melasma is not just about that. There is an inflammatory component and there are other issues in the pathogeneses,” she said. “If I give it to patients with melasma, I combine it with retinoids, because they act in a different way, or with topical or oral tranexamic acid to address the vascular component.” Avoiding sun exposure and broad spectrum sunscreen with VL cover, she added, is a vital part of the treatment armamentarium.
Enhancing the Efficacy of Laser Treatment
The 2024 review of Thiamidol studies discussed earlier recommended future research should explore the potential benefits of combining Thiamidol with laser treatment to reduce the risk of laser-induced PIH.11 Vachiramon, who has examined this question in relation to solar lentigines, explained that PIH is a common complication of laser therapy, particularly in people with darker skin types. Laser-induced PIH affects between 10–47% of people.8
“Although there are several therapeutic options available for PIH, prevention is still
the best method,” he wrote in his 2023 paper, ‘Efficacy of isobutylamido thiazolyl resorcinol for prevention of laser-induced post-inflammatory hyperpigmentation: A randomized, controlled trial’ “For laserinduced PIH, few options exist regarding the prevention of this condition. Recently, isobutylamido thiazolyl resorcinol (ITR/ Thiamidol) has been reported as an effective tool for the prevention of UVBinduced hyperpigmentation. Therefore, we hypothesised that ITR might be able to prevent PIH due to other modalities as well.”8
The study included 24 people, and researchers selected three solar lentigines of a similar size and colour on each. The lesions were then randomised into three groups: twice-daily Thiamidol application, once-daily Thiamidol application, and no application, all for 2 weeks. Next, the patients underwent 532-nm QS Nd:YAG laser therapy. The primary outcome measure was incidence of laser-induced PIH, defined by worsening of the pigmented lesion compared to 2 weeks post-laser, at 4 and 8 weeks after laser treatment. At Week 4, the incidence of PIH was significantly lower in the twice-daily Thiamidol group, compared to the no-application group (20.83% versus 50.0%; p=0.028). Incidence in the once-daily treatment group at Week 4 was 29.17%. At Week 8, there was a higher incidence of PIH in the treated groups (twice daily: 16.67%; once daily: 8.33%) than the non-treated group (4.16%) though the difference between groups was not statistically significant. The authors hypothesised that the increase could be related to the reversible tyrosinase inhibitory effect of Thiamidol. No serious adverse events or stinging, burning, or contact dermatitis were reported in the Thiamidol-treated groups. The paper also recommended Thiamidol be continued, after laser therapy, to further inhibit tyrosinase. “Longer duration of application, including continuous application after the laser treatment and co-administration with other anti-inflammatory agents may result in more effective prevention of laser-indued PIH”, they concluded.8
In another study, he examined the use of Thiamidol in combination with laser
therapy in people with symmetrical facial hyperpigmentation. Twenty-four patients were treated with five weekly sessions of low-fluence Q-switched Nd:YAG 1064nm laser (LFQS). Afterwards, one side of the face was treated with Thiamidol and the other side received a placebo cream for 12 weeks. Patients were followed for 8 weeks after the last laser treatment, and relative lightness index (RL*I), Facial Hyperpigmentation Severity Score on the malar area (FHSSm), patient satisfaction, recurrence, and adverse events were all recorded. At Week 4, there was a higher mean RL*I improvement on the Thiamidoltreated side than the placebo-treated side (62.5% versus 47.3% improvement; p<0.05). The mean FHSS m reduced at a significantly higher percentage on the ITR-treated side than the placebo-treated side (54.4% versus 40.2% reduction; p<0.05). Partial recurrence was observed on both sides, and no serious side effects were noted. The paper concluded that combined Thiamidol and LFQS therapy was superior to LFQS monotherapy in the treatment of facial hyperpigmentation, and that Thiamidol “may serve as adjuvant” in this cohort.13
Reflecting on the results of his solar lentigines, Vachiramon said: “When we applied the cream for 2 weeks before the laser therapy, the number of patients with darkened skin 4 weeks after treatment was less. I think this shows that this is a good idea. The ingredient’s mechanism of action is to inhibit tyrosinase activity at the site, so even if the skin is burned during laser therapy, it cannot produce melanin.”
He went on to say that he is increasingly using Thiamidol in clinic, as it has been shown to be effective and well tolerated. “I think it should be one of the preventative tools that we offer our patients. It helps to reduce the volume of prescription medicine they use because patients can go and buy it themselves,” he said.
Prevention
There is also emerging evidence to suggest that Thiamidol could prevent hyperpigmentation. Vachiramon’s team has conducted a randomised, single-blinded,
pilot study to evaluate the efficacy and safety of ITR in the prevention of UV-induced hyperpigmentation. Each of the 20 healthy participants applied a product containing ITR to one arm for 3 weeks, before researchers induced UVB irradiation on both arms. Compared to the control, ITR-treated arms showed a statistically significant lower mean lightness index. In addition, the ITRtreated arms improved rapidly, with normal skin colour being observed at 3 weeks after the UVB induction. Clinical evaluation by a blinded, non-treating physician and by subjects was more favourable on the ITR-treated side than the control side (p<0.05). No significant side effects were noted. “ITR is an effective agent in the prevention of pigmentary change from UVB irradiation and may serve as a promising agent for preventing other hyperpigmentary conditions,” concluded the paper.14
FUTURE DIRECTIONS
Looking to the future, Passeron said he expected a deeper understanding of the pathophysiology of hyperpigmentation disorders to lead to topical treatments that target the underlying mechanisms of disease, particularly in melasma. “I do
References
1. Passeron at al. Pigmentation disorders: prevalence, impact on QoL and social stigmatization: results of the first international survey. Abstract 20433. World Dermatology Congress, 3-8 July, 2023.
2. Plensdorf S et al. Pigmentation disorders: diagnosis and management. Am Fam Physician. 2017;96(12):797804.
3. Thawabteh AM et al. Skin pigmentation types, causes and treatment – a review. Molecules. 2023;28(12):4839.
4. Lim HW et al. Photoprotection of the skin from visible light – induced pigmentation: current testing methods and proposed harmonization. J Invest Dermatol. 2021;141(11):2569-76.
5. Passeron T. Melasma pathogenesis and influencing factors – an overview of the latest research. J Eur Acad Dermatol Venereol. 2013;27(Suppl 1):5-6.
hope that one day we will be able to cure, or at least reduce relapses, in melasma,” he said. Dlova’s hopes for the future of hyperpigmentation management focused on increasing access to what can sometimes be expensive treatments, particularly in less resourced parts of the world. She also hopes for a wider recognition of the impact of these conditions, in order for their treatment to be covered by medical insurance.
Asked the same question, Vachiramon said he hoped the community would continue to build on its recent successes. “We are moving to options that have good efficacy with a high safety profile. It is great that we have the ingredients we have nowadays, but I hope that we will have many more ingredients that target different steps of the melanin synthesis in future. That would allow us to combine each of them, and further enhance the result of treatment.”
Summing up, Vachiramon added: “Most hyperpigmentation issues are cosmetic. They may not be harmful, but they can still have a negative impact on patients’ QoL, and they can lose their self-confidence. Yet, with the tools that we have nowadays, we can combat it, we can treat it, and we can improve our patients’ QoL.”
6. Bertold C et al. Efficacy and safety of a novel triple combination cream compared to Kligman’s trio for melasma: a 24‐week double‐blind prospective randomized controlled trial. J Eur Acad Dermatol Venereol. 2023;37(12):2601-7.
7. Moolla S, Miller-Monthrope Y. Dermatology: how to manage facial hyperpigmentation in skin of colour. Drugs Context. 2022;11:2021-11-2.
8. Vachiramon V et al. Efficacy of isobutylamido thiazolyl resorcinol for prevention of laser‐induced post‐inflammatory hyperpigmentation: a randomized, controlled trial. J Cosmet Dermatol. 2024;23(7):2450-7.
9. Mann T et al. Inhibition of human tyrosinase requires molecular motifs distinctively different from mushroom tyrosinase. J Invest Dermatol. 2018;138(7):1601-8.
10. Arrowitz C et al. Effective tyrosinase inhibition by thiamidol results in significant improvement of mild to moderate melasma. J Invest Dermatol. 2019;139(8):1691-8.
11. Schuster B, Sammain A. Hyperpigmentation in skin of colour: therapeutical benefits of isobutylamido‐thiazolyl‐resorcinol (Thiamidol®), an effective tyrosinase inhibitor, in phototypes IV–VI. JEADV Clin Prac. 2024;3:801-6.
12. Roggenkamp D et al. Effective reduction of post‐inflammatory hyperpigmentation with the tyrosinase inhibitor isobutylamido‐thiazolyl‐resorcinol (Thiamidol). Int J Cosmet Sc. 2021;43(3):292-301.
13. Vachiramon V et al. Combined isobutylamido thiazolyl resorcinol and low‐fluence Q‐switched Nd: YAG laser for the treatment of facial hyperpigmentation: a randomized, split‐face study. J Cosmet Dermatol. 2021;20(6):1724-31.
14. Vachiramon V et al. Isobutylamido thiazolyl resorcinol for prevention of UVB‐induced hyperpigmentation. J Cosmet Dermatol. 2021;20(3):987-92.
Interviews
This year, EMJ is thrilled to introduce key opinion leaders Tom Davenport, Babson College, Wellesley, Massachusetts, USA, and Rick Abramson, Vanderbilt University, Nashville, Tennessee, USA, whose interviews explore the future of AI in healthcare. Covering the ways in which AI is already helping patients today, as well as the collaboration between humans and technology, these expert interviews spotlight key discussions happening in the field today.
Featuring: Tom Davenport and Rick Abramson
Distinguished Professor of IT and Management, Babson College, Wellesley, Massachusetts, USA
You are an expert on all things AI, having authored multiple books, and given several talks on the subject, both with regard to business and medicine. So, in which areas of healthcare specifically is AI already being implemented? Would readers be surprised to find out about the use of AI in certain fields or tasks?
also effective mobile app-based AI systems for primary care practitioner use that perform triage, initial diagnosis, and initial treatment plans. They are very popular in China and South East Asia, but are not widely used outside of that region yet.
Q2
I think that medical generative AI models will become very good at diagnosis and treatment recommendations
For clinical applications of AI, it’s still early; most are unlikely to be found at the patient's bedside and are still in the research lab. There are plenty of potential breakthroughs in patient care, but they need to be refined, tested further, approved by regulators, and integrated into clinical processes. There are, however, many implemented examples of AI in administrative processes, including scheduling, payer approval, payment claim adjudication, and so forth. These typically don’t require regulatory approval and don’t have to be perfect, since they don’t involve direct patient care. There are
What, in your expert opinion, is the most groundbreaking application of AI in use today in the world of healthcare?
In terms of actual benefit to patients, I would point to the mobile app platforms in Asia, because they provide care to hundreds of millions of people who wouldn’t otherwise have access to it. In terms of what’s coming out of research labs, I would vote for the AI applications that enable much earlier diagnosis of neurological conditions like Alzheimer’s and Parkinson’s disease.
Tom Davenport
Q3
How does the use of AI in healthcare settings impact patient care? How might this continue to change in the future?
As I say, not much yet. But I believe it will be very influential in the fairly near future. I think that medical generative AI models will become very good at diagnosis and treatment recommendations, and they will broaden access to care enormously. AI systems are also making it possible for clinicians to spend more time listening to patients and providing care, rather than typing in symptoms to electronic health record systems or clinical notes.
Q4
In one of your many books, ‘Advanced Introduction to Artificial Intelligence in Healthcare’, you discuss how AI might impact policymakers; can you expand on these possibilities for our readers?
It will be the job of policymakers and regulators to determine when and under what circumstances we incorporate AI into our healthcare systems and processes. There will be many voices for and against particular AI incursions, and it will be difficult to decide when to allow it. Over time, however, I believe that the combination of human clinicians and intelligent systems will provide better care than we have today. There will
be many consumers and patients who will take their care into their own hands with the help of AI if they are not allowed to work with clinicians who are augmented with the technology.
Q5
Much of your work talks about human collaboration with smart systems; what are the best examples of this that you have come across in your career? Is there a specific approach that you encourage people to take when it comes to collaboration with technology?
I almost always feel that smart humans and smart machines working together are more effective than working alone. But that collaboration will take many
different forms. Already in surgical robots, for example, the surgeon makes all the critical decisions, and the robot executes them. I think the first step is for clinicians and administrators to sit down and discuss what the desired collaboration should look like in any given situation, and work toward achieving that. The best examples that I have seen try to limit the role of an AI system so that there is a clear role for human clinicians to contribute their expertise and override the AI-based recommendation if they deem it necessary.
Q6 As a distinguished professor, do you believe that AI should now have a place in the classroom, both as a tool and a topic to learn about?
Yes, I think it’s inevitable, and I and many colleagues are already working with students
to determine how best to use it effectively. The keys to success, I believe, are the same as in health care: to maintain involvement by students and teachers, and to think critically about how to make the outputs of AI better.
Q7
Much of the discourse surrounding the increased use of AI has to do with job security, as I am sure you are aware. Do you believe there is any validity to concerns about AI one day taking jobs from humans, especially in healthcare settings?
It’s important to keep monitoring that issue, of course. However, thus far there has been little or no job loss from AI in healthcare or any other field, except from robots in manufacturing. There is a shortage of doctors and nurses in almost every part of the world these days, so anything that could improve their productivity
and give them more time with patients would be a positive step. Healthcare is also too expensive for many people and governments today, so bringing down the cost with AI would also be a positive outcome.
Thus far there has been little or no job loss from AI in healthcare
What motivated you to explore the intersection of radiology and AI, having previously worked in several different sectors?
Q2Could cutting-edge technology, including AI, ease the burden on overworked providers while simultaneously enhancing the quality of care?
I have worked previously in healthcare management consulting, health services research, clinical practice, and healthcare administration. As such, I am all too familiar with the myriad challenges we face in healthcare. A few years ago, when I was in a physician-executive role at HCA Healthcare, I had the opportunity to look out over what was transpiring within a vast USAbased for-profit health system, and I saw some disturbing trends. Volumes, whether measured in facility admissions or patient visits or procedures, were skyrocketing, but the supply of available providers was dwindling. That meant the workload on any given provider was rising exponentially, and providers were working harder and longer than ever before. This translated into both flagging morale and diminishing care quality.
At that time, I reasoned that healthcare needed to follow other industries and look to technology for a solution. Could cuttingedge technology, including AI, ease the burden on overworked providers while simultaneously enhancing the quality of care? I was so intrigued by this driving question that I left HCA and joined the startup world, where I have been for the past 3 years. I would say this is the most exciting area I’ve ever worked in, both for the opportunities and for the challenges presented by this exhilarating technology.
During your lecture at the European Congress of Radiology (ECR) earlier this year, you highlighted the limitations of AI. What do you believe are the most significant challenges that need to be addressed to advance AI in healthcare?
I am an optimist regarding the opportunities AI offers for healthcare, but we must acknowledge some significant obstacles to overcome before we can progress forward. As a community, we are now transitioning from AI as a research project into AI as a part of realworld clinical workflows. With that transition come some very important questions: are the AI tools addressing important problems, or are they merely fancy solutions to problems that have already been addressed? To advance the adoption of AI tools in the clinical setting, we cannot be satisfied with merely demonstrating the diagnostic performance of the tools. We must also evaluate their practical usefulness within realworld workflows, and we must demonstrate the incremental value of AI-enabled workflows over the status quo.
For example, let’s consider an AI tool for fracture detection. When evaluating such a tool, we cannot focus exclusively on its performance in standalone testing. We must also look at how the tool will be deployed in clinical workflows and what effect that deployment will have on the downstream outcomes we care about. If the tool is accurate for detecting easy fractures but
struggles to detect the fractures that radiologists tend to miss, the incremental value added by the AI tool might be quite small. So perhaps we need to focus on the difficult edge cases and look at fracture detection rates with the AI tool versus without. But we cannot stop there, because even if there is an improvement in fracture detection rates, we must convince ourselves that this improvement makes a long-term difference in patient care. If we can’t demonstrate such an improvement in patient care, maybe there are other reasons to adopt the AI tool, for example, perhaps the tool offers a beneficial effect on care pathway efficiency. But we can’t just assume that effect; we must demonstrate it affirmatively to justify the adoption of the tool.
Beyond evaluating AI tools and demonstrating their effect on long-term outcomes, we have other, more practical challenges to address. In most countries, AI tools are still not reimbursed by payers, which means providers must pay for these tools
themselves, and this in turn means that AI developers must show how deployment of these tools will generate a return on investment over a reasonable time horizon. In jurisdictions where AI tools are purchased by governmentrun facilities, the procurement process is often bureaucratic and cumbersome, and it may differ wildly from facility to facility.
Regulatory approval is another big challenge: most countries have not yet updated their regulatory frameworks to accommodate modern AI tools, and developers often struggle under the weight of excessive regulatory burden. But perhaps the biggest obstacle of all is ourselves; we, the healthcare community, still tend to look at AI with ambivalence and mistrust, some of us because of a fear of replacement, others because of legitimate concern for uncertainties and risks. Until we convince ourselves that AI technology is both safe and worthwhile, adoption will proceed quite slowly.
Q3
How do you balance the use of AI in radiology with the need to maintain human oversight and patient safety?
This is a crucial question, and it’s one we all need to be asking. Physicians, developers, administrators, regulators, and investors; we all share the responsibility of ensuring that AI in healthcare is adopted in an ethically responsible manner, with patient safety as our top priority. If an AI tool would make providers more efficient but at the expense of patient care quality, that’s a tool we should avoid adopting.
With that having been said, I might challenge the fundamental notion of a ‘balance’ or trade-off between technology adoption and patient safety. Of course, we want to make sure that new technology is not biasing physicians to the detriment of patient care or removing important human safeguards that keep patients safe. But we must also acknowledge that new technology might actually enhance patient safety. We know that errors are
unfortunately quite prevalent in medicine, and we are already seeing examples of how AI can prevent errors and misses; in this respect, we may actually have a moral responsibility to push AI adoption forward. We also need to be more open-minded about where human control is necessary to maintain patient safety and where automation might keep patients safer.
Q4
In your experience, what are some of the most promising applications of AI in public health screening and early cancer detection?
Well, we have archetypal examples for each: tuberculosis screening for the public health initiative and mammography for early cancer detection. Both applications are being transformed quite dramatically by AI software, to the point where I believe the workflows for both tuberculosis screening and mammography will be entirely different in 5 years from where they are today.
But we also have other emerging applications of AI for large-scale population screening. We see AI being used in early-detection initiatives for other cancers, particularly lung cancer. We see AI being deployed for early detection of chronic conditions like congestive heart failure and chronic obstructive pulmonary disease, in hopes that early identification will keep patients healthy for longer and also reduce expensive hospital admissions for acute disease exacerbations. And we even see AI being used to identify patients with low skeletal muscle mass for targeted nutrition and exercise interventions. I am optimistic that AI technology will accompany a shift in our public health focus from identifying disease that is already present to
preventing disease before it arises.
Q5
Having pioneered international teleradiology, what insights can you share about the integration of AI in teleradiology practices?
I’m not sure I would qualify as a ‘pioneer’; I would save that label for those brave entrepreneurs who introduced the world to an entirely new way of practising radiology. However, I was indeed among the first wave of international teleradiologists, before remote practice became commonplace. Back then, nobody knew whether teleradiology was just a temporary fad or whether it would become mainstream. At first, teleradiology grew and became popular simply because it allowed radiologists to avoid overnight call. But as overnight teleradiology grew more prevalent, radiology practices found they had no choice but to sign up with a teleradiology provider, because without overnight coverage they could not recruit and retain radiologists who increasingly expected overnight teleradiology as a standard part of their practice environment. In my days at HCA, daytime teleradiology coverage was becoming an important alternative to traditional on-site diagnostic radiology in those parts of the USA that were having trouble recruiting radiologists.
I think teleradiology has more growth ahead, now that we have found (in the post-Covid world) an even greater acceptance for remote diagnostic work. Regarding AI technology, I have noticed that teleradiology firms seem to be among the earliest adopters. I think that’s for a few reasons: first, teleradiology practices tend to be quite innovative, as they are continually
questioning traditional workflows and pushing the bounds of how to improve the operational side of radiology. Second, they operate at scale in an extremely competitive market environment where small differences in operational efficiency may have huge effects on profitability. I look to teleradiology as somewhat of a bellwether, an early indicator of which AI tools the market will find most useful and how quickly those tools will be adopted.
Q6 What role do you see for AI in addressing the current challenges of overworked and understaffed radiology departments?
There is enormous possibility here, but only if we can achieve the magnitude of efficiency gains we need. Current state-of-the-art AI tools can deliver 10% efficiency improvements, but that’s not enough to address the workforce staffing challenges we face. We really require efficiency gains that would double or triple our productivity, and that magnitude of workflow improvement can only come through the automation of diagnostic reporting. All the major AI software developers are working on automated ‘draft’ reporting, and the race is on to see if and when this technology will be ready for large-scale clinical deployment.
I expect we will see adoption of automated reporting not all at once, but in waves. First, we will see the integration of low-level automation into more complex, human-driven pathways, such as AI replacing the second reader in double-reader mammography workflows. Then we will see AI become the single reader in underserved regions, especially those locations that are overwhelmed with plain film
volumes. And steadily we will march on, towards more and more automated draft reporting in more regions and for more workflows, until radiology becomes much more automated than it has been in the past.
Q7
How important is interdisciplinary collaboration between clinicians, researchers, and policymakers in developing effective AI solutions in healthcare?
Interdisciplinary collaboration is absolutely crucial. Researchers are the engine for advancing technology, but they need to understand from clinicians what problems are the most pressing and what solutions will be practical for clinical workflows. Clinicians need to maintain dialogue with researchers in both the design phase and also the testing and evaluation phase, and of course, they will be the adopters of new technology as it is refined. Policymakers establish the regulatory and market frameworks needed to incentivise both development and adoption in keeping with healthcare system requirements. Co-creation of AI solutions is therefore paramount if we are to see the advancement of technically
sound, clinically effective, and policy-compliant technology.
Q8
You were formerly global Chief Medical Officer at Annalise.ai; can you elaborate on the core features of Annalise.ai’s enterprise products and how they enhance diagnostic interpretation in radiology?
Annalise.ai is a global leader in the development of advanced AI applications for medical imaging. Its software solutions are regulatory-cleared and commercially available in 40 countries. Annalise has separated itself from the competition by developing ‘comprehensive’ diagnostic support solutions, that is, solutions that report on dozens of imaging findings within a particular modality in contrast to the single-finding algorithms of some competitors.
Annalise has enjoyed rapid expansion in several markets; for example, it recently won multiple tenders within the British National Health Service (NHS) and will soon be processing one-third of all chest X-rays obtained in the UK. I recently relinquished my full-time role as Annalise’s Chief Medical Officer, but I am proud of what we accomplished as a
team during my tenure, and I look forward to serving Annalise in an advisory role going forward.
Q9 What is next for you in the field of AI and healthcare?
I’ve been going fairly hard for the last few years, so I’ll take a little bit of a break before jumping back into a full-time role. In the short term, I plan to do some clinical work, and I will also spend a fair bit of time advising investors on capital deployment and helping policymakers to focus resources. In the long term, I plan to remain focused on the intersection of technology, clinical practice, and the market and policy environments. It’s a complex space full of excitement and opportunity. I look forward to seeing what the future brings, not just for myself but for all of healthcare!
We see AI being used in early-detection initiatives for other cancers, particularly lung cancer
Lebrikizumab▼: Short and Long-Term Disease Control
IL-13 is the key cytokine in the skin of patients with AD1
IL-13, but not IL-4, shows increased gene expression in AD skin1
IL-13-producing CD4+ cells are increased with disease severity in the skin2
Mechanism of Action of Lebrikizumab
Lebrikizumab selectively targets IL-13 and inhibits its signalling3,5,6
Lebrikizumab binds to IL-13 with high affinity and slow off-rate, thereby blocking the downstream effects of IL-13 with high potency7
Lebrikizumab
IL-13 signalling: X X
Type II receptor Skin structural cells and myeloid cells
Lebrikizumab does not interfere with the IL-13 endogenous regulation mechanism of the decoy receptor3,5,6
The IL-13+lebrikizumab complex can still bind to IL-13Rα2
Lebrikizumab
Key Lebrikizumab Data: Monotherapy ADvocate
Short-term efficacy from ADvocate 1 and ADvocate 2 trials: >50% patients achieved EASI-75 at Week 16
LEB Q2W Placebo
*Missing data due to lack of efficacy or data after rescue medication usage were imputed with NRI. Other missing data were imputed with MI. **P<0.001 versus placebo
The most common adverse reactions are conjunctivitis (6.9%), injection site reactions as monotherapy through Week 52 or in combination with TCS through Week 56 is
Abbreviations
AD: atopic dermatitis; CD4: cluster of differentiation 4; EASI: Eczema Area and Severity Index; IL-13: interleukin-13; IL-13Rα: interleukin-13 receptor subunit alpha; IL4Rα: interleukin-4 receptor alpha; IGA: Investigator Global JAK: Janus kinase; LEB: lebrikizumab; mMPP: modified maintenance primary population; mITT: modified intention-to-treat; Q2W: every 2 weeks; Q4W: every 4 weeks; Rα: receptor α; SCORAD: SCORing Atopic Dermatitis;
References:
1. Tsoi LC et al. Atopic dermatitis is an IL-13-dominant disease with greater molecular heterogeneity compared to psoriasis. J Invest Dermatol. 2019;139(7):1480-9.
2. La Grutta S et al. CD4(+)IL-13(+) cells in peripheral blood well correlates with the severity of atopic dermatitis in children. Allergy. 2005;60(3):391-5.
3. Bieber T. Interleukin-13: targeting an underestimated cytokine in atopic dermatitis. Allergy. 2020;75(1):54-62.
4. Napolitano M et al. The hidden sentinel of the skin: an overview on the role of interleukin-13 in atopic dermatitis. Front Med. 2023;10:1165098.
5. Moyle M et al. Understanding the immune landscape in atopic dermatitis: the era of biologics and emerging therapeutic approaches. Exp Dermatol. 2019;28(7):756-68.
6. Lytvyn Y, Gooderham M. Targeting interleukin 13 for the treatment of atopic dermatitis. Pharmaceutics. 2023;15(2):568.
7. Okragly AJ et al. Binding, neutralization and internalization of the Interleukin-13 antibody, lebrikizumab. Dermatol Ther (Heidelb). 2023;13(7):1535-47.
8. Silverberg JI et al. ADvocate 1 and ADvocate 2 Investigators. Two phase 3 trials of lebrikizumab for moderate-to-severe atopic dermatitis. N Engl J Med. 2023;388(12):1080-91.
9. Blauvelt A et al. Efficacy and safety of lebrikizumab in moderate-to-severe atopic dermatitis: 52week results of two randomized double-blinded placebo-controlled phase III trials. Br J Dermatol. 2023;188(6):740-8.
10. European Medicines Agency (EMA). Lebrikizumab summary of product characteristics. Available at: https://www.ema.europa.eu/en/documents/product-information/ebglyss-epar-product-information_ en.pdf. Last accessed: 9 April 2024.
Moderate-to-Severe AD Through Selective IL-13 Inhibition
increased in AD2 , with levels correlating
IL-13 drives several key signs and symptoms of atopic dermatitis3,4
Moderate Severe
Severity (SCORAD)
from La Grutta S et al. 20052
ADvocate 1 and ADvocate 2 trials8,9
Long-term efficacy from ADvocate 1 and ADvocate 2 trials:†
More than 80% of Week 16 per-protocol responders maintained EASI-75 with Q4W monotherapy between Weeks 16 and 52
Week 52*
Maintenance of EASI-75 at Week 52 in lebrikizumab Week 16 responders
Indication and Posology 10
Maintenance of IGA (0/1) with ≥2 point reduction from baseline at Week 52 in lebrikizumab Week 16 responders
†Lebrikizumab per-protocol responders were re-randomised to continue lebrikizumab Q2W, or move to lebrikizumab Q4W or a placebo-withdrawal arm. Per protocol-specified criteria for having a response to lebrikizumaban: IGA score of 0 or 1 with a reduction of ≥2 points from baseline or a 75% improvement in the EASI score without rescue medication use.
reactions (2.6%), conjunctivitis allergic (1.8%), and dry eye (1.4%). The safety profile of lebrikizumab is consistent with the safety profile observed up to Week 16.10
Global Assessment; ITT: intention-to-treat; Dermatitis; TCS: topical corticosteroids.
UK-Adverse event should be reported. Reporting form and information can be found at MHRA https://yellowcard.mhra.gov.uk or search for MHRA Yellow Card in the Google Play or Apple Store. Adverse events should also be reported to Almirall Ltd. Tel. 0800 0087 399.
Lebrikizumab:
• Lebrikizumab is indicated for the treatment of moderateto-severe AD in adults and adolescents ≥12 years with a body weight ≥40 kg who are candidates for systemic therapy.
• Recommended dose of lebrikizumab is 500 mg (two 250 mg injections) at both Week 0 and Week 2, followed by 250 mg administered subcutaneously every other week up to Week 16. Once clinical response is achieved, the recommended maintenance dose of lebrikizumab is 250 mg every fourth week. Click
• Selectively binds IL-13 with high affinity and inhibits its downstream signalling
• Has demonstrated short- and long-term efficacy in signs and symptoms of moderate to severe AD
• Shows a consistent safety profile in short- and long-term use7
• Is
every 4 weeks as maintenance therapy
Improving Assessment of Steatotic Liver Disease with Non-invasive
The publication of this infographic was sponsored by GE HealthCare | EMJ. 2024;9[3]:48-49. https://doi.org/10.33590/emj/GJUN4017.
A Call to Arms
WHO, EASL, AASLD, and APASL are among the 17 organisations calling for global action on SLD,1 a leading cause of liver-related morbidity and mortality2
Early detection and management of MASLD can prevent progression to MASH, resulting in:
Better outcomes: ~10–25% of patients with MASH may develop advanced fibrosis and cirrhosis
Lower health and societal costs: In Europe, MASH was responsible for up to €1,292 million of healthcare costs and €41,536 to €90,379 million of DALY-related wellbeing costs in 20184’
Ultrasound-Guided Attenuation
SLD is the new nomenclature for the metabolic-associated fatty liver disease spectrum, including:2 MASH, formerly NASH2
MASLD, formerly NAFLD2
Caused by a build-up of fat in the liver6
Usually asymptomatic5
A ects more than one-third of adults, and more than one in 10 children1
Global prevalence increased by 50% between 1991‒20197
The Assessment Pathway
Liver biopsy remains the gold standard for detecting SLD,11 but:
MRI-PDFF is a non-invasive technique to accurately evaluate liver fat fraction,6 but: it is invasive11
it is expensive6 there is limited access6 there is inter/intraobserver variability11
The most severe form of MASLD8 Can lead to cirrhosis, liver failure, and liver cancer9
Over 16% of people with MASLD have MASH10
Traditional B-mode ultrasound: requires specialist sonographer expertise13 low sensitivity in patients who are severely obese12 intraobserver subjectivity
UGAP is well correlated to MRI-PDFF13 cheaper and more accessible than MRI6 provides staging information to guide management6
MASLD is a global health emergency. Early diagnosis is key to preventing progression to MASH
Abbreviations:
Liver
and unfeasible large-scale
AASLD: American Association for the Study of Liver Diseases; of the Liver; DALY: disability-adjusted life year; EASL: European metabolic dysfunction-associated steatohepatitis; MASLD: metabolic disease; MRI-PDFF: magnetic resonance imaging proton density disease; NASH: non-alcohol steatohepatitis; SLD: steatotic liver attenuation parameter; WHO: World Health Organization. Products mentioned
biopsy
Non-invasive Ultrasound-based Technique
Attenuation Parameter (UGAP)
Non-invasive quantifiable image guided techniques expand adoption of ultrasound
GE HealthCare’s UGAP solution, on the LOGIQ™ ultrasound portfolio:
Automated measurement algorithm for optimum measurement range14
Guided image acquisition for quantifiable, repeatable results
Well correlated to MRI-PDFF,13 with proven cut-o values16 breathing manipulations15 patient positioning15 patient diet status15 large-scale use reproducible results, even for non-ultrasound experts, including nurses and technicians
UGAP
new international nomenclature for steatotic liver disease: one step forward towards enhanced awareness for healthier life. Eur J Intern Med. 2023;117:1-2.
3. Lekakis V, Papatheodoridis GV. Natural history of metabolic dysfunction-associated steatotic liver disease. Eur J Intern Med. 2024;122:3-10.
4. Allen AM et al. Healthcare and socioeconomic costs of NAFLD: a global framework to navigate the uncertainties. J Hepatol. 2023;79(1):209-17.
5. Eskridge W et al. Metabolic dysfunction-associated steatotic liver disease and metabolic dysfunction-associated steatohepatitis: the patient and physician perspective. J Clin Med. 2023;12(19):6216.
6. Lauschke VM. Practice guidance documents for the diagnosis and management of non-alcoholic fatty liver disease-recent updates and open questions. Hepatobiliary Surg Nutr. 2023;12(5):780-4.
7. Younossi ZM et al. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): a systematic review. Hepatology. 2023;77(4):1335-47.
8. Piazzolla VA, Mangia A. Noninvasive diagnosis of NAFLD and NASH. Cells. 2020;9(4):1005.
9. Petta S et al. The first MASH drug therapy on the horizon: current perspectives of resmetirom. Liver Int. 2024;DOI:10.1111/liv.15930.
10. Pedrosa M et al. Global prevalence of nonalcoholic steatohepatitis (NASH): findings from a targeted literature review. Value in Health. 2018;21:S82.
11. Ryu H et al. Reproducibility of liver sti ness measurements made with two di erent 2-dimensional shear wave elastography systems using the comb-push technique. Ultrasonography. 2019;38(3):246-54.
12. de Moura Almeida A et al. Fatty liver disease in severe obese patients: diagnostic value of abdominal ultrasound. World J Gastroenterol: WJG. 2008;14(9):1415.
Bende F et al.
New Developments in Clinical Trials for Osteoarthritis: Are We Closer to Improving Pain Management and Disease Modification?
Editor's Pick
My editor’s pick for this issue is an insightful review article in which the authors discuss the future of therapeutic agents in osteoarthritis, targeting inflammation, pain, and cartilage regeneration. Though there are currently no effective disease-modifying anti-rheumatic drugs licensed for the treatment of osteoarthritis, which affects 10 million people in the UK, Sofat and colleagues concluded that the present Phase II and III trials show promising results for the future.
1. Institute for Infection and Immunity, St George’s, University of London, UK 2. St George’s University Hospitals NHS Trust, London, UK *Correspondence to nsofat@sgul.ac.uk
Disclosure: This work was supported by the National Institute for Health and Care Research (NIHR) Academic Clinical Fellowships to Ahmed (ACF-2021-16-002) and Feather (ACF-2023-16-003). The authors have declared no conflicts of interest.
Disclaimer: The views expressed in this publication are those of the authors and not necessarily those of the NHS, NIHR, and the Department of Health or Social Care.
Osteoarthritis (OA) is a chronic condition that can lead to pain, disability, and loss of function. There are currently few pharmacological treatments, and none are disease modifying. It is important to identify new treatments to reduce associated morbidity, as well as high costs to the individual and society. OA pathogenesis involves the cartilage, synovium, and bone, with many mediators in the immune system implicated in this process. These provide several targets for pharmacotherapy that can be divided into treatments that target pain or disease-modifying drugs that aim to maintain the joint. Previous OA trials conducted have failed to either meet efficacy or safety measures. Notably, antinerve growth factor drugs that were superior to placebo had several adverse events that subsequently limited their usage. The aim of this paper is to highlight the current treatments under investigation that are in Phase II and III of development.
This review searched trials that have been registered on clinicaltrials.gov with the term “osteoarthritis” and a primary completion date of 2021 or after that are in Phase II and III. This identified 252 studies, 52 of which were included in the review after screening and eligibility checks, that were then categorised as either targeting pain and inflammatory pathways or disease-modifying osteoarthritis drugs. Two further papers were included as they present two distinct therapies for hand OA. The results showed numerous avenues in development, with promising results, and provides hope to reduce the global burden of morbidity. It is important that these treatments are affordable for this chronic condition.
Key Points
1. Osteoarthritis (OA) is a common arthritic condition, affecting 10 million people in the UK alone. There are currently no effective disease-modifying anti-rheumatic drugs licensed for the treatment of OA.
2. This study was a narrative review of clinical trials identified from clinical trials databases to identify Phase II and III studies with a primary completion on or after December 2021. The authors identified 52 studies categorised as either targeting pain modulation /inflammatory pathways or disease-modifying OA drugs that were reviewed in this article.
3. There is a strong pipeline of drug discovery with Phase II and III trials of new therapeutic agents in OA that are targeting several pathways including inflammation, pain, and cartilage regeneration.
INTRODUCTION
Osteoarthritis (OA) is the most common arthritis worldwide, causing pain, disability, and loss of function due to chronic joint disease 1 The most affected joint is the knee, followed by the hand and hip.1 Knee OA makes up 85% of the clinical burden of disease 2 There is a higher prevalence of radiologically evidenced OA compared to symptomatic OA 2 Significant costs are associated with the disease, including direct costs such as medication and surgery, but also indirect costs due to early retirement and loss of work.2 There remains a huge unmet need to develop new treatments for OA. This narrative review will discuss the pathogenesis of OA, current management, and clinical trials exploring new treatment avenues.
Pathogenesis
OA is an active disease in which there is an imbalance of repair and destruction of the whole joint 2 It involves all structures, including hyaline articular cartilage, subchondral bone, capsule, synovium, and periarticular muscles.2 It is theorised there are numerous subtypes, such as neuropathic, inflammatory, and metabolic, which allow for different treatment targets 3
In the early stages of damaged cartilage repair, increased chondrocyte activity is apparent. By-products of this increased activity include matrix degradation compounds and pro-inflammatory mediators, which lead to dysregulation of chondrocyte function. These by-products affect the adjacent synovium leading to tissue hypertrophy and increased vascularity 4 There is a predominance of macrophages in the synovitis seen in OA, reflecting a more focused innate immune response compared to rheumatoid arthritis . 5 The effects on subchondral bone lead to increased bone turnover and subsequent vascular proliferation invades the cartilage. The development of subchondral bone marrow lesions (BML) is observed.2 BMLs can be best visualised on T2-weighted, fat-saturated MRIs as hyperdense diffuse lesions. There is a consensus now that the presence and frequency of BMLs correlate with pain.6 The abnormal loading leads to damage and remodelling, evidenced on histological analysis by subchondral bone trabecular thickening, cysts, angiogenesis, and new nerve formation.7
Degradation of cartilage is caused by IL-1β, which binds to synoviocytes, leading to the production of matrix metalloproteinases,
cyclooxygenase-2, prostaglandin E2, and nitric oxide. This accelerates degradation via nuclear factor kappa-B and MAPK signalling pathways. Cartilage destruction is further enhanced by IL-1β triggering downstream gene expression of proteolytic enzymes including the disintegrin and metalloproteinase with thrombospondin motifs (ADAMTS), also known as aggrecanases. TNF-α also plays a role in coordinating an inflammatory response and release of matrix metalloproteinases. Hence, there are many pro-inflammatory cytokines involved in OA pathogenesis that could be potential targets for novel treatments.
Current Treatment Therapies
There is good consensus on management strategies from stakeholders 8,9 First-line treatment is non-pharmacological. This includes education, exercise, weight loss, and walking aids. Encouragement of self-management is important; patient outcomes improve if interventions around non-pharmacological measures are used.10 Key messages to communicate to people with OA are about treatment approaches, the disease pathophysiology, and imaging.11 One important message is the importance of a personalised exercise plan, best delivered by a therapist, as they can consider the complexities of a patient’s situation. Two systematic reviews found exercise reduces pain, improves physical function, and improves quality of life.12,13 Another systematic review found no radiographic progression of disease or increase in pain in elderly patients who undertake low-impact exercise.14
Topical nonsteroidal anti-inflammatory drugs (NSAID) are recommended. A systematic review of 43 studies found NSAIDs superior to a placebo, with a 0.3 effect size for relieving pain and 0.35 for improving function. In the study and general population, no serious gastrointestinal and renal side effects were reported.15
Paracetamol is no longer seen as first-line after it was found to be only minimally effective when compared to placebo, while still having an adverse effect profile.16 While paracetamol can be useful in clinical practice, it should be used carefully to
avoid unwanted side-effects. Oral NSAIDs are effective in managing pain; however, they have significant cardiovascular and renal side effects that need to be noted in certain patient groups. Due to these side effects, NSAIDs should be started after medical advice and for limited time periods. Guidelines suggest using concurrent proton-pump inhibitors or cyclooxygenase-2 inhibitors in appropriate patients without co-existing conditions.17
Duloxetine has been found to be efficacious in the treatment of OA 18 Centrally acting analgesics, such as nortriptyline, were compared to a placebo in a randomised control trial (RCT) in New Zealand, where it was found to have no benefit at 14 weeks for reducing pain.19
Intra-articular steroids are used for short term pain relief and as an adjunct therapy. However, regular injections are not recommended as it is associated with a greater loss of cartilage volume when compared to placebo, which was shown in a 2-year study using triamcinolone 20 Current guidelines do not favour the repeated use of corticosteroid injections for OA.
Recent Failed Treatment Targets
Many theoretical treatments have been tried and tested, with a failure to translate into clinical efficacy from animal models.21 A meta-analysis by Singh et al.,22 looked at nine studies that used colchicine in RCTs for hand and knee OA and found there was no significant improvement in pain or function.
Nerve growth factor (NGF) is implicated in pain modulation in OA.23 NGF enhances neurotropic and nociceptive pathways by interacting with its receptor, tropomyosin receptor kinase A (TrkA), modulating the pain pathway. Due to its role in the mediation of pain, pain therapies using monoclonal antibodies have been developed (e.g. tanezumab, fulranumab, and fasinumab). Tanezumab was tested in a Phase III trial and was shown as superior compared to a placebo.23 The safety profile of NGF agents has been questioned, as a dose-dependent side effect is the development of rapidly progressive osteoarthritis (RPOA) 24,25 This
has been related to the co-prescription of NSAIDs 24,25 One possible hypothesis for this side effect is that reduction in pain leads to increased weight bearing, causing increased tissue damage to the joint. Concerns over RPOA have led to NGF-neutralising antibodies’ use being limited to those with palliative diagnoses.26
TrkA inhibitors are also being investigated due to their role in the same pathway. Despite promising pre-clinical trials, a Phase II trial using an oral TrkA inhibitor failed to meet its primary endpoint of an improvement of Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain subscale.27 A proof-of-concept study found an intra-articular injection of a TrkA inhibitor to be effective in significantly reducing WOMAC scores at 4 weeks; however, at 12 weeks the difference was no longer statistically significant. Comparably, intraarticular steroid injections demonstrated joint pain reduction for a maximum of usually 3 weeks 28 Although, 67.3% of those who received the treatment had injection joint inflammatory reactions.
The paper proposes that in the clinical setting this could be masked or ameliorated by coprescription of other analgesic medication.28 Unlike NGF inhibitors, no damage to the joints or evidence of RPOA was noted at the end of the trial 28
Since there are currently no diseasemodifying drugs available to treat OA, there has been a large growth in clinical trials investigating novel therapeutics for OA, which will be discussed further in this review.
METHODS
The authors conducted an electronic search of clinicaltrials.gov to identify clinical trials. It was chosen as the most comprehensive database for clinical trials. This was a structured search, limited to trials in Phase II and III and with a completion date on or after December 2021 to keep the review current. Initially, studies that were not regarding osteoarthritis and its treatment were excluded. A focus was put on pharmacological trials, and trials that were
addressing gene therapy/mesenchymal stem cells were removed as there was a limited word count and this could be covered in a future larger review. The exclusion criteria also included existing therapies, as they are well understood. The authors sought to describe the compounds’ mechanism of action and target receptors. Where possible they discussed the merits of the trials, the foundation on which the trial was chosen (previous Phase I data).
The search term “osteoarthritis” was used and all Phase II and III trials with a primary completion on or after December 2021 were included. They identified 252 studies in total. Trials that were terminated, withdrawn, or whose status was unknown were excluded. Trials that were beyond the scope of this review were gene therapy, mesenchymal stem cells, and surgery trials, which were excluded. They also excluded trials of nonpharmacological management of OA. The 52 remaining studies are discussed in this study. Important trials that were published during this review but not available on clinicaltrials. gov are also discussed (Figure 1).
RESULTS
The search yielded 52 studies, which were categorised as either targeting pain modulation/inflammatory pathways or disease-modifying osteoarthritis drugs. They are summarised in Table 1 with their mechanism of action and drug names.29-80
Treatments Targeting Pain and Inflammation
There are nociceptive pain receptors in the synovium and joint capsule but not in the cartilage. Pain sensitisation is indicated in OA joints, showing evidence of plasticity, as in normal ageing joints the number of nociceptive receptors should decrease. Pain pressure thresholds are decreased in people with OA, indicating central sensitisation.81-83
Botulinum Toxin Type A has a role in pain modulation. A systematic review in 2019 showed that at 4 and 8 weeks there are benefits compared to placebo in Visual Analogue Scale (VAS) and WOMAC.84 A
Table 1: Summary of potential therapies under investigation with a completion date in 2021 or later.
LNA043 ANGPTL3 protein mimetic Chondrocyte stimulation
ADAMTS: a disintegrin and metalloproteinase with thrombospondin motifs; AMP: adenosine monophosphate; ANGPTL3: angiopoietin-like 3; CCR2: chemokine receptor 2; CNS: central nervous system; GLP1: glucagon-like peptide 1; NF-κβ: nuclear factor kappa-B; NLRP3: pyrin domain-containing protein 3; PDE: phosphodiesterase; PTH: parathyroid hormone; TRPA1: transient receptor potential cation channel, subfamily A, member 1; TRPV1: transient receptor potential vanilloid subtype.
current trial is looking to check for superiority over hyaluronic acid.33
Transient receptor potential vanilloid subtype 1 antagonists and modulators have been seen as a potential target of therapy. Capsaicin can induce pain desensitisation of peripheral nociceptors after an initial transient increase in pain. Low pH and heat can also activate the channel. Previously several trials were terminated due to adverse effects associated with hypothermia and impaired noxious heat sensation 85 There are current trials with Resiniferatoxin in progress (see Table 1).
Similarly, transient receptor potential cation channel, subfamily A, member 1 is involved in pain sensitisation, triggered by temperature and noxious stimuli. A recent study testing of the drug LY3526318 in patients with osteoarthritis did not find a statistically significant difference from placebo.54
LEVI-04 is a fusion protein in which the Gc portion of human immunoglobulin is fused with the neurotrophin receptor, currently in OA trials.86
It works by binding to the excess neurotrophins, unlike the anti-NGF that blocks all NGF; therefore, it is hoped that it will not produce the same side effects.
In OA pathogenesis, there is an increase of reactive oxygen species from mitochondria due to cartilage destruction. This has proven a good target for preventing post-traumatic OA in mouse models. Amobarbital blocks mitochondrial ETC member complex I and is now being investigated as an intra-articular injection in humans 30,96
There are two current trials looking at using angiopoietin-like 3 signalling pathways that work by promoting chondrogenesis.46,47 This following a successful Phase I trial showed it preserves and regenerates cartilage in vivo in OA models and it met its primary safety endpoint.97
Chemokine ligand CCL1 7 is a T cell chemokine. Elevated levels in OA are associated with elevated pain pressure thresholds 98 As well T cell interactions, it is known to affect granulocyte-macrophage colony-stimulating factor. Animal studies have shown a lack of OA pain in CCL17
Record screened (n=252)
Trials assessed for eligibility (n=199)
Identification
Record excluded (n=53)
Trials excluded:
Reason 1: Mesenchymal stem cell or gene therapy (n=77)
Reason 2: Existing therapies (n=33)
Reason 3: Alternative medicine or supplements (n=14)
Reason 4: Non-pharmacological management (n=20)
Reason 5: Surgical treatments (n=3)
Studies included in review (n=52)
gene-deficient mice 99 The role of CCL17 in OA is not fully understood. After successful Phase I trials with anti-CCL17, there is a current Phase II trial underway to find the optimum dose for pain management 99
An IL-1 inhibitor, canakinumab, a monoclonal antibody, is in Phase II trial.34 Despite being found in small amounts in synovial fluid, posthoc analysis of the CANTOS trial showed a reduction in joint replacements of those patients on canakinumab.100 There was no difference in WOMAC pain scores of VAS in a Phase II trial of intra-articular canakinumab.101 However, a current Phase II trial is testing LNA043 and canakinumab. LNA043 is a modified version of angiopoietin-like 3, which is discussed above.
Macrophages play a role in chronic inflammation, with chemokine receptor 2 playing a major role in the migration and recruitment of monocytes into tissues.102 To target this inflammatory signalling process a small molecule antagonist, CNTX-6970, is in
a Phase II trial.60 Animal models have shown a reduction in pain.102,103
The NOD-Like receptor family, pyrin domaincontaining protein 3 (NLRP3) inflammasome pathway leads to the reduction of proinflammatory cytokines, such as IL-1β, IL-6 and TNF-α, that result in joint destruction and pain.104 Targeting this with an oral small molecule called DPV890 that binds and locks the pyrin domain-containing protein 3 inflammasome. It has been tested for various other conditions, including COVID-19, and there is a current Phase II clinical trial in patients with knee OA.41,104
Human growth hormone intra-articular injections stimulate the proliferation of chondrocytes and Type 2 collagen 105 A Phase II trial is testing growth hormone injection and will assess response to pain and cartilage regeneration.42
MEDI7352 is a monoclonal antibody which targets TNF-α and NGF, reducing the inflammatory cascade. It continues to
Figure 1: Modified prisma flow diagram.
be studied in a Phase II trial despite the halting of anti-NGF trials, which target similar pathways.57
A novel drug named MMII, a suspension of empty large multilamellar liposomes composed of dimyristoylphosphatidylcholine and dipalmitoylphosphatidylcholine, is given as an intra-articular injection and works by providing lubrication in the joint. The results of a recent Phase IIb trial did not show a persistent statistically significant result in the reduction of WOMAC pain assessment; however, there were nominally differences in pain scores of 1 mL and 3 mL preparations and it was well tolerated.106
Oxytocin is an endogenous hormone that plays a role in bone metabolism via osteoblastogenesis and chrondrogenesis. Low levels of oxytocin have been shown in patient with osteoarthritis compared to those without in an in vitro study; there are two ongoing clinical trials to understand this process.63,64,107
Semiglutide has revolutionised Type 2 diabetes and weight loss management. It decreases blood glucose, promotes satiety, and reduces hunger by mimicking glucagon-like peptide 1. A current trial, STEP-9, will compare Semiglutide against a placebo and measure their WOMAC pain scores and weight.74,108
Another avenue of pain relief is targeting somatostatin receptor 4, which is involved in pain pathways and not involved in the endocrine actions of somatostatin. Immune cells and neurons are directly inhibited 109 This novel target is being investigated in a Phase II trial.55
Teriparatide is a synthetic form of parathyroid hormone with 34 active amino acids and is used in the treatment of osteoporosis for its role in calcium homeostasis. It has a potential role in chondrocyte regeneration, which is not well understood. Furthermore, it leads to denervation in subchondral bone, reducing pain.110 There is a current Phase II trial comparing it to placebo.75
Disease-Modifying Treatments
A meta-analysis found that bisphosphonates, a class of drugs known to inhibit osteoclast action, showed limited efficacy for pain relief in OA 111 However, there are two current trials looking at intravenous zolendronate or intraarticular clondronate.31,32
WNT signalling is part of cellular homeostasis, it determines osteoblast and chondrocyte lineage specification. Lorecivivint is an intraarticular agent that is a potential diseasemodifying osteoarthritis drug.112 It modulates the WNT signally pathway by inhibiting intranuclear kinases CDC like kinase 2 and dual specificity tyrosine phosphorylation kinase 1A. In pre-clinical trials, this was effective in reducing inflammation, enhancing chondrogenesis and chondrocyte function.113
A recent Phase IIa, however, did not meet its primary endpoint of improvement in the WOMAC subscale for pain at Week 13.112 An ongoing Phase III trial has shown continued safety of the medication and an improved WOMAC pain and function scores at 12 months; despite this, at 18 months postinjection there is a loss of this effect 114
Phosphodiesterase inhibitors stop nitric oxide-mediated chondrocyte damage 115 Clitazol, normally used for the treatment of peripheral vascular disease, is a selective Type 3 phosphodiesterase, stopping the breakdown of cyclic adenosine monophosphate (AMP) and shown to prevent cartilage destruction in rats and human cartilage samples.115,116 There is a current proof-of-concept trial comparing this against conventional therapy in Egypt.117
An endpoint in OA is bone sclerosis as subchondral bone undergoes changes. Cathepsin K is primarily expressed in osteoclasts, chondrocytes, and synoviocytes, which is a cysteine protease that is involved in bone resorption.118,119 In mice with no cathepsin K, there is a high bone mass and lack of bone resorption. MIV-711 was identified as showing beneficial effects in OA and is a selective inhibitor.119 A recent RCT showed cathepsin K inhibitor had no effect on improved pain scores, but significantly reduced bone and cartilage progression 120
A potential target is ADAMTS-5 as it breaks down aggrecan. After successful Phase I trials, a Phase II trial of GLPG1972 did not meet the primary endpoint of a substantial change in the cartilage thickness compared to placebo.121 However, there are other trials currently underway with a different inhibitor, M6495, has already shown it can work ex vivo with bovine and human tissue, preserving cartilage.122 It had a successful Phase I trial showing its safety in humans, and there is now scope for further research in this area.123 There is a Phase II trial of QUC398 an intra-articular injection, targeting ADAMTS-5, which in mouse studies showed when targeted there is a reduction in pain and cartilage degeneration 79,124
A previous study of an ADAMTS-5 inhibitor failed at the Phase II stage.1 25
TPX-100 is a synthetic fragment of extracellular matrix phosphoglycoprotein, which is downregulated in OA. In animal studies, it causes articular cartilage proliferation. A Phase II clinical trial of intraarticular injection of TPX-100 found it reduced pain at 4 weeks but did not reach significance in improving patellar cartilage structure.126 It was well tolerated and there was a reduction in analgesic use. Post-hoc analysis, looking at those with moderate-to-severe bilateral tibiofemoral OA, revealed there was slower femoral bone shape change at 6 and 12 months 127
Plasma rich platelets (PRP) are an autologous blood product with a rich amount of growth factors, which has anti-inflammatory properties and reduces pain 128-130 IL-1β, TNF-α, and fibroblast growth factor are some of the catabolic cytokines that are inhibited. A systematic review comparing PRP to hyaluronic acid found it didn’t improve function but reduced pain.131 The review had issues with heterogeneity in and between studies.131 There are variations in how PRP is produced between different studies, which could account for the differences seen in efficacy outcomes.128,131 Possible variations included the amount of blood drawn, centrifuge speeds, and time. Issues with blinding in studies meant there was a possibility of a strong placebo effect.131,132 It is currently not recommended in guidelines 8,9,128
Iguratimod is a small molecule that protects the joint through immunomodulation. It inhibits NF-κβ activation, which prevents the release of inflammatory cytokines. It is used in Japan, and a current trial are looking into its effectiveness in hand OA.44
There are several clinical trials investigating metformin (Table 1). Its main action is mediated via the 5’ AMP-activated protein kinase. It leads to cartilage preservation, immunomodulation, and reduction in pain. Previous human trials were of lower quality and high risk of bias 133
Important Emerging Therapies Beyond This Search
A randomised, double-blind, placebocontrolled trial in hand OA in participants with evidence of MRI-evident synovitis showed methotrexate 20 mg once weekly had positive results. There was a moderate effect size of 0.45 at 6 months, and no effect was seen until 3 months in keeping with drug-effect in inflammatory arthritis.134 Future research could identify whether this effect persists beyond 6 months. Denosumab is anti-resorptive medication used in osteoporosis, it works by targeting RANK ligand and stopping it from activating RANK receptor found on osteoclasts. A recent Phase IIa trial of denosumab in participants with erosive hand OA showed it prevented progression of the disease 135 However, a previous study of denosumab use in knee OA showed it was not useful in symptoms or structure, although the studies had different endpoints, with the latter focusing on BMLs as a marker of progression.136
CONCLUSION
Various approaches are currently in progress to address the gap in effective therapies for OA. These range from cartilage regeneration to suppression of localised inflammation that activates inflammatory pathways inducing tissue breakdown. Since the primary symptom of OA is pain, many studies are focusing on the modulation of pain. Any treatments which are developed will need to be safe, efficacious, and cost-effective in managing this chronic condition. The enormous prevalence and chronicity mean
treatments need to be inexpensive to not burden health systems. This could focus on pain modulation and structural modification
References
1. Long H et al. Prevalence trends of site-specific osteoarthritis from 1990 to 2019: findings from the global burden of disease study 2019. Arthritis Rheumatol. 2022;74(7):1172-83.
2. Hunter D J, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393(10182):1745-59.
3. Yuan C et al. Classification of four distinct osteoarthritis subtypes with a knee joint tissue transcriptome atlas. Bone Res. 2020;8(1):38.
4. Loeser R F et al. Articular chondrocytes express the receptor for advanced glycation end products: potential role in osteoarthritis. Arthritis Rheumatol. 2005;52(8):2376-85.
5. Wood M J et al. Macrophage proliferation distinguishes 2 subgroups of knee osteoarthritis patients. JCI Insight. 2019;4(2):e125325.
6. Sofat N, Kuttapitiya A. Future directions for the management of pain in osteoarthritis. Int J Clin Rheumatol. 2014;9(2):197-276.
7. Koushesh S et al. The osteoarthritis bone score (OABS): a new histological scoring system for the characterisation of bone marrow lesions in osteoarthritis. Osteoarthr Cartil. 2022;30(5):746-55.
8. Kloppenburg M et al. 2018 update of the EULAR recommendations for the management of hand osteoarthritis. Ann Rheum Dis. 2019;78(1):16.
9. Kolasinski S L et al. 2019 American College of Rheumatology/Arthritis Foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Rheumatol. 2020;72(2):220-33.
10. Wang S Y et al. Physical Therapy Interventions for Knee Pain Secondary to Osteoarthritis. Ann Intern Med. 2012;157(9):632-44.
11. French S D et al. What do people with knee or hip osteoarthritis need to know? an international consensus list of essential statements for osteoarthritis. Arthritis Care Res. 2015;67(6):809-16.
12. Juhl C et al. Impact of exercise type and dose on pain and disability in knee osteoarthritis: a systematic review and meta-regression analysis of randomized controlled trials. Arthritis Rheumatol. 2014;66(3):622-36.
13. Fransen M et al. Exercise for osteoarthritis of the knee. Cochrane
in OA that are distinct treatment targets and how research into therapeutics needs to address both aspects.
Database of Systematic Reviews. 2015. Available at: https://doi.wiley. com/10.1002/14651858.CD004376. pub3. Last accessed: 16 March 2023.
14. Quicke J G et al. Is long-term physical activity safe for older adults with knee pain?: a systematic review. Osteoarthr Cartil. 2015;23(9):1445-56.
15. Zeng C et al. Relative efficacy and safety of topical non-steroidal antiinflammatory drugs for osteoarthritis: a systematic review and network metaanalysis of randomised controlled trials and observational studies. Br J Sports Med. 2018;52(10):642.
16. Negrini F, Negrini S. Is paracetamol better than placebo for knee and hip osteoarthritis? a cochrane review summary with commentary. Int J Rheum Dis. 2020;23(4):595-6.
17. Bannuru R R et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr Cartil. 2019;27(11):1578-89.
18. Osani M C, Bannuru RR. Efficacy and safety of duloxetine in osteoarthritis: a systematic review and meta-analysis. Korean J Intern Med. 2019;34(5):966.
19. Hudson B et al. Nortriptyline for pain in knee osteoarthritis: a double-blind randomised controlled trial in New Zealand general practice. Br J Gen Pract. 2021;71(708):e538.
20. McAlindon T E et al. Effect of Intraarticular triamcinolone vs saline on knee cartilage volume and pain in patients with knee osteoarthritis: a randomized clinical trial. JAMA. 2017;317(19):1967-75.
21. Malfait A M, Little C B. On the predictive utility of animal models of osteoarthritis. Arthritis Res Ther. 2015;17(1):1-14.
22. Singh A et al. Efficacy and safety of colchicine for the treatment of osteoarthritis: a systematic review and meta-analysis of intervention trials. Clin Rheumatol. 2023;42(3):889-902.
23. Berenbaum F et al. Subcutaneous tanezumab for osteoarthritis of the hip or knee: efficacy and safety results from a 24-week randomised phase III study with a 24-week follow-up period. Ann Rheum Dis. 2020;79(6):800-10.
24. Hochberg M C et al. When is osteonecrosis not osteonecrosis?: adjudication of reported serious adverse joint events in the tanezumab clinical development program. Arthritis
Rheumatol. 2016;68(2):382-91.
25. Teichtahl A J, Cicuttini F M. Editorial: pain relief in osteoarthritis: the potential for a perfect storm. Arthritis Rheumatol. 2016;68(2):270-3.
26. Zhao D et al. Does anti-nerve growth factor monoclonal antibody treatment have the potential to replace nonsteroidal anti-inflammatory drugs and opioids in treating hip or knee osteoarthritis? A systematic review of randomized controlled trials. EFORT Open Rev. 2022;7(7):470-80.
27. Watt F E et al. Tropomyosin-related kinase A (TrkA) inhibition for the treatment of painful knee osteoarthritis: results from a randomized controlled phase 2a trial. Osteoarthr Cartil. 2019;27(11):1590-8.
28. Krupka E et al. Efficacy and safety of intra-articular injection of tropomyosin receptor kinase A inhibitor in painful knee osteoarthritis: a randomized, double-blind and placebocontrolled study. Osteoarthr Cartil. 2019;27(11):1599-607.
29. CARE ARTHRITIS LTD. Osteoarthritis of the Knee, Inflammation, and the Effect of Adalimumab (OKINADA). NCT02471118. https://clinicaltrials.gov/ show/NCT02471118.
30. J L Marsh, University of Iowa. Translating Metabolic Responses to Mechanical Insult Into Early Interventions to Prevent PTOA. NCT04589611. https:// clinicaltrials.gov/show/NCT04589611.
31. Morten Halkjær Iversen, Martina Hansen's Hospital. The Effect of Zoledronic Acid on Patients With Osteoarthritis of the Hip. NCT04303026. https://clinicaltrials.gov/show/ NCT04303026.
32. SPA Società Prodotti Antibiotici S.p.A. Clinical Trial to Assess Efficacy, Tolerability of Rising Doses of Clodronate in Painful Knee Osteoarthritis Patients. NCT06263517. https://clinicaltrials.gov/ show/NCT06263517
33. University Hospital, Strasbourg, France. Trial Comparing Botulin Toxin Versus Hyaluronic Acid by Intraarticular Injection for the Treatment of Painful Knee Osteoarthritis (GOTOX). NCT02832713. https://clinicaltrials.gov/ show/NCT02832713.
34. Novartis Pharmaceuticals. A Safety and Efficacy Study of Anti-inflammatory (Canakinumab) and Cartilage Stimulating (LNA043) Drugs Injected Into the Knee Joint of Participants With Knee Osteoarthritis (OA). NCT04814368.
https://clinicaltrials.gov/show/ NCT04814368.
35. Steven E Harte, PhD, University of Michigan. Cannabinoid Interactions With Central and Peripheral Pain Mechanisms in Osteoarthritis of the Knee. NCT04992624. https://clinicaltrials.gov/ show/NCT04992624
36. Jonathan Vela, Aalborg University Hospital. CBD Treatment in Hand Osteoarthritis and Psoriatic Arthritis (NordCAN). NCT03693833. https:// clinicaltrials.gov/show/NCT03693833
37. NYU Langone Health. Cannabidiol (CBD) in Pain Reduction for Knee Osteoarthritis. NCT05020028. https://clinicaltrials.gov/ show/NCT05020028
38. Chad Brummett, University of Michigan. Cannabidiol for Postoperative Opioid Reduction in Primary Total Knee Arthroplasty (CORK). NCT06234631. https:// clinicaltrials.gov/show/NCT06234631
39. Mahmoud Samy Abdallah, Sadat City University. The Phosphodiesterase 3 Inhibitor Cilostazol as an Adjunct to Conventional Therapy in Patients With Osteoarthritis. NCT04789837. https:// clinicaltrials.gov/show/NCT04789837
40. Maurizio Fava, MD, Massachusetts General Hospital. A Study to Evaluate the Safety and Efficacy of CNTX-6970 in Subjects With Knee Osteoarthritis Pain. NCT05025787. https:// clinicaltrials.gov/show/NCT05025787.
41. Novartis Pharmaceuticals. Study of Efficacy, Safety and Tolerability of DFV890 in Patients With Knee Osteoarthritis. NCT04886258. https:// clinicaltrials.gov/show/NCT04886258.
42. John Sledge, BioShift Life Sciences. Human Growth Hormone Injections in the Knee Joint to Treat Osteoarthritis. NCT06354023. https://clinicaltrials. gov/show/NCT06354023.
43. GlaxoSmithKline. A Dose-Finding Study to Evaluate the Efficacy and Safety of GSK3858279 in Adults With Knee Osteoarthritis Pain (MARS-17). NCT05838742. https://clinicaltrials. gov/show/NCT05838742.
44. Peking University People's Hospital. Efficacy and Safety of Iguratimod in Patients With Hand Osteoarthritis (ESIGO). NCT05216757. https:// clinicaltrials.gov/show/NCT05216757.
45. Levicept. Clinical Trial to Evaluate the Efficacy and Safety of LEVI-04 in Patients With Osteoarthritis of the Knee. NCT05618782. https:// clinicaltrials.gov/show/NCT05618782.
46. Novartis Pharmaceuticals. Study of Safety, Tolerability, Preliminary Efficacy of Intra-articular LNA043 Injections in Patients With Articular Cartilage Lesions and Knee Osteoarthritis. NCT03275064. https:// clinicaltrials.gov/show/NCT03275064.
47. Novartis Pharmaceuticals. Study of Efficacy, Safety, and Tolerability of LNA043 in Patients With Knee
48. Biosplice Therapeutics, Inc. A Long-Term Safety and Efficacy Study of Lorecivivint in Subjects With Osteoarthritis of the Knee. NCT04520607. https://clinicaltrials. gov/show/NCT04520607.
49. Biosplice Therapeutics, Inc. A Study Utilizing Patient-Reported and Radiographic Outcomes and Evaluating the Safety and Efficacy of Lorecivivint (SM04690) for the Treatment of Moderately to Severely Symptomatic Knee Osteoarthritis (STRIDES-X-ray). NCT03928184. https://clinicaltrials. gov/show/NCT03928184.
50. Biosplice Therapeutics, Inc. A Study Utilizing Patient-Reported Outcomes to Evaluate the Safety and Efficacy of Lorecivivint (SM04690) for the Treatment of Moderately to Severely Symptomatic Knee Osteoarthritis (STRIDES). NCT05603754. https:// clinicaltrials.gov/show/NCT05603754.
51. Biosplice Therapeutics, Inc. A Study Utilizing Patient-Reported Outcomes to Evaluate the Safety and Efficacy of Lorecivivint (SM04690) for the Treatment of Moderately to Severely Symptomatic Knee Osteoarthritis (STRIDES-1). NCT04385303. https:// clinicaltrials.gov/show/NCT04385303.
52. Eli Lilly and Company. Chronic Pain Master Protocol (CPMP): A Study of LY3016859 in Participants With Osteoarthritis. NCT04456686. https:// clinicaltrials.gov/show/NCT04456686.
53. Eli Lilly and Company. A Master Protocol Study (LY900028) of Multiple Intervention-Specific-Appendices (ISAs) in Participants With Chronic Pain (CPMP). NCT05986292. https:// clinicaltrials.gov/show/NCT05986292.
54. Eli Lilly and Company. Chronic Pain Master Protocol (CPMP): A Study of LY3526318 in Participants With Osteoarthritis. NCT05080660. https:// clinicaltrials.gov/show/NCT05080660.
55. Eli Lilly and Company. Chronic Pain Master Protocol (CPMP): A Study of LY3556050 in Participants With Osteoarthritis. NCT04627038. https:// clinicaltrials.gov/show/NCT04627038.
56. Eli Lilly and Company. A Chronic Pain Master Protocol (CPMP): A Study of LY3857210 in Participants With Chronic Low Back Pain. NCT05630196. https:// clinicaltrials.gov/show/NCT05630196.
57. AstraZeneca. A Study of the Efficacy and Safety of MEDI7352 in Subjects With Painful Osteoarthritis of the Knee (BESPOKE). NCT04675034. https:// clinicaltrials.gov/show/NCT04675034.
58. Mahmoud Samy Abdallah, Sadat City University. The AMPK Modulator Metformin as a Novel Adjunct to Conventional Therapy in Patients With Knee Osteoarthritis. NCT04767841. https://clinicaltrials.gov/show/ NCT04767841.
59. Amany Abd Elaal Mohamed Aiad, Tanta University. Metformin as Adjuvant Therapy in Obese Knee Osteoarthritis Patients. NCT05638893. https:// clinicaltrials.gov/show/NCT05638893.
60. Delowar Hossain, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh. Effect of Metformin as Add-on Therapy to Ibuprofen on Disease Activity in Knee Osteoarthritis Patients. NCT06126029. https:// clinicaltrials.gov/show/NCT06126029.
61. Mostafa Bahaa, Tanta University. Metformin Safety and Efficacy in Osteoarthritis. NCT06231758. https:// clinicaltrials.gov/show/NCT06231758.
62. Sun Pharmaceutical Industries Limited. Efficacy and Safety of MM-II for Treatment of Knee Pain in Subjects With Symptomatic Knee Osteoarthritis. NCT04506463. https://clinicaltrials. gov/show/NCT04506463.
63. University of Florida. Understanding Cognition, Oxytocin & Pain in Elders (UCOPE). NCT03878589. https:// clinicaltrials.gov/show/NCT03878589.
64. Wake Forest University Health Sciences. Generate a Pharmacodynamic Model of Oxytocin for Peripheral Analgesic Effects. NCT04431206. https://clinicaltrials. gov/show/NCT04431206.
65. Paradigm Biopharmaceuticals USA (INC). Treatment Effects of Subcutaneous Injections of Pentosan Polysulfate Sodium vs Placebo in Participants With Knee OA Pain. NCT04809376. https://clinicaltrials. gov/show/NCT04809376.
66. Queen Savang Vadhana Memorial Hospital, Thailand. Intraarticular Leukocyte-rich and Leukocytepoor PRP for Osteoarthritis of the Knee (PRP). NCT05737173. https:// clinicaltrials.gov/show/NCT05737173.
67. Andrews Research & Education Foundation. Effect of Different Injection Regimens of Autologous Conditioned Plasma for Knee Osteoarthritis. NCT03889925. https:// clinicaltrials.gov/show/NCT03889925.
68. Eduardo Branco de Sousa, Instituto Nacional de Traumatologia e Ortopedia. Knee Osteoarthritis Treatment With Platelet-rich Plasma. NCT05824806. https://clinicaltrials. gov/show/NCT05824806
69. Kelly Kilcoyne, MD, Walter Reed National Military Medical Center. Comparing Platelet Rich Plasma and Corticosteroid for Military & Civilian Patients With Glenohumeral Osteoarthritis (PRP). NCT05160441. https://clinicaltrials.gov/show/ NCT05160441
70. QC Kinetix LLC. Platelet-Rich Plasma
and the Effects of NSAIDs on Pain and Functional Scores in Knee Osteoarthritis (PRPNSAIDsKOA). NCT05742763. https://clinicaltrials. gov/show/NCT05742763
71. James A. Keeney, University of Missouri-Columbia. Biological Response to Platelet-rich Plasma and Corticosteroid Injections. NCT05657496. https://clinicaltrials. gov/show/NCT05657496.
72. Bone Therapeutics S.A. Phase III Study on the Safety and Efficacy of a Single Intra-articular Administration of JTA004 in Symptomatic Knee Osteoarthritis (JTA-KOA2). NCT04333160. https:// clinicaltrials.gov/show/NCT04333160.
73. Brennan J. Boettcher, Mayo Clinic. Autologous Alpha-2 Macroglobulin Rich Plasma, Safety and Efficacy in Symptomatic Moderate Knee Osteoarthritis (A2MRP). NCT06329492. https://clinicaltrials. gov/show/NCT06329492.
74. Novo Nordisk A/S. Research Study Looking at How Well Semaglutide Works in People Suffering From Obesity and Knee Osteoarthritis. NCT05064735. https://clinicaltrials.gov/show/ NCT05064735.
75. Christopher Ritchlin, University of Rochester. Teriparatide as a Chondroregenerative Therapy in OA. NCT03072147. https://clinicaltrials.gov/ show/NCT03072147.
76. Grünenthal GmbH. Efficacy and Safety of RTX-GRT7039 in Adult Subjects With Knee Osteoarthritis. NCT05248386. https://clinicaltrials.gov/show/ NCT05248386.
77. Grünenthal GmbH. Comparison of a Single RTX-GRT7039 and Placebo Intraarticular Injection for Pain Associated With Osteoarthritis of the Knee. NCT05449132. https://clinicaltrials.gov/ show/NCT05449132.
78. Grünenthal GmbH. Open-label Trial to Check the Safety and Tolerability of RTX-GRT7039 Injections for Pain Associated With Osteoarthritis of the Knee. NCT05377489. https:// clinicaltrials.gov/show/NCT05377489.
79. Sorrento Therapeutics, Inc. Study to Evaluate Intra-articular Resiniferatoxin to Treat Moderate to Severe Pain From Knee Osteoarthritis. NCT04885972. https://clinicaltrials.gov/show/ NCT04885972.
80. Novartis Pharmaceuticals. A Proof-ofconcept Study to Examine QUC398 in Participants With Knee OA. NCT05462990. https://clinicaltrials.gov/ show/NCT05462990.
81. Phillips K, Clauw D J. Central pain mechanisms in rheumatic diseases: future directions. Arthritis Rheumatol. 2013;65(2):291.
82. Suokas A K et al. Quantitative sensory testing in painful osteoarthritis: a systematic review and meta-analysis. Osteoarthr Cartil. 2012;20(10):1075-85.
83. Fingleton C et al. Pain sensitization in people with knee osteoarthritis: a systematic review and meta-analysis. Osteoarthr Cartil. 2015;23(7):1043-56.
84. Zhai S et al. The efficacy and safety of Botulinum Toxin Type A in painful knee osteoarthritis: a systematic review and meta-analysis. J Int Med Res. 2019;48(4):0300060519895868.
85. Brown W et al. Safety, pharmacokinetics, and pharmacodynamics study in healthy subjects of oral NEO6860, a modality selective transient receptor potential vanilloid subtype 1 antago nist. J Pain. 2017;18(6):726-38.
86. Levicept. Clinical Trial to Evaluate the Efficacy and Safety of LEVI-04 in Patients With Osteoarthritis of the Knee. NCT05618782. https://clinicaltrials.gov/ show/NCT05618782.
87. Kersten C et al. Epidermal growth factor receptor – inhibition (EGFR-I) in the treatment of neuropathic pain. Br J Anaesth. 2015;115(5):761-7.
88. Yang A et al. Medical cannabis in hand surgery: a review of the current evidence. J Hand Surg Am. 2023;48(3):292-300.
89. Verrico C D et al. A randomized, double-blind, placebo-controlled study of daily cannabidiol for the treatment of canine osteoarthritis pain. Pain. 2020;161(9):2191.
90. Sophocleous A et al. The type 2 cannabinoid receptor regulates susceptibility to osteoarthritis in mice. Osteoarthr Cartil. 2015;23(9):1586-94.
91. Solanki P et al. Repurposing pentosan polysulfate sodium as hyaluronic acid linked polyion complex nanoparticles for the management of osteoarthritis: a potential approach. Med Hypotheses. 2021;157:110713.
92. Ghosh P et al. Effects of pentosan polysulfate in osteoarthritis of the knee: a randomized, double-blind, placebo-controlled pilot study. Curr Ther Pes Clin Exp. 2005;66(6):552-71.
93. Liu X et al. The effect of pentosan polysulfate sodium for improving dyslipidaemia and knee pain in people with knee osteoarthritis: A pilot study. Osteoarthr Cartil. 2023;5(2):100343.
94. Eli Lilly and Company. A Chronic Pain Master Protocol (CPMP): A Study of LY3857210 in Participants With Chronic Low Back Pain. NCT05630196. https://clinicaltrials. gov/show/NCT05630196.
95. Mehta N et al. Purinergic receptor P2X7: A novel target for antiinflammatory therapy. Bioorg Med
Chem. 2014;22(1):54-88.
96. Quarterman J C et al. HPLC-uv method validation for amobarbital and pharmaceutical stability evaluation when dispersed in a hyaluronic acid hydrogel: a new concept for posttraumatic osteoarthritis prevention. J Pharm Sci. 2022;111(5):1379-90.
97. Gerwin N et al. Angiopoietin-like 3-derivative LNA043 for cartilage regeneration in osteoarthritis: a randomized phase 1 trial. Nat Med. 2022;28(12):2633-45.
98. Lupancu T J et al. CCL17/TARC in autoimmunity and inflammation-not just a T-cell chemokine. Immunol Cell Biol. 2023;101(7):600-9.
99. Nijjar J S et al. OP0075 efficacy, safety, pharmacokinetics and immunogenicity of repeated dosing of gsk3858279 in patients with knee osteoarthritis: a phase i, randomized, double-blind, placebo-controlled study. Ann Rheum Dis. 2023;82(Suppl 1):51.
100. M R P et al. Antiinflammatory therapy with canakinumab for atherosclerotic disease. NEJM. 2017;377(12):1119-31.
101. Conaghan P et al. Intra-articular canakinumab (anti-interleukin1β) for treatment of symptomatic knee osteoarthritis: a randomized, double-blind, placebo and naproxencontrolled phase ii study. Abstract 0728. ACR Convergence, 5-9 November, 2021.
102. Jin L et al. CCR2 monocytes as therapeutic targets for acute disc herniation and radiculopathy in mouse models. Osteoarthr Cartil. 2024;32(1):52-65.
103. Longobardi L et al. Role of the C-C chemokine receptor-2 in a murine model of injury-induced osteoarthritis. Osteoarthr Cartil. 2017;25(6):914-25.
104. Duan M et al. Medicinal chemistry strategies targeting NLRP3 inflammasome pathway: A recent update from 2019 to mid-2023. Eur J Med Chem. 2023;260:115750.
105. Li Z, Li Y. Effect of growth hormone releasing hormone on chondrocytes of osteoarthritis. Korean J Intern Med. 2019;37(1):222-9.
106. Schnitzer T J et al. Intra-articular mmii, a novel suspension of large empty multilamellar liposomes, in painful knee osteoarthritis: a 26 week phase 2b placebo-controlled double blind randomized trial. Osteoarthr Cartil. 2023;31(5):688-9.
107. Roux C H et al. Oxytocin Controls Chondrogenesis and Correlates with Osteoarthritis. Int J Mol Sci. 2020;21(11):3966.
108. Bergmann N C et al. Semaglutide for the treatment of overweight and
obesity: a review. Diabetes Obes Metab. 2023;25(1):18-35.
109. Szőke É et al. Small molecule somatostatin receptor subtype 4 (sst4) agonists are novel antiinflammatory and analgesic drug candidates. Neuropharmacology. 2020;178:108198.
110. Sun Q et al. Parathyroid hormone attenuates osteoarthritis pain by remodeling subchondral bone in mice. Elife. 2021;10:e66532.
111. Davis A J et al. Are bisphosphonates effective in the treatment of osteoarthritis pain? a meta-analysis and systematic review. PLoS One. 2013;8(9):e72714.
112. Yazici Y et al. Lorecivivint, a novel intra-articular cdc-like kinase 2 and dual-specificity tyrosine phosphorylation-regulated kinase 1a inhibitor and Wnt pathway modulator for the treatment of knee osteoarthritis: a phase ii randomized trial. Arthritis Rheumatol. 2020;72(10):1694-706.
113. Deshmukh V et al. Modulation of the Wnt pathway through inhibition of CLK2 and DYRK1A by lorecivivint as a novel, potentially disease-modifying approach for knee osteoarthritis treatment. Osteoarthr Cartil. 2019;27(9):1347-60.
114. Simsek I et al. POS0278 a multicenter, observational, extension study evaluating the safety, tolerability, and efficacy of a single lorecivivint injection in knee OA subjects. Ann Rheum Dis. 2021;80(Suppl 1):363.
115. Lee S W et al. Cilostazol protects rat chondrocytes against nitric oxide-induced apoptosis in vitro and prevents cartilage destruction in a rat model of osteoarthritis. Arthritis Rheumatol. 2008;58(3):790-800.
116. Wang W et al. Cilostazol prevents the degradation of collagen Type II in human chondrocytes. Biochem Biophys Res Commun. 2014;451(3):352-5.
117. Mahmoud Samy Abdallah, Sadat City University. The Phosphodiesterase 3 Inhibitor Cilostazol as an Adjunct to Conventional Therapy in Patients With Osteoarthritis. NCT04789837. https://
clinicaltrials.gov/show/NCT04789837.
118. Ginnetti A T et al. Lead optimization of cathepsin K inhibitors for the treatment of Osteoarthritis. Bioorg Med Chem Lett. 2022;74:128927.
119. Lindström E et al. Nonclinical and clinical pharmacological characterization of the potent and selective cathepsin K inhibitor MIV-711. J Transl Med. 2018;16(1):125.
120. Conaghan P G et al. Disease-modifying effects of a novel cathepsin K inhibitor in osteoarthritis. Ann Intern Med. 2019;172(2):86-95.
121. Schnitzer T J et al. Efficacy and safety of s201086/GLPG1972, an ADAMTS-5 inhibitor, in patients with knee osteoarthritis: roccella, a 52-week, randomized, double-blind, doseranging phase 2 study. Osteoarthr Cartil. 2021;29:S264.
122. Siebuhr A et al. The Anti-ADAMTS-5 Nanobody®, M6495, protects against cartilage breakdown in cartilage and synovial joint tissue explant models. Osteoarthr Cartil. 2018;26:S187.
123. Guehring H et al. Safety, tolerability, pharmacokinetics and pharmacodynamics of single ascending doses of the antiADAMTS-5 nanobody (R), M6495, in healthy male subjects: a phase I, placebo-controlled, first-in-human study. Abstract 2175. ACR/ARP Annual Meeting, 8-12 November, 2019.
124. Brebion F et al. Discovery of GLPG1972/S201086, a Potent, Selective, and Orally Bioavailable ADAMTS-5 Inhibitor for the Treatment of Osteoarthritis. J Med Chem. 2021;64(6):2937-52.
125. Latourte A, Richette P. Inhibition of ADAMTS-5: the right target for osteoarthritis? Osteoarthr Cartil. 2022;30(2):175-7.
126. McGuire D et al. TPX-100 leads to marked, sustained improvements in subjects with knee osteoarthritis: pre-clinical rationale and results of a controlled clinical trial. Osteoarthr Cartil. 2018;26:S243.
127. McGuire D et al. Study TPX-100-5: intra-articular TPX-100 significantly delays pathological bone shape
change and stabilizes cartilage in moderate to severe bilateral knee OA. Arthritis Res Ther. 2021;23:1-9.
128. Costa L A V et al. How does plateletrich plasma compare clinically to other therapies in the treatment of knee osteoarthritis? a systematic review and meta-analysis. Am J Sports Med. 2022;51(4):1074-86.
129. Peng Y N et al. Intra-articular leukocyterich platelet-rich plasma versus intraarticular hyaluronic acid in the treatment of knee osteoarthritis: A Meta-Analysis of 14 Randomized Controlled Trials. Pharmaceuticals. 2022;15(8):974.
130. Akeda K et al. Platelet-rich plasma stimulates porcine articular chondrocyte proliferation and matrix biosynthesis. Osteoarthr Cartil. 2006;14(12):1272-80.
131. Hohmann E et al. Is platelet-rich plasma effective for the treatment of knee osteoarthritis? A systematic review and meta-analysis of level 1 and 2 randomized controlled trials. Eur J Orthop Surg Traumatol. 2020;30(6):955-67.
132. Saltzman B M et al. The therapeutic effect of intra-articular normal saline injections for knee osteoarthritis: a meta-analysis of evidence level 1 studies. Am J Sports Med. 2017;45(11):2647-53.
133. Lim Y Z et al. Metformin as a potential disease-modifying drug in osteoarthritis: a systematic review of pre-clinical and human studies. Osteoarthr Cartil. 2022;30(11):143442.
134. Wang Y et al. Methotrexate to treat hand osteoarthritis with synovitis (METHODS): an Australian, multisite, parallel-group, double-blind, randomised, placebo-controlled trial. Lancet. 2023;402(10414):1764-72.
135. Wittoek R et al. RANKL blockade for erosive hand osteoarthritis: a randomized placebo-controlled phase 2a trial. Nat Med. 2024;30(3):829-36.
136. O’Neill T et al. Effect of denosumab on knee pain and bone marrow lesions in symptomatic knee osteoarthritis. Abstract 1982. ACR Convergence, 14 November, 2023.
The Application, Safety, and Recent Developments of Commonly Used Gadolinium-Based Contrast Agents in MRI: A Scoping Review
Authors: *Moh. Tawhid Islam,1 Vera Tsnobiladze2
1. Newvision University, Tbilisi, Georgia
2. AVERSI Clinic, Tbilisi, Georgia
*Correspondence to mtislam_cu@hotmail.co.uk
Disclosure: The authors have no conflicts of interest to disclose.
Gadolinium-based contrast agents (GBCA) have played a pivotal role in enhancing the diagnostic capabilities of MRI for several decades. The application of gadolinium as a contrast agent opened new possibilities for early diagnosis with greater accuracy of a wide range of conditions, including neurologic and vascular disorders, tumours, cancers, inflammation, and more. Gadolinium is a lanthanide metal known for its strong paramagnetic properties, which produce stronger signals in MRI. The presence of GBCAs in the body alters the magnetic properties of nearby water molecules, which changes the appearance of the organs or blood vessels containing contrast when the MRI images are taken. The safety of GBCAs has been widely studied in recent years. Gadolinium is generally considered a safe and relatively nontoxic contrast agent, according to many of these studies. Many clinical studies have also shown toxic effects, allergic reactions, and gadolinium deposition in different body tissues and the brain. The rare condition of nephrogenic systemic fibrosis in adult patients with renal dysfunction has been the most popular topic of research and the main concern amongst all other risks of post-GBCA use. This review explores various research papers regarding GBCAs and focuses on providing insight into how different types of GBCAs are commonly used today in MRI scans, their properties, clinical applications, safety concerns, and recent and possible future developments in this field of medical radiology.
Key Points
1. The use of gadolinium-based contrast agents (GBCA) in MRI has been associated with adverse effects, including free gadolinium deposition, nephrotoxicity, and allergic reactions in patients. This has raised concerns about their safety and led to the development of safer MRI contrast agents.
2. In this study, applications of different GBCAs, related potential diseases, side effects, and accumulation of gadolinium were reviewed from numerous studies. Recent approaches and investigations in the development of safer MRI contrast agents were explored and discussed briefly.
3. GBCAs with a linear structure have higher risks despite their greater specificity and sensitivity. Macrocyclic GBCAs are safer and preferred, with generally low side effects, though efficacy can vary. Patients with kidney issues or frequent MRIs face higher risks. Guidelines based on the latest scientific findings are essential for improving patient safety.
INTRODUCTION
Gadolinium is an invaluable contrast agent in MRI that has various important benefits in radiology. Its unique magnetic properties allow for increased contrast in MRI images, making it easier to identify and better understand anatomical structures and pathologies. They are particularly very effective in detecting lesions as well as pathological changes in the central nervous system, cardiovascular system, and other body regions.1,2 This allows early and accurate diagnosis, appropriate treatment planning, as well as the monitoring of disease progression. Gadolinium-based contrast agents (GBCA) come in several forms, including linear and macrocyclic chelates, which are designed to increase the stability of gadolinium in the body and reduce the risk of toxic effects.3,4 Gadolinium contrast agents can be tailored to the needs of certain MRI examinations. Although gadolinium is generally considered safe, it is necessary to assess the risks of rare allergic reactions and the risk of accumulation in various body tissues. Several types of GBCA are available in today’s market, the most commonly used amongst them such as gadopentetate dimeglumine, gadobutrol, gadoterate meglumine, and gadofosveset trisodium have been reviewed and explored in line with their different application and safety profiles.
Gadopentetate Dimeglumine
Gadopentetate dimeglumine (commonly known by its brand name Magnevist [Bayer Radiology, Leverkusen, Germany]) was the first gadolinium-based contrast agent (GBCA) that became available in 1988 and is a widely used GBCA in medical imaging. It is a paramagnetic complex comprising gadolinium (Gd) ions chelated with diethylenetriamine penta-acetic acid (DTPA) and meglumine.5 This chelation enhances the stability
and solubility of the compound, making it suitable for intravenous administration in imaging procedures. The presence of unpaired electrons in Gd ions allows for the manipulation of magnetic resonance signals, improving the visualisation of anatomical structures in MRI.6,7
Gadopentetate dimeglumine enhances tissue differentiation, aids lesion detection, and provides diagnostic and treatment information. It is used in neuroimaging, musculoskeletal imaging, cardiac imaging, body imaging, and angiography. In neuroimaging, it helps visualise brain and spinal cord lesions, peripheral vascular abnormalities, demyelination diseases, and malignant tumours.8,9 In musculoskeletal imaging, it improves the visualisation of soft tissue injuries, joint disorders, and tumours. For cardiac MRI, it evaluates myocardial perfusion, viability, and cardiac function. In body imaging, it recognises liver lesions, including hepatocellular carcinoma, abdominal tumours, and assesses renal function.10 In angiography, it is used for magnetic resonance angiography (MRA) to examine blood vessels. Gadopentetate dimeglumine-enhanced MRI showed great improvement in liver lesion detection and characterisation compared to unenhanced MRI scans. A study by Attyé et al.11 used gadopentetate dimeglumine to assess blood–brain barrier permeability in patients with multiple sclerosis.11 Dynamic contrastenhanced MRI was used to monitor changes in barrier integrity. The results showed that gadopentetate dimeglumine can provide important information for evaluating disease progression and treatment response in patients with multiple sclerosis.12
While gadopentetate dimeglumine is generally safe, there are some potential risks associated with its use.13 Studies have demonstrated its efficacy while showing a low incidence of acute adverse effects, especially in paediatric patients, and its
safety profile was further improved in patients under sedation.14 Compared to macrocyclic GBCAs, linear GBCAs have a less stable molecular structure, which increases the likelihood that they would extravasate i.e., leak out of blood vessels into surrounding tissues. Extravasation can cause tissue irritation, oedema, and possibly raise the risk of compartment syndrome, especially when it happens in high volumes.15 There have been reports of rare fatal reactions associated with their use, including laryngeal oedema, hypotensive shock, respiratory arrest, arrhythmia, and bronchospasm.16
The main concern is the development of nephrogenic systemic fibrosis (NSF) in patients with kidney problems.17 NSF is a rare but serious condition characterised by skin and organ fibrosis. Several studies during the last decade reported the deposition of gadopentetate dimeglumine in the brain tissues and other organs.18-27 Adverse reactions like allergies, headaches, or nausea have also been reported, so prompt recognition and management are important.28,29 To minimise these risks, the patient’s poor kidney function must be assessed before giving gadopentetate dimeglumine, and the use of the lowest effective dose was suggested in many studies.23,30
In March 2016, the European Medicine Agency (EMA) began reviewing the GBCAs at the European Commission’s request. Following the safety evaluation in 2017, the EMA recommended the suspension of the use of linear agents such as intravenous gadopentetate dimeglumine, gadoversetamide, and gadodiamide. However, gadopentetate dimeglumine intra-articular usage was still permitted under very specific guidelines. The EMA introduced these measures according to their scientific reviews suggesting greater risks of gadolinium retention from linear GBCAs compared to macrocyclic GBCAs. Proper patient selection, monitoring, and following safety guidelines can ensure the safe and effective use of this contrast agent in clinical practice.31
Gadobutrol
Gadobutrol (commonly known in the market as Gadovist [Bayer AG, Leverkusen, Germany]), approved by the FDA in 2015, is a widely used contrast agent in MRI, recognised for its safety and effectiveness in improving the visualisation of various tissues within the body, as evaluated by a large-scale study in 23,000 patients.32 It has also been found to be well-tolerated, especially in children even under the age of 2 years, further supporting its safety profile across different age groups.33 Specifically, it is highly beneficial for vascular and soft tissue imaging. Gadobutrol is a type of GBCA that belongs to the category of macrocyclic agents. One notable advantage of gadobutrol is its lower risk of causing NSF compared to other GBCAs. As a result, it is often the preferred choice for patients with compromised kidney function.34,35
A study conducted by Prince et al.32 showcased the excellent diagnostic performance and safety record of gadobutrol in contrast-enhanced MRI scans of the brain.32 The research involved a significant number of patients and revealed that gadobutrol consistently produced highquality images, facilitating the accurate identification and characterisation of brain abnormalities. Additionally, it was observed that minimal occurrence of adverse events was associated with gadobutrol administration, further emphasising its safety in clinical settings. It was proven by studies that it is a safe and efficient GBCA for use in both MRI and MRA, enabling the visualisation of pathological lesions and abnormalities in vascular perfusion and flow across various body regions including the prostate.36,37,38 This includes a wide range of patients, such as term neonates, paediatric patients, adults of different age groups, and individuals with renal and hepatic impairment and cardiovascular disease.35
Gadobutrol can be detected in cerebrospinal fluid samples for extended periods of time, even in individuals with normal kidney function and an intact blood–brain barrier. This highlights its potential for use in the spinal canal. Clinical studies have shown that gadobutrol does not have any negative effects on kidney function, making
it a safe contrast agent for patients with impaired renal function.39,40 Furthermore, there have been studies investigating the intrathecal use of gadobutrol, specifically in relation to examining cerebrospinal fluid dynamics and enhancing glymphatic flow in conditions like idiopathic normal pressure hydrocephalus.41 These studies aimed to determine the minimum effective dose required to gather diagnostic information, showcasing the potential of gadobutrol for such applications. The extensive research conducted supports its safety and effectiveness as a contrast agent for various patient populations and clinical scenarios. Very rare cases of adverse reactions, such as fatal anaphylactic reactions, have also been reported.42 Its strong stability, safety in cases of renal impairment, and potential for intrathecal use make it a valuable tool in diagnostic imaging.43
Gadoterate Meglumine
Gadoterate meglumine (commonly known as Dotarem [Guerbet, Villepinte, France]), an MRI contrast agent, received FDA approval in 2013. It is a paramagnetic compound that enhances the visibility of blood vessels, organs, and tissues during imaging, allowing for a more detailed and accurate diagnosis.44 In terms of effectiveness, gadoterate meglumine has been widely used and proven to be effective in improving the quality and diagnostic accuracy of MRI scans. It helps to enhance the visualisation of blood vessels and abnormalities, making it easier for healthcare professionals to identify and characterise various medical conditions.45,46
Regarding the safety aspects of gadoterate meglumine, it is considered a safe contrast agent when used appropriately.47 It has a favourable safety profile and is welltolerated by most patients.48,49 However, as with any contrast agent, there are some potential risks and side effects, although they are rare. Previous studies have shown a few risks, which include allergic reactions, NSF in patients with severe kidney dysfunction, and the possibility of accumulation in brain tissue in patients with multiple administrations.44-46,50-52 Its stability plays an important role in selection. Safety
can be dependent on the structure and stability of contrast agents. Gadoterate meglumine is a macrocyclic as well as an ionic agent, which supports higher thermodynamic and kinetic stability. The high molecular stability of the agent can minimise the risk of gadolinium release from the GBCA molecule.53,54 Gadoterate meglumine has gained a significant share of the USA market and continues to be a leading choice for radiologists, with no unconfounded cases of NSF reported. It is typically administered intravenously before an MRI scan. The dosage and administration method depend on the patient’s age, weight, and the specific imaging procedure being performed.55 Furthermore, gadoterate meglumine is compatible with most MRI equipment and does not interfere with the imaging process. It provides excellent contrast enhancement and allows for clear visualisation of anatomical structures and pathological abnormalities.
Gadofosveset Trisodium
Gadofosveset trisodium (also known as Vasovist [Bayer Schering Pharma AG, Berlin, Germany]), a gadolinium-based blood pool contrast agent, was approved by the FDA in 2008 for the evaluation of aortoiliac disease in adults.56 Gadofosveset trisodium has been used mainly in the MRA of the vascular system for the diagnosis of certain disorders of the heart and blood vessels. The agent showed to have a prolonged intravascular residence time, making it particularly useful for evaluating venous, dynamic, and functional vascular diseases with a single low-dose contrast injection.57 It is considered an 'intravascular' contrast agent due to its transient, reversible, and noncovalent binding to serum albumin.58 This property allows the contrast agent to circulate for 2–3 hours after intravenous injection, making it suitable for various imaging studies.56,59
Furthermore, gadofosveset trisodium has been compared with other contrast agents, such as gadobenate dimeglumine, showing similar safety profiles and comparable image quality in certain studies.60,61 Its prolonged plasma half-life and increased relaxivity due to its ability to bind reversibly to serum albumin and form small nanoparticles
has been highlighted as a key feature, contributing to its prolonged imaging capabilities and potential applications as a negative contrast agent for discriminating metastatic from nonmetastatic lymph nodes.62,63 These unique properties of gadofosveset trisodium have been extensively studied and compared with other contrast agents, showcasing its potential advantages in specific imaging scenarios.64-66 It has been evaluated for its potential use in various medical conditions such as endometriosis, and in the preoperative evaluation of potential living kidney donors, demonstrating its versatility and potential clinical utility.67,68
Also, as a blood pool contrast agent, it has been explored in the context of equilibriumphase MRA, demonstrating its potential to overcome challenges associated with suboptimal bolus timing during whole-body vascular imaging.69 Gadofosveset trisodium is a subject of research interest due to its unique properties as a blood pool contrast agent. Studies have highlighted many advantages and the potential use of this agent. Further research may continue to explore its utility and potential.
Recent Developments
Research in developing alternative MRI contrast agents is multidisciplinary and involves chemistry, materials science, and biomedical engineering. Recent research has emphasised the necessity for alternatives to GBCAs in MRI due to concerns regarding gadolinium retention and potential toxicity.70 While GBCAs have significantly improved MRI scans for over a few decades, issues such as gadolinium deposits in the brain and NSF have led to the exploration of new contrast agents.71-74 Various materials such as manganese, iron oxide, organic molecules as small peptides, siliconbased, fluorine-based, biodegradable, and various nanoparticles including those made from gold, carbon nanotubes, fullerenes, polymers, liposomes, and viral nanoparticles have been investigated in recent years.75
Manganese has been explored as an alternative to gadolinium due to its paramagnetic properties. Manganese-based
contrast agents have shown promise as complementary agents for liver imaging, potentially serving as alternatives for specific imaging requirements.76 It has been one of the most promising and popular in research amongst the materials investigated for MRI contrast.77 Amongst paramagnetic GBCA, gadoxetate disodium (also known as primovist/eovist [Bayer Healthcare, Leverkusen, Germany)], is a hepato-specific contrast agent predominantly used for improved detection and characterisation of liver lesions, including hepatocellular carcinoma. Due to its hepatocyte-specific uptake and excretion through the biliary system, it can provide dynamic and hepatobiliary phase images.78,79 It offers unique advantages in liver MRI but has also shown challenges such as transient motion artifacts in many studies.80,81
Many efforts have also been directed towards developing gadolinium-free contrast agents, with endeavours to integrate gadolinium into nanostructures for enhanced MRI contrast imaging.82,83 These advancements aim to enhance the safety profile of contrast agents while upholding the efficacy in MRI scans. Nanoparticles, including those made from gold, carbon, or polymers, are being investigated for their potential as MRI contrast agents. These nanoparticles can be engineered to have tuneable properties and can be functionalised for targeted imaging applications.
Iron oxide nanoparticles have been investigated; most importantly, superparamagnetic iron oxide nanoparticles (SPIONs) have shown great contrast by altering the relaxation times of nearby water protons. Research is ongoing to improve their biocompatibility, imaging efficacy, and clearance from the body, which indicates a shift towards exploring novel contrast agents beyond gadolinium.84,85 Amongst SPION agents, ferumoxytol exhibited promise most recently as an alternative to GBCAs for vascular imaging.86 Ferumoxytol, a compound coated with carboxymethyldextran, was employed as a contrast agent on SPION.87 Unlike gadolinium, ferumoxytol has various features. Because of its impaired
blood–brain barrier, it is a big agent that does not go through blood arteries to reach tumours quickly. While gadolinium agents improve the lesion after minutes, the lesion is enhanced one-day following injection. Ferumoxytol has a half-life of around 14 hours; this extended half-life enables the visualisation of tumour vasculature and the determination of the relative cerebral blood volume for tumours that may be malignant. Manganese is also a significant element in the body, enso dogenous mechanisms can remove it.56,82
Organic molecules like small peptides or nanoparticles are being explored as alternatives to GBCAs. These agents can be tailored to have specific targeting capabilities and can potentially reduce the risk of toxic effects associated with metal-based contrast agents. Inorganic molecules, such as siliconbased nanoparticles have also emerged with a potential alternative to GBCAs. These nanoparticles can be functionalised with targeting ligands and have shown improvements in preclinical studies.75,88 Their contrasting effects and unique properties could position them as viable substitutes for GBCAs in future.89 Fluorine-containing compounds that contain both organic and inorganic components are also being explored for their potentials as they can provide both positive and negative contrast that may offer advantages in terms of safety and imaging sensitivity. Fluorinated agents such as theranostics have been extensively investigated for diseases like pulmonary embolism, inflammatory diseases, and cancer.90,91
Biodegradable materials that can be easily cleared from the body after imaging have also shown promise in the development of contrast agents. These agents aim to minimise long-term retention and potential toxic effects. The research on biodegradable contrast agents is diverse and promising, with studies focusing on various aspects such as cancer detection, immune response tracking, and the development of biodegradable macromolecular contrast agents.92,93
Recent studies worked on dosage reduction together with improved lesion
characterisation, clinical efficacy, and increased relaxivity.87 Gadoquatrane, a newly developed contrast agent based on tetrameric gadolinium, has significantly improved stability and relaxation.94,95 With one gadolinium ion and a non-ionic macrocyclic GBCA structure, the recently developed agent gadopiclenol was made by Robert P et al.96 with the goal of producing T1 relaxivity that is two to three times higher than that of existing gadolinium factors without sacrificing any of their physical properties. After five months of gadopiclenol treatment, the amount of gadolinium deposited in the cerebellum is comparable to that of macrocyclic gadobutrol.97 This new agent gadopiclenol (marketed as elucirem [Guerbet, Villepinte, France]), was tested on animals to see if there is cerebral deposition. It incorporates a phenyl group into DO3A, resulting in the relaxation time of Gd-DOTA without phenyl group alteration.98,99
To conclude, recent research focused on understanding their mechanisms of toxicity, distribution in the body, potential neurotoxic effects, and exploring alternative contrast agents to address safety concerns. These studies contribute to the ongoing efforts to improve the safety and efficacy of contrast agents used in MRI.
DISCUSSION
The field of MRI contrast agents is evolving, and scientists have been dedicated to the development of safer GBCAs that minimise the potential for negative impacts. A noteworthy advancement in this pursuit has been the introduction of macrocyclic chelates, which are generally linked to decreased rates of gadolinium release.100,101 Gadolinium-based contrast agents continue to serve as exceptional tools in diagnostic imaging. They allow for enhanced visualisation of anatomical structures and pathologies in MRI scans. Numerous studies have demonstrated the positive impact of GBCAs on MRI images by improving specificity, sensitivity, and visibility. This is achieved by modifying the inherent properties of tissues, leading to a significant increase in signal intensity through binding to serum proteins and creating a noticeable
contrast. However, the safety profile of GBCAs, particularly in patients with renal impairment, remains an ongoing area of research and debate. While newer and safer agents are being developed, clinicians must carefully assess the risk–benefit ratio when utilising GBCAs in their medical practice.102
Gadopentetate dimeglumine was a widely used contrast agent in MRI scans before the suspension, improving accuracy in liver and brain imaging. Multiple studies support its effectiveness.11,103 However, caution must be exercised due to the risks associated with GBCAs, particularly nephrogenic systemic fibrosis in patients with kidney issues and dialysis.86 Patients with sickle cell disease may be at higher risk of potential oxidative stress and vascular complications, and in such cases, macrocyclic GBCAs are preferred, although there is no evidence of adverse effects such as intra-vascular problems or haemolytic events induced by GBCAs in patients with sickle cell disease.104 Proper patient selection, monitoring, and adherence to safety guidelines are vital for the safe use of this contrast agent. While the risk of compartment syndrome from GBCAs is relatively rare, it is higher with linear GBCAs, especially when there is extravasation, high dosage administration, or impaired patient venous access. Minimising this risk requires close monitoring of the injection site and the use of proper injection procedures.
Both gadoterate meglumine and gadobutrol are GBCAs with comparable safety profiles, efficacies, and macrocyclic chemical structures. When it comes to gadolinium retention, macrocyclic GBCAs are regarded as safer than linear GBCAs.105 The likelihood of gadolinium being released from the complex and remaining within the body is reduced by the macrocyclic structure. As such, macrocyclic agents are usually preferred when choosing GBCAs for an MRI scan, especially for patients who are more likely to retain gadolinium, such as those with compromised renal function.106
Alternative contrast agents, such as those based on manganese, are being developed in an ongoing effort to offer
comparable diagnostic capabilities without the same safety issues.107 Although GBCAs are generally known to be safe, there are growing worries regarding possible side effects, especially in patients with compromised renal function. In these patients, the usage of GBCAs is linked to NSF, a rare but dangerous syndrome.23,30 Furthermore, although the clinical implications of this discovery are still uncertain, various recent investigations have raised doubts about the deposition of gadolinium in various tissues.98,108
Numerous research studies have also demonstrated the presence of gadolinium deposition in various organs of the human body. This occurs as a result of the release of free gadolinium into different organs and tissues, which has raised concerns about the use of gadolinium agents. The focus of this study was to investigate potential diseases and side effects associated with the accumulation of gadolinium in the patient’s body, particularly in organs such as the brain and bones where gadolinium deposition has been observed. The study also explored the development of new contrast agents that do not contain gadolinium or the invention of nextgeneration gadolinium agents, with the aim of enhancing their safety and effectiveness. One of the diseases associated with gadolinium retention is NSF, while another is gadolinium deposition disease (GDD).96,109
GBCAs continue to be popular in medical imaging, specifically in MRI scans, to enhance the contrast of images and improve the accuracy of diagnosis. These agents contain paramagnetic ions that aid in producing clearer images. In order to prevent the toxicity of free gadolinium ions, they are bound to organic ligands, forming stable chelates called Gd+3 chelates. This process reduces the release of free gadolinium ions and prevents their interaction with endogenous anions like CO3-2 and PO4-3 which could potentially result in the formation of insoluble compounds in the bloodstream and their accumulation in tissues.110 GBCAs do not worsen renal insufficiency and are generally considered safe. Nonetheless, mild adverse reactions
may occur following their administration, including nausea, vomiting, discomfort at the injection site, headache, and dizziness. Evidence exists in a few cases that confirms the presence of gadolinium deposits in various tissues such as bone, kidneys, brain, skin, and lymph nodes. The specific nature of these deposits is still unknown, and currently, there is no evidence linking gadolinium accumulation to direct tissue damage.
However, research studies have documented specific disorders associated with the retention of gadolinium, which include hypersensitivity reactions, NSF, and GDD.111-114 These conditions are uncommon and typically manifest in individuals who have pre-existing risk factors or compromised kidney function.
From the review of many studies, reports of acute and chronic adverse effects and notable concerns about GBCAs have been seen. Severe conditions like NSF, which affects people with significant kidney dysfunction and dialysis; concerns about potential long-term effects due to gadolinium retention in tissues like the brain and bones; mild-to-severe allergic reactions that require careful patient screening and monitoring; recommendations for cautious use of GBCAs during pregnancy, while breastfeeding has been deemed safe; paediatric patients are advised to use GBCAs with caution due to potential risks; GDD and any potential cancer risks are still being investigated in ongoing research for further evidence and understanding.
To reduce potential risks, it is advised to administer the lowest effective dose of GBCAs, particularly in patients with impaired renal function. The dosage calculation of GBCAs should be individualised, considering factors like age, renal function, and imaging needs. By adhering to established guidelines and incorporating the latest research on safety and efficacy, healthcare providers can optimise GBCA use while minimising risks.
The EMA guidelines provide specific dosing recommendations for various patient groups, with dosage generally calculated based on
(volume) body weight for both paediatric and adult patients. Dosage recommendations can vary depending on the specific agents. Gadobutrol and gadopentetate dimeglumine are recommended at 0.1 mmol/kg body weight, equivalent to 0.1 mL/kg body weight for a 1.0 M solution in paediatric and adult patients. For gadoterate meglumine, the recommended dose is 0.1 mmol/kg body weight, equivalent to 0.2 mL/kg body weight for a 0.5 M solution in paediatric patients including term neonates, and adults. In MRA, a dose of up to 0.3 mmol/kg body weight, or 0.6 mL/kg body weight, may be used. Gadofosveset trisodium is specifically recommended for MRA of blood vessels in adults, with a dosage of 0.03 mmol/kg body weight, equivalent to 0.12 mL/kg body weight of a 0.25 M solution. Additionally, higher doses of GBCAs have been shown to improve the detection rate of brain metastases.115 Nonetheless, it is crucial to balance the enhanced imaging benefits with the potential risks of gadolinium deposition and toxicity.
The advantages and drawbacks of employing GBCAs must be carefully evaluated. Patients, especially those at higher risk, must be monitored to ensure their safety during diagnostic procedures. As research progresses, these advancements in alternative contrast agents, along with a deeper understanding of their complexities, are anticipated to play a significant role in providing clinicians with the ability to better optimise imaging protocols and ensure accurate diagnostic outcomes.
The review was carried out on multiple previous studies, and one notable limitation of this review is that it incorporates some findings from certain studies that were published without undergoing a comprehensive scientific review process. While these papers provided valuable insights, the authors believe they require further study and analysis. Future work and the next step from this review is to conduct a detailed study and review of each type of GBCA individually, with a particular focus on safety concerns, to contribute to the development of safer MRI contrast agents.
References
1. Runge VM et al. Gadolinium: potential radiographic contrast agent. American Journal of Roentgenology. 2015;145(1):74-8.
2. Uhlig J et al. Gadolinium-based contrast agents for cardiac MRI: use of linear and macrocyclic agents with associated safety profile from 154 779 European patients. Radiol Cardiothorac Imaging. 2020;2(5):e200102.
3. Weinmann HJ et al. Characteristics of gadolinium-DTPA complex: a potential NMR contrast agent. AJR Am J Roentgenol. 1984;142(3):619-24.
4. Aime et al. Gd(III)-based contrast agents for MRI. Adv Inorg Chem. 2005;54:173-237.
5. Iyad N et al. Gadolinium contrast agents- challenges and opportunities of a multidisciplinary approach: literature review. Eur J Radiol Open. 2023;11:100503.
6. Andriyani P, Yandi Hasibuan. Potential of gadolinum as a contrast agent in MRI (magnetic resonance imaging) applications. Sriwijaya Journal of Radiology and Imaging Research. 2023;1(2):29-33.
7. Tweedle MF. Gadopentetate dimeglumine: an overview of a new magnetic resonance imaging contrast agent. Invest Radio. 1992;27(1):S2-6.
8. Jost G et al. Penetration and distribution of gadolinium-based contrast agents into the cerebrospinal fluid in healthy rats: a potential pathway of entry into the brain tissue. Eur Radiol. 2017;27(7):2877-85.
9. Kanygin V et al. Gadolinium neutron capture therapy for cats and dogs with spontaneous tumors using Gd-DTPA. Vet Sci. 2023;10(4):274.
10. Ding Y et al. Comparison of gadoxetic acid versus gadopentetate dimeglumine for the detection of hepatocellular carcinoma at 1.5 T using the liver imaging reporting and data system (LI-RADS v.2017). Cancer Imaging. 2018;18(1):48.
11. Attyé A et al. Recurrent peripheral vestibulopathy: is MRI useful for the diagnosis of endolymphatic hydrops in clinical practice? Eur Radiol. 2015;25(10):3043-9.
12. Asadollahzade E et al. The benefits and side effects of gadolinium-based contrast agents in multiple sclerosis patients. Rev Assoc Med Bras. 2022;68(8):979-81.
13. Anderhalten L et al. Different Impact of gadopentetate and gadobutrol on inflammation-promoted retention and toxicity of gadolinium within the mouse brain. Invest Radio. 2022;57(10):677-88.
14. Neeley C et al. Acute side effects of three commonly used gadolinium contrast agents in the paediatric population. Br J Radiol. 2016;89(1063):20160027.
15. Tessema G et al. Favorable outcome of hand compartment syndrome secondary to extravasation of intravenous contrast medium: a case report. Acta Scientific Orthopaedics. 2022;5(12):184-8.
16. Fang H et al. A case report of gadopentetate dimeglumine-induced cardiac arrest: resuscitation using extracorporeal membrane oxygenation. Ann Noninvasive Electrocardiol. 2023;28(3):e13039.
17. Ibrahim BM, Ismail AH. Impacts of gadolinium-based MRI contrast agent on hematological and biochemical tests for the human volunteers. Zanco Journal of Pure and Applied Sciences. 2022;34(6):37-44.
18. Tamrazi B et al. Changes in signal intensity of the dentate nucleus and globus pallidus in pediatric patients: impact of brain irradiation and presence of primary brain tumors independent of linear gadolinium-based contrast agent administration. Radiology. 2018;287(2):452-60.
19. Schlemm L et al. Gadopentetate but not gadobutrol accumulates in the dentate nucleus of multiple sclerosis patients. Mult Scler. 2017;23:963-72.
20. Flood TF et al. Pediatric brain: repeated exposure to linear gadolinium-based contrast material is associated with increased signal intensity at unenhanced T1-weighted MR imaging. Radiology. 2017;282(1):222-8.
21. Hu HH et al. Increased signal intensities in the dentate nucleus and globus pallidus on unenhanced T1-weighted images: evidence in children undergoing multiple gadolinium MRI exams. Pediatr Radiol. 2016;46(11):1590-8.
22. Cao Y et al. Signal change in the dentate nucleus on T1-weighted MR images after multiple administrations of Gadopentetate dimeglumine versus Gadobutrol. AJR Am J Roentgenol. 2016;206:414-9.
23. Kanda T et al. Gadolinium-based contrast agent accumulates in the brain even in subjects without severe renal dysfunction: evaluation of autopsy brain specimens with inductively coupled plasma mass spectroscopy. Radiology. 2015;276(1):228-32.
24. Tedeschi E et al. In vivo dentate nucleus MRI relaxometry correlates with previous administration of gadoliniumbased contrast agents. Eur Radiol. 2016;26(12):4577-84.
25. Roberts DR, Holden KR. Progressive
increase of T1 signal intensity in the dentate nucleus and globus pallidus on unenhanced T1-weighted MR images in the pediatric brain exposed to multiple doses of gadolinium contrast. Brain Dev. 2016;38:331-6.
26. Miller JH et al. MRI brain signal intensity changes of a child during the course of 35 gadolinium contrast examinations. Pediatrics. 2015;136(6):e1637-40.
27. Radbruch A et al. Gadolinium retention in the dentate nucleus and globus pallidus is dependent on the class of contrast agent. Radiology. 2015;275(3):783-91.
28. Ramalho M et al. Gadolinium retention and toxicity-an update. Adv Chronic Kidney Dis. 2017;24(3):138-46.
29. Ponrartana S et al. Safety issues related to intravenous contrast agent use in magnetic resonance imaging. Pediatr Radiol. 2021;51:736-47.
30. Kanda T et al. Brain gadolinium deposition after administration of gadolinium-based contrast agents. Jpn J Radiol. 2016;34(1):3-9.
31. Woolen SA et al. Risk of nephrogenic systemic fibrosis in patients with stage 4 or 5 chronic kidney disease receiving a group II gadoliniumbased contrast agent: a systematic review and meta-analysis. AMA Intern Med. 2020;180(2):223-30.
32. Prince M et al. Safety of Gadobutrol in over 23,000 patients: the gardian study, a global multicentre, prospective, non-interventional study. Eur Radiol. 2016;27(1):286-95.
33. Glutig K et al. Safety of Gadobutrol in more than 1,000 pediatric patients: subanalysis of the gardian study, a global multicenter prospective noninterventional study. Pediatr Radiol. 2016;46(9):1317-23.
34. Fabrega-Foster KE et al. Efficacy and safety of Gadobutrol-enhanced MRA of the renal arteries: results from GRAMS (Gadobutrol-enhanced renal artery MRA study), a prospective, intraindividual multicenter phase 3 blinded study. J Magn Reson Imaging. 2018;47(2):57281.
35. Scott LJ. Gadobutrol: a review in contrast-enhanced MRI and MRA. Clin Drug Investig. 2018;38(8):773-84.
36. Endrikat J et al. Safety of Gadobutrol: results from 42 clinical phase II to IV studies and postmarketing surveillance after 29 million applications. Invest Radiol. 2016;51:537-43.
37. Hara T et al. Prostate cancer detection with multiparametric MRI: a comparison of 1 m-concentration Gadobutrol with 0.5 m-concentration gadoliniumbased contrast agents. Curr Urol. 2018;11(4):201-5.
38. Yamada M et al. Inter-individual comparison of Gadobutrol and gadoteridol tissue time-intensity profiles for dynamic susceptibility contrast perfusion MR imaging. Magn Reson Med Sci. 2019;18(1):75-81.
39. Tombach B, Heindel W. Value of 1.0-m gadolinium chelates: review of preclinical and clinical data on Gadobutrol. Eur Radiol. 2002;12(6):1550-6.
40. Halvorsen M et al. Off-label intrathecal use of Gadobutrol: safety study and comparison of administration protocols. Neuroradiology. 2020;63(1):51-61.
41. Eide PK et al. Intrathecal contrastenhanced magnetic resonance imaging of cerebrospinal fluid dynamics and glymphatic enhancement in idiopathic normal pressure hydrocephalus. Front Neurol. 2022;13:857328.
42. Franckenberg S et al. Fatal anaphylactic reaction to intravenous gadobutrol, a gadolinium-based MRI contrast agent. Radiol Case Rep. 2018;13(1):299-301.
43. Endrikat J et al. Clinical efficacy of gadobutrol: review of over 25 years of use exceeding 100 million administrations. Invest Radiol. 2023;59(5):345-58.
44. Xiao YD et al. MRI contrast agents: classification and application (Review). Int J Mol Med. 2016;38(5):1319-26.
45. Maravilla K et al. Comparison of Gadoterate Meglumine and Gadobutrol in the diagnosis of primary brain tumors: a double-blind randomized controlled intraindividual crossover study (the REMIND Study). AJNR Am J Neuroradiol. 2017;38(9):1681-8.
46. Food and Drug Association (FDA). FDA Drug Safety Communication: FDA warns that gadolinium-based contrast agents (GBCAs) are retained in the body; requires new class warnings. 2018. Available at: https://www.fda. gov/drugs/drug-safety-and-availability/ fda-drug-safety-communication-fdawarns-gadolinium-based-contrastagents-gbcas-are-retained-body. Last accessed: 29 March 2024.
47. McWilliams RG et al. Observational study on the incidence of nephrogenic systemic fibrosis in patients with renal impairment following Gadoterate Meglumine administration: the nssafe study. J Magn Reson Imaging. 2020;51(2):607-14.
48. Pozeg P et al. Age, but not repeated exposure to Gadoterate Meglumine, is associated with t1- and t2-weighted signal intensity changes in the deep brain nuclei of pediatric patients. Invest Radiol. 2019;54(9):537-48.
49. Behzadi AH, McDonald JS. Gadoliniumbased contrast agents for imaging of the central nervous system: a multicenter European prospective
study. Medicine (Baltimore). 2022;101(34):e30163.
50. Behzadi AH et al. Immediate allergic reactions to gadolinium-based contrast agents: a systematic review and metaanalysis. Radiology. 2018;286:471-82.
51. McDonald JS et al. Acute adverse events following gadolinium-based contrast agent administration: a singlecenter retrospective study of 281,945 injections. Radiology. 2019;292(3):6207.
52. Chanana P et al. The effect of magnetic field gradient and gadolinium-based MRI contrast agent Dotarem on mouse macrophages. Cells. 2022 Feb 22;11(5):757.
53. Frenzel T et al. Stability of gadoliniumbased magnetic resonance imaging contrast agents in human serum at 37 degrees C. Invest Radiol. 2008;43(12):817-28.
54. Dotarem®. Princeton, NJ: Guerbet LLC. Highlights of prescribing information. 2019. Available at: https://guerbet.com/ media/dzgplbax/Dotarem-packageinsert.pdf. Last accessed: : 29 March 2024.
55. de Kerviler E et al. Adverse reactions to gadoterate meglumine: review of over 25 years of clinical use and more than 50 million doses. Invest Radiol. 2016;51(9):544-51.
56. Shahrouki P et al. High-resolution three-dimensional contrast-enhanced magnetic resonance venography in children: comparison of Gadofosveset Trisodium with ferumoxytol. Pediatr Radiol. 2022;52(3):501-12.
57. Sabach AS et al. (2013) Gadofosveset trisodium: abdominal and peripheral vascular applications. AJR Am J Roentgenol. 2013;200(6):1378-86.
58. Raman FS et al. 0-T whole-heart coronary magnetic resonance angiography: comparison of gadobenate dimeglumine and gadofosveset trisodium. Int J Cardiovasc Imaging. 2013;29(5):108594.
59. Mani V et al. A multicenter MRI protocol for the evaluation and quantification of deep vein thrombosis. J Vis Exp. 2015;(100):e52761.
60. Nacif MS et al. Myocardial T1 mapping and determination of partition coefficients at 3 tesla: comparison between gadobenate dimeglumine and gadofosveset trisodium. Radiol Bras. 2018;51(1):13-9.
61. Camren GP et al. A comparison between gadofosveset trisodium and gadobenate dimeglumine for steady state MRA of the thoracic vasculature. Biomed Res Int. 2014;2014:625614.
62. Ruddell A et al. Tumors induce coordinate growth of artery, vein, and
lymphatic vessel triads. BMC Cancer. 2014;14:354.
63. Yamashita K et al. Silica and titanium dioxide nanoparticles cause pregnancy complications in mice. Nature Nanotechnol. 2011;6(5):321-8.
64. Hadizadeh DR et al. Contrast material for abdominal dynamic contrastenhanced 3D MR angiography with parallel imaging: intraindividual equimolar comparison of a macrocyclic 1.0 M gadolinium chelate and a linear ionic 0.5 M gadolinium chelate. AJR Am J Roentgenol. 2010;194(3):821-9.
65. Richardson RM et al. T2 imaging in monitoring of intraparenchymal realtime convection-enhanced delivery. Neurosurgery. 2011;69(1):154-63.
66. Maki JH et al. Highly accelerated firstpass contrast-enhanced magnetic resonance angiography of the peripheral vasculature: comparison of gadofosveset trisodium with gadopentetate dimeglumine contrast agents. J Magn Reson Imaging 2009;30(5):1085-92.
67. Schreinemacher MH et al. Towards Endometriosis Diagnosis by Gadofosveset-Trisodium Enhanced Magnetic Resonance Imaging. PLoS One. 2012;7(3):e33241.
68. Kuhlemann J et al. Gadofosvesetenhanced MR imaging for the preoperative evaluation of potential living kidney donors: correlation with intraoperative findings. Rofo. 2010;182(11):1001-9.
69. Erb-Eigner K et al. Equilibriumphase MR angiography: comparison of unspecific extracellular and protein-binding gadolinium-based contrast media with respect to image quality. Contrast Media Mol Imaging.2016;11(1):71-6.
70. McDonald RJ et al. Gadolinium retention: a research roadmap from the 2018 NIH/ACR/RSNA workshop on gadolinium chelates. Radiology. 2018;289(2):517-34.
71. Werner P et al. An NMR relaxometry approach for quantitative investigation of the transchelation of gadolinium ions from GBCAs to a competing macromolecular chelator. Sci Rep. 2021;11(1):21731.
72. Khairinisa MA et al. Effects of gadolinium deposits in the cerebellum: reviewing the literature from in vitro laboratory studies to in vivo human investigations. Int J Environ Res Public Health. 2021;18(14):7214.
73. Prince MR et al. Risk factors for NSF: a literature review. J Magn Reson Imaging. 2009;30(6):1298-308.
74. Xue X et al. A nephrotoxicity-free, iron-based contrast agent for magnetic resonance imaging of tumors.
Biomaterials. 2020;257:120234.
75. Yue H et al. New class of efficient T2 magnetic resonance imaging contrast agent: carbon-coated paramagnetic dysprosium oxide nanoparticles. Pharmaceuticals (Basel). 2020;13(10): 312.
76. Brismar TB et al. Oral manganese chloride tetrahydrate: a novel magnetic resonance liver imaging agent for patients with renal impairment. Invest Radiol. 2024;59(2):197-205.
77. Henoumont C et al. Mn-Based MRI contrast agents: an overview. Molecules. 2023;28(21):7275.
78. Bickle I et al. Gadoxetate disodium. Radiopaedia. 2014;DOI:10.53347/rID26957.
79. Huh J et al. Troubleshooting arterialphase MR images of gadoxetate disodium-enhanced liver. Korean J Radiol. 2015;16(6):1207-15.
80. Well L et al. Transient severe respiratory motion artifacts after application of gadoxetate disodium: what we currently know. Rofo. 2018;190(1):20-30.
81. Pietryga J et al. Respiratory motion artifact affecting hepatic arterial phase imaging with gadoxetate disodium: examination recovery with a multiple arterial phase acquisition. Radiology. 2014;271(2):426-34.
82. Gale EM, Caravan P. Gadolinium-free contrast agents for magnetic resonance imaging of the central nervous system. ACS Chem Neurosci. 2018;9(3):395-7.
83. Marasini R et al. Integration of gadolinium in nanostructure for contrast enhanced-magnetic resonance imaging. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2020;12(1):e1580.
84. He W et al. Exceedingly small iron oxide nanoparticles as positive mri contrast agents. Proc Natl Acad Sci USA. 2017;114(9):2325-30.
85. Oberdick SD et al. Iron oxide nanoparticles as positive T1 contrast agents for low-field magnetic resonance imaging at 64 mT. Sci Rep. 2023;13(1):11520.
86. Nayak AB et al. High-resolution, whole-body vascular imaging with ferumoxytol as an alternative to gadolinium agents in a pediatric chronic kidney disease cohort. Pediatr Nephrol. 2015;30(3):515-21.
87. Knobloch G et al. Relaxivity of ferumoxytol at 1.5 T and 3.0 T. Invest Radiol. 2018;53(5):257-63.
88. Mironova A et al. Porous silicon nanoparticles with rare earth as potential contrast agents for MRI and luminescent probes for bioimaging. J biomed photonics eng. 2022;8(2): 020304.
89. Chen et al. Repurposing clinical agents for chemical exchange saturation transfer magnetic resonance imaging: current status and future perspectives. Pharmaceuticals (Basel). 2020;14(1):11.
90. Cho MH et al. Targeted, stimuliresponsive, and theranostic 19F magnetic resonance imaging probes. Bioconjug Chem. 2019;30(10):2502-18.
91. Li Y et al. 19F MRI nanotheranostics for cancer management: progress and prospects. ChemMedChem. 2022;17(4):e202100701.
92. Lizarrondo SMD et al. Tracking the immune response by MRI using biodegradable and ultrasensitive microprobes. Sci Adv. 2022;8(28):eabm3596.
93. Kermanian M et al. A novel mesoporous superparamagnetic hybrid silica/ hydroxyapatite nanocomposite as MRI contrast agent. Chemnanomat. 2021;7(3):284-91.
94. Birte MH et al. Pharmacokinetics, safety, and tolerability of the novel tetrameric, high-relaxivity, macrocyclic gadolinium-based contrast agent gadoquatrane in healthy adults. Invest Radiol. 2024;59(2):140-9.
95. Lohrke J et al. Preclinical profile of gadoquatrane. Invest Radiol. 2022;57(10):629-38.
96. Robert P et al. Contrast-to-dose relationship of gadopiclenol, an MRI macrocyclic gadolinium-based contrast agent, compared with gadoterate, gadobenate, and Gadobutrol in a rat brain tumor model. Radiology. 2020;294(1):117-26.
97. Tweedle MF. Next-generation MRI contrast agents: still including gadolinium. Radiology. 2020;294(1): 127-8.
98. Kang Y, Zhao Y. Preparation of magnetic resonance contrast agent gadolinium-containing organic nanoparticles and their electrochemical behavior investigation. Int J Electrochem Sci. 2022;17:1-10.
99. Hao J et al. A comprehensive overview of the efficacy and safety of gadopiclenol: a new contrast agent for MRI of the CNS and body. Invest Radiol. 2024;59(2):124-30.
100. Cheong BYC et al. Gadoliniumbased contrast agents: updates and answers to typical questions regarding gadolinium use. Tex Heart Inst J. 2022;49(3):e217680.
101. Idée JM et al. The role of gadolinium chelates in the mechanism of nephrogenic systemic fibrosis: a critical update. Crit Rev Toxicol. 2014;44(10):895-913.
102. Mahmood F et al. Safety of gadoliniumbased contrast agents in magnetic resonance imaging-guided radiotherapy
– an investigation of chelate stability using relaxometry. Phys Imaging Radiat Oncol. 2022;21:96-100.
103. Etemadi H et al. Iron oxide nanoparticles: physicochemical characteristics and historical developments to commercialization for potential technological applications. ACS Biomater Sci Eng. 2021;7(12):543250.
104. Dillman JR et al. Safety of gadolinium-based contrast material in sickle cell disease. J Magn Reson Imaging. 2011;34(4):917-20.
105. Jost G et al. Long-term excretion of gadolinium-based contrast agents: linear versus macrocyclic agents in an experimental rat model: Radiology. 2019;290(2):340-8.
106. Bäuerle T et al. Gadolinium-based contrast agents: what we learned from acute adverse events, nephrogenic systemic fibrosis and brain retention. Rofo. 2021;193(9):1010-8.
107. Datta A et al. Current advancement in the development of manganese complexes as magnetic resonance imaging probes J Inorg Biochem. 2022;237:112018.
108. Gulani V et al. Gadolinium deposition in the brain: summary of evidence and recommendations. Lancet Neurol. 2017;16(7):564-70.
109. Yao X et al. Gadolinium retention in the brain of mother and pup mouse: effect of pregnancy and repeated administration of gadolinium-based contrast agents. J Magn Reson Imaging. 2022;56(3):835-45.
110. Davies J et al. Gadolinium: pharmacokinetics and toxicity in humans and laboratory animals following contrast agent administration. Arch Toxicol. 2022;96(2):403-29.
111. Nucera E et al. Contrast medium hypersensitivity: a large Italian study with long-term follow-up. Biomedicines. 2022;10(4):759.
112. Shahid I et al. Use of real-life safety data from international pharmacovigilance databases to assess the importance of symptoms associated with gadolinium exposure. Invest Radiol. 2022;57(10):664-73.
113. Bara MTG et al. Hypersensitivity to gadolinium-based contrast media. Front Allergy. 2022:3:813927.
114. Harvey HB et al. Gadolinium deposition disease: a new risk management threat. J Am Coll Radiol. 2020;17(4):546-50.
115. Jin T et al. Utility of contrast-enhanced T2 flair for imaging brain metastases using a half-dose high-relaxivity contrast agent. AJNR Am J Neuroradiol. 2021;42(3):457-63.
Deep Learning-Based Approaches for Brain Tumour Segmentation and Classification
Authors: Vidya P Baiju,1 Akshitha J,1 *Namasivaya Naveen S1
1. Faculty of Engineering and Technology, Sri Ramachandra Institute of Higher Education and Research, Chennai, India *Correspondence to namasivayanaveen@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Received: 14.08.24
Accepted: 19.08.24
Keywords: Brain tumour, convolutional neural network (CNN), deep learning, segmentation.
Brain tumours are caused by the abnormal growth of cells in the brain. This occurs mainly due to genetic changes or exposure to X-ray radiation. When the tumours are detected early, they can be removed via surgery. The tumour can be removed through radiotherapy and chemotherapy if the removal of the tumour through surgery affects the survival rate. There are two main classifications of tumours: malignant or cancerous and benign or non-cancerous. Deep learning techniques are considered as they require more minimal human intervention than machine learning; they are built to accommodate huge amounts of unstructured data, while machine learning uses traditional algorithms. Though deep learning takes time to set up, the results are generated instantaneously. In this review, the authors focus on the various deep learning techniques and approaches that could detect brain tumours that were analysed and compared. The different types of deep learning approaches investigated are convolutional neural network (CNN), cascaded CNN (C-CNN), fully CNN and dual multiscale dilated fusion network, fully CNN and conditional random field, U-net convolutional network, fully automatic heterogeneous segmentation using support vector machine, residual neural network, and stacked denoising autoencoder for brain tumour segmentation and classification. After reviewing the algorithms, the authors have listed them based on their best accuracy (U-net convolutional network), dice score (residual neural network), and sensitivity score (cascaded CNN).
Key Points
1. AI technologies enable faster and more precise diagnostic capabilities by analysing large datasets from medical imaging and tests. Clinicians can use AI to complement their diagnostic expertise and improve patient outcomes.
2. The adoption of AI in healthcare presents challenges around data privacy, ethical usage, and regulation. Clinicians must be mindful of these aspects to ensure AI is integrated responsibly and aligns with medical ethics.
3. AI is a tool designed to augment clinical decision-making, not replace it. Clinicians should focus on collaborating with AI systems, ensuring that human oversight and expertise remain central to patient care.
INTRODUCTION
A brain tumour develops as a result of abnormal cell growth in the brain. Tumours are classified as malignant or benign. Malignant tumours are cancerous, whereas benign tumours are noncancerous. The other types of tumours are meningiomas, gliomas, and pituitary tumours. Meningiomas are mostly benign tumours originating from the arachnoid cap cells, representing 13–26% of all intracranial tumours. When the meningioma cannot be completely resected, radiosurgery is used to treat brain tumours.1 Gliomas are the most generally observed tumours, with different shapes and ambiguous boundaries, making them probably the hardest tumour to identify.2 Pituitary tumours are viewed as benign cancers, yet roughly 10% of them can have a forceful way of behaving, and once in a long while (0.2%) can introduce metastasis called pituitary carcinomas.3
The tumours show symptoms despite the size and part of the brain being affected. These include headaches, seizures, vomiting, and, in extreme cases, difficulty walking.4 Chemotherapy, radiation therapy, and surgery are used to treat brain tumours.5 Surgeries carry risks since the brain is a non-fungible organ. After surgery, medications are used to reduce the swelling around the tumour; seizures must be avoided, or another set of medications is needed.6 These treatments have a better success rate if tumours can be detected early and accurately. A few environmental factors that cause brain tumours are vinyl chloride or ionising radiation exposure. This leads to the mutation and deletion of tumour suppressor genes, causing brain tumours.7 Another factor is inheritance; conditions like neurofibromatosis
Type 2 carry a high risk of developing brain tumours.8,9
Deep learning techniques are frequently used for image segmentation, classification, and optimisation in the medical industry in order to detect cancers precisely. There are different scanning techniques used to detect tumours; a few of them are CT, single photon emission CT (SPECT), PET,
magnetic resonance spectroscopy (MRS), and MRI. CT has altered the course of symptomatic therapy since its invention in the 1970s. Increased radiation from patients is one of the major problems brought on by the increasing usage of CT.10 SPECT is a method generally utilised in nuclear medicine for imaging numerous organs, including the skeleton and heart, as well as for entire body imaging for the recognition of tumours.11 The advancements in PET are assessed with an accentuation on instrumentation for clinical PET imaging. PET provides good-quality images, high diagnostic accuracy, and short imaging protocols.12 The nuclear magnetic resonance principle underpins MRS. It can be used almost in any tissue of the body, but the brain is the major organ of interest in MRS. For biochemical characterisation, MRS provides an invasive diagnostic tool.13 This review uses an MRI scanning technique for comparison and analysis.
Brain MRI scans are used, and these include effective and quantitative analysis. MRI is frequently depicted as a protected methodology since it uses no ionising radiation.14 MRI is a sophisticated imaging strategy that has emerged as a clinical methodology in recent years.15 The process of image segmentation involves classification based on pixel-to-pixel techniques. There are many deep learning approaches that are used to detect these tumours such as convolutional neural network (CNN), contourlet convolutional neural networks (C-CNN), Fully Automatic Heterogeneous Segmentation using Support Vector Machine (FAHS-SVM), Fully Convolutional Neural Network and Dual Multiscale Dilated Fusion Network (FCNN and DMDF-Net), Residual Neural Network (ResNet), CNN (parametric optimisation approaches), CNN based Computer Aided Diagnostic (CAD) System approach, Cascaded CNN, FCNN and Conditional Random Field (CRF), Stacked Denoising Auto Encoder (SDAE), U-Net Convolutional Network (U-NET), and CNN (semi-supervised learning). All these approaches make use of MRI images as data input. Some pre-processing of raw MRI images is performed, such as removing unwanted parts of the image, enhancing
contrast, etc., to improve the processing time and accuracy of algorithms. This review primarily focuses on identifying the best deep learning-based approach for segmenting and classifying brain tumours.
METHODS
The research articles were obtained from Scopus, Web of Science, and PubMed using the combined keyword phrase ‘Brain Tumor Segmentation and Classification’. Fifteen research articles on the topic of ‘Brain Tumor Segmentation and Classification’, published from the year 2017 onwards, were selected and used for this study. The research articles were studied to understand the type of deep learning approach used to detect the tumour in the brain. The uniqueness of each approach, the datasets used for the research, the type of tumour detected, limitations, and accuracy/scores were also checked.
Datasets
The following are the datasets used for brain tumour segmentation and classification. From a hospital in China, Nanfang, and Tianjing Medical University, a dataset has been collected from 233 patients. The dataset includes the years from 2005–2010. It contains 3,064 slices with 708 meningiomas, 1,426 gliomas, and 930 pituitary tumours in sagittal, coronal, and axial views. With cross-validation indices, 80% of images are employed for training and the rest for performance measurements.16 A dataset consisting of multi-spectral brain MRIs includes images of benign tumours, specifically meningiomas.17 A dataset tested from The Cancer Imaging Archive (TCIA) from Thomas Jefferson University, Philadelphia, Pennsylvania, USA, includes a total of 4,069 brain images, consisting of 3,081 non-healthy images (with abnormalities) and 988 healthy brain images, which were used for testing.18 And finally, a brain tumour dataset of 253 images, of which 98 were healthy and 155 were tumouraffected. About 80% of the images were used for training the model, while the rest were for testing purposes.19 The following experiments were conducted using the
brain tumour segmentation challenge (BRATs) dataset from 2013–2020.
Experiments Conducted in BRATs 2013
This included T1, T2, fluid-attenuated inversion recovery (FLAIR) images of 30 patients. The tumour labels are annotated as (1) necrosis, (2) oedema, (3) nonenhancing tumour, (4) enhancing tumour, and 0 was denoted for normal tissue.20,21 This dataset consisted of 65 patients with glioma, including 14 low-grade gliomas (LGG) and 51 high-grade gliomas (HGG) from different centres: University of Bern, Switzerland; University of Debrecen, Hungary; Heidelberg University, Germany; and Massachusetts General Hospital, Boston, USA. The MRI scans included T2, T1, T1-c, FLAIR.22
Experiments Conducted in BRATs 2015
Training sets containing 220 patients with HGG and 54 with LGG were included. This involved all four MRI modalities. The labels were listed as follows: necrosis, oedema, non-enhancing tumour, and enhancing tumour.23 It included all modalities of MRI with an imaging size of 240x240x155. The modal images were linearly positioned to match the typical human brain.24 This included images from BRATs 2012, 2013, and TCIA. It consisted of 110 cases of unknown grades, 220 HGG, and 54 LGG for training.22 It also included images from medical image computing and computerassisted intervention (MICCAI), which has data on patients with glioma. All MRI techniques were used, and they were classified as normal brain tissue, tumour, oedema, necrosis, or increased tumour.25
Experiment Conducted in BRATs 2016
It included 220 patients with HGG and 54 patients with LGG with 191 cases with unknown grades.22
Experiments Conducted in BRATs 2017
The experiments included 146 photos from patients with brain tumours and a validation set of 46 people who had the disease, whereas the testing sets are unknown.
All the modalities of MRI were used.26 It included scans of 210 patients with HGG and 75 patients with LGG. Classifications such as a full tumour, oedema, enhancing tumour, necrosis, and non-enhancing tumour were given.27
Experiments Conducted on BRATs 2018
Patient data on histological subregions, aggressiveness, and prognosis were included, as well as multimodal MRI scans. The dimensions of the image are 240x240x150. Of 75 cases of LGG and 210 cases of HGG, 80% of it were for training, 10% for validation, and 10% for testing. It was grouped as necrosis, oedema, nonenhancing tumour, or enhancing tumour.6 It included 285 MRIs of patients with LGG or HGG. The images were acquired from 19 imaging centres. It was labelled as nontumour, contrast-enhancing core, nonenhancing core, or oedema.28 A validation set of 66 patients with brain tumours and images from 191 patients with brain tumours were included, while the testing sets are unknown. All the modalities of MRI were used (FLAIR, T1ce, T1, and T2).26
Experiments Conducted on BRATs 2020
An experiment conducted on BRATs 2020 contains 370 images of HGG and LGG tumours. Following their use, all MRI modalities were classified into peritumoural oedema, necrotic/non-enhancing tumour, or enhancing tumour tissues.29
A brain tumour segmentation and classification model using a deep CNN that includes a multiscale approach was used by Díaz-Pernas FJ et al.16 The method analyses MRI scans contained meningioma, glioma, and pituitary tumours from different viewpoints. The purpose was to develop this approach by using a T1-CE MRI scan dataset. Multi-pathway MRI scans
were processed pixel by pixel by CNN architecture to cover the full image and separate the tumour-affected areas from the healthy ones. The size of the sliding window was about 65x65 pixels and 11x11 pixels. The feature maps were classified into large, medium, and small, and the classification of three types of tumours was hence defined. A few equations were used as part of the neural network training to get the results. The dice, sensitivity, and percentage tissue type agreement score pttas (score) were calculated and graphed into a histogram. The accurate score (pttas) was identified through the histogram. After the confusion matrix was calculated, the tumour classification accuracy was also calculated (0.973). Finally, a graph was draughted between the tumour classification and confidence threshold. This approach was compared with seven other deep learning approaches, and this was concluded to be the best among the others.16
Cascaded Convolutional Neural Network
Ranjbarzadeh R et al.6 considered a preprocessing approach to work with small parts of the image rather than the whole image. C-CNN incorporates both local and global characteristics into the two routes. The distance-wise attention mechanism was used to improve the accuracy of brain tumour segmentation, and it takes into account the effect of the tumour and the brain’s centre location within the model. The experiment was carried out using the BRATs 2018 dataset. The biological arrangement of the brain’s visual cortex serves as an inspiration for the CNN model’s structure.
For the experimental results, there are three criteria, namely HAUSDORFF99 for assessing the distance between the predicted and ground-truth region; sensitivity, which measures tumour pixels; and dice similarity, which computes the overlap between the ground truth and prediction. Comparisons were made with the baseline on BRATs 2018 dataset, and even though the proposed method had outstanding results, the algorithm was able
to encounter tumours that were larger than one-third of the entire brain.6
Fully Automatic Heterogeneous Segmentation Using Support Vector Machine Approach
For segmenting brain tumours, FAHSSVM was employed by Jia Z and Chen D.17 High-level homogeneity between the adjoining brain tissue’s structure and the segmented area made the segmentation functional. An extreme learning machine algorithm was used for getting regressions and classifications. The results showed that the accuracy was almost 98.51%. These experiments were conducted on a multi-spectral brain dataset. The following steps are involved in the architecture of the proposed method. One is pre-processing, which improves the MRI’s quality and makes it appropriate for subsequent processing. Second, skull stripping makes it possible to remove more brain tissues from brain pictures. Third, morphological operation and segmentation, which uses the wavelet transformation for efficient segmentation of MRI. The set of high-level visual details, such as contrast, form, colour, and texture, make up the feature extraction. The comparison was made between CNN, U-NET, and U-net with residual connections (Unet-res).17
Residual Neural Network Approach
ResNet, an automated method, was used to segment brain tumours by Shehab LH et al.23 This method relies on addition between the output layer and its input to provide greater accuracy and faster training processes. The approach was used to locate the whole tumour area, core tumour area, and enhancing tumour area from the BRATs 2015 dataset. Since the 3x3 convolutional kernels have a larger kernel and a similar response field, they were used in the model. The three stages of the ResNet approach that were proposed here are pre-processing, segmentation by ResNet, and post-processing. In the pre-processing stage, bias field distortion on four MRI sequences is fixed, and the generated patches are normalised. ResNet 50 was used for segmentation since it has a deeper layer and lesser parameters, so the
training time would be faster. Finally, in the post-processing stage, FLAIR images were considered to locate the tumour. Evaluation metrics were used for testing the brain tumour segmentation. Comparing it with a few other methodologies, it was found that ResNet50 was the best, as the core accuracy was 0.84 and the highest among the others, and the computation time for the proposed methodology was faster (62 mins) compared to the other methodologies.23
Nayak DR et al.19 used a special CNN architecture, the CNN model, together with a parametric optimisation strategy to assess brain tumour MRI. The model’s accuracy rate remains constant throughout Taguchi’s L9 design of experiment. The collection contained 253 medical photos of the brain, 98 of which were in a healthy state and 155 of which were images with tumours. The finest solutions to engineering challenges were produced using the forensic investigation algorithm, material creation algorithm, and sunflower optimisation algorithm, producing an even or random population. Using the brain tumour MRIs dataset and the suggested CNN model, the sunflower optimisation and material creation algorithms demonstrated excellent performance throughout the simulations.19
Convolutional Neural Network Approach
The segmentation of brain tumours was automated by Annmariya E et al.29 using a deep learning model. It automated the differentiation of brain tumours using several MRI modalities. The MR sequences were independently determined by single-channel input and multi-channel input. Experiments were run on the BRATs 2015 dataset of 220 MR images.
The input image was 144x128x96 in size, and the HighRes3DNet architecture was used. The first seven levels of the 20-layer structure were derived from the input data using a 3x3x3 voxel convolutional kernel. The medium-level features from the input were encoded in the following
seven layers, while high-level features were extracted in the last six levels using a dilated convolutional kernel. In single-channel models with quantitative evaluation, FLAIR sequence produced higher segmentation accuracy. The model using FLAIR and T2W inputs produced a 0.80±0.10 dice index through dual-channel models, demonstrating better performance. The FLAIR sequence was more accurate than other sequences at segmenting brain tumours, according to the results of segmenting single-channel sequences.29
From the newly designed CNN, useful features from multi-modality images are learnt to combine multi-modality information. This technique is applied to most classifications, and the accuracy is high too. This method uses multimodal and complementary data from BRATs 2013 T1, T1c, T2, and FLAIR images. Slices from the x, y, and z axils are chosen as inputs for each voxel in the 3D picture. This design converts tri-planar 2D CNNs from 3D CNN problems because it is more effective at lowering computing complexity. Dice ratio is used for evaluation to get segmentation accuracy. In comparison with Menze et al.30 and Bauer et al.,31 the proposed approach had better mean accuracy.20
Fully Convolutional Neural Network and Dual Multiscale Dilated Fusion Approach
FCNN & DMDF techniques were used to obtain the segmentation results with appearance and spatial consistency by Deng W et al.24 The Fisher vector encoding method was used to analyse the texture features, i.e., to change the rotation and scale in the texture image. The study experimented on the BRATs 2015 dataset with a 3D size of a modal MR image of 240x240x155. The similarity of the dice segmentation results of the brain tumour were analysed using the metrics coefficient, sensitivity, and positive predictive value. Compared with the other traditional segmentation methods, this approach had improved accuracy and stability, with an average dice index of 90.98%.24
Arabahmadi M et al.21 adopted this method as its deep learning strategy since CNN (CAD) systems can help identify brain tumours from MR images. This entailed preprocessing, which included the region of interest segmentation (for brain tumours), enhancement, noise reduction, resizing, and skull stripping of MR images. The tests are performed on the BRATs 2013 dataset, which contains 50 photos of 30 patients and 30 locations labelled as necrosis, oedema, non-enhancing tumour, enhancing tumour, or everything else. Both local and global features were implemented using this technique. In contrast to the global features, which used 14x14 filters, the local features used 7x7 filters. The pace was raised by 40% by the convolutional layer, which was the last layer. The results demonstrated that deeper networks with larger patches outperform shallower networks, with dice scores of 0.88, 0.61, and 0.59 for patch sizes of 28x28, 12x12, and 5x5, respectively.21
Cascaded Convolutional Neural Network Approach
Wang G et al.26 proposed a cascaded CNN to segment brain tumours into hierarchical subregions. To increase segmentation accuracy, a 2.5D network and testtime augmentation were also applied. Experiments were conducted on the BRATs 2017 dataset. 2.5D anisotropy CNNs with a stack of slices as input with a large intraslice receptive field and a small inter-slice receptive field have been proposed. By decomposing the 3D 3x3x3 convolutional kernel, the anisotropic receptive field was made. The kernel size of the intra-slice and inter-slice convolutional kernel are 3x3x1 and 1x1x3, respectively. This method was compared with 3D U-Net, with the whole tumour by W-Net, tumour core by T-Net, and enhancing tumour core by E-Net, and adapting W-Net without using the cascade of binary prediction. The results demonstrated that uncertainty estimation aids in both improving segmentation performance and spotting probable mis-segments.26
Fully Convolutional Neural Network and Conditional Random Field Approach
FCNN and CRF approaches were used by Zhao X et al.22 to obtain segmentation with appearance and spatial consistency. These are obtained in axial, coronal, and sagittal views, and the slice-by-slice method is used for the segmentation of brain images. BRATs 2013, 2015, and 2016 were used to locate glioma tumours in patients. Compared with other methods, the evaluation results of BRATs 2013 are top-ranked.22
Stacked Denoising Autoencoders Approach
In the study by Ding Y et al.,25 multimodal MRI brain tumour pictures were segmented using SDAEs. After training, the raw parameters that feed into the classification feed-forward neural network are obtained. Then post-processing is carried out. On BRATs 2015, experiments were done, and a preliminary dice score of 0.86 was obtained. Each layer in the architecture comprises several hidden layers, an encoder and a decoder. Input and hidden layers make up encoders, and the decoder gets the output. Normal brain tissue, tumour, oedema, necrosis, and enhanced tumour are the five outputs that make classification. For further optimisation, the gradient descent method is used to classify the centre of the image. The evaluation was on true positive, false positive, false negative, dice, and Jaccard coefficients, and while comparing with other methods, SDAE showed better segmentation results than the others.25
U-NET Approach
The usage of U-NET as a deep learning approach is discussed in the study by Cherguif H et al.27 Real photos from the BRATS 2017 datasets for medical image computing and computer-assisted interventions were used. Effective segmentation was offered with a dice similarity coefficient metric of 0.81805 and 0.8103 for the utilised dataset. The architecture was composed of three sections: the encoder, which reduces the feature maps from 240x240 to the bottleneck; the bottleneck, which
compresses the feature maps to 15x15; and the decoder, which expands them back to 240x240. For ease of comparison, UNET-1 and UNET-2 are used instead. Additionally, when compared to other techniques, this one has a dice similarity coefficient (DSC) of 0.81 for brain segmentation and an accuracy of 0.99 for a whole tumour with core one.27
Mlynarski P et al.28 introduced the idea of extending the segmentation networks with image-level classification. The model was trained for segmentation and classification tasks to annotate images. The experiments were conducted on the BRATs 2018 dataset with 281 multi-scan images. An additional branch, UNET is proposed to exploit information on annotated images. The feature map size is 101x101, from which the classification branch has to output two global classification scores; i.e., tumour absent and tumour present. Initially, the kernel sizes were reduced to 8x8 and mean pooling was used to avoid information loss and optimisation problems. Once the feature map was reduced from 64 to 32, the size was 11x11 of a fully connected layer of classification. In comparison, this approach outperforms three binary segmentation problems in a multiclass setting.28
It has been found that the CNN approach has been used often. CNN is traditionally used for image-based tasks. Since images are an array of numbers indicating colour intensity, they are suitable for image classification. Hence, the CNN algorithm is the most commonly used.32 The deep learning model that is better than CNN and found in the paper is SVM. Having huge datasets separates the boundaries of two classes and provides a warning.33 It can also perform in n-dimensional space. Table 1 shows the comparison of the different deep learning methods used for brain tumour segmentation and classification with respect to accuracy, dice score, and sensitivity score. Comparing the research papers based on the accuracies and scores, the highest accuracy is found in U-NET, the highest dice score in ResNet, and the highest sensitivity score in C-CNN.
CAD: computer aided diagnostic; CNN: convolutional neural network; C-CNN: contourlet convolutional neural networks; CRF: conditional random field; FAHS-SVM: fully automatic heterogeneous segmentation using support vector machine; FCNN and DMDF-Net: fully convolutional neural network and dual multiscale dilated fusion network; ResNet: residual neural network; SDAE: stacked denoising auto encoder; U-NET: U-net convolutional network.
Hence, each algorithm has advantages and disadvantages, displaying different scores and accuracies.
CONCLUSION
The advantage of using deep learning is that it provides high-quality accuracy. It is concluded that the U-NET algorithm has the highest accuracy compared with the others (0.99). Almost every article includes dice and sensitivity scores that check the performance of the image and how a positive value can be generated correctly. Taking this into consideration, for the dice score, ResNet approach has the highest value (0.93), and for the sensitivity score, C-CNN, which includes the pre-processing approach, has the highest value of 0.97. Future studies will focus on enhancing these findings and utilising deeper architectures to boost output segmentation performance. Methods for segmenting brain tumours are anticipated to be powered by weak,
References
1. Marosi C et al. Meningioma. Crit Rev Oncol Hematol. 2008;67(2):153-71.
2. S. Hussain et al. Segmentation of glioma tumors in brain using deep convolutional neural network. Neurocomputing. 2018;282:248-61.
3. Kasuki L, Raverot G. Definition and diagnosis of aggressive pituitary tumors. Rev Endocr Metab Disord. 2020;21(2):203-8.
4. Mondia MWL et al. Brain tumor infodemiology: worldwide online health-seeking behavior using Google trends and Wikipedia pageviews. Front Oncol. 2022;12:855534.
5. Gilbert M et al. The PDQ Adult Brain Tumors Treatment. Journal of the National Cancer Institute. 2014;106(3):dju071.
6. Ranjbarzadeh R et al. Brain tumor segmentation based on deep learning and an attention mechanism using MRI multi-modalities brain images. Sci Rep. 2021;11(1):10930.
7. Kleihues P et al. Type and frequency of p53 mutations in tumors of the nervous system and its coverings. Recent Results Cancer Res. 1994;135:25-31.
8. Hodgson TS et al. Neurological
unsupervised training with fewer labels. For successful brain tumour segmentation networks, the authors anticipate combining tumour degrees such as Grade 1, 2, 3, and 4, where Grade 1 has less aggressive behaviour and tumour morphology, which records the type of tumour that has developed and how it behaves with neural architecture search algorithms. The growing role of AI in healthcare represents a paradigm shift, promising to revolutionise clinical practice, medical research, and patient care. AI’s potential to analyse vast amounts of data quickly and accurately can significantly reduce the workload of clinicians, allowing more time for patient interaction and personalised care. Nevertheless, the impact of AI will largely depend on how well it integrates with existing healthcare systems, its acceptance by medical professionals, and its ability to enhance rather than replace human judgement. Continuous education and training for healthcare professionals on AI technologies will be crucial in ensuring its safe and effective implementation.
management of Von Hippel-Lindau disease. Neurologist. 2016;21(5):73-8.
9. Rogers L et al. Meningiomas: knowledge base, treatment outcomes, and uncertainties. A RANO review. J Neurosurg. 2015;122(1):4-23.
10. Power SP et al. Computed tomography and patient risk: facts, perceptions and uncertainties. World J Radiol. 2016;8(12):902-15.
11. Warwick JM. Imaging of brain function using SPECT. Metab Brain Dis. 2004;19(1-2):113-23.
12. Bateman TM. Advantages and disadvantages of PET and SPECT in a busy clinical practice. J Nucl Cardiol. 2012;19(Suppl 1):S3-11.
13. Gujar SK et al. Magnetic resonance spectroscopy. J Neuroophthalmol. 2005;25(3):217-26.
14. Dill T. Contraindications to magnetic resonance imaging: non-invasive imaging. Heart. 2008;94(7):943-8.
15. Geva T. Magnetic resonance imaging: historical perspective. J Cardiovasc Magn Reson. 2006;8(4):573-80.
16. Díaz-Pernas FJ et al. A deep learning approach for brain tumor classification and segmentation using a multiscale convolutional neural network. Healthcare (Basel). 2021;9(2):153.
17. Jia Z, Chen D. Brain tumor identification and classification of MRI images using deep learning techniques. IEEE Access. 2020;DOI:10.1109/ ACCESS.2020.3016319.
18. Al-Hadidi MR et al. Glioblastomas brain tumour segmentation based on convolutional neural networks. Int J Electr Comput Eng. 2020;10(5):525664.
19. Nayak DR et al. Brain tumour classification using noble deep learning approach with parametric optimization through metaheuristics approaches. Computers. 2022;11(1):10.
20. Lang R et al. Brain tumor image segmentation based on convolution neural network. 9th International Congress on image and signal processing, biomedical engineering and informatics (CISP-BMEI), 15-17 October, 2016.
21. Arabahmadi M et al. Deep learning for smart healthcare-a survey on brain tumor detection from medical imaging. Sensors (Basel). 2022;22(5):1960.
22. Zhao X et al. A deep learning model integrating FCNNs and CRFs for brain tumor segmentation. Med Image Anal. 2018;43:98-111.
23. Shehab LH et al. An efficient brain tumor image segmentation based on deep residual networks (ResNets). J King Saud Univ Eng Sci. 2021;33(6):404-12.
24. Deng W et al. Brain tumor segmentation based on improved convolutional neural network in combination with non-quantifiable local texture feature. J Med Syst. 2019;43:1-9.
25. Ding Y et al. Multi-modal brain tumor image segmentation based on SDAE. Int J Imaging Syst Technol. 2018;28(1):38-47.
26. Wang G et al. Automatic brain tumor segmentation based on cascaded convolutional neural networks with uncertainty estimation. Front Comput Neurosci. 2019;13:56.
27. Cherguif H et al. Brain tumor segmentation based on deep learning. International Conference on Intelligent Systems and Advanced Computing Sciences (ISACS), 26-27 December, 2019.
28. Mlynarski P et al. Deep learning with mixed supervision for brain tumor segmentation. J Med Imaging (Bellingham). 2019;6(3):034002.
29. Annmariya E et al. Machine learning and internet of things based fruit quality monitoring system: a proof of concept implementation and analysis. IJRASET .2020;8(6):2315-23.
30. Menze BH et al. A generative model for brain tumor segmentation in multi-modal images. Med Image Comput Comput Assist Interv. 2010;13(Pt 2):151-9.
31. Bauer S et al. Fully automatic segmentation of brain tumor images using support vector machine classification in combination with hierarchical conditional random field regularization. Med Image Comput Comput Assist Interv. 2011;14(Pt 3):354-61.
32. Hasan H et al. A comparison between support vector machine (SVM) and convolutional neural network (CNN) models for hyperspectral image classification. IOP Conf Ser: Earth Environ Sci. 2019;357:012035.
33. Dehghani F et al. Joint brain tumor segmentation from multi-magnetic resonance sequences through a deep convolutional neural network. J Med Signals Sens. 2024;14:9.
Evolution of Proliferative Lupus Nephritis with Focal Extracapillary Proliferation in Latin American Patients with Lupus
Authors: José Lucas Daza,1 Yaroslad De La Cruz,1 Gerardo Gutierrez,1 Marcelo De Rosa,1 Emilio D Valenzuela,2 Verónica Remache,3 Andres Cardenas,4 *Juan Sebastián Reyes Bello5
1. University of Buenos Aires, Argentina
2. Pontificia Universidad Católica De Chile, Santiago, Chile
3. Rey Juan Carlos Madrid University, Spain
4. Department of General Medicine, University Cooperativa, Bogotá, Colombia
5. Department of General Medicine, Fundación Universitaria Sanitas, Bogotá, Colombia
*Correspondence to jureyesbe@unisanitas.edu.co
Disclosure: The authors have declared no conflicts of interest.
Objectives: This study aimed to investigate the association between the extent of focal extracapillary proliferation and the likelihood of achieving complete remission at 24 months in patients with lupus nephritis (LN).
Methods: A retrospective observational analysis was conducted on 124 patients with proliferative focal and diffuse LN. Patients were categorised into subgroups based on the extent of extracapillary involvement (Group 1: 5–24% crescents, Group 2: 25–50% crescents, Group 3: >50% crescents, and control group without extracapillary involvement). The primary outcome was the rate of achieving complete remission at 24 months, defined according to the 2021 Kidney Disease: Improving Global Outcomes (KDIGO) standards. Statistical analyses were performed using logistic regression.
Results: A total of 107 women and 17 men participated, with mean ages of 35±10 years and 34±12 years in the study and control groups, respectively. The control group exhibited a significantly higher rate of complete remission compared to the subgroups with extracapillary proliferation. Specifically, Group 1 had an odds ratio of 7.2, (95% CI: 2.3–20.2) and a p-value of 0.001, indicating a lower probability of achieving remission.
Conclusions: The presence of focal extracapillary proliferation in patients with LN was associated with a decreased likelihood of achieving complete remission at 24 months. This finding emphasises the importance of considering the extent of extracapillary proliferation in predicting treatment outcomes for LN.
Key Points
1. This study investigated the association between the extent of focal extracapillary proliferation and the likelihood of achieving complete remission at 24 months in patients with lupus nephritis.
2. Patients with extracapillary involvement greater than 5% had higher proteinuria levels and reduced likelihood of achieving remission compared to those without crescents.
3. The study highlights the importance of assessing the extent of extracapillary proliferation as a critical prognostic factor in determining lupus nephritis outcomes.
INTRODUCTION
Proliferative lupus nephritis (LN) with focal extracapillary proliferation (FEP) is a common finding in renal biopsies of patients with LN, but little is known about its progression.1 It is well established that patients with more than 50% of glomeruli showing crescents, a condition known as diffuse extracapillary proliferation (DEP), have a worse prognosis.2 However, there is limited published data on the remission rate in patients with LN Class III-IV with FEP (involving less than 50% of affected glomeruli).
Despite improvements in immunosuppressive therapies, approximately 25–35% of patients with proliferative LN progress to end-stage renal disease requiring renal replacement therapy.3 Therefore, early diagnosis; a comprehensive understanding of clinical, demographic, and histological patterns in each patient; and identifying factors influencing the disease’s progression are crucial. The presence of crescents in more than 50% of glomeruli in a renal biopsy indicates a poor prognosis,4 but there are few reports on the evolution of patients with FEP.5 Moreover, it remains uncertain whether this condition affects the patients’ outcomes and prognosis.
It is important to mention that there is little or no data on the Hispanic population that identifies or characterises the renal biopsies of patients with LN, and the presence of extracapillary involvement, and also performs a statistical analysis as a predictor of non-response to current biological therapies, such as for anti-CD20.
The data that have been extrapolated have been obtained from studies in the Asian population, where extracapillary involvement is clearly a determining predictor in the evolution and remission of the disease.
This study is based on pathology records taken from nephrology departments in only medical centres that have a high level of complexity in the countries Argentina, Colombia, Ecuador, and Bolivia. A retrospective analysis of renal biopsies was conducted from a cohort of 124 patients with proliferative LN, either focal or diffuse. The parameters analysed were demographic characteristics, disease progression, and their correlation with clinical and laboratory parameters comparing two groups with FEP (based on its magnitude) with DEP and a control group (Class III and IV LN without crescents). Table 1 displays some of these demographic characteristics: age at presentation, gender, presence of hypertension, and duration of symptoms until the time of biopsy.
METHODS
The term crescent is used to describe a lesion characterised by extracapillary hypercellularity, composed of a variable mixture of cells. Some crescents may consist predominantly of epithelial cells, while others mainly comprise monocytes and/or macrophages (Figure 1).
To distinguish crescents from the apposition of hypertrophied visceral and parietal single layers, crescents must be
Table 1: Sociodemographic characteristics and laboratory findings of patients with lupus nephritis.
Laboratory Findings
*Proteinuria expressed in g/24 hours
†Creatinine expressed in mg/dL, M, and interquartile range
‡Control group: focal or diffuse proliferative lupus nephritis without extracapillary involvement
§Group 1: 5–25% crescents
**Group 2: 25–50%
††Group 3: >50% crescents
The data is divided into a control group and three study groups based on the extent of extracapillary proliferation: Group 1 with 5–25% crescents, Group 2 with 25–50% crescents, and Group 3 with more than 50% crescents. Key characteristics such as age, gender distribution, and the prevalence of hypertension are listed alongside various laboratory findings including proteinuria, creatinine levels, ANA positivity, ds-DNA positivity, C3 and C4 levels, and urinary sediment abnormalities.
ANA: antinuclear antibodies; CR: complete regression; ds-DNA: double-stranded DNA; HTN: hypertension; IQR; interquartile range; M: mean; R: regression; SD: standard deviation expressed in absolute number and percentage; USR: urinary sediment.
PAS staining of A) endocapillary hypercellularity; B) mesangial hypercellularity and segmental sclerosis; C) karyorrhexis (HE stains), masson trichrome staining; D) cellular crescent; E) Fibrinoid necrosis and cellular crescent; and F) Segmental sclerosis.
HE: Haematoxylin and eosin stain; PAS: periodic acid–Schiff.
composed of two or more layers of cells in Bowman’s space. The International Society of Nephrology (ISN) and Renal Pathology Society (RPS) criteria define a crescent as involving 25% or more of the glomerular capsule’s circumference.8 However, in this study, it was considered a threshold of 10% or more, based on evidence from the Oxford classification of IgA nephropathy,6 considering extracapillary proliferation of more than 5%. This decision was made because not only the extension but also the pathogenic mechanism of extracapillary proliferation likely plays a significant role in the patient’s progression.
Clinical and pathological characteristics of renal biopsies from 124 patients with proliferative focal and diffuse LN who met the inclusion criteria were analysed.
Inclusion Criteria
• Diagnosis of systemic lupus erythematosus according to the 1982 American College of Rheumatology (ACR) criteria;7
• renal biopsies showing focal lupus nephritis Class III and diffuse lupus nephritis Class IV, based on the ISN and RPS classification from 2003; and8
• similar induction and maintenance treatment.
Exclusion Criteria
• Heterogeneity in treatments: patients who received different induction or maintenance treatments were excluded to maintain treatment uniformity;
• follow-up period of less than 24 months; and
• renal biopsy not processed by nephropathologists: this was considered to ensure the accuracy of histological assessment.
Data Collection
Data were collected from medical records, including demographic characteristics (age, gender, presence
Figure 1: Glomerular lesions.
of hypertension), clinical presentation, laboratory findings (proteinuria, creatinine levels, antinuclear antibodies, ds-DNA, C3, C4 levels, urinary sediment analysis), and treatment details. Renal biopsies were evaluated for the presence and extent of extracapillary proliferation.
Renal Pathology
Patients underwent a renal biopsy at the time of LN diagnosis and were classified according to the 2003 ISN/RPS criteria for LN.8 Activity index and chronicity index were calculated following the Austin criteria.9
Complete remission was considered when:
• urinary sediment was inactive (defined as less than five dysmorphic red blood cells per high-power field 40X and the absence of RBC casts);
• proteinuria was less than 500 mg in 24 hours; and
• evidence of serological inactivity (defined as the normalisation of complement factors C3, C4, CH50, and anti-DNA).
Statistical Analysis
Out of the 220 renal biopsies with proliferative focal or diffuse LN initially analysed, 96 were excluded due to lack of follow-up until 24 months or heterogeneity in induction and maintenance treatment, leaving a total of 124 histological samples.
The normality of variables was determined using the Kolmogorov-Smirnov test. The Kruskal-Wallis test with Bonferroni post hoc analysis was performed. The chi-square test was used for categorical variables, with post hoc analysis using standardised residuals. Univariate logistic regression analysis was conducted to determine complete remission of LN, calculating odds ratios (OR) and 95% CI. Dummy variables were encoded for categorical variables and incorporated into the logistic regression. Multivariate analysis was performed for statistically significant variables. A p-value of <0.05 was considered statistically
significant, and data were presented as means and standard deviation.
RESULTS
A total of 124 patients diagnosed with Class III or IV+V LN from multiple Latin American countries were included in this retrospective observational analysis. The majority of participants were female (107/124, 86.2%) with a mean age of 35±10 years (Table 1). The control group consisted of 50 patients with LN Class III and IV, without extracapillary involvement. Patients were further categorised based on the extent of extracapillary involvement into Group 1 (5–24% crescents, n=28), Group 2 (25–50% crescents, n=29), and Group 3 (>50% crescents, n=17), or control group without extracapillary involvement.
Baseline Characteristics
Sociodemographic characteristics including age, gender, and hypertension prevalence were compared among the control group and the three extracapillary involvement subgroups. Laboratory findings, including proteinuria, creatinine levels, antinuclear antibodies, ds-DNA, C3, C4 levels, and urinary sediment analysis, were analysed for the different patient groups (Table 1).
Primary Outcome Assessment
The primary outcome of achieving complete remission at 24 months was assessed based on the 2021 Kidney Disease: Improving Global Outcomes (KDIGO) standards. Univariate analysis revealed a significantly higher rate of complete remission in the control group compared to patients with extracapillary involvement. The control group had an OR of 0.04 (95% CI: 0.11–0.31), p=0.001 (Table 2), indicating a lower probability of complete remission for patients with extracapillary proliferation.
Association of Extent of Extracapillary Proliferation with Remission
Patients presenting with crescents or extracapillary involvement ranging
Table 2: Combined analysis of independent predictors for non-complete remission in lupus nephritis at 2 years.
Multivariate analysis in the different groups with respect to the control group
*Age expressed with SD and IQR
†Creatinine expressed in mg/dL
‡Proteinuria expressed in gr/L
§Control: Lupus nephritis class III-IV without extra capillary involvement
**G1: crescents 5–25%
††G2-G3: crescents 25–50%
This table presents both univariate and multivariate analyses of baseline independent predictors for non-complete remission in 124 patients with lupus nephritis over a period of 2 years. The univariate analysis compares patients who did not achieve remission with those who did, highlighting factors such as age, gender, activity index (AI), chronicity index (CI), ds-DNA positivity, haematuria, creatinine levels, proteinuria, and low complement levels.
The multivariate analysis focuses on the relationship between different patient groups and the likelihood of noncomplete remission, with particular emphasis on the extent of extracapillary proliferation. It shows that higher levels of crescents (both Group 1 and Group 2–3) and increased proteinuria are significant predictors of non-complete remission. AI: activity index; AZA: azathioprine; CI: confidential interval; CYC: cyclophosphamide; ds-DNA: double-stranded DNA; IQR: interquartile range; MMF: mycophenolate mofetil; OR: odds ratio; SD: standard deviation.
from 5–25% demonstrated a 7.2 times lower probability of achieving complete remission at 24 months (OR: 7.2; 95% CI: 2.3–20.2; p=0.001). Similarly, patients with >25–50% crescents (Group 2) and >50% crescents (Group 3) had substantially lower probabilities of achieving remission (OR: 21.2; 95% CI: 6.34–66.42; p=0.001) (Table 2).
Multivariate Analysis
A multivariate analysis was performed to evaluate the independent predictors of not achieving complete remission. The extent of extracapillary proliferation remained a significant predictor, with Group 1 having an OR of 7.2 (95% CI: 2.3–20.2; p=0.001) and Group 2 and 3 having an OR of 21.2 (95% CI: 6.34–66.42; p=0.001).
DISCUSSION
The analysis of data from 124 patients with proliferative focal and diffuse LN in various Latin American countries, considering racial differences and a 24-month followup, revealed significant findings. Patients with extracapillary involvement greater than 5% demonstrated higher levels of proteinuria and a reduced likelihood of achieving remission compared to patients without evidence of crescents in renal histology (Table 2). The most prevalent clinical presentation was microhaematuria, and the extent of extracapillary involvement correlated with greater renal dysfunction and higher proteinuria levels. Regarding remission outcomes, no significant differences were observed in chronicity indices between the group that achieved remission and the group that did not. However, there were notable differences in activity indices, particularly concerning the achievement of complete remission at 1 year. Patients with lower activity indices exhibited a higher frequency of remission (Table 2).
Glomerular crescents serve as a histopathological indicator of severe renal injury, characterised by the disruption of the glomerular capillary wall, resulting in the accumulation of macrophages and T cells in
Bowman’s space, along with damage to the glomerular capsule’s parietal cells.10,11 It is generally assumed that a higher percentage of crescent formation in glomeruli correlates with more severe clinical and pathological manifestations.12 This study’s findings support this assumption, as patients with higher extracapillary involvement exhibited more pronounced renal insufficiency and greater proteinuria compared to the control group. Although there were no significant differences in the age of patients, blood pressure levels were more frequently elevated in Groups 2 and 3. Additionally, glomerular microhaematuria was present in all groups.
Patients presenting with crescents or extracapillary involvement of more than 5% demonstrated a substantially reduced likelihood of achieving complete remission at 24 months, as indicated by a 7.2 times lower probability (Table 2). Conversely, patients without histological evidence of extracapillary proliferation had a statistically significant 70% chance of achieving complete remission at 2 years (Figure 2).
These observations emphasise the significance of evaluating extracapillary involvement in glomerular crescents as a critical prognostic factor in determining disease outcomes and response to treatment in patients with proliferative focal and diffuse LN.
The formation of glomerular crescents in LN is indeed common, and previous studies have shown a significant prevalence. In a cohort of 62 patients with rapidly progressive glomerulonephritis, 50% of them were found to have LN.13 In this current study, it was also observed that a considerable proportion of patients, more than 50%, showed extracapillary involvement of more than 5%, indicating the substantial impact of crescent formation in this cohort.14
It is crucial to emphasise that the crescent score was incorporated, which includes C0 (no crescents), C1 (crescents in less than 25% of glomeruli), and C2 (crescents in at least 25% of glomeruli), into the mesangial hypercellularity,
Proliferative lupus nephritis
Crescentic lupus nephritis (5–25%)
Crescentic lupus nephritis (25–50%)
Crescentic lupus nephritis (>50%)
Sensitivity
1-specificity
Prediction of remission at 24 months of proliferative lupus nephritis without extracapillary involvement (crescents) after a specific treatment is 70% p-value 0.01, while if the patient has crescents regardless of the extension the probability of remission at 24 months is less than 50%.
endocapillary hypercellularity, segmental glomerulosclerosis, and tubular atrophy/ interstitial fibrosis (MEST) score of the Oxford classification of IgA nephropathy.15 This addition was based on robust data and evidence derived from multicentre studies,16 ensuring the comprehensive and accurate assessment of renal histology in this investigation.
By including the crescent score, the authors aimed to enhance the precision of this evaluation and provide a more thorough analysis of the renal pathology in patients with proliferative focal and diffuse LN, considering the extent of crescent formation as an important prognostic factor.
These findings strongly indicate that the presence of extracapillary proliferation of more than 5% in glomeruli independently predicts a failure to achieve complete remission at 24 months with statistical
significance. This suggests that not only the extent of the damage but also the pathogenic mechanism of extracapillary lesions may play a crucial role in determining disease outcomes. To establish the validity of this assertion, further prospective studies are necessary.
Severe kidney involvement at diagnosis is a key risk factor for poor remission in patients with LN. Regarding the paediatric population, a recent study developed by De Mutiis C. et al.17 in a cohort of 382 patients with LN Class ≥III evaluated variables such as clinical presentation, treatment, and 24-month kidney outcomes. The study concluded that severe kidney involvement at diagnosis is a key risk factor for poor remission as LN Class III patients had a higher rate of complete remission compared to Classes IV or V.17
To the authors’ knowledge, this is the first study that evaluates the association between the extent of FEP and the likelihood of achieving complete remission at 24 months in patients with LN. However, it is worth mentioning other studies that have demonstrated specific associations among Latin American patients with LN and their outcomes.
Vinicki J. et al.18 conducted a retrospective study to evaluate treatment response in patients with proliferative and membranous LN in a cohort of 37 Latin American patients with a follow-up of 10 years. It was demonstrated that just 19% of patients could achieve complete remission after induction therapy and 30% after maintenance therapy.
In 2023, Rodelo J. et al.19 assessed the prognostic value of other pathological features such as interstitial fibrosis, tubular atrophy, and tubulointerstitial inflammation in 285 Latin American patients with LN. Moderate-to-severe interstitial fibrosis and tubular atrophy were found in 34.7% of biopsies and were linked to poorer kidney survival compared to mild or no severe interstitial fibrosis and tubular atrophy (p=0.018).19 Furthermore, patients with fibrous crescents experienced significantly worse kidney outcomes.
These studies underscore the unique challenges faced by Latin American patients with LN, highlighting lower rates of complete remission and worse kidney outcomes.
LIMITATIONS
It is essential to acknowledge the limitations of this study. First, the study design is retrospective and observational in nature, which may introduce inherent biases and limitations in the interpretation of the results. Secondly, evaluating the interobserver and intraobserver reproducibility of the anatomopathological diagnosis is necessary to ensure the reliability and consistency
of the findings. Lastly, in this study, only complete remission was evaluated, and different degrees of partial remission were not analysed, which may provide further insights into treatment responses and disease progression.
Despite these limitations, this study provides valuable insights into the relationship between extracapillary proliferation and remission outcomes in patients with proliferative, focal, and diffuse LN. Further research and welldesigned prospective studies are warranted to confirm and expand upon these findings, which could potentially lead to more targeted and effective therapeutic approaches for this challenging condition.
CONCLUSION
In conclusion, the presence of glomerular crescents or extracapillary proliferation is a clinically relevant finding and is not uncommon in patients with LN. This study’s proposed cutoff point of extracapillary proliferation of more than 5% is of particular significance, as it indicates that patients with this extent of involvement had a substantially reduced likelihood of achieving complete remission, with a 6.8 times lower probability. This finding has crucial implications for therapeutic decisions, particularly in Hispanic patients, where the presentation of this pathology can be more aggressive.20,21
These results strongly suggest that not only the extent of the damage but also the pathogenic mechanism of extracapillary lesions play a pivotal role in determining disease outcomes. Further prospective studies are essential to validate and expand upon these findings, which could potentially lead to more targeted and effective therapeutic approaches for patients with proliferative, focal, and diffuse LN.
References
1. Tang Z et al. The clinical and pathological characteristics of Chinese patients with pauci-immune crescent glomerulonephritis. Chin Med J (Engl). 2001;114(4):374-8.
2. Baqi N et al. LN in children: a longitudinal study of prognostic factors and therapy. J Am Soc Nephrol. 1996;7(6):924-9.
3. Cameron JS. Lupus nephritis. J Am Soc Nephrol. 1999;10(2):413-24.
4. Tang Z et al. Clinical features and renal outcome in lupus patients with diffuse crescentic glomerulonephritis. Rheumatol Int. 2009;30(1):45-9.
5. Oudah N et al. Glomerulonephritis with crescents among adult Saudi patients outcome and its predictors. Clin Exp Med. 2012;12(2):121-5.
6. Bajema IM et al. Revision of the International Society of Nephrology/ Renal Pathology Society classification for LN: clarification of definitions, and modified National Institutes of Health activity and chronicity indices. Kidney Int. 2018;93(4):789-96.
7. Tan EM et al. The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1982;25(11):1271-7.
8. Weening JJ et al. The classification of glomerulonephritis in systemic lupus erythematosus revisited. Kidney Int. 2004;65(3):1132. Erratum in: Kidney Int. 2004;65(2):521-30.
9. Austin HA 3rd et al. Prognostic factors in lupus nephritis. Contribution of renal histologic data. Am J Med. 1983;75(3):38291.
10. Masani NN et al. SLE and rapidly progressive glomerulonephritis. Am J Kidney Dis. 2005;45(5):950-5.
11. Yu F et al. Clinicopathological characteristics and outcomes of patients with crescentic LN. Kidney Int. 2009;76(3):307-17.
12. Chen S et al. Significance of histological crescent formation in patients with diffuse proliferative LN. Am J Nephrol. 2013;38(6):445-52
13. Zhang W et al. Clinical outcomes of LN patients with different proportions of crescents. Lupus. 2016;25(14):153241.
14. Sumethkul V et al. LN: a challenging cause of rapidly progressive crescentic glomerulonephritis. Lupus. 2000;9(6):424-8.
15. Trimarchi H et al. Oxford Classification of IgA nephropathy 2016: an update from the IgA Nephropathy
Classification Working Group. Kidney Int. 2017;91(5):1014-21.
16. Haas M et al. A multicenter study of the predictive value of crescents in IgA nephropathy. J Am Soc Nephrol. 2017;28(5):1665. Erratum in: J Am Soc Nephrol. 2017;28(5):1665.
17. De Mutiis C et al. International cohort of 382 children with LN - presentation, treatment and outcome at 24 months. Pediatr Nephrol. 2023;38(11):3699709.
18. Vinicki JP et al. LN in Latin American patients: 10-year results from a single medical center in Argentina. Lupus. 2016;25(2):217-22.
19. Rodelo J et al. Predicting kidney outcomes among Latin American patients with LN: the prognostic value of interstitial fibrosis and tubular atrophy and tubulointerstitial inflammation. Lupus. 2023;32(3):41123.
20. Garcia-Carrasco M et al. Anti-CD20 therapy in patients with refractory systemic lupus erythematosus: a longitudinal analysis of 52 Hispanic patients. Lupus. 2010;19(2):213-9.
21. Miranda-Hernández D et al. Prognostic factors for treatment response in patients with LN. Reumatol Clin. 2014;10(3):164-9.
Cytokine Profile Associated with COVID-19 Severity and Outcome: A Hospital-Based Study from Kashmir, North India
Introduction: Biomarkers of prognostic and predictive relevance are needed for the practical management of COVID-19.
Objective: The authors aimed to assess a battery of inflammatory cytokines in patients with SARS-CoV-2 to determine the cytokines of prognostic and predictive relevance in COVID-19. Methods: In a cohort of 100 patients with SARS-CoV-2 (RT-PCR confirmed), hospitalised in Shri Maharaja Hari Singh Hospital associated to Government Medical College Srinagar, India, the level of a battery of cytokines, IL-6, IL-8, IL-10, IL-1α, vascular endothelial growth factor (VEGF), TNF-α, and ferritin were estimated by ELISA on a multimode microplate reader.
Results: The deranged levels of these cytokines were mostly found in patients >60 years of age, with cough and pneumonia as the most common symptoms. A significant association was found between IL-6 and IL-8, disease severity (p=0.002; p=0.007), and poor disease outcome (p=0.040; p=0.009), respectively. A significant association was also found between decreased levels of VEGF and poor disease outcome (p=0.020). Further receiver operating characteristic analysis, univariant and multivariant (after adjusting for age, gender, and other inflammatory markers), revealed increased IL-10 (area under the curve [AUC]: 0.72) and IL-6 (AUC: 0.70) as independent markers of both disease severity (p=0.02; p=0.01) and disease outcome (P=0.03; p=0.02), respectively, and decreased VEGF (AUC: 0.69) as an independent marker of disease outcome (p=0.03). A significant association between cough and IL-8 (p=0.01) and IL-10 levels (p=0.03), and of diabetes and raised ferritin levels (p=0.01), with very high ferritin levels (>1500 ng/mL), was found in those who are likely to develop hyperinflammatory phenotype.
Conclusion: The authors conclude that ‘IL-6, IL10, VEGF, and IL-8’ are the signature inflammatory cytokine panel/profile in COVID-19, particularly in patients from Kashmir. Increased IL-10 and IL-6 levels proved to be equally significant independent prognosticators of COVID-19 severity and outcome, and decreased VEGF levels were independent predictors of poor disease outcome in patients with SARS-CoV-2. Testing of the signature inflammatory cytokine panel is, therefore, recommended for optimal clinical decision-making in patients with COVID-19 from Kashmir, India.
Key Points
1. Cytokine storm is the key pathophysiology underlying COVID-19.
2. In a cohort of 100 hospitalised patients with COVID-19 from Kashmir, India, cytokine profiling was carried out and correlated (by univariate and multivariate analysis) with COVID-19 severity and outcome.
3. The authors found ‘IL-6, IL10, vascular endothelial growth factor, and IL-8’ as particularly significant inflammatory cytokines of prognostic and predictive relevance. Testing of this cytokine panel is, therefore, recommended for clinical decision-making at least in patients with COVID-19 from Kashmir, India.
INTRODUCTION
COVID-19 is a novel β-coronavirus caused by infection with SARS-CoV-2. It is the third zoonotic disease caused by coronavirus to affect humans, following severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS).1,2 Globally, 775,615,736 confirmed SARS-CoV-2 cases and 7,051,323 deaths have been reported by the World Health Organization (WHO; as of June 2024). Symptoms of COVID-19 typically become noticeable after a 5–6-day incubation period and commonly consist of fever, cough, and fatigue. Other potential symptoms may include headache, haemoptysis, diarrhoea, dyspnoea, and leukopenia, among other signs.3,4 Elderly patients and those with pre-existing conditions such as high blood pressure, chronic obstructive pulmonary disease, diabetes, or cardiovascular disease are more likely to develop acute respiratory distress syndrome, septic shock, metabolic acidosis, coagulation dysfunction, arrhythmia, kidney damage, heart failure, liver dysfunction, and/or secondary infection, which can often lead to death.5,6
Disruption of immune homeostasis is the primary cause of mortality, morbidity, and post-COVID syndromes associated with
COVID-19. Recent studies have shown that infection spike glycoprotein of SARSCoV-2 is actually recognised or sensed by toll-like receptor 4 (TLR4), which is a type of pattern recognition receptor found on innate immune cells like circulating monocytes, macrophages, and dendritic cells. This binding activates downstream signalling pathways via MyD88, NF-κB, or interferon receptor factors that determine the expression of proinflammatory cytokines. The in situ TLR4 activation in alveolar macrophages leads to intense local inflammation, resulting in the accumulation of inflammatory factors that result in the overactivation of the innate adaptive immune response, leading to over-immunopathology known as cytokine storm. Cytokine storm ultimately causes respiratory gas exchange, breathing problems, and sometimes even death.7-9 Immune-active molecules such as IL have been suggested to contribute to the development of cytokine storm. Among the inflammatory cytokines, IL-8 is a powerful pro-inflammatory cytokine crucial in recruiting and activating neutrophils during inflammation and plays a role in the pathophysiology of COVID-19.10 Besides, IL-6 and IL-10 are other highly active inflammatory cytokines that have been associated with rapid disease progression and higher complication risk in COVID-19.11,12
Despite the information available about some inflammatory predictive and prognostic cytokines in COVID-19, it has been observed that people from geographically diverse regions and of different ethnicities and genetics behave differently against the SARS-CoV-2 virus. While some can resolve it quickly, others succumb to the disease. Furthermore, there is a possibility that SARSCoV-2 could modify host innate immune responses to avoid immune identification and weaken human defences. To find these differences, which may be unique to the population, it is essential to assess the inflammatory cytokine response in patients with SARS-CoV-2 from this part of the world. Defining the standard ranges for different cytokines and their association with clinical findings may result in the identification of some valuable biomarkers as indicators of COVID-19. The present study, therefore, aimed to evaluate the prognostic and predictive value of candidate inflammatory (pro and anti) markers in patients with SARSCoV-2 from Kashmir, India.
MATERIALS AND METHODS
The study was conducted in the Department of Biochemistry, Government Medical College, Srinagar, India, and its associated hospitals between October 2020–November 2021. A total of 100 patients (RT-PCR confirmed SARS-CoV-2 positive) and 20 control subjects (RT-PCR confirmed SARSCoV-2 negative) were included in this cohort study. The patients were diagnosed as per standard WHO/Centers for Disease Control and Prevention (CDC) criteria 2020 for COVID-19 disease. The study was initiated after obtaining approval from the Ethical Committee of Government Medical College, Srinagar (IEC/GMC-Sgr/27, 19th December). Written informed consent and response questionnaires from patients and healthy controls were documented and recorded as per hospital protocol. The study was hospital-based and included patients who were admitted to the hospital for COVID-19 complications. The samples were collected during the first week of hospitalisation, and the patients were then followed twice on the 14th day and 28th day of their admission. The clinical
staging was as per the National Institute of Health’s (NIH) guidelines.13 Individuals who showed evidence of lower respiratory disease during clinical assessment or imaging, and had an oxygen saturation measured by pulse oximetry (SpO2) ≥94% on room air at sea level were classified as moderately ill (Stage 2). Individuals who had SpO2 <94% on room air, at sea level, a ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/ FiO2) <300 mmHg, a respiratory rate >30 breaths/min, or lung infiltrates >50% were classified severely ill (Stage 3). Individuals who had respiratory failure, septic shock, and/or multiple organ dysfunction, and later failed to survive, were classified as critically ill (Stage 3). So, as far as the treatment is concerned, in this cohort, 52% of patients received piperacillin and tazobactam, 82% received dexamethasone, 47% received azithromycin, 83% received enoxaparin, and 27% received remdesivir.
The serum samples collected were stored at -70 °C until further investigations. The levels of IL-6, IL-8, IL-1α, IL-10, VEGF, TNF-α, and ferritin were estimated by ELISA on a multimode microplate reader using kits of Diaclone (DIACLONE SAS, part of Medix Biochemica, Besançon Cedex, France) or on an automated immunoanalyser (Siemens, Munich, Germant). Twenty RT-PCR-confirmed SARSCoV-2 negative subjects were taken as the control group to determine the reference range of the cytokines which were not available.
Statistical Analysis
The data were analysed using STATA software 17 (standard edition; StataCorp LLC, Lakeway Drive, College Station, USA). Correlation analysis of cytokines with socio-demographic, clinical features, comorbidities, clinical stages, and outcomes was determined by Chi-square test and Fisher exact test. Receiver operating characteristic analysis (univariate and multivariate) of various cytokines was done to determine the prognostic and predictive values of the cytokines after adjusting for various confounders.
RESULTS
Association of Inflammatory Cytokine Levels with Clinical Features and Comorbidities in Patients with SARS-CoV-2
In this cohort study, elevated levels of IL-10, IL-6, IL-8, IL-1α, TNF-α, ferritin, and decreased levels of VEGF were found
typically in patients aged >60 years. Further association of inflammatory cytokines (IL-10, IL-8, IL-6, IL1-α, VEGF, TNF-α, and ferritin) with clinical features (Supplementary Table 1A and 1B) and comorbidities (Supplementary Table 2A and 2B), revealed significant association of cough with IL-8 levels (p=0.01) and IL-10 levels (p=0.03), and of diabetes with raised ferritin levels (p=0.01).
Figure 1: Receiver operating characteristic analysis of inflammatory cytokines, IL-10, IL-6, IL-8, IL-1α, TNF-α, vascular endothelial growth factor, and ferritin with disease outcome in patients with SARS-CoV-2.
Association of Inflammatory Cytokines with Disease Severity/ Staging and Disease Outcome in Patients with SARS-CoV-2
The association of inflammatory cytokines with disease severity and outcome in patients with SARS-CoV-2 revealed significantly elevated levels of IL-8 (p=0.007; p=0.009) and IL-6 (p=0.002; p=0.040) in patients of increased disease severity and poor outcome, respectively (Figures 2B and 2D; Table 1). Further, a significant association between decreasing VEGF levels and poor disease outcomes was found (p=0.02; Table 1). An association,
though not significant, between decreasing VEGF levels and increased disease severity was found in patients (Figure 2F).
Receiver Operating Characteristic Analysis of Inflammatory Cytokines with Disease Outcome in Patients with SARS-CoV-2
In determining the predictive value of cytokines (IL6, IL-1α, IL-10, IL8, VEGF, TNF-α, and ferritin), receiver operating characteristic analysis of these inflammatory cytokines with disease outcome (followed twice on the 14th and 28th
Figure 2A–G: Correlation analysis of cytokine, IL-10, IL-6, IL-8, IL-1α, TNF-α, vascular endothelial growth factor, ferritin levels and disease severity/staging in patients with SARS-CoV-2.
Figure 2B
2C
3 (%) Stage 2 (%)
Figure 2D
2A–G continued.
Figures (2A–G) represent correlation analysis of cytokines, IL-10, IL-6, IL-8, IL-1α, TNF-α, VEGF, ferritin, and disease severity/staging in SARS-CoV-2 patients.
The clinical staging was as per the National Institute of Health (NIH) guidelines.13
Stage 2 (moderately ill): individuals who show evidence of lower respiratory disease during clinical assessment or imaging and who have an oxygen saturation measured by pulse oximetry (SpO2) ≥94% on room air at sea level.
Stage 3 (severely ill): individuals who have SpO2 <94% on room air at sea level, a ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) <300 mmHg, a respiratory rate >30 breaths/min, or lung infiltrates >50%.
Stage 3 (critically ill): Individuals who have respiratory failure, septic shock, and/or multiple organ dysfunction, which later failed to survive.
VEGF: vascular endothelial growth factor.
Figure
Table 1: Association of inflammatory cytokine IL-10, IL-6, IL-8, IL-1α, TNF-α, VEGF, and ferritin levels with disease outcome in patients with SARS-CoV-2 (N=100).
*Values considered significant when p≤0.05. VEGF: Vascular endothelial growth factor.
day) revealed raised IL-10 (area under the curve [AUC]: 0.72, at the sensitivity of 68% and specificity of 72%) and IL-6 (AUC: 0.70, at sensitivity of 70% and specificity of 62%) as equally significant predictive markers of poor disease outcome, followed by IL-8 (AUC: 0.67), TNF-α (AUC: 0.66), and ferritin (AUC: 0.66), and decreased VEGF level as predictors of poor disease outcome (AUC: 0.69, at sensitivity of 53% and specificity of 73%) (Figure 1).
Model 2
Model 3
inflammatory markers, increased IL-6 and IL-10 levels were found to be independent predictors of disease severity and poor disease outcome (Table 2), and decreased VEGF levels to be an independent predictor of poor disease outcome in COVID-19 (Table 3).
DISCUSSION
Multivariate Analysis of Inflammatory Cytokines
IL-10, IL-6, IL-8, IL-1α, TNF-α, VEGF, Ferritin, with
Disease Severity and Outcome
Using multivariate analysis models, after adjustments of age, gender, and other
Given the significance of inflammatory cytokines in predicting disease severity and outcome in patients with SARS-CoV-2, the present study evaluated a battery of inflammatory cytokines in patients with SARS-CoV-2 from Kashmir, India and found a rise in IL-8, IL-10, and IL-6, and a decrease in VEGF as particularly significant
signature inflammatory cytokine panel, as prognosticators of disease severity, and/or predictors of poor disease outcome.
Cytokine storm is a key feature of the SARS-CoV-2 infection. Upon infection binding of the SARS-CoV-2 spike protein to angiotensin-converting enzyme on Type II pulmonary alveolar epithelial cell, the damage-associated molecular patterns present on the virus get sensed by pattern recognition receptors like TLR4, which are present on innate and adaptive immune cells in alveolar cells like the macrophages, monocytes, T and B cells, and activates various signalling cascades, resulting in the production of pro-inflammatory cytokines. The in situ TLR4 activation by spike proteins of SARS and invasion of the inflammatory immune cells in the alveoli cause lung inflammation and lung
damage.7-9,14-16 Studies have shown that inflammatory cytokines play a pivotal role in the pathogenesis of severe COVID-19. Regarding IL-6, the findings from the present study are inconsistent with the meta-analysis (nine studies) that reported an over three-fold increase (≥80 pg/mL) in IL-6 levels as a mortality risk factor in SARS-CoV-2 infection.17 The efficacy of the dexamethasone and anti- IL-6 treatment in COVID-19 could be explained by the underlying mechanism of reduction of IL-6 levels in patients with moderate and severe SARS-CoV-2 as proved by Ledford.18 Consistent with worldwide studies, ferritin here has been found to be a prognosticator of COVID-19 severity, and very high ferritin (>1500 ng/mL) levels as an indicator of hyperinflammatory phenotype.19 The possible mechanism is that hyperferritinemia causes inflammatory
Model 1
Model 2
Model 3
states in SARS-CoV-2 infection, particularly in the lungs, as demonstrated by the presence of a high number of macrophages in the lung parenchyma of patients with SARS-CoV-2. Furthermore, high ferritin also potentiates the production of proinflammatory cytokine IL-6, as a feedback mechanism exists between ferritin and IL-6.20
Similar to IL-6, here IL-10 proved to be an equally significant independent predictor of disease severity and poor disease outcome after nullifying the risk contribution of variables like age, gender, and other inflammatory markers for COVID-19. The finding is consistent with various other studies, including that of Lu et al.21 and Aber et al.22 IL-10 is a pleiotropic cytokine produced by various immune cells with strong anti-inflammatory and immunosuppressive effects. It typically suppresses pro-inflammatory signals by activating the JAK1-TYK2-STAT3 pathway, leading to STAT3-mediated transcription of genes that limit the inflammatory response, as in COVID-19.23,24 During the acute phase of viral infection, IL-10 suppresses the activity of T cells, macrophages, and natural killer cells, by preventing successful viral elimination and minimising collateral tissue damage. However, during the acute phase of SARS-CoV-2 infection, and in rare cases, such as in patients with comorbidities (e.g., diabetes, cancer, those on immunosuppressants, or elderly patients), very high levels of IL-10 have been observed, impairing its anti-inflammatory function and instead potentiates pro-inflammatory action of various cytokines. High levels of IL-10 are also known to augment the proinflammatory reactions to bacterial lipopolysaccharides in human endotoxemia.25 This points to the possibility that the combination of elevated IL-10 and bacterial products (which are abundant in severe COVID-19 cases) could empower the inflammatory machinery in COVID-19.26 Consistent with the present study, high IL-10 levels found in patients with comorbidities may provide a potential link between diabetes and negative outcomes in COVID-19.27 The present study, therefore, reaffirmed the importance of considering age and comorbidities while
relating the cytokines with disease severity in COVID-19.
IL-8 is normally secreted by multiple cells, including neutrophils exposed to stimuli, and is considered the primary molecule of acute inflammation. Similar to the present study, several studies have shown neutrophilia and increased neutrophil–lymphocyte ratio as indicators of COVID-19 severity, so IL-8 is raised.28 Since IL-8 is expressed by neutrophils, therefore, consistent with the present study, IL-8 overexpression, by potentiating neutrophil chemotaxis and promoting angiogenesis, proves to be a poor prognostic biomarker for patients with SARS-CoV-2.
VEGF, apart from promoting angiogenesis, also effectively increases vascular permeability through the VEGFR2 receptormediated alterations of vascular fenestration and inter-endothelial junction.29 During a COVID-19 infection, patients frequently experience dyspnoea, which induces the activation of hypoxia-inducible factor-1alpha among which VEGF is one of the key HIF-targeted genes.30,31 Consistent with other inflammatory markers, an early rise in VEGF levels has been found; however, a decreasing trend in VEGF with severity has been observed here in COVID-19. The present study was limited by being singlecentric and included only a small number of samples. The results of the study, therefore, should be substantiated by similar multicentric studies from various parts of the country and even from other countries conducted on a large sample size. Also, the reference range of some of the cytokines was not known, so samples from healthy controls were taken in order to determine the reference range.
Taken together, the authors’ results reinforce the importance of closely monitoring the levels of cytokine panel IL-6, IL-10, VEGF, and IL-8, which might provide valuable information about the progression and changes during the treatment process of COVID-19 at the earliest.
CONCLUSION
The authors conclude that ‘IL-6, IL-10, VEGF, and IL-8’ are the signature inflammatory cytokine panel in COVID-19. Increased IL-10 and IL-6 levels proved to be equally significant independent prognosticators of COVID-19 severity and predictors of poor outcome and decreased VEGF levels as
References
1. Chen Y et al. Emerging coronaviruses: genome structure, replication, and pathogenesis, J. Med Virol. 2020;92(4):418-23.
2. Zhu N et al. China novel coronavirus investigating and research team. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382(8):727-33.
3. Guan W J et al. China medical treatment expert group for covid-1. Clinical characteristics of coronavirus disease 2019 in China. N Engl JMed. 2020;382(18):1708-20.
4. Wang W et al. Updated understanding of the outbreak of 2019 novel coronavirus (2019-nCoV) in Wuhan, China. J Med Virol. 2020; 92(4):441-7.
5. Huang C et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497-506.
6. Wang D et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061-9.
7. Zhao Y et al. SARS-CoV-2 spike protein interacts with and activates TLR41. Cell Res. 2021;31(7):818-20.
8. Choudhury A et al. In silico analyses on the comparative sensing of SARSCoV-2 mRNA by the intracellular TLRs of humans. J Med Virol. 2021;93(4):247686.
9. Choudhury A, Mukherjee S. In silico studies on the comparative characterization of the interactions of SARS-CoV-2 spike glycoprotein with ACE-2 receptor homologs and human TLRs. J Med Virol. 2020;92(10):2105-13.
10. Baggiolini M et al. Neutrophil-activating peptide-1/ interleukin 8, a novel cytokine that activates neutrophils. J Clin Invest.1989;84(4):1045-9 .
11. Wei H et al. Interleukin-10 family cytokines immunobiology and
independent predictors of poor disease outcome in patients with V-2. Considering the success of anti-IL-6 targeted therapy, profiling of the present signature inflammatory cytokine panel is, therefore, suggested as part of the inclusion criteria for optimal clinical decision-making in patients with COVID-19.
structure. Adv Exp Med Biol. 2019;1172:79-96.
12. Liu BM et al. Clinical significance of measuring serum cytokine levels as inflammatory biomarkers in adult and pediatric COVID-19 cases: a review. Cytokine. 2021;142:155478.
13. Cascella M et al, Features, Evaluation, and Treatment of Coronavirus (COVID-19) [Internet] (2023) Treasure Island: StatPearls. Available at: https://www.ncbi.nlm.nih.gov/books/ NBK554776/. Last accessed: 18 April 2024.
14. Channappanavar R, Perlman S. Pathogenic human coronavirus infections: causes and consequences of cytokine storm and immunopathology. Semin Immunopathol. 2017;39(5):52939.
15. Lu R et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet. 2020;395(10224):565-74.
16. Colling ME, Kanthi Y. COVID19-associated coagulopathy: an exploration of mechanisms. Vasc Med. 2020;25(5):471-8.
17. Aziz M et al. Elevated interleukin-6 and severe COVID-19: a meta-analysis. J Med Virol. 2020;92(11):2283-5.
18. Ledford H. Coronavirus breakthrough: dexamethasone is first drug shown to save lives. Nature. 2020;582(7813):469.
19. Jessica J M et al. COVID-19associated hyperinflammation and escalation of patient care: a retrospective longitudinal cohort study. Lancet Rheumatol. 2020;2(10):e594-602.
20. Rosario C et al. The hyperferritinemic syndrome: macrophage activation syndrome, Still’s disease, septic shock and catastrophic antiphospholipid syndrome. BMC Med. 2013;11:185.
21. Lu L et al. A potential role of Interleukin
10 in COVID-19 pathogenesis. Trends Immunol. 2021;42(1):3-5.
22. Abers MS et al. An immune-based biomarker signature is associated with mortality in COVID-19 patients. JCI Insight. 2021;6(1):e144455.
23. Moore KW et al. Interleukin-10 and the interleukin-10 receptor. Annu Rev Immunol. 2001;19:683-765.
24. Hofmann SR et al. Biological properties and regulation of IL-10 related cytokines and their contribution to autoimmune disease and tissue injury. Clin Immunol.2012;143(2):116-27.
25. Lauw FN et al. Proinflammatory effects of IL-10 during human endotoxemia. J Immunol. 2000;165(5):2783-9.
26. Islam H et al. Elevated interleukin-10 levels in COVID-19: potentiation of pro-inflammatory responses or impaired anti-inflammatory action. Front Immunol. 2021;12:677008.
27. Zhu L et al. Association of blood glucose control and outcomes in patients with COVID-19 and preexisting type 2 diabetes. Cell Metab. 2020;31(6):1068-77.
28. Chen R et al. Longitudinal hematologic and immunologic variations associated with the progression of COVID-19 patients in China. J Allergy Clin Immunol. 2020;146(1):89-100.
29. Dvorak H et al. Vascular permeability factor/vascular endothelial growth factor and the significance of microvascular hyperpermeability in angiogenesis. Curr Top Microbiol Immunol.1999;237:97-132.
30. Makino Y et al. Inhibitory PAS domain protein is a negative regulator of hypoxia-inducible gene expression. Nature. 2001;414(6863):550-4.
31. Shweiki D et al. Vascular endothelial growth factor induced by hypoxia mediates hypoxia-initiated angiogenesis. Nature.1992;359(6398):843-5.
Right Lateral Digital Rectal Examination in Men with Suspected Prostate Disease Presenting with Lower Urinary Tract Symptoms
Author: *Augustine O. Takure1
1. Department of Surgery, College of Medicine, University of Ibadan, Ibadan & University College Hospital, Nigeria *Correspondence to augusturoendo@gmail.com
Disclosure: The author reports no conflicts of interest.
Received: 02.06.24
Accepted: 07.08.24
Keywords: Efficacy, left lateral digital rectal examination, right lateral digital rectal examination (RLDRE), suitability.
Background: The prostate gland is anterior to the rectum. There are different positions for digital rectal examination, and 95% of individuals are right-handed. This study aimed to determine the suitability and efficacy of right lateral digital rectal examination (RLDRE).
Methods: A prospective cross-sectional study was conducted in a tertiary hospital on men with lower urinary tract symptoms due to benign prostate enlargement or prostate cancer. The perceptions of patients, surgical trainees, and medical students during RLDRE was assessed using the Likert scale questionnaire. The age and clinical presentation were documented. The ability to appreciate abnormal prostate disease was evaluated. The data was analysed using Statistical Package for Social Sciences (SPSS) version 24 (IBM, Armonk, New York, USA). Pearson’s correlation coefficient for non-categorical variables was performed and the level of significance was p<0.001. Ethical approval was obtained.
Results: A total of 203 patients were recruited, of which surgical trainees and medical students assessed 130 and 73 patients, respectively. The patients’ mean age was 69.5±9.1 years. The main presentations were urethral catheter in situ due to acute urinary retention in 77 patients (37.9%) and moderate lower urinary tract symptoms in 62 patients (30.5%). The number of patients with the RLDRE perception of well-tolerated, less awkward, and less painful were 161 (79.7%), 121 (59.9%), and 130 (64.4%), respectively. The perceptions of surgical trainees and medical students for ease of RLDRE were 77.7% and 74%, respectively, and for detection of abnormality were 57% and 68.5%, respectively. Detection rates for prostate cancer by surgical trainees and medical students were 87.5% and 75%, respectively, and for benign prostatic hyperplasia were 87.5% and 62.5%, respectively.
Conclusion: RLDRE was well tolerated by patients. Surgical trainees and medical students were comfortable with RLDRE with reasonable detection of benign prostatic hyperplasia and prostate cancer.
Key Points
1. There is variation in the preference for digital rectal examination (DRE) position by urologists and patients. It is difficult to teach and assess DRE skills.
2. This is a case-control prospective clinical study of right lateral DRE by surgical trainees and medical students, including their perceptions as well as patients’ perceptions.
3. Right lateral DRE is simple, based on the anterior relation of the prostate and right-handedness in 95% of individuals. Left lateral DRE for left-handed individuals.
INTRODUCTION
The worldwide prevalence of benign prostatic hyperplasia (BPH) varies between 20–60% in men over 50 years. Similarly, about 50% of men over 60 years in South Africa had BPH. In Nigeria, the incidence of BPH was 23.7% among communitydwelling men.1,2 Digital rectal examination (DRE) is important in the clinical diagnosis of BPH based on a smooth and enlarged prostate.2-8 The presence of suspicious findings doubles the risk of clinically significant prostate cancer.3 David R.H. et al,9 in a systematic review of the accuracy of DRE to measure prostate volume, reported that DRE was weak at estimating size but is good at detecting enlargement of the prostate. Studies corroborated the ability of DRE to estimate prostate size when the volume is greater than 30 mL.10 DRE was reported to detect prostate cancer in 63.4% of men in a study by Ying Y et al.11 The usefulness of DRE is well captured by the saying that: “By far your greatest aide will be the finger. The majority of diseases which affect the rectum can be made out by the educated finger.”12
Be that as it may, there are several debates as to the use of DRE as a screening tool for prostate cancer. DRE was not useful in detecting prostate cancer in men with prostate-specific antigen (PSA) 3.0–3.9 ng/mL.13 A systematic review and metaanalysis of primary care providers did not show any evidence to support the efficacy of DRE in screening for prostate cancer.14 It was argued that with the advent of a multiparametric MRI study, DRE did not fulfil the World Health Organization (WHO)
criteria for screening. In the primary health care setting, DRE was not recommended as a routine for prostate cancer screening.15 On the contrary, digital anal rectal examinations in the public health screening programme for anal cancer satisfied most of the WHO criteria as a screening examination.16
From the general practice point of view, DRE is accurate and abnormal DRE carries a 42.3% risk of prostate cancer, which is above the 3% risk threshold of the UK National Institute for Health and Care Excellence (NICE) guidelines.17 Walsh AL et al.,18 in the primary health care setting, reported that DRE alone had sensitivity, specificity, and positive predictive values of 81%, 40%, and 42%, respectively, in detecting prostate cancer in a retrospective cohort analysis. DRE is important from a contemporary cohort of patients undergoing an initial 12–18 core prostate needle biopsy.19
DRE played a limited role in the era of COVID-19 and post-COVID-19, where there was rapid adoption of virtual consultation in the form of telephone or video consultation, making DRE difficult. PSA measurement and MRI were available and were the preferred choices. DRE may detect prostate cancer in individuals who are Black. Abnormal DRE in a symptomatic patient has a positive predictive value for prostate cancer above the current NICE threshold requiring urgent referral. Therefore, DRE is important in individuals of African descent with lower urinary tract symptoms (LUTS).1,17-22
In order to increase the chances of detecting prostate cancer in men, DRE
rectal examination has been combined with serum PSA and MRI with a reasonable higher cancer detection rate.23-32
The under-utilisation of DRE alone when screening for prostate cancer has been attributed to the 61.1% of medical doctors who never performed DRE despite screening with PSA. Prostate cancer was only detected in 3–5% of the population screened with a combination of DRE, PSA, and transrectal ultrasound (TRUS).33 In a study by Teoh M et al.,34 doctors in training had a low level of confidence and comfort in performing DRE, limiting the utilisation of DRE as a critical diagnostic tool. In 2012, the United States Preventive Service Task Force (USPSTF) recommended against routine PSA screening. This led to a significant drop in the utilisation of DRE and PSA by primary physicians from 16.0% to 5.8% for DRE and 27.3% to 24.5% for PSA.35 DRE is often an overlooked part of physical examination that is informative in the hands of skilled physicians, particularly in revealing some rectal diseases.36 The preference for performing DRE on men with health insurance compared to patients who attended public hospitals in Brazil may increase overdiagnosis and overtreatment of prostate cancer.37
DRE is an essential requirement for medical practitioners, as well as a necessary skill for medical students before their exit from university. It was found across several studies that 25% of the medical students had no experience with performing DRE.38-40 The diagnostic test accuracy of DRE for prostate cancer in symptomatic patients among general practitioners in the UK was 42.3%, above the NICE 3% risk threshold.17 Of note is the observation that abnormality on DRE is not easily picked in patients who are obese, but when detected it improves the predictive value of prostate cancer, and this is significantly higher among men who are obese compared to those of a normal weight.9
Up to 50% of men with abnormal DRE before prostate needle biopsy were eventually confirmed to be prostate adenocarcinoma. The DRE features suggestive of benign prostate enlargement (BPE) include nontender, smooth, and firm prostate gland,
while in patients with malignant prostate enlargement includes hard, irregular prostates with or without obliteration of the median groove.19
During the left lateral position, the medical student is taught to rotate their index finger in the rectum to appreciate the characteristic features of a diseased prostate. This technique is not easily learnt but improves with the status of the clinician from residents to consultants.11
With increasing desire to further improve the diagnostic test accuracy of DRE, researchers and clinicians have conducted studies to standardise the ability to interpret the findings of DRE. One fingertip surface area is equivalent to 1 g of prostate tissue, which is equal to 1 cm3 volume, and this correlated well with prostate volume when assessed by ultrasound.41 Sinam LB et al.,6 also corroborated the correlation DRE estimate of prostate volume with TRUS measurement. Although there was some degree of overestimation of prostate volume by DRE, the coefficient of internal consistency was 0.851. The first attempt at standardisation of DRE in inexperienced hands established a linear correlation between DRE and ultrasound prostate volume.41 Muangpoon T et al.,42 designed the augmented reality system for digital rectal examination training and assessment to improve teaching and learning of DRE skills by providing visualisation of the finger and internal organs. The initial user study proved the applicability and usefulness. They proposed improvement of this device by using the HoloLens, which will offer a larger field of view and resolution or haptic based instead of the standard benchtop model, which is expected to generate a variety of abnormalities of prostate diseases.
In the 1990’s, the preferred position for DRE was the proctologic referred to as kneechest or prone jackknife position. However, lateral decubitus or Sim’s position is better in very ill patients.4 As R.H. Major said: “A wag once remarked, with considerable truth, that a consultant is a doctor who makes a rectal examination.”4
In the USA, the best position for DRE is the standing position or the knee-chest position.7,43 A randomised controlled study in France, analysed the lower and middle rectum and sphincter function in a DRE.44 The study concluded that the left lateral position, compared to the dorsal position, allowed the complete examination of the circumference of the rectum.44
According to a study among urologists in Brazil about their preferred position for DRE, four positions were performed in decreasing order, including lithotomy (64.3%), left or right lateral (17%), standing up (14.2%), and squatting down with elbows on the table (3.4%). However, 42.7% of the patients preferred the left lateral DRE (LLDRE) position.45 In another study in India, the cross-leg lithotomy position (78.3%) was preferred by the patient compared to the left lateral position (21.75%). It afforded the urologist to completely examine the prostate (cross-leg11.15±1.96/12 versus left lateral 9.25±2.50/12; p<0.001).46
Considering the various positions for the DRE, most individuals (95%) are righthanded, and the prostate gland is anterior to the rectum.47,48 In addition to the perceptions of patients, and medical students and doctors-in-training ability to perform DRE. 34 This study determined the patient’s perception of RLDRE compared to the LLDRE, as well as the urology trainees’ and medical students’ perceptions and ability to appreciate abnormalities of prostate diseases with the RLDRE position.
MATERIAL AND METHODS
Setting
Urology surgery outpatient clinic at the University College Hospital, Ibadan.
Study Design
The RLDRE position and LLDRE position were explained to patients who presented with LUTS. The patients were asked to compare their experience between both positions of examination. They picked a simple ballot of “R” for right or “L” for left to
determine which position was performed first. Both examinations were done on the same day.
The senior registrars (surgical trainees) and final-year medical students (medical students) were taught how to perform the RLDRE though they were quite conversant with the LLDRE. A proforma was designed and prospectively administered by surgical trainees and medical students to the patients. Two hundred and three men who voluntarily consented were enrolled in the study. The patients, urology surgical trainees, and medical perceptions on the Likert scale 1 (strongly agree) to 5 (strongly disagree) were assessed, as well as the rectal examination findings.
The Likert scale was further regrouped as Likert scores 1 and 2 were in favour, score 3 was undecided, and scores 4 and 5 were against tolerating RLDRE rather than LLDRE. In favour of RLDRE versus LLDRE, perceptions of not awkward, not more painful, and patient did not mind facing the examiner were 4 and 5, undecided was 3, and against was 1 and 2, respectively.
The regrouping of the surgical trainees and medical students’ perception using the Likert responses, RLDRE easier to perform and appreciated abnormal DRE findings was 1 and 2, undecided was 3, and did not mind facing patient scale 4 and 5, respectively.
Study Type
Cross-sectional prospective hospital-based study.
Inclusion Criteria
Men with LUTS due to suspected BPE or prostate cancer.
Exclusion Criteria
Men with urethral strictures, neurogenic bladder, and acute prostatitis.
Participants
The study included 203 patients, of which 130 and 73 were assessed by surgical trainees and medical students, respectively.
Variables
Patients’ perception; age in years; international prostate symptom score (IPSS); quality of life or bordersome score; serum PSA; prostate volume in cubic centimetres and post void in millilitres, both assessed by transrectal/abdominal ultrasound; urology trainee perception.
Data Analysis
The results of the perceptions were represented in tables. The data was analysed using SPSS version 24. The Pearson’s correlation coefficient was determined for the perceptions of the surgical trainees and medical students regarding RLDRE and LLDRE and the level of significance was p<0.01 or p<0.05, respectively. The p<0.01 and 0<0.05 corresponds to 99% and 95% CI, respectively.
Techniques of Digital Rectal Examinations
Right lateral digital rectal examination.
The patient is positioned horizontal lying on his right side on the examination couche facing the examiner. The hips are flexed at 90 degrees to the body and knees flexed at a right angle to the thigh. The examiner introduces the gloved, lubricated right index finger through the anal sphincter into the rectum and performs the examination of the prostate. The examiner appreciates the prostate that is anterior to the rectum. Then palpates the size of the prostate, the presence of a median groove, and whether the capsule is smooth, irregular, or hard. They check for tenderness and whether the rectal mucosa was fixed to the prostate or freely mobile. At the end of the examination the patient is cleaned.
Left Lateral Digital Rectal Examination
The patient lies on the left side of his body on the examination couche with back towards the examiner. The trunk is diagonal, both hip and knees are flexed, and the thigh and legs both parallel to the trunk. With the examiner standing and facing the buttocks, the right index finger is lubricated with K-Y-jelly and introduced through the anal sphincter into the rectum. The examiner then rotates his index finger anti-clockwise 180 degrees, bending down parallel to the examination couche and facing the head of the couche. The characteristics of prostate features suggestive of benign or malignancy are noted. Then they stand up, rotate their finger 180 degrees clockwise and remove their index finger. At the end of the examination the patient is cleaned.
Outcome Measures
The patients, surgical residents and medical student’s perceptions are represented by a table. The correlations between the perceptions of surgical residents and medical students as well as the correlations on the ability to appreciate abnormal DRE using the right lateral position.
Limitation
For a left-handed examiner, the patient will lay on the left side of the body with the body horizontal facing the examiner. The hips are flexed at 90 degrees to the body and knees flexed at right angle to the thigh. The examiner stands in front of the flexed knees and examines the prostate as described for the right lateral digital examination. However, there were no left-handed surgical trainees or medical students.
Ethical Issues
The patients were identified with numerical serial numbers that do not reveal their identity in compliance with the Helsinki declaration on human rights. Thereafter, a signed informed consent or fingerprint from illiterate patients was obtained. There was no malevolence with the patient. The institutional research board ethical approval was obtained UI/UCH EC registration number: NHREC/05/01/2008a.
RESULTS
A total of 203 patients were recruited into the study, of which surgical residents and medical students assessed 130 (64%) and 73 (36%) patients respectively. The mean age of the patients was 69.5±9.1 years (range: 38–99 years). The mean, standard deviation, and range for PSA, PSA density, and prostate volume were 355±1928 (0.5–20,870.0) ng/mL, 3.5±19.6 (0.01–216.00) ng/mL/mL, and 90.4±68.8 (14.6–477.0) mL, respectively. Seventy-seven (37.9%) patients presented with urethral catheter in situ and three (1.5%) had suprapubic catheter due to acute urinary retention. The others were mild, moderate, and severe LUTS were 16.3%, 30.5%, and 13.8%, respectively.
Regarding the perception of DRE positions, the patients felt that the right lateral position, compared to the left lateral position, was well tolerated, less awkward, less painful, and caused less worry about facing the examiner in 161 (79.7%), 121 (59.9%), 130 (64.4%), and 122 (60.4%) patients, respectively (Table 1).
The percentage of surgical trainees and medical students with the perception RLDRE has a higher ease of performing compared to LLDRE was 77.7% and 74%, respectively. Similarly, prostate abnormality was better appreciated in the right lateral position in 101 (57%) patients by surgical trainees and 50 (68.5%) patients by medical students. The surgical trainees and medical students were not bothered about facing the patients during RLDRE in 44.6% and 54.8% of DRE examinations, respectively (Table 1).
Table 1 also shows the statistical significance and positive correlation of the perceptions by both surgical trainees and medical students to the ease of performing RLDRE (r=0.909; p=0.000), appreciation of prostate abnormality (r=0.795; p=0.000), and that they were not bothered about facing the patients during RLDRE (r=0.836; p=0.000).
The DRE findings suggestive of prostate cancers are absent median groove, irregular prostate gland (not smooth), and attachment of rectal mucosa to the prostate gland depending on the stage of the cancer. The
chances of correctly palpating the clinical features of prostate cancer during RLDRE by surgical trainees and medical students were 87.5% and 75%, respectively (Table 2). While feeling features on RLDRE suggestive of BPE between the two groups were 87.5% and 62.5%, respectively (Table 2).
DISCUSSION
Digital rectal examination is always indicated in men with LUTS but is not recommended as a screening test for prostate cancer because 80% of those who had a biopsy done based on DRE were negative for prostate cancer.17,49 DRE is not useful in screening for prostate cancer as it is poor as a stand-alone test.50 In Prostate Research on Behavior and Education (PROBE) Survey in Europe, most urologists performed DRE on patients with LUTS due to BPH.51 The Canadian Family Physician 2019, Canadian Urological Association (CUA), American Urological Association (AUA), and European Association of Urology (EAU) guidelines all include DRE in the workup of men with LUTS due to suspected BPH.52,53,54,55 This is consistent with this study where we investigated the perception of the patients with LUTS, medical students, and surgical trainees to RLDRE. We assessed the ability of the medical students and surgical trainees to appreciate abnormalities of the prostate using the RLDRE technique compared to the left lateral position.
DRE is valuable in establishing that the prostate gland is enlarged. 9 Despite some degree of overestimation, the DRE prostate size correlated well with the TRUS volume.6,10 The European Association of Urology stated that DRE can estimate prostate volume but is less accurate compared to ultrasound. In China, patients who had a prior PSA and multiparametric MRI were sent for prostate biopsy. Experienced urologists and residents who performed the DRE before TRUS biopsy were blind to this information.
The diagnostic accuracy of DRE in patients with suspected prostate cancer referred for biopsy was 63.45%.11 Stephan et al.,3 reported that, according to rounded data without considering DRE, the risk of clinically
significant prostate cancer within 10 years is about 1%, 5%, and 20% for men with PSA levels of <2 ng/mL, 2–3 ng/mL, and >3 ng/mL, respectively. The presence of suspicious DRE doubles the risk of prostate cancer from 0.7% to 1.5%, from 3.5% to 6.5%, and from 13.7% to 23%, respectively. Thus, supporting the importance of DRE.3 However, students (33%) were less likely to accurately assess abnormalities in DRE compared to residents (64%) and clinicians (76%), with a p<0.05.56 The emphasis is for the medical students and surgical trainees to acquire this clinical skill of performing DRE as emphasised by Lass et al.52 To increase the chances of picking prostate cancer, DRE rectal examination should be combined with serum PSA, transrectal prostate ultrasound, multiparametric MRI, and prostate biopsy when the patient is fit for this last procedure.20,21,26,30,57-60
Romero et al.,45 a questionnaire-based study in Brazil, reported that the majority of the urologist preferred the lithotomy position (63.4%) for DRE, among others such as left lateral (17%), standing-up position (14.2%), and squatting down with elbow on table (3.4%). However, 42.7% of the patients preferred the left lateral position for DRE at their first visit.45 Nagathan DS et al.,46 reported that in India patients preferred the cross-leg lithotomy position, and the urologists were able to more completely examine the prostate than in the left lateral position. In the authors’ practice, all the men with LUTS routinely underwent DRE in the left lateral position at the surgical outpatient clinic. The exceptions to DRE were patients with acute prostatitis or those who were severely ill at the time of presentation.11 Furlan et al.61 reported that the majority of the patients in their study preferred a supine position for DRE. In the USA, the standing position or knee-chest position is preffered.7,43
Most patients in this study tolerated RLDRE, felt it was not awkward, less painful, and were not bothered facing the physician. This was unlike studies that reported moderateto-high discomfort and pain during LLDRE.46,57 Despite these shortcomings of DRE, more men would subject themselves to a repeat DRE for fear of late identification
of clinical prostate cancer.60 Frank J et al.,61 in a randomised study comparing the kneeelbow and left lateral position, patients were 1.9 times more comfortable with the kneeelbow position than the left lateral position. The patients also felt the knee-elbow position was twice as embarrassing as the left lateral position.60
This study demonstrated that both surgical trainees and medical students felt the RLDRE position was much easier (77.7% and 74%, respectively). This is not unrelated to the anatomic position of the prostate gland that is anterior to the rectum.48 Both surgical trainees and medical students were right-handed, consistent with Frayer D et al.,47 and both appreciated abnormalities of the prostate during RLDRE (57% and 68.5%, respectively).47 Therefore, a right-handed surgical practitioner would pick abnormal prostate features with the RLDRE position. The implication is that for left-handed surgical trainee or medical students, the patient should be placed in the LLDRE position.
Studies have shown the deficiency in the exposure of medical students to DRE in their undergraduate days. In Australia, 92% of medical students were taught, and 55% were not confident in interpreting findings of DRE because of a lack of supervision by senior colleagues.38 However, half of the medical students who studied in Pakistan and 8% in India performed DRE on mannequins. In India, 92% of medical students were taught DRE, with two-thirds performing less than five DREs before graduation due to inadequate supervision.39,40 In Ireland 24%, 20%, and 56% had no experience with DRE, did rectal examination on mannequins, and performed at least one DRE, respectively.62 It was also shown that inadequate supervision of doctors-in-training resulted in the underutilisation of DRE and that the ability to identify abnormality on rectal examination increases with experience and status. 34 This study showed that medical students were better than the surgical trainees in appreciating prostate abnormalities during RLDRE. Simulators, standardisation techniques, and augmented reality systems have been introduced to improve medical students’ skill acquisition for DRE.41,42,56 Interestingly, in this study there were
significant correlations with the perceptions of both surgical trainees and medical students regarding ease of examination, appreciation of prostate abnormalities, and not being bothered with facing the patients during RLDRE.
DRE alone detected 55.8% of prostate cancer in the screening arms of the Rotterdam, the Netherlands section of the European Randomized Study of Screening for Prostate Cancer.43 DRE was quite sensitive in identifying prostate cancer in men with a PSA value greater than or equal to 10 ng/mL. This study revealed a much higher detection rate for prostate cancer by both surgical trainees (87.5%) and medical students (75.0%). This might be related to the mean PSA of 355 ng/mL in this study, which is much higher than in the Netherlands study (52 ng/mL).43 Debansu S et al.,63 found that suspicious DRE irrespective of the serum PSA level, detected 52.18% prostate cancer compared to 45.46% using a PSA cut-off of greater than 4 ng/mL.
Increase in BMI and abnormal DRE is a strong predictor for overall prostate cancer in men who are obese, and is associated with high-grade prostate cancer.9 However, BMI was not measured in this study, which is a limitation, though subsequent studies will address this issue.
Koulikov D et al,64 documented the inability of the examining finger to reach and examine the apex, half, three quarter, and whole
prostate in 93.7%, 66.3%, 23.2%, and 3.2% of cases, respectively. The limitation of this current study is that both surgical trainees and medical students were all right-handed. There is a need to investigate the perception of the LLDRE position in left-handed medical personnel, which is different from the traditional digital rectal examination position. Another limitation was that the authors did not determine the sample size before the study. This will be addressed in a future validation of a comparative study between RLDRE and traditional LLDRE.
What this study has shown is that patients better tolerated RLDRE than left lateral DRE, and that a significant percentage of senior surgical trainees and final year medical students were able to identify abnormalities of BPH and prostate cancer. However, the long-term impact of using RLDRE on patient outcomes and generalisability to different healthcare settings will become obvious with further study.
In conclusion, the RLDRE position is well tolerated, less awkward, and less painful to the patients. Both the surgical trainees and medical students felt RLDRE was easier, and they appreciated abnormal prostate features better. There were positive correlations of RLDRE perceptions and the ability to detect BPH and prostate cancer by surgical trainees and medical students. The RLDRE position is a scientifically logical paradigm shift from the traditional DRE position.
Table 1: Patients, surgical trainee, and medical student perception of right lateral versus left lateral positions for digital rectal examinations.
Table 2: Correlations of features of prostate cancer and benign prostatic hyperplasia with right lateral digital rectal examination by surgical trainees and medical students. Symptom
1. Yeboah ED. Prevalence of benign prostatic hyperplasia and prostate cancer in Africans and Africans in the diaspora. J West Afr Coll Surg. 2016;6(4):1-30.
2. Ojewola RW et al. Prevalence of clinical benign prostatic hyperplasia amongst community-dwelling men in a south-western Nigeria rural setting: a cross-sectional study. Afr J Urol. 2017;23(2):109-15.
3. Stephan C et al. The value of digital rectal examination in clinical practice. AME Med J 2018;3:45.
4. McFarlane MJ. The Rectal Examination. In: Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations.3rd ed. Boston: Butterworths; 1990.
5. Ng M et al. Benign prostatic hyperplasia [Internet] (2024) Treasure Island: StatPearls. Available at: https://www.ncbi.nlm.nih.gov/books/ NBK558920/. Last accessed: 21 May 2024.
6. Sinam LB et al. Digital rectal grading of benign prostatic hyperplasia. Where does it stand today? J MG Inst Med Sci 2016;21(1):40-5.
7. Gerber GS, et al. Evaluation of the Urological Patient: History, Physical Exam, and Urinalysis. In: Wein AJ, Kavoussi LR et al, editors. CampbellWalsh Urology, 10th ed. Philadelphia: WB Saunders;2012. P.73-98.
8. Pearson R et al. Common questions about the diagnosis and management of benign prostatic hyperplasia. Am Fam Physician. 2014;90(11):764-74.
9. David RH et al. A systematic review of the accuracy of the digital rectal examination as a method of measuring prostate gland volume. J Clin Urol. 2019;12(5).
10. Yamamoto Y et al. Does digital rectal examination predict prostate volume greater than 30mL? Int J Urol. 2017;24: 373-6.
11. Ying Y et al. Value of digital rectal examination in patients with suspected prostate cancer: a prospective cohort analysis study. Transl Androl Urol. 2023;12(11):1666-72.
12. Mathews JM. A Treatise on diseases of the rectum, anus, and sigmoid flexure. 2nd, revised edition. New York: D. Appleton and Company; 1897.
13. Soronen V et al. Digital rectal examination in prostate cancer screening at PSA level 3.0-3.9ng/ml: long-term results from a randomized trial. Scand J Urol. 2021;55(5):348-53.
14. Naji et al. Digital rectal examination for prostate cancer screening in primary care: a systematic review and meta-analysis. Ann Fam Med. 2018;16(2):149-54.
15. Totaro A et al. Is digital rectal examination still useful in prostate cancer diagnosis? No! Urologia. 2019;86(1):32-3.
16. Nyitray AG et al. The utility of Digital Anal Rectal Examinations in a public health screening program for anal cancer. J Low Genit Tract Dis. 2020;24:192-6.
17. Jones D et al. The diagnostic test accuracy of rectal examination for prostate cancer diagnosis in symptomatic patients: a systematic review. BMC Fam Pract. 2018;19:79.
18. Walsh AL, et al. Digital rectal examination in primary care is important for early detection of prostate cancer: a retrospective cohort analysis study. Br J Gen Pract. 2014;64(629):e783-7.
19. Ricardo P et al. The digital rectal examination (DRE) remains important outcomes from a contemporary cohort of men undergoing an initial 12-18 core prostate needle biopsy. Can J Urol. 2012;19(6):6542-7.
20. Tan WS et al. Is there still a role for digital rectal examination in the prostate cancer diagnostic pathway in the COVID-19 and post COVID-19 era? Aging Male. 2021;24(1):92–4.
21. Kirby M et al. Is the digital rectal exam any good as a prostate cancer screening test? Br J Gen Pract. 2024;74(740):137-9.
22. Sajjad W et al. Diagnostic value of the abnormal digital rectal examination in the modern MRI-based prostate cancer diagnostic pathway. J Clin Urol. 2022;0(0).
23. Galic j et al. Comparison of digital rectal examination and prostate specific antigen in early detection of prostate cancer. Coll Antropol. 2003;27(1):61-6 .
24. Ojewola RW et al. An evaluation of usefulness of prostate specific antigen and digital rectal examination in the diagnosis of prostate cancer in an unscreened population: experience in a Nigerian teaching hospital. West Afr J Med. 2013;32(1):8-13.
25. Kash DP, Lal M, Hashmi AH, Mubarak M. Utility of digital rectal examination, serum prostate specific antigen, and transrectal ultrasound in the detection of prostate cancer: a developing country perspective. Asian Pac J Cancer Prev. 2014;15(7):3087-91.
26. Catalona WJ et al. Comparison of
digital rectal examination and serum prostate specific antigen in the early detection of prostate cancer: results of a multicenter clinical trial of 6.630 men. J Urol. 2017;197(25):S200-7.
27. Halpern JA et al. Use of digital rectal examination as an adjunct to prostate specific antigen in the detection of clinically significant prostate cancer. J Urol. 2018;199(4):947-53.
28. Okpua NC et al. Clinical diagnosis of prostate cancer using digital rectal examination and prostate-specific antigen tests: a systematic review and meta-analysis of sensitivity and specificity. Afr J Urol. 2021;27(32).
29. Ozah et al. The diagnostic accuracy of prostate specific antigen and digital rectal examination in the diagnosis of prostate cancer at the university of Benin teaching hospital. J West Afr Coll Surg. 2023;13(3):91-5.
30. Galosi AB et al. Detection limits of significant prostate cancer using multiparametric MR and digital rectal examination in men with low serum PSA: up-date of the Italian society of integrated diagnostic in urology. Arch Ital Urol Androl. 2021 Mar 22;93(1):92100.
31. Sarkar D et al. Correlation of digital rectal examination and serum prostate-specific antigen levels for detection of prostate cancer: retrospective analysis results from a tertiary care urology center. J Cancer Res Ther. 2022;18(6):1646-50.
32. Matsukawa A et al. Comparing the performance of digital rectal examination and prostate specific antigen as a screening test for prostate cancer: a systematic review and meta-analysis. Eur Urol Oncol. 2024;7(4):697-704.
33. Murthy GD et al. Underutilization of digital rectal examination when screening for prostate cancer. Arch Intern Med. 2004;164(3):313-6.
34. Teoh M et al. Digital rectal examination: perspectives on current attitudes, enablers, and barriers to its performance by doctors-in-training. Cureus. 2023;15(6):e40625.
35. Shoag J et al. Decline in prostate cancer screening by primary care physicians: an analysis of trends in the use of digital rectal examination and prostate specific antigen testing. J Urol. 2016;196(4);1047-52.
36. Herrero JA et al. Rectal Exam [Internet] (2024) Treasure Island: StatPearls. Available at: https://www.ncbi.nlm. nih.gov/books/NBK537356/ . Last accessed: 21 May 2024.
37. Soares SCM et al. Digital rectal examination and its associated factors
in the early detection of prostate cancer: a cross-sectional populationbased study. BMC Public Health. 2019;19(1):1573.
38. Lawrentschuk N, Bolton DM. Experience and attitudes of finalyear medical students to digital rectal examination. Med J Aust. 2004;181(6):323-5.
39. Asif M et al. Teaching and practicing rectal examination in Pakistan. Clin Teach. 2015;12(6):399-402.
40. Beena A, Jagadisan B. Digital rectal examination training among Indian medical graduates. Clin Teach. 2019;16(1):36-40.
41. Reis LO et al. Digital rectal examination standardization for inexperienced hands: teaching medical students. Adv Urol 2013:797096.
42. Muangpoon T et.al. Augmented reality system for digital rectal examination training and assessment: system validation. J Med Internet Res. 2020;22(8):e18637.
43. Schroder FH et al. Evaluation of the digital rectal examination as a screening test for prostate cancer. Rotterdam section of the European randomized study of screening for prostate cancer. J Natl Cancer Inst. 1998;90(23):1817-23.
44. Sabbagh C et al. What is the best position for analyzing the lower and middle rectum and sphincter function in a digital rectal examination? A randomized, controlled study in men. Dig Liver Dis 2014;46(12):1082-5.
45. Romero FR et al. Patient positioning during digital rectal examination of the prostate: preferences, tolerability, and results. Int Braz J Urol. 2011;37(3):37179.
46. Nagathan DS et al. Cross-leg lithotomy: is it better position for digital rectal examination of the prostate? J Clin Urol. 2013;6(5):311-6.
47. Frayer DW et al. OH-65: The earliest evidence for right-handedness in the fossil record. J Hum Evol. 2016;100:6572.
48. Singh O, Bolla SR. Anatomy, Abdomen and Pelvis, Prostate [Internet] (2023): StatPearls. Available at: https://www. ncbi.mlm.nih.gov>books>NBK540987. Last accessed: 21 May 2024.
49. Wilbur J. Prostate cancer screening: the continuing controversy. Am Fam Physician. 2008;78(12):1377-84.
50. Krilaviiute A et al. Digital rectal examination Is not a useful screening test for prostate cancer. Eur Urol Oncol. 2023;6(6):566-73.
51. Emberton M et al. Understanding patient and physician perceptions of benign prostatic hyperplasia in Europe: the Prostate Research on Behaviour and Education (PROBE) survey. Int J Clin Pract. 2008;62(1):18-26.
52. Lass E, Raveendran L. Educational implications of changing the guidelines for the digital rectal examination. Can Fam Phy. 2019;65:838-40.
53. Elterman D et al. Update-2022 Canadian urological association guideline on male urinary tract symptoms/benign prostatic hyperplasia (MLUTS/BPH). Can Urol Assoc J. 2022;16(8).
54. Sandhu JS et al. Management of lower urinary tract symptoms attributed to benign prostatic hyperplasia (BPH): AUA Guideline amendment. J Urol. 2023;211(1):11-9.
55. Gravas S et al. Summary paper on the 2023 European association of urology guidelines on the management of nonneurogenic male lower urinary tracts symptoms. Eur Urol 2023;84(2):20722.
56. Balkissoon R et al. Lost in translation: unfolding medical students' misconceptions of how to perform a clinical digital rectal examination. Am J Surg. 2009;197(4):525-32.
57. Candas B et al. Evaluation of prostatic specific antigen and digital rectal examination as screening tests for prostate cancer. Prostate. 2000;45(1):19-35.
58. Zhang A et al. Digital rectal examination in prostate cancer screening. Univ West Ont Med J. 2013;82(1):10-1.
59. Romero FR et al. Reasons why patients reject digital rectal examination when screening for prostate cancer. Arch Esp Urol. 2008;61(6):759-65.
60. Furlan et al. Patient’s reactions to digital rectal examination of the prostate. Int Braz J Urol. 2008;34:5725.
61. Frank J et al. Couch or crouch? Examining the prostate: a randomized study comparing the knee-elbow and the left-lateral position. BJU Int. 2008;87(4):331-3.
62. Fitgerald D. Digital rectal examination: national survey of undergraduate medical training in Ireland. Postgrad Med J 2007;83(983):599-601.
63. Debansu S et al. Correlation of digital rectal examination and serum prostate-specific antigen levels for detection of prostate cancer: Retrospective analysis results from a tertiary care urology center. J C Res Therap. 2022;18(6):1646-50.
64. Koulikov D et al. Why cannot I find the prostate? Behind the subjectivity of rectal exam. ISRN Urol. 2012;456821.
Prevalence of Obstructive Sleep Apnoea in Sleep Referrals and Related Medical Conditions in a Local Chest Unit in Hong Kong
Authors: *An Emmanuel Le,1 Sze Man Wong,2 Kwok Sang Wilson Yee,1 Cee Zhung Steven Tseng1
1. Department of Tuberculosis and Chest Unit, Wong Tai Sin Hospital, Hong Kong
2. Private practice, Hong Kong
*Correspondence to docteur.le.emmanuel@gmail.com
Disclosure: All authors have declared no conflicts of interest.
Received: 20.05.24
Accepted: 31.07.24
Keywords: Epworth Sleepiness Scale (ESS), Hong Kong, obstructive sleep apnoea (OSA), Patient Health Questionnaire-9 (PHQ-9), sleep epidemiology.
Objective: To understand obstructive sleep apnoea (OSA) epidemiology and associated comorbidities in a Chest Unit in Hong Kong, and to better understand sleep referrals to enhance screening assignment.
Design: A prospective, observational case-series study from a Chest Unit in Hong Kong.
Subjects: Patients, aged ≥17 years old or older and referred to Wong Tai Sin Hospital for polysomnography, were recruited from the 15th of September 2022–31st of January 2023.
Methods: Demographic, anthropometric, and phenotypic characteristics were collected. Questionnaires (Epworth Sleepiness Scale [ESS], Patient Health Questionnaire-9 [PHQ-9]) were completed and polysomnography was performed on the following night. The presence of OSA was defined as apnoea–hypopnoea index (AHI) ≥5 events·h-1.
Results: A total of 303 patients were recruited. The prevalence of OSA amongst the referred patients was 91%, and ischaemic heart disease, diabetes, and hypertension accounted for 16.3%, 34.8%, and 63.4%, respectively. In addition, 43.4% of patients fulfilled the definition of depression according to their PHQ-9 score (≥5).
Conclusion: This observational study showed that the appropriateness of referrals for sleep tests was adequate, with 91% of patients having OSA. The majority of them are overweight or obese and presented with hypertension, diabetes, and mild depression, and excessive daytime sleepiness.
Key Points
1. This article showed that referrals for sleep study based on clinician’s knowledge were appropriate, with an accuracy of 91%.
2. This case-series study tried to characterise the male and female phenotypes with obstructive sleep apnoea.
3. Primary care physicians should be aware of male and female clinical phenotypes for early diagnosis and intervention in order to lessen the burden on health outcomes.
INTRODUCTION
Obstructive sleep apnoea (OSA) is a complex and chronic disease characterised by loud snoring, daytime sleepiness, and witnessed breathing pause. It is defined by the American Academy of Sleep Medicine (AASM) as a decrease or complete cessation of airflow despite an ongoing effort to breathe,1 and it affects 4.1% and 2.4% of males and females in Hong Kong, respectively.2,3
Clinically, it is associated with the degradation of the quality of life, an increased risk of road traffic accident,4 and a detrimental effect on cardiovascular health. The pathophysiology consists of a repetitive collapse of the pharyngeal airway during sleep, leading to a transient interruption of airflow with hypoxia. It is accompanied by a central nervous system stimulation to restore upper airway patency and reoxygenation. Therefore, patients experience unrefreshing sleep with excessive daytime sleepiness due to fragmented sleep and hypoventilation.
Polysomnography (PSG) is the ‘gold standard’ to detect OSA;5 however, it is a limited and expensive test. The waiting time from referral to PSG is long. In particular, in the author’s locality, the waiting time from first consultation to PSG was 189.6 days in a teaching hospital, and in public settings the waiting time would be much more longer.6
Moreover, the referral for sleep test may not always be appropriate; the probability of making a referral for sleep apnoea can be influenced more by patient requests, regardless of physicians’ knowledge and attitudes toward OSA.7
Therefore, the use of screening questionnaire could clearly improve the prioritisation for referrals to sleep test. The STOP-BANG score, has a sensitivity from 81–86% to predict OSA in Hong Kong.8
At the Department of Tuberculosis and Chest, Wong Tai Sin Hospital, Epworth Sleepiness Scale (ESS), with an adequate reliability and validity, was mainly used to screen OSA.9 In addition, clinical presentation of OSA and depression may overlap. Signs and symptoms of fatigue, poor concentration, loss of interest, and insomnia can often be overlooked by clinicians as sleep apnoea symptoms. Among people with physician diagnosed OSA, the odds ratio for probable major depression was 2.4 among males and 5.2 among females.10 In their study, Garbarino S et al.11 showed that a pooled prevalence for depressive disorders was 35% in patients with OSA. In the author’s locality, Patient Health Questionnaire-9 (PHQ-9) is a valid tool to screen depression and has shown a sensitivity of 80% and specificity of 92%.12
OSA can also be associated with other comorbid conditions. A previous study showed that, in an OSA cohort, 34% of the patients had hypertension,13 32% suffered of diabetes,14 and 6.6% of ischaemic heart disease.14
The aim of this study was to assess the prevalence of OSA in patients referred for sleep test in a chest department and its related medical conditions. Furthermore, to aim to draw the phenotype of patients referred for sleep study.
MATERIALS AND METHODS
This prospective, observational case-series study was conducted at the Department of Tuberculosis and Chest, Wong Tai Sin Hospital from 15th of September 2022– 31st of January 2023. Ethical approval has been obtained from the Kowloon Central Cluster (KC/KE-18-0208/FR-3). Sources of the patient’s referrals were mainly from the Department of Medicine at Kwong Wah Hospital, Queen Elizabeth Hospital, Department of Otorhinolaryngology at Yan Chai Hospital, and the Department of Tuberculosis and Chest at Wong Tai Sin Hospital, Hong Kong.
For a 95% CI with 5% margin of error and with a disease prevalence of 4.1%, the sample size of the population of Hong Kong should be at least 61 patients. Most of the patients were referred for sleep test following symptoms of snoring and tiredness, while hypertension or obesity were not the main factors for referrals. All patients referred to the author’s Chest Unit who were aged ≥17 years and who did not have a known history of sleep disorders were consecutively recruited. Patients who were pregnant, in unstable conditions, on sleeping pills, or unable to fill out the questionnaires were excluded.
Patients who consented were invited to complete the two questionnaires (ESS, PHQ-9) on the day of admission prior to the sleep study. Patients with an ESS >10 were considered to have clinical daytime sleepiness.15 STOP-BANG is a score used to screen OSA. The total score ranges from 0–8, and patients can be classified for OSA risk based on their respective scores. The sensitivity of STOP-Bang score ≥3 to detect moderat-to-severe OSA is 93% and 100%, respectively.16
Anthropometric characteristics (BMI, neck circumference, and gender) were recorded. While demographic characteristics (hypertension, diabetes, and ischaemic heart disease) were retrieved from the clinical management system from hospital authority or directly from patients' clinical notes.
Level II-nocturnal PSG was performed using a Philips Respironics Alice 6 system (Philips Respironics, Murrysville, Pennsylvania, USA) in the sleep laboratory at Wong Tai Sin Hospital, Department of Tuberculosis and Chest. Recording comprised electroencephalogram channels, electrooculogram, and chin muscle electromyogram. An experienced sleep physician reviewed all the PSGs according to the AASM guidelines on sleep scoring.1 The severity of OSA was defined by the apnoea–hypopnoea index (AHI). Obstructive apnoea was characterised as complete cessation of airflow for at least 10 seconds. Hypopnoeas were characterised by a period of reduction of >30 % oronasal airflow for at least 10 seconds and associated with a ≥3% decrease of oxygen saturation and/or micro-arousal. The AHI is summarised as the sum of the total events per hour of sleep. OSA was defined using AHI as mild (5–15 events h-1), moderate (15–30 events·h-1), and severe (>30 events·h-1).1 Patients were considered to have diabetes, hypertension, or ischaemic heart disease if they were on treatment prior to admission.
The Asian phenotype has a higher body and visceral fat associated with a lower BMI, and Asian patients develop OSA at a lower BMI than those who are Caucasian.17 Modifying the STOP-BANG cut-off BMI criteria to 30 kg m−2 has improved the sensitivity without compromising specificity in OSA screening.17 The authors use the ‘modified’ STOP-BANG score, where the BMI of ≥30 kg·m−2 counts for one point.
On the day of admission, patients were asked to complete the ESS and the PHQ-9 questionnaires. The PHQ-9 is a nine‐item depression questionnaire. It is a self-report screening tool that identifies the presence and severity of depression. The severity of a depressive disorder can be divided into 5–9 (mild), 10–14 (moderate), 15–19 (moderately severe), and 20–27 (severe).18 Statistical analysis was performed using SPSS version 23 for Windows (SPSS Inc., Chicago, Illinois, USA) computer software.
Demographic data is presented with descriptive statistics. Continuous data that is normally distributed is presented as mean+/SD and student T-test is used. A p-value <0.05 was set as statistically significant.
RESULTS
From the 15th September 2022– 31st of January 2023, 303 consecutive Chinese patients were enrolled and completed the questionnaires. Of these, 267 had OSA as defined by an AHI ≥5 events/hour. The prevalence of sleep apnoea amongst patients referred was 91%, whereas only 27 patients did not experience sleep apnoea. The mean age of referred patients with obstructive sleep apnoea was 55.81±12.51 years, 204 were male (73.9%) and 72 were female (26.1%). Of the patients, 71% had never smoked, 13.8% were active smokers, and 15.2% were ex-smokers. Ninetysix patients (34.8%) were diabetic, 45 patients (16.3%) had ischaemic heart disease, and 175 patients (63.4%) were hypertensive.
The mean systolic blood pressure was 140.97±15.53 mmHg and the mean diastolic blood pressure was 87.23±11.78 mmHg. The mean BMI was 29.96±6.43 kg·m−2. The mean ESS was 10.73±5.04, while 43.5 % did not experience daytime sleepiness (ESS <10). At presentation, 41.7 % had mild-to-moderate excessive daytime sleepiness and 14.9 % had severe daytime sleepiness. The mean AHI was 40.429+/-24.23 event hour-1, and the mean ‘modified’ STOP-BANG score was 4.86±1.52. ESS was 10.73±5.04 and the mean PHQ-9 was 5.13±4.5 and 43.4% of the sample had depression (defined as PHQ-9 ≥5).
Demographics/ Phenotypes by Gender
The overall male-to-female ratio for OSA was 2.8:1 (204 versus 72). Female patients were significantly older than male patients (58.40±10.96 years verses 54.89±12.91 years, respectively; p<0.05) and heavier (BMI 31.40±9.40 kg/m2 verses 29.45±4.91 kg/m2, respectively; p=0.02).
Neck circumference in female patients, as expected, was smaller than that of males (38.01±3.78 versus 41.70±2.87, respectively; p<0.0001). Male patients tended to smoke more than female counterparts (17.6% versus 2.8%, respectively; p<0.05).
The presence of diabetes was similar between both genders, while males experienced a higher rate of hypertension and ischaemic heart disease (Table 1). As shown in Table 1, both groups presented with similar symptoms of snoring perception (80.9% for males versus 75% for females; p=0.28). Females perceived more tiredness than males (69.4% versus 55.9%; p<0.05).
Sleep Parameters by Gender
As shown in Table 2, total sleep time and sleep efficiency of PSG were significantly better in male patients. The total AHI was similar between the two groups (41.49±23.48 /h for males verses 39.33±26.34 /h for females; p=0.5).
Females tended to snore more than males (8.18±11.58% versus 13.41±17.57%, respectively; p<0.05). ESS was comparable amongst males and females (10.81±4.98 in males versus 10.50±5.23 in females; p=0.65). Table 3 shows the clinical phenotypes' difference between genders.
Table 1: Demographics/phenotypes of female and male obstructive sleep apnoea patients.
Data are presented as n (%) or mean ± standard deviation.
*Statistically significant.
N: number.
Table 2: Sleep parameters by gender.
Data are presented as n (%) or mean ± standard deviation.
*Statistically significant. N: number.
Table 3: Clinical phenotypes by gender.
Data are presented as n (%) or mean ± standard deviation.
*Statistically significant. N: number.
DISCUSSION
To the authors’ knowledge, there were no recent local studies concerning the prevalence of OSA in patients referred for sleep study, and their phenotypes, in Hong Kong.
Despite that, the majority of referrals were based on clinicians’ knowledge of OSA or patients’ requests, without formal screening tests. In this cohort, the accuracy of referral was high (91%), and only less than 10% of the patients were inappropriately referred. The systematic use of screening tools (ESS, STOP-BANG score) may help the prioritisation of sleep tests according to symptom severity.
This cohort describes the demographic, clinical aspects, and polysomnographic parameters of OSA amongst the population of Hong Kong. First, obesity played a key role in the referral of OSA. The patients were obese with a BMI of 29.96±6.43 kg.m-2 in comparison with the general population, and there was no significant difference between males and females.
However, major differences characterised the phenotypes between males and females. The series showed that female patients with OSA were older, and that BMI was rather similar in both groups (p=0.2); although, the neck circumference in female patients is smaller than that of males. The mean total AHI were similar (p=0.5). The similar rate of sleep apnoea in both genders may be related to ageing and hormonal changes due to menopause in female patients, as oestrogen and progesterone play a protective role in females with OSA.19 The mean age of the female patients was 58.40±10.96 years, while 51 years is the average age of menopause in Hong Kong.20
There is an association between OSA and diabetes, and this cohort found that 34.8% of patients were diabetic. It is similar to a French cross-sectional study with 30.1% of patients with OSA.21
The prevalence of hypertension in the general population (patients aged 65–84 years old) of Hong Kong was 57.4%.22 However, these results showed a higher proportion, with 63.4% presenting with
hypertension with a female predominance (p=0.01), attributable to a slightly higher BMI and sleep apnoea in the study. However, under treatment, the majority of them have a good control with a systolic blood pressure of 140.97±15.53 mmHg and diastolic blood pressure of 87.23±11.78 mmHg.
Ischaemic heart disease prevalence was lower than the Sleep Heart Health Study (16.3% versus 23.6%).23 The current results are consistent with the fact that the prevalence of ischaemic heart disease is lower in Chinese compared to Caucasian patients.24 In addition, 43.4% of patients fulfilled the definition of depression according to the PHQ-9 score (≥5) compared to 35%11 in the general population. Sleep apnoea can play a role in the perception of depression due to sleep disruption or hypoxemia.25
In terms of sleep duration, males significantly slept better than females, with a total sleep score 399.70±87.57 mins (p=0.025) and a sleep efficiency of 69.54±14.92% (p=0.023). However, compared to females, their sleep was more fragmented with an arousal index of 31.16±13.46 event/h (p<0.001). The authors supposed that sleep fragmentation was linked to nocturia as it was reported that males with OSA have a 1.5-fold increase in the risk of nocturia, but no significant relationship was found in females.26
Phenotypically, both males and females complained of snoring symptoms (80.9%); but, due to the different perception of symptoms between genders, females reported more tiredness and fatigue (p=0.045), although witnessed apnoea was similar (p=0.16). The study population showed mild excessive daytime sleepiness with an overall ESS of 10.73±10.73, with no difference between genders (p=0.65). Males presented with more central sleep apnoea than females (5.54±7.94 versus 1.54±2.39, respectively; p<0.0001) due to a higher prevalence in underlying ischaemic heart disease.27 Overall, both groups had some component of insomnia with sleep onset of 40.08±43.50 mins, but there is no significant difference (p=0.10).
In summary, the findings show that female and male patients have different OSA phenotypes. On average, female patients referred for sleep tests were older and had a higher BMI than their male counterparts. Despite a lower neck circumference, they tended to snore more than males, due to menopause and hormonal changes. Females tended to complain more about tiredness, and though not statistically significant, they have a longer sleep onset time. Those findings hinted that women can be misdiagnosed as having insomnia or depression instead of OSA. On the other hand, the results suggest that male patients are more likely to be smokers, younger, and have more underlying ischaemic heart disease and hypertensive disease.
Hence, primary physicians should be aware of different clinical phenotypes between males and females to make early diagnosis and intervention to lessen the burden in health outcomes.
LIMITATIONS
The current study has several important limitations. First, this study was conducted in a single centre; therefore, the number of patients recruited was rather small and results could not be generalised to the general population referred for sleep test. Another potential source of bias in the study is related to selection and recruitment; all the patients in this study have been referred by doctors, regardless of the pre-test screening questionnaire. It could therefore lead to an overestimation of the epidemiology.
In addition, time constraints precluded longterm follow-up and sleep questionnaire after continuous positive airway pressure titration and regular continuous positive airway pressure use in terms of symptoms control. Ideally, a longer follow-up period is needed to assess long term improvement of symptoms.
Nevertheless, this small cohort study is relevant in presenting the male-female distribution of OSA in the Chinese Hong Kong population, and may serve as a pilot investigation, shedding light on design and conduct for larger scale studies.
CONCLUSION
The cohort showed that the prevalence of patients referred for sleep tests is high, and referrals are generally appropriate. Phenotypically, patients are in their fifties,
References
1. Berry RB et al., The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications, Version 2.6 (2020), Darien: The American Academy of Sleep Medicine.
2. Ip MS et al. A community study of sleep-disordered breathing in middleaged Chinese men in Hong Kong. Chest. 2001;119(1):62-9.
3. Liu J et al. Prevalence of signs and symptoms suggestive of obstructive sleep apnea syndrome in Guangxi, China. Sleep Breath. 2014;18(2):37582.
4. Udholm N et al. Obstructive sleep apnea and road traffic accidents: a Danish nationwide cohort study. Sleep Med. 2022;96:64-9.
5. Kapur VK et al. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American academy of sleep medicine clinical practice guideline. J Clin Sleep Med. 2017;13(3):479-504.
6. Hui DS et al. A randomized controlled trial of an ambulatory approach versus the hospital-based approach in managing suspected obstructive sleep apnea syndrome. Sci Rep. 2017;8:45901.
7. Williams NJ et al. Factors associated with referrals for obstructive sleep apnea evaluation among community physicians. J Clin Sleep Med. 2015;11(1):23-6.
8. Ha SC et al. Evaluation and validation of four translated Chinese questionnaires for obstructive sleep apnea patients in Hong Kong. Sleep Breath. 2014;18(4):715-21.
9. Chung KF. Use of the Epworth Sleepiness Scale in Chinese patients
obese, and have hypertension, diabetes, and mild depression. Signs and symptoms of OSA differ due to gender features or perception, and physicians‘ awareness and intervention may reduce the adverse health outcomes.
with obstructive sleep apnea and normal hospital employees. J Psychosom Res. 2000;(5):367-72.
10. Wheaton AG et al. Sleep disordered breathing and depression among U.S. adults: national health and nutrition examination survey, 2005-2008. Sleep. 2012;35(4):461-7.
11. Garbarino S et al. Association of anxiety and depression in obstructive sleep apnea patients: a systematic review and meta-analysis. Behav Sleep Med. 2020;18(1):35-57.
12. Cheng CM, Cheng M. To validate the Chinese version of the 2Q and PHQ-9 questionnaires in Hong Kong Chinese patients. HK Pract. 2007;29:381-90.
13. Tao M et al. Symptom and comorbidity burden in hypertensive patients with obstructive sleep apnea. Front Endocrinol (Lausanne). 2024;15:1361466.
14. Khamsai S et al. Prevalence and factors correlated with hypertension secondary from obstructive sleep apnea. Multidiscip Respir Med. 2021;16(1):777.
15. Walker NA et al. Clinical utility of the Epworth sleepiness scale. Sleep Breath. 2020;24(4):1759-65.
16. Chung F et al. STOP-Bang questionnaire: a practical approach to screen for obstructive sleep apnea. Chest. 2016;149(3):631-8.
17. Pivetta B et al. Use and performance of the STOP-Bang questionnaire for obstructive sleep apnea screening across geographic regions: a systematic review and meta-analysis. JAMA Netw Open. 2021;4(3):e211009.
18. Kroenke K et al. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606-13.
19. Lee J et al. Sleep disorders and menopause. J Menopausal Med. 2019;25(2):83-7.
20. Family Health Service. Dealing with menopause. 2022. Available at: https:// www.fhs.gov.hk/english/health_info/ woman/14768.html. Last accessed: 1 February 2024.
21. Meslier N et al. Impaired glucoseinsulin metabolism in males with obstructive sleep apnoea syndrome. Eur Respir J. 2003;22(1):156-60.
22. Centre for Health Protection. Hypertension. 2023. Available at: https://www.chp.gov.hk/en/ healthtopics/content/25/35390.html. Last accessed: 1 April 2024.
23. Silva GE et al. Longitudinal evaluation of sleep-disordered breathing and sleep symptoms with change in quality of life: the sleep heart health Study (SHHS). Sleep. 2009;32(8):1049-57.
24. Tsai CF et al. Risk factors for ischemic stroke and its subtypes in Chinese vs. Caucasians: systematic review and meta-analysis. Int J Stroke. 2015;10(4):485-93.
25. Pesonen AK et al. REM sleep fragmentation associated with depressive symptoms and genetic risk for depression in a communitybased sample of adolescents. J Affect Disord. 2019;15(245):757-63.
26. Zhou J et al. Association between obstructive sleep apnea syndrome and nocturia: a meta-analysis. Sleep Breath. 2020;24(4):1293-8.
27. Gottlieb D.J et al. Prospective study of obstructive sleep apnea and incident coronary heart disease and heart failure: the sleep heart health study. Circulation. 2010;22:352-60.
Pelvic Atherosclerosis in Women: A Case Report of the Alleviation of Dyspareunia and Vaginal Dryness after Pelvic Artery Revascularisation
Authors: Vignes Mohan,1,2 Fatih Arslan,3 *Nicolas Diehm4,5
1. Department of Angiology of Cantonal Hospital of Graubünden, Switzerland
2. Angioviva Vascular Center, Graubünden, Switzerland
3. Leiden University Medical Center, the Netherlands
4. Vascular Center of Central Switzerland, Aarau, Switzerland
5. University of Bern, Switzerland
*Correspondence to nicolas.a.diehm@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Received: 24.05.24
Accepted: 11.07.24
Keywords: Atherosclerosis, dyspareunia, endovascular therapy, revascularisation, vasculogenic female sexual dysfunction.
Misdiagnosed and inadequately treated vasculogenic sexual dysfunction affects millions of females worldwide, highlighting the importance of a mostly overlooked pathology. Organic female sexual dysfunction, such as vaginal engorgement and clitoral erectile insufficiency, may be associated with hypogastric atherosclerosis.
In the author’s vascular medicine setting, they encountered a case of a post-menopausal female patient with symptomatic common iliac and hypogastric artery occlusion. This case highlights the diagnostic management of atherosclerosis and its secondary clinical manifestations, the differentiation between physiological post-menopausal hormonal changes and pathological vasculogenic dysfunction, as well as currently available endovascular treatment options.
The 57-year-old patient presented with symptoms indicative of bilateral peripheral artery disease, Fontaine Stage IIb, along with vaginal dryness and dyspareunia. Upon finding occlusions of the common iliac and hypogastric artery, bare metal stenting of the left distal common iliac artery and percutaneous transluminal angioplasty of the internal iliac artery was performed. At 6-week follow-up, an unlimited pain-free walking distance as well as greatly improved vaginal and clitoral erectile function was reported.
Local oestrogen application for a year showed no clinical improvement, whereas a significant difference in vaginal and clitoral erectile function was reported shortly after endovascular revascularisation. Vaginal engorgement and clitoral erection depend on increased blood inflow and pulsatile, non-calcified arterial walls. In females with cardiovascular risk factors, arterial insufficiency of the hypogastric-cavernous bed is an underestimated atherosclerotic manifestation for sexual impairment. In these patients with arteriogenic sexual dysfunction, endovascular therapy using drug-eluting stents may be considered as an effective treatment option.
Key Points
1. Vasculogenic female sexual dysfunction, a frequently overlooked consequence of atherosclerosis, impacts millions of women worldwide, leading to significant quality-of-life deterioration, especially in postmenopausal women with cardiovascular risk factors.
2. This case report examines a 57-year-old postmenopausal woman with common iliac and hypogastric artery occlusions, illustrating how endovascular revascularisation can address vasculogenic sexual dysfunction and peripheral artery disease symptoms.
3. Endovascular revascularisation emerges as a promising intervention for women with vasculogenic sexual dysfunction, providing symptom relief by restoring pelvic blood flow and highlighting the need for recognising cardiovascular contributions to female sexual health issues.
INTRODUCTION
Pathophysiology and Aetiology of Female Sexual Dysfunction
Vasculogenic female sexual dysfunction syndromes affect millions of ageing women worldwide, whose day-to-day symptoms of coital vaginal discomfort, vaginal dryness, and diminished sexual arousal are underdiagnosed and often inadequately empirically treated with hormone supplementation or simply artificial lubrication.1 As early as 1997, Park et al.2 demonstrated the root of vaginal and clitoral engorgement insufficiency to be of haemodynamic origin, showing significant changes in pelvic nerve-stimulated vaginal haemodynamics such as a decrease in blood flow and vaginal wall pressure in cases of atherosclerotic cavernosal arteries and diffuse vaginal and clitoral fibrosis. Female sexual response is assessed by the appearance of vaginal lubrication and clitoral tumescence, both associated with autonomic nerve-stimulated local increases in blood flow.3 The aetiology of female sexual dysfunction (FSD) is multifactorial, being associated with various hormonal and urogynaecological abnormalities, psychological issues, and degenerative systemic pathologies, such as metabolic syndrome and cardiovascular disease.4,5
Comparable to male erectile dysfunction (ED), the incidence of FSD has been demonstrated to rise with age and correlate bidirectionally with the existence of cardiovascular comorbidities such
as coronary heart disease, myocardial infarction, and stroke.6,7 Both conditions, vasculogenic erectile dysfunction and cardiovascular disease, are known to be associated with common predisposing risk factors such as arterial hypertension, obesity, diabetes mellitus, hypercholesterolemia, and smoking, while exhibiting similar underlying pathologies in terms of inflammation and sclerosis of arterial vessels leading to severe endothelial dysfunction.7,8 Atherosclerosis of the hypogastric-cavernous arterial bed in predisposed female patients may be an important pathophysiological factor causing organic vasculogenic erectile female sexual dysfunction.
Previous FSD treatment attempts included a range of approaches such as experimental hormone and pharmaceutical therapy, localised mechanical appliances in terms of a vacuum constriction device, and cognitive-behavioural therapy. All in all, results were often inconsistent and none of the above proved to be universally effective. By focusing on the haemodynamic origins and importance of vasculogenic etiological factors of FSD, we aimed to present and further analyse a novel therapeutic approach.
CASE DESCRIPTION
The authors present the case of a 57-year-old woman with a history of hypercholesterolemia, obesity, and smoking. Besides the above-mentioned,
no other cardiovascular risk factors were reported. The patient initially presented in January 2023 with symptoms indicative of bilateral peripheral artery disease Fontaine Stage IIb along with vaginal dryness and dyspareunia for the past year. Prior to endovascular therapy, her female sexual function index (FSFI) was as low as 30, indicating extensive deductions in the domains of desire, arousal, lubrication, orgasm, and satisfaction. Local oestrogen application prescribed by her gynaecologist brought no noticeable clinical improvement. Following a non-invasive vascular workup with oscillography and duplex ultrasound suspecting occlusions of the common iliac and hypogastric artery, bare metal stenting of the left distal common iliac artery and percutaneous transluminal angioplasty of the internal iliac artery was performed. Dual antiplatelet therapy was prescribed over the course of 4 weeks post-interventional.
After an initial period of clinical improvement, the patient’s initial complaints of peripheral leg pain after walking short distances as well as the above-described sexual dysfunction re-appeared about 1 year after the initial intervention. Duplex ultrasound confirmed the suspected diagnosis of an in-stent thrombosis in the left common iliac artery. Rotational thrombectomy using a 6F Rotarex® catheter (Rotarex, Luxembourg) was performed, followed by the placement of bare metal stents in the left common and external iliac artery and recanalisation with drug-eluting stent placement in the left internal iliac artery. At the 6-week followup, the patient reported an unlimited painfree walking distance as well as greatly improved vaginal and clitoral erectile function with an FSFI score of 80 points (indicating a maximum score of 5/5 points in the domains of desire, arousal, lubrication, orgasm, and satisfaction, whilst reporting 0/5 points in the aspect of experienced pain). Duplex ultrasound confirmed patency of the common iliac and hypogastric artery. Dual platelet inhibition using aspirin and clopidogrel was prescribed to be taken until the 3-month follow-up appointment.
DISCUSSION
It is well documented that symptoms typical of FSD increase sharply following menopause due to pathophysiological changes in vaginal tissue associated with oestrogen deprivation.2
Post-menopausal women, as well as those predisposed by the existence of cardiovascular risk factors, report noticeably more complaints of vaginal and clitoral dysfunction compared to pre-menopausal counterparts or women of the same age group devoid of cardiovascular risk factors.9 Nevertheless, a multicentre Latin American study using the FSFI, a 19-item multidimensional self-reporting measure on primary components of female sexual function quantifying potential dysfunction in six domains (desire, arousal, lubrication, orgasm, satisfaction, pain), as the main validation instrument, showed an unusually young group of women with Type 2 diabetes displaying a high prevalence of sexual dysfunction, with a decrease in vaginal lubrication being the most important associated symptom.4
Similar observations were made by a North American cross-sectional cohort study with vaginal dryness due to impaired spontaneous lubrication and a consecutive decline in the number and intensity of reported orgasms being more common amongst insulin-treated diabetic patients compared to non-diabetic women.10
The role of long-term hormone supplementation in maintaining female sexual health has been widely established. However, in view of the above, additional approaches are worth exploring. Although a vast majority of women discontinuing postmenopausal oestrogen intake develop signs of vulvovaginal atrophy, most epidemiological studies show only little increase in pre-existing dyspareunia with age,11 therefore, pointing towards a primary underlying pathology of the vaginal and clitoral arterial bed, with, irrespective of postmenopausal status, well known vascular pathogens such as dyslipidaemia being confirmed an independent risk, causing local
atrophy and the subsequent clinical symptoms.12
In the case of this patient, local oestrogen application over the course of 1 year showed no clinical improvement, whereas a significant difference in vaginal and clitoral erectile function was reported shortly after the procedure. Vaginal engorgement and clitoral erection depend on increased blood inflow and pulsatile, non-calcified arterial walls.12 Atherosclerosis, strongly associated with cardiovascular risk factors, especially in older patients, increasingly affects a younger population.13 Consequently, the age at which secondary pathologies manifest has steadily decreased within the last decade, posing a significant and long-term threat to the individuals’ quality of life if not diagnosed and treated early.14 The prevalence of male erectile dysfunction, especially of vasculogenic aetiology, has increased considerably worldwide, now considered an indicator and independent predictive marker for a disease of generalised atherosclerosis with, in turn, high cardiovascular morbidity and mortality with cardiovascular events.7 Besides nicotine abuse, diabetes mellitus is understood to be one of the most important risk that can be influenced; affected patients have shown up to a four-fold increased risk of developing vasculogenic sexual dysfunction.9,15
There is a significant disparity in recognition of vasculogenic sexual dysfunction among genders. The difference in awareness and subsequent diagnosis can largely be attributed to historical and cultural biases in research and clinical practice, in addition to the complexity of female verses male sexual anatomy and reproductive health.
By increasing the index of suspicion for vasculogenic causes of FSD, a significant gap in sexual health care is newly addressed, advocating for heightened awareness among general practitioners to assess for atherosclerosis in women with FSD; as well as to adopt a more proactive approach in evaluating FSD overall, especially in women presenting with risk factors for cardiovascular disease.
It is likely that in the case of this patient, interventional treatment could have been avoided if long-term preventative measures ensuring overall vascular health including weight loss, cessation of smoking, and statin therapy had been implemented early on. Pharmacological administration of vasodilators such as phosphodiesterase5-inhibitors (PDE-5-I), a routine primary approach in male patients with ED, has not been routinely implemented in the treatment of vasculogenic FSD, and requires further studies.
Going forward, as patients typically do not report their symptoms until the condition has progressed severely, a wider implementation and optimisation of primary and secondary preventive approaches is needed. Encouraging a healthy diet and regular exercise; routine blood sugar and lipid profile checks; and screening and assessment of potential atherosclerotic lesions in other arterial beds such as the lower limb, carotid, and coronary arteries are examples of necessary steps to be taken.
As the most frequent underlying cause is observed to be of vascular origin, a swift path to a confirmed diagnosis is crucial to monitor existing as well as potential risk factors as predictors of future burden of disease to identify patients at risk of severe cardiovascular events early.16
Male patients with severe atherosclerotic ED unresponsive to PDE-5-Is have been shown to profit greatly from endovascular drug-eluting stent therapy of erection-related arteries.17 Stable clinical outcomes were reported beyond a 1-year timeframe, proving the safety and effectiveness of this approach especially in long-term follow-up.18 While the abovedescribed case is a novelty in the field of interventional revascularisation procedures, it demonstrates current and developing endovascular therapy as an effective treatment option for pelvic atherosclerosis in its various clinical manifestations with the overall goal of routinely practised and widely accepted secondary preventive approaches.
A notable limitation of the analysis is the reliance on references that are not recent. This is primarily due to the scarcity of the current research environment. While older studies provide a foundational understanding, the scarcity of recent publications highlights the necessity for further investigation and research of a pathology becoming increasingly frequent. Also to be mentioned is the fact that insights gained from the patient case, while representing a common pathology, may not be generally applicable to primary treatment options of other patients with FSD. The authors’ analysis underscores the importance of early preventative measures; however, does not extensively explore potential barriers to implementation or how to effectively encourage patient adherence.
CONCLUSION
Organic sexual dysfunction has a significant impact on the quality of life. Despite vascular pathologies being the most frequent as well as clinically well-manageable aetiological factor, the relevance of cardiovascular integrity in female sexual health remains largely unrecognised. Once clinically manifested, endovascular revascularisation is effective and successful in restoring arterial blood flow of inner pelvic organs and may be a promising minimal-invasive treatment option for patients with severe arteriogenic FSD, improving symptoms within weeks of the intervention. Given the established direct correlation between atherosclerosis and vasculogenic sexual dysfunction, it is imperative for clinicians to consider atherosclerotic disease as
References
1. Laumann EO et al. Sexual problems among women and men aged 40-80 y: prevalence and correlates identified in the Global Study of Sexual Attitudes and Behaviors. Int J Impot Res. 2005;17(1):39-57.
2. Park K et al. Vasculogenic female sexual dysfunction: the hemodynamic basis for vaginal engorgement insufficiency and clitoral erectile insufficiency. Int J Impot Res. 1998;10(1):67. Corrected and republished from: Int J Impot Res.
a potential underlying cause of FSD in appropriate patients. Further studies are warranted to assess the role of endovascular therapy on the short- and long-term clinical improvement of FSD of atherosclerotic origin.
PATIENT PERSPECTIVE
The symptoms started over a year ago. First I noticed reoccurring leg pains after reaching a certain walking distance; later on, I additionally experienced intimate discomfort. Initially, I did not know that these two symptoms could be connected and potentially both rooted in the same cause.
My gynaecologist explained that with age and menopausal hormonal changes, vaginal dryness and its consecutive discomfort during intercourse was very common, no reason to worry, and that the prescribed oestrogen cream would help treat the underlying cause of oestrogen-derived vaginal tissue. It was not until an examination revealed blockages in my arteries that it was explained to me that those symptoms might be due to a reduced blood flow in that specific area. After the first intervention and stent placement I noticed an improvement of all the above described quite quickly before the symptoms started to re-appear. Now, 6 weeks after the obstructed artery has been re-opened, I am walking entirely pain-free and have noticed a significant improvement in libido due to almost disappeared local discomfort.
1997;9(1):27-37.
3. Berman JR. Physiology of female sexual function and dysfunction. Int J Impot Res. 2005;1(Suppl 1):S44-51.
4. Blümel JE et al. Sexual dysfunction in middle-aged women: a multicenter Latin American study using the Female Sexual Function Index. Menopause. 2009;16(6):1139-48.
5. Wheeler LJ, Guntupalli SR. Female sexual dysfunction: pharmacologic and therapeutic interventions. Obstet Gynecol. 2020;136(1):174-86.
6. Dilixiati D et al. Association between cardiovascular disease and risk of female sexual dysfunction: a systematic review and meta-analysis. Eur J Prev Cardiol. 2024;31(7): 782-800.
7. Uddin SMI et al. Erectile dysfunction as an independent predictor of future cardiovascular events: the multi-ethnic study of atherosclerosis. Circulation. 2018;138(5):540-2.
8. Shin D et al. Erectile dysfunction: a disease marker for cardiovascular disease. Cardiol Rev. 2011;19(1):5-11.
9. Slob AK et al. Sexuality and psychophysiological functioning in women with diabetes mellitus. J Sex Marital Ther. 1990;16(2):59-69.
10. Copeland KL et al. Diabetes mellitus and sexual function in middle-aged and older women. Obstet Gynecol. 2012;120(2 Pt 1):331-40.
11. Basson R. Women's sexual function and dysfunction: current uncertainties, future directions. Int J Impot Res. 2008;20(5):466-78.
12. Baldassarre M et al. Impaired lipid profile is a risk factor for the development of sexual dysfunction in women. J Sex Med. 2016;13(1):46-54.
13. Sun J et al. Global, regional, and national burden of cardiovascular diseases in youths and young adults aged 15-39 years in 204 countries/ territories, 1990-2019: a systematic analysis of Global Burden of Disease Study 2019. BMC Med. 2023;21(1):222.
14. Jacobs DR Jr et al. Childhood cardiovascular risk factors and adult cardiovascular events. N Engl J Med. 2022;386(20):1877-88.
15. Balletshofer B et al. Positionspapier zur diagnostik und therapie der peripheren arteriellen verschlusskrankheit (pAVK) bei menschen mit diabetes mellitus. Der Diabetologe. 2021;17(3):283-92.
16. Billups KL. Sexual dysfunction and cardiovascular disease: integrative concepts and strategies. Am J Cardiol. 2005;96(12B):57M-61M.
17. Mohan V et al. Long-Term outcomes of drug-eluting stent implantation for patients with atherosclerotic erectile dysfunction not responding to PDE-5inhibitors. J Endovasc Ther. 2023;DOI: 10.1177/15266028231183775.
18. Schönhofen et al. Endovascular therapy for arteriogenic erectile dysfunction with a novel sirolimuseluting stent. J Sex Med. 2021;18(2):315-26.
Amlodipine-Induced Gynaecomastia in a Patient with Spinal Cord Injury
Authors: *Vanessa J. Chow,1 Shyam Swarna1
1. Stoke Mandeville Hospital, Buckinghamshire NHS Foundation Trust, Aylesbury, UK
*Correspondence to vjchow@outlook.com
Disclosure: The authors report no conflicts of interest.
Background: Gynaecomastia is a benign enlargement of male breast tissue, often linked to disturbances in hormonal balance. Amlodipine, a calcium channel blocker widely prescribed for cardiovascular conditions, is occasionally associated with gynaecomastia, though the causal relationship is not clearly established. This report explores a unique case of amlodipine-induced gynaecomastia in a patient with spinal cord injury (SCI), a demographic that presents additional challenges due to altered neuroendocrine function and chronic inflammatory states.
Case Presentation: The authors describe a case involving a male patient in his 60s, previously treated with amlodipine following his spinal cord injury. Despite a comprehensive evaluation showing normal endocrine function and the absence of other systemic diseases, discontinuation of amlodipine led to a regression of breast enlargement, suggesting a druginduced aetiology.
Discussion: The interplay between amlodipine's pharmacological effects and the patient's SCI-related physiological changes highlights a complex pathophysiological mechanism. Amlodipine may influence the hormonal balance indirectly through vascular and metabolic effects, exacerbating the tendency towards an oestrogenic environment conducive to gynaecomastia. Furthermore, SCI-related factors such as increased adiposity and reduced physical activity may enhance the aromatisation of androgens to oestrogens, further predisposing to breast tissue proliferation.
Conclusion: This case underscores the need for heightened clinical awareness when prescribing amlodipine, particularly in patients with SCI. It prompts consideration of underlying vulnerabilities and suggests a tailored approach to pharmacotherapy to mitigate the risk of adverse drug reactions, including gynaecomastia. The reversibility of symptoms upon drug withdrawal highlights the importance of monitoring and the potential for intervention in similar cases.
Key Points
1. Gynaecomastia, affecting up to 65% of men over 65 years, can be multifactorial. Identifying iatrogenic causes is crucial, especially in patients with complex conditions like spinal cord injury (SCI).
2. This is a case report of a male patient in his 60s presenting with bilateral gynaecomastia, potentially linked to longterm amlodipine therapy, set against a background of neuroendocrine changes due to chronic SCI.
3. Amlodipine may exacerbate gynaecomastia through complex mechanisms in patients with SCI, necessitating heightened clinical vigilance and tailored management when prescribing and reviewing medications for this population.
INTRODUCTION
Gynaecomastia, the clinical term for the enlargement of the male breast, is characterised by the histological finding of increased proliferation of ductal tissue, stroma, or adipose tissue within the breast structure.1,2 The aetiology of gynaecomastia is multifactorial, with associations drawn to various medical conditions that disrupt the endocrine balance, such as pronounced obesity, hypogonadism, renal insufficiency, and hepatic dysfunction, each contributing to an altered hormonal profile conducive to breast tissue proliferation.
Pharmacological interventions, including spironolactone, antipsychotic agents, lipidlowering medications, and antiandrogens, have been recurrently linked to the aetiology of gynaecomastia.3 While less frequently associated, calcium channel blockers (CCB) such as amlodipine have also been recognised as contributing factors. Employed in the management of angina pectoris and hypertension, amlodipine was dispensed over 37 million times in 2004 within the USA.4 Its utilisation among older adults is particularly judicious, given its efficacy in blood pressure modulation and its protective role against stroke and myocardial infarction, conditions that are of paramount concern within the geriatric population.5 Consequently, acknowledging the potential adverse effects of such medication, notably the risk of gynaecomastia, is imperative. Although the direct causality between amlodipine and gynaecomastia remains to be definitively proven, the existing circumstantial evidence demands a vigilant and holistic
clinical strategy when managing patients on amlodipine therapy. This underscores the necessity for an interdisciplinary methodology that integrates pharmacology, endocrinology, and molecular biology to navigate the complexities of this clinical issue effectively.
Currently, there are only two case reports documenting amlodipine-induced gynaecomastia,6,7 along with a case series that includes two patients on long-term haemodialysis 8 This is the first report on amlodipine-associated gynaecomastia in a patient with spinal cord injury (SCI).
The changes intrinsic to SCI, such as possible altered neuroendocrine function and a chronic inflammatory state,9 play a pivotal role in the emergence and subsequent resolution of gynaecomastia in patients undergoing amlodipine therapy. This situation underscores the complex interactions at play, emphasising the need for a sophisticated approach to pharmacotherapy in this distinct patient group. A thorough medical management strategy, encompassing hormonal evaluation and adjustment, nutritional guidance, and physical rehabilitation, is essential to understand the risk of gynaecomastia among individuals with SCI.
CASE REPORT
A male in his 60s, with a history of SCI and hypertension presented with bilateral, symmetrical gynaecomastia. He noted that the onset of gynaecomastia coincided with the initiation of amlodipine (10 mg once daily)
therapy. However, the condition became more pronounced in both size and visibility following his SCI.
His medical background includes a motorincomplete cervical spinal cord injury that he sustained more than 10 years ago and hypertension. Other than amlodipine, which he had been taking for more than 10 years, he was also taking angiotensinreceptor blockers for his hypertension, anticholinergics for his neurogenic bladder, and laxatives for his neurogenic bowel. Lifestyle assessment indicated no significant concerns; he abstained from alcohol, anabolic steroids, marijuana, and whey protein supplements, and had no testicular problems. There were no records of liver disease, kidney disease, or endocrine issues. Family history did not reveal any cases of breast cancer or endocrine disorders.
Physical examination confirmed bilateral breast enlargement with tender glandular tissue beneath the areola, without detectable masses, lymphadenopathy, nipple discharge, or skin changes. He denied any breast tenderness. According to the Simon classification for gynaecomastia, he was categorised as Grade 2b, indicating moderate enlargement with excess skin.10
Laboratory tests covering liver and kidney function, thyroid function, and a hormonal profile were within normal ranges. Of note, testosterone levels were on the lower limit of normal.
Amlodipine was omitted during his stay, and regression in his symptoms was seen within a month of the drug suspension. Unfortunately, due to the inability to get into contact with the patient, there is no longterm follow-up data available to determine the potential for recurrence or reversibility of the condition.
DISCUSSION
Gynaecomastia is defined as the benign expansion of dense, subareolar male breast glandular tissue, spanning at least 2 cm.2,10,11 This condition arises from a multifaceted interaction of physiological, pharmacological,
and pathological elements that disrupt the intricate equilibrium between oestrogenic and androgenic forces within the breast tissue.2,10,11 While typically benign, and primarily a cosmetic concern rather than one of clinical significance, gynaecomastia frequently results in distress for those affected.1 Asymptomatic gynaecomastia exhibits a distinct trimodal distribution across different age groups. Initially affecting 60–90% of neonates, this condition stems from high levels of fetal oestradiol and progesterone, influenced by maternal hormones. Additionally, the early onset is linked to increased conversion of steroid precursors into sex steroids and greater aromatisation of androgens, driven by a neonatal increase in luteinising hormone.1,2 During adolescence, 50–60% experience hormonal shifts leading to gynaecomastia as they undergo physiological changes. In early puberty, the pituitary gland’s nocturnal release of gonadotropins stimulates testosterone production by the testes. Adolescents developing gynaecomastia exhibit persistently elevated serum oestradiol levels throughout the day, in contrast to those without the condition, who have a lower androgen-to-oestrogen ratio.1,2,12
In males aged more than 65 years of age, the prevalence of gynaecomastia reaches another peak, affecting up to 65% of this population 10 While the precise mechanisms remain unclear, the increase underscores the complex interplay between ageing, diminished testosterone production, and the elevated conversion of oestrogen associated with increased body fat.
Aetiological determinants of gynaecomastia encompass pathophysiological states that precipitate elevated serum oestrogen concentrations, reduce androgenic levels, or modify the mammary gland’s hormonal receptivity. Perturbations in the endocrine landscape, exemplified by conditions such as hypogonadism, hyperthyroidism, and neoplasms with augmented secretion of human chorionic gonadotropin or oestrogens, intricately disrupt the hormonal equilibrium.1,3 Hepatic pathologies, notably cirrhosis, impair the hepatic clearance of oestrogens, whereas renal dysfunction compromises the metabolic processing and
elimination of hormones.1,3 In the clinical context of this patient, these factors were meticulously evaluated and deemed noncontributory. Moreover, while adiposity is known to potentiate gynaecomastia through enhanced peripheral aromatisation of androgens within adipose depots, the authors’ patient presented with a BMI within the higher limit of normal. The role of genetic predisposition and hereditary factors, which may influence the enzymatic orchestration of steroidogenesis or the mammary gland’s sensitivity to endocrine modulation, was also considered and found to be lacking in the patient’s clinical profile.
Drug-induced gynaecomastia accounts for a minority of cases, ranging between 10–20%.13
Agents such as anti-androgens, certain antihypertensives, highly active antiretroviral therapy, and psychoactive drugs, including some antidepressants and antipsychotics, are implicated in gynaecomastia through various mechanisms, including direct oestrogenic effects, increased peripheral aromatisation, inhibition of testosterone synthesis, or prolactin elevation.3 The patient’s sole medication that might have contributed was amlodipine.
Amlodipine, a dihydropyridine CCB, modulates vascular smooth muscle contractility by selectively inhibiting L-type calcium channels, thus exerting a vasodilatory effect predominantly on peripheral arterioles, which translates into its antihypertensive and anti-anginal properties.14 The link between amlodipine and gynaecomastia, albeit not directly delineated within current literature, can be postulated through indirect pathways that alter the hormonal homeostasis, particularly the oestrogen-androgen axis, critical for maintaining mammary tissue quiescence in males.
While amlodipine itself lacks inherent hormonal activity, its long-term systemic effects could theoretically influence endocrine function indirectly.3 The vasodilatory-induced haemodynamic alterations might modulate hepatic blood flow, and consequently, the hepatic metabolism of steroids. This could disrupt the hepatic clearance of oestrogens and androgens, potentially skewing the oestrogen-to-testosterone ratio in favour of
oestrogens, thus predisposing to gynaecomastia.
Moreover, research investigating the effects of long-acting CCB on the serum steroid hormones and insulin in patients who are hypertensive and obese found that these medications significantly lowered blood pressure and reduced fasting serum immunoreactive insulin and insulin resistance index within 2–3 months of treatment.14 Concurrently, there was an observed increase in serum levels of dehydroepiandrosterone (DHEA) and DHEA sulfate, although these changes did not reach statistical significance. This study elucidates a complex mechanism by which amlodipine could potentially contribute to the onset of gynaecomastia. Specifically, elevated DHEA levels, resulting from treatment, may precipitate gynaecomastia via intricate endocrine and metabolic pathways, highlighting the intricate effects of amlodipine on hormonal dynamics and metabolic processes. Primarily, the increased substrate availability for peripheral aromatisation enhances the conversion of DHEA to oestrogenic compounds, thereby tilting the oestrogen-androgen ratio in favour of oestrogenic predominance, a pivotal factor in mammary gland proliferation. This process is further compounded by the intricacies of insulin resistance, where DHEA’s role is nuanced, potentially affecting adipose tissue distribution and hormonal profile, indirectly influencing breast tissue sensitivity.1 Moreover, the augmented levels of DHEA could perturb the hypothalamic-pituitarygonadal axis feedback loop, modulating gonadotropin secretion and thus altering gonadal steroidogenesis 14 The resultant hormonal dysregulation, characterised by an oestrogenic shift, underpins the pathogenesis of gynaecomastia.
It is also crucial to note that while elevated DHEA levels could contribute to the development of gynaecomastia, the exact outcomes are highly dependent on individual factors including metabolic status, comorbidities, genetic predisposition, and overall hormone balance. A crucial comorbidity in the authors’ patient’s history is SCI, which may indirectly facilitate the onset of gynaecomastia via a series of interrelated
physiological mechanisms. These mechanisms predominantly involve disruptions in hormonal balance, changes in body composition, and decreased physical activity.15,16
Individuals with SCI often experience significant changes in body composition, including increased adiposity and decreased lean muscle mass.9 Adipose tissue expresses aromatase, an enzyme that converts androgens to oestrogens. An increase in body fat percentage can, therefore, lead to elevated levels of circulating oestrogens, contributing to the oestrogen-androgen imbalance that favours the development of gynaecomastia.17 Especially in the context of reduced mobility and physical activity leading to muscle atrophy and increased fat accumulation.
SCI often leads to significant changes in the neuroendocrine axis due to the disruption of the hypothalamic-pituitary-gonadal axis communication. This can result in decreased levels of gonadotropin-releasing hormone and subsequently lower luteinising hormone and follicle-stimulating hormone secretion.18-20 The reduction in luteinising hormone and follicle-stimulating hormone can lead to decreased testosterone production by the Leydig cells in the testes 20 Allison and Ditor21 outline that SCI precipitates a state of chronic inflammation and immune dysfunction, marked by elevated levels of proinflammatory cytokines, whereby this sustained inflammatory state exacerbated by secondary health complications and metabolic disorders inherent to SCI, such as atherosclerosis, obesity, and diabetes, contributes to an altered hormonal profile.9,16,21 Additionally, the altered sympathetic nervous system activity post-SCI may affect adrenal function, potentially influencing androgen and oestrogen levels 9,15,21
The resultant hormonal imbalance, skewed towards oestrogenic dominance due to factors like increased adipose tissue (a rich source of aromatase enzyme for oestrogen synthesis), compounded with reduced motor activity and metabolic alterations, creates a conducive environment for the development of gynaecomastia. Notably, males with SCI had a 3.7-fold higher prevalence of lower testosterone with an overall prevalence of 33% based on free testosterone
levels.18 Other studies also found an association between SCI and testosterone deficiency,9,22-25 and in the authors’ patient, his testosterone was noted to be in the lower limits of normal. Thus, the chronic inflammatory state following SCI, coupled with the cascading effects on hormonal regulation and adipose tissue functionality, underlines a plausible pathway through which patients with SCI, particularly those on medications like amlodipine that influence vascular and adipose tissue dynamics, might develop gynaecomastia.
CONCLUSION
Amlodipine, a calcium channel blocker used for its antihypertensive and antianginal efficacy, inadvertently impacts the hormonal equilibrium, rarely but potentially instigating gynaecomastia by indirectly modifying the neuroendocrine axis or the distribution and function of adipose tissue. This pharmacological influence, coupled with the systemic disturbances induced by SCI, characterised by chronic inflammation and neuroendocrine disruptions, heightens the individual’s vulnerability to such medications. The SCI-associated shifts towards increased adiposity and reduced physical activity predispose to enhanced aromatisation of androgens into oestrogens, a process potentially accentuated by amlodipine’s effects on adipose tissue, thereby fostering an oestrogenic dominance conducive to gynaecomastia.
Moreover, the underlying chronic inflammatory state inherent to SCI, intertwined with amlodipine’s immunomodulatory actions, might catalyse glandular breast tissue proliferation. The observed reversibility of gynaecomastia upon cessation of amlodipine underscores the drug’s role in this complex interplay and underscores the critical need for clinical vigilance and personalised management in prescribing such medications to patients with SCI, taking into consideration the multifaceted systemic alterations and advocating for an integrated approach to medication management.
References
1. Swerdloff RS, Ng JCM, Gynecomastia: etiology, diagnosis, and treatment [Internet] (2023) Endotext. Available at: https://www.ncbi.nlm.nih.gov/ books/NBK279105/. Last accessed: 17 April 2024.
2. Johnson RE, Murad MH. Gynecomastia: pathophysiology, evaluation, and management. Mayo Clin Proc. 2009;84(11):1010-5.
3. Nuttall FQ et al. Gynecomastia and drugs: a critical evaluation of the literature. Eur J Clin Pharmacol. 2015;71(5):569-78.
4. Statista. Number of amlodipine prescriptions in the U.S. from 2004 to 2021. 2024. Available at: https://www.statista.com/ statistics/781586/amlodipinebesylate-prescriptions-number-inthe-us/#:~:text=Number%20of%20 amlodipine%20prescriptions%20 in%20the%20U.S.%20 2004%2D2021&text=In%202004%2C%20amlodipine%20was%20 prescribed,for%20hypertension%20 and%20angina%20pectoris. Last accessed: 17 April 2024.
5. Ismail Z et al. The impact of population ageing: a review. Iran J Public Health. 2021;50(12):2451-60.
6. Cornes PGS, Hole AC. Amlodipine gynaecomastia. The Breast. 2001;10(6):544-5.
7. Zochling J et al. Gynaecomastia and amlodipine. Med J Aust. 1994;160(12):807.
8. Komine N et al. Amlodipine-induced gynecomastia in two patients on longterm hemodialysis therapy. Clin Exp Nephrol. 2003;7(1):85-6.
9. Boehl G et al. Endocrinological and inflammatory markers in individuals with spinal cord injury: a systematic review and meta-analysis. Rev Endocr Metab Disord. 2022;23(5):1035-50.
10. Thiruchelvam P et al. Gynaecomastia. BMJ. 2016;354:i4833.
11. Robeva R et al. Causes and metabolic consequences of gynecomastia in adult patients. Int J Endocrinol. 2019;2019:6718761.
12. Reinehr T et al. Sex hormone profile in pubertal boys with gynecomastia and pseudogynecomastia. J Clin Endocrinol Metab. 2020;105(4):e1025-32.
13. Braunstein GD. Gynecomastia. N Engl J Med. 2007;357(12):1229-37.
14. Ueshiba H, Miyachi Y. Effects of the long-acting calcium channel blockers, amlodipine, manidipine and cilnidipine on steroid hormones and insulin resistance in hypertensive obese patients. Intern Med. 2004;43(7):561-5.
15. Wulf MJ, Tom VJ. Consequences of spinal cord injury on the sympathetic nervous system. Front Cell Neurosci. 2023;17:999253.
16. Farkas GJ, Gater DR. Neurogenic obesity and systemic inflammation following spinal cord injury: a review. J Spinal Cord Med. 2018;41(4):378-87.
17. Mair KM et al. Obesity, estrogens and adipose tissue dysfunction
- implications for pulmonary arterial hypertension. Pulm Circ. 2020;10(3):2045894020952019.
18. Sullivan SD et al. Prevalence and etiology of hypogonadism in young men with chronic spinal cord injury: a cross‐sectional analysis from two university‐based rehabilitation centers. PM&R. 2017;9(8):751-60.
19. Bauman WA et al. Provocative stimulation of the hypothalamicpituitary-testicular axis in men with spinal cord injury. Spinal Cord. 2016;54(11):961-6.
20. Itodo OA et al. Early changes in androgen levels in individuals with spinal cord injury: a longitudinal SwiSCI study. J Clin Med. 2022;11(21):6559.
21. Allison DJ, Ditor DS. Immune dysfunction and chronic inflammation following spinal cord injury. Spinal Cord. 2015;53(1):14-8.
22. Clark MJ et al. Testosterone levels among men with spinal cord injury. Am J Phys Med Rehabil. 2008;87(9):758-67.
23. Safarinejad MR. Level of injury and hormone profiles in spinal cord-injured men. Urology. 2001;58(5):671-6.
24. Bauman WA et al. Age-related prevalence of low testosterone in men with spinal cord injury. J Spinal Cord Med. 2014;37(1):32-9.
25. McLoughlin RJ et al. A systematic review of testosterone therapy in men with spinal cord injury or traumatic brain injury. Cureus. 2023;15(1):e34264.
Primary Parotid Tuberculosis Presenting as a Malignancy: An Exceptional Occurrence
Tuberculosis is a well-known endemic disease in India; however extra-pulmonary tuberculosis in the form of single parotid gland involvement is exceptionally unusual. Nevertheless, in instances involving slow-growing, prominent parotid gland enlargement, where malignancy is our major speculation, it should never be eliminated as a differential. There have been very few previously reported cases of tuberculosis involving salivary glands, and at times imaging has proven it difficult to diagnose such a condition and differentiate it from a benign mass or a malignancy. With that in mind, the authors present a case of tuberculosis involving just a single parotid gland in a 49-year-old woman who had been experiencing unilateral infra-auricular swelling and pain for a month. Apart from evening rise in temperature and generalised weakness, the patient had no additional symptoms suggestive of tuberculosis infection. Ultrasound represents the initial imaging modality of choice for assessment of the parotid gland. A sonographic examination of the authors' patient revealed a diffusely enlarged left parotid gland with peripherally vascular hypo-echoic areas within. On contrast-enhanced CT the left parotid gland was seen to be replaced by a heterogeneously enhancing lesion, with an abscess-like appearance. The tubercular aetiology was established after a USGguided tru-cut biopsy from the infra-auricular region revealed numerous loose granulomas with few langhans-type multinucleate giant cells amidst foci of necrosis and a salivary duct. Anti-TB medication was initiated for the patient subsequent to the presence of acid-fast bacilli on Ziehl-Neelsen staining. The patient has now received 3 months of AKT and there has been complete resolution of the symptoms.
Key Points
1. Since tuberculosis is a prevalent endemic illness with a high incidence rate in India, the diagnosing clinician should be suspicious of unusual extrapulmonary tuberculosis cases such as salivary gland infections.
2. The authors address one such uncommon instance of unilateral parotid involvement in this case report, which involved a patient without any other radiological features suggestive of tuberculous infection and a normal chest X-ray.
3. The case report highlights the value of imaging tests such as CT, ultrasound, and biopsy, as well as the need for pathologist involvement in the diagnosis of such uncommon illnesses.
INTRODUCTION
Tuberculosis is a well-known endemic disease in India; however, extra-pulmonary tuberculosis in the form of single parotid gland involvement is exceptionally unusual. Nevertheless, in instances involving slow-growing, prominent parotid gland enlargement, where malignancy is the major speculation, it should never be eliminated as a differential. Having a strong index of suspicion by the diagnosing physician is crucial for the ultimate diagnosis. Tuberculosis as a cause of parotitis is typically disregarded by otolaryngologists, and the majority of cases are unnecessarily operated.
CASE PRESENTATION
A 49-year-old female patient, a known case of hypertension and diabetes, was referred to the authors’ ear, nose, and throat department with suspicion of acute unilateral parotitis. The patient complained of gradually increasing swelling and associated pain in the left infra-auricular region for 1 month. Initially, the swelling was pea-sized and nontender, without any secondary skin changes. The swelling gradually increased for 1 month and was associated with mild pain.
On inspection, the swelling was 5x4x2 cm in size, firm-to-hard in consistency, non-mobile, non-fluctuating, and with no local rise of temperature. There was no discharging sinus or fistula. There were no dental complaints, and the oral hygiene of the patient was also good. Apart from the evening rise in temperature and generalised
weakness, the patient had no additional symptoms suggestive of tuberculosis infection. She denied any recent orodental surgical procedures, as well as any personal or contact history of tuberculosis. On investigation, the routine blood counts including the erythrocyte sedimentation rate, fasting blood sugar, liver and kidney function tests, urine analysis, electrocardiogram, and abdominal ultrasound revealed no abnormalities. HIV serology came up negative as well. The chest radiograph was also unremarkable (Figure 1A).
On ultrasonography of the left parotid region, the gland was enlarged, and a welldefined, heterogeneously hypo-echoic, oval mass lesion was noted within its architecture. It was approximately 4.7x2.1 cm in size (Figure 1B). No ductal dilatation, cystic degeneration, or intraparenchymal calcifications were observed. The colour doppler study revealed a notable degree of arterial vascularity with relatively high resistance in the periphery of the lesion (Figure 1C). In the left upper cervical area (Level II) and left sub-mental and submandibular region (Level I), a few enlarged sub-centimetric reactive lymph nodes were observed. There was noticeable vascularity and a retained fatty hilum in these lymph nodes. A tentative diagnosis of either neoplasm or granulomatous infection was made. Given the lesion’s accessibility, ultrasound-guided biopsy and contrastenhanced CT were recommended to rule out the differentials.
On contrast-enhanced CT, a distinct, lobulated mass lesion with heterogeneous enhancement was noted involving the left
1: Chest radiography and ultrasonography of the left parotid region.
A) Chest radiograph posteroanterior view depicts no significant findings. B) Ultrasonography image shows a well-defined heterogeneously hypo-echoic oval lesion measuring 4.7x2.1 cm with no calcification or cystic areas within. C) On colour doppler, vascularity is noted in the periphery of the same lesion.
2: Contrast-enhanced CT of parotid and neck region.
A) Axial image and B) coronal image show a well-defined, heterogeneously enhancing, lobulated lesion involving the superficial and the deep lobe of the left parotid gland. The posterior and superior low attenuation peripherally enhancing region of the parotid gland s/o necrosis (white arrow). The anterior and inferior intensely enhancing portion of the lateral lobe is compressed due to inflammation (blue arrow). No focal areas of calcifications, cystic changes, or ductal dilatations can be seen within the lesion.
parotid gland’s superficial and deep lobes. The lesion measured 2.7x2.2x2.7 cm in the superficial lobe and 2.8x1.7x2.3 cm in the deep lobe of the gland (Figures 2A and 2B). There were no calcifications or cavitations within the lesions. The main parotid duct was normal in calibre. Sialolitiasis was absent.
There were no signs of fistulisation or any sinus tracts. The underlying bones were normal without any signs of erosion. Left Levels I, II, and III showed few reactive lymph nodes. The right parotid gland was normal.
Figure
Figure
The fine needle aspiration cytology results were inconclusive; hence, an abdominal ultrasound-guided biopsy of the lesion was performed with an 18 g Bard biopsy needle, and histopathology revealed granulomatous inflammation with infiltrates of foamy and epithelioid lymphocytes with a focus on necrosis and salivary duct within. On highpower microscopy, occasionally Langhans and multi-nucleate giant cells of the foreign body type encircling a caseous form of necrosis were observed (Figure 3A and 3B). No cancerous cells were found. According to the histology report, the salivary gland had necrotising granulomatous inflammation that was suggestive of tuberculosis. A
A
few acid-fast tubercle bacilli were seen on the Ziehl Neelsen stain (Figure 3C). Another sample from the lesion that was sent for Cartridge-Based Nucleic Acid Amplification Test came out to be positive for Mycobacterium tuberculosis.
There have been very few previously reported cases of tuberculosis involving salivary glands, and at times imaging has proven it difficult to diagnose such a condition and differentiate it from a benign mass, granulomatous disease, or a malignancy.
A) Histopathology image, haematoxylin and eosin, 400x, high power depicts an epithelioid granuloma containing a Langhans giant cell (blue arrow). B) Granulomatous inflammation with a focus of necrosis and a salivary duct seen in the upper right-hand corner (blue arrow). A) Zeihl-Neelsen stain of the samples taken from the same patient show acid-fast dye-positive tubercle bacilli (black arrowhead).
DISCUSSION
Tuberculosis is a common endemic disease and a major cause of suffering in developing countries such as India. It is a necrotising granulomatous infection that affects several organs, exhibiting a wide range of clinical manifestations. The lungs are often the most frequently affected organ. Extra-pulmonary organs affected include cervical lymph nodes, ileocaecal junction, bones, meninges, brain, and numerous other organs;1 however, parotid gland involvement is extremely uncommon.2 In
1893, the first case of tubercular parotitis was diagnosed by C De Paoli.1,3,7
As with this case, parotid tuberculosis can develop either primarily in the absence of pulmonary tuberculosis or concurrently with pulmonary tuberculosis.3 The lymph nodes or parotid gland can become involved in either of the two ways. First, a mycobacterial infection in the oral cavity releases the bacilli, which then ascend through the salivary gland duct and enter the gland or the lymph nodes that are connected to it through lymphatic drainage. The second
Figure 3: Histopathology image and Zeihl-Neelsen stain.
B C
channel originates from a distant primary lung focus and is either haematogenous or lymphatic in nature.2-8 Latter is the more common pathway.3-5 Seventy percent of the time, the parotid gland is involved when the main afflicted glands are the salivary glands.5
Primary parotid tuberculosis is cumbersome to diagnose in the absence of clinical symptoms of lung involvement or any systemic findings due to the resemblance of the presentation to that of a tumour.2,9,10 The majority of these cases manifest as slowly growing masses that progressively get larger over months and are arduous to distinguish from neoplasm or other granulomatous diseases through imaging. Physical examination is usually unfruitful. It is only in cases of concomitant primary pulmonary tuberculosis that chest radiography can be beneficial. In this instance, there was no chest radiological indication of ongoing or past pulmonary tuberculosis. In his research, Maynard J.11 revealed that a histological investigation was the only way to differentiate between this infection and a gland tumour. Histopathology in parotid lesions has a 94–100% specificity and an 81–100% sensitivity.5 Thus, when evaluating a parotid tumour, fine needle aspiration cytology or biopsy should be done initially.
In this patient, the primary source of the infection could not be identified as there were no molar caries nor other tubercular focus anywhere else. The confirmation of the parotid tuberculosis diagnosis was made possible by ultrasonography-guided tru-cut biopsy of the intraparotid lesions. Though strong suspicion of the same was made on contrast-enhanced CT, histopathology gave the final diagnosis.
This case is unique because, unlike the majority of tubercular parotitis cases that have been documented in the past, the patient’s diagnosis came before any kind of surgery. On the other hand, the
diagnosis was previously verified on postsurgery parotidectomy tissues because early imaging and histology were unable to provide a diagnosis.7,10 In this case, since the biopsy was conclusive, surgical intervention was avoided, and early therapeutic management in the form of antituberculosis treatment was initiated. After 3 months of medication, there was complete resolution of the symptoms.
CONCLUSION
The patient was diagnosed with unilateral tubercular parotitis, and since then, treatment has been going well. A recent follow-up scan revealed only a few reactive cervical lymph nodes, and the infection in the gland had receded. The patient has been put on regular anti-tubercular medication for 6 months and has been advised a repeat chest X-ray after 3 months to look for signs of pulmonary tuberculosis. There has been constant monitoring of her health condition. The goal is to maintain or improve patient wellbeing. The authors’ wish to highlight the vital role and diligence of a radiologist and the use of imaging investigations like ultrasonography, CT, and biopsy, as well as the involvement of a pathologist in diagnosing such unusual conditions. Furthermore, saving time and accurately diagnosing the ailment ensures that the patient receives suitable treatment at an appropriate time.
Take-Home Message
Even though tuberculosis has historically been a prevalent cause of a wide range of medical disorders in India, recognising such a rare entity as tubercular parotitis requires a high level of clinical suspicion, expertise, and understanding.
References
1. Garg R et al. Parotid tuberculosis. Lung India. 2010;27(4):253-5.