10 Review of the American Thoracic Society (ATS) 2024 International Conference, May 19ᵗʰ–24ᵗʰ 2024
Congress Features
22 Transforming Lung Cancer Care: Advancements in Screening, Treatment, and Survivorship
Aleksandra Zurowska
Abstract Reviews
26 How Did Respiratory Support Management and Patients’ Demographics Change in the Intensive Care Unit Before, During, and After the Pandemic?
Karakurt et al.
29 Improvements in Skeletal Muscle Mass in Select Patients with Chronic Obstructive Pulmonary Disease Undergoing Lung Volume Reduction Interventions
Nanah et al.
31 The Use of an Electronic Order Set to Improve Latent Tuberculosis Screening Among Hospitalized Patients Who Are Initiating Immunosuppression: A Cross-Sectional Analysis
Ferland et al.
33 Sarcoid Versus Tuberculosis, or Both? Disseminated Tuberculosis in the Setting of Sarcoidosis
Janoczkin et al.
35 Epidemiological Study of Overall Survivability of Individuals Diagnosed with Lung and Bronchus Cancer in Michigan Between the Years 1996–2017
Nader et al.
36 Genitourinary Tuberculosis Resulting in Hydronephrosis
Alsheimer et al.
38 Daptomycin: A Rare Cause of Acute Eosinophilic Pneumonia
Bains et al.
Interviews
41 Michael Boyle
46 Julie Brahmer Infographic
50 Nebulization and Viral Spread: Knowns and Unknowns in the Healthcare Setting Articles
52 Sex Differences in Exercise-Induced Effects on Respiratory Infection and Immune Function
Rodriguez Bauza and Silveyra
60 High Frequency of Cystic Fibrosis-Related Endocrinopathies in a Population of Colombian Children: A Cross-Sectional Study
Gómez Rojas et al.
"ATS Strategic Goals were shared: to lead scientific discoveries, advance professional development, transform patient care..."
Editorial Board
Editor-in-Chief
Prof Robert C. Hyzy
University of Michigan, USA
Professor of Medicine, Division of Pulmonary and Critical Care Medicine, University of Michigan, Ann Arbor, USA
Prof Dr Rohan Thompson Indiana University, USA
Dr Kelly Pennington Mayo Clinic, USA
Prof Laren Tan
Loma Linda University School of Medicine, USA
Prof Michal Senitko
University of Mississippi Medical Centre, USA
Prof Dr Jacques Bouchard
Université Laval, Canada
Dr Jezreel Pantaleón García
The University of Texas MD Anderson Cancer Center, USA
Aims and Scope
American Medical Journal - Respiratory is an open-access, peer-reviewed eJournal committed to helping elevate the quality of healthcare in respiratory medicine by publishing high quality content on all aspects of lung function and respiratory diseases.
The journal is published annually, 6 weeks after the American Thoracic Society (ATS) 2024 International Conference, and features highlights from this congress, alongside interviews with experts in the field, reviews of abstracts presented at the congress, as well as in-depth features on congress sessions. Additionally, this journal covers advances within the clinical and pharmaceutical arenas by publishing sponsored content from congress symposia, which is of high educational value for healthcare professionals. This undergoes rigorous quality control checks by independent experts and the in-house editorial team.
American Medical Journal - Respiratory also publishes peerreviewed research papers, review articles, and case reports in the field. In addition, the journal welcomes the submission of features and opinion pieces intended to create a discussion around key topics in the field and broaden readers’ professional interests. American Medical Journal - Respiratory is managed by a dedicated editorial team that adheres to a rigorous doubleblind peer-review process, maintains high standards of copy editing, and ensures timely publication.
Our focus is on research that is relevant to all healthcare professionals in pulmonary medicine. We do not publish veterinary science papers or laboratory studies not linked to patient outcomes. We have a particular interest in topical studies that advance research and inform of coming trends affecting clinical practice in the respiratory field.
Editorial Expertise
AMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors are recognised authorities from their respective fields.
• Peer review, which is conducted by AMJ’s Peer Review Panel as well as other experts appointed due to their knowledge of a specific topic.
• An experienced team of editors and technical editors.
Peer Review
On submission, all articles are assessed by the editorial team to determine their suitability for the journal and appropriateness for peer review.
Editorial staff, following consultation with either a member of the Editorial Board or the author(s) if necessary, identify three appropriate reviewers, who are selected based on their specialist knowledge in the relevant area. All peer review is double blind.
Following review, papers are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected. Editorial staff have final discretion over any proposed amendments.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects.
We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial@americanmedicaljournal.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in AMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
AMJ is distributed through controlled circulation to healthcare professionals in the relevant fields globally.
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
This Publication Launch Date: 2023 Frequency: Yearly Online ISSN: 2976-7873
American Medical Journal - Respiratory is published once a year. For subscription details please visit: www.emjreviews.com
All information obtained by AMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, AMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. AMJ is completely independent of the review event (ATS 2024 International Conference) and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever.
Victoria Antoniou, Helena Bradbury, Ada Enesco, Laith Gergi, Katrina Thornber, Aleksandra Zurowska
Creative Director
Tim Uden
Design Manager
Stacey Rivers
Senior Designers
Roy Ikoroha, Steven Paul
Designer
Owen Silcox
Junior Designers
Dillon Benn Grove, Shanjok Gurung
Senior Vice President of Business Development
Robert Hancox
Vice President of Customer Success
Alexander Skedd
Marketing Director
Kristina Mestsaninova
Chief Content Officer
Justin Levett
Chief Commercial Officer
Dan Healy
Founder and CEO
Spencer Gore
Welcome
Dear Readers,
I am delighted to welcome you to the second issue of AMJ Respiratory. It’s incredible that a whole year has passed since the launch of AMJ with the first issue of this journal, and once again it was a pleasure for our team to attend the ATS 2024 International Conference. The 20th anniversary of ATS was very much the centrepiece of this year’s events. We have handpicked a number of abstracts on topics ranging from the trends in respiratory support management and patient demographics before, during, and after the pandemic; tuberculosis screening; and a rare cause of acute eosinophilic pneumonia, among others.
We have also secured exclusive interviews with experts that explore cystic fibrosis and lung cancer immunotherapy, and have delved into one of the congress sessions that explored advancements in screening, treatment, and survivorship in lung cancer. A compelling study on the frequency of cystic fibrosis-related endocrinopathies in a pediatric population is among our peer-reviewed articles, as well as a compelling literature review examining experimental and clinical evidence on how exercise affects the immune response to infection in a sex-specific manner.
In closing, I would like to thank everyone who worked tirelessly in bringing this issue together, namely our peer reviewers, contributors, and Editorial Board. I do hope you enjoy reading this issue, and would welcome your submissions until our next issue!
Permissions and copyright: accountsreceivable@emjreviews.com
Editor
Reprints: info@emjreviews.com
Media enquiries: marketing@emjreviews.com
Evgenia Koutsouki
We provoke conversation around healthcare trends and innovation - we also create engaging educational content for healthcare professionals. Join us for regular conversations with physician & entrepreneur, Jonathan Sackier. Listen Now
Foreword
Welcome to this year’s edition of AMJ Respiratory, which features highlights from the annual American Thoracic Society (ATS) International Conference, held from May 17th–22nd, in San Diego, California, USA.
Attendance, especially among European and Asian–Pacific attendants, has continued to be strong, reaching over 14,000 this year. This continues to establish the ATS International Conference as the premier venue for attendees and investigators to share new knowledge in pulmonary, critical care, and sleep medicine.
As is the case each year at the ATS International Conference, the results of multiple new investigations were presented. Charles Daley, National Jewish Health in Denver, Colorado, USA, announced results from the ARISE trial, demonstrating the benefit of adding inhaled liposomal amikacin to a macrolide in patients with Mycobacterium avium complex lung disease. Surya P. Bhatt, University of Alabama, Birmingham, USA, presented the results of the 3 NOTUS trial, which showed that subcutaneous administration of dupilumab every 2 weeks resulted in fewer exacerbations and better lung function in patients with chronic obstructive pulmonary disease patients having an elevated blood eosinophil count (i.e., Type 2 inflammation).
In critical care, the results of the Prevention and Early Treatment of Acute Lung Injury (PETAL) Network ASTER trial were announced by Michael Matthay, University of California San Francisco, USA, which failed to show the benefit of intravenous acetaminophen administration in septic patients. Meanwhile, Guofei Zhou, National Institutes of Health (NIH), Bethesda, Maryland, USA, and Michelle Gong, Montefiore Medical Center, New York, USA, moderated a session on the new NIHsponsored ARDS, Pneumonia and Sepsis (APS) Consortium, an observational network that will phenotype 4,000 hospitalized patients with APS over the next 5 years.
Attendance, especially among European and Asian–Pacific attendants, has continued to be strong, reaching over 14,000 this year
I encourage my professional colleagues to attend next year’s ATS International Conference in San Francisco, California, USA, from May 16th–21st, 2025; and to submit their conference reviews and case reports to the journal for review, and for potential inclusion in our next issue. See you in San Francisco!
Robert C. Hyzy
Professor of Medicine, Division of Pulmonary and Critical Care, University of Michigan, Ann Arbor, USA
ATS 2024
ATS
Strategic Goals were shared: to lead scientific discoveries, advance professional development, transform patient care...
Review of the American Thoracic Society (ATS) International Congress 2024 Congress Review
THIS year, the 2024 International Conference of the American Thoracic Society (ATS) took place in San Diego, California, USA, from May 17th–22nd. The opening ceremony began with a powerful sentiment from Maria Patricia Rivera, ATS President, spotlighting the ATS research program, which celebrates its 20th anniversary.
This initiative was launched in 2004, and since then, has successfully raised and granted approximately 24,000,000 USD in research funding to 302 investigators around the world. As stated by Rivera, these investigators have gone on to garner over 880 million USD in National Institutes of Health (NIH) funding, accelerating the research careers of many of those starting out. Projects encompassed the fields of asthma, chronic obstructive lung disease, lung cancer, epigenetics, interstitial lung disease, lung transplantation, sleepdisordered breathing, and more. The quantity and versatility of research funded is truly staggering!
These investigators have gone on to garner over 880 million USD in NIH funding
Rivera subsequently welcomed all leaders of fellow international respiratory societies and past ATS presidents, board members, and committee and assembly leaders. She
drew attention to the 30th anniversary of the Methods in Epidemiologic, Clinical, and Operations Research (MECOR) Program, and the 120-year anniversary of the American Lung Association (ALA). The 2023–2024 ATS Strategic Goals were shared: to lead scientific discoveries, advance professional development, transform patient care, impact global health, and strengthen the ATS community.
The 2024 Respiratory Awards included the ATS Public Service Award to Rajkumar Savai, Justus Liebig University Giessen, Germany; the ATS World Lung Health Award to Sundeep Salvi, Chest Research Foundation, Pune, India; and the Jo Rae Wright Award for Outstanding Science to Georgios Kitsios, University of Pittsburgh, Pennsylvania, USA. Furthermore, Thanh Neville, University of California, Los Angeles, USA, was awarded the J. Randall Curtis Humanism Award. All of these awards recognized the exceptional work done in the field, and the continued commitment to innovation and improved patient care.
year anniversary of the ATS research program
year anniversary of the Methods in Epidemiologic, Clinical, and Operations Research Program
Finally, William Flanary, famously known as satirist ‘Dr Glaucomflecken’, took the stage, sharing a particularly moving story about his experience with testicular cancer. He had also suffered a cardiac arrest, for which his wife had to perform cardiopulmonary resuscitation. From this story, he emphasised the need for greater compassion for the partners and responders on patients, termed ‘forgotten patients’ by Flanary. He drew the audience’s attention to the emotional distress of these medical events, and the aftershock that follows.
120 year anniversary of the American Lung Association
He emphasized the need for greater compassion for the partners and responders on patients termed, 'forgotten patients'
Stay tuned for more insights of the ATS Congress, and come back next year for our coverage of the 2025 ATS Congress, taking place in San Francisco, California from May 16th–21st .
Switching to E-Cigarettes Post-Smoking Cessation Increases Lung Cancer Risk
RESEARCH presented at ATS 2024 found that former cigarette smokers that switched to electronic cigarettes (e-cigarettes) faced higher cancer risks and mortality rates, particularly among high-risk individuals.
High-risk ex-smokers who had quit for <5 years and used e-cigarettes showed a higher risk of lung cancer
E-cigarettes have gained popularity in the recent years, particularly in conventional cigarette smokers as an alternative to conventional cigarettes. The research study led by Yeon Wook Kim from the Division of Pulmonary and Critical Care Medicine at Seoul National University, Repulic of South Korea, revealed that switching to e-cigarettes after quitting conventional smoking does not eliminate the risk of lung cancer but, in fact, increases it. The nationwide populationbased study followed over 4.3 million individuals with a history of smoking who participated in the National Health Screening Program for two periods: 2012–2014 and 2018. The study aimed to assess lung cancer risk and lung-cancer specific death (LCSD) associated with smoking habit changes from e-cigarette use among conventional cigarette smokers, stratified by the length of smoking cessation.
Results showed that ex-smokers who had quit for ≥5 years and used e-cigarettes had a significantly higher risk of LCSD (adjusted hazard ratio [aHR]: 2.69; 95% CI: 1.12–6.46) compared to those who did not
use e-cigarettes. Ex-smokers who had quit for 5 years and used e-cigarettes showed a higher risk of lung cancer development (aHR: 1.23; 95% CI: 1.09–1.39) and LCSD (aHR: 1.71; 95% CI: 1.10–2.66) than those who did not use e-cigarettes. Additionally, high-risk individuals (aged 50–80 years with ≥20 pack-years of smoking history) who had quit for ≥5 years and used e-cigarettes reported higher risks of lung cancer (aHR: 1.65; 95% CI: 1.05–2.58) and LCSD (aHR: 4.46; 95% CI: 1.85–10.75) compared to those who did not use e-cigarettes. Similarly, high-risk ex-smokers who had quit for <5 years and used e-cigarettes showed a higher risk of lung cancer (aHR: 1.26; 95% CI: 1.03–1.54) compared to those who did not use e-cigarettes.
The results showed that switching to e-cigarette use after conventional smoking cessation was associated with higher risk of developing lung cancer and higher mortality. This emphasizes the need for clinicians to caution patients about risks associated with conventional smoking alternatives and explore different strategies.
Extreme Heat Increases Risk of Asthma Hospitalizations in Children
RESEARCH presented at ATS 2024 presented by Morgan Ye, Department of Medicine and Epidemiology and Biostatistics, University of California San Francisco, USA, revealed significant links between extreme heat events and asthma exacerbations in pediatric patients.
Increased odds of asthma related hospital visits by
83 during extreme heat events %
The study, conducted at the University of California San Francisco Benioff’s Children Hospital, Oakland, USA, has found a significant association between extreme heat events and increased hospitalization and emergency department visits related to asthma among children. The study focused on a pediatric population served by a Federally Qualified Health Center in California.
Researchers analyzed electronic health record data from 2017–2020, which covered asthma related hospital visits and demographic data, including the patients’ zip codes. Temperature data were obtained from the PRISM Climate Group of Oregon State University, which provided daily maximum and minimum temperatures for each zip code’s population-weighted centroid. The study focused on the warm season (June–September) and evaluated 18 different heat wave definitions, including temperatures exceeding the 99th, 97.5th , and 95th percentiles of the total distribution of the study period for 1, 2, or 3 days. Time-stratified casecrossover design and conditional logistic regression models were used to assess the association between heat waves and asthma hospital visits. The analysis was further stratified by geographic regions within Central California and the Bay Area.
Results showed that daytime heat waves were significantly associated with increased odds of asthma hospital visits. More specifically, 1-day heat waves at the 95th percentile of temperature increased the odds of asthma hospital visits by 21%, and 3-day heat waves at the 99th percentile showed a nearly 80% increase in the odds of hospital visits. Data stratified by region showed a strong association in the Bay Area, with 83% increased odds of asthma related hospital visits during extreme heat events.
Results showed that daytime heat waves were significantly associated with increased odds of asthma hospital visits
This study highlights the impact of extreme heat events on asthma exacerbations among children, particularly in the Bay Area. The study's findings underscore the need for implementing more targeted public health interventions to protect vulnerable pediatric populations during heatwaves. These measures could include increasing awareness about the associated health risks and enhancing asthma management plans during periods of extreme heat.
Suboptimal Adoption of Updated Guidelines in Asthma Management
A RECENT study presented at the ATS 2024 International Conference revealed that only 14.5% of adult patients with asthma receive the recommended Single Maintenance And Relief Therapy (SMART) combination inhaler regimen, despite its endorsement in updated guidelines.
The National Asthma Education and Prevention Program and the Global Initiative for Asthma updated their guidelines in 2021, advocating for the use of a single inhaler containing both an inhaled corticosteroid (ICS) and formoterol, a long-acting betaagonist (LABA). SMART has been proven to significantly reduce asthma exacerbations in patients with moderate and severe asthma. Before the development of SMART, asthma management relied on using separate maintenance and rescue inhalers. However, researchers from Yale University School of Medicine noted that there has been limited data describing changes in SMART uptake and prescription since the update in management guidelines.
Researchers examined trends in SMART prescription for patients diagnosed with asthma, prescribed a maintenance inhaler containing ICS-LABA or ICS alone, and who had at least one visit to a pulmonary or allergy clinic between January 2021–August 2023. The study analysis comprised 2,016 patients from an academic healthcare system and excluded any patients with alternative pulmonary diagnoses. Statistical analyses were employed to evaluate the relationship
between patient characteristics and prescription of SMART.
It was found that 87% of patients who were prescribed SMART were also given a rescue inhaler, despite SMART inhalers being suitable for rescue use. Results revealed that patients prescribed ICS-formoterol as a maintenance inhaler were more likely to be prescribed SMART. Moreover, patients older and receiving Medicare insurance were less likely to be prescribed SMART. Researchers hypothesized that medical providers are less inclined to modify treatment regimens for older patients who are typically more resistant to changes and have been using the same inhalers for many years.
The study highlighted the need for further efforts to address barriers to SMART adoption, including insurance coverage issues, patient education, and clinician support. The results echoed findings from past studies demonstrating that clinicians can take over 15 years to widely adopt guideline updates. "This discordance between guidelines and practice is important to recognize and remedy as SMART can improve asthma outcomes," the authors concluded.
New Clinical Tool to Prioritize High-Risk Infants for Respiratory Syncytial Virus Immunization
AT THE ATS 2024 International Conference, researchers introduced a clinical prediction tool designed to prioritize high-risk infants for respiratory syncytial virus (RSV) immunization, particularly in light of the limited availability of nirsevimab in the USA.
Brittney M. Snyder, the lead author from Vanderbilt University Medical Center, Nashville, Tennessee, USA, emphasized the importance of timely identification of infants at the highest risk for RSVrelated morbidity to optimize prevention efforts. This personalized risk prediction tool aims to effectively allocate limited immunoprophylaxis resources, such as nirsevimab and palivizumab, to achieve maximum benefit and promote RSV prevention among high-risk infants' families.
The study included 429,365 infants insured by the Tennessee Medicaid Program, out of which 713 developed severe RSV lower respiratory tract infections (LRTI) requiring intensive care unit (ICU) admission. Researchers, including biostatistician Tebeb Gebretsadik, developed a multivariable logistic regression model using 19 demographic and clinical variables collected at or shortly after birth. These variables included prenatal smoking, delivery method, maternal age, and assisted breathing during birth hospitalization. The model demonstrated good predictive accuracy and internal validation.
The necessity of this tool became apparent during the nirsevimab shortage in October 2023, when the CDC recommended prioritizing high-risk infants who were not eligible for palivizumab. Nirsevimab, a longacting monoclonal antibody, and palivizumab, a short-acting monoclonal antibody requiring monthly injections, are both used to prevent RSV LRTI in newborns and young children.
Tina V. Hartert, the principal investigator, highlighted the tool's potential to prioritize
RSV prevention products effectively and to persuade vaccine-hesitant families by demonstrating their newborn's high risk for severe RSV infection. Co-author Niek Achten suggested the tool could be valuable in countries with budgetary constraints, ensuring the highest-risk infants receive necessary immunizations.
This tool represents a significant advancement in the strategic allocation of RSV prevention
Next steps for the tool include external validation, further cost-effectiveness analyses, and decision curve analyses to ensure its optimal usefulness in preventing severe RSV LRTI among infants during periods of limited immunization availability. This tool represents a significant advancement in the strategic allocation of RSV prevention resources, potentially improving outcomes for high-risk infants.
Increased Hospital Diversity Linked to Higher Ventilation Mortality Rates
NOVEL findings presented at ATS 2024 have shown that mortality rates for patients receiving mechanical ventilation for pneumonia or sepsis increase with the diversity of hospital patient populations.
This trend indicates that systemic factors, such as resource allocation and income levels, may significantly influence patient outcomes. Historically, health disparities research has focused on individual patient factors like race and income, with less attention given to the hospital systems where these disparities occur. Previous research indicated that Black women receiving mechanical ventilation for pneumonia or sepsis face the highest risk-adjusted mortality rates, while White men have the lowest.
To understand and address the systemic issues, the team conducted a study using data from the Healthcare Cost and Utilization Project State Inpatient Databases from 2018–2019. This dataset included nonsurgical patients with pneumonia or sepsis from 1,045 hospitals, encompassing over 16 million hospitalizations. After excluding hospitals with fewer than 25 patients of color, the researchers categorized hospitals into quartiles based on racial diversity and analyzed outcomes for 161,560 eligible patients.
The study found that Black women had a 37.6 percent mortality rate, compared to 36 percent for White men. While the adjusted odds of death for Black women versus White men did not significantly vary between
hospital diversity quartiles, overall mortality rates were higher in more racially diverse hospitals. The researchers noted that this increased strain might result from factors like hospital resources, staffing, insurance types, and neighborhood income levels.
The study supports previous research on hospital racial diversity and its impact on mortality following heart attacks and ICU outcomes. Gwenyth Day, University of Colorado Anschutz Medical Campus, Aurora, USA, stressed the importance of examining systemic contributors to adverse patient outcomes. “This data highlights the need for a careful evaluation of factors contributing to these outcomes and suggests adjusting resource allocation to reduce inequity and improve patient care,” Day stated. Future research by Day and colleagues will focus on understanding the variability in mortality rates from mechanical ventilation across different hospitals, aiming to identify the root causes of these disparities. They plan to use qualitative and survey methodologies to explore patient and provider experiences of bias, discrimination, and practice variability. This mixed-methods approach will hopefully help dissect the observed differences in outcomes and contribute to strategies for reducing health disparities in hospital settings.
37.6 mortality rate, compared to %
The study found that Black women had a 36 % for White men
Hormone Replacement Therapy May Improve Pulmonary Hypertension
BREAKING research presented at ATS 2024 investigates the impact of hormone replacement therapy (HRT) on pulmonary hypertension (PH) in women, a disease affecting blood vessels between the heart and lungs.
Specifically, it explores whether endogenous and exogenous HRT influence right ventricular function and PH severity across different classifications of the disease.
Longer duration of menses and HRT use were associated with lower mean pulmonary artery pressure
Researchers enrolled with G1, G2, G3, G4, or G5 PH (classified by the World Symposium on Pulmonary Hypertension [WSPH]), or mixed diseases, were categorized by their predominant subclass. Overall, 742 women with G1–G5 PH, and healthy controls were included. The research team quantified endogenous hormone exposure by assessing the duration of self-reported lifetime duration of menses and exogenous exposure by HRT usage. Right ventricular function was assessed using echocardiography, and pulmonary vascular disease was measured by mean pulmonary artery pressure during right heart catheterization. Two statistical analyses were conducted to evaluate differences in pulmonary vascular disease
and right ventricular function.
Results indicted that a longer duration of menses and HRT use were associated with lower mean pulmonary artery pressure and improved right ventricular function across all PH groups. Use of HRT was associated with a lower mean pulmonary artery pressure and higher right ventricular ejection fraction. In the G1 PH group, HRT exposure correlated with lower pulmonary artery pressure and pulmonary vascular resistance, and higher right ventricular ejection fraction. However, no significant differences were observed in WSPH Groups 2–5.
The findings suggest that hormone exposure, particularly HRT, may have a beneficial effect on pulmonary vascular disease and right ventricular function in women with PH. The results indicate a potential synergistic effect of age and HRT, supporting the theory that a threshold of estrogen exposure is necessary for a protective effect. Further research is encouraged to explore the mechanisms of female reproductive hormones as therapeutic targets for PH.
Improving Patient Outcomes for Veterans After Critical Illness
VETERANS who received care via the Post-acute Recovery Center (PARC) model after critical illness experienced better patient outcomes, with fewer deaths and more days spent at home, according to research presented at the ATS 2024 International Conference.
There was a 16.1 %
absolute reduction in mortality risk in the PARC group
Each year, over 100,000 veterans who survived critical illnesses, such as sepsis and acute organ failure, transition from intensive care units to their homes whilst classed as high-risk with ongoing acute medical issues. PARC is a telehealth care model led by nurse practitioners that aims to improve patientcentred outcomes for veterans transitioning from intensive care units to home.
Hiam Naiditch, a pulmonary and critical care fellow at the University of Pittsburgh Medical Center, Pennsylvania, USA, and colleagues conducted a retrospective analysis of 32,060 veterans from the Department of Veterans Affairs Pittsburgh Healthcare System who were classified as at risk of 1-year mortality based on their PREDICT score (a validated risk assessment tool). To assess the impact of PARC, the research team calculated the number of hospital-free days during the first 90 days after discharge. The research
team discovered that high-risk veterans who received PARC care had a median of four more days at home compared to matched controls. Furthermore, there was a 16.1% absolute reduction in mortality risk in the PARC group.
The researchers concluded that PARC is a viable post-acute care model that has the potential to improve care and reduce mortality risk in high-risk veterans after critical illness. Furthermore, this study highlights the importance of utilising models to improve patient-centred outcomes for high-risk survivors of critical illness in the broader population. The next step for Naiditch and colleagues is to conduct a randomised trial across several veteran facilities in the northeastern USA to validate the results seen so far with PARC care, and to provide further information on its effectiveness and scalability.
Insufficient Home Health Nursing for Children Who Require Ventilation
FAMILIES with children who require tracheostomy and mechanical ventilation often have to make significant employment changes due to a lack of home health nurses in their area.
Research led by Brian Jordan, Director of advanced mechanical ventilation and Associate Professor of Pediatrics, Division of Neonatology, Oregon Health & Science University, Portland, USA, explored the medical, social, and financial costs caused by a lack of home health nursing for children who are supported by tracheostomy and mechanical ventilation.
Jordan and colleagues conducted the first study to focus on in-home nursing from the perspective of the families with medicallycomplex children who require tracheostomy and mechanical ventilation. Between May–July 2023, 242 families in 34 states and the District of Columbia answered survey questions regarding home health nursing. It was reported that 86.8% of families had home health nursing hours approved by their insurers. However, 47.5% indicated that less than half of the approved hours were covered. Furthermore, 28.3% mentioned that no in-home nursing was available at the time of hospital discharge and 37.9% noted that their child's discharge was delayed due to the lack of in-home nursing care in their area.
The results also indicated that 87.8% of families had to make considerable
employment adjustments because of insufficient in-home nursing. These employment changes were not equally distributed between parents, impacting 78.4% of mothers surveyed. A total of 31.8% of families reported an annual household income reduction between 50,000 and 100,000 USD.
The medical, social, and financial costs caused by a lack of home health nursing
These findings emphasize the impact of a lack of accessible and sufficient home health nursing on families, including delays in hospital discharge, the need for major career changes, and significant income loss. Improvements in at-home care will reduce the burden on families and enhance the care for children with various pulmonary conditions that require tracheostomy and mechanical ventilation. A possible solution would be to implement more supportive legislation and services that assist families of children who require complex care.
Impact of Race-Neutral Equations on COPD Trial Eligibility
AT THE ATS 2024 International Conference, research revealed that using race-neutral spirometry reference equations for determining eligibility for chronic obstructive pulmonary disease (COPD) clinical trials may increase the enrolment of Black patients.
This study addresses a gap in understanding the impact of these equations on clinical trial inclusion criteria. Frank Sciurba from the University of Pittsburgh, Pennsylvania, USA, led the investigation, highlighting the shift from racially adjusted spirometry interpretations, which traditionally required lower values for Black patients.
These new guidelines suggest a more uniform approach, potentially altering the severity levels and eligibility for COPD clinical trials
In 2023, the ATS recommended discontinuing the use of race and ethnicity in spirometry interpretations, endorsing the Global Lung Function Initiative (GLI) race-neutral equations instead. These new guidelines suggest a more uniform approach, potentially altering the severity levels and eligibility for COPD clinical trials.
The study analysed spirometry data from the Combined Pittsburgh Lung Cohort, including 3,716 participants (3,474 White and 242 Black). The researchers compared the results using GLI ethnic-adjusted and GLI global race-neutral equations to determine the percent of forced expiratory volume in 1 second and GOLD stage for each individual. They found that using race-neutral equations resulted in a significant shift: 5.8% of individuals became ineligible, while 2.1% gained eligibility. Specifically, 1.6% of White and 8.3% of Black patients gained eligibility, while 6% of White and 2.9% of Black patients lost eligibility.
The findings suggest that race-neutral spirometry equations could reduce the severity classification for White subjects while increasing it for Black subjects, thereby impacting clinical trial enrolment criteria. The research team anticipates that these results will prompt further discussion and investigation into developing appropriate inclusion criteria, potentially enhancing the diversity and fairness of COPD clinical trials. Future research will explore the implications of these shifts and evaluate the role of raceindependent classification in clinical trial selection.
Transforming Lung Cancer Care: Advancements in Screening, Treatment, and Survivorship
Matthew Triplette, Fred Hutchinson Cancer Center and University of Washington, Seattle, USA, delivered an insightful talk at the American Thoracic Society (ATS) International Conference 2024 on how landmark studies in lung cancer screening can affect recommendations and standards of care for pulmonary medicine specialists. Triplette highlighted that lung cancer remains the leading cause of cancer-related deaths, with 85% of all lung cancer cases related to tobacco smoke worldwide.
EPIDEMIOLOGY
Introducing the epidemiology of lung cancer, Triplette explained that, according to recent studies, lung cancer mortality rates are declining faster than incidence rates in the USA. A comprehensive analysis of registry data from the National Cancer Institute (NCI), Centers for Disease Control and Prevention (CDC), and the North American Association of Central Cancer (NAACCR; covering 90% of the USA population) between 2015–2019 demonstrated a significant decrease in lung cancer mortality rates compared to incidence rates for both men (5.0% versus 2.6% annually) and women (4.3% versus 1.1% annually), with a 1.4% annual improvement in 2-year relative survival.1 Men showed greater annual incidence declines, but women experienced nearly twice the rate of annual mortality decline. These outcomes are attributed to advancements in treatments
and better access to care, partly due to the Patient Protection and Affordable Care Act. However, disparities persist, with 5-year survival rates ranging from 26% among Asian American/Pacific Islanders to 19% among American Indian/Alaskan Natives. States with higher smoking rates, such as Mississippi and Kentucky, also have higher mortality rates. The study highlights the need for targeted tobacco control, smoking cessation programs, and increased lung cancer screening to improve outcomes and address these disparities.1
SCREENING GUIDELINES
Current low-dose CT (LDCT) screening guidelines vary among organizations like the United States Preventive Services Task Force (USPSTF), Centers for Medicare & Medicaid Services (CMS), National Comprehensive Cancer Network (NCCN), the American Cancer Society, and the UK National Screening Committee. While USPSTF and CMS require a smoking cessation period of 15 years, NCCN and the American Cancer Society have removed this criterion to broaden eligibility. The UK guidelines use a risk-based approach, including any current or former smokers. Triplette explained that dropping the restrictive smoking criteria might make it easier to identify patients for screening and thus increase screening rates.
A study by Choi et al.2 examined the effectiveness of risk-based screening using data from the Multiethnic Cohort Study. The
study demonstrated that the 2021 United States Preventive Services Task Force (USPSTF) guidelines created significant disparities, especially for individuals who are African American, whose eligibility was 53% lower than that of individuals who are White. Conversely, the risk-based PLCOₘ2012 model was more sensitive and equitable. These findings underscore the potential benefits of adopting risk-based criteria to improve lung cancer screening efficiency and reduce racial and ethnic disparities. This aligns with the goals of the new screening studies to enhance early detection and ensure more inclusive and effective screening practices.
REAL-WORLD SCREENING
Triplette went on to question the applicability of clinical trial results in real-world settings. A study by Slivestri et al.3 addressed this by analyzing individuals undergoing baseline LDCT for lung cancer screening (LCS) from 2015–2019. The study compared outcomes from the American College of Radiology’s LCS Registry with those from the National LCS Trial (NLCST). The study demonstrated that 14.3% of over one million screened individuals had positive results, similar to NLCST data. However, the cancer detection rate (0.56%) was half that of NLCST (1.1%). Additionally, only 22.3% of participants with negative baseline scans followed up within 11–15 months, highlighting a gap in adherence that impacts real-world effectiveness.
Another study by Rendle et al.4 investigated downstream procedures and complications in real-world LCS across five American healthcare systems between 2014–2018. Among nearly 10,000 patients, 15.9% had abnormal LDCT results, with a 9.5% lung cancer diagnosis rate within 12 months. The positive predictive value was 9.5%, and the negative predictive value was 99.8%, with high sensitivity (92.7%) and specificity (84.4%). Despite the effectiveness of LDCT in detecting lung cancer, there were significant rates of follow-up imaging (31.9%) and invasive procedures (2.8%), with higher complication rates than NLCST, suggesting a need for improved diagnostic management to balance the benefits and harms of screening.
Despite the effectiveness of LDCT in detecting lung cancer, there were significant rates of follow-up imaging
SCREENING: ON THE HORIZON
According to Triplette: “New screening methods, technologies, and adjuvant approaches are on the horizon.” Two new studies highlight significant advancements in LCS and multi-cancer early detection, which promise to revolutionize how we approach early cancer detection, potentially leading to better outcomes and more personalized screening strategies.
A recent study introduced a deep learning model named 'Sybil', which accurately predicted lung cancer from a single LDCT.5 Validated on three independent datasets (National Lung Screening Trial, Massachusetts General Hospital, and Chang Gung Memorial Hospital), Sybil demonstrated high accuracy with area under the receiver-operator curves of 0.92, 0.86, and 0.94, respectively.
This model’s capability to run in real-time on radiology stations showcases its potential to enhance personalized screening efforts.5 Triplette also discussed a significant National Health Service (NHS)-Galleri trial led by Neal et al.,6 which evaluates a multi-cancer early detection blood test. This randomized controlled study, involving over 140,000 participants aged 50–77 in the UK, aims to assess the test’s effectiveness in reducing late-stage cancer incidence, helping the NHS decide on its potential implementation in routine screening programs. The results are anticipated in 2026. Additionally, the NCI Cancer Screening Network, with Triplette as the Health Equity and Access Chair, is investigating non-steroidal anti-inflammatory drugs and other screening technologies through a flexible research framework,
including a Vanguard pilot RCT study involving 24,000 individuals randomized to different multi-cancer early detection tests.
TREATMENT
Triplette explained that there is ongoing evidence to refine treatment for early-stage non-small cell lung cancer (NSCLC), especially with the emergence of more precision approaches to multimodal therapy in NSCLC. Additionally, the role pulmonologists play is the key to expanding the role of neoadjuvant therapy and multi-disciplinary management. Triplette mentioned two new studies in particular, that he expects to have significant implications for lung cancer treatment and screening. The first study compared sublobar resection to lobectomy in patients with small (≤2 cm), node-negative peripheral NSCLC.7 The study showed that sublobar resection was non-inferior to lobectomy in terms of disease-free and overall survival, suggesting that less invasive surgery might be a viable option for early-stage NSCLC, potentially preserving more lung function. The second study, the ADAURA trial, demonstrated that adjuvant osimertinib significantly improved
5-year overall survival rates in patients with resected, EGFR-mutated stage IB to IIIA NSCLC compared to placebo (88% versus 78%).8 These findings highlight the potential of personalized treatments based on genetic markers and less invasive surgical options to improve patient outcomes and reduce the burden of late-stage lung cancer, reinforcing the importance of early detection and tailored treatment strategies in lung cancer management.
SURVIVORSHIP
Triplette noted that there aren’t many studies on survivorship, and with that physicians and researchers need to consider interventions to support lung cancer survivors through treatment and beyond. Triplette mentioned one study as an example, in which physicians investigated the sleep quality of patients with lung cancer, who often experience sleep disturbances. A randomized trial in Hong Kong compared aerobic exercise and tai chi in 226 patients with advanced lung cancer.9 Over 16 weeks, both aerobic exercise
References
1. Kratzer TB et al. Lung cancer statistics, 2023. Cancer. 2024;130(8):1330-48.
2. Choi E et al. Risk model–based lung cancer screening and racial and ethnic disparities in the US. JAMA Oncol. 2023;9(12):1640-8.
3. Silvestri et al. outcomes from more than 1 million people screened for lung cancer with low-dose CT imaging. Chest. 2023;164(1):241-51
4. Rendle KA et al. Rates of downstream procedures and complications associated with lung cancer
and tai chi groups showed significant improvements in sleep quality, psychological distress, physical function, and circadian rhythm compared to a control group. Tai chi provided greater benefits in sleep and survival rates.9 These results suggest that incorporating physical activities, especially tai chi, can enhance lung cancer care and survivorship. This study is just one of the examples of continued efforts of physicians to improve the survivorship of patients with lung cancer.
CONCLUSION
In his concluding remarks, Triplette highlighted the ongoing advances and challenges in LCS and treatment. He noted that the decline in mortality rates can be attributed to improved treatments and access to care. However, there is still a need to address the significant disparities among different racial and ethnic groups. Triplette advocated for broader LDCT screening guidelines and emphasized the potential of risk-based models.
screening in routine clinical practice: a retrospective cohort study. Ann Intern Med.2024;177:18-28.
5. Mikhael P G et al. Sybil: a validated deep learning model to predict future lung cancer risk from a single low-dose chest computed tomography. J Clin Oncol. 2023;41(12):2191-200.
6. Neal RD et al. Cell-free DNA–based multi-cancer early detection test in an asymptomatic screening population (NHS-Galleri): design of a pragmatic, prospective randomised controlled trial. Cancers. 2022;14(19):4818.
7. Altorki et al. Lobar or Sublobar resection for peripheral stage IA nonsmall-cell lung cancer. N Engl J Med. 2023;388(6):489-98.
8. Tsuboi et al. Overall survival with osimertinib in resected EGFR-mutated NSCLC. N Engl J Med. 2023;289(2):13747.
9. Takemura N et al. Effectiveness of aerobic exercise and tai chi interventions on sleep quality in patients with advanced lung cancer: a randomized clinical trial. JAMA Oncol. 2024;10(2):176-84.
Abstract Reviews
The abstracts that follow were presented at the ATS 2024 International Conference. They have been have been carefully selected to invoke debate and discussion on the latest research and data aimed at improving patient outcomes in respiratory medicine.
How Did Respiratory Support Management And Patients’ Demographics Change in the Intensive Care Unit Before, During, and After the Pandemic?
1. Intensive Care Unit, University of Health Sciences Sureyyapasa Chest Diseases and Thoracic Surgery Research and Teaching Hospital, Istanbul, Türkiye
2. Pulmonary Department, University of Health Sciences İlhan Varank Sancaktepe Research and Teaching Hospital, Istanbul, Türkiye
*Correspondence to zuhalkarakurt@hotmail.com
Disclosure: The authors have declared no conflicts of interest.
Acknowledgements: The authors would like to thank all the nurses and other healthcare workers for their valuable data.
The SARS-CoV-2 2019 pandemic has resulted in a rise in the need for intensive care units (ICU) and mechanical ventilation due to respiratory failure. There is little evidence available on the demographic
features of patients in the ICU, as well as changes in respiratory support in the ICU for the management of chest diseases before, during, and after the pandemic. In this research, the team determined whether there was any change in the respiratory support and demographic features of ICU patients with respiratory failure.
MATERIALS AND METHODS
A retrospective observational cohort study was designed in a tertiary teaching respiratory ICU between January 1, 2017–December 31, 2023. Definitions of periods used include pre-pandemic: January 1, 2017–March 10, 2020; pandemic: March 11, 2020–May 5, 2022; and post-pandemic: May 6, 2022–December 31, 2023. During the study period, all patients accepted into the ICU were included in the study. Patient demographics, comorbid diseases, reason for respiratory failure, types of respiratory support (invasive and non-invasive mechanical ventilation, and high flow oxygen [HFO] nasal cannula), length of ICU stay, and mortality were recorded from ICU files. Joinpoint (National Cancer Institute [NCI], National Institutes of Health [NIH], Bethesda, Maryland, USA) and descriptive analysis were done.
Figure 1A & 1B: Female mortality in the intensive care unit in pre-pandemic, pandemic, and post-pandemic periods. All: 0 Joinpoints
*Indicates that the APC is significantly different from zero at the alpha=0.05 level. Test statistic and p-value not available for the empirical quantile method. Final selected model for Figure 1A is 0 Joinpoint and for Figure 1B is 1 Joinpoint. APC: annual percent change.
Table 1: Characteristics in pre-pandemic, pandemic, and post-pandemic years of Level 3 intensive care unit patients.
Patient Demographics
ICU Data, All Variables
*Values median (25–75%).
AF: atrial fibrillation; APACHE 2: acute physiologic and chronic health evaluation 2; ARDS: acute respiratory distress syndrome; CAD: coronary artery diseases; CHF: congestive heart failure; CRF: chronic renal failure; HFO: high flow oxygen; HT: hypertension; ICU: intensive care unit; T-IMV: total invasive mechanical ventilation (IMV after NIVM or IMV alone); T-NIMV: total noninvasive mechanical ventilation (NIMV after IMV or NIMV alone).
RESULTS
Patient demographics and ICU data over the 7-year period were summarized (Table 1). Diabetes, chronic renal failure, and cardiovascular diseases increased in pandemic and post-pandemic periods. The proportion of patients in the ICU that are female (Figure 1A), as well as the rate of female mortality (Figure 1B), had a gradually increasing annual percent of changes (APC) of 2.5 from 2017–2023 (Figure 1A), and during the pandemic, this increased to an APC of 12.5 (Figure 1B). Mechanical ventilation (invasive and noninvasive) gradually decreased in pandemic and post-pandemic periods; whereas, HFO use increased. Mortality of patients had an APC of 11.49 after 2019.
CONCLUSION
While the proportion of female patients in ICUs has increased over the years, and female mortality continues to increase during and after the pandemic, cardiovascular and renal diseases are more prominent post-pandemic. As HFO increased in use with the pandemic, a decrease in mechanical ventilation applications was seen, marking the most prominent difference in respiratory ICU during the pandemic.
References
1. González-Castro A et al. Non-invasive mechanical ventilation or high-flow oxygen therapy in the COVID-19 pandemic: dead heat broken. Medicina Intensiva (Engl Ed). 2023;47(3):178-80.
2. Buell KG et al. Individualized treatment effects of oxygen targets in mechanically ventilated critically ill adults. JAMA. 2024;331(14):1195-204.
Improvements in Skeletal Muscle Mass in Select Patients with Chronic Obstructive Pulmonary Disease Undergoing Lung Volume Reduction Interventions
Authors: Abdelrahman Nanah,1 Yvonne Meli,2
Fatima Abdeljaleel,1 Uddalak Majumdar,2,3 Avantika Nathani,2,3 Umur Hatipoğlu,2,3 *Amy Attaway2
1. Department of Internal Medicine, Cleveland Clinic Foundation, Ohio, USA
2. Department of Pulmonary Medicine, Cleveland Clinic Foundation, Ohio, USA
3. Department of Critical Care Medicine, Cleveland Clinic Foundation, Ohio, USA
*Correspondence to attawaa@ccf.org
Disclosure: The authors have declared no conflicts of interest.
Lung volume reduction is performed in a highly select population of patients with chronic obstructive pulmonary disease (COPD) and severe hyperinflation to improve survival, exercise capacity, and quality of life.1,2 Skeletal muscle loss is a frequent complication in severe COPD that contributes to adverse clinical outcomes, including mortality.3 The authors hypothesized that interventions to ameliorate hyperinflation in severe COPD would improve exercise capacity and restore skeletal muscle mass in these patients.
MATERIALS AND METHODS
Data from the Cleveland Clinic COPD center, Ohio, USA, were analyzed from 2008–2022. Patients were included if they had a CT of the thorax prior to and after bronchoscopic lung volume reduction (BLVR; n=19) or lung volume reduction surgery (LVRS; n=23). An initial CT scan must have been performed within 6 months of the intervention, and a follow-up CT scan must have been performed at least 6 months after the intervention.
Pectoralis muscle cross-sectional area (PMcsa), an imaging surrogate for muscle mass, was manually selected using Aquarius iNtuition (TeraRecon, Durham, North Carolina, USA) software based on an attenuation range of -50 to +90 Hounsfield units. Data were compared pre- and post-intervention using paired t-tests with a significant p-value of <0.05. Youden’s optimal cut-off criteria were used to predict an increase in PMcsa post intervention.
RESULTS
Patients with COPD who underwent interventions were 65.3±6.4 (mean±standard deviation) years old, 60.5% male, and 97.7% White. Average forced expiratory volume pre-procedure was 28±7% predicted, total lung capacity was 126±9% predicted, residual volume was 227±40% predicted, and 6-minute walk test (6MWT) was 959.33±307.4 ft. Of the subjects, 57.1% were on supplemental O2, with a mean partial pressure of oxygen in the arterial blood of 67.2±8.2 mmHg. In those patients who underwent BLVR, postprocedure PMcsa was significantly increased by approximately 9% (pre: 23.1+7.1 cm2; post: 25.5+7.3 cm2; paired t-test p=0.03). In those who underwent LVRS, PMcsa was increased by approximately 3%, which was not statistically significant (pre: 26.3+9.2 cm2; post: 27.2+10.1 cm2; paired t-test p=0.58; Figure 1). The average time between intervention and post-CT scan for BLVR and LVRS was not significantly different (BLVR:
Figure 1: Patients with chronic obstructive pulmonary disease with low 6-minute walk distance at baseline who underwent bronchoscopic lung volume reduction showed improvements in pectoralis muscle cross-sectional area post-procedure.
0.93+0.53 years versus LVRS: 1.12+0.45 years; p=0.22). Youden’s criteria determined that a 6MWT <1,050 ft was associated with a positive increase in PMcsa post-intervention in all patients (area under the curve: 0.676).
CONCLUSION
While BLVR and LVRS were both associated with increased pectoralis muscle mass in follow-up CT scans, BLVR was associated with a larger and statistically significant increase. Potential reasons may include the authors’ study’s patients with LVRS being more nutritionally robust than patients with BLVR, or experiencing delayed postoperative response in restoring skeletal muscle mass. The authors’ study also demonstrates that patients with lower exercise capacity, evidenced by a baseline 6MWT of <1,050 ft, may experience significant improvements
after lung volume reduction. This echoes the results of the NETT trial, where patients with low exercise capacity had improved outcomes. Further research is needed to identify clinical factors that predict improvements in muscle mass in patients with COPD undergoing lung volume reduction.
References
1. Criner GJ et al. A multicenter randomized controlled trial of zephyr endobronchial valve treatment in heterogeneous emphysema (LIBERATE). Am J Respir Crit Care Med. 2018;198(9):1151-64.
2. Fishman A et al. A randomized trial comparing lung-volume-reduction surgery with medical therapy for severe emphysema. N Engl J Med. 2003;348(21):2059-73.
3. Attaway AH, Welch N, Yadav R, et al. Quantitative computed tomography assessment of pectoralis and erector spinae muscle area and disease severity in chronic obstructive pulmonary disease referred for lung volume reduction. COPD. 2021;18(2):191-200.
The Use of an Electronic Order Set to Improve Latent Tuberculosis Screening Among Hospitalized Patients Who Are Initiating Immunosuppression: A Cross-Sectional Analysis
Before 2021 in Calgary, Canada, hospitalized inpatient latent tuberculosis infection (LTBI) screening, with a QuantiFERON assay (QFT),
for immunosuppression, required approval from a tuberculosis physician. This may have delayed testing, thereby resulting in QFT collection after immunosuppression initiation. An inpatient QFT order set was implemented in November 2020, permitting screening without approval for patients tested due to immunosuppression. The impact of the order set on local LTBI screening practices is yet to be investigated. Additionally, there are limited published data on inpatient QFT testing. The study’s objectives were to assess the impact of the order set on the timing of QFT collection in relation to immunosuppression initiation; describe characteristics of patients undergoing QFT testing and their test results; and assess the relationship between administration of inpatient immunosuppression and QFT results.
MATERIALS AND METHODS
A cross-sectional analysis was completed with a chart review of all adult inpatients who underwent a QFT at four acute care hospitals in Calgary, Canada, from January 1–October 31, 2020, and January 1–December 31, 2021. November 1–December 31, 2020 were excluded due to the roll-out of the order set. Z test was used to assess the proportion of pre-immunosuppression QFT testing pre- and post-order set implementation; associations were analyzed using logistic regression.
RESULTS
A total of 639 inpatients had QFT testing, of which 534 (191 pre-order set, 343 post-order set implementation) were for immunosuppression screening. Of those
tested due to immunosuppression, there was a significant decrease in the initiation of inpatient immunosuppression before collection of QFT following implementation of the order set (103/191 [54%] versus 153/ 343 [45%] in 2020 and 2021, respectively [p=0.0388]). Among all inpatients, there were 34 positive (5%), 496 negative (87%), and 109 indeterminant (17%) QFT results. Indeterminate results were more frequent among those who were administered immunosuppression in-hospital before QFT testing (either new start of immunosuppression, new medication, and/or increased dose if taking home immunosuppression; 76/279 [27%]) compared to those without new, or escalation of, immunosuppression before QFT (33/360 [9%]; p=0.0004). Univariable logistic regression analysis of variables potentially associated with indeterminate results is shown in Table 1
*Defined as either a new start of immunosuppression and/or increased dose administered before QFT collection. CRP: c-reactive protein; N/A: not applicable; QFT: QuantiFERON assay.
Table 1: Univariable logistic regression analysis of variables potentially associated with indeterminate results.
CONCLUSION
To the authors’ knowledge, this is the largest review of in-hospital QFT results. Immunosuppression started in-hospital before QFT collection was associated with a high rate of indeterminate QFT, which limits its utility. Implementing an order set significantly reduced the proportion
of QFT testing done after in-hospital immunosuppression initiation (i.e., reduced delay in testing). However, QFT collection still occurred frequently after initiation of immunosuppression. While beneficial, an order set alone may be insufficient to drastically alter practice patterns with regard to LTBI screening; a multimodal approach to this problem is required.
Sarcoid Versus Tuberculosis, or Both?
Disseminated Tuberculosis in the Setting of Sarcoidosis
Authors: Alexis Janoczkin,1 Anna Klele,1 *Ashley Vojtek,2 Dylan Soller,2 Christopher Lenivy2
1. Internal Medicine Residency, Lehigh Valley Health Network, Allentown, Pennsylvania, USA
2. Pulmonary Critical Care Fellowship, Lehigh Valley Health Network, Allentown, Pennsylvania, USA
*Correspondence to ashley.vojtek@lvhn.org
Disclosure: The authors have declared no conflicts of interest.
Acknowledgements: The authors would like to thank Lehigh Valley Health Network for the opportunity to care for patients with such breadth of pathology.
Keywords: Active pulmonary tuberculosis, caseating granulomas, pulmonary sarcoidosis, tuberculosis (TB).
Sarcoidosis and tuberculosis (TB) share similar clinical, histological, and radiographical characteristics, and can be difficult to differentiate.1 Early recognition and diagnosis of TB is imperative, as treatment modalities differ substantially. Similarly, immunosuppression in patients with sarcoidosis can be catastrophic in patients infected with TB.1,2 The authors present
a case of biopsy-proven sarcoidosis with subsequent development of multi-organ system failure secondary to disseminated TB.
CASE PRESENTATION
A 58-year-old female with recently diagnosed COVID-19 pneumonia was found to have a dry cough and dyspnoea in the setting of persistent bilateral hilar and mediastinal lymphadenopathy associated with bilateral nodular infiltrates. Of note, she immigrated to the USA from India 10 years prior, with the most recent travel to India 2 years ago. Quantiferon testing upon return to the USA was negative at that time. Workup included bronchoscopy with endobronchial ultrasound revealing non-caseating granulomas with negative stains for acid-fast bacilli (AFB). She was diagnosed with Stage 3 sarcoidosis and initiated on prolonged steroid taper with improvement of symptoms. With taper of steroid dose, however, she developed lymphocyte-predominant exudative effusion with negative cultures, and was reinitiated on a protracted steroid course with rapid symptom resolution. At 4-month follow-up, she had worsening CT findings upon steroid taper, and was started on azathioprine. One month later, she required hospital admission for worsening dyspnoea and fatigue. She was noted to be febrile, tachycardic, and tachypnoeic with worsening
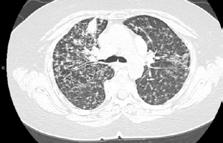
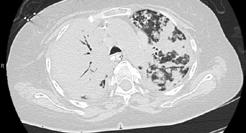
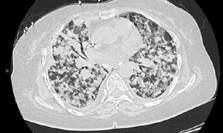
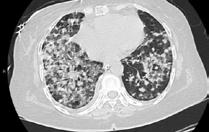
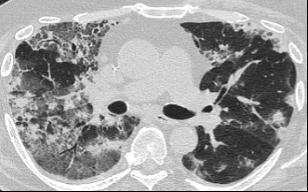
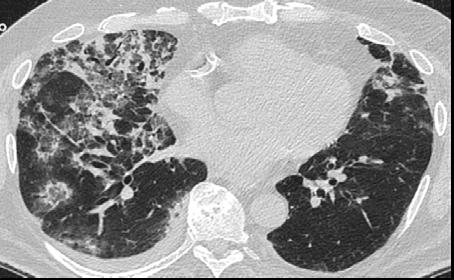
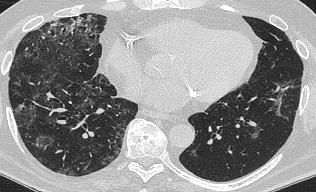
hypoxia. Subsequent CT chest showed progression of bilateral nodular infiltrates with new right upper lobe consolidation and air bronchograms concerning for multifocal pneumonia (Figure 1). Incidentally, she was also noted to have calcified splenic granulomas. She developed rapid clinical deterioration, ultimately requiring mechanical ventilation, pressor support, and continuous renal replacement therapy. Repeat bronchoscopy revealed diffuse alveolar haemorrhage with multiple AFB smears positive for Mycobacterium tuberculosis. She was immediately initiated on quadruple therapy, but unfortunately, despite treatment, developed refractory shock and passed away 2 weeks after initial presentation.
CONCLUSION
TB and sarcoidosis share synonymous manifestations, making differentiating between progression of sarcoidosis and the development of TB difficult, especially in patients who have biopsy-proven sarcoidosis. This patient’s initial negative Quantiferon testing and AFB stains, CT scan findings, pathology, and rapid symptom resolution with steroids support the initial diagnosis of sarcoidosis. Given her history and no recent identifiable risk factors, TB was lower on the differential at initial presentation to the hospital. While findings of lymphocytepredominant pleural effusions3 and splenic granulomas may be seen with sarcoidosis, this should raise suspicion for tuberculosis
A) Initial adenopathy with peripheral patchy ground glass opacities in the right lung following COVID-19 pneumonia. B) Persistent bulky adenopathy 1 year after initial presentation. C) Extensive nodularity throughout the right lung with increasing confluent opacities in the right upper lobe and stable mediastinal lymphadenopathy 2 years after initial presentation. D) Tuberculosis superimposed on sarcoidosis with progression of nodular infiltrates, worsening right upper lobe consolidation, and air bronchograms with incidental calcified splenic granulomas (not pictured).
Figure 1: CT progression of patient’s sarcoidosis and tuberculosis.
and prompt further investigation. This case highlights diagnostic challenges and the need to keep TB on the differential in patients with previous risk factors, despite negative testing and progressive CT findings with biopsyproven sarcoidosis.
References
1. Pedroso A et al. Tuberculosis and sarcoidosis overlap: a clinical challenge from diagnosis to treatment. Cureus. 2020;12(11):e11662.
2. Narasimhan P et al. Risk factors for tuberculosis. Pulm Med. 2013;2013:828939.
3. McNally E et al. The tuberculous pleural effusion. Breathe. 2023;19:230143.
4. Agrawal R et al. Tuberculosis or sarcoidosis: opposite ends of the same disease spectrum? Tuberculosis (Edinb). 2016;98:21-6.
5. Kaur H et al. Co-existence of pulmonary tuberculosis with sarcoidosis. Int J Mycobacteriol. 2021;10(3): 341-3.
6. Mortaz E et al. Common features of tuberculosis and sarcoidosis. Int J Mycobacteriol. 2016;5(Suppl 1):S240-1.
Epidemiological Study of Overall Survivability of Individuals Diagnosed with Lung and Bronchus Cancer in Michigan Between the Years 1996–2017
1. University of Michigan Health Sparrow Hospital-Michigan State University, Lansing, USA
2. Henry Ford Hospital, Detroit, USA
3. University of New Mexico, Albuquerque, USA
4. Michigan State University, East Lansing, USA
*Correspondence to nadergeo@msu.edu
Disclosure: Abdelsamia is licensed by the American Board of Internal Medicine and has received honoraria for lecture by the Binaytara Foundation. All other authors have declared no conflicts of interest.
Acknowledgements: The authors would like to thank their significant others for the relentless support they have received throughout their careers.
Keywords: Lung cancer, lung cancer screening, Michigan, survivability.
As a leading cause of death in the USA, lung and bronchus cancer has
claimed the lives of many individuals across the nation.1 However, considerable variability exists regarding risk factors and treatment of lung cancer across each state.2 The authors’ study aimed to explore the epidemiological trends of patients diagnosed with lung and bronchus cancer in Michigan, USA, between 1996–2017, including variables for patient demographics, primary tumor location, stage at diagnosis, and overall survival.
MATERIALS AND METHODS
Data was obtained through the Michigan Cancer Surveillance Program (MCSP) and the Surveillance, Epidemiology, and End Results (SEER) database. The study was determined to be exempt by the Michigan State University Institutional Review Board and adhered to all ethical guidelines. The team hypothesized that overall survival would increase following the implementation of more inclusive lung screening guidelines in 2013, and that overall survivability would be affected by age, race/ ethnicity, and stage.
RESULTS
The data showed that the mean age of diagnosis was 69 years with a median interquartile overall survival of 8 months. Log rank showed no significant difference in each of the time periods. Overall survival was reduced for individuals with an older age at diagnosis, male sex, American Indian heritage, and living in rural or urban areas. Tumor location associated with reduced overall survival included the mainstem bronchus (including the bronchus intermedius), lung base, and overlapping lesions of lung lobes. The presence of distant sites/nodes was associated with reduced overall survivability, and approximately 44.44% of Michigan residents were initially diagnosed at this stage.
CONCLUSION
This data highlight an unexpected trend of reduced overall survivability among Michigan residents diagnosed with lung cancer between the years 1996–2017, and suggest that in addition to tumor, node, and metastasis staging, other factors influence the overall survivability. Consideration of these factors may be helpful as a community outreach tool to help increase early detection and reduce overall mortality.
References
1. State of Michigan. Invasive Lung Cancer Incidence & Mortality Trends, Michigan Residents 1985-2021. 2023. Available at: https://vitalstats.michigan.gov/osr/ cancer/stateinc.asp?CDxID=IncTrendsLung. Last accessed: 17 March 2024.
2. National Cancer Institute Surveillance, Epidemiology, and End Results Program (SEER). Cancer Stat Facts: Common Cancer Sites. 2024. Available at: https:// seer.cancer.gov/statfacts/html/common.html. Last accessed: 17 March 2024.
Genitourinary Tuberculosis Resulting in Hydronephrosis
Authors: *Katie Alsheimer,1 Faraz Siddiqui,1 Jonathan Burgei,1 Julia Lantry1
1. Department of Pulmonary and Critical Care Medicine, Guthrie Clinic Robert Packer Hospital, Sayre, Pennsylvania, USA
*Correspondence to katie.alsheimer@guthrie.org
Disclosure: The authors have declared no conflicts of interest.
Genitourinary tuberculosis (GUTB) results from hematogenous spread of chronic latent pulmonary tuberculosis of 5–40 years.1 The diagnosis is typically delayed, as it can mimic a urinary tract infection.1,2 Only 5–45% of cases of tuberculosis have extrapulmonary manifestation, and of these, only 30–40% involve the urogenital tract.1
CASE PRESENTATION
This is a case of a male in his 60s who was immunocompromised due to rheumatoid arthritis, requiring methotrexate and chronic prednisone. He was diagnosed with GUTB requiring orchiectomy secondary to recurrent epididymo-orchitis. The pathology following his epididymo-orchitis showed
necrotizing granulomatous infection with negative cultures. However, urine culture was significant for pyuria and acid-fast bacilli. Cystoscopy was notable for bilateral hydronephrosis associated with significant bladder inflammation and ureteral strictures. He was treated with levofloxacin 750 mg daily for 6 months, rifampin 600 mg daily for 6 months, pyrazinamide 1,500 mg daily for 2 months, ethambutol 1,200 mg daily for 2 months, and pyridoxine 50 mg daily for 6 months as it was resistant to isoniazid (Figure 1).
CONCLUSION
Prompt diagnosis of GUTB can prevent the need for invasive procedures and improve the quality of life of patients that have GUTB. Improved awareness of the diagnosis can improve diagnosis time. Patients who require prolonged immunosuppression should be screened not only for tuberculosis, but also monitored and/or receive prophylactic therapy against opportunistic infections.
References
1. Jha SK, Rathish B, Genitourinary Tuberculosis [Internet] (2023) Treasure Island: StatPearls Publishing. Available at: https://www.ncbi.nlm.nih. gov/books/NBK557558/. Last accessed: 23 April 2024.
2. Muneer A et al. Urogenital tuberculosisepidemiology, pathogenesis and clinical features. Nat Rev Urol. 2019;16(10):573-98.
3. World Health Organization (WHO). WHO consolidated guidelines on tuberculosis: module 2: screening: systematic screening for tuberculosis disease. 2021. Available at: https://www.who.int/publications/i/ item/9789240022676. Last accessed: 23 April 2024.
4. World Health Organization (WHO). WHO consolidated guidelines on tuberculosis: module 3: diagnosis: rapid diagnostics for tuberculosis detection, 2021 update. 2021. Available at: https://www.who.int/ publications/i/item/9789240029415. Last accessed: 21 April 2024.
5. World Health Organization (WHO). Catalogue of mutations in Mycobacterium tuberculosis complex and their association with drug resistance. 2021. Available at: https://www.who.int/publications/i/ item/9789240028173. Last accessed: 21 April 2024.
6. Centers for Disease Control and Prevention (CDC). Tuberculosis (TB). Available at: https://www.cdc.gov/ tb/index.html. Last accessed: 23 April 2024.
Figure 1: CT of abdomen shows severe hydronephrosis in the right ureter.
Daptomycin: A Rare Cause of Acute Eosinophilic Pneumonia
Authors: *Sandeep S. Bains,1 Caroline McCormick,1 Anu Brixey,2 Kelly C. Vranas,1,3 Suil Kim1,3
1. Division of Pulmonary, Critical Care, and Allergy Medicine, Oregon Health & Science University, Portland, USA
2. Division of Diagnostic Radiology, Section of Cardiothoracic Imaging, VA Portland Healthcare System, Oregon Health & Science University, Portland, USA
3. Section of Pulmonary, Critical Care, Sleep, and Allergy Medicine, VA Portland Healthcare System, Portland, USA
*Correspondence to Bainss@ohsu.edu
Disclosure: The authors have declared no conflicts of interest.
Acknowledgements: The Department of Veterans Affairs did not have a role in the conduct of the study; in the collection, management, analysis, or interpretation of data; or in the preparation of the manuscript. The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs or the U.S. Government.
Acute eosinophilic pneumonia (AEP) is a rare, potentially fatal lung condition. It can vary in presentation and severity, but classically presents as an acute, febrile respiratory illness that is rapidly progressive. The pathophysiology of this disease is poorly understood. Diagnosing AEP relies on an extensive review of clinical history, data, imaging, and physical examination. The severity of illness highlights the importance of understanding its triggers, risk factors, and mechanism of action. One rare, known trigger of AEP is daptomycin.
CASE PRESENTATION
The patient was a 75-year-old male with a past medical history of Stage IIIb chronic kidney disease and a former tobacco smoker. He presented with 1 week of recurrent fevers, dry cough, and worsening shortness of breath. Approximately 2 weeks prior, he had been hospitalized for right metatarsal osteomyelitis with a positive wound culture for methicillin-resistant Staphylococcus aureus. After consultation with infectious disease physicians, he was discharged on a 4-week course of intravenous daptomycin and ceftriaxone.
On presentation, notable vitals were a temperature of 98.4 °F, heart rate of 108 bpm, blood pressure of 164/42 mmHg, and O2 saturation of 75% on room air requiring 10 L non-rebreather. Initial notable labs were a creatinine of 2.5 mg/dL (at baseline) and a white blood cell count of 12.3x109 /L, with 2% bandemia. He did not have peripheral eosinophilia on his blood work. His initial chest radiography was concerning due to right greater than left bilateral scattered opacifications, and ground glass infiltrates. A chest CT was obtained, showing dense bilateral consolidations in the upper lobes and scattered ground glass opacities throughout both lung fields, as seen in Figure 1
His O2 requirements prompted admission to the medical intensive care unit. His daptomycin was stopped immediately and he was started on a treatment for bacterial pneumonia. Unfortunately, his respiratory status worsened, eventually requiring a high-flow nasal cannula. Bronchoscopy was not safe to perform given his tenuous respiratory status. Empiric steroids with methylprednisolone 60 mg every 6 hours were started on Day 4 in the intensive care unit. After 3 days, his
A) Axial lung image of the upper lobes demonstrates striking peripheral involvement in the right lung. B) Axial lung image of the lower lobe demonstrates presence of a focal area of ground glass with a rim of consolidation known as the “reversed halo sign” or “atoll sign” (red arrow), a finding characteristic of organizing pneumonia. Axial lung images of the upper C) and lower lobes D) after treatment with prednisone shows marked interval resolution of consolidations and ground glass opacities.
chest radiograph showed considerable improvement. Eventually, bronchoscopy with bronchoalveolar lavage (BAL) was able to be performed, showing an eosinophil count of 11%.
The patient was discharged home with a 4-week prednisone taper and plans to repeat his chest CT in 4 weeks with pulmonary follow-up. At this follow-up appointment, his repeat chest CT showed remarkable improvement as seen in Figure 1C and 1D
DISCUSSION
AEP remains an uncommon, potentially life-threatening condition that requires prompt recognition. Daptomycin is a rare trigger of AEP.
Daptomycin-induced AEP follows a particular criterion: known daptomycin exposure, fever, hypoxic respiratory failure, new opacities on chest radiography, bronchoalveolar lavage >25% eosinophils, and clinical improvement following the removal of daptomycin.1-4 Risk factors for development of the condition include male sex, chronic kidney disease, and receipt of at least 4 g of daptomycin in 4 weeks.5
Figure 1: Chest CT at admission and at 4-week follow-up.
The patient fit all of the risk factors for daptomycin-induced AEP. By the time of his admission, he had received approximately 10 g of daptomycin for methicillin-resistant S. aureus osteomyelitis. Additionally, he also fit the average age and sex consistent with previous literature reviews.
It is suspected that daptomycin binds to pulmonary surfactant, resulting in the release of IL-5 cytokines. This prompts the migration of eosinophils.6 While peripheral eosinophilia is seen in 77% of daptomycin-induced AEP cases,4 this patient was among the 23% that did not present with this particular lab finding. A lack of peripheral eosinophilia does not exclude the diagnosis of AEP.
References
1. Miller BA et al. Acute eosinophilic pneumonia secondary to daptomycin: a report of three cases. Clin Infect Dis. 2010;50(11):e63-8.
2. Rachid M et al. Daptomycin-induced acute eosinophilic pneumonia: late onset and quick recovery. Case Rep Pulmonol. 2017;DOI:10.1155/2017/8525789.
3. Storandt MH, Matta A. acute eosinophilic pneumonia: a rare complication of daptomycin therapy. Cureus. 2020;12(1):e6803.
4. Uppal P et al. Daptomycin-induced eosinophilic pneumonia - a systematic review. Antimicrob Resist Infect Control. 2015;5:55.
5. De Giacomi et al. Acute eosinophilic pneumonia. Causes, diagnosis, and management. Am J Respir Crit Care Med. 2018;197(6):728-36.
6. Silverman JA et al. Inhibition of daptomycin by pulmonary surfactant: in vitro modeling and clinical impact. J Infect Dis. 2005;191(12):2149-52.
Interviews
The AMJ is honored to present the following interviews with two distinguished leaders in their respective fields of respiratory medicine. Our first interview features Michael Boyle from the Cystic Fibrosis Foundation. Boyle's leadership and vision have been instrumental in transforming the landscape of cystic fibrosis research. Our second interview showcases the expertise of Julie Brahmer, Cancer Immunotherapy at Johns Hopkins University in Baltimore, a trailblazer in the field of cancer immunotherapy, with a particular focus on innovative treatments for lung cancer and other malignancies of the upper aerodigestive tract.
Featuring: Michael Boyle and Julie Brahmer
Michael Boyle President and Chief Executive Officer, Cystic Fibrosis Foundation, Bethesda, Maryland, USA
Readers of our Respiratory journal would recognize you as a vital figure in cystic fibrosis (CF) research and care. What led you to specialize in respiratory medicine, and specifically CF?
I originally went into adult respiratory medicine because of an interest in critical care, and I rarely encountered CF. All individuals with CF at Johns Hopkins Hospital, Baltimore, Maryland, USA, in the 1990s were taken care of by pediatricians. But one fortuitous morning, when I attended a pediatric CF clinic and met four young adults with CF, changed everything. All four were very ill, but I was taken by their bravery and absolute determination to live fulfilling lives, despite their disease and shortened life expectancy. I left clinic that day energized,
and wanting to learn more. I was next taken by CF science; the cystic fibrosis transmembrane conductance regulator (CFTR) gene had recently been discovered, and the concept of using small molecules to restore CFTR protein function was just starting to emerge. When I subsequently obtained my first research grant from the CF Foundation, I fully committed to a career focusing on CF. The combination of a growing number of adults with CF and exciting new therapeutic science made the timing perfect.
Q2
You founded the Johns Hopkins University Adult Cystic Fibrosis Program, which is now one of the largest in the country. Can you tell our readers about the initiation of this project, and the journey to where it is now?
As I mentioned earlier, all individuals with CF at Johns Hopkins in the 1990s were cared for by pediatricians, and the Pediatric Program was large and extremely well-run. However, a growing number of individuals with CF were living well into their 20s and 30s, and only having pediatric care didn’t seem appropriate. After spending 2 years training with the Johns Hopkins Pediatric CF Team in the mid-1990s, I hired a nurse and an administrative assistant, put 40 medical charts of adults with CF in a wheelchair, rolled them over to the adult hospital, and officially opened the Johns Hopkins Adult Cystic Fibrosis Program. Within a few years, the program had grown to over 300 patients, and had developed a very active research program, driven by a wonderful team of caregivers and researchers. Today, the program has four full-time adult CF physicianresearchers, and an entire multidisciplinary team devoted to adult CF care and research.
Q3In 2015, you left your full-time faculty role at Johns Hopkins to join the CF Foundation. What led to you to make this change?
I loved my work and team at Johns Hopkins; I had been there for 29 years, and fully expected to spend my full career there. At the same time, I was always immensely impressed by the impact that the CF Foundation had on every aspect of CF: research, care, training, advocacy, and community support. So, when they asked me to come and oversee their clinical research work, I decided that it was a unique opportunity to make a difference for thousands of individuals with CF worldwide, not just my own patients. Taking over as President and Chief Executive Officer of the CF Foundation in 2020 provided an additional great opportunity to serve people with CF, and the CF community worldwide. While I still do see patients once a month at Johns Hopkins, my full focus is
We’re focused on accelerating the development of therapies that will benefit all people living with the disease
now on curing CF, and continuing the Foundation’s long tradition of serving and supporting patients with CF, their families, and the science community.
Q4
How does the CF Foundation work to improve research and care in CF?
All our work is grounded in our mission: to cure CF and to provide all people who have the disease the opportunity to lead long, fulfilling lives, through funding research and drug development, partnering with the CF community, and advancing high-quality, specialized care.
People with CF and their families are at the center of our work
Since 2020, the CF Foundation has invested more than 1.5 billion USD to address the needs of individuals with CF today, while developing the CF therapeutics of tomorrow. These therapeutics include the breakthrough CFTR modulators, which address the underlying cause of the disease, transforming the lives of people with CF by improving lung function and slowing disease progression. It is important to remember, however, that modulators are not a cure, and that 10–15% of people with CF cannot benefit from them, because either their CF mutations won’t respond or because they cannot tolerate side effects.
This is why we’re focused on accelerating the development of therapies that will benefit all people living with the disease, no
matter what type of CF mutations they have. This work is the focus of our ‘Path to a Cure’ initiative, which has a 500 million USD initial commitment over 5 years, to attract the world’s best genetic technologies to focus on CF. We announced this initiative upon my starting as Chief Executive Officer. This work is also supported by our therapeutics development ecosystem, which includes funding research; cultivating a robust drug development pipeline; conducting clinical trials in the CF Therapeutics Development Network, the largest CF clinical trial network in the world; sharing data from our patient registry; and providing companies access to the CF Foundation Therapeutic Lab’s incubation space, in which they collaborate with our scientists and are able to tap into unique CF-specific resources. By funding early research, and providing meaningful support to researchers and companies at all stages of the drug development cycle, we’re bringing more people into CF research, and accelerating the development of new therapies.
The CF Foundation provides significant support for multidisciplinary care teams at more than 130 accredited CF care centers across the USA. These care teams partner closely with patients to address complications associated with CF, including infection, CF-related diabetes, gastrointestinal issues, advanced CF lung disease, and mental health issues. As the experience of living with CF evolves for many, we are working to determine the best way to continue to tailor this care model.
Q5
What are you most proud of achieving, with regards to CF care and treatment during your time at the CF Foundation?
Perhaps the thing that I am most proud of since joining the Foundation in 2015 is seeing how much the lives of people with CF have changed for the better, because of therapies that we have helped to develop. What started as a pediatric disease with short survival has been turned into a disease with more adults than children, and those adults are feeling better; they’re spending much less time in the hospital and taking medications, and are now more able to live fulfilling lives. But I am also proud that at the same time we celebrate this progress, we are more committed than ever before to developing therapies that will transform the lives of all people with CF, no matter what type of CF they have, and will lay the groundwork for a true cure for CF.
Q6
How do you incorporate community into your work at the CF Foundation?
People with CF and their families are at the center of our work, and are the driving force behind all our progress. With the CF population including more adults with CF than ever before, we have created a whole department at the Foundation dedicated to engaging with, listening to, and supporting individuals with CF. This department, appropriately called Community Partnerships, leads numerous programs that allow the CF community to directly inform our work, by partnering with us and advising on projects. Examples include patient-centered workgroups on research and care; our Adult Advisory Committee, which advises our Board; and Community Voice, a program for CF community members to inform, shape, and advance Foundation programs and research
prioritization. Community Voice currently has nearly 2,000 members.
The CF Foundation also supports the community through Compass, a personalized, one-on-one patient navigation service that partners with people living with CF and their families to deal with challenges related to life with CF. In addition, Compass identifies access issues, and helps to shape our federal and state policy work.
In 2022, our Board of Trustees elected KC White, an adult living with CF, as Chair of the Board of Trustees. This marks the first time in the Foundation’s history that an adult with CF has led the National Board of Trustees.
Q7
Which of the various research projects being conducted at the CF Foundation are you most passionate about, and how might this go on to change CF treatment?
CF is a complex disease, and while we have made incredible progress, developing a genetic therapy that can treat the underlying cause, no matter which CFTR mutations a person with CF has, will be our most challenging, and rewarding, work yet. For those who are not able to benefit from CFTR modulator medicines, there is an especially pressing urgency to move this work forward. That is why I am particularly passionate about the Path to a Cure work I mentioned earlier, a research initiative to deliver treatments for the underlying cause of the disease, and a cure for every person with CF by applying the world’s most innovative science to CF. This is done through funding research programs at leading and emerging biotech companies.
One other thing that I am particularly excited about is that the genetic technologies we have been working on for the last several years are now emerging from preclinical development, and moving into clinical trials. There are five different CF genetic therapies moving into clinical trials in the next 18 months, including three inhaled CFTR ribonucleic acid trials, two gene therapy trials, and one antisense oligonucleotide trial. These therapies that we once thought of as ‘someday’ are now on our doorstep.
A final project I must mention is our recent investment in Prime Medicine, Cambridge,
Massachusetts, USA, of up to 15 million USD to pursue gene editing for CF. This is one of the Foundation’s largest investments in CF gene editing, and we are especially excited about the Prime Medicine science. If successful, it would lay the groundwork for a permanent repair of the CFTR gene.
Q8
Taking into account all research being done at the CF Foundation, and new therapies being developed, which developments do you hope to see in the near future for CF care and research?
As much progress as there has been with CFTR modulators to date, the years ahead will lead to even better, next-generation CFTR modulators. These modulators will be able to restore CFTR function in people with CF to near wildtype levels and, when started early in life, will prevent many of the complications we currently take for granted as part of CF. This will include not only the prevention of lung disease, but also pancreatic insufficiency.
The next few years will also provide a great deal of insight into the potential for genetic therapies to benefit all people with CF, no matter the mutations they have. I have no doubt that we will eventually get there, but the question is, how quickly? I am confident that the combination of the expertise of the CF science community, with the passion and commitment of the patients with CF and their family and community, will keep the rate of progress brisk, and will result in not only treatment for all people with CF, but eventually a true cure for CF.
Co-director of the Upper Aerodigestive Department, Bloomberg~Kimmel Institute for Cancer Immunotherapy, Johns Hopkins University, Baltimore, Maryland, USA
What was it that initially inspired you to go into the field of thoracic oncology?
I was initially inspired due to my grandfather’s non-Hodgkin lymphoma diagnosis when I was in high school. I found the care of a patient with cancer fascinating, and it is amazing to be part of one of the hardest times in someone’s life, no matter the outcome. Once I finally entered into my medical oncology fellowship, years later, I gravitated to thoracic oncology, due to the need to improve treatment options for patients with lung cancer. At the time, 5-year survival in patients with advanced disease was not even talked about. My mentor, a titan in the field, opened many doors for me in order to become a driving force in the care of patients with lung cancer at Johns Hopkins University, Baltimore, Maryland, USA.
Q2
You advocate for a multidisciplinary approach in the field. In what ways are you ensuring your research and practice reflects this, and what are the advantages?
Q3
You serve as a board member in multiple thoracic oncology associations and research foundations. Do you think this has granted you any opportunities in your career, and how have you utilised these positions?
Being involved in thoracic professional societies and patient advocacy groups has enabled me to help increase the awareness that lung cancer deserves increased research, funding, and support. I also get the chance to mentor other professionals, to advocate for their work and career growth
Q4
As one of the investigators on the Phase I trial of the PD-1 blocking antibody nivolumab, which went on to change immunotherapy, what did it feel like to see the treatment you had been working on impact medicine so significantly? What was the process like?
It is amazing to be part of one of the hardest times in someone’s life, no matter the outcome
I advocate for a multidisciplinary approach to patient care and research for many reasons. We are learning that more and more patients with cancer require the multiple disciplines to co-ordinate care during their cancer journey. Also, in order to truly advance the field, all disciplines are important in order to really implement research discoveries.
Being part of the development of PD-1 pathway antibodies was an amazing experience. My dream was to be part of the drug development of something significant in the cancer field. Little did I know what power these antibodies would have, and how many cancers could be controlled with these drugs. As someone who has been trained in drug development, I enjoy being part of first-in-human trials, where we give drugs coming out of the lab to patients for the first time. There is such a learning curve. Then, to see this type of drug elicit tumor responses in patients, particularly in
Julie Brahmer
cancers not felt to even be immune responsive, was amazing.
I was also proud to advocate for the development in lung cancer, which was once thought not to be immune responsive. Phase III trials have demonstrated the power of this pathway blockade, which can cause significant lung cancer shrinkage and control. What a huge win for our patients! We have patients who typically would not live very long, but now are living for years after treatment with antiPD-1 antibodies. However, there is so much more work to do in order to increase response, and combat resistance.
Q5 Have you continued your work on analysing the efficacy of nivolumab since the initial trials?
Our team at Johns Hopkins, and within the thoracic oncology community, has focused on how,
and why, drugs like nivolumab work, or do not work. Obviously, this is a very complex problem that is multifaceted. We are looking at the host immune system, gut microbiome, tumor microenvironment, and genome, which all play a part in the response and resistance to immunotherapy.
This is a very complex problem that is multifaceted
Q6 Which clinical trials, currently underway in the field of immunotherapy for lung cancer, are you most excited about?
There are many trials of immunotherapy ongoing for patients with lung cancer. I am excited about immunotherapy
In order to truly advance the field all disciplines are important, in order to really implement research discoveries
continuing to be developed in the early-stage treatment prior to surgery, where we can learn so much about the patient, cancer and drug interactions, and how to capitalize on that. Also, I am excited about bispecific antibodies that can block immune checkpoint pathways, and also potentially bring T cells into the tumor to have an effect. I think these molecules will have the power to treat, and bring immunotherapy to, more patients with lung cancer whose cancer may not otherwise respond to these treatments.
Q7
Do you think there is a place for artificial intelligence (AI) or deep learning models yet in the treatment of lung cancer and mesothelioma?
AI and deep learning will revolutionize cancer care, improve day-to-day care, and recognize patterns in patients to improve care. Also, AI and deep learning will help us take into account more precise data regarding patients’ tumors, and allow us to tailor therapy to those changes/genomics, etc.
Q8 What is next for you in the world of lung cancer immunotherapy?
That is a great question. I want to continue to work with our team at Johns Hopkins to improve care for our patients, which can be translated into meaningful improvements in long-term survival and quality of life, and broaden the application of immunotherapy to more patients. I also want to continue to mentor early career investigators and faculty, to ensure we foster future research focus on thoracic oncology.
If you like it,why not share it...
Share with a colleague today
Nebulization and Viral Spread: Knowns and Unknowns in
The publication of this infographic was supported by an Independent Medical Education Grant from Viatris and Theravance Biopharma. Respir AMJ. 2024;2[1]:50-51. https://doi.org/10.33590/respiramj/BAAZ9654.
Why is nebulizer use important?
• To deliver medications to people with acute and chronic respiratory/ pulmonary conditions1,2
• For patients who cannot use an inhaler or where a drug formulation requires nebulization3
Aerosol terminology4
Bioaerosol
• Generated by patients coughing, breathing, talking, and laughing
• Can contain infectious agents
During the COVID-19 pandemic, discordant advice from professional bodies around whether nebulization was an AGP led to preferences for, but then deficits in, other delivery systems such as pMDIs and DPIs5,6
Nebulization clearly not classed as an AGP
International Society of Aerosols in Medicine7
• No evidence that nebulizer use increases infective load of bioaerosols
Uncertain classification of nebulization as an AGP
Centers for Disease Control and Prevention
• UNCERTAIN whether aerosols from nebulizer use are infectious8
• Recommended continuing nebulizer use during COVID-19 pandemic but with AGP precautions (PPE)9
World Health Organization10
• Nebulization NOT classed as AGP but sputum induced by ‘nebulized hypertonic saline’ is
Global Initiative for COPD11
• Risk of exhaling contaminated aerosol/droplets if coughing during nebulizer use, so where possible, use inhalers
American Association for Respiratory Care12
• Nebulizer use ‘may increase transfer of particles into environment’
Medical aerosol
• Generated by aerosol devices
• Does not contain infectious agents
Fugitive emissions
• Medical aerosols + bioaerosols released during nebulizing
• Can contain infectious agents
Key:
• Use pMDIs to deliver bronchodilators
European Centre for Disease Prevention and Control13
• Infection risk linked to nebulizer use unclear so no AGP classification consensus
Nebulization clearly classed as an AGP
Global Initiative for Asthma2
• Nebulizers transmit respiratory viral particles at least 1 m so follow strict infection control procedures if nebulizer needed where COVID-19 possible
Surviving Sepsis Campaign14
• Nebulization categorised as AGP; use appropriate PPE
Spanish Multidisciplinary Group15
• Nebulization is an AGP with higher risk of COVID-19 transmission
AGP: aerosol-generating procedure; CDC: Centers for Disease Control and Prevention; CNC: COPD Foundation Nebulizer Consortium; COPD: chronic obstructive pulmonary disease; COVID: coronavirus disease; DPI: dry-powder inhaler; HCP: healthcare professional; MERS: Middle East respiratory syndrome; PCR: polymerase chain reaction; pMDI: pressurised metered-dose inhalers; PPE: personal protective equipment; SARS: severe acute respiratory syndrome; SARS-CoV-2: severe acute respiratory syndrome-covariant-2; WHO: World Health Organization.
The COPD Foundation Nebulizer advocates) was formed in 2020 solutions that ensure patient,
CNC conclusions and advice:
• Current evidence ‘insufficient
• Most published literature is inconclusive relationships between nebulizer
1. Biney IN et al. Guidance on mitigating the risk of transmitting respiratory infections during nebulization by the COPD Foundation Nebulizer Consortium. Chest. 2024;165(3):653-68.
2. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention. 2023. Available at: https://ginasthma.org/wp-content/uploads/2023/07/ GINA-2023-Full-report-23_07_06-WMS.pdf. Last accessed: 13 June 2024.
3. Ari A et al. Treating COPD patients with inhaled medications in the era of COVID-19 and beyond: Options and rationales for patients at home. Int J Chron Obstruct Pulmon Dis. 2021;16:2687-95.
4. Ari A. Practical strategies for a safe and effective delivery of aerosolized medications to patients with COVID-19. Respir Med. 2020;167:105987.
6. American Association for Respiratory Available at: https://www.aarc.org/wp-content/uploads/2020/03/guidancedocument-SARS-COVID19.pdf.
7. Fink JB, et al. Reducing aerosol-related An interim guidance endorsed Aerosol Med Pulm Drug Deliv.
5. Peeler KR, Ratzan RM (eds.), Voices from the front lines: The pandemic and the humanities (2022), San Francisco:
the Healthcare Setting
Nebulizer Consortium (CNC) (including HCPs, professional societies, industry partners, and patient 2020 to improve understanding of potential nebulization-associated infection risks and develop patient, caregiver, and HCP safety.1
The CNC examined whether studies showed that drug delivery by nebulization was an AGP and if nebulization increases infection transmission
• Neither the CDC nor WHO consider current evidence sufficient to class nebulizer therapy as an AGP associated with COVID-19 transmission8,10
• Contamination of medical aerosol in lungs was not found to be supported by evidence7
• Some studies examined suggested increased infection risk during nebulization, others did not1, 17
• A 2024 Italian study of 11 patients with COVID-19 receiving 0.9% saline nebulization did not show increased SARS-CoV-2 spread17
• Increased infection risk might be through increased HCP/ caregiver and patient contact time during nebulization8
• In a 2024 USA study of 11 patients hospitalized with COVID-19, MDI and nebulizer delivery did not impact the viral load levels or dispersion of virus inpatient rooms17
Scientific limitations in studies examined by the CNC included:
Small HCP numbers
Variable PPE usage
No differentiation between AGPs
Particle size limitations for air sampling
HCP interaction with COVID-19 prior to testing positive
Lack of virus viability verification as detection through PCR only
Different nebulizer types
Data for SARS/MERS outbreaks
advice:1
to classify nebulized therapy as an AGP’ inconclusive or did not substantiate direct nebulizer therapy and infection transmission discouraged when clinically indicated safety measures observational studies with microscopic analysis of needed to better understand aerosol science and presents additional infection risk
Francisco: UC Health Humanities Press. Respiratory Care. SARS CoV-2. Guidance document. https://www.aarc.org/wp-content/uploads/2020/03/guidanceLast accessed: 13 June 2024.
aerosol-related risk of transmission in the era of COVID-19: by the International Society of Aerosols in Medicine. J 2020;33(6):300-4. and Prevention. Interim infection prevention and control healthcare personnel during the coronavirus disease 2019 Available at: https://www.cdc.gov/coronavirus/2019-ncov/ hcp/infection-control-recommendations.html#print. Published 2024. Last accessed: Transmission of COVID-19 to health care personnel during patient - Solano County, California, February 2020. MMWR Morb Mortal Wkly Rep. 2020;69(15):472-6.
Key messages1-3
• Nebulization should not be discouraged when clinically indicated
• It is an important route of administration, especially for patients with dexterity issues, cognitive impairment, or low inspiratory flow
• PPE use should be emphasized
10. World Health Organization. Infection prevention and control in the context of coronavirus disease (COVID-19): A living guideline. Available at: https://iris.who. int/bitstream/handle/10665/372250/WHO-2019-nCoV-IPC-guideline-2023.2-eng. pdf?sequence=1. Published 2023. Last accessed: 13 June 2024.
11. Global Initiative for Chronic Obstructive Pulmonary Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Available at: https://goldcopd.org/wp-content/uploads/2024/02/GOLD-2024_v1.211Jan24_WMV.pdf. Published 2024. Last accessed: 13 June 2024.
CC BY-NC 4.0 Licence
12. American Association of Respiratory Care. SARS CoV-2. Guidance document. Available at: https://www.aarc.org/wp-content/uploads/2020/03/guidance-document-SARSCOVID19.pdf. Published 2020. Last accessed: 13 June 2024.
Copyright
13. European Centre for Disease Prevention and Control. Infection prevention and control and preparedness for COVID-19 in healthcare settings. Sixth update.
Available at: https://www.ecdc.europa.eu/sites/default/files/documents/Infectionprevention-and-control-in-healthcare-settings-COVID-19_6th_update_9_Feb_2021. pdf. Published 2021. Last accessed: 13 June 2024.
14. Alhazzani W et al. Surviving Sepsis Campaign: Guidelines on the management of critically ill adults with Coronavirus Disease 2019 (COVID-19). Intensive Care Med. 2020;46(5):854-87.
15. Luján M et al. Multidisciplinary consensus on the management of non-invasive respiratory support in the COVID-19 patient. Archivos de Bronconeumología. 2024;60(5):285-95.
16. Buttini F et al. Effects of saline nebulization on SARS-CoV-2 RNA spreading and exhaled bioaerosol particles in COVID-19 patients. J Hosp Infect. 2024;145:77-82.
17. B Clemency et al. Impact of nebulization versus metered-dose inhaler utilization on viral particle dispersion in patients with COVID-19. J Infect Prev. (In press).
Sex Differences in Exercise-Induced Effects on Respiratory Infection and Immune Function
Authors: Daniel E. Rodriguez Bauza,1 *Patricia Silveyra2
1. Department of Family Medicine, Conemaugh Memorial Medical Center, Johnstown, Pennsylvania, USA
2. Department of Environmental and Occupational Health, Indiana University Bloomington, School of Public Health, USA *Correspondence to psilveyr@iu.edu
Disclosure: The authors have declared no conflicts of interest.
A physically active lifestyle has health benefits, including enhanced vaccination responses, improved neutrophil and macrophage function, increased T cell proliferative capacity, lower numbers of senescent T cells, and lower levels of inflammatory cytokines. Therefore, exercise or physical activity is effective for preventing and treating chronic diseases. A more robust immune response is generally thought to be exerted in females than males in response to various challenges. Sex hormones in both sexes have been suggested as mediators of immune function, but research on this topic has not been designed with a sex-specific lens. The authors reviewed and summarized the experimental and clinical evidence in the available literature linking exercise, immune function, and risk of upper respiratory infections, as well as associated mechanisms. Collectively, the available literature indicates that moderate exercise improves immune function and risk for upper respiratory infections in both sexes. In contrast, prolonged and high-intensity exercise temporarily impairs immune responses and upper respiratory infection risk at a higher degree in females than males. Therefore, moderate exercise and activity may enhance immune function regardless of sex, whereas prolonged and high-intensity exercise temporarily impairs immune responses, predominantly in females more than their male counterparts.
Key Points
1. For far too long, the study of exercise and its effects on the immune system has overlooked a crucial factor: sex. This article delves into this critical gap by investigating sex-specific responses to exercise in the context of respiratory infections and immune function, a topic with far-reaching implications for public health, and personalized exercise guidelines.
2. This article reviews experimental and clinical evidence available in the literature, revealing how exercise interacts with the immune response to infection in a sex-specific manner.
3. Prolonged and high-intensity exercise temporarily impairs immune responses and increases the incidence of respiratory infections, with more predominant effects in female than male subjects. Therefore, sex-specific personalized interventions that optimize immune benefits, and minimize infection risk, should be implemented to improve public health outcomes.
INTRODUCTION
Physical activity is an efficient drug-free strategy which has been associated with multiple health benefits, including mental and physical health, in subjects from both sexes.1 More than 100 years ago, Larrabee2 observed a marked leukocytosis after violent exercise, including many polymorphonuclear neutrophils. Since then, research on exerciseinduced effects on the immune system has advanced tremendously, and reports about positive effects on health, particularly in delaying disease-related mortality, have flourished.3 Studies conducted in patients of all ages, but particularly middle-aged and older adults, have consistently shown that physical activity delays cellular aging (e.g., telomere length, immunosenescence), and reduces the risk of metabolic, respiratory, and cardiovascular disease.4,5 Overall, the practice of regular exercise has been associated with changes in immune profiles, resulting in lower inflammatory states, improved mitochondrial function, and enhanced innate and adaptive immune responses.6,7
Many factors in males and females, including sex hormones and their receptors, regulate immune system function, immune cell profiles, and response to immune challenges.8-13 Generally speaking, females have been reported to have stronger immune responses than males.14 Furthermore, female sex hormones such as estrogen, progesterone, and chorionic gonadotropin have been shown to modulate function, differentiation, and both cytokine and antibody production in various immune cells, including monocytes, dendritic cells, and lymphocytes, across the life span.15-18
On the other hand, dominant male gonadal hormones, such as testosterone, also play important roles in regulating immune responses.19
The available literature on this topic suggests that the immune system’s response to exercise strongly depends on the duration and intensity of the physical activity performed, and involves changes in multiple immune cells. This idea has taken root in the scientific literature, to an extent by which aerobic exercise, particularly moderateintensity exercise, can be beneficial for the immune system, but vigorous and prolonged exercise, on the other hand, can interfere with immunocompetence. The current study explores these scenarios in the context of male- and female-specific responses.
Here, the authors focus on acute respiratory illness, which is one of the leading causes of global morbidity. Before the COVID-19 pandemic, the incidence of upper respiratory infections reached 17.2 billion people in 2019, accounting for 42.83% of cases from all causes globally. The average adult has approximately one to six colds yearly.20 Therefore, in this review, the authors aim to provide updated and concise information on the impact of exercise on respiratory infection as immune responses to moderate and vigorous exercise, with a lens to specific sex differences.
MATERIALS AND METHODS
Databases and Key Terms Searched
The authors used both Google Scholar
and PubMed databases to identify eligible papers in their search. They used the following search terms and logic to select articles: physical activity OR exercise AND exercise-induced immune response AND immune response OR sex differences AND sex hormones OR male OR female.
Inclusion Criteria
The authors conducted the search without limit of the year of publication, limited to papers written in English. The final search was updated to November 2023. Articles were selected if they assessed the effects of moderate-intensity exercise (30–45 min/day) or vigorous exercise (endurancetrained athletes) on the immune system, through the incidence of acute respiratory illness, including study populations of 18–65 years old of both sexes. Upper respiratory tract infection (URTI) incidence was assessed by self-reporting (using health logs), or diagnosis reported by a physician.
Search Process and Study Selection
All articles were selected based on the search criteria. Articles were de-duplicated using built-in mechanisms of the authors’ university’s library services, and assessed by their titles and abstracts for inclusion. Final selections were determined after thoroughly reading the articles’ methodological design, methods, risk for bias, and data analysis, to meet the authors’ inclusion criteria and answer their research questions, as well as by the ability of the results presented to be generalized for all selected studies. To minimize bias, all articles were reviewed independently by each author following the inclusion and exclusion criteria explicitly, which were established prior to the search process and study selection.
Data Extraction and Organization
The information extracted from the studies was as follows: the first author of the study, the year of publication, the study design
and/or details of the intervention, the sample size (number and/or percentage of population), and the study’s critical outcomes. Upon review of the information presented, articles were categorized and organized in tables according to the reported response to moderate-intensity or vigorous exercise. No statistical analyses were conducted as part of this process.
RESULTS
Search Results
A total of 984 studies (Figure 1) were identified using the aforementioned key terms searched, of which 132 were duplicates. Of the remaining 852 studies, 759 had irrelevant study design or settings, or did not explicitly define the sample size or interventions, and were excluded. The full text of the remaining 93 articles was reviewed. The final selection, excluding studies that did not meet the inclusion criteria, comprised 32 articles. These were subsequently divided into articles studying moderate-intensity exercise (10 articles, listed in Supplementary Table 1) versus vigorous exercise (23 articles, listed in Supplementary Table 2).
Effects of Moderate Physical Activity Intensity on Immune Responses in Female and Male Subjects
The literature review identified 10 publications linking moderate-intensity exercise with immune response and URTI outcomes. The moderate-intensity exercise studies consisted of brisk walking, stretching, jogging, or mild aerobic exercise, and the main results, study design, participant information, and study goals are summarized in Supplementary Table 1. The authors identified four studies including only female participants,21-24 six papers that included both male and female subjects,25-30 and zero studies that included only males. Overall, enrolment of subjects ranged from 32–1,509 for the selected studies. The combined total of participants from all studies was
1: Summary of literature search and article selection.
Potentially relevant articles through database searching (n=984)
Records after duplicates removed (n=852)
759 studies irrelevant
Records after screened by title and abstract (n= 93)
Records included after full-text review (n=32)
Moderateintensity exercise (n=10)
Vigorous exercise (n=22)
5,284 (including 3,442 females and 1,842 males), and 0.93% (n=32) to 23% (n=791) were female participants. Interestingly, in all studies enrolling only females, it was reported that moderate physical activity was associated with lower rates of URTI. Also, in all four studies that included females, subjects were sedentary, overweight, or obese. Only one study that compared the effect in highly conditioned females found a reduced effect in this group versus the sedentary group.22
On the other hand, the studies that enrolled participants from both sexes found that moderate-intensity physical activity was associated with solid reductions in URTIs, and
fewer symptomatic days when compared with subjects that were sedentary. Unfortunately, while these studies included subjects of both sexes, comparisons between effects in males and females were not provided, except for one study that showed a more substantial effect in females than males in reducing URTIs.28
Effects of Vigorous Physical Activity Intensity on Immune Responses in Females and Males
The literature review identified 22 publications linking vigorous exercise (e.g., long-distance running, swimming, endurance training, triathlon, track and field, athletics, Olympic sports, and cross-
Figure
country skiing) and immune-related outcomes (Supplementary Table 2). Of these, five studies did not report the sex of the participants,31-35 whereas the remaining 17 studies enrolled both sexes.36-45 These studies enrolled a range of participants, from as low as 20 to as much as 11,274 subjects, of whom 0.12–26.00% were female. Interestingly, participants engaging in vigorous exercise displayed an increased incidence of illness compared to controls. For example, during periods of heavy training, or after a race, marathon runners had higher rates of infectious episodes. In these associations, female sex was recognized as a risk factor for athletes, as illness incidence was higher in females in nine studies that compared effects in both sexes.39,42-49
DISCUSSION
An extensive volume of peer-reviewed studies in exercise immunology has established links between immune function and exercise.50 High levels of physical activity have sometimes been associated with decreased circulating sex hormones in pre- and postmenopausal females, and alterations in susceptibility to infection and disease.51,52 Hence, it is evident that biological sex plays a vital role as an essential immune response modulator. Sex hormones, including estrogens, can act as enhancers of humoral immunity, and androgens and progesterone (and glucocorticoids) can act as natural immunosuppressants.53 Therefore, it was not surprising to find that multiple studies had identified sex differences in immune responses in both exercising and nonexercising conditions.54,55
In the current study, the authors sought to identify sex differences in the effects that various exercise modalities exert on immune responses, particularly on the association of URTI incidence, by reviewing the available literature in the topic. Overall, the authors confirmed that multiple studies conducted in the field are not designed or powered to test for sex as a biological variable, nor attempted
to evaluate the contributions of sex hormones to measured outcomes. However, the authors’ literature search identified many effects of exercise on immune function that appear to correlate with the intensity of the bouts of exercise, and modulated by sex.
The search revealed that, regardless of sex, individuals engaging in moderate-intensity exercise displayed fewer episodes of URTIs, and experienced fewer days with symptoms when compared to subjects who were sedentary. Moderate-intensity exercise was associated with an improvement in immune function in individuals who were previously sedentary. It is important to note that most of the studies reviewed here did not account for the sex variable in the design, analysis, or data reporting. Only one study indicated a higher incidence of URTIs in female subjects, when compared to males, although this effect was mild.28 Together, the available literature supports the notion that moderate exercise is beneficial to prevent infection and improve immunity in both male and female individuals.
In contrast, when reviewing the literature on vigorous exercise and its effects on immune function, and incidence of URTIs, the authors repetitively found that different forms of intense and vigorous exercise were reported to exert a negative effect on the immune system’s phenotypic makeup and functional capacity. In most cases, it was found that both URTIs and symptomatic days were higher in individuals involved in vigorous exercise, as shown in Supplementary Table 2. Interestingly, studies incorporating both male and female individuals reported that females displayed a higher incidence of illness in most studies, indicating that female sex represents an additional risk factor for the negative effect of intense exercise. Despite these findings, most studies were not designed to detect sex-specific effects, or disaggregate all data by sex. Thus, it is essential to emphasize that future work should follow the guidelines for Sex and Gender Equity in Research (SAGER) in the design, analysis, and reporting of findings.56
In sum, the available literature in this topic indicates that both the duration and intensity of exercise may affect the immune system’s response to infection, and that these effects may be influenced by fitness level and circulating sex hormone levels. This work suggests a modulatory crosstalk of female sex hormones and exercise-induced physiological responses. However, many of these studies have significant limitations, because both sex differences and the role of sex hormones were not elaborated on, or investigated, or because the geographic scope of participants differed across studies, and was more global in studies assessing vigorous exercise than moderate exercise. Despite this, the present study has solid implications for public health, as athletes, who are often considered healthier than the average population, are more prone to infection due to immune system alterations that occur during, and after, periods of heavy training. The current literature review confirms this, and indicates that female sex represents a risk factor in multiple exercise modalities and populations. Hence, medical personnel, coaches, and athletes must be aware of the increased risk of illness during vigorous exercise, particularly in females.
While the current study provides a comprehensive assessment of the relationship between exercise and immunity, it also has several limitations. First, while the reports reviewed were conducted in different countries, most studies investigating moderate exercise effects on immune function were conducted in the USA. In contrast, studies investigating vigorous exercise were conducted in multiple countries. Second, this study focuses on studies addressing the effects of URTIs in professional athletes,
References
1. Scheffer DDL, Latini A. Exercise-induced immune system response: antiinflammatory status on pe-ripheral and central organs. Biochim Biophys Acta Mol Basis Dis. 2020;1866(10):165823.
2. Larrabee RC. Leucocytosis after violent
which may limit its generalizability to other populations. Finally, information about participants’ BMI, medication use, and other medical conditions was only sometimes available in the studies consulted. This limited the authors’ ability to assess their impact on the effects reported in males and females. Clinically, this manuscript is relevant, as it confirms that there is solid evidence for the effectiveness of moderate physical activity in supporting the immune system, especially in previously sedentary people, but also found an increased risk of URTIs in females compared to males, in those who partake in vigorous exercise. Therefore, clinicians who care for females need to be aware of these findings to develop individualized exercise training programs. The authors also encourage further research on the underlying factors and potential roles of sex hormones in immunity and respiratory infection risk.
Overall, the body of literature summarized in the current study suggests that promoting training programs with increased lowto-moderate intensity training volumes, and ensuring sufficient rest and recovery, may help maintain immune health, and decrease the incidence of infection. More research must be done to fully elucidate the contributions of sex-specific factors to these outcomes, and the mechanisms underlying sex-specific immune responses to exercise. In conclusion, the available literature suggests that moderate exercise may enhance immune function, regardless of sex. In contrast, both prolonged and highintensity exercise regimes are associated with temporary impairment of immune responses, with more predominant effects in female than male subjects.
exercise. J Med Res. Jan 1902;7(1):7682.
3. Garber CE et al. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently
healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43(7):1334-59.
4. Duggal NA et al. Can physical activity ameliorate immunosenescence and thereby reduce age-related multi-morbidity? Nat Rev Immunol. 2019;19(9):563-72.
5. Arsenis NC et al. Physical activity and telomere length: impact of aging and potential mechanisms of action. Oncotarget. 2017;8(27):45008-19.
6. Lippi L et al. Impact of exercise training on muscle mitochondria modifications in older adults: a systematic review of randomized controlled trials. Aging Clin Exp Res. 2022;34(7):1495-1510.
7. Khakroo Abkenar I et al. The effects of acute and chronic aerobic activity on the signaling pathway of the inflammasome NLRP3 complex in young men. Medicina (Kaunas). 2019;55(4):105.
8. Reyes-García J et al. Sex hormones and lung inflammation. Adv Exp Med Biol. 2021;1304:259-321
9. Laffont S et al. Estrogen receptordependent regulation of dendritic cell development and function. Front Immunol. 2017;8:108.
10. Kovats S. Estrogen receptors regulate innate immune cells and signaling pathways. Cell Immunol. 2015;294(2):63-9.
11. Lang TJ. Estrogen as an immunomodulator. Clin Immunol. 2004;113(3):224-30.
12. Kadel S, Kovats S. Sex hormones regulate innate immune cells and promote sex differences in respiratory virus infection. Front Immunol. 2018;9:1653.
13. Moulton VR. Sex hormones in acquired immunity and autoimmune disease. Front Immunol. 2018;9:2279.
14. Libert C et al. The X chromosome in immune functions: when a chromosome makes the difference. Nat Rev Immunol. 2010;10(8):594-604.
15. Umair M et al. Biological sex as a critical variable in CD4+ effector T cell function in preclinical models of multiple sclerosis. Antioxid Redox Signal. 2022;37(1-3):135-49.
16. Chiarella SE et al. Sex, cells, and asthma. Mayo Clin Proc. 2021;96(7):1955-69.
17. Markle JG, Fish EN. SeXX matters in immunity. Trends Immunol. 2014;35(3):97-104.
18. Cunningham M, Gilkeson G. Estrogen receptors in immunity and autoimmunity. Clin Rev Allergy Immunol. 2011;40(1):66-73.
19. Lee T-P, Chiang B-L. Sex differences in spontaneous versus induced animal models of autoimmunity. Autoimmun Rev. 2012;11(6-7):A422-9.
20. Jin X et al. Global burden of upper respiratory infections in 204 countries and territories, from 1990 to 2019. EClinicalMedicine. 2021;37:100986.
21. Nieman DC et al. The effects of moderate exercise training on natural killer cells and acute upper respiratory tract infections. Int J Sports Med. 1990;11(6):467-73.
22. Nieman DC et al. Physical activity and immune function in elderly women. Med Sci Sports Exerc. 1993;25(7):823-31.
23. Nieman DC et al. Immune response to exercise training and/or energy restriction in obese women. Med Sci Sports Exerc. 1998;30(5):679-86.
24. Chubak J et al. Moderate-intensity exercise reduces the incidence of colds among postmenopausal women. Am J Med. 2006;119(11):937-42.
25. Barrett B et al. Meditation or exercise for preventing acute respiratory infection: a randomized controlled trial. Ann Fam Med. 2012;10(4):337-46.
26. Barrett B et al. Meditation or exercise for preventing acute respiratory infection (MEPARI-2): a randomized controlled trial. PLoS One. 2018;13(6):e0197778.
27. Fondell E et al. Physical activity, stress, and self-reported upper respiratory tract infection. Med Sci Sports Exerc. 2011;43(2):272-9.
28. Matthews CE et al. Moderate to vigorous physical activity and risk of upper-respiratory tract infection. Med Sci Sports Exerc. 2002;34(8):1242-8.
29. Zhou G et al. Smoking, leisure-time exercise and frequency of self-reported common cold among the general population in northeastern China: a cross-sectional study. BMC Public Health. 2018;18(1):294.
30. Nieman DC et al. Upper respiratory tract infection is reduced in physically fit and active adults. Br J Sports Med. 2011;45(12):987-92.
31. Peters EM, Bateman ED. Ultramarathon running and upper respiratory tract infections. An epidemio-logical survey. S Afr Med J. 1983;64(15):582-4.
32. Raysmith BP, Drew MK. Performance success or failure is influenced by weeks lost to injury and illness in elite Australian track and field athletes: a 5-year prospective study. J Sci Med Sport. 2016;19(10):778-83.
33. König D et al. Upper respiratory tract infection in athletes: influence of lifestyle, type of sport, training effort, and immunostimulant intake. Exerc Immunol Rev. 2000;6:102-20.
34. Rama L et al. Changes in natural killer cell subpopulations over a winter training season in elite swimmers. Eur J Appl Physiol. 2013;113(4):859-68.
35. Hellard P et al. Training-related risk of common illnesses in elite swimmers over a 4-yr period. Med Sci Sports Exerc. 2015;47(4):698-707.
36. Nieman DC et al. Infectious episodes in runners before and after the Los Angeles Marathon. J Sports Med Phys Fitness. 1990;30(3):316-28.
37. Heath GW et al. Exercise and the incidence of upper respiratory tract infections. Med Sci Sports Exerc. 1991;23(2):152-7.
38. Alonso JM et al. Determination of future prevention strategies in elite track and field: analysis of Daegu 2011 IAAF Championships injuries and illnesses surveillance. Br J Sports Med. 2012;46(7):505-14.
39. Timpka T et al. Preparticipation predictors for championship injury and illness: cohort study at the Beijing 2015 International Association of Athletics Federations World Championships. Br J Sports Med. 2017;51(4):271-6.
40. Alonso JM et al. Occurrence of injuries and illnesses during the 2009 IAAF World Athletics Championships. Br J Sports Med. 2010;44(15):1100-5.
41. Gleeson M et al. Influence of training load on upper respiratory tract infection incidence and antigen-stimulated cytokine production. Scand J Med Sci Sports. 2013;23(4):451-7.
42. Soligard T et al. Sports injuries and illnesses in the Sochi 2014 Olympic Winter Games. Br J Sports Med. 2015;49(7):441-7.
43. Palmer-Green D, Elliott N. Sports injury and illness epidemiology: Great Britain Olympic Team (TeamGB) surveillance during the Sochi 2014 Winter Olympic Games. Br J Sports Med. 2015;49(1):259.
44. Engebretsen L et al. Sports injuries and illnesses during the London Summer Olympic Games 2012. Br J Sports Med. 2013;47(7):407-14.
45. Soligard T et al. Sports injury and illness incidence in the Rio de Janeiro 2016 Olympic Summer Games: a prospective study of 11274 athletes from 207 countries. Br J Sports Med. 2017;51(17):1265-71.
46. Drew M et al. Prevalence of illness, poor mental health and sleep quality and low energy availability prior to the 2016 Summer Olympic Games. Br J Sports Med. 2018;52(1):47-53.
47. Mountjoy M et al. Competing with injuries: injuries prior to and during the 15th FINA World Cham-pionships 2013 (aquatics). Br J Sports Med. 2015;49(1):37-43.
48. Mountjoy M et al. Sports injuries and illnesses in the 2009 FINA World Championships (Aquatics). Br J Sports Med. 2010;44(7):522-7.
49. Engebretsen L et al. Sports injuries and illnesses during the Winter Olympic Games 2010. Br J Sports Med. 2010;44(11):772-80.
50. Simpson RJ et al. Exercise and the regulation of immune functions. Prog Mol Biol Transl Sci. 2015;135:355-80.
51. Bertone-Johnson ER et al. Recreational physical activity and steroid hormone
levels in postmenopausal women. Am J Epidemiol. 2009;170(9):1095-104.
52. Jasienska G et al. Habitual physical activity and estradiol levels in women of reproductive age. Eur J Cancer Prev. 2006;15(5):439-45.
53. Bouman A et al. Sex hormones and the immune response in humans. Hum Reprod Update. 2005;11(4):411-23.
54. Bird MD et al. Sex differences and estrogen modulation of the cellular immune response after injury. Cell Immunol. 2008;252(1-2):57-67.
55. Bouman A et al. Gender difference in the non-specific and specific immune response in humans. Am J Reprod Immunol. 2004;52(1):19-26.
56. Heidari S et al. Sex and gender equity
in research: rationale for the SAGER guidelines and recom-mended use. Res Integr Peer Rev. 2016;1:2.
57. Prien A et al. Injury and illness in aquatic sport: how high is the risk? A comparison of results from three FINA World Championships. Br J Sports Med. 2017;51(4):277-82.
58. Spence L et al. Incidence, etiology, and symptomatology of upper respiratory illness in elite athletes. Med Sci Sports Exerc. 2007;39(4):577-86.
59. Svendsen IS et al. Effect of an intense period of competition on race performance and self-reported illness in elite cross-country skiers. Scand J Med Sci Sports. 2015;25(6):846-53.
High Frequency of Cystic FibrosisRelated Endocrinopathies in a Population of Colombian Children: A Cross-Sectional Study
Authors: Susana Gómez Rojas,1 María del Pilar Pereira Gómez,1 Nora Alejandra Zuluaga Espinosa,2 Adriana Carolina Forero Torres,2 Olga Lucia Morales Múnera,3 Silvia Palacio Petri,3 Laura Fernanda Niño Serna,4 *Carlos E. Rodriguez-Martinez5,6
1. Department of Pediatric Endocrinology, School of Medicine, Universidad de Antioquia, Medellín, Colombia
2. Department of Pediatric Endocrinology, Universidad de Antioquia, Hospital San Vicente Fundación, Medellín, Colombia
3. Department of Pediatric Pulmonology, Universidad de Antioquia, Hospital San Vicente Fundación, Medellín, Colombia
4. Department of Pediatrics, Hospital Pablo Tobón Uribe, Medellín, Antioquia, Colombia
5. Department of Pediatrics, School of Medicine, Universidad Nacional de Colombia, Bogota, Colombia
6. Department of Pediatric Pulmonology, School of Medicine, Universidad El Bosque, Bogota, Colombia
*Correspondence to carerodriguezmar@unal.edu.co.
Disclosure: The authors have declared no conflicts of interest.
Received: 01.17.24
Accepted: 05.14.24
Keywords: Cystic fibrosis (CF), endocrine system diseases, morbidity, quality of life, vitamin D deficiency.
Objective: The median length of survival for cystic fibrosis (CF) has significantly increased in recent years; however, this means that endocrine complications are more frequently observed in affected patients. This research was aimed at evaluating the frequency, clinical and paraclinical features, and the treatment of linear growth and pubertal disturbances, vitamin D insufficiency/deficiency, CF-related bone disease, and adrenal and thyroid function disturbances in patients with CF, as well as to explore their association with lung function and colonization.
Method: A cross-sectional study with a retrospective collection of information from patients under 18 years of age with a confirmed diagnosis of CF, evaluated on an outpatient or in-hospital basis by a pediatric pulmonologist or endocrinologist, or in a multidisciplinary CF consultation, between January 2011–December 2020.
Results: A total of 87 patients were included. A high frequency of endocrinopathies was found. Vitamin D insufficiency/deficiency was persistent despite cholecalciferol
supplementation in 72%, short stature in 38%, pubertal delay in 26%, and thyroid axis disorders in 8% of cases. Bone disease involving densitometry and adrenal insufficiency secondary to chronic corticosteroid use were also frequent among the screened subjects (44% [n=16] and 12% [n=51], respectively). No significant differences were found for pulmonary function or bacterial lung colonization in the context of any endocrinopathies.
Conclusion: Endocrine comorbidities are frequent in patients with CF, and early recognition improves the prognosis and quality of life in these patients. The findings for this cohort ratify the importance of multidisciplinary management of patients with CF.
Key Points
1. The present study reveals that pediatric patients with cystic fibrosis (CF) have a high prevalence of endocrine abnormalities that should be recognized early by treating clinicians.
2. This article describes the prevalence, clinical and paraclinical features, and management of linear growth and pubertal disorders, vitamin D insufficiency/deficiency, CF-related bone disease, and adrenal and thyroid dysfunction in patients with CF, as well as their association with lung function and colonization.
3. Endocrine abnormalities in pediatric patients with CF should sensitize clinicians to the need for early and timely multidisciplinary management to improve the prognosis and quality of life of affected patients.
INTRODUCTION
Advances in the medical and nutritional care of patients with cystic fibrosis (CF) have increased life expectancy in recent years; for this reason, more patients develop disease-related endocrine comorbidities.1 Globally, the presence of endocrine disruption is associated with a negative impact on the clinical outcomes and mortality of those affected.2
There is still not enough data to show the frequency of endocrinopathies in the pediatric population. Therefore, the present study was aimed at evaluating the frequency of vitamin D insufficiency/deficiency, bone disease involving densitometry, thyroid and adrenal axis disorders, short stature, and pubertal delay in a population of children with CF in Medellín, Colombia. Additionally, the authors intended to describe the screening and management of these pathologies over the last 10 years, and explore the relationship between pulmonary function impairment, bacterial pulmonary colonization, and the presence of endocrinopathies.
METHODS
A cross-sectional study was conducted at the Hospital San Vicente Fundación in Medellín, Colombia. Patients under 18 years of age who were evaluated in a multidisciplinary CF consultation involving endocrinology, pulmonology, gastroenterology, and nutrition, or patients who had been assessed by pulmonology or pediatric endocrinology on an outpatient or in-hospital basis from January 2011–December 2020, were identified.
Only those who met the criteria for a confirmed diagnosis of CF were included in the analysis, which was defined as evidence of two CF-causing CFTR gene mutations in the molecular test, and/or positive results of two iontophoresis with direct Gibson and Cooke’s test >60 mmol/L, or indirect tests with values >80 mmol/L.3
An instrument was designed to collect the information, including sociodemographic aspects, assessment of pulmonary condition, frequency and characteristics of linear growth, pubertal disturbances, vitamin D insufficiency/deficiency, CF-related bone
disease, and adrenal and thyroid function disturbances.
The socioeconomic stratum was evaluated according to the stratification system of the Colombian National Planning Department; classifying 1 and 2 as low, 3 and 4 as medium, and 5 and 6 as high.
Standard deviation (SD) values were used for anthropometric assessment according to World Health Organization (WHO) charts.4 Low height risk was defined as a height/age ≥-2 to <-1 SD, and low height <-2 SD. The nutritional status classification was assessed according to resolution 2,465 of 2016. For those <5 years of age, with weight/age z-score: moderate undernutrition <-2 to ≥-3 SD, and severe undernutrition <-3 SD; and for ≥5 years with BMI/age z-score: risk of thinness ≤-1 to ≥-2 SD, and thinness <-2 SD. Mammary and testicular development were assessed by the Tanner scale (pre-pubertal <2 and pubertal ≥2).5,6
Lung function impairment was evaluated in children ≥6 years by forced expiratory volume in the first second (FEV1) measured by spirometry. Percent predicted values of FEV1 of 70–80% were considered mild, 60–70% moderate, 50–60% moderate-severe, <50% severe, and 35–50% very severe.7
Pulmonary colonization was defined as the presence of two or more cultures of respiratory secretions positive for one or more micro-organisms.8
Bone mineral density (BMD), measured by bone densitometry (DXA) of the total body without head and lumbar spine adjusted for age, gender, and height, was evaluated in patients >8 years in accordance with the recommendation of the European Society for Clinical Nutrition and Metabolism (ESPEN), the European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN), and the European Cystic Fibrosis Society (ECFS) guidelines.9
The following definitions were established for the classification of endocrinopathies:
Delayed puberty: absence of thelarche in young females at 13 years of age, and absence of testicular volume of 4 ccs or greater in young males at 14 years of age.10
Vitamin D deficiency: serum 25-hydroxyvitamin D (25[OH]D) concentrations <20 ng/mL.11 Vitamin D insufficiency: serum 25(OH)D concentrations between 20.0–29.9 ng/mL.11
Bone disease: DXA of the lumbar spine or total body without head <-2DE of BMD z-score.9
Impaired thyroid function: Thyroidstimulating hormone values persistently above the upper limit of the reference range for age associated with low T4L (primary hypothyroidism) or normal T4L (subclinical hypothyroidism).12
Adrenal insufficiency: 8 am cortisol level <3 μg/dL. Those with levels between 3–10 μg/dL were classified as indeterminate, and a low-dose adrenocorticotropin (ACTH) stimulation test was requested. A cortisol peak <18 μg/dL was considered diagnostic of adrenal insufficiency.13
Risk of adrenal insufficiency due to prolonged glucocorticoid use: oral corticosteroid use at supraphysiologic doses (>12 mg/ m2/day of hydrocortisone equivalent) for >2 consecutive weeks or >3 weeks cumulative over the past 6 months, or inhaled corticosteroid (ICS) use at high doses (beclomethasone dipropionate >400 mcg/ day, budesonide >400 mcg/day for children up to 11 years of age, and >800 mcg/day for those >11 years, fluticasone propionate >500 mcg/day) for more than 1 year.13,14
The data obtained were recorded in Microsoft Excel (Windows7®️, Redmond, Washington, USA) and subsequently analyzed with R Project version 4.1.3. To explore the association between lung colonization and lung function with the different endocrinopathies, χ2 association tests or
Fisher’s exact test were performed. A P-value of less than 0.05 was considered significant.
The protocol of the study was approved by the local ethical board.
RESULTS
A total of 386 histories were reviewed, of which 87 met the inclusion criteria. A higher percentage of affected males were found with CF, usually with pre-pubertal Tanner stage, along with a mean z-score for risk of short stature (Table 1). Regarding nutritional status, 6.2% of children <5 years, and 21% of children ≥5 years had malnutrition.
Concerning pulmonary involvement, 10% of the patients had a permanent requirement for oxygen. Of the 65 patients ≥6 years, 58 exhibited spirometry with a mean FEV1 of 70% (±20.4).
Delayed puberty was assessed in young females ≥13 years and young males ≥14 years; it was observed more frequently in males than in females, with a 3:1 ratio. Short stature was also observed more frequently in males (20 males [60.6%] versus 13 females [39.4%]).
The authors measured 25(OH)D levels in all patients, 8 am cortisol levels in 51 patients, and a stimulation test with low doses of ACTH in three children who had 8 am cortisol levels <3. An indeterminate result was obtained in the 8 am cortisol test in 19 patients, of whom 15 were at risk of adrenal insufficiency due to prolonged use of glucocorticoids. An adrenocorticotropic hormone (ACTH) stimulation test was not performed in any of them for confirmation.
Of the 49 patients >8 years old, 16 underwent DXA, with greater BMD involvement of the total body without head (n=6) for the lumbar spine (n=4), and no pathological fractures were observed in any patient.
The phosphocalcic profile was evaluated in all patients with serum levels of 25(OH) D, calcium, phosphorus, and alkaline phosphatase. Intact parathyroid hormone levels were assessed in 78 patients. Mean vitamin D levels were 24.9 ng/mL (±7.73 SD) with insufficiency/deficiency in 63 patients (67% with insufficiency and 33% with deficiency), all of whom were receiving cholecalciferol supplementation, with a median dose of 2,000 international units per day (interquartile range: 1,000–3,000).
All patients showed exocrine pancreatic insufficiency, defined as the presence of pancreatic enzyme replacement. The mean calcium was 9.6 mg/dL (±0.69 SD), phosphorus 5.29 mg/dL (±0.59 SD), alkaline phosphatase 256.6 U/L (±103.3 SD), and intact parathyroid hormone 33.57 pg/mL (±12.73 SD). These values were compared with patients who were presented with bone disease measured by DXA (Figure 1).
The association between the endocrinopathies with bacterial lung colonization is presented in Table 2
Regarding the treatment of short stature, three patients had biochemical confirmation of hormone deficiency according to a clonidine test. They received recombinant human growth hormone at a median dose of 35 mcg/kg/day. Of the seven patients diagnosed with hypothyroidism, six had subclinical hypothyroidism, five received levothyroxine supplementation due to hypogrowth (short stature with poor growth velocity), and one patient had primary hypothyroidism.
Of the 87 patients, 70 (80.5%) received inhaled or systemic corticosteroid therapy, six received supraphysiological doses of oral corticosteroid for more than 2 consecutive weeks, 40 (46%) received a high-dose ICS for more than 1 year, 30 (75%) received beclomethasone dipropionate, seven fluticasone propionate, and three budesonide.
Figure 1. Frequency distribution of serum 25-hydroxyvitamin D, phosphate, parathyroid hormone, and alkaline phosphatase levels in the total population compared to children with bone disease measured by bone densitometry.
DISCUSSION
In the present study, the authors found a high frequency of endocrinopathies in the population of CF patients evaluated, with a frequency similar to that reported in studies worldwide.1,15 Although not completely comparable given the disparity in population and methodology, the findings agree with other authors who have reported that vitamin D insufficiency/deficiency was most frequently found in endocrinopathy. In a retrospective study evaluating 101 children, adolescents, and young adults with CF, vitamin D insufficiency and deficiency, defined as 25(OH)D concentrations <30 ng/mL and <11 ng/mL, were documented in 90% and 7% of patients, respectively.16 In this cohort, deficient vitamin D levels were more frequently described, possibly because a higher cut-off point was used to define vitamin D deficiency (<20 ng/ mL). Similar results were reported by Aziz et al.17 who retrospectively evaluated 69 children with CF: 40.5% were vitamin D deficient and 31.8% were insufficient, for 72% of the
population with vitamin D levels below 30 ng/ mL. However, there was a discrepancy among the results of different studies secondary to multiple factors determining suboptimal vitamin D levels, such as deficient nutritional intake, decreased outdoor activity, altered vitamin D hydroxylation, corticosteroid use, and decreased intestinal absorption secondary to exocrine pancreatic insufficiency.18 In this population, all subjects had exocrine pancreatic insufficiency, with a significant percentage of patients reported with malnutrition, and chronic glucocorticoid use.
The second most frequent endocrinopathy was short stature. In a study that evaluated growth status in 13,116 children (age range: 0–18 years) seen at Cystic Fibrosis Foundation-accredited centers in the USA in 1993, 22% were below the 5th percentile for height-for-age based on the National Center for Health Statistics (NCHS)/Centers for Disease Control (CDC) growth.19 Also, they observed significant sex differences in the incidence of stunting (height-for-age <5th
Table 2. Endocrinopathies according to lung colonization.
a: Fisher's exact test.
percentile) during adolescence; young males aged 11–14 years showed a lower incidence of stunting (19%) than young females (29%), while the opposite trend was observed between the ages 15–18 (34% in male patients versus 28% in female patients).19 The authors found a higher frequency of short stature in this cohort despite presenting a lower percentage of malnutrition (21% >5 years of age and 6.2% <5 years of age) compared to the previous study, which reported weight-for-age <5th percentile in 47% of infants and 34% of adolescents.19 There could be a contribution of other growth-related factors that explain a higher frequency of short stature in this population, such as fat and micronutrient malabsorption, chronic infection, and chronic glucocorticoid treatment, which were frequent.19 In addition, some data support the relationship between short stature and pubertal delay in the male population. Landon et al.20 evaluated the growth rate and pubertal status of 54 adolescent and young adult males with cystic fibrosis, of whom 39% were below the 5th percentile for height, and 28% between the ages of 14–18 had delayed pubertal development.20 The frequency of short stature and delayed puberty in the authors’ study was similar to that described, with greater incidence in the male sex possibly explained by more significant involvement in malnutrition, which was three times higher in males than females. Newer data in more recent cohorts of patients with CF show normalization of pubertal timing that may be secondary to better nutrition.21 However, most of this study's patients were from low and middle socioeconomic strata, with a significant proportion of rural residents with economic and administrative difficulties in accessing nutritional supplements, and insufficient caloric intake.
Although CF-related bone disease (CFBD) screening of the entire population was not performed, among children who were screened with DXA, CFBD was frequent. In a systematic review, less than 5% of children with CF had CFBD, but this proportion increased to 20% in adolescence, with
55–65% of patients >45 years of age affected.22 Several studies have reported decreased BMD in children and adolescents with CF.23-25 Furthermore, peak mineralization has been reported to be significantly reduced in adolescents.26 In the authors’ cohort, all patients screened with DXA were adolescents, had vitamin D insufficiency/ deficiency, and were receiving chronic steroid therapy, which may have contributed to a higher frequency of bone disease in this population.
Concerning alterations in adrenal function, a retrospective study diagnosed iatrogenic adrenal insufficiency in 20.5% of their cohort. The use of high-dose ICS (beclomethasone >400 μg and fluticasone >500 μg per day), especially fluticasone, appeared to be the significant risk factor.27 The percentage of patients who were diagnosed with adrenal insufficiency in the authors’ cohort was lower (12%); however, this was similar to that reported by Préville-Ratelle et al.,28 who indicated that only 8% of the adult population with CF had adrenal insufficiency. This suggests a possible underdiagnosis secondary to difficulties in the recognition, and lack of systematic detection, of this entity.28 In the authors’ study, deficiencies in the screening of adrenal insufficiency were also evidenced. The main limitation was the difficulty in interpreting indeterminate results due to the lack of an ACTH stimulation test, which is the confirmatory test. In the authors’ environment, the lack of availability of the ACTH analog, due to a shortage, added to limited authorizations by the National Institute of Drug and Food Surveillance (INVIMA), hindering the generalized performance of this test.
Finally, the prevalence of thyroid dysfunction in patients with CF remains controversial. Some studies have reported normal thyroid function, while others have reported subclinical hypothyroidism.29,30 Serum triiodothyronine (T3) values are often decreased due to impaired conversion of thyroxine (T4) to T3 in secondary to acute and chronic illnesses that frequently occur in patients with CF. The authors findings reflect
the presence of subclinical hypothyroidism in children with CF, but with lower frequency than that reported in previous studies, probably because of a lower prevalence of iodine deficiency in the authors’ study population. According to the latest report of the National Survey of Nutritional Status (ENSIN) 2015, iodine deficiency in Colombian children aged 1–4 years was 8.1%, and in children aged 5–12 years was 4.4%.31
One of the most critical limitations was the need for more information from unscreened patients, which contributed to the lack of a sample with non-significant findings. Nevertheless, it is important to consider that part of the lack of significant differences in the presence of endocrinopathies according to lung colonization may be due to small sample size, and lack of power to prove differences. In addition, the economic and administrative barriers that limited the performance of the requested studies,
References
1. Kelly A et al. Endocrine Complications of Cystic Fibrosis. Clin Chest Med. 2022;43(4):773-89.
2. Sharma PB et al. Year in Review 2020: Multisystemic impact of cystic fibrosis. Pediatr Pulmonol. 2021;56(10):3110-19.
3. Smyth AR et al. European Cystic Fibrosis Society standards of care: best practice guidelines. J Cyst Fibros. 2014;13(Suppl 1):S23-42.
4. Curvas OMS. Resolución número 2465 del Ministerio de Salud y Protección social, 14 de junio de 2016. 2022. Available at: https://www.icbf.gov.co/ sites/default/files/resolucion_no._2465_ del_14_de_junio_de_2016.pdf. Last accessed: 10 April 2023.
5. Marshall WA, Tanner JM. Variations in pattern of pubertal changes in girls. Archives of disease in childhood. Arch Dis Child. 1969;44(235):291-303.
6. Marshall WA, Tanner JM. Variations in the pattern of pubertal changes in boys. Archives of disease in childhood. Arch Dis Child. 1970;45(239):13-23.
7. Pellegrino R et al. Interpretative strategies for lung function tests. Eur Respir J. 2005;26(5):948-68.
and the continuity of the established treatments in many patients, could have generated confusion bias by increasing or decreasing the prevalence of CF-related endocrinopathies. However, though limitations were found, this is the first study in the authors’ setting to show a high frequency of endocrinopathies in a population of children with CF.
CONCLUSION
Endocrine comorbidities are frequent in pediatric patients with CF. This investigation reinforces the importance of a multidisciplinary follow-up of pediatric patients with CF to identify affected children and those most vulnerable, and to take appropriate preventive treatment and followup measures to impact clinical outcomes, pulmonary function, and quality of life in this population group.
8. González Jiménez D et al. Vitamin D and chronic lung colonization in pediatric and young adults cystic fibrosis patients. Nutr Hosp. 2015;32(4):1629-35.
9. Ullal J et al. Treatment of cystic fibrosis related bone disease. J Clin Trans Endocrinol. 2022;27:100291.
10. Dye AM et al. Delayed puberty. Pediatr ann. 2018;47(1):e16-22.
11. Farahbakhsh N et al. Vitamin D deficiency in patients with cystic fibrosis: a systematic review and meta-analysis. J Health Popul Nutr. 2024;43(1):11.
12. Salerno M. Subclinical hypothyroidism in childhood - current knowledge and open issues. Nat Rev Endocrinol. 2016;12(12):734-46.
13. Rayas MS et al. Adrenal function in cystic fibrosis. J Cyst Fibros. 2019;18(Suppl 2):S74-s81.
14. Global initiative for asthma (GINA). Global strategy for asthma management and prevention. 2022. Available at: www. ginasthma.org. Last accessed: 10 April 2023.
15. Blackman SM, Tangpricha V. Endocrine disorders in cystic fibrosis. Pediatr Clin North Am. 2016;63(4):699-708.
16. Rovner AJ et al. Vitamin D insufficiency in children, adolescents, and young adults with cystic fibrosis despite routine oral supplementation. Am J Clin Nutr. 2007;86(6):1694-99.
17. Aziz DA et al. Vitamin D status and pulmonary exacerbations in children and adolescents with cystic fibrosis: experience from a tertiary care center. Lung India. 2021;38(4):326-29.
18. Lark RK et al. Diminished and erratic absorption of ergocalciferol in adult cystic fibrosis patients. Am J Clin Nutr. 2001;73(3):602-6.
19. Lai HC et al. Growth status in children with cystic fibrosis based on the National Cystic Fibrosis Patient Registry data: evaluation of various criteria used to identify malnutrition. J Pediatr. 1998;132(3 Pt 1):478-85.
20. Lavi E. Somatic growth in cystic fibrosis. Curr Opin Endocrinol Diabetes Obes. 2020;27(1):38-46.
21. Goldsweig B et al. Puberty in cystic fibrosis. J Cyst Fibros. 2019;18(Suppl 2):S88-94.
22. Paccou J et al. The prevalence of osteoporosis, osteopenia, and fractures among adults with cystic fibrosis: a
systematic literature review with metaanalysis. Calcif Tissue Int. 2010;86(1):1-7.
23. Anabtawi A et al. Cystic fibrosis bone disease: Pathophysiology, assessment and prognostic implications. J Cyst Fibros. 2019;18 Suppl 2:S48-55.
24. Chedevergne F, Sermet-Gaudelus I. Prevention of osteoporosis in cystic fibrosis. Curr Opin Pulm Med. 2019;25(6):660-65.
25. Douros K et al. Bone mass density and associated factors in cystic fibrosis patients of young age. J Paediatr Child Health. 2008;44(12):681-85.
26. Buntain HM et al. Controlled longitudinal study of bone mass accrual in children and adolescents with cystic fibrosis. Thorax. 2006;61(2):146-54.
27. Woods CP et al. Adrenal suppression in patients taking inhaled glucocorticoids is highly prevalent and management can be guided by morning cortisol. Eur J Endocrinol. 2015;173(5):633-42.
28. Préville-Ratelle S et al. Adrenal Insufficiency in Cystic Fibrosis: A Rare Phenomenon? Can Respir J. 2018;2018:3629031.
29. Segall-Blank M et al. Thyroid gland
function and pituitary TSH reserve in patients with cystic fibrosis. J Pediatr. 1981;98(2):21822.
30. Siwamogsatham O et al. Diagnosis and treatment of endocrine comorbidities in patients with cystic fibrosis. Curr Opin Endocrinol Diabetes Obes. 2014;21(5):422-29.
31. Ministerio de Salud de Colombia. Encuesta Nacional de la Situación Nutricional – ENSIN. 2015. Available at: www.ensin.gov.co. Last accessed: 10 April 2023.
FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM