


Well summer flew by pretty fast this year! I hope you all had a great one I had the opportunity to spend some time in the Arctic this summer It was an amazing experience, featuring sightings of polar bears, musk ox, beluga whales, Arctic fox, and fishing for Arctic char. Some of us can never get enough winter!
There have been a lot of great changes at BVS over the summer. Dr. Chele Lathroum, our critical care specialist, started in July and hit the ground running! It has been great to see all the positive changes she has made in helping manage some of our most needy patients Drs Dan Thomsen and Jane Mittelsteadt have taken a joint leadership role in our ER department and look forward to continually improving this vital service to the community. Dr. Bergman and Dr. Valerio have organized a symposium with over 120 veterinary neurosurgeons from all over the world for the first-ever BVS Neurosurgical symposium It is an honor to sponsor this meeting to help continue to drive excellence in this rapidly changing field.
In this issue, Dr Matthew Evans will highlight guided tissue regeneration I didn’t even know that was a thing, but another one of the cool ways he is saving teeth I saw him put on a really cool blue crown the other day. Kind of makes me want to chip one of my own teeth. I didn’t know you could pick colors. Dr. Ashley Mitek will also share some new options for pain management
I hope to see you all at our Fall Symposium on October 18th. We have added a day of technician CE on the 19th this year. A great opportunity for free, local, RACEapproved CE, and we even throw in a free lunch and surprise gift for those that dare to give up a valuable hunting day in October!
Thank you all for your continued support of BVS It is truly an honor and a privilege to be trusted with your clients As always, feel free to reach out if there is anything we can do better for you or your clients.
Dr Joshua Jackson, DVM, DACVS
Bridger Veterinary Specialists & Emergency invites you to our Fall Symposium on Saturday, October 18 , 2025, at the beautiful Riverside Country Club in Bozeman There is also a brand new Technicians CE day on Sunday, October, 19 . This full-weekend event brings together veterinary professionals, specialists, technicians, and thought leaders to discuss advancements in veterinary medicine and foster professional well-being th th
�� Doctor Symposium: October 18, 2025
�� NEW Tech Symposium: October 19, 2025
�� Time (both days): 8:30 AM – 4:30 PM
�� Location: Riverside Country Club, Bozeman
�� RACE Approved CE
�� Meeting and Lunch Complimentary
Our expert speakers will cover a range of topics in veterinary medicine, including:
DVM Sessions:
�� Decoding DKA
�� Management of Seizure Disorders
�� Current Studies about When to Neuter Dogs
�� Feline Dentistry
☢ Outcome of Radiation Therapy
�� Top 10 Anesthesia Questions Answered
Technician Sessions: Cytology
Tips and Tricks for Better Radiographs
�� Oral Assessment
�� Anesthesia- 3 sessions with Dr. Ashley Mitek!
�� Special Speaker: Paul Osincup, author of The Humor Habit, will discuss well-being in veterinary medicine
By Dr. Matt Evans, DVM, DAVDC
The oral microbiome of dogs and cats is composed of hundreds of different bacterial species, archaea, viruses, and microscopic eukaryotes that cover all mucosal and dental surfaces as a biofilm. These biofilms are dynamic and ever changing, working to create a microenvironment that is optimized for microorganism thriving and protected from host immune response.
They are polymicrobial colonies with different members serving different functions within the community and evolving as the biofilm matures. After about 72 hours, portions start to mineralize into calculus, and a shift begins from gram-positive to more virulent, gram-negative anaerobic species. In health, there is an equilibrium between host and biofilm that doesn’t evoke a substantial inflammatory response. If the equilibrium is disturbed, immune tolerance shifts to a proinflammatory response resulting in tissue destruction.
Most attachment loss is caused by host response as opposed to direct microbial virulence factors, which is why some animals (and people) have genetic predispositions for periodontal disease.
Gingivitis is a reversible inflammation confined to the gingiva that is not associated with attachment loss. Periodontitis is a complex inflammatory process that causes irreversible damage to the dental attachment apparatus. Gingivitis does not always lead to periodontitis; some pets can have dental deposits on their teeth for years without significant attachment loss. Periodontal disease encapsulates both gingivitis and periodontitis.
Normal (PD0): Clinically normal; gingival inflammation or periodontitis is not clinically evident.
Stage 1 (PD1): Gingivitis only without attachment loss; the height and architecture of the alveolar margin are normal.
Stage 2 (PD2): Less than 25% attachment loss or, at most, stage 1 furcation involvement in multirooted teeth.
Stage 3 (PD3): 25-50% attachment loss or, at most, stage 2 furcation involvement in multirooted teeth.
Stage 4 (PD4):
Greater than 50% attachment loss or stage 3 furcation involvement in multirooted teeth. This is end-stage disease.
A healing periodontal pocket is invaded by cells from four different sources: 1) gingival epithelium, 2) gingival connective tissue, 3) alveolar bone, and 4) periodontal ligament. Restoring healthy attachment only occurs if periodontal ligament cells are the first to repopulate a pocket. Cells from any other source create problems if they are the first to the pocket.
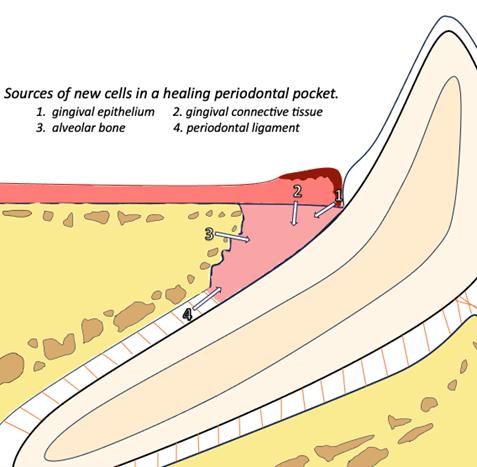
Unfortunately, epithelial cells migrate approximately 10x faster than other cell types. This creates something called a long junctional epithelium, which is highly unstable and prone to pocket reformation. In other words, simply cleaning and debriding a pocket results in reparative healing by the formation of a long junctional epithelium rather than regenerative healing, which restores periodontal ligament, cementum, and bone.
Guided tissue regeneration is a technique used to exclude unfavorable cell types and allow time for the periodontium to heal. It has the potential to SAVE TEETH that otherwise would be lost due to disease or extraction.
In GTR, flap procedures allow us to gain access to the pocket for thorough debridement of all hard and soft tissues.
Then, a barrier membrane is placed, typically along with graft materials, that acts as a chemical or mechanical prevention for migrating epithelial cells. A space is maintained for clot stabilization, which allows for periodontal regeneration. GTR selectively excludes the cell types we don’t want while encouraging periodontal ligament cells to migrate and differentiate.
Then, a barrier membrane is placed, typically along with graft materials, that acts as a chemical or mechanical prevention for migrating epithelial cells. A space is maintained for clot stabilization, which allows for periodontal regeneration. GTR selectively excludes the cell types we don’t want while encouraging periodontal ligament cells to migrate and differentiate.
Not all teeth or pocket types are good candidates for GTR, but in the right circumstances it can allow for huge and lasting improvement in probing depths. We often see teeth that started as PD34 improve to PD2, which is a more sustainable situation for the tooth long term. The tooth is protected with more innate ability to keep periodontal disease under control. GTR is a great option for strategically important teeth and with owners who are motivated to maintain teeth.

Figure 4. Same tooth from previous figures 1 year post treatment. Reduction in pocket depth from 12 mm to 3 mm.
Extraction doesn’t always have to be the first treatment option! Guided tissue regeneration is another arrow in the quiver in the fight against the common condition of periodontal disease seen in all of our patients.
Coming Soon: We Want Your Feedback!
Keep an eye out for our upcoming practice partner survey your input matters! We're always looking to improve, and your feedback helps us do just that. The survey will only take a few minutes, and your voice will help shape what's next. Stay tuned!

By Dr. Ashley Mitek, DVM, DACVAA

If you or a family member have had recent surgery, you've probably noticed the growing use of ultrasoundguided regional anesthesia in people. The American Society of Anesthesiology projects that by 2026, 50% of all knee and hip replacements will be out patient in the USA. That's thanks to the adoption of regional anesthesia that keeps patients totally pain free for 1872 hours. The benefits of these blocks are numerous, but include an enhanced patient experience, limited or no need for opioids, and a more rapid return to normal ambulatory, psychological, and gastrointestinal function. Locoregional anesthesia reduces nausea and infection rates too.
This emerging field of human interventional pain medicine has been translated into veterinary medicine, and we now have a treasure trove of peer reviewed research that supports the use of ultrasound guided regional anesthesia in cats and dogs. At BVS, we offer interventional pain medicine services to hospitalized and outpatients. Approximately 80% of our surgical patients receive ultrasoundguided local blocks prior to surgery. We also offer ultrasound-guided regional anesthesia to painful out patients as well.

These blocks take about 10 minutes to perform and can be done under sedation. Some of the blocks we offer are:
Saphenous and Sciatic nerve blocks for pain in the stifle or distal to it
Axillary Sheath Blocks for pain in the elbow or distal to it
Transversus Abdominis Plane Blocks for visceral (organ) and somatic (skin) abdominal pain (from a laparotomy, or pancreatitis, etc...)
Serratus Plane Blocks for chest wall pain (broken ribs, skin wounds, thoracotomy, etc...)
Psoas Compartment blocks for Iliopsoas pain
Epidurals (steroid and/or preservative free morphine)
There are several drugs that can be used in the block based upon the patient's needs Some options are:
1.Bupivicaine + Dexmedetomidine, which lasts about 12-18 hours
2.Nocita (Liposomal encapsulated bupivicaine), which lasts about 3 days
3.Bacteriostatic Saline + Triamcinolone + Bupivicaine, which provides 2-3 weeks of sensory blockade (off label use, for terminal patients only. Example: Osteosarcoma patients not pursuing amputation)
Last but not least, we offer a 4-hour ketamine intravenous infusion (also known as a "Pain Vacation") for patients with chronic pain from oncological disease, osteoarthritis, cervical radiculopathy and intervertebral disc disease. A case series of over 200 dogs was presented at the veterinary anesthesia conference by Fry et al., "Preliminary study of intravenous ketamine infusions for the management of chronic pain in dogs" showing significant improvements in owner reported quality of life after the infusion. Nearly all owners elected to bring their dog in for a repeat infusion two weeks later. The infusions can be repeated every other week, monthly, or as needed. There are no behavioral side effects from this low dose infusion. All dogs continue to eat, drink, walk and act normal during and after the infusion.
If you have any questions about our Interventional Pain Medicine Services including ultrasound-guided regional anesthesia or ketamine infusions, you can reach out to our anesthesiologist at ashley@bvspets.com or give us a call. We'd love to numb something for you!