

May everybody be happy May every one of us see to it That nobody suffers from any pain or sorrow I do not ask for crown Nor wish to be in Heaven or reborn I only want to alleviate the suffering of those people Who are burning in fire of sorrow
http://www.ima-india.org/ima/left-side-bar.php?scid=14

We, the members of Indian Medical Association Stand here to salute our National Flag Its honour and glory shall be our light and strength And its course shall be our course. We pledge our allegiance to it And realizing our responsibilities as the accredited members of this national organization, We swear We will dedicate everything in our power To see it fly high in the comity of nations.




1. IMARareBloodGroupOnlineBloodBankDirectory ima-india.org/Rare
2. IMAOnlineTBNotificationinitiative ima-india.org/tbnotify
3. IMAOnlineEventsReportinginitiative http://www.ima-india.org/ima/left-side-bar.php?scid=228
4. ProformaforHypertensionScreening http://module.ima-india.org/
5. IMAOnlineSentinelEventsReportingInitiative ima-india.org/sentinel
6. IMADiseaseNotification http://disnotif.ima-india.org/
7. IMARISEandSHINE http://imariseandshine.com/
8. IMABloodDonationInitiative http://www.ima-india.org/ima/left-side-bar.php?scid=289
9. IMAFlagSalutation http://www.ima-india.org/ima/left-side-bar.php?scid=14
10. IMAPrayer http://www.ima-india.org/ima/left-side-bar.php?scid=14
11. IMADigitalTV http://www.ima-india.org/imalive/ 12. IMASlideShare http://www.ima-india.org/ima/free-way-page.php?scid=287 13. IPledgeMyOrgan http://module.ima-india.org/ipmo/ 14. IMALive http://www.ima-india.org/imalive/ 15. eMedinexus/ART http://emedinexus.com/artbill/ 16. eMedinexus/Satyagraha http://emedinexus.com/satyagraha 17. IMA/ART http://ima-india.org/artbill 18. IMA/Satyagraha http://ima-india.org/satyagraha
19 IMA/Webcast http://ima-india.org/ima/ 20 IMADigitalTV http://ima-india.org/digitaltv
Office bearers for the year 2015-16
IMAAMS
IMAHeadquarters
DrSSAgarwal (National President)
Prof(Dr)AMarthandaPillai (Imm Past National President)
DrShailendraNVora (National Vice President)
DrKPrameelaSurenderRao (National Vice President)
DrOmParkashSinghKande (National Vice President)
DrSharadKumarAgarwal (National Vice President)
DrKKAggarwal (Hony Secretary General)
DrRNTandon (Hony Finance Secretary)
DrRajeevArdey (Hony Jt. Secretary)
DrRaviMalik (Hony Jt. Secretary),
DrRameshKumarDatta (Hony Jt. Secretary)
DrSanjoyBanerjee (Hony Jt. Secretary Calcutta)
DrPravinGogia (Hony Jt. Secretary)
DrHansRajSatija (Hony Asst. Secretary)
DrManjulMehta (Hony Asst. Secretary)
DrHarishGupta (Hony Jt. Fin. Secretary)
DrUjjwalKrSengupta (Hony Jt. Fin. Secretary Calcutta) IMACGP
DrVinodKumarMonga (Dean of Studies)
DrARajaRajeshwar (Hony Secretary)
DrKranshankarWDeoras (Chairman)
DrPullaraoPasumarthy (Hony Secretary)
IMAAKN Sinha Institute
DrShivkumarUtture (Hony Director)
DrArbindKumarSinha (Hony Executive Secretary)
JIMA
DrDebasishMukherjee (Hony Editor)
DrRanjanKumarChakraborty (Hony Assoc. Editor)
DrMinakshiGangopadhyay (Hony Assoc. Editor)
DrSantanuSen (Hony Secretary)
DrSukomolDas (Hony Asst. Secretary)
Your Health
DrAmitabhaBhattacharya (Hony Editor)
DrRahulDutta (Hony Secretary)
Apka Swasthya
DrPrabhatKumarTewari (Hony Editor)
DrArvindSingh (Hony Secretary)
IMANSS Scheme
DrKirtiMPatel (Chairman)
DrYogendraSModi (Hony Secretary)
IMANPPScheme
DrKrishnaMParate (Chairman)
DrJayairishnanAV (Hony Secretary)
IMAHospital Board of India
DrRVAsokan (Chairman)
DrRaviWankhedkar (Hony Secretary)
DrAnilSPachnekar (HQs. Secretary)
IMANational Health Scheme
DrAshokSAdhao(Chairman)
DrAlexFranklin(Hony Secretary)
IMANational Pension Scheme
DrSudiptoRoy(Chairman)
DrKVDevadas(Hony Secretary)
CONTENTS
Editorial :
Epistaxis —An Emergecy in day to day Practice — Debasish Mukherjee ................................4
OriginalsandPapers: Practitioners’Series :
Experience of botulinum toxin therapy in cervical dystonia, blepharospasm and hemifacial spasm — Satish Chandra, Ritu Agarwal, Jayantee Kalita, Usha K Misra ......................................................................................................7
Role of nasal endoscopy in the management of intractable epistaxis : our experience — Dwaipayan Mukherjee, Chiranjib Das ......................................................11
Incidenceofurinarytractinfectionandurologicalsymptomsin depot-medroxyprogesteroneusers— B Nisha, Sunita Malik, Jagdev Kaur, Archana Aggarwal...................................................................................................14
Acomparativestudybetweenskinsuturesandskinstaplesinabdominal surgicalwoundclosure— Chandrashekar N, Prabhakar GN, Vivek PO, Shivakumarappa GM, Fahad Tauheed .........................................................................................17
PreliminaryReports : GP Forum: CaseNote:
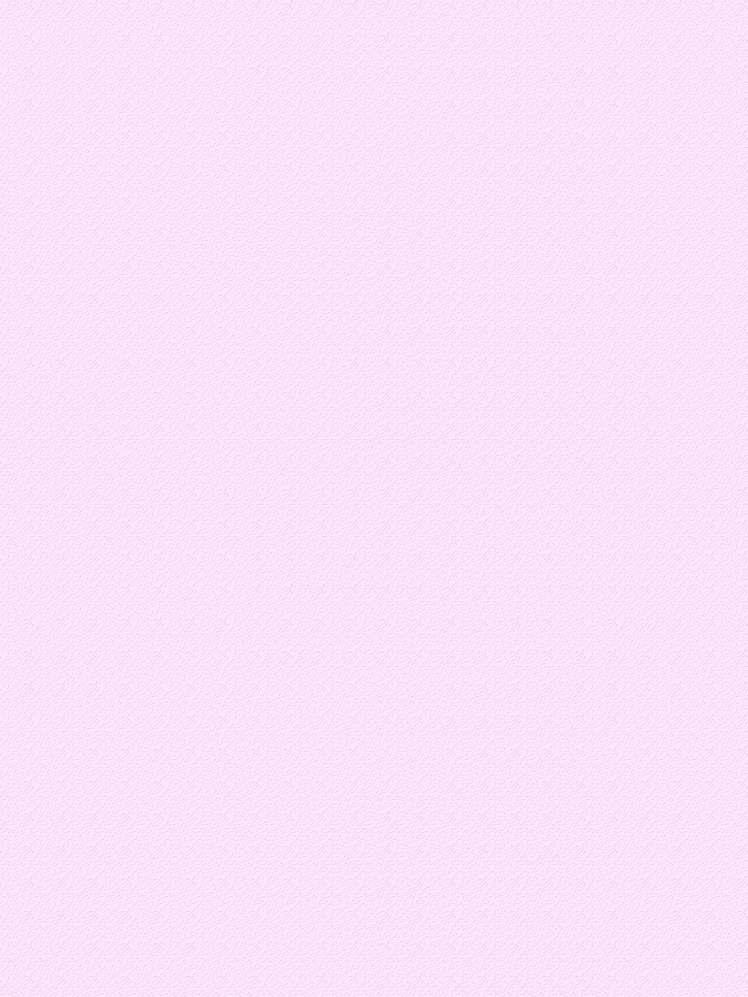
Rhinosporidiosisofdifferentorgans—astudyof57caseswithreviewof literature— Palash Kumar Mandal, Nirmal Kumar Bhattacharyya, Sumedha Dey, Pranab kumar Biswas, Subrata Mukhopadhyay, Dibyendu Gautam ...............21
Vasculartumoursofthefemalegenitaltract:aclinicopathologicstudyof11cases
— Sainath K Andola, Uma S Andola .............................................................................................25
Dupattainjuries:anidentifiablehazardousentityinavarietyofworkplace andsocialscenarios Ashok Kumar, Pritish Singh, S K Babhulkar, Pramod Jain, Bhavya Sirohi, C M Badole ....................................................................................31
Recurrentcryptomenorrhoea—asuccessfuloutcome
— Pradip Kr Saha, Dipak Kr Giri, Haricharan Roy, Satabdi Majhi .........................................33

Dr Debasish Mukherjee MBBS, DLO, MS Honorary Editor, JIMA
Epistaxis — An Emergecy in day to day Practice
Epistaxis, or bleeding from the nose, is a common complaint. It is rarely life threatening but may cause significant concern, especially among parents of small children.Most nosebleeds are benign, self-limiting, and spontaneous, but somecanberecurrent.Manyuncommoncausesarealsonoted.
Anatomy
The nose has a rich vascular supply, with substantial contributions from the internal carotidartery(ICA)andtheexternalcarotidartery(ECA).
TheECAsystemsuppliesbloodtothenoseviathefacialandinternalmaxillaryarteries.Thesuperiorlabialarteryis one of the terminal branches of the facial artery This artery subsequently contributes to the blood supply of the anterior nasalfloorandanteriorseptumthroughaseptalbranch.
The internal maxillary artery enters the pterygomaxillary fossa and divides into 6 branches: posterior superior alveolar,descendingpalatine,infraorbital,sphenopalatine,pterygoidcanal,andpharyngeal.
Thedescendingpalatinearterydescendsthroughthegreaterpalatinecanalandsuppliesthelateralnasalwall.Itthen returnstothenoseviaabranchintheincisiveforamentoprovidebloodtotheanteriorseptum.Thesphenopalatineartery enters the nose near the posterior attachment of the middle turbinate to supply the lateral nasal wall. It also gives off a branchtoprovidebloodsupplytotheseptum.
The ICA contributes to nasal vascularity through the ophthalmic artery This artery enters the bony orbit via the superior orbital fissure and divides into several branches. The posterior ethmoid artery exits the orbit through the posteriorethmoidforamen,located2-9mmanteriortotheopticcanal.Thelargeranteriorethmoidarteryleavestheorbit throughtheanteriorethmoidforamen.
Theanteriorandposteriorethmoidarteriescrosstheethmoidrooftoentertheanteriorcranialfossaandthendescend into the nasal cavity through the cribriform plate. Here, they divide into lateral and septal branches to supply the lateral nasalwallandtheseptum.
The Kiesselbach plexus, or Little’s area, is an anastomotic network of vessels located on the anterior cartilaginous septum. It receives blood supply from both the ICA and the ECA. Many of the arteries supplying the septum have anastomoticconnectionsatthissite.
Pathophysiology
Bleedingtypicallyoccurswhenthemucosaiserodedandvesselsbecomeexposedandsubsequentlybreak.
More than 90% of bleeds occur anteriorly and arise from Little’s area, where the Kiesselbach plexus forms on the septum.TheKiesselbachplexusiswherevesselsfromboththeICA(anteriorandposteriorethmoidarteries)andtheECA (sphenopalatine and branches of the internal maxillary arteries) converge. These capillary or venous bleeds provide a constant ooze, rather than the profuse pumping of blood observed from an arterial origin. Anterior bleeding may also originateanteriortotheinferiorturbinate.
Posterior bleeds arise further back in the nasal cavity, are usually more profuse, and are often of arterial origin (eg, from branches of the sphenopalatine artery in the posterior nasal cavity or nasopharynx).Aposterior source presents a greaterriskofairwaycompromise,aspirationofblood,andgreaterdifficultycontrollingbleeding.
Etiology
Causesofepistaxiscanbedividedintolocalcauses(eg,trauma,mucosalirritation,septalabnormality,inflammatory diseases, tumors), systemic causes (eg, blood dyscrasias, arteriosclerosis, hereditary hemorrhagic telangiectasia), and idiopathic causes. Local trauma is the most common cause, followed by facial trauma, foreign bodies, nasal or sinus infections, and prolonged inhalation of dry air Children usually present with epistaxis due to local irritation or recentupperrespiratoryinfection(URI).
In a retrospective cohort study of 2405 patients with epistaxis (3666 total episodes), Purkey et al used multivariate analysis to identify a series of risk factors for nosebleeds. The likelihood of epistaxis was found to increase in patients with allergic rhinitis, chronic sinusitis, hypertension, hematologic malignancy, coagulopathy or, as mentioned, heredi-
tary hemorrhagic telangiectasia. The investigators also found increased nosebleeds in association with older age andcolderweather.
Trauma
Self-induced trauma from repeated nasal picking can cause anterior septal mucosal ulceration and bleeding. This scenario is frequently observed in young children. Nasal foreign bodies that cause local trauma (eg, nasogastricandnasotrachealtubes)canberesponsiblefor rarecasesofepistaxis.
Acute facial and nasal trauma commonly leads to epistaxis. If the bleeding is from minor mucosal laceration, it is usually limited. However, extensive facial traumacan result in severe bleeding requiring nasal packing. In these patients, delayed epistaxis may signal thepresenceofatraumaticaneurysm. Patientsundergoingnasalsurgeryshouldbewarnedofthe potentialforepistaxis.Aswithnasaltrauma,bleedingcan range from minor (due to mucosal laceration) to severe (duetotransectionofamajorvessel).
and symptoms of nasal obstruction and rhinosinusitis, oftenunilateral.
Intranasal rhabdomyosarcoma, although rare, often begins in the nasal, orbital, or sinus area in children. Juvenile nasal angiofibroma in adolescent males may causeseverenasalbleedingastheinitialsymptom.
Blooddyscrasias
Congenital coagulopathies should be suspected in individualswithapositivefamilyhistory,easybruising,or prolonged bleeding from minor trauma or surgery Examples of congenital bleeding disorders include hemophiliaandvonWillebranddisease.
Dryweather Drugs
Acquired coagulopathies can be primary (due to the diseases) or secondary (due to their treatments). Among the more common acquired coagulopathies are thrombocytopeniaandliverdiseasewithitsconsequential reduction in coagulation factors. Even in the absence of liver disease, alcoholism has also been associated with coagulopathy and epistaxis Oral anticoagulants predisposetoepistaxis.
Low humidity may lead to mucosal irritation. Epistaxis is more prevalent in dry climates and during cold weather due to the dehumidification of the nasal mucosa by home heatingsystems.
Topical nasal drugs such as antihistamines and corticosteroids may cause mucosal irritation. Especially when applied directly to the nasal septum instead of the lateral walls, they may cause mild epistaxis. Medications such as nonsteroidal anti-inflammatory drugs (NSAIDs) arealsofrequentlyinvolved.
Septalabnormality
Septal deviations (deviated nasal septum) and spurs may disrupt the normal nasal airflow, leading to dryness and epistaxis.Thebleedingsitesareusuallylocatedanteriorto thespursinmostpatients.Theedgesofseptalperforations frequently harbor crusting and are common sources of epistaxis.
Inflammation
Bacterial, viral, and allergic rhinosinusitis causes mucosal inflammation and may lead to epistaxis. Bleeding in these cases is usually minor and frequently manifestsasblood-streakednasaldischarge.
Granulomatosisdiseasessuchassarcoidosis,Wegener granulomatosis,tuberculosis,syphilis,andrhinoscleroma often lead to crusting and friable mucosa and may be a causeofrecurrentepistaxis. Young infants with gastroesophageal reflux into the nose mayhaveepistaxissecondarytoinflammation.
Tumors
Benign and malignant tumors can manifest as epistaxis. Affected patients may also present with signs
Vascularabnormalities
Arteriosclerotic vascular disease is considered a reason for the higher prevalence of epistaxis in elderly individuals.
Hereditary hemorrhagic telangiectasia (HHT; also known as Osler-Weber-Rendu syndrome) is an autosomal dominant disease associated with recurrent bleeding from vascular anomalies. The condition can affect vessels ranging from capillaries to arteries, leading to the formation of telangiectasias and arteriovenous malformations. Pathologic examination of these lesions reveals a lack of elastic or muscular tissue in the vessel wall. As a result, bleeding can occur easily from minor traumaandtendsnottostopspontaneously
Various organ systems such as the respiratory, gastrointestinal, and genitourinary systems may be involved. The epistaxis in these individuals is variable in severitybutisalmostuniversallyrecurrent.
Other vascular abnormalities that predispose to epistaxis include vascular neoplasms, aneurysms, and endometriosis.
Migraine
Childrenwithmigraineheadacheshaveahigherincidence of recurrent epistaxis than children without the disease. The Kiesselbach plexus which is part of the trigeminovascular system, has been implicated in the pathogenesisofmigraine.
Hypertension
Therelationshipbetweenhypertensionandepistaxisis often misunderstood. Patients with epistaxis commonly presentwithanelevatedbloodpressure.Epistaxisismore
common in hypertensive patients, perhaps owing to vascularfragilityfromlong-standingdisease.
Hypertension, however, is rarely a direct cause of epistaxis. More commonly, epistaxis and the associated anxiety cause an acute elevation of blood pressure. Therapy therefore, should be focused on controlling hemorrhage and reducing anxiety as primary means of bloodpressurereduction.
A study by Sarhan and Algamal, which included 40 patients with epistaxis and 40 controls, reported that the numberofattacksofepistaxiswashigherinpatientswitha history of hypertension, but the investigators were unable to determine whether a definite link existed between nosebleeds and high blood pressure. They did find, however, that control of epistaxis was more difficult in hypertensive patients; patients whose systolic blood pressure was higher at presentation tended to need management with packing, balloon devices, or cauterization.
Excessive coughing causing nasal venous hypertension maybeobservedinpertussisorcysticfibrosis.
Idiopathiccauses
The cause of epistaxis is not always readily identifiable. Approximately 10% of patients with epistaxis have no [14] identifiablecausesevenafterathoroughevaluation.
Prognosis
For most of the general population, epistaxis is merely anuisance.However,theproblemcanoccasionallybelifethreatening, especially in elderly patients and in those patients with underlying medical problems. Fortunately, mortality is rare and is usually due to complications from hypovolemia, with severe hemorrhage or underlying diseasestates.
Overall,theprognosisisgoodbutvariable;withproper treatment,itisexcellent.Whenadequatesupportivecareis
providedandunderlyingmedicalproblemsarecontrolled, most patients are unlikely to experience any rebleeding. Others may have minor recurrences that resolve spontaneously or with minimal self-treatment. A small percentage of patients may require repacking or more aggressivetreatments.
Patientswithepistaxisthatoccursfromdrymembranesor minor trauma do well, with no long-term effects. Patients with HHT tend to have multiple recurrences regardless of the treatment modality Patients with bleeding from a hematologic problem or cancer have a variable prognosis. Patients who have undergone nasal packing are subject to increased morbidity. Posterior packing can potentially cause airway compromise and respiratory depression. Packinginanylocationmayleadtoinfection.
PatientEducation
Forpatienteducationresources,seetheBreaks,Fractures, andDislocationsCenter,aswellasBrokenNose.
The following precautions should be imparted to the patient:
Usenasalsalinespray.
Avoidhardnoseblowingorsneezing.
Sneezewiththemouthopen.
Donotusenasaldigitalmanipulation.
Avoidhotandspicyfoods.
Avoidtakinghotshowers.
AvoidaspirinandotherNSAIDs.
The following simple instructions for self-treatment for minorepistaxisshouldbeprovided:
Applyfirmdigitalpressurefor5-10minutes.
Useanicepack.
· Practicedeep,relaxedbreathing.
Useatopicalvasoconstrictor
Disclaimer
The information and opinions presented in the Journal reflect the views of the authors and not of the Journal or its Editorial Board or the Publisher Publicationdoesnotconstituteendorsementbythejournal.
JIMA assumes no responsibility for the authenticity or reliability of any product, equipment, gadget or any claim by medical establishments/institutions/manufacturersoranytrainingprogrammeintheformofadvertisementsappearinginJIMAandalsodoesnotendorse orgiveanyguaranteetosuchproductsortrainingprogrammeorpromoteanysuchthingorclaimsmadesoafter — Hony Editor
Experience of botulinum toxin therapy in cervical dystonia, blepharospasm and hemifacial spasm
Satish Chandra , Ritu
1 2 3 4
Agarwal , Jayantee Kalita , Usha K Misra
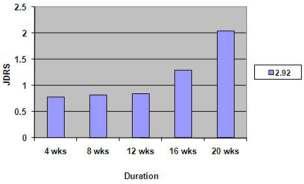
Botulinum toxin-A (BTx-A) has been recommended for cervical dystonia (CD) blepharospasm and hemifacial spasm (BHS). There are only few reports from developing countries. This study evaluates the efficacy and safety of BTx in 11 patients with CD and 22 patients with BHS from a teaching hospital. The severity of CD was assessed by Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS) and BHS by Jankovic Disability Rating Score (JDRS). Patient’s satisfaction was graded on 0-100 scale. BTx was injected as per standard protocol. The response was noted at 4 weeks. The side effects were recorded. The median age was 46 years and 13 were females. The median duration of illness was 24 (range 4-120) months. In CD group,only2patientshadtorticollisandremaininghadvariouscombinationsofretrocollis,anterocollisand laterocollis.Morethan50%improvementwasnotedin87%BHSand70%CDpatients.Theimprovementwas relatedtothedoseofBTxinCDbutnotinBHS.Theresponsewasrelatedtoseveritybutnottothedurationof dystonia. 50% patients had mild transient side effect. More than two third patients of CD and BHS responded toBTxwhichwasrelatedtoseverityofdystonia.
J Indian Med Assoc 2016; 114: 7-10]
Key words : Cervical dystonia, blepharospasm, hemifacial spasm, botulinum toxin, response, side effect.
Dystonia is a neurological disorder characterized by involuntary repetitive and sustained muscle contraction producing twitching, squeezing or other movements and abnormal postures. The dystonia may be due to underlying degenerative, vascular, toxic, metabolic or infective causes or may be idiopathic. Topographically dystonia may be generalized or focal. TheprevalenceofprimarydystoniareportedfromIndiais 43.9/100,000 population. The crude prevalence of primaryfocalorsegmentaldystoniareportedfromItalyis 127.4 per 1,000,000 populations. Blepharospasm is the commonest (prevalence 68.2), followed by cervical 3 dystonia (prevalence 44.8). The average prevalence of hemifacialspasmis7.4per100,000populationinmenand 14.5per100,000inwomen.
Dystonia not only causes functional disability but also cosmetic and emotional disturbances. Very few patients with dystonia have a good response to medical treatment, therefore,theroleofbotulinumtoxin-A(BTx-A)hasbeen explored in various focal dystonia for two decades. There is class I evidence about the efficacy of BTx-Ain cervical
Department of Neurology, Sanjay Gandhi Post Graduate Institute of MedicalSciences,Lucknow226014
1DM,Post-DoctoralFellow
2DM,Post-DoctoralFellow 3DM,Professor 4DM,Professor&Head
dystonia and class II evidence in hemifacial spasm and blepharospasm. The disadvantage of BTx-A is transient paralysis, wearing off therapeutic response, high cost and need of repeated injections. From South East Asia large series have reported in CD and BHS especially from 6-10 Thailand, Singapore and Taiwan and only small series 1-14 from India. In this communication we report our experience of BTx-A injection in focal and segmental dystonia.
MATERIALSAND METHODS
The patients with disabling focal and segmental dystonia despite optimal pharmacological therapy for 3 monthswereincludedinthestudy.Thepatientswithdoparesponsive dystonia, generalized dystonia, pregnancy, lactation, peripheral neuropathy, neuromuscular disorders,bleedingorcoagulationdisordersandrenaland hepaticfailurewereexcluded.
A detailed medical history and clinical examination were carried out The patients were evaluated neurologically including mental status by Mini-Mental State Examination (MMSE). Cranial nerve palsy, muscle power,tone,reflexandsensationswereexamined.
The topography, type and severity of dystonia were noted.Allthepatientswerevideotapedandtheseverityof dystoniawasscored.Forcervicaldystonia,TorontoWest-
15 ern Spasmodic Torticollis Rating Scale (TWSTRS) and for hemifacial/blepharospasm Jankovic Disability Rating 16Score were used. Overall satisfaction of the patients was rated on a 0-100 scale. Two different preparations of botulinum toxin type A (Dysport, Speywood Pharmaceuticals Ltd., UK and Botox, Allergan, Inc, Irvine, CA) were used as per availability of the drug. In practice, experience has shown that one unit of Botox is 17 equivalent to 4 units of Dysport ; therefore we have used 1:4conversioninbotoxtodisport.100Ubotoxwasdiluted in 2ml or 500U dysport in 2.5 ml of normal saline and 18 administered within few minutes. Cervical dystonia was categorized into laterocollis, anterocollis, retrocollis, and torticollisorcombinations.
BTx-Ainjection for the treatment of cervical dystonia was injected in splenius capitis, semispinalis capitis, trapezius, levator scapulae, sternocleidomastoid and 1 scalenus medius as per a fixed protocol. For blepharospasm injection sites included the upper medial and lateral eyelid margins, lower middle and lateral lid 20 margins, and separate injections above the eyebrow The muscleswhichcontractmostwasinjectedtotreatHFSand included orbicularis oculi, corrugator, frontalis, zygomaticus major, buccinators, and depressor anguli 21oris.
The patients were followed up at 1, 4, 12, 16 and 20 weeks The onset to peak time and duration of response were noted. The disability rating scale was used to objectively document the dystonia. The outcome of the injectionhoweverwasbased4weekresponse.
Adverse events :
Pain, hematoma, weakness, speech andswallowingdifficulty,wateringfromtheeyesandany othersymptomsfollowinginjectionwerenotedalongwith itsseverityandduration.
nia, 10 hemifacial spasm and 12 blepharospasm. The median duration of symptoms was 24 (range 4 to 120) months. These patients were on various anti-dystonia drugswhichincludedanticholinergicin28,baclofenin10 and tetrabenazine in 9 patients for a median duration of 3 months. Cranial and cervical MRI was carried out in 15 and did not reveal any abnormality In these patients, 54 sessions of BTx-A therapy were undertaken. The mean dose of botulinum toxin-A for blepharospasm and hemifacialspasmwas44units,forcervicaldystonia112.5 unitsofbotoxorequivalentdysport.
Blepharospasm/Hemifacial spasm (BHS) :
In this
group 22 patients received 38 sessions of BTx-A. Their medianagewas50.5(28-78)years.Hemifacialspasmwas present in 10 and blepharospasm in 12 patients. One patient with hemifacial spasm also had trigeminal neuralgia.The median duration of onset of action of BTxAwas4(range3to8)daysandpeakeffectwasachievedin th the 4 week. More than 50% improvement was present in 86.9% patients and lasted for median duration of 16 weeks. One patient each in hemifacial spasm and blepharospasm did not improve. The side effects were noted in 50% sessions and included ptosis in 6, facial weakness in 5, lid swelling in 3, ptosis with facial weakness in 3, lid swelling with blurred vision in 1, ptosis and lid swelling in 1. The change in Jankovic dystonia scaleisshowninFig1.
Case report :
EXPERIENCE OF BOTULINUM TOXIN THERAPY — CHANDRA ET AL 9
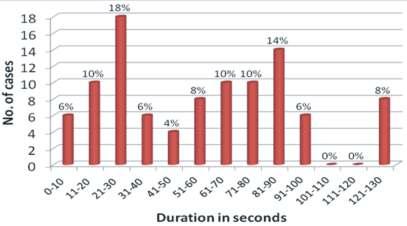
+retrocollisin2,anterocollis+laterocollisin2,torticollis + retrocollis in 2, torticollis + laterocollis in 1, torticollis+ anterocollis in 2 and only torticollis in 2 patients. These patients received 16 sessions of BTx-A. 11 cases of CD received 16 sessions, two patients recovered completely after single session. In the remaining 9 patients, two patients received 3 sessions, 1 received 2 and remaining only 1. Repeated injections in most patients were not possible because of high cost. The improvement started after a median duration of 7.5 (5-20) days and lasted for a median duration of 20 (2 to 24) weeks in all except 5 sessions in which the improvement was less than 50%. Twopatientsafter2injectionsremainedasymptomaticfor 2 years. The side effects were noted in 50% sessions and included dryness of mouth in 2, dysphagia in 2, pain and swelling at the injection site in 2 and dizziness and uneasiness in 1 patient each. These side effects improved in2weeks.ThechangeinTWSTRSscoreatdifferenttime pointsisshowninFig2.
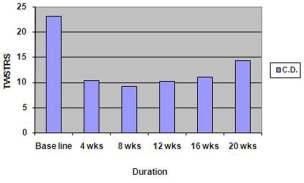
87% patients in BHS responded comparedto70%inCD(P=0.006).Theimprovementwas related to the dose of BTx-Ain cervical dystonia (r=0.54, P=0.037) but not in BHS (r=0.07, P=0.94). The response was related to severity of dystonia (r=0.55, P=0.03) but nottodurationofillness(r=-0.47,P=0.34).
Investigations : Statisticalanalysis:
Blood count, hemoglobin, ESR, blood sugar, serum creatinine, bilirubin, transaminase, calcium, phosphorus, albumin and ceruloplasmin were estimated. In cervical dystonia, cranial and cervical MRI wascarriedout.
Thepatientswereclassifiedinto 2 major groups- 1) cervical dystonia (CD) and 2) blepharospasm and hemifacial spasm (BHS). The responses of BTx-A in CD and BHS groups were compared from baseline to 4 weeks and 12 weeks using one way analysis of variance. The comparison of efficacy of BTx-Ain BHS versus CD was done by Mann Whitney Utest.Thevariableswereconsideredsignificantif2tailed p-valuewas<0.05.Allthestatisticaltestsweredoneusing SPSSversion12.0.
OBSERVATION
Thirty three patients aged 18 to 78 (median 48) years were included; 20 of whom were males.All these patients had primary dystonia. Eleven patients had cervical dysto-
A 55 years old lady had left sided hemifacial spasm and trigeminal neuralgia for last 10 years.HerMRIheadwithfiestasequencewasnormal.She received botulinum injection twice (35U-botox first time and 120 U dysport in second time) and response in hemifacial spasm was 70% in each injection and the duration of response was 12 months following first and 5 months following second injection. There was mild short lasting left sided facial palsy in first and no side effect in the second injection. There was no response in neuralgic pain.
Cervical dystonia (CD) :
Eleven patients had CD whose median age was 41 (18-58) years and only 1 was a female The duration of illness was 16 (range 4 to 72) months The pattern of CD included torticollis + laterocollis
Comparison : DISCUSSION
In the present study, the response of BTx-A in BHS was 87% and that of CD in 70% patients. Various studies ofhemifacial/blepharospasmhaveshownimprovementin 6, 9, 22-24 80.3%-100% and in cervical dystonia up to 85% of 25,26patients. The effects of BTx-A depend on the correct identification of the affected muscle and optimal dose. Cervical dystonia is a complex movement disorder with a group of overactive muscles resulting in various combinations of neck dystonia. Identification of muscle for injection in torticollis, retrocollis, laterocollis and anterocollis is essential. The muscles are targeted after observing the pattern of shift, tilt and rotation of neck.We havenotusedEMGfortargetingthemuscles.Thedoseof BTx-Ain our study ranged between 17.5 and 50 (median 27.5) units of botox or equivalent dysport for a single muscle, which is within the recommended dose of 20-60 units for different cervical muscles. Anterocollis is 27 associated with spreading of dystonia to other parts. In ourstudy,4patientshadanterocolliswithheadprotrusion and 2 of them improved more than 50%. Only 2 of our patients had cervical torticollis and the remaining 9 patients had different combinations of neck dystonia whichmayberesponsibleforrelativelypoorerresponseto BTx-A.Thesuboptimalresponsemaybeduetoantibodymediated resistance, vial-to-vial variability in response, variability in injection location and technique, change in pattern of muscle involve-
28 ment and inadequate dose. Many of our patients with severe dystonia may have suboptimal dose because of financial reason. The selection of muscles was carefully done by experienced neurologist and all the patients had some degree of improvement, therefore, it is unlikely that correct muscles were not targeted for BTx-A injection. The BTx-A was obtained from the company maintaining the cold chain. The better response in BHS could be attributed to better dosing of target muscles. The subjective improvement was more with cervical dystonia compared to hemifacial spasm as BTx-A is highly effective in controlling pain associated with cervical 19dystonia. Though the objective measurements in our study revealed a lower improvement in cervical dystonia but patients felt better subjectively which highlight the greaterfunctionalimprovement.
Repeatedinjectionsweregivento8patientswithBHS and 3 patients with cervical dystonia. On repeated injections decay of response was noted is 2 sessions. Antibodies against BTx-A may have led to secondary therapeutic failure particularly in patients who had 29 previously received high doses of toxin and were 30 reinjected within a short period. The prevalence of immuno-resistance ranges in different studies, but it is 31-32 usually less than 10%. Currently available BTx-Ahas 5 ng of neurotoxin complex per 100 U; therefore the formation of neutralizing antibody and subsequent 33 wearing off effects has significantly reduced. We had mildtomoderatesideeffectsin50%ofsessionslastingfor about 2 weeks and the reported side effects of BTx-A in hemifacial spasm and that in cervical dystonia is also similar. The higher frequency of muscle weakness in our study in BHS may be due to smaller muscle bulk and conversionofbotoxtodisportin1:4.Thecomplicationsin theliteraturewereencounteredinupto63.4%inHFSand 34 up to 72.7% in BS. BTx-A therapy is regarded as a symptomatic treatment and repeated injections are needed. Two of our patients with cervical dystonia after 2 injections remained asymptomatic for 2 years. Both these patientshowever had short durationof illness.The patient who had both trigeminal neuralgia and BHS, BTxA
injection relieved blepharospasm but not the neuralgic pain. The efficacy of BTxA in trigeminal neuralgia has 35-37 beenreportedin72.7to100%patients.
In our study, more than two-third patients with BHS andCDrespondtoBTx-Atherapywithmildtransientside effects.AbetterresponseinBHSwasrelatedtotheshorter durationofillness.
REFERENCES
1 Fahn S, Jankovic J — Practical management of dystonia. Neurol Clin 1984;2:555-69.
2 DasSK,BanerjeeTK,BiswasA,RoyT,RautDK,Chaudhuri A, et al Community survey of primary dystonia in the city ofKolkata,India. Mov Disord 2007;22:2031-6.
3 Papantonio AM, Beghi E, Fogli D, Zarrelli M, Logroscino G, Bentivoglio A, et al Prevalence of primary focal or segmental dystonia in adults in the district of foggia, southern Italy: a service-based study. Neuroepidemiology 2009;33:117-23.
4 Auger RG, Whisnant JP — Hemifacial spasm in Rochester and Olmsted County, Minnesota, 1960 to 1984. Arch Neurol 1990;47:1233-4.
5 SimpsonDM,BlitzerA,BrashearA,ComellaC,DubinskyR, Ha e M, e a Therapeut cs and Technology Assessment Subcommittee of the American Academy of Neurology. Assessment: Botulinum neurotoxin for the treatment of movement disorders (an evidence-based review): report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 2008;70:1699-706.
6 Poungvarin N, Devahastin V, Chaisevikul R, Prayoonwiwat N, Viriyavejakul A — Botulinum A toxin treatment for blepharospasm and Meige syndrome: report of 100 patients. J Med Assoc Thai 1997;80:1-8.
7 Poungvarin N, Devahastin V, Viriyavejakul A — Treatment of various movement disorders with botulinum A toxin injection: an experience of 900 patients. J Med Assoc Thai 1995;78:281-8
8 Poungvarin N, Viriyavejakul A — Botulinum A toxin treatment in spasmodic torticollis: report of 56 patients. J Med Assoc Thai 1994;77:464-70.
9 Supu ti ada A, Phanthumch nda K, Locharernkul C, Suwanwela NC — Hemifacial spasm: results of treatment with low dose botulinum toxin injection. J Med Assoc Thai 2004;87:1205-11.
10 Jamora RD, Tan AK, Tan LC — A 9-year review of dystonia fromamovementdisordersclinicinSingapore. Eur J Neurol 2006;13:77-81.
11 Behari M, Singh KK, Seshadri S, Prasad K,Ahuja GK — Botulinum toxin A in blepharospasm and hemifacial spasm. J Assoc Physicians India 1994;42:205-8.
12 Bhaumik S, Behari M — Botulinum toxin A—injection for cervical dystonia. J Assoc Physicians India 1999; 47: 26770.
13 Thussu A, Barman CR, Prabhakar S — Botulinum toxin treatment of hemifacial spasm and blepharospasm: objective response evaluation. Neurol India 1999; 47: 2069.
14 Gupta M, Singh G, Khwaja G — Botulinum toxin in the treatment of dystonias—a hospital based study. J Assoc Physicians India 2003;51:447-53.
15 CrownerBE—Cervicaldystonia:diseaseprofileandclinical management. Phys Ther 2007;87:1511-26.
16 Brin MF, Jankovic J, Comella C — Treatment of dystonia usingbotulinumtoxin.In:Treatmentofmovementdisorders. KurlanR,J.B.(Ed.)LippincottCompany1995;183-230.
17 Elston JS — Botulinum toxin for blepharospasm In: Therapy
with botulinum toxin. Jankovic J, Hallet M, (Eds.) Marcel Dekker, IncNewYork1994;191-7.
18 Shetty MK IADVL Derma osurgery Task Force Guidelines on the use of botulinum toxin type A. Indian J Dermatol Venereol Leprol 2008;74:S13-22.
19 Camargo CH, Teive HA, Becker N, Baran MH, Scola RH, Werneck LC — Cervical dystonia: clinical and therapeutic featuresin85patients. Arq Neuropsiquiatr 2008;66:15-21
20 Pang AL, O’Day J — Use of high-dose botulinum A toxin in benign essential blepharospasm: is too high too much? Clin Experiment Ophthalmol 2006;34:441-4.
21 Frei K, Truong DD, Dressler D — Botulinum toxin therapy of hem facia spasm compar ng different therapeutic preparations. Eur J Neurol 2006;13:30-5.
22 Berardelli A, Carta A, Stocchi F, Formica A, Agnoli A, Manfredi M — Botulinum A toxin injection in patients with blepharospasm, torticollis and hemifacial spasm. Ital J Neurol Sci 1990;11:589-93.
23 Novis SA, De Mattos JP, De Rosso AL — Botulinum toxin in blepharospasm, in hemifacial spasm, and in cervical dystonia: results in 33 patients. Arq Neuropsiquiatr 1995; 53:403-10.
24 Jankovic J, Schwartz K, Donovan DT — Botulinum toxin treatment o cran al-cervica dyston a, spasmodic dysphonia, other focal dystonias and hemifacial spasm. J Neurol Neurosurg Psychiatry 1990;53:633-9.
25 Comella CL, Jankovic J, Brin MF — Use of botulinum toxin typeAinthetreatmentofcervicaldystonia. Neurology 2000; 55:S15–S21.
26 Ceballos-Baumann AO — Evidence-based medicine in botulinum toxin therapy for cervical dystonia. J Neurol 2001; 248:14-20.
27 Godeiro-Junior C, Felício AC, Aguiar PM, Borges V, Silva SM, Ferraz HB — Retrocollis, anterocollis or head tremor maypredictthespreadingofdystonicmovementsinprimary cervicaldystonia. Arq Neuropsiquiatr 2009;67:402-6.
28 Smith AG — Pearls and pitfalls in the therapeutic use of botulinumtoxin. Semin Neurol 2004;24:165-74.
29 Göschel H, Wohlfahrt K, Frevert J, Dengler R, Bigalke H — Botulinum A toxin therapy: neutralizing and nonneutralizing antibodies—therapeutic consequences. Exp Neurol 1997; 147:96-102.
30 Clinical use of botulinum toxin. National Institutes of Health Consensus Deve opment Conference Statement, November12-14,1990. Arch Neurol 1991;48:1294-98.
31 Kessler KR, Skutta M, Beneke R — Long-term treatment of cervical dystonia with botulinum toxin A: efficacy, safety, and antibody frequency. German Dystonia Study Group. J Neurol 1999;246:265-74.
32 Jankov c J, Schwartz K Response and immunoresistance to botulinum toxin injections. Neurology 1995;45:1743-6.
33 Jankovic J, Vuong KD, Ahsan J — Comparison of efficacy and immunogenicity of original versus current botulinum toxinincervicaldystonia. Neurology 2003;60:1186-8.
34 Park YC, Lim JK, Lee DK — Botulinum a toxin treatment of hemifacial spasm and blepharospasm. J Korean Med Sci 1993;8:334-40.
35 Borodic GE, Acquadro MA — The use of botulinum toxin for thetreatmentofchronicfacialpain. J Pain 2002;3:21-7.
36 Piovesan EJ, Teive HG, Kowacs PA, Della Coletta MV, Werneck LC, Silberstein SD — An open study of botulinumA toxin treatment of trigeminal neuralgia. Neurology 2005; 65:1306-8.
37 Zúñiga C, Díaz S, Piedimonte F, Micheli F — Beneficial effects of botulinum toxin type A in trigeminal neuralgia. Arq Neuropsiquiatr 2008;66:500-3.
Role of nasal endoscopy in the management of intractable epistaxis : our experience
Dwaipayan Mukherjee , Chiranjib Das
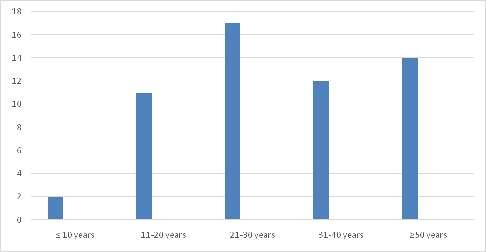
Epistaxis is the most frequent emergency in Otorhinolaryngology. Intractable epistaxis is traditionally managedwithmultiplenasalpacking.Thisisduetothecovertareasofthenose.Theavailabilityofthenasal endoscope has been a boon to the otolaryngologist, since it not only helps in proper visualization of bleeding points, but also offers a direct mode of treatment to the area. The present work was undertaken to elicit the role of nasal endoscopy in detecting the site and the possible hidden causes of the intractable epistaxis and their treatment with comparison to conventional management. We conducted this prospective study in the Otorhinolaryngology department of a tertiary care hospital of West Bengal from March 2013 to February 2015. Cases where no apparent local or systemic cause of epistaxis could be detected, were included in this study. Patients who were not willing to give consent, patients with cardiovascular disease, bleeding disorder or receiving anticoagulant drugs were excluded. When no bleeding points were seen on anterior rhinoscopy and no systemic cause was found out, nasal endoscopy wasperformedwithrigidnasalendoscopes.Patientsweretreatedwithendoscopicnasalcautery,selective nasal packing, polypectomy, excision of angioma, sphenopalatine artery cauterization, spurectomy or excision of angiofibroma. Among total 56 patients there were 15 female patients and 41 male patients. Most patientswereintheagegroupof21-30years.Themostcommoncauseofepistaxiswasbleedingpointinthe crevices of the lateral nasal wall (32%). All patients had successful control of epistaxis. Seven patients had anterior epistaxis in follow up period, which were managed with conventional treatment. Endoscopic examination of the nasal cavity has the advantage of providing better view of the nasal cavity and also aids in appropriate management of epistaxis based on their merit. It is a cost-effective and less invasive procedure.Ithasminimalmorbidityandfailurerates.
[J Indian Med Assoc 2016; 114: 11-3 & 20]
Key words : Intractable Epistaxis, Endoscopy, Selective nasal cautery, Selective nasal packing.
Epistaxis is the most frequent emergency in Otorhino-laryngology, presenting with a prevalence of about 10% to 12% Intractable epistaxis is a challenging problem due to the covert areas situated in the posterior and lateral part of the nose, which 2 are difficult to access by anterior rhinoscopy. It is traditionally managed with multiple nasal packing and prolonged hospital stay and associated with significant 3 patient morbidity and high health care costs The availability of the nasal endoscope has been a boon to the otolaryngologist, since it not only helps in proper visualization of bleeding points, but also offers a direct 2 modeoftreatmenttothearea(Kennedyetal,1985).Nasal endoscopy enables targeted haemostasis of the bleeding pointsusingelectrocautery,directpressurewithminiature targeted packs, endoscopic ligation or cauterization of the
1MS (ENT)Associate Professor KPC Medical College & Hospital, Kolkata700032
2MS (ENT) RMO cum Clinical tutor Bankura Sammilani Medical College&Hospital,Bankura722102
sphenopalatine artery, endoscopic ligation of ethmoidal arteries,cryotherapyandlasers
Aimsandobjectives:
The present work was undertaken to elicit the role of nasalendoscopyin
1. Detecting the site and the possible hidden causes of intractableepistaxis.
2. Treatmentofepistaxiswithcomparisontoconventional management.
MATERIALSAND METHODS
We conducted this prospective study in the Otorhinolaryngology Department of a tertiary care hospital of West Bengal from March 2013 to February 2015.
InclusionCriteria:
(1) Cases where no apparent local or systemic cause of epistaxiswasfound.
ExclusionCriteria:
(1) Patientswhowerenotwillingtogiveconsent.
(2) Patientswithcardiovasculardisease.
(3) Patients with bleeding disorder or receiving anticoagulantdrugs.
Based on the above criteria, 56 patients were selected in our study First of all vitals were checked. In severe epistaxis, first of all bleeding was controlled by nasal packing and patient was made haemodynamically stable. When the bleeding was controlled, detailed history of the patient was taken followed by general and otorhinolaryngology examination including thorough anterior rhinoscopy Laboratory investigations were done to rule out any systemic causes for epistaxis Investigations like haemoglobin estimation, total and differentialleucocytecount,plateletcount,ESR,bleeding time, clotting time, prothrombin time, a PTT, renal function tests, liver function tests, blood grouping were done routinely When no bleeding points were seen on anterior rhinoscopy and no systemic cause was found out; nasalendoscopywasperformedwithnasalendoscopes.
0 and 30 rigid nasal endoscopes of 2.7 mm and 4 mm diameterwereused.Lightcottonpledgetssoakedwith4% lidocainewasused.Noadrenalineorpriornasaldropswas usedandnoextrapressurewasexertedtoavoidmissingof the bleeding points.Then diagnostic nasal endoscopy was undertaken in three steps. The first step consisted of an inspection of nasal vestibule, nasopharynx and inferior nasal meatus. This was followed by an examination of sphenoethmoidal recess and superior meatus Finally, an examination of middle meatus was done. If nasal mass was found, CT scanwasdoneafterwards.
When the bleeding point was identified, endoscopic nasal cautery was done with insulated sucker cum cauteryorbipolarcautery Whenthe bleeding point was located in the posterior part of nasal cavity, endoscopic sphenopalatine artery cauterization was done If the bleedingpointwasnotreachablefor cauterization then selective nasal packing was done with gelfoam. If bleeding was coming from an ulcer, gelfoam was tightly packed between the ulcer and the nasal septum or the turbinates. Patients having septal spur were undergone endoscopic spurectomy When congested polyp was found in the middle meatus endoscopic polypectomy was done and sent for histopathological examination. The patients who were diagnosed to have angiofi-
bromas were subjected to excision of the angiofibromas and the specimens were sent for histopathological examination.
Thepatientswerefollowedupinthepost-operativeperiod at 1 week, 2 weeks, 1 month, 3 months, 6 months and 1 yearwithendoscopy
Results:
Mostpatientsinoursrudywereintheagegroupof2130 years (Fig 1). There were 15 female patients and 41 male patients. The most common cause of epistaxis was bleeding point in the crevices of the lateral nasal wall (32%),followedbybleedingulcerinthecrevicesoflateral nasal wall (16%), bleeding ulcer posterior to deviation of septum (14%), angioma in lateral nasal wall (13%), septal spur (11%), congested polyp in middle meatus (9%), angiofifbroma just posterior to middle turbinate (5%) (Table 1).All of them were treated with endoscopic nasal cautery,selectivenasalpacking,polypectomy,excisionof angioma,sphenopalatinearterycauterization,spurectomy or excision of angiofibroma (Table 2). All patients had successful control of epistaxis No significant complication or morbidity has been noted in the postoperative follow-up period of 1 year Seven patients hadanteriorepistaxisinfollowupperiodeitherduetonose picking or nose blowing.All of them were managed with conservativetreatment(Fig2&3).
Table 1— Distribution of patients according to Endoscopic findings
Endoscopicdiagnosis Numberof Percentage patients
Bleedingpointinthecrevicesoflateralnasalwall 18 32%
Bleedingulcerinthecrevicesoflateralnasalwall 9 16%
Congestedpolypinmiddlemeatus 5 9%
Angiomainlateralnasalwall 7 13%
Angiofibromajustposteriortomiddleturbinate 3 5%
Bleedingulcerposteriortodeviationofseptum 8 14%
Septalspur 6 11%
Table 2 — Distribution of patients according to treatment
Endoscopictreatment Numberof Percentage patients
Endoscopicnasalcautery 10 18%
Endoscopicselectivenasalpacking 17 30%
Endoscopicpolypectomy 5 9%
Endoscopicexcisionofangioma 7 13%
Endoscopicsphenopalatinearterycauterization 8 14%
Endoscopicspurectomy 6 11%
Excisionofangiofibroma 3 5%


DISCUSSION
The anterior and posterior rhinoscopies give a very restricted view of the nasal cavity, resulting in poor visualizationofcertainareas.Duetothisreason,thecause of the epistaxis many a times remains an enigma Even if the area is seen, it is difficult sometimes to apply direct pressuretoensurestoppageofbleeding.Traditionallythe treatmentoptionswereoneormoreofthefollowing:nasal packing, septoplasty, and ligation of external carotid artery or internal maxillary artery Apart from high failure rates ranging from 26-52%, these procedures have 5-6 significant morbidity . Conventional nasal packing is associated with considerable discomfort, mucosal trauma and morbidity due to hypoxia. The large size of the packing material exerts pressure not only on the point of bleedingbutalsoonthenormalmucosa.Sometimeshaste instrumentationmaycauseafreshbleed Externalcarotid artery ligation is associated with risk of damage to hypoglossalandvagusnerve Thetransantralapproachto internal maxillary artery may cause damage to 5, nasolacrimal duct or infraorbital nerve Recently angiography and embolization of bleeding vessels have been added to treatment option. But it requires expertise of an experienced interventional radiologist, which is not uniformly available. Moreover, it is also associated with serious 9,10 neurologicalcomplications Regularuseofnasal endoscopy during the last decade amplified the knowledge on the aetiology and treatment of epistaxis. The bleeding source inside the nasal cavity could be more easily and accurately identified. Cauterization of the bleeding point, which was previously limited to anterior portions of the nasal cavity, could be applied to posterior regionswiththeadventofendoscope . Moreover, nasal endoscopy is the only way for preventing trauma to the normal mucosa due to Fig 3 — Clinical photograph of bleeding point over middle turbinate
conventional packing Other less invasive procedures, such as selective nasal packing and endoscopic cauterization of sphenopalatine artery could be done with high efficacy rates. When selective cauterization of bleeding point is not feasible as in inferior meatus, high in the lateral nasal crevices and bleeding ulcer; a selective nasal packing is done with gelfoam. It is a dissolvable synthetic matrix that has a procoagulant effect. The gelfoam becomes nonadherent and it begins to dissolve in 12 a matter of weeks The detection of angiofibroma on endoscopy was a great source of relief as it would have normally been missed. The small mass which was later confirmedonaCTscan,wassituatedinasitewhichcould have not been possible to detect with anterior rhinoscopy We feel it is important to do a regular endoscopy in the vulnerableagegroupwithepistaxistoseeifthebleedingis notduetoanangiofibroma.Therearemanyothermethods that can be applied for the treatment of epistaxis; like lasers, cryotherapy, endoscopic ligation of the s
[2]arteries. Due to lack of facilities, these procedures
(Continued on page 20)
INCIDENCE OF URINARYTRACT INFECTIONAND UROLOGICAL SYMPTOMS — NISHA ET
Practitioners' Series Practitioners' Series
Incidence of urinary tract infection and urological symptoms in depot-medroxyprogesterone users
1 2 3 4
B Nisha , Sunita Malik , Jagdev Kaur , Archana Aggarwal
Progesterone due to its facilitatory effect on the b-receptors present in the urinary system may decrease the tone and peristalsis of urethra and ureter, causing dilatation of the urinary collecting system, decreased flow, relative stasis and defective clearance of the bacteria which can lead to urinary tract infection in women using Depot-medroxyprogesterone acetate. The other contributory factor for urinary tract infection seen recently is that use of progesterone may decrease the production of human beta defensin-2 receptor in the vaginal epithelium and may increase the susceptibility to urinary tract infection. In this study, 50 cases who opted for depot-medroxyprogesterone acetate for contraception after medical terminationofpregnancywerecomparedwith50controlswhounderwentconcomitanttuballigationalong with medical termination of pregnancy after 3 months for urinary symptoms and urinary tract infection. None were given antibiotic after the procedure. Women found to have urinary tract infection were treated accordingtoantibioticsensitivityreport.Therateofurinaryinfection(p-0.031)andurologicalsymptomsin the study group were higher than in the control group. Escherichia coli was the most common microorganism that caused urinary tract infection and second was Staphylococcus aureus. We recommend routine screening for presence of urological symptoms, urinary tract infection and asymptomatic bacteriuria in women using depot-medroxyprogesterone acetate in order to avoid complicationsofuntreatedinfection.
J Indian Med Assoc 2016; 114: 14-6]
Key words : Urinary tract infection, depot-medroxyprogesterone acetate, urological symptoms.
Depot-medroxyprogesterone acetate (DMPA) has been the most widely studied injectable contraceptive. Since its introduction many studieshavebeendonetoevaluateitsbenefitsandadverse effects. Among them urinary tract infection (UTI) is a recentlyobservedshorttermeffect.
It has been seen that progesterone has a facilitatory effect on the b-receptors present in the urinary system thereby, decreasing the tone and peristalsis of urethra and 1-4ureter due to its relaxant effect on the smooth muscles. These features contribute to UTI due to the dilation of the urinary collecting system, with decreased flow, relative stasisanddefectiveclearanceofthebacteria.
Progesterone also decreases the vascularity of the urinary system by counter acting the effect of estrogen, which helps in preparation of the tissue to combat infectionasseeninanimalexperimentbyBatraS et al . Human beta defensin-2 receptor (HBD-2) plays an
DepartmentofObstetricsandGynaecology,VardhmanMahavirMedical CollegeandSafdarjangHospital,NewDelhi110029
1MBBS,MD,SeniorResident
2MBBS,MD,FICOG,ProfessorandConsultant
3MBBS,MD,AssociateProfessorofMicrobiology
4MBBS,DMRD,ConsultantRadiodiagnosis
importantroleattheinnatedefenseongenitourinarytract. This receptor remains unaffected during the normal state.
It is seen that during infection estrogen increases the production of this receptor whereas progesterone decreasesit Hence,lackofestrogenduringmenopauseor use of progesterone based oral contraceptive in sexually active women may influence the production of HBD-2 receptor in vaginal epithelium and may increase susceptibilitytobacterialvaginitisorrecurrentUTI.
In addition to the above feature it has also been seen that progesterone dominance to some degree may also be responsible for increased incidence of genuine stress incontinence as progesterone counteracts the effect of 7-9estrogen .
Based on the above observations, due to the possible effect of progesterone on urinary tract, the present study wasundertakentodeterminewhetherDMPAincreasesthe rate of urinary tract infection in those who received this drug for contraception after medical termination of pregnancy(MTP).
MATERIALSAND METHODS
A pilot study was conducted in the family welfare
in the Department of Obstetrics and Gynecology,
wing, Safdarjang Hospital, New Delhi, India, to observe the effect of DMPAon the urinary tract, which was compared withmatched(basedonage,gravidity,socioeconomicand educationalstatus)control.However,expectingthehigher dropout, more than 100 women were recruited and 2 groupswereformed.
Study Group
78 postabortal women who had undergone MTP with suction and evacuation method, received injection Depot-medroxyprogesterone acetate 150mg intramuscularly before discharge from the hospital.These women formed the study group. Out of 78 subjects, 23 were lost to follow up, 5 were excluded (4 subject had bacterial growth in urine culture at 0 month and 1 took antibiotic) and the rest 50 subjects were comparedwithmatchedcontrol.
Control Group
69 postabortal women who had undergone MTP with concomitant tubal ligation formed thecontrolgroup.Outof69subjects,15werelosttofollow up, 4 were excluded (3 took antibiotic 1 had bacterial growth in urine at 0 month), and the rest 50 subjects were comparedwiththestudygroup.
The inclusion criteria were: (1) Apparently healthy women aged between 20-40 years, (2) no medical or surgicalillness,and(3)intendedtocomeforfollowupat3 months.
The exclusion criteria were: Any history of (1) UTI more than twice per year, (2) presence of UTI, urinary stone, urinary tract anomaly, or asymptomatic bacteriuria, urological symptoms (3) diabetes mellitus, hypertension, (4) use of any hormonal contraceptive or intrauterine device in the past 3 months, (5) presence of vaginitis or abnormal vaginal discharge, and (6) consumption of any antibioticinthepast3months.
Preliminary contact was made on the day of MTP and informed consent was taken. Questionnaires were used to evaluateurologicalsymptomsandrelevanthistory Patient then immediately received injection DMPA, 150 mg intramuscular after MTP by suction and evacuation method.Noantibioticwasgiveninbothgroups.
Mid-stream urine sample was collected on the day of procedure and sent for routine microscopy examination and bacteriological culture and sensitivity test using MacConkeyAgarmedia.
However, women showing UTI and asymptomatic bacteriuria were appropriately treated as per the antibiotic sensitivitytestandwereexcludedfromthestudy
At 3 months, women in the two groups were followed and evaluated for urological symptoms such as frequency (ie, daily void >8 times), burning micturition, urinary incontinence (urge/stress) and UTI. Bacterial count > 105 org./ml.wasconsideredassignificant.
Pearson Chi-Square and Fisher-exact test were used to compare parameters between the two groups.Value of p < 0.05wasconsideredsignificant.
RESULT
At the beginning of study there were no significant differences in age, educational status, occupation and gestationalage.
At3months,theeffectofDMPAontherateofUTIand urologicalsymptomsareshowninTable1.
The results showed that rate of UTI in the study group (p - 0.031) were significantly higher than in the control group. Frequency of urological symptom though not statistically significant but were found be higher in the DMPAusers. In the control none had increased frequency of micturition. Urinary incontinence was not reported by anyone.
The most common organism responsible for causing UTI was Escherichia coli (5 cases out of 8). The other micro-organisms were Staph aureus (2 cases out of 8) and Klebsiella (1casesoutof8).
At the beginning of the study, among 117 subjects significant bacteriuria was found in 4 who were excluded. However, these 4 subjects did not report any urological symptoms, showing prevalence of ASB as 3.42% which is close to the value seen in another study done on pregnant population 10 belonging to same geographical area 4.34% At 3 months out of 50 subjects of study group significant bacteriuria withoutanyurologicalsymptomswerefoundin2subjects, showingincidenceofASBwithDMPAas4%.
Asymptomatic bacteriuria (ASB) DISCUSSION
We have seen in the present study that women using DMPAarepredisposedtoUTI,possiblyduetotheeffectof progesterone on muscle tone, peristalsis of the ureter and also urinary vasculature. ASB, UTI, increased bladder capacity hydroureter, increased bladder capacity, and urinary incontinence have been seen during pregnancy, due to the possible effect of progesterone on the smooth 11-13 muscleoftheurinarysystem
With this background that the progesterone causes dilatation of ureter, high dose progesterone have shown 14,15 beneficial effect in patients with ureteral stone and
Table 1 — Comparison of the parameters in the two group after 3 months
16 J INDIAN
benign
prostatic hypertrophy in men Raz and
17colleagues havereportedthatoralmedroxyprogesterone acetate 20 mg daily exacerbated stress incontinence in 60% of women treated with corresponding changes in urethralpressure.
Increased incidence of bacteriuria has also been reported in women taking oral contraceptives, especially 18,19 thosewithhighdoseprogesteronecontent
20 S Ziaei et al has reported significantly higher rate of UTIandurologicalsymptomsintheDMPAusersthanthe control. As so far only one study of this kind has been published, its comparison with present study is shown in Table2.
The comparison between two studies after 3 months of DMPAuseshowsthat-
(i) DMPA may be responsible for urological symptoms andUTI.
(ii) Inourstudyurinaryincontinencewasnotseeninany subject.
(iii)The most common organism of urinary infection was Escherichiacoliinboththestudies.
CONCLUSION
DMPA, although quite safe and effective method of contraception, may be responsible for increase in the frequency of urinary infection. Hence, women who have any history of current or recurrent UTI, UTI during pregnancy, presence of urological symptoms (such as frequency and burning micturition), urinary stone or urinary tract anomaly or diabetes mellitus should be offeredanalternativemethodofcontraception. We recommend routine screening for presence of urological symptoms, urinary tract infection and asymptomatic bacteriuria in women using depot-
medroxyprogesterone acetate in order to avoid complicationsofuntreatedinfection
REFERENCES
1 Raz S, Zeigler M, Caine M — The Effect of Progesterone on the Adrenergic Receptors of the Urethra. Br J Urol 1973; 45: 131-135.
2 BatraSandIosifS—ProgesteroneReceptorsinthefemale lowerurinarytract. J Urol 1987;138:1303-4.
3 Raz S, Caine M — Adrenergic Receptors in the female canineurethra. Invest Urol 1972;9:319-23.
4 Raz S, Zeigler M, Caine M. Hormonal influence on the adrenergic receptors of the ureter. Br J Urol 1972; 44: 40510.
5 Batra S, Bjellin L, Iosif S, Martensson L, Sjogren C — Effect of estrogen and progesterone on the blood flow in the lower urinarytractofrabbit. Acta Physiol Scand 1985;123:191-4.
6 Han JH, Kim MS, Lee MY, Kim TH, Lee MK, Kim HR et al Modulation of human beta-defensin-2 expression by 17beta-estradiolandprogesteroneinvaginalepithelialcells. Epub2009Oct9.Cytokine.2010;49:209-14.
7 Grady D Brown, Brown JS, Vittinghoff E, Applegate W, Varner E, Snyder T — Postmenopausal hormones and incontinence:theheartandestrogen/progestinreplacement study. Obstet Gynecol 2001;97:116-20.
8 Cardozo LD, Kelleher CJ — Sex hormones, the menopause andurinaryproblems. Gynecol Endocrinol 1995;9:75-84.
9 Hextall A — Estrogen and lower urinary tract function. Maturitas 2000;36:83-92.
10 Bandyopadhyay S, Thakur JS, Reny P, Kumar R — High prevalence of Bacteriuria in Pregnancy and its screening methods in North India. J Indian Med Assoc 2005; 103: 25962,266.
11 Emil A, Jack W — Smith's general urology. New York: McGraw-Hill,2000:254.
12 Marchant DJ — Effects of pregnancy and progestational agents on the urinary tract. Am J Obstet Gynecol 1972; 112: 487-98.
13 WaltzerWC—Reviewarticle:theurinarytractinpregnancy. J Urol 1981;125:271-6.
14 Perlow DL — The use of Progesterone for ureteral stones: a preliminaryreport. J Urol 1980;124:715-6.
15 Mikkilsen AL, Meyhoff HH, Lindahl F, Christensen J — The effect of hydroxyprogesterone on ureteral stones. Int Urol Nephrol 1988;20:257-260.
16 Onu PE — DMPA in the management of BPH. Eur Urol 1995;28:229-35.
17 Raz S — Female Urology. Philadelphia; W.B. Saunders 1996: 304-544.
18 Marshall S, Linfoot J — Influence of hormones on Urinary tractinfection. Urology 1977;9:675-9.
19 Zahran M M, Kamel M, Mooro H, Osman M, Fayad M, Youssef AF — Effects of contraceptive pills and intrauterine devicesonurinarybladder. Urology 1976;8:567-74.
20 Ziaei S, Ninavaei M, Faghihzadeh S — Urinary Tract Infection in the Users of Depot-Medroxyprogesterone Accetate. Acta Obstet Gynecol Scand 2004;83:909-911.
We request you to send QualityArticles addressed to : Hony. Editor, Journal of IMA(JIMA), 53, Sir Nilratan Sircar Sarani (Creek Row), Kolkata 700 014
Dr. Debasish Mukherjee
Dr. Santanu Sen Hony. Editor, JIMA Hony. Secretary, JIMA Hony. Secretary, IMA Bengal
Practitioners' Series Practitioners' Series
A comparative study between skin sutures and skin staples in abdominal surgical wound closure
1 2 3 4 5
Chandrashekar N , Prabhakar GN , Vivek PO , Shivakumarappa GM , Fahad Tauheed
The skin stapling devices have revolutionized surgery for the purpose of rapid closure of abdominal wounds. However, staples have their own drawbacks. In view of this, this prospective study has been undertaken to highlight the outcomes of closure by staples and sutures with respect to speed of closure, costeffectivenessandpostoperativewounddehiscence,acceptanceofscarandpostoperativepain.Thisis a prospective hospital based study conducted in our hospital from October 2009 to September 2011 involvingatotalof200patientswhounderwentabdominalsurgerybothonanemergencyandelectivebasis. Results were analyzed and compared with previous studies. It has been found that the use of staples in abdominal surgical wound closure gives faster speed of closure, less postoperative pain, and better cosmeticresults.Staples,however,arecostlier,andwhenusedinemergencycases,associatedwithhigher ratesofwounddehiscenceandalessacceptablescar.
J
AMed Assoc 2016;114: 17-20]
Key words : Skin staples, nylon suture material, post operative wound infection, operative scar.
ny surgical intervention will result in a wound in ordertogetaccesstoanddealwiththeunderlying pathology In this situation, the surgeon’s task is to minimize the adverse effects of wounds, remove or repair the damaged structures and harness the process of woundhealingtorestorefunction.
The principle aims of tissue repair of surgical skin incisions are rapid acquisition of strength and minimum tissue damage, with minimum inflammation and a good scar.Manyfactorsincludingthechoiceofsuturematerials and its placements influence these aims; of particular relevance is the accurate co-optation of dermal edges; eversionorinversionleadstosuboptimalhealing. Formanyyearssutureshavebeenusedtoapproximate the skin edges, and also to hold the cut tissues together until the wound has healed sufficient enough as to be self supportive. Throughout antiquity many materials have been used to approximate the skin edges. Suture technology and suture sterilization have kept pace with advancement in surgical techniques and provided the surgicalfraternityawiderangeofsuturesindifferentsize asfineas30microns.Nowthesurgeonhasathisdisposal a wide variety of suture materials like natural and synthetic, non absorbable and absorbable, monofilament to poly filament. However, sutures have the disadvantage
Department of General Surgery Sree Siddhartha Medical College, Hospital&ResearchCentre,Tumkur572107
1MS,FIAGES,FAMS,AssociateProfessor
2MS,FIAGES,Professor
3MS,AssistantProfessor
4MS,ProfessorandHead
5MBBS,Postgraduate(MS)student
of consuming more time in applying and with a cosmetically inferior scar The use of other methods to approximate the wound edges like stapling devices, glue or adhesive tapes have becoming more popular of late to overcome these disadvantages At present, cost effectivenessisdebatable.
MATERIALAND METHODS
This proposed study was conducted at Sree Siddhartha Medical College, Hospital and Research Centre,Tumkur,Karnataka,overaperiodof2yearsfrom October2009toSeptember2011.
The study included 200 patients who underwent abdominal surgeries, including both emergency and electivesurgicalprocedures.Allpatientswithabdominal surgical wounds were included, but excluded from the studywerepatientswithskininfection,patientswithpost burst abdomen, wounds secondary to burns, all patients with anemia and diabetes. The patients were allotted alternately into two groups of 100 each. In group 1, abdominal wound closure was done (using 2-0/3-0 monofilament nylon) with mattress sutures. In group 2, abdominal wounds were closed with surgical skin staplingdevice.
Theoutcomewasmeasuredintermsof:
(1) Speedofclosure.
(2) Costeffectiveness.
(3) Postoperativepain.
(4) Postoperativewounddehiscence.
(5) Acceptanceofthescar
Results were analyzed and compared with the previousstudies.
Speed of closure
RESULTS
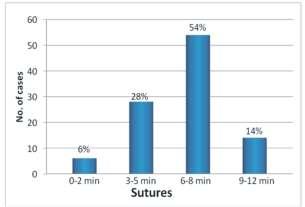
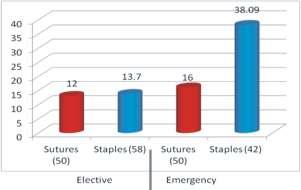
— Speed of closure was faster with staples. The average duration of closure was 8minutes in suture group and 60 to 70 sec in staples group. The abdominal wound closure in case of staples group was hence5to7timesfasterincomparisontosuturegroup(on anaveragethelengthofabdominalsurgicalwoundwas12 to15cms)(Fig1).
Postoperative pain
— Post operative pain assessment was done using visual analog score. Immediate post operativepainscoreswerehigherwiththeuseofsuturesas comparedtostaplesinbothelectiveandemergencycases. 56% of elective cases in whom suture closure was used hadapainscoreof3orhigher,comparedtoonly17.2%in staple closure group. For emergency cases, the figures were 84% for the sutures group and 14.3% for the staples group(Fig2).
Post operative wound infection and dehiscence
—
Post-operative wound infections were marginally higher (almost comparable) in staples group (13.7%) compared to sutures group (12%) in elective cases; but significantly higher in staples group (38.09%) compared to sutures group(16%)inemergencycases(Fig3).
Cosmetic results
— Cosmetic results were better with staplesinelectivecases.Howeverwhenstapleclosurewas used in emergency cases, post operative wound infection and dehiscence were higher and hence healing was with secondary intention; the resultant scar was thick and cosmeticallylessacceptable.(scarswerecomparedafter3 monthsofsurgery)(Figs4-7).
Cost
— The average median cost in suture group was Rs 100/- and in staple group Rs 310/-. Staple closure was hencethriceascostlierassutures.
DISCUSSION
Wound closure is a vital step for producing a healthy andstrongscarandalsoforensuringaestheticallypleasing appearance.
Surgical stapling was developed in 1908 by a Hungariansurgeon,HumerHultl Theoriginalinstrument was massive by today’s standards weighing 7.5 pounds. Modifications performed by Von Petz provided a lighter andsimplerdevice,andin1934FredrickofUlmdesigned an instrument that resembled the modern linear stapler In 1958,Ravich,refinedtheinstrumentstotheircurrentstate 2 andwidespreadusetoday
Staplers are made up of stainless steel. They are virtually inert. They have uniform shape and constant staple depth providing even wound tension. Rectangular shape design minimizes the trauma and minimizes the tissue compression thereby causing minimal tissue reaction and trauma and leads to wound healing with minimumscar.
Thedevelopmentofdisposableskinstaplershasmade this method of wound closure an increasingly popular technique. Skin staplers are quick and easy to use and numerous studies have confirmed the speed and efficacy ofstapingcomparedwithsuturerepair.
Eldrup et al (1981) analysed 137 patients undergoing abdominal or thoracic surgeries, and concluded that the main advantage of using staples was the time saved, as closure with mechanical suture took one third of the time required for the conventional method. On the other hand closure with staples resulted in the major disadvantage of


additional expenses, as the cost was forty seven times higherthanthatofthesuturewithDermalon
Meiring et al (1982) reported slightly better cosmetic results in a group of 40 patients undergoing laparotomy with an 80% in time saving. They also concluded that the final cost of the stapler was crucial for selecting the method
Gatt et al (1985) concluded from a controlled trial of staples for wound closure that the speed and convenience oftheskinstaplesoutweightheextracost.
Lubowski and Hunt (1985) consider proximate staple closureasuitableandfastermethodforverticalabdominal woundcomparedtosutures
Stockey and Elson (1987) compared the results of closure with staple and nylon sutures found a higher incidence of inflammation, discomfort on removal and spreading of the healing scar with staples. The only advantage of stapleswasspeedofwoundclosure.
Ranabaldo and Rowe-Jones (1992) compared staple with subcuticular sutures in 48 patients undergoing laparotomy and concluded that the difference in time was significant, nevertheless,thecostwasfivetimesgreaterwith staples
LuizRMedinadosSantosetal(1995)intheir
tients
study of 20 pa concluded that the use of skin staplers speed up closure by 80%, with better 9 cosmeticresults
JohnTKanagaye,Cheryl W Vance, Linda Chan, and Nancy Schonfeld (1997) at the Children hospital, Los Angeles, USA, reported that stapleclosurewassafe,rapid and cost effective and resulted in a cosmetically 10 acceptablescar
Iavazzo et al (2011)from a met
sis of randomized controlled trials comparing sutures with staples for the management of surgical wounds reported that staples were faster, with fewer wound infections but associated with more pain compared with sutures. Cosmetic results were 1comparable
In our present prospective study comparing skin sutures and skin staples for abdominal surgical wound closure, it has been noted that though the method of closure by the staples was significantly faster in comparison to sutures, it is met with certain drawbacks such as post operative infection with wound gaping , and subsequent prolonged duration of hospital stay posing economic burden on patients and doubling the cost factor inemergencyinfectivecasesascomparedtocleanelective cases.
Inelectivecases,thescarwasfoundtobecosmetically superior with better patient acceptance in staples group in comparison to sutures group But in emergency


20
cases, due to post operative wound dehiscence the patient acceptance of the scar was poorer in staples group as comparedtosuturesgroup.
The sutures were more cost effective compared to staples; the immediate post operative pain was comparativelyhigherinthesuturesgroup.
CONCLUSION
In our present study, we conclude that though the staples cost higher in comparison to sutures, the wound closure time was much faster which was statistically significant and in agreement with the literature reviewed.
This has a great impact on post operative recovery as the patient can be weaned off from the anaesthesia faster and thereby reducing overall operating time and hence decreasingpostoperativemorbidityandmortality.
In terms of patient acceptance of scar, we conclude that staples have good acceptance in clean elective cases and they are met with significant post operative wound infection in contaminated and emergency cases. Since staples are easier and faster to apply compared to sutures, the study showed that staples form an important surgical armamentarium for wound closure for elective and clean cases.
REFERENCES
1 Baker RS, Foote J, Kemmeter P, Brady R, Vroegop T, Serveld M — The science of stapling and leaks. Obes Surg 2004;14:1290-8.
2 RavitchMM,LaneR,CornellWP,RivarolaA,McEnanyT
(Continued from page 13)
werenotdoneinourhospital.
Closure of duodenal, gastric and intestinal stumps with wire staples: experimental and clinical studies. Ann Surg 1966; 163:573-9.
3 Eldrup J, Wied U, Andersen B — Randomised trial comparingProximatestaplerwithconventionalskinclosure. Acta Chir Scand 1981;147:501-2.
4 Meiring L, Cilliers K, Barry R, Nel CJ — A comparison of a disposableskinstaplerandnylonsuturesforwoundclosure.
S Afr Med J 1982;62:371-2.
5 Gatt D, Quick CR, Owen-Smith MS — Staples for wound closure: a controlled trial. Ann R Coll Surg Engl 1985; 67: 318-20.
6 LubowskiD,HuntD—Abdominalwoundclosurecomparing theproximatestaplerwithsutures. Aust N Z J Surg 1985;55: 405-6.
7 StockleyI,ElsonRA—Skinclosureusingstaplesandnylon sutures:acomparisonofresults. Ann R Coll Surg Engl 1987; 69:76-8.
8 Ranaboldo CJ, Rowe-Jones DC — Closure of Laparotomy wounds: skin staples versus sutures. Br J Surg 1992; 79: 1172-3.
9 Luiz R Medina dos Santos, Carlos AF Freitas, Flavio C Hojaij, Vergilius JF Araújo Filho, Claudio R Cernea, Lenine G Branda, Alberto R Ferraz — Prospective study using skin staplers in head and neck surgery. Am J Surg 1995; 170: 451-2.
10 John T Kanagaye, Cheryl W Vance, Linda Chan, Nancy Schonfeld — Comparison of skin stapling devices and standard sutures for ped a r c scalp lacerat ons: A randomized study of cost and time benefits. J Paediatrics 1997;130:808-13.
11 Iavazzo C, Gkegkes ID, Vouloumanou EK, Mamais I, Peppas G, Falagas ME — Sutures versus staples for the management of surgical wounds: a meta-analysis of randomizedcontrolledtrials. Am Surg 2011;77:1206-21.
neous epistaxis. American Journal of Rhinology & Allergy. January–February2012,26:55-60.
Preliminary Report Preliminary Report
Rhinosporidiosis of different organs — a study of 57 cases with review of literature
1 2 3
Palash Kumar Mandal , Nirmal Kumar Bhattacharyya , Sumedha Dey , 4 5 6
Pranab Kumar Biswas , Subrata Mukhopadhyay , Dibyendu Gautam
Rhinosporidiosis is a chronic granulomatous disease caused by Rhinosporidium seeberi, an aquatic parasite of class mesomycetozoa. It affects most commonly nasal cavity and rarely aerodigestive tract, tracheobronchial tree, conjunctiva, skin, penis, parotid duct and bone and mostly present as polypoid, reddish,friable mass mimicking neoplastic mass. As the lesion is increasing in our hot climate, our aim of study is to show how different organs including nasal cavity were affected by the infection. Total 57 cases werestudiedinlastfiveyearsinwhich45caseswereseenasnasalmass,4caseswereinconjuctiva,4cases were in oropharynx and one case each in larynx, skin, anus and penis. The formalin-preserved specimens appeared as friable, polypoid mass and histopathology of each case revealed classical microscopic appearance of rhinospoidiosis. To exclude from other fungal infections like coccidioidomycosis we performed periodic acid Schiff (PAS) stain and Gomori’s methenamine silver stain besides routine stain. We collectedoccupationalhistoryofeachpatientandmostofthemwerefarmersorcattleshedworkers.Similar reports are available in international literature which showed that most cases of rhinosporidiosis were seen innasalcavityandrarelyothersiteslikeconjunctiva,skin,bone,anusandpeniswerealsoinvolved.Surgical removal followed by dapsone therapy is the mainstay of treatment and recurrence is rare. Increasing incidence of this rare infection indicates that hot ,humid weather of our country and poor hygiene of cattle shed workers are the main culprit. So, health administration should take necessary steps to minimize this infection.
J Indian Med Assoc 2016;114: 21-4]
Key words : Rhinosporidiosis, Nose, Extranasal sites.
Conclusion: REFERENCES
Though anterior and posterior rhinoscopy is done routinelyasapartofclinicalexaminationofepistaxis,they havetheirownlimitations.Endoscopicexaminationofthe nasal cavity has the advantage of providing better view of the nasal cavity and also aids in appropriate management of epistaxis based on the merit. It is an effective and less invasive procedure. It has minimal morbidity and failure rates.Italsohasanaddedadvantageofpreventingdamage tonasalmucosabyblindlypackingandinstrumentation.It reduces need for prolonged hospitalization.We conclude that if the bleeding source is not identified by anterior rhinoscopy,nasalendoscopyismandatoryinmanagement ofepistaxis.
1 Rodrigo P Santos, Fernando D Leonhard, Ricardo G Ferri, Luiz C Gregorio — Endoscopic endonasal ligation of the sphenopalatine artery for severe epistaxis, Brazilian Journal ofOtorhinolaryngology,2002;68:edition4.511-4.
2 Safaya A, Venkatachalam VP, Chaudhary N — Nasal Endoscopy-Evaluation in Epistaxis, Indian Journal of Otolaryngology and Head and Neck Surgery. 2000; 52: 1336.
3 RudmikLandSmithT—Managementofintractablesponta
4 Babu M, Gowda B, Satish HS — Role of Rigid Nasal Endoscopy in the Diagnosis and Management of Epistaxis. IOSR Journal of Dental and Medical Sciences. 2014, 13: 405.
5 Schaitkin B, Strauss M, Houck JR. Epistaxis — Medical versus Surg cal therapy Comparison o efficacy, complications and economic considerations. Laryngoscope 1987;97:1392-5.
6 Shaw CB, Wax MK, Wetmore SJ — Epistaxis: a comparison oftreatment.OtolaryngolHeadNeckSurg1993;109:60-5.
7 Thakar A, C J Sharan — Endoscopic sphenopalatine artery ligation for refractory posterior epistaxis. Indian Journal of Otolaryngology and Head and Neck Surgery, 57: 2005, 2158.
8 Spafford P, Durham JS — Epistaxis: efficacy of arterial ligationandlongtermoutcome.JOtolaryngol1992;21:2526.
9 Siniluoto TM, Leinonen AS, Kartunnen AK — Embolization for management of posterior epistaxis. Arch Otolaryngol 1993;119:837-41.
10 Metson R, Hanson DG — Bilateral facial nerve paralysis following arterial embolization for epistaxis. Otolaryngol HeadandNeck1983;91:299-301.
11 O’dnnell M, Robertson G, Mcgarry GW — A new bipolar diathermy probe for the outpatient management of adult acuteepistaxis.ClinOtolaryngol1999;24:537-41.
12 Bhatnagar RK, Berry Sandeep — Selective Surgicel Packing for the Treatment of Posterior Epistaxis Ear, Nose andThroatJournal2004;83:633-4.
Rhinosporidiosis is a chronic granulomatous diseasecausedbyfungus–likeorganismknownas Rhinosporidium seeberi, an aquatic parasite of classmesomycetozoa Thelesionisgrosslycharacterized by reddish, polypoidal or sessile and friable mass. It affects most commonly different parts of nasal cavity (70%) such as anterior part of nasal septum, vestibule and nasopharynx because of affinity of the organism for mucous membrane of nasal cavity and nasopharynx. Besides nasal cavity, it may rarely affect lower aerodigestive tract, tracheobronchial tree, lips, 2,3 uvula, conjunctiva, penis, parotid duct and bone The infection is more commonly observed in
Department of Pathology, North Bengal Medical College, Darjeeling 734012
1MD(Pathol),AssociateProfessor
2MD (Pathol), Associate Professor Department of Pathology MedicalCollege&Hospital,Kolkata700073
3MD(PGT),DepartmentofPathology MedicalCollege&Hospital, Kolkata700073
4MD(Pathol),Professor DepartmentofPathology,MedicalCollege &Hospital,Kolkata700073
5MS (ENT), Professor and Head, Department of ENT Medical College&Hospital,Kolkata700073
6DMRT MS (Gen Surg), Professor, Department of General surgery MedicalCollege&Hospital,Kolkata700073
hot tropical climates of the endemic zones such as India and SriLanka It usually affects males of age group of 15 years to 40 years. The diagnosis in nasal cavity is easier, but delayed in extranasal sites which often clinically mimick neoplasm. Besides classical histopathological appearances, occupational and personal history are also needed for diagnostic corroboration. Aim of this study is to show how different organs may be affected by Rhinosporidium seeberi and increasing incidence of it in Kolkata.
MATERIALSAND METHODS
The study is a retrospective one and done in department of Pathology, Medical College, Kolkata from July 2007 to June 2012. The formalin preserved specimens appeared as friable, lobulated mass (Fig 1) which were routinely processed and stained by Haematoxylin and Eosin (H&E), Periodic acid Schiff (PAS)andGomori’smethenaminesilver Totalof57cases were retrieved within the study period which included mostly nasal masses and fewer of other different organs (Table1).
Microscopically each case showed thick-walled, rounded cysts called sporangia containing endospores. Sporangium measures 0.5mm in diameter while each endosporemeasures6-7micron.(Fig2).
RESULTS
Outof57totalcases,45casesareseeninnasalcavity,4 caseswereinconjunctiva,4casesinoropharynx,onecase each in larynx, skin, penis and anal region. All cases except one were observed in males. The only female patient had it in nasal cavity The clinical features of nasal rhinosporidiosis commonly were nasal obstruction, epistaxis, polyp. Occupational history revealed that most patients were farmers, 6 had domestic cattles in their houses all used to bath in community ponds. In extranasal sites, most patients were seen to be affected by autoinoculation from nasal mass. The rhinosporidiosis in extranasal sites presented as polypoidal, friable mass which bled on touch and so excised as suspicious neoplastic lesions but histopathology revealed the nature oflesion.
DISCUSSION
Rhinosporidiosis reviewed in 1998, has been known for more than a century since its first description in Argentina and was described as a chronic granulomatous disease with frequent recurrence after surgery and occasional dissemination from the initial focus which is most commonly seen in upper respiratory sites. It occurs universally, although it is endemic in south Asia, notably southernIndiaandSriLanka.
The literature on rhinosporidiosis and on the different morphological stages of R seeberi contains many synonymous, overlapping terms. For example, the morphological element for which the proposed term is “
Electron- dense body” were earlier termed variously as spherule, electron-dense circular structure, protrusion of
Table 1 — Showing Nasal Masses and Fewer of Other Different Organs
Site No Sex ClinicalFeatures Spread Diagnosis Treatment Follow-up(3yrs) Causeof Recurrence
Nasal 45 44 Nasal 38farmers,6had Histopathology Excisionof 10lostfollow-up, Seedingof Cavity M,1F obstruction, cattlesinhouse, oftheexcised themassf/b 32hadno endospores epistaxis, allusedtobathe mass electro- recurrence, duringsurgery polyp incommunity cauterisation 3presentedwith pond ofthebase similarsymtoms
Conjunctiva 4 M Reddishpolyp Historyof Clinically do none overpalpebral traumafrom suspicious. conjunctiva, dust&vegetable confirmedby epiphora, particles HPEofthe Photophobia excisedmass
Oropharynx 4 M Foreignbody Allhad Clinicalfeatures do none sensationin associated &historywas throat, polypin suggestive, dysphagia theirnose confirmationby histologyof excisedmass
Larynx 1 M Hoarsenessof Orotracheal confirmationby Excisionof none voice,h/onasal intubation histologyof themassf/b polypectomy excisedmass electro3yrsago cauterisation+ underGA Dapsone
Skin 1 M Polypoidleison abrasion, FNACofthe do Satelliteleisons Maybebecause onbackrecurrence FNACneedle nodule, developed ofFNAC atthesamesite injuryinc/o histologywas atthesame needleinjury afterremoval. recurrence. confirmatory site
Penis 1 M Difficultyin Autoinoculation Confirmedby do none micturation, fromnasal histologyof bleedingfrom mass theexcised meatus,growthin mass thedistalurethra
AnalRegion 1 M Growthinthe Autoinoculation Confirmedby do none analregionwhich fromnasal histologyof bleedsontouch. mass theexcised B/Lnasalpolyps mass

cell-wall, sporozoitespore,sporuleandsphericalbody.
In addition to numerous cases in human, it has been documented to occur in several species of domestic and wild animals also such as cattle, buffaloes, dogs, cats and goats.Majoritycasesaresporadicwithonlyonehistoryof epidemic in 1990 in humans and swans. Another short outbreakwasreportedinpeopleofSerbiawherenasaland ocular rhinosporidiosis were observed and a lake was incriminated as source of infection where all the patients usedtobath
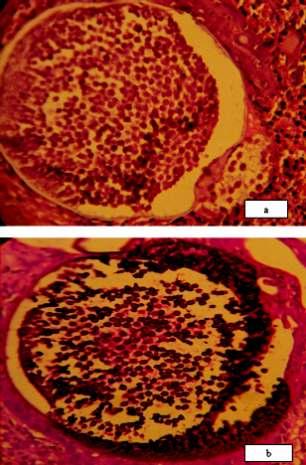
electron-dense inclusion, germinative body, or sur spread of disseminated granuloma in subcutaneous tissue
The presumed mode of infection from the aquatic habitat of R.seeberi is through the traumatized epithelium most commonly in nasal sites The occurrence of Rhinosporidiosis in river-sand workers in India and Sri Lanka is particularly relevant to such a mode of infection through abrasions caused by sand particles followed by infection by the pathogen in the putative habitat ground water Trauma from R.seeberi contaminated stones used for mopping up residual drop of urine is claimed to be responsible for anterior urethral rhinosporidiosis in the males.AutoinoculationwasconsideredbyKarmaratne in his monogram on rhinosporidiosis where he explained the occurrence of satellite lesions adjacent to granulomatous lesion especially by spillage of endospores from nasal polypoidal lesion to upper aerodigestive tract after trauma
10 as reported by Kumari R et al , Shenoy et al andTolat et 12al
Clinically, the majority of cases occur in upper respiratory tract, less commonly in upper aerodigestive tract and conjunctiva and rarely in skin, penis, anus and bones. Other than bony lesion, everywhere the infection presents as polypoidal, friable mass grossly resembling a neoplastic lesion. Though the organism has predilection for moist mucous membrane of different parts, one case 13 hasbeenreportedinparotidduct
Diagnosisisbestdonebyitshistopathologybyroutine haematoxylin and eosin stain, periodic acid Schiff stain and Gomori’s methenamine silver stain. Differential diagnosis includes spherulocystic disease caused by 14 endosporulating fungus that cannot be stained by silver stain.Another differential diagnosis includes coccidiodes immitis which cause formation of endospores of much smallersize. gery. Haematogenous spread is another way of
Cytodiagnosis of rhinosporidiosis are not of much help as the endospores in smear resemble epithelium of 15nasopharynx
Regarding treatment of polypoidal rhinosporidiosis –surgery with electrocautery is recommended by which recurrence is rare. In other cases- dapsone, primarily an antileprosy drug , has also effect in gradual elimination of R.seeberi by arresting maturation of organism and cause 16fibrosis Most of our cases have been treated by surgery followed by dapsone therapy for six months and however noneofourcaseshavehistoryofrecurrence.
CONCLUSION
Rhinosporidiosis, though most commonly seen in nasopharynx, rarely may affect other mucosal surfaces with presentation resembling neoplasm It is not uncommon in our hot climate, so elimination is needed to be oriented particularly for those patients who work in cattle-sheds or farmhouse. Surgery followed by dapsone therapyissufficienttocurethelesion.
REFERENCES
1 EmmonsCD,BinfordCH,UtzJP,Kwon-ChungKJ—In:Lea and Feb ger, ed ors Med cal Mycology, 3rd edn Philadelphia1977:464-70.
2 Franca GV Jr, Gomes CC, Sakano E, Altermeni AM, Shimizu LT— Nasal rhinosporidiosis in children. J Pediatr 1994;70:299-301.
3 Makannavar JH, Chavan SS Rh nospor d osis: Clinicopathological study of 34 cases. Indian J Pathol Microbiol 2001;44:17-21.
4 Khoo JJ, Kumar KS — Rhinosporidiosis presenting as recurrentnasalpolyps. Med J Malays 2003;58:282-5.
5 Arseculeratne SN, Ajello L — Rhinosporidium seeberi- In:
Preliminary Report Preliminary Report
RJ, Ajello L,editors. Topley & Wilson’s Microbiology & Microbial Infections, vol.4, 9th ed.London, Edward Arnold 1998:595-615.
6 Kennedy FA, Buggage RR, Ajello L — Rhinosporidiosis: A description of an unprecedented outbreak in captive swans(Cygnus spp.) and a proposal for revision of the ontogenic nomenclature of Rhinosporidium seeberi. J Med Vet Mycol 1995;37:157-65.
7 Vukovic A, Bobic-Radovanovic A, Latkovic Z, Radovanovic Z— An epidemiological investigation of the first outbreak of rhinosporidiosis in Europe. J Trop Med Hygiene 1995; 98: 333-57.
8 Karunaratne WAE — The pathology of Rhinosporidiosis. J Path Bact 1934;XLII:193-202.
9 Karunaratne WAE — Rhinosporidiosis in Man: (the Athlone Press,London)1964.
10 Kumari R, Nath AK, Rajalakshmi R, Adityan B, Thappa DM D ssem na ed cu aneous rh nospor dios s: var ed morphological appearances in the skin. Indian J Dermatol venerol Leprol 2009;75:68-71.
11 Shenoy MM, Girisha BS, Bhandari SK, Peter R — Cutaneous rhinosporidiosis. Indian J Dermatol Venerol Leprol 2007;73:179-80.
12 Tolat SN, Gokhale NR, Belgaumkar VA, Pradhan SN, Birud NR — Disseminated cutaneous rhinosporidiosis in an immunocompetent male. Indian J Dermatol Venerol Leprol 2007;73:343-5.
13 Kini U, Amirtham V, Shetty SC, Balasubramanya AM — Rhinosporidiosis of the parotid duct cyst: cytomorphological diagnosis of an unusual extranasal presentation. Diagn Cytopathol 2001;25:244-7.
14 McClatchie S Bremner AD — Unusual subcutaneous swellings in African patients. East Afr Med J 1969; 46: 62533.
15 Arseculeratne SN — An update on rhinosporidiosis and Rhinosporidium seeberi. 2nd SAARC ENT Congress 2000, Kathmandu,Nepal;Guestlecture.
16 Job A, Venkateswaran S, Mathan M, Krishnaswamy H, Raman R — Medical therapy of rhinosporidiosis with dapsone. J Laryngol Otol 1993;107:809-12.
Vascular tumours of the female genital tract : a clinicopathologic study of 11
cases
Sainath K Andola , Uma S Andola
Vascular tumours of the female genital tract are very rare. The aim of this study was to analyse the distributionofvasculartumorsinfemalegenitaltractandtocorrelatetheirclinicopathologicalfeatures.Ina retrospective study of ten years, clinical features, imaging studies, gross and microscopic features of elevencasesofbenignvasculartumoursoffemalegenitaltractwerereviewed.Theagerangeinthepresent study was 22 to 95 years. The presenting complaint was abdominal pain/mass, postcoital bleeding, vaginal and vulval mass. The duration of symptoms varied from 3 months to 10 years. A diagnosis of vascular tumour was not considered in any of these on clinical grounds. The vascular tumours occurred most commonly in ovary (five cases), followed by vulva (three cases), and one each in cervix, vagina and placenta. Clinical diagnoses ranged from cystadenoma in ovaries to endocervical polyp in cervix, Bartholin’s cyst in vulva and carcinoma in vagina. Histologically, all were benign vascular neoplasms, ranging from haemangioma (five cases), lymphangioma (two cases), lymphangioma circumscriptum (one case) and chorangioma (one case). Two recently described very rare vulval soft tissue tumours angiomyofibroblastoma (one case) and aggressive angiomyxoma of the vulva (one case) were also encountered. Benign vascular tumours in the female genital tract can present with symptoms similar to gynaecological tumours and epithelial malignancies and may lead to unwarranted radical surgery. Pathological examination is necessary in all such cases to exclude the possibility of malignancy. Angiomyofibroblastoma and aggressive angiomyxoma of the vulva are very rare and both shared similar clinicalandhistopathologicfeaturescausingdiagnosticproblems.
J Indian Med Assoc 2016; 114: 25-30]
Key words : Female genital tract, vascular tumours, haemangioma, lymphangioma, angiomyofibroblastoma, aggressive angiomyxoma, chorangioma, lymphangioma circumscriptum.
Vascular tumours are rarely found in the female genital tract (FGT). The ovaries have a rich vascular supply and the rarity of the vascular tumours in the ovary is therefore surprising. It is postulatedthattherarityofthistumourisduetothecyclic changes that the ovary undergoes during the reproductive 2years. Most of the vascular tumours are incidental 3,4 findingsduetotheirsmallsizeandasymptomaticnature. However, large lesions present clinically with features mimickingthecommongynaecologicaltumours,evenon ultrasonographic examination. Most literature contain short series of these tumours confined to one organ of 1,3,4 FGT Theobjectiveofthepresentstudyistodescribethe clinical profile and pathological features of eleven cases ofbenignvasculartumoursoftheFGT.
Department of Pathology, Mahadevappa Rampure Medical College, Gulbarga585105 MD,DCP FICP FIAMS, ProfessorandHeadoftheDepartment MD,DNB,AssociateProfessorofObstetricsandGynaecology
MATERIALSAND METHODS
Eleven cases diagnosed as having vascular tumour of FGT in the department of obstetrics and gynaecology and pathology during a period of ten years from 2000-2009, were retrieved. The clinical features, imaging studies and gross findings were analysed and the microscopic slides werereviewedforhistopathologyfeatures.
OBSERVATIONS
Clinical features and physical examination findings have been presented in Table 1. The age of the patient ranged from 22 to 95 years (mean 45.5 years). The duration of symptoms varied between 3 months to 10 years. Five patients had tumours in ovary (3 left, 1 right, 1 bilateral),threeinthevulvaandoneeachincervix,vagina and placenta (Table 2). These cases presented with nonspecific symptoms ranging from abdominal mass and/or pain, postcoital bleeding and vaginal and vulval mass. A diagnosisofvasculartumourwasnotconsideredinanyof thesecasesonclinicalgrounds.
Age Presentingcomplaints Localexamination Histopathologydiagnosis (Yrs)
38 AbdominallumpandPain Leftadnexalmass CavernoushaemangiomaofLeftOvary
45 AbdominallumpandPain Leftadnexalmass LymphangiomaofLeftOvary
50 Vulvalgrowth WartyVulvalgrowth. LymphangiomaCircumscriptum
55 Postmenopausalbleeding Cervicalgrowth Cacervixwithmetastasistopelvic lymphnodes,smallintramuralleiomyoma, TBlymphadenitisandBilateral ovarianhaemangiomas
40 Postcoitalbleeding Cervicalgrowth Cavernoushaemangiomacervix
95 Vaginalmass Vaginalgrowth Cavernoushaemangiomavagina
35 GrowthinLabia Vulvalgrowth majora –10years measuring7x6x4cm Angiomyofibroblastomaofvulva
35 Abdominalpainandmass Haemorrhagiccyst Cavernoushaemangioemaofleftovery
50 Vulvalswelling Vulvalmass DeepAggressiveAngiomyxoemavulva
35 Pain,abdominalmass Rightovarianmass, Lymphangiomaovary inrightiliacfossa acuteappendicitis
22 Pregnancy Hydramnioswith ChorangiomaofPlacenta prematureseparation ofplacenta
Clinical differential diagnosis in the present series included tubo-ovarian mass (case 1, 2, 10), haemorrhagic cyst(case8),endocervicalpolyp(case5),Cavagina(Case 6) Ca cervix with metastasis (case 4) and Bartholin’s cyst (case 7, 9). Bilateral ovarian tumour in case 4 was an incidental finding in the Panhysterectomy specimen in a case diagnosed as carcinoma cervix. The vulval lesion in case7and9,wereclinicallythoughttobeBartholin’scyst. In case 10, USG report showed acute appendicitis with bulky uterus and enlarged right ovary with clinical diagnosisofacuteappendicitis.
USGinthreecaseswithovariantumourshowedcystic ovarian mass with variable echogenecity The imaging reportsofothercaseswerenotavailableforreview.Incase 4, USG reports suggested enlargement of both ovaries probablybecauseofmetastasis.Theanatomicdistribution ofthetumourshasbeenshowninTable2.
Three of the patients with ovarian tumour underwent total abdominal hysterectomy with salphingooophorectomy. In one case panhysterectomy was performed and bilateral pelvic lymph nodes excised. In case 2, left sided salphingo-oophorectomy was done. Endocervical polypectomy was done in case 5 and excisionofmass(vagina)wasdoneincase6.Incase7&9, Vulval masses were excised completely In case 3, excision was done. In case-10, appendicectomy was done along with hysterectomy In case 11, placentawas sent for examination after delivery as the patient had hydramnios withprematureseparationofplacenta.
T h e g r o s s a n d microscopic features have beensummarizedinTable3.
Three cases with ovarian tumour showed variably enlarged ovaries with honeycomb appearance on cut section with dark brown areas. Microscopy revealed cavernous haemangioma. In Case 2 and 10, the ovaries were enlarged and cut section showed multiple cystic areas and solid areas.
Microsco
wed numerous dilated lymphatic spaces filled with lymph fluid and lymphocytic infiltrates and diagnosis of lymphangioma was made. The cervical lesion in case-5 was received as cervical polyp which was haemorrhagic and microscopy revealed cavernous haemangioma. In case6,theexcisionofvaginalmassclinicallysuspectedto be Ca vagina revealed cavernous haemangioma. The vulval lesion in case 3, revealed the features of lymphangiomacircumscriptum.
Case 7, had mass in the labia for last 10 years and clinically diagnosed as Bartholin’s Cyst.As the mass was progressively increasing in size, total excision was done and microscopy revealed tumour consisting of alternate hypo and hypercellular areas with numerous delicate capillary sized blood vessels lined by endothelial cells. The stromal cells were plump to spindle cells with moderate amount of eosinophilic cytoplasm and having round to oval to spindly nucleus with fine chromatin and inconspicuous nucleoli These cells were numerous in hyper cellular areas and were
Table 2 — Anatomic Distribution of Vascular Tumours
AnatomicSite Histopathologic Numberof Diagnosis Cases(%)
Haemangioma 02(18.18) Left Lymphangioma 01(9.09)
Ovary Right Lymphangioma 01(9.09) Bilateral Haemangioma 01(9.09) Total 05(45.45)
Cervix Haemangioma 01(9.09)
Vagina Haemangioma 01(9.09)
Vulva
Lymphangioma 01(9.09)
Angiomyofibroblastoma 01(9.09)
DeepAggressiveAngiomyxoma 01(9.09)
Total 03(27.27)
Placenta Chorangioma 01(9.09)
Total 11(100)
Table 3 — Gross and Microscopic Features of the Tumours of Female Genital Tract
SurgicalProcedure Gross Microscopy
UterocervixwithrightSalphingooophorectomy Ovary5x3x2cm. Cavernoushaemangioma(Right) LeftSalphingooophorectomy Ovary8x5x3cm.C/smultiplecysticspaces CysticLymphangioma(Left)
Excisionoflesion Greyish-brownmass 1x0.5cminvulva Lymphangiomacircumscriptum–vulva
Panhysterectomy Ovaries–both6x5x4cm.c/sdarkbrown BilateralCavernoushemangioma
Polypectomy Irregularfriablemass-cervixmeasuring2x1.5cm. Cavernoushaemangiomacervix
Excisionofvaginalmass Irregularnecroticandpurplereddishmassmeasuring4x3x2cm Cavernoushaemangiomavagina
Excisionoflabialmass Globulargrey-whitemassmeasuring7x6x5cm.c/s wellencapsulatedgrey-whitehomogenous Angiomyofibroblastomaofthevulva
Hysterectomywithleft salphingooophorectomy Ovarymeasuring4x6cm.c/shoneycombappearance. CavernoushaemangiomaOvary(Left)
Vulvalmass Pedunculatedmasscoveredwithskin.Lesion6x4cm, peduncle3x1cm.c/ssoftgelatinousreddish togrey-brownunencapsulated. Deepaggressiveangiomyxomaofvulva
Uterinecervixwithadnexa RightOvary6x4x3cm. C/scysticspacesandsolidareas. CysticLymphangioma(Right)
Placenta Placentameasuring15x13x6cm.withbrownarea measuring6x5cm.withmyxoidandvariegatedappearance Chorangiomaofplacenta
clusteredaroundthebloodvessels.Therewasnoatypiaor mitoses. A diagnosis of angiomyofibroblastoma of vulva wasmade.
In case 9, a clinical diagnosis of Batholin’s cyst was madeandexcisiondone.Grosslyitshowedsoftgelatinous reddish-brown areas. Microscopically, the lesion was moderately cellular with predominant stellate cells and few spindle cells in an abundant myxoematous stroma. The stromal cells were bland oval, showed no atypia. Amidst these were seen numerous medium to large sized blood vessels with thickening of the walls and hyalinisation. Plently of pigmented macrophages were present. A diagnosis of deep aggressive angiomyxoma of vulvawasmade.
In case 11, the placenta was submitted after the delivery of the baby by caesarean section. Placenta was measuring 15x13x6 cms. Cut section showed a large nodular lesion measuring 6x5 cms and dark brown in appearance. Microscopically the lesion composed of numerous thin walled foetal vessels of capillary or sinusoidal calibre with scant intervening stroma with fibrousandmyxoidareas.
In case 4, bilateral cavernous haemangioma were detected as an incidental finding during the procedure of panhysterectomydoneinadiagnosedcaseofcarcinomaof cervix. Interestingly in this patient, small leiomyoma was present in the myometrium. The pelvic lymph nodes showed metastatic deposits. In addition, the lymph nodes showed necrotising granulomatous inflammation compatible with tuberculous lymphadenitis. Both the ovaries were enlarged and showed features of cavernous haemangioma.
In all the eleven cases, there was no atypia, no mitoses andnonecrosis.
DISCUSSION
Vascular tumours of FGT, especially of ovary 4 constitute a very small percentage of all tumours of FGT There are only a few case reports and short series of these 1,4 tumours in the literature. Vascular tumours have been reported in a wide age group ranging from 4 months to 81 years.4 In the present series, age of the patients ranged from 22 years to 95 years with a mean of 45.5 years. Majority of the patients were in the age group of 35-50 years(8cases).Therewasnospecificclinicalpresentation suggestive of vascular tumor noted in the present series. However, these tumours can mimic other common FGT neoplasms. One of the cases was highly suspicious of malignancy(case6).
Haemangioma of ovary
Haemangioma of ovary was first described by Payne in 1869 Ovarian haemangiomas are commonly discovered incidentally at autopsy or surgery. Sometimes they present with abdominal mass and/or pain, acute abdomen or ascites, simulating commoner ovarian neoplasms. All the cases in the present series were symptomatic except one (case 4), where panhysterectomy was done in a case of primary cervical cancer which showed incidental findings of bilateral ovarian haemangioma (Fig 1) Ovarian haemangiomas are usually unilateral, though bilateral cases have been reported. Present series also showed incidentalfindingofbilateralhaemangiomaofovary Ovarian haemangiomas are usually situated in the medulla and hilus. The lesion has smooth outer surface andisredorpurplishoncutsurface.Incontrasttovascular
tumours in the other parts of the body, the most common histologic type in ovary is cavernous or mixed cavernouscapillary type. In the present series all the 5 cases were cavernous type (Fig 2, H&E, x 200). Both the cortex and medulla of the ovaries were involved in all the cases. Histopathologicexaminationisdiagnosticforthelesion.
Pre-operative diagnosis of ovarian haemangioma may befacilitatedbyradiologicmethods,thusavoidingradical surgery. In the present series, 4 cases were diagnosed as ovarian cyst on ultrasound examination and thus underwent radical surgery Simple oophorectomy is curative for ovarian hemangioma. Thus clinicopathologic correlationisusuallyessential.
Lymphangioma of ovary
— Lymphangioma of ovary is extremely rare with approximately 16 cases reported in 4,5,6 the english literature In the present series, 2 cases of ovarian lymphangioma were encountered. Clinically they simulated other cystic tumours of the ovary similar to haemangioma. Therefore pathologic examination was necessary to reach the correct diagnosis. Lymphangioma has to be differentiated from teratoma with a prominent vascular component, haemangioma and adenomatoid tumour The contents in cystic spaces, characteristic morphology with lymphocytic infiltrates and immunohistochemistry may help to differentiate these conditionsindifficultcases.
Cervical haemangioma
— Fewer than 40 cases of 2,4,7 haemangioma of cervix are present in the literature. In the present study, one case of cavernous haemangioma of cervix presented clinically with post coital bleeding and diagnosed as endocervical polyp on examination. Although cervical haemangiomas are generally asymptomatic,35%ofreportedcaseswereassociatedwith abnormal vaginal bleeding. In one of the reported case, there was rapid growth of the lesion during two 7 pregnancies,necessitatingdeliverybycaesareansection.

Cavernous haemangioma of vagina
— Cavernous hemangioma of the vagina is extremely rare and no cases have been reported in the literature over the past 35 years. Acase of cavernous haemangioma during pregnancy was 8 reportedbyRezvaniin1997. Thepresentcasewasseenin 95-years-old female who presented with a mass in the para-urethral region of the vagina which bled on touch. It was clinically diagnosed as vaginal carcinoma and excised.Themasswasvascular,necroticandfriablewitha sessile base. Microscopically, the mass revealed hyperplastic squamous epithelium with large dilated cavernous vascular channels lined by flattened endotheliumanddiagnosedascavernoushaemangiomaof vagina(Fig3,H&E,x200).
Lymphangioma circumscriptum
Lymphangioma circumscriptum is characterised by clusters of thin walled vessels filled with clear fluid. However epithelial hyperplasia and hyperkeratosis give rise to firm lesions, which are clinically suspected for genital warts or mol
circumscriptum may be congenital or acquired. To date about 11 cases of congenital and 23 cases of acquired lymphangioma circumscriptum of vulva have been 4,9,10 reportedinEnglishliterature. Acquiredcasesaremostly seen after radiotherapy to pelvis for carcinoma cervix, hence the cases are diagnosed to exclude metastatic deposits. The present case presented with a small nodular warty lesion in the labia without any previous history of malignancy Excision biopsy revealed feature of lymphangioma circumscriptum covered by hyperkeratotic hyperplastic squamous epithelium (Fig 4, H&E,x200).
Angiomyofibroblastoma of vulva
Angiomyofibroblastomaisarare,benignmesenchymaltumorthatoccurs mainly in the vulval region of middle aged (35-45years)
1 1 women In 1992, Fletcher et al proposed angiomyofibroblastoma a clinicopathological entity based on the detailed observation of vulval soft tissue
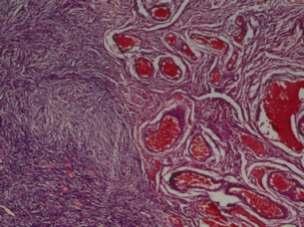
VASCULAR TUMOURS OF THE FEMALE GENITALTRACT —ANDOLA AND ANDOLA

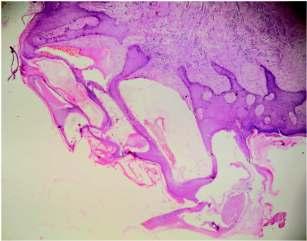
tumours.
Different studies suggest that mesenchymal histologically
vulval tumour in women of reproductive age group, angiomyo-fibroblastoma, aggressive angiomyxoema, cellular angiofibroma, fibro-epithelial stromal polyp and superficial angiomyxoema probably arise on a common pluripotential primitive cell located around the vessels of connective tissue, which could show the capacity for modulating its phenotype towards similar but distinctive 13,14 maturecells. Thiscanresultindiagnosticdifficultiesfor pathologists because of the relative rarity and their overlapping morphologicfeatures.Thereareonlyover70 1 cases reported in the English literature to date Angiomyofibroblastomaarewellcircumscribedandrange from 0.5 to 12cm, but usually measure <5cm.They can be 12,13,14 adequately treated by wide local excision. On histologic examination, angiomyofibroblastoma are composed of alternating hypercellular and hypocellular oedematousareasinwhichnumerousthinwalled,smallto medium sized vessels are regularly distributed. Tumour cellswhicharedescribedasstromalcells,haveaspindleto rounded or epithelioid appearance. Tumour cells are characteristically aggregated around the vessel or loosely dispersed in the hypocellular areas. Nuclear atypia and mitoses are not seen. The oedematous area typically containswavycollagenfibresbutlittleornomucin(Fig5, H&E, x 200). Differentiation between angiomyofibroblastoma and aggressive angiomyxoema may be very 14 difficultbothclinicallyandhistologically
In the present study, one case of angiomyofibroblastomawasdiagnosedwhichpresentedclinicallyas Bartholin’s cyst and was present for last 10 years. She came to the hospital because the mass was progressively increasing in size. Grossly, it was globular grey-white mass measuring 7x6x5 cms. Cut section was well encapsulatedgrey-whitewithsoftrubberyconsistencyand
— Aggressive
15 angiomyxoema was first described by Steeper and Rosai in1983.Thisisararelocallyinfiltrativetumourthatarises 15 in the pelvic and perineal soft tissues of young women. 14 Approximately100caseshavebeenreported. Aggressive angiomyxoemahasahighrateoflocalrecurrencebecause of its infiltrative growth and anatomical location. The treatment of choice is wide local excision. The local 15,16 recurrence rate in the range of 50-70% is reported. Grossly, Aggressive angiomyxoema is non-encapsulated gelatinous tumour with infiltrative edge. Histologic examinationshowshypocellulartumourwithsmallovoid, spindled or stellate cells that exhibit minimal nuclear atypia if any (Fig 6, H&E, x 400). Mitotic figures are not common. Numerous blood vessels are present and vary diagnosedasangiomyofibroblastoma. Aggressive angiomyxoema of vulva
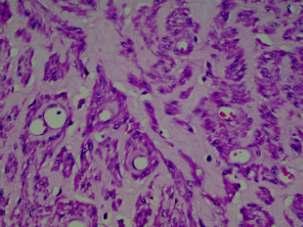
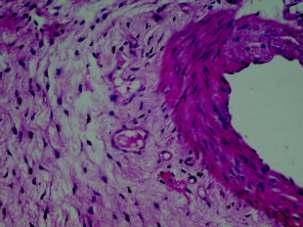
Fig 6 — Microphotograph of aggressive angiomyxoma of vulva showing abundant myxoid stroma with bland oval stromal cells with no atypia.Also seen is large blood vessel with thickening and hyalinization of the walls. (H&E X 400)
from thin walled capillary like vessels to large vessels 16 with thick muscular walls. There is no specific immunohistochemical marker of aggressive angiomyxoema yet. Tumour cells uniformly express vimentin and heterogeneously express muscle specific actin and 13,14desmin.
17 Srinivasan et al reported aggressive angiomyxoma presenting as a vulval polyp. A case of Aggressive angiomyxoema in a 50-year-old-female with a clinical presentation as Bartholin’s cyst was encouned in this study Grossly it was a pedunculated mass covered with skin measuring 6x4 cm with gelatinous cut section appearance.Basedonthecharacteristichistologicfeatures a diagnosis of deep aggressive angiomyxoema was made. Therewasnorecurrenceupto9monthsoffollow-up. The case of angiomyofibroblastoma and aggressive angiomyxoema in the present series illustrate that the differential diagnosis can be difficult. The tumour was rather similar in clinical presentation as well as at surgery andonhistopathologicexamination.Bothcasespresented as a soft non-tender swelling in the vulva and were preoperatively diagnosed as Bartholin’s cyst. Atypical and diagnostically misleading clinical features were the large size of angiomyofibroblastoma and near absence of local infiltrationofaggressiveangiomyxoema.Similarfeatures 14 wereobservedbySchiotz et al .Thesetumoursaresorare 14 thatmanygynaecologicalsurgeonsmayneverseeone. The chorangioma (haemangiomaorsocalledangiomyxomaoftheplacenta) is a benign neoplasm present in approximately 1% of 18placenta. Most chorangiomas are solitary firm solid nodules upto several cms in diameter, located in the superficialparenchymanearthefoetalsurface.Cutsection reveals a smooth myxoid consistency and tan, dark red or variegated appearance. Small solitary chorangioma are usually clinically insignificant. Large chorangioma
particu
larly those exceeding 5cm in diameter can cause
foetal hydrops, congestive cardiac failure and thrombo19cytopaenia. Inthepresentseries,acaseofchorioangioma was seen in the placenta submitted from a patient who had hydramnios.
REFERENCES
1 Uppal S, Heller DS, Majmudar B — Ovarian hemangiomaReport of three cases and review of the literature. J Arch Gynecol Obstet 2004;270:1-5.
2 Talerman A — Hemangioma of the ovary and the uterine cervix. Obstet Gynecol 1967;30:108-13.
3 Gerbie AB, Hirsch MR, Greene RR — Vascular tumors of femalegenitaltract. Obstet Gynecol 1955;6:499-507.
4 Gupta R, Singh S, Nigam S, Khurana N — Benign vascular tumors of female genital tract. Int J Gynecol Cancer 2006; 16:1195-200.
5 Ahluwalia J, Girish V, Saha S, Dey P — Lymphangioma of theOvary, Acta Obstet Gynecol Scand 2000;79:894-5.
6 Evans A, Lytwyn A, Urbach G, Chapman W — Bilateral Lymphangiomas of the ovary: an immunohistochemical characterization and review of the literature. Int J Gynecol Pathol 1999;18:87-90.
7 Cherkis RC, Kamath CP — Hemangioma of the uterine cervixandpregnancy:acasereport. J Reprod Med 1988;33: 393-5.
8 Rezvan FF Vagina cavernous hemang oma n pregnancy. Obstet Gynecol 1997;89:824-5.
9 Vlastos AT, Malpica A, Follen M — Lymphangioma circumscriptum of the vulva: a review of the literature. Obstet Gynecol 2003;101:946-54.
10 Kondi-Pafiti A, Kairi-Vassilatou E, Spanidou-Carvouni H, KontogianniK,DimopoulouK,GoulaK—Vasculartumorsof the female genital tract: a clinicopathologic study of nine cases. Eur J Gynaecol Oncol 2003;24:48-50.
11 F e cher CDM Tsang WY Fischer C Angiomyofibroblastoma of the vulva. Am Surg Path 1992; 16:373-82.
12 Fukunaga M, Nomura K, Matsumoto K, Doi K, Endo Y, Ush gome S Vu val angiomyo broblastoma: Clinicopathologic analysis of six cases. Am J Clin Pathol 1997;107:45-51.
13 Ducarme G, Valentin M, Davitian C, Felce-Dachez M, Luton D — Angiomyofibroblastoma: a rare vulvar tumor. Arch Gynecol Obstet 2010;281:161-2.
14 Schio z HA, Myhr SS, Chan KF K ngen TA AngiomyofibroblastomaandAggressiveangiomyxoma:Two Rare Tumors of the Vulva. J Pelvic Med Surg 2006; 12: 2258.
15 Steeper TA, Rosai J — Aggressive angiomyxoma of the female pelvis and perineum. Report of nine cases of a distinctive type of gynecologic soft-tissue neoplasm. Am J Surg Pathol 1983;7:463-75.
16 Begin LR, Clement PB, Kirk ME, Jothy S, McCaughey WT, Ferenczy A — Aggressive angiomyxoma of the pelvic soft parts: A clinicopathologic study of nine cases. Human Pathol 1985;16:621-8.
Placental chorangioma
Dupatta injuries : an identifiable hazardous entity in a variety of work place and social scenarios
Ashok Kumar , Pritish
Dupatta is a long loose piece of cloth worn around neck .It is flaunted by both males and females. Despite theculturalassociationofthisapparel,itispartofnumerousinjuryepisodesofvaryingenormity.Severityand enormity of dupatta related injuries range from mild contusions to strangulations, paraplegias, scalp avulsions, miscarriages, traumatic amputations, and burns to even death. These common forms of injury patternsassociatedwithdupattaareobservedbothinsocialandindustrialmilieu.Inallsuchinjuries,common component observed is that the long loose piece of cloth gets entangled in a machine part or the wheels and result in a entanglement of hair, limb part etc. Its constant and devastating consequences in cases dictate for apreventionplancomprisingbotheducationalandlegislativemeasures.
[J Indian Med Assoc 2016; 114: 31-2]
Key words : Dupatta, scalp avulsion, traumatic amputations, industrial milieu.
Dupatta(scarf),apieceoflongclothwornaroundneck,is part of a traditional apparel in eastern culture. It is uniformly attired by masses in Indian subcontinent due to its cultural associations. The loose and long floating ends of thisattireinvitetroubleinvaryingcommonunforeseensituations in the work place, at home, infarmyards, public places etc. The spectrum of harm may range from cautionary abrasions to dire 1,2,3 quadriplegiasandevenunattendedstrangulationstodeath .This sporadic but constantly reported hazardous entity calls for a diversified intervention both in the social and occupational surroundings.
School Girl Strangulation :
14-year-old girl student of the 7th standard was returning from her school along with her school friends riding on a cycle rickshaw She lost attention to her dupatta and it got entangled in wheel spokes The moment in waiting was horrible enough to remind her of some impending doom. She was strangulated hard with neck and face thrust against metal bars and dupatta choking her neck. Fortunately she was rescued by timely efforts and all this left her with a circumferential constriction mark and frighteningmemories(Fig1).
17 Srinivasan R, Mohapatra N, Malhotra S, Rao SK — Aggressiveangiomyxomapresentingasavulvalpolyp. Ind J Cancer 2007;44:87-9.
18 Wallenburg HCS, Chorangioma of the Placenta: Thirteen new cases and review of literature from 1939 to 1970 with special reference to clinical complications. Obstet Gynecol Survey 1971;26:411-25.
19 ElderGevaT,HochnerCelnikierD,Ariel—Fetalhighoutput cardiac failure and acute hydramnios caused by large placental chorangioma: case report. Br J Obstet and Gynecol 1988;95:1200-2.
thresher machine his neck cloth got entangled. He was alone at the moment, and the pulling force of the thresher hit him hard against the rotating machine and avulsed his scalp and hair from the head before helping hands arrived. He was rescued but sufferedfrommutilatingandghastlyscalpavulsion.(Fig2).
Bilateral Forearm Amputation
:
A sugar factory daily wedge labourer was feeding raw material in a cane crushing machine. He was distracted for a minute and his loose neck cloth got entangled in the rotating machine part along with sugarcanes and rotating momentum of the machine stopped only after severely crushing both his forearms. His life was saved but he underwent bilateral fore-arm amputation leaving him devoidofbothhisforearmsforlife(Fig3).

A 32-year-old male farmyard labourer was preparing to feed his cattle. While cuttinggreencrop forcattlebyamotorised
Department of Orthopedics &Traumatology, Mahatma Gandhi Institute ofMedicalSciences,Sewagram442102
1MS(Orth),AssociateProfessor
2MS(Orth),PostgraduateStudent
3MCh(Neurosurg),AssociateProfessor
4MS(Orth),ProfessorandHeadoftheDepartment
Pregnancy Loss
:
A young expecting mother with advanced gestation was travelling by a cycle rickshaw on her way back home. Events turned on the wrong side soon, and her loose long scarf got entangled in uncovered wheel spokes and the jerk she endured before the rickshaw halted gave her a severe pain abdomen and a circumferentia constriction mark She was immediately hospitalised to a trauma centre, where a sonographic scan revealed a dead foetus, which was evacuated on emergency basis.
Conclusion :
Dupatta is an integral part of the traditional attire of women
Case Note Case Note
of cloth worn like a scarf around the neck attired bymassesowingtoitsculturalassociation.Itis popularly worn with long loose ends hanging fromshoulderstobackonbothsides.Thislong loose piece of cloth is part of many continental types of attire like saree. Males are not shy of using a similar type of cloth around neck or head with clandestine thoughts of social supremacy, averting heat etc. Turban is part of traditionalattireofmalesintheIndiansociety These articles of clothing are not only part of social surroundings but are equally part of occupational surroundings. Persons use such clothes in differing proportions depending on theirworkplacesituationsalso.
Indian subcontinent. It is a long piece of

Fig 2 — Showing Severe Scalp Avulsion Sustained after being Pulled in Farmyard Grass Chopping Machine
The persons wearing this piece of cloth are vulnerable to varieties of injuries at both social scenarios and workplace situations. This peculiar form of in ury is sporadic but constantly reported. This particular variety of occupational hazard gains importance not only by virtue of its enormity but also by its occurrence in common unforeseen situations and it's scopeofprevention.
Therearevariousscenariosfromwhichsuchincidenceshave been reported. Uncovered wheel spokes of cycle rickshaws, motor cycles, poorly protected thresher machines, grass chopping machines, sugarcane juice extracting machines and 1-6 flour mills are potential origin for such injuries . Roller machines, and conveyer belts are par of numerous manufacturing units Protective measures prescribed in legislation are practiced in a compromised manner in manufacturing units whether they are small scale or large scale units. Small scale units in semi-organised sector put their workers more at risk. Cohorts at risk are many eg, household members,schoolchildren,millworkersetc.
Modeofinjuryisidenticalinalmostallsituations.Theloose longpieceofclothisoftenentwinedinrotatingcomponentofthe machinery and momentum of the moving part pulls body part towardsitcausingavarietyofinjuriestovictims. Thelimbparts areoftencrushedafterfutileeffortsofescapefromtheaccident.
Spectrum of injuries by this mechanism is diverse. One end of the spectrum constitutes simpler injuries like abrasions, contusions,orsomeblunttraumatothebodypart.Butgraverpart of spectrum has injuries like crush injuries of limbs, traumatic amputations, strangulations near to death, scalp avulsions, traumatic quadriplegias, post-traumatic foetal demise etc.
5,6,7 Deathsarealsoinlistfromsuchbizarreincidents
Thehistoryalsodescribesthestrangulationbyalongscarfof the world famous dancer Isadora Duncan in 1929. She is acclaimedasarespectedfigureinmoderndanceandwasfondof flaunting long scarves. She died due to accidental strangulation and laryngeal rupture by a long loose scarf which got entangled inthespokesofhercar
This peculiar type of injury with almost singular common mechanism is very amenable for preventive actions. The ever increasing number of such incidents both from public and industrial milieu and amount of morbidity and burden attached
withitdic

Fig 3 — Showing Bilateral forearm crush sustained in a sugar factory related to neck cloth salvaged by a bilateral forearm amputation
7,8 tatesscopeforintervention
The intervention plan has to be directed both in public and occupationaldomains.Thereisaneedtoraiseawarenesslevelof the public about increased alertness for such avoidable injuries. Incriminating factors like public transport system, poorly shielded machines for households can be deemed safe with a blendofeducationandlegislation.
Industrial environment can be made safer with the help of uniform safety measures, awareness of personal protection, protective barrier application in roller machines, conveyer belts etc. Increasing the amount of automation in high risk industrial processeswillalsobeapromisingstepagainstthisbizarreformof workplace harm. More and more participation of semi-organised small scale industrial units will promise more prevention. To summarise,thisparticularformofinjuryneedstobeidentifiedas a separate entity in public and industrial work fields and interventionplansshouldbeaccordinglydirectedtowardsit.
REFERENCES
1 Aggarwal NK, Agarwal BB — Accidental strangulation in a cyclerickshaw. Med Sci Law 1998;38:263-5.
2 Kohli A, Verma SK, Agarwal BB — Accidental strangulation inarickshaw. Forensic Sci Int 1996;78:7-11.
3 Siddiqui AA, Shamim MS, Jooma R, Enam SA — Long scarf injuries. J Coll Physicians Surg Pak 2006;16:152-3.
4 Shetty M, Shetty BS — Accidental ligature strangulation due toelectricgrinder.JClinForensicMed2006;13:148–50.
5 TaffML,BoglioliLR—Variantsoflongscarfsyndrome. Am J Forensic Med Pathol 1991;12:359-61.
6 Habal MB, Meguid MM, Murray JE — “The long-scarf syndrome”—a new health hazard. N Engl J Med 1971; 284: 734-36.
7 Gupta BD, Jani CB, Datta RG — Accidental strangulation: a casereport. Med Sci Law 2004;44:359-62.
8 Gowens PA, Davenport RJ, Kerr J, Sanderson RJ, Marsden AK — Survival from accidental strangulation from a scarf resulting in laryngeal rupture and carotid artery stenosis: the ‘‘Isadora Duncan syndrome’’. A case report and review of literature. Emerg Med J 2003;20:391-3.
Recurrent cryptomenorrhoea — a successful outcome
1 2 3 4
Pradip Kr Saha , Dipak Kr Giri , Haricharan Roy , Satabdi Majhi
Primary amenorrhoea with well developed secondary sexual character with cyclical lower abdominal pain in a postpubertal girl points more towards concealed menstruation. Imperforate hymen and transeverse vaginal septum are the two most common congenital causes of cryptomenorrhoea. Thick transverse vaginal septum if improperly treated, may recur. Successful surgery with proper postoperative careleadtoagoodpermanent outcome.
[J Indian Med Assoc 2016; 114: 33-4]
Key words : Cryptomenorrhoea, transverse vaginal septum.
Acomplete transverse vaginal septum leads to haematocolpometra in the pubescent girls. Though small but important component of gynaecological 2,3 practice is correction of congenital anomalies Transeverse vaginal septum is rare and its coexistence with cervical dysgenesis is even more rare. Transverse vaginal septum results from incomplete fusion between the vaginal components of the Mullerian ducts and the urogenital sinus. The septum varies in thicknessandmaybelocatedatanylevelinthevagina,although most are found in the upper and mid-vagina Clinical presentation depends on whether it is complete or partial. With complete septa, menstrual blood accumulates and distends structures above the septum after puberty, resulting in hematocolpos and haematometra. Such patients usually present with cyclic lower abdominal pain and ultrasonic findings of haematocolpometra. Occasionally a lower abdominal mass (haematometra) is palpable. Clinical diagnosis is usually difficultbeforesurgery
CASE REPORT
MissMDaged16yearsoldunmarriedgirlwasreferredfrom a subdivision hospital on 10.2.2011 with a hypogastric mass of 14 weeks size with well developed secondary sexual character Speculam examination revealed, a blind short vagina of 1 cm depth. On per rectal examination, a soft, globular mass at pouch of douglas, with overlying free rectal mucosa. She had normal complete haemogram, blood sugar, urea, chest x-ray and ECG report. She gives history of drainage of haematocolpos on 10-82010, at private nursing home without any prior USG report. Followingdrainageshedidnotmenstruateinthenextcycle.She visited gynaecologist of subdivision hospital and advised USG (2-11-2010)whichshows(Fig1),mildcollectionatendometrial cavity and huge thick collection in distended endocervical canal suggestive of mild haematometra & large haematocolpos but bothovaries&kidneyswerenormal.Sheunderwentre-drainage thereanddischarged10daysafterthedrainagebutunfortunately shedoesnotmenstruateinthenextcycle.
Department of Obstetrics and Gynaecology Midnapore Medical College,PaschimMidnapore721101
MBBS,DCH,MD(ObstetandGynaecol)AssistantProfessor MBBS,MD,DNB,RMO cum ClinicalTutor
MBBS, DGO, MD (Obstet and Gynaecol), RMO cum Clinical Tutor
MBBSHouseSurgeon

Following admission to our medical college, a provisional diagnosisofTransverseVaginalseptumwithvaginalatresiawas made & she underwent operation for the 3rd time on 26-2-2012. Her HIV screening was negative. Keeping Foley's catheter in bladderandurethra,andexertingtractiononcatheter,probingof thick vaginal septum is done by stillet of IV cannula. Once the sac of haematocolpos is reached, a verres needle followed by gradually increasing size of Hegars dilator upto size no. 8 is introduced in the same tract towards posterosuperior direction, keeping a finger guide at rectum. A 14 Fr Foley's catheter is placed in the sac of haematocolpos and a continuous catheter drainageofaccumulatedbloodisallowedfor4days(Fig2).The vagina was atretic and dissection was done in the loose areolar space between the bladder and rectum towards the cervix and vaginalseptalexcisionandvaginoplastywascarriedoutkeeping the Foley's catheter in situ. A 20ml syringe half cut out on nozzle-side, which is gauze and condom wrapped, over which amnion graft is placed and through inner side of syringe the Foley'scatheterispassedandthismouldstructureisplacedinthe neo-vagina (Fig 3), and kept for 7 days. A follow up USG was done for re-evaluation (Fig 4). The mould is removed after 7 days when amnion graft is taken up but the Foley's


catheteriskeptinsitufor3months.OCpillwasgivenfor3cycles and withdrawl bleeding occured at regular interval. The menstrual blood comes out 80% through foley's catheter & 20% throughneo-vaginain1stcycle,50%eachin2ndcycle,Whereas in 3rd cycle, 75% blood comes out through neo-vagina and only 25% through Foley's catheter After 3 month, catheter was taken out but OC pill was continued for another 3 month to enhance regeneration of endometrium and to have regular menstruation. She was under cover of Doxycycline & Metronidazole. After 6 month, a satisfactory vaginal length of 3 inches was achieved. Wide area above neo-vagina but no clearly demarcated external os like structure. After a year, a HSG was done, which shows elongated cervix & uterine cavity and without any bilateral peritonealspillage.Sheisfollowedupatourgynaecologyclinic.
DISCUSSION
The case presented a transverse vaginal septum which get cured after successful management. Diagnosis of such case is usually arrived at from the history of cyclic pain and primary amenorrhea with or without the clinical finding of a bulging vaginalseptum Bulgeinthevaginaonrectalexaminationraised thesuspicionofhaematocolps.Thiswasconfirmedbyultrasound findings. A simple excision and dissection through loose tissue was done to create a neo-vagina. A simpler flap method is applied Topreventstenosisduringthephaseofepithelialization, a male condom filled with gauze was inserted in the vagina

and removed after one week. Canalization procedures for the cervix have been documented to be successful especially where thecervicalbodyisintactasevidencedbyHSG.Theneo-vagina created has remained patent for 12 months without need for any dilatation.
REFERENCES
1 Stewart AD — Cryptomenorrhoea due to Transeverse vaginal septum. Online library. Wiley.com/doi/10.1111/j. 1479-828X.1968.....x/pdf.
2 Rock JA, Azziz R — Genital anomalies in childhood. Clin Obstet Gynecol 1987;30:682.
3 Deppisch LM — Transverse vaginal septum: histologic and embryologic considerations. Obstet Gynecol 1972; 39: 1938.
4 Levy G, Warren M, Maidman J. Transverse vaginal septum: case report and review of literature. Int Urogynecol J 1997; 8:173-6.
5 Brenner P, Sedis A, Cooperman H — Complete imperforate transverse vaginal septum. Obstet Gynaecol 1965; 25: 1358.
6 Wenof M, Reniak JV, Novendstern J, Castadot MJ — Transverse vaginal septum. Obstet Gynecol 1979; 54: 60454.
If you want to send your queries and receive the response on any subject from JIMA, please use the E-mail facility.
Website : www.ejima.in
ForEditorial : jima1930@rediffmail.com
ForCirculation : jimacir@gmail.com
ForMarketing : jimamkt@gmail.com
General : j_ima@vsnl.net

JOURNALOFTHE INDIAN MEDICALASSOCIATION:
IMAHouse, 53 Sir Nilratan Sarkar Sarani (Creek Row), Kolkata 700 014 Phones: (033) 2236-0573, 2237-8092, Fax: (033) 2236-6437, E-mail jima1930@rediffmail.com, Website: www.ejima.in ; www.ima-india.org, www.ima-india.org/ejima
Head office: Indian MedicalAssociation, IMAHouse, Indraprastha Marg, New Delhi - 110 002 Telephones: +91-11-2337 0009, 2337 8680, Fax: +91-11-2337 9470, 2337 0375, Telegram: INMEDICI, New Delhi 110 002, Email: hsg@ima-india.org; Website: www.ima-india.org
Date of Publication : 30th Every Month
POST BOX NO 11249
SEPTEMBER 2016
Regd. No. WBENG/2557/57
Our Respectful Homage
Bharat Ratna Dr. Bidhan Chandra Roy to
If not delivered please return to
Journal of the IMA (JIMA)
IMA House, 53 Sir Nilratan Sarkar Sarani (Creek Row), Kolkata 700 014 (India)
Published and Printed by Dr Santanu Sen on behalf of Indian Medical Association and printed at Prabaha, 45A, Raja Rammohan Roy Sarani, Kolkata 700009, Editor: Dr Debasish Mukherjee, National President (IMA): Dr SS Agarwal, Honorary Secretary General (IMA): Padma Shri Dr KK Aggarwal. E-mail: hsg@ima-india.org; Website: www.ima-india.org 36