





Volume 114 Number 06 Kolkata June 2016
CONTENTS
Editorial :
Environmental pollution and its effects — Debasish Mukherjee .....................................................85
OriginalsandPapers:
Efficacy of low dose cyclophosphamide induction regimen in proliferative lupus nephritis : a prospective study — Ananta Kumar Datta, Manoj Soren, Jyotirmoy Pal, Prasun Roy, Anirban De, Sattik Siddhanta, Partha Pratim Mukherjee ...................87
Knowledge, attitude and practice of contraception : a study from rural tertiary care centre — Beenu Kushwah, Sonal Agrawal ...............................................................................90
Ocular manifestations of thalassaemia patients with repeated blood transfusion and long term use of chelating agent — Badal Chandra Gorain, Piyali Sarkar, Kumaresh Chandra Sarkar, Jyotirmoy Dutta....................................................................................94
Practitioners’Series :
Humanoto-acariasis:440casesofintra-auraltickinfestationmanagedinruralbelt ofSullia— Sudhir M Naik, Sarika S Naik...........................................................................................98
CurrentTopic:
Co-formedconsent:acaseofrightfulapplication— Munawwar Husain, Arshad Anjum, Amir Usmani, Mubarak Alshraim, Jawed A Usmani ................................................101
GP Forums: CaseNotes: Supplement
Drugreview:febuxostat— Kiran Kumar Singal, Sunder Goyal, Parveen Gupta, Ram Gopal Sharma ................................................................................................103
Retrospectiveanalysisondiagnosisofmalaria—aneedfordeveloping community— Nilotpal Banerjee, Sujit Bhattacharjee.....................................................................105
Emphysematouspyelonephritis–inanon-diabeticyoungwomen
—arareassociation— Y S Ravikumar, K M Srinath, L S Adarsh, Manjunath S Shetty, Subrahmanyam Karuturi, B Balaji Kirushnan .................................................108 Rhinocerebralmucormycosis:reportoftwocasesandreviewofliterature — Gopee E Makwana, Vikash Jain, Nandini Bahri, Mala Sinha, Manish Kumar Mathur.................110 Harlequinichthyosis—acasereport— Sendhil Coumary A, Seethesh Ghose .................................113 ..............................................................................................................................................116

May everybody be happy May every one of us see to it
That nobody suffers from any pain or sorrow I do not ask for crown
Nor wish to be in Heaven or reborn I only want to alleviate the suffering of those people Who are burning in fire of sorrow
http://www.ima-india.org/ima/left-side-bar.php?scid=14
Editorial

We, the members of Indian Medical Association Stand here to salute our National Flag Its honour and glory shall be our light and strength And its course shall be our course. We pledge our allegiance to it And realizing our responsibilities as the accredited members of this national organization, We swear We will dedicate everything in our power To see it fly high in the comity of nations.

Environmental pollution and its effects
One of the greatest problems that the world is facing today is that of environmental pollution, increasing with every passing year and causing grave and irreparable damage to the earth. Environmental pollution consists of five basic types of pollution, namely,air,water,soil,noiseandlight.
1. IMARareBloodGroupOnlineBloodBankDirectory ima-india.org/Rare
2. IMAOnlineTBNotificationinitiative ima-india.org/tbnotify
3. IMAOnlineEventsReportinginitiative http://www.ima-india.org/ima/left-side-bar.php?scid=228
4. ProformaforHypertensionScreening http://module.ima-india.org/
5. IMAOnlineSentinelEventsReportingInitiative ima-india.org/sentinel
6. IMADiseaseNotification http://disnotif.ima-india.org/
7. IMARISEandSHINE http://imariseandshine.com/
8. IMABloodDonationInitiative http://www.ima-india.org/ima/left-side-bar.php?scid=289
9. IMAFlagSalutation http://www.ima-india.org/ima/left-side-bar.php?scid=14
10. IMAPrayer http://www.ima-india.org/ima/left-side-bar.php?scid=14
11. IMADigitalTV http://www.ima-india.org/imalive/ 12. IMASlideShare http://www.ima-india.org/ima/free-way-page.php?scid=287 13. IPledgeMyOrgan http://module.ima-india.org/ipmo/ 14. IMALive http://www.ima-india.org/imalive/ 15. eMedinexus/ART http://emedinexus.com/artbill/ 16. eMedinexus/Satyagraha http://emedinexus.com/satyagraha 17. IMA/ART http://ima-india.org/artbill 18. IMA/Satyagraha http://ima-india.org/satyagraha 19 IMA/Webcast http://ima-india.org/ima/ 20 IMADigitalTV http://ima-india.org/digitaltv
IMAHeadquarters
DrSSAgarwal (National President)
Prof(Dr)AMarthandaPillai (Imm Past National President)
DrShailendraNVora (National Vice President)
DrKPrameelaSurenderRao (National Vice President)
DrOmParkashSinghKande (National Vice President)
DrSharadKumarAgarwal (National Vice President)
DrKKAggarwal (Hony Secretary General)
DrRNTandon (Hony Finance Secretary)
DrRajeevArdey (Hony Jt. Secretary)
DrRaviMalik (Hony Jt. Secretary),
DrRameshKumarDatta (Hony Jt. Secretary)
DrSanjoyBanerjee (Hony Jt. Secretary Calcutta)
DrPravinGogia (Hony Jt. Secretary)
DrHansRajSatija (Hony Asst. Secretary)
DrManjulMehta (Hony Asst. Secretary)
DrHarishGupta (Hony Jt. Fin. Secretary)
DrUjjwalKrSengupta (Hony Jt. Fin. Secretary Calcutta)
IMACGP
DrVinodKumarMonga (Dean of Studies)
DrARajaRajeshwar (Hony Secretary)
IMAAMS
DrKranshankarWDeoras (Chairman)
DrPullaraoPasumarthy (Hony Secretary)
IMAAKN Sinha Institute
DrShivkumarUtture (Hony Director)
DrArbindKumarSinha (Hony Executive Secretary)
JIMA
DrDebasishMukherjee (Hony Editor)
DrSantanuSen (Hony Secretary)
Your Health
DrAmitabhaBhattacharya (Hony Editor)
DrRahulDutta (Hony Secretary)
Apka Swasthya
DrPrabhatKumarTewari (Hony Editor)
DrArvindSingh (Hony Secretary)
IMANSS Scheme
DrKirtiMPatel (Chairman)
DrYogendraSModi (Hony Secretary)
IMANPPScheme
DrKrishnaMParate (Chairman)
DrJayairishnanAV (Hony Secretary)
IMAHospital Board of India
DrRVAsokan (Chairman)
DrRaviWankhedkar (Hony Secretary)
DrAnilSPachnekar (HQs. Secretary)
IMANational Health Scheme
DrAshokSAdhao(Chairman)
DrAlexFranklin(Hony Secretary)
IMANational Pension Scheme
DrSudiptoRoy(Chairman)
DrKVDevadas(Hony Secretary)
Air pollution is by far the most harmful form of pollution in our environment. Air pollution is cause by the injurious smoke emitted by cars, buses, trucks, trains, and factories, namely sulphur dioxide, carbon monoxide and nitrogen oxides. Even smoke from burning leaves and cigarettes are harmful to the environment causing a lot of damage to man and the atmosphere. Evidence of increasing air pollution is seen in lung cancer, asthma, allergies, and variousbreathing problems along with severe and irreparable damage to flora and fauna. Even the most natural phenomenon of migratory birds has been hampered,withsevereairpollutionpreventingthemfromreachingtheirseasonalmetropolitandestinationsofcenturies.
Chlorofluorocarbons(CFC), releasedfromrefrigerators,air-conditioners,deodorantsandinsectrepellentscausesevere damagetotheEarth’senvironment. Thisgashasslowlydamagedtheatmosphereanddepletedtheozonelayerleadingto globalwarming.
Environmentalpollutionhasexistedforcenturiesbutonlystartedtobesignificantfollowingtheindustrialrevolutionin the 19th century Pollution occurs when the natural environment cannot destroy an element without creating harm or damagetoitself.Theelementsinvolvedarenotproducedbynature,andthedestroyingprocesscanvaryfromafewdays tothousandsofyears(thatis,forinstance,thecaseforradioactivepollutants).Inotherwords,pollutiontakesplacewhen naturedoesnotknowhowtodecomposeanelementthathasbeenbroughttoitinanunnaturalway.
Pollution must be taken seriously, as it has a negative effect on natural elements that are an absolute need for life to exist on earth, such as water and air Indeed, without it, or if they were present on different quantities, animals – including humans–andplantscouldnotsurvive.WecanidentifyseveraltypesofpollutiononEarth:airpollution,waterpollution andsoilpollution.
Causes of Environmental Pollution :
(1) Industries:
Industries have been polluting our environment especially since the beginning of the industrial revolution,asmentionedabove,notablyduetotheincreasinguseoffossilfuels.Inthe19thcenturyandforasignificant part of the 20th century, coal has been use to make machines work faster, replacing human force. Though pollution by industriesmainlycausesairpollution,soilandwatercontaminationcanalsooccur Thisisparticularlythecaseforpowergenerating industries, such as plants producing electricity (May they be a dam, a nuclear reactor or some other type of plant). Also, the transportation of this energy can be harmful to the environment. We can take as an example the transportationofpetrolthroughpipelines;ifthereisaleakinthepipeline,soilwillautomaticallybepolluted.Atthesame time, if the tanker transporting the petrol from its production plant to the place where it will be consumed leaks or sinks, thewaterwillgetcontaminated.
(2) Transportation :
Ever since men abandoned animal power to travel, pollution of the environment has become higherandhigher Itslevelshaveonlybeenincreasinguntilnow Similarlytoindustries,pollutioncausedbytransportcan mainly be attributed to fossil fuels. Indeed, humans went from horse carriages to cars, trains (which, before electricity usedtobepropelledbycoal),andairplanes.Asthetrafficisincreasingeveryday,pollutionfollowsthatevolution.
(3)AgriculturalActivities:
Agricultureismainlyresponsibleforthecontaminationofwaterandsoil.Thisiscaused by the increased use of pesticides, as well as by the intensive character of its production. Almost all pesticides
are madefrom chemicalsubstances and are meantto keep diseases and threatening animals away from the crops. However, by keeping these forms of life away, harm is almost always made to the surrounding environment as well. Furthermore, as agriculture gets more and more intensive to feed the increasing world population, more environmentsandecosystemsaredestroyedtomakespace for the crops. Some of them, like rapeseed –used to make oil–demandalotofspaceforarelativelysmalloutput.
(4) Trading Activities:
Trading activities including the production and exchange of goods and services. Concerning goods, pollution can be caused by packaging (which often involves the use of plastic, which is made fromfossilfuels)ortransport,mainly.
(5)Residences:
Finally,residentialareasprovidetheir fair share of pollution as well. First, to be able to build homes, natural environment has to be destroyed in one way or another Wildlife and plants are driven away and replaced by human constructions.As it requires the work of industries, construction itself is also a source of contamination of the environment. Then, when people settle in, they will produce waste every day, including a part that cannot be processed by the environment without harmyet.
Effects of Environmental Pollution
Now that we have identified the main causes of environmentalpollution,letusstudythenegativeeffectsit has:
(1) Effects on Humans:
The effects of environmental pollutiononhumansaremainlyphysical,butcanalsoturn into neuro-affections in the long term. The best-known troubles to us are respiratory, in the form of allergies, asthma, irritation of the eyes and nasal passages, or other
formsofrespiratoryinfections.Notably,thesewellspread affections can be observed when air pollution is high in cities, when the weather gets hot, for instance. On top of that, environmental pollution has been proven to be a major factor in the development of cancer This can happen for example when we eat reminiscences of pollutants used in the production of processed foods, or pesticides from the crops. Other, rarer, diseases include hepatitis, typhoid affections, diarrhoea and hormonal disruptions.
(2) Effects on Animals:
Environmental pollution mainly affects animal by causing harm to their living environment,makingittoxicforthemtolivein.Acidrains can change the composition of rivers and seas, making themtoxicforfishes,animportantquantityofozoneinthe lower parts of the atmosphere can cause lung problems to all animals. Nitrogen and phosphates in water will cause overgrowth of toxic algae, preventing other forms of life to follow their normal course. Eventually, soil pollution will cause harm and sometimes even the destruction of microorganisms, which can have the dramatic effect of killingthefirstlayersoftheprimaryfoodchain. As for animals, plants, and especially trees, can be destroyed by acid rains (and this willalsohaveanegativeeffectonanimalsaswell,astheir naturalenvironmentwillbemodified),ozoneinthelower atmosphere block the plant respiration, and harmful pollutantscanbeabsorbedfromthewaterorsoil.
(3) Effects on Plants :
Efficacy of low dose cyclophosphamide induction regimen in proliferative lupus nephritis : a prospective study
1 2 3 2 4
Ananta Kumar Datta , Manoj Soren , Jyotirmoy Pal , Prasun Roy , Anirban De , 5 6 Sattik Siddhanta , Partha Pratim Mukherjee
An extended course of high-dose (cumulative dose usually > 6g over 6 months) intravenous (IV) cyclophosphamide (CYC), in combination with glucocorticoid, had been the standard treatment regimen (NIH protocol) for proliferative lupus glomerulonephritis. An alternative to prolonged intense immunosuppression, there are studies which showed successful treatment with low dose IV CYC (cumulative dose 3 g in 3 months) and IV glucocoticoid as a remission-inducing agent, followed by azathioprine (AZA) as a long-term remission-maintaining agent. Thirty consecutive patients with Lupus Nephritis class III and IV (RPS/ISN) or class V with III or IV were included. They were given Induction therapy by6cyclesoflowdose(500mg)i.v.pulsecyclophosphamideand3dosesof1gmethylprednisolonefollowed by maintenance azathioprine. The present study is a “before and after comparison study”. Mean age of patients was 25.3 ±6.2 years. All were female. Of them, 73.3 %( n=22) were of stage 4, 23.3 %( n=7) of stage 3 and 3.33 %( n=1) of stage 5. At the end of induction regimen, creatinine reduced significantly from 1.06±0.54 to 0.74±0.17 (p= 0.0041) and urine became free from any active sediments (p<0.05). The urinary 24 hour protein excretion reduced significantly (4206.3±1155.5 mg vs 155.6±72.7 mg; p<0.0001). Induction regimen withlowdosecyclophosphamidewasfoundtobeeffectiveinproliferativelupusnephritisinourpopulation.
[J Indian Med Assoc 2016;114: 87-9&93]
Key words : Lupus, Nephritis, Cyclophosphamide, Low dose.
I(4) Effects on the Ecosystem :
In short, environmental pollution, almost exclusively created by human activities, has a negative effect on the ecosystem, destroying crucial layers of it and causing an even more negativeeffectontheupperlayers.
Disclaimer
TheinformationandopinionspresentedintheJournalreflecttheviews of theauthorsandnotof theJournalor itsEditorial BoardorthePublisher Publicationdoesnotconstituteendorsementbythejournal.
JIMAassumesnoresponsibilityfortheauthenticityorreliabilityofanyproduct,equipment,gadgetoranyclaimbymedical establishments/institutions/manufacturers or any training programme in the form of advertisements appearing in JIMA and also does not endorse or give any guarantee to such products or training programme or promote any such thing or claims madesoafter
— Hony Editor
n established SLE median life expectancy is less than general population. While disability in patients with SLEiscommondueprimarilytochronicfatigue,arthritis, and pain, the leading causes of death in the first decade of disease are systemic disease activity, renal failure, and infections.
To date, most experts agree that the treatment of moderate-to-severe SLE consists of a period of intensive immunosuppressive therapy (induction therapy) followed by a longer period of less intensive maintenance therapy Patients with proliferative forms of glomerular damage (ISN III and IV) usually have microscopic hematuria and proteinuria (>500 mg per 24 h); If untreated, virtually patients develop ESRD within 2 years of diagnosis.
MD (Gen Med) Associate Professor, Department of General Medicine,IPGME&R,Kolkata700020
MD (Gen Med) RMO Cum Clinical Tutor, Department of General Medicine,BurdwanMedicalCollege&Hospital,Burdwan713104
MD (Gen Med) Professor Department of General Medicine, RG KarMedicalCollege&Hospital,Kolkata700004
MD (Gen Med) RMO Cum Clinical Tutor, Departmet of General Medicine,NRSMedicalCollege&Hospital,Kolkata700014
MD (Gen Med) Assistant Professor, Department of General Medicine,IPGME&R,Kolkata700020
MD (Gen Med) Professor, Department of General Medicine, CalcuttaNationalMedicalCollege&Hospital,Kolkata700014
Therefore, aggressive immunosuppression is indicated (usually systemic glucocorticoids plus a cytotoxic drug). An extended course of high-dose intravenous(IV) cyclophosphamide (CYC), in combination with glucocorticoids, has become the standard treatment of proliferative lupus glomerulonephritis since the pioneering prospective trials performed by the National Institutes of Health (NIH) group that demonstrated the 2-4 superiorityofthisregimenoveroralorIV glucocorticoid therapyalone.Severalinvestigatorshave,however,raised some concerns about the indiscriminate use of the so5,6 called “NIH regimen” to treat all lupus nephritis patients First, the results of the NIH studies, as well as a recent 7 meta-analysis of all randomized trials in lupus nephritis, failed to demonstrate that an extended course of IV CYC was superior in terms of renal outcome and survival to other regimens of oral or IV cytotoxic drug(s). Second, high-dose IVCYC treatment is highly toxic; up to 25% of patients develop herpes zoster infection, up to 26% experience a severe infection, and up to 52% of women at 2-5 risk have ovarian failure As an alternative to prolonged intense immunosuppression, there are studies which
EFFICACY OF LOW DOSE CYCLOPHOSPHAMIDE INDUCTION REGIMEN — DATTA ET AL 89
treatment of lupus nephritis patients
showed successful with a sequential regimen consisting of low dose IVCYC (cumulative dose 3 gm) and IV glucocoticoid as a remission-inducing agent, followed by azathioprine (AZA) as a long-term remission-maintaining agent Hence this study is undertaken to find out the response to such low dose cyclophosphamide plus corticosteroids in patients with proliferative glomerulonephritis for remissioninduction.
MATERIALSAND METHODS
Location: Thirty consecutive patients fulfilling the criteria and willing to participate in the study were selectedfrompatientsadmittedinGeneralmedicineward and attending Rheumatology clinic of Calcutta National MedicalCollegeandHospital.
Inclusion criteria: Lupus Nephritis class III and IV (RPS/ISN)orclassVwithIIIorIV
Exclusion criteria: Patients with any other form of renal disease like associated diabetes mellitus, preexisting hypertension, and chronic kidney disease due to causesotherthanSLEwereexcluded.
Patients having bone marrow suppression, very low platelet count, or who had taken CYC or AZAduring the previousyearorhadtaken>15mg/dayofprednisolone(or equivalent) during the previous month were excluded (except for a course of glucocorticoids for a maximum of 10 days before referral were also excluded. Patients with agelessthan12yearsandpregnancywereexcluded.
Study methodology:All the patients thus diagnosed to have lupus nephritis of class III and class IV, as well as class V accompanied by III or IV disease were given Induction therapy by 6 cycles of chemotherapy each consisting of low dose (500mg) i v pulse cyclophosphamide and 3 doses of 1gm methylprednisolone. Thiswasfollowedbymaintenancetherapy consist of prednisolone and azathioprine in the treatment protocol .Each patient was counselled about this therapy and consent taken. Evaluation for disease activity is performed by using renal function, urine microscopy and 24hoururinaryalbuminexcretion.
The present study is a “before and after comparison study” in which different laboratory parameters before theintroductionofLowdosepulsecyclophosphamideand methylprednisolonewerecomparedwiththeirvaluesafter 3monthsofthesametherapy Significanceofdifferencein meanswascalculatedby“pairedttest”.Avalueofp<0.05 wasconsideredsignificant.
RESULTSANDANALYSIS
Total 30 patients of SLE with grade III or IV were included. The mean age of the patients was 25.33yrs± 6.177yrs, maximum age is 38 yrs and minimum is 17 yrs.
Allpatientswerefemale.73.3%(n=22)areofstage4, 23.3 %( n=7) are of stage 3 and 3.33 %( n=1) is of stage 5. TheresultsaresummarisedinTable1.Themeanureawas 46.3± 25.775 mg/dl with a maximum of 120mg/dl and minimum of 17 mg/dl. The mean creatinine was 1.062± 0.538 mg/dl with a maximum of 2.85mg/dl and minimum of0.4mg/dl.Atinitialvisit,themean24Hrurinaryprotein was 4206.33± 1155.51with a maximum of 8100mg and minimum of 3600 mg. At the end of remission induction regimen, the mean 24Hr urinary protein was 155.567± 72.72with a maximumof 436 mg and minimumof 80 mg. The mean urea was 28± 12.98 mg/dl with a maximum of 70mg/dl and minimum of 16 mg/dl. The mean creatinine was0.742±0.172mg/dlwithamaximumof1.2mg/dland minimum of 0.4 mg/dl. At initial visit urine microscopy revealed 3 patients have urinary cast and 10 have microscopic hematuria. At the end of intensive phase (3 months)urinemicroscopyrevealednocastorhematuriain anyofthepatient.
Cytotoxic/immunosuppressive agents added to glucocorticoidsarerecommendedtotreatseriousSLElike nephritis. Almost all prospective controlled trials in SLE involving cytotoxic agents have been conducted in combination with glucocorticoids in patients with lupus nephritis.InpatientswhoserenalbiopsiesshowISNgrade III or IV disease, early treatment with combinations of glucocorticoids and cyclophosphamide reduces progression to ESRD and improves survival . If cyclophosphamide is used for induction therapy, the recommended "National Institutes of Health (NIH)" dose (based on clinical trials at that institution) is 500–750 mg/m intravenously, monthly for 6 months, followed by maintenance with daily oral mycophenolate or azathioprine.
2-5
Since cyclophosphamide has many adverse effects and is generally disliked by patients, alternative approaches using lower doses have been tested. European studies have shown that IV cyclophosphamide at doses of 500 mg every 2 weeks for six doses ("low dose") is as effective as the recommended higher dose given for a longerdurationintheNIHregimen("highdose") Followupstudieshaveshownnodifferencesinthehigh-doseand low-dosegroups(deathorESRDin9–20%ineachgroup).
Table 1 — Results of the study
Baseline(n=30) After3months(n=30) Pvalue
Serum
Urinemicroscopy: Redcells;Cast 10;03 0;0 <0.05 Urinary24h protein 4206.33±1155.51 155.567±72.72 <0.0001
The Euro-Lupus Nephritis Trial studied 90 SLE patients with proliferative glomerulonephritis who were assigned to a high-dose IV CYC regimen (6 monthly pulsesand2quarterlypulses;dosesincreasedaccordingto the white blood cell count nadir) or a low-dose IV CYC regimen (6 fortnightly pulses at a fixed dose of 500 mg), eachofwhichwasfollowedbyAZA.Followupcontinued for a median of 41.3 months in the low-dose group and 41 months in the high- dose group. Renal remission was achieved in 71% of the low-dose group and 54% of the high-dosegroup(notstatisticallysignificant).Renalflares were noted in 27% of the low-dose group and 29% of the high-dose group. Although episodes of severe infection were more than twice as frequent in the high-dose group, the difference was not statistically significant.The results of the trial indicate that there was no significantly greater cumulative probability of treatment failure in patients taking a low-dose IV CYC regimen than in those taking a high-dose regimen, and the cumulative probability of achieving renal remission was similar in both groups. In 12 another study done in Egypt by SabryA,Abo-Zenah H Fourtysix SLE patients with diffuse proliferative glomerulonephritis were asigned to either a high-dose (a maximum of 1 g/dose) of IV CYC (HD-CYC) for six monthlypulsesfollowedbytwoquarterlypulsesorafixed low-dose (500 mg/dose) of IV CYC (LD-CYC) for six fortnightlypulseswithacumulativedoseof3g.Attheend of the study (1 year after starting therapy), there was no difference either in patients' or in renal survival in both groups.Another study was conducted by M.A. Frutos,A. 13 MartínGómez wheretheystudiedwithintermittentpulse therapy with intravenous cyclophosphamide (IC) in 97 patients (75 female) aged over 20 years. The series was divided into three groups. Group A (n = 39) received monthlyICpulses(begin1g)forupto24monthsbetween 1985-1991, Group B (n = 47) received monthly IC pulses (1g) for six months with additional quarterly doses for a maximum of 18 months, depending on the therapeutic response (from 1991) and from 1999, Group C (n = 11) patients were treated with low-dose IC (3 g in three months) followed by azathioprine (2 mg/kg) or mycophenolate mofetil (1.5-2.0 g/day) for 12-18 months. Comparison of the values at baseline and after 24 months showed that the serum creatinine (mg/dl) fell in Group A from 1.77 ± 1.06 to 1.09 ± 0.63, in Group B from 1.22 ± 0.85 to 0.95 ± 0.45, and in Group C from 0.90 ± 0.23 to 1.17 ± 0.54 (p < 0.05). In the same period, proteinuria (g/day) fell in GroupAfrom 6.19 ± 4.31 to 0.79 ± 1.76, in Group B from 4.43 ± 3.17 to 2.08 ± 3.65, and in GroupC from 5.43 ± 3.37 to 3.22 ± 4.00 (p < 0.05). There was no differences between the three groups in both variables .In our study; there is significant fall in proteinuria from 206.33± 1155.51 with a maximum of 8100mg and
minimum improvement for mean 24 Hr urinary protein is 96.3% (n=30,p<0.0001).
14 However another study from Puerto Rico has shown that the standard dose cyclophosphamide therapy appears to be more effective, and similar in terms of drug safety, than the low-dose regime for lupus nephritis. In fact, poor outcomes have been reported in African Americans and Hispanics compared to Caucasians with lupus nephritis 15 and thus might merit high or standard dose regimen Further, genetic polymorphism of cytochrome P450 may also lead to differential results of two regimens of cyclophosphamide in different ethnic groups. However, our study showed both groups to be similar, which is consistentwithearlierlargerstudies,alludedabove.
CONCLUSION
Thus before and after comparative study with induction regimen of 6 doses of 500 gms IV cyclophosphamide along with intravenous methylprednisolone for patients with proliferative lupus nephritis showed significant improvement in renal function.
REFERENCES:
1 Boumpas DT, Sidiropoulos P, Bertsias G — Optimum therapeutic approaches for lupus nephritis: What therapy andforwhom? Nat Clin Pract Rheumatol 2005;1:22-30.
2 Austin HA iii,Klippel JH,Balow JE, le Riche NG, Steinberg AD, Plotz PH, et al Therapy of lupus nephritis: controlled trial of prednisone and cytotoxic drugs. N Engl J Med 1986;314:614-9.
3 Boumpas DT, Austin HA III, Vaughan EM, Klippel JH, Steinberg AD, Yarboro CH, et al — Controlled trial of pulse methy predniso one versus wo reg mens of pulse cyclophosphamide in severe lupus nephritis. Lancet 1992; 340:741–5.
4 Gourley MF, Austin HA III, Scott D, Yarboro CH, Vaughan EM, Mu r J, e a Methy predn solone and cyclophosphamide, alone or in combination, in patients with lupusnephritis. Ann Intern Med 1996;125:549-57.
5 Urowitz MB. Is “aggressive” therapy necessary for systemic upus erythematosus? Rheum Dis C in North Am 1993;19:263-70.
6 Ponticelli C. Treatment of lupus nephritis: the advantages of a flexible approach Nephrol D a Transp an 1997;12:2057–9.
7 Bansal VK, Beto JA — Treatment of lupus nephritis: a metaanalysisofclinicaltrials. Am J Kidney Dis 1997;29:193-9.
8 HoussiauFA,VasconcelosC,D’CruzD—Earlyresponseto immunosuppressive therapy predicts good renal outcome in lupus nephritis: lessons from long-term followup of patients in the Euro- Lupus Nephritis Trial, Arthritis Rheum 50: 393440,2004.
9 Bevra H Hahn —Treatment of life-threatening SLE: Proliferative forms of lupus nephritis. Longo, Fauci, Kasper, Hauser, Jameson, Loscalzo. Harrison’s Principles of InternalMedicine.18thedition,volume-2,319:2733.
10 Steinberg AD, Steinberg SC — Long-term preservation of renal function in patients with lupus nephritis receiving treatment that includes cyclophosphamide versus those treatedwithprednisoneonly. Arthritis Rheum 1991;34:94550.
11 Houssiau FA, Vasconcelos C, D’Cruz D, Sebastiani GD GarridoE,Daniel MG, et al Immunosuppressivetherapyin of 3600 mg to 155.567± 72.72. So average
(Continued on page 93)
Originals and Papers Originals and Papers
Knowledge, attitude and practice of contraception : a study from rural tertiary care centre
1 2
Beenu Kushwah , Sonal Agrawal
Realizing the ill effects of increasing population, India was the first country to have started a state sponsored Family Planning Programme, long back in 1952; India is the second most populous country of the world only after China. To attain the required targets India needs nationwide surveys to assess the practices of contraception especially in poor performing states in order to utilize the available resources according to local needs. Hospital based, cross-sectional survey conducted amongst the women of post natalwardofareferralhospitalmainlycateringruralpopulation.Knowledge,AttitudeandPracticesurveyof family planning was conducted amongst these women. A total of 4221 subjects were interviewed.58% of these women were aware of contraceptive methods, mostly Permanent followed by IUCD, Condom, least of oralpills.Spacingmethodsarelessknownamongstruralwomenwhiletheuseisevenlowerwhichcallsfor furtherstrengtheningoftheexistingawarenessprogrammes.
J Indian Med Assoc 2016;114: 90-3]
Key words : Contraception, Total Fertility Rate, Family planning.
On First March 2011, Indian’s population stood at 1.21 Billion which is projected to be 1.4 Billion in 2026.Indiawhichaccountsforworld’s17.5%population isthesecondmostpopulouscountryintheworldnextonly toChina(19.4%).Ofthe1.21BillionIndians,68.84%live in rural area while 31.6% live in Urban areas, as per the census 2011 Therefore more than half of the total populationresideinruralareasinthiscountry
DespitethefactthatIndiawasthefirstcountrytohave started state sponsored Family Planning Programme in 1952, decline in the rate of Total Fertility Rate (TFR) has not been to the extent as was aimed, especially in rural areas For historicalreasonssomestatesinIndiadepicted a tendency of higher growth of population. In order to facilitate the creation of area specific programmes, Government of India in 2001 constituted a group of eight states which were lagging behind in improving their fertility indicators. This group is called as Empowered ActionGroup(EAG).
Present study was conducted in the state of Madhya Pradesh(MP),oneofthemembersofEAG.TotalFertility Rate (TFR) of MP in 2009 was 3.3, against the National average of 2.6 with even bigger difference between Rural and Urban areas, Rural TFR being3.6 and Urban TFR
Department of Obstetrics and Gynaecology, Shyam Shah Medical College and Associated Sanjay Gandhi and Gandhi Memorial Hospital,Rewa486001 MD,DNB,Assistantprofessor, MBBS,JuniorResident
being 1respectively
2.3 against the National average of 2.9 and 2
One of the main objectives of the family planning programme is to spread the knowledge of contraceptive methods and develop, among the people, an attitude favourable for adoption of contraceptive method. The progressachievedinthissphereisnormallyassessedfrom theresultsofKnowledge,AttitudeandPracticesurvey
Present study was conducted amongst the women of post natal ward of one of the Tertiary Health care Centres of Madhya Pradesh. Department of Obstetrics and GynaecologyofGandhiMemorialHospitalhadtotal4927 deliveries (Vaginal and caesarean both) during last 6 months period, 90% of these women come from rural areasasthereisnootherequippedgovernmentrunHealth CareCentreisavailableacrossawidearea.
MATERIAL
This was a Hospital based, Cross Sectional, Observational, Descriptive study during a period of 6 months from June to November 2011. After taking informed consents and briefing about the aim of study, A Totalof4221womenofpostnatalwardofourdepartment consented to be interviewed. A20 point, Semi-structured questionnaire was read out to the subjects. Data were collected regarding socio-demographic features, knowledge, attitude and practices of various family planningmethods.
Womenofagegroup18-35years,wereincludedinthe
study, 78% belonged to 18-22 years age group. Sixtytwo per cent women were illiterate, 24% were literate but without any formal schooling, 11% were literate till primaryandresthadstudiedaboveprimary.Only3%were employed with regular source of income, 16% were running some home business, 12% were working as helper’s at others’houses both with irregular income and 20%werefarmersandwerehelpingtheirhusbands(Table 1).
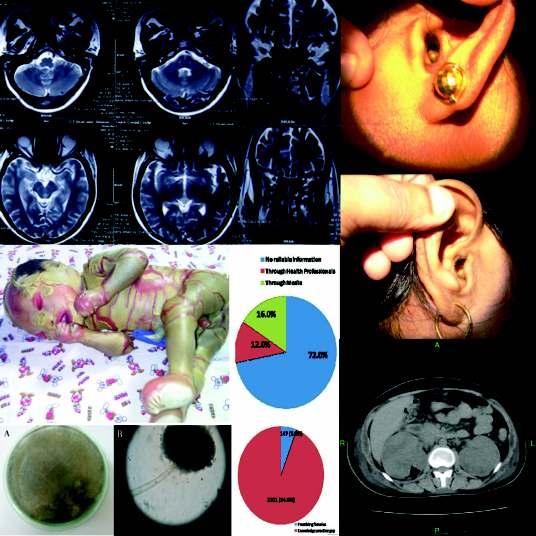
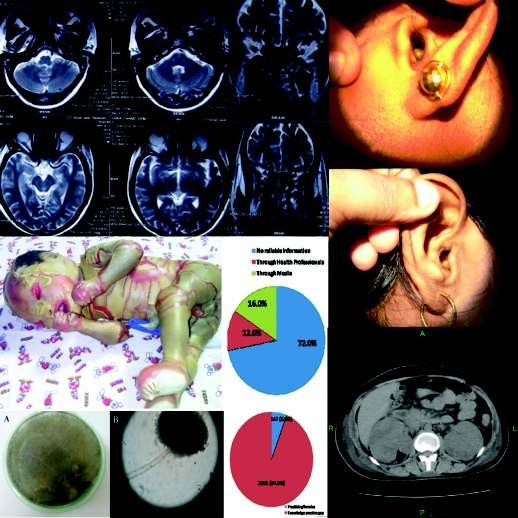
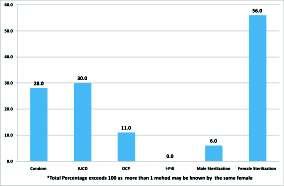
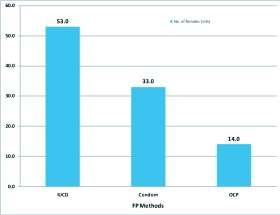
On assessing the knowledge it was found that 58% of women were aware of at least one of the available family planning methods, maximum knowledge was for permanent method (Tubectomy-56%, Vasectomy-6%), followed by IUCD (30%), Condoms (28%), and oral pills (11%) (Fig 1). Although majority (71%) of all women who had knowledge of any family planning methods showed positive attitude towards use but only 6% of these had actually used any method ever of which majority (53%) had used IUCD, 33% condoms and only 14% had usedoralpillsresultinginaveryhighknowledge-practice gap i.e. 96%. None of the Participants were aware of emergencycontraceptivemethod(i-pill)(Figs2and3).
There was no reliable source of information for majorityofparticipants(72%),whileHealthprofessionals contributedtoonly12%andmediato16%.Only7%were satisfiedwiththeircurrentmethodofuse(Fig4).
Main reason for not practicing any one of family planning methods was inefficient accessibility to right information and follow up facility if needed (69%), rest were not using any method because of non cooperation by theirhusbandsandlesserroleindecisionmaking.
While majority of participants (67%) were willing to use contraceptive method in future, 9% refused to use any methodwhile24%werenotabletodecide.Amongstthose who had positive attitude, majority (64%) wanted to use condomfollowedbyIUCD(28%)andonly8%likedpills.
DISCUSSION
In our study maximum awareness was for permanent method of family planning and nil for emergency contraceptionwhileKnowledgefortemporarymethodsin present study was relatively low, which is comparable 3 with another study from India, while it was almost same 4-6 forallmethodsindevelopedregionsofworld
In present study oral pills were used by only 4% womenincontrasttothewomenoftheUnitedState where oral pills are the most popular reversible method of contraception. Other study from ICMR also showed low use of oral pills by Indian females, which is com-
2448)
9-1 parabletootherstudies
The huge knowledge and practice gap of our study has 12-14 also been observed by others , factors which could be identified for this were; wrong information regarding side effects,scarcityofhealthcarefacilitytoconsultifrequired and lesser role in decision making, all of these are directly relatedwithlowliteracylevelsandinadequateinclusionof the educational sessions related with family planning methods by the health professionals. Findings of study fromIndiaobservedsimilargapbecauseoffactorsdirectly 15 relatedwithsocioeconomicdevelopment
6 A study from Reddy showed relatively low contribution of health care personnel in providing family planning knowledge, which was observed in our study as well. The role of health care personnel in providing contraceptive knowledge should be emphasized as it’s a twowaycommunicationprocess.
Sixtyone per cent women of our study were Para three and above and 46% had underwent unconventional methods for terminationof pregnancy at least once before present pregnancy, while 26% had actually wished for termination of present pregnancy but had to continue because of non availability of the facilities nearby These findings from our study are an indirect reflection for the need of termination of pregnancy because of poor knowledge and even lesser practice of contraception. According to one study on an average 5 million legal and illegalabortionsperannumcouldbeabortionrateofIndia 9 for current decade The Indian Survey of Death reports that nearly 18% of maternal deaths result from abortion.Majority of these abortions were illegal and indirectly reflect the significant burden of unmet need of family planning methods available to the women from ruralandremoteareas.
CONCLUSION
In recent years, the need for studies for assessing prevailingcontraceptivepracticesisveryimportantacross various regions of this country to know about regional needs. Results of present study clearly reflect an urgent need for facilitating the access to more information, education and communication with the reproductive couples according to individual needs. This study indicates a pressing need for effective intervention strategies, both at the community and clinic level, backed with efficient counselling, motivation and provision of servicesinRuralandRemoteareas.
REFERENCES
1 Family Welfare Statistics in India 2011: Statistics Division, MinistryofHealthandFamilyWelfare,GovernmentofIndia.
2 J Mao: Knowledge, Attitude and Practices of Family Planning: A study of Tezu Village, Manipur (India). The Internet Journal of Biological Anthropology, 2007 Volume 1 (1).
3 Srivastava Reena, Srivastava Dhirendra Kumar, Jina Radha, Sr vastava Kumkum, Sharma Nee a Saha Sushmita—Contraceptiveknowledge,attitudeandpractice (KAP) survey. Journal of Obstet Gynecol India 2005; 55: 546-50.
4 Young LK, Farguhar CM, Mc Cowan LME — The Contraceptive practice of women seeking termination of pregnancyinAuklandclinic. NZ Med J 1994;107:189-91.
5 Aneblom G, Larson M, Odlind V — Knowledge, use and attitudes towards emergency contraceptive pills among Swedish women presenting for induced abortion. BJOG 2002; 109: 155-60.
6 Bromham DR, Cartmill RS — Knowledge and use of secondary contracept on among pat en s request ng terminationofpregnancy. BMJ 1993;306:556-7.
7 Johansson ED — Future developments in hormonal contraception. Am J Obstet Gynecol 2004;4:s69-s71.
8 Baveja R, Buckshee K, Das K, Das SK, Hazra MN, Gopalan S et al — Evaluating contraceptive choice through the method –mix approach (An ICMR Task Force Study). Contraception 2000;61:113-9.
9 Takkar N, Goel P, Saha PK, Dua D — Contraceptive practices and awareness of emergency contraception in educated working women. Indian J MedSci 2005; 59: 14349.
10 Mittal S, Bahadur A, Sharma JB — Survey of knowledge, attitudeandpracticeofcontraceptionandmedicalabortionin women attending family planning clinic. J Turkish German Gynecol Assoc 2007;8:3.
11 Kanojia JK, Nirbhavane NC, Toddywala VS, Betrabet SS, PatelSB,DatteS, et al Dynamicsofcontraceptivepractice amongst urban Indian women. Natl Med J India1996; 9: 10912.
12 Mahawar Priyanka, Anand Shweta, Raghunath Deepa, Dixit Sanjay — Contraceptive Knowledge, Attitude and Practices
(Continued from page 89) upus nephr tis The Euro-Lupus Nephr tis Trial, a Random zed Tria of Low-Dose Versus High-Dose Intravenous Cyclophosphamide. Arthritis Rheum 2002; 46: 2121-31.
12 Sabry A, Abo-Zenah H, Medhat T — A comparative study of two intensified pulse cyclophosphamide remission-inducing regimensfordiffuseproliferativelupusnephritis:anEgyptian experience. Int Urol Nephrol 2009;41:153-61.
13 MA Fru os, A Martín Gómez Intravenous Cyclophosphamide for lupus nephritis: twenty years reducing the dose. NEFROLOGÍA. Volumen 27. Número 1. 2007
in mothers of Infants: A Cross Sectional study. National Journal of Community Medicine 2011;2:105-7.
13 SharmaA,SharmaV—Trainingofopinionleadersinfamily planning in India: Does it serve any purpose. Rev Epidemiol Sante Publique 1996;44:173-80.
14 Sharma V, Sharma A — Family planning practices among tribals of South Rajasthan, India. J Res Educ Indian Med 1991;10:5-9.
15 Gautam AC, Seth PK — Appraisal of the knowledge, attitude and practices (KAP) of family control devices among rural rajputs and Scheduled caste of Hatwar area of Bilaspur district, Himachal Pradesh. Anthropologist 2001; 4(4):289-292.
16 R Reddy S, K C Premrajan, K A Narayan, Akshaya Kumar Mishra — Rapid appraisal of knowledge, attitude and practices related to family planning methods among men within5yearsofmarriedlife. J Prev Soc Med 2003;34:63-6.
14 Castro-Santana LE, Colón M, Molina MJ, Rodríguez VE, Mayor AM, Vilá LM — Efficacy of two cyclophosphamide regimens for the treatment of lupus nephritis in Puerto Ricans:lowversusstandarddose. Ethnicity & disease 2010; 20:S1-116-21.
15 Contreras G, Lenz O, Pardo V, Borja E, Cely C, Iqbal K, Nahar N, de La Cuesta C, Hurtado A, Fornoni A, BeltranGarcia L, Asif A, Young L, Diego J, Zachariah M, SmithNorwood B — Outcomes in African Americans and Hispanicswithlupusnephritis. Kidney Int 2006;69:1846-51
OCULAR MANIFESTATIONS OF THALASSAEMIAPATIENTS WITH REPEATED BLOOD TRANSFUSION
Ocular manifestations of thalassaemia patients with repeated blood transfusion and long term use of chelating agent
1 2 3 4
Badal Chandra Gorain , Piyali Sarkar , Kumaresh Chandra Sarkar , Jyotirmoy Dutta
To study the ocular manifestations in beta-thalassaemia major patients with multiple blood transfusions, ocular side-effects of iron chelating agents and to find out any correlation of the side-effects of iron chelating agents with age and sex, a prospective observational study was undertaken which included 100 bthalassaemia major patients, who were divided into 2 groups based on thalassaemia treatment regimens receivedatthetimeofpresentation.Propermedicalhistory,thoroughphysicalandocularexaminationswere done to determine the prevalence of ocular manifestations and to correlate these manifestations with iron chelating agents. In 100 patients (56 males, 44 females) with age ranging between 6 months and 15 years, ocular involvements were detected in 52 cases in the form of lens opacity, decreased visual acuity, retinal pigment epithelium degeneration and disc hyperaemia, more in group receiving blood and deferriprone therapy. Retinal pigment epithelium degeneration and mottling were found significantly associated with patients receiving oral chelating agents but there was no significant correlation with lens opacity or decreased visual acuity. A large number of thalassaemic children were found to have ocular complications despite moderate doses of deferriprone and in the presence of high serum ferritin levels, which implicate a role of iron in ocular pathology in thalassaemia. Most of the ocular changes of beta-thalassaemia were attributed to longer duration of disease. These changes had slight male preponderance. Retinal pigment epithelium degenerations and mottling, venous tortuosity, disc hyperaemia were found significantly more in patientsonlongtermoralchelatingagents(deferriprone). [J Indian Med Assoc 2016;114: 94-7]
Key words : Beta-thalassaemia, deferriprone, ocular complications.
Thalassaemia is a heterogeneous group of genetic dis orderresultingfromdefectsingenesproducing -or -globin chains of haemoglobin. Beta-thalassaemia results from a defect in -globulin chain production and ranges from clinically silent heterogeneous thalassaemia minor to severe transfusion-dependent thalassaemia major These are the most common single gene disorder worldwide Mutations involving the beta-globin gene in beta-thalassaemia cause disruption in red blood cell maturation leading to ineffective erythropoiesis and 1 multisysteminvolvement.Itisestimatedthat1.5%ofthe worldpopulation,ie,200millionpeoplearecarriersofthe -thalassaemia gene. In India, the mean prevalence of the -thalassaemiageneis3.3%;1,000childrenarebornwith -thalassaemia major each year in India. Worldwide incidence is 60000 per year which are mostly in developingworld.
Department
Although blood transfusions therapy alleviates anaemia,theyleadtomassivetissuedepositionofironand may eventually result in multiorgan dysfunction. Iron overload occurs either due to excess gastro-intestinal absorption or secondary to repeated blood transfusions. Transfusional iron leads to iron deposition in the reticuloendothelial system of the spleen, liver, bone marrow and eye. In advanced cases, iron also accumulates in parenchymal cells of the liver, heart, pancreas and endocrine organs, which are sensitive to the toxic effects of iron. Adverse ocular changes include cataract, pigmentary retinopathy, optic neuropathy, thinning and tortuosity of retinal vessels and vitreoretinal haemorrhages which are due to the disease itself or as side-effectsoftheironchelatingagents
MATERIALAND METHOD
This prospective observational study was conducted on 100 beta-thalassaemia major patients who attended thalassaemia clinic, Calcutta National Medical College & Hospital, Kolkata during the period of September 2010 to March 2012. All patients were informed about the nature of the study and an informed consent for participation obtained. In case of minors, consent was taken from their parents. The diagnosis of beta-thalassaemia major was
confirmedbyclinicalandhaematologicalexaminationsat CNMC paediatric outpatient's department (OPD). All patients received scheduled blood transfusions at three to four weeks intervals. The study included children aged <15years who were diagnosed as cases of betathalassaemiamajor,receivingmultiplebloodtransfusions with or without chelating therapy. Patients >15 years of age, or having haemoglobinopathies other than betathalassaemia major, anaemia due to other causes or other congenital diseases were excluded from the study The patients were divided into 2 groups. Group A received blood transfusion but no iron chelating therapy and group B received combination regimen of blood transfusion and oral deferriprone. Paediatrician elicited a complete general history (including family history and details of previous blood transfusions and iron chelation therapy) and performed systemic examination, especially for presence of pallor, icterus, frontal bossing, prominent maxilla, skin hyperpigmentation and hepatosplenomegaly Laboratoryinvestigationsincludedbaseline complete blood counts and serum ferritin estimation. The ophthalmologist elicited a complete ophthalmic history andperformedocularexamination.
Ocular examination included near and distance visual acuity assessment with and without glasses in all children usingpreferentiallookingtest,picturecardsandSnellen's charts as applicable, external examination with diffuse illumination, slit-lamp examination, direct and indirect ophthalmoscopy and fundus fluorescein angiography (FFA)inselectedpatients. Thepatientswerefollowedup at three-monthly intervals during which complete ocular assessmentwasdoneandprogressioninocularchanges,if any, noted. Serum ferritin levels were assessed at sixmonthly intervals. Ocular findings at follow-up visits were correlated with the age and sex of the patient, serum ferritin level and use of iron chelating agent (deferriprone).
A p-value less than 0.05 was considered statistically significant. Statistical analyses were performed using software SPSS (version 12). For correlation of sex with lenticular opacities, retinal pigment epithelium (RPE) degeneration and RPE mottling, Chi test was used. Correlation of lens opacities, RPE degeneration and RPE mottlingwithserumferritinlevels,wasdonebyPearson's correlational analysis with p-value <0.05 taken as significant. Correlation of lens opacities, RPE degeneration and RPE mottling with dose of deferriprone in various groups too was obtained by Pearson's correlationalanalysis.
OBSERVATIONS
Inthisstudy,therewere56malepatients(56%)and44 females(44%)(Table1).Theiragerangedfromsixmonths to fifteen years. Among them, 21 patients were <5 years, 44 between 6 -10 years and 35 between 11-15 years.They were assigned in two groups according to treatment regimens.
GroupAincluded45patients(45%)whoreceivedonly blood transfusion but no iron chelating agents. Group B included 55patients (55%) who received blood transfusionsandoralchelatingagent(deferriprone75-100 mg/kg/day). Eighteen (85.71%) and 3 patients (14.29%) below five years of age, 17 (38.63%) and 27 patients (61.37%) between 6 and 10 years of age and 10 (28.57%) and 25 patients (71.43%) between 11 and 15 years of age were in group A and B respectively (Table 1). Ocular involvement was observed in 52 patients (52%), whereas 48 patients (48%) showed no ocular involvement. It had beenseenthatocularchangeswereincreasedinolderthan inyoungerchildren(91.42%in11-15yearsand19.04%in <5 years of age groups). The fundus changes (68.57%) werealsomorein11-15yearsagegroup(Table2).Ocular involvements in relation to sex are not significant (p=0.125).There were 30 male patients (57.69%) and 22 female patients (42.31%) having ocular involvement respectively
It had been seen that ocular involvements were more commoningroupB(n=45;81.82%)thaningroupA(n=7, 15.56%). Ocular involvements were significant (p<0.0001) in relation to treatment regimen groups. Decrease in visual acuity were more in group B (n=16; 29.09%) than group A (n=6; 13.33%) thalassaemia patients. Significant correlation of deferriprone therapy with RPE degeneration (p=0.003) and RPE mottling (p=0.001)was observed but not with decreased visual acuity (p=0 058), lens opacity (p=0 928), venous tortuosity (p=0.093) and disc hyperaemia (p=0.249) (Table3).
Thestudyshowedthattheaverageserumferritinlevels were increased in thalassaemia patients who had ocular changes and decreased visual acuity. It was observed that ocular changes (p<0.001) were significantly associated with high serum ferritin level in the form of decreased
Table 1 — Distribution of Thalassaemia Cases according to Treatment Regimen in Various Age and Sex Groups
Age/sex GroupA(without GroupB(with Total ironchelating chelatingagent- (n=100) agent)(n=45) deferriprone)(n=55)
Agegroup(inyears)
<5 18(85.71%) 3(14.29%) 21(21%) 6-10 17(38.63%) 27(61.37%) 44(44%) 11-15 10(28.57%)
Table 2 — Distribution of Cases according to Ocular Manifestations Age(years) Ocular Decreased Lens Fundus involvement(%) VA(<6/9)(%) opacity(%) changes(%) <5(n=21) 4(19.04%) 1(4.76%) 0 3(14.28%) 6-10(n=44) 16(36.36%) 3(6.81%) 7(15.91%) 4(9.09%) 11-15(n=35) 32(91.42%) 18(51.42%) 6(17.14%) 24(68.57%)
Total(n=100) 52(52%) 22(22%) 13(13%) 30(30%)
Table 3 — Groupwise Distribution of Thalassaemia Patients with Ocular Manifestations in the Two Treatment Regimen Groups
Manifestations GroupA GroupB Total(%) P-value (withoutiron (withdeferriprone) chelating)(n=45) (n=55)
Ocularinvolvement
Present 7(15.56%) 45(81.82%) 52(52%) <0.0001
Absent 38(84.44%) 10(18.18%) 48(48%)
Bestcorrectedvisualacuity
Normal 39(86.67%) 39(70.91%) 78(78%) 0.058
Decreased 6(13.33%) 16(29.09%) 22(22%)
Lensopacity:
Present 6(13.33%) 7(12.73%) 13(13%) 0.928
Absent 39(86.67%) 48(87.27%) 87(87%)
RPEdegeneration:
Present 1(2.22%) 12(21.82%) 13(13%) 0.003
Absent 44(97.78%) 43(78.18%) 87(87%)
RPEmottling:
Present 2(4.44%) 16(29.09%) 18(18%) 0.001
Absent 43(95.56%) 39(70.91%) 82(82%)
Venoustortuosity
Present 2(4.44%) 8(14.55%) 10(10%) 0.093
Absent 43(95.56%) 47(85.45%) 90(90%)
Dischyperaemia:
Present 1(2.22%) 4(7.27%) 5(5%) 0.249
Absent 44(97.78%) 51(92.73%) 95(95%)
BCVA(P<0.001), RPE degeneration (p<0.001), RPE mottling (p<0.01) and venous tortuosity(p<0.025)(Table4).
DISCUSSION
Thalassaemia is a hereditary disorder characterised by reduction in the synthesis of globin chains ( or ). Reduced globin chain synthesis causes reduced haemoglobin synthesis and eventually produces a hypochromic microcytic anaemia because of defective hemoglobinisation of red blood cells. Patients suffering from beta-thalassaemiamajorpresent with varied ocular and systemic manifestations.
OCULAR MANIFESTATIONS OF THALASSAEMIAPATIENTS WITH REPEATED BLOOD TRANSFUSION — GORAIN ET AL 97
world had also been performed in patients of up to 45 years of age. This age disparity can be attributed to lower survival rates among thalassaemia patients in India;reasonsforthisseemtobepoorcompliancewith therapy, difficulty in obtaining regular blood transfusionsandhighcostofironchelationtherapy
This study showed a slight male preponderance 6 (1.25:1).This is consistent with studies of Gartaganis, Gaba and Taneja where ratios of 1.07:1, 1.33:1 and 1 25:1 respectively, were observed Ocular 6 involvementwasseenin52%ofpatients.Gartagantis, 8 9 10 Gaba, Taneja, Dewan and Abdel-Malak , reported figures of 41.3%, 58% , 71.4%,36% and 68% 6 8 respectively Gartaganis Gaba and Taneja in their studies, found lens opacities in 13.85%, 45.7% and 40%respectively.
Table 4 — Relation of Mean Serum Ferritin Level with Different Ocular Manifestation among Different Thalassaemia Patients
Manifestations Noof Meanserum P-value cases ferritin(ng/ml)
Ocularinvolvement: Yes 52 2509.92±480.508 <0.001 No 48 2036.67±675.656
Bestcorrectedvisualacuity:
Decreased 22 2699.55±529.492 <0.001
Normal 78 2165.21±603.395
Lensopacity
Present 13 2330.77±664.700 0.769
Absent 87 2275.59±256.611
RPEdegeneration
Present 13 2889.62±549.873 <0.001
Thirteen out of 100 subjects in this study had lenticular opacities (13%). No significant correlation was found between the occurrence of lens opacity and deferriprone therapy Lens opacities were correlated significantlywithhigheraverageserumironlevelsand serum ferritin levels.This is in contrast with studies of 6Gartaganis where no correlation between the occurrence of lens opacity and raised serum ferritin was found. Dewan found that 20% of patients had cataract that was associated with raised serum ferritin levels. Decreased visual acuity was found in 22 patients (22%). Sixteen patients receiving deferriprone had decreased visual acuity (29.1%). Six patients not receiving iron chelation had decreased visual acuity (13 4%) Thus, iron chelation showed minimal statistical significance regarding decreased visual acuity (p=0.058).
Absent 87 2192.08±587.569
RPEmottling
Present 18 2628.61±580.580 0.010
Ocular findings range from decreased visual acuity, colour vision anomalies and night blindness, cataract, visual field defects and optic neuropathy Iron-chelating agents like d e s f e r r i o x a m i n e a n d deferriprone are reported to cause many of these ocular changes. In this study, various ocular manifestations of -thalassaemia and the effects of various iron chelating agents on the eyes were found. The results of this study were based on data obtainedfrom 100 thalassaemiacases(56%malesand44%females).
Absent 82 2206.84±613.287
Venoustortuosity:
Present 10 2516.67±441.942 0.025
Absent 90 2163.90±641.000
Dischyperaemia
Present 5 2635.00±553.286 0.212
Absent 95 2264.22±626.915
Inthisstudy patientsbelongedtoagegroupsixmonths to fifteen years. However, similar studies in the western
This observation is consistent with 1 the findings of Taneja and Taher . Regarding the fundus changes of the thalassaemia patients in this study, RPE degeneration was observed in 13% (p=0.003), RPE mottlingin18%(p=0.001)anddisc hyperaemia in 5% of patients (p=0.249).
This observation is consistent 10 with the findings of Abdel-Malak who found RPE degeneration in 17.7% and RPE mottling in 25%. RPE degenerations were found in 21.82 % of the patients 10 receivingdeferripronetherapy(Abdel-Malak foundRPE degenerations in 27 8% of patients) Deferriprone may be contributory to the occurrence of RPE degeneration These findings are consistent with
Taher who found that patients on deferriprone were four timesmorelikelytohaveRPEdegenerationsascompared to patients on desferrioxamine. RPE mottling was detected more in the patients receiving deferriprone therapy (29.09%). This result was found to be consistent 9 10 with Taneja (10%) and Abdel-Malak (33.3%). Retinal venous tortuosity was observed in 10% of patients. This incidenceislesswhencomparedtotheincidencereported byGaba (17.14%)andTaher (17.9%)butquitesimilarto Taneja (11%). Disc hyperaemia was found in 5% of patients which is consistent with the findings of Taneja 9 and Dewan who found it in 7% and 8% patients respectively.
It has been seen that the average serum ferritin levels were increased in thalassaemia patients who had ocular changesanddecreasedvisualacuity Correlationofserum ferritin levels with retinal venous tortuosity was statistically significant (p=0.03). This is consistent with 8 observations of Gaba and Taneja Patients with thalassaemia have been found to have a higher labile iron pool, and it has been proposed that this mediates cellular damage.
Iron causes oxidative damage to proteins, lipids and DNAthrough the generation of free radicals in the Fenton reaction,andithasbeenshowntodisruptthebloodretinal barrier Iron is potentially related to several ocular diseases, including glaucoma, cataract, age related macular degeneration and intra-ocular haemorrhage. Raised serum ferritin is a surrogate marker of transfusion haemosiderosis, which may predispose thalassaemia patientstothetoxiceffectsofiron.Thespecificroleofiron in ocular involvements in thalassaemia needs to be studied. A larger number of thalassaemic children were foundtohaveocularabnormalitiesdespitemoderatedoses of deferriprone and presence of high serum ferritin levels, which implicate a role of iron in ocular pathology in thalassaemia.Alarger study to evaluate the role of iron in ocularinvolvementinthesepatientsisrecommended.The reversibility of ocular changes should also be studied by
changingthechelatingagentoralteringits'dose.
A limitation of the present study is that it cannot conclusivelyestablish whether ocular changes are a result of the disease or due to iron chelating agents. It may be kept in mind that iron overload and iron chelating agents bothmaybemutuallyconfoundingfactorsinthecausation ofocularchangesofthalassaemia.
REFERENCES
1 Chaston TB, Richardson DR — Iron chelators for the treatment of iron overload disease relationship between structure,redoxactivityandtoxicity. Am J Hematol 2003;73: 200-10.
2 Lokeshwar MR, Shah N, Kanika S, Manglani M, editors — IAP Textbook of Paediatrics. 3rd ed. New Delhi: Jaypee Publishers,2006:622-30.
3 Greer JP, Foerster J, Lukens JN, editors — Wintrobe's Clinical Hematology. 11th ed. Vol 1. Phladelphia: Lippincott WilliamsandWilkinsPublishers,2009:1083-131.
4 Choudhry VP, Naithani R — Current status of iron overload and chelation with deferasirox. Indian J Pediatr 2007; 4: 5964.
5 WongRW,RichaDC,HahnP,GreenWR,DunaiefJL—Iron toxicity as a potential factor, in AMD. Retina 2007; 27: 9971003.
6 Garataganis SP, Zoumbos N, Koilopoulos JX, Mela EK — Con ras sens t v ty function in pa ents with beta thalassemiamajor. Acta Ophththalmol 2000;78:512-5.
7 Gaba A, Souza PD, Chandra J, Narayan S, Sen S — Ocular abnormalities in patients with beta thalassemia. Am J Ophthalmol 1998;108:699-703.
8 Taneja R, Malik P, Sharma M, Agarwal MC — Multiple transfused thalassemias major: ocular manifestations in a hospital based population. Indian J Ophthalmol 2010; 58: 125-30.
9 Dewan P, Gomber S, Chawla H, Rohatgi J — Ocular changes in multi-transfused children with b- thalassaemia receiving desferrioxamine: a case control study. SAJCH 2001;5:11-4.
10 Abdel-Malak DSM, Dabbous OAE, Saif MYS, Saif ATS — Ocular manifestations in children with b- thalassemia major andvisualtoxicityofironchelatingagents. J Am Sci 2012;8: 633-8.
11 Taher A, Bashshur Z, Shamseddeen WA, Abdulnour RE, Aoun E, Koussa S, et al — Ocular findings among thalassemiapatients. Am J Ophthalmol 2006;142:704-5.
Practitioners' Series Practitioners' Series
Human oto-acariasis : 440 cases of intra-aural tick infestation managed in rural belt of Sullia
1 2
Sudhir M Naik , Sarika S Naik
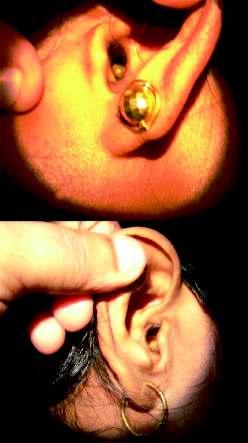
Soft tick in the ear is a very common acute painful and distressing condition in the flowering months of October to March. It’s a common condition in the rubber growing belt of Sullia. The mouthparts of the tick gripsfirmlytheskinoftheexternalauditorycanalorthetympanicmembraneandsucksbloodandswellsup.
Otoscopy and removal of the tick from the ear can be done in outpatients in adults and is difficult in a frightened irritable child. To emphasise the need for prompt management by an experienced otolaryngologistinallsuchcasesofintra-auraltickinfestation,aretrospectivestudyof440cases(173males and 267 females) who attended the department of ENT, KVG Medical College, Hospital, Sullia with history of intra-aural ticks was conducted over a period of 48 months. Out of 440 cases of intra-aural ticks, 215 cases were treated in the outpatient department and 223 cases under short general anaesthesia with otomicroscopy.Intra-auraltickinfestationisanacutepainfulconditionwhichneedspromptmanagementby an experienced otolaryngologist. Proper visualisation and instrumentation is necessary to avoid complications.
J Indian Med Assoc 2016; 114: 98-100 & 107]
Key words : Intra-aural tick, otalgia, otomicroscopy, general anaesthesia.
Humanoto-acariasisistheinfestationoftheearcanal 1-3 by ticks or mites It is rare in humans and 1-3 commonlyseeninlivestockanddomesticanimals These intra-aural ticks can perforate the tympanic membrane, cause suppurative otitis media, subluxation of the incudomalleal or incudostapedial joints and the dislocation of the stapes from the oval window, bleeding 4-6 fromtheearcanalandrarelyfacialparalysis
Thisintra-auraltickinfestationisacommoncondition seen in rubber growing population of Sullia. It is a common painful condition presenting to the otologist during the flowering months of October to March (Fig 1).
Animate foreign bodies are comparatively rare and inanimate foreign bodies account to around 84%. Majority 7 oftheanimateforeignobjectsaresmallcockroaches
Most of the patients present with acute severe pain in the ear The condition affects all age groups It is diagnosed by performing an otoscopic canal examination or ear endoscopy which will show the presence of tick or its' blackish faecal particle (Fig 2). The intense pain is because of firm gripping of the skin of the external auditory canal and the tympanic membrane by its' 8mouthparts
Department of ENT Head and Neck Surgery, KVG Medical College, Sullia574327
MBBS,MS(ENT),AssociateProfessor
MBBS,DA,SeniorResident,DepartmentofAnaesthesia
Comments :
Ticks are obligate bloodsuckingarachnids a n d a r e e a s i l y transmitted through domestic animals and pets to humans The twomajortypesofticks, basedonthepresenceor absence of a hard shield called scutum, are ixodidae (hard ticks) and argasidae (soft 10ticks)
Childrenandanxiousadultswillnotco-operateforear examination or otoscopy and forceful examination may 8 cause damage to the external ear and tympanum So, examination of the ear using an otoscope or otomicroscope and exact visualisation of the tick is very 8 important before attempting to remove it Its an acute painful condition which needs urgent intervention Cooperative patients can be managed in the outpatient only meanwhile anxious and paediatric patients were managed withoto-microscopyundergeneralanaesthesia.
The
Study :
Aretrospectiveanalysisof440patientswhohadintraaural tick infestation were included in the study One hundred and seventy-three males and 267 females wereincludedunderthestudy Theyoungestpatientwasa 3-year-old girl and oldest was a 79-year-old woman. The studyperiodwasof48monthsfromJanuary2007toApril 2011. All patients with intra-aural tick infestation were includedinthestudy Allpatientshadexcruciatingpainin ear as presenting complaint. Otoscopic examination was donetoconfirmthelivingtickforeignbody
Tick removal was done under 4% topical anaesthesia inco-operativeadultpatientsintheoutpatientdepartment. General anaesthesia was preferred for anxious and younger patients Under short general anaesthesia otomicroscopywasdoneandtheticksremovedbycupped
forceps under All the patients managed in OPDwereobservedforanhour anddischargedwithantibiotics and analgesics for one week. Patients managed under general anaesthesia were observed for a day and discharged on next day with antibioticsandanalgesics.
Analysis :
magnification.
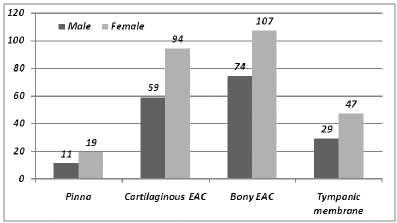
All the ticks located on the pinna were removed in the OPD (11 males and 19 females). Out of the 153 cases of ticks in the cartilaginous external auditory canal 92 cases co-operated for removal in OPD (62%) and in 58 cases ticks were removed under general anaesthesia with otomicroscopy (38%). Out of the 181 cases of ticks in the bony external auditory canal, 90 co-operated for removal in OPD (49.72%) and in 91 cases ticks were removed under general anaesthesia with otomicroscopy (50 28%) (Table1andFig3).
Allticks(76cases)locatedonthetympanicmembrane were removed under general anaesthesia with otomicroscopy Here 2 females refused removal under general anaesthesia. Small perforations were seen after removalofthetickslocatedonthetympanicmembranesin 2 males and 4 females. No other complications were seen inrestofthecases.
Soft tick attaches to its' host with its mouthpart, which not only is embedded in the skinbutisalsogluedintoplacewith a cement like secretion The tick can voluntarily detach from its' host, but when forced off, it may leave the attached mouthpart embedded in the skin As long as the mouthpart is attached to the patient, the patient remains at risk 1 for tick borne diseases Removal of an intra-aural tick is a painful experience to patients, especially 1children Most of the times, the removal is made difficult by the swollen and narrowed canal from previous multiple attempts by inexperienced medical personnel 1 withinadequateinstruments
The tick swells up after sucking blood and the engorged tick is easy to detect in narrow ear canal. The unfed tick situated at the anterior fornix of the external ear canal is 2 seen with difficulty on otoscopy. The anterior bony hump of the ear canal may block the view to that particulararea
Cerumen(wax) in the canal can hinder tick visualisation The tick stands out as a shiny surface making it conspicuous within the wax The dark brown colour of the tick faecal matter which is digested blood might mix with the wax and create a confusing 8picture Otomicroscopy should be done to confirm the diagnosis A tick which is easily visualised should be graspedbyacrocodileorcuppedearforcepsandpulledout steadily . Rotating the tick during removal may break off the mouthparts leaving the sequelae of infection and 1 irritationoftheearcanal
100
Tick removal is a very painful experience to the patient because of 12 the sensitivity of the ear canal Patients in the paediatric age group never allow removal without 12anaesthesia Swollen and narrowed ear canal due to tick bite trauma and previous attempts at removal by inexperienced medical personnel with inadequate instruments make removal even in experienced hands 1difficult . Always institutional management where adequate facilities and expertise are available
12 shouldbesought
Tickscanberemovedbymanual forceps or by applying noxious stimuli so that the tick detaches
s
Current Topic Current Topic
12spontaneously Manyreagentshavebeenusedtoinducea 12 noxiousstimuluswithvaryingresults Somepractitioners usedspiriteardropsfor3daysbeforesyringingthetickout 13 on day 4 Some used 4% lignocaine instead, but only instilled the canal for 10 4minutes Olive oil, sodium bicarbonate, petroleum jelly and liquid paraffin are among various preparations used to facilitate tick removal with none of them proven to be 4 superiortoanother
Table 1 — Showing Distribution of Cases according to Method of Removal of Intra-aural Ticks
Location Noofcases
OPD Otomicroscopic removal removal(GA)
Pinna 30 0
CartilaginousEAC 95 58
BonyEAC 90 91
In the above study 4% lidocaine was instilled in the patient’s ear canal for 10 minutes and it was found that the tick can be removed easily by doing ear suction or using forceps under microscopy. Cocaine if available can be instilled which anaesthetises and disengages the tick from the tympanic membrane and also decongests the swollen canal and reduces the pain, thus calming the 12 patient down However in non-cooperative children, removal under general anaesthesia is safer and less traumatic to the patients The most commonly recommended and successful tick removal method is 14 manualextractionofthetick Itisseenthatthetickwould best be removed by grasping it close to the skin and 11 exertingasteady,evenpressurewithoutrotating Another author proposed a technique of mechanical removal involving rotation instead of traction, which he claimedmorereliableforrapidandpainlessremovalofthe entire tick, including the head, not leaving the mouthpart 15behind .Aftertheremovaloftick,itsfaecalparticleshould also be cleared off the ear canal since tick faeces and body
Tympanicmembrane 0 74 Total 215 223
localised manifestation such as facial nerve paralysis. Tick paralysis is a known complication of tick infestation anywhereinthebodyandhasbeenreportedparticularlyin northern America and Australia, but wasrarelyencounteredinthisregion People from this tropical climate are more frequently exposed to tick bite and have developed some immunity to it's toxin However, cases of isolated local paralysis; usually involving facial nerve, have been reported although less commonly reportedintheliterature.
The tick salivary secretions contain a neurotoxin and the 10 paralysingeffectofthetickisattributedtoit Thistoxinis found to interfere with the liberation or synthesis of 10 acetylcholineatthemotorendplateofmusclefibres The severity of paralysis is independent of the number of ticks 15infested But a correlation between the duration of tick attachment and the likelihood of transmission of toxin or 16 infectionisreported Severaltheorieshavebeenputforth to explain the pathophysiology of localised facial nerve 16 palsyinanintra-auraltickinfestation .
Co-formed consent : a case of rightful application
Munawwar
Husain , Arshad Anjum , Amir Usmani , Mubarak Alshraim , Jawed A Usmani
Informed consent has its roots on certain principles of bioethics and law. It has succeeded in eliminating discrepancies in medical practice. However, lately certain misgivings have started creeping in this hypothesis and therefore it was felt to revisit it. In the process a new concept has emerged which of course needstobedebated.ThereisaninstanceinwhichtheConsumerCourtinIndiaheldthesurgeonnegligentfor conducting sterilization operation during caesarian section without obtaining prior consent, particularly when there was no urgency for the same. This raises another question on the chivalry of the doctor. The authors are sure that the concept of co-formed consent is more robust and would stand a better chance of survival in the highly meshed world of technology and suspicion. Incidences of obtaining consent as an eye washshalldecreaseifnottotallyeliminated.Theconceptisdiscussedbelow.
[J Indian Med Assoc 2016; 114: 101-2]
Key words : Consent, informed consent, co-formed consent, consent audit, truth commission, reformed consent
W15 fluids can also be contaminated Antibiotics and analgesics should be prescribed for a week to reduce secondaryinfectioninthesiteoftrauma.
The neurological complications of intra-aural tick infestation may occur, where they usually present as a
The presence of tympanic membrane perforation may enable the tick saliva (with toxin) to enter the middle ear and reach the facial nerve probably through a natural dehiscence of the fallopian canal causing paralysis In cases where the tympanic membrane is intact, direct extension of the inflammatory process to the fallopian canal is via persistent dehiscence or direct invasion of the infectious organisms into the facial canal through the middle ear which results in oedema of the inflamed nerve 17 withinthecanal
AbundantcattleticksintheagriculturalareasofSullia, 7 18 is the cause of these abundant intra-aural ticks. Marina
(Continued on page 107)
hen a patient interacts with the doctor for treatment, whether it is medical or surgical, it involves interference with human body. To avoid legal ensnarement for battery which is “the application of force to the person of another without lawful justification”, and that of an assault which is “an act of the defendant which causes to the plaintiff reasonable apprehension of the 3 infliction of a battery on him by the defendant”, it is obviously transparent that informed consent should be taken by the treating doctor to satisfy the appetite of law The origin of informed consent can be traced to the 4 principle of autonomy and self-bodily integrity The concept caught on partly propelled by the advent of high 6,7 technology in medical sphere and the cost involved The physician as well as the patient benefited because it created choice for the patient. However, in due course of time it was realized that medical profession has become complicated with too many stakes involved. Professionalism got a down-beating Some where along the line the patient became conscious of his
Department of Forensic Medicine, Jawaharlal Nehru Medical College, Aligarh202002
MD, DNB, MNAMS, Associate Professor, Chairman & Former MedicalSuperintendent
DCH,AssistantProfessor
MD(Psychiatry),AssistantProfessor,DepartmentofPsychiatry MBBS FRCP (Path), Associate Professor Department of Pathology,KingKhalidUniversity,Abha,KingdomofSaudiArabia MD(Path),MD(Med),Professor
101
ownrightsandtheBillofPatients’Rightswasintroduced Since everything came at a price the patient became 9 demanding leading to the creation of hostile patient The concept and practice of defensive medicine came into 10existence The patient was the end loser. Subsequently a need was felt to reform the informed consent which did not prove a panacea. During this commotion of mental conflict, allegiance wrestling and the compulsion to incorporate ethics into practice, the informed consent lost some of its sheen. Convention now faced rock stable contradiction. The essential ingredients of informed consentlikefullandtimelydisclosureofrisksandbenefits by the physician to the patient and then obtaining the 12 voluntary consent after adequate supply of information became a legal embodiment rather than a crusade against unprofessionalism. This has sown the seed of co-formed consentwhichisdiscussednext.
Co-formed Consent :
Co-formed consent may be defined as “a mutually formed consent between the physician and the patient basedontheunderstandingthatallegiancetoone’sinterest would be subservient to end-goal and in the process protecting the institution of professional ethics, humane endeavorandautonomywithoutresortingtoill-conceived chivalry in a bid to establish one’s own genuineness of desire and action”. A large chunk of onus rests on the shouldersofthephysician.
102
The essential elements of co-formed consent would includethefollowing:
(1) Full disclosure by the physician to the patient without encumbranceofone’sowninterest.
(2) The doctor’s allegiance to his professional body must notholdswaywhileelicitinginformedconsent.
(3) The conflict of interest must never be involved. The trickydomainsinthiscontextwouldbethehospitalto which the physician is attached and to which he is obligated,theunsolicitedmarketingofproducts,abid to raise the banner of reputation high, desire to oblige one’s own brothers-in-profession, and above all the urgetoinflateone’sowncoffer
(4) Whileobtainingco-formedconsentthereshouldnotbe an iota of lingering doubt that consent has not been cleanly obtained Medicomoral duty and obligation mustbemetindisputably
Process of Evaluation and Re-evaluation
:
Redundancysetsinwheneverchangeisnottimelybrought or sought. Similar to informed consent now being questioned the concept and practice of principles of co-formed consent would also receive a beating if safeguards are not created for its healthy flourishing. Inthiscontexttwosuggestionsareputforth.
(a) Consent Audit: Similar to the audit of inventory and stock, clinical audit in large hospitals and the audit of the procedure and practice of biomedical research there should be the audit of co-formed consent. A proforma may be designed which would have the capacity to evaluate the covert and overt action of the physician. Likewise the patient informed consent couldbeevaluatedonanacceptablescale.
(b) Truth Commission: A periodical Truth Commission couldbeaskedtoconveneandevaluatetheco-formed consent audit itself. This Truth Commission could be inlinewiththeTruthandReconciliationCommission formed at the end of apartheid government in South Africa.Theretheguiltyandthesuspectweregiventhe chance to come out clean and disclose voluntarily their involvement in racial discrimination and debasedactionduringpre-Mandelaerawithanoption 13 of receiving an amnesty . The mandate of Truth Commissioninthiscasewouldbetotrackincorrigible cases violating co-formed consent procedure repeatedly while at the same time giving a chance to reformforfirsttimeoffenders.
Conclusion :
Co-formedconsentisanotaproductoffantasy Infact it is one step forward to informed consent. This would expose the subtle desire and motivation – seen and unseen – of the physician and would be able to question his sin
cerity in getting the consent. Provision for legal action should be incorporated. Meticulous record keeping is a mustfortheco-formedconsentproceduretosucceed.
REFERENCES:
1 Dr Janaki S — Kumar v Mrs Sarafunnisa 1999 (3) CPR 472 (ker); (2000)CPJ66(Ker).
2 Salmond & Heuston on The Law of Torts [20th ed, 1992, ThirdIndianReprint(1999)]
3 Winfield&Jolowiczonort,15thed,p63.
4 Mallardi V — The origin of informed consent. Acta OtorhinolaryngolItal.2005;25:312-27.
5 Francisco V — Ethical problems of medical technology. BulletinofPAHO,1990;24: 379-85.
6 Kumar L, Husain M, Ahmad I — Level of accessibility of radiologicaldiagnostic toolsofhightechnologyanditseffect on human health: study of Ultrasonography, CT scan and MRI in different perspective. J Ind Med Assoc 2012; 110: 148-52.
7 Judith LW — The implications of cost-effectiveness analysis of medical technology. Office of Technology Assessment, US Government Printing Office, Washington, DC, 1981; pp 1-24
8 Patients Bill of Rights. Declaration of Lisbon on the Rights of thePatient. Adopted bythe34thWorldMedicalAssociation (Lisbon,September/October1981)
9 Kramer CH, Kramer JR — Managing the hostile patient. Geriatr Nurs 1976;2:35-7.
10 John EM, Arnold RJ — Physician responsibility for the cost of unnecessary medical services (special article). NEJM 1978;299:76-80.
11 Henry J, Balmer PW, Lawrence P — Reformed Consent: Adap ng o new media and research participant preferences Accessed at h p://has ngscenter org/ Publications/IRB/detail.aspx?id=3288
12 Informed Consent. Stanford Encyclopedia of Philosophy. Accessed at ht p:/ p ato stanford edu/en r es/ n ormedconsent/
13 United States Institute of Peace. Truth and reconciliation Commission (TRC). Accessed at http://www.usip.org/ publications/truth-commission-south-africa
If you want to send your queries and receive the response on any subject from JIMA, please use the E-mail facility.
Website : www.ejima.in
ForEditorial : jima1930@rediffmail.com
ForCirculation : jimacir@gmail.com
ForMarketing : jimamkt@gmail.com
General : j_ima@vsnl.net
GP Forum GP Forum
Drug review : febuxostat
1 2 3 4 Kiran Kumar Singal , Sunder Goyal , Parveen Gupta , Ram Gopal Sharma
Gout is the most common type of inflammatory arthritis in men over the age of 40 years affecting approximately0.8%ofthepopulation.Therehavebeenrelativelyfewadvancesintreatmentandpreventionof gout over the last forty years. Febuxostat has been recently approved by FDA. Febuxostat is a selective and potent inhibitor of xanthine oxidase. The drug has come 40 years after the commonly used drug allopurinol. Nodoseadjustmentsarerequiredinpatientswithmildtomoderaterenalorhepaticimpairment. [J Indian Med Assoc 2016; 114: 103-4]
Key words : Gout, uric acid, febuxostat, allopurinol, xanthine oxidase inhibitor.
Gout is the most common type of inflammatory arthritis in men over the age of 40 years. It affects approximately 0.8 % of population It is a chronic, often progressive condition characterised by attacks or flares, that are marked by intense pain, redness and swelling in affected joints Symptoms result from an acute inflammatoryresponsetoelevateduricacidlevelinjoints. Significant amount of the pathogenesis of gout is known but despite the prevalence and morbidity of this disease, there have been relatively few advances in treatment and prevention of gout over the last forty years. At this time, therapies for gout are divided roughly into those for acute treatment namely non-steroidal anti-inflammatory drugs (NSAIDs), colchicines, corticosteroids and preventive therapies namely prophylactic colchicines or corticosteroids, probenecid, allopurinol. Unfortunately, these medications are often misused for gout or have significant adverse reactions. For treatment of acute gout, gastro-intestinalandrenalsideeffectsofNSAIDsarewell known.Colchicinegivenorallyforacutetreatmentofgout can lead to significant gastro-intestinal toxicity, and the intravenous (IV) form of colchicine has been associated withserioussafetyconcerns,includingdeath,especiallyin elderly patients or those with renal failure. Systemic corticosteroids are effective but have serious side effects, and not all physicians are comfortable with potentially saferintra-articularuseofcorticosteroids.
Most patients with gout under excrete uric acid; therefore, probenecid is often indicated for preventing acute gout in patients without tophi or renal stones. However, this uricosuric agent is seldom used, and is poorly tolerated because of rash or gastro-intestinal side-
Department of Medicine, MM Institute of Medical Sciences and Research,Ambala134203
MBBS,MD(Med),AssistantProfessor MBBS,MS(GenSurg),Associate ProfessorofSurgery MBBS,MD(Med),Associate Professor MBBS,MS(GenSurg),AssistantProfessorofSurgery
effects Al
lopurinol, the most commonly used drug for
gout prevention, can be effective at decreasing uric acid levels and reducing acute flares. Rare but serious adverse events can occur from allopurinol, including a potentially fatal hypersensitivity syndrome (rash, fever, hepatitis), more commonly seen in patients with renal failure and thosereceivingdiuretics.Dosingofallopurinolisdifficult in patients with renal failure, those most in need of uric acidloweringtherapy Evenifallopurinoliswelltolerated, it is often ineffective for gout because it is used intermittently or its' dose is not adequately adjusted to achieve appropriately low uric acid levels (usually<6 mg/dl).
Thus, the medical community needs to be better educated about the use of current drugs for gout as we need more effective and safer drugs for management of gout For treatment of hyperuricaemia and gout, febuxostat has been recently approved by FDA Febuxostat is similar to allopurinol as it also inhibits the enzymexanthineoxidase. 4 Febuxostat is a non-purine xanthine oxidase inhibitor for the long term management of hyperuricaemia in patients of gout. Its' major goal in the management of hyperuricaemia and gout is long term reduction in serum urate concentrations to levels below the limit of urate solubility (about 6.8mg/dl) because such a reduction over time will prevent or reverse the formation and deposition ofuratecrystals.
Mechanism of Action :
Febuxostat is a selective and potent inhibitor of xanthine oxidase, the drug setting in the access channel to the molybdenumpterin active site of the enzyme. It has minimal effects on other enzymes involved in purine and pyrimidine metabolism [5,6]. Febuxostat does not have a purine like backbone, unlike allopurinol and oxypurinol. Xanthine oxidase is needed to successively oxidate both hypoxanthineandxanthinetouricacid,henceinhibitionof xanthine oxidase by febuxostat reduces the production of uricacid.
104 J INDIAN MED ASSOC,
Spectrum :
FebuxostathasbeenapprovedofuseingoutinEurope and USA. Febuxostat is a particularly appropriate second line option to allopurinol where this uricosuric is contraindicated, as in stage three or worse chronic renal disease andinpatientswithahistoryofurolithiasis,aninabilityto adequately increase hydration or with identified uric acid overproduction.
Pharmacokinetics :
Like allopurinol, febuxostat lowers plasma uric acid levels by inhibiting enzyme xanthine oxidase. Febuxostat is about 50% absorbed, giving a Cmax at 1 to 1.5 hours. It ismetabolisedbyconjugationviatheuridinedephosphate glucorosyl transferase (UGT) iso-enzymes UGT1A1, 1A3, 1A9 AND 2B7 and by oxidation via CYP450 isoenzymes 1A2, 2C8 and 2C9.Metabolism leads to four active metabolites. Febuxostat undergoes hepatic elimination(45%)andrenalelimination(49%).
Indications :
The only indication for febuxostat usage is in managementofhyperuricaemiainpatientswithgout.The drug is not recommended for the management of asymptomatic hyperuricaemia. The drug has come 40 yearsafterthecommonlyuseddrugallopurinol.Thisdrug was approved in the year 2009 in Europe and USA for managementofhyperuricaemia.
Precautions and Contra-indications
Febuxostat can cause allergic reactions and should be avoidedinpatientsallergictoit.
During pregnancy this drug should be used only when clearlyindicated.
This drug should be used with caution in patients with underlying cancer, heart disease, liver disease, kidney disease,organtransplantandstroke.
Febuxostat is contra-indicated in patients taking theophylline,azathiapurineandmercaptopurine.
Adverse Effects :
Mostfrequent:Skinrash
Lessfrequent:Abdominalpainwithcramps,abnormal hepaticfunctiontests
Rare : Allergic dermatitis, alopecia, anaemia, angina, angiodema, appetite changes, biliary calculus, blurred vision, bone marrow depression, cerebrovasular accident, conduction disorders of the heart, constipation, dehydration,disordersofhaircolour,hepatitis,dyspepsia, oedema, epistaxis, fatigue, flu like symptoms, gastritis, general weakness, hearing disorder, haematuria, hypersensitivitydrugreaction,kidneystone,leucocytosis, libido changes, mood changes, myalgia, pancreatitis, parasthesias, peptic ulcer, pruritis of skin, purpura, renal
failure, photosensitivity, thrombocytopaenic disorder, thrombo-embolic disorder, tremors, urticaria, vertigo. vomiting,xerostomia.
Dosage and Administration :
Febuxostatissuppliedas40mgand80mgtablets.The tablet can be taken without regard to food or antacid use. Recommendedstartingdoseis40mgoncedaily Thedose may be increased to 80 mg/day in patients who do not achieve uric acid level <6 mg/dl after two weeks on lower dose.
Febuxostat significantly reduces uric acid levels within2weeksafterinitiationoftherapyandupto48%by the end of 104 weeks of therapy The main aim of therapy istoachievetheprimarygoalofserumuricacidlessthan6 mg/dl,60%ofpatientsachievedthisgoalwithadoseof80 7 mg/dayor120mg/dayinthestudy
Nodoseadjustmentsarerequiredinpatientswithmild to moderate renal or hepatic impairment. Caution is recommendediffebuxostatisadministeredinsevererenal orhepaticimpairment.
Place in Therapy :
Theonlyindicationforthisdrugisintreatmentofgout.
GP Forum GP Forum
Retrospective analysis on diagnosis of malaria — a need for developing community
Nilotpal Banerjee , Sujit Bhattacharjee
Today the attention has shifted from the slide examination to newer methods on Malaria. The methods today, based on newer techniques have not produced any signifant impact on health care. Most newer methods are difficult for 80% of population. Statistics prove the diagnostic value of the slides. Business on healthcarehavemadetheservicescostlywithoutsignificantchangeforthemasses.Astheattentionshifted today, we find that the skilled Malaria technicians have virtually disappeared to the point of extinct. Though training courses obviously include slide examination on Malaria, the institutions seem to have lost interest and consequently attitude, aptitude for meticulous slide examination on Malaria. Economic pressure of the newer tests for Malaria on the masses are huge but doctors too, have been advising newer test methods, finding lack of quality in slide methods. Malaria exists more than ever before. The drug resistance problem is ofcourseanotherimportantconcernforMalaria.Preventionaspectsaremultisectoral.TheGov’tofIndiahas rightlymaintainedslidemethodsforMalariaasthegoldstandard.Thereexistsseparatevalueofsupplement and substitute for the benefit of the masses as the very aim is appropriate service. The substitutes are requiredtobefoundfortreatment,notfordiagnosisonMalaria,asrecordsofservicestudiesspeakvolumes onsuccessprojectedinthisanalysis.
[J Indian Med Assoc 2016; 114: 105-7]
Inarandomtrialof762patients,febuxostat,atadaily dose of 80 mg or 120 mg, was more effective than allopurinol at the commonly used fixed daily dose of 300 mginloweringserumurate
Recommendations : REFERENCES
1 Lawrence RC, Helmick CG, Arnett FC — Estimates of the prevalence of arthritis and selected musculoskeletal disorders in the United States (Abstract). Arthritis Rheum 1998;41:778-99.
2 Ferraz MB — An evidence based appraisal of the management of non-tophaceous interval gout (Abstract). J Rheumatol 1995;22:1618-9.
3 Singer JZ, Wallace SL — The allopurinol hypersensitivity syndrome. Unnecessary morbidity and mortality (Abstract). Arthritis Rheum 1986;29:82-7.
4 Sundy JS, Hershfield MS — Uricase and other novel agents for the management of patients with treatment-failure gout (Abstract). Curr Rheumatol Rep 2007;9:258-64.
5 Okamoto K, Eger BT, Nishino T, Kondo S, Pai EF, Nishino T — An extremely potent inhibitor of xanthine oxidoreductase: crystal structure of the enzyme inhibitor complex and mechanismofinhibition. J Biol Chem 2003;278:1848-55.
6 BeckerMA,KisickiJ,KhosravenR—Febuxostat(TMX-67), a novel, non-purine, selective inhibitor of xanthine oxidase, is safe and decreases serum urate in healthy volunteers. Nucleos Nucleol 2004;23:1111-6.
7 Bruce SP — Febuxostat: a selective xanthine oxidase inhibitor for the treatment of hyperuricaemia and gout. Ann Pharmacother 2006;40:2187-94.
8 Becker MA, Schumacher HR Jr, Wortmann RL, MacDonald PA, Eustace D, Palo WA, et al —Febuxostat compared with allopurinol in patients with hyperuricaemia and gout. N Engl
Key words : Slide methods, Immune fluorescence, Rapid diagnostic tests.
This study of comparison was attempted, driven by sheer need of the masses which probably is the nuchcusthatcannotbeignoredconsideringthepovertyof healthcaretakergroupsinIndianscenario.
Projection on 7 years of Retrospective scenario on Tripura State service result on Malaria slide examination
Year Blood Blood Positive P.Fcasesand slideslide cases percentage collection examination
1998 244080 231187 12595 10507 83%
1999 212056 212056 14408 11889 82%
2000 204322 204322 12245 9480 77%
2001 291652 291652 18502 14629 79%
2002 245406 245406 13319 10863 81%
2003 252339 252339 13807 10800 78%
2004 251146 251146 17455 15182 87%
Source: Gov’t of Tripura release- 7years of “Success” A Health Bulletin.
Department of Microbiology, Tripura Medical College & Dr BRAM TeachingHospital,Agartala799014 MD(Microbol), Assistantprofessor MD,ProfessorandHead
Scenario mentioned above, reveal serious magnitude ofMalariafevercasesinthisgeographicallyisolatedstate. The network from the city to the periphery reveal the laboratory diagnosis of Malaria that was commendable successstoryofcost-effectivediagnosis.
Shifting of Attention
Today various types of diagnostic procedures have been adopted along with availability in the market and theiradoption.Lessofskillandmoreofrelaxationcomfort have been achieved. The rapid test methods have almost replaced the old golden labour The eyestrain lessened, moreparamedicsandmedicsarebeingproducedbutthese developments have brought the skill of this laboratory technique to “drop test service” in tertiary care hospitals too.Theslideskillhasalmostvanished,ananticommunity development and matter of concern as at least 400 million acute cases of Malaria occur worldwide each year, causes atleast100milliondeathseveryyear.
: Why Amear Method Ideal :
A method of choice for masses is evaluated, selected onthebasisofthefollowingyardsticks:
(1) Themethodthatiseasytoperform.
(2) Themethodthatissimpletoperform.
(3) Themethodthatisrapidtodeliver
106 J INDIAN MED ASSOC, VOL 114, NO 6, JUNE 2016
(4) Themethodthatgivesgoodsensitivity
(5) Themethodthatgivesgoodspecificity
(6) Amethodthatneedsminimumgeneralandtechnical infrastructuralbackupsupport.
(7) Amethodthatiseasilyavailablebytheinstititions.
(8) A method that is easily affordable both by the institutionsandthemasses.
(9) Amethod that can be quickly supported depending onthelocationoftesting.
(10) A method that involves inner skill, culminating in “Eureka”jubilationonsuccess-selfmotivating.
(11) Amethodthatmaynotdependonpowersupply
(12) Amethodthatiseasilydemonstrable.
(13) A method that invites the art and science of search findingtocreateinterestamonglearners.
(14) Amethodthatgiveslesserfalseresult.
(15) A method that gives satisfaction among professionals.
(16) Amethod that has the faithstrength for adoption by clinicianforprescriptionrequest.
(17) A method that invokes inner quality to be rapidly spreadandcommunicated.
(18) Amethodthatautomaticallycreatesinterestamong production personnel to capture market because of mass need requirement both for business houses of production, its marketing availability and health careteacherandprovidergroups.
(19) Above all, cost-effectivity and cost-benefit aspects fortheIndiancommunity.
A comparative analysis highlighted in Clinical Microbiologyreviewisasbelow:-
ANALYSISAND INTERPRETATION
Along with the introduction of newer diagnostic systems, the slide methods have lost the zeal and lustre of searching and finding aspects, by the laboratory Technician, supervised by the branch specialist that always carried adventurous life saving effort, lingering prognostic enquiry, hardly pulsed today The inbuilt process of achievement was seen peeping through. Involvementwasatreattowatch.Nospecialinfrastructure was required. Today, the high cost systems including maintenance engulfed by the institutions, do save the patient but absorb the pocket of the families with no special advantage for the customer Bending and benting for newer methods and techniques therefore have serious adverse effect on the community of a country like India. Thrustupontestproceduresneedstobeseriouslyreviewed and debated upon by the Institutions, equally also to produceskilledtechnicianforslidemethodssothat,desert surroundingthegoldstandard,canbeavertedfromquality pointofview,probablyfeltasneedofthehour.
Nevertheless, all the systems have specific areas of application. So nothing is discredited upon, rather encouraged on its area of use and application whether screeningordiagnosticorsurveyorresearchfields.
DISCUSSIONAND SUGGESTIONS
India is classified under developing nation. The population is plagued with multi dimensional problems and Malaria is one rampant. So, the health care providers need to review seriously about the cost of laboratory diagnosis. The rapidity in diagnosis, the easy procedural pattern, the simple procedure need to be balanced with
Specificity
Source : Reference number 01 of references.
P falciparum P falciparumand good,othersdifficult only p.vivaxgood,and ovaleandp.malariae onlywithPldh
economic burden
of the health care taker coccooned in
the shell of care service. Money earning and Malaria care cannot tune together Another option may be reduction of the cost of modern diagnosis of Malaria by the private sectors, by keeping a very thin profit margin considering the magnitude gasped, by the Indian community. Cost –effectiveness may be redefined, because many sufferers do not come for the second time or return on hearing the cost in the first consultation. These lot become non responder to care service and prefer to suffering as they cannotaffordto.
CONCLUSION
(1) The institutions today probably lack interest to producegoodslide technicianforMalaria.
(2) Qualified technicians today, therefore lack skill for slideexamination.
(3) Indiancommunitycannotaffordhighcostsystems.
(4) There is no substitute to slide skill and slide service care.
(5) Equallyeasy,simple,rapidmethodstodayareloaded with economic burden particularly for the community.
(6) Our apathy cannot and should not engulf the patient andcommunity.
(7) The country needs to adopt and adapt patient –friendlycheaperapproach.
(8) Turning away faces from golden basics have disastrouseffectoncommunity
(9) The conclusion is more inscribed as the dreadful Plasmodium Falciparum is so rampant in the community, already a store house of poverty, ignoranceandunemployment,huntingfortwosquare mealsaday
(10) Growth without targetted focus on basics is no growth,onlyimbalancesthecommoncareservices.
REFERENCES
1 Anthony Moody — 2002 Rapid Diagnostic Tests for Malaria Parasites. Clinical Microbiology Reviews. Vol 15. No 1, page-66-78.
2 Henry’s Clinical Diagnosis and Management by Laboratory Methods.21stedition.Page-1134.
3 Wallach’s — Interpretation of Diagnostic tests. 9 edition, Page-1030.
4 “Saphalya”Bulletin.Gov’tofTripura.Page-30
5 HitendrasinhGThakor—October2000;JIndianMedAssoc Vol98.No-10.Page623-7.
(Continued from page 100)
found the abundance of cattle ticks in Malaysian villages as cause for high incidence of human intra-aural ticks in the region. Also during the study unfed tick larvae in the surrounding forested habitats, suggest an extra 18 domiciliarymodeofinfestationrelatedtocattlerearing REFERENCES
1 Naude TW, Heyne H, van der Merwe IR, Benic MJ — Spinose ear tick, Otobius megnini (Duges, 1884) as the cause of an incident of painful otitis externa in humans. J S Afr Vet Assoc 2001;72:118-9.
2 Huchzermeyer HF — Another human ear tick case. J S Afr Vet Assoc 2002;73:2.
3 van der Merwe IR, Benic MJ, Naude TW, Heyne H — Spinose ear tick as the cause of an incident of painful otitis externa. S Afr Med J 2002;92:712-3.
4 Indudharan R, Ahamad M, Ho TM, Salim R, Htun YN — Human otocariasis. Ann Trop Med Parasitol 1999; 93: 1637.
5 CampbellNA—Anunusualcaseoffacialparalysis. Cent Afr J Med 1977;23:141-5.
6 Indudharan R, Dharap AS, Ho TM — Intra-aural tick causing facialpalsy. Lancet 1996;348:613-4.
7 SomayajiKSG,RajeshwariA—Humanotoacariasis. Indian J Otolaryngol 2007:59:237-9.
8 Srinoviant N, Raja Ahmad RLA — Intra-aura tick infestation:thepresentationandcomplications. Intern Med J 2003;2:21.
9 SpachDH,LilesWC,CampbellGL,QuickRE,AndersonDE, Fritsche TR — Tick-borne disease in the United States. N Engl J Med 1993,329:936-47.
10 Vedanarayanan V, Sorey WH, Subramony SH — Tick paralysis. Semin Neurol 2004; 24:181-4.
11 Needham GR — Evaluation of five popular methods for tick removal. Pediatrics 1985;75:997-1002.
12 Zamzil AA, Baharudin A, Shahid H, Din Suhaimi S, Affendie MJ — Isolated facial palsy due to intra-aural tick (ixodoidea) infestation: Arch Orofac Sci 2007;2:51-3.
13 Fegan D, Glennon J — Intra-aural ticks in Nepal. Lancet 1996;348:1307-22.
14 Gammons M, Salam G — Tick removal. Am Fam Physician 2002;66:643-7.
15 Schultheis L — A novel technique to remove the common dogtick. Am Fam Physician 1998;58:354.
16 Sood SK, Salzman MB, Johnson BJ, Happ CM, Feig K and Carmody L — Duration of tick attachment as a predictor of the risk of Lyme disease in an area in which Lyme disease is endemic. J Infect Dis 1997;175:996-9.
17 Miller MK —. Massive tick (Ixodes holocyclus) infestation with delayed facial-nerve palsy. Med J Australia 2002; 176: 264-5.
18 Mariana A, Ho TM, Saleh I, Indudharan R — Species distribution of ticks in two localities in Kelantan. Trop Biomed 1996;13:185-7.
EMPHYSEMATOUS PYELONEPHRITIS – INANON-DIABETIC YOUNG WOMEN — RAVIKUMAR
Emphysematous
pyelonephritis – in a non-diabetic
young women — a rare association
Y S Ravikumar , K M Srinath , L S Adarsh , Manjunath S Shetty , 4 5
Subrahmanyam Karuturi , B Balaji Kirushnan
EmphysematousPyelonephritisisalifethreateninginfectionthatresultsfromcomplicatedpyelonephritis by gas producing organisms. It is an acute necrotizing infection of the kidney that occurs predominantly in diabeticpatients.Patientsfrequentlypresentwithsepsisandketoacidosis.EscherichiaColiappearstobethe most frequent organism responsible for this infection. We present a case of emphysematous pyelonephritis in a women with intrauterine death of fetus at 20 weeks gestation who did not have features of obstruction of theurinarytractandanondiabetic,managedconservatively.
[J Indian Med Assoc 2016; 114: 108-9]
Key words : Emphysematous pyelonephritis, Intrauterine death, non-diabetic patient, conservative management.
A22 year old female patient who had PGE induced delivery of dead fetus 4 days back presented to us with severe, noncolicky pain in the right flank along with abdominal distension, fever and oliguria since 4 days. She had no history of vomiting, trauma, dysuria, hematuria, or bleeding per vaginum. She was notaknowndiabetic,hypertension,tuberculosisorrenaldisease inthepast.Hergeneralphysicalexaminationrevealedpallorand bilateral pitting pedal edema. Pulse rate was 112/min, blood Pressurewas100/70mmofHg,Respiratoryratewas34/minand temperature was 100.F Abdominal examination revealed distended abdomen with right renal angle tenderness. On Ausculation of the respiratory system patient had bilateral basal crepitations. Cardiac examination was unremarkable except for tachycardia. Per vaginum examination showed closed os and wellcontracteduterus.
Investigations
— Blood investigations showed Hb-8.8 gm%,TLC–14,300with79%neutrophilsandaplateletcountof 49,000cells/dl.RenalparametersatadmissionwereaCreatinine of4.2mg%,Ureaof103.9mg%.Serumelectrolytesatadmission werenormal.Urineroutineshowed200-300puscells/Hpf,40-60 RBC’s per hpf and albuminuria. Liver function test was normal except for low serum albumin of 2.6 gm/dl. Bleeding time and clottingtimewaswithinnormallimits.PT INRwas1.18.Patient hadaHbA1Cof5.5%.Fastingbloodsugarwas89mg%andPost Prandialsugarwas119mg%
Ultrasound abdomen and KUB revealed bilateral enlarged kidneys with emphysematous pyelonephritis of the right kidney withperinephriccollection.
Department of Medicine, JSS Medical College & Hospital, Mysore 570015
MD,AssociateProfessor
MD,AssistantProfessor
MD,DNB(Nephro),ProfessorofNephrology
MBBS,JuniorResident
MBBS,JuniorResident
CT abdomen showed diffuse enlargement of both kidneys with small pockets of air in the right kidney which is suggestive ofemphysematouspyelonephritisontherightside.(Fig1)
A diagnosis of Emphysematous Pyelonephritis of the right kidney Huang Class II was made. Patient was treated with intravenous antibiotics (Piperacillin+Tazobactum) and Clindamycin. Patient underwent percutaneous drainage for the collectionintheperinephricspaceoftherightkidney Inviewof decreasing urine output and elevated renal parameters, patient was also initiated on hemodialysis through jugular intravenous catheter
Patient underwent 3 sessions of hemodialysis, continued on supportive management and percutanoeus drainage. Repeat renalfunctionswereshowingsignificantimprovement.
Urine culture showed E.Coli (>10 colonies) sensitive to the above antibiotics. Blood culture was sterile. Patient was continuedwiththeaboveantibioticsfor3weeks.
Two weeks after admission Patient became better with normal renal functions and good urine output. She was transferredoutoftheIntensivecareunitanddischargedfromthe hospital3weeksafteradmission.
DISCUSSION
Emphysematous pyelonephritis is a severe necrotizing infection of the renal parenchyma caused by gas producing organisms. The clinical course can be devastating if not recognizedearlyandtreated
Emphysematous pyelonephritis is not a common condition. ThereportedincidenceoftheconditionfromIndiaisnotexactly known.Theconditionisclassicallydescribedindiabeticwomen whopresentwithpyelonephritis.
The most common predisposing condition is diabetes mellitus.95%ofthepatientshavediabeteswhichisuncontrolled
levels of glycosylated hemoglobin or high blood
with high sugars. Rare cases have been reported in patients who are nondiabetic. Of these 22% had obstructed upper urinary tracts, 4% had polycystic kidney disease and 4% had end-stage renal disease Renal cell adenocarcinoma compl cated by emphysematouspyelonepritishasbeenreported. Theleftkidney is more commonly affected than the right. Bilateral cases of emphysematouspyelonephritishavebeenreported.
The clinical manifestations of EPN appear to be similar to those encountered in classical cases of upper urinary tract infections.AccordingtoHuangandTseng,feverwas encountered in 79% of the patients, abdominal or back pain in 71%, nausea and vomiting in 17%, lethargy and confusion in 19%,dyspneain13%andshockin29%.
The most common organisms isolated are E.coli, klebsiella andproteus.
Among the imaging studies, CT scan has been the most sensitive. In 2000, Huang et al proposed a staging system of emphysematouspyelonephritis.
Class1–Gasconfinedtocollectingsystem
Class2–Gasconfinedtorenalparenchymaalone
Class3A–PerinephricextensionofgasorAbscess
Class3B–ExtensionofthegasbeyondGerota’sFascia
Class4–BilateralEPNorEPNinasolitarykidney
Our patient was not a diabetic and failed to show an features ofobstructionoftheurinarytractbyimagingstudies.E.Coliwas isolated from the urine cultures which was consistent with the most common pathogens isolated. A rare case of Post-Partum renal failure due to emphysematous pyelonephritis has been reported. The success of treating the condition conservatively with flank drainage and percutaneous nephrostomy have been reported to be better than nephrectomy Our patient with Huang Class II emphysematous pyelonephritis was treated conservatively and recovered completely To the best of our knowledge Emphysematous pyelonephritis complicating IUD deliveryinpregnancyhasnotbeenreportedinliterature.
REFERENCES
1 Sean TG, Sheshadri S, Saravu K — Emphysematous pyelonephritis. J Assoc Physicians India 2002;50:1413-5.
2 Shokeir AA, El-Azab M, Mohsen T, El-Diasty T — Emphysematous pyelonephritis: a 15-year experience with 20cases. Urology 1997;49:343-6.
3 Lin CH, Huang JJ, Liu HL, Lee SY, Hsieh RY, Tseng CC — Renal cell carcinoma complicated by emphysematous pyelonephritis in a non-diabetic patient with renal failure. Nephron 2002;92:227-9.
4 Huang JJ, Tseng CC — Emphysematous pyelonephritis: clinicoradiological classification, management, prognosis, andpathogenesis. Arch Intern Med 2000;160:797-805.
5 Lee IK, Hs eh CJ, L u JW B a era extensive emphysematous pyelonephritis. A case report. Med Princ Pract 2009;18:149-51.
6 Kumar N, Singh NP, Mittal A, Valson AT, Hira HS — An uncommon cause of postpartum renal failure—bilateral emphysematous pyelonephritis. Ren Fail 2009;31:171-4.
7 AswathamanK,GopalakrishnanG,GnanarajL,ChackoNK, Kekre NS, Devasia A — Emphysematous pyelonephritis: outcome of conservative management. Urology 2008; 71: 1007-9.

Fig 1 : CT abdomen showing diffuse enlargement of both kidneys with small pockets of air in the right kidney which is suggestive of emphysematous pyelonephritis on the right side
Case Note Case Note
Rhinocerebral mucormycosis : report of two cases and review of literature
Gopee E Makwana , Vikash Jain , Nandini Bahri , Mala Sinha , Manish Kumar Mathur
Mucormycosis is an infection caused by fungi of the order Mucorales in the phylum Zygomycota. Rhinocerebral mucormycosis is the most common form of the disease and typically develops in diabetic or immunocompromised patients and presents as an acute fulminant infection, which is often lethal. Sinusitis, orbital cellulitis and rapidly progressing opthalmolplegia in the context of diabetes and immunosuppression should prompt the diagnosis. Early diagnosis and prompt treatment is the key. We herein present two patients with microbiologically proven rhinocerebral mucormycosis. A comprehensive review of the literaturehasbeendonetoupdatethepathophysiologyandthediagnosis.
[J Indian Med Assoc 2016;114: 110-2&114]
Key words : Mucormycosis, rhinocerebral, diabetes mellitus, opthalmoplegia.
Mucormycosis (zygomycosis, phycomycosis) is one of the most common forms of the opportunistic fungal infections and the disease may present with pulmonary rhinocerebral, gastrointestinal, cutaneous, haematogenous or mixed manifestations Rhinocerebral mucormycosis (RCM) typically affect diabetic or immunocompromised patients 2,3,4 disease with a high mortality rate It usually begins in the nasal mucosa and paranasal sinuses, and extends towards the orbits and cranial cavity and causes necrotizing vasculitis The most characteristic feature of mucormycosis is invasion of a blood vessel resulting in hemorrhage, thrombosis, infarction and necrosisoftissue.Generally,theinfectionisrapidlyprogressive, withlocalandperineuralspreadbut,occasionallyhematogenous [6] dissemination with multiorgan involvement can be seen We herein present two case of RCM who presented at our hospital withcharacteristicfeaturesandprogression.
1 :
A 40 years old male patient with diabetes mellitus (DM) presentedtoalocalhospitalwith5dayshistoryofheadache,left hemi facial pain and difficulty in deglutition since 3 days. MRI brain of the patient was done outside which showed mild left maxillarysinusmucosalthickening(Fig1).Restoftheparanasal sinuses, orbit and brain were normal. He was symptomatically treatedwithNSAIDsonoutpatientbasis.
Subsequently three days later he presented to our hospital withinabilitytoopenlefteye,diplopiaandgraduallyprogressive painful left sided vision loss and left hemi facial swelling and severeheadache. Therewasnohistoryoffever Onexamination the patient was having left sided proptosis, opthalmoplegia with
MPShahMedicalCollege&GGHospital,Jamnagar361008
MD,TutorinMicrobiology DepartmentofMicrobiology
MD,DNB,SeniorResident,DepartmentofRadiodiagnosis MD,HeadoftheDepartmentofRadiodiagnosis MD,HeadoftheDepartmentofMicrobiology MD(Microbiol)SeniorResident,DepartmentofMicrobiology

RHINOCEREBRAL MUCORMYCOSIS — MAKWANA ET AL 111
when spores reach 8,9 patient to patient spread has been reported In a predisposed hostthesesporesareconvertedintofungalhyphae.
The principal predisposing factors are DM (especially with acidosis) and hematologic malignancies with neutropenia. Acidosis rather than hyperglycemia appear to be important predisposing factor Other identified risk factors are chronic steroid treatment, organ transplant, chemotherapy, chronic renal insufficiency, ferrum intoxication (desferoxamine treatment in dialyzed patients), burns patient. However, it is not frequent in 10 HIVpatientsastheysufferalymphociticimmunitydisorder
Mucormysois is caused by one of the members of the mucoraceal family, including Absidia, Mucor, and Rhizopus.Histologic distinction of the Mucor fungi from the more common Aspergillus is based on the characteristically broad, ‘‘empty-appearing,’’ nonseptated hyphae of these fungi, which are readily visible after routine hematoxylin and eosin 11,12staining .
left 3 , anterior rhinoscopy revealed no evidence of any eschar or suppuration Laboratory findings showed neutrophilic leucocytosis with random blood glucose level 360 mg/dl. Renal functionandelectrolyteswerenormal.MRIwasrepeated(Fig2) which revealed left sided sinusitis & premaxillary soft tissue swelling, left sided orbital cellulitis with proptosis. There was subtle asymmetry involving bilateral cavernous sinus with T2 hypointense non enhancing soft tissue on left side. On the basis of rapid progression of imaging findings over 3 days and the clinicalprofile,apossibilityofmucormycosiswasconsideredin spite of the patient being afebrile and non toxic. Nasal swab was taken and sent for microbiological examination which revealed broad, non-septate, ribbon like hyphae with wide angle branching at irregular intervals on KOH wet mount preparation suggestive of fungal etiology with likely diagnosis of mucormycosis.
On emergency basis the patient was operated under general anesthesia and extended radical left maxillectomy and orbital exenteration was performed. Post operatively the patient was in alteredsensoriumwithdecreasedgagandcouldnotbeextubated immediately On examination he had left 7 , 9 and 11 cranial nerve palsy and right sided hemiplegia. MRI was done which showed presence of acute infarct involving left MCA territory with T2 hypointense non enhancing soft tissue involving left cavernoussinuswithocclusionofleftInternalcarotidartery(Fig 3). The patient was treated with intravenous high-dose amphotericinB(15mg/kg/day).CultureonSabourad’sdextrose agar and lacto-phenol cotton blue preparation confirmed the diagnosis of mucormycosis (Fig 4). Clinical improvement was noted and the patient was discharged after 1 month. The patient remainedclinicallystableatthetimeofsubmissionofthisreport.
Case 2 : 110
A 30 year old female patient with poorly controlled Type 1 DM presented with 5 days of worsening nasal discharge, left facial pain and erythema, headache and fever. Neutropenia was 4 and 6 cranial nerves palsy Local nasal examination by
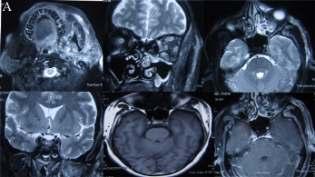
Fig 2 (A)Axial T2WI shows soft tissue swelling involving left temporal and infratemporal region, masseteric, parotid, buccal and parapharyngeal space. (B)Axial T2WI shows left maxillary bilateral ethmoidal sinusitis. T2 hyperintensity with swelling involving left extraocular muscle, stranding of orbital fat and proptosis. (C-F) [T2FS axial, T2FS coronal, T1 axial, post gadolinium (gd) T1 axial] Subtle asymmetry involving bilateral cavernous sinus with T2 hypointense non enhancing soft tissue on left side
In case of RCM, after inhalation the fungus causes necrotizingvasculitisofthenoseandsinuses,andrapidlyextend 13 into the orbits, deep face, and cranial cavity . This results from perivascular, perineural, or direct soft-tissue invasion causing a suppurative arteritis, vascular thrombosis, and infarction of surrounding tissues. Patients often present acutely with headache, fever, facial swelling, sinusitis, and unilateral orbital apex syndrome. Neurologic deficits and obtundation may occur secondary to intracerebral abscess formation and septic 5,11,13 thrombosis of major intracranial vessels . The necrotic nasal eschar is very suggestive but it only appears in 20-40% of the 10 patients,andisconsideredabadprognosissign
blood count and blood glucose level was
detected in the 435mg/dl. MRI was performed and demonstrated inflammatory changes involving paranasal sinuses, nasopharynx, face and neck spaces. T2 hypointense lesion causing a filling defect and lateral bulging of left cavernous sinus was seen with narrowing of cavernous ICAand resultant acute infarct involving left basal ganglia.The diagnosis was based on the microbiological evaluation of the biopsy specimen obtained via endoscopic examination of the paranasal sinuses. Urgent left sided extended radical maxillectomy and ethmoidectomy was performed. She was treated with amphotericin B. However the patient succumbed to cardio respiratory compromise 5 days after surgery
DISCUSSION
Mucormycosis (also known as zygomycosis or phycomycosis), was first described by Paulltauf in 1885. Phycomycetes are ubiquitous fungi occurring in soil, air skin, body orifices, manure,spoiledfoodanddust.Inoculationoccursbyinhalation,
Management of chronic RCM is not well established. Widesurgical debridement where feasible, prolonged high-dose systemic liposomal amphotericin B, control of underlying the nasal cavity and/or nasopharynx No
In the appropriate clinical context, the imaging findings of RCMonCTandMRimagingarediagnostic.Theseincludesofttissueopacificationofsinuseswithhyperdensematerial,nodular mucosal thickening, and an absence of fluid levels in the maxillary ethmoid, frontal, and sphenoid sinuses, in decreasing 14 order of incidence . Sinus contents have a variety of MR signal characteris ics, including T2 hyperin ensi y or marked hypointensity on all sequences, possibly secondary to the 13 presence of iron and manganese in the fungal elements Softtissue infiltration of the deep face and obliteration of the normal fat planes in the infratemporal fossa, pterygopalatine fossa, 14 pterygomaxillary fissure, and periantral fat are often present Typically, proptosis occurs because of enhancing soft-tissue 15 masses crowding the orbital apex and the cavernous sinuses . Thickeningandlateraldisplacementofthemedialrectusmuscle are characteristic of orbital invasion from disease in the ethmoid sinuses.Lackofenhancementofthesuperiorophthalmicveinor ophthalmic and internal carotid arteries may be seen and is relatedtovasculitisandthrombosis.Intracranialfindingsinclude infarcts related to vascular thrombosis, mycotic emboli, and 5,11,16 frontal lobe abscesses Mnif and colleagues suggested that the association between orbital cellulitis and sinusitis in the context of immunosuppression should prompt the diagnosis of 17mucormycosis
factors, and hyperbaric oxygen are used Survival
comorbid rates range from 21% to 70%, with higher mortality among patients without DM and even higher in patient with intracranial 2,3,4,11,18extension Surgical treatment is always necessary, with extended resection until bleeding tissue is found. Efforts to save the ocular globe with conservative resections usually lead to a delayed enucleation and worsening of the patient. Adequate paranasal sinuses drainage must be ensured. Liposomal amphotericinB,althoughmoreexpensivehaslessrenaltoxicity fewer adverse effects, and a better solubility in the CNS. Hence thedosecanbesafelyincreased.Theinitialdoseis1mg/kg/day whichcanbeincreasedto3oreven5mg/kg/day Renalfunction as well as potassium and magnesium must be rigorously 10 monitoredduringtreatment,thatusuallylastsfor3to7months The fungistatic and angiogenic effects of hyperbaric oxygen could enhance the effect of amphotericin B and improve the vascularization. Its value is not well established but it is thought toimproveprognosisinCNScases,withtheuseof100%oxygen for90to180minutesatpressuresfrom2to2.5atmosphereswith 10 1or2exposuresdailyforatotalof40treatments
Rhinocerebral mucormycosis should be suspected in the setting of rapidly progressive ophthalmoplegia and blindness in patientswithDM.Computedtomography(CT)andtheMagnetic resonanceimaging(MRI)mayplayanimportantrolefrominitial suspicion of the diagnosis to determining its extension. The treatmentmustfocusincorrectingthegeneralstatus,appropriate antimicrobial treatment and surgical resection. Because of its rapid evolution and severe consequences which include a high mortality rate, a high index of suspicion should be maintained. Earlydiagnosisandaggressivetreatmentmaybelifesaving.
REFERENCES
1 Franquet T, Gimenez A, Hidalgo A. Imaging of opportunistic fungal infections in immunocompromised patient Eur J Radiol 2004;51:130-8.
2 Rumboldt Z, Cas llo M Indo ent in racrania mucormycosis: case report. AJNR Am J Neuroradiol 2002; 23:932-4
3 Warwar RE Bu lock JD Rhino-orb ta -cerebra mucormycosis:areview. Orbit 1998;17:237-45
4 Yohai RA, Bullock JD, Aziz AA — Survival factors in rhinoorbital-cerebral mucormycosis. Surv Ophthalmol.1994; 39: 3-22.
5 Haliloglu NU, Yesilirmak Z, Erden A — Rhino-orbitocerebral mucormycosis: report of two cases and review of theliterature. Dentomaxillofacial Radiology 2008;37:161-6.
6 McLean FM Perineura spread of rh nocerebra mucormycosis. Am J Neuroradiol 1996;17:114-6
7 Paulltauf A — Mycosis mucorina. Virchows Arch 1885; 102: 543
8 Naussbaum ES, Holl WA. Rhinocerebral mucormycosis: changingpatternsofdisease. Surg Neurol 1994;41:152-6.
9 Hopkins MA, Treloar DM. Mucormycosis in diabetes. Am J Crit Care 1997;6:363-7.
10 Javier González Martín-Moro, Jose María López-Arcas Calleja, Miguel Burgueño García — Rhinoorbitocerebral
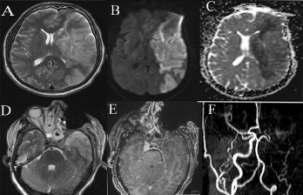
Fig 3 : (A-C, axial T2WI, diffusion,ADC)Acute infarct involving left MCAterritory with (D,E axial T2WI and Post gd T1WI)T2 hypointense non enhancing soft tissue involving left cavernous sinus with(F TOF MR angiography) occlusion of left Internal carotid artery
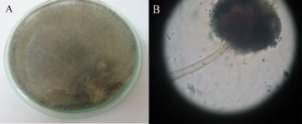
Fig : 4 (A) Culture on Sabourad’s dextrose agar incubated at 25C and 37C showed rapidly growing, fluffy cottony colony which was white initially and turned greyish brown over a week. (B) Lactophenol cotton blue preparation of culture colony showing erect sporangiophores forming terminal spherical multispore sporangia
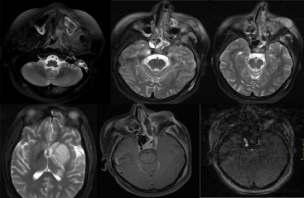
Fig 5 (A-D: T2W FS axial, E: T1W axial post gd. F: TOF MR angiography) MRI showing inflammatory signal alteration in the paranasal sinuses, nasopharynx, left mastoid air cells, left mastigator space, infratemporal space, premaxillary space (A-C) with peripherally enhancing collection (E). T2 hypointense punctuate foci are seen in nasal cavity and ethmoid sinuses (B,C).T2 hypointense lesion causing a filling defect and lateral bulging of left cavernous sinus(B,C,E).
Narrowing of left cavernous ICAwith resultant acute infarct involving basal ganglia (F,D)
(Continued on page 114)
Harlequin ichthyosis — a case report Case Note Case Note
Sendhil Coumary A , Seethesh Ghose
Harlequin ichthyosis is a potentially lethal congenital disorder of the skin characterized by an extremely thickenedlayerofkeratin.Thoughprimarilyaskindisease,itsmanifestationscompromiseothersystemsas well.Inundiagnosedcases(usuallyarule)itcomesasashocktoboththeparentsandthecareprovider.
[J Indian Med Assoc 2016; 114: 113-4]
Key words : Congenital Ichthyosis, ABCA12, Pre-natal sonogram.
Ichthyosis describes a dry, rough skin with scaling over the body Thereareseveralcongenitalorgenetic,icthyosiformor ichthyotic syndromes and acquired ichthyoses which are a complication of several systemic and malignant diseases. They range from mild ichthyosis vulgaris to the often lethal harlequin ichthyosis. Harlequin ichthyosis (HI) is one of the first genodermatoses recorded with an incidence of 1: 300000 live births. Its mode of inheritance is autosomal recessive. It can be diagnosed prenatally by skin biopsy, amniotic fluid analysis and by ultrasound. Long term multidisciplinary approach can help theseneonatessurvivetoadulthood.
CASE REPORT
Twenty year old unbooked primigravida at 34 weeks gestationalagepresentedtothecasualtywithdrainingpervagina of 6 hours duration. She conceived spontaneously two months after a second degree consanguinous marriage. There was no significant past, personal or family history especially in relevance to dermatological disorders. Her antenatal period was uneventful.
At admission her general physical examination was unremarkable. Obstetric examination revealed a singleton live fetus with breech presentation in early labour The CTG showed a distress pattern and a caesarean was planned and executed. A live preterm male fetus weighing 2100 grams with thick yellow plaques separated by deep red fissures and contractures of the extremities was born (Fig 1).An urgent dermatological opinion revealedtheglaringdiagnosisofHI.Thenewbornwasshiftedto NICU where it succumbed to severe respiratory distress. She recovered well. The parents were counseled about the need for early amniotic fluid analysis and 3D ultrasound in the subsequentpregnancy
DISCUSSION:
HIisasevereerythrodermicichthyosis,withanincidenceof one in three lakh births, which may be an under-estimate. It causesadistinctiveandalarmingappearanceatbirth.
HI cultured keratinocytes show excessive cornification and
Department of Obstetrics & Gynaecology, Mahatma Gandhi Medical College&ResearchInstitute,Puducherry607402 MD,DNB(Obs&Gyn),AssociateProfessor MD(Obs&Gyn)Professor&Head
fail development of epidermal barrier function and desquamation. ResearchhasidentifieddeletionofABCA12geneinthefamilies affected with HI They also demonstrated recovery after corrective ABCA 12 gene transfer into patient keratinocytes. Histopathology of the skin showed marked compact orthohyperkeratosis, extending to the hair follicles and pilosebaceous units.Parakeratosisisalsomarked
ure of desquamation. ABCA 12 is responsible for the
Clinically the affected infant is usually pre-mature. The neonate appears to be encased in a yellow-brown rigid, thick hyperkeratotic coat, covering the whole body surface. This inflexible cast splits at sites of stress, producing deep red fissures, resembling a Harlequin’s costume. Facial features are distorted due to severe ectropion, conjunctival oedema eclabium (everted lips). The nose and external ears are tethered and appear rudimentary Hand and feet are oedematous and encased in mitten-like casts. Movement is restricted, so respiratory insufficiency results from limited chest expansion. They also have feeding difficulties, leading to hypoglycaemia, dehydration and renal failure. Temperature instability and infection commonly supervene leading to rapid demise. The distinctive clinical features of HI are unlikely to be confused, with less severe presentation of a colloidion baby or restrictive dermatopathy
Detailed genetic counseling is required for affected families and pre-natal diagnostic testing should be offered in future pregnancies. Second trimester fetal skin biopsy was the earliest and the only confirmatory investigation available. Hair canal keratinisation appears around 15 weeks. Electron microscopic studies can show abnormal vacuoles in keratinized cells and malformation of lamellar granules in the hair However, the timing for foetal skin biopsy is very elusive. Amniotic fluid analysis revealed intra-cellular lipid vesic es in shed keratinocytes. Pre-natal sonographic features like a flat facial profile with absent nose, wide gaping mouth, dysplastic ears, abnormal fixed position of hands and IUGR Three and four dimentionalultrasoundshowsextremelythickenedkeratinlayer of skin, along with the above mentioned abnormalities The successful identification of the specific ABCA 12 mutation in affected families has opened the way for early DNAbased tests. Pre-natal chorionic villous sampling or amniocentesis can be done.Pre-implantationgeneticdiagnosisisalsobeingstudied.

long ichthyosis has to be explained gently to the parents. Care giversshouldbetrainedtocopewiththepredictableproblemsof hypothermia, feeding, respiratory problems, sepsis and dehydration. The benefit of retinoids is not very clear as not all survivors have received it. Early introduction of actiretin, probablyacceleratessheddingofplaques,withinfirstfewweeks. Survivorsareatahighriskforosteopenia,vitamin-Ddeficiency, chronic ectropion, constrictive deformities of hand and feet. Genetherapymayeventuallybecomepossible
REFERENCES:
1 Akiyama M, Sugiyama-Nakagiri Y, Sakai K — Mutation in lipid transporter ABCA 12 in HI and functional recovery by correctivegenetransfer. J Clin Invest 2005;115:1777-84.
2 Tapalwowicz K, Wygledowska G —Harlequin ichthyosis –difficultyinprenataldiagnosis. J Appl Genet 2006;47:195-7.
3 Shimizu A, Akiyama M, Ishiko A, Yosklke T — Prenatal exclusion of harlequin ichthyosis; Potential pitfalls in timing ofskinbiopsy. Br J Dermatology 2005;153:811-4.
Outcome was poor until in early 1980’s. Several babies have been reported to have long term survival. The dilemma of providing intensive neonatal care and accepting a severe life
(Continued from page 112)
Fig 1 Alive preterm male fetus and literature review. Med Oral Patol Oral Cir Bucal 2008;13:E792-5.
4 Berg C, Geipel A, Kohl M — Prenatal sonographic features of harlequin ichthyosis. Arch Gynecol Obstet 2003; 268: 4851.
5 Vohra N, Rochelson B, Smith LM — Three dimensional sonographic findings in harlequin ichthyosis. J Ultrasound Med 2003;22:737-9.
mucormycosis: A case report Cran ofacial mucormycos s: assessmen with CT Radiology 1986;160:207-12
11 Chan LL, Singh S, Jones D — Imaging of mucormycosis skullbaseosteomyelitis. AJNR Am J Neuroradiol 2000;21: 828-31.
12 FotterpekarG,MukherjiS,ArbalezA—Fungaldiseasesof theparanasalsinuses. Semin Ultrasound CT MR 1999;20: 391-401.
13 Terk MR, Underwood DJ, Zee C — MR imaging in rhinocerebral and intracranial mucormycosis with CT and pathologicalcorrelation. MRI 1992;10:81-7
14 Gamba JL, Woodruff WW, Djang WT, Yeats AE —
15 Press GA, Weindling SM, Hesselink JR — Rhinocerebral mucormycosis:MRmanifestations. JCAT 1988;12:744-9
16 Jain KK, Mittal SK,Kumar S — Imaging features of central nervous sytem fungal infection. Neurology India 2007; 55: 241-50.
17 Mnif N, Hmaied E, Oueslati S — Imaging of rhinocerebral mucormycosis. J Radiol 2005;86:1017-20.
18 Horger M, Hebart H, Schimmel H — Disseminated mucormycosis in haematological patients: CT and MRI findings with pathological correlation. BJR 2006; 79: e88–e95.
We request you to send QualityArticles addressed to : Hony. Editor, Journal of IMA(JIMA), 53, Sir Nilratan Sircar Sarani (Creek Row), Kolkata 700 014
Dr. Debasish Mukherjee
Dr. Santanu Sen Hony. Editor, JIMA Hony. Secretary, JIMA Hony. Secretary, IMA Bengal
SUPPLEMENT
Branch Notes
Durg (Chhattisgarh) NursesDayCelebrated
Chennaicity (Tamil Nadu) BloodDonationCamp
Virudhunagardist. (Tamil Nadu) BloodDonationCamp
Chennaicity (Tamil Nadu) FreeEyeCamp
Madurai (Tamil Nadu) CME
Attur (Tamil Nadu) AaoGaonChale
Salem (Tamil Nadu) AaoGanonChale
Virudhunagardist. (Tamil Nadu) BloodDonationCamp
Chennaicity (Tamil Nadu) BloodDonationCamp
Bangalore (Karnataka) GeneralBodyMeeting
Chennaicity (Tamil Nadu) EyeDonation
Bhavnagar (Gujarat) PanelDiscussion
Mundargi (Karnataka) WorldAsthmaDay
Mysore (Karnataka) WorldAsthmaDay
Bangalore (Karnataka) — ExecutiveMeeting
Ludhiana (Punjab) TheWorldAsthmaDay
Ludhiana (Punjab) APanelDiscussion
Ludhiana (Punjab) CelebrateWorldAsthamaDay
Chennaicity (Tami Nadu) Lecture On Amaem a In Pregnancy
Ambalacantt (Haryana) Ima Hbi Chapter Of Haryana State Was Launched
Bangalore (Karnataka) CommitteeMeeting
Kota (Rajasthan) — InternationalThalassemiaDayAwarenessProgram
Kancheepuram (Tamil Nadu) Annual Free C rcumc sion Camp
Poonamallee (Tamil Nadu) CMEProgrammeOn“EyeDisorders A HolisticApproach”
Poonamallee (Tamil Nadu) CMEOnDisorders
Salem (Tamil Nadu) WorldRedCrossDay
Serampore (West Bengal) CME Conducted On The Occassion On 2ndAnnualConferenceOfImaSimacon2016
Serampore (West Bengal) 2nd Annuaual Conference-SIMACON2016
Mumbai (Maharashtra) AsthmaDay
Nizamabad (Andra Pradesh) CME On Recent Advances In ManagementOfArthritis
Mundargi (Karnataka) InternationalNursesDay
Ludhiana (Punjab) SeminarOn“ViolenceAgainstWomen”(Vaw)
Chennaicity (Tamil Nadu) NursesDayCelebrated
Kancheepuram (Tamil Nadu) IMAInternationalNursesDay2016
Salem (Tamil Nadu) — WorldNursesDay
Poonamallee (Tamil Nadu) — InternationalNurses’Day
Salem (Tamil Nadu) FreeDiabeticCamp
Chennaicity (Tamil Nadu) CMEOnRecentCancerTrends
Coimbatore (Tamil Nadu) NursesDayProgramme
Telangana —CmeProgramOnRecentAdvancesInSurgicalOncology
Mumbai (Maharashtra) — AmsCME
Mumbai (Maharashtra) CMEOnAms
Poonamallee (Tamil Nadu) InternationalFamilyDa Nizamabad (Andra Pradesh) Awareness On World Blood Pressure Day
Bangalore (Karnataka) NoTobaccoDay
Tellicherry (Kerala) ExecutiveMeeting
Poonamallee (Tamil Nadu) Workout Session On “Physical And MentalWellnessForTheElderly”
Chennaicity (Tamil Nadu) WorkshopOnAdolescentProblemM
Mumbai (Maharashtra) CMEOnHypertension
Kota (Rajasthan) InvestorAwarenessProgram
Salem (Tamil Nadu) FreeDiabeticAwarenessCamp
Salem (Tamil Nadu) CMEOnDiabeticNeuropathy
Poonamallee (Tamil Nadu) FreeRuralMedicalCamp
Poonamallee (Tamil Nadu) MothersDay
Tellicherry (Kerala) — GeneralBodyMeeting
Salem (Tamil Nadu) CMEOnInfertilitySpecialist
Dehradun (Uttarakhand) CME Cum GBM In InternetAddictionAn VisibleMonsterInEveryhome
Sathyamangalam (Tamil Nadu) — CME On Interpretation Of Xray
FindingsForGps
Mumbai (Maharashtra) AaoGaonChale
Virudhunagardist. (Tamil Nadu) CMEOnDiabetesManagement
Salem (Tamil Nadu) CME On “Osteoporosis -the SilentYet Costly Epidemic
Salem (Tamil Nadu) GeriatricScreeninginOpd-ABird’sEyeView
Poonamallee (Tamil Nadu) IMA World No Tobacco Day Commemorative
Poonamallee (Tamil Nadu) — WorldNoToobaccoDay
Chhatarpur (Madya Pradesh) — CMEOnHaemophiliaInChildren
Durg (Chhattisgarh) AntiTobaccoDay
Bhavnagar (Gujarat) — WorldTobaccoDay
Mundargi (Karnataka) WorldNoTobaccoDay
Mumbai (Maharashtra) WorldNoTobaccoDay
Berhampur (Orissa) CMEOnWorldNoTobaccoDay
Punjab BloodDonationCampAtChandigarh
Ludhiana (Punjab) —WorldNoTobaccoDay
Kota (Rajasthan) AwarenessTalkOnTobaccoAndHealth
Kota (Rajasthan) NoTobaccoDay
Salem (Tamil Nadu) WorldNoTobaccoDay
Kancheepuram (Tamil Nadu) IMAWorldNoTobaccoDay2016:
Kancheepuram (Tamil Nadu) Empower ng Students Program
Bhavnagar (Gujarat) WorldEnvironmentDay
Cuttack (Orissa) WorldEnvironmentDay
Ludhiana (Punjab) EnvironmentDay
Sathyamangalam (Tamil Nadu) FreeCardiacCamp
Salem (Tamil Nadu) CMEOnCancerSurvivors
Kancheepuram (Tamil Nadu) WorldEnvironmentDay
Kancheepuram (Tamil Nadu) “BmdDetectionCamp”
Kancheepuram (Tamil Nadu) AwarenessProgramOnOsteoporosis
Cuttack (Orissa) AcademicMeet
Chennaicity (Tamil Nadu) HeathCamp
Chennaicity (Tamil Nadu) — WorldEnvironmentDay
Tiruchirapalli (Tamil Nadu) — CMEOnVariousTopic
Kerala BloodDonationCamp
Kancheepuram (Tamil Nadu) CMEOnVitaminD
Kancheepuram (Tamil Nadu) CME On Women Doctors Wing
Kota (Rajasthan) InternationalYogaDay
Te angana On To
Management
Hyderabad City (Andra Pradesh) MegaHealthCamp
Salem (Tamil Nadu) MedicalCamp
Chennaicity (Tamil Nadu) BloodDonationCamp
Chennaicity (Tamil Nadu) CMEOnRecentAdvanceInHip&Knee ReplacementSugery
Kancheepuram (Tamil Nadu) — CME On Management Of Diabetic Nephropathy
Kancheepuram (Tamil Nadu) CMEOnNephrology
Coimbatore (Tamil Nadu) InternationalYogaDay
Kancheepuram (Tamil Nadu) Internationa Day Of Yoga 2016
Ludhiana (Punjab) CME On Standard Care Of Tuberculosis
Mundargi (Karnataka) CMEOnAlcohal
Sathyamangalam (Tamil Nadu) Camp On Bone Mineral Density DetectingCamp
Kancheepuram (Tamil Nadu) DrugAwarenessRally
Kancheepuram (Tamil Nadu) Rewarding The Acievers & MotivatingOtherStudent
Chennaicity (Tamil Nadu) InternationalYogaDay
Kancheepuram (Tamil Nadu) DrugAwarenessRally
Kancheepuram (Tamil Nadu) Rewarding The Achievers & Motivating
Kancheepuram (Tamil Nadu) —DrugAwarenessRally


JOURNALOFTHE INDIAN MEDICALASSOCIATION:
IMAHouse, 53 Sir Nilratan Sarkar Sarani (Creek Row), Kolkata 700 014 Phones: (033) 2236-0573, 2237-8092, Fax: (033) 2236-6437, E-mail jima1930@rediffmail.com, Website: www.ejima.in ; www.ima-india.org, www.ima-india.org/ejima
Head office: Indian MedicalAssociation, IMAHouse, Indraprastha Marg, New Delhi - 110 002 Telephones: +91-11-2337 0009, 2337 8680, Fax: +91-11-2337 9470, 2337 0375, Telegram: INMEDICI, New Delhi 110 002, Email: hsg@ima-india.org; Website: www.ima-india.org
Date of Publication : 30th Every Month
POST BOX NO 11249 JUNE 2016
Regd. No. WBENG/2557/57

If not delivered please return to Journal of the IMA (JIMA) IMA House, 53 Sir Nilratan Sarkar Sarani (Creek Row), Kolkata 700 014 (India)
Published and Printed by Dr Santanu Sen on behalf of Indian Medical Association and printed at Prabaha, 45A, Raja Rammohan Roy Sarani, Kolkata 700009, Editor: Dr Debasish Mukherjee, National President (IMA): Dr SS Agarwal, Honorary Secretary General (IMA): Padma Shri Dr KK Aggarwal. E-mail: hsg@ima-india.org; Website: www.ima-india.org 120