— G R Ekbote, Sharad K Waje, Pankaj Bhalerao ...............................................................................18
Preliminary Report: MalariainfectionandABObloodgroups:astudyconductedinthecentralIndian stateofMadhyaPradesh— Sherly T D, G Vyas ..................................................................................22
CurrentTopic: Currentandfuturetrendsinthemanagementofthyroidassociated ophthalmopathy— Garima Agrawal, D C Mehta ..............................................................................24
—acasereport— Asha R Prasad, S P Jakhanwal......................................................................................33 Supplement................................................................................................................................................36 3
Dr Debas sh Mukherjee Honorary Ed or JIMA
Dr Santanu Sen Honorary Secretary JIMA
May everybody be happy May every one of us see to it
That nobody suffers from any pain or sorrow I do not ask for crown
Nor wish to be in Heaven or reborn I only want to alleviate the suffering of those people Who are burning in fire of sorrow
We, the members of Indian Medical Association Stand here to salute our National Flag Its honour and glory shall be our light and strength And its course shall be our course. We pledge our allegiance to it And realizing our responsibilities as the accredited members of this national organization, We swear We will dedicate everything in our power To see it fly high in the comity of nations.
EDiabetes : scale up prevention, strengthen care, and enhance surveillance
veryyear,theWorldHealthOrganizationselectsapriorityareaof global public health concern as the themeforWorldHealthDay,whichfallson7April,thebirthdayoftheOrganization.
The theme for World Health Day 2016 will be diabetes, a noncommunicable disease (NCD) directly impacting millionsofpeopleofglobally,mostlyinlow-andmiddle-incomecountries.
The prevalence of diabetes have been steadily increasing in the past few decades, in particular in low- and middleincomecountries.Knowledgeexiststoreversethistrendthroughtargetedpreventionandappropriatecare.
Working to prevent, detect and treat diabetes is also criticalto development.Within the 2030Agenda for sustainable Development,GovernmentshavesetanambitioustargettoreduceprematuremortalityfromNCDs–includingdiabetes –byonethird;achieveuniversalhealthcoverage;andprovideaccesstoaffordableessentialmedicines–allby2030.
Diabetes is one of four priority NCDs targeted by world leaders in the 2011 Political Declaration on the Prevention and Control of NCDs and the SDGs 2016-2030.The GlobalAction Plan for the Prevention and Control of NCDs 20132020providesaroadmapandmenuofpolicyoptionstoattainninevoluntaryglobaltargets,includinganadditionaltarget tohalttheriseindiabetesandobesityby2025.
Diabetes, therefore, is an issue relevant to people around the world, as well as multiple stakeholders, including government,civilsociety,theprivatesector,andintergovernmentalagencies.
Whileeverycountryandcommunityisatadifferentstageinaddressingitsdiabeteschallenge,thereareanumberof activities that could be considered at national and local level onWorld Health Day 2016 to help achieve its objectives to increaseawarenessandtriggerasetofactionstotacklediabetes.
Diabetes is a chronic, metabolic disease characterized by elevated levels of blood glucose (or blood sugar), which leads over time to serious damage to the heart, blood vessels, eyes, kidneys, and nerves. The most common is type 2 diabetes, usually in adults, which occurs when the body becomes resistant to insulin or doesn't make enough insulin. In the past three decades the prevalence of type 2 diabetes has risen dramatically in countries of all income levels. Type 1 diabetes, is a chronic condition in which the pancreas produces little or no insulin by itself. For people living with diabetes,accesstoaffordabletreatment,includinginsulin,iscriticaltotheirsurvival.Thereisagloballyagreedtargetto halttheriseindiabetesandobesityby2025.
The mission of the WHO Diabetes Programme is to prevent diabetes whenever possible and, where not possible, to minimizecomplicationsandmaximizequalityoflife.
Dr Debasish Mukherjee MBBS, DLO, MS Honorary Editor, JIMA
Dr Dalia Chatterjee MBBS, DTM&H, MD Guest Editor
The above goal is addressed by focusing on the following core functions. These functions are in close alignmentwiththecorefunctionsofWHO:
• To oversee the development and adoption of internationally agreed standards and norms for the diagnosisandtreatmentofdiabetes,itscomplications andriskfactors.
• To promote and contribute to the surveillance of diabetes, its complications and mortality, and its risk factors.
• To contribute to building capacity for the prevention andcontrolofdiabetes.
• To raise awareness about the importance of diabetes asaglobalpublichealthproblem.
The main goals of the World Health Day 2016 campaignaimsto:
• Increase awareness about the rise in diabetes, and its staggering burden and consequences, in particular in low-andmiddle-incomecountries;
• Trigger a set of specific, effective and affordable actions to tackle diabetes.These will include steps to prevent diabetes and diagnose, treat and care for peoplewithdiabetes;and
• LaunchthefirstGlobalreportondiabetes,whichwill describetheburdenandconsequencesofdiabetesand advocate for stronger health systems to ensure improved surveillance, enhanced prevention, and moreeffectivemanagementofdiabetes.
There are two main forms of the diabetes. People with type 1 diabetes typically make none of their own insulin and therefore require insulin injections to survive. People withtype2diabetes,theformthatcomprisessome90%of cases,usuallyproducetheirowninsulin,butnotenoughor they are unable to use it properly People with type 2 diabetes are typically overweight and sedentary, two conditions that raise a person’s insulin needs. It may also beseenduringpregnancy.
The diabetes epidemic is rapidly increasing in many countries, with the documented increase most dramatic in low-andmiddle-incomecountries.
A large proportion of diabetes cases are preventable. Simplelifestylemeasureshavebeenshowntobeeffective in preventing or delaying the onset of type 2 diabetes. Maintaining normal body weight, engaging in regular physical activity, and eating a healthy diet can reduce the riskofdiabetes.
Diabetes is treatable. Diabetes can be controlled and managed to prevent complications. Increasing access to diagnosis, self-management education and affordable treatmentarevitalcomponentsoftheresponse.
Efforts to prevent and treat diabetes will be important to achieve the global Sustainable Development Goal 3 target of reducing premature mortality from noncommunicablediseases(NCDs)byone-thirdby2030. Many sectors of society have a role to play, including governments, employers, educators, manufacturers, civil society, private sector, the media and individuals themselves.
We request you to send QualityArticle addressed to : Hony. Editor, Journal of IMA, 53 Sir Nilratan Sarkar Sarani (Creek Row), Kolkata 700 014
Dr. Debasish Mukherjee Dr. Santanu Sen Hony. Editor Hony. Secretary
Disclaimer
The information and opinions presented in the Journal reflect the views of the authors and not of the Journal or its Editorial Board or the Publisher Publicationdoesnotconstituteendorsementbythejournal. JIMA assumes no responsibility for the authenticity or reliability of any product, equipment, gadget or any claim by medical establishments/institutions/manufacturersoranytrainingprogrammeintheformofadvertisementsappearinginJIMAandalsodoesnotendorse orgiveanyguaranteetosuchproductsortrainingprogrammeorpromoteanysuchthingorclaimsmadesoafter — Hony Editor
Purpose of this study is to perform Retinopathy of Prematurity (ROP) screening, to identify infants who have or are likely to develop ROP and to suggest recommendations based on it. This hospital based prospectivestudywascarriedoutin50pretermbabiesover18monthsperiod.
Indirect ophthalmoscopy was performed in infants with gestational age < 36 weeks and/or birthweight < 2000 gm. Maternal and neonatal risk factors were noted and data analyzed statistically. The patients were divided into two groups A and B, Group A comprising of babies with stage 1 and 2 ROP and Group B comprisingofStage3-5ROP.
TwentytwopercentbabiesdevelopedROP.Onethirdpositivecaseswereweighing<1500gm. 39%were < 30 weeks gestation .Sepsis and Intra Ventricular Haemorrhage (IVH) were independent and statistically significantriskfactors(p<0.05).Antenatalsteroidadministration(p=0.001),reducedtheoccurrenceofROP. WerecommendROPscreeningat4-6weeksofpostnatalageinallpretermbabieswithbirthweight<2000 gm and/or gestational age < 36 weeks. Judicious use of oxygen has a significant effect on reduced incidence ofROP.
[J Indian Med Assoc 2016; 114: 7-11]
Key words : Retinopathy of prematurity, preterm babies, oxygen therapy, low birth weight babies.
Retinopathy of Prematurity (ROP), a potentially blinding condition is a proliferative disorder of the developing retinal vasculature seen in the preterm and 1 low birthweight infants, first described by Terry as RetrolentalFibroplasia.
The outcome ranges from minimal sequel to bilateral, irreversible and total blindness. Incidence of this condition is rising rapidly in developing countries with improvements in neonatal care and increasing survival of verylowbirthweightinfants.
The most important determinant of any ROP management program is an effective screening strategy Three questions: Whom to screen? When to screen? and How to screen? are important questions which we must answerintheIndianScenario.
Hence the present study was undertaken to screen the preterm infants for ROP which if untreated may cause severevisualdisability
Ahospital based, prospective observational study was conducted in Department of Ophthalmology in collaboration with Department of Pediatrics, in a rural based hospital of Central India, between 2008-2011. All relevantperinataldataincludingriskfactors(Maternaland Neonatal)weredocumented.
Inclusion Criteria
:
2,3 1) Gestationalageatbirthoflessthan36weeks
2 2) Birthweightlessthan2000gms
3) Extraordinarysupportofoxygen
4) Complete documentation of hospital records including details regarding other factors that can increase theriskofROPandwherescreeningshouldbeconsidered werepretermbabieswith:
a. RespiratoryDistressSyndrome
b. Sepsis
c. SicklySurvivors
d. Pneumonitis
e. MultipleBloodTransfusions
f. Multiplebirths(twins/triplets,etc.)
g. Apnoeicepisodes
h. Intraventricularhemorrhages
RETINOPATHY OF PREMATURITY SCREENING INARURAL BASED HOSPITAL OF CENTRAL INDIA
Exclusion Criteria:
1) Babieswithcongenitalanomaliesoftheeye
2) Babieswithchorioretinitis
3) Babieswithbirthtrauma
4) Babieslosttofollowup
FirstexaminationwascarriedoutinNICUbetween4-6 weeks postnatally under all aseptic precautions and followingstandardROPscreeningguidelines.Subsequent examinations were done at 2-3 weeks interval or even earlier, if necessary till retina was fully vascularised. Classification of ROP was done according to the 4,5 InternationalClassification(ICROP).
Babieswithstage1-2diseasewerekeptinROPGroup A and those with (more severe disease) stage 3 - 5, were kept in ROP Group B. Neonatal and maternal risk factors weredocumented.
Babies were examined by dilating the pupils with diluted Tropicacyl Plus (0.5% Tropicamide+ 2.5% Phenylephrine) eye drops in 1:2 dilution using distilled water. Eyes were examined 30 minutes after application of the first drop. Excess drops spilling over were wiped with sterile cotton to prevent systemic complications. Eyes were examined by indirect ophthalmoscopy with a condensinglensof+20D. Aninfantileeyespeculumwas used to keep the eyes open. Oculocephalic reflex and scleraldepressionwereusedtoexamineperipheralretina.
Babies with ROP were scheduled for screening as follows: the examinations were performed weekly for stage 1-2 disease and more frequently for stage 3 disease, till the disease started resolving or progressed to threshold stage. Babies showing evidence of regression were followed up weekly till vascularisation was complete. Babies progressing to threshold stage were treated with laser Screening was continued till term gestation and subsequentfollowupwasdonein3to6months.
Neonatal risk factors like sex, birthweight (in grams), gestational age (in weeks), details of oxygen saturation, blood transfusion, sepsis, apnoea, intraventricular hemorrhage, Indomethacin used for Patent Ductus Arteriosus Aminophylline, acidosis (PH<7 3), phototherapy, necrotizing enterocolitis, seizures were recordedforriskfactoranalysis.Maternalriskfactorslike type of delivery, twin pregnancy, premature rupture of membranes, maternal diabetes, pregnancy induced hypertension, antenatal steroids, oligohydramnios and whetherthebabywasinbornoroutborn,wererecorded.
All infants receiving Oxygen therapy had continuous monitoring with Pulse Oximetry and Arterial Blood Gas Analysis through umbilical or peripheral arterial blood sampling. Apnoea was defined as cessation of respiration for > 20 seconds which required resuscitation with BagMask and Oxygen. Sepsis was diagnosed by clinical
picture, changes in the leucocytes count, elevated Creactive proteins and positive culture report. Follow up screening and management of ROP was done as per guidelinesgivenbyAmericanAcademyofPediatrics.
Aprospective statistical analysis was done on the data usingtheExcelandRprogrammingsoftwarepackage.
RESULTS
During the study period of 18 months, the total no of babies <36 weeks gestation and <2000 gms at birth was 138. However 50 babies fulfilled all the inclusion criteria and were included in the study, rest were lost to follow up/diedandwereexcludedfromthestudy
Problemsencounteredduringscreeningwereminimal and related to scleral indentation. None developed conjunctivitis, apnoea, cyanosis or hypothermia during examination. No problems were encountered due to mydriaticuse.
Elevenofthe50pretermbabies(22%)developedROP and all had bilateral disease. There were 10 males and 1 female infant with ROP Eight babies were in Group A (Stage1-2)and3wereinGroupB(Stage3-5).
The birthweight of ROPbabies ranged from 968-1650 gramswithmeanweightof1260.90±215.52gramswhile thatofnon-ROPbabiesrangedfrom900-2900gramswith meanweightof1517.07±419.04grams.Onsimilarlines, mean weight of babies in group A was 1309.75 ± 226.19 gramsandgroupBwas1130.66±134.84grams.
The gestational age of ROPbabies ranged from 28-36 weeks with mean gestational age of 30.54 ± 2.54 weeks while that of non-ROP babies ranged from 28-39 weeks withmeanageof33.12±3.05weeks.Alsothegroupwise tendencies were obtained. The mean gestational age of babies in Group A was 30.75 ± 2.81 weeks and Group B was30±2.81respectively
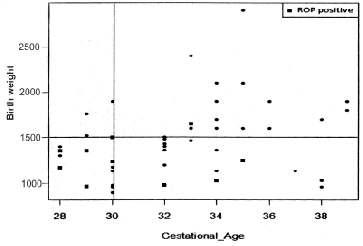
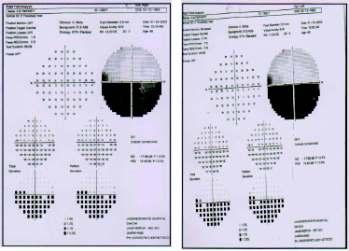
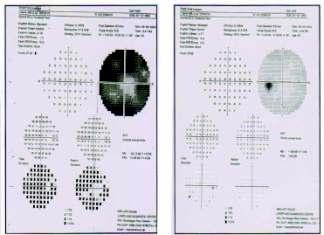
TheScatterPlotasshowninFigure1revealedthat,for a cut-off weight of 1500 gm, the incidence of ROP was statistically significant (p=0.045). Nearly, 31% of the babiesweighinglessthan1500gmwereaffected.Further, a cut-off gestational age of 30 weeks indicated significant numberofincidences(p=0.040).Nearly39%ofthebabies wereaffectedwithagelessthanorequalto30weeks.
The statistical significance of difference between the ROP+ve and ROP–ve cases was compared and analyzed using independent t-test. The results are shown in Table 1.Various neonatal risk factors were studied and their significanceisshowninTable2.Theimpactofsomeofthe key factors of interest was studied on ROP and shown in Table 3. The factors identified were either singleton or in combinationwiththe‘inborn’or‘outborn’category.
DISCUSSION
ROPisanavoidablecauseofchildhoodblindnessand
in WHO's VISION 2020 it is given high priority. Early treatment to prevent blindness due to ROP requires qualified and trained ophthalmologist, who can do ROP screeninginbabiesatriskinNICUsoonafterbirth.
The incidence of prematurity has increased over the few years. With increasing incidence of prematurity and bettersurvivalofsmallerbabies,theincidenceofROPwas expected to increase. Hence an attempt was made in the current study to look at the incidence of ROP in a rural basedhospital.
In the present study, 50 babies admitted to NICU and satisfying the inclusion criteria during the study period werescreenedforROP
Flynn and others have highlighted the fact that if retinal examination is too soon after birth, acute retinopathy of prematurity is missed as changes often develop later in more preterm infants. Equally if the examination is too late any acute changes may have regressed and no sequeale can be detected. According to American Academy of Ophthalmology guidelines, the first examination should normally be performed between 4 and 6 weeks of chronologic (postnatal) age or, alternatively, within the 31st to 33rd week of postconceptionalorpostmenstrualage(gestationalageatbirth plus chronological age), whichever is later, as determined bytheinfant’sattendingpediatricianorneonatologist.
The incidence of ROP in the present study is 22.00% which is well within the range reported from other studies as shown in Table 4. An Indian study by Gupta et. al. in 2004 reportedincidenceof21.7%.
Lowerbirthweight(<1250grams)wasassociatedwith stageIIIandaboveROP MaximumnumberofROPcases were seen in birthweight between 1000-1500 grams.ROP stage I and II (Group A) was found in eight babies(72.72%) where as advanced ROP stage III and above(GroupB)wasfoundinthreebabies(27.27%).
RekhaetalreportedROPin46%infantsweighingless than 1500 grams and less than 34 weeks. We reported seven ROPpositive cases (63.63%) between 28-30 weeks of gestation which forms the majority group of ROP Hence, lower gestational age was significantly associated withincreasedincidenceofROP.
Various studies as shown in the table 4 have taken variableinclusioncriteria.Insomestudieslessgestational age and/or weight is taken and in others they have taken either gestational age or only weight as inclusion criteria. In order to include all ROP positive cases we have includedallbabieswithgestationalagelessthan36weeks and /or birthweight less than 2000 gms as suggested by Jalali et al.
In our setup we have found ROP positive cases both above and below the gestational age of 32 weeks and birthweightof1500grams.Astheinclusioncriteriawere
NS–NonSignificant
differentit’snotpossibletocompareresultsfully Thusthe screening criteria should be less rigid than described in reports from long established centres. Therefore, every country and particularly, different regions should make guidelinesbasedoncurrentandlocaldata.
Lower gestational age and low birthweight are the mostimportantriskfactorsfortheetiologyforROPinour study and it is well recognized that the incidence and severity of ROP are inversely proportional to gestational ageandbirthweight.
In our study mean gestational age of infants who developed ROP(30.54±2.54 weeks) was lower than those who did not develop ROP (33.12±3.05 weeks) and was statistically significant with p=0.0105. The mean birthweight of babies who developed ROP (1260.90±215.52grams)waslesserthatthosewhodidnot develop ROP (1517.07±419.04 grams) and was statisticallysignificantwithp=0.0097.
Various neonatal risk factors for ROP were studied. Out of all preterm babies (n=50) we reported 23 babies (46.00%) with sepsis and eight babies (34.75%) among them developed ROP which was statistically significant (p=0.04). Six out of these eight preterm babies were outborn i.e. they were delivered outside our hospitalandwerereferredhere,which explains the high incidence of sepsis inthesecases.
Another important risk factor in our study was IVH which was also statisticallysignificant(p=0.029).
The present study clearly highlights the importance of antenatal steroids in the prevention of ROP Antenatal steroid use has been recommendedforpregnanciesof24to 34 weeks of gestation with threatened premature delivery to decrease the risk of RDS and neonatal death in pretermneonates.
Inourstudy,21pretermcaseshad history of antenatal steroid administration.Outofthese,18babies did not develop ROP which showed antenatal steroid administration helps in non occurrence of ROP and was statistically significant (p=0.0014). Antenatal steroids administration to reduce the incidence of ROPwas also 10 reportedbyHiggins et al
The causal link between ROP and supplemental oxygen has been confirmed by controlled trials and 1 clinical studies. Preliminary work has suggested that continuous oxygen monitoring may reduce the incidence of ROP In our NICU, oxygen administration, its flow rate and duration are not based solely on clinical findings like cyanosis, respiratory distress or heart rate, but are closely monitored by pulse oxymetry and oxygen saturation is kept between 88-94% Although oxygen administration was a significant independent risk factor of ROP, but in our study, 14 out of 17 inborn babies (i.e. babies born in our hospital) were given oxygen judiciously and so they did not develop ROP which was statistically significant (p=0.0127) as compared to babies deliveredandmanagedoutsideourhospital(outborn)who showedincreasedincidenceofROP.
Fig 1 — Scatter Plot Showing the Distribution of CasesAccording to GestationalAge and Birth Weight
The management of ROP basically depends on findings of ROP screening and follow up screening once ROPis detected .In our series of eleven cases ,three cases were in Group B ( ROP stage III and above) and needed lasertherapy
GroupA(ROPStageIandII)includedeightpatientsof ROP and were followed up closely Asignificant number of babies (n=8, 72.72%) regress without reaching threshold disease in our study and is comparable to other 12 studiesinliteratureasreportedbyAzadRV et al
The decreased incidence of ROP in the present study could be attributed to the improved neonatal nutritional support, continuous pulse oxymetry, and judicious use of Oxygen.Thereducedincidencecouldalsobeduetolow 10
RETINOPATHY OF PREMATURITY SCREENING
survival of extreme preterm babies and limited sample size.
Since ROP is essentially asymptomatic in the early stages, standards of practice now demand carefully timed retinal examinations of at risk infants. Guidelines for ROP screening in Indian scenario should be gestational age of lessthan36weeksandbirthweightlessthan2000gramsto avoidmissingROPcases GoodteamworkofObstetrician, Neonatologist and an Ophthalmologist is vital and they should work in close cooperation to detect ROP early and manage it Parents of at risk babies should be properly counselled so that they understand the severity of blinding complicationsandtheneedoflifelongfollowup
REFERENCES
1 Terry TL “Extreme prematur ty and fibrob ast c overgrowth of persistent vascular sheath behind each crystalline less 1. Preliminary Report. American Journal of Ophthalmology 1942;25:203-204.
2 Jalali S, Matalia J, Hussain A, Anand R — Modification of screening criteria for ROP in India and other Middle Income Countries. American Journal of Ophthalmology 2006; 141: 966-8.
3 Jalali S, Anand R, Kumar H, Dogra MR, Azad R, Gopal L — Programme planning and screening strategy in retinopathy of prematurity. Indian Journal of Ophthalmology 2003; 51: 89-99.
4 Comm ttee for the c ass fica on of retinopathy of prematurity. An international classification of retinopathy of prematurity. Archives of Ophthalmology 1984;102:1130-4.
5 Comm ttee for the c ass fica on of retinopathy of prematurity. An international classification of retinopathy of prematurity, II: the classification of retinal detachment. Archives of Ophthalmology 1987;105:906-12.
6 Maheshwari R, Kumar H, Paul VK, Singh M, Deorari AK, Tiwari AK — Incidence and risk factors of retinopathy of prematurity in a tertiary care newborn unit in New Delhi. National Medical Journal of India 1996;9:211-4.
7 FlynnJT,O’Grady,GE,HerreraJ—“Retrolentalfibroplasias clinicalObservation” Archives of Ophthalmology 1977;95: 217-23.
8 Gupta VP, Dhaliwal U, Sharma R, Gupta P, Rohatgi J — Retinopathy of Prematurity-Risk Factors: Indian Journal of Pediatrics 2004;71:887-92.
9 Rekha, Battu S, RR, Chandrashekhara, MK — “Retinopathy of Prematurity- A Preliminary report”. Indian Journal of Pediatrics 1992;29:623-6.
10 Higgins, RD, Mendelsohn, AL, Defeo, JJ — “Antenatal Dexamethasone and decreased Severity of Retinopathy of Prematurity”. Archives of Ophthalmology 1998;116:601-6.
11 Charan, R, Dogra, MR, Gupta, A — “The incidence of retinopathy of prematurity in a neonatal care unit”. Indian Journal of Ophthalmology 1995;43:123-6.
12 Raj VA — Retinopathy of Prematurity; A Text and Atlas, In: RajVA;NewDelhi. Jaypee Brothers 2006:41-2.
ARANDOMIZED STUDY COMPARING EFFICACYAND SAFETY OF MILNACIPRAN — DALAI ET AL 13
A Randomized
study comparing efficacy and safety of milnacipran versus escitalopram on patients of major depressive disorder
Sayanti ghosh , Sushobhan Pramanik , Madhumita Ray
Theobjectiveofthestudywastocomparetheefficacyandsafetyofmilnacipranandescitalopraminthe treatmentofpatientsofmajordepressivedisorder(MDD).Thestudywasconductedin60patientssuffering from major depressive disorder as per Diagnostic and Statistical Manual of Mental Disorders IV (DSM-IV) criteria. Patients were randomized into two groups and were given either milnacipran (50mg OD) or escitalopram (10mg OD) for 8 weeks. The primary efficacy parameter was the change in Hamilton Depression Rating Scale -17 items (HDRS-17) where as the change in Montgomery –Asberg Depression Rating Scale (MADRS) was the secondary parameter. Safety evaluation was based on the treatment emergentadverseeffectsandlaboratoryinvestigations. There was significant decrease in HDRS-17, MADRS from baseline to endpoint (p<0.001) in both the groups. However the difference in scores between two groups was not statistically significant. The mean HDRS-17 score decreased from26.28 (SEM 0.48) to 9.88 (SEM 0.52) in milnacipran group and from 25.70 (SEM 0.64) to 11.08 (SEM 0.46) in escitalopram group at the end of therapy. There was no significant difference in adverse effects and laboratory parameters between the two groups. So these findings of this study indicate that milnacipran 50mg is equally effective to escitalopram (10mg) in patients of major depressivedisorder(MDD).
[J Indian Med Assoc 2016;114: 12-6]
Key words : Milnacipran, Escitalopram, Major Depressive Disorder
Major depressive disorder (MDD) is defined as depressedmoodonadailybasisforaminimum duration of 2 weeks.An episode may be characterized by sadness, indifference, apathy, or irritability and is usually associated with: changes in sleep patterns, appetite, and weight; motor agitation or retardation; fatigue; impaired concentration and decision-making; feelings of shame or guilt;andthoughtsofdeathordying.
MDD is a common and serious mental illness with sometimes fatal consequences that imposes a significant disease burden on the individual in terms of impaired functioningandhealth-relatedqualityoflife(HR-QOL).
FinalYear MD PGT (Pharmacol), Department of Pharmacology, R GKarMedicalCollege,Kolkata700004
MD (Pharmaco ), Assoc a e Professor, Departmen of Pharmacology NRSMedicalCollege,Kolkata700014
MD (Psychiatry), Associate Professor, Department of Psychiatry, RGKarMedicalCollege,Kolkata700004
MD (Psychiatry), Assistant Professor, Department of Psychiatry, RGKarMedicalCollege,Kolkata700004
Second year MD PGT (Anaesthes o ogy), Department of Anaesthesiology,NationalMedicalCollege,Kolkata700014
MDD
continues to be a considerable problem, both for
clinician and the public health level. It is currently the fourth leading cause of disease and disability worldwide andisprojectedtorisetosecondin2020.
Various groups of antidepressant medication available in the market, namely monoamine oxidase inhibitors (MAOs), tricyclic antidepressants (TCAs), selective serotonin reuptake inhibitors (SSRIs) and selective serotonin-norepinephrinereuptakeinhibitors(SNRIs).
MAOIs are not used regularly due to its side effectslikeorthostatichypotensionandweightgainetc.
TCAs are not preferred these days because of their adverse effect profile i.e. anticholinergic effects, cardiac arrhythmiasandseizureprecipitation.
SSRIs are presently the most widely used antidepressants because of their better safety profile and tolerability. SSRIs selectively blocks neuronal transport of serotonin and increase synaptic availability of 4serotonin. Escitalopram, the S-enantiomer of citalopram, isan(SSRI)antidepressantthatisthemostselectiveofthe SSRIs. The efficacy and safety of escitalopram has been 5,6 wellestablishedinthetreatmentofMDD.
SNRIsinhibitreuptakeofneurotransmitters,serotonin and norepinephrine. This results in an increase in the extracellular concentrations of serotonin and norepinephrine in the brain that are known to play an important role in mood. Among the SNRIs milnacipran has the best 5-HT/NA inhibition ratio irrespective of the dosage(5HT:NA-1.6:1) and has ideal pharmacokinetic parameters,alleveationofallsymptomsofdepression. Ina meta-analysisoftwostudiescomparing milnacipranwith SSRIs- fluoxetine and paroxetine, milnacipran was found 9,10 tobesignificantlymoreeffectivethan SSRIs.
So till now we didn’t know which is the better choice for the treatment of MDD with respect to efficacy and safety,eitherescitalopramormilnacipran.
Medline search at the inception of this study did not show any published data on the efficacy and safety of milnacipran vs escitalopram amongst major depressive population.
Hence, the present study was designed to compare short term efficacy and safety of milnacipran and escitalopraminthetreatmentofmajordepressivedisorder
MATERIALAND METHODS
Ethical Considerations :
The study protocol, along with the informed consent form (in Bengali, Hindi& English) was submitted to the Institutional Ethics Committee, R. G. Kar Medical College, Kolkata, for approval. Subject recruitment commenced only after such approval was obtained in writing.
Informed written consent was taken from each participant. Illiterate patients gave their left thumb impression instead of signature in the presence of an appropriatewitness.
Study Setting :
• Screening: Through out-patient department (OPD) R.G.KarMedicalCollege,Kolkata(R.G.K.M.C).
• Recruitment and Drug dispensing: Through PsychiatryOPDofR.G.K.M.C.
• Data compilation and Statistical analysis: In DepartmentofPharmacology,R.G.K.M.C.
Study Duration :
For each enrolled subject the total duration of therapy waseightweeks(8wks).
Study Design :
The current study was designed as a prospective, interventional, randomized, assessor blind, activecontrolled, fixed dose with two parallel treatment groups wascarriedoutatasingleCentre.
Subject Selection Criteria :
Patients attending the psychiatry OPD of R.G.K.M.C. with clinical features of major depressive disorder fulfillingtheDSM-IVcriteriawererecruitedinthestudyif they fulfilled the following inclusion and exclusion criteria.
Inclusion Criteria :
• Age:18-65years
• Sex:Eithersex
• Major Depressive disorder based on DSM-IV criteriabaselinescoreof=17of17itemHDRS-17.
Exclusion Criteria :
• Patients with clinically significant renal or hepatic diseaseoranyotherchronicmedicalillness
• alcoholordrugabusewithinthepastoneyear
• history of myocardial infarction or unstable heart diseasewithinpast6months
• acutecoronarysyndromewithinpast6months
• knownorsuspectedpregnancyorbreastfeeding
• Use of any antidepressant within past 30 days or participationinanyotherclinicaltrialwithin3month
Sample Size :
For the purpose of sample size calculation, changes in the Hamilton Depression Rating Scale-17 Items12, 13 (HDRS-17) was taken as the criteria. The study was designedtodetectatleastadifferenceof2HDRS-17score between the two treatment groups, considering level of significance 5% ( a of 0.05) and 80% power, we required 48patients(24ineachgroup).Assumingadropoutrateto be 20% we included a total of 60 patients. Sample size calculationwasdonebyusingWinPepiver11.1software.
Blinding :
Study was designed as assessor-blind study so that assessor was not aware of the group allocation of individualsubjects.
Randomization :
The estimated sample size for the study (including dropouts) was 60 (30 in each group).A random number table generated by computer was used to allocate patients to treatment groups, and the study coordinator was the onlypersonwithaccesstotherandomization.
Treatment Schedule :
Patients were randomized (generated by computer) into two groups and were started on either milnacipran 50mg orally with a glass of drinking water after dinner or escitalopram 10 mg in the same manner The follow up visits were at the end of 2nd week (FU-1) and after end of
8th week (end of the study-EOS). At each visit efficacy and safety was evaluated and drug was supplied. Compliance was checked by pill countmethod at each follow up visit. The drop outs or withdrawal if any along with reasons for the same were recorded. Data was collected in a specially designed case report form (CRF) by conducting a personal interview with each patient duringtheclinicvisit.
ASSESSMENT PARAMETERS
The following parameters were assessed at the visits specified:
Efficacy Parameters :
Primaryefficacyparameter
Change of the score of Hamilton Depression Rating Scale-17 Items12, 13 (HDRS-17) – baseline of the study (BS),firstfollowupatendof2ndweek(FU-1)andendof thestudyatendof8thweek(EOS).
Secondaryefficacyparameters
Change of the score of Montgomery –Asberg DepressionRatingScale14(MADRS)–BS,FU-1,EOS
Safety evaluation was based on spontaneously reported adverse effects at any time (by telephone also) andthelaboratoryinvestigationsatbaselineandattheend ofstudytimei.e.endof8thweek.
STATISTICALANALYSIS
The statistical analysis was done in accordance with the guidelines of modified intention to treat (MITT) analysis. Descriptive statistics were reported as percentages, mean± S.E.M (standard error mean) for continuous parametric variable, and median for continuous nonparametric variables. Fisher’s exact test was employed to test the association of study characteristics between the two treatment groups for categorical variables. Unpaired‘t’ test was employed to find the significance in different treatment over the study period of 8 weeks (p<0.05). Friedman’s ANOVA test followed by Dunn’s Multiple Comparison test was employed to find the significance in the same treatment group in various time period in the study period of 8 weeks, The computer software graph pad inStat version 3.06.wasusedforallthestatisticalanalysis.
RESULTANDANALYSIS
A total of 60 patients suffering from MDD as per DSM-IV criteria were enrolled in the study Finally 49 patients(25subjectsintreatedwithmilnacipran-GroupM and 24 subjects were treated by escitalopram -Group E) completedthestudyasperprotocol.
The patients in both the groups had comparable demographicprofilesasshowninTable1.
HDRS-17 SCORE
As observed from Table 2, there was significant de
cline in HDRS-17 score in both the study groups over the period of treatment of 8 weeks when any of the follow-up visits was compared with the corresponding baseline (p value <0.001 by FriedmanANOVAtest followed by post hoc analysis of Dunn’s Multiple Comparison test).However there was no statistically significant difference of HDRS-17 score between the group M and groupEatanypointoftimeanalyzedbyUnpaired‘t’test.
MADRS SCORE
AsseenfromTable3,boththegroupsshowsignificant declinein MADRS score over the periodof treatmentof 8 weeks, when compared with the corresponding baseline. Again, there was no statistically significant difference of MADRS score across the groups at any point of the study analyzedbyunpaired‘t’test.
Table 1 — Demographics and Mean Baseline Scores
Parameters GroupM GroupE p
(n=25) (n=24)
Age(inyears): Range 18-55 25-56 Mean±SEM 36.04±2.09 35.75±1.63 >0.05
Sex Male 11(44%) 12(50%) >0.05 Female 14(56%) 12(50%) >0.05
Baselinescores(Mean±SEM),Median: HDRS-17: (Mean±SEM) 26.28±0.48 25.70±0.64 >0.05 Median 26 26 >0.05 MADRS: (Mean±SEM) 39.92±0.69 39.83±0.56 >0.05 Median 40 40 >0.05
p value for comparison between the study groups for age and baseline score is from Student’s unpaired t test, while for sex distributionisfromFisher’sexacttest.
Table 2 — Changes in HDRS-17 SCORE (decreasing score means improvement)
Visits GroupM GroupE pvalue (n=25) (n=24)
Baseline
Mean±SEM 26.28±0.48 25.70±0.64 0.48
Median 26 26
FU-1(after2weeks):
Mean±SEM15.04±0.66*** 15.95±0.57** 0.30
Median 15 16
EOS(after8weeks):
Mean±SEM 9.88±0.52*** 11.08±0.46*** 0.09
Median 10 12
*** means p<0.001, **means p<0.01. p value for comparison between the study groups was from Unpaired‘t’test.While p value for within group comparison of any of the follow up visits to the corresponding baseline is Friedman ANOVA test with Dunn’s MultipleComparisontestasposthoctest.
TREATMENT EMERGENTADVERSE EVENTS
During the 8 weeks treatment period, the recruited subjects experienced and spontaneously reported the following adverse events represented in Table 4. None of theeventsweresevereenoughtowarrantwithdrawalfrom the study, and all resolved spontaneously There were no hospitalizations owing to adverse events and no serious adverse events. The adverse events were comparable in bothgroups.
Laboratory investigations of hematological and biochemical parameters did not show any significant change at the end of treatment as compared to baseline in boththegroupsasshowninTable5.
DISCUSSION
Although there are a number of therapeutic choices available for the treatment of major depression, it is generallyacknowledgedthatthecurrentfirstlinetherapies provide less than satisfactory outcome in many instances. This is because nearly two-third of all patient are either partially or completely non responsive, only one-third experience full remission and many have tolerability concerns that limit long term treatment .Thus the development of new agents that can meaningfully expand the expected therapeutic effect and tolerability of antidepressant therapy option is an important medical need.
Thepresentstudywasarandomizedcontrolledclinical trial to evaluate the efficacy and safety of a new group of antidepressant-milnacipran (SNRI) in comparison to escitalopram (SSRI) in the patients of major depressive disorder. They are assigned to two treatment groups by randomization. The groups were comparable at baseline with respect of age, sex, weight and baseline scores of HDRS-17, MADRS scale. Both treatments were effective inimprovingthevarioussymptomsofthedisease.
Theprimaryefficacyvariablewasthescoringobtained on the HDRS-17 scales. And the secondary efficacy variablewasthescoringobtainedontheMADRSscales.
The changes of score of HDRS-17 from baseline to after 8 weeks were significantly less for both milnacipran (mean ± SEM,baseline-26.28 ± 0.48, study end-9.88 ± 0.52 ,p value-0.001 ) and escitalopram(mean ± SEM, baseline-25.70 ±0.64,study end- 11.08 ± 0.46,p value,0.001 ). But there were no significant difference in HDRS-17scoreattheendof the study between the two treatmentgroups.
Thechangesofscoreof
Table 3 — Changes in MADRS SCORE (decreasing score means improvement) Visits
Baseline
*** means p<0.001, **means p<0.01. p value for comparison between the study groups was from Unpaired‘t’ test. While p valueforwithingroupcomparisonofanyofthefollowupvisits to the corresponding baseline is Friedman ANOVA test with Dunn’sMultipleComparisontestasposthoctest.
Table 4 —Adverse events encountered in study subjects
Adverseevents GroupM GroupE
Nausea 16 12
Vertigo 8 4
Sweating 10 8
MADRS scale from baseline to study end were significantly less for both milnacipran (mean ± SEM,baseline-39.92 ± 0.69,study end-15.6 ± 0.88,p value-,0.001 ) and escitalopram(mean ± SEM,baseline39.83 ±0.56,study end- 16.5 ± 0.87,p value-0.001 ) drugs. But there were no significant difference between the two MADRS score at study end between the two treatment groups.
Regarding safety and tolerability in our study, both treatments were well accepted as assessed by clinical and laboratoryparameters.
Table 5 — Laboratory test profile in the study groups (Values are Mean ±SEM)
16 J INDIAN MED ASSOC, VOL 114, NO 4, APRIL 2016
The result of the study corroborates with the previous 15 clinical trials like trials on escitalopram vs duloxetine or 16 escitalopram vs venlafexine .No significant difference of efficacy and safety of escitalopram vs duloxetine or venlafexine (SNRIs) was observed in both the above mentionedtrials.
The results of this study contradict with the previous trials based on comparison of milnacipran with other SSRIsindepression.Inastudyitwasseenthattheefficacy of milnacipran was significantly better than fluoxetine (SSRI)althoughsideeffectswerenotsignificantlydiffer Another study it was seen that milnacipran was superior in efficacy to SSRIs (fluoxetine, fluvoxamine) 17 andequallytolerated.
Adverse drug reactions were encountered in both the treatmentgroups,mainlyinthefirstweekbutmostofthem were well tolerated after two to three weeks. The most common events were nausea (16 out of 25 patients in group M, 12 out of 24 in group E).No statistically significant difference was found between the two groups intermsofadverseevents.
None of the treatment emergent adverse events was severeenoughtowarrantwithdrawalfromthestudy.
The present study had some limitations like the treatment period was relatively short (8weeks). Due to time constraint escalation to higher doses was not possible. Though we all know that depression is sometimes self-limiting, in the present study it was not possibletoaddaplacebogroup.
In conclusion, the findings of this study indicates that milnacipran,at the dose of 50 mg/dayis an effective and safe antidepressant in comparison to escitalopram at the doseof10mg/dayinthepatientofMDD.
REFERENCES
1 Victor, Reus: part 16 neurologic disorders: 386 mental disorder Kasper, Braunwald, Fauci, Harrison’s Principles of Internal Medicine 17 th edition: McGraw-Hill Medical Publishing:2008:2716.
2 Xie F, Despiegel N, Danchenko N ,Hansen K — Cost effectiveness ana ysis o esc talopram compared to ven afaxine and f uvoxamine n treatment o major depressive disorder. International Journal of Psychiatry in Clinical Practice 2009;13:59-69.
3 Grover S, Dutt A , Avasthi A — An overview of Indian research in depression Indian journal of psychiatry 2010; 52:178-88.
4 Dinesh K Badya Prem P Khos a Ra inder S Deswal,Prithpal S Matreja — Safety and Efficacy of Duloxetine Versus Venlafaxine in Major Depression in Indian Patients JK Science Journal of Medical Education & Research:2006:8:95-199.
5 Burke WJ, Gergel I, Bose A — Fixed-dose trial of the single isomer SSRI escitalopram in depressed outpatients. J Clin Psychiatry 2002;63:331-6.
6 Wade A, Lemming OM, Hedegaard KB — Escitalopram 10mg/day is effective and well tolerated in a placebocontrolledstudy in depression in primary care. Int Clin Psychopharmacol 2002;17:95-102.
7 Stahl SM — SNRIs: Their Pharmacology, Clinical Efficacy, and Tolerability in Comparison with Other Classes of Antidepressants. CNS Spectrum 2005;10:732-47.
8 Puozzo C — Pharmacology and pharmacokinetics of milnacipran.Int.Clin. Psychopharmacol 2002;17:S25-S35.
9 Guelfi JD — A double-blind comparison of the efficacy and safety of milnacipran and fluoxetine in depressed inpatients. Int.Clin. Psychopharmacol 1998;13:121-8.
10 Sechter D — A comparative study of milnacipran and paroxetine in outpatients with major depression. J Affect Disord 2004;83:233-6.
11 DiagnosticandStatisticalManualofMentalDisorder,4thed. tex revision (DSM- V-TR) Wash ng on DC: AmericanPsychiatricAssociation,2000:356.
12 Hamilton M — Rating scale for depression. J Neurosur Psychiatry 1960;23:56–62.
13 Hamilton M — Development of a rating scale for primary depressiveillness.BrJSocClinPsychol1967;6:278–296.
14 Montgomery SA, Åsberg M — A new depression scale designed to be sensitive to change. Br J Psychiatry 1979; 134:382–9.
15 Khan A, Bose A, Alexopoulos G S, Gommoll C, Li D, Gandhi C — Double-Blind Comparison of Escitalopram and Duloxetine in the Acute Treatment of Major Depressive Disorder. Clin Drug Investig 2007;27:481-92.
16 Bielski R J,Ventura D ,Chang C — A Double-Blind Comparison of Escitalopram with Venlafaxine XR in the Treatment of Major Depressive Disorder. J Clin Psychiatry 2004;65:1190-6.
17 Lopez IJ, Guelfi JD, Pletan Y, Tournoux A, Prost JF — Milnacipran and selective serotonin reuptake inhibitors in majordepression. Int Clin Psychopharmacol 1996;11:41-6.
If you want to send your queries and receive the response on any subject from JIMA, please use the E-mail facility.
Practitioners' Series Practitioners' Series
To study the effects of hyperbaric oxygen therapy in chronic diabetic foot lesions
1 2 2
G R Ekbote , Sharad K Waje , Pankaj Bhalerao
To Study the effects of hyperbaric oxygen therapy in chronic diabetic foot lesions, a prospective controlled study was undertaken. Thirty diabetics with chronic foot lesions were randomized to study group (conventionalmanagementand40sessionsofhyperbaricoxygentherapy)andcontrolgroup(conventional management). The patients were assessed for average hospital stay, control of infection and wound healing. The control of infection spread was quicker. Positive cultures decreased from initial 19 to 3 in study group as against from 16 to 12 in the control group. (p < 0.05). This difference was most pronounced for Escherichia coli. Also, the need for major amputation wa significantly less in the study group (n= 20 as against the control group (n=7) (p< 0.05). The average hospital stay was not affected. We conclude that hyperbaric oxygen therapy can be safely used and is beneficial as an adjuvant therapy in chronic diabetic footlesions.
J Indian Med Assoc 2016; 114: 18-20]
Key words : Chronic diabetic foot lesions, amputations, Hyperbaric Oxygen (HBO) Hyperbaric oxygen therapy (HBOT), wound healing, complication of diabetic foot, infections in diabetic foot.
Diabetes mellitus is the most common of the serious metabolic disorders characterized by long-term complications involving eyes, kidneys, nerves 1-6 and blood vessels . Diabetic angiopathy leads to chronic foot lesions and has a higher risk of amputation than nondiabeticsduetopoorcontrolofinfection. Theemergence of hyperbaric oxygen therapy (HBOT) as an adjunct to therapyofdiabeticfootlesionshasitsbasisinthefactthat it can reduce anaerobic infection, can improve blood supply and can decrease ischaemic damage to nerves This prospective study was carried out to evaluate the effectofhyperbaricoxygenindiabeticfootlesionsandits useasanadjunctivemeasure.
MATERIALAND METHOD :
Thirtydiabeticswithchronicfootlesionswerestudied over a period of 2 years at our hospital. All patients were admitted. All patients received regular surgical treatment consisting incision and drainage of abscesses and debridementofwound. Locally,thewoundsweredressed with eusol (1.25% w/v boric acid and 1.25% w/v of bleaching powder) and / or povidone iodine. In those patientsinwhomthegangrene/infectionascendedabove theankle,amputationwasperformedtolimitthespreadof infection and resulting toxemia. Major amputation was definedas
anamputationdone,abovetheanklejoint. Allotherswere considered as minor amputations. Antibiotics were administered along with metronidazole. Antibiotics commonly used were cep
aminoglycosides and were changed according to sensitivity patterns. Diabetic control was achieved with insulin given subcutaneously. Two patients with diabetic ketoacidosis were initially treated with intravenous regularinsulin.
The patients were randomly allotted to one of the two groups. One received a complete course of HBOT as an adjunct to the above mentioned treatment (the study group) and the other group (control) received only conventional therapy The HBOT was given in a monoplace hyperbaric oxygen chamber at Sassoon General Hospital, Pune over a period of 8 weeks. The HBOT was administered at 3 atmospheres pressure for a period of 45 minutes at each sitting. The patient is slid completelyintothechamberandthechamberisconnected to the patient monitoring panel. Oxygen flow is started (flushing phase) for 2-3 minutes till high oxygen concentration is achieved. The chamber pressure is graduallyraisedto3atmosphericpressuresafterselecting closed circuit mode. After the therapy, the chamber pressureisgraduallyreducedtonormal.
TostudytheeffectsofHBOTthefollowingparameters were evaluated : (1) wound cultures-before and after each sitting (2) assessment of local wound daily In case of amputations, skin flaps were assessed. The other parametersstudiedwerehospitalstay,needforamputation
III
TO STUDYTHE EFFECTS OF HYPERBARIC OXYGEN THERAPY IN CHRONIC DIABETIC FOOT LESIONS — EKBOTE ET AL 19
andlevelofamputationifnecessary
Patients were also investigated with complete hemogram, liver and renal profile, X ray chest, ECG and serialbloodsugars. Urinesugarchartwasmaintainedasa guidetodailydiabeticcontrol.
The two groups were matched for age and sex as shown in (Table 1). The average hospital stay and amputation rates are depicted in (Table 2). The average hospital stay in the study group was less but this was statistically not significant. The need for major amputationinthestudygroupwassignificantlyless. The mode of wound healing is shown in (Table 3). The number of patients requiring skin grafts was higher in the study group as there was better local control of infection withHBOandlesseramputations. Theresults of pre and post procedural wound cultures are charted in Table-4. In the study group, there was a significant overall control of wound infections, especially of Pseudomonas and E.coli. Though there was reduction in the staphylococcal and anaerobic infections, it wascomparablewiththecontrolgroup. There werenocomplicationsrelatedtotheHBOT
DISCUSSION :
Table 1 — Clinical data of patients with diabetic foot
*Difference in the groups were not significant; IDDM : insulin dependent diabetes mellitus; NIDDM : non-insulin dependent diabetesmellitus
Table 2 — Hospital stay, types of amputations and their indications in patients with diabetic foot
Studygroup Controlgroup Significance Hospitalstay(days) Average
One of the most destructive complications ofdiabetesislossofalimb. Threefactorslead to tissue necrosis in the diabetic foot viz. neuropathy, infection and ischaemia. Peripheral ischaemia may also result from small vessel disease. However, it is unlikely that the microvascular 1 disease itself is responsible for foot ulcers. Anaerobic bacteriacoexistwithaerobicbacteriainmostofthecases IncreasedpartialpressureofoxygenintissueswithHBOT bypasses the specific oxygen making haemoglobin 9superfluous Whether HBOT is useful is diabetic foot lesionswherethemicrovasculardiseasecompromisesthe deliverysystemisnotknown.
Uncontrolleddiabetes n=0 n=5 gangrene n=1 n=1
AK:aboveknee,BKbelowknee,n=No.ofpatients
Table 3 — Data regarding wound healing in patients with diabetic foot
Studygroup(n) Controlgroup(n)
Skingraft 6 2
Stumphealing 5 6
Persistentinfection 1 3
n=No.ofpatients
In the present study, a reduction in hospital stay was found in patients receiving HBOT Though not statistically significant, it shows that aggressive medical and surgical management remains essential if the effects ofHBOaretoberealized Consequently,thisgrouphada higher rate of skin graftings, minor amputations and repeated debridements in the salvaged limb. The major effectofHBOwasseenasthesignificantlyreducedrateof major amputations in the study group. This is because HBO may have successfully achieved local control and prevented spread of the infection proximally Patients were therefore able to maintain a bipedal gait, with a greatly reduced morbidity The effect on bacteriology were rather surprising. Overall, HBO controlled the woundinfection.
Specifically Pseudomonas and Ecoli were eliminated betterthaninthecontrolswithconventionaltherapy
ThebeneficialeffectsofHBOmaybeexplainedonthe followinggrounds. HBOimprovesmicrovascularsupply by increasing the amount of oxygen so that gaseous diffusion can occur in relatively avascular or ischaemic 9areas Normal fibrobiast proliferation and collagen production requires a local oxygen tension level of 20-40 mmofHg.Raisingthisthresholdlevelto40-50mmofHg stimulates greater degree of neovascularisation which may favour definitive local healing. Oxygen is bactericidal to certain anaerobic or microaerophilic organisms because they lack the appropriate enzymes (superoxide dismutase and catalase) necessary to protect theminhighlyoxygenatedenvironments.
5 Barnes AJ, Dormandy TL, Dormandy JA, Slack J — Is hyperv sco y a treatab e component of diabe c
microcirculatorydisease. Lancet 1977;ii:789-91.
6 Peterson CM, Jones RL, Koenig BS, Melvin ET, Lehrman MD— Reversible hematological sequelae of diabetes. Ann Int Med 1977;86:425-9.
7 Olodart RM, Seitz CR — Effrect of hyperbaric oxygen on Gramnegativebacilli.ClinRes1964;12:37.
8 Louie TJ, Barlett JG, Tally FP, Gorbach SL — Aerobic and anaerobicbacteriaindiabeticfootulcers. Ann Int med 1976; 85:461-63.
9 Camporesi EM, Moon RE, Grande CM — Hyperbaric medicine: an integral part of trauma care. Crit Care Clin 1990;6:203-17.
Preliminary Report Preliminary Report
Malaria infection and ABO blood groups : a study conducted in the central Indian state of Madhya Pradesh
1 2
Sherly T D , G Vyas
Thisstudywasundertakentofindthepossiblecorrelationbetweenthefrequencyofmalariainfectionand ABO blood groups. Three hundred and fifty one malaria infected subjects were studied. Blood group A has been found to be most vulnerable to malaria infection. This finding corroborates with other studies which showedthe relativedisadvantageofbloodtypeAwhenitcametomalaria.
J Indian Med Assoc 2016; 114: 22-3]
Key words : Malaria,ABO blood group correlation.
There has been increasing evidence that ABO blood- group antigens play some significant role 1-9 in the aetiology and prognosis of malaria As malaria continues to be a big threat to public health safety, any knowledge of possible correlation between malaria infection and blood groups can be of great use in the diagnosisandtreatmentofmalaria.
The aim of this research was to examine the rate (frequency) of malaria infection among ABO blood groups.An effort has been made to find out the likelihood of different ABO blood types for infection by different plasmodium types.
MATERIALAND METHOD
The study included 351 malarial parasite positive patients who were treated for malarial infection at Ujjain Charitable Trust Hospital, Ujjain, and RD Gardi Medical College Hospital, Ujjain, from August 2008 to January 2010. The study population was a cross-section of the general population in and around the city of Ujjain, Madhya Pradesh, a low transmission malaria endemic region.
The data was collected by using a proforma. The collected data was analysed using correspondence analysis. The observed relations between different malarial infections andABO blood groups were tabulated and the statistical significance of each table was assessed andinterpreted.
Department of Medicine, Ujjain CharitableTrust Hospital and Research Centre,Ujjain456006
MBBS,DNBFinalYearResident MD, FICP, FICA, FRIPHH, Professor of Medicine, RD Gardi MedicalCollege,Ujjain456006
sidered as complicated malaria, with severe anaemia (Hb <5 g/dl), jaundice (serum bilirubin >3 mg/dl) and hypoglycaemia (blood glucose < 40 mg/dl). Of these 14 cases, blood groupAaccounted for 7 cases (50%). Blood groups B and O claimed 3 (21.43%) and 4 cases (28.57%) respectively.Among 337 cases of uncomplicated malaria, there were 33 incidents of mild (Hb <10 g/dl) to moderate (Hb<8 g/dl) anaemia. Blood groupAconstituted 20 such cases (60.61%), leaving only 8 to group B (24.24%), 4 to groupO(12.12%),and1togroupAB(3.03%).
DISCUSSION
The available statistics suggest that the most common blood groups in India are O (37%) and B (33%), with O havingpredominanceinthesouth(38%)andBinthenorth 10,1(37%) Inprevalence,OandBarefollowedbyA(22%).
OBSERVATIONS
Regarding malaria infection and ABO blood types in general, the present research found that (1) blood groupA wasmoresusceptibletomalariainfectionthanotherblood groups and (2) that the rate of susceptibility to malaria infection for people of blood groups B, O and AB was more or less equal. Out of the total 351 subjects, 144 belonged to blood group A (41.03%). Group A was followed by group B and group O, accounting for 103 (29.35%) and 87 subjects (24.78%)respectively. Seventeen subjects had AB blood type, making only 4.84%ofthetotalnumber
On the frequency of plasmodium types in the study population, it was noticed that blood groupAranked high in both P falciparum and P vivax infections, although blood group B rated slightly higher for P falciparum, if mixed infections were excluded. Among 19 unmixed P falciparum subjects, 7 belonged to groupA(36.84%) and 9 to group B (47.37%). Group O claimed 2 subjects (10.53%)andgroupAB,1(5.26%).
The vast majority of the study subjects were infected with P vivax (93.16%). This is to say, 327 subjects out of 351had P vivax infection.Ofthese327vivaxsubjects,133 were of groupA(40.67%), 93 of group B (28.44%), 85 of groupO(26%),and16ofgroupAB(4.89%).
It was also noticed that blood group A topped in the likelihoodofmixedinfectionaswell.Of5mixedinfection cases,4weregroupA(80%)and1wasgroupB(20%).
Coming to complications associated with malaria, the present research showed that blood group A had higher frequency of complicated malaria. Out of the total 351cases,therewere14cases(3.99%)thatmaybecon
TheleastcommonbloodgroupisAB(7%).Goingbythese statistics, the overall distribution ofA, B, O andAB blood groupsinUjjain(theplaceofthisresearch)wouldmoreor lessbe,22%,37%,34%,and7%respectively
Inthisstudy,however,thepeoplewithtypeAbloodare the largest group affected by malaria infection (41.03%).
In other words, while blood groupAmade up only 22% of the general population, it accounted for more than 41% of the study subjects. Blood group A topped in both P falciparum and P vivax infections. GroupAaccounted for 40.67% of P vivax infections. If mixed infections were included as well, the rate of P falciparum infection for blood type A rose to 45.83%. It was also found that the likelihoodofmixedinfectionishighforbloodgroupA.All these show that blood group A is more susceptible to malaria infection than other blood groups. This finding agrees with some earlier studies which have found blood type A to be more predisposed than other groups to 4-6,12 malarial infection Maybe, antigen A works as a coreceptorformalarialinfection.
WithregardtobloodgroupO,thisstudy’sfindingsare at variance with earlier studies. It has been suggested by several studies that blood group O is fairly resistant to 1-6,8,12 severe malaria, due to reduced RBC rosetting This relativeadvantagewhichbloodgroupOenjoysisthemost significant finding so far in the study of malaria and blood group correlation. In the present study, however, this advantageofbloodtypeOcouldnotbeconfirmed. Itwas found that blood group O, like blood group A, has higher frequency of complicated malaria. But it should be noted
that there were only 14 cases of complicated malaria among351subjectsunderstudy Noreliableinferencecan be drawn from the observation of such a small number of samples.
ACKNOWLEDGMENT
Sherly TD would like to thank Dr G Vyas, Dr JP Bhagwat, Dr VK Sharma, and Dr BL Bamboria for their helpwiththisresearch.
REFERENCES
1 Car son J, Wah gren M Plasmod um falc parum erythrocyte rosetting is mediated by promiscuous lectin like interactions. J Exp Med 1992;176:1311-7.
2 Udomsangpetch R, Todd J, Carlson J, Greenwood BM — The effects of hemoglobin genotype and ABO blood group on the formation of rosettes by Plasmodium falciparum infected red blood cells. Am J Trop Med Hyg 1993; 48: 14953.
3 Rowe A, Obeiro J, Newbold CI, Marsh K — Plasmodium falciparum rosetting is associated with malaria severity in Kenya. Infect Immun 1995;63:2323-6.
4 Fischer PR, Boone P — Short report: severe malaria associated with blood group. Am J Trop Med Hyg 1998; 58 122-3.
5 Barragan A, Kremsner PG, Wahlgren M, Carlson J — Blood group A antigen is a coreceptor in Plasmodium falciparum rosetting. Infect Immun 2000;68:2971-5.
6 Rowe JA, Handel IG, Thera MA, Deans AM, Lyke KE, Koné A, et al — Blood group O protects against severe Plasmodium falciparum malaria through the mechanism of reducedrosetting. Proc Natl Acad Sci 2007;104:17471-6.
7 Uneke CJ — Plasmodium falciparum malaria and ABO blood group: is there any relationship? Parasitol Res 2007; 100:759-65.
8 RoweJA,OpiDH,WilliamsTN—Bloodgroupsandmalaria: fresh insights into pathogenesis and identification of targets forintervention. Curr Opin Hematol 2009;16:480.
9 DeepaM,AlwarVA,RameshkumarK,RossC—ABOblood groups and malaria related clinical outcome. J Vector Dis 2011;48:7-11.
10 Nanu A, Thapliyal RM — Blood group gene frequency in a selected north Indian population. Indian J Med Res 1997; 106:242-6.
11 KumarH,MishraDK,SarkarRS,JaiprakashM—Difficulties in immunohaematology: the weak D antigen. Med J Armed Forcees India 2005;6:348-50.
12 Cserti CM, Dzik WH — The ABO blood group system and Plasmodium falciparum malaria. Blood 2007;110 2250-8.
MALARIAINFECTIONANDABO BLOOD GROUPS — SHERLYAND VYAS 23
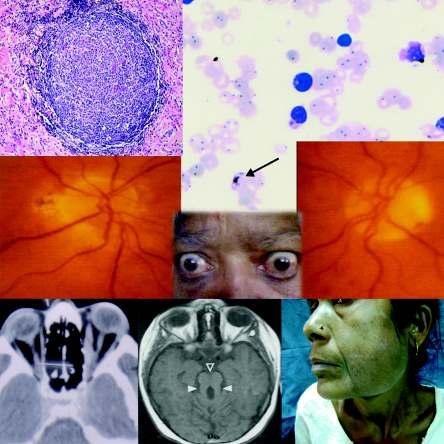
Current and future trends in the management of thyroid associated ophthalmopathy
1 2
Garima Agrawal , D C Mehta
Thyroid associated ophthalmopathy is common in patients with thyroid dysfunction. The present articlereviewsthecurrentandfutureconceptsinthemanagementofthyroidassociatedophthalmopathy. ManyoftheguidelinesinthepresentarticlearebasedontheconsensusstatementoftheEuropeanGroup onGrave’sOrbitopathy.
The present article was written after reviewing the articles on the net and journals as mentioned in the references.
J Indian Med Assoc 2016;114: 24-7]
Key words : Thyroid associated ophthalmopathy, management.
Ocular involvement is common in patients with thyroid disease. In these patients the status of the thyroid is variable. The majority are hyperthyroid, some are hypothyroid while a few are euthyroid.In many it may be difficult to demonstrate any thyroid abnormality at all. Thus the management of the thyroid dysfunction and the threat to vision requires close co-operation between the 1 ophthalmologist and the physician/endocrinologist.The presentarticle reviewsthecurrentandfuturetrendsinthe managementofthyroidassociatedophthalmopathy
Thepresentarticlewaswrittenafterreviewingarticles on the internet and the journals as mentioned in the references.Itwaskeptinmindtoincludetherecentstudies and updates on the subject .The authors experience in treating patients of Thyroid associated ophthalmopathy (TAO)intheclinicswasinvaluableinwritingthearticle.
Pathogenesis :
TAO is initiated by autoreactiveTcells that react with one or more antigens shared by the thyroid and the orbit.These T lymphocytes after reaching the orbit react with the shared auto-antigen and trigger a cascade of events.There is secretion of cytokines which cause proliferation of fibroblasts, expansion of adipose tissue andsecretionofhydrophilicglycosaminoglycansfromthe fibroblasts.There is a resultant increase in orbital content 1,2 whichexplainsmanyfeaturesoftheophthalmopathy
Those individuals younger than forty years are considerablymore likely to manifest orbital fat expansion related proptosis in the absence of muscle infiltration,
M & J Institute of Ophthalmology, BJ Medical College, Ahmedabad 380016
The shared auto-antigen may be the thyrotropin receptorortheinsulinlikegrowthfactor1receptor
B cells act as antigen presenting cells and autoantibodyproducingcells.
Genetic factors in Graves' ophthalmopathy remain poorly understood.Environmental factors play a major role in the development and progression of the ophthalmopathy These include smoking as an important riskfactor Microbial infectionshavealsobeenpostulated asariskfactor
Clinical Features
:
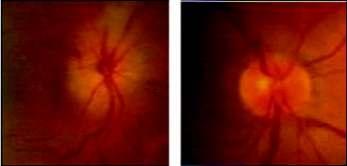
The clinical features include lid retraction lid lag,proptosis, extra-ocular muscle involvement, optic neuropathy,conjunctivalcongestionandchemosis(Fig1).
The natural course of thyroid ophthalmopathy is variable.Usuallythereisanactivephasethatlastsforonetwo years followed by a plateau phase when the disease becomesstableandfinallytheinactivephasewhenthereis 1 remission.Theremissionisgenerallyincomplete
Diagnosis and Investigations
:
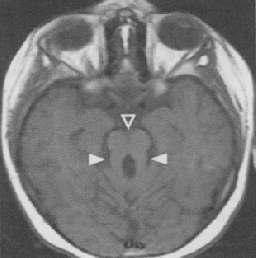
The diagnosis is certain in patients with bilateral ophthalmopathy and thyroid dysfunction Thyroid dysfunction is evident by serum levels ofT3,T4 andTSH. In those with doubt orbital imaging and measurement of thyrotropin receptor antibodies is warranted. Presence of high levels of serum thyrotropin receptor antibodies are highly specific and sensitive for thyroid associated ophthalmopathy Orbital imaging with CT scan or MRI willrevealenlargementoftheextra-ocularmuscleswith
dons and an increase in fibro-adipose
sparing of the ten tissue (Fig 2). In patients with optic neuropathy there may be compression of the optic nerve by the enlarged extraocularmusclesespeciallyattheapex(apicalcrowding)
Activity and Staging :
The clinical activity score helps in classifying TAO as active or inactive Components of the clinical activity score are spontaneous retrobulbar pain,painwitheyemovement,redness of the eyelids, redness of the conjunctiva, swelling of the eyelids, swelling of the caruncle, conjunctival oedema (chemosis). Each component isgivenascoreof1.Atotalscoreof0-2 indicates inactive throid associated ophthalmopathy while a score from 37 indicates active Graves' ophthalmopathy
Patients with active disease will show a good response to immunosuppressive therapy while those with inactivediseasewillnot.
In addition TAO has been classified as mild, moderate or severe 5 (Table 1) Dysthyroid optic neuropathy and keratopathy both indicate that the ophthamopathy is sightthreateningandshouldbetreated immediately.
Treatment :
Thyroid dysfunction should be corrected in all patients Thyroid dysfunction may be treated with antithyroid drugs or with radio-iodine therapy In randomised trials, radioiodine t
Another method of classification developed in Vancouver is the VISA classification This is a clinical recording form which separates the clinical features of thyroid ophthalmopathy into the following four p
; I (inflammation,congestion); S (strabismus motility restriction); A (appearance, exposure). International ThyroidEyeDiseaseSocietyhasmodifiedtheserecording forms by consensus of its members and adopted them as theirstandardisedofficerecord
Table 1 — Showing Features of Mild and Moderate to Severe 5,6 Graves’ Ophthalmopathy
*Intermittent diplopia occurs when the patient is fatigued or awakening in the morning. Inconstant diplopia occurs at extremes of gaze.Constant diplopia occurs both when the patient is looking straightaheadandwhenthepatientislookingdown
hyperthyroidism caused progression of ophthalmopathy in about 15% of patients, whereas antithyroid drugs did not modify the natural course of G
Prophylactic treatment with glucocorticoid agents may be appropriate for many patients with Graves’ ophthalmopathy whose hyperthyroidism has been treated with radio-iodine therapy especially those withhighriskfactors.Riskfactorsfor progression of Graves’ ophthalmopathy after radio-iodine therapy include cigarette smoking, severe hyperthyroidism (serum triiodothyronineconcentration,>5nmol per liter), high levels of thyrotropinreceptor antibodies, and uncontrolled hypothyroidism after radio-iodine therapy.
Anyriskfactorfortheprogressionofophthalmopathy if present should be controlled. Smoking (if present) should be stopped.Any concurrent infections should be treated The treatment of ophthalmopathy includes supportive treatment, glucocorticoids, other immunosuppressiveagents,orbitalradiotherapy surgery. Supportive therapy : This includes lubrication with topical tear supplements and non-steroidal antiinflammatorydrugs,darkglassesandtapingoftheeyelids at night to reduce the symptoms of dry eye. Prism glasses are used for the correction of diplopia Mild ophthalmopathymaybetreatedwithlocalmeasuresalone with follow-up every 3 to 6 months as there is a 25% chanceofitprogressingtomoderatetoseveregrade
Glucocorticoids : Vision threatening optic neuropathy requires treatment with glucocorticoids.The usual regimen is to give methylprednisolone in a dose of one gram intravenously for initial three days.This is followed by oral corticosteroids If there is no improvement after one to two weeks the patient should 5,6 undergopromptsurgicaldecompression
Fig 2 — CECT Scan (Axial Section) Showing Exophthalmos and Enlarged Medial Rectus and Inferior Rectus Muscles
Fig 1 — Showing Bilateral Exophthalmos and Marked Retraction of the Upper Eyelid CURRENT
Moderate to severe and active ophthalmopathy also requires treatment with glucocorticoids The recommended regimen consists of twelve weekly infusionsofmethylprednisolonewithacumulativedoseof 4.5 grams (500mg weekly for 6 weeks, then 250 mg weeklyfor6weeks) Intravenoustherapyshouldbegiven only with close monitoring (specially of liver function) in 8 specialisedcentres Tominimisetheriskofhepatotoxicity 5,6,9 courses exceeding 8 grams are not recommended . Rare casesofsevereandacuteliverdamagehavebeenreported 10-12 withtheuseofhighdosesofintravenoussteroids
High dose oral glucocorticoids in a dose of 40mg or higherinitiallyfollowedbytaperinguntilwithdrawalafter 4-6 months are also used. They are a reasonable option in patientswithliver disease
Patients should be closely monitored for other potential aspects of glucocoticoid therapy as high blood pressure, hyperglycaemia,gastric side-effects,infection 1 andelectrolyteabnormalities.
Two randomised controlled trials have shown that intravenous therapy has a higher rate of favourable response as compared to oral therapy.Intravenous therapy is also well tolerated with reduced risk of development of cushingoid features.However a close watch on liver 1 functionsasmentionedaboveismandatory
Orbital radiotherapy : Orbital irradiation may be used as an additional therapy.It has been found to be beneficial particularly when eye motility is impaired though it has been observed that patients with certain features, including exophthalmos, eyelid retraction, and soft-tissue changes, tend to have a poor response to 13treatment Radiation is given in ten sessions over a two weeks period with a total cumulative dose of 10-20 Gy. It should be avoided in patients with diabetic retinopathy or severe hypertension (as may cause retinal damage)and in patients younger than 35 years of age (due to long term 5,6 potentialcarcinogeniceffects) Combinedtreatmentwith glucocorticoids and radiotherapy has been found to be more effective than either treatment alone as suggested by datafromrandomisedtrials
Surgery : Orbital decompression surgery is required for sight threatening optic neuropathy and for sight threatening exposure keratopathy.Orbital decompression is indicated in sight threatening optic neuropathy if high dose glucocorticoids do not result in improvement in one 5,6 totwoweeks
It is also indicated in vision threatening exposure keratopathy which does not improve with supportive 5,6measures
Cosmetic surgery for Graves ophthalmopathy should be performed after the disease has been consistently inactive for at least six months.Here the order to be followedisorbitaldecompression followedbystrabismus 5,6 surgeryfollowedbyeyelidsurgery
Other immunosupressive agents : Steroid sparing agentssuchasazathioprine,50-150mg/dayorcyclosporin A, 5-7 mg/kg for 4-12 months may be used in the treatment of cases with persistent diplopia despite steroid therapyorthoseintoleranttosteroids
Recent Advances And Future Trends
:
Rituximab is an anti CD20 monoclonal antibody that induces transient B cell depletion that modifies the active inflammatory course of thyroid associated 14,15 14 ophthalmopathy In an open label study Mario et al found that rituximab significantly decreased proptosis andinflammationinpatientswithactiveTAO.
Etanercept is an inhibitor of tumour necrosis factor. 16 Paridaens et al in a pilot study found etanercept to decrease inflammation and the clinical signs of Graves ophthalmopathy
:
The management of thyroid ophthalmopathy requires a multidisciplinary approach involving the ophthalmologist and the endocrinologist. The above review gives the current recommendations in the managementofthisdiseaselargelybasedontheconsensus statement of the European Group on Graves’Orbitopathy 5,6 (EUGOGO) on management of Graves ophthalmopathy. Newer drugs as rituximab and TNF inhibitors await randomised controlled trials. They may well open a new paradigm in the management of this complex disorder in thenearfuture.
REFERENCES
1 LuigiB,LauraTM—Grave’sophthalmopathy. N Engl J Med 2009;360:994-1001.
2 Bednarczuk T, Hiromatsu Y, Inoue Y, Yamamoto K, Wall JR, Nauman J — T-cell mediated immunity in thyroid associatedophthalmopathy. Thyroid 2002;12:209-15.
3 PrabhakarBS,BahnRS,SmithTJ—Currentperspectiveon the pathogenesis of Graves’ disease and ophthalmopathy. Endocr Rev 2003;24:802-35.
4 Mourits MP, Prummel MF, Wiersinga WM, Koornneef L — Clinical activity score as a guide in the management of patients with Graves’ ophthalmopathy. Clin Endocrinol 1997;47:9-14.
5 Bartalena L, Baldeschi L, Dickinson A — Consensus statement of the European Group on Graves’ Orbitopathy (EUGOGO) on management of Graves' ophthalmopathy. Eur J Endocrinol 2008;158:273-85.
6 Bartalena L, Baldeschi L, Dickinson A — Consensus statement of the European Group on Graves’ Orbitopathy (EUGOGO)onmanagementofGraves’orbitopathy. Thyroid 2008;18:333-46.
7 Dolman PJ, Rootman J – VISA classification for Graves orbitopathy. Ophthal Plast Reconstr Surg 2006;22:319-24.
8 Kahaly GJ, Pitz S, Hommel G, Dittmar M — Randomized, single blind trial of intravenous versus oral steroid monotherapy in Graves’ orbitopathy. J Clin Endocr Metab 2005;90:5234-40.
9 Van Gees RJ Sasim IV Koppeschaar HPF Methy predn so one pulse herapy for pat en s with moderately severe Graves’ orbitopathy: a prospective, randomized, placebo-controlled study. Eur J Endocrinol 2008;158:229-37.
10 Marinó M, Morabito E, Brunetto MR, Bartalena L, Pinchera A, Marcocci C — Acute and severe liver damage associated with intravenous glucocorticoid pulse therapy in patients withGraves’ophthalmopathy. Thyroid 2004;14:403-6.
11 LeMoliR,Baldeschi L,SaeedP,Regenburg N,MouritsMP, Wiersinga WM — Determinants of liver damage associated with intravenous methylprednisolone pulse therapy in Graves’ophthalmopathy. Thyroid 2007;17:357-62.
12 Weissel M, Hauff W — Fatal liver failure after high-dose glucocorticoid pulse therapy in a patient with severe eye disease. Thyroid 2000;10:521.
13 Bradley EA, Gower EW, Bradley DJ — Orbital radiation for Graves ophthalmopathy: a report by the American Academy ofOphthalmology. Ophthalmology 2008;115:398-409.
14 Salvi M, Vannucchi G, Campi — Treatment of Graves’ disease and associated ophthalmopathy with the anti-CD20 monoclonal antibody rituximab: an open study. Eur J Endocrinol 2007;156:33-40.
15 El Fassi D, Nielsen HC, Hasselbalch HC, Hegedüs L — Treatmentresistant,severe,activeGraves’ophthalmopathy successfully treated with B lymphocyte depletion. Thyroid 2006;16:709-10.
16 ParidaensD,vandenBoschWA,vanderLoosTL,Krenning EP, van Hagen PM — The effect of etanercept on Graves’ ophthalmopathy:apilotstudy. Eye 2005;19:1286-9.
ARARE CASE OF KIMURA’S DISEASE OF CHEEK — MISHRA AND JOSHI 29
A rare case of Kimura’s disease of cheek
Mukesh Mishra, Sandhya Joshi
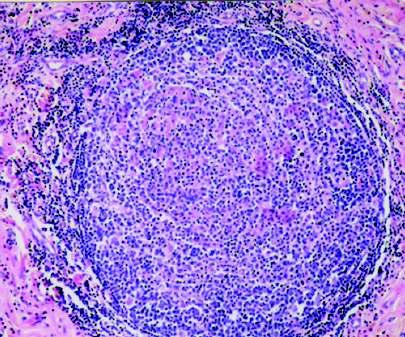
Kimura’s disease is a rare benign chronic inflammatory disorder of unknown cause that mostly presents as painless unilateral cervical lymphadenopathy or solitary/multiple masses in the head –neck region. Here, a case of swelling in cheek, anterior to parotid gland which was later found to be due to Kimura’sdiseasehasbeendescribed.
[J Indian Med Assoc 2016; 114: 28-9]
Key words : Kimura, eosinophilia, angiolymphoid hyperplasia, lymphadenopathy.
ThefirstreportofKimura'sdisease(KD)wasfromChina in1937,inwhichKimmandSzeto described7cases of a condition they termed “eosinophilic hyperplastic lymphogranuloma”. The disorder received its current name in 1948, when Kimura et al noted the vascular component and referred to it as an “unusual granulation combined with hyperplasticchangesinlymphoidtissue”.
The disease is endemic in Asia especially in China and Japan.ThereisamalepredominancewithaM/Fratioof3.5:1to 9:1inmostseriesreported.
Kimura’s disease involves the skin, lymph nodes and salivary glands in the head –neck area and is reported to be associatedwithnephriticsyndromeinapproximately15-19%of cases.
CASE REPORT
A 47-year-old female, a native of Nepal, presented in ENT OPD at General Hospital, Dahod with a painless, slow growing left sided cheek swelling for 3 years.She complained of occasional itching over the lesion with disfigurement of the cheek.
Examination — The swelling was ill-defined with no definite margins, non-tender immobile, soft to firm in consistency in the subcutaneous plane anterior to the parotid region (Fig 1). Skin over the swelling was mildly darkened in colour Clenching of the teeth would slightly demarcate the swelling which was not fixed to the underlying muscle. Comparedtotheright sideofthecheektherewasfullnessonthe left side. Intra-orally the mucosa was normal. No neck lymphadenopathy was noted. No other abnormality was detected.
Investigations — Routine blood investigations revealed eosinophilia. A provisional diagnosis of soft tissur tumour was made.The patient was prepared for general anaesthesia and excisionoftheswellingwasplannedbyexternalroute.
Treatment — A8 cm long skin incision was made over the swelling at the level of an imaginary line connecting tragus
DepartmentofENT GovernmentGeneralHospital,Dahod389151 MS(ENT),ConsultantENTSurgeon MD (Anaesthesiol), Consultant Anaesthetist, Department of Anaesthesiology
1 — Showing an Ill-Defined SwellingAuterior to the Parotid Region
to oral
commisure.Asubcutaneousyellowish-brownswellingof
size 5x4x1 cm approximately with irregular margins was exposed,overlyingbutadherenttomuscleand theparotidtissue. After careful dissection from the Wharton's duct, the lesion was excised in toto. Haemostasis was achieved. Wound was closed with a small drain which was removed on the 2nd postoperative day Pressuredressingwasapplied.Nopostoperativefacialnerve paresis was noted. The patient was put on tab cetirizine 10 mg oncedaily
Histopathology — Histopathological study of the specimen showed extensive sclerotic areas punctuated by lymphoid follicles and alarmingly large number of eosinophils even forming micro-abscesses.This picture is classical of KD (Fig 2, H&Ex20).
Follow-up Follow-upwasdoneafter2 and6months.No recurrence of swelling was seen and fullness over the cheek had subsided.
DISCUSSION
The aetiology of this chronic disease is unknown. An
immune reaction to an
aberrant unknown antigenic stimulus has been suggested, perhaps implicating a role for Candida albicans, but no formal demonstration has been made to date. It can be suggested that prolonged immunologic stimulation can lead to clonal lympho d proliferation in occasional cases. Mast cells, a major source of interleukin 4 and 5, might play an important role in the pathogenesis of Kimura’s disease, by regulating IgE synthesis and orchestrating eosinophilicinfiltration.
However measurements of IgE levels were not done in this case.
Other mechanisms postulated aretraumaandpersistentparasitic antigenicstimulation.
The onset of KD is insidious and lesions are benign, following an indo ent course, gradually increasing in size over years. The prognosis is good and no malignant transformationhasbeenreported.
Diagnosis of KD is frequently difficult A biopsy and/or excision of the involved lymph node or the lesion itself is required for definitive histopathological diagnosis, and is often therapeutic as well. The histopathological picture is same regardless of the site involved and is characterised by lymphoid follicles formation with prominent germinal centres, infiltration of eosinophils, sometimes forming micro-abscesses, fibrosis, increased postcapillary venules and vascular proliferation. Vessels remain thin-walled with cuboidal endothelial cells. Polykaryotic giant cells of the Warthin-Finkeldey type are a common feature. The role of fine needle aspiration cytology (FNAC)isforthediagnosisofrecurrentlesions.
Clinical differential diagnosis for KD include reactive lymphadenopathy, lymphoma, salivary gland tumour, nodal metastasis (breast, colorectal and nasopharyngeal cancer), lymphangioma,haemangiomaandMikulicz’sdisease.
Although not diagnostic, CT and MRI can help in distinguishing Kimura’s disease from other conditions and delineatingtheextentofdisease.
The treatment of Kimura’s disease is problematic. Surgical excision has been found to be curative although recurrence is
common. Localised initial regrowth can be managed with surgical excision, other therapeutic options include radiation in cases refractory to medical and surgical therapy systemic corticosteroids especially in frequent relapses or cases complicated with nephritic syndrome Cytotoxic agents, cyclosporineandpentoxyphyllinecanalsobeentried.
REFERENCES
1 Kimm HT, Szeto C Eosinoph ic hyperplast c lymphogranuloma,comparisonwithMikulicz'sdisease. Prof Chin Med Soc 1937;7:329.
2 Kimura T, Yoshimura S, Ishikawa E — On the unusual granulat on combined w th hyperplas ic changes of lymphatictissues. Trans Soc Pathol Jpn 1948;37:179-80.
3 LarrocheC,BletryO—Kimura’sdisease.GuillevinL,editor. O r p h a n e t E n c y c o p e d a , 2 0 0 5 www.orpha.net/data/patho/uk_kimura.pdf:1-3(access20).
4 Yuen HW, Gah YH, Low WK, Lim-Tan SK — Kimura’s disease: a diagnostic and therapeutic challenge. Singapore Med J 2005;46:179-83.
5 Kohli A, Singh G — Kimura’s disease. JK Science 2008; 10: 149-50.
Fig
Fig 2 — Microphotograph Showing Extensive ScleroticAreas Punetuated by Lymphoid Follicles and Large Number of Eosinophils
Joubert syndrome : a case report
1 2 3
P A Fazal Ghafoor , Sajeer K T , Jamaludheen C V
Here is reported a child with developmental delay, hypotonia during infancy, rotator nystagmus, dysarthriaandmentalretardationwhowasdiagnosedtohaveJoubertssyndromeat8yearsofage. [J Indian Med Assoc 2016; 114: 30 & 32]
Key words : Joubert syndrome, molar tooth sign, magnetic resonance imaging
Joubert syndrome (JS) is an autosoma recessive neurodevelopmental disorder, which is characterised by the molar tooth malformation (MTM), a complex brainstem malformation that reflects aplasia or marked hypoplasia of the cerebellar vermis, thickened and elongated superior cerebellar peduncles and a deepened interpeduncular fossa that is apparent on axial MRI at the midbrain–hindbrain junction Clinically, classic JS is associated with neonatal hypotonia (loss of muscle tone),ataxia,developmentaldelay mentalretardation,andoften neonatal apnoea/hyperpnoea (irregular breathing) and/or ocular motor apraxia (difficulties in initiating rapid horizontal eye 2,3 movements or saccades) Autistic features have also been 4,5 reportedasarelativelycommoncomponentofJS CASE REPORT
An 8-year-old malnourished girl with motor and mental retardationpresentedwiththecomplaintsofinabilitytofixgaze, failure to gain weight and weakness and ataxia. She was the first child of a first degree consanguineous marriage. There was no historyofsimilarillnessinthefamily Herpasthistorydisclosed developmentalretardation.
Examination Major retardation was seen involving the gross motor system. She was able to sit without support by the age of one year and she could walk a few steps by herself by the age of two. Speech could be understood clearly when she was 5 years old. She had been a hypotonic and hypo-active baby all throughout her childhood, and had nystagmus in the form of rotatory eye movements noticed by her parents since she was a few months old. She was born as a full term vaginally delivered child with a birth weight of about 2.5 kg. She had dysarthria, rotatorynystagmusandgaitataxia.
Investigations An Magnetic resonance imaging (MRI) brain study was done which revealed vermian agenesis. Isthmus was hypoplastic together with thickening and elongation of the superior cerebellar peduncles giving “molar tooth” appearance (Fig1).Also,theshapeofthe4thventriclehadbeenchangedinto
MD (Gen Med), DM (Neurology), Associate Professor and ConsultantNeurologist MD(GenMed),AssistantProfessor MBBS,DHSc(PublicHealth),MHSc(PublicHealth),Registrar
what may be described as “bat wing appearance.” Size of the posterior fossa was normal with cerebrospinal fluid filling the ventricular space All these findings suggested Joubert syndrome.
DISCUSSION
Joubert syndrome was first identified by pioneering paediatric neurologist Marie Joubert and associates in 1969 in four siblings and one sporadic case that exhibited episodic hyperpnoea, abnormal eye movements, ataxia and mental retardation with agenesis of cerebellar vermis and dilatation of fourth ventricle in typical batwings configuration Approximately 10% of individuals with Joubert syndrome have abnormalcollectionsofcerebrospinalfluidinthefourthventricle ortheposteriorfossathatresembleDandy-Walkermalformation. Worldwide around 200 cases of Jouberts' syndrome have been reported. In the syndrome midline structures of the brain stem have both anatomic and functional defects. Neuropathological studies reveal agenesis of the cerebellar vermis, malformation of several brainstem nuclei and dysplasia of structures at the pontomesencephalic junction. Extensive brain stem malformation couldexplaintheoculomotorapraxiaandhyperpnoea;anomalies ofgracilienucleiandsolitarytractarethoughttocontributetothe abnormal respiratory pattern The eye abnormalities observed in this disease usually wane off with age. The eye abnormalities observed in this disease include complete oculomotor apraxia in horizontal and vertical directions and ocular coloboma. Hypotonia and mental retardation are non-variable features of Joubert syndrome. Long term follow-up of the children with this disease reveals majority having severe mental and motor developmental impairments. Inheritance of this disease is said to be autosomal recessive. Recent studies have shown that it is a genetically heterogeneous disorder with one locus pointing to chromosome9q
The striking structural defects of Joubert syndrome in imaging studies are dysgenesis of the isthmus (part of the brainstem between pons and inferior colliculus) which is seen as elongation and thinning of ponto-mesencephalic junction, and deep interpeduncular fossa; thickening of superior cerebellar peduncles;hypoplasiaofthevermischaracterisedbyincomplete lobulation and enlarged fourth ventricles; incomplete fusion of the halves of the vermis creating a sagittal cleft seen on coronal MRI planes. Combinations of the first three features produce the characteristic“molartoothsign”
(Continued on page 32)
Case Note Case Note
A rare case of leukaemoid reaction in Plasmodium falciparum infection : a case report
Haematological presentation of malaria is usually in the form of leucopaenia along with increased number of monocytes and macrophages. Rarely, cases have been reported in which initial presentation of malaria is in the form of leukaemoid reaction. No cases have been found on websearch from Indian subcontinent.Becauseoftheapparentrarityofleukaemoidreactionin Plasmodium falciparum infection,the followingcasehasbeenreported. [J Indian Med Assoc 2016;114: 31-2]
Key words : Leukaemoid reaction, malaria, Plasmodium falciparum.
Themajorityofmalariapatientsatpresentationhavetotal white blood cell (WBC) count in the normal range.
Leucopaenia (WBC count < 4 × 10/l) may affect up to 15% of patients. Rateofleucocytosis(WBCcount>10×10/l)inadults range between 1 and 7%. Reportedly, malaria induced changes in the differential white cell count include neutropaenia, neutrophilia, immature neutrophils(leftshift),neutrophiltoxicgranulation, lymphopaenia, lymphocytosis, atypical lymphocytes, monocytosis, eosinopaenia, posttreatment eosinophilia and leukaemoid reactions. The underlying mechanisms include a shift in neutrophils from the circulatory to the marginal pool to sites of inflammation, splenic localisation, serum lymphotoxic factors and intercurrent bacterialinfections
Irving et al reported a case of a 4-year-old patient with Plasmodium falciparum infection.The blood picture was that of a leukaemoid reaction withsevereanaemiaandhightotalleucocytecount.
Similar cases were reported by Soe et al and CaptainJames et al
Because of the difficulties of diagnosis posed by a leukaemoid picture in malaria and the rarity of thisfinding,thiscasehasbeenreported.Itispossible that the increased haemolysis and the attending anaemia are responsible in certain cases for sufficient bone marrow stimulationtocausethischange
CASE REPORT
hepatosplenomegaly, both two fingers below the respective costalmargins.
Investigations — Peripheral smear and bone marrow aspiration was done. Total leucocyte count was 19,600
A10-month-old female child presented with fever with chill andrigoursincetwodaysandprogressivelyincreasingpallor.
Examination The patient was anaemic and had
DepartmentofPathology CSMMedicalUniversity,Lucknow226003 MD(Pathol),Professor MD(Pathol),AssistantProfessor MD(Microbiol),ProfessorofMicrobiology MD (Microbiol), Professor and Head of the Department of Microbiology
cells/cmm. Differential count revealed 21% polymorphs, 63% lymphocytes and 4% cells of immature granulocyte series mainly myelocytes, 1% eosinophils and 11% monocytes. Platelet count was 84,000/cmm. Few nucleated red blood cells were also present. Plasmodium falciparum gametocyte and ring forms were present (Fig 1, Leishman stain, x 40). Haemoglobin was8g/dl.Reticulocytecountwasreduced.
Bonemarrowsmearswerecellularwithincreasednumberof lymphocytes(41%),majoritywithlarge‘activated’morphology Granulocytic precursors (40%) showed heavy toxic granules. Erythropoesis was normoblastic (19%). Megakaryocytes were present in normal number. Macrophages with phagocytosed brown pigment were seen in increased number Smears also showedpresenceof Plasmodium falciparum gametocyte.
Her liver function test showed increased billirubin, increasedaspartateandalaninetransferase.
Management and Follow-up — The patient was given injection artesunate 2.4 mg/kg body weight intravenously at diagnosis, then at 12 hours and 24 hours, then once a day for 24 hours. This was followed by artemisinin based combination therapy (ACT) consisting of artesunate and amodiaquine; 4 mg/kgbodyweightofartesunateand10mgbase/kgbodyweight of amodiaquine was given once a day for 3 days orally in tablet form.
Following treatment his peripheral smear was made at 6th day and 28th day after treatment and they showed complete disappearanceofparasites.
DISCUSSION
The blood stage of falciparum malaria may cause lifethreatening anaemia. The anaemia is typically normocytic and normochromic, with a notable absence of reticulocytes. Red blood cells are destroyed as parasites complete their growth cycle; although some parasites may be removed from erythrocytes as immature ring forms by phagocytic cells. Infected ery hrocytes may also be phagocytosed by macrophages following opsonisation by immunoglobulins and/orcomplementcomponents
Case Note
Haematologicalpresentationofmalariaisusuallyintheform of leucopaenia along with increased number of monocytes and macrophages. Rarely, cases have been reported in which initial presentation of malaria is in the form of leukaemoid reaction. Such cases pose difficulties in diagnosis. It is possible that the increased haemolysis and the attending anaemia are responsible in certain cases for sufficient bone marrow stimulation to cause thischange
REFERENCES
1 TaylorWR,WidjajaH,BasriH,OhrtC,TaufikT,TjitraE, et al
Changes in the total leukocyte and platelet counts in Papuan and non Papuan adults from northeast Papua infected with acute Plasmodium vivax or uncomplicated Plasmodium falciparum malaria. Malar J 2008;7:259.
2 Irving KG, Kemp E, Olivier BJ, Mendelow BV — Unusual presentation of malaria as a leukaemoid reaction a case report. S Afr Med J 1987;71:597-8.
3 Soe S, Tin S, Than S — Myeloid leukemoid reaction in malaria infection. Southeast Asian J Trop Med Public Health 1991;22:677-8.
4 JamesAR,GeorgeMR—LeukemoidReactionduetoMixed Malarial Infection. NewJersey. Medical Service, Tilton GeneralHospital,FortDix,1946:283-7.
Reticulocytopaenia has been observed in numerous clinical studies of malarial anaemia. This is due to an increased proportionoftheerythroidprognitorsintheG2phase Thrombocytopaenia is almost invariable in malaria and so may be helpful as a sensitive but non-specific marker of active infection. Increased removal of platelets may follow absorption ofimmunecomplexes.
(Continued from page 30)
on axial MRI or CT planes. Tecto cerebellar dysplasia and Dandy –Walker syndrome , two other situations which may be the source of confusion, also may accompany Joubert syndrome
REFERENCES
1 Maria BL, Hoang KB, Tusa RJ, Mancuso AA, Hamed LM, Quisling RG, et al — ‘Joubert syndrome’ revisited: key ocular motor signs with magnetic resonance imaging correlation. J Child Neurol 1997;12:423-30.
2 Joubert M, Andermann F — Familial agenesis of the cerebellar vermis: a syndrome of episodic hyperpnea, abnormal eye movements atax a and retardat on Neurology 1969;19:813-25.
3 Boltshauser E, Isler W — Joubert syndrome: episodic hyperpnea, abnormal eye movements, retardation and ataxia, associated with dysplasia of the cerebellar vermis. Neuropaediatrics 1977;8:57-66.
4 Maria BL, Boltshauser E, Palmer SC, Tran TX — Clinical features and revised d agnostic criteria n Joubert syndrome. J Child Neurol 1999;14:583-90.
5 Holroyd S, Reiss AL, Bryan RN — Autistic features in Joubert syndrome: a genetic disorder with agenesis of the cerebellarvermis. Biol Psychiat 1991;29:287-94.
6 JoubertM,EisenringJJ,RobbJP,AndermannF—“Familial agenesis of the cerebellar vermis: a syndrome of episodic hyperpnea abnorma eye movements, a axia, and retardation”. Neurology 1969;19:813-25.
5 Weatherall DJ, Miller LH, Baruch DI, Marsh K, Doumbo OK, Casals-Pascual C, et al — Malaria and the red cells. Hematology 2002;1:35-57.
Bilateral non-arteritic anterior ischemic optic neuropathy (NAION) — a case report
1 2
Asha R Prasad , S P Jakhanwal
Non-arteritic Anterior Ischemic Optic Neuropathy (NAION) is due to ischemia of the optic nerve head. This is one of the causes of blindness or seriously impaired vision among middle aged and elderly population.Ophthalmoscopicexaminationinactivestageshowsasectoraldiscswellingandperipapillary haemorrhage.
Wereportacaseofa50yearoldmalewhopresentedwithcomplaintsofsomeblurringofvisioninright eye.Fundusexaminationhadsimilarpictureasdescribedabove.Heunderwentthoroughocular,systemic and haematological evaluation after which he was diagnosed to be suffering from Non-arteritic AION. Nocturnal hypotension was diagnosed to be the cause for his condition. While on treatment with steroids hedevelopedsimilarpictureinhisfelloweye.Antimetaboliteswasthenaddedtohistreatmentregimeand continuedforsixmonthstillhisopticdiscswellingsubsidedanddiseaseprogressionwashalted.Though his central vision remained as 6/9 and 6/6 respectively, his visual field showed marked altitudinal defects. The patient was followed for two years. No further deterioration of vision was seen but his field of vision remainedimpaired.
[J Indian Med Assoc 2016; 114: 33-5]
Key words : Non-arteriticAnterior Ischemic Optic Neuropathy, optic nerve head.
Non-arteritic AION is characterised by visual loss associated with optic disc swelling and subsequently varying degrees of optic atrophy Sometimes flame shaped haemorrhage is seen on the swollen disc or nearby neuroretinal layer The incidence of AION is estimated to be 2.3 – 10.3 per 100.000 Nocturnal arterial hypotension is found to have an important role in producing Non arteritic AION and most patients experience visual disturbances immediately on waking up in the morning. Hypotension causes hypoperfusion of optic nervehead Thebloodsupplytotheanterior head of the optic nerve is mainly by the posterior cilliary arteries and it is these arteries which are affected thus producing ischemia of optic nerve head and causing nerveconductiondefects (Fig1).
We report a case who observed sudden visual disturbances in one eye on waking up in the morning, followed by a similar observation in the other eye just after a month and a half. After all necessary investigationshewasfinallydiagnosedtobe suffering from bilateral NAION due to nocturnalhypotension.
CASE REPORT
soonaftergettingupthismorning.Soonasheopenedhiseyes,he was momentarily only seeing scenes which had occurred the previous day, like his wife wearing a green sari and opening cupboard,which was a scenethathad occurredtheprevious day This was then followed by decrease in his clarity of vision in sameeye.
Fig 1 – Blood supply of the optic nerve head
9 Chance PF, Cavalier L, Satran D, Pellegrino, Koeing M, Dobyns WB — Clinical and genetic aspects of Joubert and relatedsyndromes. J Child Neurol 1999;14:660-6. Fig 1 — MRI of Brain Showing Molar Tooth Sign
A 50 year old man presented with blurring of vision in right eye since morning.Henarratedapeculiarsymptomwhichhehadobserved
8 Tusa RJ, Hove MT — Ocular and occulomotor signs in Joubertsyndrome. J Child Neurol 1999;14:621-7.
Department of Ophthalmology, Tata Main Hospital, Jharkhand 831001
MS (Ophthalmol), Specialist
MS (Ophthalmol), Head of the Department & Sr Specialist
He was not a known diabetic or hypertensive.The only drug patient was taking was Allopurinol because of hyperuricaemia. His blood pressure was 110/88mmHg. There was no past ocular history or relevant family history, but personal history revealed thathewasasmoker
On examination his visual acuity was 6/18 in Right eye (RE) and 6/6 in Left eye(LE). He had a slight brightness perception defect and an afferent papillary defect in right eye
Ophthalmoscopically there was blurring of right disc margin with single splinter hemorrhage in peripapillary region (Fig 2).
Humphrey’s visual field demonstrated marked peripheral field defect with visual field reduced to tubular vision in right eye whereas visual field in left eye was normal (Fig 3).Differential diagnosis was optic neuritis , multiple sclerosis, neuromyelitisoptica. MRI of the brain and orbits was normal. A diagnosis of optic neuritis was made and he was given Pulse Methyl prednisolone 250 mg four times a day for 4 days; followed by oral prednisolone 40mg per day for 14 days. Symptoms did not improve significantly but disc oedema subsided. A month and a half later patient started observing similardisturbanceinvisualacuityandclarityinlefteye.Similar sectoral disc oedema was seen in this eye also.Visual acuity was 6/9.Pupilsweresluggishlyreactingtolightinbotheyesandright eyenowshoweddiscpallor
On general examination there was no pallor or icterus or palpable lymph nodes. Pulse was 84/min regular and blood pressure was 120/78mm Hg. Examination of CVS, respiratory system and abdomen was normal. Thorough neurological
evaluation was done. There was no history or symptoms to suggest any cranial nerve involvement. There was no motor or sensory impairment or cognitive decline. Higher functions were normal. Motor system showed normal bulk and tone and grade 5 powers in all four limbs. Motor nerve conduction of median nerve, ulnar nerve, peroneal nerve, tibial nerve and fascial nerve werenormal. Abdominalreflexeswerepresentandplantarswas downgoing. Sensory system was normal. There were no cerebellar signs. Rhomberg’s test was normal. Skull and spine was normal. Visual Evoked Potential showed bilateral optic nervedysfunction.
Hematological reports showed Hb 18.2gm%, Platelet count 16700/cu mm. WBC differential – Neutrophils – 82%, Lymphocytes 15%, ESR 20mm at end of one hour.hr CSF examination showed sugar 63mg%, protein 26mg%, WBC – 4 lymph,RBCnormal.Faecesexaminationshowednoovaorcyst. MCV-81.8fl; MCH- 28.1pg; MCHC-34.3 g/dl; S creatinine 0.9mg%; TSH 2.30Uiu/ml; Fasting blood sugar 99mg%; Postprandial blood sugar 103mg%; Serum Sodium-140m mol /L; Serum Potassium 3.3m mol/L; Cholesterol 252mg% ; CRP 30.3ug/l , ANA was negative. A nonreactive fluorescent treponemalantibodyabsorptiontestandanormaltuberculinskin testwerepresent.
atherosclerosis where nocturnal hypotension may act as final insult leading to NAION . On both occasions our patient experienced symptoms on waking up in morning. He was found tohaveamarginallyhighcholesterollevelandhewas also a smoker which could have added to the hypoperfusion of nerve head by causing vasoconstriction. Patients with small disc have an anatomical predisposition for NAION as the Initial oedema compromises circulation producing further neuronal damage, but in our patient the disc appeared tobefairlynormalsizeandhewasemmetropic.
About 15% of patients experience NAION in the second eye. Involvement of second eye is sequential and never simultaneous and visual loss usually 10 stabilizes in few days Decompression trials have 11 beentriedtosalvagevisioninthefelloweye Thedisc swelling and hemorrhage ultimately resolves with residual optic atrophy Many of these patients are left legally blind. Unfortunately our patient was among themwhereofabilateralinvolvementwaspresentbut probably with our treatment some good functional visioncouldbesalvagedinbotheyes.
Hewasstarted Azathioprimtablet50mgper day soon after involvement of second eye, and adviced to check haemoglobin, total count and platelet count once monthly, while on Azathioprim, and to stop the medicine if Hb<8mg%; total count <4000/cu mm platelet count < 100,000/cu mm. Azathoprim and Prednisolone was continued for 6 months and steroid was gradually tapered off. Atorvastatin 10mgperdaywasgivenandhewasadvisedlow fat diet and low cholesterol diet. Disc oedema was seen to subside in 3 weeks. Both eyes showed disc pallor (Fig 4) though Visual acuity remained as 6/9. Improvement from initial loss of field of vision in right eye was seen and Humphrey’s visual field testing showed an altitudinal field defect in both eyes typical for NAION was seen (Fig 5). He was followed up till10yearsafterstoppingthemedicineandwas found to be stable. Because of the persisting inferior fields defects patient faced difficulty in walking reading and dressing up and was compelledforacompromisedlifestyle.
DISCUSSION
Non-arteritic AION usually occurs spontaneously and is known to occur following acute hypotension Sevilla et al reported cases of NAION secondary to hypotension episodes related to hemodialysis, rapid correction of mal gnant hypertension and systemic hypovolaemia.Chronic hypoperfusion of small end arterial blood vessels, that is the posterior ciliary vessels that supply the optic nerve head, may occur in blood loss during surgical 6,7 procedures and can predispose to NAION It hasbeenhypothesizedthatifanopticnervehead has been rendered vulnerable to ischemia by various predisposing factors such as aging, hypertension,diabetes,hypercholesterolaemia,
4 Sevilla K, Groggel G — Anterior ischemic optic neuropathy as a complication of hemodialysis. Am J Kidney Dis 1986; 8: 61-636
NAION produces an ischemic insult in the nerve head which inturn leads to release of vascular endothelial growth factor (VEGF). This causes rapid and reversible increase in vascular permeability and vasogenicedema of the affected nerve head. This edema cause compression and infarction of previously affected part of optic nerve and create a sort of compartment syndrome. Recent case reports have described a significant improvement in visual acuity and visual field in patient treated with intravitrealBevacizumab an anti vascular growth 12 factor agent(Anti-VEGF) Intravitreal bevacizumab maybeabooninhaltingtheprogressionofvisualfield lossandimprovethechancesofpreventingblindness, We also considered he possibility of an inflammatoryopticneuropathyandthereforeinitiated anevaluationforpossibleinflammatorycausesbutall Laboratory testing were within normal limits.ABlood pressure of 110/88 mmHg, elevated cholesterol level and smoking habit ledustoadiagnosisofNAIONwhichwasconfirmedbyarepeat visual field after 2 weeks of involvement of second eye. An Altitudinal defect was seen in both eyes and this feature is diagnosticofNAION.AsecondattackofNAIONinsameeyeis unlikely and no further deterioration of vision was seen in the patientevenuntil10yearsoffollowup.
ACKNOWLEDGEMENT
We are thankful to Lt. Gen Dr G. Ramdas (GM, Medical Services)andDrDPSamaddar(CIMS)ofTataMainHospitalfor their perpetual encouragement and guidance in every clinical activities.
REFERENCES
1 Hayreh SS — Ischemic Optic Neuropathy. Indian J Ophthalmol 2000;48:171-9,1.
2 Hayreh SS — The blood supply of the optic nerve head and the evaluation of it- Myth and Reality. Prog Retina Eye Res 2001;20:563-93
3 Hayreh SS, Podhajsky PA, Zimmerman B — Role of nocturnal arterial hypotension in optic nerve head ischemic disorgders. Ophthalmologica 1999;213:641-7
4 Hayreh SS. Blood flow in the optic nerve head and factors that may influence it. Prog Retina Eye Res 2001; 20: 595-624.
6 Johnson MW, Kincaid MC, Trobe JD Bilateral retrobulbar optic nerve infarctions after blood loss and hypotension. A clinicopathological case study. Ophthalmology 1987; 94: 1577-84.
7 Jaben SL, Glaser JS, Daily M — Ischemic optic neuropathy fol owing genera surg ca procedures J ClinNeuroophthlmol 983;3:239-44.
8 Hayreh SS, Joos KM, Podhajsky PA — Systemic diseases assoc a ed with nonar erit c an erior schem c opt c neuropathy. Am J Ophthalmol 1994;18:766-80.
9 Beck RW, Servais GE, Hayreh SS — Anterior ischenmic optic neuropathy-IX Cup -to –disc ratio and its role in pathogenesis. Ophthalmology 1987;94:1503-8.
10 Beri M, Klugman MR, Kohler JA, Hayreh SS — Anterior ischemic optic neuropathy VII. Incidence of bilaterality and various influencing factors. Ophthalmology 1987; 94: 10208.
11 Newman NJ, Scherer R, Langenberg P, Kelman S, Feldon S,KaufmanD, et al ThefelloweyeinNAION;Reportfrom the ischemic optic neuropathy decompression trial follow up study. Am J Ophthalmol 2002;134:317-28.
12 Hosseini H, Razeghinejad MR — Anterio Ischemic Optic Neuropathy after intravitreal injection of bevacizumab.J Neuroophtalmol 2009;29:160-1.
Right eye Left eye
Fig 2 – Blurring of right disc margin with splinter hemorrhage while disc margins of Left eye is normal
Right eye Left eye
Fig 3 – Visual field of Right eye showing almost tubular vision while visual field of left eye is normal
Right eye Left eye
Fig 4 – Pallor of both optic disc
Right eye
Left eye Fig 5 –Altitudinal field defects in both eye
SUPPLEMENT
B
Branch Notes
IMA Badagara — The activities of May was evaluated by Dr.K.M.Subhash and Dr.C.Vijayaraghavan.World environment day activities were planned for June 6th. Doctors day to be celebrated on July 1st. The program is to be charted out later Ifthar sangamam was decided to be held on 19th, Sunday CME program “BASICON 2016” on 05-06-2016 : A one day CME Program “BASICON 2016” for General Practitioners was held on 05-06-2016 at Dazzle Banquet Hall,Vadakara.The program was organized by Ceeyam Academy in association with IMA –AMS. There was good participation with nearly 150 delegates attending the program. SWC meeting at Thalasseryon05-06-2016:IMA
participated in the SWC meeting held on 05-062016 at Thalassery The President Dr M Muraleedharan, Dr PM Saleem, Dr C.Vijayaraghavan and Dr K. M. Abdulla attended the meeting and actively participated in the discussions. World Environment DaywasobservedbyIMABadagaraon06-06-2016atIMAHall at8pm.Aftertheprogram,SaplingswereplantedattheIMAHall compound to observe the Environment Day IMA Badagara organizedan‘IftharSangamam’on19-06-16atIMAHall. IMA Perinthalmanna Branch On 01.06.2016 : In connection with ‘Pravesanotsavam’ IMA Perinthlmanna Branch donated school kits for 40 tribal inmates of Sai Snehatheeram Boys Hostel on 1st of June, 2016. IMA also handed over Rs 10,000 to the hostel authorities. On 05.06.2016 the occasion of ‘World Environment Day’ WIMA members distributedtreesaplingsandalsoplantedsomefruittreesaplings at the District Hospital premises. IMA Perinthalmanna branch celebrated ‘World Blood Donor Day’on 14th June, 2016 at the Perinthalmanna Blood Bank Auditorium. IMA Perinthalmanna branch members actively participated in ‘World Yoga Day’ observed on 21st June, 2016. Doctors Day to be celebrated on July1st,2016. Asapartof‘DrugAbuseandAnti-narcoticDay’, WIMA Perinthalmanna arranged a talk for students at Govt. Higher Secondary School, Perinthalmanna on 27th June, 2016. As a part of ‘Drug Abuse and Anti-narcotic Day’, WIMA Perinthalmanna arranged a class for students of CCST College, Karalmanna on 28th June, 2016. It celebrated Doctor’s Day along with Ifthar Meet on 1st July 2016. The program was a familygettogetherofIMAPerinthalmannabranchmembers.
IMA Kozhikode Branch — On 5-6-2016: world environmental day: Planting Trees at IMA Premises. Medical CampforPoliceForceatPoliceClub, Kozhikodeinassociation with MIMS & BMH State Working Committee meeting at Thalassery President, Secretary and other State leaders are attended. On 12-6-2016: Medical Camp for Police Force at PoliceClub, KozhikodeinassociationwithMIMS&BMH On 15-6-2016: IMA AMS CME, 75 members participated in the CME. Topic: A Nephrologists perspective on Hypertension by Dr S.Vinugopal, ConsultantNephrologist, Kozhikode.On 166-2016: IMA District Task Force MEET at IMA Hall, Kozhikode. On 18-6-2016: IMA MBS family meet. On 19-62016:MedicalCampforPoliceForceatPoliceClub, Kozhikode in association with MIMS & BMH. On 23-6-2016: IMA GB
CUM CME,Topic: Revascularization Strategies in Unprotected LeftMainCoronaryArteryCriticalLesions:IsthereaParadigm Shift ? by Dr K.P Balakrishnan, MD, DM, FICC, HOD, Dept. ofCardiology,KIMS-AlshifaHospital,Perinthalmanna.On 266-2016: Observation of INTERNATION DAY AGAINST DRUG ABUSE & ILLICIT TRAFFICKING. Press Meet at Calicut Press Club reg. Doctors’ day celebration on 1st July 2016.
IMA Cochin Branch 1stJune, 2016 Karuthal Cancer Detection Camp in BPHC Cheranalloor On 11th June IMA Cochin Special CME on Bariatric Surgery IMA Lagoon Nite.
21st June International Yoga Day at General Hospital Ernakulam,18thJune.On26thJuneIFTHARmeetatIMA.29th June Special CME. General body meeting with CME was conducted in association with Indian Association of Psychiatry on recent advances in psychiatry Presented ‘Ethics Pearls’ in Monthly meeting by Dr Joy Joseph. Conducted three CMEs altogather in the month of June. Advances in Bariatric Surgery, Medicine, Science and Law Cochin Clinical Society Meeting at Sunrise Hospital.Yoga day celebration and various activities by WIMA.
IMA Kunnamkulam Branch — In June 3rd, connection with WORLD ENVIRONMENT DAY, IMA Kunnamkulam in association with WIMA conducted a program at adopted IMMNUEL LP SCHOOL, Chittanjoor IMA donated Waste Baskets and Tree saplings to the school. Workshop for the volunteers of ACCIDENT CARE & TRANSPORT SERVICE(ACTS) of Thrissur District. Doctors Day to be celebrated on July 1st. CME and Ethical pearls for the month of June was discussed. In June 22nd, IMA Kunnamkulam and Police Department of Kunnamkulam division conducted First Aid Class and DrugAbuse and TrafficAccidents to the students of Vivekananda College Kunnamkulam.
IMA Kuthuparamba Branch Celebrating Doctors' Day on 1st July, 2016 and in the evening program began with an ‘Iftar’ party which was well attended by the IMA familyandguests.
JIMA Guidelines for Authors
Communicationsintendedforpublicationshouldbesentto the Editor, Journal of the Indian Medical Association (JIMA). JIMA will consider manuscripts prepared in accordance with 1 theVancouverstyle . Articles are considered for publication on condition that these are contributed solely to JIMA, that they have not been publishedpreviouslyinprintandarenotunderconsiderationby another publication. In the selection of papers and in regard to priority of publication, the opinion of the Editor will be final. TheEditorshallhavetherighttoedit,condense,alter,rearrange or rewrite approved articles, before publication without referencetotheauthorsconcerned.
Authorship: All persons designated as authors should qualifyforauthorship.Authorshipcreditshouldbebasedonly on significant contributions to (a) conception and design, or analysisandinterpretationofdata;andto(b)draftingthearticle orrevisingitcriticallyforimportantintellectualcontent;andon (c) final approval of the version to be published. Conditions (a), (b) and (c) must all be met. Authors may include explanationofeachauthor’scontributionseparately
Manuscript and CD : Scripts of articles should be typewritten, double-spaced on one side ofA4 size paper with at least 2.5 cm margin at the top and on left hand side of the sheet and should be submitted in triplicate.Also sending CD in Microsoft Word (Window) is a must. Manuscripts not accepted for publication will not be returned to the authors. Authors should keep one copy of their manuscripts for reference.Separatepagesshouldbeusedfordifferentsections.
Title page— The title page should include the title of the article which should be concise but informative, name(s) of author(s) with his/her (their) academic qualification(s) and designation(s), and complete postal address including pin code oftheinstitution(s)towhichtheworkshouldbeattributed.
Abstract— The 2nd page should carry an abstract of no more than 250 words and should contain the purposes of the study or in-vestigations, basic procedure, main findings and theirimplicationsalongwithKeywords.
Text— The text of Originals and Papers should conform to theconventionaldivisionofabstract,introduction,materialand method,observations,discussionandreferences.Othertypesof articles such as Practitioners’ Series, Case Notes, Current Topics,GPForum,etc,arelikelytoneedotherformats.
Statistical evalua on Description of the statistical methods used should either be given in detail in the “material and method” section of the article or supportive reference may becited.
Abbreviations— Standardabbreviationsshouldbeusedand be spelt out when first used in the text.Abbreviations should notbeusedinthetitleorabstract.
Units of measurement— Metric units should be used in scientific contributions. If the conventional units or SI units wereactuallyfollowedinmeasurementsthatshouldbegivenin parentheses.
Drugs— The generic names of the drugs (and not proprietary names) including dose(s), route(s) and period of administrationshouldbementioned.
Length of manuscripts— For Originals and Papers, Practitioners’Series, Preliminary Report, GP Forum and Current Topics: Maximum 2000-2200 words, 2-3 figures, and/or 2-4 tables, for Case Notes: Maximum 800 words, 2 figures,1table,forLettertotheEditor:300-500words.
Tables— Tables should be simple, self-explanatory and should supplement and not duplicate the information given in thetext.
Illustrations— Graphs, charts, diagrams or pen drawings must be drawn by professional hands in Indian ink (black) on white drawing paper In case of x-ray, miniature photoprints should be supplied. Photographs should be supplied in high quality glossy paper not larger than 203 mm x 254 mm (8"x 10") In case of m crophotograph stains used and magnification should be mentioned. Each illustration should bear on its back the figure number and an arrow indicating the top.All illustrations should be black and white and should be submittedintriplicatewithsuitablelegends.
References— Referencesshouldbenumberedintheorder in which they are first mentioned in the text. The full list of references at the end of the communication should be arranged in the order mentioned below (names and initials of all authors and/or editors up to 6; if more than 6, list the first 6 followed by et al):
Referencefromjournal: 1Cogo A, Lensing AWA, Koopman MMW Piovella F, SivagusaS,WellsPS, et al Compressionultrasonographyfor diagnostic management of patients with clinically suspected deep vein thrombosis: prospective cohort study BMJ 1998; 316:17-20.
Referencefrombook:
2Handin RI— Bleeding and thrombosis. In: Wilson JD, Braunwald E, Isselbacher KJ, Petersdorf RG, Martin JB, Fauci AS, et al editors Harrison's Principles of Internal Medicine. Vol1.12thed.NewYork:McGrawHillInc,1991:348-53.
Referencefromelectronicmedia:
3NationalStatisticsOnline—Trendsinsuicidebymethodin E n g l a n d a n d W a l e s , 1 9 7 9 - 2 0 0 1 www.statistics.gov.uk/downloads/theme_health/HSQ 20.pdf (accessedJan24,2005):7-18.
Only verified references against the original documents should be cited. Authors are responsible for the accuracy and completeness of their references and for correct text citation. Thenumberofreferenceshouldbekeptlimitedto20incase ofmajorcommunicationsand10forshortcommunications.
Dual publication : If material in a submitted article has been published previously or is to appear in part or whole in anotherpublication,theEditormustbeinformed.
Forwarding letter: The covering letter accompanying the article should contain the name, complete postal address along withe-mailidentityofoneauthorascorrespondentandmustbe signed by all authors. The correspondent author should notify changeofaddress,ifany,intime.
Declaration:Adeclarationshouldbesubmittedstatingthat the manuscript represents valid work and that neither this manuscript nor one with substantially similar content under the presentauthorshiphasbeenpublishedorisbeingconsideredfor publication elsewhere and the authorship of this article will not be contested by any one whose name (s) is/are not listed here, and that the orderof authorship as placed in the manuscript is final and accepted by the co-authors. Declarations should be signed by all the authors in the order in which they are mentionedintheoriginalmanuscript.
Matters appearing in the Journal are covered by copyright but no objection will be made to their reproduction provided permission is obtained from the Editor prior to publication and dueacknowledgmentofthesourceismade.
Head office: Indian MedicalAssociation, IMAHouse, Indraprastha Marg, New Delhi - 110 002 Telephones: +91-11-2337 0009, 2337 8680, Fax: +91-11-2337 9470, 2337 0375, Telegram: INMEDICI, New Delhi 110 002, Email: hsg@ima-india.org; Website: www.ima-india.org
Date of Publication : 30th Every Month
POST BOX NO 11249 APRIL 2016
Regd. No. WBENG/2557/57
If not delivered please return to
Journal of the IMA (JIMA)
IMA House, 53 Sir Nilratan Sarkar Sarani (Creek Row), Kolkata 700 014 (India)
Published and Printed by Dr Santanu Sen on behalf of Indian Medical Association and printed at Prabaha, 45A, Raja Rammohan Roy Sarani, Kolkata 700009, Editor: Dr Debasish Mukherjee, National President (IMA): Dr SS Agarwal, Honorary Secretary General (IMA): Padma Shri Dr KK Aggarwal. E-mail: hsg@ima-india.org; Website: www.ima-india.org