13396 New biomarkers for diagnosis of bladder cancer : A bibliometric analysis
Roberto Falabella, Valentina De Simone, Felice Crocetto, Francesco del Giudice, Angelo Porreca, Nazario Foschi, Biagio Barone, Luca Di Gianfrancesco, Valentina Di Pasquale, Vincenzo Francesco Caputo
13301 Management of forgotten double J stents: Insight from a systematic review of case repor ts Antonius Galih Pranesdha Putra, Yufi Aulia Azmi, Soetojo Wirjopranoto, Nadya Rahmatika, Agustin Junior Nanda De Niro, Alviano Satria Wibawa, Kevin Muliawan Soetanto
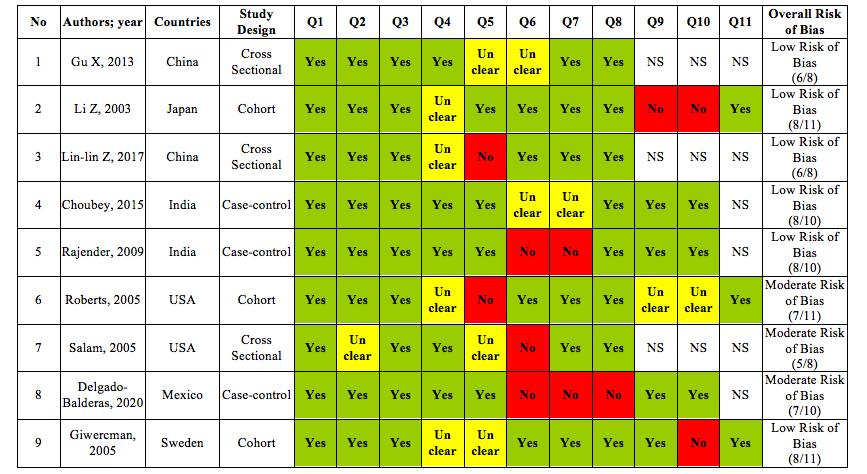
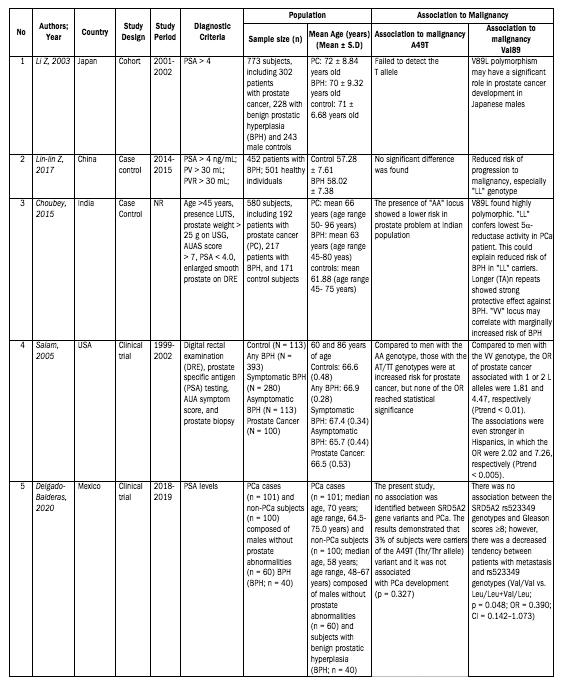
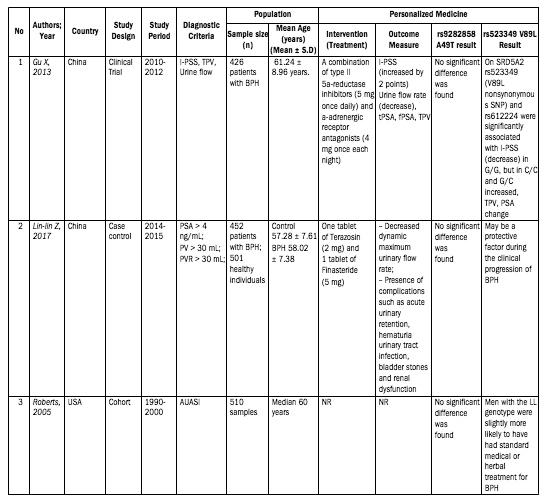
13318 A comprehensive systematic review of studies on the potential of A49T and V89L polymorphism in SRD5AR2 as high susceptibility gene association with benign prostate hyperplasia and prostate cancer
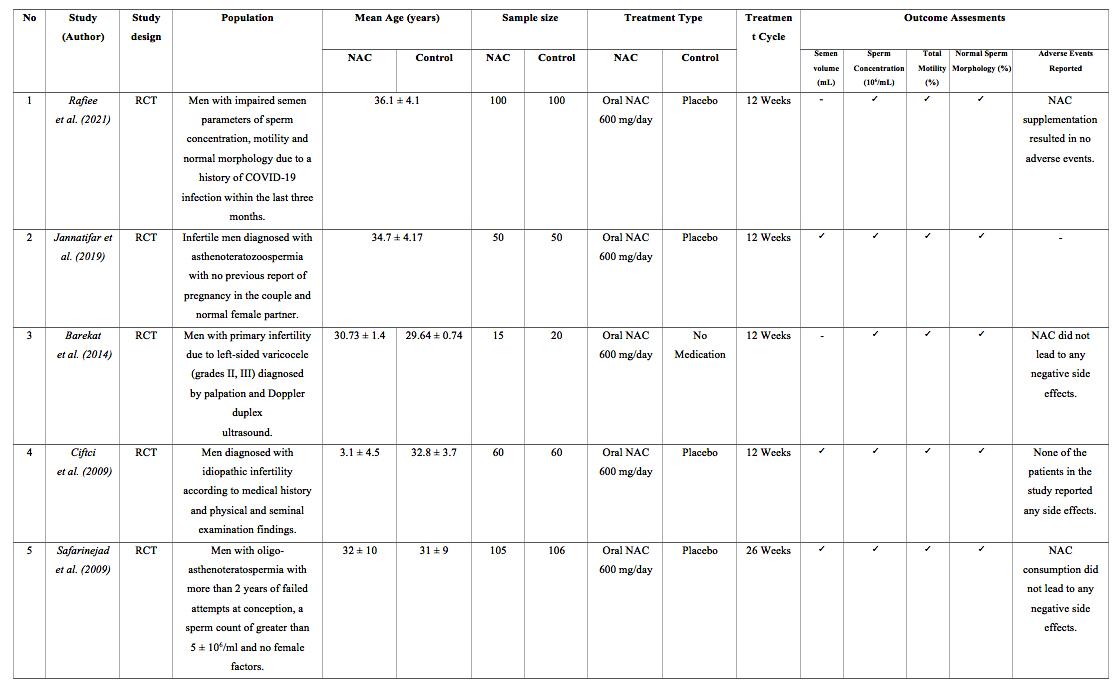
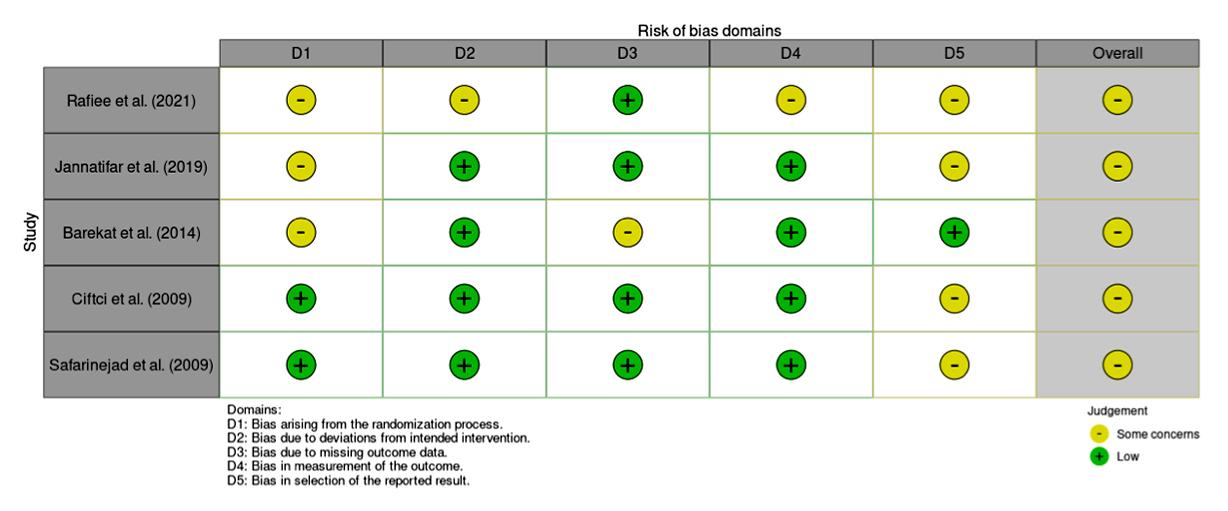
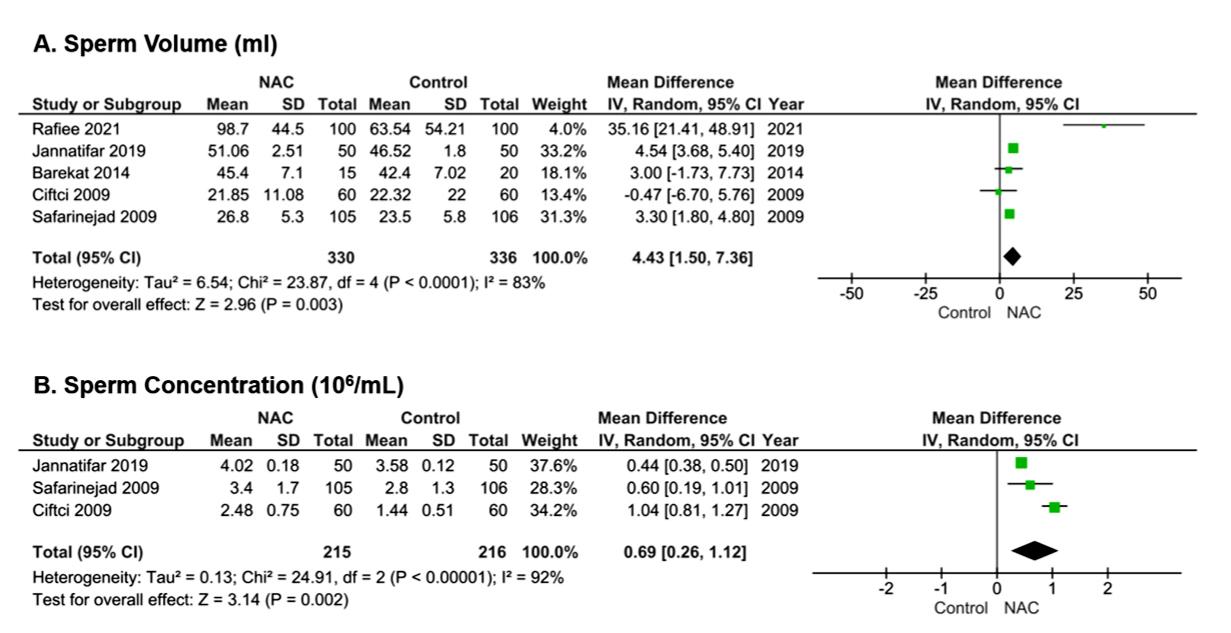
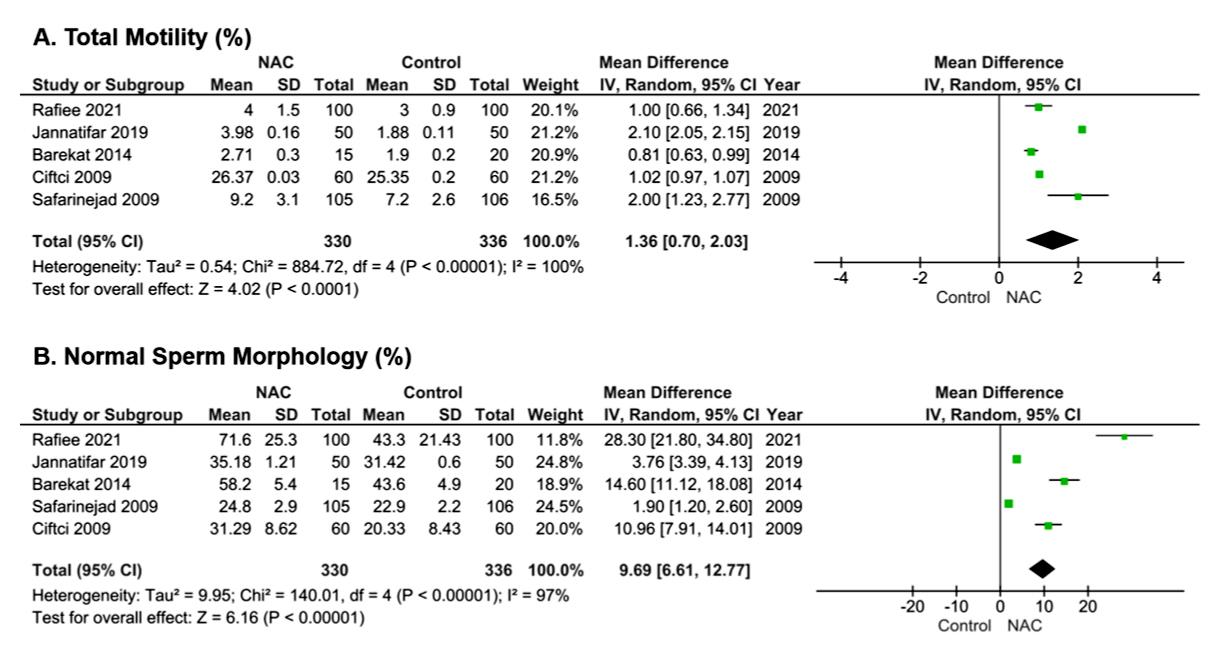
13750 Unlocking the potential of antioxidant supplementation with N-acetylcysteine to improve seminal parameters and analysis of its safety: A systematic review and meta-analysis of randomized controlled trials
12658 Sur vival and oncological outcomes for young men (≤ 55 years) undergoing radical prostatectomy for localized prostate cancer
Shahryar Zeighami, Ali Ariafar, Alireza Makarem, Faisal Ahmed, Mohammadreza Askarpour
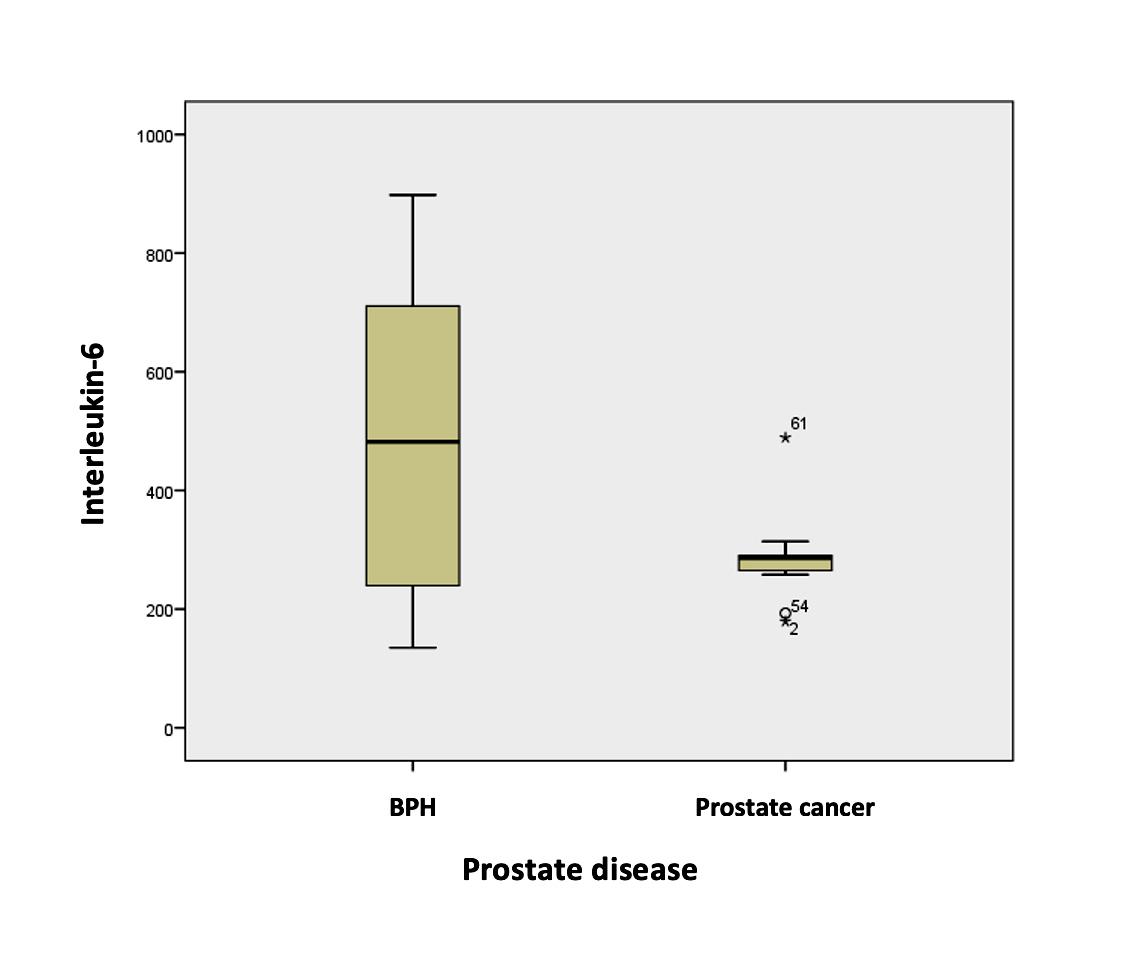
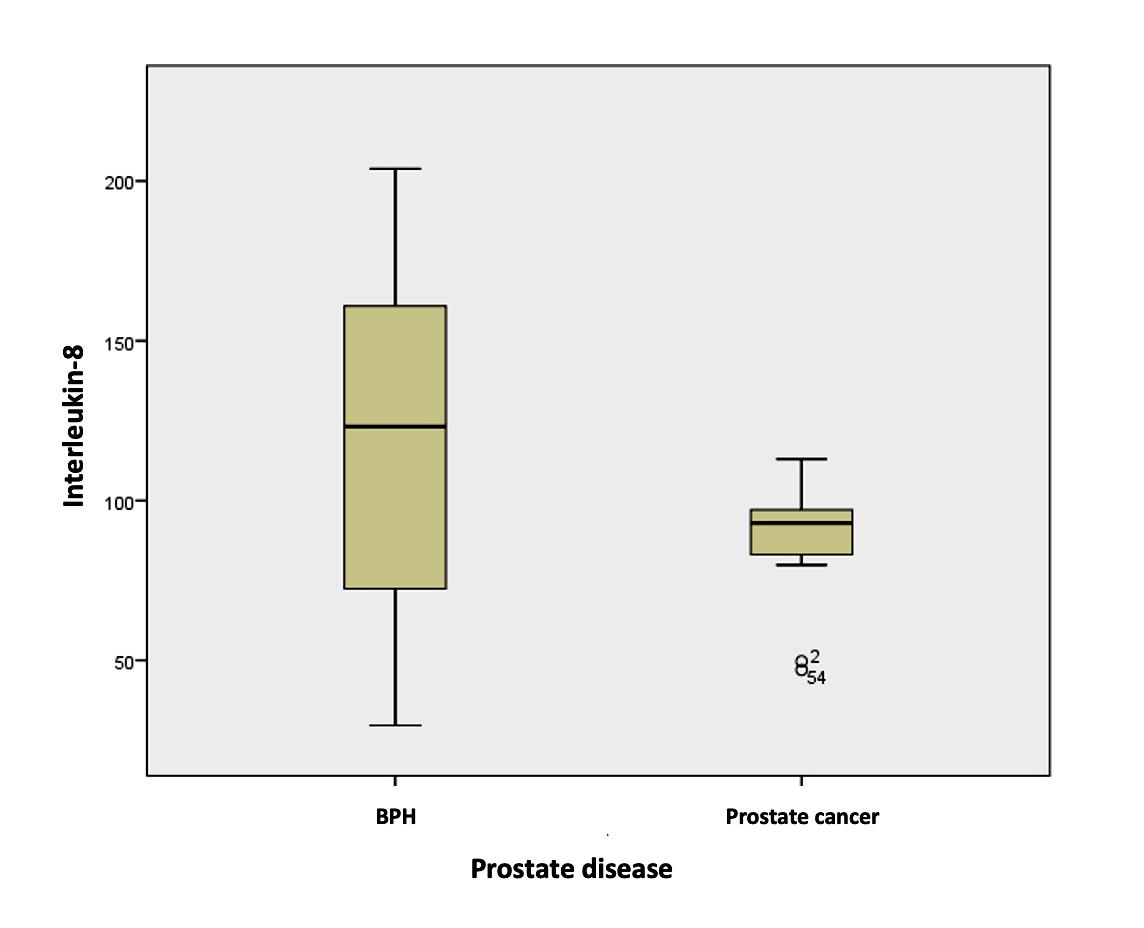
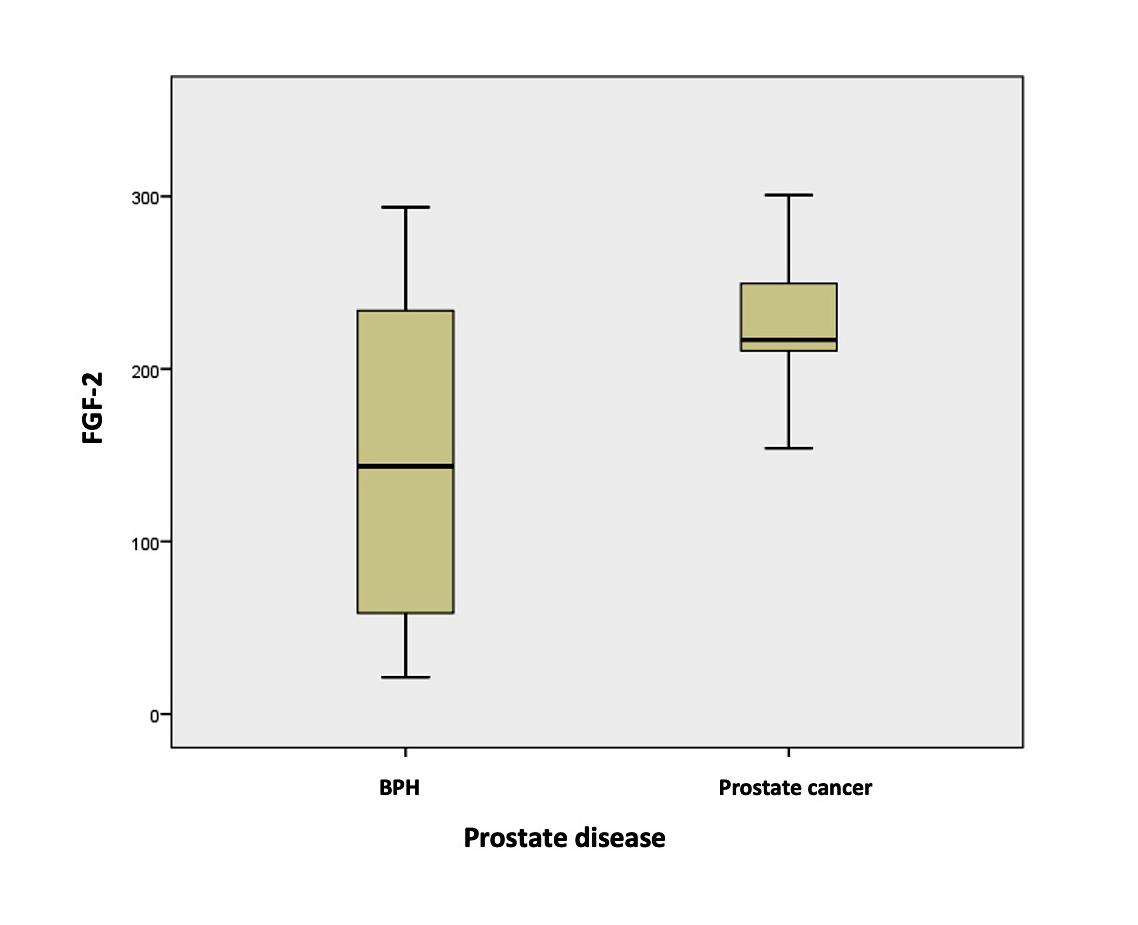
13353 The impact of inflammation on prostate tumor dynamics: A pathological perspective on prostate cancer and benign prostatic hyperplasia
Syakri Syahrir, Muhammad Asykar Palinrungi, Mochammad Hatta, Khoirul Kholis, Syarif, Abdul Azis, Muhammad Faruk
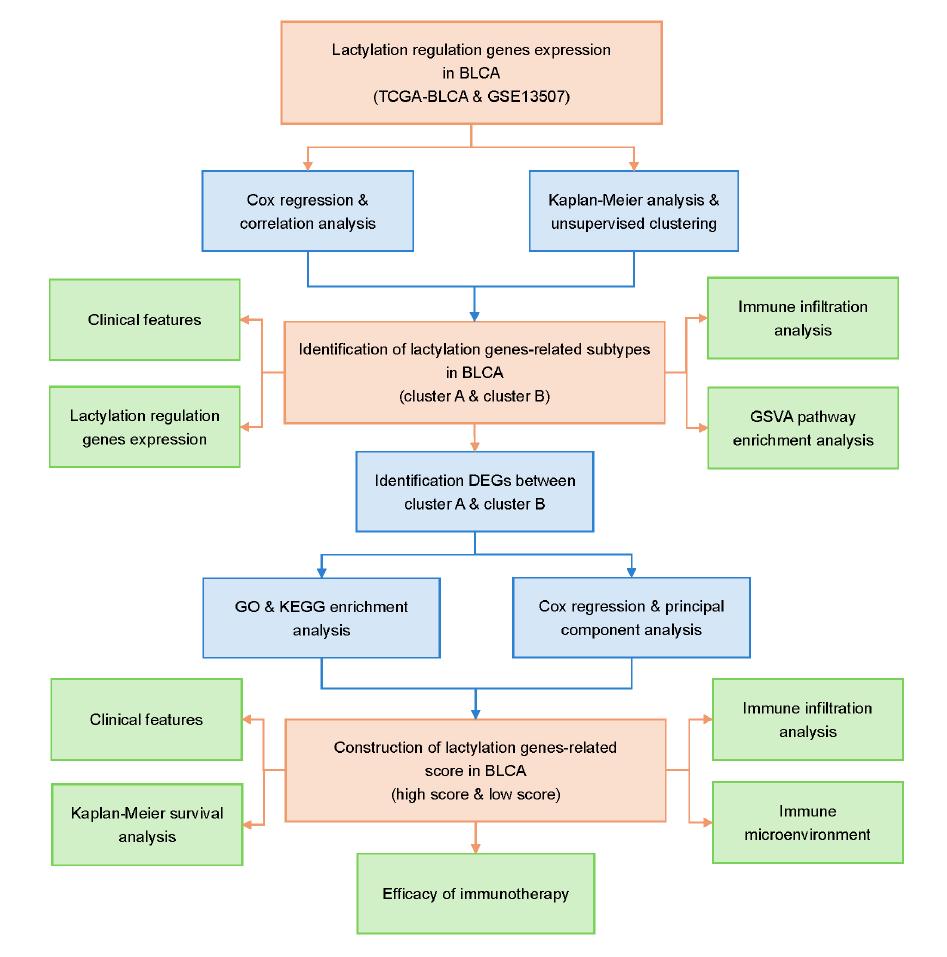
13516 Predictive role of lactylation-related gene signature in the prognosis and immunotherapy response in bladder cancer
Guoyuan Liu, Ting Hong, Xinyu Liu, Xuanhao Lin, Peixiu Yao, Xifeng Chen, Yonghai Zhang, Kemal Sarica, Xuwei Hong
13428 Preoperative platelet-to-lymphocyte ratio as a predictor of inguinal lymph node metastasis in penile cancer
Francesco Passaro, Antonio Tufano, Gianluca Spena, Alessandro Izzo, Flavio Antonino Scarlata, Biagio Barone, Luigi Napolitano, Gabriele Pezone, Pierluigi Alvino, Achille Aveta, Savio Domenico Pandolfo, Simone Cilio, Lorenzo Romano, Francesco Di Bello, Alessandro Calarco, Rosario Leonardi, Carlo Buonerba, Sisto Perdonà
13336 Comparative evaluation of the efficacy and safety of antegrade minimally percutaneous nephrolithotomy (mPCNL) and retrograde intrarenal surger y (RIRS) in the treatment of upper ureteral impacted stones: A retrospective cohor t study
Kequan Cheng, Xuwei Hong, Gang Wang, Zepai Chi, Kemal Sarica, Guoyuan Liu, Yonghai Zhang
13824 Urine alkalinization for dissolution of uric acid stones and treatment of other urological diseases with a treatment combining potassium magnesium citrate and theobromine
Celia Abad Rodriguez-Hesles, Hassan Alkhatatbeh, María Belén Alonso Bartolomé, Carmen Arai Valladares Ferreiro, Hector Ricardo Ayllón Blanco, Cristina Calzas Montalvo, Daniel Carrasco Gómez, Marta Casadevall Rubau, Elena Maria Casas Martinez, Sara Esturo Sacristan, Miguel Gómez Garberí, Blanca Gómez-Jordana Mañas, Rosa Maria Gras Martinez, Ana Morales Martínez, Pedro Hernandez-Peñalver, Silvia Juste Alvarez, Alberto López Sierra, Rafael Maria Mas Lucas, Isabel Mohedano Sánchez, Isabel Montuenga Fernandez, Baraa Nakdali Kassab, Maria Negueroles-Garcia, Leticia Ruibal Gago, Laura Sánchez, Bernat Isern, Alberto Trinchieri
13412
Discovering a new nutraceutical based on pollen extract and teupolioside: A prospective monocentric study evaluating its role in alleviating lower urinar y tract symptoms in benign prostatic hyperplasia patients
Mattia Lo Re, Marta Pezzoli, Anna Cadenar, Elettra Fuligni, Leonardo Gajo, Andrea Minervini, Andrea Cocci
13268 Ten years’ single surgeon experience of excision and primar y anastomosis (EPA) urethroplasty for traumatic urethral stricture: An analysis of risk factors for urethral stricture recur rence
Paksi Satyagraha, Edi Wibowo, Besut Daryanto, Gede Wirya Diptanala Putra Duarsa, Adrianus Gupta Wijaya, Fauzan Kurniawan Dhani
EDITORIAL BOARD
EDITOR IN CHIEF
Alberto Trinchieri (Milan, Italy)
ASSOCIATE EDITORS
Emanuele Montanari, Department of Urology, IRCCS Foundation Ca’ Granda Ospedale Maggiore Policlinico, University of Milan, Italy – Gianpaolo Perletti, Department of Biotechnology and Life Sciences, Section of Medical and Surgical Sciences, University of Insubria, Varese, Italy; Department of Human Structure and Repair, Ghent University, Ghent, Belgium - Angelo Porreca, Robotic Urology and Mini Invasive Urologic Surgery Unit, Abano Terme Hospital, Abano Terme, Italy
EXECUTIVE EDITORIAL BOARD
Alessandro Antonelli, Department of Urology, Azienda Ospedaliera Universitaria Integrata (A O U I ), Verona, Italy - Antonio Celia, Department of Urology, San Bassiano Hospital, Bassano del Grappa, Italy - Luca Cindolo, Department of Urology, Villa Stuart Hospital, Rome, Italy - Andrea Minervini, Department of Urology, University of Florence, Unit of Oncologic Minimally-Invasive Urology and Andrology, Careggi Hospital, Florence, Italy - Bernardo Rocco, Department of Urology, University of Modena and Reggio Emilia, Modena, Italy - Riccardo Schiavina, Department of Urology, University of Bologna, Bologna, Italy
ADVISORY EDITORIAL BOARD
Pier Francesco Bassi, Urology Unit, A Gemelli Hospital, Catholic University of Rome, Italy – Francesca Boccafoschi, Health Sciences Department, University of Piemonte Orientale in Novara, Italy – Alberto Bossi, Department of Radiotherapy, Gustave Roussy Institute, Villejuif, France –Tommaso Cai, S Chiara Hospital, Trento, Italy –Paolo Caione, Department of Nephrology-Urology, Bambino Gesù Pediatric Hospital, Rome, Italy – Luca Carmignani, Urology Unit, San Donato Hospital, Milan, Italy –Liang Cheng, Department of Urology, Indiana University School of Medicine, Indianapolis, IN; Department of Pathology and Laboratory Medicine, Indiana University School of Medicine, Indianapolis, IN – Giovanni Colpi, Retired Andrologist, Milan, Italy – Giovanni Corona, Department of Urology, University of Florence, Careggi Hospital, Florence, Italy – Antonella Giannantoni, Department of Surgical and Biomedical Sciences, University of Perugia, Italy – Paolo Gontero, Department of Surgical Sciences, Molinette Hospital, Turin, Italy – Steven Joniau, Organ Systems, Department of Development and Regeneration, KU Leuven, Belgium – Frank Keeley, Bristol Urological Institute, Southmead Hospital, Bristol UK – Laurence Klotz, Division of Urology, Department of Surgery, Sunnybrook Health Sciences Centre, University of Toronto, Toronto, Ontario, Canada – Börje Ljungberg, Urology and Andrology Unit, Department of Surgical and Perioperative Sciences, Umeå University, Umeå, Sweden –Nicola Mondaini, Uro-Andrology Unit, Santa Maria Annunziata Hospital, Florence, Italy – Gordon Muir, Department of Urology, King's College Hospital, London, UK –Giovanni Muto, Urology Unit, Bio-Medical Campus University, Turin, Italy – Anup Patel, Department of Urology, St Mary's Hospital, Imperial Healthcare NHS Trust, London, UK – Glenn Preminger, Division of Urologic Surgery, Duke University Medical Center, Durham, NC, USA – David Ralph, St. Peter's Andrology Centre and Institute of Urology, London, UK – Allen Rodgers, Department of Chemistry, University of Cape Town, Cape Town, South Africa – Francisco Sampaio, Urogenital Research Unit, State University of Rio de Janeiro, Rio de Janeiro, RJ, Brazil – Kemal Sarica, Department of Urology, Kafkas University Medical School, Kars, Turkey – Luigi Schips, Department of Urology, San Pio da Pietrelcina Hospital, Vasto, Italy – Hartwig Schwaibold, Bristol Urological Institute, Southmead Hospital, Bristol, UK – Alchiede Simonato, Department of Urology, University of Verona, Azienda Ospedaliera Universitaria Integrata, Verona, Italy – Carlo Terrone, Department of Urology, IRCCS S Martino University Hospital, Genova, Italy – Anthony Timoney, Bristol Urological Institute, Southmead Hospital, Bristol, UK – Andrea Tubaro, Urology Unit, Sant’Andrea Hospital, “La Sapienza” University, Rome, Italy – Richard Zigeuner, Department of Urology, Medical University of Graz, Graz, Austria
BOARD OF REVIEWERS
Maida Bada, Department of Urology, S Pio da Pietrelcina Hospital, ASL 2 Abruzzo, Vasto, Italy - Lorenzo Bianchi, Department of Urology, University of Bologna, Bologna, Italy - Mariangela Cerruto, Department of Urology, Azienda Ospedaliera Universitaria Integrata (A O U I ), Verona, Italy - Francesco Chessa, Department of Urology, University of Bologna, Bologna, Italy - Daniele D’Agostino, Robotic Urology and Mini In-
vasive Urologic Surgery Unit, Abano Terme Hospital, Abano Terme, Italy - Fabrizio Di Maida, Department of Urology, University of Florence, Unit of Oncologic Minimally-Invasive Urology and Andrology, Careggi Hospital, Florence, Italy - Antonio Galfano, Urology Unit, Niguarda Hospital, Milan, Italy - Michele Marchioni, Department of Medical, Oral and Biotechnological Sciences, "G. d'Annunzio" University of Chieti, Laboratory of Biostatistics, Chieti, Italy - Andrea Mari, Department of Urology, University of Florence, Unit of Oncologic Minimally-Invasive Urology and Andrology, Careggi Hospital, Florence, Italy - Luigi Napolitano, Unit of Urology, Department of Neurosciences, Reproductive Sciences, and Odontostomatology University of Naples “Federico II”, Naples, Italy - Antonio Porcaro, Department of Urology, Azienda Ospedaliera Universitaria Integrata (A O U I ), Verona, Italy - Stefano Puliatti, Department of Urology, University of Modena and Reggio Emilia, Modena, Italy - Daniele Romagnoli, Robotic Urology and Mini Invasive Urologic Surgery Unit, Abano Terme Hospital, Abano Terme, Italy - Chiara Sighinolf, Department of Urology, University of Modena and Reggio Emilia, Modena, Italy - Tommaso Silvestri, Urology Clinic, Department of Medical, Surgical and Health Science, University of Trieste, Trieste, Italy - Petros Sountoulides, Aristotle University of Thessaloniki, Department of Urology, Thessaloniki, Greece - Alessandro Tafuri, Department of Urology, Vito Fazzi Hospital, Lecce, Italy
SIEUN EDITOR
Pasquale Martino, Department of Emergency and Organ Transplantation-Urology I, University Aldo Moro, Bari, Italy
SIEUN EDITORIAL BOARD
Emanuele Belgrano, Department of Urology, Trieste University Hospital, Trieste, ItalyFrancesco Micali, Department of Urology, Tor Vergata University Hospital, Rome, ItalyMassimo Porena, Urology Unit, Perugia Hospital, Perugia, Italy – Francesco Paolo Selvaggi, Department of Urology, University of Bari, Italy – Carlo Trombetta, Urology Clinic, Cattinara Hospital, Trieste, Italy – Giuseppe Vespasiani, Department of Urology, Tor Vergata University Hospital, Rome, Italy – Guido Virgili, Department of Urology, Tor Vergata University Hospital, Rome, Italy
UrOP EDITOR
Carmelo Boccafoschi, Department of Urology, Città di Alessandria Clinic, Alessandria, Italy
UrOP EDITORIAL BOARD
Renzo Colombo, Department of Urology, San Raffaele Hospital, Milan, Italy – Roberto Giulianelli, Department of Urology, New Villa Claudia, Rome, Italy – Massimo Lazzeri, Department of Urology, Humanitas Research Hospital, Rozzano (Milano), Italy – Angelo Porreca, Department of Urology, Polyclinic Abano Terme, Abano Terme (Padova), Italy –Marcello Scarcia, Department of Urology, "Francesco Miulli" Regional General Hospital, Acquaviva delle Fonti (Bari), Italy – Nazareno Suardi, Department of Urology, San Raffaele Turro, Milano, Italy
GUN EDITOR
Arrigo Francesco Giuseppe Cicero, Medical and Surgical Sciences Department, Sant’Orsola-Malpighi University Hospital, Bologna, Italy
GUN EDITORIAL BOARD
Gianmaria Busetto, Department of Urology, Sapienza University of Rome, Italy –Tommaso Cai, Department of Urology, Santa Chiara Regional Hospital, Trento, Italy –Elisabetta Costantini, Andrology and Urogynecological Clinic, Santa Maria Hospital of Terni, University of Perugia, Terni, Italy – Angelo Antonio Izzo, Department of Pharmacy, University of Naples, Italy – Vittorio Magri, ASST Nord Milano, Milano, Italy – Salvatore Micali, Department of Urology, University of Modena and Reggio Emilia, Modena, Italy – Gianni Paulis, Andrology Center, Villa Benedetta Clinic, Rome, Italy – Francesco Saverio Robustelli della Cuna, University of Pavia, Italy – Giorgio Ivan Russo, Urology Department, University of Catania, Italy – Konstantinos Stamatiou, Urology Department, Tzaneio Hospital, Piraeus, Greece – Annabella Vitalone, Department of Physiology and Pharmacology, Sapienza University of Rome, Rome, Italy
Un’opera completa sul microbiota, il complesso consorzio di batteri che abita il nostro organismo e ne influenza lo status di salute o malattia. Centinaia di illustrazioni a colori, contenuti multimediali, aggiornati in progress continuo ed accessibili mediante QR code. Un Trattato imprescindibile per chi si occupa di salute interpretando i referti sul microbiota.
Costo di copertina €120,00, IVA e spese di spedizione incluse. Per informazioni ed eventuali ordini, scrivere a: info@edizioniscriptamanent.eu
ORIGINAL PAPERS
13383 Factors associated with erectile dysfunction in traumatic urethral strictures following EPA urethroplasty: A single center experience
Paksi Satyagraha, Gede Wirya Diptanala Putra Duarsa, Fauzan Kurniawan Dhani, Adrianus Gupta Wijaya, Besut Daryanto
13342 The effect of hyperbaric oxygen therapy on hypospadias reconstr uction: A preliminar y randomized controlled trial study of VEGF levels and HOPE score analysis
Mendy Hatibie Oley, Maximillian Christian Oley, Ari Astram Adhiatma Iskandar, Chaula Luthfia Sukasah, Indri Aulia, Fima Lanra Fredrik G Langi, Harsali Fransicus Lampus, Irawan Sukarno, Vania Sukarno, Muhammad Faruk
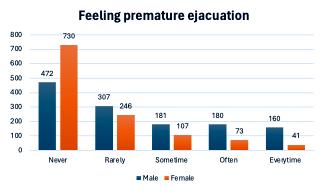
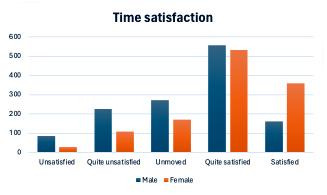
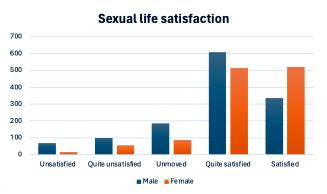
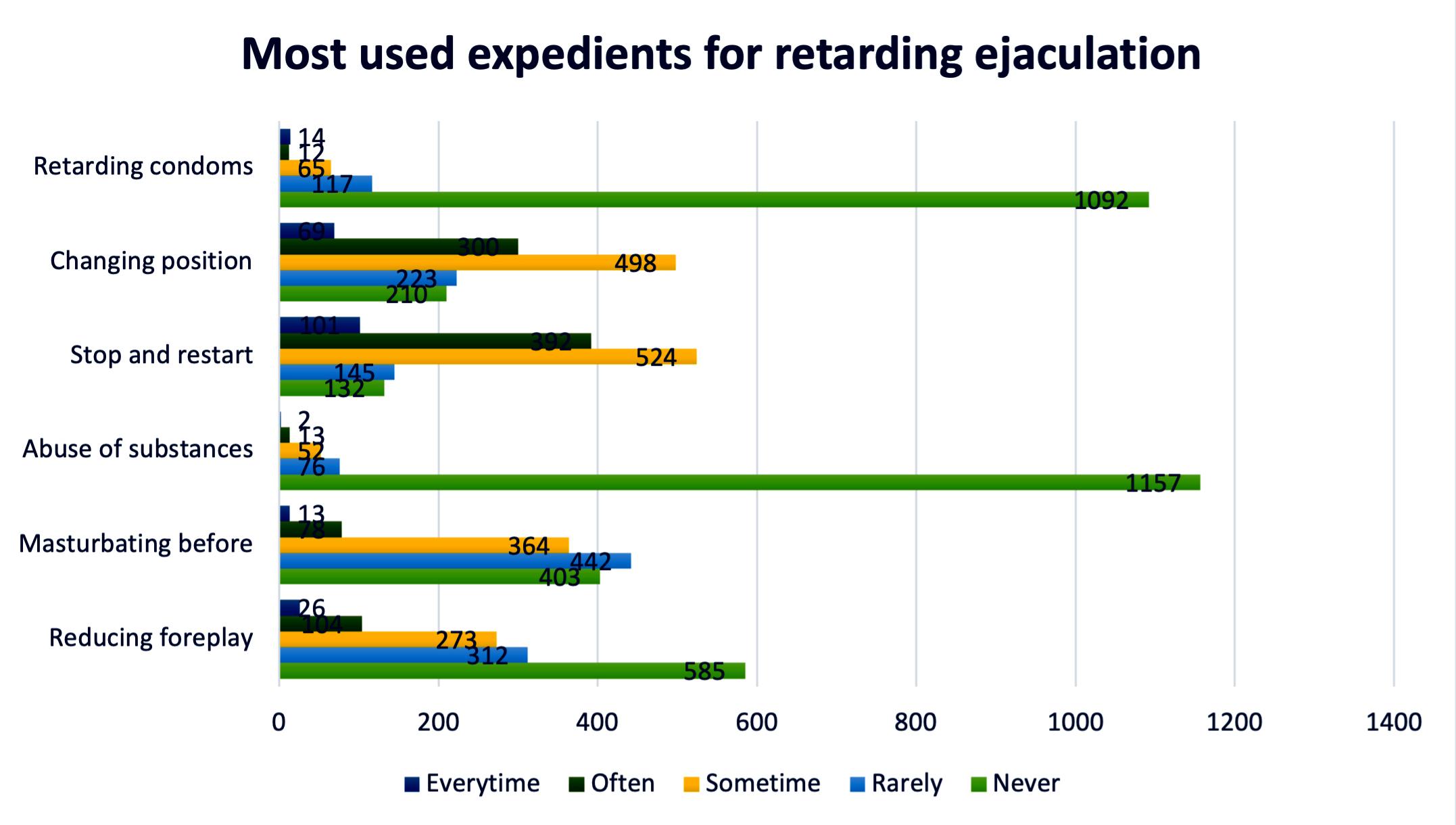
13445 Discrepancy between male and female perceptions of ejaculation latency and sexual satisfaction: Results from an online open sur vey Andrea Cocci, Marta Pezzoli, Arturo Lo Giudice, Gaia Polloni, Giorgio Ivan Russo, Leonardo Gajo, Daniel Giunti, Michele Di Dio, Borja Garcia Gòmez, Manuel Alonso Isa, Agustin Fraile Poblador, Javier Romero Otero, Andrea Minervini, Mattia Lo Re
13541 Laparoscopic radical prostatectomy with the simultaneous implant of a penile prosthesis: Ten years follow up Nicola Mondaini, Andrea Abramo, Caterina Romeo, Fabio Crocerossa, Francesco Cantiello, Rocco Damiano, Riccardo Bartoletti
13207 Enhanced patient recover y with ear ly extensive surgical debridement in Four nier's gangrene: Evaluation of perioperative outcomes in a multicentric experience
Giovanni Cochetti, Alessio Paladini, Luca Lepri, Andrea Vitale, Raffaele La Mura, Miriam Russo, Paolo Mangione, Matteo Mearini, Andrea Fabiani, Emanuele Iacobone, Lucilla Servi, Ettore Mearini, Michele Del Zingaro
12832 Cor relation between seminal alpha-Glycer ylphosphor ylcholine and semen parameters in infer tile patients pre and post sub-inguinal micro-varicocelectomy: A prospective study
Ahmed Fathy Aboseif, Nashaat Nabil, Sameh Fayek GamalEl Din, Shaimaa Ali Abdelkareem, Aya Ahmed Onsi M M B c H, Ahmad Zaghloul, Amgad Elseginy
13128 Sper m DNA fragmentation: Focusing treatment on seminal transpor t fluid beyond sper m production
Moises Abraham Adel Domínguez, Walter D Cardona Maya, Andrés Mora Topete
LETTERS
13525 Treatment with perilesional injections of Pentoxifylline in patients with Peyronie's disease improves the therapeutic effect of oral and topical antioxidant therapy
Gianni Paulis, Andrea Paulis, Giovanni De Giorgio
13343 Lady urologist and male patients with prostate cancer
Rodolfo Montironi, Antonio Lopez-Beltran, Meredith C Wasserman, Alessia Cimadamore, Liang Cheng
13324 Urogenital and extra genital mutilation in gender-affir ming surger y: Are we violating primum non nocere?
Zeki Bayraktar
EDITORIAL COMMENTS
13708 “Lady urologist and male patients with prostate cancer”
13379
Elisabetta Costantini, Ester Illiano
Urogenital and extra genital mutilation in gender-affir ming surger y: Are we violating primum non nocere?
Tommaso Cai, Alessandro Palmieri on behalf of Italian Society of Andrology
Edizioni Scripta Manent s.n.c.
Via Melchiorre Gioia 41/A - 20124 Milano, Italy
Tel +39 0270608060
e-mail: scriman@tin.it
web: www edizioniscriptamanent eu
Registrazione: Tribunale di Milano n 289 del 21/05/2001
Direttore Responsabile: Pietro Cazzola
Direzione Marketing e PR: Donatella Tedeschi
Comunicazione e Media: Ruben Cazzola
Grafica e Impaginazione: Stefania Cacciaglia
Affari Legali: Avv Loredana Talia (MI)
Ai sensi della legge 675/96 è possibile in qualsiasi momento opporsi all’invio della rivista comunicando per iscritto la propria decisione a: Edizioni Scripta Manent s n c - Via Melchiorre Gioia, 41/A - 20124 Milano
The Publisher is not liable for the opinion expressed by the Authors of the articles and for images used by them
GENERAL INFORMATION
AIMS AND SCOPE
“Archivio Italiano di Urologia e Andrologia” publishes papers dealing with the urological, nephrological and andrological sciences
Original articles on both clinical and research fields, reviews, editorials, case reports, abstracts from papers published elsewhere, book rewiews, congress proceedings can be published
REVIEW
New biomarkers for diagnosis of bladder cancer: A bibliometric analysis
Roberto Falabella 1 , Valentina De Simone 2 , Felice Crocetto 3 , Francesco del Giudice 4 , Angelo Porreca 5 , Nazario Foschi 6 , Biagio Barone 7 , Luca Di Gianfrancesco 5, 6 , Valentina Di Pasquale 2 , Vincenzo Francesco Caputo 1
1 Unit of Urology, San Carlo Hospital, Potenza, Italy;
2 Department of Industrial Engineering, University of Salerno, Italy;
3 Unit of Urology, Department of Neurosciences, Reproductive science and Odontostomatology, University of Naples Federico II, Naples, Italy;
4 Department of Maternal infant and Urological Sciences, Sapienza University Rome, Policlinico Umberto 1 Hospital, Rome, Italy;
5 Oncological Urology, Veneto Institute of Oncology (IOV), IRCCS, Padua, Italy;
6 Department of Urology, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Università Cattolica del Sacro Cuore, Rome, Italy;
7 Department of Urology, P O San Paolo, Asl Na1 Centro, Naples, Italy
Summary
Background/Objectives: Bladder cancer is a multifactorial disease, ranking as the 10th most common cancer globally and the fourth most common cancer in men and the ninth in women in the Western world
This bibliometric analysis aims to identify and evaluate scientific literature addressing new biomarkers for bladder cancer diagnosis, as well as to identify the most prolific organizations, authors, journals, countries, and keywords within this research domain.
Methods: An electronic search was conducted using Elsevier's Scopus database From a total of 940 retrieved papers (published between 2019 and 2024), 493 were selected For data analysis and visualization, the titles of articles, year of publication, countries, authors, journals, articles, and keywords were analyzed using Microsoft Excel, VOSviewer, and Biblioshiny
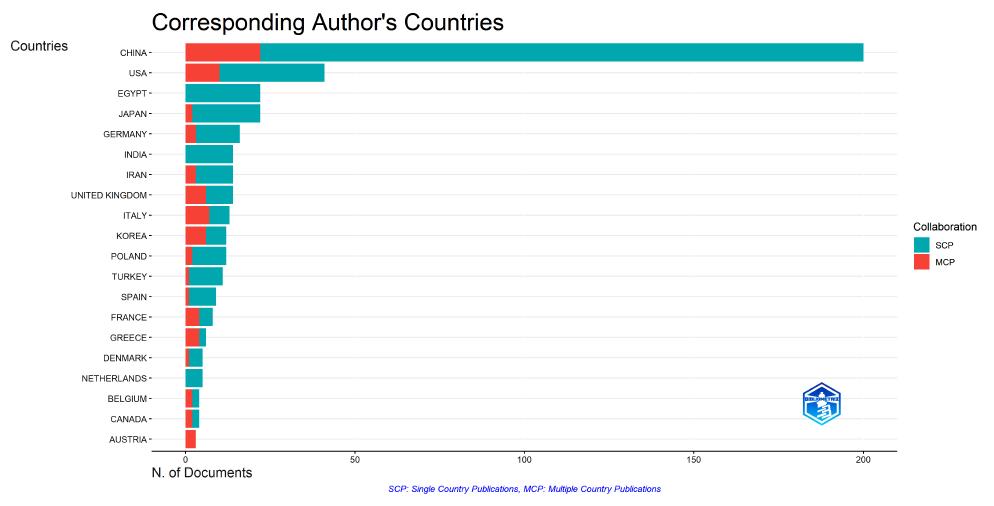
Results: China published the most papers (200 articles) and received the highest number of citations, followed by the USA
While some countries, such as Egypt and India, published exclusively Single Country Publications (SCPs), others demonstrated a higher level of international collaboration, with at least half of their publications being Multi-Country Publications (MCPs). Countries with higher rates of MCPs were Greece (66 6%), Italy (53 8%), Korea, and France (50%) The journals that produced the most publications and received the highest number of citations were Cancers, International Journal of Molecular Sciences, and Frontiers in Oncology, confirming their role in producing high-impact research
Conclusions: The consistent distribution of publications over the years considered indicates a sustained interest in this field
Submitted 17 November 2024; Accepted 13 December 2024
INTRODUCTION
Bladder cancer (BC) diagnosis has traditionally relied upon different diagnostic tests, both invasive and non-invasive, including imaging-based, molecular, urine-based, and
histopathological tests Invasive tests include cystoscopy and fluorescence cystoscopy which remain the gold standard for detecting bladder cancer Non-invasive tests include urine cytology (a standard test with high specificity but low sensitivity especially for low-grade cancers) (13) Urine-based tests are the most common non-invasive methods for detecting bladder cancer, including protein, transcriptomic, and epigenetic markers Multiple studies have assessed cell-free DNA, DNA mutation, methylated DNA, circulating tumour cells, miRNA, mRNAs, cell-free proteins and peptides in urine specimens and blood (4) Circulating urinary tumour DNA (utDNA) has shown a major sensitivity over traditional urine cytology and offers genomic and epigenetic insights (5) Four urinary biomarkers have FDA approval, but they have not replaced cystoscopy and cytology due to limitations in sensitivity and specificity (6) Several studies have identified several proteins in urinary extracellular vehicles (EVs) that show potential, such as MASP2, C3, A2M, CHMP2A, and NHERF1 (7)
Advances in next-generation sequencing have highlighted genomic, transcriptomic, and epigenetic markers as promising candidates (8) Furthermore, in the current literature, multitarget biomarker panels offer better diagnostic accuracy compared with single biomarkers (9, 10) Research has focused on identifying new biomarkers capable of reducing the use of invasive diagnostic methods or to be complements of traditional methods (1-3), however, their clinical utility is still under investigation due to varying sensitivity and specificity
For this reason, the aim of our work is, through a bibliometric analysis of the literature, to evaluate the typology, methods, diffusion, and evolution of published papers to orient towards more aware research of the available material Currently, bibliometric analysis has turned into an accepted method to present the research patterns of scientific literature (11) It provides evidence regarding the progress of a specific domain, accentuating the most relevant country, journals, authors, and institutes involved in
the research area (12, 13) During these years, the results of bibliometric analyses were used in orthopaedics, gynaecology, and other medical fields (14-17), providing a guide for further research on disease prevention and treatment (18, 19) However, there is a paucity of bibliometric studies examining biomarkers in bladder cancer Therefore, this study systematically analyzed the research of biomarkers in BC, to assess frontiers and hotspots in this field In summary, the aim of this study was to analyze global developments in biomarker studies, providing a valid analysis that projects the researcher towards new directions such as personalized medicine, liquid biopsy or the use of combinations of markers to improve diagnostic accuracy, sensitivity and specificity of tests and personalized treatment of the patient
MATERIALS AND METHODS
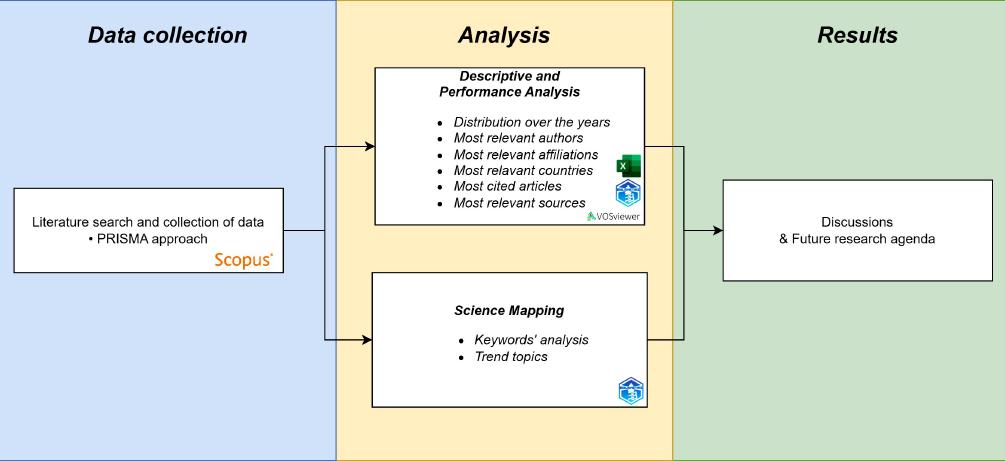
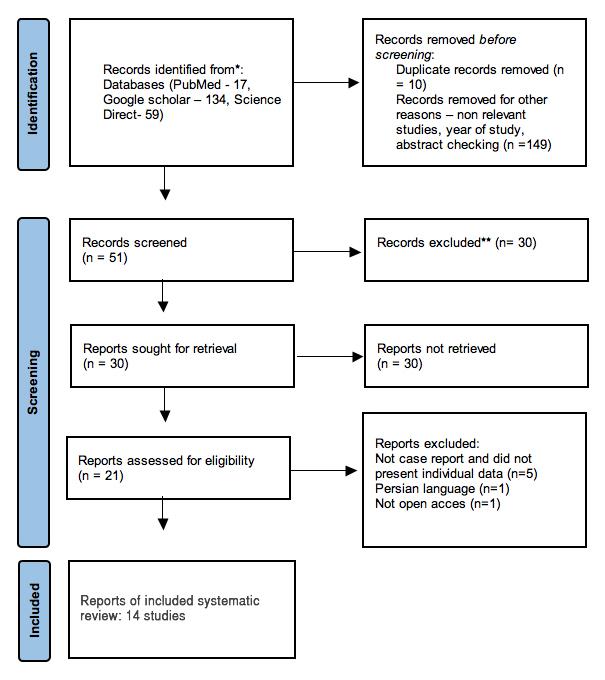
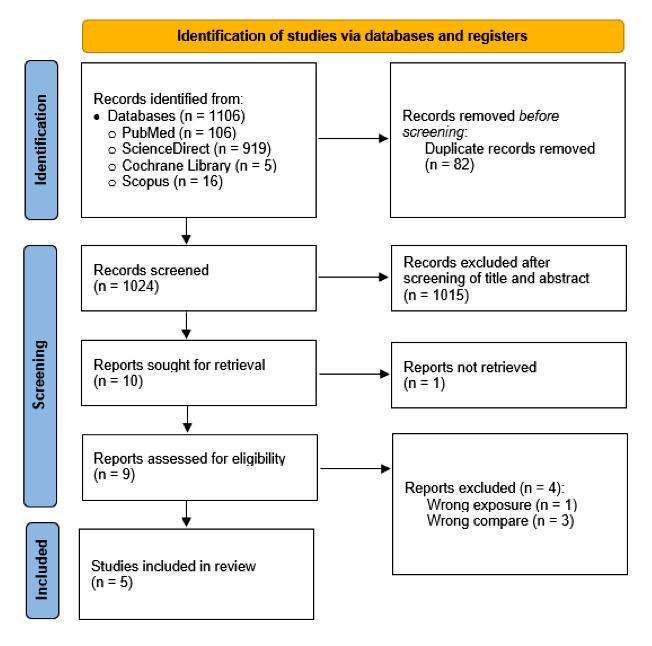
The overall methodology followed to perform the bibliometric analysis has been reported in Figure 1
Data collection
The Scopus database, one of the largest peer-reviewed databases of multidisciplinary research publications, was used to search for the relevant literature related to the research topic of this study The search was conducted in August 2024 and the search string was developed using terms in line with the aim of this research study Search terms associated with (1) bladder cancer, (2) biomarkers, and (3) diagnosis have been combined using Boolean Operators (“OR”, “AND”) The overall string developed is reported below
TITLE-ABS-KEY( ["bladder cancer" OR "bladder carcinoma") AND (biomarkers OR markers) AND (diagnosis)]
The Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA), i e , a technique that provides a roadmap to study systematic reviews objectively, clearly,
and transparently, has been adopted in this research study for the establishment of an eligible set of articles to analyze (20) All articles related to the use of biomarkers for diagnosis of bladder cancer have been considered relevant if they met the following criteria: (1) written in the English language, (2) focused on bladder cancer (3) involving biomarkers for diagnosis and not follow up of bladder cancer
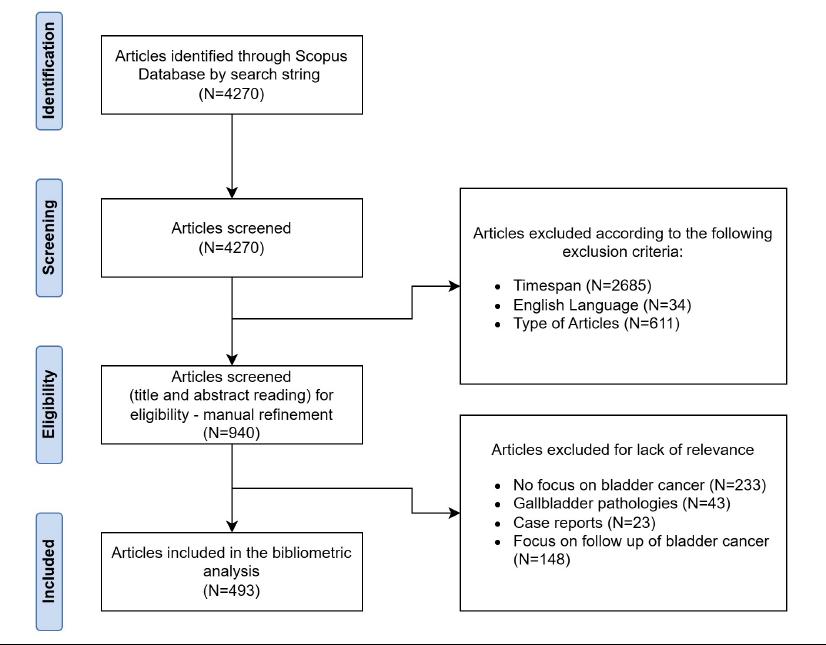
The authors decided to include only research articles from peer-reviewed journals This choice was mainly related to the quality of publications The timespan was limited to the last six years (2019-2024) The period has been chosen to provide a detailed analysis of the topic focusing on the most recent publications trying to highlight how the research topic is changing Two authors conducted the screening process following the PRISMA method as reported in Figure 2 following the inclusion criteria just discussed In the analysis of the searched works, the following were excluded from the analysis: Articles not relevant to bladder cancer (233 articles), articles related to gallbladder pathologies (43 articles), case reports (23 articles), articles dedicated to the analysis of new biomarkers only for the follow up of bladder cancer (148 articles) Finally, data from the selected articles were gathered and stored in ** csv formats
Analysis
After having defined the final set of articles, the bibliometric analysis was carried out using Microsoft Excel and t
Biblioshiny is an R statistical programming language tool developed by Aria and Cuccurullo (2017) (21) and designed for quantitative evaluation The user-friendly interface of Biblioshiny makes it simple for users to import, modify, and generate interactive visualizations of data Also, VosViewer, freely available software developed for constructing and viewing bibliometric maps with significant attention to graphical representation, was employed for some of the analyses carried out
R Falabella, V De Simone, F Crocetto, et al
Figure 1. Research methodology.
As reported in Figure 1, a descriptive and performance analysis was defined
This analysis, focused on the publications and their main characteristics, aimed to examine the contribution of researchers in a given field (22) The most relevant authors, sources, affiliations, articles, etc have been identified objectively Subsequently, a more detailed analysis in the field of science mapping was performed Focusing on keywords as a unit of analysis, the existing and possible future relationships between the topics were investigated
Keywords and their trends revealed the main themes on which researchers have focused over the years and that dominate the research landscape
RESULTS
Figure 2
PRISMA flow chart for the screening process
493 included articles from a starting value of 4270 papers.
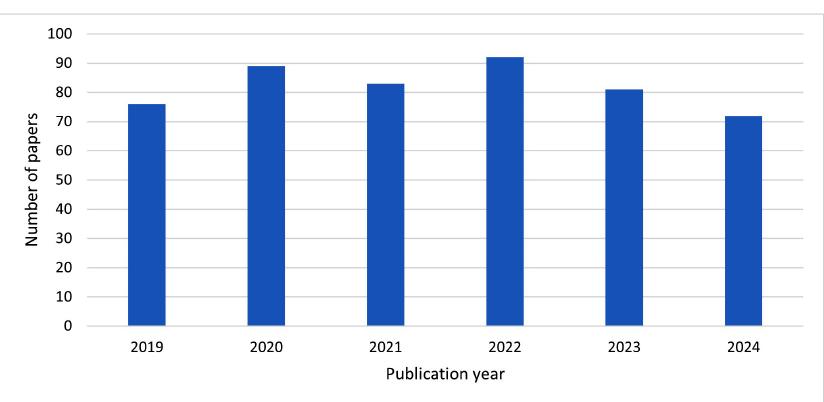
Figure 3
Distribution of the number of papers per year
Figure 3 shows the annual change of studies from 2019 to 2024 The number of papers remains stable overall, highlighting a constant attention to the topic
The 493 publications identified are distributed across 253 different sources
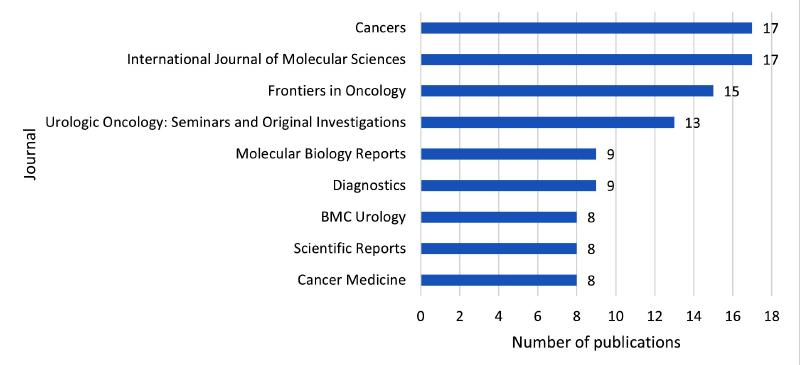
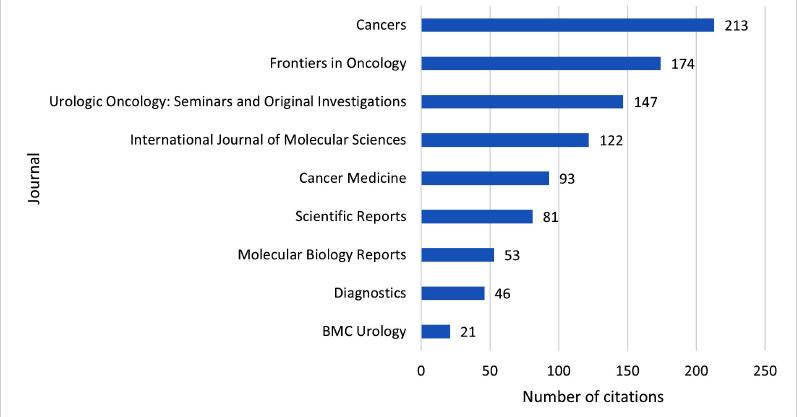
Figure 4 exhibits the top 10 journals that contributed to the domain of bladder cancer biomarkers and in Figure 5 the citations received are reported Cancers, International Journal of Molecular Sciences and Frontiers in Oncology published the highest number of articles (17 in the first 2 and 15 in the third), that received a high number of citations (respectively 213, 122 and 174) Urologic Oncology:
Figure 4. Journals number of publications over the last 5 years.
Figure 5. Journals number of citations over the last five years.
Seminars and Original Investigations is the first journal in the purely urological sector for the number of papers published, that is 13 with 147 citations With 104 total publi-
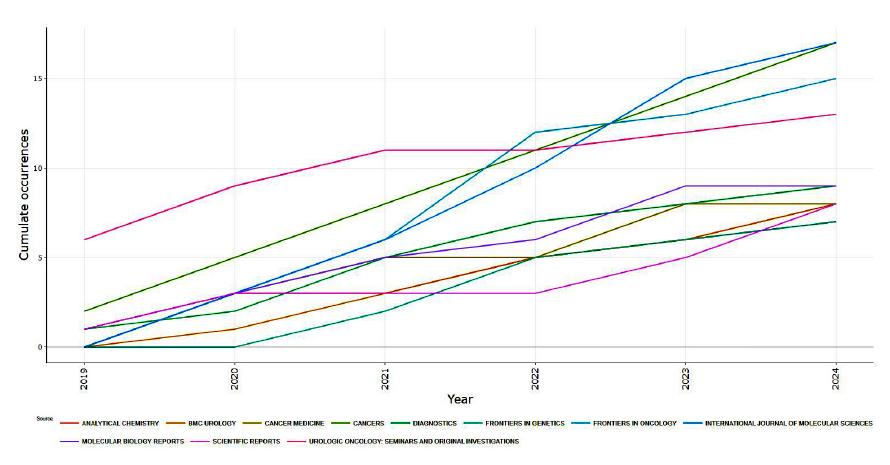
Figure 6. Distribution of Sources over the last 5 years
cations, the top 10 journals published 21% of all publications identified in the last 5 years Figure 6, instead, shows the evolution over time of publications on leading sources
Archivio Italiano di Urologia e Andrologia 2025; 97(1):13396
R Falabella, V De Simone, F Crocetto, et
Figure 7. Journals number of citations over the last five years
Table 1.
Number of country publications and distribution of SCP and MCP articles in percentage.
* Number of art c es based on the correspond ng authors ** Populat on in mi lions of inhab tants
Performance of countries/regions on global output
Table 1 and Figure 7 show the leading countries (the first 15) that published the highest number of papers related to bladder cancer biomarkers based on the nationality of the corresponding author All articles were analyzed also considering the difference between SCP (Single country publication) and MCP (multi country publication) to indicate in addition to the corresponding authors also the other authors belong to the identified country China published the highest number of papers (200) which represents 40 6% of all the articles identified, followed by the USA which published 41 articles (8 3% of the sample), although this primacy goes to Greece, followed by Poland,
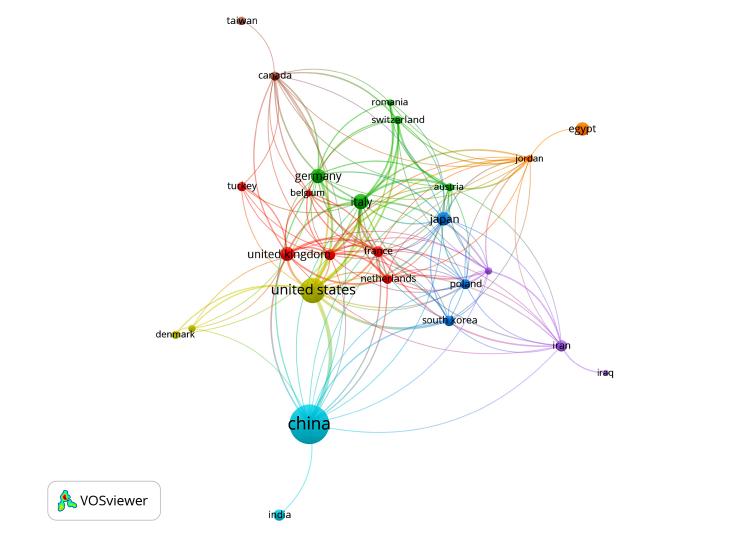
Korea, and Italy considering the ratio between the articles published and the population (expressed in millions of inhabitants) of the countries considered Some countries, such as Egypt and India, published exclusively SCP-type articles The countries with at least half of MCP articles and therefore greater collaboration at an international level are Greece (66 6%), Italy (53 8%), Korea (50%), and France (50%) With respect to collaborations between authors from different countries, Figure 8 highlights the collaboration network identified in the selected papers The different colors highlight the main clusters of co-authorship collaborations identified It is clear that there are countries that have numerous collab-
orations (China, USA, Italy, Germany, Japan) and others with very limited collaborations (Egypt only with Jordan; India only with China; Iraq only with Iran; Taiwan only with Canada)
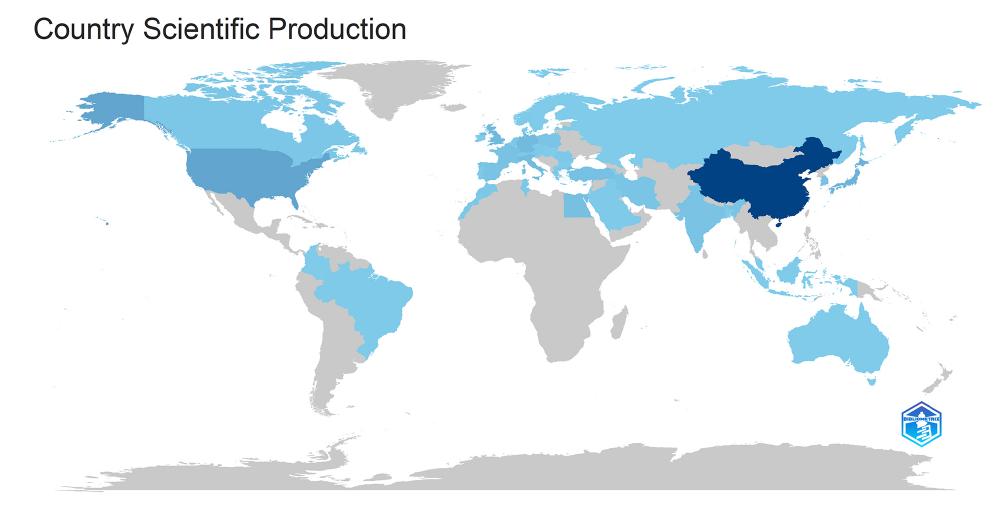
The Country Scientific Production (Figure 9 and Table 2) was also calculated by measuring the total number of Authors by country affiliation
The number was obtained by considering the number of Corresponding Authors plus the number of co-authors of the same nationality who authored each paper
As a result, the sum of values of Scientific Production of all the countries is higher than the total number of papers considered (each paper contributing with more authors apart from papers with a single authorship)
The results obtained numerically for the first 20 countries are reported in Table 2, where the overall production and total number of citations were also related to the population of the countries (millions of inhabitants in the year 2023) China and the USA are the top countries with respectively 1660 and 430 authors identified, however,
R Falabella, V De Simone, F Crocetto, et al
Figure 9. Country scientific Production The highest saturation for the major number of publications
Figure 8. Clusters of international collaborations
Table 2.
Results of top ten countries based on the country scientific production
considering the Country Scientific production per million inhabitants, Denmark, Greece, Tunisia, Netherlands, UK, and Italy are the countries with the highest scientific production
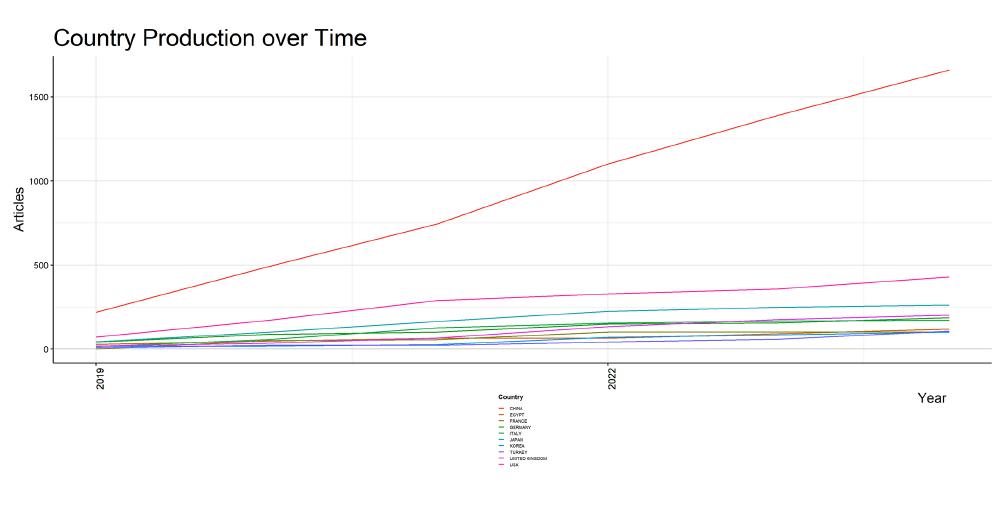
Figure 10 shows the trend of publications over time, showing strong growth for China and much slower growth for the remaining countries
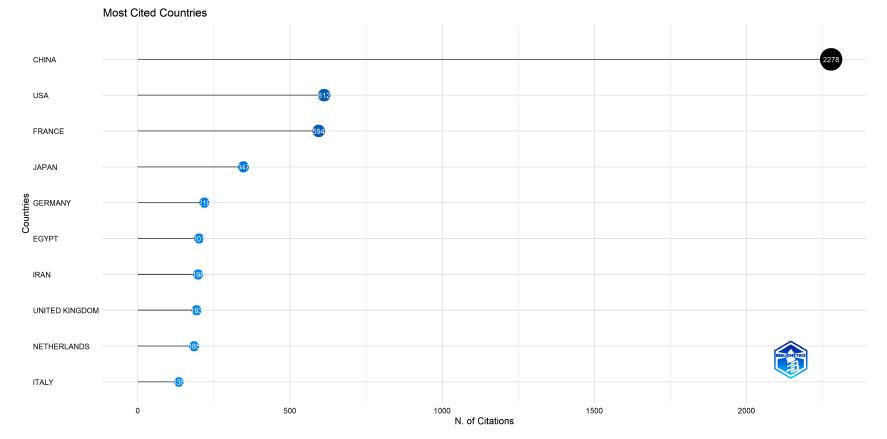
Focusing, instead, on the citations received by the different countries (Figure 11 and Table 2), a different trend is noted China, the USA and Japan maintain the first positions, followed by countries such as France, or Iran which obtained a high number of citations despite a lower production This aspect could depend on numerous factors: a greater or lesser quality of the published papers, different possibilities of access to the papers (open access or subscription), or a different temporal distribution of the works with relative impact on the recorded citations
Table 3 analyses the results of the different countries compared to European and non-European countries
Although with a lower overall number, 94 corresponding authors and 921 Country scientific production for EUcountries and 380 and 3300 for the others, the works published at the European level show a higher ratio between the citations received and the works published (respectively 1 69 versus 1 31)
Furthermore, as also highlighted in Table 2 considering
Table 3. Results of the EU- countries and no EU-countries
the overall population of the countries considered, at the European level the number of publications and citations received per million inhabitants is higher
Affiliations performance analysis
Going into the details of the authors’ affiliations, 1011 affiliations were identified for the 493 papers
Figure 11 Country Distribution of the number of citations
Population in mil ions of inhabitants
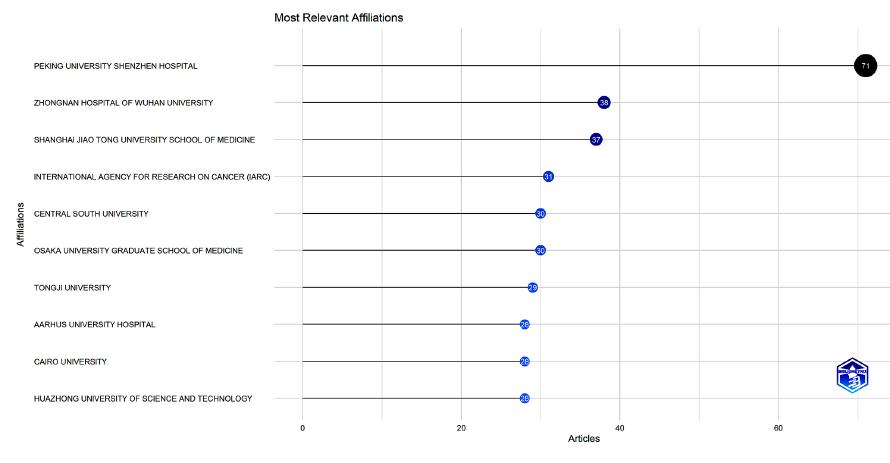
Figure 12. Most relevant affiliations
Figure 12 displays findings of the most relevant institutes, based on the corresponding authors, that are pub-
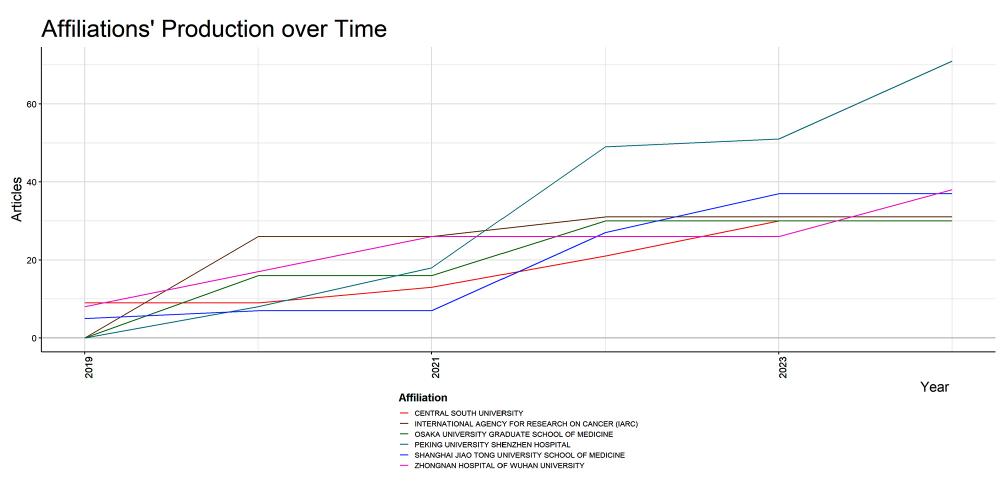
Hospital published 71 papers, followed by Zhongnan Hospital of Wuhan University and Shangai Jiao Tong University School of Medicine with 38 and 37 papers respectively These main institutes also show (Figure 13) an increase in publications in the last 5 years Extending the evaluation to all the authors of the papers, the first five institutes are reported in Table 4, with evidence also of the increase over time
Table 4
Affiliations’ publications over timeDetails
Figure 13
Affiliations’ production over time
Figure 14.
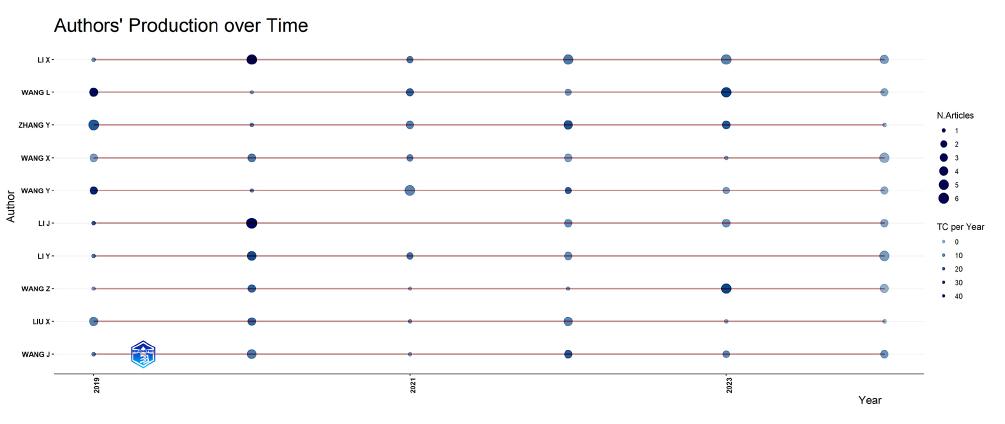
Most relevant authors based on the number of document over times
Authors performance analysis
For 493 papers, a total of 3373 different authors were identified with an average of 9 42 authors per paper Only 3 articles are published by a single author Furthermore, the international co-authorship is equal to 20 08%
Table 5 identifies the leading authors who published papers related to bladder cancer biomarkers in the last 5 years
Li X published 21 papers, followed by Wang L, Wang X Wang, Y and Zhang Y, who published 17 articles each Li X was the highest cited author (345), followed by Wang C
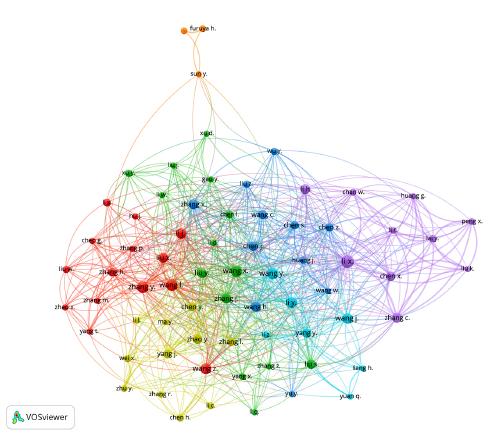
and Wang Y, who received 336 and 333 citations, respectively (Table 5, Figure 14) The co-occurrence of authors is shown in Figure 15
Documents performance analysis
Table 6 displays the highly cited papers on bladder cancer biomarkers Among these, a paper Alix-Panabieres C et al published in 2021, received the highest citation (457) The subsequent most highly cited articles were by Usuba W et al 's paper, which was published in 2019 and received 174 citations (Table 6)
Table 5. Most leading authors (number of papers and citations).
Author Number of documents Total citations
Li X 21 345
Wang L 17 261
Wang X 17 139
Wang Y 17 333
Zhang Y 17 278
Li Y 15 249
Wang Z 15 164
Li J 14 294
Wang J 14 206
Wang H 13 262
Zhang C 13 91
Zhang J 13 257
Li H 12 124
Liu X 12 141
Zhang X 12 259
Zhao Y 12 229
Chen J 11 311
Chen X 11 295
Liu S 11 167
Liu Y 11 90
Yang Y 11 221
Chen Y 10 67
Wang C 10 336
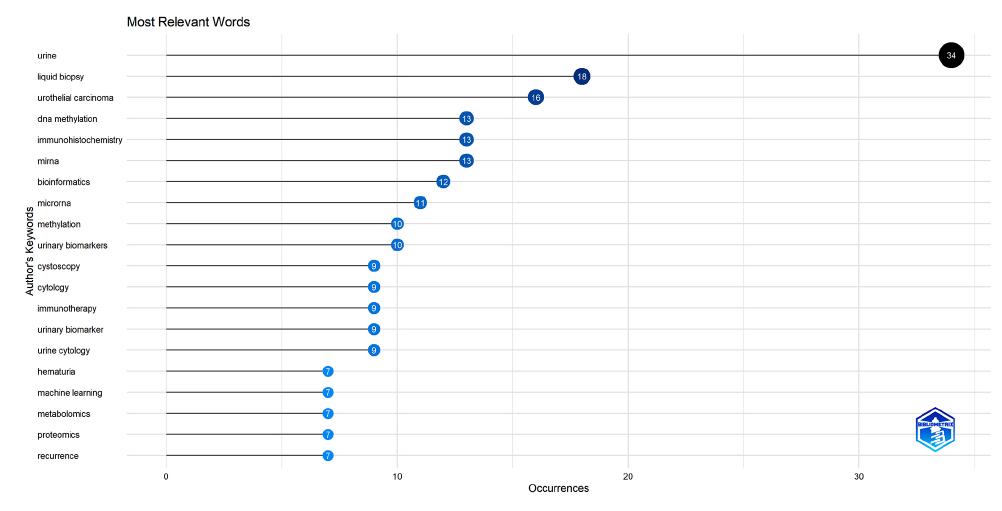
Figure 16. Most relevant keywords.
Figure 15. Co-authorship distribution
papers identified (for example review, meta-analysis) were excluded In this way, the top relevant keywords found in this analysis, according to the level of occurrence, were
Keywords performance analysis
In the present analysis, various keywords were used in the domain of bladder cancer diagnostic biomarkers
Keyword performance analysis was carried out excluding the keywords used for primary research for example bladder cancers, biomarker, and all similar The keywords related to the methods applied in the
urine (34 papers), liquid biopsy (18 papers), urothelial carcinoma (16 papers), DNA methylation (13 papers) and miRNA (13 papers) (Figure 16) Considering the frequency over the years considered, there is a growing use of the world urine, liquid biopsy, methylation, and miRna that confirm the interest in mini-invasive research of novel biomarkers for the diagnosis of BC (Figure 17)
Archivio Italiano di Urologia e Andrologia 2025; 97(1):13396
R Falabella, V De Simone, F Crocetto, et al
Table 6. The top ten most cited papers.
Liquid biopsy: From discovery to clinical application
Circulating miRNA panels for specific and early detection in bladder cancer
Urine DNA methylation assay enables early detection and recurrence monitoring for bladder cancer
Evaluation of serum exosomal LncRNA-based biomarker panel for diagnosis and recurrence prediction of bladder cancer
The systemic immune-inflammation index is associated with an increased risk of incident cancer – A population-based cohort study
A renal-clearable macromolecular reporter for near-infrared fluorescence imaging of bladder cancer
Permutation-based identification of important biomarkers for complex diseases via machine learning models
Highly sensitive detection of bladder cancer-related miRNA in urine using time-gated luminescent biochip
LncRNA PVT1 regulates VEGFC through inhibiting miR-128 in bladder cancer cells
Diagnostic accuracy of novel urinary biomarker tests in non-muscle-invasive bladder cancer: A systematic review and network meta-analysis
Authors
Al x-Panabières C , Pantel K
Usuba W , Urabe F , Yamamoto Y , Matsuzaki J , Sasaki H , Ich kawa M , Takizawa S , Aoki Y , N ida S , Kato K , Egawa S , Chikaraishi T , Fuj moto H , Ochiya T
Chen X , Zhang J , Ruan W , Huang M , Wang C , Wang H , Jiang Z , Wang S , Liu Z , Liu C , Tan W , Yang J , Chen J , Chen Z , Li X , Zhang X , Xu P , Chen L , Xie R , Zhou Q , Xu S , Irwin D L , Fan J -B , Huang J , Lin T
Zhang S , Du L , Wang L , J ang X , Zhan Y , Li J , Yan K , Duan W , Zhao Y , Wang L , Wang Y , Shi Y , Wang C
Fest J , Ruiter R , Mulder M , Groot Koerkamp B , Ikram M A , Stricker B H , van Ei ck C H J
Huang J , J ang Y , Li J , He S , Huang J , Pu K
Mi X , Zou B , Zou F , Hu J
Wang Y , L Z , Lin Q , We Y , Wang J , Li Y , Yang R , Yuan Q
Yu C , Longfei L , Long W , Feng Z , Chen J , Chao L , Peihua L , X ongbing Z , Hequn C
Laukhtina E , Sh m S R , Mori K , D'Andrea D , Soria F , Rajwa P , Mostafaei H , Compérat E , Cimadamore A , Moschini M , Teoh J Y -C , Enikeev D , Xylinas E , Lotan Y , Palou J , Gontero
P , Babjuk M , W tjes J A , Kamat A M , Roupret M , Shariat S F , Pradere B , European Association of Uro ogy-Young Academic Urologists (EAU-YAU): Urothelial Carc noma Working Group
Source title
Cancer Discovery
Cancer Dcience
Journal of Cinical Investigation
Journal of Cellular and Molecular Medicine
International Journal of Cancer
Angewandte Chemie - International Edition
Nature Communications
ACS Sensors
Journal of Cellular Physiology European Urology Oncology
Figure 17. Keywords frequency over time.
DISCUSSION
To the best of the authors’ knowledge, this is the first bibliometric analysis focusing on research based on new biomarkers in the diagnosis of bladder cancer from 2019 to 2024 over the last 6 years The Scopus database was used to generate an eligible set of articles related to the topic field including only research articles from peer-reviewed journals to guarantee the high level of the publications analyzed
The six-year time interval taken into consideration was chosen with the aim of evaluating how research has evolved in the last period, how it is changing, and which are the most important and recent results Several parameters have been taken into consideration such as journals, the contribution of nations and organizations, citations, leading countries, author’s contributions and keywords
With the support of the bibliometric analysis and mapping a better visualization of organizations and dynamics of science domains have been done to make a deep description of this scientific field and to provide predictions for future trends
The analysis revealed that the distribution of publications over the 6-year interval remained almost constant, highlighting an ever-present interest in the field under study
An interesting finding of this bibliometric analysis was that most of the papers were published in the most influential and pertinent journals, having a high impact factor, this underlining that the papers published are characterized by a lot of citations
Even if some countries, like Egypt and India, published exclusively SCP-Type articles, other nations showed at least half of MCP-articles showing greater collaborations at an international level This is the case of Greece with 66 6%, Italy with 53 8%, and Korea and France with 50% of MCP article The number of citations of these MCP articles underlined also the strong value of the publications on the field in analysis and the high impact on research
The main clusters of international collaborations and coauthorship were shown in Figure 8 and underlined how nations like Italy, the USA, China, Germany, and Japan had numerous collaborations while Egypt, Taiwan, Iraq, and India showed limited collaborations, this confirming the results of our analysis on their propension to SCParticles
The journals which produced the greatest number of works were Cancers, International Journal of Molecular Sciences, and Frontiers in Oncology and they received a high number of citations, confirming their role in producing highly impactful publications Urologic Oncology: Seminars and Original investigations was the first purely urological Journal for publications in this field, with 13 works and 147 citations It should be noted that the top ten journals published 21% of all publications identified by our analysis
Considering the number of national publications (Figure 9), China was the best publisher, with the highest number of papers in this field (200), representing the 40% of all articles The second country for the number of publications was the USA with 41 articles (8 3%) Considering the pure number of citations, China is in the first place, but considering the country's production over time, Figure 10 showed how China, the USA, and Japan were
the first publishers with a growing interest, followed by France and Iran that on the contrary obtained a high number of citations despite a lower production of articles
The explanation for this phenomenon is probably linked to different factors including, better or worse quality of the works, the different possibilities of accessing these works or the different temporal distribution of the articles with a consequent different impact on citations
However, considering the overall population of the different countries, it is above all the European countries that have the greatest scientific production and also the greatest capillarity and resonance of the published works, as evidenced by the greater number of citations received Affiliation Performance analysis details on author’s affiliat i o n s a n d m o s t r e l e v a n
research Peking University Shenzhein Hospital was the first publisher with 71 papers, followed by Zhongnan Hospital of Wuhan University and Shangai Jiao Tong University School of Medicine with respectively 38 and 37 papers, thus confirming that the main institutes correspond to the main country publisher (China) The analysis also confirmed the growing trend of publications of these institutes over the last 5 years, confirming the constant interest in the field of study
The Authors performance analysis showed the highest cited authors, underlining how there was a correspondence between the author with the greatest number of publications and the one with the greatest number of citations, as shown in Table 5
A piece of fundamental importance in our research is repr e s e n t e d b y d o c u m e n t p e r f o r m a n c e a n a l y s i s w h i c
showed the most cited works
In the study of Alix-Panabierès C et al (2021), enormous attention was given to the role of Circulating Tumor Cells (CTC) and Circulating Tumor DNA (ctDNA) as new biomarkers with clinical application in early cancer detection, improved cancer staging, detection of relapse and monitoring of therapeutic efficacy (23)
Usuba W et al. (2019) underlined the role of miRNa profiles as a tool for liquid biopsy in bladder cancer screening and performed a global miRNA profiling of 392 serum samples of bladder cancer patients with 100 non-cancer samples and 480 samples of other cancers as controls, thus demonstrating that the 7-miRNA panel could be a biomarker for the specific and early detection of bladder cancer (24) In this research study, a careful choice of keywords (bladder cancer; circulating microRNA; diagnosis; early detection; liquid biopsy) has shown the real importance and great impact of the topic of work
In the third most cited paper, Chen X et al (2020) developed a diagnostic model capable of identifying Bca-specific methylation markers and compared it with cytology and FISH (25) With this model, they showed how urine tumor DNA methylation assessment for early diagnosis but also for minimal residual tumor detection and surveillance in Bca could be proposed as a rapid, noninvasive, and promising approach to reduce the burden of invasive methods
The keyword performance analysis showed the most relevant words used in the papers and their frequency over time Considering also the frequency over the years, there was a growing use of the words urine, liquid biopsy,
R Falabella, V De Simone, F Crocetto, et al
methylation, and miRna that confirm that the research hotspots are supported by the interest in novel biomarkers for the diagnosis of BC
In this analysis, the choice to exclude the keywords used in the first search was dictated by the desire to increase the appropriateness of the article selection In this way, it was possible to highlight keywords such as liquid biopsy, miRNA, and urine, useful for understanding which type of research the various authors were leaning towards These results have underlined the trend of research towards non-invasive diagnostic approaches such as urinalysis and liquid biopsy
The growing use of these words is also confirmed by the analysis of the frequency of their use in literature over the years, thus underlining that the research hotspots are supported by the interest in identifying new diagnostic methods and new biomarkers in the diagnosis of BC
CONCLUSIONS
This bibliometric analysis demonstrated that research on biomarkers in BC is in rapid evolution Nonetheless, this study has limitations, since we have used only one database, namely the Scopus database which does not represent the entire literature, and some articles not indexed could not be included However, bibliometric analyses are a precise instrument in the field of medicine, giving us the possibility to better understand the evolution of literature, the collaborations, and the value of the papers published Furthermore, it highlighted the links between the various nations, institutes, and authors, bringing to light the great value of collaboration between the different structures
From a clinical point of view, this bibliometric analysis has shown, through the articles taken into consideration, the propensity of the research towards non-invasive methods of diagnosis of bladder carcinoma that could support or replace conventional diagnostic methods It has also underlined the possibility that the combination of different biomarkers could potentially improve diagnostic accuracy and contribute to increasing the accuracy (sensitivity and specificity) of the tests Although large-scale clinical trials are necessary to validate the effectiveness of these biomarkers and also evaluation of the costs of developing urinary biomarkers tests should be taken into account
REFERENCES
1 Karam JA, Lotan Y, Shariat SF Urine Cytology and Commercially Available Urine-Based Markers for Monitoring of Bladder Urothelial Carcinoma Lab Med 2007; 38:48-52
2 Feil G, Stenzl A Tumor marker tests in bladder cancer Actas Urol Esp 2006; 30:38-45
3 Mitropoulos D, Adamakis I, Perimenis P Contemporary diagnosis of bladder cancer Expert Opin Med Diagn 2008; 2:713-20
4 Lopez-Beltran A, Cheng L, Gevaert T, et al Current and emerging bladder cancer biomarkers with an emphasis on urine biomarkers Expert Rev Mol Diagn 2020; 20:231-43
5 Linscott JA, Miyagi H, Murthy PB, et al From Detection to CureEmerging Roles for Urinary Tumor DNA (utDNA) in Bladder Cancer Curr Oncol Rep 2024; 26:945-58
6 Lee HH, Kim SH Review of non-invasive urinary biomarkers in bladder cancer Transl Cancer Res 2020; 9:6554-64
7 Jordaens S, Oeyen E, Willems H, et al Protein Biomarker Discovery Studies on Urinary sEV Fractions Separated with UF-SEC for the First Diagnosis and Detection of Recurrence in Bladder Cancer Patients Biomolecules 2023; 13:932
8 Satam H, Joshi K, Mangrolia U, et al Next-Generation Sequencing Technology: Current Trends and Advancements Biology 2023; 12:997
9 Gogalic S, Sauer U, Doppler S, et al Validation of a protein panel for the noninvasive detection of recurrent non-muscle invasive bladder cancer Biomarkers 2017; 1-8
10 Tan WS, Tan WP, Tan MY, et al Novel urinary biomarkers for the detection of bladder cancer: A systematic review Cancer Treat Rev 2018; 69:39-52
11 Ellegaard O, Wallin JA The bibliometric analysis of scholarly p r o d u
105:1809-31
12 Hossain MM Current status of global research on novel coronavirus disease (COVID-19): a bibliometric analysis and knowledge mapping F1000Research 2020; 9:374
13 Chahrour M, Assi S, Bejjani M, et al A Bibliometric Analysis of COVID-19 Research Activity: A Call for Increased Output Cureus 2020; 12:e7357
14 Kelly JC, Glynn RW, O’Briain DE, et al The 100 classic papers of orthopaedic surgery: A BIBLIOMETRIC ANALYSIS J Bone Joint Surg Br 2010; 92-B:1338-43
15 Vaishya R, Gopinathan P, Gupta BM, et al Scholarly trends in g l o b a l o r t h o
orthopaedics: A bibliometric analysis from 2013 to 2024 J Orthop 2025; 60:35-43
16 Zhang Y, Xiao F, Lu S, et al Research trends and perspectives of male infertility: a bibliometric analysis of 20 years of scientific literature Andrology 2016; 4:990-1001
17 Akbari R, Hantoushzadeh S, Panahi Z, et al A bibliometric review of 35 years of studies about preeclampsia Front Physiol 2023; 14:1110399
DECLARATIONS
Ethical approval: This study did not require ethical approval, considering its nature as a bibliometric analysis
Availability of data and material: All data generated or analyzed during this study are included in this published article
Competing interests: The authors declare that they have no competing interests
Funding: This research received no external funding
Authors' contributions: Conceptualization: V d S , V d P , R F and V F C ; Methodology: V d P , V d S ; Software: V d S ; Validation: N F , B B and F C ; Investigation: V F C and V d S ; Resources: L d G , A P and F d G ; Data curation: V d P ; Writing original draft preparation: V d S and V F C ; Writing-review and editing: R F , V d P and V F C ; Project administration: V d P and V F C All authors have read and agreed to the published version of the manuscript
Acknowledgments: Not applicable
18 Alam BF, Nayab T, Ali S, et al Current Scientific Research Trends on Salivary Biomarkers: A Bibliometric Analysis Diagnostics 2022; 12:1171
19 Wu CC, Islam MdM, Poly TN, Weng YC Artificial Intelligence in Kidney Disease: A Comprehensive Study and Directions for Future Research Diagnostics 2024; 14:397
20 Moher D, Liberati A, Tetzlaff J, Altman DG Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement Int J Surg 2010; 8:336-41
21 Aria M, Cuccurullo C bibliometrix: An R-tool for comprehensive science mapping analysis J Informetr 2017; 11:959-75
22 Han J, Kang HJ, Kim M, Kwon GH Mapping the intellectual structure of research on surgery with mixed reality: Bibliometric network analysis (2000-2019) J Biomed Inform 2020; 109:103516
23 Alix-Panabières C, Pantel K Liquid Biopsy: From Discovery to Clinical Application Cancer Discov 2021; 11:858-73
24 Usuba W, Urabe F, Yamamoto Y, et al Circulating miRNA panels for specific and early detection in bladder cancer Cancer Sci 2019; 110:408-19
25 Chen X, Zhang J, Ruan W, et al Urine DNA methylation assay enables early detection and recurrence monitoring for bladder cancer J Clin Invest 2020; 130:6278-89
26 Zhang S, Du L, Wang L, et al Evaluation of serum exosomal Lnc RNA-based biomarker panel for diagnosis and recurrence prediction of bladder cancer J Cell Mol Med 2019; 23:1396-405
27 Fest J, Ruiter R, Mulder M, et al The systemic immune-inflammation index is associated with an increased risk of incident cancer A population-based cohort study Int J Cancer 2020; 146:692-8
28 Huang J, Jiang Y, Li J, et al A Renal-Clearable Macromolecular Reporter for Near-Infrared Fluorescence Imaging of Bladder Cancer Angew Chem Int Ed 2020; 59:4415-20
29 Mi X, Zou B, Zou F, Hu J Permutation-based identification of important biomarkers for complex diseases via machine learning models Nat Commun 2021; 12:3008
30 Wang Y, Li Z, Lin Q, et al Highly Sensitive Detection of Bladder Cancer-Related miRNA in Urine Using Time-Gated Luminescent Biochip ACS Sens 2019; 4:2124-30
31 Yu C, Longfei L, Long W, et al LncRNA PVT1 regulates VEGFC through inhibiting miR-128 in bladder cancer cells J Cell Physiol 2019; 234:1346-53
32 Laukhtina E, Shim SR, Mori K, et al Diagnostic Accuracy of Novel Urinary Biomarker Tests in Non-muscle-invasive Bladder Cancer: A Systematic Review and Network Meta-analysis Eur Urol Oncol 2021; 4:927-42
Correspondence
Roberto Falabella, MD rfalabella@libero it
Vincenzo Francesco Caputo, MD (Corresponding Author) vincitor@me com
Unit of Urology, AOR San Carlo, Potenza, Italy
Via Potito Petrone 85100 Potenza, Italy
Valentina De Simone vadesimone@unisa it
Valentina Di Pasquale vdipasquale@unisa it
Department of Industrial Engineering, University of Salerno, Italy
Felice Crocetto, MD
Felice crocetto@unina it
Unit of Urology, Department of Neurosciences, Reproductive Science and Odontostomatology, University of Naples Federico II, Naples, Italy
Francesco Del Giudice, MD
Francesco delgiudice@uniroma1 it
Department of Maternal infant and Urological Sciences, Sapienza University Rome, Policlinico Umberto 1 Hospital, Rome, Italy
Angelo Porreca, MD angeloporreca@gmail com
Oncological Urology, Veneto Institute of Oncology (IOV) IRCCS, Padua, Italy
Biagio Barone, MD
Biagio barone@aslnapoli1centro it
Department of Urology, P O San Paolo, Asl Na1 Centro, 80125, Naples, Italy
Nazario Foschi, MD
nazario foschi@policlinicogemelli it
Luca Di Gianfrancesco, MD dr lucadigianfrancesco@gmail com
Department of Urology, Fondazione Policlinico Universitario Agostino Gemelli, IRCCS, Università Cattolica del Sacro Cuore, Rome, Italy
R Falabella, V De Simone, F Crocetto, et al
Management of forgotten double J stents: Insight from a systematic review of case reports
Antonius Galih Pranesdha Putra 1* , Yufi Aulia Azmi 2* , Soetojo Wirjopranoto 1 , Nadya Rahmatika 3 , Agustin Junior Nanda De Niro 1 , Alviano Satria Wibawa 1 , Kevin Muliawan Soetanto 4
1 Department of Urology, Faculty of Medicine, Universitas Airlangga; Dr Soetomo General Academic Hospital, Surabaya, Indonesia;
2 Department of Health Sciences, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands;
3 Faculty of Medicine, Universitas Wijaya Kusuma, Surabaya, Indonesia;
4 Department of Immunology, Faculty of Medicine Siriraj Hospital, Mahidol, University, Bangkok, Thailand
* These authors shared first author
Summary
Background: Double J Stent is one of the procedures frequently performed in the field of urology Forgotten DJ Stent is a problem that can cause serious complications. This systematic review aims to explore complications and management of patients with forgotten double J stents.
Methods: Scientific literature was obtained from PubMed, ScienceDirect, and Google Scholar with a publication year limited to 2013-2023 The search string included ‘forgotten DJ stent, case report, complication’. Inclusion criteria were as follows: (1) case report or series, (2) available individual patient data, and (3) English language. Data are presented descriptively. Results: Of the 210 records, 14 articles published were analyzed after the full-text assessment. Forgotten DJ stent sufferers vary from age 7 years to 88 years Male gender was predominant The initial symptoms were flank pain and micturition disorders. The complications experienced were encrustation, multiple stones formation, emphysematous pyelonephritis, emphysematous perinephric abscess, fragmentation, and vesical calculus In management, it was found that procedures were selected according to patient's situation at that time and the condition of the stent There are case reports that report management that differed from those initially planned All the patients were alive after treatment
Conclusions: A forgotten DJ stent can have serious consequences The management approach requires a combination of various endourological procedures In consideration of potential complications, urologists need to be careful in making decisions about the choice of technique used
Submitted 26 October 2024; Accepted 9 December 2024
INTRODUCTION
The DJ Stent is one of the tools that urologists need to drain and divert upper urinary tract Over the past few decades, there have been continued advances in placement techniques and materials used for ureteral stent This technique has gained recognition from urologists worldwide as a necessary procedure in urology surgical
practice The DJ stent is the most frequently applied indwelling stent in the treatment of symptoms of upper urinary tract obstruction (1)
The DJ stent is essential and frequently employed in various procedures It helps keep the ureters open, ensuring the reduction of swelling and the healing of any potential injuries Therefore, it is considered a useful tool in the postoperative therapy of patients with retroperitoneal tumours or fibrosis, ureteropelvic junction stenosis, ureteral strictures, ureteral stones, or iatrogenic ureteral injury, A DJ stent is typically the preferred treatment option for patients suffering from obstructive uropathy caused by urinary tract stones
Nevertheless, the use of DJ stents can causes some complication (2) Forgotten DJ stent is one of the problems associated with the use of DJ stents which have become a challenging problem for urologists As a consequence of h widespread use of stents, in association to lack of information and compliance with routine follow up visits, patients may forget for years that they have had the placem e n t o f a D J s t e n t i n t h e p e l v i c - u r e
e r a l s y s t e m Hematuria, stent occlusion, migration, fragmentation, encrustation, stone formation, recurrent urinary tract infections (UTI), obstruction of the urinary tract, kidney failure, fistula formation in the iliac arteries, and even fatal complications can result from a forgotten DJ stent (3)
Management of the forgotten DJ stent varies depending on the complications experienced and differs from patient to patient (1) This management requires an individual approach in view of possible long-term and shortterm complications secondary to the use of DJ stents Comparison of complications and assessment of outcomes of management in different cases can provide new insights into managing forgotten DJ stents Managing a forgotten DJ may be time-consuming, complex, complicated, risky, and expensive, so the treatment choice must be precise and accurate (4)
METHODS
Preferred Reporting Items for Systematic Reviews and MetaAnalyses (PRISMA) were adhered to in the present study (5)
Ethics statement
Ethical approval was not crucial for this study, as it did not involve direct patients, and all included data were previously published
The Protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) by PRISMA-P guidelines (PROSPERO CRD42024577367)
Eligibiliy
A systematic search focused on case reports and a series about forgotten double J stents, which featured information on individual patients Case reports published in 2013-2023 having complete individual data, written in English, discussing appropriate topics, namely management and complications of forgotten DJ stents, were included in the analysis Exclusion criteria were being not case report manuscript, lack of individual data, not written in English and not open access Article duplication were eliminated prior to the screening of titles and abstracts
Search strategy and selection of studies
On August 23, 2023, we performed a systematic database search in PubMed, ScienceDirect, and Google Scholar
A n e x h a u s t i v e e x p l o r a t i o n w a s a l s o a c c
through a manual or bibliography search of relevant papers
The keywords "forgotten/neglected double J stent, complication, case report" were used in the search The titles and abstracts of the articles were assessed independently for prospective eligibility as studies for the full-text review
Article extraction
We independently extracted essential information from the included studies using a structured and standardized form The extracted information includes author, year, country, number of patients, age, sex, symptoms, history, forgotten DJ stent time duration, complication, management and outcome
Quality assessment
We independently assessed the risk of bias in included studies by implementing Joanna Briggs Institute (JBI) checklist, that is used for critical appraisal of case studies
We categorized the results as 'yes, cannot tell, and no' (6)
Statistical analysis
A meta-analysis was not feasible because this systematic review evaluated a rare condition which relies on pub-
lished case reports Similar findings of variables, such as symptoms, are grouped to evaluate their frequency
RESULTS
Study selection
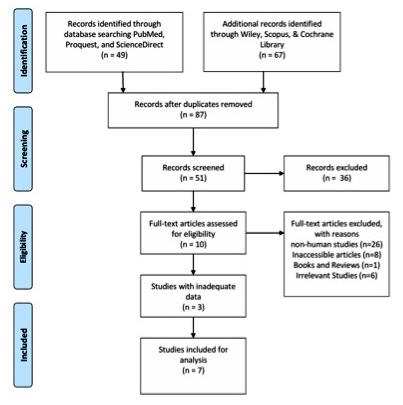
Ten of the 210 records returned by the search were duplicates After sifting through titles and abstracts, we eliminated 149 articles Following the full-text assessment, we included 14 published articles in this systematic review The PRISMA flow diagram (Figure 1) presents the procedure for selecting studies and the exclusion justifications
Quality assessment
We evaluated each included case report using the JBI critical appraisal checklist (Table 1) The summarized critical appraisal checklist shows that the studies were generally of moderate to good quality
Study and demographic characteristics
This systematic review of published cases included 14 case reports (Table 2) Most research was conducted in developing countries, including India (4 studies) Forgotten DJ stent sufferers range in age from 7 to 88 Male gender predominated in most of the studies (10 studies)
A Galih Pranesdha Putra, Y Aulia Azmi, S Wirjopranoto, et al
Figure 1.
Flowchart study selection
Table 1.
Article quality assessment
No Author Were patient’s Was the patient’s Was the current Were diagnostic Was the Was the Were adverse Does the demographic history clearly clinical condition tests or assessment intervention(s) post-intervention e vents (harms) case repor t characteristics described of the patient on methods and the or treatment clinical condition or unanticipated provide clearly described? and presented presentation results clearly procedure(s) clearly described? e vents identifie akeaway as a timeline? clearly described? described? clearly described? and described? lessons?
1 Aboutaleb, et al, 2021, UAE (12) Yes Yes
2 Ahmed, et al, 2021, Yemen (13) Yes
3 Sigdel et al, 2021, Nepal (14) Yes
4 Hee lee et al, 2022, Republ c of Korea (15)
5 Prihadi et al, 2018, Indonesia (16)
6 Alwesali et al, 2022, Saudi Arabia (17)
7 Sharma, 2018, India (18) Yes
8 Ghorai et al, 2022, India (19) Yes
9 Kandem r et al, 2019, Turkey (20) Yes Yes
10 Nihal Er et a , 2023, Turkey (21)
11 Aam ir, et a , 2022, India (22)
12 Gupta et al, 2017, Ind a (23)
13 Yan Gu et al, 2016, China (24)
14 Kumsa, et a , 2022, Ethiopia (25)
Table 2
Research characteristics
NAuthor, year, country
Aboutaleb, et al, 2021, UAE (12)
Ahmed, et a , 2021, Yemen (13)
Sigdel et al, 2021, Nepal (14)
Hee lee et a , 2022, Republic of Korea (15)
Prihad et al, 2018, Indonesia (16)
Alwesali et al, 2022, Saudi Arabia (17)
Sharma, 2018, India (18)
Ghorai et al, 2022, India (19)
Kandemir et al, 2019, Turkey (20)
Nihal Er et al, 2023, Turkey (21)
Aamiir, et al, 2022, India (22)
Gupta et al, 2017, India (23)
Yan Gu et al, 2016, Ch na (24)
Kumsa, et al, 2022, Ethiopia (25)
Symptoms
Most people complain of flank pain and micturition disorders as their initial symptoms Diarrhea and nocturia are sporadic The duration of symptoms varies depending on their appearance
History and forgotten DJ stent time duration
The patient's medical history varies, including procedures related to ureteric/pelvic/kidney stone treatment, ureteral stricture with UTI, a surgical procedure to remove a giant uterine myoma, renal transplant, muscle-invasive bladder
tumour, sigmoid colon cancer, partial resection of the bladder and nonspecific flank surgery In addition, there were patients with a history of previously forgotten DJ stent treatment DJ stents were forgotten per periods ranging from 1 to 17 years
Complications
The complications experienced were encrustation, multiple stones formation, emphysematous pyelonephritis, emphysematous perinephric abscess, fragmentation, and vesical calculus
A Galih Pranesdha Putra, Y Aulia Azmi, S Wirjopranoto, et al
Management and outcome
Procedures used for treatment were based on the patient's situation Sometimes procedures differed from those initially planned
For example, a percutaneous nephrolithotomy (PCNL) was performed in a patient who was originally scheduled for ureterorenoscopy lithotripsy, that was not effective in
Table 3
Management and outcome
Author, year, country
Aboutaleb, et al, 2021, UAE
Ahmed, et a , 2021, Yemen
Sigdel et al, 2021, Nepal
Hee lee et a , 2022, Republic of Korea
Prihad et al, 2018, Indonesia
Alwesali et al, 2022, Saud Arabia
Sharma, 2018, India
Ghorai et al, 2022, India
Kandemir et al, 2019, Turkey
History
Post ureteric stone treatment
Right open nephrolithotomy with double j stent placement due to obstructed right renal pelvis stone
History of extracorporeal shock wave lithotripsy (ESWL)
Ureteral stricture with UTI
Surgical procedure to remove a giant uterine myoma
Renal transplant 13 years ago in India for end stage renal disease of unknown etiology
History of right-sided laparoscopic Anderson-Hynes dismembered pyeloplasty with double J (DJ) stenting performed for right pelviureteric junction obstruction 5 years back
ureterolithotomy with left sided DJ stenting elsewhere 17 years ago for a ureteral stone
Endoscopic stone surgery due to right ureteral stone and kidney stone 11 years ago
DJ stent
removing the DJ stent In another case, the planned cystoscopic laser lithotripsy was not feasible because the preoperative endoscopic examination showed a bladder stone with a radius of about 2 cm at the tip of the double-J catheter from the right kidney
All the patients remained alive after treatment for DJ stent removal
The whole stent was covered with a thick layer of encrustation with multiple stones formation
Double-J stent was separated into four parts and the stones were observed in the total parts of the right urinary tract system from the renal pelvis to the bladder with a 20 £ 15 mm stone impacting the left renal pelvis huge radiolucent bladder stone around the double j stent
Emphysematous pyelonephritis
Encrustation, Emphysematous perinephric abscess
No
No encrustation
Right DJ stent without encrustation and radiopaque shadow in left renal region
Management
Endorse cystolithotripsy with Holmium YAG laser for the bladder calculus and semirigid/flexible ureteroscopy with Holmium YAG laser lithotripsy for ureteral stones and encrusted stent
The left ureteroscopic ureterolithomy and double j stent placement were done under spinal anesthesia during the first operation. Then, right open nephroureterolithotomy with open cystolithotomy were performed after 1 month of previous surgery to remove the stone and forgotten double j stent
Surgical drainage to control the sepsis Few days later after control of sepsis and optimization, left nephrectomy and removal of retained DJ stent was done
Retained DJS removal and vesicolitholapaxy A piece of fractured stent was removed via open ureterolithotomy
Ureterorenoscopic lithotripsy, but it failed to remove the remaining encrusted double-J stent As a result, percutaneous nephrolithotomy was performed successfully
Nephrostomy was performed and antegrade pyelogram
Two weeks later, the patient became hemodynamically stable and underwent a DJ stent removal without any stenting due to stricture
Ureteric stent removal followed by placement of right-sided percutaneous nephrostomy (PCN)
He underwent right nephrectomy followed by left percutaneous nephrolithotomy
An abdominal X ray revealed an encrusted left sided DJ stent with its lower end showing a large radio opacity suggestive of a vesical calculus fragmented and severely encrusted ureteral
Nihal Er et al, 2023, Turkey
A history of kidney stones, and a double-j catheter was placed in her right kidney as a treatment for kidney stones
A bladder stone about 2 cm in size was formed around the double-J catheter
underwent percutaneous cystolithotomy using pneumatic lithotripsy along with removal of the forgotten DJ stent under intravenous antibiotic cover
Cystoscopy was made under general anesthesia
The foreign object was removed with forceps
Then with ureterorenoscope, the stones integrated with the stent at the end of the piece of DJ stent in the ureter were fragmented with pneumolithotriptor
Stone pieces and the second removed part of the stent were extracted with foreign object forceps Then using nephroscope through percutaneous intervention, the stones at the end of the third torn piece of DJ stent were fragmented with pneumolithotriptor They were extracted with forceps
The patient was planned cystoscopic laser lithotripsy
After the pre-operative examinations and follow-up results came out normal, the patient was taken to operation Because a bladder stone with a radius of approximately 2 cm on the end of a double-J catheter from the right kidney was spotted, It was decided that it was no suitable for lithotripsy because of the size of the stone
Therefore, transition to open surgery was decided
Aamiir, et al, 2022, India
The stent placed 11 years back as a part of Percutaneous Nephrolithotomy (PCNL) for right renal stone, had forgotten
Large urinary baldder stone with encrusted Double J stent and calculus deposits along the entire length of the stent
The patient was then managed in two sittings, as an open cystolithotomy, followed a few months later by a combination of uretroscopic lithotripsy and percutaneous lithotomy
it for 6 years, underwent open cystolithotomy for the encrusted DJ stent and concomitant urinary bladder stone, was again lost to follow up
Passage of tube like structure (lower end of right DJ stent) through ileal conduit 15 days back He had undergone radical cystectomy with ileal conduit for muscle invasive bladder tumor six years back in another hospital
Approximately 6 years prior, the patient had undergone simultaneous radical resection of sigmoid colon cancer and partial resection of the bladder
Nonspecific flank surgery 15 years ago
5 years 6 years 6 years 15 years
Bilateral Staghorn Calculus with Forgotten Double J Stent in Ileal Conduit Patient
Patient was successfully treated with minimally invasive therapy in the form of combined bilateral PCNL (Percutaneous Nephrolithotomy) and ESWL (Extracorporeal Shock Wave Lithotripsy) therapy
Presence of an entire coiled double-J stent with calculi from the kidney to the bladder
Severe stent encrustation at the presentation He also had a solitary bladder stone and many pelvic stones discovered
DISCUSSION
Demographic characteristics
Most cases were observed in developing countries, including India (4 cases) A forgotten DJ stent is frequent in developing nations, with patients from lower socioeconomic classes being more susceptible (7) in fact, patients from lower socioeconomic backgrounds may have less access to quality healthcare They need to receive adequate counselling, to avoid misunderstandings about their treatment Individuals from lower socioeconomic classes often face financial constraints that can affect their ability to seek medical care or to attend follow-up appointments Delays in stent removal can increase the risk of complications (26)
The age of patients with forgotten DJ stent ranged from 7 to 88 Male gender predominated in most studies (10 studies) A review of hospital data from 2000 to 2013, including 28 cases of forgotten DJ stents, revealed that the average age of patients was 37 7 ± 14 years (3) A retrospective study on forgotten DJ stent patients between January 2009 and December 2019 reported an average age of 32 1 years (1) Patil et al reported an average age of 56 66 years 2 and Adanur et al. of 38 2 ± 25 06 years (range from 2 to 86 years) (4) Ali observed an average age of 59 12 ± 9 8 years, ranging from 34 to 70 8 The majority of these cases involved men In Adanur’s study, 39 out of 54 patients were men, while 15 were women (4) This contrasts with the findings on another study, where the majority were women, with 9 out of 16 patients (56 25%) (8) Lin et al observed that patients over 60 were 3 6 times more likely to forget their DJ stent than younger patients (27)
Symptoms
Most patients complained of flank pain and micturition disorders as their initial symptoms Diarrhea and nocturia are sporadic The duration of symptoms was variable A study identified urinary irritation and hematuria as the most frequent complaints (3) In another study, pain and dysuria
A computed tomography scan revealed mild hydronephrosis of the left kidney and one J end of the stent in the bladder. The stent was removed successfully by cystourethroscopy and holmium laser lithotripsy
Cytolithotrity and semirigid ureteroscopy with laser lithotripsy were performed, and the encrusted stent was removed Subsequently, an open cytolitotomy was done Followed by an ultrasound-guided PCNL at which time the remaining stones were removed
were the most common issues (1) Patil et al reported that patients typically presented with low back pain, dysuria, hematuria, and fever (2) Additionally, another study indicated that pelvic pain with lower urinary tract symptoms were reported by most patients, with 9 out of 16 (56 25%) experiencing these symptoms Recurrent urinary tract infections were found in 2 patients (12 5%), while 4 cases (25%) showed no symptoms (8)
History and forgotten DJ stent time duration
The medical history of patients varies, including procedures related to ureteric/pelvic/kidney stone treatment, ureteral stricture with UTI, surgical removal of a giant uterine myoma, renal transplant, muscle-invasive bladder tumour, sigmoid colon cancer, partial resection of the bladder and nonspecific flank surgery In addition, there are patients with a history of previously forgotten DJ stent treatment DJ stents remained forgotten for a period ranging from 1 to 17 years Other studies reported an average stent indwelling time of 38 96 months1, 22 6 ± 30 3 (6144) months 4 and 1 73 ± 0 9 (0 11-3 4) years (8) DJ stents generally must be replaced or removed within six weeks to 6 months to avoid complications (2)
Complications
The complications observed were encrustation, multiple stones formation, emphysematous pyelonephritis, emphysematous perinephric abscess, fragmentation, and vesical calculus (1) The study of Hajjaj reported several complications occurring during or after stent removal, including stent fragmentation (20%), fever (16%), sepsis (8%), and hematuria requiring a transfusion (4%) (9) In a series of 16 cases, severe stent encrustation was seen in ten cases; two cases involved urinary tract obstruction, one involved stent migration, and two involved stent fragmentation8 Another study reviewed 50 000 procedures performed on 36 688 patients between 1996 and 2021 Complications were related to malposition of the DJ stent, migration and obstruction of the ureteral stent, and symptoms of bladder i r
Gupta et al, 2017, Ind a
Yan Gu et al, 2016, China
Kumsa, et a , 2022, Ethiop a
demanding blood transfusion in 7 instances 10 The severity of symptoms depends on the duration of stent indwelling time and the degree of encrustation and stone formation Longer forgotten stents are more likely to cause significant morbidity (28)
The treatment of case reported in our review yielded the encouraging result that every patient survived, whereas three of the twenty-eight patients involved in another investigation passed out due to complications following the intervention for stent removal (3)
Management and outcomes
The treatment should be multimodal and individualized and often the initial planned treatment has to be changed due to unexpected situations Sometimes the DJ stent cannot be removed with the planned procedure, so a different procedure has to be performed In addition, during the examination, other unexpected problems, such as stones, can be found requiring making adjustments The procedure performed also depends on the patient's condition Many procedures can be performed for the removal of forgotten stents, such as cystoscopic extraction of the stent, percutaneous cystolithotomy (PCLT), percutaneous n e p h r o l i t h o t o m y ( P C N L ) , u r e t e r o r e n o s c o p y l i t h o t r i p s y (URSL), extracorporeal shock wave lithotripsy (ESWL) with cystoscopic stent removal (1) The choice of procedure depends on variables such as location and extent of calcification and associated stent injury All patients with stents should receive counseling regarding potential longterm complications Especially if stents are forgotten for more than a year, they may have a very thick layer of deposits on their surface and may require additional procedures such as shock wave lithotripsy, ureteroscopy (URS), and PCNL, alone or in combination, with great caution to prevent related morbidities (2)
The procedure to be carried out requires accurate preoperative evaluation Preoperative evaluation is critical, involving a thorough history and physical examination, evaluation through urine culture and sensitivity tests, appropriate radiological imaging, such as Kidney Ureter Bladder (KUB) X-ray, ultrasound, or non-contrast CT (NCCT), and serum creatinine assessment (26-28)
Sohrab et al described removal of stent using endourology techniques and extracorporeal shock wave lithotripsy (ESWL) (3) Mahmood et al reported ureteroscopy as the most common primary surgery (1) Another paper reported that 14 children experienced retention of DJ stent retention that were removed using ESWL, cystolithotripsy (CLT), and PCNL (11) In Nawaz Ali's study, four patients underwent cystoscopic stent removal, four CLT, three had CLT followed by PCNL, two had their fragmented stents removed by ureteroscopy and one by open pyelolithotomy (8)
Prevention
Prevention remains a critical aspect of managing forgotten stents, emphasizing the importance of proper patient counseling regarding the stent's indwelling time and the necessity of follow-up Establishing a stent registry with patient details and scheduled removal dates coupled with automated reminders via social media to patients and healthcare providers can significantly reduce the inci-
dence of forgotten stents Additionally, engaging patients and relatives in the follow-up process is essential to prevent complications and mitigate the associated morbidity and healthcare costs The effective management of forgotten DJ stents hinges on a comprehensive approach that integrates timely intervention, meticulous follow-up, and proactive prevention strategies (26-28)
Limitation of the study
This review considered case report data, so further research needs to be carried out prospectively This research also has not been able to explore long-term complications from stent removal management due to forgotten DJ Stent Future research is recommended to investigate complications from stent removal management
CONCLUSIONS
A forgotten DJ stent can lead to significant consequences, necessitating a management approach that combines various endourological procedures while carefully considering potential complications Urologists must exercise caut i o n w h e n
Healthcare providers must inform all patients with an implanted stent about the long-term risks of prolonged stenting and stress the need for timely removal or replacement
REFERENCES
1 Mahmood K, Singh KH, Upadhyay R, et al Management of forgotten double-J stent in a tertiary care center with ten years of experience: a retrospective study Int Surg J 2020; 7:2615
2 Patil S, Raghuvanshi K, Jain DK, Raval A Forgotten ureteral double-J stents and related complications: a real-world experience African J Urol 2020; 26:8
DECLARATIONS
Ethical approval: Ethical approval was not crucial for this study, as it did not involve direct patients, and all included data were previously published
Availability of data and material: Availability of Data and Materials Data and materials used in our study are open to access by request
Competing interests: No conflict of interest was declared by the authors
Funding:A u t h o r s ' c o n t r i b u t i o n s : Y A A , S W , N R , A G P P , A J N D N a n d K M S ; M e t h o d o l o g y : Y A A , S W , N R , A G P P, A J N D N and K M S; Investigation: Y A A, S W, N R, A G P P, A J N D N, A S W, and K M S; Writing Original Draft: Y A A, S W, N R, A G P P, A J N D N, A S W, and K M S; Writing review & editing: Y A A, S W and K M S; Resources: Y A A, S W, N R, A G P P, A J N D N and K M S; Visualization: N R, and A G P P; Supervision: Y A A and S W
Acknowledgments: None
Conference presentation: This article has never been presented at any conference before
A Galih Pranesdha Putra, Y Aulia Azmi, S Wirjopranoto, et al
3 Sohrab A, Aneesh S, Sureka SK, et al Forgotten Reminders: an Experience with Managing 28 Forgotten Double-J Stents and Management of Related Complications Indian J Surg 2015; 77:1165-1171
4 Adanur S, Ozkaya F Challenges in treatment and diagnosis of forgotten/encrusted double-J ureteral stents: the largest single-center experience Ren Fail 2016; 38:920-926
5 Page MJ, McKenzie JE, Bossuyt PM, et al The PRISMA 2020 statement: an updated guideline for reporting systematic reviews BMJ 2021; 372: n71
6 Joanna Briggs Institute Critical Appraisal Tools Checklist for Case Reports Available from: https://jbi global/sites/default/files/202008/Checklist for Case Reports pdf
7 Jhanwar A, Bansal A, Prakash G, Sankhwar S Endourological Management of Forgotten Double J Ureteral Stents: A Single Centre Study SM J Urol 2017; 3:1-3
8 Ali N, Somarendra K, Ali A Forgotten Double-J Stent: Evaluation and Management in a Tertiary Hospital in the North East India International Journal of Scientific Study 2021; 9:103-8
9 Al-Hajjaj M, Alam OA, Abu-Hussein B, et al Forgotten Double-J ureteral stent: An analysis of 25 cases in a tertiary hospital Ann Med Surg 2022; 80:104223
10 Geavlete P, Georgescu D, Mul escu R, et al Ureteral stent complications - experience on 50,000 procedures J Med Life 2021; 14:769-775
11 Nerli RB, Magdum PV, Sharma V, et al Forgotten/retained double J ureteric stents: A source of severe morbidity in children African J Paediatr Surg 2016; 13:32-35
12 Aboutaleb H A neglected double J ureteral stent for 10 years: A rare case report Urol Case Reports 2021; 36:101570
13 Ahmed F, Al-Wageeh S, Ghabisha S, et al A case report of forgotten double J stent with giant calculus formation from the renal pelvis to the bladder J Emerg Med Trauma Acute Care 2021:13
14 Sigdel B, Shrestha S, Maskey P Forgotten DJ stent presenting with emphysematous pyelonephritis: A life threatening complication Int J Surg Case Rep 2021; 87:106405
15 Lee IH, Shin HS, Ahn DJ A forgotten double-J ureteral stent resulting in an emphysematous perinephric abscess: A case report Medicine (Baltimore) 2022; 101:E29418
16 Prihadi JC, Kusumajaya C Double-J stents forgotten for four years: A case report Med J Indones 2019; 28:280-283
17 Alwesali SM A long forgotten ureteral stent for 13 years post renal transplantation Urol Case Reports 2022; 44:102156
18 Sharma A, Garg G, Sharma D, Singh M Fungal bezoar in an immunocompetent patient: A rare complication of forgotten double J stent BMJ Case Rep 2018; 2018:bcr2018226904
19 Ghorai RP, Talwar HS, Mittal A, et al A 17-year-old indwelling ureteral stent with large vesical calculus at one end: The tombstone of a forgotten Double “J” stent J Fam Med Prim Care 2022; 11:796-798
20 Kandemir A, Sönmez MG Treatment of fragmented and severely encrusted ureteral double-J stent forgotten for 11 years through multimodal endourological methods Urol Ann 2019; 11:310-313
21 Er ZN, Tiryaki SE, Erdener Çeliktürk C, Avlan D Forgotten Double-J Stent With Bladder Stone Formation: a Pediatric Case Turkish Med Student J 2023; 10:133-135
22 Aamir S Forgotten double J stent with maximum stone burden J Clin Images Med Case Reports 2022; 3:128-133
23 Gupta R, Dey RK, Sharma R, Gupta S Bilateral staghorn calculus with forgotten double j stent in ileal conduit patient - A rare urological challenge J Clin Diagnostic Res 2017; 11:PD9-10
24 Gu Y, Zhang J, Wang G Use of cystourethroscopy to remove an indwelling double-J ureteral stent 6 years following simultaneous radical sigmoid colon cancer and partial bladder resection: A case report Exp Ther Med 2016; 11:2467-2469
25 Kumsa ID, Gebreamlak AL, Leul MM, et al A case report on the management of neglected and forgotten DJ stent for 15 years with severe encrustation and multiple renal and bladder stones Int J Surg Case Rep 2023; 103:107859
26 Vajpeyi V, Chipde S, Khan FA, Parashar S Forgotten double-J stent: Experience of a tertiary care center Urol Ann 2020; 12:138143
27 Lin TF, Lin WR, Chen M, et al The risk factors and complications of forgotten double-J stents: A single-center experience J Chin Med Assoc 2019; 82:767-771
28 Cheng W, Chiu YC, Fan YH, et al Risks of forgotten double-J ureteric stents after ureterorenoscopic lithotripsy in Taiwan: a nationwide population-based study Sci Rep 2020; 10:20711
Correspondence
Soetojo Wirjopranoto (Corresponding Author) stjowirjopranoto@gmail com
Department of Urology, Faculty of Medicine, Universitas AirlanggaDr Soetomo General Academic Hospital, Jl Mayjen Prof Dr Moestopo No 6-8, Surabaya, East Java, Indonesia, 60286
Antonius Galih Pranesdha Putra galihpranesdha@gmail com
Agustin Junior Nanda De Niro deniro nanda@yahoo co id
Alviano Satria Wibawa alvianosw65@gmail com
Department of Urology, Faculty of Medicine, Universitas AirlanggaDr Soetomo General Academic Hospital, Surabaya, Indonesia
Yufi Aulia Azmi yufiazmi@gmail com; y aulia azmi@umcg nl
Department of Health Sciences, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands
Nadya Rahmatika nadyasaham@gmail com
Faculty of Medicine, Universitas Wijaya Kusuma, Surabaya, Indonesia
Kevin Muliawan Soetanto kmskevinmuliawan@gmail com
Department of Immunology, Faculty of Medicine Siriraj Hospital, Mahidol, University, Bangkok, Thailand
A comprehensive systematic review of studies on the potential of A49T and V89L polymorphism in SRD5AR2 as high susceptibility gene association with benign prostate hyperplasia and prostate cancer
1 Medical Faculty, Universitas Brawijaya, Malang, Indonesia;
2 Urology Department, Faculty of Medicine Universitas Brawijaya, Dr Saiful Anwar General Hospital, Malang, Indonesia
Summary
Introduction and objectives: Being the most common disease in aged men, the etiology of Benign Prostatic Hyperplasia (BPH) is not fully defined. Recent studies have reported that the association between Benign Prostate Hyperplasia and metabolic genes is still inconsistent
A gene connected with BPH is SRD5AR2, whose polymorphisms, A49T and V89L, have distinct enzyme activity This systematic review examines SRD5AR2 polymorphisms within two alleles (A49T and V89L), assessing their roles as prognostic indicators of malignancy, and response to medication
Materials and methods: We conducted a search on six different databases, including PubMed, Scopus, Wiley, ProQuest, Cochrane Central, and Science Direct using as string of keywords (BPH) AND [(rs523349) OR (V89L)] AND [(rs9282858) OR (A49T)]. We finally selected seven articles to be extracted. Quality appraisal of clinical trials was evaluated using the Joanna Briggs Institute Approach for systematic reviews
Results: We sorted nine clinical studies from various countries examining SRDA52 polymorphism and its association of BPH and prostate cancer About V89L we found that the "LL" genotype, indicating reduced 5α-reductase activity, is linked to a lower BPH risk, while the "VV" genotype may slightly increase BPH risk About A49T, compared to “AA” genotype, “AT” tends to be associated to higher risk in developing prostate cancer A49T polymorphism does not show any effect on medical treatment while V89L showed a protective effect on the clinical progression of BPH when treated with 5a-reductase inhibitors, aadrenergic receptor antagonists, and alpha blockers.
Conclusions: SRD5A2 polymorphisms could be a good indicator for prognostic malignancy and a potential tool for personalized medicine of BPH The findings strongly support the recommendation for further study about SRD5AR2 to enhance its use for screening and prevention and to optimize the medical treatment of Benign Prostatic Hyperplasia
Submitted 30 October 2024; Accepted 5 December 2024
INTRODUCTION
Benign prostatic hyperplasia (BPH) is the most common cause of lower urinary tract symptoms (LUTS) in men due to bladder outlet obstruction (1) Symptoms range from increased urinary hesitancy, urgency, and frequency to acute urinary retention Histologic BPH is found in approximately 50% of men aged 50 years, and its prevalence increases about 10% each subsequent decade (2) Likewise, significant LUTS are documented to occur in about 10%20% of men aged 50-59 and increase to one-third of men by ages 70-79 In parallel, prostate volume increases between age 40 and age 79, with the greatest increases appearing in the sixth and seventh decades of life (3) Recent studies have uncovered several genes linked to both BPH and prostate cancer For instance, Li et al (4) investigated the V89L and A49T SRDA52 polymorphisms, while Zhang et al expanded the search by examining genotype distributions of SRD5A2, CYP17, CYP19, and VDR genes in Chinese populations (4, 5) Additionally, Choubey et al (5) focused on polymorphisms at the (TA)n locus Together, these investigations, alongside others exploring c
enhanced our understanding of the genetic factors that may impact the development of BPH and prostate cancer Previous researchers have noted the presence of alleles with low catabolic activity including two polymorphic sites: an alanine to threonine substitution at codon 49 (A49T) and a valine to leucine substitution at codon 89 (V89L) (6) The V89L polymorphism correlates with reduced concentrations of androstanediol glucuronide, free testosterone, and testosterone (7) Individuals with the “LL” genotype exhibit a slight, nonsignificant, decrease in androstanediol glucuronide concentrations compared to those with the “VV” genotype The L allele's moderate reduction in SRD5A2 activity results in lower dihydrotestosterone (DHT) levels, although the biological mechanism behind this genotype's connection with decreased DHT production remains unclear (4) However, DHT levels in the prostate are influenced by various factors, including testosterone metabolism and DHT inactivation Testosterone, not DHT, appears to be the primary androgen promoting prostate
carcinogenesis (8) In addition to the V89L polymorphism, the SRD5A2 A49T is linked to a significantly lower concentration of androstanediol glucuronide, indicating its impact on androgen metabolism (9) The SRD5A2 polymorphism likely represents a crucial point in DHT metabolism, possibly explaining its association with prostate cancer risk This underscores the complexity of genetic factors influencing prostate cancer susceptibility Both polymorphisms likely contribute to variations in androgen levels, potentially influencing prostate cancer development (10) To the best of our knowledge, there has been limited r e s e a r c h a b o u t A 4 9 T a n d V 8 9 L p o l y m o r p h i s m s o f
SRD5AR2 as BPH risk factor Considering the role in benign prostatic hyperplasia and in the risk of malignancy and in their treatment, the Authors were interested in reviewing evidence about SRD5AR2 polymorphisms A49T and V89L, in order to assess their roles as prognostic indicators for malignancy and response to medication
MATERIALS AND METHODS
Data sources and search strategy
The systematic review was carried out based on the Preferred Reporting Items for Systematic Reviews and Meta Analysis (PRISMA) guidelines by utilizing the PubMed, Scopus, Wiley, ProQuest, Cochrane Central, and Science Direct Article search for papers in English was done using boolean operators with the following keywords: [(Benign Prostatic Hyperplasia) OR (BPH) OR (Prostate Cancer)] AND [(rs523349 OR V89L) AND (rs9282858 OR A49T)]
The inclusion criteria were: case-control or cohort study; study investigating gene polymorphisms A49T and V89L in SRD5AR2 and their association with BPH and prostate cancer; written in English Quality appraisal of clinical trials was evaluated using the Joanna Briggs Institute Approach for systematic reviews
Selection process
The authors individually evaluated findings of literature search, beginning with the titles and abstracts of papers which passed eligibility criteria screening Any disagreement was freely discussed with one senior author to settle them The entire text was then examined to weed out research that were not relevant
Data extraction
The selected articles were extracted by the Authors, who then assessed their suitability Disagreements were discussed and ultimately settled after each author reviewed the articles on his own Name of the author, year of publication, country, study design, number of samples, sample characteristics, intervention, comparison, length of followup, and desired outcomes were taken from eligible studies
RESULTS
Study selection
After the literature search, 116 articles were retrieved by the six databases Several articles were excluded due to duplication of studies (n = 29) Some papers were exclud-
ed because they did not adhere to inclusion criteria (n = 36) There were 41 articles excluded due to ineligible data, such as review articles and books, and inaccessible articles due to subscriptions Finally, nine articles were included in the systematic review to be analysed qualitatively and quantitatively
Figure 1 shows the PRISMA flowchart
Study design
This review consists of 9 clinical studies with varying designs: 1 cross-sectional, 3 case-control, 2 cohort studies, and 3 clinical trials The total number of participants across all studies includes 1,226 individuals, comprising prostate cancer patients, BPH patients, and healthy controls Methods of diagnosis and assessment included blood diagnostic criteria, prostate-specific antigen (PSA) testing, digital rectal examination (DRE), and biopsy
includes Bulgaria, China, Japan, the USA, India, and Sweden The review emphasizes the impact of gene polymorphism and its associations with prostate diseases, explores and discusses their implications for personalized medicine
Risk of bias summary
The risk of bias for various study designs; case-control, cohort, and cross-sectional was evaluated using the JBI Critical Appraisal Tools According to the risk of bias assessment, three studies were found to have a moderate risk of bias, primarily due to ambiguous statements in areas such as the identification of confounding factors and the strategies used to address them, as well as incomplete data throughout the studies
The remaining studies (n = 6) were classified as having a low risk of bias (see Figure 2)
Despite the varying levels of bias across the included studies, most of the data have been thoroughly examined and discussed The reviewers concluded that, overall, the studies are sufficiently suitable for analysis
Study result summary
Gene polymorphism
Results for V89L variant of SRD5A2 are reported in Table 1 For the A49T, men with the AT/TT genotypes were at increased risk for BPH, asymptomatic, and symptomatic BPH and prostate cancer compared to men with the AA genotype, although none of the OR reached statistical significance
Association to malignancy
Based on the studies on V89L polymorphism that were evaluated, it was shown that “LL” allele, that confers a low activity of 5 alpha reductase, was less common in patients with prostate cancer On the other hand, “VV” locus, which is commonly found in the Hispanic population, is associated with a higher risk of BPH
The A49T gene consists of “AA” locus and “TT” locus producing “AA”, “AT”, and “TT” genotypes All of the genotypes mentioned have no statistically significant correlation to malignancy, although “AT” and “TT” genotypes have a higher risk of developing prostate cancer “AT”
R Maharani, H Lestari, P Mahakarya Dewa, et al
the literature selection
Figure 1. PRISMA flowchart of
Figure 2. Risk of bias assessment
Table 1
Gene polymorphism
variants were more frequently found among Prostate Cancer patients while “AA” variants were least likely to be found on patients with prostate cancer and BPH
Response to drugs
Both genes demonstrated a protective effect against the clinical progression of BPH when treated with 5α-reductase inhibitors, α-adrenergic receptor antagonists, and alpha blockers Populations with the “LL” genotype were likely more suitable to have a standard or herbal treatment for BPH
DISCUSSION
The results of the present study, when contextualized with previous research (11-16), provide a deeper understanding of the role of genetic polymorphisms in the SRD5A2 gene, particularly V89L and A49T, in the development and progression of prostate pathological condi-
tions like BPH and prostate cancer (PCa) The associations between these polymorphisms and disease risk highlight the genetic mechanisms that may influence prostate enlargement and malignancy, as well as the potential for personalized treatment strategies based on these genetic markers
Our findings on the V89L polymorphism align with previous studies showing that the SRD5A2 gene encoding an enzyme responsible for converting testosterone into dihydrotestosterone (DHT), plays a key role in prostate growth
The activity of this enzyme also known as 5-alpha reductase type 2 is linked to the severity of BPH The V89L polymorphism shows distinct enzyme activity variations that influence androgen levels and drive prostate growth, potentially leading to prostate cancer
Our review found that the "LL" genotype is less common in prostate cancer patients, suggesting that this allele may have a protective effect by lowering 5-alpha reductase activity and, consequently, DHT production
R Maharani, H Lestari, P Mahakarya Dewa, et al
Table 2. Prognostic to Malignancy
Archivio Italiano di Urologia e Andrologia 2025; 97(1):13318
These results are consistent with a study by Konwar et al (17), which reported that the LL genotype is associated with lower androstanediol glucuronide concentrations, thereby reducing free testosterone and DHT levels
This may explain the reduced prostate volume and lower cancer risk in individuals with the "LL" genotype com-
pared to those with the "VV" genotype Furthermore, the higher risk of BPH associated with the "VV" allele was also supported by Lunn et al (18) research, which indicated ethnic differences in V89L polymorphism prevalence
In Asian populations, such as those in India and Japan, the polymorphism was found at higher rates, contribut-
Archivio Italiano di Urologia e Andrologia 2025; 97(1):13318
R Maharani, H Lestari, P Mahakarya Dewa, et al
Table 3. Response to medical treatment
ing to an increased risk of BPH This suggests that the genetic impact of the V89L variant may vary across different ethnicities, with certain populations exhibiting a higher predisposition to prostate diseases
Regarding the A49T polymorphism, our review found no statistically significant association with malignancy, though the "AT" and "TT" genotypes tended to be associated with a higher risk of developing prostate cancer compared to the "AA" genotype This aligns with Giwerchman et al (15), who estimated that the A49T polymorphism could be found in approximately 8% of prostate cancer patients and 6 3% of BPH patients, indicating its role in increasing the probability of developing BPH and prostate cancer Although not as prominent in Asian populations, this polymorphism is commonly observed in Hispanic populations, as well as in certain countries like Turkey and China
While the statistical significance of the A49T polymorphism in relation to malignancy remains inconclusive in our review, these findings emphasize its potential importance as a genetic marker for prostate cancer susceptibility This warrants further research, especially in nonHispanic populations, to determine whether the A49T variant can be used as a predictive tool for prostate disease risk in other ethnic groups
The study findings on gene polymorphisms in the SRD5A2 gene also underscore the potential for personalized medicine in treating prostate-related conditions
According to Li et al (14), the SRD5A2 gene regulates critical hormonal pathways, influencing prostate growth and function This insight into the biochemical pathways driven by V89L and A49T polymorphisms supports the idea of genotype-driven therapeutic approaches
Both V89L and A49T polymorphisms demonstrated protective effects against the clinical progression of BPH when treated with 5-alpha reductase inhibitors and αadrenergic receptor antagonists
These findings imply that personalized treatment strategies based on genetic markers could optimize therapeutic outcomes and reduce the likelihood of disease progression, offering a more tailored approach to managing BPH and prostate cancer
A study by Daryanto et al (19) showed that combination of dutasteride with tamsulosin could give a more significant effect in terms of lowering the contractility of prostate smooth muscle
While the findings of this review are compelling, they also reveal the need for further research The prevalence of V89L and A49T polymorphisms in Hispanic populations has been well-documented, but additional studies in Asian populations are necessary to understand their role in diverse genetic backgrounds For example, as noted by Lunn et al (18), the V89L polymorphism shows high prevalence in India and Japan, suggesting a population-specific effect Expanding genetic studies to include other Asian regions may yield valuable insights into the global relevance of these polymorphisms
Additionally, larger cohort studies and more diverse population sampling are needed to strengthen the associations between these polymorphisms and prostate cancer or BPH risk A more detailed exploration of the mechanistic pathways involved in DHT production and androgen activity, particularly in relation to the SRD5A2 gene,
will be essential for translating these genetic insights into clinical practice
This study confirms the significant role of the SRD5A2 gene and its V89L and A49T polymorphisms, in influencing the risk of prostate disease and its progression
Both variants have distinct effects on the enzyme activity and androgen levels, impacting on prostate growth and the likelihood of developing BPH or prostate cancer
Ethnic differences in polymorphism prevalence further highlight the importance of population-specific genetic research By integrating genetic profiling into clinical practice, personalized medicine approaches may offer
prostate-related conditions, improving patient outcomes while minimizing unnecessary interventions
CONCLUSIONS
In conclusion, this systematic review proves that SRD5A2 is a high susceptibility gene that is linked to BPH A49T and V89L are the polymorphism of the gene involved ninBoth polymorphism varies in different ethnic populations Further studies are required to evaluate different risk factors and outcomes after medical treatment in different geographical situation in order to provide a better theoretical basis to study the role of genetic in the pathogenesis of BPH and prostate cancer
2 Goodarzi D, Cyrus A, Khoddami Vishteh HR, et al Effect of celecoxib on benign prostatic hyperplasia: Results of a preliminary study Urological Science 2011; 22:147-150
3 Middleton LW, Shen Z, Varma S, et al Genomic analysis of benign prostatic hyperplasia implicates cellular re-landscaping in disease pathogenesis JCI Insight 2019; 5:e129749
4 Li Q, Zhu Y, He J, et al Steroid 5-alpha-reductase type 2 (SRD5A2)
DECLARATIONS
Ethical approval: Not applicable
Availability of data and material: All inquiries can be directed to the corresponding author
Competing interests: The authors declare that they have no competing interests
V89L and A49T polymorphisms and sporadic prostate cancer risk: a meta-analysis Molecular biology reports 2013; 40:3597-3608
5 Choubey VK, Sankhwar SN, Carlus SJ, et al SRD5A2 gene polymorphisms and the risk of benign prostatic hyperplasia but not prostate cancer Asian Pac J Cancer Prev 2015; 16:1033-1036
6 Salam MT, Ursin G, Skinner EC, et al Associations between polymorphisms in the steroid 5-alpha reductase type II (SRD5A2) gene and benign prostatic hyperplasia and prostate cancer Urol Oncol 2005; 23:246-253
7 Zeng XT, Su XJ, Li S, et al Association between SRD5A2 rs523349 and rs9282858 Polymorphisms and Risk of Benign Prostatic Hyperplasia: A Meta-Analysis Front Physiol 2017; 8:688
8 Price DK, Chau CH, Till C, et al Association of androgen metabolism gene polymorphisms with prostate cancer risk and androgen concentrations: Results from the Prostate Cancer Prevention Trial Cancer 2016; 122:2332-2340
9 Elzanaty S, Giwercman YL, Giwercman A Significant impact of 5alpha-reductase type 2 polymorphisms on sperm concentration and motility Int J Androl 2006; 29:414-20
10 Neslund-Dudas C, Bock CH, Monaghan K, et al SRD5A2 and HSD3B2 polymorphisms are associated with prostate cancer risk and aggressiveness Prostate 2007; 67:1654-1663
11 Allen NE, Forrest MS, Key TJ The association between polymorphisms in the CYP17 and 5α-reductase (SRD5A2) genes and serum androgen concentrations in men Cancer Epidemiol Biomarkers Prev 2001; 10:185-9
12 Van Gils CH, Onland-Moret NC, Roest M, et al The V89L Polymorphism in the 5-α-Reductase Type 2 Gene and Risk of Breast Cancer Cancer Epidemiol Biomarkers Prev 2003; 12:1194-9
13 Wang C, Tao W, Chen Q, et al SRD5A2 V89L polymorphism and prostate cancer risk: A meta-analysis Prostate 2010; 70:170-8
14 Li J, Coates RJ, Gwinn M, Khoury MJ Steroid 5-α-reductase type 2 (SRD5a2) gene polymorphisms and risk of prostate cancer: A HuGE review Am J Epidemiol 2010; 171:1-13
15 Giwercman YL, Abrahamsson PA, Giwercman A, et al The 5alpha-reductase type II A49T and V89L high-activity allelic variants are more common in men with prostate cancer compared with the general population Eur Urol 2005; 48:679-85
16 Tekin Neijmann S, Kural A, Tinay I, et al Association of missense substitution of A49T and V89L in the SRD5A2 gene with prostate cancer in Turkish patients Turkish Journal of Biochemistry 2017; 42:37-43
17 Konwar R, Chattopadhyay N, Bid HK Genetic polymorphism and pathogenesis of benign prostatic hyperplasia (BPH) BJU international 2008; 5:536-44
18 Lunn RM, Bell DA, Mohler JL, Taylor JA Prostate cancer risk and polymorphism in 17 hydroxylase (CYP17) and steroid reductase (SRD5A2) Carcinogenesis 1999; 20:1727-31
19 Daryanto B, Naim HY, Budaya TN The Effect of Tamsulosin, Dutasteride Monotherapy and Tamsulosin-Dutasteride Combination on Prostate Smooth Muscle Contractility in BPH Model Wistar Strain Rattus Novergicus Medical Archives 2023; 77:13
Correspondence
Revina Maharani 10maharanirevina@gmail com
Hotma Lestari hotlesmo67@gmail com
Putra Mahakarya Dewa putramahakaryadewa25@gmail com
Dewangga Yudisthira dewanggay369@gmail com
Nasim Amar nasemamar2003@gmail com
Medical Faculty, Universitas Brawijaya, Malang, Indonesia
Besut Daryanto (Corresponding Author) urobes fk@ub ac id
Urology Department, Faculty of Medicine Universitas Brawijaya, Dr Saiful Anwar General Hospital, Malang, Indonesia
R Maharani, H Lestari, P Mahakarya Dewa, et al
Unlocking the
potential of antioxidant supplementation with N-acetylcysteine to improve seminal parameters and analysis of
its safety: A systematic review and meta-analysis of randomized
1 Division of Urology, Department of Surgery, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia;
2 Faculty of Medicine, Hasanuddin University, Makassar, Indonesia;
3 Department of Urology, Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia
Summary
Introduction and objectives: N-acetyl-cysteine (NAC) is one of the oldest and most powerful antioxidants used to treat various diseases It plays an important role in protecting cells against oxidative damage and has the potential to improve seminal parameters in male with infertility. This systematic review and meta-analysis aim to comprehensively evaluate the efficacy and safety profile of antioxidant supplementation with NAC in male with infertility or impaired semen parameters
Materials and methods: This systematic review and meta-analysis adhered to Cochrane Handbook guidelines A literature search across PubMed, ScienceDirect, Cochrane Library and Scopus on February 21, 2024 of studies evaluating NAC supplementation for male infertility or impaired semen parameters was conducted Study quality was assessed using Revised Cochrane's risk of bias (RoB 2 0) and RevMan 5 4 was used for meta-analysis.
Results: Search yielded 1 106 articles and 5 studies were included in this meta-analysis. Our study showed that patients who received NAC had statistically significant results in improving sperm volume [MD: 0.69 (0.26-1.12), P = 0.002], sperm concentration [MD: 4 43 1 50-7 36), P = 0 003], sperm total motility [MD: 9.69 (6.61-12.77), P < 0.00001], and normal sperm morphology [MD: 1 36 (0 70-2 03), P < 0 0001] compared to control. Additionally, patients given NAC had no reported side effects based on our included studies
Conclusions: We found NAC supplementation significantly improves seminal parameters and has a favorable safety profile These findings highlight the potential role of NAC as a safe supplementation for male with infertility or in male with impaired semen parameters.
Submitted 18 February 2025; Accepted 24 February 2025
INTRODUCTION
The male component significantly accounts for around 50% of all infertility cases (1) Male fertility is primarily influenced by spermatogenesis, the process of spermatozoa formation from spermatogonia within the testes Male
infertility is caused by defective sperm parameters (spermatogenic failure), including total absence (azoospermia), low count (oligozoospermia), abnormal morphology (teratozoospermia), and/or impaired motility (asthenozoospermia) The failure in dealing with male infertility is mostly because of the multifaceted etiology that arises from the interaction of genetics, lifestyle choices, environmental influences, and concomitant conditions (2) Reactive oxygen species (ROS) are normal products of cellular metabolism, mainly produced in the mitochondria during oxidative phosphorylation Free radicals form during oxygen reduction for energy production When oxidants increase, the balance shifts toward oxidative stress, which is linked to over 100 disorders, including infertility ROS can induce protein degradation, lipid peroxidation, DNA damage and apoptosis Evidence indicates that ROS-mediated damage to sperm significantly contributes to 30%-80% of all cases (3, 4)
N-acetyl-cysteine (NAC) is a dietary supplement and mucolytic drug utilized in the treatment of acetaminophen and paracetamol overdoses As a thiol-based derivative of the amino acid L-cysteine and a precursor to glutathione peroxidase, it has potent anti-inflammatory, mucolytic, and antioxidant properties Numerous studies indicate that NAC supplementation can elevate sperm counts, improve motility, diminish abnormal morphology, minimize DNA fragmentation, promote acrosomal activity, and function as a potent semen antioxidant (5)
This review investigates the potential of NAC supplementation in the latest studies on seminal parameters and its safety in male with infertility or impaired semen parameters
METHOD
Search strategy
Two authors independently searched for and reviewed all randomized controlled trial describing the efficacy and safety of NAC in male with infertility or impaired semen parameters from inception until February 21, 2024 from several databases comprised of PubMed, ScienceDirect,
2 , Ponco Birowo 3 , Widi Atmoko 3
M A Giffari Makkaraka, A Taufik Fadillah Zainal, et al
Scopus and Cochrane Library The subsequent keywords were generated by integrating several terms, including “N-acetyl-cysteine” AND “Semen quality” OR “seminal parameters” OR “Semen” This study applied no restrictions regarding country or publication year The protocol o f t h i s m e t a - a n a l y s i s w a s r e g i s t e r e d i n P R O S P E R O (CRD42024516001) This study also followed the guideline of PRISMA 2020 (6)
Eligibility criteria
This systematic review and meta-analysis examined studies of randomized controlled trials that met the specified criteria The studies were included into this meta-analysis if they fulfilled the following criteria (1) Evaluated NAC supplementation for male with infertility or impaired semen parameters; (2) Each article provided precise data, mostly involving the subject count and indicator outcomes of: semen volume, sperm concentration, total motility, normal sperm morphology and adverse event (AE) reported; and (3) Full-text article in English language and related data can be obtained Studies presented as abstracts, review articles, and case reports were removed
Selection process
Duplicate studies were identified and excluded after the initial search The titles and abstracts of the remaining literature were screened by at two independent reviewers to determine eligibility Studies meeting the criteria were included, while those not meeting requirements were excluded Conflicts in study classification were resolved through group discussion The results of the literature screening adhere to the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA guidelines)
Data extraction
The following data were collected for each study by different reviewers: (1) First author’s name; (2) Published time; (3) The type of study design; (4) Patients description; (5) Patient’s received therapy, dosage and treatment period; (6) Number of patients in each group; (7) age, and (8) Data on semen volume (mL), sperm concentration (106/mL), total motility (%), normal sperm morphology (%) and AE reported
Quality assessment
Two authors independently assessed all identified inclusion studies, and any disagreements that emerged were addressed with the input of a third reviewer Cochrane Risk of Bias (ROB) Tools 2 was used to assess the quality of each study ROB 2 instrument was utilized to assess the risk of bias in randomized controlled trials (RCTs), focusing on five domains (7) Overall risk-of-bias judgement of these instruments was classified into 3 groups which low risk of bias (if the study is judged to be at low risk of bias for all domains for this result), some concerns (if there is some concern at least in one domain) and high risk of bias (if the study is judged to be at high risk of bias in at least one domain for this result) Risk-of-bias Visualization (ROBVIS) was used for the visualization of risk of bias graph (8)
Statistical analysis
The acquired data was analyzed with Review Manager 5 4
(Cochrane Collaboration, UK) Variations between baseline (study entrance) and study completion (end-point measure) were utilized to indicate changes in the results Mean difference (MD) was used to explain continuous data and odds ratio (OR) for dichotomous results with the corresponding 95% confidence interval (CI) I2 value refers to statistical analysis of heterogeneity The fixed-effects model is used if I2 < 50%, while the random-effects model is used if I2 ≥ 50% The results will be presented in a forest plot, and the overall effect is considered significant if p < 0 05 Asymmetry tests, including Egger’s test for assessing potential publication bias via funnel plots, will not be performed if the meta-analysis comprises fewer than 10 studies due to their restricted reliability (9) Furthermore, subgroup analysis and sensitivity analysis will also not be conducted if there is a small number of studies (10)
RESULTS
Literature search, screening results and characteristic of studies
From various databases, 1 106 studies were initially identified using keywords After excluding 82 duplicates, two reviewers independently screened the remaining 1 024 study titles and abstracts, which excluded 1 015 articles according to the inclusion and exclusion criteria After reviewing only nine full texts, we excluded four studies because they lacked sufficient data or did not meet our study criteria
Finally, 5 RCT studies (11-15) were included in our analysis with a total of 666 patients Full details of the search and selection process are presented in the PRISMA flow diagram (Figure 1) and the characteristics of these studies are stated in Table 1
Quality assessment result
Three studies (11-13) raised concerns regarding the randomization process (domain 1), while one study (11) indicated issues related to the lack of personnel and patient blinding, which pertains to deviations from intended interventions (domain 2) and bias in outcome measurement (domain 4) Additionally, one study (13) expressed concerns about missing outcome data due to a significant number of patient withdrawals, resulting in an imbalance in sample sizes between groups (domain 3) Four studies (11, 12, 14, 15) raised concerns about bias in the selection of reported results due to the absence of a published protocol (domain 5) A detailed assessment of the risk of bias is presented in Figure 2
Sperm volume
Sperm volume from two studies assessing the efficacy of NAC showed a marked improvement of sperm volume (MD: 0 69; 95% CI: 0 26-1 12; P = 0 002), NAC demonstrated a markedly larger enhancement in sperm volume in relation to the control group (Figure 3A)
Sperm concentration
Five studies evaluating the efficacy of NAC exhibited that the NAC group had a significant improvement (MD: 4 43; 95% CI: 1 50-7 36; P = 0 003) (Figure 3B), it
Syarif,
Figure 1
Flow of literature search and selection based on Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA)
demonstrated that NAC is more effective in increasing sperm concentration compared to the control (Figure 3B)
Total sperm motility
Four studies revealed that patients who received NAC intervention had a significant improvement in total sperm motility (MD: 9 69; 95% CI: 6 61-12 77; P < 0 00001) (Figure 4A), which shown that NAC was more effective in enhancing sperm motility than the control (Figure 4A)
Normal sperm morphology
There were four studies that assessed normal sperm morphology The random effects model showed that there was significant increase in normal sperm morphology in the NAC group (MD: 1 36; 95% CI: 0 70-2 03; P < 0 0001),
which demonstrated that NAC resulted in a much higher enhancement in sperm normal morphology relative to the control (Figure 4B)
Safety profile
The included studies reported that patient receiving NAC supplementation at a dosage of 600 mg/day for twelve weeks or 26 weeks, resulted in improved sperm quality without any reported side effects
DISCUSSION
The results of this meta-analysis showed that NAC supplementation significantly increased sperm volume, sperm concentration, total sperm motility and normal sperm mor-
Risk of bias assessment using the revised Cochrane risk-of-bias tool algorithm for randomized trials (RoB 2 0)
Archivio Italiano di Urologia e Andrologia 2025; 97(1):13750
Syarif, M A Giffari Makkaraka, A Taufik Fadillah Zainal, et al
Figure 2.
phology in male with infertility or impaired semen parameters Wei et al previously carried out a meta-analysis assessing the effectiveness of L-carnitine/L-acetyl-carnitine (LC/LAC) and NAC in males with idiopathic asthenozoospermia The findings indicated that supplementation with LC/LAC and NAC significantly enhanced sperm motility, normal morphology, sperm concentration, and ejaculate volume (16) Different from that study, this metaanalysis included 5 RCT studies evaluating NAC supplementation and providing new insights into the effective-
Archivio Italiano di Urologia e Andrologia 2025; 97(1):13750
Figure 3
Forest plots of seminal parameters of (A) Semen volume (B) Sperm concentration
CI: Confidence interval; IV: Inverse variance; SD: standard deviation
Figure 4
Forest plots of seminal parameters of (A) Total motility (B) Normal sperm morphology
CI: Confidence interval; IV: Inverse variance; SD: standard deviation
M A Giffari Makkaraka, A Taufik Fadillah Zainal, et al
ness of NAC for improving semen parameters Several previous studies have shown that around 30-80% of male infertile patients have increased ROS in their semen (17) An increase in ROS that surpasses the antioxidant capacity in semen leads to an imbalance between pro-oxidants and antioxidants, resulting in oxidative stress (OS) conditions that damage the spermatozoa plasma membrane and sperm DNA This explains why increased ROS can have a negative impact on sperm parameters and cause infertility in men (18) One way to prevent OS is to increase the antioxidant capacity of semen by providing antioxidant supplements
NAC is a derivative of the natural amino acid L-cysteine, which has an important role in cellular protection against oxidative damage (19) NAC is one of the oldest and most powerful antioxidants in treating several diseases, including its application in decreasing the viscosity and flexibility of mucus due to its capacity to break disulfide bonds
In addition, NAC has the potential to interact directly with oxidants and with some thiols, which are excellent hydroxyl radical scavengers (20) The results of this metaanalysis show that NAC administration can improve the quality of sperm parameters This is thought to be related to the main role of NAC as a stem-form antioxidant, which has the ability to increase intracellular glutathione concentration, the most crucial biothiol responsible for cellular redox imbalance (21) NAC administration can also increase the total antioxidant capacity (TAC) in semen fluid (20) Increased TAC will prevent OS due to overproduction of ROS This is proven by the study of Barekat et al , who reported that patients given NAC reduced the percentage of ROS in semen (13) Preventing OS in semen can prevent damage to spermatozoa and enhance the integrity of sperm DNA, leading to a significant increase in the number of sperm in the semen (19) Several studies have reported that the antioxidant effect in semen can also increase the mitochondrial function of spermatozoa, thereby providing more energy and increasing their motility (22) Jannatifar et al. indicated that following NAC administration, the levels of seminal malondialdehyde (MDA) drastically reduced MDA served as a particular indicator of lipid peroxidation, whereas TAC exhibited a considerable rise NAC mitigates the intensity of oxidative stress, therefore diminishing lipid peroxidation (12) The theoretical basis and mechanisms explain the results of this meta-analysis, which show that NAC is effective and safe in improving sperm parameters In addition, NAC is relatively safe and well tolerated, even at high doses (21) Of all the included studies, none reported any significant side effects of NAC administration on male with infertility or impaired semen parameters The primary goal of infertility therapy is to achieve pregnancy In a study conducted by Barekat et al , NAC was administered to men following varicocelectomy, leading to significant improvements in semen quality and a higher reported clinical pregnancy rate in the NAC group compared to the control group This indicates a notable enhancement in fertility outcomes associated with NAC supplementation (13) Unfortunately, our analysis could not assess pregnancy rates because the studies we included did not provide sufficient data for further evaluation The dosage and duration of NAC supplementation
have been extensively evaluated in studies related to male fertility Most studies have administered NAC at a dosage of 600 mg each day for three months, which has consistently resulted in significant improvements in sperm quality and oxidative stress markers Jannatifar et al reported enhanced sperm parameters following this regimen (12), while Rafiee et al observed similar benefits in men with impaired semen parameters (11) In a larger trial by Safarinejad et al , participants received 600 mg of NAC daily for 26 weeks, leading to significant improvements in multiple semen parameters (15) Comhaire et al also noted improvements in sperm concentration and acrosome reaction at similar dosages (23) These studies suggest that NAC supplementation at dose of 600 mg each day for durations of three to six months should be preferred for enhance seminal parameters
Several studies have reported on the safety profile of NAC supplementation Erkkilä et al found no cytotoxic effects of NAC on human male germ cells in vitro, supporting its safety for reproductive health applications (24) A systematic review by Zafarullah et al highlighted that NAC is also safe in various clinical applications, being generally well-tolerated even at higher doses used for treating conditions such as chronic obstructive pulmonary disease and acetaminophen overdose (25) This study suggests that NAC is a safe and effective antioxidant supplement for enhancing male fertility parameters without a significant risk of adverse events
DECLARATIONS
Ethical approval: This study did not need ethical approval
Availability of data and material: All data and materials from this research are available to the researcher and we will provide it upon request if the researcher needs it
Competing interests: The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript
Funding: All funding for this research comes from researchers without receiving reimbursement of research costs or research grants from third parties
Authors' contributions: Contribution Details (to be ticked marked as applicable):
Definition of intellectual content
search
Data acquisition
Data analysis
Statistical analysis
Manuscript preparation
Manuscript editing
Manuscript review
Guarantor
Acknowledgments: We as authors would like to thank all parties involved in this study, including the Department of Urology, Faculty of Medicine, Hasanuddin University and also Hasanuddin University Hospital
Conference Presentation: This article has been oral presented in the 21st Urological Association of Asia Congress (UAA) on September 7th 2024
Syarif,
We need to acknowledge some limitations of this study First, there are only a few trials included in our study However, all studies used in this research are randomized controlled trials, hence augmenting the robustness of the findings In addition, bias due to deviations from intended interventions may affect the final results of this study Secondly, this meta-analysis is limited by the limited number of RCT studies Based on these limitations, it is important to interpret the findings of this review cautiously, as they may warrant further studies Additionally, future studies should analyze and compare the combination of NAC and other types of antioxidant supplements to improve sperm parameters Based on our analysis, we recommend NAC supplementation for males experiencing impairment of semen parameters, either at a dose of 600 mg or at a dose of 200 mg NAC three times a day for a minimum of 12 weeks, and up to 26 weeks
CONCLUSIONS
A significantly improvement of seminal parameter was found in male with infertility or impaired semen parameters who received NAC supplementation NAC supplementation has also been proven to be safe These findings highlight the potential role of NAC as a safe supplementation for males with infertility or impaired semen parameters
REFERENCES
1 Schlegel PN et al Diagnosis and Treatment of Infertility in Men: AUA/ASRM Guideline Part I J Urol 2021; 205:36-43
2 Assidi M Infertility in Men: Advances towards a Comprehensive and Integrative Strategy for Precision Theranostics Cells 2022; 11:1711
3 O’Flaherty C Reactive Oxygen Species and Male Fertility Antioxidants 2020; 9:287
4 Agarwal A et al Male Oxidative Stress Infertility (MOSI): P
T
Management of Idiopathic Male Infertility World J Mens Health 2019; 37:296-312
5 Tenório MCDS, Graciliano NG, Moura FA, et al N-Acetylcysteine (NAC): Impacts on Human Health Antioxidants (Basel) 2021; 10:967
6 Page MJ, et al The PRISMA 2020 statement: an updated guideline for reporting systematic reviews The BMJ 2021; 372:n71
7 Sterne JAC, et al RoB 2: a revised tool for assessing risk of bias in randomised trials BMJ 2019; 366:l4898
8 McGuinness LA, Higgins JPT Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments Res Synth Methods 2021; 12:55-61
9 Egger M, Smith GD, Schneider M, Minder C Bias in meta-analysis detected by a simple, graphical test BMJ 1997; 315:629-634
10 Higgins JPT Cochrane Handbook for Systematic Reviews of Interventions https://training cochrane org/handbook (2024)
11 Rafiee B, Bagher Tabei SM The effect of N-acetyl cysteine consumption on men with abnormal sperm parameters due to positive history of COVID-19 in the last three months Arch Ital Urol Androl 2021; 93:465-467
12 Jannatifar R, Parivar K, Roodbari NH, Nasr-Esfahani MH Effects of N-acetyl-cysteine supplementation on sperm quality, chro-
matin integrity and level of oxidative stress in infertile men Reprod Biol Endocrinol RBE 2019; 17, 24
13 Barekat F, et al A Preliminary Study: N-acetyl-L-cysteine Improves Semen Quality following Varicocelectomy Int J Fertil Steril 2014; 10:120-126
14 Ciftci H, Verit A, Savas M, et al Effects of N-acetylcysteine on Semen Parameters and Oxidative/Antioxidant Status Urology 2009; 74:73-76
15 Safarinejad MR, Safarinejad S Efficacy of Selenium and/or NAcetyl-Cysteine for Improving Semen Parameters in Infertile Men: A Double-Blind, Placebo Controlled, Randomized Study J Urol 2009; 181:741-751
16 Wei G, et al A Meta-Analysis of the Efficacy of L-Carnitine/LAcetyl-Carnitine or N-Acetyl-Cysteine in Men With Idiopathic Asthenozoospermia Am J Mens Health 2021; 15:15579883211 011371
17 Agarwal A, et al Male Oxidative Stress Infertility (MOSI): Proposed Terminology and Clinical Practice Guidelines for Management of Idiopathic Male Infertility World J Mens Health 2019; 37:296-312
18 Bui AD, Sharma R, Henkel R, Agarwal A Reactive oxygen species impact on sperm DNA and its role in male infertility Andrologia 2018; 50:e13012
19 Rafiee B, Bagher Tabei SM The effect of N-acetyl cysteine consumption on men with abnormal sperm parameters due to positive history of COVID-19 in the last three months Arch Ital Urol Androl 2021; 93:465-467
20 Ciftci H, Verit A, Savas M, et al Effects of N-acetylcysteine on semen parameters and oxidative/antioxidant status Urology 2009; 74:73-76
21 Tenório MCDS, Graciliano NG, Moura FA, et al N-Acetylcysteine (NAC): Impacts on Human Health Antioxidants (Basel) 2021; 10:967
22 Hirata S, Hoshi K, Shoda T, Mabuchi T Spermatozoon and mitochondrial DNA Reprod Med Biol 2002; 1:41-47
23 Comhaire FH, et al The effects of combined conventional treatment, oral antioxidants and essential fatty acids on sperm biology in subfertile men Prostaglandins Leukot Essent Fatty Acids 2000; 63:159-165
24 Erkkilä K, Hirvonen V, Wuokko E, et al N-acetyl-L-cysteine inhibits apoptosis in human male germ cells in vitro J Clin Endocrinol Metab 1998; 83:2523-2531
25 Zafarullah M, Li WQ, Sylvester J, Ahmad M Molecular mechanisms of N-acetylcysteine actions Cell Mol Life Sci CMLS 2003; 60:6-20
Correspondence
Syarif Syarif (Corresponding Author) syarifbakri@hotmail com Perintis Kemerdekaan St KM 10, Tamalanrea, Makassar, Indonesia (Postal Code: 90245)
Moh Anfasa Giffari Makkaraka fasagifari@gmail com
Ahmad Taufik Fadillah Zainal ahmadtaufik2014004@gmail com Faculty of Medicine, Hasanuddin University, Makassar, Indonesia
Ponco Birowo ponco birowo@gmail com
Widi Atmoko dr widiatmoko@yahoo com Department of Urology, Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia
ORIGINAL PAPER
Survival and oncological outcomes for young men (≤ 55 years) undergoing radical prostatectomy for localized prostate cancer
Shahryar Zeighami 1 , Ali
Ariafar
1 ,
Alireza Makarem
1 ,
Faisal Ahmed 2 , Mohammadreza Askarpour 1
1 Department of Urology, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran;
2 Department of Urology, School of Medicine, Ibb University, Ibb, Yemen
Summary
Objectives: This research aimed to compare the prostate cancer (PCa) features, survival rate, and functional outcomes after open suprapubic Radical Prostatectomy (RP) between younger men (≤ 55 years) and older men (> 55 years)
Methods: In this retrospective cohort study, we studied 134 patients with clinically localized PCa who underwent RP at our centers between 2011 and 2019, with 26 (19.40%) patients aged ≤ 55 Pathological parameters, survival rate (at 5 and 10 years), and functional outcomes such as erectile function and continence rate (at two years from RP) were evaluated retrospectively, and the two groups were compared. The Chi-square test, KaplanMeier, and Cox proportional hazards method were used for statistical analysis.
Result: Men aged ≤55 had greater rates of organ-confined tumors, lower D’Amico risk grouping and pathologic Gleason grade than their older counterparts (all p < 0 05) The median follow-up was 81 months. The survival rate at five and ten years were higher in younger men versus older counterparts (96 15% vs. 93.47% and 92.15% vs. 82.13% ) but difference was not statistically significant (p = 0 1539) Five-year biochemical recurrence-free and metastasis-free survival rates in younger men versus older counterparts were 96 2% vs 81 5% and 75 7% vs 51 5% Men > 55 years were associated with worse BCR-free and metastasis-free survival in univariate analysis and with worse BCR in multivariate analysis The continence rate was significantly better in men aged ≤ 55 compared to older counterparts (OR: 5 08; 95% CI: 1 61-22 61; p = 0 013) However, erectile function was not statistically significant between groups [for moderate ED: (OR: 1 08; 95% CI: 0 43-2 79, p = 0 865), for severe ED (OR: 1.60; 95% CI: 0.35-11.50, p = 0.579)].
Conclusions: Our study showed that survival rates were similar in younger men (≤ 55 years) and their older counterparts. However, older patients who underwent RP had more advanced disease, worse BCR-free survival, and a worse continence rate. For localized prostate cancer patients under 55 years of age, radical prostatectomy is an excellent treatment option with excellent long-term survival outcomes Given the relatively small number of patients younger than 55, a large cohort study with long-term postprocedural follow-up is needed to validate this observation.
KEY WORDS: Radical prostatectomy; Survival outcome; Oncological outcomes; Young men
Submitted 13 May 2024; Accepted 6 June 2024
INTRODUCTION
Prostate cancer (PCa) is a male malignancy seen mainly in the older population Eighty percent of cases are diagnosed after the age of 65 years, yet PCa identification in younger males aged less than 50 has risen from 1% in the 1970s to 5% (1) Various autopsy investigations show a considerable rate of latent PCa in the third, fourth, and fifth decades of life, ranging between 20% and 30% (2)
In younger men, latent PCa prevalence varies in autopsy series reports, ranging from 34% occurrence in the United States to 27% occurrence in Hungary and 2 6% occurrence in the Greek series (3-5) The increasing prevalence of PCa detection at a young age raises concerns about the natural course of this disease and treatment options In low-risk, elderly PCa patients with a Gleason score of about (6), active surveillance is a good option (6) This is not the case with patients under the age of 55, who might require urgent intervention in the majority of instances due to the more aggressive behavior of the disease in younger patients, which leads to an increased number of patients undergoing radical prostatectomy (RP) (7)
The data regarding the outcomes of young men who suffered from PCa are contentious According to Tjaden et al , the disease in younger patients is more aggressive, with worse prognoses (8) However, recent studies mentioned that young men with low-risk PCa have better outcomes after RP (9, 10) A common limitation in these surveys was the use of prostate-specific antigen (PSA) relapse to measure the endpoint of the oncological outcome At the same time, the progression of the disease or mortality seems to be the optimal outcome for reaching a better judgmental conclusion In this article, we studied PCa patients who underwent RP and compared the pathological findings, oncological outcomes, and survival rates between younger men (≤ 55 years) versus older patients
MATERIALS AND METHODS
Study design: In this retrospective cohort study, we studied 134 PCa patients who underwent retropubic RP in our referral teaching centers (Ali-Asghar Hospital and Namazi Hospital, Shiraz, Iran) between March 2011 and March 2019 The mean age of patients was 62 6 ± 9 2
y e a r s ( r a n g e : 2 9 0 - 7 7 0 y e a r s ) T w e n t y - s i x ( 1 9 4 % ) patients were aged ≤ 55 years, while 108 (80 6%) patients were aged > 55 years The study was approved by the Ethics Committee of Shiraz University of Medical Sciences (ID: IR SUMS MED REC 1398 493) and was conducted per the Declaration of Helsinki Additionally, written informed consent was obtained from patients for participation in our study
We included all patients diagnosed with localized PCa who underwent Radical Prostatectomy and filled the standardized self-administrated questionnaires before and one year after the surgery Patients with missed information r e g a r d i n g c l i n i c a l a n d p a r a c l i n i c a l p a r a m e t e r s w e r e excluded Patient characteristics, such as family history of disease, age, and clinical parameters, such as clinical stage, biopsy Gleason score, and PSA level, were gathered before surgery After surgery, pathological data (surgical margin status, lymph node status, pathological stage, and Gleason score) were obtained The PSA level was evaluated every three months in the initial year post-RP This frequency was reduced to biannually for the subsequent two years, and from the fourth year onward, the check-ups were conducted annually In two successive readings, biochemical recurrence (BCR) was defined as a PSA of more than 0 2 ng/ml The RECIST criteria were used to evaluate the progression of the disease: CT, MRI, and bone scan were used to confirm skeletal lesions Following the pathological analysis of prostate cancer (PCa), supplementary treatment, either radiation therapy (RT) or a combination of RT and androgen deprivation therapy, was given within four months post-RP If BCR was identified, a rescue treatment, either RT alone or combined with androgen deprivation therapy, was administered
We used histological examination following surgery or biopsy to confirm a local recurrence The pathological result was evaluated using the AJCC 2002 staging system From 1992 to 2005, we utilized the Gleason Grading system for tumor grading, and after 2 0 0 5 , w e a d o p t e d t h e u p d a t e d Gleason grading system (11) Urine continence was considered to use a 0-1 protective pad
The evaluation of erectile function was carried out using a uniform questionnaire, which incorporated the International Index of Erectile Function (IIEF-5) Patients who had an IIEF-5 score greater than 16, indicating no erectile dysfunction or only mild erectile dysfunction, were classified as potent We assessed clinical and pathological data, along with followup information (such as time to BCR, detected metastasis or local recurrence, urinary continence, and erectile function) comparing the two groups
Table 1
Statistical analysis
We utilized the mean ± standard deviation (SD) to represent the quantitative variables, and the frequency (percentage) was employed to describe the qualitative variables Chi-squared tests were used to compare the characteristics of patients and tumors Kaplan-Meier survival c u r v e s a n d C o x - p r o p o r t i o n
applied for univariate and multivariate BCR-free survival, metastasis-free survival, and overall survival analyses
Functional outcome (24-month continence and potency) was analyzed using multivariable logistic regressions A p-value less than 0 05 was deemed statistically significant All the data were processed using the SPSS version 20 software (SPSS Inc , Chicago, IL, USA)
RESULT
Patient and tumor characteristics
Table 1 presents all the cases' pathological and clinical features and compares age-related variables Among our 134 cases, 26 (19 40%) patients were aged ≤ 55 years, while 108 (80 6%) patients were aged > 55 Young patients had greater rates of organ-confined tumors, lower D'Amico risk grouping and pathologic Gleason grade group than their older counterparts (all p < 0 05) However, the younger group aged ≤ 55 years have a higher rate of positive family history of prostatic cancer (p < 0 001)
Oncological outcome
Biochemical recurrence occurred in 21 (16%) patients over a median of 44 months [Min: 23 - Max: 65 months] of follow-up, with no statistically significant difference between groups (p = 0 0588) (Figure 1) During a follow-up of 84 6 ± 23 1 months (median: 81 [min: 27 - max: 120]), metastases were discovered in 32 (23 9%) patients, with no sig-
PSA:
S Zeighami, A Ariafar, A Makarem, et al
Figure 1.
Figure 2
Biochemical recurrence-free survival stratified by age groups
3.
nificant difference between groups (p = 0 1539) (Figure 2)
Five-year biochemical recurrence-free and metastasis-free survival rates in younger men versus older counterparts were 96 2% vs 81 5% and 75 7% vs 51 5% Median survival was 87 months (95% CI: 81-90 months) The disease's progression time was 82 8 ± 24 7 months (median: 80 [min: 27 - max: 120 months]) and did not differ significantly between groups (p = 0 1348) (Figure 3)
The survival rate for the age group ≤ 55 years at five and ten years was 96 15% (95% CI: 89 04%-100 0%) and 92 15% (95% CI: 82 27%-100 0%) The survival rate for the age group > 55 years at five and ten years was 93 47% (95% CI: 88 92%-98 3%) and 82 13% (95% CI: 3 76%91 4%) The Kaplan-Meier analysis showed a similar biochemical progression-free survival (BPFS) rate without statistically significant difference (log-rank p = 0 152) The uni- and multivariable Cox-regressions analysis showed that in univariate analysis, older patients were more likely to develop BCR (HR: 26 04; 95% CI: 8 42-80 54, p < 0 001) and metastasis (HR: 2 60; 95% CI: 1 02-6 60, p = 0 045)
The multivariable Cox-regressions analysis showed that nearly all parameters, both before and after surgery, were similar except for biochemical recurrence (HR: 88 70; 95% CI: 14 19-554 43, p < 0 001) and was a predictor for disease progression However, after adjusting for further prognostic factors (Gleason score, preoperative PSA, lymph node status, surgical margin, pathologic stage), patients' age (≤ 55 vs > 55 years) was not a statistically significant predictor for mortality (p = 0 949) (Table 2)
Table 2
Uni- and multivariable Cox-regressions predicting mortality-free survival
Figure
Table 3.
Postoperative continence and potency rates stratified by age groups
Regarding postoperative functional outcome, the continence rate was significantly influenced by age in univariate analysis (OR: 4 88; 95% CI: 1 57-21 47, p = 0 014) and multivariate analysis (OR: 5 08; 95% CI: 1 61-22 61; p = 0 013) The erectile function was more improved in younger age [2 (16 7%) vs 10 (83 3%)] However, the rate was not statistically significant in univariate [for moderate: (OR: 0 89; 95% CI: 0 36-2 21, p = 0 792) and for severe (OR: 1 16; 95% CI: 0 26-8 14, p = 0 858)] or multivariate analysis [for moderate: (OR:1 08; 95% CI: 0 43-2 79, p = 0 865), for severe (OR: 1 60; 95% CI: 0 35-11 50, p = 0 579=)] (Table 3)
DISCUSSION
Age at cancer diagnosis is a well-known prognostic factor in the majority of malignancies Although few studies have found a worse prognosis in earlier high-stage PCa patients (12-15), Interestingly, evidence from recent research has also revealed that early diagnosis of PCa in younger cases is related to lower stage and grade or perhaps to better results (9, 10, 16) A recent comprehensive review also discovered that younger age was associated with positive clinicopathological features and a more favorable prognosis for BCR in patients with low to intermediate risk However, in high-risk groups, younger patients often experienced notably poorer oncological results (17) In this research, we examined the characteristics of PCa, functional results, and survival outcomes in young men 55 years old or below after RP and then compared these findings with those of men older than 55 Selecting candidates for radical prostatectomy is a challenging task for both the physician and the patient The patient’s life expectancy, the natural history and curability of prostate cancer, as well as the morbidity of treatment and deferred treatment, must all be carefully evaluated Although the existing clinical data containing this information has inherent flaws, all these factors can be calculated with good precision A concentrated effort should be made to present the patient with prognostic information that is appropriate for his age, health status, and the stage and grade of cancer Because not all men who choose radical
prostatectomy will require or benefit from surgical intervention, the patient must be fully involved in the decision-making process (18) In our study, it is probable that younger individuals underwent more intensive screening, resulting in more frequent diagnoses at an early stage of the disease Furthermore, younger patients were more likely to prefer surgery over older patients
It is crucial to seek a better understanding of the correlation between younger age and prostate cancer occurrence and progression, which will aid strategic approaches when t
patients in the PSA era (17) Salinas et al observed that prostate cancer
However, men in this age group are more likely to die from higher grade/stage disease, indicating a demographic difference between early-onset and older male prostate cancer patients (19) Similar to our study design, several studies on clinicopathological characteristics of prostate cancer chose the age of 55 as a cutoff point (13, 20, 21) However, there is no agreement on the age at which these tumors become most aggressive or on the characteristics that make these tumors more aggressive in young individuals A recent meta-analysis suggested that age 50 is often used as the cutoff to separate younger and older patients in RP cohorts, which contradicts our choice of 55 as the cutoff (17) However, with our limited number of cases, choosing a lower age cutoff threshold of less than 55 years would result in an unbalanced sample size per group, increasing the possibility of mistakes during the matching and making statistical analysis challenging Family history, age, and race are all established risk factors for prostate cancer While family history accounts for just 9% of cases, early-onset prostate cancer has a higher likelihood of being hereditary compared to late-onset prostate cancer This increase in the risk of prostate cancer can be explained by the higher number of alleles in those patients (22, 23) Similarly, in our study, family history was found in 0 9% of older males (> 55 years) and 23 1% of younger men (≤ 55 years), which was statistically significant (< 0 001) Several other studies also show a strong link between family history and early-onset prostate cancer detection in young men (9, 12) Future research on rare cases is essential to finding additional risk alleles and better understanding the disease's etiology
In this study, men aged ≤ 55 had greater rates of organconfined tumors, lower D'Amico risk grouping, and pathologic Gleason grade than their older counterparts The findings of this report were similar to Milonas et al report, which mentioned younger men (≤ 55 years old) tend to have less aggressive clinical and pathological PCa characteristics than older men (24) According to several investigations, older men are more likely to have advanced malignancy features Ji and colleagues analyzed the pathological characteristics of PCa patients divided into three age groups: 55 or younger, between 56 and 75, and older than
S
75 They found that the percentage of Gleason pattern five tumors varied significantly across the groups (44 4%, 32 3%, and 36 8%, respectively), indicating a significant difference (χ2 = 11 641, p = 0 003) (25) This study's bivariate regression analysis demonstrated that greater pathological GS were indicators of illness development However, this conclusion might arise from the considerable imbalance in the patient group ages, with just 26 participants aged ≤ 55 and 108 patients aged 55-75 All of these data lead us to believe that preconceptions regarding cancer's aggressiveness at a young age play a significant influence in choosing a surgical treatment decision Various studies have shown a high long-term BiochemicalFree Survival Rate (BFSR) in the young male group For example, Tan et al showed greater 5- and 10-year survival rates among younger individuals (97 9% vs 95 9% and 94 9% vs 85 3, respectively) (13) Freedland and colleagues examined 1 753 male patients post-RP in their research They discovered that men under 50 had a significantly higher BFSR than other age groups 16 In contrast, Milonas et al found that young men had a 5- and 8year BFSR of 77 9% and 72 4%, although this difference was not statistically significant compared to males over 55 (12) Song and colleagues found that patients aged 55 or younger had better survival rates in the first year after treatment but poorer outcomes in the second, third, and fifth years compared to older age groups (20) In our study, the survival rate at five and ten years in younger men versus older counterparts was 96 15% vs 93 47% and 92 15% vs 82 13% but was not statistically significant (p = 0 1539) Five-year BCR-free and metastasis-free survival rates in younger men versus older counterparts were 96 2% vs 81 5% and 75 7% vs 51 5%, and men > 55 years were associated with worse BCR-free and metastasis-free survival in univariate analysis and worse BCR in multivariate analysis However, the patient's age at surgery was not proven to be an independent predictor in multivariable analysis Similarly, in most studies, the patient's age at surgery was not proven to be an independent predictor in multivariable analysis, indicating a significant role of other factors (12, 16) In the current study, young individuals had less erectile dysfunction (16 7% vs 83 3%), but it was not statistically significant in regression analysis Our findings were similar to those of other studies in the literature Brajtbord and colleagues studied the recovery of erectile function after RP in two age groups (≤ 60 years old and those older than 60) They found that older men were more likely to experience a notable decrease in sexual outcomes, specifically discomfort (26) In another study, Alemozaffar et al also showed a correlation between increasing age and a lower chance of erectile function despite controlling for baseline performance (27) Tilki et al reported the one-year sexual function after RP in patients aged less than 45 years, between 45-65 years, and over 65 years They found that 75 6%, 58 6%, and 45 3% of patients had a potent sexual function, respectively (28) However, the better recovery of erectile function in our study might result from the differences in community settings and specialists Indeed, the restoration of continence should be viewed as a process Although information on early continence is rare, it has been observed that most men regain conti-
nence three months post-RP Furthermore, the recovery rate increases to approximately 90% after one year and continues improving (29, 30) A recent report by Theissen et al investigated the factors impacting early continence in post-radical prostatectomy The authors revealed reduced urine loss in younger patients or those with organ-confined tumors and those in whom the bilateral nerve-sparing technique was successfully used in RP In the current study, younger individuals had statistically significantly better continence rates Our findings were similar to those of other studies in the literature (31, 32)
Study limitations
Our research had some limitations First, as a retrospective study with a small sample size, especially in the young age group (less than 55 years), it inherits some inevitable confounders related to these studies, which could cause gaps in clinical information Second, due to limitations in the data archive, factors such as detailed treatments and multimodality treatments were not evaluated We also could have benefited from a larger group of younger patients in our study to strengthen our results As a result, more high-quality studies with larger sample sizes are required to validate our findings further
CONCLUSIONS
Our study showed survival rates were similar in younger men (≤ 55 years) and their older counterparts However, older patients who underwent RP had more advanced disease, worse BCR-free survival, and worse continence rate For that, in localized PCa patients under 55 years, radical prostatectomy is an excellent treatment option with excellent long-term survival results Given the modest number of patients under 55, extensive cohort studies with long-term post-procedural follow-up are necessary to validate this observation
DECLARATIONS
Ethical approval: Registry and the Registration No of the study/trial: Not applicable All patient’s parents or legal guardians provided written informed consent before enrolment
Availability of data and material: All inquiries can be directed to the corresponding author
Competing interests: The authors declare no conflict of interest
Funding: None
Authors' contributions: SZ and AM: designed the study and were involved in the record collection FA and MA: wrote the manuscript SZ and AA: edited the manuscript, and provided guidance, and formal analysis AA: conceptualized the study, designed the study, edited the manuscript, provided guidance, and approved the final version of the manuscript
Acknowledgments: The authors would like to thank Shiraz University of Medical Sciences, Shiraz, Iran, and also the Centre for Development of Clinical Research of Nemazee Hospital and Dr Nasrin Shokrpour for editorial assistance
REFERENCES
1 Milonas D, Venclovas Z, Gudinaviciene I, et al Long-Term O n c o l o g i c a l O
Prostatectomy for Localized Prostate Cancer Biomed Res Int 2017; 2017:9858923
2 Hussein S, Satturwar S, Van der Kwast T Young-age prostate cancer J Clin Pathol 2015; 68:511
3 Soos G, Tsakiris I, Szanto J, et al The Prevalence of Prostate Carcinoma and Its Precursor in Hungary: An Autopsy Study Eur Urol 2005; 48:739-44
4 Stamatiou K, Alevizos A, Agapitos E, Sofras F Incidence of impalpable carcinoma of the prostate and non-malignant and pre carcinomatous lesions in Greek male population: An autopsy study Prostate 2006; 66:1319-28
5 Sakr WA, Haas GP, Cassin BF, et al The Frequency of Carcinoma and Intraepithelial Neoplasia of the Prostate in Young Male Patients J Urol 1993; 150:379-85
6 Ariafar A, Zeighami S, Salehipour M, et al An Investigation of the P a
Prostatectomy in Southern Iran: A Cross-sectional Study Middle East J Cancer 2021; 12:69-78
7 Kinnear NJ, Kichenadasse G, Plagakis S, et al Prostate cancer in men aged less than 50 years at diagnosis World J Urol 2016; 34:1533-9
8 Tjaden HB, Culp DA, Flocks RH Clinical adenocarcinoma of the prostate in patients under 50 years of age J Urol 1965; 93:618-21
9 Parker PM, Rice KR, Sterbis JR, et al Prostate cancer in men less than the age of 50: a comparison of race and outcomes Urology 2011; 78:110-5
10 Becker A, Tennstedt P, Hansen J, et al Functional and oncological outcomes of patients aged < 50 years treated with radical prostatectomy for localized prostate cancer in a European population BJU Int 2014; 114:38-45
11 Gleason DF, Mellinger GT Prediction of prognosis for prostatic adenocarcinoma by combined histological grading and clinical staging J Urol 1974; 111:58-64
12 Milonas D, Venclovas Z, Gudinaviciene I, et al Long-Term O
Prostatectomy for Localized Prostate Cancer Biomed Res Int 2017; 2017:9858923
13 Tan L, Wang LL, Ranasinghe W, et al Survival outcomes of younger men (< 55 years) undergoing radical prostatectomy Prostate Int 2018; 6:31-5
14 Hong SK, Nam JS, Na W, et al Younger patients have poorer b
prostate cancer Asian J Androl 2011; 13:719-23
15 Dantanarayana ND, Hossack T, Cozzi P, et al Men under the age of 55 years with screen detected prostate cancer do not have less significant disease compared to older men in a population of patients in Australia BMC Urol 2015; 15:124
16 Freedland SJ, Presti JC, Jr , Kane CJ, et al Do younger men have better biochemical outcomes after radical prostatectomy? Urology 2004; 63:518-22
17 Zheng Y, Lin SX, Wu S, et al Clinicopathological characteristics of localized prostate cancer in younger men aged ≤ 50 years treated with radical prostatectomy in the PSA era: A systematic review and meta-analysis Cancer Med 2020; 9:6473-84
18 Lepor H Selecting candidates for radical prostatectomy Rev Urol 2000; 2:182-9
19 Salinas CA, Tsodikov A, Ishak-Howard M, Cooney KA Prostate cancer in young men: an important clinical entity Nat Rev Urol 2014; 11:317-23
20 Song P, Peng Z, Shu M, et al Reduced survival of young patients under 55 years with metastatic prostate cancer: a population-based study J Cancer 2021; 12:4985-92
21 Lu Y, Huang HH, Lau WKO Survival outcomes of Asian younger men (< 55 years) undergoing radical prostatectomy: a review of prostate cancer database in a tertiary hospital in Singapore Int Urol Nephrol 2020; 52:1885-91
22 Carter BS, Beaty TH, Steinberg GD, et al Mendelian inheritance of familial prostate cancer Proc Natl Acad Sci USA 1992; 89:3367-71
23 Lange EM, Salinas CA, Zuhlke KA, et al Early onset prostate cancer has a significant genetic component Prostate 2012; 72:147-56
24 Milonas D, Venclovas Z, Jievaltas M Age and aggressiveness of prostate cancer: analysis of clinical and pathological characteristics after radical prostatectomy for men with localized prostate cancer Cent European J Urol 2019; 72:240-6
25 Ji G, Huang C, Song G, et al Are the Pathological Characteristics of Prostate Cancer More Aggressive or More Indolent Depending upon the Patient Age? Biomed Res Int 2017; 2017:1438027
26 Brajtbord JS, Punnen S, Cowan JE, et al Age and baseline quality of life at radical prostatectomy--who has the most to lose? J Urol 2014; 192:396-401
27 Alemozaffar M, Regan MM, Cooperberg MR, et al Prediction of erectile function following treatment for prostate cancer JAMA 2011; 306:1205-14
28 Tilki D, Maurer V, Pompe RS, et al Tumor characteristics, oncological and functional outcomes after radical prostatectomy in very young men ≤ 45 years of age World J Urol 2020; 38:95-101
29 Kuehhas FE, Naegele R, Eckersberger E, et al Urinary continence after radical prostatectomy: the patient perspective Can J Urol 2011; 18:5811-8
30 Zorn KC, Wille MA, Thong AE, et al Continued improvement of perioperative, pathological and continence outcomes during 700 robot-assisted radical prostatectomies Can J Urol 2009; 16:4742-9
31 Theissen L, Preisser F, Wenzel M, et al Very Early Continence After Radical Prostatectomy and Its Influencing Factors Front Surg 2019; 6:60
32 Cano Garcia C, Wenzel M, Humke C, et al Impact of Age on Long-Term Urinary Continence after Robotic-Assisted Radical Prostatectomy Medicina (Kaunas) 2023; 59:1153
Correspondence
Shahryar Zeighami zeyghamishahryar@yahoo com
Ali Ariafar
ariafar76@gmail com
Alireza Makarem alirezamakarem2001@gmail com
Mohammadreza Askarpour askarvip2@gmail com
Department of Urology, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran
Faisal Ahmed (Corresponding Author) fmaaa2006@yahoo com
Department of Urology, School of Medicine, Ibb University of Medical Sciences, Ibb, Yemen
S
ORIGINAL PAPER
The impact of inflammation on prostate tumor dynamics: A pathological perspective on prostate cancer and benign prostatic hyperplasia
Syakri Syahrir 1, 2 , Muhammad Asykar Palinrungi 1 , Mochammad Hatta 3 , Khoirul Kholis 1, 2 , Syarif 1 , Abdul Azis 1 , Muhammad Faruk 4
1 Division of Urology, Department of Surgery, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia;
2 Dr Wahidin Sudirohusodo Hospital, Makassar, Indonesia;
3 Department of Clinical Microbiology, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia;
4 Department of Surgery, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia
Summary
Introduction: Chronic inflammation is associated to the pathogenesis of prostate cancer (PCa) and benign prostatic hyperplasia (BPH)
This study evaluated the correlation between inflammatory markers fibroblast growth factor-2 (FGF2), interleukin (IL)-8, and IL-6 in PCa and BPH tissues to understand their involvement in disease progression
Methods: A cross-sectional investigation was carried out, examining prostate specimens from 62 male patients diagnosed with PCA or BPH Specimens were taken via transurethral resection of the prostate (TURP) and stained with hematoxylin and eosin to look for inflammatory infiltrates and aggressiveness
The levels of FGF2, IL-8, and IL-6 were evaluated using ELISA Chi-square and logistic regression tests were used in the statistical analysis
Results: High-grade inflammation was found in all BPH cases (100%), but not in PCa cases. In BPH tissues, elevated levels of IL-8 and IL-6 had a significant correlation with high-grade inflammation (p < 0.05). On the other hand, PCa tissues had considerably greater FGF2 levels than benign tissues (p < 0 05) Elevated FGF2 levels and the lack of high-grade inflammation in PCa tissues point to different pathogenic processes in PCa and BPH.
Conclusions: This study emphasizes the importance of chronic inflammation in BPH development, with IL-8 and IL-6 playing essential roles The results imply that treating BPH by focusing on IL-8 and IL-6 may be beneficial. Increased levels of FGF2 in PCa tissues suggest that this protein may be used as a biomarker and therapeutic target for PCa. These findings highlight the importance of targeting both inflammatory and growth factor pathways for treating prostatic disorders.
Submitted 6 November 2024; Accepted 27 January 2025
INTRODUCTION
Prostate cancer (PCa) and benign prostatic hyperplasia (BPH) are increasingly significant health issues, with their prevalence likely to rise due to an aging population (1, 2)
A deeper understanding of the natural history of prostate tumors is crucial for improving early detection and devel-
oping effective therapeutic strategies (3) The development of prostate tumors has been linked to a range of factors, including race, age, heredity, diet, and environment
Recent research suggests that prostatic inflammation may play a key role in both PCa and BPH (4-6), highlighting the need for further investigation into this connection (5, 6)
The hypothesis that inflammation can drive cancer cell proliferation has been explored for over 150 years Recent preclinical research supports the idea that inflammation plays a role in the development and progression of PCa The correlation between prostatic inflammation and BPH has been recognized since as early as 1937 (7) Despite these historical and preclinical insights, there remains a scarcity of comprehensive clinical data directly linking prostatic inflammation with tumor development and progression Understanding the immune pathways associated with prostate tumors could lead to novel therapeutic strategies (3,8) The inflammatory infiltrates found in prostate glands differ in type, intensity, and location, indicating the participation of various molecular processes (9)
Pathological research is particularly valuable in this context, as it can provide more reliable insights into the association between inflammation and prostate tumors compared to epidemiological studies alone (5, 10)
Recent studies have identified inflammatory cytokines such as fibroblast growth factor-2 (FGF2) interleukin (IL)-8, and IL-6 as potential contributors to prostate tumor development (11, 12) FGF2 is known for its role as a potent growth factor, promoting abnormal prostate growth and the proliferation of basal epithelial cells, thus contributing to the pathogenesis of both PCa and BPH IL-6 and IL-8 are also critical in stromal growth associated with BPH and cancer progression (11, 13) This study aims to explore the correlation between inflammation and prostate tumor development and progression by investigating these inflammatory markers and their roles in both PCa and BPH
METHODS
Study population and tissue collection
A cross-sectional study was carried out to examine the
association between prostatic inflammation and the development of tumors The study involved 62 prostate samples from patients with symptoms of obstruction who were diagnosed with either PCa and BPH These samples were acquired during TURP procedures between April and September 2018 Participants were recruited from four major Hospitals in Makassar: Universitas Hasanuddin Hospital, Ibnu Sina Hospital, Awal Bros Hospital, and Wahidin Sudirohusodo Hospital The investigation was granted authorization by the Institutional Review Board, and informed consent was gathered from all individuals prior to their participation in the study
Prostate processing and histological analysis
All collected prostate specimens were processed and subjected to histological analysis Hematoxylin and eosin staining was performed on all samples A qualified pathologist examined the specimens to assess the presence and extent of inflammatory infiltrations and their aggressiveness
Degree of inflammation
Morphological description (typical inflammatory cell density, cells/mm2) was classified as low grade (individual inflammatory cells, most of which separated by distinct intervening spaces [< 100]), moderate grade (confluent sheets of inflammatory cells with no tissue destruction or follicle formation/ lymphoid nodule [100-500]), and high grade (confluent sheets of inflammatory cells with tissue destruction or follicle/nodule formation [> 500]) (14)
Inflammatory aggressiveness
Inflammation was assessed using a 4-point scale: grade 0 indicates no interaction between glandular epithelium and inflammatory cells; grade 1 denotes contact between glandular epithelium and inflammatory cells, with minimal epithelial dissociation present; grade 2 involves interstitial inflammatory infiltration with limited glandular epithelium disruption (less than 25%); grade 3 reflects glandular epithelium disruption exceeding 25% of the examined material (15) In this study, grades 0 and 1 were classified as having no glandular disruption, and grades 2 and 3 were classified as glandular disruption groups
Inflammatory location
Stromal inflammatory cells are located in the prostatic stroma, distant from prostatic glands Periglandular inflammatory infiltrates are centered around glands and ducts, approaching glands and ducts closely Glandular inflammatory infiltrates are found within the epithelium and/or lumens of glands and ducts (14)
Inflammatory markers evaluation
The inflammatory cytokines FGF2, IL-8, and IL-6 levels in prostate samples were quantified using ELISA kits from R&D Systems (Minneapolis, MN) The procedure followed the manufacturer’s instructions In summary, 100 μL of each sample was added in duplicate to the wells and incubated at room temperature for 1 5 hours Subsequently, 100 μL of biotinylated antibodies was added to each well and incubated for one hour at 37°C After this step, streptavidin-horseradish peroxidase was applied for 45 minutes, followed by a 30-minute incubation with 3,3’,5,5’-
TMB The reaction was terminated with sulfuric acid, and absorbance was recorded at 450 nm using a PHERAstar microplate reader (BMG LABTECH, Durham, NC) FGF2, IL-8, and IL-6 concentrations were quantified in ng/mL
Prostate-specific antigen (PSA) examination
A 3 cc blood sample was taken from the vein, then centrifuged to take the blood serum Then, the blood serum was examined by the Architech Plus device from Abbott (Chicago, Illinois, USA) using a Monoclonal antibody PSA reagent from Meridian Bioscience (Memphis, TN, USA) with catalog #M86806M The PSA concentrations was quantified in ng/mL
Statistical analysis
The data were evaluated to distinguish BPH from PCa based on their pathological characteristics The chi-square test was utilized to evaluate the correlation between inflammatory infiltrates and the presence of prostate diseases To examine the association between inflammatory infiltrates and prostate diseases aggressiveness, the Kruskal-Wallis test was conducted Additionally, Spearman correlation test was performed to determine the correlation between PSA, inflammatory markers and age A p-value of less than 0 05 was deemed statistically significant, with a confidence interval set at 95% All statistical analyses were conducted using SPSS software
RESULTS
Baseline characteristics of patients
The study included 62 prostate glands from male subjects (Table 1), with 51 glands (82 3%) diagnosed as BPH and 11 glands (17 7%) as prostate cancer The average age of the patients was 69 ± 9 years, while the median volume of the glands measured 65 ± 35 cm³ Inflammatory aggressiveness showed glandular disruption in 49 glands (79%) and no glandular disruption in 13 glands (21%) The mean PSA level for PCa was 92 16 ± 39 35
Table 1.
Characteristics of participants
Variables n (%) Age (years), mean (± SD)
Glands
Benign prostate hyperplasia
(± 9)
(82.3)
Prostate carcinoma 11 (17 7)
Degree of inflammation
Low grade
(72 6)
Moderate grade 0 (0)
High grade 17 (27 4)
Inflammatory aggressiveness
No glandular disruption 13 (21)
With glandular disruption 49 (79)
PSA level (ng/mL), mean (± SD)
PCa 92 16 (± 39 35)
BPH 20 54 (± 24 53)
Prostate volume (cc), mean (± SD) 65 (± 35)
PSA: Prostate specific antigen; PCa: Prostate cancer; BPH: benign prostatic hyperp asia
S Syahrir, M Asykar Palinrungi, M Hatta, et al
Table 2
Pathological features of inflammation in 62 prostate glands
Variables BPH PCa P-value
Degree of inflammation
Low grade 34 (75 6) 11 (24 4) 0 026
Moderate grade 0 (0) 0 (0)
High grade 17 (100) 0 (0)
Inflammatory location
Stromal 9 (69 2) 4 (30 8) 0 22
Periglandular 0 (0) 0 (0)
Glandular 42 (85 7) 7 (14 3)
PCa Prostate cancer; BPH: ben gn prostat c hyperp asia
Pathological features of inflammation
Table 2 summarizes the pathological features of inflammation in the prostate glands as observed in patients with PCa and BPH Out of the 62 patients, 45 exhibited low-grade inflammation (low-grade inflammation was present in 34 [75 6%] BPH glands and 11 [24 4%] PCa glands) In contrast, all 17 cases of high-grade inflammation were found in BPH glands, showing significant difference (p < 0 05)
Regarding inflammation location and aggressiveness, 13 glands had stromal-only inflammation (9 in BPH and 4 in PCa), and 49 glands had glandular involvement (42 in BPH and 7 in PCa) The differences in inflammation locations were not statistically significant (p > 0 05)
Classification and degree of inflammation
Figure 1 illustrates the classification and degree of inflammation Low-grade inflammation was the most prevalent pattern, characterized by a scattered infiltrate of inflammatory cells within the stroma It was found in 34 (75 6%) BPH glands and 11 (24 4%) PCa glands In contrast, high-grade inflammation, involving extensive areas of confluent infiltrate, was less common and observed in 17 (100%) BPH glands A significant correlation was o b s e r v e d b e t w e e n t h e d e g r e e o f i n fl a m m a t i o n a n d prostate diseases aggressiveness (rho = 0 786, p < 0 05)
High-grade inflammation was linked to glandular disruption, whereas low-grade inflammation was associated with the absence of glandular disruption
Figure 1
Table 3.
The comparison of clinical data and inflammatory marker between patients with low and high grade of inflammation
Variable Degree of inflammation P-value Low grade High grade
PSA: Prostate specif c ant gen; IL-6: nterleukin-6; IL-8: inter euk n-8; FGF: f brob ast growth factor-2
Comparison of clinical data and inflammatory markers
Table 3 compares clinical data and inflammatory markers between patients experiencing low-grade and high-grade inflammation Patients with high-grade inflammation exhibited higher serum PSA levels than those with lowgrade inflammation (114 vs 38), this difference was statistically significant (p < 0 05)
Association between inflammatory markers (IL-6, IL-8, and FGF-2) and age with serum PSA levels
In table 4, no correlation was shown between the inflammatory markers (IL-6, IL-8, and FGF-2) and serum PSA
Table 4.
Correlation between PSA, inflammatory markers and age.
Spearman corre at on test
Degree of inflammation based on histopathological examination: A Low-grade inflammation [presence of scattered inflammatory cells (arrow)] (HE staining, magnification 10x); B. High-grade inflammation [extensive areas of inflammation with the formation of lymphoid nodules (arrow)] (HE staining, magnification 4x)
levels (rho = 0 157, p = 0 322; rho = 0 113, p = 0 475; and rho = -0 077, p = 0 630, respectively) Additionally, serum PSA levels did not show a correlation with the patients' age (rho = 0 069, p = 0 626)
Increased inflammatory marker concentration in prostate diseases tissue
The levels of FGF2, IL-8, and IL-6 were measured in p r o s t a t e d i s e a s e s s a m p l e s P a t i e n t s w i t h h i g h - g r a d e inflammation had significantly higher concentrations of
IL-6 compared to those with low-grade inflammation (638 vs 382, p < 0 05) The mean IL-6 concentration in benign tissues was recorded at 493 pg/ml, whereas in cancerous tissues, it was 264 pg/ml, indicating a significant difference (p < 0 05; Figure 2)
Likewise, IL-8 levels were found to be greater in highgrade inflammation cases compared to low-grade inflammation (149 vs 99, p < 0 05) The mean IL-8 concentration was 120 pg/ml in benign tissues and 83 pg/ml in cancer tissues (p < 0 05; Figure 3)
Figure 2.
The comparison of IL-6 tissue levels between prostate diseases (p-value < 0.05).
Figure 3.
The comparison of IL-8 tissue levels between prostate diseases (p-value < 0.05).
S Syahrir, M Asykar Palinrungi, M Hatta, et al
Interestingly, FGF2 concentration was higher in lowgrade inflammation compared to high-grade inflammation (190 vs 94, p < 0 05) The mean FGF2 concentration was higher in cancer tissues compared to benign tissues (238 vs 148, p < 0 05; Figure 4)
DISCUSSION
Chronic inflammation is associated to the development of various prostatic conditions, but the precise roles and mechanisms of inflammatory markers like FGF2, IL-8, and IL-6 are still not well understood In this study, prostate samples from patients with PCa and BPH were examined, with a focus on inflammation presence and severity, and the concentrations of FGF2, IL-8, and IL-6 High-grade inflammation was found in all BPH cases, but not in PCa cases Elevated IL-8 and IL-6 levels were detected in BPH tissues with high-grade inflammation, while FGF2 concentrations were significantly higher in cancerous tissues compared to benign tissues The presence of high-grade inflammation in all BPH cases and its absence in PCa cases suggest a strong link between inflammation and BPH pathogenesis Chronic inflammation appears to be a critical driver of hyperplastic growth in the prostate, as indicated by the elevated levels of IL-8 and IL-6 in inflamed tissues This finding implies that targeting inflammatory pathways could be a potential therapeutic strategy for BPH
One potential reason for the lack of significant inflammation in PCa tissues is that inflammation's role in PCa may be intricate and influenced by the context In the initial phases of PCa, inflammation may be a key factor in fostering carcinogenesis However, as the cancer advances, elements like genetic mutations and epigenetic alterations may take precedence in facilitating tumor
Figure 4.
The comparison of FGF-2 tissue levels between prostate diseases (p-value < 0.05).
growth According to De Marzo et al , inflammation may trigger the onset of cancer, but further oncogenic developments are necessary for the progression to full malignancy (16)
IL-6 and IL-8 levels
The elevated levels of IL-8 and IL-6 in BPH tissues highlight their significant role in promoting an inflammatory microenvironment IL-6 is known for its multifunctional role in immune response and cell proliferation, while IL8 is involved in the recruitment of inflammatory cells and angiogenesis These findings indicate that IL-8 and IL-6 are key mediators in the inflammatory processes contributing to BPH development The heterogeneity of inflammatory responses might also influence the overall impact of inflammation on prostate disease progression (17) As the inflammatory infiltrates in prostate tissues are heterogeneous in nature, severity, and location hence it is a possible explanation to why the elevated IL-6 and IL-8 are significant in BPH but not uniformly present in PCa tissues (17, 18)
FGF2 levels
The markedly elevated levels of FGF2 found in PCa tissues compared to benign tissues suggest that growth factors could be more critical in the advanced stages of cancer development FGF2 contributes to cell growth, differentiation, and angiogenesis, all of which are vital processes for tumor progression and metastasis (19) This finding suggests that FGF2 could be a potential biomarker for PCa and a target for therapeutic interventions The elevated levels of FGF2 in PCa tissues support the idea that as PCa progresses, growth factors like FGF2 become more critical in sustaining tumor growth and promoting metastasis (20-22)
Inflammation’s Role in BPH vs PCa: Where are we now?
In their study, Inamura and Terada highlighted the roles of IL-8 and IL-6 in benign prostatic hyperplasia (BPH), explaining how these cytokines facilitate tissue remodelling and smooth muscle contraction, which can affect the progression of the disease This finding aligns with our results, which demonstrate elevated levels of IL-8 and IL6 in BPH tissues with marked inflammation (23) Based on our observations, it seems likely that these cytokines are key players in the inflammatory process, acting as the molecular pathways through which chronic inflammation influences prostatic diseases
Other research has also pointed to this, linking it to the pro-inflammatory environment created by increased levels of IL-8 and IL-6 (10, 24)
We also found in our observation that high-grade inflammation is found predominantly in BPH cases, as proposed by Kramer et al who stated BPH might be an immune inflammatory disease, validating the association between inflammation and prostatic diseases They found that inflammatory infiltrates are common in BPH tissues and are associated with disease severity (24, 25)
Robert et al also found that inflammatory infiltrates are common in BPH tissues and are associated with disease severity (26) Further reinforcing the idea that inflammation plays a crucial role in the severity and progression of BPH
De Marzo et al discussed how chronic inflammation in the onset and progression of prostate cancer They emphasized that chronic inflammation could foster a microenvironment conducive to cancer development, which aligns with our findings of increased FGF2 levels in prostate cancer tissues (16)
Their study suggested that inflammation could drive genetic and epigenetic changes that promote malignancy, aligning with our findings regarding the role of inflammatory markers
Bridging the current gap
Our findings further reinforce the theory that chronic inflammation is a key factor in the development of BPH The significant association between high-grade inflammation and BPH also supports the idea that targeting specific inflammatory pathways could be a potential therapeutic strategy Increased levels of IL-8 and IL-6 suggest these cytokines are critical mediators of the inflammatory processes driving BPH, providing a deeper explanation of t h e d i s e a s e ' s p a t h o g e n e s i s T h e i n fl a m m a t i o n - d r i v e n model of disease was also proposed by as Kramer et al who suggested that BPH might be fundamentally an i m m u n e i n fl a m m a t o r y d i s e a s e ( 2 5 ) M o r e o v e r , t h e absence of high-grade inflammation in PCa tissues, contrasted with the higher levels of FGF2, indicating that different mechanisms may be at play in PCa and BPH This supports the hypothesis that while inflammation initiates BPH, other factors such as growth factors like FGF2 become more critical in later stages of PCa (5, 16, 27)
The differential expression of FGF2, IL-8, and IL-6 in PCa and BPH and tissues has significant clinical implications Anti-inflammatory treatments targeting IL-6 and IL-8 may offer therapeutic benefits for patients with BPH by mitigating the inflammatory processes that drive
hyperplasia For instance, agents that block IL-6 signalling, such as tocilizumab, have shown efficacy in treating inflammatory diseases and might be repurposed for BPH treatment (28, 29) Furthermore, the elevated FGF2 levels in PCa suggest that therapies aimed at inhibiting FGF2 could be more relevant for managing PCa Anti-FGF2 therapies, such as the use of FGFR inhibitors, are being explored in various cancers and could potentially be adapted for PCa (30) These targeted approaches could lead to more effective treatments tailored to the underlying pathophysiology of each condition (31) Overall, our findings suggest that a dual approach targeting both inflammation and growth factors might be necessary to effectively manage prostatic diseases, aligning with the multiple approaches for the treatment strategies proposed by recent clinical (31, 32) A limitation of this study is that it included only 62 prostate glands, with 51 diagnosed with BPH and 11 with PCa This relatively small sample size may limit the generalizability of the findings to a broader population The study found no high-grade inflammation in PCa tissues, which raises questions about the role of inflammation in the later stages of cancer This absence may indicate that other factors, such as genetic mutations, play a more significant role in PCa progression, but the study does not explore these factors in depth
CONCLUSIONS
This study deepens our understanding of the distinct roles of FGF2, IL-8, and IL-6 in PCa and BPH A signific
inflammation and BPH, characterized by increased levels of IL-8 and IL-6, while such inflammation was not present in PCa tissues Conversely, FGF2 levels were found to be notably elevated in PCa tissues These findings suggest different pathogenic mechanisms in BPH and PCa, with growth factors like FGF2 becoming more prominent in cancer progression Future studies should focus on longitudinal designs to clarify the causal correlation between inflammation and prostate disease progression Investigating the molecular mechanisms underlying the differential expression while exploring other inflammatory cytokines Conducting multicenter studies could be highly beneficial for several reasons: multicenter studies can recruit participants from various geographical locations and demographics, leading to a more diverse patient population This diversity can help ensure that the findings are generalizable across different groups, which is crucial for understanding the broader implications of inflammation in prostate diseases Researchers can significantly increase the sample size by pooling data from multiple centers A larger sample size enhances the study's statistical power, allowing for more robust conclusions regarding the associations between inflammatory markers and prostate conditions
REFERENCES
1 Tang J, Yang J Etiopathogenesis of benign prostatic hypeprlasia Indian J Urol 2009; 25:312-7
S Syahrir, M Asykar Palinrungi, M Hatta, et al
2 Zlotta AR, Egawa S, Pushkar D, et al Prevalence of inflammation and benign prostatic hyperplasia on autopsy in Asian and Caucasian men Eur Urol 2014; 66:619-622
3 Sampson N, Madersbacher S, Berger P Pathophysiology and therapy of benign prostatic hyperplasia Wien Klin Wochenschr 2008; 120:390-401
4 Guner E, Danacioglu YO, Arikan Y, et al The presence of chronic inflammation in positive prostate biopsy is associated with upgrading in radical prostatectomy Arch Ital Urol Androl 2021; 93:280284
5 De Nunzio C, Kramer G, Marberger M, et al The controversial relationship between benign prostatic hyperplasia and prostate cancer: The role of inflammation Eur Urol 2011; 60:106-117
6 Jones SA, Jenkins BJ Recent insights into targeting the IL-6 cytokine family in inflammatory diseases and cancer Nat Rev Immunol 2018; 18:773-789
7 Moore RA Inflammation of the Prostate Gland1 J Urol 1937; 38:173-182
8 Gandaglia G, Briganti A, Gontero P, et al The role of chronic prostatic inflammation in the pathogenesis and progression of benign prostatic hyperplasia (BPH) BJU Int 2013; 112:432-441
9 Delongchamps NB, de la Roza G, Chandan V, et al Evaluation of Prostatitis in Autopsied Prostates: Is Chronic Inflammation More Associated with BPH or Cancer? J Urol 2008; 179:1736
10 Oseni SO, Naar C, Pavlovic M, et al The Molecular Basis and C l i n i c a l C o n s e q u e n c e s o f C h r o n i c I n fl
Diseases: Prostatitis, Benign Prostatic Hyperplasia, and Prostate Cancer Cancers (Basel) 2023; 15:3110
11 Penna G, Fibbi B, Amuchastegui S, et al Human Benign Prostatic Hyperplasia Stromal Cells As Inducers and Targets of Chronic Immuno-Mediated Inflammation J Immunol 2009; 182:4056-4064
DECLARATIONS
Ethical approval: This protocol was approved by the Institutional Review Board at our institution (no UH18010030) All procedures involving human participants were performed in accordance with the ethical standards of the 1964 Helsinki declaration and its later amendments or comparable ethical standards Informed consent was obtained from all participants included in the study
Availability of data and material: The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request
Competing interests: The authors declare that they have no competing interests
Funding: This research received no specific grant from any funding agency in the public, commercial, or not for- profit sectors
Authors' contributions: All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work
Acknowledgments: None
12 Fibbi B, Penna G, Morelli A, et al Chronic inflammation in the pathogenesis of benign prostatic hyperplasia Int J Androl 2010; 33:475-488
13 Elkahwaji JE The role of inflammatory mediators in the development of prostatic hyperplasia and prostate cancer Res Rep Urol 2013; 5:1
14 Nickel JC, True LD, Krieger JN, et al Consensus development of a histopathological classification system for chronic prostatic inflammation BJU Int 2001; 87:797-805
15 Irani J, Levillain P, Goujon JM, et al Inflammation in benign prostatic hyperplasia: correlation with prostate specific antigen value J Urol 1997; 157:1301-1303
16 De Marzo AM, Platz EA, Sutcliffe S, et al Inflammation in prostate carcinogenesis Nat Rev Cancer 2007; 7:256-269
17 Sfanos KS, de Marzo AM Prostate cancer and inflammation: the evidence Histopathology 2012; 60:199-215
18 Murtola TJ, Gurel B, Umbehr M, et al Inflammation in benign prostate tissue and prostate cancer in the finasteride arm of the prostate cancer prevention trial Cancer Epidemiol Biomarkers Prev 2016; 25:463-469
19 Stone L FGF2 causes genomic instability Nat Rev Urol 2018; 15:528-528
20 Inamura S, Terada N Chronic inflammation in benign prostatic hyperplasia: Pathophysiology and treatment options Int J Urol 2024; 31:968-974
21 Syahrir S, Hatta M, Warsinggih W, et al Propionebacterium acnes associated with inflammation in benign prostatic hyperplasia Int Med J 2020; 25:13412051
22 Gurel B, Lucia MS, Thompson IM, et al Chronic inflammation in benign prostate tissue is associated with high-grade prostate cancer in the placebo arm of the prostate cancer prevention trial Cancer Epidemiol Biomarkers Prev 2014; 23:847-856
23 Pecqueux C, Arslan A, Heller M, et al FGF-2 is a driving force for chromosomal instability and a stromal factor associated with adverse clinico-pathological features in prostate cancer Urol Oncol 2018; 36:365 e15-365 e26
24 Ropiquet F, Giri D, Lamb DJ, Ittmann M FGF7 and FGF2 are increased in benign prostatic hyperplasia and are associated with increased proliferation J Urol 1999; 162:595-9
25 Kramer G, Mitteregger D, Marberger M Is benign prostatic hyperplasia (BPH) an immune inflammatory disease? Eur Urol 2007; 51:1202-1216
26 Robert G, Descazeaud A, Nicolaïew N, et al Inflammation in benign prostatic hyperplasia: a 282 patients’ immunohistochemical analysis Prostate 2009; 69:1774
27 De Marzo AM, Nakai Y, Nelson WG Inflammation, atrophy, and prostate carcinogenesis Urol Oncol 2007; 25:398-400
28 Rose-John S, Jenkins BJ, Garbers C, et al Targeting IL-6 transsignalling: past, present and future prospects Nat Rev Immunol 2023; 23:666-681
29 Bechis SK, Otsetov AG, Ge R, Olumi AF Personalized medicine for the management of benign prostatic hyperplasia J Urol 2014; 192:16-23
30 Turner N, Grose R Fibroblast growth factor signalling: from development to cancer Nat Rev Cancer 2010; 10:116-129
31 Schaeffer EM, Srinivas S, Adra N, et al Prostate Cancer, Version 3 2024 Featured Updates to the NCCN Guidelines J Natl Compr Canc Netw 2024; 22:140-150
32 Schaeffer E, Srinivas S, Antonarakis ES, et al NCCN Guidelines Insights: Prostate Cancer, Version 1 2021 J Natl Compr Canc Netw 2021; 19:134-143
Correspondence
Syakri Syahrir (Corresponding Author) drsyakrisyahrir@gmail com
Division of Urology, Department of Surgery, Faculty of Medicine, Hasanuddin University - Dr Wahidin Sudirohusodo Hospital, Makassar, Indonesia
Jalan Perintis Kemerdekaan KM 11, Makassar, 90245, South Sulawesi, Indonesia
Muhammad Asykar Palinrungi apalinrungi@yahoo com
Khoirul Kholis khoirulkholis@yahoo com
Syarif Syarif syarifbakri@unhas ac id
Abdul Azis
abdul azis031@gmail com
Division of Urology, Department of Surgery, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia
Mochammad Hatta hattaram@yahoo com
Department of Clinical Microbiology, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia
Muhammad Faruk muhammadfaruk@unhas ac id
Department of Surgery, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia
S Syahrir, M Asykar Palinrungi, M Hatta, et al
ORIGINAL PAPER
Predictive role of lactylation-related gene signature in the prognosis and immunotherapy response in bladder cancer
Guoyuan Liu 1* , Ting Hong 2* , Xinyu Liu 2* , Xuanhao Lin 3 , Peixiu Yao 3 , Xifeng Chen 3 , Yonghai Zhang 1 , Kemal Sarica 4, 5 , Xuwei Hong 1
1 Department of Urology, Shantou Central Hospital, Shantou, China;
2 Clinical Medical Research Center, Shantou Central Hospital, Shantou, China;
3 Department of Biobank, Shantou Central Hospital, Shantou, China;
4 Department of Urology, Health Sciences University, Prof Dr Ilhan Varank Education and Training Hospital, Istanbul, Turkey;
5 Department of Urology, Biruni University, Medical School, Istanbul, Turkey
* These authors contributed equally to this work
Summary
Objective: Lactylation is a type of chemical modification involving the introduction of lactyl groups to a molecule which can affect the interactions between tumor cells and their microenvironment
This study aims to evaluate the possible role of lactylation-related gene signature in the prediction of both prognosis and immunotherapy response in bladder cancer (BLCA).
Methods: Lactylation-related genes were obtained from the published work and two subtypes (cluster A and B) were identified through unsupervised clustering The differences including clinical features, differentially expressed genes (DEGs), pathways, and immune cell infiltration between these two clusters were thoroughly examined
Results: By utilizing the DEGs between the two clusters, a lactylation score was identified to predict the overall survival status and the response of BLCA patients receiving immunotherapy Our results demonstrated that patients with a high lactylation score tended to have a worse survival period and increased immune cell infiltration level Further analysis showed that high lactylation score may be associated with higher sensitivity to immune checkpoint inhibitor (ICI) treatment which is crucial in the identification of the suitable candidates for ICI therapy
Conclusions: Our results emphasize the possible predictive role of lactylation-related gene signature both in the survival rates of BLCA and its implications for treatment strategies.
Submitted 22 December 2024; Accepted 3 January 2025
INTRODUCTION
Bladder cancer (BLCA) is one of the most common malignant pathologies of the genitourinary tract, with approximately 573,000 new cases and 212,000 deaths per year worldwide The incidence of BLCA is still increasing owing to population growth and ageing (1-3) In recent years, immune checkpoint inhibitors (ICIs) took attention as
an effective alternative for advanced BLCA due to their better tolerance especially by older patients with more c o m o r b i d i t i e s H o w e v e r ,
shown in a subset of patients with BLCA, the overall response rate of ICI’s is only 15%~25%, which increases the demand for biomarkers of response and therapeutic strategies that can overcome resistance to ICIs (4, 5)
Lactylation modification has been well studied for its potential role in cancer progression (6-8) The tumor microenvironment is characterized by low pH, hypoxia, and increased lactate production Lactate, a product of pyruvate metabolism, is known to play an important role in promoting tumor growth and metastasis by modulating the extracellular matrix, angiogenesis, and immune evasion (9-11)
Lactylation has also been found to alter the activity and stability of intracellular proteins, leading to changes in certain cellular processes including glycolysis (12, 13) and apoptosis (14) In addition, lactylation can further affect the interactions between tumor cells and their microenvironment by promoting or inhibiting tumor progression (15-17)
These findings suggest that lactylation may serve as a potential target for the development of novel cancer therapeutics to interfere with lactate signaling pathways and disrupt tumor progression However, the role of lactylation in BLCA remains still unclear
In this present study, we aimed to identify lactylationrelated gene subtypes of BLCA through unsupervised clustering in order to compare clinical features, differentially expressed genes (DEGs), pathways and immune cell infiltration between the lactylation-related gene subtypes identified
Furthermore, by establishing a special lactylation score we also aimed to predict the overall survival of BLCA patients Lastly, we investigated the correlation between the lactylation score and the tumor immune microenvironment, as well as the potential for immunotherapeutic efficacy
MATERIALS AND METHODS
Sources of sample
The Cancer Genome Atlas Urothelial Bladder Carcinoma (TCGA-BLCA) is a data collection initiative that is part of a larger effort to connect cancer phenotypes to genotypes The data includes clinical, genetic, pathological, and radiological information of 412 tumor samples and 19 normal samples GSE13507 is a public gene expression dataset that identifies prognosis-related gene signatures in BLCA It contains 165 primary tumors, 23 recurrent tumors, 58 normal bladder mucosae surrounding cancer and 10 normal bladder mucosae, the clinical characteristics of included samples are attached as well
Data collection
The mRNA expression profile and clinical data for TCGABLCA (412 tumor tissues) were downloaded from the University of California Santa Cruz (UCSC)-Xena database (https://xenabrowser net/datapages/), while GSE13507 (165 tumor tissues) was obtained from the Gene Expression Omnibus (GEO) database (https://www ncbi nlm nih gov/ geo/) The clinical characteristics and survival outcomes of BLCA patients from these two datasets were shown in supplementary Table S1 R package “limma” was executed to normalize the expression data for nonuniform matrix distribution To improve the reliability, the two datasets were merged and batch effects were removed using the R package “sva” The gene set for lactylation was acquired from the published work (18)
Online analysis
The genetic alteration of selected genes, including copy number variant (CNV), methylation and mutation, were conducted using Gene Set Cancer Analysis (GSCA) database (http://bioinfo life hust edu cn/GSCA/#/), which is an integrated platform for genomic, pharmacogenomic, and immunogenomic gene set cancer analysis The platform has four main functional modules for cancer GSA to explore, analyze and visualize expression, genomic variations, tumor immune infiltration, drug sensitivity and their associations with clinical outcomes
Enrichment analysis
Gene Ontology (GO) analysis and Kyoto Encyclopedia of Genes and Genomes (KEGG) analysis are two common functional annotation methods, which are mainly used to study the functions of genes and proteins GO analysis is performed by classifying the function of a gene or protein into three distinct levels: Molecular Function, Cellular Component and Biological Process to describe their different functions and interactions within cells KEGG analysis is a functional annotation method based on metabolic pathways and biological signaling networks By correlating genes or proteins with metabolic pathways and signaling networks in KEGG databases, it is possible to understand their functional roles and interrelationships in the cells To obtain the pathways used in Gene Set Variation Analysis (GSVA), the HALLMARK, Reactome, and KEGG pathways were downloaded from version 7 5 1 of the Msigdb database The R package "GSVA" was used to calculate the pathway score for each sample The R package "clusterprofiler" was used to carry out GO and KEGG analysis of DEGs
Immune cell infiltration analysis
The R package "ESTIMATE" was used to assess the BLCA samples' tumor microenvironment, including stromal score, immune score, and ESTIMATE score In order to measure the 23 immune cell infiltrations, the GSVA R package's ssGSEA function was used Following that, the various groups were compared based on their immune cell level
Construction of Lactylation score
Using the R package "limma" , we identified 275 DEGs distinguishing between cluster A and B with |logFC| > 0 5 and p < 0 05 Subsequently, we conducted univariate regression analysis, which revealed 11 DEGs significantly associated with overall survival at p < 0 001 Based on these 11 DEGs, we performed principal component analysis (PCA) Using principal components 1 and 2, we constructed the lactylation score (19)
Statistical analysis
All data are presented as the mean ± Standard Deviation (SD) Statistical analysis was performed using R software (https://www r-project org/, version:4 1 1) P < 0 05 (two-tailed) was considered statistically significant: *p < 0 05, **p < 0 01, ***p < 0 001, and ****p < 0 0001
RESULTS
Identification of lactylation genes-related subtypes of BLCA
The flow chart of the study is show in Figure 1 At first, we combined the expression profiles of tumor tissues from TCGA-BLCA and GSE13507, and then used univariate Cox regression and Kaplan-Meier analysis to evaluate the prognostic significance of lactylation genes (Supplementary Table S2) Figure 2A depicts the results of univariate Cox regression and correlation analysis of lactylation genes 10 lactylation genes were revealed to have some correlation with each other Among them, 9 genes were identified as risk factors and one was favorable factor While Figure 2B illustrates 7 lactylation genes that were significantly associated with the prognosis of BLCA patients revealed by Kaplan-Meier analyses Next, we divided BLCA into two subtypes, cluster A and B, based on the expression pattern of lactylation genes (Figure 3A), and found that there was a clear distinction between cluster A and B according to the PCA plot (Figure 3B) We also presented the distribution of clinical features and lactylation gene expression in each cluster (Figure 3C, D)
Furthermore, we assessed the immune infiltration in BLCA samples, and found that the stromalscore, immunescore, and ESTIMATEscore were all higher in cluster A (Figure 3E), and most immune cell levels were more highly infiltrated in cluster A than in cluster B (Figure 3F)
We also investigated the differences between the two clusters in terms of various pathways using GSVA We discovered that most of the HALLMARK pathways, KEGG pathways, and Reactome pathways had higher scores in cluster B (Supplementary Figure S1) For HALLMARK pathways, the scores TGF BETA signaling pathway and MTORC1 signaling pathway were higher in cluster B For KEGG, the scores of TGF BETA signaling pathway, WNT signaling
G Liu, T Hong, X Liu, et al
pathway, and MTOR signaling pathwaywere higher in cluster B For Reactome results, most pathways were observed to be higher in cluster B These findings suggested that the biggest difference between the two subtypes was in the pathways associated with carcinogenesis
Identification of gene subtypes and construction of lactylation score
By employing the "limma" package, 275 DEGs were screened between cluster A and cluster B (Figure 4A) The GO enrichment analysis highlighted that these DEGs were enriched in cell growth and G1/S transition of mitotic cell cycle in Biological Process (BP), cell leading edge and nuclear speck in Cellular Component (CC), and DNA binding transcription factor binding in Molecular Function (MF) (Figure 4B-D) In terms of KEGG, the DEGs were predom-
inantly enriched in Cell cycle, p53 signaling pathway, and Nicotinate and nicotinamide metabolism (Figure 4E)
Furthermore, we utilized univariate Cox regression analysis to determine the prognostic significance of the 275 DEGs and identified 11 genes associated with overall survival (p < 0 001) (Figure 5A, Supplementary Table S3)
To confirm above findings, unsupervised clustering separated patients into two subtypes based on these 11 prognostic genes, geneCluster A-B (Figure 5B) Patients categorized in geneCluster A had worse survival rates compared to those in geneCluster B (Figure 5C) The expression of the 11 lactylation-related genes was depicted in Figure 5D, while Figure 5E showed the distribution of clinical features and expression of the 11 prognostic genes in the two geneClusters Using the PCA algorithm, the 11 prognostic genes were used to establish the lacty-
Figure 1. Flow chart of the study.
Figure 2.
Correlation and prognostic value of lactylation genes in BLCA: A Network diagram showing the interaction of lactylation genes in BLCA The line connecting the lactylation genes represents their correlation, with the line thickness indicating the strength of the correlation between lactylation genes Blue and pink represent negative and positive correlations, respectively B Kaplan-Meier analysis of indicated genes
lation score Figure 5F suggested that patients with a high lactylation score have worse survival The correlation between cluster, geneCluster, lactylation score, and survival status is depicted in Figure 5G using a Sankey dia-
gram We analyzed the correlation of lactylation score with immune cell infiltration and found that patients with high lactylation score have elevated immune cell infiltration level (Figure 5H)
Archivio Italiano di Urologia e Andrologia 2025; 97(1):13516
G Liu, T Hong, X Liu, et al
Lactylation-related gene signature in bladder cancer
Figure 3.
Identification of lactylation genes-related subtypes of BLCA:
A Consensus matrix heatmap defining various clusters and their correlation area B PCA plot of BLCA patients in two clusters
C Distributions of clinical features and expression levels of lactylation genes between two clusters D The expression of lactylation genes in cluster A and cluster B E The tumor microenvironment difference in two clusters F The difference of immune cell infiltration level in two clusters.
Archivio Italiano di Urologia e Andrologia 2025; 97(1):13516
Figure 4
Enrichment analysis of DEGs between two lactylation subtypes:
A. Volcanic map of DEGs between two clusters. B-D. GO enrichment analysis of DEGs, including BP, CC, and MF.
E The correlation of DEGs with top5 terms of KEGG results
Archivio Italiano di Urologia e Andrologia 2025; 97(1):13516
G Liu, T Hong, X Liu, et al
Lactylation-related
Figure 5. Construction of lactylation score in BLCA: A Forest plot presenting results of univariate Cox regression analysis B Consensus matrix heatmap defining various clusters and their correlation area. C. Kaplan-Meier analysis of BLCA patients in two geneClusters. D. The expression of indicated genes in two geneClusters E Distributions of clinical features and expression levels of 11 DEGs between the two geneClusters F Kaplan-Meier analysis of lactylation score in BLCA G The sankey diagram visualized the correlation between cluster, geneCluster, lactylation score, and survival status of BLCA patients H The correlation between lactylation score and immune cell infiltration Red color represents positive correlation, blue color represents negative correlation
Genetic alteration of prognostic genes
We further explored the expression and genetic alterations of 11 prognostic genes The SNV frequency of these genes was generally low, with TBX3 having the highest SNV fre-
quency (Supplementary Figure S2A-B) Supplementary Figure S3A displays the percentage of copy number variation (CNV) for each gene TP53INP1 had the highest amplification CNV frequency, while LGALS1 showed a significant
CNV deletion We also represented the percentage of heterozygous and homozygous CNV of each gene in BLCA, including heterozygous amplification, heterozygous deletion, homozygous amplification, and homozygous deletion (Supplementary Figure S3B) The linear CNV levels of TCIRG1, TP53INP1, and TBX3 were positively correlated with their mRNA expression (Supplementary Figure S3C) The expression of these genes was generally negatively correlated with their DNA methylation level (Supplementary Figure S3D)
The association of lactylation score with clinical features
Additionally, we discovered that patients who are alive have lower lactylation scores compared to those who have passed away (Figure 6A) The proportion of patients who are alive in the high lactylation score group (43%) was lower than that in the low lactylation score group (63%)
Figure 6
Furthermore, a higher lactylation score was strongly associated with other clinical features, including gender, grade, WHO stage, N stage, and T stage in BLCA (Figure 6B-F)
The correlation of lactylation score with immune microenvironment and efficacy of immunotherapy The correlation between the immune microenvironment and lactylation score was evaluated As illustrated in Figure 7A, chemokine and receptor expression were notably elevated in the high lactylation score category The lactylation score exhibited a favorable correlation with immune-related pathways such as inflammatory response, IL6-JAK-STAT3 signaling pathway, IL2-STAT5 signaling pathway, and interferon GAMMA response (Figure 7B) Additionally, the high lactylation score group demonstrated an elevated immune checkpoint expression, including
The association of lactylation score with clinical features: A Left: The lactylation score in alive and dead groups
Right: The percentage of alive and dead patients in high and low lactylation score groups B Left: The lactylation score in various gender Right: The percentage of various gender patients in high and low lactylation score groups C Left: The lactylation scores in high- and low-grade groups. Right: The percentages of high- and low-grade patients in high and low lactylation score groups. D Left: The lactylation score in high- and low-stage groups Right: The percentage of high and low stage patients in high and low lactylation score groups E Left: The lactylation score in high and low N stage groups Right: The percentage of high and low N stage patients in high and low lactylation score groups F Left: The lactylation score in high and low T stage groups Right: The percentage of high and low T stage patients in high and low lactylation score groups
G Liu, T Hong, X Liu, et al
Lactylation-related
CD274, CTLA4, LAG3, PDCD1, and TIGIT (Figure 7C)
Moreover, the high lactylation score group presented a higher frequency of gene mutations (Supplementary Figure S4A-C) These findings further support the theory that cancer patients with a high lactylation score may respond well to immunotherapy
Figure 7.
To verify our hypothesis, further analysis was performed u
patients with a high lactylation score were responsive to ICI treatment in the IMvigor210 cohort (20) (Figure 7DE; Urothelial carcinoma) and NCT02684006 cohort (21) (Figure 7F-G; Renal clear cell carcinoma)
The correlation of lactylation score with immune microenvironment and efficacy of immunotherapy: A. The expression of chemokines and chemokine receptors in high and low lactylation score group in BLCA B The correlation of lactylation score with HALLMARK pathway scores C The expression of immune checkpoints in high and low lactylation score group D Kaplan-Meier analysis of patients in high and low lactylation score groups in IMvigor210 cohort. E. The percentage of patients with different progress status after ICI treatment in high and low lactylation score groups in IMvigor210 cohort F Kaplan-Meier analysis of patients in high and low lactylation score groups in NCT02684006 cohort. G. The percentage of patients with different progress status after ICI treatment in high and low lactylation score groups in NCT02684006 cohort
Apart from immunotherapy, we also analyzed other antitumor drugs Based on the predicted results using the R package “pRRophetic” , we displayed 6 commonly used chemotherapeutic agents for BLCA, including gemcitabine, cisplatin, vinblastine, doxorubicin, docetaxel, and paclitaxel, may be resistant to patients with a high lactylation score Furthermore, 5 targeted agents, including sunitinib, pazopanib, gefitinib, erlotinib, and tipifarnib, were also revealed to be resistance in high lactylation score group (Supplementary Figure S5)
DISCUSSION
Lactylation modification seems to have an important place in cancer therapeutics research It has been well shown that tumor cells undergo metabolic reprogramming, resulting in increased lactate production and alterations in the microenvironment (22-24) Related with this issue, lactate has been shown to play a critical role in tumor growth and progression by promoting angiogenesis, immune evasion, and metastasis (25) Moreover, lactylation of proteins has been found to modulate cellular processes involved in carcinogenesis regarding the survival, proliferation, and invasion status (26, 27) These findings suggest that lactylation modification may offer novel therapeutic targets in the management of cancer
However, further studies are needed to identify specific lactylated targets and explore the possible underlying mechanisms of this process in different types of tumors
In recent years, increasing attention has been focused on the possible role of lactylation modification in carcinogenesis of different tumor types such as bladder cancer (28), lung cancer (29), liver cancer (27, 30), and gastric cancer (31) A recent study indentified a unique cluster of cisplatin-resistant epithelial cells by constructing a BLCA single-cell atlas The elevated lactylation was founded in the cisplatin-resistant cluster and verified in BLCA cell lines with cisplatin resistance Furthermore, H3K18la was up-regulated in cisplatin-resistant BLCA cell lines, and heightened transcription factor expression such as YBX1 and YY1, ultimately driving cisplatin resistance in BLCA (28) More and more studies demonstrated the emerging evidence suggesting that lactylation modification plays a critical role in the pathogenesis and progression of cancer However, further research is certainly needed to explore the exact underlying mechanisms of lactylation in different types of tumors and to develop novel lactylation-based therapies for the treatment of cancer
In this study, firstly we evaluated 11different lactylation genes By examining the expression of these lactylation genes, we identified two subtypes of BLCA (cluster A and B) Additionally, we observed the difference in malignant cancer-promoting pathways and immune-related pathways between cluster A and B, such as TGF BETA SIGNALING, MTORC1 SIGNALING, and WNT SIGNALING PATHWAY Based on these findings, in the second stage we investigated the immune infiltration in BLCA samples The stromal, immune, and ESTIMATE scores were all higher in cluster A, and most immune cell levels were found to be highly infiltrated in cluster A than in cluster B
Based on this information in our study we aimed to develop a lactylation score for quantifying patient risk
Initially, we screened 275 DEGs across two clusters and later we conducted univariate Cox regression analysis to determine the prognostic value of these 275 DEGs 11 genes being identified at the last stage have been found to be correlated with overall survival period (p < 0 001) Following this critical evaluation based on the PCA algorithm used , we established a lactylation score depending on these 11 prognostic genes In addition to the poorer survival rates observed in patients with high lactylation scores; the correlation between the lactylation score and immune cell infiltration suggested a positive association between these two variables Among the 11 genes included in the established lactylation score, CLIC3 TCIRG1 S100A8 and LGALS1 were found to be related to glycolysis and lactate regulation in tumor cells CLIC3 and TCIRG1, as a member of the chloride intracellular channel protein family and a subunit of a large protein complex known as a vacuolar H+-ATPase (V-ATPase) respectively, play important roles in regulating the pH of cells and their surrounding environment (32, 33) The acidification of the tumor microenvironment (TME) can regulate glycolysis in cells and mediate the production of lactate, thereby regulating the lactylation modification of proteins (34) S100A8 is a member of the S100 family of proteins containing 2 EF-hand calcium-binding motifs It is involved in the regulation of a number of cellular processes such as cell cycle progression and differentiation According to a recent study, S100A8 also play a critical role in promoting macrophage perturbation and glycolysis through the TLR4/MyD88/NF-κB signaling pathway (35) LGALS1, also known as Gal-1, is a member of the family of beta-galactoside-binding proteins implicated in m o d u l
Previous study had revealed that the TLR4/Gal-1 signali n g p a t h w
E M T processes in CRC cells (36) Although no studies have revealed that the other seven genes are directly or indirectly related to lactylation modification, many studies have reported that they are closely related to the occurrence and development of bladder cancer Among them, SPHK1, RCN3, CDA, TBX3, AEBP1 and KRT16 are widely reported oncogenes It can regulate cell apoptosis, promote cell proliferation, migration, or resist immune killing by activating STAT3 and NF-κB signaling pathways, participating in collagen biosynthesis, inducing specific gene mutations, or acting as transcriptional promoters (37-43) TP53INP1 has been reported to be a tumor suppressor gene in bladder cancer, which can inhibit the migration and invasion of bladder cancer cells by inducing autophagy and inhibiting the activation of extracellular regulated kinase (ERK) (44)
The effectiveness of an ICI treatment can be predicted by chemokines, chemokine receptors, and immune checkpoints (45, 46) Chemokines are critical in directing immune cell migration necessary to mount and deliver an effective antitumor immune response Chemokine secretion is often altered in the TME, and an aberrant chemokine profile can facilitate the differentiation and infiltration of immunosuppressive pro-tumorigenic cells into the tumor, namely Treg cells, MDSCs and TAMs Due to their multifaceted role in the tumor immune response and tumor biology, the chemokine network has emerged as a potential
G Liu, T Hong, X Liu, et al
Lactylation-related
immunotherapy target (47) In addition, immune checkpoints are another key regulator of the tumour immune response Normally, the presence of immune checkpoints avoids the damage caused by excessive immune response, but tumour cells can escape from the immune system by expressing corresponding ligands that bind to them, activating inhibitory pathways or inhibitory immune checkpoints within the immune cells, inhibiting immune cell activity or mediating apoptosis of immune cells Immune checkpoint inhibitors can enhance the immune attack against tumours by blocking the interaction of these immune checkpoint proteins with their ligands and preventing the inactivation of T-cell function (48) Our results reveal that high expression levels of chemokines, chemokine receptors, and immune checkpoints were observed in the group with high lactylation scores, which indicated although high lactylation score is a poor prognostic factor for BLCA, patients with high lactylation score may respond better to an ICI treatment This finding is highly valuable in an attempt to predict the efficacy of ICI treatment in a reliable manner in cases with BLCA The analysis of immunotherapy datasets confirmed that patients with high lactylation scores had positive responses to ICI treatment in the IMvigor210 and NCT02684006 cohorts These findings again further supported our findings However, as a bioinformatics-based analysis, the findings of this study are subjected to several limitations First and foremost, as research in the protein lactylation field is still in its preliminary stages, there are relatively few genes directly related to lactylation modification reported Therefore, the lactylation gene subtypes and lactylation score identified based on these genes may not be able to fully describe the characteristics of lactylationrelated gene signature Furthermore, the experimental validation of all signature genes currently faces practical difficulty due to the lack of corresponding lactylation antibodies Another potential limitation of this study is that the findings of this study rely mainly on retrospective data collected from public databases The accuracy of the lactylation score in predicting the response to ICI treatment by BCa still needs to be verified by large-scale clinical trials
CONCLUSIONS
In the light of our findings and the limited data published so far in the literature, we may state that lactylation genes have a significant control over the immune microenvironment of tumors, clinical traits and treatment outcomes in cases with BLCA Moreover, a lactylation score has been well established by our group and this scoring has proven its reliability in the prediction of the prognosis and efficacy of ICI treatment All these observations indicated well the vital role of lactylation in clinical practice which could enable the physicians to potential customization of the applied treatments in BLCA patients
REFERENCES
1 Sung H, Ferlay J, Siegel RL, et al Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries CA Cancer J Clin 2021; 71:209-49
2 Lobo N, Afferi L, Moschini M, et al Epidemiology, Screening, and Prevention of Bladder Cancer Eur Urol Oncol 2022; 5:628-39
3 Chen X, Zhang J, Ruan W, et al Urine DNA methylation assay enables early detection and recurrence monitoring for bladder cancer J Clin Invest 2020; 130:6278-89
4 Bellmunt J, Powles T, Vogelzang NJ A review on the evolution of PD-1/PD-L1 immunotherapy for bladder cancer: The future is now Cancer Treat Rev 2017; 54:58-67
5 Boegemann M, Aydin AM, Bagrodia A, Krabbe LM Prospects and progress of immunotherapy for bladder cancer Expert Opin Biol Ther 2017; 17:1417-31
6 Zhang D, Tang Z, Huang H, et al Metabolic regulation of gene expression by histone lactylation Nature 2019; 574:575-80
7 Fan H, Yang F, Xiao Z, et al Lactylation: novel epigenetic regulatory and therapeutic opportunities Am J Physiol Endocrinol Metab 2023; 324:E330-8
8 Rong Y, Dong F, Zhang G, et al The crosstalking of lactateH i s t o n e l a c t y l a t i o n a n
17:e2200102
9 P é r e z - T o m á s R , P é r e z - G u i l l é n I
Microenvironment: An Essential Molecule in Cancer Progression and Treatment Cancers (Basel) 2020; 12:3244
10 Ippolito L, Morandi A, Giannoni E, Chiarugi P Lactate: A Metabolic Driver in the Tumour Landscape Trends Biochem Sci 2019; 44:153-66
11 Certo M, Tsai CH, Pucino V, et al Lactate modulation of immune responses in inflammatory versus tumour microenvironments Nat Rev Immunol 2021; 21:151-61
12 Xie J, Hong S, Zhang X, et al Inhibition of glycolysis prevents behavioural changes in mice with MK801-induced SCZ model by alleviating lactate accumulation and lactylation Brain Res 2023; 1812:148409
13 Gaffney DO, Jennings EQ, Anderson CC, et al Non-enzymatic Lysine Lactoylation of Glycolytic Enzymes Cell Chem Biol 2020; 27:206-13 e6
14 Liu J, Du J, Li Y, et al Catalpol induces apoptosis in breast cancer in vitro and in vivo: Involvement of mitochondria apoptosis pathway and post-translational modifications Toxicol Appl Pharmacol 2022; 454:116215
15 Yao G, Yang Z Glypican-3 knockdown inhibits the cell growth, stemness, and glycolysis development of hepatocellular carcinoma cells under hypoxic microenvironment through lactylation Arch Physiol Biochem 2023; 2:1-9
16 Miao Z, Zhao X, Liu X Hypoxia induced β-catenin lactylation promotes the cell proliferation and stemness of colorectal cancer through the wnt signaling pathway Exp Cell Res 2023; 422:113439
17 Gu J, Zhou J, Chen Q, et al Tumor metabolite lactate promotes tumorigenesis by modulating MOESIN lactylation and enhancing TGF-β signaling in regulatory T cells Cell Rep 2022; 40:111122
18 Liu X, Zhang Y, Li W, Zhou X Lactylation, an emerging hallmark of metabolic reprogramming: Current progress and open challenges Front Cell Dev Biol 2022; 10:972020
19 Yang Z, Ming X, Huang S, et al Comprehensive Analysis of m(6)A Regulators Characterized by the Immune Cell Infiltration in Head and Neck Squamous Cell Carcinoma to Aid Immunotherapy and Chemotherapy Front Oncol 2021; 11:764798
20 Balar AV, Galsky MD, Rosenberg JE, et al Atezolizumab as firstline treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: a single-arm, multicentre, phase 2 trial Lancet 2017; 389:67-76
21 Motzer RJ, Robbins PB, Powles T, et al Avelumab plus axitinib versus sunitinib in advanced renal cell carcinoma: biomarker analysis of the phase 3 JAVELIN Renal 101 trial Nat Med 2020; 26:1733-41
22 Sgarra R, Battista S, Cerchia L, et al Mechanism of Action of Lactic Acid on Histones in Cancer Antioxid Redox Signal 2023; 40:236-49
23 Xu Y, Hao X, Ren Y, et al Research progress of abnormal lactate metabolism and lactate modification in immunotherapy of hepatocellular carcinoma Front Oncol 2022; 12:1063423
24 Zhang Q, Liu S, Wang H, et al ETV4 Mediated TumorAssociated Neutrophil Infiltration Facilitates Lymphangiogenesis and Lymphatic Metastasis of Bladder Cancer Adv Sci (Weinh) 2023; 10:e2205613
25 Wang L, Li S, Luo H, et al PCSK9 promotes the progression and metastasis of colon cancer cells through regulation of EMT and PI3K/AKT signaling in tumor cells and phenotypic polarization of macrophages J Exp Clin Cancer Res 2022; 41:303
26 Wang X, Ying T, Yuan J, et al BRAFV600E restructures cellular lactylation to promote anaplastic thyroid cancer proliferation Endocr Relat Cancer 2023; 30:e220344
27 Wu X In-depth discovery of protein lactylation in hepatocellular carcinoma Proteomics 2023; 23:e2300003
DECLARATIONS
Ethical approval: The study was approved by the Institutional Review Board of Shantou Central Hospital and carried out following the Declaration of Helsinki
Availability of data and material: The data that support the findings of this study are available with the article and its supplementary material, or are available from the corresponding authors upon reasonable request
Competing interests: The authors declare that there is no conflict of interest
Funding: This study was supported by the National Natural Science Foundation of China (Grant No 82372685), Basic and Applied Basic Research Foundation of Guangdong Province (Grant No 2023A1515220213), Science and Technology
Shantou City (Grant No sfk[2023] No 68-1)
Authors' contributions: Conceptualization: X H and Y Z ; Investigation: G L , T H ; and X L Data curation: T H and X L ; Formal analysis: G L ; Methodology: X L ; Resources: P Y ; Software: X C ; Writing - original draft: G L and T H ; Writing - review & editing: X H , K S and Y Z Funding acquisition: X H and Y Z
Consent for publication: All authors have read and approved the content and agree to submit for consideration for publication in the journal
Acknowledgments: None
28 Li F, Zhang H, Huang Y, et al Single-cell transcriptome analysis reveals the association between histone lactylation and cisplatin resistance in bladder cancer Drug Resist Updat 2024; 73:101059
29 Yang YH, Wang QC, Kong J, et al Global profiling of lysine lactylation in human lungs Proteomics 2023; 23:e2200437
3 0 K o t s i l i t i E L a c t y l a t i o n a n d H C C p r o
Gastroenterol Hepatol 2023; 20:131
31 Yang H, Zou X, Yang S, et al Identification of lactylation related model to predict prognostic, tumor infiltrating immunocytes and response of immunotherapy in gastric cancer Front Immunol 2023; 14:1149989
32 Suh KS, Yuspa SH Intracellular chloride channels: critical mediators of cell viability and potential targets for cancer therapy Curr Pharm Des 2005; 11:2753-64
33 Flinck M, Hagelund S, Gorbatenko A, et al The Vacuolar H(+) ATPase α3 Subunit Negatively Regulates Migration and Invasion of Human Pancreatic Ductal Adenocarcinoma Cells Cells 2020; 9:465
34 Chen L, Huang L, Gu Y, et al Lactate-Lactylation Hands between Metabolic Reprogramming and Immunosuppression Int J Mol Sci 2022; 23:11943
35 Ji X, Nie C, Yao Y, et al S100A8/9 modulates perturbation and glycolysis of macrophages in allergic asthma mice PeerJ 2024; 12:e17106
36 Park GB, Kim D TLR4-mediated galectin-1 production triggers epithelial-mesenchymal transition in colon cancer cells through ADAM10- and ADAM17-associated lactate production Mol Cell Biochem 2017; 425:191-202
37 Qin Z, Tong H, Li T, et al SPHK1 contributes to cisplatin resistance in bladder cancer cells via the NONO/STAT3 axis Int J Mol Med 2021; 48:204
3 8 G i l d a C o s t a R M , L e v e s q u e C , B i a n c h i - F r i a s D , e t a l Pharmacological NF-κB inhibition decreases cisplatin chemoresistance in muscle-invasive bladder cancer and reduces cisplatininduced toxicities Mol Oncol 2023; 17:2709-27
39 Ding J, Meng Y, Han Z, et al Pan-Cancer Analysis of the Oncogenic and Immunological Role of RCN3: A Potential Biomarker for Prognosis and Immunotherapy Front Oncol 2022; 12:811567
40 Liu W, Newhall KP, Khani F, et al The Cytidine Deaminase A P O B E C 3 G C o n t r i b u t e s t o C a n c e r M u t a g
C
l Evolution in Bladder Cancer Cancer Res 2023; 83:506-20
41 Huang L, Shao W, Wang X, et al TBX3 stimulates proliferation and stem cell self-renewal in bladder carcinoma Histol Histopathol 2023; 38:65-72
42 Majdalawieh AF, Massri M, Ro HS AEBP1 is a Novel Oncogene: Mechanisms of Action and Signaling Pathways J Oncol 2020; 2020:8097872
43 Somji S, Cao L, Mehus A, et al Comparison of expression patterns of keratin 6, 7, 16, 17, and 19 within multiple independent isolates of As(+3)- and Cd (+2)-induced bladder cancer: keratin 6, 7, 16, 17, and 19 in bladder cancer Cell Biol Toxicol 2011; 27:38196
44 Liu X, Zhou Z, Wang Y, et al Downregulation of HMGA1 Mediates Autophagy and Inhibits Migration and Invasion in Bladder Cancer via miRNA-221/TP53INP1/p-ERK Axis Front Oncol 2020; 10:589
45 Pinato DJ, Howlett S, Ottaviani D, et al Association of Prior
G Liu, T Hong, X Liu, et al
Antibiotic Treatment With Survival and Response to Immune Checkpoint Inhibitor Therapy in Patients With Cancer JAMA Oncol 2019; 5:1774-8
46 Liu L, Bai X, Wang J, et al Combination of TMB and CNA Stratifies Prognostic and Predictive Responses to Immunotherapy Across Metastatic Cancer Clin Cancer Res 2019; 25:7413-23
Correspondence
Guoyuan Liu liugyst@126 com
Yonghai Zhang zhang yonghai@126 com
Department of Urology, Shantou Central Hospital, Shantou, China
Ting Hong 695594973@qq com
Xinyu Liu lxy19971116@163 com
Clinical Medical Research Center, Shantou Central Hospital, Shantou, China
Xuanhao Lin stbiobank@126 com
Peixiu Yao yaopeixiu0646@qq com
Xifeng Chen
cxf8282@163 com
Department of Biobank, Shantou Central Hospital, Shantou, China
Kemal Sarica saricakemal@gmail com
Department of Urology, Health Sciences University, Prof Dr Ilhan Varank
Education and Training Hospital, Istanbul, Turkey
Xuwei Hong (Corresponding Author) hong xuwei@sina cn
Shantou Central Hospital, 114th Waima Road, Shantou 515031, P R China
47 Bule P, Aguiar SI, Aires-Da-Silva F, Dias JNR ChemokineD i r e c t e d T u m o r M i c r o e n v
Immunotherapy Int J Mol Sci 2021; 22
48 Peng Q, Qiu X, Zhang Z, et al PD-L1 on dendritic cells attenuates T cell activation and regulates response to immune checkpoint blockade Nat Commun 2020; 11:4835
Predictive role of lactylation-related gene signature in the prognosis and
immunotherapy
response in bladder cancer
Guoyuan Liu 1* , Ting Hong 2* , Xinyu Liu 2* , Xuanhao Lin 3 , Peixiu Yao 3 , Xifeng Chen 3 , Yonghai Zhang 1 , Kemal Sarica 4, 5 , Xuwei Hong 1
1 Department of Urology, Shantou Central Hospital, Shantou, China;
2 Clinical Medical Research Center, Shantou Central Hospital, Shantou, China;
3 Department of Biobank, Shantou Central Hospital, Shantou, China;
4 Department of Urology, Health Sciences University, Prof Dr Ilhan Varank Education and Training Hospital, Istanbul, Turkey;
5 Department of Urology, Biruni University, Medical School, Istanbul, Turkey
* These authors contributed equally to this work
SUPPLEMENTARY TABLES
Table S1.
Clinical characteristics and survival outcomes of BLCA patients from TCGA-BLCA and GSE13507 cohorts
(n)
Gender Male, n (%)
Age >
(73 8)
(81 8) Female, n (%)
n (%)
≤ 60, n (%)
T stage
T1T2, n (%)
T3T4, n (%)
N stage
(26 2)
(26 2)
(29 9)
(61 9)
n (%) 34 (8 2)
N0, n (%)
Table S2.
Univariate Cox regression and Kaplan-Meier analysis of lactylation genes
(67 3)
(18 2)
(14 5)
(58 0)
(90 3) N1, n (%) 47 (11 4) 8 (4 9) N2, n (%)
n (%)
M stage
M0, n (%)
State
(3.6) N3, n (%) 8 (2 0)
(10 2)
(47 5)
(0)
(1 2)
(95 8) M1, n (%) 11 (2 7)
Grade
n (%)
n (%)
(4 2)
(49 8)
(94 2)
n (%) 21 (5 1)
n (%) 3 (0 7) 0 (0)
Table S3.
Univariate Cox regression analysis of 275 DEGs screened between cluster A and cluster B
The score of pathways in two clusters, including HALLMARK, KEGG, and Reactome pathways
Archivio Italiano di Urologia e Andrologia 2025; 97(1):13516
S2.
The SNV of prognostic DEGs
A The frequency of deleterious mutations of lactylation genes in BLCA
B The mutations waterfall plot of indicated genes in BLCA
G Liu, T Hong, X Liu, et al
Figure
Figure S3
The CNV and methylation of DEGs
A The CNA percentage of DEGs in BLCA B The homozygous and heterozygous CNV of DEGs in BLCA
C The correlation of CNV with mRNA expression in BLCA D The correlation of methylation level with mRNA expression
Figure S4.
The gene mutation differences in high and low lactylation score group
A The gene mutation frequency in high lactylation score group in BLCA B The gene mutation frequency in low lactylation score group in BLCA. C. The gene mutation differences in high and low lactylation score group.
Archivio Italiano di Urologia e Andrologia 2025; 97(1):13516
G Liu, T Hong, X Liu, et al
Lactylation-related
Figure S5.
The analysis of curative effect of anti-tumor drugs
The IC50 of indicated anti-tumor drugs in high and low lactylation score groups
ORIGINAL PAPER
Preoperative platelet-to-lymphocyte ratio as a predictor of inguinal lymph node metastasis in penile cancer
Francesco Passaro 1* , Antonio Tufano 1* , Gianluca Spena 1 , Alessandro Izzo 1 , Flavio Antonino Scarlata 1 , Biagio Barone 2 , Luigi Napolitano 2 , Gabriele Pezone 2 , Pierluigi Alvino 2 , Achille Aveta 2 , Savio Domenico Pandolfo 2, 3 , Simone Cilio 2 , Lorenzo Romano 2 , Francesco Di Bello 2 , Alessandro Calarco 4 , Rosario Leonardi 5 , Carlo Buonerba 6, 7 , Sisto Perdonà 2
1 Department of Urology, Istituto Nazionale Tumori, IRCCS, “Fondazione G Pascale”, Naples, Italy;
2 Department of Neurosciences and Reproductive Sciences and Odontostomatology, University of Naples “Federico II”, Naples, Italy;
3 Department of Urology, University of L’Aquila, L’Aquila, Italy;
4 Urology Unit, San Carlo di Nancy Hospital, GVM Care and Research, Rome, Italy;
5 Department of Medicine and Surgery University of Enna KORE, Enna, Italy;
6 Department of Public Health, University of Naples “Federico II”, Naples, Italy;
7 Associazione O R A -Oncology Research Assistance, Somma Vesuviana, Italy
* These authors contributed equally to this work
Summary
Background: Penile cancer (PC) is a rare malignancy with poor prognosis. To date, reliable preoperative biomarkers for lymph node status and prognosis are still lacking This study aims to explore the potential role of preoperative platelet-to-lymphocyte ratio (PLR) as a predictor of inguinal lymph node invasion in PC patients
Methods: Retrospective analysis was conducted on anamnestic, clinical, and laboratory data of PC patients who underwent surgical treatment between January 2016 and October 2023
Inguinal lymphadenectomy was performed as per EAU guidelines. PLR, calculated as the ratio between platelet-to-lymphocyte values obtained from preoperative blood analyses, was assessed within 30 days before surgery Patients were categorized into pN- (no lymph node metastasis) and pN+ (lymph node metastasis confirmed pathologically) Statistical analyses included Kruskal-Wallis and Mann-Whitney U tests, univariate logistic regression, and ROC curve analysis with Youden index, assuming p < 0 05 as statistically significant
Results: Overall, 60 PC patients were retrospectively involved in the study. A total of 36 (60%) patients reported ILN metastases, confirmed by inguinal lymphadenectomy (pN+), while no ILN metastases (pN-) were reported in 24 (40%) patients The AUC for predicting ILN metastasis by preoperative PLR was 0 71 (p = 0.014). According to the ROC curve analysis and the Youden Index, a cut-off for PLR was set at 122.4.
On Univariable logistic regression analysis, the presence of T stage ≥ 2 (OR = 3 21; 95% CI: 1 43-7 47, p = 0 011), lymphovascular invasion (OR = 3 78; 95% CI: 1 56-5 90, p = 0 003), clinical node-positive disease (OR = 19.86; 95% CI: 5.91-41.03, p < 0 001) and PLR ratio > 122 4 (OR = 7 22; 95% CI: 1 4122 71, p = 0 0148) were independent predictors of pN+ disease
Conclusions: The current study confirms the relationship between cancer and inflammation. When elevated preoperatively, PLR may be associated with inguinal lymph node invasion in PC patients
Submitted 26 November 2024; Accepted 8 December 2024
INTRODUCTION
Penile cancer (PC) is a rare cancer with a prevalence of 0 1-1 per 100,000 men in high-income countries (1) Several risk factors have been reported, including the absence of childhood circumcision, phimosis, chronic inflammation, inadequate penile hygiene, smoking, immunosuppression and human papillomavirus (HPV) infection (2) Lymph node status represents an important prognostic factor, in association with primary tumor grade, pathologic T stage, histologic subtype, and lymphovascular invasion (3) Several treatments for localized early-stage disease are available, ranging from topical 5-Flurouracil therapy and laser therapy to glans resur-facing and glansectomy with reconstruction (4, 5) As the disease progresses to more advanced stages, recommendations include partial or total penectomy with or without reconstruction, or radiotherapy (6, 7) However, radical surgical treatment represents the gold standard for high-grade and high-stage disease (8)
PC displays aggressive behavior and tends to metastasize primarily to locoregional lymph nodes (LN) Metastatic progression typically affects inguinal LNs (ILN) and then extends to pelvic LN (PLN), following the anatomical drainage route (9) Consequently, after local treatment for the primary lesion, inguinal lymph node dissection (ILND) is recommended if there is evidence of lymph node invasion or in high-risk patients (10) Despite significant advancements in imaging and surgical techniques, the absence of reliable biomarkers for diagnosis, prognosis, and follow-up remains a challenge (11) In this scenario, recent studies have underscored the pivotal role of inflammation in various tumorigenic processes, including proliferation, invasion, metastasis, and angiogenesis (12, 13) Hence, several inflammatory indexes such as neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), Albumin-to-Alkaline Phosphatase Ratio (AAPR), have emerged and proposed as potential prognostic biomarkers in different cancers including genitourinary tumors (14-16) These biomarkers, char-
acterized by different sensitivity and specificity, represent a low-cost yet powerful tool in stratifying cancer patients Interestingly, platelet-to-lymphocyte ratio (PLR) has recently gained widespread recognition as a valuable prognostic factor in various types of tumors, including lung, colorectal, and esophageal cancer (17) However, the prognostic impact of PLR on PC remains poorly explored Interestingly, Wu et al developed a reliable nomogram based on clinicopathologic and laboratory data incorporating PLR, squamous cell carcinoma antigen SCC-Ag, lymphovascular invasion (LVI), and pT-stage for the prediction of lymph node extranodal extension in patients with PC (18) Moreover, Hu et al in their single center experience found that PLR was a significant independent predictor for OS and PFS in patients treated with ILND (12) Based on these findings we aimed at investigating the utility of preoperative PLR as a prognostic indicator of inguinal lymh node (ILN) invasion in PC patients
MATERIALS AND METHODS
We retrospectively analyzed anamnestic, clinical and laboratory data retrieved from patients who underwent surgical treatment for penile cancer at IRCCS Hospital “Pascale” of Naples between January 2016 and October 2023 According to EAU guidelines, sentinel lymph node biopsy and/or inguinal lymphadenectomy (modified/standard) was performed in patients with high-risk tumors (≥ T1G3) and/or patients with cN+ In case of pT1G1/G2 status a ILND following a modified template was reserved for those patients with either lymphovascular or peri-neural invasion Due to the retrospective nature of the study and the use of procedures included in the common clinical practice, no ethical committee was required The inclusion criteria were: (1) primary tumor treated surgically, (2) tumor pathology confirmed by an expert uro-oncology pathologist and (3) available data to calculate PLR Exclusion criteria from the study were (1) presence of pelvic lymph node involvement or the presence of distant metastasis at diagnosis, (2) patients with conditions affecting the number of platelets such as liver diseases, hemolytic anemia, chronic infectious and inflammatory diseases, splenectomy, and alcoholism (Figure 1) Routine venous blood samples were obtained within 30 days before scheduled primary surgery PLR was calculated as the ratio between platelet-to-lymphocyte values Demographic, clinical and pathological data were collected in a single, customized dataset Evaluated preoperative demographic and clinical characteristics included age, smoking status, hypertension status, body mass index (BMI), Charlson Comorbidity Index, American Society of Anesthesiologists (ASA) score and PLR calculated using the platelet and lymphocyte counts, obtained via routine complete blood counts in peripheral blood samples before primary surgery Oncological outcomes variables included surgical margin status, final histology, staging (according to TNM classification system), grading tumor, lymph vascular and perineural invasion Patients were further divided into two categories: pN- (i e those without ILN metastasis identified at the histopathological analysis after inguinal lymphadenectomy) and pN+ (i e those with ILN metastasis at the histopathological analysis after inguinal lymphadenectomy) Means and standard deviations were reported for con-
tinuous variables while frequencies and percentages were reported for categorical variables The KolmogorovSmirnov test was used to assess the normality of data before proceeding to further analysis A Mann-Whitney U Test was used to evaluate continuous variables, while Chi-square test was used for categorical variables analysis Univariable logistic regression analysis was used for calculating odds ratio (OR), 95% confidence interval (CI) calculations, and to estimate pathologic node-positivity Statistical analysis was conducted using IBM SPSS software (version 25, IBM Corp, Armonk, NY, USA) A p value < 0 05 was considered to be statistically significant
RESULTS
Overall, 60 PC patients met the inclusion criteria Descriptive characteristics and preoperative laboratory data of the overall cohort are reported in Table 1
Table 1.
Baseline and pathological characteristics.
Pathologic T stage, n (%)
Grading , n (%)
F Passaro, Antonio Tufano, G Spena, A Izzo, et al
Overall n = 26 patients had cN- status Of those, sentinel lymph node biopsy and modified inguinal lymphadenectomy was performed in n = 6 and n = 20 patients, respectively A total of n = 34 patients with a cN+ status underwent ILND following a standard template The mean age at the time of surgery was 66 9 ± 14 4 years A total of 36 (60%) patients reported ILN metastases (pN+), confirmed by ILND following a standard or modified template Conversely, no ILN metastases (pN-) were reported in 24
Receiver operating characteristic (ROC) curve and area under the curve (AUC) to define the optimal PLR cutoff.
AUC: 0 71 (p = 0 014)
(40%) patients No statistically significant differences were reported for baseline characteristics, except for preoperative lymphocytes (pN- vs pN+: 1 9 ± 0 8 vs 1 4 ± 0 4; p = 0 04) and PLR (pN+ 193 8 ± 79 5 vs pN- 122 5 ± 54 2; p= 0 02)
The AUC for predicting ILN metastasis by preoperative PLR was 0 71 (p = 0 014) According to the ROC curve analysis and the Youden Index, a cut-off for PLR was set at 122 4 (Figure 1)
On Univariable logistic regression analysis, the presence of T stage ≥ 2 (OR = 3 21; 95% CI: 1 43-7 47, p = 0 011), lymph vascular invasion (OR = 3 78; 95% CI: 1 56-5 90, p = 0 003), clinical node-positive disease (OR = 19 86; 95% CI: 5 91-41 03, p < 0 001) and PLR ratio > 122 4 (OR = 7 22; 95% CI: 1 41-22 71, p = 0 0148) were independent predictors of pN+ disease (Table 2)
DISCUSSION
In PC patients, nodal metastasis emerges as the foremost predictor of a poor clinical outcome, with tumor grade and lymph vascular invasion also serving as significant prognostic indicators (10, 19) According to EAU guidelines, sentinel lymph node biopsy and/or inguinal lymphadenectomy is crucial for patients with intermediate or high-risk tumors (≥ T1G2) and/or those with clinically positive lymph nodes (cN+) (10) In spite of unequivocal endorsements advocating the adoption of these potentially life-saving interventions, several authors have underscored suboptimal adherence to clinical guidelines (20, 21) This phenomenon may be ascribed to the foreseen m o r b i d i
drainage in the lower extremities and scrotum, with reported morbidity rates reaching as high as 50% (9)
Moreover, the poor compliance may also be caused by the lack of reliable biomarkers and a small number of predictors included in the current guidelines
It is well established that cancer-related inflammation and systemic inflammatory responses contribute to tumor initiation and progression, including neo-angiogenesis, tumor progression, and metastasis Several studies have investigated the role of PLR in various types of cancers Jiang et al found that a high PLR was associated with poorer survival prognosis in ovarian cancer (OS: HR 1 80 (95% CI 1 37-2 37), p = 0 000; PFS: HR 1 63 (95% CI 1 38-1 91), p = 0 000) and cervical cancer (OS: HR 1 36 (95% CI 1 10-1 68), p = 0 005; PFS: HR 1 40 (95% CI 1 16-1 70), p = 0 002) (22) Moreover, when examining urological malignancies, Wang et al demonstrated that an elevated PLR predicted poor overall survival (OS; HR = 1 85, 95% CI = 1 51-2 25, p < 0 001) and disease-free survival (DFS; HR = 1 4, 95% CI = 1 1-1 79, p = 0 007) in prostate cancer patients (23) Nevertheless, subgroup analyses showed that the PLR remained a significant prognostic factor for OS irrespective of ethnicity, tumor stage, or cut-off value (23)
To the best of our knowledge our study is the first to explore the predictive value of preoperative PLR in ILN invasion within a PC cohort Several noteworthy findings emerged from the analysis
Firstly, the cut-off of the PLR set by the ROC analysis was 122 4 in the present study
Similar PLR cut-offs points were found for other urological tumors Herraiz-Raya and colleagues discovered that germ cell tumor patients with a PLR > 150 were more likely to experience disease progression, advanced stage II and III, and residual disease Additionally, they found that PLR levels were significantly higher in seminoma patients compared to non-seminoma patients (24) Moreover, Imamoglu observed a PLR > 104 to be a significant predictor of advanced disease (stage II and III) with a sensitivity of 71% and a specificity of 88%, exclusively in nonseminoma patients (25) Conversely, a higher PLR (> 212) was depicted by Peksa et al in a testis cancer cohort
Authors examined the correlation between immune checkpoint proteins microenvironments and systemic inflammatory reactions In their study elevated PLR was associated with the presence of nodal and distant metastases as well as an advanced disease stage (26)
Furthermore, patients with high PLR showed significantly better five-year event-free survival compared to those with low PLR (89% vs 69%, p = 0 018) (26) Notably, a combination of high PLR and low expression of immune checkpoint regulators (V-domain Ig suppressor of T cell activation) in tumor-infiltrating and peritumoral lymphocytes and macrophages was identified as a sole predictor of relapse and disease progression in multivariate analysis These findings support the idea that the clinical behavior of tumors is influenced by a complex interaction between the local tumor immune environment and systemic inflammation
Secondly, the predictive role of PLR in the prediction of ILN invasion was confirmed on univariable analysis (OR = 7 22) However, given the absence of comparative data, we must view our study as an introductory investigation into the potential of PLR as a prognostic biomark-
er for ILN invasion, as this outcome has not been previously addressed in the literature
Third, our analysis confirmed the role of lymphovascular invasion as a crucial prognostic indicator (OR = 3 78, p = 0 018 univariable analysis) These ORs are similar to the study by Winters et al (OR = 3 10), where lymphovascular invasion emerged as the primary independent predictor of occult lymph node metastasis (27) Similar findings have been reported by other studies, corroborating the significance of lymphovascular invasion as a substantial risk factor for occult micro metastases (28, 29) Taken together, these findings imply a potential enhancement in current risk stratification schemes Specifically, the presence of LVI, irrespective of tumor stage or grade, warrants consideration as high-risk disease
The precise role of PLR in oncological patients remains largely unexplored Nevertheless, several theories have been proposed Platelets serve as a crucial source of cytokines, binding to FGF, PDGF, VEGF, and TGF-β family proteins, and thereby acting as a reservoir for secreted growth factors that promote tumorigenesis and metastasis development Tumor cells can activate and aggregate platelets through both direct and indirect mechanisms, which play a crucial role in metastatic spread Platelets function as key transporters of both proangiogenic and antiangiogenic factors (30, 31) Moreover, they influence the process of angiogenesis, including platelet-derived microparticles, microRNA, lipids, and surface receptors
They are active in both the early and late stages of angiogenesis (32) This understanding raises the potential for targeting platelet functions as a promising strategy for cancer treatment On the other hand, inflammatory response is linked to conditions such as lymphocytopenia, neutrophilia, and thrombocytosis Lymphocytes are essential for immune function and play a significant role in suppressing cancer progression Hence, a lower lymphocyte count, reflected by a high PLR, may translate in a reduced immune surveillance, thus allowing tumor progression (33-35) We acknowledge several limitations of our study These include its retrospective, single-center design, and the relatively small sample size, which may introduce selection and treatment biases Additionally, the restricted cohort size and limited number of events precluded multivariable analysis, preventing identification of more reliable predictors for ILN involvement Furthermore, the absence of follow-up data limits our ability to assess patient prognosis, and certain critical variables, such as tumor multifocality, tumor cell koilocytosis, and keratinization, were not included Our results should be validated by exter nal cohorts with multi-center studies prior to considering PLR for clinical use as an adjunctive biomarker in the diagnostic setting of inguinal lymph node metastasis
CONCLUSIONS
The current study must be considered as an initial experience regarding the role of PLR as a potential biomarker in this setting of population We identified potential predictors of ILN invasion in PC patients However, further investigations and larger cohorts are required to confirm the clinical utility of PLR in patients’ outcomes
F Passaro, Antonio Tufano, G Spena, A Izzo, et al
Preoperative platelet-to-lymphocyte ratio as a predictor of inguinal lymph node metastasis in penile cancer
REFERENCES
1 Thomas A, Necchi A, Muneer A, et al Penile cancer Nat Rev Dis Primers 2021; 7:11
2 Morrison BF Risk factors and prevalence of penile cancer West Indian Med J 2014; 63:559-60
3 Fankhauser CD, de Vries HM, Roussel E, et al Lymphovascular and perineural invasion are risk factors for inguinal lymph node metastases in men with T1G2 penile cancer J Cancer Res Clin Oncol 2022; 148:2231-2234
4 Cilio S, Tufano A, Pezone G, et al Sexual outcomes after conservative management for patients with localized penile cancer Curr Oncol 2023; 30:10501-10508
5 Babbar P, Yerram N, Crane A, et al Penile-sparing modalities in the management of low-stage penile cancer Urol Ann 2018; 10:1-6
6 Manjunath A, Brenton T, Wylie S, et al Topical therapy for noninvasive penile cancer (Tis)-updated results and toxicity Transl Androl Urol 2017; 6:803-808
7 Shabbir M, Muneer A, Kalsi J, et al Glans resurfacing for the treatment of carcinoma in situ of the penis: surgical technique and outcomes Eur Urol 2011; 59:142-7
8 EAU-ASCO Penile Cancer Guidelines Edn presented at the EAU annual congress Milan 2023 ISBN 978-94-92671-19-6
9 Teh J, Duncan C, Qu L, et al Inguinal lymph node dissection for penile cancer: A contemporary review Transl Androl Urol 2020; 9:3210-3218
10 Hakenberg OW, Compérat EM, Minhas S, et al EAU guidelines on penile cancer: 2014 Update Eur Urol 2015; 67:142-150
11 Flammia RS, Tufano A, Antonelli L, et al Diagnostic performance of magnetic resonance imaging for preoperative local staging of penile cancer: a systematic review and meta-analysis Appl Sci 2021; 11:7090
12 Hu C, Bai Y, Li J, et al Prognostic value of systemic inflammatory factors NLR, LMR, PLR and LDH in penile cancer BMC Urol 2020; 20:57
DECLARATIONS
Ethical approval: Retrospective study exempt from ethics committee approval
Availability of data and material: https://zenodo org/ records/14223575
Competing interests: The authors declare no conflicts of interest
Funding: This research received no external funding
Authors' contributions: Conception and design, B B , P A , A A , F A S , R L , F D B , G S , A I and A T ; Analysis and interpretation of data, G P , L R , C B , S D P , F P , S C , S P , A C and L N ; drafting the article B B , P A , A A , F A S , F P , S C , S P , A C and L N ; revising the article critically R L , F D B , G S , A I , A T , G P , L R , C B and S D P ; final approval of the version to be published B B , P A , A A , F A S , R L , F D B , G S , A I and A T ; agreement to be accountable for all aspects of the work G P , L R , C B , S D P , F P , S C , S P , A C and L N All authors have read and agreed to the published version of the manuscript
Acknowledgments: Not applicable
Consent for publication: Not applicable
13 Liu S, Fang J, Jiao D, Liu Z The predictive value of inflammatory markers for pathological response of ipsilateral supraclavicular lymph nodes and for prognosis in breast cancer after neoadjuvant chemotherapy Gland Surg 2020; 9:1354-1362
14 Azizi M, Peyton CC, Boulware DC, et al Prognostic value of neutrophil-to-lymphocyte ratio in penile squamous cell carcinoma patients undergoing inguinal lymph node dissection Eur Urol Focus 2019; 5:1085-1090
15 Xu Z, Zhang J, Zhong Y, et al Predictive value of the monocyteto-lymphocyte ratio in the diagnosis of prostate cancer Medicine (Baltimore) 2021; 100:e27244
16 Tufano A, Napolitano L, Barone B, et al Preoperative albuminto-alkaline phosphatase ratio as an independent predictor of lymph node involvement in penile cancer Medicina 2024; 60:414
17 Wu Y, Li C, Zhao J, et al Neutrophil-to-lymphocyte and plateletto-lymphocyte ratios predict chemotherapy outcomes and prognosis in patients with colorectal cancer and synchronous liver metastasis World J Surg Oncol 2016; 14:289
18 Wu C, Li Z, Guo S, et al Development and validation of a nomogram for the prediction of inguinal lymph node metastasis extranodal extension in penile cancer Frontiers In Oncology 2021; 11:675565
19 Kultravut K, Siriboonrid S Characteristic of penile cancer and prognostic factors of inguinal and pelvic lymph node involvement Urol Ann 2023; 15:278-284
20 Lebentrau S, Wakileh GA, Schostak M, et al Does the identification of a minimum number of cases correlate with better adherence to international guidelines regarding the treatment of penile cancer? Survey results of the European prospective penile cancer study (EPROPS) Front Oncol 2021; 11:759362
21 Kirrander P, Sherif A, Friedrich B, et al Steering committee of the Swedish national penile cancer register Swedish national penile cancer register: incidence, tumour characteristics, management and survival BJU Int 2016; 117:287-292
22 Jiang S, Liu J, Chen X, et al Platelet-lymphocyte ratio as a potential prognostic factor in gynecologic cancers: a meta-analysis Arch Gynecol Obstet 2019; 300:829-839
23 Wang J, Zhou X, He Y, et al Prognostic role of platelet to lymp h o c y t e r a t i o i n p ro s t a t e c a
(Baltimore) 2018; 97:e12504
24 Herraiz-Raya L, Moreillo-Vicente L, Martínez-Ruiz J, et al Leukocyte and platelet counts as prognostic values of testicular germ cell tumours Actas Urol Esp 2019; 43:284-292
25 Imamoglu G I, Eren T, Baylan B, Karacın C May high levels of systemic immune-inflammation index and hematologic inflammation markers suggest a further stage in testicular tumours? Urol Int 2019; 103:303-310
26 Peksa R, Kunc M, Popeda M, et al Combined assessment of immune checkpoint regulator VISTA on tumor-associated immune cells and platelet-to-lymphocyte ratio identifies advanced germ cell tumors with higher risk of unfavorable outcomes Cancers 2021; 13:1750
27 Winters BR, Mossanen M, Holt SK, et al JL Predictors of nodal upstaging in clinical node negative patients with penile carcinoma: a national cancer database analysis Urology 2016; 96:29-34
28 Ficarra V, Akduman B, Bouchot O, et al Prognostic factors in penile cancer Urology 2010; 76(2 Suppl 1):S66-73
29 Zekan DS, Dahman A, Hajiran AJ, et al Prognostic predictors of lymph node metastasis in penile cancer: a systematic review Int Braz J Urol 2021; 47:943-956
30 Filippelli A, Del Gaudio C, Simonis V, et al Scoping review on platelets and tumor angiogenesis: do we need more evidence or better analysis? Int J Mol Sci 2022; 23:13401
31 Tufano A, Perdonà S, Viscuso P, et al The impact of ethnicity and age on distribution of metastases in patients with upper tract urothelial carcinoma: analysis of SEER data Biomedicines 2023; 11:1943
32 Wojtukiewicz MZ, Sierko E, Hempel D, et al Platelets and cancer angiogenesis nexus Cancer metastasis Rev 2017; 36:249-262
33 Wakefield LM, Smith DM, Flanders KC, Sporn MB Latent transforming growth factor-beta from human platelets A high molecular weight complex containing precursor sequences J Biol Chem 1988; 263:7646-54
34 Iacopino F, Pinto F, Bertaccini A, et al Soluble E-cadherin and IL6 serum levels in patients affected by prostate cancer before and after prostatectomy Oncol Rep 2012; 28:370-4
35 Gay LJ, Felding-Habermann B Contribution of platelets to tumour metastasis Nat Rev Cancer 2011; 11:123-34
Correspondence
Francesco Passaro, MD francescopassaro1996@gmail com
Antonio Tufano, MD (Corresponding Author) antonio tufano91@gmail com
Gianluca Spena, MD gianlu spena@gmail com
Alessandro Izzo, MD a izzo@istitutotumori na it
Flavio Antonino Scarlata, MD scarlataflavioantonino@gmail com
Sisto Perdonà, MD s perdona@istitutotumori na it
Department of Urology, Istituto Nazionale Tumori, IRCCS, “Fondazione G Pascale”, 80131 Naples, Italy
Biagio Barone, MD biagio193@gmail com
Luigi Napolitano, MD dr luiginapolitano@gmail com
Gabriele Pezone, MD gabrielepezone94@gmail com
Pierluigi Alvino, MD
pierluigi alvino@gmail com
Achille Aveta, MD achille-aveta@hotmail it
Savio Domenico Pandolfo, MD pandolfosavio@gmail com
Simone Cilio, MD simocilio av@gmail com
Lorenzo Romano, MD loryromano@hotmail it
Francesco Di Bello, MD fran dibello12@gmail com
Department of Neurosciences and Reproductive Sciences and Odontostomatology, University of Naples “Federico II”, 80131 Naples, Italy
Alessandro Calarco, MD alecalarco@gmail com
Urology Unit, San Carlo di Nancy Hospital, GVM Care and Research, Rome, Italy
Rosario Leonardi, MD leonardi r@tiscali it
Department of Medicine and Surgery University of Enna KORE, Enna, Italy
Carlo Buonerba, MD carbuone@hotmail com
Department of Public Health, University of Naples “Federico II”, 80131 Naples, Italy
F Passaro, Antonio Tufano, G Spena, A Izzo, et al
ORIGINAL PAPER
Comparative evaluation of the efficacy and safety
of antegrade minimally percutaneous nephrolithotomy (mPCNL) and retrograde intrarenal surgery (RIRS) in the treatment of upper ureteral impacted stones:
A retrospective cohort study
Kequan Cheng 1, 2* , Xuwei Hong 1* , Gang Wang 1, 2 , Zepai Chi 1 , Kemal Sarica 3, 4 , Guoyuan Liu 1 , Yonghai Zhang 1
1 Department of Urology, Shantou Central Hospital, Shantou, Guangdong, P R China;
2 Department of Urology, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, Guangdong, P R China;
3 Department of Urology, Health Sciences University, Prof Dr Ilhan Varank Education and Training Hospital, Istanbul, Turkey;
4 Department of Urology, Biruni University, Medical School, Istanbul, Turkey
* These authors contributed equally to this work
Summary
Objective: To compare the safety and efficacy of retrograde intrarenal surgery (RIRS) versus minimally invasive percutaneous nephrolithotomy (mPCNL) in the minimal invasive management of impacted upper ureteral stones along with the evaluation of predictive radiological parameters.
Patients and methods: A retrospective analysis was done in 124 patients, undergoing RIRS (n:61) and mPCNL (n:63) for the management of impacted upper ureteral stones Both operative (success and complication rates, operative time, postoperative hospital stay) and radiological (ureteral wall thickness (UWT), stone volume (SV), and stone density (Hounsfield unit, HU) factors were all evaluated and recorded Comparative evaluation of stone free status in both groups was done following 72 hours and 4-weeks after the procedures to calculate the primary stone-free as well as final stone clearance rates Additionally, the outcomes of RIRS group were categorized based on the intraoperative findings (presence or absence of stone encasement by a polyp) and preoperative radiological parameters. All data were well analyzed for statistical significance A significance level of P<0.05 was considered statistically significant. Results: Baseline patient and stone related characteristics were similar in two groups. The success rates after a single session for RIRS and mPCNL were 73 77% and 93 65%, respectively (p = 0.003), indicating a significantly higher success rate for mPCNL However the final stone clearance rates were 96 72% and 100.00%, respectively (p = 0.147), with no significant difference observed among the groups The RIRS group demonstrated higher rate of need for auxiliary treatments (p < 0.001), shorter hospital stay (p < 0 001) and lower incidence of bleeding (p < 0.001). Radiological evaluation showed no significant differences in stone volume, HU and UWT values between patients with and without residual stones after RIRS (Pstone volume = 0 151, PHU = 0 451, PUWT = 0 083) Similarly, no significant differences were observed with respect to these values also in mPCNL patients, (Pstone volume = 0 532, PHU = 0 455, PUWT = 0 658) However, a significant difference has been noted regarding the mean value of UWT between the stones surround-
ed by a polypoid alterations and the ones without such changes with values 5.23 ± 0.65 mm, to 4.10 ± 0.82 mm respectively (p = 0 001)
Conclusions: Our results demonstrated that antegrade mPCNL achieves faster stone clearance and a lower re-treatment rate without serious complications in impacted upper ureteric stones However, RIRS could be a valuable and safe alternative with comparable success rates particularly in cases with contraindications to or unwillingness for mPCNL Preoperative assessment of ureteral wall thickness (UWT) value may be a good predictor for the possible tissue changes in ureteral wall at stone site to guide the decision making of the most appropriate surgical approach
Submitted 4 November 2024; Accepted 28 November 2024
INTRODUCTION
Around 5-10% of the general population suffer from urolithiasis (1, 2) Majority of the cases presenting with obstructive ureteral calculi require a prompt management to preserve functional and structural status of the involved kidneys which may cause some irreversible changes if not removed on time (3-5)
Regarding the management of such cases, ureteroscopy (URS) with laser lithotripsy and percutaneous nephrolithotomy (PNL) are the available options applied in the mana g e m e n t o f o b s t r u c t i n g l a r g e u r e t e r a l c a l c u l i ( 6 )
Antegrade percutaneous approach is being applied in a certain per cent of the cases with the complete removal of all stone(s) in a single session However, this procedure is more invasive than other endourological approaches for the risk of certain severe complications (bleeding, perforation, infection, etc) even in experienced hands In the
light of the risk for such complications endourologists began to use smaller instruments in an attempt to limit both the extent of renal injury and also the risk of above mentioned complications (7, 8) Miniaturized PCNL techniques are being utilized with higher success and limited complications in the majority of cases presenting with large upper tract stones (9)
On the other hand, based on its less invasive nature and successful outcomes compared with PCNL, flexible ureteroscopic management gained more popularity in the last 2-3 decades as a result of the evident advances in instrument technology Based on these improvements and acceptable outcomes obtained the joint clinical guidelines of the AUA and the EAU Nephrolithiasis Panel on the Management of Ureteral Calculi recommend URS in patients with proximal ureteral stones smaller than 2 cm (10) Additionally, the most recent EAU and AUA guidelines also recommend URS as the primary modality for stones > 10 mm (1, 11)
This modality may serve as a viable alternative treatment particularly in patients with contraindications to PCNL or whom do not prefer to undergo such a more invasive intervention (12) However, accumulated data have shown that despite its evident minimally invasive nature, ureteroscopic manipulation may be associated with certain complications such as ureteral injuries and subsequent ureteral stricture formation (13)
Additionally, relatively lower stone-free rates (SFR) and the need for additional auxiliary procedures (14, 15) remain significant challenges for this technique when particularly dealing with large stones Some stone related parameters have been identified and used to predict the outcomes of Retrograde Intrarenal Surgery (RIRS) in the management of large, impacted ureteral stones causing certain degree of obstruction Related with this issue in addition to the size, volume, density and chemical composition of the stones treated, the thickness of the ureteric wall surrounding the impacted stone(s) have been used with great success to predict both the success as well as complications of RIRS in such cases (16)
Taking the advantages and disadvantages of both modalities into account, in this study we aimed to compare the clinical results of RIRS and mPCNL in the management of single impacted upper ureteral stones less than 2 cm in diameter Also, the potential value of some radiological parameters in the prediction of success after RIRS were evaluated to select the most appropriate surgical method in these stones
PATIENTS AND METHODS
A retrospective analysis was conducted in 124 patients with upper ureteral impacted stones (< 2 cm) admitted to our urology department from April 2020 to December 2023 Based on the type of intervention applied, patients were divided into two groups: Group 1 (n:61) including patients undergoing RIRS with laser lithotripsy and Group 2 (n:63) including patients undergoing mPCNL An informed consent was obtained in all cases undergoing both interventions
Inclusion criteria were unilateral single upper ureteral stones (< 2 cm) confirmed by non-contrast computed tomog-
raphy (NCCT) Exclusion criteria included patients with active urinary tract infections, previous renal-ureteral interventions, renal functional deterioration and anatomical abnormalities contraindicating surgery In addition to a detailed history and through urogenital examination, blood/urine analyses were done in all patients Patients with urinary tract infections were previously treated according to the outcomes of culture-sensitivity tests Radiological evaluation consisted of kidney-ureter-bladder (KUB) film, sonography and NCCT in all cases An intravenous urography was performed in cases requiring further anatomical information for making a proper decision
Demographic data, including age and sex, medical history, and stone side, size, and location, were recorded (see Table 1) Surgical duration, length of hospital stays, perioperative complications, and treatment outcomes were evaluated and compared between groups Additionally, Hounsfield units (HU) value of the stone, ureteral wall thickness (UWT) and maximum transverse and longitudinal diameter of the stones were measured on NCCT and noted KUB X-ray was obtained within 72 hours of post-operative period to confirm the correct placement of double-J stents and to assess residual stone status Surgical success was defined as the absence of fragment or presence of residual stone fragments smaller than 3 mm following the procedures Residual stones were treated with extracorporeal shock wave lithotripsy (ESWL) or external physical vibration lithotripsy (EPVL) DJ stents were removed after two weeks, and all patients were followed up one month postoperatively in the outpatient or inpatient department to outline the status of final stone clearance
Definitions of outcome measures
Surgical efficacy: Assessed the results of 72-hour and onemonth follow-up, including technical success rate and stone-free rate Operative Time: For RIRS, timing commenced with the placement of the flexible ureteroscope sheath, or the guidewire passing the stone and concluded with the successful placement of the ureteral stent For mPCNL, timing began with the percutaneous puncture and ended with the successful placement of the nephrostomy tube
Postoperative Hospital duration: The duration from the day
Treatment Rate: Number of cases requiring ESWL and EPVL based on follow-up KUB results Postoperative Complications: Postoperative Complications were classified according to the Clavien-Dindo system, including the number of cases requiring hemostatic agents, those with postoperative fever, and those needing pain medication within 24 hours of surgery
Surgical procedure
RIRS: The procedure was performed in the lithotomy position under general or combined spinal-epidural anesthesia
A 0 035-inch Wolf guidewire was passed into the ureter through the rigid Fr 8 0 to 9 8 Wolf ureteroscope was and stone localization was confirmed by using low-pressure irrigation Fragmentation of the stone was performed with the help of either holmium laser or pneumatic ballistic lithotrip-
K Cheng, X Hong, G Wang, et al
sy The holmium laser settings were arranged with a frequency value of 10 Hz, energy value of 800 J, and pressure value of 14 kPa While larger fragments were extracted with the help of stone forceps, dust and smaller fragments were flushed out The procedure was finished with the routine placement of a 5-Fr double-J stent in the affected ureter A urethral catheter was left in place for 1 to 2 days mPCNL: Following the placement of a 5Fr open end ureteral catheter during cystoscopic evaluation in lithotomy position under general anesthesia, later the patient was turned into prone position and renal puncture was performed with a 18-gauge puncture needle under ultrasound guidance Upon achieving puncture to the dependant calyx, a 0 035-inch guidewire was inserted into the collecting system whit following a 1 cm skin incision, fascial dilation and placement of a 18-Fr working sheath A 17-Fr nephroscope was introduced through the working sheath for stone fragmentation Stones were disintegrated using either a holmium laser or pneumatic ballistic lithotripsy and all fragments were removed A nephrostomy tube was inserted if necessary Following the removal of all stone fragments a 5-French double-J stent was placed antegradely into the affected ureter A urethral catheter was placed and retained for 1 to 2 days as needed
Radiologic evaluation of the stones and relevant parameters
NCCT images were analyzed by two radiologists to measure the ureteral wall thickness (UWT) at the stone location by taking the maximum value from cross-sectional images Hounsfield unit (HU) value of the stone was measured at the stone's central region, avoiding the boundary with surrounding soft tissue Maximum longitudinal and transverse diameter of the stones were measured in coronal and transverse planes Stone surface area (SA) and volume (V) were estimated using the following formulas based on EAU guidelines (10):
SA (mm²) = l × w × π × 0 25 (Formula 3-1)
V (mm³) = 0 6 × SA1 27 (Formula 3-2) (l = maximum longitudinal diameter, w = maximum transverse diameter)
Degree of hydronephrosis was classified based on preoperative ultrasound or CT measurements of renal pelvis separation as mild, moderate, or severe
Statistical analysis
Data were analyzed using SPSS 26 0 software For quantitative data, independent samples t-tests were used for normally distributed data, and Wilcoxon rank-sum tests for non-normally distributed data Categorical data were analyzed using chi-square tests Statistical significance was set at p < 0 05
RESULTS
Comparative evaluation of the efficacy rates
A total of 124 adult patients were included in the study There were no statistically significant differences between the two groups in terms of demographic characteristics such as sex, age, medical history, stone side, location, and size (Table 1)
Table 1.
Preoperative baseline characteristics of patients in the MPCNL and RIRS groups
Sex/cases (%)
Side of the stone/cases (%)
Medical history/cases (%)
Comparative evaluation of the peri- and postoperative parameters are given in Table 2 Although there was a significant difference in the operative success rates between the two groups (p < 0 05), no significant difference could be noted in the stone-free rates of two groups Of the 61 cases in RIRS group, 14 required additional procedures (ESWL or EPVL) to achieve a complete stone-free status The auxiliary treatment rate was higher in the RIRS group compared to the mPCNL group (p < 0 05)
Table 2
Complications were classified by using the Clavien-Dindo grading system and no Grade IV complication was noted in any case of this study There was no statistically significant difference regarding the postoperative pain between the two groups However, use of the hemostatic drugs was more frequent (30 16%) in the mPCNL group where one patient received blood transfusion and one underwent interventional treatment for bleeding demonstrating a statistically significant difference (p < 0 05) between two groups with respect to this complication There was no significant difference between the two techniques regarding the postoperative need for pain medication within 24 hours and infective complication rates
Last but not least, the average hospital stay was 2 98 ± 1 58 days in the RIRS group and 4 76 ± 2 32 days for the mPCNL group respectively, indicating a relatively longer recovery time observed in the mPCNL group (p < 0 05)
Evaluation of the radiological parameters
Comparative analysis of the possible relationship between treatment outcomes and mean stone related parameters (volume and HU) as well as mean UWT values revealed no statistically significant differences between two group of cases (PRIRS-stone volume = 0 151 > 0 05, PRIRS-HU = 0 451 > 0 05, PRIRS-UWT = 0 083 > 0 05; PmPCNLstone volume = 0 532 > 0 05, PmPCNL-HU = 0 455 > 0 05, PmPCNL-UWT = 0 658 > 0 05) (Tables 3, 4)
A retrospective analysis of our data revealed that the RIRS group had a lower success rates in a single session compared to the mPCNL group, often requiring additional ESWL or EPVL Further analysis of success rates in RIRS group demonstrated that stone free rates were significantly affected by the changes in the ureteral wall characteristics (Table 5)
While 36 out of 61 cases in this group had inflammatory
Table 5.
Comparison of imaging data for cases with and without polyp encapsulation in RIRS group.
Stone Stone t-value P-value without polyp with polyp encapsulation encapsulation (n = 54) (n = 7)
HU stands for Hounsfield Units, a measure used in CT scans; UWT stands for ureteral wall thickness; Mean SD nd cates the mean standard dev ation
polyps noted during the procedure, 6 had strictures and 7 had stones encased by polyps, which could complicate guidewire placement, increase the risk of intraoperative bleeding, and necessitate multiple ureteroscope manipulations causing additional trauma Based on this fact, further detailed analysis on the preoperative imaging findings and the presence of intraoperative polyps encasing stones was conducted, as demonstrated in Table 5
The mean preoperative UWT value detected in NCCT imaging was significantly higher in cases with stones encased by polyps (5 23 ± 0 65 mm), (P UWT = 0 001)
In contrast, there was no statistically significant difference in the mean stone volume and mean HU values (P stone volume = 0 441, P HU = 0 711)
DISCUSSION
Currently both anterograde PCNL and RIRS are acceptable options for the minimal invasive management of impacted proximal ureteral stones with varying rates of success and complications in different series (17) Each modality has its own advantage and disadvantages and accumulated experience so far demonstrated that despite its higher stone free rates in a single session, even miniPCNL could be associated with severe complications (1820) On the other hand, with the use new generation flexible scopes with Ho-YAG laser technology, RIRS was found to reveal comparable stone free rates with limited rate of complications particularly in risk group of cases for PCNL (21)
HU stands for Hounsfield Units, a measure used in CT scans; UWT stands for ureteral wall th ckness; Mean SD nd cates the mean standard dev ation
Table 4.
Comparison of imaging data of residual stones after MPCNL surgery
HU stands for Hounsfield Un ts, a measure used n CT scans; UWT stands for uretera wal th ckness; Mean SD indicates the mean standard deviation
Taking all these facts into account, in this present study we aimed to evaluate the efficacy and safety of both modalities in the management of impacted upper ureteral stones causing obstruction Additionally, we evaluated the some certain radiological parameters in an attempt to predict the outcomes of RIRS in such stones and their possible role in the preoperative decision making phase to outline the best modality
Evaluation of our obtained data revealed the following findings
Evaluation of success rates and the need for auxiliary treatment
O u r r e s u l t s d e m o n s t r a t e d a s i g n i fi c a n t d i f
between success rates in terms of stone free status during short term evaluation between the two modalities where RIRS approach seemed to be less effective Additionally,
K Cheng, X Hong, G Wang, et al
Table 3.
Comparison of imaging data of residual stones after RIRS surgery
mPCNL vs RIRS for upper ureteral impacted stones
patients undergoing RIRS procedure required higher need for adjunctive treatments to achieve outcomes similar to mPCNL As a certain advantage, mPCNL was associated with the advantage of effective fragmentation of the stones from above enabling rapid expulsion of residual fragments under high-pressure irrigation coupled with the enhanced clarity Despite marked advances in RIRS technology, such as improved irrigation systems and larger working channels, flexible ureteroscopy technique remains less effective in stone fragmentation compared to mPCNL (22)
Related with this issue, Faruk et al , found that flexible ureteroscopic management is effective for upper ureteral stones (average size of 1 24 cm), with a 96 4% single-session success rate (23) However, flexible ureteroscopic stone management was found to exhibit promising results in challenging cases such as obese and pediatric patients In their original study Best et al were able to demonstrate a single-session success rate of 91% obese patients undergoing flexible ureteroscopic lithotripsy (24) Regarding the disadvantages of RIRS compared to mini-PCNL, the complex nature of the procedure with its high equipment costs and maintenance expenses seemed to limit the widespread use of RIRS (25) Stone fragmentation and removal may also be less practical and effective during RIRS compared to mPCNL where dust forming during the procedure can cause blurred vision making the identification of small fragments hard for the surgeon However, recent technological advancements with the introduction of new effective laser types and suction device will certainly help to improve the success rates of RIRS, as in studies indicating good results for relatively larger stones (26) In fact Mult¸escu et al and Cho et al were able to demonstrate that stones larger than 1 cm could be well pulverized in a successful manner with flexible ureteroscopic approach (27)
Evaluation of the procedure related complications
Complications with mPCNL are primarily linked to puncture and stone fragmentation, including severe risks like bleeding, upper urinary tract perforation, renal function deterioration and injury to adjacent organs (28, 29)
In the retrospective study of 10 413 cases of F-URL treatment patients by Xu et al (30) the incidence rate of complications with electronic ureteroscopy soft mirrors did not exceed 1%
In our study, 8 patients in the RIRS group experienced postoperative infective problems, which were well treated with appropriate antibiotic treatment Among these, 3 cases experienced fever possibly due to bacteremia from stone fragmentation Regarding the bleeding complication while postoperative hematuria generally improved well within one day after the procedure in RIRS cases, cases in mPCNL group required more hemostatic drugs, with one case requiring interventional treatment for severe bleeding Thus, mPCNL generally involves more postoperative complications and higher management demands
Evaluation of ureteral wall thickness value on the outcomes of RIRS
Mean ureteral wall thickness (UWT) values did not show any statistically significant difference between the two
groups with or without residual stones for either specific technique Possible reasons include: 1) UWT measurements can be influenced by factors such as the surgeon ’ s experience, scan thickness, and CT image quality; (31) 2) Large stones are frequently associated with ureteral anomalies, which can lead to measurement errors In this study, 5 cases in the RIRS group exhibited significant ureteral tortuosity, necessitating image aggregation from three planes to achieve more accurate UWT values
Subgroup analysis revealed that stones encased by polyps in the RIRS group had significantly mean higher UWT values, indicating that preoperative measurement of UWT may be an effective predictor for the presence of polyps encasing stones Elevated UWT was found to be associated with ureteral inflammatory proliferation (16) Our results indicate that measurement of UWT value may help to predict stone related ureteral changes and guide urologists in decision making phase to choose the most appropriate option for a successful and complication free procedure Mini PCNL approach could be a reasonable alternative in such cases by avoiding RIRS for polyp-encased stones to minimize the risk of procedure related complications
Limitations
Our study is not free of limitations First of all the retrospective, single-center nature of the study design could be stated as the main limitations Additionally, relatively small size of the sample along with a shorter follow-up period (one month) are additional limitations We believe that further randomized controlled trials would further support the validity of these findings Clinical observations indicate that impacted stones are often accompanied by varying degrees of ureteral tortuosity, which may introduce measurement errors Additionally, inflammatory reactions leading to congestion and edema can cause the ureteral wall to have a density similar to surrounding soft tissues, resulting in measurement bias Utilizing imaging techniques to accurately measure ureteral wall area (UWA) and extract imaging features could provide new insights for developing individualized treatment plans for patients with upper ureteral impacted stones (32)
CONCLUSIONS
Our findings demonstrated that mini-PCNL could provide higher stone free rates and lower need for auxiliary treatments compared to RIRS in the management of impacted upper ureteral stones However, RIRS was found to be safer with limited rate of complications associated with faster postoperative recovery Our findings did also point out the predictive role of UWT value on the presence and severity of polypoid formation surrounding the stones Thus, this radiological parameter may be helpful for the endourologists during decision making phase to choose the appropriate modality for the management of such stones to limit procedure related complications and increase the stone free rates
REFERENCES
1 Türk C, Petrík A, Sarica K, et al EAU Guidelines on interventional treatment for urolithiasis Eur Urol 2016; 69:475-82
2 Knoll T, Wezel F, Michel MS, et al Do patients benefit from miniaturized tubeless percutaneous nephrolithotomy? A comparative prospective study J Endourol 2010; 24:1075-9
3 Sunaryo PL, May PC, Holt SK, et al Ureteral strictures following ureteroscopy for kidney stone disease: a population-based assessment The JPN J Urol 2022; 208:1268-75
4 May PC, Hsi RS, Tran H, et al The morbidity of ureteral strictures in patients with prior ureteroscopic stone surgery: multi-institutional outcomes J Endourol 2018; 32:309-14
5 Sammon JD, Ghani KR, Karakiewicz PI, et al Temporal trends, practice patterns, and treatment outcomes for infected upper urinary tract stones in the united states Eur Urol 2013; 64:85-92
6 Schuster TG, Hollenbeck BK, Faerber GJ, et al Complications of ureteroscopy: analysis of predictive factors JPN J Urol 2001; 166:538-40
7 Ruhayel Y, Tepeler A, Dabestani S, et al Tract Sizes in miniaturized percutaneous nephrolithotomy: a systematic review from the european association of urology urolithiasis guidelines panel Eur Urol 2017; 72:220-35
8 Clayman R From knife to needle to nothing: The waning of the wound Int Braz J Urol 2001; 27
9 Ghani KR, Andonian S, Bultitude M, et al Percutaneous nephrolithotomy: update, trends, and future directions Eur Urol 2016; 70:382-96
10 Preminger GM, Tiselius HG, Assimos DG, et al 2007 Guideline for the management of ureteral calculi Eur Urol 2007; 52:1610-31
11 Assimos D, Krambeck A, Miller NL, et al Surgical management of stones: american urological association/endourological society guideline, part I JPN J Urol 2016; 196:1153-60
12 Aboumarzouk OM, Somani BK, Monga M Flexible ureteroscopy and holmium:YAG laser lithotripsy for stone disease in patients with
DECLARATIONS
Ethical approval: The study was approved by the Institutional Review Board of Shantou Central Hospital
Availability of data and material: The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request
Competing interests: These authors declare that they have no conflict of interest
Funding: This study was supported by the Special Fund Project for Science and Technology Innovation Strategy of Guangdong Province (Grant No STKJ202209068)
Authors' contributions: Conception and design: YZ, KS and GL; Data analysis and interpretation: KC and GW; Data acquisition: XH and ZC; Critical revision of the manuscript: YZ, KS and GL; Drafting the manuscript: KC and XH; Statistical analysis: KC, XH; Supervision: YZ All authors read and approved the final version of the manuscript
Acknowledgments: Not applicable
Consent for publication: Not applicable
bleeding diathesis: a systematic review of the literature Int Braz J Urol 2012; 38:298-305; discussion 6
13 Roberts WW, Cadeddu JA, Micali S, et al Ureteral stricture formation after removal of impacted calculi JPN J Urol 1998; 159:723-6
14 Soderberg L, Ergun O, Ding M, et al Percutaneous nephrolithotomy versus retrograde intrarenal surgery for treatment of renal stones in adults Cochrane DB Syst Rev 2023; 11:Cd013445
15 Akman T, Binbay M, Ozgor F, et al Comparison of percutaneous nephrolithotomy and retrograde flexible nephrolithotripsy for the management of 2-4 cm stones: a matched-pair analysis BJU Int 2012; 109:1384-9
16 Dean NS, Millan B, Uy M, et al Ureteral wall thickness is an effective predictor of ureteral stone impaction and management outcomes: a systematic review and meta-analysis JPN J Urol 2023; 210:430-7
17 Lai S, Jiao B, Diao T, et al Optimal management of large proximal ureteral stones (>10 mm): A systematic review and meta-analysis of 12 randomized controlled trials Int J Surg 2020; 80:205-17
18 Wu C, Hua LX, Zhang JZ, et al Comparison of renal pelvic pressure and postoperative fever incidence between standard- and minitract percutaneous nephrolithotomy Kaohsiung J Med Sci 2017; 33:36-43
19 Yang Z, Song L, Xie D, et al Comparative study of outcome in treating upper ureteral impacted stones using minimally invasive percutaneous nephrolithotomy with aid of patented system or transurethral ureteroscopy Urology 2012; 80:1192-7
20 Sakr A, Salem E, Kamel M, et al Minimally invasive percutaneous nephrolithotomy vs standard PCNL for management of renal stones in the flank-free modified supine position: single-center experience Urolithiasis 2017; 45:585-9
21 Gökce M, Akpinar Ç, Obaid K, et al Comparison of retrograde ureterorenoscopy (URS) and percutaneous anterograde ureteroscopy for removal of impacted upper ureteral stones >10 mm in the elderly population Int Braz J Urol 2021; 47:64-70
22 Goodman TM Ureteroscopy with pediatric cystoscope in adults Urology 1977; 9:394
23 Yencilek F, Canguven O, Albayrak S, et al A comparison of shock wave lithotripsy, semirigid and flexible ureteroscopy in the management of proximal ureteral calculi Turk J Urol 2009; 35:101-107
24 Best SL, Nakada SY Flexible ureteroscopy is effective for proximal ureteral stones in both obese and nonobese patients: a two-year, single-surgeon experience Urology 2011; 77:36-9
25 Lildal SK, Andreassen KH, Baard J, et al Consultation on kidney stones, Copenhagen 2019: aspects of intracorporeal lithotripsy in flexible ureterorenoscopy World J Urol 2021; 39:1673-82
26 Prabhakar M Retrograde ureteroscopic intrarenal surgery for large (1 6-3 5 cm) upper ureteric/renal calculus Indian J Urol 2010; 26:46-9
27 Multescu R, Geavlete B, Georgescu D, et al Holmium laser intrarenal lithotripsy in pyelocaliceal lithiasis treatment: to dust or to extractable fragments? Chirurgia-Bucharest 2014; 109:95-8
28 Sun H, Zhang Z, Yuan J, et al Safety and efficacy of minimally invasive percutaneous nephrolithotomy in the treatment of patients with medullary sponge kidney Urolithiasis 2016; 44:421-6
29 de la Rosette JJ, Opondo D, Daels FP, et al Categorisation of
K Cheng, X Hong, G Wang, et al
mPCNL vs RIRS for upper ureteral impacted stones
complications and validation of the Clavien score for percutaneous nephrolithotomy Eur Urol 2012; 62:246-55
30 Xu G-b, Li X-z, He Y-z, et al Ten years experience in treatment of upper urinary calculi withRIRS: clinical analysis of 10 413 cases in single center Chin J Endosc 2020; 26:64-8
31 Popiolek M, Lidén M, Georgouleas P, et al Radiological signs of stone impaction add no value in predicting spontaneous stone passage Urolithiasis 2024; 52:114
Correspondence
Kequan Cheng, MD chengkq2021@163 com Xuwei Hong, MD hong xuwei@sina cn
Gang Wang, MD 1031020787@qq com
Zepai Chi, MD zepaichist@126 com
Guoyuan Liu, MD liuguoyuan91@sohu com
Department of Urology, Shantou Central Hospital, Shantou, Guangdong, P R China
Kemal Sarica, MD saricakemal@gmail com
Department of Urology, Health Sciences University, Prof Dr Ilhan Varank Education and Training Hospital, Istanbul, Turkey
Yonghai Zhang, MD (Corresponding Author) zhang yonghai@126 com
Department of Urology, Shantou Central Hospital 114th Waima Road, Shantou, Guangdong, P R China
32 Yamashita S, Kohjimoto Y, Iguchi T, et al Ureteral wall volume at ureteral stone site is a critical predictor for shock wave lithotripsy outcomes: comparison with ureteral wall thickness and area Urolithiasis 2020; 48:361-8
Urine alkalinization for dissolution of uric acid stones and treatment of other urological diseases with a treatment combining potassium magnesium citrate and theobromine
Celia Abad Rodriguez-Hesles 1 , Hassan Alkhatatbeh 2 , María Belén Alonso Bartolomé 3 , Carmen Arai Valladares Ferreiro 4 , Hector Ricardo Ayllón Blanco 3 , Cristina Calzas Montalvo 5 , Daniel Carrasco Gómez 6 , Marta Casadevall Rubau 7 , Elena Maria Casas Martinez 8 , Sara Esturo Sacristan 9 , Miguel Gómez Garberí 10 , Blanca Gómez-Jordana Mañas 11 , Rosa Maria Gras Martinez 12 , Ana Morales Martínez 1 , Pedro Hernandez-Peñalver 7 , Silvia Juste Alvarez 5 , Alberto López Sierra 13 , Rafael Maria Mas Lucas 14 , Isabel Mohedano Sánchez 15 , Isabel Montuenga Fernandez 16 , Baraa Nakdali Kassab 10 , Maria Negueroles-Garcia 12 , Leticia Ruibal Gago 17 , Laura Sánchez 10 , Bernat Isern 18, 19 , Alberto Trinchieri 20
1 Hospital Universitario Clínico San Cecilio, Grenada, Spain;
2 Department of General Surgery, Urology and Anaesthesia, The Hashemite University, Zarqa, Jordan;
3 Hospital Universitario La Paz, Madrid, Spain;
4 Hospital de Valme, Endourology and Urolithiasis Section, Sevilla, Spain;
5 Hospital Universitario 12 de Octubre, Madrid, Spain;
6 Hospital Regional Universitario de Málaga, Malaga, Spain;
7 Fundacio Puigvert, Barcelona, Spain;
8 Hospital Universitario Rey Juan Carlos, Madrid, Spain;
12 Hospital General Universitario de Valencia, Valencia, Spain;
13 Hospital Nuestra Señora de Sonsoles, Avila, Spain;
14 General Hospital of Segovia, Segovia, Spain;
15 Hospital Juan Ramón Jiménez, Huelva, Spain;
16 Hospital Universitario Príncipe de Asturias, Alcala de Henares (Madrid), Spain;
17 Complexo Hospitalario Universitario de Pontevedra, Pontevedra, Spain;
18 Devicare, Barcelona, Spain;
19 Laboratori d’Investigació en Litiasi Renal, Universitat de les Illes Balears, Spain;
20 CDC Ambrosiana, Milano, Italy
Abstracts were presented at 1st-2nd-3rd-4th-5th Edition of the Clinical Cases Contest related to the non-surgical clinical management of renal lithiasis Full texts are available at https://professional devicare com/concurso-casos/en/
Summary
Background: Urine alkalinization can be used for the treatment of some urological diseases.
Methods: A series of cases showing the beneficial effects of urine alkalinization with combination of potassium magnesium citrate and theobromine for the dissolution of uric acid stones and the treatment of other urological pathological conditions is presented.
Results: Alkalinization was effective in the dissolution of uric acid renal stones in various clinical conditions Two cases of bilateral renal stone, four cases of staghorn renal stone, seven patients with unilateral renal stone, and five cases of ureteral stone were described. In this group the age ranged from 46 to 91 years, the M/F ratio was 7/11, the density of the stones ranged between 300 and 528 In most cases the urinary pH ranged from 5 to 5 5 Diabetes was observed in 4 cases, obesity in 4 cases and hyperuricemia in 7 Alkalinizing treatment achieved complete dissolution of the stone in 12 cases and almost complete or partial dissolution in other 6 A combination of potassium magnesium citrate and theobromine was used in all the cases In 4 cases the administration of allopurinol was associated In one case with obstructive ureteral stones, stone
dissolution was obtained with the combined administration of bicarbonate via nephrostomy and intravenous bicarbonate and oral treatment with citrates Stone dissolution of uric acid stones has also been described in some specific clinical conditions such as Crohn's disease with ileostomy, outcome of partial nephrectomy, cross-fused renal ectopia
Alkalinization was also used to prevent encrustation of a self-expanding metallic ureteral stent Alkalinization has also been employed during the period of Mitomycin administration for the treatment of non-muscle infiltrating bladder tumors and for the treatment of overactive bladder
Conclusions: The findings of these case reports demonstrate that urinary alkalinization with frequent monitoring of urinary pH can be successfully employed in the non-surgical treatment of uric acid stones of different sizes in various locations
The physiological value of urinary pH varies between 4 5 and 8 0, although the urine pH over 24 hours usually ranges between 5 7 and 6 3 so minimizing the risk of pHdependent crystal formation (1) Urinary pH depends on d i e t a r y i n t a k e , m e t a b o l i s m a n d p o s t - re n a l u r i n a r y changes due to infection by some bacterial species
Urinary pH values lower than 5 5 cause the formation of crystals or stones of uric acid which are poorly soluble in acidic urine For this reason, products based on bicarbonate or citrate have long been used for the treatment and prevention of uric acid stones (2, 3) However, excessive alkalinization can increase the value of urinary pH above a threshold beyond which the precipitation of sodium urate and especially phosphate salts are favored The target value of urinary pH for the dissolution of uric acid stones is between 6 and 6 5 and it must be carefully monitored (4, 5) The concomitant administration of theobromine, which has a pH-independent solubilizing action on uric acid crystals, may be useful to avoid excessive alkalinization (6, 7)
Alkalizers are also effective in dissolving crystals and stones consisting of certain drugs such as sulphadiazine
Table 1.
Bilateral renal uric acid stones
RENAL BILATERAL STONES (N = 2)
Patient & Stone 71 yrs F
Bilateral stones Obstructive left stone 23 6 mm
73 yrs F
Right kidney 9 mm UPJ stone+ calyceal stones + partial coralliform of pelvis and lower calix Left kidney non-ostructive stone
Urine alkalinization has also found application in the treatment of other urological diseases Alkalizers are used for the symptomatic treatment of uncomplicated urinary tract infections in some countries (8), although the efficacy of this treatment has not been confirmed by randomized trials The administration of alkalizing agents has also been proposed for the treatment of urinary frequency and pain in patients with interstitial cystitis because afferent C-fibers in the bladder wall could be activated by H+ ions frum acidic urine (9, 10)
Finally, urine alkalinization has been associated with intravesical Mitomycin treatment of non-muscle infiltrating bladder tumors to stabilize the drug and increase its absorption into the bladder wall (11)
CASE SERIES
Bilateral renal stone (Table 1) Lit-Control® pH Up as a great alternative for uric acid stones (María Belén Alonso - 2nd Ed 2021)
We report the case of a 71-year-old obese woman diagnosed with bilateral uric acid lithiasis who required
Lit-Control® pH Up x 2 + bicarbonate Right DJ stent
Lit-Control® pH Up x 3
Outcome
3 months complete left stone dissolution decreased size of right stone
4 months
Residual stone in right lower calix. Microliths in left middle and lower calyces
8 months
No stones
Metabolic
Obesity
Dyslipidemia
Ur pH 5 5
Diabetes Obesity sCr 3 61 at admission
Ur pH 5 5
urgent urinary referral, after which alkalinising treatment with potassium citrate was prescribed without benefit The patient had to undergo percutaneous nephrolitectomy, a procedure which failed to remove all the kidney stones After this, the patient was treated with LitControl® pH Up, achieving almost a total resolution of her kidney stones (Figure 1)
Effective alkalinizing chemolysis in multiple uric acid nephrolithiasis and coralliform calculi (Alberto López - 4th Ed 2023)
A 73-year-old diabetic woman with high cardiovascular morbidity was referred to the emergency department with c l i n i c a l a n d l a b o r a
Urinalysis showed urinary pH 5 and abundant amorphous urates in the sediment The CT scan showed multiple bilateral nephrolithiasis and a large pseudo-coralliform stone in the right kidney, causing ipsilateral obstructive uropathy Urgent placement of a double J catheter
Celia Abad Rodriguez-Hesles, Hassan Alkhatatbeh, M Belén Alonso Bartolomé, et al
Author María Be én Alonso 2021
A berto López 2023
Figure 1.
stone in the lower calyx of the left kidney and a kidney stone in the right kidney before and after treatment
Figure 2.
Dissolution of almost all multiple bilateral renal stone including a large pseudo-coralliform stone in the right kidney after 4 months of alkalinizing treatment with Lit-Control® pH Up
and admission to the intensive care unit was performed
Once the septic process was concluded, she was reviewed in consultation and alkalinizing treatment with LitControl® pH Up was decided After four months, she presented a satisfactory evolution, good tolerance to treatment, and dissolution of almost all uric acid lithiasis
Subsequent control showed normal renal ultrasound, and the metabolic study showed normal uric acid and citrate excretion in urine, as well as improvement of renal function and urinary pH with a current value of 6 (Figure 2)
Staghorn renal stones (Table 2)
Combined medical approach for uric acid staghorn lithiasis (Laura Sánchez - 1st Ed 2020)
Medical treatment for uric acid lithiasis comprises two modalities: stone formation prevention and chemolysis with curative intent The Authors present the results of the combined medical treatment of uric acid lithiasis for the purpose of stone size reduction The case of a 54-yearold man was presented who, after an episode of mild, self-limited hematuria, was diagnosed by CT scan with staghorn renal stone in the left kidney The metabolic study showed hyperuricemia and hyperuricosuria Given the normal renal function and the disappearance of the symptoms, it was decided to start combined therapy by alkalizing the urine using Lit-Control® pH Up, allopurinol and dietary measures After four months of treatment, the patient presents with uremia and uricosuria within nor-
mal values, as well as a reduction in the stone size, completely disappearing the stone that was in the upper calyx of the right kidney The combined medical treatment for uric acid stones can dissolve the stone or reduce its size, avoiding or facilitating surgical treatment (Figure 3)
Figure 3. Partial dissolution of left kidney staghorn stone.
Medical management of uric acid kidney stones, after a case report (Ana Morales Martínez - 1st Ed 2020)
Urinary uric acid stones are a frequent and important pathology in our clinical practice Conservative treatment by means of hygienic-dietary measures and correct urinary alkalinization by means of citrate and theobromine seems to be a promising combination for the treatment and resolution of these lithiasis A case with complete resolution of a coralliform uric acid lithiasis was observed after 12 weeks of treatment with Allopurinol and Lit-Control® pH Up without adverse reactions and avoiding the need for invasive surgical measures This case has been presented elsewhere as a self-standing case report after participating in the 1st Edition of Clinical Case Contest (12)
Medical treatment of staghorn uric acid lithiasis with Lit-Control® pH Up (Baraa Nakdali Kassab - 3rd Ed 2022)
A 65-year-old Caucasian female who was evaluated for pain in the right renal fossa of 10 days evolution, is presented During her follow-up appointment, an abdominal/pelvic CT scan was requested where a right staghorn lithiasis of 4 5 cm x 3 2 cm was observed, occupying the upper, middle, and lower calyces, with growth towards the renal pelvis, with an average density of 450 Hounsfield Units (HU) An alkalizing medical treatment was started using Lit-Control® pH Up (potassium citrate, magnesium citrate and theobromine) After being treated for three months, the resolution of lithiasis was observed
Author Laura Sánchez 2020
Ana Morales Martínez 2020
Baraa Nakdali
Table 2
Staghorn uric acid stones
RENAL STAGHORN STONES (N = 4)
Kassab 2022
Mohedano 2023
Chemolytic treatment for uric acid lithiasis, even for staghorn stones, should be considered as the first treatment option This case has been presented elsewhere as a self-standing case report after participating in the 3rd Edition of Clinical Case Contest (13)
Chemolysis of large coralliform lithiasis with Lit-Control® pH Up (Isabel Mohedano - 4th Ed 2023)
A case report showing the usefulness of medical treatment in coralliform lithiasis of uric acid despite its large size A 52-year-old woman referred to our office for hematuria An abdomino-pelvic CT scan was performed showing a 6 cm right renal lithiasis, of coralliform mor-
Unilateral uric acid renal stones
RENAL UNILATERAL STONES (N = 7
Author
Patient & Stone
83 yrs F
Right kidney stone 17x5 mm pelvis +lower pole stone
Calzas Monta vo 2022
Celia Abad Rodríguez-Hassles 2023
46 yrs M
two stones in right pelvis (15 mm + 16 mm) + dilatation right upper-middle calyces at 6 month follow up after PCNL 27 mm stone right pelvis + two stones in lower calix (7 and 8 mm)
56 yrs F
6-7 mm stone lower left calix
67 yrs F
Multiple stones in right kidney (4 mm pelvis, upper, middle calix)
66 yrs F
4 mm obstructive left ureteral stone + 15 mm non-obstructive right renal pelvis stones
60 yrs F
two left kidney stones 15 mm in the renal pelvis and 21 mm in lower calyx
59 yrs F
impacted right renal pelvis stone secondary hydronephrosis 16 x 9 mm
phology, extending from the renal pelvis towards the middle and lower calicial groups, producing mild ectasia of the excretory system After 11 months of urinary alkalinization using Lit-Control® pH Up (potassium citrate, m
achieved almost complete chemolysis with a pH around 6 We should consider alkalinizing pharmacotherapy as the first treatment option in patients with uric acid lithiasis (Figure 4)
Unilateral renal stones (Table 3)
Oral chemolysis as an effective treatment in the resolution of uric acid kidney stones (Blanca Gómez-Jordana Mañas - 2nd Ed 2021)
Kidney stone disease is a highly prevalent pathology that is still increasing and is composed of uric acid in 10 and 15% of cases A clear relationship has been established between the formation of this type of stones with the presence of an acid urinary pH Therefore, the current treatment is based on the use of urine alkalizers to prevent the crystallization of uric acid It seems that the assoc i a t i o n o f t h e o b ro
increase its efficacy We reviewed a clinical case from our center that presents uric acid nephrolithiasis resolved by medical treatment (Figure 5)
Lit-Control® pH Up x 2 Lit-Control® pH Up x 2 Lit-Control® pH up
Lit-Control® pH Up x 2 300 mg of Allopurinol DJ stent
Spontaneous left stone passage + Lit-Control® pH Up 1 x 2-3 + Allopurinol 300 mg once day + DJ stent
Flexible left URS
Partial fragmentation Lit-Control® pH Up 2 x 2 + left DJ stent
Unsuccessful Mini-PCNL (purulent urine) nephrostomy+ Lit-Control® pH Up Lit-1 x 2
Outcome 6 months complete dissolution
3 months
No evidence of stone 6 months
Decreased to 2 mm 4 months
Complete resolution 3 months
Slight decrease
6 months very significant reduction
12 months
No lithiasis
3 months
Dissolution residual stone in the lower calix
2 months
No evidence of stone
sUA
Previous bariatric surgery
Breast cancer mastectomy + chemotherapy + adjuvant hormone therapy
sUA normal urUA 752 mg/day
Diabetes Obesity
High purine diet
Mild hyperuricosuria sUA 8 5
Ur pH 5 2
Low ur citrate
Celia Abad Rodriguez-Hesles, Hassan Alkhatatbeh, M Belén Alonso Bartolomé, et al
Figure 4. Complete chemolysis of a 6 cm right renal staghorn stone.
Table 3.
Blanca Gómez-Jordana Mañas 2021 Silvia Juste A varez 2024
Rafael Maria Mas Lucas 2024
Cristina
Hassan Akhenaten 2024
E ena Mª Casas Martínez 2024
Breaking the cycle: Successful oral treatment of recurrent uric acid stones after early post-surgical relapse (Silvia Juste Alvarez - 5th Ed 2024)
We present a case report of an early uric acid nephrolithiasis recurrence after surgery which was successfully dissolved by oral alkalinization We collect clinical data, laboratory studies, imaging studies (mostly CT scan) and analysis of the stone composition after surgery Two treatments were administered sequentially during the patient's management: percutaneous nephrolithotomy was first performed, then, after an early recurrence, oral chemolysis was performed Percutaneous nephrolithotomy was first performed due to high stone burden and obstructive uropathy
Stone composition analysis revealed uric acid as its main component The patient suffered from early recurrence (6 months later) Oral chemolysis was decided and lithiasis was completely dissolved after alkalinization of urine with Lit-Control® pH Up for 3 months The patient remains asymptomatic (Figure 6)
The power of dietary supplements and urinary pH regulation in the treatment of kidney lithiasis (Rafael Maria Mas Lucas - 5th Ed 2024)
To evaluate the effectiveness of treatment with Lit-Control® pH Up in reducing uric acid kidney stones and normalizing urinary pH in a patient with left renal colic A patient with uric acid kidney stones was diagnosed through abdominal CT scan and urine analysis After 6 months, a significant reduction in the size of the kidney stones was observed (from 6-7 mm to 2 mm), and urinary pH was normalized The patient remained asymptomatic during this period
Treatment with Lit-Control® pH Up was effective in reducing kidney stone size and normalizing urinary pH, with favorable results and no new episodes of renal colic The treatment was adjusted to maintain long-term control with a dose of 2 capsules per day
Complete resolution of multiple nephrolithiatic pathology using conservative management with alkalizing oral chemolysis (Cristina Calzas Montalvo - 3rd Ed 2022)
Clinical case presentation to demonstrate that uric acid lithiasis can be completely dissolved using alkalizing oral chemolysis We describe evaluation, diagnosis, treatment, and follow-up of a 67-year-old female patient with multiple renal lithiasis who was assessed in the emergency department and later through the urology outpatient consultation After urinary pH alkalization with Lit-Control® pH Up for 4 months, all the lithiasis located in the right kidney disappeared completely according to the abdominal-pelvic CT scan and the patient remains without urinary symptoms Oral chemolysis based on urine alkalization by administration of Lit-Control® pH Up allows to dissolve uric acid stones if the urinary pH is kept above 7 Urinary alkalinization can be combined with allopurinol if there is hyperuricemia and/or hyperuricosuria and with urinary drainage in case of complicated renal colic or with tamsulosin to favor spontaneous expulsion (Figure 7)
Pharmacological chemolysis of uric acid lithiasis in a patient undergoing bariatric surgery and chemotherapy (Celia Abad Rodríguez-Hesles - 4th Ed 2023)
A woman underwent bariatric surgery and was subsequently diagnosed with breast cancer undergoing mastectomy and chemotherapy + adjuvant hormone therapy The patient was referred from the oncology department with left lumbar pain and an imaging test showing 4 mm of obstructive lithiasis in the left ureteral meatus together with 15 mm of non-obstructive urolithiasis in the right renal pelvis After spontaneous expulsion of obstructive lithiasis, treatment of the right lithiasis with a composition suggestive of uric acid is proposed The patient did not wish surgical treatment It was decided to alkalinize the urine using Lit-Control® pH Up and dietary recommendations, achieving complete chemolysis The patient currently remains asymptomatic (Figure 8)
Partial
of a 15
Figure 5.
Complete dissolution of right kidney stone 17x5 mm of the pelvis and lower pole and 3 mm stone of lower calix of left kidney
Figure 6
Dissolution of residual stones after PCNL in the right pelvis (27 mm) and in the lower calix (7 and 8 mm).
Figure 7. Complete chemolysis of multiple stones of the right kidney.
Figure 8.
dissolution
mm non-obstructive stone in the right renal pelvis
9.
Dissolution of two stones of the left kidney (15 mm in the renal pelvis and 21 mm in lower calyx)
The role of urine alkalinization on using Lit-Control® pH Up in the treatment of uric acid kidney stones post failed endoscopic procedure A clinical case report (Hassan Alkhatatbeh - 5th Ed 2024)
U r i c a c i d k i d n e y s t o n e s a r e a c o m m o n f o r m o f nephrolithiasis and are primarily associated with conditions such as hyperuricosuria, acidic urine pH, and obesity The management of uric acid stones requires addressing the underlying causes, including urine alkalinization, which plays a crucial role in preventing stone formation and promoting the dissolution of existing stones This case report explores the therapeutic benefits of urine alkalinization using Lit-Control® pH Up in the treatment of a patient with recurrent uric acid kidney stones with previously failed endoscopic procedure (Figure 9)
Ureteral uric acid stones
URETERAL STONES (N = 5)
mm stone in an ureter loop with uretero-hydronephrosis
of anterograde and retrograde URS
60 yrs M
19 mm right lumbar ureter stones
+ left ureteral lithiasis of 2 mm
+ bilateral retrograde dilatation
+ lower calix microlithiasis
68 yrs M
Anuria & bilateral obstruction
91 yrs M
15 mm pelvic
obstructive stone of 15 mm
Three obstructive ureteral stones (25 mm of length)
Lit-Control® pH Up prevents morbidity and mortality in Mini-PCNL treatment of large obstructive uric acid stones (Elena Mª Casas Martínez - 5th Ed 2024)
The objective of this clinical case is to evaluate the effectiveness of Lit-Control® pH Up in the treatment of large uric acid stones, thus avoiding the surgical risks and complications of more invasive procedures We present the case of a 59-yearold woman who, during an incidental imaging test, was found to have a large impacted stone in her right renal pelvis, causing secondary hydronephrosis After an unsuccessful attempt at Mini-PCNL due to the presence of purulent urine and the visualization of a radiolucent stone on fluoroscopy, the patient was treated with Lit-Control® pH Up until the next surgical intervention was scheduled During follow-up, a reduction in stone size was observed, eventually leading to its complete disappearance Therefore, LitControl® pH Up could be considered an effective alternative therapy for the treatment of large stones, instead of more invasive interventions (Figure 10) (Table 3)
Ureteral stones (Table 4)
Clinical case presentation: pharmacological management of uric acid urolithiasis (Miguel Gómez Garberí - 1st Ed 2020)
The prevalence of uric acid stones represents 10% of all
Dissolution of a stone of the right pelvis after failed mini-PCNL
Lit-Control® pH Up
Allopurinol
DJ stenting Nephrostomy
oral treatment Lit-Control® pH Up 1 x 2 local chemolysis with 1/6 molar sodium bicarbonate through the nephrostomy Lit-Control® pH Up x 2 + DJ stent
Canoxidin x 3 and Lit-Control® pH Up 2 x 2 Initially DJ stent (R) PCN (L) Then Bilateral PCN Lit-Control® pH Up (2 x 2 day) and sodium bicarbonate 500 mg per day Allopurinol 100 mg Low purine diet Fluid intake
Outcome 4 months
complete dissolution of the ureteral stone and partial of the stone in the lower calix) 1 month disappearance of the lithiasis
3 months complete chemolysis
Stone reduction
At 4 months right RIRS
At 5 months left RIRS 3 months
complete dissolution of all the stones
Celia Abad Rodriguez-Hesles, Hassan Alkhatatbeh, M Belén Alonso Bartolomé, et al
Table 4
Author Miguel Gómez Garberí 2020
María Negueroles-García 2021
Daniel Carrasco Gómez 2024
Letic a Ruibal Gago 2024
Carmen Arai Valladores Ferreiro 2024
Figure
Figure 10.
urolithiasis and its pharmacological management has an established role in both treatment and prevention The objective of this case presentation was to show the pharmacological management of uric acid stones We presented a case of a 67-year-old male patient with a personal history of uric stones who attended outpatient consultation presenting kidney function deterioration and a grade III ureterohydronephrosis affecting the left kidney caused by a 15 mm obstructive stone in the proximal ureter and a 22mm non-obstructive stone in the lower calyx It was decided to place a double-J stent and to prescribe pharmacological treatment with Lit-Control® pH Up and allopurinol The complete dissolution of the intraureteral stone and a reduction of the intracalyceal stone were achieved Pharmacological treatment can facilitate and even avoid surgical interventions in patients with uric stones
Oral and local chemolysis via nephrostomy for treatment of radiolucent stones (María Negueroles-García - 2nd Ed 2021)
A clinical case about the use of oral and local chemolysis by nephrostomy catheter for the treatment of radiolucent stones is reported The case of a 90-year-old multi-pathol o g i c a l m a l e , w h o re q u i re d n e p h ro s t o m y d u e t o pyelonephritis secondary to radiolucent stones in the proximal ureter, is described After resolution of the infectious condition, surgery was attempted by anterograde and retrograde ureterorenoscopy without success because the kidney stone was found in a ureteral loop It was decided to perform an oral treatment with Lit-Control® pH Up and local chemolysis with 1/6 molar sodium bicarbonate through the nephrostomy, which led to the disappearance of the lithiasis We considered alkalizing oral chemolysis together with local nephrostomy, a useful treatment option in patients with radiolucent calculi (Figure 11)
11.
Disappearance of proximal right ureteral stone after oral treatment with Lit-Control ® pH Up and local chemolysis with 1/6 molar sodium bicarbonate through the nephrostomy
Use of Lit-Control® pH Up as alkalinizing agent for the treatment of large ureteral uric acid lithiasis
(Carrasco-Gomez Daniel - 5th Ed 2024)
To evaluate the use of medical treatment with Lit-Control® pH Up as a useful non-invasive alkalinizing supplement for urolithiasis We presented the case of a 60-year-old male who came to the emergency department with typical colic caused by a 19 mm left ureteral lithiasis, producing mild ureteropelvic ectasia After diversion of the urinary tract, CT scan control performed 3 months later
just after medical expulsive treatment and Lit-Control® pH Up use successfully lead to resolution of that lithiasis After 3 months of urinar y alkalinization using LitControl® pH Up (potassium citrate, magnesium citrate and theobromine), the patient achieved complete chemolysis with a pH around 6 We should consider alkalinizing pharmacotherapy as the first treatment option in patients with uric acid lithiasis (Figure 12)
Figure 12
Dissolution of right ureteral stone after DJ stenting
Lit-Control® pH Up as a treatment for uric acid lithiasis (Leticia Ruibal Gago - 5th Ed 2024)
This is the case of a 68-year-old man with multiple comorbidities (type 2 diabetes, epilepsy, frontotemporal dementia) He was admitted for anuria and obstructive renal failure caused by bilateral reno-ureteral stones Initially, a right double-J stent and a left nephrostomy were placed for urinary diversion A month later, he was readmitted due to acute renal failure and catheter obstruction, requiring replacement and the addition of a right nephrostomy Given the urinary pH of 5 and recurrent catheter obstruction, treatment with Canoxidin® and Lit-Control® pH Up was initiated, raising the urinary pH to 6 A scheduled retrograde intrarenal surgery on the right side was performed Following medical treatment, a reduction in left side stones was observed Finally, retrograde intrarenal surgery on the left side was scheduled, achieving complete stone clearance The patient remains on preventive treatment with Lit-Control® pH Up, with no evidence of stone recurrence (Figure 13)
13.
Reduction of size of bilateral reno-ureteral stones before RIRS
Chemolysis in elderly and renal failure patient (Carmen Arai Valladores Ferreiro - 5th Ed 2024)
We presented the case of 91 years old patient with personal story of frequents renal colic pain and spontaneous expulsion of lithiasis, diagnosed with multiple ureteral and renal obstructive stones compatible with uric acid composition The patient also suffered chronic kidney failure, with creatinine clearance of 33 ml per min and potassium level of 5 3 mEq/L We proposed chemolysis
Figure
Figure
with Lit-Control® pH Up (2 tablets twice a day) and sodium bicarbonate 500 mg per day, with complete dissolution of all the stones in 3 months (Table 4)
Urinary alkalinization in other pathological conditions (Table 5)
Pharmacological chemolysis of uric acid lithiasis in a patient with Crohn's disease (Rosa Maria Gras Martínez - 3rd Ed 2022)
A male patient with Crohn's disease and an ileostomy carrier, was diagnosed with uric acid lithiasis after visiting the emergency room during an episode of left renal colic After urinary alkalization using Lit-Control® pH Up and dietary recommendations, the patient achieved a complete chemolysis, maintaining the stability of his underlying condition, without showing side effects throughout the treatment After the stone dissolution, the patient remains asymptomatic and under follow-up through outpatient visits This case has been presented elsewhere as a self-standing case report after participating in the 3rd Edition of Clinical Case Contest (14)
OTHERS (N = 6)
Author Rosa Maria Gras Martínez 2022
Hector Ricardo Ayllón 2022
Sara Esturo 2023
Isabel Montuenga 2023
Patient & Stone
54 M
Crohn disease and ileostomy
11 mm left PUJ stone
54 M partial nephrectomy left pelvic 16 mm stone
64 yrs M
Recurrent endoscopies for stone treatment resulting in critical ureteral stenosis
68 yrs M
Single left kidney (crossed and fused renal ectopia)
high volume renal lithiasis upper and middle calyces + pyelocaliceal dilatation
Marta Casadevall 2024
Pedro Hernández-Peñalver 2024
70 yrs M with detrusor overactivity
77 yrs M
recurrent intermediate risk non-muscle invasive bladder cancer (NMIBC)
64 yrs M
multiple Ta Low Grade tumours
Lit-Control® pH Up in the medical management of uric acid lithiasis (Hector Ricardo Ayllón - 3rd Ed 2022)
Clinical case report of a 54-year-old male, who is diagnosed with a single 16 mm kidney stone as an incidental finding in a control CT scan due to a previous left radical nephrectomy The low Hounsfield units, urinary pH and the nonvisibility of the lithiasis in simple X-ray suggested that it was a uric acid stone After the patient’s consent, chemolyt-
ic treatment of lithiasis using potassium citrate was planned The patient showed partial improvement using the treatment but referred GI discomfort, so the medication was changed to Lit-Control® pH Up and allopurinol + colchicine, since the patient also presented hyperuricemia in control tests Once the treatment is changed the patient showed a complete resolution of the lithiasis (Figure 14)
Figure 14.
Dissolution of left kidney stone after partial nephrectomy.
Celia Abad Rodriguez-Hesles, Hassan Alkhatatbeh, M Belén Alonso Bartolomé, et al
Table 5.
Urinary alkalinization in other pathological conditions
ization by Lit-Control® pH Up and dietary recommendations The underlying pathology of the patient was stabilized with no adverse effects, good tolerance and adherence to treatment (Figure 15)
Figure 15.
Patency of a self-expanding ureteral stent was maintained with urinary alkalinization (Lit-Control® pH Up).
Chemolysis of uric acid lithiasis in a patient with crossed renal ectopia (Isabel Montuenga - 4th Ed 2023)
A case is presented of a male patient with crossed and fused renal ectopia, who following an episode of abdominal pain, was diagnosed with high volume renal lithiasis disease associated with pyelocaliceal dilatation Given the characteristics of the patient and the lithiasis, urinary alkalinization by using Lit-Control® pH Up and dietary recommendations was decided The patient presented a clear decrease in the lithiasis load and pyelocaliceal dilatation, with no side effects Currently, he remains with the same treatment and is being followed up in outpatient clinics (Figure 16)
Figure 16.
Almost complete dissolution of a high volume renal stone in crossed fused renal ectopia
Urinary alkalinization for the management of overactive bladder (Marta Casadevall - 5th Ed 2024)
Overactive bladder has a global prevalence of 10 8-35 6% and a negative impact on patient’s quality of life There is limited evidence in the literature regarding the effects that a variation in urinary pH may have on symptoms associated with overactive bladder The aim of our study was to evaluate the clinical changes related to bladder overactivity following a treatment for urinary alkalinization We present the case of a 70-year-old male with detrusor overactivity and acidic urinary pH (pH 6), who underwent urinary alkalinization treatment with Lit-Control® pH Up, monitored by an electronic device Upon completing the treatment, clinical improvement was observed, primarily
in the patient’s urinary frequency, significantly enhancing his quality of life
Urine alkalinization and measurement in patients undergoing Mitomycin instillations for intermediate risk non-muscle invasive bladder cancer (Pedro Hernández - Peñalver-5th Ed 2024)
To explore the urine alkalinization and its measurement in patients with intermediate risk NMIBC undergoing instillations with mitomycin Two patients were given Lit-Control® pH Up 1-2 times a day with a target pH ≥ 6 during the weeks prior to the instillations Every day, they measured their urine pH with lab sticks, recording the measurements and one patient used the digital Lit-Control® pH Meter Lit-Control® pH Up is a safe and tolerated option for improving the urine alkalinization, which aims to reduce recurrence rates in patients undergoing mitomycin instillations The digital pH Meter could give more information to the patient to guide the urine alkalinization (Table 5)
CONCLUSIONS
This case series confirms the effectiveness of alkalizing therapy with citrates (Lit-Control® pH Up) for the dissolution of uric acid stones at any site and of any size The time required for dissolution varied between 3 and 12 months Side effects were mild and infrequent High-dose citrates can cause gastro-intestinal disorders and sodium salts can aggravate urinary hypertension The addition of theobromine may allow the dose of citrates to be reduced, increasing the efficacy and tolerability of the drug
REFERENCES
1 Corder CJ, Rathi BM, Sharif S, et al 24-Hour Urinalysis [Updated 2024 Oct 6] In: StatPearls [Internet] Treasure Island (FL): StatPearls Publishing; 2025 Jan- Available from: https://www ncbi nlm nih gov/ sites/books/NBK482482/
DECLARATIONS
Ethical approval: Ethics Committee (EC) was not required for a retrospective review of cases Patient consent was obtained by the institution of each Author
Availability of data and material: All inquiries can be directed to the corresponding author
Competing interests: B I is an employee of Devicare The remaining authors have no conflicts of interest to declare
Funding: Devicare provided for the APC
Authors' contributions: Conceptualization, B I and A T ; methodology, A T ; software, N/A ; validation, B I ; formal analysis, A T ; investigation, A T ; resources, N/A ; data curation, A T ; writing C A R-H , H A , M B A B , C A V F , H R A B , L B , C C M , N C G , D C G, M C R , E M C M , S E S , L G M , B GJ M , R M G M , P H-P , S J A , A L S , R M M L , I M S , I M F , B M de H , M N-G , L R G ; writing-review and editing, A T ; visualization, A T ; supervision, B I ; project administration, N/A; funding acquisition, N/A All authors have read and agreed to the published version of the manuscript”
Acknowledgments: N/A
2 Kamphuis GM, Wouter van Hattum J, de Bie P, Somani BK Method of alkalization and monitoring of urinary pH for prevention of recurrent uric acid urolithiasis: a systematic review Transl Androl Urol 2019; 8(Suppl 4):S448-S456
3 Trinchieri A, Esposito N, Castelnuovo C Dissolution of radiolucent renal stones by oral alkalinization with potassium citrate/potassium bicarbonate Arch Ital Urol Androl 2009; 81:188-91
4 Sanz-Gómez I, Angerri O, Baboudjian M, et al Role, Cost, and Availably of Urinary pH Monitoring for Kidney Stone Disease-A Systematic Review of the Literature Curr Urol Rep 2023; 24:381-388
5 Grases F, Rodriguez A, Berga F, et al A new device for simple and a c c u
H
Springerplus 2014; 3:209
6 Hernandez Y, Costa-Bauza A, Calvó P, et al Comparison of Two Dietary Supplements for Treatment of Uric Acid Renal Lithiasis: Citrate vs Citrate + Theobromine Nutrients 2020; 12:2012
7 Trinchieri A Theobromine for treatment of uric acid stones and other diseases Arch Ital Urol Androl 2024; 96:13277
8 O'Kane DB, Dave SK, Gore N, et al Urinary alkalisation for symptomatic uncomplicated urinary tract infection in women Cochrane Database Syst Rev 2016; 4:CD010745
Correspondence
Celia Abad Rodriguez-Hesles celiaabadrh@gmail com
Ana Morales Martínez anamorales891@hotmail com Hospital Universitario Clínico San Cecilio, Grenada, Spain
Hassan Alkhatatbeh dr23hak@yahoo com
Department of General Surgery, Urology and Anaesthesia, The Hashemite University, Zarqa, Jordan
María Belén Alonso Bartolomé mery ab95@hotmail com Hector Ricardo Ayllón Blanco hector ayllonb@gmail com Hospital Universitario La Paz, Madrid, Spain
Carmen Arai Valladares Ferreiro Spainarailo79@hotmail com Hospital de Valme, Endourology and Urolithiasis Section, Sevilla
Cristina Calzas Montalvo cristinacm179@gmail com
Silvia Juste Alvarez sjustealvarez@gmail com Hospital Universitario 12 de Octubre, Madrid, Spain
Daniel Carrasco Gómez
Hospital Regional Universitario de Málaga, Malaga, Spain diabliyocarrasco@gmail com
Marta Casadevall Rubau casadevallm28@gmail com
Pedro Hernandez-Peñalver pedrohp964@gmail com Fundacio Puigvert, Barcelona, Spain
Elena Maria Casas Martinez elena casasmrtz@gmail com Hospital Universitario Rey Juan Carlos, Madrid, Spain
Sara Esturo Sacristan saraesturosacristan@gmail com Hospital Universitario Galdakao-Usansolo, Galdakao, Spain
9 Ueda T, Yoshida T, Tanoue H, et al Urine alkalization improves the problems of pain and sleep in hypersensitive bladder syndrome Int J Urol 2014; 21:512-7
11 Au JL, Badalament RA, Wientjes MG, et al ; International Mitomycin C Consortium Methods to improve efficacy of intravesical mitomycin C: results of a randomized phase III trial J Natl Cancer Inst 2001; 93:597-604
12 Morales Martínez A, Melgarejo Segura MT, Cano García MC Manejo médico de los cálculos renales de ácido úrico, a próposito de un caso [Medical management of uric acid renal stones, case description ] Arch Esp Urol 2021; 74:442-445
13 Nakdali Kassab B, Budia Alba A Medical treatment of coralliform uric acid lithiasis with Lit-Control® pH Up Kenya Journal of Urology 2024; 2:18-20
14 Gras Martínez RM, Diranzo García M, Álvarez Barrera A, et al Pharmacological Chemolysis of Uric Acid Lithiasis in A Patient with Crohn's Disease Arch Esp Urol 2023; 76:823-828
Miguel Gómez Garberí miguelggarberi@gmail com
Baraa Nakdali Kassab baranakdali@hotmail com
Laura Sánchez laurasanchezc10@gmail com Department of Urology, Hospital Universitario San Juan de Alicante, Alicante, Spain
Blanca Gómez-Jordana Mañas blanca gomezj@quironsalud es, blanca gomezj@fjd es Hospital Universitario Fundación Jiménez Díaz, Madrid
Rosa Maria Gras Martinez rosagrasma@gmail com
Hospital General Universitario de Valencia, Valencia, Spain
Alberto López Sierra albertoyedok@gmail com
Hospital Nuestra Señora de Sonsoles, Avila, Spain
Rafael Maria Mas Lucas rafamaslucas@hotmail com General Hospital of Segovia, Segovia, Spain
Isabel Mohedano Sánchez isabel-ms5@hotmail com
Hospital Juan Ramón Jiménez, Huelva, Spain
Isabel Montuenga Fernandez isabel montuenga@gmail com Hospital Universitario Príncipe de Asturias, Alcala de Henares (Madrid), Spain
Maria Negueroles-Garcia
maria negueroles@gmail com
Hospital Clínico Universitario de Valencia, Valencia, Spain
Leticia Ruibal Gago
leticia ruibal gago@sergas es Complexo Hospitalario Universitario de Pontevedra, Pontevedra, Spain
Bernat Isern bernat isern@uib cat Laboratori d’Investigació en Litiasi Renal, Universitat de les Illes Balears, Spain
Alberto Trinchieri (Corresponding Author) alberto trinchieri@gmail com CDC Ambrosiana, Milan, Italy
Archivio Italiano di Urologia e Andrologia 2025; 97(1):13824
Celia Abad Rodriguez-Hesles, Hassan Alkhatatbeh, M Belén Alonso Bartolomé, et al
ORIGINAL PAPER
Discovering a new nutraceutical based on pollen extract and teupolioside: A prospective monocentric study evaluating its role in alleviating lower urinary tract symptoms in benign prostatic hyperplasia patients
1 Unit of Oncologic Minimally Invasive Urology and Andrology, University of Florence, Careggi Hospital, Florence, Italy;
2 Department of Experimental and Clinical Medicine, University of Florence, Florence, Italy
* These authors contributed equally to this work
Summary
Background: Benign prostatic hyperplasia (BPH) is a common condition in men over 50, leading to lower urinary tract symptoms (LUTS). A nutraceutical containing pollen extract (Graminex® G96®) and teupolioside has shown potential in alleviating LUTS by targeting inflammation and dihydrotestosterone production This prospective, monocentric study enrolled 60 patients with mild to moderate LUTS due to BPH
Methods: Participants received one tablet daily for three months Assessments included the International Prostate Symptom Score (IPSS), quality of life (QoL), uroflowmetry, postvoid residual (PVR), and sexual function (IIEF-5, MSHQ EjD)
Results: Fifty-three patients completed follow-up. Significant improvements were observed in IPSS and QoL (p < 0 001), with scores decreasing from 14 (11-16) at baseline to 10 (8-12) at three months and decreasing from 3 (2-3) to 2 (2-2), respectively. Uroflowmetry parameters (Qmax and PVR) improved, increasing from 12 (11-16) ml/s to15 (11-17) ml/s and decreasing from 50 (30-55) ml to 35 (25-45) ml, respectively, without statistical significance (p > 0 05) Sexual function and PSA levels remained stable, with no significant adverse effects reported
Conclusion: The combination of pollen extract and teupolioside effectively alleviates LUTS in BPH patients with a favorable safety profile, particularly in avoiding sexual dysfunction
Submitted 21 Nvember 2024; Accepted 12 December 2024
INTRODUCTION
Benign prostatic hyperplasia (BPH) is a prevalent condition among men over 50 years old, often leading to lower urinary tract symptoms (LUTS) (1) Chronic inflammation is pivotal in the pathogenesis and progression of BPH, where immune cells in the prostate release pro-inflammatory cytokines and free radicals, exacerbating the inflammatory process (2)
α1-blockers and 5α-reductase inhibitors are established therapies, yet their impact on erectile and ejaculatory function can be bothersome (3, 4) Consequently, there is a growing interest in nutraceutical agents for managing BPH Within this context, Xipag® (IDI Integratori Dietetici Italiani S r l , Aci Bonaccorsi, CT, Italy), formulated with pollen extract (Graminex® G96®; 500 mg) and teupolioside (Teupol 25P; 60 mg), has emerged as a promising BPH treatment, supported by research into its key components (5)
Graminex®, derived from Secale cereale, has demonstrated anti-inflammatory, anti-edema, and antioxidant effects in ex vivo studies on rat prostate specimens, owing to its complex composition rich in amino acids, enzymes, minerals, and bioactive compounds (6) Pollen extracts have been researched for their efficacy in managing prostatitis and pelvic pain, with animal models showing effectiveness in reducing stromal proliferation and glandular inflammation (7, 8) Furthermore, clinical trials have highlighted significant improvements in chronic pelvic pain and LUTS with pollen extract, often surpassing the efficacy of tadalafil (9)
Teupolioside, derived from Ajuga reptans cell cultures, has shown promise in preliminary in vitro studies by reducing dihydrotestosterone (DHT) production through NADPH oxidation and exhibiting notable anti-inflammatory properties (5)
This combined approach offers a novel therapeutic strategy for alleviating LUTS in BPH patients, targeting both inflammation and DHT production This study aims to assess the efficacy of Xipag® in managing LUTS among BPH patients
MATERIALS AND METHODS
Study design and protocol
This single-center observational study was conducted from March to September 2024
This study was awarded at the 97th SIU Congress in Bari on October 11th-13th, 2024
Mattia Lo Re 1, 2* , Marta Pezzoli 1, 2* , Anna Cadenar 1, 2 , Elettra Fuligni 1, 2 , Leonardo Gajo 1, 2 , Andrea Minervini 1 , Andrea Cocci 1, 2
Patients presenting mild or moderate LUTS related to BPH were enrolled after signing a written informed consent
All enrolled patients completed three baseline (T0) questionnaires: the International Prostatic Symptoms ScoreQ u a l i t y o f L i f e ( I P S S - Q o L ) , t h e M a l e S e x u a l H e a l t h
Questionnaire Ejaculatory Dysfunction (MSHQ EjD - Short Form), and the International Index of Erectile Function-5 (IIEF-5) Additionally, patients underwent a blood examination to evaluate prostate-specific antigen (PSA) levels and performed uroflowmetry with post-void residual (PVR) evaluation
Patients who consented to participate in the study received one tablet per day of Xipag® for three months Clinical evaluations, using the same four baseline questionnaires, PSA dosage, and uroflowmetry with PVR assessment, were conducted at one month (T1) and three months (T2) after the start of the treatment At T2, patients were also asked about their willingness to continue the use of Xipag®
The study was conducted in line with Good Clinical Practice guidelines and with the ethical principles of the Declaration of Helsinki Before the beginning of the study, all participants signed the written informed consent No placebo run-in period was performed
Inclusion and exclusion criteria
Inclusion criteria were age over 40 years, diagnosis of LUTS related to BPH, mild to moderate LUTS (IPSS score 819), sexually active patients (IIEF-5 score ≥ 17) and any prostate volume
Exclusion criteria included clinical suspicion of prostatic cancer (based on rectal examination or suspicious elevation of PSA levels) or bladder cancer, neurological bladder, urethral stricture, bacterial prostatitis or recurrent urinary tract infections, previous pelvic radiation therapy, use of alpha-blockers, 5-alphareductase inhibitors, or phosphodiesterase-5 inhibitors (PDE5i), and allergies to components of Xipag®
Outcomes
The primary objective was to evaluate the efficacy of Xipag® in improving urinary symptoms and function, as measured by IPSS, maximum urinary flow rate (Qmax), and PVR
The secondary objective was to assess changes in sexual function, using IIEF-5 and MSHQ-EjD scores, and analyze any changes in PSA levels
Statistical analysis
Values for quantitative variables are expressed as median and interquartile range (IQR)
Comparisons between pairs of values (baseline - each time point) were per-
formed using a Wilcoxon signed rank test, with a p-value < 0 05 deemed to be statistically significant All statistical a n a l y s e s w e r e c o n d u c t e d u s i n g S P S S 2 1 0 ( I B M Corporation, Armonk, NY, USA)
RESULTS
A total of 60 patients were consecutively enrolled in this study Of these, 6 were lost to follow-up and 1 was excluded due to starting alpha-blocking therapy on his family doctor's advice Consequently, 53 patients completed both the 1 and 3-month follow-ups The age of participants was 55 (45-64) years, with a body mass index (BMI) of 24 5 (23 2-26 3) Significant improvements in urinary symptoms were observed at both time points (p < 0 001) (Table 1) IPSS score decreased from 14 (11-16) at baseline to 11 (9-13) at 1 month and 10 (8-12) at 3 months IPSS Q u a l i t y o f L i f e (QoL) parameter also improved, decreasing from 3 (2-3) at T0 to 2 (2-2) at T1 and 2 (2-2) at T2 Uroflowmetry parameters improved, even without a statistical significance (p < 0 05): Qmax increased from 12 (11-16) ml/s at T0 to 14 (11-16) ml/s at T1 and 15 (11-17) ml/s at T2 meanwhile PVR decreased from 50 (30-55) ml at T0 to 35 (25-40) ml at T1 and 35 (25-45) ml at T2 (Figure 1)
Table 1
Functional outcomes at different timepoints
IQR: nterquarti e range; Qmax: max mum f ow rate; PVR: post-void res dua ; IPSS: Internat onal Prostat c Symptoms Score; QoL: Qua ity of L fe; MSHQ: men sexual health questionna re
Figure 1.
Graphical representation of functional outcomes over different time points
Qmax: maximum flow rate; PVR: post-void residual; IPSS: International Prostatic Symptoms Score; QoL: Quality of Life
M Lo Re, M Pezzoli, A Cadenar, et
Regarding sexual function, there was a slight increase in both IIEF5 and MSHQ EjD scores, though these changes were not statistically significant (p > 0 05) PSA levels remained stable at T1 and showed a slight decrease at T2, but no statistically significant changes were detected (p > 0 05)
After 3 months of treatment, 44 patients (83 2%) expressed their willingness to continue Three patients (5 7%) reported no significant improvement in LUTS and expressed the desire to switch to another therapy Six patients (11 3%) with initially mild LUTS experienced intolerance to daily therapy, leading them to want to discontinue the treatment, with the possibility of reevaluation if symptoms worsened
Overall, no ADRs were recorded After three weeks of using Xipag®, one patient developed a mild skin rash, which was resolved spontaneously The patient continued the treatment, and no similar events occurred, suggesting that the rash was not likely an ADR related to the nutraceutical
DISCUSSION
In this study, we evaluated the efficacy and safety of a novel nutraceutical, Xipag®, which contains Teupolioside (Teupol 60 mg) and Pollen Extract (Graminex® G96® 500 mg), for the treatment of LUTS associated with BPH
As previously documented in the literature, the effectiveness of Teupolioside in addressing prostatic hypertrophy and that of Pollen Extract in alleviating symptoms such as chronic pelvic pain and irritation are well established (10), making this product particularly promising for managing moderate LUTS
Our findings offer several insights into the potential utility of this product
First, only three patients (5 7%) reported no significant improvement in LUTS and expressed a desire to switch to alternative therapies Conversely, all other participants experienced a significant improvement in symptoms as measured by the International Prostate Symptom Score (IPSS), alongside a non-significant improvement in urinary flow rate (Qmax) Our study corroborates the findings of Muraca et al , who first demonstrated the potential benefits of Xipag® in a pilot study (11), noting an IPSS improvement from a mean baseline score of 13 3 ± 6 1 to a 3-month decrease of 22 7-88 9% (mean 55 2 ± 23 6%)
This consistency with prior research bolsters the credibility of our results and suggests that Xipag® may represent an effective therapeutic option for patients with BPH
Secondly, while nutraceuticals have garnered attention in the management of BPH, their efficacy remains a subject of debate A recent systematic review by Franco et al (12) did not find significant evidence supporting the efficacy of nutraceuticals in various trials However, another systematic review by Novara et al (13) reported significant efficacy on outcomes such as IPSS, IPSS QoL, and Qmax in patients treated with Permixon, which also exhibited a favorable safety profile In this context, our study demonstrates that a phytotherapeutic agent like Xipag® can achieve symptom improvements in selected patients, comparable to those observed in studies of nutraceuticals like Serenoa repens
Thirdly, although the symptom relief observed with Xipag® was less pronounced than that reported in studies of alphablockers, our study is noteworthy for the absence of adverse effects on sexual function, as we do not detect a significant change in the IIEF and MSHQ ED questionnaire
This is a considerable advantage, as conventional alphablocker treatments are often associated with side effects, such as ejaculatory dysfunction, which can lead to therapy discontinuation (14, 15) The tolerability of Xipag® thus positions it as an attractive option for patients seeking symptom relief – particularly those with mild symptoms –without the risk of side effects
Nonetheless, our study is not devoid of limitations One notable limitation is the relatively short follow-up period of three months While significant improvements were observed within this timeframe, longer follow-up is necessary to assess the sustainability of Xipag®'s effects
Additionally, the observational nature of our study introduces potential biases, as it lacks the rigor of a randomized controlled trial (RCT) Future research should aim to utilize RCT methodologies to further validate the efficacy of Xipag® and compare its performance against placebo and established BPH treatments in a controlled environment
CONCLUSIONS
In conclusion, this study represents the largest cohort to date evaluating the effects of Xipag® on BPH-related symptoms, with 53 patients completing the study The size of our cohort enables a more robust analysis and provides valuable data to the limited existing literature on Xipag® and contributes to the growing body of evidence supporting the use of nutraceuticals in managing BPHrelated symptoms, particularly in cases where conventional therapies may lead to undesirable side effects
DECLARATIONS
Ethical approval: The procedures used in this study adhere to the tenets of the Declaration of Helsinki The patients/participants provided their written informed consent to participate in this study
Availability of data and material: All inquiries can be directed to the corresponding author
Competing interests: The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript
Funding: The authors report no involvement in the research by the sponsor that could have influenced the outcome of this work
Authors' contributions: MLR and MP have given substantial contributions to the conception and the design of the manuscript AC, LG AND EF to the acquisition of the data; MLR to the analysis and interpretation of the data MLR, and MP have participated to drafting the manuscript, AM and AC revised it critically All authors read and approved the final version of the manuscript
Acknowledgments: Not applicable
REFERENCES
1 Kevin T McVary MF BPH: Epidemiology and Comorbidities 2006; 12 Accessed August 26, 2024 https://www ajmc com/view/ apr06-2288ps122-s128
2 Nickel JC, Roehrborn CG, O’Leary MP, et al The relationship between prostate inflammation and lower urinary tract symptoms: examination of baseline data from the REDUCE trial Eur Urol 2008; 54:1379-1384
3 Zhou Z, Cui Y, Wu J, et al Meta-analysis of the efficacy and safety of combination of tamsulosin plus dutasteride compared with tamsulosin monotherapy in treating benign prostatic hyperplasia BMC Urol 2019; 19:17
4 Liguori G, Trombetta C, De Giorgi G, et al Efficacy and safety of combined oral therapy with tadalafil and alfuzosin: an integrated approach to the management of patients with lower urinary tract symptoms and erectile dysfunction Preliminary report J Sex Med 2009; 6:544-552
5 Korkina LG, Mikhal’chik EV, Suprun MV, et al Molecular mechanisms underlying wound healing and anti-inflammatory properties of naturally occurring biotechnologically produced phenylpropanoid glycosides Cellular and Molecular Biology TM 2007; 53:84-91
6 Locatelli M, Macchione N, Ferrante C, et al Graminex Pollen: Phenolic Pattern, Colorimetric Analysis and Protective Effects in Immortalized Prostate Cells (PC3) and Rat Prostate Challenged with LPS Molecules 2018; 23:1145
7 Cai T, Gallelli L, Cione E, et al The efficacy and tolerability of pollen extract in combination with hyaluronic acid and vitamins in the management of patients affected by chronic prostatitis/chronic pelvic pain syndrome: a 26 weeks, randomized, controlled, singleblinded, phase III study Minerva Urol Nephrol 2022; 74:780-788
8 Habib FK, Ross M, Lewenstein A, et al Identification of a prostate inhibitory substance in a pollen extract Prostate 1995; 26:133-139
9 Matsukawa Y, Naito Y, Funahashi Y, et al Comparison of cernitin pollen extract vs tadalafil therapy for refractory chronic prostatitis/chronic pelvic pain syndrome: A randomized, prospective study Neurourol Urodyn 2020; 39:1994-2002
10 Cai T, Verze P, La Rocca R, et al The role of flower pollen extract in managing patients affected by chronic prostatitis/chronic pelvic pain syndrome: a comprehensive analysis of all published clinical trials BMC Urol 2017; 17:32
11 Muraca L, Scuteri A, Burdino E, et al Effectiveness and Safety of a New Nutrient Fixed Combination Containing Pollen Extract Plus Teupolioside, in the Management of LUTS in Patients with Benign Prostatic Hypertrophy: A Pilot Study Life (Basel) 2022; 12:965
12 Franco JVA, Trivisonno L, Sgarbossa NJ, et al Serenoa repens for the treatment of lower urinary tract symptoms due to benign prostatic enlargement Cochrane Database Syst Rev 2023; 6:CD001423
13 Novara G, Giannarini G, Alcaraz A, et al Efficacy and Safety of Hexanic Lipidosterolic Extract of Serenoa repens (Permixon) in the Treatment of Lower Urinary Tract Symptoms Due to Benign Prostatic Hyperplasia: Systematic Review and Meta-analysis of Randomized Controlled Trials Eur Urol Focus 2016; 2:553-561
14 Cindolo L, Pirozzi L, Fanizza C, et al Drug Adherence and Clinical Outcomes for Patients Under Pharmacological Therapy for Lower Urinary Tract Symptoms Related to Benign Prostatic Hyperplasia: Population-based Cohort Study Eur Urol 2015; 68:418-425
15 Bapir R, Bhatti KH, Eliwa A, et al Effect of alpha-adrenoceptor antagonists on sexual function A systematic review and meta-analysis Arch Ital Urol Androl 2022; 94:252-263
Correspondence
Mattia Lo Re, MD mattialore1994@gmail com
Marta Pezzoli, MD (Corresponding Author)
marta pezzoli@unifi it
University of Florence, Careggi Hospital, 50100 Florence, Italy
Anna Cadenar, MD
anna cadenar@unifi it
Elettra Fuligni, MD
elettra fuligni@unifi it
Leonardo Gajo, MD
leonardo gajo@unifi it
Andrea Minervini, MD
andrea minervini@unifi it
Andrea Cocci, MD
cocci andrea@gmail com
ORIGINAL PAPER
Ten years’ single surgeon experience of excision and primary anastomosis (EPA) urethroplasty for traumatic urethral stricture: An analysis of risk factors for urethral stricture recurrence
Paksi Satyagraha, Edi Wibowo, Besut Daryanto, Gede Wirya Diptanala Putra Duarsa, Adrianus Gupta Wijaya, Fauzan Kurniawan Dhani
Urology Department, Faculty of Medicine, Universitas Brawijaya, Saiful Anwar General Hospital, Malang, Indonesia
Summary
Introduction: Excision and Primary
Anastomosis (EPA) urethroplasty is the standard treatment for traumatic urethral strictures, but managing them remains challenging for urologists. Identifying factors leading to EPA urethroplasty failure benefits both patients and surgeons. This study aims to analyze risk factors for urethral stricture recurrence after one-year follow-up of EPA urethroplasty
Materials and methods: Data on male patients undergoing EPA urethroplasty at the Urology Department of Saiful Anwar General Hospital from January 2013 until December 2023 were prospectively recorded Successful urethroplasty, defined as the absence of additional treatment necessity, was assessed until 12 months follow-up Demographic data, time to surgery, stricture etiology, comorbidities, prior urethral interventions, and operation steps were recorded Univariate and multivariate coxregression analyses were performed using IBM SPSS Statistics version 21
Result: Total 95 patients were observed, and 89 patients were included, averaging 41 2 ± 15 59 years old EPA urethroplasty succeeded in 91% of cases over a median follow-up of 16.3 months Pelvic fracture urethral injury (PFUI) was the predominant etiology in 74% of cases, with an average stricture length of 25 4 ± 16 3 mm The average time to surgery was performed on average 6.67 ± 4.07 months after diagnosis. In univariate analysis, body mass index (BMI), time to surgery, and stricture length were associated with urethral stricture recurrence. However, only time to surgery showed a significant association in multivariate analysis.
Conclusions: Obesity, the length of the stricture, and delayed surgical intervention are associated with an increased risk of urethral stricture recurrence in patients following EPA EPA urethroplasty demonstrates a high success rate in managing traumatic urethral strictures
Submitted 18 October 2024; Accepted 1 November 2024
INTRODUCTION
Excision and Primary Anastomosis (EPA) urethroplasty is recognized as a gold standard surgical technique for the
management of traumatic urethral strictures, particularly in cases involving the bulbar urethra Traumatic urethral strictures are a significant clinical challenge, often resulting from various forms of trauma, particularly in males
The etiology of these strictures is multifaceted, with trauma being a predominant cause Various mechanisms of injury contribute to the development of urethral strictures, including pelvic fractures, straddle injuries, and direct trauma to the urethra during accidents (1)
The incidence of motorcycle road accidents leading to pelvic fractures and urethral injury in Indonesia is a significant public health issue, exacerbated by the country's high reliance on motorcycles as a primary mode of transportation (2) The prevalence of this condition varies, with estimates suggesting that it affects 229 to 627 individuals per 100,000, and can be particularly pronounced in certain demographics (3, 4) The management of these strictures has evolved, with EPA urethroplasty being favored for its high success rates and low complication profiles, particularly for strictures shorter than 2 cm (5-7)
The technique of EPA urethroplasty involves the excision of the diseased segment of the urethra followed by direct end-to-end anastomosis This method is particularly effective for short, isolated bulbar strictures, yielding success rates upwards of 90% (5, 6, 8) However, the risk of recurrence remains a significant concern in the management of urethral strictures post-trauma Factors influencing recurrence include the length of the stricture, the presence of underlying conditions, and the surgical technique employed (8-11) Identifying factors leading to EPA urethroplasty failure benefits both patients and surgeons This study aims to analyze risk factors for urethral stricture recurrence after one-year follow-up of EPA urethroplasty
METHODS
Pre operative patients assessment
We conducted a retrospective analysis of the medical records of 95 male patients diagnosed with traumatic urethral stricture who were referred from nearby hospital and all across Indonesia We reviewed demographic
details, educational status, underlying causes, comorbidities, smoking history, previous procedures, as well as the duration of the disease, interventions, and outcomes based on both inpatient and outpatient records Patients were classified as highly educated if they had completed an undergraduate degree All patients underwent EPA urethroplasty performed by a single surgeon (PS) at Saiful Anwar General Hospital in Malang, Indonesia, between January 2013 and December 2023 Patients with penile strictures, a history of hypospadias, or those requiring tissue substitution techniques were excluded from this study The duration of the disease was defined as the time elapsed from the initial diagnosis of the urethral stricture to the date of the EPA procedure Each patient had a suprapubic catheter placed to allow for urethral rest To assess the location and length of the stricture, a Bipolar Voiding Cysto-Urethrography (BVCUG) was performed
Surgical technique
All patients underwent EPA urethroplasty under general anesthesia while positioned in the lithotomy position via the perineal approach After mobilizing the bulbar urethra, the stricture location was identified intraoperatively using rigid cystoscopy, and the urethra was transected at the stricture site with sharp scissors The scar tissue at both urethral ends was then completely excised until healthy urethral mucosa was reached A wide-caliber, spatulated, tension-free anastomosis was performed using six 4-0 PGA sutures EPA urethroplasty consists of several adjunctive surgical steps to achieve a tension-free anastomosis, including bulbar mobilization, crural separation, inferior pubectomy, supracrural rerouting, and total pubectomy, particularly when the stricture is too long for a tension-free anastomosis Finally, a 14Fr silicone Foley catheter was inserted, which remained in place for four weeks postoperatively If the procedure for EPA urethroplasty consists only in bulbar mobilization, this was classified as bulbar mobilization On the contrary, if the procedure includes steps beyond bulbar mobilization, it was categorized as over bulbar mobilization
Postoperative follow-up and outcome definition
Patients were followed up at 1, 3, and 12 months after surgery, and then annually, with evaluations including uroflowmetry and residual urine volume measurements Urethrography was conducted whenever a recurrent stricture was suspected, indicated by a decrease in urinary flow rate and/or worsening symptoms Successful urethroplasty was defined as the absence of the need for further treatment Paired T-Test was used to assessed patient outcome parameters Both univariate and multivariate Cox regression analyses were conducted using IBM SPSS Statistics version 21 P values < 0 05 were considered statistically significant
RESULTS
A total of 95 patients were observed, and 89 were included in the study, with an average age of 41 2 ± 15 59 years The patients had a mean body mass index (BMI) of 23 05 kg/m² Hypertension and diabetes mellitus (DM) were present as comorbidities in 10 1% and 16 9% of the patients,
respectively The most common aetiology of urethral strictures was pelvic fracture urethral injury (PFUI), followed by straddle injury, iatrogenic causes related to transurethral surgery, and direct trauma The bulbo-membranous urethra had the highest incidence of strictures, followed by the bulbar urethra More than 35% of patients had undergone endoscopic treatment 1-2 times previously, while about 39% had never received endoscopic treatment The average time to surgery was performed on average 6 67 ± 4 07 months after diagnosis EPA urethroplasty was successful in 91% of cases, with a median follow-up of 16 3 months Eight patients reported had recurrent stricture, two patients at 3 months after the surgery and six patients at 12 months after the surgery For recurrent strictures, treatments included redo EPA urethroplasty in 3 cases, urethral dilatation in 4 cases, and redo non-transecting urethroplasty in 1 case (Table 1)
The uroflowmetry outcomes from 1 month, 3 months and 12 months after the surgery of the patient did not show any different such as Qmax, Voided Volume and post void residual volume (PVR) (Table 2, Figure 1) In univariate analysis, body mass index (BMI) (OR 4 45, 95%CI
Table 1. Patient characteristics
P Satyagraha, E Wibowo, B Daryanto, et al
1 36-28 1, p = 0 007), time to surgery (OR 3 89, 95%CI 1 63-13 24, p = 0 003), and stricture length (OR 2 14, 95%CI 1 05-1 62, p = 0 01) were associated with ure-
thral stricture recurrence However, only time to surgery (OR 2 44, 95%CI 1 06-12,93, p = 0 04) showed a significant association in multivariate analysis (Table 3)
Table 2 Uroflowmetry outcomes.
vs no
Non PFUI vs PFUI Surgical steps 1.5
Bulbar mobilization vs over bulbar mobilization
* Significant resu t BMI: Body Mass Index; CI: Conf dence Interval;
Table 3
Uni- and multivariate Cox regression analysis for risk factor recurrence rate EPA urethroplasty
Figure 1. Changes in Qmax (A), Voided volume (B), Post void residual (C) from 1, 3, and 12 months
DISCUSSION
EPA urethroplasty is widely regarded as the gold standard for treating traumatic urethral strictures, particularly those caused by pelvic fractures or direct trauma In Indonesia, motorcycle accidents often result in pelvic fractures and associated urethral injuries (2) This finding is consistent with our cohort, where PFUI accounted for 74% of the causes of traumatic urethral strictures Our cohort achieved a high success rate of 91% in EPA urethroplasty, comprising 89 patients, making it one of the largest series of patients undergoing this procedure in Southeast Asia, despite the relatively short follow-up period (median of 16 3 months) This outcome is consistent with previous studies that report success rates ranging from 85% to 95% (12) However, the definition of a successful urethroplasty remains a topic of debate, with no clear agreement on the best postoperative follow-up approach In our study, successful urethroplasty was defined as the absence of the need for further treatment, which has been widely used in most previous research (13) At our center, postoperative followup typically involves catheter removal four weeks after surgery, followed by uroflowmetry We do not routinely perform postoperative cystoscopy due to the unavailability of flexible cystoscopy, as well as concerns about cost-effectiveness and the geographical burden, which requires patients to travel to our center Despite this positive result, the potential for stricture recurrence remains a concern, with various factors influencing the risk of recurrence One of the primary risk factors identified in the literature is the length of the stricture Studies have shown that longer strictures, particularly those exceeding 2 cm, are associated with higher recurrence rates following urethroplasty (14, 15) This is likely due to the increased complexity of surgical repair and the potential for inadeq u a t e v a s c u l a r i z a t i o n o f t h e a n a s t o m o s e d s e g m e n t Furthermore, the presence of dense periurethral fibrosis, often seen in long strictures, can complicate the surgical approach and contribute to poorer outcomes (16) In our cohort, strictures longer than 2 cm were associated with a greater risk of recurrence Two patients experienced recurrence within the first 3 months, and six within 12 months after surgery This is in line with the findings of Kinnaird et al , who reported an average recurrence time of 11 7 months, with occurrences ranging from 2 weeks to 77 months (17) Similarly, Barbagli et al , observed that recurrences in their cohort of both anastomotic and substitution urethroplasty patients were evenly distributed over time, with a plateau reached only after 5 years (18) BMI has been identified as a potential risk factor influencing the recurrence of urethral strictures following EPA urethroplasty The relationship between BMI and surgical outcomes is multifaceted, as obesity can impact both the surgical procedure and the healing process (19) In our cohort, patients with BMI over 25 significantly had higher risk of recurrence the technical challenges posed by a h i g h e r B M I c a n c o m p l i c a t e t h e s u r g i c a l a p p r o a c h
Increased adipose tissue in the perineal region may hinder access to the urethra, making it more difficult to achieve a tension-free anastomosis, which is crucial for successful outcomes (20) Additionally, the presence of excess tissue may lead to increased tension at the anastomosis site, further contributing to the risk of recurrence (21)
One notable finding from this cohort is that delayed surgical intervention exceeding 6 months is a significant predictor of recurrence in patients undergoing EPA urethroplasty As we know, Indonesia is one of the largest archipelagic countries in the world, comprising numerous islands, which makes accessing adequate healthcare facilities time-consuming and costly (22) Furthermore, the limited distribution of reconstructive urologists is a major factor contributing to the prolonged time before patients r e c e i v e t r e a t m e n t T h i s c o r r e l
d e
h e importance of prompt evaluation and management of urethral strictures, as timely surgical intervention is linked to better healing conditions and outcomes (23)
Comorbidities such as DM and hypertension have been shown to influence stricture recurrence in some studies These conditions may predispose patients to recurrence due to poor microvascular circulation and impaired wound healing associated with DM and hypertension (24) However, this finding contrasts with the results of our cohort study, where DM and hypertension were not statistically significant risk factors for recurrence We believe this discrepancy may be attributed to the relatively young average age of patients undergoing EPA urethroplasty in our study, which was 41 2 years, at an age when few individuals have developed degenerative diseases
The location of the stricture is another critical factor A study by Bagchi et al identified the bulbar urethra as the most common site of stricture, which is generally associated with better outcomes compared to membranous urethral strictures, where recurrence rates tend to be higher due to the complexity of the anatomical region and the proximity to the external urinary sphincter (7) In our cohort, the bulbomembranous urethra exhibited the highest incidence of strictures; however, there was no significant difference in recurrence risk based on the location of the stricture Several studies indicate that prior urethral procedures can impact outcomes These patients tend to have a slightly higher incidence of recurrence, likely due to the cumulative trauma resulting from previous dilatations or urethrotomies (12, 18) In our cohort, over 35% of patients had undergone one or more endoscopic treatments before opting for EPA urethroplasty; however, interestingly, this finding does not align with the results of our study
Limitations of the present study include its retrospective nature, limited follow-up duration, single institution and surgeon, relatively small sample size, and subjectivity in outcome assessment While our criteria for defining recurrence were somewhat subjective and relied on patient-reported symptoms that prompted urethrography, we believe this approach is clinically valid due to the lack of consensus on how to define stricture recurrence following urethroplasty Addressing these limitations through larger, multicenter, and prospective studies will be essential for optimizing surgical techniques and improving patient outcomes
CONCLUSIONS
Obesity, the length of the stricture, and delayed surgical intervention are associated with an increased risk of urethral stricture recurrence in patients following EPA EPA
P Satyagraha, E Wibowo, B Daryanto, et al
urethroplasty demonstrates a high success rate in managing traumatic urethral strictures Careful patient selection, along with prompt and appropriate surgical intervention, is crucial to improving long-term outcomes and reducing the risk of re-stricture
REFERENCES
1 Yücetürk CN, Keseroglu BB Etiology of Posterior Urethral Strictures: Analysis of 116 Cases Ankara Education and Research Hospital Medical Journal 2020; 53:76-80
2 Djoeworo WR, Tasono Hadi DP, Darjoko ST Motorcycle accident injuries are more severe than other land transportation injuries Univ Med 2018; 37:105-14
3 Ma YC, Lin L, Luo Z, Jin T Smoking is an independent risk factor for stricture recurrence after the urethroplasty: a systematic review and meta-analysis Int Braz J Urol 2023; 49:8-23
4 Hussain M, Khan MS, Lal M, et al Stricture of Urethra: Patterns and Outcomes of Management from a Single Centre in Pakistan Over 7 Years J Coll Physicians Surg Pak 2020; 30:79-84
5 Waterloos M, Verla W, Oosterlinck W, et al Excision and Primary Anastomosis for Short Bulbar Strictures: Is It Safe to Change from the Transecting towards the Nontransecting Technique? Biomed Res Int 2018; 2018:3050537
6 D'hulst P, Floyd MS Jr, Castiglione F, et al Excision and Primary Anastomosis for Bulbar Urethral Strictures Improves Functional Outcomes and Quality of Life: A Prospective Analysis from a Single Centre Biomed Res Int 2019; 2019:7826085
7 Bagchi P, Pratihar S, Rajeev T, et al An audit of management of male urethral stricture and its outcome: a single centre retrospective review Int Surg J 2020; 7:774
8 Elsayed M, Wahab A, Sallem E, Riad A Outcome of non-transected anastomotic urethroplasty for management of short bulbar urethral stricture Sohag Med J 2019; 23:187-193
9 Shalkamy O, Elsalhy M, Alghamdi SM, et al Erectile function after different techniques of bulbar urethroplasty: does urethral transection make a difference? BMC Urol 2023; 23:140
10 Siegel J, Panda A, Tausch TJ, et al Repeat excision and primary anastomotic urethroplasty for salvage of recurrent bulbar urethral stricture J Urol 2015; 194:1316-1322
DECLARATIONS
Ethical approval: This study was approved by the Health Research Ethics Commission of Saiful Anwar General Hospital Number: 400/214/K 3/102 7/2024
Availability of data and material: The datasets used and/or analyzed during the current study are available upon reasonable request
Competing interests: The authors declare no conflict of interest
11 Kumar S, Kapoor A, Ganesamoni R, et al Efficacy of holmium laser urethrotomy in combination with intralesional triamcinolone in the treatment of anterior urethral stricture Korean J Urol 2012; 53:614
12 Han J, Liu J, Hofer M, et al Risk of urethral stricture recurrence increases over time after urethroplasty Int J Urol 2015; 22:695-699
13 Horiguchi A, Ojima K, Shinchi M, et al Single-surgeon experience of excision and primary anastomosis for bulbar urethral stricture: analysis of surgical and patient-reported outcomes World J Urol 2021; 39:3063-3069
14 Sikpa KH, Botcho G, Sewa E, et al Male urethral stricture: epidemiological, clinical, and therapeutic aspects in Kara Open J Urol 2023; 13:101-107
15 Topaktas R, Ürkmez A, Tokuç E, et al Hematologic parameters and neutrophil/lymphocyte ratio in the prediction of urethroplasty success Int Braz J Urol 2019; 45:369-375
16 Selukar D, Pothare AN, Meshram K, et al A case series of standard surgical management of bulbo-membranous stricture Int Surg J 2017; 4:1299
17 Kinnaird AS, Levine MA, Ambati D, et al Stricture length and etiology as preoperative independent predictors of recurrence after urethroplasty: A multivariate analysis of 604 urethroplasties Can Urol Assoc J 2014; 8:E296-300
18 Barbagli G, Kulkarni SB, Fossati N, et al Long-term followup and deterioration rate of anterior substitution urethroplasty J Urol 2014; 192:808-813
19 Wiegand LR, Brandes SB The UREThRAL stricture score: A novel method for describing anterior urethral strictures Can Urol Assoc J 2012; 6:260-4
20 Akyüz M, Sertkaya Z, Koca O, et al Adult urethral stricture: practice of Turkish urologists Int Braz J Urol 2016; 42:339-345
21 Ansari IS, Islam SU, Ali W, Haq IU Urethrotomy and end-toend urethroplasty in anterior urethral strictures up to 1 5 cm Dept of Urology Mayo Hospital, Lahore Pak J Med Health Sci 2022; 16:174-175
22 Leosari Y, Uelmen JA, Carney RM Spatial evaluation of healthc a r e a c c e s s i
Province, Indonesia PLOS Glob Public Health 2023; 3:e0001600
23 Desai D, Harrison W, Raveenthiran S, et al Urethronav: the aetiology and extent of idiopathic urethral stricture in an Australian population Transl Androl Urol 2024; 13:423-432
24 Blaschko SD, McAninch JW, Myers JB, et al Repeat urethroplasty after failed urethral reconstruction: outcome analysis of 130 patients J Urol 2012; 188:2260-2264
Correspondence
Paksi Satyagraha (Corresponding Author) uropas fk@ub ac id
Edi Wibowo eddiewibowo283@gmail com
Besut Daryanto urobes fk@ub ac id
Gede Wirya Diptanala Putra Duarsa diptaduarsa@gmail com
Adrianus Gupta Wijaya guptawijaya@gmail com
Fauzan Kurniawan Dhani fauzankurniawandhani@gmail com
Urology Department, Saiful Anwar General Hospital Malang, Jalan Jaksa Agung Suprapto 2, Klojen, Malang, East Java 65112, Indonesia
ORIGINAL PAPER
Factors associated with erectile dysfunction in traumatic urethral strictures following EPA urethroplasty: A single center experience
Paksi Satyagraha, Gede Wirya Diptanala Putra Duarsa, Fauzan Kurniawan Dhani, Adrianus Gupta Wijaya, Besut Daryanto
Urology Department, Faculty of Medicine, Universitas Brawijaya, Saiful Anwar General Hospital, Malang, Indonesia
Summary
Introduction: Urethral repair with Excision and Primary Anastomosis (EPA) urethroplasty offers excellent outcome in managing traumatic urethral strictures However, its impact on erectile function (EF) is largely unknown Study to evaluate EF outcome post-operatively is still limited worldwide. We report factors associated to EF following EPA Urethroplasty performed by single surgeon in tertiary hospital. In this study, we aim to evaluate the risk of erectile dysfunction (ED) following EPA Urethroplasty
Materials and methods: This is a retrospective study on patients with traumatic urethral strictures who underwent EPA Urethroplasty from 2013 to 2023. Variables including age, body mass index, systemic disease, etiology, stricture length, prior procedures and erection hardness score (EHS) score prior and 12 months after surgery were recorded Pre-Operative ED was determined using Penile Doppler Ultrasound, which was defined as a peak systolic velocity of less than 25 cm/s Univariate and Multivariate logistic regression analysis were performed using IBM SPSS Statistic
Results: A total of 89 patients were included. Among them, 33 patients (33 7%) suffered from initial ED prior to surgery
Pelvic fracture urethral injury (PFUI) was the predominant etiology (74%); 29% of the patients were active smokers, and 68 5% had prior endoscopic treatment Among the 48 patients without ED prior to surgery, 7 of them (14 6%) developed ED following surgery in 12 months of follow up After EPA, there was a reduction of mean EHS score from 2 70 to 2 53 (p = 0 176)
Multivariate analysis showed that smoking status (p = 0 035; OR 4 41), PFUI as the mechanism of injury (p = 0 007; OR 2 89), prior urethrotomy (p = 0 020; OR 4 69), and prior dilatations (p = 0.046; OR 0.18) were related as risk factors of ED following EPA urethroplasty
Conclusions: Risk of ED following EPA is inevitable, although the number is not high as expected Smoking, PFUI and prior treatment rather than EPA, emerge as predominant risk factors associated with the development of ED subsequent to surgical repair
Submitted 14 November 2024; Accepted 2 December 2024
INTRODUCTION
The rate of traffic accidents in Indonesia is alarmingly high, which significantly impacts the incidence of pelvic
trauma A study on pelvic fractures in Indonesia from 2016 to 2018 involved 229 patients with pelvic injuries that lead to developing of traumatic urethral strictures especially Pelvic Fracture Urethral Injury (PFUI) Traffic accidents were responsible for 76% of these cases (1-6) Excision and Primary Anastomosis (EPA) Urethroplasty is a reconstructive technique for traumatic urethral strictures, involving the complete removal of the affected urethral segment followed by tension-free anastomosis that offering excellent clinical outcomes (7) However, the impact of EPA Urethroplasty on erectile function (EF) has raised concerns Existing studies on erectile dysfunction (ED) both prior and after EPA Urethroplasty for traumatic urethral strictures are limited Research evaluating EF outcomes post-operatively remains scarce worldwide The exact cause of ED in men following urethroplasty remains poorly studied (8, 9) There is lack of available data in Indonesia concerning about EF following such procedure This gap in information limits the understanding of the risks and effectiveness of this interventions Our study aims to address this gap by examining the factors associated with EF following EPA Urethroplasty performed by a single surgeon at a tertiary hospital
METHODS
Study sample and design
This study employs a retrospective design focusing on patients with traumatic urethral stricture who underwent EPA Urethroplasty at Dr Saiful Anwar General Hospital in Malang, a tertiary referral hospital Study sample consists of patients with traumatic urethral stricture who received EPA-Urethroplasty treatment at Dr Saiful Anwar General Hospital between 2013 and 2023 The inclusion criteria for this study are as follows (1) Male patients diagnosed with traumatic urethral stricture, confirmed through Bipolar Voiding Cysto-Urethrography (BVCUG); (2) Patients with no prior EPA Urethroplasty Repair The exclusion criteria for this study are (1) Male patients with urethral stricture caused by factors other than trauma; (2) Patients loss of follow-up before 12 months; (3) Patient who underwent Redo-Urethroplasty
P Satyagraha, G Wirya Diptanala Putra Duarsa, F Kurniawan Dhani, et al
The research utilizes medical records to evaluate sexual function outcomes before and after the procedure The variables recorded in this study include age, BMI, systemic diseases, etiology, stricture length, prior procedures, and EHS scores both prior to and 12 months after surgery We excluded all the patients who suffered preoperative ED from the study Pre-operative ED was determined using Penile Doppler Ultrasound, and a Peak systolic velocity of less than 25 cm/s indicate initial ED P o s t o p e
Hardness Score (EHS) and the International Index of Erectile F
Urethroplasty procedure
Postoperative follow-up and outcome definition
We followed all the patients with no prior ED following surgery up to 12 months of follow-up using EHS score and IIEF-5 assessment at 1, 3, 6 and 12 months following the surgery We included and analyzed all the patient who develop ED during this period of follow-up
Statistical analysis
Univariate and multivariate logistic regression analyses were performed using IBM SPSS Statistics to analyze the data This statistical approach allowed for the examination of potential predictors and the impact of various factors on the outcomes of ED in patients undergoing EPAUrethroplasty
RESULTS
Characteristics of the research sample
The study included 89 patients with a mean age of 41 24 years (SD ± 15 59) The median follow-up period was 16 3 months (SD ± 3 15) The mean BMI was 23 05 kg/m² (SD ± 2 57) Among the patients, 29 2% were current smokers, 10 1% had type 2 diabetes mellitus, and 16 9% had hypertension The average length of stricture was 25 4 mm (SD ± 16 3), with the mean time to surgery being 6 67 months (SD ± 4 07) Types of injuries included straddle injury (12 35%), iatrogenic (11 23%), direct (2 24%), and PFUI (74 15%) The stricture site was bulbar in 62% of cases and membranous in 27% of cases There were 34 patients (38 20%) who had performed internal urethrotomies and 33 patients (37 07%) had performed urethral dilatation prior to surgery Fourteen patients (15 73%) did not undergo any types of endoscopic treatment following the surgery Types of surgery performed were bulbar mobilization (39 33%), crural separation (32 58%), inferior pubectomy (26 96%), and supracrural rerouting (1 12%) The success rate of EPA was 91%, with an 8% recurrence rate ED was noted in 40 74% of patients pre-operatively, and 49 39% postoperatively (Table 1) Among the 48 patients without ED prior to surgery, 7 of them (14 6%) developed ED postoperatively
Erectile function outcome following EPA urethroplasty
The statistical analysis was performed using the MannWhitney test The mean EHS Score decreased slightly from 2 70 (SD ± 0 798) pre-operatively to 2 53 (SD ±
Table 1.
Patient characteristics.
Number of patient
(year) (SD)
(%)
Stricture aetiology, n (%)
site, n (%)
(± 15.59)
dysfunction (ED), n (%)
(n: 81)
0 823) at 12 months post-operatively, but this change was not statistically significant (p = 0 176) Similarly, the mean IIEF-5 score showed a minor increase from 19 35 (SD ± 4 547) to 19 73 (SD ± 4 174) over the same period, which was also not statistically significant (p = 0 444) (Table 2 and Figure 1)
Table 2. Erectile function outcome
Pre-operative (n: 48) 12 months of follow-up (n: 41)
Factors associated with the risk of ED post-operatively
In the univariate analysis, smoking significantly increased the odds of occurrence of erectile dysfunction (OR 6 78, 95% CI 1 32-34 81, p = 0 022) The type of PFUI injury also emerged as a significant predictor of occurrence of erectile dysfunction (OR 2 76, 95% CI 1 13-6 72, p = 0 026) Additionally, the number of procedures prior to EPA Urethroplasty significantly increased the risk of erectile dysfunction after EPA (OR 0 19, 95% CI 0 04-0 90, p = 0 036)
In the multivariate analysis, smoking remained a significant risk factor for occurrence of erectile dysfunction (OR 4 41, 95% CI 1 11-17 57, p = 0 035)
The PFUI injury type continued to significantly predict recurrence erectile dysfunction occurrence (OR 2 89, 95% CI 1 34-6 21, p = 0 007) The number of urethrotomies also significantly increased the odds of ED following EPA Urethroplasty (OR 4 69, 95% CI 1 28-17 24, p = 0 020), and prior procedures remained a significant factor in postoperative ED (OR 0 18, 95% CI 0 05-0 68, p = 0 011) (Table 3)
DISCUSSION
Figure 1. EHS (A) and IIEF-5 Score (B) in 12 months of follow up
The prevalence of ED after pelvic fractures ranges from 528%, but it is significantly higher after PFUI, varying between 26-76% (10-12) ED after PFUI typically results from direct injury to the posterior urethra, penile nerves, and arteries There is ongoing debate about whether neurogenic or vascular injury is the primary cause Evidence leans towards neurogenic causes, with high response r
abnormal electromyograms in affected patients, despite normal vascular flow Some studies, however, report high occlusion rates in penile arteries, suggesting a vascular component (13)
The mechanism of ED following PFUI typically involves direct trauma that both lacerates and often avulses the posterior urethra, concurrently damaging the penile nerves and arteries as they traverse the pelvic floor behind the prostate before entering the penis Literature debates whether neurogenic or direct vascular injury is the primary cause of ED, with more evidence pointing towards neurogenic ED (14, 15) Both vasculogenic and neurogenic causes have been proposed for ED after PFUI, and various studies have attempted to identify the specific pathophysiologic factors involved to better guide treatment There is no clear consensus on the primary cause of organic ED after PFUI Feng et al found that only 28% of men with ED post PFUI had organic ED, most of which was neurogenic (16) Studies by Mark et al and Machtens et al support the predominance of neurogenic factors, noting high response rates to neurogenic treatments and evidence of nerve damage (17, 18) Guan et al 's study of 120 patients found that 80% had organic ED, with 30% vasculogenic, 43% neurogenic, and 27% mixed Most vasculogenic cases involved veno-occlusive dysfunction rather than arterial insufficienc (19) These findings highlight the variability in ED etiology post PFUI and emphasize the need for a tailored, stepwise diagnostic approach to treatment
Table 3.
and multivariate Cox regression analysis for ED following EPA urethroplasty
P Satyagraha, G Wirya Diptanala Putra Duarsa, F Kurniawan Dhani, et al
Differentiating between ED due to PFUI and de novo ED from urethral realignment or delayed urethroplasty requires multiple assessments before and after injury and repair (20) Studies show that delayed urethroplasty increases the risk of ED by 3% over the 34% associated with PFUI alone, resulting in a 37% incidence of de novo ED The higher rate of ED after delayed urethroplasty compared to primary endoscopic alignment likely reflects differences in injury severity and ED reporting (21) Men undergoing primary realignment generally have less severe PFUIs, as indicated by a lower ED rate compared to those needing delayed urethroplasty However, the association is unclear due to variability in institutional practices regarding primary realignment and delayed urethroplasty (20) Our study utilized four techniques include bulbar urethral mobilization, crural separation, inferior pubectomy, and supracrural rerouting Despite employing these methods, the results showed no significant impact on postoperative erectile dysfunction Using only bulbar urethral mobilization and crural separation is considered a simple perineal approach Including either an inferior pubectomy or supracrural rerouting is classified as an elaborated perineal approach (22) In a previous study, 74 patients (30 2%) underwent transecting bulbar urethroplasty, while 171 patients (69 8%) underwent non-transecting techniques Both groups had similar success rates (87 8% vs 86 5%, p = 0 93) and postoperative complications (8 1% vs 7%, p = 0 73) Transient ED was more common in the transecting cohort (8 1% vs 2 9%, p = 0 07), but de novo permanent ED rates were comparable (4 1% vs 2 9%, p = 0 65)
Transecting techniques can lead to transient ED that typically improves within a year, while permanent ED is uncommon and not significantly influenced by the type of urethroplasty technique used (23)
A previous meta-analysis involving 21 studies with 6 791 patients showed consistent results across two stages In the univariate analysis (18 studies, 5 811 patients), smoking was associated with a higher risk of stricture recurrence (RR = 1 32, p = 0 001) The multivariate analysis (11 studies, 3 176 patients) also found smoking linked to increased stricture recurrence (RR = 1 35, p = 0 049) Smoking may increase the risk of stricture recurrence after urethroplasty Quitting smoking is recommended for patients undergoing urethroplasty (24) Smoking adversely impacts ED through several mechanisms It disrupts the nitric oxide (NO) pathway by impairing both endothelial and neuronal NO synthase (NOS) activities
Specifically, components of burned tobacco inhibit neuronal NOS, while cigarette smoke damages the endothelium, reducing endothelial NOS-mediated vasodilation
Additionally, smoking produces superoxide anions that decrease free NO levels in the corpora cavernosa These superoxides activate NADH oxidase enzymes, diverting NO into a peroxynitrite pathway and reducing its vasoactive availability Smoking also affects Rho-associated kinase (ROK) signaling by decreasing NO levels, which leads to increased ROK activity and worsens ED
Finally, smoking causes intrinsic vascular damage, altering elastin in the extracellular matrix and inducing calcification of medial elastic fibers, resulting in arterial stiffness and impaired vessel dilation (24) Unlike our study, previous study found no significant correlation between
postoperative ED and smoking history (25), Waddel et al reported a higher incidence of ED associated with smoking history (26)
In our study, we found that previous treatment had significant results in post-operative ED Potential mechanisms for erectile dysfunction following DVIU include direct injury to the cavernous nerve caused by the urethrotomy knife, fibrosis resulting from fluid and urine leakage into the periurethral space, infection, or the creation of a shunt between the corpora cavernosa and the corpus spongiosum (27) Despite its lower success rates c o m p a
Urethrotomy (DVIU) remains the most used treatment for anterior urethral stricture (28)
Erickson et al used the BMSFI to assess ED following urethral reconstruction and discovered that patients over 50 years old experienced a notable decline in the mean EF domain score, unlike their younger counterparts (29) Similarly, Anger et al indicated that both age and preoperative EF can negatively impact postoperative sexual outcomes Their prospective review found that men with postoperative EF scores ≤ 20 on the IIEF questionnaire were older (mean age 47 vs 36 8 years, p = 0 17) and had poorer preoperative EF values (mean 20 vs 29, p = 0 11) compared to those with EF scores > 20, though these differences were not statistically significant (30) In contrast, other studies found no clear link between age and the incidence of ED, though older men generally had lower preoperative IIEF scores and experienced a greater decline in these scores Chapman et al also found no significant association between age and sexual dysfunction i n t h e i r m u l t i v a r i a t e a n a l y s i s ( 3 1 - 3 3 ) A g e s h o w e d insignificant results in our study on postoperative ED due to a potentially small sample size, narrow age range, variability in preoperative function, and confounding factors Statistical methods may not have detected subtle age effects, and the follow-up duration might have been too short Additionally, the complex relationship between age and ED could have diluted the impact of age alone Coursey et al suggested that stricture length could be a predictive factor for postoperative erectile function, finding that men with poorer erectile outcomes had significantly longer strictures compared to those with improved or stable erections (mean 6 8 cm vs 4 cm) (34) However, subsequent research has contradicted this association (29, 32, 35) ED is approximately 3 5 times more prevalent in men with diabetes mellitus (DM) compared to those without the condition (36) In a previous study involving 878 men, logistic regression was used to examine the relationship between ED and body mass index (BMI) The incidence of ED was 53 1% Men in the ED group had significantly higher BMIs compared to those in the nonED group (p = 0 01) Obese men had a higher risk of ED compared to those with normal weight (OR = 1 97, 95% CI = 1 25-3 14, p = 0 004), even after adjusting for potential confounding factors (OR = 1 78, 95% CI = 1 10-2 90, p = 0 02) Overall, these findings indicate a positive correlation between obesity and the risk of moderate to severe ED (37) In our study, the variable BMI did not yield significant results This lack of significance may be attributed to the fact that the average BMI of the participants was 23 05, which falls within the normal weight
range Additionally, the study sample did not include a wide range of BMI values, leading to a limited distribution of data that could have impacted the ability to detect a significant effect of BMI on erectile function outcomes
The limitation of the study is its retrospective design, which relies on historical medical records This approach can lead to incomplete or inconsistent data collection, potentially affecting the accuracy and reliability of the findings Additionally, the study's reliance on patientreported outcomes, such as the EHS Score and the IIEF5 score, may introduce bias due to subjective interpretations by the patients To strengthen the findings, a prospective cohort study design could be implemented in future research This approach would allow for more controlled and consistent data collection, including real-time assessments of erectile function and other relevant variables Additionally, incorporating objective measures, such as penile Doppler ultrasound or other physiological assessments of erectile function, could provide more a c c u
Urethroplasty on erectile dysfunction
CONCLUSIONS
The risk of ED following EPA Urethroplasty, while present, is generally lower than anticipated Smoking, PFUI, and prior treatments rather than the EPA procedure itself emerge as significant risk factors contributing to the development of ED after surgical repair Despite the inherent risk of ED associated with any urethral surgery, these factors play a more prominent role in influencing post-operative erectile function
REFERENCES
1 Smith T Current management of urethral stricture disease Indian J Urol 2016; 32:27
2 Waterloos M, Verla W Female Urethroplasty: A Practical Guide Emphasizing Diagnosis and Surgical Treatment of Female Urethral Stricture Disease Biomed Res Int 2019; 2019:1-13
DECLARATIONS
Ethical approval: This study was approved by the Health Research Ethics Commission of Saiful Anwar General Hospital Number: 400/214/K 3/102 7/2024
Availability of data and material: The datasets used and/or analyzed during the current study are available upon reasonable request
Competing interests: The authors declare that they have no competing interests
3 Alwaal A, Blaschko SD, McAninch JW, Breyer BN Epidemiology of urethral strictures Transl Androl Urol 2014; 3:209-13
4 Smith T Current management of urethral stricture disease Indian Journal of Urology 2016; 32:27
5 Ramadana Y, Chilmi MZ Epidemiology of pelvic fracture in the emergency room at Dr Soetomo General Hospital between 20162018 Qanun Medika - Medical Journal Faculty of Medicine Muhammadiyah Surabaya 2022; 6(1)
6 Agung Nugroho TS, Adi K Five years characteristic of urethral
Indonesian Journal of Urology 2021; 28:30-4
7 Nilsen OJ, Holm HV, Ekerhult TO, et al To Transect or Not Transect: Results from the Scandinavian Urethroplasty Study, A Multicentre Randomised Study of Bulbar Urethroplasty Comparing Excision and Primary Anastomosis Versus Buccal Mucosal Grafting Eur Urol 2022; 81:375-82
8 Sangkum P, Levy J, Yafi FA, Hellstrom WJG Erectile dysfunction in urethral stricture and pelvic fracture urethral injury patients: diagnosis, treatment, and outcomes Andrology 2015; 3:443-9
9 Kałuzny A, Krukowski J, Matuszewski M Erectile dysfunction after urethroplasty Cent European J Urol 2019; 72:402-7
10 Schulman JE, O’Toole RV, Castillo RC, et al Pelvic Ring Fractures Are an Independent Risk Factor for Death After Blunt Trauma J Trauma 2010; 68:930-4
11 Demetriades D, Karaiskakis M, Toutouzas K, et al Pelvic Fractures: Epidemiology and Predictors of Associated Abdominal Injuries and Outcomes1 J Am Coll Surg 2002; 195:1-10
12 Johnsen NV, Dmochowski RR, Young JB, Guillamondegui OD Epidemiology of Blunt Lower Urinary Tract Trauma With and Without Pelvic Fracture Urology 2017; 102:234-9
13 Mazzone A, Anderson R, Voelzke BB, et al Sexual function following pelvic fracture urethral injury and posterior urethroplasty Transl Androl Urol 2021; 10:2043-50
14 Barratt RC, Bernard J, Mundy AR, Greenwell TJ Pelvic fracture urethral injury in males mechanisms of injury, management options and outcomes Transl Androl Urol 2018; 7:S29-62
15 Johnsen NV, Kaufman MR, Dmochowski RR, Milam DF Erectile Dysfunction Following Pelvic Fracture Urethral Injury Sex Med Rev 2018; 6:114-23
16 Feng C, Xu Y-M, Yu J-J, et al Risk Factors for Erectile Dysfunction in Patients with Urethral Strictures Secondary to Blunt Trauma J Sex Med 2008; 5:2656-61
17 Mark SD, Keane TE, Vandemark RM, Webster GD Impotence following pelvic fracture urethral injury: incidence, aetiology and management Br J Urol 1995; 75:62-4
18 Machtens S, Gänsslen A, Pohlemann T, Stief CG Erectile dysfunction in relation to traumatic pelvic injuries or pelvic fractures BJU Int 2001; 87:441-8
19 Guan Y, Wendong S, Zhao S, et al The vascular and neurogenic factors associated with erectile dysfunction in patients after pelvic fractures International Braz J Urol 2015; 41:959-66
20 Bhowmik P, Sharma G, Sharma P, et al Prospective study of de novo sexual dysfunction after anterior urethroplasty: Causative factors, incidence, and recovery of function - A single-center experience Urol Ann 2022; 14:60
21 Blaschko SD, Sanford MT, Schlomer BJ, et al The incidence of erectile dysfunction after pelvic fracture urethral injury: A systematic review and meta-analysis Arab J Urol 2015; 13:68-74
P Satyagraha, G Wirya Diptanala Putra Duarsa, F Kurniawan Dhani, et al
22 Koraitim MM Post-traumatic posterior urethral strictures: Preoperative decision making Urology 2004; 64:228-31
23 Shalkamy O, Elsalhy M, Alghamdi SM, et al Erectile function after different techniques of bulbar urethroplasty: does urethral transection make a difference? BMC Urol 2023; 23:140
24 Kovac JR, Labbate C, Ramasamy R, et al Effects of cigarette smoking on erectile dysfunction Andrologia 2015; 47:1087-92
25 Ma Y, Lin L, Luo Z, Jin T Smoking is an independent risk factor for stricture recurrence after the urethroplasty: a systematic review and meta-analysis International Braz J Urol 2023; 49:8-23
26 Waddell O, Mclauchlan J, McCombie A, et al Quality of life in early-onset colorectal cancer patients: systematic review BJS Open 2023; 7:zrad030
27 Sangkum P, Levy J, Yafi FA, Hellstrom WJG Erectile dysfunction in urethral stricture and pelvic fracture urethral injury patients: diagnosis, treatment, and outcomes Andrology 2015; 3:443-9
28 Siegel JA, Morey AF Opinion: Anastomotic Urethroplasty International Braz J Urol 2015; 41:615-8
29 Erickson BA, Wysock JS, McVary KT, Gonzalez CM Erectile function, sexual drive, and ejaculatory function after reconstructive surgery for anterior urethral stricture disease BJU Int 2007; 99:607-11
30 Anger JT, Sherman ND, Webster GD The Effect of Bulbar Urethroplasty on Erectile Function J Urol 2007; 178:1009-11
31 Dogra PN, Saini AK, Seth A Erectile Dysfunction After Anterior Urethroplasty: A Prospective Analysis of Incidence and Probability of Recovery Single-center Experience Urology 2011; 78:78-81
32 Chapman DW, Cotter K, Johnsen NV, et al Nontransecting Techniques Reduce Sexual Dysfunction after Anastomotic Bulbar U r e t h r o p l a s t
Analysis Journal of Urology 2019; 201:364-70
33 Haines T, Rourke KF The effect of urethral transection on erectile function after anterior urethroplasty World J Urol 2017; 35:839-45
34 Coursey JW, Morey AF, McAninch JW, et al Erectile function after anterior urethroplasty J Urol 2001; 166:2273-6
35 Xie H, Xu Y-M, Xu X-L, et al Evaluation of erectile function after urethral reconstruction: a prospective study Asian J Androl 2009; 11:209-14
36 Defeudis G, Mazzilli R, Tenuta M, et al Erectile dysfunction and diabetes: A melting pot of circumstances and treatments Diabetes Metab Res Rev 2022; 38:e3494
37 Liu Y, Hu X, Xiong M, et al Association of BMI with erectile dysfunction: A cross-sectional study of men from an andrology clinic Front Endocrinol (Lausanne) 2023; 14:1135024
Correspondence
Paksi Satyagraha uropas fk@ub ac id
Gede WIrya Diptanala Putra Duarsa diptaduarsa@gmail com
Fauzan Kurniawan Dhani fauzankurniawandhani@gmail com
Adrianus Gupta Wijaya guptawijaya@gmail com
Urology Department, Faculty of Medicine, Universitas Brawijaya, Saiful Anwar General Hospital, Malang, Indonesia
Besut Daryanto, MD (Corresponding Author) urobes fk@ub ac id
Urology Department, Saiful Anwar General Hospital Malang, Jalan Jaksa Agung Suprapto 2, Klojen, Malang, East Java 65112, Indonesia
ORIGINAL PAPER
The effect of hyperbaric oxygen therapy on hypospadias
reconstruction: A preliminary randomized controlled trial study of VEGF levels and HOPE score analysis
Mendy Hatibie Oley 1 , Maximillian Christian Oley 2 , Ari Astram Adhiatma Iskandar 3 , Chaula Luthfia Sukasah 4 , Indri Aulia 4 , Fima Lanra Fredrik G Langi 5 , Harsali Fransicus Lampus 6 , Irawan Sukarno 7 , Vania Sukarno 8 , Muhammad Faruk 9
1 Division of Plastic Reconstructive and Aesthetic Surgery, Department of Surgery, Faculty of Medicine, Sam Ratulangi UniversityR D Kandou Hospital, Manado, Indonesia;
2 Division of Neurosurgery, Department of Surgery, Faculty of Medicine, Sam Ratulangi University - R D Kandou Hospital, Manado, Indonesia;
3 Division of Urology, Department of Surgery, Faculty of Medicine, Sam Ratulangi University - R D Kandou Hospital, Manado, Indonesia;
4 Division of Plastic Reconstructive and Aesthetic Surgery, Department of Surgery, Faculty of Medicine, Universitas IndonesiaDr Cipto Mangunkusumo Hospital, Jakarta, Indonesia;
5 Department Epidemiology and Biostatistics, Public Health Faculty, Sam Ratulangi University, Manado, Indonesia
6 Division of Pediatric Surgery, Department of Surgery, Faculty of Medicine, Sam Ratulangi University - R D Kandou Hospital, Manado, Indonesia;
7 Department of Surgery, Faculty of Medicine, Sam Ratulangi University, Manado, Indonesia;
8 Siloam Hospital, Manado, Indonesia;
9 Department of Surgery, Faculty of Medicine, Hasanuddin University - Hasanuddin University Hospital, Makassar, Indonesia
Summary
Introduction: Hypospadias is a congenital abnormality of the urethral meatus in males Hypospadias can be corrected by two-stage urethroplasty
Hyperbaric oxygen therapy (HBOT) can accelerate wound healing after surgery by increasing oxygenation, angiogenesis, and collagen synthesis This study aimed to measure the effectivity of HBOT based on serum vascular endothelial growth factor (VEGF) level and Hypospadias Objective Penile Evaluation (HOPE) score in hypospadias reconstruction patients. Methods: This was a randomized controlled trial study. Hypospadias reconstruction was performed using the SidikChaula and Manset Flap techniques Each HBOT session ranged from 30-60 minutes, administered at 1-3 atm Twenty subjects were divided into two groups: the HBOT and control groups
VEGF serum levels were measured 1 hour after the operation and 1 hour after every HBOT session The HOPE score was assessed at the bedside by the attending physician, consisting of six items: the position of the meatus, the shape of the meatus, the shape of the glans, the shape of the penile skin, and the shape of the penile axis, including penile torsion and penile curvature The data were analyzed with SPSS version 28, using the Shapiro-Wilk and independent t-test methods
Results: There was a trend of increasing VEGF levels as the number of HBOT sessions increased, with significant increase found in patients who underwent three (p = 0 038), four (p = 0.002), and five (p = 0.008) HBOT sessions. We found a significant increase in the total HOPE score (p = 0.028) and penile torsion score (p = 0.006) in the HBOT group.
Conclusions: HBOT can accelerate wound healing after urethroplasty Three or more HBOT sessions are recommended after the repair of hypospadias
Submitted 4 November 2024; Accepted 3 January 2025
INTRODUCTION
Hypospadias is a congenital abnormality of the male external genital tract, with the characteristic anatomic position of the urethral meatus at the ventral or anterior part of the penile body, often accompanied by urethral spongiosum, widened dorsal prepuce, ventral foreskin, penile chordee, and deviation of the ventral penile body (1) The main treatment remains surgical correction with various techniques, one of which is the two-stage urethroplasty technique, also known as the Sidik-Chaula technique In the first stage, the chordee is released and a neourethra is created using the distal intraglandular tunnel removed from the preputial vascularized flap The full-length urethra is then reconstructed in a second stage, using a locally transposed cutaneous flap with minimal manipulation (2)
Hyperbaric oxygen therapy (HBOT) is a therapeutic modality to improve tissue hypoxic conditions by providing high-pressure oxygen so that tissue oxygen tension increases It thereby improves oxygen delivery to hypoxic tissue because dissolved oxygen can pass through tissue fluids even if the tissue is damaged and has poor blood circulation Increased oxygen availability in tissue promotes angiogenesis, collagen synthesis, increased reactive oxygen species for bacterial clearance, inhibition
of inflammation, and inhibition of leukocyte adhesion to endothelium This correlates with increased wound healing, damaged tissue regeneration, and fibroblast scar tissue remodeling (3)
Various reports state that wound healing accelerated with hyperbaric oxygen, including hypospadias reconstructive surgery scars, by increasing the vascular endothelial growth factor (VEGF) stimulation of angiogenesis through proliferation Neheman et al (4) evaluated the use of HBOT to increase the success rate of staged tubularized autograft (STAG) repair in repeatedly failed correction cases They showed that hyperbaric adjuvant therapy in a pediatric population improved the result of previously failed hypospadias surgery and led to better graft uptake Chang et al (5) also used HBOT as an adjuvant therapy for hypospadias patients undergoing two-stage correction using buccal mucosal grafts to repair glans penis dehiscence and urethroplasty for urethral strictures after hypospadias correction They obtained successful outcomes in these cases with HBOT administration
The optimum scoring system for cosmetic outcomes following hypospadias surgery should be an objective, repeatable, and validated tool measuring each relevant and surgically correctable component of the hypospadias (6) The Hypospadias Objective Penile Evaluation (HOPE) score has good validity and reliability, which supports its use as an objective indicator of cosmetic appearance foll o w i n g h y p o s p a d i a s s u r g e r y ( 6 - 9 ) T h e i n c r e a s e i n hypospadias cases and the use of HBOT, which plays a role in the wound healing process, has led researchers to examine the effect of HBOT on the success of hypospadias surgery This study aimed to measure the effectivity of HBOT based on the serum VEGF level and HOPE score in patients after hypospadias reconstruction
METHODS
This was a randomized controlled trial study conducted between December 2021 and December 2022, and conducted per CONSORT guideline 2010 (10)
The data collection and processing were performed at R D Kandou Hospital and Siloam Manado Hospital The study population inclusion criteria were patients with all types of hypospadias who would undergo surgery and were willing to be participants in the research We excluded patients with tympanic perforation, endocranial implants, or hearing problems; patients with epilepsy or other types of seizures; patients in chemotherapy; patients with alcoholism or users of psychoactive drugs; heart pacemaker users; patients with claustrophobia or other psychiatric problems; patients with uncontrolled hypertension, heart failure, respiratory failure, pneumothorax, or asthma; and non-cooperative patients
Urethroplasty procedure
The control and HBOT groups both underwent surgery for hypospadias Distal, middle, and proximal hypospadias were all repaired using a modified two-stage urethroplasty: the Sidik-Chaula technique An additional approximation of the bilateral subgranular flap, called the Manset flap, which is especially useful in cases of middle hypospadias, was also used (11)
HBOT Group
Patients in the HBOT group received standard wound dressings, as did the control group Additionally, they underwent one session of 100% oxygen therapy within 24 hours postoperatively, for 5 consecutive days Each HBOT session lasted 30-60 minutes and was administered at 2 4 ATM
Control group
The control group received only standard wound dressings, changed every 2 days with moist sterile gauze, and a 5-day course of oral broad-spectrum antibiotics
Outcome
The primary outcomes include differences in VEGF levels and HOPE scores before and after hyperbaric oxygen therapy (HBOT) Secondary outcomes were the assessment of baseline characteristics of hypospadia repair patients and the number of HBOT sessions required to significantly impact VEGF levels and HOPE scores
VEGF examination
In the control group, VEGF serum levels were measured once, 1 hour after the operation In the HBOT group, VEGF serum levels were measured 1 hour after each of the 5 HBOT sessions (HBOT 1, 2, 3, 4, and 5), with a blood sample taken after every session
The VEGF serum levels were measured in guanidium thiocyanate L6 buffer The samples were centrifuged for 60 minutes until coagulated, then kept in a -80 ºC container until analysis
All samples were examined using the human VEGF ELISA kit protocol of the SimpleStep ELISA kit from AssayGenie Human VEGF-A with catalog no HUES01397 The results are expressed in ng/ml
HOPE score
The HOPE score was assessed at the bedside by the attending physician, consisting of six items: the position of the meatus, the shape of the meatus, the shape of the glans, the shape of the penile skin, and the shape of the penile axis including penile torsion and (if erection was observed) penile curvature The possible HOPE scores range from 1 to 10 (12) A standardized photograph was taken pre-operatively (under general anesthesia) and six months post operative Two researchers individually assessed the HOPE score of the patients based on the photograph taken, without knowing the patient's identity The final HOPE score was taken from mean HOPE score from both assessors
Randomization
The participants were randomly and equally divided into HBOT and control group using a computer sequence generator Patients in the HBOT group were allocated to a multichamber hyperbaric unit; therefore, patient blinding was not possible However, the patients' identities were blinded to the author responsible for allocation, as well as to the assessor who evaluated the HOPE score preoperatively and the assessor who assessed the HOPE score postoperatively
Statistical analysis
Univariate evaluation was carried out according to the
M Hatibie Oley, M Christian Oley, A Astram Adhiatma Iskandar, et al
type of variable: numeric or categorical The descriptive tabulation of numeric variables is shown as mean, range, and standard deviation The distribution normality was assessed by the Shapiro-Wilk test The difference between the two groups in VEGF levels was tested with the independent t-test and Mann-Whitney test Results are shown for fixed effects in the form of estimates of 95% confidence interval (CI) and p-value The statistical analysis was carried out with SPSS version 28 (Armonk, NY, USA: IBM Corp ) and R Software version 3 5 1, assisted by the use of Microsoft Excel spreadsheets
RESULTS
Kandou Hospital had 20 cases of hypospadias repair within 1 year Ten were treated with HBOT as an adjuvant treatment, and the other half had conventional post-operation procedures The patient characteristics are shown in Table 1
Table 1.
Baseline characteristics of the study population Parameter
Type of hypospadias
Subcoronal
Distal
2 (10)
Penoscrotal [n (%)] 1 (10.0) 1 (10.0) 2 (10)
Scrotal [n (%)] 0 (0 0) 1 (10 0) 1 (5)
HBOT: Hyperbar c oxygen therapy; SD: standard deviation
The mean age of the participants was 12 6 years (SD 7 3), ranging from 2 to 32 years old The most common type of hypospadias found was subcoronal (35%), and the least frequent was scrotal (5%)
Table 2
The comparison of VGEF serum levels between the control and HBOT groups 1 hour after hypospadias reconstruction is shown in Table 2
The mean serum VEGF level of the control group was 394 49 ± 107 88 ng/mL Significant increases in serum VEGF levels were observed in the patients given three (mean difference [MD]=122 0, p = 0 038, 95% CI 7 74236 26), four (MD 223 6, p = 0 002, 95% CI 94 92352 27), and five (MD 292 71, p = 0 008, 95% CI 90 13495 30) HBOT sessions Overall, the patients in the control group had a lower mean VEGF level compared to the HBOT group, regardless of the number of sessions Although not significant, a slight increase also occurred in serum VEGF levels after the first (MD 1 73) and second (MD 54 00) HBOT sessions
Importantly, the concentration of serum VEGF constantly increased after each session of HBOT, despite the wide range of 95% CI
Ten participants came for follow-up and assessment of the HOPE score The difference in HOPE scores between both groups is shown in Table 3 A significant difference in favor of the HBOT group was found in penile torsion (p = 0 006) and total HOPE score (p = 0 014) Further, the HBOT group had a higher mean score for all six item variables
Table 3.
Hypospadias Objective Penile Evaluation (HOPE) scores of hypospadias repair patients
of meatus
of meatus
torsion
HBOT: Hyperbar c oxygen therapy; SD: standard dev
Serum vascular endothelial growth factor (VEGF) of hypospadias repair patients
DISCUSSION
A total of 20 patients who met the inclusion criteria and were willing to participate in the study were divided equally into the control and HBOT groups However, only five patients in the control group and five patients in the HBOT treatment group attended follow-up to assess the HOPE score
HBOT: Hyperbaric oxygen therapy; SD: standard deviation;
interva
The minimum age of the subjects participating in our study was 3 years and the maximum age was 32 years, with an average age of 12 6 years If detected early, hypospadias can be corrected surgically at 6 to 18 months of age, depending on the severity (13) No standard age exists for hypospadias repair surgery although if it is performed too early, the penis may be too
Hyperbaric
small and cause technical difficulties Some studies suggest that patients should take testosterone supplements until the penis size is sufficient to operate However, this method is not supported by strong evidence (14)
Performing surgery at an early age is more beneficial in terms of psychology because patients tend not to remember their previous condition, so their body image is more positive In addition, surgery at an older age is associated with more complications due to increased urethral secretions and nocturnal erections (15)
Several similar studies have recorded younger ages at surgery than the present study, such as Kocherov et al (29 4 months), Nabil et al (17 months), and Shenoy et al (50 4 months) (16-18)
Our study presented a significant difference of age between the HBOT group (17 4 years) and the control group (7 7 years), which complicates result interpretation Older participants may exhibit different biological responses, while younger ones face surgical challenges These differences, due to randomization in a small sample size, represent a key limitation of the study
The type of hypospadias in this study was most often subcoronal (35%), followed by penile (30%) and glandular (20%), and the least common was posterior (15%) This is in accordance with the theory that states that almost 50% of cases are anterior, 20% are penile, and the rest are posterior Overall, the subcoronal position is the most common for hypospadias (19, 20)
Conditions of oxygen deprivation in tissues often occur after hypospadias reconstruction surgery due to the large number of incisions and flaps on a relatively small area The placement of skin flaps in hypospadias repair surgery usually requires flap rotation, thus damaging the vascularization of epithelium and inducing vascular spasm in it Vasospasm is thought to be the main trigger of flap ischemia Tissue hypoxic conditions complicate the healing process, reduce the success rate of surgery, and increase postoperative complications (21)
HBOT is a therapeutic modality to improve tissue hypoxic conditions by increasing oxygen supply to damaged tissues Naturally, the process of angiogenesis occurs due to stimulation of the release of growth factors, cytokinases, and lipid mediators produced during injury One of the proangiogenesis mediators is VEGF HBOT helps accelerate the process of angiogenesis characterized by an increase in VEGF, which causes an acceleration of the wound healing process (3, 4)
Our study found that VEGF levels in patients who underwent HBOT were higher than in the control group (394 49 ± 107 88 pg/mL) Notably, the gradual increase in VEGF levels was directly proportional to the number of HBOT sessions given to patients The VEGF level was 392 76 ± 107 50 pg/mL after the first HBOT session, 448 49 ± 88 68 pg/dL after the second HBOT session, 516 49 ± 133 94 pg/mL after the third HBOT session, 618 09 ± 141 63 pg/dL after the fourth session, and 687 20 ± 687 20 pg/dL after the fifth session
A significant increase in VEGF (p < 0 05) was found after the third (p = 0 038), fourth (p = 0 002), and fifth (p = 0 008) HBOT sessions
The results of this study support previous research by Oley et al , who conducted a study on crush injury patients,
who were divided into HBOT and placebo treatment groups VEGF levels in the HBOT group were 1,505 9 ng/mL and higher that in patients undergoing debridement only
Similarly, VEGF mRNA expression was 1 2-fold higher in the group receiving HBOT therapy (22) A study by Chang et al on patients who underwent repair of recurrent hypospadias found that the group treated with 2% nitroglycerin and HBOT had a higher success rate (88 8%) compared to the group only given 2% nitroglycerin (69 6%)
Fewer complications were found in the HBOT group than in the control group (5)
Hypospadias reconstructive surgery aims to improve functional and cosmetic outcomes for patient satisfaction
The HOPE scoring system objectively evaluates hypospadias surgery outcomes, including complications, cosmetic appearance, and function (12) However, the system has limitations, such as the lack of perioperative assessment of hypospadias severity (23)
This study found that the HBOT group had a significantly better outcome in terms of penile torsion and total HOPE score compared to the control group
The p-value for both of these findings was less than 0 05, indicating that the differences were statistically significant This suggests that HBOT may have a positive effect on the clinical appearance of the wound after hypospadias reconstructive surgery Patients who received HBOT had better cosmetic appearance for meatal torsion variable and the total HOPE score
Complication rates are high for hypospadias reconstructive surgery, with nearly 40% of surgeries being repeat operations performed to improve cosmetic results Risk factors include scar tissue, ischemic tissue, negligence in surgical technique, improper sutures, improper suture tension, hematoma, and infection (24) Wound healing has four phases, with chronic tissue hypoxia disrupting the balance of collagen secretion and causing hypertrophy of scar tissue, resulting in wound deformities (25)
Another study found that the neovascularization of tissue through the process of HBOT, characterized by an increase in VEGF, resulted in faster wound healing, avoiding the formation of scar tissue and keloids (26-29)
The study demonstrates that HBOT accelerated wound healing after urethroplasty by increasing serum VEGF levels However, the study has some limitations, including the relatively high rate of loss to follow-up (50%) for the HOPE score evaluation (due to the COVID-19 pandemic situation)
The study also did not include measurement of the VEGF level before each HBOT session, so we do not know exactly how much the VEGF level increased after each H B O T s e s s i o n F u t u r e w o r k w i t h l a r g e r s t u d i e s i s required to determine the exact mechanism of action, with a 2-month post-operation follow-up to measure the clinical and functional outcomes
CONCLUSIONS
This study demonstrated that HBOT accelerated wound healing after urethroplasty by increasing the serum VEGF level Three or more HBOT sessions are recommended after hypospadias repair
M Hatibie Oley, M Christian Oley, A Astram Adhiatma Iskandar, et al
REFERENCES
1 T u r k y i l m a z Z , K a r a b u l u t R , A t a n A , S o n m e z K R e d o Hypospadias Repair: Comparison of Three Different Methods Urol Int 2020; 104:391-5
2 Snodgrass W, Bush N Staged Tubularized Autograft Repair for Primary Proximal Hypospadias with 30-Degree or Greater Ventral Curvature J Urol 2017; 198:680-6
3 Shinomiya N Molecular Mechanisms of Hyperbaric Oxygen Therapy In: Shinomiya N, Asai Y (eds) Hyperbaric Oxygenation Therapy Springer, Singapore 2020
4 Neheman A, Rappaport YH, Verhovsky G, et al Hyperbaric oxygen therapy for pediatric “hypospadias cripple” evaluating the advantages regarding graft take J Pediatr Urol 2020; 16:163 e1163 e7
5 Chang C, White C, Katz A, Hanna MK Management of ischemic tissues and skin flaps in Re-Operative and complex hypospadias repair using vasodilators and hyperbaric oxygen J Pediatr Urol 2020; 16:672 e1-672 e8
6 Ghahestani SM, Ahmadi A, Pashazadeh F, Lotfi B Validity and Reliability of the Persian Version of Hypospadias Objective Penile Evaluation (HOPE) Questionnaire J-Res-Urol 2022; 6:15-20
7 Krull S, Rissmann A, Krause H, et al Outcome after Hypospadias R e p a i r : E v a l u a t i o n U s i n g t h e H y p o s p a d i a s O b j e c t i v e P e n i l e Evaluation Score Eur J Pediatr Surg 2018; 28:268-272
8 Neheman A, Carr N, Beberashvili I, et al Predictors for cosmetic outcomes in hypospadias repair: prospective assessment based on validated questionnaires J Urol 2022; 207(Suppl 5):e128
9 van der Toorn F, de Jong TPVM, de Gier RPE, et al Introducing the HOPE (Hypospadias Objective Penile Evaluation)-score: A vali-
DECLARATIONS
E t h i c a l a p p r o v a l : This protocol was approved by the Institutional Review Board at our institution (no 149/EC/KEPKKANDOU/IX/2021) All procedures involving human participants were performed in accordance with the ethical standards of the 1964 Helsinki declaration and its later amendments or comparable ethical standards Informed consent was obtained from all child's parents or guardians participants included in the study
Availability of data and material: The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request
Competing interests: The authors declare that they have no competing interests
Funding: This research received no specific grant from any funding agency in the public, commercial, or not for- profit sectors
Authors' contributions: All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work
Acknowledgments: We acknowledge Fred van der Toorn et al for the development of the HOPE SCORE
dation study of an objective scoring system for evaluating cosmetic appearance in hypospadias patients J Pediatr Urol 2013; 9:100616
10 Schulz KF, Altman DG, Moher D CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials BMJ 2010; 340:c332-c332
11 Sukasah CL, Supit L Sidik-Chaula Urethroplasty and the Manset Flap for Non-Glanular Hypospadias Repair Jurnal Plastik Rekonstruksi 2012; 1:74-81
12 van der Toorn F, de Jong TPVM, de Gier RPE, et al Introducing the HOPE (Hypospadias Objective Penile Evaluation)-score: A validation study of an objective scoring system for evaluating cosmetic appearance in hypospadias patients J Pediatr Urol 2013; 9:100616
1 3 A n a n d S , L o t f o l l a h z a d e h S H y p o s p a d
Reconstruction 2023 Jun 3 In: StatPearls [Internet] Treasure Island (FL): StatPearls Publishing; 2024
14 Ahmad R, Chana R, Ali S, Khan S Role of parenteral testosterone in hypospadias: A study from a teaching hospital in India Urol Ann 2011; 3:138
15 Skarin Nordenvall A, Norrby C, Butwicka A, et al Nishimura W, editor Psychosocial outcomes in adult men born with hypospadias: A register-based study PLoS One 2017; 12:e0174923
16 Kocherov S, Lev G, Chertin B Use of BioGlue Surgical Adhesive in Hypospadias Repair Curr Urol 2014; 7:132-5
17 Shenoy NS, Tiwari C, Gandhi S, et al Efficacy of fibrin sealant as waterproof cover in improving outcome in hypospadias surgery Afr J Paediatr Surg India; 2021; 18:215-8
18 Sultan TA, Faktry TA, Nabil A, Shenishn MZ Prospective comparative study of hypospadias surgical repair with and without the use of fibrin sealant International Surgery Journal 2019; 6:2722
19 Atici A, Celikkaya M, El C, Akcora B Results of Surgery P e r f o r m e d o n 1 5 1 P
2 1 A p p e a d u - M e n s a h W , H e s s e A J , G l o v e r - A d d y H , e t a l Complications of hypospadias surgery: Experience in a tertiary hospital of a developing country Afr J Paediatr Surg 2015; 12:211
22 Oley MH, Oley MC, Noersasongko AD, et al Effects of hyperbaric oxygen therapy on vascular endothelial growth factor protein and mRNA in crush injury patients: A randomized controlled trial study International Journal of Surgery Open 2021; 29:33-9
23 Springer A Assessment of Outcome in Hypospadias Surgery - A Review Front Pediatr 2014; 2:2
24 Agrawal K, Misra A Unfavourable results in hypospadias Indian Journal of Plastic Surgery 2013; 46:419
25 Hong WX, Hu MS, Esquivel M, et al The Role of HypoxiaInducible Factor in Wound Healing Adv Wound Care (New Rochelle) 2014; 3:390-9
26 Xue M, Jackson CJ Extracellular Matrix Reorganization During Wound Healing and Its Impact on Abnormal Scarring Adv Wound Care (New Rochelle) 2015; 4:119-36
27 Liu Z-J, Velazquez OC Angiogenesis in Wound Healing In: DA Dartt (Ed)Encyclopedia of the Eye Academicc Press 2010, pp 99105
28 Peña-Villalobos I, Casanova-Maldonado I, Lois P, et al Hyperbaric Oxygen Increases Stem Cell Proliferation, Angiogenesis and Wound-Healing Ability of WJ-MSCs in Diabetic Mice Front Physiol 2018; 9:995
29 Shams F, Moravvej H, Hosseinzadeh S, et al Overexpression of VEGF in dermal fibroblast cells accelerates the angiogenesis and wound healing function: in vitro and in vivo studies Sci Rep 2022; 12:18529
Correspondence
Mendy Hatibie Oley (Corresponding Author) mendy hatibie@unsrat ac id
Division of Plastic Reconstructive and Aesthetic Surgery, Department of Surgery, Faculty of Medicine, Sam Ratulangi University, Jalan Raya Tanawangko No 56, Malalayang Satu Barat, Malalayang, Manado, North Sulawesi, 95162, Indonesia
Maximillian Christian Oley max oley@unsrat ac id
Division of Neurosurgery, Department of Surgery, Faculty of Medicine, Sam Ratulangi University - R D Kandou Hospital, Manado, Indonesia
Ari Astram Adhiatma Iskandar ari astram urologi@dosenlb unsrat ac id Division of Urology, Department of Surgery, Faculty of Medicine, Sam Ratulangi University - R D Kandou Hospital, Manado, Indonesia
Chaula Luthfia Sukasah chaula luthfia@ui ac id Indri Aulia drindriaulia@gmail com
Division of Plastic Reconstructive and Aesthetic Surgery, Department of Surgery, Faculty of Medicine, Universitas Indonesia - Dr Cipto Mangunkusumo Hospital, Jakarta, Indonesia
Fima Lanra Fredrik G Langi flangi2@unsrat ac id Department Epidemiology and Biostatistics, Public Health Faculty, Sam Ratulangi University, Manado, Indonesia
Harsali Fransicus Lampus harsali lampus@unsrat ac id
Division of Pediatric Surgery, Department of Surgery, Faculty of Medicine, Sam Ratulangi University - R D Kandou Hospital, Manado, Indonesia
Irawan Sukarno drirawan120@gmail com
Department of Surgery, Faculty of Medicine, Sam Ratulangi University, Manado, Indonesia
Vania Sukarno vaniasung03@gmail com Siloam Hospital, Manado, Indonesia
Muhammad Faruk muhammadfaruk@unhas ac id
Department of Surgery, Faculty of Medicine, Hasanuddin UniversityHasanuddin University Hospital, Makassar, Indonesia
M Hatibie Oley, M Christian Oley, A Astram Adhiatma Iskandar, et al
ORIGINAL PAPER
Discrepancy between male and female perceptions of ejaculation latency and sexual satisfaction: Results from
an online open survey
Andrea Cocci 1 , Marta Pezzoli 1,2 , Arturo Lo Giudice 3 , Gaia Polloni 4 , Giorgio Ivan Russo 3 , Leonardo Gajo 1, 2 , Daniel Giunti 5 , Michele Di Dio 6 , Borja Garcia Gòmez 7 , Manuel Alonso Isa 8 , Agustin Fraile Poblador 9 , Javier Romero Otero 10 , Andrea Minervini 1 , Mattia Lo Re 1, 2
1 Unit of Oncologic Minimally Invasive Urology and Andrology, University of Florence, Careggi Hospital, Florence, Italy;
2 Department of Experimental and Clinical Medicine, University of Florence, Florence, Italy;
3 Urology Section, Department of Surgery, University of Catania, Catania, Italy;
4 Centre of Psychology, Como, Italy;
5 Centro Integrato di Sessuologia Il Ponte, Florence, Italy;
6 Department of Surgery, Division of Urology, SS Annunziata Hospital, Cosenza, Italy;
7 Hospital Universitario 12 Octubre, Instituto de Investigación Sanitaria Hospital 12 de Octubre, Madrid, Spain;
8 Department of Urology, Hospital Universitario HM Puerta del Sur, Instituto Investigación Sanitaria HM Hospitales and ROC Clinic, Madrid, Spain;
9 Department of Urology, Hospital Universitario HM Rivas, Instituto Investigación Sanitaria HM Hospitales and ROC Clinic, Madrid, Spain;
10 Department of Urology, Hospital Universitario HM Sanchinarro, Instituto Investigación Sanitaria HM Hospitales and ROC Clinic, Madrid, Spain
Summary
Background: Premature ejaculation is a sexual dysfunction that can impact both men and women. This study aimed to shed light on this condition within a cohort as extensive as possible
Materials and methods: We conducted an online open survey, distributed via social media, proposing a questionnaire regarding various aspects including the duration of ejaculatory latency, perceptions of premature or delayed ejaculation, as well as lifestyle and psychological aspects of sexuality The questionnaire comprised 77 questions for male participants and 16 for female participants, with responses structured on a Likert scale ranging from 1 to 5
Results: A total of 1300 men and 1197 women participated in the survey, completing the entire questionnaire The median age (IQR) of male participants was 27 (23-32) years, while that of female participants was 22 (19-35) years. Men reported a median (IQR) ejaculatory latency time of 17 (8-20) minutes during sexual intercourse, compared to 20 (15-20) minutes reported by women Only 7 5% (98) of men and 5% (60) of women reported an ejaculatory latency time of less than 3 minutes in their last five sexual encounters (p = 0 0001) Twelve percent (160) of men believed they consistently experienced premature ejaculation, whereas only 3% (41) of women reported this sensation (p = 0.0001). Regarding satisfaction with ejaculatory latency time, 7% of men (85) expressed dissatisfaction, whereas only 2% of women (28) reported the same (p = 0.0001). Conversely, only 12% of men (160) considered themselves completely satisfied, compared to 30% of women (358) (p = 0.0001).
Conclusions: These analyses highlight a dissonance between male and female perceptions of premature ejaculation, not only in terms of actual intercourse duration but also in terms of psychological perception and sexual well-being This should suggest a need to increase awareness among the population regarding the contrast between idealized sexual experiences and reality
KEY WORDS: Premature ejaculation; Delayed ejaculation; Sexual satisfaction
Submitted 1 December 2024; Accepted 13 December 2024
INTRODUCTION
Premature ejaculation (PE) is a common sexual dysfunction that significantly impacts individuals' sexual experiences and overall well-being (1-3) PE is traditionally categorized into lifelong and acquired forms, with definitions often revisited by the scientific community According to the current definition by the International Society for Sexual Medicine (ISSM), acquired and lifelong PE are male sexual dysfunctions characterized by: (i) an intravaginal ejaculatory latency time (IELT) that always or nearly always is about one minute of vaginal penetration from the first sexual experience (lifelong PE), or a clinically significant and bothersome reduction in latency time, often to about three minutes or less (acquired PE); (ii) the inability to delay ejaculation on all or nearly all vaginal penetrations; and (iii) negative personal consequences, such as distress, bother, frustration, and/or the avoidance of sexual intimacy (4) The true prevalence of PE remains ambiguous, evidenced by a wide range of different multinational studies (5-8) Numerous studies have evaluated satisfaction with sexual life, considering both patients and their partners, in cases of sexual dysfunctions such as PE or erectile dysfunction (ED), as well as in the general population, underscoring the adverse effects of PE on relationships and sexual satisfaction (9-11) The primary aim of this study is to assess the ejaculatory latency time with a focus on the prevalence of PE in a large cohort of young patients, to
understand how it affects satisfaction with sexual intercourse for both males and their partners Secondary objectives include evaluating factors that may influence PE and examining behaviors adopted by the population in reallife experiences to enhance their quality of sexual life
MATERIALS AND METHODS
Study population
Participants were recruited via nonpaid posts of a survey link on Instagram, Facebook and Telegram, correlated to the webpage “Sessuologia” of Daniel Giunti (https://www instagram com/sessuologia/?hl=it) No advertising campaigns or giveaway incentives were utilized for patient recruitment, and all responses were kept completely anonymous Inclusion criteria included being 18 years of age or older, proficiency in the Italian language, and providing informed consent before accessing the survey, with the explicit option to terminate participation at any time by closing the webpage Data from participants who did not complete the survey were omitted from the analysis Additionally, measures were implemented to prevent individuals from participating in the survey more than once A completed checklist following the CHERRIES criteria (12) is provided as Supplementary material 1
Questionnaire
Institutional Review Board (IRB) approval was not required from our center for this kind of survey, but an informed consent was provided before the start of the questionnaire with information on the topics of the survey, the anonymity of the responses and the possibility to terminate participation at any time by closing the webpage The survey encompassed a variety of questions, and two models were developed (refer to Supplement Material 2): one targeting the male population, comprising 77 questions that were more complex and detailed regarding aspects of masturbation (age of onset, frequency, ejaculation latency), lifestyle (consumption of alcohol, drugs, and their influence on ejaculation time), and psychological aspects of sexuality; the other tailored to the female population, consisting of 16 questions, primarily addressing the frequency and duration of sexual intercourse and its impact on sexual life satisfaction Ejaculatory latency time was documented as the average duration across the last five penetrative and masturbatory episodes PE patients were identified as individuals with an IELT of less than three minutes and who exhibited distress related to this condition, as evidenced in the psychological questions
Statistical analysis
Descriptive statistics were utilized to examine the responses from the questionnaire The sample was one of convenience, without the conduct of a power analysis The estimations of IELTs did not follow a normal distribution; therefore, summarized data are presented as medians and interquartile ranges
Response frequencies were compared between male and female groups using the Chi-square test A multivariate logistic regression was employed to analyze the association between the condition of PE and factors such as abnormal
sexual habits or trauma, lifestyle, and psychic dysfunction
Statistical analyses were performed using STATA (StataCorp 2023 Stata Statistical Software: Release 18 College Station, TX: StataCorp LLC)
RESULTS
Demographic characteristics
A total of 2,497 respondents were included in this study, with 1,300 men and 1,197 women The male sample comprised individuals who identified as heterosexual straight
Table 1.
Demographic characteristics
A Cocci, M Pezzoli, A Lo Giudice, et
(n = 1,148, 88 3%), homosexual gay (n = 65, 5 0%), bisexual (n = 74, 5 7%), and other or unspecified orientations (n = 13, 1 0%) We included female participants who had sexual intercourses with male subjects, independently from their sexual orientation
The median age (IQR) for the two groups was 27 (23-32) for men and 22 (19-35) for women The participation of principally young subjects was probably due to the use of social media At the time of the survey, 83 3% (n = 1083) of men and 83 7% (n = 1002) of women reported being in a stable relationship The most frequent rate of sexual intercourse reported was 1-2 times per week by 43 5% (n = 566) of men and 58 1% (n = 695) of women
Median (IQR) ejaculatory latency time (ELT) declared by men during sexual intercourse was 17 (8-20) minutes versus 20 (15-20) minutes by women
Additional demographic and sexual life-related characteristics are reported in Table 1
Regarding the perception of suffering from delayed ejaculation, 44 5% (n = 578) of men and 52 3% (n = 626) of women declared that they had never experienced it (Table 2)
Conversely, 8 3% (n = 108) of men believed they always suffered from delayed ejaculation, while only 2 1% (n = 25) of women reported that they partners never suffered if it (p < 0 01)
In terms of perceived suffering from PE, 36 3% (n = 472) of men reported never experiencing it, in contrast to
Table 2
60 9% (n = 730) of women who reported that they partners never suffered if it (p < 0 01) While 12 3% (n = 160) of men believed they always suffered from PE, only 3 4% (n = 41) of women reported this feeling (p < 0 01) (Figure 1) However, only 7 5% (n = 98) of men and 5% (n = 60) of women declared an ejaculatory latency time of under 3 minutes in their last five sexual encounters (p < 0 01)
Regarding satisfaction with ejaculatory latency time, 6 5% (n = 85) of men considered themselves unsatisfied, compared to 2 3% (n = 28) of women (p < 0 01) Moreover, only 12 3% (n = 160) of men reported being fully satisfied, versus 29 9% (n = 358) of women (p < 0 01) (Figure 2) In terms of overall sexual satisfaction, only 25 9% (n = 337) of men considered themselves fully satisfied, compared with 43 5% (n = 521) of women (p < 0 01) (Figure 3)
Figure 1. Feeling premature ejaculation
Figure 2
Satisfaction with ejaculatory latency time
Figure 3. Overall sexual satisfaction
Figure 4
Graphical representation of most used expedients for retarding ejaculation
Finally, most men often or always use expedients to delay ejaculation, most used the "stop and start" technique, and the change of intercourse position (Table 4) (Figure 4)
Factors associated with premature ejaculation
In Table 3 we reported the result of the multivariate logistic regression analysis
In the analysis, the odds ratio in predicting PE during sexual intercourse for "age", "substance abuse" and "porn use frequency” was 1 00 (p = 0 46) 0 76 (p = 0 24) and 0 88 (p = 0 66), respectively
The odds ratio in predicting PE for "masturbation frequency" , "penetrating frequency" and "erection quality" was 0 76 (p = 0 02), 0 75 (p < 0 01) and 0 73 (p < 0 01)
The odds ratio in predicting PE during sexual intercourse for "premature ejaculation during masturbation" was 6 74 (p < 0 001)
The odds ratio for "alcohol abuse" is 1 60 (p = 0 019), suggesting that alcohol use has a positive effect, increasing the risk of PE
The odds ratio for "sex desire" is 1 02 (p = 0 903), indicating that sexual desire does not significantly affect PE
DISCUSSION
Here, we presented our work in which we subjected the largest population cohort presented in a study from a single center to the best of our knowledge, to a questionnaire regarding the sexual life of both men and women
In this study, the IELT reported by male patients was a median (IQR) of 17 (8-20) minutes This finding is corroborated by female partners, who reported a median IELT of 20 (15-20) minutes, indicating an increased dura-
tion of intercourse compared to that reported in the literature For instance, Nguyen et al (13) recently observed a perceived IELT of 6 09 (± 6 59) minutes (median 3 minutes, range 0 5-45 minutes), which was 2 01 (± 1 21) minutes for the PE-affected group and 11 69 (± 6 83) minutes for the control group, in a population with a mean age of 30 9 (±6 84) years, similar to our study's population (median 27 (23-32) years) Conversely, Giuliano et al (14), in a multicentric study, reported a median IELT in the group of Italian subjects not affected by PE of 15 0 (1 5-45 0) minutes, more in line with our data, although our series did not differentiate between patients affected by PE and those who were not Moreover, Patrick et al (15), in a study of a large population sample (1,587 patients), noted a median IELT of 1 8 (range, 0-41) minutes for PE subjects and 7 3 (range, 0-53) minutes for
Table 3.
Multiple logistic regression of factors associated with premature ejaculation
non-PE subjects, with a mean age of 35 4 (± 10 7) years
Our results, therefore, offer an update on the average IELT among the population, particularly in younger individuals
Regarding the prevalence of PE, we observed a global prevalence of 7 5% in our study population, which aligns with the results of two large observational studies included in the ISSM evidence-based definition of PE, where the prevalence of lifelong and acquired PE was 6 2% and 8 0%, respectively (2, 3)
The implementation of multivariate logistic regression analysis enabled the assessment of predictive factors for PE Factors such as masturbation frequency, penetration frequency, and quality of erections were identified as having a negative impact on PE The association between penetration frequency and PE is well-documented in the literature This was highlighted in a study by Verze et al (16), which found that Italian men with PE experienced a significant reduction in sexual intercourse attempts A comparable decline in sexual frequency was observed among men with PE versus non-PE men in a study based on the Korean general population (17) Consistently, the current study found an inverse correlation, indicating that a higher frequency of sexual intercourse was associated with a reduced probability of experiencing PE (Table 3) The correlation between ED and PE is equally evident, with a higher incidence of PE noted in patients with ED (18-20), a finding that is consistent with observations from the current research (Table 3)
Concerning sexual desire, our results were contrasting While the study was based on the Korean general population (17), low libido was more frequent in men with PE compared to men without, we did not find those association
Our questionnaire incorporated five questions related to potential PE prevention techniques (Male Questionnaire, Questions 58-62, Supplementary Material 2) Behavioral therapy is recognized as a critical component in the management of PE (21-24) As indicated in Table 4, the "start and stop" method, along with "changing position, " emerged as the most frequently utilized technique in our sample, reported as sometimes or often by 40% and 30% for the former, and 38% and 23% for the latter, respectively Given that "changing position" could be considered another variant of the "start and stop" method, a considerable segment of the population employs these techniques
This suggests that a majority of the population, even those not diagnosed with PE, use behavioral strategies to extend the duration of sexual encounters, which in turn
Table 4. Most used expedients for retarding ejaculation
indicates a high prevalence of subjective PE On one hand, this finding may explain the higher IELT observed in our cohort compared to that documented in the literature; on the other hand, it could imply a degree of discomfort with the duration of intercourse, despite exceeding the 3-minute threshold defined by the ISSM
Concerning the latter point, this study facilitates the assessment of both men's and their partners' satisfaction with sexual activity and their expectations The link between PE and personal distress is well-established (25), with varying impacts on men and their partners Patrick et al (15) reported that partners' perceptions of PE are typically less problematic than those of the affected individuals This was also supported by Verze et al (16), although a significantly higher proportion of partners of men with PE reported personal distress (44% vs 3%) and interpersonal difficulties (25% vs 2%) compared to partners of non-PE men Graziottin & Althof (10), in a 2011 review, identified significantly greater sexual problems, decreased satisfaction, and heightened distress and interpersonal difficulties among partners of men with PE than those of non-PE men
In our dataset, as depicted in Table 2, there is a notable disparity in terms of satisfaction between men and women concerning the duration of intercourse and related sensations Specifically, only 26% of men reported full satisfaction, compared to 44% of women This discrepancy, alongside the fact that the study involved a younger population with fewer comorbidities that could impair sexual activity, should prompt reflection on the psychological pressures faced by young men regarding sexual performance and may direct educational interventions toward a more accurate understanding of sexual realities and the adjustment of expectations to prevent a dysfunctional misperception of sexual life
This research offers a fresh outlook on the perception of ELTs among the young, male and female, population, and its influence on the behavioral and emotional facets of sexual life, and encompasses the largest mixed cohort yet assessed with this method, to the best of our knowledge
The substantial case series also enabled us to evaluate various factors associated with PE, corroborating existing literature (26, 27) Additionally, through the questionnaire focused on the psychological domain, this study offers a preliminary view into the perceived differences in sexual life satisfaction between men and women
The interpretations of our findings must consider the study's limitations Primarily, the employed questionnaire is not internationally validated, though it is akin to other instruments, such as the SCS-M (28) or the Female Sexual Distress Scale-Revised-Premature Ejaculation (FSDS-R-PE) devised by Limoncin et al (29) Nonetheless, the use of a multi-item questionnaire enabled us to explore various aspects not assessable by any single questionnaire available in the literature to date Secondly, it should be acknowledged that the study relies on voluntary participation in a questionnaire disseminated by a page addressing these types of issues Consequently, it must be recognized that there is no explicit distinction between users who actively seek out the page, presumably for concerns pertaining to the sexual sphere, and those who encounter the page through sponsored content without perceiving themselves
to have such issues Additionally, due to the specific clinical setting we employed, we did not differentiate whether the subjects had lifelong or acquired PE Since the different clinical expressions of PE rarely require different treatment strategies, this bias does not significantly impact our results An additional significant limitation is that the study participants were not evaluated by a professional, such as a sexologist or psychosexologist, which would have permitted a more precise objectification of the feelings described by the population Regrettably, this limitation is intrinsic to the study design, which was structured as a survey The inclusion of a predominantly young sample may introduce biases, especially concerning the prevalence of ED and its impact on PE (30)
CONCLUSIONS
In conclusion, our findings, given the extensive sample size and the range of assessed items, provide new insights into the prevalence of subjective premature ejaculation and its psychological consequences for both patients and their partners within the Italian population Moreover, these results affirm the documented correlations between PE and its risk factors
REFERENCES
1 Rosen RC, Althof S Impact of Premature Ejaculation: The Psychological, Quality of Life, and Sexual Relationship Consequences J Sex Med 2008; 5:1296-1307
2 Gao J, Zhang X, Su P, et al Prevalence and Factors Associated with
DECLARATIONS
Ethical approval: This research has been conducted in the public arena using only publicly available or accessible records without contact with the individual/s and it does not require ethics reviews according to Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans Articles 2 2 to 2 4
Availability of data and material: The datasets used and/or analyzed during the current study are available upon reasonable request from the corresponding author
Competing interests: The authors declare that they have no competing interests
Funding: The authors report no involvement in the research by the sponsor that could have influenced the outcome of this work
Authors' contributions: AC and MLR have given substantial contributions to the conception and the design of the manuscript ALG, MP, GP, MDD, MAI, AFP, GL and DG to the acquisition of the data; MLR and ALG to the analysis and interpretation of the data MLR, AC, ALG have participated to drafting the manuscript, BGG, JRO, AM revised it critically
All authors read and approved the final version of the manuscript
Acknowledgments: Not applicable
Consent for publication: Not applicable
the Complaint of Premature Ejaculation and the Four Premature Ejaculation Syndromes: A Large Observational Study in China J Sex Med 2013; 10:1874-1881
3 Serefoglu EC, Yaman O, Cayan S, et al Prevalence of the Complaint of Ejaculating Prematurely and the Four Premature Ejaculation Syndromes: Results from the Turkish Society of Andrology Sexual Health Survey J Sex Med 2011; 8:540-548
4 Serefoglu EC, Mcmahon CG, Waldinger MD, et al An EvidenceBased Unified Definition of Lifelong and Acquired Premature Ejaculation: Report of the Second International Society for Sexual Medicine Ad Hoc Committee for the Definition of Premature Ejaculation Sex Med 2014; 2:41-59
5 Laumann EO, Paik A, Rosen RC Sexual dysfunction in the United States: prevalence and predictors JAMA 1999; 281:537-44
6 Basile Fasolo C, Mirone V, Gentile V, et al Premature Ejaculation: Prevalence and Associated Conditions in a Sample of 12,558 Men Attending the Andrology Prevention Week 2001 A Study of the Italian Society of Andrology (SIA) J Sex Med 2005; 2:376-382
7 Gospodinoff ML Premature ejaculation: clinical subgroups and etiology J Sex Marital Ther 1989; 15:130-134
8 Santillán-Romero AS, Valladares-Garrido MJ, Juarez-Ubillus A, et al Prevalence and associated factors of premature ejaculation and erectile dysfunction in young, single men who have sex with men in Lima, Peru Sex Med 2024; 12:qfae013
9 Burri A, Giuliano F, Mcmahon C, Porst H Female Partner’s Perception of Premature Ejaculation and Its Impact on Relationship Breakups, Relationship Quality, and Sexual Satisfaction J Sex Med 2014; 11:2243-2255
10 Graziottin A, Althof S What does premature ejaculation mean to the man, the woman, and the couple? J Sex Med 2011; 8(Suppl 4):304-309
11 Waldinger MD, Quinn P, Dilleen M, et al A multinational population survey of intravaginal ejaculation latency time J Sex Med 2005; 2:492-497
12 Eysenbach G Improving the quality of web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES) J Med Internet Res 2004; 6:e34
13 Nguyen HB, Nguyen CT, Pham MQ, et al Perceived intravaginal ejaculation latency time: The diagnosis of premature ejaculation among Vietnamese men Andrology 2024; 12:618-623
14 Giuliano F, Patrick DL, Porst H, et al Premature Ejaculation: Results from a Five-Country European Observational Study Eur Urol 2008; 53:1048-1057
15 Patrick DL, Althof SE, Pryor JL, et al Premature ejaculation: An observational study of men and their partners Journal of Sexual Medicine 2005; 2:358-367
16 Verze P, Arcaniolo D, Imbimbo C, et al General and sex profile of women with partner affected by premature ejaculation: results of a large observational, non-interventional, cross-sectional, epidemiological study (IPER-F) Andrology 2018; 6:714-719
17 Lee SW, Lee JH, Sung HH, et al The prevalence of premature ejaculation and its clinical characteristics in Korean men according to different definitions Int J Impot Res 2013; 25:12-7
18 Corona G Erectile dysfunction and premature ejaculation: a continuum movens supporting couple sexual dysfunction J Endocrinol Invest 2022; 45:2029-2041
19 Moussa M, Papatsoris AG, Chakra MA, et al Erectile dysfunction in common neurological conditions: A narrative review Arch Ital Urol Androl 2020; 92:371-385
A Cocci, M Pezzoli, A Lo Giudice, et al
20 Metz ME, Pryor JL Premature ejaculation: A psycho physiological approach for assessment and management J Sex Marital Ther 2000; 26:293-309
21 Ia AH, Naggar E, Gilany AH El Assessment of as needed use of pharmacotherapy and the pause-squeeze technique in premature ejaculation Int J Impot Res 2001; 13:41-5
22 Yuan P, Dai J, Yang Y, et al A comparative study on treatment for premature ejaculation: Citalopram used in combination with behavioral therapy versus either Citalopram or behavioral therapy alone 2008; pp 35-38 https://www researchgate net/publication/ 292872130
A comparative study on treatment for premature ejaculation Ci talopram used in combination with behavioral therapy versus eit her Citalopram or behavioral therapy alone
23 Dogan K, Keçe C Comparison of the results of stop-start technique with stop-start technique and sphincter control training applied in premature ejaculation treatment PLoS One 2023; 18:e0283091
24 Cooper K, James MMS, Kaltenthaler E, et al Interventions to treat premature ejaculation: A systematic review short report Health Technol Assess (Rockv) 2015; 19:1-180
25 Russo GI, Cocci A Do we have put a new cornerstone for the
treatment of premature ejaculation? Int J Impot Res 2018; 30:272273
26 Ventus D, Jern P Lifestyle Factors and Premature Ejaculation: Are Physical Exercise, Alcohol Consumption, and Body Mass Index Associated with Premature Ejaculation and Comorbid Erectile Problems? J Sex Med 2016; 13:1482-1487
27 Herkommer K, Meissner VH, Dinkel A, et al Prevalence, lifestyle, and risk factors of erectile dysfunction, premature ejaculation, and low libido in middle-aged men: first results of the Bavarian Men’s Health-Study Andrology 2024; 12:801-808
28 Gündüz A, Sertçelik S, Gündogmus I, et al Turkish validity and reliability of the sexual complaints screener for men Turkish validity and reliability of the sexual complaints screener for men Psychiatry and Clinical Psychopharmacology 2018; 29:1-6
29 Limoncin E, Tomassetti M, Gravina GL, et al Premature ejaculation results in female sexual distress: Standardization and validation of a new diagnostic tool for sexual distress J Urol 2013; 18:1830-1835
30 Jannini EA, Lombardo F, Lenzi A Correlation between ejaculatory and erectile dysfunction Int J Androl 2005; 28(Suppl 2):40-45
Correspondence
Andrea Cocci, MD (Corresponding Author) cocci andrea@gmail com
Unit of Oncologic Minimally Invasive Urology and Andrology, University of Florence, Careggi Hospital, 50100 Florence, Italy
Marta Pezzoli
marta pezzoli@unifi it
Leonardo Gajo leonardo gajo@unifi it
Unit of Oncologic Minimally Invasive Urology and Andrology, Department of Urology, University of Florence, Careggi Hospital, 50100 Florence, Italy
Arturo Lo Giudice arturologiudice@gmail com
Giorgio Ivan Russo giorgioivan russo@unict it
Urology Section, Department of Surgery, University of Catania, Catania 95131, Italy
Gaia Polloni info@gaiapolloni com Centre of Psychology, Via Cadorna, 22100 Como, Italy
Daniel Giunti danielgiunti@gmail com Centro Integrato di Sessuologia Il Ponte, 50100 Florence, Italy
Michele Di Dio m didio@aocs it
Department of Surgery, Division of Urology, SS Annunziata Hospital, Cosenza, Italy
Borja Garcia Gòmez borjagarciagomez@gmail com
Hospital Universitario 12 Octubre, Instituto de Investigación Sanitaria Hospital 12 de Octubre, Madrid 28041, Spain
Manuel Alonso Isa manuel alonso@rocclinic com Department of Urology, Hospital Universitario HM Puerta del Sur, Instituto Investigación Sanitaria HM Hospitales and ROC Clinic, Madrid, Spain
Agustin Fraile Poblador agustin fraile@rocurologia com Department of Urology, Hospital Universitario HM Rivas, Instituto Investigación Sanitaria HM Hospitales and ROC Clinic, Madrid, Spain
Javier Romero Otero jromerootero@rocclinic com Department of Urology, Hospital Universitario HM Sanchinarro, Instituto Investigación Sanitaria HM Hospitales and ROC Clinic, Madrid, Spain
Andrea Minervini andrea minervini@unifi it Mattia Lo Re mattialore1994@gmail com Unit of Oncologic Minimally Invasive Urology and Andrology, University of Florence, Careggi Hospital, 50100 Florence, Italy
Discrepancy between male and female perceptions of ejaculation latency and sexual satisfaction: Results from an online open survey
Andrea Cocci 1 , Marta Pezzoli 1,2 , Arturo Lo Giudice 3 , Gaia Polloni 4 , Giorgio Ivan Russo 3 , Leonardo Gajo 1, 2 , Daniel Giunti 5 , Michele Di Dio 6 , Borja Garcia Gòmez 7 , Manuel Alonso Isa 8 , Agustin Fraile Poblador 9 , Javier Romero Otero 10 , Andrea Minervini 1 , Mattia Lo Re 1, 2
1 Unit of Oncologic Minimally Invasive Urology and Andrology, University of Florence, Careggi Hospital, Florence, Italy;
2 Department of Experimental and Clinical Medicine, University of Florence, Florence, Italy;
3 Urology Section, Department of Surgery, University of Catania, Catania, Italy;
4 Centre of Psychology, Como, Italy;
5 Centro Integrato di Sessuologia Il Ponte, Florence, Italy;
6 Department of Surgery, Division of Urology, SS Annunziata Hospital, Cosenza, Italy;
7 Hospital Universitario 12 Octubre, Instituto de Investigación Sanitaria Hospital 12 de Octubre, Madrid, Spain;
8 Department of Urology, Hospital Universitario HM Puerta del Sur, Instituto Investigación Sanitaria HM Hospitales and ROC Clinic, Madrid, Spain;
9 Department of Urology, Hospital Universitario HM Rivas, Instituto Investigación Sanitaria HM Hospitales and ROC Clinic, Madrid, Spain;
10 Department of Urology, Hospital Universitario HM Sanchinarro, Instituto Investigación Sanitaria HM Hospitales and ROC Clinic, Madrid, Spain
Table 1. Checklist for Reporting Results of Internet E-Surveys (CHERRIES).
No need for IRB is required from our center for this kind of survey and informed consent process
Informed consent was registered before the questionnaire People were informed on the length and the thematic of the survey
Data protection Data were anonymized and stored in private server, accessible from the investigators only
Development and pre-testing Development and testing Survey was developed as a Google questionnaire, from a drive create for the occasion Recruitment process and description of the Open survey
An “open survey” is a survey open for each visitor of a site sample having access to the questionnaire
Contact mode
Survey administration
Questionnaire was proposed via social media from the page “Sessuologia – di Daniele Giunti”
Advertising the survey Survey was published via Instagram Stories, Instagram posts, Facebook posts, Tik Tok posts, reaching firstly follower of the page and then common contact
Web/E-mail
Posted as previously said, then people get redirected in a Google surveys
Context The page “Sessuologia – di Daniele Giunti” is mainly oriented on discussing sexulogy topic, from serious and real problems to lighter topics As a sexual-oriented page, people visiting it could be affected from some kind of problem, and that could lead to a selection bias
Mandatory/voluntary Voluntary survey
Incentives NO
Time/Date
One month 1 October 2023 – 1 November 2023
Randomization of items or questionnaires No randomization was needed
Adaptive questioning
Number of Items 7
Questions were mainly closed, with a Likert scale of answers Open questions were specified
Number of screens (pages) 11
Completeness check
Response rates
All items provided a non-response option such as “not applicable” or “rather not say”, and selection of one response option was mandatory to go on to other questions
Review step through a Back button
Unique site visitor
Unique visitors were assured using IP and cookies
View rate (Ratio of unique survey No data regarding view rate are available visitors/unique site visitors)
Participation rate (Ratio of unique visitors No data regarding participation rate are available who agreed to participate/unique first survey page visitors)
Completion rate (Ratio of users who finished No data regarding completion rate are available the survey/users who agreed to participate)
Preventing multiple entries from Cookies used
Cookies were not used as a unique identifier Entering with Google account is required to take the assessment to prevent the same individual duplicate submissions
IP check IP address was not used as a unique identifier Entering with Google account is required to take the assessment to prevent duplicate submissions
Log file analysis None used.
Registration Registration was performed via Google account Analysis
Handling of incomplete questionnaires Only completed questionnaire were analyzed
Questionnaires submitted with an atypical Time for completing the assessment is not tracked We estimate it takes 10 minutes to complete the survey
timestamp
Statistical correction No weighting was done on the users’ responses
A Cocci, M Pezzoli, A Lo Giudice,
Discrepancy between male and female perceptions of ejaculation latency and sexual satisfaction: Results from an online open survey
Andrea Cocci 1 , Marta Pezzoli 1,2 , Arturo Lo Giudice 3 , Gaia Polloni 4 , Giorgio Ivan Russo 3 , Leonardo Gajo 1, 2 , Daniel Giunti 5 , Michele Di Dio 6 , Borja Garcia Gòmez 7 , Manuel Alonso Isa 8 , Agustin Fraile Poblador 9 , Javier Romero Otero 10 , Andrea Minervini 1 , Mattia Lo Re 1, 2
1 Unit of Oncologic Minimally Invasive Urology and Andrology, University of Florence, Careggi Hospital, Florence, Italy;
2 Department of Experimental and Clinical Medicine, University of Florence, Florence, Italy;
3 Urology Section, Department of Surgery, University of Catania, Catania, Italy;
4 Centre of Psychology, Como, Italy;
5 Centro Integrato di Sessuologia Il Ponte, Florence, Italy;
6 Department of Surgery, Division of Urology, SS Annunziata Hospital, Cosenza, Italy;
7 Hospital Universitario 12 Octubre, Instituto de Investigación Sanitaria Hospital 12 de Octubre, Madrid, Spain;
8 Department of Urology, Hospital Universitario HM Puerta del Sur, Instituto Investigación Sanitaria HM Hospitales and ROC Clinic, Madrid, Spain;
9 Department of Urology, Hospital Universitario HM Rivas, Instituto Investigación Sanitaria HM Hospitales and ROC Clinic, Madrid, Spain;
10 Department of Urology, Hospital Universitario HM Sanchinarro, Instituto Investigación Sanitaria HM Hospitales and ROC Clinic, Madrid, Spain
MALE QUESTIONNAIRE (ORIGINAL – ITALIAN LANGUAGE)
1. Quanti anni hai?
2 In quale genere ti identifichi?
3. Qual è la tua etnia?
4 Qual è il tuo livello di istruzione?
5 Qual è la tua professione?
6. In che parte d'Italia vivi?
7 Quanto sei alto (in centimetri)?
8 Quanto pesi (in kg)?
9. BMI?
10 Fumi?
11. Fai uso di bevande alcoliche?
12 Fai uso di sostanze stupefacenti?
13 Se fai uso di sostanze stupefacenti, indica quali utilizzi (possibili una o più risposte)
14. Assumi farmaci antidepressivi?
15 Soffri di malattie alla tiroide?
16 Soffri di malattie neurologiche?
17. Reputi di soffrire di ansia?
18 Reputi di soffrire di sintomi depressivi (es apatia, affaticabilità, tristezza pervasiva, pianti ricorrenti)?
19. Il tuo sonno è sufficiente e riposante?
20 Hai fratelli?
21 Hai sorelle?
22. Sei circonciso?
23 In caso di risposta affermativa a che età hai eseguito la circoncisione (se invece non sei circonciso indica " ")?
24 Soffri di frenulo corto?
25 hai difficoltà ad abbassare la pelle del pene (il prepuzio) durante l'erezione o durante il rapporto?
26. Soffri regolarmente di prostatiti o infezioni/infiammazione dei genitali?
27 Descrivi il tuo orientamento sessuale
28 Relazione sentimentale
29. Con quale frequenza utilizzi materiale pornografico (di qualsiasi genere)?
30 Ti capita di masturbarti utilizzando esclusivamente fantasie sessuali?
31. Con quale frequenza pratichi sexting e/o camming? (Sexting: invio e ricezione di messaggi, testi, video e/o immagini sessualmente espliciti; Camming: insieme di pratiche sessuali che si possono sperimentare mentre si è in contatto con una persona in videochat)
32 Sei a conoscenza di essere stato tradito?
33. A quanti anni ti sei masturbato per la prima volta?
34 Ritieni di aver avuto la giusta privacy durante le tue prime esperienze con la masturbazione?
35 Sei mai stato sgridato a seguito dell'essere stato scoperto mentre ti masturbavi?
36 Quando hai iniziato a praticare la masturbazione o i primi rapporti sessuali, solitamente eri costretto a doverlo fare in fretta (es perché in casa c'erano i genitori, avevi paura di essere scoperto, ecc )?
37. Solitamente ti masturbi:
38 Utilizzi il lubrificante quando ti masturbi?
39 Con quale frequenza ti masturbi?
40. Quanto spesso ti capita di essere interrotto mentre ti masturbi?
41 Riferendoti alle ultime cinque volte in cui ti sei masturbato, quanti minuti sono intercorsi tra l’inizio della masturbazione e l’eiaculazione?
42. Hai rapporti sessuali con...
43 Hai rapporti sessuali con partner
44 Con quale frequenza hai rapporti sessuali penetrativi?
45. Utilizzi il preservativo durante i rapporti sessuali?
46 Riesci a raggiungere e mantenere l'erezione fino alla fine del rapporto sessuale
47 Reputi il tuo desiderio sessuale:
48. Quanto spesso fai preliminari prima di iniziare un rapporto sessuale? (i preliminari possono includere baci, carezze, masturbazione reciproca, sesso orale, interpretazione di ruoli sessuali e pratiche fetish o BDSM)
49. In media quanto tempo dedichi ai preliminari?
50 Eviti o limiti al minimo i preliminari ricevuti per paura di venire ancora prima?
51 Ti capita di provare fastidio o dolore al pene durante i rapporti sessuali?
52. In quali luoghi ti capita più frequentemente di avere rapporti sessuali? (possibili una o più risposte)
53 Se hai risposto altro, specifica dove , altrimenti scrivi NO
54 Quanto spesso vieni interrotto durante i rapporti sessuali?
55. Quanto spesso riesci a eiaculare durante i rapporti sessuali?
56 Hai mai simulato l'orgasmo durante un rapporto sessuale penetrativo?
57. Ti è mai capitato di masturbarti prima di un incontro sessuale con lo scopo di riuscire a durare più a lungo?
58 Hai mai utilizzato sostanze stupefacenti prima di un rapporto sessuale con lo scopo di riuscire a durare più a lungo?
59 Durante un rapporto sessuale penetrativo, ti è capitato di fermare i movimenti coitali, riprendere il controllo e ripartire, con lo scopo di durare più a lungo?
60. Durante un rapporto sessuale penetrativo, ti è capitato di cambiare frequentemente posizione sessuale con lo scopo di riuscire a durare più a lungo?
61 Utilizzi preservativi ritardanti, creme anestetiche oppure farmaci come paroxetina o dapoxetina con lo scopo di riuscire a durare più a lungo?
62 Riferendoti agli ultimi cinque rapporti sessuali penetrativi che hai avuto, in media dopo quanti minuti dallinizio della penetrazione hai eiaculato?
63. Quanto spesso hai la sensazione di impiegare TROPPO tempo ad eiaculare durante i rapporti sessuali?
64 Quando hai la sensazione di impiegare troppo tempo ad eiaculare, provi
65. Quanto spesso hai la sensazione di impiegare TROPPO POCO tempo ad eiaculare durante i rapporti sessuali?
66 Quando hai la sensazione di impiegare troppo poco tempo ad eiaculare, provi
67 Sei soddisfatto del tempo che intercorre tra l'inizio della penetrazione e l'eiaculazione?
68. Secondo te quanto influiscono i preliminari nel tempo che intercorre tra l'inizio della penetrazione e l'eiaculazione?
69 Credi che il/la/i tuo/a/oi partner sia/siano soddisfatto/a/i del tempo che intercorre tra l'inizio della penetrazione e l'eiaculazione?
70. In generale, sei soddisfatto dei rapporti sessuali che hai avuto negli ultimi sei mesi?
FEMALE QUESTIONNAIRE (ORIGINAL – ITALIAN LANGUAGE)
1 In quale genere ti identifichi?
2 In quale fascia d'età ti collochi?
3. Qual è la tua etnia?
4 Qual è il tuo livello di istruzione?
5. Hai rapporti sessuali regolari con un partner di genere maschile?
6 Hai una relazione stabile con un partner di genere maschile?
7 Con quale frequenza hai rapporti sessuali con il tuo partner?
8. Quanto spesso il tuo partner riesce ad eiaculare durante i rapporti sessuali?
9 Quanto spesso tu e il tuo partner fate preliminari prima del rapporto sessuale? (i preliminari possono includere baci, carezze, masturbazione reciproca, sesso orale, interpretazione di ruoli sessuali e pratiche fetish o BDSM)
10. Quanto tempo tu e il tuo partner dedicate ai preliminari?
11 Riferendoti agli ultimi 5 rapporti sessuali che hai avuto, in media dopo quanti minuti dall'inizio della penetrazione il tuo partner ha eiaculato?
12. Quanto spesso hai la sensazione che il tuo partner impieghi TROPPO tempo ad eiaculare durante i rapporti sessuali?
13 Quanto spesso hai la sensazione che il tuo partner impieghi TROPPO POCO tempo ad eiaculare durante i rapporti sessuali?
14 Sei soddisfatto/a del tempo che intercorre tra l'inizio della penetrazione e l'eiaculazione del tuo partner?
15. Secondo te quanto influiscono i preliminari nel tempo che intercorre tra l'inizio della penetrazione e l'eiaculazione del tuo partner?
16 Secondo te i preliminari influiscono:
17 In generale, sei soddisfatto/a dei rapporti sessuali che hai con il tuo partner?
MALE QUESTIONNAIRE (TRANSLATED)
1 How old are you?
2 What gender do you identify with?
3. What is your ethnicity?
4 What is your level of education?
5. What is your profession?
6 In which part of Italy do you live?
7 How tall are you (in centimeters)?
8. What is your weight (in kg)?
9 BMI
10 Do you smoke?
11. Do you consume alcoholic beverages?
12 Do you use narcotics?
13. If you use narcotics, please indicate which ones (possible multiple responses).
14 Do you take antidepressant medications?
15 Do you suffer from thyroid diseases?
16. Do you suffer from neurological diseases?
17 Do you consider yourself to suffer from anxiety?
18 Do you consider yourself to suffer from depressive symptoms (e g , apathy, fatigue, pervasive sadness, recurrent crying)?
19. Is your sleep sufficient and restful?
20 Do you have brothers?
21. Do you have sisters?
22 Are you circumcised?
23 If yes, at what age did you undergo circumcision (if not circumcised, indicate " ")?
24. Do you suffer from a short frenulum?
25 Do you have difficulty retracting the penile skin (foreskin) during erection or intercourse?
26 Do you regularly suffer from prostatitis or infections/inflammation of the genitals?
27 Describe your sexual orientation
28 Relationship status
29. How often do you use pornographic material (of any kind)?
30 Do you masturbate using exclusively sexual fantasies?
31 How often do you practice sexting and/or camming? (Sexting: sending and receiving sexually explicit messages, texts, videos, and/or images; Camming: engaging in sexual practices while in contact with someone in video chat)
32 Are you aware of being betrayed?
33. At what age did you masturbate for the first time?
34 Do you believe you had the right privacy during your first experiences with masturbation?
35 Have you ever been scolded after being discovered masturbating?
36. When you started practicing masturbation or engaging in sexual activities, were you usually forced to do it quickly (e.g., because parents were at home, fear of being discovered, etc )?
37 How do you usually masturbate?
38. Do you use lubricant when you masturbate?
39 How often do you masturbate?
40. How often are you interrupted while masturbating?
41 Referring to the last five times you masturbated, how many minutes passed between the start of masturbation and ejaculation?
42 Do you have sexual intercourse with
43. Do you have sexual intercourse with partners...
44 How often do you have penetrative sexual intercourse?
45 Do you use condoms during sexual intercourse?
46. Can you achieve and maintain an erection until the end of sexual intercourse?
47 How do you rate your sexual desire?
48. How often do you engage in foreplay before starting sexual intercourse? (Foreplay may include kissing, caressing, mutual masturbation, oral sex, role-playing, and fetish or BDSM practices)
49 On average, how much time do you dedicate to foreplay?
50. Do you avoid or minimize received foreplay for fear of ejaculating too soon?
51 Do you experience discomfort or pain in the penis during sexual intercourse?
52 In which places do you most frequently have sexual intercourse? (Possible multiple responses)
53. If you answered "other," specify where; otherwise, write NO.
54 How often are you interrupted during sexual intercourse?
55. How often can you ejaculate during sexual intercourse?
56 Have you ever faked orgasm during penetrative sexual intercourse?
57 Have you ever masturbated before a sexual encounter to last longer?
58. Have you ever used narcotics before a sexual encounter to last longer?
59 During penetrative sexual intercourse, have you ever stopped coital movements, regained control, and resumed to last longer?
60 During penetrative sexual intercourse, have you ever changed sexual positions frequently to last longer?
61. Do you use delaying condoms, anesthetic creams, or medications such as paroxetine or dapoxetine to last longer?
62 Referring to the last five penetrative sexual encounters you had, on average, after how many minutes from the start of penetration did you ejaculate?
63. How often do you feel that it takes TOO LONG to ejaculate during sexual intercourse?
64 When you feel that it takes too long to ejaculate, do you
65 How often do you feel that it takes TOO LITTLE time to ejaculate during sexual intercourse?
66. When you feel that it takes too little time to ejaculate, do you...
67 Are you satisfied with the time between the start of penetration and ejaculation?
68 In your opinion, how much do foreplay influence the time between the start of penetration and ejaculation?
69. Do you believe that your partner(s) is/are satisfied with the time between the start of penetration and ejaculation?
70 In general, are you satisfied with the sexual encounters you have had in the last six months?
FEMALE QUESTIONNAIRE (TRANSLATED)
1 What gender do you identify with?
2 In which age group do you place yourself?
3. What is your ethnicity?
4 What is your level of education?
5 Do you have regular sexual relations with a male partner?
6. Do you have a stable relationship with a male partner?
7 How often do you have sexual relations with your partner?
8. How often does your partner ejaculate during sexual relations?
9 How often do you and your partner engage in foreplay before sexual intercourse? (Foreplay may include kissing, caressing, mutual masturbation, oral sex, role-playing, and fetish or BDSM practices)
10. How much time do you and your partner dedicate to foreplay?
11 Referring to the last 5 sexual encounters you had, on average, after how many minutes from the start of penetration did your partner ejaculate?
12 How often do you feel that your partner takes TOO LONG to ejaculate during sexual relations?
13. How often do you feel that your partner takes TOO LITTLE time to ejaculate during sexual relations?
14 Are you satisfied with the time between the start of penetration and your partner's ejaculation?
15. In your opinion, how much do foreplay influence the time between the start of penetration and your partner's ejaculation?
16 In your opinion, do foreplay influence:
17 In general, are you satisfied with the sexual relations you have with your partner?
ORIGINAL PAPER
Laparoscopic radical prostatectomy with the simultaneous implant of a penile prosthesis: Ten years follow up
1 Department of Urology, Magna Graecia University, Catanzaro, Italy;
2 Department of Experimental Medicine, Magna Graecia University, Catanzaro, Italy;
3 Department of Urology, University of Pisa, Italy
Summary
Introduction: Even today, despite technological evolution, erectile dysfunction remains the most feared complication after radical prostatectomy surgery expecially for patients who report pre-existent refractory erectile dysfunction (ED) and patients in whom there is a high risk of extracapsular disease, such as any cT2c or cT3, who undergo non-nerve sparing radical prostatectomy (RP). To overcome this issue, Khoudary et al performed the first simultaneous placement of a penile prosthesis during open RP in 1997, aiming at an early return to sexual function without any impact on oncological outcomes and without significant adverse effects Ten years ago we performed laparoscopic extraperitoneal RP and simultaneous penile prosthesis implantation (PPI) on ten patients in order to preserve the full length of the penis and to improve their satisfaction and quality of life (QoL) increasing the chances of ED resolution
Objectives: Aim of this study is to illustrate the ten years follow up of this case series which has no terms of comparison in the world. Oncological and functional results were analyzed. Materials and Methods: In 2013 10 patients underwent simultaneous PPI (with an AMS InhibiZone prosthesis). Patients were evaluated by means of urological visits, questionnaires, and objective measurements before surgery, at discharge from the hospital, on postoperative days 21 to 28, each 3 months for the first year, and each year thereafter The main outcome measures were biochemical recurrence-free rate, penile length and quality of life
Results: Eight patients with mean age 71 (range 66-75) were reached at the 10-year follow-up; one patient died of acute infarction 10 years after surgery and another one died of disease 7 years after surgery Partners had, currently, mean age 60 (range 37-71). Mean preoperative PSA was 9.3 (6.3-13.7) and mean PSA at 10 years was 0 08 (range 0 01-1 2)
International index erectile function IIEF before surgery was 11 (range 9-14) and 23 (range 22-25) at 10 years Partner satisfaction rating increased from 7 (post-surgical) to 8 at 10 years Penis length was unchanged after 10 years: mean intraoperative length was 9 cm (range 8.5-9.5) and mean length at 10 years was 8 8 cm (range 8-9 5)
Conclusions: In our cases, laparoscopic radical prostatectomy with the simultaneous implant of a penile prosthesis demonstrate to be an interesting option to offer to selected and highly motivated patients Outcomes like preservation of the penis length, resuming of normal sexual activity 21 days after surgery, partner satisfaction and oncological safety at 10-year fol-
low-up make it a valid surgical technique to be proposed in clinical practice if performed by an experienced team in prosthetic surgery
KEY WORDS: Radical Prostatectomy; Erectile dysfunction; Penile prosthesis; Andrology; Quality of life
Submitted 28 December 2024; Accepted 3 January 2025
INTRODUCTION
Radical prostatectomy (RP) is the most common treatment option for men with localized prostate cancer worldwide, being related to excellent and reproducible cancer control rates Although progress has been made in nerve sparing (NS) surgery, erectile dysfunction (ED) still remains a common long-term complication after RP To overcome this issue, Khoudary et al performed the first simultaneous placement of a penile prosthesis during open RP in 1997, aiming at an early return to sexual function without any impact on oncological outcomes and without significant adverse effects (1) We describe a case series of patients who underwent laparoscopic extraperitoneal RP combined with PPI (during 2013) to evaluate the impact of this treatment strategy on preserving the full dimensions of the penis and improving patients’ sexual Quality of life (QoL) (2) Aim of this study is to illustrate the ten years follow up of this case series which has no terms of comparison in the world Oncological and functional results were analyzed
MATERIALS AND METHODS
Ten patients underwent simultaneous penile prosthesis implantation (PPI) (with an AMS InhibiZone prosthesis) and laparoscopic RP in 2013 They were evaluated by means of urological visits, dedicated questionnaires inherent in QoL and sexual function, objective measurements before surgery, at discharge from the hospital, on postoperative days 21 to 28, each 3 months for the first year, and each year thereafter for 10 years The main outcome measures were biochemical recurrence-free rate, penile length, and quality of life 1 All procedures were performed according our standard practice All patients and their partners underwent sexual counselling with a
N Mondaini, A Abramo, C Romeo, et al
clinical sexologist, both before surgery, in order to assess their motivation to undergo such a procedure, and after surgery, in order to investigate their level of satisfaction with the results The study was conducted in line with the STROBE statement (http://www strobe-statement org) Due to the retrospective nature of the study in Italy, it did not require approval by the local ethics committee Nevertheless, it was conducted in line with the Good Clinical Practice guidelines and the ethical principles laid down in the latest version of the Declaration of Helsinki
Data collection
All patients were evaluated with penile measurements and questionnaires which were administered before surgery, at discharge from the hospital, on postoperative days 21 to 28, each 3 months for the first year, and each 6 months thereafter At the time of surgery, the following parameters were recorded: the patient’s and partner’s age, the Charlson comorbidity index, preoperative prostatespecific antigen levels, Gleason score, penile length, clinical prostate cancer stage (through an abdominal computed tomography (CT) scan and skeletal scintigraphy), estimated blood loss, visual analogue scale (VAS) pain scores, analgesic use, duration of hospital stay, and surgical complications, according to the Clavien-Dindo classification
Penile length measurements
Penile length was evaluated through a manual measurement of the fully stretched penis in the flaccid state The length was obtained from the pubis to the tip of the penis and made in centimeters (3)
Questionnaires
Patients completed dedicated questionnaires for satisfaction and the 36-Item Short Form Health Survey (SF-36) questionnaire Patients’ satisfaction was evaluated using patient-reported outcomes (PROs) QoL was measured using an Italian version of the SF-36 Health Survey, a test particularly suitable for chronic conditions A year after surgery patients and their partners were also asked to rate their level of sexual satisfaction on a scale of 1 to 10, with 1 meaning “completely unsatisfactory” and 10 meaning “maximum level of satisfaction” We decided to use the PROs tool instead of the International Index of Erectile Function questionnaire because the aim of the present study was to evaluate the impact of laparoscopic extraperitoneal RP with simultaneous PPI on patients’ satisfaction (1)
Surgical procedure
All laparoscopic RP procedures were performed by a single experienced uro-oncological surgeon (RB) All penile prostheses were placed by a single surgeon with high-volume experience in PPI surgery (NM) Upon conclusion of the prostatectomy and after removing the prostate via access through a Hasson trocar we manually positioned the reservoir The pneumo-Retzius was redetermined and the positioning of the reservoir optimized between the bladder and pubis We then made a penile-scrotal incision and isolated the internal inguinal ring with a blunt incision as far as the external fascia of the rectal-abdominal muscles that was crossed by fine-tip forceps, the path of which was simultaneously monitored from the laparoscopic access The reser-
voir tube, previously plugged with a special titanium plug, was then dislocated to the penile-scrotal incision The reservoir was then inflated and its location checked once again A pelvic drain was positioned and removed on day 1 After ensuring haemostasis, the implant was positioned The two cylinders were initially positioned following bilateral cavernosotomy, followed by the pump that was placed at the level of the scrotum, and subsequently tubing were connected The prosthesis was then almost fully activated for the first 24 hours with a compressive bandage All patients stayed for 4 hours in a nurse-operated recovery room The drain was removed on day 1 and patients were discharged from the hospital on day 4 On day 10, retrograde and voiding cystography was carried out after removing the bladder catheter Activation of the prostheses took place between day 21 and day 28
Ethical
considerations
The present study was conducted as a consecutive case series in which patients who received a similar treatment were followed and all outcomes were recorded and analyzed Even though the case series had a descriptive study design, the local ethical committee was informed about the study
RESULTS
Among patients that were enrolled in this study with a median age of 71 years, one died of acute infarction 10 years after surgery (group no adjuvant therapy) and another died of disease 7 years after surgery (group radiotherapy after surgery) According to the Clavien-Dindo classification, the first patient reported a severe complication: migration of the reservoir into the bladder, which was resolved without prosthesis removal This occurred even though the reservoir had been placed under vision A CT scan was carried out, and it demonstrated a lesion on the superior wall of the bladder due to a pressure ulcer formed by the reservoir near a bladder diverticulum The reservoir was then removed from the bladder and changed through laparotomic access The bladder wall was then repaired and a catheter was placed 2 After 7 days, the catheter was removed and the patient was discharged after cystography No prosthesis infections occurred (Table 1)
Table 1
Post-surgery penile lenght measurements
Oncological outcomes
Over a median follow-up of 120 months 3 patients were disease-free without adjuvant therapy, and 4 were on hormonal therapy; 1 of the latter group had to undergo radiotherapy after surgery
Penile length at the time of surgery and at the follow-up visits
The median penile length at the time of the surgery was 9 cm Post-surgery penile length measurements showed the preservation of the full dimensions of the penis compared to the preoperative measurements No statistically significant differences were found between the preoperative penile length measurements and the follow-up measurements However, a reduction of 0 5 cm was observed in only 20% of the patients, although no patients described having problems with their penile dimensions (Table 2)
Table 2.
Clinical, laboratory and demographic characteristics.
Characteristic
Patients
Age (y) (at 120 mo)
PSA (pre-surgery)
PSA (post surgery) (at 120 mo)
IIEF score (pre-surgery)
10 (2 died)
71 (66-75)
9 3 (6 3-13 7)
0 08 (0 01-1 2)
11 (9-14)
IIEF score (post-surgery) (at 120 mo) 23 (22-25)
Partner’s age (y) (at 120 mo)
60 (37-71)
Values are presented as number only or median (range) PSA: prostate-specif c ant gen;
IIEF: Internat onal Index of Erectile Funct on
Quality of life evaluation
The pre-surgery SF-36 median value was 97 (range, 9698) According to post-surgical sexual counselling with a clinical sexologist, all patients were satisfied with their penile implants, and the couples’ level of sexual satisfaction was rated a median of 8 (range, 7-10) at follow-up 1
The median post-surgery SF-36 score was 99 (range, 9799) A statistically significant difference was found between the pre-surgery and post-surgery SF-36 scores (p = 0 02) (Table 3)
Table 3.
Questionnaire and quality of life results at enrolment and at last follow-up
Variable Quality of life result
SF-36
Pre-surgery (enrolment)
Post-surgery (120 m)
Sexual satisfaction scale
Values are presented as med an (range) SF-36: 36-Item Short Form Health Survey
97 (96-98)
99 (97-99)
8 (7-10)
DISCUSSION
In the 1990s, Clough et al suggested the integration of plastic surgery techniques with breast-conserving treatments for breast cancer In the urological setting, in 1997 Khoudary et al performed a combination procedure of
open non-nerve-sparing retropubic RP and PPI in 50 men This group was compared with a group of 72 men who went RP alone during the same time interval No significant differences were noted in the preoperative patient variables The mean operative time for prosthesis insertion was 82 minutes, and the mean time to sexual interc o u r s e w a s 1 2 7 w e e k s
n s occurred, with a mean follow-up of 1 7 years Four men (8%) required revision of their inflatable penile prosthesis There were no significant differences between the combination procedure and RP alone with regard to estimated blood loss, length of hospital stay or analgesic use
Men who chose the simultaneous placement of a penile prosthesis with RP reported greater overall QoL (1) In the present paper we reported the results of simultaneous PPI and RP performed from June 2013 to June 2014 in 10 patients who completed the study follow-up period (median, 32 2 months) ” No difference was found between the time of surgery and the 2-year follow-up evaluation in terms of penile length The pre-surgery 36Item Short Form Health Survey (SF-36) median score was 97 The and median postoperative SF-36 score was 99 at 3 months follow-up (2) Patients were satisfied with their penile implants, and couples’ level of sexual satisfaction was rated median 8 Post-surgery penile lenght measurements showed the preservation of the full dimensions of the penis compared to the preoperative measurements
No prosthesis infections occurred, over a median followup of 120 months In light of these results, laparoscopic extraperitoneal RP with simultaneous PPI could be proposed to selected and very motivated patients because:
a) medicated AMS InhibiZone [American Medical Systems, Inc (AMS), Minnetonka, MN, USA] penile prostheses reduce the risk of prosthesis infections Moreover, the extraperitoneal approach is preferable in order to keep the prosthesis reservoir located in a place with a low risk of infection (3);
b) simultaneous PPI preserves penile length; c) combined procedure reduces the duration of hospitalization and allows patients to quickly resume sexual activity A faster return to a satisfactory sexual life could have a positive impact on QoL and on the couple’s well-being (4)
Some aspects of this study should be considered, in particular the fact that all surgical oncological procedures were performed by a single dedicated surgeon and all prosthesis implantations were performed by the same surgeon with a high-volume experience Moreover, the psychological counselling support and the involvement of the partner in the surgical decision-making process should be considered strengths of this study The main limitation of this study is the fact that it was a consecutive case series However, our findings could serve as a basis for planning future studies The majority of our patients had low- or intermediate-risk cancers and they could have undergone complete nerve-sparing resection, which in experienced hands, does not result in high positive margin rates However, all patients reported stable ED with no benefits from PDE5i or intracavernous therapy For this reason, we did not consider this treatment strategy to be overtreatment Finally, the inclusion of a psy-
N Mondaini, A Abramo, C Romeo, et al
chologist in the patients’ care should be considered a strength of this study Psychological support during the PPI is a key means of improving adherence to the followup and overall outcomes
We believe that laparoscopic extraperitoneal RP can be considered an optimal surgical technique that offers considerable safety margins for the simultaneous implantation of a tricomponent penile prosthesis, even though simultaneously performing 2 surgical procedures may increase the risk of complications The hospitalization length is no longer than that required for normal surgery, and the additional costs of the prostheses can be easily amortized by avoiding the costs of a second surgical operation for the penile implant and avoiding the postoperative use of prostaglandins for penile erection
The main complications of prostate cancer surgery are ED and urinary incontinence Several patients received an artificial sphincter for urinary incontinence The presence of a penile implant is not a contraindication for artificial sphincter implantation The cuff can be placed through the perineal approach in the bulbar urethra or over the bladder neck in particular cases The reservoir can be placed on the opposite site of the penile implant reservoir and the pump in the opposite part of the scrotum
CONCLUSIONS
The aim of this study is to evaluate the outcome of simultaneous PPI and RP The ideal candidates are those who report pre-existent refractory ED and patients in whom there is a high risk of extracapsular disease, such as any cT2c or cT3, who undergo non-nerve sparing RP A simultaneous procedure would avoid two admissions, reduce hospitalization time and guarantee a faster recovery of sexual function, preventing the otherwise unavoidable loss of penile length Since the urologist does not need to preserve the neurovascular bundles, as the penile implant will take care of postoperative rigidity, RP can be
DECLARATIONS
Ethical approval: The case series has been approved by the local medical research ethics committee Protocol number 78901
Availability of data and material: The datasets used and/or analyzed during the current study are available upon reasonable request from the corresponding author
Competing interests: The authors declare that they have no competing interests
Funding: There are no sources of funding for the research
Authors' contributions: NM, study concept, data analysis and interpretation, manuscript original drafting; statistical analyses; AA, statistical analyses, contribution to manuscript writing and editing; CR, participated in writing FC, participated in writing, language editing; FC, participated in writing, language editing; RD, critically reviewed the study proposal; RB, proofreading All the authors read and approved the final version of the manuscript and agreed to be accountable for all aspects of the work
Acknowledgments: Not applicable
performed more radically from an oncological point of view, thus reducing the risk of recurrence and metastasis, especially in patients with high risk disease In conclusion, simultaneous PPI with RP provides early sexual rehabilitation, improving patients' QoL, without compromising surgical outcomes However, larger series will be necessary, to better identify the patients who are more likely to benefit from nerve sparing surgery and postoperative penile rehabilitation from those who would are more likely to develop refractory ED post RP and would therefore benefit from simultaneous PPI
REFERENCES
1 Khoudary KP, DeWolf WC, Bruning CO 3rd, Morgentaler A Immediate sexual rehabilitation by simultaneous placement of penile prosthesis in patients undergoing radical prostatectomy: initial results in 50 patients Urology 1997; 50:395-9
2 Mondaini N, Cai T, Sarti E, et al A Case Series of Patients Who Underwent Laparoscopic Extraperitoneal Radical Prostatectomy with the Simultaneous Implant of a Penile Prosthesis: Focus on Penile Length Preservation World J Mens Health 2018; 36:132-138
3 C a k i r O O , P o z z i E , C a s
Measurement: Methodological Challenges and Recommendations, a Systematic Review J Sex Med 2020; 18:433-439
4 Cocci A, Cito G, Romano A, et al Radical prostatectomy and simultaneous penile prosthesis implantation: a narrative review Int J Impot Res 2020; 32:274-280
Correspondence
Nicola Mondaini, MD (Corresponding Author) n mondaini@unicz it
Andrea Abramo, MD a abramo10@gmail com
Fabio Crocerossa, MD crocerossa@unicz it
Francesco Cantiello, MD cantiello@unicz it
Rocco Damiano, MD damiano@unicz it
Department of Urology, Magna Graecia University, 88100 Catanzaro Italy
Caterina Romeo, MD cateromeo93@hotmail it Department of Experimental Medicine, Magna Graecia University, Catanzaro, Italy
Riccardo Bartoletti, MD bartoletti@unipi it
Department of Urology, University of Pisa, Italy
ORIGINAL PAPER
Enhanced patient recovery with early extensive surgical debridement in Fournier's gangrene: Evaluation of perioperative outcomes in a multicentric experience
Giovanni Cochetti 1 , Alessio Paladini 1 , Luca Lepri 1 , Andrea Vitale 1 , Raffaele La Mura 1 , Miriam Russo 1 , Paolo Mangione 1 , Matteo Mearini 1 , Andrea Fabiani 2 , Emanuele Iacobone 2 , Lucilla Servi 2 , Ettore
Mearini 1, 3 , Michele Del Zingaro 1
1 Department of Medicine and Surgery, Urology Clinic, University of Perugia, Perugia, Italy;
2 Surgery Department, Urology Unit, Macerata Civic Hospital, Area Vasta 3 Asur Marche;
3 Department of Medicine and Surgery, Urological Andrological Surgery and Minimally Invasive Techniques Unit, S Maria Hospital, University of Perugia, Terni, Italy;
Summary
Objective: Fournier's gangrene (FG) is a rare, life-threatening necrotizing fasciitis primarily affecting the perineal, genital, and perianal regions. This rapidly progressing bacterial infection predominantly affects middleaged and elderly men This multicenter study aims to describe the management in a wide cohort of Fournier's gangrene cases that presented to three tertiary centers with early extensive surgical debridement
Materials and methods: We retrospectively collect data from patients with FG who were referred to the Urology Clinic of the Department of Medicine and Surgery (Perugia), the Urological Andrological Surgery and Minimally Invasive Techniques Unit (Terni) of the University of Perugia, and the Urology Unit of the Surgery Department of the Macerata Civic Hospital between January 2019 and March 2024 for onset of classic signs and symptoms of FG. Extensive surgical debridement was immediately performed under general anesthesia to reach normochromic and vascularized tissue in wide and depth extension, assuring vital and healthy margins For all patients, intravenous daptomycin plus piperacillin/tazobactam were administered
Results: 28 male patients with FG underwent early surgical debridement. In two cases, orchidectomy and partial penectomy were required during surgical debridement due to extensive necrosis Colon diversion and urinary diversion were not necessary for any of the patients 32 1% complications were recorded in according to the Clavien Dindo classification; 6 patients died in the perioperative Excluding death data, the average duration of antibiotic therapy was 22 0 ± 9 1 days, and the average length of stay was 17.6 ± 11.8 days.
Conclusions: Fournier's gangrene has high mortality rates. It requires timely surgical debridement and antibiotic therapy to achieve positive outcomes This study shows that a primary extensive debridement can help reduce the need for further intervention and shorten the hospital stay
Submitted 7 October 2024; Accepted 20 October 2024
INTRODUCTION
Necrotizing soft tissue infections are serious conditions caused by bacterial toxins that activate a severe systemic inflammatory response Fournier's gangrene (FG) is a rare and severe form of necrotizing fasciitis that affects the perineum, exter nal genitalia, and adjacent tissues
It was first described in 1764 by Baurienne, but the French physician Jean Alfred Fournier is more widely credited with its identification In 1883, Four nier presented a case series of 5 young men with this condition, highlighting its sudden onset and potentially fatal nature (1) FG progresses rapidly, affecting the subcutaneous and fascial planes (2) According to Sorensen et al , FG affects less than 0 02% of hospital admissions, with an incidence rate of 1 6 cases per 100 000 people (3) It mainly affects men, with an average age of 60 years, and the male-to-female ratio is 10:1 (2, 4)
Several risk factors have been associated with the development of FG, including immunosuppression, diabetes, HIV, malignancies, inflammatory bowel disease, renal and hepatic failure, recent trauma, and medical procedures (2, 4) The use of antihyperglycemic drugs, such as sodiumglucose cotransporter 2 inhibitors (SGLT2i), has also been linked to FG in some cases (5)
Inflammation and edema result in obliterating endarteritis, leading to thrombosis of subcutaneous blood vessels
This causes ischemia and necrosis along the dartos fascia, Colles' fascia, Scarpa's fascia, and the abdominal wall (6)
Diagnosis of FG usually involves a clinical examination, radiological tests, and laboratory analyses The onset of necrotizing fasciitis can be slow, with up to 40% of cases showing no symptoms When symptoms do appear, they may include pain in the genital and perineal areas, with little to no visible skin damage in the early stages As the condition progresses, the skin may become red and dusky, and there may be a foul-smelling discharge from the genital and perineal areas, along with a crackling sensation under the skin (7)
Treatment usually involves a combination of broad-spectrum antibiotics, fluid resuscitation, and multiple surgical
debridements, with an average of 3 5 procedures per patient (8) In severe cases, intensive supportive care may be necessary for hours or days (9) Delayed diagnosis and treatment can lead to high mortality rates, which can reach up to 30% or more in some instances (3, 10, 11)
To further explore this rare and deadly condition, we conducted a retrospective analysis of patients admitted and treated for FG with typically extensive surgical debridement in three tertiary referral centers in the last 5 years
MATERIALS AND METHODS
We included all patients who were referred to Urology Clinic of the Department of Medicine and Surgery (Perugia) and the Urological Andrological Surgery and Minimally Invasive Techniques Unit (Terni) of the University of Perugia, and the Urology Unit of the Surgery Department of the Macerata Civic Hospital between January 2019 and March 2024 for onset of classic signs and symptoms of FG
All patients signed an informed consent form to anonymously treat their medical data for scientific purposes at the hospital admission
For each patient, vital signs and parameters, the Charlson Comorbidity Index, medical history, blood exams, urinary samples, and blood cultures were recorded A local ultrasound and a thoracic-abdomen CT scan were performed in all cases
We included in the patient’s evaluation the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) introduced in 2004 by Wong et al to help distinguish necrotizing fasciitis from other soft tissue infections (12)
We also performed the Fournier’s Gangrene Severity Index (FGSI) as a mortality predictor tool for FG patients, created by Laor et al (13)
All patients underwent prompt fluid resuscitation and broad-spectrum intravenous antibiotics within one hour of emergency department admission If there was suspicion of FG, extensive surgical debridement was immediately performed under general anesthesia in the operative theatre, considering reaching normochromic and vascularized tissue in wide and depth extension, assuring vital and healthy margins Subsequent debridements were performed only when signs of local necrosis or de-vascularized tissue appeared in the next few days
Patients were assumed to be cured once they achieved normalized vital signs, had negative blood cultures and wound microbiological examinations, and had normal levels of C-reactive protein and procalcitonin
Additionally, their surgical wounds needed to heal completely without any discharge or pain Follow-up care involved periodic visits with specialists and medication, if necessary
Complications were recorded and reported according to the Clavien-Dindo classification
A descriptive analysis was conducted, with continuous variables reported as mean with standard deviation (SD) and categorical variables reported as frequencies (%)
RESULTS
The study involved 28 male patients, with an average age of 59 6 ± 14 3 years and a mean Charlson Comorbidity Index
of 4 7 ± 2 4 All patients displayed local edema and necrotized skin (Figure 1) as the primary clinical presentation, with additional symptoms including erythema (78 5%), fever (57 1%), local pain (42 8%), subcutaneous crepitation (32 1%), and purulent exudate (10 7%) (Figure 2)
In all cases, the blood exams revealed a neutrophilic leukocytosis, a mean C-reactive protein of 32 7 ± 16 2 mg/L, and procalcitonin of 27 41 ± 12 7 ng/ml
The ultrasound showed a significant thickening of the area involved with fluid intrafascial film and several hyperechoic spots with posterior echoes as for the aerial components The CT scan confirmed the presence of a large amount of air and gas in the surrounding soft tissues and served to better explore the tissues involved
The mean FGSI and LRINEC scores were 3 6 ± 1 4 and 6 3 ± 2 1, respectively The most common comorbidities were diabetes (64 3%), hypertension (57 1%), and cardiac disease (57 1%) Polymicrobial flora with aerobic and anaerobic bacteria was the dominant report (67 8%), followed by Staphylococcus (21 4%) and Enterococcus faecium (7 1%) wound culture
For all patients, intravenous daptomycin plus piperacillin/ tazobactam were administered: 3 (10 7%) and 2 (7 1%) patients required a switch from piperacillin/tazobactam to
G Cochetti, A Paladini, L Lepri, et al
Figure 1. Left emiscrotal necrotizing fasciitis
Figure 2. Fournier’s gangrene with purulent discharge.
imipenem-cilastatin due to infection by Enterococcus faecalis and Escherichia Coli extended-spectrum beta-lactamase (ESBL) producer, respectively
On average, patients underwent surgery 14 2 ± 5 7 hours after accessing the emergency department (Figure 3) In two cases, orchidectomy and partial penectomy were required during surgical debridement due to extensive necrosis Colon diversion and urinary diversion were not necessary for any of the patients
Six patients (21 4%) required blood pressure support with intravenous noradrenaline after surgery and were admitted to the intensive care unit (ICU) for 26 ± 4 3 hours Five patients (17 8%) required subsequent debridement, with a mean of 0 3 ± 0 5 further surgical debridements performed before discharge; all surgical debridements were performed bedside with local anesthesia
Reconstructive surgery by a plastic surgeon was performed on 14 3% of in-patients to improve tissue and skin restoration in the treated site One patient, affected by diabetes mellitus, chronic kidney disease, and immunosuppression due to the assumption of Everolimus for transplanted kidney required the use of Vacuum-Assisted Closure (VAC) therapy for the scrotal skin for approximately 20 days with gradual recovery and complete re-epithelialization
Complications were recorded in nine patients (32 1%) according to the Claviend Dindo classification; 3 (10 7%) patients underwent blood transfusion (grade II), and six patients (21 4%) died (grade V), with an average time to death of 3 5 ± 2 1 days Of those, one patient had multiple comorbidities, a patient had Duchenne syndrome and succumbed to acute respiratory distress syndrome One of these patients was admitted to the operating theatre 36 hours after symptom onset due to an unstable clinical condition The other three pateints died in the 48 hours after debridment due to the compromission of the cardiovascole system due to septic shock
Excluding death data, the average duration of antibiotic therapy was 22 0 ± 9 1 days, and the average length of stay was 17 6 ± 11 8 days
DISCUSSION
Prompt fluid resuscitation, broad-spectrum intravenous antibiotics, and primary extensive surgical debridement are safe and effective procedures that help reduce mortality, re-interventions, and hospital length of stay
FG constitutes a rare disease, accounting for only 0 02% of hospital admissions (3) Initially considered idiopathic, the cause of FG is now identifiable in most cases, often coming from aerobic and anaerobic bacterial infections in the ano-rectum (30-50%), uro-genitalia (20-40%), and genital surface (20%) (2, 11) It predominantly affects immunocompromised individuals and those with compromised microcirculation, with risk factors including diabetes, obesity, chronic alcoholism, smoking, drug abuse, renal and liver failure, pelvic malignancies, inflammator y bowel diseases, HIV infection, recent trauma, and recent urethral and perineal surger y FG is more prevalent in individuals with malnutrition and lower socioeconomic status (2) Diabetes, in particular, has been associated with 32-66% of FG cases, with uncontrolled diabetes linked to a poorer prognosis and necessitating more aggressive treatment (11)
The use of SGLT2i drugs in diabetic patients has been initially correlated with increased FG cases, although subsequent studies have disputed this correlation, warranting further investigation
Our case series is in line with previous studies, which highlight diabetes as a significant risk factor for the development of FG Around 64% of the patients in our study had type II diabetes mellitus, and all of them were male
The average age at diagnosis was consistent with recent literature It is well known that males are more susceptible to developing FG However, females, despite being less affected, are at a higher risk of FG-related mortality due to anatomical differences that enable rapid infection spread in women (14)
Histological examination of patients with FG shows necrosis of the superficial and deep fascia, fibrinoid coagulation in the blood vessels, infiltration of tissues by various types of cells, and necrotic tissue debris A key identifying feature is the presence of blood vessel thrombosis in the affected area Interestingly, even when there are significant pathological changes in the deep tissues, the skin can remain intact for a prolonged period (4) Up to 40% of FG cases manifest with no symptoms initially, making early diagnosis challenging Symptoms include genital and perianal pain, erythematous and dusky skin, subcutaneous crepitation, and malodorous and purulent exudates Differential diagnosis involves distinguishing FG from conditions such as gangrenous balanitis in males with diabetes and ulcerative forms of inguinal lymphogranulomatosis, gangrenous diabetic vulvitis, acute genital ulcers, and soft cancer in women The LRINEC score aids in diagnosis, with scores ≥ 6 indicating suspicion of necrotizing fasciitis and ≥ 8 strongly suggestive (15, 16)
In our study, we started the antibiotic therapy with intravenous daptomycin plus piperacillin/tazobactam, according to the empiric treatment of necrotizing fasciitis, and only after microbiological culture did we decide to switch the therapy according to the sensitivity The primary goal of antibiotic therapy in FG is to control the systemic
Figure 3. Surgical debridement of the necrotic tissue
infection and reduce the bacterial load in the affected area Because the infection is polymicrobial, broad-spectrum antibiotic coverage is essential until specific bacterial cultures can guide more targeted therapy Antibiotic treatment should begin immediately upon diagnosis, as any delay can result in the worsening of the infection and an increased risk of mortality Initial antibiotic therapy typically involves broad-spectrum agents covering aerobic and anaerobic bacteria This often includes a combination of agents such as a carbapenem (e g , meropenem or imipenem) or piperacillin-tazobactam, which provide broad coverage against gram-positive, gram-negative, and anaerobic bacteria In some cases, an aminoglycoside (e g , gentamicin) or fluoroquinolone may be added to c o v e r re s i s t a n t g r a m - n e g a t i v e b a c t e r i a A d d i t i o n a l l y, metronidazole or clindamycin is often included to target a n a e ro b i c b a c t
, which can produce dangerous toxins (4) Once culture results and antibiotic sensitivity profiles are obtained, the treatment can be adjusted to target the specific bacteria responsible for the infection This strategy helps minimize antibiotic resistance development while maintaining effective control over the infection
The duration of antibiotic therapy varies depending on the severity of the infection and the patient’s response to treatment The management of FG with antibiotics presents several challenges First, the condition often occurs in patients with underlying health issues, such as diabetes, immunosuppression, or chronic kidney disease, which complicate the selection and dosing of antibiotics
These patients may require adjusted dosages or alter native agents to avoid drug toxicity while ensuring effective antimicrobial coverage Additionally, the rise of antibiotic-resistant organisms poses a growing threat to the treatment of necrotizing infections like FG Methicillin-resistant Staphylococcus aureus (MRSA) and multidrug-resistant gram-negative bacteria, such as ESBL-producing E coli and Klebsiella, are increasingly implicated in these infections More specialized antibiotics may be required to combat resistant strains, such as vancomycin, linezolid, or daptomycin Careful monitoring of antibiotic effectiveness and resistance patter ns is essential to ensure successful treatment
An urgent debridement is necessary to improve outcomes According to Lin et al , surgery should be performed within 15 hours of the onset of symptoms to avoid an increased risk of major complications (17) Moreover, multiple further surgical debridements are usually needed in the operative theatre to the rapid disease relapse In our study, the average time to surgery was approximately 14 hours, which explains the survival rate in line with the literature Surgery aims not only to remove damaged tissue but also to drain the infection completely The full extent of the disease may not be apparent from the areas of skin involvement, which is typically less than the involvement of tissue beneath the skin It's important to be careful not to unintentionally open up deeper facial layers that were not originally affected Our case series differs from the findings in the literature, as only 17 8% of patients required additional debridement after 24 hours, and 14 3% under went reconstructive surgery This result could be reached with
a primarily extensive debridement in hemodynamically stable patients
Our hospitals did not use hyperbaric oxygen therapy (HBOT) for wound healing due to logistical constraints According to the literature, HBOT has been found to have lower mortality rates compared to conventional therapy However, its impact on the length of stay and number of debridements is inconclusive HBOT has emerged as a promising adjunct in the management of necrotizing fasciitis By increasing the partial pressure of oxygen in tissues, HBOT can significantly enhance the body's natural defense mechanisms The elevated oxygen levels create a hostile environment for anaerobic bacteria, often the primary culprits in necrotizing fasciitis, particularly in conditions like FG Additionally, HBOT stimulates the production of reactive oxygen species, which can directly damage bacterial cells Beyond its direct antimicrobial effects, HBOT promotes angiogenesis and tissue granulation, accelerating wound healing This is achieved by improving local blood flow, enhancing the delivery of nutrients to damaged tissues, and stimulating the growth of new blood vessels Furthermore, HBOT can modulate the immune response, reducing inflammation and enhancing the body's ability to fight infection While the evidence supporting the use of HBOT in necrotizing fasciitis is growing, its application has limitations The optimal timing, duration, and frequency of HBOT treatments remain subjects of ongoing research Moreover, the cost of HBOT and the logistical challenges associated with its delivery can limit its accessibility in many healthcare settings (18) Our experience, on the other hand, suggests that a multimodal treatment strategy, which includes daily site cleansing, can achieve complete restoration without the need for HBOT or surgical grafting while maintaining optimal outcomes despite comparable mortality rates One of the modern advancements in wound care is the use VAC therapy, also known as Negative Pressure Wound Therapy (NPWT) VAC therapy has become a valuable tool in managing the large, complex wounds that follow the debridement of necrotizing fasciitis, offering several benefits that promote healing and reduce complications (19) VAC therapy offers several key advantages in the management of necrotizing fasciitis First and foremost, it accelerates wound healing by creating an optimal environment for tissue regeneration Large wounds, such as those caused by necrotizing fasciitis, are often slow to heal Still, applying negative pressure can speed up the process by improving blood flow and promoting healthy tissue growth This is particularly important in reducing the need for additional surgeries or skin grafts (20) Despite its many advantages, VAC therapy is not without challenges The cost of the equipment and the need for specialized training to properly administer the therapy can limit its accessibility in some healthcare settings (21) In the case of FG, which poses a significant risk of mortality (20-30%), medical emergency measures should be taken These measures include fluid resuscitation, broadspectrum antibiotics, and urgent surgical debridement The timely execution of these measures is crucial, and various validated scores, such as the FGSI and Uludag FGSI (UFGSI) (13, 22, 23) can predict mortality rates associated with FG (24-26) Our experience shows that the death rate (21 4%) is consistent with existing litera-
G Cochetti, A Paladini, L Lepri, et al
ture, with only one death attributed to the progression of Duchenne syndrome and not FG In one case, delays in diagnosis and treatment were observed, highlighting the significance of timely intervention
The length of hospital stay (LOS) has decreased significantly The first study was conducted by Carroll et al in 1986 (27) reported a LOS of 48 days, whereas the latest review by Bowen et al (28) showed a reduced LOS of 18 5 days
Our study also reported a lower LOS, which we attribute to the small number of re-debridements
CONCLUSIONS
FG is a rare but serious health condition that still has high mortality rates It requires prompt and comprehensive intervention that should include timely surgical debridement and antibiotic therapy to achieve posi-tive outcomes
The study emphasizes the difficulties involved in managing this complex condition However, it also shows that a primary extensive debridement can help reduce the need for further intervention and shorten the hospi-tal stay
REFERENCES
1 Singh A, Ahmed K, Aydin A, et al Fournier’s gangrene A clinical review Arch Ital Urol Androl 2016; 88:157
2 Paladini A, Cochetti G, Tancredi A, et al Management of Fournier’s gangrene during the Covid-19 pandemic era: make a virtue out of necessity Basic Clin Androl 2022; 32:12
3 Sorensen MD, Krieger JN Fournier’s Gangrene: Epidemiology and Outcomes in the General US Population Urol Int 2016; 97:249-59
4 Chernyadyev SA, Ufimtseva MA, Vishnevskaya IF, et al Fournier’s Gangrene: Literature Review and Clinical Cases Urol Int 2018; 101:91-7
5 Ellegård L, Prytz M Fournier’s gangrene under SGLT-2 inhibitor therapy: A literature review and case report Int J Surg Case Rep 2020; 77:692-4
6 Del Zingaro M, Boni A, De Vermandois JAR, et al Fournier’s gan-
DECLARATIONS
Ethical approval: Institutional Review Board Statement not applicable
Availability of data and material: Data reported in this article are all available at location cited in the reference section
Competing interests: The authors declare no conflicts of interest
Funding: This research received no external funding
Authors’ contributions: Conceptualization, G C and A V ; Methodology, E M and L S ; Formal analysis, L L ; Investigation, M R ; Data curation, M D Z and E I ; Writing-original draft preparation, A P and M M ; Writing-review and editing, A V , R L M and A F ; Supervision, M D Z and P M ; project administration, G C All authors have read and agreed to the published version of the manuscript
Acknowledgments: Not applicable
Informed consent statement: Not applicable
grene and intravenous drug abuse: an unusual case report and review of the literature Open Medicine 2019; 14:694-710
7 Del Zingaro M, Boni A, Paladini A, et al Fournier’s gangrene secondary to locally advanced prostate cancer: case report and review of the Literature G Chir 2019; 40:481-96
8 Molla YD, Assefa MA, Abraha AY Fournier’s gangrene with retroperitoneal extension, a case report Int J Surg Case Rep 2023; 105:107984
9 Ioannidis O, Kitsikosta L, Tatsis D, et al Fournier’s Gangrene: Lessons Learned from Multimodal and Multidisciplinary Management of Perineal Necrotizing Fasciitis Front Surg 2017; 4:36
10 Auerbach J, Bornstein K, Ramzy M, et al Fournier Gangrene in the Emergency Department: Diagnostic Dilemmas, Treatments and Current Perspectives Open Access Emerg Med 2020; 12:353-364
11 Singh A, Ahmed K, Aydin A, et al Fournier’s gangrene A clinical review Arch Ital Urol Androl 2016; 88:157
12 Wong C-H, Khin L-W, Heng K-S, et al The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: A tool for distinguishing necrotizing fasciitis from other soft tissue infections* Crit Care Med 2004; 32:1535-41
13 Laor E, Palmer LS, Tolia BM, et al Outcome prediction in patients with Fournier’s gangrene J Urol 1995; 154:89-92
14 Czymek R, Frank P, Limmer S, et al Fournier’s gangrene: is the female gender a risk factor? Langenbecks Arch Surg 2010; 395:173-80
15 Kincius M, Telksnys T, Trumbeckas D, et al Evaluation of LRINEC Scale Feasibility for Predicting Outcomes of Fournier Gangrene Surg Infect (Larchmt) 2016; 17:448-53
16 Wang T-L, Hung C-R Role of tissue oxygen saturation monitoring in diagnosing necrotizing fasciitis of the lower limbs Ann Emerg Med 2004; 44:222-8
17 Lin T-Y, Cheng I-H, Ou C-H, et al Incorporating Simplified Fournier’s Gangrene Severity Index with early surgical intervention can maximize survival in high-risk Fournier’s gangrene patients Int J Urol 2019; 26:737-43
18 Raizandha MA, Hidayatullah F, Kloping YP, et al The role of hyperbaric oxygen therapy in Fournier’s Gangrene: A systematic review and meta-analysis of observational studies Int Braz J Urol 2022; 48:771-81
19 Assenza M, Cozza V, Sacco E, et al VAC (Vacuum Assisted Closure) treatment in Fournier’s gangrene: personal experience and literature review Clin Ter 2011; 162:e1-5
20 Zhang R, Zhang Y, Hou L, Yan C Vacuum-assisted closure versus conventional dressing in necrotizing fasciitis: a systematic review and meta-analysis J Orthop Surg Res 2023; 18:85
21 Agarwal P, Kukrele R, Sharma D Vacuum assisted closure ( VAC ) / n e g a t i ve p re ssu re w ou n d t h e r a p y ( N P W T ) for d i ffi c u l t wounds: A review J Clin Orthop Trauma 2019; 10:845-8
22 Yilmazlar T, Isik O, Ozturk E, et al Fournier’s Gangrene: Review of 120 Patients and Predictors of Mortality Ulus Travma Acil Cerrahi Derg 2014; 20:333-7
23 Sparenborg JD, Brems JA, Wood AM, et al Fournier’s gangrene: a modern analysis of predictors of outcomes Transl Androl Urol 2019; 8:374-8
24 Al-Kohlany K, Baker K, Ahmed F, et al Treatment outcome of Fournier’s gangrene and its associated factors: A retrospective study Arch Ital Urol Androl 2023; 95:11318
25 Ghabisha S, Ahmed F, Al-wageeh S, et al Prognostic determi-
nants and treatment outcomes of Fournier’s Gangrene treatment in a resource-limited setting: A retrospective study Arch Ital Urol Androl 2023; 95:11450
26 Wirjopranoto S, Affandi MR, Ashari FY, et al Evaluating prognostic indicators for in-hospital mortality in Fournier’s gangrene: a 7year study in a tertiary hospital Arch Ital Urol Androl 2024; 96:12387
27 Carroll PR, Cattolica E V, Turzan CW, McAninch JW Necrotizing soft-tissue infections of the perineum and genitalia Etiology and early reconstruction West J Med 1986; 144:174-8
28 Bowen D, Juliebø-Jones P, Somani BK Global outcomes and lessons learned in the management of Fournier’s gangrene from highvolume centres: findings from a literature review over the last two decades World J Urol 2022; 40:2399-410
Correspondence
Giovanni Cochetti giovanni cochetti@unipg it
Alessio Paladini alessiopaladini89@gmail com
Luca Lepri
lucalepri3@libero it
Andrea Vitale (Corresponding Author) andrea vitale69@yahoo it
Raffaele La Mura lamura@specializzandi unipg it Miriam Russo miriam russo@specializzandi unipg it Paolo Mangione paolo mangione@specializzandi unipg it Matteo Mearini matteo mearini@outlook it
Michele Del Zingaro michele delzingaro@unipg it
Department of Medicine and Surgery, Urology Clinic, University of Perugia, Perugia, Italy
Andrea Fabiani andreadoc1@libero it
Emanuele Iacobone emanuele iacobone@sanita marche it
Lucilla Servi lucilla servi@sanita marche it
Surgery Department, Urology Unit, Macerata Civic Hospital, Area Vasta 3 Asur Marche, Italy
Ettore Mearini
ettore mearini@unipg it
Department of Medicine and Surgery, Urological Andrological Surgery and Minimally Invasive Techniques Unit, S Maria Hospital, University of Perugia, Terni, Italy
G Cochetti, A Paladini, L Lepri, et al
ORIGINAL PAPER
Correlation between seminal alpha-Glycerylphosphorylcholine and semen parameters in infertile patients pre and post sub-inguinal micro-varicocelectomy: A prospective study
Ahmed Fathy Aboseif 2 , Nashaat Nabil 2 , Sameh Fayek GamalEl Din 1 , Shaimaa Ali Abdelkareem 3 , Aya Ahmed Onsi M.M.B.c.H 4 , Ahmad Zaghloul 1 , Amgad Elseginy 1
4 Egypt Ministry of Health & Population, Cairo, Egypt
Summary
Background: Varicocele (Vx) which is the most treatable cause of male infertility, is also associated with low sperm count, decreased sperm motility and increased sperm abnormal morphology. We aimed in the current study to evaluate the correlation between seminal Alpha-Glycerylphosphorylcholine (αGPC) and semen parameters in infertile patients pre and post sub-inguinal micro-varicocelectomy
Methods: The current comparative prospective study was carried out on 20 male patients who presented to Kasr Al-Ainy Hospitals from March 2022 to March 2023 as well as 20 healthy controls The participants were divided into groups as follow: group (1) included fertile normozoospermic men (n = 20) who served as controls Group (2) included infertile oligoasthenoteratozoospermia (OAT) men with varicocele (n = 20)
Patients in group (2) were followed up to 3 months after microsurgical sub-inguinal Varicocelectomy. The examination included assessment of Vx with scrotal Duplex Semen analysis was done according to the 5th Edition of WHO manual for semen analysis
Results: The study demonstrates that αGPC level was significantly higher among fertile normozoospermic control group and infertile OAT men post varicocelectomy when compared to infertile OAT men preoperative (p < 0 001) Moreover, it demonstrates that on follow up of infertile OAT group 3 months after sub-inguinal micro-varicocelectomy, all semen parameters showed significant improvement compared to the corresponding semen parameters pre-operatively among Vxs grade II and grade III (p < 0.001, p < 0.001, respectively). A significant positive correlation was found between αGPC level and semen parameters including sperm normal forms, sperm count and sperm motility Using ROC curve, αGPC protein showed a sensitivity of (100%) and a specificity of (100%) at cut off value (≤ 1 975 pg/ml) in differentiation between infertile OAT patients with Vx and control fertile normozoospermic men (p < 0 001)
Conclusions: αGPC may play an important role in infertility in men with Vx and correction of Vx improves the seminal αGPC level
Infertility is defined as the inability to conceive after at least 12 months of regular unprotected sexual intercourse Infertility is a worldwide complaint and is projected to involve 8-12% of couples in the fertility period (1) Males are responsible for 20-30% of cases of infertility and are participating in a further 20% Male subfertility is a wide range problem with almost unknown cause in most cases (1) Although various diagnostic tests are available, their interpretation is imprecise and often subjective Varicocele (Vx) which is the most treatable cause of male infertility with a prevalence of 40%, is also associated with low sperm count, decreased sperm motility and increased sperm abnormal morphology (2-4) The main hypotheses were that hyperthermia, venous pressure, hormonal imbalance, toxic substances and reactive oxygen radicals were involved in the pathophysiology and that varicocelectomy improved the number and motility of sperms (2-4) Vx causes a progressive decline in fertility with upwards of 80% of men presenting with secondary subfertility having a Vx (5) Several studies tried to answer how Vx causes infertility Factors included increased oxidative stress due to increased pressure on venous walls, scrotal hyperthermia, hypoxia, reflux of renal and adrenal metabolites, hormonal imbalances, the formation of antisperm antibodies and change in the seminal fluid composition including epididymal proteins (68) Miyaoka and Esteves found that patients with both clinical and subclinical Vxs benefited from varicocelectomy because their sperm counts went up by a lot (9) Alpha-glycerylphosphorylcholine (αGPC), one of the major phosphorus containing-choline compounds of seminal plasma, is secreted mainly by the epididymal epithelium under androgenic control (10) The organic fraction of human seminal plasma contains phosphate esters, particularly αGPC, phosphorylcholine (PCh) and inorganic phosphate (11) αGPC is synthesized by the epididymis It originated from phosphatidylcholine (PC) and broke down into choline and α-glycerophosphate (12) PC synthesis in mammalian tissue occurs by Kennedy pathway with choline as one of the pillar substances that necessitates the removal of fatty acids by phospholipase activity
(12) Also, the synthesis of αGPC entails sequential activity of a phospholipase A or alternatively, activity of a single phospholipase B Notably, αGPC is water soluble and degraded by hydrolysis to glycerol-3-phosphate and choline catalysed by GPC phosphodiesterase activity (12) Evaluation of αGPC activity may also help find out if the epididymis is open and if sperm isn't normal Unfortunately, there are different opinions in the literature about how useful the assay is for male infertility (13) The epididymal function in semen analysis has been prev i o u s l y r
Alpha-glucosidase, αGPC and L-carnitine were measured in sperm-free seminal plasma to determine the exact importance of these proteins in male fertility but with conflicting results (14) The objective of this study was to evaluate the effectiveness of evaluation and assessment of seminal of αGPC in infertile men before and after subinguinal micro-varicocelectomy
PATIENTS AND METHODS
The current comparative prospective study was carried out on 20 male patients who presented to Kasr Al-Ainy Hospitals from March 2022 to March 2023 as well as 20 controls The institutional ethical committee of Beni suef university approved the work that conforms to Helsiniki declaration 2013 (15) (FMBSREC/08032022)
Inclusion criteria
Any infertile case with oligoasthenoteratozoospermia (OAT) and Vx aged 20 to 30 years old
Exclusion criteria
Patients suffering from azoospermia and subclinical Vx, smoking, patients with congenital anomalies or leukocytospermia, history of blood transfusion, iron therapy or anemia were excluded from the study
Inclusion criteria of the controls
They were healthy age matched individuals who were companions to the cases
The participants were divided into groups as follows: group (1) was fertile normozoospermic men (n=20) served as controls Group (2) was infertile OAT men with Vx (n = 20) Patients in group (2) were followed up to 3 months after sub-inguinal micro-varicocelectomy
General and clinical examinations were done The examination included assessment of Vx with scrotal Duplex Semen analysis was done according to the 5th Edition of WHO manual for semen processing (2010) (16)
Clinical examination was carried out in a warm room at the standing position with/without Valsalva maneuver Color Doppler Ultrasonography was conducted for assurance of Vx and its grade when one or more veins had a maximal diameter >3 mm with a retrograde flow at rest or under Valsalva maneuver Vx was classified according to Chiou et al (1997) and Kim et al (2008) characterization (17-18)
The ejaculates were obtained after 4-5 days of sexual abstinence into sterile containers More than one sample was provided 2 weeks apart Sub-inguinal micro-varicoc-
electomy was done under general anaesthesia (19) Also, it was done using a surgical microscope HB Surgitech [5 Step Magnifications (4x, 6x, 10x, 16x & 25x) 45 degree Inclined Binocular Tubes, 12 5x Wide Field Eye Pieces, F = 200 mm Objective Lens, Aadesh Complex, Court Road, Near CJM Court, Ambala-134003, Haryana, India]
After hospital discharge, patients were invited to attend to follow-up visit 3 months after sub-inguinal micro-varicocelectomy Semen samples were obtained as described above Fertile men infertile delivered one sample only, while infertile OAT men delivered 2 samples pre and post sub-inguinal micro-varicocelectomy
Measurement of αGPC
Quantitative detection of seminal αGPC was assayed by enzyme linked immunosorbent assay (ELISA) sandwich principle Human PC/CPG (Choline Phosphoglyceride ELISA kit supplied by the American research products, USA (Cat no EELH0730) according to manufacturer’s instructions
Statistical analysis of the data
Data were fed to the computer and analysed using IBM SPSS software package version 20 0 (Armonk, NY: IBM Corp) Qualitative data were described using number and percent The Shapiro-Wilk test was used to verify the normality of distribution Quantitative data were described using range (minimum and maximum), mean and standard deviation The significance of the obtained results was judged at the 5% level F-test (ANOVA) was used for normally distributed quantitative variables, to compare between more than two groups with Post Hoc test (Tukey) for pairwise comparisons Pearson coefficient was used to correlate between two normally distributed quantitative variables Chi-square test was used to examine the relationship between two qualitative variables T Test was to assess the statistical significance of the difference between two study group means Finally, receiver operating characteristic curve was used to evaluate the sensitivity and specificity for quantitative diagnostic measures that categorize cases into one of two groups
The optimum cut off point was defined as that which maximized the AUC value The area under the ROC curve (AUC) results were considered excellent for AUC values between 0 9-1, good for AUC values between 0 8-0 9, fair for AUC values between 0 7-0 8, poor for AUC values between 0 6-0 7 and failed for AUC values between 0 50 6
RESULTS
The sociodemographic characteristics of the participants are shown in Table 1 The study demonstrates that αGPC level was significantly higher among fertile normozoospermic control group and infertile OAT men post subinguinal micro-varicocelectomy when compared to infertile OAT men preoperative (p < 0 001) (Table 2) Moreover, it was demonstrated that on follow up of infertile OAT group 3 months after sub-inguinal micro-varico c e l e c t o m y , s e m e n p a r a m e t e r s s h o w e d s i g n i fi c a n t improvement compared to the corresponding semen parameters pre-operatively among Vxs grade II and grade
A Abo Sief, N Nabil, S F GamalEl Din, et al
Table 1
Descriptive data of the controls and group IIa (pre-operative infertile OAT with varicocele) and group IIb (Infertile OAT after sub-inguinal micro-varicocelectomy).
Table 2. Comparison between controls and groups IIa and IIb regrading αGPC level and normal forms
Sperm normal forms (%)
SD = Standard dev at on; IQR: Inter Quart le Range; F: F for ANOVA test, pa rw se compar son bet each 2 groups were done using Post Hoc Test (Tukey); p: p value for comparing between the 3 groups (group I and group II a and group IIb); p1: p value for comparing between group I and group IIa (pre-operative) and Group Ib (post-operative); p2: p value for comparing between group IIa (pre-operative) and group IIb (post-operat ve)
Patients with Vx grade II
(years)
Table 3
Data of infertile men with varicocele grade II pre and post sub-inguinal micro-varicocelectomy.
GPC level (pg/ml)
Sperm normal forms (%)
SD = Standard deviat on; t: Student t-test; p: p va ue for compar ng between the stud ed categories
III (p < 0 001, p < 0 001, respectively) (Tables 3-4)
There were no significant differences among patients with Vx grade II and Vx grade III, pre and post sub-inguinal micro-varicocelectomy regarding age (Tables 3-4) Furthermore, there was a significant positive correlation between αGPC level and semen parameters including sperm normal forms, sperm count and sperm motility (Table 5) Using ROC curve, αGPC protein showed a sensitivity of (100%) and a specificity of (100%) at a cut off value of ≤ 1 975 pg/ml in differentiation between infertile OAT patients with Vx and control fertile normozoospermic men (p < 0 001) (Figure 1)
Figure 1
ROC curve showing α-GPC level (pg/ml) to discriminate between infertile OAT patients with varicocele and controls.
+DISCUSSION
In our study, analysis of semen parameters revealed that infertile OAT men with Vx showed statistically significant decrease regarding sperm counts and percentage of
Table 4
Data of infertile men with varicocele grade III pre and post sub-inguinal micro-varicocelectomy
Table 5. Correlations between different parameters in the current study
Figure 2.
ROC showing α-GPC level (pg/ml) to discriminate between infertile OAT patients with varicocele before and after varicocelectomy
motile sperms when compared to fertile normozoospermic men who had normal basic semen paramaters On follow up of infertile OAT group 3 months after subi
showed significant improvement compared to the corresponding semen parameters pre-operatively In agreement with our results, Shabana et al reported that sperm count and progressive motility significantly improved after varicocelectomy compared to pre-operative analysis (20) Consistently, Rehman et al reported that sperm count, motility and normal morphology were significantly lower in Vx patients in comparison to normal individual (21) This result agreed with a large-scale study of 7035 healthy young men from general European populations demonstrated that the presence of Vx was associated with poorer semen quality (22) Evidence from both animal and human studies show that varicocele affects sperm quality Experimental Vx has been associated with impairment of testicular and epididymal endocrine and exocrine function, which may contribute to infertility seen in men with Vx (23) Moreover, we found that normal forms of sperms significantly improved in cases of Vx grade III compared to cases of Vx grade II after subinguinal micro-varicocelectomy Consistently, Pasqualotto et al did a study on 61 men with Vx (24) They found that men with large varicoceles have worse sperm parameters before surgery, but they improve more after surgery than men with small or medium-sized varicoceles (24) Krishna Reddy et al showed that patients with grade III Vx not only have better sperm parameters after surgery than those with grades I and II, but also have a significant increase in testicular volume, which goes along with improvement in sperm parameters (25)
In our current study, on follow up of infertile OAT group 3 months after sub-inguinal micro-varicocelectomy, semen parameters and αGPC showed significant improvement compared to the corresponding semen parameters preoperatively among Vx grades II and III In our study, we believe that αGPC levels decrease in infertile men with Vx this may be related to hyperthermia, venous pressure and reactive oxygen radicals which could be involved in the pathophysiology of the devastating impact of Vx on spermatogenesis In the current study levels of seminal αGPC were significantly higher post sub-inguinal micro-varicocelectomy compared to pre-operative in infertile males with Vx Seminal αGPC were nearly matching to levels of fertile normozoospermic men after sub inguinal micro-varicocelectomy Statistically significant positive correlation was found between αGPC level and semen parameters Also, the current study did not demonstrate a relation between age and αGPC level Seminal αGPC showed 100% sensitivity and 100% specificity in differentiation between infertile OAT patients with Vx and fertile normozoospermic men Same values of sensitivity and specificity were obtained when comparing seminal αGPC between infertile OAT patients with Vx and post sub-inguinal micro-varicocelectomy Camargo et al conducted a study to determine the seminal plasma lipid fingerprints in adults with Vx before and after varicocelectomy (26) They reported that αGPC levels improved in the post-varicocelectomy group (26) Seminal αGPC is one of the three main epididymal markers important for proper spermatogenesis One of the physiological functions attributed to αGPC is a possible role in respiration and motility of sperm (27) In the same context, Mieusset et al (2020) reported significantly lower levels of αGPC in azoospermic men (28) This finding indi-
cated the possible significant role played by αGPC in male fertility In contrast, Mieusset et al previously reported (1988) no major difference in the total seminal content of αGPC among fertile and infertile men (29) Furthermore, Zhang et al reported that levels of αGPC in asthenozoospermic men were significantly higher compared to healthy controls (30) Admittedly, small sample size is considered the main limitation of the current study as well as short follow up period However, the prospective nature of the study can add strength to the current findings
CONCLUSIONS
Seminal αGPC may play an important role in infertility in men with Vx and correction of Vx improves seminal αGPC level
REFERENCES
1 Agarwal A, Baskaran S, Parekh N, et al Male infertility Lancet 2021; 397:319-333
2 Mostafa T, Rashed LA, Osman I, Marawan M Seminal plasma oxytocin and oxidative stress levels in infertile men with varicocele Andrologia 2015; 47:
3 Jensen CFS, Østergren P, Dupree JM, et al Varicocele and male infertility Nat Rev Urol 2017; 14:523-533
4 Choy JT, Eisenberg ML Male infertility as a window to health Fertil Steril 2018; 110:810-814
5 Fang Y, Su Y, Xu J, et al Varicocele-mediated male infertility: From the perspective of testicular immunity and inflammation Front Immunol 2021; 12:729539
6 Al Bakri A, Lo K, Grober E, et al Time for improvement in semen parameters after varicocelectomy J Urol 2012; 187:227-231
7 Nork JJ, Berger JH, Crain DS, Christman MS Youth varicocele and varicocele treatment: a meta-analysis of semen outcomes Fertil Steril 2014; 102:381-387
8 Elbardisi H, El Ansari W, Majzoub A, Arafa M Does varicocelectomy improve semen in men with azoospermia and clinically palpable varicocele? Andrologia 2020; 52:e13486
DECLARATIONS
Ethical approval: This study was approved by the institutional ethical committee of Beni Suef University Additionally, informed consent was obtained from the patients
Availability of data and material: All inquiries can be directed to the corresponding author
Competing interests: The authors declare no competing interests
Funding: This study did not receive any fund
Authors' contributions: SFG drafted the initial manuscript; SFG revised the article critically; SFG reviewed and edited the article; NN designed the study; SAA performed the lab work of the study; AO, AE, AZ, AAS collected and analyzed the data All authors reviewed the manuscript
Acknowledgments: We would to thank the surgeons who performed the sub inguinal micro-varicocelectomy
9 Miyaoka R, Esteves SC A critical appraisal on the role of varicocele in male infertility Adv Urol 2012; 2012:597495
10 Ma JY, Lee MY, Kim HM, et al Shibimijihwang-tang elevates intracellular ATP and choline content in the cerebral cortex of ovariectomized rats J Ethnopharmacol 2000; 72:77-85
11 López Rodríguez A, Rijsselaere T, Beek J, et al Boar seminal plasma components and their relation with semen quality Syst Biol Reprod Med 2013; 59:5-12
12 Gallazzini M, Burg MB What’s new about osmotic regulation of glycerophosphocholine Physiology 2009; 24:245-249
13 Ramm SA Seminal fluid and accessory male investment in sperm c o m p e t i t i o n P h
375:20200068
14 Dacheux JL, Dacheux F, Druart X Epididymal protein markers and fertility Anim Reprod Sci 2016; 169:76-87
1 5 W o r l d M e d i c a l A s s o c i a t i o n W o r l d M e d i c a l A
Declaration of Helsinki: ethical principles for medical research involving human subjects JAMA 2013; 310:2191-2194
16 World Health Organization (WHO) WHO laboratory manual for the examination and processing of human semen 5th ed Geneva: WHO: 2010 271 p
17 Chiou RK, Anderson JC, Wobig RK, et al Color-Doppler ultrasound criteria to diagnose varicoceles: correlation of a new scoring system with physical examination Urology 1997; 50:953-956
18 Kim HH, Goldstein M Adult varicocele Curr Opin Urol 2008; 18:608-612
19 Lee JY, Yu HS, Ham WS, et al Microsurgical intermediate subinguinal varicocelectomy Int Surg 2014; 99:398-403
20 Shabana W, Teleb M, Dawod T, et al Predictors of improvement
in semen parameters after varicocelectomy for male subfertility: A prospective study Can Urol Assoc J 2015; 9:E579
21 Rehman KU, Zaneb H, Qureshi AB, et al Correlation between testicular hemodynamic and semen quality indices in clinical varicocele patients in Pakistan BioMed Res Int 2019; 2019:7934328
22 Damsgaard J, Joensen UN, Carlsen E, et al Varicocele is associated with impaired semen quality and reproductive hormone levels: a study of 7035 healthy young men from six European countries Eur Urol 2016; 70:1019-1029
23 Birowo P, Tendi W, Widyahening IS, et al The benefits of varicocele repair for achieving pregnancy in male infertility: A systematic review and meta-analysis Heliyon 2020; 6:e05439
24 Pasqualotto FF, Lucon AM, Sobreiro BP, et al Effects of medical therapy, alcohol, smoking, and endocrine disruptors on male infertility Rev Hosp Clin Fac Med Sao Paulo 2004; 59:375-82
25 Krishna Reddy SV, Basha Shaik A, Sailaja S, Venkataramanaiah M Outcome of varicocelectomy with different degrees of clinical varicocele in infertile male Advances in Andrology 2015; 2:5-9
26 Camargo M, Montani DA, Gozzo FC, et al Lipid fingerprinting profile of seminal plasma of patients perfomingsubinguinal microsurgery of varicocelectomy Fertil Steril 2012; 98:S146-S147
27 Cooper TG, Weidner W, Nieschlag E The influence of inflammation of the human male genital tract on secretion of the seminal markers α-glucosidase, glycerophosphocholine, carnitine, fructose and citric acid Int J Androl 1990; 13:329-336
28 Mieusset R, Bieth E, Daudin M, et al Male partners of infertile couples with congenital unilateral absence of the vas deferens are mainly non-azoospermic Andrology 2020; 8:645-653
Correspondence
Ahmed Fathy Aboseif, MD ahmed Fathy mohamed@med bsu edu eg Nashaat Nabil, MD nashaatnabil70@gmail com
Egypt Ministry of Health & Population, Cairo, Egypt
A Abo Sief, N Nabil, S F GamalEl Din, et al
ORIGINAL PAPER
Sperm DNA fragmentation: Focusing treatment on seminal transport fluid beyond sperm production
Moises Abraham Adel Domínguez 1 , Walter D Cardona Maya 2 , Andrés Mora Topete 1
1 Centro de Uro-Andrología S C , Guadalajara, Jalisco, México; 2 Grupo Reproducción, Departamento de Microbiología y Parasitología, Facultad de Medicina, Universidad de Antioquia, Medellín, Colombia
Summary
Aim: To determine the effects of oral antibiotics and anti-inflammatory agents on semen parameters and the sperm DNA fragmentation index (DFI). Methods: Ninety-eight men with infertility diagnosis were included. The participants submitted two semen samples, before and at least two months after treatment Macroscopic and microscopic semen parameters were evaluated following the World Health Organization (WHO) guidelines In addition, the sperm DFI was evaluated using the sperm chromatin dispersion (SCD) technique Subsequently, a treatment regimen was administered, including daily oral doses of ciprofloxacin (1000 mg) and doxycycline (100 mg) for 21 and 10 days, respectively. In addition, non-steroidal anti-inflammatory drugs (15 mg of meloxicam) were used for 10 days After treatment, the same parameters were re-evaluated for new semen samples taken under the same initial conditions
Results: After treatment, significant increases in pH, sperm count, total concentration, and normal sperm morphology were observed, but no significant differences were found in the seminal volume parameter or progressive motility After treatment, a significant decrease in the concentration of immature cells was observed, and although not statistically significant, a reduction in the concentration of leucocytes was observed After treatment, the mean sperm DFI significantly decreased from 28 24 ± 12 39% to 16 2 ±7 1%
Conclusions: Treatment with antibiotics and anti-inflammatories significantly reduced the sperm DFI and improved semen quality.
KEY WORDS: Male fertility; Infertility; DNA fragmentation index; Semen; Spermatozoa
Submitted 19 September 2024; Accepted 6 October 2024
INTRODUCTION
Infertility is a problem that affects an increasing number of people around the world, regardless of gender (1, 2) When studying semen to evaluate and diagnose male fertility, it is considered that male factors are responsible for 50% of infertility cases (3), and specialists focus primarily on the macroscopic and microscopic parameters of semen (4) However, although these parameters can be considered essential for determining the success of a pregnancy, it is crucial that, in the presence of infertility, sperm functional alterations that could affect embryonic
development are also evaluated (5-7) A high sperm DNA f r a g m e n t a t i o n i n d e x ( D F I ) h a s b e e n a s s o c i a t e d w i t h decreased male fertility and an increased risk of spontaneous abortions (8, 9) Therefore, it has become an essential parameter in fertility studies for evaluating sperm quality
Sperm DNA fragmentation can occur for different reasons, such as oxidative stress, DNA lesions, infections, and other factors (10) Different techniques are used to evaluate the sperm DFI, including the single-cell gel electrophoresis (comet) assay, the sperm chromatin structure a s s a y , D N A b r e a k a g
u hybridization (DBD-FISH), and terminal deoxynucleotidyl transferase deoxyuridine triphosphate (dUTP) nick end labeling (TUNEL) assay, among others These methodologies have shown promising results but require specialized equipment and high-cost reagents, making those tests unavailable for all populations (11) In contrast, the sperm chromatin dispersion assay (SCD) offers many advantages, such as its low cost compared to other techniques and its simplicity, practicality, speed, and reproducibility (11-13)
The most explored treatment for reducing sperm DFI is the chronic use of oral antioxidants, based on the evidence that DNA fragmentation is frequently associated with states of oxidative stress (14-16) However, the presence of bacteria in semen can also affect semen quality, and consequently, identifying the presence of bacteria in couples with fertility problems could be beneficial for improving semen parameters and increasing the chances of successful conception (17)
Therefore, antibiotics could also improve sperm DFI in some instances in which DNA fragmentation is caused by a bacterial infection in the male reproductive tract; treatment with appropriate antibiotics could clear the infection and reduce inflammation, which could help improve sperm DNA integrity (18)
This study aimed to determine the effects of oral antibiotics and anti-inflammatory agents on semen parameters and the sperm DFI
MATERIALS AND METHODS
Ninety-eight men with the diagnosis of primary or secondary infertility, either directed for advanced and non-
advanced reproductive techniques were included (Centro de Uro-Andrología S C , Guadalajara, Jalisco, México) Each patient was invited to participate in the study, and authorization was requested under current ethical standards; each participant also provided informed consent
The study participants provided two semen samples under similar conditions of sexual abstinence (3-5 days), one before treatment and one at least two months after treatment Both semen samples were analyzed in the same laboratory by the same expert technician
Basic macroscopic and microscopic sperm parameters were evaluated following the WHO guidelines (19), and the sperm DFI was determined using the sperm chromatin dispersion test (SCD, Sperm DNA kit, Obi biotek) following the manufacturer's instructions In addition, the concentrations of leukocytes and immature cells were also evaluated
After the initial semen evaluation, the patients were invited to receive daily oral doses of ciprofloxacin (1000 mg) or doxycycline (100 mg) for 21 or 10 days, respectively
In addition, non-steroidal anti-inflammatory drugs (15 mg of meloxicam) were used for 10 days
Statistical analysis
The data distribution was evaluated with the normality test of residuals, and the descriptive analysis was carried out according to the distribution of the variables Paired t tests were carried out for related samples when the data met normality, and the Wilcoxon test was used for nonnormal distributed samples A p value of < 0 05 was considered to indicate statistical significance
RESULTS
Ninety-eight men with infertility diagnosis participated in the study The median age was 36 ± 6 7 years, with an interquartile range (25-75) of 32-41 years
As shown in Table 1, no significant differences were found regarding seminal volume or progressive motility
However, after treatment, a significant increase in pH, sperm count, total concentration, and normal sperm morphology was observed
In addition, a decrease, although not statistically significant, in the concentration of immature cells and leucocytes was observed after treatment: 1 4 ± 2 0 million/mL vs. 0 85 ± 1 6 million/mL (p = 0 2613) and 1 9 ± 2 2 vs. 1 2 ± 1 8 million/mL (p = 0 4541), respectively
Changes in the sperm DFI after treatment
Finally, after treatment, the mean sperm DFI significantly decreased from 27 2 ± 10 7% to 16 9 ± 7 6% (p < 0 001) (Figure 1)
DISCUSSION
The results of this study support the effectiveness of an antibiotic and anti-inflammatory treatment approach in male patients diagnosed with infertility, consistent with previously published preliminary results (20) Initial evaluation of semen samples revealed various parameters essential for determining sperm quality, such as volume, pH, viscosity, sperm concentration and sperm DFI (7) We hypothesize that the sperm DFI problem lies not in the quality of the sperm itself during spermatogenesis but in the factors that promote the degradation of its integrity once it has reached maturity and in the seminal tract
Following this approach, we have implemented a treatment plan based on dual-scheme antibiotics accompanied by anti-inflammatories to improve the quality of the t r a n s p o r t m e d i u m r a t h e r t h a n t h e s p e r m a t o g e n e s i s process in the seminal fluid used for spermatogenesis
A few years ago, there was no consensus on how to manage high prostate-specific antigen (PSA) levels that have occasionally been detected during PSA screening, because PSA levels can increase for several reasons, including trauma, ejaculation, rectal and urethral procedures, and numerous noncancerous etiologies such as benign prostatic hyperplasia, inflammation, and infection (21); therefore most urologists make decisions based on their training and experience, and the use of antibiotics to reduce high PSA is
M A Adel Domínguez, W D Cardona Maya, A Mora Topete
Table 1.
Changes in semen parameters before and after treatment
Figure 1
an alternative (22), although it is not safe to discard biopsies in patients who achieve a satisfactory PSA response to antibiotics (22), because if it has been observed that the use of antibiotics delays the diagnosis of prostate cancer
In the same way, most of the seminal fluid is composed of by secretions of accessory glands, which comprise the prostate, the seminal vesicles, and the bulbourethral glands, and it is possible that the presence of bacteria in this fluid and in its places of origin (23, 24) could negatively affecting the semen and sperm quality
Therefore, as bacteria are present in the semen, safe from its origin, the use of antibiotics will eradicate the local inflammatory effect that promotes tissue damage and release of more prostate antigen, as is happening in patients with increased PSA However, given that the fragmentation of sperm DNA don’t occur during its formation, eliminating bacteria from the seminal pathways would allow the elimination of local inflammation and its deleterious effects on sperm DNA
Bacteria may release soluble factors, such as lipopolysaccharides, hemolysins, and other soluble spermatotoxic factors that can affect sperm physiology (23, 25) The effects of bacterial infection may be multiple, comprising reduction in motility, induction of teratozoospermia (abnormal sperm morphology), apoptosis, DNA fragmentation, sperm agglutination, and exposure to oxidative stress through forming reactive oxygen species (ROS) (23, 25)
Altogether, the use of low-potency steroids is necessary because antibiotics do not affect the mucosa of the urothelium or the urethra, but steroids can generate an anti-inflammatory effect on mucous membranes (26)
Therefore, using antibiotics and steroids can impact both the tissue of the epididymis, prostate and seminal vesicles as well as the urothelial mucosa of the urethra and prostatic urethra, where the semen is expelled
A key finding in this study was the high sperm DFI observed in the samples, with a mean of 28 24 ± 12 39%
This result highlights the presence of significant sperm DFI in the infertile patient population According to the literature, a cutoff of 20% can differentiate between fertile and infertile men (27) Previous evidence from a comparative study carried out with fertile and infertile patients showed that the average sperm DFI was 29 95% (26 6-34 3%) in infertile patients and 19 90% (15 6-24 4%) in fertile patients; moreover, a sperm DFI > 26 1% was associated with a 2 8-fold increased risk of infertility (28)
Furthermore, orally administered ciprofloxacin and etoricoxib for 15 days reduced the sperm DFI from 36 ± 3% to 24 9 ± 1% (20)
The implemented treatment, which included antibiotics and anti-inflammatories, led to significant changes in semen parameters A significant increase in pH and total sperm concentration was observed at the end of treatment, suggesting an improvement in sperm quality Although the semen volume did not significantly change, these other indicators support the effectiveness of the therapeutic approach (29)
Furthermore, a reduction in the concentration of leukocytes and round cells, which are markers of inflammation, is an important finding Although the decrease in leukocyte concentration did not reach statistical significance, the reduction in the number of round cells was sta-
tistically significant Since round cells are a marker of t r a n s i e n t i n fl a m m a t i o n s e c o n d a
y
o s p e r m a
g e n i c aggression, their decrease is positive and could be related to a decrease in sperm DNA fragmentation (30)
The most striking finding was the significant decrease in the DFI at the end of treatment
This indicates a substantial improvement in sperm DNA integrity and, therefore, in sperm quality Taken together, these results support the initial hypothesis that male infertility problems do not reside solely in the quality of the sperm themselves but rather in the factors that may promote the degradation of their integrity once they have reached maturity Antibiotic and anti-inflammatory treatments effectively address these factors, substantially improving semen parameters, including significantly reduced sperm DFI (20)
The proposed hypothesis is that a significant percentage of sperm DFI can be generated during its passage through the seminal pathway rather than being an exclusive process of spermatogenesis In essence, factors present in the epididymis, seminal vesicles, and prostate can substantially contribute to fragmentation, even in the absence of clinical symptoms or semen culture findings These factors include inflammatory changes in the epididymis, asymptomatic bacterial colonization, subclinical prostatitis, infrequent ejaculation and others Evaluating and managing these conditions in the seminal pathway could improve, to a certain extent, the quality of the seminal sample before deciding on Intracytoplasmic sperm injection (ICSI)
Therefore, in this way, the possibility of optimizing sperm quality through a therapeutic approach targeting the seminal pathway, as a strategy before considering assisted reproduction techniques, has to be considered, intending to improve natural pregnancy rates or reduce the need for ICSI in some cases
CONCLUSIONS
These findings are promising and may have significant implications for managing male infertility aiming to the quality of the seminal transport fluid beyond spermatogenesis, in order to obtain a non-hostile environment where sperm DNA fragmentation is reduced However, it is essential to highlight the need for additional research and longterm studies to validate these results and better understand the underlying mechanisms involved in this treatment
DECLARATIONS
Ethical approval: Authorization was requested under current ethical standards; each participant also provided informed consent
Availability of data and material: All inquiries can be directed to the corresponding author
Competing interests: None
Funding: None
Authors’ contributions: M A A D , W D C M , A M T
Acknowledgments: None
REFERENCES
1 Eisenberg ML, Esteves SC, Lamb DJ, et al Male infertility Nat Rev Dis Primers 2023; 9:49
2 Kimmins S, Anderson RA, Barratt CLR, et al Frequency, morbidity and equity - the case for increased research on male fertility Nat Rev Urol 2024; 21:102
3 Schlegel PN, Sigman M, Collura B, et al Diagnosis and Treatment of Infertility in Men: AUA/ASRM Guideline Part I J Urol 2021; 205:36
4 Abayomi BA, Afolabi BM, Victor DA, Oyetunji I Semen parameters associated with male infertility in a subsaharan black population: The effect of age and body mass index J Gynecol Infertility 2018; 1:1
5 Gil-Villa AM, Cardona-Maya W, Agarwal A, et al Role of male factor in early recurrent embryo loss: do antioxidants have any effect? Fertil Steril 2009; 92:565
6 Gil-Villa AM, Cardona-Maya W, Agarwal A, et al Assessment of sperm factors possibly involved in early recurrent pregnancy loss Fertil Steril 2010; 94:1465
7 McQueen DB, Zhang J, Robins JC Sperm DNA fragmentation and recurrent pregnancy loss: a systematic review and meta-analysis Fertil Steril 2019; 112:54
8 Álvarez JG Aplicaciones clínicas del estudio de fragmentación del ADN espermático Revista Internacional de Andrología 2007; 5:354
9 Robinson L, Gallos ID, Conner SJ, et al The effect of sperm DNA fragmentation on miscarriage rates: a systematic review and metaanalysis Hum Reprod 2012; 27:2908
10 Evenson DP Sperm chromatin structure assay (SCSA®) for fertility assessment Current Protocols 2022; 2:e508
11 Cicaré J, Avila A, Caille A, Munuce MJ Incorporación del test de dispersión de la cromatina espermática al laboratorio andrológico Revista Internacional de Andrología 2016; 14:137
12 Fernández JL, Muriel L, Goyanes V, et al Simple determination of human sperm DNA fragmentation with an improved sperm chromatin dispersion test Fertil Steril 2005; 84:833
13 Fernández JL, Muriel L, Rivero MT, et al The sperm chromatin dispersion test: a simple method for the determination of sperm DNA fragmentation J Androl 2003; 24:59
14 Aitken RJ, De Iuliis GN Origins and consequences of DNA damage in male germ cells Reprod Biomed Online 2007; 14:727-33
15 Greco E, Iacobelli M, Rienzi L, et al Reduction of the incidence of sperm DNA fragmentation by oral antioxidant treatment J Androl 2005; 26:349
16 Saldarriaga Monsalve LJ, Cardona Maya WD Efecto del zumo de sandía (Citrullus lanatus) en el estrés oxidativo en espermatozoides humanos Revista chilena de obstetricia y ginecología 2020; 85:423
17 Ocampo Flórez GM, Calle Correa E, Carvajal Obando A, Cardona Maya WD En búsqueda de la fertilidad, tratamiento con antibiótico resuelve el problema de una pareja infértil Reporte de caso Revista Médica de Risaralda 2022; 28:138
18 Gallegos G, Ramos B, Santiso R, et al Sperm DNA fragmentation in infertile men with genitourinary infection by Chlamydia trachomatis and Mycoplasma Fertil Steril 2008; 90:328
19 World Health Organization WHO Laboratory Manual for the Examination and Processing of Human Semen, 6th ed ed2021
20 Bibancos M, Rocha AM, Hassun PA, et al Sperm DNA frag-
mentation decreases after oral anti-inflammatory and antibiotic treatment Fertil Steril 2008; 90:S467
21 Schaeffer AJ, Wu SC, Tennenberg AM, Kahn JB Treatment of chronic bacterial prostatitis with levofloxacin and ciprofloxacin lowers serum prostate specific antigen J Urol 2005; 174:161
22 Atalay HA, Canat L, Alkan I, et al Prostate-specific antigen reduction after empiric antibiotic treatment does not rule out biopsy in patients with lower urinary tract symptoms: prospective, controlled, single-center study Prostate Int 2017; 5:59
23 Zuber A, Peric A, Pluchino N, et al Human Male Genital Tract Microbiota Int J Mol Sci 2023; 24
24 La Vignera S, Condorelli RA, Vicari E, et al Markers of semen inflammation: supplementary semen analysis? J Reprod Immunol 2013; 100:2
25 Tvrda E, Duracka M, Benko F, Lukac N Bacteriospermia - A formidable player in male subfertility Open Life Sci 2022; 17:1001
26 Jayakumar S, Pringle K, Ninan GK Idiopathic urethritis in children: Classification and treatment with steroids J Indian Assoc Pediatr Surg 2014; 19:143
27 Santi D, Spaggiari G, Simoni M Sperm DNA fragmentation index as a promising predictive tool for male infertility diagnosis and treatment management - meta-analyses Reprod Biomed Online 2018; 37:315
28 Wiweko B, Utami P Predictive value of sperm deoxyribonucleic acid (DNA) fragmentation index in male infertility Basic Clin Androl 2017; 27:1
29 Sergerie M, Laforest G, Bujan L, et al Sperm DNA fragmentation: threshold value in male fertility Hum Reprod 2005; 20:3446
30 Zhou J, Chen LI, Li J, et al The semen pH affects sperm motility and capacitation PloS one 2015; 10:e0132974
Correspondence
Moises Abraham Adel Domínguez, MD moises adel@gmail com
Andrés Mora Topete, MD drandresmora@hotmail com
Centro de Uro-Andrología S C , Guadalajara, Jalisco, México
Walter D Cardona Maya, PhD wdario cardona@udea edu co
Grupo Reproducción, Departamento de Microbiología y Parasitología, Facultad de Medicina, Universidad de Antioquia, Medellín, Colombia
ORIGINAL PAPER
Evaluation of in vivo supplementation of 2660 mg D-aspartic acid and 200 mg ubiquinol and 10 mg zinc on different semen parameters in idiopathic male infertility: A randomized double blind placebo controlled study
Sameh Fayek GamalEl Din 1 , Elnashar A M 1 , Yasser Elkhiat 1 , Tarek Hussein 2 , Mohamed Ahmed AbdElSalam 1 , Ayman Alam 1 , David Ramzy 1 , Islam Moatamed 1 , Ashraf Zeidan 1 , Amr Elahwany 1 , Mohamed Wael Ragab 1 , Omar Zahran 1 , Hany Saad 3
1 Department of Andrology, Sexology, and STDs, Faculty of Medicine, Cairo University;
2 Department of Andrology, Sexology, and STDs, Faculty of Medicine, Alexandria University;
3 Department of Andrology, Sexology, and STDs, Faculty of Medicine, Suez Canal University
Summary
Introduction: About 20-30% of cases of infertility are attributed to male factor and males are also contributing to infertility in a further 20% Idiopathic male subfertility is the commonest cause in most cases D-aspartic acid (D-Asp) is an endogenous amino acid occurring in several tissues and cells of both invertebrates and vertebrates
The current study is one of the first to evaluate the in vivo supplementation of D-aspartic acid in idiopathic male infertility
Thus, we aimed in the current study to evaluate the in vivo effect of D-aspartic acid, zinc and co-enzyme Q 10 supplementation on different semen parameters and serum testosterone level in idiopathic male infertility
Methods: A total of 75 infertile patients were recruited from the outpatient andrology clinic from March 2023 to June 2024. The current study was registered at the UMIN clinical registry trials prior to initiating the study (UMIN000050023). Group (A) included 24 infertile patients who received 2660 mg d-aspartic acid plus 200 mg of ubiquinol plus 10 mg zinc once daily for 3 months Group (B) included 24 infertile patients who received placebo (starch granules) daily for 3 months. Results: Interestingly, patients in group (A) who received 2660 mg d-aspartic acid plus 200 mg of ubiquinol plus 10 mg zinc once daily for 3 months showed significant improvement in progressive sperm motility after 3 months (10.63 ± 8.64 vs 15.21 ± 12 11, p = 0 047) Also, they showed highly significant increase in total testosterone level (5.06 ± 1.74 vs 5.89 ± 1.62, p = 0 009)
Conclusions: D-aspartic acid plus ubiquinol plus zinc are promising ingredients that showed good results when administrated once daily to infertile males.
KEY WORDS: Idiopathic male infertiliy; Total testosterone; Progressive sperm motility; D-aspartic acid; Ubiquinol; Zinc.
Submitted 30 December 2024; Accepted 17 January 2025
INTRODUCTION
About 20-30% of cases of infertility are attributed to male factor and males are also contributing to infertility in a
further 20% Idiopathic male subfertility is the commonest cause in most cases (1) D-aspartic acid (D-Asp) is an endogenous amino acid occurring in several tissues and cells of both invertebrates and vertebrates (2) It was first detected in the brain and optic lobes of the cephalopod mollusy Octopus vulgaris and later in the nervous and endocrine systems of various animal phyla such as crustaceans, amphibians, reptiles, fish, chicken, rat, and man (3-14) Topo et al conducted a clinical trial on 23 healthy male volunteers who consumed 3 12 gram of sodium DAsp for 12 consecutive days (15) They found significant increase in LH and testosterone levels after 12 days by 33% and 42%, respectively (15) Thus, Topo et al postulated that consumed D-Asp may also be remained in the testis and it continued to stimulate the testosterone production in the testis (15) In the aforementioned study the mean baseline testosterone were within 25% of the lower clinical range (3-10 ng/mL) and D-Asp supplementation elevated testosterone levels to approximately 50% of the clinical range (4 5-6 4 ng/mL) (15) These findings can be explained by the fact that D-Asp acts directly on the pituitary gland inducing an increase of LH releasing (15-16) Furthermore, two in vitro studies had demonstrated a beneficial effect of Zn, D-Asp and Co-enzyme Q10 (Co-Q10) on sperm motility, recovery of spermatozoa by swim-up and lipid peroxidation (17, 18)
On the contrary, Willoughby et al who conducted a study on twenty apparent healthy and heavy resistance-trained men (19) The participants trained 4 times/week while orally taking either 3 gram of placebo or D-Asp in the morning upon waking (19) There was no effect on muscle strength, body mass and serum hormones after 28 days of D-Asp supplementation (19)
To the best of our knowledge, the current study is one of the first to evaluate the in vivo supplementation of D-Asp in male infertility
Thus, we aimed in the current study to evaluate the in vivo effect of D-Asp, zinc and Co-Q10 supplementation on different semen parameters and serum testosterone level in idiopathic male infertility
Fayek GamalEl Din, Elnashar A M , Y Elkhiat, et al
MATERIALS AND METHODS
A total of 75 infertile patients were recruited from the outpatient andrology clinic from March 2023 to June 2024 The recruited patients were assessed for eligibility to join the study (Figure 1) The institutional ethical committee of Alexandria University approved the study on 23/1/2023 that conforms to Helsinki declaration 2013
(20) Also, the current study was registered at the UMIN c l i n i c a l
(UMIN000050023) Twenty-three patients were excluded from the study The remaining 52 patients were equally randomized by simple numbering method into 2 groups Unfortunately, 4 patients dropped out of the study, 2 patients were from group (A) and 2 patients were
S
Figure 1 Study flow chart
from group (B) (Figure 1) Group (A) included 24 infertile patients who received Spertility® that consists of 2660 mg D-aspartic acid plus 200 mg of ubiquinol (active form of Co-Q10) plus 10 mg zinc once daily for 3 months Group (B) included 24 infertile patients who received placebo (starch granules) daily for 3 months Five cc blood was withdrawn for total testosterone evaluation at the beginning of the study and after 3 months All participants brought 2 semen samples at the beginning and at the end of the study Semen analysis was processed according to the 5th guidelines of the WHO (21)
Inclusion criteria of the patients
Any infertile male aged 25 to 40 years old suffering from idiopathic infertility was included
Exclusion criteria of the patients
Any idiopathic infertile male suffering from varicocele or l
excluded Also, any infertile patient with hormonal imbalance was excluded Finally, any infertile patient with small testicular volume < 8 ml was also excluded
RESULTS
The current study did not show any significant difference in the mean age of the participants of both groups (31 25 years, ± 7 86; 33 96 years, ± 8 11, respectively, p = 0 062) Interestingly, patients in group (A) who received Spertility showed significant improvement in progressive sperm motility after 3 months of daily supplementation of D-aspartic acid (10 63 %, ± 8 64, 15 21 %, ± 12 11, p = 0 047, respectively) (Table 1)
They also showed significant increase in total testosterone level after 3 months of daily supplementation of D-aspartic acid (5 06 ng/dl, ± 1 74; 5 89 ng/dl, ± 1 62, respectively, p = 0 009) (Table 1)
Conversely, total sperm concentration and sperm motility and abnormal forms did not show any improvement after daily supplementation of D-aspartic acid in patients of group (A) (Table 1) Furthermore, patients in group (B) who received placebo did not show any improvement in total sperm concentration, sperm motility, progressive sperm motility, abnormal forms and total testosterone (Table 2)
Despite, significant improvement in progressive sperm motility and significant increase in total testosterone in patients in group (A), yet, pregnancy rate was 8 3% only Owing to the fact that only 2 patients out of 24 patients in group (A) succeeded to impregnate their wives
Statistical methods
Data management and statistical analysis were performed using the Statistical Package for Social Sciences (SPSS) version 25
Numerical data were summarized using means and standard deviations or medians and ranges Data were explored for normality using Kolmogrov-Smirnov test and ShapiroWilk test Mann-Whitney U and Wilcoxon Signed Ranks Tests were used for the comparison between groups All pvalues are two-sided P-values ≤ 0 05 were considered significant
DISCUSSION
The current study had demonstrated significant improvement in progressive sperm motility in group (A) patients who received Spertility daily for 3 months Similarly, two previous studies demonstrated beneficial effects of in vitro supplementation of D-Asp on progressive sperm motility (17, 18) Moreover, an animal study revealed an improvement in sperm function of rabbits after being adminstered D-Asp (22) In the same context, D’Aniello et al (2005) was one of the first to demonstrate lower levels of this amino acid in the semen of patients with oligoastenoteratozoospermia than in fertile men (23) The significant improvement in sperm motility in the current study can also be explained by the presence of zinc and Co-Q10 in the ingredients of Spertility Several studies had shown the beneficial effects of zinc in male inferility (18, 24-26) In contrats, Foresta et al (2014) failed to demonstrate any correlation between zinc and sperm motility (27)
Table 1.
Changes in semen parameters and total testosterone in group (A) before and after spertility
Table 2
Changes in semen parameters and total testosterone in group (B) before and after placebo.
Additionally, Co-Q10 has a well-established dual action as electron/proton carrier in mitochondrial bioenergetic chain and antioxidant agent (18) In the same context, Li et al (2006) found significant different concentrations of this antioxidant in the seminal plasma of fertile men and infertile patients (28) Conversely, Nadjarzadeh et al (2014) had revealed that this molecule had a potent antioxidant effect (29) Furthermore, Spertility contains ubiquinol which is the active form of Co-Q10 that facilitates its gastro-intestinal absorption Similarly, GarridoMaraver et al (2014) demonstrated the effect of different f o r m u
REFERENCES
1 Agarwal A, Baskaran S, Parekh N, et al Male infertility The Lancet 2021; 397:319-333
2 D'Aniello A D-Aspartic acid: an endogenous amino acid with an important neuroendocrine role Brain Res Rev 2007; 53:215-234
3 D'Aniello A, Giuditta A Identification of D-aspartic acid in the brain of Octopus vulgaris lam J Neurochem 1977; 29:1053-1057
4 Okuma E, Fujita E, Amano H, et al Distribution of Free D-Amino Acids in the Tissues of Crustaceans Fisher Sci 1995; 61:157-160
( 3 0 )
Another interesting finding of the current study was the highly significant increase in total testosterone level in group (A) patients who received Sperility once daily for 3 months Consistently, a study had reported a steroidogenic role of D-Asp in humans and rats (15)
Quite the reverse, Willoughby et al (2014) failed to demonstrate any change in serum testosterone level in resistance-trained men after being resistance trained 4 times weekly for 1 month and after ingesting 3 g daily of D-aspartic acid (19) It should be mentioned that the dose of D-Asp in the aforementioned study was higher than the concentration of D-Asp in Spertility Notably, the role of testosterone in male infertility is well established by two important reviews showing the pivotal role of androgen in spermatogensis (31, 32) In the same context, Carvalho et al (2022) had revealed that eugenol administration to Wistar rats reduced serum testosterone and sperm viability (33) On the contrary, a previous study had stated that serum testosterone levels demonstrate no relationship to sperm concentration (34) To wrap up, Spertility administration in the form of once daily sachet for 3 months had shown significant improvement in progressive sperm motility and highly significant increase in serum total testosterone To the best of our knowledge, the current study is one of the first to demonstrate the i m p a c t o f i
s ubiquinol plus zinc to infertile males Despite such achievements that were shown in the current study, yet, the pregnancy rate was very low as two patients only from group (A) succeeded to conceive naturally This disappointing finding could be attributed to the small sample size and the short period of follow up Admittedly, there are several limitations of the current study Firstly, the small sample size and short duration of follow up are seen as major limitations of the current study Nevertheless, the proper and consistent study design and being a prospective one added strength to the current findings Also, we were not able to measure luteinizing hormone and sperm DNA fragmentation index adding further limitations of the current study Finally, we were not able to utilize the 6th edition of the WHO for semen analysis processing (35)
CONCLUSIONS
D-aspartic acid plus ubiquinol plus zinc are promising ingredients that showed good results when administrated once daily to infertile males Future cohort studies that evaluate these ingredients versus l-carnitine are needed to affirm these findings
5 Di Fiore M, Assisi L, Botte V, D'Aniello A D-Aspartic acid is implicated in the control of testosterone production by the vertebrate g o n a d S t u
Endocrinol 1998; 157:199-207
6 Raucci F, Assisi L, D'Aniello S, et al Testicular endocrine activity is upregulated by D-aspartic acid in the green frog, Rana esculenta J Endocrinol 2004; 182:365-376
7 Assisi L, Botte V, D'Aniello A, Di Fiore M Enhancement of aromatase activity by D-aspartic acid in the ovary of the lizard Podarcis s sicula Reproduction 2001; 121:803-808
8 Raucci F, D’Aniello S, Di Fiore M Endocrine roles of D-aspartic acid in the testis of lizard Podarcis s sicula J Endocrinol 2005; 187:347-359
9 D’Aniello A, Di Fiore M, Fisher G Occurrence of Daspartic acid in animal tissues and its role in the nervous and endocrine systems Trends Comp Biochem Physiol 1998; 4:1-24
10 Neidle A, Dunlop DS Developmental changes in free D-aspartic acid in the chicken embryo and in the neonatal rat Life Sci 1990; 46:1517-1522
11 Dunlop DS, Neidle A, McHale D, et al The presence of free Daspartic acid in rodents and man Biochem Biophys Res Com 1986; 141:27-32
DECLARATIONS
Ethical approval: The study was prospectively registered at UMIN under the following serial number 000050023
Availability of data and material: All inquiries can be directed to the corresponding author
Competing interests: The authors declare no competing interests
Funding: This study did not receive any fund
Authors' contributions: SFG, AEN, TH and YE developed the conception and study design; MAA, IM, AZ, MWR, AA, DR and OZ recruited the cases; HS performed the statistics of the study; SFG intellectually drafted the manuscript and critically revised the data All authors approved the final draft
SFG drafted the initial manuscript; SFG revised the article critically; SFG reviewed and edited the article; NN designed the study; SAA performed the lab work of the study; AO, AE, AZ, AAS collected and analyzed the data All authors reviewed the manuscript
Acknowledgments: We would like to thank Parkville Pharmaceutical Company for their provision of the drug and placebo once daily for 3 months
We would thank the surgeons who performed the sub inguinal micro-varicocelectomy
S Fayek GamalEl Din, Elnashar A M , Y Elkhiat, et al
12 Hashimoto A, Nishikawa T, Oka T, et al Widespread distribution of free Daspartate in rat periphery FEBS Lett 1993; 331:4-8
13 Hashimoto A, Kumashiro S, Nishikawa T, et al Embryonic development and postnatal changes in free D-aspartate and D-serine in the human prefrontal cortex J Neurochem 1993; 61:348-351
14 Fisher GH, D'Aniello A, Vetere A, Padula L, Cusano GP, Man EH Free D-aspartate and D-alanine in normal and Alzheimer brain Brain Res Bulletin 1991; 26:983-985
15 Topo E, Soricelli A, D’Aniello A, et al The role and molecular mechanism of D-aspartic acid in the release and synthesis of LH and testosterone in humans and rats Reprod Biol Endocrinol 2009; 7:1482-1488
16 D’Aniello A, Di Fiore MM, Fisher GH, et al Occurrence of Daspartic acid and N-methyl-D-aspartic acid in rat neuroendocrine tissues and their role in the modulation of luteinizing hormone and growth hormone release FASEB J 2000; 14:699-714
17 Talevi R, Barbato V, Fiorentino I, et al Protective effects of in vitro treatment with zinc, d-aspartate and coenzyme q10 on human sperm motility, lipid peroxidation and DNA fragmentation Reprod Biol Endocrinol 2013;11:81
18 Giacone F, Condorelli RA, Mongioì LM, et al In vitro effects of zinc, D-aspartic acid, and coenzyme-Q10 on sperm function Endocrine 2017; 56:408-415
19 Willoughby DS, Leutholtz B D-Aspartic acid supplementation combined with 28 days of heavy resistance training has no effect on body composition, muscle strength ,and serum hormones associated with the hypothalamo-pituitary-gonadal axis in resistance-trained men Nutr Res 2013; 33:803-810
2 0 W o r l d M e d i c a l A s s o c i a t i o n W o r l d M e d i c a l
n Declaration of Helsinki: ethical principles for medical research involving human subjects JAMA 2013; 310:2191-2194
21 World Health Organization (WHO) WHO laboratory manual for the examination and processing of human semen 5th ed Geneva WHO 2010; 271 p
22 Macchia G, Topo E, Mangano N, et al DLAspartic acid administration improves semen quality in rabbit bucks Anim Reprod Sci 2010; 118:337-343
23 D’Aniello G, Ronsini S, Guida F, et al Occurrence of D-aspartic acid in human seminal plasma and spermatozoa: possible role in reproduction Fertil Steril 2005; 84:1444-1449
24 Hadwan MH, Almashhedy LA, Alsalman AR Oral zinc supplementation restores high molecular weight seminal zinc binding protein to normal value in Iraqi infertile men BMC Urol 2012; 13:1232
25 Mocchegiani E, Costarelli L, Giacconi R, et al Zinc-binding proteins (metallothionein and alpha-2 macroglobulin) and immunosenescence Exp Gerontol 2006; 41:1094-107
26 Macanovic B, Vucetic M, Jankovic A, et al Correlation between sperm parameters and protein expression of antioxidative defense enzymes in seminal plasma: a pilot study Dis Markers 2015; 2015:436236
27 Foresta C, Garolla A, Cosci I, et al Role of zinc trafficking in male fertility: from germ to sperm Hum Reprod 2014; 29:1134-45
28 Li K, Shi Y, Chen S, et al Determination of coenzyme Q10 in human seminal plasma by high-performance liquid chromatography and its clinical application Biomed Chromatogr 2006; 20:1082-6
29 Nadjarzadeh A, Shidfar F, Amirjannati N, et al Effect of Coenzyme Q10 supplementation on antioxidant enzymes activity
and oxidative stress of seminal plasma: a double-blind randomised clinical trial Andrologia 2014; 46:177-83
30 Garrido-Maraver J, Cordero MD, Oropesa-Avila M, et al Clinical applications of coenzyme Q10 Front Biosci (Landmark Ed) 2014; 19:619-33
31 Holdcraft RW, Braun RE Hormonal regulation of spermatogenesis Int J Androl 2004; 27:335-42
32 Smith LB, Walker WH The regulation of spermatogenesis by androgens Semin Cell Dev Biol 2014; 30:2-13
33 Carvalho RPR, Lima GDA, Ribeiro FCD, et al Eugenol reduces serum testosterone levels and sperm viability in adult Wistar rats Reprod Toxicol 2022; 113:110-119
34 Jackaman R, Ghanadian R, Ansell ID, et al Relationships between spermatogenesis and serum hormone levels in subfertile men Br J Obstet Gynaecol 1977; 84:692-6
35 World Health Organization WHO Laboratory Manual for the Examination and Processing of Human Semen, 6th ed ; WHO Press: Geneva, Switzerland, 2021 Available online: https://www who int/publications/i/item/9789240030787 (accessed on 3 December 2021)
Correspondence
Sameh Fayek GamalEl Din, MD (Corresponding Author) samehfayek@kasralainy edu eg
Department of Andrology and STDs Kasr Al-Ainy, Faculty of Medicine Cairo University, Al-Saray Street, El Manial, Cairo, 11956, Egypt
Elnashar A M , MD abdelrahmanelnashar@kasralainy edu eg
Yasser Elkhiat, MD elkhiat@hotmail com
Mohamed Ahmed AbdElSalam, MD moh 756@cu edu eg
Ayman Allam, M M B c H aymanallam085@gmail com
David Ramzy, M M B c H davidramzy1994@gmail com
Eslam Meatmed, M M B c H eslammeatmed@gmail com
Ashraf Zeidan, MD zidana2000@gmail com
Amr Alahwany, MD amralahwani@hotmail com
Mohamed Ragab, MD m w ragab@kasralainy edu eg
Omar Zahran, M M B c H omar5b2007@gmail com
Department of Andrology, Sexology, and STDs, Faculty of Medicine, Cairo University, Cairo, Egypt
Tarek Hussein, MD tarekmhaa@hotmail com
Department of Andrology, Sexology, and STDs, Faculty of Medicine, Alexandria University, Alexandria, Egypt
Hany Saad, MD hanysaad@med suez edu eg
Department of Andrology, Sexology, and STDs, Faculty of Medicine, Suez Canal, Egypt
LETTER TO EDITOR
Treatment with perilesional injections of Pentoxifylline in patients with Peyronie's disease improves the therapeutic effect of oral and topical antioxidant therapy
Gianni Paulis 1 , Andrea Paulis 2 , Giovanni De Giorgio 3
1 Department of Urology and Andrology, Peyronie’s Care Center, Castelfidardo Castelfidardo Clinical Analysis Center, Rome, Italy;
2 Bambino Gesù Children’s Hospital, IRCCS (Istituti di Ricovero e Cura a Carattere Scientifico), Rome, Italy;
3 Department of Urology and Andrology, Section of Ultrasound Diagnostics, Castelfidardo Clinical Analysis Center, Rome, Italy
KEY WORDS: Peyronie’s disease; Antioxidants; pentoxifylline; Injections, oral drug administration, topical drug administration
Submitted 25 December 2024; Accepted 3 January 2025
To the Editor,
We conducted a retrospective study to demonstrate that it is possible to achieve better therapeutic outcomes through combining perilesional injections of pentoxifylline (PTX) with oral antioxidants and the local application of a cream containing antioxidants and a gel containing diclofenac in patients with Peyronie's disease (PD) We compared two similar groups of patients with PD using the two treatments mentioned above The typical symptoms of PD commonly include penile deformity, penile pain, erectile dysfunction, and psychological distress such as anxiety and depression (1, 2) PTX is a synthetic methylxanthine derivative that has structural similarities to caffeine and theophylline Originally created as a hemorheological agent, it was first used to treat peripheral vascular diseases, cerebrovascular insufficiency, diabetic neuropathy, sickle cell disease, and various inflammatory and fibrotic conditions Brant et al (2006) were the pioneers in utilizing PTX for PD PTX possesses antifibrotic, anticalcific, antioxidant, anti-inflammatory, antiplatelet, and vasorelaxant properties (3) While some guidelines do not recommend the use of antioxidants such as PTX for treating PD, there have been numerous published therapeutic cases involving PTX, either on its own or in combination with other antioxidant and non-antioxidant therapies (3-6) All of these clinical studies in the literature, in which PTX has been used, have demonstrated that this drug is able to counteract PD due to its ability to interfere with the pathogenetic mechanisms of the disease and reduce the most important symptoms of the disease In our most recent clinical practice we discontinued oral administration of PTX as we observed a high prevalence (15 7%) of side effects that impact the circulatory system, blood pressure, and intestinal system (6) For these reasons, we are now using PTX only through perilesional penile injections We have not found other studies in the literature where penile injections of PTX have been used to treat PD
We performed a retrospective analysis of the clinical database of a single uro-andrology clinic From the database, we extracted 263 patients with active PD (first stage) who had visited our Peyronie's care center between December 2019 and October 2024 In our clinical archive, all clinical information (medical history and physical examination) and diagnostic tests were available, both before and after treatment Of these 263 patients, 152 had already undergone combined therapy with oral antioxidants + topical therapy, as well as perilesional penile injections with PTX The remaining 111 patients had undergone the same oral and topical antioxidant therapy but had not received penile injections with PTX This latter group of patients decided not to undergo penile injections due to a fear of penile pain and/or logistical reasons related to the great distance between their residence and our treatment center All 263 patients had undergone at least one 6-month treatment cycle and were potentially able to be divided into two treatment groups, as planned for our study However, after analyzing the data of all these patients, a clear heterogeneity between the two groups was detected To ensure statistical homogeneity between the two treatment groups and ensure a similar number of participants in these groups, we conducted further selection and excluded another 159 cases from the study These cases were excluded based on their clinical characteristics, such as the degree of penile curvature, plaque volume, presence of ED or penile pain, age, onset of the disease, and comorbidities Finally, after this further selection, we included 104 cases in the study, which we divided into two treatment groups (group A and group B), each consisting of 52 cases
Treatment characteristics for each group were as follows: Group A received a combination of oral antioxidants and topical creams for 6 months, along with peri-lesional penile injections with PTX every 2 weeks Group B received the same oral and topical treatments as Group A, but without the penile injections with PTX, for 6 months The detailed characteristics of the treatment for each therapeutic group are shown in the “legend” of the Table 1
G Paulis, A Paulis, G De Giorgio
This retrospective study was conducted in compliance with the principles contained in the Declaration of Helsinki (Fortaleza, 2013); all study subjects were contacted and provided informed consent for study inclusion All patients were informed that treatment with penile injections of pentoxifylline is an "off-label" therapy Sensitive data were anonymized to warrant patients’ privacy according to Legislative Decree 10 August 2018, n 101, published in the Official Gazette of the Italian Republic, General Series, issue 205, 09/04/2018 All 104 PD patients underwent photographic documentation of penile curvature (according to Kelâmi) and dynamic Penile dynamic Doppler ultrasound (PDDU) with plaque and volume measurements and answered the following questionnaires: the Generalized Anxiety Disorder-7 (GAD-7), the Patient Health Questionnaire-9 (PHQ-9), the Visual Analog Scale (VAS) for penile pain measurements, the International Index of Erectile Function (IIEF), and the Peyronie's Disease Questionnaire (PDQ, Symptom Bother Domain) for the evaluation of the psychosexual impact of the disease
Table 1
Clinical results (related to the reduction and/or the regression of PD symptoms, plaque volume, and its internal calcification) after 6 months of treatment
Clinical results Group A
Decrease in plaque volume
Decrease in calcification within the plaque
Decrease of the penile curvature angle
Mean decrease (in degrees °)
Mean decrease in the VAS score
increase in the IIEF score in patients with ED
Mean decrease in the PDQ-bother score in patients with psychosexual impact by PD
decrease in the GAD-7 score in patients with anxiety
the PHQ-9 score
patients with complete plaque regression
B
n. 52 cases treated with n. 52 cases treated only with Group A oral and topical antioxidants oral and topical antioxidants versus Group B + PTX injections without PTX injections P-value
N patients with disappearance of significant depression
A: Oral y: L-carnitine
dai y for 6 months; Topical y: cream w th propol s and hyaluronic acid 2x dai y + d c ofenac ge 4% dai y for 6 months; Per - esiona pen
Group B: The same ora antioxidants and topica treatments as Group A for 6 months (without peri-lesional peni e injections with PTX)
PD Peyronie’s disease ED erect le dysfunct on; PTX Pentoxify l ne; SD standard deviation; χ2 test chi-squared test t-test Student's t-test
VAS Visual ana og scale, for pain assessment, score range 0–10 Interpretation of score: mi d to moderate pa n 1–5, severe pain 6–7, very severe pain 8–10
IIEF Internationa Index of Erect le Function, score range 0–30 Interpretation of score: severe ED 0–10, moderate ED 11–16, m ld to moderate ED 17–21, m ld ED 22–25, and no ED 26–30
PDQ symptom-bother Peyronie’s Disease Quest onnaire symptom bother, to evaluate the psychosexual impact, score range 0–16 nterpretation of score: mild bother 1–4, med um bother 5–8, high bother 9–12, severe bother 13–16
GAD-7 General zed Anxiety D sorder-7 questionnaire, for the assessment of anxiety, score range 0–21 Interpretat on of score: m nimal anx ety 0–4, mild anxiety 5–9, moderate anx ety 10–14, and severe anxiety 15–21
S gnificant anx ety when GAD-7 score > 9
PHQ-9 = Patient Health Questionna re-9, for depress ve d sorder, score range 0–27 Interpretation of score: min ma depress on = 0–4, mi d depression = 5–9, moderate depression = 10–14, moderately severe depression = 15–19, severe depress on = 20–27
S gnificant depression present when PHQ-9 score > 9
P-va ue: if the p-va ue s < 0 05, it is judged as sign f cant; f the p-value is > 0 05, t is judged as not significant
Treatment with perilesional injections of Pentoxifylline in patients with Peyronie's disease
The endpoints of this study were related to the reduction and/or regression of PD symptoms, plaque volume, and its internal calcification
Our results show that patients in the two treatment groups did not differ in age and most of the associated conditions and comorbidities At the end of the treatment, we visited all patients again and subjected them to the same diagnostic tests that were performed before treatment
Statistical analysis of the results after 6 months of treatment highlighted significant differences between the outcomes of the two groups (Group A versus Group B), in terms of improvement in penile pain, effective reduction in plaque size, improvement in penile curvature, improvement in IIEF score, and reduction in the psychological impact of PD
Significantly better reduction of PD symptoms, plaque volume, and its internal calcification, was always observed by the addition of perilesional penile injections with PTX (group A) when compared to the oral and topical administration of antioxidants and diclofenac gel alone (group B) (see Table 1) An higher statistically significant regression rate of PD symptoms, plaque, and its internal calcification was observed for Group A (compared to Group B) only for three clinical evaluations: disappearance of penile pain, disappearance of ED, and disappearance of significant depression (see Table 1)
We did not observe any side effects after the use of oral and topical substances
We only observed in one case a small bruise at the site of PTX injection, which resolved at about 5 days after the injection
The results of our present study revealed that the combination of periodic perilesional penile injections with PTX significantly increases the therapeutic efficacy, when compared to oral and topical antioxidant therapy alone Although the therapeutic response to the combination of oral and topical antioxidants (Group B) after 6 months was certainly good, in terms of improvement of all PD symptoms, penile injections with PTX combined with other oral and topical antioxidants (Group A) allowed us to achieve results that were unequivocally superior to those obtained without penile injections (Group B)
The limitations of our study are related to the absence of a control group comprising PD patients not receiving any therapy As PD is a chronic progressive disease, it would be deemed unethical to withhold treatment, even for the purpose of a research study
We believe that our therapeutic success in treating PD was mainly due to the addition of penile perilesional injections with PTX to the oral and topical antioxidant therapy We also consider the following factors to be important: careful selection of antioxidants to use, performing penile ultrasound examination with a modern ultrasound device with an elastography module that allows for very precise measurements of the plaque, and assigning the ultrasound examination to a physician with extensive experience in PD cases
As we observed high rates of significant anxiety and depression in PD patients, we believe that psychotherapy should be associated with medical treatment for PD patients, in order to improve their quality of life
Although the treatment results obtained in this study were highly statistically significant, we believe that further randomized and controlled studies with a larger number of cases are needed to confirm the effectiveness of penile injection therapy with PTX
REFERENCES
1 Pryor JP, Ralph DJ Clinical presentations of Peyronie’s disease Int J Impot Res 2002; 14:414-417
2 Garaffa G, Trost LW, Serefoglu EC, et al Understanding the course of Peyronie's disease Int J Clin Pract 2013; 67:781-788
3 Brant WO, Dean RC, Lue TF Treatment of Peyronie's disease with oral pentoxifylline Nat Clin Pract Urol 2006; 3:111-115
4 Smith JF, Shindel AW, Huang YC, et al Pentoxifylline treatment and penile calcifications in men with Peyronie’s disease Asian J Androl 2011; 13:322-325
DECLARATIONS
Ethical approval: Our study, being a retrospective study, does not require approval from an ethics committee according to current regulations, and in any case it received approval from the Castelfidardo Ethical Commission (protocol code #00243, date of approval 10 September 2024) for studies involving human
Availability of data and material: All inquiries can be directed to the corresponding author (paulisg@libero it)
Competing interests: The authors declare no conflicts of interest
Funding: This research received no external funding
Authors' contributions: All authors contributed equally to the conceptualization, investigation, data curation, analysis of results, and writing of this article
Acknowledgments: We are grateful to the patients who took part in our study, allowing us to observe and analyze the good outcomes of the treatments they received
5 Ibrahim A, Gazzard L, Alharbi M, et al Evaluation of Oral Pentoxifylline, Colchicine, and Penile Traction for the Management of Peyronie's Disease Sex Med 2019; 7:459-463
6 Paulis G, Barletta D, Turchi P, et al Efficacy and safety evaluation of pentoxifylline associated with other antioxidants in medical treatment of Peyronie’s disease: A case-control study Res Rep Urol 2016; 8:1-10
Correspondence
Gianni Paulis (Corresponding Author) paulisg@libero it
Department of Urology and Andrology, Peyronie’s Care Center, Castelfidardo Castelfidardo Clinical Analysis Center, Rome, Italy
Andrea Paulis
Bambino Gesù Children’s Hospital, IRCCS (Istituti di Ricovero e Cura a Carattere Scientifico), Rome, Italy
Giovanni De Giorgio
Department of Urology and Andrology, Section of Ultrasound Diagnostics, Castelfidardo Clinical Analysis Center, Rome, Italy
LETTER TO EDITOR
Lady urologist and male patients with prostate cancer
Rodolfo Montironi 1 , Antonio Lopez-Beltran 2 , Meredith C Wasserman 3 , Alessia Cimadamore 4 , Liang Cheng 5
1 Molecular Medicine and Cell Therapy Foundation, c/o Polytechnic University of the Marche Region, Ancona, Italy;
2 Department of Surgery, Cordoba University Medical School, Cordoba, Spain;
3 Division of Urology, Department of Surgery, The Warren Alpert Medical School of Brown University, Providence, RI, USA;
4 Institute of Pathological Anatomy, Department of Medicine, University of Udine, Udine, Italy;
5 Department of Pathology and Laboratory Medicine, Department of Surgery (Urology), Brown University Warren Alpert Medical School, Brown University Health, and the Legorreta Cancer Center at Brown University, Providence, RI, USA
KEY WORDS: Female and male; Medical student; Lady urologist; Male patient; Self-respecting man
Submitted 4 November 2024; Accepted 29 November 2024
To the Editor
In 2022 Dr Suzanne Koven published a book entitled Letter to a Young Female Physician, Notes from a Medical Life W W Norton & Company, Inc, New York (1) The book starts with a letter written by the author while participating in a 2017 orientation session at Harvard Medical School during which new interns were asked to write self-addressed essays expressing “their hopes and anxieties” (1) In the first part of her letter, Dr Koven writes: “On your urology rotation in medical school, you were informed that your presence was pointless, since, as you were told by an attending, no self-respecting man would go to a lady urologist” (1)
Co-authors of the present contribution (ALB, MCW, AC, and LC) put forward a series of questions on such a quotation: 1 Female and male medical students and postgraduate trainees: 2 “Lady urologist” ; 3 Male patients; and 4 “Self-respecting man” The answers reported hereafter were given by the other co-author (RM, a uropathologist whose training included urologic oncology), to some extent representing his personal view or experience
Female and male medical students and postgraduate trainees
Over the years, an extensive series of lectures on clinically oriented uropathology were delivered to medical students Teaching included practical sessions Basically, both female and male students – the former outnumbering their male peers – were very good in terms of proficiency, i e , no differences between the students of the two genders were noticed Occasionally, an attempt was made, with very little success, to encourage female and male students to apply for postgraduate training in pathology They were never discouraged from applying for other specialties, including urology An idea of what being in a non-pathology specialties would have meant, in terms of advantages and disadvantages, was given The same approach was adopted when teaching uropathology to interns, residents and fellows in urology as well as to other non-urology postgraduate trainees It was pointed out that both female and male have the same chances to succeed in their future professional and academic career as well as with patients, the latter independently of being selfrespecting or not (See below) It was also explained to them, women and men, not to tolerate the belief that one sex is superior to or more valuable than another sex
“Lady urologist”
Despite the relatively equal number of female and male graduating from medical school, in some countries the proportion of women in the urology services, both academic and not academic, has been lower than that of male urologists Mayer et al investigated the gender differences in publication productivity among academic urologists in the United States (2) The authors found that “Women represent a growing proportion of academic urology faculty, but despite the recent increase in number entering the field, relatively few women occupy senior leadership positions” (2) Probably, this has reflected an older approach of a basically male profession, an approach that has changed rapidly over times However, the female contributions are not of a lower level compared with those of male urologists in all the settings: office, ward and operating room as well as academically A recent study by Wallis et al showed that “patients treated by female surgeons have lower rates of adverse postoperative outcomes including death at 90 days and 1 year after surgery compared with those treated by male surgeons ” (3) Female urologists are not mentioned here by name; it would appear a kind of discrimination or personal preferences They can be easily found on the websites of national and international urology and uro-oncology societies and meetings
R Montironi, A Lopez-Beltran, M C Wasserman, et al
Male patients
When reviewing the histological slides sent by patients with prostate cancer, the answer to major questions from them concerned the importance of morphologic and molecular features in terms of diagnosis, prognosis and therapeutic options (4) Most patients were in touch with male urologists, a minority being with female urologists The recollection from those patients was that female and male urologists were considered to be at a comparable level, from the human and professional levels They said that they were not afraid of discussing with female urologists all aspects of their disease, including potency and continence, in a way similar to that with male urologists Some patients said that they preferred male urologists: they had nothing to be ashamed of, but they felt uncomfortable with a female urologist (5) It was heard from them that women urologists did not dislike having male patients
CONCLUSIONS
“Self-respecting man”
Concerning “self-respecting man” (1), Dr Koven was probably referring to men/patients of a certain social class, depending on education, occupation and income To the best of the co-author’s experience (RM), the patients were dealt with independently from their social class The same did the lady urologists in relation to the social class of their male patients
REFERENCES
1 Koven S Letter to a Young Female Physician: Thoughts on life and work (Notes from a Medical Life) New York, NY: W W Norton & Company, Inc; 2022
2 Mayer EN, Lenherr SM, Hanson HA, et al Gender Differences in Publication Productivity Among Academic Urologists in the United States Urology 2017; 103:39-46
3 Wallis CJD, Jerath A, Aminoltejari K, et al Surgeon Sex and Long-Term Postoperative Outcomes Among Patients Undergoing Common Surgeries JAMA Surg 2023; 158:1185-1194
4 Cimadamore A, Cheng L, Lopez-Beltran A, et al Patients ask and pathologists answer: ten questions around prostate cancer grading Virchows Arch 2024 Aug 17 doi: 10 1007/s00428-024-03891-9 Epub ahead of print PMID: 39153109
Competing interests: The authors have nothing to disclose
Funding: The authors report no involvement in the research by the sponsor that could have influenced the outcome of this work
Authors' contributions: Author ALB and author LC have given substantial contributions to the conception or the design of the manuscript, author MW and author AC to acquisition, analysis and interpretation of the data All authors have participated in drafting the manuscript, author RM revised it critically All authors read and approved the final version of the manuscript
Acknowledgments: Not applicable
Correspondence
Rodolfo Montironi, MD (Corresponding Author) rodolfo montironi51@gmail com
Molecular Medicine and Cell Therapy Foundation, c/o Polytechnic University of the Marche Region, Via Tronto 10, 60126 Ancona, Italy
Antonio Lopez-Beltran, MD em1lobea@gmail com
Department of Surgery, Cordoba University Medical School, Cordoba, Spain
Meredith C Wasserman, MD meredith wasserman@gmail com
Division of Urology, Department of Surgery, The Warren Alpert Medical School of Brown University, Providence, RI, USA
Alessia Cimadamore alessiacimadamore@gmail com
Institute of Pathological Anatomy, Department of Medicine, University of Udine, Udine, Italy
Liang Cheng liang cheng@yahoo com
Department of Pathology and Laboratory Medicine, Department of Surgery (Urology), Brown University Warren Alpert Medical School, Brown University Health, and the Legorreta Cancer Center at Brown University, Providence, RI, USA
LETTER TO EDITOR
Urogenital and extra genital mutilation in gender-affirming surgery: Are we violating primum non nocere?
Zeki Bayraktar Department of Urology, Sancaktepe Sehit Prof Dr Ilhan Varank Training and Research Hospital, University of Health Sciences, Istanbul, Turkey
Submitted 31 October 2024; Accepted 29 November 2024
INTRODUCTION
In transgender individuals, there is a mismatch between biological sex and gender (sex-gender discordance), and this mismatch is often attempted to be resolved by changing the sex (1) However, sex cannot be changed through surgery or hormones, because sex has immutable components such as genetic/chromosomal (XX/XY), gonadal (testis/ovary), skeletal-pelvic (androgenic/gynecoid), gametic (sperm/oocyte), pregnancy (possible/not possible), lactation (possible/not possible), and internal-external genital structures Removing or destroying sexual organs does not change sex; it only leads to urogenital mutilation On the other hand, the perception of gender (or gender dysphoria) can change at any time, especially during adolescence (2)
Gender-affirming surgery and mental health
Gender-affirming surgery (GAS) is not performed to treat a congenital anatomical or functional disorder (since transgender individuals do not have such a pathology) but to address the psychological issues of transgender individuals This is the justification put forward for GAS (1) However, there is no conclusive evidence in the literature to support this justification The U S Centers for Medicare & Medicaid Services reviewed all relevant studies to assess whether these surgeries should be covered by insurance and prepared a comprehensive report, ultimately rejecting the request The report states that the studies are inconsistent; when taken collectively, the evidence is insufficient Most studies are not longitudinal, or they do not include concurrent pre- and post-operative controls/tests Many studies have reported positive outcomes, but the strength and reliability of these results are low due to the aforementioned potential issues Four welldesigned and executed studies were identified (2-6), but these also did not show a clinically significant difference in quality of life measured by psychometric tests before and after surgery (7)
GAS does not improve the psychological issues of transgender individuals; on the contrary, it worsens them A community-based study conducted in Sweden found that transgender individuals who underwent surgery had more mental health problems and treatment requests compared to those who did not undergo surgery The use of anxiolytics and antidepressants, as well as suicide rates, were higher in the surgery group-hospitalizations due to suicide attempts were nearly twice as high (8)
When this study was first published, it claimed that GAS improved mental health, but after objections and a re-analysis of the data, it was revealed that this was not the case, and in fact, the opposite was true The authors and the journal acknowledged this and published a correction (9) How could such a major analytical error have been overlooked by the reviewers of a journal like the American Journal of Psychiatry? Normally, this would not be possible, but it happened Why? Are academic publications that promote GAS being positively biased?
Other studies also show that GAS does not improve psychological issues and even worsens them in some patients
A study conducted at New York University found that in about one-fifth of cases, mental health worsened after surgery (10) Another study conducted at the University of California reported that 53% of individuals who underwent GAS visited the emergency department within the first year, and 17 3% of these cases were due to psychiatric issues (11) A study at the University of Texas examined millions of patient records and found that individuals who underwent GAS had 12 times higher suicide rates, 10 times higher rates of self-harm and suicide attempts, 8 times higher rates of post-traumatic stress disorder (PTSD), and 3 3 times higher mortality rates (12)
The Swedish cohort, which has about 30 years of follow-up (the longest and most comprehensive study on this topic), confirms these findings, showing that mental health issues persist even after GAS and continue throughout life In this cohort, the overall mortality rate of transgender individuals who underwent surgery was three times higher compared to the general population, hospital admission rates were three times higher, and completed suicide rates were 19 times higher (13)
Urogenital and extra-genital mutilation in gender affirming surgery
GAS does not improve the psychological issues of transgender individuals, and in addition, it results in urogenital and extra-genital mutilation (Figures 1-3) Male-to-female (MtF) surgical procedures result in urogenital mutilation, while female-to-male (FtM) procedures result in both urogenital and extra-genital mutilation (if phalloplasty is performed) (1419) Transgender individuals who undergo GAS lose their reproductive function completely and almost entirely lose their sexual function, while their urinary function is also significantly impaired Surgical complications requiring revision, which reduce the quality of life, are common (20)
A meta-analysis conducted by Wang et al reported an overall complication rate of 76 5% after phalloplasty, with a urethral fistula rate of 34 1% and a urethral stricture rate of 25 4% (14) Veerman et al (15) also reported a urethral stricture rate of 63% and a revision requirement due to fistula or stricture in 73% of cases, concluding that genital genderaffirming surgery with urethral lengthening is a complex procedure with a high complication rate After addressing complications, no clinically significant differences in urological functioning were observed Even after additional surgeries, 30% of patients lost the ability to urinate from the tip of the penis
When phalloplasty is performed, the arm or leg from which the flap is taken is also mutilated (Figure 4) These limbs are damaged not only cosmetically, but also neurologically and functionally, and all develop pain (16)
In a meta-analysis by Horbach et al , complications of MtF procedures were listed as follows; changes in urinary function 32%, urinary incontinence 19%, wound dehiscence 12-33%, vaginal stenosis 12%, genital pain 3-9%, vaginal necrosis 2 7-4 2%, rectal injury 2-4 2%, rectovaginal fistula 1-17%, urethral stricture 1-6%, local abscess 5%, hematoma 3%, clitoral necrosis 1-3%, vaginal prolapse 1-2% (17)
Urogenital and extra genital mutilation in a FtM case
[A FtM patient who applied with a complaint of total incontinence, a flap was taken from the left arm in another center and a neophallus was performed, but flap necrosis developed, a flap was taken from the right leg and a neophallus was performed again, but this time urethral necrosis developed, perineal externalization was performed, the patient received periurethral submucosal injections twice by us, he partially benefited, his incontinence decreased –this patient had 14 surgeries for FtM procedures – including revisions]
Urogenital and extra genital mutilation in other FtM case
[A FtM patient presented with severe pain in the left leg and inability to urinate/urethral obstruction; the dysfunctional penile prosthesis was removed, urethrotomy was performed internally but was unsuccessful, urethral externalization was performed; this patient underwent 17 surgeries for FtM procedures – including complications]
Figure 1.
Figure 2.
Figure 3
An MtF case presenting with complaints of difficulty urinating and pain. The patient, who had undergone surgery at another center, exhibited swelling, pain, and tenderness below the urethral meatus The patient frequently experienced infections, pain, and swelling, was unable to engage in sexual intercourse, and had persistent urination problems (in MtF cases, the urethra is severed at the level of the bulbar urethra; therefore, the visible meatus in this case is actually a severed bulbar urethra This urethra remains in continuous contact with neighboring tissues and the atmosphere, much like an open wound, leading to frequent infections)
Deterioration in quality of life and shortening of lifespan
Figure 4. Sequels (extra-genital mutilation) in the arm and leg from which the flap was harvested in cases of phalloplasty
Kuhn et al found a significantly reduced quality of life in transgender individuals 15 years after vaginoplasty, listing complications as follows: urinary dysfunction 47%, urgency 25%, stress incontinence 23%, inability to achieve sexual satisfaction 23%, urgency 17%, fecal incontinence 9 4%, difficulty or inability to fully empty the bowels 7 6%, vaginal prolapse 7 5%, and revision surgery due to prolapse 3 4% (18)
Kuhn et al also report that the urogenital complications of GAS are underreported in the literatüre (these rates are actually higher) Because transgender individuals who undergo GAS are quite reluctant to express their urogenital issues, so these problems are likely underreported (18), (19) Indeed, Kamran et al , who examined patient-reported outcome measures (PROMs) in 286 studies representing over 85,395 transgender cases in more than 30 countries, found that patient reports were absent or incomplete in most studies (21)
One of the dramatic outcomes of GAS is the shortening of life expectancy For instance, while the expected average life span in the Danish population is 81 9 years for women and 78 years for men, the average age of death for transgender individuals who underwent GAS was found to be 53 5 years (22) These data indicate that transgender individuals who undergo GAS die on average 25-28 years earlier, meaning their lives are shortened by about one-third due to psychiatric issues, the side effects of hormones used, cancers, lung, cardiovascular diseases, infections, and surgical complications (22, 23)
Is gender affirming surgery systematic iatrogenic harm?
These data show that GAS violates the medical principle of "first, do no harm" (primum non nocere) and systematically harms transgender individuals In my opinion, GAS is the greatest systematic iatrogenic harm in the history of medicine Transgender individuals have serious mental health issues and need psychosocial support because of these problems (24) However, GAS does not provide them with any tangible benefit; on the contrary, it harms them As surgeons, we are not improving the mental health issues of transgender individuals with GAS; instead, we are collaborating with their mental health issues and, by engaging in consent engineering, mutilating them urogenitally In short, we do not treat
them; we victimize them GAS does not change sex; it results in sexual mutilation GAS is partially feminization or masculinization, but predominantly mutilation Transgender individuals do not need mutilating surgeries but treatments that provide concrete benefits based on a risk-benefit analysis When and how will transgender individuals access these treatments? As specialists, we need to conduct new studies to develop the treatment options transgender individuals need and, more importantly, discuss this issue independently of ideology (based on medical evidence) Transgender individuals need treatments based on biological evidence, not ideological views Current medical practices, particularly GAS procedures, are mutilating transgender individuals, and they must be reviewed
In ancient times, it was believed that mental illnesses were caused by demons and that drilling holes in the skull would allow them to escape this led to cranial trepanation (25) Just as today we look back on cranial trepanation with mockery and astonishment, I believe that future medical professionals will look at GAS the same way, saying, "It's hard to believe, but in the 21st century, doctors-surgeons tried to treat gender dysphoria with surgery and attempted to change sex by removing urogenital organs, resulting in urogenital mutilation "
CONCLUSIONS
In conclusion, transgender individuals who undergo GAS lose their reproductive function irreversibly and almost entirely lose their sexual function, while their urinary function is also significantly impaired If phalloplasty is performed, the arm or leg is also mutilated In addition, many complications from surgeries arise So what do they gain for all these losses? Nothing (it is claimed that their mental health improves, but there is no definitive evidence in the literature to support this claim, and in fact, there is evidence to the contrary) So, what is the reason for this insistence on GAS?
As a surgeon/urologist licensed to perform GAS, I find these surgical procedures unethical and follow current medical practice with concern I am making these reminders to fulfill my professional and moral responsibility and to recommend that GAS procedures that harm transsexuals be reviewed We must act according to the principle of "First, do no harm" and our priority should be to avoid harming our patients
REFERENCES
1 Coleman E, Radix AE, Bouman WP, et al Standards of care for the health of transgender and gender diverse people, version 8 Int J Transgend Health 2022; 23(Suppl 1)-S259
2 Kuo JH, Carrera RA, Mulyani LC, et al Exploring the interaction effects of gender contentedness and pubertal timing on adolescent longitudinal psychological and behavioral health outcomes Front Psychiatry 2021; 12:660746
3 Heylens G, Verroken C, De Cock S, et al Effects of different steps in gender reassignment therapy on psychopathology: a prospective study of persons with a gender identity disorder J Sex Med 2014; 11:119-26
4 Ruppin U, Pfäfflin F Long-term follow-up of adults with gender identity disorder Arch Sex Behav 2015; 44:1321-29
5 Smith YL, Van Goozen SH, Kuiper AJ, Cohen-Kettenis PT Sex reassignment: outcomes and predictors of treatment for adolescent and adult transsexuals Psychol Med 2005; 35:89-99
6 Udeze B, Abdelmawla N, Khoosal D, Terry T Psychological functions in male-to-female people before and after surgery Sex Relatsh Ther 2008; 23:141-45
7 Jensen TS, Chin J, Rollins J, et al Gender dysphoria and gender reassignment surgery 2016 https://www cms gov/medicare-coverage-database/view/ncacal-decision-memo aspx?proposed=N&NCAId =282&bc=ACAAAAAAQAAA&
8 Bränström R, Pachankis JE Toward rigorous methodologies for strengthening causal inference in the association between gender-affirming care and transgender individuals' mental health: response to letters Am J Psychiatry 2020; 177:769-72
9 Correction to Bränström and Pachankis Am J Psychiatry 2020; 177:734
10 Robinson IS, Blasdel G, Cohen O, et al Surgical outcomes following gender-affirming penile reconstruction: patient-reported outcomes from a multi-center, international survey of 129 transmasculine patients J Sex Med 2021; 18:800-11
11 Zhang TR, Harel D, Rivera A, et al Incidence, complications, and long-term outcomes of gender-affirming phalloplasty: analysis of a large statewide population-based dataset Urology 2024; 185:27-33
12 Straub JJ, Paul KK, Bothwell LG, et al Risk of suicide and self-harm following gender-affirmation surgery Cureus 2024; 16:e57472
13 Dhejne C, Lichtenstein P, Boman M, et al Long-term follow-up of transsexual persons undergoing sex reassignment surgery: cohort study in Sweden PLoS One 2011; 6:e16885
14 Wang AMQ, Tsang V, Mankowski P, et al Outcomes following gender-affirming phalloplasty: a systematic review and meta-analysis Sex Med Rev 2022; 10:499-512
15 Veerman H, de Rooij FPW, Al-Tamimi M, et al Functional outcomes and urological complications after genital gender-affirming surgery with urethral lengthening in transgender men J Urol 2020; 204:104-109
16 Peters BR, Sikora Z, Timmins BH, Berli JU Nerve morbidity at the radial forearm donor site following gender-affirming phalloplasty J Plast Reconstr Aesthet Surg 2022; 75:3836-44
17 Horbach SER, Bouman MB, Smit JM, et al Outcome of vaginoplasty in male-to-female transgenders: a systematic review of surgical techniques J Sex Med 2015; 12:1499-512
18 Kuhn A, Hiltebrand R, Birkhäuser M Do transsexuals have micturition disorders? Eur J Obstet Gynecol Reprod Biol 2007; 131:226-30
19 Kuhn A, Santi A, Birkhäuser M Vaginal prolapse, pelvic floor function, and related symptoms 16 years after sex reassignment surgery in transsexuals Fertil Steril 2011; 95:2379-82
20 Bayraktar Z Urogenital complications that decrease quality of life in transgender surgery New J Urol 2024; 19:52-60
21 Kamran R, Jackman L, Chan C, et al Implementation of patient-reported outcome measures for gender-affirming care worldwide: a systematic review JAMA Netw Open 2023; 6:e236425
22 Simonsen RK, Giraldi A, Kristensen E, Hald GM Long-term follow-up of individuals undergoing sex reassignment surgery: psychiatric morbidity and mortality Nord J Psychiatry 2016; 70:241-7
23 Simonsen RK, Hald GM, Kristensen E, Giraldi A Long-term follow-up of individuals undergoing sex reassignment surgery: somatic morbidity and cause of death Sex Med 2016; 4:e60-8
24 Heylens G, Elaut E, Kreukels BP, et al Psychiatric characteristics in transsexual individuals: multicentre study in four European countries Br J Psychiatry 2014; 204:151-6
25 Gualdi-Russo E, Lefebvre P, Arnaud J Cranial surgery in antiquity: the size of trepanations during the Neolithic period in France World Neurosurg 2024; 190:131-40
DECLARATIONS
Ethical approval: Not applicable
Availability of data and material: Not applicable
Competing interests: There is no conflict of interest in the study
Funding: There is no funding in the study
Authors' contributions: ZB wrote the text
Acknowledgments: Not applicable
Correspondence
Zeki Bayraktar, MD (Corresponding Author) dr zekibay@gmail com
Department of Urology, Ilhan Varank Training and Research Hospital, University of Health Sciences, 34895, Sancaktepe, Istanbul, Turkey
EDITORIAL COMMENT ON
“Lady urologist and male patients with prostate cancer”
Elisabetta Costantini, Ester Illiano
Andrological and Urogynecological Clinic, Santa Maria Terni Hospital, University of Perugia, Terni, Italy
KEY WORDS: Female and male; Medical student; Lady urologist; Male patient; Self-respecting man
Submitted 12 January 2025; Accepted 13 January 2025
As a member of the Editorial Board and a pioneering woman in the world of urology, I would like to make some comments on the letter from Prof Montironi and his team published in the present issue of Archivio Italiano di Urologia e Andrologia (1) about Suzanne Koven's book published in 2021 (2)
After her inter nship and medical residency at Johns Hopkins Hospital, Suzanne Koven joined the Harvard Medical School and practiced basic inter nal medicine at Massachusetts General Hospital for more than 30 years Of particular interest is her “Letter to a Young Woman Physician,” an essay describing the challenges faced by women physicians, including her personal struggle with “imposter syndrome, ” a long-held secret belief that she is not smart or good enough to be a “real” doctor Consulted by thousands of readers around the world, Koven's “Letter” tur ned into a heartfelt reflection on her medical career
Montironi's letter focused on 4 points, which I commented on separately
1) Male and female medical students and residents
In Italy, the admission tests for medicine and especially for graduate school have changed things a lot If we look at the entrance exams today, we do not find big gender differences; in fact, perhaps it is women who get in more easily It used to be that before entering resident schools it was almost mandatory to attend the department in which one then wanted to attend resident school for a certain period of time; and in that case female students were discriminated against in that they did not always get in by simple “choice”of the committee In some Urology schools they were known to be asked not to show up I entered in resident school in 1987 and the opinion of all my colleagues was that I could never become a surgeon, at best I could be an instrumental nurse in the operating room or alter natively I could only do urodynamic examinations or work on prostate biopsy slides
Today, in fact, the situation has changed, and the real first obstacle for women is to establish themselves in the world of work in the surgical environment, and this is mainly because mentoring is practically exclusively male Female residents are hardly trained in the operating room, as being often more precise and willing than male residents they are mostly employed in the outpatient setting
In academia, especially in the surgical branches, there are no women full professors except in negligible numbers In Urology today, 2024, we have only one female full professor out of more than 40 men Therefore, in Urology the pyramid is extremely gender biased, with few female researchers and very few female associate professors who are often unfairly denied academic progression even with impeccable curricula The fact that the Authors state that in their realities “both women and men have the same chances to succeed in their future professional and academic careers and with patients” shows a new and certainly promising opening for a better future for women uropathologists, but I do not see the same situation in the surgical branches
2) Women urologists
It is evident that the percentage of women in urology services, academic and otherwise, has been lower than that of male urologists Why? The decision to become a urologist today is a difficult and not very popular choice In general, the number of students enrolled in surgical residence schools is lower than in medical schools, and the reasons may be different Surgery involves specific and more complex reasons, first and foremost the risks, including medico-legal and well known to all, inherent in the profession that are undoubtedly higher and the training that is often difficult
The choice to become a surgeon today is often uneconomical, and many students prefer branches that allow for greater profits even in private freelancing Currently, students in the period of the competition for admission to resident schools, no longer attend the hospital ward and the operating room
The student goes from being a “medical student” to a “resident, ” without knowing the realities of the department, much less the operating room Being a resident in a surgical branch means having different goals and expectations Many come
E Costantini, E Illiano
to resident school without knowing their aptitudes; academia does not always help the resident discover them and understand what their practical skills are Women residents, for the most part, have little opportunity to experience the operating room and are often referred to super-specialties that involve a more clinical than surgical approach This makes it increasingly difficult for women urologists to get a grip on and demonstrate surgical skills, if any, once they enter the workforce
Montironi et al reported Mayer's statement (3), “Relatively few women hold leadership positions in the session, and this reflects an old approach of a fundamentally male profession, an approach that has changed rapidly over time ” It is not yet clear to me how it is changing My experience is similar to that of Suzanne Koven, reported in her book “Letter to a Young Woman Physician, Notes from a Medical Life ” We are of the same generation, and I can only agree with at least some of what she says I too have experienced many of her difficulties, although we probably have different characters, and I never felt like an impostor and always believed in myself In some ways my situation was even worse because in the urological world, when I started working, I was the “only” woman, unlike in Inter nal Medicine or Gynecology where sometimes women outnumber men The urological world was, moreover, one of the most difficult for a woman to experience: all the colleagues were men and most of the patients were also men In addition to this, the real discrimination was the fact that surger y was almost always precluded to women Surger y was always reser ved for men The reasons? They are unclear
For a long time, optimistically, I thought the reason was mainly based on the long-standing belief that long and sometimes demanding Open surgery was not suitable for the female physique: surgeries that were too long and tiring Unfortunately, however, the reality, also based on my personal history, was more discriminatory, and the male belief was that women did not have the surgical ability in their hands Today, however, many women are proving that this ability is not exclusive to the male gender
Today, many women urologists are unable to understand some of Suzanne's considerations because they experience a different situation Two elements are tur ning the tables on women in Urology and in surgical branches in general The first is the introduction of new technologies and the robotic surgical approach that are completely changing the scenario Surgeries are no longer so physically strenuous and the ability to maneuver the robot is proving that the female gender has capabilities equal to those of the male gender, and I don't want to say better because I would discriminate in the opposite sense
On the other hand, it is true that in both gender surgical skill is related to individual factors Just as we are not all inclined to play the violin, so we are not all predisposed to surgery, as well as to mathematics, singing, or dancing The second factor is the increase in jobs where women have somehow managed to emerge, which has prompted many more women to become urologists and follow suit Almost as if to say that if one did it, so can others That's why today's new generations do not feel the gender difference significantly, and this is especially true where there is female leadership
Finally, regarding Wallis's study (4), it is interesting because it shows that empathy, which is considered a predominant female characteristic, can improve outcomes after surgery This is important because it underscores the importance of shared decision making as part of the physician-patient relationship and how today this approach should be considered a must for any therapeutic approach
3) Male patients
Both male and female patients can decide which physician to follow I think it is important that in every field there are specialists of both genders, so that each patient can choose the gender he or she feels comfortable with I think the patient is sovereign in his or her choice
In my opinion, the fact that men do not want to be seen by women has been used, in an exaggerated way, as a discriminatory element Actually, I don't think any particular comments are necessary We found this news in the newspapers, but no one ever wrote that some women do not want to be visited by men Yet it happens and it is not news A few years ago, there were no women urologists It was normal for the male patient to find it strange to be seen by a woman, just as it was normal for a woman to be seen by a male gynecologist because there was no alter native Today, patients consciously choose the specialist physician based on their professional considerations and preferences To find many women in urology clinics today means that the population is adapting, and fortunately this is no longer new So today everything is changing for the better and it is nice to have the opportunity to choose freely I don't see why I should be offended if a man prefers not to be seen by me The important thing is that in the end the patient finds the right solution to his urological problem Perhaps I am a bit presumptuous to think that those who choose differently will not necessarily choose the best!
4) Self-respecting man
I agree with Montironi (1) of course patients are treated equally both for regardless of gender and social class I think this has always been the case, independent of the historical era and the gender of the physician
REFERENCES
1 Montironi R, Lopez-Beltran A, Wasserman MC, et al Lady Urologist and Male Patients with Prostate Cancer Arch Ital Urol Androl 2025; 97:13343
2 Koven S Letter to a Young Female Physician: Thoughts on life and work (Notes from a Medical Life) New York, NY: W W Norton & Company, Inc; 2022
3 Mayer EN, Lenherr SM, Hanson HA, et al Gender Differences in Publication Productivity Among Academic Urologists in the United States Urology 2017; 103:39-46
4 Wallis CJD, Jerath A, Aminoltejari K, et al Surgeon Sex and Long-Term Postoperative Outcomes Among Patients Undergoing Common Surgeries JAMA Surg 2023; 158:1185-1194
DECLARATIONS
Ethical approval: Not applicable
Availability of data and material: Not applicable
Competing interests: The authors have nothing to disclose
Funding: The authors report no involvement in the research by the sponsor that could have influenced the outcome of this work
Authors' contributions: Author ALB and author LC have given substantial contributions to the conception or the design of the manuscript, author MW and author AC to acquisition, analysis and interpretation of the data All authors have participated in drafting the manuscript, author RM revised it critically All authors read and approved the final version of the manuscript
Acknowledgments: Not applicable
Correspondence
Elisabetta Costantini (Corresponding Author)
elisabetta costantini@unipg it
Professor of Urology
Chief of Andrological and Urogynecological Clinic - AOU Terni
Chief of Department of Surgery and Surgical Specialty
President of Bachelor's degree in Midwifery
Dept of Medicine and Surgery - University of Perugia - Italy
Andrological and Urogynecological Clinic, Santa Maria Terni Hospital, University of Perugia 05100 Terni (Italy)
Ester Illiano, MD, PhD
ester illiano@inwind it
Andrological and Urogynecological Clinic,Santa Maria Terni Hospital, University of Perugia 05100 Terni (Italy)
EDITORIAL COMMENT ON
Urogenital and extra genital mutilation in gender-affirming surgery: Are we violating primum non nocere?
Tommaso Cai 1, 2 , Alessandro Palmieri 3 on behalf of Italian Society of Andrology
1 Department of Urology, Santa Chiara Regional and Teaching Hospital, Trento, Italy;
2 Institute of Clinical Medicine, University of Oslo, Oslo, Norway;
3 Department of Neurosciences and Reproductive and Odontostomatological Sciences, Urologic Unit, Università Federico II, Naples, Italy
Submitted 6 February 2025; Accepted 6 February 2025
In Arch Ital Urol Androl, Zeki Bayraktar presented the results of a review of all published research on the quality of life, satisfaction, patient-reported outcomes, and short- and long-term problems of patients who had gender-affirming surgery (GAS) (1) According to the Author, transgender people who have GAS virtually completely lose their sexual function and irreversibly lose their reproductive function, and their urinary function is also severely compromised (1) According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR), gender dysphoria has been defined as a marked incongruence between one ’ s experienced/expressed gender and their assigned gender, lasting at least 6 months (2) Strong desires to be of the other gender and to be treated as such (or any alter native gender different from one's assigned gender) are linked to gender dysphoria (2) On the basis of these considerations, is clear that transgender people experience an impairment in quality of life in terms of clinically significant distress or impairment in social, occupational, or other important areas of functioning (3, 4) Gender dysphoria-related distress might include anxiety, sadness, low self-esteem, self-harm, suicidality, or trauma reactions, including hypervigilance, brought on by social mistreatment
These facts make it abundantly evident that gender dysphoria is a mental illness that needs specialized care because it has a major detrimental influence on social and familial life Gender dysphoria is not only a psychological issue but is a complicated mental illness that typically affects individuals and their families Transgender individuals may need genderaffirming surgery in a number of situations to enhance their overall quality of life All urologists certified to do this type of surgery must attend to these patients' requirements and works to enhance their quality of life
These crucial aspects of treating gender dysphoria are not included in Zeki Bayraktar's paper
1) The lack of recognition of high volume and highly qualified centres; 2) The lack of agreement among surgeons regarding surgical procedures and the management of complications; and 3) The absence of a long-lasting and beneficial partnership between patient associations and the Uro-andological Scientific Society are the unmet needs for bettering the care of transgender individuals who need gender-affirming surgery
In conclusion, it is clear that gender dysphoria is a complicated mental illness that requires specific treatment such as several times gender-affirming surgery The question not is: “So, what is the reason for this insistence on GAS?” but “How we can improve the management of gender-affirming surgery in terms of quality of care, patients’ satisfaction and quality of life?”
REFERENCES
1 Bayraktar Z Urogenital and extra genital mutilation in gender-affirming surgery: Are we violating primum non nocere? Arch Ital Urol Androl 2025; 97:13324
2 Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) American Psychiatric Association 2022
DECLARATIONS
Ethical approval: Not applicable
Availability of data and material: Not applicable
Competing interests: None
Funding: Not applicable
Authors' contributions: T C and A P writing
Acknowledgments: Not applicable
3 Turban JL, Beckwith N, Reisner SL, Keuroghlian AS Association between recalled exposure to gender identity conversion efforts and psychological distress and suicide attempts among transgender adults JAMA Psychiatry 2020; 77:68-76
4 Cai T, Verze P, Bjerklund Johansen TE The Quality of Life Definition: Where Are We Going? Uro 2021; 1:14-22
Correspondence
Tommaso Cai - ktommy@libero it Department of Urology, Santa Chiara Regional Hospital, Trento, Italy Alessandro Palmieri - info@alessandropalmieri it Department of Urology, Federico II University, Naples, Italy
INSTRUCTIONS TO AUTHORS – ARCHIVIO ITALIANO
OPEN ACCESS
Open access publishing does have its costs. Information regarding authors’ payment are not made available to editors and reviewers ensuring that they cannot be influenced in their selection of papers for publication by payment conditions or limitations. The Article Processing Charge for publication in this journal is EUR 300,00 (plus VAT, if applicable).
Our fees cover the costs of peer review, copyediting, publication, different format of publication (HTML, PDF), inclusion in many Open Access databases.
All bank charges shall be borne by the payer. Please note that our fees do not include taxes (VAT):
- Private or public ITALIAN customers (individuals, universities, hospitals, other organizations) must ALWAYS add VAT (IVA) at standard rate (4%);
- European Union PRIVATE customers must add the standard rate of their own country VAT tax;
- European Union private/public ORGANIZATIONS (universities, hospitals, others with regular VAT number) should not add any taxes at standard rate, provided that they indicate their VAT number;
- Outside the European Union, individuals and organizations should not add any taxes at standard rate.
Important: Authors are NOT required to pay at the moment of submission. If the paper is accepted, the Managing Editor of Open Access Edition will guide the Authors through the payment procedure. No article will be published before waiver or payment.
According to the United Nations list of Least Developed Countries (LCDs) available from: http://www.un.org/en/development/desa/policy/cdp/ldc2/ldc_countries.shtml Authors coming from those countries are entitled to ask for a discount.
A “Formal Request for discount” has to be forwarded to the Managing Editor of Open Access Edition, after receiving the acceptance letter. The Editorial Committee will then evaluate the merits of each individual case.
Any other informal request (such as comments at the moment of submission, or made in the covering letter of the revised version) will not be taken into consideration.
FAST-TRACK PEER REVIEW
All papers published in Archivio Italiano di Urologia e Andrologia (AIUA) are peer reviewed. Fast-track peer review (4 weeks) can be obtained by supplementary fee of € 488 (VAT included).
METHODS OF PAYMENT Authors can pay their fees by: PayPal is the most recommended and secure payment system. It enables you to pay getting your payment receipt immediately and without sharing your financial information. Other methods of payment are:
Bank transfer
BANK NAME: Banca Popolare di Sondrio, Branch #1, Strada Nuova 75, I-27100 Pavia, Italy
ACCOUNT HOLDER: PAGEPress Srl
BIC/SWIFT: POSOIT22
IBAN: IT85Y0569611301000005086X83
Credit Card The credit card form to be filled and returned either via e-mail or via fax is available for download here.
Check sent by surface mail Checks must be made payable to PAGEPress Srl and must be sent to our full postal address: PAGEPress Publications, via A. Cavagna Sangiuliani 5, 27100 Pavia, Italy.
Note: In any method of payment you choose, kindly specify: 1. journal name; 2. paper ID number; 3. first author.
IMPORTANT TO KNOW
REGISTERED DRUGS, DIET SUPPLEMENTS, NUTRACEUTICALS, MEDICAL DEVICES
Authors of papers that contain references to registered drugs, diet supplements, nutraceuticals and medical devices are requested to buy a minimum amount of 100 reprints at a cost of € 1.500 (1 to 4 pages) or € 2.000 (5 to 8 pages). Prices for the purchase of number of reprints greater than 100 can be negotiated with Edizioni Scripta Manent At present, Edizioni Scripta Manent let everyone to read, print and download papers from website, but retains copyright for republishing and distribution rights for commercial purpose.
TRANSLATION
Translation of manuscripts in Italian language is offered on payment.
Translation and reprints can be requested to Edizioni Scripta Manent by e-mail to info@edizioniscriptamanent.eu
AUTHORS’ RESPONSIBILITIES
Manuscripts are accepted with the understanding that they have not been published or submitted for publication in any other journal.
Authors must submit the results of clinical and experimental studies conducted according to the Helsinki Declaration on clinical research and to the Ethical Code on animal research set forth by WHO (WHO Chronicle 1985; 39:51). The Authors must obtain permission to reproduce figures, tables and text from previously published material. Written permission must be obtained from the original copyright holder (generally the Publisher).
MANUSCRIPT PRESENTATION
Authors must submit their manuscripts (MAC and WINDOWS Microsoft Word are accepted) after registration and login to the link: http://www.aiua.it. Surface or e-mail submission are not accepted.
Manuscripts must be written in English language in accordance with the “Uniform Requirements for Manuscripts submitted to biomedical journals” defined by The International Committee of Medical Journal Editors (http://www.ICMJE.org). Manuscripts
in Italian language can be published after translation (expenses will be charged to the Authors). Manuscripts should be typed double spaced with wide margins. They must be subdivided into the following sections:
TITLE PAGE
It must contain: a) title; b) a short (no more than 40 characters) running head title; c) first, middle and last name of each Author without abbreviations; d) University or Hospital, and Department of each Author; e) last name, address and e-mail of all the Authors; f) corresponding Author; g) acknowledgement of conflict of interest and financial support.
SUMMARY
Authors must submit a summary (300 words, 2000 characters) divided by subheadings as follows: Objective(s), Material and method(s), Result(s), Conclusion(s). After the summary, three to ten key words must appear, taken from the standard Index Medicus terminology.
TEXT
For original articles concerning experimental or clinical studies, the following standard scheme must be followed: Summary - Key Words - Introduction - Material and Methods - Results - Discussion - Conclusions - References - Tables - Legends - Figures.
Case Report should be divided into: Summary - Introduction (optional) - Case report(s) - Conclusions - References
Supplementary Materials can be added for online publication.
SIZE OF MANUSCRIPTS
Literature reviews, Editorials and Original articles should not exceed 3500 words with 3-5 figures or tables, and no more than 30 references.
Case reports, Notes on surgical technique, and Letters to the editors should not exceed 1000 words (summary included) with only one table or figure, and no more than three references. No more than five authors are permitted.
REFERENCES
References must be sorted in order of quotation and numbered with arabic digits between parentheses. Only the references quoted in the text can be listed. Unpublished studies cannot be quoted, however articles “in press” can be listed with the proper indication of the journal title, year and possibly volume. References must be listed as follows.
JOURNAL ARTICLES
All Authors if there are six or fewer, otherwise the first three, followed by “et al.”. Complete names for Work Groups or Committees. Complete title in the original language. Title of the journal following Index Medicus rules. Year of publication; Volume number: First page. Example: Starzl T, Iwatsuki S, Shaw BW, et al. Left hepatic trisegmentectomy Surg Gynecol Obstet. 1982; 155:21.
BOOKS
Authors - Complete title in the original language. Edition number (if later than the first). City of publication: Publisher, Year of publication. Example: Bergel DIA. Cardiovascular dynamics. 2nd ed. London: Aca de mic Press Inc., 1974.
BOOK CHAPTERS
Authors of the chapters - Complete chapter title. In: Book Editor, complete Book Title, Edition number. City of publication: Publisher, Publication year: first page of chapter in the book. Example: Sagawa K. The use of central theory and system analysis. In: Bergel DH (Ed), Cardiovascular dynamics. 2nd ed. London: Aca demic Press Inc., 1964; 115.
TABLES
Tables must be numbered in Arabic digits and referred to in the text by progressive numbers. Every table must be accompanied by a brief title. The meaning of any abbreviations must be explained at the bottom of the table itself.
FIGURES
(Graphics, algorithms, photographs, drawings). Figures must be numbered and quoted in the text by number. The meaning of symbols or abbreviations must be indicated. Histology photograph legends must include the enlargement ratio and the staining method. Legends must be collected in one or more separate pages.
• Do not include any illustrations as part of your text file. • Do not prepare any figures in Word as they are not workable. • Line illustrations must be submitted at 600 DPI.
• Halftones and color photos should be submitted at a minimum of 300 DPI. • Power Point files cannot be uploaded. • If possible please avoid transmitting electronic files in JPEG format or save the JPEG at the highest quality available • PDF files may be uploaded.
MANUSCRIPT REVIEW
Manuscripts are evaluated by the Editorial Board and/or by two referees designated by the Editors. The Authors are informed in a time as short as possible on whether the paper has been accepted, rejected or if a revision is deemed necessary. The Editors reserve the right to make editorial and literary corrections with the goal of making the article clearer or more concise, without altering its contents. Submission of a manuscript implies acceptation of all above rules.
PROOFS
Authors are responsible for ensuring that all manuscripts are accurately typed before final submission. Galley proofs will be sent to the first Author. Proofs should be returned within seven days from receipt.