Table of Contents CHAPTER 1 Tooth Wear in General Practice 1 Does Tooth Wear Matter? 2 Early Recordings of Tooth Wear 4 Education and Tooth Wear for General Practitioners 6 Is It Just Aging? Demographic Patterns 10 Population Trends in Tooth Wear 13 Should I Treat or Refer? 14 CHAPTER 2 Etiology of Tooth Wear: Causes and Recognition .................................... 15 Recognizing Patterns of Wear 16 An International Grading System and Risk Assessment of Tooth Wear ................................. 18 Common Indices for Assessing Tooth Wear .......................................................... 22 Active Wear or Adapted Wear? ...................................................................... 25 Tooth Wear Definitions and Clinical Appearance ..................................................... 28 The Role of Gastric Acid in Tooth Wear ............................................................... 41 Recreational Drug Use 60 Sports and Tooth Wear 63 Diet and Tooth Wear 64 Occupational Tooth Wear 70 Sleep-Related Breathing Disorders 73 The Role of Saliva 75 CHAPTER 3 Occlusion and Tooth Wear 77 Early Occlusal Concepts 78 Engrams and Adaptation 79 Key Occlusal Concepts 80
MANAGING TOOTH WEAR VIII CHAPTER 4 Diagnosis of Tooth Wear: The Clinical Exam 133 Thinking Laterally .................................................................................. 134 Initial Interview: Gathering a History ................................................................ 134 Medical History ..................................................................................... 141 Lifestyle Clues 143 Conditions and Medication Associated with Tooth Wear 144 Drug-Induced Bruxism 145 Diseases Associated with Hyposalivation 147 The Changing Medical Status of a Patient 148 Discussing Sensitive Issues in a Dental or Medical History 150 X-ray Appearance of Tooth Wear 153 Is It Active or Passive? 156 Intraoral Evaluation of Tooth Wear 157 Clinical Records at the New Patient Examination 160 CHAPTER 5 The Team and Tooth Wear: The Role of the Hygienist and Therapist .....183 Introduction 184 The Role of the Hygienist/Therapist 184 Planning a Separate Appointment for Tooth Wear Diagnosis and Prevention 185 Establishing Awareness of the Condition 186 Saliva Testing ...................................................................................... 187 Dietary Analysis, Frequency, and Habits .............................................................. 191 Risk Assessment Questionnaires .................................................................... 194 Tooth Wear Risk Assessment Appointment .......................................................... 197 Remineralization Strategies 199 Improving Saliva Quality and Quantity 202 Dentifrices and Prophylaxis Techniques 203 Fluorides 204 High pH Protective Solutions 205 Sports 206 Supplements 206
IX CHAPTER 6 Developing the Blueprint for Restorative Tooth Wear Management 207 Facially Driven Planning ........................................................................... 208 Smile Design Rules, Attractiveness, and Biology ..................................................... 210 Starting the Blueprint ............................................................................... 211 An Interdisciplinary View in Planning 226 Tooth Wear Blueprint: Establishing the Functional Starting Point 243 Articulation: Analog and Virtual Assessment of Tooth Wear 251 Assessing the Need for an Increase in Vertical Dimension 258 CHAPTER 7 Testing Your Design: The Pretreatment Mock-up 267 The New Standard for Case Approval 268 New Materials for Test-Driving a Design 269 Starting the 3D Design: The Additive Wax-Up 270 How to Deliver a Mock-up 283 The Functional Mock-up 286 The Orthodontic/Restorative Mock-up 295 Presenting the Options 298 Flipping Treatment Planning on Its Head: The Emotional Mock-up 299 Integrating Interdisciplinary Care 302 The Bonded Functional and Aesthetic Mock-up 302 Steps to Create an Index for a Motivational Mock-up 309 Mock-up Delivery Steps ............................................................................ 312 The Mock-up Photo Shoot ......................................................................... 314 The Mock-up Presentation ......................................................................... 315 Important Aesthetic and Functional Tests after the Presentation ..................................... 316 Informed Consent 317 Moving to Treatment After the Mock-up 318 CHAPTER 8 Restorative Options: Material Selection in Tooth Wear Cases 319 Building a Framework for Restorative Treatment 320 Remaining Enamel: An Important Biomechanical Factor in Restorative Solutions 321 Restorative Materials 325 Transitional or Temporary Restorations? 353
MANAGING TOOTH WEAR X CHAPTER 9 Treatment 357 About Treatment ..................................................................................358 Where Do I Start? .................................................................................. 359 A Risk Assessment Approach to Care .............................................................. 360 A Classification of Tooth Wear 361 Sequencing Treatment in Complex Cases 442 Managing NCCLs 469 Composite or Porcelain? 476 CHAPTER 10 Longevity in Tooth Wear Cases 483 The Importance of Continuing Care in Case Stability 484 Digital Monitoring in Tooth Wear Cases 485 Aging of Restorations: Survival Rates of Different Materials 486 Imbrication of Lower Incisors and Orthodontic Relapse 501 Aging and Medication 501 Review of Temporary and Transitional Restorations 502 Occlusal Splints 505 Preventive Trays 507 The Patient Relationship and Continuing Care 510 Bibliography 511 Acknowledgments 523 The Author 525
Tooth Wear in General Practice
CHAPTER 1
Does Tooth Wear Matter?
In recent years I’ve visited the University of Otago School of Dentistry and presented to fourth – and final – year students. It’s a chance to share a little of what lies ahead for our future dentists and my thoughts on the future in our rapidly developing profession. General dental practice has never been more interesting, and the field of tooth wear satisfies so many aspects of the skills we are trained to use: applying a medical diagnostic model to dentistry, design and artistry, sculpture and engineering, use of innovative technology, and the science of dental materials. It requires detective work and lateral thinking, empathy, and listening. Most of all, it’s about offering confidence and reassurance to patients who are often discovering for the first time that chemical and physical forces are damaging their teeth.
One year we were discussing the concept of facially based treatment planning. The case presentation was a 40-year-old woman who had an inverse smile curve and significant tooth wear. It had been hard to capture a facial photograph for analytical purposes—her reluctance to smile was borne by shame and embarrassment. She could only grimace, hesitant to reveal worn, damaged teeth. The students laughed when it was pointed out that she was a beautiful woman. We went on to examine the ability to see through a patient’s disability and visualize the beauty in a reluctant smile.
We walked through the diagnostic and technical elements, but more importantly the human context associated with loss of confidence and self-esteem. My host was an esteemed forensic expert and dental anthropologist, Professor Jules Keiser. He complimented me on the case, and we reflected on the need to open vertical dimension and restore upper and lower teeth in a conservative manner.
Professor Keiser then put his anthropological hat on and commented that not all tooth wear needs treatment, outlining the biomechanical consequences of removal of aprismatic enamel from teeth. Professor Keiser was correct—not all tooth wear needs treatment. How, then, does a clinician make the distinction, and what drives us to intervene? Does a patient believe they have a problem, and what is the distinction between physiologic and pathologic wear?
I go back to that day often as I reflect on longevity and dental outcomes in my patient base of 35 years. When you have had the privilege of serving patients for more than 3 decades, it is possible to see what time and circumstance do to the mouth. Professor Keiser raised the rhetorical question, “Are we overreacting to tooth wear in practice?” and this question sits at the back of my mind and has driven a practice with early recognition and prevention as a focus. We often see tooth wear before the patient sees it; what is our responsibility to raise it and address it? After all, patient awareness frequently lags the severity of tooth wear. By the time the patient is aware, wear can be severe and solutions complex and costly.
MANAGING TOOTH WEAR 2
Reflecting on cases delivering aggressive restorative solutions had resulted in more enamel loss with crowns on every tooth. Was it necessary when more conservative interdisciplinary solutions would be more appropriate? Until the last three decades, our only option for the severely worn dentition was rehabilitation with extensive crown and bridgework or removal of teeth. Thankfully, developments in adhesive dentistry and improvements in modern-day composites have allowed more conservative solutions.
How do we determine pathological from physiological wear? It can be challenging for general dentists. How and when to intervene is at times subjective depending on the case, the extent of the wear, the mechanisms at work (i.e., attrition, abrasion, erosion), and also how the patient perceives wear, which may be asymptomatic and gradual.
Changing life expectancy, a drive by dentists and patients to retain teeth for life, and social expectations of beauty and aesthetics have a role to play in treatment decisions too. Tooth wear can be historical or active, and making sense of the dynamic nature of tooth wear can be confusing. How can we combine interdisciplinary dentistry, such as orthodontics, to offer less aggressive alternatives to patients?
The discipline of tooth wear presents many dilemmas and raises questions:
QUESTION
� Does it matter?
� Is it active?
� Does the patient see it as an issue?
� Will it change?
� When is it appropriate to intervene?
� What will happen if we do nothing?
This book weighs all aspects of the treatment options and the motivation for managing tooth wear. Above all, we focus on biologic, functional, and aesthetic rationale with the goal of enamel conservation and protection at the forefront.
CHAPTER 1 TOOTH WEAR IN GENERAL PRACTICE 3
Early Recordings of Tooth Wear
Tooth wear has existed since the beginning of humankind. For centuries the human dentition has worn because of frictional contact of teeth in an abrasive hunter-gatherer diet. Forensic odontology shows skulls of traditional populations with flat, worn tooth surfaces, perfectly adapted to a diet of tough or abrasive food, which had to be ground and macerated (Fig. 1.1)

Dental anthropologists have long considered human tooth wear a normal physiological phenomenon—an adaptive response to the use of teeth as tools or an abrasive hunter-gatherer diet, where teeth remain functional in their worn state throughout life.1, 2 Genetic factors influence tooth morphology and occlusion and, in turn, occlusion and food consistency influence the chewing pattern. The resulting gradual tooth wear is accompanied by physiological adaptation involving bone remodeling, arch shortening, and compensatory tooth eruption.
Tooth wear had health implications for early civilizations. Periapical lesions and bony fenestrations occurred in some preliterate populations, influenced by extreme wear. Kieser et al. examined 225 skulls of precontact New Zealand Maori.3 Tooth surface loss can result in pulpal exposure with subsequent formation of intra-bony lesions in response to periapical infection. Their study showed that 83% of the skulls examined had at least one fenestrated lesion.
They also noted periapical lesions in intact teeth, the so-called closed periapical lesion (Fig. 1.2) 4 These are found on teeth that are clinically isolated from any direct communication

MANAGING TOOTH WEAR 4
Figure 1.2 – Illustration of periapical lesions and fenestrations because of tooth wear.
Figure 1.1 – Illustration of a flat, worn hunter-gatherer dentition.
with the oral cavity and its associated microorganisms. Heavy use of teeth as tools or traumatic injury can cause enamel-dentine cracks, allowing bacterial ingress to pulpal tissue. 5 Both male (2.4%) and female (4.7%) specimens had lesions associated with minimal observable enamel wear.
What is physiologic wear, and what is pathologic wear? When do we need to be concerned in general practice?
In evaluating the mechanisms of wear, attrition and abrasion are physiological. Attrition and abrasion become pathologic when the rate and nature of wear increases the risk of associated pathology.
For example, a patient with symptoms of pain, fracture, or infection associated with attrition has adverse health implications. Endodontic sequelae have been found in 11% of tooth wear patients as late stages of dental erosion. A patient affected psychologically by visible tooth wear, loss of teeth, facial collapse, and an aging smile may exhibit pathological wear. This reflects changing aesthetic norms in modern society, where there is a stronger drive to restore teeth to their unworn state, irrespective of age. Erosion is generally considered as pathologic and was rarely seen in hunter-gatherer skulls. Erosion was first described by Pierre Fauchard, French dentist and surgeon, who was widely acknowledged as the father of modern dentistry. He published Le Chirurgien Dentiste in 1728 and first described tooth wear as follows:
The enamel of teeth is subject to disease which simulates caries, but it is however not caries. The external surface becomes uneven and rough like a grater but more irregular. I call this erosion of the surface of the enamel, or disposition to caries. From this it comes that the enamel is eaten by some corrosive, in the same way as rust corrodes the surface of metals. The cure for this is to polish the surface of the tooth.6
While there was inevitably some acidic food in the diet of the hunter-gatherer, a change to farming by humans and an increase in carbohydrate consumption meant human biome diversity changed. Biofilm biodiversity shifted toward acid-producing organisms in human plaque, and this tipped the chemistry of the mouth toward net mineral loss, or caries.7
The consumption of sugar-sweetened beverages, the loss of the protective biofilm through acid washing, and changes in biofilm diversity have resulted in a modern-day form of tooth wear where erosion plays a significant role independently of, or in conjunction with, other forms of tooth wear.
CHAPTER 1 TOOTH WEAR IN GENERAL PRACTICE 5
QUESTION
� What is the “normal” rate of wear for the modern man or woman?
� What are our modern-day expectations about retention of teeth, beauty, and aging or antiaging?
Education and Tooth Wear for General Practitioners
Despite identification of erosion by Fauchard nearly 300 years ago, the subject of tooth wear hasn’t had a distinct focus in undergraduate education until recently. Operative dentistry taught mechanical concepts of GV Black, with a focus on treatment of caries, until the last 30 years.8
In the 1980s and 1990s, adhesive dentistry emerged as a reliable restorative technique, and cariology became a distinct branch of dentistry; caries risk assessment became a focus in undergraduate education and general practice in the 2000s.9 Operative dentistry became conservative dentistry, with a focus on enamel and dentine conservation, and tooth wear gained more focus for undergraduate students and general dentists alike.
Some forms of tooth wear gained exposure as an offshoot of caries risk assessment. The role of saliva in tooth wear and the relationship between erosive tooth wear and systemic diseases, such as gastroesophageal reflux disease and salivary gland impairment, created a focus on oral medicine and tooth wear.10
Dental students and general practitioners learned the etiology of tooth wear and applied preventive strategies, but the restorative techniques were more complex reconstructions that often fell into the realm of the prosthodontist.
Other forms of tooth wear were often labeled as “bruxism,” and dentists learned how to make a bite splint or protective night guard. That was often the restorative extent of new graduate strategies for managing tooth wear.
Even today, when sharing this image of tooth wear in Figure 1.3, it is not uncommon to have dentists jump to the conclusion that the patient is grinding their teeth.
A closer look at the presence of thin, fragile enamel surfaces, with brittle transparent remnants, signals that this case is unlikely to involve any abnormal attrition or tooth grinding (Fig. 1.4). This case has all the hallmarks of erosion.
MANAGING TOOTH WEAR 6
The risk of ignoring tooth wear and carrying out extensive restorative treatment in a worn dentition without exploring the cause, rate of wear, or raising the consequences with the patient creates the potential for:
� Ongoing tooth wear and structural fatigue in the presence of chemical or biomechanical forces;
� Failure of newly placed restorations;
� The risk of sensitivity, pulpal involvement, or tooth loss;
� Aesthetic compromise;
� Anterior teeth under increasing load and risk of failure, where posterior wear is active; and

� Costly re-treatment for the patient.

CHAPTER 1 TOOTH WEAR IN GENERAL PRACTICE 7
Figure 1.3 – Acid erosion, demonstrating thin transparent enamel, cupping, and yellowing of teeth as enamel is lost.
Figure 1.4 – Transparent brittle enamel remains, indicating bruxism is unlikely to be a factor in tooth wear in this case with acid erosion.
CLINICAL CASE CRUMBLING BOTTOM TEETH


This patient presented with concerns about “crumbling bottom teeth.” She had evidence of erosion and attrition (Fig 1.5). She noticed her lower teeth were becoming more chipped and fragile in the last five years. In addition, she had chipped veneering ceramic from a crown on her upper left central incisor. Implants had been placed two years earlier and restored to a flat, worn occlusion at lower premolar and first molar sites (Figs. 1.5, 1.6)
Further investigation revealed the use of a vitamin C powder used daily with water, lemon juice in water, and diet sodas contributing to wear. Treatment involved redesign of the occlusal scheme, using conservative additive dentistry with composite resin to open the occlusal vertical dimension, and crowns in the upper arch. At the completion of initial treatment, the implant crowns remained out of occlusion (Fig. 1.7), highlighting the challenge of an implant that behaves like an ankylosed tooth. Continuous eruption won’t occur from the implant crowns; opposing teeth will over-erupt, disrupting the maxillary occlusal plane and altering contact points and interproximal contours. Implant crown replacement needed to be done on all four fixtures to maintain occlusal stability and prevent over-eruption of the opposing teeth.
The point of this case is that the underlying etiology was not managed before significant and costly treatment with implants for the patient. Consideration of wear, the overall occlusal scheme, and the patient’s concerns about longevity of her teeth may have saved her the cost and time for re-treatment as part of a wider plan to manage her concerns.
MANAGING TOOTH WEAR 8
Figure 1.6 – Altered anterior relationship, with an active extrinsic acidic etiology contributing to ongoing wear.
Figure 1.5 – Wear is evident on lower teeth, and implant crowns have been designed to a worn occlusal scheme.
CLINICAL TIP Before embarking on any indirect dentistry, which is a significant investment for most patients, consider the overall functional relationships and wear patterns, in addition to the normal periodontal, caries, and endodontic assessments made during an examination.

CHAPTER 1 TOOTH WEAR IN GENERAL PRACTICE 9
Figure 1.7 – Initial reconstruction, restoring worn lower teeth in composite resin, with new crowns in the upper arch. Implant crowns were finally replaced to restore posterior occlusal contact.
Implants out of occlusion
While the diagnosis of tooth wear may be more widely recognized and discussed today, the management is not, presenting a dilemma for the general dentist:
� Do I need to intervene?
� Where do I start?
� What material do I use?
� Can I do harm?
� Will it last?
� Is there a system or protocol that I can follow?
Many dentists in general practice are challenged by the presence of tooth wear, uncertain how to manage tooth wear restoratively when required, particularly where it involves many teeth and entire arches. It is work that is deferred to prosthodontists, who are trained to manage complex occlusal and aesthetic issues. Tooth wear is commonplace, however, and with a heightened awareness, and the use of systematic processes to provide lasting solutions for patients, the general practitioner can manage patients with confidence and predictability.

This book aims to provide tools for any general dentist to understand more about tooth wear and offer preventive strategies and restorative solutions to patients. We define when to intervene and when tooth wear is pathological, as well as provide a system of classification and planning and a range of restorative solutions.
Is It Just Aging? Demographic Patterns
The following image shows some sign of tooth wear (Fig. 1.8). How old do you think this patient is?
MANAGING TOOTH WEAR 10
Figure 1.8 – Example of patient with early signs of tooth wear.
There are some diagnostic clues: glossy anterior teeth with loss of secondary anatomy, slight incisal edge wear. Restorations are more traditional—porcelain fused to metal and gold, with metal margins visible. Cusp tips appear to be intact. Teeth are yellow, a color change associated with aging, and dentine lobes are becoming visible on central incisors. So what was your guess? 55, 65?
The patient was 80 when the photo was taken in 2022, having been cared for in my office for 30 years. Wear was minimal in the context of his age; the color didn’t bother him, he functioned without an awareness of his teeth, and had virtually no periodontal attachment loss apart from slight mucogingival recession throughout his life.
The notion that wear is commensurate with age is reasonable. The more significant question might be, How much tooth wear is commensurate with age?
Many studies have been done to assess the rate of tooth wear in populations and the relationship of tooth wear to age. Tooth wear and the attrition patterns are used for estimates of age in anthropological studies and in forensic dentistry. Several qualitative methods and indices have been proposed to measure tooth wear.
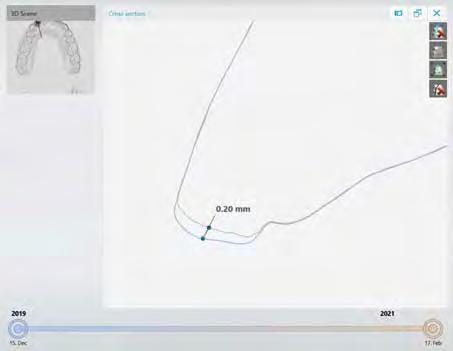
Intraoral scanners allow digital comparative technology and superimposition of timestamped scans within dental software. These methods promise an estimation of tooth wear over time, allowing tooth height (linear) or volume loss (volumetric) and may be useful in the general practice setting (Fig. 1.9)
CHAPTER 1 TOOTH WEAR IN GENERAL PRACTICE 11
Figure 1.9 – Comparative scans showing tooth surface loss in a 22-year-old patient over 2 years.
Further research is needed to assess the practicality of digital comparative technology in large-scale epidemiologic tooth wear studies. Some of the challenges include differences in trueness and precision among different scanners and operator techniques and the accuracy of scan correlation and matching of digital models in which many variables may change. It may not be suitable for teeth that undergo morphological alterations over time. Any site that has had restorations, decay, orthodontic tooth movement, compensatory eruption, or tooth replacement since a baseline scan may create correlation challenges in large-scale studies.
However, quantitative three-dimensional results are likely to become the norm in general practice, where a patient’s history is well known.
QUESTION
� What is a normal rate of wear?
� Is there a threshold level at which we decide the rate of wear is a red flag or pathological for an individual based on their age?
The rate of removal of a mineralized tissue undergoing any kind of wear process in a normal functioning individual will vary enormously, with much human variability. Likewise, the clinical interpretation of a threshold level by a dentist could be variable and subjective, based only on clinical judgment.
Smith and Robb examined 1,007 patients with only 9 having completely unworn dentitions, suggesting that some tooth wear is expected in all age groups.11 Dentine exposure became more common in older cohorts. They identified that 5–7% of adults in all age cohorts had wear that could justify treatment. What was the threshold for justifying treatment? In many instances, the threshold is determined by the experience of the clinician and remains a subjective decision for many dentists.
How much wear is normal for an age group? How do we define pathological or unacceptable wear? The evidence for a relationship between pathological wear and age is not clear, and while some wear is expected for age, severe wear is not age dependent.12
Lambrechts measured the attrition contact wear of human enamel over a 4-year period. 13 Slightly higher wear rates (38 microns) were measured during the first year of restoration placement (running in wear), followed by steady-state wear after two years. Quantitatively, 15 to 29 microns of steady state enamel wear was recorded per year. If we use an average of 20 microns per year, that equates to about 1mm over 50 years.
Ray et al. quantified tooth wear and used conventional digital radiography to estimate the rate of tooth wear of maxillary and mandibular central incisors.14 The crown length of 1,239 permanent maxillary and mandibular central incisors from 346 persons (age groups: 10, 25,
MANAGING TOOTH WEAR 12
40, 55, and 70 years ±3) were measured by 3 calibrated dentists. Study teeth were intact incisally, had clearly visible incisal edges and cementoenamel junction (CEJ), and had natural tooth antagonists.
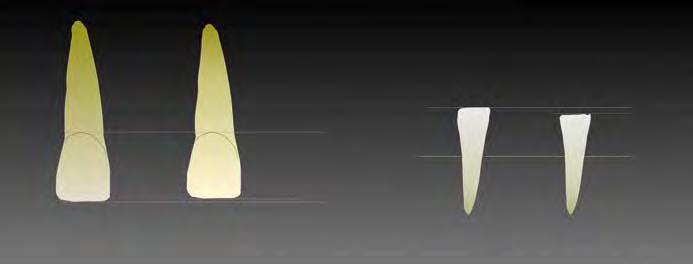
Tooth wear was estimated to average 1.01 mm for maxillary central incisors and 1.46 mm for mandibular central incisors by 70 years of age (Fig. 1.10). Incisor crown length decreased at a linear rate in both arches over the 60 years represented by the age groups.
Observing wear rates beyond 1 mm in a younger patient could highlight wear that is not commensurate with age, triggering further investigation.
Population Trends in Tooth Wear
Tooth wear is a significant oral health issue. Erosive tooth wear is the third-most commonly observed oral condition after caries and periodontal disease, with a prevalence similar to that of dentine hypersensitivity.15
Gillborg et al. reviewed tooth wear in 831 adults in Sweden, using the Basic Erosive Wear Examination (BEWE), photographs, saliva samples, and questionnaires.16 Almost 80% of the individuals had signs of erosion, and over 90% had signs of attrition. A high level of tooth wear was found in 4.6% of the individuals. Significantly, more men had tooth wear. Daily consumption of fruit had a stronger correlation to tooth wear than acidic drinks.
CHAPTER 1 TOOTH WEAR IN GENERAL PRACTICE 13
Figure 1.10 - A schematic of tooth wear estimates by age 70, as per Ray et al.14
1.46 mm for maxillary central incisors
1.01 mm for maxillary central incisors
Should I Treat or Refer?
General dentists are at the forefront of diagnosis and early detection of disease. If you are reading this book, it’s probably because you want to know more about tooth wear. The implications for your practice are to:
� Highlight a growing health issue to your patients;
� Identify tooth wear early, before treatment becomes complex and costly;
� Offer solutions to prevent further tooth surface loss;
� Provide longevity and health through maintenance of the dentofacial system;
� Ensure the longevity of any restoration you might place;
� Expand the range of services in your office; and
� Restore confidence and well-being to your patients and satisfaction to you and your team.
Restorative management of tooth wear can range from simple treatments to complex fullmouth rehabilitation, and the decision is often whether to restore or not.
Single tooth dentistry is well within the scope of every general dentist. When we are confronted with treatment of multiple teeth, the prospect can be daunting.
Some dentists, after reading this book, may feel they want to refer to colleagues with more experience and confidence in delivery of complex restorative procedures involving an entire arch or multiple restorations. Systematic application of the principles in this book should give general dentists the confidence to explore the field of tooth wear further, starting with simple preventative options, followed by reversible restorative solutions, and moving to more complex cases with experience.
MANAGING TOOTH WEAR 14
