
15 minute read
The relationship between germline mutations and the incidence of pancreatic cancer

The relationship between germline mutations and the incidence of pancreatic cancer
Bronte Elliott
Wollumbin High School
Abstract
Pancreatic adenocarcinoma is one the most aggressive forms of cancer. Up to 20% of cases are due to inherited deleterious germline mutations meaning that 1 in 5 people have been capable of significantly improving their prognosis through means of an earlier diagnoses as a result of genetic screening. This research paper aims to determine the relationship between specific deleterious germline mutations and the incidence rate and development of pancreatic cancer in individuals. The data generated within this study looked at factors such as age, sex, ethnicity, and patient history. Genetic screening was employed to ascertain predetermined cancer-causing genes in patients. It was found that individuals with a positive family history of pancreatic cancer were more likely to carry deleterious germline mutations and consequentially develop familial pancreatic cancer in their lifetime. The mutations found to hold the strongest association in developing pancreatic cancer were BRAC2, ATM, and PMS2.
Literature review
In Australia, pancreatic cancer (PC) is the third most common cause of cancer-related death. Accounting for >95% of pancreatic cancer cases, pancreatic adenocarcinoma, (aka: cancer of the pancreatic ducts) hereafter known as PAC, is one of the most aggressive forms of cancer.
When considering the genetics, more specifically, the genetic mutations surrounding PAC, it has been found that certain deleterious genes carry a higher risk of developing the disease than others. Through research, strong associations have been found between specific germline mutations and the susceptibility of an individual developing PC and other related syndromes and diseases. This information is of vital importance when it comes to cancer screening and early diagnosis, and can mean the difference between recovery and remission, or death as a result of the disease.
This literature review attempts to collate and present current findings relating to the associations between population incidence rates and genetic germline mutations.
Current research is focused on identifying relations between a person’s genetic mutations and their susceptibility to PC. The identification of high-risk PC gene mutations gives health practitioners and researchers a panel of markers to aid in the identification and surveillance of individuals who are at a high risk of developing PC and other associated diseases of that same ilk.
Are there any associations between an individual’s genetic information and the incidence rate of developing PAC?
Clinical Practice Guidelines in Oncology (Tempero 2010 et al) reported that 5-10% of PAC cases arise from a genetic vulnerability. It is still with major uncertainty that contemporary research can account for the majority of PC associated germline mutations. A lack of known pathogenic mutations suggests further unnamed mutations. These findings mean that up to 1 in 5 people with PAC are able to receive an earlier diagnosis therefore improving their prognosis dramatically when compared to the average diagnosis timeframe.
One study (Hu et al. 2018b) took a population of 1,819 individuals with PC from a larger group of 140,000 who underwent multigene panel testing. This study found that 97.7% of PC’s were PAC’s. The study reported that 20.73% (combined frequency) of all patients carried at least one type of genetic mutation relating to the onset of this particular cancer.
What deleterious germline mutations are linked with PAC?
Knowing there is an association between PC and inherited germline mutations, research is now directed towards finding the specific deleterious germline mutations responsible for the onset of PC. Deleterious germline mutations escalate one’s predisposition to certain disorders, diseases, and syndromes.
Genes that influence tumour suppression pose an increased risk of cancer if mutated, damaged, or missing. The study found that 5.5% of PC patients carried mutations in 6 genes linked with PC. Limitations to this data include the usage of public reference controls, the fact that the panel of 21 genes did not represent all deleterious germline mutations associated with cancer, and the geographical location cases came from restricted areas therefore not accurately representing all races regarding the data collected.
In another study (Salo-Mullen 2015 et al). Again, the genes BRAC2 and BRAC1 were found to be the most common mutation, along with the presence of 22 other mutations found to be associated with PC and its related syndromes. The study acknowledged its limitations, the main being a patient selection bias during recruitment and testing, that being said, the population was one of the largest current published studies in its area, giving real-world depictions and applicable data.
The most prevalent of these deleterious genes was BRAC2 (BReast CAncer gene 2). Upon further examination, the BRCA1 and BRCA2 gene mutations were found to have higher recorded prevalence rates in the Ashkenazi Jewish (AJ) race. The AJ population in each study has consistently recorded higher risk ratios, cases of PC, and, consequentially, cases of familial PC along with mutations in the BRCA genes. For instance, PAC patients with positive family history as well as AJ heritage had a BRCA1/2 mutation prevalence of 13.7%, this figure is extremely high when compared to patients with no family history or AJ heritage with a mutation prevalence rounded to 0%.
How do these specific mutations relate to PAC in terms of familial heredity?
Familial history is another tool that can be used to estimate an individual’s risk of developing PC. Though we do not yet understand the reasons why certain groups of people are more likely to carry specific mutations, we can recognise and apply the patterns we are presented with and can use this information to aid the current forms of treatment and research concerning PC.
In a study focused on familial PC (Shi, Hruban & Klein 2009), it was stated that 5-10% of all patients with PC had a positive family history. This data supports links between inherited deleterious germline mutations and population incidence rates concerning the occurrence of PC.
Similar findings were presented in a separate study (Lal 2015) concerning inherited susceptibility to pancreatic cancer, it was found that 13% of patients with a high/intermediate risk of familial PC had mutations in their germlines. These groups came from classifications of threegenerational pedigrees, where the high and intermediate risks of familial PC were analysed for germline mutations. These histories are a direct result of the increased likelihood of carrying mutated BRAC2 and BRAC1 genes.
A notable similarity between numerous studies was the data surrounding genetic syndromes and their relevance to PC. The family of associated PC syndromes includes hereditary breast and ovarian cancer, pancreatitis, colorectal cancer, melanoma, and adenomatous polyposis. The papers linked the high risk associated with both familial and personal histories of such syndromes, as individuals with such histories were more likely to carry PC-associated germline mutations.
The small scope of the known pathogenic mutations associated with PC across all current literature as it stands, begs to suggest additional, currently uncatalogued genes that contribute to a person’s susceptibility to PC and its other related syndromes and conditions. This point addresses the direction of new research, and where the effort is currently being placed towards in order to increase our knowledge regarding the determining of pathogenic mutations.
Summary
This review of current literature found that certain deleterious germline mutations are associated with the development of pancreatic cancer with roughly 1/5 of PAC patients being carriers. The most prevalent of these genes, were mutations in the BRCA2, followed closely by the BRCA1 germlines. Persons of AJ descent were found more likely to be carriers of such mutations, evidenced through more frequent familial cases of PAC. Current research only accounts for the most common deleterious germline mutations, with more obscure, rare mutations left undiscovered. Future research is focusing on identifying any unknown high-risk pathogenic mutations and developing precise predictive genetic testing regarding PAC and its relative syndromes.
Scientific research question
Are specific germline mutations an influential factor in the incidence rate and development of pancreatic cancer in individuals?
Scientific hypothesis
Germline mutations are an influential factor in the incidence rate of pancreatic cancer in individuals
Null hypothesis
Germline mutations are not an influential factor in the incidence rate of pancreatic cancer in individuals.
Methodology
The dataset utilized was generated by a pancreatic cancer researcher at the Garven Institute. Due to ethical regulations surrounding the use of actual patient data, a ‘mock’ dataset was generated that reflected patterns commonly found in clinical practice that did not contain actual patient information.
The dataset shows a case-series from a metropolitan location in Sydney Australia over a 3-year period. Information was based on the same hospital, to ensure demographical similarities. Two cohorts of 114 patients were generated, one with PC & one without PC. The variables tested on were as follows:
• Age at diagnosis
• Ethnicity
• Personal history of other cancers
• Family history of other cancers
• Family history of pancreatic cancer
• Genetic status
These variables were selected in the aim of determining a relationship (if any) between germline mutations and the incidence rate of pancreatic cancer.
Appropriate descriptive statistics were used to calculate and compare the means, modes, medians, standard deviations, ranges or the variables investigated within this study.
Chi-squared tests were then utilized to determine whether two categorical variables held a measurably significant association, one that contrasted the expected null hypothesis. Microsoft Excel was utilized to perform the Chi-squared tests. Expected frequency tables were constructed and compared to the observed frequencies.
Results
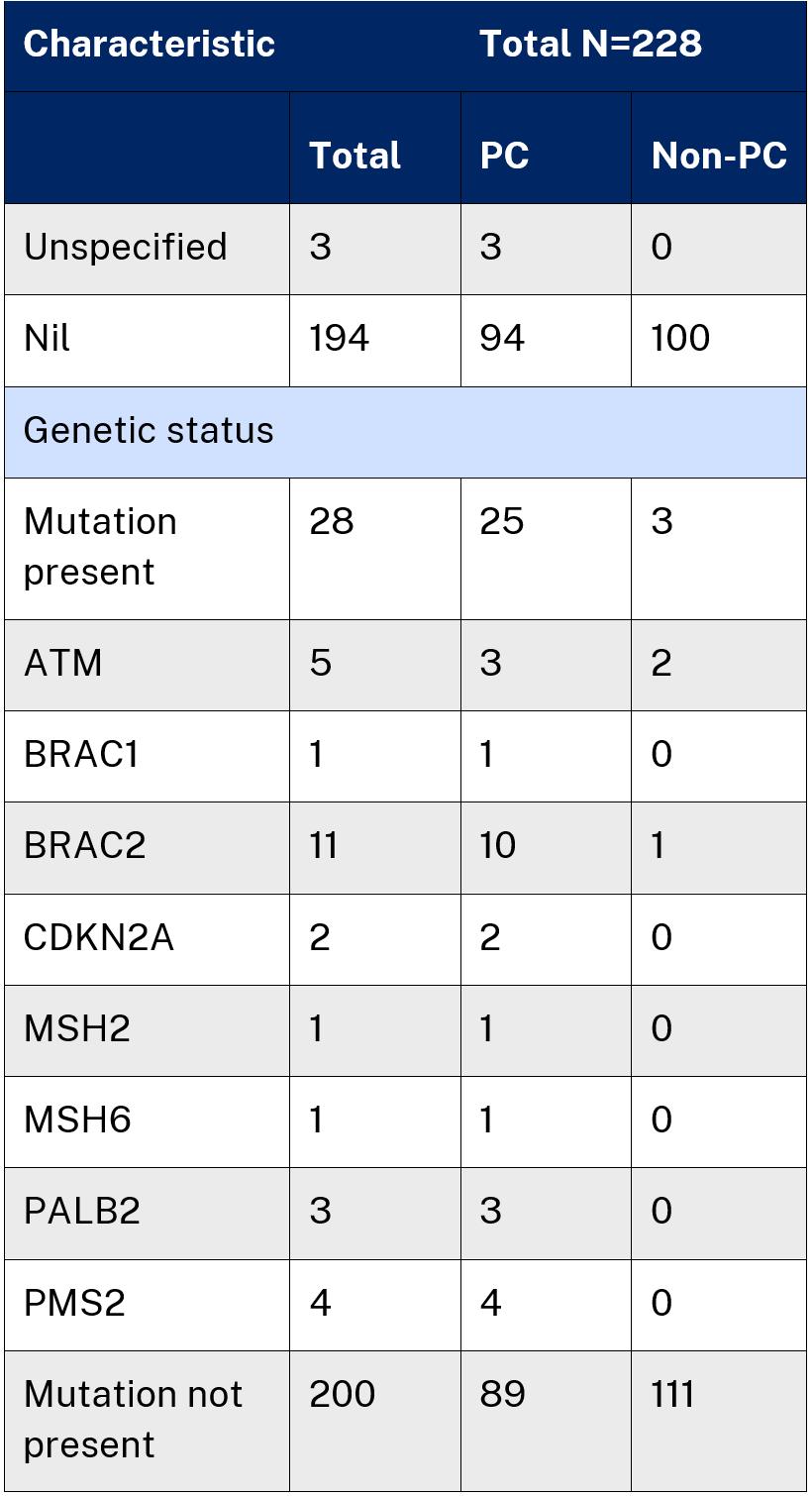
Table 1 depicts an overview of the data collated from the dataset generated by the Garven Institute. A frequency count of sex, ethnicity, age of diagnosis, family and personal history of cancer and genetic status has been provided. The table contains information on both the cohort diagnosed with pancreatic cancer and the case-control cohort of those not diagnosed with pancreatic cancer. All these patients had pancreatic adenocarcinoma.




Discussion
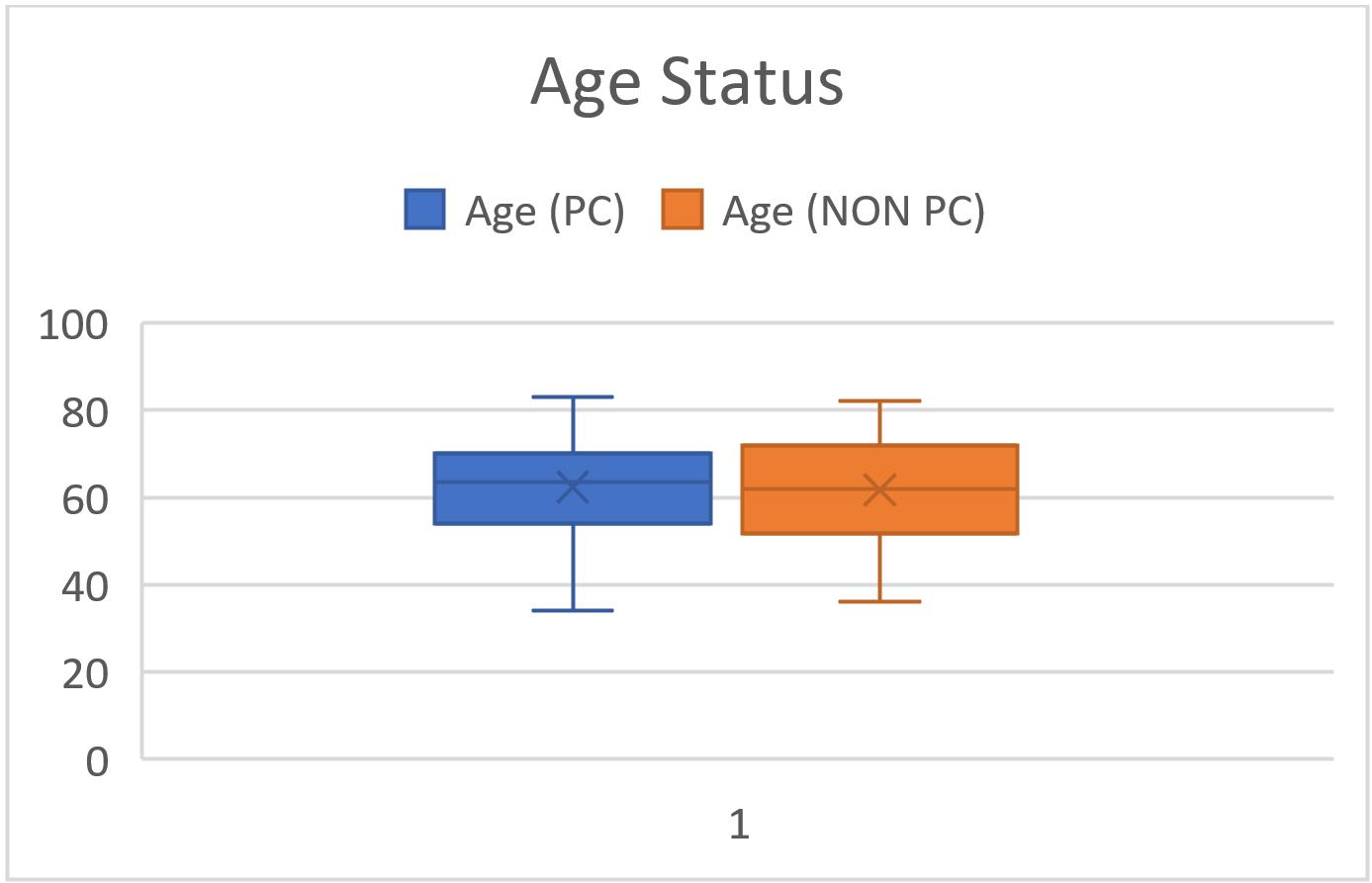
The dataset provided encompassed a cohort of 228 individuals. It was partitioned into two distinct groups each comprising 114 subjects. These groups were designated as 'PC' (denoting pancreatic cancer) and 'non-PC' (signifying non-pancreatic cancer). While a significant portion of the data collected consisted of qualitative variables, notably, the age (figure 1) parameter was available in a quantitative form.
In light of the largely categorical nature of the data, Chi-squared tests were employed to assess the statistical significance of disparities between the variable ‘Cancer’ and other variables identified as potentially exhibiting a pronounced association based on the preliminary descriptive statistics.
A Chi2 test was performed between Cancer and Ethnicity. The returned p-value of .353 was higher than the standard p-value of 0.05 indicating that this data was statistically insignificant and held no relation whatsoever thus not rejecting the alternate hypothesis.

It was found that 21.9% of PC individuals carried germline mutations selected for screening, whereas only 2.6% of non-PC individuals the germline mutations selected for screening within the dataset. This figure is supported by another study 1 2, that reported that 20.73% of all patients carried at least one type of genetic mutation relating to the onset of pancreatic cancer.
1 Hu et al. 2018b
2 Tempero et al. 2010
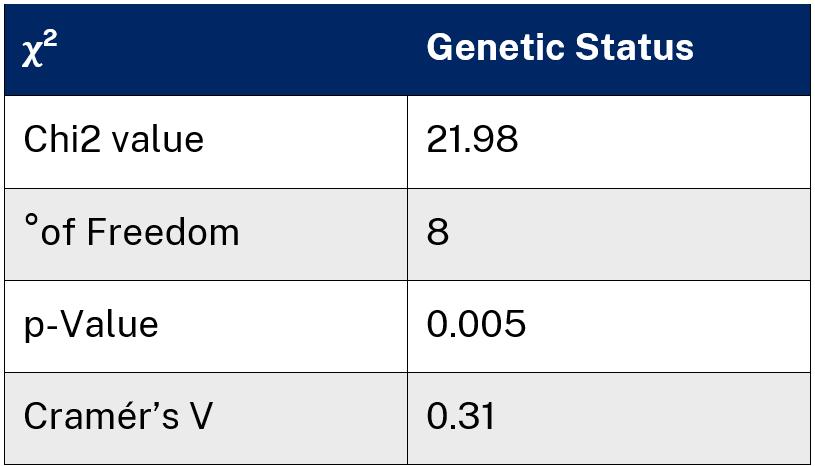
A second Chi2 test was performed between Cancer and Genetic status. Genetic Status referring to presence of specific mutations across both cohorts (PC and Non-PC). The returned p-value of 0.005 was lower than the standard p-value of 0.05 resulting in a 99.995% level of confidence in rejecting the null hypothesis. This indicates a statistically significant relationship between the two variables, henceforth leading to the rejection of the null hypothesis.
These results most compellingly address the research question. The genetic disparity between PC and Non-PC individuals suggesting that germline mutations indeed play a crucial role in the development of pancreatic cancer in certain individuals.
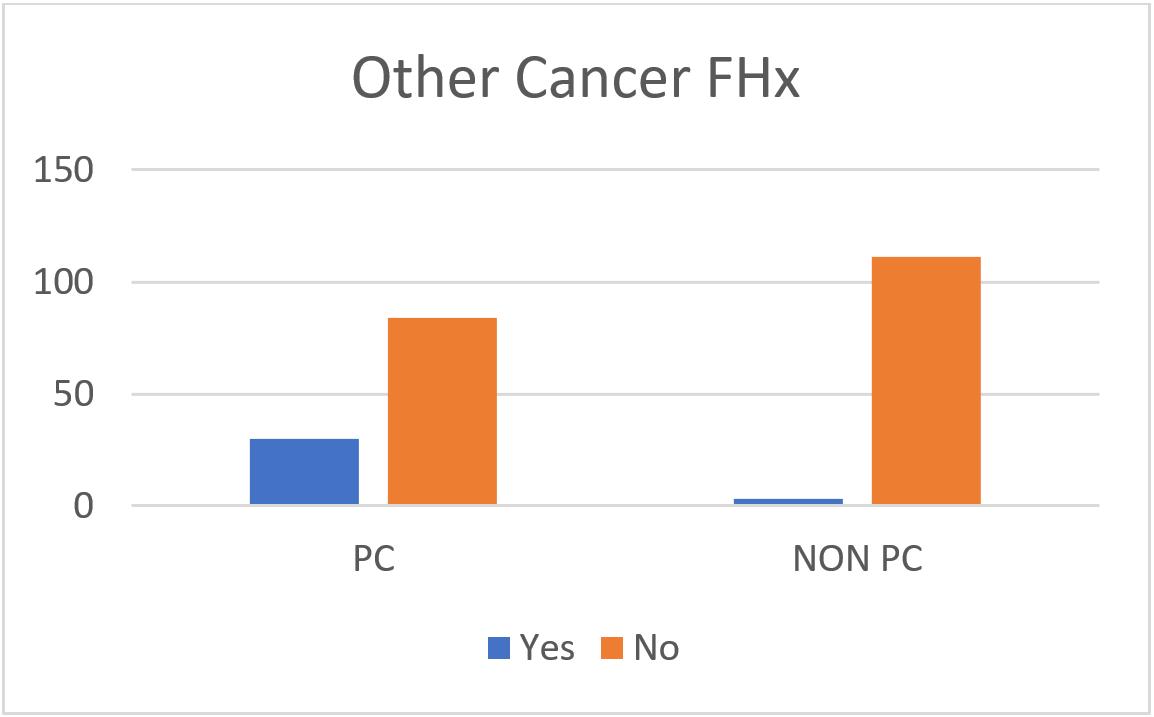
Most remarkable was the Chi2 test performed between Cancer and FHx PC (Family History of Pancreatic Cancer). Out of the PC cohort, 14.5% of patients had a positive family history. Most relevant literature reports that 5-10% of PC patients have a positive family history 3 4 The resulting p-value of <0.001 was lower than the defined significance level of 0.05 giving a >99.999% confidence level in rejecting the null hypothesis. Such a result underscores the exceptionally remote likelihood of the observed variable being a product of mere chance.
Family history (figure 3) played a significant role, as a substantial proportion of individuals had no familial ties to pancreatic cancer, while a smaller subset had a family history of the disease. This duality emphasizes the potential germline hereditary aspect of pancreatic cancer susceptibility.
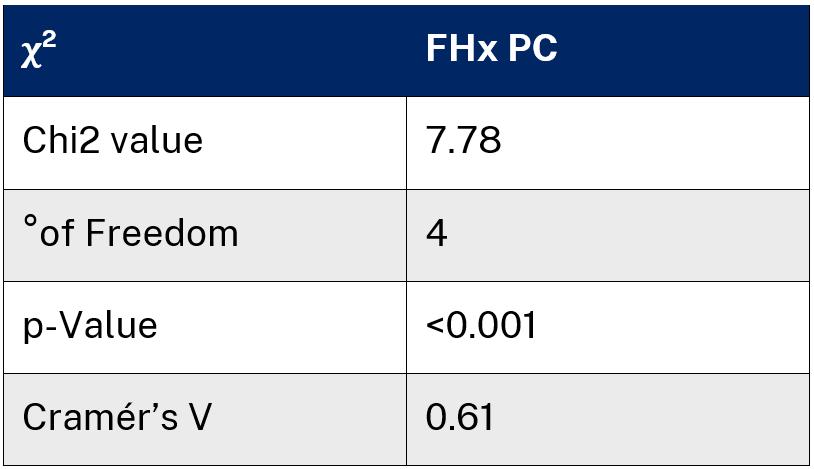
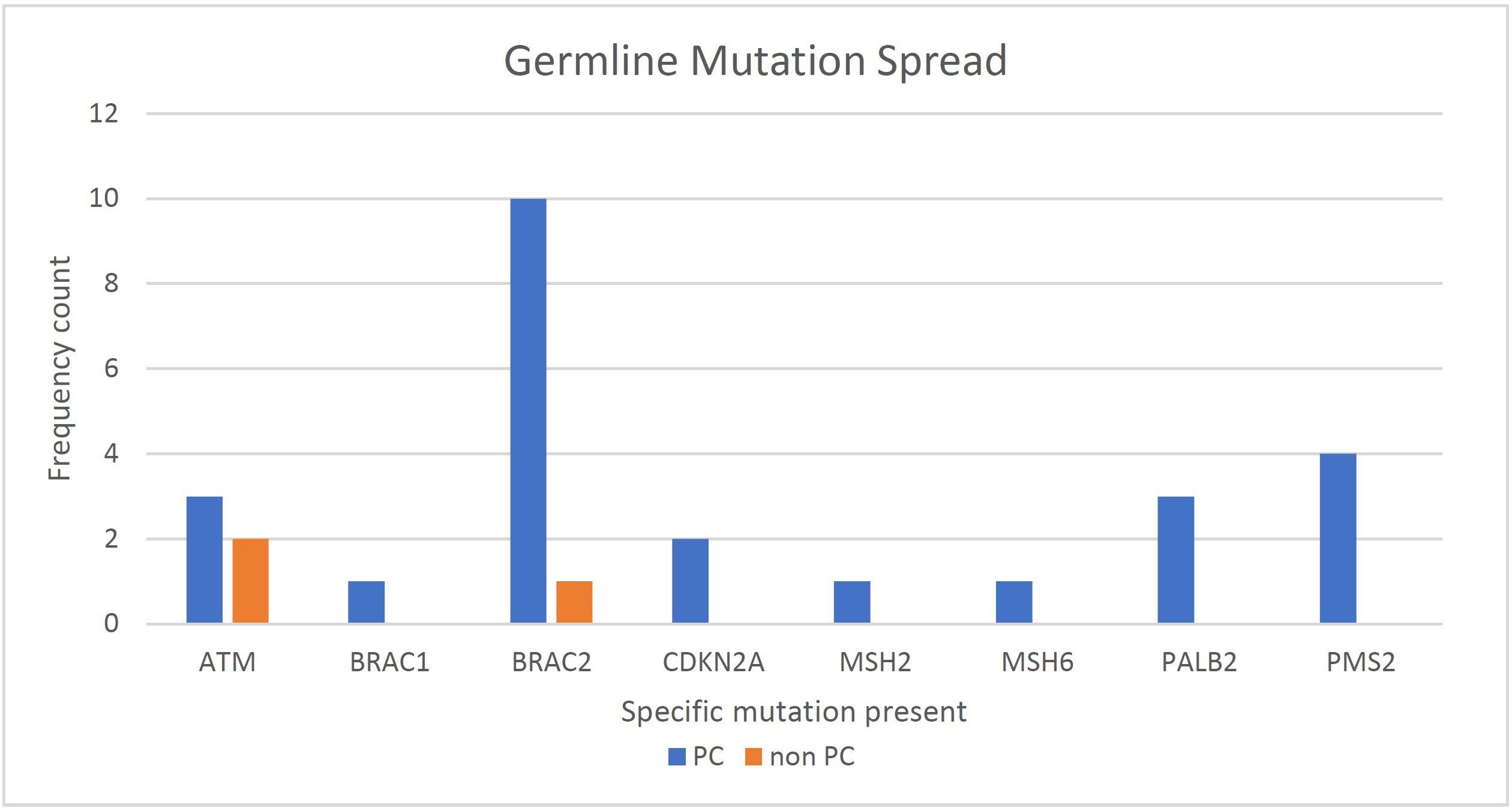
Figure 5 (Germline Mutation Spread) displays the frequencies of the identified germline mutations selected for screening within the dataset. The strong presence of BRAC2 closely followed by BRAC1, and ATM as deleterious germline mutations is concurrent with current literature 55 , . PMS2, PALB2, CDKN2A, and MSH2 are all frequently suggested to have an association with the development of PC as well. These findings provide strong statistical evidence for the observed associations, making their emergence highly unlikely. They make a substantial contribution to our understanding of the complex dynamics involved in pancreatic cancer, thereby enhancing the ongoing scientific discussion in this field of research.
3Shi, Hruban & Klein 2009
4 Lal 2015
5 Salo-Mullen et al. 2015
The main limitation of this study was the fact that the data used came from a single hospital in a metropolitan area. The small demographic resulted in a limited scope of practicality within the research. To remedy this, a wider range of patients from varying geographical locations, ethnicities, and economical demographics should be employed in order to make the results applicable to the general population.
Next steps to take should aim to breach the gap of knowledge in regard to what types of genetic mutations lead to the development of pancreatic cancer. Doing so would greatly decrease the prognosis of familial pancreatic cancer as well as significantly contribute to the ongoing scientific discourse surrounding this disease.
Conclusion
In conclusion, this report sought to investigate the influence of specific germline mutations on the incidence rate and development of pancreatic cancer in individuals. The analysis of a cohort of 228 subjects, divided into ‘PC” and “Non-PC) groups revealed significant insights.
Firstly, the Chi2 test conducted between ‘Cancer’ and various variables highlighted a substantial genetic disparity. Notably, 21.9% of PC individuals carried one or more of germline mutations selected for screening, in contrast to only 2.6% among the non-PC individuals. This stark contrast led to the rejection of the null hypothesis and indicated a statistically significant relationship, suggesting that germline mutations play a pivotal role in the development of pancreatic cancer.
Furthermore, the investigation into Family History of Pancreatic Cancer revealed an extremely low likelihood of the aforementioned variable being a product of chance, emphasising the likely potential hereditary aspect of pancreatic cancer susceptibility.
The frequencies of germlines mutation within this experiment combined with existing literature added substantial evidence to the associations between these mutations and pancreatic cancer.
Acknowledgements
Special thanks to Tanya Dwarte who is the Clinical Research Coordinator and part of the Australian Pancreatic Cancer Genome Initiative at the Garvan Medical Research Institute. Tanya acted as my mentor throughout this process, as well as supplying the generated mock data set.
Reference list
Chaffee, KG, Oberg, AL, McWilliams, RR, Majithia, N, Allen, BA, Kidd, J, Singh, N, Hartman, A-R, Wenstrup, RJ & Petersen, GM 2018, ‘Prevalence of germ-line mutations in cancer genes among pancreatic cancer patients with a positive family history’, Genetics in Medicine, vol. 20, no. 1, pp. 119–127, viewed 20 January 2023,
Hu, C, Hart, SN, Polley, EC, Gnanaolivu, R, Shimelis, H, Lee, KY, Lilyquist, J, Na, J, Moore, R, Antwi, SO, Bamlet, WR, Chaffee, KG, DiCarlo, J, Wu, Z, Samara, R, Kasi, PM, McWilliams, RR, Petersen, GM & Couch, FJ 2018a, ‘Association Between Inherited Germline Mutations in Cancer Predisposition Genes and Risk of Pancreatic Cancer’, JAMA, vol. 319, no. 23, p. 2401, viewed 20 January 2023, .
Hu, C, LaDuca, H, Shimelis, H, Polley, EC, Lilyquist, J, Hart, SN, Na, J, Thomas, A, Lee, KY, Davis, BT, Black, MH, Pesaran, T, Goldgar, DE, Dolinsky, JS & Couch, FJ 2018b, ‘Multigene Hereditary Cancer Panels Reveal High-Risk Pancreatic Cancer Susceptibility Genes’, JCO Precision Oncology, no. 2, pp. 1–28.
Lal 2015, ‘Inherited predisposition to pancreatic adenocarcinoma: role of family history and germline p16, BRCA1, and BRCA2 mutations’, Cancer research, vol. 60, Cancer Res, no. 2, viewed 20 January 2023, .
Salo-Mullen, EE, O’Reilly, EM, Kelsen, DP, Ashraf, AM, Lowery, MA, Yu, KH, Reidy, DL, Epstein, AS, Lincoln, A, Saldia, A, Jacobs, LM, Rau-Murthy, R, Zhang, L, Kurtz, RC, Saltz, L, Offit, K, Robson, ME & Stadler, ZK 2015, ‘Identification of germline genetic mutations in patients with pancreatic cancer’, Cancer, vol. 121, no. 24, pp. 4382–4388, viewed 20 January 2023, .
Shi, C, Hruban, RH & Klein, AP 2009, ‘Familial Pancreatic Cancer’, Archives of Pathology & Laboratory Medicine, vol. 133, no. 3, pp. 365–374, viewed 20 January 2023, .
Tempero, M, Chair, Arnoletti, J, Behrman, S, Ben-Josef, E, Benson Iii, A, Lurie, R & Berlin, J 2010, Pancreatic Adenocarcinoma: Clinical Practice Guidelines in Oncology, September, viewed 5 February 2023, .
