Regardless of how you review smears, Sysmex and CellaVision have the right tools for your unique workflow. With solutions ranging from slide preparation and staining to complete hematology automation, peripheral blood imaging has never been so flexible. And CellaVision Remote Review software and Database Server allow consultation with your experts, no matter where they are. Visit Sysmex.com/CellaVision
Unistik® Safety Lancets are designed with you and your patient in mind. They are engineered with Comfort Zone Technology® to help reduce pain during the sampling process while consistently delivering the results you expect. Three activation methods are available in a variety of gauge sizes to provide solutions for all of your capillary sampling needs.
Choosing Unistik Safety Lancets ensures: Comfort for your patients
Supply Continuity
Sten Westgard
By Priya Sivaraman, PhD
Kurec, MS, MASCP, H(ASCP)DLM
Ankit Gupta, Mike Heydlauf, Nivedita Mitra, Artem Boltyenkov
Meghan W. Starolis, MS, PhD, HCLD(ABB)
Jimmy Lowery MBA, MLS(ASCP)SBBCM and Justin Cox, MBA, MLS
Results traceable to the WHO International Standard for result harmonization through standardization across laboratories and hospitals
Three tests from a single sample - critical transplant virus testing (CMV, EBV, BKV) from <1ml of a single plasma sample; one of the lowest processing volumes required in fully-automated systems 1, 2
Multiplex target design provides quantitative accuracy, reliable, and reproducible results for reassurance to aide in clinical decision making diagnostics.roche.com
cobas® CMV, cobas® EBV, and cobas® BKV on cobas® 5800/6800/8800 Systems
Happy new year
By Christina Wichmann
Editor in Chief
Ithink we have a great issue to start your new year off! Our Continuing Education article on page 6 was written by Sten Westgard, Director of Client Services and Technology at Westgard QC. He provides a summary of some of the CLIA proficiency testing (PT) changes that will be enforced on January 1, 2025, along with guidance on preventing PT failures using the analytical Sigma metric. The full CLIA final rule in the Federal Register can be viewed at: https://www. federalregister.gov/documents/2022/07/11/2022-14513/ clinical-laboratory-improvement-amendments-of1988-clia-proficiency-testing-regulations-related-to and the updated interpretive guidelines and survey procedures can be viewed here: https://www.cms.gov/ files/document/qso-25-10-clia.pdf.
There are many new analytes that will now be regulated and there are revised scoring criteria for currently regulated analytes. In our March and November 2025 issues, experts from the American Proficiency Institute will be answering your confidential questions in our “Dear API Abby” column. Questions for them can be sent to editor@mlo-online.com.
I love the article,“Tough-minded optimism: Strategies to thrive not just survive” on page 20. I think it’s a great read to start the new year off — especially if you’re a new year goal setter (like me). This article gives wonderful guidance on how to stay positive when things get rough and includes 12 characteristics of tough-minded optimists based on the book, The Power of Optimism by Alan Loy McGinnis. The second one really resonated with me: “Tough-minded optimists look for partial solutions…One of the greatest obstacles to success is perfectionism.”
MLO staff met the author of this article, Patty Eschliman, at the KnowledgeLab conference this past April. Patty was a lab manager and lab director for many years and is also a certified professional coach. She is president and CEO of Lab Leader Coach. Patty will be contributing to MLO throughout the year in a new “Coaching Corner” series in our April, September, and November issues where she will be answering your questions related to teamwork, leadership, personal growth, and more. Those questions can also be sent to editor@mlo-online.com.
Finally, new year goals often involve money. Saving more money, evaluating our spending, getting more money somehow. Anthony Kurec, Clinical Associate Professor at SUNY Upstate Medical University has provided you an article on page 16 titled,“Reimbursement for laboratory services: Are you leaving money on the table?”This educational article on laboratory billing provides information on CPT codes and ICD codes, along with guidance on resolving denials and errors. Anthony’s article will help lab managers minimize denials, improve cash flow, and reduce potential compliance issues.
And while you are in a goal-setting state of mind, do not forget to nominate your lab for MLO’s Lab of the Year Award. The winning labs are featured in the April 2025 issue, and this is always one of the most exciting issues of the year to see the wonderful work being done in your clinical labs. The submission requirements are at: https://www.mlo-online.com/55234457.
I welcome your comments and questions — please send them to me at cwichmann@mlo-online.com.
PUBLISHER Chris Driscoll cdriscoll@endeavorb2b.com
EDITOR IN CHIEF Christina Wichmann cwichmann@mlo-online.com
MANAGING EDITOR Erin Brady ebrady@endeavorb2b.com
PRODUCTION MANAGER Edward Bartlett
ART DIRECTOR Kermit Mulkins
AUDIENCE DEVELOPMENT/LIST RENTALS Laura Moulton | lmoulton@endeavorb2b.com
John Brunstein, PhD, Biochemistry (Molecular Virology) President & CSO PathoID, Inc., British Columbia, Canada
Lisa-Jean Clifford, COO & Chief Strategy Officer Gestalt, Spokane, WA
Barbara Strain, MA, SM(ASCP), CVAHP Principal, Barbara Strain Consulting LLC, Formerly Director, Value Management, University of Virginia Health System, Charlottesville, VA
Jeffrey D. Klausner, MD, MPH Professor of Preventive Medicine in the Division of Disease Prevention, Policy and Global Health, Department of Preventive Medicine at University of Southern California Keck School of Medicine. Donna Beasley, DLM(ASCP), Director, Huron Healthcare, Chicago, IL
Anthony Kurec, MS, H(ASCP)DLM, Clinical Associate Professor, Emeritus SUNY Upstate Medical University, Syracuse, NY
Medical Laboratory Observer USPS Permit 60930, ISSN 0580-7247 print, ISSN 2771-6759 online is published 10 times annually (Jan, Mar, Apr, May, Jul, Aug, Aug-CLR, Sep, Oct, Nov) by Endeavor Business Media, LLC. 201 N Main St 5th Floor, Fort Atkinson, WI 53538. Periodicals postage paid at Fort Atkinson, WI, and additional mailing offices. POSTMASTER: Send address changes to Medical Laboratory Observer, PO Box 3257, Northbrook, IL 60065-3257. SUBSCRIPTIONS: Publisher reserves the right to reject non-qualified subscriptions. Subscription prices: U.S. $160.00 per year; Canada/Mexico $193.75 per year; All other countries $276.25 per year. All subscriptions are payable in U.S. funds. Send subscription inquiries to Medical Laboratory Observer, PO Box 3257, Northbrook, IL 60065-3257. Customer service can be reached toll-free at 877-382-9187 or at MLO@ omeda.com for magazine subscription assistance or questions. Printed in the USA. Copyright 2025 Endeavor Business Media, LLC. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopies, recordings, or any information storage or retrieval system without permission from the publisher. Endeavor Business Media, LLC does not assume and
opinions by the authors of said articles.
Fast Facts
Cancer prevention and screening save lives
Improvements in cancer prevention and screening have averted more deaths from five cancer types combined over the past 45 years than treatment advances, according to a modeling study led by researchers at the National Institutes of Health (NIH). The individual contributions of prevention, screening, and treatment varied by cancer site:
1 million breast cancer deaths (out of 2.71 million that would have occurred in the absence of all interventions) were averted from 1975 to 2020, with treatment advances contributing to three-quarters of the deaths averted and mammography screening contributing to the rest.
Important
information about the CLIA proficiency testing final rule
The Centers for Medicare & Medicaid Services (CMS) updated their Proficiency Testing (PT) and PT Referral brochure on their CLIA Brochures website to assist laboratories in preparing for the new regulations. The brochure will help laboratories complete PT enrollment and place orders with their PT providers for 2025. This guidance will inform laboratories of the upcoming changes necessary for compliance prior to the January 1, 2025 implementation date.
The Clinical Laboratory Improvement Amendments of 1988 (CLIA) Proficiency Testing Regulations Related to Analytes and Acceptable Performance (CMS-3355-F) final rule became effective on July 11, 2024; however, it will not be implemented until January 1, 2025.
New report highlights need for sustained investment in infection prevention and control programs
A new global report on infection prevention and control (IPC) by the World Health Organization (WHO) shows there has been slow progress in addressing critical gaps to prevent healthcare-associated infections (HAIs).
98% of the 3.45 million lung cancer deaths averted (out of 9.2 million) were due to prevention through tobacco control efforts and treatment advances accounted for the rest.
160,000 cervical cancer deaths averted (out of 370,000) were entirely through cervical cancer screening (i.e., Pap and HPV, or human papillomavirus, testing) and removal of precancerous lesions.
The report finds that though 71% of countries now have an active IPC program, just 6% met all of the WHO IPC minimum requirements in 2023-2024. This is well behind the target of more than 90% by 2030 set in the WHO Global action plan and monitoring framework on IPC. The report also highlights that patients in low- and middle-income countries (LMICs) have up to 20 times higher risk of acquiring infections during healthcare delivery than in high-income countries (HICs).
The report found that healthcare facilities face significant financial and resource challenges, including a lack of IPC professionals and budgets, especially in LMICs. Nearly a quarter of countries reported shortages in their supply of personal protective equipment in 2023.
New data from WHO and the Organisation for Economic Cooperation and Development (OECD) estimates that up to 3.5 million patients could die each year from HAIs without urgent action. Improving IPC measures at every level will help to reduce the number of deaths. The modelling estimated that IPC interventions at the point of care in health facilities, coordinated by Ministries of Health or established networks, could avert up to 821,000 deaths per year by 2050. Such an intervention would also yield annual savings in healthcare expenditure as high as US$ 112 billion and generate economic gains of up to US$ 124 billion.
California confirms first clade I mpox case
The California Department of Public Health confirmed, through laboratory testing, the first known case of clade I mpox in the United States. The risk of clade I mpox to the public remains low, and there continue to be sporadic clade II mpox cases in the United States, according to the Centers for Disease Control and Prevention (CDC).
940,000 colorectal cancer deaths were averted (out of 3.45 million). 79% were due to screening and removal of precancerous polyps, with treatment advances accounting for the remaining 21%.
360,000 prostate cancer deaths were averted (out of 1.01 million). Screening via PSA testing contributed 56% and treatment advances contributed 44%.
The case was diagnosed in a person who recently traveled from Eastern Africa. The individual was treated shortly after returning to the United States at a local medical facility and released. Since then, the person has isolated at home, is not on treatment specific for mpox, and symptoms are improving. Based on their travel history and symptoms, patient specimens were tested and confirmed for the presence of clade I monkeypox virus. Casual contact, like you might have during travel, is unlikely to pose significant risks for transmission of mpox.
The anticipated overall risk of clade I mpox to the general population in the United States from the outbreak in Central and Eastern Africa is low. Earlier this year CDC conducted a risk assessment which included epidemiologic data from Central and Eastern Africa, data from the ongoing mpox outbreak in the United States caused by clade IIb, and historical data on clade I mpox outbreaks in DRC and other affected countries. In addition, CDC has simulated clade I mpox outbreaks. These simulations indicate that close-contact transmissions within and between households are unlikely to result in a large number of mpox clade I cases in the United States.
Have you heard about the (other) major regulatory change this year?
CLIA changed its proficiency testing criteria — and almost no one is talking about it
By Sten Westgard
If you got lost in last year’s labyrinth of laboratory-developed tests (LDTs), or caught up in the latest CLIA changes to personnel requirements, you can be forgiven if you missed the update to the CLIA proficiency testing criteria.1 In a quirk of timing, the new criteria became effective on July 11, 2024, but were not yet enforced. The actual teeth of the new rules didn’t bite until January 1, 2025, when the proficiency testing programs must implement the changes.
Why is CLIA changing PT criteria?
Proficiency (PT) testing criteria were established in 1992, as part of the implementation of the CLIA 1988 regulations. For the last 33 years, those PT criteria have stood unchanged, even as everything else in the laboratory rapidly evolved. As instruments improved, the 1992 PT goals became easier to hit, so much so that criticisms began to be voiced about their relevance. The ’92 goals were too broad, no longer reflective of modern instrumentation, and more importantly, no longer reflected modern use and interpretation of test results. CLIA PT began to seem less like a true test of laboratory performance and more like a rubber stamp. Belatedly, laboriously, CLIA updated the goals. The new goals are meant to reflect the method performance and clinical use of the 21 st century. It seems uncontroversial that instruments from this century should not be judged by the standards of the last century.
Even the implementation of these changes has rolled out in a kind of slow motion. After a proposed set of criteria were issued in 2019, the official changes were only announced on July 11, 2022 — with a full two years allocated for labs to prepare for the changes. By the time these criteria go into effect, it will have been almost two and a half years since they were announced.
Earning CEUs
See test online at https://ce.mlo-online.com/ courses/have-you-heard-aboutthe-other-major-regulatorychange-this-year/ Passing scores of 70 percent or higher are eligible for 1 contact hour of P.A.C.E. credit.
LEARNING OBJECTIVES
Scan code to go directly to the CE test.
Upon completion of this article, the reader will be able to:
1. List the reasons why CLIA is changing PT criteria.
2. Discuss the changes that may make a difference in PT results.
3. Describe the Sigma metric and its utility in PT success.
4. Discuss the reasons for PT failures in the newly applied CLIA rules.
Changes that will make no difference?
For many laboratories, proficiency testing has been pro-forma, a routine activity without risk of failure, a motion to go through to maintain compliance, but never something reflective of true performance or quality. For years, it’s been so easy to pass the surveys that laboratories have been assuming that, even with new changes, they are still guaranteed to pass. But look over the size of the changes that will go into effect on January 1st:
Why haven’t we heard more about this?
While CMS published all of these rule changes in the Federal Register, the proficiency testing providers haven’t aggressively publicized them. While alerts have been sent out, and notifications have been posted on various websites, no one has offered laboratories a detailed preview of the impact of these goals on their future survey results.
Overburdened, understaffed laboratories — the most common type of laboratory in the United States — have not had the bandwidth to contemplate their future failures or successes in proficiency testing. The LDT controversy and CLIA personnel changes have drowned out the PT notices.
Magnesium 25% 15% 40% reduction
Uric acid 17% 10% 41% reduction
Hemoglobin 7% 4% 42.8% reduction
C3 complement 3 SD 15% varies by method
T3 Uptake 3 SD 18% varies by method
Triiodothyronine 3 SD 30% varies by method
HbA1c NDR: 20% or 3 SD (API) 8% 60% reduction
CA 125 NDR: 3 SD (CAP) / 2 SD (API) 20% varies by method
Key abbreviations. CAP: College of American Pathologists. API: American Proficiency Institute.
A full list of these changes can be found in the Federal Register, 1 as well as an annotated version on Westgard Web.2
There are three main kinds of changes:
• Directly regulated tests where defined goals are being tightened. In the table, hematocrit, potassium, magnesium, uric acid, and hemoglobin are examples. For these, we can calculate how much smaller the new goals will be.
• Directly regulated tests without fully defined goals, now have newly defined goals. In the table, C3 complement, T3 uptake, and triiodothyronine are examples. It’s not possible to state how large the reduction is, because each method was previously judged by a method-specific group SD. For a method that has a large group SD, the reduction will be more significant than a method that has a small group SD.
• Previously unregulated methods now being directly regulated with defined goals. In the table, HbA1c, CA 125, and estradiol are examples. It’s even harder to determine the size of the reduction because not only were the previous goals method-specific, the previous goals were also PT-provider-specific. For unregulated methods, each PT provider was able to set their own goals. HbA1c is a curious example of the impact of CLIA 2024 requirements. The new CLIA requirement is 8%, and the old goal for API was 20%, while the goal for CAP, following the National Glycohemoglobin Standardization Program (NGSP) program, was a goal of 6%. In this one instance, CAP users may find it easier to pass proficiency testing if they adjust to the CLIA requirement.
Conventional wisdom is that these changes aren’t going to impact labs significantly. But if CMS reduces a goal by 60%, where is the concrete evidence that this won’t impact at least a few laboratories? Why change goals if they have no impact at all? Surely some labs are going to feel a new pain come January 1 st. The question is, will it be felt by your laboratory?
What predicts your PT future? The analytical Sigma metric
One simple technique to predict PT failure is to calculate the analytical Sigma metric of your method. This calculation has been around for over 20 years and doesn’t require any additional resource or study. You simply tap into the performance data you are already collecting — and many of the major control vendors have already built it into their QC or peer comparison software.
The Six Sigma approach has been around even longer. While it’s long past the peak of its popularity, when it was closer to a cult than a management technique (Remember black belts, master black belts, and champions?), the core utility from Six Sigma is still there. A universal scale of zero to six, where Six Sigma is the most desirable outcome.
There are three ingredients to the analytical Sigma metric:
• Your cumulative imprecision — something like intermediate reproducibility, basically a few months of your QC performance.
• Your bias — which you can obtain several ways. Using peer comparison software (the difference between your cumulative mean and the peer group cumulative mean) is a convenient way. But you could also use the very PT surveys that we’re concerned about — again finding the difference between your survey results and those of your peer group. If you’re lucky and well-funded, you might be able to benchmark your method in an accuracy-based survey, or test some reference materials, or compare against a reference method — these ways will give you a more traceable, “true” bias.
• The allowable total error (TEa). This is not something from your laboratory — it’s from CLIA. These are the requirements that just changed. These variables get arranged in this order: Analytical Sigma metric = [ TEa% - |bias%|] / CV% [You can also work this equation out in units instead of percentages, where the CV is replaced by the SD.] Think of it this way: CLIA gives you a target to hit (TEa), and your imprecision and bias determine whether or not you hit the bullseye or miss the target completely. If you achieve Six Sigma, you’ve hit the bullseye and achieved world class performance and there’s no danger of PT failure in your future. Five Sigma means excellent performance and also no worry of PT failure. Four Sigma is good performance, with PT failure
unlikely. Three Sigma is considered the minimum acceptable performance by theory, but if you achieve it, your PT failure worries are still very low. Because CLIA allows a 20% failure rate, the Sigma metric you worry about doesn’t emerge until 2.3 or lower. Sigma metrics of 2.3 and lower indicate higher likelihood of future PT failures.
Who will suffer most under the new CLIA PT rules? Since 2022, when the changes were announced, Westgard QC has analyzed real-world data from hundreds of instruments across the United States. What we’ve found confirms what every laboratory suspects: methods, instruments, and laboratories are not created equally.3 While it’s convenient for those at administrative and executive levels to pretend that all diagnostic manufacturers are the same, and analytical quality is simply a commodity (thereby justifying the selection of the cheapest box), those closer to the bench level know the ground truth: some instruments are better than others, some methods are more imprecise than others, and some laboratories are plagued by QC and PT failures more than others.
The pain of the tighter CLIA PT requirements will not be felt equally across laboratories. If you choose the wrong method or instrument, you’ll see an increase in PT failures in 2025. However, if you’ve selected a method or instrument with high Sigma quality, these new PT criteria may not even make you blink.
For poor-quality methods, the suffering (and PT failures) will stretch out over time. It will manifest as a slow-motion disaster, where in any given survey, the low Sigma method might be spared failure because the PT samples didn’t test the vulnerable part of the range, where one failure in PT is not automatically followed by another PT failure in the next survey, because the samples and levels tests change with each survey. Labs with poor instruments and methods have one management approach for PT: hoping for good luck.
For high-quality methods, there’s an extra bonus: knowing the analytical Sigma metric allows you to streamline your QC. Using Westgard Sigma Rules,4 a 2019 evolution of the
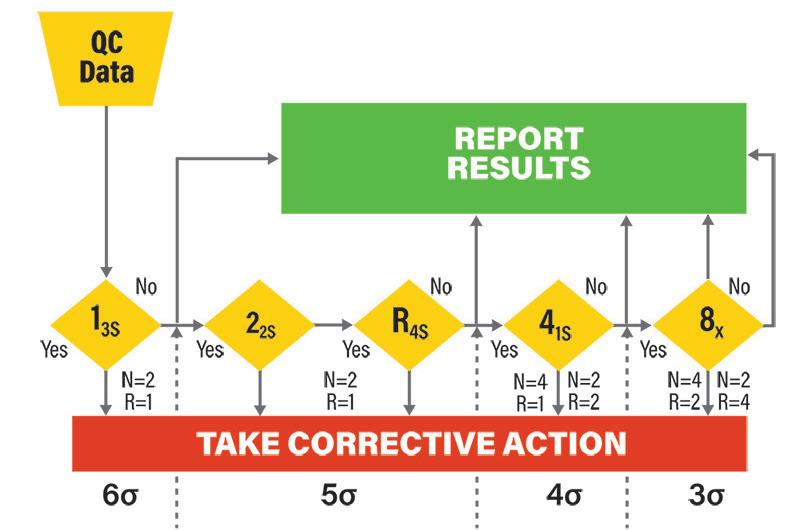
Figure 2. In this Westgard Sigma Rules flowchart, the traditional Westgard Rules are cut into sections by dashed vertical lines, each one designated at the bottom by a Sigma metric. For example, the 6 Sigma vertical line means that only the 1:3s rule is necessary for QC. As the Sigma metric declines, more Westgard Rules are needed, until 3 Sigma is reached. At that point the minimum acceptable quality (3 Sigma) requires the maximum Westgard Rules. Below 3 Sigma? The Westgard Rules can’t save you — you’ll need all of them and more — and those are also the assays that are vulnerable to future PT failure.
Westgard Rules introduced back in 1981, you can reduce the number of rules, levels, and even (if you’re in the mood for advanced strategies) frequency of QC, as your analytical Sigma metric increases (See Figure 2). If you find your assays are achieving Six Sigma, you can even stop using Westgard Rules altogether and rely on something as simple as a 1:3s control rule.
One last question: Are you ready? Or are you just hoping to be lucky?
All the tools to help you predict your PT failures are available free. Most of the proficiency testing providers allow you to review your old survey data and manipulate it to impose different performance specifications. But if you don’t enjoy resurrecting old data to run a simulation, you can use your current data to estimate the Sigma metric today.
Remember, any Sigma metric over 2.3 will be unlikely to face more failures in PT surveys. But while you breathe a sigh of relief over the surveys, remember that you can take advantage of higher Sigma metrics to reduce your overall QC effort.
This year’s PT constriction doesn’t have to become a crisis: it can also be the opportunity for your laboratory to bring its QC practices into the 21st century.
At Westgard QC, we’ve spent the last two years accumulating real-world data from hundreds of instruments across the diagnostic landscape. We have identified which instruments are going to be happy on January 1st and which ones are going to have a bad hangover. If you’re interested in participating in our national performance database (and seeing how your results compare to the national spectrum), don’t hesitate to reach out to benchmarking@ westgard.com.
Scan code to go directly to the CE test.
References
1. Centers for Medicare & Medicaid Services. Clinical Laboratory Improvement Amendments of 1988 (CLIA) proficiency testing regulations related to analytes and acceptable performance. Federal Register. Published July 11, 2022. Accessed November 6, 2024. https:// www.federalregister.gov/d/2022-14513.
2. Westgard S. 2024 CLIA Acceptance Limits for Proficiency Testing - Westgard. Westgard.com. Accessed November 6, 2024. https://westgard.com/clia-a-quality/quality-requirements/2024-clia-requirements. html.
3. Westgard S. Beckman Coulter DxI 9000 immunoassay analyzer assay performance meets new CLIA 2024 PT goals with highest proportion of Six Sigma performance amongst manufacturers. Presented at: ADLM 2024. https://www.researchgate.net/publication/383058141_ Beckman_Coulter_DxI_9000_immunoassay_analyzer_assay_performance_meets_new_CLIA_2024_PT_goals_with_highest_proportion_of_Six_Sigma_performance_amongst_manufacturers.
4. Westgard JO, Westgard SA. Establishing Evidence-Based Statistical Quality Control Practices. Am J Clin Pathol. 2019;1;151(4):364-370. doi:10.1093/ajcp/aqy158.
Sten Westgard is Director of Client Services and Technology for Westgard QC . Sten has presented at conferences and workshops worldwide on topics such as the “Westgard Rules,” IQCP, Six Sigma, method validation, and quality management, and received an Outstanding Speaker award from the AACC for 2008 through 2012, and 2016. Sten is an adjunct faculty member at the Mayo Clinic School of Health Sciences in Rochester, Minnesota; an adjunct faculty member at the University of Alexandria, Egypt; an adjunct visiting faculty member at Kastruba Medical College of Manipal University, Mangalore, India; and an honorary visiting professor at Jiao Tong University, Shanghai.
Importance of awareness of elevated fetal hemoglobin (HbF) in HbA1c testing
By Priya Sivaraman, PhD
Elevated fetal hemoglobin (HbF) in adults, though welldocumented, remains a point of interest in clinical diagnostics, particularly in HbA1c testing. HbF is a type of hemoglobin made of two alpha and two gamma subunits, in contrast to adult hemoglobin (HbA), which consists of two alpha and two beta subunits. Typically present in fetuses and newborns, HbF production usually decreases by six months of age. However, several conditions lead to elevated HbF levels in adults, potentially affecting the accuracy of A1c test results, a key tool for monitoring diabetes.1 The illustration in Figure 1 (on page 12) describes the process. 2
Some conditions and situations associated with elevated HbF in adults
• Sickle cell disease (SCD): Sickle cell disease, a genetic disorder affecting hemoglobin, causes red blood cells to become rigid and sickle-shaped, obstructing blood flow. This condition is prevalent in African and African American populations, with 1 in 365 African American babies born with sickle cell disease. HbF, which typically accounts for less than 1% of total hemoglobin in adults, is elevated in individuals with SCD, ranging from 5% to 8%. Higher HbF levels in these patients may provide some protection against the severe effects of sickle cell anemia by reducing red cell sickling. 3
• β -thalassemia: β -thalassemia is an inherited blood disorder caused by mutations in genes responsible for hemoglobin production. There are two main types: β -thalassemia major, characterized by severe anemia requiring regular blood transfusions, and β - thalassemia minor, which leads to mild anemia. In some forms of β -thalassemia, such as HbE/ β -thalassemia, HbF levels are elevated, potentially providing a survival advantage by increasing the number of red blood cells with HbF (F cells). This elevation is driven by increased erythropoietin production, a hormone that promotes red blood cell production.4,5
• Hereditary persistence of fetal hemoglobin (HPFH): HPFH is a benign condition characterized by the continued production of significant levels of HbF into adulthood. This occurs due to mutations in genes that regulate hemoglobin production, allowing HbF levels to remain elevated even after birth. 6
• Malignancies: Elevated HbF levels can also be seen in individuals with certain malignancies and among specific ethnic groups. For example, some populations of Mediterranean, Southeast Asian, or African descent may naturally have higher HbF levels.7
• Therapeutic factors: HbF is being explored as a potential treatment option in certain conditions. Recent research
Improved Workflow. Better A1c Results.
Fully automated A1c testing, simply load racks and walkaway, reduce your hands on labor time
A1c by Sebia provides high-resolution separation so detecting interfering hemoglobin variants is effortless
Uncompromised results, free from analytical and clinical interferences, providing confidence in your testing
Multi-Assay analyzer capable of running A1c, Hb, and Myeloma testing on a single instrument
has identified a protein, hypoxia-inducible factor 1α (HIF1α), that activates the production of fetal hemoglobin (HbF) in adult blood cells. Additionally, CRISPR-Cas9 gene editing can be used to increase HbF levels in patients with β-thalassemia and correct the primary gene mutations causing the condition. Methods to enhance the transcription of the gamma-globin (HBG) gene are being explored, allowing patients with β-hemoglobinopathies to produce more HbF. HbF is also being investigated as a potential treatment for severe inherited blood disorders like sickle cell disease and β-thalassemia. 8,9,10
Does elevated HbF affect HbA1c results?
Whether it is a condition that may or may not cause health problems or a therapy approach considered in treating a condition, it is important to be aware that the presence of elevated HbF in individuals can impact the accuracy of HbA1c test results. Since HbA1c testing measures glycated hemoglobin to estimate average blood glucose levels, elevated HbF may lead to either falsely high or falsely low HbA1c values, depending on the testing method used.11
This raises challenges for laboratories, as not all HbA1c testing methods can detect or account for elevated HbF and hence show HbF interference. Methods for HbA1c testing include cation-exchange HPLC, boronate affinity, capillary electrophoresis, immunoassays, and enzymatic methods. Boronate affinity, immunoassay, and enzymatic methods have been reported to exhibit lower tolerance to elevated HbF levels compared to ion-exchange HPLC and capillary electrophoresis. Boronate affinity and immunoassay methods leverage structural differences in hemoglobin molecules.12
Boronate affinity methods measure total glycated Hb and results are reported as a corrected HbA1c equivalent. HbF has gamma chains, for which the terminus is a glycine residue, in place of β-chains where the valine terminal residues can be glycated to form HbA1c. Thus, for boronate affinity methods, since HbF is glycated to a lesser extent, the glycated fraction will be lower than for people without elevated HbF. The interference of HbF with HbA1c results is likely due to a lower glycation rate for HbF compared with HbA. Because boronate affinity measures the ratio of glycated to non-glycated hemoglobin regardless of species, the presence of elevated HbF causes a false lowering of the HbA1c result. With boronate affinity methods, HbF at levels of 10–15% interfere with HbA1c results. Even though the user is able to detect the glycated and the non-glycated peak in the form of a chromatogram, the method lacks the ability to detect or presumptively
identify HbF, making it impossible to know if the HbA1c results needs a second opinion and/or verification.13,14,15
Immunoassays for HbA1c measurement also leverage structural differences between hemoglobin molecules. The system measures both A1c and total hemoglobin (THb), using antibodies that specifically bind to the HbA1c epitope, which includes the glycated N-terminal valine and the next three amino acids of the β-chain. The system detects the antigen–antibody complex; and the HbA1c percentage is calculated as the ratio of measured glycated HbA to THb. In patients with elevated HbF, lack of glycation at the terminus of the gamma chain of HbF results in less antibody binding, while the total hemoglobin measurement includes HbF as well as HbA, leading to a lower HbA1c result.14 This limitation is acknowledged in the instructions for use of immunoassay systems. With immunoassays, HbF as low as 10–15% can interfere with HbA1c results.16
Primitive Erythropoiesis
Definitive Erythropoiesis
of gestation, embryonic globin (ε) is silenced and fetal globin (γ) starts to be expressed. Perinatally the switch to adult globin (β) occurs. (B) Erythropoiesis occurs in the blood islands of the yolk sac in the first 8 weeks of gestation, then in the fetal liver between 8 and 32 weeks, and finally in the bone marrow from 32 weeks on. (C) Structure of the main human hemoglobins expressed during development. Embryonic globin, fetal hemoglobin and adult hemoglobin.
Yolk Sac
Figure 1. (A) Around week 6
“Just want to get my instrument results to my EMR”
“ We need a full-function lab system that is Quick to install and easy to learn”
Designed specifically for labs that simply want to “send results to their EMR/EHR without breaking the bank”, xEmr Plus is ideal for small office practices, waived labs, oncology practices, and hospitals with bedside testing.
Full-function Laboratory Information System designed for the most demanding moderately and highly complex laboratories providing the most complete Laboratory Information System a il bl t d . A cloud-based, full function Laboratory Information System suitable for moderately and highly complex laboratories.
“We need a ‘Cloud-based’ LIS l ti ”
“How can I provide my nursing homes and physician clients Web-Access to place their orders and see their results”
“In my state, consumers are allowed to order testing from my lab without a physician. I see a great revenue opportunity!”
Internet Outreach providing full web-based Order Entry and In-box for your physicians, nursing homes, or, for that matter, any type of client you may have. When it’s time to grow your business, Web Portal is your solution.
Hosted at a HIPAA-compliant Datacenter, Consumer Portal is a public facing, customizable website for your lab. It provides consumers the ability to order testing, schedule collections, pay for their testing, and see their results. An excellent opportunity for increasing revenue and improving cash flow!
Some immunoassay manufacturers notify users that their method interferes with HbA1c results at levels as low as 7% HbF, leading to inaccurately lower reported HbA1c values.17
Enzymatic methods measure HbA1c and total hemoglobin (THb) from whole blood specimen. Some methods specifically measure N-terminal fructosyl dipeptides of the β -chain of HbA1c cleaved by a fructosyl peptide oxidase. The HbA1c concentration is calculated from the ratio of HbA1c and THb: HbA1c. These methods like immunoassays provide the laboratorian with just a HbA1c number with no detection of HbF or other variant hemoglobins. Just as in immunoassays, enzymatic assays also show interference with HbA1c results at HbF concentration of 10–15%.16
Cation exchange HPLC for HbA1c testing separates hemoglobin molecules based on charge. The method employs a column with negatively charged stationary phases that interact with the positively charged amino groups of hemoglobins. As the sample passes through the column, hemoglobin fractions are separated based on their charge differences. HbA1c elutes at a specific retention time and is detected via absorbance, typically at 415 nm. An HPLC chromatogram is a graphical representation of the separation of compounds as they pass through the HPLC system. Each peak on the chromatogram corresponds to a different fraction in the sample.12 In the context of HbA1c testing, the chromatogram shows distinct peaks for various hemoglobin fractions including HbF.
A laboratory within the Texas hospital system uses a cation exchange HPLC analyzer for HbA1c testing in their laboratory. They see a fair amount of adult patient whole blood samples that are presumptively identified as HbF on their HPLC analyzer. The analyzer claims no interference with HbA1c results from HbF at levels up to 25% (Figure 2). At levels beyond 25%, the analyzer will provide a presumptive identification of the HbF, however, it will not provide an HbA1c result (Figure 3). The advantage of an ion exchange HPLC analyzer is the ability to detect a peak in the HbF window highlighted on the chromatogram.
Summary
As the incidence of elevated HbF in testing samples rises, laboratories need to remain vigilant and assess the potential impact on HbA1c measurements. Accurate diagnostics ensure appropriate diabetes management and reduce the risk of misdiagnosis or inadequate treatment.
References
1. Linch D. Encyclopedia of Immunology (Second Edition): Bone Marrow and Hematopoiesis. Published online 1998:374-377.
2. Cantú I, Philipsen S. Flicking the switch: adult hemoglobin expression in erythroid cells derived from cord blood and human induced pluripotent stem cells. Haematologica. 2014;99(11):1647-9. doi:10.3324/ haematol.2014.116483.
3. Akinsheye I, Alsultan A, Solovieff N, et al. Fetal hemoglobin in sickle cell anemia. Blood. 2011;118(1):19-27. doi:10.1182/blood-2011-03-325258.
4. Rees DC, Porter JB, Clegg JB, Weatherall DJ. Why are hemoglobin F levels increased in HbE/beta thalassemia? Blood 1999;94(9):3199-204.
5. Rochette J, Craig JE, Thein SL. Fetal hemoglobin levels in adults. Blood Rev. 1994;8(4):213-24. doi:10.101 6/0268-960x(94)90109-0.
6. Sharma DC, Singhal S, Woike P, et al. Hereditary persistence of fetal hemoglobin. Asian J Transfus Sci 2020;14(2):185-186. doi:10.4103/ajts. AJTS_71_16.
7. Wolk M, Martin JE, Reinus C. Development of fetal haemoglobin-blood cells (F cells) within colorectal tumour tissues. J Clin Pathol. 2006;59(6):598-602. doi:10.1136/ jcp.2005.029934.
8. Feng R, Mayuranathan T, Huang P, et al. Activation of γ-globin expression by hypoxia-inducible factor 1α Nature 2022;610(7933):783-790. doi:10.1038/ s41586-022-05312-w.
9. Finotti A, Gambari R. Combined approaches for increasing fetal hemoglobin (HbF) and de novo production of adult hemoglobin (HbA) in erythroid cells from β-thalassemia patients: treatment with HbF inducers and CRISPR-Cas9 based genome editing. Front Genome Ed. 2023;5:1204536. doi:10.3389/ fgeed.2023.1204536.
10. Demirci S, Leonard A, Tisdale JF. Genome editing strategies for fetal hemoglobin induction in beta-hemoglobinopathies. Hum Mol Genet. 2020;29(R1):R100-R106. doi:10.1093/hmg/ddaa088.
11. Chen Z, Shao L, Jiang M, et al. Interpretation of HbA1c lies at the intersection of analytical methodology, clinical biochemistry and hematology (Review). Exp Ther Med 2022;24(6):707. doi:10.3892/etm.2022.11643.
12. Sivaraman P. Choosing a test method to measure HbA1c. Medical Laboratory Observer. June 26, 2020. Accessed November 20, 2024. https://www.mlo-online. com/disease/diabetes/article/21142641/ choosing-a-test-method-to-measure-hba1c.
13. Rhea JM, Molinaro R. Pathology consultation on HbA(1c) methods and interferences. Am J Clin Pathol. 2014;141(1):5-16. doi:10.1309/AJCPQ23GTTMLAEVL.
14. Little RR, Rohlfing CL. The long and winding road to optimal HbA1c measurement. Clin Chim Acta. 2013;418:63-71. doi:10.1016/j. cca.2012.12.026.
15. Little RR, Roberts WL. A review of variant hemoglobins interfering with hemoglobin A1c measurement. J Diabetes Sci Technol. 2009;3(3):446-51. doi:10.1177/193229680900300307.
17. 510(k) substantial equivalence determination decision summary assay only template. FDA. Accessed November 21, 2024. https://www.accessdata.fda.gov/ cdrh_docs/reviews/K121610.pdf.
Priya Sivaraman, PhD is a Senior Product Manager at Tosoh Bioscience Inc based in Grove City, Ohio. She specializes in HbA1c testing. With more than 15 years of experience in the diagnostic industry, she supports a broad profile of A1c clients in the hospital and laboratory setting.
Haptoglobin
Insulin
Krebs
Lipoprotein(a)
Microalbumin
Prealbumin
Transferrin
Reimbursement for laboratory services
Are you leaving money on the table?
By Anthony Kurec, MS, MASCP, H(ASCP)DLM
The traditional view of the total testing process (TTP) consists of pre-analytic, analytic, and post-analytic phases. However, one must also consider a post-post-analytic phase — the process needed to get paid. Understanding the reimbursement process can mean whether a laboratory is profitable or a money loser. Medical billing is complex with many opportunities for denials and rejections. In the United States, 15%-17% of medical private payor claims are initially denied.1,2 It has been reported that up to 80% of medical bills contain errors amounting to $68 billion annually. There are many sources for errors including chronic staffing shortages, from clinician burnout to support staff shortages, all contributing to payment denials. 3,4 Laboratory managers must understand billing practices, for failure to do so can significantly impact a laboratory’s revenue stream.
What laboratory managers need to know
The players
There are over 1,100 third-party health insurance payors in the United States, all with different reimbursement plans and requirements. Knowing who the third-party payors are (payor mix) sets the playing field for understanding the
rules in how charges are submitted and reimbursed. Table 1 lists the payor mix.
CPT and ICD codes®
Every laboratory has a chargemaster — a list of all laboratory tests by CPT code (Current Procedural Terminology) that is updated annually. In addition, ICD-10 codes (International Classification of
Diseases, 10th revision) are also used to identify specific medical diagnoses/ procedures. ICD-10 codes are currently used in the United States, however, ICD-11 codes were approved and released in 2022 by the WHO and adopted by more than sixty countries. The United States’ transition to ICD-11 will occur between 2025 and 2027.
Denials
and what to do with them?
Up to 65% of medical billing claims are not reworked resulting in a 20% to 30% loss in revenue.5 The laboratory is a high-volume service with many more CPT codes than other healthcare services thus greater opportunities for errors can occur. Further, reworking denied payments for services such as MRIs, surgeries, etc. often takes priority over less expensive laboratory tests.2 Figure 1 lists some common denials with some main ones discussed below.
CPT issues
The following are a few procedural errors that may occur in up to 45% of charges due to the misuse or omission of a CPT code. Note: Attempting to enhance reimbursements by manipulating CPT codes is a compliance issue.6
• Modifiers are codes appended to CPT codes indicating additional information about a service is available. Table 2a lists some common modifiers used for laboratory services. Improper use of modifiers may account for 8% of billing errors.
• Duplicate billing occurs when the same test/service is billed twice. If a repeat test is medically necessary, a modifier is required. (13% of errors)
• Unbundling is when the components of a panel are billed separately. Table 2b is an example of unbundling an electrolyte panel that incorrectly enhances reimbursements. (10% of billing errors)
• Upcoding occurs when a more complex and expensive CPT code is used when a less complex and cheaper test was actually performed (15% of billing errors). Table 2c illustrates how a qualitative test was performed but charged as a quantitative test getting a higher reimbursement.
ICD coding issues
ICD coding requires communication between the healthcare provider and the laboratory. A submitted ICD code must medically support why a specific test was ordered, i.e., medical necessity. Up to 60% of medical bills may be in error due to improper diagnosis codes (ICD codes).
Modifier Definition
• Non-FDA-approved tests, experimental tests, and screening tests are generally not covered and will be denied unless an Advanced Beneficiary Notice (ABN) is obtained. Example: modified or noncommercially available kits used to test for glucose or protein tests on body fluids.
25 Significant, separately identifiable evaluation and management service by the same physician or other healthcare professional on the same day of the procedure or other service
26 Used to bill the professional component of service provided, i.e., pathology diagnosis of a biopsy
50 Used to report a bilateral procedure during the same operative session, by the same provider in two anatomically different areas
59 Identifies distinct procedural services. These services are different such as an allergen testing regimen performed on the same day.
77 Repeat procedure by another provider on the same day such as a biopsy read by a surgical pathologist and a cell block by a cytopathologist
90 Specimen sent to outside laboratory (reference laboratory) for evaluation
Repeat laboratory test on the same day to check on any changes; does not include confirming test results TC Reflects the technical component performed by a non-physician; i.e., preparation of histology slides to be read by a pathologist GT or 95 Codes for all diagnoses, evaluations, or treatments via telemedicine when used via an interactive audio and video telecommunication system.
Table 2c. Example of
• Laboratory tests that are not explicitly covered by a third-party payor will require a pre-authorization. Many molecular and genetic tests fall into this category.7
• National Correct Coding Initiative (NCCI) edits were developed by Medicare to promote appropriate coding methodologies and minimize improper billing submissions. Though mainly used by Medicare, many insurance companies use similar edits. The following are some key components.
• NCDs (National Coverage Determinations): There are twenty-three policies covering some common tests, listing the CPT code(s) and the acceptable ICD codes. The claim will be denied if the ICD code is not on the list. Table 3a shows an example of a patient with acute myocardial infarction (ICD10= I21.9) who had two tests performed: PTT and Digoxin.
• PTP (Procedure to Procedure Edits) identifies certain tests (CPT) that cannot be billed at the same patient encounter. Table 3b shows two panels that cannot be ordered/performed at the same patient encounter. Generally, the least expensive of the two will be reimbursed.
• MUE (Mutually Unlikely Edits) identifies the maximum number of times a specific test can be ordered during the same date of service. Table 3c shows a few examples.
• LCDs (Local Coverage Determinations) supplement NCDs in covering medically necessary items or services that are managed locally and vary from location to location. Similar to MUEs, some LCD policies may further define the frequency of testing, e.g., lipids, thyroid testing, glucose testing, or glycated hemoglobin.
• Laboratories using outdated or deleted ICD codes will result in a denial. Of note, ICD-11 contains four times more codes than ICD10, thus opening up opportunities for miscoding.
Other sources of error
• Typographic errors or omissions account for 27% of denials. 5 Examples include misspelled names, common surnames (Smith, Jones, etc.), and generational designations (II, III, Jr., Sr.) that can be easily confused. Wrong birthdates, dates of service, or insurance numbers are also major sources of errors. Failure to notify a change of address or last name (due to marital status) will also lead to a denial.
• Change in employment often means a change in healthcare plans, thus a patient needs to ensure that they submit the correct insurance to their provider. Patients seeking healthcare services from a non-participating provider (out-of-network provider) will receive a denial of payment.1
• Timely filing is dictated by an insurance company specifying the period within which a claim must be received, and if not, will be denied (6% of errors). Timely filing cutoffs vary by payor ranging from 90 days to a year. Denied charges that are not promptly worked and resubmitted can miss the deadline especially when payors are slow to respond (up to 60 days) with a denial. 8
• Place of Service (POS) — these two-digit codes are required on the claim forms to indicate where the patient was at the time of service, i.e., hospitals, clinics, emergency facilities, hospices, etc. (4% of errors). If a patient is transferred from a nursing facility (POS 31) to a hospital (POS 21) and the POS was not changed, all hospital services will be denied. 6
Appeals
Denials interrupt laboratory cash flow and if not followed up promptly can be a significant loss of revenue. It has been reported that up to 60% of returned claims were not corrected and resubmitted, yet two-thirds of these denials are appealable. Denials take time to review and investigate as to why they were denied/rejected. The average cost to initially file a claim correctly is less
Table 3a. Example of patient with acute myocardial infarction (ICD10=I21.9).
Table 3b. Example of upcoding.
Table 3c. Examples of laboratory MUEs
than $7, while the cost to review and fix a denial ranges from $25 to over $100. Submitting a clean claim is the goal.5,9 Often, charges for a denied claim are passed on to the patient with almost 44% having problems paying their medical bills; 64% of these specifically had problems paying for laboratory services.10
Conclusion
Laboratory managers must educate themselves about laboratory billing and take the lead in resolving and fixing denial problems. Failure to do so leads to loss of revenue and potential compliance concerns. CPT codes are updated annually and ICD codes in April and October of each year. Purchasing CPT and ICD manuals can help laboratory managers identify coding changes. Errors in Medicare/Medicaid billing, whether accidental or intentional, can result in an audit, the consequences of which can include repayment, penalties, criminal charges, and exclusion from all federally funded programs. Government-based insurance can account for as much as 50% of a laboratory’s revenue. Understanding Medicare/Medicaid rules is critical since they serve as a model for commercial payors. Knowing the payor mix and reimbursement rates allows a manager to focus on the best and highest payors and can play an important part in developing an annual budget. Looking at the reimbursement rates for the top 25 high-volume tests by payor is a good start in ensuring correct billing practices. Review the chargemaster for current CPT codes. Any recent price increases in reagents, equipment, controls, salaries, or overhead should be reflected in assessing charges by performing a test cost analysis (TCA) if needed, especially for the more complex, time-consuming, or expensive tests such as genetic, molecular, and mass spectrometry assays.11
Contacting the laboratory’s billing agent to find out denial claim statistics and routinely reviewing them can help identify trends or other systemic problems, whether it’s a personnel problem or software issue. Proactively train and educate personnel in billing procedures. A bi-directional relationship with the billing department can educate billers about unique differences in laboratory procedures and conversely, educate laboratorians about billing rules and regulations. Also developing a relationship with office personnel from high-volume clinics/providers can be useful in obtaining diagnosis and pre-authorization information. Ensuring
Common Denial Codes
CO4: Missing modifier
CO11: Coding error
CO15: Missing or invalid authorization number
CO18: Duplicate claim
CO22: Bill sent to secondary insurance instead of the primary
CO27: Charges after insurance expired
CO29: Past the time limit for filing
the phlebotomy staff collects the right/ correct information at the time of service can eliminate potential errors. Finally, commercial insurance companies have used rule-based artificial intelligence (AI) algorithms and machine learning to sort claims and initiate denials. It has been noted that some algorithms fail to evaluate claims accurately, thus improperly initiating denials. Some laboratories have integrated AI with their laboratory information system (LIS), which can manage various functions including time-consuming repetitive tasks, processing of claims, and flagging errors before they are released. AI uses past denial experiences to predict future denial issues. However, even with the aid of AI, it is still necessary to perform regular internal audits to ensure billing practices are accurate and legal, thus minimizing denials, improving cash flow, and reducing potential compliance issues.3,8,12
REFERENCES
1. Pollitz K, Lo J, Wallace R, Mengistu S. Claims denials and appeals in ACA Marketplace plans in 2021. KFF. February 9, 2023. Accessed November 20, 2024. https:// www.kff.org/private-insurance/issue-brief/ claims-denials-and-appeals-in-acamarketplace-plans/.
2. Trend alert: Private payers retain profits by refusing or delaying legitimate medical claims. Premier. March 21, 2024. Accessed November 20, 2024. https://premierinc.com/ newsroom/blog/trend-alert-private-payersretain-profits-by-refusing-or-delayinglegitimate-medical-claims.
3. Leveraging AI and automation to minimize claim denials in healthcare. Experian Health. Published August 1, 2024. Accessed November 20, 2024. https://www.experian.com/ blogs/healthcare/prevent-claim-denials-withai-and-automation/#.
4. Moneypenny M. Over 20 woeful medical billing error statistics — etactics. Etactics | Revenue Cycle Software. October 20, 2020. Accessed November 20, 2024. https://etactics.com/blog/medical-billing-error-statistics.
5. Reduce denials and increase your lab’s revenue and net collections. Ligolab. September 23, 2024. Accessed November 20, 2024. https://www.ligolab.com/post/ reduce-denials-and-increase-your-labsrevenue-and-net-collections.
CO55: Considered experimental/ investigational
CO96: Non-covered charge(s)
CO97: Submitted multiple claims for bundled services
CO151: Information submitted does not support the number of services
CO167: Diagnosis is not covered
6. Lindner J. Study reveals shocking medical billing errors statistics impacting Americans. Gitnux. July 17, 2024. Accessed November 20, 2024. https://gitnux.org/ medical-billing-errors-statistics/.
7. Bonislawski A. Prior authorization a growing headache for labs as payors clamp down on molecular, genetic testing. 360Dx. May 16, 2024. Accessed November 20, 2024. https:// www.360dx.com/clinical-lab-management/ prior-authorization-growing-headachelabs-payors-clamp-down-molecular.
8. Williams J. Battle of the Bots: As payers use AI to drive denials higher, providers fight back. HFMA. March 28, 2024. Accessed November 20, 2024. https://www.hfma. org/revenue-cycle/denials-management/ health-systems-start-to-fight-back-against-aipowered-robots-driving-denial-rates-higher/.
9. Poland L, Harihara S. Claims denials: A step-by-step approach to resolution. J AMIHA. April 25, 2022. Accessed November 20, 2024. https://journal.ahima.org/page/ claims-denials-a-step-by-step-approach-toresolution.
10. Hamel L, Norton M, Pollitz K, Levitt L, Claxton G, Brodie M. The burden of medical debt: Results from the Kaiser Family Foundation/New York times medical bills survey. KFF. January 5, 2016. Accessed November 20, 2024. https://www.kff.org/health-costs/ report/the-burden-of-medical-debt-resultsfrom-the-kaiser-family-foundationnew-yorktimes-medical-bills-survey/view/ print/.
11. WHO Laboratory test costing tool. (World Health Organization; 2019). Published 2019. Accessed November 20, 2024. https://iris. who.int/bitstream/handle/10665/346135/ WHO-EURO-2019-3484-43243-60604-eng. pdf?sequence=3.
12. Mello MM, Rose S. Denial—artificial intelligence tools and health insurance coverage decisions. JAMA Health Forum. 2024;5(3):e240622. doi:10.1001/ jamahealthforum.2024.0622.
13. Emerson J. Payer mix in the nation’s largest for-profit health systems. August 9, 2023. Accessed November 20, 2024. https://www. beckershospitalreview.com/hospital-finance/ payer-mix-in-the-nations-largest-for-profithealth-systems.html.
14. Novitas. Modifiers. Novitas Solutions. Updated April 17, 2023. Accessed November 20, 2024. https://www.novitas-solutions. com/webcenter/portal/MedicareJH/ pagebyid?contentId=00003604.
Anthony Kurec, MS, MASCP, H(ASCP)DLM is Clinical Associate Professor, Emeritus, at SUNY Upstate Medical University in Syracuse, NY. He is also a member of the MLO Editorial Advisory Board.
Tough-minded optimism Strategies to thrive, not just survive
By Patty J. Eschliman, MHA, MLS(ASCP), DLM, CPC
Dale Carnegie, writer and author of such famous books as How to Win Friends and Influence People, said, “One of the most tragic things I know about human nature is that all of us tend to put off living. We are all dreaming for some magical rose garden over the horizon instead of the roses that are blooming outside our windows today.”1 This hesitation to live life, the inability to see the value in what we have, and the frustration of not having what we want seems to be pervasive in today’s world. As a professional coach, many reach out to me with feelings of despair, confusion, and pessimism. These are very powerful feelings that can make any of us put off living, lose hope, and wish for more rose gardens. In these challenging times, no one wants to hear a Pollyanna hear-no-evil, see-no-evil comeback such as “Oh you’re just having a bad day, tomorrow will be better!” Instead, we are searching for understanding. We need a more practical approach to rise us out of our darkness. We need realism — to see things as they are and yet find a path forward. We long to feel optimistic but it feels like a bridge too far.
Tough-Minded Optimism is a way of thinking presented in the book The Power of Optimism written by Alan Loy McGinnis, 1990.2 Although written 34 years ago and long out of print, McGinnis’s book provides an evergreen approach to addressing and tackling problems head-on. As a respected psychologist and researcher, McGinnis studied the intellectual habits of people who faced significant setbacks but still became extremely successful. He summarized his findings into 12 characteristics that can easily become habits embedded into our lives today.
Tough-minded optimists are seldom surprised by trouble.
The world is full of problems. Do you think of yourself as a problem solver? Think back to any setback in your life. While at the time, you may have thought it impossible to succeed, did life go on? Did you find another way? Of course you did because you were forced to look at other options. Our biggest breakthroughs often come after our biggest breakdowns. Paul Romer, Nobel Laureate Economist said, “A crisis is a terrible thing to waste.”3 A mistake is only a mistake if we do not learn from it. Anticipate problems and try to find the lesson when bad things happen.
Tough-minded optimists look for partial solutions. It is easy to feel overwhelmed by a challenge. One of the greatest obstacles to success is perfectionism. Brené Brown, in her book The Gifts of Imperfection, describes perfectionism as a defense mechanism that people use, thinking that if they look perfect or if everything they do or say is perfect, they can avoid or minimize the pain of shame, judgement, or blame. But there is no such thing as perfect. Studies show the drive to be perfect actually impedes achievement and is correlated with depression, anxiety, addiction, and life paralysis.4 Don’t let perfect get in the way of good enough.
Tough-minded optimists believe they have control over their future.
When Albert Einstein was a boy, he received this comment from his teacher,“Albert is a very poor student. He is mentally slow, unsociable, and is always daydreaming. He is spoiling
it for the rest of the class. It would be in the best interests of all if he were removed from school at once.”5 Think of all the scientific discoveries that would not have happened if Einstein let that discourage him. Instead, he continued his passion and believed in himself.You cannot control what happens to you, but you can control how you react to it.
Tough-minded optimists allow for regular renewal. Author Anne Lamott said, “Almost everything will work again if you unplug it for a few minutes, including you.”6 Keeping your energy high and understanding what you need for regular renewal is essential to building and sustaining resiliency in today’s challenging world. Whether you enjoy socializing with friends, spending time with children, eating healthy food, or taking a nap, find out what fills your bucket and make the time to mindfully enjoy it.
Tough-minded optimists interrupt their negative trains of thought. This can be very challenging. Do you have an unconscious train of negative thoughts taking over your brain? We are certainly our own worst critic, but the continuous put-downs do nothing to increase confidence or success. One tip for improvement is to pay attention to the words you use. Do you unintentionally catastrophize things by using words like “always” and “never”? Do you tend to jump to worst case scenarios? Mark Twain said, “I’ve had a lot of worries in my life, most of which never came true.”7 Don’t let the past or future rob you of your peace today.
Tough-minded optimists heighten their powers of appreciation. There is always something to be thankful for. Increase your awareness of the beauty around you. The rain, the sunshine, a blooming flower, the food on your plate, the support of a friend or loved one, a kind gesture. In the words of Oprah Winfrey,“Gratitude can transform any situation. It alters your vibration, moving you from negative energy to positive. It’s the quickest, easiest, most powerful way to effect change in your life, this I know for sure.”8
Tough-minded optimists use their imaginations to rehearse success.
Professional athletes use visualization and imagery to create an increase in mental awareness, which boosts
confidence and overall well-being. Repeatedly, this has shown to provide a competitive advantage in performance.9 If you want to pitch a new idea to your supervisor, or need to have a difficult conversation with someone, visualize it going well, see the look on their faces, and feel your confidence rise as they listen intently. From there, it also becomes easier to develop strategies to turn the conversation around if it is not going well.
Tough-minded optimists are cheerful even when they can’t be happy. It is realistic to know that life is not all rainbows and unicorns, but it is equally realistic to understand that we all have the conscientious ability to choose how we think. You can choose to think the worst, or you can choose to see what is good in any situation. “What lies behind us and what lies before us are tiny matters compared to what lies within us,” Ralph Waldo Emerson. 10 Choose wisely.
Tough-minded optimists believe they have an almost unlimited capacity for stretching. Contrary to popular belief that humans only use 10% of their brain, recent studies using functional magnetic resonance imagining (fMRI) show that most of our brain is in use most of the time, even when performing simple tasks, resting, or sleeping.11 Staying active both physically and mentally, eating well, exercising our brains through solving puzzles, and the very nature of our jobs as laboratory scientists allow for increased cognitive function and brain synapsis renewal.12
Tough-minded optimists build lots of love into their lives. In a study performed at University of California, Berkeley, seven thousand adults were studied over nine years. They found that people with weak social ties had a death rate two to five times higher than those with strong social ties.13 We are the sum average of the people we hang out with. Tip the scales in your favor by reducing the amount of time you spend with negative people and surround yourself with those who love, encourage, and challenge you in a positive way.
Tough-minded optimists like to swap good news.
When was the last time you heard a speech that moved you, a book you read that made you cry, a movie so compelling you lost track of all reality. These are all examples of impactful story telling. Artist and film director Phillipp Humm said, “Through the art of storytelling, we can preserve our heritage, educate future generations, and inspire change.”14 Tough-minded optimists understand that constant complaining only brings themselves and others down.
Tough-minded optimists accept what cannot be changed.
Charles Darwin, who developed the Theory of Evolution said, “It is not the strongest of the species that survives, nor the most intelligent. It is the one that is most adaptable to change.” 15 Many of us go through life beating our heads against the wall, trying to force our own plans for the future when often, the future has other plans. Flexibility is a virtue and the one thing we can all
OTHER PEOPLE'S ACTIONS
OTHER PEOPLE'S OPINIONS OTHER PEOPLE'S MISTAKES
count on is change. Stay curious and be a life-long learner. Remember the things you can control and the things you cannot (See Figure 1).
Conclusion
This article gives a brief outline of each of the 12 characteristics that make a Tough-Minded Optimist. If even one or two of these characteristics resonate, I feel confident that with practice, your life will feel a little lighter and the future will seem a little brighter. Be real, be tough, and stay optimistic.
References
1. Carnegie D. A quote by dale Carnegie. Goodreads.com. Accessed November 19, 2024. https://www.goodreads.com/ quotes/180216-one-of-the-tragic-things-i-know-about-human-nature.
2. Loy McGinnis A. The Power of Optimism. San Francisco:Harper & Row; 1990.
3. Manzo P. A crisis is a terrible thing to waste. Stanford Social Innovation Review. Published online 2010. doi:10.48558/KYJD-P694.
4. Brown B. GIFTS of IMPERFECTION : 10th Anniversary Edition. Hazelden. Published online 2022:74-77.
5. Loy McGinnis A. The Power of Optimism. San Francisco:Harper & Row; 1990: 39.
6. Lamott A. A quote by Anne Lamott. Goodreads.com. Accessed November 19, 2024. https://www.goodreads.com/ quotes/6830146-almost-everything-will-work-again-if-you-unplug-it-for.
7. Twain M. A quote by Mark Twain. Goodreads.com. Accessed November 19, 2024. https://www.goodreads.com/ quotes/201777-i-ve-had-a-lot-of-worries-in-my-life-most.
8. Website-files.com. Accessed November 19, 2024. https:// cdn.prod.website-files.com/5f6cc9cd16d59d990c8fca3 3/6515752583b692abb91d04db_gratitude-quotes-famous-2.jpg.
9. Elizabeth Quinn MS. How imagery and visualization can improve athletic performance. Verywell Fit. Updated July 4, 2021. Accessed November 19, 2024. https://www.verywellfit.com/ visualization-techniques-for-athletes-3119438.
10. Krstic Z. 103 quotes about managing anxiety to help comfort you through tough days. Good Housekeeping. January 28, 2023. Accessed November 19, 2024. https://www.goodhousekeeping.com/health/ wellness/a42396674/anxiety-quotes/.
11. Burgess L. How much of our brain do we actually use? Brain facts and myths. Medicalnewstoday.com. Updated July 17, 2024. Accessed November 19, 2024. https://www.medicalnewstoday.com/ articles/321060.
12. Johnson J. Brain exercises: 22 ways to improve memory, cognition, and creativity. Medicalnewstoday.com. Updated April 4, 2023. Accessed November 19, 2024. https://medicalnewstoday.com/articles/ brain-exercises?.
13. Loy McGinnis A. The Power of Optimism. San Francisco:Harper & Row; 1990:114-115.
14. Humm P. 23 inspirational storytelling quotes. Power of Storytelling. November 25, 2021. Accessed November 19, 2024. https://power-ofstorytelling.com/storytelling-quotes/.
15. Meah A. 25 inspirational quotes on Adaptability. AwakenTheGreatnessWithin. October 16, 2023. Accessed November 19, 2024. https://www.awakenthegreatnesswithin. com/25-inspirational-quotes-on-adaptability/.
Patty J. Eschliman, MHA, MLS(ASCP), DLM, CPC is a Certified Professional Coach who specializes in laboratory leadership growth and professional support. As President and CEO of The Lab Leader Coach, Patty coaches many lab professionals in all roles in the areas of building leadership skills, preventing burnout, improving communication, building cohesive teams, and how to be a positive influencer. She has 39 years of experience as a Medical Laboratory Scientist, the last 29 spent in leadership.
Teamwork:
Leadership:
Personal growth:
COACHING CORNER
with Patty Eschliman, MHA, MLS(ASCP)DLM, CPC New article series coming soon!
In Coaching Corner, you are invited to ask questions about anything
How should I deal with a toxic co-worker?
How can I stay positive when the team seems so negative?
How can I ensure our ideas are heard by leadership?
How do I hold that difficult conversation?
What can I do to change the culture of my team or my organization?
What skills are needed to build a cohesive team?
What do I need to do to get ahead? How can I ask for a raise?
How can I increase my strengths and work with my weaknesses to be more successful?
What do I need to do to ensure I get that promotion or new job?
Send your questions to editor@mlo-online.com
Patty’s answers to your confidential questions will be published in the April, September, and November 2025 issues.
Your laboratory plays a crucial role in the healthcare ecosystem.
When your Laboratory Information System falters, it ultimately impacts patient care. Partner with a vendor who understands the critical nature of your work. e that ve
Orchard Software
is proud to be that vendor.
47 97% 9.8
Net Promoter Score (NPS)* Customer Satisfaction Rating Top Ranking in Support & Customer Care in 2024 Black Book Survey
84 % of all inbound support calls were answered within two minutes of all inbound support calls were answered within five minutes 96 %
Don’t let technical issues stand in the way of quality care. Choose Orchard and experience the difference.
Precision partners: AI in diagnostic labs for clinical decision support
By Ankit Gupta, Mike Heydlauf, Nivedita Mitra, Artem Boltyenkov
Clinical decision support (CDS) systems can streamline the diagnostic process by assessing the appropriateness of ordered tests, identifying critical values, and minimizing treatment delays through automated decision-making support for clinicians. CDS has had a longstanding presence in diagnostics, exemplified by features like reflex testing and autoverification, which have aimed to optimize laboratory workflows and improve diagnostic outcomes. However, diagnostics are on the precipice of a significant shift in the landscape of CDS, marked by the emergence of a new generation of systems leveraging artificial intelligence (AI) technologies. This new generation of systems could improve laboratory testing by introducing advanced capabilities for data analysis, pattern recognition, and patient-centric interpretations. By harnessing the power of AI, next-generation CDS systems promise to deliver more sophisticated insights, enable faster and more accurate diagnoses, and enhance the overall quality of patient care. Here, we explore the potential impact of AI-backed CDS on diagnostic testing and emphasize its capacity for patientcentric interpretations to provide insights into how these advancements will reshape the field of laboratory medicine and improve healthcare outcomes.
rule-based predefined criteria. Autoverification algorithms utilize data filters based on instrument error and quality control flags, serum indices, critical values, result range limits, delta checks, and consistency checks. These rules detect abnormal results and verify them for possible errors before release. They fall into two categories: comparing test results with predefined limits for the test type or comparing them with prior results for the same patient to ensure consistency.
Applying AI decisioning in lab workflows
Recent studies have shown that up to 70% of laboratoryrelated errors occur in the preanalytical phase of laboratory testing.1 AI-based CDS systems have shown significant potential in the pre-analytical phase. For instance, a neural network algorithm effectively detected clots that could skew coagulation test results.2 Similarly, a recent study revealed that a machine learning (ML) algorithm can detect mislabeled samples with 92.1% accuracy, surpassing human performance by approximately 14%.3 Another application in the pre-analytical phase is assessing serum quality based on hemolysis, icterus, and lipemia (HIL). A recent study used convolutional neural network–based deep learning models to analyze sample images to determine their HIL status and by extension their quality.4 Similar models are being integrated into vision systems on diagnostic instruments to detect HIL errors in real-time, preventing costly analytical cycles from being wasted on unsuitable samples.
One of the most critical roles of clinical laboratories is the test report verification process at the post-analytical phase. This process identifies potential errors before releasing test results. To streamline this, clinical laboratories historically employed techniques, such as autoverification, which use computer-based algorithms to evaluate and validate test results by following
Autoverification rules are very time consuming to implement and vary between laboratories. In addition, reports that are labeled ‘invalid’ by an autoverification system, will need manual verification. The promise of an AI-based autoverification system was demonstrated in a Chinese hospital where the AI autoverification system outperformed the traditional rule-based system by reducing the number of invalid reports by 80% thus reducing the need for manual intervention and workload.5
Similar to autoverification, reflex testing typically relies on simple “if-then” rules; for example, thyroid stimulating hormone (TSH) followed by reflex testing for free thyroxine (FT4) if TSH is above or below established criteria. However, this limits their scope since most test ordering decisions involve more complexity than a simple rule will allow. With the emergence of electronic medical records and AI, it appears plausible that future laboratory services could include an advanced reflex testing system with a wider scope and greater impact that can take multiple data points into consideration. In a recent study, the concept of smart reflex testing using an ML model was introduced where upon getting a complete blood count (CBC) result, the model predicted the need for ferritin testing to confirm anemia.6 The model performed moderately well in predicting ferritin testing need and demonstrated greater suitability to reflex testing than rule-based approaches.
Applying AI decisioning to lab diagnostics data
The integration of CDS systems that use AI to address various questions in healthcare using lab diagnostics data in the postanalytical phase has shown promising applications. CDS systems can help in the interpretation of multidimensional test results by providing likelihood scores for potential diseases, improving risk stratification, predicting disease outcomes, and providing differential diagnosis. These technologies can play a critical role in monitoring organ functions by tracking blood results and trends and facilitating early and accurate disease diagnosis. Furthermore, by predicting disease progression and patient outcomes, AI/ML can empower healthcare providers to make well-informed decisions regarding patient care and intervention. The use-cases cover a diverse range of medical conditions, including but not limited to infectious diseases, such as sepsis and COVID,7,8 cardiovascular diseases,9 cancer diagnostics,10 liver diseases,11 kidney diseases,12 and autoimmune diseases.13
Among all the use-cases of integration of ML into laboratory medicine for developing a CDS solution, early sepsis identification and outcome prediction is undergoing rapid advancement.14 These solutions, however, have not yet found wide clinical adoption as various challenges like population variability in biomarkers, limited access to datasets due to privacy issues, lack of external validations, and lack of large datasets with sufficient parameters to robustly train decisioning algorithms persist and prevent well-functioning algorithms from being created. Despite such challenges, some systems have overcome these hurdles. Recently, Prenosis has received a de novo FDA clearance for its AI/ML-based sepsis prediction algorithm ImmunoScore,TM which can help in assessing the risk of having sepsis or progressing to sepsis within 24 hours of patient assessment. Similarly, Smart Blood Analytics has released the CE-marked SBAS Software, which employs advanced ML algorithms to determine the most likely diagnoses based solely on an individual's blood test results.
The adoption of AI to lab data is in its early stages, but it is likely to grow considering the trajectory of similar diagnostic advancements in imaging applications. An example of the use of AI in diagnostic imaging can be found in the hematology space from Scopio Labs (Tel Aviv-Yafo, Israel). The interpretation of white blood cell (WBC) differentials, red blood cell (RBC) morphology, and platelet estimation is done using AI from a full-field peripheral blood smear image made on FDA-approved systems, thus reducing turnaround time for sample review by 60%.15
The FDA-approved list16 of AI/ML-enabled medical devices is dominated by radiology solutions, with 87% of such devices approved in 2022 belonging to this category. AI has impacted all aspects of radiology from staff scheduling and picking the correct scan settings to the imaging process itself, i.e., interpretation and identification of features in an image.17 Top diagnostics imaging manufacturers have incorporated AI in their imaging software to improve accuracy and efficiency of imaging, such as enabling shorter imaging time in MRI and reducing radiation doses in PET scanning. On the CDS front, there are multiple companies who serve different use cases like lung cancer (Aidence), breast cancer (DeepHealth), brain cancer (Cortechs.ai), and hemorrhage and aneurysm detection (Viz Neuro™). AI supported solutions can also enhance the quality of care in remote areas. An example is a solution from Qure.ai, which in conjunction with a portable X-ray, can be used to screen for tuberculosis from chest X-ray scans.18
Conclusion
While modern laboratories have significantly improved their efficiency and accuracy in processing samples and delivering results by utilizing the latest advancements in the pre-analytical and analytical space, the selection of tests and interpretation of results by clinicians still largely relies on manual cognitive processes, leaving room for human error and variability. It is highly likely that in the future CDS systems will also provide tailored recommendations of an optimal set of tests to aid clinicians in confirming the most probable diagnosis, ruling out improbable ones, and assessing the risks associated with lethal diseases. In addition, lab test interpretation, personalized analytics reporting, and tailored diagnostics based on age, gender, and co-morbidities will become more prevalent in the clinical field.19 This ensures that the correct diagnosis and therapy are provided to the patient rather than a one-for-all system, which may not fit the patient’s history, symptoms, and diagnosis. It is also worth mentioning that a vision for the future involves integrative diagnostics, where data from clinical laboratories, radiology, pathology, and electronic health records will be aggregated and contextualized by CDS systems for clinical actions.20 Although AI-driven CDS systems are still in their early stages, the potential exists to significantly transform diagnostics and enhance patient care. Given the rapid advancements in the field, the beneficial impact of AI on laboratory medicine is not merely a distant aspiration but rather a present and tangible reality.
Ankit Gupta is a Senior Key Expert in the Center for Innovation in Diagnostics at Siemens Healthineers, based in Bangalore, India. With over six years of experience in AI-driven algorithms, Ankit leads the development of AI-based clinical decision support systems, focusing on innovative solutions that enhance diagnostic accuracy and improve patient outcomes.
Mike Heydlauf is a Senior Key Expert at the Center for Innovations in Diagnostics at Siemens Healthineers . He has been working in laboratory automation and informatics for over 18 years and is a member of IFCCs Committee on Mobile Health and Bioengineering in Laboratory Medicine and an advisor on CLSI’s Expert Panel on Automation and Informatics (AUTO).
Nivedita Mitra is a Principal Key Expert in the Center for Innovation in Diagnostics at Siemens Healthineers, based in Bangalore, India. She leads several novel technology evaluation and external collaboration efforts and has expertise in start-up scouting, technology consulting, diagnostic workflow optimizations, and market/need analysis for white space identification and competitor analysis.
Artem Boltyenkov is a global head of Health Economics and Outcomes Research (HEOR) and a senior key expert in HEOR at Siemens Healthineers Diagnostics . In his current role, Artem leads HEOR collaborations with leading hospitals worldwide to show how in-vitro diagnostic tests change care pathways and improve patient outcomes.
Artem is the author of multiple books and peer-reviewed publications in medical journals on HEOR topics. He earned his PhD in Health Economics from the HHL, Leipzig (Dr. rer. oec.) University in Germany.
References are available online at mlo-online.com/55245858.
Cases of respiratory illnesses like walking pneumonia and whooping cough are surging. Why?
By Meghan W. Starolis, MS, PhD, HCLD(ABB)
Since last spring, the number of infections caused by Mycoplasma pneumoniae, a bacterial cause of ‘walking pneumonia,’ has been increasing. The U.S. Centers for Disease Control and Prevention (CDC) issued an alert advising the rate of cases, especially among young children ages 2–4, differs from previous years, when most infections were observed among school-aged children and adolescents.1
While symptoms can be mild — not necessitating staying home in bed, hence its name — serious complications can occur that may require hospitalization. These complications can also leave behind long-lasting effects, like new or worsening asthma and, in some cases, encephalitis or brain disease.
Though there is no national surveillance system in place to track cases of walking pneumonia, the CDC has observed an increase in emergency visits with a discharge diagnosis of walking pneumonia among all age groups. In addition, test positivity for the pathogen has been high, with outbreaks occurring mostly in crowded environments. On top of this, many states are reporting increasing diagnoses of pertussis (also known as whooping cough) another respiratory illness caused by the bacterium Bordetella pertussis
So, how can laboratory professionals ensure they are staying on top of testing, diagnosis, and treatment when these and other respiratory illnesses are growing in prevalence even before the traditional ‘cold and flu’ season?
2024’s post-COVID reemergence of respiratory pathogens
The United States is currently experiencing high rates of whooping cough cases, especially among children. Infection rates in 2024 are eclipsing what was seen in the prior year, with numbers returning to pre-pandemic trends.2 While the pandemic saw lower rates, likely due to mitigation measures like remote learning and masking, cases this year are higher than in 2019 before the start of the pandemic.3 Outbreaks of whooping cough also tend to be cyclical, with peaks in reported cases occurring every 2–5 years. Why are these upper respiratory pathogens reemerging, and at such high levels? During the COVID-19 pandemic, many non–SARS-CoV-2 respiratory diseases saw periods of low incidence of infection. Now that pandemic restrictions have been lifted and people have returned to their normal activities, seasonal respiratory diseases are able to spread person-to-person through droplet and aerosol routes as usual. This is affecting children particularly hard, as some have not yet been exposed to many of these respiratory pathogens, causing an ‘immunity gap.’4 Additionally, the mitigation efforts enacted during the COVID-19 pandemic to slow disease spread affected the seasonality and cyclical outbreak patterns of several respiratory pathogens.5 We are now observing a return to these outbreak patterns while simultaneously dealing with immunity gaps in the population.
Accurately identifying these infections so that patients can be properly managed is met with several unique challenges. First, these respiratory conditions often have symptoms that are similar. Respiratory pathogens can cause coughing, headaches, fever, runny nose, and a number of other common symptoms that can be difficult to differentiate. And testing for these illnesses, which are often needed to identify the specific bacteria or virus causing the infection, can be underutilized for certain populations or clinical settings.6
What to know about testing
With the increase in cases of M. pneumoniae, whooping cough, and other respiratory pathogens, laboratory testing plays a critical role in helping providers identify, differentiate, and treat these illnesses. Testing is particularly crucial for hospitalized children, who may be especially vulnerable to complications.
Testing for M. pneumoniae is often done in hospital settings, but samples can also be collected in an outpatient clinic, wherein a healthcare provider will collect an upper respiratory swab for testing. M. pneumoniae is commonly part of a panel that tests for many pathogens, including flu, COVID-19, and other viruses and bacteria (i.e., a syndromic panel). This panel approach can be useful in ruling out other diseases that may require specific antibiotics, so that patients with walking pneumonia receive access to the care needed as soon as possible, before their condition worsens. Targeted testing for M. pneumoniae is offered at several laboratories as a laboratory-developed test (LDT).
Whooping cough can be difficult to diagnose in its early stages, as its symptoms typically mirror other respiratory illnesses. Once the illness has progressed, a clinician may be able to make a diagnosis through a physical exam and by testing an upper respiratory swab for the B. pertussis bacteria using a rapid polymerase chain reaction (PCR) test.7 There are several options for PCR testing for both B. pertussis and a related pathogen, B. parapertussis, available as LDTs and FDA-approved assays. These pathogens are also a detectable target on several syndromic respiratory panels.
Fortunately, testing methods have improved over the last few years, allowing clinicians to catch more cases of these diseases. With diagnostic PCR test methods now widely available, laboratory tests can identify cases in 2024 that may have been missed in prior years.8
How to prevent the spread of respiratory illnesses
We have learned much about respiratory droplets over the last few years. Unfortunately, symptoms of these conditions, like coughing and sneezing, can accelerate the spread of pathogens. Strategies like handwashing and covering the nose and mouth can mitigate the spread.
Vulnerable patient populations can also consider avoiding crowded environments where outbreaks are likely and staying on top of their vaccines. By being aware of symptoms of walking pneumonia and whooping cough, a patient can get tested by their provider quickly and receive treatment before complications arise.
Lessons learned from the COVID-19 pandemic: What can we apply to other respiratory illnesses?
In the thick of the COVID-19 pandemic, practices like frequent handwashing, social distancing, and sanitizing shared surfaces were commonplace. Some preventative measures, like staying home when symptoms of sickness are felt and
avoiding others who might be sick, helps to prevent spread of disease. Vaccination is also critical to reducing risk from influenza, COVID-19, and whooping cough.
Throughout ‘cold and flu season,’ respiratory illnesses can become difficult to track given their prevalence. It is important for individuals to visit their doctor if they feel unwell so a test can be procured if needed and a treatment prescribed, if available. Experts have predicted a seasonal outlook similar to what was experienced last season — meaning the number of hospitalizations for flu, COVID-19, RSV, and other respiratory illnesses is expected to hold steady.9
Preventing the spread of walking pneumonia, whooping cough, and other infectious diseases this year is something we can all take steps towards together. The rising number of cases can and should encourage individuals to be more mindful about their own symptoms, so that conditions can be addressed at their onset before they are spread further. Testing for (and treating) these illnesses is vital. We can all do our part to lessen the impact of a bad respiratory illness season — even beyond when the weather warms.
REFERENCES
1. CDC. Mycoplasma pneumoniae infections have been increasing. National Center for Immunization and Respiratory Diseases. October 18, 2024. Accessed December 3, 2024. https://www.cdc. gov/ncird/whats-new/mycoplasma-pneumoniae-infections-havebeen-increasing.html.
2. CDC. Whooping cough is on the rise, returning to pre-pandemic trends. National Center for Immunization and Respiratory Diseases. October 23, 2024. Accessed December 3, 2024. https://www.cdc.gov/ ncird/whats-new/cases-of-whooping-cough-on-the-rise.html.
3. CDC. Pertussis surveillance and trends. Whooping Cough (Pertussis). December 2, 2024. Accessed December 3, 2024. https://www.cdc.gov/ pertussis/php/surveillance/index.html.
4. Ang HJ, Menegale F, Preziosi G, et al. Reconstructing the impact of COVID-19 on the immunity gap and transmission of respiratory syncytial virus in Lombardy, Italy. EBioMedicine. 2023;95:104745. doi:10.1016/j.ebiom.2023.104745.
5. Gavenčiak T, Monrad JT, Leech G, et al. Seasonal variation in SARS-CoV-2 transmission in temperate climates: A Bayesian modelling study in 143 European regions. PLoS Comput Biol 2022;18(8):e1010435. doi:10.1371/journal.pcbi.1010435.
7. American Lung Association. Pertussis symptoms and diagnosis. Lung.org. Accessed December 3, 2024. https://www. lung.org/lung-health-diseases/lung-disease-lookup/pertussis/ symptoms-diagnosis.
8. Attaway CC, Wang H. Laboratory testing for respiratory viruses for the clinician. Cleve Clin J Med. 2024;91(9 suppl 1):S42-S49. doi:10.3949/ ccjm.91.s1.07.
9. CDC. Monitoring respiratory illnesses informs decision making. National Center for Immunization and Respiratory Diseases. October 21, 2024. Accessed December 3, 2024. https://www.cdc. gov/ncird/whats-new/monitoring-respiratory-illnesses-informsdecision-making.html.
Meghan W. Starolis, MS, PhD, HCLD(ABB) is Senior Science Director of Infectious Disease at Quest Diagnostics . She oversees molecular infectious disease testing and plays a critical role in the strategic planning of diagnostic solutions for infectious diseases at Quest Diagnostics. Dr. Starolis completed a PhD in Microbiology and Infectious Diseases from George Mason University and is board-certified by the American Board of Bioanalysis (ABB). She serves as an elected councilor for the Pan American Society for Clinical Virology (PASCV) as well as chairperson of the Clinical Practice Committee. She also serves on the Clinical Practice Committee for the Association of Molecular Pathology (AMP). Dr. Starolis also has a passion for teaching and holds an adjunct faculty position at George Mason University.
Optimizing Clostridioides difficile diagnosis
Reducing overdiagnosis and enhancing antimicrobial stewardship through a two-step testing approach
By Jimmy Lowery MBA, MLS(ASCP)SBBCM and Justin Cox, MBA, MLS
Clostridioides difficile (C. diff ), a Gram-positive, sporeforming bacteria, is the most common cause of hospitalacquired infection in the United States, responsible for an estimated 12,000 deaths annually.1 Clinical presentation of C. diff infection (CDI) can vary from mild cramping and diarrhea to severe colitis, with complications including pseudomembranous colitis, toxic megacolon, and septic shock. The clinical course of CDI can be recurrent, and managing this infection is complicated by antibiotic resistance and the persistence of C. diff spores in healthcare environments.
The challenge
Diagnosis of CDI is based primarily on clinical presentation and confirmed by diagnostic testing. This is complicated in an inpatient setting because non-infectious diarrhea is common in this patient population. Approximately 10% of these patients are asymptomatic carriers of C. diff, 2 meaning their gut flora contains C. diff but does not exhibit clinical symptoms. Molecular testing methods for CDI such as nucleic acid amplification tests (NAAT) and polymerase chain reaction (PCR) are common and offer high sensitivity as a screening test, but they are unable to differentiate between asymptomatic carriers and patients with active CDI caused by toxin-producing C. diff organisms. As a result, C. diff testing by molecular methods alone has been shown to result in overdiagnosis and overtreatment with antimicrobial therapy.3 Because many people are asymptomatic carriers of C. diff, the Infectious Disease Society of America (IDSA), the Society for Healthcare and Epidemiology of America (SHEA), the European Society of Clinical Microbiology and Infectious Diseases (ESCMID), and the American College of Gastroenterology (ACG) all suggest using a toxin enzyme immunoassay test to help differentiate patients with active disease from those who are simply carriers.
Additionally, a proposed change to the National Healthcare Safety Network’s (NHSN) C. diff infection reporting guidelines was announced in 2023. Previously, the last test entered into a patient record defined a CDI event. This change is intended to improve upon the existing NHSN CDI measure by including evidence of a C. diff positive test AND antibiotic treatment and defines a healthcare facility-onset, antibiotic-treated C.
difficile infection (HT-CDI) as any positive C. diff test on day ≥4 and ≥5 days of C. diff antibiotic treatment.4 This proposed change is significant because the order of testing in the CDI testing algorithm no longer impacts whether a positive C. diff test is a reportable CDI event, allowing laboratories more flexibility in selecting the best algorithm for their specific patient population and workflow. With the addition of a treatment component to the proposed NHSN reporting guidelines, clinicians are also encouraged to consider clinical presentation as well as laboratory test results when diagnosing CDI.
The solution
To properly determine if a patient has active CDI, the American College of Gastroenterology (ACG)5 and the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA)6 guidelines recommend a multistep testing algorithm including a sensitive screening test and a specific toxin test. Glutamate dehydrogenase (GDH) is an enzyme present in all C. diff organisms that multiple independent studies7-10 have shown to be equivalent to molecular testing methods in sensitivity for ruling out CDI. Toxin enzyme immunoassay (EIA) methods provide
Perform C. difficile PCR test for evaluation & decision
Figure 1. Guidance provided to clinical staff for interpretation of results.
excellent clinical sensitivity to confirm a diagnosis of CDI. An algorithm that begins with a GDH or molecular screening test, followed by a toxin test for confirmation, has been recommended as the best performing algorithm for CDI testing.6,11
In December 2020, St. John’s Hospital, part of Hospital Sisters Health System (HSHS), transitioned from molecular screening testing only for C. diff to a complete stand-alone two-step C. diff algorithm, in a single enzyme immunoassay (EIA) test device. This change was driven by the need to comply with updated NHSN standards, aiming to lower standardized infection ratios (SIR) by improving diagnostic accuracy and reducing unnecessary isolation of colonized but uninfected patients. Additionally, the change sought to streamline infection prevention resources, as the previous method required extensive review of all orders before testing, placing a heavy burden on infection prevention teams.
The decision-making process involved key stakeholders, including the laboratory, quality improvement team, nursing, and the chief medical officer. Over a three-month period, the transition was carefully planned, encompassing validation and correlation studies, policy development, and education for both nursing and laboratory teams. Additionally, clinicians were provided with guidance on interpretation of results (See Figure 1).
The
results
Following the implementation of a two-step algorithm, there was notable reduction in CDI, with a 21% decrease from 2020 to 2021, and a further 31% drop from 2021 to 2022. Overall, this led to a 45% reduction in CDI over the two-year period. This achievement reduced unnecessary patient isolations, enhanced antibiotic stewardship, and resulted in an estimated annual savings of $65,000 for the laboratory. The dual benefit of improving patient care while reducing costs aligns with HSHS’s commitment to providing high-quality, affordable healthcare in the communities they serve.
Jimmy Lowery MBA, MLS(ASCP)SBBCM serves as Product Manager for TECHLAB . He is an experienced Clinical Laboratory Scientist and Product Marketer with over 20 years of experience in laboratory medicine. He has been actively involved with professional organizations like the AABB and has authored or co-authored multiple publications and posters related to laboratory testing.
Justin Cox, MBA, MLS is the System Laboratory Director for Hospital Sisters Health System (HSHS) , overseeing 13 hospital-based laboratories across the organization. With 18 years of experience, he has driven initiatives in process improvement and laboratory standardization. Justin holds an MBA from Greenville University and is recognized for his leadership and community involvement.
Open channel reagents
When clinical laboratories are facing challenges with proving lot-to-lot reproducibility or when their current reagents are not performing as expected, SEKURE open channel reagents can be employed to help improve clinical performance. SEKISUI
High-quality biomarkers of neurodegeneration
The Lumipulse G β -Amyloid Ratio (1-42/1-40) is an in vitro cerebral spinal fluid (CSF) test that combines the results of Lumipulse G β -Amyloid 1-42 and Lumipulse G β -Amyloid 1-40 into a ratio of ß-Amyloid 1-42 to ß-Amyloid 1-40 concentration using the LUMIPULSE G1200 Analyzer. Fujirebio
Prognostic power for cardiac care
Atellica IM High-Sensitivity Troponin I offers rapid AMI detection and is the first high-sensitivity troponin assay cleared in the U.S. for aiding in prognosis of ACM and MACE up to one year. Providing actionable results in 10 minutes, this blood test seamlessly integrates into routine workflows on Atellica IM and Atellica CI Analyzers. Siemens Healthineers
References are available online at mlo-online.com/55247144.
Simultaneous autoantibody detection assay
The KRONUS 3-Screen Islet Cell Autoantibody ELISA Assay Kit is for the simultaneous detection of autoantibodies to GAD and/or IA-2 and/or ZnT8 in human serum. Absorbance is measured and is proportional to the total amount of autoantibodies present. For Research Use Only. Not For Use in Diagnostic Procedures. KRONUS
Extend the power of HPV testing
BD Onclarity HPV Assay offers extended genotyping to identify high-risk HPV types beyond 16, 18, and 45 and is approved for self-collection in healthcare settings. Together, this provides a more specific risk assessment and enables tracking of individual HPV types over time and offers greater access to cervical cancer screening. Reagents are stored at room temperature for easier consumable loading. BD
One sample, more answers
The Aptima Multitest Swab simplifies testing for sexual and vaginal health with proven performance by detecting up to 7 infections and disease states from one vaginal swab. Hologic
Easily detect GBS
Hardy Diagnostics’ Strep B Carrot Broth One-Step is for the detection of Group B Streptococcus (GBS) in pregnant women. Color changes from white to orange represent a positive result for hemolytic GBS. Increased sensitivity over conventional methods, decreased turn-around time, and lower overall cost. Positives require no follow-up testing! Hardy Diagnostics
Independent specialty IA controls with procalcitonin
Specialty Immunoassay Plus Controls are comprehensive quality controls that monitor the precision of laboratory specialty IA testing procedures. These controls include clinically relevant analytes Procalcitonin, IL-6, Active Vitamin B12 , and more. Offered in automation-compatible InteliQ tubes and standard Liquichek vials, Specialty Immunoassay Plus Controls help streamline your lab’s workflows. Bio-Rad
Early lyme disease detection
The all-ELISA ZEUS Borrelia Modified Two-Tiered Testing (MTTT) algorithm, by Sebia Autoimmune & infectious Diseases, improves detection of early Lyme disease by up to 30% compared to the Standard Two-Tiered Testing (STTT) algorithm. The STTT algorithm requires a 2 nd tier immunoblot, which adds subjectivity and reduces sensitivity in detecting acute Lyme disease. Sebia Autoimmune & Infectious Diseases
The IDS Free Testosterone is the first fully automated FDAcleared assay that quantifies free testosterone levels in serum or plasma to support the diagnosis of androgen disorders. Suitable for low to high volume testing labs, the assay offers streamlined workflow, rapid results and cost effectiveness. Revvity
One-step syndromic RT-PCR
QIAstat-Dx Analyzer 2.0 (9002828), combined with assay cartridges, delivers precise RT-PCR results for multiple pathogens in about an hour. Choose from our gastrointestinal or respiratory assays, all easy to use with one-step preparation and no precision pipetting. View Ct values directly on the touch-screen interface for added clinical insights. QIAGEN
Resilience + Passion
We make diagnostics that matter
We recognize your passion for providing accurate and timely clinical chemistry results that help drive appropriate treatment decisions. We also know you are resilient and must navigate through numerous challenges, from declining reimbursement rates to staffing shortages.
At SEKISUI Diagnostics, we are committed to providing high quality SEKURE® Clinical Chemistry Reagents from our North American manufacturing sites to help laboratories maximize productivity while minimizing costs.
To learn more about our clinical chemistry reagent products scan the QR code or go to Clinical Chemistry Reagents
LABORATORY INNOVATOR
Tamara Kirby is the Laboratory and Quality Manager at Advanced Diagnostic Laboratory. She has over twenty years of experience in laboratories, including forensics, pharmaceutical, and clinical testing. Tamara has a Bachelor of Science degree in Chemistry from Austin College and a Master of Science degree in Forensic Science from the University of Illinois, Chicago. She began as a forensic chemist and was involved in quality audits under ASCLD-LAB. In her time in clinical labs, she has been responsible for accreditation to standards under CAP, CLIA, and ISO (15189 and 17025). Currently, she also serves as a Technical Supervisor for Molecular and Toxicology testing at ADL.
Implementing risk analysis into lab operations
By Christina Wichmann
15189, such as quality indicators and risk analysis, we have found many instances that we have been able to preemptively identify problem areas and address them before they ever occur. We continually review our procedures in all analytical stages and assess risk and improvement to patient care, accuracy of testing, and consistency of reporting.
How large is the laboratory at ADL Health and who are your primary customers?
Our current team includes twenty staff from management to technical team to customer service. We have a wide variety of customers, including rehabilitation facilities, drug monitoring, nursing and assisted living, family practitioners, home healthcare, and specialty providers like wound care physicians and urologists.
Are there particular lessons learned you can share with other laboratory managers and directors on reducing laboratory errors?
Congratulations on being the first clinical laboratory in the United States accredited to the new version of ISO 15189. For those unfamiliar with ISO 15189, would you explain how this accreditation supports the pre-analytical, analytical, and postanalytical stages of testing?
Thank you so much. We have found accreditation to ISO 15189 to truly build upon the standards that labs already follow under CLIA, and it places even more focus on continual improvement of processes. By using the tools of ISO
I have found that the process of risk analysis in the laboratory is often underrated and overlooked as a tool for reduction of laboratory error. Laboratory directors and management need to find a way to seamlessly implement risk evaluation into their current processes.
For example, in our lab this has become an ongoing conversation in our team meetings. When you involve the entire team in the evaluation of risk and improvement, it allows everyone to take responsibility for the quality of lab work, and to bring attention to potential problems that may never be seen by more than one or two people. Making this a normal conversation between staff can truly improve quality and reduce errors.
The other great opportunity we have found for risk assessment is during competencies. As a manager
or technical supervisor, observing the daily hands-on processes gives a window into possible risks in the procedures that aren’t necessarily thought of during the SOP-writing process. Observingdifferent personnel performing the same task will often provide valuable insight into potential risks that can be addressed with procedure changes.
What is a lesson learned you can share with fellow laboratory managers and directors on the accreditation process?
I think the biggest lesson is that accreditation checklists can all too easily be viewed as a long list of tedious work to be added to our already full schedule. But what we have found is that most of these processes can easily be included in what we are already doing. If we have a meeting scheduled quarterly, for example, we can use that time for periodic review of quality indicators and proficiency testing. As laboratory managers and directors, we have the freedom to implement the standard requirements in a way that works for our laboratory, and it may not look like other labs. But if we can use the tools as they are intended, the quality of all laboratory work will improve, which is the point of accreditation in the first place.
What do you see the future laboratory looking like?
The future laboratory is going to continue to become more automated, and with AI development, this will affect how data is processed, reviewed, and reported. In addition, medicine is becoming more and more personalized and local. This means that patients are expecting to be able to test ondemand, in a convenient location or even at home. These types of changes will require laboratories to be evolving continually, striving to meet these needs while ensuring the highest level of quality.
MLO LAB OF THE YEAR 2025
CALL FOR ENTRIES
MLO’s Lab of the Year Award celebrates medical laboratories that demonstrate their extraordinary commitment to quality patient care. Submissions will be judged on achievements in five areas. A panel of judges selected from MLO’s Editorial Advisory Board will select the winner and two runners-up. All will be featured in the April 2025 issue of MLO, in print and online, and awarded a display wall plaque, with the winner featured on the issue cover.
ALL SUBMISSIONS DUE BY JANUARY 13, 2025
Medical laboratories, utilizers of a lab’s service and non-vendor affilities are welcome to submit. Submission requirements are at: https://www.mlo-online.com/55234457
NEW! Choyce Urine Collection and Transport Containers
The ultimate innovation for safety and product efficacy!
Choyce Easy-Hold Handles and leak resistant containers makes it easier to urinate into the cup and not over your fingers, hands, and floor!
Choyce’s unique urine collection and transport container with recessed needle and infection control safety lid.
(compatible with BD and Greiner tubes)
Choyce’s new Easy-Pour offers you a secure, leak-proof container with infection-control lid that allows the lab to easily obtain a sample without removing the cap, consequentially less propensity for spilling urine, and safer diagnosis.
For further information and samples, please call or write.