8 > Revolutionizing Healthcare: How Automation and AI Are Shaping the Future of Supply Chains
JANETTE WIDER
28 > The Cyber Case for Supply Chain and IT Collaboration
KAREN CONWAY
Infection Prevention
12 > AI and Automation: New Tools in the Fight Against Healthcare-Associated Infections
MATT MACKENZIE
Sterile Processing
14 > Automation in the Sterile Processing Department
KARA NADEAU
20 What Sterile Processing Should Know About Multidrug-Resistant Organisms (MDRO)
HEIDE AMES AND JANET MESZAROS
24 > In-Person Continuing Education, Networking Essential for SP Professionals
JULIE E. WILLIAMSON
26 > New Educator: Where Should I Start?
ADAM OKADA
Departments
4 > Automation Nation
6 > What’s on the Web, Advertiser Index
Automation Nation
BY JANETTE WIDER
Iimagine the topics on the cover of this month’s magazine tipped off all our readers as to what this edition is all about: automation. This topic was suggested by many of our readers and listeners of our podcast, Healthcare Hodgepodge.
The three feature stories featured in this edition cover sourcing and logistics, infection prevention, and sterile processing and how automation is making an impact in these three departments across the hospital. The healthcare industry is still facing a shortage of workers and an increased demand in care due to an aging population, and many leaders at hospitals and health systems are looking to automation to ease these burdens and others.
My article this month covers automation in the healthcare supply chain. I had a lot of questions for the experts I interviewed, particularly about the landscape post COVID, as our industry moved incredibly quickly into the automation space.
Chris Luoma, chief strategy officer at GHX made an excellent point about automation and the COVID19 pandemic. He said, “As healthcare moves to a wider range of locations beyond hospital walls, extending supply chain automation is becoming increasingly important. The COVID-19 pandemic didn’t
introduce new automation, but it did significantly accelerate its adoption. Before the pandemic, it was business as usual—manual processes, face-to-face interactions, and paperbased systems. By the end of that same week, the world shut down. Suddenly, hospitals had to operate remotely, and paper was no longer an option. This forced a rapid shift toward automation solutions.”
And now that the technology is readily available, the demand for automation only continues into 2025 as hospitals are facing increasingly tight budgets. Automation can help hospitals reduce operational costs— automating tasks like inventory management can assist with ensuring that supplies are replenished in a timely manner and avoid stockouts or overstocking. This reduces waste and ensures that resources are utilized efficiently.
Most importantly, automation empowers healthcare workers to deliver more effective and compassionate care. My article can be found on page 8.
Does your hospital or health system have a success story surrounding automation? I’d love to hear your story and feature it on our podcast. Reach out to me directly at jwider@ hpnonline.com or connect with me on LinkedIn.
March 2025, Vol. 49, No. 3
VP & Market Leader
Healthcare and Dental
Chris Driscoll
cdriscoll@endeavorb2b.com | 978-880-8345
Editor-in-Chief
Janette Wider jwider@hpnonline.com
Associate Editor
Matt MacKenzie mmackenzie@endeavorb2b.com
Senior Contributing Editor Kara Nadeau knadeau@hpnonline.com
Advertising Sales
East & West Coast
Kristen Hoffman khoffman@endeavorb2b.com | 603-891-9122
Midwest & Central
Brian Rosebrook brosebrook@endeavorb2b.com | 918-728-5321
Advertising & Art Production
Production Manager | Ed Bartlett
Art Director | Kelli Mylchreest
Advertising Services
Karen Runion | krunion@endeavorb2b.com
Audience Development
Laura Moulton | lmoulton@endeavorb2b.com
Endeavor Business Media, LLC
CEO Chris Ferrell
COO Patrick Rains
CRO Paul Andrews
CDO Jacquie Niemiec
CALO Tracy Kane
CMO Amanda Landsaw
EVP Medical & Healthcare Technology Kylie Hirko
EVP Endeavor Business Intelligence Paul Mattioli
Healthcare Purchasing News USPS Permit 362710, ISSN 1098-3716 print, ISSN 2771-6716 online is published 11 times annually - Jan, Feb, Mar, Apr, Jun, Jul, Aug, Sep, Oct, Nov/Dec, Nov/Dec IBG, by Endeavor Business Media, LLC. 201 N Main St 5th Floor, Fort Atkinson, WI 53538. Periodicals postage paid at Fort Atkinson, WI, and additional mailing offices. POSTMASTER: Send address changes to Healthcare Purchasing News, PO Box 3257, Northbrook, IL 60065-3257. SUBSCRIPTIONS: Publisher reserves the right to reject non-qualified subscriptions. Subscription prices: U.S. $160.00 per year; Canada/ Mexico $193.75 per year; All other countries $276.25 per year. All subscriptions are payable in U.S. funds. Send subscription inquiries to Healthcare Purchasing News, PO Box 3257, Northbrook, IL 60065-3257. Customer service can be reached toll-free at 877-382-9187 or at HPN@omeda.com for magazine subscription assistance or questions. Printed in the USA. Copyright 2025 Endeavor Business Media, LLC. All rights reserved. No part of this publication June be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopies, recordings, or any information storage or retrieval system without permission from the publisher. Endeavor Business Media, LLC does not assume and hereby disclaims any liability to any person or company for any loss or damage caused by errors or omissions in the material herein, regardless of whether such errors result from negligence, accident, or any other cause whatsoever. The views and opinions in the articles herein are not to be taken as official expressions of the publishers, unless so stated. The publishers do not warrant either expressly or by implication, the factual accuracy of the articles herein, nor do they so warrant any views or opinions by the authors of said articles.
The Only Medical Scales with Verified Accuracy
Accurate patient weighing plays a critical role in ensuring correct medical dosages, especially in pediatrics and oncology. An NTEP-certified medical scale provides highly accurate and consistent readings, crucial in medical settings where precise weight measurements are necessary for patient care and medication dosing. DETECTO is the only medical scale manufacturer offering nationally-regulated, NTEP-certified medical scales. Why trust the most important thing in life with anything less: the life of medical patients.
Proud Partner:
What’s on the Web
Vizient Releases Spend Management Outlook for 2025-2026
Vizient has released a new Spend Management Outlook “representing the best estimate of the change in the price of pharmaceuticals, medical devices and supplies, capital equipment and services between July 1, 2025, to June 30, 2026. The report “projects a 3.84% increase in pharmacy and an increase of 2.3% in non-pharmacy spend over that timeframe.” Market prices encompassing the non-pharmacy healthcare supply chain will increase an average of 2.3% between July 2025 to June 2026. Read on: hpnonline.com/55264277
2025 Cybersecurity Supply Chain Insights with Richard Staynings
Norovirus Vaccine From Moderna Currently in Phase Three Trial
A phase three trial for a potential norovirus vaccine from Moderna is currently underway. Results are expected “as soon as later this year or 2026.” The study is enrolling 25,000 people in order to see a number of cases that would allow researchers to analyze the data and determine the efficacy of the vaccine. Norovirus is a “stomach bug that causes vomiting and diarrhea. It’s highly contagious and can spread easily in nursing homes and daycares, and on cruise ships.”
Read on: hpnonline.com/55263739
Richard Staynings is currently Chief Security Strategist for Cylera. He is also author of Cyber Thoughts, a leading healthcare cybersecurity blog, and teaches postgraduate courses in cybersecurity, health informatics and healthcare management at the University of Denver University College. On this episode, Richard and Janette Wider, Editor-in-Chief of HPN, discuss lessons learned in supply chain cybersecurity from 2024 and looks ahead to 2025. Listen at: hpnonline.com/55262378
Editorial Advisory Board
Jimmy Chung, MD, MBA, FACS, FABQAURP, CMRP, Chief Medical Officer, Advantus Health Partners and Bon Secours Mercy Health, Cincinnati, OH
Joe Colonna, Chief Supply Chain and Project Management Officer, Piedmont Healthcare, Atlanta, GA; Karen Conway, Vice President, Healthcare Value, GHX, Louisville, CO
Dee Donatelli, RN, BSN, MBA, Senior Director Spend symplr and Principal Dee Donatelli Consulting LLC, Austin, TX
J. Hudson Garrett Jr., PhD, FNAP, FSHEA, FIDSA, Adjunct Assistant Professor of Medicine, Infectious Diseases, University of Louisville School of Medicine
Melanie Miller, RN, CVAHP, CNOR, CSPDM, Value Analysis Consultant, Healthcare Value Management Experts Inc. (HVME) Los Angeles, CA
Dennis Orthman, Consulting, Braintree, MA
Janet Pate, Nurse Consultant and Educator, Ruhof Corp.
Richard Perrin, CEO, Active Innovations LLC, Annapolis, MD
Jean Sargent, CMRP, FAHRMM, FCS, Principal, Sargent Healthcare Strategies, Port Charlotte, FL
Richard W. Schule, MBA, BS, FAST, CST, FCS, CRCST, CHMMC, CIS, CHL, AGTS, Senior Director Enterprise Reprocessing, Cleveland Clinic, Cleveland, OH
Barbara Strain, MA, CVAHP, Principal, Barbara Strain Consulting LLC, Charlottesville, VA Deborah Petretich Templeton, RPh, MHA,Chief Administrative Officer (Ret.), System Support Services, Geisinger Health, Danville, PA
Ray Taurasi, Principal, Healthcare CS Solutions, Washington, DC
SMART INVENTORY
Smart, Automated Inventory Management
Save over 50 minutes per PAR location per day
No Scanning Required
Simply pull down the Reorder Flipper to trigger an order. That’s it!
Manage PAR Locations Remotely
Supply inventory is managed from the Intelli-Flip.net Web Based Portal.
ERP Integration
Fully automate your process by integrating Intelli-Flip with your ERP system.
To learn more or to request a demo, scan the QR Code or go to Intelli-Flip.com.
Revolutionizing Healthcare: How Automation and AI Are Shaping the Future of Supply Chains
Healthcare Purchasing News shares insights from three supply chain leaders on automation.
BY JANETTE WIDER
In the past decade, the healthcare supply chain has experienced a significant shift toward automation, driven by the need for greater efficiency and adaptability. From order automation to advanced logistics and inventory management, the industry’s focus has expanded to encompass both digital and physical automation. This transformation has been further accelerated by the COVID-19 pandemic, which highlighted the need for more agile and data-driven systems.
Healthcare Purchasing News spoke with several experts who have observed firsthand how the industry’s rapid adoption of automation is not just about reducing costs, but about enhancing collaboration, improving inventory visibility, and supporting a more resilient healthcare system. As automation and AI continue to evolve, the healthcare supply chain is poised for even greater innovation, offering new ways to streamline operations, improve patient care, and ensure a more sustainable future for the industry.
Chris Luoma, chief strategy officer at GHX commented on what he’s seen in his career when it comes to automation. He said, “Looking back over the past decade, the focus has been on driving automation, especially in the order-to-cash and procure-to-pay
spaces. This includes everything from order automation to invoicing and logistics notifications, whether through EDI transactions or other methods. We’ve worked to extend these processes to various parts of the healthcare supply chain, including acute and non-acute care, and to more complex areas like the implantable space, which involves multiple stakeholders from clinicians to manufacturers to device reps.”
“As healthcare moves to a wider range of locations beyond hospital walls, extending supply chain automation is becoming increasingly
important,” he added. “The COVID19 pandemic didn’t introduce new automation, but it did significantly accelerate its adoption. Before the pandemic, it was business as usual— manual processes, face-to-face interactions, and paper-based systems. By the end of that same week, the world shut down. Suddenly, hospitals had to operate remotely, and paper was no longer an option. This forced a rapid shift toward automation solutions.”
GHX’s Luoma noted, “The pandemic also highlighted the critical need for automation in inventory and logistics, especially within consolidated service centers and warehousing, which have become more important for both healthcare providers and manufacturers.”
Bill Selles, senior vice president, Transformation, Vizient said, “In the last 5-10 years, supply chain automation can be grouped into two
primary areas: physical and digital automation. Physical automation often leverages robotics to reduce the cost associated with humans moving goods in warehouses and hospitals, often in very capital-intensive investments. Digital automation has manifested through the deployment of major IT infrastructure such as enterprise resource planning (ERP) systems, point of use technology, and warehouse management systems. These applications allow for rulesbased automation where transactions are minimized and automated, whether natively by the application itself, or through robotic process automation or artificial intelligence.”
Tom Redding, executive vice president, Healthcare at St. Onge Company laid out his thoughts regarding supply chain automation over the past 5 to 10 years. He said, “In the past 5 years, the most recent advancements in automation have focused heavily on the manual and tedious tasks like requisitioning, item master maintenance, and invoice reconciliation, to name a few. Many health systems are investing in solutions to automate processes that will increase data accuracy, completeness and availability to streamline the decision-making process. Additionally, larger health systems are developing strategies to implement robotics and automation for their distribution operations. Many health systems are prioritizing the integration of automation tools with their existing ERP systems, electronic health records (EHR), and supply chain platforms to create a more seamless flow of data. This interconnectedness reduces silos and ensures better communication across departments.”
Further, he noted, “Over the last decade, health systems have continued to invest in point of use inventory management solutions to reduce the burden of manually
managing inventory across hundreds of locations. The cost to serve the ever-increasing number of clinical locations has forced supply chain leaders to think differently about how to leverage the right amount of technology and systems. The industry has continued to explore solutions that
can passively support their operations versus creating additional workload for their teams to manage their inventories.”
Regarding COVID specifically, Redding added, “COVID reminded all of us about the importance of inventory visibility across the health
system and including suppliers. It created an opportunity for health systems to leverage data automation to actively monitor demand patterns and further enhance their ability to identify shortages before they become critical for the health system. The pandemic not only drove short-term solutions but also fostered a shift toward more automated, data-driven, and agile supply chains for the future.”
Vizient’s Selles added his thoughts as well. He said, “COVID contributed to organizational understanding that the supply chain needs continual investment, including in automation. The great resignation that followed the pandemic and subsequent wage inflation has put increased pressure on health system executives and supply chain leaders to drive automation to reduce dependence on scarcer and costlier labor.”
Digital transformation
When asked about the digital transformation of supply chains, GHX’s Luoma stated, “Digital transformation in healthcare supply chains was already underway before COVID19, but the pandemic certainly accelerated it. One example is the widespread adoption of cloud ERP systems. About 60% of our customers are moving in this direction, with roughly 30% already transitioned and another 30% in progress. This shift isn’t just about moving systems to the cloud; it’s about changing how businesses operate, driving more automation, and enabling data-driven decisions.”
Indeed, he said, “Every time you automate a process, you generate data. When you rely on paper, you miss out on that opportunity. Another important driver of this transformation is workforce efficiency and satisfaction. While it may not make headlines like clinical challenges, these issues are top of mind for our customers, and automation is a key part of addressing workforce challenges, including burnout.”
Artificial intelligence
And of course, what would an article in 2025 be without mentioning AI? GHX’s Luoma said, “AI is a broad term these days, and it can mean a variety of things. When we talk about generative AI like ChatGPT, there is certainly potential for applications in areas like reporting and email drafting. But the larger scope of AI, including machine learning and predictive analytics, is already being implemented today.”
He added, “Supply chain leaders are increasingly facing a threefold challenge: tighter margins, more complex supply
chains, and greater cost transparency. Meeting these demands requires automation, data-driven decision-making, and AI capabilities. However, it’s important to note that AI isn’t a magic bullet. It requires a strong data foundation, trust in systems, and widespread adoption—sometimes even a re-imagining of business processes. If a process is inefficient or not data-driven, AI can actually make things worse by speeding up bad outcomes.”
And as for automation and AI, GHX’s Luoma explained that AI and automation are closely intertwined in healthcare supply chains. AI is driving much of the automation, helping teams focus on the most critical tasks—delivering the right supplies to the right patient at the right time and place. It’s about freeing up clinical teams to practice at the top of their licenses, with AI and automation streamlining the supply chain to support their work.
Selles also shared his insights. He said, “AI has tremendous potential to advance automation, and in some areas, it is already doing so; however, its use is certainly sub-scale compared to the impact it will have over the next 5-10 years. Much of the AI investment happening in organizations is concentrated in revenue-related areas such as physician productivity (i.e., clinical documentation) or on larger workforces within the health system (revenue cycle). That said, supply chain’s day for AI investment is quickly approaching, and even the early efforts to use AI to optimize inventory, interact with end users through large language models, or optimize order patterns are all proving useful, despite not being broadly adopted.”
And St. Onge Company’s Redding largely agreed with both., He commented, “AI has significant potential to improve how service is delivered using chatbots and virtual assistants to streamline customer service requests, to the use of real-time tracking of inventories and predicting potential shortages. We are only scratching the service when it comes to the potential benefit of AI on the use of automation.”
Looking forward
As for the impact and the future of this space, Vizient’s Selles noted, “Leading health system supply chain leaders operate with an automation mandate: to help relieve continued margin compression, and each year supply chain leaders are being asked to do more. They are piloting new techniques, measuring impact, and scaling, while also keeping a close eye on the horizon for what others are doing that may be applicable. This type of pressure necessitates automation and new ways of working.”
Bill Selles
Chris Luoma
Tom Redding
“The next 5-10 years in supply chain automation will be fascinating,” he added. “Physical automation, through the deployment of drone delivery technology, will continue to remove repetitive physical tasks from the workforce. Additionally, digital automation via agentic AI—the ability of AI to work independently—will have a transformative effect on how the supply chain works. End users will have the type of curated experiences in their working world that they will have in their home life, as people command the same ease in ordering goods and completing tasks in their business lives as they do in their consumer lives.”
GHX’s Luoma asserted, “Today, the focus isn’t just on automation for its own sake. The goal is to eliminate manual processes, but also to support broader objectives like analytics and AI-driven decision-making. Automation is a tool for achieving these goals, allowing supply chain teams to operate in a near real-time, data-driven environment.
“Automation in supply chain processes goes beyond just efficiency; it’s about enabling collaboration between supply chain, clinical, and financial teams. By automating procurement and other processes, we can provide the data needed to make informed decisions about the right supplies for optimal patient outcomes. This is where the industry is investing—moving into areas like implantable supply
chains and logistics, where automation helps ensure the right supplies are delivered at the right time, in the right place, with greater resilience.
“As the industry evolves, we’re moving toward a ‘living ecosystem’ of supply chains, where automation acts as the glue that keeps everything connected and running efficiently. This dynamic ecosystem will be key to solving for both cost efficiency and resilience in supply chains, adapting to the changing needs of healthcare delivery.”
Finally, St. Onge Company’s Redding concluded by saying that “I believe health systems will invest heavily in automated supply chain systems to enhance their ability to respond to emergencies by providing real-time inventory tracking, supplier status updates, and alternative sourcing options. This approach is critical in maintaining operations during natural disasters, pandemics, or supply chain disruptions. Additionally, health systems will invest in solutions to become more service-focused, which may include personalization of customer service, real-time monitoring and automated corrective action of potential issues, and autonomous decision-making on inventory management, to name a few. We anticipate a higher use of autonomous technologies for internal and external transport of materials.” HPN
AI and Automation: New Tools in the Fight Against HealthcareAssociated Infections
BY MATT MACKENZIE
New technologies are providing hospitals with fresh and improved tools for preventing healthcare-associated infections (HAIs).
An article from Innovation News Network lays out several advancements that have been made in socalled “smart hospitals.” Those advancements include “automated disinfection systems employing robots and UV-C light solutions…that have been proven effective in killing a wide array of pathogens, including bacteria and viruses.” Smart sensors and wearables for staff members are another tool increasingly being used to “track patient and staff hygiene compliance.”
Artificial intelligence (AI) has also seen its use increase in hospital settings. Certain “predictive analytics, powered by machine learning and AI algorithms, play a crucial role in infection modeling and outbreak prevention.” When AI
analyzes “vast amounts of data from various sources,” it can help to “identify patterns and trends that indicate a potential outbreak before it happens.”
Another tool that smart hospitals are using to try to enhance their infection control measures is real-time monitoring and data analytics. Using technologies that can track infection control measures in real time can provide “immediate insights into healthcare environments’ pathogen levels.” Emerging issues can be identified quickly, which can be leveraged to contain outbreaks before they become more problematic. Potential risks can be anticipated and proactive measures can be implemented to “safeguard patients and staff.”
In fact, using real-time monitoring tools is backed by research, including one study published in Frontiers of Public Health. This study was specifically meant to “investigate the potential risk factors for developing HAI in the ICU using real-time automatic nosocomial infection surveillance systems (RT-NISS) to surveil, and analyze the effectiveness of RT-NISS coupled with comprehensive interventions on HAI prevention and control in the ICU.” All data from inpatients in an ICU from January 2021 to December 2022 was pooled; comprehensive interventions were implemented in this ICU in 2022, the effects of the “RT-NISS application combined with comprehensive interventions on HAI prevention and control” could be evaluated.
By “implementing comprehensive interventions depending on infection surveillance by the RT-NISS in 2022, the prevalence proportion of HAI was reduced from 12.67% in 2021 to 9.05% in 2022,” and the “prevalence proportion of hospital-acquired
multidrug-resistant organisms was reduced from 5.78% in 2021 to 3.21% in 2022.” The authors of the study concluded that “the adoption of an RT-NISS can adequately and accurately collect HAI case information to analyze the relative high-risk factors for developing HAIs in the ICU. Furthermore, implementing comprehensive interventions derived from real-time automation surveillance of the RT-NISS will reduce the risk and prevalence proportions of HAIs in the ICU.” Studies like these show that automating certain processes in hospitals and operating rooms can lead to actual tangible results and reductions in HAI rates.
Healthcare Purchasing News was able to speak with Evan Sylvester, MPH, CIC/LTC, WFR, MT(ASCP), senior director of Infection Prevention, North Division, at Providence Health Services: Puget Sound & Alaska in Seattle; and Joanna Mills, RN, MSN, CNS, CIC, system director of Infection Prevention at Walnut Creek, Calif.,-headquartered John Muir Health, about the promise and potential of automation and artificial intelligence in clinical settings.
How do you feel about increasing AI technology in operating rooms? Is AI automating any tasks that were previously burdensome to employees?
Sylvester: AI technology in operating rooms is a gamechanger. It enhances efficiency by automating tasks such as scheduling, which optimizes OR times and reduces the burden on staff, allowing them to focus more on patient care. As AI continues to evolve, healthcare organizations are moving beyond the initial phases of adoption and are now focusing on leveraging AI to address staffing shortages and automate mundane tasks.
What is the potential for AI technologies to act as a tool for preventing healthcare-associated infections?
Mills: There are models already developed to identify risk associated with sepsis, utilizing numerous clinical variables. Predictive analytic models are also currently being utilized in data mining software to identify potential risk of infections. AI technology would be a great tool to determine individual patient risk and treatment tailored to the specific physiological factors and evidence (research) for validated protocols.
Sylvester: AI has significant potential to reduce healthcare-associated infections. It can be used in risk rating models, patient chatbots to guide them through their surgical journey, and frontline healthcare worker chatbots that provide quick access to internal policies and practices. Additionally, AI can enhance surveillance of
hospital-acquired infections by identifying patterns in large datasets more efficiently than humans.
Is automation benefitting staffing? What about costs?
Mills: Any and all automation related to staffing and cost is beneficial. There is a tremendous amount of time and effort dedicated to scheduling and determining patient acuity in acute care facilities. AI could significantly benefit this process by utilizing historic data related to seasonal trends and types of patient populations to determine safe staffing levels.
Sylvester: Automation can benefit many tasks, particularly those that are repetitive and time-consuming. In terms of staffing, automation helps alleviate burnout and address shortages by taking over mundane tasks, allowing healthcare workers to focus on more critical aspects of patient care where AI may not be able to be deployed. While the initial investment in AI may be substantial, the longterm benefits include reduced costs and improved efficiency.
Let’s talk about data. Are there any automated tasks in IP departments collecting data analytics? If so, what can the data be used for?
Sylvester: Currently, there are limited AI tools specifically designed to simplify the infection preventionist’s job. However, at Providence Swedish, we are developing a Central Line Blood Stream Infection (CLABSI) Machine Learning (ML) tool to identify patients at risk of infection 48 hours in advance. We are also exploring ML for more precise detection of Surgical Site Infections (SSI).
Are there any tools that are being used in IP departments to help with automation that are of particular note?
Sylvester: To my knowledge, there are no widely used AI tools in IP departments yet. However, the development of tools like the CLABSI ML tool shows promise for the future.
Are there any problem areas in general in the IP space that are on the rise / require intervention soon?
Mills: Antibiotic resistance and emergence of virulent pathogens are critical aspects of Infection control and prevention that threaten large patient populations.
Sylvester: Staff turnover has led to education gaps in Infection Prevention practices. Some organizations are using AI to create online educational modules for new hires and annual training. A more pressing concern is the rise in infectious diseases and the need for rapid detection of pathogens and their transmission. HPN
Automation in the Sterile Processing Department
Improving efficiency and quality without stressing the system
BY KARA NADEAU
Technologies that can automate manual processes in the sterile processing department (SPD), boosting efficiency, assuming physically laborious tasks, and/or contributing to improved instrument quality and safety, have been heralded as a panacea for understaffed and overworked sterile processing (SP) professionals.
In this article, SP professionals and technology/solutions providers offer an overview of where automation has taken hold and is providing benefit. This is followed by a detailed
look into the automation of surgical tray assembly where experts explain how deeply rooted problems in the perioperative realm can hold back advancements.
Exploring the landscape of SPD automation
Last year, when I asked SP professionals on LinkedIn what topics were most important to them in 2025, SPD automation was first voiced as a topic of interest by Densley Coke, MBA, BSTM, CST, CHL, CRCST, CER, SME, SPD manager of Northside
Hospital and adjunct instructor at Gwinnett Technical College.
“The future of sterile processing department automation in 2025 and beyond is poised for transformative advancements,” said Coke.
When reaching out to the broader SP community on the topic of automation, I encountered an enthusiastic response, with several experts offering up their insights for this article.
“Automation has taken a foothold in all our lives and the sterile processing departments within various healthcare facilities are no exception; in fact it’s a welcome addition,” said Nancy Kane, senior product manager, infection prevention and control, HuFriedy Group.
“SPD automation has and will continue to find ways to increase labor efficiency and make things easier for
employees to focus on quality outcomes and improve compliance,” said John Kimsey, VP, Processing Optimization and Customer Success, STERIS.
“The power of automation lies in its ability to drive proactive solutions, tackling persistent challenges in the industry,” said Brian Reed, cofounder & CEO, Ascendco Health. “It gives departments a bird’s-eye view of operations while helping staff streamline daily tasks, making it easier to identify patterns and trends effectively.
“Overall, automation will continue to support both administration and technicians in the years to come, and automated equipment will continue to change the landscape of sterile processing departments,” said Hannah Schroeder, clinical education specialist, Pure Processing.
Coke, Kane, Kimsey, Reed, and Schroeder shared examples of where SPD teams are leveraging automation in their processes today.
Data and analytics
“The biggest use of automation in 2025 will be in the data collection, workflow documentation, and decision-making areas,” said Kimsey. “Data automation to augment SPD decision making includes calculating real time priority processing needs, labor needs and productivity results, operational metrics, and even ‘stopping the line’ when an out of process step is attempted. Automation of data collection and compiling that data into real-time actionable reports and events is key to ensuring SPDs are efficient and compliant.”
Schroeder noted how she is seeing more SPD teams utilize data to improve their processes and achieve their goals, stating:
“This can include creative scheduling plans, or change to daily/weekly assignment objectives, even including new roles added to the department.
We are already seeing positions such as instrument coordinators who are responsible for maintaining tracking systems, or the added responsibility of daily maintenance for the technician.”
Coke noted how SPD teams are using predictive analytics to “foresee potential equipment failures or workflow inefficiencies, reducing downtime.”
Kane spoke to “equipment innovations with features such as predictive maintenance and cycle detection.” She cited the example of “modern tabletop sterilizers that provide automated mechanical monitoring and automated cycle recordkeeping.”
Instrument cleaning and sterilization
“While many people may envision robots, cobots or automated guided vehicles as automation, SPD has seen valuable efficiencies through simple automation of tasks such as automated dosing systems at the sink and cleaning of robotic arms with automated sonic and instrument washer cycles,” said Kimsey.
“Automated washers and sterilizers allow simultaneous batch processing, significantly reducing delays,” Coke commented. “High-capacity, automated sterilizers with integrated monitoring systems improve consistency in sterilization cycles.”
“Biological monitoring products with features like enzyme-based detection can provide results of sterilizer function in minutes rather than hours and automatically provide results, with no interpretation or recordkeeping required,” said Kane.
“It’s these meaningful but simple areas that have provided benefits to
SPDs and will continue to do so,” said Kimsey. “2025 will see continued automation of physical tasks, such as cleaning of robotic arms through robotic assisted cycles in instrument washers.”
Tray assembly
Coke spoke to automation advancements in surgical tray assembly, stating:
“Robots designed to assemble surgical trays with precision are gaining traction, especially in large hospitals. These robots use imaging and AI to detect missing or damaged instruments. Robotic tray assembly not only speeds up the process but also reduces repetitive strain injuries among staff.”
Instrument tracking
In exploring the use of automation in the SPD, Coke pointed to the use of RFID tagging for real time instrument location tracking, explaining how this ensures each item is traced throughout its lifecycle. He described the benefits of this automated technology deployment, stating:
“It enhances compliance with regulatory standards like ANSI/AAMI ST79, enables centralized monitoring through software dashboards, and minimizes errors in instrument handling, resulting in higher patient safety.”
According to Kimsey, instrument tracking systems are poised to harness the most benefits in terms of data analytics, as they “harness large amounts of data while interfacing with front line staff. Automating data collection and then automatically compiling the data to augment human decision-making is already underway.”
Nancy Kane
Densley Coke
Brian Reed
Inventory management
“Inventory management, a traditionally manual and time-consuming process, will become more proactive through digitized procurement platforms,” said Reed. “These systems will automate cross-referencing and trigger supplier selection, reducing errors and optimizing spending.”
“Automated inventory replenishment will save time, improve resource use, and enhance decision-making,” Reed continued. “These changes won’t happen overnight, but as industry professionals, we can implement
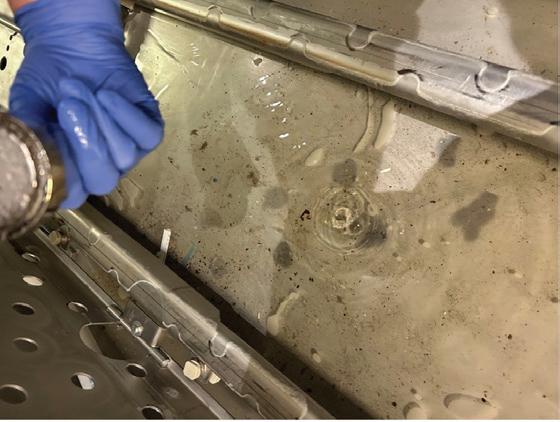
Case in Point: Automated Equipment Maintenance Failures
“Automation is critically important and has helped SPDs improve production and quality,” said Gregory Agoston, B.S., M.B.A., CRCST, LSS, VP Client Services, SpecialtyCare. “Autoclaves, instrument washer/disinfectors, and software that eliminates paper are all great examples of automation in SPD. With these advances come new challenges related
to equipment maintenance. To provide reliable service, these systems must be on a regular inspection and maintenance program.”
“Unfortunately, at multiple hospitals, we found cases where automated equipment was not properly inspected or maintained,” Agoston added. He
them gradually, ensuring they are both purposeful and sustainable for long-term success.”
IFU adherence, risk management
According to Schroeder, while most think “automation means faster,” the benefits go beyond task efficiency to improved compliance and consistency.
“Automation as a supporting tool aids in consistently meeting required steps in your sterile processing procedures and manufacturer instructions for use (IFU),” said Schroeder.
Cart washer nozzle plugged with debris; in one cart washer we found 50% of the nozzles plugged and not functioning. This resulted in inefficient cleaning of the trays.
provided the following examples and photos, noting how “In all cases, these failures to maintain equipment led to SPD quality errors.”
• Cart washers with excessive amounts of debris in the bottom of the unit
• Automated instrument and cart washers with plugged nozzles
• Chemical dispensers with blocked feed lines
• Autoclaves with plugged drains
“With the implementation of automated devices, such as conveyor systems or flushing aids, rather than a ‘faster’ approach we are opening opportunity for time reallocation, to put the manpower behind processes that require more human interaction, like visual inspection or equipment maintenance.”
Reed commented on the use of automated data capture and analytics on SPD risk management, explaining how this approach will “reshape workflows by providing real-time alerts to prevent inconsistency, ensuring adherence to best practice IFUs.”
“On a larger scale, these systems calculate departmental risks and performance metrics, offering full transparency for leadership to manage factors affecting regulatory compliance, surgical schedules, and patient outcomes,” he added.
“Having easily accessible information, like manufacturer instructions for use (MIFU) or instrument/ product sterilization parameters via something like product embedded QR codes can also save time and effort,” said Kane.
Impact on SPD teams
Coke stressed how the automation of previously manual processes in the SPD requires change management and new skill sets, stating:
“Automation reshapes job roles; manual tasks decrease, but technical oversight and problem-solving responsibilities grow. Lack of proper training is the primary cause of staff resistance to automation.”
“Department personnel will need to be trained to know and perform processes without the support of automation for when those situations do arise,” said Schroeder. “Technicians’ and leaders’ knowledge bases will continue to expand and develop as they now learn not only standards and processes but
Ferrous materials picked up from the bottom of the cart washer
also understand their equipment and how it supports compliance in completing process cycles.”
“Automation should be viewed as a reallocation of resources versus an elimination,” said Kimsey. “With current labor shortages, we need to leverage our human talent by the most effective means to add value and allow automation to handle task completion where possible.”
Reed commented on how SPD staffing models will benefit from automation, stating:
“Advanced management systems will enable SPDs to align staffing needs with instrument volume, modeling requirements based on surgical demand. This will improve resource allocation, budgeting, and operational efficiency, ensuring departments are properly staffed to meet fluctuating needs.”
Technical considerations and maintenance
Coke acknowledged how there are always challenges with new technology, including compatibility challenges between new automated systems and existing equipment or infrastructure. Lengthy downtime during system upgrades or repairs can disrupt workflows.
“These require collaboration with IT departments for cybersecurity and network stability,” he explained.
Schroeder spoke to the “large lift” of maintenance, replacement, and sometimes unexpected downtime that comes with the integration of automated technologies, stating:
“Just like any other mechanical equipment in your departments, your automation will require routine maintenance and inspection.”
She offered this example:
“Dosing and flushing systems often require daily disinfection and calibration to ensure they are performing as they should. It’s important to have a determined cadence
for maintenance and follow it so that you can negate preventable downtime.”
Automation investments
When considering where and how much to invest in automation, Kimsey offered this advice to SPD teams:
John Kimsey
“You need to review alternatives that make sense for the situation both clinically and financially. Trade shows have displayed automated tray wrapping machines or robots that are fun to watch but financially and operationally are not realistic for current day SPDs.”
The promise and potential pitfalls of automated tray assembly
While researching the topic of SPD automation, I came across a study published in the April 2024 edition of BMC Surgical on the link between errors in surgical trays and lost chargeable operating room (OR) minutes.1
The study, conducted across seven pediatric ORs on an academic healthcare campus, found nearly 87% of all tray errors resulted from failures in visualization (instrument inspection, identification, and function). Researchers estimated the annual lost charges for surgical instrument associated delays in chargeable minutes to be between $6.7M and $9.4M.
They commented on how the reporting of surgical instrument errors historically relies on cumbersome, non-automated, and humandependent data entry into a computer database that is not integrated into the electronic medical record (EMR), and called for technological advances in instrument identification, inspection, and assembly.
I spoke with lead researcher Peter F. Nichol, MD, Ph.D., Medical Director of Surgical Services, American Family
Children’s Hospital, and associate professor of Surgery, University of Wisconsin - Madison, School of Medicine and Public Health, on this study and additional research he is conducting on SPD and OR optimization.
Nichol is a fervent champion of OR and SPD optimization. He and his team work collaboratively with technology providers focused on collecting perioperative data, specifically data related to instrument inventory, usage, and quality issues. With his own data scientist, Nichol has been analyzing this data to uncover the root causes and consequences of failures, including tray errors and their impact on surgical revenue.
The promise: Efficient and accurate tray assembly supports surgical revenue growth
If 87% of all tray errors in Nichol’s study resulted from failures in humans inspecting instruments, identifying instruments, or evaluating their functionality, why not leverage technology to automate these processes?
Hospital executives want their surgical teams to perform more cases so they can generate greater revenue. Nichol spoke to technology companies that are leveraging AI to optimize OR utilization, identifying wasted time in scheduling to squeeze in more cases. He pointed to one academic medical center that has pushed its OR utilization from 80% up to 90% by using this data-driven intelligence.
Surgical teams need their SPD teams to deliver instrument trays faster to support rapid OR turnover and the ability to accommodate more cases in the surgical schedule.
Therefore, automating surgical tray assembly would reduce the risk for human error and speed the delivery
of accurate, complete, functional, and safe instruments to the OR. This supports the OR team in performing more surgical cases, maximizing OR chargeable minutes, and, in turn, generating more revenue.
On the surface, leveraging automation in tray assembly sounds like a remedy to costly perioperative problems and a driver of greater surgical revenue. But looking deeper, there are critical factors that must be addressed before widespread automation can be implemented.
Pitfall: Tackling the physician preference card conundrum
The so-called “recipe” for surgical procedures, physician preference cards are notoriously inaccurate, with SPD teams on the front-end assembling trays and carts filled with instruments and disposables that go unused – and on the back end reprocessing these items regardless of whether they were used or not.
“It is a well-known fact that the biggest bottleneck and stressor for anybody working in SPD is decontamination because the OR throws everything into a pile and sends that jumbled mess of instruments for reprocessing,” said Nichol. “The decontamination technician can’t differentiate between what was used in case and what went unused to focus their efforts of removing bioburden from used instruments because everything is mixed together with bioburden everywhere.”
Nichol acknowledged how automated technology for decontamination is far from reality, leaving the dangerous and undesirable task of manual cleaning to humans. He stated:
“It’s probably hard to come up with an AI technology that can read through a pile of completely disorganized, contaminated, and discombobulated instruments to identify what has and hasn’t been used.”
So, if decontamination is already a bottleneck in instrument reprocessing, with technicians overwhelmed by case cart disasters filled with heaps of used and unused instruments, pushing for increased OR utilization without first addressing physician preference cards bloated with unnecessary instruments will only make matters worse.
And if the SPD can’t reprocess instruments needed for surgical procedures efficiently and effectively, the OR team won’t have what it needs to perform those cases.
One case study found preference card optimization could eliminate an estimated 10,000+ hours of personnel labor across multiple departments, most notably in the SPD, by preventing unnecessary item picking, packing, returning to inventory (for unused single-use items), and reprocessing (for reusable items).2
Nichol urges healthcare organizations to invest time in understanding instrument utilization so they can cleanse
preference cards of unnecessary items. He described his own work in this area:
“We examined instrument utilization for a handful of procedures in our orthopedic hospital. When we looked at a single surgeon and the instruments they use for total hip procedures, there were three or four different patterns of trays with a 5-10% variation in instruments per tray. We determined that if we could establish a single tray that factored in these slight variations, we could eliminate 67% of instruments on that surgeon’s current trays. Downstream, that means far fewer instruments coming into decontam for reprocessing.”
Pitfall: Lack of quality issue reporting
Even with accurate physician preference cards and streamlined instrument trays, quality issues can still occur. While most OR or SPD teams acknowledge they have some level of tray errors, Gregory Agoston B.S., M.B.A., CRCST, LSS, VP Client Services, SpecialtyCare, said few truly understand the extent of the problem.
“The reality is that most hospitals don’t understand the quality of their surgical instrument trays because they lack an efficient and effective way to track quality from the standpoint of the end user, which is the OR team,” Agoston explained.
Based on data captured and analyzed by SpecialtyCare, fewer than 20% of SPD related quality issues are reported in hospitals. Agoston described the typical series of events in hospitals today:
“A tray with some kind of instrument issue arrives in the OR forcing the surgical team to fix the problem. Maybe they request a new tray or get what they need from a peel pack. Their priority is to do whatever they can to move forward with the case, perform it effectively and safely and not disrupt that day’s surgery schedule. Often, they don’t have or don’t want to take the time needed to manually report the issue.”
It is a chicken and egg scenario – perioperative teams need automated technologies that make it easy and efficient to document quality issues and identify and address root causes (e.g., a specific tray that is troublesome, a specific SPD technician who needs retraining), but they don’t have the data-driven evidence to convince hospital executives of the extent and cost associated with the errors. If hospital administrators understood the true cost of SPD related errors, they would be more willing to invest in enabling technologies.
The team at SpecialtyCare is shedding light on these issues and driving the adoption of automation in this area
Gregory Agoston
through its research and collaboration with perioperative teams throughout the U.S.
“Once we implement an automated tracking system for quality issues, a hospital’s reported error rate will generally double, and in some cases triple or quadruple,” said Agoston. “We worked with an SPD manager responsible for two large community hospitals where the OR teams reported about 10 quality issues per month. We implemented the tracking technology and in two weeks’ time, one hospital OR team alone reported 84 tray issues. That prompted a call to us from the healthcare organization’s CFO requesting help to fix the problems.”
The crisis compelling hospitals to act on SPD automation
When asked how to secure buy-in from hospital executives to invest in SPD process optimization, including automation, Nichol said, “the Boomers are going to drive all this.”
“The Baby Boomers are the largest population, they are not in great health, and they will want orthopedic, heart, and cancer procedures in the midst of the collapsing labor market,” he stated. “As they age, the Boomers are switching
over to Medicare Plus, which has terrible reimbursement. When you start adding up the math, if hospitals don’t find a way to be more efficient, they aren’t going to survive.”
Nichol estimates healthcare organizations lose about $50B a year in their SPDs, not including the cost to replace lost instruments. He stated:
“I believe the most successful non-profit healthcare organization made $560M in revenue last year. That is dwarfed by $50B in SPD losses, correct? If we could stem those losses across the board, hospitals would start running much closer to the black.”
So how do we go about driving change now?
“We start talking about it,” Nichol explained. “Using social media and other platforms to talk about the billions of dollars hospitals are leaving on the table today.”
Follow Nichol on LinkedIn to watch his video series, “The Imminent Collapse of Healthcare.” HPN
REFERENCES:
1. Observed rates of surgical instrument errors point to visualization tasks as being a critically vulnerable point in sterile processing and a significant cause of lost chargeable OR minutes. Nichol PF et al. BMC Surg 2024 Apr 15; 24(1): 110
2. Sterile Processing Department Achieves 90%+ Preference Card Accuracy with Tecsys Software, the Stanford Health Story, Tecsys, https://infohub.tecsys.com/hubfs/Case-Studies/ Sanford-Health-Tecsys-Case-Study.pdf
What Sterile Processing Should Know About MultidrugResistant Organisms (MDRO)
BY HEIDE AMES, JANET MESZAROS
Learning Objectives
1. Explain how multidrugresistant organisms (MDRO) came to exist.
2. Identify SPD tactics to protect staff and patients from MDRO.
Contributed by:
In 1929, Dr. Fleming discovered penicillin when a mold contaminated his petri dishes that were growing Staphylococcus, but it took approximately 10 years for the first human trials could begin. Thanks to collaborative efforts by British and American scientists, mass production was accomplished towards the end of World War I with wide prescription use by 1946.1 The first strains of penicillin resistant bacteria were discovered before this; E. coli in 1940 and four strains of S. aureus in 1942.
Antibiotics are found throughout the microbial world. Microorganisms
produce toxins like penicillin to protect themselves and their food sources. However, through mutation or gene transfer, organisms once susceptible to the toxins develop ways to alter the danger from toxins.
Though antibiotic resistance has always existed, the quantity of antibiotic-resistant microorganisms was low. It took the overuse and misuse of antibiotics to expedite their proliferation and set the stage for multidrugresistant organisms. What started as a single case of penicillin resistant S. aureus in 1942 grew to more than 80% of all S. aureus infections by the 1960s.2
Overuse and misuse of antibiotics has led to the selection of drug-resistant organisms, as only those with resistance can survive. Studies have shown a direct link between higher antibiotic usage and increased presence of drug-resistant organisms within the environment.5 Added to this is the impact of misuse. The CDC states that in the U.S. 28% of antibiotics prescribed by outpatient settings were not necessary.6 Using antibiotics when it is not necessary creates an opportunity for bacteria living in the body to develop resistance.
Healthcare is not the only contributor. Agriculture overuses antibiotics to prevent infections within animals. Both the antibiotics and the animals’ antibiotic-resistant organisms can be carried into the environment and to our dinner table. In a document review of drug-resistant outbreaks between 2012 and 2022, several outbreaks were attributed to antibiotic-resistant Salmonella and E. coli sourced to an animal-based food or animal fecal contamination of vegetable food sources.8
As scientists develop new antibiotics to combat drug-resistant microorganisms, the overuse and misuse of new antibiotics can lead to microbial resistance to them. The more types of antibiotics that a microorganism population is exposed to, the more drug resistances can be developed, leading to multidrug-resistant microorganisms.
Antimicrobial resistance does not always stay with the bacteria that developed it. Bacteria have the unique ability to share genetic information between different bacterial cells even if they are different kinds of bacteria. An E. coli bacterium can swap resistance mechanisms with that of Klebsiella spp. bacterium, for example. Practically, an individual harboring an antibiotic-resistant E. coli in their gut could find the other
gut bacteria becoming antibiotic resistant too.
Individuals with colonies of antibiotic-resistant bacteria often show no symptoms or signs of infection. Several studies have evaluated colonization of individuals in long term care facilities, hospital respiratory
“Studies have shown a direct link between higher antibiotic usage and increased presence of drugresistant organisms.”
patients, and a few within the community at large. The percentage of colonized individuals varies greatly but ranged between 4% and 30%.
How to reprocess devices that could have MDRO
It begins with universal precautions. Assume that every device has an MDRO. Devices should be transported in a closed, leak-proof, and puncture-resistant container. The container should be labeled as biohazardous. It’s important to remember that the container itself could also be contaminated. Always use gloves when handling containers containing soiled instrumentation.
Durable medical equipment, such as IV pumps, could become contaminated while in use. The same precautions used for handling soiled instrumentation applies to handling durable equipment.
Wear appropriate personal protective equipment (PPE) that will prevent cross contamination from the soiled instrument, contaminated spills and splashes, and aerosolization during cleaning and rinsing of the devices.
Lesson:
What Sterile Processing Should Know About Multidrug-Resistant Organisms (MDRO)
March 2025
This lesson was developed by STERIS. Lessons are administered by Endeavor Business Media.
Earn CEUs
After careful study of the lesson, complete the examination online at educationhub.hpnonline.com. You must have a passing score of 80% or higher to receive a certificate of completion.
Certification
The Certification Board for Sterile Processing and Distribution has preapproved this in-service unit for one (1) contact hour for a period of five (5) years from the date of original publication. Successful completion of the lesson and post-test must be documented by facility management and those records maintained by the individual until recertification is required. DO NOT SEND LESSON OR TEST TO CBSPD. www.cbspd.net.
Healthcare Sterile Processing Association, myhspa.org, has preapproved this in-service for 1.0 Continuing Education Credits for a period of three years, until January 13, 2027.
For more information, direct any questions to Healthcare Purchasing News editor@hpnonline.com.
Quiz Answers: 1. C, 2. A, 3. D, 4. B, 5. A, 6. D, 7. C, 8. C, 9. D, 10. A
PPE should continue to be worn until the device has undergone a disinfection process.
Cleaning and rinsing followed by disinfection and sterilization render instruments and durable medical equipment ready for use. Each step in the process is necessary to ensure the removal and/or destruc-
disinfectants. Mycobacterium and Pseudomonas bacteria that developed this resistance are also known to develop drug resistance.
Switching from a glutaraldehyde based high-level disinfectant, following equipment instructions for use, and using single dose high-level disinfectant chemistries instead of reus-
“It is possible for drug-resistant organisms to develop a disinfectant resistance.”
tion of microorganisms. Sterilization is the highest level of microbial kill. Sterilants attack multiple components and processes within the microorganisms to inactivate or kill them. Steam sterilization is known to denature (deform) and coagulate proteins. Vaporized hydrogen peroxide, another sterilant, oxidizes organic compounds such as amino acids and proteins necessary for cell function. Additionally, healthcare sterilization processes use an overkill method to ensure that no microorganisms or viruses can survive the process, thus preventing the development of resistance.
High-level disinfectants kill or inactivate many microorganisms and viruses except for bacterial spores. Often high-level disinfectants can achieve sterilization given longer exposure times, higher concentrations, or, in some cases, higher processing temperatures. Misuse of reusable high-level disinfectant solutions and failure to decontaminate automated endoscope reprocessors as described in the instructions for use have led to the development of organisms with resistance to specific types of high-level disinfectants. In both cases, bacteria exposed to sublethal conditions developed resistance to glutaraldehyde-based high-level
able can help reduce the possibility of developing a resistant population.
Intermediate-level disinfectants are used to disinfect surfaces, instrumentation, and durable medical equipment. They kill most microorganisms including Mycobacterium but are not effective on bacterial spores or some fungi spores, protozoan cysts, and non-lipid or naked viruses. Examples include phenolics, iodophors, and some chlorine compounds. The last category of disinfectants is low-level disinfectants that are also used similarly to intermediate-level disinfectants. These kill all vegetative organisms except for bacterial spores, Mycobacteria, fungi spores, protozoan cysts, and non-lipid or naked viruses.
Several bacteria have developed resistances to specific formulations of intermediate and low-level disinfectants. Reasons include overuse and misuse of the disinfectants. Intermediate and low-level disinfectants are commonly used for disinfection of items that only contact intact skin (e.g. hands), and department surfaces, such as IV poles. Thorough cleaning is very important, especially for hand hygiene, to reduce the number of microorganisms. Ensuring that surfaces remain wet with the disinfectant for the required contact time helps to
prevent sublethal exposures and the development of resistance. Lastly, rotating the intermediate or lowlevel disinfectant chemistry used will help prevent the development of resistance as each type of chemistry attacks the cells in a different way.
Do all drug-resistant microorganisms have resistance to sterilants and disinfectants?
Chemical drugs, sterilants, and disinfectants are all designed to attack and destroy microorganisms and viruses, but each does it in a different way. A bacterial mechanism that defends against penicillin will not work against an iodophor, for example.
It is possible for drug-resistant organisms to develop a disinfectant resistance. Studies on bacterial populations found in U.S. rivers showed antibiotic acquired resistance to sulfadiazine. These same bacteria showed an increased resistance to quaternary ammonium compound disinfectants.9 At the time of this article, there have been no reported drug and disinfectant resistant microorganisms detected within healthcare facilities.
Sterile processing plays a critical role in MDRO management
The development of multi-drug resistant and disinfectant resistant organisms and viruses is not anticipated to slow in the future. Sterile processing has a critical role in stopping the spread of MDRO through good processing techniques and decontamination stewardship. HPN
REFERENCES:
1. Davies J, Davies D. (2010). Origins and evolution of antibiotic resistance. Microbiology and Molecular Biology Reviews . 74(3):417-33. doi: 10.1128/MMBR.00016-10. PMID: 20805405; PMCID: PMC2937522.
2. Hunt, D. and Kates, O. (2024) A Brief History of Antimicrobial Resistance. AMA Journal of Ethics 4;26(5):E408-417. doi: 10.1001/amajethics.2024.408.
3. Lobanovska M, Pilla G. (2017). Penicillin’s Discovery and Antibiotic Resistance: Lessons for the Future? Yale Journal of Biology and Medicine. 90(1):135-145. PMID: 28356901; PMCID: PMC5369031.
4. Goossens H, Ferech M, Vander Stichele R. et al. (2005) Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. Lancet. 2005;365(9459):579–587. doi: 10.1016/S0140-6736(05)17907-0.
5. Centers for Disease Control and Prevention (CC). (2024, January 6). Outpatient Antibiotic Prescribing in the United States. CDC. https://www.cdc.gov/antibiotic-use/hcp/data-research/antibiotic-prescribing.html#:~:text=At%20least%20 28%25%20of%20antibiotics%20prescriptions%20 are%20unnecessary%20in%20U.S,the%20most%20prescribed%20antibiotics4.
6. Xu C, Kong L, Gao H, Cheng X, Wang X. (2022) A Review of Current Bacterial Resistance to Antibiotics in Food Animals. Frontiers in Microbiology 13:822689. doi: 10.3389/ fmicb.2022.822689.
7. Fastl C, De Carvalho Ferreira HC, Babo Martins S, Sucena Afonso J, di Bari C, Venkateswaran N, Pires SM, Mughini-Gras L, Huntington B, Rushton J, Pigott D, Dev-
What Sterile
leesschauwer B. (2023) Animal sources of antimicrobial-resistant bacterial infections in humans: a systematic review. Epidemiology & Infection. 14;151:e143. doi: 10.1017/ S0950268823001309.
8. Ash, R. and Iverson, J. (2025 January 6). Antibiotic and Disinfectant Resistant Bacteria in Rivers of the United States. IATP https://www.iatp.org/sites/default/ files/64_2_37588.pdf
HEIDE AMES , BS, CCSVP, CSPDT is a product manager with 28 years of healthcare and/ or laboratory experience in various roles, including as a researcher, author, instructor, tutor, and presenter. Her areas of expertise include biology, microbiology, sterilization
Processing Should Know About Multidrug-Resistant Organisms (MDRO) - Practice Quiz
1. When was penicillin widely prescribed?
A. 1929
B. 1940
C. 1946
D. 1960
2. What contributed to the proliferation of antibiotic-resistant organisms?
A. Overuse of antibiotics
B. Sterilization failures
C. Bacterial mutation
D. The use of high-level disinfectants
3. How can antibiotics enter the environment?
A. Insecticide runoff
B. Contaminated feces
C. Contaminated vegetables
D. Overuse to prevent animal infections
4. Creating new antibiotics eliminates the threat of MDROs.
A. True
B. False
5. Which microorganism can share genetic information of resistance?
A. Bacteria
B. Helminths
C. Protozoa
D. Viruses
All CEU quizzes must be taken online at: educationhub.hpnonline.com. The cost to take the quiz is $10.
validations, medical device processing, sterility assurance uses and applications, and process failure investigations.
JANET MESZAROS, BS, MS, is a lead scientist and college instructor with over 30 years of laboratory and education experience. At STERIS she has served as a researcher, author, and presenter, and at the college level she has provided instruction in the areas of chemistry, biology, biological chemistry, microbiology, and anatomy and physiology.
6. What has happened to individuals who have MDROs but do not show symptoms?
A. Synthesized
B. Sympathized
C. Matured
D. Colonized
7. What should be used to prevent staff cross contamination with MDROs?
A. Device instructions for use
B. Intermediate surface disinfection
C. Personal Protective Equipment
D. Sterilization
8. Which type of high-level disinfectant has Mycobacterium developed resistance for?
A. Peracetic Acid
B. Vaporized Hydron Peroxide
C. Glutaraldehyde
D. Ortho-phthaladehyde
9. Which tactic can be used to prevent microorganisms from developing resistance to intermediate disinfectants?
A. Thorough cleaning
B. Ensure surfaces remain wet
C. Rotate disinfectants used
D. All of the above
10. Which statement is true?
A. Some drug-resistant organisms can develop disinfectant resistance.
B. Antibiotic resistance causes disinfection resistance.
C. Many MDROs in hospitals are also disinfectant resistant.
D. Overuse of antibiotics causes disinfectant resistance.
In-Person Continuing Education, Networking Essential for SP Professionals
BY JULIE E. WILLIAMSON
Healthcare is an ever-evolving industry, with each discipline contributing uniquely and vitally to patient care and outcomes. For Sterile Processing, ensuring process quality, safety, efficiency, and consistency must be the primary goals of every technician and manager. Attaining those goals hinges on a commitment to continuing education and training and adherence to policies and procedures that are rooted in best practices and aligned with current standards, guidelines, and regulations.
Continuing education and professional advancement come in many forms, from in-department training and inservices to certification attainment, webinars, podcasts, magazine articles, journal studies, and in-depth conferences and chapter events. Each can contribute to an SP professional’s knowledge growth and skill set development; however, in-person education focused entirely on the discipline is among the most powerful ways to cultivate knowledge and new skills, learn the latest research and updates to standard and guidelines, and share ideas with peers and industry experts to improve service quality, infection prevention, and patient safety.
The Healthcare Sterile Processing Association’s (HSPA’s) annual conference is the leading in-person educational event for the profession, delivering dozens of expertled sessions on the most pertinent topics impacting the discipline. The events not only provide valuable professional development opportunities (many worth continuing education credits that can be applied toward recertification) for new and seasoned SP technicians, educators, and leaders but they also facilitate quality networking with other industry professionals and vendor representatives. Attendees consistently share with HSPA that the knowledge gained from the events can be readily passed to their departmental teammates and implemented to elevate operational performance and outcomes.
The 2025 HSPA Conference, taking place in Louisville, Kentucky, April 26–29, will bring together more than 1,500
SP professionals across all titles and experience levels and provide education at every turn. Targeted learning begins with Saturday preconference labs and workshops, most of which are included in the price of full-conference registration and allow participants to apply their new-found knowledge in a hands-on format. Beyond the traditional educational sessions, attendee learning also carries into the profession’s largest vendor Expo, with supplier representatives available to demonstrate their latest products and services and answer questions. Numerous exhibiting vendors also provide in-booth continuing education worth CE credits.
Making a case for continuing education
HSPA recognizes that many facilities and their employees face budgetary restrictions and every financial decision, including attendance at offsite professional development and educational events, must be justified. For years, the association has provided a customizable “Conference Value Letter” to help SP professionals make a compelling case for attending professional events, including chapter meetings, national conferences, or other continuing education opportunities that become available.
Although it is not uncommon for some SP professionals to pay their own way and use vacation time to attend educational events that greatly benefit their employer, HSPA has been pleased to learn that many individuals who shared the value letter with their department’s leaders and, in some cases, facility executives, were able to attain financial support for attendance. To learn more about the 2025 HSPA Conference, visit http://www.myhspa.org/2025conference. The Conference Value Letter can be downloaded at https:// s6.goeshow.com/hspa/annual/2025/attendee-documents. cfm. HSPA encourages SP professionals to keep the value letter on file and modify it as needed for future educational programs or endeavors where administrative support is required or beneficial. HPN
Clariti Solutions 4. Acadiana Rehabilitation Hospital 5. Prominence Advisors 6. Capital Blue Cross 7. TekTone Sound & Signal Mfg. Inc.
8. Village Caregiving 9. Pivot Point Consulting, a Vaco Company 10. The Surgery Center LLC
Honorable Mention:
• Pacific Asian Counseling Svcs
hcinnovationgroup.com/topcompaniestowork 1. Mott Children’s Health Center 2. HWL
St. Clair County Community Mental Health Authority 15. St. Tammany Health System 16. Wabash General Hospital 17. Metrolina Nephrology Associates 18. Midland Memorial Hospital
19. Hackensack Meridian Health
20. CoxHealth
New Educator: Where Should I Start?
BY ADAM OKADA
Q“I am a new sterile processing educator at a facility that has never had an educator before. Where should I start?”
AI have been in your exact situation, and I sympathize with it. It can be overwhelming to be the first person to “create” an SPD education program.
My first piece of advice is to start small. “Don’t try to eat the elephant in one bite,” as the saying goes (which is a disgusting analogy, now that I think about it, but I suppose the point is a good one). It’s too much to
think about the enormity of the project, so you need to start one task at a time and not try to do everything that needs to be done.
Prioritization skills will be crucial. Are there big issues looming?
One facility I worked at had major patient safety issues with blood being left inside surgical trays. We started fixing that issue right away. Starting with the proper placement of indicators inside of sets doesn’t make sense if a facility is about to be shut down.
Once all major safety issues are addressed, you can get down to
Instrument Inspection Competency
A. Able to identify potential weak spots & soil on general stainless steel instrumentation
B. Able to test scissors using testing material
(1) Able to show different testing material for shorter than 4” and longer than 4”
(2) Uses towel to test bandage
C. Able to identify wear & tear on Tungsten Carbide needle holder inserts
D. Able to use insulation tester to test inculated instrumenation. (laparoscopic, bipolar, etc.)
E. Able to utilize index cards to test rongeurs and Kerrisons
(1) Able to identify potential soil build-up Inside Kerrison working action
*Self Assessment: 1 = Experienced 2 = Need Practice 3 = Never Done
*Evaluation / Validation Methodologies: T = Tests N/A = Not Applicable D = Demonstration V= Verbal |=
Figure 1 (Image courtesy of Adam Okada)
the elephant meat and potatoes of what an educator is responsible for. Paperwork! I’m joking, of course . . . (but not really).
Competencies
For sterile processing educators, one of the primary responsibilities will be to create and maintain competencies for all sterile processing staff. From ANSI/ AAMI ST79:2017 (Sec. 4.2.2) on sterile processing personnel: “The responsibility for sterile processing should be assigned to qualified individuals who have demonstrated competence in all
aspects of sterile processing, including biohazard transportation, decontamination, preparation, packaging, sterilization, sterile storage, and distribution of sterile medical devices.”1
Later in that same section, “Documentation of competence provides verification of qualifications and workplace training, as required by regulatory and accrediting agencies.”1
One of the primary jobs of the educator will be to create and maintain these competencies to ensure all sterile processing personnel are competent to perform all aspects of their roles. You will also need to ensure that there is proper documentation of these activities. Competencies will need to be completed upon hire, at regular intervals (i.e., yearly), and whenever a new instrument/device/machine is introduced into the department.
What goes into a competency? (Fig. 1)
That will depend on your definition of “. . . all aspects of sterile processing. . ..”1 It will include required knowledge like the OSHA Bloodborne Pathogens standard 2, worker safety information including, but not limited to a) fire exits, b) extinguisher locations, c) ergonomics, d) chemical safety, and e) the SDS. You’ll need them to be competent in the required skills for the sterile processing area including, but not limited to a) decontamination, b) instrument inspection, c) packaging, d) IUSS, etc. Each machine or piece of equipment (e.g., ultrasonic, automated washer, cart washer, sterilizer) in the department will need to have training and each department will have specific competencies for their unique situations including, but not limited to a) robotics, b) high-level disinfectants, c) tracking software, and d) patient-care equipment.
There are some great resources on The Joint Commission’s website if you’re looking for help on creating
Preceptors will check off as tasks are completed
competencies; for example, the Staff Competency Policy.3
Training
Another important responsibility will be to ensure proper, comprehensive, and documented training of your employees. This will include your competency documentation, but you’ll also need to oversee the actual hands-on training of new techs and ongoing training of your existing ones.
Does the educator do the actual training of new technicians themselves?
As much as possible, sure, but more than likely the answer will be no.
As a new educator, I was overseeing three separate 24-hour-a-day sterile processing departments and routinely had training occurring at each location. There was no possibility (outside of an expensive and morally dubious cloning process) for me to be at each location on each shift training new technicians. I always tried to be there for them on their shift for week 1 of training, then I passed them along to a trusted senior “preceptor” for the remainder of their hands-on. HPN
Article conclusion and references can be found at
Figure 1 (Image courtesy of Adam Okada)
The Cyber Case for Supply Chain and IT Collaboration
BY KAREN CONWAY
Alot has changed in healthcare since the start of the pandemic, including an increased use of telehealth and the ability of employees to work remotely. All of this has been made possible by a dramatic increase in the use of cloud-based applications that have expanded where and how healthcare can be delivered by supporting remote access to critical data. As healthcare’s digital footprint increases, so, too, has the cybersecurity risk, with more than 90% of healthcare organizations reporting an attack in 2024, according to the Ponemon Institute “2024 Study on Cyber Insecurity in Healthcare.”
This is of particular interest for the supply chain, which is a prime target for cybercriminals. Nearly 70% of those participating in the Ponemon study said they experienced an average of four supply chain-directed attacks over the past 2 years, with the vast majority (82%) saying those attacks negatively impacted patient care, e.g., by delaying critical procedures. With cyberattacks in healthcare increasing faster than in other industries, it makes sense that health system executives told Guidehouse researchers in November 2023 that cybersecurity was their IT budget priority. But a little over a year later, despite some large attacks in 2024 (hitting Ascension, the Kaiser health plan, and Change Healthcare), there was little mention of cybersecurity at the recently completed JPM Healthcare Conference. At the same time, many of the investments cited by healthcare systems will only increase their cybersecurity risk. For example, many not-for-profit healthcare systems spoke about partnering more with third parties to help operate home healthcare, pharmacies, diagnostics, and other ancillary aspects of their business. Many of these steps are seen as cost-saving strategies, but they also increase the points of digital access to a healthcare system’s infrastructure and data that can be exploited by cybercriminals.
With supply chain responsible for relationships with thousands of third parties, any effective health system cybersecurity risk management program must include a strong partnership between supply chain and IT. Together, supply chain is responsible for the availability and safety of a multitude of products and services used in patient care, while IT maintains the operation and security of the
technology systems, many of which are cloud-based, that manage the procurement, distribution, storage, and payment for those resources.
Below are some recommended steps that IT and supply chain can take together to protect against costly and often life-threatening cyber attacks to both a health system’s
“As healthcare’s digital footprint increases, so, too, has the cybersecurity risk, with more than 90% of healthcare organizations reporting an attack in 2024.”
internal systems as well as those run by their partners and in turn their business partners and vendors.
• Start by identifying all of your suppliers and points of digital connectivity. Then prioritize your most strategic suppliers, based on the criticality of the products, services, and data they provide and/or manage.
• For suppliers that utilize the cloud, also assess the risk level associated with their cloud service providers.
• Develop a standardized approach to risk assessment based on the factors that raise the probability of attacks, such as the type and volume of data handled.
• Incorporate contract language that specifies supplier responsibilities for maintaining security standards, including with their vendors and business partners.
• Determine the level of risk associated with each supplier, starting with the most strategic.
• Conduct individual supplier risk assessments with the frequency and scope based on their assigned level of risk.
• Share results of assessments with the vendors and internal staff. Follow up on any outstanding issues. During the pandemic, the critical nature of supply chain to the delivery of safe and effective healthcare became apparent to both healthcare leaders and the general public. Unfortunately, it also caught the attention of cybercriminals. It is incumbent upon supply chain leaders to expand their own cybersecurity risk capabilities, in partnership with the IT experts in their own organizations and the expertise of their vendors and business partners. HPN
Bone Punches
Consistent. Comfortable. Clean. Convenient.
Engineered to meet the demands of spinal and cranial neurosurgery, SQ.line KERRISON Bone Punches deliver dependability and comfort.