











This guide includes brief descriptions of our benefit offerings and the cost. We believe that it is important for you to understand the benefits offered to you. We encourage you to take the time to educate yourself about your options and choose the best coverage options for you and your family. Please review this guide in its entirety. We urge you to keep this guide and refer to it throughout the year. If you have any questions, please contact the Human Resources Department at (269) 673-0537.
Open Enrollment
You can make changes to your benefit elections during our annual open enrollment, which is detailed below.
• Open Enrollment Period: November 7, 2022, to November 21, 2022
• Election Forms Due to Human Resources: November 21, 2022
• Benefits Effective: January 1, 2023
• Payment Coupons: To be mailed by December 19, 2022
Dependent Eligibility
If you currently have coverage on any of your eligible dependents, you can continue to cover them. Please note, if you drop coverage for any of your dependents or yourself, you can not add the coverage again in the future. Dependents are defined as:
• Your legally married spouse,
• Your natural child, stepchild, legally adopted child, a child placed for adoption, a child for whom you are required to provide health insurance by a Qualified Medical Child Support Order, or a child for whom you or your spouse have legal guardianship. The child is eligible for coverage through the end of the month in which they turn age 26. You are responsible for notifying Human Resources that your dependent is no longer eligible for coverage,
• Your disabled dependent(s) who are age 26 or older, primarily supported by you, and incapable of self-sustaining employment by reason of mental or physical handicap.
Medical Plan Choice
There are two plan options. Each utilizes the Priority Health network of providers. You can locate participating providers near you by visiting the Priority Health website at www.priorityhealth.com using the “Find a Doctor” feature. Although both plans give you the freedom to seek care outside of the Priority Health network, you will always have the highest level of coverage if you remain in-network. Please refer to your SBC for full details.
The SBC is a requirement under health care reform and replaces the benefit-at-a-glance documents. It allows you to compare your Allegan County provided benefits to other employers, such as your spouse’s plan or even Medicare options. We encourage you to use the SBC to determine which plan is right for you.
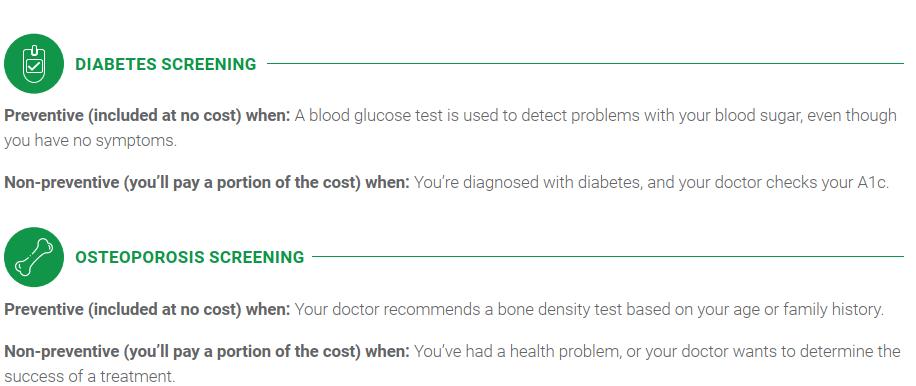
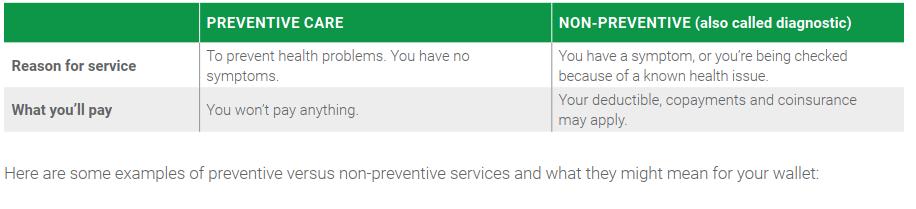
Preventive Care
Both medical plans include coverage for preventive care exams and screenings at no cost to you, as defined by the United States Preventive Services Task Force, the Health Resources and Services Administration, and the Centers for Disease Control and Prevention. Below is a list of common services that are considered preventive (subject to age and frequency guidelines which may result in cost sharing if they are not followed). Some states offer additional coverage; please review the complete list of guidelines and limitations provided by Priority Health for more details.
• Routine Physical Exam
• Routine Lab Procedures
• Well Woman Visits
• Routine Mammograms
• Routine Bone Density Test

• Routine Breast Exam
• Routine Gynecological Exam
• Routine Pap Smear
• Routine Colonoscopy
• Routine Colorectal Cancer Screening
• Routine Digital Rectal Exam
• Routine Prostate Test
• Screening for Gestational Diabetes
• Smoking Cessation
• Testing for HPV and HIV
• Immunizations

All three medical plans include coverage for preventive care exams and screenings at no cost to you. The preventive care services covered under the plans follow the recommendations from the United States Preventive Services Task Force, the Health Resources and Services Administration, and the Centers for Disease Control and Prevention.
Below is a list of common services that are considered preventive. Please note, these services may be subject to age and frequency guidelines and may result in cost sharing if they are not provided in accordance with the recommended guidelines. Some states offer additional coverage; please review the complete list of guidelines and limitations provided by Priority Health for more details.
• Routine Physical Exam
• Well Baby and Child Care
• Well Woman Visits
• Immunizations
• Routine Bone Density Test
• Routine Breast Exam
• Routine Gynecological Exam
• Screening for Gestational Diabetes
• Routine Digital Rectal Exam
• Routine Colonoscopy
• Routine Colorectal Cancer Screening
• Routine Prostate Test
• Routine Lab Procedures
• Routine Mammograms
• Routine Pap Smear
• Smoking Cessation
• Testing for HPV and HIV
We are excited to announce that as of January 1, 2023, diagnostic mammograms and colonoscopies will be paid 100% before the deductible is met, where currently they are paid after the deductible is met.

Delta Dental of Michigan
Staying healthy includes obtaining quality dental care for you and your family. Delta Dental Preferred Provider Organization (PPO) is Delta Dental’s plan that offers quality dental benefits at great savings. The Delta Dental PPO gives you access to two of the nation’s largest networks of participating dentists; Delta Dental PPO network and Delta Dental Premier network.
You can visit any licensed dentist, but you will save the most money if you see a dentist who participates in either the PPO or Premier Networks.
To find a participating dentist, use the Find a Dentist tool on the website www.deltadentalmi.com or call customer service at 800-524-0149. Delta Dental’s Automated Service Inquiry (DASI) system is available 24/7, or representatives may assist you Monday through Friday, 8:30 a.m. to 8 p.m.

Please note, this is a partial listing of benefits and services only. Please refer to the Delta Dental benefit summary or certificate of coverage for full details. All covered services are subject to the conditions, limitations, exclusions, terms and provisions of the Delta Dental certificate of coverage.
EyeMed
Vision care is an important part of your family’s health care. As such, we offer vision services through EyeMed. EyeMed has an extensive network of vision care providers who offer copayments and/or allowances for eye exams, lenses, and frames. Every twelve months the plan will cover your choice of either medically-necessary contact lenses or eyeglass lenses.
To find a participating provider, use the Find an Eye Doctor tool on the website www.eyemed.com or call customer at 866-939-3633.

Contacts (in lieu of glasses)
$130 allowance for contacts; copay does not apply Contact lens exam (fitting and evaluation) Payable every
Please note, this is a partial listing of benefits and services and reflects in-network coverages only. Please refer to the EyeMed benefit summary or certificate of coverage for full details. All covered services are subject to the conditions, limitations, exclusions, terms and provisions of the EyeMed certificate of coverage. You will receive scheduled reimbursements when using an out-of-network provider.
2023 INSURANCE RATES
Option 1 – PPO Plan 80% Rx $10/$50/$50 Ded. $1,000/$2,000 Co-Insurance 80% after deductible
Option 2 – HDHP HSA 100% Rx $10/$40/$80 after ded. Ded. $2,000/$4,000 Co-Insurance 100% after deductible Deductible applies to all services except preventative care


