


Hardy Diagnostics releases FDAcleared NG-TEST® CTX-M Multi in the United States. CTX-M Multi is an in vitro, rapid, and visual immunoassay for the qualitative detection of CTX-M enzymes (groups 1, 2, 8, 9, and 25) for the rapid detection of ESBL’s.
CTX-M-mediated ESBL-producing bacteria, primarily Escherichia coli, have been identified in various settings, including hospitals and long-term care facilities. While initially thought rare, CTX-M enzymes are now recognized as a significant cause of extended-spectrum cephalosporin resistance.
Using CTX-M Multi provides detection in just 15 minutes from isolated colonies.
















































































































































































































































































































































By Christina Wichmann
Editor in Chief
Happy Thanksgiving! I can’t believe it’s the end of the year already. One theme I’ve noticed throughout 2025 is the growing presence of artificial intelligence (AI) in laboratory medicine. Across MLO articles — from digital pathology to microbiology — AI is increasingly becoming part of the story. In case you missed any of these articles, some are as follows:
• Reimbursement for laboratory services — Are you leaving money on the table (January 2025) “Some laboratories have integrated AI with their laboratory information system (LIS), which can manage various functions including time-consuming repetitive tasks, processing of claims, and flagging errors before they are released.”
• Department of Laboratory Medicine and Pathology, Mayo Clinic Florida: Innovation, collaboration, and commitment to excellence in patient care (April 2025) “The laboratory is in the process of digitizing its archived anatomic pathology slides…Future plans will use the large, diverse datasets to build powerful artificial intelligence models in pathology.”
• Evolving paradigms in diabetes diagnosis and classification: ADA standards of care 2025 and the use of artificial intelligence (July 2025) “By analyzing data from blood sugar levels, medical history, and even retinal scans, AI tools can predict diabetes subtypes, identify high-risk patients, and tailor solutions to individual needs — with improved accuracy, reducing healthcare costs and addressing critical gaps in diagnosis, treatment, and daily management.”
• Healthcare tech visionary (July 2025) “If a pathologist needs to research a particular finding or validate a complex diagnosis, they can use AI to find similar cases and information quickly.”
• Modernizing microbiology: Achieving balance between comprehensive insights and efficiency (September 2025) “The introduction and advancement of artificial intelligence–enabled data interpretation tools is also helping increase consistency in culture media analysis.”
In response to AI’s rapid advancement, the Joint Commission and Coalition for Health AI (CHAI) published high-level guidance, The Responsible Use of AI in Healthcare, for the deployment and use of AI tools in healthcare organizations. Outlined in the guidance are seven elements of responsible use of AI. Below are some laboratory-specific considerations related to each:
• AI policy and governance structures: Lab leadership should be a part of this governance committee that provides oversight of AI tools involved in patient care.
• Patient privacy and transparency: Lab data frequently contain protected health information that needs to be protected from unauthorized disclosure.
• Data security and data use protections: Laboratory information systems must have ample protection from data leaks and cyber attacks.
• Ongoing quality monitoring: Labs must continuously monitor AI tool performance to ensure they continue to deliver accurate, reliable, and safe results.
• Voluntary, blinded reporting of AI safety-related events: Labs should have mechanisms to flag, investigate, and report incidents in which AI tools contributed to wrong or missed results or adverse outcomes.
• Risk and bias assessment: Labs should determine whether AI tools have undergone bias detection during development and monitor tools as appropriate.
• Education and training: Education and training helps to ensure safe implementation and integration of AI tools into laboratory workflows. As AI continues to evolve, these principles can help laboratories adopt new technologies responsibly — enhancing both quality and patient safety.
I welcome your comments and questions — please send them to me at cwchmann@mlo-online.com.
Vol. 57, No. 9
EDITOR IN CHIEF Christina Wichmann cwichmann@mlo-online.com
MANAGING EDITOR Erin Brady ebrady@endeavorb2b.com
PRODUCTION MANAGER Edward Bartlett
ART DIRECTOR Kelli Mylchreest
AUDIENCE DEVELOPMENT/LIST RENTALS
Laura Moulton | lmoulton@endeavorb2b.com
ADVERTISING SERVICES MANAGER Karen Runion | krunion@endeavorb2b.com
ADVERTISING
SALES DIRECTOR OF HEALTHCARE Brian Rosebrook DIRECTOR OF SALES
EAST COAST/MIDWEST SALES, CLASSIFIEDS Carol Vovcsko (941) 321-2873 | cvovcsko@mlo-online.com
SOUTH/WEST COAST/ILLINOIS SALES Lora Harrell (941) 328-3707 | lharrell@mlo-online.com
MLO EDITORIAL ADVISORY BOARD
John Brunstein, PhD, Biochemistry (Molecular Virology) President & CSO PathoID, Inc., British Columbia, Canada
Lisa-Jean Clifford, COO & Chief Strategy Officer Gestalt, Spokane, WA
Barbara Strain, MA, SM(ASCP), CVAHP Principal, Barbara Strain Consulting LLC, Formerly Director, Value Management, University of Virginia Health System, Charlottesville, VA
Jeffrey D. Klausner, MD, MPH Professor of Preventive Medicine in the Division of Disease Prevention, Policy and Global Health, Department of Preventive Medicine at University of Southern California Keck School of Medicine. Donna Beasley, DLM(ASCP), Director, Huron Healthcare, Chicago, IL
Anthony Kurec, MS, H(ASCP)DLM, Clinical Associate Professor, Emeritus , SUNY Upstate Medical University, Syracuse, NY
Suzanne Butch, MLS(ASCP)CM, SBBCM, DLMCM Freelance Consultant, Avon, OH
Paul R. Eden, Jr., MT(ASCP), PhD, Lt. Col., USAF (ret.), (formerly) Chief, Laboratory Services, 88th Diagnostics/Therapeutics Squadron, Wright-Patterson AFB, OH
Daniel J. Scungio, MT (ASCP), SLS, CQA (ASQ), Consultant at Dan the Lab Safety Man and Safety Officer at Sentara Healthcare, Norfolk, VA CORPORATE TEAM
CEO Chris Ferrell COO Patrick Rains CDO Jacquie Niemiec CALO Tracy Kane CMO Amanda Landsaw EVP INFRASTRUCTURE & PUBLIC SECTOR GROUP Kylie Hirko VP OF CONTENT STRATEGY, INFRASTRUCTURE & PUBLIC SECTOR GROUP Michelle Kopier 30 Burton Hills Blvd., Suite 185 Nashville, TN 37215 800-547-7377 | www.mlo-online.com
Medical Laboratory Observer USPS Permit 60930, ISSN 0580-7247 print, ISSN 2771-6759 online is published 10 times annually (Jan, Mar, Apr, May, Jul, Aug, Aug-CLR, Sep, Oct, Nov) by Endeavor Business Media, LLC. 201 N Main St 5th Floor, Fort Atkinson, WI 53538. Periodicals postage paid at Fort Atkinson, WI, and additional mailing offices. POSTMASTER: Send address changes to Medical Laboratory Observer, PO Box 3257, Northbrook, IL 60065-3257. SUBSCRIPTIONS: Publisher reserves the right to reject non-qualified subscriptions. Subscription prices: U.S. $160.00 per year; Canada/Mexico $193.75 per year; All other countries $276.25 per year. All subscriptions are payable in U.S. funds. Send subscription inquiries to Medical Laboratory Observer, PO Box 3257, Northbrook, IL 60065-3257. Customer service can be reached toll-free at 877-382-9187 or at MLO@ omeda.com for magazine subscription assistance or questions. Printed in the USA. Copyright 2025 Endeavor Business Media, LLC. All rights reserved. No part of this publication may be reproduced or
Rajasri Chandra,
MS,
By Kinal Bhatt, MD,
By Sue Styles, MSI; Danielle Casey, MBA, MLS(ASCP)CM; and Anita Hoeksema MS, MLS(ASCP)CM


By Alesia McKeown, PhD
Coaching
By Patty J. Eschliman, MHA, MLS(ASCP), DLM,
By Violet Nxedhlana, PhD, MLS(ASCP) and Shepherd Maingano, PhD, MLS(ASCP), GCCP
Kara Nadeau




By Rajasri Chandra, MS, MBA
According to the National Cancer Institute, oncology is a branch of medicine that specializes in the diagnosis and treatment of cancer.1 Cancer is a health challenge across the globe including in the United States. More than 2 million new cancer cases and over 600,000 deaths are projected to occur in the United States in 2025
See test online at https://ce.mlo-online.com/ courses/advancements-intechniques-and-technologiesin-oncology
Passing scores of 70 percent or higher are eligible for 1 contact hour of P.A.C.E. credit.
lEaRnIng oBJECtIVES
Upon completion of this article, the reader will be able to:
1. List the epidemiological statistics on current cancer rates and deaths in the United States.
2. Define how cancer is diagnosed.
3. Discuss laboratory testing, artificial intelligence, endoscopic exams, molecular testing, and biopsies as they relate to cancer diagnosis and treatment.
4. List new innovations in the evolution of cancer treatment.
due to cancer. 2 Thanks to advancements in the techniques and technologies in oncology, cancer mortality rates have continued to decline through 2022 averting nearly 4.5 million deaths since 1991. 2
The mechanism of cancer involves dysregulation of the cell cycle and the disruption of key checkpoint controls by manipulating and overcoming the normal regulatory processes that prevent uncontrolled proliferation.3 Cancer cells utilize different metabolic strategies to sustain rapid growth; accumulate multiple genetic changes; leave the tissue of origin and spread to other sites; evading the immune system, which typically eliminates abnormal or damaged cells; and increase the supply of nutrients and oxygen to tumors.4
Cancer can cause various symptoms, many of which are similar to that of benign tumors or other causes.5 Hence, an accurate diagnosis of cancer involves knowledge of the patient’s history, physical examination, and diagnostic testing. Cancer diagnosis is usually confirmed by tests using various methods.
The various testing methods used for cancer diagnosis are as follows: 6
• Laboratory tests
• Molecular testing
• Diagnostic imaging
• Endoscopic exams
• Tumor biopsies
Diagnostic tests for cancer are used to confirm or eliminate the presence of cancer; monitor the disease progression; and evaluate the effectiveness of treatment. In some cases, it is necessary to repeat testing when a person’s condition has changed, if a sample collected was not of good quality, or an abnormal test result needs to be confirmed.
Some of the common laboratory tests are as follows: Complete blood count (CBC): Measures levels of red blood cells, white blood cells, and platelets. Abnormally high or low counts can indicate certain cancers, such as leukemia or lymphoma.
Tumor markers: Measure substances—often proteins— made by cancer cells or by the body in response to cancer. They are usually used with other tests to help detect, monitor, or track treatment response. (See Table 1 for tumor markers and their sites.)
Molecular testing: Molecular testing is a laboratory method that uses a sample of tissue, blood, or other body fluid to check for certain genes, proteins, or other biomolecules to examine genetic and molecular characteristics. The tests are performed to provide information for diagnosis, prognosis, and treatment planning. Molecular testing for cancer can be broadly classified into three types — DNA analysis, mRNA expression analysis, and protein expression analysis.8
DNA analysis
DNA analysis looks at the genetic material of cells to find changes (mutations, amplifications, and alterations) that may cause cancer to develop, grow, or spread. Depending on the type of analysis required, the following techniques may be used:
• Polymerase chain reaction (PCR)
• Real-time PCR
• Microarray
• Sequencing – Sanger sequencing and next-generation sequencing (NGS)
Examples of point mutations are the following:
• BRAF V600E point mutation in the BRAF gene - in melanoma - the amino acid valine (V) at position 600 is replaced by glutamic acid (E).9
• EGFR L858R point mutation in the EGFR gene, specifically in exon 21 - in non-small-cell lung cancer (NSCLC) - the amino acid leucine (L) is replaced with arginine (R) at codon 858.10
Examples of insertions/deletions are as follows:
• Insertion in Exon 20 of HER2 gene in NSCLC8
• Deletion in Exon 19 of EGFR gene in NSCLC8
Examples of gene amplification/fusion are as follows:
• Amplification in HER2 gene (ERBB2) in breast cancer11
• Amplification in N-MYC in neuroblastoma12
• BCR-ABL fusion in chronic myeloid leukemia (CML)13
• ETV6-RUNX1 fusion in acute lymphocytic leukemia14
• EWSR1-FLI1 fusion in Ewing sarcoma, a bone and soft tissue cancer15
• TMPRSS2-ERG fusion in prostate cancer16
• ALK and ROS1 fusion in NSCLC17
mRNA expression analysis
This test measures the activity (expression) levels of genes in cancer cells by looking at the messenger RNA (mRNA) they produce. Some of the techniques that may be used are the following:
alpha-fetoprotein (aFP) liver, testes
Beta-human chorionic gonadotropin (β-hCg) testes
Breast cancer gene 1 & 2 (BRCa1/2) Breast
Cancer antigen (Ca) 15-3 Breast
Cancer antigen (Ca) 19-9 Stomach, colorectal, gastrointestinal, pancreas
Cancer antigen (Ca) 125 ovary
Cancer antigen (Ca) 50 Bladder, colon
Carcinoembryonic antigen (CEa) Stomach, liver, breast, ovary, gastrointestinal, lung
Cyfra 21-1 Esophagus, lung, bladder
Human epididymis protein 4 (HE4) ovary
nuclear matrix protein 22 (nMP22) Bladder
neuron-specific enolase (nSE) lung, brain, thyroid
Prostate-specific antigen (PSa) Prostate
Serum S100 Melanoma
Squamous cell carcinoma antigen (SCC) oesophagus, bronchus, lung, cervix
Table 1. tumor markers and their sites.7
Prostate-specific antigen (PSa) Prostate cancer
Carcinoembryonic antigen (CEa) Colorectal cancer, others HER2/neu Breast cancer
alpha-fetoprotein (aFP) liver cancer, germ cell tumors
Ca-125 ovarian cancer
EgFR non-small-cell lung cancer
BCR-aBl fusion protein Chronic myelogenous leukemia (CMl)
Cyclin d1 Breast, prostate, lymphoma
Table 2. Protein biomarkers and their related cancers.22
• Reverse transcriptase qPCR
• Digital PCR
• DNA microarrays
• RNA sequencing
Example tests are as follows:
1. Oncotype Dx measures mRNA expression of 21 genes for breast cancer18
2. MammaPrint Dx measures mRNA expression of 70 genes for breast cancer19
3. Decipher Prostate measures mRNA expression of 22 genes for prostate cancer20
4. ColoPrint measures mRNA expression of 18 genes for colon cancer21
Protein-based analysis
Cancer cells undergo several molecular and genetic changes that result in the overproduction, alteration, or loss of normal proteins. These changes result in new proteins or modified versions of existing proteins that are released into the
bloodstream or other bodily fluids — these act as diagnostic or prognostic biomarkers. Some key mechanisms include:
• Overexpression of growth factors: Cancer cells often overproduce growth factors, leading to uncontrolled cell proliferation.
• Loss of tumor suppressor proteins: Tumor suppressor proteins, such as p53, are often mutated or down regulated in cancer cells, contributing to uncontrolled cell growth.
• Altered post-translational modifications: Changes in protein modifications such as phosphorylation, glycosylation, or cleavage can produce altered protein isoforms detectable in blood samples.
Table 2 provides examples of protein biomarkers and related cancers.
Techniques for protein-based analysis
Proteins may be detected using the following techniques:
• ELISA
• Flow cytometry
• Immunohistochemistry (IHC)
Protein expression may be detected using the following techniques:
• Mass spectrometry
• Two-dimensional gel electrophoresis
• Protein microarrays
Diagnostic imaging is used to detect tumors and other abnormalities, determine the extent of disease, evaluate the effectiveness of treatment, and perform biopsies and other surgical procedures.
Imaging can be of three types:
• Transmission imaging
• X-ray
• Computed tomography scan (also called a CT scan or computed axial tomography or CAT scan)
• Bone scan
• Lymphangiogram (LAG)
• Mammogram
• Reflection imaging
• Ultrasound
• Emission imaging
• Magnetic resonance imaging (MRI)
Artificial intelligence (AI) in diagnostic imaging
Artificial Intelligence (AI) is revolutionizing diagnostic imaging.23 The benefits of AI technologies that use machine learning and deep learning are as follows:24-26
• Enhance the precision, efficiency, and personalization of diagnostic and therapeutic processes. 24
• Enable image classification and analysis for superior interpretation of medical images using data-driven, automated, and assistive systems to support clinical decision-making at unprecedented levels.
• Enable automated detection algorithms that can identify patterns and abnormalities challenging for the human eye to detect.
• Use quantitative imaging biomarkers to provide deeper clinical insights to help assess disease progression, predict treatment response, and personalize patient care.
As AI technology evolves, quantitative imaging will become an integral tool for precision diagnostics and evidence-based decision-making.
Circulating tumor cells (CtC) Provides information about the tumor’s genetic profile assesses metastatic potential
Evaluates drug resistance
Cell-free dna (cfdna) Provides information about the tumor’s genetic profile assesses metastatic potential
Evaluates drug resistance
Extracellular vesicles (EV) offers insights into the tumor’s molecular characteristics
Circulating tumor dna (ctdna) – subset of cell-free dna (cfdna)
Reveals intercellular communication
detects and monitors cancer identifies mutations and copy number variations aids in treatment selection
mRna identifies disease-associated mRna expression patterns
May serve as potential biomarkers for cancer and other diseases
Table 3. Analytes for liquid biopsies and their applications.
The different types of endoscopic exams are used to examine structural abnormalities or an obstruction in different parts of the body:
• Cystoscopy to examine the bladder and urinary tract
• Colonoscopy to examine the colon and rectum
• Endoscopic retrograde cholangiopancreatography (ERCP) to examine liver, gallbladder, bile ducts, and pancreas
• Esophagogastroduodenoscopy (also called EGD or upper endoscopy) to examine esophagus, stomach, and duodenum
• Sigmoidoscopy to examine the lower one-third of the large intestine
Tumor biopsies help to determine whether a tumor is malignant (cancerous) or benign. Some of the common types of biopsies are as follows:
• Endoscopic biopsy
• Bone marrow biopsy
• Excisional/wide local incision biopsy (when the entire tumor is removed) or incisional biopsy (only a portion of the tumor is removed)
• Fine needle aspiration biopsy
• Punch biopsy (involves taking a deeper sample of the skin)
• Shave biopsy (involves removing the top layers of skin by shaving it off)
• Skin biopsy
Limitations of tumor biopsies27,28
• Tissue biopsies are an invasive method and difficult to collect for some anatomical sites.
• They provide very limited information on the intratumoral and intermetastatic genetic heterogeneity and the genetic and epigenetic changes that occur with disease progression. Thus, the therapeutic decisions must be based on historical tissue biopsy results, which may be suboptimal.
• They cannot identify any lesions in different locations.
• Surgical biopsies:
• Cannot be repeated or done frequently.
• Dependent on patient’s age and health condition.
• Involve high cost.
• Can cause harmful clinical complications. 28 Depending on the tissue biopsy procedure, patients may experience excessive bleeding (hemorrhage), infection, puncture damage to nearby tissue or organs, and skin numbness around the biopsy site. 29
• However, tumor biopsies have limitations that can be circumvented by liquid biopsies.
• However, tumor biopsies have limitations that can be circumvented by liquid biopsies.
Tumor biopsy limitations can be circumvented by liquid biopsies. Liquid biopsies are based on the molecular profiling of biofluids and thus are able to overcome some of the above-mentioned limitations posed by tissue biopsy.27
Advantages of liquid biopsy tests are as follows:
• Liquid biopsy is minimally invasive and hence does not pose the challenges to the patient that invasive surgical tissue biopsies may cause.
• Specimens for liquid biopsy are body fluids and can be collected frequently.
• Analysis of liquid biopsy tests can provide various information in real-time including mutations in DNA, copy number alterations (CNAs) of crucial genes, transcriptome/proteome profiling, epigenetic alterations, metabolite profiling, etc. This analysis provides crucial longitudinal information and data for more accurate diagnosis by the pathologists regarding both primary and metastasized tumors. 30 Additionally, this information helps the pathologist understand the state of the tumor, see genetic and epigenetic changes occurring in the tumor with progression, and see possible metastatic alterations, allowing proper therapeutic management of the cancer patient. 28
The most common methods that have been used for liquid biopsy are traditional qPCR mutational testing, droplet digital PCR (ddPCR), and next-generation sequencing (NGS). 33 Newer technologies such as nanotechnology are being developed for liquid biopsy applications and have shown good promise.33,34 Table 3 provides examples of a few analytes for liquid biopsies and their applications.31
The list of FDA-approved liquid biopsy tests are as follows:32
• Cell Search Circulating Tumor Cell (CTC) Test detects CTCs. It’s used to predict the likely outcome for people with metastatic breast, prostate, or colon cancer.
• Cobas EGFR Mutation Test v2 detects ctDNA. It detects a mutation on the EGFR gene in non-small cell lung cancer (NSCLC).
• Guardant360 CDx detects ctDNA.
• FoundationOne Liquid CDx detects ctDNA. Guardant360 CDx and FoundationOne Liquid are approved both for companion diagnostics and general tumor profiling.
Cancer is treated in several ways and is dependent on the patient’s medical condition, age, health, lifestyle, and the type and stage of cancer. Possible treatment options are chemotherapy, radiation therapy, surgery, and biological therapies.35
Scan code to go directly to the CE test.
Owing to a better understanding of cancer as an evolving, heterogeneous disease, cancer treatment has progressed from radical surgeries and conventional chemotherapy to highly personalized approaches like precision oncology, 36 targeted therapies, and immunotherapies, including CAR-T cells.37 This has led to more effective, less toxic treatments focused on the patient’s specific biomarkers and the tumor’s genomic characteristics.
There have been continuous advancements in the techniques and technologies in oncology, marked by advancements in early detection, targeted therapies, and immunotherapies. Immunotherapies that harness the body’s own immune system to fight cancer (such as checkpoint inhibitors); CAR T-cell therapy;37 personalized mRNA vaccine;38 new drug delivery modalities like antibody drug conjugates (ADC);39 robotic assisted surgery;40 and combination therapies41 where different types of immunotherapies, targeted therapies, and traditional treatments may be used to enhance anti-tumor responses and overcome resistance are all transforming oncology. This evolution is leading to highly personalized, precise therapies tailored to a patient’s tumor profile. Advancements in immunology, genomics, and technology like nanotechnology42 and artificial intelligence43 are driving this new era of precision oncology, improving both patient outcomes and quality of life. There is hope that in the near future, cancer will no longer be considered a challenging disease by healthcare professionals and patients.
1. NCI Dictionary of Cancer Terms. Oncology. National Cancer Institute. Accessed October 3, 2025. https://www.cancer.gov/publications/ dictionaries/cancer-terms/def/Oncology.
2. Siegel RL, Kratzer TB, Giaquinto AN, Sung H, Jemal A. Cancer statistics, 2025. CA Cancer J Clin. 2025;75(1):10-45. doi:10.3322/caac.21871.
3. Dash BC, El-Deiry WS. Cell cycle checkpoint control mechanisms that can be disrupted in cancer. Methods Mol Biol. 2004;280:99-161. doi:10.1385/1-59259-788-2:099.
4. AACR Cancer Progress Report 2024. Understanding the path to cancer development. American Association for Cancer Research. Accessed October 3, 2025. https://cancerprogressreport.aacr.org/wp-content/ uploads/sites/2/2024/09/AACR_CPR_2024.pdf.
5. About Cancer. Diagnosis and staging. National Cancer Institute. Accessed October 3, 2025. https://www.cancer.gov/about-cancer/ diagnosis-staging.
6. How is cancer diagnosed? Stanford Health Care. Accessed October 3, 2025. https://stanfordhealthcare.org/content/shc/en/ medical-conditions/cancer/cancer/cancer-diagnosis.html/.
7. Tumour markets. The Doctors Laboratory. Accessed October 3, 2025. https://www.tdlpathology.com/specialties/tumour-markers/.
8. Pao W. Ladanyi M. Detecting gene alterations in cancers. My Cancer Genome. Updated May 26, 2019. Accessed October 3, 2025. https://www.mycancergenome.org/content/page/ detecting-gene-alterations-in-cancers/.
References are available online at https://mlo-online.com/55321223.

Rajasri Chandra, MS, MBA is a global marketing leader with expertise in managing upstream, downstream, strategic, tactical, traditional, and digital marketing in biotech, in vitro diagnostics, life sciences, and pharmaceutical industries. Raj is an orchestrator of go-to-market strategies driving complete product life cycle from ideation to commercialization.
By Kinal Bhatt, MD, MPH
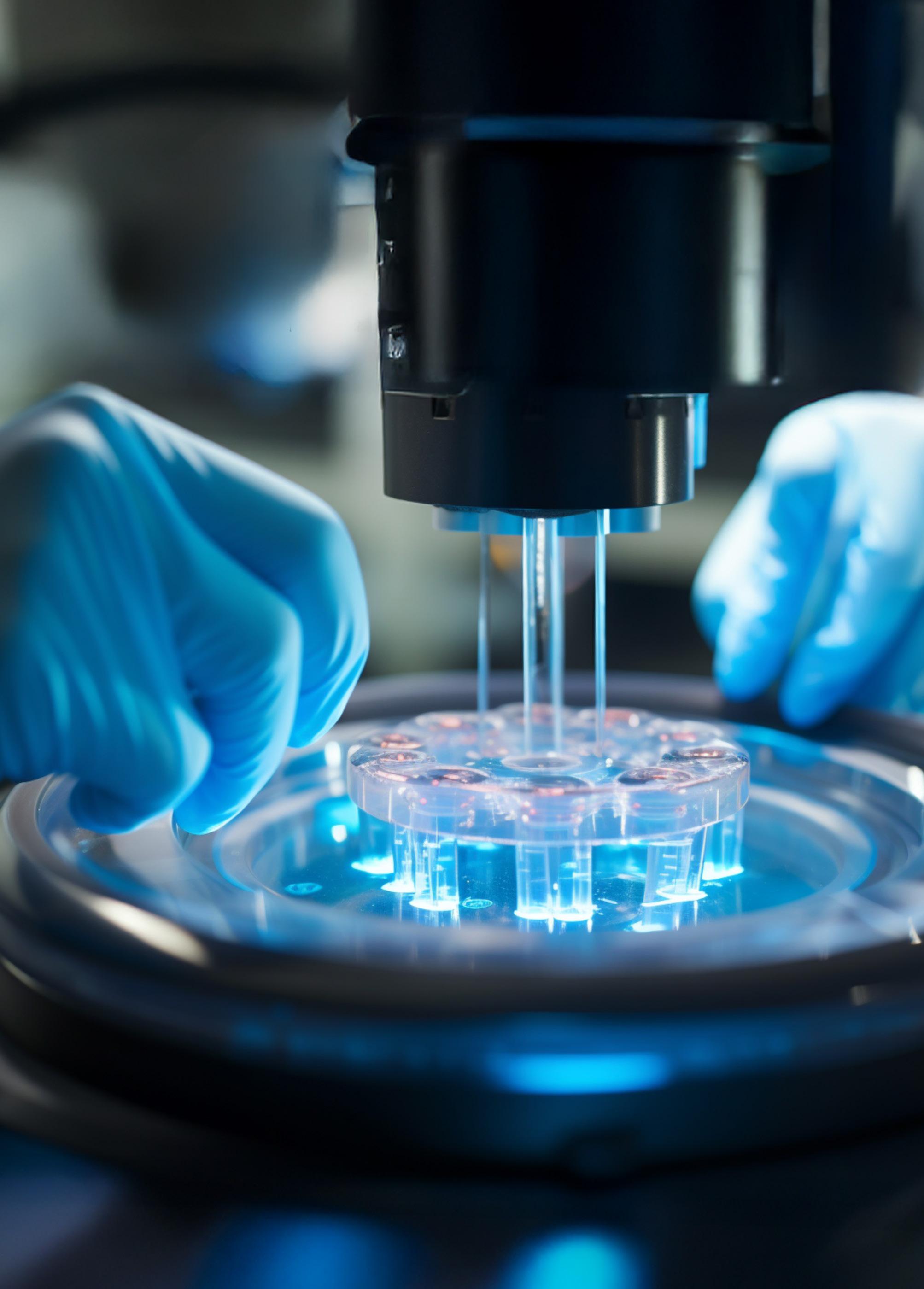
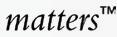
Alzheimer’s disease (AD) remains one of the most pressing public health challenges, with millions affected worldwide and numbers expected to rise. Early and accurate diagnosis of AD is critical for enabling access to emerging treatments, care planning, and supporting symptom management. Identifying the disease in its preclinical or early symptomatic stages allows clinicians to initiate interventions that may slow progression, manage symptoms more effectively, and improve quality of life. It also enables patients and families to make informed decisions about future care, legal and financial planning, and participation in clinical trials.
From a therapeutic standpoint, early diagnosis is increasingly important as disease-modifying treatments become available, many of which are most effective when administered before significant neurodegeneration has occurred. For clinical laboratories, this underscores the value of reliable, accessible testing methods that can support timely and precise diagnostic workflows.
As the demand for early and accurate diagnosis grows, clinical laboratories are increasingly positioned at the forefront of innovation—transitioning from peripheral roles to central players in neurodegenerative disease diagnostics.
From imaging to biomarkers: A shifting diagnostic landscape
Historically, AD diagnosis has relied on clinical assessments, neuropsychological testing, and advanced imaging techniques. Amyloid and tau PET scans provide direct measures of amyloid and tau pathology, while MRI is primarily used to assess structural and functional brain changes associated with neurodegeneration. Although informative, these methods are costly, invasive, and often inaccessible to many patients. Cerebrospinal fluid (CSF) analysis, another cornerstone of AD diagnostics, offers high diagnostic accuracy but requires lumbar puncture and specialized handling—limiting its scalability and routine use.
Because of these methodological constraints, clinical laboratories have traditionally played a limited role in these diagnostic workflows. However, the emergence of blood-based biomarkers is reshaping this landscape, promising scalable and minimally invasive tools that can complement, and in some contexts reduce reliance on, imaging and CSF testing.
Blood-based biomarkers: A new frontier for labs
For many years, scientists, clinicians, and diagnostic companies have been searching for an easier way to identify AD. Recent advances have identified key plasma biomarkers that reflect AD pathology with high accuracy. For example, plasma tau phosphorylated at amino acid 217 (p-Tau217) has shown similar sensitivity and specificity to CSF for identifying tau and amyloid pathologies,1 which mirrors study findings (although accuracy may vary across settings). p-Tau217 has been observed
to rise decades before cognitive symptoms and may precede detectable tau accumulation on PET.2
When used in combination, biomarkers have the potential to offer diagnostic accuracy comparable to amyloid PET imaging, which can be especially beneficial for cognitively unimpaired individuals. A ratio of p-Tau217, a marker of tau pathology, and amyloid beta 1-42 (Aβ1-42), a marker of amyloid accumulation, in the brain, has shown high accuracy (with positive and negative predictive values (PPV and NPV) ≥90%) for detecting amyloid pathology.3
In May 2025, the U.S. Food and Drug Administration granted clearance for the first blood test designed to aid in the detection of amyloid plaques—a hallmark of AD—in adults 55 and older who exhibit symptoms of cognitive decline. In clinical studies, this assay, the Lumipulse G pTau217/β -Amyloid 1-42 Plasma Ratio test, demonstrated a positive predictive value of ~92% and a negative predictive value of ~97%,


showing strong concordance with PET and CSF results and marking a major milestone in AD diagnostics.4
In July 2025, the Alzheimer’s Association issued the first evidence-based clinical practice guidelines focused on the use of blood-based biomarker tests to “assess levels of Alzheimer’s disease pathology in people with cognitive impairment.”5
The new guidelines currently only apply to patients with mild cognitive impairment who are being seen for memory disorders, and the test must meet certain criteria to apply:
• “BBM tests with ≥90% sensitivity and ≥75% specificity can be used as a triaging test, in which a negative result rules out Alzheimer’s pathology with high probability. A positive result should also be confirmed with another method, such as a cerebral spinal fluid (CSF) or amyloid positron emission tomography (PET) test.
• “BBM tests with ≥90% for both sensitivity and specificity can serve as a substitute for PET amyloid imaging or CSF Alzheimer’s biomarker testing.” 5
Note that these recommendations apply exclusively to patients with
objective cognitive impairment presenting to specialized memory care settings and should always be interpreted within the broader clinical context, with attention to test performance variability.
Despite their promise, blood-based biomarkers are not without challenges. Standardization of pre-analytical methods and guidelines for assessing these biomarkers will be required for consistent and reliable integration into clinical practice.6,7 Labs integrating AD biomarker must consider factors such as pre-analytical differences; biological variability, including age, sex, APOE ε4 carrier status; and interpret results in light of comorbidities such as kidney disease.8
Before the sample ever reaches the machine, variables such as the sample type (plasma vs. serum), collection tube type (e.g., K 2EDTA versus K 3EDTA versus lithium heparin versus sodium citrate), mixing ratios, and processing time can significantly impact results.9
For example, amyloid beta (Aß) is a relatively sticky protein. Tubes that
minimize proteolytic degradation and reduce protein binding to the surface of the tube (which can lead to artificially low levels of Aß) can decrease peptide degradation, improving accuracy.9,10 Similarly, the stability of certain biomarkers is highly dependent on proper pre-analytical handling and storage temperature of blood samples.11,12
Other than the aforementioned Lumipulse assay, plasma-based assays remain research use only (RUO) or are laboratory-developed tests (LDT). Tests must meet CLIA standards and, where applicable, FDA clearance or LDT validation under CLIA. Understanding the sensitivity and specificity of available assays—be they RUO assays or already approved—can aid in the understanding of test reliability. This is essential for evaluating diagnostic utility, minimizing false positives or negatives, and guiding clinical decision-making and research applications.7
Test sensitivity, specificity, and reproducibility must be evaluated and verified. Similarly, calibration, reference ranges,




and inter- and intra-lab harmonization are essential for clinical reliability. Misdiagnosis can lead to ineffective or potentially harmful treatments, unnecessary emotional distress, and exclusion from clinical trials that could offer therapeutic benefits.13 Labs and clinicians must be aware of the psychological impact of early diagnosis and ensure results are communicated accurately and responsibly.14,15
Workflow integration and clinical impact
With complex texting and increasing demand, laboratories must consider how blood-based biomarker tests fit into their broader clinical workflows:
• Analyzers and automation: Advantaged workflows, driven by advanced technologies, automation, and high-sensitivity analyzers, can streamline operations, reducing errors, manual touchpoints, and repetitive steps
• Ordering and reporting: Clear guidelines for patient preparation (e.g., fasting status, time of day16), test use (e.g., cognitive screening, differential diagnosis, eligibility for disease modifying therapies), and result interpretation (relative to things like disease stage and comorbidities) are needed to support clinicians
• Data integration: Results should be compatible with laboratory information systems (LIS) and electronic health records (EHR) systems to enable longitudinal tracking (needed for monitoring disease progression) and decision support (needed for evidence-based recommendations)
• Clinical utility: Biomarker testing can help identify patients eligible for disease-modifying therapies and help reduce reliance on more invasive and costly procedures such as imaging and CSF testing
As our understanding of AD and other dementias grows and more biomarkers become available, we will be better equipped to identify individuals at risk and monitor disease progression. Simultaneously, our reliance on the expertise of the clinical laboratory staff for translating results into actionable diagnostic data will grow. Collaborative models involving partnerships between clinical labs, neurology clinics, biomarker
manufacturers, research institutions, and pharmaceutical companies will be essential for refining testing protocols, validating new assays, and ultimately improving patient outcomes through more integrated and personalized diagnostic strategies.
Blood-based biomarkers represent a turning point in Alzheimer’s disease diagnostics, and clinical laboratories are poised to play a transformative role,
As the demand for early and accurate diagnosis grows, clinical laboratories are increasingly positioned at the forefront of innovation.
fundamentally reshaping the future of dementia care. Continued research, education, innovation, and ethical deployment are essential to maximizing the impact of these biomarkers. Working with the assay developer to establish comprehensive training for personnel regarding the challenges of implementing AD blood-based biomarkers will position clinical laboratories for success in the ever-evolving landscape of AD diagnostics.
1. Khalafi M, Dartora WJ, McIntire LBJ, et al. Diagnostic accuracy of phosphorylated tau217 in detecting Alzheimer’s disease pathology among cognitively impaired and unimpaired: A systematic review and meta-analysis. Alzheimers Dement 2025;21(2):e14458. doi:10.1002/alz.14458.
2. Jonaitis EM, Janelidze S, Cody KA, et al. Plasma phosphorylated tau 217 in preclinical Alzheimer’s disease. Brain Commun. 2023;5(2):fcad057. doi:10.1093/braincomms/ fcad057.
3. Wynveen P, Lengfeld J, Lim HK, et al. Performance of the Beckman Coulter prototype plasma p-Tau217 and p-Tau217/Aβ42 ratio assays in a cohort of individuals with cognitive impairment. Poster presented at the: AAIC 2025; July 28, 2025; Toronto, CA.
4. FDA clears first blood test used in diagnosing Alzheimer’s disease. FDA. May 16, 2025. Accessed September 23, 2025. https://www. fda.gov/news-events/press-announcements/ fda-clears-first-blood-test-useddiagnosing-alzheimers-disease.
5. Alzheimer’s Association releases its first clinical practice guideline for blood-based biomarker tests. Alzheimer’s Association. July 29, 2025. Accessed September 23, 2025. https://aaic.alz.org/releases-2025/ clinical-practice-guideline-bloodbased-biomarkers.asp.
6. O’Bryant SE, Gupta V, Henriksen K, et al. Guidelines for the standardization of
preanalytic variables for blood-based biomarker studies in Alzheimer’s disease research. Alzheimers Dement 2015;11(5):549-60. doi:10.1016/j. jalz.2014.08.099.
7. Mielke MM, Anderson M, Ashford JW, et al. Considerations for widespread implementation of blood-based biomarkers of Alzheimer’s disease. Alzheimers Dement 2024;20(11):8209-8215. doi:10.1002/alz.14150.
8. Torres-Torronteras J, Gouda M, Teunissen CE, Verberk IMW, del Campo M. Impact of pre-analytical factors on fluid biomarker measurements in Alzheimer disease. In: Biomarkers of Neurodegenerative Disorders Springer Nature Switzerland; 2025:475-496.
9. Alcolea D, Beeri MS, Rojas JC, Gardner RC, Lleó A. Blood biomarkers in neurodegenerative diseases: Implications for the clinical neurologist. Neurology. 2023;101(4):172-180. doi:10.1212/WNL.0000000000207193.
10. Chen Y, Zeng X, Lee J. Improving the preanalytical stability of Alzheimer’s disease plasma biomarkers: the impact of blood collection tubes supplemented with protease inhibitors. Alzheimers Dement. 2024;20(S2). doi:10.1002/alz.088796.
11. Figdore DJ, Schuder BJ, Ashrafzadeh-Kian S, Gronquist T, Bornhorst JA. Algeciras-Schimnich A. Differences in Alzheimer’s disease blood biomarker stability: Implications for the use of tau/amyloid ratios. Alzheimers Dement. 2025;21(4). doi:10.1002/alz.70173.
12. Sunde AL, Alsnes IV, Aarsland D, et al. Preanalytical stability of plasma biomarkers for Alzheimer’s disease pathology. Alzheimers Dement (Amst). 2023;15(2):e12439. doi:10.1002/dad2.12439.
13. Gaugler JE, Ascher-Svanum H, Roth DL, et al. Characteristics of patients misdiagnosed with Alzheimer’s disease and their medication use: an analysis of the NACC-UDS database. BMC Geriatr. 2013;13:137. doi:10.1186/1471-2318-13-137.
14. Bomasang-Layno E, Bronsther R. Diagnosis and treatment of Alzheimer’s disease:: An update. Dela J Public Health. 2021;7(4):74-85. doi:10.32481/djph.2021.09.009.
15. The psychological and emotional impact of dementia. Alzheimer’s Society. Updated June 27, 2022. Accessed September 23, 2025. https://www.alzheimers. org.uk/get-support/help-dementiacare/understanding-supportingperson-dementia-psychological-emotionalimpact#:~:text=Impact%20of%20a%20 dementia%20diagnosis,if%20the%20 time%20feels%20right.
16. Verberk IMW, Misdorp EO, Koelewijn J, et al. Characterization of pre-analytical sample handling effects on a panel of Alzheimer’s disease-related blood-based biomarkers: Results from the Standardization of Alzheimer’s Blood Biomarkers (SABB) working group. Alzheimers Dement 2022;18(8):1484-1497. doi:10.1002/alz.12510.

Kinal Bhatt, MD, MPH holds a Doctor of medicine degree and a master of Public health degree. she specialized in epidemiology, health policy and management, and health education and promotion. Dr. Bhatt brings her passion for advancing medical science and improving patient outcomes combined with her cross-field collaborations to her role as medical Director at Beckman Coulter






Why Choose Unistik®?



Top Activated Safety Lancets


•Three Activation Methods for flexibility


Side Activated Safety Lancets
•Multiple Gauge Sizes & Depths to match virtually every need
•Comfort Zone Technology® helps minimize pain for patients1
•Permanently Retracts for added safety and reduced risk
Trusted by Healthcare Professionals





Contact Activated Safety Lancets
Unistik® Safety Lancets provide solutions for nearly all of your capillary sampling needs. Designed with both you and your patients in mind, Unistik® delivers comfort, reliability, and ease of use.
Available on contract with major GPOs—plus agressive contracting and incentives available.
Make the Smart Choice. Choose Unistik®!


By Sue Styles, MSI; Danielle Casey, MBA, MLS(ASCP)CM and Anita Hoeksema, MS, MLS(ASCP)CM
Thank you for submitting your proficiency testing questions. API Abby is here with answers! The American Proficiency Institute (API) is pleased to share its technical expertise on all things proficiency testing. API, a global leader in proficiency testing programs, is dedicated to improving the accuracy and efficiency of clinical laboratory testing. Known for its constant innovation in the field, API offers technical expertise and checklists to help its laboratory customers become more proficient. Now let’s get to your questions!
Dear API Abby:
I’m seeking ways to enhance the performance of our laboratory. Even with a passing grade on our proficiency testing challenges, how might we use the resulting proficiency testing data to improve?
—Task Rabbit
Dear Task Rabbit:
This is a great question! I am so glad you have identified that proficiency testing
is more than just a pass or fail test. Proficiency testing can help you identify problems before they turn into critical errors. By looking at your overall trend in performance you may notice that you are starting to show a bias, and that may help you identify shifts in calibration or missed maintenance before you detect an error in your controls. Similarly, looking at your trend analysis over multiple events can help you identify if you have an issue that is slowly affecting the outcome of your result.
Because proficiency testing should be run as close as possible to a patient test, proficiency testing can help to identify pre- and post-analytical errors as well. A result that seems like it may have been one random error may actually be identifying someone who is missing a critical step in the testing process. For example, take a laboratory that reported urine susceptibility results and received a failure on a common antimicrobial drug. Upon investigation, the supervisor found that the technologist did not indicate the source when setting up susceptibility
testing on their instrument-based test system. Without the source information, the system tested a drug that was inappropriate to report for a urinary tract infection. This investigation alerted the supervisor to do a chart review to ensure that patient samples did not include reports with inappropriate antibiotics. This also led to a training opportunity for the technologist.
Dear API Abby:
I know, I know… thou shalt not share proficiency testing results! However, without revealing who performed the test, is it permissible to discuss proficiency testing results with our laboratory team after the event? Is there a teaching schematic we might use?
—All Together Now
Dear All Together Now:
Every moment can be a teaching moment, and proficiency testing is no exception. It is important that you noted “after the event.”You should never discuss your proficiency testing results
during the event, but afterwards there is much to learn.
For example, proficiency testing challenges that use virtual or paper images, such as blood cells or parasite challenges, may be shared with the laboratory team after the test event’s due date. Ask their opinions and discuss the responses. If there was a particularly challenging image or a source your laboratory does not view on a regular basis, this may be a great teaching moment.
Quantitative results can be just as educational. If you note that you are starting to trend above or below your peer group mean on a particular analyte, challenge your staff to do some problem solving. What is occurring that may cause your laboratory to trend lower or higher than your peers? As the team investigates, they will be learning about the analyte, the instrument, your control processes, and your procedures. These wonderful learning moments may benefit both new and seasoned technologists.
Dear API Abby:
Does the recent court action on laboratory-developed tests (LDTs) impact proficiency testing?
—Inquiring Izzy
Dearest Izzy:
In response to the court decision, in September 2025, the Food and Drug Administration (FDA) reverted its regulatory text for laboratory-developed tests back to what was issued prior to May 2024. So, the short answer to your question is no, proficiency testing is not impacted. Accuracy and validation though proficiency testing or alternative assessments continue to be required for LDTs under CLIA regulations.
Dear API Abby:
How should my laboratory be assessing accuracy if no proficiency testing is available? Are there ways for us to request new proficiency testing programs?
—An Enthusiast
assessments should be performed at least twice a year. The most commonly utilized options are split-sample analysis and exchanging samples with another laboratory. These exercises may document method comparability or linearity and verify accuracy.
In addition to basics like how to obtain samples and which test results will be compared, laboratories performing alternate assessments should consider the credentials of any other laboratories providing results, the clinically
allowable difference between results, and the levels of analytes to be tested. There are also services that might simplify some decisions, like a sample exchange registry that allows laboratories to obtain split samples for analytes that are complex, or for specialty testing panels, and provides results back to each participating laboratory. In any case, your laboratory director should approve and document the plan for each alternate assessment performed.
Continued on page 19













Dear Enthusiast:
Kudos to you for recognizing that validating the accuracy and reliability of your assays is essential to your laboratory’s overall quality. While proficiency testing is one valuable way to document performance, it is not the only option. Alternative assessments may also be used to demonstrate accuracy and reliability, especially when proficiency testing is not required or available. To meet regulatory expectations, these
By Alesia McKeown, PhD
Unpredictability has become a defining challenge for laboratories preparing for the annual respiratory season. With fluctuating seasonal severity, overlapping viral and bacterial threats, and emerging pathogens with pandemic potential, laboratories continue to be challenged in their ability to develop a testing strategy that meets all of these needs. The 2024–2025 respiratory season embodied all of these uncertainties. It was characterized by an especially severe influenza burden, the first high-severity season in more than seven years, along with the highest rates of hospitalizations and outpatient visits for respiratory illnesses observed in the last fifteen years.1,2 Additionally, rising cases of Mycoplasma pneumoniae 3 and Bordetella pertussis 4 further demonstrated the need to include bacterial pathogen detection within the diagnostic toolkit. Lastly, heightened surveillance of the human burden of influenza A(H5N1) challenged testing strategies, demanding many institutions to adopt additional measures for influenza A subtyping in their inpatient populations. 5

The dynamic nature of the annual respiratory burden must be met with options that offer flexibility. Customizable and flexible molecular solutions now represent a critical tool for aiding in the development of a fit-for-purpose respiratory testing strategy. These solutions, which are being developed on CLIA-waived and moderate complexity systems, now offer unprecedented ease in designing a personalized strategy that empowers institutions to maximize the diagnostic yield of each test to uniquely meet their regional needs.
Designing a respiratory testing strategy is anything but prescriptive. Labs must balance clinical needs, operational realities, and resource constraints to find the right fit. The Association for Diagnostics & Laboratory Medicine’s document on laboratory diagnosis of respiratory viruses, released in 2024, provides a framework and guidance, but real-world implementation varies.6 While there is no one-size-fits-all approach, there are several key factors for laboratories to consider when developing testing strategies:
• Seasonality and current trends: Factor in the unpredictable timing and prevalence of viral and bacterial respiratory pathogens.
• Patient populations: Consider age, demographics, immune status, and comorbidities.
• Care setting: Tailor testing approaches to the unique demands of inpatient versus outpatient environments and access to CLIA-waived and moderate complexity systems.
• Time to result and turnaround time: Ensure results are delivered quickly enough to guide clinical decisions effectively.
• Actionability of results: Focus on tests that will meaningfully influence patient management and public health decisions.
• Access/reimbursement: Evaluate whether the test is both medically necessary and accessible to the target patient population. Given all of these considerations, many laboratories have turned to multiplex testing platforms for the diagnosis of respiratory infections. Defined as a syndromic approach to diagnosis, these tests are designed to provide simultaneous results for multiple pathogens that cause similar symptoms, all from a single patient sample. Targeted multiplex tests that detect influenza A, influenza B, SARS-CoV-2, and RSV (often referred to as a respiratory 4-plex) have risen in popularity in the post-pandemic era and are becoming the standard of care for diagnosis of respiratory infections for the general population. Expanded multiplex panels that typically detect 20-plus viral and bacterial pathogens have also gained traction for their role in defining treatment plans for inpatients and high-risk individuals. However, challenges still remain in determining how best to leverage these standardized solutions within diverse patient care pathways, especially in the face of changing seasonal dynamics.
Flexible, customizable diagnostic solutions are a promising tool for laboratorians looking to evolve their testing strategies to better meet their specific needs. Potential impacts of a flexible solution include the following:
• Higher diagnostic yield: Customizable panels allow laboratorians and providers to design tests that detect only what is medically necessary for their patient population. One study showed that tailoring










During respiratory season, your patients depend on you to provide fast, accurate diagnosis and effective treatment plans. Having the right diagnostic solutions in your office can help you provide the care your patients expect.
Our product portfolio includes high-quality, point-of-care molecular and antigen tests for diagnosing respiratory illnesses. Our solutions can help you deliver answers and treatment plans for your patients which can get them on the road to recovery and improve outcomes for your clinical practice.
We make diagnostics that matter because we believe each test represents the health and well-being of a real person.






patented swabs


Puritan PurSafe Plus® Collection & Transport System,FDA-approved for the collection, inactivation and preservation of upper respiratory tract specimens suspected of containing SARS-CoV-2, featuring patented HydraFlock® flocked swabs.
VISIT US IN PERSON AMP2025, Booth #1129
LEARN MORE ONLINE info.puritanmedproducts.com/ pursafe-plus
panel composition based on local pathogen prevalence, patient age, and epidemiologic trends can greatly increase diagnostic yield.7 Another study found that adding high-prevalence targets, such as rhinovirus, to a standard 4-plex respiratory panel improved diagnostic yield from 12.5% to 26% during the study period.
• Improved diagnostic stewardship: Some flexible solutions also offer digital reflex testing, which allows a two-step approach for results reporting, all from a single test run. Clinicians can first request a subset of targets and, if those are all negative, the instrument will automatically provide results for a predefined list of additional pathogens. Manual release of additional targets may also be possible if results are requested within a pre-defined time window. Digital reflex supports diagnostic stewardship by reducing duplicate testing and decreasing reagent costs. 8
• Increased access: Flexible respiratory testing technologies are now being designed for highthroughput platforms, enabling laboratories to process larger volumes more efficiently. Expanded multiplex panels on these systems have the potential to cut costs, streamline workflows, and make comprehensive respiratory testing more affordable, increasing access for a broader patient population.
As laboratories prepare for another season marked by both familiar and unpredictable respiratory threats, the ability to adapt strategies to specific needs while maintaining vigilance for unexpected changes will be critical. Flexible, customizable testing technologies offer a way forward, helping networks expand access, refine stewardship, and respond efficiently to shifting patterns of disease. Is your institution ready for a change? Consider these questions when evaluating how these solutions may be implemented in your network:
benefit most from customizable respiratory panels?
• How could implementing digital reflex or flexible panel options support stewardship and cost efficiency?
• What partnerships across clinical teams (e.g., infection prevention, pediatrics, emergency medicine) would strengthen adoption of these solutions?
By asking these questions now, laboratorians can build a foundation of preparedness that balances flexibility, stewardship, and personalized patient care.
1. Dugan V. 2024-25 Influenza season update and seasonal influenza vaccine recommendations for the 2025-26 U.S. influenza season. CDC/NCIRD. June 26, 2025. Accessed October 3, 2025. https://www. cdc.gov/acip/downloads/slides-2025-06-2526/04-dugan-influenza-508.pdf.
2. Lewis T. Why this year’s flu season is the worst in more than a decade. Scientific American. March 6, 2025. Accessed October 3, 2025. https://www.scientificamerican. com/article/why-this-years-flu-season-isthe-worst-in-more-than-a-decade/.
3. Same RG, Gerber JS. Walking (pneumonia) down memory lane: Mycoplasma pneumoniae returns. J Pediatric Infect Dis Soc. 2025;14(2):piaf006. doi:10.1093/jpids/ piaf006.
4. Hanna S, Samies N. Clinical progress note: Pertussis. J Hosp Med. 2025;20(8):862-865. doi:10.1002/jhm.70080.
5. CDC. Technical Report: June 2024 highly pathogenic avian influenza A (H5N1) viruses. CDC. June 5, 2024. Accessed October 3, 2025. https://www.cdc.gov/bird-flu/ php/technical-report/h5n1-06052024.html.
6. Berry GJ, Jhaveri TA, Larkin PMK, Mostafa H, Babady NE. ADLM guidance document on laboratory diagnosis of respiratory viruses. J Appl Lab Med. 2024;9(3):599-628. doi:10.1093/jalm/jfae010.
• Does our current testing strategy provide enough flexibility to adapt to unexpected shifts in circulating pathogens?
• Which patient populations or care settings in our network would
7. Gonzalez K, Amicarelli G. Age-stratified epidemiology of respiratory pathogens and the value of customizable syndromic testing using the LIAISON PLEX respiratory flex assay. J Mol Diagn. 2025;27(9):809-818. doi:10.1016/j.jmoldx.2025.05.009.
8. Norton JM, Dashler G, Klein E, Mostafa HH. The utility of syndromic respiratory pathogen panels: the premise of flexible and customizable approaches. J Clin Microbiol. 2025;63(7):e0031325. doi:10.1128/ jcm.00313-25.

Alesia McKeown, PhD is a Scientific Partner for Infectious Disease in Medical and Scientific Affairs at Roche Diagnostics . She is the subject matter expert for Roche’s high-throughput and POC respiratory solutions. She also co-leads an interdisciplinary team focused on improving access and utilization of diagnostics in the respiratory disease area.
Your feedback on what you need to maintain laboratory compliance is valued by proficiency testing providers. After all, no one understands your laboratory’s needs better than you! By communicating with your proficiency testing provider via a phone call, email, request form, chat, etc., they can conduct an evaluation and begin researching the analyte, the platforms used for testing, relevant target ranges, regulatory requirements, and possible sample types to potentially offer a program. The sooner your proficiency testing provider hears of a need, the sooner they can work to create a proficiency program for that analyte.
Dear API Abby:
My reagent is on backorder, and I don’t know when more will come in. Do I still have to do the proficiency test, or should my patient samples take priority?
—Patience Counts
bodies are allowed to employ their own approaches for adding value. They may add requirements designed to further improve laboratory quality, such as additional proficiency testing, staff training, or laboratory procedures. They may monitor proficiency scores differently to help prevent small issues from becoming bigger problems. They may also use different terminology or add different expertise to the teams that visit laboratories. All these differences are allowed as long as the CLIA rules, at a minimum, are followed.
Dear API Abby:
MLO polled its readers on the following question: While reviewing proficiency test results for hemoglobin A1c, you observe your laboratory’s values are consistently lower than expected. Which of the following is the most likely source of error?
A) Problem with the most recent calibration.
B) Change in reagent manufacturer or formulation.
Dear Patience:
Of course you want to put patients first! However, sometimes that means making hard choices, and this is one of those times. Providing the best patient care means keeping up all your usual quality measures.You wouldn’t skip your routine controls, so if you are currently testing patients, you must also perform proficiency testing as scheduled. Proficiency testing may be one of the few times you test a sample with an abnormal result, or culture a bacteria species that might show up in a patient a few months from now. It is important to know that your systems are all running as intended. Backorders always happen at the worst times, though. If you do find yourself out of reagent when your proficiency testing is scheduled, the basics are to notify your proficiency testing provider, document the situation, and save your samples.You can usually notify your provider as part of reporting your other results, indicating which tests you cannot perform. This avoids a 0% score for failing to participate. Your documentation should include the dates of the proficiency testing event, when patient testing stopped, and a record of the supplies being on backorder. Finally, if you save your samples and test them when you have supplies again, it will help to document how you would have performed.
Here’s hoping your supplies come in soon!
Dear API Abby:
My friend who works in another laboratory said they made changes after a recent inspection and added a process we do not follow where I work. My manager said we do not need to change, that their process could be due to a different requirement. This made me wonder, if all laboratories follow CLIA, how can there be “different” requirements?
—Claire N. Consistent
C) Results were not transcribed onto the result forms correctly.
D) An issue with the sample storage temperature before testing.
—MLO Reader
Dear Claire:
It does seem like the rules should be the same for everyone, right? Rest assured there is no unfairness here. Different requirements can be due to differences between laboratories, but another common reason is laboratories choosing to be accredited. Accreditation usually replaces your state CLIA inspection and can include additional requirements your laboratory agrees to meet.
There are several laboratory accreditation organizations that review CLIA compliance in addition to their own accreditation requirements. CMS ensures that these approved organizations follow CLIA requirements. Other than that, the accreditation
Dear MLO Reader:
The answer is A, a problem with the most recent calibration is the most likely source of error. While all of the answers are important issues to investigate, calibration should be your first check when observing lower than expected values for hemoglobin A1c.
A majority of poll respondents (64%) answered correctly with “A.” 16% answered “B,” 2% answered “C,” and 19% answered “D.”

Sue Styles, MSI is Director of Quality and regulatory a ffairs at American Proficiency Institute she is responsible for a Pi ’s c L ia compliance and approval with regulatory organizations and oversees reporting of laboratory data to those organizations. Ms. s tyles led a Pi ’s accreditation to the iso standard for proficiency testing providers, iso / iec 17043, and has conducted international training on topics related to the standard. a s part of maintaining a Pi ’s quality management system, she is also involved with auditing, analyzing sample quality data, and setting policy.

Danielle Casey, MBA, MLS(ASCP) cM is Vendor relations Manager at American Proficiency Institute she oversees sample procurement, organizes pilot studies, and plays a critical role in the strategic planning of proficiency testing programs. Ms. casey is the primary contact for i VD manufacturers to work with a Pi to develop proficiency programs for novel test systems and analytes. she has been instrumental in researching, developing, and implementing over 30 new proficiency testing programs for a Pi including a Urinary tract infection Panel and a nail infection Panel, both of which were the first of their kind in the world.

Anita Hoeksema, MS, MLS(ASCP) cM is the technical support Manager at American Proficiency Institute. she oversees the development and maintenance of proficiency testing programs including providing participant instructions, collecting results, and generating evaluations. Ms. Hoeksema provides technical leadership to a team of medical laboratory scientists who implement a Pi programs according to c L ia requirements and provide technical support to participants.



I like your article and answers. Thank you. My comment is about the Coaching Corner in the September 2025 issue:
I just have another suggestion for this Team Building meeting situation — other than just lack of trust. As an introvert, like many science- and engineering–type people, when I am asked point blank what my concerns or questions are, I can’t think of a thing. I need to mull it over and process the question. I don’t think well “on the spot.” Because of this, I have learned to run my meetings by letting people know beforehand if I will be looking for suggestions about a particular topic. I could have them write down their thoughts to bring to the meeting. If it is a sensitive topic, I would let them email their concerns BEFORE the meeting so that I can anonymously share those thoughts with the group.
I have become very aware of how extroverts and introverts differ in their work style and the advantages of each, so that was my first thought when I read this question.
Thank you, Susan
Thank you for your email! Yes, speaking as a recovering introvert, I totally understand your perspective, and you are correct. It does take more time for some people than others to respond. I also believe that the more you meet as a team and make it safe for everyone to contribute, even the most introverted find they are valued for their input and will eventually open up. Especially those that initially send their thoughts by email after the meeting as described by the person who wrote into MLO. It is good that you take everyone into consideration before and during the meeting. I bet that makes your meetings both engaging and productive!
Thank you for reading my column and let’s keep the conversation going!
I am a new MLS graduate, and I am very excited to begin my career! I did great in training, interacted well with the teaching MLSs in the departments, am a hard worker, and received high scores on my exams. I didn’t get a perfect score on my ASCP certification, but I passed in June and was offered jobs in two of the three hospitals where I interviewed. The hospital I chose has a great reputation, and I was very excited to be offered a 12-hour day shift generalist position. I am writing because I think I made a mistake. They seem to hate me here. I can’t seem to do anything right and there is one person, in particular, that seems to run the show, and she is not even a supervisor! She is older and acts like I am an idiot and makes snide comments to the other MLSs about me. Should I quit and see if the other job is still open? Maybe this is not the right career for me.
DEAR GROWING SCIENTIST:
It really pains me to read this because I believe you have chosen an amazing career and one that, because of the learning experience you have described, is a career that you will be very successful in and find fulfilling. No one should be expected to start their career, fresh out of school, knowing everything. It takes proper training, mentoring, and both understanding and grace to grow. It doesn’t happen overnight and surely not in the very few three months since you graduated. Working only three days a week, there are probably some low volume tests that you have not even seen yet! I fear that what you are experiencing is bullying by the other scientists on the team, specifically this older “informal” leader that is being both unkind and unprofessional. Her behavior is negatively influencing others to behave in the same intolerable way, and I am especially concerned if this is going on unchecked by leadership.
Bullying is becoming a big issue in the lab. In fact, the March issue of MLO published an article titled, “How addressing bullying in medical labs will improve overall retention” written by Alex Mitchell, the Marketing Communications Manager at Lighthouse Lab Services. In the article he quotes an informal poll, sent by Jon Harol, President of Lighthouse Lab Services as part of the 2023











MLO’s Lab of the Year Award celebrates medical laboratories that demonstrate their extraordinary commitment to quality patient care. Submissions will be judged on achievements in five areas. A panel of judges selected from MLO’s Editorial Advisory Board will select the winner and two runners-up. All will be featured in the April 2026 issue of MLO, in print and online, and awarded a display wall plaque, with the winner featured on the issue cover.
Medical laboratories, utilizers of a lab’s service and non-vendor affiliates are welcome to submit. Submission requirements are at: https://www.mlo-online.com/55316888










annual wage and moral survey asking laboratory professionals if they have ever witnessed or personally experienced bullying in the lab. 75% of the 341 respondents said that bullying in the lab is a real concern. That is a huge number, which is both sad and totally unacceptable.
Please reach out to the leadership of your lab. If there is a direct supervisor over the older scientist, go to him or her first but if you don’t feel like you are taken seriously, ask to speak with the director and Human Resources. This type of behavior must not be tolerated.
”Trust is the glue of life. It’s the most essential ingredient in effective communication. It’s the foundational principle that holds all relationships.”
In my coaching, clients tell me they are reluctant to address bullying because of fear of retaliation. That is exactly the “game” that is played by bullies, and you will need to be both courageous and strong. I promise you that the effort will be worth it!
You might feel like it is just you right now, but I am sure there are other scientists on the team who feel like they have made a mistake too, but it is no mistake! You have chosen a fantastic career and since the hospital has a great reputation, I feel certain that your Human Resource department will value your concerns.
At first, talk only to leadership about this situation, and let them handle it. It is unfortunate, but you don’t know
who you can trust if the team has an informal leader, that is the cancer metastasizing the group. Leadership should take swift action to address the situation and make sure this older scientist is held accountable for her actions while also setting firm expectations for appropriate behavior with the team. Be patient as this person also deserves the opportunity to improve. If the comments continue, just say “Please stop, your comments are not helpful/appropriate/professional.” (You choose the word that you feel most comfortable with.) However, if you feel like things are not changing or are getting worse, continue to work with leadership until it does. If at any point you feel unsafe or threatened, let your leadership know and submit your resignation. There are great labs out there with fun and caring team members led by responsible and attentive leaders. These are leaders who keep this behavior out of the team by holding themselves and others accountable to an engaging work environment and positive culture. Best of luck to you and let me know how I can help!
How do I become a good leader that people will respect?
There is a quote that says “Respect: It’s hard to attain but easy to lose” ~ Anonymous. The reason it is so hard to attain is because it is so uniquely important to people in different ways. Respect is often defined by behaviors and qualities such as integrity, honesty, empathy, consistency, presence, and being an active listener but many of these can be defined differently based upon the situation or the culture of a society, workplace, or team. I also believe that respect is a reciprocal action. You give respect and earn respect in return. It is easy to lose because there can be so much emotion around the vulnerability it takes in building great relationships.











I have studied leadership for over 30 years, but I will never scratch the surface for all the qualities that make a good leader and while I might do my best to practice what I have learned, it does not always mean that I have earned the respect of others. What I might say or do for one person that adds significant value may be offensive or cause frustration for another. It all depends on how it is said, how I hold myself accountable for my actions, and the trust I have built in the relationship. Stephen R. Covey, the author of The 7 Habits of Highly Effective People said that “Trust is the glue of life. It’s the most essential ingredient in effective communication. It’s the foundational principle that holds all relationships.” I recommend you start there, building trust. Stay genuine with your intent to serve others, stay kind, look for the best in others and interact in a consistent, positive manner, giving respect and listening to understand with an open heart and open mind. It might take some time but stay the course. If you act from the foundation of a strong set of positive values, when it feels good to you, it will feel good to others too.

Patty J. Eschliman, MHA, MLS(ASCP), DLM, CPC is a certified professional c oach who specializes in laboratory leadership growth and professional support. a s president and ceo of The Lab Leader Coach, patty coaches many lab professionals in all roles in the areas of building leadership skills, preventing burnout, improving communication, building cohesive teams, and how to be a positive influencer. She has 39 years of experience as a Medical l aboratory Scientist, the last 29 spent in leadership.




















Earn continuing education credits
Stay ahead with the latest testing techniques










Navigate regulatory updates with confidence Insights in diagnostics & molecular advances
in &























By Violet Nxedhlana, PhD, MLS(ASCP) and Shepherd Maingano, PhD, MLS(ASCP), GCCP
Perhaps the most underappreciated organ in the human body is the liver. It is one of the largest organs in the body, and unlike other vital organs such as the skin and kidneys, the liver has a myriad of functions. When the liver is compromised, its functions are also impeded. This results in many symptoms, and in some cases, the patient remains asymptomatic.
The liver weighs approximately 1.4–1.5 kilogram (kg) in males and 1.2–1.4 kg in females. It has an approximate length of 15–18 centimeters (cm), 10–12 cm width, and 5–8 cm in thickness. The liver increases 5 cm every 5 years as a child gets older and thus attains a size of 15 cm by age 15.9 Three-quarters of the liver is situated in the upper right quadrant with a thickness of 2.3 cm. The left lobe is in the upper left quadrant and is 1.2 cm thick. The right lobe extends further down than the left lobe, misaligning the left and right kidneys. However, several factors influence the exact liver measurements. Research using ultrasound showed that age, sex, body shape, and size are the critical determinants of liver size. In general, the liver is larger in males than in females.1 Examination techniques, whether palpation, percussion, or radiographic, may influence the reported measurements.9 Visually, the liver is shiny and has a burgundy color. It has a smooth texture upon touch, showing its delicacy and vulnerability. Most of the liver is protected by the rib cage, and this may pose a challenge to physical examination.
The human body is an ecosystem in which many processes take place simultaneously to maintain a homeostatic balance. Organs function to sustain the life of an organism. Many of these organs, even though vital, have limited functions compared to the liver. For example, the major function of the heart is to pump blood, the lungs for gas exchange, the kidneys for water regulation, and so forth. The liver, on the other hand, is said to have over 500 functions that include hematopoiesis, nutrient storage, metabolism, digestion, gluconeogenesis, clotting factors production, detoxification, and many other functions.
When the liver is compromised, many other processes throughout the body are affected. It is, therefore, critical to evaluate the health of the liver at certain intervals depending on a person’s genetic predisposition, age, sex, and susceptibility to occupational exposure. Clinical laboratories perform several tests that aid in the diagnosis of liver complications.
One of the most common tests for liver disease disorders is a liver profile. The profile, often called the panel, is a group of tests ordered together to provide a comprehensive status of an organ or a process. The liver profile is a panel that includes four main enzyme tests that indicate a liver disorder. A liver test, such as aspartate aminotransferase (AST), also known as serum glutamic-oxaloacetic transaminase (SGOT), is a common
enzyme used to detect liver anomalies. The challenge is that this enzyme is also found in the heart and muscles. Its elevation in laboratory testing cannot be solely attributed to liver problems. Another common liver enzyme test, alkaline phosphatase (ALP), plays a role in metabolism. The enzyme, although present in the liver, is also found in various tissues that include the intestines, kidneys, and bones. Gamma glutamyl transferase (GGT) is found primarily in the liver, where it is implicated in liver functions and bile production. Although it is used to monitor liver disease or damage, it cannot be used for the diagnosis of liver disease without other tests to confirm the diagnosis. GGT can also be used to monitor the treatment of liver conditions. Perhaps one unique characteristic of the liver is that it is the only organ in a human that has the ability to regenerate. However, Forbes and Newsome2 reported that conditions such as chronic scarring, fatty liver disease, massive liver injury, and prior exposure to chemotherapy can impede regeneration, leading to liver failure.
Alanine aminotransferase (ALT), also referred to as serum glutamic-pyruvic transaminase (SGPT), completes a list of liver tests for the evaluation of liver disorders. ALT may be in other organs, such as in heart, kidney, and muscle cells; it remains an indicator of definite liver cell injury.7 ALT is a reliable and sensitive marker for liver disease.5 Concentration of ALT in the liver is 3000 times that of the blood,8 making it an ideal marker for liver-related diseases and disorders. The elevation of ALT is the first sign of liver problems, and it triggers a workup to determine the underlying disease. ALT stays elevated in diseases such as cardiovascular disease, diabetes, and obesity.6 Other diseases associated with elevated ALT include viral hepatitis, non-alcoholic fatty liver disease, as well as acute and chronic liver diseases.10 ALT can be detected in serum at low concentrations. The amount increases with injury to the hepatocyte membrane. The amount of alanine is determined by a number of factors, including age, sex, body mass index, pubertal age, and elevated levels of triglycerides.7 Researchers also reported other physiological factors that affect ALT levels. Excessive physical exertion, ethnicity, body mass index, and diurnal variation have been associated with different levels of ALT.7
Several instruments use different methods to quantify the amount of ALT in serum or whole blood. Even though these testing methods are built into different instruments, manufacturers are concerned about the accuracy of measurement. The spectrophotometric method to quantify ALT in serum is quite popular in a clinical laboratory. Serum ALT acts on L-alanine and α-ketoglutaric acid. The reaction results in the production of L-glutamate and pyruvate. Lactate dehydrogenase catalyzes the reduction of pyruvate by NADH to lactic acid. This reaction oxidizes NADH (nicotinamide adenine dinucleotide) to produce NAD+. The rate of the NADH oxidation reaction is measured as a decrease in absorbance at 340 nanometers (nm) when using a spectrophotometer. This decrease in absorbance is directly proportional to the concentration of ALT.4
The Colorimetric method was also popular in quantifying serum ALT but was replaced by the spectrophotometric method. In this method, ALT acts on L-alanine and α-ketoglutaric acid to produce L-glutamate and pyruvate. Pyruvate then reacts with a colored agent to form a hydrazone, which has a distinct color. The intensity of the color is
proportional to the concentration of ALT and is measured by a colorimeter. Several other methods are used to measure levels of ALT. Chemiluminescence is based on enzyme coupling that results in the production of hydrogen peroxide. The produced hydrogen peroxide reacts with a chemiluminescent to produce a light signal. The light signal is measured to determine ALT levels in whole blood or serum. Fluorescence and chromatography are just some of the methods used in the laboratory.3
Alanine aminotransferase (ALT) is an important indicator for liver disease or disorder. Although AST, ALP, ACP (acid phosphatase), and LD (lactate dehydrogenase) may be included in the liver panel, ALT remains the most reliable indicator of liver disease. Even though ALT is found in several organs and tissues, the highest concentration is found in the liver. The reference range for ALT is affected by many factors that include physical exertion, age, ethnicity, and body mass index. There are several methods of testing ALT. The spectrophotometric method, which replaced the colorimetric method, is the most commonly used method in the clinical laboratory.
1. Choukèr A, Martignoni A, Dugas M, et al. Estimation of liver size for liver transplantation: the impact of age and gender: Role of Age and Gender for Liver Graft Size. Liver Transpl. 2004;10(5):678-685. doi:10.1002/lt.20113.
2. Forbes SJ, Newsome PN. Liver regeneration - mechanisms and models to clinical application. Nat Rev Gastroenterol Hepatol 2016;13(8):473-85. doi:10.1038/nrgastro.2016.97.
3. Hartmann P, Schnabl B. Inexpensive, accurate, and stable method to quantitate blood alanine aminotransferase (ALT) levels. Methods Protoc 2022;5(5):81. doi:10.3390/mps5050081.
4. Hsueh CJ, Wang JH, Dai L, Liu CC. Determination of alanine aminotransferase with an electrochemical nano ir-C biosensor for the screening of liver diseases. Biosensors (Basel). 2011;1(3):107-17. doi:10.3390/bios1030107.
5. Kaplan MM. Alanine aminotransferase levels: what’s normal? Ann Intern Med. 2002;137(1):49-51. doi:10.7326/0003-4819-1371-200207020-00012.
6. Kim WR, Flamm SL, Di Bisceglie AM, Bodenheimer HC; Public Policy Committee of the American Association for the Study of Liver Disease. Serum activity of alanine aminotransferase (ALT) as an indicator of health and disease. Hepatology. 2008;47(4):1363-70. doi:10.1002/ hep.22109.
7. Moriles KE, Zubair M, Azer SA. Alanine Aminotransferase (ALT) Test. StatPearls [Internet] Treasure Island. Published online 2024.
8. Rej R. Aspartate aminotransferase activity and isoenzyme proportions in human liver tissues. Clin Chem. 1978;24(11):1971-9.
9. Wolf DC. Evaluation of the size, shape, and consistency of the liver. In: Clinical Methods: The History, Physical, and Laboratory Examinations Butterworths; 1990.
10. Yip TC, Wong VW, Wong GL. Alanine aminotransferase level: The road to normal in 2021. Hepatol Commun. 2021;5(11):1807-1809. doi:10.1002/ hep4.1788.

Violet Nxedhlana, PhD, MLS(ASCP) is the Program Director & associate Professor of the medical technology Program at John A. Burns School of Medicine, University of Hawai‘i at Manoa she oversees the day-to-day operation of the medical technology program and is responsible for the overall management, leadership, and accreditation compliance of the educational program. she also designs, reviews, and revises the curriculum to reflect current best practices in medical laboratory science.
Shepherd Maingano, PhD, MLS(ASCP), GCCP is the Program Director & associate Professor for medical l aboratory technician and Phlebotomy Programs at University of Hawai‘i’s Kapi‘olani Community College. He is responsible for the organization, administration, periodic review, records, continued development, and general policies and effectiveness of the program. He is also a professor of Hematology and clinical chemistry.

Survey of 100+ medical laboratory professionals reveals changing MDx testing patterns, improved supply stability, cautious AI adoption, and a strong focus on quality assurance.
By Kara Nadeau
The results of the 2025 MLO MDx State of the Industry Survey (SOI) are in! Over 100 medical laboratory professionals participated, answering questions on molecular diagnostics (MDx) testing modalities and trends, supply availability, and quality assurance.
New for this year, MLO queried the medical laboratory community on clinical areas driving MDx testing demand, proficiency testing for molecular assays, and the use of artificial intelligence/ machine learning (AI/ML) tools for molecular diagnostics.
We present the quantitative survey results alongside commentary from medical laboratory professionals and vendors in the MDx space.
Key 2025 survey findings
• Clinical demand drivers: Infectious disease (non-COVID) dominates MDx testing demand, cited by 77% of respondents.
• Respiratory testing trends: More than half of laboratory professionals (55%) reported a 0–25% increase in respiratory testing this year, while nearly one-quarter (24%) reported a decrease (up from 17% in 2024).
• MDx modalities: rRT-qPCR remains the top MDx modality at 54%, though reported usage fell from 64% in 2024. Rapid molecular testing rose slightly to 52% (up from 49% in 2024), while rapid antigen testing decreased to 48% (down from 49% in 2024).
• AI/ML adoption: Two-thirds (67%) of labs are not using or planning to adopt AI/ML for molecular diagnostics. About one in five (19%) are considering future adoption, while 6% are already using AI/ML tools in their workflows.
• Supply chain pressures: Supply stability has improved: 71% of lab professionals report adequate supplies to meet demand (up from 62% in 2024), although there was a slight uptick in sourcing challenges for winged blood collection sets (16% vs. 13% in 2024).
• Quality Assurance: Proficiency testing participation is strong, led by The College of American Pathologists (CAP) (48%) and American Proficiency Institute (API) (36%). Labs are stepping up efforts to reduce the number of potential false positive test results, with 90% of respondents reporting they verify pre-analytical steps (vs. 68% in 2024).
Survey participants changed little since last year, with most respondents working in Lab Manager,
Administrator, Supervisor, or Lab Director positions (53%), employed by hospital/health system labs (51%). One notable increase was participation in the survey by Medical Laboratory Scientists (MLS) (17% in 2025, up from 10% in 2024).
testing volumes and trends
Most medical laboratory professionals surveyed (64%) report their labs performing between 0-100 molecular-based tests (non-COVID-19) per day.
Percentages for other volumes are as follows:
• 101-200: 13% (unchanged from 2024)
• 201-300: 6% (up from 5% in 2024)
• 301-400: 1% (unchanged from 2024)
• 401+: 17% (down from 22% in 2024)
When asked what types of molecular diagnostic tests they use most in their labs, reverse transcriptase quantitative polymerase chain reaction (rRT-qPCR) topped the list at 54% (down from 64% in 2024), followed by rapid molecular tests at 52% (up from 49% in 2024), and rapid antigen tests at 48% (down from 49% in 2024).
Responses for the other testing MDx modalities:
• Flow cytometry: 14% (down from 21% in 2024)
• DNA/genetic testing: 11% (down from 20% in 2024)
• Next generation sequencing: 10% (down from 18% in 2024)
• Mass spectrometry: 9% (up from 8% in 2024)
• Reverse transcription loop-mediated isothermal amplification (RT-LAMP): 8% (down from 9% in 2024)
• Recombinase polymerase amplification (RPA): 6% (up from 4% in 2024)
• Liquid biopsy: 7% (up from 6% in 2024)
• None: 5% (up from 3% in 2024)
• CRISPR-based diagnostics: 2% (up from 0% in 2024)
Additionally, 5% of respondents selected “other” as a response (down from 11% in 2024), offering up these alternative testing modalities used in their labs: Lab developed tests (LDT), PCR amplification, multiplex real-time RT-PCR, and qPCR.
“At times we are asked to look into new assays or procedures,” said George Manolopoulos, Clinical Lab Manager, Pathology Reference Lab in San Antonio. “The FDA regulation of LDTs would have been an issue if it stayed in place. A decision had been made not to look
What types of molecular diagnostic tests do you use in your laboratory?
Reverse transcriptase quantitative polymerase chain reaction (rRT-qPCR)
Reverse transcription loop-mediated isothermal ampli cation (RT-LAMP)
Recombinase polymerase ampli cation (RPA)
CRISPR-based diagnostics
DNA/Genetic testing Flow cytometry
into any new LDT implementation as we didn’t have the resources or wanted to deal with an FDA submission. Nevertheless, without the FDA regulation in mind our decisions are driven solely by client demand and as such we haven’t implemented any new molecular methodology since 2020.”
Matt Easterday, CEO, Dovetail Genomics, spoke to how advances in 3D genome architecture are helping researchers uncover functional disease variants that traditional linear sequencing often misses:
“Traditional sequencing shows us the linear code of DNA, but much of disease biology lies in how that code folds and interacts in three-dimensional space. By mapping genome architecture, researchers can pinpoint structural variants, enhancer hijacking, and other regulatory events that drive disease
yet remain invisible to conventional approaches.

“At Dovetail Genomics, our LinkPrep platform integrates sequence and structure into a single workflow, enabling labs to uncover clinically relevant variants at higher sensitivity and with clearer biological context. These insights are proving especially valuable in oncology, where understanding 3D genome organization can reveal functional variants linked to disease progression, relapse, and therapeutic resistance.”

Clinical demand
New for this year, MLO asked medical laboratory professionals which clinical areas were driving the most demand for molecular testing in their labs. Over three-quarters of respondents (77%) cited infectious
disease (non-COVID) as driving the greatest demand.
About one-fifth of respondents reported oncology (22%) or reproductive health (19%) as driving the most demand for MDx.
As for other clinical categories:
• Genetic/heredity testing: 13%
• Transplant medicine: 6%
• Neurology: 5%
• Cardiology: 5%
• Pharmacogenomics: 4%
An additional 20% of respondents cited another clinical area responsible for molecular testing demand, with the top categories including:
• Emergency department
• Environmental/activities of daily living
• Gynecology
• Pediatrics
• Primary care/family practice
• Pulmonology
• Sexually transmitted diseases (STD)/sexually transmitted infections (STI)
• Stool microbiome
• Urgent care
• Urology
Antonio Vergara, senior vice president, Core Lab and Near Patient Care at Roche Diagnostics, commented on clinical lab trends and technology adoption, stating:
“Clinical laboratories are navigating a dynamic molecular diagnostics landscape, marked by a shift from high-volume, single-target assays toward comprehensive, customizable syndromic testing. This evolution, driven by the need for faster, broader answers in areas like respiratory and sexual health, is coupled with ongoing lab consolidation, reimbursement dynamics, and greater workflow efficiency.
“As test-to-treat remains ever important, laboratories are demanding faster and more expansive testing capabilities, adaptable for seasonality, patient population and care setting. Roche is directly addressing these challenges with flexible and automated solutions. Our recently 510(k) cleared cobas Respiratory 4-flex empowers labs to customize panels for specific testing needs on the cobas 5800/6800/8800 molecular systems.
Which clinical areas are driving the most demand for molecular testing in your lab?
Infectious disease (non-COVID)
Oncology
Pharmacogenomics
Genetic/hereditary testing
Reproductive health
Transplant medicine
Neurology
Cardiology
Other
“Technology adoption is also accelerating, with next-generation sequencing (NGS) and digital PCR becoming more prevalent for high-throughput and sensitive analysis. Roche’s sequencing by expansion (SBX) technology, currently in development, will provide a novel, cost-effective option for high-throughput analysis for research projects.”



Yves Dubaquie, senior vice president, Diagnostics, Revvity, spoke to the need for MDx testing that meets the broad demand for efficiency, accuracy, and access. He stated:
“Clinical laboratories are rapidly adopting COVID-era innovations—such as self-sample collection, decentralized testing, and rapid nucleic acid diagnostics—to accelerate same-day treatment decisions and expand patient access. This shift reflects a broader need for solutions that are not only faster and more accurate, but also practical and scalable across diverse healthcare settings, including low-resource and low-income regions where the burden of infectious disease remains highest.
“Revvity is supporting this transformation with innovations that directly address these evolving needs. Through streamlined workflows like the automated T-SPOT.TB test, Revvity helps laboratories simplify complex processes, reduce turnaround times, and improve consistency in results.”
“As test-to-treat remains ever important, laboratories are demanding faster and more expansive testing capabilities, adaptable for seasonality, patient population and care setting.”
“Consumers are increasingly seeking solutions that meet their needs in an evolving healthcare landscape, and we expect to continue seeing a demand for Percentage (%)
Meghan W. Starolis, MS, PhD, HCLD(ABB), Senior Science Director, Infectious Disease at Quest Diagnostics, noted the trend of patients taking a more active role in their own healthcare, specifically around testing for human papillomavirus (HPV) and STIs.


Large,

greater patient empowerment,” said Starolis.“Self-collection is something many more patients are taking an interest in, particularly for certain women’s health testing such as for HPV or STIs.
“The ability for a patient to self-collect has many advantages, like increased patient comfort and convenience. Offering self-collection for HPV primary screening has the potential to significantly increase the number of patients screened and get the care they need to prevent or treat cervical cancer. But one potential challenge as we move forward in this space, is ensuring that patients who do need follow-up care following HPV testing, such as pap smears or colposcopies, are appropriately linked to that follow-up care.”
Respiratory testing
When asked how much respiratory testing has increased in their labs since last year, the most notable response was among those reporting it had decreased, at 24% of respondents, up from 17% in 2024.
As for those reporting an increase in respiratory testing:
• 0-25% increase: 55% (up from 49% in 2024)
• 26-50% increase: 13% (down from 20% in 2024)
• 51-75% increase: 6% (unchanged from 2024)
• 76-100%: 1% (down from 7% in 2024)
• 101+% increase: 1% (up from 0% in 2024)
“There is a slow but steady growth in MDx testing volumes in areas that have always been the staple of our lab,” Manolopoulos commented. “On the contrary, respiratory testing, i.e., COVID testing, has ceased. Since there are plenty of options for clinicians’ offices for that type of testing, our lab has refrained from expanding in that area.”
“Respiratory molecular diagnostic testing has ebbed and flowed post-COVID, and not just seasonally,” said Sheridan M. Voshake, MS, MLS(ASCP)cm, Medical Laboratory Supervisor, Memorial Hospital, Carthage, Il. “While it still tends to spike in the winter months, we have also seen where it will sporadically increase during other times of the year depending on whether there is a regional outbreak occurring.”
“We have removed stand-alone COVID molecular testing and huge panels with non-clinically significant multiple targets as readily available, and now only offer it as a four-plex with Flu A/B and RSV,”Voshake added. “I believe that drilled-down panels, like the four-plex, are an appropriate middle ground between guessing at single target molecular testing and not getting reimbursed on big panels with too many clinically insignificant targets.”
With increased attention on the use of AI/ ML in healthcare, including the lab environment, MLO asked medical laboratory professionals if their labs had adopted or are planning to adopt AI/ML tools for molecular diagnostics.
Most survey respondents (67%) reported their labs are not currently using AI/ML, nor do they have plans to, nearly one-fifth
(19%) said they are not currently using these technologies but plan to use them, 8% said they are planning to adopt them, and 6% said they are already using them.
Eunsin Bae, MD, Sr. Vice President/Head of Global Communications, Seegene, commented on the need for automation in medical laboratories, stating:
“The ability for a patient to self-collect has many advantages, like increased patient comfort and convenience. Offering selfcollection for HPV primary screening has the potential to significantly increase the number of patients screened and get the care they need to prevent or treat cervical cancer.”
“Seegene views the major trend in clinical laboratories as the need for solutions that maximize efficiency while reducing costs and reliance on limited resources. Laboratories are under pressure to deliver rapid, accurate results despite workforce and budget challenges, and scalable technologies are becoming essential. Seegene supports this shift by providing fully automated platforms and multiplex assays that streamline the entire diagnostic process from sample to result, helping laboratories strengthen operational sustainability and expand access to high-quality diagnostics worldwide.”


M. Voshake, MS, MlS(aScP)cm

Nearly three-quarters of medical laboratory professionals (71%) reported having adequate testing supplies to meet testing demands (up from 62% in 2024). Conversely, 29% reported that a lack of sample-related products has impeded their testing capacity at times (down from 38% in 2024).
Delving into specific supply categories where they have experienced trouble sourcing due to supply chain issues, half of participants (50%) reported having no problem in any of the categories MLO offered as potential survey answers, up from 36% in 2024.
Commenting on improved supply chain conditions, Manolopoulos stated: “Since the peak of COVID, supply chain issues and availability of assay reagents have improved dramatically. It has been a couple of years since a needed item was delayed or on back order.”
The one supply category where there was an increase in reported sourcing issues was winged blood collection sets at 16% of respondents, up from 13% in 2024. In all others, medical laboratory professionals reported fewer sourcing problems compared with last year.
• Controls/Reagents: 22%, down from 27% in 2024
• Blood collection tubes: 17%, down from 26% in 2024
• Culture media: 8%, down from 21% in 2024
• Pipettes/pipette tips: 8%, down from 11%
• Testing kits for SARS-CoV-2: 8%, down from 11% in 2024
• PPE: 3%, down from 7% in 2024
• Swabs/Consumables: 7%, down from 10% in 2024
• Blood culture transfer devices: 3%, down from 8% in 2024 Jennifer Schneiders, Phd
Have you adopted or are you planning to adopt AI/ML tools for molecular diagnostics?
Yes, already using
Yes, planning to adopt
No, we are not currently using but plan to
No, we are not currently using and have no plans to
• Transport media: 1%, down from 10% in 2024
• Urine testing supplies: 1%, down from 3% in 2024
• Lab plastics not noted above: 12%, down from 16% in 2024
As for respondents who indicated they were experiencing sourcing issues in other product categories (3%, down from 4% in 2024), contributed answers to the question included needle holders that have the safety cap attached and polymerase chain reaction (PCR) kits.
Jennifer Schneiders, PhD, president, Diagnostic Solutions at Hologic, commented on how clinical laboratories are navigating workforce shortages and supply chain challenges while facing growing demand for faster, more accurate molecular diagnostics. She stated:
“This drives the need for automation and integrated platforms that increase throughput without compromising quality. By partnering with labs, we focus on delivering scalable solutions, like Hologic’s Panther System, a fully automated molecular diagnostics platform that enables the consolidation of a growing menu of assays for women’s health, sexually transmitted infections, respiratory infections and more. Through ongoing training, and with our combined expertise, we help labs streamline workflows and uphold the rigorous quality standards we all expect. Our commitment is to invest in the labs of the future and help them expand access to diagnostics that enhance patient care through early, accurate detection.”
Another new question for this year was around proficiency testing for molecular assays. MLO asked if their labs participate in this testing, and if so, through what organization do they participate. CAP was highest on the list at 48% of respondents, followed by API at 36%, WSLH Proficiency Testing at 6% and the Centers for Disease Control and Prevention (CDC) at 3%.
One-fifth of respondents (20%) said their labs do not participate in proficiency testing for molecular assays. Additionally, 7% of respondents who reported their labs participate in proficiency testing for molecular assays said they did so through another source. Sources cited include:
• A blinded internal PT as it is unique LDT
• Alternative assessment procedures
• CMC Vellore EQAS
• controllab (Brasil)
• PEEC (Chile)
• QCMD
• RfB
• RML
When asked how they handle questionable results with molecular tests, half of medical laboratory professionals report repeating the test (50%, up from 45% in 2024).
The other modalities reported are as follows by percentage ranking:
• 22% verify that all pre-analytical, analytical, and/or post-analytical steps are performed correctly (down from 24% in 2024)
• 16% repeat the test with a different employee/equipment/test (up from 15% in 2024)
• 4% send results to another lab for verification and second test (down from 6% in 2024)
Among the 7% who selected “other” as their response, most noted they use all the modalities listed.
Regarding steps taken to reduce the number of potential false positive test results, those surveyed reported greater use across all methodologies proposed compared with last year.
• 90% verify all pre-analysis steps are performed correctly (up from 68% in 2024)
• 67% decontaminate the work/test area per laboratory procedures (up from 59% in 2024)
• 62% repeat the test with the same sample and new extractions (up from 47% in 2024)
• 39% refer to quality assurance program (up from 34% in 2024)
• 30% repeat the test with another method and compare results (up from 14% in 2024)
A further 6% medical laboratory professionals reported that they don’t use any of these methodologies to reduce the number of potential false positive MDx test results (up from 3% in 2024), and 7% said they use another method not specified in the survey (unchanged from 2024).
Other methodologies cited by survey respondents:
• Get a new swab
• Make sure staff is well trained in all areas of molecular testing
• Monitor positivity rates
• Recollect sample and repeat test
The 2025 MLO MDx State of the Industry Survey paints a picture of laboratories that are adapting to evolving testing demands while strengthening supply resilience and quality safeguards.
Infectious disease testing continues to drive the majority of molecular work, even as respiratory testing levels off and emerging modalities make small but meaningful gains. While adoption of AI/ML remains limited, labs are proactively refining practices to reduce false positives and ensure test reliability.
Together, these findings highlight a sector that is cautiously innovating while holding fast to its core mission: Delivering accurate, timely, and high-quality molecular diagnostics to support patient care.

Kara Nadeau has 20+ years of experience as a healthcare/ medical/technology writer, having served medical device and pharmaceutical manufacturers, healthcare facilities, software and service providers, non-profit organizations and industry associations.

By Erin Brady
Medical Laboratory Observer (MLO) publishes a Laboratory Information Systems (LIS) Buyer’s Guide annually. We started including lab data products from companies outside the LIS in 2024, and this year are officially introducing the MLO LIS and Lab Data Solutions Guide.
In addition to the product tables, we interviewed seven laboratory technology experts who gave their insights on current and future technological developments in the clinical laboratory, suggestions on how vendors can help ease the process of adopting LIS and other technologies in the lab, advice for lab leaders, and the evolution of LIS.
Technological advancements
The current biggest technological advancements impacting LIS and other lab data tools in 2025 are artificial intelligence (AI), cloud-based products, and interoperability, according to the experts. Rob Brown, Head of the Scientific Office, Sapio Sciences emphasized,“The most transformative advancements impacting lab information tools are focused on intelligence, usability, and configurability. Lab information tools are moving beyond passive record-keeping to integrate AI that acts as a co-scientist, helping with experiment design, result analysis, and the recommendation of next steps.”
“Voice is also emerging as a new interface in both research and diagnostics labs, allowing scientists to interact with their LIMS using natural language. These advancements are
supported by unified platforms that connect various tools in a single environment, reducing handoff errors and enabling full traceability,” he said.
Suren Avunjian, CEO, LigoLab observed the quick adaptation and flexibility of laboratories as new technologies are rolled out. “Automation and AI are no longer experimental; they’re embedded into modern LIS platforms. Labs are utilizing agentic tools to automatically flag inconsistencies, interpret results, apply AI to digital slides, scan paper requisitions and import them as an order, voice-to-text and command control of the LIS, and generate customized reports. This reduces manual review and allows staff to focus on higher-value clinical work,” he said.
Kim Futrell Senior Strategic Marketing Manager, Clinisys said, “In 2025, cloud-based LIS platforms have become foundational to modern lab operations, offering remote access, scalability, and built-in disaster recovery. With rising concerns around data privacy, vendors are enhancing cybersecurity and compliance features to meet regulatory demands. A primary emphasis is placed on interoperability, with LIS platforms


increasingly engineered to seamlessly connect with EHRs, digital pathology, genomics, and AI diagnostics.”
She added,“Structured data frameworks facilitate seamless integration, allowing labs to function within broader healthcare ecosystems. Utilizing embedded analytics tools powered by pay-per-use cloud computing, labs can access real-time dashboards and insights into test utilization, staffing, and patient outcomes—optimizing performance and demonstrating value. Simultaneously, digital pathology and AI are revolutionizing remote collaboration, accelerating image analysis, and creating adaptive workflows that cater to evolving diagnostic needs. Moreover, AI presents innovative opportunities for enhancing service and supporting delivery models.”
Avunjian continued, “With open APIs and interoperability standards, LIS systems are now able to connect seamlessly with instruments, EHRs, billing platforms, and digital pathology solutions. This creates a more unified ecosystem and reduces the silos that have traditionally hindered lab efficiency and growth.” He noted that with all this, labs are also focusing more on cybersecurity, complying with regulations, and hardening their systems against ransomware and hacker attacks.“Modern systems incorporate embedded encryption, robust audit trails, and predictive analytics,


enabling labs to reduce both risk and waste across a range of applications, from instrument maintenance to reagent management,” he said.
Furthermore, “All of these advancements are converging into comprehensive informatics platforms, systems of action that cover the entire lifecycle of a case, from accessioning through revenue capture,” according to Avunjian.
Integration hurdles


When asked what challenges labs face when adopting or upgrading LIS and other data platforms, Gilbert Halkim, CEO, SCC Soft Computer mentioned mindset as the main obstacle. “Too often, labs try to replicate their legacy workflows in a new LIS. The best results come when labs adopt vendor best practices, streamline implementations, and leverage modern functionality without over-customization.”
Labs often face significant challenges from legacy systems that create rigid workflows, siloed data, and a frustrating user experience, Brown said. “These issues directly impact critical metrics like turnaround time, sample traceability, and regulatory compliance. A key problem often occurs in the pre-analytical phase, where manual data entry and poor sample handoffs introduce errors.”
Eric Dingfelder, President and CEO, Data Innovations pointed out another barrier. “One of the most significant
challenges laboratories encounter when upgrading their laboratory information systems (LIS) or other data platforms is achieving seamless interoperability across diverse systems, instruments, and automation technologies. Integrating these components—often from different vendors—can be complex, time-consuming, and costly,” he said.
Futrell said,“Staffing shortages often limit the time and resources available for implementation and training, delaying adoption, curtailing new feature
adoption rates and reducing onboarding effectiveness. Labs are required to maintain fast turnaround times and avoid any disruptions that could impact result delivery and provider satisfaction. Additionally, they must ensure compliance with HIPAA, CLIA, and FDA standards, including secure data transmission and audit trails. It is essential that LIS platforms connect seamlessly with lab instruments and


external systems to prevent workflow disruptions.”
How vendors can help Vendors can help ease the process of adopting LIS and other technologies in the lab by guiding labs toward proven models while still aligning with their operational goals, according to Halkim.
Brown suggested vendors offer modern platforms with out-of-the-box solutions designed for real-world lab workflows. “Configurability is essential, as it allows labs to adapt processes without relying on developers. Additionally, intuitive interfaces, including voice and natural language tools, simplify onboarding and help resolve key bottlenecks: TAT, traceability, data fragmentation, and compliance,” he said.
Futrell added,“Vendors play a crucial role in mitigating these challenges. By offering flexible and scalable solutions, they allow labs to adopt new systems gradually, minimizing disruption. Robust implementation support—including project management, training, and technical assistance—can ease the burden on lab staff. Advanced connectivity tools help eliminate middleware and ensure smooth communication between lab instruments and third-party systems.”
Dingfelder pointed to his company’s solutions when asked how vendors can help ease the integration burdens on labs. “Data Innovations offers vendor-neutral middleware solutions that simplify connectivity and data exchange. Instrument Manager middleware enables centralized integration and oversight of unlimited LIS platforms, instruments, and in vitro diagnostic devices. This allows labs to unify operations across multiple disciplines, locations, and systems—enhancing efficiency, scalability, and data consistency.”
Advice for lab leaders
Labs should look beyond current features and evaluate a vendor’s roadmap for AI, interoperability, and patient-facing tools, said Ed Price, CEO, Computer Service & Support, Inc.“Just as important, they should ensure they own and can access their data. Too many systems restrict exports or lock customers into closed databases. Avalon gives clients direct read-access, empowering them to build their own analytics, integrate external tools, and retain full control. The LIS platforms that balance compliance, innovation,

Introducing AlinIQ Insight and its family of applications— making your key diagnostic data more accessible and usable, because new levels of data visibility bring greater insight.
SIMPLE. INTUITIVE. INNOVATIVE.
• Easily sort, configure and set parameters to highlight what’s most important
• Instantly oversee application data integrated in real-time
• Quickly compare daily metrics to your own KPI targets

Is your product certified under the Health It certificate Program through the office of the national coordinator for Health Information technology?
does your platform provide aI-driven decision support or predictive analytics for diagnostics or lab performance?
are pre-configured interfaces with common lab analyzers part of your standard product offering?
are pre-configured interfaces with common inpatient electronic medicalrecord systems part of your standard product offering?
are pre-configured interfaces with common outpatient electronic medicalrecord systems part of your standard product offering?
are pre-configured interfaces with common pathology imaging systems part of your standard product offering?
do you support ingestion of a final report from a digital pathology solution provider?
do you accept discreet data from a digital pathology solution provider to fill out a report template and provide auto sign out of the case?
your product include
module for revenue cycle management?
does your product have an automated process for tracking medical necessity verification?
product include features for inventory control and supply-chain management?
your product include
module for managing Poct?
does your product have full bidirectional integration capabilities for data exchange with digital solutions?
Is your product interoperable with aPI’s or other proficiency testing providers?
does your product support multi-factor authentication (MFa) for user access?
does your product include audit trail functionality for tracking user activity and data changes?
does your product support machine learning model integration for lab operations or diagnostics?
does your product offer robotic process automation (rPa) features for administrative tasks (e.g., billing, report generation)?
does your product include a patient portal or integrate with patientfacing systems for test results and communication?
Product name Instrument Manager middleware and lab enablement software
Key Features Instrument Manager is a truly vendor-neutral lab middleware that enables enterprise laboratories to connect all sites, systems and instruments through a single platform providing end-to-end lab management that supports improved productivity, quality, compliance, and uptime performance.
atellica data Manager
• rules-based standardized testing
• realtime workflow dashboard
• Integrated Qc management
• simplified review and edit
• built-in result autovalidation
• robust traceability, audit trails, and reporting
Integration capabilities Instrument Manager middleware integrates with all lab information systems and instruments, regardless of make or manufacturer. data Innovations offers a library of over 1,200 drivers and continue to develop new drivers as new laboratory instruments enter the market.
solutions the service Provides
• Productivity solutions to optimize, automate, and standardize lab workflows –including custom autoverification (aV) solutions that enable labs to reach aV rates of 85% and higher across disciplines.
• Quality-control solutions that ensure accurate instrument performance and compliance. Qc solutions include Moving averages & Moving Medians, eP evaluator, automated caP Lab Proficiency reporting, and more.
• Performance and reliability solutions that maximize lab uptime. these include High availability & disaster recovery with automatic failover protection, and the cloud-based solution Lab GPs, which optimizes lab uptime through all-in-one connectivity monitoring, downtime alerts and troubleshooting from anywhere.
• Lab analytics software, including data Innovations’ Laboratory Intelligence program, which tracks essential KPIs in real time. Labs can track an unlimited number of KPIs, including turnaround time, Qc failures, aV rates, and much more. drill-down features for root-cause analysis give labs insights into opportunities for operational improvement.
relevant certification/ compliance data Innovations maintains soc 2 compliance, participates in the Medical device single audit Program (MdsaP), and maintains an Iso 13485 registered quality management system.
2. Lab data solutions Guide and empowerment will deliver the greatest long-term value.”
Jomah Williams, Product Manager for IT, Siemens Healthineers emphasized the importance of choosing a solution that will evolve with the laboratory. “Within any cost associated purchase, you want value and a vehicle that can handle the growth of your lab needs as well as offering innovate for the functions.”
Halkim offered clear advice, “Don’t compromise by cutting corners. Implementing systems without investing in a robust LIS can create long-term limitations. Instead, partner with a state-ofthe-art LIS that supports advanced interoperability, scalability, and modern lab workflows. This ensures labs remain agile, secure, and future-ready.”
A common observation is that a neutral platform allows for adaptation to changes in the LIS or device manufacturer without being limited by operational tools that may not align with evolving laboratory needs, Dingfelder added. “It is advisable to consider flexibility and adaptability in both purchasing and change management decisions when selecting a partner.”
The evolving LIS LIS platforms are required to evolve to support interoperability with EHRs, digital pathology, genomics tools, or AI diagnostics.
“Interoperability is now essential,” Price stressed. “Avalon LIS supports HL7, FHIR, and modern APIs to connect directly with major EHRs. We’re expanding these capabilities to integrate with digital pathology systems, genomics data, and external AI diagnostics - enabling true bi-directional data exchange rather than isolated workflows.”
Williamssaid, “Auto-verification workflows drive faster results and integration with many new devices like middleware providers and real time data streaming. Standardization of result protocols leads to consistent quality.”
The stress on laboratories to use more technologies and the need for one seamless workflow for EHRs, digital pathology tools, genomics data, RCM, and AI diagnostics was spotlighted by Avunjian. “Advanced LIS platforms are evolving to make this possible by serving as the central hub where all of these technologies come together.
atellica data Manager integrates with multi-instruments (125+), and connects to multiple laboratory information systems.
refer to key features
Digital pathology is a prime example. Moving from glass slides to high-resolution digital images allows pathologists to review cases remotely, collaborate with peers, and use AI to highlight patterns that the human eye may miss or fill out the report with the AI diagnosis in preparation for the pathologist to review and sign out. But scanners and viewers on their own do not solve the interoperability challenge. That requires a modern LIS.”
He continued, “Diagnostic accuracy improves when AI and human input are combined in a unified report. Turnaround times drop because case data, images, and results are all in one place. Collaboration becomes easier, whether within a hospital network or across the globe. Most importantly, patient care improves because clinicians receive complete, timely, and clear results. By building interoperability into the core of an advanced LIS platform, labs are provided with the foundation to adapt to the digital future.”

In the time it takes to read this headline, you could scan in 120 samples


If a hospital performs one million tests per year and loses one in 1,400 tubes at a cost of $400–600 per tube, then the annual cost could be as much as $428K—not to mention the burden on patients and hospital.1
By implementing Indexor, you can trace samples starting at patient draw, monitor key quality indicators during transportation, and automate time-consuming lab operations.






powered by






THAT’S HEMOSTASIS TESTING WITH THE ACL TOP FAMILY 70 SERIES + HEMOHUB INTELLIGENT DATA MANAGER.
Introducing an end-to-end frictionless workflow in Hemostasis testing. Powerful automation and centralized data management deliver consistent, quality-assured results while reducing manual steps and optimizing workflow.
Efficiency that performs
Experience system-wide standardization with the same software and reagents across all instruments, plus automated performance verification and continual loading with no system interruption.
Advanced quality management

Streamline quality control (QC) management with real-time HemoHub synchronization. Auto-generated reports ensure audit readiness. And optical LED technology prevents errors before they happen.
One reagent menu. Total confidence.
The HemosIL comprehensive reagent menu offers the most liquid ready-to-use routine and specialty reagents, including the only FDA-cleared liquid ready-to-use PT reagents.


Scan QR code or visit Werfen.com/70Series to learn more

The Werfen logo is a trademark of Werfen. HemosIL, ACL, ACL TOP, ACL Elite, ACL AcuStar, ReadiPlasTin, RecombiPlasTin, SynthASil, SynthAFax are trademarks of Instrumentation Laboratory Company, d.b.a Werfen, and/or one of its subsidiaries or parent companies and may be registered in the United States Patent and Trademark Office and in other jurisdictions. All other product names, company names, marks, logos, and symbols are trademarks of their respective owners. ©2025 Instrumentation Laboratory. All rights reserved.