The right hemostasis solution for your lab is more than just an analyzer--it’s the winning combination of advanced technology and reagents, proven reliability and best-in-class service. Partnering with Sysmex gives you all of that and more, allowing you to clot smarter, not harder.
www. m x. m/
Sysmex has rated highest for System Reliability & Service *
Vol. 58, No. 1
Happy new year!
By Christina Wichmann
Editor in Chief
Arecent MLO survey of 12 lab leaders from across the U.S. paints a clear picture — this year is poised to be one of transformation, reinvention, and purpose.1 The recurring theme across the experts’ voices is growth through modernization. Whether it is automation, AIassisted workflows, or unified digital infrastructures, labs are embracing innovations that allow laboratory professionals to rise above repetitive tasks and contribute to deeper, more meaningful work. What experts expect to see in 2026:
• More automation and AI, freeing up laboratory professionals for higher-level tasks that need human judgment.
• A shift toward fully integrated, networked laboratories — multi-site systems under unified governance, quality, and operations rather than siloed individual labs.
• Labs becoming strategic partners in healthcare delivery, not just “behind the scenes,” with stronger collaboration with clinicians and involvement in clinical decision-making.
• Use of digital pathology, AI-based image analysis, advanced informatics, and real-time analytics to improve quality, turnaround times, and operational efficiency.
Challenges we cannot ignore
That optimism is tempered by hard realities. Workforce shortages remain critical. Without bold steps to rebuild the pipeline — from training programs to career development — we risk bottlenecks in quality, responsiveness, and innovation. Financial pressure also persists. Declining reimbursements, rising supply costs, and unpredictable staffing expenses threaten to restrict labs’ ability to stay “cutting-edge.” Challenges experts hope will be addressed in 2026 are as follows:
• The workforce crisis — retiring laboratory scientists and too few new entrants into lab science, threatening staffing sustainability.
• The cost/reimbursement squeeze — declining reimbursements, rising supply (and staffing) costs, making it harder for many labs to afford modernization or “cutting-edge” test methodologies.
• Over-reliance on interim/traveling staff (agency staff), which can be costly, disrupt continuity, and burden training/competency maintenance.
• Pressure to build flexible, appealing career paths and workplace cultures so labs attract and retain new talent.
MLO in 2026
In the coming year, I hope our magazine will be instrumental in helping 2026 be a year of transformation! We have an exciting editorial calendar planned for you:
• Showcasing advances in automation, informatics, and AI
• Encouraging laboratories to re-evaluate their procedures and workflows
• Elevating the conversation around workforce sustainability: training, retention, career development, and workplace satisfaction
• Featuring the latest advancements in patient diagnostics
To all our readers — your work matters. The clinical laboratory field is evolving — and together, we have the opportunity to define what a modern lab should be: agile, intelligent, impactful, and deeply integrated into patient care.
I welcome your comments and questions — please send them to me at cwichmann@mlo-online.com.
REFERENCE
1. Wichmann C. Inside the lab of 2026: Insights from 12 laboratory experts. MLO Online. November 24, 2025. Accessed December 10, 2025. https://www.mlo-online.com/online-exclusives/ article/55332108/inside-the-lab-of-2026-insights-from-12-laboratory-experts.
EDITOR IN CHIEF Christina Wichmann cwichmann@mlo-online.com
MANAGING EDITOR Erin Brady ebrady@endeavorb2b.com
PRODUCTION MANAGER Edward Bartlett
ART DIRECTOR Kelli Mylchreest
AUDIENCE DEVELOPMENT/LIST RENTALS Laura Moulton | lmoulton@endeavorb2b.com
John Brunstein, PhD, Biochemistry (Molecular Virology) President & CSO PathoID, Inc., British Columbia, Canada
Lisa-Jean Clifford, COO & Chief Strategy Officer Gestalt, Spokane, WA
Barbara Strain, MA, SM(ASCP), CVAHP Principal, Barbara Strain Consulting LLC, Formerly Director, Value Management, University of Virginia Health System, Charlottesville, VA
Jeffrey D. Klausner, MD, MPH Professor of Preventive Medicine in the Division of Disease Prevention, Policy and Global Health, Department of Preventive Medicine at University of Southern California Keck School of Medicine. Donna Beasley, DLM(ASCP), Director Huron Healthcare, Chicago, IL
Anthony Kurec, MS, H(ASCP)DLM, Clinical Associate Professor, Emeritus , SUNY Upstate Medical University, Syracuse, NY
Paul R. Eden, Jr., MT(ASCP), PhD, Lt. Col., USAF (ret.) (formerly) Chief, Laboratory Services, 88th Diagnostics/Therapeutics Squadron, Wright-Patterson AFB, OH
Daniel J. Scungio, MT (ASCP), SLS, CQA (ASQ), Consultant at Dan the Lab Safety Man and Safety Officer at Sentara Healthcare, Norfolk, VA
CORPORATE TEAM
CEO Chris Ferrell COO Patrick Rains CDO Jacquie Niemiec CALO Tracy Kane CMO Amanda Landsaw EVP INFRASTRUCTURE & PUBLIC SECTOR GROUP Kylie Hirko VP OF CONTENT STRATEGY, INFRASTRUCTURE & PUBLIC SECTOR GROUP Michelle Kopier 30 Burton Hills Blvd., Suite 185 Nashville, TN 37215 800-547-7377 | www.mlo-online.com
Medical Laboratory Observer USPS Permit 60930, ISSN 0580-7247 print, ISSN 2771-6759 online is published 10 times annually (Jan, Mar, Apr, May, Jul, Jul-CLR, Aug, Sep, Oct, Nov) by Endeavor Business Media, LLC. 201 N Main St 5th Floor, Fort Atkinson, WI 53538. Periodicals postage paid at Fort Atkinson, WI, and additional mailing offices. POSTMASTER: Send address changes to Medical Laboratory Observer, PO Box 3257, Northbrook, IL 60065-3257. SUBSCRIPTIONS: Publisher reserves the right to reject non-qualified subscriptions. Subscription prices: U.S. $164.80 per year; Canada/Mexico $199.56 per year; All other countries $284.54 per year. All subscriptions are payable in U.S. funds. Send subscription inquiries to Medical Laboratory Observer, PO Box 3257, Northbrook, IL 60065-3257. Customer service can be reached toll-free at 877-382-9187 or at MLO@ omeda.com for magazine subscription assistance or questions Printed in the USA. Copyright 2026 Endeavor Business Media, LLC. All rights reserved. No part of this publication may be reproduced
By Ian Lentnek,
and Angela Neale, PA-C,
By William E. Winter,
and Christina Wichmann
Fast Facts
Lab professionals share what drives them to stay
In a recent Q&A, Michelle Westfort shared strategies for retaining skilled lab professionals. We asked 58 clinical laboratory professionals what motivates them to keep coming back to the lab every day: 7% said compensation and benefits 5% responded professional growth opportunities 12% stay because of their positive workplace culture 9% enjoy the flexibility/worklife balance of their lab 53% are motivated by making a difference in patient care 2% answered working with cutting-edge technology 12% had their own reasons such as a sense of loyalty to their lab and their patients.
Spotlight on MLO online exclusives
Medical Laboratory Observer has published several online exclusive articles in the final months of 2025 spanning several topics such as 2026 predictions, vaginitis testing, proficiency testing, staff retention, and more. Below are highlights from eight of our most recent online exclusive articles. The full version of each piece can be found at mloonline.com/online-exclusives.
What is my patient’s volume status? Leveraging plasma volume estimation to guide clinical decisions in and beyond the ICU
Assessment of a patient’s volume status is a task that clinicians do daily in managing hospitalized patients as it affects multiple systems of the body. In critically ill patients, it may be done more frequently, even hourly. It aids in determining end-organ perfusion and helps caregivers decide on interventions such as the need for intravenous fluids, diuresis, ventilator settings, blood pressure management, and kidney function, among others. The precise determination of a patient’s fluid status is something that is not clearly defined and is generally made by the clinician using a variety of modalities: physical examination, vital signs, laboratory and radiologic findings, and sometimes invasive testing or complex technological devices. Despite these many ways of determining a patient’s volume status, there is no universally accepted standard for what represents the true value. Many of these methods give conflicting results, and even experienced clinicians can disagree on what the true plasma volume in any given patient is. This can directly impact patient care—for example, does a septic patient with a low blood pressure need vasopressors or a fluid bolus? Does a patient with COPD who is difficult to wean have fluid overload? When do you stop diuresis in a heart failure patient? Answers to these questions and many others rely on accurate assessment of a patient’s fluid status, specifically their intravascular fluid status.
Authors Martin Ekiti, MD, MPHc and Matt Davis, BS, RRT discuss the utility of using estimated plasma volume (ePV) as a prognostic indicator for various disease states.
Advancing laboratory excellence: An interview with the CAP’s Joel Todd Moncur, MD, PhD, MS, FCAP
The College of American Pathologists (CAP) recently announced the offering of 21 new proficiency testing (PT) and external quality assessment (EQA) programs for 2026, including the first HIV-1/HIV-2 molecular detection and differentiation program to be accessible globally. U.S. firsts include the country’s first H5N1 avian influenza and Dengue Virus Serology (DENS) programs.
Medical Laboratory Observer (MLO) spoke with Joel Todd Moncur, MD, PhD, MS, FCAP, Chair of the CAP’s Council on Scientific Affairs about the new programs. Dr. Moncur elaborates on the new offerings and how they will promote excellence in laboratories.
These PT/EQA programs are key tools that laboratories can use to support high-quality testing and satisfy accreditation and compliance requirements, including CMS/ CLIA and CAP standards. In addition, CAP’s PT programs generate unparalleled data on laboratory practices and performance that the College uses to understand emerging challenges, support continuous improvement, and advocate for policies that strengthen laboratory quality and patient care.
Inside the lab of 2026 Insights from 12 laboratory experts
To explore what the next year may hold, MLO spoke with 12 laboratory professionals whose roles span bench operations, laboratory quality, enterprise leadership, diagnostics innovation, and health-tech entrepreneurship. They told us what they see in the future for U.S. laboratories and what challenges they hope the laboratory industry can solve in 2026.
Their predictions reflect both optimism and urgency: calls to rebuild the workforce pipeline, integrate multi-site networks, strengthen
clinical collaboration, modernize infrastructure, and streamline the process of test result to clinical action. Together, their insights offer a multifaceted view of the future of U.S. laboratories—one ready to redefine its value, expand its reach, and shape the future of patient care.
This Q&A was developed with the co-chairs of the NETEC Laboratory Workgroup:
• Vicki Herrera, MS – Research Coordinator at the University of Nebraska Medical Center and Training & Education Coordinator at the Nebraska Biocontainment Unit, and Co-Chair of the NETEC Laboratory Workgroup
• Dr. Colleen Kraft, MD – Professor, Department of Pathology and Department of Medicine, Division of Infectious Diseases, Emory University School of Medicine, and Co-Chair of the NETEC Laboratory Workgroup Laboratories play a critical role in detecting and responding to high-consequence infectious diseases (HCIDs). The National Emerging Special Pathogens Training and Education Center (NETEC), as the Coordinating Body of the National Special Pathogen System (NSPS), helps ensure hospital labs are ready for these challenges. The NSPS Level 2 Resource Guide supports this mission with practical tools, checklists, and best practices that make readiness measurable, actionable, and sustainable.
NETEC Laboratory Workgroup co-chairs Vicki Herrera, MS and Colleen Kraft, MD discuss the advantages of adopting the NSPS Level 2 Resource Guide in laboratories with MLO Editor-in-Chief, Christina Wichmann.
Giving lab workers a reason to stay
Skilled lab professionals are essential to healthcare, as 70% of medical decisions depend on diagnostic test results. Effective career paths do more than list job titles. They outline the learning and upskilling required each step along the way and make
progression criteria transparent so employees know what it takes to move forward.
Recognition isn’t just about promotions. Labs can celebrate their teams in various meaningful ways, from additional responsibilities to public acknowledgements, fully funded education opportunities, and performance awards. The key? Be genuine, timely, and consistent. When your team feels valued, they’re more engaged and motivated to bring their best to work every day.
In this MLO exclusive interview, Michelle Westfort discusses how labs can foster a motivated, skilled, and engaged workforce with MLO Editor-in-Chief, Christina Wichmann.
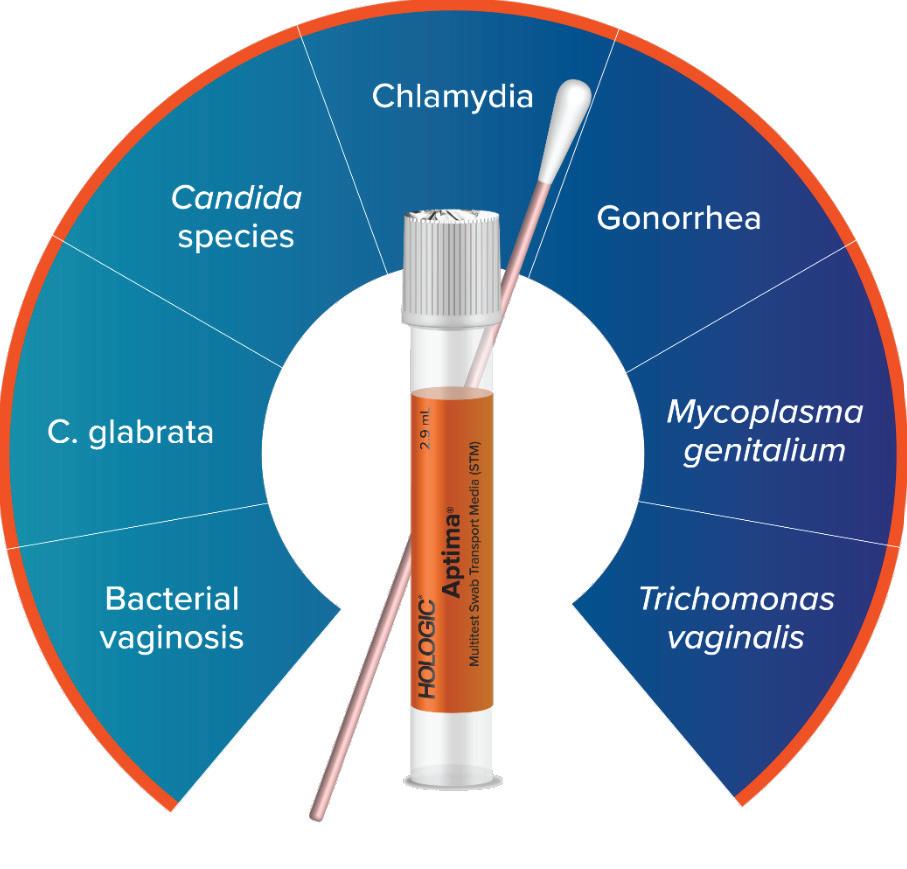
Rethinking vaginitis testing: Opportunities for improvement in laboratory-enabled care
This article highlights key challenges labs and clinicians face using traditional testing methods, how NAAT technology is improving outcomes in both lab efficiency and patient care, and why STI co-infection insights from the study should shift current diagnostic paradigms.
The landscape of vaginitis testing is evolving, and laboratories have an opportunity to lead the way by embracing more accurate guideline-based approaches. Moving beyond empirical treatment and outdated manual methods to NAAT-based testing is more than simply a technological upgrade; it is a necessary shift toward data-driven, patient-centered care.
The growing momentum of AI in digital pathology: An interview with Olga Colgan, PhD
In this exclusive interview, Olga Colgan, PhD discusses how artificial intelligence (AI) is shaping the future of digital pathology in clinical laboratories.
The pathology field, particularly diagnostic pathology, is experiencing a growing imbalance between demand and workforce capacity. On one hand, earlier screening programs and an aging global population are driving a significant increase in the number of samples requiring analysis. On the
Unmasking
anti-nuclear antibodies: The critical role of serial dilution
Systemic autoimmune rheumatic diseases (SARDs) comprise a number of autoimmune disorders, including systemic lupus erythematosus (SLE), systemic sclerosis (SSc), antiphospholipid syndrome (APS), Sjögren’s syndrome (SS), idiopathic inflammatory myositis (IIM), vasculitis, and rheumatoid arthritis (RA).
This article discusses the significance of anti-nuclear antibody (ANA) testing in diagnosing SARDS, emphasizing the need for serial dilutions to unmask masked patterns and improve diagnostic accuracy. The authors stress the importance of adhering to ICAP’s guidelines for ANA screening and highlight the potential consequences of using only a single dilution—focusing on the risk of overlooking mixed patterns amongst routine ANA samples.
other hand, advances in personalized medicine, biomarker discovery, and immunotherapy are adding layers of complexity to each diagnosis. This means not only more samples, but also more tests per sample, and more sophisticated assays overall. At the same time, the profession is grappling with a global shortage of pathologists. This workforce deficit is contributing to longer turnaround times, delayed diagnoses, and ultimately, delayed treatment for patients.
Artificial intelligence (AI)-driven digital pathology, while still in the early stages, is beginning to gain meaningful momentum as clinical labs look for scalable solutions to address these mounting challenges in diagnostic complexity and workforce capacity.
• By digitizing slides, labs can:
• Enable remote work
• Improve flexibility for pathologists
Make the field more attractive to new professionals.
Emerging uses of handheld blood gas analyzers
By Ian A. Lentnek, MD and Angela Neale, PA-C, MBA, MLS(ASCP)
Earning CEUs
See test online at https://Emerginguses-ofhandheld-blood-gas-analyzers
Passing scores of 70 percent or higher are eligible for 1 contact hour of P.A.C.E. credit.
LEarning oBJECtiVEs
Upon completion of this article, the reader will be able to:
1. Define point-of-care testing and its advantages compared to central laboratory diagnostics.
Point-of-care testing (POCT) achieved significant attention over the past several years, associated in part with technological advancement, the SARS-CoV-2 pandemic, and the growing demand for rapid test results.1 Point-of-care (POC) is defined as the ability to provide expedient lab results at or near a patient’s bedside. 2 These instruments support a broad range of clinical settings and offer an increasing array of testing analytes. Analyzers are typically small and often portable and include compact benchtop systems and handheld devices.1 Rapid and reliable results can minimize delays in clinical decision-making and support expedient patient management. Advancements in technology such as wireless connectivity, smaller devices, and microfluidics, have facilitated creation of portable and user friendly POCT devices. 3
2. List the various settings in which POC testing supports.
3. Discuss the uses and impact of POC testing in various settings.
4. Describe the benefits of POC lactate testing in sepsis. Scan code to go directly to the CE test.
POCT is routinely used for blood gas analysis and other measures of clinical assessment using sample types, arterial, venous, and capillary. Near patient devices have become an important tool in the evolving healthcare landscape, supporting assessment for blood gas levels, electrolytes, metabolites, and other analytes often within minutes.4
Respiratory season can pose a real threat to your patients, especially the elderly. Fast, accurate diagnosis and treatment is one way to protect them and get them back to doing what they love. Having the right diagnostics in your office can help you deliver a higher level of patient satisfaction and improve efficiency.
Our product portfolio includes high-quality, point-of-care molecular and antigen tests for diagnosing respiratory illnesses.
We make diagnostics that matter because we believe each test represents the health and well-being of a real person.
The quick turnaround time using POCT supports accelerated clinical decision-making in critical hospital settings including the emergency department, critical care units, and operating rooms. Handheld devices offer intriguing prospects for use outside the hospital setting, including physician offices, specialty clinics, rural community health centers, disaster sites, ambulances and paramedic services, or large social gatherings such as sport or entertainment events.1
Use of a handheld device can often minimize delays associated with workflow for critical analytes, including sample transport and processing, by providing a timely lab result near the patient’s location. This can be particularly important in time-sensitive scenarios like respiratory distress, trauma care, and other potentially life-threatening emergencies.1 However, its utility could also provide value in less critical settings, as the rapid turnaround time of a handheld analyzer could enhance workflow efficiency and support valuable cost-savings.
The role of handheld and near patient devices continues to expand, offering the potential of improved outcomes and streamlined workflow across diverse settings.5 Importantly, POCT should not be perceived as a replacement for lab-based testing but as a complimentary method of addressing needs beyond the scope or existing capabilities of the central lab.
POCT outside the hospital setting
Handheld blood gas analyzers have been widely implemented by emergency responders for the early identification of critically ill patients at the point of contact or during transport, including in ambulances, medical helicopters, or during interfacility transfer. 6 Increasingly, testing by first responders includes metabolic status, informing on critical care conditions like respiratory failure and sepsis;6 providing results such as oxygenation status, lactate levels, and electrolytes; supporting informed triage for interventions such as hemodynamic resuscitation, oxygen therapy, and ventilatory support.
In the case of sepsis, there is a profound impact of timely intervention to reduce morbidity and mortality.7 The Surviving Sepsis Campaign includes blood lactate testing as a potential aid in the diagnosis of sepsis as levels of serum lactate help to inform resuscitation measures.8 The emphasis on early recognition of sepsis and rapid initiation of treatment reflects a commitment to improving patient outcomes.7 It starts with a clinical assessment and laboratory tests such as lactate, which per the 1-Hour Bundle, Surviving Sepsis Campaign are pivotal to understanding the status of sepsis and initial intervention.9 Studies have shown that for every hour of delay in starting antibiotics in sepsis or septic shock, mortality rates can increase significantly.10 This statistic demonstrates the urgency and importance of adhering to these new guidelines.
In cases of severe illness, early blood gas results can serve as a “heads-up,” ensuring that the receiving team is ready to deliver advanced care without delay, during critical transitions.
POCT in natural disasters
While use of POCT is increasingly being utilized in the pre-hospital settings, significant potential for use in disaster situations exists.1,11 Natural disasters such as fires, floods, tornadoes, and hurricanes are increasingly impacting much of the U.S. population.12 The need for an urgent and broad response to a large number of impacted individuals necessitates
use of portable equipment in these resource-limited settings. Handheld, easy to use, compact analyzers that offer a range of analyte testing can support on-site assessment of patients and aid critical triage and transport decisions.1 Some POCT devices offer a battery-operated option, allowing access to testing at the patient’s side when infrastructure may be fractured. This could be particularly useful in situations where hospitals are on “diversion,” when a patient may require
Rapid and reliable results can minimize delays in clinical decision-making and support expedient patient management.
an admission, or when referral to either a regional or more distant tertiary care center may offer more advanced care.
For example, in the case of wildfires, first responders with a blood gas analyzer can immediately assess the respiratory status of a patient who has suffered from smoke inhalation, supporting intervention for those in most urgent need and reducing unnecessary use of precious resources such as oxygen. For burn injury victims, blood gas analysis can help with acid-base balance, guiding further hemodynamic resuscitation.11
The ability to deliver immediate, actionable data makes POCT a valuable tool for triage, treatment, and timely transport decisions during mass casualty and disaster response operations. Accurate and easy to use analyzers are essential in these settings.
Emergency department (ED) triage
In the ED and critical care settings, fast and accurate diagnostics are vital for clinical decision-making and support improved outcomes.14 Blood gas POCT analyzers are indispensable to assess metabolic status (i.e., pH), electrolyte levels (i.e., potassium and calcium), and cardiopulmonary presentation (i.e., pO2).11
While most of these tests can be conducted in the core lab, preanalytical errors, and time to results can be a barrier to prompt decision-making and a drain on resources, especially when time is of the essence.15 In contrast, a POCT analyzer offers significant utility, delivering rapid information, often within minutes, by either a venous or arterial blood draw or capillary sample. Further, POCT can help alleviate some of the common preanalytical sample errors that frequently occur in STAT samples, enabling greater efficiency and reducing the likelihood of delays resulting from rejected patient samples. This actionable data, at the point of care, can support quick clinical responses, especially in a fast moving and high-pressured environment.
Implementation of a POCT program will often require collaboration across various departments, which may include laboratory personnel, clinical staff, leadership and, in many institutions, an appointed point-of-care coordinator. This internal collaboration can help to ensure that protocols are standardized, quality controls are consistently followed, and patient results are promptly reported to clinicians.
Software solutions available with POC devices help automate labor intensive processes such as data management, monitoring of quality control trends, and user training requirements. POCT devices connected to electronic health
record systems allow data to be easily accessible to clinicians and ensure compliance with medical record storage requirements. While POCT does occasionally raise concerns about cybersecurity, engaging and aligning with IT colleagues early on can help mitigate these concerns and reduce valuable time spent evaluating vendors.
Elite athletics and large social gatherings
biking, or road racing, where having access to quick results at the point of care, could provide insight into an athlete’s condition.18
Conclusion
Scan code to go directly to the CE test.
The use of POCT within elite athletics and large social gatherings (i.e., sporting events, entertainment venues, and conventions) has gained traction. The performance of elite athletes may be optimized using POCT devices during training when relying on a distant central lab would be logistically challenging or impossible. Moreover, medical teams at large social gatherings can use POCT devices to quickly assess acutely symptomatic people including athletes, performers, event staff, spectators, and attendees. This data may be particularly helpful for conditions such as dehydration, electrolyte abnormalities, and even early sepsis.16, 17
POCT could allow on-site medical teams to determine if patient transportation to a medical facility is required. This maximizes the efficient use of emergency medical transport services, particularly under circumstances where roads are not easily navigable due to crowds or closures. The portable handheld devices have also shown great utility during remote or long-distance events such as marathons, mountain
POC diagnostics have experienced tremendous recent advances. Contemporary devices are capable of rapidly testing a broader range of analytes using convenient analyzers making them a valuable tool across diverse clinical settings. From emergency departments and critical care units to disaster zones and social gatherings, this technology supports medical care in more environments than ever before.
REFERENCES
1. The future of point-of-care testing (POCT). L2DocX. May 14, 2025. Accessed November 20, 2025. https:// blog.lab2doctors.com/2025/01/23/ the-future-of-point-of-care-testing-poct/.
3. Moore THM, Dawson S, Kirby K, et al. Point-of-care tests in the emergency medical services: a scoping review. Scand J Trauma Resusc Emerg Med. 2025;33(1):18. doi:10.1186/s13049-025-01329-y.
4. Hassan W, Martinez S. Arterial blood gas sampling [ABG machine use]. In: StatPearls. StatPearls Publishing; 2024.
6. Elrobaa IH, Khan K, Mohamed E. The role of point-of-care testing to improve acute care and health care services. Cureus. 2024;16(3):e55315. doi:10.7759/ cureus.55315.
7. Karnatovskaia LV, Festic E. Sepsis: a review for the neurohospitalist. Neurohospitalist. 2012;2(4):144-53. doi:10.1177/1941874412453338.
8. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181-1247. doi:10.1007/ s00134-021-06506-y.
9. Surviving Sepsis Campaign. Society of Critical Care Medicine (SCCM). Accessed November 20, 2025. https://www.sccm.org/ survivingsepsiscampaign.
10. Tang F, Yuan H, Li X, Qiao L. Effect of delayed antibiotic use on mortality outcomes in patients with sepsis or septic shock: A systematic review and meta-analysis. Int Immunopharmacol. 2024;129(111616):111616. doi:10.1016/j. intimp.2024.111616.
11. Tran NK, Godwin Z, Bockhold J. Point-ofcare testing at the disaster-emergencycritical care interface. Point Care. 2012;11(4):180-183. doi:10.1097/ POC.0b013e318265f7d9.
12. Smith A. 2024: An active year of U.S. billion-dollar weather and climate disasters. NOAA Climate.gov. January 10, 2025. Accessed November 20, 2025. https://www.climate.gov/news-features/ blogs/beyond-data/2024-activeyear-us-billion-dollar-weather-andclimate-disasters.
13. Eggleston FC, Feierabend TC. The early acidosis of burns: its relationship to extent of burn and management. Surgery. 1975;77(5):641-647.
14. Kapoor D, Srivastava M, Singh P. Point of care blood gases with electrolytes and lactates in adult emergencies. Int J Crit Illn Inj Sci. 2014;4(3):216-22. doi:10.4103/2229-5151.141411.
15. Romero A, Muñoz M, Ramos JR, Campos A, Ramírez G. Identification of preanalytical mistakes in the stat section of the clinical laboratory. Clin Chem Lab Med. 2005;43(9):974-975. doi:10.1515/ CCLM.2005.168.
16. Sharma A, Tok AIY, Alagappan P, Liedberg B. Point of care testing of sports biomarkers: Potential applications, recent advances and future outlook. Trends Analyt Chem. 2021;142(116327):116327. doi:10.1016/j. trac.2021.116327.
17. Mercalli C, Ghio FE, Bonizzato S, et al. Providing medical care at mass gathering sporting events: the 2023 Ryder Cup experience. BMC Emerg Med. 2025;25(1):151. doi:10.1186/s12873-025-01316-7.
18. Bermon S, Nassif M, Kapai A. Point-of-care testing: A new era for endurance medicine. MLO. 2025;57(2):16-17.
Ian A. Lentnek, MD leads Medical a ffairs for Point-ofCare testing at Siemens Healthineers
Angela Neale, PA-C, MBA, MLS(ASCP) is a Medical a ffairs o fficer for Point-of-Care testing at Siemens Healthineers.
45299370
The role of A1c and CGM testing
By William E. Winter, MD; Christina Wichmann
For more than four decades, hemoglobin A1c has served as the cornerstone of long-term glycemic assessment, guiding diabetes diagnosis, risk stratification, and treatment decisions. Its durability stems not only from its technical strengths—standardization, reproducibility, and accessibility—but from the powerful clinical evidence that cemented its role. As a single biomarker obtained from a routine blood draw, A1c provides a comprehensive, validated picture of average glycemia and remains the only measure proven to predict long-term complications and the impact of therapy.
Yet diabetes care has evolved dramatically. With the explosion of GLP-1 therapies such as Ozempic, heightened public interest in tracking glucose, and growing patient access to continuous glucose monitoring technology, there is an urgent and highly relevant need for discussion to understand how we use diagnostic technology. In this article, William E. Winter, MD answers MLO’s questions on this topic.
HbA1c testing has been around for decades. What makes it so enduring as the “gold standard” in diabetes management?
Following the discovery of insulin by Banting and Best in 1921, there was the hope that diabetes mellitus had been cured. Prior to the discovery of insulin, persons with type 1 diabetes rarely lived more than a year and certainly succumbed to the disease within 2 years of diagnosis.1 While insulin was lifesaving for persons with type 1 diabetes, as the years and decades passed, physicians and their patients realized that diabetic complications were frequent and caused blindness, kidney failure, neuropathy and premature cardiovascular death. Thus, the paramount question for all physicians and persons with diabetes was as follows: “Is the development of diabetic complications dependent on the patient’s glycemic control, or are complications independent of glycemia?” If diabetic complications did indeed result from chronic hyperglycemia, the penultimate question became: “Does improved glycemic
control decrease one’s risk of developing diabetic microvascular complications?”
Two studies published in the 1990s addressed these two questions. The Diabetes Control and Complications Trial (DCCT) 2 and the United Kingdom Prospective Diabetes Study (UKPDS)3 examined, respectively (and prospectively), persons with type 1 diabetes and persons with type 2 diabetes. Both studies came to similar conclusions: the severity of hyperglycemia, as measured by hemoglobin A1c, was correlated with the participants’ risk of developing microvascular complications (e.g., retinopathy, nephropathy, and neuropathy). Possibly even more important were their findings that improved glycemia, as measured by reductions in hemoglobin A1c, reduced the participants’ risks of developing microvascular complications. This spelled good news for the diabetes community: by maintaining plasma glucose as close as possible to the “normal range,” microvascular complications could be prevented. Thus, patients could improve their likely outcomes by reducing hemoglobin A1c levels.
These two studies demonstrate that hemoglobin A1c is an excellent marker of long-term risk for the development of complications. Since that time, researchers have discovered that modest elevations in hemoglobin A1c in persons without diabetes can predict the later development of type 2 diabetes and elevated hemoglobin A1c can be used to diagnose diabetes.
Therefore, hemoglobin A1c is the primary metric for the assessment of long-term glycemia that can predict diabetes, diagnose diabetes, and assess a person’s risk for diabetic microvascular complications. No single biomarker (obtained by a single phlebotomy) provides the diversity of information that is provided by the measurement of hemoglobin A1c. Hemoglobin A1c measurements are affordable, clinically available (being present on many highly automated platforms), highly standardized, accurate, and reproducible. There is less biological variability in hemoglobin A1c than measurements of plasma glucose. As well, hemoglobin A1c concentrations are stable throughout the day, and testing does not require fasting.
What evidence from landmark trials like the DCCT and UKPDS still resonates today in showing the importance of A1c?
The DCCT4 and UKPDS5 findings are as valid in 2026 as they were in the 1990s. Higher levels of hemoglobin A1c predict an increased risk of diabetic microvascular complications. Possibly even more important is the fact that reducing hemoglobin A1c levels reduces one’s risk of developing such complications. These facts apply to all persons with diabetes regardless of whether or not a person with diabetes is insulin-treated.
What’s the value of HPLC technology for measuring A1c?
In various locations throughout the world, there is up to a 1%-4% risk of a patient having a hemoglobinopathy or thalassemia that could yield a clinically invalid hemoglobin A1c result when measured by a structural-based method (e.g., immunoassay, enzymatic, or boronate affinity). The laboratorian and clinician caring for the patient can be assured that hemoglobin A1c measurements reported using a charge-based separation method (e.g., HPLC or capillary electrophoresis) can detect the absence of hemoglobin A and can often suggest the
presence of a hemoglobinopathy and/or thalassemia. Therefore, charge-based methods can reduce errors in reporting hemoglobin A1c, thereby improving patient care.
What has continuous glucose monitoring brought to diabetes care that wasn’t possible before?
Hemoglobin A1c and CGM are complementary and are “partners” in the care of patients with diabetes. Only hemoglobin A1c is validated as a measure of risk for the development of long-term diabetic complications, and only reductions in hemoglobin A1c have been shown to reduce the patient’s risk of developing such complications. However, hemoglobin A1c measurements do not inform the patient or their health care team as to how glycemic control can be improved (e.g., “normalized”). This is the role of self-monitoring of blood glucose (SMBG) and especially CGM. Prior to CGM, persons with diabetes might perform SMBG, at most, seven times per day, as a basis for adjusting medication dosages, diet, and exercise. With CGM, interstitial glucose can be measured every 5 minutes to develop a detailed glycemic profile. With these data in hand, the patient and their health care team can plan and implement a flexible regiment to improve glycemia measured as a reduction in hemoglobin A1c.
It should be noted that, in the U.S. at least, insurance companies will only cover the partial or full costs of CGM in persons with type 1 diabetes and persons with insulin-treated type 2 diabetes. Therefore, CGM is only available to a limited number of people with diabetes. Furthermore, the cost of CGM is not negligible. As well, wearing the CGM device, monitoring the CGM results, adjusting medications, and incorporating a healthy diet and exercise require a considerable commitment from the patient and their family. Not all CGM-eligible persons are able (or willing) to make and execute such a commitment. Lastly, while CGM is potentially a wonderful tool for improving glycemia, CGM is not used to predict or diagnose diabetes, which are functions provided by hemoglobin A1c measurements and not CGM.
How do patients respond differently when they see real-time data from CGM compared to periodic A1c results?
CGM and hemoglobin A1c assess different aspects of glycemia. CGM provides real-time data (and past data) whereas hemoglobin A1c is a summative measure of what has happened cumulatively in the last 2 to 3 months. By reducing their hemoglobin A1c concentration, patients can reduce their risk of developing diabetic complications. While it is assumed that improved glycemic control, as measured by CGM, will reduce the patient’s risk of developing diabetic complications, there are no prospective CGM studies analogous to the DCCT and UKPDS that prove this hypothesis.
A 2024 article in Clinical Diabetes reported the following key points regarding patients who use CGM (this is a direct quote from the article):6
• Ninety percent of survey respondents agreed that the majority of continuous glucose monitoring (CGM) sensors were accurate. However, only 79 and 78%, respectively, were satisfied with sensor performance on the first and last day of wear.
• Forty-two percent agreed that accuracy varies from sensor to sensor, with 54% experiencing skin reactions or irritation using sensors.
• Thirty-five percent were concerned about the impact of overthe-counter or prescription medications (e.g., cold and flu
remedies or pain relief products) on sensor accuracy.
• Thirty-six percent agreed that inaccurate CGM alarms or alerts negatively affected daily life, and 34% agreed that they negatively affected diabetes management.
Many people believe that continuous glucose monitoring (CGM) will eventually replace A1c. Do you agree with that view? Why or why not?
I do not believe that CGM should replace hemoglobin A1c measurements. As described in my previous response, CGM and hemoglobin A1c are complementary, and they provide different information. CGM provides real-time glycemic data that can be used to determine day-to-day, minute-to-minute care. Hemoglobin A1c is retrospective providing information about average glycemia over the preceding 2 to 3 months. CGM is expensive, demanding, labor-intensive and is not available to all people with diabetes. If 10% of people in the U.S. have type 1 diabetes and 90% have type 2 diabetes, with 25% of these persons using insulin (and are thus eligible for CGM), assuming that all of these insulin-treated persons indeed used CGM, approximately 2 out of 3 people with diabetes would not have access to CGM (nor should it be assumed that they would benefit from CGM). Presently 40% to 50% of people with type 1 diabetes use CGM.7
With new therapies such as GLP-1 receptor agonists (e.g., Ozempic), how does the role of A1c testing or CGM change?
Novel therapies should not change the use of CGM or hemoglobin A1c measurements.
In an era of digital health and remote monitoring, where do you see A1c fitting into the workflow of the future diabetes clinic?
Hemoglobin A1c will continue to be used as currently recommended by the American Diabetes Association.8 Persons with glycemic control at or near to target should have their hemoglobin A1c measured every 6 months whereas persons with glycemia above the target range should be tested every 3 months. Whereas point-of-care testing (POCT) devices for measuring hemoglobin A1c may be convenient, they have the following limitations: POC
testing by staff takes staff away from direct patient care. Because POCT devices generally measure hemoglobin A1c in one sample at a time, POCT is inefficient when compared to central laboratory testing where measurements are automated. POCT for hemoglobin A1c is not as accurate or precise as central laboratory testing. Unless there is a dedicated POC testing staff coordinator, staff are usually not trained to appreciate the importance of quality control and quality assurance. POCT is more expensive than central laboratory testing.
If you could leave physicians with one key message about A1c and CGM, what would it be? CGM and hemoglobin A1c are complementary measurements that are both important for the care of insulintreated persons.
REFERENCES
1. Polonsky KS. The past 200 years in diabetes. N Engl J Med. 2012;367(14):1332-40. doi:10.1056/NEJMra1110560.
2. Diabetes Control and Complications Trial Research Group; Nathan DM, Genuth S, Lachin J, et al. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329(14):977-86. doi:10.1056/ NEJM199309303291401.
3. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998;352(9131):837-53.
4. Diabetes Control and Complications Trial Research Group; Nathan DM, Genuth S, Lachin J, et al. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329(14):977-86. doi:10.1056/ NEJM199309303291401.
5. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998;352(9131):837-53.
6. Holt E, Nguyen H, Bispham J, et al. Perceptions of continuous glucose monitoring systems in the T1D exchange diabetes registry: Satisfaction, concerns, and areas for future improvement. Clin Diabetes. 2024;42(1):104-115. doi:10.2337/cd23-0005.
7. Mayberry LS, Guy C, Hendrickson CD, McCoy AB, Elasy T. Rates and correlates of uptake of continuous glucose monitors among adults with type 2 diabetes in primary care and endocrinology settings. J Gen Intern Med. 2023;38(11):2546-2552. doi:10.1007/s11606-023-08222-3.
8. American Diabetes Association Professional Practice Committee. 6. Glycemic goals and hypoglycemia: Standards of care in diabetes-2025. Diabetes Care 2025;48(1 Suppl 1):S128-S145. doi:10.2337/ dc25-S006.
Christina Wichmann editor-in-Chief Medical l aboratory Observer | endeavor business Media
William E. Winter, MD is board-certified in pediatrics, pediatric endocrinology, chemical pathology, and clinical chemistry. a Fellow of both the College of a merican Pathologists (C a P) and the academy of Diagnostics and l aboratory Medicine ( a Dl M), Dr. Winter has served in multiple leadership roles at the university of Florida, including Director of Pathology Residency and Medical Director for Clinical Chemistry, Phlebotomy s ervices, and Point-of-Care testing. He has practiced pediatric endocrinology for over 25 years and was principal investigator for several niH-funded diabetes studies, including trialnet, te DDY, and R a Diant a s an Francisco native, he earned his bs in chemistry from s anta Clara university and his MD from l oyola university Chicago.
Confident Testing Starts with Accuracy, Reliability,
and Trust
Bio-Rad’s HPLC Systems Are the Gold Standard of HbA1c Testing.
Our automated hemoglobin testing systems deliver consistent and timely results, with the added advantage of no interference with certain hemoglobin variants (HbS, HbC, HbE, and HbD).
With over 40 years of leadership in HbA1c and/or HbA2/F/A1c testing, our HPLC platforms are used in labs worldwide and are aligned with international quality standards.
Discover the Difference
How to prepare for a Joint Commission survey
By Harriet Briggs, MBA, MLS(ASCP)
Accreditation is a cornerstone of patient safety and quality care.
As a laboratory surveyor for Joint Commission, I have the privilege of working with laboratories across the country to support their quality improvement efforts. A common question I receive is how labs — whether in a small community hospital or part of a large health system — can best prepare for their Joint Commission accreditation survey. This question is even more pressing in today’s healthcare landscape, where staffing and resources are often limited.
Turn daily tasks into survey prep
The best piece of advice I like to give to my peers is simple: make survey readiness a daily habit. For example, instead of just signing and dating a document and then filing it away, take the opportunity to review its completeness and accuracy. By closely reviewing documents, one can begin to identify trends and take immediate corrective action if needed.
A good approach is to take a critical value from the daily critical value list and locate all necessary documentation in a patient’s medical record. If time allows, review proficiency testing documentation related to the critical value, continue with quality control, temperature monitoring records, etc. Such daily tasks can help labs stay prepared without feeling overwhelmed.
Use the survey guide
Another simple but important step is to review Joint Commission’s survey guide, which includes a document list. These are the documents that the surveyor will request during the survey. Work as a team to collect these documents early. And as they are gathered, ask, “Does this reflect our current practice?” This proactive review helps identify and address any gaps before survey.
Three key focus areas
There are three common areas that labs struggle with: proficiency testing, employee competency, and documenting procedures. These areas have been consistent for the past several years. By focusing on these areas, labs can address potential roadblocks before they arise.
Proficiency testing
In the laboratory world, proficiency testing is like midterms and finals. This is when a Centers for Medicare & Medicaid Services (CMS)–approved provider sends an unknown specimen to a lab for analysis two to three times a year. The results are then compared to expected values or consensus results. Unacceptable results are becoming more common, and repeated failures can put a lab at risk of losing testing capability. Joint Commission surveyors review two years or six events of proficiency testing. We do not just want
to see pending results; we also want to see completed ones. For labs that use the College of American Pathologists (CAP) proficiency programs, providing a scorecard for the past six events is more efficient than flipping through multiple binders.
Given the myriad of reasons for failing proficiency testing — clerical, technical, or random errors — I always encourage labs to conduct a thorough investigation every time a result comes back as unacceptable. Performing a root cause analysis can help identify the underlying issue and prevent recurrence. While Joint Commission does not require this step, labs that do it often take proactive corrective actions that ultimately improve performance.
Employee competency
Training and competency are two separate things but are often mistaken as the same. Training is how to do things the organization’s way, while competency is demonstrating the ability to perform tasks correctly.
I often share this analogy: when I was 16 years old, my brother trained me how to drive a stick shift. Years later, I still have not shown him competency.
Joint Commission requires initial training and initial competency to be documented separately. This is unique to Joint Commission and is not required by other accreditors or CMS. Using the same document for both is a common mistake.
During the survey, we check that competency requirements are met and review human resources (HR) files for employees included in tracers. In small labs (5-6 staff), we likely will review almost all files; in larger labs, we will choose select files.
Additionally, we verify that job descriptions meet minimum requirements for education, experience, certification and credentials.
Surveyors do not interpret documentation; we ask labs to show and explain their process. We also check compliance with the Clinical Laboratory Improvement Amendments (CLIA) six procedures of a competency assessment:
• Directly observing routine test performance, including patient preparation and, if applicable, specimen handling, processing, and testing
• Monitoring the recording and reporting of test results
• Reviewing intermediate test results or worksheets, quality control (QC) records, proficiency testing (PT) results, and preventive maintenance records
• Directly observing instrument performance, maintenance, and function checks
• Assessing test performance using previously analyzed test specimens, internal blind testing samples, or external PT samples
• Assessing problem-solving skills
Documenting procedures
Every laboratory process should have a documented procedure — and actual practice must match that procedure. I often find mismatches: a procedure exists but is not followed, or a practice exists without a procedure. Both need to align.
Best practices for documenting procedures are as follows:
• Review and update procedures annually.
• Involve staff in updates to ensure accuracy.
• Maintain version control and store documents in a centralized system for easy access.
Engage team through mock tracers
The best way to prepare for a Joint Commission survey is to make sure all team members participate and feel part of the accreditation process. Mock tracers are an excellent tool for this.
Simulate the entire process — from opening conference to exit conference — and involve other departments like respiratory, nursing, and quality. This builds collaboration and reinforces the
shared goal of patient safety and quality care for all.
Survey readiness is not a one-time event — it is a daily habit. Start small today: review one document, verify one competency, or begin to map out a
Accreditation is a cornerstone of patient safety and quality care.
mock tracer. Joint Commission is always here to help labs on their accreditation journey. For helpful resources, visit www.jointcommission.org.
Harriet Briggs, MBA, MLS(ASCP) is a Field director – Laboratory Surveyor Program at Joint Commission. in this role, she is responsible for the management and oversight of field staff who conduct laboratory accreditation surveys. Prior to her role as Field director, briggs was a laboratory surveyor.
Ready or not: Operational readiness for HCID patients The clinical laboratory perspective
By Vicki L. Herrera, MS and Colleen S. Kraft, MD
Operational readiness for high-consequence infectious diseases (HCIDs) remains one of the most critical challenges in modern healthcare. While much attention is often directed toward frontline clinical teams, the clinical laboratory plays an equally pivotal—yet sometimes underrecognized—role in protecting patients, clinicians, and the broader community. Successful patient outcomes depend on timely and accurate diagnostics, and laboratories must be prepared to safely process specimens from potentially infected individuals at any moment, regardless of their facility’s size, resources, or geographic location.
Patients with suspected HCIDs may present to any healthcare setting, from a 10-bed rural critical access hospital to a 1,000-bed tertiary care center. Illness does not respect institutional readiness. When people are unwell, they seek care wherever it is immediately accessible—ideally in their own communities. Therefore, every hospital laboratory must maintain a foundational level of competency, safety readiness, and operational fluency to manage specimens from patients under investigation for HCIDs. The literature consistently emphasizes that timely diagnostic testing is critical not only for patient stabilization but also for ensuring diagnostic accuracy and survival.1 During an HCID assessment, it is neither ethically nor clinically acceptable to withhold standard of care interventions while awaiting confirmatory testing. Even as advanced molecular diagnostics are pending, routine laboratory studies often guide early interventions that prevent deterioration.
To support national readiness, the National Emerging Special Pathogens Training and Education Center (NETEC) has established itself as the premier resource for HCID preparedness across the United States. NETEC provides comprehensive training, technical assistance, and evidence-based guidance to hospitals and laboratories. In addition, NETEC operationalizes and is the coordinating body for the National Special Pathogens System (NSPS)—a tiered network of healthcare facilities designed to address gaps in national healthcare readiness and support scalable, standardized responses during outbreaks.2 The NSPS Level 2 Resource Guide3 serves as a practical and operational framework that helps laboratories strengthen their preparedness across multiple domains, including communication systems, safety protocols, risk assessments, and testing workflows. This is in the context of organizing readiness into 11 key capability domains— spanning from physical infrastructure and PPE supply through laboratory operations, training and exercises, personnel management, infection prevention and control, waste management, decedent care, research, emergency management, treatment and care delivery, and communication/coordination. These domains reflect the breadth of systems and operational elements a
facility must address to safely receive, treat, and discharge patients with HCIDs.
High-quality care for HCID patients requires early identification and containment. NETEC’s guiding mantra—Identify, Isolate, Inform—remains foundational to safe and effective response efforts.4,5 Clinicians must first identify patients who present with epidemiologic risk factors or symptoms consistent with an HCID. Next, patients must be isolated promptly to prevent transmission. The final step—inform—is often the most crucial for laboratory safety. This notification must extend beyond infection prevention and clinical leaders to explicitly include the laboratory. When laboratory personnel are informed early that a specimen may contain a high-consequence pathogen, they can implement targeted biosafety measures,
modify workflows, and reduce unnecessary exposure risks. Numerous studies highlight that laboratories are safer and operationally more effective when communication occurs before specimen arrival.6
Mitigating risk to clinical laboratorians
Safe laboratory operations form the backbone of effective HCID management. Protecting laboratorians is not optional— it is essential to maintaining uninterrupted diagnostic capacity. Both historical evidence and contemporary HCID events demonstrate that laboratory workers face measurable risk when biosafety practices are incomplete or inconsistent.7 Even in high-volume laboratories that routinely process thousands of specimens daily, each sample carries potential risk.8 The key to risk mitigation lies in recognizing that HCID-associated hazards are not unique; rather, they often mirror risks inherent in routine laboratory tasks. What differs is the potential severity of consequences following an exposure.
Procedures that generate aerosols—centrifugation, vortexing, pipetting, opening blood tubes, or mixing specimens—are among the most common sources of exposure. These routine steps can result in aerosolization or surface contamination, especially when performed quickly or under pressure. Understanding these workflow vulnerabilities is essential when handling specimens that may contain high-consequence pathogens.9
While research laboratories working with Biosafety Level-4 (BSL-4) pathogens have established extensive biosafety protocols, they represent a specialized subset of facilities, and accidental laboratory infections have been exceedingly rare in the United States, with no recorded deaths.10,11 Importantly, advancements in therapeutics during recent Ebola, Lassa, and Marburg outbreaks have introduced viable post-exposure prophylaxis options, further enhancing safety for laboratorians when exposures occur.12
Risk assessments provide laboratories with a systematic method for evaluating their workflows, identifying potential hazards, and determining appropriate mitigation strategies.13 A robust risk assessment considers physical layout, specimen transport pathways, equipment safety, staff experience, and the complexity of laboratory procedures. When used effectively, risk assessments drive the development of targeted training, engineering controls, and evidence-based policies that safeguard employees and ensure testing continuity.
To further enhance national laboratory readiness, the NETEC Laboratory Working Group is developing a comprehensive risk assessment tool tailored specifically to special pathogen preparedness. Scheduled for release in mid-2026, this resource will provide laboratories with a structured, standardized approach to evaluating and strengthening their biosafety practices. The tool is expected to support institutions of all sizes—from small community hospitals to large academic centers—allowing them to identify gaps and systematically improve safety infrastructure.
Lessons learned: The Iowa Lassa fever case
The Iowa Lassa fever case in 2024 serves as a compelling reminder of the importance of effective communication and preparedness.14 In this event, delays in recognizing and notifying the laboratory led to unintended exposures among laboratory staff across several facilities.15 This case illustrates how routine workflows can be impacted when information is incomplete. There are instances when laboratories do not receive advance notice that a specimen may contain an HCID, which can increase the risk to staff. This incident also underscores how quickly routine laboratory processes can be disrupted when key clinical information is missing. As reported in the BMJ, the 2024 U.S. Lassa fever case involved a traveler who likely contracted the infection in West Africa and whose illness was not initially recognized as a highconsequence pathogen.14 Situations like this demonstrate how easily an HCID can enter the healthcare system without early suspicion, leaving laboratories unaware that a specimen may require enhanced biosafety measures. For readers less familiar with these workflows, laboratories rely heavily on clinical clues—such as travel history, symptom patterns, or known exposure risks—to decide when to implement specialized procedures, personal protective equipment, or containment devices. When that information is delayed or incomplete, staff may handle samples using standard methods that offer insufficient protection. Clear communication at the time of specimen submission is therefore essential to safeguarding both laboratory personnel and the diagnostic process.
This incident reinforces the fundamental message: laboratorians must remain vigilant. It’s crucial to avoid complacency, especially in high-throughput environments where speed and volume can overshadow caution. Effective communication, robust risk assessments, and sustained preparedness efforts are essential to protecting both patients and staff.
Vicki L. Herrera, MS serves as a Research c oordinator and Lab Manager at university of nebraska Medical center’s global center for Health security and the training and education c oordinator for the nebraska Biocontainment unit. she is co-chair of the Laboratory Workgroup for the national e merging special Pathogens training and education center (netec). With over 20 years of clinical- and research-laboratory experience, she has led specimen-handling, select-agent oversight, and biocontainment-unit lab operations during high-consequence outbreaks, including ebola, coVID-19, and Mpox.
Colleen S. Kraft, MD serves as a Professor in the Departments of Pathology and Medicine (Infectious Diseases) at e mory university school of Medicine, directs the clinical Virology Research Laboratory, and previously served as a ssociate chief Medical o fficer of e mory university Hospital. a s an infectious disease physician, clinical laboratorian, and a healthcare executive, Kraft played a key role during the pandemic in coVID-19 diagnostics, clinical research, and hospital preparedness.
References are available online at mlo-online.com/55335497
Reshaping the rheumatoid arthritis journey with smarter diagnostics
By Tara Bruner, MHS, PA-C, DFAAPA
Autoimmune diseases occur when the immune system mistakenly attacks the body’s own tissues. They often present with symptoms like fatigue, joint pain, muscle weakness, and skin rashes, varying considerably between patients.1 They can also evolve over time, making them challenging for laboratory professionals and healthcare providers to accurately diagnose.
It takes an average of four doctors and four years for patients to receive an autoimmune diagnosis from the first visit.2 Delays in autoimmune disease diagnosis can be harmful — worsening disease progression, leading to unnecessary treatments, and reducing quality of life.3 In fact, 99% of individuals with autoimmune diseases report fatigue impacting their quality of life, while 89% say it also hinders their ability to work.4 Studies show that delays in diagnosis not only worsen physical symptoms,3 but they also contribute to significant mental health challenges, such as anxiety, depression, and mistrust in the healthcare system.5
Rheumatoid arthritis (RA), in particular, is one of the most common and debilitating autoimmune diseases, affecting about 1.3 million Americans.6 Timely and accurate diagnosis is critical, as early treatment can prevent irreversible joint damage and improve long-term outcomes. However, diagnosing RA remains complex since symptoms overlap with many
other conditions and biomarkers are not always clear-cut, though advances in laboratory technology are beginning to close these gaps and help clinicians detect RA earlier and with greater accuracy.
Challenges associated with RA diagnostics
More than 15 million Americans live with one or more autoimmune diseases,7 but up to 76% of autoimmune patients report at least one misdiagnosis.8 Diagnosing RA can be particularly challenging because the symptoms mimic many other conditions, and clinicians who are not specialists in identifying autoimmune diseases may not spot the signs early. RA symptoms, such as fatigue, joint stiffness, and pain, are often nonspecific and can resemble other inflammatory or autoimmune conditions. For RA specifically, one recent study found that 48.3% of patients with RA were misdiagnosed before presentation to a rheumatologist.9 Additionally, up to 20% of RA patients — likely even more, depending on the study — are seronegative, meaning that they are not going to test positive for the most relevant diagnostic markers. With a shortage of rheumatologists combined with an increased need for these specialists, many patients visit multiple other healthcare providers before they reach a rheumatologist, prolonging their time to diagnosis. Primary care physicians
are often the first point of contact for patients seeking care, but they may not have a high level of familiarity with autoimmune testing protocols.
Gender bias can also contribute to delays. In fact, women are 66% more likely to be misdiagnosed compared to men10 – a stark statistic, especially considering 80% of autoimmune conditions affect women.11 The above challenges all combine to contribute to longer diagnostic timelines that can delay or altogether halt patients’ access to effective treatment.
How combined testing assays are changing the diagnostic landscape
In 2010, the American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR) released new classification criteria for RA with two of the four classification domains involving blood tests. The key blood-based markers are rheumatoid factor (RF) and anti-cyclic citrullinated peptides (anti-CCPs). Testing for RF and anti-CCP antibodies is crucial in diagnosing RA. While RF is a common marker, anti-CCP is much more specific to RA. Based on these antibodies, RA in adults can be classified as either seropositive or seronegative.
Rheumatoid arthritis (RA), in particular, is one of the most common and debilitating autoimmune diseases, affecting about 1.3 million Americans.
In seropositive RA, blood tests show unusually high levels of antibodies called anti-CCPs. These are specific markers for RA and may show up as much as a decade before symptoms do, and around 60% to 80% of people diagnosed with RA have anti-CCPs.12 By definition, people with seronegative RA don’t have these antibodies in their blood. Most people who test positive for anti-CCP antibodies also test positive for RF. However, RF can also be elevated in many other conditions, such as chronic infections, liver disease, and other autoimmune disorders, making it a less specific marker for RA.
Because of its high specificity, anti-CCP testing is now considered the preferred diagnostic marker for RA. Clinicians often order both anti-CCP and RF tests together to improve diagnostic confidence and accuracy. Combining tests for RF and anti-CCP antibodies also significantly increases the accuracy of diagnosing RA. Measuring multiple antibody isotypes — such as IgA, IgM, and IgG — can also further enhance diagnostic sensitivity. The presence of several isotypes often indicates a more active immune response, which supports a serological diagnosis of RA. Researchers have found that testing for these RF isotypes and anti-CCP results in specificity of nearly 100%.
With a comprehensive RA profile, labs can cut through the uncertainty around RA, helping clinicians get to a diagnosis faster and have a more complete interpretation for the provider. As mentioned, time to diagnosis also shortens time to treatment, which can slow the progression of RA in patients. For example, disease-modifying anti-rheumatic drugs or steroids can help ease inflammation, and rehabilitative strategies like exercise are an important part of symptom management.
However, all of these interventions follow an accurate diagnosis, which means labs must be ready to provide the most comprehensive testing for better patient care. Systems that
run this testing in parallel can improve diagnostic confidence without complicating a lab’s workflow. Providing the most comprehensive recommended testing means better support for clinicians trying to sift through RA symptoms, especially primary care physicians who may not be as familiar with autoimmune condition symptoms as rheumatologists are.
Progress toward faster, smarter, and more equitable RA diagnosis
The path to an accurate RA diagnosis has historically been long and uncertain, but new diagnostic criteria and technologies are changing this. These technologies not only increase laboratory efficiency, but also help physicians make faster, more confident decisions for patients.
Ultimately, closing the diagnostic gap in RA with these testing processes can help get patients to a faster diagnosis and intervention, improving their quality of life and giving them back time, mobility, and certainty in their care journey.
2. Diagnosis tips. Autoimmune Association. Accessed December 3, 2025. https://autoimmune.org/resource-center/diagnosis-tips/.
3. Kernder A, Richter JG, Fischer-Betz R, et al. Delayed diagnosis adversely affects outcome in systemic lupus erythematosus: Cross sectional analysis of the LuLa cohort. Lupus. 2021;30(3):431-438. doi:10.1177/0961203320983445.
4. Ladd VT. Autoimmune fatigue: what does it feel like? Autoimmune Association. Accessed December 3, 2025. https://autoimmune.org/ blog/beyond-tired-fatigue-and-autoimmune-disease/.
6. Rheumatoid arthritis treatment. Brigham and Women’s Hospital. Accessed December 3, 2025. https://www.brighamandwomens.org/ medical-resources/rheumatoid-arthritis-treatment.
7. De Widt L. New study calculates autoimmune disease prevalence in U.S. Mayo Clinic. January 6, 2025. Accessed December 3, 2025. https://newsnetwork.mayoclinic.org/discussion/ new-study-calculates-autoimmune-disease-prevalence-in-u-s/.
8. Sloan M, Harwood R, Sutton S, et al. Medically explained symptoms: A mixed methods study of diagnostic, symptom and support experiences of patients with lupus and related systemic autoimmune diseases. Rheumatol Adv Pract. 2020;4(1):rkaa006. doi:10.1093/rap/ rkaa006.
9. Javaid U, Mahmud TH, Rasheed A, et al. Factors leading to diagnostic and therapeutic delay of rheumatoid arthritis and their impact on disease outcome. Cureus. 2023;15(1):e34481. doi:10.7759/cureus.34481.
10. The Soliant Health 2024 State of Healthcare Report. Soliant Health. April 10, 2024. Accessed December 3, 2025. https://www.soliant.com/ blog/the-soliant-health-2024-state-of-healthcare-report/.
11. Goldman B. Stanford Medicine-led study shows why women are at greater risk of autoimmune disease. Stanford Medicine. February 1, 2024. Accessed December 3, 2025. https://med.stanford.edu/news/ all-news/2024/02/women-autoimmune.html.
12. Braschi E, Shojania K, Allan GM. Anti-CCP: A truly helpful rheumatoid arthritis test? Can Fam Physician. 2016;62(3):234.
Tara Bruner, MHS, PA-C , DFAAPA practices primary care at Primecare medical c linic in s earcy, a R and is manager, c linical Education, us for Thermo Fisher Scientific ImmunoDiagnostics Division. s he received a Bachelor of science in Biology degree from oklahoma c hristian university in 2000. a fter graduation she worked as a research technician in the department of a rthritis and immunology at oklahoma medical Research Foundation. in 2005 she graduated from the university of oklahoma health sciences c enter with a masters of health sciences in Physician a ssistant s tudies.
ALL SUBMISSIONS DUE BY JANUARY 13, 2026
MLO LAB OF THE YEAR 2026 CALL FOR ENTRIES
MLO’s Lab of the Year Award celebrates medical laboratories that demonstrate their extraordinary commitment to quality patient care. Submissions will be judged on achievements in five areas. A panel of judges selected from MLO’s Editorial Advisory Board will select the winner and two runners-up. All will be featured in the April 2026 issue of MLO, in print and online, and awarded a display wall plaque, with the winner featured on the issue cover.
Medical laboratories, utilizers of a lab’s service and non-vendor affiliates are welcome to submit. Submission requirements are at: https://www.mlo-online.com/55316888
Implementing AI tools: Best practices and considerations
By Fred Ashbury, PhD MASCC
If you have been to a pathology or diagnostics conference in the last couple of years, you have already encountered it: the seeming whirlwind of AI-powered tools available for clinical laboratory use. It’s a radical change from where this field was just a few years ago. Indeed, the evolution of these tools is happening so quickly that the array of potential options can differ dramatically in a matter of months.
With a rapidly changing landscape, it can be difficult to navigate best practices in AI-powered tools for interpretation and lab results. Which options are worth your time, and which are a waste? Which will lead to better care for patients, and which will end up frustrating your clinical colleagues?
These are critical questions as laboratory teams are bombarded with news
and offers about the latest AI services and products. Tools for scanning digital pathology images and suggesting molecular findings, for example, might help staff members review cases faster and deliver results to physicians sooner. The same goes for AI tools designed to accelerate literature review for variant interpretation. But some AI tools could be a burden for clinical teams, or worse, produce inconsistent, incomplete, and therefore untrustworthy results that shouldn’t be incorporated into patient care.
Amid all the uncertainty around AI tools for clinical labs, one thing is clear: demand for molecular testing will only rise in the coming years. With advances in research and new assays being developed and approved, such as minimal residual disease tests that will involve
serial testing of the same patients over time, the workload for molecular laboratorians is set to grow substantially. For many labs, AI tools may be the only effective option for meeting that demand in a resource-constrained environment.
Challenges and opportunities
In some ways, these AI tools have arrived at the perfect time. Clinicians are busier than ever. Meanwhile, the reports they’re getting from laboratory medicine practices are growing in complexity thanks to large gene panels, exome or whole genome sequencing, and an increasing number of treatment options that depend on molecular testing to match patients to drugs or to clinical trials. In addition, results are needed faster than ever to help clinical teams make time-sensitive
decisions about patient care. Generating results rapidly and then interpreting and presenting them in a clinician friendly manner are essential responsibilities for already overworked lab teams.
Using the power of AI tools to review and summarize the scientific literature, identify drug options associated with a specific biomarker, or scan through a patient’s electronic health record to pull out useful elements could help clinical lab teams get through tedious research faster and focus their time on more valuable tasks. For example, AI is a natural fit for keeping tabs on an exploding knowledge base.
But deploying AI services has to be done in a way that makes sense for both laboratories and patient-facing clinicians. Within the lab, it is important to match AI tools to the existing workflow, rather than trying to reinvent laboratory processes. Everything from sample processing to how results are communicated should be considered. A critical component to leveraging AI
Amid all the uncertainty around AI tools for clinical labs, one thing is clear: demand for molecular testing will only rise in the coming years.
tools is to ensure they fit seamlessly into the workflow. If they don’t, users are less likely to take advantage of them and more likely to view them as a burden rather than a help.
The same is true for ordering physicians. If the process of using an AI service is difficult, clinicians probably won’t adopt it. We already know that many eligible patients don’t get the molecular tests they should have simply because the ordering process is too clunky or inconvenient. If AI tools are implemented in clinical labs in a way that makes the clinician’s workflow more difficult — whether that’s how tests are ordered or how results are reported out — then these tools will not be successful.
An optimal model
When searching for AI services, it can be tempting to look for a one-stop shop to deliver on the clinical laboratories’ strategic priorities: a single solution
that can orchestrate a lab’s complete AI needs. Unfortunately, at this stage of AI product development, there is no end-to-end AI workflow. Right now, the best approach is to consider task-specific agents: a tool for reviewing patient records, another tool for summarizing the literature, and so on to build upon the goals of the laboratory’s program. Throughout the process, it is imperative to keep humans in the loop. When it comes to patient care, very few AI tools have been validated extensively enough to go unsupervised by a lab expert. After all, healthcare is still a human-to-human interaction, and we cannot lose sight of this basic fact.
Another avenue to consider, especially for labs with severe resource constraints, is the choice of tool versus partner. With the right team members and sufficient time and money, lab staff could bring in individual AI agents for many of the tasks in a molecular diagnostics workflow. But in labs without those resources, it may make more sense to find a service partner that can recommend the best tools and even help implement them. The partnership model can be even lower cost for labs willing to partner in critical research; many companies can find ways to extract value from insights to advance science and find new ways to treat diseases.
Data curation
AI is the ultimate manifestation of that old adage: garbage in, garbage out. Getting good performance from any AI tool depends on having properly curated, standardized data. This is a huge stumbling block in the healthcare
field, where even the cleanest records from two separate laboratories often aren’t concordant with each other. Consider situations where clinicians and some labs use different terms to describe the same thing — such as a position point on a chromosome versus a protein effect — and it’s easy to get a sense of how difficult it is for AI tools to mine electronic health records and emerge with useful results.
For larger laboratories looking to expand their operations into areas such as biomarker discovery or managing clinical trials, it’s important to curate available data properly. If this isn’t something that can feasibly be done by staff members, there are companies that provide data standardization and curation services to help labs get on track. Once the data sources are well organized, any AI tool implemented to help with biomarker discovery or other data mining tasks will be far more effective and reliable.
Whether labs handle data curation themselves or work with a service provider, it’s important to align these processes with how each lab expects to use that data. Standardizing electronic health records is a very different task compared to aggregating oncology test results in preparation for biomarker discovery.
Calling all innovators
Change in medicine is never easy — especially when lives are on the line. But to improve patient outcomes and advance care, we must embrace new ways of thinking. This means overcoming the challenges of transformation and
finding ways to seamlessly connect vast amounts of information across the patient journey, enabling better decisions at the point of care. AI products and services are mostly being developed and offered by third-party companies, but it’s the clinical laboratory professionals who have to be the innovators. Only this community can determine the tasks where AI will be most effective, the
Within the lab, it is important to match AI tools to the existing workflow, rather than trying to reinvent laboratory processes.
ideal ways to roll out new AI-powered services, and how to use AI responsibly with sensitive patient data and with end-user providers and other clinical team members who may be skeptical of newer technologies.
With staffing shortages, cost pressures, and overwhelming demand, it can be easy to dismiss AI tools as an unnecessary time sink. But these tools have real potential to help clinical teams increase their efficiency across the patient care continuum, such as translating test results, identifying possible action steps, listing therapies associated with a specific biomarker, suggesting alternatives when patients develop treatment toxicity, and recommending post-treatment management plans.
For all these reasons, AI tools should be considered viable options for clinical laboratories, so long as they are paired with appropriate guardrails to ensure their responsible use. In this way, they are no different from any other novel technology that lab teams evaluate, validate, and implement to enhance their workflows and help their clinician partners deliver even better patient care.
Fred Ashbury, PhD MASCC is a
co-founder and Chief Scientific Officer
at VieCure, a company dedicated to improving precision oncology care at the community level. His background is in medical oncology and behavioral sciences. He has academic appointments at The Ohio State University and the University of Calgary.
Single sample simplicity for sexual health: The diagnostic journey of a single swab
By Samantha A. Byrnes, MPH, PhD
Sexual health remains an essential pillar of care for all Americans. However, accessing timely testing is not always straightforward. For women and people with a cervix, access to healthcare providers— ncluding obstetrician-gynecologists (OB-GYNs)—can be difficult, particularly in rural settings. A recent Kaiser Family Foundation analysis found a ratio of approximately one OB-GYN for every 2,600 women in the United States, driving long wait times for appointments.1 This can reduce the frequency of sexual health specialist appointments, potentially redirecting individuals to primary- or urgent-care settings when symptoms arise.
Diagnostic solutions need to be flexible to adapt to these different healthcare
settings, patient schedules and preferences. Fortunately, a variety of innovations are helping maximize these healthcare encounters. One prime example is the wide array of testing that can now be performed using a single vaginal swab (potentially self-collected). This one specimen can be used to identify both symptomatic and asymptomatic infections at the point of care and in clinical laboratories. Ongoing innovation is also helping clinical labs efficiently process many sexual health tests on a single, fully automated platform to overcome previous complexities.
Flexible testing at the point of care
One of the challenges with sexual health testing for women is that different infections can cause overlapping symptoms
or no symptoms at all. While many infections can be readily treated, selecting the right medication is essential, as the treatment for one condition may be totally ineffective against another. Coinfections are also relatively common in certain regions and demographics.2 Accurately diagnosing the cause of the infection is therefore critical to ensure proper treatment, prompt symptomatic relief, and to stop the spread of infection. In settings such as urgent care clinics and emergency departments, point-ofcare (POC) testing with gold-standard PCR technology can return accurate results in as little as 20 minutes.3 Practitioners can use multiplex assays to test for many common sexually transmitted infections (STIs), including Chlamydia trachomatis (CT), Neisseria gonorrhoeae
(NG), and Mycoplasma genitalium (MG), simultaneously. If the sample is positive for one or more infections, the appropriate treatment and counseling can be provided within the same appointment.
With the latest technologies, specimens such as a vaginal swab that are used in point-of-care settings can also be used with laboratory-based tests, further streamlining the continuum of care.
Expanding test menus and platform consolidation in clinical labs
Point-of-care testing and patient selfcollection are excellent tools for enhancing the frontline diagnostic experience. However, it does not stop there. Many instruments today require minimal sample processing volumes, which help conserve the specimen. Combined with more standardized instrumentation, the same vaginal swab can now be used to run point-of-care assays and be sent for additional testing in a clinical lab.
In laboratories, the menu of potential assays for a single specimen continues to expand. For example, a new Bacterial vaginosis and Candida vaginitis (BV/ CV) assay is currently in development. Bacterial vaginosis is characterized by an imbalance in the vaginal microbiota caused by overgrowth of normal bacteria. More than 50% of women diagnosed with BV experience recurrence within 12 months,4 and it is associated with an increased risk of HIV infection, pelvic inflammatory disease, and adverse pregnancy outcomes. Candida vaginitis, by contrast, is a fungal infection caused by the overgrowth of Candida species in the vulvovaginal area. It can cause significant discomfort and may negatively impact quality of life.5 The overlapping symptoms of BV, CV, and other causes of vaginitis complicate diagnosis and treatment, making it an important test for symptomatic patients. Processing BV/CV assays using the same vaginal swab sample used for CT/NG/MG/TV testing provides another opportunity for healthcare practitioners to simplify the patient experience, removing the need for additional sampling events and collection devices.
The benefits of single-sample simplicity also extend to clinical laboratory operations. Many labs today are burdened with managing multiple platforms, vendors, and complex workflows for different tests. This leads to increased hands-on time, training needs, and supply chain complexity.
Fortunately, technological advances are helping to streamline these processes. Labs can now adopt a unified, high-throughput molecular assay platform for sexual health testing, so a single sample can be run on a fully automated system—increasing value without adding complexity. This provides clinically actionable results, aligned with current guidelines, for
Many labs today are burdened with managing multiple platforms, vendors, and complex workflows for different tests. This leads to increased hands-on time, training needs, and supply chain complexity. Fortunately, technological advances are helping to streamline these processes.
many thousands of patients in the most efficient way possible. Ready-to-use reagents further reduce manual tasks associated with sample preparation and cleaning maintenance, while increasing standardization across laboratories and different lab technicians.
If results are positive, reflex testing using the same vaginal swab sample can then guide which therapies may be most effective. Additionally, these streamlined systems allow additional sample characterization for research or epidemiological tracking using the same vaginal swab sample. For example, easy-to-use tests now allow labs to detect mutant DNA markers, which can be associated with antibiotic resistance.6 This allows labs to build out customized menus based on the current needs of the populations they serve.
Removing barriers to sexual health testing
We are now moving toward an era where a variety of sexual health tests can be processed using a single vaginal swab sample. Laboratories can seamlessly run many assays using the same specimen and the same unified diagnostic platform. At the point of care, single-sample simplicity allows healthcare providers to maximize patient interactions at a time when scheduling appointments
and visiting the doctor in person can be challenging. Maximizing a single sample demands less from the patient and gives the option for self-collection, overcoming barriers to access for some individuals. It paves the way for sameday treatment and for the fast relief of symptoms. Finally, given the nature of infectious organisms, timely sexual health testing and treatment can limit further spread, benefiting the broader population.
REFERENCES
1. Long M, Rae M, Winger A, Pestaina K. Access to OB-GYNs: Evaluating workforce supply and ACA marketplace networks. KFF. July 10, 2025. Accessed November 18, 2025. https://www.kff.org/affordable-care-act/ access-to-ob-gyns-evaluating-workforcesupply-and-aca-marketplace-networks/.
2. Tran A, Amamoto A, Bates M, Leonard J, Carrico V, Pride DT. Prevalence of Mycoplasma genitalium in a Southern California patient population. Diagn Microbiol Infect Dis. 2025;114(2):117130. doi:10.1016/j. diagmicrobio.2025.117130.
3. Roche receives FDA clearance with CLIA waiver for cobas liat molecular tests to aid in diagnosing sexually transmitted infections at the point of care. Roche Diagnostics. January 22, 2025. Accessed November 18, 2025. https://diagnostics. roche.com/us/en/news-listing/2025/ roche-receives-fda-clearance-with-cliawaiver-for-cobas-liat-molecular-teststo-aid-in-diagnosing-sexually-transmittedinfections-at-the-point-of-care.html.
4. Abbe C, Mitchell CM. Bacterial vaginosis: A review of approaches to treatment and prevention. Front Reprod Health. 2023;5:1100029. doi:10.3389/ frph.2023.1100029.
5. Willems HME, Ahmed SS, Liu J, Xu Z, Peters BM. Vulvovaginal candidiasis: A current understanding and burning questions. J Fungi (Basel). 2020;6(1):27. doi:10.3390/ jof6010027.
6. TIB Molbiol pre-designed assays for use on the cobas omni utility channel on cobas 5800/6800/8800 Systems: UC-TIB-MG Resistance. Roche Diagnostics Accessed November 18, 2025. https://diagnostics. roche.com/us/en/products/product-category/ tib-molbiol-pre-designed-assays-for-use-onthe-cobas-omni-utilit.html#productInfo.
Samantha A. Byrnes, MPH, PhD is a senior scientific Manager at Roche Diagnostics she has a decade of experience developing a range of diagnostic technologies for detection of sexually transmitted infections (stis) and other infectious diseases in multiple healthcare settings, including at the point of care. a t roche, Dr. Byrnes serves as the strategy lead covering sexual health and HPV/cervical cancer on the molecular Medical scientific a ffairs team. she obtained her Doctorate of Bioengineering and a Masters of Public Health from the t he university of Washington Departments of Bioengineering and global Health, respectively.
Flow cytometry controls
Veri- c ells gPI positive control provides standardized leukocytes for P nH clinical research quality control. available within Human gPI- a P d c ocktail Kit (c at# 391507) offering complete solution with liquid antibody cocktail featuring cd157, cd 64, cd15, cd 45, cd 24, cd14 markers plus F laer reagent for high-sensitivity gPI-deficient population detection.
Revvity
Reliable spinal fluid cell count control
spinalscopics is a spinal fluid cell count control for manually performed total cell counts using a hemocytometer. Made from a human protein matrix with stabilized human cells, it mimics real spinal fluid to help medical professionals validate quantitation of red and white blood cells in cerebrospinal fluid samples.
Quantimetrix
One control, many platforms
Birlinn c oV2-Flu- rs V c ontrol Panel M509 is intended for in vitro use as a quality control to monitor the performance of laboratory nucleic acid testing procedures for the qualitative detection of nucleic acid tests that target specific gene segments. Birlinn c oV2-Flu- rs V c ontrol Panel M509 is compatible with many platforms and ldts.
Maine Molecular Quality Controls
Extensive test menu on high-speed benchtop
t he d Z- l ite c270 is an exceptionally versatile, Windows 11-compatible benchtop chemistry analyzer offering 60+ moderate-complexity assays including general and special chemistry, lipid panels, cardiac and cancer markers, and toxicology. It is ideal for physician offices, pain and oncology clinics, reference labs, hospital labs, and as a backup analyzer.
Carolina Liquid Chemistries
One sample, multiple results
accurately diagnosing st Is is complicated due to asymptomatic infections, overlap in symptoms when they do present, and frequent co-infection with more than one pathogen. t he a ptima Multitest s wab simplifies testing for sexual and vaginal health with proven performance by detecting up to seven infections and disease states from one vaginal swab.
Hologic
Three-screen autoantibody assessment
t he K ronus 3- screen Islet c ell a utoantibody el Isa a ssay Kit is for the simultaneous detection of autoantibodies to gad and/or I a -2 and/or Znt 8 in human serum. a bsorbance is measured and is proportional to the total amount of autoantibodies present. For research use only. not For use in diagnostic Procedures.
KRONUS
Rapid and reliable POC hsTnI
PATHFAST provides high-sensitivity cardiac troponin I results directly at the point of care. Combining central lab accuracy with a 17-minute turnaround time, the compact PATHFAST analyzer supports faster clinical decisions for patients with chest pain (NT-proBNP, D-dimer and hsTnI). The system uses whole blood or plasma and delivers quantitative results.
Polymedco
Ultra low PSA quality control
Acusera Ultra Low PSA Control -TU10523 provides quality control material for post-operative or therapeutic PSA monitoring. It offers a target value below 0.06 ng/ml, liquid ready-to-use format, 30-day open-vial stability, and a human serum matrix, supporting laboratories measuring ultra-low PSA concentrations. Randox Laboratories
Does your company have a vitamin D product?
We’d like to invite you to showcase one applicable product in our March 2026 issue! This is a no-charge opportunity, and your submission is due by/before January 30, 2026. Reach out to ebrady@endeavorb2b. com for specs.
a-1 Microglobulin
Anti-Streptolysin O
Apolipoproteins: AI, AII, B, CII, CIII, E
b-2 Microglobulin
Complement C3, C4
CRP, hs-CRP
Cystatin C
D-Dimer
Factor XIII
Ferritin
Fibrinogen
H. pylori
Lower cost Expanded test menu
Outstanding customer support
Haptoglobin
Hemoglobin A1c
IgA, IgG, IgM
Insulin
Krebs von den Lungen-6
Lipoprotein(a)
Microalbumin
Prealbumin
Remnant Lipoprotein
Chol.
Rheumatoid Factor
Transferrin
UIBC
LABORATORY INNOVATOR
Byron Selman is President and CEO of Nova Biomedical, leading the combined Nova Biomedical and Advanced Instruments business since the July 2025 acquisition and merger. Byron previously led Advanced Instruments since joining in 2017. With deep technical and commercial expertise, Byron has built high-performing teams and driven market expansion and strategic turnarounds across hospital, blood center, and biotech sectors.
Prior to joining Advanced Instruments, Byron served as President of Global Markets at Haemonetics Corporation and spent over 20 years at Pall Corporation in executive and general management roles, including President of the Medical Division. He holds a B.S. in Mechanical Engineering from Case Western Reserve University and an M.B.A. from Hofstra University’s Frank G. Zarb School of Business.
How will the merger of Advanced Instruments and Nova Biomedical enhance the value proposition for clinical hospitals—specifically in terms of improving diagnostic accuracy, operational efficiency, and patient outcomes?
The merger of Advanced Instruments and Nova Biomedical marks a transformative step forward for clinical hospitals worldwide. By uniting two industry leaders under the Nova Biomedical name, we are combining complementary strengths in analytical instrumentation, research, and development, and global customer support. This strategic integration enhances our value to hospitals uniting best-in-class technologies and decades of expertise
Combining strengths and improving care
By Christina Wichmann
in laboratory diagnostics, enabling us to deliver more precise, reliable, and reproducible results. The potential to now combine our world class technologies onto singular platforms with expanded functionality will significantly enhance how we serve our customers and patients, empowering clinicians to make faster, more confident decisions, ultimately improving patient care and outcomes.
The merger will also help our customers streamline their workflows and provide integrated solutions that address the evolving needs of modern clinical laboratories. We support our customers with a unified global network that ensures responsive service, comprehensive training, and ensures seamless product integration. We help customers reduce downtime, optimize resource utilization, and support laboratories in delivering timely results—even in the face of staffing challenges or increased demand.
At the heart of this merger is a shared commitment to improving patient outcomes. By expanding our footprint in healthcare settings, we are better positioned to support clinicians across the continuum of care—from diagnosis to treatment monitoring. Our dedication to innovation keeps us at the forefront of life science advancements, delivering new solutions that address healthcare’s most pressing challenges. As one unified brand, we remain dedicated to delivering gold-standard solutions, supporting customer workflows, improving automation, and driving meaningful improvements in healthcare delivery. We are excited about the opportunities this merger creates and remain steadfast in our mission to support hospitals in achieving the highest standards of diagnostic excellence and patient care.
How do you approach postmarket support, training, and feedback from customers to improve products over time?
Our commitment to customers extends well beyond the initial installation of our products. We take a proactive, multi-faceted approach to post-market support, training, and continuous improvement.
From order placement through implementation, our dedicated service and support teams engage with customers to ensure seamless installation, comprehensive training, and rapid response to any question or challenge. This includes our ‘Hypercare’ program, designed to provide enhanced early-stage support and communication during the critical product implementation period.
Customer feedback is also central to our new product development process. We systematically collect and analyze input through surveys, direct conversations, and ongoing customer engagement. This feedback is reviewed by our internal teams, and it directly informs both incremental enhancements and long-term innovation. Our goal is to foster deep partnerships with clinical laboratories, ensuring that our solutions not only meet but exceed expectations for reliability, efficiency, and patient care. By maintaining open channels for feedback and investing in ongoing training and support, we help our customers deliver the highest standards of diagnostic excellence.
How does customer feedback from laboratories feed into your company’s product development?
At Nova Biomedical, customer feedback from laboratories is central to our product development process. We believe that the best innovations are born from listening closely to the needs and experiences of the clinicians and laboratory professionals who use our solutions every day.
Our approach is both proactive and systematic. We actively gather feedback through multiple channels, including direct conversations, surveys, and post-installation reviews. This input is reviewed by our quality, service, and product development teams, ensuring that every voice is heard and considered. For example, we ensure enhanced support and direct communication during the critical early stages of product adoption, allowing us to capture real-time insights and address any questions swiftly.
This feedback loop drives continuous improvement and innovation. Insights
Serving Texas beyond the call.
Tim, a Veteran and Technical Consultant with Sysmex, has called Texas home for 20 years. When devastating floods struck, it hit close to home. Taking time off for search and rescue, he faced RVs tangled in trees and supplies running scarce. With support from Sysmex, delivering everything from chainsaws to flashlights, Tim showed up with just one question: “What do you need and how can I be a part of the good?” And when it comes to your lab? Tim won’t show up with a chainsaw—just the right tools, a positive attitude and the expertise to keep things running smoothly.
Tim Rasar Sysmex Technical Consultant
from our customers directly inform incremental enhancements and long-term product roadmaps. Whether it’s refining usability, expanding automation, improving reliability, or introducing new features, our goal is to ensure that our solutions exceed the evolving expectations of clinical laboratories.
Through our open channels for feedback and investment in ongoing training and support, we foster deep partnerships with our customers. This collaborative approach enables us to deliver products that truly make a difference in diagnostic accuracy, operational efficiency, and, ultimately, patient care.
What emerging trends do you believe will reshape laboratory diagnostics in the next five years?
Over the next five years, laboratory diagnostics will undergo a significant transformation driven by several key trends. Automation and artificial intelligence (AI) will accelerate, enabling laboratories to process greater volumes of data with increased speed and accuracy. AI will enhance predictive analytics, workflow optimization, and decision support, helping labs deliver faster, more reliable results even amid staffing challenges. The rise of biologics, cell and gene therapies, and mRNA-based treatments is reshaping the clinical landscape, requiring laboratories to adopt new testing protocols and uphold higher standards for data integrity and compliance.
As laboratory operations become increasingly digitized, data integrity and cybersecurity are becoming central concerns, with hospitals and labs seeking robust solutions to protect sensitive information and keep pace with evolving regulations. There is also a growing emphasis on sustainability, including reducing single-use plastics and waste, with innovations in device design and workflow efficiency helping labs achieve both environmental and operational goals.
Finally, as experienced laboratory professionals retire and new, tech-savvy staff enter the workforce, there will be greater reliance on automation, digital tools, and integrated training to maintain quality and efficiency despite ongoing staffing shortages. At Nova Biomedical, we are committed to leading in these areas. We are investing in innovation, supporting our customers through change, and ensuring that laboratories are equipped to deliver the highest standards of patient care in a rapidly evolving healthcare environment.
What strategies have you seen labs employ to ensure quality and accuracy while addressing faster turnaround times and staffing issues?
Clinical laboratories are under increasing pressure to deliver accurate results quickly, even as they face persistent staffing challenges. The most successful labs are embracing a combination of
process optimization, automation, and robust quality management systems to meet these demands. Many have implemented advanced laboratory information systems and automated platforms
The rise of biologics, cell and gene therapies, and mRNAbased treatments is reshaping the clinical landscape, requiring laboratories to adopt new testing protocols and uphold higher standards for data integrity and compliance.
to streamline workflows, reduce manual errors, and accelerate turnaround times. Lean methodologies—focused on eliminating inefficiencies and maximizing value—are being widely adopted to optimize every step from sample intake to result reporting. Additionally, labs are investing in ongoing staff training and cross-functional teamwork to ensure that quality standards are maintained, even as teams adapt to new technologies and fluctuating workloads. By leveraging these strategies, laboratories can uphold the highest standards of accuracy and reliability, while also delivering timely results that support better patient care, even in the face of staffing shortages and increased demand.
If a hospital performs one million tests per year and loses one in 1,400 tubes at a cost of $400–600 per tube, then the annual cost could be as much as $428K—not to mention the burden on patients and hospital.1
By implementing Indexor, you can trace samples starting at patient draw, monitor key quality indicators during transportation, and automate time-consuming lab operations.
Fully Automated A1c Testing. Load racks and walk away.
More than A1c: One Platform, Multiple Assays. Consolidate HbA1c, Hb, and Myeloma testing.
Unmatched Resolution: Clearer Results, Superior Hb Variant Detection. Easy-to-interpret patterns when Hb variants are present.
Built-in Safeguards for Smart Reporting. Provide confidence in results and better patient care.