



2024-2025 Employee BenefitsGuide



Welcometothe2024-2025MidwestMoleEmployee BenefitsGuide.Thisguideoffersyouandyourfamily membersalookintoyourcomprehensivebenefits program.Weencourageyoutotakethetimeto educateyourselfaboutyouroptionsandchoosethe bestcoverageoptionsforyouandyourfamily.We haveincludedbriefdescriptionsofourbenefit offeringsandthecost.Ifyouhaveanyquestions, pleasecontactMidwestMole’sHumanResources Department.

Welcometo yourBenefits

Contents Introduction 4 Overview 5 MedicalBenefits 7 TheValueofPreventiveCare 12 SupplementalInsurance 13 LifeandDisabilityInsurance 15 DentalCoverage 16 VisionCoverage 17 VoluntaryLifeInsurance 17 EmployeeAssistanceProgram 21 ElectionForm 23 ContactInformation 27 ComplianceNotices 26 ANNUALNOTICES https://issuu.com/docs/04961995496947f9aec6f13dbc27bb4b?fr=x KAE9_zU1NQ
Benefitsfor2024-2025Introduction
AsanemployeeofMidwestMole,enjoyingyourworkandmakingvaluablecontributionsto businessareequallyvital.Thehealth,satisfactionandsecurityofyouandyourfamilyare important,notonlytoyourwell-being,butultimately,intermsofachievingthegoalsofour organization.
Forthe2024-2025planyear,MidwestMolehasworkedhardtoofferacompetitivetotal rewardspackagethatincludesvaluableandcompetitivebenefitsplans.Theseprograms reflectourcommitmenttokeepingourstaffhealthyandsecure.Weunderstandthatyour situationisunique,andMidwestMoleisofferinganoverallbenefitspackagethatcanbe shapedandmoldedbyyoutofityourneeds.
ThisbenefitsbookletisasummarydescriptionofyourMidwestMolebenefitplans.Ifthereis adiscrepancybetweenthesesummariesandthewrittenlegalplandocuments,theplan documentsshallprevail.Thisbookletandplansummariesdonotconstituteacontractof employment.
Wehopethisbenefitsbooklet,alongwithouradditionalcommunicationanddecisionmakingtools,willhelpyoumakethebesthealthcarechoicesforyouandyourfamily.
UpdateOnHealthCareReform

EffectiveJanuary1,2019theTaxCutsandJobsAct(TJCA) repealedtheindividualmandatetomaintainhealth insuranceorberesponsiblefora“sharedresponsibility payment”.Wehopetokeepofferingthesebenefitsasa valuablepartofyourtotalcompensationinthefuture. However,becauseweofferyoucoveragethatsatisfiesall thehealthreformrequirements,youwillnotqualifyforany federalassistancetopurchaseanindividualorfamilypolicy ontheopenmarket(the“marketplace”).
4
Introduction
PREPAREDBYGIBSONFORMidwestMole
2024-2025Overview
MidwestMoleprovidesanarrayofbenefitsthatcanhelpyouenjoyincreasedwell-being, dealwithanunexpectedillnessoraccident,buildandprotectyourfinancialsecurity, balanceyourpersonalandprofessionallifeandmeeteverydayneeds.Thesebenefitsare affordable,comprehensiveandcompetitive.
Thetablebelowsummarizesthebenefitsavailabletoeligiblestaffandtheirdependents.
Regularfull-timeemployeesworking30ormorehoursperweekareeligibletoenrollin benefits.
Youmayalsoenrollthefollowingfamilymembers:
•Yourlegalspouse
•Yourchildrenunderage26
•Yourunmarriedchildrenwhoareage26orolderandmentallyorphysicallydisabled
Childrenincludeyournaturalchildren,adoptedchildren,step-childrenwhoyousupport, andchildrencoveredunderachildsupportorder.
5
BenefitsAt-A-Glance Eligibility Carrier Coverage AnthemBlueCrossBlueShield*NEW! Medical Principal Dental VSP(throughPrincipal) Vision Principal BasicLife/AD&D Principal VoluntaryTermLife Principal ShortTermDisability NewAvenues EmployeeAssistanceProgram(EAP) Principal Accident*NEW! Principal CriticalIllness*NEW! Principal HospitalIndemnity*NEW!
2024-2025Overview(continued)
ChangesandQualifyingEvents
WhenCoverageBegins
Anewlyhiredemployeemaychoosebenefitplansthatwillbeeffectiveonthe1st ofthemonthfollowing30daysofemployment.Failuretoelectbenefitswithin30 daysofbecomingeligiblewillresultinforfeitureofcoverageandyouwillnot haveanotheropportunitytoenrolluntiltheannualenrollment,unlessyou experienceaQualifyingEvent.
QualifyingEvents
Eligibleemployeesmayenrollormakechangestotheirbenefitselectionsduring theannualopenenrollmentperiod.Aswithmostbenefits,onceyouelectan optionyouareboundtothatchoicefortheentireplanyearunlessyou experiencea“QualifyingEvent”.Thesemayinclude,butarenotlimitedto:
Changesinemploymentstatus
Changesinlegalmaritalstatus
Changesinnumberofdependents
Takinganunpaidleaveofabsence
Dependentsatisfiesorceasestosatisfyeligibilityrequirement
FamilyMedicalLeaveAct(FMLA)leave.
ACOBRA-qualifyingevent
EntitlementtoMedicareorMedicaid
Achangeintheplaceofresidenceoftheemployee,resultinginthe currentcarriernotbeingavailable
6
MedicalBenefits

7
AnthemBlueAccessPPOHSA-Qualified AnthemBlueAccessPPOHSAOptionE3 Non-Network In-Network N/A BlueAccess Network Individuals:$12,000 Families:$24,000 Individuals:$4,000 Families:$8,000 Deductibles (Individual/Family) Individuals:$15,000 Families:$30,000 Individuals:$5,000 Families:$10,000 Out-of-PocketMax (Individual/Family) 30%AfterDeductible 0%AfterDeductible CostSharingAfterDeductible 30%AfterDeductible 0%AfterDeductible PrimaryCareVisit 30%AfterDeductible 0%AfterDeductible Telemedicine/OnlineVisit 30%AfterDeductible Plancovers100% PreventiveCare 50%AfterDeductible $10copayafterded(Pref. Pharm.) $20copayafterded(In-Network) Pharmacy/RX(Generic) 50%AfterDeductible $25copayafterded(Pref. Pharm) $45copayafterded(In-Network) Pharmacy/RX(Preferred) 50%AfterDeductible $75copayafterded(Pref. Pharm) $85copayafterded(In-Network) Pharmacy/RX(Non-Preferred) 50%AfterDeductible 25%upto$350(Preferred) 25%upto$450(InNetwork) Pharmacy/RX(Specialty) 30%AfterDeductible 0%AfterDeductible OutpatientProcedure CoveredasIn-Network 0%AfterDeductible EmergencyRoom 30%AfterDeductible 0%AfterDeductible UrgentCare 30%AfterDeductible 0%AfterDeductible InpatientVisit Standard Non-Tobacco Weekly Contributions $19.00 $17.00 Employee $63.00 $57.00 Employee+Spouse $61.00 $55.00 Employee+Child(ren) $93.00 $84.00 Employee+Family
HealthSavingsAccount(HSA)
ThisishowanHSAworks:
Ahealthsavingsaccount(HSA)isahealthcareaccountandsavingsaccountinone.Themain purposeofthisaccountistooffsetthecostofaqualifyinghighdeductiblehealthplan(HDHP)and providesavingsforyourout-of-pocketeligiblehealthcareexpenses–thoseyouandyourtax dependentsmayhavenow,inthefuture,andduringyourretirement.
Thisisa“portable”account.YouownyourHSA!It’sincludedinyouremployeebenefitspackage,but afteryousetupyouraccount,it’syourstokeep,evenifyouchangejobsorretire.
OnceyourHSAisestablished,moneyiscontributedtoyouraccountbyyou,friendsand/orfamily, andyoucanthenuseyourHSAdollarstax-freetopayforeligiblehealthcareexpenses.Yousave moneyonexpensesyou’realreadypayingfor,likedoctors’officevisits,prescriptiondrugs,and muchmore.Bestofall,youdecidehowandwhentouseyourHSAdollars.
AnnualContributionLimit:
Forthe2024planyeartheIRShassetthemaximumHSAcontributionforasingleat$4,150and familyat$8,300.Forthoseage55+,theIRSallowsanadditional$1,000“catch-up”contribution.
WhyisitagoodideatohaveanHSA?
HSAsbenefiteveryonewhoiseligibletohavethisaccount–singleindividuals,families,andsoonto-beretirees.Yousavemoneyontaxesinthreeways:
•Tax-freedeposits–ThemoneyyoucontributetoyourHSAisn’ttaxed(uptotheIRSannuallimit).
•Tax-freeearnings–Yourinterestandanyinvestmentearningsgrowtax-free.
•Tax-freewithdrawals–Themoneyusedtowardeligiblehealthcareexpensesisn’ttaxed–nowor inthefuture.
•Settingasidepre-taxdollarsintoyourHSAmeansyoupayfewertaxesandincreaseyourtakehomepaybyyourtaxsavings.Yousavemoneyoneligibleexpensesthatyouarepayingforoutof yourpocket.Theamountyousavedependsonyourtaxbracket.Forexample,ifyouareinthe30 percenttaxbracket,youcansave$30onevery$100spentoneligiblehealthcareexpenses.
HSAfundsrolloverfromyeartoyearandaccumulateinyouraccount.Thereisno“use-it-or-lose-it” rulewithHSAs,andyoudecidehowandwhentouseyourHSAfunds,whichcanbeusedfor eligibleexpensesyouhavenow,inthefuture,orduringretirement.Andwhenyouhaveacertain balanceinyourHSA,investmentopportunitiesareavailable.
8

9
AnthemBlueAccessPPOOption14 Non-Network In-Network N/A BlueAccess Network Individuals:$6,000 Families:$18,000 Individuals:$2,000 Families:$6,000 Deductibles (Individual/Family) Individuals:$15,000 Families:$30,000 Individuals:$5,000 Families:$10,000 Out-of-PocketMax (Individual/Family) 40%AfterDeductible 20%AfterDeductible CostSharingAfter Deductible 40%AfterDeductible $25copayforPrimaryCare $50copayforSpecialist PrimaryCareVisit 40%AfterDeductible $25copay Telemedicine/OnlineVisit 40%AfterDeductible Plancovers100% PreventiveCare 50%Coinsurance $10copay(Pref.Pharmacy) $20copay(In-NetworkPharm.)Pharmacy/RX(Generic) 50%Coinsurance $35copay(Pref.Pharmacy) $45copay(In-NetworkPharm.)Pharmacy/RX(Preferred) 50%Coinsurance $75copay(Pref.Pharmacy) $85copay(In-NetworkPharm.) Pharmacy/RX(NonPreferred) 50%Coinsurance 25%upto$350(Pref.Pharm.) 25%upto$450(In-Network)Pharmacy/RX(Specialty) 40%AfterDeductible 20%AfterDeductible OutpatientProcedure CoveredasIn-Network $250copaythen20% EmergencyRoom 40%AfterDeductible $75copayafterDeductible UrgentCare 40%AfterDeductible 20%AfterDeductible InpatientVisit AnthemBlueAccessPPONon-HSAQualified Standard Non-Tobacco Weekly Contributions $36.00 $32.00 Employee $90.00 $82.00 Employee+Spouse $82.00 $74.00 Employee+Child(ren) $135.00 $124.00 Employee+Family
MedicalBenefits
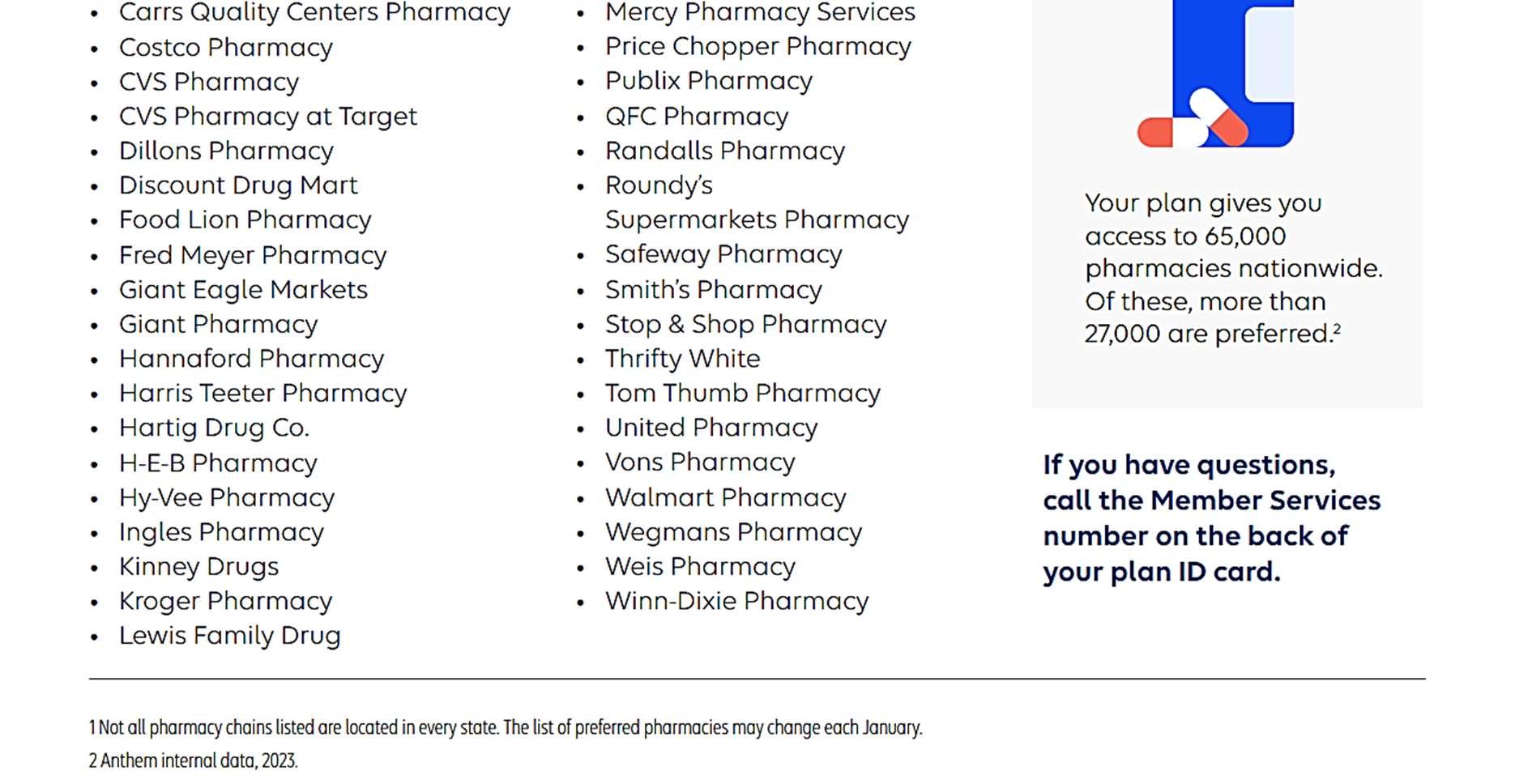
PrescriptionDrugChanges
InmovingourmedicalandpharmacycoveragetoAnthemthefollowing medicationswillchangetiers.Ifyoutakeanyofthesemedications,you’llwant tobepreparedforthesechangeseffectiveJuly1,2024.Ifthemedicationisin green,itisatalowercosttoyou,ifitisred,youwillexperienceapossible increaseincost.
11 ChangestoCommonMedications Improvement AnthemNewTier UHCTier Medication No 4 3 SkyriziPen NoChange 2 2 Eliquis Yes 2 3 Trulicity NoChange 2 2 SynjardyXR Yes 2 3 Rybelsus NoChange 1 1 Lamotrigine NoChange 1 1 Buspirone No N/A 1 BupropionHCL NoChange 1 1 Levothyroxine Yes 3 4 Vraylar
TheValueofPreventativeCare
Understandingthefullvalueofcoveredbenefitsallowsyoutotakeresponsibilityfor maintaininggoodhealthandincorporatinghealthyhabitsintoyourlifestyle.Some examplesincludegettingregularphysicalexaminations,mammogramsand immunizations.
ThroughtheplansofferedbyMidwestMole,allcoveredindividualsandfamilymembersare eligibletoreceiveroutinewellnessserviceslikethese,atnocost;allcopays,coinsurance,and deductiblesarewaived.
WhichPreventiveCareServicesAreCovered?
TheUSPreventiveServicesTaskForcemaintainsaregularlistofrecommendedservices thatallACA-compliantinsuranceplansshouldcoverat100%within-networkproviders. Belowisalistofcommonservicesthatareincludedintheplansofferedthisyear:
RoutinePhysicalExam
WellBabyandChildCare
WellWomanVisits
Immunizations
RoutineBoneDensityTest
RoutineBreastExam
RoutineGynecologicalExam
ScreeningforGestational Diabetes
ObesityScreeningand Counseling
RoutineDigitalRectalExam
RoutineColonoscopy
RoutineColorectalCancerScreening
RoutineProstateTest
RoutineLabProcedures
RoutineMammograms
RoutinePapSmear
SmokingCessationPrograms
HealthEducation/CounselingServices
HealthCounselingforSTDsandHIV
TestingforHPVandHIV
ScreeningandCounselingforDomestic Violence
12

13 SupplementalInsurance Principal Accident Accidentinsuranceismeanttopayyouacashbenefitshouldyouoracoveredfamily memberisinjuredinanaccident Coverage PlanFeatures Upto$5,000 InjuryBenefitAmount Upto$7,500 Dislocation Upto$10,000 Fracture PlanRatesforOff-The-JobAccidentCoverage $9.04 EmployeeOnly $14.90 Employee+Spouse $16.85 Employee+Child(ren) $26.59 Family HospitalIndemnity MidwestMoleprovidesyouwiththeopportunitytofurtherprotectyourfamilywitha HospitalIndemnityPlan,whichpaysyouasetamountshouldyoubeplaceinahospital. Coverage PlanFeatures $1,000FirstDay Admission $100 DailyHospital $2,00 DailyICU PlanRatesforOff-The-JobAccidentCoverage $13.29 EmployeeOnly $45.59 Employee+Spouse $24.84 Employee+Child(ren) $59.30 Family
SupplementalInsurance
Principal CriticalIllness

CriticalIllnessinsuranceismeanttopayyouacashbenefitbasedontheselectedamount ofcoveragechosenduringenrollmentshouldyouoracoveredfamilymemberdevelops certainillnesses.Examplesofcertaincoveredillnessesarelistedbelow.
Childrenareautomaticallycoveredfor25%ofanemployee’sbenefitatnocosttoyou GuaranteeIssueisthemaximumscheduledbenefitavailableduringtheinitial enrollmentperiodwithnoproofofgoodhealthrequired.
14
%OfElectedAmountGiven Illness 100% HeartAttack 100% InvasiveCancer 100% MajorOrganFailure 100% Stroke 25% LymeDisease
Spouse Employee $2,500Increments $5,000Increments Increments $,10,000 $20,000 GuaranteedIssueAmount
$50,000 MaximumAmount
VoluntaryCriticalIllnessMonthlyRateper$1000Coverage Employee/SpouseRate Age $.490 24&Under $.631 25-29 $.780 30-34 $.940 35-39 $1.296 40-44 $1.840 45-49 $2.796 50-54 $3.692 55-59 $5.818 60-64 $8.312 65-69 $11.934 70+
ScheduledBenefit
$25,000or50%ofEmployee ElectedAmount
Principal
BasicLife/AD&D

LifeInsuranceisanimportantpartofyourfinancialwell-being,especiallyifothersdepend onyouforsupport.MidwestMoleprovidesBasicTermLifeandAD&Dinsuranceatno costtoyou.
ShortTermDisability
MidwestMoleprovidesshorttermdisabilitycoveragetohelpprovidepaycheckreplacement moniesintheeventyouaredisabled.Thisinsuranceisprovidedatnocosttoyou.
15 Life/AD&DandDisabilityInsurance
Coverage PlanFeatures $25,000 EmployeeLifeBenefitAmount $25,000 EmployeeAD&DBenefitAmount $25,000 GuaranteeIssue Thefollowingshowshowmuchbenefitsarereducedatcertainages: BenefitReduction AgeBand 35% 65 50% 70
PlanFeatures 60% EmployeeBenefitAmount $1,000 MaximumWeeklyBenefitAmount 7days EliminationPeriod(Accident) 7days EliminationPeriod(Sickness) 25weeks BenefitDuration
DentalCoverage
Principal

DentalcoverageisofferedthroughPrincipalandutilizesthePrincipalDPPO network.ToFindaProviderinyourarea,pleasevisitwww.principal.com/dentist
16
COREPLAN In-Network BUY-UPPLAN In-Network Service $50/$150 $50/$150 CalendarYearDeductible(Individual/ Family) MaximumAllowable Charge 90%ofUsual& Customary Out-of-NetworkReimbursementLevel Covered100% Covered100% PreventiveCare(deductiblewaived) 100%AfterDeductible80%AfterDeductible BasicProcedures(Fillings,etc.) 60%AfterDeductible50%AfterDeductibleMajorProcedures(Crowns,Dentures,etc.) $1,000 $1,500 CalendarYearMaximumBenefit 50%upto$1,000peryear MaximumBenefitRollover NotCovered 50%upto$1,000lifetimeOrthodontiaBenefit(uptoage19) EmployeeWeekly Contributions (COREPLAN) EmployeeWeekly Contributions (BUY-UPPLAN) ParticipationLevel $2.00 $3.00 Employee $6.00 $7.00 Employee+Spouse $6.00 $11.00 Employee+Child(ren) $11.00 $12.00 Employee+Family
VisionCoverage VSP(throughPrincipal)

VisioncoverageisofferedthroughPrincipalandutilizestheVSP(VisionServicePlan) network.ToFindaProviderinyourarea,pleasevisitwww.vsp.com
17
Non-Network In-Network Service Reimbursedupto$45 $10copay VisionExam Lenses Reimbursedupto$30 $25copay Single Reimbursedupto$50 $25copay Bifocal Reimbursedupto$65 $25copay Trifocal Reimbursedupto$100 $25copay Lenticular Reimbursedupto$70 $25copay.combinedwith lenses
Frames Reimbursedupto$105 $150Allowance ElectiveContactLenses Reimbursedupto$210 $25copay MedicallyNecessaryContact Lenses Frequency(Months) Every12Months Every12Months Exam Every12Months Every12Months Lenses Every24Months Every24Months Frames Every12Months Every12Months Contacts EmployeeWeeklyContributions $2.00 Employee $4.00 Employee+Spouse $4.00 Employee+Child(ren) $6.00 Employee+Family
($150Allowance+20%off balance)
VoluntaryLifeInsurance

VoluntaryGroupTermLife
MidwestMolealsoprovidesyouwiththeopportunitytopurchaseadditionallifeinsurance throughPrincipal.Premiumsarebasedonageandamountofinsurance.
$110,000Employee/$30,000spouse
AvailableinIncrementsof$5,000 Employeemustelectcoveragetocovera spouse
$100,000(NottoExceed100%ofEE election)
$5,000or$10,000 Employeemustelectcoveragetocover dependentchildren
18
Principal-SummaryofCoverage
VoluntaryLifeInsurance PlanFeatures AvailableinIncrementsof$10,000 EmployeeBenefitAmount $10,000 MinimumBenefitAmount $300,000 MaximumBenefitAmount
GuaranteeIssue
SpouseBenefitAmount
SpouseMaximumBenefitAmount
DependentChild(ren)Benefit Thefollowingshowshowmuchbenefitsarereducedatcertainages: BenefitReduction AgeBand 35% 65 50% 70
VoluntaryLifeInsurance


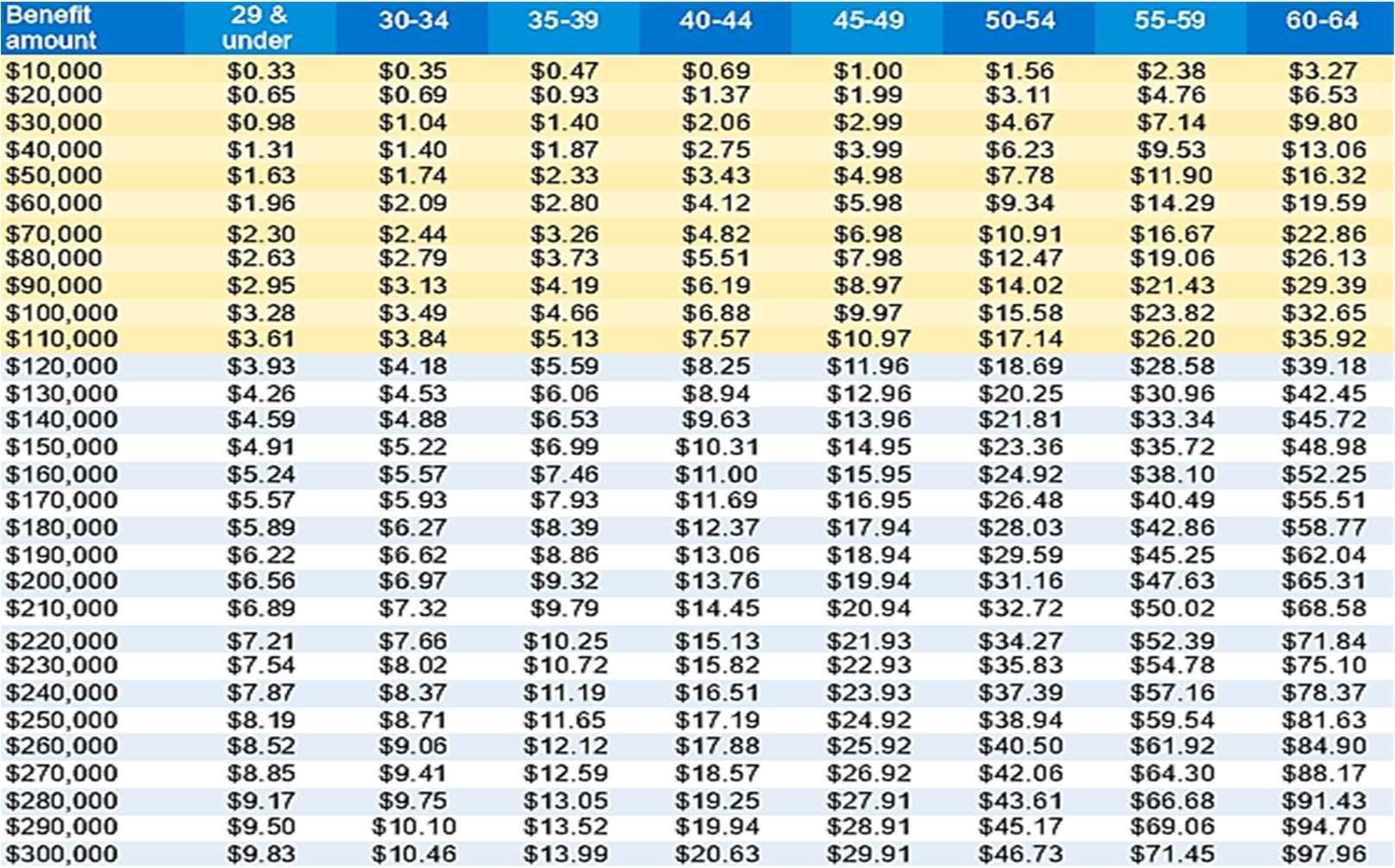
Note:Proofofgoodhealth/evidenceof insurabilityisrequiredtoapplyforbenefit amountsgreaterthanthosehighlightedhere.
Ifyouragechangestoadifferentrateband duringtheguaranteeperiod,yourpremium willchangetoreflectthenewrateband effectiveofonthenextpolicyanniversary date.
Thissummaryisnotacompletestatement oftherights,benefits,limitationsand exclusionsofthecoveragedescribedhere. Forcostandcoveragedetails,contact PrincipalLifeInsuranceCompany.

PrincipalisissuedbyPrincipalLife InsuranceCompany,711HighSt,Des Moines,IA50392
19
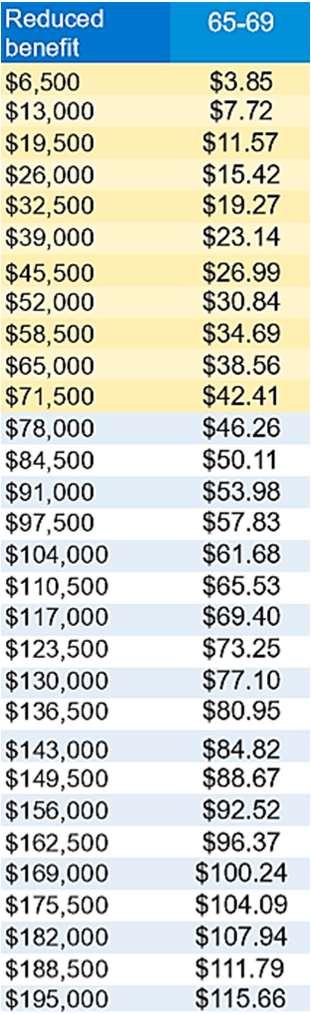
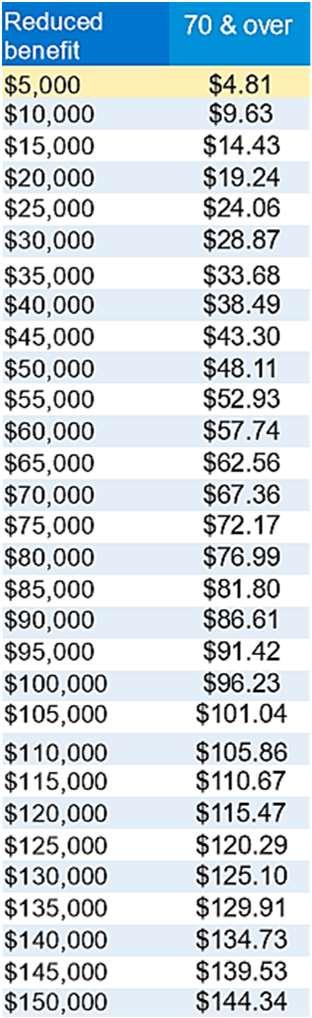
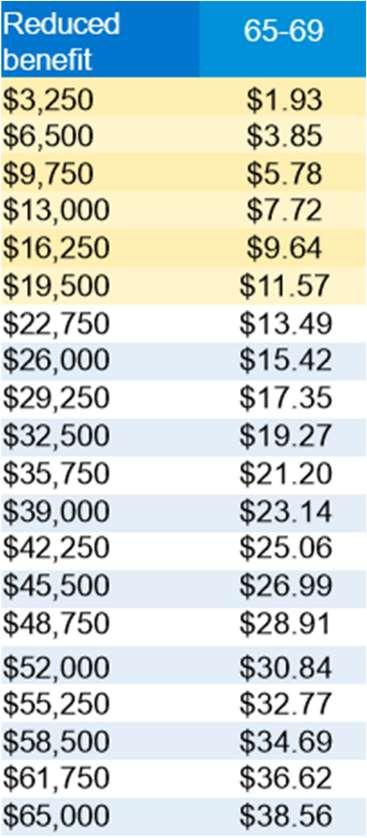
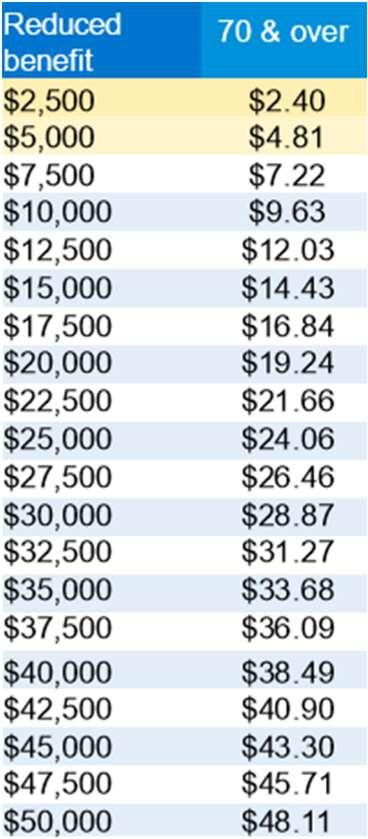
Age-BasedReductions
VoluntaryTermLifeInsurancefrom
GP55136-10
|03/2019|©2019PrincipalFinancialServices,Inc.
VoluntaryLifeInsurance
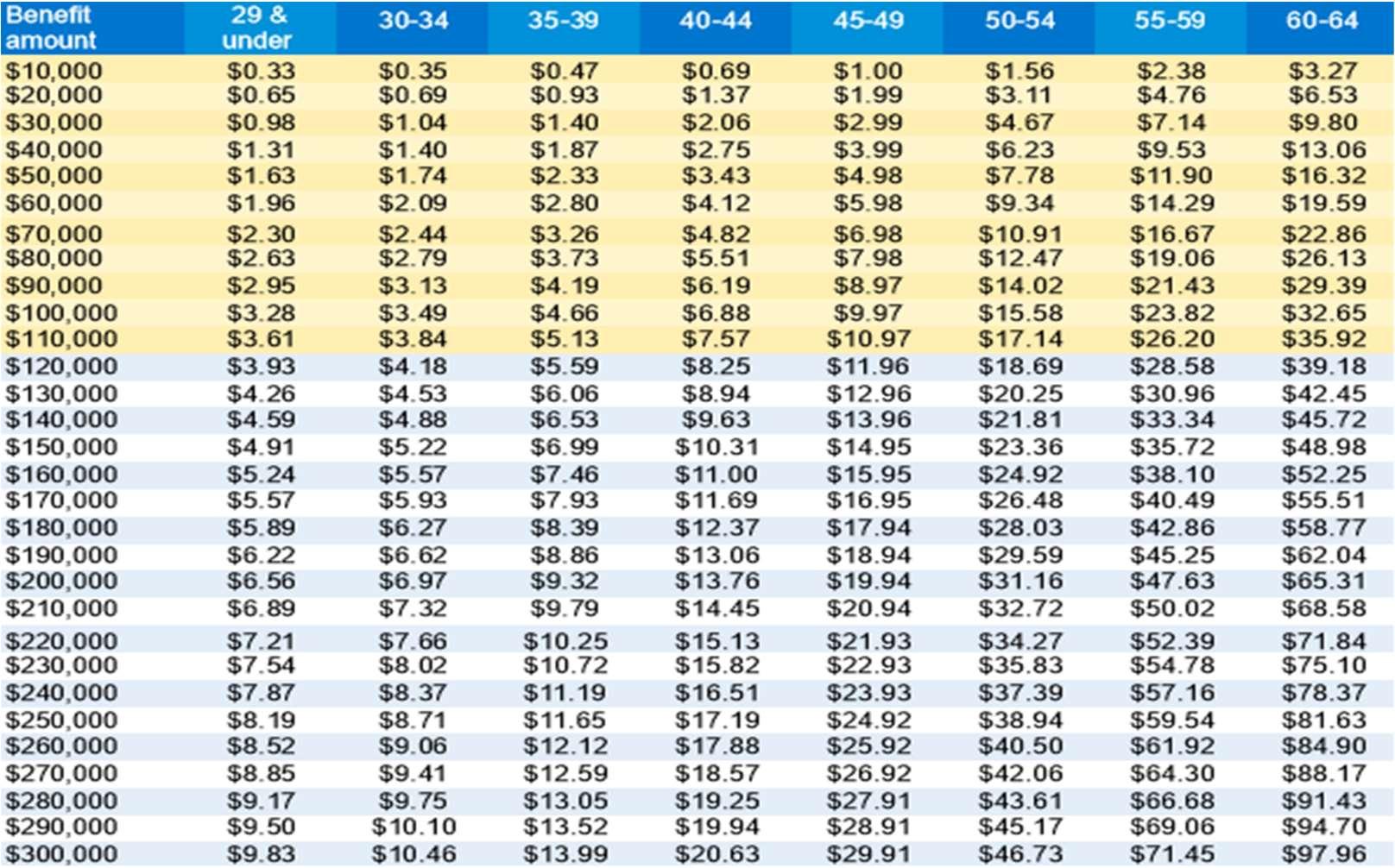
Note:Proofofgoodhealth/evidenceof insurabilityisrequiredtoapplyforbenefit amountsgreaterthanthosehighlightedhere.
Ifyouragechangestoadifferentrateband duringtheguaranteeperiod,yourpremium willchangetoreflectthenewrateband effectiveofonthenextpolicyanniversary date.
Thissummaryisnotacompletestatement oftherights,benefits,limitationsand exclusionsofthecoveragedescribedhere. Forcostandcoveragedetails,contact PrincipalLifeInsuranceCompany.
PrincipalisissuedbyPrincipalLife InsuranceCompany,711HighSt,Des Moines,IA50392
20
Age-BasedReductions
VoluntaryTermLifeInsurancefrom
GP55136-10
SpouseWeeklyRates
|03/2019|©2019PrincipalFinancialServices,Inc.

MidwestMoleofferseligibleemployeesandthefamilymemberslivingintheirhouseholdsan EmployeeAssistanceProgramwithNewAvenues,Inc.
NewAvenuesoffersconfidentialcounselingthroughanetworkoflicensedclinicianslocated closetoyourhomeorworkplace.Thesetrainedprofessionalsarereadytohelpyoudealwith familyorwork/lifeissuesthatmaybecausingyourlifetofeeloutofbalance.
Allservicesarestrictlyconfidentialandatnocosttotheemployeeorfamilymembers.
CommonQuestions…
WHOISELIGIBLE?
•Allfull-timeandpart-timeemployeesandthefamilymemberslivingintheirhouseholds.
•Dependentsuptoage26,notlivinginthehomeoftheemployee,areeligibleifonthe employee’shealthinsurance.
•PerDiem,temporaryemployees,volunteers,andstudent/internsareexcluded.
•Startsfirstdateofactiveemployment.
•Eligibilityrunsthroughthelastdayofemployment.
•ServiceswillonlybecoverediftheemployeecallsNewAvenuesforauthorizationpriortotheir firstsession.
WITHWHATTYPESOFPROBLEMSCANNEWAVENUESCOUNSELORSHELP?
•StressAnxietyWorkplaceIssues



•Marriage/Family/Relationshipproblems

•PersonalConcernsSubstanceAbuseGrief
HOWMANYCOUNSELINGSESSIONSDOIHAVE?
Thereare3Face-to-FaceEAPsessionsperemployeefamilypercontractyear. ThecontractyearrunsfromApril1stthroughMarch31st.
www.NewAvenuesOnline.com NewAvenuesTollFree#800-731-6501
WHATIFINEEDMORETHAN3SESSIONS?
OnceyouhaveusedyourEAPsessions,youareresponsibleforfeesincurredforadditional sessions.Youmaychoosetocontinueservicesunderthetermsofyourhealthplanbenefit. (SeeyourhealthplanSPDforadescriptionofcoveredservices).NewAvenuesmakesevery attempttoarrangeyourEAPsessionswithacounselorwhoisinyourhealthplannetworkso youmaycontinuewiththesameperson.
HOWDOIACCESSMYFACE-TO-FACEEAPSESSIONS?
JustcallNewAvenuesat:800-731-6501or574-232-2131.Selectoption#2.Servicesarestrictly confidentialandthereisnoout-of-pocketcosttoyouortoyourfamilymembers.
Inadditiontoface-to-facecounseling,NewAvenuesofferstelephoniccounseling(855-492-3625) aswellasanarrayofonlinesupportservicesavailable24/7.
YoumayalsodownloadtheiCONNECTYOUAppfromtheAppStore(iphone)orGooglePlay (android)andregisterusingthepasscode34952tohave24/7accesstomentalhealth professionals.
Aweb-basedinformationcentercontainingawealthofarticles,usefultips,interactivetoolsand linksaswellasaccesstoStructuredTelephonicCounseling(855-492-3625)offeringlivecounselors thatcanbeaccessed24/7fromthecomfortofyourhome.
NEWAVENUESPROVIDERDIRECTORY:
AlistingoflicensedandcredentialedcounselorsandtherapistsintheNewAvenuesEAPNetwork.
Visitourwebsiteatwww.NewAvenuesOnline.com NewAvenuesTollFree#800-731-6501 WORK-LIFERESOURCECENTER:YourPasswordis:CompleteEAP.
.
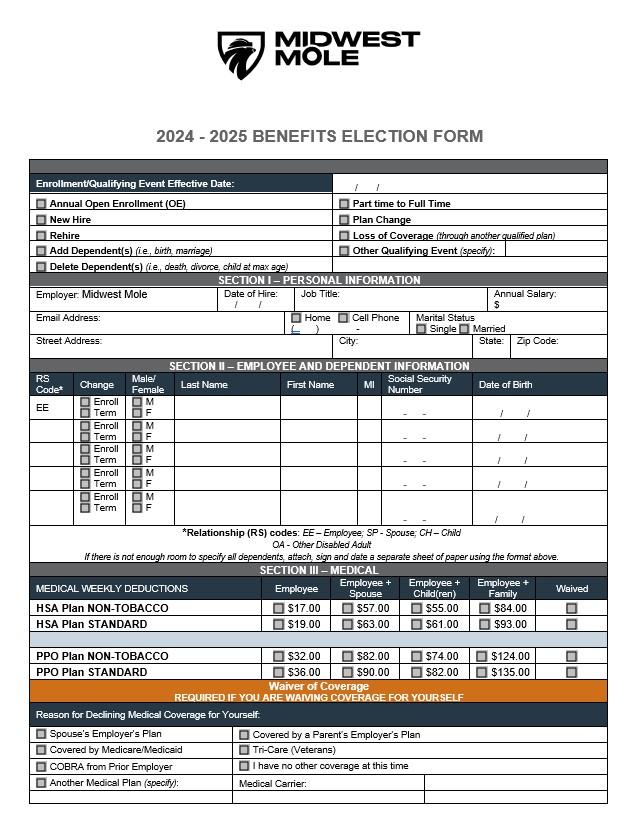
ElectionForm 23
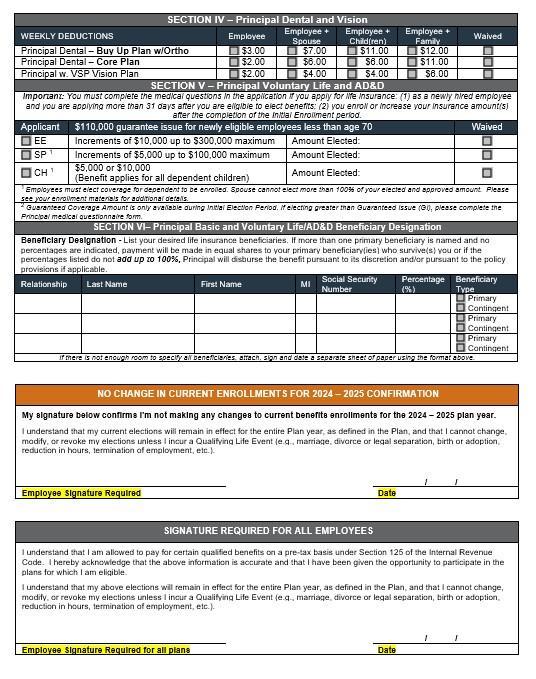
ElectionForm 24


MidwestMoleHumanResources|P317.545.1335ext.119Emphillips@midwestmole.com WEBSITE PHONENUMBER CARRIERCONTACTINFO www.anthem.com 1-833-945-2663 Medical—Anthem www.principal.com 1-800-986-3343 Dental—Principal www.principal.com 1-800-986-3343 Vision—VSP(throughPrincipal)
1-800-731-6501 EmployeeAssistanceProgram—NewAvenues www.principal.com 1-800-986-3343 LifeInsurance—Principal www.principal.com 1-800-986-3343 DisabilityInsurance—Principal www.principal.com 1-800-986-3343 SupplementalInsurancePlans—Principal https://www.midwestmole.com ImportantContactInformation
www.NewAvenuesOnline.com
ComplianceNotices
NoticeofSpecialEnrollmentRights
Ifyouaredecliningenrollmentforyourselforyourdependents(includingyourspouse)becauseofotherhealthinsuranceor grouphealthplancoverage,youmaybeabletoenrollyourselfandyourdependentsinthisplanifyouoryourdependents loseeligibilityforthatothercoverage(oriftheemployerstopscontributingtowardyouroryourdependents’othercoverage). However,youmustrequestenrollmentwithin30daysafteryouroryourdependents’othercoverageends(orafterthe employerstopscontributingtowardtheothercoverage).Inaddition,ifyouhaveanewdependentasaresultofmarriage, birth,adoption,orplacementforadoption,youmaybeabletoenrollyourselfandyourdependents.However,youmust requestenrollmentwithin30daysafterthemarriage,birth,adoption,orplacementforadoption.
Ifyouaredecliningenrollmentforyourselforyourdependents(includingyourspouse)whilecoverageunderMedicaidora stateChildren’sHealthInsuranceProgram(CHIP)isineffect,youmaybeabletoenrollyourselfandyourdependentsin thisplanifyouoryourdependentsloseeligibilityforthatothercoverage.However,youmustrequestenrollmentwithin60 daysafteryouroryourdependents’MedicaidorCHIPcoverageends.Ifyouoryourdependents(includingyourspouse) becomeeligibleforastatepremiumassistancesubsidyfromMedicaidoraCHIPprogramwithrespecttocoverageunder thisplan,youmaybeabletoenrollyourselfandyourdependents(includingyourspouse)inthisplan.However,youmust requestenrollmentwithin60daysafteryouoryourdependentsbecomeeligibleforthepremiumassistance.
NoticeofPatientProtection
Ifyourhealthplangenerallyrequiresthedesignationofaprimarycareprovider,youhavetherighttodesignateanyprimary careproviderwhoparticipatesinournetworkandwhoisavailabletoacceptyouoryourfamilymembers.Forchildren,you maydesignateapediatricianastheprimarycareprovider.Untilyoumakethisdesignation,thehealthplangenerallymay designateoneforyou.Forinformationonhowtoselectaprimarycareprovider,andforalistoftheparticipatingprimary careproviders,contactyourplanadministratororyourHumanResourcesDepartment.
Youdonotneedpriorauthorizationfromthehealthplanorfromanyotherperson(includingaprimarycareprovider)in ordertoobtainaccesstoobstetricalorgynecologicalcarefromahealthcareprofessionalinournetworkwhospecializesin obstetricsorgynecology.Thehealthcareprofessional,however,mayberequiredtocomplywithcertainprocedures, includingobtainingpriorauthorizationforcertainservices,followingapre-approvedtreatmentplan,orproceduresfor makingreferrals.Foralistofparticipatinghealthcareprofessionalswhospecializeinobstetricsorgynecology,contactyour planadministratororHumanResourcesDepartment.
Women’sHealthandCancerRightsActNotice
Ifyouhavehadoraregoingtohaveamastectomy,youmaybeentitledtocertainbenefitsundertheWomen’sHealthand CancerRightsActof1998(WHCRA).Forindividualsreceivingmastectomy-relatedbenefits,coveragewillbeprovidedina mannerdeterminedinconsultationwiththeattendingphysicianandthepatient,for:
•Allstagesofreconstructionofthebreastonwhichthemastectomywasperformed;
•Surgeryandreconstructionoftheotherbreasttoproduceasymmetricalappearance;
•Prostheses;and
•Treatmentofphysicalcomplicationsofthemastectomy,includinglymphedema.
Thesebenefitswillbeprovidedsubjecttothesamedeductiblesandcoinsuranceapplicabletoothermedicalandsurgical benefitsprovidedunderthisplan.IfyouwouldlikemoreinformationonWHCRAbenefits,contactthePlanAdministrator.
Newborns’andMothers’HealthProtectionActNotice
Grouphealthplansandhealthinsuranceissuersgenerallymaynot,underFederallaw,restrictbenefitsforanyhospital lengthofstayinconnectionwithchildbirthforthemotherornewbornchildtolessthan48hoursfollowingavaginaldelivery, orlessthan96hoursfollowingacesareansection.However,Federallawgenerallydoesnotprohibitthemother'sor newborn'sattendingprovider,afterconsultingwiththemother,fromdischargingthemotherorhernewbornearlierthan48
26
27 ComplianceNotices
hours(or96hoursasapplicable).Inanycase,plansandissuersmaynot,underFederallaw,requirethataproviderobtain authorizationfromtheplanortheinsuranceissuerforprescribingalengthofstaynotinexcessof48hours(or96hours).
Michelle’sLawNotice
Michelle’sLawwassignedintolaweffectiveJanuary1,2010.Thislawgenerallyallowsseriouslyillorinjuredfulltime collegestudents,whoarecoveredundertheirparent’shealthinsuranceplan,totakeuptooneyearofmedicallynecessary leaveofabsenceiftheleavenormallywouldcausethedependentchildtoloseeligibilityforcoverageundertheplandueto lossofstudentstatus.FortheMichelle’sLawextensionofeligibilitytoapply,adependentchild’streatingphysicianmust providewrittencertificationofmedicalnecessity(i.e.,certificationthatthedependentchildsuffersfromaseriousillnessor injurythatnecessitatestheleaveofabsenceorotherenrollmentchangethatwouldotherwisecauselossofeligibility).
*UnderthePatientProtectionandAffordableCareAct,grouphealthplansarerequiredtooffercoveragetodependent childrenuptoage26,regardlessofstudentstatus.
HIPAANoticeofPrivacyPractices
TheHealthInsurancePortabilityandAccountabilityActof1996("HIPAA")requiresthatwemaintaintheprivacyofprotected healthinformation,givenoticeofourlegaldutiesandprivacypracticesregardinghealthinformationaboutyouandfollowthe termsofournoticecurrentlyineffect.Participantsininsuredgrouphealthplansmayalsoreceiveanoticeofprivacy practicesfromthoseplans.YoumayrequestacopyofthecurrentPrivacyPractices,explaininghowmedicalinformation aboutyoumaybeusedanddisclosedandhowyoucangetaccesstothisinformation.
AsRequiredbyLaw.WewilldiscloseHealthInformationwhenrequiredtodosobyinternational,federal,stateorlocallaw. Youhavetherighttoinspectandcopy,righttoanelectroniccopyofelectronicmedicalrecords,righttogetnoticeofa breach,righttoamend,righttoanaccountingofdisclosures,righttorequestrestrictions,righttorequestconfidential communications,righttoapapercopyofthisnoticeandtherighttofileacomplaintifyoubelieveyourprivacyrightshave beenviolated.
GeneticInformationNondiscriminationActof2008(GINA)
TheGeneticInformationNondiscriminationActof2008(“GINA”)prohibitsthePlanfromdiscriminatingagainstindividualson thebasisofgeneticinformationinprovidinganythebenefitsunderincludedbenefitplans.GINAgenerally:
•ProhibitsthePlanfromadjustingpremiumorcontributionamountsforagrouponthebasisofgeneticinformation;
•ProhibitsthePlanfromrequestingormandatingthatanindividualorfamilymemberofanindividualundergoagenetic test,providedthatsuchprohibitiondoesnotlimittheauthorityofahealthcareprofessionaltorequestanindividualto undergoagenetictest,orprecludeagrouphealthplanfromobtainingorusingtheresultsofagenetictestinmakinga determinationregardingpayment;
•AllowsthePlantorequest,butnotmandate,thataparticipantorbeneficiaryundergoagenetictestforresearch purposesifthePlandoesnotusetheinformationforunderwritingpurposesandmeetscertaindisclosurerequirements; and
•ProhibitsthePlanfromrequesting,requiring,orpurchasinggeneticinformationforunderwritingpurposes,orwithrespect toanyindividualinadvanceoforinconnectionwithsuchindividual’senrollment.
MentalHealthParityActNotice
TheMentalHealthParityAct(“MHPA”)requiresthattheannualorlifetimedollarlimitsonmentalhealthbenefitsmaynotbe lowerthananysuchdollarlimitsforhealthandsurgicalbenefitsofferedbyagrouphealthplanorhealthinsuranceissuer offeringcoverageinconnectionwithagrouphealthplan.ThelifetimelimitceasedtoapplyeffectiveJanuary1,2011andthe annuallimitceasedtoapplyeffectiveJanuary1,2014.Beginningwiththe2010planyear,federallawalsowillrequirethat plansprovidingbothhealth/surgicalandmentalhealthbenefitsmaynotimposemorerestrictivefinancialrequirements(such asdeductiblesandcopayments)andtreatmentlimitations(suchaslimitsondaysofcoverage)onmentalhealthbenefits thanareimposedonhealth/surgicalbenefits.
ComplianceNotices
AQualifiedMedicalChildSupportOrder(QMCSO)isacourtorderoranorderissuedbyastateadministrativeagencyin accordancewithfederalandstatelawsthatrequiresanalternatebeneficiary(forexample,achildorstepchild)tobe coveredbyaplanparticipant’sgrouphealthplan.ThePlanhonorsQMCSOsthatmeetthelegalrequirementsforsuch orders.ItisimportanttonotethataQMCSOcannotrequireaplantoprovideatypeorformofbenefit,oranoption,thatis notcurrentlyavailablefromtheplantowhichtheorderisdirected,unlessreceivingthisbenefitoroptionisnecessaryto meettherequirementsoftheSocialSecurityAct,whichrelatestotheenforcementofstatechildsupportlawsand reimbursementofMedicaid.AQMCSOmustbeprovidedtothePlanAdministratortodetermineifitmeetsthelegal requirementsforaQMCSO.Ifitdoes,thealternatebeneficiaryisconsideredabeneficiaryforthepurposesofERISAandis enrolledasadependentoftheemployeeparticipant.IfthePlanAdministratorreceivesamedicalchildsupportorderthat relatestoyou,youwillbenotifiedandtheninformedofthedecisionastowhethertheorderisqualified.
UniformedServicesEmploymentandReemploymentRightsAct(USERRA)
Continuationandreinstatementrightsmayalsobeavailableifyouareabsentfromemploymentduetoserviceinthe uniformedservicespursuanttotheUniformedServicesEmploymentandReemploymentRightsActof1994(USERRA).If youtakeleaveunderUSERRA,totheextentrequiredbyUSERRA,yourEmployermaycontinuetomaintainyourbenefits onthesametermsandconditionsasifyouwerestillanactiveemployee.
EmployeesgoingintoorreturningfromserviceintheuniformedservicesmayhavePlanrightsmandatedbyUSERRA. TheserightsapplyonlytoemployeesandtheirdependentscoveredunderthePlanbeforetheemployeeleftformilitary service.TobeentitledtoUSERRArights,theemployeemustgivetheemployeradvancednoticeoftheemployee’sabsence fromemploymentforuniformedservice,unlessprecludedbymilitarynecessityorifitisotherwiseimpossibleor unreasonableunderallthecircumstances.Additionally,subjecttocertainexceptions,theemployee’sabsencefromwork maynotexceedfiveyears.
USERRArightsincludeupto24monthsofcontinuedhealthcarecoverage.Forperiodsofleavelessthan31days,the employeeonlyneedstopayhisorhernormalportionofthepremium.Forperiodsofleave31daysormore,coveragewill onlybeextendeduponpaymentoftheentirecostofcoverageplusareasonableadministrativefee.
IfyoucomplywithUSERRAuponreturningtoactiveemploymentaftermilitaryservice,youmayre-enrollyourselfandyour eligibledependentsinhealthcoverageimmediatelyuponreturningtoactiveemployment,evenifyouandyoureligible dependentsdidnotelectUSERRAcontinuationcoverageduringyourmilitaryservice.Reinstatementwilloccurwithoutany waitingperiodsorpre-existingconditionexclusions,exceptforillnessesorinjuriesconnectedtothemilitaryservice.
USERRArightsterminateiftheemployee’sdischargefromtheuniformedservicewasaresultof“dishonorable”orother undesirableconduct,theemployeefailstoreportbacktoworkorapplyforreemploymentwithinthetimeperiodrequired underUSERRA,oriftheemployeefailstopaycoveragepremiums.
ThetimeperiodswithinwhichtoelectandpayforUSERRAcontinuationofcoverageshallbethesametimeperiodswithin whichtoelectandpayforCOBRAcoverageunderthePlan.IfbothUSERRAandCOBRAapply,anelectionfor continuationcoveragewillbeanelectiontotakeconcurrentCOBRA/USERRAcoverage.Notealsothatstatelawmay providecontinuationand/orconversioncoverage.
QualifiedMedicalChildSupportOrderNotice
28
ComplianceNotices
PremiumAssistanceUnderMedicaidandtheChildren’sHealthInsuranceProgram(CHIP) IfyouoryourchildrenareeligibleforMedicaidorCHIPandyou’reeligibleforhealthcoveragefromyouremployer,your statemayhaveapremiumassistanceprogramthatcanhelppayforcoverage,usingfundsfromtheirMedicaidorCHIP programs.Ifyouoryourchildrenaren’teligibleforMedicaidorCHIP,youwon’tbeeligibleforthesepremiumassistance programsbutyoumaybeabletobuyindividualinsurancecoveragethroughtheHealthInsuranceMarketplace.Formore information,visitwww.healthcare.gov.
IfyouoryourdependentsarealreadyenrolledinMedicaidorCHIPandyouliveinaStatelistedbelow,contactyourState MedicaidorCHIPofficetofindoutifpremiumassistanceisavailable.
IfyouoryourdependentsareNOTcurrentlyenrolledinMedicaidorCHIP,andyouthinkyouoranyofyourdependents mightbeeligibleforeitheroftheseprograms,contactyourStateMedicaidorCHIPofficeordial1-877-KIDSNOWor www.insurekidsnow.govtofindouthowtoapply.Ifyouqualify,askyourstateifithasaprogramthatmighthelpyoupay thepremiumsforanemployer-sponsoredplan.
IfyouoryourdependentsareeligibleforpremiumassistanceunderMedicaidorCHIP,aswellaseligibleunderyour employerplan,youremployermustallowyoutoenrollinyouremployerplanifyouaren’talreadyenrolled.Thisiscalleda “specialenrollment”opportunity,andyoumustrequestcoveragewithin60daysofbeingdeterminedeligiblefor premiumassistance.Ifyouhavequestionsaboutenrollinginyouremployerplan,contacttheDepartmentofLaborat www.askebsa.dol.govorcall1-866-444-EBSA(3272).
Ifyouliveinoneofthefollowingstates,youmaybeeligibleforassistancepayingyouremployerhealthplan premiums.ThefollowinglistofstatesiscurrentasofJanuary31,2024.ContactyourStateformore informationoneligibility.
ALABAMA-Medicaid
Website:http://myalhipp.com/ Phone:1-855-692-5447
ARKANSAS–Medicaid
Website:http://myarhipp.com/ Phone:1-855-MyARHIPP(855-692-7447)
COLORADO–HealthFirstColorado(Colorado’s MedicaidProgram)&ChildHealthPlanPlus(CHP+)
HealthFirstColoradoWebsite: https://www.healthfirstcolorado.com/ HealthFirstColoradoMemberContactCenter: 1-800-221-3943/StateRelay711 CHP+:https://hcpf.colorado.gov/child-health-plan-plus CHP+CustomerService:1-800-359-1991/StateRelay711 HealthInsuranceBuy-InProgram (HIBI):https://www.mycohibi.com/ HIBICustomerService:1-855-692-6442
ALASKA-Medicaid
TheAKHealthInsurancePremiumPaymentProgram Website:http://myakhipp.com/ Phone:1-866-251-4861
Email:CustomerService@MyAKHIPP.com MedicaidEligibility: https://health.alaska.gov/dpa/Pages/default.aspx
CALIFORNIA–Medicaid
HealthInsurancePremiumPayment(HIPP)Program Website:http://dhcs.ca.gov/hipp Phone:916-445-8322
Fax:916-440-5676
Email:hipp@dhcs.ca.gov
FLORIDA–Medicaid
Website: https://www.flmedicaidtplrecovery.com/flmedicaidtplrecovery. com/hipp/index.html Phone:1-877-357-3268
29
ComplianceNotices
GEORGIA–Medicaid
GAHIPPWebsite:https://medicaid.georgia.gov/healthinsurance-premium-payment-program-hipp
Phone:678-564-1162,Press1
GACHIPRAWebsite:
https://medicaid.georgia.gov/programs/third-partyliability/childrens-health-insurance-program-reauthorization-act2009-chipra
Phone:(678)564-1162,Press2
IOWA–MedicaidandCHIP(Hawki)
MedicaidWebsite:
https://dhs.iowa.gov/ime/members
MedicaidPhone:1-800-338-8366
HawkiWebsite:http://dhs.iowa.gov/Hawki HawkiPhone:1-800-257-8563
HIPPWebsite:https://dhs.iowa.gov/ime/members/medicaid-ato-z/hipp
HIPPPhone:1-888-346-9562
KENTUCKY–Medicaid
KentuckyIntegratedHealthInsurancePremiumPayment Program(KI-HIPP)Website: https://chfs.ky.gov/agencies/dms/member/Pages/kihipp.aspx Phone:1-855-459-6328
Email:KIHIPP.PROGRAM@ky.gov
KCHIPWebsite:https://kidshealth.ky.gov/Pages/index.aspx Phone:1-877-524-4718
KentuckyMedicaidWebsite:https://chfs.ky.gov/agencies/dms
MAINE–Medicaid
EnrollmentWebsite: https://www.mymaineconnection.gov/benefits/s/?language=en_ US
Phone:1-800-442-6003;TTY:Mainerelay711 PrivateHealthInsurancePremiumWebpage: https://www.maine.gov/dhhs/ofi/applications-forms Phone:1-800-977-6740;TTY:Mainerelay711
MINNESOTA–Medicaid
Website: https://mn.gov/dhs/people-we-serve/children-andfamilies/health-care/health-care-programs/programs-andservices/other-insurance.jsp
Phone:1-800-657-3739
INDIANA–Medicaid
HealthyIndianaPlanforlow-incomeadults19-64 Website:http://www.in.gov/fssa/hip/ Phone:1-877-438-4479
AllotherMedicaid
Website:https://www.in.gov/medicaid/ Phone1-800-457-4584
KANSAS–Medicaid
Website:https://www.kancare.ks.gov/ Phone:1-800-792-4884
HIPPPhone:1-800-967-4660
LOUISIANA–Medicaid
Website:www.medicaid.la.govorwww.ldh.la.gov/lahipp Phone:1-888-342-6207(Medicaidhotline)or 1-855-618-5488(LaHIPP)
MASSACHUSETTS–MedicaidandCHIP
Website:https://www.mass.gov/masshealth/pa Phone:1-800-862-4840
TTY:711
Email:masspremassistance@accenture.com
MISSOURI–Medicaid
Website: http://www.dss.mo.gov/mhd/participants/pages/hipp.htm Phone:573-751-2005
NEBRASKA–Medicaid MONTANA–Medicaid
Website: http://dphhs.mt.gov/MontanaHealthcarePrograms/HIPP Phone:1-800-694-3084
Email:HHSHIPPProgram@mt.gov
Website:http://www.ACCESSNebraska.ne.gov
Phone:1-855-632-7633
Lincoln:402-473-7000
Omaha:402-595-1178
NEWHAMPSHIRE–Medicaid NEVADA–Medicaid
MedicaidWebsite:http://dhcfp.nv.gov
MedicaidPhone:1-800-992-0900
Website:https://www.dhhs.nh.gov/programsservices/medicaid/health-insurance-premium-program Phone:603-271-5218
TollfreenumberfortheHIPPprogram:1-800-852-3345, ext.5218
30
ComplianceNotices
NEWJERSEY–MedicaidandCHIP
MedicaidWebsite:
http://www.state.nj.us/humanservices/ dmahs/clients/medicaid/ MedicaidPhone:609-631-2392
CHIPWebsite:http://www.njfamilycare.org/index.html CHIPPhone:1-800-701-0710
NORTHCAROLINA–Medicaid
Website:https://medicaid.ncdhhs.gov/ Phone:919-855-4100
OKLAHOMA–MedicaidandCHIP
Website:http://www.insureoklahoma.org Phone:1-888-365-3742
PENNSYLVANIA–MedicaidandCHIP
Website:https://www.dhs.pa.gov/Services/Assistance/Pages/H IPP-Program.aspx
Phone:1-800-692-7462
CHIPWebsite:Children'sHealthInsuranceProgram(CHIP) (pa.gov)
CHIPPhone:1-800-986-KIDS(5437)
SOUTHCAROLINA–Medicaid
Website:https://www.scdhhs.gov Phone:1-888-549-0820
Website:http://gethipptexas.com/ Phone:1-800-440-0493
VERMONT–Medicaid
Website:HealthInsurancePremiumPayment(HIPP)Program |DepartmentofVermontHealthAccess Phone:1-800-250-8427
WASHINGTON–Medicaid
Website:https://www.hca.wa.gov/ Phone:1-800-562-3022
WISCONSIN–MedicaidandCHIP
Website: https://www.dhs.wisconsin.gov/badgercareplus/p-10095.htm Phone:1-800-362-3002
NEWYORK–Medicaid
Website:https://www.health.ny.gov/health_care/medicaid/ Phone:1-800-541-2831
NORTHDAKOTA–Medicaid
Website:https://www.hhs.nd.gov/healthcare Phone:1-844-854-4825
OREGON–Medicaid
Website:http://healthcare.oregon.gov/Pages/index.aspx Phone:1-800-699-9075
RHODEISLAND–MedicaidandCHIP
Website:http://www.eohhs.ri.gov/ Phone:1-855-697-4347,or 401-462-0311(DirectRIteShareLine)
SOUTHDAKOTA-Medicaid
Website:http://dss.sd.gov Phone:1-888-828-0059
MedicaidWebsite:https://medicaid.utah.gov/ CHIPWebsite:http://health.utah.gov/chip Phone:1-877-543-7669
VIRGINIA–MedicaidandCHIP
Website:https://coverva.dmas.virginia.gov/learn/premiumassistance/famis-select
https://coverva.dmas.virginia.gov/learn/premiumassistance/health-insurance-premium-payment-hippprograms Medicaid/CHIPPhone:1-800-432-5924
WESTVIRGINIA–MedicaidandCHIP
Website:https://dhhr.wv.gov/bms/ http://mywvhipp.com/ MedicaidPhone:304-558-1700
CHIPToll-freephone:1-855-MyWVHIPP(1-855-699-8447)
WYOMING–Medicaid
Website:https://health.wyo.gov/healthcarefin/medicaid/prog rams-and-eligibility/ Phone:1-800-251-1269
ToseeifanyotherstateshaveaddedapremiumassistanceprogramsinceJanuary31,2024,orformoreinformationon specialenrollmentrights,contacteither:
U.S.DepartmentofLabor EmployeeBenefitsSecurityAdministration www.dol.gov/agencies/ebsa 1-866-444-EBSA(3272)
U.S.DepartmentofHealthandHumanServices CentersforMedicare&MedicaidServices www.cms.hhs.gov 1-877-267-2323,MenuOption4,Ext.61565
31
UTAH–MedicaidandCHIP TEXAS–Medicaid
32 ComplianceNotices
YourRightsandProtectionsAgainstSurpriseMedicalBills
Whenyougetemergencycareoraretreatedbyanout-of-networkprovideratanin-networkhospitalorambulatorysurgical center,youareprotectedfrombalancebilling.Inthesecases,youshouldn’tbechargedmorethanyourplan’scopayments, coinsuranceand/ordeductible.
Whatis“balancebilling”(sometimescalled“surprisebilling”)?
Whenyouseeadoctororotherhealthcareprovider,youmayowecertainout-of-pocket-costs,likeasuchasacopayment, coinsurance,ordeductible.Youmayhaveadditionalcostsorhavetopaytheentirebillifyouseeaproviderorvisitahealth carefacilitythatisn’tinyourhealthplan’snetwork.
“Out-of-network”meansprovidersandfacilitiesthathaven’tsignedacontractwithyourhealthplantoprovideservices.Outof-networkprovidersmaybepermittedtobillyouforthedifferencebetweenwhatyourplanpaysandthefullamount chargedforaservice.Thisiscalled“balancebilling.”Thisamountislikelymorethanin-networkcostsforthesameservice andmightnotcounttowardyourplan’sdeductibleorannualout-of-pocketlimit.
“Surprisebilling”isanunexpectedbalancebill.Thiscanhappenwhenyoucan’tcontrolwhoisinvolvedinyourcare—like whenyouhaveanemergencyorwhenyouscheduleavisitatanin-networkfacilitybutareunexpectedlytreatedbyanoutof-networkprovider.Surprisemedicalbillscouldcostthousandsofdollarsdependingontheprocedureorservice.
Youareprotectedfrombalancebillingfor: Emergencyservices
Ifyouhaveanemergencymedicalconditionandgetemergencyservicesfromanout-of-networkproviderorfacility,the mosttheycanbillyouisyourplan’sin-networkcost-sharingamount(suchascopayments,coinsurance,anddeductibles). Youcan’tbebalancebilledfortheseemergencyservices.Thisincludesservicesyoumaygetafteryou’reinstable condition,unlessyougivewrittenconsentandgiveupyourprotectionsnottobebalancedbilledforthesepost-stabilization services.
Certainservicesatanin-networkhospitalorambulatorysurgicalcenter
Whenyougetservicesfromanin-networkhospitalorambulatorysurgicalcenter,certainproviderstheremaybeout-ofnetwork.Inthesecases,themostthoseproviderscanbillyouisyourplan’sin-networkcost-sharingamount.Thisappliesto emergencymedicine,anesthesia,pathology,radiology,laboratory,neonatology,assistantsurgeon,hospitalist,orintensivist services.Theseproviderscan’tbalancebillyouandmaynotaskyoutogiveupyourprotectionsnottobebalancebilled.
Ifyougetothertypesofservicesatthesein-networkfacilities,out-of-networkproviderscan’tbalancebillyou,unlessyou givewrittenconsentandgiveupyourprotections.
You’reneverrequiredtogiveupyourprotectionsfrombalancebilling.Youalsoaren’trequiredtogetout-ofnetworkcare.Youcanchooseaproviderorfacilityinyourplan’snetwork.
Whenbalancebillingisn’tallowed,youalsohavethefollowingprotections:
•You’reonlyresponsibleforpayingyourshareofthecost(likethecopayments,coinsurance,anddeductiblethatyouwould payiftheproviderorfacilitywasin-network).Yourhealthplanwillpayanyadditionalcoststoout-of-networkprovidersand facilitiesdirectly.
•Generally,yourhealthplanmust:
oCoveremergencyserviceswithoutrequiringyoutogetapprovalforservicesinadvance(alsoknownas“prior authorization”).
oCoveremergencyservicesbyout-of-networkproviders.
oBasewhatyouowetheproviderorfacility(cost-sharing)onwhatitwouldpayanin-networkproviderorfacilityand showthatamountinyourexplanationofbenefits.
oCountanyamountyoupayforemergencyservicesorout-of-networkservicestowardyourin-networkdeductibleand out-of-pocketlimit.
Ifyoubelieveyou’vebeenwronglybilled,contactthefederalNoSurprisesHelpDeskat1-800-985-3059.Visit www.cms.gov/nosurprises/consumersformoreinformationaboutyourrightsunderfederallaw.
33 ComplianceNotices
FamilyandMedicalLeaveAct(FMLA)
LeaveEntitlements.Eligibleemployeeswhoworkforacoveredemployercantakeupto12weeksofunpaid,job-protected leaveina12-monthperiodforthefollowingreasons:
•Thebirthofachildorplacementofachildforadoptionorfostercare;
•Tobondwithachild(leavemustbetakenwithinoneyearofthechild’sbirthorplacement);
•Tocarefortheemployee’sspouse,child,orparentwhohasaqualifyingserioushealthcondition;
•Fortheemployee’sownqualifyingserioushealthconditionthatmakestheemployeeunabletoperformtheemployee’s job;
•Forqualifyingexigenciesrelatedtotheforeigndeploymentofamilitarymemberwhoistheemployee’sspouse,child,or parent.
Aneligibleemployeewhoisacoveredservicemember’sspouse,child,parent,ornextofkinmayalsotakeupto26weeks ofFMLAleaveinasingle12-monthperiodtocarefortheservicememberwithaseriousinjuryorillness.Anemployeedoes notneedtouseleaveinoneblock.Whenitismedicallynecessaryorotherwisepermitted,employeesmaytakeleave intermittentlyoronareducedschedule.
Employeesmaychoose,oranemployermayrequire,useofaccruedpaidleavewhiletakingFMLAleave.Ifanemployee substitutesaccruedpaidleaveforFMLAleave,theemployeemustcomplywiththeemployer’snormalpaidleavepolicies.
BenefitsandProtections.WhileemployeesareonFMLAleave,employersmustcontinuehealthinsurancecoverageasif theemployeeswerenotonleave.UponreturnfromFMLAleave,mostemployeesmustberestoredtothesamejoborone nearlyidenticaltoitwithequivalentpay,benefits,andotheremploymenttermsandconditions.Anemployermaynot interferewithanindividual’sFMLArightsorretaliateagainstsomeoneforusingortryingtouseFMLAleave,opposingany practicemadeunlawfulbytheFMLA,orbeinginvolvedinanyproceedingunderorrelatedtotheFMLA.
EligibilityRequirements.Anemployeewhoworksforacoveredemployermustmeetthreecriteriainordertobeeligiblefor FMLAleave.Theemployeemust:
•Haveworkedfortheemployerforatleast12months;
•Haveatleast1,250hoursofserviceinthe12monthsbeforetakingleave;*and
•Workatalocationwheretheemployerhasatleast50employeeswithin75milesoftheemployee’sworksite.*Special “hoursofservice”requirementsapplytoairlineflightcrewemployees.
RequestingLeave.Generally,employeesmustgive30-days’advancenoticeoftheneedforFMLAleave.Ifitisnotpossible togive30-days’notice,anemployeemustnotifytheemployerassoonaspossibleand,generally,followtheemployer’s usualprocedures.Employeesdonothavetoshareamedicaldiagnosisbutmustprovideenoughinformationtothe employersoitcandetermineiftheleavequalifiesforFMLAprotection.Sufficientinformationcouldincludeinformingan employerthattheemployeeisorwillbeunabletoperformhisorherjobfunctions,thatafamilymembercannotperform dailyactivities,orthathospitalizationorcontinuingmedicaltreatmentisnecessary.Employeesmustinformtheemployerif theneedforleaveisforareasonforwhichFMLAleavewaspreviouslytakenorcertified.Employerscanrequirea certificationorperiodicrecertificationsupportingtheneedforleave.Iftheemployerdeterminesthatthecertificationis incomplete,itmustprovideawrittennoticeindicatingwhatadditionalinformationisrequired.
EmployerResponsibilities.Onceanemployerbecomesawarethatanemployee’sneedforleaveisforareasonthatmay qualifyundertheFMLA,theemployermustnotifytheemployeeifheorsheiseligibleforFMLAleaveand,ifeligible,must alsoprovideanoticeofrightsandresponsibilitiesundertheFMLA.Iftheemployeeisnoteligible,theemployermust provideareasonforineligibility.EmployersmustnotifyitsemployeesifleavewillbedesignatedasFMLAleave,andifso, howmuchleavewillbedesignatedasFMLAleave.
Enforcement.EmployeesmayfileacomplaintwiththeU.S.DepartmentofLabor,WageandHourDivision,ormaybringa privatelawsuitagainstanemployer.TheFMLAdoesnotaffectanyfederalorstatelawprohibitingdiscriminationor supersedeanystateorlocallaworcollectivebargainingagreementthatprovidesgreaterfamilyormedicalleaverights.
ComplianceNotices
Pleasereadthisnoticecarefullyandkeepitwhereyoucanfindit.Thisnoticehasinformationaboutyourcurrent prescriptiondrugcoveragewithMidwestMoleGroupHealthPlanandaboutyouroptionsunderMedicare’s prescriptiondrugcoverage.ThisinformationcanhelpyoudecidewhetherornotyouwanttojoinaMedicare drugplan.Ifyouareconsideringjoining,youshouldcompareyourcurrentcoverage,includingwhichdrugsare coveredatwhatcost,withthecoverageandcostsoftheplansofferingMedicareprescriptiondrugcoveragein yourarea.Informationaboutwhereyoucangethelptomakedecisionsaboutyourprescriptiondrugcoverageis attheendofthisnotice.
TherearetwoimportantthingsyouneedtoknowaboutyourcurrentcoverageandMedicare’sprescriptiondrug coverage:
1.Medicareprescriptiondrugcoveragebecameavailablein2006toeveryonewithMedicare.Youcangetthis coverageifyoujoinaMedicarePrescriptionDrugPlanorjoinaMedicareAdvantagePlan(likeanHMOor PPO)thatoffersprescriptiondrugcoverage.AllMedicaredrugplansprovideatleastastandardlevelof coveragesetbyMedicare.Someplansmayalsooffermorecoverageforahighermonthlypremium.
2.MidwestMolehasdeterminedthattheprescriptiondrugcoverageofferedbytheMidwestMoleGroupHealth Planis,onaverageforallplanparticipants,expectedtopayoutasmuchasstandardMedicareprescription drugcoveragepaysandisthereforeconsideredCreditableCoverage.Becauseyourexistingcoverageis CreditableCoverage,youcankeepthiscoverageandnotpayahigherpremium(apenalty)ifyoulaterdecide tojoinaMedicaredrugplan.
WhenCanYouJoinAMedicareDrugPlan?
YoucanjoinaMedicaredrugplanwhenyoufirstbecomeeligibleforMedicareandeachyearfromOctober15th toDecember7th
However,ifyouloseyourcurrentcreditableprescriptiondrugcoverage,throughnofaultofyourown,youwill alsobeeligibleforatwo(2)monthSpecialEnrollmentPeriod(SEP)tojoinaMedicaredrugplan.
WhatHappensToYourCurrentCoverageIfYouDecidetoJoinAMedicareDrugPlan?
IfyoudecidetojoinaMedicaredrugplan,yourcurrentMidwestMoleGroupHealthPlancoveragewillnotbe affected.IfyoukeepyourcurrentcoverageandelectMedicarePartD,yourMidwestMoleGroupHealthPlan coveragemaycoordinatewithyourMedicarePartDcoverage.IfyoudodecidetojoinaMedicaredrugplanand dropyourcurrentMidwestMoleGroupHealthPlancoverage,beawarethatyouandyourdependentswillnot beabletogetthiscoverageback,unlessyouhaveaqualifyinglifeeventoruntilthenextopenenrollment.
WhenWillYouPayAHigherPremium(Penalty)ToJoinAMedicareDrugPlan?
YoushouldalsoknowthatifyoudroporloseyourcurrentcoveragewithMidwestMoleanddon’tjoina Medicaredrugplanwithin63continuousdaysafteryourcurrentcoverageends,youmaypayahigherpremium (apenalty)tojoinaMedicaredrugplanlater.
Ifyougo63continuousdaysorlongerwithoutcreditableprescriptiondrugcoverage,yourmonthlypremiummay goupbyatleast1%oftheMedicarebasebeneficiarypremiumpermonthforeverymonththatyoudidnothave
ImportantNoticefromMidwestMoleAboutYourPrescriptionDrugCoverageand
Medicare(CREDITABLE)
34
ComplianceNotices
thatcoverage.Forexample,ifyougonineteenmonthswithoutcreditablecoverage,yourpremiummay consistentlybeatleast19%higherthantheMedicarebasebeneficiarypremium.Youmayhavetopaythis higherpremium(apenalty)aslongasyouhaveMedicareprescriptiondrugcoverage.Inaddition,youmayhave towaituntilthefollowingOctobertojoin.
ForMoreInformationAboutThisNoticeOrYourCurrentPrescriptionDrugCoverage Contactthepersonlistedbelowforfurtherinformation.
NOTE:You’llgetthisnoticeeachyear.YouwillalsogetitbeforethenextperiodyoucanjoinaMedicaredrug plan,andifthiscoveragethroughMidwestMolechanges.Youalsomayrequestacopyofthisnoticeatany time.
ForMoreInformationAboutYourOptionsUnderMedicarePrescriptionDrugCoverage
MoredetailedinformationaboutMedicareplansthatofferprescriptiondrugcoverageisinthe“Medicare&You” handbook.You’llgetacopyofthehandbookinthemaileveryyearfromMedicare.Youmayalsobecontacted directlybyMedicaredrugplans.
FormoreinformationaboutMedicareprescriptiondrugcoverage:
•Visitwww.medicare.gov
•CallyourStateHealthInsuranceAssistanceProgram(seetheinsidebackcoverofyourcopyofthe “Medicare&You”handbookfortheirtelephonenumber)forpersonalizedhelp
•Call1-800-MEDICARE(1-800-633-4227).TTYusersshouldcall1-877-486-2048.
Ifyouhavelimitedincomeandresources,extrahelppayingforMedicareprescriptiondrugcoverageis available.Forinformationaboutthisextrahelp,visitSocialSecurityonthewebatwww.socialsecurity.gov,or callthemat1-800-772-1213(TTY1-800-325-0778).
Remember:KeepthisCreditableCoveragenotice.IfyoudecidetojoinoneoftheMedicaredrug plans,youmayberequiredtoprovideacopyofthisnoticewhenyoujointoshowwhetherornot youhavemaintainedcreditablecoverageand,therefore,whetherornotyouarerequiredtopaya higherpremium(apenalty).
EffectiveDate:07/01/2024
NameofEntity/Sender:MidwestMole
Contact--Position/Office:MaxPhillips,HumanResourcesManager
Address:6814W350North,GreenfieldIN46140
PhoneNumber:317-545-1335ext.119
35



https://www.midwestmole.com