DIFFICULTSOCIETYAIRWAY MEMBERS EZINE September 2022 Edition


Difficult Airway Society E-Zine September 2022 Contents 2 REMINDER TO DAS MEMBERS Please remember to update your details if your address or email address changes! Members can update their details by emailing WEdas@anaesthetists.orgWANTTOHEARFROMYOU DAS encourages member participation we would love to read your comments, contributions and suggestions for future E-Zines. Have you been involved in an interesting airway case? Is there an article that has changed your practice? Do you have an idea for improving airway anaesthesia that you would like to collaborate on? All formats welcome: text, video, photo, infographic… We know you are a creative bunch! Send us your thoughts at ezine@das.uk.com @dasairway @dastrainees

Difficult Airway Society E-zine May 20223Executive Updates Editorial 4 Letters to the editors 6 DAS Executive Update 7 DAS Scientific Officer Report 9 DAS 2022 13 In Memory Of Dr Ronnie Cormack 11 ClinicalEducationDilemma 14 Educational Series: Perioperative Medicine Part 2 22 #JanuAIRWAY - The Compilation 41 Masterclass with DAS: Abstracts 43 TraineeTraineesCompetition Winners 46 Journal Club - Recommended Reads CONTENTS52MiscellaneousAirwayManagementinMajor Trauma - an Australian Perspective 54 New patient information for awake tracheal intubation: June 2022 59 Difficult Airway Database - an update 61 Conference Corner WAMM 63 Proposals to host DAS 2024 64
Welcome to the September 2022 edition of the Difficult Airway Society E-Zine. We would like to start by expressing our sadness to hear of the death of Dr Ronnie Cormack. There is no anaesthetist in the UK (or in fact, globally) who hasn’t used the Cormack and Lehane classification: a teamunderstanding of your view is a crucial part of safety in airway management. We have a very fitting tribute to Dr Cormack from Dr Ellen O’Sullivan (Past President of DAS) and Dr Adrian Pearce (Founding Member of WeDAS).have the second of our three-part educational series focusing on peri-operative medicine, this time with exceptional authors covering Frailty, Cardio-Pulmonary Exercise Testing, and Risk Assessment*. We are lucky to have the team from the Alfred Hospital in Melbourne writing an exciting article about traumatic airway management and their fantastic trauma service. We continue the trend of popular educational webinars run by the inimitable Dr Gunjeet Dua. Most recently this was ‘A Masterclass with DAS: Abstracts’: a must watch to get your CV up to scratch as a trainee or | Helen Aoife Iliff | Natalie Silvey | Moon-Moon Majumdar |
Ms Kate Rivett, DAS patient representative, writes an important article about the need for high quality written information for our patients during the process of consent. She reveals the new DAS awake tracheal intubation patient information leaflet, easily available on the DAS website for you to print for your own patients.
Thisdoctor.month’s clinical dilemma pays due respect to ‘the compromised airway’ and covers a range of dire circumstances (what if they’re hypoxic? What if they’re agitated? What if they’re six?). Our airway experts have risen to the challenge, and we hope you find their thought processes as useful as we do.
It is obvious that anaesthetic trainees are an incredibly creative bunch, and we had a wealth of submissions for this year’s Difficult Airway Society trainee competition. For the first time in 2022, we had two categories to enter: creative writing and creative media. We are ecstatic to award the first prize for creative writing to Dr Asya Veloso Costa, and the first prize for creative media to Dr Helena Jennison. In fact, the standard of
Difficult Airway Society E-Zine September 2022 Contents 4
EDITORIALan
equivalently experienced locally-employed


Difficult Airway Society E-Zine September 2022 submissions was so high the judges ended up awarding 3 extra prizes for: 1. Best podcast - Dr Eoin Dore and Dr Duncan Brouwer-Kemp 2. Best video - Dr Jo Lau 3. Best photography - Dr Hannah Leaman We cannot wait to showcase all their amazing work to you in this edition. Finally, it’s the DAS 2022 ASM from the 5-7th October. Book your leave, get your trains/ flights sorted … because this year we are going to Newcastle! Get ready for some insightful learning, and a wonderful opportunity to catch up with colleagues in person after a long time apart. If you have any feedback or article contributions please get in touch with our editorial team by emailing ezine@das.uk.com or tag us on Twitter @dasairway or *IfHelenNatalieMoon-Moon@dastrainees.MajumdarSilveyIliffyoumissedthefirst in the peri-op series, don’t be shy! You can find the May 2022 Ezine here, go back and have a peruse. You’re welcome

DAS has an important place in the lives of anaesthetists as they all have to take care in airway management, the prime source for things going astray. All anaesthetists faced with fatal complications in airway management have still sleepless nights years after such an event. It is therefore of utmost importance to train the skills of airway management in all its aspect to help the anaesthetist to do a good job if confronted with a major difficult to prevent mishaps from happening. Furthermore, DAS has other issues to offer, such as monitoring of the airway during induction, maintenance and emergence of the anaesthetic. Short written information in the DAS E-zine are well-appreciated as they give us tips and tricks to improve our practice in the interest of better patient care.
To: trainee@das.uk.com
Editors Note: The E-Zine is something we are passionate about and it is lovely to receive such feedback. We want it to be as useful to members as possible so please do get in contact with any suggestions and/ or feedback - ezine@das.uk.com or tag us on Twitter @dasairway or @dastrainees. Please get in touch, we love hearing from you! |
Subject: DAS E-Zine - May 2022
I appreciate this very much. It is easy to download and the content is worth reading and helps to better understand airway problems. Congratulations to the whole team.
From: Professor André van Zunder, Professor and Chairman Discipline of Anesthesiology, The University of Queensland.
Difficult Airway Society E-Zine September 2022 Contents 6
Editors Response: Thank you for your kind feedback it is much appreciated. We've put a lot of work into the formatting and content of the eZine to try and make it as easily accessible to members as possible while simultaneously curating content. We're delighted to hear our members find it easy to access and the content of interest.
Thank you for sending the May edition of the Difficult Airway Society E-Zine.
LETTERS TO EDITORSTHE |
|
Ronnie was also the very deserved recipient of the DAS Macewen Medal in 2013, acknowledging his contribution to airway management and patient safety. As the DAS Executive team we would like to express our sincere condolences to Ronnie’s family from the DAS committee and the DAS membership, all of whom have been impacted by Ronnie’s work.
|
A lot has happened since our last Ezine report – alleged lies and misinformation, lots of resignations, calls for change of leadership and even some sinus surgery! Fortunately none of that drama applied to the DAS committee, who have continued to work hard as always. There has been progress made in some key areas of DAS business, in particular the DAS Website, educational events, eFONA and dif fi cult airway databases, DAS Professorships and DAS guidelines. And of course we mustn’t forget to mention all the excellent work by the DAS surveys coordinator, trainee and lay Sadly,representatives.wehave to share the news of the recent death of Dr Ronnie Cormack. Ronnie will always be remembered for the extraordinary impact of his famous publication and grading scale of direct laryngoscopy, which he wrote with John Lehane. This was one of the highest cited papers in anaesthesia history and the most commonly used airway grading scale worldwide, there simply can’t be an anaesthetist out there who hasn’t referred to or used the Cormack and Lehane grading.
Difficult Airway Society E-Zine September 2022 Contents 7 EXECUTIVE UPDATE |
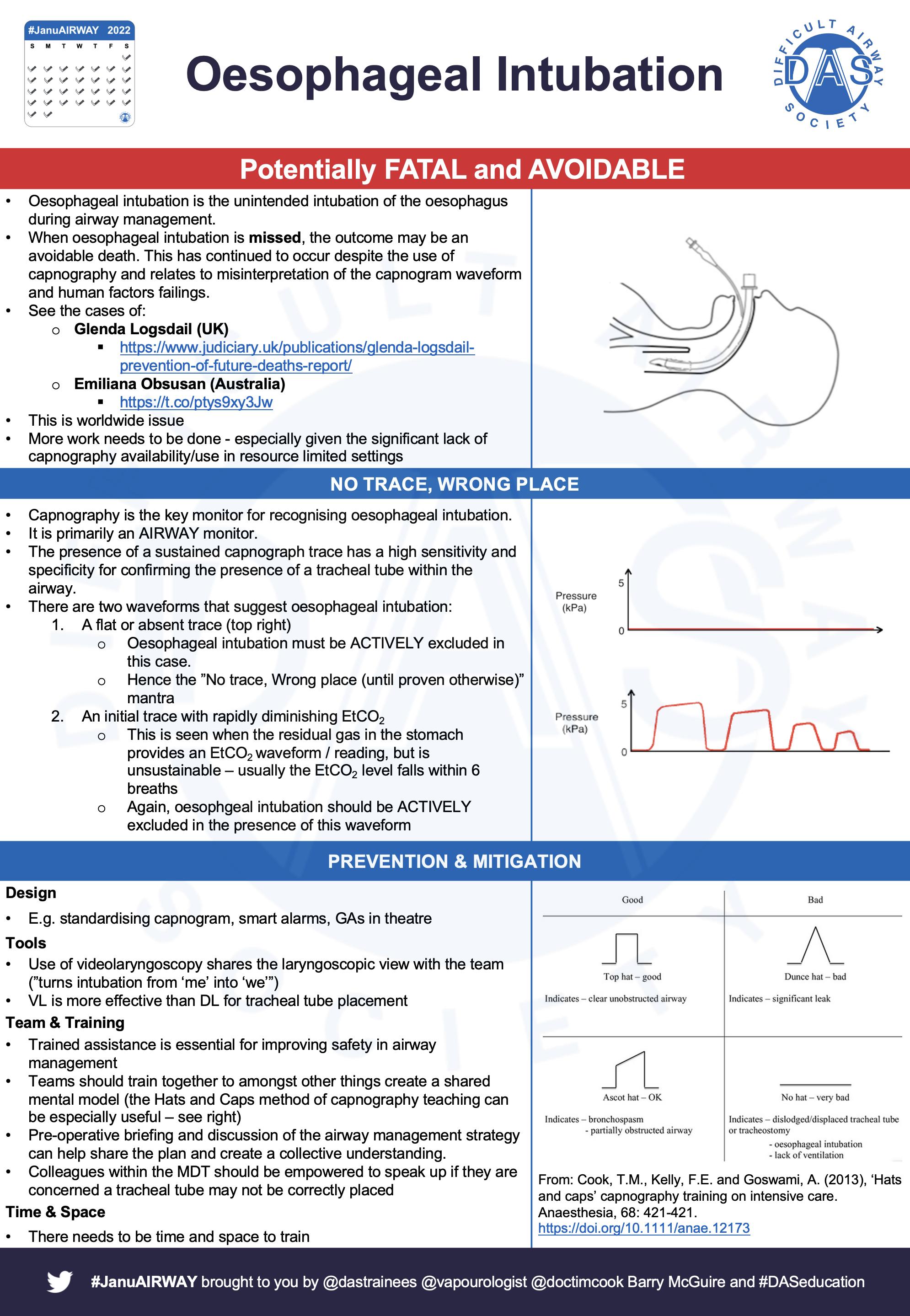
There has been a lot of work done nationally and locally to highlight the ‘no trace, wrong place’ campaign and reduce the incidence of undetected oesophageal intubation. DAS has been heavily involved in promoting this important work with the RCoA, we also have representation on various working parties and have recently been asked to endorse a consensus document on this. The DAS committee encourage our membership to promote the ‘no trace, wrong place’ campaign at their local hospitals and we would be very happy to be contacted to help. We have been working on upgrading the DAS website for a while now, progress has unfortunately been slow with many unexpected issues arising along the way, we
Ravi Bhagrath | Imran Ahmad Fauzia Mir


Difficult Airway Society E-Zine September 2022 Contents 8 have been dealing with them which is why it has taken so long to complete the upgrade. We cannot give you a timeline, however what we can say is that we are making good progress and our DAS website leads and subcommittee will see this through!
An excellent programme has been put together with outstanding speakers and sessions planned, there is also an excellent social programme in store too, so do please join Imranus!Ahmad, DAS President Ravi Bhagrath, DAS Secretary Fauzia Mir, DAS Treasurer
Finally, DAS central and the local organising team at Newcastle, lead brilliantly by Dr Iftikar Pervez, are looking forward to welcoming you in October at the first DAS ASM for 3 years.
As conferences start up again following a 2 year hiatus, DAS has been well represented amongst many of them, both nationally and internationally, including the Qatar conference on airway management in Doha, the RCOA updates in Manchester, ISAIC conference in Milan, GAMC meeting in London and the IAMS on line conference. There are many more to come over the rest of the year, this just highlights the excellent and important work DAS continues to produce.
DAS is always involved in important projects all of which are at different stages in their timelines. We are delighted to share that the final manuscript for the guidelines on human factors and ergonomics has been submitted for peer review. The guidelines on the ethics of airway management is close to completion and work has started on the paediatric, obstetric and intubation/extubation guidelines. The safer pre-hospital anaesthesia working group will have their first meeting soon and there are other potential guidelines in the pipeline. We would like to thank everyone involved in the planning and writing of all these guidelines, it is a huge amount of work which takes up a lot of time and we do appreciate your commitment in ensuring they are done. We are delighted to share the fabulous news that our Scienti fi c Of fi cer, Kariem ElBoghdadly, has been awarded the Featherstone Professorship by the Association of Anaesthetists. This is a very prestigious award and Professor El-Boghdadly is very deserving of it, he has produced some award winning and highly cited work over the past few years including the consensus guidelines on airway management of COVID patients, the IntubateCOVID series of papers and DAS guidelines on Awake Tracheal Intubation and management of haematoma post thyroid surgery, just to name a few! Many many congratulations Professor El-Boghdadly!
Kariem El-Boghdadly |
|
SCIENTIFIC OFFICER REPORT
Difficult Airway Society E-Zine September 2022 Contents 9
As we emerge from the darkest days of the pandemic, without forgetting that we are still not out of the woods, we have yet again seen academia in airway management thriving. Several practice-changing publications have emerged with more on the way. More grants have been applied for than ever before, and I am in no doubt that we will see invaluable evolution in patients safety. DAS has continued to play a vital role in supporting academic anaesthesia, with a renewed interest in some of our academic support through a number of exciting academic opportunities.
1. Direct DAS Grants. To ensure continuity and sustainability of grass-roots airway management research, we have a rolling process of grant funding via direct application to DAS. Applications for funding of up to £5,000 for studies broadly related to airway management will be peerreviewed. Further details are available on the DAS website or by contacting me directly. We have already had a number of applications, and we hope to receive more. Reach out for more information on this today!
2. DAS Grants via the NIAA. DAS funds up to £20,000, split between large Project Grants (up to £15,000) and Small Grants (up to £5,000). Last year saw a single application round, with one application of £15,000 being received. The first round of 2022 applications saw 5 applications for a


3. DAS PhD Programme. This Programme gives support to researchers who have a list of publications that may be suitable to put together as a PhD. DAS will support applicants throughout the process of a PhD by publication, including funding support.
Difficult Airway Society E-Zine September 2022 Contents 10 total of more than £26,000 requested and, although none were funded, highlights the energy around airway management research. The next round is now openmore information and details on how to apply are available here
standing in the field of airway management as established by outstanding contributions through publications, creative work or other appropriate forms of scholarship, and through teaching and administration. The award will be announced at DAS ASM – be there! Our vision remains to continue to cultivate academia through DAS and airway management, and to begin to support, design and develop our own projects with our enthusiastic, creative and brilliant membership. Don’t hesitate to reach out and get ScientiDASKarieminvolved!El-BoghdadlyScientificOfficerfic-officer@das.uk.com
4. DAS Faculty of Professors. This is an untapped resource that is open to any DAS Member to reach out to for guidance, support or advice on any academic matters, including grant applications and study design. DAS Professor of Anaesthesia and Airway Management for 2022 is an award conferred in recognition of a member’s national/international
IN MEMORY OF DR RONNIE CORMACK (1930-2022)
Ellen O'Sullivan | Adrian Pearce |
Difficult Airway Society E-Zine September 2022 Contents 11
|
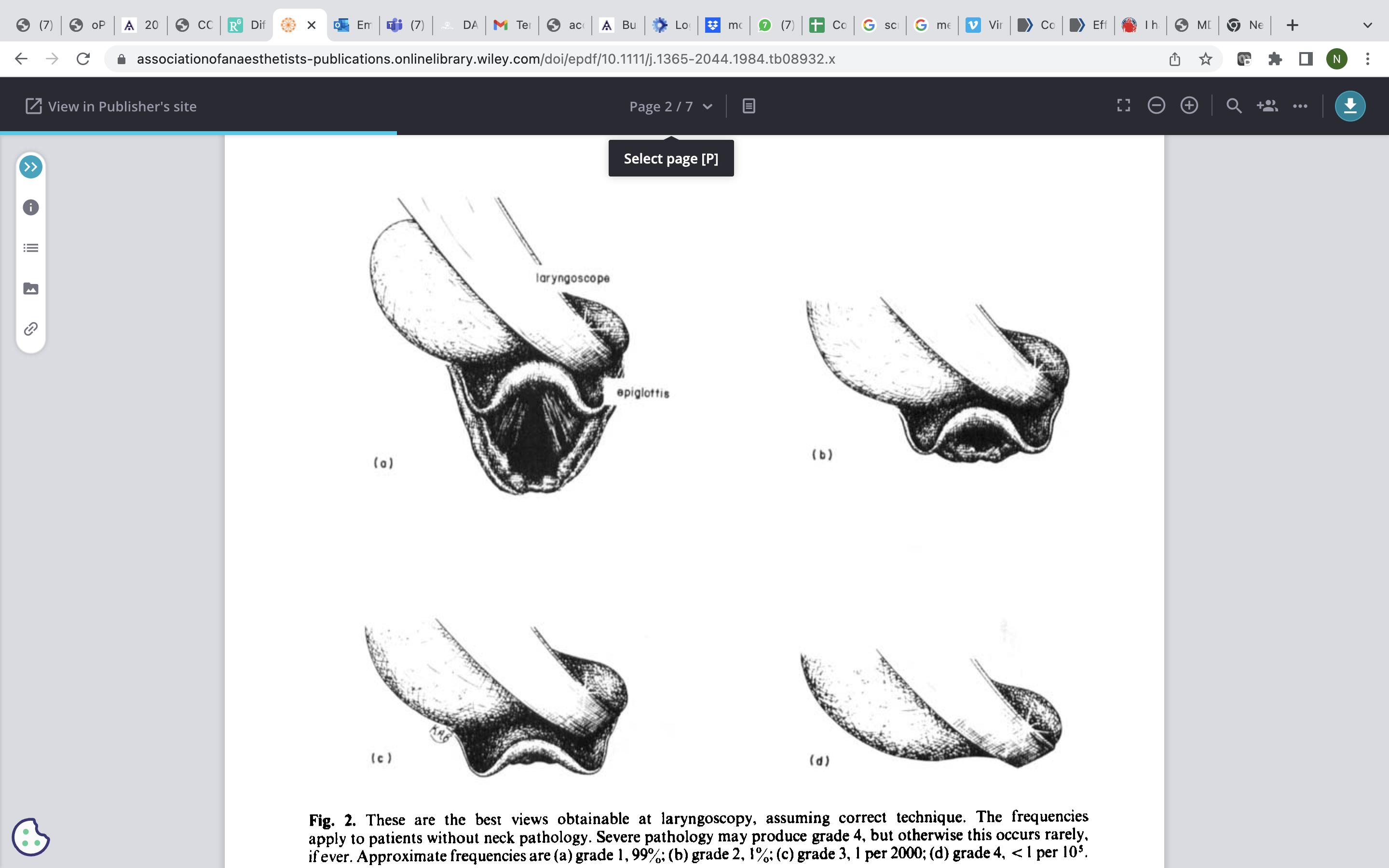
Cormack's great contributions to airway management, for which the Dif Society awarded him the Macewen medal in 2013, are contained within his 1984 seminal paper 'Dif fi cult tracheal intubation in obstetrics' which he co-authored with Dr John Lehane. Until the early 1980s virtually all obstetric anaesthesia cases were undertaken under general anaesthesia. Cormack and Lehane first proposed that it was possible to classify or sub-divide difficult intubation by the degree of laryngeal exposure under direct laryngoscopy and this legacy has endured.
Difficult tracheal intubation in obstetrics. Anaesthesia 1984; 39: 1105 – 1111
Ronnie Cormack was born in 1930 in Rangoon, Burma where his surgeon father was head of military services. He graduated from Oxford in 1961 and was an anaesthetic senior lecturer at Bristol. He was appointed to the new MRC unit at Northwick Park in 1972 and it was there that he met Dr John Lehane, a fellow Consultant. Dr Cormack took early retirement to focus on his research interests which included statistics.
Cormack clearly identified the problem that needed solving – dif fi culty was mostly encountered in a patient with a Grade 3 view and the frequency of this was low enough that many (trainee) anaesthetists were unfamiliar and inexperienced with the situation. Their solution was the adoption of the most likely intubation technique to be successful (the Macintosh method of a bougie inserted into the endotracheal tube), its universal adoption within training, practising the technique by not adequately lifting the epiglottis to simulate a Grade 3 view and keeping records. This didactic teaching was very uncommon at that time but was part of the culture which was the basis of great change in airway management over the next 35 years. In later conversations he revealed It is in the nature of 'seminal' papers that succeeding generations examine them critically and possibly to the point of rejection. But without the genius of the initial paper, the Fig 1: The original illustration of the 4 best views obtainable at laryngoscopy, assuming correct technique from the seminal paper by Cormack and Lehane.
The more important messages are often overlooked, but form a very important landmark within UK airway management.
Ellen O’Sullivan, Past President Diffi cult Airway Society
Difficult Airway Society E-Zine September 2022 Contents 12
Dr Ronnie Cormack receiving the DAS Macewen Medal in October 2013. His citation for the medal by Jaideep J Pandit describes him as “someone who has contributed so much to anaesthesia and in particular in the area of airway management and improved patient safety.” His work, along with that of Lehane, has influenced the life of every single anaesthetist in immeasurable scale.
detailed discussion could not have taken place. Cormack persistently and bravely defended his 'solution' over the next 25 years despite changing times and opposition. He had an exceptional, methodical, scientific mind and 20 years after he retired, at the age of 77, he wrote a blistering editorial supporting the Northwick Park drill. It was an opportunity for 'modern-era' anaesthetists to propose different solutions with equal vigour and to promote them with confidence. Next time you intubate by direct or indirect laryngoscopy you will inevitably proceed according to the view of the laryngeal inlet. It was Cormack and Lehane that codified that approach. The CL grading system has given us a universal language to communicate and research laryngoscopy & tracheal intubation. Although various techniques have subsequently evolved, this simple system has stood the test of time and Cormack’s name will always be associated with this seminal paper from 1984. The Society remembers a gentle, caring and enthusiastic teacher.
Adrian Pearce, Founding member Difficult Airway Society

BOOK YOUR LEAVE AND REGISTER TODAY
B.
2.
A 26 year-old man presents with a one-day history of fever, sore throat, and change in voice, and is now extremely anxious and unable to swallow. He is normally fit and well, with no regular medications. He has no allergies. On examination: Stridulous and spitting saliva into a cup. Normal mouth opening. RR 34, Sats 96% on room air. Working hard with accessory muscle use and leaning forwards. Unable to lie HR 124, BP 80/40, sweating profusely. GCS 15, very anxious – on the cusp of becoming agitated. Temp 39.9℃ ED have applied 100% O2 via a non-rebreathe mask, given a bolus of 1L Hartmann’s, and started appropriate IV antibiotics and given 8mg dexamethasone. They have called you because they think he needs urgent definitive airway management. What would you do? What would you do if this patient becomes hypoxic (sats 88% on RA) and profoundly agitated/distressed? What would you do if this patient was 6 years old? is your plan? What Would You Do? us on twitter with your thoughts! @dastrainees
flat. C.
Difficult Airway Society E-Zine September 2022 Contents 14 CLINICAL DILEMMA | What Would You Do? |
1.
What
@dasairway
Contact
A.
D.
E.
. The
3.


Difficult Airway Society E-Zine September 2022
3. What would you do if this patient was 6? I would contact the most skilled paediatric anaesthetist and ENT surgeon, and proceed similarly, recognising that it will be impractical to prepare the patient for tracheostomy awake.
My first choice device would be a videolaryngoscope with a screen that is visible to others in the operating theatre, and I would use the smallest tracheal tube that would be suitable for ICU management. I would have a bougie opened and ready to be used. If I am unable to successfully intubate the patient’s tracheal rapidly, I would insert a supraglottic airway device (iGel) and attempt ventilation through this whilst the surgeon proceeds with a tracheostomy. I would not spend time with multiple attempts at tracheal intubation, and would promptly move forward with tracheostomy insertion if unsuccessful in the first instance.
Airway Expert 1: 1. What would you do?
2. What would you do if this patient becomes hypoxic (sats 88% on RA) and profoundly agitated/ distressed? This might require airway management in the ED, and thus I would do the same as in the operating theatre (HFNO, surgeon ready for tracheostomy, videolaryngoscopy for first attempt intubation). I would not attempt to provide sedation for agitation, as this may worsen airway obstruction.
WHATWOULDYOUDO? DAS Expert Corner
I would start by ensuring the patient is somewhere safe. I would ensure we contact the operating theatres and on-call ENT surgeons, getting theatres ready to receive the patient for definitive airway management. I would assess if the patient is safe for transfer, and if so, take all airway equipment and drugs that I might need for the transfer, including RSI medications, supraglottic airway devices, disposable video laryngoscope, a range of tracheal tube sizes, and a front-of-neck airway kit comprising a scalpel, bougie and size 6.0 tracheal tube.
Following safe transfer to the operating theatre, I would immediately commence HFNO and increase flow rates to >50 l.min-1 and ensure IV fluids are running at the maximum rate. The patient is likely to be unable to tolerate awake tracheal intubation, so I would proceed with full pre-oxygenation whilst getting all of the required equipment ready for an emergency tracheostomy: scrubbed skilled surgeon with the site of tracheostomy marked (ideally using ultrasound), equipment opened and ready to be used, and infiltration with lidocaine with adrenaline. I would have the surgeon ready for the tracheotomy, then after adequate pre-oxygenation, I would induce anaesthesia with high-dose rocuronium, fentanyl and propofol, with a metaraminol ‘chaser’.
Once the airway is secured, I would confirm with capnography, and secure the tracheal tube or tracheostomy, before stabilising the patient with additional lines etc. before transferring to ICU to allow the inflammation and infection to be treated in a more controlled fashion.
In both scenarios I will get ready for a front of neck access as a secondary plan if securing the airway is not as planned and have all the equipment ready with a surgeon in theatres. I will intubate this patient in theatres to avoid any delays in transfer if needed in the event of a failed intubation. In case of a 6 year old patient, I will seek help from a Paeds anaesthetist who are more experienced with difficult airways in that age group.
Initial impression of this patient is that of someone with impending airway obstruction. He has a high respiratory rate with accessory muscle use. Drooling of saliva, change in voice and unable to swallow are all indicators of airway obstruction/ swelling. Although his saturations are holding well I will ask for a blood gas to assess whether he is getting tired (eg high CO2), and therefore needing intubation sooner rather than waiting for the medical interventions to show their effect and risking his observations getting worse.
Airway Expert 2:
do an awake tracheal intubation at this stage with minimal sedation and the operator being the senior, most experienced anaesthetist. I will liaise with HDU/ ITU for post intubation/ operation care for this patient and not extubate him until his airway oedema has settled.
If the saturations drop and his condition worsens I will plan for a general anaesthetic and secure his airway.
I will prepare to intubate him but in a safe environment with help around and an ODP. I will also ask for an ENT surgeon to be present during attempts to secure the airway. Depending on the condition and level of co operation I will consider doing an Fibreoptic nasendoscopy preIintubation.willplanto
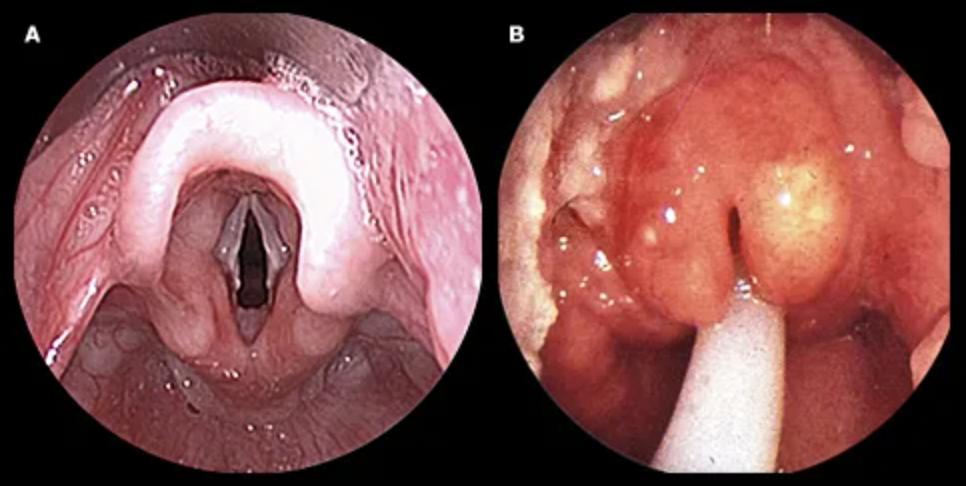
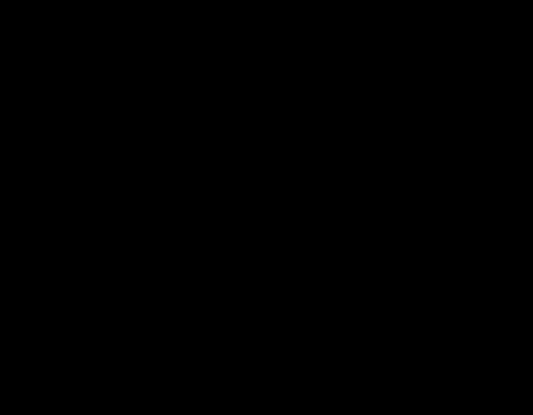
A: normal airway, compared to B: swollen epiglottis in the context of epiglottitis. Image credit: UpToDate http:// uptodate.com
Difficult Airway Society E-Zine September 2022 Contents 16
Airway Expert 3:
One of the first differential diagnoses would be epiglottitis. What seems obvious is that this patient has a worsening airway and is septic.
1. Is the ED the correct place to manage this patient? If yes then:
A/B: apply HFNO at 70 L/min
D: do not sedate, attempt to reassure E: IV paracetamol in addition to the antibiotics
Have ENT attempted a nasendsocopy to determine to degree/site of the airway obstruction?
a) In theatre with HFNO on at 70L/min, Concurrently have the surgical and nursing team prepared for an emergency tracheostomy (set open, surgeons scrubbed). Set up for a GA - full monitoring, BIS if patient b)compliant.Induce anaesthesia with remifentanil TCI and low rate propofol TCI and cricoid pressure. 1.2mg/kg rocuronium then one attempt at VL . If you have a view then place a 5.0mm ID MLT. If this fails some centres may choose to place a suspension laryngoscope to attempt a view and proceed to HFJV. This has the advantage of avoiding a potentially damaging tracheostomy.
If you have time to move to a theatre setting that is best. This is a high-risk scenario and the most experienced people are needed - Consultant Anaesthetist, Consultant ENT surgeon, experienced ODP and nursing team (who are familiar with head and neck surgery).
3. I'd call my paediatric colleagues!
If the patient stabilises with the above manoeuvres transfer to ICU with a low threshold for an airway intervention (to be done in theatre). There may be a place for an elective ATI either VL or FB.
C: consider vasoconstrictors (metaraminol, phenyephrine)
2. If despite applying HFNO the patient is hypoxic and agitated your options are limited.
c) However, if the above is unsuccessful then a surgical tracheostomy is needed
Difficult Airway Society E-Zine September 2022 Contents 17
[1]Mymanagement.thoughtsare:ATIifpatientis cooperative enough [2] GA intubation with a VL and a FB to hand I would perform this in theatre, pre-mark the cricothyroid membrane (using US) and ensure that an experienced ENT surgeon and scrub team were present in theatre. I would explain to the patient that in my hands and practice an ATI is the safest option, but for this to be successful I would need his cooperation.
Plan B: If the ATI fails or it is not appropriate then I would move to a high risk GA intubation using a VL and have a FB at hand if I need to do a combined VL/FB intubation.
My working diagnosis is acute epiglottitis. The patient has a compromised airway, which is resulting in worsening agitation, cooperation and hypoxia. The voice change, increased work of breathing, inability to swallow and inability to lie flat are worrying signs and highlight the need for urgent airway
Difficult Airway Society E-Zine September 2022 Contents 18 Airway Expert 4:
PlanC/D: If Plans A&B fail then I would immediately move to a surgical cricothyroidotomy or if I had time ask the surgeon to perform a surgical tracheostomy.
Plan A: I would start with an ATI and use minimal sedation (as I wouldn’t want to risk over sedation), use HFNO for procedural oxygenation, and take care with topicalisation as there is a risk of inducing laryngospasm and having inadequate topicalisation. I would also downsize the ETT and use a 6.0 tube. I would do this with the patient sitting bolt upright with suction immediately to hand.
E. Quickly discuss as MD team and agree strategy. Options include:
2. What would you do if this patient becomes hypoxic (sats 88% on RA) and profoundly agitated/ distressed?
3. What would you do if this patient was 6?
1. What would you do?
Again, awake option not available. Pre-oxygenation very difficult so either do so with parental help or even consider small (sedative) dose of Ketamine to facilitate pre-induction oxygen delivery.
4. eFONA - prophylactic cric could be performed pre-induction (narrow or wide) but again probably unwise with risk of complete airway obstruction during procedure.
2. ATI. High risk of failure would make this a relatively poor choice in my view - poor tolerance; failure of LA topicalisation; high risk of complete obstruction.
D. Neb Adrenaline + HFNO + lots of reassurance (leave sitting of course!). Assessment so far(infective) acute upper airway obstruction + sepsis with CVS compromise. Locate and mark CT membrane
Use Critically Ill Intubation Checklist. Actively manage human factors and ergonomics (HFE).
Other main difference is increased risk of eFONA failure (particularly if lack of paeds head & neck ENT surgeon available) so generally favour ETT or SGA attempts over eFONA. RSI. I WOULD paralyse although i know others would not.
5. Rescue (failed intubation) - SGAs available (choice of device and size); eFONA - scalpel cric by ENT/OMFS/ED (neck already marked); final option is upper airway access by surgeons e.g. rigid laryngoscope/bronchoscope.
Very little time before cardiac arrest. So, as above but no awake option - straight to GA intubation attempts with rescue options as above; less time perhaps to get the ‘best people’ and ‘best HFE'.
Difficult Airway Society E-Zine September 2022 Airway Expert 5:
A. immediate resus + assessment
1. Awake FONA (probably a poor choice owing to patient’s mental state);
This man is [a] pretty sick and [b] has a critical airway. So he needs
B. mobilisation of the best team immediately available to ED [must not attempt to move him] - this will depend on where you work, but ideally Senior ENT [or OMFS] with appropriate kit for upper airway + eFONA
3. RSI (Fent, Ketamine, Roc/Sux) with MacVL (personal choice, but don’t see obvious indication for hyper-angulated VL) + bougie (expect poor laryngeal view) - this is my likely choice. Ideally, I would use HFNO during prep; then tight-fitting FM + CPAP pre-RSI; then BVM ventilation prior to intubation; then HFNO during airway management
C. preparation for CVS resus (IV fluids; Adrenaline IV bolus + infusion, CVC)
The pathogens responsible are now more varied and can be polymicrobial. There have even been recent case reports of epi/supraglottitis associated with severe COVID-19 disease. For this reason, the term "supraglottitis" is often preferred, as the infections may affect the supraglottic structures more generally.
When first setting this case, acute epiglottitis was at the forefront of our minds, and our experts generally thought the same. Since the addition of the Haemophilus influenzae type b (HIB) vaccine to the infant immunization schedule in many countries worldwide, the annual incidence of epiglottitis in children has decreased overall. However, the incidence in adults has remained stable, and it is now much more likely we will encounter this disease in adults as well.
Oedema due to infection of the epiglottis and supraglottic structures can be gradually progressive until there is rapidly deterioration, respiratory distress, airway obstruction, and death.
FROM OUR CASE SETTER | Moon-Moon Majumdar |
With anti-vax sentiment brought to the fore by the pandemic, previously rare, life-threatening diseases are rearing their heads once again. Australia has seen a recent case of an unvaccinated toddler with severe diphtheria requiring intensive care admission, and in the UK there was a recent case report of similar disease in a 76 year old woman. The above presentation is not dissimilar to a respiratory presentation of diphtheria (just add in the hallmark greyish-white pseudomembrane over the mucous lining of the tonsils, pharynx, larynx, or nares that can extend into the trachea, and severe cervical lymphadenopathy — sometimes so severe there is a 'bull neck' appearance). Cardiovascular instability is a frequent feature in both epiglottitis and diphtheria, in the former this tends to be septic shock, in the latter predominantly cardiogenic shock from diphtheria toxin myocarditis. Early diptheria antitoxin (DAT), antibiotics, and early airway management are the mainstays of treatment: the latter allows mechanical removal of tracheobronchial membranes, and prevents the risk of sudden asphyxia. We felt this case was a good opportunity to remind ourselves of the urgent management of acute impending airway obstruction. As you can see from our airway experts: there is frequently more than one safe way to skin the proverbial cat. Depending on the situation, some of our experts would transfer to theatre and some would stay in ED to manage the airway. Some would prefer an awake approach — and some think an asleep approach is safer in their hands. The prevailing concepts throughout everyone's answers are clear communication with your team, and careful planning (as far as time allows, depending on how unstable the patient is), so that it's easier to make cognitive progression towards more invasive approaches (for example front of
THOUGHTSneck).
Difficult Airway Society E-Zine September 2022 Contents 20
Difficult Airway Society E-Zine January 2022 Contents 21
In this September 2022 edition of the DAS E-Zine, we are proud to present the second in our three part perioperative medicine series. You can find the first part in our May 2022 edition here, where we had three articles: 'Perioperative Medicine: an Introduction', 'The National Emergency Laparotomy Audit Project', and 'Shared Decision Making'. This time, we present another three excellent articles. As a starter for 10, we have an in-depth discussion of risk assessment from the Perioperative Medicine group at University College London. Dr Alexander Gibson (ST5 anaesthestic trainee at University College London NHS Foundation Trust) and Dr Matt Oliver (consultant in anaesthesia and perioperative medicine at UCLH, and associate professor at UCL division of surgery and interventional science) talk us through why risk assessment matters, how we can approach it, and how to talk to our patients about it.
Difficult Airway Society E-Zine September 2022 Contents 22
Following on from the theme of risk assessment, we delve into the details of CPET with our very own Dr Tom Lawson, DAS Education lead, and consultant anaesthetist at Morriston Hospital in Swansea. Tom looks at the history and process of CPET and shares a practical | Moon-Moon Majumdaruseful| approach to interpreting the '9 panel plot'.
PERI-OPERATIVEand MEDICINE SERIES: PART 2
Finally we finish with a fascinating article on frailty from Dr Anthi Andrianou (an anaesthetist/ intensivist in a former life, she is now a POPS [Perioperative medicine for Older People undergoing Surgery] fellow at Guy's and St Thomas' NHS Foundation Trust) and Dr Jugdeep Dhesi (consultant geriatrician, and POPS clinical lead at Guy's and St Thomas' NHS Foundation Trust). They discuss a gentleman who was referred to the POPS team prior to his head and neck surgery, where comprehensive geriatric assessment and assessment of frailty were key to his surgical pathway. We hope very much that you enjoy reading and learning from these fantastic resources as much as we have.
PERIOPERATIVE
Alexander Gibson Oliver
Why is it important?
Difficult Airway Society E-Zine September 2022 Contents 23
| Matt
Chance is a statement of probability or odds. Most people feel more comfortable thinking about probability which is expressed as a fraction by dividing the event in question by the total number of possible outcomes. This is often presented as a frequency which should strictly include a time period in its description. By its nature risk involves uncertainty and the way we perceive risk is governed by our own experiences and personality as well as wider social factors. Risk should also be considered a product of the probability of the event occurring and the severity of the implications of this outcome.
Risk assessment is an essential facet of multidisciplinary and shared decision making. It allows the identi fi cation and management of modifiable risk factors pre-operatively, the tailoring of anaesthetic and surgical technique to the patient and the safest allocation of resources for postoperative care. As many as 15-30% of surgical inpatients suffer from morbidity of some form postoperatively. This likely represents a complex interaction between the indication, nature and extent of the surgical insult, patient factors and the quality of care.1 The development of post-operative morbidity is associated with increased post-operative mortality, a decline in physical function and quality of life as well as extra healthcare costs. 2 Indeed, the development of postoperative morbidity is a greater determinant of long-term survival following major surgery than pre- or intra-operative Datafactors.3from the National Confidential Enquiry into Patient and Death and Intensive Care National Audit and Research Centre has demonstrated that approximately 80% of all
|
MEDICINE: RISK ASSESSMENT |
What is risk? As doctors and anaesthetists the assessment of risk is fundamental to our dayto-day care of patients. However, as a concept we are often poor at understanding and incorporating risk into our decisions and often poor at explaining it to others. Risk can be considered the chance that something will happen or the chance that an outcome will differ from that which was expected. It usually refers to the negative implications of an intervention or encounter. In a healthcare setting this commonly means failure or harm including side effects and complications.


✦
✦
Surgical factors include: organ system operated on; operative approach and invasiveness; blood loss, duration; intraoperative complications; urgency of surgery (30-day mortality of emergency surgery is 10-fold that of Functionalelective).1,4capacity, is an important predictor of how a patient will respond to the overall stress of surgery. This is based on the observation that the increase in oxygen consumption seen after major surgery can only be sustained at approximately 30% of a patient’s maximal capacity (VO2 max or VO2 peak). Multiple studies have demonstrated that a VO2 peak < 15 ml/kg/min and/or an anaerobic threshold < 11 ml/kg/min place a patient in a high risk category in terms of morbidity and mortality (See POETTS Guidance for a summary of current evidence).7 Whilst formal cardiopulmonary exercise testing with a metabolic cart may not be available to all, surrogates such as the incremental shuttle walk test can be used. Failing a measured assessment, scoring systems such as the Duke Activity Status Index allow estimation of functional capacity from a protocoled assessment of activities of daily living, which may improve upon some of the limitations of self-reported functional Aftercapacity.athorough history and examination there then exists a plethora of tools that can be used to guide ongoing decision making and patient care. Biomarkers are playing an emerging role in the risk assessment of patients undergoing surgery and are now included in national guidelines in North America and Europe 8,9 Raised pre-operative BNP and NT-proBNP have been shown to be
perioperative deaths occur in a high-risk cohort accounting for 13% of the overall surgical workload.4,5 This high-risk group’s overall risk of hospital mortality is as high as 12% and post-operative morbidity as high as 50%.4,6 do we identify risk factors and predict the risk of adverse outcomes?
Identifying risk starts with a good understanding of the patient presenting for surgery and the nature of the procedure they are presenting for. This should start with a review of the comorbidities of the patient and an assessment of functional status. Repeated studies have demonstrated that several patient and surgical factors independently predict post-operative morbidity and mortality. These include: age (increasing incidence of mortality > 65years); frailty; ✦ reduced functional capacity; American Society of Anaesthesiologists Physical Status (ASA-PS); co-morbidities including anaemia, obesity, diabetes, congestive cardiac failure and cirrhosis (which can increase mortality three to five fold); history of smoking.
✦
✦
Difficult Airway Society E-Zine September 2022 Contents 24
✦
✦
✦
✦
How
✦
The are multiple ways to estimate the risk of adverse postoperative outcomes including an assessment of frailty and functional capacity (covered elsewhere in this edition), the use of biomarkers and the use of risk scoring systems and risk prediction models.
✦
Difficult Airway Society E-Zine September 2022 Contents 25 associated with increased post-operative mortality and cardiac events. Post-operative elevation in troponin is also an important prognostic marker and an independent predictor of cardiovascular outcomes and mortality. With ever larger populations examined and validated against and with the ease at which they can be accessed on mobile devices, risk scoring systems and risk prediction models should now be part of everyday anaesthetic practice. These tools use multivariate analysis to examine the association between patient
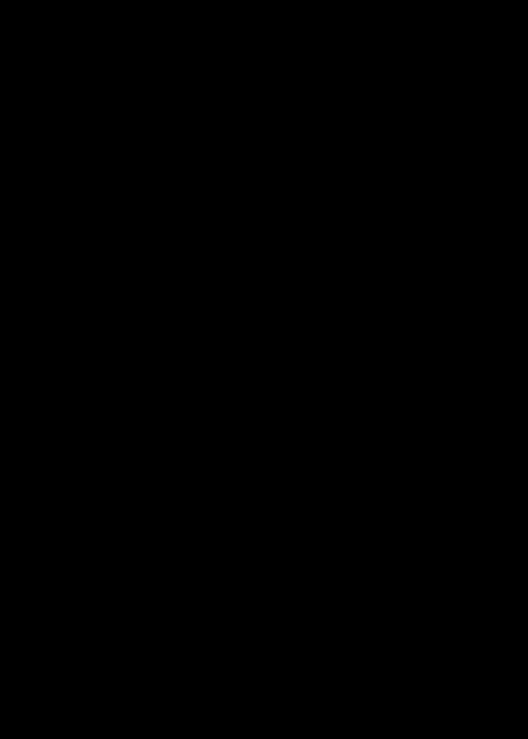
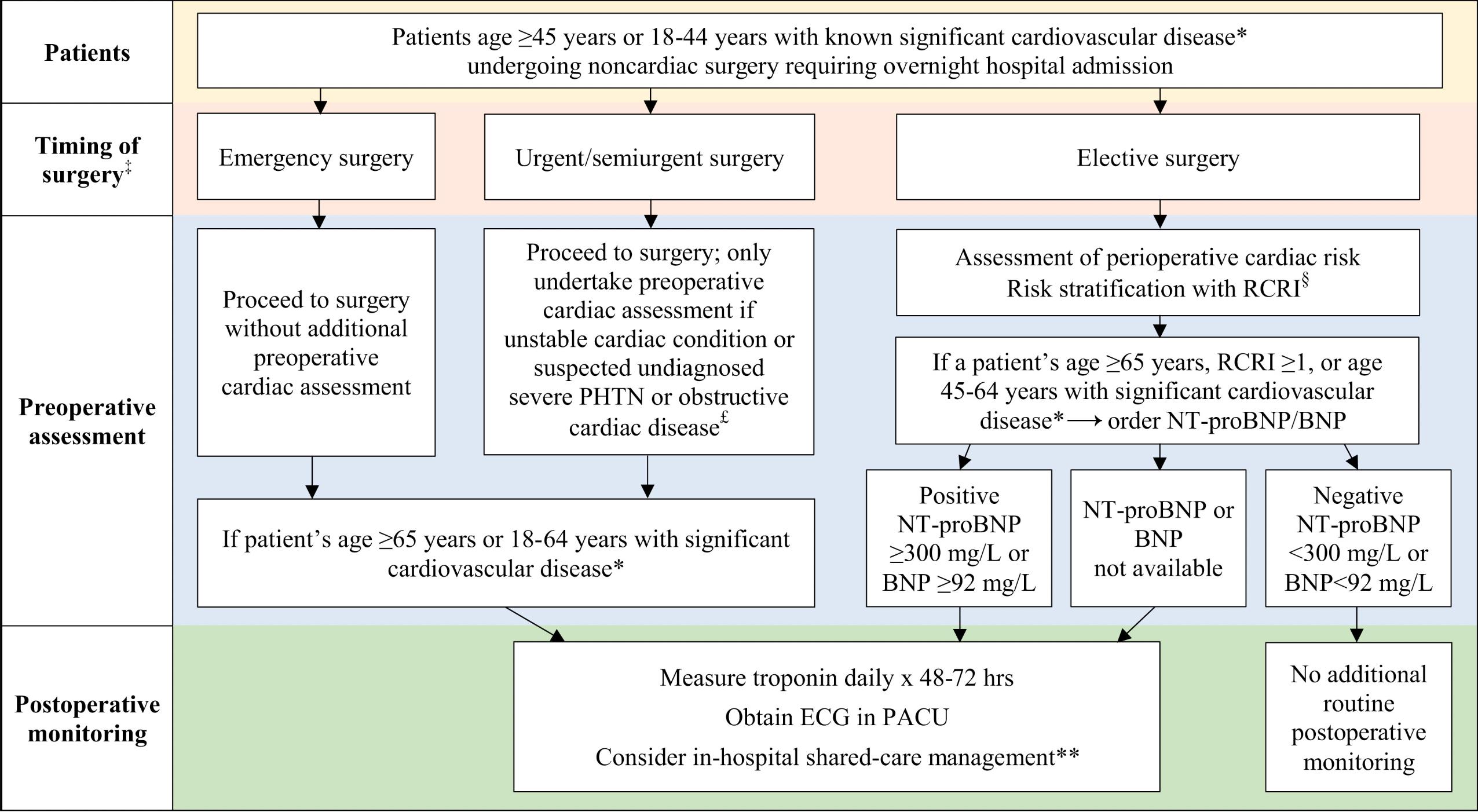
Fig 1. Preoperative risk assessment and postoperative monitoring flow diagram, from the 2016 Canadian Cardiovascular Society Guidelines on Perioperative Cardiac Risk Assessment and Management for Patients Who Undergo Noncardiac Surgery8
BNP, brain natriuretic peptide; ECG, electrocardiogram; NT-proBNP, N-terminal pro-brain natriuretic peptide; PACU, postanesthesia care unit; PHTN, pulmonary hypertension; RCRI, Revised Cardiac Risk Index. ∗ Significant cardiovascular disease includes known history of coronary artery disease, cerebral vascular disease, peripheral artery disease, congestive heart failure, severe PHTN or a severe obstructive intracardiac abnormality (eg, severe aortic stenosis, severe mitral stenosis, or severe hypertrophic obstructive cardiomyopathy). ‡ Timing of surgery refers to emergency surgery (eg, severe trauma, ruptured aortic aneurysm), urgent surgery (eg, hip fracture, bowel obstruction), semiurgent surgery (eg, cancer with potential to metastasize), or elective surgery (eg, knee arthroplasty).
£ If physical examination suggests there is an unknown severe obstructive intracardiac abnormality (eg, severe aortic stenosis, severe mitral stenosis, or severe hypertrophic obstructive cardiomyopathy) or severe PHTN, then obtain an echocardiogram before surgery to inform the anesthesiologist, surgeon, and medical team of the type and degree of disease. If the history suggests the patient has an unstable cardiac condition (eg, unstable angina) then discussion with the patient and surgical/medical team is required to decide whether to delay, cancel, or proceed with surgery.
§ RCRI score (each worth 1 point): history of coronary artery disease, cerebrovascular disease, congestive heart failure, preoperative insulin use, preoperative creatinine > 177 μmol/L, and high-risk surgery (ie, intraperitoneal, intrathoracic, or suprainguinal vascular surgery). Shared-care management refers to a multidisciplinary approach to inpatient postoperative care; this includes the surgeon and a medical specialist (eg, internist, cardiologist, gerontologist), who will help with perioperative monitoring and management of cardiovascular complications.
∗∗
Difficult Airway Society E-Zine September 2022 Contents 26 characteristics and specified post-operative outcomes in large cohorts of patients.10
Finally, the assessment of cardiac risk deserves special focus as post-operative cardiovascular morbidity is associated with particularly poor survival and other measures such as hospital length of stay. American and European guidance involve a stepwise approach to cardiac risk assessment involving an initial assessment using the RCRI and/or knowledge of the nature of the surgical risk. If the case is considered intermediate or high risk (> 1% probability of a Major Adverse Cardiac Event) then the functional capacity of the patient should be considered. If less than or equal to 4-metabolic equivalents (approximately 15ml/kg/min) then further tests including non-invasive tests can be considered to aid decision making or inform perioperative care.23,24
The statistical presentation of risk is a subject in itself, but the importance of clear descriptions and framing of risk should not be underestimated. Numbers should be presented as event rates, using frequencies, rather than as probabilities using percentages. Using a common denominator should be used where a choice between various treatments may affect the risk of the same event occurring. Supplementing the use of numbers with verbal risk descriptors, such as high and low, may also aid understanding but they should not be used in isolation.
Standardised numerical definitions of these terms should be used as presented in The
Scoring systems such as the Revised Cardiac Risk Index (RCRI) use group stratification or aggregates of weighted risk factors to predict the risk of an adverse outcome which can be applied to a group of patients. 11 Risk prediction models allow patient-speci fi c parameters to be entered into a model created from the initial logistical regression providing individual probabilities of risk.12
Communicating risk is an important part of decision making and consent and this is reflected in updated General Medical Council guidance on the subject. 25 Information discussed should be objective and should focus on factors that are important to the patient. Individually tailoring how we discuss risk with our patients is likely to enhance decision making.
Specific surgical procedures have their own risk prediction models to estimate 30-day mortality including EUROSCORE (cardiac), Nottingham Hip Fracture Score (hip fracture repair) and the National Emergency Laparotomy Audit risk prediction model (emergency abdominal surgery).13,14,15 There are also tools for specific post-operative morbidity including ARISCAT (pulmonary) and SPARK (renal).16,17 Many guidelines now also recommend screening for risk of psychological distress, malnutrition and post-operative cognitive dysfunction.18 There are many other wellvalidated tools which have been validated in mixed (multi-specialty) populations including P-POSSUM, SORT, and the ACS NSQIP.19,20,21 These three models are recommended by the National Institute for Health and Care Excellence for use as part of perioperative patient assessment and consent.22 The ACS NSQIP model also generates risk estimates for 13 non-mortality outcomes including systemspecific insults, re-admission, and discharge to a post-acute care facility. However, due to its proprietary nature, this model has not been validated outside its derivation cohort.
How is risk best communicated?
Royal College of Anaesthetists’ infographic on Common events and risks in anaesthesia (RCoA).26 This tool also frames these numbers in a context that might be more familiar to people, which particularly helps when numbers involved are very small. In terms of framing risk, it is worth noting that as humans we tend to be more risk averse when risk is framed as negative outcome or loss. Describing the risk in different ways, such as 99 in a 100 people are unlikely to experience an accidental dural puncture during insertion of an epidural, may help patients understand the risk more without intending to convince them one way or another.
Difficult Airway Society E-Zine September 2022 Contents 27
Glossary: ✦ European System for Cardiac Operative Risk Evaluation ✦ ARISCAT - Assess Respiratory Risk in Surgical Patients in Catalonia ✦ SPARK – Simple Postoperative AKI Risk ✦ P-POSSUM – Portsmouth- Physiological and Operative Severity Score for enumeration of Mortality and Morbidity ✦ SORT – Surgical Outcome Risk Tool ✦ ACS NSQIP – American College of Surgeons National Surgical Quality Improvement Program
The risk of adverse postoperative outcomes is not uniform, varying by patient, surgical and process factors. Assessment of risk should now be a routine part of the care of patients undergoing surgery. Combining a review of co-morbidities and an assessment of the type and magnitude of surgery, frailty and functional capacity along with the use of a risk prediction model will allow a comprehensive appraisal of the case to emerge. For it to impact meaningful, patient-centred outcomes it needs to be discussed carefully with both patient and colleagues and acted upon by targeting interventions and resources at highrisk individuals throughout their perioperative Linkjourney.toreferences
Difficult Airway Society E-Zine September 2022 Contents 28
Tom Lawson |
PERIOPERATIVEcinematography.
|
MEDICINE: CPET
Bouny began testing and improving a dynamometer that Marey had constructed in 1895 at the Champ de Mars winter cycle track. The result was the first bicycle ergometer1; the front wheel connected to a brake dynamometer and the rear replaced with an iron flywheel (Figure 1).
The current bicycle ergometers used in CPET are much the same, albeit more advanced versions. They generate a measurable workload by adding resistance (the method of which can vary depending on the bicycle).
Together with a metabolic cart (a device that allows for the breath-by-breath analysis of gas exchange parameters) and with the use of flow Fig 1: Bouny’s Bicycle Ergometer (dated 1896) - From a 2003 PhD dissertation by Yaser Mahfouz Atwa Saad Elgohari.
If life imitates art, then perhaps medicine imitates sport. As I write this article, riders from 34 countries tackle stage 11 of the Tour de France, battling from Albertville, up the southern approach to the top of Col du Granon in the Serre Chevalier. So, it’s fitting that this article about the basics of cardiopulmonary exercise testing (CPET), begins with a Frenchman; Elisée Bouny.
Born 26th June 1872 in Sainte-Foy-LaGrande, Bouny was described as a rare spirit (‘Un si rare esprit’). Despite studying medicine at the Paris medical faculty in 1890, he would not however practice clinical medicine; a chronic, and hitherto, unnamed illness that claimed his life at the young age of 28 was responsible for cutting short his medical career. He was, however, fascinated by bicycles (as was most of France in the late 19th century), writing his doctoral thesis on the physiology of the lower extremities in cycling. Whilst a medical student, Bouny came into the orbit of the renowned polymath, Étienne-Jules Marey. One of Marey’s principal concerns was the physiology of motion, an obsession with which would lead him to invent the ‘chronophotographic gun’; in essence the first ‘video camera’, becoming a pioneer in the emerging field of

✦
✦
In the realms of anaesthesia, the assessment of exercise capacity and peri-operative risk stratification go hand-in-hand, although more recently CPET services and peri-operative physicians are seeing more medical patients, not just for investigation of dyspnoea, but also the assessment of long-COVID, determination of baseline function in patients with progressive cardiac disease, etc.
So why CPET?
✦ Green light – low risk, normal recovery expected and can proceed.
✦ Amber light – intermediate risk, either in terms of degree/complexity of surgery, or in terms of fitness and comorbidities. Potential for prolonged / incomplete recovery and need for further investigation, optimisation and appropriate post-operative support.
✦
CPET fulfils a key part of the pre-operative risk discussion and can help inform shareddecision making. As part of a dialogue with patients, it is important to explain to them that ‘when someone undergoes major surgery, their body incurs a debt. The ability to repay that debt depends on several factors; age, fitness, co-morbid state, type of surgery, etc’ which CPET can help determine. Whilst CPET may not necessarily be able to determine a specific percent risk of certain complication, it can be useful more generally to stratify patients into broad risk groups. A traffic light model can be helpful for patients to conceptualise what this means: -
✦
✦ Red light – high risk. Potential that surgery poses a greater threat to life than underlying Increasingly,condition. CPET is being adopted by various surgical specialties as part of their guidelines for the pre-operative work-up of patients for surgery. Historically, colorectal, vascular and thoracic surgery have led the way in requesting CPETs for their patients. It might seem odd, for an article on CPET to appear in an e-zine primarily aimed at those interested in airway or head and neck anaesthesia, but there is growing evidence that CPET can be performed for patients with head and neck cancers2,3. Indeed, airway obstruction and head and neck cancer do not appear in the lists of absolute or relative contraindications for CPET from the American Thoracic Society/American College of Chest Physicians joint statement on CPET4, although it is clear that care and caution should be taken when testing such patients. Whilst CPET for such patients may be unusual outside of major specialist centres, it may prove to be a growing area in the future. What follows is a basic introduction to what a CPET is and how a non-expert can interpret a test.
Difficult Airway Society E-Zine September 2022 Contents 29 sensors and other monitoring equipment such as ECG, blood pressure cuffs and pulse oximetry, a whole host of physiological parameters can be measured and derived.
The use of CPET has expanded greatly in the last two decades and is used by professionals across a wide array of disciplines. Principally, the main uses of CPET are: Assessment of exercise capacity and / or limitation; Peri-operative risk stratification; Investigation of dyspnoea of unexplained origin; Disease prognostication.
including: ✦ Oxygen
activity;
✦ Respiratory Exchange
✦ Partial
Carbon Dioxide ✦ Heart
ischaemic changes. ✦ Oxygen Pulse
‘9-panel
Let’s
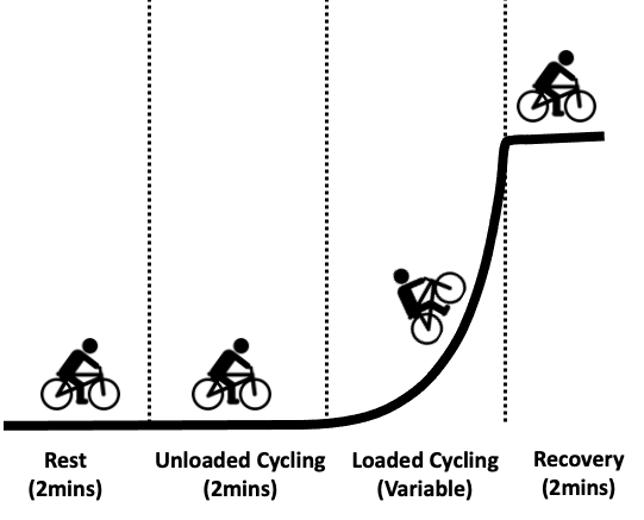
they
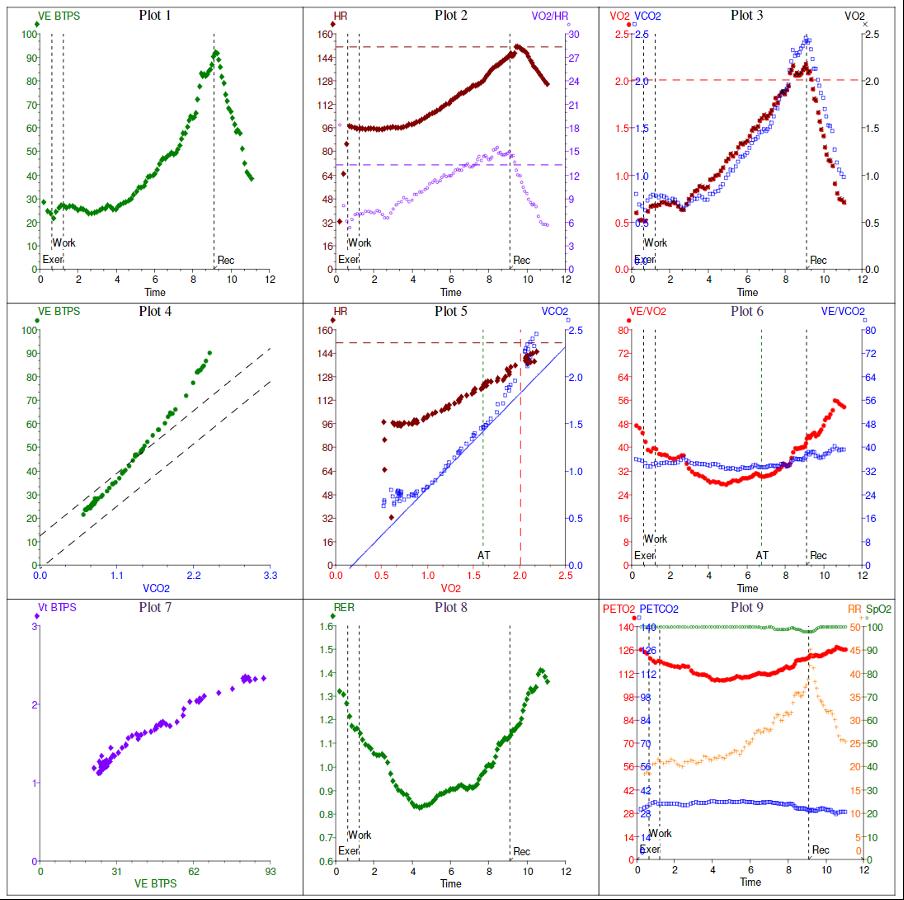
4. Recovery – 2-5 minutes of measurements to assess the response to stopping exercise (e.g. autonomic tone leading to heart rate to decrease at an appropriate rate). essence the normal response to exercise is to increase the various physiological mechanisms required to match increased energy demands from increased muscular cardiac output, pulmonary blood flow, ventilation, pulmonary gas transfer and peripheral blood flow. Thus, measure and derive a variety of parameters consumption (VO2) dioxide production (VCO2) Ratio (VCO2/ for (VEVO2) (VEVCO2) End-Tidal Pressures of Oxygen and rate (HR), rhythm and potential (VO2/HR) rate parameters are presented as a set of 9 each with a different plot. There are several different plots’, but effectively present largely the same information in different orders. For simplicity will examine the standard Wasserman 9-panel plot which is commonplace in the literature (figure 3), most of the parameters are plotted against time (but some can also be plotted against workload). look at each plot in order.Schematic representation of of
Difficult Airway Society E-Zine September 2022 Contents 30 A CPET consists of 4 basic (and largely standardised) phases (shown in figure 2):1. Rest – 2-3 minutes of baseline measurements 2. Unloaded cycling – 2-3 minutes of cycling with no pedal resistance. Start to measure response to movement and allow patient to attain needed pedal cadence (approximately 60 revolutions per minute). 3. Loaded cycling – workload increases in a ramped fashion. Patient continues until unable to maintain adequate pedal cadence (usually due to leg fatigue or joint pain, less common reasons include breathlessness or test terminated by clinician).
we
✦ Work
CPET
Oxygen
(WR) ✦ ΔVO2/WR ✦ Oxygen saturations (SpO2) ✦ Blood pressure These
we
In
panels,
different phases
Fig 2:
✦ Carbon
and CO2
VO2) ✦ Tidal volume (VT) ✦ Respiratory rate (RR) ✦ Minute ventilation (VE) ✦ Ventilatory equivalents
✦
Plot 2 – VO2/HR and HR vs time Usually, both VO2 and HR should increase with increasing workload.
Plot 1 – VE vs time
Heart rate/cardiac output are the factors that usually limit exercise capacity. HR should reach >80% predicted (usually >90%).
✦
✦
Difficult Airway Society E-Zine September 2022 Contents 31
The oxygen pulse (VO2/HR) is a surrogate marker of stroke volume. CPET for a normal subject
✦
✦
✦
Figure 3: a
✦
Normally, minute volume should increase with increasing workload. VE should reach >80% predicted. Failure to do so implies ventilatory limitation e.g. COPD.
A low oxygen pulse or early plateau can indicate cardiac disease
Of note, in figure 3 resting VCO2 is actually greater than VO2 and this is likely due to a degree of anticipatory hyperventilation before exercise.
A shallow VO2 rise usually points to a cardiovascular abnormality.
Normally, VO2/HR increases with exercise, but the gradient may start to flatten off towards peak exercise as any increase in cardiac output is due to increasing HR and not stroke volume.
✦
The gradient of this curve should be <35. A shallow curve may be seen in CO2 retention.
✦
Plot 5 – VCO2 (and HR) vs VO2 This is the primary plot that is used to determine the AT. VCO 2 should steadily increase with increasing exercise until the AT is reached. After which VCO2 abruptly increases, as a way of compensating for the metabolic acidosis that ensues due to the increase in lactic acid production associated with increased anaerobic metabolism.
✦
✦
Plot 3 – VO2 and VCO2 vs time
✦
The AT is the VO2 at the inflection point on the VCO2 curve at which the gradient steepens. This is normally >40% of the predicted peak VO2 Failure of AT to exceed 40% implies cardiovascular abnormality (e.g. low cardiac output, anaemia, peripheral vascular disease, etc).
Normally, there is a fairly linear relationship between minute ventilation and VCO2 which represents efficient CO2 clearance.
Whereas, a steep curve (i.e. high minute ventilation with low VCO2) implies poor ventilatory function with an inability to clear CO2 - which is either pulmonary in origin (from increased in dead space / tidal volume ratio) or cardiac in origin (seen with a low PaCO2, in which there is a low ‘driving pressure’ to remove CO2 from alveolar gas – i.e. cardiac failure is unable to maintain an adequate diffusion gradient for CO2).
✦
✦
✦
Difficult Airway Society E-Zine September 2022 Contents 32 ✦
✦
An abrupt flattening of VO2 slope can suggest the onset of cardiac ischaemia and needs to be correlated with the exercise ECG.
✦
✦
Under normal circumstance, VO2 is greater than VCO2 at rest, and remains so during exercise until the anaerobic threshold (AT) is reached. Peak VO2 should be >80% predicted (<80% suggests reduced exercise capacity).
✦
✦
✦
✦
✦
✦
A curve with a gradient >36 indicates ineffi cient ventilation and has been shown to be a good predictor of morbidity and mortality.
Plot 4 – VE vs VCO2
✦
Sometimes this curve has work rate superimposed, this can be useful as a means of seeing how VO2 varies in the face of increasing exercise. VO2 should rise in a linear fashion, in-line with work rate slope.
The two curves are essentially mirror images of each other.
The VEVO 2 plot can be used as an additional means of cross-checking the accuracy of the AT from plot 5.
✦
Plot 7 – VT vs VE
Plot 8 – RER vs time
VEVO2 begins to rise at the AT, because VO2 cannot rise further.
✦
✦
Plot 9 – PETO2 and PETCO2 (with RR and SpO2) vs time This plot shows how the end-tidal partial pressures of oxygen and carbon dioxide change time during exercise.
A failure of RER to rise above 1.0 implies the failure or inability to mount a lactic acidosis.
The respiratory exchange ratio (RER) is the ratio of VCO2 to VO2 Normally, VCO2 is slightly less than VO2 at rest and resting RER is <1.0 As exercise progresses both VCO2 and VO2 increase, and beyond the AT RER must be >1.0 due to the increase in VCO2.
✦
✦
✦
Difficult Airway Society E-Zine September 2022 Contents 33
Ventilatory equivalents are unitless values that are used to express the efficiency of the lungs in terms of volume of ventilation required to either consume or eliminate a volume of gas (oxygen and carbon dioxide respectively).
✦
At rest lung apices are better ventilated than perfused. As exercise increases, apical pulmonary vessels are recruited and as such their V/Q ratios improve. The result is a gradual fall in VEVCO 2 and VEVO 2 showing improving V/Q matching.
✦
Of note in figure 3 the resting RER is >1.0 –this is likely due to anticipatory hyperventilation – if we correlate this with RR shown on plot 9, we can see a resting RR of 18-20.
✦
Plot 6 – VEVCO2 and VEVO2 vs time
✦
✦
✦
After the AT, lactic acidosis is initially buffered by HCO3- - this is known as isocapnic buffering, as VEVCO2 is largely unchanged. However, at some point ventilation must increase to eliminate CO2 as a means of dealing with the metabolic acidosis, because the buffering capacity of blood has been exhausted – this is the respiratory compensation point (RCP) –which can be very subtle on this plot.
Usually, at lower intensity exercise, minute ventilation increases primarily due to increasing tidal volume, rather than respiratory rate. As intensity increases, a point arrives at which tidal volume cannot increase any further (lung units are maximally recruited), hence any increase in minute ventilation is due to increasing respiratory rate – the result is a ‘dogleg’ curve.
PETO 2 should fall as more oxygen is extracted from air, until the AT after which end-tidal O2 increases because ventilation
✦
Additionally, the nadir of both VEVO2 and VEVCO2 represents the point at which the lungs are most efficient. If the lowest value for VEVCO2 is >30 it implies poor gas exchange (e.g. pulmonary vascular disease) or ineffi cient ventilation (e.g. COPD).
A shallow curve implies obstructive disease.
✦
✦
✦
Difficult Airway Society E-Zine September 2022 Contents 34 increases without an additional increase in VO2 ✦ PETCO 2 however, gradually rises with exercise due to increased production. After the RCP, ventilation increases to compensate for acidaemia and end-tidal CO2 begins to fall. ✦ This plot can also be used to correlate AT, which occurs at the nadir of PETO2 and highest PETCO2.
CPET is a fascinating topic and an area within anaesthesia / perioperative medicine, in which anaesthetists can indulge in watching physiology change in real-time (without the need of a syringe of propofol or a surgeon’s knife), can aid in the appropriate allocation of healthcare resources and can help patients to make informed decisions about their care. I hope you’ve found this helpful and if you’d like more information, please feel free to email me (thomas.lawson@wales.nhs.uk) or tweet me (@vapourologist). to references
Link
Preoperative assessment of frailty in surgical cancer
Deliveringpatients:
Frailty Assessment Frailty is de fi ned as a progressive, multidomain deterioration in functional reserve
The treatment of most head and neck malignancies includes a combination of major/complex surgery and/or chemo/ radiotherapy. These interventions are effective in achieving cure with 19 - 59% 10year survival but can be difficult to tolerate for older patients.1 Surgical management of head and neck cancer can be particularly problematic, as there is permanent alteration of the anatomy and physiology of essential structures and function including airway and eating and those crucial to maintaining quality of life including communication. This can mean that patients need to manage tracheostomies, speaking valves, feeding tubes and pumps and may have to re-learn skills such as speaking. These issues can generate interesting dilemmas which can be more complex in the context of old age, frailty and multimorbidity, as demonstrated in this case presentation. Case presentation
An 87 year old male patient was referred to the Perioperative medicine for Older People undergoing Surgery (POPS) preoperative clinic in preparation for hemiglossectomy with neck dissection and free flap for a T3N0M0 tongue squamous cell carcinoma. The tumour was sizeable (4 cm), located at the right side of the tongue causing problems with breathing (patient had to sleep sitting up and had suffered incidents of saliva aspiration) and swallowing (he had lost a significant amount of weight). Both of these symptoms had led to significant functional Indeconditioning.termsofco-morbidities, he had well controlled hypertension on Bendro fl umethiazide and had stopped smoking more than 20 years previously. From a social perspective, he lived alone with no relatives in the United Kingdom and although he had some older friends they were unable to provide support. He remained independent in personal care and was able to manage his affairs but had reported recent subtle deterioration in day-to-day function.
Difficult Airway Society E-Zine September 2022 Contents 35
Perioperative medicine for Older People undergoing Surgery (POPS) care for a patient with head and neck cancer. Introduction It is well known that the incidence of most malignancies increases with age. This is also true for head and neck cancer (which is the 8th most common cancer in the UK with) 22% of all new head and neck malignancy diagnoses presenting in people aged 75 years and over.1
PERIOPERATIVE MEDICINE: FRAILTY | Anthi Andrianou | Jugdeep Dhesi |


Difficult Airway Society E-Zine September 2022 Contents 36 which increases vulnerability to even minor external stressors resulting in adverse outcomes (mortality, prolonged hospital stay, loss of independence, increased costs of care etc).2,3 Frailty needs to be considered by all healthcare professionals as it can affect decision making at every step of the perioperative pathway.
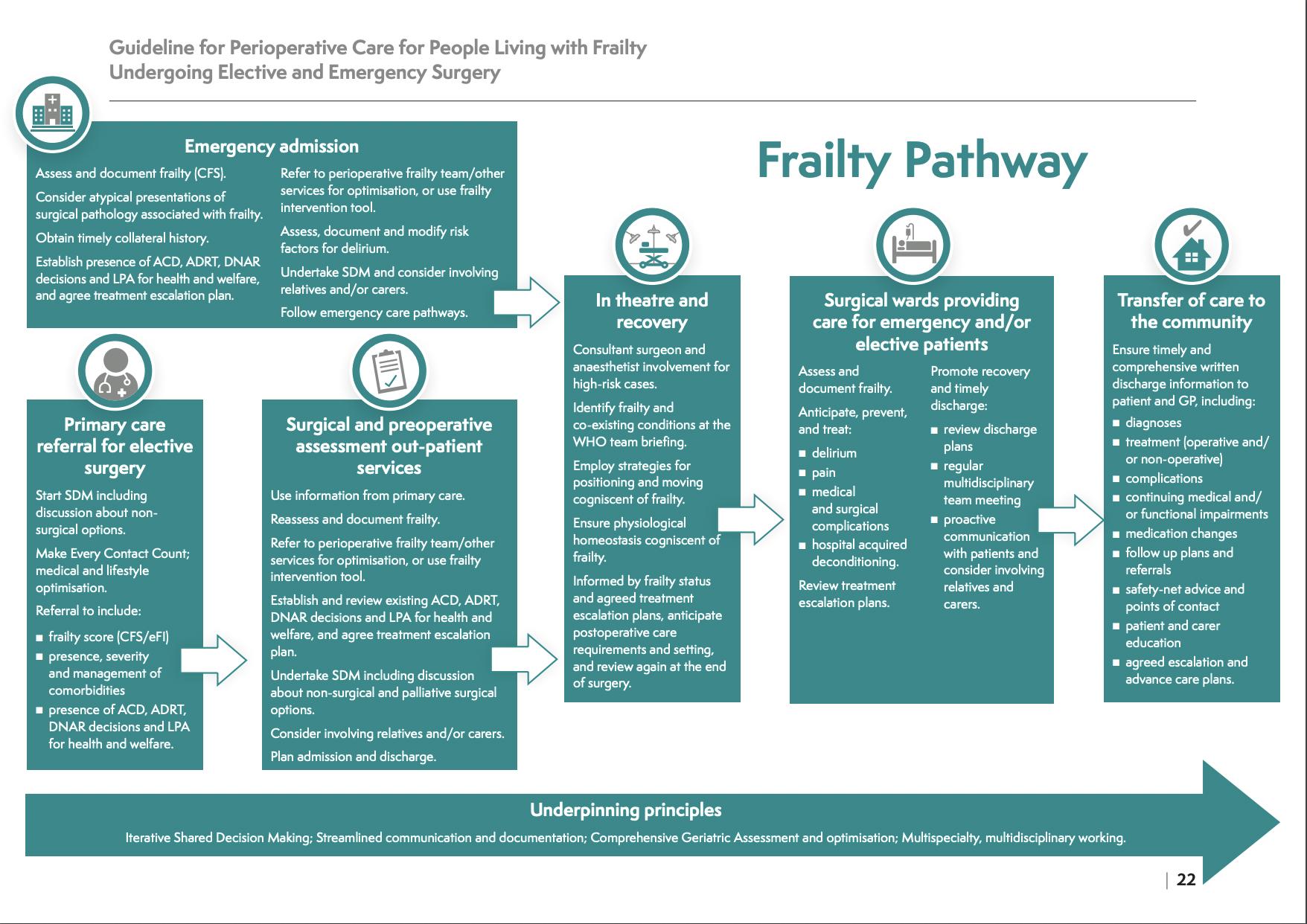
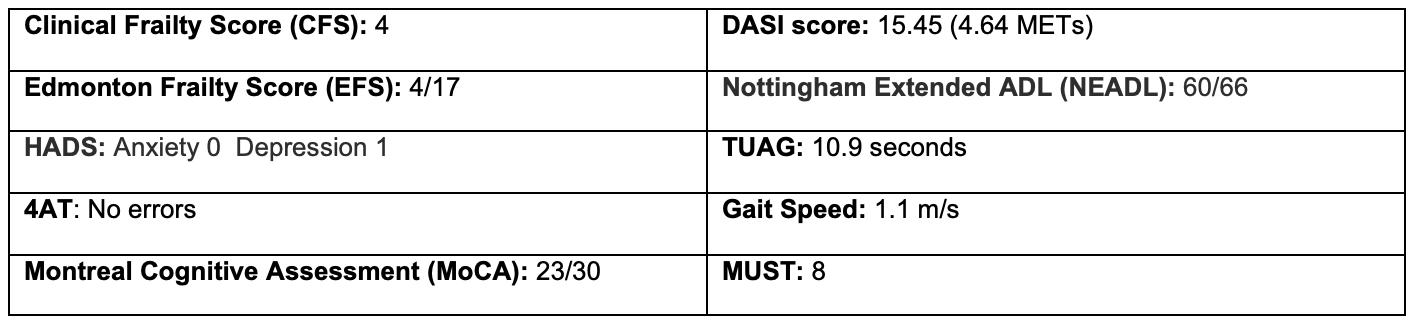
Frailty Scores Clinical Frailty Score (CFS): Expressed as Scale 1 – 9 (1 – very fit, 9 – terminally ill) and accompanied by a visual aid, (Rockwood et al., 2005). Clinical Frailty is defined as CFS > 4 and is associated with higher risk of Fig 1. Guideline for Perioperative Care for People Living with Frailty Undergoing Elective and Emergency Surgery. Joint guideline Centre for peri-operative care/British Geriatrics Society, 2021.
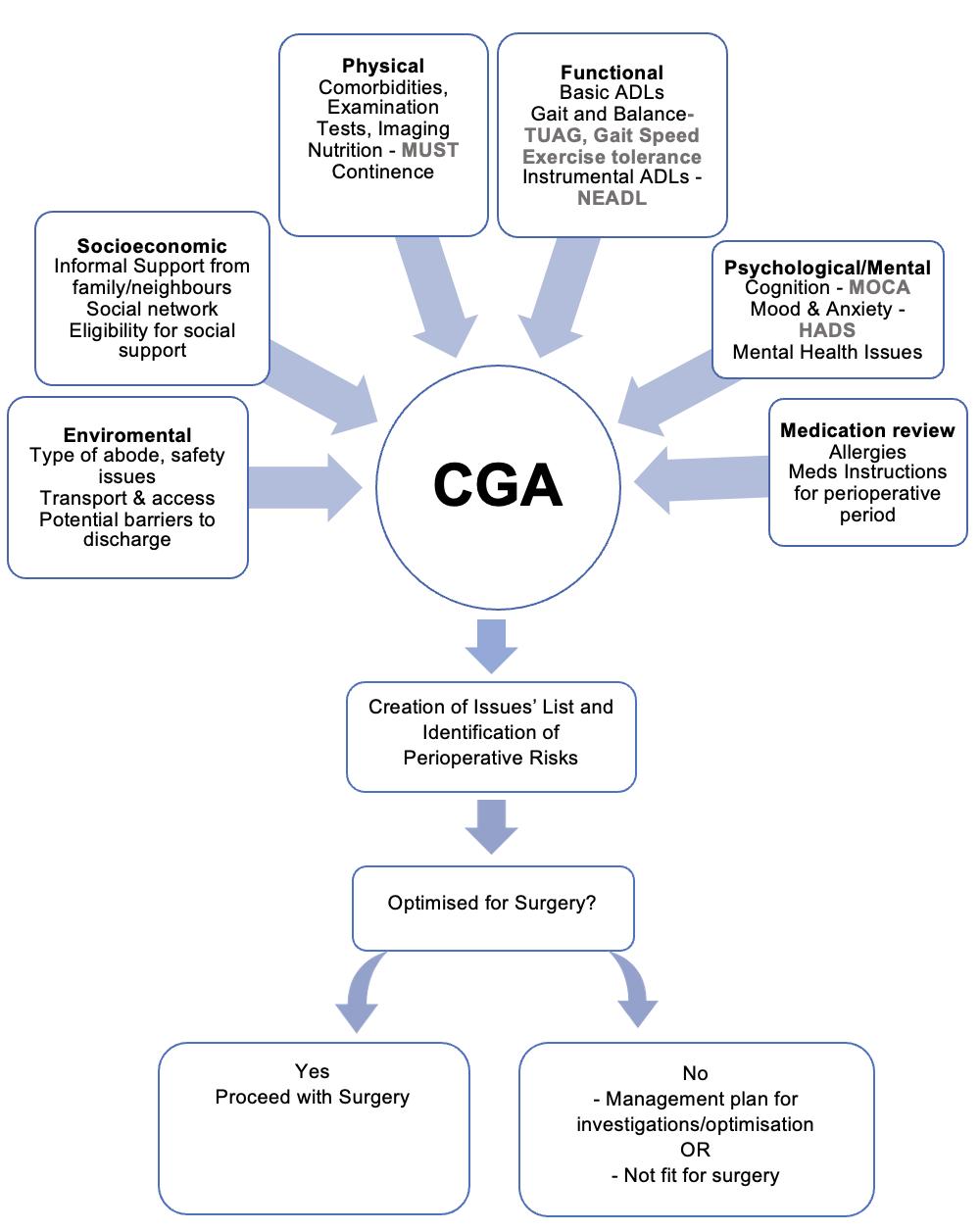
In 2021, the Centre for Perioperative Care (CPOC) and British Geriatrics Society (BGS) published guidelines on perioperative care for people living with frailty undergoing elective and emergency surgery.4 Applying the recommendations of the guideline in this case, the patient underwent preoperative Comprehensive Geriatric Assessment and optimisation (CGA). CGA is the underpinning methodology in geriatric medicine and is the gold standard for assessing frailty. It is a multidimensional and ideally multidisciplinary tool, through which the following components are assessed and optimised.5 CGA Scores and Interpretation This list is not exhaustive, but provides a flavour of frequently tools and scores used in CGA based services.
Difficult Airway Society E-Zine September 2022 Contents 37 Fig 2. Comprehensive Geriatric Assessment and various Frailty Scores
Difficult Airway Society E-Zine September 2022 Contents 38
Activity of Daily Living Index (NEADL): expressed as a scale of 0 –66, this self-administered questionnaire provides an extended ADL score that is correlated with more complex measures of disability. It assesses 21 activities in four categories: mobility, kitchen activities, domestic and leisure activities.33,34,35 Time Up And Go (TUAG): a timed test used to assess mobility, balance and gait. Patients are instructed to raise from a chair, walk 3 meters, turn and return to the chair. Patients with TUAG of greater than 20 seconds are at increased risk of falls.36,37
Gait Speed: Timed test where an individual is timed walking 4m. Gait speed less than 0.8m/ sec is associated with adverse postoperative outcomes (morbidity, mortality, institutionalisation).38,39,40
Mood/Anxiety: Hospital Anxiety and Depression Scale (HADS): Expressed as scale 0 – 21 for each component, was developed in 1983 to identify anxiety and depression among patients in nonpsychiatric hospitals. This scale excludes physical symptoms of anxiety and depression which can overlap with physical illness. High HADS scores have been associated with higher risk of postoperative delirium and increased mortality and major morbidity in some surgical populations.15,16,17,18 Cognition: 4As Test (Arousal, Attention, Abbreviated Mental Test – 4, Acute change): Screening tool for the detection of delirium, designed for routine Montrealuse.19,20,21,22,23Cognitive Assessment (MoCA): Expressed as a scale of 0 – 30, is a brief screening tool with high sensitivity and speci fi city for detecting mild cognitive impairment. Scores below 24 are considered abnormal.24,25,26,27
postoperative complications.6,7,8,9,10 Edmonton Frailty Score (EFS): Expressed as Scale 0 – 17 , this is a multidimensional, performance based frailty assessment tool, designed to be used by non-geriatricians in a variety of settings (outpatients’ clinics, at the bedside etc). EFS>6 is associated with higher risk of postoperative complications in a heterogenous vascular surgical population.11,12,13,14
Fig 3. Case scores for this patient
Functional status: Duke Activity Status Index (DASI): Expressed as a scale of 0 – 58.2, this self-administered questionnaire examines 12 types of physical activity and correlates well with oxygen uptake and therefore Metabolic Equivalents Nottingham(METs).28,29,30,31,32Extended
✦
✦
✦
Shared decision making: The case was discussed the same day with the surgical team, above concerns were considered and the patient was scheduled to be admitted in the hospital that same week to monitor the airway and start enteral nutrition via NJT. Admission and discharge: successful operation, admitted to intensive care for 48 hours for monitoring mainly of airway and respiratory function, but he did not require any organ support. Eventually discharged back to his own house with carers’ support, dietitian, speech and language, and physiotherapy input in the community.
Nutrition Malnutrition: Universal Screening Tool (MUST): is a screening tool used to identify adults who are malnourished, at risk of malnutrition or obese. A score > 2 signifies high risk of malnutrition.41,42
New diagnosis of COPD: increased risk of postoperative pulmonary complications. Started on LAMA/LABA according to national guidelines, advice on nebulised therapy to be used post procedure; taught respiratory exercises by physiotherapist.
✦
Lack of social support: with increased risk of delayed discharge from hospital. Proactive occupational therapy involvement to facilitate effective timely discharge.
Conclusion As shown, the CGA provided all involved professionals with a list of issues that could be optimised, monitored, or anticipated during the perioperative period, in order to avoid complications, increased length of stay or barriers to discharge. Moreover, this detailed assessment gave the patient the opportunity to understand better and in depth the implications of a major operation like this and the special demands of having to manage a variety of equipment and learn new skills. His admission date was expedited, he had a successful operation, and he was discharged to his own house with support, eventually returning to previous baseline in approximately four months.
✦
Normocytic anaemia: deplete in vitamin B12 folate and iron. Coeliac screen negative and attributed to poor nutrition. Optimised using intramuscular vitamin B12, oral folate and intravenous iron.
Link to references
Mild cognitive impairment: with implications regarding capacity to consent and ability to manage post-operative devices and equipment. Risk of delirium reduced through optimisation of mild hyponatraemia by stopping Bendroflumethiazide and introducing Amlodipine. Delirium pathway used and shared with patient and ward team.
Difficult Airway Society E-Zine September 2022 Contents 39
Malnutrition: Hospital dietitian involved, provided supplements and an NJT insertion was organised.
Case Discussion: Assessment and optimisation Following Comprehensive Geriatric Assessment, the major issues were identified.
Difficult Airway Society E-Zine September 2022 Contents 40 Further Learning Course: Perioperative Care of Older People Undergoing Surgery | British Geriatrics Society (bgs.org.uk) –E learning Podcasts: Anaesthesia 2018 podcast | geriatric care and the value of teamwork | The Royal College of Anaesthetists (rcoa.ac.uk) – Prof Weller and Prof Dhesi - 2018 TopMedTalk - Perioperative Frailty with Jude Partridge | EBPOM 2020 London (google.com) Podcast: Frailty | The Faculty of Intensive Care Medicine (ficm.ac.uk) – Frailty and Critical Care Episode 1.1 – Comprehensive Geriatric Assessment – The Hearing Aid Podcasts Episode 1.2 Delirium – The Hearing Aid Podcasts Episode 2.1 Frailty – The Hearing Aid Podcasts Episode 3.08: Peri-operative care – The Hearing Aid Podcasts Episode 7.02 ‘Silver’ Trauma – The Hearing Aid Podcasts


Difficult Airway Society E-Zine Contents 42
✦
submit.MASTERCLASS WITH DAS:
✦ Be
✦
✦
✦
✦
✦
Difficult Airway Society E-Zine September 2022 Contents 43
Kariem El-Boghdadly, our Scientific Officer at DAS, kicked things off with a talk on 'How to Write a Good Abstract'. His key principles to abide by: Know your audience – review the author guidelines carefully and follow them. Pitch your work for your reviewers and readers. concise – less is more. it simple – simplicity is key to making sure your message is clear and absorbed by the audience. selective – think about what you are delivering so your message isn’t lost in a sea of information and do not overreach in your conclusions. check – wrong spelling can undermine your work, run through a spell check before you
Abstracts for the DAS conference will be judged usually by 3 different people and all are scored independently. There is a quality assurance process to make sure the marks are consistent. For those abstracts which score particularly highly, 15 –20 are reviewed to select the oral presentations. This takes a huge amount of time, and I would like to give a personal thank you to all involved in the process.
✦ Keep
✦ Spell
ABSTRACTS|NatalieSilvey|AlistairMcNarry,Joint DAS and RCoA Lead for Airway Leads and a veteran of abstract judging then took us through an enlightening look at what happens when you press submit on your abstract and the judging process. His top tips around the submission process: Check you have followed the instructions Make sure you have carefully typed in your email address so you receive any correspondence. If you have any questions ask before you submit. For DAS 2022 submissions – check you get a con fi rmation email: everyone who successfully submits an abstract will get one. Make sure you have clear consent, clear results and check your punctuation.
Submitting an abstract to a conference can be a daunting process but it is a great way of highlighting the amazing work you are doing, and also valuable points for applications and the all important evidence for sign off of curriculum competencies.
May saw the first of our planned webinar series, Masterclass with DAS, and we kicked off with a really insightful session on Abstracts.
✦ Be
✦
The webinar received excellent feedback, and a huge thanks to Helen Aoife Illiff for managing everything behind the scenes and Rebecca Davenport, Specialities Societies Manager, for her invaluable support.
Please watch out for the announcement of our next Masterclass with DAS as well as other webinars and events from DAS education. Let us know what topics you wish to learn about in the future! Tweet us @dastrainees @dasairway or email us at trainee@das.uk.com
Difficult Airway Society E-Zine September 2022 Contents 44
Our very own DAS education lead Gunjeet Dua and immediate past president of DAS Barry McGuire, gave their insights on what makes a great abstract, poster and oral presentation. In short – sell yourself and your work. This is your opportunity to show what fantastic work you have been doing and it a part of the conference we really value because it is an opportunity for us to learn from each other.
Some key pearls of wisdom: Originality is a benefit so think about your project in advance before you even start. Put your mind in that of the audience so you don’t lose your audience when presenting your project. Try to present locally first, this gives you an opportunity to practice and refine your Wepresentation.finishedwith a panel discussion which included Sharim Khan, the abstract lead for DAS 2022. One thing our panel all agreed on whether you are submitting an abstract, producing your poster or giving an oral presentation, focus on your one clear message from your work and focus on the impact of this. A piece of key information was given by Kariem El-Bogdadly - if you submit something as an abstract you can then submit it for publication in a journal as long as you declare that the work has been presented before and give details of this. You cannot do it the other way around, i.e. you cannot have data published and then submit an abstract of the same work. The abstract submission for DAS 2022 is now closed and the judging process is ongoing. We are looking forward to our first in-person meeting since 2019 and I particularly will be looking out for the posters and oral presentations to see the incredible work that will be presented at the conference.
✦
✦
Difficult Airway Society E-Zine September 2022 Contents 45 MORE ANNOUNCEMENTSPROGRAMMECOMING SOON! DAS WEBINARS 2022 | Gunjeet Dua | #LearnTogether @dastrainees #DASeducation For all members of the multidisciplinary team Members will be emailed details of upcoming webinars including registration details from the DAS Secretariat. Please ensure your email address is up to date so as not to miss information on events.


Difficult Airway Society E-Zine September 2022 Contents 46 This year, the standard of entries to the DAS trainee competition has been incredibly high. This year's title was 'Airway Training of Dreams', and we invited trainees to interpret that however they wished — in whatever media they wished. For the first time in 2022, we had two categories to enter: creative writing, and creative media. 1st Prize Creative Writing: Dr Asya Veloso Costa 1st Prize Creative Media: Dr Helena Jennison However, the standard of submissions was so high the judges ended up awarding 3 extra prizes for: 1. Best podcast - Dr Eoin Dore and Dr Duncan Brouwer-Kemp 2. Best video - Dr Jo Lau 3. Best photography - Dr Hannah Leaman We, as fellow trainees, are extremely proud to present their work here in the eZine. Enjoy! DAS TRAINEEWINNERSCOMPETITION2022 | Congratulations to everyone who entered! |
Simulation is well-established within medical education as it allows the same opportunity to learn by doing without harming patients. It is a powerful tool which is proven to advance educational goals via experiential learning.4 Simulation is also incredibly well-received by anaesthetic trainees, with 90% of trainees supporting its use.5 The Royal College of Anaesthetists (RCOA) Simulation strategy calls for an increasing role of simulation in training, with a view to integrate simulation where possible into the new 2020 curriculum.6
“For the things we have to learn before we can do them, we learn by doing them.”
The RCOA hopes to eventually introduce a system where minimum standards for essential clinical skills including failed intubation drill and front-of-neck access (FONA) should be demonstrated using simulation-based resources. This could occur prior to first performance of the skill or as part of continuing assessment and development in
Difficult Airway Society E-Zine September 2022 Contents 47
Classically,Aristotle2 airway training was acquired “on the job”, within an apprenticeship model of learning. For an incredibly practical discipline, learning by doing is fundamental, and having OF DREAMS
Asya Veloso Costa | exposure to clinical cases allows doctors to develop their own judgement. However, this model results in significant variability based on the skill and engagement of the supervising anaesthetist. Case mix, and time pressures in theatre also have a role to play, resulting in dissimilar learning experiences between trainees.3 There is also concern that with the increasing use of supra-glottic airway devices (SADs), trainees are having fewer opportunities to strengthen core airway skills such as mask ventilation and intubation.
|
Airway training shouldn’t be difficult. Yet numerous trainees feel inadequately experienced in what is arguably one of the most fundamental areas of anaesthesia. Airway emergencies have the potential to have foundNationalinjuryconsequencescatastrophicsuchasbrainanddeath.ThefourthAuditProject(NAP4)thateducationandtraining was a causal or contributory factor in approximately half of the adverse airway events studied.1 Their findings recommended airway training for both trainees and trained anaesthetists. So how do we maximize training opportunities when these difficult airway events are rare, and when we cannot guarantee uniform experience across the board? Ultimately, it comes down to repeated exposure and familiarity with the equipment and human factors in emergency situations, which can be achieved via simulation. Additionally, empowering trainees and trainers to make the most of the opportunities that do arise and creating a positive learning culture is crucial.
1ST PRIZE CREATIVE WRITING AIRWAY TRAINING

The argument against simulation is that it is just not the real thing. Simulators have been progressively increasing in fidelity, and these come at a price. However, simulation has the potential to be incredibly cost-effective if aimed intelligently,4 and it can integrate equipment, procedures, guidelines, and human factors into one learning experience.
The ideal airway training would use all these factors in a cohesive and safe experiential learning environment at regular intervals in structured courses. Currently, airway workshops and courses run by major organisations such as DAS are available, but for limited numbers, and local training is encouraged. Despite this, a recent national survey found that 16% of hospitals did not offer any airway training workshops. Of those that did, over half were run less frequently than annually. 12 Ultimately, repetition is the key to mastering any expert technique, and skills that are not used will decline.13 This again makes a case for having regular simulations throughout training.
“The only real mistake is the one from which we learn nothing” Henry SimulationFord2is bene fi cial not only at the individual level, but to enhance team-based working. Human factors are recognised as vital contributors to any emergency scenario and expecting trainees to manage difficult airways without factoring this in is unrealistic. These simulation workshops would ideally be multidisciplinary and encourage discussion on human factors in debrief. They should involve trainees, operating department practitioners (ODPs) & anaesthetic nurses. Debrief with
Difficult Airway Society E-Zine September 2022 Contents 48 different stages of training. This would not only improve patient safety but provide a set provision of airway opportunities nationally. Technology is becoming increasingly advanced, and we are seeing this reflected in the equipment available for anaesthesia in the last few decades. Videolaryngoscopes, which are becoming increasingly prevalent, are recommended by the Difficult Airway Society (DAS) as part of their difficult airway algorithm but can also be powerful teaching tools.7
There is evidence to show that novice anaesthetists who were taught using videolaryngoscopy had more rapid acquisition of intubation skills.8 Recording of intubations can also be used for structured feedback.9 New devices and techniques are becoming increasingly available, but has training kept up with this pace? NAP 4 highlighted several cases where awake fibre-optic intubation, now commonly referred to as awake tracheal intubation (ATI), was not used where it was indicated despite being the gold-standard technique in diffi cult airways. This may potentially be down to inexperience because of lack of opportunity and resulting reluctance to use an unfamiliar technique. Simulation would provide opportunities for trainees to work on this core skill. We are also seeing the emergence and renewing of increasing numbers of national guidelines, such as the DAS guidelines for ATI and for unanticipated difficult intubation in adults.7,10 These provide widespread access to best-practice and useful cognitive aids, which have the power to improve technical performance and decision making in anaesthesia. 11 Guidelines also promote consistency in training, and these can be reinforced in simulation.
Learning is an experience, one that should be stress-free and enjoyable. Learning therefore occurs best in a system which looks after doctors. A work satisfaction survey of anaesthetic trainees in 2019 found that roughly one fi fth of trainees had high depression risk. Prevalence of perceived stress (37%) and burnout risk (25%) were even higher and these often co-existed.15
Wellbeing is a buzzword that comes up time and time again, and it is important we take a holistic view of training. Doctors can be empowered to be better and take control of their training if they are treated better. Looking after staff wellbeing is not only a moral responsibility but has a significant impact on performance and productivity in organisations.16 This is important not only at an organizational level but also at a more personal one. Educational supervisors should regularly check in with trainees to reflect on challenging cases where there are lessons to be Whatlearnt.constitutes the ideal airway training? My experience is one that I will not forget – it has encouraged me to write this essay, take control of my training and sign up to an airway course. Key ingredients include a motivated trainee, a passionate trainer, maximization of a clinical case where there is learning opportunity available, and targeted training based on level and experience. Regular simulation focusing on equipment, guidelines and human factors is essential to ensure core skills are maintained. Airway training shouldn’t be difficult, and when done right it can really feel like a dream.
Link to references
Being able to observe the registrar performing a fibre-optic intubation was also beneficial for me at my level of training. There was effective communication within the anaesthetic team, with the surgical team, and the atmosphere was an incredibly positive one. I went home that day feeling exhilarated, but this isn’t a common feeling in the current climate.
“Study without desire spoils the memory, and it retains nothing that it takes in” Leonardo Da Vinci2
Difficult Airway Society E-Zine September 2022 Contents 49 self-re fl ection and observer feedback promotes learning in this environment.14 So, this brings me on to reflect on one of my own experiences as a core trainee. I recently had a fantastic training experience during an airway list in a large tertiary centre. I was asked to assess an elderly patient with severe neck fi brosis secondary to previous radiotherapy following an oral squamous cell carcinoma excision. This was an airway like none I had seen before. After my assessment, I presented my findings to the consultant, who then proceeded to give me structured feedback and describe their strategy for assessing such an airway. We agreed the safest plan for this patient would be an awake tracheal intubation. The consultant identified one of the senior registrars who required airway experience and asked them to join us to perform the awake intubation whilst I topicalised the airway. What was striking was the different levels of training that were occurring in tandem during this case. I had performed an airway assessment, obtained useful feedback, and learnt about topicalisation using the DAS ATI guidelines, whilst the consultant actively identified a great learning opportunity for one of the registrars to perform a procedure.
Difficult Airway Society E-Zine September 2022 Contents 50 1ST PRIZE CREATIVE MEDIA AIRWAY TRAINING OF DREAMS | Helena Jennison |


Difficult Airway Society E-Zine September 2022 Contents 51 TRAINEE COMPETITION|Extraprizes| The judges were so impressed with the standard of entries, particularly in the creative media category, they have decided to award 3 additional prizes Best podcast - Dr Eoin Dore and Dr Duncan Brouwer-Kemp https://t.co/Q3F0B566GS Best video - Dr Joanna Lau Best photographyDr Hannah Leaman





Difficult Airway Society E-Zine September 2022 Contents 52 JOURNAL CLUB | Recommended Reads | Welcome to the DAS Journal Club - Recommended Reads. Papers are chosen by members of the DAS committee, with short citations/summaries by members of the ezine editorial team. This edition's recommended reads come from Kariem El-Boghdadly with summaries by Natalie Silvey. We welcome members feedback and thoughts on the papers featured - please tweet us @dastrainees or @dasairway or email us at ezine@das.uk.com Effect of Non-Invasive Respiratory Strategies on Intubation or Mortality Among Patients With Acute Hypoxemic Respiratory Failure and COVID-19: The RECOVERY-RS Randomised Clinical Trial. ✦ Perkins GD, Ji C, Connolly BA et al. Effect of Non-Invasive Respiratory Strategies on Intubation or Mortality Among Patients With Acute Hypoxemic Respiratory Failure and COVID-19: The RECOVERY-RS Randomised Clinical Trial. JAMA. 2022; 327(6): 546-558 doi:10.1001/ jama.2022.0028 PMID: 35072713; PMCID: PMC8787685. Think back to the early days of the COVID-19 pandemic, the scramble to find out information, webinars with colleagues treating patients to glean treatment strategies, the uncertainty of what we were facing. Luckily we are now in a much better place, in no small part thanks to some incredible pieces of research that gave us treatment options and of course, the amazing speed at which safe and effective vaccines were produced and rolled out. But...what about our management of acute hypoxic respiratory failure in patients with COVID-19.
Theefficacy.RECOVERY-RS trial is a randomised, prospective, multi-centre trial conducted at 75 hospitals across the UK and was designed to determine whether either CPAP or HFNO, compared with conventional oxygen therapy, improves clinical outcomes in hospitalised patients with COVID-19 related acute hypoxaemic respiratory failure.
There has been increasing and widespread use of continuous positive airway pressure (CPAP) and high-flow nasal oxygenation (HFNO), but there have been conflicting results regarding their
The authors conclusion - “our study did not demonstrate a significant difference in efficacy between the McGrath X-blade and the CMAC video laryngoscope”. But is that the full story? Delve into this paper and have a look at the exclusion criteria - does this reflect the type of patients we see when confronted with a patient requiring cervical spine immobilisation?
Interestingly the study was underpowered to detect a difference between the two blade types, this is a perfect opportunity in a journal club to refresh our knowledge on power calculations and why these matter when designing a study.
This two centre randomised control trial compared blades from two brands of video laryngoscopes, the hyperangulated McGrath X-blade and the Macintosh-type CMAC blade in patients undergoing anaesthesia who had manual inline stabilisation undertaken with the primary outcome measure being first-attempt tracheal intubation success.
The conclusion - “among patients with acute hypoxaemic respiratory failure due to COVID-19 an initial strategy of CPAP significantly reduced the risk of tracheal intubation or mortality compared with conventional oxygen therapy, but there was no significant difference between an initial strategy of HFNO compared with conventional oxygen therapy.”
So does this study change your practice? Will you no longer use HFNO in this patient group, instead reaching for the CPAP mask first? Or is it a bit more complicated than that? This is a brilliant paper with some very interesting points to lead a discussion with, for example the study did not meet its pre-planned sample size due to a fall in cases and recruitment ending.
Difficult Airway Society E-Zine September 2022 Contents 53
Whilst we all hope that the worst days of the pandemic are behind us, studies like this remind us of the incredible work done to date - rapidly improving the care our patients received and will receive thanks to studies such as this, RECOVERY and REMAP-CAP. That is truly something to be celebrated. Comparing the first-attempt tracheal intubation success of the hyperangulated McGrath® X-blade vs the Macintosh-type CMAC videolaryngoscope in patients with cervical immobilization: a twocentre randomised control trial.
✦ Zhang J, Tan LZ, Toh, H, Foo CW, Wijeratne S, Hu H and Seet E. Comparing the first-attempt tracheal intubation success of the hyperangulated McGrath® X-blade vs the Macintosh-type CMAC videolaryngoscope in patients with cervical immobilization: a two-centre randomised control trial. AJ Clin Monit Comput. 2022; 36 (4) : 1139 - 1145. doi: 10.1007/ s10877-021-00746-5 Epub 2021 Aug 4. PMID: 34347225. Patients with cervical spine precautions present a challenging airway even in the absence of other factors that increase the risk of a difficult airway. Whilst the debate around the use of manual in-line stabilisation during airway management in this patient group carries on, evaluation of different devices continues. What type of blade should we be reaching for when managing such patients, a hyperangulated blade or a MAC blade?
Difficult Airway Society E-Zine September 2022 Contents 54 AIRWAY MANAGEMENT IN MAJOR TRAUMA, AN AUSTRALIAN PERSPECTIVE | Peter Forrest | Christopher Groombridge | Simon Hendel | Pierre Bradley
Victoria is the second most populous state in Australia and geographically is a similar size landmass to the island of Great Britain. There has been an integrated State Trauma System in place since 2000.1 This system prioritises the early identification, treatment, and transfer of severely injured patients (Injury Severity Score (ISS) > 12) to one of three major trauma centres (2 adult and 1 paediatric). The system incorporates regional (Level-2) trauma centres, and a system for primary retrieval from point-of-injury to a major trauma centre, Fig 1: Structure of trauma services in Victoria, Australia.1




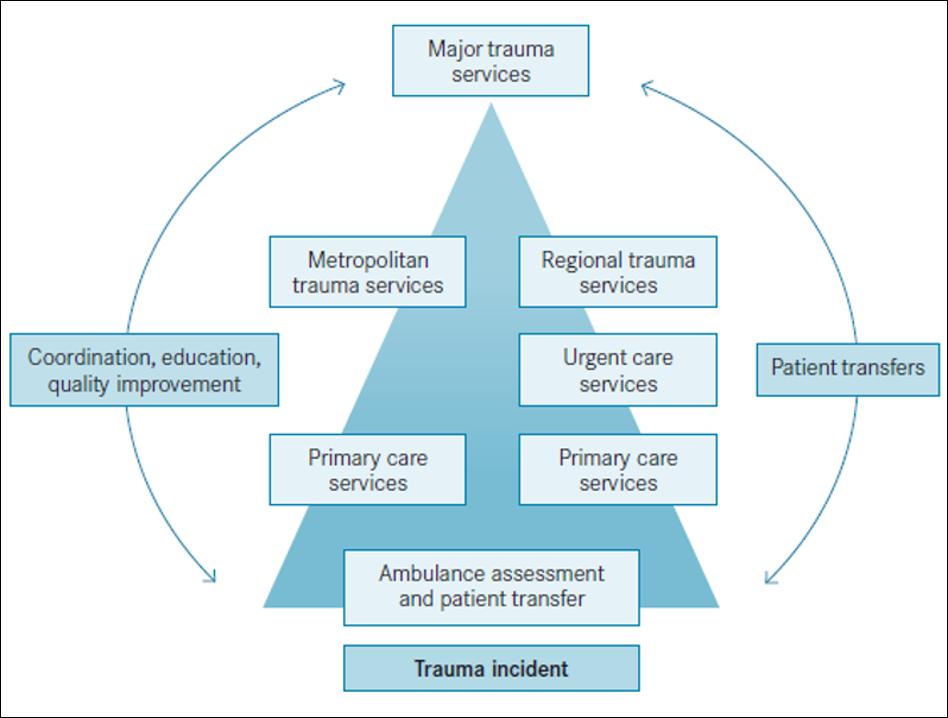
Difficult Airway Society E-Zine September 2022 Contents 55 and secondary retrieval from lower to higher levels of in-hospital care. This is a hub and spoke model of trauma retrieval which is appropriate to the geography and demography of Victoria. Comparable approaches are employed throughout Australia, to prioritise transfer to definitive
Victoria’s Helicopter Emergency Medical Service is staffed by MICA paramedics with advanced practice guidelines. Unlike much of the UK and other Australian states, there are no joint physician-paramedic prehospital teams. In-hospital airway management in major trauma patients
Thecare.2Alfred Hospital is one of the adult major trauma centres and state referral centre for major burns and Extra Corporeal Life Support. In 2021, the service had 9915 trauma admissions of which 14% had an ISS > 12.3 As with most jurisdictions outside the USA, blunt trauma represents greater than ninetyfi ve percent of trauma presentations in Victoria, with the majority occurring outside of metropolitan Melbourne.4 Airway management begins at the scene by paramedics of varying skillsets (community volunteers, quali fi ed ambulance paramedics, and mobile intensive care ambulance (MICA) paramedics).
The NAP4 study has highlighted the dangers of emergent airway management in the nontheatre environment, especially in the out of hours period.5 The Alfred has had a specialist anaesthetist on site 24-7 (known as the consultant in charge; CIC) for over 20 years and has moved towards a continuous specialist emergency physician presence since the advent of COVID-19. Trauma call alerts are received by the full trauma team, with anaesthesia medical provider Fig 2: Top 10 causes of Injury for all trauma admissions at The Alfred in 2021.3
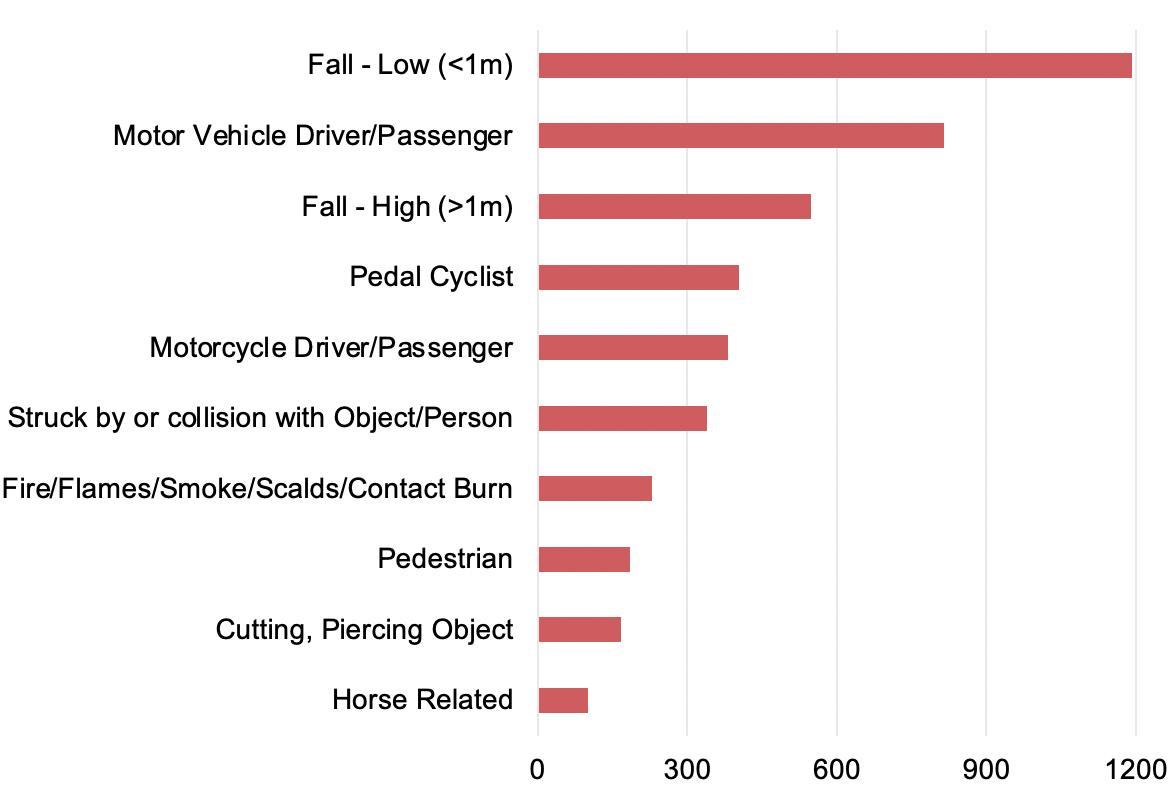
In the emergency department, the first attempt laryngoscopist is usually an emergency medicine trainee, under the supervision of a Specialist Emergency Physician or Specialist Anaesthetist. There is an established education program, associated protocols, and a tailored checklist for these patients, with videolaryngoscopy using Karl-Stortz C-MAC and a bougie being the preferred first-line technique.6 As far as possible, induction of anaesthesia is standardised (using pre-drawn syringes of ketamine, fentanyl and rocuronium). This has previously caused controversy between anaesthesia and the emergency department, but it is largely accepted as a safer combination of drugs in most patients allowing for a range of anaesthesia skills. The induction drug combination can be tailored to patient need and should be discussed within the team, ideally prior to patient arrival.6
Difficult Airway Society E-Zine September 2022 Contents 56 involvement 24-hours a day. Between 0730 and 2300, the CIC receives the alert and designates appropriate personnel to the trauma bay. Outside these times, the initial alert is received by anaesthesia registrars and response is escalated to the CIC as required. This system ensures early, senior anaesthesia presence for major trauma (and burns), and serves as an early warning for operating suite
2. The injured airway Complex maxillofacial and trachea-bronchial injury is rarely the primary indication for airway management. When it occurs, speci fi c attention to the airway assessment allows for a careful collaborative decision-making approach, ensuring safe airway management in the appropriate location with correct Developingstaff.9,10 an airway and oxygenation strategy is essential in managing trauma patients with these injuries. It is in this group that the use of video-laryngoscopy may prove difficult, with the presence of blood in the airway potentially impairing visualisation of the glottis. MacIntosh geometry video-
Airwayreadiness.management in trauma falls into 3 broad categories: non airway trauma, airway injury (including burns), and intubation to facilitate definitive care. Irrespective of reason, airway management is the primary responsibility of the CIC in conjunction with the trauma team leader. The role of primary laryngoscopist may be delegated to trainees depending on urgency, perceived complexity, staff experience, or other competing resuscitation priorities. The Alfred is a quaternary trauma teaching hospital, so ensuring safe, supervised opportunities for developing advanced airway skills in trainees is an important health-service role.
1. Emergent management of the nontraumatised airway Emergent endotracheal intubation for nonairway trauma in the emergency department is most commonly due to head injury.6 Drugaffected individuals are overrepresented in trauma presentations and within Victoria, 13% of individuals presenting to a major trauma centre tested positive for an illicit substance. Of these patients, 77% tested positive to methamphetamines – a reflection of Australia’s challenges in addressing methamphetamine use in the community. 7,8 Induction of anaesthesia and intubation to achieve situational control and facilitate on-going investigations (along with ensuring staff safety) is common.
Difficult Airway Society E-Zine September 2022 Contents
Human factors in airway management
The importance of human factors in airway management is not new and in the management of major trauma, clear communication is a key precondition for Table 1: Predictors of inhalation injury in Burns Patient.13
11
In patients requiring airway control for definitive care, there is time to plan, prepare, and then perform. While airway management for definitive care should be timely and made in the context of other treatment priorities, there is reduced time-pressure than in the emergency airway. In planning airway management for definitive care, anaesthetists should consider the surgical access required and whether the plan is suitable for ongoing intensive care, or whether a post-operative plan (e.g. tube exchange) may be required.
57
laryngoscopes, which also allow direct laryngoscopy (such as CMAC / Glidescope Direct view), are preferred. I-Gels (Intersurgical, UK) have recently been introduced as the supra-glottic airway of choice in the difficult airway trolley and are easily accessible across all locations where advanced airway management occurs.
Patients with significant airway burns fall into this category. Early identification of airway involvement and intubation is required to prevent a very difficult situation developing, however predicting inhalation injuries can be dif fi cult. A predictive model has been developed at The Alfred based on 1148 presentations over a 7-year period to the Victorian Adult Burns Service. Seven variables have been identified (Table 1), although it is yet to undergo prospective validation.13
As with all effectively executed plans, multidisciplinary communication is key to success.
3. Airway management for definitive care
Equipment is available for both needle and surgical cricothyroidotomy on the difficult airway trolley.12 However, in the non-fasted non-elective patient, surgical cricothyroidotomy is the rescue technique of choice, if a primary front of neck approach was not employed.
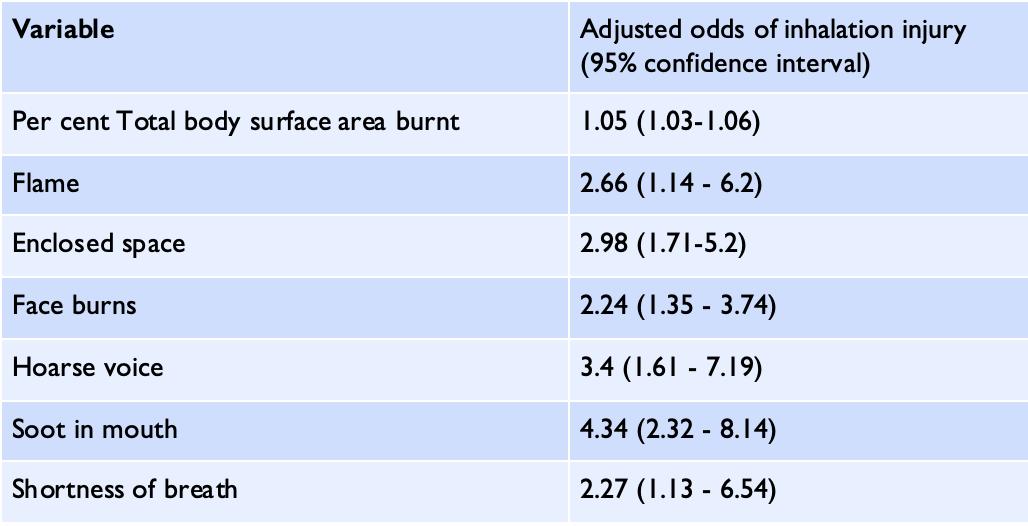
The establishment of an ongoing airway audit and teaching program in our emergency department has contributed to consistent high-quality care, especially with the rotation of anaesthesia and emergency registrars every 6 months. The introduction of the program found a significant improvement in first attempt success rate (95% vs 89%) without a change in adverse events.6 The Alfred has developed a trauma-anaesthesia clinical fellowship and is coordinated by the two specialist anaesthetists who are also employed as trauma consultants. The fellowship focuses on individual and collective trauma-team training, clinical exposure across the patient journey (from point of injury to hospital discharge), quality improvement, and clinical Opportunitiesresearch.exist
The trauma service at the Alfred is not run by the general surgical team of the day (as in many other centres). Instead, ‘trauma’ is its own multidisciplinary admitting unit and is staffed by specialist trauma consultants, junior medical staff, and crucially supported by expert nursing and allied health professionals. Trauma consultants are recruited from a range of specialties including surgery, emergency medicine, and anaesthesia (although intensive care specialists are eligible for recruitment, none are currently employed as trauma consultants). This team approach is invaluable in enabling smooth inter-disciplinary prioritization and decision-making. It also centralizes a breadth of expertise across surgery and critical care (in both military and civilian settings) under the one banner.
for senior trainees to spend six months of a twelve-month fellowship in the trauma service (as a trauma fellow alongside emergency medicine and surgery fellows). Alternatively, a full year in anaesthesia is also possible. Interested trainees can contact S.Hendel@Alfred.org.au for further information. Applications open in May each year, for employment from the following February. August commencement is available by mutual negotiation.
Professor Pierre Bradley, Adjunct Clinical Associate Professor, Monash University, Victoria; Anaesthesiologist, The Alfred, Melbourne, Australia Link to references
Difficult Airway Society E-Zine September 2022 Contents 58 success.
Conclusions Airway management in trauma can provide significant challenges to the trauma team, both in the decision to intubate and the complexity and timing of the intubation itself. Despite these challenges, a multi-disciplinary approach within a major trauma service can foster a proactive approach in safely managing severely injured patients while simultaneously providing training opportunities for trainees from multiple craftDrgroups.Peter Forrest, Anaesthesia Registrar, The Alfred, Melbourne, Australia Dr Christopher Groombridge, Emergency Medicine Physician and Trauma Consultant; Emergency Department Airway Lead, The DrAlfredSimon Hendel, Anaesthesiologist and Trauma Consultant; Head of Trauma Anaesthesia, The Alfred; Clinical Research Fellow, National Trauma Research Institute, AssociateAustralia.
NEW PATIENT INFORMATION FOR AWAKE TRACHEAL INTUBATION: JUNE 2022 | Kate Rivett |
procedure with reference to patient experience. Clear explanations are given for terms such as intubation and awake intubation, together with brief descriptions of fl exible bronchoscopes and video laryngoscopes and how their usage might differ. There is a constant message that the anaesthetist and the clinical team are available to offer advice and answer questions, in addition to their involvement in the technical aspects of the Whilstprocedure.signposting to the relevant section of the DAS website might be the preferred option for some patient groups, consideration should also be given to those members of the public who prefer to have a hard copy.
Provision of hard copy ensures that the patient does have the correct DAS version (rather than possibly accessing information from an internet source where clinical content is not necessarily accurate or approved).
Difficult Airway Society E-Zine September 2022 Contents 59
The aim of the new ATI patient guidance is to provide a brief explanation of the process, rationale, equipment and risks whilst providing a basic knowledge of the
DAS is currently investigating how it might be possible to offer a wider variety of language options.
DAS have updated their patient information for Awake Tracheal Intubation (ATI) for patients. The June 2022 version is now available here A recent patient panel lead by DAS highlighted that patients would generally prefer to have access to detailed information about anaesthetic or airway management topics well in advance of the day of surgery. If the need for ATI is identi fi ed at preassessment then this is the ideal time for the patient to be made aware of the extensive patient materials that are available. The ATI information helps patients to understand the nature of the procedure and how this might differ from previous anaesthetic experiences.
The provision of any patient information in an emergency setting will always be balanced against the acuity of the patient, and the likelihood of their ability to comprehend any aspects of their emergency care. For those patients however who are allocated to an emergency list (CEPOD) there may well be an opportunity to discuss the preferred anaesthetic technique and provide accurate and timely information as part of their perioperative care.
Access to the internet within Trusts is variable (at best) and hard copy allows the patient adequate time to re-read, reflect and possibly question the content before undergoing any procedure. The June 2022 version is currently only available in English and Welsh.

Difficult Airway Society E-Zine September 2022 Contents 60
Whilst clinical involvement is a requirement to establish a patient on the DAS database, the patient information appertaining to this project supports the initiative and clearly identifies the patient benefits.
Kate Rivett, DAS patient representative
In addition to the new ATI patient information the DAS website now has a link to a joint DAS/RCoA leaflet ‘Your airway and breathing during anaesthesia’ (February 2020). This patient information, produced with the RCoA, is widely translated.
For those patients who have been identified as having a difficult airway necessitating an ATI, the patient information also provides a link to the DAS Airway Alert Card Project.
The concept of ATI is familiar to airway specialists and anaesthetists, however this level of knowledge is not representative of the wider population. Whilst the Covid pandemic might have heightened awareness of the need for mechanical ventilation, the associated airway management would not generally be understood as integral to this process. The key aspects of general anaesthesia remain a mystery to many people with the specific concepts of any intubation technique or associated airway management not even being considered as part of having a general anaesthetic; this level of comprehension should be considered when outlining the need for ATI. The provision of patient information is designed to support the consultation for both the patient and the DASclinician.continues to work to improve the patient information available. An infographic, with a glossary on ATI is currently in the review process and we hope to be able to publish this early in the Autumn.
Difficult Airway Society E-Zine September 2022 Contents 61 DIFFICULT AIRWAY DATABASE - AN UPDATE | Achuthan Sajayan | DAS Difficult airway database is continuing its expansion across the country and several national organisations have confirmed their official support to the project in the last few months. The following is the list of organisations supporting us: ✦ Society for Obesity and Bariatric Anaesthesia (SOBA) ✦ Association of Anaesthetists (AoA) ✦ Obstetric Anaesthetists Association (OAA) ✦ Royal College of Anaesthetists (RCoA) ✦ Safe Anaesthesia Liaison Group (SALG) ✦ Association for Perioperative Practice (AfPP) ✦ College of Operating Department Practitioners (CODP) ✦ Society for Education in Anaesthesia (SEAUK) ✦ UK Society for Computing and Technology in Anaesthesia (SCATA-UK) ✦ Intensive Care Society (ICS) Here is the comparison of current figures with those from September 2021: Sept 21 Current Status 150 Hospital sites 190 820+ submissions 1200+ 1935 Access logins 2500+ The analysis of the data collected over the fi rst fi ve years has very recently been published in Anaesthesia! Here's the link DAS Airway Alert Card and Difficult Airway Database - How to join the project? ----------------------------------------------------Check if your hospital is already on the project https://das uk com/content/dad sites If not, please follow the steps below If your hospital is not yet part of this project and you are interested in taking the lead role locally, please do get in touch with us via dad@das.uk.com. If you work in a hospital which is already a part of the project, please encourage your colleagues to submit the data promptly and let us know if you have any feedback about the project or the process of submission. Some useful links are: DAS Database main page and the list of Trusts currently taking part in the project. Other project related documents can be found here Dr Achuthan Sajayan dad@das.uk.com Co-Lead, DAS Difficult Airway Database
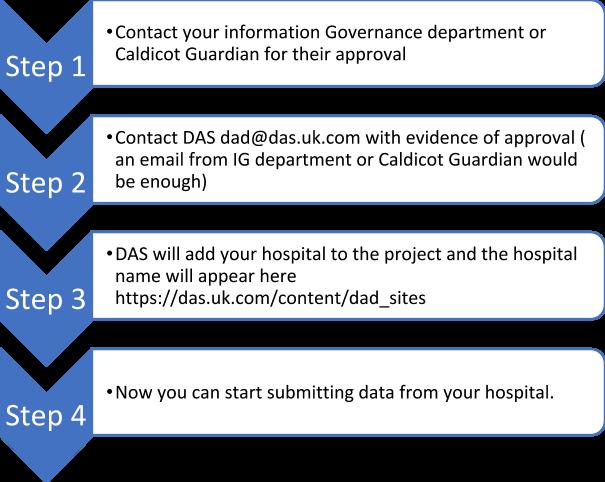
If are not a DAS need to register with the database before submitting data. is free and only takes few
you
Registration
minutes. Please follow this acaregisterhttps://das.uk.com/das_user/link https://das.uk.com/dad
Difficult Airway Society E-Zine September 2022 Contents 62 If you are a trainee or specialty doctor, please discuss with your supervising consultant before submitting the data and provide their name How to submit a case to the DAS Database? Download the patient information and consent form from the DAS isanaesthesia.frompatienPleaseaDiscusssent_formhttps://das.uk.com/aac/conwebsitewiththepatientndobtaintheconsent.makesurethethasrecoveredfullytheeffectsofRecoveryroomnota recommended place for Giveconsenting.onecopyto the patient and keep one in the records Once the data is submitted, there will be an option to print out the summary of the event. Please print two copies, give one to the patient and keep the other in the patient records. There will also be an option to print out a letter to the GP. This can either be sent directly to the GP or give it to the patient with instructions to hand over to their GP. Consent Data submission Summary document GP letter
member, you
Difficult Airway Society E-Zine January 2022 Contents 63 WORLD MANAGEMENTAIRWAYMEETING|EllenO’Sullivan|FollowingonfromthesuccessofWAMM1,heldinDublinin2015,andWAMM2inAmsterdamin2019weplantorunaWAMM3.Datesandvenuesarepresentlybeingdiscussed. WATCH THIS SPACE! FURTHERCOMINGANNOUNCEMENTSSOON!



Difficult Airway Society E-Zine September 2022 Contents 64 @dasairway @dastrainees #DASeducation DAS expect all those considering a bid to contact us and discuss what is involved in hosting prior to submission. Email: secretary@das.uk.com for more details. We are delighted to welcome proposals from those interested in hosting the DAS ASM in 2024. Proposals should contain information on the proposed venue(s) and costs, hotel accommodation nearby and transport links as a minimum. Key Dates: Submission of Proposals Window Opens: 1st July 2022 Deadline for Submissions: Midnight, 16th September 2022 Shortlisted proposals will be invited for presentation in October 2022 Submissions should be emailed to the DAS Secretariat at: das@anaesthetist.org PROPOSALS TO HOST OUR ANNUALMEETINGSCIENTIFICIN2024!!
8. Duceppe E, Parlow J, MacDonald P, Lyons K, McMullen M, Srinathan S, et al. Canadian Cardiovascular Society guidelines on perioperative cardiac risk assessment and management for patients who undergo noncardiac surgery. Can J Cardiol. 2017; 33:17-32.
14. Maxwell MJ, Moran CG, Moppett IK. Development and validation of a preoperative scoring system to predict 30 day mortality in patients undergoing hip fracture surgery. Br J Anaesth. 2008 Aug 21; 101(4):511–17.
10. Oliver CM, Walker E, Giannaris S, Grocott MPW, Moonesinghe SM. Risk assessment tools validated for patients undergoing emergency laparotomy: a systematic review. Br J Anaesth. 2015 Nov 3; 115(6): 49–60.
ASSESSMENT|References1/2|
3. Khuri SF, Henderson WG, DePalma RG, Mosca C, Healey NA, Kumbhani DJ, et al. Determinants of long-term survival after major surgery and the adverse effect of postoperative complications. Ann Surg. 2005 Sept; 4.242(3):326-343.Findlay GP, Goodwin APL, Protopapa K, Smith NCE, Mason M. National Confidential Enquiry into PeriOperative Outcomes and Deaths. Knowing the Risk. A review of peri-operative care of surgical patients. 2011. Available from: https://www.ncepod.org.uk
PERIOPERATIVE MEDICINE: RISK
9. De Hert S, Staender S, Fritsch G, Hinkelbein J, Afshari A, Bettelli G, et al. Pre-operative evaluation of adults undergoing noncardiac surgery: Updated guideline from the European Society of Anaesthesiology. Eur J Anaesthesiol. 2018; 35:407–465.
1. Pearse RM, Holt PJE, Grocott MPW. Managing perioperative risk in patients undergoing elective non-cardiac surgery. BMJ. 2011 Oct 5; 343:d5759.
11. Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 1999; 12.100:1043–9.Stones J, Yates D. Clinical risk assessment tools in anaesthesia. BJA Educ. 2019 19(2):47-53.
13. Nashef SAM, Roques F, Sharples LD, Nilsson J, Smith C, Goldstone AR, et al. EuroSCORE II. Eur J Cardiothorac Surg. 2012; 41: 734–745
Difficult Airway Society E-Zine September 2022 Contents 65
2. Moonesinghe SM, Mythen MG, Das P, Rowan KM, Grocott MPW. Risk stratification tools for predicting morbidity and mortality in adult patients undergoing major surgery. Anesthesiology. 2013 Oct; 119(4):959–81.
5. Pearse RM, Harrison DA, James P, Watson D, Hinds C, Rhodes, A, et al. Identification and characterisation of the high-risk surgical population in the United Kingdom. Critical Care. 2006 June 2; 10:R81.
6. Royal College of Surgeons. The high-risk general surgical patient: raising the standard. 2018. Available from: 7.https://www.rcseng.ac.ukLevettDZH,Jack S, Swart M, Carlisle J, Wilson J, Snowden C, et al. Perioperative cardiopulmonary exercise testing (CPET): consensus clinical guidelines on indications, organization, conduct, and physiological interpretation. British Journal of Anaesthesia. 2018 Nov 24; 120(3): 484-500.
15. Eugene N, Oliver CM, Bassett MG, Poulton TE, Kuryba A, Johnston C, et al. Development and internal validation of a novel risk adjustment model for adult patients undergoing emergency laparotomy surgery: the National Emergency Laparotomy Audit risk model. Br J Anaesth 2018;121:739–48.
PERIOPERATIVE MEDICINE: RISK
20. Protopapa KL, Simpson JC, Smith NCE, Moonesinghe SR. Development and validation of the Surgical Outcome Risk Tool (SORT). Br J Surg. 2014; 101:1774-1783.
21. Bilimoria KY, Liu Y, Paruch JL, Zhou L, Kmiecik TE, Ko CY, et al. Development and evaluation of the universal ACS NSQIP surgical risk calculator: a decision aid and informed consent tool for patients and surgeons. Am Coll Surg. 2013 Nov; 217(5):833-842.
ASSESSMENT|References2/2|
22. National Institute for Health and Care Excellence (NICE). Perioperative care in adults: Evidence review for perioperative risk stratification tools. NICE. 2020 Aug 19. Available from: https://www.nice.org.uk
18. El-Boghdadly K, Lockwood S, Crawshaw A, McNally S, Summerton D, Mercer N et al. Preoperative assessment and optimisation for adult surgery, including consideration of COVID-19 and its implications. 2021.
19. Prytherch DR, Whiteley MS, Higgins B, Weaver PC, Prout WG, Powell SJ. POSSUM and Portsmouth POSSUM for predicting mortality. Physiological and operative severity score for the enumeration of mortality and morbidity. Br J Surg. 1998; 85(9):1217–1220.
Difficult Airway Society E-Zine September 2022 Contents 66
23. American College of Cardiology (ACC)/American Heart Association (AHA) Task Force. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery. Circulation. 2014;130:e278-e333.
24. Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA) Joint Task Force: 2014 ESC/ ESA Guidelines on non-cardiac surgery: cardiovascular assessment and management. Eur Heart J. 2014;35:2383–25.2431. General Medical Council (GMC). Decision making and consent. 2020 September 30. Available from: 26.www.gmc-uk.orgRoyalCollege of Anaesthetists. Common events and risks in anaesthesia. 2019 September. Available from: https://rcoa.ac.uk
17. Park S, Cho H, Park S, Lee S, Kim K, Yoon HJ, et al. Simple Postoperative AKI Risk (SPARK) Classification before Noncardiac Surgery: A Prediction Index Development Study with External Validation. J Am Soc Nephrol. 2019 Jan; 30 (1):170-181.
16. Canet J, Gallart L, Gomar C, Paluzie G, Valles J, Castillo J, et al. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology. 2010 Dec; 113:1338–1350.
Difficult Airway Society E-Zine September 2022 Contents 67 PERIOPERATIVE MEDICINE: CPET | References 1/1 | 1. Prinz JP. Elisee Bouny. The inventor of the bicycle ergometer. In: Kurt Tittel, Karl-Hans Arndt, Wildor Hollmann (eds.): Sports medicine. Yesterday Today Tomorrow. Report from the anniversary symposium of the German Association of Sports Physicians, Oberhof from September 25th to 27th, 1992 2. Lalabekyan BB, et al. Cardiopulmonary exercise testing and cardiopulmonary morbidity in patients undergoing major head and neck surgery. J Oral Maxillofac Surg. 2021 Apr;59(3):297-302 3. Bedin DCC et al . Is it possible to perform cardiopulmonary exercise test in laryngectomized patients? European Respiratory Journal 2018 52: PA2485 4. American Thoracic Society. ATS/ACCP statement on cardiopulmonary exercise testing. Am J Respir Crit Care Med 2003; 167: 211e77
Difficult Airway Society E-Zine September 2022 Contents 68 PERIOPERATIVE MEDICINE: FRAILTY | References 1/3 | 1. Head and neck cancers statistics | Cancer Research UK 2. Frailty in the older surgical patient: a review - PubMed (nih.gov)- Partridge et al. – 2012 3. Effects of preoperative frailty on outcomes following surgery among patients with digestive system tumors: A systematic review and meta-analysis - ScienceDirect – Ding - 2021 4. Guideline for the care of people living with frailty undergoing elective and emergency surgery | British Geriatrics Society (bgs.org.uk) 5. Comprehensive Geriatric Assessment Toolkit for Primary Care Practitioners | British Geriatrics Society 6.CFS:(bgs.org.uk)Aglobal clinical measure of fitness and frailty in elderly people - PMC (nih.gov) – Rockwood et al. original paper – 2005 7. The role of illness acuity on the association between frailty and mortality in emergency department patients referred to internal medicine - PubMed (nih.gov) – Pulok et al. 2020 8. Using the Clinical Frailty Scale in Allocating Scarce Health Care Resources - PubMed (nih.gov) – Version 2.0 –Rockwood, Theou, 2020 9. Clinical frailty scale as a point of care prognostic indicator of mortality in COVID-19: a systematic review and meta-analysis - eClinicalMedicine (thelancet.com) – Kastora et al – 2021 10. rockwood_cfs.pdf (bgs.org.uk) – CFS pdf 11.EFS: Frailty and poor functional status are common in arterial vascular surgical patients and affect postoperative outcomes - PubMed (nih.gov) – Partridge, Fuller, Dhesi – 2015 12. Frailty is associated with postoperative complications in older adults with medical problems - PubMed (nih.gov) – Dasgupta et al. – 2007 13. Assessment of predictive validity and feasibility of Edmonton Frail Scale in identifying postoperative complications among elderly patients: a prospective observational study | Scientific Reports (nature.com)- He et al. –14.2020 efs.pdf (bgs.org.uk) – EFS questionnaire pdf 15.HADS: Preoperative Anxiety as a Predictor of Mortality and Major Morbidity in Patients >70 Years of Age Undergoing Cardiac Surgery - PMC (nih.gov) Williams et al. – 2013 16. Is the Hospital Anxiety and Depression Scale (HADS) a valid measure in a general population 65–80 years old? A psychometric evaluation study - PMC (nih.gov) Djukanovic et al. – 2017 17. Effects of Preoperative Anxiety on Postoperative Delirium in Elderly Patients Undergoing Elective Orthopedic Surgery: A Prospective Observational Cohort Study - PMC (nih.gov) Ren at al. – 2021 18. Microsoft Word - Document1 (svri.org) – HADS questionnaire pdf
31. The effect of age on mechanisms of exercise tolerance: Reduced arteriovenous oxygen difference causes lower oxygen consumption in older people - ScienceDirect – Fuller et al. 2021 32. Duke Activity Status Index (DASI) - MDCalc – DASI Calculator An extended activities of daily living scale for stroke patients - FM Nouri, NB Lincoln, 1987 (sagepub.com) 34. Rasch analysis of the Nottingham extended activities of daily living scale - PubMed (nih.gov) – Das Nair et al. –35.2011 Microsoft Word - EADL 3.doc (nottingham.ac.uk) – NEADL pdf
33.NEADL:
The effect of baseline cognition and delirium on long-term cognitive impairment and mortality: a prospective population-based study - The Lancet Healthy Longevity – Tsui et al. – 2022 27. MoCA-Test-English_2009 (mocatest.org) – MoCA pdf Exercise Tolerance: 28. A brief self-administered questionnaire to determine functional capacity (The Duke Activity Status Index)ScienceDirect – Hlatky - 1989 29. Integration of the Duke Activity Status Index into preoperative risk evaluation: a multicentre prospective cohort study - ScienceDirect - Wijeysundera et al - 2020 30. A simplified (modified) Duke Activity Status Index (M-DASI) to characterise functional capacity: a secondary analysis of the Measurement of Exercise Tolerance before Surgery (METS) study - British Journal of Anaesthesia (bjanaesthesia.org.uk) – Riedel et al - 2021
Difficult Airway Society E-Zine September 2022 Contents 69 PERIOPERATIVE MEDICINE: FRAILTY | References 2/3 | 19.4AsT: 4AT - Rapid Clinical Test for Delirium Detection (the4at.com) – official site 20. Protocol for validation of the 4AT, a rapid screening tool for delirium: a multicentre prospective diagnostic test accuracy study | BMJ Open – Shenkin et al – 2018 21. The 4 ‘A’s test for detecting delirium in acute medical patients: a diagnostic accuracy study - NCBI Bookshelf (nih.gov) – McLullich – 2019 22. (9) 4AT delirium assessment tool on admission links to outcomes: 2 centre study of 82,770 patients - YouTube – 4AT presentation – McLullich 23. 4 A’s Test for Delirium Screening - MDCalc – 4AT calculator 24.MoCA: The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment - PubMed (nih.gov) – Nasreddine et al. – 2005 25. Montreal Cognitive Assessment (MoCA) | Occupational Medicine | Oxford Academic (oup.com) – Hobson 26.2015
Difficult Airway Society E-Zine September 2022 Contents 70 PERIOPERATIVE MEDICINE: FRAILTY | References 3/3 | 36.TUAG: Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test - PubMed (nih.gov) – Shumway-Cook - 2000 37. Prognostic validity of the Timed Up-and-Go test, a modified Get-Up-and-Go test, staff's global judgement and fall history in evaluating fall risk in residential care facilities | Age and Ageing | Oxford Academic (oup.com) Nordin et al –38.Gait2008speed:Gait speed as a measure in geriatric assessment in clinical settings: a systematic review - PubMed (nih.gov)Peel et al 2012 39. Gait speed as a test for monitoring frailty in community-dwelling older people has the highest diagnostic value compared to step length and chair rise time - PubMed (nih.gov) – Schoon – 2014 40. Gait Speed and 1-Year Mortality Following Cardiac Surgery: A Landmark Analysis From the Society of Thoracic Surgeons Adult Cardiac Surgery Database - PubMed (nih.gov) – Afilalo et al. - 2018 41.MUST: Introducing 'MUST' (bapen.org.uk) 42. Evaluation of nutritional status as an independent predictor of post-operative complications and morbidity after gastro-intestinal surgery - ScienceDirect – van Der Kroft et al – 2015
13. Dyson K, Baker P, Garcia N, Braun A, Aung M, Pilcher D, Smith K, Cleland H, Gabbe B. To intubate or not to intubate?
2. Cameron PA, Fitzgerald MC, Curtis K, McKie E, Gabbe B, Earnest A, Christey G, Clarke C, Crozier J, Dinh M, Ellis DY, Howard T, Joseph AP, McDermott K, Matthew J, Ogilvie R, Pollard C, Rao S, Reade M, Rushworth N, Zalstein S; Australian Trauma Quality Improvement Program (AusTQIP) collaboration. Over view of major traumatic injury in Australia--Implications for trauma system design. Injury. 2020 Jan;51(1):114-121. doi: 10.1016/j.injury.2019.09.036. Epub 2019 Oct 3. PMID: 3.31607442.Fitzgerald M, The Alfred Trauma Audit: 1st July 2020-30th June 2021 [PowerPoint presentation]. The Alfred Hospital, Melbourne. Presented 21 Nov 2021 4. Victorian State Trauma Outcomes Registry and Monitoring Group. Victorian State Trauma Registry Annual Report 2019–2020. [Online]. Available from: https://www.monash.edu/__data/assets/pdf_file/0008/2706047/VSTR-Annual-Report-2019-20[Accessed 17 July 2022].
Predictors of inhalation injury in burn-injured patients before arrival at the burn centre. Emerg Med Australas. 2021 Apr;33(2):262-269. doi: 10.1111/1742-6723.13604. Epub 2020 Aug 27. PMID: 32856398.
Difficult Airway Society E-Zine September 2022 Contents 71 AIRWAY MANAGEMENT IN MAJOR TRAUMA: AN AUSTRALIAN PERSPECTIVE | References |
7. Peacock A, Leung J, Larney S, Colledge S, Hickman M, Rehm J, Giovino GA, West R, Hall W, Griffiths P, Ali R, Gowing L, Marsden J, Ferrari AJ, Grebely J, Farrell M, Degenhardt L. Global statistics on alcohol, tobacco and illicit drug use: 2017 status report. Addiction. 2018 Oct;113(10):1905-1926. doi: 10.1111/add.14234. Epub 2018 Jun 4. PMID: 29749059.
8. Knott J, Yap C, Mitra B, Gerdtz M, Daniel C, Braitberg G. Screening major trauma patients for prevalence of illicit drugs. Drug Alcohol Rev. 2022 Jan;41(1):285-292. doi: 10.1111/dar.13355. Epub 2021 Jul 15. PMID: 34263497.
12. Chrimes N, Bradley WPL, Gatward JJ, Weatherall AD. Human factors and the 'next generation' airway trolley. Anaesthesia. 2019 Apr;74(4):427-433. doi: 10.1111/anae.14543. Epub 2018 Dec 14. PMID: 30548998.
5. Cook TM, Woodall N, Harper J, Benger J; Fourth National Audit Project. Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 2: intensive care and emergency departments. Br J Anaesth. 2011 May;106(5):632-42. doi: 10.1093/bja/aer059. Epub 2011 Mar 29. PMID: 21447489.
1. Atkin in C, Freedman I, Rosenfeld JV, Fitzgerald M, Kossmann T. The evolution of an integrated State Trauma System in Victoria, Australia. Injury. 2005 Nov;36(11):1277-87. doi: 10.1016/j.injury.2005.05.011. PMID: 16214472
WEB_FINAL.pdf
9. Bradley P, Chapman G, Crooke B, Greenland K. Airway Assessment. 2016. [Online] Available from: https:// www.anzca.edu.au/getattachment/eff1ab5d-46cf-46db-95ef-5e65ecb88c26/PU-Airway-Assessment-20160916v1 [Accessed 12 July 2022].
10. Rehab A. Managing Airway Trauma: Applying logic and structure to the anaesthetic decision making process.In: R Riley, Australasian Anaesthesia [e-book]. ANZCA, 2019. Available from: https://www.anzca.edu.au/getattachment/ 220cc6da-3eee-463b-9b66-4e8b33861d7e/Australasian-Anaesthesia-2019 [Accessed 17 July 2022)
6. Groombridge C, Maini A, Olaussen A, Kim Y, Fitzgerald M, Mitra B, Smit V. Impact of a targeted bundle of audit with tailored education and an intubation checklist to improve airway management in the emergency department: an integrated time series analysis. Emerg Med J. 2020 Sep;37(9):576-580. doi: 10.1136/emermed-2019-208935. Epub 2020 Jun 17. PMID: 32554746.
11. Endlich Y, Hore PJ, Baker PA, et al. Updated guideline on equipment to manage difficult airways: Australian and New Zealand College of Anaesthetists. Anaesthesia and Intensive Care. June 2022. doi:10.1177/0310057X221082664
1.T. M. Cook, N. Woodall, C. Frerk, on behalf of the Fourth National Audit Project, Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 1: Anaesthesia. British Journal of Anaesthesia. 2011;106(5):617–631.
7.Frerk C, Mitchell VS, McNarry AF, et al. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. British Journal of Anaesthesia 2015;115: 827–48.
3.Marshall SD, Chrimes N. Time for a breath of fresh air: Rethinking training in airway management. Anaesthesia. 4.Al-Elq,2016;71(11):1259-1264.A.Simulation-based medical teaching and learning. Journal Of Family And Community Medicine.2010;17(1), 5.Bruce35. R, McLeod A, Smith G. A Survey of UK anaesthetic trainee attitudes towards simulator-based training experience. Royal College of Anaesthetists Bulletin 2005;34:1722-3.
8.Howard Quijano KJ, Huang YM, Matevosian R, Kaplan MB, Steadman RH. Video assisted instruction improves the success rate for tracheal intubation by novices. British Journal of Anaesthesia. 2008;101: 568–72, e1.
12.Lindkær Jensen, NH, Cook, TM and Kelly, FE. A national survey of practical airway training in UK anaesthetic departments. Time for a national policy?. Anaesthesia. 2016; 71:1273-1279.
10.Ahmad I, El-Boghdadly K, Bhagrath R et al. Difficult Airway Society guidelines for awake tracheal intubation (ATI) in adults. Anaesthesia, 2020;75: 509-528.
Difficult Airway Society E-Zine September 2022 Contents 72 AIRWAY TRAINING OF DREAMS, 1ST PRIZE CREATIVE WRITING | References |
2.Dashe & Thomson. 35 Inspiring Quotes about learning. 2022 Available: https://www.dashe.com/blog/motivation/ inspiring-learning-quotes/ [Accessed 14/04/22]
6.Royal College of Anaesthetists (RCOA). Simulation Strategy 2018-2023. (2018) Available: https://www.rcoa.ac.uk/ sites/default/files/documents/2019-07/Simulation-Strategy-FINAL.pdf [Accessed 13/04/2022].
11.Marshall SD. Use of cognitive aids during emergencies in anesthesia: A systematic review. Anesthesia and Analgesia 2013;117: 1162–71.
15.Looseley A, Wainwright E, Cook TM, et al. Stress, burnout, depression and work satisfaction among UK anaesthetic trainees; a quantitative analysis of the Satisfaction and Wellbeing in Anaesthetic Training study. Anaesthesia. 16.Sauerteig2019;74(10):1231-1239.S,Wijesuriya J, Tuck M, Barham-Brown H. Doctors’ health and wellbeing: at the heart of the NHS’s mission or still a secondary consideration? Intl Rev Psychiatry. 2019;31(7-8):548-554.
9.McGaghie WC, Issenberg SB, Barsuk JH, Wayne DB. A critical review of simulation based mastery learning with translational outcomes. Medical Education 2014;48: 375–85.
13.Marshall SD, Chrimes N. Time for a breath of fresh air: Rethinking training in airway management. Anaesthesia. 14.Bhagwat2016;71(11):1259-1264.M.Simulation and anaesthesia. Indian J Anaesth. 2012;56(1):14-20.
Difficult Airway Society www.das.uk.com@dasairway@dastrainees