
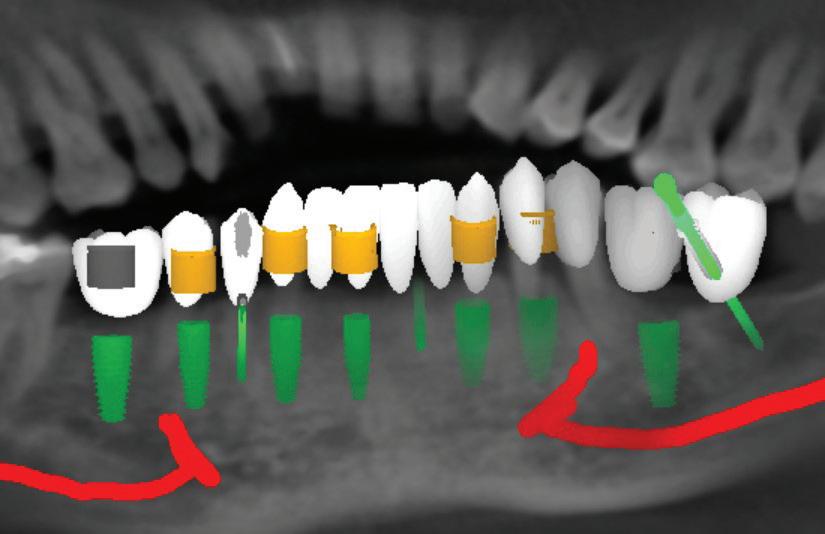
Instantaneously receive patient scans to deliver optimal
Patients capture videos of their teeth at home using the Grin Scope and intuitive smartphone app
Grin Care Specialists check every scan for treatment progress and problems and communicate with patient and doctor when needed
AI treatment tracker analyses and compares actual treatment progress with digitally planned treatment
Doctors and their teams have complete control and oversight of all patients using the intuitive dashboard
Progress and milestones easily shared with referring doctors
40% to 60%
Fewer in-person visits.
240%
$266->$640
Increased revenue per visit.
16hrs per week
Time that has been saved.
$200K+
Practice ROI*
Average practice return.
*based on average practice ROI calculator
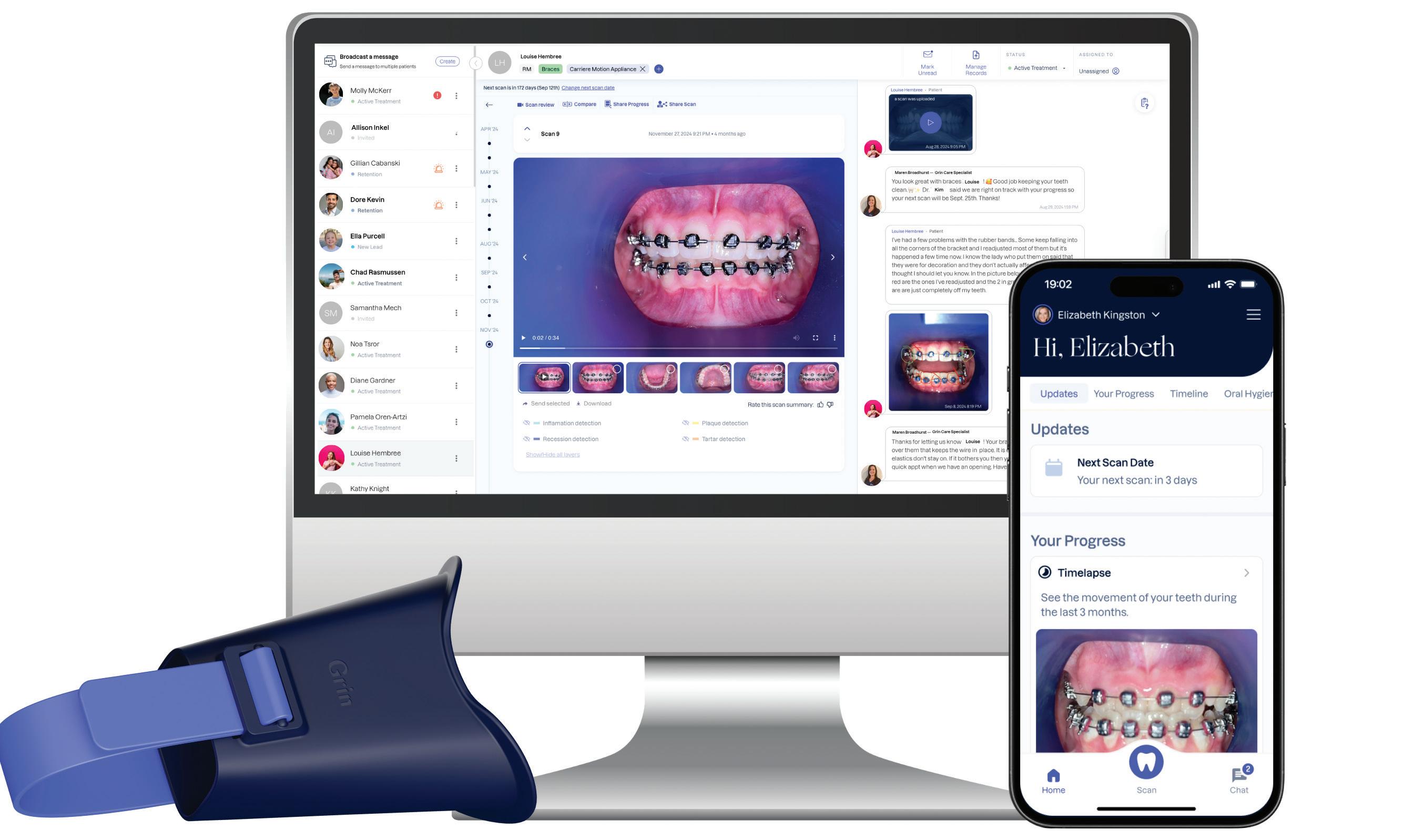
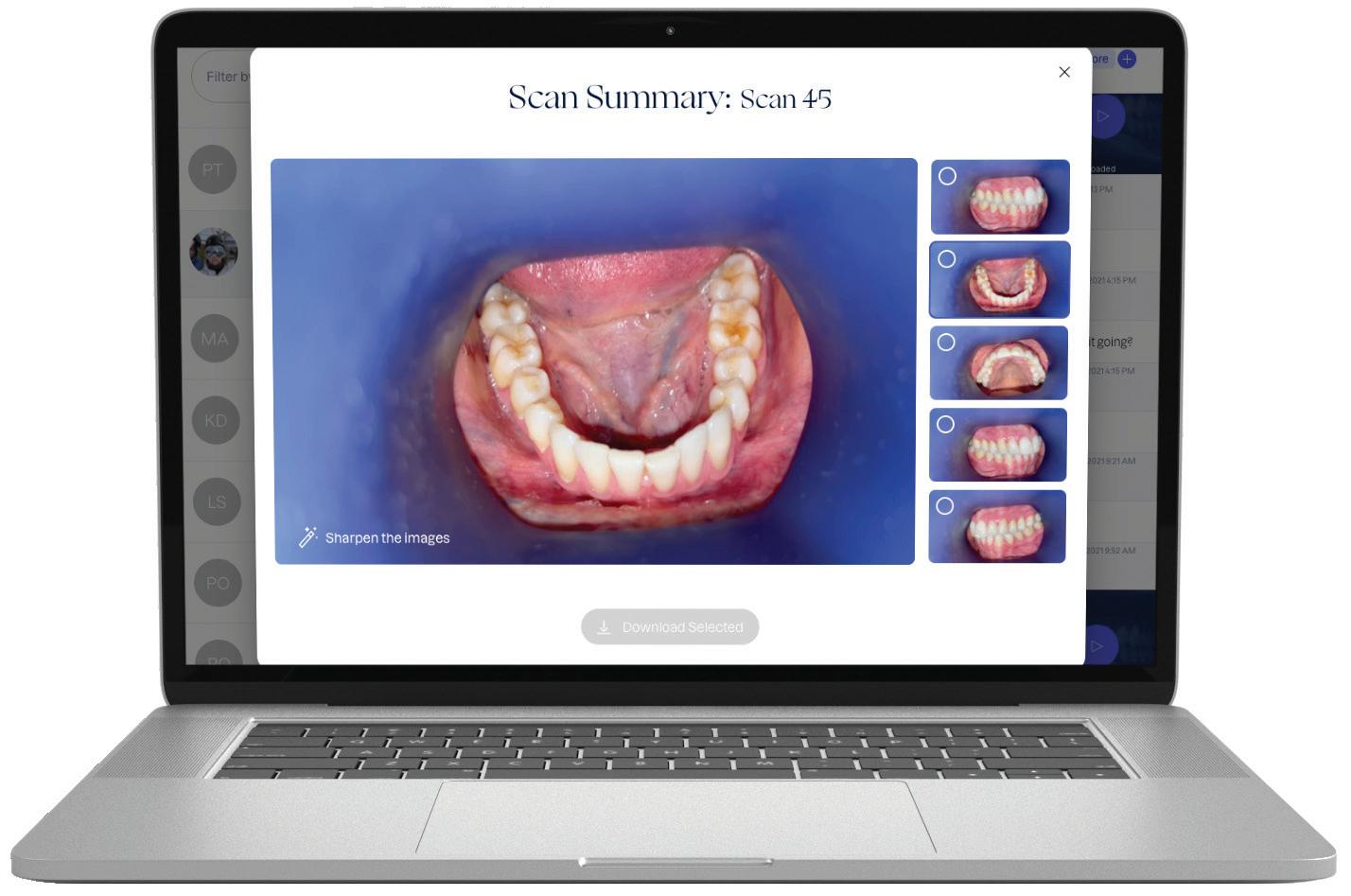
The easy way to monitor your orthodontic patients remotely

Increase your clinical excellence and enhance your patient experience without the need for unnecessary in-chair consults.
* Active treatment monitoring capped at 3 years












the
Dental practice transactions, smart negotiators and dumb decisions
Trust builders: Strengthening patient confidence in you
Practice buyer mythbusters
A better way to follow up your patients and get results

82 Beyond the chair: Smart marketing moves for dentists in 2025



facebook.com/dentalpracticenow twitter.com/adpmagazine instagram.com/dentevents
www.dentalpractice.com.au
Publisher & Editor: Joseph Allbeury Clinical Editor: Dr David Roessler Technology Editor: Prof. Laurence J. Walsh Infection Control Editor: Prof. Laurence J. Walsh Senior Contributing Editor: Dr Christopher CK Ho Columnists: Dr Georges Fast, Dr Jesse Green, Garry Pammer, Phillip Win, Dr David Moffet, Graham Middleton, Simon Palmer, Julie Parker, Jayne Bandy, Angus Pryor Design & Production: Jasper Communications Australasian Dental Practice™ ISSN 1445-5269 is printed in Australia and published six times per year by Main Street Publishing Pty Limited ABN 74 065 490 655 PO Box 586, Cammeray NSW 2062 Tel: (02) 9929-1900 Fax: (02) 9929-1999 Email: info@dentist.com.au © 2025 All rights reserved. The contents of this magazine are copyright and must not be reproduced without the written permission of the publisher. Permission to reprint may be obtained upon application. Correspondence and manuscripts for publication are welcome. Although all care is taken, the editor and publisher will not accept responsibility for the opinions expressed by contributors to this magazine, or for loss or damage to material submitted for publication
Subscriptions: Australia and NZ: A$99.00 per year includes OralHygiene™ and eLABORATE™ magazines; Overseas Airmail: A$220.00 per year.


NovaMin delivers superior* coverage of exposed dentine tubules1, with a reparative^ layer that is 50% harder than natural dentine.2

To find out more and order free samples, scan the QR code or visit at www.haleonhealthpartner.com/en-au/ or www.haleonhealthpartner.com/en-nz/ NZ AU
ALWAYS READ THE LABEL AND FOLLOW THE DIRECTIONS FOR USE.
*In lab testing vs stannous fluoride toothpaste.1
^Forms a protective layer over the sensitive areas of the teeth. Brush twice a day for lasting sensitivity protection.
1. Cambridge, 2013. Haleon Data on File: Surface coverage and tubule occlusion of dentine treated with competitor products after 12 hrs immersion in AS. Richard Langford, Cambridge University, July 2023. 2. Parkinson, C. R. and Willson, R. J. (2011) ‘A comparative in vitro study investigating the occlusion and mineralization properties of commercial toothpastes in a four-day dentin disc model’, J Clin Dent, 22(3), pp. 74-81.
Trademarks are owned by or licensed to the Haleon group of companies © 2024 Haleon group of companies or its licensor. Sydney, Australia. Auckland, New Zealand. TAPS BG3819 PM-AU-SENO-24-00046.

and control – a


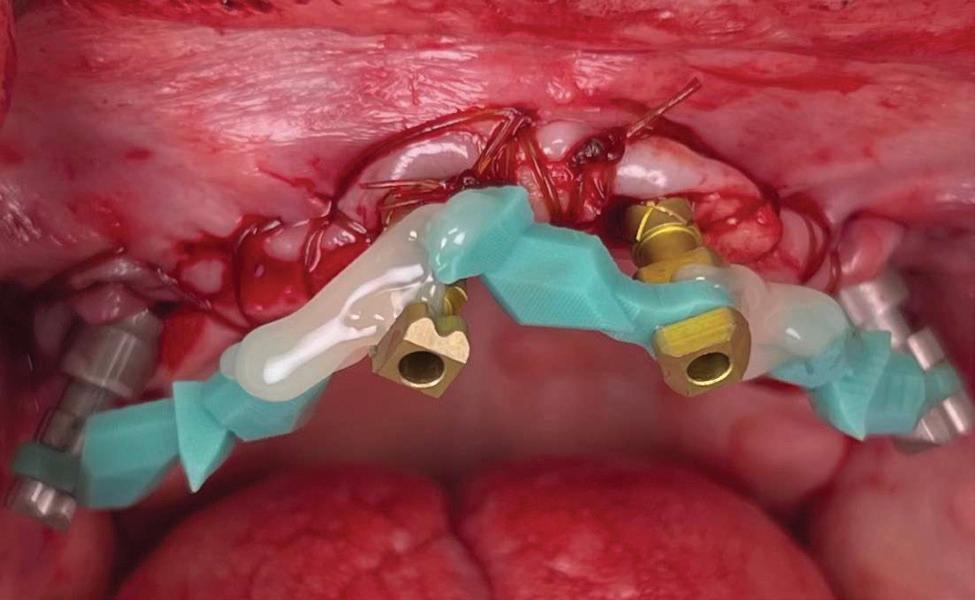
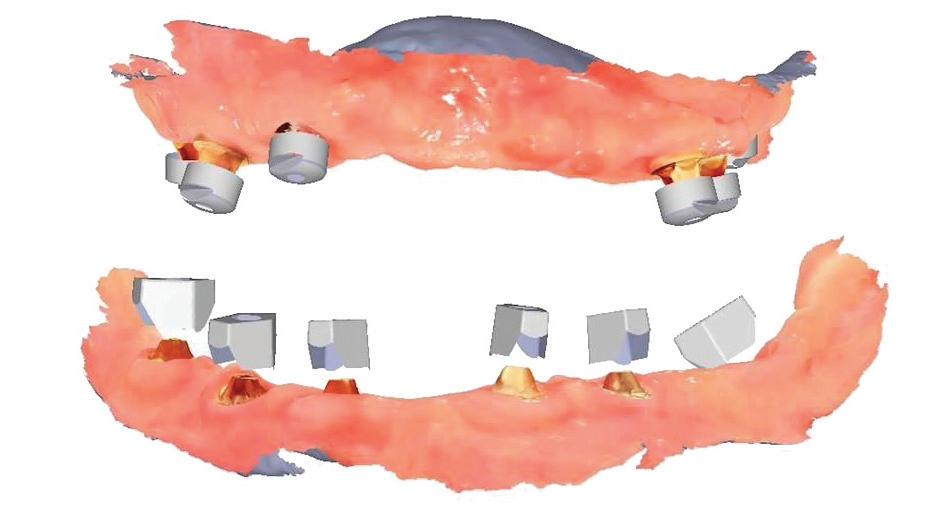
194 Comprehensive full-arch restoration: From extractions to immediate load with 3D-printed long-term provisional 198 New Aoralscan Elite Wireless and Metismile MR Face Scanner
Real jaw movements and face morphing on the digital patient: production of functional restorations in only two chairside appointments
Biodentine™ in Bio-Bulk Fill procedure as a core material for indirect restoration


By Joseph Allbeury
For the thirteenth time, almost in a row except for the COVID mess, I joined hundreds of other Australians and thousands - 135,000 to be exact - of dental colleagues from across the globe in descending on Cologne, Germany for the greatest show on Earth. And once again, it delivered and then some.
The 41st IDS concluded with 135,000 visitors from 156 countries having come together to see the latest and greatest from 2,010 exhibitors from 61 countries.
The exhibition - there is no accompanying education program - covered 180,000 square metres with stands big and small on show from every dental manufacturer you know and love and thousands you have never heard anything about at all and never will.
From a dentists’ perspective, the IDS is often a bucket list trip to see how big “dentistry” actually is [it’s massive]. Much of what is on show will never be available in Australia, however, it’s certainly the place to stay on trend with the latest in diagnostic technology, radiography, intraoral scanning and the like.
Dental technicians and prosthetists, conversely, flock to the IDS to keep up with the trends in manufacturing solutions. Big ticket items like milling machines are plentiful at the IDS as are 3D printing solutions and the exhibition is a great place to find out exactly what’s coming next. Manufacturing dentures digitally remains a key area of interest.
Most of all, however, IDS is where the dental industry comes together to deal. The dental trade from Australia meets with the agencies they represent to renew relationships and see what’s coming next. Equally, manufacturers are often on the look out for new distributors and distributors for new agencies. With everything all in one place, the event attracts dental dealers from across the globe.
Digital Dentistry & Dental Technology 2025 is coming up on August 1-2 and many of the new products from IDS 2025 will already be on show.
We’ve been working hard to firm up the education program and if you visit www.dentaltechnology.com.au, 80% of the sessions are now locked in with 30+ speakers confirmed presenting across six streams. Expect lots on full arch restorations, digital dentures, 3D printing, milling, CAD and CAM software, artificial intelligence, automation, intraoral scanning, 3D facial scanning, milling, orthodontics, photogrammetry, materials, smile design, implantology, CBCT, cosmetic dentistry, aligners and more.
The venue is looking pristine following the conclusion of renovations and the new ballroom will bring the exhibition together in a single location. The format is once again the same but there will be some changes we hope will enhance the delegate experience.
So register now and don’t miss out!
Enjoy the edition...
Joseph Allbeury, Editor and Publisher

Practice Sale Search, Australia’s leading dental practice brokerage, is excited to announce the appointment of Simon Moore as its new Account Manager, based in Queensland. Mr Moore brings over 15 years of experience in medical and dental finance to the team, having worked with some of Australia’s most prominent specialist lenders, including Investec, BOQ Specialist and most recently, Credabl. With a deep understanding of the financial landscape and long-standing relationships within the dental profession, Simon is uniquely equipped to support practice owners through the complex process of selling their dental practice.“We’re thrilled to welcome Simon Moore to our growing team,” said Simon Palmer, Managing Director of Practice Sale Search. “His long background in dental and medical finance, combined with his relationship-driven approach, makes him an invaluable asset to both our business and our clients.” Mr Moore said “Queensland is an exciting and evolving market and I look forward to helping our clients achieve the best results and terms for the sale of their practice.” Simon’s appointment strengthens Practice Sale Search’s national presence and further reinforces its position as the most trusted name in dental practice sales across Australia. Mr Moore can be contacted by emailing simon.moore@practicesalesearch.com.au or call 1300-282-042.
Each year, millions of people get dental implants as a longterm, natural-looking fix for missing teeth. But traditional implants don’t fully mimic real teeth.
Researchers from Tufts University School of Dental Medicine and Tufts University School of Medicine recently described a new approach to dental implants that could better replicate how natural teeth feel and function. Their study, published in Scientific Reports, shows early success with both a “smart” implant and a new gentler surgical technique in rodents.
“Natural teeth connect to the jawbone through soft tissue rich in nerves, which help sense pressure and texture and guide how we chew and speak. Implants lack that sensory feedback,” said Jake Jinkun Chen, DI09, a professor of periodontology and director of the Division of Oral Biology at the School of Dental Medicine and the senior author on the study.
Traditional dental implants use a titanium post that fuses directly to the jawbone to support a ceramic crown, and the surgery often cuts or damages nearby nerves. To tie these inert pieces of metal into the body’s sensory system, the Tufts team developed an implant wrapped in an innovative biodegradable coating. This coating contains stem cells and a special protein that helps them multiply and turn into nerve tissue. As the coating dissolves during the healing process, it releases the stem cells and protein, fueling the growth of new nerve tissue around the implant.
The coating also contains tiny, rubbery particles that act like memory foam. Compressed so that the implant is smaller than the missing tooth when it’s first inserted, these nanofibers gently expand once in place until the implant snugly fits the socket. This allows for a new minimally invasive procedure that preserves existing nerve endings in the tissue around the implant.
Siddhartha Das et al, Surgical considerations towards inducing proprioceptive feedback in dental implants, Scientific Reports (2025). DOI: 10.1038/s41598-025-99923-8


Gunz Dental is back, with a proud 89 year trading history in the dental industry supported by trusted products, innovative solutions, and reliable service Now proudly owned by the Miller Dental Group, a well-respected name in the dental industry, we are proud to be a leading national dental supply company
Gunz Dental stands for quality, innovation, and a commitment to helping practices deliver the best patient care Gunz Dental is proud to be the longest standing Australian-owned dental brand. We’re committed to supporting the dental community with exceptional service, reliable products, and high-quality equipment Our focus is on innovation, bringing in new and advanced solutions to meet the evolving needs of dental professionals across Australia, New Zealand, and the Pacific




portfolio of solutions matching the needs of your
Gunz Dental has most recently added DC Air Sensor systems, Monet Laser Curing Light, The Premier Dental Product and material range, iVeneer and a number of other agencies to compliment our existing agencies from Kulzer to Carestream dental equipment











By Georges Fast
“There is an old saying that ‘the only people who like change are wet babies’ and in our profession, much of the way that dentistry has to be delivered is working against the interests of the dentist and more importantly, the patient. It appears that much of the change has occurred just for the sake of change...”
aving spent the first 2 months of the year in enforced rest as a result of spinal surgery, I had time to reflect on how our profession has changed over the past half century. Most would agree that generally, the changes have been positive. Our materials are better, our knowledge is more research-based, treatment options have increased exponentially and patients are keeping their teeth for longer. And yet, do patients have better access to treatment when they need it and do they receive the same level of care?
There is an old saying that “the only people who like change are wet babies” and in our profession, much of the way that dentistry has to be delivered is working against the interests of the dentist and more importantly, the patient.
It appears that much of the change has occurred just for the sake of change, driven by market imperatives and a quest for aesthetics dictated by current fashion.
The standardisation of treatment procedures has resulted in less emphasis on craftmanship. I have quite a few gold restorations in my own mouth, two of which were placed there by a very fine dentist in 1968, both are still intact with no breakdown around the margins and both the teeth are functioning well, despite one of them having been root treated with silver points at the time. I take regular radiographs and there are absolutely no problems. I placed a number of gold restorations in my wife’s mouth before we were married in 1973 and they, too, are all still functioning well. And yet my laboratory, which
employs more than 30 technicians, has only one person who is still capable of producing good metal margins and despite all the emphasis on digital restorations and aesthetics, the dentists that I treat as patients prefer gold in their own mouths and for their families wherever possible.
Automation in our profession has made it easier to treat teeth without having to think too much about what we are doing. The exponential growth of design software means that dentists with a limited understanding of the process can produce adequate restorations.
The growth of third parties and of health funds running corporate practices and employing dentists to deal with one aspect of a treatment process, effectively absolves the dentist from responsibility for any procedure other than the one they performed. Other dentists or hygienists in the same practice deal with other aspects and thus the only person who owns any problem that may arise is the patient. Yet as long as the right forms were signed and the patient was informed of any potential risks and offered the choice of seeking a second opinion, no one will be held accountable.
“We started on the downward trajectory when third parties worked hard to convince the public that dentistry was a product and not a service. Their biggest impediment was patient loyalty and they have been committed to getting rid of it. Thus, preferred provider schemes, special pricing, bonus of the month, have crept into our profession. And sadly, many of our new graduates will not experience the joy of treating several generations of the same family and having their patients think of them as friends...”
We started on the downward trajectory when third parties worked hard to convince the public that dentistry was a product and not a service. Their biggest impediment was patient loyalty and they have been committed to getting rid of it. Thus, preferred provider schemes, special pricing, bonus of the month, have crept into our profession. And sadly, many of our new graduates will not experience the joy of treating several generations of the same family and having their patients think of them as friends. Continued 88


Place your order before June 22nd to enjoy savings of up to $3,300* in tax in this financial year!






Ends June 22nd. T&C's apply. Scan the QR code to check out our deals



The cliche that “when you are green you grow and when you are ripe you rot” has never been more relevant. We have a public sector structure (and in this I include academia) that is mostly concerned with keeping itself employed and thus benefits from producing an ever-increasing regulatory burden without having to prove that this is to anyone’s benefit other than their own.
When I was working and studying in the U.K. in the very early 70s, I became interested and then became involved in implant dentistry. I was lucky to have mentors like Hans Orlay, Ron Cullen, Lou Caplan and others. One of my most vivid memories is of Leonard Linkow opening the First World Implant Congress in Paris in October 1972 with the words: “Behold the turtle, he only makes progress when he sticks his neck out”.
We already knew at that time that Titanium was biocompatible and that cells could grow towards it without needing an intermediary and this resulted in osseointegration. One of the practices where I worked was across the road from the Hawker Sidley aircraft factory which gave me access to pure Titanium. I obtained some pure Titanium, cylindrical wire which I planned to use if I ever decided to try doing some endodontic stabilisers as I figured that this would be better than the CoCr wire that Hans Orlay was using at the time.
I brought this back to Melbourne with me, together with my rather primitive implant kit, as well as a Kurer Post kit - no TGA rules in those days.
dry heat furnace, cut it to length less some 5 mm, coated it in endodontic sealer 10 mm short of the end to make sure that I didn’t extrude sealer past the apex, tapped it into place using my implant hammer and a Unitek pin placement tool and then using G.P. points, I sealed the tapering part of the root canal. I placed an amalgam seal on the lingual. The tooth became discoloured, the patient got married and moved to Queensland. I lost contact with him in the late 70s.
Fifteen years ago, I had to refer an elderly patient to an Oral Surgeon to have some teeth removed. We got a phone call at the surgery from her daughter who wanted to understand what was happening. I called back what was a Queensland number and identified myself to the man who answered the phone. On hearing my name, he identified himself and asked whether I remembered him. Of course I did. I asked him whatever happened to that tooth. He said that it didn’t cause any problems but that it had turned jet black and he and his wife got sick of looking at it. He’d had it extracted some 5 years earlier and it was replaced by a conventional implant. I asked him about the teeth either side of it and he said that they were still there and perfectly OK.
“The cliche that ‘when you are green you grow and when you are ripe you rot’ has never been more relevant. We have a public sector structure (and in this I include academia) that is mostly concerned with keeping itself employed and thus benefits from producing an ever-increasing regulatory burden without having to prove that this is to anyone’s benefit other than their own...”
In 1975, one of my patients who was 18 years old became involved in a car accident; he hit the steering wheel with his chin and sustained 2 horizontal fractures in his 31, both quite a way subgingivally. The 41 and 32 were intact. The normal treatment at that time would have required extraction of the 31 and the placement of a partial denture or a bridge to replace the missing tooth.
Knowing that he had nothing to lose, he agreed to let me experiment on him. I extirpated the 31, drilled 10mm past the apex using a sterile Kurer Post spiral drill that matched the diameter of my titanium wire. I sterilised the Titanium using a
Yes, I did stick my neck out, but the result ended being a lot better for the patient than if we had opted for a bridge or a partial denture. The biological cost was negligible and we bought him 30 years of function until a better and more modern treatment became available.
In the current regulatory environment, treatment such as I described is not only illegal and would result in crippling fines being imposed by the TGA, but possibly result in losing one’s right to practice. If I had made a conventional bridge, the teeth either side would have been compromised and possibly lost by now, a partial denture would have caused periodontal problems.
One case does not prove anything, but the result speaks for itself and sadly the option to use our knowledge and initiative is no longer open to us.
The fun is gone!


By David Moffet
EA journey built on smoke and mirrors will always end badly...
“Imagine telling a new patient on the phone that the fee for their cleaning was $150.00 and then finding out when you meet them that they are a chronic smoker with advanced periodontitis in a mouth that hasn’t seen the inside of a dental office for forty years...”
very procedure and protocol in your office needs to operate with 100% crystal clear clarity.
When your dental practice skips essential steps, you create liabilities and time bombs that come back to haunt you at a significant multiple of devastation that massively outweighs the cost or imposition of simply doing things correctly in the first instance.
Recently, one of my clients found this out the hard way.
Let me explain...
I’ve always said...
I’ve always said, both as a dental practice owner and also as a dental practice coach, that when a new patient phones your office for an appointment for a check-up examination and a dental cleaning, the dental office needs to clarify politely to the caller, that there may be a possibility that their teeth may need two [or sometimes more] appointments to completely clean their teeth properly.
This is because if we do not frame this “variation” up from the get-go, then we can end up with a very irate customer inside our practice who says:
“Why can’t you clean my teeth in one visit?”
Or
“Do I have to pay for another visit so you can finish the job?”
Or
“You mean I have to come back? Why can’t you finish it all now?”
It is unreasonable…
It is unreasonable for any logical or sane person to believe that a dirty mouth and a cleaner mouth having a professional dental cleaning should take the same amount of time and also should incur the same fee.
Why would that be so?
Would an unruly tenant expect to pay a house cleaner a fee for an end of lease clean of the property that they have rented for two years [and trashed] that was equal to what a homeowner pays their weekly cleaning lady who visits every week?
Of course not… so why should mouths be different to houses?
You’re absolutely correct...
You’re right.
They should not be charged the same fee.
Because one requires far more work than the other.
We developed a perfect script...
At Active Dental, we developed a perfect script for our receptionists to use to inform every patient [new or existing] who was
well and truly overdue for a dental cleaning, that there may be a chance that a second visit could possibly be required.
This script worked well every time with no exceptions.
And that’s what your dental practice needs...
Imagine telling a new patient on the phone that the fee for their cleaning was $150.00 and then finding out when you meet them that they are a chronic smoker with advanced periodontitis in a mouth that hasn’t seen the inside of a dental office for forty years...
As my client said today...
When we don’t pre-qualify the patient [on the phone] that because it has been a while between visits for them, that they may need extra visits to complete their cleaning, then one of the following three scenarios will occur:
• We rush the cleaning and fail to complete it properly; or
• We only do a superficial cleaning and so the patient receives incomplete treatment; or
• We defer necessary treatment to a later date and the patient carries on without knowing that they have active periodontitis inside their mouth.
And all of these scenarios are unsatisfactory and unprofessional results for our valued patients.
It is our role and duty…
It is our role and duty as healthcare professionals first and foremost to be looking after the health of our patients thoroughly and completely.
Cutting corners now as an attempt to build unearned popularity is a sham and a house of cards.
Your patients will respect you more for your honesty.
Any deception displayed towards your patients will return ten-fold and bite you where it hurts.
A reputation built on smoke and mirrors will always end badly...
Dr David Moffet is a dentist and a #1 Amazon Bestselling author. He is the inventor of The Ultimate Patient Experience ™, a simple to implement patient retention system he used to build and subsequently sell (for several million dollars) his very successful practice [of 28 years] in working class western Sydney. David has now retired from wet-fingered dentistry and spends his time lecturing and coaching private dental clients in the USA, Canada, Great Britain, Europe and Australia and New Zealand on how to improve their practices. David can be contacted at david@theUPE.com or visit www.TheUltimatePatientExperience.com.

• Universal: For anterior and posterior region
• No layering: up to 4 mm increment thickness
• Highest stability: 91% filler content
• Excellent aesthetics: Outstanding polishability
• 5 Cluster-Shades: Cover all 16 VITA® classical shades


The specialist perspective on common surgical and restorative quandaries BRISBANE - JUNE 20-21 2025 MELBOURNE - AUGUST 8-9 2025
Presented by Specialists Prof. Axel Spahr and Dr Tom Giblin

Professor Axel Spahr
Specialist Periodontist in Private Practice and Head of the Discipline of Periodontics and Program Director of the Doctor of Clinical DentistryPeriodontics post-graduate program at The University of Sydney Dental School.
Doctor Thomas Giblin
Specialist Prosthodontist in Private Practice
President, International Congress of Oral Implantologists, Diplomate ICOI, Board Member of Australian Society of Implant Dentistry (ASID), Member of ADA, ACP, IAG, AARD.
This advanced course is tailored for dentists with prior experience in implant surgery, aiming to further refine their expertise and clinical proficiency. The program is designed to deepen participants’ understanding and enhance their skills in both the surgical and restorative aspects of implant procedures. It emphasizes essential clinical topics to optimise outcomes and success rates, including practical insights into common challenges and solutions.

n Evaluating the digital workflow in implant dentistry: practical benefits versus technological novelty.
n Digital shade analysis and lab communication.
n Prosthetic design single / bridge /full arch / removable.
n Restorative materials.
n Impressions vs scanning.
n Optical and biomechanical properties of natural teeth and restorative materials and why it matters.
n Restoration design and preparation geometry.
n Fitting and delivery of indirect adhesive restorations.
n Verification of treatment sequences and outcome validation.
n Breaking down complex cases with novel solutions to restorative dilemmas.
n Practical clinical applications and case studies.


n Patient selection and comprehensive treatment planning.
n The effects of systemic diseases and medications on surgical outcomes, healing and implant success.
n Risk assessment (SAC), and the influence of implant type, material, surface characteristics and implant/abutment connections.
n The use of short and reduced-diameter implants.
n Guidelines for implant planning, key parameters and management of peri-implant tissues.
n Immediate, early and late implant placement strategies.
n One-stage versus two-stage implant surgery techniques.
n Surgical instruments, materials, and common complications.
n Freehand versus guided implant placement methods.
n Implant maintenance to avoid problems.

Grin’s full virtual care ecosystem, offering personalised care, revenue boosting and AI-powered optimisation solutions, is now available to doctors and patients across both countries
GRIN, the leading remote monitoring and care platform for digital oral healthcare solutions, announced that its comprehensive system is now available to oral care professionals across Australia and New Zealand. This marks a major milestone in the company’s mission to create the next era of orthodontics globally. Grin now delivers AI-powered, human-first care across the US, Canada, Brazil, the EU, Israel and now Australia and New Zealand.
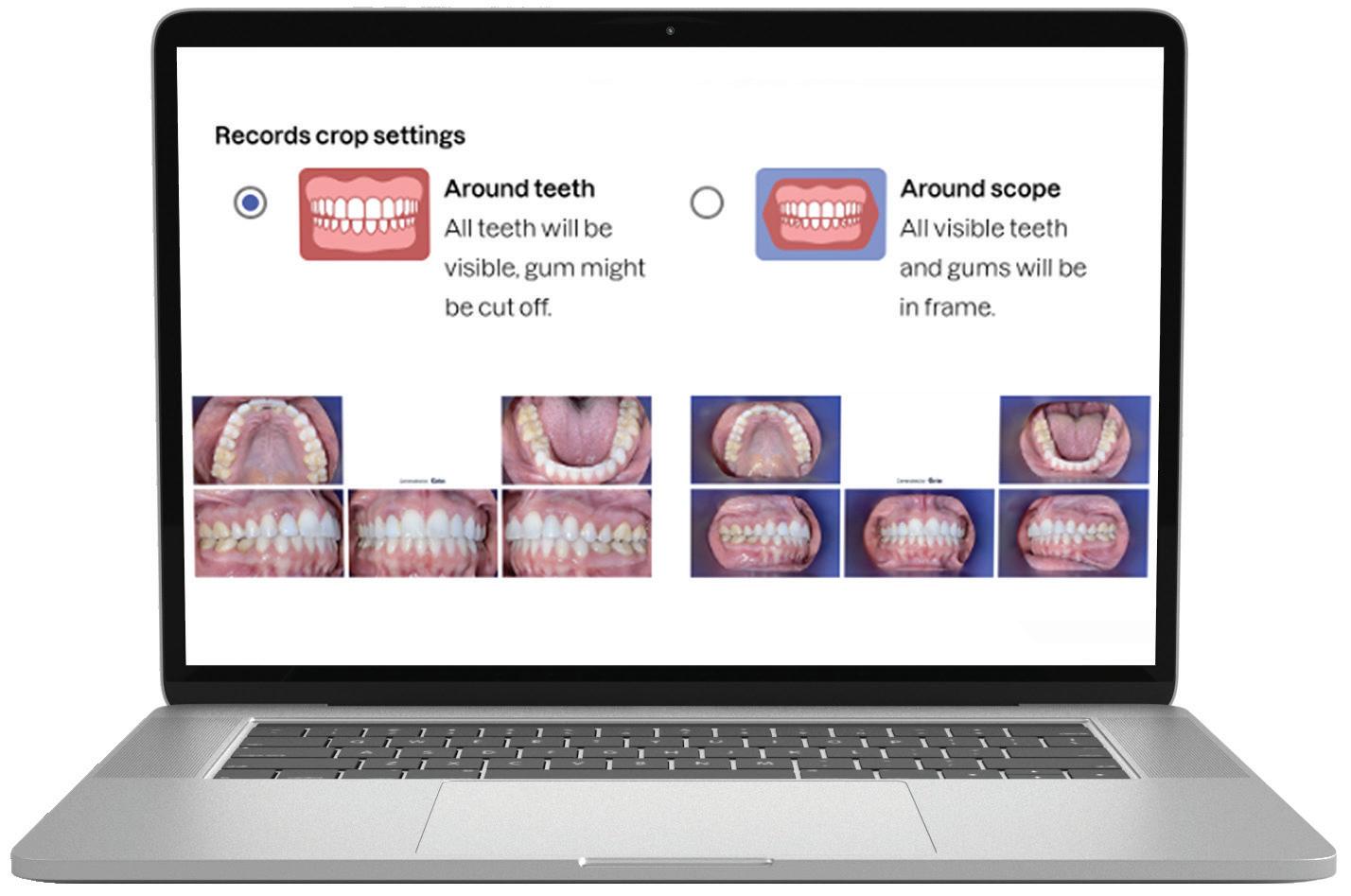
Grin’s full platform—including the FDA- and TGA-listed Grin Scope® and Scope Mini, now approved in Australia—features a powerful app, doctor portal and AI-enabled tools that strengthen patient relationships through virtual monitoring, human intelligence and realtime communication.
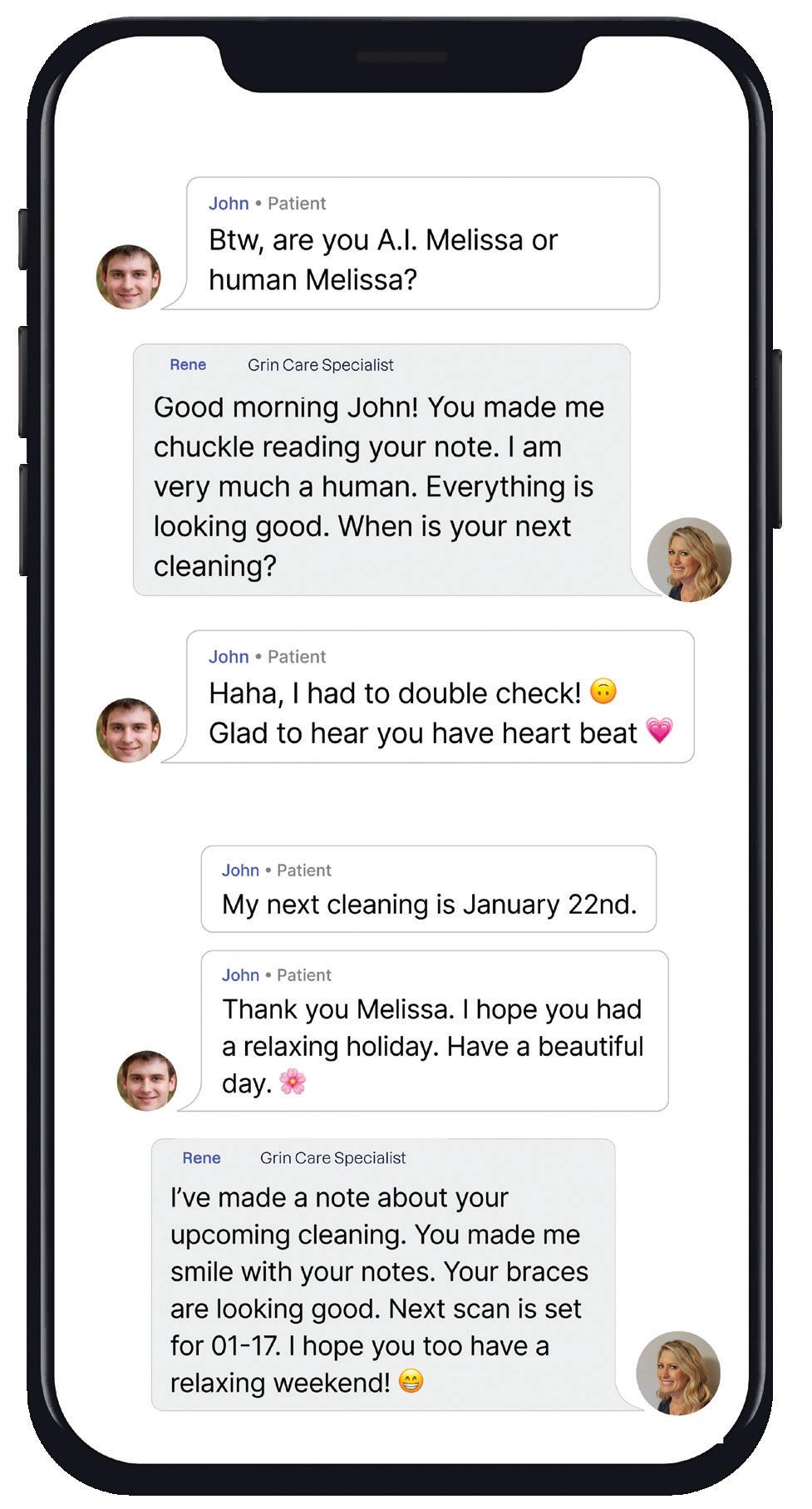
Typically, Grin Doctors provide patients undergoing orthodontic treatment, whether with brackets and wire or aligners, with a Grin Scope that attaches to their smartphone. The innovative Grin app then guides patients to video scan their teeth in treatment in front of a mirror. These scans are then immediately available to the clinician for review via the doctor portal to monitor treatment progress and address any clinical issues.


Importantly, at the heart of it all is the Grin Care Specialist—an extension of your team who ensures virtual care is seamless, your workflows stay efficient and your patients remain connected, engaged and on track every step of the way. Human Grin Care Specialists are able to maintain a dialogue with patients and alert Grin Doctors when required, increasing efficiency.
With features like Grin CoPilot™, Grin 3D Tx Tracker™, Grin RapidReferral™ and other enhanced AI-enabled tools, as well as a new integration with Clarity™ by Solventum, Grin’s platform offers an unmatched, scalable, patient-first solution.
“At Grin, our mission is to simplify care and make quality oral health more accessible to patients everywhere,” said Dr Adam Schulhof, CEO and Co-Founder of Grin. “We’re excited to extend this mission to providers across Australia and New Zealand, who, until now, haven’t had access to a comprehensive platform that combines AI-powered technology with human clinical oversight to deliver precision, streamline operations and foster stronger patient connections.”
Grin’s Australasian launch also sets the stage for greater access in rural and remote regions, reducing barriers to care. Grin’s ecosystem allows doctors to continue to scale while maintaining care with remote patients.
“I’ve watched Grin evolve over the past several years,” said Dr Vas Srinivasan, specialist orthodontist and practice owner at Invisible Orthodontics in Hervey Bay, Queensland. “I value its sleek, intuitive design that enables me to monitor progress, step in when necessary and minimise unnecessary appointments. Most importantly, I feel confident scaling my practice with Grin, knowing it was built by Dr Adam Schulhof—an orthodontist who truly understands what it takes to grow successfully.”
“Grin brings something truly fresh to the ANZ market— a smart, clinically driven platform that meets the evolving needs of both providers and patients,” said Andrew Holmes, CEO of Liift Dental, distributor of Grin in Australia and New Zealand.
“Having seen the challenges practices face in balancing growth with efficiency, I believe Grin’s combination of AI-powered tools and human clinical oversight offers a practical, scalable solution. Its flat-fee pricing model that includes the Grin Scope and what amounts to lifetime monitoring delivers real financial value to Australian practices—providing cost predictability, supporting increased patient volume and helping improve the bottom line without the burden of rising fees. It’s a smarter way to grow and exactly the kind of innovation this region has been waiting for.”
Based in New York, Grin is a comprehensive digital platform that provides solutions for all oral health needs. The Grin App and Grin Scope® allow doctors to access a full patient management suite. Patients can access quality professional care from the convenience of their smart devices. Doctors can remotely monitor patients via virtual check-ins for complete visibility—reducing chair time, increasing patient volume, and ensuring safety and beautiful smile results.
For more information on Grin ®, visit www.get-grin.com or call ANZ Country Manager Andrew Holmes on 0420-985-661, email grin@liift.dental or call (02) 8355-2200.
The Ivoclar Group is launching Tetric® plus, a new simplified composite specially designed to set new standards in universal composites. Tetric plus takes its name from the Greek prefix “tetra”, meaning “four” and this number is central to its key product features. It incorporates four essential elements: simplified shade matching with just 4 shades, increments of up to 4mm for greater efficiency, versatile application options in all 4 quadrants and an optimised 4-filler technology for excellent handling and aesthetic results.
Tetric plus revolutionises shade selection in dentistry, allowing for easy shade matching with its innovative colour cloud concept. Just 4 shades cover the entire spectrum of the classical VITA shades. Thanks to its exceptional shade adaptation, Tetric plus creates an outstanding chameleon effect: In its cured state, the material absorbs and scatters light in a way that closely mimics natural tooth structure, allowing it to blend almost seamlessly with the surrounding tooth structure. This high level of adaptation is achieved through the perfect combination of monomers, fillers and pigments.
Another remarkable feature of Tetric plus is its ability to accommodate variable layer thicknesses ranging from 0.1 to 4mm, allowing for greater flexibility while also reducing material consumption. Another notable advantage is its reliable curing time of just 3 seconds,1 that allows for a fast and easy application. These short curing times streamline workflows, minimise interruptions for dentists and enhance treatment efficiency. By enabling faster and more efficient restorations, Tetric plus not only saves valuable time but also improves the overall patient experience.

Tetric plus is a simplified universal composite that is suitable for all cavity classes, from Class I to V. With just one product, dentists can treat a wide range of indications in all 4 quadrants, significantly reducing material consumption and streamlining the workflow. For maximum handling convenience, Tetric plus is available in two viscosities: sculptable and flowable.
Tetric plus Fill is characterised by a sculptable viscosity. The viscosity can be adjusted, if desired, by heating the material up to 68°C, without compromising its mechanical properties.
Tetric plus Flow, by contrast, offers a universal viscosity that stands out due to its exceptional thixotropic properties. This flowable composite combines precision and high stability with excellent flowability, enabling quick and efficient volume replacements. Furthermore, Tetric plus Flow adapts smoothly to cavity walls and has a self-levelling effect, providing for ideal cavity adaptation.
The quality of Tetric plus is defined by its innovative 4-filler technology, which integrates a combination of nano-
and micro-particles to deliver outstanding mechanical properties. Tetric plus ensures reliable curing for layers of up to 4mm while offering high radiopacity to facilitate accurate detection during diagnosis. The mechanical properties include high flexural strength (133 MPa), high compressive strength along with low wear and low shrinkage stress, reducing the risk of marginal gaps.
Tetric plus is more than just another composite: it is designed to simplify the daily workflow of dentists and optimise their treatment efficiency. With easy shade selection and short curing times, dentists can focus entirely on patient care, while delivering efficient and high-quality work. In summary, Tetric plus combines 4 shades with 4mm layer thicknesses, universal applicability in all 4 quadrants and an innovative 4-filler technology, making it the ideal solution for the demands of modern dentistry.
For more information on Tetric® plus, visit https://www.ivoclar.com/tetric-plus or 1300-486-252, orders.au@ivoclar.com NZ: 0508-486-252 orders.nz@ivoclar.com
1. With Bluephase PowerCure in the 3sCure mode

Tetric® plus Simplified universal composite
– 5 cavity classes
– 4 shades
– 3 seconds curing time
– 2 viscosities
– 1 universal composite

dentevents presents...
SYDNEY 1-2 AUGUST 2025
NOVOTEL SYDNEY BRIGHTON BEACH
TWO DAYS OF LECTURES AND WORKSHOPS ON DIGITAL DENTISTRY FOR DENTISTS, SPECIALISTS,
DENTAL TECHNICIANS AND DENTAL PROSTHETISTS
ONLY $880 FOR 2 DAYS OF EDUCATION











Join us again or for the first time at Digital Dentistry & Dental Technology No 6 for a fun, exciting and fully immersive learning experience with the best of the best in the new age of dentistry. This year’s program will again cover Digital Smile Design • Digital orthodontics • Intraoral scanning • 3D Facial Scanning • Digital implantology • Digital full arch restorations and full mouth rehabilitations • Digital Dentures • 3D Printing • Milling • CBCT • Materials and applications • Software and more with MORE Hands-on Sessions • MORE Advanced Sessions
REGISTRATION FEES
$880 inc gst
EARLY BIRD PRICING
$440 before 5 apr 2025 price increases $110 on the 2nd of every month
$440 before 24 Jan 2024 price increases $110 on the 2nd of every month INCLUSIONS Registration fee includes participation in TWO full days of education (12 CPD hours), all catering and Friday drinks. Multiple lectures and workshops are being run concurrently to allow you to build your own program to suit your specific interests. Price is all inclusive.
VENUE DETAILS
VENUE DETAILS
and more!
Join us again or for the first time at Digital Dentistry & Dental Technology No 5 for a fun, exciting and fully immersive learning experience with the best of the best in the new age of dentistry. This year’s program will again cover Digital Smile Design • Digital orthodontics • Intraoral scanning • 3D Facial Scanning • Digital implantology • Digital full arch restorations and full mouth rehabilitations • Digital Dentures • 3D Printing • Milling • CBCT • Materials and applications • Software and more with MORE Hands-on Sessions • MORE Advanced Sessions • MORE New Products • NEW Masterclasses... and more! ONLY $440 FOR 2 DAYS OF EDUCATION (12 HOURS OF CPD) IF YOU REGISTER BEFORE 24 JANUARY 2024 (SAVE 50%) TWO DAYS • 6 CONCURRENT EDUCATION STREAMS 39 TOP SPEAKERS • 80 EDUCATION SESSIONS THE
PROGRAMME DETAILS
PROGRAMME DETAILS
FRIDAY 24 MAY 2024 9.00am - 5.00pm - education 5.00pm - 7.00pm - happy hour SATURDAY 25 MAY 2024 9.00am - 5.00pm - education
FRIDAY 1 AUGUST 2025 9.00am - 5.00pm - education 5.00pm - 7.00pm - happy hour SATURDAY 2 AUGUST 2025 9.00am - 5.00pm - education
12 HOURS CPD
Novotel Sydney Brighton Beach - The Grand Parade, Brighton-Le-Sands NSW 2216 - Close to Sydney Domestic and International Airports Check the website for details of discounted accommodation rates for the conference • Ample parking available at the hotel
Street Publishing Pty Ltd ABN 74 065 490 655 www.dentevents.com • info@dentist.com.au • Tel: (02) 9929 1900 • Fax: (02) 9929 1999



































By Angus Pryor
The Chicago Dental Society (CDS) Midwinter Meeting has long been a cornerstone of the dental industry and in 2025, it celebrated a remarkable 160 years, making it the oldest dental conference in the US. This milestone was not just about longevity but also about the continuous evolution of the event—keeping pace with technological advancements, fostering community and providing an unmatched platform for education and networking.
We had the pleasure of speaking with Dr Denise Hale, President of the Chicago Dental Society, to get an insider’s perspective on what made this year’s meeting special.
Dr Hale credits the event’s success to the tight-knit nature of the dental profession. Unlike some other medical fields, dentistry thrives on collaboration rather than competition. She highlighted how CDS actively scouts globally—from Canada to Mexico and even Australia—to bring in fresh voices, cuttingedge research and new technology. “There’s a lot of camaraderie in dentistry,” she explained. “We travel far and wide to bring the best speakers and exhibitors to Chicago.”
The Midwinter Meeting is one of the biggest dental trade shows in North America, making it a prime location for companies to unveil new products.
“Many companies use the Chicago show to launch products,” Dr Hale confirmed. “It’s one of the top meetings in the country and getting a speaking slot here can launch a speaker’s career.”
This reputation attracts international attendees, including a growing number from Australia. One Australian dentist put it simply: “Whatever I see on the exhibit floor here, I know will be coming to Australia in the next year or two. It helps me stay ahead of the curve.”
Beyond the tech and education, this year’s keynote speaker left a lasting impact. Chef Grant Achatz of the renowned Michelin-starred Chicago restaurant, Alinea, shared his courageous journey battling stage IV tongue cancer and detailed his groundbreaking treatment and recovery as well as discussing the vital role dentists played in his oral cancer detection
Grant faced multiple hospitals that suggested radical surgery; he found an alternative treatment path that saved his speech, taste, and ultimately, his career.
“I wasn’t ready to accept that. On the advice of a friend, I went to the University of Chicago. There, I was offered a different path—an experimental trial with chemotherapy and radiation. No surgery. No amputation of my tongue. It was a risk, but I took it. And it worked. That was 2008. Now, 16 years later, I stand here, cancer-free, still doing what I love—still tasting, still creating, still speaking.”
With 500 people in attendance, his story was a powerful reminder of resilience and innovation—values that resonate deeply with the dental community.
The Midwinter Meeting is known for its robust Continuing Professional Development (CPD) program, but this year, the buzz was also about new technology.
Dr Hale was particularly fascinated by 3D printing and digital scanning, which she believes will revolutionise dentistry.
“If I were 20 years younger, I’d be all over that,” she admitted. “In the future, labs might become obsolete because everything can be made in-office.”
To support learning, CDS increased its hands-on workshops, which proved to be hugely popular; many sold out quickly.
Achallenge for any long-standing event is keeping it fresh and relevant and CDS has tackled this head-on. One key focus has been engaging younger dentists.
To attract new generations, the event introduced a more vibrant social scene, including a disco night with a DJ—a sharp contrast to the formal President’s Dinner Dance.
“We want to keep young people engaged,” Dr Hale said. “The dance floor was full—it was fantastic!”
Another major takeaway from the pandemic was the importance of in-person events. Exhibitors made it clear: they wanted a physical show, not a hybrid event. Dentists, too, preferred handson experiences—touching materials, testing equipment and interacting with products firsthand.
For those considering attending next year, Dr Hale’s message is simple: “The energy here is electric. If you want to see where dentistry is heading, network with industry leaders and experience the latest innovations firsthand—Chicago is the place to be.”
With its rich history, forward-thinking approach and commitment to community, the CDS Midwinter Meeting continues to be a must-attend event for dental professionals worldwide.
Internationally award winning composites.
50+ years of innovation, serving dentists in over 100 countries.



William Green are taking inspiration from the automotive industry with the launch of its new Diplomatic Immunity deal, offering a 6-year warranty and fixed price service on its full range of Diplomat dental units.
“The Diplomat range are ultra-reliable, fully-featured, high-quality Europeanmade dental units at a variety of attractive price points,” said Ryan Green, managing director of local distributor, William Green Pty Ltd. “However, the Diplomat brand is not as well-known as some in Australia and as a result, buyers may be wary in regard to their reliability and service support.
“So we looked around at other markets and there are a lot of synergies with the automobile industry and the trend towards long warranties and low cost of ownership being used to put buyers’ minds at ease.
“As a result, we’re now reinforcing the Diplomat range with a real 6-year warranty and fixed price servicing during that same period, backed by William Green, the company my grandfather started 78
years ago. In short, trust the brand and we’ll back you 100%.”
Mr Green said that once customers are introduced to the Diplomat range, they are surprised by its ergonomic design combined with lux-level comfort for patients.
“The Diplomat range has a dental unit model suitable for every dental practice – whether you’re on a budget or looking for a fully featured unit with smart connectivity, advanced technology and a full range of options and accessories. There is the perfect unit in the range for every practice.
“And now, Diplomat also has an industry leading ‘real’ 6-year warranty.”
Mr Green said that with most dental equipment being financed, the Diplomatic Immunity deal effectively caps your expenditure over that period. You have the lease payment and the annual fixed price service fee. That’s it. If you’re fitting out a multi-chair clinic, then that becomes even more attractive.
Mr Green said William Green has been selling Diplomat for over a decade and they have hundreds of satisfied customers in Australia already.
Diplomat has been engineering dental units that outlast and outperform the competition for 60 years and are recognised in Europe for superior reliability, advanced technology and award-winning design.
Features include smart handpiece recognition, brushless micromotors with endodontic functions, 3D pneumatic headrests, customisable water, speed and torque controls and a truly open, limitless Smart Display that lets you use any iPad or Android tablet for full access to your imaging software, practice management system, web browsing and even patient education on YouTube.
The Diplomatic Immunity deal is a simple proposition, according to Mr Green.
“Purchase a Diplomat dental unit and commit to the annual fixed price service plan and we will guarantee the product for six years. A fully-featured, high-quality European-made dental unit guaranteed for 6 years… What more could you ask for?”.
For more information on the new Diplomatic Immunity 6-year warranty with fixed price servicing deal, visit www.williamgreen.com.au

Your guaranteed solution for dental unit reliability across the entire Diplomat range
l Available on the full range of dental units from budget to high-tech ultra-lux.
l 6-year warranty on parts and labour.
l Fixed price annual servicing (required to validate warranty).
l Made in the European Union (Slovakia) by Diplomat (established 60 years).
l Serviced nationwide by William Green Pty Ltd (established 78 years).
l Open, Limitless Smart Display with iPad or Android tablet compatibility (Pro Model).
l Brushless micromotors with endo functions, 3D pneumatic headrest, smart handpiece recognition, customisable water, speed & torque controls and more...
Visit our Sydney showroom to try the Diplomat range before you consider buying any other dental unit for your practice!
William Green Pty Ltd
47- 49 Mary Parade
Rydalmere NSW 2116
Ph + 61 2 8865 0300



Presented by Dr Angelo Lazaris
SYDNEY • SEP 19-20 |
• OCT 24-25

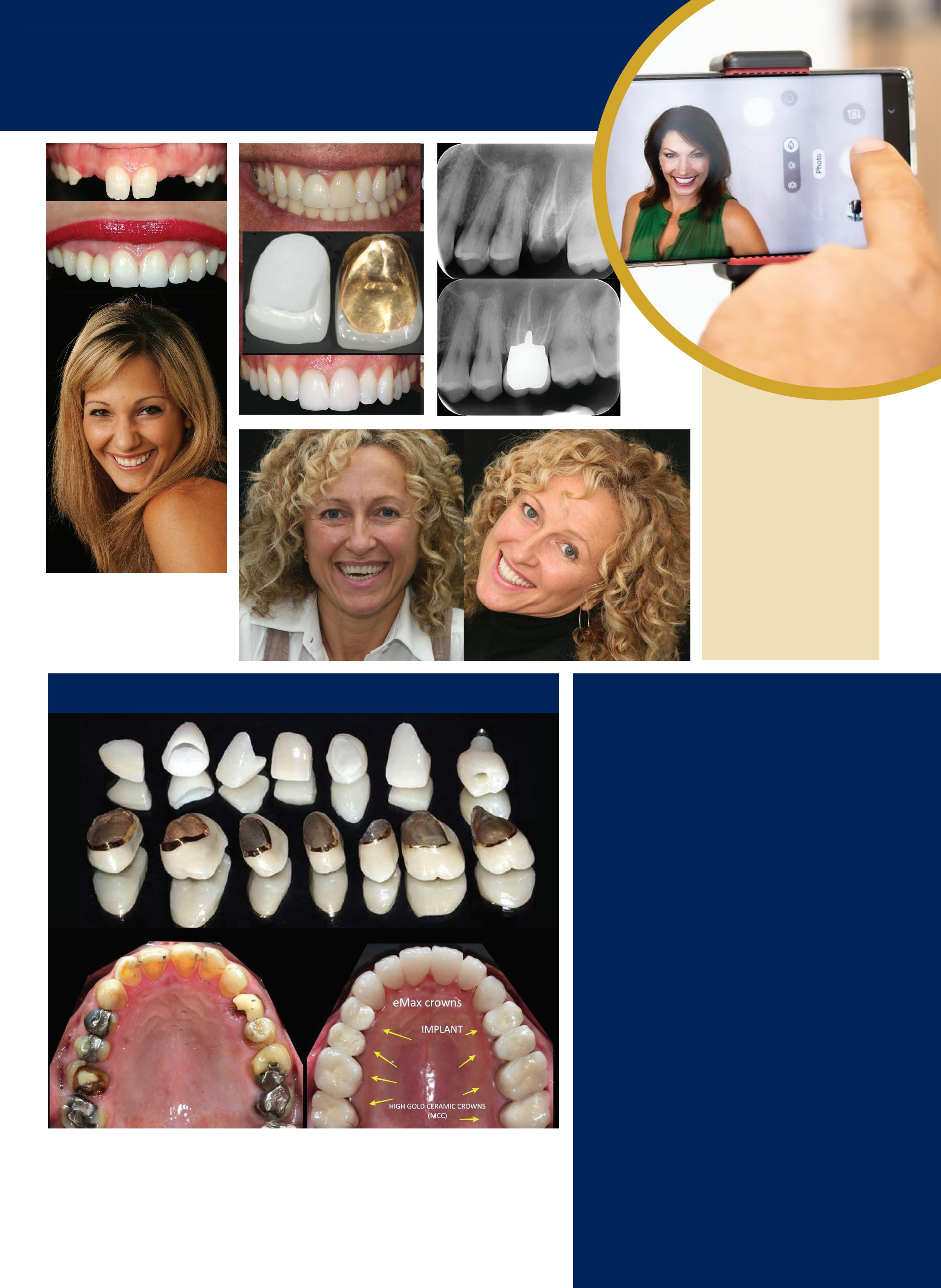
Dr Angelo Lazaris is renowned as the doyen of dental veneers... Celebrities, professionals, billionaires and every day Australians seek out Dr Lazaris when they want outstanding aesthetic excellence...
In the ALPHA TO OMEGA OF VENEERS, Dr Lazaris shares his unique, aesthetically-driven protocols and digital workflows as a unified system developed specifically to enhance clinical efficiency and predictability and eliminate any margin for error. Structured in a modular sequence, each topic is delivered as a step in a methodical, reverse-engineering process that maps out a logical pathway to achieving superior treatment outcomes with precision and confidence. Honed through comprehensive critical analysis and evolution, these protocols are universally applicable to every dentist, every patient and every case...
VENEERS are the #1 requested cosmetic dentistry procedure - LEARN TO DELIVER EXCELLENCE!





BDS (Hons) (Syd), MSc (Aes) (Kings College)
Angelo has developed his own complete digital protocols from inception and design through to delivery and integrated these with biomimetic adhesive dentistry and contemporary restorative materials to create a complete clinical workflow that is equally applicable to single restorations, through to complex full mouth rehabilitations, culminating in outstanding clinical outcomes in a real-world commercial environment. His innovative approach to clinical dentistry is to start at the desired
endpoint, deconstruct complex treatments and develop solutions have made him a sought after KOL, educator and mentor. With appointments including honorary senior lecturer for Kings College London and the University of Sydney, Angelo has recently been assigned as course director for a post graduate diploma and masters degree in digital dentistry; a testament to his expertise and the influence of this discipline in dental practice.


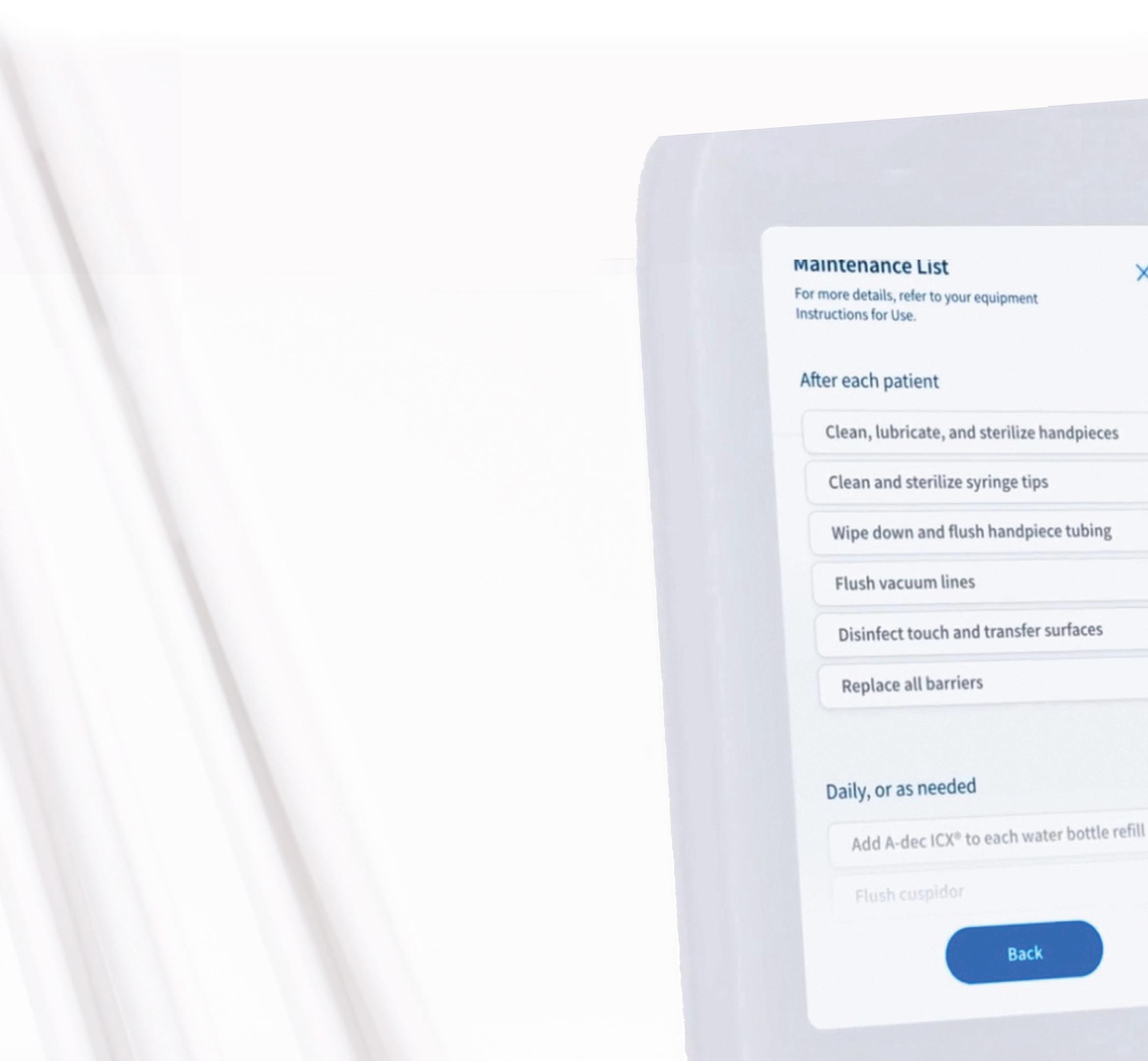
We depend on technology in our everyday lives to make things easier. From smartphones and home automation to park-assist on our cars. Now life can be just as easy using your dental equipment, thanks to the latest A-dec Pro delivery systems enabled with “A-dec+” –available on new A-dec Pro dental units.
“A-dec+” is an updatable software program, giving you a new level of connection to make your work life easier and enable you to be better prepared, day after day, patient after patient.
In turn, both you and your patients will enjoy the exceptional comfort, access and support that only an ergonomically designed and highly awarded A-dec patient chair can provide.
The flagship A-dec Pro combines the proven A-dec 500 patient chair with a new delivery system, the most obvious of which is a new control head and larger touchscreen with its stunning graphics and a host of intuitive built-in features.
A-dec Pro’s A-dec+ platform brings your dental units right up to the 21st Century with these key features:


Designed to be viewed from any angle, the Dynamic Screen 7 (DS7) touchpad provides a clear visual (and audio) connection with your equipment.
The intuitive settings are right at your fingertips and are easy to customise for the way you work.
From initial setup of the touchpad in your preferred language and displaying your actual chair colour on the screen; to graphically displaying the exact chair position (selectable with a single touch on the graphic icon); to setting a timer when working with light-cured composites.
With the DS7 touch screen, you’ll see just what you need, depending on the selected function so that you can stay focused on your patient. For example, dynamic presets change when you pick up an instrument, showing the instrument type and things like motor speed (or speed at the bur if desired) on the active screen.

Dedicated memory buttons let each user personalise their instrument presets for endodontics, electric motors, scalers and timers. Clear, visual onscreen confirmations of the selected function help you work with confidence, automatically showing the chosen instrument and its settings.
Multi-user capabilities let each user select their preferred chair and instrument settings. This can move with you to another chair in each connected surgery. At the end of the day, maintenance schedules and software updates are available on the touchscreen for your review.
The DS7 touchscreen displays daily maintenance checklists and diagnostic equipment alerts right there on your touchscreen without having to remove equipment covers.
Y
ou can monitor all your A-dec equipment’s data through the A-dec+ app. With a scalable platform, you can manage and monitor you’re A-dec+ enabled equipment across a single practice or a multi-clinic organisation.
While A-dec 500 chairs are dependable and extremely long lasting, technology is ever-changing which makes A-dec+ so important in helping future-proof your practice. The ability to integrate new clinical capabilities with the existing A-dec Pro delivery platform means your equipment can continually evolve with you – and your practice.
New ancillaries like electric motors, cameras, 3D scanners and scalers can be easily added to the DS7 touchpad for seamless integration. Once added, the settings for each instrument can be displayed on the touchscreen, such as the colour-coded intensity of Satelec scalers for example.


Once you register on the A-dec+ app, new product features, enhancements and integrations will be available over time through software updates.
In the future, A-dec+ will offer evolving equipment management options for your entire suite of A-dec connected equipment for better equipment performance and utilisation.
The A-dec Pro delivery system is built on the award-winning A-dec 500 patient chair platform. Features that make this dental unit so popular are its superior ergonomics and comfort for both operator and patient, now with the enhanced A-dec Pro delivery system.
With six instrument positions on the A-dec 500 Pro, you can integrate many existing and future combinations, from turbines and electric handpieces to intraoral cameras, scalers and curing lights.
You can smoothly and precisely place the delivery system where you want it and count on it to stay there without drifting thanks to A-dec 500 Pro’s inbuilt capacitive-touch brake which automatically activates as soon as you release the grab handle.

hoosing the right dental equipment increases your personal comfort, productivity and ultimately, success. To help guide you in this process, A-dec has produced a helpful booklet: What to Look for When Buying Dental Equipment”. With the wide array of flexible dental unit configurations suited to general dental and different specialties, this handy guide includes information based on input from doctors, dental industry experts, dealers and technical specialists – all designed to help you choose the right dental equipment with confidence.
To find your nearest A-dec dealer contact 1800-225-010 or visit australia.a-dec.com.
Asmall but much-admired feature is the new LED coolant indicator that lights up when a handpiece is lifted so you can adjust the coolant flow without having to second guess which knob to touch.
The segment leading A-dec Pro 300 Pro, with it’s more compact head and 5” Control Pad 5i (CP5i) and simplified graphics, can be upgraded with the optional A-dec+ Gateway module to also enable you to also add new capabilities and future products on the open platform A-dec+ software.
A-dec 300 Pro’s innovative 4-position control block design is enough to accommodate most surgeries with their lowspeed, high-speed, scaler and Triplex syringe needs, together with an optional electric motor or accessory such as an intraoral camera.
All of this new technology is backed by A-dec’s unbeatable 10-year warranty for total peace of mind. Experience the best in quality, reliability and ergonomics with today’s and tomorrow’s technology built right in.
Find out about the exciting new world of A-dec Pro delivery systems and A-dec+ software at your authorised A-dec dealer. Phone 1800-225-010 or visit australia.a-dec.com.






Which A-dec® delivery is right for you?
Whatever your practice style, A-dec has a delivery that’s made for you, from the leading-edge A-dec 500 Pro to the efficiently compact A-dec 300 Pro. And with updatable A-dec+ software on board*, you’ll have the flexibility to integrate the latest clinical products anytime. For a delivery that’s truly your own, scan the QR code on the left to speak with your A-dec Territory Manager.


ICOI World Congress
ICOI World Congress
September 11–13, 2025
ICOI World Congress
September 11–13, 2025
September 11–13, 2025
“Modern Implantology — Is the Latest Really the Greatest or Can We Learn from History?”
“Modern Implantology — Is the Latest Really the Greatest or Can We Learn from History?”
“Modern Implantology — Is the Latest Really the Greatest or Can We Learn from History?”
Sheraton Grand Sydney Hyde Park

Sheraton Grand Sydney Hyde Park
161 Elizabeth St.
161 Elizabeth St.
Sheraton Grand Sydney Hyde Park
161 Elizabeth St.
Sydney, Australia
Sydney, Australia
Sydney, Australia
Sheraton Grand Sydney Hyde Park
161 Elizabeth St.
Sydney, Australia
September 11–13, 2025
“Modern
At the forefront of innovation and excellence in implant dentistry, our mission is to convene the premier gathering of professionals from around the globe, united by a shared commitment to advancing the field and improving patient care. Through cutting-edge research, unparalleled education, and meaningful collaboration, we strive to inspire, empower, and equip our attendees with the knowledge, skills, and insights necessary to achieve excellence in every aspect of clinical implantology. By fostering a culture of continuous collaborative learning, innovation and excellence, we aim to shape the future of implant dentistry, driving positive change and making a lasting positive impact on the lives of patients we treat worldwide.
Sheraton Grand Sydney Hyde Park
At the forefront of innovation and excellence in implant dentistry, our mission is to convene the premier gathering of professionals from around the globe, united by a shared commitment to advancing the field and improving patient care. Through cutting-edge research, unparalleled education, and meaningful collaboration, we strive to inspire, empower, and equip our attendees with the knowledge, skills, and insights necessary to achieve excellence in every aspect of clinical implantology. By fostering a culture of continuous collaborative learning, innovation and excellence, we aim to shape the future of implant dentistry, driving positive change and making a lasting positive impact on the lives of patients we treat worldwide.
161 Elizabeth St.
At the forefront of innovation and excellence in implant dentistry, our mission is to convene the premier gathering of professionals from around the globe, united by a shared commitment to advancing the field and improving patient care. Through cutting-edge research, unparalleled education, and meaningful collaboration, we strive to inspire, empower, and equip our attendees with the knowledge, skills, and insights necessary to achieve excellence in every aspect of clinical implantology. By fostering a culture of continuous collaborative learning, innovation and excellence, we aim to shape the future of implant dentistry, driving positive change and making a lasting positive impact on the lives of patients we treat worldwide.

Sydney, Australia
Dr Louie Al-Faraje
General Practitioner
Dr. Louie Al-Faraje
San Diego, California
General Practitioner
San Diego, California

Dr Ady Palti
General Practitioner
Edgewater, New Jersey
Dr Ophir Fromovich
Mastery of Advanced Techniques: Equip attendees with the knowledge and skills to master advanced gical and restorative techniques.
Dr. Ady Palti
General Practitioner
Adamin, Israel
Deciphering of Emerging Technologies: Explore implant dentistry’s latest innovations and emerging technologies, providing insights into cutting-edge treatment modalities and materials.
General Practitioner

Edgewater, New Jersey
• Comprehensive Treatment Planning: Enhance your ability to develop comprehensive treatment plans tailored to individual patient needs and maximise predictable outcomes.

Dr Rachel Schallhorn
Periodontist
Dr Teruaki Homma
General Practitioner
Dr. Ophir Fromovich
Denver, Colorado
General Practitioner

Prof. Dong-Seok Sohn
Mastery of Advanced Techniques: Equip attendees with the knowledge and skills to master advanced gical and restorative techniques.
Tokyo, Japan
Management of Complications: Doing is one thing, but effectively managing complications and challenges that may arise is another.
Mastery of Advanced Techniques: Equip attendees with the knowledge and skills to master advanced gical and restorative techniques.
Oral & Maxillofacial Surgeon
Dr. Rachel Schallhorn
Periodontist

Daegu, Korea
Deciphering of Emerging Technologies: Explore implant dentistry’s latest innovations and emerging technologies, providing insights into cutting-edge treatment modalities and materials.
Multidisciplinary Collaboration: Foster collaboration among dental specialists, including prosthodontists, periodontists, oral surgeons and implantologists, to optimise superior results.
Adamin, Israel

Denver, Colorado
• Deciphering of Emerging Technologies: Explore implant dentistry’s latest innovations and emerging technologies, providing insights into cutting-edge treatment modalities and materials.
Dr Jedediah Huss
General Practitioner
Prof. Axel Spahr Periodontist,
Comprehensive Treatment Planning: Enhance your ability to develop comprehensive treatment plans tailored to individual patient needs and maximise predictable outcomes.
Santa Rosa, California
Dr. Teruaki Homma
Prof. University of Sydney
Sydney, Australia
Dr Dean Licenblat General Practitioner
Patient-Centred Care: Emphasize the importance of effective communication, informed consent, and patient education, to enhance patient satisfaction and treatment success. Address ethical / legal considerations and adherence to professional standards and regulations.
Comprehensive Treatment Planning: Enhance your ability to develop comprehensive treatment plans tailored to individual patient needs and maximise predictable outcomes.
Prof. Dong-Seok Sohn
Sydney, Australia
Management of Complications: Doing is one thing, but effectively managing complications and challenges that may arise is another.
Management of Complications: Doing is one thing, but effectively managing complications and challenges that may arise is another.
General Practitioner Tokyo, Japan


Oral & Maxillofacial Surgeon

Evidence-Based Practice: Promote the integration of evidence-based principles into clinical decision-making, critically evaluate research literature and apply the latest scientific findings.
Daegu, Korea
• Multidisciplinary Collaboration: Foster collaboration among dental specialists, including prosthodontists, periodontists, oral surgeons and implantologists, to optimise superior results.
Dr Larissa Steigmann
Periodontist
Dr. Jedediah Huss
Tel Aviv – Yafo, Israel
Dr Justin Moody General Practitioner
Scottsdale, Arizona
Multidisciplinary Collaboration: Foster collaboration among dental specialists, including prosthodontists, periodontists, oral surgeons and implantologists, to optimise superior results.
Dr Konstantinos Valavanis
General Practitioner
Prof. Axel Spahr
Athens, Greece
Patient-Centred Care: Emphasize the importance of effective communication, informed consent, and patient education, to enhance patient satisfaction and treatment success. Address ethical / legal considerations and adherence to professional standards and regulations.
General Practitioner Santa Rosa, California


Patient-Centred Care: Emphasize the importance of effective communication, informed consent, and patient education, to enhance patient satisfaction and treatment success. Address ethical / legal considerations and adherence to professional standards and regulations.
Periodontist; Prof. University of Sydney
• Evidence-Based Practice: Promote the integration of evidence-based principles into clinical decision-making, critically evaluate research literature and apply the latest scientific findings.

Dr Alvaro Ordonez
ICOI designates the Scientific Program for 20 continuing education credits. All Scientific Session presentations are lecture format and qualify for AGD Subject Code 690 Implant.
Orofacial Pain/Implants Specialist
Elanora Heights, NSW, Australia
Evidence-Based Practice: Promote the integration of evidence-based principles into clinical decision-making, critically evaluate research literature and apply the latest scientific findings.
Prof. Man Yi
Dr. Dean Licenblat
South Miami, Florida

Oral & Maxillofacial Surgeon; Prof. Sichuan University Sichuan, China
Dr. Larissa Steigmann
Periodontist
General Practitioner Sydney, NSW, Australia
ICOI is an ADA CERP Recognized Provider. ADA CERP is a service of
CERP at www.ada.org/cerp.
Tel Aviv – Yafo, Israel
International Congress of Oral Implantologists (ICOI). Nationally Approved PACE Program Provider for FAGD/MAGD credit. Approval does not imply acceptance by any regulatory authority or AGD endorsement. April 1, 2024 to March 31, 2028. Provider ID# 217378.
ICOI designates the Scientific Program for 20 continuing education credits. All Scientific Session presentations are lecture format and qualify for AGD Subject Code 690 Implant.
ICOI designates the Scientific Program for 20 continuing education credits. All Scientific Session presentations are lecture format and qualify for AGD Subject Code 690 Implant.
Dr. Justin Moody
General Practitioner
Scottsdale, Arizona
Dr. Alvaro Ordonez
Dr. Konstantinos Valavanis
General Practitioner
Athens, Greece
Prof. Man Yi
For more information and registration visit https://icoi.world/upcoming-events
Orofacial Pain/Implants Specialist
South Miami, Florida
Oral & Maxillofacial Surgeon; Prof. Sichuan University
Sichuan, China
TikTok, Instagram Reels and YouTube Shorts are taking over and they’re not just for dance trends. Quick, 15-60 second videos are a powerful way to showcase patient stories, answer common questions or introduce your team. Keep it simple, keep it authentic and keep it under a minute.
Real vs perfect: Authenticity wins
Over-polished, ad-style posts are fading fast. Patients want to see the real side of your practice - the friendly banter between team members, the behind-the-scenes of a busy clinic, even the honest answers to patient questions. Raw, relatable content builds trust faster than any stock image ever will.
BY ANGUS PRYOR
your audience but also encourages them to seek your services for their dental needs.
Community content: Your patients are your best creators Encourage happy patients to share their experiences, tag your practice and leave reviews. User-generated content isn’t just free marketing, it’s social proof. Whether it’s a selfie with their new smile, a shoutout for a painless visit, or a thank-you message, their stories are more convincing than any ad you can create.

Educational content: Establishing authority
Providing informative content, like explaining procedures or debunking dental myths, positions your practice as a knowledgeable and trustworthy source. This not only educates
Collaborative content with local businesses
Partnering with local businesses for co-branded social media posts can enhance your community presence. For example, collaborating with a nearby gym or health food store for a wellness campaign can introduce your practice to a broader audience, fostering community ties and mutual promotion.







When choosing Ampac Dental, your getting More Than Equipment. Your gaining a dependable partner that provides genuine, personalised support, and collaboration in the success of your practice.
1.Diagnostics & Photography
2.Treatment Planning
3.Occlusion & TMD/facial pain
4.Composite Reconstructions
5.Tooth Wear Management/ Restorative Treatment options
6.Periodontics & Aesthetic Dentistry
7.Minimal Intervention Ultra Thin Porcelain Technology
8.Fixed Prosthodontics - Tooth Supported Crown & Bridgework Impressions, Preps, Posts
9.Removable Prosthodontics
10.Implant Prosthodontics & Surgical Planning
11.Dentofacial Aesthetics
12.Full-mouth Reconstructions
Course starts in Mid 2025
Certificate 14,500.00 + GST (Module 1-6)
Diploma 25,000.00 + GST (Module 1-12)
Each Module is 100 Hours
20 hours face to face teaching, 20 hours of online lectures and 60 hours of self-directed guided learning.
This would include 40 hours of CPD per module which equals 240 CPD hours across 6 modules or 480 CPD hours over 12 modules.
2 Year Programme Level 7
Qualification
Prosthodontist & Implant Surgeon Visiting







In its continuing commitment to reimagine and improve solutions for the dental industry, Carestream Dental has launched the Advance Edition of the CS 8200 3D, along with the latest updates in automated implant planning. The CS 8200 3D Advance Edition is the newest addition to the CS 8200 3D Family and builds on the success of its award-winning predecessors with extended fields of view—including two new larger FOVs—and AI-powered software that streamlines and automates the implant planning workflow.*
The CS 8200 3D’s Advance Edition: Expertly designed to let practices expand patient care and their businesses
As a leader in CBCT technology, Carestream Dental is always developing new ways for practitioners to do more for their patients and their businesses. That’s why the CS 8200 3D Advance Edition is ideal for practitioners looking to expand their treatment options with a scalable solution that grows with their practice.
• Flexible configurations for greater scalability: The CS 8200 3D’s Advance Edition is available in three FOV configurations - 8 x 9 cm, 12 x 10 cm and 16 x 10 cm - that can be easily upgraded so the system can grow with practice needs.
• Broadest range of FOVs in its category: With up to 11 FOVs, the system supports a wide range of clinical indications including implants, endodontics, periodontics, oral surgery, TMJ and airway analysis.
• High-resolution imaging : With a maximum resolution of 75 microns, the CS 8200 3D delivers high-precision scans, ideal for endodontic cases.
• AI-powered implant planning:* The enhanced implant planning module automates the implant workflow, allowing practitioners to plan implants faster and with greater precision.
• Enhanced workflow integration: The system’s open architecture facilitates seamless integration with third-party intraoral scanners and software, ensuring a smooth digital workflow.
• Award-winning compact design: The CS 8200 3D’s Advance Edition retains the industry-recognised compact footprint of the CS 8200 3D and CS 8100 3D Families, making it easy to install in any practice.

Want to add a new dimension to your dental practice?
Offer more treatment types? Or simplify your workflow?
One solution now can help you do it all… and more.
Want to add a new dimension to your dental practice? Offer more treatment types? Or simplify your workflow? One solution now can help you do it all… and more.
Want to add a new dimension to your dental practice? Offer more treatment types? Or simplify your workflow? One solution now can help you do it all… and more.
Discover the CS 8200 3D Advance Edition CBCT with unparalleled versatility that lets you advance your practice’s future. With a category-leading FOV range from 4x4 to 16x10cm, and AI-powered software, the CS 8200 3D creates countless possibilities.
Discover the CS 8200 3D Advance Edition CBCT with unparalleled versatility that lets you advance your practice’s future. With a category-leading FOV range from 4x4 to 16x10cm, and AI-powered software, the CS 8200 3D creates countless possibilities.
Discover the CS 8200 3D Advance Edition CBCT with unparalleled versatility that lets you advance your practice’s future. With a category-leading FOV range from 4x4 to 16x10cm, and AI-powered software, the CS 8200 3D creates countless possibilities.




“If you’re a practitioner who wants to improve your diagnostic capabilities and expand your treatment options, this is the system that delivers the high-powered imaging, upgraded FOVs, intuitive software and compact design that makes it easier than ever to start using CBCT imaging or to replace existing equipment,” Stephane Varlet, Global Business Line Manager for Extraoral Imaging, Carestream Dental, said.
Additionally, new AI-assisted software accelerates the entire implant planning process by automating time-consuming tasks. Now, preparing data for implant cases— like merging CBCT volumes with digital impressions—designing virtual crowns and digitally placing implants is all handled automatically, making implant planning faster and easier. When combined with a prosthetic-driven approach, these software updates improve treatment predictability and give doctors the confidence to deliver precise and successful implant outcomes.
“The CS 8200 3D’s Advance Edition, with intuitive AI-driven imaging software, represents Carestream Dental’s commitment to provide innovative solutions that evolve to meet the ever-changing demands of the industry,” Philippe Maillet, General Manager of the Global Equipment Business, Carestream Dental, said. “Carestream Dental has made it easy for practitioners to deliver more confident diagnoses, enhance treatments and grow their practice in an efficient manner with a trusted partner.”
With more than 25,000 CS 8200 3D and CS 8100 3D systems installed around the world, the CS 8200 3D Advance Edition continues the legacy of Carestream Dental solutions designed to help dental practitioners successfully make the move to CBCT imaging, no matter the treatment they offer or the size of their practice.
*Work in progress, available for sale starting Q3 2025.
To learn more about the CS 8200 3D Advance Edition, visit carestreamdental.com or contact Carestream Dental at info.apac@csdental.com.

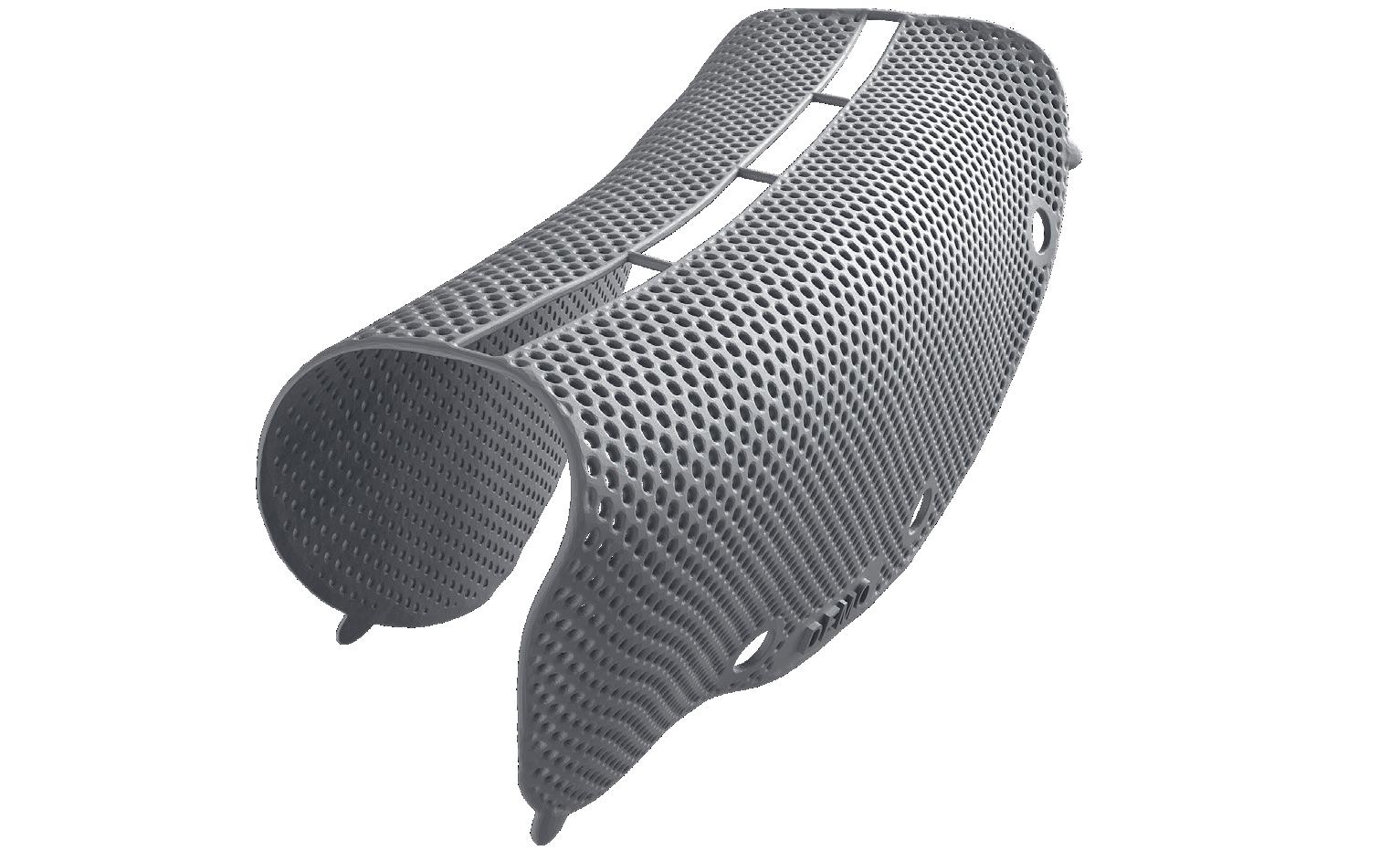
Titanium for reliable stability and space maintenance
Precise patient-specific
Precise patient-specific
3-D printing
3-D printing
Titanium for reliable stability and space maintenance
Titanium for reliable stability and space maintenance
Less surgery time due to perfect fit without shape adaptation
Precise patient-specific
Precise patient-specific
3-D printing
3-D printing
Less surgery time due to perfect fit without shape adaptation
Less surgery time due to perfect fit without shape adaptation
due to perfect fit without shape adaptation
much easier and faster to be installed.
Fully microstructured surface protects from tissue ingrowth
Calculation of augmentation volume (optional)
Calculation of augmentation volume (optional)
Less surgery time due to perfect fit without shape adaptation Integrated implant positioning (optional)
Fully microstructured surface protects from tissue ingrowth
”I have been using the new Yxoss with a dense structure for the last 2 years and I can state that they are very effective and predictable devices for horizontal and vertical ridge augmentation. When associated with 70% of autogenous bone chips and 30% of DBBM their efficacy is comparable withthe one of traditional PTFE non-resorbable membranes, but much easier and faster to be installed.“
Prof. Massimo Simion
Prof. Massimo Simion Fully microstructured surface protects from tissue ingrowth
”I have been using the new Yxoss with a dense structure for the last 2 years and I can state that they are very effective and predictable devices for horizontal and vertical ridge augmentation. When associated with 70% of autogenous bone chips and 30% of DBBM their efficacy is comparable withthe one of traditional PTFE non-resorbable membranes, but much easier and faster to be installed.“
Prof. Massimo Simion
Prof. Massimo Simion
”I have been using the new Yxoss with a dense structure for the last 2 years and I can state that they are very effective and predictable devices horizontal and vertical ridge augmentation. When associated with 70% of autogenous bone chips and 30% of DBBM their efficacy is comparable withthe one of traditional PTFE non-resorbable membranes, but much easier and faster to be installed.
”I have been using the new Yxoss with a dense structure for the last 2 years and I can state that they are very effective and predictable devices for horizontal and vertical ridge augmentation. When associated with 70% of autogenous bone chips and 30% of DBBM their efficacy is comparable withthe one of traditional PTFE non-resorbable membranes, but much easier and faster to be installed.“
Integrated implant positioning (optional)
Calculation of augmentation volume (optional)
Calculation of augmentation volume (optional)
of autogenous bone chips and 30% of DBBM their efficacy is withthe one of traditional PTFE non-resorbable membranes, but much easier and faster to be installed.
Integrated implant positioning (optional)
Integrated implant positioning (optional)
Integrated implant positioning (optional)
Head-to-head comparison as assessed by Dr. Seiler and Dr. Ronda
comparison as assessed by Dr. Seiler and Dr. Ronda
Head-to-head comparison as assessed by Dr. Seiler and Dr. Ronda
Head-to-head comparison as assessed by Dr. Seiler and Dr. Ronda
Head-to-head comparison as assessed by Dr. Seiler and Dr. Ronda
Head-to-head comparison as assessed by Dr. Seiler and Dr. Ronda
Head-to-head comparison as assessed by Dr. Seiler and Dr. Ronda
Head-to-head comparison as assessed by Dr. Seiler and Dr. Ronda
Prof. Massimo Simion
Prof. Massimo Simion Fully microstructured surface protects from tissue ingrowth
”I have been using the new Yxoss with a dense structure for the last 2 years and I can state that they are very effective and predictable devices for horizontal and vertical ridge augmentation. When associated with 70% of autogenous bone chips and 30% of DBBM their efficacy is comparable withthe one of traditional PTFE non-resorbable membranes, but much easier and faster to be installed.“
”I have been using the new Yxoss with a dense structure for the last 2 years and I can state that they are very effective and predictable devices horizontal and vertical ridge augmentation. When associated with 70% of autogenous bone chips and 30% of DBBM their efficacy is comparable withthe one of traditional PTFE non-resorbable membranes, but much easier and faster to be installed.“
Prof. Massimo Simion
Prof. Massimo Simion
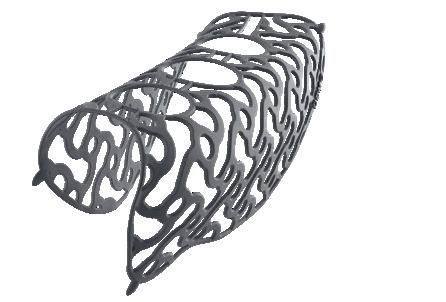
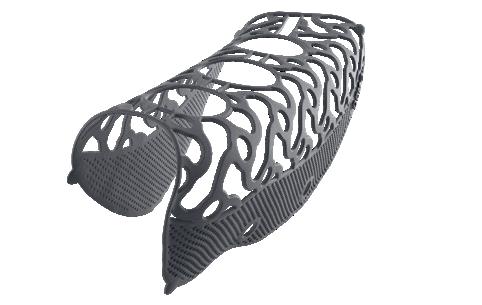

Head-to-head comparison as assessed by Dr. Seiler and Dr. Ronda
Head-to-head comparison as assessed by Dr. Seiler and Dr. Ronda
Head-to-head comparison as assessed by Dr. Seiler and Dr. Ronda
Head-to-head comparison as assessed by Dr. Seiler and Dr. Ronda
Properties
Bone maturation
Soft tissue quality
Removal
Removal
Bone maturation
Uniformly open
CBR protect
CBR fully-protect
Occlusal part: open
Apical area: micropores
Micropores across complete scaffold No micropores


The Ivoclar Group is celebrating the 20th anniversary of its IPS e.max family. Since its market launch in 2005, IPS e.max has revolutionised dentistry, setting new standards in quality, efficiency and aesthetics.
With more than 230 million restorations* worldwide, IPS e.max has proven its clinical success and lasting impact on modern dentistry.
The IPS e.max family was introduced in 2005 with a range of different products, including the two high-strength lithium disilicate glass-ceramics IPS e.max Press and IPS e.max CAD; the zirconium oxide ceramic IPS e.max ZirCAD; and the fluorapatite veneering ceramic IPS e.max Ceram. This comprehensive solution has given dental technicians and dentists a high level of flexibility and aesthetics from day one. The all-ceramic materials have driven advancements in monolithic techniques for durable dental restorations, enabling minimally-invasive treatment approaches.
The innovative power of IPS e.max is especially evident in the advancement of minimally invasive dental treatments. While in the past extensive preparations were necessary, the highstrength materials of the IPS e.max range have enabled a more conservative approach.
Generally, more and more patients are looking for metal-free, highly aesthetic restorations that offer both functional reliability and natural appearance. With the IPS e.max product family, dental technicians and dentists have access to a wide range of solutions designed to meet these evolving demands.
OMilestones in the evolution of IPS e.max
ver the past two decades, four flagship IPS e.max products have established themselves as key pillars of modern dentistry:
• IPS e.max Press: The proven lithium disilicate press ceramic for highly accurate, esthetically impressive restorations.
• IPS e.max CAD: The high-strength lithium disilicate glassceramic for the CAD/CAM production of restorations with highly aesthetic characteristics.
• IPS e.max ZirCAD: Innovative zirconia that, thanks to GT technology, combine high strength with exceptional aesthetics.
• IPS e.max Ceram: A veneering ceramic suitable for both lithium disilicate and zirconium oxide, offering natural light dynamics and excellent shade effects.
Future developments of IPS e.max will focus on enhancing efficiency and aesthetics even further. New material generations and digital workflows will help dentists and dental technicians to achieve outstanding results with even less effort. Following the mission “All ceramic. All you need”, Ivoclar will continue to drive innovation in all-ceramics and build on the success of the IPS e.max family.
For further information on the IPS e.max family, please visit: https://www.ivoclar.com/de_li/landing-pages/20-jahre-ips-e.max or call AU: 1300-486-252 or email orders.au@ivoclar.com or in NZ: 0508 486 252 orders.nz@ivoclar.com
Works in 3 mins Material compatibility1,2


Removes+ 99.9% of odour-causing bacteria*3-5
Lifts stains, removes discolouration6,7
Helps keep appliances looking clear1,2
Compatible with common dental appliance material1,2
For more information, visit www. haleonhealthpartner.com/enau/, www.haleonhealthpartner. com/en-nz/ or scan the QR code


Comparison of water flosser and interdental brush on reduction of gingival bleeding and plaque: A randomized controlled pilot study

Objective
To determine the efficacy of a Waterpik Water Flosser vs interdental brushes for plaque and gingivitis reduction.
Methodology
Twenty-eight subjects completed this two week study. Subjects were assigned to one of two groups: the Waterpik Water Flosser (WF) plus a manual toothbrush or interdental brushes (IDBs) plus a manual toothbrush. Gingival health was evaluated by measuring bleeding on probing (BOP) at six sites per tooth. Plaque removal was measured using the Rustogi Modification of the Navy Plaque Index (RMNPI).
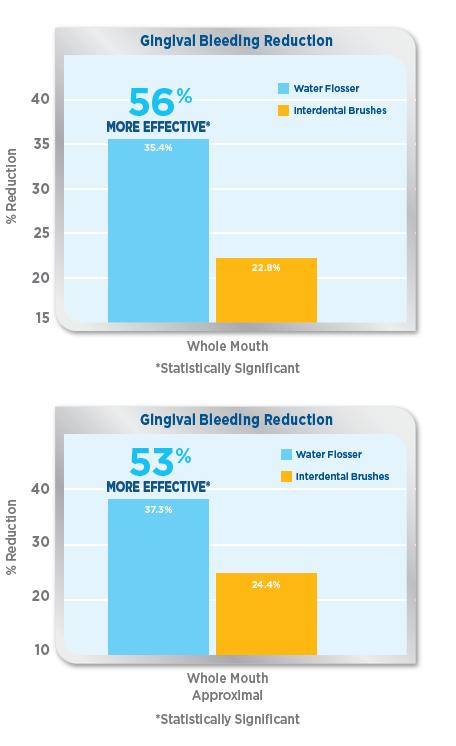
Results
The Waterpik Water Flosser was significantly more effective than the interdental brushes for reducing gingival bleeding. Notably, the Water Flosser was 56% more effective for reducing whole mouth bleeding and 53% more effective for reducing whole mouth approximal bleeding
Conclusion
The Waterpik Water Flosser is significantly more effective than interdental brushes for improving gingival health.
To book your free Professional Education Waterpik Lunch & Learn Session or to try Waterpik yourself at Professional Trial rates, visit www.waterpikshop.com.au or email professionalAU@waterpik.com
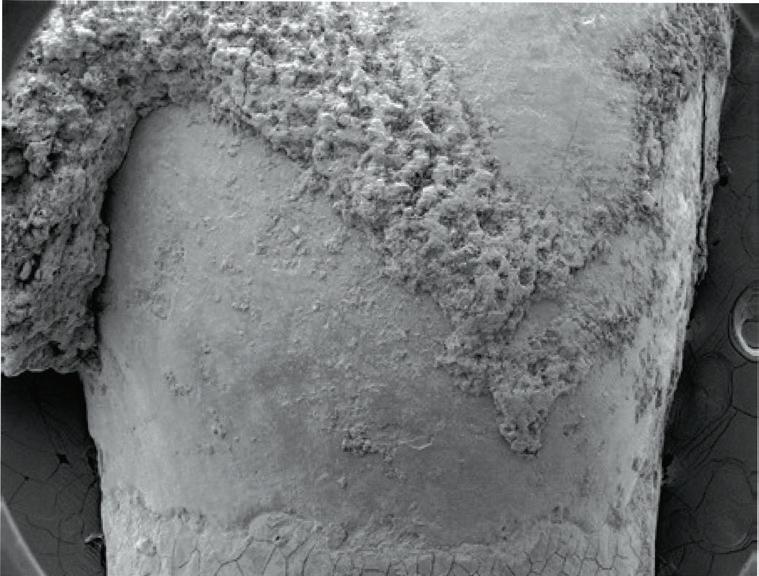



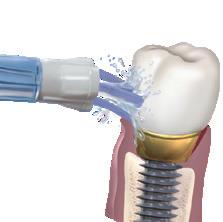

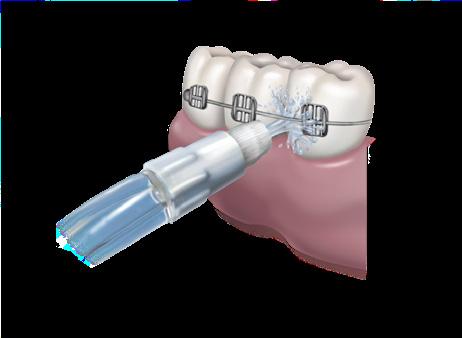




The International Dental Show (IDS) 2025 in Cologne, Germany again showcased groundbreaking dental innovations, ranging from digital technologies to traditional tools and materials. The integration of proven and emerging products is having a significant impact on dental practices.
135,000 visitors from 156 countries attended the event where more than 2,000 companies from over 60 countries presented a comprehensive range of dental medicine and dental technology products – with visibly high levels of motivation, expertise and diversity.
The 41st IDS that concluded on March 29, 2025, with a convincing overall result that not only surpassed the key figures of IDS 2023, but also confirmed its claim to be an international benchmark in terms of
quality, reach and professional relevance. Once again, it became clear: Germany is a key innovation hub in the dental world – and the Cologne trade fair location is an active driver for the future of the industry.
IDS 2025 showcased a host of innovations that ranged from digital technologies and their extension in the direction of Cloud computing and Artificial Intelligence (AI), through to aids for classic dental medicine and dental technology methods. The combination between trusted and innovative products proved to be especially strong.
Software assistance is proving to be invaluable in dentistry. It enables caries to be detected more accurately, the acceleration of a cephalometric analysis
through the automatic designation of orientation points in the X-ray or the preparation of decisions for extractions and orthognatic surgery. The dentist can fall back on Artificial Intelligence with fullyautomated X-ray imaging for diagnosis and treatment planning.
In this way, AI can already recognise caries on bite wing X-rays better than a human being. Based on a panoramic X-ray, current software makes a pre-classification, depicts it in a classic odontogram and in a detection list: “Bridge from 47 to 45, caries on 44, 43 intact, etc.” - the dentist “only” needs to check this and where necessary correct it.
A coloured depiction of the findings generated at the same time is easier to discuss with the patient than a black and white X-ray. Moreover, all of these evaluations are available electronically and can thus be shared among colleagues.
The matching together of intraoral scans, 3D X-rays and computer tomography scans serves as the basis for today’s backward planning, particularly in the area of implantology. This is now also enhanced by magnetic resonance imaging (MRT), an imaging method that does not emit ionising radiation. This particularly makes it easier to diagnose secondary and occult caries compared to conventional methods. This will above all enable the dimensions of carious lesions to be determined more accurately in future.
The MRT could also play a bigger role in periodontal diagnostics because it detects bone loss earlier than bleeding-onprobing and X-rays.
Combined prophylaxis method – many ways lead to the same goal
There is a trend towards convenient multifunctional systems in the field of professional prophylaxis: An ultrasonic handpiece and a powder jet handpiece in one, all of which provide the highest level of treatment comfort. For instance, the ultrasonic handpiece oscillates elliptically and can, just like the powder jet handpiece, be finely adjusted to twelve different settings (amount of water, dosage applied). The water temperature can also be set to four different levels for a painfree procedure.
Beyond this, there is a choice of hand instruments, ultrasonic systems and airpolishing devices for the professional, mechanical removal of plaque including subgingival debridement. And contraangles with a particularly narrow neck and small head as well as the matching polishing cups enable easy access, even to “difficult” regions of the oral cavity.
Many different ways lead to the desired goal: One for example is using a set of modern hand instruments, one of which has a solid material tip that promises especially good precision. This enables both the decontamination of periodontal pockets and the smoothing of the root surfaces.
The periodontology teams already profit from modern digital technology during the diagnosis stage. In this way, the depth of the pockets is determined in the
traditional way using a probe, digitallysupported special models allow automatic documentation. Diagnostics can also be carried out without chairside assistance using such “computer PA probes”.
movement
Endo motors with more and more “safety” functions are being introduced in dental practice. It is a similar principle to the ABS system, the brake assist system and the electronic stability programme in cars: The endo team can fall back on the support of different assistance systems. These include the automatic torque control system; it is connected to an automatic stop should the critical torque limit be exceeded. An automatic stop also occurs if the apex is reached. In a special mode, continual and reciprocal movements are combined with each other and alternated depending on the situation. This relieves the files time and again, reducing the risk of breakage. Sensorless motor controls (a further development compared to conventional brush and sensor-based motor controls) ensure fast reaction times to undesirably high rotational speed and torque deviations or break-offs. The ensuing possible “immediate reaction” allows a stable setting for the files and the dynamics of a continual electronic length determination during the active processing in combination with a – if necessary – automatic change of rotation direction helps the dentist always keep the file on the desired target.
The production of large volumes makes the additive manufacturing of dental technology items really effective. Up to 100 crowns fit on a standard build platform with a 100 millimetre radius, which can then be printed in five hours – in three hours indeed using a double laser system. Apart from crowns, the printable items also include bridges, bars and supraconstructions as well as all implant-supported items like single abutments, telescopic crowns, primary and secondary parts, orthodontic appliances, model casting dentures with clasps and partial dentures.
The business models are also shifting due to the additive construction of metal structures. In the individual case, it often has to be decided where the items should be produced: in one’s own laboratory, in the cooperation lab, at the central manufacturers or industrial service.
In the area of additive manufacturing of plastics, restorations can be printed out of high-filled composites using the DPS technique (digital press stereolithography). The liquid resin is classically found in a tray that contains a vertically movable construction platform.
Initially it is moved up to the surface of the liquid so that a thin layer of resin forms on top of the construction platform. The thin layer is hardened according to the “construction plan” by applying light to certain points.
The construction platform then moves down slightly so that another thin initially still liquid layer of resin collects on top of the hardened layer. This is hardened and the construction platform moves down a bit further and the procedure is repeated again and again.
As an alternative to the tray, the resin can be administered in vacuum-sealed capsules. This can simplify and accelerate the work process and also works in a large range of viscosities particularly with highly viscous ceramic-filled resins.
The speed is a huge advantage here. This means supplying several teeth (or several patients) after fillings have failed will become a “totally normal” therapy option.
Because several crowns, inlays, onlays and veneers can be produced simultaneously within a few minutes and delivered to the respective practices.
As well as metals and plastics, ceramics can also be manufactured using additive production. In this way, in the course of a pilot project a subperiosteal jaw implant has already been printed and inserted into the patient’s mouth in one single intervention without bone augmentation.
A novel digital workflow especially for total prosthesis is available. It involves a two-step milling process.
It combines a tooth-coloured PMMA disc with a classic denture resin and eliminates time-consuming bonding. An efficient aesthetic design can be achieved based on tooth libraries. The full dentures are ready after possible (minor) manual adjustments.
Treated in a single session - combination of everything in the Cloud
The number of production options is increasing in the practices: Crowns, inlays and more can be produced “chairside” for treatment in one single session or quickly sent over to the practice laboratory. As such, the patient is often treated in one single session. This is becoming of great importance for more and more people and it is even also possible for (three-unit) bridges made of zirconia. A well-interlinked digital procedure including fast milling systems and speed sintering furnaces is advantageous. Alternatively, the dentures can be produced using the 3D printing technique.
However, the biggest innovative power across all different areas of dentistry lies in the consolidation of all relevant information in secure Cloud systems. Uploading files instead of sending them per e-mail of Wetransfer, downloading software and thus benefitting from the progress in Artificial Intelligence – this idea is no longer a vague vision today, but (almost) tangible reality.
How different Cloud services are designed depends on the interior of the respective devices and their connectivity. This can be discussed in detail in the course of technical discussions at the exhibition stands. In the case of some Cloud services the focus lies on the predictive maintenance of the supply systems of a practice (i.e. compressors, suction systems, waterlines). For example, the competent external technician will automatically inform the practices about having maintenance carried out on time and alarm them if there are signs of a problem that needs repairing.
Attachments in 3D printing –biofeedback from the splint
Many different developments are coming together in the field of orthodontics. For instance, there are the first 3D printed attachments. Their advantages include high precision, durability and colour stability. These attachments are among other things used for correcting slightly misaligned teeth prior to restorative treatments.
For children and youths as well as for patients with narrow jaws, a specially
developed splint for relief from acute TMD symptoms is now available. It fulfils several functions at the same time, offers both neuromuscular relief, helps correct adapted postures and balances occlusal interferences. Beyond this, it can also be used as diagnostics for recognising TMDrelated symptoms at an early stage.
For the bruxism therapy, special splints bring along an integrated biofeedback mechanism. If the wearer grinds his teeth while sleeping they vibrate and subtle tone (similar to a mobile phone) at precisely the right intensity so they don’t wake the bruxers, but gently encourage them to stop grinding their teeth. This protects the teeth, implants and jaw bones against damage and prevents resulting painful symptoms. An integrated data retrieval enables a precise analysis of individual grinding patterns and opens up new possibilities of stress prevention and patient awareness.
A peculiarity that refers to teeth grinders or occlusal splints and which also applies to gum shields: The high precision of a classic elastomeric impression is not required here. Hence, at this point the effort is reduced by taking a squeeze bite. Thanks to the pre-formed wax bites with an “ideal” size and thickness and without an intermediate layer, they only have to be heated slightly. Hence, the user has better control of the centres during the bite registration and because the bite is shorter and narrower, it frequently doesn’t have to be trimmed.
The team’s efforts to ensure sustainable, environment and climate-friendly operations becomes increasingly more important both for the environment and also for the identification of the entire team and the patients with a practice. It is thus good news that innovations are continually introduced in this section.
For example, in the hygiene section for bottle disinfection: Completely plasticfree natural fibre cloths from certified forestry are combined with alcohol solutions without aldehyde and perfume. Or for the disinfection of suction systems: Instead of aggressive cleaning agents that only ensure the optical cleanliness, the hygiene teams rely on special preparations for the practice and laboratory. Even a neutral pH value (=7) is possible - full effect, gentle on the devices.
The energy consumption of a suction system can also be influenced. Modern executions disposing of the so-called radial technique (instead of side channel compression) are significantly more energy efficient. This reduces the practice’s CO2 footprint and also has a positive effect on the economic outcome.
Moreover, digital technology can also improve the sustainability: Appointments can be pooled using a digitally-supported practice administration (i.e. check-ups for parents and their children). The practice website can inform the patients about attractive means of arrival by bus and the train. Both reduce the number of arrivals and departures by car and thus the CO2 footprint of the practice.
In combination a benefit for the IDS visitors
The concepts, methods and products exhibited at the International Dental Show 2025 enabled the dentists, dental technicians and their teams to update their knowledge on state-of-the art techniques fast. Depending on the region and positioning of the individual practices or laboratory, the selection of the suitable devices, instruments and further auxiliary aids varied.
Dental practices and laboratories can definitely make a targeted investment decision on the well-founded basis of information gained from a visit to the 41st IDS 2025 in accordance with the high goals of the World Health Organisation WHO, the Global Dentists Association FDI and the regional dentists associations and in this way make contemporary dental medicine available to all people. This is a realistic claim for the entire world today!
In this connection, the dental industry showcased the entire spectrum of therapy options from solid basic care through to high-end dentistry at IDS - trusted and innovative products and technologies for the entire world.
With the aid of the information gained at IDS, the practices and laboratories are now optimising their equipment and their positioning. Ultimately, the patients will profit from the new concepts, techniques and products they integrate into their daily work.
IDS Cologne 2027 will be held on March 16-20, 2027. See www.ids-cologne.de
AESTHETIC MONOLITHIC ZIRCONIA

Discover unmatched aesthetics and strength in one Zirconia solution. Perfect fit, biocompatible, for all restorations.
That’s the Avant Advantage


VITA Zahnfabrik is expanding its range of products for digital prosthetics with the innovative 3D printing materials from the VITA VIONIC SOLUTIONS portfolio. The new VITA VIONIC RESINS offer users high-quality materials and reliable shades, making 3D printing in the laboratory costefficient and dependable.
With VITA VIONIC RESINS, a completely printed workflow becomes reality: from VITA VIONIC TRY-IN RESIN for try-ins to the definitive denture base with VITA VIONIC BASE RESIN IMPACT, to the tooth elements made from VITA VIONIC DENT RESIN and the final customisation. This workflow is at the heart of the new VITA VIONIC ECONOMY level, making it possible to print dentures quickly, efficiently and with impressive quality, saving both time and money.
VITA VIONIC BASE RESIN IMPACT offers a new level of quality for fabricating final denture bases. Thanks to its durability, the material has a high load capacity and a low risk of fractures. The balanced property profile promises longlasting results.
VITA VIONIC DENT RESIN is used to create highly abrasion-resistant, shade-stable dental arches and elements: as of April 2025, resins in eight VITA classical A1–D4 shades and the bleach shade 0M3 will be available. Thanks to its high strength, the new resin is suitable for final dentures, as well as temporary crowns and bridges. The very low wear values of the printed denture teeth made with VITA VIONIC DENT RESIN, make them comparable to milled work in terms of durability
The new VITA VIONIC TRY-IN RESIN completes the portfolio. It is an ideal material for functional try-ins in partial and full dentures. It offers fast and material-efficient production and easy processing. It also sets new standards for durability, thanks to its long shelf life of three years.

High-level disinfection and sterilisation are complex processes, requiring initial and ongoing training of frontline staff. A key component of appropriate disinfection and sterilisation is point-ofuse precleaning performed by front-line staff. The removal of gross soil at the point of use and keeping items moist until cleaning are important to prevent the hardening of debris or the development of biofilm due to processing delays which can lead to less effective decontamination. Infection outbreaks have occurred when one or more steps of reusable device processing are missed or done incorrectly. For this study, training and competencies for staff precleaning reusable devices prior to processing were developed. Precleaning requirements were reviewed and updated if indicated. A train-the-trainer approach was employed. Staff were required to understand the device function and the specifics of the manufacturer’s instructions for use, be knowledgeable on processing best practices and be able to provide practical application of best practices to their respective devices. In total, 254 participants attended the training program from 2018 through 2021. Median test scores improved from pre-test to post-test for all participants. Overall test scores significantly improved after participants completed the training each year. The results also showed that basic knowledge does not degrade over a 1-year period. These results show that welldesigned hands-on training is an effective way to train health care workers on precleaning of reusable devices that require processing.
Fox J et al. Impact of COVID-19 pandemic on reusable device precleaning training for front-line staff.
American Journal of Infection Control 2025;53:269-271.
Internationally award winning glass ionomers.
Ionglass formula
Choice of viscosity
Choice of setting time
50+ years of innovation, serving dentists in over 100 countries.


Mastication – the threefold implications of chewing well for long enough

Question 1. Which of the following is not a direct benefit of prolonged chewing cycles?
a. Enhanced release of nutrients during digestion.
b. Increased appetite and food intake.
c. Suppression of ghrelin levels.
d. Improved insulin responsiveness.
Question 2. Why is prolonged chewing thought to have a positive impact on cognitive function?
a. It increases salivary amylase levels only in older adults.
b. It reduces appetite and leads to more sleep.
c. It stimulates cerebral blood flow, activating brain areas.
d. It prevents tooth loss, which directly improves memory.
Question 3. According to the article, what is one hormonal mechanism by which chewing helps regulate hunger?
a. Chewing increases cortisol and decreases leptin.
b. Chewing stimulates ghrelin, which reduces hunger.
c. Chewing decreases ghrelin and increases GLP-1 and insulin.
d. Chewing inhibits insulin secretion to maintain glucose levels.
Question 4. What factor contributes to individual differences in salivary amylase concentration?
a. The type of food consumed.
b. The number of teeth present.
c. The frequency of chewing gum.
d. The number of amylase gene copies.
Question 5. What is one major limitation of research studies on the effects of chewing, as highlighted in the article?
a. All studies are based only on children and teenagers.
b. The studies used artificial foods instead of real meals.
c. Blinding is difficult because participants are aware of their chewing activity.
d. The results are inconclusive due to extremely small sample sizes.
INSTRUCTIONS:
Question 6. What is one of the main reasons ozonated water is preferred over gaseous ozone in dental settings?
a. It is less costly and more convenient to use.
b. It has a longer half-life than gaseous ozone.
c. It is more corrosive, providing better sterilization.
d. It penetrates deeper into bacterial cell walls.
Question 7. Why does ozonated water act more quickly on Gram-negative bacteria than Gram-positive bacteria?
a. Gram-negative bacteria are smaller.
b. Gram-positive bacteria lack a cell wall.
c. Gram-negative bacteria have thinner cell walls.
d. Ozonated water selectively targets Gram-negative species.
Question 8. What is a major limitation of ozonated water as a disinfectant?
a. It causes irreversible damage to human tissues.
b. It degrades rapidly into oxygen, reducing its effectiveness over time.
c. It corrodes dental appliances.
d. It is toxic if ingested in small quantities.
Question 9. Compared to sodium hypochlorite (NaOCl), ozonated water is advantageous for disinfecting impressions because...
a. It increases surface wettability.
b. It creates a protective plastic coating.
c. It preserves impression surface detail better.
d. It forms stable chlorine compounds on the surface.
Question 10. Which of the following is NOT a documented application of ozonated water in dentistry, as mentioned in the article?
a. Treating periodontal pockets.
b. Disinfecting toothbrushes.
c. Decontaminating dental impressions.
d. Polishing dental prostheses.

By Terry Whitty

Question 11. Which of the following is a key advantage of the Shining 3D Elite Wireless scanner’s design?
a. It is the fastest scanner on the market.
b. It is lightweight, weighing only 194 grams.
c. It comes with a larger scanning tip.
d. It requires no battery charging.
Question 12. What unique technology allows the Shining 3D Elite Wireless scanner to scan implants with precision?
a. IntraOral Photogrammetry (IPG)
b. High-Resolution Imaging (HRI)
c. Bluetooth Technology
d. 3D Imaging Sensor
Question 13. What is the purpose of the “Cap Scan Bodies” feature in the Shining 3D Elite Wireless scanner?
a. To help align soft tissues in immediate loading cases.
b. To improve scan speed.
c. To help detect dental caries.
d. To create more accurate impressions for crowns.
Question 14. What additional function does the MetiSmile MR face scanner provide?
a. It helps design digital dentures.
b. It captures high-quality facial scans for treatment planning.
c. It improves scanning accuracy for crowns and bridges.
d. It tracks jaw movements for implant placement.
Question 15. What is the significance of the “Place-Connect technology” in the Shining 3D Elite Wireless scanner?
a. It allows the scanner to connect to any WiFi network.
b. It enables automatic pairing with multiple receiver cradles across different surgeries.
c. It helps scan soft tissues more accurately.
d. It reduces the battery consumption of the scanner.
Real jaw movements and face morphing on the digital patient: production of functional restorations in only two chairside appointments

Question 16. What is the primary benefit of using the Zirkonzahn diagnostic tools and design automations in the patient workflow?
a. Faster patient consultation times.
b. Shortened restoration production time, with fewer appointments.
c. Reduced cost of dental treatments.
d. Simplified storage of patient data.
Question 17. In the first chairside appointment, what type of data does the dentist collect from the patient?
a. X-rays and CT scans.
b. Physical impressions and facial photographs.
c. 2D pictures of the face and digital impressions.
d. Intraoral photos and tooth color analysis.
Question 18. What is the purpose of the Smile Creator module in the Zirkonzahn.Modellier software?
a. To create a virtual version of the patient’s mouth for analysis.
b. To analyze the patient’s occlusion for treatment planning.
c. To simulate the effect of the restoration on facial symmetry.
d. To design a preview of the potential new smile based on patient data.
Question 19. What does the “Real Movement” function in the Zirkonzahn.Modifier design software achieve?
a. It simulates the patient’s facial expressions to evaluate aesthetics.
b. It displays the patient’s mandibular movements to customize the prosthetics’ function.
c. It imports patient data from other software systems.
d. It automatically designs a smile for the patient.
Question 20. What role does the Face Hunter 3D facial scanner play in the diagnostic process?
a. It records the patient’s occlusal plane.
b. Photorealistic digitalisation of the face for integration into the design.
c. It simulates various tooth movements.
d. It analyzes the patient’s bite relationship for prosthetics design.
By Emer. Prof. Laurence Walsh AO
Source control refers to the use of a face-worn product that covers a person’s mouth and nose to reduce the spread of large respiratory droplets to others when the person talks, sneezes or coughs. Members of the general public wear masks of various types to provide source control and reduce the spread of viral particles through airborne transmission. Masks sold to the public often do not meet any standards, raising concerns about their effectiveness in reducing the spread of respiratory viruses.


TMost cloth masks, whether homemade or those existing in the market, have not been evaluated to determine how well they perform. To assess the effectiveness of face-worn products used for source control, this study assessed the total outward leakage (TOL) for products from 9 categories to determine how much products reduced the leakage of exhaled aerosol. This was calculated by dividing the concentration outside the face-worn product by the concentration inside the face-worn product. The TOL accounts for leakage around the edges and through the filter material (i.e., penetration). Testing used a benchtop system with 2 different-sized headforms with silicone elastomer skin. Each unit was donned 5 times per headform. TOL varied from 10% to 58% and was significantly affected by both product category and headform size. TOL was greater for the medium headform than the large headform. Overall, single-layer cloth masks were the least effective measure for source control, with the highest TOL. Medical level 2-compliant 3-layer masks had a lower mean TOL of 16.4%, while level 1 masks 27.4% to 35.4%, due to poorer fit on the headform, thus indicating the importance of fit. Overall, these data suggest that 3-layer disposable level 2 face masks would be preferred for source control for the public. Single-layer cloth masks should be selected with caution as a source control measure for reducing airborne transmission of virus-laden aerosols, given the high total TOL observed in this study.
Yang W et al. Total outward leakage of face-worn products used by the general public for source control. American Journal of Infection Control 2025;53:239-244.
he need for effective respiratory protection in health care settings is paramount, particularly in light of the ongoing challenges posed by airborne pathogens. N95/P2 particulate filtering respirators (PFRs) are widely used to protect health care workers from infectious aerosols. The fit of PFRs and halfface respirators is critical. Fit-testing is done so that individual health care workers can achieve the required protection factor (PF). PF 10 is desired, which means a 10-fold reduction in the dose of pathogen respired (inside the respirator) compared with the environment. At present, no objective ways exist to evaluate the implementation of respirators at the point of use. Previously, it was shown that 26% of health care workers achieve appropriate fit at point of use. This study developed a prototype infrared (IR) kiosk that can be deployed in the health care setting to increase the efficacy of fit-checking. The kiosk is intended to be used as a visual aid with real-time feedback on areas of air leak and if leaks are present, guide the user where they may need to adjust their respirator. A total of 657 quantitative fits were conducted on 166 subjects using 4 different respirator styles (cup style, tri-fold, flat-fold and duckbill style). Randomisation was performed, with controls employing a standard “fit-check” and the intervention group using the infrared video kiosk. In the latter group, participants had 1 minute to use the IR kiosk to detect and adjust for thermal gradient leaks. The kiosk provided real-time visual feedback, highlighting areas where the respirator might be leaking. Participants could adjust their respirators based on this feedback before undergoing the fit test. The primary outcome was passing rates of quantitative fit, with secondary outcomes of respirator type, gender, ethnicity and previous experience. In the kiosk group, there was a significantly higher pass rate (50.6%) compared with controls (30.8%), with an odds ratio for passing of 2.3 (95% confidence intervals [CI] 1.8-2.9, P < .001). The duckbill style improved the greatest (OR 4.1, 95% CI 2.1-7.9, P < .001), and Tri-fold also showing substantial benefit (OR 2.66, 95% CI 1.45.2, P < .001). Gender and ethnicity did not influence outcomes when using the kiosk, nor did previous experience. Thus, the point-of-use kiosk improved the odds of achieving a satisfactory fit of common respirator styles, independent of participant demographics. This approach could address a gap in PFR use by providing individual assessment and interventions that improve worker safety.
Chapman D et al. Evaluation of a point-of-use kiosk for improving the fit of N95/P2 respirators in health care settings: A randomized controlled trial. American Journal of Infection Control 2025;53:36-43.


Powerball is specifically designed for screwing PMMA and printed resin direct to the multiunit abutment. The Powerball screw has a 2.6mm screw head with parallel sides and a unique radius on the screw head, optimised to distribute stress through the polymer.

Speedball is specifically designed for screwing PMMA and printed resin direct to the multi-unit abutment. The Speedball screw has a 2.6mm screw head with wine glass sides and a unique radius on the screw head. It has been designed to work with all screws from M1.4 through to M2.0.

Vortex, aka LA VIS screw, is specifically designed for screwing PMMA and printed resin direct to the multi-unit abutment. The Vortex screw has a 2.2mm screw head with tapering sides and a unique radius on the screw head. It is optimised to distribute stress through the polymer.

to Aerospace

By Emeritus Professor Laurence J. Walsh AO

In clinical practice, we often have discussions with patients about their occlusal function and the need to ensure sufficient opposing pairs of natural teeth, or their relevant prosthetic replacements.
We assume that patients understand the importance of proper chewing for effective eating.
Within dentistry, there is not a broad understanding of the benefits of chewing activities beyond the obvious connection to the mastication of food. The purpose of this article is to summarise recent concepts on the importance of chewing, beginning with its obvious purpose in mastication and nutrition, then moving on to discuss the
impact of chewing on appetite and finally, the impact of chewing on cerebral blood flow and the development of dementia.
Chewing food – using more cycles
Performing more chewing cycles before swallowing can provide a number of benefits. Using a greater number of chewing cycles helps to break the physical substrate of the food down further, enhancing subsequent digestion by facilitating the release of nutrients.1,2 This occurs because mastication increases the surface area to volume ratio of the food. It also reduces the maximum dimensions of the food and thus aids swallowing.
Variables such as the amount taken in one bite, the number of chews per bite and the rate of stimulated saliva production all influence the extent to which a food bolus is deformed, fragmented and lubricated with saliva during mastication. With longer chewing, the extended exposure to salivary amylase enzymes allows for greater breakdown of complex starches into simple carbohydrates, thus aiding digestion.
Each individual has habitual masticatory processes and there are also inter-individual variations in bite force. Both the normal number of chewing cycles and the bite force applied can vary by a twofold range between different adults.3 Using more chewing cycles slows the pace of eating and provides more satisfaction from eating and a greater sense of satiety. As a result, less food is required to gain the same sense of fullness at mealtimes. This strategy reduces the intake of energy and so will aid in weight control and in the prevention of obesity. Following this logic, there is a compelling argument that extended mastication could be one simple strategy to reduce the risk of lifestyle-related diseases.3-5
At the end of a meal, the process that terminates eating is influenced by a range of feedback mechanisms and one of these is the duration of chewing. The literature shows a considerable influence of the number of chewing cycles on both the level of satisfaction with eating and the extent to which the sensation of hunger is suppressed. This leads to the conclusion that moderate chewing (e.g. 25 chewing cycles) is likely to be the most comfortable, with less than 10 cycles being insufficient and more than 40 chewing cycles being impractical.3-5 Eating at a slower rate with more chews per bite gives smaller particles to swallow, while eating at a faster rate is associated with larger bite sizes, a shorter mastication time and fewer chews per bite.5
As an example of these principles in action, chewing sugar-free gum increases the sensation of fullness and reduces the sensation of hunger and the desire to eat.3-5 Of note, this effect occurs even when the gum has no flavour, but the impact is enhanced when a suitably pleasant mint or fruit flavour is present in the gum. One explanation for this beneficial effect of chewing is that a greater number of chewing cycles is more likely to change the level of hormones, leading to increased levels of glucagon-like peptide (GLP-1) and insulin and suppressed levels of ghrelin.
Increased early insulin secretion is associated with better glucose absorption. The relationship between extended chewing and a stronger initial insulin response probably occurs because a longer chewing time extends the period for taste perception for the food. Ghrelin is the appetite hormone and is elevated in the blood between meals in the fasting state and then is reduced in response to food intake. Prolonged chewing suppresses the levels of ghrelin and thus reduces appetite.
As a simple, inexpensive and non-pharmacological approach, it seems difficult to argue against the benefits of using longer chewing cycles (Table 1). On the other hand, faster eating is often associated with poorer glucose tolerance and insulin responsiveness and an increased prevalence of metabolic syndrome.3-5
These types of beneficial relationships for prolonged chewing have been shown for chewing gum as well as for conventional foods such as pizza.3-5
For chewing gum, a period of chewing suppresses the return of hunger following a meal and reduces cravings for sweet and salty snacks between meals. For pizza, more chewing cycles can positively influence palatability. Of particular interest, prolonged chewing tends to dramatically reduce the intake of food in the parts of the meal which follow.
Some practical advice that follows from this is that patients could be advised to increase the number of chewing cycles for their food. The same advice could be given for sugar-free chewing gum, if they are using this. More chewing cycles per bite requires relatively little additional effort. Rather than counting individual chewing actions, it will be more practical to advise patients to chew each bite for 20 to 30 seconds before swallowing.
The advice on chewing must be tailor-made to the individual patient situation, since for some patients, implementing this as an approach may not be practical or appealing, e.g. because of a lack of suitable opposing teeth, mobile teeth, unstable prostheses, etc. As well, there can be considerable variations between one person in the next, since individuals have different expectations and habits around their eating practices. This means it is necessary to titrate in an individual patient the influence of chewing time when their end goal is to achieve a reduction in appetite or in food intake.
When giving advice about chewing for longer, one must take into account that the textures of different types of food can vary enormously. A ranking of foods by category is shown in Table 2, which incorporates descriptors from the International Dysphagia Diet Standardisation Initiative (IDDSI) Guidelines. The higher the category number, the greater the masticatory force and the number of chewing cycles that are required.
Do not suggest to patients that they need to attempt to chew soup or other low viscosity or liquid foods. Softly textured foods require minimal chewing. On the other hand, foods with considerable hardness or a high viscosity have a microstructure which is more difficult to chew and this reduces the average bite size.1-3 Foods with thicker textures require longer processing in the mouth and this slows the eating rate. They also give higher than expected levels of fullness, meaning that the caloric intake is less overall. This is one of the obvious benefits of eating unprocessed fruit and raw vegetables.
On the other hand, foods which can be consumed very rapidly are associated with a greater overall intake of energy and consequently with adipose deposition and with higher body weight. Adding to this, individuals who eat very quickly not only consume more within a given meal, but they also tend to have greater consumption of snacks in the post meal period. They experience less of the sensation of fullness after the meal has finished.
Within the oral cavity, the food breakdown process is an interaction between time, the physical structure of the food and the degree of lubrication. Hence, foods with different characteristics have quite different breakdown dynamics. Foods that are physically large will take some time to chew to the point where the particles are below the threshold for size which is safe to swallow for that particular individual.
A further important consideration is that individuals vary greatly in terms of their ability to produce stimulated saliva when chewing. This causes variation in the number of cycles required. For hard foods with a low moisture content, those with very high production rates of stimulated saliva can reach the threshold where the food is suitable to swallow after a relatively small number of chewing cycles.
The reverse is true for those with salivary gland hypofunction who have a deficit in the production of stimulated saliva. The author refers to this as “Sao biscuit” test, where this particular hard dry biscuit is the challenge item that the patient must attempt to chew and then swallow, without taking any liquid.
One of the most interesting aspects of the literature on the topic of chewing is that forms of oral stimulation other than chewing can also lower the levels of ghrelin in the blood and suppress appetite.4-5
This effect has been explained in terms of vagal efferent nerve stimulation. It remains to be seen how such actions could be applied to practical protocols for oral stimulation that patients could perform themselves at home. Likewise, there could be an opportunity to alter the structure of chewing gum to enhance some of these effects on ghrelin.
An important limitation of the literature regarding the relationship between chewing cycles, appetite, food intake and hormone levels is that many studies have been done on individuals within the healthy weight range and relatively few studies have included individuals who are overweight.
A further issue is that it is not possible to have true blinding in such studies, as participants will be aware whether they have chewed or not, whether the gum is flavoured or not and how long they have chewed for.
A meta-analysis of the effect of chewing on self-reported hunger4 has identified that the longer the period of fasting, the greater the impact of prolonged chewing on satiety.
As already mentioned, chewing is a powerful stimulus for the production of saliva from the major glands, particularly the parotid glands. As a consequence of this, as the flow increases and reabsorption of ions through the ductal structure of the saliva glands is altered, there is a dramatic elevation in the concentration of bicarbonate ions and therefore an increase in the pH. The pH can change from typically around 6.5 for saliva at rest, to 8.0-8.5 for stimulated saliva. This represents a 100-fold reduction in the concentration of hydrogen ions.
Stimulated saliva helps to create a favourable environment for remineralisation, since the isotherms which dictate the formation of various mineral species from calcium and phosphate ions are all driven to mineral formation under high pH (alkaline) conditions. Increased salivary flow also accelerates the clearance of substrates from the mouth and enhances the antimicrobial actions of saliva. These well-known benefits underpin the oral health benefits of chewing sugar-free gum.
Table 1. The rationale behind extended chewing
n Improved processing of food
n Smaller size and increased number and surface area of food bolus particles
n Extended contact with saliva
n Greater salivary amylase pre-digestion of starches
n Enhanced salivary clearance
n Enhanced initial insulin response
n Suppressed ghrelin levels, lowered appetite and decreased intake of food
n Increased glucagon-like peptide-1
n Increased satisfaction from eating
Table 2. A ranking for food texture according to the difficulty of mastication
0 Thin drinks (water, tea, coffee)
1 Slightly thick drinks (cream soup)
2 Mildly thick drinks (nectar)
3 Liquidised, moderately thick drinks or foods (honey)
4 Able to swallow without chewing; tines of a fork make a clear pattern on the surface; pureed foods and extremely thick drinks (purees, cooked cereals, mashed bananas, thick pudding)
5 Able to smash with the tongue; minced and moist foods; particles easily come through the tines of a fork (meat loaf, baked beans, casseroles)
6 Able to smash with edentulous ridges; soft and bite-sized foods; can be broken down with pressure from a fork (cheese, pizza, bagels)
7 Regular foods that are able to be chewed easily; can be broken down with pressure from a fork (muffins, tuna)
8 Hard and crunchy foods, tough raw fruits and vegetables
9 Dry and crusty breads, dry tough meats, hard nuts
Types 0-7 are designed for inclusion in the diets of people with dysphagia. Adapted from The International Dysphagia Diet Standardisation Initiative 2019 https://iddsi.org
As already mentioned, the salivary enzyme amylase plays a key role in hydrolysing the alpha bonds of starch and glycogen to release glucose. The concentration of salivary amylase varies widely between individuals, because of differences in the number of copies of the amylase gene. Higher numbers of gene copies are found in ethnic groups that historically were farmers rather than hunter gatherers, because of their greater reliance on starch-based foods as their primary energy source. Individuals who carry more copies of the amylase gene and who therefore have higher salivary amylase levels will be able to extract more energy from the same load of complex carbohydrates and will do so quite quickly after eating starchy foods.
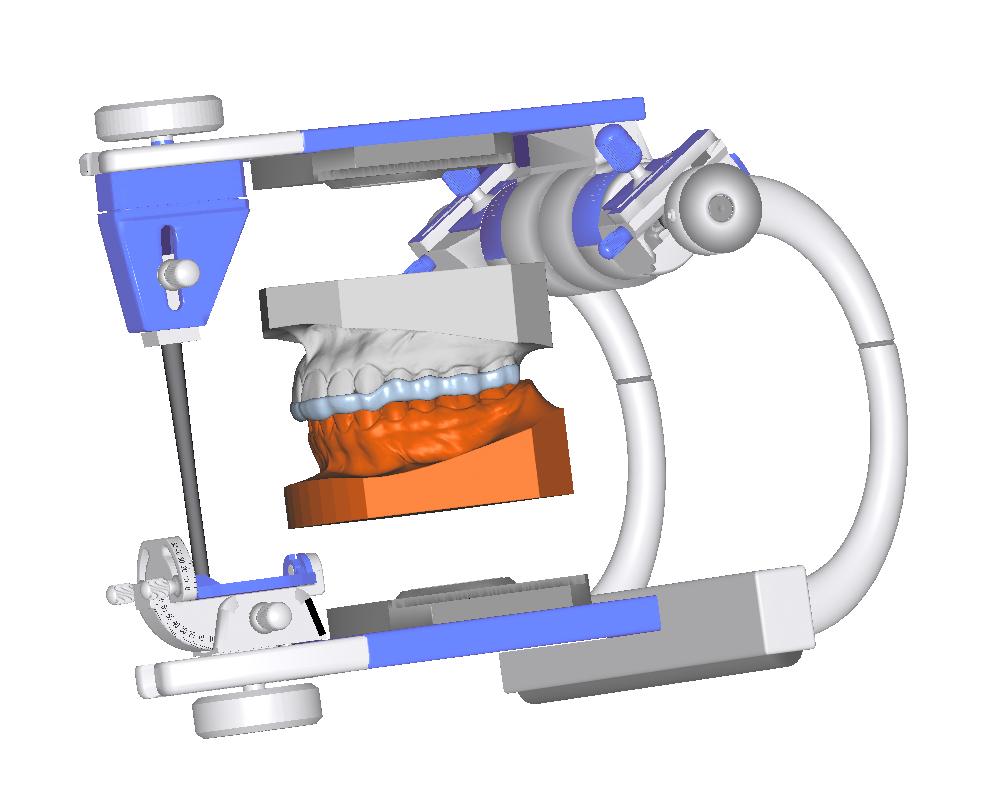
• Any Design
• HD PMMA Milled
• Flexion Milled
• POM Resin Milled
• 3D Print Option
• Perfect Fit
• Upper or Lower
• All scans accepted



There is evidence that the loss of teeth is associated with cognitive decline in the later years of life, with a gradient dose-response effect for missing teeth and the risk of cognitive decline. This effect has been seen in population studies in South America and in North America.6,7
Tooth loss is positively associated with an increased risk of dementia in adults.8
Conversely, having more remaining teeth is associated with having a lower risk of dementia in later life.9
There is accumulating evidence that tooth loss and occlusal dysfunction may affect brain function and trigger the onset of dementia.10
This could mean that poor oral function could be a contributing factor to the onset of dementia.
While part of any such connection between tooth loss and dementia could be due to periodontitis and ongoing chronic subclinical inflammation, it is also possible that a decline in chewing due to edentulism could contribute.
The reason for this is that chewing increases cerebral blood flow bilaterally, which in turn positively affects cognitive function.11-13
Following this line of argument, there is an active discussion in the recent geriatric dentistry literature of the benefits of effec-
tive and prolonged chewing to ensure sufficient activation of masticatory muscles, as well as for the proper mastication of food, whether that chewing involves natural teeth, dental implants or dental prostheses.
Appropriate and sufficiently long chewing then enhances cerebral blood flow and activates specific brain areas. Together, these prevent amyloid-beta plaque formation, which is an essential event in the development of neurodegenerative diseases.14-16
The most recent concepts around the importance of chewing stress that all the components of the masticatory system must work together in order to ensure adequate nutrition, appropriately regulate the desire for food and preserve cognitive function.
Dental professionals can make powerful arguments around the importance of maintaining teeth for their chewing function. Hopefully the recent evidence summarised in this article provides a steppingstone for people to explore the sizeable literature which has accumulated around the importance of chewing in the maintenance of health.
1. Witt T, Stokes JR. Physics of food structure breakdown and bolus formation during oral processing of hard and soft solids, Curr Opin Food Sci. 2015;3:110-117.
2. Prinz JF, Lucas PW. An optimization model for mastication and swallowing in mammals, Proc Roy Soc London B 1997;264:1715-1721.
3. Robinson E, Almiron-Roig E, Rutters F, de Graa CF, et al. A systematic review and meta-analysis examining the effect of eating rate on energy intake and hunger. Am J Clin Nutr. 2014;100(1):123-151.
4. Miquel-Kergoat S, Azais-Braesco V, Burton-Freeman B, Hetherington MM. Effects of chewing on appetite, food intake and gut hormones: A systematic review and meta-analysis. Physiol Behav. 2015;151:88-96.
5. Forde CG, Stieger M. Metabolic Impacts of food oral processing. Food Chemistry, Function and Analysis No. 30. Oral Processing and Consumer Perception: Biophysics, Food Microstructures and Health. Eds. Wolf B, Bakalis S, Chen J. The Royal Society of Chemistry, 2022. London. Pp. 137-186.
6. Peres MA, Bastos JL, Watt RG, Xavier AJ, Barbato PR, D’Orsi E. Tooth loss is associated with severe cognitive impairment among older people: findings from a population-based study in Brazil. Aging Ment Health. 2015;19(10):876-84.
7. Galindo-Moreno P, Lopez-Chaichio L, Padial-Molina M, Avila-Ortiz G, O’Valle F, Ravida A, Catena A. The impact of tooth loss on cognitive function. Clin Oral Investig. 2022;26(4):3493-3500.
8. Fang WL, Jiang MJ, Gu BB, Wei YM, Fan SN, Liao W, Zheng YQ, Liao SW, Xiong Y, Li Y, Xiao SH, Liu J. Tooth loss as a risk factor for dementia: systematic review and meta-analysis of 21 observational studies. BMC Psychiatry. 2018;18(1):345.
9. Oh B, Han DH, Han KT, Liu X, Ukken J, Chang C, Dounis K, Yoo JW. Association between residual teeth number in later life and incidence of dementia: A systematic review and meta-analysis. BMC Geriatr. 2018;18(1):48.
10. Nakamura T, Zou K, Shibuya Y, Michikawa M. Oral dysfunctions and cognitive impairment/dementia. J Neurosci Res. 2021;99(2):518-528.
11. Hasegawa Y, Ono T, Hori K, Nokubi T. Influence of human jaw movement on cerebral blood flow. J Dent Res. 2007;86(1):64-8.
12. Ono T, Hasegawa Y, Hori K, Nokubi T, Hamasaki T. Task-induced activation and hemispheric dominance in cerebral circulation during gum chewing. J Neurol. 2007;254(10):1427-32.
13. Hasegawa Y, Tachibana Y, Sakagami J, Zhang M, Urade M, Ono T. FlavorEnhanced Modulation of Cerebral Blood Flow during Gum Chewing. PLoS One. 2013;8(6):e66313.
14. Miquel S, Aspiras M, Day JEL. Does reduced mastication influence cognitive and systemic health during aging? Physiol Behav. 2018;188:239-250.
15. Lopez-Chaichio L, Padial-Molina M, O’Valle F, Gil-Montoya JA, Catena A, Galindo-Moreno P. Oral health and healthy chewing for healthy cognitive ageing: A comprehensive narrative review. Gerodontology. 2021;38(2):126-135.
16. Da Silva JD, Ni SC, Lee C, Elani H, Ho K, Thomas C, Kuwajima Y, Ishida Y, Kobayashi T, Ishikawa-Nagai S. Association between cognitive health and masticatory conditions: a descriptive study of the national database of the universal healthcare system in Japan. Aging 2021;13(6):7943-7952.
About the author
Emeritus Professor Laurence J. Walsh AO is a specialist in special needs dentistry who is based in Brisbane, where he served for 36 years on the academic staff of the University of Queensland School of Dentistry, including 21 years as Professor of Dental Science and 10 years as the Head of School. Since retiring in December 2020, Laurie has remained active in hands-on bench research work, as well as in supervising over 15 research students at UQ who work in advanced technologies and biomaterials and in clinical microbiology.
Laurie has served as Chief Examiner in Microbiology for the RACDS for 21 years and as the Editor of the ADA Infection Control Guidelines for 12 years. His published research work includes over 400 journal papers, with a citation count of over 20,000 citations in the literature. Laurie holds patents in 8 families of dental technologies. He is currently ranked in the top 0.25% of world scientists. Laurie was made an Officer of the Order of Australia in January 2018 and a life member of ADAQ in 2020 in recognition of his contributions to dentistry.
Minimise discomfort with extra access. The Micross Curve represents the next evolution in the Micross family, making minimally invasive bone harvesting even easier. Just like the Micross, it was developed for minimally invasive techniques. Thanks to the curved design, it is even easier to use in hard-to-reach areas. Collect only the bone that is absolutely needed and reduce invasiveness – your patients will love it.

The ergonomic design enables clinicians to effortlessly access retromandibular, palatal, and other hard-to-reach areas. New 27° curvature

By Graham Middleton

“Ultimatums invariably have the opposite effect to what was intended, being regarded as offensive and often rejected...”
From 1987 onwards, I observed a multitude of dental and veterinary business buy/sell and partnership/associateship transactions and valued hundreds of practices both personally and with colleagues. They carried many lessons. All names used below and practice identifiers have been altered to preserve confidentiality.
An aggressive individual prepares a buy-out proposal and presents it to a practice owner as being not negotiable. Ultimatums invariably have the opposite effect to what was intended, being regarded as offensive and often rejected or ignored with the offeror leaving the practice. Attempts to coerce owners causes rejection.
I f there are signs that a practice principal is looking to slow down, it is best that the employed dentist/ dentists ask politely whether they are amenable to a discussion about the future. Care must be taken not to back the principal into a corner. It is important to ask questions such as whether, if they are inclined to sell, they wish to continue as a clinician post sale? For how many days per week and how many holiday breaks they would like?
In the advent of the sale of a practice, it’s best that no notice of change of ownership occurs. Patients will make appointments and if their preferred dentist is unavailable, a receptionist will book them to another.
The approach must not be rushed. Forcing a negotiation can result in the principal resisting and usually fails. The usual reaction of owners is to ignore unacceptable offers. I observed that, on many occasions, dentists left practices within months of failed buy-outs.
What happens if the not negotiable offer is from a partner or associate owner with a deadline?
Most recipients ignore hostile partners deadlines as it displays strength. Intending buyers need to find a way to politely open discussion of possible sale. The greater the provocation, the longer the time to a buyout and the more damage to the practice.
Consider a situation where the younger associate takes care to maintain friendly relations and politely enquires about the older associate’s longer-term needs, including need for relief of administrative responsibility and a period of reversion to a part-time contractor status without notifying the change to patients. As an older partner begins to crave more leisure time, this option becomes attractive. Patience and good manners are required. Treat the staff similarly and take care to thank receptionists for booking new patients and chairside assistants. Principals are more likely to sell if buyers have the staff’s respect.
Simon, a proficient assistant dentist, concentrates on building his communication skills with patients, practice staff and the practice owner, Louise. Gradually his patient list, follow up appointments and personal referrals increase. He greets Louise each morning and in spare moments shares dental information and professional news. He establishes her confidence in him, covers for her absence on holidays and takes care to rebook the patients back to her for follow up appointments. He plays a long game positioning himself as the logical buyer of the practice or of an associateship within. As his fees grow, his position becomes stronger and Louise comes to realise that her best long-term option is to sell to Simon. He will not agree to be employed by a corporate buyer. Patience and diplomacy are the pathway to a deal.
The lessons for intending buyers
1. Young dentists succeed best by concentrating on building their worth to the practice to a point at which no corporate would buy it without their agreement to a long-term contract.
2. Young dentists must not agree to having their contract transferred to a corporate. 3. If you want to buy a practice, don’t work for a corporate. Search for employment in the type of practice you would like to own.
4. Successful practice owners end up millions of dollars better off over their dental careers than do those who worked for dental corporates.
“Young
dentists succeed best by concentrating on building their worth to the practice to a point at which no corporate would buy it without their agreement to a long-term contract. Young dentists must not agree to having their contract transferred to a corporate. If you want to buy a practice, don’t work for a corporate. Search for employment in the type of practice you would like to own...”
The owner who shot himself in the foot
Tom was the long-term assistant dentist in “Harold’s” practice. Harold wished to sell and Tom was a willing buyer at a fair price. Harold quoted corporate buy-out prices. Tom’s advice was that the relevant comparison was of sales to assistant dentists rather than to corporates with onerous work out conditions. Harold decided to sell to a corporate but the corporate indicated that a condition of purchase was that Tom sign a contract with them. Tom refused to assist a corporate to bid against his own offer and left the practice. Through taking poor advice, Harold lost his sale to Tom and the corporate was no longer interested. Tom moved to another practice and a trickle of patients followed him.
1. Practice principals with a single effective long-term employed dentist must be careful when making offers to sell. If the deal is not completed, the employed dentist usually leaves.
2. Practice owners who dangle the carrot and then change their offer or deal with other parties after the offer has been made risk worse outcomes.
Greene and Greedy practised as associates in an established practice in a regional city with four surgeries, one each for the associates and two for assistant dentists. Greene and Greedy had roughly equivalent fees. Their two assistant dentists each produced about 60 percent of the fees of an associate.
The premises were rented at arm’slength. Having signed up for a dental “pathways to wealth” program, Greedy announced that he wanted to practice “up-market dentistry” elsewhere in the same city.
He intended to depart the practice and expected Greene to buy out his interest in it. He was renting premises through local real estate agents known to Greene and had elaborate fit out plans for a state-ofthe-art practice.
Greene consulted me initially asking for a practice valuation but it was not a valuation issue.
As Greedy was leaving, a telephone arrangement was agreed upon whereby patients making appointments would press button A to make an appointment with Greene or Greene’s assistant dentist or press button B for Greedy or Greedy’s assistant was the fair solution.
Greedy could take with him two surgeries of equipment and half the consumable stock, one assistant dentist and half of the non-clinical staff—essentially his half of the practice.
Greene discussed with the landlord taking over the lease. Inexplicably, Greedy’s solicitors had expected Greene to buy his share of equipment and goodwill and assumed his acceptance of a situation forced upon him. Buying Greedy’s goodwill was untenable as he would be practising locally.
I advised Greedy’s solicitors that it was their client’s decision to move which had imposed on Greene an effective doubling of his rental cost and that they were wasting their time if they thought that they had a basis for his demands. Greedy was too deeply committed to pull back and moved. Greene changed the locks and subsequently ran a successful practice. How successful Greedy was is uncertain as economic conditions in the regional centre were not supportive of the type of expensive dentistry he aspired to.
The lessons
1. Attempts to force a financial settlement on an associate for a situation not of their making can backfire badly; and 2. Early consultation is essential before making unilateral decisions.
Attempts to rob a practice vendor (1)
Aveteran dentist in an inner-city suburb sold his practice to a younger dentist with normal non-compete conditions. Shortly thereafter, he began work in a practice about 4 kilometers distant. On my advice, the employing practice was put on notice that they would be held liable for being a party to his breach of contract. They promptly dispensed with his services.
The lesson.
Speed is critical in such instances.
Attempts to rob a practice vendor (2)
An outer suburban practice owner sold her practice then blatantly set up within the exclusion zone shortly afterwards. She had acted in bad faith. Threat of legal action supported by expert practice valuation advice resulted in cessation and damages payment.
How the ex-practice owner and subsequent employed assistant dentist robbed a practice owner
“Cunning” sold his CBD practice to “Easy” with a two year non-compete agreement and became the practice assistant dentist. Soon, after two years had elapsed,
Cunning advised Easy that he was finishing up immediately. Cunning’s patients quickly cancelled appointments.
Initially, Easy was confronted with poor legal advice from a Queens Counsel to the effect that as the two year noncompete time had expired, he could do nothing. Desperately, Easy sought my advice. He also engaged a forensic IT expert who reported that on a succession of nights leading up to his departure Cunning had been recorded by the practice security system entering the practice for several hours. The IT specialist identified that records of patients previously treated or who had forthcoming appointments with him had been downloaded to a computer at the employer of his son and from there, transferred onwards to his
“Employed dentists have a duty of care toward the property of their employer including with respect to patient details and the employer’s goodwill. Transferring of patient records by an employee is theft. Transfers of records between IT systems are traceable...”
home computer. Discovery revealed that forthcoming appointments had reappeared in the practice to which he had moved on the identical dates and times of the cancelled appointments in Easy’s practice. My advice was that the matter was not a breach of non-compete condition but the theft by an employee of patient records belonging to their employer with the intention of profiting from the diversion of patients. Cunning also compromised his son’s employers who were potentially liable for his actions and the dental practice to which he shifted patients. Lawyers promptly changed their advice and the matter moved to a legal mediation.
Cunning agreed to pay Easy a substantial sum and would also have had huge legal bills. Easy received the payment but had substantial legal costs. Cunning was ostracised by dental colleagues.
1. Employed dentists have a duty of care toward the property of their employer including with respect to patient details and the employer’s goodwill.
2. Transferring of patient records by an employee is theft.
3. Transfers of records between IT systems are traceable.
Long ago (1985-1987), I spent two years as HR Director of the Victorian Attorney General’s Department. There I learned that court backlogs were a perennial issue. Judges and courts infrastructure are costly.
There were regular efforts to reduce court waiting lists. Getting a dispute between two dentists to a Supreme Court civil list hearing is a time consuming and expensive process. It involves the cost of top solicitors, senior barristers and expert witness reports and attendances. Court lists are forever changing as important matters take priority, judges take leave or time out to write judgements. The judges are quick to refer disputes which they don’t perceive have much public interest to mediation if it has not been there. Nor do judges have much interest in disputes between dentists. They are content to see them delayed until the parties decide that they will settle out of court due to growing legal costs. Most don’t proceed beyond mediation.
As most disputes between dentists are resolved before reaching court, examples of case law with respect to breach of exclusion arrangements are difficult to find. A consensus among lawyers experienced in preparing buy-sell and associate agreements for metropolitan dentists is that a two-year exclusion covering a distance of eight kilometers is enforceable. Where a vendor works in the practice following sale, the exclusion condition
should start from the date that they leave the practice. Making exclusion conditions much greater weakens them as there is a legal view concerning the right to ply one’s trade.
The law does not excuse attempts to cheat on a buyer: The vendor who set out to steal back patients
Adentist sold his practice in an outer suburb of Sydney to two young dentists who performed normal due diligence. Shortly afterwards, there was a big decline in patient bookings and the vendor dentist’s patients were noticeably avoiding the practice. Enquiries revealed that the vendor had circulated them with details of his new dental practice location conveniently located near a railway station but beyond the exclusion zone limit. He had induced patients to make appointments with him at the new location and had acted in bad faith in selling them his practice goodwill. The matter was settled in the buyers’ favour in legal arbitration. The issue was one of acting in bad faith. The fact that the perpetrator set up outside the exclusion zone was irrelevant. Having sold his practice, he had no right to induce the patients to follow him to his new location.
“Dr
Excitable” and “Dr Calm”:
Two dental specialists at war!
Two dental specialists—“Dr Excitable” and “Dr Calm”—came to me to resolve a situation of which the solution was so obvious as to defy logic as to why it had not occurred to them already. Their practice had two locations relatively distant from each other and additionally, both visited a couple of general practices to treat specialist patients for short periods on a monthly basis. Their relationship had broken down. They had settled into a routine where they worked distantly from each other and the fees earned through each location were approximately equal. The obvious solution was for each to take that part of the practice at which they were the dominant provider. Calm wanted that solution but Excitable threw up inconsequential arguments against it. In a joint meeting with myself and a member of my staff, it was obvious that Excitable detested Calm.
Excitable wanted detailed goodwill valuations but we advised that valuations made no sense as the fee base of each practice location was near even.
He then demanded that all equipment be valued. We pointed out that the large items had been depreciated to zero and that as there was a full set in each location, it was pointless.
The market in second hand dental equipment is so negligible as to be an unreliable value guide.
Excitable then demanded that all the small hand instruments be valued.
Our suggestion was that on a Saturday, all the small instruments at location one would be emptied out of cabinetry.
They would toss a coin for first pick of the small instruments, then choose
Often when approached to perform a valuation, I found that practice valuation was not appropriate to the situation. In my lengthy time since founding Synstrat Group in 1994, I had long established a dental valuation service but found that many enquiries about valuation were a way of seeking advice on another critical issue. I put those valuation requests aside and advised them concerning the underlying problem. In many cases, they had received incompetent business advice from an accountant.
court proceedings. “Dodgy Don’s” accounting valuation tricks
“A consensus among lawyers experienced in preparing buy-sell and associate agreements is that a two-year exclusion covering a distance of eight kilometers is enforceable. Where a vendor works in the practice following sale, the exclusion condition should start from the date that they leave the practice...”
Family separation and financial settlements are common among the professions. Where a dental financial settlement occurs, the point of difference to be argued by family law professionals, who too often profit by prolonging settlement agreements, is the value of a dentist’s practice, as while shares and superannuation fund balances are easily demonstrated, a practice has an intangible quality and value that can be disputed.
alternatively until the lot was exhausted. On the Sunday, they would repeat the exercise at location two.
A similar approach was taken with the consumable supplies at each location.
There was an argument about patients requiring extended treatment. Our advice was that the specialist concerned was expected to continue treatment or if professional ethics so dictated, he would, pay for another specialist to continue treatment.
No money changed hands and they were to jointly pay for the accounting and other costs involved in their separation. They proceeded on their separate ways.
Some individuals styled as forensic accountants will value any type of business regardless as to whether they have expert knowledge concerning the industry or profession concerned. They offer their services via family lawyers but they have rarely had sufficient relevant knowledge of dental practice financials to value them accurately. I regularly refused to do valuations outside of the dental and veterinary professions with whom we dealt on a regular basis and of which I had a great deal of industry knowledge.
Confronted with a dental practice, “Dodgy Don” valued it well above market value or well below depending on which side of a dispute he was valuing it for. He did this by substantially misquoting the owner’s market value salary and by using multiples of the resulting EBITDA which were far removed from practice market value. He contrived unrealistic values but as long as there were lawyers who had no idea as to true value but had figures they could argue in settlement, he received work to value a variety of businesses.
When I came across him, he was grossly overvaluing a badly rundown dental practice in decrepit premises on behalf of the lawyers representing the non-dental spouse in a family court dispute. In doing so, he enabled lawyers to prolong the property settlement at great cost to the parties. There is no victory, other than to lawyers, if costs cause distress to both parties.
If requiring a practice valuation for legal purposes, be sure that the valuer you use is experienced in valuing dental practices and has appeared in court as an expert on the value of dental practices. Many accountants claim to be “forensic accountants” but the only dentist they know is the one that drilled their teeth. Don’t accept a recommendation as to the expert valuer to use unless they have proven experienced valuing dental practices.
Irarely stepped beyond the bounds of dental and veterinary practices but in a particular instance, a desperate medical specialist asked me to examine a valuation done for family court purposes in support of his estranged wife. As I knew from experience that many medical specialists have little goodwill because of the nature of their referrals and that most of their surgery is done in hospitals, I was intrigued as to how a valuer had arrived at a value of nearly $1 million.
I asked the specialist whether the valuer had made any enquiries of him concerning the procedures he performed or the source of his patients. He had had no such enquiries. He was one of a numerically small medical specialist category but in actual fact others in that category referred patients to him for a particular procedure.
He was one of three specialists performing that procedure, one in Melbourne, one in Sydney and one in a regional centre. There was no identifiable market in practices of his sub-specialty. There was no goodwill value and the only other assets of the practice were a modest amount of used furniture and instruments. His operations were done in hospital. I noted that the valuer, an accountant, had listed his valuation experience in his report, consisting of a total of eight assignments in miscellaneous businesses. The case set-
“A qualification is far less important than having had extensive experience in advising and valuing dental practices....”
tled on my report with the other valuer, a chartered accountant, withdrawing his report in embarrassment.
Many of those purporting to have valuation expertise lack knowledge of the type of business they are valuing. Demand of valuers, suggested by lawyers, that they summarise their experience of valuing and of advising dental practices before you agree to their appointment. A qualification is far less important than having had extensive experience in advising and valuing dental practices. Remember it is you, not a lawyer, who pays the valuer’s fees.
Best wishes to all dentists, Graham Middleton
The information contained in this article is unsolicited general information only, without regard to the reader’s individual financial objectives, financial situation or needs. The information contained in this article is general in nature and you should consider whether the information is appropriate to your needs and where appropriate, seek professional advice from an accountant or financial adviser. It is not specific advice for any particular individual and is not intended to be relied upon by any person. Before making any decision about the information provided, you should consider the appropriateness of the information in this article, having regard to your objectives, financial situation and needs and consult your professional adviser. Any indicative information and assumptions used here are summarised, are not a product illustration or quote and also may change without notice to you, particularly if based on past performance. This notice must not be removed from this article.
Graham Middleton disposed of his interest in Synstrat group on 30 June 2020 and won’t be starting another business; he spent the later 33 years of his working life advising health professionals on business and financial matters. Dentists were the most numerous of his clients. He is the author of the recently published Financial Success for Dentists.
Dentists may obtain a copy by making a donation of minimum $60 to the Delany Foundation a registered charity which assists schools in Ghana, Kenya and Papua New Guinea then email Graham at graham. george.middleton@ gmail.com. A copy will be sent to you. All proceeds go to the Delany Foundation for its good work. Graham has paid for the printing and mail costs personally.

predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. when it comes to the perfect fit, Hu-Friedy is just right. DENTISTS LOVE OUR STAINLESS STEEL PEDO CROWNS:
predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. it comes to the perfect fit, Hu-Friedy is just right. DENTISTS LOVE OUR STAINLESS STEEL PEDO CROWNS:
Septanest : the first choice of dentists with over 150 million injections per year, provides you high quality you can trust



: MARCH 9 |
: SEPT 13
: JUNE 1 |
: SEPT 20 |
*organised in conjunction with the australian dental association in new south wales and victoria
A dental practice is usually one of the most valuable assets in a dentist’s life.
When it comes time to sell, many will do so with little understanding of the value of what they are selling and how to present it effectively to a buyer.
Others delay putting their practice on the market at an optimal time, fearful of what to do next and afraid of a loss of their identity.
This course explains:
• How to prepare your practice for sale to optimise the price, terms and compatibility with a purchaser
• Which exit strategy is right for your practice and why
• When is an optimal time to maximise the return for your asset
• Pitfalls owners fall into that devalue their practice in the final years of ownership
• Steps owners can take to improve the outcome in the final years of ownership
for anyone within 5 years of EXITING


With more than 20 years’ experience in dental practice sales, Simon Palmer has extensive knowledge of and insight into the complexities and sensitivities involved in buying and selling dental practices. Simon’s business - Practice Sale Search - sells more than 100 practices per year. He is a regular writer/contributor to dental publications and journals, and is regarded as an expert on dental practice purchases and sales in Australia and New Zealand.
n Exit planning: how do you get your practice ready to sell?
n What are the pros and cons of the exit options/ strategies available to you?
n Succession Planning: What do you need to do now to prepare?
n What is the likely profile of the buyer for your practice and what will they be looking for?
n Valuing Dental Practices: What/ where is the value in your practice?
n How do you handle staff discretion, confidentiality and disclosure?
n Legal agreements
n Effective strategies for transferring patients effectively from seller to buyer
n What to do next post sale: post-sale strategies
n Tax implications and strategies when selling
n Expert finance, legal, accounting speakers


By Julie Parker
In the world of dentistry, trust is the basis on which successful patient-practitioner relationships are built. Without trust, dental professionals risk encountering obstacles such as reduced treatment acceptance, limited word-of-mouth referrals and diminished team morale. Therefore, nurturing trust with patients is not only crucial but also indispensable for the sustained success of any dental practice.
Let’s delve deeper into the impact of trust in dentistry and what you can do as a practitioner to build strong and maintainable trust with your patients.
Trust is the patients’ confidence in their dentist’s competence, integrity and commitment to their oral health and well-being. It represents the belief that the dentist will act ethically, provide honest guidance and deliver high-quality care tailored to the patient’s specific and unique needs and preferences. When patients trust their dentist, they feel empowered to make informed decisions about their dental care, communicate openly about their concerns and engage in long-term partnerships with the practice. Trust serves as the cornerstone of positive patient experiences, driving treatment acceptance, satisfaction and loyalty.
The impact of trust in dentistry
T he importance of trust in dental practice cannot be overstated, as it underpins these critical aspects of patient care and practice success:
Patients are more likely to accept treatment recommendations from a dentist they trust. Confidence in the dentist’s expertise and integrity instils patients with the assurance that they are receiving the best possible care, leading to greater compliance with treatment plans and improved clinical outcomes. Improved clinical outcomes also lead to more referrals.
Trusting relationships foster higher levels of patient satisfaction and engagement. Patients feel valued, respected and genuinely cared for when they perceive that their dentist has their best interests at heart. This positive experience enhances patient loyalty and encourages them to maintain ongoing relationships with the practice.
S atisfied and trusting patients are highly inclined to refer friends, family and colleagues to their dentist. Positive wordof-mouth referrals serve as a powerful endorsement of the practice’s quality of care and integrity, attracting new patients and contributing to practice growth and sustainability. Referred patients do not need to be attracted through discounted fees!
Dental anxiety and fear are significant barriers to seeking dental care for many patients. Building trust with patients creates a supportive, empathetic and safe environment that alleviates anxiety and
fosters a sense of comfort and confidence. Patients who trust their dentist are more likely to feel relaxed and at ease during dental visits, leading to more positive treatment experiences.
Patient trust not only impacts the patientdentist relationship but also extends to the dental team. When patients trust their dentist, team members are less defensive and feel validated and motivated in their roles, leading to improved morale, job satisfaction and teamwork.
Given the high importance of trust, here are seven actionable strategies that you can implement that give your patients many reasons to trust you.
N
othing builds trust like evidence that you know what you are doing! Continuously refine your clinical skills, stay abreast of advancements in dental technology and technique.
G
eorge Bernard Shaw said, “The single biggest problem in communication is the illusion that it has taken place”. Communication is a skill that we learn. So read books, watch informational videos, enrol in courses (Toastmasters is a terrific communication development avenue), conduct team role-playing - anything to bring awareness around how you
communicate and how others receive your messages. Continual improvement in the area of communication will benefit many aspects of your life, not just trust-building with your patients.
Recruit, train and empower team members who share the practice’s commitment to excellence, professionalism and patient-centred care. Foster a positive team culture that prioritises patient satisfaction, teamwork and continuous improvement.
We don’t always deliver positive news to patients. Occasionally, we may recommend services that some perceive as costly. Moreover, treatment success can sometimes be compromised, or treatment may even fail. Embracing these difficult discussions enables us to communicate openly and honestly with patients about their prospects and what they can anticipate.
Implement effective systems to ensure consistent service delivery and meet or exceed patient expectations at every touch-point of the patient journey.
Prospective patients rely on patient reviews of your practice and your expertise to guide their decision-making until they have the opportunity for direct interactions with you. It’s essential to monitor your reviews closely and encourage satisfied patients to share their positive experiences, as these reviews play a significant role in shaping prospective patients’ perceptions and early trust-building.
While many dental practices typically assign post-operative follow-up duties to auxiliary team mem-
bers, if you’re a practitioner striving to strengthen trust with your patients, consider personally conducting these follow-up communications.
When patients receive a call directly from their dentist, it demonstrates your genuine commitment to ensuring successful treatment outcomes.
By implementing these trust-building strategies, dental professionals can cultivate strong, enduring and mutually beneficial relationships with their patients.
Julie Parker is a Dental Practice Management Consultant and Team Educator. At the age of 33, Julie became the first non-dentist to own a dental practice in Australia. Julie is Co-Founder of Julie Parker Practice Success and CoFounder of Dental Business Mastery. Visit julieparkerpracticesuccess.com.au and dentalbusinessmastery.com.au to find how Julie can help your dental practice be more successful through consulting programs, online courses, podcasts and more.
Synstrat has spent many years collecting data on dental practices. We provide you with the best available knowledge on the performance of your practice relative to others. Our proven service has assisted many dentists Australia wide to create significant wealth. We are able to provide you with business accounting, practice valuation and financial advice services tailored to the dental profession.
•Do you need us to value the practice? •What rent can it afford?
How do you structure to meet tax planning

By Simon Palmer

As experienced dental practice brokers in Australia, my team and I are always amazed at the misconceptions that some dentists have about the process of buying and selling a practice. In this series of articles, we thought we would address some of the more commonly heard and persistent misconceptions that practice buyers have.
Buyer Misconception 1: My perfect practice is out there waiting for me
M any buyers have a rigid list of success criteria of what they are looking for in a practice and what it will cost and won’t look at opportunities that lie outside of these criteria. What they don’t realise is:
1. You pay for perfection. When something perfect or close to perfect appears, there is a lot of demand. A lot of the time, everyone is looking for the same criteria and, when it appears, the demand can push the price up beyond what you feel is reasonable.
2. Potential perfection is far cheaper than proven perfection. Sometimes, if you look slightly outside of your wish list, you can find “diamonds in the rough”. The foundation and potential for perfection is there, behind a lessperfect exterior, waiting for someone to come in and smooth over the rough edges.
3. You may not know what “perfect” looks like yet. If you start looking at things outside of your initial criteria, you may find that what equals “perfect” changes. You may find that some things that you previously thought were a “must have” become less important and you find other things to prioritise in your wish list.
Misconception 2: A lawyer is a lawyer and a source of finance is a source of finance
When you’re selecting a lawyer and financier, please look for one who is:
1. Available and quick to respond. There is a saying that “Time kills deals”. When you have a deal on the table and both sides are eager to accept, you want that excitement to help carry the deal to the finish line. Any delay can break that momentum and allow circumstances inside or outside the practice (another offer comes in, changes in economic circumstances, etc) to interfere with that momentum. Lawyers and banks that can work on your matter and respond quickly are much more likely to get you to the finish line.
2. Professional and polite in their approach. A lawyer who is antagonistic and combative or rude in their correspondence can kill a deal.
3. Experienced in medical/dental practice sales. Most dentists would cringe to hear of someone in their profession overselling their expertise and trying to do complex clinical work that is outside of their abilities, work that should be referred to a specialist. This is how I feel when a buyer tells me that they:
• Will be using a lawyer to help them buy a practice that they used for their divorce, immigration or buying their house;
“There is a saying that ‘Time kills deals’... When you have a deal on the table and both sides are eager to accept, you want that excitement to help carry the deal to the finish line. Any delay can break that momentum and allow circumstances inside or outside the practice to interfere with that...”
• Have a lawyer that “does a bit of everything”; or
• Are going to use a financier to help them buy their practice that has never financed a business before.
Buying a practice is an expensive and complex transaction, with many moving parts. To give yourself the best chance of success, you need specialised help from a bank and lawyer that have deep knowledge of the profession you are in and the type of business that you are buying.
The best way to negotiate the price is to criticise what is being sold
There is a school of thought that, in a price negotiation, the buyer should point out every fault, weaknesses, minor flaw and imperfection of the acquisition and talk down any strengths in order to justify giving the vendor a lower-thanexpected price.
This negotiating strategy may seem like a logical way to communicate your lower appraisal of the asset in question. It may be honest feedback and it may even work when buying assets like a second-hand car from a used car salesman. However, when buying a business from someone who has owned, worked in and built it up for years (sometimes decades), this type of negotiation is more likely to be completely ineffective and counterproductive.
Time and again I have seen a vendor be more likely to bend their price expectations for the purchaser who expresses appreciation and respect for them and their practice, than the one who does not.
Simon Palmer is the Managing Director of Practice Sale Search, Australia’s largest dental practice brokerage.
If you’d like more information on practice sales or want to have a confidential discussion about your practice’s circumstances, email Simon Palmer at info@practicesalesearch.com.au or call 1300-282-042.
If you’re intending to sell your practice in the next 5 years, hear Simon’s advice at www.exitacademy.com.au
By Jayne Bandy
You follow up with your patients when they don’t have another appointment. This means an appointment for their preventive care/hygiene or dental treatment.
There are two ways you follow up with your patients.
The first way is to send out a generic and impersonal letter, postcard, email or SMS asking patients to call your office.
And the second way to follow up with your patient is to call your patient and have a personal conversation with them about them and the appointment they need.
I’m sure you can see which is the better choice.
When dental teams let me read their follow up letters, they usually start with:
“Our records show...”
Or
“In a recent examination of your dental records...”
This is simply not personal and just looks like something generic from your dental software.
I know some patients will always respond and make an appointment after receiving this type of letter, but how many of your patients don’t respond to this letter.
What happens next?
You then send another follow up letter. Usually, the same one again and again and most patients will just continue to ignore the letter.
You end up with a systematic cycle of follow up letters with hardly any response.
This then becomes a system in your practice and a belief that you are following up with your patients when in actual fact, there is no real follow up happening.
Why not call your patient. You know most of the patients very well because you have built a relationship with them already. Call your patient!
Here’s a far better way to start your patient follow up conversation:
“Hi John, this is Jayne from Active Dental. How are you today? (A conversation will often begin at this point).
“Dr Green has asked me to give you a call.” (pause and listen to your patient).
“Dr Green is very concerned because you have not made your appointment for... Let’s make you an appointment.”

Call Tracking Excellence is not a product IT’S A RESULT!
With Call Tracking Excellence your team will learn the SAME exact processes Jayne used to:
1. Dramatically improve new patient call-in conversions to booked appointments.
2. Retain existing patient appointments
3. Prevent ongoing losses from appointment cancellations.
Visit the website to find out how to get started. It’s that easy! www.calltrackingexcellence.com
Can you see how the call is now personalised? It is about the patient and their dental needs and about the relationship between the dentist and the patient.
Once you call your patient, you can ask questions, answer questions, try to remove anything getting in the way of the patient going ahead and making their appointment.
You can’t do this in an email, SMS, letter or postcard.
The more follow up letters I read, the more I see how impersonal they are.
I know following up on a call with a patient can be a little uncomfortable at first.

It helps to keep in mind that the reason your patient didn’t originally make the appointment or cancelled their appointment, is often still the same reason they have not made another appointment.
Be prepared to have a conversation with your patient on the phone about what is still in their way of going ahead with treatment and know what solutions you can offer your patient.
This is what you do when you are truly helping your patients.
Once you start making follow up calls the RIGHT way it becomes easier and you get better and better at making appointments for your patients.
To find out how I can teach your team to know what to say and ask your patients, to help them make more kept appointments and prevent cancellations, call me on 1300-378-044 or email jayne@thedpe.com
Jayne began her career as an educator. After spending several years teaching, she made the jump to practice management, serving as a Practice Manager for a renowned dentist in Sydney for more than 25 years, giving her first-hand experience at what works when it comes to building and maintaining patient relationships, how to convert leads over the phone and most importantly - what it takes to reach your practice goals. As the CEO and Founder of Dental Phone Excellence, Jayne helps practices convert more calls into appointments, reduce cancellations and nurture effective patient communication that will result in increased profitability. Her past experience as an educator combined with her passion for practice management gives her a unique set of skills that allows your team to fully understand and take advantage of the tools she presents.


• Computer Designed
• Perfect Fit
• Patented Material
• Laser Cut
• Smooth edges
• 3D Printed Model
• Perfect Fit
• Upper &/or Lower
• All scans accepted


By Angus Pryor, MBA (Marketing)
Walk into any dental practice and you can feel the difference in an instant.
Some are alive with energy, phones ringing, patients chatting with familiar faces, appointments consistent. Others feel flat, with empty chairs and an (unsurprisingly) unmotivated team.
What makes the difference? It’s not luck and it’s not just location. It’s consistent marketing, but not the kind you see in flashy ads. It’s small, everyday things that build patient trust, keep your schedule full and make your practice the one patients choose and return to, again and again.
Yet too many practices make marketing complicated. They chase trends, try every new tool, or post to social media without a plan. But the best practices? They stick to what works. They don’t need gimmicks because they focus on the fundamentals, the same basics that work just as well in 2025 as they did a decade ago.
IFirst impressions that stick
f you want to know how a patient feels about your practice, look at what they see first. It’s probably not your front desk or your friendly smile, it’s your website. That’s your digital front door and it’s where many patients decide if they even want to visit you.
But here’s the problem: Too many dental websites feel like an afterthought. They’re slow, outdated, full of technical medical jargon or just plain confusing. Patients don’t need a lecture on dental technology, they don’t care about your degree or accolades: they want to know three things:
• Who are you? Real photos of your team, a warm welcome, and a simple message that shows you care;
• What do you offer? Clear, plain-language explanations of your services. Instead of “Scaling and Root Planing,” say “Deep Clean for Gum Health”;
• How can they book? A big, easy-tofind “Book Now” button. No one wants to search.

But a website is just the beginning. Your Google Business Profile is often the first thing a patient sees. If your reviews are old, your photos are stiff or your contact details are out of date, you’re missing an opportunity.
• Keep it updated: Check your contact information, opening hours and services regularly.
• Respond to reviews: Every review is a chance to show you care. “Thanks for visiting, Sarah! We’re glad you had a great experience.”
• Use real photos: Your team, your space - not stock images that look like a bank! Patients decide in seconds whether they trust you. Make those seconds count.
Adecade ago, a happy patient told a friend. Today, they tell Google and Google tells everyone else. Online reviews are the new word of mouth and they’re often the first thing patients check before choosing a dentist.
Too many practices leave reviews to chance however. They hope for good feedback but rarely ask for it. The best practices have a simple approach:
• Ask at the right moment: Just finished a whitening session with a thrilled patient? That’s the time to ask.
• Make it easy: Use a direct link in a follow-up text or email. The fewer steps, the better.
• Train your team: A receptionist can simply say, “If you enjoyed today’s visit, we’d love it if you could share a review online”.
• Respond to everything: Whether it’s a glowing review or a complaint, always reply. Show you care. However, it’s not just about stars. Think about how you respond. When patients see a practice that takes the time to thank happy patients or resolve a complaint, they see a team that cares. Plus, less than 5-star reviews are one of the best ways to take a hard look at what you’re doing and make adjustments as needed.
Most practices think of social media as a chore, something to tick off the list. But the best practices know it’s not just about posting; it’s about connecting, following up and connecting again. Instead of endless posts about services or promotions, they share stories. They introduce team members, share patient milestones (with permission) and give information that patients actually want to consume.
• Be consistent, not constant: Two or three good posts a week beat daily fillers.
• Highlight real stories: Did a young patient lose their first tooth? Did a long-time patient finish their Invisalign journey? Share it.
• Answer questions: Use your comments section as a place for free advice. “How often should I change my toothbrush?” “Every three months, or sooner if the bristles look worn”.
• Show you care: It’s not just about being seen, it’s about making followers feel seen. Interact with patients and their accounts. 5 minutes a day will significantly boost your engagement and reach. Reach = more eyes on your business.
Attracting new patients is great, but keeping the ones you have is even better. Patient retention is where real growth happens. Loyal patients don’t just come back — they trust your advice, they accept treatments and they refer friends.
The best practices know that retention starts with staying connected.
• Reminders that feel personal: A friendly text, an email or a quick call. Not just “You have an appointment”, but “We’re looking forward to seeing you”.
• Follow up after visits: “Hi James, just checking in after your filling. Any
“Think of retention like a garden. Neglect it and it withers. Nurture it and it thrives. So many practices focus all their energy on planting new seedsspending on ads to attract new patients - but forget to care for the ones they’ve already grown...”
connections that build trust
Marketing isn’t just digital. For many patients, trust starts with seeing you as part of their world. Smart practices go beyond the treatment room and the front desk.
• Support local events: Sponsor a school sports team, join community health fairs, or run free dental hygiene talks.
• Partner with local businesses: Gyms, cafes, local allied health clinics; look for opportunities for cross-promotion with likeminded local businesses.
• Show up: Be visible. When patients see your name around town, it’s a reminder that you’re part of their community. Patients notice practices that make a contribution to their community and they’re more likely to choose a dentist they see as part of their world.
Consistency is the real secret
Bdiscomfort?” It’s two minutes that can mean the world.
• Celebrate milestones: Birthdays, dental anniversaries, even a patient’s first visit. Small touches make a big difference.
• Reach out to inactive patients: “We haven’t seen you in a while. Your smile deserves some care”.
Think of retention like a garden. Neglect it and it withers. Nurture it and it thrives. So many practices focus all their energy on planting new seeds - spending on ads to attract new patients - but forget to care for the ones they’ve already grown.
The irony? Those “new seeds” are the most expensive ones. You pay for every click, every ad impression, every promotion. But the patients already in your database? They’re the low-hanging fruit, the ones who already know you, trust you and are far more likely to book again.
ut for all the marketing tips and tactics, there’s one truth that’s often missed: Consistency beats everything. A practice that does a few things well, over and over, will always outperform one that tries to do everything, badly. You must be consistent and reliable. Patients remember a practice that shows up, in their inbox, on social media, at the local footie and with a simple reminder call. They remember the team that knows their name, the dentist who remembers their last conversation, the interaction that feels genuine. Keep your messaging clear, your connections strong and your patient experience unforgettable. Because in 2025, the practices that thrive aren’t just the ones with the biggest ads. They’re the ones patients remember.
Multi-award-winning Practice Growth Specialist, Angus Pryor, is an author, marketer and international speaker. He is the #1 Google-ranked dental marketer in Australia. In 2023, Angus’ team at Dental Marketing Solutions received the ADIA’s marketing award. More details are at www.DentalMarketingSolutions.com.au. For a smarter, cheaper solution to finding great team members doing particular tasks, there is a solution. To find out how to unlock the gold in your practice from incomplete treatment plans, reactivations and more, visit www.DentalStars.com.au.
Presented by Emeritus Professor Laurence Walsh AO BDSc, PhD, DDSc, GCEd, FRACDS, FFOP (RCPA), FFDT (RCS Edin)
8
Learn from Australia’s leading authority on infection prevention and control in dentistry about recent changes in infection control including from the Dental Board of Australia (July 2022), the ADA (4th edition guidelines August 2021 and the ADA Risk management principles for dentistry during the COVID-19 pandemic (October 2021)), the new guidelines from NHMRC (May 2019), Hand Hygiene Australia (Sept 2019) and the CDNA (Dec 2018) as well as recent changes in Australian Standards and TGA regulations that are relevant to infection control. The course provides a summary of how those changes interlink with one another and also covers practical implementation of the new requirements and what it means for everyday dental practice. Hear about the why and the how and keep up-to-date with the changes that are happening.
This one day course will cover changes in regulations and guidelines from 2018 to 2022 including:
n Risk-based precautions.
n Hand hygiene and hand care practices.
n Addressing common errors in personal protective equipment.
n Biofilm reduction strategies.
n Efficiency-based measures to improve workflow in instrument reprocessing and patient changeover.
n Correct operation of mechanical cleaners and steam sterilisers.
n Wrapping and batch control identification.
n Requirements for record keeping for instrument reprocessing.
n Correct use of chemical and biological indicators.






Laurie Walsh is a specialist in special needs dentistry who is based at the University of Queensland in Brisbane, where he is an emeritus professor. Laurie has been teaching and researching in the areas of infection control and clinical microbiology for over 25 years and was chief examiner in microbiology for the RACDS for 21 years. His recent research work includes multiple elements of infection control, such as mapping splatter and aerosols, COVID vaccines and novel antiviral and antibacterial agents. Laurie has been a member of the ADA Infection Control Committee since 1998 and has served as its chair for a total of 8 years, across 2 terms. He has contributed to various protocols, guidelines and checklists for infection control used in Australia and represented dentistry on 4 committees of Standards Australia and on panels of the Communicable Diseases Network of Australia and of the Australian Commission on Safety and Quality in Health Care.
n On-Demand access to 29 Online Learning Videos (Over 8 hours of education).
n Watch and re-watch at your leisure 24/7
n Digital Online Learning Companion.
n Digital Suggested Reading Material.
n Online Questionnaire to earn 8 Hours of CPD.
By Emeritus Professor Laurence J. Walsh AO
With improvements in the technology for generating ozonated water, the potential applications of this technology continue to expand.
This article is an update to a 2021 comprehensive review of the applications of ozonated water, 1 with particular emphasis on applications related to infection prevention and control in the area of prosthodontics.
zone dissolved into water has been used for many years in various fields of dentistry due to its well-known antimicrobial effects and high biocompatibility. Ozonated water is highly effective in killing both Gram positive and Gram negative bacteria, working more quickly on the latter than the former.1,2 The reason for this difference relates to variations in cell wall, which then affect the sensitivity of different species of bacteria to oxidising agents. A Gram-positive cell wall is thicker and provides greater resistance.
The antibacterial action of ozone occurs through oxidation of glycoproteins, glycolipids, amino acids and other components of the cell membrane, resulting in increased membrane permeability, leakage of cell contents, damage to intracellular components and eventually microbial lysis.3,4
The rapid timeframe within which cell membrane damage occurs to bacteria means that ozonated water works more quickly than biocides and disinfectants that need to penetrate into the bacterial cell cytoplasm. A further advantage of the pattern of membrane attack to bacteria is that this type of action cannot lead to the development of resistance by bacteria. This is because ozone attacks multiple types of molecules and inhibits numerous enzymatic pathways and control systems of bacteria.
When ozone is dissolved into water, the powerful oxidising actions of the solution also make it effective against other forms of pathogens beyond bacteria, including viruses and protozoa. It is also effective against fungi, fungal spores and bacterial spores. Of the various species of fungi that can be found within the normal oral mycobiome, isolated water is highly effective against Candida species, including C. albicans, C. krusei and C. tropicalis 5
The wide antimicrobial spectrum of ozonated water explains the breadth of its documented applications in dentistry, which range from the treatment of caries, through to its use as an irrigant in root canal treatment and for periodontal pockets,6-11 and its use for treating dental unit waterlines.1,12,13
An important trend over the past two decades has been a greater emphasis in research on the applications of ozonated water as opposed to gaseous ozone. There are several reasons behind the shift including lower cost and greater convenience, including the development of compact handheld battery-powered devices for generating ozonated water on demand. Adding to these obvious practical benefits, dissolving ozone into water lowers the potential for oxidative injury to human tissues, while still maintaining the antimicrobial actions. Ozonated water has been used as a mouthwash, in both children and adults.14 It is not toxic for use and no negative gastrointestinal effects have been found from its accidental or deliberate ingestion.15 Cell culture studies have revealed that minor and reversible dose-related changes can occur on keratinocytes and fibroblasts of the gingival tissue, but that prolonged exposure times are needed for significant changes to occur. Moreover, all changes seen were reversible after 48 hours.16 This underscores its high biocompatibility. Indeed, of the available biocides and disinfectants, ozonated water is considered one of the safest for direct contact with the tissues of humans.17
One of the most important limitations of ozonated water is its short half-life. Under normal room temperature conditions, the half-life of ozonated water is only about 20 minutes, after which time the dissolved ozone will degrades back into normal diatomic oxygen. This is why ozonated water must be used within the first 5-10 minutes after being produced.18
There is a considerable body of research being undertaken internationally to extend the applications of ozonated water. A comprehensive review undertaken in 2021 of major patent databases identified a total of 620 individual patents and 134 patent families.17 South Korea and United States were the countries of origin for the largest number of patent applications, with a total of 103 and 91 applications, respectively.

Figure 1. The Hydrozone Health Ozone Rinse Tumbler generates ozonated water in 90 seconds and is ideal for mouth rinsing, impression disinfection and other applications including surface cleaning using the built-in spray feature.
Some of the more notable applications that are documented for ozonated water include as a sanitising material to be used as a component of hand hygiene. The strong actions of ozone on enteric bacteria and enteric viruses,19-21 as well as respiratory viruses22 underpin such clinical applications. Several clinical studies conducted in Japan and Sweden have shown strong performance for ozonated water when used for hand hygiene, especially for individuals with severe forms of dermatitis who are unable to tolerate alcohol-based products.23,24 At the present time, the National Hand Hygiene Initiative in Australia does not include the use of ozonated water as a substitute for the existing TGAlisted alcohol-based hand gel products with proven antimicrobial activity. This gap does not prevent in any way the use of ozonated water for physical handwashing and a number of dental practices have installed taps for physical handwashing with ozonated water.


An important responsibility of clinicians is to prevent contamination spreading from the patient treatment area to other parts of the practice and to external locations. Regardless of whether the clinic has its own laboratory or whether items are being sent to an external laboratory, the responsibility of limiting the spread of contamination remains nonetheless. A typical patient will have in their oral microflora about 280 bacterial species and numerous species of fungi. A 1 mL volume of the resting saliva from a healthy patient with good oral hygiene contains approximately 750 million microorganisms.25 A dental impression will pick up around 1 mL of saliva. This reinforces the need for appropriate decontamination of impressions before they are poured up or scanned.
Microbiological studies of impressions have shown that the most common species of microbes present are Streptococcus, Staphylococcus, Actinomyces and Candida, 26 all of can be readily transferred through to the dental laboratory when decontamination procedures are inadequate.27-29 Organisms transferred on impressions can then contaminate study models and working models.30
Typical procedures for impression decontamination include vigorous rinsing under running water followed by the application of a detergent and further rinsing. Based on assessment of risk, many clinicians choose to use a disinfection solution as a further step in the protocol. This can lead to issues since the antimicrobial agents that are present may alter the impression and reduce the surface quality of the resulting cast or scan. Hence, it is critical to consider the extent to which ozone may influence impression materials, when compared to other commonly used agents such as sodium hypochlorite (NaOCl).
Several studies have examined the use of gaseous ozone for the disinfection of elastomeric impression materials, including
condensation silicones and addition silicones of various consistency (e.g. Panasil putty, medium and light). The typical approach used is to measure the reductions of Pseudomonas aeruginosa, Staphylococcus aureus and Candida albicans by counting colony-forming units (CFU) on the surface of treated samples.
One study of this type undertook ozonation for 10 minutes (15 ppm, at an ozone flow rate of 800 mg/hour in a box with a volume of 8 L). This approach gave a 6-log reduction in S. aureus, P. aeruginosa and C. albicans 32 A second study using gaseous ozone reported reductions in Escherichia coli, S. aureus, P. aeruginosa and Enterococcus faecalis on the surface of addition silicone impression materials and noted a positive effect on the wettability of the material.33 Similar positive results were seen in a third study which used an exposure time of 5 minutes.34
A potential concern with all types of disinfecting agents is that there may be subtle changes on the impression surface. With the elastomeric materials, the polymers can degrade through a polymer chain scission process, during which oligomers and finally monomers are formed, which then leave the polymer.35 This issue has been well described for NaOCl, when used at a tenfold dilution (i.e. 0.525% final concentration) on vinyl polysiloxane impressions. This causes surface degradation with emergence of silica crystals on the surface. Unlike NaOCl, a 5-minute exposure to gaseous ozone (10 mins at 4L/min with ozone production of 2.61 g/h) does not cause significant or visible surface degradation. This means that, when compared with common disinfectants, ozone treatment of impressions is more likely to lead to highly accurate prosthetic restorations. Careful inspection of the ozone-exposed impression surface using scanning electron microscopy has revealed subtle wavy-wrinkling surface structures. These result from surface oxidation and the subsequent formation of a stiff silicon dioxide film.36-38 Despite these minor changes to the surface, the utility of the impression is not impaired significantly.39


Figures 4-5. Ozonated water is an ideal pre-procedural mouth rinse particularly before implant or periodontal treatments.
Several studies have demonstrated the usefulness of ozonated water for impression decontamination, for both irreversible hydrocolloid materials,40 as well as for elastomeric materials, including PVS, vinyl polyethers, addition silicones and condensation silicones in light body, medium body or putty variants.40-43 Ozonated water caused comparatively less changes to the surface than the reference materials of 0.5% NaOCl and 2% glutaraldehyde, making it a desired alternative as it was better able to preserve surface detail, whilst still being highly effective at reducing the load of microorganisms present. Of note, one study showed that treatment with ozonated water had no effect on the wettability and hydrophilicity of the surface. This was in contrast to NaOCl, which caused a reduction in surface wettability.43
Inadequate impression decontamination can lead to the persistence of microorganisms from the patient which then survive on the surface of the study model or working model.44 Inactivating these microorganisms without damaging the surface of the cast is a significant challenge. Most agents that have been used to disinfect dental casts, including NaOCl, increase the surface roughness of the cast.45 On the other hand, ozonated water does not adversely affect the surface roughness or its topography at the microscopic scale. In addition, there is no chemical reaction between the calcium sulphate of the cast and the ozone in the water, meaning that the presence of gypsum does not accelerate the decomposition of the ozone that has dissolved. Hence, ozonated water can be used to disinfect dental stone casts.45
The rapid antimicrobial action of ozone dissolved in water makes it suitable for use for situations where a rapid sanitising action is required. This includes treating toothbrushes to prevent overgrowth of normal oral microflora 46 and disinfecting removable appliances and dentures.47-50 An important advantage of this approach is that it does not cause corrosion, unlike NaOCl. Microorganisms that may be found on dentures, including Streptococcus spp., C. albicans and S. aureus, are readily inactivated by ozonated water.
This article has updated and extended the information summarised in the earlier 2021 review.1 It is clear from the information presented that there are a number of useful applications for water in everyday clinical practice, particularly for procedures involving impressions, appliances and prostheses, where there is a need for rapid and effective decontamination without the risks of corrosion to any metallic components which may be present. The availability of modern handheld ozonated water devices can assist in improving infection prevention and control, by limiting the spread of contamination from the patient’s mouth and the chair side to the dental laboratory. Ozonated water also provides a convenient solution to the challenge of a working castle study model that has become contaminated, and can augment physical handwashing when used as a final step after ordinary tap water.
1. Walsh LJ. Ozone in water: let the recent evidence speak. Australas Dent Pract. 2021;31(4):86-90.
2. Bialoszewski D, Bocian E, Bukowska B, et al. Antimicrobial activity of ozonated water. Med Sci Monit. 2010;16:MT71-MT75.
3. Nagayoshi M, Fukuizumi T, Kitamura C, et al. Efficacy of ozone on survival and permeability of oral microorganisms. Oral Microbiol Immunol 2004;19:240 246.
4. Almaz ME, Sönmez IS. Ozone therapy in the management and prevention of caries. J Formos Med Assoc. 2015;114:3-11.
5. Naito S, Shiga I. Microbiocidal properties of ozone on various microorganisms suspended in water. J Jpn Soc Food Sci Technol. 1982;29(1):1-10.
6. Azarpazhooh A, Limeback H. The application of ozone in dentistry: A systematic review of literature. J Dent. 2008;36:104 116.
7. Gopalakrishnan S, Parthiban S. Ozone – A new revolution in dentistry. J Bio Innov. 2012;1:58-69.
8. Case PD, George R, Bird PS, Walsh LJ. Treatment of root canal biofilms of Enterococcus faecalis with ozone gas and passive ultrasound activation. J Endod. 2012;38(4):523-526.
9. Hubbezoglu I, Zan R, Tunc T, et al. Antifungal efficacy of aqueous and gaseous ozone in root canals infected by Candida albicans. Jundishapur J Microbiol. 2013;6:1–3.
10. Goztas Z, Onat H, Tosun G, et al. Antimicrobial effect of ozonated water, sodium hypochlorite and chlorhexidine gluconate in primary molar root canals. Eur J Dent. 2014;8:469-474.
11. Giuroiu CL, Andrian S, Stoleriu S, et al. The combination of diode laser and ozonated water in the treatment of complicated pulp gangrene. Appl Sci. 2020;10:4203.
12. Walsh LJ. Disinfection of dental unit water with ozone. Australas Dent Pract. 2006;17(3):68-70.
13. Walsh LJ. Electrolytic ozonation of water: a new solution to the problem of dental unit waterline biofilms. Australas Dent Pract. 2011;22(1): 114-116.
14. D’Amario M, Di Carlo M, Natale SM, et al. Application of ozone therapy in paediatric dentistry. Appl. Sci. 2022;12:11100.
15. Durgapal S, Shetty M. Effectiveness of ozone against common dental problems: a literature review. J. Clin. Diagnostic Res. 2022;16:14-19.
16. Floare AD, Scurtu AD, Balean OI, et al. The biological effects of ozone gas on soft and hard dental tissues and the impact on human gingival fibroblasts and gingival keratinocytes. Processes 2021;9:1978.
17. Mascarenhas LAB, Oliveira FO, da Silva ES, et al. Technological advances in ozone and ozonized water spray disinfection devices. Appl Sci. 2021;11:3081.
18. Gupta S, Deepa D. Applications of ozone therapy in dentistry. J Oral Res Rev. 2016;8:86.
19. Shin GA, Sobsey MD. Reduction of Norwalk virus, poliovirus 1, and bacteriophage MS2 by ozone disinfection of water. Appl Environ Microbiol. 2003;69:3975-3978.
20. Suchomel M, Lenhardt A, Kampf G, Grisold A. Enterococcus hirae, Enterococcus faecium and Enterococcus faecalis show different sensitivities to typical biocidal agents used for disinfection. J Hosp Infect. 2019;103:435-440.
21. Walsh LJ. Handling the challenges of Norovirus and C. difficile infection. Australas Dent Pract. 2020;31(1):106-108.
22. Jia-min Z, Chong-yi Z, Geng-fu X, et al. Examination of the efficacy of ozone solution disinfectant in inactivating SARS virus. Chin J Disinfect. 2004;21:27-28.
23. Nakamura K, Saito K, Kashiwazaki J, et al. Evaluation of ozonated water using ASTM E1174 for standardized testing of handwash formulations for healthcare personnel. J Hosp Infect. 2018;100: 211-213.
24. Breidablik HJ, Lysebo DE, Johannessen L, et al. Ozonized water as an alternative to alcohol-based hand disinfection. J Hosp Infect. 2019;102:419-424.
25. Mantena SR, Mohd I, Sajjan S, Ramaraju A. Disinfection of impression materials: a comprehensive review of disinfection. Int J Dent Mater. 2019;1:7-16.
26. Egusa H, Abe K. Clinical evaluation of the efficacy of removing microorganisms to disinfect patient-derived dental impressions. J Prosthet Dent. 2009;102:56.
27. Powell GL, Runnells RD, Saxon BA, Whisenant BK. The presence and identification of organisms transmitted to dental laboratories. J Prosthet Dent. 1990;64:235-237.
Emeritus Professor Laurence J. Walsh AO is a specialist in special needs dentistry who is based in Brisbane, where he served for 36 years on the academic staff of the University of Queensland School of Dentistry, including 21 years as Professor of Dental Science and 10 years as the Head of School. Since retiring in December 2020, Laurie has remained active in hands-on bench research work, as well as in supervising over 15 research students at UQ who work in advanced technologies and biomaterials and in clinical microbiology.
28. Samaranayake LP, Hunjan M, Jennings KJ. Carriage of oral flora on irreversible hydrocolloid and elastomeric impression materials. J Prosthet Dent. 1991;65:244 249.
29. Rice CD, Dykstra MA, Gier RE, Cobb CM. Microbial contamination in four brands of irreversible hydrocolloid impression materials. J Prosthet Dent. 1991;65:419 423.
30. Mitchell DL, Hariri NM, Duncanson MG, et al. Quantitative study of bacterial colonization of dental casts. J Prosthet Dent. 1997;78:518 521.
31. Amin WM, Al Ali MH, Al Tarawneh SK, et al. The effects of disinfectants on dimensional accuracy and surface quality of impression materials and gypsum casts. J Clin Med Res. 2009;1:81 89.
32. Wezgowiec J, Wieczynska A, Wieckiewicz M, et al. Evaluation of antimicrobial efficacy of UVC radiation, gaseous ozone, and liquid chemicals used for disinfection of silicone dental impression materials. Materials 2022;15:2553.
33. Celebi H, Büyükerkmen EB, Torlak E. Disinfection of polyvinyl siloxane impression material by gaseous ozone. J Prosthet Dent. 2018;120:138-143.
34. Poulis N, Kyriacou A, Kotsou M, Bezirtzoglou E, Prombonas A, Drakoulis N. Effectiveness of low-flow high-ozone concentration disinfection of dental impressions: A comparative study to immersion disinfection. Br J Appl Sci Technol. 2014;4:2528-2537.
35. Evensen HT, Jiang H, Gotrik KW, et al. Transformations in wrinkle patterns: Cooperation between nanoscale cross-linked surface layers and the submicrometer bulk in wafer-spun, plasma-treated polydimethylsiloxane. Nano Lett. 2009;9:2884-2890.
36. Hillborg H, Karlsson S, Gedde UW. Characterisation of low molar mass siloxanes extracted from crosslinked polydimethylsiloxanes exposed to corona discharges. Polymers 2001;42:8883-8889.
37. Efimenco K, Wallace WE, Genzer J. Surface modification of Sylgard-184 Poly (dimethyl siloxane) networks by ultraviolet and ultraviolet/ozone treatment. J Colloid Interface Sci. 2002;254:306-315.
38. Zhu Y, Otsubo M, Honda C. Degradation of polymeric materials exposed to corona discharges. Polym Test. 2006;25:313-317.
39. Poulis N, Prombonas A, Yannikakis S, et al. Preliminary SEM observations on the surface of elastomeric impression materials after immersion or ozone disinfection. J Clin Diagnost Res. 2016;10 (12):ZC01-ZC05.
40. Savabi O, Nejatidanesh F, Bagheri KP, et al. Prevention of cross-contamination risk by disinfection of irreversible hydrocolloid impression material with ozonated water. Int J Prev Med. 2018;9:37.
41. Abinaya K, Muthu Kumar B, Ahila S. Evaluation of surface quality of silicone impression materials after disinfection with ozone water: an in vitro study. Contemp Clin Dent. 2018;9(1):60-64.
42. Shankar K, Dandekeri S, Shetty R, et al. Comparative evaluation of ozone water and glutaraldehyde on surface detail reproduction of vinyl polyether silicone impression materials at different time intervals. J Pharm Bioallied Sci. 2024;16(Suppl 4):S3837-S3839.
43. Fulsundar PD, More V, Bhadekar R, Bhola J. Comparative evaluation of ozonated water and 0.5% sodium hypochlorite for their effect of disinfection and surface wettability on polyvinyl siloxane impression material. World J Dent. 2022;10:5005.
44. Ivanovski S, Savage NW, Brockhurst PJ, Bird PS. Disinfection of dental stone casts: antimicrobial effects and physical property alterations. Dent Mater. 1995;11:19-23.
45. Nishikori R, Sawajiri M, Okuda T, et al. Effect of ozonated water on the surface roughness of dental stone casts. Dent Mat J. 2018;37(5):740-745.
46. Bezirtzoglou E, Cretoiu SM, Moldoveanu M, et al. A quantitative approach to the effectiveness of ozone against microbiota organisms colonizing toothbrushes. J Dent. 2008;36:600-605.
47. Murakami H, Sakuma S, Nakamura K, Ito Y, Hattori M, Asai A, et al. Disinfection of removable dentures using ozone. Dent Mater J. 1996;15:220 225.
48. Arita M, Nagayoshi M, Fukuizumi T, et al. Microbicidal efficacy of ozonated water against Candida albicans adhering to acrylic denture plates. Oral Microbiol Immunol 2005;20: 206-210.
49. Murakami H, Sakuma S, Nakamura K, et al. Disinfection of removable dentures using ozone. Dent Mater J. 1996;15:220 225.
50. Murakami H, Mizuguchi M, Hattori M, et al. Effect of denture cleaner using ozone against methicillin resistant Staphylococcus aureus and E. coli T1 phage. Dent Mater J. 2002;21:53 60.
Laurie has served as Chief Examiner in Microbiology for the RACDS for 21 years and as the Editor of the ADA Infection Control Guidelines for 12 years. His published research work includes over 400 journal papers, with a citation count of over 20,000 citations in the literature. Laurie holds patents in 8 families of dental technologies. He is currently ranked in the top 0.25% of world scientists. Laurie was made an Officer of the Order of Australia in January 2018 and a life member of ADAQ in 2020 in recognition of his contributions to dentistry.
Simply fill with tap water and turn it on

Ideal for...
Mouth rinsing prior to invasive treatments
Hand washing
Waterline disinfection
Surface disinfection
Impression disinfection
Rinsing of dentures, splints & appliances
When ozone is dissolved into water, the powerful oxidising actions of the solution make it effective against pathogens including bacteria, viruses, protozoa, fungi, fungal spores and bacterial spores.
The Aqueous Ozone Tumbler with built-in sprayer...
Generates up to 300ml of ozonated water - Dimensions 220mm x ø 60mm
Rechargeable (USB-C)
3 settings - 1ppm for oral rinsing (90 seconds)
2ppm for oral appliances (180 seconds)
3ppm for surface spraying (270 seconds)




> Protects you and your staff from needle stick injuries
> Complies with latest regulations
> Intuitive device
> Available with either sterile single use or sterilisable handle


Passive or active aspiration: security for the patient
Transparent barrel: aspiration is clearly visible
Sliding protective sheath: protection from needle stick injuries


Two different positions:
first Holding Position (reversible)
final Locking Position (irreversible)



for you. when it comes to the perfect fit, Hu-Friedy is just right.
A study demonstrated that when introduced in a dental school, Ultra Safety Plus was a the key success factor for avoiding needle stick injuries. With Ultra Safety Plus, needle stick injuries decreased from an average of 11.8 to 0 injuries per 1,000,000 hours worked(1)
STEEL PEDO CROWNS:
Septanest : the first choice of dentists with over 150 million injections per year, provides you high quality you can trust





By Dr Ryan Dunlop, DMD (USA)
ull-arch implant rehabilitation with immediate loading continues to redefine standards in restorative dentistry, offering patients rapid functional and aesthetic improvements. Achieving consistent clinical success, however, requires a comprehensive, patient-specific approach—one that integrates precise planning, surgical expertise and cutting-edge digital workflows.
In many treatment protocols, excessive bone reduction (FP3 design) is still commonly employed to simplify prosthetic
alignment. Yet, this approach can jeopardize long-term outcomes by complicating future revisions and increasing biological risk. Bone preservation should be prioritised, particularly when immediate function is the goal.
This case study, presented by Dr Ryan Dunlop, showcases a complete treatment sequence from extractions to immediate loading using TRI® matrix implants and a 3D-printed long-term provisional restoration. It underscores the advantages of a digitally driven, minimally invasive protocol that maintains anatomical integrity while delivering high aesthetic and functional results.

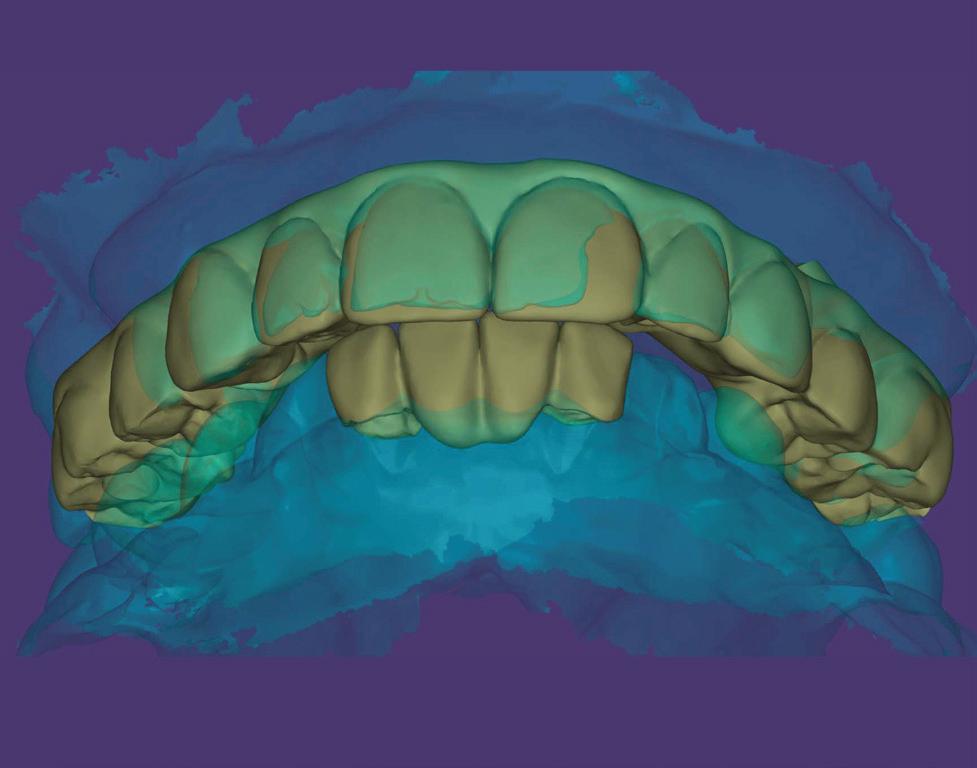
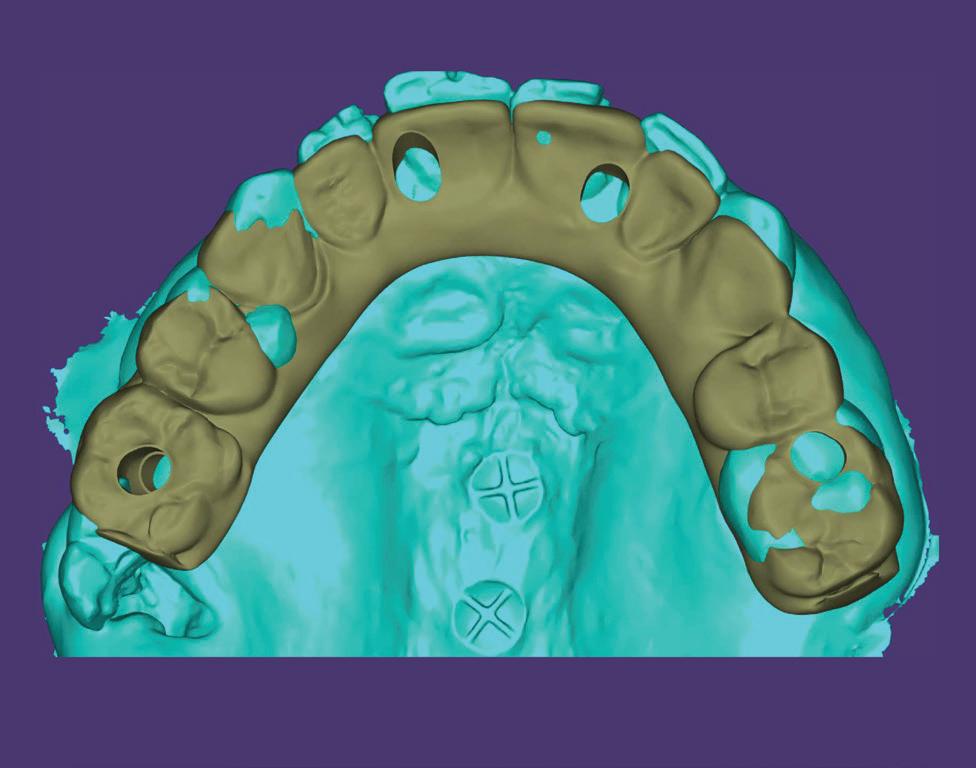
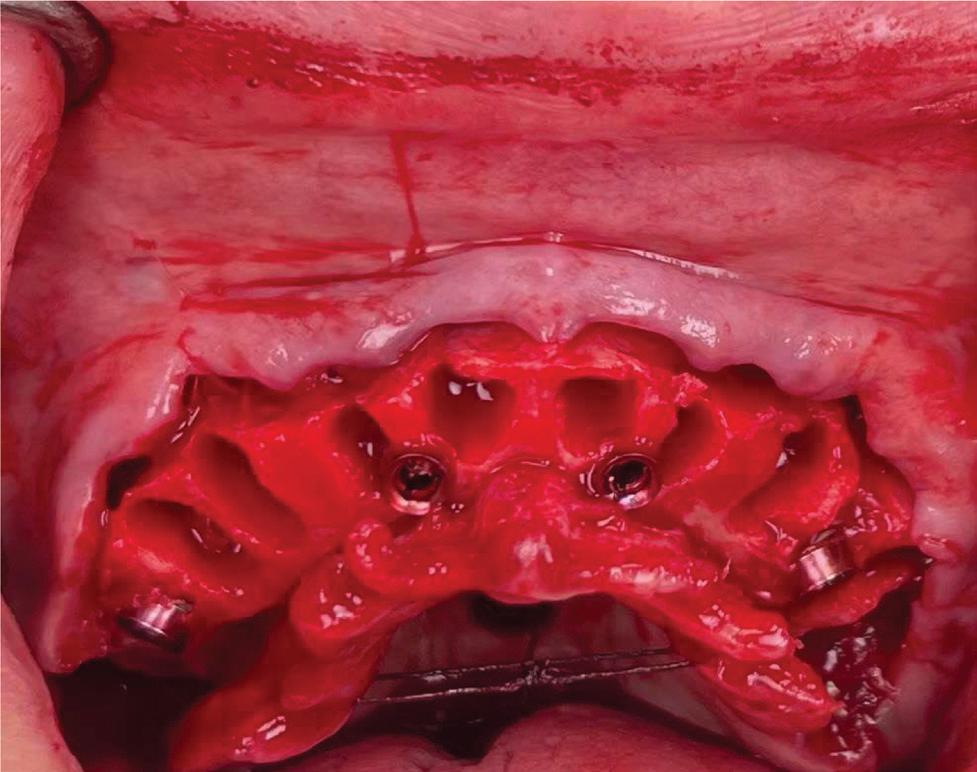
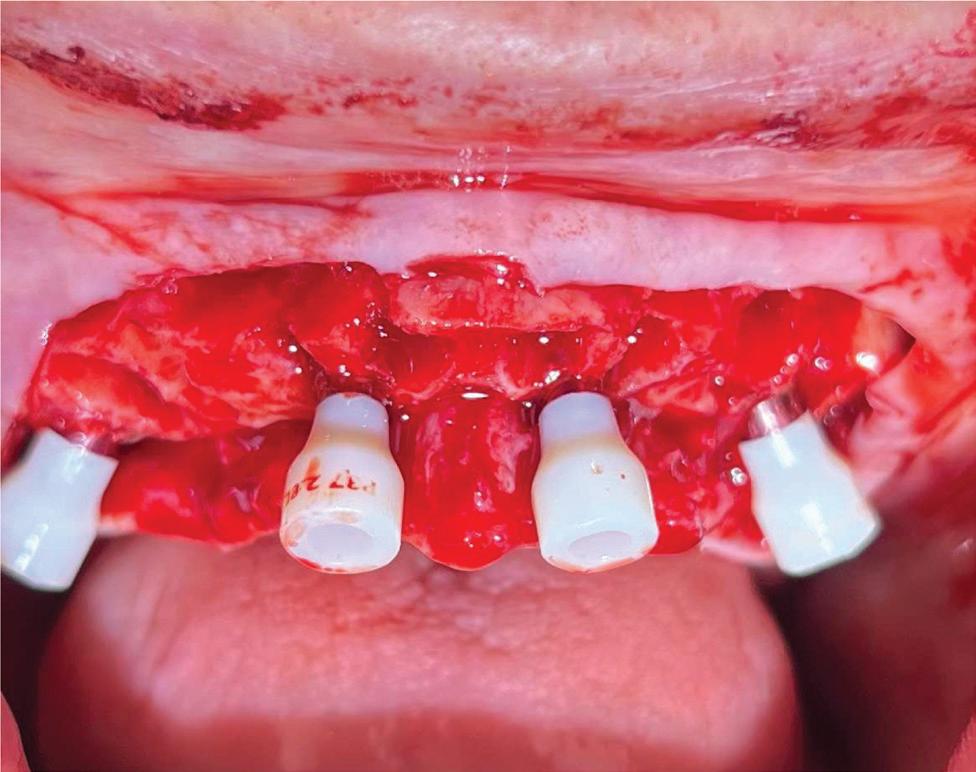
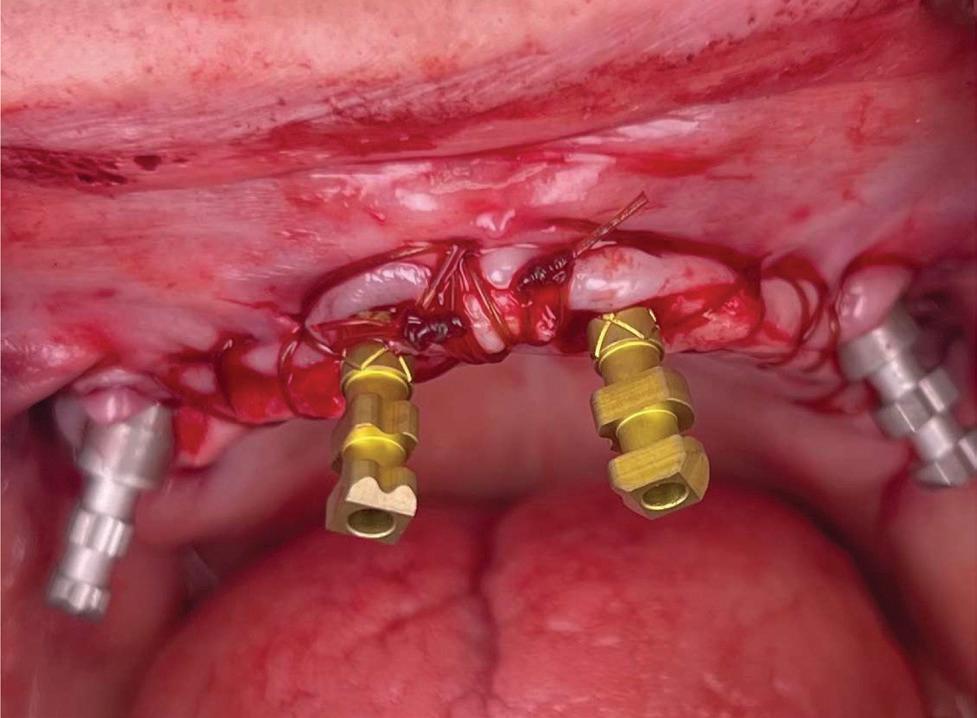
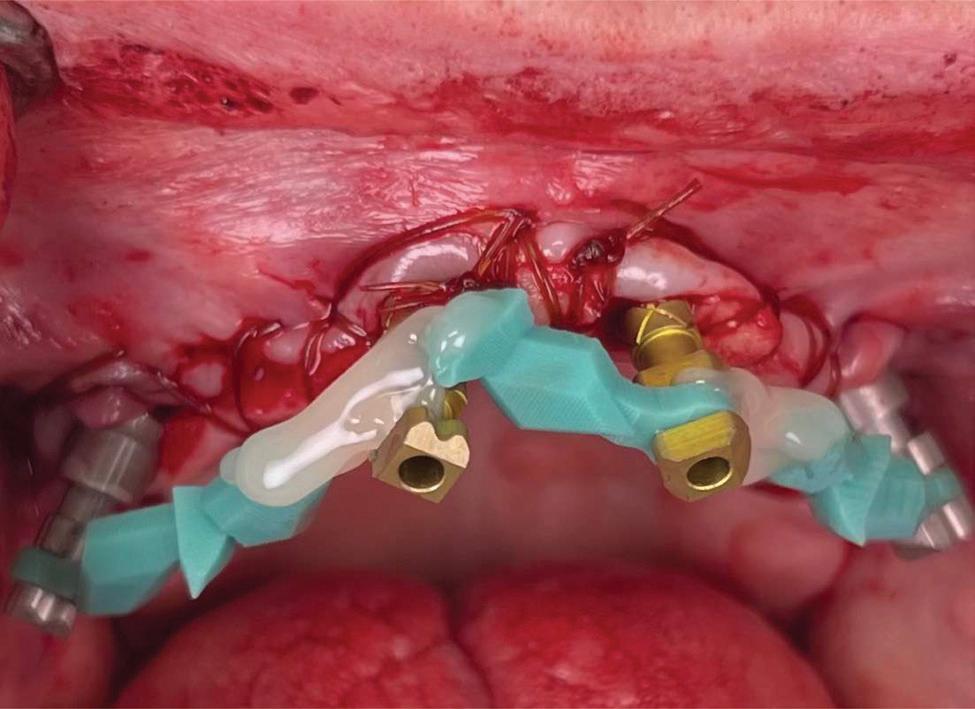
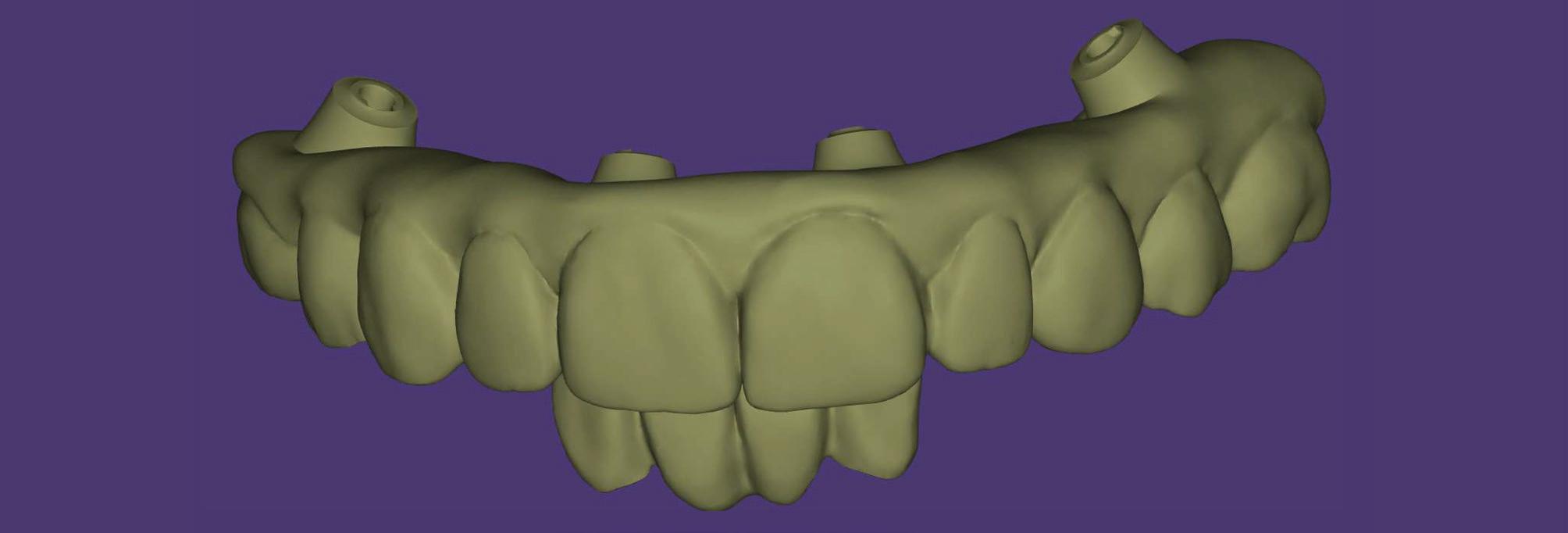
Figure 10. Implant position matching with wax-up. Provisional ready to be 3D-printed.


Figures 10-11. Immediate placement of 3D-printed provisional restoration.
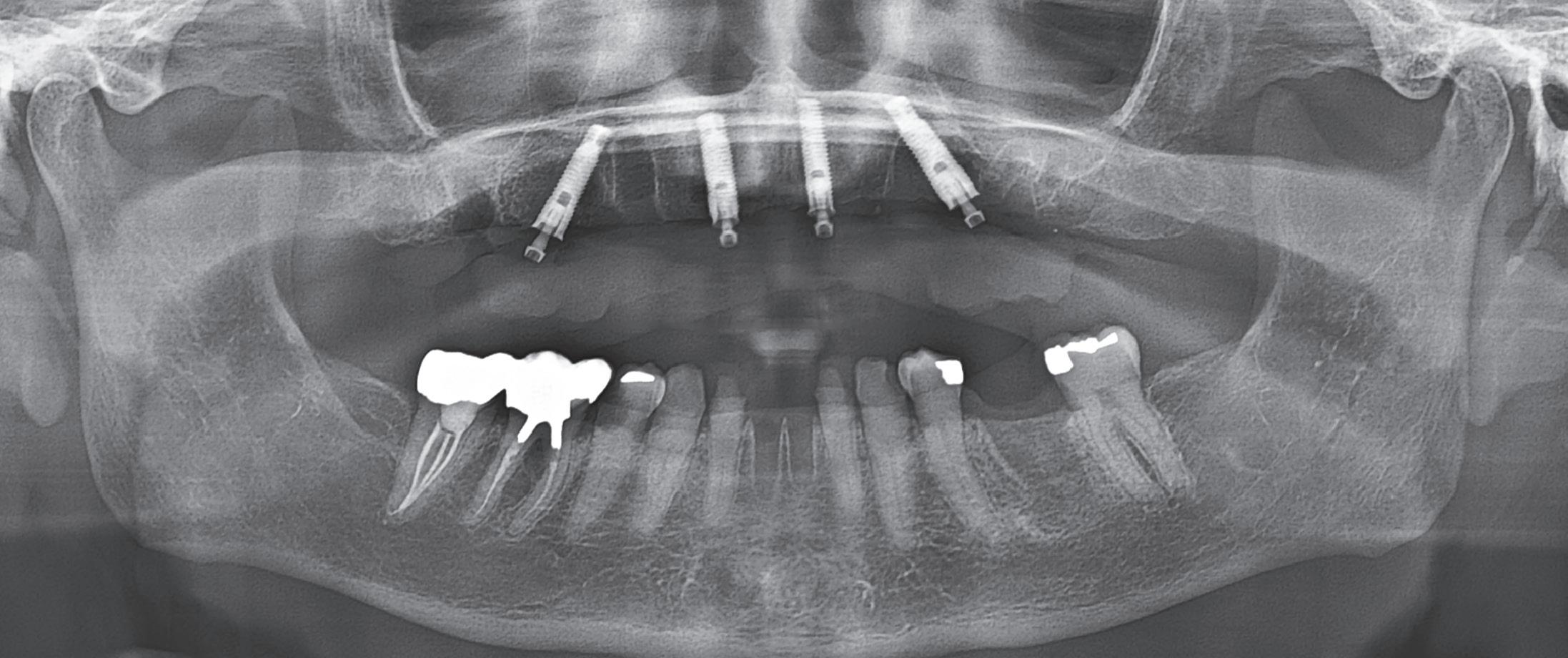
Figure 12. Post-op radiograph of immediate loading on day of placement.
About the author
Dr Dunlop wanted to be a dentist from a young age. At UCLA, he studied Anthropology and conducted research on Burning Mouth Syndrome at the UCLA School of Dentistry. He attended Harvard Dental School, won numerous clinical and research awards and was Class President for 3 years.
His research on trends in postgraduate dental education was published in the prestigious Journal of Prosthodontics in 2007. He was Chief Resident during his two-year residency at the Mt Sinai Medical Center in New York City, overseeing thousands of implant cases.

The world’s first implant approved for full digital restorations without abutment
The world’s first implant approved for full digital restorations without abutment
The matrix® is the first-ever dental implant connection that has been specifically designed for the new digital manufacturing technologies such as CAD/CAM milling or 3D printing. The implant concept allows to plan the restoration directly on the implant without the use of the abutment and without manual cementation. NO
The matrix® is the first-ever dental implant connection that has been specifically designed for the new digital manufacturing technologies such as CAD/CAM milling or 3D printing. The implant concept allows to plan the restoration directly on the implant without the use of the abutment and without manual cementation. NO ABUTMENT. NO CEMENT. NO LIMITS.
The world’s first implant approved for full digital restorations without abutment
The matrix® is the first-ever dental implant connection that has been specifically designed for the new digital manufacturing technologies such as CAD/CAM milling or 3D printing. The implant concept allows to plan the restoration directly on the implant without the use of the abutment and without manual cementation.

www.tri.swiss 0297

By Terry Whitty

It’s been the the most successful new intraoral scanner on the market to date and by new, we mean it’s not just an intraoral scanner as one would traditionally know it; it’s also a Photogrammetry scanner as well. Of course it’s the Shining 3D Elite Scanner and its been buzzing all over the internet in chat groups, Facebook and all other forms of social media, showing how truly remarkable this scanner is.
We did a review of the wired Elite scanner in Australasian Dental Practice back in an earlier edition, so what is new you say? Well now not to be resting on their laurels, Shining 3D have just released a wireless version of the Elite scanner and not only does it have all the features of the wired scanner, it has a few more new and compelling features that if you were thinking about buying a scanner surely this will make you run out and get one without question!
Firstly, the wireless Elite is a tiny and lightweight scanner at only 194 grams, arguably the lightest wireless scanner on the market today and that’s with the battery loaded! Compare it to a Trios 6 at 308 grams or a Medit i700 at 328 grams or even the highly publicised Allied Star at 245 grams and the Elite wins it hands down, but weight is not all it wins.
The Elite wireless is ergonomic, easy to holdeven in small hands - and it’s simple one button operation lets you control all the functions of the software when scanning easily without touching a screen or a mouse via “ motion sensing” on-screen tracking tracking.
Of course it still comes with 3 tip sizes, standard for general use, paediatric for kids and those adults with limited access and what they call the “Big” tip for photogrammetry use.
For communication, it’s equipped with WIFI 6 technology which is it’s own built in system.



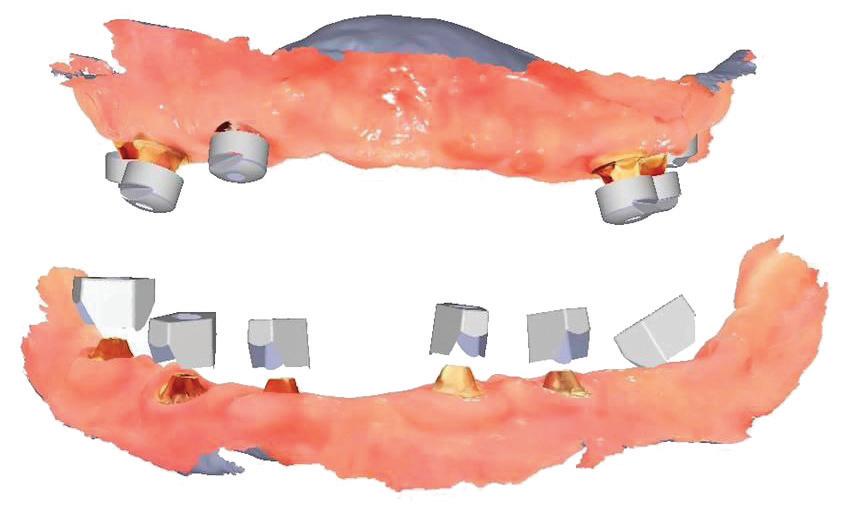





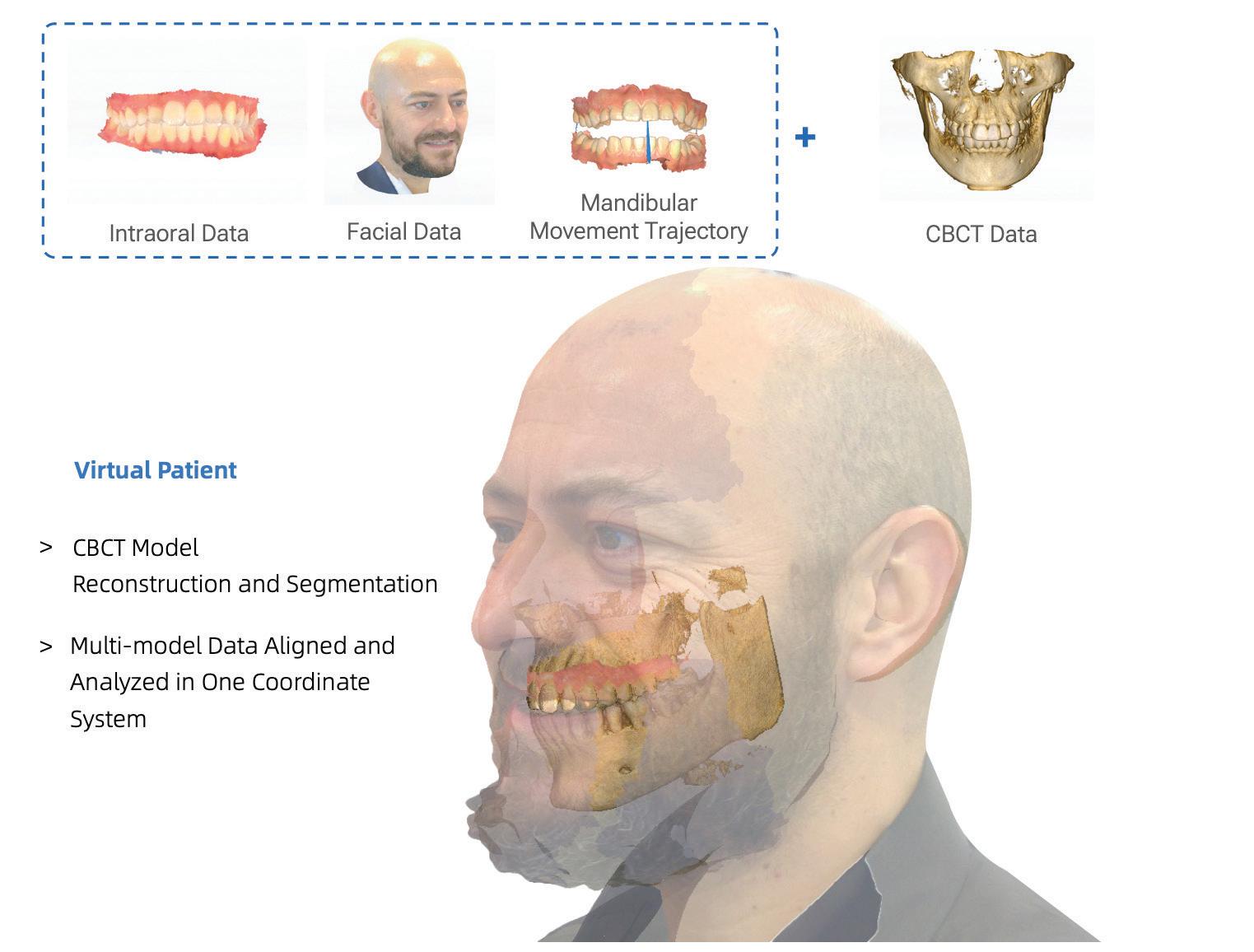
Now don’t be confused with your wireless system at home or at work for the internet, this is nothing to do with it at all. It uses its own dedicated transmitter (the scanner) and receiver/cradle (the base station) to make the connection to your computer in a wireless fashion. Speaking of the receiver, you can have multiple receivers in your other surgeries so all you need to do is pick up the scanner from one receiver cradle and take it to your next surgery, place it on the next receiver cradle and it will pair automatically and you’re ready to go. That’s amazing and they call it Place-Connect technology. By the way, the receiver is also the charging station! Speaking of charging, you receive 2 batteries each with a capacity of 2 hours. If you always leave it on the cradle, you will never have a problem being out of charge and no one I know scans for 2 hours non-stop as there is no need. This is a very fast scanner so often the scanning time will only be a few minutess depending on your experience and the clinical situation. You can scan anything with this scanner - your usual meat and potatoes Crowns, Bridges, Inlays onlays, veneers, splints, surgical guides mouthguards, smile design, etc - and it does the scanning with Ferrari speed and accuracy second to none. Now what of implants? Well this is where we separate this scanner from everything else on the market. Sure you can scan your traditional scan bodies to do an all digital crown or bridge, no problem
at all, however full arch or All-on-X cases traditionally pose problems. The Elite wireless is capable, via some amazing inbuilt tech and the use of some cleverly designed scan bodies - what they call High Accuracy Coded Scanbodies (HACS)you can scan the relative implant position across a full arch with accuracy of less than 5 microns ! This is thanks to IPG technology - IntraOral Photogrammetry. It sounds a bit like Star Trek speak but its available today with the Shining 3D Elite Wireless scanner. Can you imaging the time and headaches this solves? Never having to worry if things will “fit”, no more try-ins, no more verification jigs, just the confidence to know things will fit and its all done with one device so the workflow is smooth, intuitive and best of all accurate and repeatable case after case.
To make matching of soft tissue even more simple and reliable, Shining 3D have also released Cap Scan Bodies. The Cap scan body is a fantastic solution to resolve the difficulties and problems occurring when aligning soft tissues and coded scan bodies in immediate loading cases. In immediate loading cases, some factors such as mobile tissues can lead to the failure of automatic alignment, requiring further manual alignment. The Cap scan body solves this problem as it captures the alignment of the soft tissues to the Cap scans, then relates this to the HACS, a perfect match every time.

The New ELITE IntraOral Scanner from Shining 3D uses patented IntraOral Photogrammetry Technology to be the most accurate scanner available.
• Small form factor
• Lightweight 124 grams!
• Ultra fast scanning
• Dual mode IPG scanner
• Complete software suite
• Scan All On X Cases accurately
• Suitable for all IntraOral Scanning
• 3-year Warranty







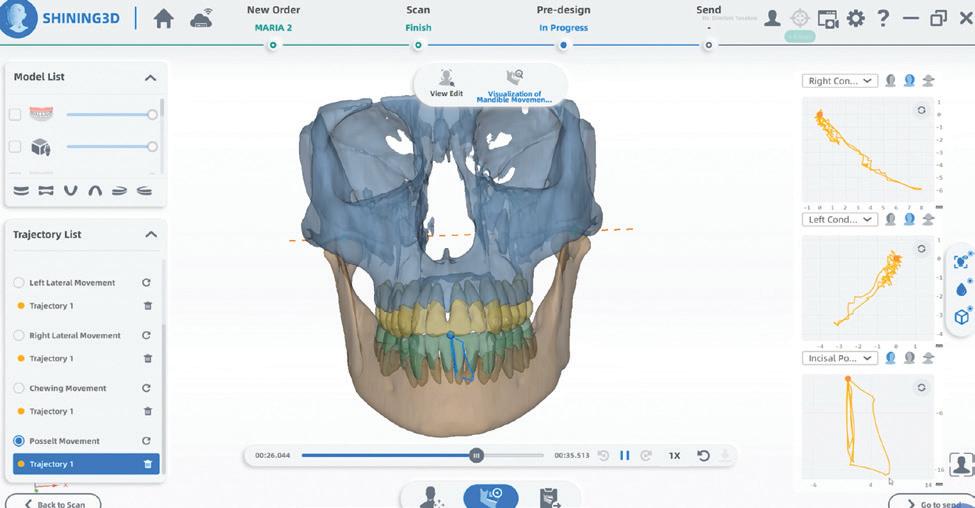
If this is not enough, there is now an “edentulous” mode that will capture soft tissues of edentulous arches with amazing capability. Those of you who are into removable prosthetics should at least try this as the world is changing fast and the clinical techniques of removable dentures is changing with it to help make your job easier and more predictable. I’d love to tell you more but I could write a whole article on just this function. Suffice to say, get a demo of the scanner in office and try it out but make sure you have soft floor covering to cushion the blow of your jaw hitting the floor. Did I mention you can capture Jaw motion tracking? Well it can and this can be exported to exocad CAD software so you can get a very accurate state of play of the actual movements of the patient and use this while designing restorations – real groundbreaking stuff.
We have not even ventured into the software of the Wireless Elite scanner. Suffice to say, you get a full suite of software that will make everyone happy. Besides the scanning software, there is an Oral Health Report generator where the software can pick up caries, pigmentations calculus, etc and you guessed it, with the help of Mr AI. This can also be sent to the patients phone via a QR code for them to ponder over.
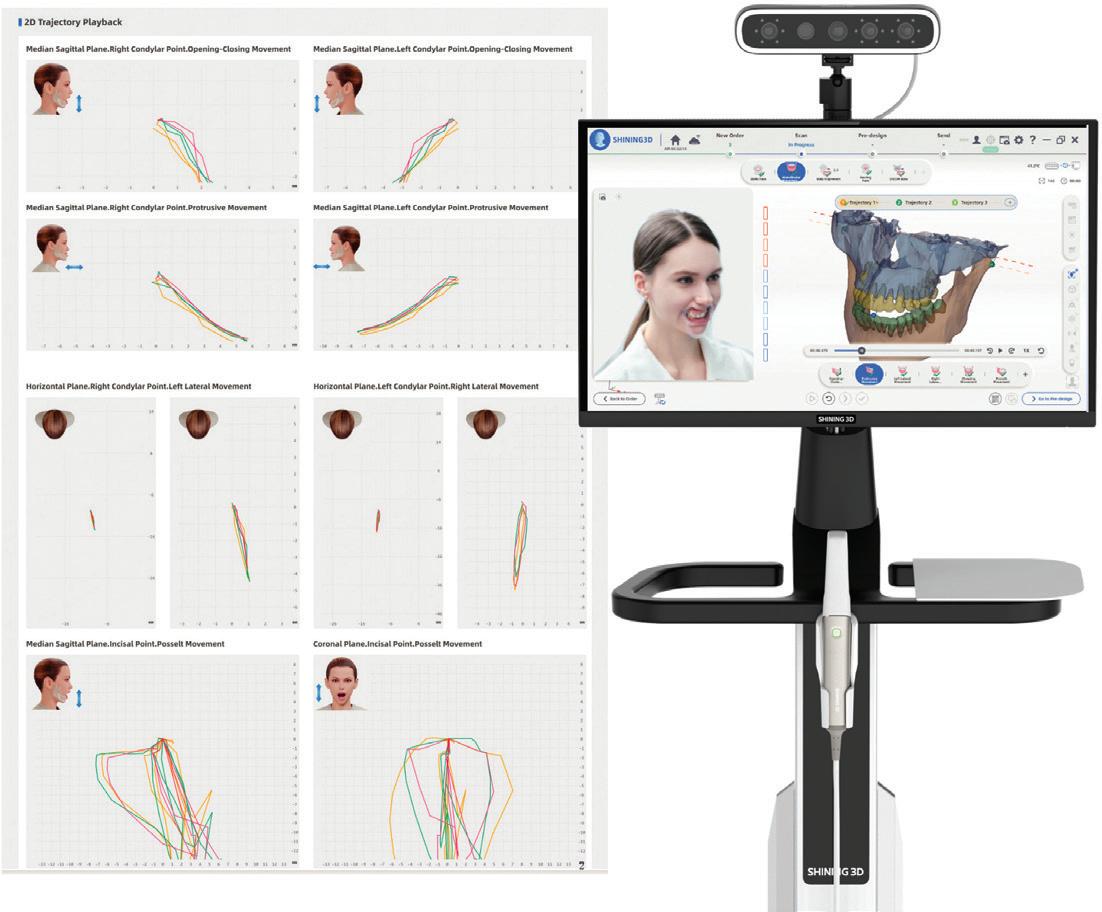
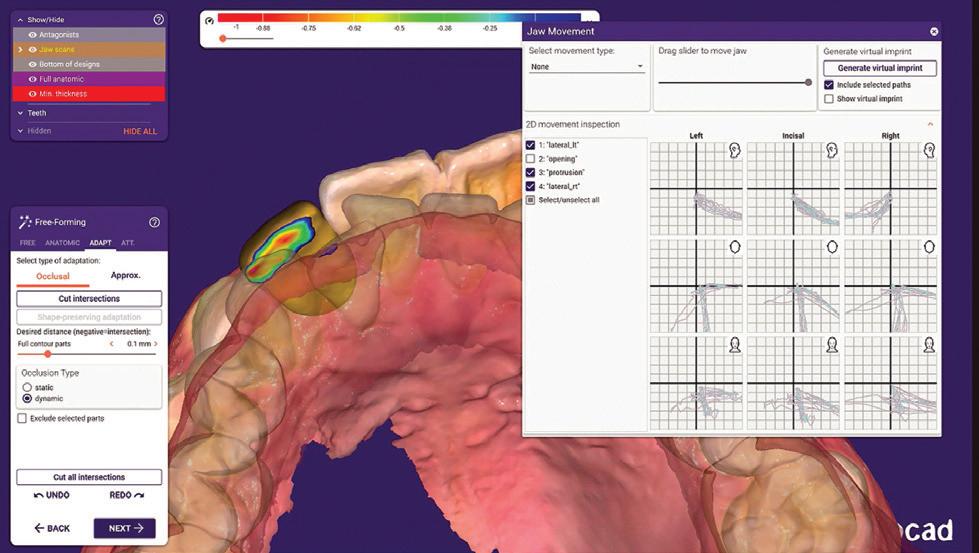
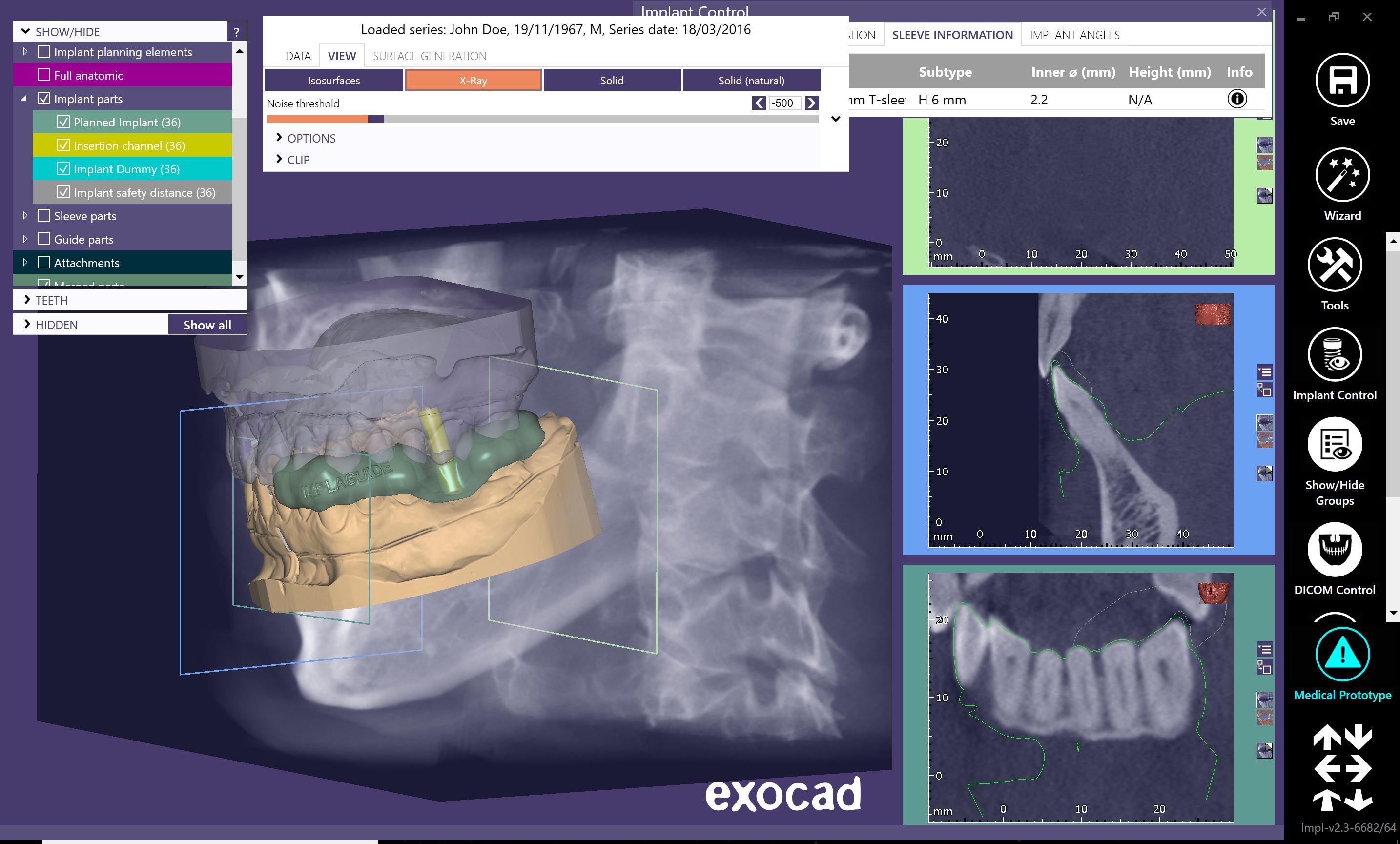
Free Case Evaluation Send


All implant surgical guides
• Edentulous Cases
• Scan Appliances
• Free Planning Software


The scanner also doubles as an intraoral camera so you can take snaps along the way and add to this report. There is margin line detection, undercut measurement, occlusion heat mapping and bite analysis, an orthodontic simulator, scan comparison and you can design models, splints, temporaries, indirect bonding trays ready to send to your 3D printer and, BTW, Shining 3D have 3D printers as well and they are great.
The Shining 3D Elite Wireless is again another groundbreaking device that has the power to do everything and is the only intraoral scanner with built-in photogrammetry if you want it, as its also available now without that option at a sharper price. You can of course upgrade it later if you wish. Match it with a face scanner and you have a perfect pair.
Speaking of facial scanners, a new release from Shining 3D, the MetiSmile MR face scanner, represents a substantial upgrade to the previous model both in terms of hardware capability and clinical application. As facial scanning continues to take on a more central role in treatment planning, the Metismile MR provides practitioners with a faster, more detailed and a more stable platform for capturing facial data with a high degree of accuracy.
The significance of this upgrade extends well beyond aesthetics. A high-quality facial scan is increasingly essential for developing treatment plans that are not only functionally sound but also harmonised with the patient’s natural facial features.
With the Metismile MR, clinicians can now adopt an holistic imaging approach, integrating facial symmetry, soft tissue dynamics and overall facial balance into the planning process. This allows for more predictable outcomes and better patient communication, key factors in contemporary multidisciplinary care.
Three new modules take the Metismile MR beyond what many would expect a facial scanner to do and integrates it with any intraoral scanner and now any DICOM file from a CBCT scan. Of course, the ideal setup would be to pair the MR with the recently release Elite photogrammetry intraoral scanner but it will work with any scanner capable of outputting STL files.
Firstly and foremost the scanner is compact and lightweight and can be used in two modes, hand held or fixed on the supplied mini tripod stand. This dual function makes it very easy to adapt to the way you wish to work. I have also seen it adapted to be fixed on to dental units and it works very well like this as well so having the flexibility of taking the basic facial scan in many different ways is accomodating. The scan only takes a few seconds and you can take multiple scans, open mouth, closed mouth, smiling, etc and the scans can be easily matched together by the software. If that’s all you wish to do, then these files are easily exported and can be imported into you favourite CAD software such as exocad. However, there is much more if you wish.
The Optimal jaw relationship module is an interesting take on the the traditional Vertical Dimension measurement. By taking measurements of Vertical Dimension of Occlusion and Vertical Dimension at Rest, the freeway space can be calculated. This is essential in edentulous cases to then make the full dentures but can be very useful in dentate cases too, especially when restoring a worn occlusion. Through AI and standard measurements, the optimal jaw relationship can be detected.
The next module is Mandibular Movement Analysis. It contains two parts - dentition movement trajectory and mandibular movement analysis. The mandibular motion trajectory can help collect the user’s mandibular motion trajectory and allow the user to export the motion trajectory for the design of the restoration, effectively preventing problems such as premature contact and jaw interference, thereby improving the functionality and adaptability of the restoration. The Mandibular motion trajectory analysis supports users to import CBCT data and project the trajectory data onto a 2D plane, assisting users in diagnosing and analysing patients’ functionality, symmetry and stability.
The third module is the motion tracker. This can be achieved with dentate or edentulous patients with the use of marker devices adhered to the teeth or registration trays depending on the type of case. This will accurately track the motion of the jaws and give a plethora of data that can be analysed for the individual patient.
And if that is not enough, it all comes on the optional new e-Motion cart where the two scanners, computer and touch screen all can live and be ergonomically accessed.
Shining 3D are really going all out to bring you the best, most innovative quality products at realistic prices so there is no excuse not to check these out at your dealer today.
About the author
Terry Whitty is a dental technician and noted commentator and KOL on digital dentistry. He lectures globally on subjects related to digital dentures, 3D printing and orthodontics.
• Any Design
• HD PMMA Milled
• Flexion Milled
• POM Resin Milled
• 3D Print Option
• Perfect Fit
• Upper or Lower
• All scans accepted
Example of a full-digital workflow based on the production of a demo mock-up. The tools for patient diagnostic as well as the design automations used allow for a precise functionalisation of the prosthetics in the digital world, providing patients with customised restorations in only two chairside appointments.

The latest technologies and software innovations in terms of patient data acquisition permit the production of functionalised and aesthetic restorations in considerably shorter times. Through a mockup demo case, this article describes a workflow based on Zirkonzahn patient diagnostic tools and design automations allowing for the manufacture of precise, individual dental prostheses in only two chairside appointments. A comparison between the produced demo mock-up and the natural teeth is also displayed, to show the mock-up’s high level of customisation and naturalness achieved with the workflow.
During the first appointment with the patient, the practitioner records the patient’s data and oral situation by taking 2D pictures of the face as well as digital impressions through the intraoral scanner. After the visit, the dentist sends the recorded data to the dental technician, who creates a virtual patient folder in the archive software, saving and storing all patient information for future usage. Based on the 2D pictures and intraoral scans, the dental technician designs a first set-up by means of the Smile Creator module included in the Zirkonzahn.Modellier software, in order to create a preview of the potential new smile.
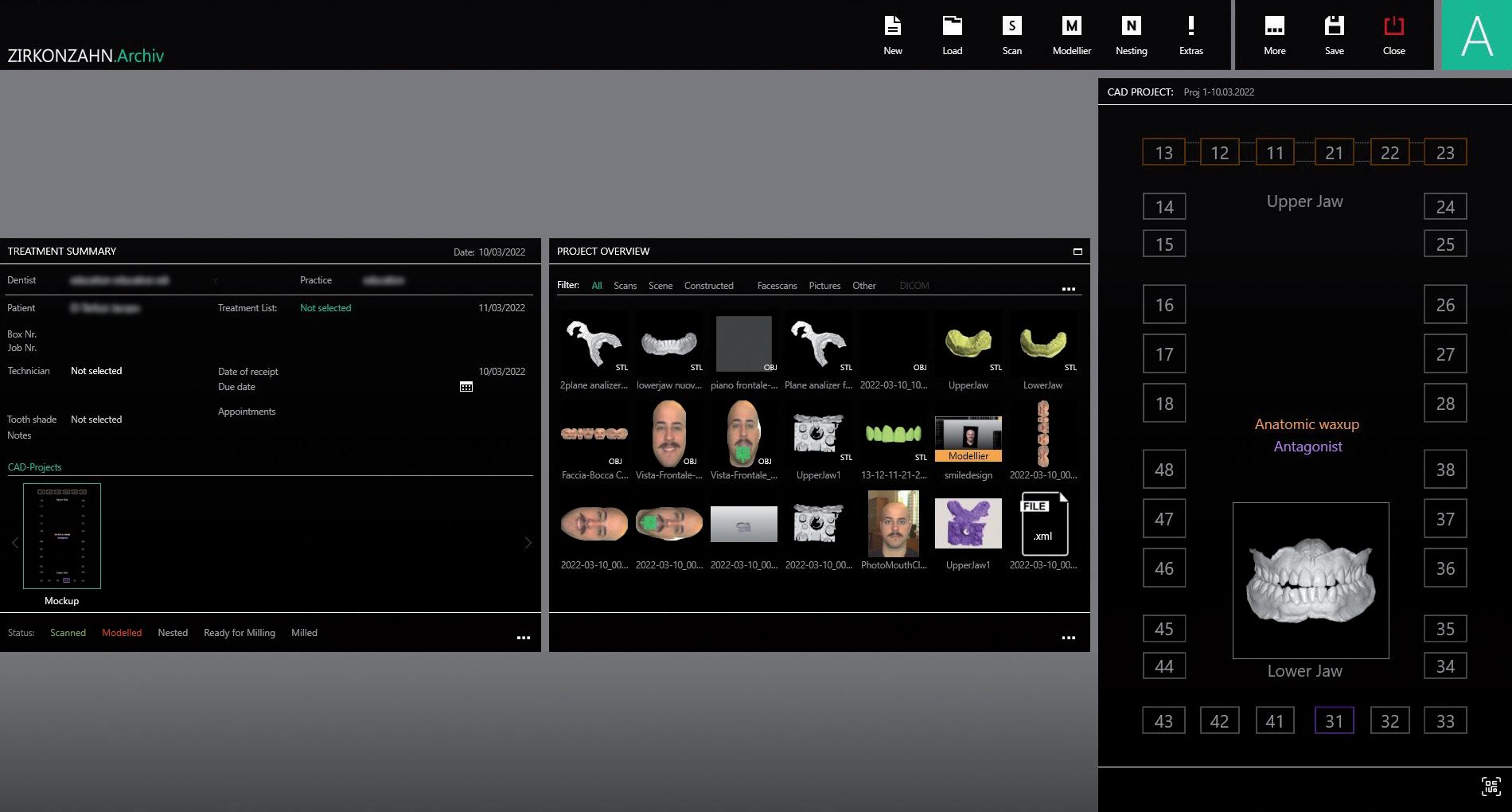
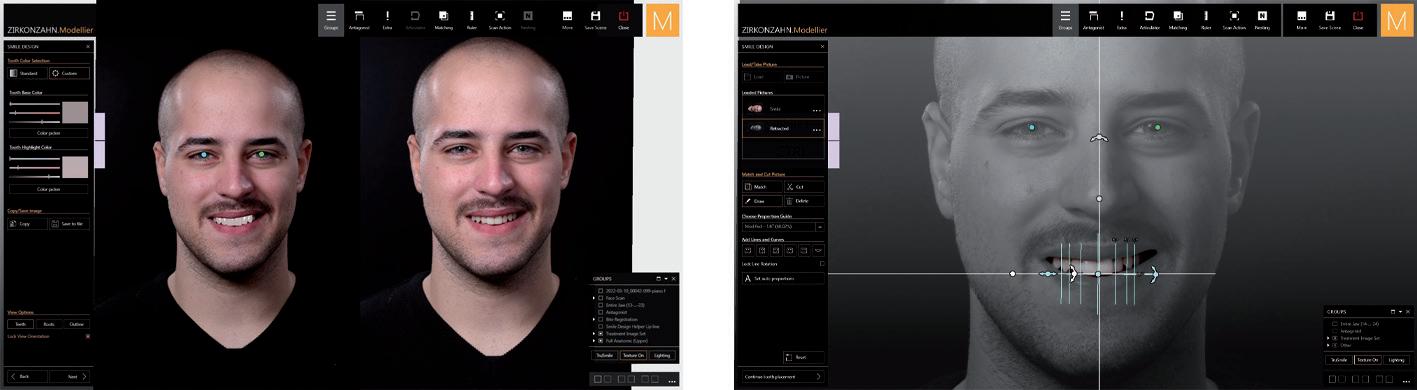



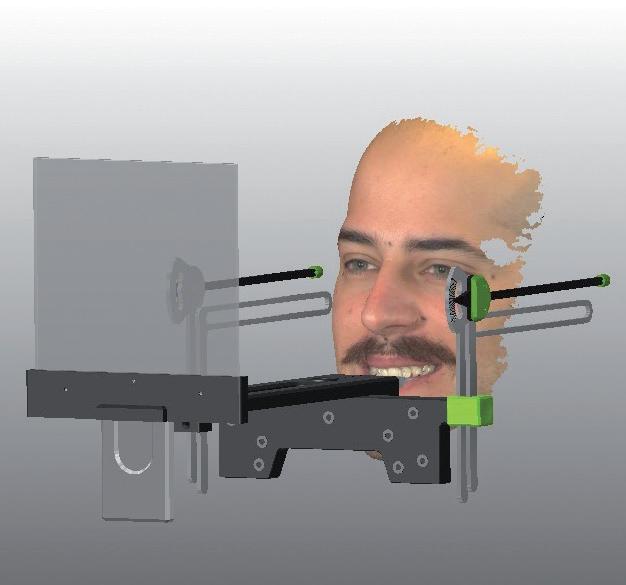
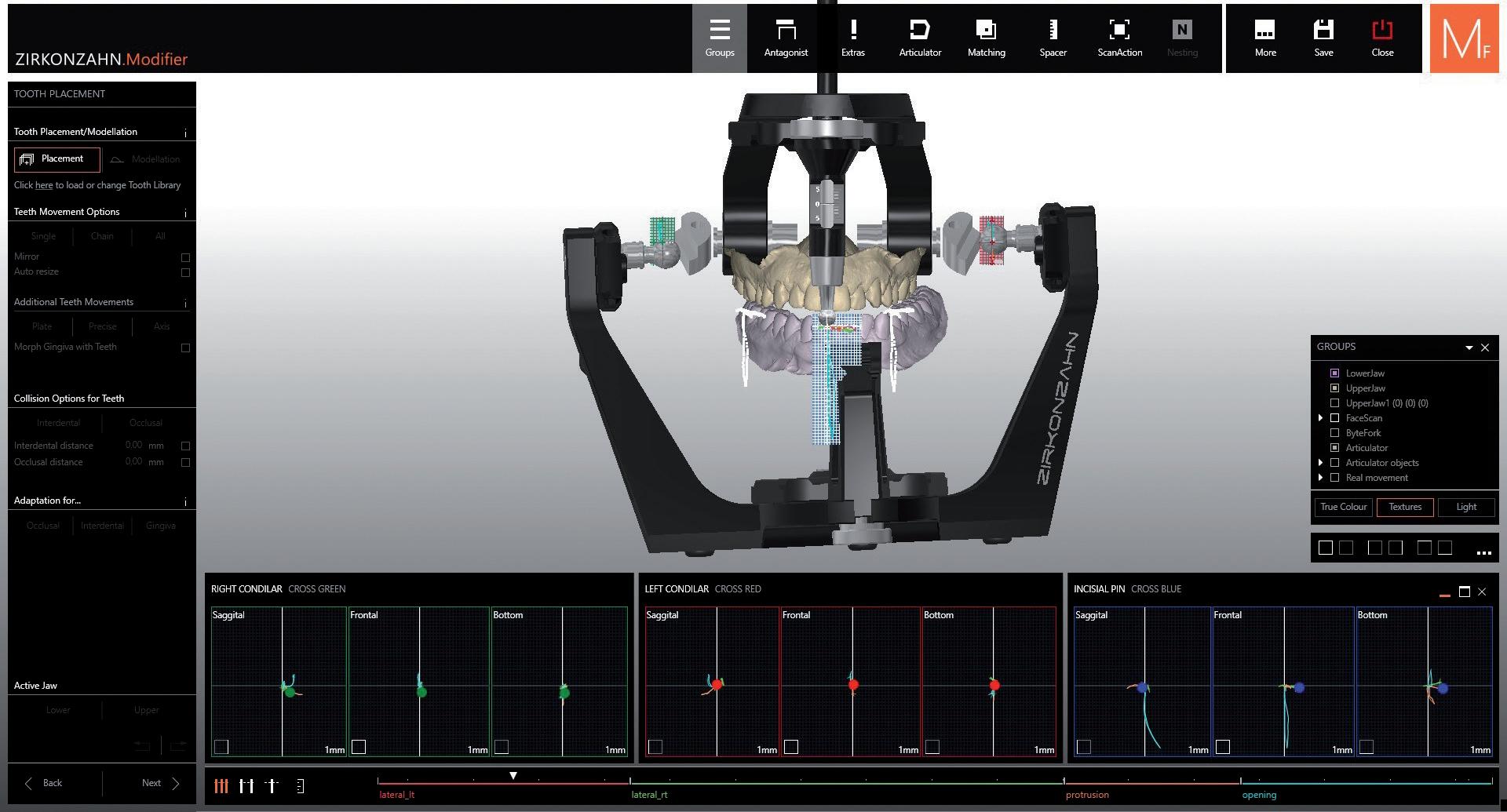
With the Smile Creator, the dental technician can design the tooth setup based on the natural teeth of the patient; alternatively, the virtual libraries of natural tooth sets available in the software can be used.
In addition, the dental technician can apply different tooth sizes, display the teeth in a real tooth colour, as well as integrate different reference lines into the 2D pictures for better tooth alignment (e.g. the smile line). The completed setup can then be exported as a 2D or 3D file and saved in the software for future designs.
uring the second appointment, the dentist and the dental technician show the digital smile preview to the patient. If the patient is satisfied with the aesthetic result, the dentist continues the treatment according to the restoration type. This demo case for the creation of a mock-up shows the workflow generally used for treating complex cases on implants. In such situations, the dentist employs the following patient diagnostic tools:
• The PlaneSystem® (MDT Udo Plaster), which records patient’s occlusal plane and oral situation in Natural Head Position;
• The PlaneAnalyser II, which detects patient’s real mandibular movements for a detailed and customised functionalisation of the prosthetics; and
• The Face Hunter 3D facial scanner, for a photorealistic digitalisation of patient’s face physiognomy.


Monolithic full arches made of Prettau® 2 Dispersive® Bleach zirconia on anodised titanium bases, veneered only in the gingival area.
DT Janka Gregorics – Zirkonzahn Education Center Brunico, South Tyrol, Italy
NATURAL REPRODUCTION OF WHITE AND BRIGHT TEETH
- Pre-shaded zirconia with natural colour gradient, optimal flexural strength and particularly high translucency
- No limitations! Ideal for monolithic full arches, but also for single crowns, inlays, onlays, veneers, bars and multi-unit bridges (reduced or monolithic)
- No ceramic chipping (thanks to monolithic design), no abrasion of the antagonist
- Can be characterised individually for each patient with Colour Liquid Prettau® 2 Aquarell Intensive, ICE Ceramics, Fresco Ceramics, ICE Stains Prettau® and ICE Stains 3D by Enrico Steger
- Also available in three Bleach shades




































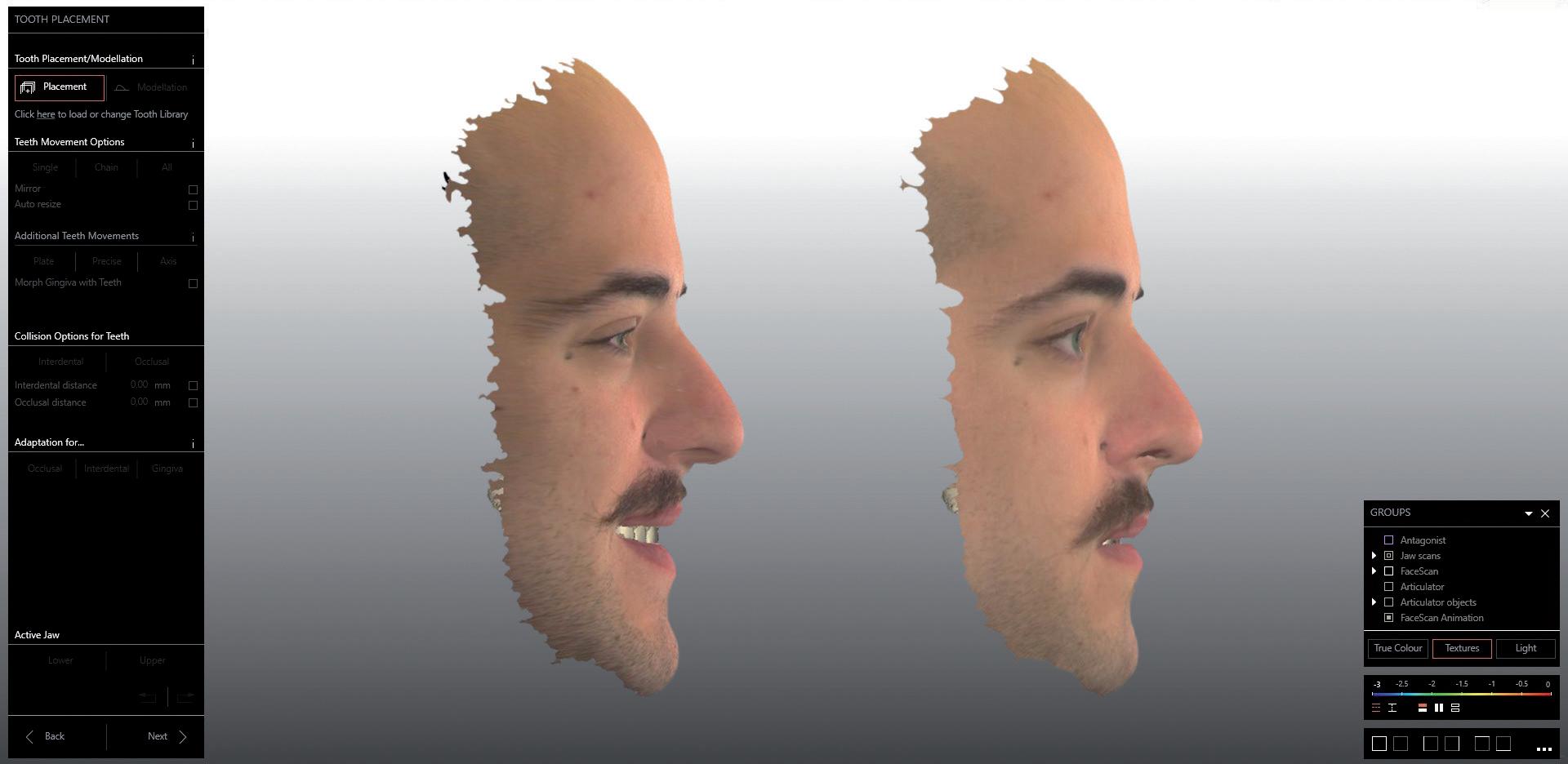

Such technologies permit the 1:1 reproduction of patient’s physiognomy and oral situation into the virtual world with no loss of precious information. In this way, the techno-clinical team can continue the workflow with no need for further chairside appointments to perform functional and aesthetics checks. This is possible thanks to the integration of the recorded information into the Zirkonzahn.Modifier design software. Indeed, by means of a specific software function (“Real Movement”), the dental technician can display with accuracy all mandibular movements recorded with the PlaneAnalyser II (opening, closing, protrusion, retrusion and laterotrusive movements) achieving an optimal functionalisation of the design. Subsequently, with another function (“Face Morphing”), the functional movements can be associated with the patient physiognomy in order to simulate several face expression (e.g. smiling) and evaluate the restoration in terms of aesthetics.
Movements can also be imported into the virtual articulator, which is adjusted automatically in relation to the case, for a possible switch to the analogue workflow with milled or printed models.
At this point, the dental technician sends to the dentist a PDF file including all information concerning the design as well as the software-generated functional movements. After the dentist’s final approval, the dental technician proceeds with the manufacture of the prosthetics.
The patient goes to the dental practice to receive the restoration. No functional or aesthetic changes have to be applied, since all checks were performed on the digital patient by means of the Real Movement and Face Morphing functions.







DESIGNED USING THE “SNORING” FUNCTION IN THE ZIRKONZAHN.MODIFIER SOFTWARE
- Selection of the “Snoring” function and creation of all upper and lower margins
- Generation of a digital plane to separate the upper and lower bite
- Loading anchors considering the distance between the first molar of the lower jaw and the canine of the upper jaw. Slight insertion of the anchor into the bite to leave enough space for the connectors
- Creation of a breathing gap between upper and lower incisors. This portion is calculated digitally and subtracted from the upper and lower bite by creating a split which improves patient’s breathing


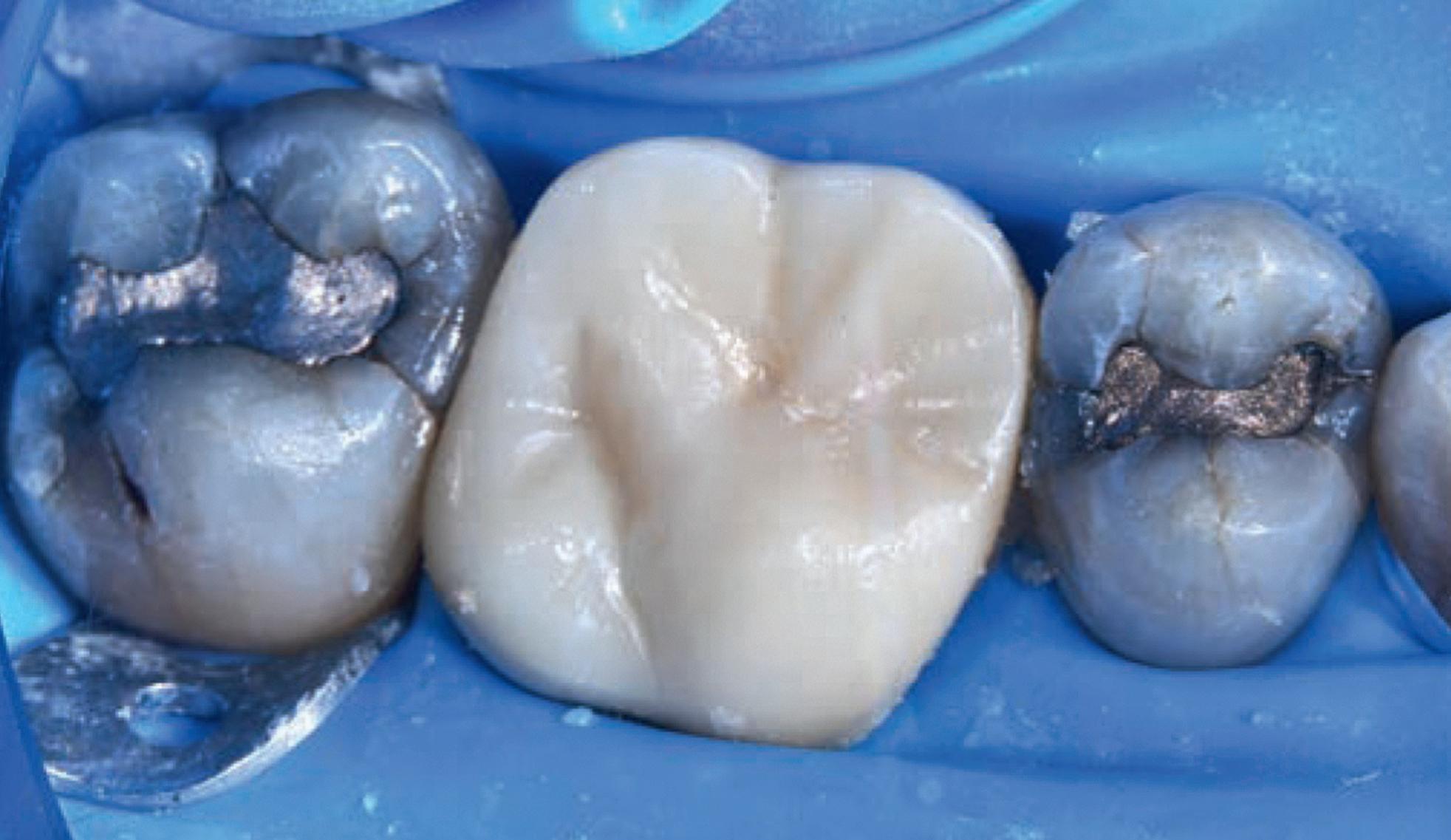
By Dr M Paul Renner

Teeth with cracks that exhibit symptoms of moderate to severe pulpitis have historically been treated by pulpectomy, root canal treatment and then restoration with fullcoverage indirect restorations. With the success of pulpotomies using calcium silicate cements, many of these teeth have been able to retain their vitality and arguably increase their longevity.


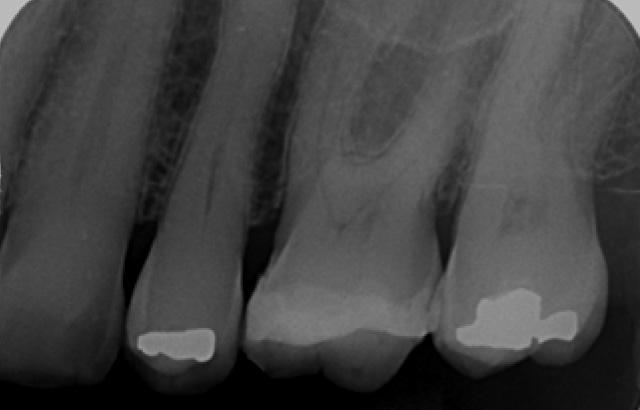

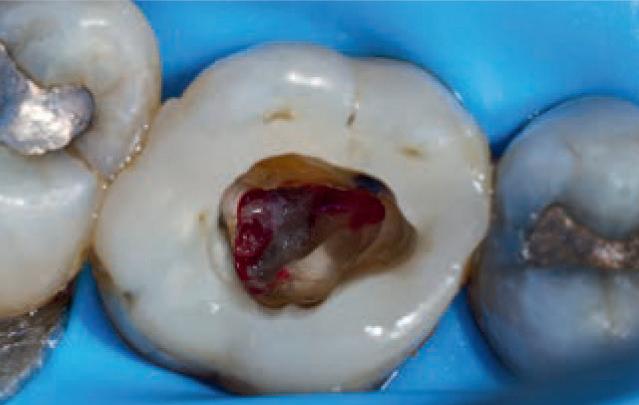


In this case, a full pulpotomy was performed on tooth 26 using Biodentine™ (Septodont, France) with the Bio-Bulk Fill technique, with a permanent dentine restoration and interim enamel restoration to allow time to assess the success of the vital pulp therapy. The Biodentine then acted as a core for the indirect restoration.
Numerous studies have demonstrated that the success rate of partial and full pulpotomies ranges from 75-100%.2,3 It has been advocated as the preferred option for treating teeth with symptoms once described as irreversible pulpitis.4,5
While there is little published data on the use of pulpotomy in cracked teeth, my own professional experience has shown this to be a viable treatment option for these symptomatic teeth.
Full pulpotomy and restoration with an indirect full-coverage restoration is a viable treatment option for cracked teeth with symptoms of moderate to severe pulpitis.
How long have you been using Biodentine?
I switched from MTA to Biodentine five years ago.
Why do you use the Bio-Bulk Fill procedure with Biodentine? What are the main advantages for you?
Firstly, if I have sufficient time at the appointment, I can wait for the Biodentine to fully set (12 minutes) and then complete the permanent restoration without fear of damaging the
Symptomatic teeth that are found to have cracks are one of the more difficult situations for which to plan treatment. Many articles have been published regarding these teeth and unfortunately, there has been no consensus on the best course of treatment. In my experience, it is best to treat these teeth conservatively as this allows for further treatment options if the conservative treatment fails.
Biodentine. Secondly, in what is usually the case, if I have insufficient time to wait for the set and then complete the restoration, I can simply fill the cavity completely with Biodentine, wait for the complete set (12 minutes), discharge the patient and then reappoint them at a later date to cut back the Biodentine and cover it with the final restoration. I often use this latter technique to allow time to assess Biodentine’s effect on the pulp tissue, whether it be a pulpotomy, deep cavity or symptomatic crack, before committing to the final restoration, especially if an indirect restoration is planned.
Clinical signs and symptoms
I n 2018, a 59-year-old patient presented with vague pain in the upper left region. He had difficulty locating which tooth was painful, but he reported that he thought it was one of the last two teeth (26 or 27). No teeth were tender to percussion. Tooth 26 reacted strongly to cold testing while the other teeth reacted normally.




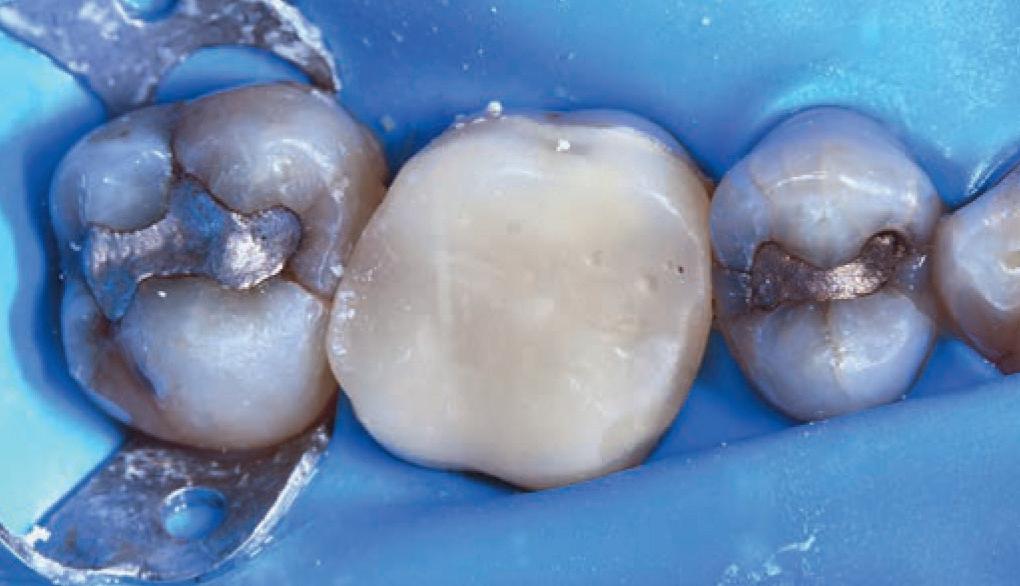


Tooth 26 tested positive to biting on damp gauze but the sensation did not linger. Both tooth 27 and 25 were negative to the bite test. The composite resin restoration in tooth 26 was removed under rubber dam and crack lines could be seen under the restoration (Figure 1), with the most obvious running from the lingual to the centre of the tooth and another from the mesiobuccal to the centre. A number of other minor cracks were visible, including one that ran under the buccal cusps (Figure 1).
These crack lines were discussed with the patient and he was given the option of either restoring the tooth with direct composite resin or with a full-coverage indirect restoration. The patient chose to have the tooth restored with a direct composite resin and so this was performed at this appointment. The patient returned annually for examination and reported the tooth was asymptomatic.
In 2024, the patient presented again with pain in tooth 26. He reported the tooth was very sensitive to cold, with
the pain lasting several minutes. He also reported that the tooth had ached spontaneously at times.
On examination, the tooth reacted very strongly to cold, which lasted for almost one minute. The tooth was also slightly tender to percussion. The composite resin restoration appeared sound (Figure 2).
A PA radiograph (Figure 3) revealed no periapical radiolucency (PARL), but the pulp chamber was reduced in size when compared to a previous bitewing radiograph.
predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. it comes to the perfect fit, Hu-Friedy is just right.
predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. comes to the perfect fit, Hu-Friedy is just right.
Septanest : the first choice of dentists with over 150 million injections per year, provides you high quality you can trust
Given the tooth’s previous history of visible cracks running into the tooth and the current symptoms of moderate to severe pulpitis, a decision was made after discussion with the patient to enter the pulp chamber to assess the condition of the pulp and the depth of the cracks. The plan was to either perform a full pulpotomy or, if no viable pulp tissue was present, extirpate the pulp.
Using local anaesthetic and rubber dam isolation, access was obtained through the composite resin restoration. While the cracks were visible, they appeared similar to the image from 2018 (Figure 4). The roof of the pulp chamber was removed and vital tissue was found, which did not appear to be heavily inflamed (Figure 5). A pulp stone was also present (Figure 6). Removing this revealed bleeding pulp tissue at the opening of the root canals. A cotton pellet soaked in NaOCl was placed on the pulp tissue at the opening of the root canal and after five minutes the bleeding had ceased (Figures 7 and 8).
As the plan was to restore the tooth with a full-coverage indirect restoration, the entire pulp cavity was filled with Biodentine with the Bio-Bulk Fill technique. (Figure 9).
The patient returned after twelve weeks and reported that the tooth had been asymptomatic (Figure 10).
At this appointment, a preparation for a ¾ crown was performed (Figure 11). The Biodentine was left in situ, cut back and used as a core for the restoration. A PVS impression was recorded and a BISAcrylic temporary crown cemented with provisional cement (Figure 12).
Three weeks later, a monolithic zirconia crown (Figure 13) was bonded onto the tooth (Figure 14). The tooth will be monitored and a review radiograph taken after six months.
Discussion
This case highlights a number of elements of pulpotomies in teeth with cracks. Firstly, many teeth with deep cracks have a long-standing mild pulpitis, to which the pulp has responded by producing reparative dentine that
often appears in the form of a pulp calcification. The operator must be careful when performing vital pulp therapy on these teeth as it is often difficult to differentiate the pulp calcification from the floor of the pulp chamber. Any pulp calcifications must be removed before assessing the condition of the radicular pulp tissue.
Secondly, in teeth with pulp symptoms resulting from cracks, it is best to perform a coronal pulpotomy. This allows the floor of the pulp chamber to be examined for
“The ability to use Biodentine in the Bio-Bulk Fill technique has a number of advantages in cases like the above. The initial vital pulp therapy appointment can be shortened by completely filling the cavity and using the Biodentine as a permanent dentine replacement and an interim enamel replacement...”
any extension of the crack across the floor, which would greatly reduce the prognosis for the tooth.
The ability to use Biodentine in the BioBulk Fill technique has a number of advantages in cases like the above.
The initial vital pulp therapy appointment can be shortened by completely filling the cavity and using the Biodentine as a permanent dentine replacement and an interim enamel replacement. The fact that the material can be left for up to six months allows time to assess the success of the procedure before committing to the final indirect restoration. The strength of Biodentine means there is no requirement to place a separate core material.
I would like to thank my DAs, Ms Ellen Gordon and Ms Julie Schefe, for their assistance with the procedures and photography.
Paul graduated from the University of Queensland with a BDSc in 1981. He has worked in general practice since, first in government service and then in his private practice in Dalby, Queensland from 1991 onwards. For the last 15 years, Paul has been employed as a part-time clinical supervisor at the University of Queensland, supervising final year students. Additionally, he currently holds the title of Associate Lecturer at the university. Paul has been active in the Australian Dental Association Queensland, where he served as president for two terms and was awarded lifetime membership. Since starting to treat symptomatic carious teeth using vital pulp therapy eight years ago, it has become an increasingly important part of Paul’s practice. Due to the inability of many patients to afford root canal therapy and restoration with an indirect restoration, Paul has been able to save many teeth from extraction using this approach. Apart from vital pulp therapy, his other areas of interest are the diagnosis and treatment of cracked teeth and dental photography.
1. Wei Shang ,1 Zeliang Zhang,1 Xicong Zhao,1 Qingquan Dong,2 Gerhard Schmalz ,3 and Shaonan Hu 2 The Understanding of Vital Pulp Therapy in Permanent Teeth: A New Perspective. BioMed Research International, 2022, 1–11. https://doi. org/10.1155/2022/8788358.
2. McHugh, H.;Wright, P.P.; Peters, C.I.; Peters, O.A. Diagnostic and Prognostic Predictors for the Success of Pulpotomy in Permanent Mature Posterior Teeth with Moderate to Severe Pulpitis: A Scoping Review. Oral 2023, 3, 545–571. https://doi.org/10.3390/oral3040045.
3. Al-Ali M. and Camilleri J. (2022) The scientific management of deep carious lesions in vital teeth using contemporary materials—A narrative review. Front. Dent. Med 3:1048137. doi: 10.3389/ fdmed.2022.1048137.
4. https://www.aae.org/wp-content/uploads/2021/05/ VitalPulpTherapyPositionStatement_v2.pdf.
5. European Society of Endodontology (ESE) developed by: Duncan HF, Galler KM, Tomson PL, Simon S, ElKarim I, Kundzina R, Krastl G, Dammaschke T, Fransson H, Markvart M, Zehnder M., Bjørndal L. European Society of Endodontology position statement: Management of deep caries and the exposed pulp. International Endodontic Journal, 52, 923–934, 2019.


predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy


Biodentine™ saves pulps EVEN with signs and symptoms of irreversible pulpitis*
Biodentine™ saves pulps EVEN with signs and symptoms of irreversible pulpitis*
saves pulps EVEN with signs and symptoms

saves pulps EVEN with signs and symptoms
Biodentine™ brings one-of-a-kind benefits for the treatment of up to 85%** of irreversible pulpitis cases:
For vital pulp therapy, bulk- lling the cavity with Biodentine™ makes your procedure better, easier and faster:
Biodentine™ brings one-of-a-kind benefits for the treatment of up to 85%** of irreversible pulpitis cases:
tooth
Biodentine™ brings one-of-a-kind benefits for the treatment of up to 85%** of irreversible pulpitis cases:
As the first all-in-one biocompatible and bioactive dentin substitute, Biodentine™ fully replaces dentin wherever it’s damaged.
• Vital Pulp Therapy allowing complete dentin bridge formation
brings one-of-a-kind benefits for the treatment of
• Vital Pulp Therapy allowing complete dentin bridge formation
brings one-of-a-kind benefits for the treatment of up to 85%** of irreversible pulpitis cases:
Pulp healing promotion: proven biocompatibility and bioactivity
• Minimally Invasive treatment preserving the tooth structure
Reduced risk of failure: strong sealing properties
• Vital Pulp Therapy allowing complete dentin bridge formation
• Minimally Invasive treatment preserving the tooth structure
• Immediate Pain relief for your patients’ comfort
Vital Pulp Therapy allowing complete dentin bridge formation
Only one material to fill the cavity from the pulp to the top
• Immediate Pain relief for your patients’ comfort • Bio-Bulk filling procedure for an easier protocole
• Minimally Invasive treatment preserving the tooth structure
• Bio-Bulk filling procedure for an easier protocole
• Immediate Pain relief for your patients’ comfort

New Biphasic Formulations allowing you to manage the pace of your bone grafting procedures:
Similar mechanical behavior as natural dentin: ideal for bulk filling
Minimally Invasive treatment preserving the tooth structure
Immediate Pain relief for your patients’ comfort
Biodentine™ helps the remineralization of dentin, preserves the pulp vitality and promotes pulp healing. It replaces dentin with similar biological and mechanical properties.
• Bio-Bulk filling procedure for an easier protocole
(80% ß-TCP / 20% Hydroxyapatite)
The final enamel restoration will be placed within 6 months.
Improving on Biodentine the composite onto Biodentine full restoration in a single session
Bio-Bulk filling procedure for an easier protocole
Bio-Bulk filling procedure for an easier protocole
40/60 (40% ß-TCP / 60% Hydroxyapatite)

Please visit our
Please visit our website for more information
www.septodont.com
Please visit our website for more information www.septodont.com







To enjoy the clinical benefits of the first and only dentin in a capsule, ask your dental distributor for Biodentine™.




Success in orthodontics doesn’t have to be difficult, tedious and slow.
Dr Daniel Sable and Dr Andrew Pepicelli mixed the right elements, advice and attitude for a winning formula.
If you’re a quality professional who creates great outcomes for your patients but you’ve reached a growth plateau, this story is an amazing insight into how expansion, consolidation and outstanding practice growth can be achieved.
For almost 15 years, Drs Sable and Pepicelli ran successful orthodontic practices. Both were dedicated professionals with strong academic backgrounds and as a result, had more clients than they could handle. But each practice had reached its “chair capacity” and could no longer grow.
However, they were friends who shared a common vision, one that could only be achieved by collaboration. The vision was to create a combined super practice. They started by working together, which itself wasn’t enough.
Then, in 2016, they bought a block of land next to their practice in Chadstone, Melbourne and were joined by Dr James Newby to bring in some fresh young talent.
They engaged a local architect, Lou Antonino, to build the structure, based on their belief of what was the perfect practice space and their preference for a minimalist design.
The next move was significant.
They avoided the usual suspects like dental fit-out companies. From years of practice they knew what quality elements were essential to success and who to consult.

After getting the basic design right with the architect, they knew the principal quality element was the purchase of the practice chair. Working long hours over each chair every day and having clients both comfortable and correctly positioned was vital to success. And in every chair they expected state-of-the art technology and correct ergonomics for both patient and practitioner.
So it was a no-brainer to continue their successful partnership with an industry leader, Belmont Chairs.
Dr Pepicelli reasoned: “Having used Belmont chairs since 2007, we knew they were supremely reliable and first class quality. The practice chair is not an area to ever have second best.”










Settling on no less than 14 new Belmont Chairs, they then consulted with dental expert John Borg of Borg Dental for the refinement of the designs and the remainder of the fit out.
With Borg it was an authentic collaboration.
As well as genuinely objective advice on all the equipment requirements, Borg offered design insights into plumbing, plant room layouts, correct space rations and patient flow. Sable, Pepicelli and Newby, now trading as “Chadstone Orthodontics,” have exceeded their dreams of success. An expert practice team now allows them more time to give back to the profession as part-time lecturers at Melbourne Dental School, which in turn keeps Chadstone Orthodontics at the cutting edge of procedures and best practice. But that wasn’t the goal, as Pepicelli explains: “We’re now in a privileged position, helping even more people improve their health and wellbeing. This can have a positive impact on their development as a person.”
It started with a dream, and a collaboration not just with each other, but with hand-picked consultants creating the perfect practice: architect Lou Antonino, the experts at Belmont Chairs and John Borg of Borg Dental.
And it’s a dream every quality practitioner can achieve.
The Practice
The Practice Chadstone Orthodontics
Principals Dr Daniel Sable and Dr Andrew Pepicelli
Type of Practice Specialist Orthodontic
Location Murrumbeena, Melbourne, Victoria
No of chairs 14
The Team
Architect Lou Antonino
Installer John Borg, Borg Dental
Equipment
Dental Units 14 x Belmont Clesta II
Autoclaves Melag
Imaging Dentsply Sirona Aexos CBCT with Ceph
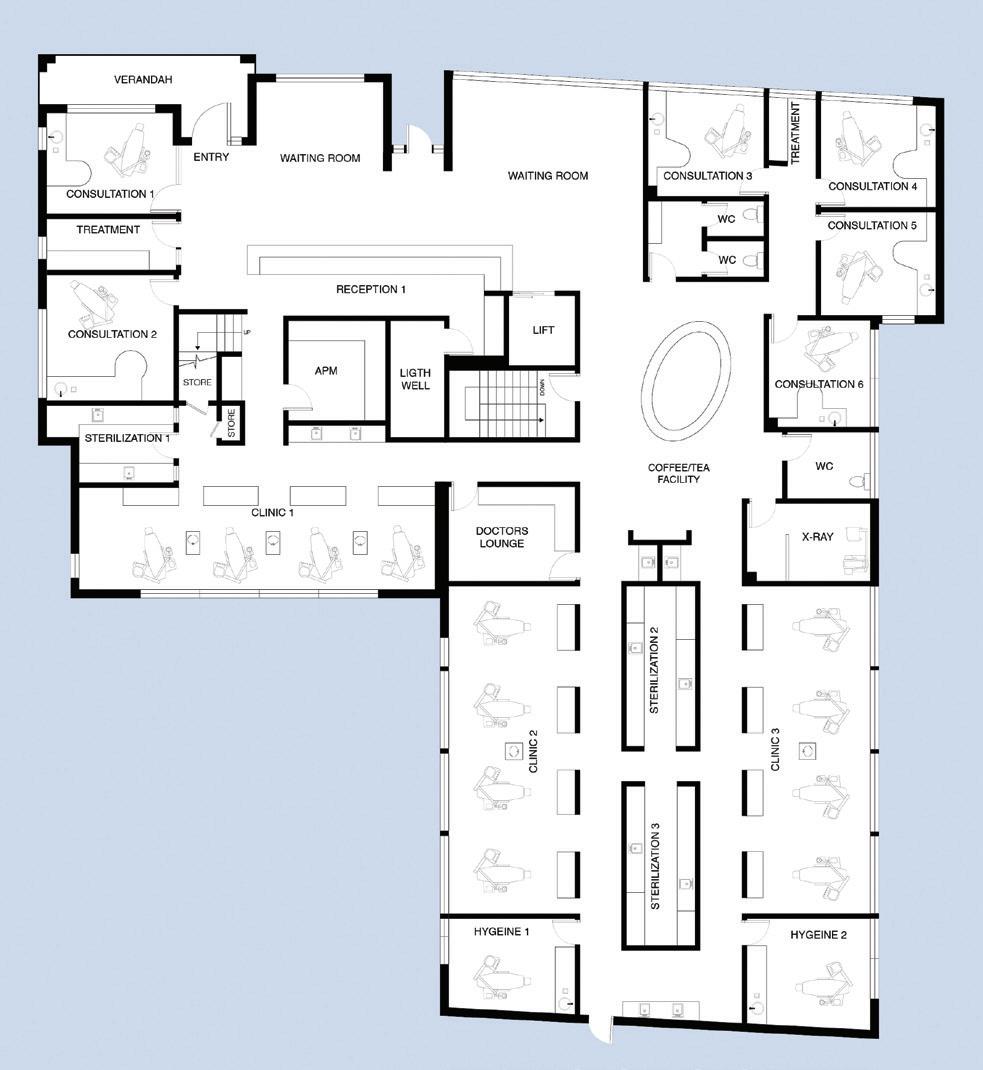


















By David Petrikas
Arenowned Adelaide paediatric dentist has created a dental haven for parents and children living in the picturesque Adelaide Hills and surrounding country areas.
Dr Gabrielle Smart (nee Allen) recently established Hills & Country Paediatric Dentistry in Hahndorf after a brief stint working in Murray Bridge and the Adelaide Hills followed by many years of training and specialising in paediatric dentistry at the Women’s & Children Hospital in Adelaide.
Having spent 12 years in public and private practice, Gabrielle felt it was time to be her own boss and wanted to bring paediatric services – and potentially other dental specialists – to Hahndorf for those not wanting to travel all the way into the city to access them.
Her practice now provides a local specialist hub for Hahndorf and surrounding country centres areas extending from Victor Harbor to McLaren Vale, Stirling, Murray Bridge and the Barossa, enabling local families to avoid travelling down the hill into Adelaide on the South Eastern Freeway.
It also continues a family tradition of paediatric dentistry as her great uncle, Dr Kevin Allen – who trained in Boston, was the first paediatric dentist in South Australia, later teaching paediatric dentistry at Adelaide Dental Hospital.
The move to Hahndorf also enabled a better work-life balance for Gabrielle and her family with two young children. Having looked at five commercial properties in Mount Barker and one in Hahndorf, she found most drawn to the historic beauty of Hahndorf but many buildings on the main street had parking restrictions or challenges associated with historic buildings.




This led her to a stylish new build tucked away just behind the main street. The new building has a typically steep gabled roof with timber façade and lime mortared brickwork, providing a nod to the town’s historic past.
Best of all, the site has ample parking in a carpark behind and is also right next to a chemist and general medical practice, providing complementary healthcare services.
Having a brother as an architect proved to be a bit of a bonus, as he was able to sketch a floor plan to allow Gabrielle to secure a lease before she gave her ideas to an architectural firm, Cheesman Architects, who are highly skilled and experienced in dental practice design. They went on to design a practice that would cater to her paediatric patients, taking into account their specialised needs.
She decided on having two oversized clinical rooms to provide plenty of disabled access and room for prams. A family-sized bench in the surgery enables children to be close to their parents while she is working.
One of the pillars of the practice that Gabrielle was focused on was that her patients and their families could be cared for
in a space that did not feel too “clinical”. This was achieved with a cool, calming, but varied colour palette selected to avoid warm colours that can be potentially triggering for neurodivergent patients, together with natural timber features, “wombat” and floral themed graphics, including in a large mural on the surgery walls.
Other thoughtful touches include lots of beautiful mini canvas artworks created by her children, a well-stocked play area with toys, bean bag, low stools and bench and of course, the obligatory television in the waiting room.
The next challenge was to find a dental chair that would work best for her and her young patients, some of whom have special needs.
Having only ever used A-dec chairs and A-dec dental carts in theatre, it’s little surprise that Gabrielle wanted an A-dec chair for her own practice.
She was chatting to a mentor dentist, Dr Brian Lange, who was putting retirement plans in place and although he was at the end of his career, he had a beautiful A-dec 500 chair that still had plenty of years left in it.

This is where Adelaide A-dec dealer, Dental Concepts, were able to help out.
Having made a significant investment taking over the new site and fitting it out to a very high standard, up cycling this chair provided an economical and also sentimental solution to equipping the new surgery.
Dental Concepts completely refurbished the A-dec 500 chair, including removing the light and spittoon and installing brand new “Cyan” soft blue seamless upholstery.
Gabrielle said the A-dec 500 chair is very flexible and that the seat shape and unique A-dec adjustable headrest design held the patients in position, which enabled her to fit a mask comfortably to get an effective seal under nitrous oxide sedation and also allowed parents to sit comfortably in the chair supporting their young ones on their lap too when needed.
She said the chair was also very “inviting” because of its soft, pastel colour and the very smooth and gentle recline action. She could also swing the delivery system out of the way to make it less intimidating and that by doing so, there was nothing that young patients could accidently break.
Most often she found kids responded to the challenge of her asking if they could climb and proving it by climbing up onto the patient chair.
Gabrielle opted for a ceiling mounted A-dec LED light which reaches to the patient bench, enabling her to do an examination on the patient bench if needed, which was great for anxious patients who could be a bit tricky if they’d had a bad experience in the past––or for treating patients in wheelchairs (sometimes using the A-dec headrest in an inverted position).
The new A-dec LED light also has “touchless” controls which has proved to be another advantage.“Not having to turn light on and off and just being able to swipe your hand in front of it is a game-changer,” she said. “The yellow ‘cure-safe’ function gives you longer to work with the composite and the kids like the yellow light”.
When using nitrous oxide sedation, Gabrielle often tells a story about going on a snorkelling adventure at the beach and will use imagery of the light being the “sun” warming the children up as they watch relaxing underwater fish videos on the ceilingmounted TV.

Gabrielle said the A-dec 500 chair also contributed to her own comfort and ease of working. “It’s a very comfortable chair and I can tuck my legs in under the backrest much easier. That gives me good reach with small patients and the range of height means I can do stand-up extractions.”
The headrest design was also excellent for supporting the patient and putting the oral cavity at the ideal angle to work on them. “I had a nine-year-old patient with a supernumery tooth right back in the palate which we were able to access well for extraction here in the clinic recently and it’s also great for patients (parents) with neck issues as you can always find a comfortable position for them.”
Hills & Country Paediatric Dentistry has grown significantly since opening, with a dedicated practice manager and three dental assistants along with another paediatric dentist one to two days a week and an hygienist one day a week having joined the team.
The practice now also has a second A-dec 500 chair in sage green sewn upholstery and an Orthodontist that hires the rooms out on Mondays, making it a real paediatric/adolescent hub in the town.
Gabrielle is understandably pleased with her new practice and also the positive sentiment associated with using her mentor, Brian Lange’s, chair every day and which is also a testament to the longevity of A-dec quality and design.
The Practice
Hills & Country Paediatric Dentistry
The Principal Dr Gabrielle Smart
Practice Type Specialist Paediatric
Location Hahndorf, South Australia
Size 117 square metres
No of chairs 2
The Team
Design Cheesman Architects & Dental Concepts
Architect James Allen
Builder Leske Building
Project Manager Dental Concepts
Installer Dental Concepts, Adelaide
Equipment
Dental Units A-dec 500 with A-dec 576 Ceiling Mount LED Light
Sterilisation
W&H Lisa 22VA with Traceability
W&H Assistina Twin
Imaging Vatech A9 CBCT
Vatech EzRay Air wall x-ray
Kavo Scan eXam phosphor plate scanner
Vatech sensor for theatre
Compressor Cattani A200
Suction Cattani Micro SMART Cube
Software Core Practice


Information contained in this section is provided by the manufacturers or distributors. Australasian Dental Practice does not assume responsibility for the accuracy of the data.

The MICROSS and MICROSS Curve Cannula are single-use devices designed for manual cortical bone harvesting. With a unique shape and a compact 5 mm diameter, they support a minimally invasive approach and are easy to use, even in narrow or hard-to-access areas — making bone harvesting a straightforward procedure. Now with a new 27° curvature, the ergonomic design of the MICROSS Curve allows clinicians to easily access retromandibular, palatal and other challenging anatomical areas. The instruments collect
only the amount of bone that is strictly necessary for the treatment of minor periodontal and peri-implant defects. Advantages of the disposable semicircular blade include sterile, ready to use; minimally invasive; chamber capacity 0.25 cc; ergonomical design; and allows you to easily reach retromandibular, palatal and other challenging areas.
Available: Geistlich Pharma Tel: 1800-776-326 info@geistlich.com.au www.geistlich.com.au

TRI Dental Implants new TRX Guided Surgery Kit offers a radically reduced workflow with an unmatched precision due to the sharp cutting properties of the drills. Enjoy the highest level of precision, even in challenging cases, with TRX’s lateral cutting abilities and patented 2-level depth stop. With its simple and unique

Grin remote monitoring offers a safer and more convenient approach to orthodontic care. Grin includes an easy-to-use Scope that, when attached to your patient’s smart phone, enables them to take self-scans of their mouth. You can then remotely monitor treatment progress, answer questions and effectively address any emergency situations without a necessitating a face-to-face
appointment. With Grin, you are able to keep an even closer eye on your patients oral hygiene and overall treatment progress without the need for additional appointments.
Available: TRI Dental Implants ANZ Tel: (02) 8355-2200 grin@liift.dental www.liift.dental www.get-grin.com
design, color-coding, and compatibility with major software providers, TRX is the ultimate solution for seamless and precise dental surgery.
Available: TRI Dental Implants ANZ Tel: (02) 8355-2200 info@tri-implants.com.au www.tri-implants.com.au
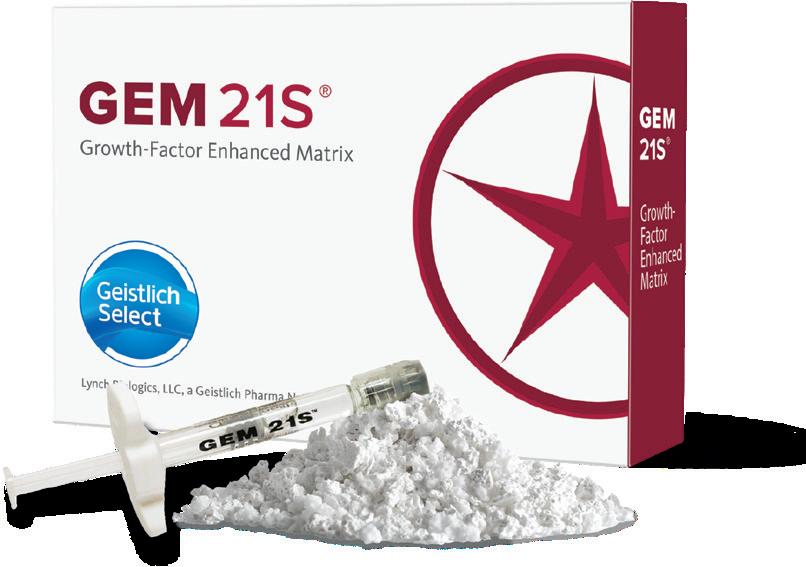
GEM 21S ® Growth-factor
Enhanced Matrix is crafted to boost the patient’s naural healing capacity, promoting the restoration of lost bone and gingiva. Extensive in vitro and in vivo studies have demonstrated that rhPDGF-BB is a powerful stimulant of angiogenesis that also stabilises newly formed blood vessels. GEM 21S® is the only dental therapy containing rhPDGFBB, one of the main growth
factors found in the human body and well known for its stimulatory role in wound healing. GEM 21S increases the amount of PDGF at the grafted site to aid in faster, more bone and better healing.
Available: Geistlich Pharma Tel: 1800-776-326 info@geistlich.com.au www.geistlich.com.au

Tru-line® Invisible Orthodontics celebrates 20 years of Australian made clear aligners with the last innovation - Tru-Line X-tra 48 hour ALIGNERS™
s Precision CAD designed and CNC manufactured, Laser Cut
s Free case evaluation
s Free online training course
s Free viewing software
s Realistic treatment setupsNo Cartoonodontics!



Mention this ad for 50% off your first case
s Free Click retainers
s 48 hour turnaround on request
s Trusted experience, Australia’s first established Aligner brand in 2004
s Satisfaction guaranteed
s 100% value