100 | Resources for Addiction Treatment and Crisis Response in Delaware
101 | Index of Advertisers
102 | Delaware Journal of Public Health Submission Guidelines
The Delaware Journal of Public Health (DJPH), first published in 2015, is the official journal of the Delaware Academy of Medicine / Delaware Public Health Association (Academy/DPHA).
Submissions: Contributions of original unpublished research, social science analysis, scholarly essays, critical commentaries, departments, and letters to the editor are welcome.
Questions? Contact managingeditor@djph.org
Advertising: Please contact ksmith@delamed.org for other advertising opportunities. Ask about special exhibit packages and sponsorships. Acceptance of advertising by the Journal does not imply endorsement of products.
Any report, article, or paper prepared by employees of the U.S. government as part of their official duties is, under Copyright Act, a “work of United States Government” for which copyright protection under Title 17 of the U.S. Code is not available. However, the journal format is copyrighted and pages August not be photocopied, except in limited quantities, or posted online, without permission of the Academy/DPHA. Copying done for other than personal or internal reference use-such as copying for general distribution, for advertising or promotional purposes, for creating new collective works, or for resale- without the expressed permission of the Academy/DPHA is prohibited. Requests for special permission should be sent to managingeditor@djph.org
Substance Use, Abuse, Treatment, and Recovery
Substance use disorder (SUD) encapsulates a complex set of conditions that affect a person’s brain and behavior, and can lead to an inability to control the use of an illegal (or legal!) drug or medicine.1 Although the risk of addiction and how fast someone can become addicted varies by the drug, some drugs and medications are known to have a high risk, and cause addiction more quickly. SUD can start simply enough, with an experimental use of a recreational drug like alcohol, nicotine, or marijuana, which then becomes more frequent. Others may be prescribed pain medication—particularly opioids—and may find they need more and more to get the same level of pain relief.
As time passes, a person may need a larger dose to feel the “high,” or effect of the drug. They may find they need the drug just to feel good, or merely to function. As their use of the drug or medication increases, they may find it is increasingly challenging to go without the drug, and thus, attempts to stop using it may lead to physical illness and withdrawal.
SUD is not unique to Delaware, nor indeed to the United States. Anyone, anywhere can find themselves addicted to a substance. It is not a moral failing, and individuals may need help to overcome this disorder. Fortunately, help is available, in many forms. The Substance Abuse and Mental Health Services Administration (SAMHSA) has a National Helpline that is free, entirely confidential, and operates 24 hours a day, 7 days a week (1-800-662-HELP | 1-800-6624357), offering treatment referrals and information in both English and Spanish.
Help Is Here Delaware (http://helpisherede.com) offers Narcan (Naloxone) nasal spray training to treat a narcotic overdose, as well as emergency and crisis resources like the Delaware Hope Line (883-9-HOPEDE | 883-946-7333) and Prevention Helpline (302-633-2680).
This issue of the Delaware Journal of Public Health on substance use, abuse, treatment, and recovery offers information on many more programs and connections in Delaware, all with the goals of helping people out of substance use and into treatment and recovery. As always, we would like to thank our Guest Editors for this issue, Joanna R. Champney (Director of the Delaware Division of Substance Abuse and Mental Health) and Dr. Vishesh Agarwal (Chief of Addiction Services at ChristianaCare) for curating an excellent issue on such an important topic.
Help is here. If you are struggling with substance use, please reach out.
REFERENCES
1. Volkow, N. D., & Blanco, C. (2023, June). Substance use disorders: A comprehensive update of classification, epidemiology, neurobiology, clinical aspects, treatment and prevention. World Psychiatry, 22(2), 203–229. https://doi.org/10.1002/wps.21073 PubMed Free full-text: https://onlinelibrary.wiley.com/doi/10.1002/wps.21073
Omar A. Khan, M.D., M.H.S. Editor-in-Chief, Delaware Journal of Public Health
Katherine Smith, M.D., M.P.H. Publisher, Delaware Journal of Public Health
Gu t Editors
A Word from the Guest Editors
Joanna R. Champney, M.A.
Director, Division of Substance Abuse and Mental Health, Delaware Department of Health and Social Services
Delaware’s fatal drug overdoses have declined for the last two years (2% between 2022 and 2023 and 36% between 2023 and 2024), bringing the total to 338 drug deaths at the end of 2024. While we are gratified that our state’s death rates have been reduced (mirroring the regional and national downward trend), now is not the time to lose focus.
It is within this context of progress that we curate this special issue on substance use disorder in Delaware. Health practitioners and policymakers alike remain focused on preventing addiction and overdose, enhancing screening, linking patients to care, creating program options that reach underserved people, and removing barriers to recovery.
This issue highlights the multifaceted efforts to build a robust and effective addiction treatment ecosystem in Delaware. At its core, substance use treatment is about acknowledging the dignity and worth in the people we serve and treat, and offering care and support that can help them recover and thrive. You’ll find powerful examples of this in four featured programs in this issue: paramedics offering buprenorphine to patients after nonfatal overdoses, outreach to unhoused individuals, postoverdose response street outreach, and recovery housing.
We also explore the intersection of substance use and the justice system, exploring the effectiveness of programs that reframe addiction as a matter of public health concern rather than solely a criminal one. The public health system is also preparing for the onset of recreational cannabis being legally available for retail purchase this August, and this issue includes two articles dedicated to cannabis (both medical and recreational).
Furthermore, as our health system strives for parity in treating behavioral health, this issue also emphasizes the critical need for more robust addiction medicine training for medical students and residents. Discussions also include effective nonopioid pain management strategies and using effective patient engagement strategies in treating addiction.
Regardless of your role in responding to the overdose epidemic, we trust you will find this specially curated issue on substance use disorder to be both useful and informative.
The NATION’S HEALTH
September 2025
The Nation’s Health headlines
Online-only news from The Nation’s Health newspaper
Public Health harnessing AI to boost research https://www.thenationshealth.org/content/55/7/1.1
Teddi Nicolaus
U.S. immigration detention scale-up sets stage for public health crisis https://www.thenationshealth.org/content/55/7/1.2
Sophia Meador
Community resilience, safety endangered by cuts at FEMA https://www.thenationshealth.org/content/55/7/1.3
Mark Barna
Indiana congregations tackling loneliness in older adults https://www.thenationshealth.org/content/55/7/8.1
Natalie McGill
New York City residents get paid to report polluting commercial vehicles https://www.thenationshealth.org/content/55/7/8.2
Natalie McGill
WHO report: Loneliness, social isolation rising around the globe https://www.thenationshealth.org/content/55/7/11.1
Arushi Dogra
Too good to be true? Don’t be fooled by health scams https://www.thenationshealth.org/content/55/7/16
Teddi Nicolaus
New APHA lawsuit challenges HHS on COVID-19 vaccine guidance https://www.thenationshealth.org/content/55/7/2.2
Sophia Meador
Nation’s capital a fitting host for APHA 2025, rally on National Mall https://www.thenationshealth.org/content/55/7/3.2
Mark Barna
Newsmakers: September 2025 https://www.thenationshealth.org/content/55/7/e7
Arushi Dogra
Many other articles available when you purchase access
Entire Issue $12
Visit https://www.thenationshealth.org/user
Cannabis Use in Adolescents
Gurkirat K. Bhangu, D.O.; Aakanksha Singh, M.B.B.S.; Avni Shah, D.O. & Narpinder Malhi, M.D. Department of Psychiatry, ChristianaCare
ABSTRACT
As cannabis legalization expands across the United States, its use among adolescents remains a pressing public health concern. This analytic essay analyzes the current prevalence, patterns, and consequences of cannabis use in adolescents. While legalization has not substantially increased adolescent use, it has contributed to normalization and greater access, ultimately lowering perceived risk and complicating prevention efforts. Increasing product potency and diversified consumption methods (e.g., vaping, dabbing, edibles) add to these challenges. Adolescent cannabis use is associated with adverse outcomes in brain development, mental health, and physical health including its effects on the gastrointestinal, cardiovascular, respiratory and endocrine systems of body. Cannabis Use Disorder (CUD) is underdiagnosed and undertreated in youth, with no FDA-approved pharmacological treatments. Psychosocial interventions such as contingency management and cognitive behavioral therapy (CBT) show modest efficacy, particularly when involving families. This paper highlights the urgent need for targeted education, policy measures, and accessible evidence-based interventions specifically tailored to adolescent populations to address the evolving challenges of cannabis use and its long-term consequences.
CURRENT STATE AND PREVALENCE
Cannabis ranks as the most frequently used illicit drug and the third most common psychoactive substance, following alcohol and nicotine among adolescents.1 As of 2024, cannabis use among middle and high school students in the United States remained at historically low levels compared to the previous three decades, with a significant decline during the period of the COVID-19 pandemic. According to the Monitoring the Future 2025 (MTF) report, despite the reduction, prevalence remains notable, with 26% of 12th graders, 16% of 10th graders, and 7% of 8th graders reporting marijuana use in the past year. Daily use (defined as use on 20 or more days in the past month) also remained low, particularly among younger students, with just 0.7% of 8th graders and 5.1% of 12th graders reporting such frequent use.2 Notably, a higher prevalence of cannabis use has been observed among adolescents identifying as LGBTQ+ (30.9%), mixed race (27.1%), and Native Hawaiian or Pacific Islander (23.1%), and smoking cannabis was the most common method of consumption. Evidence indicates that coping-related motivations for cannabis use have become more prevalent among adolescents, with over half (53%) reporting its use to relax. Girls were more likely than boys to endorse coping reasons, and Black and Hispanic adolescents reported such motivations at higher rates than their White peers.3
Similarly, cannabis vaping, which had been increasing in previous years, has stabilized, with approximately 17.6% of 12th graders reporting past-year use.2 The MTF 2025 report also highlighted the emergence of Delta-8 Tetrahydrocannabinol (THC), also known as “marijuana light” due to its intoxicating effects. Unlike adolescents, cannabis use has continued to rise among young adults aged 19–30, reaching record-high levels for both smoking and vaping cannabis.2 According to a report from the Substance Abuse and Mental Health Services Administration (SAMHSA), 10% of individuals who use marijuana develop a dependence, and this risk increases significantly for those who begin using marijuana before the age of 18, with approximately 16-17% becoming addicted.4
Cannabis is derived from the dried parts of the Cannabis sativa or Cannabis indica plant, including its leaves, flowers, stems, and seeds. While “cannabis” refers to the plant material itself, “cannabinoids” include both naturally occurring and synthetic compounds that interact with the body’s endocannabinoid system. In recent years, the growing legalization of cannabis for medical use and the commercialization of recreational use have expanded access and led to a wider variety of available products.5 These modern cannabis products, whether natural or synthetic, often contain much higher concentrations of THC than in the past, with average potency rising from about 1%–4% in the mid-20th century to over 19% today. This increase in potency has raised concerns about adverse health effects, especially among frequent or inexperienced users. New methods of consumption, such as vaping high-potency concentrates like wax and shatter or ingesting edibles, have further elevated these risks.5–7 However, cannabis and cannabinoids also offer important therapeutic benefits. The FDA has approved specific cannabinoids for medical use; including, dronabinol and nabilone for chemotherapy-induced nausea and vomiting in 1985, dronabinol for appetite stimulation in wasting conditions such as HIV in 1992, and cannabidiol for treating seizures associated with Dravet syndrome and Lennox-Gastaut syndrome in 2018, as well as other seizure disorders in 2020.5
LEGALIZATION AND ITS IMPACT ON ADOLESCENT CANNABIS USE
Policy Landscape
Despite cannabis’s continued classification as a Schedule I drug under federal law, U.S. cannabis policies have undergone a significant shift from prohibition to broader acceptance over the last two decades. As of February 2025, 39 states and the District of Columbia have allowed the medical use of cannabis products. Additionally, 24 states, 3 territories, and the District of Columbia allow or regulate recreational use of cannabis for individuals aged 21 and older.8–10 With cannabis legalization, potential benefits, such as reduced incarceration for drug-related offenses, reduced opioid-related harms in those with chronic pain, decreased racial disparities in law enforcement, and increased tax revenue generation, have been observed.5,11,12
Regulatory Challenges
Different states have implemented various safeguards to mitigate the exposure and use of cannabis in adolescents. For example, in the state of Colorado, cannabis regulations include strict advertising restrictions, prohibiting outdoor signage within 500 feet of schools, places of worship, and playgrounds. The use and possession of cannabis is banned on all school properties statewide. Local jurisdictions retain the authority to ban or limit retail cannabis businesses. Direct advertising to minors is prohibited, and media advertising via TV, radio, print, and the internet is permitted only when less than 30% of the audience is under 21 years old. Individuals under 21 are also not allowed inside dispensaries. Despite these safeguards, youth remain exposed to cannabis through adult normalization, media coverage, dispensary visibility near high-traffic venues like sports arenas, and a strong presence on social media.8Youth under 20 are required to be diagnosed with severe medical conditions by two independent physicians to qualify for the use of medical cannabis. Those with CUD are more likely to seek access, especially in states without legal recreational use. Youth with chronic illnesses, such as inflammatory bowel disease or chronic pain, often use cannabis for symptom relief, primarily pain. However, many also met the criteria for CUD, highlighting the overlap between therapeutic use and misuse risk.5,8,10
Shifting Public Opinion
Public opinion has shifted markedly toward acceptance of cannabis use, influencing policy changes.8 According to MTF 2025, the perceived risk of regular cannabis use among 12th graders has declined significantly from 58% in 2000 to 36% in 2024.2 Despite this, evidence suggests that medical cannabis laws (MCLs) have had little to no effect on adolescent use overall. In contrast, cannabis use in adults has significantly risen. The effects on other substances such as alcohol, opioids, and tobacco vary, with some evidence that MCLs may reduce opioid-related harms, but inconclusive effects on alcohol and tobacco use. The impact of cannabis legalization on CUD is mixed; however, more permissive laws, such as those allowing dispensaries, are associated with higher rates of CUD among adults. Research on recreational cannabis laws (RCLs) is still emerging, but early findings indicate minimal changes in adolescent use, though some increase may occur among college students.8,11,12 A national study of 149,383 adolescents aged 12–17, examining recreational marijuana law enactment between 2012 and 2015, found no significant increase in marijuana use or frequent use among adolescents, suggesting that legalization primarily increases cannabis use among adults who gain legal access. Notably, the study observed a small increase in CUD among adolescents who were already using marijuana, highlighting greater vulnerability among youth with psychiatric or familial risk factors and those exposed to more potent cannabis products after legalization.11 Overall, the public health impact of cannabis legalization is complex and depends heavily on how specific laws are designed and implemented.10
Shifting cannabis policies have also contributed to lowered risk perception among vulnerable populations like pregnant women.13,14 A systematic review found that cannabis legalization was associated with increased maternal cannabis use during pregnancy and postpartum, as well as greater parental use and approval of adult cannabis use.15 The review noted an increase
in unintentional pediatric cannabis exposures post-legalization, which has led to higher rates of emergency department visits and critical care admissions compared to other types of poisonings. The American Academy of Pediatrics (AAP) cautioned against adult cannabis use in the presence of minors; evidence remained inadequate to establish a causal relationship between legalization, parenting behavior, and child outcomes. Authors also emphasized that the impact of legalization might vary based on individual factors, such as genetic vulnerability to substance use, indicating that higher-risk families could be disproportionately affected.5,15 Similarly, legalization of cannabis has been linked to higher rates of positive urine drug screens (16.2% vs 20.2%; OR, 1.3 (1.0-1.7); p<.048) in young women aged 12-22 years old which could have a detrimental impact on the prenatal development of babies.16,17
Potency Trends
Since legalization, cannabis products have become significantly more potent. This trend directly contradicts Cowan’s “Iron Law of Prohibition,” which predicted that tougher enforcement would increase potency while legalization would lower it. Instead, lower enforcement risks have spurred innovation in extraction methods and expanded access to materials for producing high-THC products.18
Legal cannabis flower typically contains 20–25% THC, nearly double the THC concentration found in black-market flower before legalization. Even more concerning are cannabis concentrates like wax, shatter, and oils, which often range from 80–90% THC, making them about four times stronger than legal flower and more than seven times stronger than black-market flower.18–20 Some state-level monitoring has found concentrates with THC levels as high as 95%.20 Legalization and commercialization have increased the availability and diversity of these products, but research has not kept pace with their rapid evolution.20
The increase in THC levels raises public health concerns, particularly as new consumption methods like edibles, vaping, and dabbing now allow users to consume even higher doses of THC. A study done in 2019 in Colorado showed that about 24% of adolescents reported lifetime use of concentrate, which accounts for 72% of all adolescent cannabis users. Among these, 35.6% consumed edibles, 34.4% used dabbing, and 20.3% used vaping. With commercialization fueling rapid market growth, concentrate sales in Colorado increased by 480% between 2014 and 2017. Their market share nearly doubled from 17% to 32%.20
Traffic Safety
The impact of cannabis policies on traffic accidents has shown mixed results. In the first three states to legalize recreational cannabis, there was a combined 5.2% increase in police-reported traffic crashes and a 6% rise in auto insurance collision claims compared to neighboring states where cannabis remains illegal. Between 2012 and 2017, the number of drivers involved in fatal crashes who tested positive for THC more than doubled in Washington State. It was unclear whether cannabis impairment caused these accidents. In contrast, Colorado experienced a decline in cannabis-impaired traffic fatalities, dropping from 12% in 2016 to 8% in 2017.21–23
CANNABIS USE DISORDER
The Diagnostic and Statistical Manual (DSM) of Mental Health Disorders, fifth edition, defines criteria for CUD as cannabis use with at least 2 or more of 11 specific symptoms within a 12-month period, encompassing four main categories:
1. Impaired control such as using larger amounts or longer than intended, unsuccessful efforts to cut down and spending excessive time related to use, and cravings
2. Social impairments such as failure to fulfill major roles, continued use despite interpersonal problems, and giving up important activities.
3. Risky use including the use of cannabis in physically hazardous situations and continuing use despite known physical or psychological problems
4. Pharmacological criteria for tolerance and withdrawal symptoms.
The disorder’s severity is specified as mild (2–3 symptoms), moderate (4–5), or severe (6 or more).24
Regular cannabis use before age 17 is linked to an increased risk of developing CUD in young adulthood.20 A significant risk factor for developing CUD is early age of initiation, particularly before age 16. This is likely related to the fact that the brain, including the endocannabinoid system, is actively developing during adolescence and is more vulnerable to environmental exposures at this time.13 Other risk factors include high frequency of use, male gender, and concurrent tobacco or alcohol use.8
Although males are more frequently diagnosed with CUD, when the frequency of cannabis use is controlled, the rates of CUD are similar between both sexes. Females may develop CUD more rapidly (a phenomenon known as “telescoping”), experiencing more intense withdrawal symptoms, and showing higher rates of comorbid anxiety or mood disorders. The gender gap is narrowing, potentially due to the increased use and use of higherpotency products among females.20
Cannabis Withdrawal Syndrome
Cannabis Withdrawal Syndrome (CWS) particularly affects heavy and regular cannabis users. Symptoms typically begin within 24 hours of cessation, peak during the first week, and may last up to a month.19 To meet DSM-5 criteria, individuals must exhibit at least three of seven symptoms, developing within seven days of stopping or significantly reducing use. These symptoms include irritability, anger or aggression; nervousness or anxiety; sleep difficulties such as insomnia or vivid dreams; decreased appetite or weight loss; restlessness; depressed mood; and at least one physical symptom causing discomfort (e.g., headaches, sweating, nausea, vomiting, or abdominal pain).25
Studies estimate that approximately 47% of regular or dependent cannabis users experience withdrawal symptoms, with higher prevalence in clinical populations and those with concurrent tobacco or other drug use disorders. The biological basis involves the downregulation of CB1 receptors due to chronic cannabis use, leading to neurotransmitter disruptions during withdrawal. CWS symptoms often overlap with anxiety and depression, which many users attempt to manage by resuming cannabis use, thereby complicating cessation and treatment efforts. Recognizing CWS is crucial because its symptoms interfere with daily functioning and act as negative reinforcers that contribute to relapse and continued cannabis use.26
Routes of Consumption
The rise in CUD and cannabis withdrawal reflects broader shifts in how cannabis is consumed, highlighting the need to examine the expanding variety of high-potency cannabis products and routes of administration. Dabbing refers to the practice of vaporizing high-potency cannabis concentrates such as wax or shatter at high temperatures (typically between 400–600°F) using a device called a dab rig. Common cannabis products include dried flower, oils, solid concentrates like hash and shatter, edibles such as gummies or baked goods, and topicals like creams and balms applied to the skin. These products are consumed using a range of devices, including joints, blunts, bongs, vape pens, and dab rigs.12
The route of administration and the type of product used have a significant impact on the health effects and psychoactive experience. Smoking and vaping generally produce rapid but short-lived effects, while edibles result in a slower onset with longer-lasting effects. High-potency concentrates, such as those used for dabbing, tend to produce more intense psychoactive effects than lower-potency forms. Although smoking dried cannabis flower remains the most common method of consumption in the United States and Canada, the popularity of other forms, such as edibles and concentrates, continues to rise, especially in areas where recreational cannabis is legally available.12
Electronic cigarettes (e-cigarettes), initially developed for nicotine delivery, are now frequently modified by adolescents to vaporize cannabis products like hash oil, THC-infused wax, and dried buds or leaves. This method of consumption is particularly attractive to youth due to its discreet nature, with a less pungent odor than smoking. A 2014 study conducted in five high schools in Connecticut revealed, through an anonymous survey, that 27.9% of lifetime e-cigarette users and 29.2% of cannabis users reported using e-cigarettes to vape cannabis. Notably, the use of e-cigarettes to vape cannabis was 27 times more common among high school students than among adults, again likely due to its discreet nature. Although these findings are based on self-reported data, and thus may be underestimated, they highlight a concerning trend in adolescent cannabis consumption. Moreover, school-specific factors like cannabis culture and anti-vaping policies may also play a more significant role in influencing cannabis.26
Cannabis Use and Brain Development
Adolescents who initiate cannabis use early tend to consume it in greater amounts and with greater frequency than those who begin later in life. Specifically, initiating cannabis use before the age of 16 has been associated with more pronounced short- and long-term detrimental effects on brain development, including higher dependence compared to individuals who begin using cannabis in adulthood.5,27
The human endocannabinoid system regulates a variety of physiological processes through endogenous cannabinoids that interact with two primary G-protein-coupled receptors known as Cannabinoid receptors (CB-Rs): CB1 and CB2. CB1 receptors are mainly located in the brain, while CB2 receptors are found on peripheral immune cells and dopaminergic terminals in the striatum. Tetrahydrocannabinol (THC), the psychoactive component of cannabis, acts as a partial agonist at both CB1 and CB2 and is associated with euphoria, psychosis, and motor
and cognitive dysfunction, along with therapeutic properties such as analgesia and anti-inflammatory effects. In contrast, cannabidiol (CBD) demonstrates a more complex pharmacology. It antagonizes CB1, negatively modulates CB2, and activates TRPV1 and 5-HT1A receptors, producing therapeutic anxiolytic, antipsychotic, and anti-inflammatory effects. CBD also inhibits GPR55 signaling via modulation of calcium and adenosine signaling, a mechanism linked to antiepileptic and antipsychotic activity.28–30
Several studies have implicated both acute and chronic impairments in memory, learning, attention, motor skills, and executive functioning associated with cannabis use. These cognitive effects are believed to result from the direct activation of CB1 receptors, which are in key brain regions such as the prefrontal cortex, globus pallidus, substantia nigra, hippocampus, striatum, and cerebellum leading to poor academic outcomes. These impairments tend to be more pronounced in younger individuals who use cannabis regularly.31–33 Another longitudinal study of 799 adolescents found a dose-dependent association between cannabis use over five years and neurodevelopmental abnormalities, including accelerated cortical thinning, particularly in the prefrontal regions of the brain.26 Early exposure to THC during the prenatal and adolescent periods has been associated with impaired neural connectivity in the hippocampus, explaining the link between early and regular cannabis exposure with decreased IQ.34,35
CANNABIS USE AND PSYCHIATRIC COMORBIDITIES
Psychosis
Adolescent cannabis use has an established association with an increased risk of psychotic disorders, particularly among those with early-onset and heavy use.36,37 Although acute cannabisinduced psychosis is relatively rare in adolescents, up to 75% of individuals who experience these brief episodes go on to develop chronic psychotic disorders.38 The risk is highest for those with a pre-existing vulnerability to psychosis, such as those with a family history of schizophrenia, high-potency THC product use, and daily or near-daily cannabis use.19 Studies have suggested that cannabis use increases the risk of developing a psychotic disorder by approximately 2 to 4-fold.38,39 Early-onset users also have an increased risk of developing symptoms of psychosis earlier than those who do not use cannabis.38
Although the lifetime prevalence of psychosis has remained stable in recent years, cannabis use has increased. This suggests that lifetime prevalence may not be a sensitive enough measure to detect the impact of adolescent cannabis consumption on the development of psychosis. Additionally, because CUD is significantly underdiagnosed, the true overlap between CUD and psychosis may be underestimated.38
Internalizing and Externalizing Disorders
The psychological effects of cannabis use, specifically internalizing and externalizing disorders, are highlighted in Table 1. A systematic review and meta-analysis of 11 studies involving 23,317 individuals found that adolescent cannabis use was associated with an increased risk of developing depression and suicidal behaviors in later life, even in individuals without preexisting mental health conditions. Furthermore, younger
adolescents aged 14-15 were at a significantly higher risk of developing suicidal behaviors. This risk was prominent in girls as compared to boys with an additional impact on academic performance and delinquency.42 Individuals who were using cannabis before age of 18 experienced markedly reduced odds of high-school completion (adjusted odds ratio AOR = 0.37, 95% CI 0.20–0.66) and lower odds of achieving a university degree (AOR = 0.38, 95% CI 0.22–0.66) when compared to those who had never used cannabis along higher odds of suicide attempt (6·83, 2·04-22·90).53
Table 1: Adverse Effects of Cannabis Body System Associated Effects
Impairment in memory, learning, attention, motor skills, and executive functioning31–33
The overall relationship between depression and cannabis use is still unclear. Some studies suggest cannabis may provide symptom relief for certain individuals with depression, while others indicate it can worsen symptoms by causing emotional blunting and anhedonia. Cannabis use may interact with the brain’s reward system, potentially playing a role in the development of
Major Depressive Disorder (MDD). This conflicting evidence is especially concerning given the possible link between cannabis use and increased risk of suicidal behaviors in young people, warranting more nuanced research.39
CUD is a commonly found comorbidity in individuals with Attention Deficit Hyperactivity Disorder (ADHD), with an estimated prevalence of 33%-38%.43 Both CUD and ADHD are associated with academic challenges including disruptive behaviors and difficulties with time management, which often result in poor grades.54 Although less intuitive than other stimulating drugs such as cocaine, cannabis’s role in the dopaminergic pathway may be potentially why individuals with ADHD are more prone to use cannabis.55
Individuals with childhood ADHD not only tend to initiate cannabis use earlier but may also follow distinct usage trajectories compared to their non-ADHD peers. Whereas adolescents without ADHD who engage in cannabis and alcohol use often show a decline in substance use as they transition into adulthood, individuals with a history of childhood ADHD exhibit sustained or increasing patterns of use into adulthood.56 These findings suggest that ADHD may be a risk factor for prolonged or escalating substance use.
Cannabis Use and Physical Health
With the most common method of cannabis consumption being smoking, with vaping gaining more popularity among adolescents, the effects of cannabis use on the respiratory system are of particular interest. Several studies suggest an increased prevalence of respiratory symptoms, even when nicotine use was controlled for, as highlighted in Table 1
Existing literature on asthma is primarily from adult studies and reports a significant association between cannabis use and asthma; for instance, one study found that emerging adult cannabis users had a 1.71-fold increased odds of filling prescriptions for asthma medications, even after adjusting for confounding factors such as body mass index and tobacco use. These findings underscore the need for further investigation, particularly in adolescent populations, to clarify causal relationships and long-term pulmonary outcomes.45
Furthermore, there is some evidence linking cannabis use with cancer. A longitudinal study following over 49,00 men in Sweden for 40 years starting in 1969-1970 found that “heavy” cannabis smoking, defined as over 50 uses over a lifetime, was significantly associated with more than a twofold risk of developing lung cancer (hazard ratio 2.12, 95% CI 1.08-4.14) over the 40-year follow-up period, even after statistical adjustment for baseline tobacco use, alcohol use, respiratory conditions, and socioeconomic status.47
Low doses of cannabis are antiemetic and have been FDAapproved for chemotherapy-induced nausea, but chronic high doses can paradoxically cause hyperemesis. Cannabis Hyperemesis Syndrome (CHS) is a functional gut-brain disorder marked by episodic nausea and vomiting. Considered a variant of cyclical vomiting syndrome (CVS) in cannabis users, CHS is uniquely associated with compulsive hot bathing or showers for symptom relief and has been linked to heavy cannabis use, with symptoms improving after sustained cessation. First reported in 2004, the incidence of CHS cases has increased in parallel with increasing global cannabis use and legalization.50
Notably, in 2019, there was a multistate E-cigarette or Vaping product use-associated Lung Injury (EVALI) outbreak, with a report of approximately 2,506 hospitalized cases reported to the CDC. Of these, over 859 were young adults (18-24) and 360 were adolescents.48 Approximately 77-80% of these adolescents reported using THC-containing products.8,48 Common pulmonary symptoms in EVALI include shortness of breath, chest pain, cough, and rarely hemoptysis, with lung images showing ground glass opacities.57 Many of these cases involved acute lung injuries requiring intensive care/intubation. Adolescents with EVALI more frequently have a history of asthma and mental, emotional, or behavioral disorders, such as ADHD, compared with adults.48
Studies have shown adverse cardiac effects stemming from THC, including increased heart rate and moderate increases in blood pressure.46 While there are several documented case studies in young adults, as documented in Table 1, many of which are without prior cardiovascular risk factors,49 reports are rare in adolescents. One case report documents a 16-year-old who experienced an MI shortly after acutely inhaling cannabis. Extensive toxicology had confirmed the presence of a THC metabolite and ruled out exposure to other substances. One month after the event, an MRI showed a severely dilated left ventricle and moderately to severely depressed global systolic function, indicating there may be long-term effects of cannabis use on the cardiovascular system.58
Studies of the endocrine effects of cannabis use in adolescents are limited. The Tracking Adolescents’ Individual Lives Survey (TRAILS), a non-clinical cohort study, provided some insight into the relationship between cannabis use and stress reactivity in adolescents. Adolescents with a history of lifetime cannabis use demonstrated reduced physiological stress reactivity compared to non-users, even after adjusting for sociodemographic variables. Additionally, early-onset cannabis users (ages 9–12) exhibited lower morning cortisol levels relative to non-users and those with later-onset use (ages 13–14). Furthermore, adolescents who had used cannabis at least once showed elevated evening cortisol levels compared to never-users. These findings suggest that adolescent cannabis use, especially with early initiation, may dysregulate diurnal cortisol patterns, causing potential disruption of the hypothalamic-pituitary-adrenal (HPA) axis.44
Studies on chronic cannabis users have also noted detrimental effects on sleep architecture, as highlighted in Table 1. Notably, one study demonstrated a temporal shift in how cannabis use is associated with sleep patterns in adolescents over time. At initial assessment (mean age of 15), cannabis use correlated with weekend oversleeping, whereas at follow-up (mean age of 17), it was associated with reduced weekend sleep duration.59 Evidence suggests a bidirectional relationship: early sleep disturbances and an evening chronotype may predict future cannabis use, while early cannabis use is linked to later sleep problems such as reduced sleep duration, poor sleep quality, and insomnia.45
Treatment of CUD
Cannabis use can lead to impairment, addiction, and other serious consequences, yet treatment rates for CUD remain low. Despite rising use overall, there was no increase in the percent of substance use treatment admission where cannabis was the primary drug between 2003 and 2013. Data from the National
Epidemiologic Survey on Alcohol and Related Conditions (NESARC) shows that only a small proportion of individuals with CUD received cannabis-specific interventions; just 7.2% with current cannabis abuse and 13.7% with lifetime use in NESARCIII (2012–2013).19
Despite increasing cannabis use and CUD prevalence, treatment options remain inadequate. To date, no pharmacological treatments have received FDA approval for use in managing CUD in either adolescents or adults. There is also limited success of off-label psychotropic medications particularly in relapse prevention.60 In several studies, N-acetylcysteine (NAC) has shown promise. A youth-focused randomized controlled trial found that NAC doubled the odds of abstinence when paired with contingency management (CM), but NAC alone (without CM) was not effective in a more recent trial. CM is a robust behavioral approach providing extrinsic motivation, which is important in youth where treatment motivation may be limited or fleeting. This suggests CM may be essential for NAC’s efficacy, particularly in adolescents.61 Miranda and colleagues conducted a randomized controlled trial to test the potential efficacy of topiramate plus motivational enhancement therapy (MET) for treating cannabis use among adolescents. Topiramate was titrated over 4 weeks and continued at 200 mg for 2 weeks. Greater reductions in cannabis use was seen in topiramate groups suggesting it is a promising treatment intervention.62 Gabapentin, oxytocin and chronic dosing of naltrexone have also similarly shown reductions in CUD or prevention of relapse in small or targeted patient samples but have not yet shown efficacy in larger samples.25 Cannabinoid replacement therapies such as nabilone, nabiximols, or dronabinol have not yet proven consistently effective, adding to the challenge of finding reliable pharmacological treatments for CUD.26
Current treatments, especially in youth, rely on psychosocial and behavioral interventions. Evidence suggests adolescents benefit most from externally reinforced, family-involved interventions like CM, MET, and CBT compared to other age groups. Brief motivational interviewing and family-based programs significantly improve abstinence outcomes. Emerging evidence also suggests gender may moderate response to treatment. Personalized feedback interventions have reduced cannabisrelated problems among women but not men, suggesting sexspecific tailoring may enhance outcomes.60
Overall, medications aimed at treating CUD show promise, especially when combined with behavioral interventions. However, as noted above, their success has been limited and currently no FDA-approved medications exist for CUD in adolescents or adults. As seen in tobacco cessation, combining medications with behavioral counseling may offer more effective treatment outcomes.25
In contrast, current placebo-controlled trials for CUD suggest that certain medications may help manage withdrawal symptoms. For withdrawal management, mirtazapine and quetiapine show some efficacy for withdrawal symptoms, while zolpidem and benzodiazepines may help with sleep disturbances. Cannabinoidbased treatments like oral THC, nabiximols, and nabilone appear promising for addressing withdrawal globally; however, further research is needed. These medications may reduce discomfort during cessation but are generally insufficient for achieving abstinence or reducing long-term use.25
CONCLUSION
The evolving landscape of cannabis legalization, increasing product potency, and diversified modes of consumption present complex challenges to adolescent health and public policy. In contrast to adults, cannabis legalization has not led to a dramatic increase in adolescent cannabis use. However, it has resulted in greater social acceptance and reduced perceived risk in adolescents. While cannabis offers therapeutic potential for certain medical conditions, there is overwhelming evidence to demonstrate significant health risks associated with its consumption in adolescents. Early and frequent use, particularly with access to high-potency products, has been associated with various adverse outcomes, including detrimental effects on brain development, mental health, and physical health in adolescents. Effective prevention strategies require targeted education, robust policy measures, and continued research into adolescent vulnerability. Likewise, current treatment options for CUD are limited, emphasizing the urgent need for evidence-based interventions specifically tailored to adolescents.
Dr. Bhangu may be contacted at gurkirat.bhangu@christianacare.org
REFERENCES
1. Ross, J. A., & Levy, S. (2023, June). The impact of cannabis use on adolescent neurodevelopment and clinical outcomes amidst changing state policies. Clinical Therapeutics, 45(6), 535–540. https://doi.org/10.1016/j.clinthera.2023.03.009
2 Miech, R. A., Johnston, L. D., Patrick, M. E., & O’Malley, P. M. (2025). Monitoring the Future national survey results on drug use, 1975–2024: Overview and detailed results for secondary school students. Monitoring the Future Monograph Series. Institute for Social Research, University of Michigan. https://monitoringthefuture.org/results/annual-reports
3 Patrick, M. E., Peterson, S. J., Terry-McElrath, Y. M., Rogan, S. E. B., & Solberg, M. A. (2024, January). Trends in coping reasons for marijuana use among U.S. adolescents from 2016 to 2022. Addictive Behaviors, 148, 107845. https://doi.org/10.1016/j.addbeh.2023.107845
4 SAMHSA. (2024, November). Know the effects, risks and side effects of marijuana. https://www.samhsa.gov/marijuana
5 Hill, K. P., Gold, M. S., Nemeroff, C. B., McDonald, W., Grzenda, A., Widge, A. S., Carpenter, L. L. (2022, February). Risks and benefits of cannabis and cannabinoids in psychiatry. The American Journal of Psychiatry, 179(2), 98–109 https://doi.org/10.1176/appi.ajp.2021.21030320
6 Chandra, S., Radwan, M. M., Majumdar, C. G., Church, J. C., Freeman, T. P., & ElSohly, M. A. (2019, December). Correction to: New trends in cannabis potency in USA and Europe during the last decade (20082017). European Archives of Psychiatry and Clinical Neuroscience, 269(8), 997–997 https://doi.org/10.1007/s00406-019-01020-1
7 Hall, W., & Degenhardt, L. (2008). Cannabis use and the risk of developing a psychotic disorder. World Psychiatry, 7(2), 68–71 https://doi.org/10.1002/j.2051-5545.2008.tb00158.x
8. Hinckley, J., Bhatia, D., Ellingson, J., Molinero, K., & Hopfer, C. (2024, March). The impact of recreational cannabis legalization on youth: the Colorado experience. In European Child and Adolescent Psychiatry (Issue 3, pp. 637–650). Springer Science and Business Media Deutschland GmbH.
9. Hoffmann, D. E., & Weber, E. (2010, April 22). Medical marijuana and the law. The New England Journal of Medicine, 362(16), 1453–1457 https://doi.org/10.1056/NEJMp1000695
10 Smart, R., & Pacula, R. L. (2019). Early evidence of the impact of cannabis legalization on cannabis use, cannabis use disorder, and the use of other substances: Findings from state policy evaluations. The American Journal of Drug and Alcohol Abuse, 45(6), 644–663 https://doi.org/10.1080/00952990.2019.1669626
11. Cerdá, M., Mauro, C., Hamilton, A., Levy, N. S., Santaella-Tenorio, J., Hasin, D., Martins, S. S. (2020, February 1). Association between recreational marijuana legalization in the United States and changes in marijuana use and cannabis use disorder from 2008 to 2016. JAMA Psychiatry, 77(2), 165–171. https://doi.org/10.1001/jamapsychiatry.2019.3254
12 Wadsworth, E., Craft, S., Calder, R., & Hammond, D. (2022, June). Prevalence and use of cannabis products and routes of administration among youth and young adults in Canada and the United States: A systematic review. Addictive Behaviors, 129, 107258 https://doi.org/10.1016/j.addbeh.2022.107258
13. Volkow, N. D., Baler, R. D., Compton, W. M., & Weiss, S. R. B. (2014, June 5). Adverse health effects of marijuana use. The New England Journal of Medicine, 370(23), 2219–2227. https://doi.org/10.1056/NEJMra1402309
14 Volkow, N. D., Han, B., Compton, W. M., & McCance-Katz, E. F. (2019, July 9). Self-reported medical and nonmedical cannabis use among pregnant women in the United States. JAMA, 322(2), 167–169 https://doi.org/10.1001/jama.2019.7982
15 Wilson, S., & Rhee, S. H. (2022, March). Causal effects of cannabis legalization on parents, parenting, and children: A systematic review. Preventive Medicine, 156, 106956 https://doi.org/10.1016/j.ypmed.2022.106956
16. Gunn, J. K. L., Rosales, C. B., Center, K. E., Nuñez, A., Gibson, S. J., Christ, C., & Ehiri, J. E. (2016, April 5). Prenatal exposure to cannabis and maternal and child health outcomes: A systematic review and meta-analysis. BMJ Open, 6(4), e009986 https://doi.org/10.1136/bmjopen-2015-009986
17 Rodriguez, C. E., Sheeder, J., Allshouse, A. A., Scott, S., Wymore, E., Hopfer, C., Metz, T. D. (2019, November). Marijuana use in young mothers and adverse pregnancy outcomes: A retrospective cohort study. BJOG, 126(12), 1491–1497. https://doi.org/10.1111/1471-0528.15885
18 Smart, R., Caulkins, J. P., Kilmer, B., Davenport, S., & Midgette, G. (2017, December). Variation in cannabis potency and prices in a newly legal market: Evidence from 30 million cannabis sales in Washington state. Addiction (Abingdon, England), 112(12), 2167–2177. https://doi.org/10.1111/add.13886
19 Hasin, D. S. (2018, January). US epidemiology of cannabis use and associated problems. Neuropsychopharmacology, 43(1), 195–212 https://doi.org/10.1038/npp.2017.198
20. Hinckley, J. D., Ferland, J. M. N., & Hurd, Y. L. (2024, May). The developmental trajectory to cannabis use disorder. In American Journal of Psychiatry (Issue 5, pp. 353–358). American Psychiatric Association.
21 Monfort, S. (2018). Effect of recreational marijuana sales on policereported crashes in Colorado, Oregon, and Washington (pp. 1–24). Insurance Institute for Highway Safety, Highway Loss Data Institute. https://www.iihs.org/topics/bibliography/ref/2183
22 Reed, J. K. (2021). Impacts of marijuana legalization in Colorado. Colorado Division of Criminal Justice. https://cdpsdocs.state.co.us/ors/docs/reports/2021-SB13-283Report.pdf
23 Tefft, B., & Arnold, L. (2020). Cannabis use among drivers in fatal crashes in Washington State before and after legalization. AAA Foundation for Traffic Safety. https://aaafoundation.org/cannabis-use-among-drivers-in-fatalcrashes-in-washington-state-before-and-after-legalization/
24 Hasin, D. S., O’Brien, C. P., Auriacombe, M., Borges, G., Bucholz, K., Budney, A., . . . Grant, B. F. (2013, August). DSM-5 criteria for substance use disorders: Recommendations and rationale. The American Journal of Psychiatry, 170(8), 834–851 https://doi.org/10.1176/appi.ajp.2013.12060782
25 Brezing, C. A., & Levin, F. R. (2018, January). The current state of pharmacological treatments for cannabis use disorder and withdrawal. Neuropsychopharmacology, 43(1), 173–194 https://doi.org/10.1038/npp.2017.212
26 Morean, M. E., Kong, G., Camenga, D. R., Cavallo, D. A., & KrishnanSarin, S. (2015, October). High school students’ use of electronic cigarettes to vaporize cannabis. Pediatrics, 136(4), 611–616. https://doi.org/10.1542/peds.2015-1727
27. Chen, C.-Y., Storr, C. L., & Anthony, J. C. (2009, March). Early-onset drug use and risk for drug dependence problems. Addictive Behaviors, 34(3), 319–322 https://doi.org/10.1016/j.addbeh.2008.10.021
28. Iffland, K., & Grotenhermen, F. (2017, June 1). An update on safety and side effects of cannabidiol: A review of clinical data and relevant animal studies. Cannabis and Cannabinoid Research, 2(1), 139–154 https://doi.org/10.1089/can.2016.0034
29 Moehle, M. S., & Conn, P. J. (2019, August). Roles of the M4 acetylcholine receptor in the basal ganglia and the treatment of movement disorders. Mov Disord, 34(8), 1089–1099. https://doi.org/10.1002/mds.27740
30 Sylantyev, S., Jensen, T. P., Ross, R. A., & Rusakov, D. A. (2013, March 26). Cannabinoid- and lysophosphatidylinositol-sensitive receptor GPR55 boosts neurotransmitter release at central synapses. Proceedings of the National Academy of Sciences of the United States of America, 110(13), 5193–5198 https://doi.org/10.1073/pnas.1211204110
31 Casey, J. L., & Cservenka, A. (2020, January 28). Effects of frequent marijuana use on risky decision-making in young adult college students. Addictive Behaviors Reports, 11, 100253. https://doi.org/10.1016/j.abrep.2020.100253
32 Crean, R. D., Tapert, S. F., Minassian, A., Macdonald, K., Crane, N. A., & Mason, B. J. (2011, March). Effects of chronic, heavy cannabis use on executive functions. Journal of Addiction Medicine, 5(1), 9–15 https://doi.org/10.1097/ADM.0b013e31820cdd57
33. Gruber, S. A., Dahlgren, M. K., Sagar, K. A., Gönenc, A., & Killgore, W. D. S. (2012, March 9). Age of onset of marijuana use impacts inhibitory processing. Neuroscience Letters, 511(2), 89–94 https://doi.org/10.1016/j.neulet.2012.01.039
34 Meier, M. H., Caspi, A., Ambler, A., Harrington, H., Houts, R., Keefe, R. S. E., . . . Moffitt, T. E. (2012, October 2). Persistent cannabis users show neuropsychological decline from childhood to midlife. Proceedings of the National Academy of Sciences of the United States of America, 109(40), E2657–E2664 https://doi.org/10.1073/pnas.1206820109
35 Zalesky, A., Solowij, N., Yücel, M., Lubman, D. I., Takagi, M., Harding, I. H., . . . Seal, M. (2012, July). Effect of long-term cannabis use on axonal fibre connectivity. Brain, 135(7), 2245–2255 https://doi.org/10.1093/brain/aws136
36 Chadwick, B., Miller, M. L., & Hurd, Y. L. (2013, October 14). Cannabis use during adolescent development: Susceptibility to psychiatric illness. Frontiers in Psychiatry, 4, 129. https://doi.org/10.3389/fpsyt.2013.00129
37 Englund, A., Morrison, P. D., Nottage, J., Hague, D., Kane, F., Bonaccorso, S., Kapur, S. (2013, January). Cannabidiol inhibits THC-elicited paranoid symptoms and hippocampal-dependent memory impairment. Journal of Psychopharmacology (Oxford, England), 27(1), 19–27 https://doi.org/10.1177/0269881112460109
38 Levine, A., Clemenza, K., Rynn, M., & Lieberman, J. (2017, March). Evidence for the risks and consequences of adolescent cannabis exposure. Journal of the American Academy of Child \&. Journal of the American Academy of Child and Adolescent Psychiatry, 56(3), 214–225 https://doi.org/10.1016/j.jaac.2016.12.014
39. Urits, I., Gress, K., Charipova, K., Li, N., Berger, A. A., Cornett, E. M., . . . Viswanath, O. (2020, May 19). Cannabis use and its association with psychological disorders. Psychopharmacology Bulletin, 50(2), 56–67. https://pubmed.ncbi.nlm.nih.gov/32508368
40 Abush, H., Ghose, S., Van Enkevort, E. A., Clementz, B. A., Pearlson, G. D., Sweeney, J. A., Ivleva, E. I. (2018, June 30). Associations between adolescent cannabis use and brain structure in psychosis. Psychiatry Res Neuroimaging, 276, 53–64 https://doi.org/10.1016/j.pscychresns.2018.03.008
41. Albaugh, M. D., Ottino-Gonzalez, J., Sidwell, A., Lepage, C., Juliano, A., Owens, M. M., . . . Garavan, H., & the IMAGEN Consortium. (2021, June 16). Association of cannabis use during adolescence with neurodevelopment. JAMA Psychiatry, 78(9), 1–11 https://doi.org/10.1001/jamapsychiatry.2021.1258
42 Gobbi, G., Atkin, T., Zytynski, T., Wang, S., Askari, S., Boruff, J., Mayo, N. (2019, April 1). Association of cannabis use in adolescence and risk of depression, anxiety, and suicidality in young adulthood. JAMA Psychiatry, 76(4), 426–434 https://doi.org/10.1001/jamapsychiatry.2018.4500
43 Zaman, T., Malowney, M., Knight, J., & Boyd, J. W. (2015, Jul-Aug). Co-occurrence of substance-related and other mental health disorders among adolescent cannabis users. Journal of Addiction Medicine, 9(4), 317–321 https://doi.org/10.1097/ADM.0000000000000138
44. van Leeuwen, A. P., Creemers, H. E., Greaves-Lord, K., Verhulst, F. C., Ormel, J., & Huizink, A. C. (2011, August). Hypothalamic-pituitaryadrenal axis reactivity to social stress and adolescent cannabis use: The TRAILS study. Addiction (Abingdon, England), 106(8), 1484–1492. https://doi.org/10.1111/j.1360-0443.2011.03448.x
45 Tuvel, A. L., Winiger, E. A., & Ross, J. M. (2023, January). A review of the effects of adolescent cannabis use on physical health. Child and Adolescent Psychiatric Clinics of North America, 32(1), 85–105 https://doi.org/10.1016/j.chc.2022.07.005
46. Bechtold, J., Simpson, T., White, H. R., & Pardini, D. (2015, September). Chronic adolescent marijuana use as a risk factor for physical and mental health problems in young adult men. Psychol Addict Behav, 29(3), 552–563 https://doi.org/10.1037/adb0000103
47 Callaghan, R. C., Allebeck, P., & Sidorchuk, A. (2013, October). Marijuana use and risk of lung cancer: A 40-year cohort study. Cancer Causes Control, 24(10), 1811–1820 https://doi.org/10.1007/s10552-013-0259-0
48 Adkins, S. H., Anderson, K. N., Goodman, A. B., Twentyman, E., Danielson, M. L., Kimball, A., Wiltz, J. L., & the Lung Injury Clinical Task Force and the Lung Injury Epidemiology/Surveillance Task Force. (2020, July 1). Demographics, substance use behaviors, and clinical characteristics of adolescents with e-cigarette, or vaping, product use–associated lung injury (EVALI) in the United States in 2019. JAMA Pediatrics, 174(7), e200756 https://doi.org/10.1001/jamapediatrics.2020.0756
49. Ladha, K. S., Mistry, N., Wijeysundera, D. N., Clarke, H., Verma, S., Hare, G. M. T., & Mazer, C. D. (2021, September 7). Recent cannabis use and myocardial infarction in young adults: A cross-sectional study. CMAJ, 193(35), E1377–E1384 https://doi.org/10.1503/cmaj.202392
50 Perisetti, A., Gajendran, M., Dasari, C. S., Bansal, P., Aziz, M., Inamdar, S., Goyal, H. (2020). Cannabis hyperemesis syndrome: An update on the pathophysiology and management. In Annals of Gastroenterology (Issue 6, pp. 571–578). Hellenic Society of Gastroenterology.
51 Schierenbeck, T., Riemann, D., Berger, M., & Hornyak, M. (2008, October). Effect of illicit recreational drugs upon sleep: Cocaine, ecstasy and marijuana. Sleep Medicine Reviews, 12(5), 381–389 https://doi.org/10.1016/j.smrv.2007.12.004
52 Hasler, B. P., Franzen, P. L., de Zambotti, M., Prouty, D., Brown, S. A., Tapert, S. F., Clark, D. B. (2017, June). Eveningness and later sleep timing are associated with greater risk for alcohol and marijuana use in adolescence: Initial findings from the National Consortium on Alcohol and Neurodevelopment in Adolescence Study. Alcoholism, Clinical and Experimental Research, 41(6), 1154–1165 https://doi.org/10.1111/acer.13401
53. Silins, E., Horwood, L. J., Patton, G. C., Fergusson, D. M., Olsson, C. A., Hutchinson, D. M., Mattick, R. P., & the Cannabis Cohorts Research Consortium. (2014, September). Young adult sequelae of adolescent cannabis use: An integrative analysis. The Lancet. Psychiatry, 1(4), 286–293. https://doi.org/10.1016/S2215-0366(14)70307-4
54 Hogue, A., Evans, S. W., & Levin, F. R. (2017). A clinician’s guide to co-occurring ADHD among adolescent substance users: Comorbidity, neurodevelopmental risk, and evidence-based treatment options. Journal of Child \& Adolescent. Journal of Child & Adolescent Substance Abuse, 26(4), 277–292 https://doi.org/10.1080/1067828X.2017.1305930
55 Loflin, M., Earleywine, M., Leo, J. D., & Hobkirk, A. (2014). Subtypes of attention deficit-hyperactivity disorder (ADHD) and cannabis use. Substance Use \& Misuse, 49(4), 427–434. https://doi.org/10.3109/10826084.2013.841251
56 Kennedy, T. M., Howard, A. L., Mitchell, J. T., Hoza, B., Arnold, L. E., Hechtman, L. T., Molina, B. S. G. (2019, December). Adult substance use as a function of growth in peer use across adolescence and young adulthood in the context of ADHD: Findings from the MTA. Addictive Behaviors, 99, 106106 https://doi.org/10.1016/j.addbeh.2019.106106
57 Thakrar, P. D., Boyd, K. P., Swanson, C. P., Wideburg, E., & Kumbhar, S. S. (2020, March). E-cigarette, or vaping, product use-associated lung injury in adolescents: A review of imaging features. Pediatric Radiology, 50(3), 338–344 https://doi.org/10.1007/s00247-019-04572-5
58 Toce, M. S., Farias, M., Powell, A. J., Daly, K. P., Vargas, S. O., & Burns, M. M. (2019, Jan-Feb). Myocardial infarct after marijuana inhalation in a 16-year-old adolescent boy. Pediatr Dev Pathol, 22(1), 80–86. https://doi.org/10.1177/1093526618785552
59. Pasch, K. E., Latimer, L. A., Cance, J. D., Moe, S. G., & Lytle, L. A. (2012, September). Longitudinal bi-directional relationships between sleep and youth substance use. Journal of Youth and Adolescence, 41(9), 1184–1196.
https://doi.org/10.1007/s10964-012-9784-5
60. Ghafouri, M., Correa da Costa, S., Zare Dehnavi, A., Gold, M. S., & Rummans, T. A. (2024, February 28). Treatments for cannabis use disorder across the lifespan: A systematic review. Brain Sciences, 14(3), 227 https://doi.org/10.3390/brainsci14030227
61. Gray, K. M., Tomko, R. L., Baker, N. L., McClure, E. A., McRae-Clark, A. L., & Squeglia, L. M. (2025, April). N-acetylcysteine for youth cannabis use disorder: Randomized controlled trial main findings. Neuropsychopharmacology, 50(5), 731–738 https://doi.org/10.1038/s41386-025-02061-y
62. Miranda, R., Jr., Treloar, H., Blanchard, A., Justus, A., Monti, P. M., Chun, T., Gwaltney, C. J. (2017, May). Topiramate and motivational enhancement therapy for cannabis use among youth: A randomized placebo-controlled pilot study. Addiction Biology, 22(3), 779–790 https://doi.org/10.1111/adb.12350
O ctob er 2 025
Par t nership U p d ate
ACS and Epic Content Integration Webinar
Join the American Cancer Society (ACS) and Epic Systems for an insightful over view of the patient education materials developed by ACS and their integration into Epic electronic health systems. The webinar will provide an update on the content available for usage, what to expect next, and a demo on platforms like eSyM highlighting how to access materials from your Epic Foundation System.
The webinar will take place at 12 p.m. ET on Thursday, October 16, 2025.
Regis ter for the webinar
New Videos Available from ACS
Preser ving Fer tility During Cancer Treatment
This video explains fer tility preser vation options for women, men, and adolescents undergoing cancer treatment Viewers can learn about available techniques and how to make a plan with their health care team. Coming soon in Spanish!
Watch and share
Understanding Lung Cancer Staging Video Series
This in-depth video series on lung cancer staging shows how tumor size, lymph node involvement, and metastasis impact diagnosis and treatment planning Viewers can learn who per forms staging, when it’s done, and how biopsy procedures guide care decisions Coming soon in additional languages!
Upcoming ECHO Webinars
Building Pathways to Fer tility Preser vation in Cancer
ACS is proud to par tner with the Alliance for Fer tility Preser vation on an ECHO program to assist health care professionals in building systems to increase access to fer tility preser vation for people with cancer. The target audience for this program is multidisciplinar y care teams, including cancer care, reproductive endocrinolog y, hospital administration, and advocacy organizations
Sessions will begin at 12 p.m. ET on Tuesday, September 23, 2025.
Regis ter here
Prostate Cancer Screening in Primar y Care (Cohor t 2)
This ECHO program is designed to suppor t primar y care clinicians navigating the complexities of prostate cancer screening. It tackles key challenges, including when to initiate screening, how to identif y appropriate candidates, how to minimize harm and overdiagnosis, how to interpret prostate-specifc antigen (PSA) results, and how to determine the right time for referral. MDs, DOs, NPs, and PA s in adult primar y care who handle PSA testing and specialty referrals are the target audience for this program.
Sessions will begin at 12 p.m. ET on Tuesday, September 23, 2025.
Regis ter here
Addressing Breast Density & Risk in Primar y Care (Cohor t 2)
This program is designed to help primar y care clinicians gain clarity on screening and risk management for patients with dense breasts, family histor y of breast cancer, or genetic markers for breast cancer. The ECHO program will cover topics including supplemental screening recommendations, risk assessment models, and using shared decision-making to help patients arrive at informed decisions.
Sessions will begin at 4 p.m. ET on Tuesday, October 7, 2025.
Regis ter here
Understanding Multi-cancer Detection Testing
ACS has developed an ECHO program to help equip primar y care clinicians and multidisciplinar y cancer care teams with a foundational understanding of multi-cancer detection (MCD) tests The sessions will also help attendees understand how to use evidence-based communication about potential risks, benefts, and uncer tainty o MCD tests and their results in cancer screening.
Sessions will begin at 11 a m ET on Tuesday, October 14, 2025
Regis ter here
A Look at Substance Use Diversion Programs in the Delaware Criminal Justice System Using the Sequential Intercept Model
Ellen Donnelly, Ph.D.
Center for Drug and Health Studies, University of Delaware
Joanna Champney, M.A.
Director, Division of Substance Use and Mental Health, Delaware Health and Social Services
Michael Records Bureau Chief, Bureau of Healthcare, Substance Abuse, and Mental Health Services, Delaware Department of Correction
ABSTRACT
This commentary describes approaches by Delaware health and justice practitioners that divert justice-involved individuals presenting with substance use disorder (SUD) symptoms out of the criminal justice system and enhance connections to treatment and supportive services. It applies the Sequential Intercept Model (SIM) used by the U.S. Substance Abuse and Mental Health Services Administration (SAMHSA) to discern opportunities for intervention at various stages of criminal processing. Examples of deflection/diversion programs at six of the SIM points are presented. Such cross-system collaborations are helping to redefine criminal justice reform and pathways of care after contact with the criminal justice system.
INTRODUCTION
Evolving substance use problems in Delaware’s communities are fundamentally transforming criminal justice processing practices in the State. Since 2019, Delaware has consistently ranked among the top five states with the highest drug overdose mortality rates. The State experienced a 69% increase in overdose deaths from 2016 to 2021.1 Drug poisoning deaths remain high despite declines in fatalities (338 in 2024 versus 527 in 2023) that reflect national patterns.2 According to internal drug monitoring data, between 2023 and 2024, Delaware’s fatal drug overdoses fell 36% (527 vs. 338).3 Nonfatal suspected overdose rates have been more stable, impacting 2.7 per 10,000 individuals as of 2022.3 Substance use contributes to disproportionate rates of contact with the criminal justice system. An estimated 9% of people with a substance use disorder (SUD) diagnosis will experience arrest in a given year.4 A recent systematic review estimates that 37% of men and 48% of women who entered U.S. jails and prisons met the diagnostic criteria for a drug use disorder.5
THE SEQUENTIAL INTERCEPT MODEL
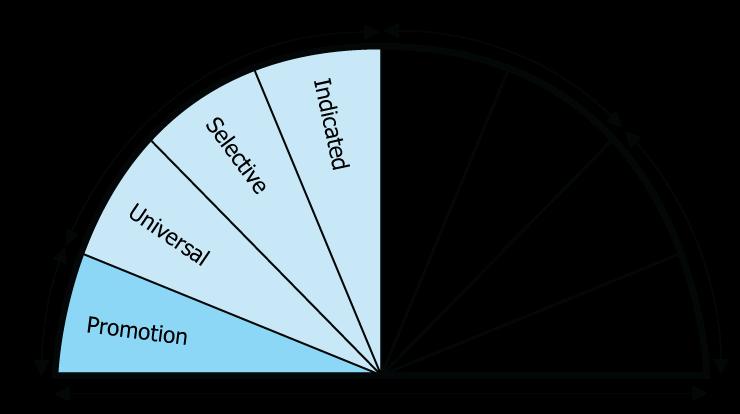
The Sequential Intercept Model (SIM) is a linear model of movement through the criminal justice system.6 It features six “intercepts” of criminal processing called Intercepts 0-5. Individuals may not necessarily engage with every point due to the nature of their justice contact, though, and may cycle through points due to recurrent interactions with law enforcement, courts, probation, or corrections. The overarching goal is deflection, or diversion, of individuals presenting with substance use or mental health disorder symptoms out of the justice system and toward treatment and supportive services in communities. We detail each stage in the following.
• Intercept 0 is the first stage of the SIM, representing community-level interactions before contact with the justice system occurs. It features 911 dispatch, crisis line or crisis intervention team, and law enforcementbased pre-arrest efforts that prioritize treatment or service referral before an arrest can take place.
• Intercept 1 refers to arrest diversion or arrest deflection initiatives. Once police or emergency personnel are deployed, Intercept 1 responses prioritize referrals or hand-offs to community services in lieu of taking an individual into custody, setting formal charges, or placing them into jail until their initial court appearance.
• Intercepts 2 and 3 pertain to detention and court processing decisions. The former determines whether someone should be released to the community and under what conditions, as well as whether they should face criminal charges. An emphasis is placed on diversion to community-based services through coordination by members of the court, clinicians, and social workers soon after booking or shortly before their initial court appearance. The latter characterizes diversion initiatives that occur after someone’s pretrial detention. It likewise includes programs to ensure people have access to appropriate care while waiting in jail for their cases to work their way through the courts or after being sentenced to incarceration following adjudication. Jail/prison health care and access to medication are legally required to ensure people remain in stable health during their stay.
• The last two intercepts characterize the coordination of treatment and care as part of the transitions out of the justice system and into the community. Intercept 4 involves efforts that provide treatment and supportive programming following an individual’s incarceration. Programs help to coordinate care plans, access to recovery programs and medication, and other supports that encourage reintegration into communities after someone has been released from jail or prison. Intercept 5 provides a role for communitybased supervision (e.g., probation) that decreases offenses or violations of sentencing conditions that result in jail or prison stays as a consequence.
EXAMPLES OF SIM MODEL INTERVENTION
IN DELAWARE
Pre-Arrest Diversion at Intercepts 0 and 1
The possibility of intervention before arrest has inspired numerous law enforcement agencies to start unique deflection initiatives. One of the earliest programs in Delaware– Hero Help in New Castle County– represents part of the State’s earliest efforts to address substance use issues through treatment referral amid growing overdose death rates in the 2010s. Developed in 2016, the Hero Help program was designed to give Delaware residents aged 18 and older without convictions or serious offenses or major pending charges the opportunity to receive immediate treatment with a local provider.7,8 Individuals could enter the program through voluntary self-referrals, in lieu of arrest, or by officer recommendation. With grant support from the University of Baltimore’s Combating Opioid Overdoses through CommunityLevel Intervention (COOCLI) Initiative, Hero Help hired a full-time civilian coordinator embedded in the police department. This coordinator led efforts to connect participants to direct (i.e., detox) and indirect services (e.g., housing, transportation, mental health) and manage care plans. Likewise, the coordinator actively led outreach campaigns and invited people to the Hero Help program as a follow-up to a non-fatal overdose. Funding from the Bureau of Justice Assistance expanded Hero Help’s team to include a mental health professional, case manager, nurse, and child victim advocate.9
The Hero Help program has demonstrable impacts. At the individual level, the addition of a coordinator increased detox completion rates from 56% to 77% and next-level care acceptance rates from 51% to 76%.10 Arrests decreased, too.10 At the community level, the program may have contributed to decreases in aggregated overdose rates in the jurisdiction that the New Castle County Division of Police serves. According to a Center for Drug and Health Studies study that compared forecasted and actual overdose rates, the expansion of the Hero Help team led to a decrease of 7.5 nonfatal and 1.85 fatal overdoses per month. Such reductions in overdoses contributed to a cost-savings of $21.5 million per month, based on Centers for Disease Control calculations11 of the costs of Opioid Use Disorder and other health economic data.12
Other early intercept interventions have emerged across Delaware. The Angel program in Dover was developed at the same time as Hero Help. Under this initiative, sworn officers and volunteers known as Angels would connect people with SUD to a local treatment provider for intake and clinical evaluation for needs.13 At present, the Delaware Comprehensive Opioid, Stimulant, and Substance Abuse (COSSAP) Saving Lives Initiative has multiple models of deflection, with sites in diverse locales, such as New Castle City, Seaford/Laurel, Georgetown, and Newark.
The Division of Substance Abuse and Mental Health (DSAMH) has also embedded behavioral health clinicians and peer support specialists in all Delaware State Police troops statewide.14
Individuals who have contact with the Delaware State Police due to underlying substance use disorders are offered the opportunity to access behavioral health treatment services in lieu of their criminal charges progressing. Program metrics compiled by DSAMH indicate that9,599 referrals have been made by Delaware State Police to the program since the program’s launch in 2021. Thirty-five percent of these individuals have accepted the program, with 2,201 people accepting the referral to addiction or psychiatric treatment.
SUD Programs in Delaware’s Correctional Institutions at Intercepts 2 through 5
Amid robust early-stage diversion opportunities, efforts to address substance use are also being undertaken towards the later stages of the SIM. As of June 30, 2024, 6% of individuals incarcerated in Delaware’s Level 5 institutions had a lead criminal charge that involved drugs.15 This finding is based on screenings of all people incarcerated in Delaware, regardless of charge type. The Delaware Department of Correction (DOC) operates nine inpatient SUD programs for its incarcerated populations. As a unified correctional system, DOC operates both jails and prisons for the State. Individuals who are incarcerated before adjudication (i.e., pretrial detention populations) are housed in the same prison facilities, but remain in distinct areas from those who are incarcerated after conviction (i.e., sentenced populations). Sentencing in Delaware is also differentiated by level, with Level 4 being work release/home confinement and Level 5 being incarceration.
Three of DOC’s SUD programs target pretrial populations, allowing people to access therapeutic communities, or specialized housing units focused on group-based healing, while waiting for the resolution of their cases. Its 6 for 1 program was first developed in 2002 for men incarcerated in Howard R. Young Correctional Institution, until it was expanded to include women housed in Baylor Women’s Correctional Institution in 2013. The program’s name initially reflected receiving one day of credit time for every six days of therapy, but now encompasses the program operating seven days a week, with six days of therapy and one day of reflection.16
In 2020, DOC introduced the Road to Recovery (R2R) program for its sentenced populations. R2R is based on the therapeutic community model and incorporates cognitive behavioral therapy into its curriculum. Therapy is group-based. As former DOC Commissioner Claire DeMatteis observed, “it’s more of a dormitory-style setting” where R2R participants “have classes together, counseling together, they rec together, and they eat together, and they help one another through the process.”17 A counselor leads CBT group sessions targeting one’s thinking and ways of changing their thought processes when similar situations arise. The program includes individual counseling sessions, peer-led treatment sessions, self-help groups, and interactive journaling exercises.
R2R features three tracks. Track 1 is a residential program with 30-35 hours weekly for 9 to 12 months for Level 5 and 25-30 hours for 6-9 months at Level 4. Track 2 is an intensive outpatient care program with 9-15 hours weekly for 4 to 6 months at Levels 4 and 5. Track 3 is an outpatient program with 9 hours weekly for 3 to 6 months at Levels 4 and 5. An assessment tool called the Addiction Severity Index (ASI) is used in conjunction with drug screens and multidisciplinary clinical reviews by DOC, helps to determine individual needs as well as placement within R2R. The program permits participants to also take “electives,” addressing trauma, anger management, co-occurring disorders, and relationships.18 A preliminary report on cognitive behavioral therapy interventions by the Center for Drug and Health Studies suggests that participation in R2R diminishes arrest rates at the 6-month and 1-year marks relative to a control group without programming.19
Since 2017, DOC has introduced medication-assisted treatment programming for opioid use disorder (MOUD) in its facilities. DOC can continue medications given to individuals in the community prior to their incarceration as well as prescribe medications at intake. Currently, DOC administers daily forms of Methadone and Buprenorphine through a nurse and long-acting injections of Buprenorphine and Naltrexone. Individuals who are identified as having OUD may access medication regardless of their participation in a DOC SUD program. Individuals with OUD in the general population also have the opportunity to engage in one MOUD/SUD group session and a one-on-one mental health session per month.
MAT is a key strategy for reentry as well. Before individuals with OUD are released from prison, plans are developed in the three months before release to continue medication and treatment within the community. Post-release plans depend on the type of medication as well as the needs of the individual. To illustrate, newly released individuals who were prescribed methadone receive a warm handoff to a community provider for an immediate appointment, those prescribed oral Buprenorphine receive a week’s supply before seeing a community provider, and those with long-acting medications receive an injection a month before release. The goal is to provide a continuum of care to prevent recidivism, improve treatment linkage, and encourage successful transitions to the community.
CONCLUSION
Substance use problems require appropriate care and robust interventions within the criminal justice system. The SIM is a useful framework to locate opportunities where treatment initiation and engagement, service integration and linkages, diversion from jail and prison, and crime prevention can all occur. Examples of SUD-focused programmatic developments in Delaware underscore the importance of justice and healthsystem collaborations. These partnerships rely on referral networks, case management, therapy, supportive clinicians, and other social services. Criminal justice institutions– police, courts, jails, and prisons– will be differentially positioned to develop SUD responses in their communities, largely due to disparities in resources and available behavioral health services. The task of addressing SUD may feel overwhelming to criminal justice agencies. Still, thriving health and justice partnerships combined with evidence of deflection program effectiveness in Delaware are changing the narrative about what criminal justice reform and the treatment of justice-involved persons presenting with SUD can look like.
Dr. Donnelly may be contacted at done@udel.edu .
REFERENCES
1. My Healthy Community. (2025). Drug Overdose Deaths. Delaware.gov https://myhealthycommunity.dhss.delaware.gov/topics/ drug-overdose-deaths/death-certificates/state
2. Delaware News. (2025, April 28). State agencies announce substantial reduction in drug overdose deaths. State of Delaware News. https://news.delaware.gov/2025/04/28/state-agencies-announcesubstantial-reduction-in-drug-overdose-deaths/
3. My Healthy Community. (2025). Mental health & substance use. https://myhealthycommunity.dhss.delaware.gov/topics/mental-healthsubstance-use/state
4. Pew Charitable Trusts. (2023, February 6). More than 1 in 9 adults with co-occurring mental illness and substance use disorders are arrested annually. https://pew.org/3HWryCL
5. Fazel, S., Yoon, I. A., & Hayes, A. J. (2017, October). Substance use disorders in prisoners: An updated systematic review and metaregression analysis in recently incarcerated men and women. Addiction (Abingdon, England), 112(10), 1725–1739. https://doi.org/10.1111/add.13877
6. Substance Abuse and Mental Health Services Administration. (2020, June 29). The sequential intercept model (SIM). https://www.samhsa.gov/criminal-juvenile-justice/sim-overview
7 Horn, B. (2016, May 20). As Delaware heroin deaths rise, more treatment options sought. The News Journal. https://www.delawareonline.com/story/news/local/2016/05/20/ delaware-heroin-deaths-continue-more-treatment-optionssought/82899870/
8 Horn, B. (2017, December 21). Now hiring: Coordinator for county’s addiction program, Hero Help. Delaware News Journal. https://www.delawareonline.com/story/news/local/ heroindelaware/2017/12/22/now-hiring-coordinator-countysaddiction-program-hero-help/975105001/
9 Donnelly, E. A., Stenger, M., Streisel, S., O’Connell, D. J., & Arnold, J. (2021). Addressing opioid misuse: Hero Help as a recovery and behavioral health response. Journal of Community Safety & Well-being, 6(3), 142–147. https://doi.org/10.35502/jcswb.191
10 Streisel, S., O’Connell, D. J., Visher, C., & Martin, S. S. (2019). Using law enforcement to improve treatment initiation and recovery. Federal Probation, 83(2), 39–44
11. Centers for Disease Control and Prevention. (2020, December 3). Cost of injury & violence. Centers for Disease Control and Prevention. https://www.cdc.gov/injury/features/health-econ-cost-of-injury/index.html
12 Donnelly, E. A., O’Connell, D. J., Stenger, M., Arnold, J., & Gavnik, A. (2023). Law enforcement-based outreach and treatment referral as a response to opioid misuse: Assessing reductions in overdoses and costs. Police Quarterly, 26 https://doi.org/10.1177/10986111221143784
13 Horn, B. (2016). Dover police start Angel program to combat heroin. The News Journal. https://www.delawareonline.com/story/news/local/ heroindelaware/2016/06/29/dover-police-start-angel-program-combatheroin/86428350/
14. Delaware Division of Substance Abuse and Mental Health. (2023). State of Delaware Police Diversion Program (PDP). State Epidemiological Outcomes Workgroup (SEOW) Summer Meeting, Delaware Health and Human Services Department, Division of Substance Abuse and Mental Health. https://bpb-us-w2.wpmucdn. com/sites.udel.edu/dist/9/12983/files/2023/09/For-Posting_PDP_ PresentationSEOW_8_29_23.pdf
15. Delaware Department of Corrections. (2024). Annual Report. Retrieved from https://doc.delaware.gov/assets/documents/annual_ report/DOC_2024AnnualReport.pdf
16 Barrish, C. (2015). Baylor prison: Women find new way in this cell block. The News Journal. https://www.delawareonline.com/story/ news/local/2015/08/28/women-find-new-way-cell-block/71323096/
17. Cherry, A. (2020, October 22). Road to recovery: Delaware prisons revamp drug treatment programs. WDEL 101.7 FM. https://www.wdel. com/news/road-to-recovery-delaware-prisons-revamp-drug-treatmentprograms/article_c2363fd8-14a7-11eb-81b9-5fd8b9cff6df.html
18 Delaware Department of Correction. (2020). Road to recovery. https://doc.delaware.gov/assets/documents/newsroom/2020/20press1022.pdf
19 O’Connell, D. J., Rell, E., Visher, C., & Donnelly, E. A. (2024). Cognitive behavioral interventions and misconduct behind bars: a randomized control trial of CBI-CC (Final Report to National Institute of Justice (Award Number: 2018-75-CX-0020) 308692). Center for Drug and Health Studies. https://www.ojp.gov/pdffiles1/nij/grants/308692.pdf
The Delaware Healthcare Association, in a Joint Providership with the Healthcare Leadership Network of Th e Delaware Valley, and Bayhealth, presents
The 29 th Delaware Healthcare Forum on Wednesday, Decemb er 10, 2025, 8:30 AM to 4:30 PM at Bally’s Dover Casino Resort, Rollins Center, Dover, Delaware
The Healthcare Forum is expected to have over 500 healthcare leaders from provider organizations throughout Delaware for our one day educational and networking conference.
Registrations are now open.
Sponsor opportunities:
You don’t want to miss this opportunity to showcase your products and services to decision makers in the healthcare industry. Sponsor participation, over the years, has been greatly appreciated, both by us and by the Forum attendees. We are sure you, too, will benefit from the exposure your company receives through these events. With your Sponsorship, the Delaware Healthcare Association is able to provide Healthcare Education at a reasonable cost.
The Forum Offers Continuing Education Credits to Attendees:
Bayhealth is approved as a provider of nursing continuing professional development by the Maryland Nurses Association, an accredited approver by the American Nurses Credentialing Center’s Commission on Accreditation. (MNA#4003178).
Click here for more information
Rethinking Pain Relief After Surgery: What We Can Learn from Knee Replacements
Asim Trimzi Medical Student, Sidney Kimmel Medical College, Thomas Jefferson University
ABSTRACT
This paper offers a clear, evidence-based look at how we can reduce opioid use after knee replacement surgery without sacrificing pain relief. This review focuses specifically on total knee arthroplasty (TKA)—one of the most commonly performed and most painful surgeries—and asks whether opioids are truly necessary. By analyzing results from 21 clinical trials, the paper shows that non-opioid medications like NSAIDs and gabapentinoids can provide similar pain control with fewer side effects, such as nausea, dizziness, constipation, and sedation. Lower risk of long-term use is an added benefit. A recent RCT found that after knee/shoulder arthroscopy, 72% of patients in an opioid-sparing protocol remained opioid-free over six weeks—compared to just 5.4% in the traditional opioid group.8 Given how many people receive their first opioid prescription after surgery, the findings have major public health implications. They highlight a growing opportunity for clinicians and hospitals to shift away from default opioid prescribing toward safer, evidence-based pain management protocols. This transition is not only clinically feasible, but also urgently needed to reduce unnecessary opioid exposure, prevent avoidable side effects, and lower the risk of long-term use or diversion. With the right combination of education, clinical tools, and systemlevel support, many surgical patients may recover successfully with minimal or no opioid use when supported by effective multimodal protocols.
INTRODUCTION
Opioid prescribing after surgery has been a major contributor to long-term opioid use in the United States. With orthopedic procedures accounting for a substantial proportion of surgical opioid prescriptions, efforts to reframe how pain is managed postoperatively have gained urgency. Total knee arthroplasty (TKA) is one of the most common and painful elective surgeries, making it a particularly important procedure to analyze when considering alternatives to traditional opioid-based analgesia. Patients undergoing TKA often receive significant amounts of opioids both during their hospital stay and in the weeks that follow, a practice that can increase the risk of prolonged use and dependency.1
The issue of postoperative opioid prescribing gained national attention in the early 2000s, when clinical norms began to emphasize aggressive pain control as a measure of quality care. This shift was fueled in part by the adoption of pain as the ‘fifth vital sign’ and the introduction of patient satisfaction metrics tied to pain control, which created pressure on clinicians to prescribe opioids more liberally.2
As a result, opioids were commonly prescribed in large quantities after routine procedures, sometimes for weeks at a time. Unfortunately, many patients transitioned from short-term postoperative use to long-term dependence. Persistent opioid use is commonly defined as continued opioid consumption for more than 90 days following surgery. Studies have shown that 6% of opioid-naive patients still use opioids three to six months after surgery, and the risk increases with each additional day of prescription (figure 1).3 The overprescription of opioids in surgical settings became one of the initial entry points for many individuals into chronic use and, in some cases, addiction.
This review explores whether non-opioid analgesics— including NSAIDs, acetaminophen, and gabapentinoids—can offer equivalent pain relief to opioids while reducing risks of dependence, adverse effects, and prolonged use. TKA was chosen as a representative procedure because of its high surgical volume, well-documented pain burden, and standardized recovery protocols. It provides a clear and replicable lens through which to assess pain management strategies that might also benefit patients undergoing other types of surgery.
METHODS
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, a widely accepted framework that enhances transparency and rigor in systematic reviews. PRISMA was used in this review to ensure consistent study selection, clear reporting, and reproducibility of methods—important features when synthesizing clinical trial data on pain management strategies. A comprehensive literature search was conducted using PubMed, Scopus, and the Cochrane Library to identify randomized controlled trials published between January 2010 and April 2024. Search terms included combinations of: “total knee arthroplasty,” “TKA,” “postoperative pain,” “opioid,” “NSAID,” “acetaminophen,” “gabapentin,” “non-opioid analgesia,” and “multimodal pain management.”
Studies were included if they (1) enrolled adult patients undergoing primary total knee arthroplasty, (2) compared opioidbased regimens to at least one non-opioid analgesic (NSAIDs, acetaminophen, or gabapentinoids), and (3) reported outcomes such as pain scores, morphine milligram equivalent (MME) use, opioid-related side effects, or length of hospital stay. Studies that did not provide quantifiable data on these outcomes or used opioids in both control and intervention groups were excluded.
Data were extracted and synthesized narratively and graphically to highlight key trends and treatment effects. No new statistical analysis was performed. A meta-analysis from the search results was not conducted due to heterogeneity in study designs, outcome measures, medication combinations, and follow-up durations across trials. This variability limited the ability to produce a meaningful pooled estimate, and thus a narrative synthesis was determined to be the most appropriate and transparent way to present the findings.
RESULTS
Pain Control
There was no statistically significant difference in pain scores between the groups within the first 48 hours after surgery, meaning that patients who received non-opioid regimens experienced pain relief comparable to those who received traditional opioid-based protocols.4 In fact, several studies noted that patient-reported pain scores fell within clinically acceptable ranges across both groups, suggesting that opioids may not be necessary as a first-line option for managing early postoperative discomfort after TKA. Additionally, multimodal regimens combining two or more non-opioid medications often provided enhanced control of both resting and movement-related pain.
One patient, a 64-year-old retired teacher who underwent knee replacement last year, shared that her care team used a nonopioid regimen including celecoxib, acetaminophen, and a nerve block. “I was nervous at first, thinking the pain would be unmanageable,” she said. “But honestly, I never felt like I needed anything stronger. I was able to start walking the next day.”
This aligns with the growing trend of patient empowerment through education. When individuals understand that pain control can be achieved without relying solely on opioids, they are more likely to embrace alternatives and feel satisfied with their recovery process. Many patients report less fear about side effects, increased ability to participate in physical therapy, and a greater sense of autonomy in their recovery.
Opioid Use
Patients in the non-opioid groups used significantly fewer opioids overall—especially when NSAIDs and gabapentinoids were included in the regimen. Some studies reported a 30–60% reduction in total morphine milligram equivalents (MME) consumed during hospitalization and post-discharge followup.5 This reduction is clinically meaningful, as it not only limits patient exposure to addictive substances, but also reduces the risk of long-term opioid use and lowers the chance of leftover pills being diverted or misused in the community.
Another patient described her previous experience with opioids after an earlier hip procedure: “They made me nauseous, dizzy, and I couldn’t focus. When my surgeon said we could try fewer opioids this time around, I was relieved. The new protocol actually worked better and I didn’t have that foggy feeling.”
The community impact of reduced prescribing should not be understated. Fewer pills prescribed means fewer opportunities for misuse by others in the household, accidental ingestion by children, or diversion into illicit markets. Surgeons who adopt opioid-sparing protocols aren’t just protecting individual patients—they’re helping mitigate a wider public health risk.
Side Effects
The non-opioid groups consistently experienced fewer opioidrelated side effects such as nausea, vomiting, constipation, and sedation—symptoms that can delay mobilization and negatively impact patient experience.6 Importantly, concerns about NSAIDrelated complications like gastrointestinal bleeding or renal impairment were not substantiated in the short-term followup periods included in these trials. When used appropriately, NSAIDs proved to be both safe and effective within the context of a controlled perioperative protocol.
Patients commonly cited the ability to think clearly and move early after surgery as a major benefit. One individual noted, “It felt empowering to be alert and in control of my body. That wasn’t the case after my last surgery when I was on oxycodone.”
Providers have echoed these observations, with many noting that patients on non-opioid protocols are more engaged during rounds, more motivated in physical therapy, and more confident about returning home.
Hospital Stay
While not statistically significant across all studies, there was a slight trend toward shorter hospital stays in patients managed with multimodal, opioid-sparing protocols (figure 2).7 This trend is likely influenced by faster return to mobility and fewer medication-related complications. Shorter hospital stays can reduce healthcare costs and lower the risk of hospital-acquired complications such as infections or delirium in older adults. Additionally, patients on non-opioid protocols were less likely to experience delays in discharge due to issues like opioid-induced constipation or disorientation. Several studies noted improved
coordination of care and earlier mobilization milestones in these patients, helping them transition more smoothly to outpatient rehabilitation or home-based recovery.
WHY THIS MATTERS BEYOND ORTHOPEDICS
Although this review focuses on TKA, its findings are relevant to a broad range of surgical specialties. Procedures such as cesarean sections, colorectal surgeries, spinal operations, and even outpatient orthopedic interventions like arthroscopy have similarly benefited from non-opioid, multimodal pain management strategies.8 The common thread across these procedures is the effectiveness of targeting multiple pain pathways—rather than relying on opioids alone—to achieve adequate pain relief.
In gynecological and general surgery, for instance, combining acetaminophen with NSAIDs has shown similar reductions in opioid use, while regional blocks and local anesthetics are gaining traction in laparoscopic procedures. As in TKA, patients in these settings report higher satisfaction and fewer complications when opioids are minimized.
Furthermore, the adoption of these strategies supports public health goals to reduce opioid exposure at the population level. Many patients receive their first opioid prescription in the perioperative setting, and minimizing that exposure could prevent progression to misuse. Hospitals and surgical teams that prioritize evidence-based, opioid-sparing approaches are playing a direct role in reshaping how pain is treated and how risk is managed.
Figure 2. Hospital Stay Duration by Pain Management Strategy
FUTURE STEPS
Looking ahead, more research is needed to evaluate long-term outcomes, including the risk of persistent opioid use, quality of life, and functional recovery. There is also an opportunity to investigate how patient education, particularly around realistic pain expectations and the safety and effectiveness of non-opioid options, can influence patient buy-in and recovery. Expectationsetting and preoperative screening can enhance the success of non-opioid regimens. Multidisciplinary collaboration between surgeons, anesthesiologists, pharmacists, and physical therapists will be key in expanding the reach and impact of opioid-sparing strategies.
Mr. Trimzi may be contacted at trimziasim@gmail.com
REFERENCES
1. Brummett, C. M., Waljee, J. F., Goesling, J., Moser, S., Lin, P., Englesbe, M. J., . . . Nallamothu, B. K. (2017, June 21). New persistent opioid use after minor and major surgical procedures in US adults. [PubMed]. JAMA Surgery, 152(6), e170504. https://doi.org/10.1001/jamasurg.2017.0504
2 Rudd, R. A., Aleshire, N., Zibbell, J. E., & Gladden, R. M. (2016, January 1). Increases in drug and opioid overdose deaths—United States, 2010–2014. MMWR. Morbidity and Mortality Weekly Report, 64(50-51), 1378–1382 https://doi.org/10.15585/mmwr.mm6450a3
3 Alam, A., Gomes, T., Zheng, H., Mamdani, M. M., Juurlink, D. N., & Bell, C. M. (2012, March 12). Long-term analgesic use after low-risk surgery: A retrospective cohort study. [PubMed]. Archives of Internal Medicine, 172(5), 425–430 https://doi.org/10.1001/archinternmed.2011.1827
4 Memtsoudis, S. G., Poeran, J., Zubizarreta, N., Cozowicz, C., Mörwald, E. E., Mariano, E. R., & Mazumdar, M. (2018, May). Association of multimodal pain management strategies with perioperative outcomes and resource utilization: A population-based study. [PubMed] Anesthesiology, 128(5), 891–902 https://doi.org/10.1097/ALN.0000000000002132
5 Zywiel, M. G., Stroh, D. A., Lee, S. Y., Bonutti, P. M., & Mont, M. A. (2011, November 2). Chronic opioid use prior to total knee arthroplasty. [PubMed] The Journal of Bone and Joint Surgery. American Volume, 93(21), 1988–1993 https://doi.org/10.2106/JBJS.J.01473
6. Chou, R., Gordon, D. B., de Leon-Casasola, O. A., Rosenberg, J. M., Bickler, S., Brennan, T., Wu, C. L. (2016, February). Management of Postoperative Pain: A Clinical Practice Guideline From the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. [PubMed] The Journal of Pain, 17(2), 131–157 https://doi.org/10.1016/j.jpain.2015.12.008
7 Kehlet, H., & Dahl, J. B. (2003, December 6). Anaesthesia, surgery, and challenges in postoperative recovery. [PubMed] Lancet, 362(9399), 1921–1928 https://doi.org/10.1016/S0140-6736(03)14966-5
8 Ladha, K. S., Neuman, M. D., Broms, G., Bethell, J., Bateman, B. T., Wijeysundera, D. N., Wunsch, H. (2019, September 4). Opioid prescribing after surgery in the United States, Canada, and Sweden. [PubMed] JAMA Network Open, 2(9), e1910734 https://doi.org/10.1001/jamanetworkopen.2019.10734
Planning to attend the APHA 2025 Annual Meeting in DC in November?
If so, join us for the Mid-Atlantic 2025 Breakfast Convening on Sunday, November 2 from 8:00-10:30 AM at the Walter E. Washington Convention Center.
At this convening, you will hear from public health professionals and leaders representing the Mid-Atlantic Region and have an opportunity to network among colleagues.
This is a great way to:
• Meet leaders from your state’s public health association
• Expand your network in the region
• Learn how we can collaborate to support our shared goals
Cost: $25 per person
Location: 801 Allen Y. Lew Place NW, Washington, DC 20001
Statewide Prehospital Buprenorphine in Delaware:
Two-Years of Paramedic-Initiated Medication for Opioid Use Disorder After Overdose
Gregory K. Wanner, D.O., F.A.C.E.P.
Emergency
Medical Services and Preparedness Section, Delaware Division of Public Health; ChristianaCare
Mollee Dworkin, M.S.
Emergency Medical Services and Preparedness
Robert A. Rosenbaum, M.D., F.A.E.M.S., F.A.C.E.P.
Section, Delaware Division of Public Health
Emergency Medical Services and Preparedness Section, Delaware Division of Public Health
ABSTRACT
The Delaware Division of Public Health, Office of Emergency Medical Services (EMS) implemented the first statewide program enabling paramedics throughout the state to initiate buprenorphine treatment for opioid use disorder (OUD) in the prehospital setting. Building on a model from Camden, New Jersey, this protocol was approved in 2022 in response to rising overdose deaths and was fully implemented across Delaware’s advanced life support (ALS) EMS agencies in April 2023. Eligible patients—those 18 years or older, resuscitated with naloxone, and able to consent—received up to 24 mg of sublingual buprenorphine along with ondansetron for nausea. Between April 2023 and May 2025, paramedics administered 118 buprenorphine doses to 105 patients, with improvement in withdrawal symptoms reported after 63.6% of doses. Despite a rise in patient ineligibility due to altered mental status—likely linked to sedating adulterants,such as xylazine and medetomidine,in regional street drugs—paramedics increased the percentage of eligible patients accepting offered buprenorphine from 19.0% to 22.8% between the first and second year of the program. This protocol not only addresses acute overdose management in the field but also connects patients to ongoing care, aiming to reduce mortality and expand access to medications for opioid use disorder.
INTERVENTION
The opioid crisis has ravaged our communities in recent years. With escalating overdose deaths and healthcare systems strained, innovative methods of starting medications for opioid use disorder (MOUD)—such as buprenorphine—became a focus of Delaware’s Division of Public Health (DPH) and Division of Substance Abuse and Mental Health (DSAMH). Buprenorphine, an opioid receptor partial agonist medication with high receptor binding affinity, is an established and effective treatment for opioid use disorder (OUD).1,2 However, paramedics starting buprenorphine in a prehospital setting after an opioid overdose is a novel and innovative approach.2,3 The Delaware prehospital buprenorphine program incorporated the experiences from an emergency medical service (EMS) agency in Camden, New Jersey to produce a statewide protocol in Delaware.2,3 The Delaware protocol authorizes county advanced life support (ALS) agency paramedics to administer buprenorphine for patients under the following protocol and criteria:
Delaware ALS Buprenorphine Protocol4
Indications: Opioid overdose 18 years of age or older, requiring administration of naloxone. After explanation of the treatment, the patient expresses interest in buprenorphine administration and is agreeable to treatment for opioid addiction. Agency is approved to participate in the buprenorphine program by OEMS.
Exclusions: Patient is unwilling to give name AND date of birth, pregnancy, methadone dose less than 48 hours ago,* altered mental status and unable to give consent.
Perform Clinical Opioid Withdrawal Scale (COWS).1 If COWS score is greater than 5 OR the patient was opiate-free for 72 hours prior to the overdose, Administer Buprenorphine bundle.
• Administer 16 mg buprenorphine sublingual (SL)
• Administer 4-8 mg ondansetron (Zofran) oral disintegrating tablet (ODT) or intravenous (IV) as needed for nausea.
If after 10 minutes the symptoms worsen or persist, Contact Medical Control to administer 8 mg buprenorphine SL.
• Maximum of 24 mg buprenorphine.
Provide the patient Medication Assisted Treatment (MAT) brochure and provide a clinic appointment; transport to hospital, or obtain refusal of service.
*NOTE: Guidance was issued by the Delaware Office of EMS (OEMS) in November 2024 increasing the methadone exclusion period to 5 days since last methadone dose--rather than 48 hours--to further decrease the risk of precipitated withdrawal. Buprenorphine is administered as the combination product 8mgbuprenorphine/2mg-naloxone (Suboxone®) sublingual film.
Goals
The goals of the Delaware prehospital buprenorphine protocol are twofold:
1. Safely start patients on buprenorphine after opioid overdose, avoiding buprenorphine precipitated withdrawal (BPW), and 2. Link patients to ongoing care
BPW is a rapid worsening of opioid withdrawal symptoms which can occur when buprenorphine displaces a full opioid agonist, such as fentanyl. Risks of BPW appear related to chronic fentanyl use, methadone use, time frame from last use of opioids, and starting dose of buprenorphine.1,2,5 Based on prior research, the risk of BPW is very low when buprenorphine is administered shortly after naloxone resuscitation of an opioid overdose.2,3,5
Using this protocol, Delaware paramedics can start patients on buprenorphine—a potentially life-saving medication— and link the patient to ongoing care through a local MOUD provider if the patient declines transportation to the emergency department (ED).
Place and Time
In 2022, Delaware EMS providers recognized the potential to provide additional assistance to patients after an opioid overdose. Information was obtained from regional experts and through the efforts of EMS field providers, county ALS agencies, and the Delaware Office of EMS, a protocol for prehospital buprenorphine was drafted and approved in November of 2022.4 Training was provided to all county-based paramedics in Delaware over the following months. In April of 2023, the prehospital buprenorphine protocol was implemented throughout the State of Delaware through the cooperation of all county-based ALS agencies, making Delaware the first state to fully implement prehospital buprenorphine by all emergency response ALS agencies statewide.
Population
People throughout the State of Delaware who experience an opioid overdose and receive naloxone to reverse the effects of the overdose are eligible for inclusion in the prehospital buprenorphine protocol. As previously mentioned, additional criteria include at least 18 years of age, ability to consent to the treatment, and a COWS score greater than 5, unless they have been opioid-free for at least 72 hours prior to the overdose. Excluded from receiving buprenorphine are patients who are unwilling to provide their name and date of birth, pregnancy, have recently received methadone, or have altered mental status (AMS) and are unable to give consent.4 Regarding methadone and as stated above, the protocol initially required at least 48 hours since the last dose of methadone, however, guidance was issued in November 2024 increasing this period of time since last methadone to 5 days to further reduce the risk of precipitated withdrawal.
Purpose
Delaware EMS providers see the consequences of the opioid crisis every day, and they are trying to help. Basic life support (BLS) providers have been administering naloxone to overdose victims since 2014, and EMS agencies across Delaware have been distributing “leave behind” naloxone rescue kits since 2020. The naloxone rescue kits, provided by the Delaware Department of Health and Social Services, include two doses of naloxone, a pocket mask, and resources for OUD treatment. These efforts have saved countless lives in Delaware. Unfortunately, the number of overdose-related deaths associated with synthetic opioids (fentanyl) and polysubstance use continued to rise.6 In 2019, there were 431 overdose deaths in Delaware, increasing to 447 deaths in 2020, 514 deaths in 2021, and 537 deaths in 2022.7 The need for additional pathways to OUD treatment became clear.
IMPLEMENTATION
In 2019, an innovative treatment pathway with prehospital buprenorphine after overdose was developed and studied by Cooper University Hospital EMS in Camden, New Jersey.2 With the increasing numbers of overdoses and deaths in Delaware, a statewide effort to increase the availability of OUD care and MOUD was undertaken. The Delaware Office of EMS, paramedic agencies, and medical directors, with the input of experts from Cooper University Hospital, drafted a prehospital buprenorphine protocol, approved in November 2022. Following approval of the protocol, a coordinated training effort took place for all of Delaware’s county-based paramedics. Training included four hours of instruction in:
• Pharmacology of buprenorphine-naloxone
• Benefits and risks of prehospital buprenorphine
• Stigma reduction
• Discussions with patients about starting MOUD
• Referral planning, including county-specific resources
Training topics were chosen to assist paramedics in understanding how buprenorphine can help with OUD, the benefits of MOUD, and the difficulties stigma can have related to engagement and treatment of this patient population. Following training, the Delaware prehospital buprenorphine program was fully implemented throughout the State of Delaware in April of 2023 as the first statewide EMS buprenorphine program in the country. With this program, Delaware paramedics can administer buprenorphine after an opioid overdose and provide followup appointment resources for ongoing OUD care.
During a similar timeframe, the Delaware Overdose System of Care (OSOC) Acute Stabilization Subcommittee— consisting of representatives from emergency departments, EMS, MOUD providers, DPH, and DSAMH—worked to develop MOUD referrals pathways and guidelines to improve OUD care across the acute care system, benefitting EMS and ED patients. Delaware OSOC was created through legislation in 2018 to “ensure that consistent, humane, evidencebased treatment and care is available and provided to those requiring acute management for overdose or substance use disorder” and “improve care, treatment, and survival of the overdose patient in the State of Delaware.”8
EVALUATION
Within the first week of implementation, patients in all Delaware counties received prehospital buprenorphine after opioid overdose. We tracked the number of eligible patients, ineligible patients, doses given, COWS scores, and demographics. From April 2023 through May 2025 there were 118 doses of buprenorphine administered by paramedics to 105 patients. Eighty (76.2%) of these patients were transported to the ED and 25 (23.8%) declined transportation and received MOUD follow-up appointment resources. Demographics, dispositions, dosages, and COWS Scores are reported in Table 1
Table 1. Patient Demographics, Disposition, Buprenorphine Dose, and COWS Scores
Buprenorphine Dose and Response
The average dose per patient was 16.5 mg, doses administered are reported in Table 1. The specific initial COWS score was
documented for 81 (77.1%) of patients receiving buprenorphine, and a second optional COWS score was documented in 71 (68%) of patients that received buprenorphine. Under documentation of medication response, 75 (63.6%) doses were documented as the patient feeling “Improved,” 42 (35.6%) doses were documented as “Unchanged,” and 1 (0.8%) was documented as feeling “Worse.”
Eligibility and Offers for Prehospital Buprenorphine
Between April 2023 and April 2025 there were 3,000 patients that received naloxone after overdose and treated by paramedics; of these 504 patients were eligible for prehospital buprenorphine and 1,933 patients were ineligible. In 563 cases either the patient would not discuss or the EMS provider did not discuss buprenorphine for various case-specific reasons. Over this time frame the number of eligible patients decreased and ineligible patient numbers increased (Figure 1). The decreasing eligibility and increasing cases with “altered mental status and unable to consent” appear to correspond to the regional increase in sedating adulterants in the street drug supply, including xylazine and medetomidine.
Even with the total number of eligible patients decreasing in the second year of the program (Figure 1), paramedics increased the percentage of buprenorphine offers accepted by eligible naloxone patients from 19.0% in year one (April 2023-March 2024), to 22.8% in year two (April 2024-April 2025), as shown in Figure 2.
Of the 2,496 cases in which the patient was ineligible for buprenorphine or buprenorphine was not offered or discussed (Figure 3), “altered mental status and unable to consent” was the most common reason for ineligibility (61.2%), followed by “patient would not discuss” (12.3%), “COWS score <5” (10.7%), “provider chose not to discuss” (10.3%), “currently on methadone” (3%), “patient left the scene prior to discussion” (1.4%), and several “other” exclusions such as age less than 18 years or pregnancy (1.2%).
Figure 1. Number of Paramedic Naloxone Encounters with Ineligible and Eligible for Buprenorphine Patients, Delaware, Monthly, April 2023-April 2025
2. Number of Paramedic Naloxone Patients Eligible for Buprenorphine and Acceptance, Delaware, Quarterly, April 2023-March 2025
3. Prehospital Buprenorphine Ineligibility and Reasons Buprenorphine Not Offered, Delaware, April 2023-April 2025
Figure
Figure
Adverse Effects
Based on prior studies, high-dose buprenorphine initiation in the prehospital or ED settings appears to be safe, and few adverse effects would be expected, including a very low risk of precipitated withdrawal.2,3,5 Few adverse effects of buprenorphine were reported in Delaware, however, followup after EMS contact was unavailable in most of our cases. As stated above, in 41 of our cases, withdrawal was documented as “unchanged” and one case documented as feeling “worse” after a second dose of buprenorphine. Recent methadone use was identified as a potential concern in a few cases with ongoing withdrawal symptoms. While 75 patients were excluded due to taking methadone within 48 hours prior to overdose and EMS contact, with the prolonged half-life and potentially high doses of methadone being received, we updated guidance to exclude patients who have taken methadone in less than 5 days.
CONCLUSION
Sustainability
Prehospital buprenorphine initiation is one part of our multifaceted public health response to the opioid crisis. Funding for the Delaware prehospital buprenorphine program was provided through the First Responders—Comprehensive Addiction and Recovery Act (FR-CARA) Grant. In addition to funding, we recognized that ongoing education is an important part of program sustainability. To further improve prehospital buprenorphine acceptance rates, we will continue providing education for paramedics, emergency department staff, community members, and patients. Additionally, we intend to increase the use of EMS physicians and Post-Overdose Response Teams (PORT)—outreach teams with the ability to assist overdose patients who decline EMS transport--to help educate and engage patients in OUD care and treatment. The need for OUD treatment is expected to continue into the future. With continued funding and education, EMS providers are well-positioned to continue “meeting patients where they are” to provide care.
Public Health Significance
The complicated impact of the opioid crisis on individuals, families, and communities cannot be understated. In Delaware, the public health response has been coordinated by Delaware Health and Social Services, including the Division of Public Health (DPH), Division of Substance Abuse and Mental Health (DSAMH), and Delaware Overdose System of Care (OSOC), along with Delaware medical and OUD treatment providers, hospitals, emergency departments, and EMS organizations. Prehospital buprenorphine is only one aspect of this response. Over the first 2 years of this program, 105 patients were started on buprenorphine by paramedics in Delaware. However, the number started on buprenorphine alone does not fully account for the impact of this program. For opioid use disorder, research suggests that it takes between 3 and 8.5 recovery attempts to enter OUD remission.9 Every contact after an overdose and every discussion of treatment can help bring a patient one step closer to OUD treatment, recovery, and remission. Delaware paramedics from all three county paramedic agencies have initiated well over 500conversations with patients about OUD treatment. Whether starting buprenorphine in the field or initiating conversations and providing resources for treatment, the Delaware prehospital buprenorphine program has brought care for OUD directly to the patient—literally meeting the patient where they are.
Dr. Wanner may be contacted at Gregory.wanner@delaware.gov .
ACKNOWLEDGEMENTS
We acknowledge the vitally important teamwork of our partners in EMS administration and paramedics in Kent, New Castle, and Sussex counties, MOUD providers, hospital emergency departments, Delaware Overdose System of Care (OSOC), Overdose Response Center (ORC), Division of Public Health (DPH), and Division of Substance Abuse and Mental Health (DSAMH).
FUNDING DISCLOSURE
Funding for the Delaware prehospital buprenorphine program was provided through the First Responders—Comprehensive Addiction and Recovery Act (FR-CARA) Grant.
REFERENCES
1. American Society of Addiction Medicine. (2020). The ASAM national practice guideline for the treatment of opioid use disorder: 2020 focused update. Journal of Addiction Medicine, 14(2S Suppl 1), 1–91. https://doi.org/10.1097/ADM.0000000000000633
2 Carroll, G. G., Wasserman, D. D., Shah, A. A., Salzman, M. S., Baston, K. E., Rohrbach, R. A., Haroz, R. (2021, Mar-Apr). Buprenorphine field initiation of rescue treatment by emergency medical services (Bupe First EMS): A case series. Prehospital Emergency Care, 25(2), 289–293. https://doi.org/10.1080/10903127.2020.1747579
3. Carroll, G., Solomon, K. T., Heil, J., Saloner, B., Stuart, E. A., Patel, E. Y., Haroz, R. (2023, February). Impact of administering buprenorphine to overdose survivors using emergency medical services. Annals of Emergency Medicine, 81(2), 165–175. https://doi.org/10.1016/j.annemergmed.2022.07.006
4. Delaware Department of Health and Social Services. (2024). Delaware advanced life support protocols, guidelines, policies, and standing orders. Office of Emergency Medical Services. https://dhss.delaware.gov/dhss/dph/ems/files/ALSProtocols2024.pdf
5. Joiner, A. P., Wanthal, J., Murrell, A. N., Cabañas, J. G., Carroll, G., Hern, H. G., . . . Glenn, M. (2025). A scoping review and consensus recommendations for emergency medical services buprenorphine (EMS-Bupe) programs. Prehospital Emergency Care, 29(4), 384–406. https://doi.org/10.1080/10903127.2024.2445739
6. Garnett, M.F., Minino, A.M. (2024). Drug overdose deaths in the United States, 2002-2023. NCHS Data Brief, Number 522. https://dx.doi.org/10.15620/cdc/170565
7. Delaware Division of Forensic Science. (2024). Division of Forensic Science 2023 annual report. State of Delaware Department of Safety and Homeland Security. https://forensics.delaware.gov/resources/ contentFolder/pdfs/2023%20DFS%20Annual%20Report.pdf
8. An Act to Amend Title 16 of the Delaware Code Relating to the Creation of an Overdose System of Care, H.B 440. 149th General Assembly. (2018). https://legis.delaware.gov/BillDetail?legislationId=26746
9. Kelly, J. F., Greene, M. C., Bergman, B. G., White, W. L., & Hoeppner, B. B. (2019, July). How many recovery attempts does it take to successfully resolve an alcohol or drug problem? Estimates and correlates from a national study of recovering u. S. Adults. Alcoholism, Clinical and Experimental Research, 43(7), 1533–1544. https://doi.org/10.1111/acer.14067
Enhancing Client Engagement in Substance Use Treatment Through the Perspective of Recovering Professionals
Jesse Tallyen, L.M.S.W., L.C.D.P
Doctor of Social Work Student, Delaware State University
Amy Habeger, Ph.D., L.C.S.W.
Doctor of Social Work Program Director and Associate Professor of Social Work, Delaware State University
ABSTRACT
Objective: To explore how the experiences of recovering professionals reveal insights that improve and influence the goals and outcomes of clients in substance use treatment. Methods: In the Summer of 2024, a qualitative study investigated the observations and experiences of six recovering Delaware residents working in the field of addiction treatment. Semi-structured interviews conducted over Zoom discussed treatment experiences, with subsequent coding focused on the domains of experience, practice, and challenges. Results: Coding of the interviews revealed four themes: relationships, levels of care, and understanding, which aid in clinical understanding of client motivations, plus systemic issues. Stronger relationships increased client commitment, functioning as a form of mentorship that reinforced the client’s willingness to trust and build confidence. Levels of care that solved real-life problems were deemed very effective but faced funding challenges. Self-determination was paramount, with the clients willing to participate, but sometimes in a manner that permits them to maintain control. Finally, treatment failure may be a systemic flaw preventing clients from accessing essential resources necessary to gain recovery. Conclusion: Recovering professionals reported on the use of personal skills to enhance therapeutic relationships with clients and inform their clinical practice by facilitating and executing discussions and goals. This study expounded on the numerous ways in which professionals recognize encoded information within client interactions, such as willingness and self-determination, and tailor treatment decisions to enhance client engagement. It is essential that the skills and power of the therapeutic relationship be maximized to make treatment as effective as possible. Policy Implications: This study provides additional evidence of missed opportunities to address the needs of individuals lacking essential services, such as transportation or housing. Furthermore, reserving resources to protect agency interests damages the client’s prognosis for continued treatment.
INTRODUCTION
Between 2011 and 2021, drug overdose deaths in Delaware soared by over 300%, increasing from 17.6 to 54 per 100,000 individuals.1 These statistics demonstrate the impact of substance use in Delaware and the urgent need for improvement in the realm of substance treatment.
A national shortage of mental health and substance treatment providers is adversely affecting access to treatment. Nearly one-third of the U.S. population lives in a designated Health Professional Shortage Area.2 Factors such as rising costs, a lack of services, and providers refusing to accept new patients result in wait times lasting up to 48 days.2 Clients that experience stigma or feeling misunderstood by their treatment team are less likely to seek services. The shortage of professionals working in the field emphasizes the importance of maximizing available services.3
Recent developments in the field of alcohol and drug treatment include using the experiences of professionals already in recovery to aid clients who are seeking recovery. Utilizing the experiences of individuals in recovery has been gaining traction in the clinical world through peer services and self-disclosure. Theoretically, these services enhance the therapeutic alliance and improve treatment outcomes for clients currently in treatment, sometimes by lending credibility to treatment or making it more appealing.4
BOUNDARIES AND RESPONSIBILITIES FOR RECOVERING PROFESSIONALS
Recovering professionals work in the field of alcohol and drug treatment at numerous levels and positions. The scope of this article is direct service contact with clients, such as a peer specialist, counselor, or licensed social worker. Professionals and paraprofessionals are defined by regulatory bodies and restrained by professional codes of ethics.5 Some essential factors associated with helping positions include role responsibilities and personal boundaries.
Role Responsibilities
When dealing with an intimate and complex issue such as drug and alcohol use, clear responsibilities for professionals are vital. White addressed the development of the peer helper role, as well as accreditation standards that establish what falls within the scope of each role.6 White argued that role confusion must be avoided, such as the professional accepting the role of a sponsor or other responsibilities outside their job description. Some roles are designed for a flexible environment, while others are more rigid. For example, therapy typically takes place in a confidential office, whereas peer support specialists might work in group or residential settings.
Enhancing engagement is particularly important for community field workers and peer support specialists, who assist underserved populations at lower levels of reimbursement and salary compensation. Community field workers and peer support specialists often work with the clients in nontraditional settings, often in locations like those from which they originated.3
Personal Boundaries
Professionals who are recovering may experience strong emotional ties with the clients with whom they are working.7 Personal boundaries ensure the restriction of actions to those considered best for the client, maintaining the integrity of the treatment modality. Common boundary issues include sexual relationships and dual relationships, which could result in disturbing the power structure of the therapeutic alliance. Former clients joining an agency as employees may be concerned about their privacy and confidentiality.7
Leveraging Lived Experience in Treatment
Sharing one’s personal experience is a powerful tool in the treatment field, involving the sharing of lived experiences to benefit clients facing similar challenges.8 This process is known as storytelling, a tool primarily used by peer support specialists to offer evidence of change and emotional support to clients who may doubt their ability to succeed. Storytelling guidelines require that disclosed material be selected based on its relevance to the client’s needs, being both trauma- and culturally sensitive, and suitable for the treatment environment. Hearing a peer’s story bolsters confidence and cultivates feelings of empowerment and motivation.8
Members of Alcoholics Anonymous use storytelling in a non-professional capacity to pass on a program of recovery. Members attend meetings to discuss messages of abstaining from alcohol, sharing on life progress, the beginning or end of their drinking careers, and overcoming their denial about their problem. These messages form the narrative through which new members learn the AA recovery model.9
The theoretical framework for this study capitalizes on dynamics of the therapeutic relationship. Could recovering professionals share their experience, strength, and hope with new clients to encourage commitment? Figure 1 demonstrates the concept this study explores.
Figure 1. The Narrative of Personal Experience
REVIEW OF THE LITERATURE
Despite numerous studies offering quantitative analyses on recovering professionals, there is a rarity of qualitative studies, lending credence to the need for more research. Studies primarily focused on negative aspects of recovering professional providing substance use treatment, such as protection from relapse and maintaining personal safety.4 For example, in Denmark,10 twentyfive treatment centers out of thirty-eight agencies participating in a 2001 study reported using recovering counselors. That study revealed risk factors associated with relapses and dual relationships, again focusing on protection instead of enhancement.
A Canadian study with twenty-six participants found that personal experience with addiction offered credibility to treatment, permitting influence in the decision-making process.11 Personal experience of addiction proved a strong influential factor in administrating treatment.
Racz and his colleagues in Hungary examined the transition of the six recovering persons into professional colleagues.12 Four themes related to the realm of professional work came to light: “1. the recovering self and the helping self, 2. the wounded helper, 3. the skilled helper, and 4. the experience of helping.” Each archetype assists the client differently, described as helping the spiritual journey but without giving directions.
A study in Indonesia with six recovering professionals discussed overcoming the stigma of addiction and reclaiming their identity as professionals.13 They uncovered the importance of establishing personal value in recovery and feeling understood by those with whom they interact. However, the authors claimed data saturation after six interviews and passive observations. Vital data related to the experiences of recovering professionals might still be available. These discussions are also prevalent in the United States. Recently, McNeely focused on healthcare professionals recovering from substance dependence in Colorado.14 Those professionals acknowledged that stigma inhibited their initiation of treatment and discussed their observations on improving treatment options. One such recommendation was the provision of long-term mentoring for professionals to maintain discreet treatment.
Seeking Improvements to Service Delivery
The literature is clear on the value of the recovering professional’s experience, while also setting necessary parameters on ethical regulations. However, personal experience may lead to different decisions or approaches than traditional clinical practices, potentially leading to updates or improvements in treatment.
This study explores the perspective of recovering professionals in Delaware to inform the community of substance abuse treatment. These qualitative interviews investigated the research question: How can recovering individuals working in addiction treatment utilize their perspective to enhance services?
METHODS
A semi-structured interview guide explored personal and professional treatment experiences among recovering professionals. Questions focused on three domains: experience, practice, and challenges. A Zoom platform created a consistent meeting experience for each interview, with all meetings recorded and transcribed. Institutional Review Board approval was received from Delaware State University (2024-JT-723).
Participants
Convenience sampling was utilized to select six recovering professionals living in Delaware. Inclusion criteria included active employment in a treatment agency, and a minimum of seven years of abstinence from drugs and alcohol. Seven years is appropriate to witness changes or improvements between personal experience and current practice, as well as developed skills of observation and self-awareness. Eligibility in employment included providing direct care to clients, such as peer specialists or counselors, rather than administrative or medical roles. Composite demographics are summarized below in the Results section.
Data Collection
After completing the informed consent and demographic survey, participants received a Zoom link for the interview. Interviews lasted approximately 20 minutes, beginning with a brief introduction to their experiences in the field, then addressing the questions outlined in the guide.
The questions covered in the interviews captured three domains of experience from the participants. Participants reflected on how past experiences guided their understanding of treatment, influenced their knowledge of current treatment practices, and helped identify service barriers to address. Questions included in the discussion included defining client success, identifying personal challenges to providing effective services, and observations in the field of substance treatment over time.
The audio files were transcribed and scrubbed of any identifying information. Transcripts were assigned a number in order of completion, thereby maintaining the confidentiality of each participant.
Data Analysis
Data analysis followed Paul Ricoeur’s interpretative philosophy, which focuses heavily on the unique value of each individual’s experiences.15 Ricoeur’s work enhanced the theoretical underpinnings when valuing individual experiences with specific methods of data analysis. Ricoeur recommended shifting back and forth between handling the text as is and interpreting the underlying narratives.
Ricoeur’s method analyzes threads in the data behind the narrative.15 The three phases are explanation, naïve reading, and interpretive reading, establishing a hermeneutic arc, which establishes the given text and then focuses inward on its significance to develop the interpretive value.
The researcher read through each interview in what Ricoeur referred to as the explanation, with impressions acquired from the material but without interpretation.15 Segments of the interviews were extracted from the text, serving as the nodes to which subsequent steps were applied. In the following reading, emerging patterns divulged the themes of experience, current practice, and challenges. The final, critical reading linked the text’s themes back to the study’s design, thereby forming the hermeneutic arc emphasized by Ricoeur’s philosophy.
Ricoeur also acknowledged the researcher as part of the environment in which data is collected.15 During interviews, the researcher confined interactions to asking questions and offering reflective statements to ensure comprehension of the participants’ statements. Some familiarity was present, as the participants were all known by the researcher, but his influence on participant testimony remained minimal.
A graduate research assistant participated in the coding process to reinforce interrater reliability. The assistant coded independently and then discussed her findings with the researcher to establish a consensus. The data were refined, with the resulting themes incorporated into the study’s discussion.
RESULTS
A diverse group of six participants provided data on their experiences as recovering professionals. Diversity in participants encompassed gender, race, education, credentialing, and the levels of care encountered in professional practice. Composite demographics are summarized in Table 1.
The participants engaged in the discussions, addressing observations and experiences from various treatment settings, that they reported as both challenging and rewarding. Although the topic of professional expectations surfaced periodically, it was often accompanied by insights into best practices, such as this statement from Participant #2: “You have to really think where the client is at and what they’re really going through. But I do know that if they’re not 100 percent surrendered to this addiction, then they’ll keep coming back.” She recognized the client’s right to self-determination, even though the client might continue to use drugs or alcohol.
Though initially sorted by categories of experience, practice, and challenges, themes emerged that ran across the dimensions. The four most common themes are presented in Table 2, along with their corresponding subthemes, and textual examples.
Table 1. Participant Composite Demographics
Table 2. Themes and Subthemes from Recovery Interviews
Themes Subthemes
Gain Trust
Self-Determination
Relationships
Levels of Care
Understanding
Defiance vs. Willingness Distractions & Commitments
Types of Service
Medication-Assisted Treatment
Responding to Increased Risk Multidimensional Needs of Care
Social Control Resources – lack of, control of, accessing Agency Conditions
The most commonly recurring theme throughout the interviews was the value of relationships. Several instances occurred in which a relationship sparked a segment of a participant’s journey. As stated by Participant #2, “I knew that I wanted to help other people because there was always someone here to help me.” Participant #3 mentioned the critical role relationships played in establishing his recovery: “While in sober living, I happened to have a few people who refused to allow me to leave their presence until we had had a chance to have a conversation.” Later, he referred to developing his practice. “I would not have acknowledged that about myself had I not had some people who are really respected point those types of things out to me.” Both examples demonstrate an increase in personal motivation based on interactions with others.
Barriers to Trust
Many difficulties prevent the therapeutic relationship, blocking the client’s ability to form trust. These difficulties include distractions, obligations, and trauma. Participant #2 acknowledged the significant barrier that trauma represents:
Sometimes, not being able to get or meet them where they’re at. Because you can’t…They’re so closed. They’re so closed off. They have so much trauma going on in their life. They don’t know how to trust. So, it’s hard for you to get in to even actually see where they’re at. That’s a challenge. Because you want the best for all of them.”
Trust was also brought up by Participant #4, who said, “You have to really gain the trust of your client. And I want to always make that abundantly clear to them when they come in that this is tough work.”
Several participants mentioned that the client’s honesty was necessary to reinforce the therapeutic relationship. Participant #6 said, “If you’re honest, I know I can work with that. Like, you messed up, OK, but you are honest about it. That I can work with because I know that means that we have a shot.” Similar sentiments were shared by Participant #5: “Sometimes it makes it easier for me to cipher through the BS. You know what I mean? It
Textual Examples
“…it’s hard for you to get in…”
“If you’re honest, I know I can work with that.”
“…people who are really respected point those types of things out.”
IOP, Prison, Outpatient, Residential Settings
“…they’re learning how to live without doing drugs.”
“…so many people are dying, every single day.”
“…due to my trauma history, I can relate with them…”
“Immediately, defenses up.”
“One session is not going to take care of child trauma.”
“a lot of places will keep their resources close… so they don’t have to share.”
“They put a lot of obligations on them that make it very difficult.”
allows me to be able to hold them accountable in a healthy way.” He referred to the client’s dishonesty, saying, “We both know that’s not the case right now; this is kind of what it is. So, let’s just focus on what we can do to make it better.”
Willingness Versus Defiance
The duality between willingness and defiance established itself repeatedly. Willingness was associated with behaviors such as compliance with rules, adapting to changes in the social environment, learning new behaviors, and giving effective effort. Defiance was conjectured to mean not following the rules, such as falsifying drug screens or stopping treatment once the client starts feeling better. Participant #4 described how differences in priorities affect treatment.
We have to talk to them about…what their priority is at the moment. If it is working in therapy, let’s do it… If it’s my kids are going back to school next week, I can’t make it for another month. I’ve got too much to do. My baby daddy just ran off, and I’ve got no time to come in. These are things I’ve heard today, actually.
Some actions that could be inferred as defiance, in that they add to the possibility of treatment failure, might actually be systemic issues blocking their progress.
Levels of Care
Experience within the treatment field covered a myriad of locations, describing services offered in recovery houses, prisons, Intensive Outpatient Programs, inpatient settings, case management, drug diversion, and MAT clinics.
Types of Service
When asked which setting was most impactful, Participant # 1 identified the prisons, saying, “I learned how to read people because they learn how to read you real quick. So, with that population, it was very enlightening. I grew a lot in that field.”
Participant #2 shared: “When they’re doing IOP, they’re out there in the real world. ... And so, they’re learning how to live without doing drugs…You gotta deal with outside life, and then you gotta come back here.” Intuitive learning occurs in various settings.
One pattern in the data revolved around the prevalence of IOP, specifically mentioned during four out of the six interviews. Participant #3 said, “I had two facilitators for IOP who were both peers, both of whom gave me things that I still carry with me today.” That sentiment was also shared by Participant #5, saying, “I know how much that IOP helped me in the beginning.” Finally, Participant #6 was emphatic when describing her experience, saying, “They suggest IOP, I go to IOP. I was there at eleven and a half months. And it saved my life. It absolutely saved my life.” Though levels of care are varied, these individuals held IOP treatment in high regard.
Medication-Assisted Treatment
The participants highlighted Medication-assisted treatment (MAT) as a significant shift in the treatment field. In some cases, participants admitted to hesitancy before accepting the harm-reduction principles of MAT. Levels of acceptance varied by person, with MAT (primarily methadone) carrying the risk of abuse. Participant #1 described it this way:
I was always an abstinence-based person, all or nothing, but I really learned some of the benefits and importance of MAT - that it works for some people. It can be abused, like everything can, but I really learned how to respect, you know…It’s a tool…You use any tool that’s available to benefit your recovery.
Clients with opiate use disorder funnel through the MAT clinics instead of outpatient care.
Responding to Increased Risk
Drugs associated with more recent crises in Delaware –namely Xylazine and Trank – were also touched on during the discussions, funneling through the same channels as the users of opioids and fentanyl. Regarding the sudden increase in overdose rates, Participant #5 said, “In the beginning, it, it like, nobody really kind of knew what was going on, cause, for me anyway, and you know, I’m even in the field and it still kinda came out of nowhere.” He discussed how treatment responded: “I think we’ve caught up to at least treating it…Where I work now, we’ve got a wound specialist cause the stuff eats your flesh and all that.” Participant #6 spoke of the sudden adjustment also, saying, “I never thought I would see when small towns and things like that were, are overcome by addiction, and so many people are in the grips, and so many people are dying, every single day.” They recognize the escalation in the crisis despite improvements in the response.
Multidimensional Needs of Care
Finally, levels of care also reflected the multidimensional facet of treatment. Difficulties related to addiction, such as physical and mental health, must be attended to, or other services, such as establishing stable housing and family services, and with legal consequences. These interviews indicated the need to consider that addiction affects the whole person and requires a multitude of treatment settings. Participant #4 said, “…I always have to include that dual diagnosis of mental health because we have to work on both pieces and here; we also work on the physical health as well. You see the multidimensionality of it all.”
Understanding
Understanding was the connection between the recovering professionals and how they guide their clinical practice and decision-making. Such decisions could be considered best practices, with personal experience offering insight into maximizing the clinical potential of the session.
Similarities exist between the categories of relationships and understanding. Distinguishing between them requires consideration that the relationship builds trust between the professional and the client. Within the theme of understanding, professionals utilize their knowledge to enhance the effectiveness of treatment, even during times when the relationship has yet to be established. Understanding helps to tailor professional behaviors based on knowledge or intuition.
Sharing
Some of these techniques involve appropriate disclosure when sharing or the awareness of how clients meet or do not meet treatment goals. Participant #1 described the trauma-informed approaches she employs in group therapy. She expressed her views this way:
I do a trauma group called Seeking Safety…And due to my trauma history, I can relate with them and give a platform where they can share and feel comfortable sharing traumatic experiences…I can share my experience with them and help guide them – the group – to stay on topic and to focus on the core aspects of the topic.
Her experience lends credibility to her facilitation of the group discussion, allowing her to redirect the conversation when necessary to enhance its value and effectiveness.
That sentiment was shared by Participant #6, who said, “Don’t ever act like you have all the answers, and you know it all…you need to do exactly what I say…Immediately, defenses up. I’m not gonna listen to you. You don’t know what I’ve been through - those kinds of things.” Occupying the role of the expert is not deemed helpful.
Guidance
Participant #2 recognized the impact of childhood trauma, speaking on her belief that trauma must be handled carefully during sessions when handling the treatment goals.
You may have…set their treatment plan up…only, you may not be able to meet all those goals, especially if they’re dealing with childhood trauma. So, you’re gonna focus on childhood trauma. One session is not going to take care of child trauma. You may have to have two or three sessions on childhood trauma.
She established that healing takes time and willingness but moves at the client’s rate rather than that of the program.
Self-Determination
One factor particularly prevalent was defining client success. The context of defining success centered on self-determination, enabling clients in treatment to set goals at their own pace. Coercing goals or setting expectations often creates friction, as noted by Participant # 3. He argued that quantifying statistics for progress in such an intimate and individualized line of work damages the client’s investment, saying:
I’ve gotten to a point now, especially with what I do currently, I define client success by asking the client what is considered successful…What I discovered is that you do want to do things that are going to benefit you, but you want to do them on your terms—got it.
Systemic Issues
Along with ways to streamline the treatment process, the interviewees shared the challenges their clients face. Systemic issues include the accessibility of resources within the treatment system. Although somewhat predictable, these challenges included a need for more affordable housing, involvement in the legal system, and staffing issues. However, deeper layers of information revealed that they involved acquiring resources and systemic failures in responding effectively to individuals involved in the process.
Lack of Cooperation
Participant #3 discussed the damage caused by the siloing of resources and the lack of interagency collaboration.
Perhaps I could help a person get to the next stage, but one of these other silos will not communicate that they have access to a service that I need for a person that I’m providing services to. Maybe I don’t know about this program. Maybe I’ve not heard of it, and a lot of places will keep their resources close to the vest, so they don’t have to share with anyone else…It doesn’t matter where they get the help. That is the person who’s without.
If the process of passing the baton fails to materialize, the forward momentum of the client’s treatment is lost. When the client is the focus of attention, providing appropriate resources should be the top priority.
Dependence
Another area for improvement involves the system’s handling of individual needs. Participant #1 discussed the client’s dependence on family or friends, such as transportation to appointments or providing housing for family court. She emphasized the risk of the client relying on others to meet their housing and transportation needs for treatment, probation, or family court purposes.
A lot of times, they have to rely on family members if they’re willing to help them out. Otherwise, it’s very challenging. … They put a lot of obligations on them that make it very difficult for even someone in sobriety to achieve. Instead of providing a framework for success, the conditions are almost insurmountable unless the client becomes dependent on others.
Treatment failure may be a systemic flaw preventing clients from accessing the necessary resources when needed. Funding was raised as a systemic issue that needs to be addressed, with Participant #5 stating, “…especially in Delaware if a person does not have insurance, it is so hard to get somebody into treatment.” Insurance was addressed in different ways, but the participants shared creative ways that providers navigated those barriers. Participant #4 looked at pro bono work to maintain the client’s treatment, saying, “We can always either write it off or back bill it when they get their insurance back.” Participant #6 took a different approach, mentioning grant funding from the state that permits her autonomy from insurance restrictions. “Luckily, right now, the grant allows me that, which is wonderful, but a short period of time. The insurance companies, that’s a hurdle.”
DISCUSSION
The findings from this study support the existing international literature, suggesting that conditions relevant to this topic in the United States run parallel to those in Canada and Europe. The testimony of the participants verified that many agencies employ recovering individuals in clinical roles, validating their lived experiences and observations. This study explored the range of settings in which recovering professionals serve, with all participants having experienced numerous levels of care. When applied to the research questions, personal recovery experiences at different levels provide the necessary context toward professional competence. Recovering professionals are versatile, demonstrating the ability to adapt to various environments.
The participants described their transitions from active clients to recovering professionals, frequently disclosing the impact of guidance and mentorship on their journeys. In addiction treatment, professionals guide clients toward empowerment, coaching them to achieve personal goals, such as earning a degree, pursuing a career change, and fulfilling their potential. As found by Simbolon’s team,13 this process validates the professional’s recovery while increasing job satisfaction and enriching the treatment experience for both the client and the clinician.
A recovering professional’s intuition interprets client willingness, indicating when and how hard to encourage a client and when distance is needed. Clinical insight into the value of client willingness – or lack thereof – is a critical factor when tailoring services, such as group topics and curriculum use at an agency level, and deepening the quality of conversations. In effect, personal experience enhances the clinician’s ability to translate the client’s motivational cues.
The quality of personal exchanges impacts the types of treatment recommendations a client receives. During the interviews, participants with experience in IOP claimed that they found it effective. Therefore, their recommendations most likely include programs they found effective. Conversely, if a person’s experience in a program was not to their liking, they would describe it in negative terms, discouraging others from attending. Recovering professionals recognize that personal experience impacts factors such as recruitment, retention, and successful completion rates. Agency policies and treatment decisions must remain focused on the client. Recovering professionals emphasize the importance of navigating the network of treatment agencies when helping clients access scarce or highly sought-after resources. They value empathy, as many clients struggle with external factors such as childcare, transportation, or employment, which were challenges they once faced. Rather than considering treatment goal compliance, recovering professionals acknowledge the life challenges facing clients and work to establish achievable objectives.
Public Health Implications
Many of the challenges facing clients in substance use treatment are systemic. This study provides findings of missed opportunities to support individuals who lack essential services, such as transportation or housing. Furthermore, reserving resources to protect agency interests damages the client’s prognosis for continued treatment. Involving recovering professionals when drafting new programs would increase the effective use of limited funds.
Although various best practices, evidence-based models, and publications are readily available, barriers continue to hinder the dissemination of information to where it is needed.16 Communicating this information within the treatment network highlights the importance of relationships with legislative stakeholders may lead to shifts in both the legal system and insurance payments, prompting them to address client challenges more effectively. Accommodations such as consolidating or reducing the burden of office visits offers hope to clients struggling to comply. Evidence-informed practices are effective when sufficient time is allocated for the message to be fully absorbed.
Future policy change could examine the qualitative impact of legislation that responds to systemic obstacles. One example includes legislative changes that are already in effect with Delaware Senate Bill #4. The State of Delaware proposed reforms in probation and legal sentencing, including investing in reentry and housing programs, and reducing probation sentences for lower-priority cases.17 It is vital to remain current on whether legislation validates study results by demonstrating a reduction in barriers faced by clients.
Recommendations
Incorporating the experiences of recovering professionals during individual and group therapy sessions validates the client’s feeling understood and improves the quality of person-centered care. Treatment goals would be person-centered rather than based on expectations to achieve quantified results. Clients are more likely to commit to goals that are relevant.
Providing the professionals an opportunity to use their experience, strength, and hope increases job satisfaction. By nurturing the professional’s experience in the workplace, retention will improve, reducing the impact of the shortage of mental health and substance use providers.18 This is of particular importance in rural areas, where options for treatment are severely limited.
Effective supervision and training are essential to promote sharing and disclosure that remain appropriate, and client centered. Revised treatment regulations can renew how professionals interact in the field while avoiding the stigma and misinformation that could potentially damage the client’s experience.19 The increased focus on peer-centered roles indicates the need to review agency staffing. Recovering social workers and therapists would be instrumental to removing systemic barriers, with a personal bank of rich experience to share.
Future Research
The lack of qualitative studies and the critical need to increase the effectiveness of alcohol and drug treatment suggest a significant gap and need for future research. Areas for potential study include expanding the results of this study in a treatment agency and applying leadership theory to maximize the therapeutic relationship’s influence. Future research could explore the therapeutic alliance as a form of leadership, influencing and encouraging clients to strive towards their treatment goals. Partnering the therapeutic alliance with leadership theory may help determine a pathway toward navigating difficult situations. In Leader-Member Exchange Theory, leaders influence a team by recognizing and enhancing employee potential.20 Adapting this
trait would enhance therapeutic transactions between the client and the team, leading to higher-quality increased responsibilities and client benefits, plus reducing disruptive behaviors, such as early treatment termination.
Another area worthy of exploration is the range of opinions involving Medication-Assisted Treatment. One participant in this study admitted that she was hesitant to accept MAT as an effective tool. Exploring these personal biases may assist in removing the stigma referred to within these interviews.
Limitations
There are inherent limitations in qualitative methodologies, such as small sample size and lack of generalizability. However, steps were taken to mitigate these limitations. The data analysis had a thematic underpinning applied to numerous layers of coding. Involving a research assistant in the coding process increased the trustworthiness of this study. Finally, cultural differences between this study in Delaware and those found in the literature, specifically in European countries and Canada, may influence the interpretation of the data. Comparison or replication studies across the United States to further explore this topic would further strengthen the application of the findings.
CONCLUSION
This paper fills a gap in the literature through a small qualitative interview study of recovering professionals working in the State of Delaware. Recovering professionals use personal skills to enhance therapeutic relationships with clients and inform their clinical practice by facilitating and executing discussions and goals. Through recorded interviews, the participants expounded on the numerous ways in which they recognize encoded information available from client interactions, such as willingness and selfdetermination, and then respond through appropriate sharing and guiding discussions. This study demonstrated the importance of developing responsive policies and legislation to foster therapeutic alliances to enhance treatment outcomes.
Mr. Tallyen can be contacted at: JTallyen@desu.edu
FUNDING ACKNOWLEDGEMENT
AH received partial funding for this manuscript through an Institutional Development Award (IDeA) from the National Institute of General Medical Sciences of the National Institutes of Health under award number U54GM104941.
REFERENCES
1. KFF. (2024). Mental Health in Delaware. Mental Health and Substance Use State Fact Sheets: https://www.kff.org/statedata/mental-health-and-substance-use-statefact-sheets/delaware/
2. Health Resources and Services Administration. (2024). State of the Behavioral Health Workforce, 2024. U.S. Department of Health and Human Services. https://bhw.hrsa.gov/sites/default/files/bureau-health-workforce/stateof-the-behavioral-health-workforce-report-2024.pdf
3 Beck, A., Page, C., Buche, J., Rittman, D., & Gaiser, M. (2018). Scopes of practice and reimbursement patterns of addiction counselors, community health workers, and peer recovery specialists in the behavioral health workforce. University of Michigan School of Public Health, Behavioral Health Workforce Research Center, Ann Arbor. https://www.healthworkforceta.org/wp-content/uploads/2023/07/BHWRC_SOPs.pdf
4 Doukas, N., & Cullen, J. (2010, June). Recovered addicts working in the addiction field: Pitfalls to substance abuse relapse. Drugs Education Prevention & Policy, 17(3), 216–231. https://doi.org/10.3109/09687630802378864
5. Kiepek, N., & Ausman, C. (2023, March). “You are you, but you are also your profession”: Nebulous boundaries of personal substance use. Contemporary Drug Problems, 50(1), 63–84. https://doi.org/10.1177/00914509221132301
6. White, W. (2006). Sponsor, recovery coach, addiction counselor: The importance of role clarity and role integrity. Selected Papers of William L. White: https://www.chestnut.org/resources/06ddde83-ee41-4efa-80c1141e1857a4c0/2006-Sponsor-Recovery-Coach-Addiction-Counselor.pdf
7. Pietkiewicz, I., & Skowronska-Wloch, K. (2017). Attitudes to professional boundaries among therapists with and without substance abuse history. Polish Psychological Bulletin, 48(3), 411–422. https://doi.org/10.1515/ppb-2017-0047
8. Substance Abuse and Mental Health Services Administration. (2023). Incorporating peer support into substance use disorder. In Treatment Improvement Protocol (TIP) Series, No.34. Rockville, MD, US: Substance Abuse and Mental Health Services Administration. https://library.samhsa.gov/sites/default/files/pep23-02-01-001.pdf
9. Rankine, J. (2020). Negotiating an alcoholic identity within the Alcoholics Anonymous twelve-step recovery model: A narrative inquiry. University of the West of England, Faculty of Health and Applied Sciences, Bristol. doi: https://uwe-repository.worktribe.com/OutputFile/5963854
10 Hecksher, D. (2007). Former substance users working as counselors. A dual relationship. Substance Use & Misuse, 42(8), 1253–1268 https://doi.org/10.1080/10826080701446711
11 Novotna, G., Dobbins, M., Jack, S., Sword, W., Niccols, A., Brooks, S., & Henderson, J. (2013). The influence of lived experience with addiction and recovery on practice-related decisions among professionals working in addiction agencies serving women. Drugs Education Prevention & Policy, 20(2), 140–148 https://doi.org/10.3109/09687637.2012.714015
12 Racz, J., Kassai, S., Pinter, J., Benedeczki, P., Dobo-Nagy, Z., Horvath, Z., & Gyarmathy, V. (2015). The therapeutic journeys of recovering helpers - an interpretive phenomenological analysis. International Journal of Mental Health and Addiction, 13, 751–757 https://doi.org/10.1007/s11469-015-9560-3
13 Simbolon, M., Zulkarnain, I., & Ridho, H. (2024). Identity negotiation in recovering addicts who work as addiction counselors (phenomenological study on the Indonesian Addiction Counselors Association North Sumatra Region). 4(6), 795-810. doi:10.55927/mudima.v4i6.9802 https://journal.formosapublisher.org/index.php/mudima/article/view/9802
14 McNeely, H. L., Nelson-Brantley, H., Teel, C., Wright, S., Peterson, M., & Brooks, J. V. (2025, January-March 01). Substance use treatment providers’ perspectives on barriers and facilitators for treatment, recovery, and returning to work for healthcare professionals with nonmedical substance use. Journal of Addictions Nursing, 36(1), 27–35 https://doi.org/10.1097/JAN.0000000000000606
15 Tan, H., Wilson, A., & Olver, I. (2009). Ricoeur’s theory of interpretation: An instrument for data interpretation in hermeneutic phenomenology. International Journal of Qualitative Methods, 8(4), 1–15 https://doi.org/10.1177/160940690900800401
16 Magill, M., Maisto, S., Borsari, B., Glass, J. E., Hallgren, K., Houck, J., Kuerbis, A. (2023, May). Addictions treatment mechanisms of change science and implementation science: A critical review. Alcohol Clin Exp Res (Hoboken), 47(5), 827–839 https://doi.org/10.1111/acer.15053
17 Delaware, A. C. L. U. (2024). Senate bill 4: Probation reform. ACLU Delaware: https://www.aclu-de.org/en/legislation/senate-bill-4-probation-reform
18. Clary, E., Ribar, C., & Weigensberg, E. (2020). Challenges in providing substance use disorder treatment to child welfare clients in rural communities. U.S. Department of Health and Human Services. Office of the Assistant Secretary for Planning and Evaluation. https://aspe.hhs.gov/sites/default/files/private/pdf/263216/ ChallengesIssueBrief.pdf
19 Bensaid, B., Machouche, S., & Tekke, M. (2021). An Islamic spiritual alternative to addiction treatment and recovery. Al-Jāmi‘ah. Journal of Islamic Studies, 59(1), 127–162 https://doi.org/10.14421/ajis.2021.591.127-162
20. Lunenburg, F. (2010). Leader-Member Exchange Theory: Another perspective on the leadership process. International Journal of Management. Business Administration (London), 13(1), 1–5.
Advancing Harm Reduction through Data Mapping: The Role of Delaware’s Overdose Response Center
Brent Waninger, M.Ed. & Edward Schiavi, B.A.
Delaware Division of Substance Abuse and Mental Health
ABSTRACT
Designed in 2022, the Overdose Response Center, was created to provide a centralized, near real-time center for raw data and street intelligence analytics, and deployment operations and coordination of community response assets across the state. As the center began to operate during 2023, it became clear that the utilization of geospatial mapping software was a critical component to providing targeted direction and responses. Today, the center regularly maps relevant data, providing staff with multi-layered analysis of the current situation around the state, allowing us to provide clearly targeted (and personally walk-able) zones for both internal state field teams and partner programs, organizations, and outreach teams.
During the height of the opioid epidemic and related overdose crisis, collectively, Delaware made great strides in becoming data-informed in the use of federal grant funding for our response and actions. Naloxone became widely available to the public, and initiatives were designed and implemented in response to available data. However, more recently there was a desire to shift from being data-informed and become “data-responsive.” This strategy would accelerate beyond just analyzing what happened last year or last quarter, to also look at what was happening last week and last night to direct the actions of today and tomorrow. The Overdose Response Center (ORC) under the Delaware Division of Substance Abuse and Mental Health was the embodiment of that strategic shift. Beginning operation in mid-2023, the ORC provides a statewide hub for both near real-time surveillance and analysis, as well as the coordination of community-level responses to the ongoing opioid/overdose epidemic. A critical component of being ‘data-responsive” leverages modern software tools to complete geospatial mapping and trend analysis. Using these tools, the ORC is able to more effectively support harm reduction strategies by targeting outreach interventions and efforts across the state. In Figure 1, sample overdose data shows the mapping visualization of different types of overdoses and the ability to highlight areas for or targeted previously for outreach.
The ORC securely collects and manages overdose-related data from various emergency medical service agencies, law enforcement agencies, treatment providers, and communitybased organizations. This information is compiled with “street intelligence” collected directly from individuals suffering from Opioid Use Disorder, outreach teams, and treatment facilities across the state. The ORC also incorporates all related information from other state partnerships or sponsored initiatives related to the epidemic, including wastewater testing and drug residue sample testing, to create the most complete picture of the opioid epidemic possible.
Leveraging the state’s existing access to the ArcGIS suite of software products, the ORC analyzes and uploads relevant pieces into a restricted portion of that platform specifically created for ORC use. Each component of information allows the center to create multiple map layers to be added and removed as needed to conduct various types of analysis and trend monitoring. This consolidated information and mapping is then used to create “deployment plans” that guide staterun teams (including the Bridge Clinic and Post-Overdose Response Teams) and our community partners’ outreach efforts to the areas of highest need or of emerging concern across the state. This coordination not only addresses the direct need, it also minimizes duplication of numerous teams self-responding to an area just because they are familiar with it.
Activation and response of these community-level assets can take many forms, but all support harm reduction activities. This can be as simple as conducting naloxone training and distribution to help with the state’s saturation goals, or delivery and discussion of educational materials, to the provision of assessment and treatment services on-site, or training on self-care of wounds triggered by xylazine contamination in the drug supply. The ORC supports data-responsive direction to both general outreach activity or “canvassing” of an entire area, and the targeted response to an individual to offer support and services after a non-fatal overdose. Outreach data sent back to the ORC allows real-time mapping of outreach and harm reduction efforts (figure 2).
Using this approach, the ORC is not only able to identify the areas of the state in the most need of outreach and engagement, but also provide those outreach teams with additional layers of information about that area like population census information, local naloxone training/ distribution partners, and nearby treatment provider locations/offices. With two-way feedback from the variety of outreach teams and partners, the ORC is also able to track trends and changes over time, ensuring coverage of Delaware’s unhoused populations and the movement of encampment sites.
In addition to deployment plans, the ORC publishes bulletins and reports to ensure up-to-date knowledge and understanding of the broadest range of partners. This includes brief one-page summaries of new or emerging substances of concern like xylazine and medetomidine (figure 3), and more recently the monthly Delaware Street Drug Report that identifies trends in street drugs that were sampled and analyzed from across the state (figure 4). This information, combined with the deployment plans gives individuals responding on the ground the best understanding of what they should expect and what they must be prepared for when attempting outreach work (figure 5).
The security protocols and design of the ORC allows the center to receive and digest raw data and street intelligence as rapidly as partners can (or are permitted) to share that information. In addition, the ORC has recently begun
piloting software tools that provide feedback loops directly from workers in the field into the ArcGIS mapping systems being utilized in the center. This allows the ORC to map back over the deployment plans and map layers to know where outreach was successful and impactful. Evaluation of this feedback loop over the next year will be used to directly measure the impact of harm reduction and outreach efforts. This feedback also allows for constant evaluation and reassessment of the deployment plans and pivoting to address emerging areas almost as soon as they arise. This extra layer of feedback and analysis from the field, advances the ORC above most other forms of data-driven and data-informed efforts across the country, and allows the center to truly be “data-responsive,” while enhancing harm reduction efforts of and for Delawareans in all corners of the state.
Mr. Waninger may be contacted at brent.waninger@delaware.gov .
4. The Delaware Street Drug Report.
Figure
Figure 5. Recent Emerging Substances Identified in Recent Delaware Street Drug Reports
Dear Medical Provider ,
The American Cancer Society National Lung Cancer Roundtable (ACS NLCRT), American College of Radiology® (ACR®), Radiology Health Equity Coalition (RHEC) , and Go2 For Lung Cancer have partnered once again for the annual National Lung Cancer Screening Day (“National LCS Day”).
This year’s National Lung Cancer Screening Day is on Saturday, November 8, 2025 In Delaware, we will be encouraging lung screening during the entire month of November The goal of this event is to reduce disparities, promote access to care, and save lives.
Lung cancer is one of the deadliest forms of cancer and is estimated to claim the lives of over 125, 070 Americans this year. Did you know that even though survival rates can be improved significantly by screening, only a small percentage of eligible individuals get screened for lung cancer . In Delaware in 2022, only 24% of those that are eligible reported having a CT scan for lung cancer screening within the past 12 months. Most cases continue to be diagnosed at distant stage, which is harder to treat and decreases survival. In 2017-2021, 45% of new lung cancer cases were diagnosed at the distant stage.
Our purpose for this focus in November is to increase screening access for people who cannot take time off during their weekly schedules to get screened for the early detection of lung cancer.
Primary c are p roviders are the backbone of successful lung screening programs . Join us by supporting National Lung Cancer Screening Day on November 8th and all month long , by referring your eligible patients for screening . Show them you care about their health. Refer them to a nearby screening center today. We appreciate your support this November.
Together, we can make a difference and create a nation where lung cancer is screened for, detected early, treated effectively, not stigmatized, and conquered!
Let’s work together to save lives!
Find a screening site near you : Lung Cancer Screening Locator
For more information visit the National Lung Cancer Roundtable and the National Lung Cancer Screening Day to register for free resources!
FOCUS Fogarty-supported researchers use food as medicine to address tuberculosis & type 2 diabetes
NATIONAL
PROFILE
Gwenyth Lee, PhD, works at the intersection of infectious disease & nutrition
Q & A
Christine Sizemore, PhD, provides a pragmatic perspective on global health
NEWS
LAUNCH orientation presentations address capacity building and career development
INSTITUTES OF HEALTH • DEPARTMENT OF HEALTH AND HUMAN SERVICES
Global Health Matters
FOGARTY INTERNATIONAL CENTER
Dietitians in Benin develop meal plans tailored to local culture and local tastes.
BUILDING CAPACITY FOR Research on Sexually Transmitted Infections
IN LOW- AND MIDDLE-INCOME COUNTRIES
By providing funding and protected time for both mentors and trainees, Fogarty has played and continues to play a crucial role in the development of research capabilities worldwide.
I STARTED MY FEDERAL GOVERNMENT CAREER three decades ago in the CDC Division of Sexually Transmitted Disease Prevention, so I was excited to travel to Montreal in July for the World Congress of the International Society for Sexually Transmitted Diseases Research and the International Union against Sexually Transmitted Infections.
For the convention, I’d organized a symposium that emphasized how the burden of sexually transmitted infections (STIs) in low- and middle-income countries (LMICs) is eight-fold higher than in high-income countries. This means the need for STI research in LMICs is substantially higher, yet opportunities are increased as well. Research priorities include developing affordable pointof-care diagnostics as well as novel antibiotics, antivirals, and vaccines; investigating antibiotic resistance; optimizing behavioral interventions; integrating STI services with other
health programs; using digital health solutions; and conducting research of at-risk groups such as teens, sex workers, men who have sex with men, and people living with HIV.
The symposium attracted a standing-room-only crowd and began with a presentation by Dr. Le Minh Giang and his mentee, Dr. Bùi Thị Minh Hảo, from Hanoi Medical University in Vietnam. Their Fogarty D43 research training grant is building on the national HIV prevention program (with support from PEPFAR).
Next, Dr. Jenell Stewart from Hennepin Healthcare in Minnesota spoke on behalf of herself and Dr. Elizabeth Bukusi, a former Fogarty trainee and current Fogarty grantee. They’ve been building research capacity in Kisumu, Kenya, based on the work of the late Dr. King Holmes, a former Fogarty grantee and board member and an early leader in AIDS care and research.
Next up was Dr. Patty Garcia, a
former Fogarty trainee and grantee from Universidad Peruana Cayetano Heredia, Peru, who spoke about her own early research as a mentee of Holmes. Their work led to the development of a robust HIV and STI clinical care and research infrastructure in Peru. The final presenter, Dr. Álisson Bigolin, described how, with the support of mentors, he now leads STI diagnostics development in the Brazilian Ministry of Health.
Co-moderator Dr. Francis Ndowa, director of the Skin & Genito-Urinary Medicine Clinic in Zimbabwe, underscored the need for translating evidence-based research findings into practice, while co-moderator Dr. Kees Reitmeijer, an editor of the journal Sexually Transmitted Diseases, highlighted the role of journals in supporting early-career researchers worldwide.
Perhaps surprisingly, these various presenters from Asia, Africa, and Latin America shared commonalities. Notably, they all started by developing public health and clinical infrastructure and later added a research component, which could then support research training. All believe the commitment of both U.S. and LMIC mentors as well as the dedication of their mentees has been instrumental for growth.
By providing funding and protected time for both mentors and
trainees, Fogarty has played and continues to play a crucial role in the development of research capabilities worldwide.
Undoubtedly, STI research conducted by former Fogarty trainees in all corners of the globe has improved health not only worldwide, but also in the United States, where it has informed STI prevention and treatment guidelines and practices and contributed to the development of STI diagnostics and vaccines that benefit all humanity.
Afterwards, Bigolin introduced me to his mentor, Dr. Angelica Espinosa Miranda, STI Unit Coordinator in the Brazilian Ministry of Health, who mentioned that she is also a former Fogarty trainee. Later, I met Dr. Sunil Sethi, a professor at the Post Graduate Institute of Medical Education and Research in Chandigarh, India. He’ll be hosting the 2027 World STI & HIV Congress and we discussed including a day-long session on research capacity building. He is also a former Fogarty trainee!
Such chance conversations underscore the ways in which Fogarty, by pursuing its vision of capacity building, has extended the frontiers of health research and disseminated scientific advances across the globe. I expect more former Fogarty trainees will be attending the 2027 World STI & HIV Congress in India.
Fogarty International Center
National Institutes of Health Department of Health and Human Services
July/August 2025
Volume 25, Issue 4
ISSN: 1938-5935
Publishing Director Andrey Kuzmichev
Editor-in-Chief
Susan Scutti
Contributing Writers/Editors
Mariah Felipe-Velasquez Amanda Stearns
Digital Analyst Merrijoy Vicente
Graphic Designer Carla Conway
CONNECT WITH US
The Fogarty International Center is dedicated to advancing the mission of the National Institutes of Health by supporting and facilitating global health research conducted by U.S. and international investigators, building partnerships between health research institutions in the United States and abroad, and training the next generation of scientists to address global health needs.
profile
IQUITOS,
PERU,
IS OFTEN DESCRIBED AS THE LARGEST CITY IN THE WORLD THAT’S INACCESSIBLE BY ROAD,
says Gwenyth Lee, PhD, assistant professor in the Department of Biostatistics and Epidemiology at the Rutgers School of Public Health.
“So if you take a big boat up the Amazon, Iquitos is about as far as you can go before the river gets a lot shallower and you have to switch to a small boat.” Situated east of the Andes in Loreto province, it is home to more than 150,000 people and served as a major port for the global
4
4 GLOBAL HEALTH MATTERS
rubber trade during the 19th Century.
“All of my formative research— master’s, PhD, postdoc—has been in the general area of early child health,” says Lee, who lived in Iquitos on and off for more than two years while working on her PhD. “Spending that amount of time there allowed me to
Gwenyth Lee PhD, MPH
Fogarty Fellow 2014-2015
U.S. institution
Johns Hopkins Bloomberg School of Public Health
Foreign institution
Asociacion Benefica Prisma (NGO)
Project
Impact of enteric infections on the growth and development of children living in the Peruvian Amazon
Current affiliation
Rutgers School of Public Health
make certain connections to child health and become interested in questions based on observations or discussions with people.”
Iquitos, then, was a natural setting for her Fogarty LAUNCH Fellowship.
Investigative independence
Lee’s project examined the impact of enteric (intestinal) infections on the growth and development of a cohort of children in Iquitos. Specifically, she looked at how enteric infections, and other exposures related to nutrition, impact child growth and development. Her work used social network analysis to evaluate how social ties within communities function to improve food security.
The project allowed her to continue her research in a familiar field, yet it also enabled her to transition to nutritional epidemiology, which examines child development in relation to diet, a field of interest to Lee. “My fellowship was very much a building block, scientifically, to the projects that I work on now.”
Photo courtesy of Gwenyth Lee
Gwyneth Lee gathers with her colleagues while working on the EcoMiD project in Ecuador.
Her Fogarty project also pushed her towards independence. “Field work wasn’t completely new to me, but what was new is that, increasingly, I was left to figure out what I wanted to do and then run with it.” She also managed her own administrative paperwork, a significant advance. “It was the first project where I had a large number of people working directly for me—during my PhD, I had two people helping me collect data, for the Fogarty project, eight or 10. My mentors started to, in an appropriate way, step back and make me responsible as a project manager.”
Results of her fellowship year also include publications, presentations, and landing a post-doctoral position.
“Being in-country was very helpful for finding those opportunities and networking and disseminating my research more readily.” She continued working with her Peruvian colleagues at UPCH during her postdoc training funded by Fogarty’s Inter-American Training for Innovations in Emerging Infectious Diseases program.
Subsequently, she began a research faculty position at University of Michigan School of Public Health, where she received a K01 award from the National Institute of Allergy and Infectious Diseases. Her Ecuadorbased project, Dynamic modeling of antagonism between enteric infection and undernutrition in infancy, officially ended in May but continues under a no-cost extension.
“I work as a co-investigator with Dr. Joseph Eisenberg and Dr. Karen Levy for Enteropatógenos,
Crecimiento, Microbioma, y Diarrea (EcoMiD), a pediatric cohort study that looks at environmental exposures and child health outcomes with a specific focus on the microbiome across rural and urban communities in Ecuador.” (The microbiome is the community of microorganisms that can be found living together in your gut.) Offered a position at Rutgers University, Lee transferred and began working with another early career investigator, Shauna Downs, an associate professor in the Department of Health Behavior, Society and Policy. Combining interests, they received funding from the Eunice Kennedy Shriver National Institute of Child Health and Human Development for a project in Kenya that aims to reduce teen malnutrition.
One year into that project, Lee has begun to steer students and colleagues to apply for LAUNCH fellowships. “It’s invaluable for people interested in research, especially global health research, but even research in general.”
Traditional diets
The fruits of global health research recompense Americans in two ways, says Lee. “It provides training
opportunities for American students while advancing general scientific knowledge.”
One example of this is her Ecuador project. “It’s increasingly understood that the American microbiome is affected by our diets and exposures to our environment. Now that is not necessarily representative of the way humans have lived for thousands of years, right?” Researchers who study the microbiome in Ecuador encounter an urban-to-rural gradient, with part of the population eating a more westernized diet and living a more westernized lifestyle, while the diet and lifestyle of river communities, including residents of Iquitos, reflect regional traditions.
“ SO THERE’S A VARIETY THERE THAT WOULD BE HARD TO FIND IN THE U.S. AND WE CAN LEARN FROM THAT AND POTENTIALLY APPLY LESSONS LEARNED BACK IN THE STATES.”
Gwenyth Lee’s global work focuses on infectious disease and nutrition.
(Left) Lee outside Hospital Esmeraldas in Ecuador (Right) Lee (in front, writing) contributes to sample collection for the EcoMiD project in Ecuador.
FOCUS I NUTRITION
Mon plan de repas OSanDiaBé
RESEARCH EXPLORES FOOD AS MEDICINE
GLOBALLY & IN THE U.S.
“My meal plan” is a dietary guide tailored to the tastes and preferences of patients in Benin. Courtesy of Halimatou Alaofè
Good nutrition is crucial for maintaining health. A balanced diet fuels the body and also lowers the risk of illness, including type 2 diabetes, heart disease, and infectious diseases.
Earlier this year, the U.S. Department of Health and Human Services (HHS) crafted a plan for ending chronic disease in the U.S. The Make Make America Healthy Again (MAHA) initiative aims to ensure that all
Americans live longer, healthier lives, supported by systems that prioritize prevention, wellbeing, and resilience.
In particular, the HHS’ report, Make Our Children Healthy Again: Assessment, summarizes the decline in children’s health and identifies potential drivers of rising disease where progress is most likely. First among these is “poor diet.”
In light of the MAHA agenda, this
CULTURALLY RELEVANT MEAL PLANS LEAD TO BETTER HEALTH
STANDARD NUTRITION ADVICE OFTEN FAILS TO RESONATE WITH LOCAL PREFERENCES AND PRACTICES IN LOWER-INCOME NATIONS. Unfortunately, this leads to poor diet adherence and suboptimal health outcomes, says Halimatou Alaofè, PhD, associate professor at the University of Arizona. Her International Research Scientist Development Award (IRSDA) Program project in her native Benin aims to “bridge that gap between advice and practice by designing a culturally relevant, sustainable nutrition intervention that can empower patients in low resource settings to improve their dietary adherence.”
Specifically, her research focuses on long-term nutritional management of type 2 diabetes, which develops when the body cannot use insulin correctly, leading to excess sugar in the blood, in turn causing damage to the eyes, kidneys, nerves and heart.
Tailored plans
An alarming increase in type 2 diabetes-related illness and mortality is occurring in Benin, a west African country that borders Nigeria and sits just south of the Sahara. Diabetes prevalence has quadrupled in this French-speaking country of 14.7 million people, from 3% to 12.4% over the last decade, reaching as high as 22% in some regions. The negative effects impact not only those who live with the condition, but also their families and the healthcare system, says Alaofè.
Small scale studies of nutritional interventions for type 2 diabetes conducted in Benin have found very low adherence to the recommended diet. “Just 20%, but it might be even lower,” says Alaofè, who suspects that the suggested food plans are difficult to adhere to or unacceptable for patients. When developing a dietary intervention, researchers need to include general guidelines yet also consider the many
issue’s FOCUS: Nutrition spotlights two Fogarty-supported projects centered on using food as medicine—one seeking to improve the health of patients with type 2 diabetes in Benin, the other aiming to prevent and treat tuberculosis in Tanzania.
The researchers believe that these nutritional studies, despite their far-off locations, have direct implications for Americans.
Dietitians learn how to measure blood pressure.
additional factors that encourage uptake of an eating plan.
For example, medical nutrition therapy, which is formulated by a registered dietitian or nutritionist, helps patients manage specific health conditions. The evidence based process begins with a clinical assessment, followed by a diagnosis and intervention plan, and then requires monitoring. For this to work, personalization is required.
“Culturally tailored nutrition therapy has proven particularly effective with type 2 diabetes. It recognizes the connection between food, dietary habits and culture, and understands that effective behavior change necessitates that an intervention be both meaningful and relevant to each patient,” says Alaofè.
Courtesy of Halimatou Alaofè
In short, food preferences and cultural beliefs are baked into each individual plan.
Challenges
Alaofè sees a chasm between the official guidelines and actual patient behavior. When listening to people, she often hears a “lack of awareness at the patient level, but also at the healthcare provider level.”
Before beginning her IRSDA project, she conducted formative research which included focus group interviews with stakeholders. She found that nutritionists often “present the idea that Benin doesn’t have good local resources. But it’s not true. We have seasonal fruits and vegetables and many of our national dishes are vegetable-based.”
Her formative research also showed that patients don’t want to participate in projects delivered via healthcare systems because “healthcare means death. Can you imagine? If you provide a service at the healthcare level, the population will never come and listen to you,”
FOCUS
In turn insufficient patient interaction leads to out-of-touch recommendations. “We still say, ‘eat five portions of fruit and vegetables.’ We still say, ‘one spoon of oil.’ What does that even mean, when in Africa the food is shared?”
Alaofè asked one patient focus group: Why don’t you eat more fruits and vegetables?
The answer: “Fruits and vegetables are for the poor. When you have a guest, you have to put out a rice dish or spaghetti.” Carb-based, westernized food confers prestige, she notes.
“In the media, everywhere, nutritionists talk about obesity and a good diet, but how do you convince people to eat good food, when they believe that eating a particular carb means they belong to a higher status?”
Having examined perceptions of obesity, she found that people reject the negative connotations of “obesity” because for them, weight “is related to wealth and to attraction and to fertility. Women say, ‘I have to gain weight when I’m pregnant,’ so how do I convince those who are overweight to lose pounds to help with glycemic control [lowering blood sugar]?”
Nutritional communication strategies need to change, says Alaofè. “We need to adjust so our patients don’t run from us.”
Family matters
Alaofè, who previously worked as a lab technician in both rural and urban areas of Benin, saw first-hand how nutrition intersects with disease prevention and long-term health outcomes. Overall she hopes to better understand the biological,
“ MOST PEOPLE DIE DUE TO UNDERNUTRITION, NOT BECAUSE OF THE DIABETES—THEY DIE BECAUSE THEY DON’T KNOW WHAT TO EAT.”
social and policy dimensions of diet, while contributing to evidence based solutions to improve population health.
Alaofè believes her project will be relevant to many U.S. citizens on whose behalf her research is funded.
“We have low health literacy and under-resourced communities facing food insecurity who need help to access adequate and nutritious food.”
Although her project is not yet complete—it will end in 2027—Alaofè has already published three papers. One paper examines best practices for engaging social networks in nutrition interventions. Another shows how both culture and family relate to diets.
“Most people die due to undernutrition, not because of the diabetes—they die because they don’t know what to eat. Families don’t know how to support the patient, so we have to help them do that.”
It’s not necessary to require the entire family’s constant participation, but family members need to be invited along whenever there’s crucial information to be shared, says Alaofè. “People become isolated when they have diabetes. They feel they have to solve it alone, when, really, they need the support of their families.”
Halimatou Alaofè, PhD.
NUTRITIONAL RESEARCH IN TANZANIA MAY HELP COAL MINERS
IN THE U.S.
Chronic respiratory disease, including asthma, is a common diagnosis in the United States—in fact, it’s the fifth most common cause of death. By contrast, tuberculosis (TB) is an unusual diagnosis in the U.S.
Yet TB research conducted in Tanzania will likely prove very beneficial for Americans, say Dr. Scott Heysell, a professor of international medicine at University of Virginia (UVA), and Dr. Stellah Mpagama, a physician-scientist at Kibong’oto Infectious Diseases Institute in Tanzania. They are co-principal investigators of a Fogarty Global Infectious Diseases Research Training Program project.
“In the U.S. and where I work in Appalachia, there’s a lot of coal mining,” explains Heysell. In Tanzania, there’s a roughly equal rate of mining as in Appalachia (though for different commodities), and so people develop lung disease from silicosis or other environmental aspects of the industry just as they do in the U.S.
This shared history of similar environmental exposures and chronic lung disability suggests Tanzanian research will likely translate to the American context. Studying how a targeted nutritional intervention, given either before or during a TB episode, impacts chronic lung disease “will possibly have direct implications for any nation where chronic lung disease is common,” says Heysell.
Learning by doing
Ancient in origin, tuberculosis is a serious infectious illness affecting the lungs. It’s caused by bacteria that spreads via droplets propelled into the air when an ill person coughs or sneezes.
Some people who inhale TB germs have strong immune systems, so their bodies successfully fight off disease. Others have weaker systems and so disease develops, leading to weight loss and possibly wasting.
“Malnutrition is a consequence yet also a cause of tuberculosis—it is the leading risk factor for developing tuberculosis,” says Heysell. People who are undernourished lack a healthy immune response, so, following exposure to germs, they’re likely to progress to disease, which leads to a worsening of their famished condition.
This bidirectional relationship
between sustenance and disease is where Heysell and Mpagama center their TB project.
Mpagama says, “Our research explores all forms of nutritional status in TB patients to understand how nutrition influences disease outcomes.” Undernutrition and poor nutrition are closely related but distinct, she explains. Undernutrition is defined as inadequate food intake that leads to deficiencies in essential nutrients and then presents as wasting, stunting, or being underweight.
“Malnutrition is a consequence yet also a cause of tuberculosis—it is the leading risk factor for developing tuberculosis.”
Photos courtesy of Scott Heysell
Drs. Stellah Mpagama & Scott Heysell
Grant writing workshop and data science bootcamp, Moshi, Tanzania 2024
Courtesy of Scott Heysell
“Malnutrition is a broader term that includes both undernutrition and overnutrition—where excessive or imbalanced intake (such as too much sugar, salt, or fat), often without meeting essential nutrient needs, leads to overweight and obesity.”
Overnutrition can lead to diabetes, where high levels of blood sugar affect immune cell function, impairing the body’s ability to defeat infections.
Heysell’s and Mpagama’s project will train six post-doctoral candidates to become independent researchers at leading institutions across the country including Kibong’oto Infectious Diseases Hospital, the Kilimanjaro Christian Medical University College and Kilimanjaro Clinical Research Institute, Muhimbili University of Health and Allied Sciences, and the University of Dodoma. Pursuing separate research plans, each trainee will investigate how the gut microbiome, nutritional interventions, pulmonary rehabilitation, chronic lung disease, and the bacterial infection of TB interact and intertwine.
“Our role is to provide guidance, mentorship, and encouragement to help them build confidence and pursue their professional goals,” says Mpagama.
Why Tanzania?
Mpagama’s and Heysell’s training grant began in March 2022 and ends in February 2027, by which time each
FOCUS
trainee should be capable of competing for National Institutes of Health grants and other global funding, setting research agendas, and overall contributing to policymaking and to the community. “Two of the six total postdocs in the earliest cohort are just finishing their projects and the latest cohort just started,” says Heysell.
Metrics of success include academic promotion, development of a research team, and grant submission and receipt. Heysell says, “So we’ve had a fair amount of success; those who started at the beginning have been academically promoted and their research teams have grown. They’ve published scientific papers and submitted research grant proposals to NIH and other funders. They haven’t yet received word back, so it’s too early to determine the success of those grants.”
Training in Tanzania, a country with a high burden of TB, is crucial because TB needs to be studied in endemic areas (where it’s most common). “While tuberculosis exists in the United States—for instance, a little over 10,000 people were diagnosed with the disease in 2024—we need a much greater scale of impact and severity of disease presentation to really understand scientifically how to intervene,” says Heysell.
Tanzania is also a country with high rates of undernutrition. “We need to understand how undernutrition leads to TB disease, and then how we might target and treat undernutrition either before tuberculosis develops or during the disease course itself,” Heysell explains.
Building the research workforce in Tanzania is an equally important goal. “The approaches, findings, and the
frameworks we develop are designed to be transferable and applicable to other diseases, including pandemics and other health threats on and outside the continent,” Mpagama says.
Conducting research in Tanzania provides opportunities not found in the U.S., but there are snags as well, says Heysell. “Getting the timeline right is one challenge. For instance, we think we’ll be able to do this in two months when in fact it takes six because of the regulatory environment or getting something shipped and having it arrive on time with the proper paperwork.”
“The long-term relationship that UVA has established with partners in the region facilitates a lot of the work that would be more difficult if we were starting from scratch,” says Heysell.
Nutritional challenges
Mpagama says the current U.S. administration is addressing poor nutrition as a national health concern, “so the methodologies and key insights generated from our work may be applicable—either directly or indirectly—in the American context.”
She adds, “There is also an opportunity to expand this research to the U.S. to address its own malnutrition challenges. This would produce valuable cross-country comparisons that help reveal common, underlying mechanisms and inform more effective strategies for addressing malnutrition in both local and global settings.”
Heysell concludes, “Through the work we’re doing in Tanzania, we’ll be able to understand how a nutritional intervention affects the immune system in an important way.”
10 GLOBAL HEALTH
Scott Heysell at a Tanzanian research symposium.
Christine F. Sizemore, PhD
Q A&
A pragmatic perspective on global health
Christine Sizemore retired from her position as the director of Fogarty’s Division of International Relations (DIR) on April 30. Her career began in the biopharmaceutical industry, where she worked in drug discovery and development. Prior to joining Fogarty in 2018, she spent 18 years at the National Institute of Allergy and Infectious Diseases (NIAID) as chief of the Tuberculosis, Leprosy and Other Mycobacterial Diseases section. Sizemore received her Master’s degree in Biology and her Ph.D. in Bacterial Genetics from the Friedrich Alexander Universität in Erlangen, Germany.
What was your first job at NIH?
AI started as a program officer in the tuberculosis (TB) program at the National Institute of Allergy and Infectious Diseases (NIAID) in 2000. It was an opportunity to work on a much larger scale and on the full spectrum of research and product development for TB and other mycobacterial diseases. The job fit me to a T. Along with being practical, I’m a big picture person. I like seeing and making connections and figuring out strategy to fill gaps in knowledge in the most straightforward and practical way. At first, there were just two of us, but once we began to strategically grow the program and more program officers and medical officers joined the team, we became a Section within the Division of Microbiology and Infectious Diseases and I was named Section Chief. I remained in that role until I became the director of DIR in 2018.
Do Americans benefit from NIHfunded research in low- and middle- income countries (LMICs)?
When I was at NIAID, I worked a lot with LMICs, because TB is a
disease of poverty. I learned very quickly that the way scientists from lower resource countries think and the way they approach challenges is more pragmatic and often more outcome-oriented. What we call “neglected diseases” are very real for them and any solutions they can develop will have real impact for their communities. They see interventions or programs that work at the local level as worthwhile even if they do not scale globally. This has been a challenge for some very innovative projects criticized for not being “global enough” despite making a huge difference for local communities.
This practical thinking is a great complement to the science that is conducted in richer countries where doing research is not uncommon.
If we want to crack the hard nuts in research, then the two sides must work together—the pragmatists and the technologists. Collaborations between low- and high- income countries give investigators a lot of technological access, including large data centers and large infrastructure,
all of which are necessary to holistically tackle a problem. But when it comes to direct patient outcomes and impact, you need to start with the pragmatism of LMIC researchers who have the experience and insights into what is needed to make prevention, diagnosis or cure a reality.
What do you tell global health researchers?
We would do well by communicating outside a narrowly-focused cluster of like-minded individuals. For example, try to explain the relevance of your scientific work to your non-scientific neighbors and take their questions seriously. If you can’t answer, “Why does that matter?” in a way that resonates with them, then more introspection may be needed.
To really understand a disease and what it means, you need to go to where it is. My first trip to Africa showed me what it means to have TB as a patient, as a community and what TB means for healthcare providers— what infrastructure is available, what it takes to get your drugs and finish months’ worth of treatment, and what nurses and doctors, as well as community health workers and families do, to help patients. That immediately puts a different perspective on the utility of a fancy, sensitive diagnostic machine vs. a low tech, easy to use, fast diagnostic test. After that trip, I never thought about my job the same way again.
NEWS&Updates
Resolute
vision:
Caring for casualties in low-resource conflict settings
“When people think of military trauma care, they often think of what existed in Iraq and Afghanistan. But that paradigm has shifted,” says Hannah Binzen Wild, a former Fogarty fellow whose project in Burkina Faso focused on improving casualty care for patients with conflict-related injuries.
Unlike the wars in the Middle East, irregular warfare as well as large-scale combat operations between great powers will not be characterized by air superiority or intact echelons of care. Instead, U.S. military trauma care personnel may face conditions resembling those seen in Burkina Faso: specifically, prolonged transportation times, restricted supply chains, and severe resource limitations.
Solutions devised by trauma care personnel in Burkina Faso reflect long years of experience with warfare in a context that might more closely resemble what the U.S. may face in the future. “It would be ideal to synthesize these lessons, which can be beneficial to the U.S. for the planning and preparedness of its military, while also providing more resources and technical advisory support to personnel in lowresource conflict settings,” says Wild. Providing care during conflicts Wild, now a general surgery resident at the University of Washington, spoke at July’s orientation for Fogarty’s Launching Future Leaders in Global Health Research Training Program. As part of her own Fogarty fellowship in Burkina Faso, she worked on a range of proposals, all focused on trying to
improve casualty care for patients with conflict-related injuries.
“The formal project was piloting integration of explosive ordnance risk education with community first aid responder training in communities affected by the threat of IEDs (improvised explosive devices),” says Wild.
Led by Dr. Nicolas Meda, a professor at University of Ouagadougou in Burkina Faso, Wild’s team conducted this pilot through a collaboration with the Mines Advisory Group, a global advocacy group. (Mine action generally comprises explosive ordnance detection and clearance, risk education, and victim assistance.)
With their networks of community liaisons, charitable mine action programs already possess a platform to deliver community first-responder training in conflict and post-conflict settings. Programs like the Burkina Faso pilot are now underway in Syria, Afghanistan, and Mozambique. The Antipersonnel Mine Ban Convention recognized the value of merging community first responder training with explosive ordnance risk education and added an integrated program to its most recent action plan.
During her Fogarty fellowship Wild also collaborated closely with local military surgeons including Dr. Yves Sanou and Dr. Yves Aziz Nacanabo. The team conducted one of the largest analyses of local casualties in the Sahel to date (roughly 1,400), filling a longstanding evidence gap on casualty care within local health systems.
The team is also studying other key casualty care problems such as tourniquet application and blood availability.
One life’s mission
Wild discovered her passion in life at a young age and never wavered from it.
“I was five years old during the Rwandan genocide and, being an early reader, I learned about it and could not comprehend how people knew that this was happening in the world and moved on with their lives.” As she grew older, Wild read about conflicts taking place in Bosnia and in the Middle East. “I decided to spend my life trying to be useful in this type of setting.”
Though her passion places her in harm’s way, Wild does not dwell on this. “I calculate and moderate risk as much as I can. But the purpose of my existence is making a contribution in this environment, so when you’re lucky enough to be doing exactly what you’re built to do and want to do, personal risk factors differently.” She notes that her colleagues in low-resource conflict settings provide care for the wounded under extraordinarily challenging conditions with little recognition. “I follow the path that I think will make me most effective in mitigating human suffering,” says Wild.
Courtesy of Hannah Binzen Wild
Wild and Colonel Bassinga in the operating room
NEWS&Updates
What do you mean when you say capacity building?
“I didn’t know what capacity building meant until I went to Uganda, and then someone said that phrase to me every hour,” says Dr. Yukari Manabe, a professor of medicine at Johns Hopkins University School of Medicine. Between 2007 and 2012, she served as head of research at the fledgling Infectious Diseases Institute (IDI), founded in Kampala in 2002.
“The research capacity building pyramid became the focus and the guide of everything that occurred at the institute when I worked there,” says Manabe. At the top are the easy things to accomplish, such as bringing in tools, equipment, and research money. The next step on the pyramid is skills. “So equip the person, right? We all know how to do that with courses and training,” says Manabe. Harder tasks to complete—such as developing a core staff, infrastructure and systems—requires the help of international faculty to fill specific gaps and to provide mentorship. The final step encompasses the most difficult goals, including comprehending and interpreting local context (to appropriately assist the country’s Ministry of Health) and building enduring partnerships.
As it matured, the institute necessarily updated its strategic plan, says Manabe. The first plan reflects “the era of dependence. It’s narrowly focused. You’re still trying to build a critical mass of talent and training key staff abroad. Grants are led by external partners.”
The second strategic plan reflects a new era, that of independence. “We
could replicate most things in-country. We’d partnered with policymakers. We had key staff and a larger group of funders. We started to disseminate knowledge to others on the continent.” With its third strategic plan, the institute entered the era of interdependence. “We’ve become a national node within continental networks. We have global and regional links and sustainable funding. We get major grants directly. Talent comes to us.”
Today, IDI is considered a true center of excellence able to foster independent researchers, says Manabe, who spoke to Fogarty fellows attending the Fogarty’s Launching Future Leaders in Global Health Research Training Program orientation in July. “Now people try to steal [talent] from us, which is the surest sign of success.”
Cascade effect
U.S. research dollars go farther in places where things happen at a much higher frequency, says Manabe. For example, congenital syphilis has risen precipitously over the last decade in the U.S., still it’s more efficient and less expensive to study syphilis in a hot spot where the prevalence is up to 30% compared to 0.01% in the U.S. “Money going overseas actually comes back to benefit people in the U.S. afterwards.”
Currently, as director of Johns Hopkins’ Center for Innovative Diagnostics for Infectious Diseases, Manabe focuses on point-of-care diagnostics, which enable health
care providers to test and treat patients within a single visit, rather than waiting days for test results (with patients needing to make additional visits).
Point of care diagnostics “exploded” during COVID, says Manabe. (The NIH’s Rapid Acceleration of Diagnostics program was a multi-billion-dollar investment in COVID-19 testing methods.) She now urges companies to consider using the platforms created during the pandemic when creating new diagnostics for other diseases instead of wasting “this investment that American taxpayers have already made.”
So how does Manabe define capacity building today? “It means friends and colleagues—cultivating your network through training. It also means just getting things done and having a public health impact. You train a few who go on and train 10 and that leads to hundreds of people trained who have an impact on thousands.”
This cascade effect is the joy of capacity building, she says.
“IN SOME PLACES, THEY NO LONGER NEED US AS MUCH AS THEY USED TO, AND THAT MAY BE DIFFICULT EGOTISTICALLY, BUT MAYBE THE SIGN OF REALLY HAVING MADE A DIFFERENCE IS WHEN YOU TEACH YOURSELF OUT OF A JOB.”
Courtesy of Yukari Manabe
Yukari Manabe, MD
The Infectious Diseases Institute in Kampala, Uganda, used this capacity building pyramid as a guide.
people
Community
Adnan Hyder tapped by BU School of Public Health
Boston University has appointed Dr. Adnan Hyder the Robert A. Knox Professor and next dean of its School of Public Health beginning fall 2025. Hyder’s Fogarty- and National Institutes of Health-funded research has contributed to the global understanding of the epidemiological burden, risk factors, potential interventions, economic impact, and socio-cultural correlates of noncommunicable diseases and injuries globally. Currently, Hyder is senior associate dean for research and innovation and professor of global health at The George Washington University Milken Institute School of Public Health.
Simone Badal honored with a Sabga Award
The Anthony N. Sabga Caribbean Awards for Excellence has selected Simone Badal, MD, for this year’s Science & Technology laureate. Badal, a senior lecturer at The University of the West Indies, Mona, has been recognized for her work in developing Caribbean-specific cancer cell lines. Her research led to the creation of the first prostate cancer cell line derived from a Caribbean man, addressing a gap in cancer research, where models have historically focused on Caucasian populations. Badal, a Fogarty Emerging Global Leader, has more than 45 peer-reviewed publications.
Katherine O’Brien wins Albert B. Sabin Gold Medal
The 2025 recipient of the Albert B. Sabin Gold Medal is Katherine O’Brien, MD, for her work in the licensure and global introduction of vaccines against pneumococcal disease, rotavirus, and respiratory syncytial virus. O’Brien is widely considered a pioneering global health leader whose innovative work in vaccine access and policy has transformed immunization programs worldwide. Previously, she served as an Epidemic Intelligence Service officer at the U.S. Centers for Disease Control and Prevention and led vaccine research and development initiatives at the Johns Hopkins Bloomberg School of Public Health. Her past work includes large-scale vaccine impact studies and clinical trials.
Abdoulaye Djimdé wins Hideyo Noguchi Africa Prize
The Hideyo Noguchi Africa Prize in Medical Research has been awarded to Abdoulaye Djimdé, MD, director of the Parasites & Microbes Research & Training Center at the University of Science, Techniques and Technologies of Bamako, Republic of Mali. Djimdé is a Fogarty grantee who has also been supported by the National Institute of Allergy and Infectious Diseases for his efforts to combat infectious and other diseases in Africa. The award recognizes his work in the areas of treatment and control of malaria as well as training of young researchers in African countries.
Barbara Sina secures bioethics leadership award
The 2025 Oxford Global Health & Bioethics International Conference honored Barbara Sina, PhD, with a Global Health Ethics Leadership Award. Sina serves as acting director of Fogarty’s Division of International Training and Research. This annual award recognizes a member of the bioethics community who has made immense contributions to the advancement of the field, often under challenging circumstances. The selection committee noted that Sina’s efforts have shepherded vital initiatives across the training, research and policy/practice spectrum while also yielding lasting benefits for many.
HEALTH Briefs Global
Gut microbiome study includes previously under-sampled populations
In 2007, the Human Microbiome Project (HMP) set the goal of characterizing the human microbiome and measuring its contribution to disease. Large cohorts in high income countries have been well represented in HMP studies, yet low- and middle-income nations, which account for nearly 84% of total population, have been under-represented; this reduces the generalizability of HMP’s conclusions. To help rectify this, Stanford’s Dr. Dylan G. Maghini conducted a cross-sectional gut microbiome study sampling 1,801 women from Burkina Faso, Ghana, Kenya, and South Africa for her Fogarty fellowship project. Using shotgun metagenomic sequencing—a technique that enables microbiologists to detect both the bacterial diversity and the abundance of microbes in the gut—Maghini’s team identified taxa (hierarchical groups of microbes) with geographic and lifestyle associations and also an HIV infection signature defined by taxa not previously linked to HIV. The study is published in Nature.
How do newly approved vaccines affect RSV hospitalizations?
Each year respiratory syncytial virus (RSV), which usually causes mild, cold-like symptoms, leads to 1,500 to 2,800 hospitalizations per 100,000 infants in the U.S.
A research team, led by Fogarty’s Chelsea Hansen, used mathematical modeling to examine impacts of newly introduced immunization strategies on RSV hospitalizations in King County, Washington. (Beginning in 2023, the CDC’s Advisory Committee on Immunization Practices recommended a monoclonal antibody or passive vaccine, nirsevimab, for routine use in infants and a single dose of either one of the two approved active vaccines for older adults.) The team estimate that vaccination cut RSV hospitalizations by two-thirds in babies less than 6 months old and by a third in seniors over age 75 during the 2024-25 season (when compared to no vaccination). Fogarty’s Dr. Cécile Viboud is senior author of the paper published in JAMA Network Open.
Researchers identify a new diabetes subtype in sub-Saharan Africa
Type 1 diabetes results from autoimmune destruction of insulin-secreting cells— according to studies of mostly European populations. Now a new study published in Lancet Diabetes and Endocrinology provides evidence that many young people in Africa, and some in the U.S., may have a non-autoimmune form of type 1 diabetes. Dr. Dana Dabelea of University of Colorado, who receives funding from the National Institute of Diabetes and Digestive and Kidney Diseases, participated in this project. The researchers enrolled 894 participants with young-onset diabetes from Cameroon, Uganda, and South Africa and assessed their blood levels of antibodies against insulinproducing cells and calculated their genetic risk of developing diabetes. Next, the team compared findings with similar, age-matched studies performed in the U.S. Discovery of a form of type 1 diabetes that is not caused by immune system dysregulation could change how diabetes is diagnosed, treated and managed, while paving the way for more effective medicines and better outcomes.
Fogarty alumnus co-leads study of cardiovascular health in southeast U.S.
Each year, rural areas in the U.S. experience 60,000 more cardiovascular-disease related deaths than urban areas due, in part, to a lack of specialists and cardiac imaging machines that are required to detect, diagnose, and manage cardiovascular disease. The RURAL (Risk Underlying Rural Areas Longitudinal) Cohort Study aims to address critical gaps in awareness and knowledge related to heart and lung disorders in several southeastern states. RURAL mobile exam units, which are outfitted with a lab, private exam rooms, and cardiovascular assessment and imaging tools, travel to the counties where the study’s more than 3,000 enrolled participants live. Dr. Gerald Bloomfield, a former Fogarty fellow and associate professor at Duke University School of Medicine, is co-lead of the study’s Imaging Core, which is responsible for obtaining CT scans and also storing, processing, and accessing the images.
All text produced in Global Health Matters is in the public domain and may be reprinted. Please credit Fogarty International Center. Images must be cleared for use with the individual source, as indicated. In rare cases when a correction is needed after an issue’s printed version has been finalized, the change will be made and explained in the online version of the article.
FUNDING NEWS
On behalf of the Fogarty International Center at the U.S. National Institutes of Health (NIH), the following funding opportunities, notices and announcements may be of interest to those working in the field of global health research.
Funding Announcement
International Research Scientist Development Award (IRSDA) (K01 Independent Clinical Trial Not Allowed) (K01 Independent Clinical Trial Required)
Mobile Health: Technology and Outcomes in Low and Middle Income Countries (R21/R33 Clinical Trial Optional)
Global Infectious Disease Research Training Program (D43 Clinical Trial Optional)
Deadline Details
March 9, 2026
March 9, 2026
August 6, 2026
Fogarty fellows gather in Bethesda
Once again, Fogarty welcomes trainees from across the U.S. and the globe!
Orientation for Fogarty’s Launching Future Leaders in Global Health (LAUNCH) Research Training Program took place on July 7-11 at the Hyatt Regency in Bethesda, Maryland, near the National Institutes of Health (NIH) campus.
LAUNCH supports one-year mentored research training opportunities
for U.S. and international scholars at biomedical research institutions and established project sites in low- and middle-income countries.
The orientation included workshops, presentations, lectures, and panel discussions featuring global health leaders and experts as well as NIH leadership, including NIH Director Dr. Jay Bhattacharya. This year’s trainees are supported by 24 NIH Institutes, Centers, and Offices.
Fogarty International Center
National Institutes of Health
31 Center Drive
Bethesda, MD 20892
NIH Director Dr. Jay Bhattacharya talks with a scientist following his fireside chat.
Speakers, left to right: Ellie Dehoney (Research!America); Dr. Wafaie Fawzi (Harvard T.H. Chan School of Public Health); Jane Simoni, PhD (NIH); Fred Ssewamala, PhD (Washington University School of Medicine); and Dr. Magaly Blas (Universidad Peruana Cayetano Heredia)
Photos courtesy of Fogarty staff
Boots on the Ground: DSAMH’s Bridge Clinic Encampment Outreach Team
Nicholas Panunto Delaware Division of Substance Abuse and Mental Health
This photo essay documents an afternoon with the Division of Substance Abuse and Mental Health’s (DSAMH) Bridge Clinic Encampment Response Team. It is a visual representation of the conditions and environments the Bridge Clinic Encampment Team experiences daily. Funded by the State Opioid Response (SOR) grant that the state receives from the Substance Abuse and Mental Health Services Administration (SAMHSA), a federal agency, the team seeks to engage individuals who are unhoused (homeless) who may be experiencing substance use disorder or mental health challenges.
The Bridge Clinic Encampment Team is active in all three counties in Delaware. Existing homeless encampments are visited routinely, and the team receives frequent tips about new encampments that have sprung up. When visiting encampments, the team focuses on building relationships with the individuals residing there. Practical supports such as food, hygiene items, or weather-specific items are offered. Narcan kits for overdose reversal are also provided. The team discusses individuals’ behavioral health needs and offers connections to care, including transportation if the individual is ready to enter treatment or access services on the spot. Unhoused clients who are actively using street drugs may have skin wounds that need medical attention; DSAMH provides a mobile nurse to assist clients with basic would care, provides supplies to patients to properly clean and dress their wound, and offers referrals to higher levels of care.
Donations for unhoused individuals are accepted by the Bridge Clinic.
New Castle County Bridge Clinic Encampment Outreach Team (Heather, Dwight, Nurse Amy, Mel, Chelsi, & Ty), our boots on the ground, take a photo with their vehicle fleet before heading out to perform outreach with local encampments.
Ty stands next to a hand-dug shelter pit at a Christiana homeless encampment.
The Encampment Outreach Team (Ty, Dwight, & Mel) engages with individuals at a New Castle County Encampment.
Dwight, Ty, & Mel leave a New Castle County encampment.
New Castle County Bridge Clinic Encampment Outreach Team (Ty, Dwight, Heather, Nurse Amy, & Chelsi) engage with an individual to help them to seek medical services.
New Castle, Kent, & Sussex County Bridge Clinic Encampment Outreach Teams (Mel, John, Joey, Jazmin, Ty, Keyonna, & Chelsi) put their boots on the ground in Dover.
Joey & Ty walk through a tick-infested wooded area to perform outreach. When leaving this encampment, Joey had to remove multiple ticks from his clothing.
An empty encampment in Kent County.
Encampment Team makes their way through a Kent County encampment.
A discarded, empty Narcan Kit rests next to an old tarp within an encampment.
Medical Marijuana in the Mid-Atlantic Region
Marym Khan, D.O. & Vishesh Agarwal, M.D. Department of Psychiatry, ChristianaCare.
BACKGROUND & INTRODUCTION
Cannabis, or marijuana, is one of the most widely used psychoactive agents globally, with an estimated 188 million people using it annually,1 for both recreational and medicinal use. Delta-9-tetrahydrocannabinol (THC) is the principal psychoactive substance responsible for the effects of cannabis on a person’s cognitive abilities. Another widely studied cannabinoid is cannabidiol (CBD).2 Ongoing research is currently being done on therapeutic uses of cannabis. As of December 2022, 37 states, three territories and the District of Columbia (D.C.) allow the medical use of cannabis.3 At the federal level, cannabis is classified as a Schedule I substance under the US Comprehensive Drug Abuse Prevention and Control Act of 1970, which is determined to have a high potential for abuse and no accepted medical use, conferring the use of cannabis a federal offense.4 The purpose of this paper is to serve as a medical commentary on the medical use of cannabis in the Mid-Atlantic region, which is defined as: New York, New Jersey, Pennsylvania, Delaware, Maryland, Virginia, West Virginia, and the D.C. The paper will explore the differences surrounding the laws that support the use of medical cannabis, and the variability in the way it is prescribed and utilized by patients.
METHODS
Search Term Strategy
The online databases that were utilized to retrieve articles were: PubMed, Web of Science, PsycInfo, and Scopus. The following search terms were used to identify peerreviewed articles in each database: “medical marijuana AND legal status,” “medical cannabis AND United States,” “medical cannabis AND risk factors,” “medical cannabis AND adverse effects,” “medical cannabis AND therapeutic use”, and “Cannabinoid ratio.” Bibliographies of pertinent articles and studies were examined methodically to identify relevant articles.
Inclusion Criteria
In this medical commentary, secondary data was the primary information source utilized and they were of various types, such as: meta-analysis, systematic reviews, cross-sectional, prospective cohort, and observational studies. Systematic reviews were the most common type of study analyzed. Studies done in states in the Mid-Atlantic region were accessed.
Data Analysis
The results and data acquired from the research studies will be utilized to critically analyze the literature, and establish ideas for future research. Topics including examining state legislation on medical cannabis licensing, therapeutic use of cannabis, and differences in the ratios of CBD and THC may be used as the groundwork for additional studies.
RESULTS
After reviewing and analyzing the current literature and state legislature on medical cannabis use in the MidAtlantic region, a table was created to outline the results found (see table 1 starting on page 68). One major finding from examining state legislation was the differences in approval for medical cannabis for particular conditions in these states. For example, from among the eight areas evaluated, it was found that some states specify a list of diseases for the use of medical cannabis, while other states leave it up to the physician’s discretion. The states that specify a list of conditions overlap with the diagnoses listed in the February 2017 report, The Health Effects of Cannabis and Cannabinoids, published by the Center for Medicinal Cannabis Research, which some states have used as reference. This report summarizes recent studies that display therapeutic efficacy of cannabis for a wide array of conditions. The studies range from double-blind, placebocontrolled trials to systematic reviews. The report concludes that there is clinical evidence that cannabis is effective for the treatment of chronic pain, chemotherapy- induced nausea/vomiting, multiple sclerosis spasticity symptoms, and sleep disturbances affiliated with obstructive sleep apnea, fibromyalgia, chronic pain, and multiple sclerosis. There is limited clinical evidence that cannabis is effective for improving appetite/decreasing weight loss in HIV/AIDS, Tourette Syndrome, Anxiety, and PTSD.16
CONCLUSION & DISCUSSION
This commentary serves to create a concise review of the medical cannabis laws and regulations that are implemented in the Mid-Atlantic region. The analysis identifies similarities and differences in how Delaware’s neighboring states permit medical cannabis to be utilized. Each state has its own regulatory body charged with creating its unique medical cannabis guidelines. Most of these governing departments establish the clinical use of cannabis for conditions that are widely accepted in the medical community such as neuropathic and chronic pain. However, it can also be seen that there are conditions listed for some states that do not have substantial evidence to support cannabis use, such as epilepsy or IBS. Continued research in the medical community is imperative to determine whether this product can be used as a stand-alone therapy or in conjunction with other treatment modalities for various disease states. In the future, if enough research is conducted, there may be a standardized manner in which medical cannabis is recommended for patients, ranging from the dosing route to the THC/CBD ratio.
Dr. Khan may be contacted at marym.khan@christianacare.org
REFERENCES
1. Hindley, G., Beck, K., Borgan, F., Ginestet, C. E., McCutcheon, R., Kleinloog, D., . . . Howes, O. D. (2020, April). Psychiatric symptoms caused by cannabis constituents: A systematic review and meta-analysis. The Lancet. Psychiatry, 7(4), 344–353. https://doi.org/10.1016/S2215-0366(20)30074-2
2 U.S. Department of Health and Human Services. (n.d.). Cannabis (marijuana) and cannabinoids: What you need to know. National Center for Complementary and Integrative Health. https://www.nccih.nih.gov/health/cannabis-marijuana-andcannabinoids-what-you-need-to-know
3 Karmen Hanson, A. G. (n.d.). State medical cannabis laws. https://www.ncsl.org/research/health/state-medical-marijuanalaws.aspx#3
4 Ebbert, J. O., Scharf, E. L., & Hurt, R. T. (2018, December). Medical Cannabis. [PubMed] Mayo Clinic Proceedings, 93(12), 1842–1847 https://doi.org/10.1016/j.mayocp.2018.09.005
5 New York State. (n.d.). Office of cannabis management. https://cannabis.ny.gov
6 State of New Jersey. (n.d.). Cannabis Regulatory Commission. https://www.nj.gov/cannabis/
7 Coogan, T. A. (2019, December 26). Analysis of the cannabinoid content of strains available in the New Jersey Medicinal Marijuana Program. Journal of Cannabis Research, 1(1), 11. https://doi.org/10.1186/s42238-019-0011-z
8 Commonwealth of Pennsylvania. (n.d.). Pennsylvania Medical Marijuana Program. https://www.pa.gov/agencies/health/programs/medicalmarijuana.html
9. State of Delaware. (n.d.). Medical Marijuana Program. https://dhss.delaware.gov/dhss/dph/hsp/medmarhome.html
10. State of Maryland. (n.d.). Maryland Cannabis Administration. https://cannabis.maryland.gov/Pages/home.aspx
11. State of West Virginia. (n.d.). Office of Medical Cannabis. https://omc.wv.gov/Pages/default.aspx
12. Commonwealth of Virginia. (n.d.). Cannabis Control Authority. https://cca.virginia.gov/
13. Norml. (n.d.). Medical Marijuana Laws. https://norml.org/laws/medical-laws/
14 Virginia Norml. (n.d.). Virginia Medical Cannabis Dispensaries. https://www.vanorml.org/dispensaries
15 District of Colombia. (n.d.). Alcoholic beverage and cannabis administration. https://abra.dc.gov/page/medical-cannabis-program
16. National Academies of Sciences, Engineering, and Medicine. (2017). The health effects of cannabis and cannabinoids: the current state of evidence and recommendations for research. Washington, DC: The National Academies Press. https://doi.org/10.17226/24625
Table 1. Current Literature and Legislature on Medical Marijuana in the Mid-Atlantic Region
State Medical Cannabis Statutes
State Medical Cannabis Statutes
NY A6357 (2014) Signed by governor 7/5/143
NY A6357 (2014) Signed by governor 7/5/143
In 2014, New York State passed the Compassionate Care Act to create a program to safely and e ectively provide medical cannabis to eligible state residents.5
In 2014, New York State passed the Compassionate Care Act to create a program to safely and e ectively provide medical cannabis to eligible state residents.5
Legalization
Legalization of Medical/ Recreational cannabis/ Both
of Medical/ Recreational cannabis/ Both
Medical Conditions Approved for Use of Medical Cannabis
Medical Conditions Approved for Use of Medical Cannabis
Both Alzheimer muscular dystrophy
Both Alzheimer muscular dystrophy
Amyotrophic lateral sclerosis (ALS)
Certification of Health Care Practitioner
Certification of Health Care Practitioner
# of Medical cannabis Dispensaries Maximum Amount Dispensed
NJ New Jersey Compassionate Use Medical Marijuana Act (CUMMA), January 20106
NJ New Jersey Compassionate Use Medical Marijuana Act (CUMMA), January 20106
Jake Honig Compassionate Use Medical Cannabis Act, July 2019
Jake Honig Compassionate Use Medical Cannabis Act, July 2019
Autism
Amyotrophic lateral sclerosis (ALS)
Cancer
Autism
Cancer
Chronic pain
Practitioners must be licensed, registered or certified by New York state to prescribe controlled substances within the state.
Practitioners must be licensed, registered or certified by New York state to prescribe controlled substances within the state.
Pain that degrades health and functional capability as an alternative to opioid use
A minimum of a two-hour approved course must be completed by practitioners who wish to certify patients for medical cannabis as determined by the OCM.
A minimum of a two-hour approved course must be completed by practitioners who wish to certify patients for medical cannabis as determined by the OCM.
Pain that degrades health and functional capability as an alternative to opioid use
Parkinson disease
Parkinson disease
Post-traumatic stress disorder (PTSD)
Post-traumatic stress disorder (PTSD)
Rheumatoid arthritis (RA)
Rheumatoid arthritis (RA)
Substance use disorder
Substance use disorder
Spinal cord injury with spasticity
Spinal cord injury with spasticity
Any other condition at the discretion of the care provider
Any other condition at the discretion of the care provider
Both ALS
Both ALS
Anxiety
Physician, PA, and NP
Physician, PA, and NP
9 No more than 3 oz/1 month
9 No more than 3 oz/1 month
Anxiety
Cancer
Cancer
Chronic pain
Hold active medical license in good standing issued by the NJ Board of Medical Examiners
Hold active medical license in good standing issued by the NJ Board of Medical Examiners
Chronic pain
Dysmenorrhea
Glaucoma
Dysmenorrhea
HIV & AIDS
Glaucoma
HIV & AIDS
Inflammatory bowel disease, including Crohn’s disease
Inflammatory bowel disease, including Crohn’s disease
Intractable skeletal muscular spasticity
Possess active controlled dangerous substance registration issued by the NJ Division of Consumer A airs not subject to limitation
3 broad groups in NJ medical market7:
3 broad groups in NJ medical market7: Those with < 1% CBDA and with THCA concentration from 10 to 30%;
Those with < 1% CBDA and with THCA concentration from 10 to 30%;
Practice in New Jersey.
Possess active controlled dangerous substance registration issued by the NJ Division of Consumer A airs not subject to limitation
Practice in New Jersey.
Intractable skeletal muscular spasticity
Migraine
Migraine
MS
MS
Muscular dystrophy
Muscular dystrophy
Opioid Use Disorder
PTSD
Opioid Use Disorder
PTSD
Seizure disorder, including epilepsy
Seizure disorder, including epilepsy
Terminal illness with prognosis of less than 12 months to live
Terminal illness with prognosis of less than 12 months to live
Tourette Syndrome
Tourette Syndrome
Those with both THCA and CBDA concentrations in the 5–10% range;
Those with both THCA and CBDA concentrations in the 5–10% range; Those with < 1% THCA and with CBDA concentration > 10%.
Those with < 1% THCA and with CBDA concentration > 10%.
State Medical Cannabis Statutes
State Medical Cannabis Statutes
PA Passage of Act 16 of 2016 created the Medical Marijuana Program Fund8
PA Passage of Act 16 of 2016 created the Medical Marijuana Program Fund8
Legalization of Medical/ Recreational cannabis/ Both
Legalization of Medical/ Recreational cannabis/ Both
Medical Conditions Approved for Use of Medical Cannabis
Medical Conditions Approved for Use of Medical Cannabis
Certification of Health Care Practitioner
Passage of Act 44 of 2021 created the Medical Marijuana Assistance Program.8 Medical ALS
Passage of Act 44 of 2021 created the Medical Marijuana Assistance Program.8
Medical ALS
Anxiety disorders
Anxiety disorders
Physician that has an active license with the Pennsylvania Department of State
Autism
Autism
Cancer, including remission therapy
Physician that has an active license with the Pennsylvania Department of State
Apply for registration with the Department of Health
Cancer, including remission therapy
Crohn’s disease
Crohn’s disease
Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
Apply for registration with the Department of Health
170 The dosage will be determined by a pharmacist and patients may receive up to a 30-day supply at a time.
170 The dosage will be determined by a pharmacist and patients may receive up to a 30-day supply at a time.
Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
Complete the required Department of Health-approved training.
Complete the required Department of Health-approved training.
Dyskinetic and spastic movement disorders
Dyskinetic and spastic movement disorders
Epilepsy
Epilepsy
Glaucoma
Glaucoma
HIV / AIDS
HIV / AIDS
Huntington’s disease
Huntington’s disease
Inflammatory bowel disease
Inflammatory bowel disease
Intractable seizures
Intractable seizures
MS
MS
Neurodegenerative diseases
Neurodegenerative diseases
Neuropathies
Neuropathies
Opioid use disorder for which conventional therapeutic interventions are contraindicated or ine ective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions;
Parkinson’s disease
PTSD
Opioid use disorder for which conventional therapeutic interventions are contraindicated or ine ective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions; Parkinson’s disease
PTSD
Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain;
Sickle cell anemia;
Terminal illness; and Tourette syndrome
Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain; Sickle cell anemia; Terminal illness; and Tourette syndrome
State Medical Cannabis Statutes Legalization of Medical/ Recreational cannabis/ Both Medical Conditions Approved for Use of Medical Cannabis
DE Medical Marijuana Law, Title 16, Ch 49A (2011)9
Medical Agitation of Alzheimer’s Disease
ALS
Anxiety (CBD Rich Card Only)
Autism with aggressive behavior
Cancer
Chronic Debilitating Migraine
Decompensated Cirrhosis
Glaucoma
HIV/AIDS
PTSD
Terminal Illness
A chronic or debilitating disease or medical condition or its treatment that produces one or more of the following;
1. Cachexia or Wasting Syndrome
2. Severe debilitating pain that has not responded to previously prescribed medication or surgical measure for more than three months, or for which other treatment options produced serious side e ects.
3. Intractable Nausea
4. Seizures
5. Severe and persistent muscle spasms, including but not limited to those characteristic of Multiple Sclerosis.
Certification of Health Care Practitioner # of Medical cannabis Dispensaries
Physician, Advanced practice registered nurse (APRN)/PA
Must be licensed to work in DE
No specific medical marijuana training required by law in order to certify patients for the program
4 Patients are authorized to purchase three ounces of usable marijuana every 14 days, for a total of six ounces per month
Medical marijuana oil means:
Cannabidiol oil which is a processed Cannabis plant extract that contains at least 15% cannabidiol but no more than 7% tetrahydrocannabinol.
THC-A oil which is a processed Cannabis plant extract that contains at least 15% tetrahydrocannabinol acid but not more than 7% tetrahydrocannabinol
MD Senate Bill 923 signed 4/14/1410
Both Anorexia
Cachexia
Chronic or debilitating disease or medical condition that results in being admitted into hospice or receiving palliative care.
Glaucoma
PTSD
Severe or chronic pain
Severe nausea, Seizures
Severe or persistent muscle spasms
Wasting syndrome
another chronic medical condition which is severe and for which other treatments have been ine ective.
Physician, dentist, podiatrist, NP, PA
Practitioner with an active state controlled dangerous substances registration Is registered with the Commission
102 The standard amount certification issued by a provider for a patient identifies the quantity of dried flower and/ or THC that the patient can purchase in a given 30-day period. The standard amount is 120 grams of dried flower or 36 grams of a THC product, however, a provider may certify a patient for more or less than the standard amount.
State Medical Cannabis Statutes
WV Senate Bill 386, signed into law on April 19, 2017 created the Medical Cannabis Act.11
Legalization of Medical/ Recreational cannabis/ Both
VA Code of Virginia § 18.2251.1. A. HB93312
Medical Conditions Approved for Use of Medical Cannabis
Medical Cancer
HIV/AIDs
ALS
Parkinson’s disease
Multiple sclerosis
Damage to the nervous tissue of the spinal cord with objective neurological indication of intractable spasticity
Epilepsy
Neuropathies
Huntington’s disease
Crohn’s disease
PTSD
Intractable seizures
Sickle cell anemia
Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
Terminally ill (medical prognosis of life expectancy of approximately one year or less if the illness runs its normal course)
Both Any diagnosed condition or disease determined by the practitioner to benefit from such use.13
Certification of Health Care Practitioner
Physician
Physician must apply for registration in the form and manner required by the Bureau for Public Health within the West Virginia Department of Health and Human Resources.
Dispensaries
37 May not exceed a 30day supply of individual doses
Physician, NP, PA12
D.C. Legalization of Marijuana for Medical Treatment
Amendment Act of 201015
Act Number: A18-0429
Law Number: L18-0210
E ective from Jul 27, 2010
Both “Qualifying medical or dental condition” means any condition for which treatment with medical marijuana would be beneficial, as determined by the patient’s authorized practitioner.
Qualifying medical or dental treatment” means:
(A) Chemotherapy; (B) The use of azidothymidine or protease inhibitors; (C) Radiotherapy; or
(D) Any other treatment, as determined by rulemaking, whose side e ects require treatment through the administration of medical marijuana in the same manner as a qualifying medical or dental condition
Health care practitioners must register with Alcoholic Beverage Regulation Administration
1314 No more than 4 oz/1 month12
Products may contain up to 10 mg THC per dose. “Dose” means a single unit, like one capsule or one dropperful. “Dosage” is the total amount taken each time, for example 2 sprays 4 time per day. There are no limits on dosage.14
7 May possess at any moment 8 oz of dried medical marijuana.
Upstream Solutions: Building Delaware’s Future Through Prevention Science
Amy M. Herb Planner IV, Division of Substance Abuse and Mental Health, Delaware Department of Health and Social Services
INTRODUCTION
Delaware faces urgent and growing challenges in behavioral health, with rising rates of substance use disorders (SUD) and mental health conditions leading to adverse impacts on individuals, families, and communities. These increases come after a decade of major declines in tobacco use and modest declines in other substance use in Delaware. In addition to the public health crisis of COVID-19, the pandemic disrupted social, economic, and healthcare systems, significantly affecting the delivery of services and coordination among providers, particularly in the realm of substance use prevention. According to data collected for the National Survey of Drug Use and Health (NSDUH), SUD affects over 17% of individuals aged 12 and older, with rates nearing 30% among young adults aged 18–25. Nearly one in five adults in Delaware has experienced a mental illness, and almost 18% of youth aged 12–17 have had a major depressive episode.1
The need for an effective prevention strategy in Delaware is especially urgent given the ongoing opioid epidemic plaguing Delaware families and communities, and the increasing normalization of marijuana use, particularly among youth and young adults, following Delaware’s 2015 decriminalization and 2023 legalization of recreational use for those 21 and older. As marijuana becomes more widely accepted, the perception of risk has declined, with over half of 12th graders in Delaware reporting lifetime marijuana use and 39% of all high school students doing the same.2 Early initiation is a strong predictor of long-term substance use problems, and most adults in SUD treatment report beginning use during adolescence, reinforcing the critical importance of targeting youth and young adults with focused prevention strategies.
These realities, combined with national data showing increased co-occurring mental health and substance use disorders underscore the critical role prevention has in implementing a comprehensive approach that recognizes multiple opportunities to address behavioral health problems and highlights the urgency to implement effective, science-based prevention strategies before the behavioral health crisis deepens further.
PREVENTION SCIENCE
Prevention science plays a vital role in addressing the intertwined public health challenges of addiction and mental health. Broadly speaking, prevention science is oriented toward promoting health and well-being. At the forefront of prevention science, practitioners focus on strategies, practices, policies, and programs designed to intervene before a problem or condition emerges or worsens to reduce adverse outcomes. At the core of prevention science, practitioners focus on the development of evidence-based strategies that reduce risk factors and enhance protective factors to improve the health and well-being of individuals, families,
and communities, and the promotion of health equity and the reduction of disparities. This approach offers a data-driven, costeffective framework that proactively fosters resilient individuals, families, and communities before they require intensive treatment.
For the past 50 years, prevention science has drawn from a diverse range of disciplines including the behavioral, social, psychological, and neurosciences. Practitioners are skilled in approaches that support science-based strategies to understand the origins of social problems at the individual, community, and societal levels (e.g., substance use, mental health, juvenile delinquency, criminal behavior, violence, trauma, human trafficking, and poverty).3 By drawing on multiple disciplines, including epidemiology, psychology, sociology, and education, prevention science develops interventions that are targeted, effective, and measurable. Its goal is not only to prevent the onset of mental health challenges and substance use, but to promote the health and resilience of entire populations.
Prevention science fosters social capital and health equity, two essential components for sustainable communities. It focuses on reducing modifiable risk factors and enhancing protective factors across biological, psychological, familial, community, and societal levels. Prevention science uses an upstream approach to addressing problems, which can reduce costs by halting or redirecting collateral consequences of outdated, downstream, reactionary approaches.4 Unlike treatment, which often responds to harm after it has occurred, prevention science is proactive, evidence-based, and aimed at sustaining wellness and equity over time. By focusing on the root cause of social problems, prevention science aims to improve the well-being of individuals and communities through approaches that identify risk factors and build resiliency by increasing protective factors, all while continuing to assess and evaluate the efficiency and effectiveness of the programs.
Prevention science is not only morally compelling but fiscally responsible. Evidence shows that every dollar spent on effective prevention yields multiple dollars in societal savings from reduced healthcare costs to decreased criminal justice involvement and increased educational attainment.
APPROACH TO PREVENTION
The Division of Substance Abuse and Mental Health (DSAMH) is one of the nine divisions within Delaware’s Department of Health and Social Services (DHSS) and is the single state agency (SSA) for the State of Delaware. DSAMH’s mission is to promote health and recovery by ensuring that Delawareans have access to quality prevention and treatment for mental health, substance use, and gambling conditions. DSAMH is the lead agency in Delaware and is dedicated to addressing substance use prevention, treatment,
and recovery. DSAMH collaborates with other state agencies, schools, community-based organizations, healthcare providers, and other key stakeholders, ensuring that all Delawareans across the lifespan have the opportunity to live healthy, fulfilling lives. DSAMH has adopted a “No Wrong Door” policy to ensure all individuals, at any time, can access an array of behavioral health services. This policy embeds a philosophy across the agency that emphasizes every staff person within the agency participates in assuring the availability of services for individuals in need. Individuals can contact or go to any of the staff within an agency to find the information, direct service, or referral they need, and be assisted no matter where they enter the system.
Delaware uses SAMHSA’s Strategic Prevention Framework (SPF) as the process and basis for this prevention strategy.5 The SPF is based on a comprehensive model for planning, implementation, and evaluation of prevention practices and programs, and outlines five key steps, detailed below, including:
• Assess Needs: Profile population needs, resources, and readiness to address needs and gaps in service delivery.
• Build Capacity: Identify, enhance, or build competency and resources for state and community partners to sufficiently detect and address identified needs.
• Plan: Develop an iterative, responsive, and practical strategic and implementation plan for prevention policies, practices, and programs.
• Implement: Implement evidence-based prevention policies, practices, and programs
• Evaluate: Systematically monitor, assess, and adjust all prevention policies, practices, and programs.
INSTITUTE OF MEDICINE’S CONTINUUM OF CARE MODEL
Delaware’s prevention approach aligns with the Substance Abuse and Mental Health Services Administration’s (SAMHSA) Behavioral Health Continuum of Care Model, derived from an Institute of Medicine (IOM) report (figure 1).6 This comprehensive approach to behavioral health recognizes the multiple opportunities to address behavioral health problems. Utilizing this model framework supports DSAMH’s mission to promote health and recovery by ensuring that Delawareans have access to quality prevention and treatment for mental health, substance use, and gambling conditions.
Figure 1. SAMHSA Behavioral Health Continuum of Care Model
The IOM’s risk-based classification enhances the effectiveness, precision, and scalability of prevention efforts. By applying this framework, DSAMH can strategically allocate resources, match interventions to the appropriate population, and maximize impact by addressing needs at every stage of risk. This model also supports coordination across providers, promotes health equity, and helps ensure that no group, whether at low or high risk, is overlooked.
Based on this model, Delaware’s approach to preventing behavioral health challenges and outcomes focuses on strategies that target populations with different levels of risk which classifies preventive interventions according to the targeted population. The IOM population classifications are:
• Universal: The general public or a whole population group that has not been identified on the basis of individual risk
• Selective: Individuals or a subgroup of the population whose risk of developing a disorder is significantly higher than average
• Indicated: Individuals in high-risk environments who have minimal but detectable signs or symptoms foreshadowing disorder or have biological markers indicating predispositions for the disorder but do not yet meet diagnostic levels
Delaware views prevention as a continuum, even if individuals or populations have engaged in risky behaviors or have been diagnosed with a mental health condition and/or substance use disorder. While Delaware supports an upstream approach through primary prevention efforts, the state increasingly recognizes the importance of a comprehensive approach to behavioral health, including the implementation of secondary and tertiary prevention strategies. These strategies focus on early intervention to reduce the severity and impact of mental health and substance use disorders, and to manage the impact of chronic behavioral health conditions, aiming to prevent worsening outcomes and improve the quality of life for individuals already experiencing significant mental health conditions or substance use disorders.
RISK AND PROTECTIVE FACTORS
Although behavioral health challenges can vary substantially from mental health conditions and substance use, research demonstrates that some common elements are effective in preventing or mitigating the effects of these issues. SAMHSA defines risk factors as the “conditions in people’s lives that make them more or less likely to use alcohol, tobacco, or illicit drugs.”7 These factors are characteristics at the biological, psychological, family, community, or cultural level and are associated with a higher likelihood of problem outcomes. These include characteristics such as genetic predisposition, child abuse, trauma, familial substance abuse, norms favorable to drug and alcohol use, including substance-abusing peers, social isolation or alienation, lack of employment opportunities, and prenatal exposure.
Researchers and health advocates have identified several risk and protective factors associated with substance use, many of which develop during childhood. Understanding and identifying these factors is essential for effective prevention, as it enables the early implementation of interventions that can significantly reduce the likelihood of substance use in the future. In the absence of
protective factors, certain conditions, experiences, and societal factors can combine to increase the risk for behavioral challenges in individuals and communities, including but not limited to behavioral health concerns.
Overarchingly, prevention efforts enhance protective factors and reduce risk factors at the individual, relationship, community, and societal levels. These efforts must be comprehensive and complementary rather than conducted in isolation. In other words, interventions at each of these levels are necessary, but insufficient when undertaken in isolation. Characteristic at the biological, psychological, family, or community (including peers and culture) level that is associated with a lower likelihood of problem outcomes or that reduces the negative impact of a risk factor on problem outcomes.
For optimal behavioral health, protective factors include:
• Positive Social Connections: This includes prevention efforts aimed at building strong relationships with family, friends, and community members who can provide emotional support and reduce feelings of isolation.
• Healthy Social and Emotional Skills: This includes providing skills-based education on prevention efforts to develop skills such as empathy, emotional regulation, and effective communication, which can enhance resilience and coping mechanisms.
• Engagement in School and Community Activities: This includes fostering communities and schools that encourage and promote participation in educational and community-based programs. These programs can foster a sense of purpose and belonging, contributing to positive mental health outcomes.
• Access to Mental Health Care: This includes addressing community needs and enhancing access to and awareness of mental health services and support systems that can aid in early identification and treatment of mental health issues, promoting recovery and well-being. Connectedness to and positive relationships with individuals, family, friends, community, and social institutions.
To achieve effective outcomes in primary prevention, it is critical to understand the risk and protective factors that contribute to local behavioral health challenges. Prevention practitioners do not directly reduce rates of SUD or other behavioral health issues; rather, they influence these outcomes by targeting the underlying factors that drive them. Once a community identifies its priority problem behaviors—such as cannabis use or binge drinking—it must then determine which risk and protective factors most strongly influence those behaviors. With this understanding, communities can select and implement evidence-based programs, policies, and practices designed to address those factors and, in turn, reduce the occurrence of the targeted behaviors.7
DELAWARE’S BEHAVIORAL HEALTH PREVENTION STRATEGY AND PLAN
In late 2023, to address the state’s fragmented prevention infrastructure and service delivery drift impacted by the increase in the incidence and prevalence of substance abuse and the public health crisis of COVID-19, DSAMH leveraged the State Epidemiological Outcomes Workgroup (SEOW) to produce a State Prevention Portfolio to explore the current landscape of
prevention in Delaware. The assessment included a community provider survey, and content areas included communities served, services provided, and access to resources. Findings from this assessment described four main themes: financial resources, geographic area served, description of prevention services, and community perceptions of risk.
Concurrently, a cross-sector body of prevention stakeholders began to convene to develop a coordinated statewide behavioral health prevention strategy. The convoy of stakeholders assessed the state’s prevention landscape and identified the following objectives to serve as the foundation for the 2025 – 2030 Delaware Behavioral Health Prevention Strategy and Plan. These objectives included:
• Increase protective factors through education and development for individuals, families, and communities with evidence-informed prevention and early intervention strategies to prevent adverse outcomes of behavioral health challenges, the use and misuse of drugs, and the development of substance use disorders;
• Increase the capacity to implement data-driven decision-making;
• Support educational institutions (K-12 and higher education) to increase their capacity to implement and deliver effective prevention programs and strategies focused on risk and protective factors; and
• Increase the capacity of the prevention workforce to plan, implement, deliver, and evaluate quality prevention services to individuals, families, and communities.
Delaware has begun to address these objectives to build a comprehensive, collaborative, data-driven, and sustainable prevention infrastructure, committed to fostering healthy and resilient individuals, families, and communities. This infrastructure is grounded in reducing risk factors, strengthening protective factors, building resilience, and promoting well-being. Since 2023, guided by Prevention Science and the Strategic Prevention Framework, a committee composed of state officials, education and research institutions, and community-based prevention providers has met regularly to develop a multi-faceted approach. Some of the initiatives that have begun including:
• Formalized the role and membership of the Delaware Addiction Action Committee (AAC) Prevention Subcommittee housed as a subcommittee of the AAC (16 DE Code § 5198), which is a legislative committee charged with developing and monitoring a coordinated and comprehensive approach to Delaware’s addiction epidemic. This subcommittee will be charged with ensuring coordination to meeting the objectives of the State Behavioral Health Prevention Strategy and Plan.
• Assessed the prevention landscape in Delaware to develop a comprehensive Statewide Behavioral Health Prevention Strategy and Plan
• Established a plan for a statewide cannabis prevention peer to peer media campaign using the grassroots hashtag #MyReasonWhyDE
• Developed a Statewide Cannabis Prevention Workgroup to align strategies across agencies and providers.
• Supported the restructuring of the Delaware Prevention Partners, a coalition of prevention providers, to build capacity across the prevention workforce through training and collaboration to increase competencies in evidence-based planning, implementation, delivery and evaluation of prevention services.
• Since the restructuring, the DPP has expanded reach and information sharing through a network of over 60 prevention professionals and social media; hosted monthly prevention provider sharing and collaboration sessions; established a quarterly prevention workforce training series, Prevention Professionals Have Power; organized and hosted the largest annual Delaware Prevention Day at Legislative Hall; and hosted Delaware’s largest Community Service and Prevention project, The Party.
• Supported the expanded capacity within the Delaware Department of Education to include a dedicated prevention specialist in each county to coordinate substance use prevention education across public and charter schools and to build partnerships between community providers and coalitions with K-12 schools.
The future and ongoing efforts to addressing the Delaware prevention landscape include:
• Expansion of the integrations of the SEOW with the collection and assessment of substance abuse consumption and consequence patterns at the state and local levels will be conducted and disseminated.
• Increase substance use prevention education efforts in K-12 schools to ensure coordination and efficiency of mandated substance use prevention education under regulation 551 and increase social and emotional learning.
• Provide technical assistance and capacity building across community-based organizations and prevention coalitions.
• Identify strategies and implementation plans to build the capacity across the state to address gaps and needs, and identify training and technical assistance integration for prevention subrecipients, prevention providers, and prevention coalitions
• Establishment of a youth coalition (for young people games 16 –25) to provide youth voice and advocacy to the state’s prevention efforts.
• Continued support for expansion of the DPP through the development of a state technical assistance and training plan, and events to foster collaboration and networking
• The development of a dedicated repository of prevention resources and evidence-based programming on the Help is Here website.
• Increase capacity across the state for the #MyReasonWhyDE peer to peer prevention campaign through a train-the-trainer series in the curriculum.
• Provide ongoing support for secondary, tertiary, and harm reduction prevention efforts to reach those who may need more intense intervention services.
• Expand integration of substance use screening tools in primary health care and community-based settings.
• Monitor and evaluate the effectiveness of programs and services utilizing outcome measures to inform decision-making for prevention services throughout Delaware.
• Ensure cultural competency through all substance abuse prevention programs, policies, and practices to reduce health disparities among diverse populations related to substance abuse.
• Meet regularly with Delaware’s prevention stakeholders/partners through the AAC Prevention Workgroup to develop/monitor the Behavioral Health Prevention Strategy and Plan to ensure the mobilization of community resources and ongoing collaboration, thereby sustaining the desired outcomes of programs, policies, and practices developed through the plan.
Delaware stands at a critical crossroads, where proactive, evidence-based prevention strategies can chart a new course toward healthier individuals, stronger families, and more resilient communities. Guided by prevention science and empowered by cross-sector collaboration, the state is laying a robust foundation to address behavioral health challenges before they take root. As Delaware advances its 2025–2030 Behavioral Health Prevention Strategy and Plan, the commitment to a data-driven, equityfocused, and youth-engaged approach offers more than hope; it offers a blueprint for transformation. By investing in prevention today, Delaware is not only mitigating risk but cultivating a future where well-being is the norm, not the exception.
Dr. Herb may be contacted at amy.herb@delaware.gov .
REFERENCES
1. Substance Abuse and Mental Health Services Administration. (n.d.). Key substance use and mental health indicators in the United States: Results from the 2022 National Survey on Drug Use and Health. HHS Publication No. PEP23-07-01-006, NSDUH Series H-58 Center for Behavioral Health Statistics and Quality. https://www.samhsa.gov/Data/Report/2022-Nsduh-Annual-National-Report
2. Centers for Disease Control and Prevention. (2025). Youth online: Middle school YRBShttps://nccd.cdc.gov/youthonline/App/Default.aspx?SID=MS
3. National Prevention Science Coalition to Improve Lives. (2025). The impact of prevention science https://www.npscoalition.org
4. Prevention Technology Transfer Center (PTTC) Network. (n.d.). Home. Pttcnetwork.org. Retrieved July 2025, from https://pttcnetwork.org/
5. Substance Abuse and Mental Health Services Administration. (2019). Substance abuse and mental health services administration: A Guide to SAMHSA’s Strategic Prevention Framework. Center for Substance Abuse Prevention. https://library.samhsa.gov/product/guide-samhsas-strategic-preventionframework/pep19-01
6. Strategic Prevention Technical Assistance Center. (2024). the institute of medicines continuum of care. Strategic Prevention Technical Assistance Center. https://www.samhsa.gov/sites/default/files/resourcefiles/sptaccontinuum-of-care.pdf
7. Substance Abuse and Mental Health Services Administration. (2020). Focus on prevention: Strategies and programs to prevention substance use. Choice Reviews Online, 49(03), 49–150749–1507. https://doi.org/10.5860/choice.49-1507
Building Competence and Compassion: Addiction Education for Medical Students
Amy Modi Medical Student, Philadelphia College of Osteopathic Medicine
INTRODUCTION
As a medical student navigating my clerkships, the opioid epidemic shifted from an abstract concept to a painful reality. I witnessed a young woman from Hockessin tossing in her bed, sweat beading on her forehead as her body grappled with the physical torment of withdrawal. I took the history of a Wilmington resident whose years of legitimate pain, initially alleviated by an innocent prescription, fell prey to an insidious dependence. I watched a mother of two come to terms with the horrifying truth that immediate amputation was her only means of survival. I faced the stark reality that my community was a microcosm of a national crisis.
Despite its size, Delaware has become one of the states most severely impacted by the opioid epidemic. In 2022, Delaware recorded the nation’s third-highest rate of drug overdose mortality, resulting in 549 lives lost. This marked a 24% increase in deaths compared to just two years prior.1 Reflecting on these concerning statistics and my current role as a medical student, I wonder: are medical schools equipping future physicians with the tools and knowledge to address this complex crisis?
GAPS IN MEDICAL EDUCATION
The harsh truth is that medical education has not evolved alongside the escalating substance use disorder (SUD) epidemic. The accrediting bodies for MD and DO medical schools do not require a standardized curriculum on SUD.2 The current state of medical education is perplexing. We dedicate significant time to understanding rare blood dyscrasias, conditions so uncommon that many physicians may never encounter them. Meanwhile, our emergency departments are overwhelmed, treating hundreds of patients struggling with opioid overdose and withdrawal every day. It is puzzling that such a widespread and devastating disease receives so little focus from those entrusted with healing.
Rotating medical students and residents often find themselves ‘learning on the job,’ particularly when their foundational training in specific areas could be more extensive. However, the sensitive conversations, detailed assessments, and thoughtful treatment strategies unique to addiction medicine are an art form that requires intentional instruction. As these future healthcare professionals enter the workforce, they must be prepared to engage in crucial discussions about addiction, recognize the subtle signs of SUDs, and confidently make referrals for treatment. Some may argue that comprehensive SUD knowledge should primarily reside with internal or family medicine specialists. However, individuals suffering from SUDs are human beings who, like any other patient, may present with a myriad of health concerns spanning every medical specialty. Therefore, regardless of their chosen field, every physician should possess fundamental competence and compassion in addressing addiction. The current limited focus on addiction education is a disservice to the patients we are sworn to serve.
THE PCOM ADDICTION MEDICINE ELECTIVE
Seeing the room for improvement in our traditional curriculum, students at the Philadelphia College of Osteopathic Medicine (PCOM) enthusiastically stepped up to develop a unique Addiction Medicine elective for secondyear DO students in 2022. Guided by Dr. Frederick Goldstein, this elective offers engaging weekly two-hour evening sessions that effectively combine classroom learning with enriching hands-on experiences.
In the first week, the elective focused on understanding the disease model of addiction, emphasizing the complex biological, psychological, and social factors involved in SUDs. In the following weeks, students had the opportunity to engage directly with addiction medicine psychologists and physicians. Outside the classroom, students were fortunate to shadow support group meetings, such as Narcotics Anonymous. Hearing real-life stories from individuals in recovery provided a deeply personal and relatable perspective on addiction. Students also connected with community organizations like Prevention Point in Kensington, Philadelphia. Their volunteers walked students through hands-on opioid overdose simulations, giving them an opportunity to practice administering naloxone. This enriching curriculum taught students valuable skills and deepened their understanding of the local resources available to those facing addiction challenges.
OUTCOMES AND IMPACT
The PCOM Addiction Medicine Elective made a significant impact, providing a clear direction for the future of medical education. Fifty students participated in the pilot elective and completed detailed pre- and post-course surveys that evaluated their comfort and competence in dealing with SUDs.3 The results showed marked improvements, illustrating a new generation of empowered physicians:
• Comfort in assessing patients for addiction increased dramatically from 20% to 100%.
• Comfort in discussing addiction with patients rose from 41% to 95%.
• Understanding of addiction as a disease improved from 66% to 100%.
• Knowledge of accessing community resources for treatment referrals surged from a mere 2% to 91% (p<0.01).3
BROADER IMPLICATIONS FOR MEDICAL EDUCATION
With the escalating costs of medical education, it is imperative for medical schools to improve their curriculum to address the present healthcare challenges, particularly the SUD and opioid crisis. The success of PCOM’s elective highlights the growing need for more standardized and interactive addiction education in medical schools across the country. At the very least, foundational training should encompass the neurobiology of addiction, screening tools, evidence-based treatments, and insights into community resources.
In addition, medical training should address stigma and foster a compassionate, patient-centered approach to SUD. Connecting with individuals in recovery, engaging in community outreach, and observing support group meetings provide invaluable experiences. These interactions offer a genuine glimpse into the lives of those affected by addiction, helping students foster a deeper respect, empathy, and understanding that goes far beyond what they might read in textbooks.
CULTIVATING DELAWARE’S PHYSICIAN WORKFORCE
PCOM is proud to be one of Delaware’s medical schools through the Delaware Institute of Medical Education and Research (DIMER) program. DIMER students are warmly encouraged to return to Delaware to practice in both primary care and specialty areas. Since Delaware has been deeply affected by the opioid crisis, our future physicians who receive their training at PCOM through DIMER are set to play a crucial role in tackling this critical challenge and making a positive impact in our community.
This elective holds special meaning for many of us DIMER students, particularly because we are eager to give back to our hometowns. By delving into the challenges our communities face firsthand, we are not just honing our clinical skills; we are also learning how to support our neighbors. Enhancing addiction education offers an immediate and profound benefit to healthcare in Delaware, equipping future physicians with the tools they need to confront addiction, reduce stigma, and ultimately improve health outcomes.
Ms. Modi may be contacted at am2961@pcom.edu
REFERENCES
1. for Disease Control and Prevention. (2025, Jan 10). Drug overdose mortality by state. Centers for Disease Control and Prevention.
2. Morford, K. L., Tetrault, J. M., & Fiellin, D. A. (2024, June). The MATE Act: Progress for substance use education, but is checking a box enough? Journal of General Internal Medicine, 39(8), 1496–1498. https://doi.org/10.1007/s11606-024-08652-7
3. Caulkins, R., Klunk, A., Suttera, C., VanDuzer, K., & Goldstein, F. J. (2023). Outcomes from an Addiction Medicine Elective for 2nd Year PCOM DO Students. DigitalCommons@PCOM. https://digitalcommons.pcom.edu/research_day/research_day_ PA_2023/researchPA2023/29/
OpiRescue Delaware is a FREE overdose rescue application that provides:
• Step-by-step instructions to reverse an opioid overdose
• Resources for family and friends
Download the OpiRescue Delaware App at:
• HelpIsHereDE.com/App
• Your mobile device App store
Emily Smith, M.D.
Addiction Psychiatry Training Within the State of Delaware: Need of the Hour
Chief Resident, Department of Psychiatry, ChristianaCare
John Q. Berlin, D.O.
Associate Program Director, Department of Psychiatry, ChristianaCare
Ram A. Sharma M.D.
Associate Program Director, Department of Psychiatry, ChristianaCare
Humans across cultures have been consuming addictive substances for centuries, and the health, social, and economic consequences associated with use of these substances, whether legal or illicit, are certainly not new phenomena. Despite increasing knowledge regarding neurobiological changes that occur with substance use disorders (SUDs) and policy changes aimed at reducing the consequences of substance use in varying ways (ranging from criminalizing use of certain drugs to promoting harm reduction), SUDs remain a significant public health problem throughout the United States. According to the 2023 National Survey on Drug Use and Health (NSDUH), 48.5 million people aged 12 or older, over 17% of this population, met criteria for a substance use disorder in the past year.1 SUDs range from mild to severe (addiction), and recent decades have been marred by increasing rates of death due to overdose (OD), often associated with opioids.2 The U.S. Congress Joint Economic Committee estimated that opioid misuse and OUD cost the country close to $1.5 trillion in 2020, and that is not including the economic burden stemming from alcohol use disorder and other substance use disorders. Costs of health care, the criminal justice system, public safety, lost productivity, decreased quality of life and lives lost (such as due to overdose) all contribute to the economic toll of addiction.3 Despite increasing awareness that addiction touches individuals from all backgrounds and growing acceptance that compulsive use represents an aspect of a biological illness rather than a moral failing, many affected individuals do not receive potentially life-saving treatment. While there are a number of barriers to treatment – including but not limited to availability and accessibility of treatment, cost concerns, insurance coverage of services, and stigma – studies suggest that physicians’ limited knowledge and skills in the realm of addiction treatment contribute to limited use of evidencebased practices to identify, assess, and effectively treat patient with SUDs.4 Ensuring that all US medical schools provide sufficient training on recognizing, evaluating, and providing compassionate care to individuals with SUDs is a crucial step in providing our workforce with the knowledge and skills needed to address this public health crisis.
Delaware has not been spared from rising rates of SUDs and overdose deaths. In recent years Delaware has surpassed the national average in terms of SUD prevalence and overdose rates.2,5 In 2017-2019, the annual average prevalence (among people aged 12 and older) of past-year substance use disorder was 9.6% in Delaware compared to a national average of 7.4%
during that same time period.5 Our state has also suffered a higher rate of drug overdose deaths (many secondary to opioids) than the national average between 2011 and 2021. In 2021, there were 54.0 drug overdose deaths per 100,000 population in Delaware compared to 34.4 per 100,000 in the United States.5 While Delaware’s strategic state-level policies are showing a positive impact on reducing overdose deaths in recent years, the success of these efforts is being tested by a critical shortage of healthcare providers.6 This scarcity of qualified professionals means that despite the state’s commitment, many Delawareans struggling with substance use disorders (SUDs) continue to face significant barriers to accessing the care they need. In this opinion article we will explore some of the areas where medical training can be expanded to include treatment of substance use disorders and to improve access of care for the patients in the state of Delaware. We propose a multilayered approach to incorporate exposure to train future physicians who are empathetic, confident, and follow evidence-based care to treat SUD population.
1. Including a required addiction rotation as a core component for medical students. Integrating in depth knowledge and skill-based training for medical students will serve as a strong foundation for the future healthcare workforce. The curriculum should include evidence-based practices for the identification, intervention, and treatment of SUDs, including but not limited to approaches such as Screening, Brief Intervention, and Referral to Treatment (SBIRT) and motivational interviewing. The neurobiological basis of addiction and pharmacology of Medication Assisted Treatment should also be topics of discussion. This education will provide early career physicians, regardless of their specialties, with the basic tools to identify at risk patients and early withdrawal symptoms and to incorporate preventative strategies. Equipping physicians with these basic skills can facilitate brief intervention and timely referral from any medical office, which can potentially prevent overdose. Furthermore, the more healthcare settings that adopt these approaches, the greater the extent to which harm reduction can be achieved at a broader scale in the community.
2. Offering an Addiction rotation as a required block to training programs. Advocating for training programs, particularly primary care training residencies (Pediatrics, Family Medicine and Internal Medicine) to add a required Addiction rotation can have a significant impact in reducing the barriers to access to care. Hands on training during these rotations can substantially reduce the hesitancy to prescribe many life-saving medicines for this population at the primary care level (such as Buprenorphine, which evidence has shown can decrease risks of OD and relapse).7
3. Creating an addiction psychiatry training program. This is the last, but perhaps most critical, step to feedback into the cycle of training. The establishment of an addiction psychiatry fellowship in Delaware would be instrumental in recruiting and ideally retaining psychiatrists passionate about the specialty. In addition to serving as an opportunity for Delaware physicians to receive further addiction training, a fellowship could recruit other physicians to the area to provide care to our community throughout residency, and these trainees may choose to continue serving this population after completing fellowship. With more addiction specialists in Delaware, a critical mass could be achieved, which could open up the bottle neck of supply and demand. It would also naturally create a space of collaboration between medical centers, community treatments centers, health agencies, and even policy makers; the fellows could rotate through various care settings and, with the support of their faculty mentors, could learn how to effectively advocate for their patients by discussing barriers to treatment and exploring potential solutions with the state government agencies and policy makers. Furthermore, a training program could foster a culture of research and lead to more tailored and effective interventions specifically for the state.
The establishment of an Addiction Psychiatry fellowship in Delaware would be a meaningful step towards providing Delawareans with access to physicians equipped with the skills to treat SUDs and the comorbid psychiatric conditions that commonly accompany addiction. By proactively addressing the gaps in medical school and residency training, and by establishing a dedicated Addiction Psychiatry Fellowship program in Delaware, we can empower our future physicians with the knowledge, skills, and compassion necessary to effectively combat this public health epidemic. Dr. Sharma may be contacted at drramabhisheksharma@gmail.com
REFERENCES
1. Substance Abuse and Mental Health Services Administration. (2024). 2023 National survey on drug use and health (NSDUH): Main highlights. U.S. Department of Health and Human Services. https://www.samhsa.gov/data/sites/default/files/reports/ rpt46356/2023-nsduh-main-highlights.pdf
2 KFF. (2024, May 29). Mental health and substance use state fact sheets: Delaware. KFF. https://www.kff.org/statedata/mental-health-and-substance-use-statefact-sheets/delaware/
3 U.S. Congress Joint Economic Committee. (2022, September 28). The Economic Toll of the Opioid Crisis Reached Nearly $1.5 Trillion in 2020. Jec.Senate.Gov. Retrieved July 16, 2025, from https://www.jec.senate.gov/public/_cache/files/67bced7f-423240ea-9263-f033d280c567/jec-cost-of-opioids-issue-brief.pdf
4 Campopiano von Klimo, M., Nolan, L., Corbin, M., Farinelli, L., Pytell, J. D., Simon, C., Compton, W. M. (2024, July 1). Physician reluctance to intervene in addiction. JAMA Network Open, 7(7), e2420837. https://doi.org/10.1001/jamanetworkopen.2024.20837
5 Substance Abuse and Mental Health Services Administration. (2020). Behavioral health barometer: Delaware, volume 6. U.S. Department of Health and Human Services. https://www.samhsa.gov/data/sites/default/files/reports/rpt32824/ Delaware-BH-Barometer_Volume6.pdf
6 Delaware Department of Health and Social Services. Drug Overdose Deaths Overview Data for Delaware. My Healthy Community. Updated May 29, 2024. Accessed July 21, 2025. https://myhealthycommunity.dhss.delaware.gov/topics/drug-overdosedeaths/overview/state
7 Wakeman, S. E., Larochelle, M. R., Ameli, O., Chaisson, C. E., McPheeters, J. T., Crown, W. H., Sanghavi, D. M. (2020, February 5). Comparative effectiveness of different treatment pathways for opioid use disorder. JAMA Network Open, 3(2), e1920622. https://doi.org/10.1001/jamanetworkopen.2019.20622
Are Substance Use Deflection Programs Seen as Effective? Exploring Police Attitudes on Program Implementation
Jullianne Regalado, M.A.
PhD Research Assistant, Center for Drug and Health Studies, Department of Sociology and Criminal Justice, University of Delaware
Ellen Donnelly, Ph.D.
Associate Professor, Center for Drug and Health Studies, Department of Sociology and Criminal Justice, University of Delaware
Emalie Rell, Ph.D
Research Associate, Center for Drug and Health Studies, Department of Sociology and Criminal Justice, University of Delaware
Adam Gavnik, M.A.
Ph.D. Research Assistant, Center for Drug and Health Studies, Department of Sociology and Criminal Justice, University of Delaware
Madeline Stenger, Ph.D.
Postdoctoral Fellow, Department of Psychiatry and Behavioral Science, Duke University School of Medicine, Wilson Center for Science and Justice, Duke University School of Law
Daniel J. O’Connell, Ph.D.
Senior Scientist, Center for Drug and Health Studies, Department of Sociology and Criminal Justice, University of Delaware
ABSTRACT
Objective: To determine the prevalence and determinants of beliefs in substance use deflection programs’ effectiveness among police officers working in agencies with diversion initiatives. Methods: We present responses from an anonymous online survey about deflection programs fielded to all law enforcement officers in the State of Delaware in January 2025. A total of 111 officers reported working in an agency with a substance use deflection program and completed relevant survey questions. Descriptive statistics summarize police officers’ views on program effectiveness, attitudes toward leadership, beliefs in enforcing the law, occupational experiences, and personal characteristics. Logistic regression models isolate the factors associated with beliefs in program effectiveness. Descriptive statistics identify common barriers to deflection program implementation. Results: A majority (59%) believe their programs are effective. On average, over three-quarters of respondents express that deflection programs are appropriate, feasible, and implementable. Tough-on-crime attitudes and being in a position for less than five years diminish the likelihood of stating that a deflection program is effective. Knowing someone who has a substance use or mental health disorder and working in a larger police department increases perceptions of program effectiveness. The three most commonly cited barriers to program implementation were having people interested in treatment, homelessness/housing issues, and the potential ineffectiveness of diversion. Conclusions: Police officers generally believe their departments’ substance use deflection programs are successful. Even more officers think programs can be easily and appropriately implemented. Commonly cited barriers highlight the difficulties in addressing substance use in communities. Policy Implications: This overall support for deflection underscores the potential for further cross-system collaborations with public health practitioners. Such partnerships may also be vital in addressing barriers that inhibit law enforcement-based deflection efforts. Further evaluation and research efforts can demonstrate the impacts of substance use deflection and the practices that make deflection programs more successful.
INTRODUCTION
Across the United States, substance-involved overdoses pose a major challenge for public health officials and emergency responders to address. The Centers for Disease Control and Prevention revealed that fatal drug overdose deaths were at an estimated 105,007 in 2023.1 Despite national rates decreasing from 2022, overdose incidents remain prevalent in various states. Delaware holds one of the highest drug overdose fatality figures in the U.S., with a rate of 55.3 deaths per 100,000 people in the total population.2 Issues of substance use, including opioid misuse, continue to be pronounced at the state and county levels, creating pressure toward criminal justice responses.3
With greater criminal justice contact among those inhibiting substance use disorders (SUD), efforts toward interventionist and harm reduction approaches provide an alternative model away from the criminalization of substance use.4
To redress Delaware’s high number of fatal and non-fatal drug overdose incidents,5 Delaware law enforcement agencies have embraced substance use deflection programs as a strategy. Deflection, also known as police diversion or pre-arrest diversion, aims to refer individuals presenting with substance use to treatment or supportive services before arrest and other crises necessitating police response occur.6 Deflection programs typically feature one or more pathways to care:
self-referral, active outreach by treatment providers following officer recommendation, naloxone plus as a post-overdose or acute risk of overdose response, officer prevention through treatment initiation, and officer intervention by holding charges in abeyance.7 Although programs vary in form, all share a primary interest in diminishing criminal justice involvement and improving connections to care.
Police officers’ attitudes can influence the success of a deflection intervention. This study examines the beliefs and opinions of police officers who worked in Delaware law enforcement agencies that have deployed a substance use-focused deflection program as of 2025. We present the results of a January 2025 survey inviting all police officers to share their views on deflection practices. We explore three research questions:
1. Do police officers think that their deflection programs are effective?
2. What are the predictors of officer beliefs in deflection program effectiveness? and
3. What are the barriers to the implementation of a successful deflection program?
We rely on descriptive statistics and logistic regression to address these questions. This research offers a contemporary and local look at law enforcement perspectives in an evolving landscape of public health and criminal justice collaborations targeting substance use and other behavioral health issues.
BACKGROUND
Substance Use-focused Deflection Programs and Practices
In recent years, deflection programs have gained traction among U.S. law enforcement agencies, as well as caught the attention of many government legislators.8 Although deflection practices are not a new phenomenon, social and political factors, such as the rise of drug overdoses, changing community relations with the police, and renewed pushes to take a public health approach to mitigate mental health and substance use crises, have shifted their practice to meet the needs of community members.9 In a report for the National Conference of State Legislatures, Widgery (2023) defined deflection as,
“Deflection programs occur before arrest or prior to initiation of a law enforcement or other justice system contact. These programs generally provide a path to treatment for individuals with mental health or substancerelated needs with the goal of averting the need for an emergent response from law enforcement or health services. Programs typically involve law enforcement, peer support specialists, recovery coaches, clinical staff, case managers, or social workers.”8
The overarching goal of deflection programming is to utilize community-based and public health approaches to prevent crime and address the needs of community members, rather than using the traditional, punitive, criminal justice system strategies of reacting to criminal offenses. Deflection programs are voluntary and usually happen before being charged with a crime. There are varying types of substance use deflection programming, including co-responder models, community outreach teams, post-overdose interventions, and officer
routine activity prevention. In particular, substance use deflection programs aim to direct community members to treatment or resources for their substance use in an attempt to solve the underlying mechanisms leading to frequent substance use.10 Examples of pre-arrest deflection programs include New Castle County Division of Police’s Hero Help Program,11 Dover Police Department’s Angel Program,12 and the Delaware State Police’s Police Diversion Program.13
Police Attitudes
Amid the growth of deflection programs, attention should be given to the buy-in of law enforcement officers tasked with implementing these efforts. We consider how police officers’ perceptions and attitudes view the effectiveness and implementation of deflection programs. We specifically evaluate the role of four factor sets (i.e., leadership, tough-on-crime attitudes, occupational experiences, and personal characteristics) in potentially shaping beliefs. First, leadership’s stance on deflection programs and practices may influence officers’ willingness to engage in alternative policing practices14,15 Early deflection programs responding to rising overdose rates have demonstrated chiefs’ energy and hard work made programs possible in the first place (see the example of the Gloucester, MA Police Department’s Angel Program16).
Second, tough-on-crime views may impact views on deflection as a non-traditional alternative. Literature suggests officers can take on more “warrior” or “guardian” policing styles.17 The former emphasizes a strong “crime-fighting” strategy that prioritizes law and order through officer control, while the latter focuses more on service through community engagement and building relationships.18 These worldviews affect officer cynicism (or optimism) towards the rehabilitation of people in treatment, even impacting their everyday decisions to refer qualifying individuals to treatment.19
Third, the occupational experiences of police officers may shift attitudes toward deflection programs. Deflection training, including education about substance use and naloxone administration, has a profound range of impact on perceptions about police officer skills or readiness,20 people who experience overdoses,21 and overall programmatic interventions.22 Experience in larger departments reflects differences in resources and opportunities to perform their jobs. Moreover, an officer’s tenure and length of service in their current position as a police officer can change identification, relationships, and involvements with their departments.23 Longer service can further expose officers to issues of substance use and outcomes following police encounters with individuals diagnosed with SUD.24
Fourth, an officer’s personal identity may serve as a lens to perceive the effectiveness and implementation of deflection programs. Gender25,26 and race/ethnicity27,28 are associated with differences in officers’ willingness to engage in more empathetic, communication-focused, and community-oriented policing practices. Personal relationships with others diagnosed with behavioral health disorders could also lend to different understandings of and feelings toward people affected by substance use disorder.22,29
A main critique of literature on deflection and other servicecentered approaches to policing is that studies largely do not consider whether police deflection programs have an impact in
the community.30 A more recent analysis of the effectiveness of police-involved overdose outreach programs in New England found police thought outreach and conversations with people who use drugs (PWUD) about treatment options successfully encouraged individuals to be involved in treatment, but place less weight on the idea that these mechanisms impact a person’s decision regarding entering treatment.31 This study’s analysis of police buy-in and perceived effectiveness adds to the growing knowledge on treatment and public health approaches to reducing substance use and substance use-related issues.
METHODS
Data
This study presents descriptive and multivariate regression results derived from an original survey of Delaware police officers to gauge their attitudes on deflection programs. The survey is part of a series of surveys launched on behalf of the Criminal Justice Council’s Delaware Comprehensive Opioid, Stimulant, and Substance Abuse (COSSAP) Saving Lives project, supported by the U.S. Bureau of Justice Assistance (15PBJA-22GG-04461-COAP). All surveys are anonymous and voluntary. This approach allows officers to confidentially answer questions. The research team, though, is unable to perform longitudinal data analysis because we do not track respondents and their responses over time.
Data for this study derives from a 2025 online survey disseminated via a link embedded in an email to all police officers working in state and local law enforcement agencies. The survey was available for six weeks from January to February 2025. All responses were captured by REDCap, a secure data collection and record management system. Respondents were not compensated for completing the survey, and completion of the survey was voluntary.
A total of 369 police officers completed the survey. Among the completed surveys, 131 officers (36% of the sample) reported working in an agency with a substance use deflection program. Our final sample contains 111 respondents, who answered all deflection program and demographic questions.
Dependent Variables
Our study has 14 dependent variables associated with our research questions. The first variable measures deflection program effectiveness. We asked respondents, “How effective do you think a substance use deflection program will be in your community?” and gave them a four-point scale ranging from “extremely ineffective,” “ineffective,” “effective,” and “extremely effective.” Due to skew in the response category, we collapse this question into two categories: “ineffective” (=0) and “effective” (=1).
Then, we use 12 dependent variables to measure police officer attitudes towards the implementation of their department’s substance use deflection program in more detail. We replicate the 12 implementation outcome questions provided by the National Institutes of Health’s Justice Community Opioid Innovation Network (JCOIN).32 Such survey questions were originally developed by Weiner et al. (2017) as part of a psychometric assessment strategy for program implementation.3 We ask respondents to rate on a four-point scale whether they “strongly disagree,” “disagree,” “agree,” or “strongly agree” with 12 statements. Nine statements ask if
“ our agency’s deflection program…” “seems fitting”, “seems suitable”, “seems applicable,” “seems like a good match”, “seems implementable,” “seems possible,” “seems doable,” “seems easy to use,” “meets my approval,” “is appealing to me.” We likewise ask two individual-centered questions: “I like our agency’s deflection program,” and “I welcome our agency’s deflection program.” These sentiments tap into the acceptability, appropriateness, and feasibility of the program.
Our last dependent variable measures perceived barriers to deflection programs. We ask police officers, “Do you perceive any barriers to implementing a diversion program?” and ask them to check off all potential barriers from a list of 17 options. These options included: “working with service providers,” “having people interested in treatment,” “officer ‘buy-in’ with the program,” “a lack of diversion training,” “creating partnerships with treatment centers,” “the potential ineffectiveness of diversion,” “the potential for diversion to be time-consuming,” “not enough officers employed,” “a lack of available treatment services/options,” “staffing shortages at treatment centers,” “housing issues/homelessness,” “transportation to services,” “overcoming addiction,” “addressing trauma/PTSD,” “the potential complexity of diversion,” “the potential financial costs of diversion,” and “Other.” If a respondent selected “Other,” they had the opportunity to add another barrier as free-text in a space provided below.
Independent Variables
We introduce 11 independent variables to measure attitudes toward leadership, approaches to crime, occupational experiences, and personal characteristics of police officers participating in our survey. Our first variable of police officer attitudes toward leadership was captured through a leadership index. Respondents were asked to provide their level agree with the statements: “Leadership within my department encourages thinking about problems in new ways,” “Leadership within my department gives encouragement and recognition to staff,” “Leadership within my department communicates a clear and positive vision of the future for our department,” “Leadership within my department encourages my professional development,” “Leadership within my department fosters trust, involvement, and cooperation among staff” “Leadership within my department is supportive of police-led diversionary programs (i.e., substance use, mental health).” A six-item scale was created based on a factor analysis using polychoric correlations. Cronbach’s alpha results demonstrated a high internal reliability between items (alpha=0.90). An appendix table presenting these factor loadings is available upon request. Our second independent variable concerns the approaches of police officers when enforcing the law and addressing crime. A tough-on-crime index was generated by asking participants their level of agreement with the following items: “If police don’t arrest for minor offenses, it will only encourage more serious crime,” “It is the police officer’s job to enforce the law ‘by the book.’” “ The only way for police to get respected is to get tough on offenders,” and “Police should be enforcing the law, rather than engaging with substance use or mental health issues.” Factor analysis using polychoric correlations confirmed that items loaded onto one factor. Cronbach’s alpha demonstrated acceptable internal reliability for this measure (alpha=0.58). Factor loading estimates are also reported in an appendix table that is available upon request.
Next, several characteristics of police officers’ occupational background are analyzed. Dichotomous variables were included to capture exposure to deflection training (1= received, 0= not received), large department size (1= more than 51 officers, 0= 50 officers or less), length of time serving as an officer (1= more than 10 years, 0= less than 10 years), and the length of time in the officer’s current position (1= five years or less; 0= six years or more). Lastly, we account for the personal characteristics of police officers. A dichotomous measure was utilized for sex (1 = male, 0 = female). Race and ethnicity are also captured through a dichotomous variable (1= non-Hispanic, white, 0= other racial/ethnic group). We also include if they have any close friends or family members who have or had a substance use disorder (SUD) or mental health illness (MHI) (1 = yes, 0 = no).
Analysis
We performed four sets of analysis on this final sample. First, we present descriptive statistics describing the sample of police officers working in departments with substance use deflection programs and their overall beliefs about their programs’ effectiveness. Next, we summarize descriptive statistics about the implementation of their department’s substance use deflection program. We replicate JCOIN’s implementation outcomes measures introduced by Weiner and colleagues (2017) to solicit perceptions of program acceptability, appropriateness, and feasibility. Third, we display the results of a logistic regression model that predicts officer beliefs about deflection program effectiveness based on their beliefs towards leadership, approaches to enforce the law, occupational experiences, and demographic characteristics. Finally, we show proportions of officers who agreed to survey-identified barriers to the implementation of deflection programs. The research team identified these barriers based on prior research4 and informal conversations with key informants participating in the COSSAP project.
RESULTS
Descriptive Results for Overall Deflection Program Effectiveness, Attitudes, and Characteristics of Respondents in the Sample
Table 1 provides descriptive statistics for the overall attitudes and characteristics of police officers in agencies with deflection programs. A majority (59%) of these officers believe that their department’s substance use deflection program was effective. These respondents have generally positive views toward leadership (3.03 out of a possible maximum of 6 in agreement). On average, they tend not to have strongly tough-on-crime views when enforcing the law (average index value is 2.61). Approximately half (48%) of the sample received some form of deflection training within the last year. Over three-quarters of the respondents work in departments with 50 or more officers, have least ten years of service, and have been in their current position for 5 years or less. Demographically, police officers were predominantly male and white. Almost two-thirds of respondents express that they know a close friend or family member with substance use or a mental health disorder.
Descriptive Results for Respondent Views on Deflection Program Implementation
With considerable support for deflection programming, we then explore police officers’ beliefs about the acceptability, appropriateness, and feasibility. Table 2 details responses concerning the character of their agency’s substance use deflection program using twelve psychometric measures of program implementation. When considering acceptability, four out of five officers welcome deflection programs and approve of them. A strong, but slightly lower proportion (67%) find deflection programs appealing. About 75% of respondents state that they like their agency’s deflection programs.
Substance use deflection programs score high on metrics of appropriateness and feasibility. Over 80% of police officers agree or strongly agree that these initiatives seem fighting, suitable, applicable, and like a match. Similar levels of support are found for beliefs that the program is implementable, possible, doable, and easy to use. Only a small percentage (less than 5%) of police officers strongly disagree with the appropriateness and feasibility of their department’s program.
Logistic Regression Results Predicting Beliefs in Deflection Program Effectiveness
Table 3 presents estimates of a logistic regression analysis predicting police officers’ beliefs in the effectiveness of their department’s substance use deflection program. Attitudes towards leadership do not appear to have a strong impact on views towards deflection programming. Police officers who take on tougher-on-crime perspectives are significantly less likely to believe in the effectiveness of deflection programs. Occupational experience has mixed effects on police officers’ perspectives on deflection initiatives. Results suggest that training does not strongly influence views. Those working in larger departments are more likely to express that the agency’s deflection efforts are effective. Tenure, as measured by length of service, also does not play a significant role in shaping attitudes; however, staying in one’s position for less than 5 years reduces the odds of believing in a deflection program’s efficacy by 68%. Personal characteristics of officers also matter. Gender and race/ethnicity do not
substantially change beliefs about deflection programs. Knowing someone with substance use or a mental health disorder, however, makes an officer significantly more likely (i.e., 130% increase) to agree with the effectiveness of a deflection program.
Descriptive Results of Police Officers on Barriers to Deflection Program Implementation
Table 4 summarizes descriptive results of perceived barriers to implementing a substance use deflection program among police officers. The table ranks barriers from most to least frequently reported. The most common barrier to program success is having people interested in treatment. Approximately 65% of police officers identify individuals’ interest in treatment as an obstacle. The second most cited barrier among police officers is housing issues or homelessness, with 60% of the sample identifying this as an issue. Almost a majority (49.5%) names the potential
ineffectiveness of deflection as a barrier. Other considerable barriers include logistical concerns, such as staffing shortages at treatment centers (42%), transportation to services (36%), and a lack of available treatment options (36%). About a third of police officers distinguish “buy-in” and not enough officers employed in deflection programs as problems. Offices have fewer operational concerns about a lack of diversion training and the financial costs of diversion. A large portion of the sample (42%) believes that overcoming addiction challenges affects deflection efforts.
Deflection has become an attractive alternative to traditional methods of arrest, formal charging, and incarceration when police encounter individuals presenting with substance use disorder symptoms. The opinions of law enforcement officers should be given special attention, as they shape the legitimacy of a deflection program and expectations for its outcomes. This study explored the beliefs of Delaware police officers working in agencies with deflection programs to discern general attitudes about program effectiveness, implementation, and barriers to program success. We summarized 111 responses about deflection programs from a survey fielded to Delaware police officers in January 2025 using descriptive statistics and a logistic regression model to predict beliefs in the effectiveness of their agency’s deflection program. Our study points to four findings. Police officers generally believe their departments’ deflection programs are effective. We found that 59% of officers ranked their program as “effective” or “extremely effective.” We then determined that police officers express stronger beliefs in the acceptability, appropriateness, and feasibility in the implementation of deflection programs. Four out of five officers agreed with statements that deflection programs seemed “doable,” “fitting,” “possible,” “easy to use,” “implementable,” and “like a match,” among other metrics. Twothirds of the sample reported “liking” deflection programs. Next, we established drivers of beliefs in program effectiveness. Results of a logistic regression model show that knowing someone with behavioral health issues and working in a larger department increase the likelihood of describing deflection programs as effective. Conversely, tough-on-crime attitudes and being in a position diminish beliefs in program efficacy. Our study found less support for the potential roles of leadership, tenure, training, race/ethnicity, or gender on police officers’ opinions toward deflection initiatives. Finally, police officers agree that a range of barriers inhibit deflection programs. While interest in treatment and homelessness appear to be common issues related to enrollment, almost half (49.5%) of police officers cited the potential ineffectiveness of diversion as a concern.
The study has several limitations to be kept in mind. Due to concerns for privacy and confidentiality, we were unable to ask questions about the details of officers’ positions or their departments. For example, we cannot determine whether a respondent was directly involved with a deflection program. We also could not ask officers to name their departments or the communities that they serve. Substance use problems, including overdose death and opioid-related arrest rates, and available behavioral health services vary across geographic space.33 It is possible that perceptions of program effectiveness relate to underlying conditions in their jurisdictions and their exposure to everyday deflection program operations. Next, we do not know how deflection program perceptions relate to the specifics of the problems. We also do not know when a deflection program began or the nature of the intervention (e.g., staffed with volunteers, full-time clinicians, part-time case managers, or specially trained officers, etc.). More advanced or fully resourced programs, such as Hero Help, may encourage police officers to think differently about substance use deflection relative to newer or smaller initiatives. Furthermore, our survey derives from a smaller sample of officers in Delaware. The views of over a hundred officers may differ from those of their colleagues, as officers who do not
have strongly positive or negative feelings about substance use deflection may not have completed the survey. Our findings of program effectiveness and predictors of these views may also not generalize to areas without knowledge of, exposure to, or training for deflection programs.
PUBLIC HEALTH IMPLICATIONS
Results of this study point to two implications for public health. Because police officers generally believe that deflection programs work, we can expect that deflection as a practice has legitimacy among the ranks of law enforcement. Such positive responses to deflection may be an indication of evolving understandings of the role of police in combating high overdose death rates in their communities. Likewise, it may suggest that deflection programs may have buy-in from ordinary officers over time. Police leadership and public health practitioners may be reasonably hopeful that officers may eventually see the utility of new deflection programs. This study further underscores that officers understand the real barriers to deflection programs. Commonly cited issues to implementing deflection programs — interest in treatment, housing or homelessness, staffing shortages, and fears of program ineffectiveness — are not simple to resolve. Indeed, these issues point to the need for cross-system collaboration to encourage connection to direct and indirect supportive services. Deflection has considerable promise, underscoring an evolution in how law enforcement officers perceive their responsibilities and how police can better serve their communities.
Dr. Donnelly may be contacted at done@udel.edu
ACKNOWLEDGMENTS
This work was supported by the Comprehensive Opioid Abuse Site-based Program (COSSAP) (15PBJA-22-GG-04461-COAP) through the State Criminal Justice Council. Views expressed in this article are those of the authors.
REFERENCES
1. Garnett, M. F., & Miniño, A. M. (2024). Drug overdose deaths in the United States, 2003–2023. Centers for Disease Control and Prevention. https://doi.org/10.15620/cdc/170565
2 Centers for Disease Control and Prevention. (2022, March 1). Drug overdose mortality by state https://www.cdc.gov/nchs/pressroom/sosmap/drug_poisoning_ mortality/drug_poisoning.htm
3 Weiner, B. J., Lewis, C. C., Stanick, C., Powell, B. J., Dorsey, C. N., Clary, A. S., . . . Halko, H. (2017, August 29). Psychometric assessment of three newly developed implementation outcome measures. Implementation Science : IS, 12(1), 108 https://doi.org/10.1186/s13012-017-0635-3
4 Blais, E., Brisson, J., Gagnon, F., & Lemay, S.-A. (2022, July). Diverting people who use drugs from the criminal justice system: A systematic review of police-based diversion measures. The International Journal on Drug Policy, 105, 103697. https://doi.org/10.1016/j.drugpo.2022.103697
5 My Healthy Community. (2025). Drug overdose deaths Delaware.gov https://myhealthycommunity.dhss.delaware.gov/topics/drug-overdosedeaths/death-certificates/state
6 Charlier, J. (2014). Law enforcement deflection frameworks: A decision making tool for police leaders. Center for Health and Justice at Treatment Alternatives for Safe Communities.
7 Police Treatment and Community Collaborative. (2021). Pre-Arrest Diversion: Pathways to Community. Police, Treatment, and Community Collaborative. https://ptaccollaborative.org/
8 Widgerly, A. (2023). The legislative primer series for front-end justice: deflection and diversion. National Conference of State Legislatures. https://documents.ncsl.org/wwwncsl/Criminal-Justice/DeflectionDiversion-f02.pdf
9 Charlier, J. (2022, July 31). Deflection: a powerful crime-fighting tool that improves community relations. Police Chief Magazine https://www.policechiefmagazine.org/deflection-a-powerful-crimefighting-tool-that-improves-community-relations/?ref=659e399c2000a 873d104f964920a672b
10 Charlier, J., & Reichert, J. (2020). Introduction: deflection—police-led responses to behavioral health challenges. National Association of Drug Court Professionals.
11 Donnelly, E. A., Stenger, M., Streisel, S., O’Connell, D. J., & Arnold, J. (2021). Addressing opioid misuse: Hero help as a recovery and behavioral health response. Journal of Community Safety & Well-being, 6(3), 142–147 https://doi.org/10.35502/jcswb.191
12 Horn, B. (2016). Dover police start Angel program to combat heroin The News Journal. https://www.delawareonline.com/story/news/local/ heroindelaware/2016/06/29/dover-police-start-angel-program-combatheroin/86428350/
13. Division of Substance Abuse and Mental Health. (2023). State of Delaware Police Diversion Program (PDP). State Epidemiological Outcomes Workgroup (SEOW) Summer Meeting, Delaware Health and Human Services Department, Division of Substance Abuse and Mental Health.
14 Myhill, A., & Bradford, B. (2013). Overcoming cop culture? Organizational justice and police officers’ attitudes toward the public. Policing, 36(2), 338–356 https://doi.org/10.1108/13639511311329732
15 Donnelly, E. A., Stenger, M., O’Connell, D. J., Gavnik, A., Regalado, J., & Bayona-Roman, L. (2024). Police officer attitudes toward pre-arrest behavioral health diversion programs: Identifying determinants of support for deflection using a machine learning method. Policing, 47(4), 648–662.
https://doi.org/10.1108/PIJPSM-11-2023-0158
16. Schiff, D. M., Drainoni, M.-L., Weinstein, Z. M., Chan, L., BairMerritt, M., & Rosenbloom, D. (2017, November). A policeled addiction treatment referral program in Gloucester, MA: Implementation and participants’ experiences. Journal of Substance Abuse Treatment, 82, 41–47 https://doi.org/10.1016/j.jsat.2017.09.003
17 McLean, K., Wolfe, S. E., Rojek, J., Alpert, G. P., & Smith, M. R. (2020). police officers as warriors or guardians: Empirical reality or intriguing rhetoric? Justice Quarterly, 37(6), 1096–1118 https://doi.org/10.1080/07418825.2018.1533031
18 Murphy, K., & McCarthy, M. (2024). Guardian versus warrior cops: Predicting officers’ support for procedural justice and coercive policing. Policing and Society, 34(10), 1011–1030. https://doi.org/10.1080/10439463.2024.2357653
19. Schaible, L., Gant, L., & Ames, S. (2021). The impact of police attitudes towards offenders on law-enforcement assisted diversion decisions. Police Quarterly, 24(2), 205–232 https://doi.org/10.1177/1098611120960714
20 Purviance, D., Ray, B., Tracy, A., & Southard, E. (2017, Apr-Jun). Law enforcement attitudes towards naloxone following opioid overdose training. Substance Abuse, 38(2), 177–182. https://doi.org/10.1080/08897077.2016.1219439
21. Winograd, R. P., Stringfellow, E. J., Phillips, S. K., & Wood, C. A. (2020, September 2). Some law enforcement officers’ negative attitudes toward overdose victims are exacerbated following overdose education training. The American Journal of Drug and Alcohol Abuse, 46(5), 577–588
https://doi.org/10.1080/00952990.2020.1793159
22 Kruis, N. E., McLean, K., & Perry, P. (2021, December). Exploring first responders’ perceptions of medication for addiction treatment: Does stigma influence attitudes? Journal of Substance Abuse Treatment, 131, 108485
https://doi.org/10.1016/j.jsat.2021.108485
23 Shafiq, N., Ohlsson, I. M., & Mathias, P. (2016). Predictors of punitive attitudes among police officers. Journal of Forensic Practice, 18(1), 76–86
https://doi.org/10.1108/JFP-04-2015-0025
24 Rouhani, S., Schneider, K. E., Rao, A., Urquhart, G. J., Morris, M., LaSalle, L., & Sherman, S. G. (2021, December). Perceived vulnerability to overdose-related arrests among people who use drugs in Maryland. The International Journal on Drug Policy, 98, 103426 https://doi.org/10.1016/j.drugpo.2021.103426
25 Rabe-Hemp, C. E. (2009). POLICEwomen or PoliceWOMEN?: Doing gender and police work. Feminist Criminology, 4(2), 114–129. https://doi.org/10.1177/1557085108327659
26. McCarthy, D. J. (2013). Gendering ‘soft’ policing: Multi-agency working, female cops, and the fluidities of police culture/s. Policing and Society, 23(2), 261–278 https://doi.org/10.1080/10439463.2012.703199
27 Paoline, E. A., Myers, S. M., & Worden, R. E. (2000). Police culture, individualism, and community policing: Evidence from two police departments. Justice Quarterly, 17(3), 575–605 https://doi.org/10.1080/07418820000094671
28 Jenkins, M. J. (2016). Police support for community problem-solving and broken windows policing. American Journal of Criminal Justice, 41(2), 220–235 https://doi.org/10.1007/s12103-015-9302-x
29 Green, T. C., Zaller, N., Palacios, W. R., Bowman, S. E., Ray, M., Heimer, R., & Case, P. (2013, December 1). Law enforcement attitudes toward overdose prevention and response. Drug and Alcohol Dependence, 133(2), 677–684 https://doi.org/10.1016/j.drugalcdep.2013.08.018
30 Shapiro, G. K., Cusi, A., Kirst, M., O’Campo, P., Nakhost, A., & Stergiopoulos, V. (2015, September). Co-responding police-mental health programs: A review. Administration and Policy in Mental Health, 42(5), 606–620 https://doi.org/10.1007/s10488-014-0594-9
31 Becker, L. T. (2021). Police perceptions of police-involved overdose outreach program effectiveness. Journal of Drug Issues, 51(4), 611–627. https://doi.org/10.1177/00220426211016324
32. JCOIN Coordination and Translation Center. (2025). JCOIN core measures. Justice Community Overdose Innovation Network Coordination and Translation Center https://www.jcoinctc.org/resources/core-measures/
33. Donnelly, E. A., Brown, C. L., McBride, A., Beletsky, L., & Anderson, T. L. (2023). Emerging disparities in the placement of law enforcementbased treatment referral and recovery programs. Criminal Justice Review, 48. https://doi.org/10.1177/07340168221117109
DELAWARE’S CHILD RESTRAINT LAW HAS CHANGED
Ensure your child’s safety and obey the law by following the requirements below.
• Children under the age of 2 and 30 pounds must ride in a rear-facing car seat.
• Children under the age of 4 and 40 pounds must ride in a harnessed car seat.
• Children who are old enough to ride in booster seats must remain in the booster seat until they reach the height or weight maximum listed by the booster seat manufacturer. While booster seat maximums vary, it will never be lower than 4'4".
OHS FITTING STATIONS
To schedule a FREE car seat check, please contact one of our fitting station coordinators.
OHS General Contact Information: Email: DSHS_OHS@Delaware.gov
Phone: 302-744-2740
Susan’s Recovery Story: A Journey of Rediscovery and Renewal
Ashley Reed Sober Living Program Manager, Limen Recovery + Wellness
SUSAN’S RECOVERY STORY: IN HER OWN WORDS
For much of my life, addiction overshadowed everything. I was a daughter, a friend, and a hairstylist who found joy in helping others feel beautiful. But behind every haircut and smile, I hid a growing struggle with substance use disorder—one that followed me from Delaware County to Philadelphia and eventually to Wilmington. I experienced periods of sobriety and hope, times when I believed I was finally turning a corner. But addiction kept pulling me back, eroding my spirit piece by piece.
Then came the pandemic. The world shut down, and so did my last threads of stability. The loneliness, fear, and chaos of COVID-19 pushed me to a devastating relapse. I fell deeper into addiction—this time using fentanyl laced with xylazine. It ravaged my body, leaving my legs covered in deep, infected wounds. I was starving, emotionally shattered, and spiritually hollow. I lost everything—my relationships, my career, and any vision I had for the future. I was surviving, but barely.
In 2022, I arrived at Saint Francis Hospital at what I believed was the end of my road. I was admitted in critical condition, wracked with pain, caught in the throes of withdrawal, and consumed by hopelessness. But something unexpected happened—a moment that changed everything. A nurse looked me in the eye and gently said, “Stay. Take care of your body.”
Those few words stirred something in me. For the first time in a long time, I felt seen. That spark of human connection became the start of something new.
I spent months in the ICU undergoing surgeries and intensive wound care. It was excruciating—physically, emotionally, spiritually. But in that painful stillness, something within me began to heal. The staff didn’t just care for my wounds; they treated me like a person who mattered. Their compassion helped me reconnect with my own humanity. I stopped just surviving. I began to imagine what it might feel like to truly live.
That’s when I found Limen Recovery + Wellness.
At Limen, I finally found space to breathe—to be still, safe, and seen. I stayed for over a year, immersing myself in therapy, community, and healing. The women there became my chosen family. Day by day, I rebuilt my foundation. I faced hard truths, made amends, forgave myself, and reclaimed the woman I thought I had lost. Recovery isn’t just about stopping the use of substances. It’s about rediscovering who you really are. Limen gave me structure and hope—but more than anything, it gave me back to myself. I found my voice. I found purpose. I found strength.
Today, I’m an active member of a 12-step fellowship, and I’ve celebrated multiple years of continuous sobriety— something I never thought possible. I’m creating a life filled with connection, service, and intention. I still face challenges, but now I have the tools, support, and faith to meet them head-on.
This journey has not been easy. But it has been beautiful. And I am forever grateful—for Saint Francis, for Limen, for Ashley, and for the second chance I was given.
A PARTNER IN HEALING: FROM THE PERSPECTIVE OF LIMEN HOUSE STAFF PERSON ASHLEY REED
I first spoke to Susan while she was still at Saint Francis Hospital, preparing for discharge and searching for her next step. She was physically fragile and emotionally depleted, and she shared that she had already been turned away from numerous rehabilitation centers and housing programs due to her extensive medical needs.
Even through the phone, I could sense her desperation and deep desire for change. I knew we would need to make adjustments to our program to meet her unique medical and emotional needs. And we did. We admitted Susan and immediately began tailoring our support around her. This wasn’t hard to do because Susan was ready. She was grateful, determined, and willing to do the work to rebuild her life.
I had the privilege of working with her one-on-one, supporting her physical recovery, her sobriety, her mental health, and— perhaps most profoundly—her spirit. During her time with us, Susan connected deeply with a 12-step fellowship. She got a sponsor and experienced her own spiritual awakening. She also began to give back, volunteering with Meals on Wheels, and we helped her secure disability support to provide some financial stability.
When she completed our program and moved on to live independently, she was no longer the same woman who had first called me. Saint Francis had helped heal her body—but at Limen, Susan healed her soul. Watching her journey has been one of the greatest honors of my career.
Providers are on the front lines of behavioral health care: WHO: Pediatricians, family physicians, nurse practitioners, physician assistants, and OB-GYNs serving patients 21 and under.
CHALLENGE: Many providers feel unequipped to diagnose, treat, or manage behavioral health conditions.
DCPAP equips providers with expert guidance, training, and resources to navigate behavioral health challenges with confidence:
• Immediate access to a child and adolescent psychiatrist during office hours: Tuesdays and Thursdays, 12–2 p.m.
• Consultations within 24 hours for screening, diagnosis, and treatment.
• Ongoing training and education through live and recorded webinars, clinical guidelines, and more.
• Referral assistance to connect patients with specialized care.
Timely behavioral health support is critical:
· DCPAP’s provider-to-provider collaboration model connects you with child and adolescent psychiatrists for expert guidance.
· With timely support, you can confidently address behavioral health concerns, improving patient outcomes.
• ADHD, anxiety, depression, and other mental health concerns
• Medication management and treatment considerations
• Disruptive behavioral problems
COMMON TOPICS FOR DCPAP CONSULTATIONS: FOR PATIENTS 21 AND UNDER.
Innovation Collaboration: Harnessing the Power of Nurse Scientist and Bedside Nurse Partnerships
The nursing profession is deeply rooted in the life and behavioral sciences, having evolved from the historical image of white dresses and caps to modern scrubs and lab coats. Despite its strong foundation in scientific processes, nursing is not yet recognized as a STEM profession. Nurses trained in research and PhD-prepared nurse scientists are paving the way for academia and healthcare to acknowledge the contributions of nursing to science through research, promotion of evidence-based practice, and dissemination of curated knowledge. Nurse scientists play a crucial role in involving more clinical nurses in research efforts. However, clinical nurses face several challenges in participating in research. To address these challenges, ChristianaCare launched the Nursing Fellowship in Robotics and Innovation in 2024. This fellowship provides clinical nurses with research opportunities and mentorship from nurse scientists. It successfully bridges the gap between clinical practice and research, fostering a future where nurses are integral contributors to scientific advancement.
BACKGROUND
Close your eyes and envision a nurse during their shift. What comes to mind? For some, it may be the classic white, crisp dress and cap, emblematic of the deep-rooted history of nursing. For others, it may be more modern scrubs, possibly in a fashionable style, reflective of the agility and forward progress in nursing. Or perhaps it’s the iconic pandemic nurses, depicted with capes as ‘healthcare heroes.’1 But what about wearing a lab coat?
Clinical nurses utilize assessment skills, deductive reasoning, and pharmacokinetic knowledge, while consistently leveraging evidence-based practices in their daily work. Despite nursing being deeply rooted in sciences such as biology, chemistry, physics, behavioral psychology, pharmacology, and pathophysiology, it is not traditionally classified as a science or considered a STEM (science, technology, engineering, and mathematics) profession. Nurses are regularly engaged in a scientific process that mirrors that of researchers; however, they are not typically viewed as a profession made up of scientists.2,3 The discipline of nursing science emerged during the era of Florence Nightingale and has progressively evolved throughout the 20th century to the present day. Today, nurse scientists are integral to academia, hospitals, and joint academic-practice roles.4 These professionals are nurses who have completed a PhD in nursing science. Their roles encompass conducting original research, building and fostering a culture of inquisitive scholars, and championing knowledge uptake and application to drive innovation and enhance practice.5
Nurse scientists play a pivotal role in enhancing healthcare and the role of clinical nurses. They strengthen the visibility and value of PhD-prepared nurses, foster inquiry, and promote scholarly activities within the nursing profession.6 As the role of nurse scientists continues to evolve, institutions are increasingly able to leverage their expertise to further advance nursing practice and research.7
Despite the expanding field of nursing science and the increasing presence of nurse scientists within healthcare systems, clinical nurses face various barriers to participating in research. These barriers include insufficient knowledge and skills, lack of mentorship, and inadequate protected time for research activities.8
CHRISTIANACARE’S NURSING FELLOWSHIP IN ROBOTICS AND INNOVATION
To address these challenges, ChristianaCare established a new Nursing Fellowship in Robotics and Innovation. This fellowship aims to enable clinical nurses to engage in technology-based research and acquire essential knowledge and skills that are often inaccessible to those nurses working at the bedside or in the clinic. Launched in mid-2024, the fellowship consists of a weekly four-hour commitment dedicated to asynchronous learning, lectures, and robust discussions. The fellows also participate in ongoing robotics research, including an IRB-approved study examining the value of a co-bot within the hospital.
To enhance their learning experience, the fellowship is led by a nurse scientist within the hospital system, with a second PhDprepared clinical nurse scientist assisting. These nurse scientists provide a more enriching mentorship experience. They offer greater guidance in the research process, career advice, and networking opportunities, further exposing fellows to the world of health researchers.
The pioneering cohort of the fellowship is comprised of four diverse nurses from various practice areas with differing lengths of bedside careers. All fellows entered the program with at least a baccalaureate degree, with one currently enrolled in a Doctor of Nursing Practice program, and minimal hands-on research experience or knowledge.
A key feature of the program is its flexibility, designed to accommodate the fluid schedules of clinical nurses. The time commitment is financially compensated through prestigious
external funding from a national nursing foundation. This protected time enables fellows to engage in data collection and analysis, as well as literature exploration, thereby pursuing academic opportunities. Without such protected time, nurses often face the dilemma of sacrificing self-care to engage in research and professional advancement.9
CONCLUSION
The ChristianaCare Nursing Fellowship has further illuminated the need to fill the fountain of nursing knowledge, especially if we want more people to drink from it. If we do not create a stronger pipeline where bedside nurses can expose themselves to research with the mentorship of nurse scientists, eventually, the fountain will run dry. We must focus on creating a future in which, when the average person considers what does it means to be a nurse, they no longer see the white, crisp uniform of yesterday, but instead, the white, crisp lab coat driving the science of nursing forward.
Ms. Abernathy may be contacted at: briana.abernathy@christianacare.org
ACKNOWLEDGEMENT
We are deeply grateful to the American Nurses Foundation Reimagining Nursing Initiative and ChristianaCare leadership for their support and funding of this transformative fellowship, thoughtfully created for clinical nurses.
REFERENCES
1. Einboden, R. (2020, July). SuperNurse? Troubling the hero discourse in COVID times. Health (London), 24(4), 343–347. https://doi.org/10.1177/1363459320934280
2. Green, C., & John, L. (2020, April). Should nursing be considered a STEM profession? Nursing Forum, 55(2), 205–210 https://doi.org/10.1111/nuf.12417
3 Dreisbach, C., Wright, M. L., Walker, R. K., Byon, H. D., & KeimMalpass, J. (2022, June 26). Nursing science as a federally-recognized STEM degree: A call to action for the United States with global implications. International Journal of Nursing Studies Advances, 4, 100084 https://doi.org/10.1016/j.ijnsa.2022.100084
4 Stolley, J. M., Buckwalter, K. C., & Garand, L. (2000, Spring). The evolution of nursing research. J Neuromusculoskelet Sys, 8(1), 10–15. https://pubmed.ncbi.nlm.nih.gov/31511759
5 Vessey, J. A., McCabe, M., & Lulloff, A. J. (2017, February). Nurse scientists: One size doesn’t fit all. Nursing Management, 48(2), 26–34 https://doi.org/10.1097/01.NUMA.0000511917.44775.95
6. Birkhoff, S. D., Nair, J. M., Monturo, C., Molyneaux, D., Rochman, M. F., Sawyer, A. M., & Moriarty, H. (2020, October). Increasing nursing research capacity: The roles and contributions of nurse scientists within healthcare systems in the Greater Philadelphia region. Appl Nurs Res, 55, 151288 https://doi.org/10.1016/j.apnr.2020.151288
7. Allen, D. H., Arthur, E. K., Blazey, M., Brassil, K., Cahill, J. E., Cooley, M. E., Yoder, L. H. (2023, February). A scoping review on the nurse scientist role within healthcare systems. Worldviews on Evidence-Based Nursing, 20(1), 47–55 https://doi.org/10.1111/wvn.12624
8. Mulkey, M. A. (2021, May-June 01). Engaging bedside nurse in research and quality improvement. Journal for Nurses in Professional Development, 37(3), 138–142. https://doi.org/10.1097/NND.0000000000000732
9 Elias, R., Sawatsky, A., & Ratelle, J. (2024, April). Protected time for research among academic hospitalists: A qualitative study of hospitalist group leaders. Journal of General Internal Medicine, 39(5), 723–730 https://doi.org/10.1007/s11606-023-08525-5
Reimagining Nursing Through Innovation and Design Thinking
Hannah Rackie, B.S.N., R.N., C.-E.F.M. & Patricia C. Pawlow, Ph.D., A.C.N.P.-B.C. ChristianaCare Health System
ABSTRACT
Recruitment and retention of nurses is a national health issue with implications for patients, nurses, and other healthcare providers. This article describes an innovative opportunity for the professional development of nurses at a local health system. This Nursing Research and Innovation Fellowship provided participating nurses with the knowledge of a design thinking framework and fostered the application in the context of complex challenges they face in their daily work. The potential impact of such programs on job satisfaction, retention, and relevance to public healthcare issues is discussed.
INTRODUCTION
This article explores the growing nursing shortage and the need to attract and retain nurses in the setting of current challenges in the healthcare environment. It describes an innovative initiative at a local Delaware health system that engages nurses, teaching them skills that build resilience and support a problem-solving mindset. Sabine and Gibbs, in their article titled “Unraveling Healthcare Shortages in Delaware and Charting a Course for Equity and Resilience,” which appeared in the December 2023 issue of the Delaware Journal of Public Health (DJPH), noted the growing shortage of healthcare workers, including nurses.1 The gap between the number of new nurses entering the workforce and the open positions continues to increase. There is evidence that inadequate nurse staffing has a negative impact on both patient and nursing outcomes. Dr. Aiken and colleagues reported that high patient-to-nurse ratios are associated with increased patient mortality and nurse burnout.2 The public needs to be aware of this growing challenge.
A Delaware-based health system recently offered a unique professional development opportunity for nurses through the Nursing Research and Innovation Fellowship. In this yearlong training, nurses learned about research, innovation, and design thinking—a solution-oriented, patient-centered approach to addressing challenges. When nurses are engaged and feel valued, health systems are more likely to retain them. Exposing nurses to unique opportunities like this fellowship may contribute to the development of a more sustainable and resilient workforce.
REIMAGINING NURSING THROUGH INNOVATION AND DESIGN THINKING
If someone were to ask you to describe a nurse, what would you say? Typically, people think of a woman, often in scrubs, typically in a hospital setting. Although this may have been accurate many years ago, the image of nursing is evolving. Nursing is the largest component of the healthcare workforce, with over four million nurses nationwide3 and
nearly 40% practicing4 outside of direct bedside care. Nurses are increasingly serving in a wide range of roles – from public health to policy, education, and research. This ability to care for people in diverse settings empowers nurses to have a profound impact on all areas of the nation’s health, especially when they are given the proper support and tools. Although nurses are the largest portion of the healthcare workforce, the United States is currently facing a national nursing shortage crisis. Over 100,000 nurses left the profession during the pandemic, and data suggests that annually, the number of new nurses entering the workforce is approximately 20,000 less than anticipated openings.5 Additionally, a recent survey through the National Council of State Boards of Nursing (NCSBN) found that one-fifth, equivalent to approximately 900,000 nurses in the U.S., indicated they plan to leave the nursing profession by 2027.6 Inadequate nurse staffing leads to errors, increased patient morbidity and mortality, and increased nurse burnout.2 Nurse turnover is not only costly to the hospital systems but also negatively impacts patient outcomes. It is essential to create an environment where nurses of all levels of expertise can grow and thrive, allowing them to develop professionally and remain successful in their positions. Changes are needed to recruit and retain these essential members of our healthcare system.
Healthcare organizations nationwide are developing and implementing various strategies to retain nurses. Last August, ChristianaCare Health System established a unique Nursing Research Fellowship in Robotics and Innovation (NRFRI), bringing the topic of innovation and research to clinical nurses at the bedside. The fellowship was part of a larger project funded by the American Nurses Foundation Reimagining Nursing Initiative examining the use of robotics in nursing care. Through this fellowship, the four fellows were not only immersed in the research process and innovation experience but also allowed to network outside their clinical area and bolster skills not typically utilized in their current nursing role. The immensely positive feedback
received regarding the fellowship after such a short period reinforces nurses’ desire for continued education and growth in their daily work and throughout their careers.
Topics discussed during this program included survey design, abstract writing, health equity, and many other subjects. One of the most impactful topics discussed was the integration of design thinking in healthcare. Given the ever evolving and complex needs of patients, no two days at work are ever the same for nurses. Each patient presents distinct challenges that require thoughtful, individualized care. This day-to-day problem-solving fosters nurses to become natural innovators. One powerful way to support this was to introduce a framework, design thinking that aligns with the way nurses already think and work. While there are several ways to solve the same problem, there are also many ways to think about how to solve the same problem.
Design thinking is a problem-solving approach that originated in the 1970s in fields such as industrial and academic design, computer science, psychology, business, and engineering.7 Over recent years, design thinking has been increasingly integrated into the healthcare system due to its emphasis on human-centered, practical innovation. Given the current challenges the healthcare industry is facing, this new approach is gaining popularity. In fact, a title and abstract search for “design thinking” through PubMed in 2007 yielded zero papers, but the same search 13 years later resulted in over 60 papers.7 Unlike traditional approaches that focus solely on fixing the problem itself, design thinking is solution-focused and centered on the individual.8 This ensures that innovations are not just new and novel but usable and meaningful to the people they are designed for, typically patients, caregivers, or staff. The framework consists of five phases – empathize, define, ideate, prototype, and test. When performing the empathize step, nurses and healthcare team members set aside their own biases, observing and interviewing patients to pinpoint the problems accurately, ensuring that the end user ultimately benefits. Once they better understand the lens of the end user, they can more clearly define the challenge, create innovative ideas, propose a process or model to address the issue, and test or measure outcomes. While listed in chronological order, the process is designed to be iterative and flexible, allowing teams to revisit and refine ideas as they evolve.8 The focus on empathy and adaptability makes it a natural fit for nursing, where these traits are foundational to clinical care. When nurses focus on the needs of those most affected by healthcare challenges, they are addressing real-life problems in a practical, sustainable, and impactful way.
Many nurses remain unfamiliar with the design thinking framework despite the increasing utilization in healthcare environments. ChristianaCare is working to change that by embracing the idea of innovation and instilling it into its organizational culture. In addition to the externally funded and internally developed Nursing Research Fellowship,
two of Christiana Care’s nursing leaders were selected to participate in the prestigious Johnson & Johnson Nursing Innovation Fellowship in partnership with Penn Nursing and the Wharton School. Throughout this year-long program, participants and their teams apply design thinking to address problems specific to their practice areas, ultimately creating a more effective environment where nurses and patients can thrive. With two of the system’s top leaders participating in this fellowship, they exemplify nursing’s innovative approach to problem-solving patient care issues. Nurses who know their patients and the health care system are well-positioned to apply design thinking and drive the change they want to see.
Nurses who are more equipped with the skills to address challenges proactively are more engaged in their work and empowered to improve the work environment. They report increased job satisfaction, reduced burnout, and improved desire to remain in their current role.9,10
CONCLUSION
Christiana’s Nursing Research Fellowship is one example of how offering nurses opportunities to develop new skills and embrace change and innovation can make a difference. Introducing these skills early in a nurse’s career can foster a mindset that emphasizes patient-centered solutions. Even for those who eventually transition away from the bedside, these skills extend well beyond hospital walls, ultimately benefiting the nation’s health. Providing nurses with the tools they need to think creatively, approach problems differently, and act proactively can lead to significant health initiatives that address some of our most challenging issues in healthcare, particularly the retention of our largest healthcare workforce and the most trusted profession.11
My exposure to the Christiana Nursing Research Fellowship and the design thinking framework has changed my image of nursing. Nursing goes far beyond the bedside. Nurses can be researchers and innovators, solving complex problems related to patients and the healthcare system. My experience through this fellowship has not only better equipped me to care for my patients, but also opened my mind to future opportunities for my ongoing professional growth.
Ms. Rackie may be contacted at Hannah.rackie@christianacare.org .
ACKNOWLEDGEMENT
The authors would like to acknowledge the American Nurses Foundation Reimagining Nursing Initiative for funding this fellowship, and ChristianaCare leadership for supporting this program.
REFERENCES
1. Sabine, N & Gibbs, T.E. (2023). Unraveling healthcare shortages in Delaware and charting a course for equity and resiliency. Delaware Journal of Public Health. 9(5), 14-18. https://doi.org/10.32481/djph.2023.1
2. Aiken, L. H., Clarke, S. P., Sloane, D. M., Sochalski, J., & Silber, J. H. (2002). Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. JAMA, 288(16), 1987–1993. https://doi.org/10.1001/jama.288.16.1987
3. Rosseter, R. (2024, April). Nursing workforce fact sheet. American Association of Colleges of Nursing. https://www.aacnnursing.org/news-data/fact-sheets/nursingworkforce-fact-sheet
4. U.S. Department of Labor. (2025, April 18). Bureau of Labor Statistics, Occupation outlook handbook: Registered nurses. https://www.bls.gov/ooh/healthcare/registered-nurses.htm
5. Hoover, M., Lucy, I., & Mahoney, K. (2024, January 29). Data Deep Dive: A National Nursing Crisis. U.S. Chamber of Commerce. https://www.uschamber.com/workforce/nursing-workforce-datacenter-a-national-nursing-crisis
6. Suran, M. (2023). Overworked and understaffed, more than 1 in 4 US nurses say they plan to leave the profession. JAMA, 330(16), 1512–1514. https://doi.org/10.1001/jama.2023.10055
7. Krolikowski, K.A., Bi, M., Baggott, C.M., Khorzad, R., Holl, J.L., & Kruser, J.M. (2022). Design thinking to improve healthcare delivery in the intensive care unit: Promise, pitfalls, and lessons learned. J Crit Care. 69, 153999. https://doi.org/10.1016/j.jcrc.2022.153999
8. Han, E. (2022, January 18). What is design thinking & why is it important? Harvard Business School Online: Business Insights Blog. https://online.hbs.edu/blog/post/what-is-design-thinking
9. Cicolini, G., Comparcini, D., & Simonetti, V. (2013). Workplace empowerment and nurses’ job satisfaction: A systematic literature review. Journal of Nursing Management, 22(7), 855–871. https://doi.org/10.1111/jonm.12028
10. Gu, L., Wang, L., Pan, B. (2022). Psychological empowerment and job satisfaction in nurses: A systematic review and meta-analysis. Front Public Health, 10, 1022823. https://doi:10.3389/fpubh.2022.1022823 PMID: 36438239; PMCID: PMC9692104.
11. Saad, B. L. (2025, March 27). Americans’ ratings of U.S. professions stay historically low. Gallup.com https://news.gallup.com/poll/655106/americans-ratings-professionsstay-historically-low.aspx
Workforce
DSAMH Naloxone Access Training
New Castle County: Kent County: Sussex County:
Appoquinimink Community Library
2nd Thursday of each month
Training: 11:00am-12:00pm
POD:12:00pm- 1:00pm
Bear Public Library
4th Monday of each month
Training: 5:00pm- 6:00pm POD: 6:00pm-7:00pm
Claymont Public Library
1st Wednesday of each month
Training: 11:00am-12:00pm
POD:12:00pm- 1:00pm
Rt. 9 Library and Innovation Center
4th Friday of each month
Training: 11:00am-12:00pm
POD:12:00pm- 1:00pm
Dover Public Library
3rd Saturday each month
Training: 2:00pm - 3:00pm POD: 3:00pm - 4:00pm
4th Thursday Each Month
Training: 5:00pm - 6:00pm
POD: 6:00pm - 7:00pm
Harrington Public Library
1st Tuesday each month
Training: 12:00pm - 1:00pm POD: 1:00pm - 2:00pm
James Wiliams State Service Center
2nd Tuesday of each month
Training: 11:00am-12:00pm
POD:12:00pm- 1:00pm
What is Narcan
Narcan (Naloxone) is a medication that is effective in reversing the effects of an opioid overdose in an individual.
Learning Objectives:
• Recognize and effectively respond to an opioid overdose
• What Naloxone is, how to store it & to administer Relevant laws and legislation around Naloxone, including the statewide standing order
Georgetown Public Library
1st Tuesday each month
Training: 3:00pm - 4:00pm POD: 4:00pm - 5:00pm
Laurel State Service Center
1st Monday each month
Training: 12:00am - 12:00pm
POD: 12:00pm - 1:00pm
Lewes Public Library
2nd Saturday each month
Training: 12:00pm - 1:00pm
POD: 1:00pm - 2:00pm
Training:
Classroom-style. This is the most informative training for any member of the public offering an in depth presentation to a small group in 30-45 minutes with plenty of time for questions and answers.
POD (Point of Distribution):
This training is best for returning trainees, or those who have used their Naloxone kit previously. Only requires a few minutes per person.
Bedside Brain Breaks: How Stepping Back into Education Can Step Healthcare Forward
Morgan Tallo, B.S.N., R.N., C.C.R.N. and Susan Smith Birkhoff, Ph.D., R.N. ChristianaCare
ABSTRACT
Historically nurses have been drivers of innovation, from Florence Nightingale’s sanitation movement in the 1850’s to Anita Dorr creation of the code cart. This article explores the ingenuity of nursing and emphasizes the importance of education and professional development of bedside nurses. Amid the demands of increasing patient acuity and healthcare challenges, equipping bedside nurses with specialized education can yield improved patient outcomes alongside bedside nurse retention. The pioneering Nursing Research Fellowship in Robotics and Innovation at a local Delaware hospital is leading the way for nurses to engage in research, acquire new skills and become voices of change on their units. This fellowship demonstrates how a structured investment in nurses fosters curiosity and innovation, by offering nurses the tools, time, and support to ask “why not” and unlock solutions to today’s healthcare challenges.
Did you know a nurse initially developed what we know as the code cart in the mid-1960s? Anita Door was the innovative nurse who changed the way we approach and bring care to critically ill patients.1 Another nurse innovator was Sister Jean Ward, who recognized that jaundiced neonates improved at a faster rate when they were placed in direct sunlight.2 This innovation went on to become bilirubin lights that are still used in neonatal intensive care units to this day. These two nurses--along with countless others--are examples of how nursing ingenuity has the potential to profoundly change healthcare. These nurses recognized there could be a better way to take care of their patients.
This innovative spirit in nursing dates back to Florence Nightingale in 1854 who focused on cleaner environments, fresh fruit, and clean water that decreased mortality rates from 60% to 2.2% in her assigned military hospital.3 Clean spaces and fresh food seem like an obvious beneficial change to us today but back then when sanitation was not a standard of care, these changes directed by a nurse were groundbreaking. Today with increasing workforce challenges, could nurses have the time and space to be just as innovative with similar impacts on the future of our healthcare?
Patients today are sicker and require more sophisticated care than ever before. Experienced nurses are the backbone to provide this care, yet many may leave the bedside to pursue other opportunities. How can we keep them at the bedside to continue providing excellent care and to tap into their expertise to solve our challenging problems? One tried and true solution has been to invest in bedside nursing through professional development and education. Investing in nurses not only increases retentions rates, it reinvests into the organization and community, but most importantly has a positive impact on patient care.4 Nurses are one of patients’ strongest advocates, often supporting patients and their families through the worst times in their lives. From medication administration to discharge planning, nurses are there through it all and impact every part of the patient care process. Yet with the increasing complexities of the healthcare system,
nurses are in need of unique formalized training that can keep pace with the rapidly changing healthcare landscape that is also increasingly integrating technology to support and augment the healthcare workforce.
A local Delaware hospital did just that with nurses leading the research and implementation of delivery robots. What is more futuristic than a delivery robot cruising through hospital halls to offload specific tasks humans normally perform? This delivery robot is designed to be a collaborative robot or also known as a cobot. It is programmed to safely assist humans in shared and collective workspaces.5 For the past three years, these cobots have delivered thousands of medications, supplies, and equipment requests to most areas of the hospital. Nurses at different levels, led by a PhD trained nurse, conducted multiple research studies to better understand how a delivery cobot may be changing the work environment. Who is better equipment to investigate the practice environment than nurses themselves?
An extension of this research morphed into a formalized training program titled, “Nursing Research Fellowship in Robotics and Innovation.” Four bedside nurses from different practice areas were selected after a rigorous interview process to become the inaugural nurse fellow cohort. This ‘one of a kind, first of its kind’ fellowship provided a unique opportunity to invest in bedside nurses through rigorous education, inter-professional connections, and resources that will equip them with new skillsets, potentially leading to implementing research and evidence-based practice projects in their practice areas. Because the curriculum is anchored in researching robotics in the hospital setting, the fellows are exposed to studying this type of cuttingedge technology, which is not typically led by nurses.
Over the course of eight months, the fellows dedicated two hours a week to didactic presentations that introduced them to research designs, theoretical frameworks, protocol development, health equity, and grant funding. Special guest lectures about health inequity and assistive robotics in healthcare helped expose
nurse fellows to areas of healthcare not often talked about at the bedside. Another 2-4 hours a week were dedicated to applying their research knowledge directly to an active robotics study as co-investigators. This “brain break” from a typical patient care assignment allowed the fellows to gain a new perspective on how they can personally be innovative on their units (e.g., mentoring colleagues in the research process, advocating for implementing evidence-based practices, and determining areas of improvement in their specific patient population).
Gaining diverse skills from this unique fellowship program each week, these fellows became more empowered to think differently and to recognize their greater contribution within and beyond the bedside. These nurse fellows are now equipped with tools and professional connections to tackle a problem and start working on a solution that can impact the whole hospital system. For instance, the fellows began projects aimed at addressing opportunities for improvement in patient care on their respective units. Without this fellowship, the fellows would not have had the resources or support to start asking the “why not?” questions and advocating for change. These fundamental changes to their perspectives through formalized education have the potential to increase nurses’ professional commitment and decrease their intent to leave.4
The “why not” mindset is critical to be a catalyst for change not only healthcare but any workforce position. What would patient care look like if nurses like Anita Dorr and Sister Jean Ward left the bedside prematurely and took their genius ideas with them? What if Florence was not a pioneer for cleaner practice environments in hospitals back when that critical factor was overlooked? She is dubbed the mother of nursing2 and most likely she would be quite proud of the ingenuity of nurses who came after her.
Investing in professional bedside nurses’ development is one way to ensure that healthcare as a whole moves forward into the future. Nurses developing innovative ideas is nothing new, but acquiring many seats at the table to move ideas forward is a work in progress. Anita Dorr recognized a more efficient way to immediately respond to coding patients and then, went on to co-found the Emergency Nurses Association.1 Imagine the pioneering insights could be made to today’s high-tech healthcare if nurses like Anita and Jean could have been a part of research and innovation early on in their careers through professional development offered to bedside nurses. Florence, Anita, and Jean set a magnificent table for nurses and now, it is time to add more seats.
Ms. Tallo may be contacted at morgan.tallo@christianacare.org
ACKNOWLEDGEMENT
Thank you to the American Nurses Foundation Reimagining Nursing Initiative and ChristianaCare leadership for this incredible opportunity to create a career energizing fellowship for bedside nurses.
REFERENCES
1. Emergency Nurses Association. (n.d.). Honoring the legacy of Anita Dorr, RN, FAEN - Emergency nursing innovator. New York State Council Emergency Nurses Association. https://nysena.org/library/news_archive/2021/211025.html
2. Neonatal Nursing Hall of Fame - Academy of Neonatal Nursing Academy of Neonatal Nursing. (n.d.). https://www.academyonline.org/page/halloffame
3. Karimi, H., & Masoudi Alavi, N. (2015, June). Florence Nightingale: The mother of nursing. Nursing and Midwifery Studies, 4(2), e29475. https://doi.org/10.17795/nmsjournal29475
4 Chang, H.-Y., Lee, I.-C., Chu, T.-L., Liu, Y.-C., Liao, Y.-N., & Teng, C.-I. (2019, September). The role of professional commitment in improving nurses’ professional capabilities and reducing their intention to leave: Two-wave surveys. Journal of Advanced Nursing, 75(9), 1889–1901 https://doi.org/10.1111/jan.13969
5 El Zaatari, S., Marei, M., Li, W., & Usman, Z. (2019). Cobot programming for collaborative industrial tasks: An overview. Robotics and Autonomous Systems, 116, 162–180 https://doi.org/10.1016/j.robot.2019.03.003
Stop The Bleed: How a Standardized Policy and Reporting May Assist Healthcare Organizations with Tackling the Workplace Violence Crisis
Workplace violence in healthcare settings is a growing concern, with healthcare workers facing significantly higher risks of physical and verbal assaults compared to other professions. Despite the prevalence and severity of these incidents, there remains a critical lack of standardized policies across institutions and jurisdictions to address and mitigate workplace violence. This inconsistency contributes to underreporting, inadequate preventive measures, and insufficient support for affected staff. This article highlights the urgent need for comprehensive, evidencebased national standards and policy frameworks to ensure the safety and wellbeing of healthcare workers, improve reporting mechanisms, and foster a culture of zero tolerance for violence in healthcare environments.
Violence against nurses and healthcare workers has become increasingly prevalent within the United States, as evidenced by the recent tragic assaults in both Pennsylvania and Florida. Only 33% of nurses report feeling safe within their work environment,1 with many experiencing long-term impacts, including PTSD, anxiety, and depression. National Nurses United (NNU) conducted a survey of nearly 1000 nurses, with data gathered between January 1 and December 31, 2023.2 More than 67% of nurses surveyed responded they were verbally threatened, and 38.7% reported being physically threatened.2 Currently, no standardized national system for tracking and reporting incidents exists within the United States, posing challenges to reporting, tracking, and follow-up systems.1 Has a societal shift occurred that contributed to the acceptance of violence against healthcare workers, or is the lack of policy and tracking systems creating that perception?
While no federal law currently exists to protect healthcare workers from workplace violence (WPV), legislation has been established at the state level. Federal policy has been established in WPV prevention efforts by encouraging security protections, recognition of behavior indicators, employee assistance, and education initiatives.3 However, they do not require WPV protections, though some states have sought legislative solutions, including mandatory establishment of a comprehensive prevention program for healthcare employers, and increased penalties for those convicted of assaults of a nurse and/or other healthcare personnel. Delaware Nurses Association supported DE House Bill 324, which was enacted in June 2022 making it an assault in the 2nd degree, class D felony, to intentionally cause physical injury to an ambulance operator, a rescue squad member, licensed practical nurse, registered nurse, paramedic, or licensed medical doctor while such person is performing a work-related duty.4
The Joint Commission also developed WPV prevention standards because of increased violent attacks within the healthcare setting, often attributed to inadequate staff training, lack of follow-
through regarding threatening behaviors, and lack of standardized policies to address these events. The WPV standards serve as a framework that organizations may apply based on their interpretation and available resources. However, variations in how the framework is implemented can occur. An urban hospital located in a major metropolitan area will have access to additional resources (i.e., increased staff and revenue) when compared to more rural hospitals. Thus, the framework does not account for disparities despite similar threats and potential for WPV.
A standardized policy with a streamlined reporting capability would allow organizations to collect data and analyze trends. The lack of a centralized database makes it challenging to track incidents. The collection of robust data, or “data dashboards,” would better allow organizations to identify opportunities for the implementation of prevention and de-escalation practices that better promote the safety and wellbeing of staff. In addition, the data would allow organizations to identify trends or culminating factors that may enable them to better prepare and prevent violence from escalating.
According to the Occupational Safety and Health Administration (2023), 75% of all reportable workplace violence events occur in healthcare.5 Without a standardized system for tracking and reporting, there is no way to accurately trend occurrences of violence in the workplace. Opportunities exist to develop and implement reporting standards, both physical and non-physical, when they occur. Multiple barriers exist that do not allow for appropriate reporting and follow-up actions. Barriers may include fear of retaliation, financial burden of missed work, and perceptions that reporting will not lead to change. Reporting can also be time-consuming and tedious, particularly when staff feel overwhelmed with daily tasks. Reporting can also be viewed as “just one more thing” to add to a daunting list of things to do. Leadership may overcome reporting barriers by engaging and encouraging staff to report incidents and providing supportive resources. Staff should receive regular education and updates regarding reporting and follow-up policies and procedures.
Reporting should not simply identify an incident but lead to meaningful change within the organization. Once staff begin to observe positive changes in workplace safety, they may feel more empowered and inclined to report future incidents. As policies are further developed, increased engagement and improved staff perception regarding workplace safety may be realized. It is also critical to identify potential violent behavior through early intervention and de-escalation strategies, as well as implementing follow-up protocols. It is not enough to simply say there is a “no tolerance policy” without any implementation and adherence to consequences. Nursing is a team sport, and WPV requires a hands-on approach to empower staff to use their voices. As nursing burnout rates continue to increase, the negative impacts can be observed in patient safety, quality of care, provider wellbeing, and nurse retention.6 A NCSBN 2023 survey reported nearly half of surveyed nurses experienced stress and burnout, with over 600,000 expected to leave the workforce by 2027 because of these factors.6 It would be irresponsible and foolish to assume that the perceived or actual threat of violence is not a contributing factor to feelings of burnout. According to an article from Clinical and Transitional Research regarding workplace violence against nurses, “more than 70% of nurses are constantly worried about being a victim of WPV. These stresses decrease job satisfaction and increase constant psychological stress, which negatively affects nurses’ work and personal life. All forms of violence result in psychological stress.”7
Workplace violence against nurses is a serious and growing concern that demands immediate and unified action. Without standardized national policies and effective reporting systems, healthcare workers remain at risk, and meaningful change is delayed.
While I was generally aware of WPV, the Nursing Research Fellowship in Robotics and Innovation at ChristianaCare provided me with an opportunity to grow as a leader and gain new knowledge that can be applied to this topic. My fellowship mentors helped me to explore the issue, which led to my ability to recommend strategies to address WPV in my workplace environment.
Ms. Mitchell may be contacted at elmitchell@christianacare.org.
ACKNOWLEDGEMENT
Thank you to the American Nurses Foundation Reimagining Nursing Initiative and ChristianaCare leadership for the incredible opportunity to participate in the Nursing Research Fellowship in Robotics and Innovation at ChristanaCare. Special thanks to Dr. Susan Smith for your leadership throughout the fellowship, and to my coauthor, Dr. Julie McCulloh Nair for your contributions, mentorship, and support.
REFERENCES
1. American Organization for Nursing Leadership. (2024, December 12). Workplace Violence Prevention Leadership Symposium https://www.aonl.org/foundation/workplace-violenceprevention-symposium
2. National Nurses United. (2024, Feb 5). NNU report shows increased rates of workplace violence experienced by nurses https://www.nationalnursesunited.org/press/nnu-report-showsincreased-rates-of-workplace-violence-experienced-by-nurses
3. American Nurses Association. (2025, Mar 13). American Nurses Association position statement on workplace violence. https://www.nursingworld.org/practice-policy/nursingexcellence/official-position-statements/id/incivility-bullyingand-workplace-violence/
4. Delaware, H. B. 324. An Act to Amend Title 11 of the Delaware Code Relating to Assault. 2022. https://legis.delaware.gov/BillDetail/79181
5. Security Magazine. (2023, Apr 28). Delaware hospital cited by OSHA for failing to stop workplace violence. https://www.securitymagazine.com/articles/99273-delawarehospital-cited-by-osha-for-failing-to-stop-workplace-violence
6. National Council of State Boards of Nursing. (2023, Apr 13). NCSBN research projects significant nursing workforce shortages and crisis. https://www.ncsbn.org/news/ncsbn-research-projectssignificant-nursing-workforce-shortages-and-crisis
7. Kafle, S., Paudel, S., Thapaliya, A., & Acharya, R. (2022, September 13). Workplace violence against nurses: a narrative review. U.S. National Library of Medicine. https://pmc.ncbi.nlm.nih.gov/articles/PMC9536186/
RESOURCES FOR ADDICTION TREATMENT AND CRISIS RESPONSE IN DELAWARE
To reach the 988 Suicide and Crisis Lifeline, call or text 988 on your phone or visit https://dhss.delaware.gov/988-2/
To reach Delaware’s adult mobile crisis programs, call: 800-652-2929 (Northern Delaware) or 800-345-6785 (Southern Delaware)
To reach Delaware’s child and youth mobile crisis program, call: Delaware Guidance Services at 800-969-HELP (4357)
To receive free Narcan to reverse overdose, visit the Help is Here webpage at https://www.helpisherede.com/ to request Narcan at no cost through the mail, to find a regularly scheduled kit training and distribution session in your county, or to find the location of one of five harm reduction vending machines in the state that distributes Narcan, fentanyl and xylazine test strips, and other harm reduction items at no cost.
For immediate assistance with a substance use disorder or mental health concern, visit a Bridge Clinic. Locations and hours of each county’s clinic are listed at https://www.helpisherede.com/ . Click on “Get In Person Access to Services” on the homepage.
For a searchable list of addiction treatment providers in Delaware, visit Treatment Connection at https://www.treatmentconnection.com/
For information about Narcan training, accessing treatment (including a special guide for patients without insurance), and substance abuse information toolkits for healthcare providers and parents, visit Help is Here DE at https://www.helpisherede.com/
For information about treating opioid use disorder, grants available to support opioid response activities, and news and statistics about addiction response in Delaware, visit the Addiction Treatment Resource Center website at https://atrc.dhss.delaware.gov/
Public Health Delaware Journal of Submission Guidelines
updated March, 2024
About the Journal
Established in 2015, e Delaware Journal of Public Health is a peer-reviewed electronic publication created by the Delaware Academy of Medicine/Delaware Public Health Association. e publication acts as a repository of news for the medical, dental, and public health communities, and is comprised of upcoming event announcements, past conference synopses, local resources, peer-reviewed content ranging from manuscripts and research papers to opinion editorials and personal interest pieces, relating to the public health sector. Each issue is largely devoted to an overarching theme or current issue in public health.
e content in the DJPH is informed by the interest of our readers and contributors. If you have an event coming up, would like to contribute an Op-Ed, would like to share a job posting, or have a topic in public health you would like to see covered in an upcoming issue, please let us know.
If you are interested in submitting an article to the Delaware Journal of Public Health, or have any additional inquiries regarding the publication, please contact the managing editor at managingeditor@djph.org, or the publisher at ksmith@delamed.org.
Information for Authors Submission Requirements
e DJPH accepts a wide variety of submission formats, including brief essays, opinion editorials pieces, research articles and ndings, analytic essays, news pieces, historical pieces, images, advertisements pertaining to relevant, upcoming public health events, and presentation reviews. Additional types of submission not previously mentioned may be eligible, please contact a sta member for more information.
e initial submission should be clean and complete, without edits or markups, and contain both the title and author(s) full name(s). Submissions should be 1.5 or double spaced with a font size of 12. Once completed, articles should be submitted via the submission page at https://djph.org/submissions/submit-an-article/ Graphics, images, info-graphics, tables, and charts are welcome and encouraged to be included in articles. Please ensure that all pieces
are in their nal format, and all edits and track changes have been implemented prior to submission. To view additional information for online submission requirements, please refer to the DJPH website: https://djph.org/submissions/submit-an-article/
Trial registration information is required for all clinical trials and must be included in the nal article and/or abstract.
Abstracts
Authors must submit a structured or unstructured abstract along with their article. Abstracts will have a maximum of 200 words, including headings. Structured abstracts should employ 4-5 headings, and may include Objectives, Methods, Results, and Conclusions. A fth heading, Policy Implications, may be used if relevant to the article. All abstracts should provide the date(s) and location(s) of the study if applicable, as well as any trial registration information.
Submission Length
While there is no prescribed word length, full articles will generally be in the 2,500-4,000word range, and editorials or brief reports will be in the 1,500-2,500-word range. If there are any questions regarding the length of a submission or APA guidelines, please contact a sta member.
Copyright
e journal and its content is copyrighted by the Delaware Academy of Medicine / Delaware Public Health Association (Academy/DPHA). e contents are licensed under Creative Commons License – CC BY-NC-ND (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Images are NOT covered under the Creative Commons license and are the property of the original photographer or company who supplied the image.
Opinions expressed by authors of articles summarized, quoted, or published in full within the DJPH represent only the opinions of those authors and do not necessarily re ect the o cial policy of the Academy/DPHA, the DJPH, or the institution with which the authors are a liated.
Con icts of Interest
Any con icts of interest, including political, nancial, personal, or academic con icts, must be declared prior to the submission of the article, or in conjunction with a submission. Con icts of interest are any competing interests that may leave readers feeling misled or deceived, and/or alter their perception of subject matter. Declared con icts of interest will be published alongside articles in the nal publication.
Nondiscriminatory
Language
Use of nondiscriminatory language is required in all DJPH submissions. e DJPH reserves the right to reject any submission found to be using sexist, racist, or heterosexist language, as well as unethical or defamatory statements.