Review achievement of 2025 goals Plan for 2026 conference commenced
Plan for 2026 goals, education mapped
Business Card
Editor’s Message
Kiaora, and welcome to the February 2025 edition of Supplyline. I hope you all had a wonderful Christmas and New Year. The time has certainly flown by.
I’m delighted to let you all know that Donna Dador, NZSSA Vice President will be helping me with putting together the NZSSA Supplyline from now on. The front cover of Supplyline – the NZSSA Road Map –will identify key events that will be happening this year. Like this year’s conference in Rotorua and various study days around NZ. Donna created this Road Map and it does look really good.
One of the hardest pieces of information to source for Supplyline are articles. So if you have seen any relevant articles in your travels that you think would be good to include in Supplyline, please let Donna or myself know.
Included in this edition are updates on this year’s conference; course information; and changes to the NZSSA Website. The NZSSA Executive Body contact list has been updated as well.
Ngā mihi
Aileen Derby Editor NZSSA Supplyline
I am happy to be of assistance to our Chief Editor Aileen Derby. I am trying to leverage my clinical experience and passion for healthcare, dedicated to promoting best practices and continuous improvement in healthcare sterilization through informative and engaging content. I am very excited to be journeying with you at this time of digital age. I would like to encourage you to take part in promoting education by sharing a paper that you have worked on and have it publish in our Supplyline issue. And because we are so passionate with education, we are also giving you the schedules of our steam meeting around the country. So see you in one of them!
President’s Message
We are now into the new year and things are underway for the conference in Rotorua on September 3rd - 5th September 2025.
We will soon be calling for abstracts and hopefully we will have the itinerary out by the end of May. We are also in the planning stage for what we are doing this year.
• Shelagh and Aileen are working hard on getting us regulated as we are currently self-regulated - we will keep you updated with any new information.
• Charanjeet Sidhu, Donna Dador, and Maureen Scott will be marking the registration portfolios and replacing Kelly Swale who has done a great job, so thanks Kelly.
• We are forming a collaboration with the DAA (Designated Audit Agency) so they can audit sterile Sciences and certificate us. High performing units’ won’t have to be audited yearly, instead 4/5 years.
• Aileen and Shelagh are working on our scope of practise for level 4 and once its complete we will send it out to the members
• The Association is now on LinkedIn which will help our profile.
• We have also put the scholarship on our web site.
• The leaders meeting is on the 28th of March and will be a team’s meeting more information to come.
Regards
Donna Dador Co-Editor NZSSA Supplyline
Martin Bird NZSSA President
All rights reserved. No reuse allowed without permission. (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. The copyright holder for this preprint this version posted February 5, 2025. https://doi.org/10.1101/2025.02.03.25321618;
Validating sporicidal efficacy of ultrasound probe high-level disinfection devices in clinical settings
David Bellamya,*, Karen Vickeryb
a Sterilising Services Department (SSD) Manager, St George Hospital; Vice President, World Federation for Hospital Sterilization Sciences (WFHSS)
b Faculty of Medicine, Health and Human Sciences, Macquarie University, Sydney, Australia
* Corresponding author: St George Hospital, Gray Street, Kogarah, NSW, 2217, Australia.
Email address: David.Bellamy@health.nsw.gov.au (D. Bellamy).
The copyright holder for this preprint this version posted February 5, 2025. https://doi.org/10.1101/2025.02.03.25321618; doi: medRxiv preprint
(which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.
All rights reserved. No reuse allowed without permission.
Abstract
Introduction: In accordance with AS5369:2023 and ISO 15883-1:2024 Standards, in-field validation testing of automated high-level disinfection (HLD) devices in clinical settings is necessary to qualify their performance. Responding to reports that some ultraviolet-C (UV-C) devices were failing to achieve sporicidal efficacy during routine in-field validation, we evaluated the sporicidal efficacy of these devices via a performance qualification test.
Methods: Sporicidal efficacy was assessed using commercially available stainless steel biological indicators (BIs) inoculated with 10 6 Geobacillus stearothermophilus spores (ATCC® 7953). BIs were clamped in top and bottom locations inside chambers of devices [UV-C light-emitting diode (LED), UV-C lamp and hydrogen peroxide (H 2O2) mist]. BI test conditions included packaged, unwrapped and non-flamed and unwrapped and flame sterilised on the clamped coupon end. Results were evaluated on a pass (no growth) or fail (growth) basis.
Results: The results showed that the UV-C LED device failed to inactivate spores in all tested positions and conditions (n=18). The UV-C lamp device passed 2/6 tests in the flamed condition but failed all other tests (n=12). The H 2O2 mist system passed all tests, inactivating spores for all conditions and chamber positions (n=18).
Conclusion: Our findings show that despite claiming sporicidal efficacy, the UV-C devices both failed in-field validation tests using bacterial endospores. These results indicate that the UV-C devices were not sporicidal in these tests. The H 2O2 mist device was the only system in this study that passed all tests, achieving sporicidal efficacy.
The copyright holder for this preprint this version posted February 5, 2025. https://doi.org/10.1101/2025.02.03.25321618; doi: medRxiv preprint
(which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.
All rights reserved. No reuse allowed without permission.
Introduction
The appropriate reprocessing of reusable medical devices before individual patient use is essential for the prevention of infection transmission (1). Ultrasound probes that contact nonintact skin or mucous membranes during patient procedures are classified as semi-critical devices and, at a minimum, require high-level disinfection (HLD) (2,3).
There are three automated systems intended to provide HLD of ultrasound probes currently in clinical use in Australia and New Zealand (ANZ). All of these devices claim efficacy against bacterial endospores according to their product literature (4-6). The Therapeutic Goods Administration (TGA) standards for sporicidal efficacy require demonstrated inactivation of 106 spores (7) and sporicidal products should be able to achieve a 6-log reduction of any bacterial endospore, including species such as Geobacillus stearothermophilus. The three devices available in ANZ utilise ultraviolet-C (UV-C) lightemitting diodes (LEDs), UV-C lamps, or hydrogen peroxide (H 2O2) mist in enclosed systems.
Routine in-field validation testing of disinfection devices in clinical use is required under both Australian (AS 5369:2023) (8) and International Standards (ISO 15883-1:2024) (9).
Performance qualification reflects one stage of in-field validation and requires testing the biological inactivation of microorganisms using a biological indicator (BI) test (AS 5369:2023) (8).
Performance qualification of automated disinfection devices is required after installation, upon servicing and requalification annually under Australian standards (AS 5369:2023) (8). We became aware of data showing that some UV-C devices were failing to achieve sporicidal efficacy during routine validation in hospitals located in Australia and set out to test the efficacy of these devices ourselves in a rigorous in-field validation process using BIs.
We assessed the sporicidal efficacy of the disinfection processes through the destruction of 106 bacterial endospores (G. stearothermophilus), consistent with TGA requirements (7). These BIs were chosen on the basis that manufacturers of all three technologies evaluated in this study claim sporicidal efficacy (4-6).
Materials and methods
Automated disinfection devices
The performance of three commercially available automated disinfection devices was evaluated in clinical settings across ANZ. The devices included two UV-C systems [UV-C LED (Lumicare ONE, Lumicare) and UV-C lamp (Hypernova Chronos ®, Germitec)] of different wavelengths and dimensions, and a hydrogen peroxide mist system (H 2O2 mist: trophon®2, Nanosonics) (Table 1). All devices were operated according to the manufacturer’s Instructions for Use (IFU).
Table 1. Specifications of the assessed disinfection devices.
Disinfection device
UV-C LED (Lumicare ONE, Lumicare)
Manufacturer HLD method
Lumicare, Drummoyne, New South Wales, Australia
UV-C, LED (265-275nm wavelength)
Compatible medical devices for HLD
Semi-critical or critical endocavitary and surface ultrasound probes
Cycle duration Dimensions (mm)
90 seconds (1.5 minutes)
Height=620
Width=360
Depth=325
The copyright holder for this preprint this version posted February 5, 2025. https://doi.org/10.1101/2025.02.03.25321618; doi: medRxiv preprint
(which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.
All rights reserved. No reuse allowed without permission.
UV-C lamp (Hypernova Chronos®, Germitec)
H2O2 mist (trophon®2, Nanosonics)
Procedures
Germitec, Bordeaux, NouvelleAquitaine, France
Nanosonics Ltd, Macquarie Park, New South Wales, Australia
UV-C, mercury lamps (254nm wavelength)
Sonicated hydrogen peroxide mist (35%)
Semi-critical or critical endocavitary and surface ultrasound probes
Semi-critical or critical endocavitary and surface ultrasound probes
90 seconds (1.5 minutes)
420 seconds (7 minutes)
Height=1020 Width=380 Depth=430
Height=535 Width=360 Depth=317
BIs containing 106 G. stearothermophilus (ATCC® 7953) spores inoculated onto stainless steel coupons (dimensions: 34.0mm × 7.0mm × 0.8mm) (Terragene ®, BT93/6) enclosed in a glassine package/ Tyvek® (dimensions: 25mm × 70mm) were used.
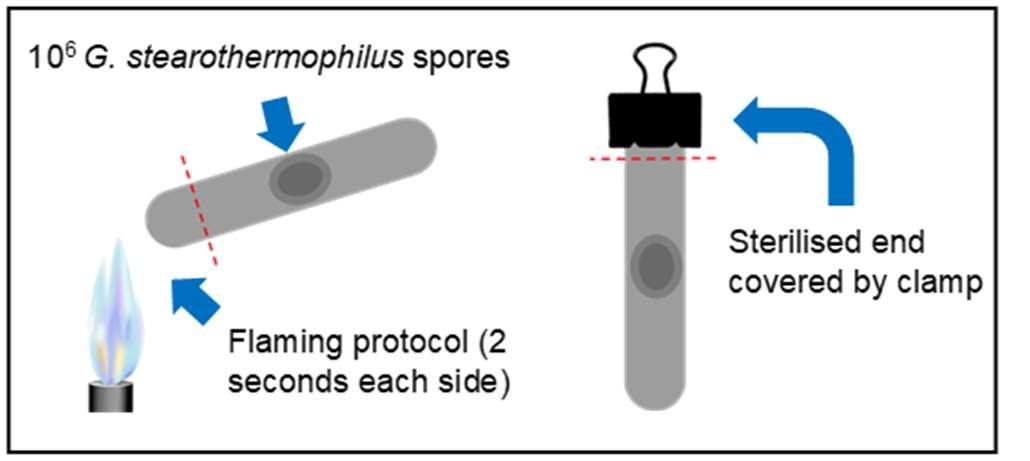
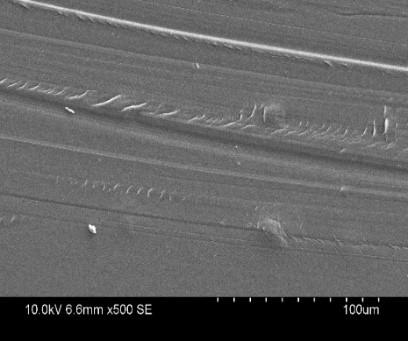
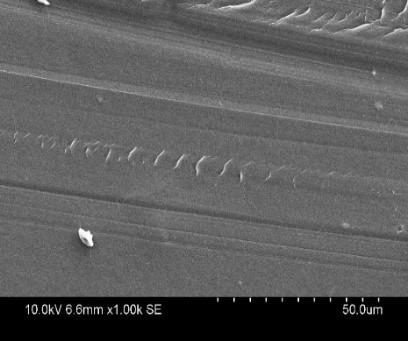
Given that UV-C light has limited penetration and is subject to shadowing, we opted to test three conditions; 1) The BI in its typical glassine packaging/ Tyvek ®; 2) The BI with packaging removed and; 3) The BI with packaging removed plus flame sterilisation of the coupon end which was later clamped (Figure 1A-1C).
D)
The copyright holder for this preprint this version posted February 5, 2025. https://doi.org/10.1101/2025.02.03.25321618; doi: medRxiv preprint
All rights reserved. No reuse allowed without permission. (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.
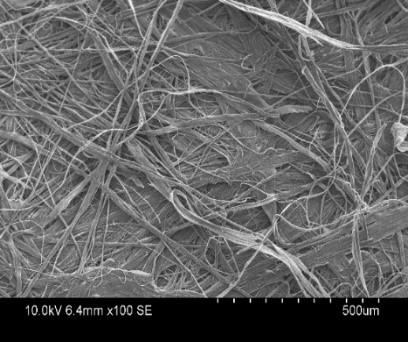
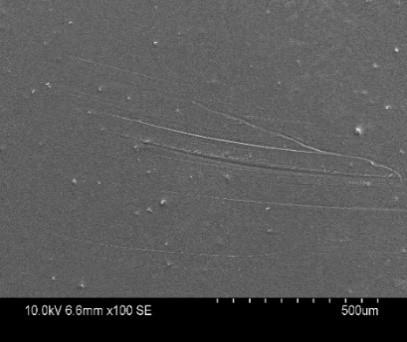
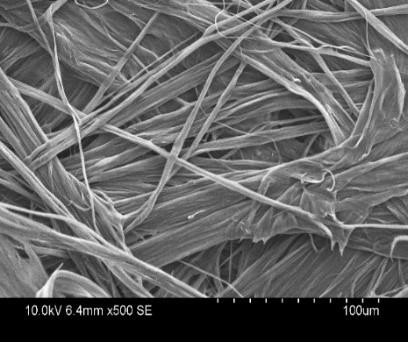
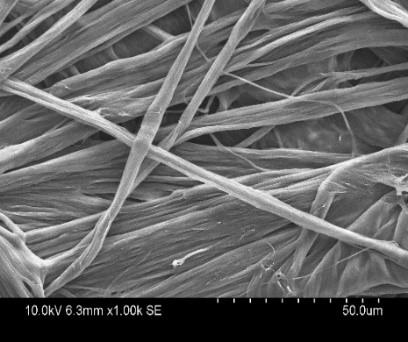
Figure 1. Three BI test conditions and scanning electron microscopy (SEM) images of BI (Terragene®, BT93/6) glassine packaging/ Tyvek® A) BI coupon contained within a glassine package/ Tyvek®. B) BI coupon without packaging. C) A diagram of the BI with a flamed sterilised coupon end. D) SEM images showing the structure of the high-density polyethylene side of the BI package is fibrous in nature, allowing the penetrability of very small particles. E) SEM images showing that the structure of the plastic side of the BI package is non-permeable in nature with no visible pores.
BIs corresponding to the test conditions were suspended in the disinfection chambers via a sterilised clamp which was attached to one end of the coupon or packaging. Due to potential shadowing effects on the coupon from the clamp, a flame sterilisation technique of the clamped coupon end was employed to account for any shadowing, where the shadowed areas would not be accessible to UV-C radiation. This was performed by flame sterilising 5mm (0.5cm) of the BI coupon ends for 2 seconds on each side of the same end (1 minute cooling time in between) (see S1). The sterilised end of the coupon was then clamped onto the coupon holder inside the respective disinfection device.
For the non-flamed BI test condition without glassine packages/ Tyvek ® (stainless steel BI coupon only), BIs were aseptically removed from the packaging and directly clamped onto the holder. For the BIs tested with glassine packages/ Tyvek ®, the edge of the package was clamped and suspended inside the disinfection device using the holder (BI coupon itself was not clamped when inside the package).
BIs were positioned, with the inoculation site facing outwards, in the top and bottom positions inside the disinfection chamber to represent locations within the chamber corresponding to where a clinical probe would be placed (Figure 2). Three replicates were used for each test condition for both top and bottom positions in the chamber, totalling 6 replicates per device. The holder was suspended in each disinfection device and exited from the chamber via the cavity located at the top where an ultrasound probe cable would typically emerge.
Figure 2. Set up of the BIs clamped onto the holder positioned in the top and bottom of the tested disinfection chambers. A) BI coupons without glassine packages/ Tyvek ® (flame sterilised coupon end or non-flamed). B) BI coupons contained within glassine packages/ Tyvek®.
A standard disinfection cycle was carried out according to the disinfection device manufacturer’s IFU. Three cycles were conducted per test condition, with each BI placed in the top and bottom positions (2 BIs) for each cycle, for a total of 6 replicates per condition. After the disinfection cycle, each BI coupon was aseptically collected into suitable culture media according to the manufacturer’s IFU.
Three positive controls were included for both the flamed and non-flamed test conditions (total of 6 positive controls per device) and were prepared by aseptically transferring the BI
A)
B)
The copyright holder for this preprint this version posted February 5, 2025. https://doi.org/10.1101/2025.02.03.25321618; doi: medRxiv preprint
All rights reserved. No reuse allowed without permission. (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.
directly into the corresponding culture media vial. The inclusion of positive controls ensured that the incubation process did not contribute to a false-negative result.
All vials were then shipped to an accredited, independent test laboratory and incubated and assessed for growth/no growth according to the manufacturer’s IFU. Growth indicated failure of the test, and no growth indicated a pass result.
Data analysis was performed using R-Studio software (version 4.1.1). To examine the relationship between disinfection devices and test conditions (flame sterilised, non-flamed, glassine package/ Tyvek®), a Fisher’s exact test was performed to assess independence. A p-value less than 0.05 indicated statistical significance.
Results
The study assessed a total of 72 BIs across the three disinfection devices (UV-C LED, UV-C lamp and H2O2 mist), three test conditions (flamed, non-flamed and glassine package/ Tyvek®), with 18 positive controls for the flamed and non-flamed conditions. The H 2O2 mist device exhibited the highest sporicidal efficacy with a 100% pass rate across all tested conditions and chamber positions overall (18/18 replicates) (Table 2).
The UV-C lamp demonstrated partial efficacy under the flamed condition, with a 66.67% pass rate (2/3 replicates) in the bottom position, but a 0% pass rate (0/3 replicates) in the top position, with a 33.33% pass rate for the overall flamed condition (2/6 replicates). The UV-C lamp failed to inactivate spores across any of the non-flamed and glassine/Tyvek ® package conditions (0/12 replicates), with an 11.11% overall pass rate across all tested conditions (2/18 replicates).
In contrast, the UV-C LED device failed in inactivating spores across all tested conditions and positions (0/18 replicates) (Table 2).
Statistical analysis under all test conditions revealed significant differences in the pass/fail rate between the devices, χ2(2, N=6), p<0.0021, p<0.0002, p<0.0002, for flamed, non-flamed and glassine package/ Tyvek® conditions, respectively. All positive controls demonstrated spore growth, validating incubator function and spore viability.
Table 2. BI testing results for each of the evaluated disinfection devices.
The copyright holder for this preprint this version posted February 5, 2025. https://doi.org/10.1101/2025.02.03.25321618; doi: medRxiv preprint
All rights reserved. No reuse allowed without permission. (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.
package/ Tyvek®
control- Flamed
control- Nonflamed
Discussion
The in-field validation results showed that the H 2O2 mist system was effective at sporicidal disinfection in all cases, while the UV-C LED and UV-C lamp systems were largely ineffective. Two of the six replicates were successfully disinfected by the UV-C lamp system when using a BI without packaging with the flame sterilised end. However, these successful tests only occurred in the bottom chamber position, while all replicates in the top position failed.
The UV-C lamp device performed better than the UV-C LED device, achieving sporicidal efficacy for 2 of 6 flame sterilised BIs, while the UV-C LED device was ineffective in all tested cases, irrespective of the BI condition or chamber position (Table 2). On reviewing the literature, we identified a manufacturer-funded study on the UV-C LED system. This study reported a >7-log10 reduction of Bacillus subtilis spores after undergoing UV-C disinfection (10). In the previous study, the spores were spread over a very large area compared to the standard BIs used in the present study. The lower density of the inoculum could pose a lesser challenge and may explain the differences in results to the present study.
The differences observed between the UV-C devices may be attributable to the varied wavelength, dose, temperature, reflectivity of the chamber wall material and configuration of light sources in the chamber (11,12,13). Overall, the results show that the automated UV-C disinfection devices did not consistently achieve sporicidal inactivation. As the validation of disinfection devices is a requirement according to Australian and international standards (8,9), automated disinfection devices, particularly UV-C disinfection devices, should be successfully validated to ensure they are meeting claims such as sporicidal efficacy.
In order for a UV-C device to achieve a pass result under these test conditions, it must deliver a sufficient dose of UV-C radiation to the BI to effectively inactivate all spores present. It is evident in the study that the UV-C devices were unable to deliver an adequate dose to the relatively uniform, flat surface of the BI coupons to achieve sporicidal efficacy. While there are several known factors that can impact sporicidal efficacy of UV-C based technologies, the dose received by an area of a probe is dependent on the irradiance level on the target surface and the duration of exposure. As the duration of exposure is dictated by the pre-set cycle time, it is critical that the irradiance level on the surface is sufficient to inactivate the spores.
UV-C requires a direct path of light to disinfect the target surface, with intensity falling with the square of distance from the target (inverse square law), impacting the amount of UV-C radiation that is received (11). As such, the distance of the BI from the light source may have
The copyright holder for this preprint this version posted February 5, 2025. https://doi.org/10.1101/2025.02.03.25321618; doi: medRxiv preprint
All rights reserved. No reuse allowed without permission. (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.
resulted in a sub-efficacious dose. Mercury lamps have been shown to exhibit less variability in irradiance distributions compared to UV-C LEDs at shorter distances from the surface plane (14). Given that areas closer to the source of light receive greater irradiance (11), it may be the case that the configuration and distance of light sources in the bottom location of the UV-C lamp chamber were better able to irradiate an appropriate dose onto the BIs, although inconsistently. This finding, coupled with the failing of all the BIs located in the top position, demonstrates that irradiance is not equally distributed within the entire chamber.
In addition to the above considerations, the dosage of UV-C irradiated onto the coupon surface may have been affected by variables such as the surface topography and potential micro-shadowing on the surface of the coupon (15). The potential for shadowing effects may impact disinfection efficacy, which increases the risk of microorganisms surviving in areas of low irradiance (11). As the potential for large variation in irradiance distribution has been noted, testing is needed to demonstrate efficacy in areas of least irradiance (16). Despite employing flame sterilisation on the clamped coupon end in the present study to account for potential shadowing in the clamped area, UV-C was still unable to effectively inactivate the spores, even in non-shadowed areas on the coupon. These limitations of uneven irradiance distributions and potential shadowing underscore the challenges of UV-C disinfection devices in achieving adequate disinfection, particularly for complex surfaces.
Several recent studies investigating the use of UV-C for the disinfection of semi-critical devices found that the HLD criteria were not consistently met as microorganisms remained on the devices following HLD (10,17-20), suggesting that UV-C technology may not be able to deliver effective HLD in all cases.
The current study found that the H 2O2 mist system passed all tests, inactivating spores across all replicates, in all conditions tested. This demonstrates that the H 2O2 mist device met the TGA standards for sporicidal efficacy by achieving the inactivation of 10 6 bacterial endospores (7). These findings may be attributable to the ability of the H 2O2 mist device to distribute H2O2 mist across the carrier surface which ensures greater surface coverage and spore inactivation, even in shadowed areas around the clamp. These data align with existing literature on the efficacy of the H2O2 mist system for sporicidal disinfection (1).
Interestingly, the H2O2 mist device inactivated the spores on the BIs contained in glassine packages/ Tyvek®, whereas the UV-C devices were ineffective in penetrating the packages to inactivate the spores. This demonstrates that the H2O2 mist device provided more effective penetration of difficult-to-reach areas, such that there is adequate saturation and coverage of the entire surface of a contaminated device, and thus sporicidal efficacy. While the transparent plastic side of the glassine package/ Tyvek ® is non-permeable to molecules, the glassine package/ Tyvek® side of the package contains high-density polyethylene fibres designed to allow penetration of gases and very small particles (Figure 1D and 1E), while maintaining an effective barrier to microorganisms such as bacterial cells (≈1µm diameter) and fungal spores (>1µm diameter) (21). Given that the glassine package/ Tyvek® is hydrophobic in nature, it is apparent that the H 2O2 mist effectively permeates the glassine package/ Tyvek® to inactivate the spores on the BI coupon.
A limitation of the study is that BI coupons containing different surface materials and bacterial spores were not investigated. However, a standardised and commercially available BI test was employed in the study and these BIs are used widely to validate the sporicidal efficacy of disinfectors or sterilisers. Furthermore, the implication and claims of sporicidal efficacy made by the manufacturers represent that the devices used within this study would demonstrate efficacy regardless of the BI chosen. In this regard, it is worth noting that the spores used within this study are not worst-case spores for UV-C technology, and therefore
The copyright holder for this preprint this version posted February 5, 2025. https://doi.org/10.1101/2025.02.03.25321618; doi: medRxiv preprint
(which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.
All rights reserved. No reuse allowed without permission.
additional testing with worst-case microorganisms is warranted. In addition to the above, there may have been some variation in the positioning of the BI coupons in the top and bottom locations of the disinfection chamber across the devices due to differences in device sizes. Future studies on automated HLD devices in clinical use, including quantification methods such as colony forming units with testing directly on ultrasound probe surfaces, may be beneficial to corroborate the current findings on sporicidal efficacy.
In conclusion, the results show that the H2O2 mist device passed the sporicidal tests, whereas the UV-C devices failed most or all of the tests, depending on the system tested. Failure of in-field validation in these cases corresponded to a failure in sporicidal efficacy. This raises questions as to whether UV-C devices are able to consistently ensure effective inactivation of spores on ultrasound probes in clinical settings. Periodic and successful infield validation of automated disinfection devices is crucial to protect the health and safety of healthcare professionals and patients.
Ethical considerations
Ethical approval and informed consent were not required as there were no patients or volunteers involved in this study.
Authorship statement
D.B: conceptualisation, writing – review and editing. K.V: conceptualisation, methodology, writing – review and editing.
Acknowledgements
The authors would like to thank the hospitals for use of their facilities.
Funding
This study was funded by Nanosonics Ltd, Sydney, Australia.
Conflicts of interest
D.B declares no conflicts of interest relevant to this study. K.V has previously received consulting fees from Nanosonics Ltd.
Supplementary information
S1. Flame sterilisation method validation.
The copyright holder for this preprint this version posted February 5, 2025. https://doi.org/10.1101/2025.02.03.25321618; doi: medRxiv preprint
(which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.
All rights reserved. No reuse allowed without permission.
References
1. Vickery K, Gorgis VZ, Burdach J, Patel D. Evaluation of an automated high-level disinfection technology for ultrasound transducers. J Infect Public Heal. 2014;7(2):153–60.
2. Australasian Society for Ultrasound in Medicine (ASUM), Basseal JM, Westerway SC, et al. Guidelines for Reprocessing Ultrasound Transducers. Australas J Ultrasound Medicine. 2017;20(1):30-40.
3. Carrico RM, Furmanek S, English C. Ultrasound probe use and reprocessing: Results from a national survey among U.S. infection preventionists. Am J Infect Control. 2018;46(8):913–20.
4. Germitec website, 2024 [internet]. Available from https://www.germitec.com/enus/chronos.
5. Lumicare website, 2024 [internet]. Available from https://lumicare.one/clinical.
6. Nanosonics website, 2024 [internet]. Available from https://www.nanosonics.com.au/products/trophon-2/microbial-defence.
7. Therapeutic Goods Administration. TGA Instructions for Disinfectant Testing; Department of Health, Australian Government. 2021.
8. AS 5369:2023 Reprocessing of reusable medical devices and other devices in health and non-health related facilities. Standards Australia.
9. ISO 15883-1:2024. Washer-disinfectors — Part 1: General requirements, terms and definitions and tests. International Organization for Standardization.
10. Yasir M, Willcox MDP. The use of ultraviolet light generated from light-emitting diodes for the disinfection of transvaginal ultrasound probes. PLOS ONE. 2024;19(2):e0298449.
11. Demeersseman N, Saegeman V, Cossey V, Devriese H, Schuermans A. Shedding a light on ultraviolet-C technologies in the hospital environment. J Hosp Infect. 2023;132:85–92.
12. Sheikh J, Swee TT, Saidin S, Malik SA, Olmedo JJS, Chua LS, et al. Comparative multivariate analysis for high-touch surface disinfection using optimized ultraviolet-C LEDs configuration. Hyg Environ Heal Adv. 2024;11:100101.
13. Stojalowski P de S, Fairfoull J. Comparison of Reflective Properties of Materials Exposed to Ultraviolet-C Radiation. J Res Natl Inst Stand Technol. 2021;126:126017.
14. Fredes P, Raff U, Gramsch E, Tarkowski M. Estimation of the Ultraviolet-C Doses from Mercury Lamps and Light-Emitting Diodes Required to Disinfect Surfaces. J Res Natl Inst Stand Technol. 2021;126:126025.
15. Ratliff K, Oudejans L, Calfee W, Abdel-Hady A, Monge M, Aslett D. Evaluating the impact of ultraviolet C exposure conditions on coliphage MS2 inactivation on surfaces. Lett Appl Microbiol. 2022;75(4):933–41.
16. Yeoh L, Cogar L, Barak M, Tan LY, Spargo G, Burdach J. UV-C disinfection of ultrasound probes: Challenges of uneven irradiance on complex surfaces. PLOS ONE. 2024;19(10):e0312931.
17. Chen L, Zhang H, Chang F, Yu H, Lu M, Zhao J, et al. A multicenter study on the effects of different methods of disinfecting medical external-use ultrasound probes. Am J Infect Control. 2024;52(2):167–75.
18. Ezeh UC, Achlatis E, Crosby T, Kwak PE, Phillips MS, Amin MR. The Effectiveness of Ultraviolet Smart D60 in Reducing Contamination of Flexible Fiberoptic Laryngoscopes. Laryngoscope. 2023;133(12):3512 –9.
19. Rudhart SA, Günther F, Dapper L, Thangavelu K, Gehrt F, Stankovic P, et al. UV light-based decontamination: an effective and fast way for disinfection of endoscopes in otorhinolaryngology? Eur Arch Oto-Rhino- Laryngol. 2020;277(8):2363–9.
The copyright holder for this preprint this version posted February 5, 2025. https://doi.org/10.1101/2025.02.03.25321618; doi: medRxiv preprint
(which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity.
All rights reserved. No reuse allowed without permission.
20. Schmitz J, Kossow A, Murcia KO de, Heese S, Braun J, Möllmann U, et al. Disinfection of Transvaginal Ultrasound Probes by Ultraviolet C – A clinical Evaluation of Automated and Manual Reprocessing Methods. Ultraschall Med - Eur J Ultrasound. 2019;41(06):681–7.
21. Gonzalez-Martin C. Airborne Infectious Microorganisms ☆. Encycl Microbiol. 2019;52–60.
7A Pacific Rise, Mount Wellington, Auckland 1060, New Zealand
The NZSSA is committed to bringing education opportunities your way. Below are some of the activities planned for the year ahead.
NZSSA Annual Conference
Wednesday 3rd – Friday 5th September 2025
Energy Event Centre Rotorua
Watch the NZSSA website conference page for more details: https://nzssa.co.nz/conferences/
Regional education meetings:
Planning is underway for regional meetings. These are held on a Saturday and are open to everyone working in reprocessing. These meetings are a great way to connect with people in the industry while learning.
Keep up with the actual dates and programmes on the NZSSA website: https://nzssa.co.nz/meetings-staff-development/
South Island Dunedin, 22nd March
Christchurch, 3rd week of May
North Island Palmerston North, June or July
Waikato, late April
Auckland, July
Leaders Meetings – These have previously been held as online meetings. The executive is looking at reintroducing these in 2025. If you have any topics you would like discussed please contact Donna Dador.
The NZSSA Conference Committee are excited to invite you to the 2025 Annual Conference.
Mark your calendars!
Ever wanted to share your knowledge or story at NZSSA Conference?
The Call for Abstracts invites researchers, practitioners, and industry professionals to submit their work for consideration as part of the conference program. Authors are encouraged to present innovative research, case studies, or insights that align with the conference themes. Call for Abstracts will open on Monday 17 March.
For any conference queries, please contact Britta van Uden, Event Manager, Britta@mtanz.org.nz
LACK OF KEY DATA
WHITE PAPER
ELLA ORGAIN
Applied M athematics ( BS )
U niversity of N orth C arolina at C hapel H ill
L eaves areas of uncertainty within set level tracking Facts
Set level tracking of surgical instruments can collect vast amounts of data.
The problem is the data collected at the set level is not all-encompassing Vital information regarding the individual instruments is missing. Without key data about specific instruments, accuracy and reliability is lost in exchange for uncertainty and convenience.
Data is a powerful tool that can improve the quality of decisionmaking. It can help institutions identify trends, optimize solutions, and create a better plan for the future, subsequently saving time, money, and even lives. However, being accurate in judging what is known and unknown is critical for data-driven decision-making. Incomplete or inaccurate data about a subject allows for assumptions and human error Consequently, this leaves room for uncertainty in areas where reliability and zero defects are imperative, such as in hospital operating rooms
The current standard for surgical instrument management is set level tracking. The issue is that surgical instruments within a set may be
packaged incorrectly, become mixed up in their sets, migrate to other sets, or become lost altogether. How does this prevailing standard introduce uncertainty that leads to these errors?
At the Sterile Processing Department (SPD), instruments are compiled into a set by manually clicking a checkbox for each instrument as it is identified and assembled into its set. Given that there are hundreds of thousands of surgical instrument catalog references and variations by different manufacturers, a large assumption is made that the SPD technician can correctly distinguish
similar instruments By this system it is impossible to know with absolute certainty that the correct instrument is selected and placed in the correct set Further assumptions are made during the decontamination process. Instruments may be mixed up
Set level tracking cannot trace unique surgical instruments with absolute certainty. There are hundreds of thousands of instruments and variations with different manufacturers and unique catalog numbers Instruments migrate from their original set, whether intentionally or not “Good data provides indisputable evidence while anecdotal evidence, assumptions, or abstract observation might lead to wasted resources due to taking action based on an incorrect conclusion” [1]
either within their own set or with other sets during this step [2]
Instruments may migrate to other sets in various scenarios. An instrument may need to be borrowed from a set for a different procedure at the last minute, for a surgeonbased preference, or to replace an instrument in need of repair Additionally, there is no guarantee that a borrowed instrument or an instrument needing repair makes it back into its original set At any point in the multi-stage life cycle of an instrument, any number of people could influence what happens to the instrument regardless of the set level tracking. This reality that set level tracking cannot ensure with confidence the identification and history of a single, unique instrument exposes the institution to the possibility of errors and wasted resources due to assumptions and uncertainty.
Consequences of decisions based on assumptions rather than reliable data extend beyond wasted resources to the potential exposure of patients to disease and institutional liability. For example, the contraction of diseases like Creutzfeldt-Jakob disease (CJD) and toxic anterior segment syndrome (TASS) are associated with the inadequate cleaning of contaminated surgical instruments [3]-[6] A lack of adequate (and potentially inaccurate) data regarding the unique instruments associated with a potential exposure incident risks patient safety. Further, exposure incidents may have been minimized or even avoided if the specific
instruments in question could be traced and decontaminated according to appropriate protocol. Without reliable data about key variables for each potentially contaminated instrument (successive patients and procedures, sterilization procedures undergone, etc.), informed decisions about transmission risk and patient notification are left to uncertainty. The basis of these decisions becomes a matter of conjecture. Moreover, exposure incidents like CJD and TASS may necessitate the suspension of hospital procedures for the quarantining of potentially exposed instruments [6]. The result is disruption to scheduled services and risk to patients in emergencies Sometimes, if there are no readily functional alternative instruments, hospitals must make the difficult decision between halting operations and continuing despite the exposure risk to patient safety [1]. Again, these decisions may be difficult to make as there is not reliable data to help identify and trace the potentially contaminated instruments.
Surgical preferences and idiosyncrasies may also be subject to errors due to a lack of reliable data Whether learned from surgical instructors, amassed with years of experience, or to keep up with advances in medicine, surgeonspecific instrument preferences are important to approach with accuracy. If a requested instrument is not in a set, time must now be spent searching for a correct instrument Besides the disruption of a procedure, there may not be an
In a study of 19 incidents of patient exposure to potentially CJD-contaminated instruments reported to the CDC, “[a]t least 12 of the hospitals had multiple neurosurgical sets [T]he CJDcontaminated instruments could not be identified in 11 of the 19 hospitals” [3].
Research has found that individual instrument preferences play a significant role in procedural outcomes [7].
Under 21 CFR 801.45(a), “[a] device that must bear a unique device identifier (UDI) on its label must also bear a permanent marking providing the UDI on the device itself if the device is intended to be used more than once and intended to be reprocessed before each use” [8], [9].
The Global Unique Device Identification Database (GUDID) recorded over 4 million device identifier records as of July 2024 (GUDID download) [10].
easily locatable and correct instrument readily available for use
At risk are time, money, patient outcome, tension in the operating room, and surgeon performance to the highest degree of excellence. The elimination of uncertainty regarding surgical instruments is crucial for the safety of patients and the effectiveness of surgeons performing procedures
Instrument level tracking identifies pivotal data for the life of an instrument involving the specific processing methods performed on the instrument (temperatures and pressures), the instrument’s procedural history (sterilization batch, operating room, surgeon, patient), and its location at any given time (operating room, clinic, room, cart, shelf, set) These key datasets enable hospitals to identify the exact
References
instruments associated with specific patients and surgeons
It is important to collect meaningful data tracked at the instrument level to ensure accuracy Beyond accuracy in what information is known, it is critical to determine what is not known to avoid assumptiondriven decision-making An absence of data at the instrument level may lead to uncertainty. Therefore, to achieve a higher level of reliability, accuracy at the instrument level is imperative for making data-driven decisions.
Regarding CJD, when asked “[s]hould hospitals track the use of surgical equipment to determine which instruments were used for which patients?” the North Carolina Division of Public Health responded “Yes ” [4]
Instrument level tracking procedures should be implemented to reduce uncertainty and inform decisions with relevant, reliable data
[1] “12 Reasons Why Data Is Important,” The Council on Quality and Leadership Inc , Mar. 2018. [Online]. Available: https://www.c-q-l.org/resources/guides/12-reasons-why-data-is-important/ [Accessed Aug. 14, 2024]
[2] E G. Smyth, M. Farrell, D. G. Healy, C. Finn, D. O’Brien, D. F. O’Brien, R Howley, P. Turner, and H. Humphreys, “Managing the Consequences of Neurosurgical Intervention in a Patient with Previously Undiagnosed Creutzfeldt-Jakob Disease,” Infection Control and Hospital Epidemiology, vol. 35, no. 7, pp. 907-908, Jul. 2014. [Online]. Available: Cambridge University Press, https://www.cambridge.org/core/journals/infection-control-and-hospital-epidemiology/article/managing-theconsequences-of-neurosurgical-intervention-in-a-patient-with-previously-undiagnosed-creutzfeldtjakobdisease/5697C7992144B54DABB0FD271664408B [Accessed Aug. 13, 2024].
[3] E. D. Belay, J. Blase, L M. Sehulster, R. A. Maddox, and L. B. Schonberger, “Management of neurosurgical instruments and patients exposed to Creutzfeldt-Jakob disease,” Infection Control and Hospital Epidemiology, vol. 34, no. 12, pp. 12721280, Dec. 2013. [Online]. Available: PubMed Central, https://pubmed.ncbi.nlm.nih.gov/24225612/. [Accessed Aug. 13, 2024].
[4] North Carolina Division of Public Health, “Frequently Asked Questions about Creutzfeldt-Jakob Disease (CJD),” North Carolina Department of Health and Human Services, Feb 2014 [Online]. Available: https://epi.dph.ncdhhs.gov/cd/diseases/cjd.html [Accessed Aug. 13, 2024].
[5] S. Cetinkaya, Z. Dadaci, H. Aksoy, N. O Acir, H. I. Yener, and E. Kadioglu, “Toxic anterior-segment syndrome (TASS),” Clinical ophthalmology (Auckland, N.Z.), vol. 8, pp 2065–2069, Oct. 2014. [Online]. Available: PubMed Central, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4199838/ [Accessed Aug. 13, 2024].
[6] C. Y. Park, J. K. Lee, and R. S. Chuck, “Toxic anterior segment syndrome-an updated review,” BMC Ophthalmology, vol. 18, no. 276, Oct. 2018. [Online]. Available: PubMed Central, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6203205/ [Accessed Aug. 13, 2024]
[7] H. Mohamadipanah, C. A Perumalla, L. E. Kearse, S. Yang, B. J Wise, C. K. Goll, A. K. Witt, J. R. Korndorffer, and C. M. Pugh, “Do Individual Surgeon Preferences Affect Procedural Outcomes?” Annals of surgery, vol. 276, no. 4, pp. 701-710, Oct. 2022. [Online]. Available: PubMed Central, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10254571/. [Accessed Aug. 14, 2024]
[8] 21 CFR 801.45. Available: The Electronic Code of Federal Regulations, https://www.ecfr.gov/current/title-21/chapterI/subchapter-H/part-801/subpart-B/section-801.45 [Accessed Aug. 16, 2024].
[9] Food and Drug Administration, “Unique Device Identification System,” Department of Health and Human Services, Sep. 2013. [Online]. Available: Federal Register, https://www.federalregister.gov/documents/2013/09/24/2013-23059/unique-deviceidentification-system [Accessed Aug. 16, 2024].
[10] Global Unique Device Identification Database. 2018- National Library of Medicine [Online]. Available: https://accessgudid.nlm.nih.gov/download [Updated Aug. 1, 2024; accessed Aug. 14, 2024]
Hospital Compliance Made
Toi Ohoma i Inst itute of Technol ogy Ltd.
Delivery changing to semesters in 2025
• From Semester 1 2025 the Certificate and Diploma will be delivered in 2 semesters per year. This change only applies to new students starting in Semester 1 2025
• All students will need to enrol in two courses in their first semester of the year, then one course in their second semester of the year.
• Fees for both courses in the first semester of study will need to be paid prior to the semester start.
• New students can enrol in Semester 2.
The Certificate will still be completed in 1 year of study (2 semesters)
PUBH4011 Safe sterilisation work practice
Enquiries regarding your application: email: SterilisationApps@toiohomai.ac.nz Semester 1
PUBH4013 Applied sterilisation practice project
PUBH4012 Application of standards for sterilisation practice
The Diploma will still be completed in 2 years of study (4 semesters)
PUBH5009 Continuous improvement of reprocessing services
PUBH5010 Validation for the sterilisation reprocessing cycle
PUBH5008 Quality management systems for reprocessing facilities Year 2
Semester 1 Semester 2
PUBH5011 Monitoring for the reprocessing cycle
PUBH5012 Leadership skills for sterilisation management
PUBH5013 Evidence based practice for the sterile sciences
Heliyon 10 (2024) e37281
Contents lists available at ScienceDirect Heliyon
journal homepage: www.cell.com/heliyon
Research article
Microbiological evaluation of ultraviolet C light-emitting diodes for disinfection of medical instruments
Hannah Siwe a, b , Annelies Aerssens c , Mieke V. Flour b , Silke Ternest a, c , Leen Van Simaey d , Duncan Verstraeten b , Alain F. Kalmar e , Isabel LerouxRoels c, f, 1, * , Philip Meuleman a, 1, ** , Piet Cools d, 1, ***
a Laboratory of Liver Infectious Diseases, Department of Diagnostic Sciences, Faculty of Medicine and Health Sciences, Ghent University, Corneel Heymanslaan 10, entrance 38, Medical Research Building 2, 9000, Ghent, Belgium
b Research and Development, eLEDricity, Hundelgemsesteenweg 446A, 9820, Merelbeke, Belgium
c Department of Infection Control, Ghent University Hospital, Corneel Heymanslaan 10, entrance 12, Clinical Building 12E, 9000, Ghent, Belgium
d Laboratory Bacteriology Research, Department of Diagnostic Sciences, Faculty of Medicine and Health Sciences, Ghent University, Corneel Heymanslaan 10, entrance 38, Medical Research Building 2, 9000, Ghent, Belgium
e Department of Electronics and Information Systems, IBiTech, Ghent University, Technologiepark-Zwijnaarde 126, 9052, Ghent, Belgium
f Department of Diagnostic Sciences, Faculty of Medicine and Health Sciences, Ghent University, Corneel Heymanslaan 10, entrance 38, Medical Research Building 2, 9000, Ghent, Belgium
ARTICLE INFO
Keywords:
UVC LED
Sustainability
Staphylococcus aureus
Reprocessing
ABSTRACT
Background: Despite the many guidelines for reprocessing of medical instruments, challenges persist such as microbial resistance to biocides, corrosive effects on materials, and timeconsuming reprocessing procedures. Ultraviolet (UV) C light-emitting diode (LED) chambers might provide a solution but the integration in healthcare is still in its infancy. Here, we evaluated the efficacy of a novel ZAPARAY™ UVC LED chamber as a time and energy-efficient alternative for reprocessing of medical instruments for which current disinfection protocols exhibit limitations.
Methods: We verified the disinfection efficacy of the UVC LED chamber on a Petri dish and contaminated several medical devices with Staphylococcus aureus ATCC 25923. The bacterial reduction was assessed after 5 min of UVC LED exposure. Additionally, we investigated the impact of rinsing before UVC exposure.
Results: We demonstrated a bacterial reduction of 9 log10 on a Petri dish. Non-rinsed dental tools exhibited varied reduction levels ranging from a 3.23 log10 to a 6.25 log10 reduction. Rinsing alone yielded an average reduction of 2.7 log10 and additional UVC exposure further reduced the bacterial load by an average of 3.65 log10 We showed an average 4.90 log10 reduction on thermistors, 2 log10 or less on orthodontic pliers, and no reduction on handpieces.
Conclusions: This study demonstrates that UVC LED chambers may be used as a standardized substitute for specific (manual) disinfection procedures of certain medical devices, offering a
time-efficient and more sustainable alternative. However, its use should be preceded by efficacy testing for each specific type of instrument.
1. Introduction
Correct reprocessing of reusable medical devices is an essential cornerstone of a good infection prevention and control program in healthcare facilities [1]. Reprocessing entails cleaning, disinfection and/or sterilization procedures to ensure the safe reuse of medical instruments [2]. This can be obtained through (the combination of) a variety of physical and chemical methods that include the use of detergents, oxidizing agents, aldehydes, radiation, and/or heat [3,4]. Spaulding’s classification is a commonly used system to assess which procedure is required for adequate reprocessing [4]. This classification defines non-critical (in contact with intact skin), semi-critical (in contact with non-intact skin or mucosae), or critical instruments (in contact with blood or sterile tissues), with the latter posing the highest risk for infection [3].
Despite the many reprocessing guidelines and protocols, device-associated outbreaks have been increasingly reported [5–7] and several challenges and limitations remain. Critical devices (e.g. surgical instruments) and some semi-critical devices, such as heat-sensitive flexible endoscopes, undergo a largely automated process of sterilization or high-level disinfection (HLD) [3] but these procedures are often time-consuming. Many non- and semi-critical medical instruments still undergo (semi-) manual reprocessing, but these manual procedures are not standardized and therefore highly error-prone, particularly when it concerns devices with a complex design [8–11]. The use of chemical disinfectants is associated with a high environmental burden [12,13], and the risk of inducing or increasing microbial resistance to biocides and cross-resistance to antibiotics [14,15]. The recommended dwell time of disinfectants may also be compromised under time pressure [16]. Furthermore, corrosive effects on instruments have been reported as a result of heat sterilization or chemical disinfection [17,18].
Disinfection by ultraviolet (UV) C generated by mercury discharge lamps is well established in the context of environmental disinfection [19–21] and might provide an answer to some of these challenges. UVC inactivates microorganisms either by direct absorption or indirectly via reactive oxygen species, targeting their DNA, RNA, proteins, and lipids [22–24]. However, there are more energy-efficient alternatives available including UVC light-emitting diodes (LEDs). These LEDs offer various other advantages such as being more compact and eco-friendly as they are free of toxic mercury [25,26]. Nevertheless, UVC LEDs are at present not widely used which could be as a result of their lower irradiance efficiency as compared to mercury discharge lamps [26]. However, UVC LEDs remain highly effective in deactivating pathogens and the technology is continuously evolving, as forecasted by Haitz’s law [27]. Ongoing research aims to further enhance their efficiency [28], indicating a promising future for UVC LEDs in various applications.
The implementation of UVC chambers for instrument disinfection in healthcare is still in an early stage due to several limitations that need to be considered such as the low quality of available research, the lack of standardization for UVC chambers, the low penetration depth of UVC, and the necessity for optimal exposure of the instrument without shadow formation [29]. UVC mercury chambers have been researched and shown to be effective for disinfection of electronic devices such as tablets [30,31] used in hospitals, and to some extent on medical devices including intravaginal probes [32–34], flexible fiberoptic laryngoscopes [35] and silicon dental impressions [36]. UVC LED has been investigated for stethoscope disinfection, revealing its potential for effective decontamination of these medical devices [37].
To the best of our knowledge, the efficacy and broad applicability of UVC LED chambers for instrument disinfection have not been thoroughly investigated, highlighting the need for further research to ensure their correct and optimal implementation. We aimed to evaluate the efficacy of a novel UVC LED chamber for disinfection of non- or semi-critical instruments, particularly those instruments for which current disinfection protocols exhibit limitations. In this study, we focused on how the shape and technical characteristics of the medical instruments influence the disinfection efficacy, using Staphylococcus aureus as a clinically relevant model pathogen.
2. Methods
2.1. Identification and selection of instruments
As an initial market survey, open interviews were held with potential end-users in health care (e.g. head nurses, dentists ), which led to the selection of dental tools (hammer shaped needle, sawtooth needle, and chisel needle) as proof of concept for microbiological testing (Table 1). At 14 departments of the Ghent University Hospital, semi-structured interviews, and questionnaires (Supplementary Figure A1) were used to identify those instruments for which there is a high need for an alternative disinfection strategy. In total, 29 identified instruments were given a high, medium, or low score for six parameters (i.e. correct implementation of current protocol, impact of current protocol on lifespan of instrument, processing time of current protocol, use frequency, cost of instrument and risk of a healthcare-associated infection (HAI)) (Supplementary Tables A1 and A2) and plotted in two heatmaps displaying instrument clusters sharing similar characteristics (Supplementary Figure A2). Based on feasibility and accessibility, a subset of instruments were selected for microbiological testing, more specifically, a nasal/oral thermistor (sensor) (REF: P1222, Pro-Tech, Downers Grove, Illinois, USA), a dental handpiece (REF: SYNEA WA-99 LT, W&H Dentalwerk, Bürmoos, Austria), a round ended orthodontic plier (REF: 4151-640, Masel Orthodontics, Carlsbad, California, USA), and a sharp ended orthodontic plier (REF: 678-106, Hu-Friedy, Chicago, Illinois, USA) (Table 1).
H. Siwe et al.
Heliyon 10 (2024) e37281
2.2.
UVC LED device
The UVC LED disinfection device evaluated in this study was the ZAPARAY™ RAY-ONE prototype 0/102 (eLEDricity, Merelbeke, Belgium) and further designated in this manuscript as “UVC LED chamber” . The device consists of an enclosed chamber with a drawer made of a quartz bottom in which objects can be placed with a maximum size of 200 mm × 300 mm x 70 mm (width x depth x height). The chamber and drawer are lined with UVC reflective material. This reflective material, along with LEDs mounted at the top and bottom of the chamber that emit UVC radiation at 275 nm, ensure homogenous UVC exposure with an irradiance of approximately 0,395 mW/cm2
2.3.
Contamination
Staphylococcus aureus (ATCC 25923) was aerobically cultured at 37 ◦ C for 24 h on tryptic soy agar with 5 % sheep blood (TSA-5% SB) (BD, Franklin Lakes, New Jersey, USA). For each experiment, an inoculum suspension was freshly prepared by resuspending S. aureus colonies in 0.9 % sterile NaCl solution (saline). The optical density (OD) at 600 nm was measured using the Denovix DS-11 spectrophotometer (Denovix, Wilmington, USA) with the OD ranging between 1,0 and 1,7 to obtain a concentration of approximately 109 colony forming unit (CFU)/mL. As initial verification and reference, a 10 μL droplet of the inoculum suspension was pipetted onto the center of a sterile 60 × 15 mm polystyrene Petri dish and then immediately exposed to UVC. Dental tools, orthodontic pliers and handpieces were steam sterilized before the start of each experiment and thermistors were decontaminated with 70 % ethanol. Dental tools were contaminated by applying the inoculum through partial submersion in 7 mL of inoculum suspension in a 15 mL tube. Orthodontic pliers were partially submerged in 80 mL inoculum suspension in a 100 mL multipurpose beaker. Handpieces were contaminated through partial submersion of the instrument in 10 mL of inoculum suspension in a 50 mL tube. All instruments were incubated for 10 min at room temperature. Afterward, a tapping motion was applied to the instruments to remove the excess liquid by tapping the instrument four times against the border of its container, used during contamination. Thermistors were contaminated around the three sensor tips by rubbing a cotton swab that had been soaked with inoculum in a circular motion around the tips. To investigate whether rinsing before UVC exposure would improve the outcome of the disinfection procedure; dental tools, handpieces, and orthodontic pliers, were rinsed for 3 s under a jet of water as a simplified cleaning step. Pliers were held in an open orientation during rinsing for water to flow through the hinge. Afterward, instruments were dapped on tissue paper to remove excess liquid. All instruments were exposed to UVC immediately after the contamination procedure without allowing the instruments to dry up.
2.4. UVC disinfection
Petri dishes and medical devices were positioned directly in the center of the drawer, except for dental tools which were positioned in a fixture for stability. Orthodontic pliers were placed in an open orientation. Petri dishes and medical devices were subjected to a 5min disinfection cycle which equated to a UVC dose of approximately 118 mJ/cm2 Contaminated Petri dishes and instruments that did not undergo UVC treatment were handled in parallel and served as an untreated control.
2.5. Assessment of log reduction factors
2.5.1. Bacterial recovery
The 10 μL droplet in the Petri dish was collected by locally rinsing the area of the droplet with 1 mL of saline which was then added to 9 mL saline and resuspended. Afterward, it was locally rinsed for a second time with 1 mL originating from the already collected volume to apply additional friction for the collection of residual material on the surface of the Petri dish. Bacteria on dental tools were recovered by partial submersion in 7 mL saline in a 15 mL tube. Handpieces were placed in a 50 mL tube containing 10 mL saline. All tubes with objects inside were vortexed for 20 s. Orthodontic pliers were placed in an open orientation inside a 100 mL multipurpose beaker and rinsed five times with the same 10 mL saline. Thermistors were positioned in a fixture above a 60 × 15 mm polystyrene sterile Petri dish. Subsequently, the three sensor tips were each rinsed with 1 mL saline. Finally, all rinse fluids were collected in a 15 mL tube and vortexed.
2.5.2. Bacterial enumeration
The bacterial load was quantified by performing a tenfold serial dilution of the collected suspension. A droplet of 5 μL was pipetted onto TSA-5%SB for each dilution, and afterward, plates were slanted vertically at a nearly 90◦ angle to create a droplet line. Subsequently, plates were incubated at 37 ◦ C for 18–24 h and colonies were manually counted. The dilution with the highest countable value within the range of 0–100 CFU was used to calculate the bacterial concentration of the original suspension. The log reduction was calculated as followed:
2.6. Confirmation of the absence of bacterial growth after UVC exposure
To confirm the lack of viable bacteria in the absence of growth with the droplet line technique, a 10 μL droplet was spotted on a Petri dish and treated as previously described. The droplet was then collected by locally rinsing the area with 90 μL saline. This total volume of 100 μL was plated onto TSA-5%SB according to the spread plate technique. Similarly, thermistors and dental tools were prepared and handled as previously described and after bacterial recovery, the instruments were directly imprinted onto TSA-5%SB.
2.7. Statistical analysis
Statistical analysis was performed using GraphPad Prism version 8.0.1. Bar charts in all figures were depicted as mean ± standard deviation with dots representing individual data points. Data was verified for normal distribution using the Shapiro Wilk test. A paired t-test was used when the data was normally distributed, otherwise, the Wilcoxon matched-pairs signed rank test was used. Statistical significance was expressed as * (p < 0.05), ** (p < 0.01), *** (p < 0.001), **** (p < 0.0001), or ns (non-significant).
3. Results
3.1. Verification of the UVC LED chamber as a disinfection device
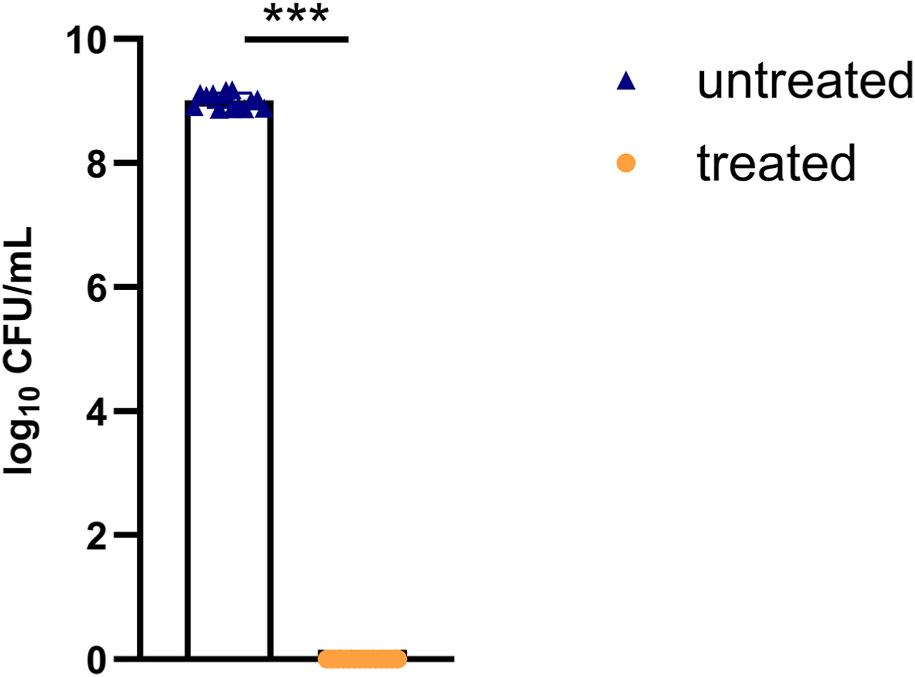
Before we initiated the evaluation of the device to disinfect medical instruments, we wanted to assess its usefulness in a disinfection experiment using Petri dishes as a simple surface. Collected suspensions from the untreated control (n = 14) had an average bacterial concentration of 1.02 × 109 CFU/mL (Fig. 1). Exposure of the droplet to a 5-min disinfection cycle resulted in a complete reduction below detectable levels across all experiments (Fig. 1), with an average log10 reduction factor of 9. The absence of growth was confirmed when the treated droplet was spread-plated (Supplementary Figure A3).
3.2. Evaluation of the efficacy of the UVC LED chamber for disinfection of non-rinsed medical instruments
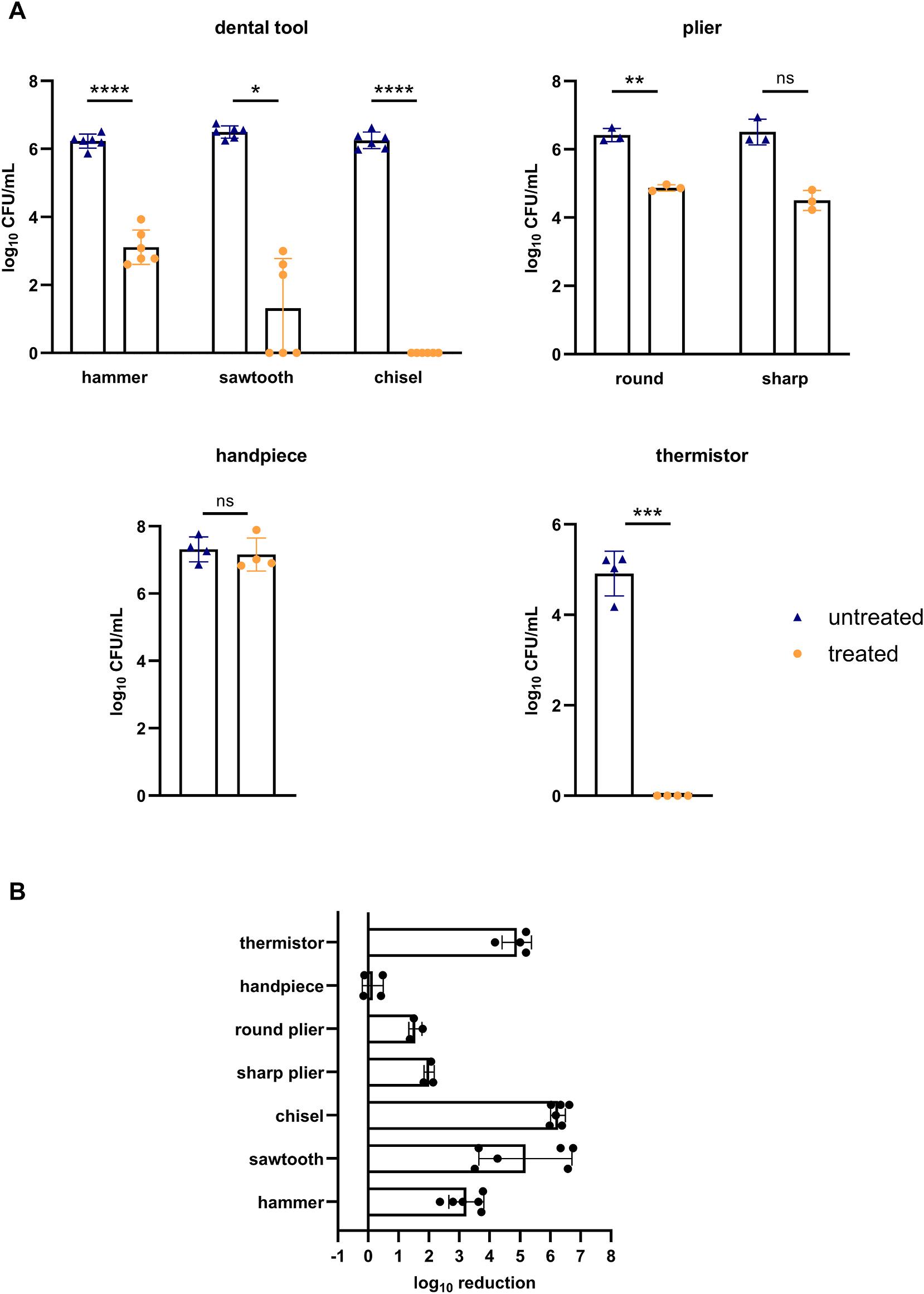
To evaluate the efficacy of the device for disinfection of medical instruments, various identified instruments were artificially contaminated with S. aureus and exposed to UVC. The bacterial load of the collected suspensions of the different dental tools and pliers was highly comparable for the untreated conditions, resulting in an average concentration of 106 CFU/mL (Fig. 2A). UVC exposure yielded significantly lower bacterial concentrations for all three dental tools, with a complete reduction for the chisel needle (Fig. 2A). Remarkably, for the sawtooth needle results varied from partial to complete reduction across different experiments. The average log10 reduction factor was 3.23, 5.18 and 6.25 for the hammer-shaped needle, sawtooth needle, and chisel needle, respectively (Fig. 2B). Pliers showed a significant, but lower reduction of the bacterial load after UVC exposure with a log10 reduction factor of 2 or less (Fig. 2B). UVC exposure of handpieces did not result in any bacterial reduction whereas thermistors showed the absence of growth after exposure, resulting in an average log10 reduction factor of 4.90 (Fig. 2A and B). Additionally, the agar imprinting method confirmed the absence of bacterial growth on the UVC treated thermistors (Supplementary Fig. A4). However, a few colonies were observed for the treated chisel needle as compared to the dense growth of S. aureus for the untreated control (Supplementary Fig. A4).
Fig. 1. Bacterial load of a contaminated Petri dish without UVC exposure (untreated) and after 5 min of UVC exposure (treated). Log-transformed colony forming units (CFU)/mL of S. aureus under control and treatment conditions. Dots represent individual data points. Bar charts are shown as mean ± standard deviation (n = 14 treated and 14 untreated) (14 independent experiments), *** (p < 0.001) (Wilcoxon matched-pairs signed rank test).
H. Siwe et al.
Heliyon 10 (2024) e37281
Fig. 2. Bacterial load and log reduction factors of non-rinsed medical instruments. Dots represent individual data points. Bar charts are shown as mean ± standard deviation (SD). (A) Log-transformed colony forming units (CFU)/mL of S. aureus under control and treatment conditions collected from dental tools (n = 6) (6 independent experiments), round and sharp ended orthodontic pliers (n = 3) (3 independent experiments), handpieces (n = 4) (2 independent experiments), and thermistor (n = 4) (2 independent experiments). * (p < 0.05), **p < 0.01), *** (p < 0.001), **** (p < 0.0001), ns (non-significant) (paired t-test except for data on sharp ended plier and sawtooth, Wilcoxon matched-pairs signed rank test) (B) Log10 reduction factors for the different medical instruments.
H. Siwe et al.
Heliyon 10 (2024) e37281
Heliyon 10 (2024) e37281
3.3. Evaluation of the efficacy of the UVC LED chamber for disinfection of rinsed medical instruments
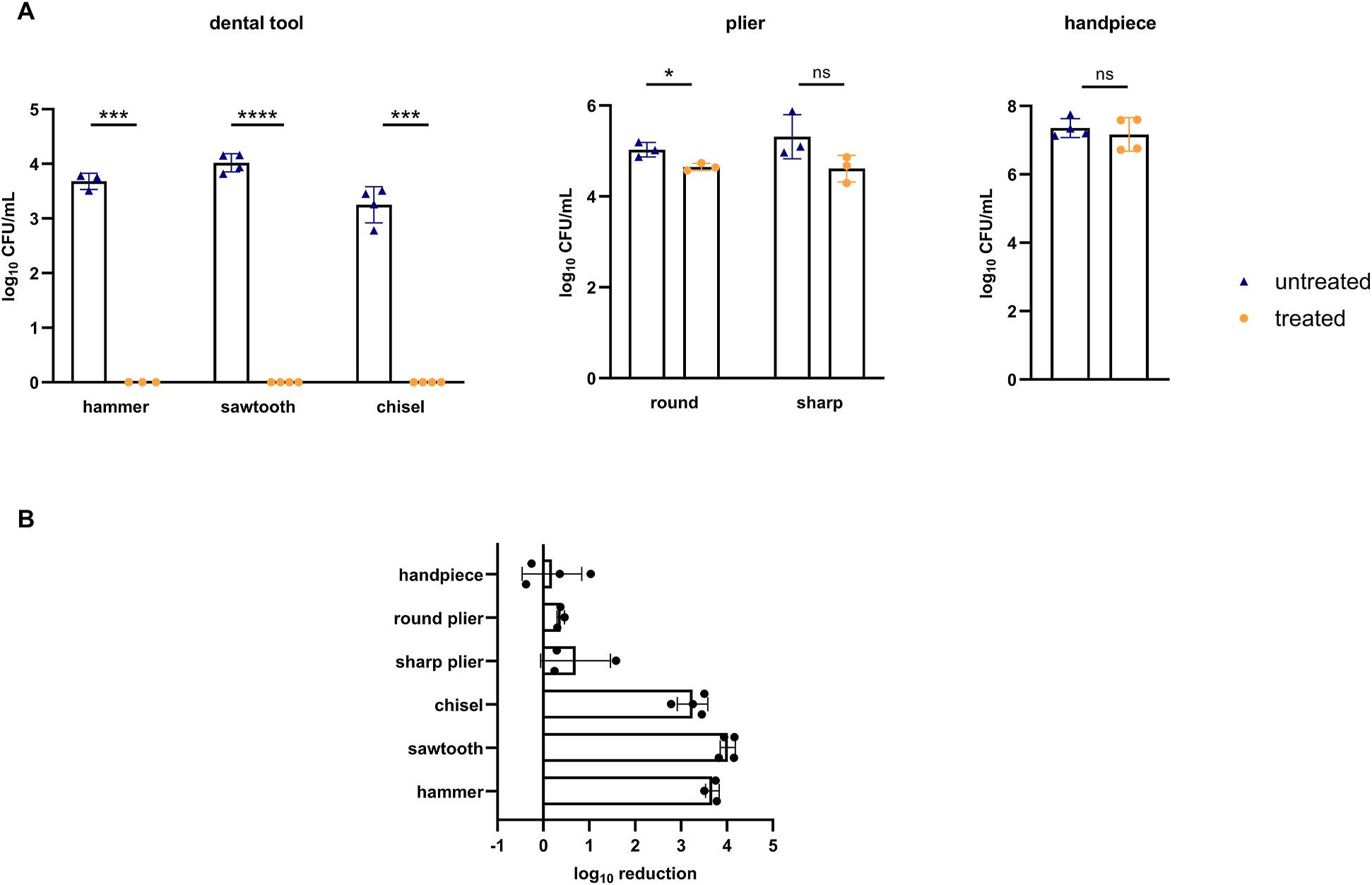
To evaluate whether rinsing improves the overall disinfection procedure for those instruments where complete reduction was not obtained, a short rinsing step was included before UVC treatment. Rinsed untreated controls showed on average 2.7 and 1.3 log10 lower bacterial loads (CFU/mL) for dental tools and pliers, respectively, compared to unrinsed counterparts (Fig. 3A and 2A). Rinsing followed by UVC exposure resulted in undetectable growth for the hammer shaped needle, sawtooth needle, and chisel needle with an average log10 reduction factor of 3.68, 4.02, and 3.25 respectively, resulting in an overall average log10 reduction factor of 3.65 (Fig. 3B). However, no rinsing effect was observed for pliers and handpieces for the treatment conditions (Fig. 3A and 2A). This resulted in an average log10 reduction factor of less than 1 for pliers and no reduction for handpieces (Fig. 3B). Instrument imprinted plates of the rinsed dental tools showed a few colonies for all treated objects as compared to untreated objects (Supplementary Figure A5).
4. Discussion
In this study, we evaluated the performance of the novel ZAPARAY™ UVC LED chamber for the disinfection of artificially contaminated simple surfaces (i.e. Petri dishes) as well as of complex medical instruments. First, we have shown that the device was able to induce complete reduction (9 log10 reduction) of S. aureus on a standard Petri dish that has a smooth, flat, non-porous surface without any cavities.
The results obtained on medical devices varied considerably depending on the instrument. In literature, research has been described where instruments were artificially contaminated and disinfected with UVC [38,39]. However, these studies employed limited contamination through several inoculated sites of 1 cm2 across the device, including a blood pressure gauge and N95 respirators. Post-exposure, these areas were sampled with a pre-moistened cotton swab and placed in a solution for bacterial recovery, or in the case of respirators, the areas were cut out. Another study evenly distributed a small inoculum onto the membranes of stethoscopes which were placed onto plate count agar for bacterial recovery [37]. These approaches are unfeasible to demonstrate the efficacy of a UVC chamber for medical devices that are more complex in shape or technical design. Therefore, this study employed a different
Fig. 3. Bacterial load and log reduction factors of rinsed medical instruments. Dots represent individual data points. Bar charts are shown as mean ± standard deviation (SD). (A) Log-transformed colony forming units (CFU)/mL of S. aureus under control and treatment conditions collected from dental tools (n = 3 or 4) (4 independent experiments), round and sharp ended orthodontic pliers (n = 3) (3 independent experiments), handpieces (n = 4) (2 independent experiments). * (p < 0.05), ** (p < 0.01), *** (p < 0.001), ns (non-significant) (paired t-test except for data on handpieces, Wilcoxon matched-pairs signed rank test) (B) Log10 reduction factors for the different medical instruments.
H. Siwe et al.
methodology through partial submersion of the devices (with exception of the thermistors), thereby enabling a more accurate representation of natural contamination. Studies using UVC mercury chambers for disinfection of devices naturally contaminated during routine use, have been described for some medical devices such as electronic devices [30,31], intravaginal probes [32–34] and flexible fiberoptic laryngoscopes [35]. This approach could result in a more thorough understanding of the effectiveness as well as the practical implementation of the UVC chamber in daily practice as compared to artificial contamination in laboratory setting. However, the complexity of this study design may render on-site studies for each potential instrument of interest impractical and may not always be necessary depending on the result obtained on an artificially contaminated instrument.
The instruments subjected to UVC LED disinfection in our study were semi-critical devices that require at least HLD [3]. For this reason, the devices (with exception of the thermistors) were contaminated with a high inoculum, such that upon disinfection a log10 reduction factor of 6 could be demonstrated, which is the endpoint for HLD recommended by the Food and Drug Administration [40]. Using different types of dental tools, all having the same rod-like structure but with variable ends, we demonstrated that the efficacy of the UVC LED chamber for disinfection of medical instruments was influenced by their technical and/or structural characteristics as reduction levels varied from a 3 log10 to 6 log10 reduction for the non-rinsed dental tools. For instance, UVC disinfection of the chisel needle, the dental tool with the lowest complexity, consistently resulted in undetectable growth, averaging a reduction of 6.25 log10 with the droplet line technique. In contrast, the sawtooth needle and hammer shaped needle demonstrated an average reduction of 5.18 log10 and 3.23 log10, respectively. The conflicting results of the sawtooth needle could potentially be explained by the different volumes of inoculum remaining between the ridges after excess droplet removal. Rinsing for 3 s under a stream of water as a simplified cleaning process reduced the bacterial load by 2.7 log10 and improved the final outcome of the disinfection procedure for all dental tools. Bacterial growth remained undetected with the droplet line technique for all dental tools. However, a few colonies were still observed when the rinsed and treated instruments were imprinted onto agar. Thorough cleaning before HLD or sterilization is required to ensure the subsequent technique is effective at inactivating microorganisms [3]. The incorporation of a more thorough cleaning method may further improve the outcome, and when combined with UVC LED, may offer an effective disinfection alternative. UVC was unable to decontaminate handpieces, both in the rinsed and non-rinsed conditions. These instruments are complex in nature due to technical characteristics and therefore require a multistep decontamination process [41,42]. This complexity likely prevented UVC from accessing the internal part of the device, leading to the absence of bacterial reduction. However, this does not negate the possibility of the use of a UVC chamber as an alternative disinfection step for the exterior of the device prior to lubrication and HLD or sterilization, as the exterior is commonly cleaned/disinfected through a manual procedure involving a disinfectant cloth [43]. A similar trend was observed with the orthodontic pliers, where only partial reduction (2 log10 or less) was obtained as the contaminating bacteria inside the hinge were likely not accessible to UVC. Implementation of an adequate disinfection alternative would be beneficial as these instruments frequently experience corrosion through heat sterilization, the commonly used technique in practice [18]. We were able to show a complete reduction of the bacterial load on an oral/nasal thermistor, demonstrating an average reduction of 4.90 log10, which was further confirmed using the instrument imprinting procedure. Currently, these instruments are either single-use or reusable provided they are manually disinfected. A UVC disinfection chamber may offer the possibility for reprocessing single-use thermistors, on condition that it complies with guidelines and regulations which could contribute to more sustainable practices [44,45]. Although the reuse of single-use devices is performed worldwide, it remains a matter of controversy and is unauthorized in several countries [3,46,47]. In addition, the error-prone manual disinfection of reusable thermistors could be replaced by a standardized process utilizing UVC chambers, if preceded by a manual cleaning step.
Standardization of UV disinfection is still under development whereby a variety of other standards are currently being used, such as the EN14885 standard developed for chemical disinfection [29]. However, the recent British standard BS8628:2022 [48] specifically developed for validation of UV(C) disinfection systems is increasingly used and entails laboratory tests conducted on stainless steel disc carriers. Here, we demonstrated that the disinfection efficacy on a simple surface (i.e. a standard Petri dish or stainless-steel disc) does not necessarily reflect the disinfection performance on a contaminated instrument. This highlights the importance of assessing the efficacy on real-life instruments and the standards used to validate UVC chambers should consider this.
Here, we evaluated the efficacy of a UVC LED chamber for disinfection of medical instruments, focusing on how the shape and technical characteristics of these instruments influence the disinfection efficacy. While the study was limited to the clinically relevant pathogen S. aureus in the absence of organic soling, our results on medical devices, combined with existing literature on bacterial species [49–51] suggest that variations in the design of instruments have a greater impact on the reduction efficacy than variations between bacterial species. However, future research should include a broader variety of microorganisms such as yeasts, molds, and viruses to provide more insight into the required dose for effective decontamination of medical devices. Additionally, only a limited subset of instruments was examined, while an extensive list of unexplored devices remains. These instruments could be investigated in follow-up research. The use of UVC as an alternative disinfection strategy for medical devices should be preceded by efficacy testing for each candidate device to ensure the safe use of UVC chambers in medical settings, mitigating the risk of acquiring a nosocomial infection.
5. Conclusions
This study evaluated the efficacy of UVC LED for disinfection of a range of medical instruments that have not been previously assessed. Using S. aureus as the test organism, we demonstrated the high disinfection capacity of the novel ZAPARAY™ UVC LED chamber on a simple surface, such as a Petri dish which is smooth, flat, non-porous, and without cavity. However, varying results obtained from medical instruments indicate that instrument shape and technical characteristics may substantially influence the efficacy of UVC disinfection. These factors should be considered, along with the initial level of contamination after routine use, cleaning
H. Siwe et al.
Heliyon 10 (2024) e37281
Heliyon 10 (2024) e37281
steps, and the desired level of disinfection (non-critical vs. semi-critical devices). Our findings highlight the potential of UVC chambers as a standardized substitute for specific (manual) disinfection procedures, but they may not be suitable for all instruments. Given the variability in efficacy, it is essential that their use is preceded by efficacy testing for each specific type of instrument. In this manner, the study provides novel insights into the broad applicability of UVC LED chambers and offers a benchmark for future research in exploring the potential of UVC LED.
Funding
This work was supported by the Flanders Innovation and Entrepreneurship (VLAIO) [Grant numbers HBC.2022.0304 and HBC.2021.0849]. The funding source was not involved in any aspects of the study design, the execution, the analysis, the writing, or the decision to submit for publication.
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: H.S. is an employee of eLEDricity, M.V.F. was an employee and shareholder of eLEDricity until halfway through the study. D.V. and A.F.K. are shareholders of eLEDricity but were not involved in the analysis or interpretation of the data. All other authors declare they have nothing to disclose.
Acknowledgements
We thank the staff of the departments at the Ghent University Hospital, and the private practice end-users for their contribution to the study.
Appendix A. Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.heliyon.2024.e37281.
References
[1] World Health Organization, Global report on infection prevention and control, Retrieved 21 November 2023, from, https://www.who.int/publications/i/item/ 9789240051164, 2022.
[2] World Health Organization, "Minimum Requirements for Infection Prevention and Control programmes.", 2019
[3] Center for Disease Control and Prevention, Guideline for disinfection and sterilization in healthcare facilities, Retrieved 20 November 2023, from, https://www. cdc.gov/infectioncontrol/pdf/guidelines/disinfection-guidelines-H.pdf, 2008, May 2019.
[4] G. McDonnell, P. Burke, Disinfection: is it time to reconsider Spaulding? J. Hosp. Infect. 78 (3) (2011) 163–170
[5] P.M. Southworth, Infections and exposures: reported incidents associated with unsuccessful decontamination of reusable surgical instruments, J. Hosp. Infect. 88 (3) (2014) 127–131
[6] W.A. Rutala, D.J. Weber, Reprocessing semicritical items: outbreaks and current issues, Am. J. Infect. Control 47 (2019) A79–A89
[7] A.M. Laheij, et al., Healthcare-associated viral and bacterial infections in dentistry, J. Oral Microbiol. 4 (2012)
[8] M.J. Alfa, et al., Manual methods are suboptimal compared with automated methods for cleaning of single-use biopsy forceps, Infect. Control Hosp. Epidemiol. 27 (8) (2006) 841–846
[9] N. Kenters, et al., Infectious diseases linked to cross-contamination of flexible endoscopes, Endosc. Int. Open 3 (4) (2015) E259–E265
[10] J.T. Walker, et al., Cleanability of dental instruments – implications of residual protein and risks from Creutzfeldt-Jakob disease, Br. Dent. J. 203 (7) (2007) 395–401
[11] D.L. Buescher, et al., Disinfection of transvaginal ultrasound probes in a clinical setting: comparative performance of automated and manual reprocessing methods, Ultrasound Obstet. Gynecol. 47 (5) (2016) 646–651
[12] N. Musee, et al., Occurrence, effects, and ecological risks of chemicals in sanitizers and disinfectants: a review, Environmental Chemistry and Ecotoxicology 5 (2023) 62–78
H. Siwe et al.
[13] K. Romero Starke, et al., Are healthcare workers at an increased risk for obstructive respiratory diseases due to cleaning and disinfection agents? A systematic review and meta-analysis, Int J Environ Res Public Health 18 (10) (2021)
[14] J.-Y. Maillard, Resistance of bacteria to biocides, Microbiol. Spectr. 6 (2) (2018), https://doi.org/10.1128/microbiolspec.arba-0006-2017
[15] A.D. Russell, Bacterial resistance to disinfectants: present knowledge and future problems, J. Hosp. Infect. 43 (1999) S57–S68
[16] B.F. Leas, et al., AHRQ comparative effectiveness technical briefs, in: Environmental Cleaning for the Prevention of Healthcare-Associated Infections, Agency for Healthcare Research and Quality (US), Rockville (MD), 2015
[17] M. Dioguardi, et al., Management of instrument sterilization workflow in endodontics: a systematic review and meta-analysis, Int J Dent 2020 (2020) 5824369
[18] A. Wichelhaus, et al., Corrosion of orthodontic pliers using different sterilization procedures, J. Orofac. Orthop./Fortschritte der Kieferorthopadie 65 (6) (2004) 501–511
[19] N.G. Reed, The history of ultraviolet germicidal irradiation for air disinfection, Publ. Health Rep. 125 (1) (2010) 15–27
[20] W.A. Hijnen, E.F. Beerendonk, G.J. Medema, Inactivation credit of UV radiation for viruses, bacteria and protozoan (oo)cysts in water: a review, Water Res. 40 (1) (2006) 3–22
[21] J. Henderson, et al., Field study of early implementation of UV sources and their relative effectiveness for public health and safety, J. Occup. Environ. Hyg. 19 (9) (2022) 524–537
[22] S.E. Beck, et al., Comparison of UV-induced inactivation and RNA damage in MS2 phage across the germicidal UV spectrum, Appl. Environ. Microbiol. 82 (5) (2015) 1468–1474
[23] C.A. Juan, et al., The chemistry of reactive oxygen species (ROS) revisited: outlining their role in biological macromolecules (DNA, lipids and proteins) and induced pathologies, Int. J. Mol. Sci. 22 (9) (2021)
[24] A. Rodger, UV absorbance spectroscopy of biological macromolecules, in: G.C.K. Roberts (Ed.), Encyclopedia of Biophysics, Springer Berlin Heidelberg, Berlin, Heidelberg, 2013, pp. 2714–2718
[25] L.T. Budnik, L. Casteleyn, Mercury pollution in modern times and its socio-medical consequences, Sci. Total Environ. 654 (2019) 720–734
[26] T. Nicolau, et al., A comprehensive analysis of the UVC LEDs’ applications and decontamination capability, Materials 15 (8) (2022)
[28] T. Bhattarai, A. Ebong, M.Y.A. Raja, A review of light-emitting diodes and ultraviolet light-emitting diodes and their applications, Photonics 11 (6) (2024) 491
[29] N. Demeersseman, et al., Shedding a light on ultraviolet-C technologies in the hospital environment, J. Hosp. Infect. 132 (2023) 85–92
[30] E.M. Allen, et al., The effectiveness of germicidal wipes and ultraviolet irradiation in reducing bacterial loads on electronic tablet devices used to obtain patient information in orthopaedic clinics: evaluation of tablet cleaning methods, J. Hosp. Infect. 105 (2) (2020) 200–204
[31] M. Resendiz, et al., Comparative effectiveness of rapid-cycle ultraviolet decontamination to chemical decontamination on high-touch communication devices, Am. J. Infect. Control 47 (9) (2019) 1135–1139
[32] M. Pichon, et al., Decontamination of intravaginal probes infected by human papillomavirus (HPV) using UV-C decontamination system, J. Clin. Med. 8 (11) (2019)
[33] C. Kyriacou, et al., Time-effectiveness and convenience of transvaginal ultrasound probe disinfection using ultraviolet vs chlorine dioxide multistep wipe system: prospective survey study, Ultrasound Obstet. Gynecol. 60 (1) (2022) 132–138
[34] G. Kac, et al., Evaluation of a new disinfection procedure for ultrasound probes using ultraviolet light, J. Hosp. Infect. 65 (2) (2007) 163–168
[35] U.C. Ezeh, et al., The effectiveness of ultraviolet smart D60 in reducing contamination of flexible fiberoptic laryngoscopes, Laryngoscope 133 (12) (2023) 3512–3519
[36] J. Wezgowiec, et al., Evaluation of antimicrobial efficacy of UVC radiation, gaseous ozone, and liquid chemicals used for disinfection of silicone dental impression materials, Materials 15 (7) (2022)
[37] G. Messina, et al., A new UV-LED device for automatic disinfection of stethoscope membranes, Am. J. Infect. Control 43 (10) (2015) e61–e66
[38] G. Moore, et al., Use of UV-C radiation to disinfect non-critical patient care items: a laboratory assessment of the Nanoclave Cabinet, BMC Infect. Dis. 12 (2012) 174
[39] J.L. Cadnum, et al., Effectiveness of ultraviolet-C light and a high-level disinfection cabinet for decontamination of N95 respirators, Pathog Immun 5 (1) (2020) 52–67
[40] Food and Drug Administration, Medical washers and medical washer-disinfectors - class II special controls guidance document for the medical device industry and FDA review staff, Retrieved 17 November 2023, from, https://www.fda.gov/medical-devices/guidance-documents-medical-devices-and-radiation-emittingproducts/medical-washers-and-medical-washer-disinfectors-class-ii-special-controls-guidance-document-medical, 2002.
[41] G. Smith, A. Smith, Microbial contamination of used dental handpieces, Am. J. Infect. Control 42 (9) (2014) 1019–1021
[42] E.C. Deasy, et al., Effective cleaning and decontamination of the internal air and water channels, heads and head-gears of multiple contra-angle dental handpieces using an enzymatic detergent and automated washer-disinfection in a dental hospital setting, J. Hosp. Infect. 128 (2022) 80–88
[43] G.W.G. Smith, et al., Survey of the decontamination and maintenance of dental handpieces in general dental practice, Br. Dent. J. 207 (4) (2009). E7-E7
[44] Food and Drug Administration, Enforcement priorities for single-use devices reprocessed by third parties and hospitals, Retrieved 25 November 2023, from, https://amdr.org/wp-content/uploads/2021/03/1168-.pdf, 2000.
[45] A. Molero, et al., Sustainability in healthcare: perspectives and reflections regarding laboratory medicine, Ann Lab Med 41 (2) (2021) 139–144
[46] European Commision, National rules on reprocessing of single-use devices, Retrieved 25 November 2023, from, https://health.ec.europa.eu/medical-devicestopics-interest/reprocessing-medical-devices/national-rules-reprocessing-single-use-devices_en, 2022.
[47] W. Popp, et al., What is the use? An international look at reuse of single-use medical devices, Int. J. Hyg Environ. Health 213 (4) (2010) 302–307
[48] 8628 Bs, Disinfection using ultraviolet radiation. Methods for quantitative testing of automated ultraviolet disinfection activities by direct illumination. Determination of Bactericidal, Mycobactericidal, Sporicidal, Yeasticidal, Fungicidal, Virucidal and Phagocidal Activities. 2022, British Standard Institution, 2022
[49] H. Schobel, et al., Antimicrobial efficacy and inactivation kinetics of a novel LED-based UV-irradiation technology, J. Hosp. Infect. 135 (2023) 11–17
[50] D.-K. Kim, D.-H. Kang, J.L. Schottel, UVC LED irradiation effectively inactivates aerosolized viruses, bacteria, and fungi in a chamber-type air disinfection system, Appl. Environ. Microbiol. 84 (17) (2018)
[51] D.-K. Kim, S.-J. Kim, D.-H. Kang, Bactericidal effect of 266 to 279nm wavelength UVC-LEDs for inactivation of Gram positive and Gram negative foodborne pathogenic bacteria and yeasts, Food Res. Int. 97 (2017) 280–287
H. Siwe et al.
Heliyon 10 (2024) e37281
UPDATE on the NZSSA WEBSITE
A website is the window into the NZSSA and the time has come where the website currently in use (for many years) is now looking dated and with a format that is lacking the ability to meet the requirements of 2025.
The NZSSA are in the process of refreshing our website to meet the needs of our members in 2025. We are currently finalising the finer details with the provider, to ensure a format which allows a wider range of potential functionalities available to us.
As our members will be aware, we have made the first step of changing the domain name from www.nzssa.org to www.nzssa.co.nz. Issues encountered with the domain name provider required the change, however the change does create an easier to remember and more relatable domain name for the NZSSA going forward. Please remember that only the .co.nz domain name is correct, as the search engines begin to count more visits to the new domain name, the old (.org) site will cease to be located. Please remember to update the new domain name if you have saved NZSSA on your device
The new website will have a more modern feel, a bright colour palette and enable the NZSSA to look at improving
the online experience when visiting the site. The change of platform will provide the web administrators an easier to manage service which will allow the website to stay up to date with information our members require.
The functionality improvements will allow the expansion of the website to offer a focused member only experience, provided educational/learning opportunities such as training videos and online learning sessions. The website will also provide direct links to the NZSSA social media pages allowing effective multi-platform integration.
The development and creation of a totally new website does take more time than just a re-skin of the existing site, however, the aim is to have the new website launched during Q1 of 2025, with rebuilding and growth of content throughout 2025 leading up to the NZSSA Conference and beyond.
Thanks,
Ants Owens NZSSA Executive Member SSD Team Lead Southern Cross Gillies Hospital Auckland
Sonidet Supplyline NZ
Appl y no w for a N ZS SA Sch ol arsh ip 2025
Appl icati ons clo se 30 Apri l 2025, 5pm
Education
Course & administration fees are covered for the student
NZSSA Conference, Rotorua Conference registration, return flights, 3 days accommodation
WFHSS Congress, Conference registration, return flights, 5 days accommodation
For full details of the scholarships and application forms visit the Scholarship page: https://nzssa.co.nz/scholarship/
Contact Details NZSSA Executive Body:
Martin Bird (President) CSSD Manager Dunedin Hospital Dunedin martin.bird@southendhb.govt.nz