
19 minute read
Creative Corner


Go Places in My Mind
So far away and long ago.
Advertisement
We were free to explore the deepest ocean, climb the tallest mountain.
Now, a voice of sadness looms over the world.
Two years and counting isolation, two years and waiting, building frustration.
I pick up a pen, begin to write it all down, painting in the streets of Italy.
The roaring pyramids of Egypt, I want to see you soon.
Sandy white beaches, of Jamaica, Dancing until the sun goes down, I have yet to meet you.
Pictures in my mind of places I long to go.
This autistic poet misses seeing the world.
I close my journal as I breathe into the moment.
As I wait, let’s hope COVID-19 does not intend to stay, this deadly virus, only allows me to travel In my mind.
By Amanda Harrinauth
Amanda Harrinauth is a poet, author and life coach with disabilities. She is a disability empowerment coach. She discovered the power of poetry in 2016, after being diagnosed with autism, saying it allows her “to dance with life.” She also believes poetry has healing properties.
Aging AND Dementia

By Seth Keller, MD
People with Intellectual and Developmental Disabilities (IDD) are living longer than ever before. Over the past 50 years, there have been a growing personal, social and cultural awareness and sensitivity to the rights and needs for those with IDD and to those that support them throughout their lifetime.
Growing older allows all of us to enjoy life as it unfolds and to gain from it as much as we can. We can all appreciate that aging also will have an impact upon us physically and mentally. One aspect of aging is how our minds will change. Short-term memory and the ability to pull out of our minds information that is stored will naturally be slower, which is all a part of the normal aging process. We even have an expectation of what the aging process is like, based on these experiences and knowledge “normal” aging.
But what of those who have had a life-long disability, and what of those in particular, who have Down syndrome? What do we expect for them as they grow older? Supporting people with IDD has always focused on early intervention, but the focus on adult care and supports, and in particular on geriatrics, has not gained attention until very recently. This absence of awareness has led to a tremendous amount of ignorance as to what the aging process is like and on how to best support it.
The National Task Group on Intellectual Disabilities and Demen-
tia Practices (NTG) was created in 2010 to fill in the wide knowledge and supports gap which had existed until that point. Individuals, their families/ caregivers, support organizations, and healthcare supports, all were in the dark when decline of function began to occur—specifically, what to do, how to provide assessments, diagnostics and care, especially if Alzheimer’s disease (AD) was found to be the cause of the decline. This tremendous lack of sup-
ports leads to a great level of frustration, uncertainties, and often significant turmoil as the progression of the disease continues, ultimately leading to a tragic end…death. Many people with IDD who have had some degree of a baseline cognitive or intellectual dysfunction throughout their lifetime, will most notably also have additional normal cognitive decline as they age. This decline may be subtle and some may not be so. The ability to know the change is part of the normal aging process or a sign of an illness or disease, including Alzheimer’s disease or some other form of dementia which may be very difficult to determine. People with Down syndrome have a very high risk of developing early onset AD due to their genetic predisposition of having an extra copy of chromosome 21, which leads to an early accumulation of beta amyloid protein in the brain. This protein is thought to be one of the main contributors leading to AD. People with DS will develop AD, with some estimates as high as 60% by age 60.
The NTG needed to ensure it had the expertise and dedication of its leaders to be able to provide the much-needed level of education, training and supports. We absolutely needed people who had a personal vested interest in the issues at hand. Family advocacy has become a prominent part of the NTG.
We were thrilled to meet Marianne Barbera, who has been involved in special education and supporting her aging father, as well as her sister with Down syndrome. Nothing prepared her for when her sister began to show signs of decline.
Marianne’s story about her sister, Susan, is very similar to many others who were shocked and dismayed about the decline and the realization of what came next. Many families and caregivers across the country and around the world who support individuals aging with IDD, and in particular DS, will often face some level of decline of function.
The NTG will help to provide the much-needed education, training, and advocacy that is sorely needed, as there are significant barriers and ongoing disparities that remain. Working together with national, state and local I/DD and aging organizations is instrumental in being able to help further along the important care and supports required—as the number of individuals with age-related decline and dementia increase. We personally appreciate the issues, and are sensitive to the needs and concerns that aging has to those with IDD and especially those with Down syndrome.
Seth M. Keller, MD is a board-certified neurologist in private practice with Neurology Associates of South Jersey. He specializes in the evaluation and care of adults with Intellectual and Developmental Disabilities (IDD) with neurologic complications. Dr. Keller is on the Executive Board of the Arc of Burlington County, as well as on the board for The Arc of New Jersey Mainstreaming Medical Care Board. Dr. Keller is the Past President of the American Academy of Developmental Medicine and Dentistry (AADMD). He is the co-president of the National Task Group on Intellectual Disabilities and Dementia Practices (NTG).

My SisterSusan’s StoryBy Marianne Barbera

Truth be told, my family and I thought we had everything in place for my sister Susan, or at least this is what we thought. Local agencies provided services for my sister and we felt, “if it ain’t broke, don’t fix it.” In other words, if my sister was receiving the proper care and services for all aspects of her life, and we were satisfied with them, why look elsewhere?
In fact, other than The Arc, we were unaware of other national organizations specific to Down syndrome. What we never knew was that looming in the background was my sister’s accelerated aging due to the greater propensity of individuals with Down syndrome to age sooner and develop dementia at a much earlier age than neurotypical individuals. Had we known about the National Task Group on Intellectual Disabilities and Dementia Practices (NTG), we would have had an idea of what might be part of my sister’s life in her later years.
In January 2016, just a few weeks after celebrating Christmas and my sister’s birthday - her most favorite

Susan with heart facepaint
day of the Marianne and Susan year - it was mentioned to me by her group home manager that she and other staff had been noticing changes in my sister’s ability, and they wanted to know my thoughts. They were also interested in having her checked medically for early onset of dementia.
I was shocked and in disbelief as this didn’t make sense to me. My sister was in her 40s and, to me, dementia was something that happened to the elderly, not my spry, vivacious, loving sister. Especially not at her current age. My sister actually looked the same as she did in her mid-20s! And, of course, her vibrant, carefree personality was the same too. To me, there were no signs of aging. She didn’t develop wrinkles and gray hair, nor did she do anything differently since her late 20s - she had her day program, residence, family, and friends. She reached her potential and we were all satisfied and content with her life, especially my sister. The only aging that was noticeable was with my father, a World War II veteran, who did develop increased medical issues and physically showed signs of aging. But not my sister.And there was no reason for me to even consider the notion that she was aging internally at an accelerated rate.
If anything was different, it was my belief that if my sister had any changes, it was attributed to her having
Susan and her dance award
an off day and I would modify things to accommodate her, which was what I always had been doing so it didn’t seem any dif- ferent now. I visited my sister weekly, whereas her day program staff, and group home staff, spent many more hours and days with her each week; they noticed the changes I didn’t see.
In fact, it wasn’t until she declined that I learned that individuals with Down syndrome and/or other intellectually developmentally disabilities weren’t expected to have the same longevity as neurotypical individuals. Throughout the years that my sister lived in her group home, some of the older women developed dementia. I always felt sad for them and their families but had no reason to ever conclude that this could happen to my sister. To me, there was zero connection. But I was wrong - oh, so wrong.
So, in the beginning, when I first heard the news, it felt like I was run over by a truck - I was completely shocked and unprepared and had so much concern for what might lie ahead for my beautiful baby sister. This concept was extremely difficult to comprehend, confront and accept. It wasn’t like hearing that she may have asthma or something else that was controllable or curable.
I eventually comforted myself by thinking that since dementia is a very slow progressing disease, that it would be many, many years until my sister

Susan’s 40th birthday would experience major decline. Sadly, this wasn’t how the disease progressed; my assumption was wrong.
Besides the shock of the potential reality, finding a reputable neurologist that I felt confident with was my primary concern so my sister could receive the best care available. Simultaneously and subsequently, I searched for reliable resources specific to IDD and dementia to guide me, as I felt totally unprepared for what might lie ahead. My quest to find this help, knowledge, and resources was ongoing for years. Much to my surprise, it was extremely difficult to find. My persistence never wavered but, believe it or not, finding a needle in a haystack would have been easier! It just shouldn’t be this way.
Fast forward to February 2021, approximately five years after the initial conversation about my sister’s decline and concern of dementia, I learned about the NTG. I was ecstatic that I finally found an organization that had information and a family support group specific to IDD and dementia. Oh, how I wish I had known
about the NTG sooner, and how I wish it hadn’t been so difficult to find.
Prior to finding out about the NTG, my sister’s doctors and staff, along with myself, did our best. Yet, we surely would have benefitted from the knowledge and expertise of the NTG. My sister exhibited all the signs that many individuals with Down syndrome experience when aging. If we had the specific knowledge from the NTG sooner, it would have helped us to know what to expect and how to handle it. What I learned upon finding the NTG and reading their vast resources, many aspects of my sister’s decline fit all the tell-tale signs that I read about. It would have been so valuable to have had this information long ago, for not even her neurologist knew about how my sister’s journey would fit into a predictable pattern, and her neurologist was definitely an extremely knowledgeable doctor and open to learning, including my input.
Fortunately, my sister’s primary care provider was specialized in providing care for individuals with IDD. So, when there were signs of cognitive decline, the primary care provider was aware of other potential medical conditions that could be the cause of decline that often mimic dementia. Because of this, other medical conditions were ruled out before seeking medical treatment from a neurologist. Had the primary care provider not been experienced with working with individuals with IDD, there would have been the assumption that the symptoms she had caused dementia, when indeed it could have been possible that it was something else.
The NTG’s resources provide information and insight into this, which can be of huge help to families trying to navigate what to do and where to go for help for their loved one exhibiting signs of cognitive decline. It is also an organization that has extensive information for medical professionals.
The NTG is on the cutting edge of information pertaining to aging and dementia, especially for IDD individuals. This information won’t prevent the illness from occurring, but will inform and guide families on how to
best proceed with the diagnosis, possible treatment, and an idea of what may lie ahead. Unfortunately, my sister lived only an additional six months after my learning about the NTG. Each month, I attended the family support group, which was so incredibly helpful and supportive for that time period; in fact, I continue to attend the monthly meetings - to receive and give support. I have made it my priority to become more involved with the NTG, so I can inform family members The NTG’s resources provide information and insight into this, which can be of huge help to families trying to navigate what “ of what may be included in their loved one’s lives as they age. I never want anyone to be without the information, resources, and support that is available through the NTG. The NTG has become an organization that is now very near and to do and where to go for help for dear to my heart. The NTG cannot prevent a family their loved one exhibiting signs of member’s loved one from cognitive decline. aging and/or declining, but it can be a tremendous source of abundant, invaluable information and support. So, every day, I am dedicated to spreading the word, with my only intent to help others have an easier path on an extremely difficult journey by making families aware of the resources and support readily available to them, and to educate them about NTG and the wealth of abundant, invaluable information available on their website. Marianne Barbera is a passionate family advocate for IDD individuals, families, and caregivers. This role was shaped by her lifelong relationship and unbreakable bond with her sister who had Down syndrome. Ms. Barbera was her sister’s advocate, legal guardian, and cheerleader throughout her sister’s life. As a result of her sister’s journey with dementia and eventual passing, Ms. Barbera has become driven to bring awareness and resources to help others so that they are better prepared for what may be included in their loved-one’s life as they age. Marianne Barbera serves on the board of the National Task Group on Intellectual Disabilities and Dementia Practices and is chair of the Family Support Committee.
ARoyalShame
The Hidden Cousins of Queen Elizabeth
By Rick Rader, MD FAAIDD, FAADM
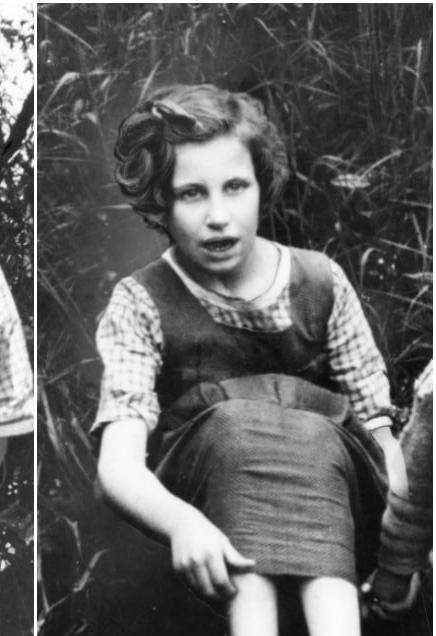

Nerissa Bowes-Lyon (left) and Katherine Bowes-Lyon (right)

This year marked a major milestone for the British monarchy. The United Kingdom threw a historic celebration for Queen Elizabeth II’s Platinum Jubilee. The 96-year-old queen is the first British monarch in history to reach a Platinum Jubilee, which marks 70 years on the throne. She ascended to the throne on February 6, 1952, following the death of her father, King George VI.
As expected, the celebration included everything from the Trooping of the Color Guard, to parades, star-studded concerts, street parties across the country, and a final appearance by the queen herself. No doubt, Queen Elizabeth has been a much loved, respected and revered monarch, and has done much to fortify the significance of the royals when their very existence has been argued as being archaic or dinosaurian.
Like many families, the Windsors had some hidden secrets. One of which is particularly significant to readers of our publication, HELEN: The Journal of Human Exceptionality. The Queen had two cousins that had intellectual disabilities, and while one would think that they received royal treatment, protection and support, the truth is that they were secretly institutionalized, ignored and abandoned.
The first cousins were named Nerissa and Katherine; they were the daughters of John and Fenella Bowes-Lyon, with the former being the older brother of Elizabeth (the Queen Mother). Both of the sisters were institutionalized in 1941 at the Earlswood Institution for Mental Defectives. At the time, Nerissa was 15 and Katherine was 22.
In 1986, the British newspaper The Sun published an expose about the Royal Family and revealed that the girls were at the institution for 45 years and that the Royals
never visited them or acknowledged their existence. The report indicated that the sisters were born with severe “learning disabilities” and were committed to the “asylum” at the height of World War II and remained in the care of medical professionals for the remainder of their lives. To add insult to injury, the two were listed as dead in the 1963 edition of esteemed royal genealogy guide, Burke’s Peerage.
In addition to the two sisters, three other second cousins of the Queen, Idonea, Ethelreda and Rosemary Fane, were also admitted to the Royal Earlswood Hospital in Surrey. All five of the Royals were diagnosed with genetic disorders exhibiting severe and profound cognitive impairments. In 2011, in a British documentary called The Queen’s Hidden Cousins, medical records from the institution reported that Nerissa, “makes unintelligible noises all the time… very affectionate…can say a few babyish words.” Nerissa passed away on January 22, 1986, at age 66, having spent more than 40 years in the institution.
In an interview with retired caregiver Dot Penfold, she offered this vision of Katherine, “She was no problem to look after, but she was mischievous, like naughty children. Katherine was a scallywag. You could scream at her and she’d turn a deaf ear.” Both sisters had no vocalic communication, but they would point and make noises, “and when you knew them, you could understand what they were trying to say. They understood more than you’d think.” Reports of the caregivers revealed that they formed meaningful relationships with the sisters and provided more than custodial care. This is a testimony to the long-standing commitment of direct support professionals and, despite little or no formal training, their humanism often guided them even in institutionalized settings. Of course, that is not to ignore the many instances of brutality and deprivation that occurred in institutions all over the world.
While the Royals disavowed the existence of the sisters during their lives, their deaths were also ignored and unacknowledged. In an article in 2020, reporter Phil Boucher recounts that “Nerissa was buried in a humble plot in Redhill, Surrey, with her grave marked by a six-inch plastic marker reading simply “M11125 Bowe4s-Lyon.” Only hospital staff attended the ceremony. Katherine died 28 years later on February 23, 2014, having relocated to a Surrey care home following the closure of the Royal Earlswood in 1997, which has now been converted into luxury apartments. “Aged 87 when she passed, Katherine also rests in Redhill, alongside her sister and their cousins Idonea, Ethelreda and Rosemary.”
When the story broke about the cousins, the Royals released statements that the sisters were never ignored and that they (members of the Royal family) paid numerous visits to see them and spend time with them. Inspection of the reports from the institution indicated that no one had visited them in the years spent at Earlswood.
In “The Crown”, a carefully researched television series about Queen Elizabeth’s life, there is a scene in which the Queen’s sister, Princess Margaret first learns about her cousins’ plight and shouts at the Queen Mother, “It’s wicked and it’s cold-hearted and it’s cruel and it’s entirely in keeping
with the ruthlessness, which I myself have experienced in this family. Darwin had nothing on your lot – shame on all of you.” In response, the Queen Mother tells Margaret, “Don’t be so naïve. We had no choice.” While no one can definitely say if this conversation was accurately depicted, and if indeed it every took place, it is safe to say that the Royal’s response to distancing themselves from the five cousins was a strategic decision to “protect” the family from the shame, embarrassment and indignity that embracing them was thought to foster. This was the tragedy of not supporting, including and embracing family members with disabilities. In doing so, the Royals missed an opportunity to The Queen had two cousins with intellectual disabilities. One would think they received “ royal treatment, protection and demonstrate to British society how they can elevate the fabric support, but the truth is they of society by acknowledging the were secretly institutionalized, value and role of people with disabilities, and how people can ignored and abandoned. enrich their own lives by caring for and about them. Queen Elizabeth proposed the following to her subjects, “Families, friends and communities often find a source of courage, rising up from within. Indeed, sadly, it seems that it is tragedy that often draws out the most and the best from the human spirit.” In the case of the royals, their belief that the existence of Nerissa and Katherine was a tragedy was overshadowed by the tragedy of their indifference, neglect and abandonment; for this was a case of royal shame. Rick Rader, MD, FAAIDD, FAADM, DHL (hon) is Director, Habilitation Center, Orange Grove Center; President, American Association on Health and Disability; Member, National Council on Disability; Board, American Academy of Developmental Medicine and Dentistry; National Medical Advisor, National Alliance for Direct Support Professionals; Board, National Task Group on Intellectual Disabilities and Dementia Practices.


