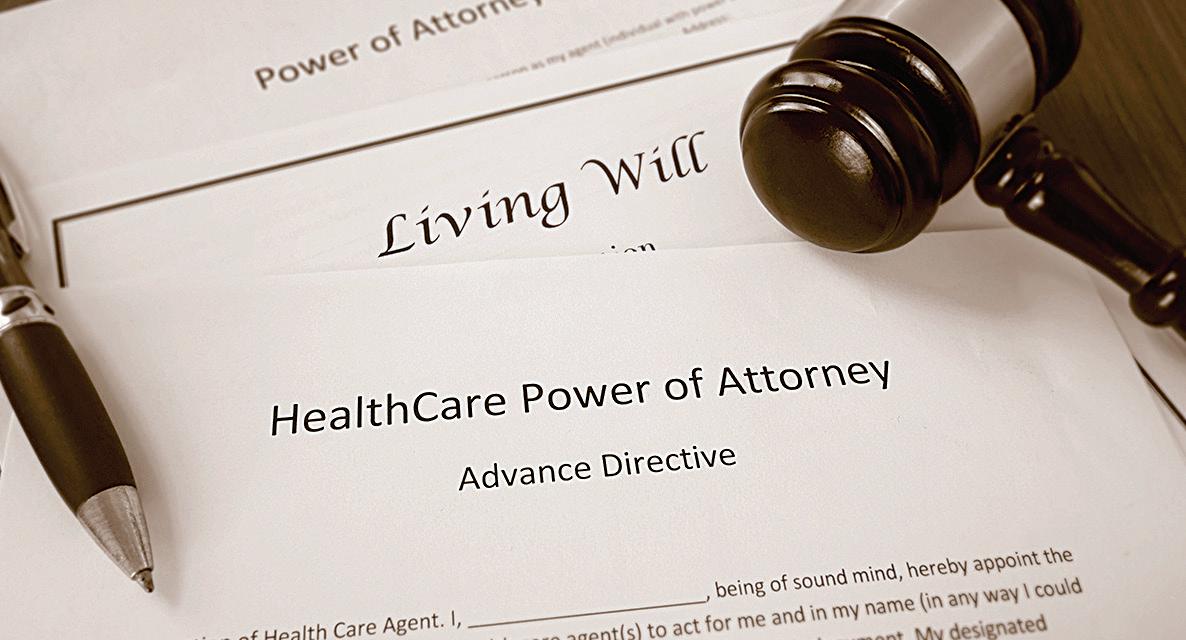
What kind of legal documents or arrangements about your end-of-life medical care should you have?
An “Advance Medical Directive” and “Durable Power of Attorney for Health Care” (or “Health Care Proxy”) are legal documents that take effect if the patient becomes incompetent. Even though these documents can be written without the assistance of an attorney, some states give them considerable legal weight.
An Advance Medical Directive specifies what medical procedures the patient wishes to receive or to avoid. (An Advance Medical Directive sometimes is called “A Living Will,” but because of its association with the advocacy of euthanasia, we have chosen to avoid this phrase.)
Durable Power of Attorney specifies a particular individual (variously called a “proxy,” “agent,” or “surrogate”) to make medical decisions on behalf of the patient (or the “principal”) when the patient is no longer able to do so.
When neither of these instruments is drawn up, the task of making important medical decisions usually falls to the family. Most states have laws governing the use
Caring for Charlotte Area Catholic Families in Their Hour of Need Since 1926
FUNERAL SERVICE, INC.
Charlotte 704-334-6421
Pineville 704-544-1412
Mint Hill 704-545-4864
Derita 704-596-3291
and implementation of the Advance Medical Directive and Durable Power of Attorney. All hospitals and health care facilities are required by law to provide written information to the patient about the right to accept or refuse medical treatment and the right to formulate an Advance Directive and/or designate Durable Power of Attorney. The health care facility must also provide written policies stating how the patient’s Advance Directive or Durable Power of Attorney will be implemented. People should remember that they do not have to sign any Advance Directive given to them by the hospital.
WHICH ONE SHOULD YOU CHOOSE?
Make certain that your Advance Directive forbids any action that the Catholic faith considers to be immoral, such as euthanasia or physician-assisted suicide.
(A Catholic hospital, in any case, will not follow a directive that conflicts with Church teaching.)
Once a directive is made, copies should be distributed to the agent and anyone else the patient deems appropriate. One
Please pray for the following priests who died during the month of November:
Msgr. Richard Bellow – 2023
Abbot Oscar Burnett, OSB – 2017
Rev. John P. Bradley – 2003
Rev. Raphael Bridge, OSB – 1996
Rev. Brian Cook – 2023
Rev. Msgr. John P. Manley – 1981
Rev. Bernard A. Manley Jr. – 2016
Rev. Charles T. Reese – 2017
Rev. John A. Regan – 1976
Rev. D. Edward Sullivan – 2009
Rev. Stephen A. Sullivan - 1989

At www.ncbcenter.org : What are the Church’s teachings on end-of-life decisions and how difficult will it be to follow them? Must we endure a great deal of pain? What if I am no longer able to make medical decisions for myself? Order or download a copy of “A Catholic Guide to End-of-Life Decisions,” which describes how you might approach end-of-life decisions in light of the teachings of the Church.
should periodically review the provisions of an Advance Directive and, when there is a revision, all previous copies should be destroyed.
The usefulness of an Advance Directive, which gives specific instructions for care, is limited because of its inflexibility. If circumstances change significantly between writing the Advance Directive and its implementation, the instructions may be of little value to those acting on a patient’s behalf, or may even hinder their freedom to make good decisions. There may also be a problem of interpreting the document when it is not clearly written. An Advance Directive oftentimes does not allow for adequate informed consent because one must make a decision about a future medical condition which cannot be known


in advance.
When drawing up an Advance Directive, therefore, one should focus on general goals rather than on specific medical procedures.
Assigning Durable Power of Attorney is preferable to an Advance Directive because it leaves decisions in the hands of someone whom the patient has personally chosen.
A proxy agent also can be more sensitive and responsive to the decision-making that is necessary for a given case. When assigning Durable Power of Attorney one should choose an agent of good moral character – someone who is known to be capable of making sound decisions under stressful circumstances. The agent should know the teachings of the Church and possess the practical wisdom to apply them to changing circumstances.
An agent, of course, must also survive the patient. One may designate alternate agents in case one’s first choice, for some reason, is unable to act.
A good agent makes decisions for the patient in light of what the patient would choose if able to do so. The proxy, therefore, should be very familiar with your moral convictions and wishes. When there is an Advance Directive from you, this should be the guide. When there is not, the agent must act on the oral instruction that has been given. Sometimes, however, acting in your best interests means ignoring instructions that are obviously unwarranted or clearly immoral. No agent is bound to carry out actions that conflict with morality and the faith.
ALSO NOTE
When formulating any Advance Directive and discussing end-of-life issues, avoid using the expression “quality of life” because it is used by advocates of euthanasia to suggest that some lives are not worth living. While illness and other circumstances can make life very difficult, they cannot diminish the inestimable worth of each human life created by God. Life itself is always a good, and is a quality that can never be lost. Still, we need not cling to this life at all costs (what’s called “therapeutic obstinacy”), since the life to which we have been called in Christ is incomparably better. — National Catholic Bioethics Center
St. Matthew’s Parishioner
What is the difference between foreseeing death and intending death?
The difference ultimately lies in the intentionality of the patient or health care professional. A person should never intend in any way the death of a patient or the hastening of a patient’s death. Sometimes it is difficult to determine whether a medical decision made during end-of-life care includes such an intention. Certain means can be used to alleviate a patient’s pain, for example, by a physician who foresees that the patient’s life may be shortened as a result (as an indirect, non-intended but tolerated effect of the therapy), but similar means could be used to intentionally shorten a patient’s life.
Are proportionate or ordinary means the same for everyone?
Basic care (such as nutrition and hydration, pain relief, antibiotic treatment, and postural change) is generally the same for all patients and should always be provided. The evaluation of proportionate or disproportionate means, however, is based on objective and subjective factors for an individual patient. For example, total parenteral nutrition may be a proportionate means in an industrialized country but a disproportionate means in a developing country, where it is not affordable or is technically too difficult to administer. A treatment may also be disproportionate because it is futile or because it causes complications that are too hard for the patient or the patient’s family to bear.
What ethical problems are there with advance directives?
The right of patients to self-determination can lead them to include morally illicit requests in advance directives, such as requests to have ordinary care withdrawn.
An effective therapeutic alliance between a physician, a patient and the patient’s proxy is the best way to address end-of-life issues. Requests made by a patient in an advance directive may preclude therapeutic dialogue, preventing such an alliance.
A patient may react to an illness or a specific therapy differently than expected, or medical advances occurring after a directive was written may change the patient’s treatment options in unexpected ways. In such situations, an advance directive may prevent objective moral analysis.
Advance directives are often difficult to interpret and apply in the actual circumstances encountered by health care professionals, relatives and proxies. Advance directives that do not differentiate between proportionate and disproportionate treatments may be promoted by pro-euthanasia associations as a first step toward acceptance of euthanasia.
What is a Provider Orders for Life-Sustaining Treatment (POLST)?
A Provider Orders for Life-Sustaining Treatment (POLST) is a medical order specifying whether life-sustaining treatment is to be used or withheld for a specific patient in various circumstances. It carries the signatures of the health care provider and sometimes the patient.
It differs from a do-not-resuscitate order
Frequently Asked Questions

and a traditional advance directive in that it is actionable from the moment it is signed by the health care provider, even if the patient is still competent and is not terminally ill.
One reason given for use of a POLST and similar instruments is the avoidance of futile or unwanted treatment. Even without a POLST, however, patients are never obligated to submit to health care procedures whose burdens outweigh therapeutic benefits.
Decisions about forgoing life-sustaining treatment should be made at the time and in the circumstances in which the decisions are needed (not years ahead), and they should be made by the patient or the patient’s surrogate in consultation with the patient’s attending physician, in line with the patient’s known wishes and best interest (not by health care workers who are strangers to the patient but have access to his POLST).
The details of a patient’s medical condition at a specific time need to be considered when such decisions are made, including the imminence of anticipated death, the likely risks
and side effects of treatment, the suffering treatment is likely to cause, and the expense to the patient’s family and community.
An optimal advance directive is written in very general terms. Instead of specifying treatment, it designates a health care proxy or surrogate who will make decisions if the patient is incompetent, someone who knows the will of the patient
and the teachings of the Catholic Church.
What is the difference between an advance directive and a POLST?
An advance directive is a legal document that allows a person to identify a proxy or surrogate decision maker and express his wishes about receiving or forgoing health care, including life-sustaining treatment, in the event that he is no longer able to communicate such wishes. An optimal advance directive is written in general terms that identify principles on which a surrogate is to base decisions, made with the assistance of a physician, in the specific health care situation encountered by the patient.
A POLST is a medical order about receiving or forgoing lifesustaining treatment that takes effect from the moment the health care provider signs it, even if the patient is competent and not terminally ill.
Why is the designation of a health care proxy or surrogate morally preferable to use of a POLST?
Unless death is imminent, it is virtually impossible to compare the benefits and burdens of treatment before a patient has encountered a specific health care situation. Thus, pre-signed checklists of treatments to be received or withheld are not helpful for making decisions based on the best interest of the patient and consistent with the patient’s wishes.
A well-informed proxy who knows the patient, understands the values held by the patient, and respects the natural moral law can provide a far better understanding of how the patient’s wishes are to be respected than can a general checklist that is not tied to any specific patient care situation.
— National Catholic Bioethics Center

LISA M. GERACI | CATHOLIC NEWS HERALD
A new statue of Christ the King graces the columbarium at Christ the King parish in High Point. The statue was purchased from Vietnam by parishioners and friends at St. Joseph Vietnamese Church in Charlotte just in time for All Souls’ Day.