26 minute read
The Open Apex Challenge

The Open Apex Challenge
A Case Series
Joseph C. Stern, D.D.S.
ABSTRACT
Aim: To describe different endodontic techniques for managing immature necrotic teeth. Managing immature necrotic teeth has always posed challenges because of the unpredictable nature of treating roots with wide open apices that lack an apical stop. Traditionally, treatment involved placement of long-term calcium hydroxide, which was often tedious and required multiple visits. Compliance was frequently an issue, especially since many patients in this category are children and as a result, many teeth were lost due to infection or fracture. Recently, with the introduction of more biocompatible materials, a shorter treatment approach has been advocated using calcium silicate materials, such as MTA, which can be placed at the apex to provide a suitable seal. However, this technique remains challenging when encountering a blunderbuss apex, where placing the material without pushing it past the apex can be extremely difficult. More recently, pulp regeneration has emerged as a viable alternative to apexification for managing blunderbuss apices. This case series explores various techniques and methods for managing an open apex.
Apexification is a procedure aimed at inducing an apical hard-tissue barrier in a root with an open apex and promoting the continued apical development of an immature root in teeth with necrotic pulp. In simpler terms, apexification is a root canal treatment for teeth with an open apex, but with several key differences.
Due to the thin root structure and open apex, root canal debridement is primarily achieved through chemical means, with minimal or no mechanical instrumentation. Because there is no defined “apical stop,” using an apex locator to determine working length is often unreliable, making radiographs the most accurate method for measuring working length.
The main challenge in apexification is creating an apical stop that allows for successful obturation. Unlike conventional endodontic treatment, where gutta-percha is typically used as the primary obturating material, it is less effective in teeth with an open apex.
Traditionally, for apexification, long-term calcium hydroxide (CH) was used to induce an apical hard-tissue barrier. After conventional disinfection, CH was placed in the canal as an inter-visit medicament to help stimulate a hard-tissue barrier at the apex. Completion of endodontic therapy was usually delayed until apical barrier formation was achieved. Often, multiple CH dressing changes were needed to allow for an apical bridge to form. Once a barrier formed, which could take more than 12 months, the canal was obturated in a conventional manner with guttapercha and sealer. The disadvantage to this approach was the variability in treatment time and the unpredictability of the formation of a total and impervious apical seal.[1-2]
More recently, the apical plug technique has been employed, in which a bioceramic (BC) material such as MTA or BC Putty (Brasseler, USA) is placed at the apex to provide an apical seal, rather than waiting for CH to induce the seal. The biggest advantage of this approach is treatment is carried out over a much shorter period, generally over one or two visits. It has also been shown to have a high long-term success rate.

While this approach works well for open apex cases, there remains the challenge of filling an open apex, with a risk of overfilling the canal. With the periapical bone and ligament gone in these open apex cases, there is no physical barrier to help resist an overfill. An extra-radicular apical matrix (barrier) of calcium sulfate (ACE Surgical Supply Co, Inc, Brockton, MA) can be placed to prevent extrusion of the BC material past the apex.[3-17]
Due to the challenges mentioned above, pulp regeneration—or more accurately, pulp revascularization—has gained popularity in recent years. In pulp regeneration, the goal is not to fill or obturate the canal at the apex but, rather, to use a scaffold, such as a blood clot, within the canal to stimulate the formation of new tissue (Case 3). However, a drawback of this approach is the lack of reinforcement in the pericervical area of the tooth, which can increase the risk of microleakage, especially if the tooth fractures.[18-39]

A modified regeneration approach strikes a unique balance by placing a blood clot scaffold at the apical end, minimizing the risk of overfilling the canal. A BC plug is placed on top of the blood clot and the remainder of the canal is then sealed with a restorative material, which not only strengthens the pericervical region, but also helps prevent microleakage of bacteria should the tooth develop coronal cracks.[40-41]

A major challenge in treating infected immature teeth with a blunderbuss apex (Figure A) is the inability to predictably fill the root canal to the apex without risking significant overfilling (Case 2). In recent years, pulp regeneration has gained popularity as a treatment option for these teeth. Instead of attempting to fill the apex with gutta-percha, we draw healthy blood into the canal after disinfection, using it as a scaffold to promote tissue growth and further root development (Case 3).
The blood is drawn into the canal by over-instrumenting the apex with a file. There are generally three goals to the regenerative procedure: eliminate infection; add additional root length; and add additional thickness to the root walls. Classically, continued root growth was thought to be possible only in vital cases (apexogenesis). Recent studies on pulp regeneration have clearly shown that some continuation of root growth is also possible in necrotic infected cases, even when significant periapical pathology is present. The key to achieving this success is thorough disinfection of the root canal and then leaving some space at the apex for continued root growth.

What differentiates a modified regeneration procedure from a “classic” pulp regeneration procedure is the approach to filling the canal space. In modified regeneration, most of the canal, including the pericervical area, is filled with a restorative material to reinforce the root and provide additional mechanical strength. In contrast, in pulp regeneration, most of the canal is left empty, or more specifically, filled with a blood clot, to allow for continued tissue growth (Case 3).
In modified regeneration, only the apical 3 mm to 5 mm is used as a scaffold for the blood clot. Filling the majority of the canal space with restorative material helps prevent bacterial microleakage, particularly in cases where there is significant loss of coronal tooth structure, as it provides additional protection in the event of a crown fracture. At the interface with the blood clot, or “empty space” in the canal, a bioceramic (BC) material is placed. This material acts as a stimulator to encourage continued tissue growth. The restorative material is then placed on top of the BC material (Figure AC).
Another important factor that supports root growth is hertwig’s epithelial root sheath (HERS), the tissue at the apex responsible for stimulating root development. In the presence of infection, HERS becomes dysfunctional and can only be “reawakened” to play a role in regeneration once the root canal has been thoroughly disinfected. Case 1 demonstrates the modified regeneration procedure, where the root canal was disinfected and filled close to the apex with a combination of BC and restorative materials. No attempt was made to fill the blunderbuss apex to its full length, as doing so would have risked an overfill (Case 2).
Case 1: Modified Regeneration (Figure 1)
A 12-year-old girl presented with her mom with a chief complaint of pain and swelling of the lower left mandibular vestibule. Radiographic imaging revealed a periapical radiolucency (PARL) associated with tooth #20, which had an incompletely formed blunderbuss apex. No caries or restorations were noted, but the tooth was very painful to the touch and did not respond to vitality testing. A diagnosis of pulp necrosis with acute apical access was made.
The likely cause of the necrotic pulp was a worn-down dens evaginatus. The recommended treatment was root canal therapy, more specifically, apexification. After access preparation, bloody and purulent discharge was noted. To obtain working length, a large size 80k-file was placed in the canal to an estimated length and a radiograph taken.
The canal was irrigated with 3 ml of 5.25% sodium hypochlorite. The EndoActivator (Dentsply, Tulsa, OK) was used to sonically agitate the irrigant in the canal to ensure thorough disinfection. Light instrumentation with both rotaries and hand files was completed. The canal was dried with a surgical microsuction tip. CH (Ultracal XS, Ultradent Products Inc, South Jordan, UT) was used as an inter-visit medicament. The tooth was temporarily restored with intermediate restorative material (IRM).
The patient returned after four weeks for completion of treatment. She reported that all symptoms had subsided. Clinical examination revealed that the swelling had resolved. CH was removed from the canal with irrigation and activation with the EndoActivator. The canal was irrigated with a combination of 3 ml of 5.25% sodium hypochlorite and 3 ml of 17% EDTA (ethylene diamine tetra-acetic acid). The canal was dried with a surgical microsuction tip. Red, healthy-looking blood was noted in the apical third of the canal. EndoSequence BC putty (Brasseler USA, Savannah, GA) was used as the material of choice due to its biocompatibility. Care was taken to make sure it was placed 5 mm from the apex. Multiple radiographs were needed to confirm proper placement of the putty.
Once the BC putty was in place for 15 minutes, to allow it to set, the canal was etched, rinsed, dried, and a dual-cure composite placed deep into the canal and allowed to selfcure for about five minutes. The access opening was restored with regular composite (Dentsply Sirona, Charlotte, NC), and the patient was put on a recall schedule to monitor healing.
At the one-year recall visit, the patient was completely asymptomatic, and radiographic examination revealed almost complete healing of the periapical radiolucency. A significant increase in root length and thickness was noted.
Case 2: Apexification (Figure 2)
A 12-year-old boy presented with his dad with a chief complaint of mild discomfort in the upper anterior maxilla. The patient reported a history of trauma around three years ago in which teeth #7 and #8 were luxated while playing in the park. For a couple of weeks after the trauma, the teeth were loose but firmed up over time and were generally asymptomatic. Only recently did he report experiencing some minor discomfort in the area.
Clinical exam revealed mild discomfort to percussion on tooth #8, while teeth #7, #9 and #10 tested within normal limits. Teeth #7 and #8 did not respond to vitality testing, while teeth #9 and #10 did. A fistula was present on the buccal aspect, which traced to the apex of tooth #8. Radiograph exam revealed the root of tooth #8 to be immature with a blunderbuss apex and a large periapical radiolucency. The radiolucency extended to the apex of tooth #7. The root canal space of tooth #7 appeared very calcified and did not respond to vitality testing.
As most of the lesion was attached to tooth #8, the plan was to treat #8 and monitor #7. A diagnosis of pulp necrosis with chronic apical abscess was made for tooth #8. Once the tooth was accessed, a necrotic pulp was confirmed. No drainage was noted from the canal. Most of the disinfection was carried out with irrigation rather than instrumentation due to the thin canal walls.
To obtain working length, a large size 80k-file was placed in the canal to an estimated length and a radiograph taken. The canal was irrigated with 3 ml of 5.25% sodium hypochlorite. The EndoActivator (Dentsply, Tulsa, OK) was used to sonically agitate the irrigant in the canal to achieve thorough disinfection. Light instrumentation with both rotaries and hand files was completed. The canal was dried with a surgical microsuction tip, and CH (Ultracal XS, Ultradent Products Inc, South Jordan, UT) was used as an inter-visit medicament. The tooth was temporarily restored with IRM.

The patient returned after one month for completion of treatment. He reported that all symptoms had subsided. The fistula had healed. CH was removed from the canal with irrigation and activation with the EndoActivator. The canal was irrigated with a combination of 3 ml of 5.25% sodium hypochlorite and 3 ml of 17% EDTA. The canal was dried with a surgical microsuction tip. EndoSequence BC putty (Brasseler USA, Savannah, GA) was used as the material of choice due to its biocompatibility. Care was taken to make sure it was placed as close to the apex as possible. Multiple radiographs were needed to confirm proper placement of the putty.

The BC putty was left in place at the apex for 15 minutes. The plan was to use a size 100 gutta-percha as a master point with a coating of BC sealer (Brasseler, USA), which would be heated and condensed lightly up against the apical BC putty. During the condensing process, the gutta-percha point was pushed past the apex, likely due to the blunderbuss apex with no apical stop. The tooth was temporarily restored with IRM. In retrospect, a modified regeneration approach would have been more appropriate.
When the patient returned for the re-evaluation visit, he was generally asymptomatic but with some slight apical tenderness above tooth #8. The access was restored with composite, and a surgical flap was made to remove the excess guttapercha and smooth out the apex. No bone graft or membrane was used. The patient returned for a one-year recall. The radiographic exam revealed almost complete healing of the periapical radiolucency. The lesion that had at one point encompassed both teeth #7 and #8, now had almost completely healed. No further treatment was necessary.
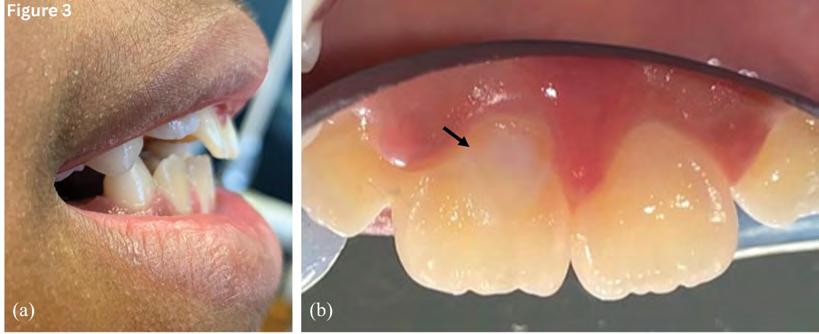
Case 3: Pulp Regeneration (Figure 3)
A 9-year-old girl presented with her mom for endodontic treatment for tooth #20. The patient was generally asymptomatic but reported a “bubble” on her gums. A gutta-percha point was used to trace the fistula on the buccal aspect to the apex of tooth #20. Radiographically, the apex was blunderbuss with a periapical radiolucency. The likely cause was caries, noted on the distal aspect extending proximal to the pulp.

Clinically, the tooth was negative to percussion, palpation and vitality testing. A diagnosis of pulp necrosis with chronic apical abscess was made. Treatment options were discussed with the patient and her parents. The planned treatment was pulp regeneration, in hopes of having further root growth.
Local anesthesia was administered, and the tooth isolated with a rubber dam. The caries was excavated and the pulp chamber accessed. After working length was confirmed radiographically, the canal was irrigated with 3 ml of 5.25% sodium hypochlorite. The EndoActivator (Dentsply, Tulsa, OK) was used to sonically agitate the irrigant in the canal to achieve thorough disinfection. Light instrumentation with both rotaries and hand files was completed. The canal was dried with a surgical microsuction tip, and CH (Ultracal XS, Ultradent Products Inc, South Jordan, UT) was used as an inter-visit medicament. The tooth was temporarily restored with IRM.
The patient missed a couple of appointments in the interim and was seen only after four months. At that time, the sinus tract healed, and the periapical radiolucency was significantly smaller. The root also looked to have grown in both length and width.
At the second visit, CH was removed from the canal with irrigation and activation with the EndoActivator. The canal was irrigated with a combination of 3 ml of 5.25% sodium hypochlorite and 3 ml of 17% EDTA. A size 20k-file was used to over-instrument the canal enough to trigger bleeding. The blood was allowed to reach close to the CEJ. BC putty was lightly condensed against the blood clot using a plugger and then allowed to set for about 15 minutes. A definitive composite restoration was placed.
At the 13-month recall from when the treatment was initiated, radiographic exam showed almost complete healing of the periapical radiolucency and continued root growth. The tooth was healthy and fully functional.
Case 4: Apexification (Figure 4)
A 24-year-old male presented with a chief complaint of pain in the upper anterior maxilla. The patient reported a history of trauma more than 10 years ago in which teeth #7 and #8 were luxated while playing sports. Tooth #8 had a crown fracture and was restored with a composite. The patient reported that after the trauma, he experienced occasional discomfort in the area but not enough for him to present to the dentist for evaluation. More recently, the pain had worsened.
The clinical exam revealed mild discomfort to percussion on teeth #7 and #8. Neither tooth responded to vitality testing, while teeth #6, #9 and #10 did. Radiograph exam revealed the root of tooth #8 to be immature, with an open apex and a large periapical radiolucency. The radiolucency extended to the apex of tooth #7. Apical inflammatory root resorption was noted on tooth #7. A diagnosis of pulp necrosis with symptomatic apical periodontitis was made for both teeth #7 and #8.
Once the teeth were accessed, necrotic pulps were confirmed. No drainage was noted from the canals. Conventional endodontic treatment was performed for tooth #7. Most of the disinfection for tooth #8 was carried out with irrigation rather than instrumentation due to the thin canal walls and open apex. To obtain working length, a size 35k-file was placed in the canal to an estimated length and a radiograph taken.
The canal was irrigated with 3 ml of 5.25% sodium hypochlorite. The EndoActivator (Dentsply, Tulsa, OK) was used to sonically agitate the irrigant in the canal to ensure thorough disinfection. Light instrumentation with both rotaries and hand files was completed. The canal was dried with a surgical microsuction tip, and CH (Ultracal XS, Ultradent Products Inc, South Jordan, UT) was used as an inter-visit medicament. The tooth was temporarily restored with IRM.
The patient returned after one month for completion of treatment. He reported that all symptoms had subsided. CH was removed from the canals with irrigation and activation with the EndoActivator. The canal was irrigated with a combination of 3 ml of 5.25% sodium hypochlorite and 3 ml of 17% EDTA. The canal was dried with a surgical microsuction tip. EndoSequence BC putty (Brasseler USA, Savannah, GA) was used as the material of choice due to its biocompatibility. Care was taken to make sure it was placed as close to the apex as possible. Multiple radiographs were needed to confirm proper placement of the putty. The putty was slowly condensed to the apex with a plugger. Once it was confirmed that the putty was set at the apex, the remaining canal space and access was restored with a dual-cure composite.
At the eight-month recall, radiographic exam showed significant healing of the periapical radiolucency around both teeth #7 and #8. The teeth were healthy and fully functional.
Conclusion
Treating an immature permanent tooth can be both an endodontic and restorative challenge. In the past, apexification was the treatment of choice for an immature and necrotic tooth.
More recently, pulp regeneration has been discussed as an alternative treatment modality, the advantage being a shorter treatment time and continued root growth. A modified regeneration approach, where the coronal root structure is reinforced with restorative materials, has the benefit of adding strength to an already thin and weakened coronal root structure while also allowing continued root growth at the apical third.
Queries about this article can be sent to Dr. Stern at Joseph.stern18@touro.edu.
REFERENCES
1. Sheely EC, Roberts GJ. Use of calcium hydroxide for apical barrier formation and healing in non-vital immature permanent teeth: a review. Br Dent J 1997;183:241–6.
2. Cvek M. Treatment of non-vital permanent incisors with calcium hydroxide. I. Follow-up of periapical repair and apical closure of immature roots. Odontol Rev 1972;23(1):27-44. PMID: 4504474.
3. Shabahang S, Torabinejad M, Boyne PJ, et al. A comparative study of root-end induction using osteogenic protein-1, calcium hydroxide, and mineral trioxide aggregate in dogs. J Endod 1999;24:1–5.
4. Holden DT, Schwartz SA, Kirkpatrick TC, Schindler WG. Clinical outcomes of artificial root-end barriers with mineral trioxide aggregate in teeth with immature apices. J Endod 2008;34:812–7.
5. Moore A, Howley MF, O’Connell AC. Treatment of open apex teeth using two types of white mineral trioxide aggregate after initial dressing with calcium hydroxide in children. Dent Traumatol 2011;27:166–73.
6. Huang GT. Apexification: the beginning of its end. Int Endod J 2009 Oct;42(10):855-66. doi: 10.1111/j.1365-2591.2009.01577.x. Epub 2009 Jun 22. PMID: 19549154.
7. Purra AR, Ahangar FA, Chadgal S, Farooq R. Mineral trioxide aggregate apexification: a novel approach. J Conserv Dent 2016;19:377–80.
8. Pace R, Giuliani V, Nieri M, Di Nasso L, Pagavino G. Mineral trioxide aggregate as apical plug in teeth with necrotic pulp and immature apices: a 10-year case series. J Endod 2014;40:1250–4.
9. Chang SW, Oh TS, Lee W, Cheung GS, Kim HC. Long-term observation of the mineral trioxide aggregate extrusion into the periapical lesion: a case series. Int J Oral Sci 2013;5:54–7.
10. Albadri S, Chau YS, Jarad F. The use of mineral trioxide aggregate to achieve root end closure: three case reports. Dent Traumatol 2013;29:469–73. [PubMed] [Google Scholar].
11. Damle SG, Bhattal H, Loomba A. Apexification of anterior teeth: a comparative evaluation of mineral trioxide aggregate and calcium hydroxide paste. J Clin Pediatr Dent 2012;36:263–8. [PubMed] [Google Scholar].
12. Park M, Ahn BD. Immature permanent teeth with apical periodontitis and abscess treated by regenerative endodontic treatment using calcium hydroxide and MTA: a report of two cases. Pediatr Dent 2014;36:107–10. [PubMed] [Google Scholar].
13. Bonte E, Beslot A, Boukpessi T, Lasfargues JJ. MTA versus ca(OH)2 in apexification of nonvital immature permanent teeth: a randomized clinical trial comparison. Clin Oral Investig 2015;19:1381–8. [PubMed] [Google Scholar].
14. Mente J, Leo M, Panagidis D, Ohle M, Schneider S, Lorenzo Bermejo J, et al. Treatment outcome of mineral trioxide aggregate in open apex teeth. J Endod 2013;39:20–6. [PubMed] [Google Scholar].
15. Frank AL. Therapy for the divergent pulpless tooth by continued apical formation. J Am Dent Assoc 1966 Jan;72(1):87-93. doi: 10.14219/jada.archive.1966.0017. PMID: 5215726.
16. Steiner JC, Van Hassel HJ. Experimental root apexification in primates. Oral Surg Oral Med Oral Pathol 1971 Mar;31(3):409-15. doi: 10.1016/0030-4220(71)90163-0. PMID: 5277393.
17. Ree MH, Schwartz RS. Long-term success of nonvital, immature permanent incisors treated with a mineral trioxide aggregate plug and adhesive restorations: a case series from a private endodontic practice. J Endod 2017 Aug;43(8):1370-1377. doi: 10.1016/j.joen.2017.02.017. Epub 2017 Jun 1. PMID: 28578893.
18. Lin J, Zeng Q, Wei X, Zhao W, Cui M, Gu J, Lu J, Yang M, Ling J. Regenerative endodontics versus apexification in immature permanent teeth with apical periodontitis: a prospective randomized controlled study. J Endod 2017 Nov;43(11):1821-1827. doi: 10.1016/j. joen.2017.06.023. Epub 2017 Aug 30. PMID: 28864219.
19. Huang GT. The coming era of regenerative endodontics: what an endodontist needs to know. Alpha Omegan 2011 Spring;104(1-2):46-51. PMID: 21905366.
20. Chen MY, Chen KL, Chen CA, Tayebaty F, Rosenberg PA, Lin LM. Responses of immature permanent teeth with infected necrotic pulp tissue and apical periodontitis/abscess to revascularization procedures. Int Endod J 2012 Mar;45(3):294-305. doi: 10.1111/j.13652591.2011.01978.x. Epub 2011 Nov 14. PMID: 22077958.
21. Iwaya SI, Ikawa M, Kubota M. Revascularization of an immature permanent tooth with apical periodontitis and sinus tract. Dent Traumatol 2001;17:185–7.
22. Banchs F, Trope M. Revascularization of immature permanent teeth with apical periodontitis: new treatment protocol? J Endod 2004;30:196–200.
23. Kling M, Cvek M, Meja` re I. Rate and predictability of pulp revascularization in therapeutically reimplanted permanent incisors. Endod Dent Traumatol 1986;2:83–9.
24. Law AS. Considerations for regeneration procedures. J Endod 2013 Mar;39(3 Suppl):S44-56. doi: 10.1016/j.joen.2012.11.019. PMID: 23439044.
25. Huang GT. A paradigm shift in endodontic management of immature teeth: conservation of stem cells for regeneration. J Dent 2008 Jun;36(6):379-86. doi: 10.1016/j.jdent.2008.03.002. Epub 2008 Apr 16. PMID: 18420332.
26. Chrepa V, Pitcher B, Henry MA, Diogenes A. Survival of the apical papilla and its resident stem cells in a case of advanced pulpal necrosis and apical periodontitis. J Endod 2017 Apr;43(4):561-567. doi: 10.1016/j.joen.2016.09.024. Epub 2017 Feb 9. PMID: 28190588.
27. Liao J, Al Shahrani M, Al-Habib M, Tanaka T, Huang GT. Cells isolated from inflamed periapical tissue express mesenchymal stem cell markers and are highly osteogenic. J Endod 2011 Sep;37(9):1217-24. doi: 10.1016/j.joen.2011.05.022. Epub 2011 Jul 16. PMID: 21846537; PMCID: PMC3499979.
28. Thibodeau B, Trope M. Pulp revascularization of a necrotic infected immature permanent tooth: case report and review of the literature. Pediatr Dent 2007 Jan-Feb;29(1):47-50. PMID: 18041512.
29. Iwaya S, Ikawa M, Kubota M. Revascularization of an immature permanent tooth with periradicular abscess after luxation. Dent Traumatol 2011 Feb;27(1):55-8. doi: 10.1111/j.16009657.2010.00963.x. PMID: 21244629.
30. Lovelace TW, Henry MA, Hargreaves KM, Diogenes A. Evaluation of the delivery of mesenchymal stem cells into the root canal space of necrotic immature teeth after clinical regenerative endodontic procedure. J Endod 2011 Feb;37(2):133-8. doi: 10.1016/j.joen.2010.10.009. PMID: 21238791.
31. Iwaya SI, Ikawa M, Kubota M. Revascularization of an immature permanent tooth with apical periodontitis and sinus tract. Dent Traumatol 2001 Aug;17(4):185-7. doi: 10.1034/j.16009657.2001.017004185.x. PMID: 11585146.
32. Jeeruphan T, Jantarat J, Yanpiset K, et al. Mahidolstudy 1: comparison of radiographic and survival outcomes of immature teeth treated with either regenerative endodontic or apexification methods: a retrospective study. J Endod 2012;38:1330-6.
33. Torabinejad M, Faras H. A clinical and histological report of a tooth with an open apex treated with regenerative endodontics using platelet-rich plasma. J Endod 2012;38:864-8.
34. Shimizu E, Jong G, Partridge N, et al. Histologic observation of a human immature permanent tooth with irreversible pulpitis after revascularization/regeneration procedure. J Endod 2012;38:1293-7.
35. Thibodeau B, Teixeira F, Yamauchi M, et al. Pulp revascularization of immature dog teeth with apical periodontitis. J Endod 2007;33:680-9.
36. Wang X, Thibodeau B, Trope M, et al. Histologic characterization of regenerated tissues in canal space after the revitalization/revascularization procedure of immature dog teeth with apical periodontitis. J Endod 2010;36:56-63.
37. Tong HJ, Rajan S, Bhujel N, Kang J, Duggal M, Nazzal H. Regenerative endodontic therapy in the management of nonvital immature permanent teeth: a systematic review-outcome evaluation and metanalysis. J Endod 2017 Sep;43(9):1453-1464. doi: 10.1016/j.joen.2017.04.018. Epub 2017 Jul 22.PMID: 28743431.
38. Shaik I, Tulli M, Unnam P, Karunakaran S, Vaddi DS, Jabeen R, Tiwari RVC. Regenerative endodontic therapy in the management of nonvital immature permanent teeth: a systematic review and metaanalysis. J Pharm Bioallied Sci 2021 Jun;13(Suppl 1):S36-S42. doi: 10.4103/ jpbs.JPBS_807_20. Epub 2021 Jun 5. PMID: 34447039; PMCID: PMC8375786.
39. Murray PE. Review of guidance for the selection of regenerative endodontics, apexogenesis, apexification, pulpotomy, and other endodontic treatments for immature permanent teeth. Int Endod J 2023 Mar;56 Suppl 2:188-199. doi: 10.1111/iej.13809. Epub 2022 Aug 15. PMID: 35929348.
40. Songtrakul K, Azarpajouh T, Malek M, Sigurdsson A, Kahler B, Lin LM. Modified apexification procedure for immature permanent teeth with a necrotic pulp/apical periodontitis: a case series. J Endod 2020 Jan;46(1):116-123. doi: 10.1016/j.joen.2019.10.009. Epub 2019 Nov 21. PMID: 31761331.
41. Desai S, Chandler N. The restoration of permanent immature anterior teeth, root filled using MTA: a review. J Dent 2009;37:652–7.

Joseph C. Stern, D.D.S., is director of endodontics and clinical assistant professor of dental medicine at Touro College of Dental Medicine at New York Medical College, Hawthorne, NY. A diplomate of the American Board of Endodontics, he is in private practice in Clifton, NJ.