11 minute read
Supporting elective recovery through a short stay arthroplasty pathway


Jonathan Howell and Mary Stocker
Jonathan Howell has been a Consultant orthopaedic surgeon in Exeter since 2004. He has been Clinical Director of Orthopaedics, Trauma and Rheumatology at Exeter, andis currently joint clinical lead at the Southwest Ambulatory Orthopaedic Centre. He is a Past President of the British Hip Society, and has published multiple scientific papers in the field of hip replacement and revision surgery.
Advertisement
Mary Stocker is joint clinical lead for SWAOC and is a Consultant Anaesthetist at Torbay and South Devon NHS Foundation Trust. She has a strong interest in day surgery and was the clinical lead for day surgery in South Devon for 14 years working, at the helm of their nationally recognised day surgery unit. She has been a member of the Council of the British Association of Day Surgery (BADS) since 2009 and served as their president for three years. She is currently their representative on the International Association of Ambulatory Surgery (IAAS), General Assembly.
Waiting lists for elective orthopaedic surgery have been rising across the United Kingdom for several years, due to a combination of factors that include issues of demand, facilities and staffing. A lack of access to ring-fenced orthopaedic in-patient care in acute hospital sites has been one of the contributors to waiting list growth, and this pressure on facilities has become more acute since the COVID-19 pandemic, exacerbated by seasonal peaks in other infectious diseases.
One way in which elective care might be protected from the influence of acute pressures is to make more efficient use of the resources that are allocated to orthopaedic surgery. In 2021 we were given the opportunity to address the elective waiting list in Devon through the development of a new protected elective site, and to maximise the benefit gained by our system we undertook to transform the way in which elective arthroplasty surgery was delivered in our area.
Background
In March 2020, as the NHS faced an uncertain and potentially overwhelming need for acute care because of the COVID-19 pandemic, the NHS in England responded with several secondary care initiatives that included establishing a number of new medical units, known collectively as the ‘Nightingale’ hospitals [1] The Exeter Nightingale Hospital was the smallest and the last of these units to be opened; it was established on the site of a disused home improvements store (Figure 1), and during the COVID-19 pandemic it treated 247 patients from eight acute Trusts across three counties.

Figure 1: Transformation from DIY store to hospital; the building prior to transformation

Figure 1: a mural from one of the inside walls of the COVID-19 facility; one of the seven wards in the Exeter Nightingale Hospital.

Figure 1: one of the seven wards in the Exeter Nightingale Hospital.
In May 2021, Devon Integrated Care System (ICS) was awarded funding from the National Accelerator Systems Programme, to support reduction in waiting times in key target areas. This funding was utilised to transform the site of the Exeter Nightingale Hospital for use by four specialities across the Devon system: elective orthopaedics, radiology, ophthalmology and rheumatology.
Building an elective orthopaedic centre
New ways of working
At the inception of the project, we assembled a multi-disciplinary team (MDT) that included anaesthetic and orthopaedic clinical leads, as well as senior management, nursing and therapy leads, architects, estates, information technology and governance. The MDT set out to go beyond simple considerations of waiting lists numbers, and to use the Nightingale transformation as a test of change for new ways of working. The ambition was to revisit every aspect of our existing patients’ journeys, to solve many of the challenges experienced at the base hospitals, and to implement new state-of the-art pathways for elective orthopaedic care. In particular, we were keen that improvements in our patient care would enable us to make drastic reductions in patients’ length of stay, an intention reflected in the name chosen for the new unit, The Southwest Ambulatory Orthopaedic Centre (SWAOC). As a starting point the MDT gathered examples of best practice from within Devon and across the country, and we visited several other units to learn from their experience in short stay elective care. At a time when recruitment of clinical colleagues was very challenging, we undertook a campaign to attract candidates who had a stated interest for working in new ways, and across the clinical teams we built a culture of challenge and innovation. In line with Getting it Right First Time (GIRFT) recommendations, we have set a benchmark of a minimum four joints per all day list, and recognising that these primary surgeries at a protected elective site represent valuable training opportunities, we have worked with regional consultant colleagues to ensure that trainees have the opportunity to work at SWAOC.
New facilities
The Exeter Nightingale Hospital already had seven wards on site but planning laws and building regulations prevented us from placing theatres within the existing structure. We therefore commissioned modular units that included two theatres, each of which had separate anaesthetic and lay-up rooms, a recovery area and stores (Figure 2). The layout of the unit was optimised with patient flow and working efficiency at the heart of the design, as well as considerations necessary for establishing a green area within the theatre complex. The building and commissioning work was completed in January 2022, and despite the challenges of the winter of 2021/22, with the flexibility and willingness of clinical and management colleagues, SWAOC opened to patients in March 2022.

Figure 2: Delivery and installation of the modular theatre complex.
The SWAOC Pathway
To reduce some of the challenges in redesigning all aspects of an elective orthopaedic pathway, and with the need to make an immediate significant impact on a substantial segment of the orthopaedic waiting list, the MDT decided that the project would initially focus on primary hip and knee replacement surgery. The success of the project has since allowed us to extend the scope of surgery to foot and ankle, with soft tissue knees, hip arthroscopy and spinal surgery also currently in advanced stages of planning for introduction at SWAOC. A summary overview of the primary knee and hip pathway is shown in Figure 3; every stage of the patient journey was redesigned, some selected aspects of which are discussed in more detail in this section.
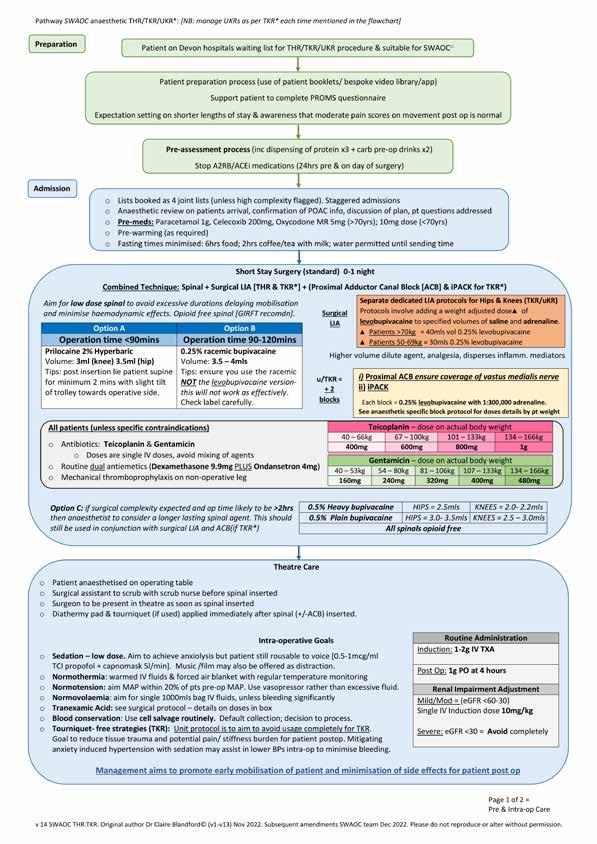
Figure 3 (part 1): Summary document showing an overview of the SWAOC pathway.
Patient selection
SWAOC is a remote site, physically separated from the nearest acute hospital, and this created some potential difficulties with medical cover and the management of emergencies. As a result, the MDT designed a Red/ Amber/Green (RAG) rating system, based on a systemic review of patients’ comorbidities, and used this to select patients suitable for surgery at SWAOC. In the interests of safety, we limited our initial experience to patients deemed to be ‘Green’, with minimal co-morbidities, but in light of the safety and success of the unit we have been able to extend the facilities to those rated ‘Amber’ and even to some rated ‘Red’. The important thing to note is that every patient passing through SWAOC is placed on the same ambulatory pathway, so that everyone has the same chance of benefitting from day case arthroplasty.
Preparation for surgery
Short stay arthroplasty demands that a patient’s medical condition is optimised for their operation, that their physiology is disturbed as little as possible during their stay, and that each patient receives consistent messaging and treatment along their pathway. We have created written and video patient information resources designed to promote day case or one night stay. Patients receive carbohydrate drinks the night before surgery and their food starvation period is limited to a maximum of six hours, with tea and coffee allowed up to two hours before and water to the point of their surgery. Premedication with a combination of Paracetamol, Celecoxib and Oxycodone helps to reduce post-operative pain and to promote early mobilisation.
Intra-operative care
Short stay arthroplasty care is promoted through highly protocolised anaesthetic techniques, augmented by surgical infiltration of local anaesthetic. General anaesthetics are avoided, and sedation minimised, to ensure patients recover rapidly; they spend just a few minutes in primary recovery before moving to the rehabilitation area. In consultation with anaesthetic colleagues, we developed two spinal protocols, based on either prilocaine or racemic bupivacaine, which wear off rapidly after surgery thus promoting early mobilisation.
Preoperative fluid balance is optimised and a maximum of 1,000 mls crystalloid is administered intraoperatively; we routinely perform cell salvage, with homologous transfusion in cases justified by collected volumes.
Theatre efficiency is promoted through agreed triggers for lay-up of the next case, communication with the admission area, and sending for patients. Anaesthesia is performed in a dedicated room, on the operating table, following which surgeons position patients before they are transferred tothe operating theatre.
Postoperative care and discharge
In the primary recovery area intravenous fluids are discontinued and patients are given a carbohydrate drink. After a brief period of monitoring, they are transferred to secondary recovery, where mobilisation starts as soon as the spinal has worn off. Pain scores and nausea are reviewed regularly with a low threshold for treatment, food is introduced early, post-operative X-rays are performed, and patients are encouraged to get dressed in their own clothes as soon as possible.
Discharge from the unit is protocolised and nurse led, and discharge paperwork is populated by different elements of the patient’s electronic pathway record. Patients receive a standardised pack of discharge medication that includes a strictly limited period of oxycodone use. Telephone calls are made to the patients on day one and day seven after discharge, and pain scores and patients’ opiate use are audited regularly.
SWAOC results
The first patients were treated in March 2022 and at the time of writing (January 2023), 740 primary hip and knee replacements have been carried out at the unit (Figure 4). The length of stay at SWAOC for all primary hip and knee replacements is shown in Figure 5, with the mean length of stay by procedure shown in Figure 6; 52% of primary arthroplasties performed at SWAOC have been day cases. Data from the author’s (JH) base trust shows that, in the year 2021/22, the median length of stay for both primary hip and knee replacements was three days. The data shown in figures 5 and 6 therefore represent a significant downward shift in length of stay, which might be interpreted as resulting from patient selection. Indeed, the treatment of more complicated and frail patients has remained at the base trusts and SWAOC has treated more straightforward cases. However, learning from the pathways described has been incorporated into base trusts, and data from 2022/23 shows, that in the author’s (JH) Trust, the median length of stay for primary hip and knee replacement is now two days, even amongst this population of sicker, more complex patients.
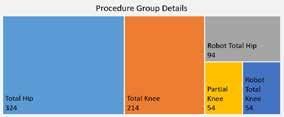
Figure 4: Numbers of primary hip and knee replacements performed at SWAOC (data last accessed 20th January 2023).

Figure 5: Length of stay for primary hip and knee arthroplasty at SWAOC

Figure 6: Mean length of stay at SWAOC by procedure.
Of course, length of stay is only one metric of interest, and we must ensure that patients’ care is not compromised by a relentless drive to reduce their time in hospital. Figure 7 shows the overall pain scores reported by SWAOC patients, demonstrating that only a very small proportion have severe pain, and the data in Figure 8 shows a high rate of patient satisfaction with the service they received at SWAOC.

Figure 7: Overall pain experience of SWAOC patients.

Figure 8: SWAOC patient satisfaction scores.
Conclusion
SWAOC provided the Devon ICS, not only with an opportunity to reduce its waiting times for elective orthopaedic surgery, but also to develop new pathways for elective care that have allowed us to drastically improve our length of stay for high-volume low complexity procedures. This has been achieved through a multidisciplinary re-design of all aspects of our patients’ journey and through a greater protocolisation of the treatment that they receive. In this article the authors have discussed some aspects of these protocols, and we would like to thank all members of our MDT, and all those teams around the country, whose shared expertise helped us to achieve these results. The SWAOC MDT is in turn completely open to sharing our protocols with anyone interested in obtaining further information about them.
References
1. Coronavirus: How NHS Nightingale was built in just nine days. Available at: www.bbc. co.uk/news/health-52125059