14 minute read
‘Oops!’ Designing and implementing a novel peer-to-peer training session on learning from surgical mistakes

Adam Stoneham, Simon Williams, John Hardie, Greg Neal-Smith and Fransiska Guerreiro
Adam Stoneham is a post-CCT senior fellow in hand surgery at University Hospitals Southampton. His interests are in upper limb surgery and medical education. He is also the holder of a Guinness World Record. He developed the ‘Oops’ Programme after participating in a serious medical error as a junior trainee.
Advertisement
Simon Williams is a Core Surgical Trainee working towards a career in orthopaedics. He has an interest in medical education and has a PGCert in Medical Education.
John Hardie regularly publishes, speaks, and directs courses in Human Factors in surgery. His early work was informed by his initial pilot training with the RAF, and subsequent General Aviation flying. He is a T&O registrar in the Wessex deanery.
Greg Neal-Smith is a T&O registrar in the Wessex Deanery. Outside of medicine he is an avid cook and has been trained by a Michelin starred chef in London. He is also a keen rugby player and is risking his surgical career once again when he captains his rugby sevens team in the Bournemouth Sevens this year!
Fransiska Guerreiro is an ST5 in the Wessex Deanery. She won awards as a business manager, won the RCS Surgical Skills competition and Core Surgical Trainee of the year, and a prize at the European Society of Sports Knee Arthroscopy 2022 Congress. In her spare time she enjoys playing piano, guitar, and exploring the great outdoors with her husband and daughter.
Mistakes in surgery are exceptionally common; they can harm surgeons as well as patients and are a major burden on healthcare systems in terms of wasted resources and the cost of litigation. Surgeons are not prone to seeking support for their mistakes and there are few forums available for them to discuss them with their peers. The aim of this article is to share our experience of developing and running a novel peer support training session and provide a blueprint for others to do the same. The session was entitled ‘Oops!’ (Optimising Outcomes through Peer Support) and was specifically targeted at Speciality Registrars. The objective was to provide a safe and confidential forum for participants to discuss their own mistakes and learn from each other’s.
What are mistakes and why do they happen?
We defined a mistake as a decision or action which produced an unwanted result, either for the surgeon or the patient or both. The occurrence of errors in any human system is inevitable, but mis-management of these errors may lead to surgical incidents. Surgical incidents often result from complex interactions, decisions, and events rather than isolated, individual mistakes.
When workload exceeds the personal capacity of the surgeon, the likelihood of error increases [1].
This may be particularly applicable to surgical trainees who may not have performed the procedure recently (indeed sometimes at all). Other potential factors such as fatigue, distraction, or external pressures may further reduce capacity.
In surgery, a person’s experience (or lack of it) is critical. Whereas one would expect an individual’s competence to increase over their career, their perception of their own ability may in fact decrease. In 1999, Dunning and Kruger devised an experiment which showed that less skilled individuals consistently overestimated their ability whereas more highly skilled individuals were prone to underestimate it (see Figure 1 and 2) [2]. Appreciation of this effect both in ourselves – and just as importantly in those we supervise – may be strategic in predicting and avoiding mistakes [3].
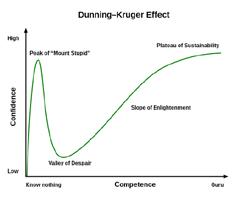
Figure 1: The original work of Dunning and Kruger [2] showing actual vs. perceived ability. Low ability individuals consistently overestimated their performance whereas high ability individuals were prone to underestimate it.

Figure 2: How Dunning and Kruger’s work is more commonly represented to show how inexperienced individuals do not appreciate their lack of knowledge (‘you don’t know what you don’t know’).
What is the scope of the problem in the NHS?
One in 20 hospital admissions results in avoidable patient harm [4]. So-called ‘never-events’ such as wrong site surgery and retained surgical instruments may happen as often as 1:100,000 and 1:10,000 respectively [5].
Threat of litigation is highly present in UK practice. Surgical mistakes contribute to the significant burden of NHS clinical negligence claims, with spending on pay-outs and settlements increasing rapidly in recent years, resulting in a bill of around £2.4 billion in 2018-19 [6]. Surgical specialties are documented to have the greatest number of litigious claims, with 2,847 over a ten-year period to 2019, though obstetrics and gynaecology has the highest total value of pay-outs [7].
Over 90% of surgeons report experiencing an intraoperative adverse event, most commonly within the last year. Whilst this can harm patients, the effect on the surgeon themselves can be significant and often overlooked. Amongst those surveyed they almost unanimously expressed strong feelings of anxiety, guilt, sadness, anger, shame, and/or embarrassment but few sought professional psychological counselling [8].
How can we avoid them?
It is estimated that there are over 500 million interactions between patients and the NHS a year [9]. Although some mistakes are inevitable we believe this number could be reduced.
The study of Human Factors (HF) – or how systemic and individual characteristics influence behaviour – has been shown to improve safety and outcomes for those giving and receiving care. In recent years, healthcare has adopted proven HF concepts from the aviation, maritime and rail industries [10]. Examples include the WHO surgical checklist [11,12], pre-operative planning techniques, standardised communication for safety-critical moments [13], structured team briefings, and dual surgeon operating [14].
Peer-to-peer teaching has proven benefits in medical education [15]. The aim of this session and the pre-course survey was to identify factors which had led to mistakes, as well as to share specific technical details which would enable other participants to anticipate and avoid the same thing happening in the future.
Box 1: Mistakes in orthopaedic surgery. Experience from a leading UK indemnity provider:
• Average claims for a new consultant: 1 in every 2.5 years
• A surgeon’s worst mistakes tend to occur in the first 3-5 years of autonomous practice
• 25% of consultants participate in wrong site surgery in their career
Peer-to-peer training session
An anonymous pre-course survey was circulated to all Orthopaedic Registrars in the Wessex Deanery. This collected basic information on level of training, sex, number of surgical errors encountered, and the factors which contributed to mistakes. Free text boxes were provided to cite examples of mistakes in which trainees had personally participated or directly observed.
Trainees were invited to prepare a brief 10-15 minute presentation of a particular error which they felt had relevant learning points for their peers. It was reinforced to colleagues that there was no requirement to submit a case, and any information provided would only be used with their consent. The day was hosted at a central but deliberately non-clinical venue. Only Speciality Registrars were invited in an attempt to create a safe atmosphere in which participants could be candid in their opinions. A single exception was made for a respected (recently retired) NHS Consultant with significant experience in medical education, surgery, and medical negligence. His role as mentor and mediator proved instrumental in the success of the day.
Well-known General Practitioner and comedian, Phil Hammond, was invited to present to the group on learning events throughout his career and his collaboration with mainstream and social media to highlight wider failings in the National Health Service. This featured a degree of comedy to engage the group, ‘break the ice’ and provoke discussion.
The session adapted peer-to-peer teaching model – a format with proven benefits demonstrated in medical education research [15]. Psychological safety was established at the outset by agreeing to discuss all cases in confidence and adhere to Just Culture principles [16]. These principles include accountability for actions and an openness to learn from incidents but rejection of uncontextualised blame. Cases for discussion were anonymised by the presenters, and included incidents leading to adverse outcomes, and ‘near misses’ which did not lead to harm. As well as ‘technical mistakes’, presenters were encouraged to consider the wider context of the incidents and address learning points.
Pre-course survey results
Trainees reported a total of 76 ‘serious’ mistakes (e.g. missed diagnoses, wrong treatment, significant complications). The median number was three each over their career to date (range 1-10).
The nature of the mistakes varied greatly from misplaced hardwear, to wrong operation / wrong site surgery, to avoidable revision. A representative sample are displayed in Box 2.
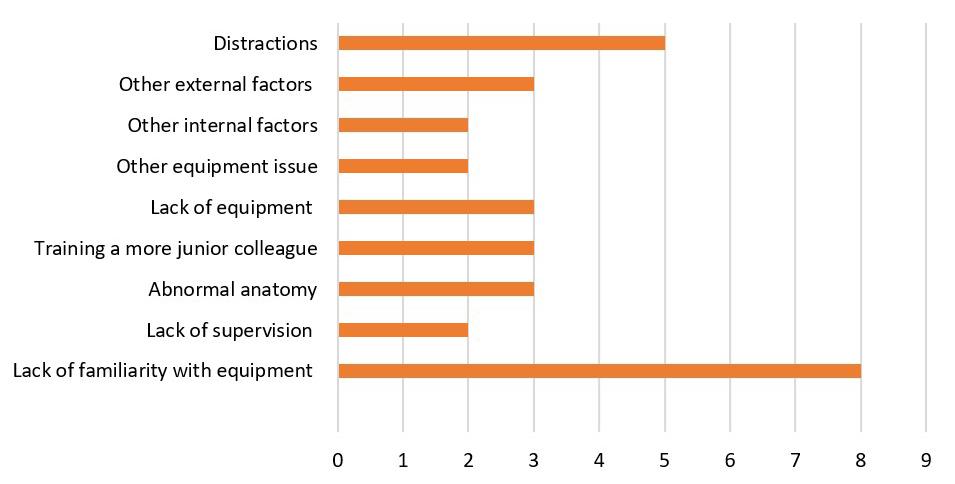
The commonest reason cited for mistakes was lack of familiarity [n=8, 42%] followed by distractions [n=5, 26%]. Other reasons are shown in Figure 3.

Figure 3: Factors contributing to a serious error or near miss.
In general, responders lamented their lack of preparation, failure to communicate effectively between junior and senior colleagues, and not ‘listening to their gut’ when they thought something was wrong.
Box 2: Sample of errors which Registrars reported:
• Lag screw passed behind IM femoral nail, unnoticed intra-operatively
• Reverse oblique proximal femoral fracture inappropriately treated with DHS with early failure
• Injury to superficial peroneal nerve during ankle ORIF
• Knee arthroplasty popliteal nerve injury, not subsequently recognised
• Hemiarthroplasty positioned too long
• Equipment not available due to holes in sterile sets
• DHS screw protruded medially into a calcified artery
• Too many passes of guidewire during DHS led to fracture of lateral wall whilst inserting lag screw
• Ankle Fixation in which the syndesmotic screws missed the tibia
• Inadvertent scaphoidectomy during routine trapeziectomy
What did we learn?
“Success is going from one failure to the next without losing enthusiasm” Unknown; sometimes attributed to Winston Churchill and cited by John Charnley
100% rated the course as ‘very beneficial to training’. The sessions delivered by Registrars, a recently retired Consultant, and Phil Hammond were the best received.
Certain specific cases were presented which highlighted particular equipment issues or ‘banana skins’ to avoid with individual operations. Some participants had never heard of some of the complications discussed and so left much better informed and able to avoid them themselves. It was refreshing to hear a balanced and realistic appraisal of our speciality including our less glamorous and less talked-about moments. There was a genuine feeling of comradery and whilst it is good to share our triumphs, participants took significant comfort in knowing they were not alone in their disasters.
Some themes came up repeatedly in the discussion. These included unfamiliarity with certain pieces of equipment and a lack of training and resources in some areas. The ‘quick Dynamic Hip Screw (DHS)’ was a particular cause of angst and it was suggested that this phrase be banned outright. Performing the procedure a few times on simulators (e.g. ‘Sawbones’) could be a minimum requirement for certain reproducible operations.
Consultant supervision was an important topic of conversation. Most of the cases presented had occurred when Registrars were operating unsupervised. It was the opinion of the senior Consultant present that on the whole this is no longer acceptable and indefensible in legal terms should a complication ensue. One of the more challenging errors had occurred because the consultant was inexperienced, and the trainee regretted that he had felt unable to speak out. Another serious mistake happened despite a very experienced surgeon being scrubbed in the room and the trainee felt their presence had in fact given them a false sense of reassurance.
The training of junior trainees by senior trainees was keenly debated. Many Registrars enjoy teaching and feel that it is necessary to facilitate to transition from trainee to Consultant trainer. Most agreed that it needs to be done in a safe environment and some expressed disappointment that they were not able to teach due to lack of senior support themselves. The extent to which trainees are ‘given enough rope by which to hang themselves’ is, of course, a matter of context and personal discretion, which develops with experience.
Learning from our practice (good and bad) is already a core curriculum outcome. Generic professional capabilities (GPC), established by the General Medical Council (GMC), which must be included in all post-graduate training curricula, include doctors learning from their “…own performance, that of others, human factors and cognitive biases”17. This session was unanimously welcomed as a rare opportunity to put this into practice and we believe it would be a very welcome addition to any regions’ regular teaching programme as well as an incorporated or standalone annual national event.
Box 3: Some surgical truisms were aired:
• “See one, do one, teach one” is dead
• If you have never heard of it you can’t avoid it
• You don’t know what you don’t know
• Big mistakes happen through small holes
• Check twice cut once
• If it feels wrong it probably is
• Remember the seven P’s: proper prior planning prevents piss poor performance
Conclusion
“If you ain’t getting complications you ain’t operating” Anon
We were wary that this concept presents enormous scope with limited time. Therefore we had to be very selective regarding the content included. We tried to touch on legal aspects of medical errors and could easily have gone in many other directions including as human factors, psychology, non-technical skills etc. Other courses do exist in these areas.
Our peer-to-peer learning approach is not intended to replace departmental or national methods for clinical governance or incident investigation.
Wessex has traditionally had a very even split of the gender of trainees so it was surprising how few female Registrars participated in the survey or submitted cases to present on the day. Presuming men and women make equal numbers of mistakes (?) it would be worthwhile exploring whether this is a genuine trend and the factors underlying it.
We all make mistakes. Sometimes because we just lack technical ability but more often because of a litany of factors both within and beyond our control in any given context. Although we know we should – indeed we are professionally obliged to – reflect and learn from these events, there are currently very few forums in which to do so.
BOX 4: Words of advice from a senior surgeon upon making a serious mistake:
• Take a deep breath and step away from the table – obviously if safe to do so.
• Take another deep breath and tell someone senior and sensible in theatre there is a problem. Be cautious about just announcing in theatre, the patient may be awake, rumour control will have it out in the corridor before you can blink and by the time it comes back you will have removed the wrong hand and leg.
• Phone a friend or your boss. Preferably get them to come immediately to the theatre if on site, but if not, un-scrub and spend five minutes or longer talking to them about your options.
• Get them to join you if feasible and complete case with them there – you will be pretty unsettled and do not want any more issues.
• Write a full operation note.
• Have a cup of tea and large quantity of chocolate.
• Consider cancelling the rest of the list.
• Debrief team in theatre – don’t forget they will be upset and will be called on by investigation.
• Write a full account immediately and email to yourself and friend +/- Clinical Director/Lead clinician.
• Fill in Datix.
• Contact your defence union.
• Phone your friend/mentor/someone who knows the operation and talk about it. Most complications have been done before.
This all-new peer-to-peer training day was a great success; we would strongly encourage other regions getting in touch to replicate and share our experience.
Acknowledgements
We are very grateful to Nigel Rossiter, Simon Hodkinson, Sophie Phillips, Alex Marshall-Lewis, Portia Ross, Alex Thomas, Sam Shamoon, and Jack Hurst.
References
References can be found online at www.boa.ac.uk/publications/JTO
