Health and care services report
Sponsored by


Groundbreaking Research – saving and improving lives

Sponsored by
Groundbreaking Research – saving and improving lives

The British Heart Foundation (BHF) is the largest independent funder of heart and circulatory disease research in Northern Ireland. Formed over 60 years ago, the leading heart charity has revolutionised the treatment and care of heart and circulatory disease.
Its ground-breaking research has saved countless lives and the charity continues to fight for the 225,000 people living here with heart or circulatory conditions such as coronary heart disease, heart failure, and stroke.
Head of British Heart Foundation Northern Ireland, Fearghal McKinney, tells agendaNi about the progress the charity is making in heart health and why its life-saving research is more vital than ever.
We have come a long way since the BHF began over 60 years ago. In the 1960s, more than seven out of 10 heart attacks in the UK were fatal. Today, over seven in 10 people survive. This is tremendous progress, but our work is far from over.
In Northern Ireland, despite all the good progress, around 225,000 people are living with heart and circulatory disease.
These conditions are responsible for nearly a quarter of all deaths here, tragically claiming an average of 11 lives every single day.
And alarmingly, more people under the age of 75 are now dying from these diseases than at any time in the last 14 years. This is a wake-up call that means we must act now, to continue that vital research journey.
Innovation and determination were the focus of one remarkable story that highlights the lifesaving impact of BHF research. Professor Frank Pantridge and his team, who were modestly funded by the BHF in Belfast in the 1960s, revolutionised emergency care worldwide.
He developed the first portable defibrillator, a device that has since saved countless lives. His legacy is a testament to the power of research –and to the vital role your support plays in funding it.
Today, thanks to our supporters’ generosity, we are funding pioneering research at Queen’s University Belfast into conditions like heart failure and heart attack recovery.
Recently, we brought together researchers from Queen’s and Ulster University with our new Chief Scientific and Medical Officer, Professor Bryan Williams, to chart an exciting new direction for research here in Northern Ireland.
But our research is needed now more than ever. Earlier this year, we launched a campaign on the urgency of tackling sudden cardiac death. Twelve poignant murals were created across the UK by the BHF to highlight the tragic reality that 12 young people under the age of 35 are lost every week to sudden cardiac death in the UK.
One of these striking artworks was unveiled on Linenhall Street, Belfast and depicted popular barman and electrician Joseph Burns, who suffered a sudden cardiac arrest at his parents’ home 10 years ago in July 2014.
Too many lives, like Joseph’s, are being taken too soon by sudden cardiac death. No one should have to experience the sudden loss of their child, sibling, or parent, but sadly that is the cruel reality of heart disease – it does not discriminate.
The BHF is already carrying out groundbreaking research, to treat and prevent the causes of sudden cardiac death.
BHF researcher, Kathryn McGurk, whose family hail from Northern Ireland,

“BHF continues to work every day on tackling health inequalities within cardiovascular care.”
is one of a team of scientists working to develop a cure for inherited heart muscle diseases which affect around 8,000 people here.
BHF’s £30 million CureHeart programme – the most ambitious research grant in the BHF’s history –aims to develop the first cures for inherited heart muscle diseases.
BHF can only invest in transformational research like this thanks to the generosity of our loyal supporters – so it is vital we have continued and increased support if we are to keep backing lifesaving research like CureHeart – but there is still more to do.
Our efforts also extend beyond research. We successfully campaigned for CPR training to become a mandatory part of the school curriculum here and worked with the Department of Education and the Northern Ireland Ambulance Service to make that happen.
Every year, we distribute 28,000 heart health resources across Northern Ireland, and our life-saving tool RevivR, offers free CPR training in just 15 minutes – available to anyone, anywhere, with just a cushion and a phone.

We are also working closely with sports teams, community groups, schools and businesses to expand this lifesaving training. Earlier this year, during Heart Month, we teamed up with the Northern Ireland Football League to train football clubs in CPR, and we have plans to work with many other organisations in the coming year.
Our influencing work over the last number of years has helped deliver significant change, most recently in the area of organ donation legislation. As of June 2023, all adults in Northern Ireland are considered potential organ donors unless they choose to opt out or are in an excluded group. The Organ and Tissue Donation (Deemed Consent) legislation, known as ‘Dáithí’s Law’ in honour of young Dáithí Mac Gabhann, changed the way consent is granted and follows similar law changes in Wales, England, and Scotland.
Over the past year we have been working with the NI Agri-Rural Health Forum and Farm Families Health Checks team to drive work on blood pressure awareness amongst the farming community. This culminated in an event we held at the Balmoral Show with attendance from the health and agriculture ministers as well as many
agri-rural stakeholders. We continue to work with this important community in Northern Ireland through driving awareness of lifesaving skills.
Our ambition in influencing government and the health system is to achieve the best outcomes for patients. We are working with the cardiology network and leading cardiologists and heart nurses to, amongst other things, prevent heart disease by targeting blood pressure and cholesterol, improve treatment and care for those with heart failure, and increase opportunities so everyone can take part in cardiac rehabilitation.
Critical to the survival journey is the defibrillator but knowing where to find one in an emergency can be the difference between life and death. That is why we developed The Circuit in partnership with the Association of Ambulance Chief Executives, Resuscitation Council UK, St John Ambulance, and NHS England.
The Circuit is the national defibrillator network that maps defibrillators across the UK. This system allows ambulance services to direct bystanders to the nearest defibrillator, potentially saving lives in those critical moments.
But there is still work to be done. We have registered over 98,000 defibrillators on The Circuit, and more than 3,500 in Northern Ireland, but we know there are many more out there that remain unregistered. In the coming months, we will be campaigning to reach 100,000 defibrillator registrations, ensuring that more lives can be saved in emergencies.
BHF continues to work every day on tackling health inequalities within cardiovascular care. Our focus has been on primary care with blood pressure and cholesterol checks as well as women’s health.
We recently launched our Bias and Biology: The Heart Attack Gender Gap report timed to coincide with development of a women’s health action plan by the Department of Health to highlight that there can be no consideration of any health without considering heart health as a vital component.
This is the first BHF report into women’s heart attack outcomes in Northern Ireland that addresses socio-economic differences and makes recommendations across themes of awareness, diagnosis and treatment.
Non-communicable diseases (NCDs) such as heart disease, cancer, stroke, diabetes, lung disease, and liver disease are some of the leading causes of death and disability.
In fact, research commissioned by BHF Northern Ireland in 2023, estimates the overall annual cost to society of smoking, alcohol consumption and obesity in Northern Ireland is around £1.9 billion – equivalent to 4.5 per cent of the Northern Ireland economy.
NCDs place a huge burden on society and our health and social care system. They also disproportionately affect the most deprived in our communities, contributing to health inequalities.
Many of these deaths and lost years of healthy life could be prevented through public health action to address NCD risk factors. Investing in population-wide action to reduce rates of smoking, harmful alcohol consumption, and overweight and obesity is also important for the longer-term resilience of our health service and the wider economy.
As Chair of the NI NCD Alliance, BHF NI is working alongside a number of key stakeholders to help prevent heart and circulatory disease and other NCDs by campaigning for urgent, population-level action to reduce rates of smoking, harmful alcohol consumption, and overweight and obesity.
Heart and circulatory diseases cause nearly a quarter (24 per cent) of all deaths in Northern Ireland but there is a gap in the strategic direction to addressing cardiovascular conditions. The previous service framework for cardiovascular health and wellbeing expired in 2017. Despite the prevalence of heart and circulatory disease in Northern Ireland, there has been no updated strategic approach for improvement of the care of patients with heart and circulatory disease.
At the end of last year BHF NI brought together over 150 local staff, patients, and leading voices in heart and circulatory diseases from across UK, Ireland and Europe, to shine a spotlight on heart disease within Northern Ireland and the need for a renewed strategic approach.
“Lifesaving research is more vital now than ever and your support in that ambition is vital too.”
The audience was made up of clinicians, some stakeholders and officials as well as a panel of MLAs. We had a range of high-profile speakers including Professor Rafael Bengoa, alongside international speakers from the European Society of Cardiology, Scotland, Ireland and England.
Our health and policy teams are working to identify gaps in services and map out a range of actions and interventions that are practical and cost effective that can form the core of a heart disease campaign.
We will aim to support and enhance the cardiac network, produce recommendations to reduce the Northern Ireland postcode lottery of services, reduce demand on stretched services, improve life expectancy and reduce the burden on care.
At a national level, BHF is calling on the new UK Government to make a meaningful difference to the lives of people affected by heart disease by committing to bold co-ordinated action on three fronts; better prevention of heart disease and stroke by addressing drivers like obesity and smoking, prioritisation of heart care and supercharging research to unlock future treatments and cures.
None of what we do would be possible without public support – all our income comes from the public, whether it be face to face fundraising events organised by our local fundraisers, charity partnerships, contributions from wealthy donors, or those who think of us kindly in their wills.
And we also have seven shops across Northern Ireland where we sell clothing, jewellery, books, games and much more, donated to us by the public.
We recently held a supporter event at Belfast City Hall, with over 100 of our amazing supporters in attendance. It offered the opportunity to connect and share stories on the lifesaving work the BHF does in heart and circulatory research and strengthen our collective commitment.
Many of the wonderful families we work with closely were in attendance as well as new supporters who we are excited to get to know better.
Our supporters’ contributions whether through fundraising, volunteering, or simply by spreading awareness, have made the British Heart Foundation the largest independent funder of heart and circulatory disease research in Northern Ireland.
Lifesaving research is more vital now than ever and your support in that ambition is vital too.
Contact BHF NI
Órla Copeland, Fundraising Manager T: 07714 069129
E: copelando@bhf.org.uk
Liam Duggan, Policy and Public Affairs Manager T: 07974 901087
E: dugganl@bhf.org.uk
Karen McCammon, Health Service Engagement Lead
T: 028 9002 3545
E: mccammonka@bhf.org.uk

Minister of Health Mike Nesbitt MLA has outlined his primary policy pieces to complete the health reform jigsaw, the details of which have been met with some scepticism by Executive partners and opposition colleagues alike.
In July 2024, the Health Minister issued a Written Ministerial Statement to update MLAs on his policy priorities. In a previous speech, his first to the Assembly since assuming the portfolio in May, Nesbitt identified health inequalities as his predominant focus. Outlining his intention to “reboot the public conversation about health reform”, the Minister announced his intention to publish two associated documents:
1. a draft hospital reconfiguration framework; and
2. a three-year strategic plan for health and social care focusing on stabilisation, reform, and delivery, with an overriding objective of producing better outcomes for patients.
Furthermore, the Basque public health and management specialist, Rafael Bengoa was invited by the Minister to return to Northern Ireland where he
was the keynote guest speaker at the October 2024 ‘Health and Social Care Reform: Accelerating Change’ conference.
Speaking ahead of the conference, Bengoa said: “The analysis in Systems Not Structures [the Bengoa report] is just as valid today as when it was published. The need for transformation, backed by sustained resources, is ever more pressing.”
After eight years, Bengoa’s one-day return was showcased as a significant component of the health reform “reboot”.
In the same month, the Health Minister published Hospitals: Creating a Network for Better Outcome, a draft reconfiguration framework for hospitals
which outlines the principles informing the creation of an interdependent hospital network. The foremost principle of the draft framework is that while all existing hospitals will have a role to play, they cannot provide all services.
With modern medicine driving increasing clinical specialisation and subspecialisation, change, Nesbitt argues, is inevitable. As such, while stressing that “no acute hospitals will close”, he asserts that not every hospital can provide every service, and the roles of specific hospitals must change.
The Minister said: “We need to see each of our hospitals as part of something bigger and wider – fitting into a network in which each plays a key part. This is essential if we are to deliver better outcomes for patients and staff.”
Referencing Bengoa’s 2016 report, Systems, Not Structures: Changing
Health and Social Care and the 10-year plan produced in response, Health and Wellbeing 2026: Delivering Together, the draft framework places acute hospitals into four main categories within a wider network.
1. Local: delivering primary, secondary, and community care services in support of general and area hospitals. This includes Ards Hospital, Bangor Hospital, Dalriada Hospital, Downe Hospital, Lagan Valley Hospital, Lurgan Hospital, Mid-Ulster Hospital, Moyle Hospital, Omagh Hospital and Primary Care Complex, Robinson Hospital (Ballymoney), South Tyrone Hospital, Waterside Hospital, and Whiteabbey Hospital.
2. General: delivering defined secondary care services, including the delivery of some unscheduled care alongside elective care for a specific geographic location. This includes Causeway Hospital, Daisy Hill Hospital, and Southwest Acute Hospital.
3. Area: delivering a full range of secondary care services within a geographic area defined by the five health and social care trusts. This includes Altnagelvin Hospital, Antrim Area Hospital, Craigavon Area Hospital, Belfast Hospitals Campus, and Ulster Hospital.
4. Regional: delivering specialist inpatient services for the entire population. This includes: Altnagelvin North West Cancer Centre, Belfast City Hospital including the Cancer Centre, Musgrave Park Hospital, Royal Belfast Hospital for Sick Children, Royal Jubilee Maternity hospital, Royal Victoria Hospital, and Ulster Hospital Regional Centre for Plastic Surgery and Maxillofacial Surgery.
Furthermore the draft framework establishes five enablers and 13 actions to support the delivery of a connected hospital network.
The five enablers are: workforce, funding, communities and people, digital solutions, and cross-HSC trust collaboration, while actions include consideration of:
• available travel supports;
• maintaining core general hospital services in the short to medium term;

“Reconfiguring hospital services remains an important part of the overall jigsaw.”
Minister of Health, Mike Nesbitt MLA
• moving specific activities out of specialist regional centres into area hospitals;
• aligning clinical training with projected population health demand;
• reviewing how vulnerable specialist services might be consolidated via closer collaboration with Britain and the Republic.
The draft was opened to public consultation on 2 October 2024 and closes on 22 January 2025.
In a letter addressed to all MLAs on 30 September 2024, the Minister promised MLAs that his department would publish the three-year plan determining the health and social care strategy for the Assembly’s remaining mandate within weeks of Bengoa’s departure. At the time of writing, this document has yet to be published.
In the same letter, Nesbitt warned: “The current financial position makes progress all the more difficult... While the Programme for Government sets out the limits that the present budgetary situation places on efforts to reduce waiting lists, I will continue to make the case for significantly more funding for health.
“I have no time for the argument that money alone is the solution to the health service’s ills. Equally, anyone who suggests it is not part of the answer is sadly mistaken.”
As such, the public now awaits the publication of the three-year plan as the final piece of the health reform jigsaw, and its subsequent implementation alongside the hospital reconfiguration.
In the meantime, considering the one element of reform that has been published to date – the draft hospital reconfiguration framework – the response of the Minister’s Assembly and Executive colleagues has been less than positive.
From an opposition perspective, the SDLP’s health spokesperson Colin McGrath MLA commented on the proposed reconfiguration saying: “We cannot escape the fact that there is very little detail in the Minister’s statement today about what transformation will look like or what form it will take.”
Likewise, while welcoming the announcement, Alliance Health spokesperson Danny Donnelly MLA asserted: “We do not need more reviews and frameworks... We need decisions now. There is some concern around the lack of detail on how this will work in practice.”
At the same time, Sinn Féin MLA Liz Kimmins insisted: “Consideration must also be given to ensure those in more rural areas are able to access hospital services in a timely manner when they need to.”

An uncosted plan to reform Northern Ireland’s hospital network will require “every square inch of current acute hospital capacity”, Health Minister Mike Nesbitt MLA has outlined.
“According to Professor Bengoa, the cost of not doing reform is that, by 2040, health will absorb the entire – the entire – Northern Ireland Executive Budget. There will be nothing for schools or infrastructure — nothing for anything except health. We have to do it,” declared Health Minister Mike Nesbitt MLA when asked about the cost of not transforming the health service.
Nesbitt was taking questions from MLAs in the Assembly shortly after the publication for consultation of a new plan to reform Northern Ireland’s hospital network.
Hospitals: Creating a Network for Better Outcomes navigates away from the politically sensitive subject of hospital closures – despite that being the recommendation of successive health reviews stretching back to 2001 – through a reconfiguration of services provided by existing hospitals, rather than closing facilities.
In essence, patients will be asked to travel further for certain types of care but will be seen faster, as some services are consolidated in a bid to avoid duplication and competition for resources.
Details of exactly what this consolidation will look like is absent from the plan, as is any form of costing – with critics understandably cynical given the framework is the latest in a line of healthcare reviews, all of which have been unsuccessfully implemented.
The Minister has stated that the framework should not be viewed in isolation “but as an important piece of the overall puzzle that will deliver better outcomes”.
Interestingly, the framework was published shortly before a visit to Northern Ireland by Raphael Bengoa who led the delivery of the 2016 Systems, Not Structures review, a foundation for the 10-year Health and Wellbeing 2026: Delivering Together strategy
Bengoa’s visit could be read as an attempt by those leading health reform to emphasise that work remains ongoing, and perhaps re-energise the conversation around why change is necessary.
Talk of radical reform to the hospital network first emerged in 2001, when the Maurice Hayes



review recommended, amongst other things, reducing the total number of hospitals. The 2011 Compton Review included a recommendation to cut the number of acute hospitals from 10 to five, while in 2014, the Donaldson report suggested closing some local hospitals in recognition that expertise was being too thinly spread across Northern Ireland’s network.
Bengoa’s report was the fourth health review in less than a quarter of a century that has suggested cutting or changing the number of acute hospitals, but change to date has been piecemeal.
A number of barriers have curtailed health transformation, primarily, political instability as well as a shortage of public finances. A further recognised barrier is that closing services is deemed politically unpopular.
Navigating this, Nesbitt has made it clear in his foreward to the new framework that “no acute hospital will close”. Instead, the framework indicates the need to develop regional centres of excellence or surgical hubs for some inpatient services.
“The reality is that we will continue to need every square inch of current acute hospital capacity,” the framework states, adding: “The roles of some hospitals will change to better deliver the health needs of the community and keep pace with modern medicine, as well as contribute to regional delivery. Services may be relocated in some cases from their existing locations, but all hospitals will continue to play a central and vital role in our health service and in their local communities.”
The framework categorises Northern Ireland’s acute hospitals into four specific main types: local hospitals; general hospitals; area hospitals; and regional centres. Outlining that it is unsustainable for all hospitals to provide all services, the Department of Health says that the framework will seek to identify the core services in each of these types of hospitals and consider the key challenges to sustainably deliver these. However, while the framework proscribes a future action plan, no timeline has been set for delivery.
Importantly, the framework highlights that hospital network reform is not without challenges, and pinpoints three key areas where action will be required.
1. On workforce challenges, the plan says that actions will need to be taken to proactively address challenges in working across HSCT areas such as travel, recruitment, retention, and equity in the division of workloads.
2. In relation to transport and travel challenges, including ambulance services, the plan recognises that the movement of both patients and staff between services and sites will require crossdepartmental working alongside other key partners to address challenges around road infrastructure, the public transport network, and digital connectivity in rural areas.
3. On patient pathways, the plan states: “Patient pathways or a person’s route to treatment must be at the heart of system reconfiguration and discussed at the earliest possible opportunity. Pathways must be mapped with serious consideration given to stakeholders required to ensure pathways work in a seamless way and in the end create a more efficient and effective outcome for both patients and staff.”
Hospitals: Creating a Network for Better Outcomes proposes a total of 13 actions ranging from a review of the Department of Health’s Transport Strategy, through to designating Causeway as an elective care centre, and the definition of a suitable level of protected bed base, diagnostic and theatre capacity for regional specialist services.
Opening the consultation to the plan in early October 2024, Minister Nesbitt said: “While every hospital cannot provide every service, each hospital will still play a vital role, not just in their local communities but as a valued part of a planned regional system.
“This document can help assure communities that reconfiguration of services is not about cutting costs or closing hospitals. It is about managing change in a controlled way and demonstrating the benefits. It’s about showing how each hospital can fit into the network and best serve patients.
“Change is happening. We see that with the increasing shift towards centres of excellence such as standalone elective care hubs. This is reform in action but there is much more to do. A collaborative approach can better sustain our network to the benefit of patients and staff.”
However, publication of the document was met with some scepticism from MLAs. Diane Dodds, the DUP’s health spokesperson described the plan as “underwhelming”, and pointed to a lack of detail in the publication.
“Eight years on from the Bengoa Report, why is the focus still on principles? Surely we have had all the frameworks we need?” she stated.
Similarly, the SDLP’s Health Spokesperson Colin McGrath MLA said: “Without concrete proposals or timescales there is genuine concern that transformation could once again be allowed to drift. We have heard

multiple health ministers pay lip service to the notion of transformation but what we need now is delivery to transform our health service and make it fit for purpose to provide patients with the care they need.”
Health Minister Nesbitt has indicated that Hospitals: Creating a Network for Better Outcomes was the first of a series of planned announcements and publications aimed at setting health and social care services on a clear path to recovery.
Following the publication of the plan, the Minister has set out plans to publish a major review of maternity services and a three-year strategic plan for the remainder of the mandate.
Highlighting that the current financial position makes progress more difficult, he adds: “While the Programme for Government sets out the limits that the present budgetary situation places on efforts to reduce waiting lists, I will continue to make the case for significantly more funding for health.
“I have no time for the argument that money alone is the solution to the health service’s ills. Equally, anyone who suggests it is not part of the answer is sadly mistaken.”

Action 1: The Department will work with the Executive departments to consider carefully the travel support available for our population.
Action 2: DoH to review 2007 Transport Strategy for Health and Social Care services in Northern Ireland.
Action 3: HSC Trusts to continue to consider how their local hospitals can best and most sustainably meet local population needs.
Action 4: Consideration to be given as to how in the short to medium term HSC Trusts can work in collaboration to maintain these core general hospital services.
Action 5: Consideration to be given to designating Causeway as an Elective Care Centre.
Action 6: Consideration to be given as to the most sustainable allocation of resources across area hospitals to minimise inequities in access to services.
Action 7: Consideration to be given to moving suitable activity out of specialist regional centres into area hospitals.
Action 8: Consider approach to clinical training to ensure that job roles best match current and future population health needs.
Action 9: Consider how the allocation of doctor training places and development of new roles such as advance practice roles can best support service sustainability across the hospital network.
Action 10: Continue with a rolling programme of speciality specific workforce reviews, to encompass all skill mix roles.
Action 11: Review regional specialist services and identify those most vulnerable. Consider how vulnerabilities can be mitigated, for example through strengthening links with colleagues in Britain and the Republic.
Action 12: Define a suitable level of protected bed base, diagnostic and theatre capacity for regional specialist services.
Action 13: DoH to explore with HSC Trusts and NICON how provider collaboration might help to support and sustain the hospital network.
2001 Maurice Hayes Review:
The review recommended reducing the hospitals, amalgamating health boards into one, integrating health and social care, removing accident and emergency services from five of Northern Ireland’s smallest acute hospitals.
2011 Compton review:
Transforming Your Care: A Review of Health and Social Care in Northern Ireland offered a range of proposals including a 50 per cent reduction of Northern Ireland’s 10 acute hospitals and the opening of new health and care centres in Banbridge, Ballymena and Omagh.
2014 Donaldson Report:
The review recommended closing local hospitals and self-management of chronic disease based on an understanding that there too many hospitals and expertise was being too thinly spread.
2016 Bengoa Report:
The basis of a 10-year plan introduced by then Health Minister Michelle O’Neill, the review set out 18 timespecific action points aiming to improve services, cut waiting list times and improve care for an ageing population. Underpinning the review was the need to transform heath and care service delivery on the understanding that the existing model was unsustainable.
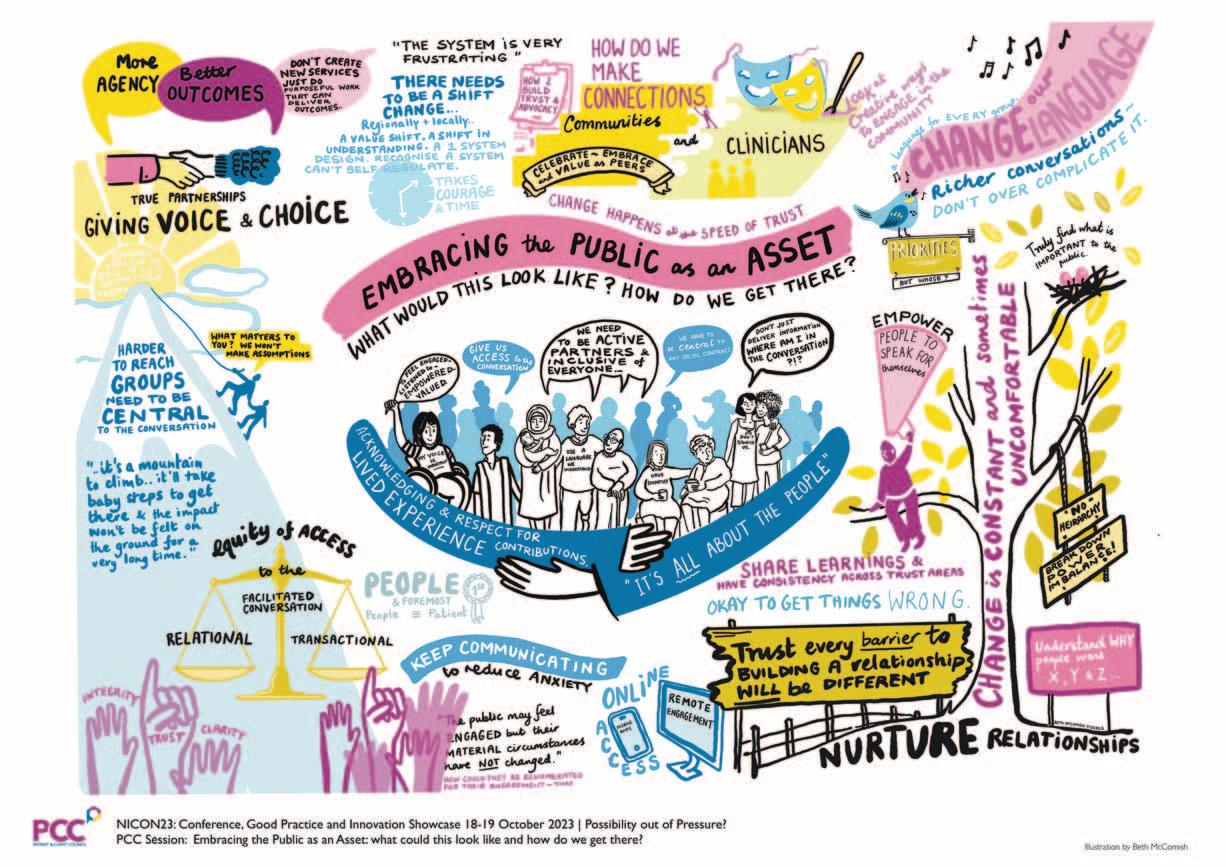
Being able to hear, understand, and strategically address people’s issues is vital to tackling the causes of persistent health inequalities, writes Patient and Client Council (PCC) CEO, Meadhbha Monaghan.

One of Health Minister Mike Nesbitt MLA’s key areas of focus is tackling the persistent health inequalities which exist in Northern Ireland. The draft Programme for Government and the Live Better initiative place a clear and welcome focus on this issue.
We know there are numerous social and economic determinants of health inequalities and it is right to recognise that addressing these will require a cross-cutting and cross governmental approach.
Through their lived experience, the public know what their needs and those of their communities are, what has worked and what has not. To this end, there is a growing recognition of the need to more effectively involve the public in policy development, public sector reform, and in delivering effective and safe services.
This is underpinned by the need to change the nature of the relationship between the public and services, from one of passive recipients to active partnership.
A strategic and cross-governmental approach to public participation, which embraces the public as assets and has the ethos of partnership at its core, has the potential to shift the dial on delivering much needed public sector reform and sustainably tackling health inequalities. With the statutory duty of Involvement that exists across the health and social care (HSC) system, there is the potential for the HSC to lead in this area.
Being able to hear, understand, and strategically address people’s issues is vital to shaping services which meet the diverse range of people’s needs and to tackle the causes of persistent health inequalities. People who are facing health inequalities often face difficulties accessing, navigating, and resolving issues about HSC services, which can be extremely complex. They can often go unheard.
The PCC provides independent advocacy support to the public who may have an issue in health and social care. Our focus is on working with HSC organisations to find a resolution to people’s issues.
Advocacy support is not only vital for individuals and families, it is a key part of assurance within the HSC system; it can reduce the potential for compounded harm, build trust in services, enhance potential learning, and address inequality and inequity in complaint and engagement processes.
In an effort to make our services more accessible, over the coming months PCC are working with voluntary and community organisations and others already embedded in local communities, to bring our trained practitioners to different locations across the region. Our aim is to reach members of the public who may not usually access our services. By building relationships with local communities and voluntary and community organisations, we aim to work collaboratively to do our part in helping reduce health inequalities through accessible advocacy support.
The overall landscape of advocacy service provision is, however, fragmented. At the PCC we are making the case for regionally commissioned independent advocacy services. Such an approach would give assurance that the public has consistent access to advocacy support. This, in turn, would help develop a strategic approach to public participation and tackling longstanding health inequalities.
T: 0800 917 0222
E: info@pcc-ni.net
W: www.pcc-ni.net
X: @PatientClient


With such an enormous impact now and into the future, we cannot afford to ignore dementia

Many of you reading this will personally know the impact of dementia on those living with it. It is a profound personal and family challenge, but the impact does not end behind closed doors. The pressure on the health and social care (HSC) system, and the huge personal and economic costs present the most urgent health challenge of our time, writes Ruth
Barry, National Influencing Manager at Alzheimer’s
Society.
The numbers are daunting. The cost of dementia in Northern Ireland is £1 billion a year now, forecasted to reach £2 billion in just 15 years. Tragically, that cost falls most heavily on those living with the condition and their carers (63 per cent). We, at Alzheimer’s Society, are determined to change this and, not only shine a light on the scale and urgency of the challenge but – for the first time –clear, evidence-based actions to ease pressure and reduce cost.
Around 25,000 people are living with dementia in Northern Ireland today, and at least a third of these people do not have a diagnosis. Research commissioned by Alzheimer’s Society estimates the number of people living with dementia will increase from approximately 25,000 to 37,500 by 2040. The scale of the increase is the highest amongst equivalent figures for England and Wales.
We can, and must, challenge the status quo. Policymakers have not prioritised dementia, and the rising costs and pressures are relentless. There are clear, positive choices that can be made NOW and must be made to support the HSC system to address the challenge presented by dementia, now and into the future.
At the recent NICON conference, Heath Minister Mike Nesbitt MLA stated that if we do not make radical changes within the next 15 years; the health service will swallow up all public funding.
Let us choose to take a different path.
Today, across the UK, almost one million people with dementia access A&E every year, one in every six hospital beds are occupied by someone with dementia, and people with dementia make 16.2 million visits to GPs every year.
We are not simply pointing out problems in the system, we are presenting an overwhelming, evidence and policybased case for change. Our evidence shows that people who are undiagnosed are disproportionately drawing on healthcare resources. Those who are undiagnosed are three times more likely to visit A&E than people without the condition. Undiagnosed people with dementia visit A&E more than people with mild, moderate, and severe dementia. If we do not act now, the health service will be completely overwhelmed.
The current diagnostic pathway is slow and disjointed, with significant variation in the quality of diagnosis services across Northern Ireland, including speed of delivery, accuracy and referral to support services. On average, a dementia diagnosis takes 3.5 years from the onset of symptoms, with no specific national target included in the Regional Dementia Pathway published in 2018 (which remains to be fully funded and implemented).
We have clear evidence that demonstrates the importance of early and accurate diagnosis yet spending on diagnosis and treatment in the UK is equivalent to just 1.4 per cent of dementia healthcare costs – in contrast, a third of all dementia health spend is in unplanned hospital admissions. We need to invest in dementia diagnosis through enhancing access to diagnosis services and collecting national and local

diagnosis data. Without this, people will not be able to access existing treatments and interventions to help manage their symptoms today or be ready for the disease-slowing treatments of tomorrow.
Diagnosing someone with the UK’s biggest killer is more than just a moral duty. It unlocks access to support and potential treatments or interventions which directly translates into reduced system pressure.
We now know, through the research Alzheimer’s Society commissioned from Carnall Farrar, that the average annual cost of dementia per person increases as the condition progresses, going from £29,000 for mild dementia to £81,000 for severe dementia. These are enormous cost differences and anything we can do to intervene early and effectively is critical.
By diagnosing people just one year earlier and providing access to these NICE-approved treatments where they are effective, modelling suggests there could be savings of tens of thousands of pounds by delaying the onset of severe symptoms. By delaying the impact, people with dementia can enjoy their independence and a better quality of life for longer, meaning that nursing home admission and expensive, intensive care required for more severe dementia, comes later down the line.
More research is needed to fully understand the impact of the available treatments. What we do know is that they are most effective the earlier they are given. To achieve these savings, we first need to diagnose people and diagnose them earlier.
Minister Nesbitt has set out his priorities, an intention to ‘reboot Bengoa’ and a renewed focus on dementia through the Regional Dementia Project Board. We know in starker terms than ever before that the foundations for delivering better care for people, for easing pressure, for reducing cost – begin with improving diagnosis.
As Lord Darzi says, citing our evidence in his recent report on the state of the NHS in England: “There is an important challenge to improve the quality and quantity of care for people with dementia.”
I could not agree more.
It will take a society to beat dementia. This is a challenge which must be faced and faced now. It will take all of us together.
Call: 0333 150 3456. If you are affected by dementia, worried about a diagnosis or a carer, trained staff are ready to give you the support you need.



Chief Digital Information Officer at the Department of Health, Dan West, discusses the current and future benefits of ongoing digital transformation in the health and social care sector.
Outlining the vision of the Department of Health’s 2022 Digital Strategy to deliver, before the end of the decade, the transformation of health and social care into a highly integrated and personalised system, with services tailored to an individual’s genetics, being data driven, and optimised by advancements in digital technology, West is quick to point out an existing projection that, without successful interventions, by 2040 the entirety of Northern Ireland’s block grant would need to be dedicated to health and social care services, due to the current trajectory of healthcare inflation.
“It is a stark figure and driving the digital transformation of health and social care in that financial context is not straightforward,” he explains.
The Department of Health’s Digital Strategy, alongside underpinning data, cyber security, and innovation
strategies, outlines the strategic intent to 2030 and represents a £1.3 billion investment portfolio. Outlined in the strategy is an overarching vision of “making lives better for the people of Northern Ireland, using digital to transform the way we deliver health, care and wellbeing services”.
Underpinning this vision, West explains, is a recognition that without transformation: “Our children will not be able to get health and care in the way we expect to get it, unless we do something bold and different in the way we deliver those services.
“We need to change experiences, both for staff who give the care, and for service users who receive the care, and we need to drive transformation in a very different way than we have done over the last few years. This strategy helps us to understand that,” he says.
Currently, says West, the Department is
doing a lot of “programmatic delivery”, which he explains is aimed at addressing technical debt and historic underinvestment.
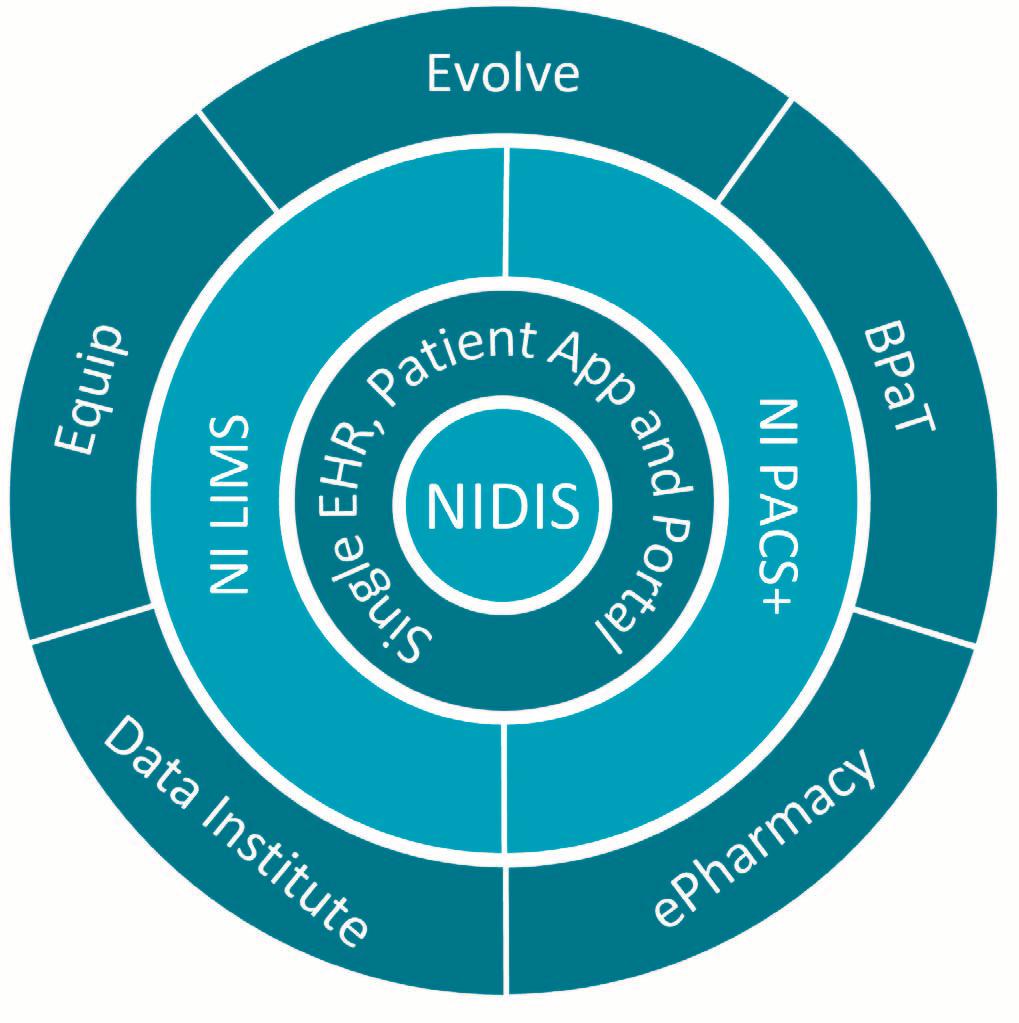
Offering a high level look at the investment portfolio, he points to the development of the ‘Encompass’ single electronic health record (EHR) being delivered on top of the Northern Ireland Digital Identity Service (NIDIS), both of which launched in 2023. This has enabled the ongoing rollout of converged clinical platforms, including Northen Ireland Laboratory Information Management System (LIMS) and the Northern Ireland Picture Archive and Communication System (NIPACS+), across secondary hospital care, mental health, community and social care services.
Wider again is the current delivery of some 80 projects in the enterprise portfolio delivery phase, with a further
Source: Department of Health
80 in earlier stages of discovery, business case development, procurement or design –all aiming to improve care services and data capabilities. Included in the next wave of transformation are two investments that replace significant and outdated IT infrastructure and systems: the Northern Ireland Blood Production and Tracking project, to build a new vein to vein blood product tracking platform, and the Equip programme, which replaces current backoffice systems with the new Oracle Cloud platform.
“Equip is a hugely impactful programme, and a really important next step for Northern Ireland – it will drive convergence and modernisation in our back office and provide a new technology platform for delivery of finance, procurement, logistics, HR and payroll”, explains West.
Highlighting recognition that much of the early work has been centred on technology, but that technology is not the end in itself, he stresses that improved services are about improved economic outcomes and improved health and social care for society.
“We need to pivot away from the big delivery activities of the last few years, and having broken the back of our technical debt, start thinking more about how we leverage the new platforms, build our capabilities to do transformation at the front line of service delivery, and make care better for people in this region.
“Building a new digital transformation and innovation capability collectively from the centre out to all of the care delivery organisations and care professionals is a large area of focus for my team currently.”
Reflecting on the successes of the last few years, West outlines what has been a busy implementation roadmap.
Since 2019, the Department has been developing a range of business cases, and working with stakeholders, particularly financial leaders with economic responsibility to approve the investment portfolio. While the outbreak of Covid-19 served to disrupt the planned digital journey, West explains that much progress was made on digital transformation during this time.
Pointing to the rollout of a completely new Microsoft environment, the CIO explains that this underpinned the convergence of clinical services and the enablement of remote working during the pandemic.
West goes on to explaining that by May 2025, the Department will have completed the roll out of Encompass, which will be “globally unique” as a single, national platform including both health and social care services being supported by a single system.
Discussing the impact of progress to date, West says: “‘Once of Northern Ireland’ should not be overlooked.
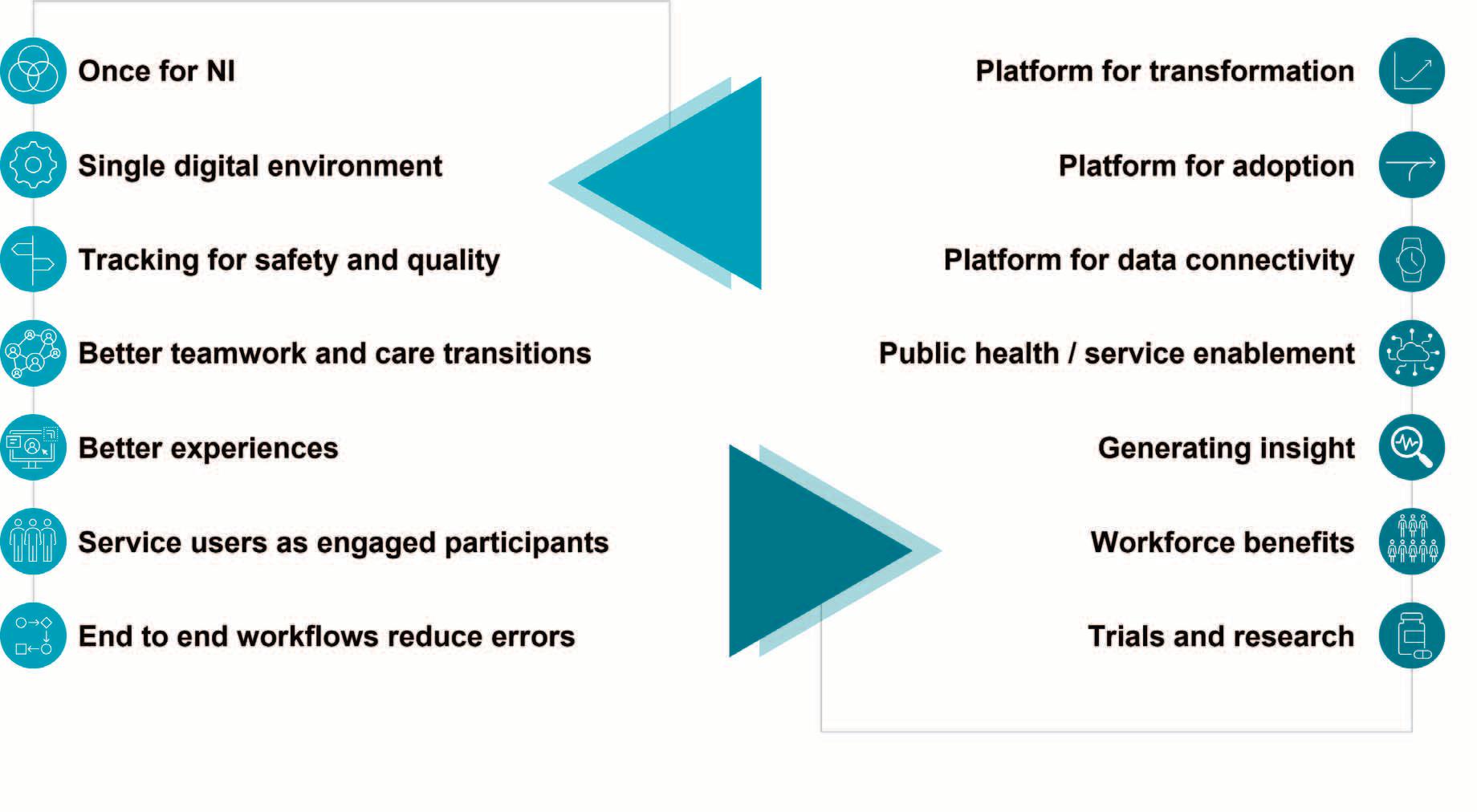

“The fact that we now have a single converged platform for all organisations and services in secondary care, mental health, community services, and social care, to deliver care models and care outcomes, is a huge accomplishment. Health and social care delivery is understandably complex, so the ability to simplify this by delivering a single platform brings a lot of benefits.
“The single digital environment brings all professions and services into one information environment, digitally enabling a range of workers who would not previously have had access to technology. We have rolled out masses of end user devices and end points to staff who otherwise would not have interacted with digital records as part of the way they do their jobs.
“A second advantage is the ability to track for safety and quality. We now have a single place to automate the movement of work around our system. Diagnostic tests in laboratories and in medical imaging currently move digitally through the system, based on the new platform. Now, we can bring diagnostic results into clinical workflows and provide protocolised alerts to clinicians involved in the care of an individual.”
Other benefits outlined by West include better teamwork and efficient care transitions; better service user experiences; service users as engaged participants; and the reduction of errors in end-to-end workflows.
Returning to the vision of helping clinicians to transform the services they
Source: Department of Health
deliver, West recognises that between 80 to 90 per cent of all healthcare interactions occur in primary care, he says: “Having made some headway in digitising secondary care, we need to shift focus to think about how we are going to work with stakeholders to help transform primary care, including community pharmacies – there is huge benefit in working with GPs to continue to improve digital capabilities in practices and in how our GPs enable services for citizens.”
West reflects on the fact that the investments are not about digitising the current operations “What we have built and bought for ourselves is an ability to drive change in a very different way than we did before. Converged platform and converged capabilities allow us to influence change more easily than we were able to before.
“We have got better connectivity, and will be able to ingest a broader range of data sources, including wearables, in order to manage chronic diseases, without putting the burden onto clinicians for dealing with that data.”
Concluding, West says: “The goal is not the technology, the technology is a means to an end – the ultimate goal is improved care outcomes, better care experiences for service users and staff, and a more sustainable health and care economy for our children. Healthcare is not about technology, it is about people.”

Although more than 28 per cent of individuals who died by suicide in 2022 were in contact with the relevant authorities before their deaths, the Department of Health has extended Protect Life 2, its existing suicide prevention strategy, by three years.
In October 2024, the Department of Health extended Protect Life 2: A Strategy for Preventing Suicide and Self Harm in Northern Ireland 20192024. When it was published in 2019, the Protect Life 2 Strategy aimed to achieve a 10 per cent reduction in suicide rates across Northern Ireland by 2024, a figure which may have been achieved, but classification of deaths means that the data thus far is too unreliable to decipher whether this target has been met.
Despite this potential progress, the most recent statistical release on deaths by suicide by the Northern Ireland Statistics and Research Agency (NISRA) shows that more than 28 per cent of individuals who died by suicide were in contact with relevant authorities before their deaths.
Furthermore, suicide rates in Northern Ireland’s most deprived communities remain three-times higher than in the least deprived areas, even after the efforts initiated under Protect Life 2. The strategy’s broad-based initiatives, have failed to meaningfully address these community-specific vulnerabilities, such as poverty, limited access to mental health services, and
higher social isolation. More targeted, and adequately funded, interventions tailored for at-risk populations are essential to address these gaps effectively.
Although Protect Life 2 underscores the importance of a multi-agency approach, evidence suggests weak levels of collaboration between health, education, and social services, particularly in rural and economically disadvantaged areas. The progress report indicates that while local groups met to advance strategy goals, a coordinated, overarching structure for cross-departmental action remains lacking. As a result, existing initiatives are fragmented, leaving many at-risk individuals without cohesive, accessible support systems.
The strategy’s extension suggests a continued need for robust crisis and postvention support, especially in rural areas where crisis intervention resources are sparse. Services like the Multi-Agency Triage Team (MATT) and the Lifeline helpline have helped address acute mental health crises, but analysis shows that these programmes are limited by underfunding and are not universally accessible. Effective,
region-wide crisis response remains crucial for de-escalating crises and supporting those bereaved by suicide, yet this component is currently underresourced.
Protect Life 2’s funding – £8.7 million annually – has proven insufficient to meet the needs of Northern Ireland’s most vulnerable populations. Additionally, data limitations hinder timely responses and targeted adjustments, with a recent review of suicide data from 2015 to 2020 revealing inconsistent classifications of deaths, thus complicating long-term tracking of suicide trends and areas needing immediate attention.
Speaking upon publication of a review designed to examine these failures – in spite of the review coinciding with the extension of the existing strategy –Health Minister Mike Nesbitt MLA stated that it is “clear that the research supports the need for collective action and sustainable funding and investment if the Executive is to deliver on the Protect Life 2 Strategy”, and further committed to develop a new draft action plan to be taken forward by Executive departments and delivery partners.

With its mission of a healthy and sustainable district, which provides better economic, environmental and social outcomes for all, Newry, Mourne and Down District Council is blessed with both significant natural assets and an enviable level of outside investment.
Key projects ranging from the multi-million pound Newry City Park to the Be Active for Life programmes in local leisure centres are being delivered to equip and encourage its citizens to improve their health and wellbeing by becoming more active.
Improving the health and wellbeing of its approximately 181,363 residents and reducing health inequalities has been a key strategic objective for the Council area, which spans the south east of Northern Ireland, bordered by a 150km coastline. Overlooked by three Areas of Outstanding Natural Beauty, it is an area now proudly home to the Mourne Gullion Strangford UNESCO Global Geopark.
As per the Council’s Corporate Plan (2021-2023), to “continue to improve the health and wellbeing of everyone in the district and reduce health inequalities” and to “enable and support people to engage in inclusive and diverse activities in their community” were two key drivers for investment into a series of projects. This resulted in more people participating in targeted health programmes and facilities to encourage more active lifestyles. Improving the health and wellbeing of everyone in the
district will also remain a key priority of the new Corporate Plan being delivered for 2024 to 2027.
By way of a stocktake, and in identifying the needs of the district, Newry, Mourne and Down District Council has worked with partners and stakeholders in the public, private, community and voluntary sectors to create key strategies which have shaped the direction of investment. These include a Sports and Physical Activity Strategy 2024-2029, Play Strategy Review, Sports Facilities Strategy and Sports Hub Review. Through these strategies, key areas for enhancements have been identified and the Council will be working with external funders to support the projects.
One key project is the development of Newry City Park, to be located on a 15acre site at the Albert Basin within the heart of Newry city centre.
The Council’s Outline Business Case for Newry City Park was approved by the Department for Communities and a Contract for Funding was issued in December 2023 — opening access to £16.2 million from the Executive’s City Deal Complementary Fund. The Council is providing £2.4 million of match funding
to deliver the 15-acre City Park as part its Newry City Centre Regeneration Programme of works, and it is anticipated a planning application for the park will be submitted in the coming months.
The park is set to provide a state-of-theart facility encompassing a sensory garden, urban sports areas, an inclusive play park, water sports facilities, an events plaza and woodland trails. With an absence of any such provision currently within the city, this facility will significantly attract footfall from across the district and beyond whilst increasing participation amongst an array of sport and leisure amenities.
With more of our residents spending a greater amount of time outdoors, the Council in conjunction with the Department of Agriculture, Environment and Rural Affairs (DAERA), Sport NI and the Woodland Trust have invested £1.9 million from 2017 to the present day in creating and updating 13 walking trails, covering 40km.
The trails are located in Glendesha Forest in Forkhill, Seaforde Plantation Wood, Corry Wood and Bunkers Hill near Annsborough, Drumkeeragh Forest, Windmill Hill/Lough Park near Ballynahinch and Ballynahinch Rugby Club, Glasswater Wood and Tobar Mhuir Wood near Crossgar, St Patrick’s GAC in Saul, Aughrim Hill Trail near Kilkeel, Tievenadarragh Wood near Drumaness, and Daisy Hill Wood in Newry. 263,364 visitors accessed the trails in 2023/24.
The Council's Play Strategy (2017) was established to create an effective strategic framework for decision making in relation to the development, maintenance and roll-out of play opportunities across the district.
Following a £3.2 million investment between 2017-2024 by the Council and the Northern Ireland Rural Development Fund (DAERA), six new play parks have been developed and over 30 existing parks have received significant enhancements which has increased the Council’s Play Value by 23 per cent amongst low value play parks and 23 per cent also amongst mid value play parks.


Newry, Mourne and Down District Council recently completed a Play Strategy Review, which has identified another 14 parks that will be upgraded over the next four years, demonstrating both Council and funders’ clear commitment to supporting the Child’s Right to Play as articulated in the UN’s Convention of the Rights of the Child, Article 31.
The Sports Facility Strategy commissioned in 2017 also identified sporting facilities throughout the district which required upgrades. Having completed this assessment, £1.8 million was invested both directly by Council through Capital Projects and via the Council’s Financial Assistance Grants, to upgrade facilities. On completion of the Sports Facilities Strategy, the Council carried out a Multi Sports Hub Review in 2022 addressing the need of eight sports such as association football, Gaelic games, rugby and athletics.
A projected budget of £3.5 million has been set to deliver large multi-sports hubs in each of the seven district electoral areas, for example The Donard Park Project in Newcastle and Jennings Park multi-sports Project, Newry.
In terms of targeted, measurable health improvements, Newry, Mourne and
Down District Council deliver a bespoke programme called Be Active for Health and Be Active for Life.
The latter is a Newry, Mourne and Down District Council initiative which delivers physical activity classes to a broad demographic from teenagers, to parent and baby, to older and less active residents. The programme, funded fully through the Council, delivers a series of low-to-moderate intensity classes. It attracts those who are new to physical fitness or want to embark on a journey of increased movement and physical and mental wellbeing.
In relation to the Be Active for Health programme, the Council is committed to the Physical Activity Referral Scheme (PARS), a GP referred, 12 week physical activity programme which is delivered in partnership with the Public Health Agency.
Those on the programme benefit from prescribed physical activity such as walks, group-based exercise classes and gym based programmes in a social setting, which collectively aid the rehabilitation of health conditions such as hypertension, elevated cholesterol, diabetes, heart disease, asthma, bronchitis or COPD, musculoskeletal disorders and mild or moderate mental health problems.
Through the delivery of the Council’s Be Active for Life and Be Active for Health programmes, over 10,805 participants have benefitted from targeted physical activity programmes in 2023/24.
Whilst such investment from government departments and organisations has delivered quantifiable outputs against health and wellbeing objectives, this investment is having a positive impact on other strategies. Through the provision of these facilities and programmes, it contributes to other objectives such as increased activity tourism, investing in job creation, enhancing our environment and promoting the revitalisation of our city, towns, villages and rural communities.
The Belfast Region City Deal, together with complementary fund investment, will see almost £200 million invested in the Newry, Mourne and Down area over the next 10 years, in what is a once-in-ageneration opportunity for the district.
It is a district positioning itself as one of the best places to live, work and visit, and improving the health and wellbeing of its residents will remain central to the quality of life to be enjoyed in Newry, Mourne and Down as it transforms over the next decade.
T: 0330 137 4000
E: info@nmandd.org
W: www.newrymournedown.org


In May 2024, the Health and Social Care (HSC) announced that it would broaden care service provision through the integrated care model, unique to Northern Ireland.
An integrated model is a single, joined-up system, based on bringing different parts of the health and social care system together with others who have a role in the wellbeing of the Northern Ireland population to understand what is needed, and how we can best deliver that with the resources we have.
In a review in June 2024, the British Medical Association (BMA) asserted that the significant pressures in social care in Northern Ireland is “a direct result of inadequate resourcing”.
The BMA adds that “there does not appear to be a mechanism to capture and disaggregate spending on social care, despite the integrated structure”. Aiming to overcome challenges such as rising demand, resource constraints, and significant health inequalities, the Integrated Care System (ICS) Framework shifts away from traditional, fragmented healthcare models towards a collaborative and population-focused system.
The ICS Framework emphasises the roles of preventive care, early intervention, and empowering communities in their health management. A key priority is to reduce health inequalities by targeting social determinants such as socioeconomic status and environment. This framework is anchored in a population health approach, which aims to enhance the wellbeing of entire communities rather than solely focusing on individual health outcomes.
Structurally, the ICS Framework operates through five area integrated partnership boards (AIPBs), each aligned with health and social care trust areas. These boards consist of representatives from various sectors, including HSC trusts, GPs, pharmacies, local councils, and the voluntary sector. AIPBs will create localised health and wellbeing plans based on a population health needs assessment, ensuring resources are directed toward the most pressing needs within communities. They work closely with the Strategic Planning and
Performance Group (SPPG) and the Public Health Agency (PHA) to align with regional priorities while maintaining local responsiveness.
At the regional level, the ICS Framework Partnership Forum aims to foster coordination across AIPBs and identifies opportunities for broader collaboration. This body provides AIPBs with strategic guidance and enables shared learning and best practice exchange, promoting a cohesive approach to addressing common challenges and scaling effective solutions across Northern Ireland.
The framework’s governance model ensures that each partner organisation maintains its statutory responsibilities while promoting accountability through outcome-based metrics tied to the overarching Strategic Outcomes Framework (SOF). The SOF guides longterm population health goals, while the System Oversight Measures (SOMs) offer short-term performance metrics to ensure progress toward these outcomes.
Budget 2023/2024 allocation: £7.3 billion
Over 73,000 HSC staff (as of December 2023)
Over 300 GP practices and over 1,400 GPs (excluding locums) with over two million registered patients (as of 31 March 2023)
Over 540,000 inpatient and day case admissions in 2022/23
Over 750,000 attendances at emergency departments (March 2023)
Over 119,000 patients waiting to be admitted to hospitals –over 77 per cent waiting more than 13 weeks (June 2023)
Over 22,500 people receiving 296,000 hours of domiciliary care each week in 2022/2023
Almost 23,000 children in need and over 3,800 children in care in 2022/2023
Source: HSC
The 2024/2025 Delivery Plan, published in July 2025 by the Social Care Collaborative Forum – a collaboration between the Department of Health and the Northern Ireland Social Care Council – is grounded in three primary themes: workforce sustainability, innovative care models, and improved commissioning and contracting. These themes inform each workstream’s actions and objectives, balancing immediate, actionable reforms with foundational steps for a robust future social care system.
1. Workforce sustainability: The social care sector’s workforce challenges are welldocumented, from recruitment hurdles to retention challenges exacerbated by Covid-19 pandemic pressures. The action plan’s workforce initiatives include implementing a new Social Care Workforce Strategy to guide workforce planning over the next decade, offering clear career pathways and opportunities for ongoing professional development. Efforts also include expanding international recruitment and enhancing support for foreign-trained staff, aiming to alleviate critical workforce gaps by March 2025.
2. Innovative care models: Recognising the need for capacity expansion, the SCCF is pioneering new models of home care delivery that go beyond traditional task-based approaches. A statutory digital home care solution is set for completion by December 2024 across all trusts,


promising efficiencies that could significantly reduce delays in service delivery. Additionally, the action plan aims to advance a regional brokerage system to streamline independent sector home care provision, facilitating quicker response times across trust boundaries.
3. Enhanced commissioning and contracting: Ensuring value and consistency in social care services is a central focus. By December 2024, the Department of Health aims to complete a comprehensive review of care home contracts, aligning standards with recent legislative and operational changes. The action plan further underlines that preparation is underway for preprocurement processes to facilitate streamlined, regionally consistent contracts that trusts can deploy starting in 2025. This reform aims to offer clearer contractual guidelines for providers, including potential VAT reclaim facilitation for restructuring independent sector providers.
Speaking in the Assembly in July 2024, Health Minister Mike Nesbitt MLA emphasised the critical role of integrated care in transforming healthcare quality and health outcomes.
He stated: “We need to reorganise hospital services and how we will manage our hospital system as an integrated network. This requires a shift from viewing individual hospitals as discrete units to embracing the idea of a network of interdependent hospitals.”

Despite a 10-year blueprint for mental health service improvement, “derisory” funding means that it will be impossible for this strategy to achieve its objectives, writes Deirdre Heenan, Professor of Social Policy at Ulster University.
Prior to the restoration of the devolved government, our politicians rarely missed an opportunity to reassure the public that addressing poor mental health was one of their key priorities. Notwithstanding these worthy pronouncements mental health services in Northern Ireland are being left to fail.
Patients and service users struggle to access both routine and urgent care. Their inability to access the help that is required is having a severe knockon effect on other parts of the health service. Frequently, people in crisis are forced to go to emergency departments in search of assistance. These busy, noisy, and challenging environments are completely inappropriate for those presenting with mental health issues.
In a recent report, the Northern Ireland Audit Office (NIAO) warned that Northern Ireland’s mental health crisis is costing the region more than £3 billion per year. Escalating waiting lists, underfunding, a depleted workforce, fragmented services, and lack of access to services are just some of the challenges.
Current waiting times have led to an increased level of stress for those living with chronic conditions, or acute conditions leading to a spiral of worsening physical and psychological health. The inability of the system to cope with demand in an appropriate way, means tragic stories of anguish to individuals, families, and communities are all too commonplace.
Recommendations from seriously critical reviews have not been implemented and the same errors are repeated. A lack of independent oversight means follow-ups do not happen and change is not followed through.
The voluntary and community sector which provides essential services, is under unsustainable pressure. A number of organisations are at a risk of closure as budget constraints mean that they are stretched beyond their limits. Their frustration is palpable. Despite their best efforts they are unable to secure appropriate care and support for those who had reached out for help. They describe a system that is profoundly broken.
Figures for December 2023 record a total of just over 17,500 people awaiting a first appointment to access mental health services. Within this, psychological therapies represent a disproportionate share, with around 6,500 people waiting to access services.
Alongside this, performance against waiting time targets has also continued to deteriorate. Worryingly, around threequarters of those on psychological therapies waiting lists, as of December 2023, had been waiting longer than the 13-week target time. As a result, service users and their families feel that they cannot get the help that they need.
Without timely treatment, however, peoples' conditions will deteriorate, becoming more difficult and costly to treat.
“Mental
Deirdre
Many mental health challenges are preventable and therefore the costs to society could be reduced or avoided. Research has shown that early intervention works and is cost effective. Yet, in March 2023 the only funded primary school counselling programme Healthy Happy Minds was axed due to budget cuts.
Waiting until someone is in crisis and asking them to navigate a system not designed for their needs is bound to end in failure. People are not getting the help that they need, they are not assessed quickly enough, and often are unable to contact crisis teams directly. Being turned away because you are not ‘suicidal enough’ or waiting for hours in a hospital to be told to contact your GP in the morning, is not unusual. There should be no wrong door for people seeking help and assistance.
Northern Ireland is reported to have the highest prevalence of mental illness in the UK. Yet, at 7 per cent, the proportion of the health budget allocated to mental health remains significantly lower than that of the other regions. The most recent figures indicate that the proportion in England is 11.39 per cent, in Wales it is 13.32 per cent and in Scotland it is 9.41 per cent.
In June 2021, the Department of Health published a 10-year mental health strategy; a blueprint to modernise and
transform services. In a welcome development, this strategy was accompanied by a funding plan which set out the money required to execute the actions.
To date, progress in implementation has been deeply disappointing. Given the lack of momentum, it defies belief that the Programme for Government states that “we will redouble our efforts to improve the physical and mental health outcomes of Northern Ireland’s population and reduce inequalities, through continued implementation of, for example, the Mental Health Strategy 2021-2031”.
This year the Department of Health have committed just one-eighth of the necessary investment to implement the plan. This derisory level of funding means it will be impossible for this strategy to achieve its objectives. Worse, if timescales and objectives must be revisited, money that has already been spent has essentially been wasted.
Vulnerable people and their families are being repeatedly failed, causing avoidable suffering and distress. We have a blueprint for change but without drive and funding, the devastating consequences of mental illness will continue to blight this society.

The reduction of waiting lists and delivery of excellent care is a shared goal, it is time for a plan that enables NHS patients to immediately access private sector resources, writes Mark Regan, CEO, Kingsbridge Private Hospital Group.
Our NHS ambulances are built by Mercedes, our drugs are manufactured by Glaxo/Pfizer and dispensed by Medicare and Boots. The very buildings that make up the NHS estate in Northern Ireland are built by Farrans and Lagan, so why does the narrative “NHS good, private bad” still exist locally?
In England almost 60 per cent of all cataract surgery is delivered by private hospitals and as a result, less than 1 per cent of the population wait a year or more. In Northern Ireland, more than 14 per cent of patients wait 12 months or more for treatment – 20 times worse than
England. Yet, we are still so opposed to embracing a partnership with the private sector that worked so well during the Covid pandemic.
It is time to change the narrative of NHS versus private healthcare. We both share the same end goal – to reduce waiting lists while delivering excellent, timely, and effective diagnosis and treatment for patients.
In times of crisis, we pull together. Why should it be any different when it comes to tackling the ever-increasing waiting lists we face in Northern Ireland? Our
colleagues in the NHS face an uphill battle with the trajectory getting steeper by the day and the independent sector (IS) can help.
I am not proposing anything radical. In fact, Kingsbridge Healthcare Group has been the principal partner to the public sector NHS/HSC since 2005, accounting for the majority of outsourced procedures during that period. We currently have over 100 live contracts, in all specialties, with the HSC, meaning that should funding become available, patients can be outsourced within days to Kingsbridge, and as per NHS core
principles, it would be free at the point of delivery to the patient.
Working in partnership with the NHS, Kingsbridge delivered more than 15 per cent of all surgery that took place in Northern Ireland last year.
During the Covid pandemic, we facilitated trusts by providing all of the main hospital beds and theatres on a not-for-profit, cost recovery basis to perform lifesaving operations for cancer patients whilst Belfast City Hospital was a nightingale hospital.
But there is an opportunity and a need to do more. We will only start to see any improvement when we move past the ‘private healthcare bad guys’ argument and recognise that efficient joint use of resources and capacity, in both the NHS and private healthcare providers is the only way forward.
The statistics speak for themselves. In Northern Ireland, 14 per cent of the total population are waiting more than a year for a consultation or surgery. To put that figure in perspective, this is 20 times higher than in England, where only 5 per cent are on waiting lists for this period of time.
In relation to cancer and specifically areas such as bowel, oesophageal, and stomach cancer, we know that 70 to 80 per cent of patients in Northern Ireland do not start treatment within two months of an urgent referral from a GP. Patients deserve better, and solutions only come with investment. Over the last two decades we have expanded our capacity as well as clinical capabilities and facilities through acquisition, capital expenditure, and new site development.
We pride ourselves on being pioneers bringing a number of firsts to Northern Ireland including the first private GP practice in 2008, a dedicated training academy for healthcare professionals including surgeons, new surgical techniques such as the Mako robotic surgery for hips and knee surgeries, and the very first private ICU opening at Kingsbridge in Belfast – that would allow us to assist the NHS in completing complex cardiac surgery.
Our team saw the opportunities in medical tourism and since 2015, under the Northern Ireland Planned Healthcare Scheme, we have treated over 61,222 cross border patients from the Republic.

In 2021, the HSCB, now the SPPG agreed that there was a need for a regionally accessible endoscopy centre. Despite the inability to secure any contracts from the public sector, Kingsbridge invested in a Diagnostic and Treatment Centre at the Kings Hall Complex. We now have the capacity to offer endoscopy to over 1,500 patients every month with urgent referrals able to access screening within seven days of referral from their GP.
These innovations should increasingly be made available to NHS patients, free at the point of delivery. The question is, how do we make this a reality?
The recent UK Autumn Budget saw an unexpected windfall of an extra £130 million for the Stormont Executive to spend on public services over the next two years with just under £100 million available for spending in the 2024/25 financial year.
While we all recognise the competing needs across the board, health should be a priority for the wellbeing of our local population if we are to meet the targets for increased productivity, and getting people back into work to secure our future economic growth and prosperity as outlined in the draft Programme for Government.
I would encourage our political leaders to seriously consider a plan of action that would allocate additional funding to health in a way that would allow NHS patients to immediately access private
sector resources, while the public sector takes the time to build its own capacity in the longer term. This move would effectively forge a path where, in partnership we can collectively make some serious headway in reducing waiting lists and delivering tangible benefits to the people of Northern Ireland.
The clock is ticking and the time for decisions is now. Let’s see some affirmative action that will allow us to move into 2025 with some much-needed good news and a positive plan for making a real impact.
Mark Regan
CEO Kingsbridge Healthcare Group reganm@kingsbridgehealthcaregroup.com
T: 028 9066 7878 W: www.kingsbridgeprivatehospital.com


The Department of Health’s Shaping the Future of Nursing and Midwifery in Northern Ireland: A Strategic Vision for 2023–2028 aims to establish a healthcare system where nurses and midwives operate “to their full potential” has no budget allocated and it is unclear how the proposed reforms will be implemented.

The Department of Health states that its mission is to support and enable nurses and midwives in providing safe, effective, and compassionate care. Central to this mission is a “healthful culture” defined by collaborative decision-making, innovative leadership, and continuous improvement. This environment creates a workplace fostering well-being and professional respect, going beyond healthcare delivery to include meaningful, supportive interactions among healthcare staff, patients, and families.
However, while the goals for the future cultural workspace for healthcare professionals have been outlined, the means through which this will take place is less clear, as there is no budget allocation for the strategy and there has been no public comment by Minister of Health Mike Nesbitt MLA.
Three strategic themes structure the vision: workforce stabilisation, a population health approach, and role transformation within multidisciplinary teams. Each theme represents a pillar aimed at creating a resilient nursing and midwifery workforce capable of meeting the needs of Northern Ireland’s population.
1. Stabilising the workforce: Workforce stabilisation is essential to achieving safe and effective care. Addressing workforce shortages, optimising workload management, and providing structured career pathways are fundamental to this priority. Creating stable and supportive working conditions prevents burnout and encourages retention, especially given growing healthcare demands. This theme prioritises workload planning and staff well-being, both critical for enabling providers to deliver consistent, highquality care.

2. Implementing a population health approach: Adopting a population health approach allows the Department to integrate public health, prevention, and early intervention into nursing and midwifery practice. This approach aligns with global practices prioritising the social determinants of health, promoting healthy behaviours, and reducing disparities. By focusing on public health and prevention, Northern Ireland’s workforce can proactively improve community health and reduce the demand on acute services over time.
3. Transforming roles within multidisciplinary teams: Recognising the evolving nature of healthcare, the vision seeks to empower nurses and midwives by expanding their roles within multidisciplinary teams. This approach creates a healthcare environment that values each profession’s unique contributions. By broadening roles, the Department enables these professionals to become essential members of patient care teams, fostering comprehensive, patient-focused care. This also offers significant opportunities for career development and job satisfaction.
To bring the vision’s themes to life, the Department outlines four immediate priority actions:
1. Workforce and workload planning
Effective workforce and workload management are crucial to meet current demands. A stable, wellsupported workforce enables care continuity and allows providers to give the time and attention required for person-centred care. Addressing workload pressures and improving resource allocation supports sustainable, high-quality care delivery.
2. Education and training
Continuous education and training equip nursing and midwifery professionals with the skills necessary for changing healthcare demands. Investment in high-quality education ensures professionals deliver safe, evidence-based care. Additionally, training that adapts to new healthcare needs enables providers to expand their competencies, preparing them for a multidisciplinary care model.
3. Career pathways
Clear career pathways attract and retain skilled professionals. By providing structured opportunities for advancement, the Department aims to foster a resilient workforce with a long-term commitment to the profession. Defined pathways allow providers to develop specialisations, pursue leadership roles, and broaden skills, contributing to personal and professional fulfilment.
4. Quality assurance framework
A quality assurance framework ensures care standards remain consistently high, fostering public trust in the healthcare system. Through structured quality control, this framework enables continuous improvement to meet evidence-based standards and community needs. Emphasising cultural respect, safety, and compassionate care, a quality assurance framework ensures equity and accountability in healthcare delivery.
At the core of this strategic plan is establishing a ‘healthful culture’ that promotes shared decisionmaking, transformational leadership, and innovation. This culture fosters empowerment and value for both staff and patients. Transformational leadership, combined with a supportive, inclusive work environment, encourages providers to take initiative, share insights, and work collaboratively.
A ‘healthful culture’ is cited by the Department as “essential for addressing psychological safety, morale, and retention”. By creating an environment where staff feel secure and appreciated, the Department states that it aims to prevent burnout and support mental wellbeing. This approach reflects a broader understanding of healthcare delivery that values patients and those who care for them.
The 2023–2028 vision aims to foster a culture by stabilising the workforce, embracing a population health approach, and enhancing roles within multidisciplinary teams, with the broad vision of ensuring healthcare providers are well-prepared, supported, and valued.
While the Minister has yet to comment on the strategy, Chief Nursing Officer, Maria McIlgorm, at the time of publication, said: “It is important that we will continue to work together to provide the resources and conditions to ensure that everyone involved in providing nursing and midwifery care can confidently and safely provide high quality evidence-based care.”

A public consultation on a prospective replacement public health bill has now closed amid much recrimination from within the Executive and beyond. Whether it results in new legislation within the remaining mandate of this Assembly mandate is questionable.
Following a review of the current Public Health Act (Northern Ireland) 1967, it was determined that the legislative framework for public health should be updated to respond to modern public health emergencies.
As such, Policy underpinning the Public Health Bill (Northern Ireland), a 79-page consultation document was published by the Department of Health in July 2024, remaining open to public consultation until mid-October 2024.
This follows the framework provided by the Department of Health’s March 2016 review of the existing legislation, which concluded that “the 1967 Act is deficient in a number of respects”. Among its 18 proposals, the previous review recommended that “the
Executive should include a public health bill in its legislative programme for the next Assembly mandate” as an “entirely new piece of legislation”.
Now, in his July 2024 foreword to Policy underpinning the Public Health Bill (Northern Ireland), Minister for Health asserts: “The overarching principle of the draft Bill is to protect the population against various forms of infection and contamination including biological, chemical and radiological, in addition to infectious diseases.
“This all-hazards approach will enable broader surveillance, supporting more timely and effective interventions, controlling the further spread of infection and contamination.”
On top of this, the summary
recommendations of the proposal document indicate that the new legislation should:
• update specific powers in relation to restrictions on employment, quarantine, isolation, and medical examination;
• detail the roles and responsibilities of relevant authorities; and
• determine the “underlying human rights-based principles” guiding the implementation of “powers of intervention”.
Given the significant public interest generated by the consultation, the Department of Health subsequently published a ‘fact file’ at the beginning of October 2024 to address “some misunderstandings” surrounding the document.
In this fact sheet, the Department emphasises:
• existing public health legislation is obsolete;
• a public health bill has yet to be published (though this contradicts the document’s foreword);
• public health powers relating to households, businesses, and schools already exist and are rarely applied;
• individual rights would be protected by comprehensive safeguards;
• existing legislation already provides for infected persons to be detained via a magistrates’ court order; and
• the Health Minister is opposed to mandatory vaccination.
In late September 2024, amid significant public interest – and what the Minister referred to as “some misunderstanding” – the consultation was extended by two weeks, with





emphasis placed on the subsequent Assembly scrutiny that any resulting draft legislation would face.
“I am determined that the planned ill will strike the correct balance between the state’s responsibility to protect the public’s health, our collective responsibility to protect each other, and the autonomy, rights and dignity of individuals,” he said.
Later, upon the closure of the consultation, the Minister insisted: “Public health interventions require legal backing, he says, adding: “Unless we are to seriously argue that individuals have the right to knowingly or unknowingly cause biological, chemical and radiological contamination or otherwise put the health and lives of others at risk.”
Following the closure of the consultation, the Minister acknowledged that “the public consultation on a proposed new public health bill was always going to be controversial” and suggested that it had “aggravated the scars” imprinted by the Covid-19 pandemic and associated public health measures.
Now, the consultation responses must be evaluated before a public health bill is drafted. “Then it will fall to me to bring forward a bill and seek Assembly
support. I look forward to further robust debate, which will offer opportunities for amendments which remove proposals and add others,” the Minister explains.
Indeed, the “robust debate” is already well underway and will continue for some time. For example, in an oral response to the SDLP’s Colin McGrath MLA during an Assembly questions session in October 2024, Nesbitt indicated that he had “not yet had a briefing on the number of responses” and added: “No bill has been written, and the Bill’s composition will be dictated to an extent by the public’s reaction to that consultation process. However, it will also be up to the Assembly and the Committee for Health to decide the shape of the Bill.” The Minister also remarked that he is “personally not in favour of forced vaccinations”.
Likewise, in a written response to the DUP’s Stephen Dunne MLA, who queried the timescale between the reviewing the public consultation findings and formulating a new public health bill, Nesbitt was reticent.
“My department have received a high volume of responses,” he said, adding: “The process to consider the responses has commenced, the timeframe to complete this review, given the high volume of responses, is
still under consideration.”
However, the Minister’s consultation document came under criticism from several quarters, not least from his Executive partners. Referencing her party’s response to the consultation, Sinn Féin health spokesperson, Liz Kimmins MLA, says: “Any proposals from the health department for a new public health bill must be consistent with people’s human rights and equality requirements.
“The absence of both an Equality Impact Assessment and a Human Rights Impact Assessment from this consultation document is a serious and unacceptable omission.
“The Department of Health’s proposals and the consultation are not fit for purpose and Sinn Féin does not support the approach being pursued by the Minister for Health.”
Likewise, the DUP accused the Department of Health of “huge overreach” and published its sevenpage response to the consultation. The party’s health spokesperson, Diane Dodds MLA, asserts: “The Health Minister’s refusal to scrap this consultation – despite bizarrely distancing himself from some of its most divisive elements - has undermined public confidence...
“We do not believe the proposals currently under consideration strike a fair balance between fulfilling public health objectives and defending personal liberty... All of this represents a huge overreach and must be rejected. The Department must go back to the drawing board.”
However, speaking with the BBC Radio Ulster’s Evening Extra, Chair of the British Medical Association (BMA) Northern Ireland, Alan Stout asserted that the proposed legislation “is very broad reaching” and should not examined “simply through the lens of Covid or actually vaccination itself”.
In the meantime, given the scrutiny that lies ahead, it remains to be seen whether the Executive can formulate a new legislative framework for responding to a future public health crisis, in a timely manner. Certainly, in the absence of a indicated timeframe, this journey – which began in 2015 – is likely to be an odyssey.


Following scenes of racist violence in August 2024 in parts of Northern Ireland, which left some healthcare staff feeling anxious, frightened, and unwelcome, Permanent Secretary for the Department of Health, Peter May, outlines the hugely valuable contribution of internationally educated and recruited professionals.
The landscape of society in Northern Ireland is evolving and our population is becoming increasingly diverse, reflecting the globalised world we live in. This diversity is perhaps most apparent within our health and social care (HSC) workforce.
It is important therefore that we foster a healthcare environment that is truly inclusive: we want all staff, regardless of their background or country of origin, to have the opportunity to thrive and excel in their careers, to deliver better outcomes for patients and to make a positive impact on the health and wellbeing of the community.
Our workforce is highly dedicated and resilient in the face of tremendous pressures. However, there are growing demands being placed on our health services, due to factors including population ageing and patients’ needs becoming
more medically complex. The current level of vacancies across professional disciplines is also a major challenge: at the end of June 2024, there were more than 5,300 vacancies actively being recruited across the HSC, with the highest number of vacancies being in registered nursing and midwifery. There was a total of 378 medical and dental vacancies.
Therefore, the utilisation of international recruitment is a key avenue in addressing our resource issues, enabling the strengthening of our HSC workforce and delivery of a sustainable health and social care system.
Since 2016, 1,700 international nurses have been recruited and remain in post regionally across the five HSC trusts through the well-established and highly successful International Nurse Recruitment project. Of those recruited 1,649 are in adult nursing roles and 51 in mental health roles. A
further 51 mental health nurses are scheduled to arrive in the coming months.
International supply now makes up 28 per cent of the doctors joining the HSC workforce in Northern Ireland – up from 7 per cent in 2014. Over the last three years, a total of 207 international doctors have been recruited to HSC trusts.
In the Southern Health and Social Care Trust, for example, a group of doctors recruited from India is working across a range of grades and specialties including general surgery, emergency medicine, urology, gynaecology, radiology, and orthopaedics. With significant vacancies and challenges recruiting and retaining doctors, the Trust’s human resources team launched an international recruitment drive and travelled to Mumbai, India, to interview candidates.
Work is now progressing to develop the potential for international recruitment for other healthcare professions including pharmacy, social work, and allied health professionals. That will, of course, be dependent on the availability of funding as well as the availability of recruits within specific professionalisms.
In recent years, there has been a marked increase in the number of trainees requiring a visa to commence medical training programmes in Northern Ireland, both general practitioners and specialists. Currently, there are 369 trainees requiring visa sponsorship (up from 270 in August 2023).
As part of NIMDTA’s VALUED Strategy, a ‘New to Northern Ireland (N2NI)’ project was established in 2021. A working group has helped to develop strategies to provide support to trainees and improve their training experience, including welcome events, enhanced induction programmes, and peer mentoring.
The health and social care system in Northern Ireland strives to provide excellent pastoral care for newly arrived international recruits, underpinned by adherence to ethical international recruitment principles outlined in the Department’s Code of Practice for International Recruitment, which aims to protect the rights of international


recruits across health and social care, including those employed within the independent sector.
Our HSC trusts have received recognition for their efforts to ensure that diversity is valued and celebrated within the workforce. In September 2024, Belfast Trust became the first health trust in the UK to be awarded the prestigious ‘Trust of Sanctuary’ Award, marking its commitment to providing a safe, welcoming environment for everyone, regardless of background, ethnicity, or origin.
The South Eastern Trust’s recent Diversity Celebration Fun Day, attended by more than 1,000 people, was
arranged for trust staff and their families to celebrate the richness of diversity within the Trust and to promote unity, inclusion, and cross-cultural understanding.
Such events are important to show the abiding commitment of the HSC to the principles of inclusion and unity as we respect the diversity of all our staff who by their dedication and skill are enhancing the quality of patient care every day.

Investment in Northern Ireland’s general practice remains the lowest in the United Kingdom.
A new report published by the Department of Health (DoH) entitled Investment in General Practice, Northern Ireland 2019-20 to 2023-24, shows that the total investment in general practice throughout the region has seen a continued cut in real terms following the significant cut of 7 per cent in the previous financial year.
In 2023/24, the total investment in general practice, including the reimbursement of drugs dispensed in general practice was £388.2 million.
Compared to 2022/2023, which seen £374.7 million, this represented an increase in the total investment in GP practices of 3.6 per cent in Northern Ireland. However, in real terms and accounting for inflation, it equates to a decrease
of 2.48 per cent, as the final figure of investment for 2022/23 (in real terms) stood at £398.1 million.
The Northern Ireland Audit Office (NIAO) published a report in March 2024 entitled Access to General Practice in Northern Ireland. The report found that investment in general practice has increased steadily since the introduction of the General Medical Services (GMS) contract in 2004/05, and overall by just under 37 per cent in real terms between 2004/05 and 2022/23.
However, the 2022/23 financial year marked a slight reduction in investment compared to 2021/22 which saw £377.8 million in investment (£428.4 million in real terms). Similarly, funding per patient also fell slightly (from £188 to £185), marking the first reduction in funding since

2007/08 and given the levels of inflation in 2022/23, it represented a real term cut in of 7 per cent compared to 2021/22.
In response to the recommendation in the report of the Review Body on Doctors’ and Dentists’ Remuneration (DDRB), a 6 per cent uplift was applied for GP pay. In addition, there was a 6 per cent uplift for practice staff expenses and a 7.3 per cent uplift for other expenses (3 per cent recurrent) were also applied, representing an investment of £16.624 million (of which £2.182 million is non-recurrent).
However, the British Medical Association (BMA) Northern Ireland GP committee chair Alan Stout states that general practice is in “absolute crisis”, and criticised the Department of Health’s attitude towards the figures.
“Right across Northern Ireland, GP practices are facing spiralling costs, rocketing inflation, a huge increase in the need for appointments and everincreasing complexity and yet we see a real time reduction in funding to general practice,” Stout states.
“It is astonishing to see it clearly laid out that we are delivering so much while facing a real terms decrease in funding of 6.92 per cent.”
Per capita, investment in general practice in Northern Ireland has traditionally been lower compared to the other regions in the UK. There is evidence of some convergence in recent years (particularly with Wales), but the region is still lower than England and Scotland.
Nearly £68 million other payments were made during the 2022/23 financial year. Of this, almost £24 million related to premises and IT costs and a further £17 million covered other central and administered funds and services e.g., the cost of treatment room nurses. Another £28 million was allocated to GP out-of-hours services.
Published UK-wide data on investment in general practice was discontinued from 2018 due to changes in contractual arrangements in each country, meaning payment categories are no longer directly comparable.
Furthermore, the lower investment in general practice is reflected in lower earnings for GPs in Northern Ireland. While not taking account of hours worked, the latest available data for 2021/22 year indicates that on average, GPs in Northern Ireland earned £104,400 (after expenses but before tax) similar to GPs in Wales. This however, was £6,000 less that GPs in Scotland and nearly £14,000 less than GPs in England. Data for earlier years indicates that average GP earnings in Northern Ireland have been the lowest across the UK since 2016/17.
Moreover, the Labour Government’s first Budget in 14 years has drawn stark criticism among GP practices throughout the region. As part of the Budget, the Northern Ireland Executive has been provided with a £18.2 billion settlement in 2025/26. While the Budget did not specify spending on health, this includes a £1.5 billion top-up through the Barnett Formula, with a £1.2 billion for day-today spending and £270 million for capital investment.
According to the BMA, this means that the Northern Ireland Executive has “run out of reasons” not to “properly” cover GP indemnity costs. In addition, the UK Budget has been criticised for increasing the National Insurance which has left GP practices vulnerable.
Stout states that GP surgeries would be negatively affected by the Budget, saying that it would not be feasible for some surgeries to meet the National Insurance increase and the minimum wage increase. He warned that practices throughout the region were already under pressure and that there was a possibility that practices could close. Just one week after the Budget was announced, a surgery in County Derry announced it would close, with more than 2,300 patients being transferred to surgeries in the surrounding area.
Chair of the Northern Ireland General Practitioners Committee Frances O’Hagan says: “The Budget looks like it could be good and bad news for GPs. While we hope the allocation to Northern Ireland can address some of the issues, the costs GPs as employers will now face in terms of changes to the increase in National Insurance will be an additional financial pressure.”