

Gather insights into the status of cardiovascular disease (CVD) prevention and control programs and enabling drivers to design an intervention package that will reduce the cardiovascular risk for Ho Chi Minh City population health.
1. Vietnam country profile, CVD health burden, and directions to move forward
2. Review the outcome of the previous CVD program in Ho Chi Minh City
3. Baseline assessment of existing CVD health care services of health facilities in the project’s three priority districts
4. SwipeRx Survey Results: insights to inform pharmacy client selfScreening for CVD Risk in Viet Nam
5. The assessment of the current maturity level of using Artificial Intelligence in health care
Demographic
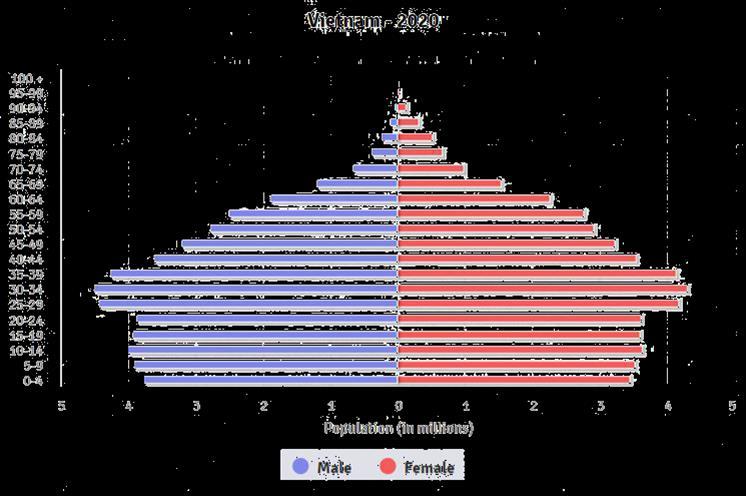
Population: 98.685.363 (2022 est.)
Ethnic groups: Kinh 85.7%, others 14,3%
Religions: none 81.8%, Buddhist 7.9%, Catholic 6.6%, others. Disparities across regions, groups can be a challenge to health services
Urban population: 37.3% (2020)
Population growth rate: 1% (2021 est.)
Fertility rate: 2.06 children born/woman (2021 est.)
Early marriage: 10.6% of women aged 20-24 married or in union before 18
Economy
GDP growth rate: 7.02% (2019 est.)

GDP: $271.158 billion (2020 est.)
GDP per capita: $8,65 (2020 est.)
Population below poverty line: 6.7% (2018 est.)
Unemployment rate: 3.1% (2018)
Employment: 37.2% in agriculture, 27.4% in industry, 35.3% in services (2019 est.)
Internet users: 70.35% (July 2018 est.)

Government
Type of government: one-party socialist republic
Administrative divisions: 63 provinces and municipalities
Chief of state: President Nguyen Phu Trong
Head of government: PM Pham Minh Chinh
Political party: Communist Party of Vietnam
VIETNAM COUNTRY PROFILE, CVD HEALTH BURDEN AND DIRECTIONS TO MOVE FORWARD
Government Ministry of Health (MOH
• MOH’s departments
• Institutions under management of MOH (NIHE, Pasteur Institutes, etc.)
• Medical colleges
• Central hospitals (General and Specialized)


provincial Department of Health
• Provincial General/Specialized hospitals
• Centers for Preventive Medicine
• Provincial Secondary Medical school
• Pharmaceutical company
health administrative units
• District Health Centers
• Region polyclinics
(commune/ward)
VIETNAM COUNTRY PROFILE, CVD HEALTH BURDEN AND DIRECTIONS TO MOVE FORWARD
Provincial District Commune 63
District
Health facilities and other ministries and sectors CHS
Village health workers
HEALTH BURDEN AND DIRECTIONS TO MOVE FORWARD
Source: https://www.healthdata.org/vietnam
VIETNAM COUNTRY PROFILE, CVD
VIETNAM COUNTRY PROFILE, CVD HEALTH BURDEN AND DIRECTIONS TO MOVE FORWARD HTN 12,500,000 All NCD Case 17,000,000 50% undetected Diabetes 3,000,000 70% undetected COPD 2,000,000 Cancer 300,303
31% 19% 6%4% 18% 11% 11% Cardiovascular diseases Cancers Chronic respiratory diseases Diabetes Other NCDs Communicable, maternal, perinatal and nutritional conditions VIETNAM COUNTRY PROFILE, CVD HEALTH BURDEN AND DIRECTIONS TO MOVE FORWARD Data and graph from WHO NCD Country Profile 2018. The mortality estimates have a high degree of uncertainty because they are not based on any national NCD mortality data. NCDs are estimated to account for 77% of all deaths 2016 total population: 94,569,000 2016 total death: 549,000
Source of hypertension & diabetes
Commune health stations
District health facility
Health care
Private health
19% 34% 27% 10% 8% 2%
facilities at provincial level Central hospitals
facilities VIETNAM COUNTRY PROFILE, CVD HEALTH BURDEN AND DIRECTIONS TO MOVE FORWARD General Department of Preventive Medicine MoH. National Survey on NCD risk factors 2015
medications 6% 39% 35% 14% 5% 1%
1National Strategy for Prevention and Control of NCDs 2015–2025, National NCD Plan 2022 - 2025 and the Vietnam Health Program recognize the need for outreach services and management systems to promote early detection of CVDs in PHC.
3The government has shown a solid commitment to:
► Achieving 100% online public services across sectors, ► the nationwide introduction of electronic medical records (EMRs) for outpatients.
► Developing digital data storage, AI at all health care establishments to build national health databases.
2The national agenda for digital transformation emphasized a people-centered approach and the need to foster a digital culture
► Develop telemedicine platforms to provide remote medical services.
► Gradually develop and strengthen digital disease prevention and health care systems.
► Strive to achieve the “one doctor for each citizen” idea to create a digital personal health dossier.
► Establish easy access to telemedicine and electronic medical prescriptions.
VIETNAM COUNTRY PROFILE, CVD HEALTH BURDEN AND DIRECTIONS TO MOVE FORWARD

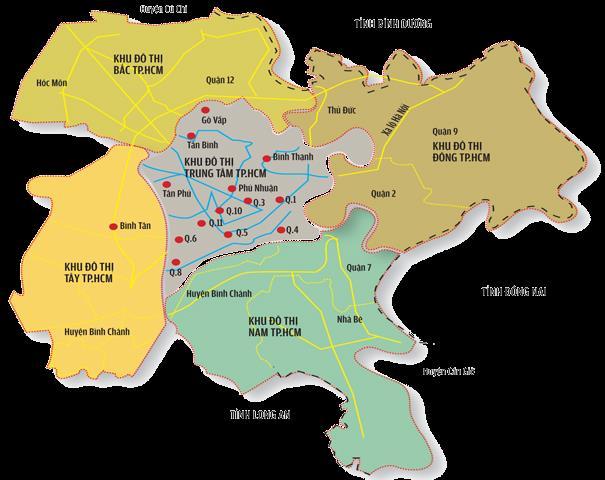
Before January 1st, 2021, HCMC had 24 districts with 319 wards and communes. Thu Duc City was established when District 2, District 9, and Thu Duc District merged. HCMC has 22 districts (including 21 districts and 1 city) with 312 wards and communes and 310 commune health stations.1
Source:
1.https://thongtinduan.com/thi-truong-24h/9242-phuong-an-sap-nhap-cac-quan-huyen-tai-tphcm.html;
2. Census of the HCMC population (No. 223/UBND VX, dated Jan 21,2022);
3. https://worldpopulationreview.com/world cities/ho chi minh city population;
4 HCMC demographic yearbook 2019;
5. https://saigoneer.com/saigon-news/19291-saigon-aims-to-reach-over-$12,000-in-gdp-per-capita-by-2030;
6.https://en.wikipedia.org/wiki/Ho_Chi_Minh_City;
7. https://www.hcmcpv.org.vn/tin tuc/ty le nguoi hut thuoc la thu dong cao nhat tai cac dia diem quan bar ca phe tra 1491854799;
8. https://vnexpress.net/80 dan ong tp hcm uong ruou bia 3447585.html; 9. https://congluan.vn/685 dan so tp hcm luoi tap the thao-post58322.html
Urban profile
Population 9,053,710 (2022 est)2
Population growth rate 2.71%3
Life expectancy 76.6 years old (2019 est)4
GDP per capita US$ 6,862 (2019 est)5
Literacy rate: (adult 15+) 99% (2019 est)4
Unemployment rate: 5.45% (2022 est)3
Ethnic demographics Vietnamese: 93.52%, Chinese: 5.78%, Khmer: 0.34%, Cham: 0.1%, other nationalities Koreans, Japanese, Americans, South Africans, Filipinos and Britons6
Rates of smoking, alcohol consumption, physical exercise
Smoking rate in males: 46.6% (2018 est)7 Alcohol assumption: 80% in males, 22% in females (2016 est)8 Physical exercise: 31.5% (2018)9
REVIEW THE OUTCOME OF THE PREVIOUS CVD PROGRAM IN HO CHI MINH CITY
1HCMC plan on the implementation of the National Strategy for NCDs prevention and control in HCMC aims to control the increase of morbidity and mortality due to NCDs in which prioritizes for prevention and control of cancers, CVD, DM, Chronic obstructive pulmonary disease and asthma
The HCMC DOH issued regulations and mandates for sharing and managing data related to CVDs/hypertension (HTN) and diabetes mellitus (DM) between public hospitals and preventive medicine centers at district and commune levels.
5-year operation plan of the health sector in HCMC for the period of 2021-2025 highlights the goal of strengthening the NCD management and preventing of risk factors affecting population health.
Plan on EHR deployment citywide period 2019-2025 across 22 districts.
The “smart city” agenda entails developing and applying digital technologies in all sectors to improve public administration and ensure a sustainable, knowledge-based economy.
VIETNAM COUNTRY PROFILE, CVD HEALTH BURDEN AND DIRECTIONS TO MOVE FORWARD
2
3
4
5
HCMC People Committee HCMC Department of Health
AND DIRECTIONS TO MOVE
District People Committee
District health administrative units
• Provincial General/Specialized hospitals
• Centers for Preventive Medicine
• Provincial Secondary Medical school
• Pharmaceutical company
Commune People Committee
• District Health Centers
• Region polyclinics
CHS (commune/ward) Village health workers
Tran Thi Mai Oanh, Tran Van Tien, Duong Huy Luong, Khuong Anh Tuan, Nguyen Khanh Phuong, Le Quang Cuong, Amy Taye, Gilbert Kombe, and Saul Helfenbein. March 2009. Assessing Provincial Health Systems in Vietnam: Lessons from Two Provinces.

VIETNAM COUNTRY PROFILE, CVD HEALTH BURDEN
FORWARD
Health program

VIETNAM COUNTRY PROFILE, CVD HEALTH BURDEN AND DIRECTIONS TO MOVE FORWARD
20 disease prevention, medical examination and treatment, reproductive health care, supply of essential drugs, community health management, communication and health education. 310 CHS 2,014 staffs of which 23% are doctors CHS main functions Source: Ho Chi Minh City Department of Health’s plan on capacity building of the grassroots health system in the period of disease control in Ho Chi Minh City; a meeting on October 8, 2021
prevention, primary health care and medical examination and treatment.
out of
professional medical examinations as well as treatment and PHC
VIETNAM COUNTRY PROFILE, CVD HEALTH BURDEN AND DIRECTIONS TO MOVE FORWARD disease
16
22 DHCs have established polyclinics to perform
activities. 22 DHCs 4,445 health care staff DHCs main functions 712 doctors 59 public health staff 866 assistant doctors 540 pharmacists 1,471 nurses, midwives, and medical technicians 797 others. Source: Ho Chi Minh City Department of Health’s plan on capacity building of the grassroots health system in the period of disease control in Ho Chi Minh City; a meeting on October 8, 2021
22 DHs
Level I: 3
Level II: 16 Level 3: 1
health workers
2,285 doctors 85 public health staff 204 are assistant doctors 590 are pharmacists 3,754 are nurses, midwives, medical technicians 1,409 others.
DHCs main functions
diagnosis and treatment services.
Source: Ho Chi Minh City Department of Health’s plan on capacity building of the grassroots health system in the period of disease control in Ho Chi Minh City; a meeting on
VIETNAM COUNTRY PROFILE, CVD HEALTH BURDEN AND DIRECTIONS TO MOVE FORWARD
8,327
October 8, 2021
• 2010 - now
• HTN, DM
• Capacity building, awareness raising, screening
• 2016 -2021
• HTN, DM
• Capacity buiding, awareness raising, screening, early diagnosis, treatment linkage, case management, stakeholder engagement (PPP, community collaborators, checkpoints), e-tracker

MOVE
HCMC PATH

• 2016-2020
• HTN, DM
• Awareness-raising, early diagnosis, treatment and management
Tran Thi Mai Oanh, Tran Van Tien, Duong Huy Luong, Khuong Anh Tuan, Nguyen Khanh Phuong, Le Quang Cuong, Amy Taye, Gilbert Kombe, and Saul Helfenbein. March 2009. Assessing Provincial Health Systems in Vietnam: Lessons from Two Provinces.
VIETNAM COUNTRY PROFILE, CVD HEALTH BURDEN AND DIRECTIONS TO
FORWARD
FHI 360
Project Year # of districts intervened*
3/2016 3/2017 1 district (at 5 CHSs)
Abundant Health (Pfizer Foundation)
6/2017 5/2018 1 district (at 11 CHSs)
9/2018 7/2019 24 districts (at 151 CHSs)
8/2019 9/2020 23 districts (at 292 CHSs)
Community for Healthy Hearts (Novartis Foundation)
Transforming the NCD response (Access Accelerated)
AND DIRECTIONS TO MOVE
98,903
Not analyzed Newly: 1,414 (1.4%)
6/2016 6/2019 4 districts (at 16 CHSs) 121,273 29,908 (for patients with known and unknown conditions)
6/2019 3/2021 1 district (at 16 CHSs) 16,739 7,940 (for patients with known and unknown conditions)
Previously: 18,412 (18.6%)
13,078 patients were treated at CHSs, including people screened by the CHSs and people who self-referred treatment from the hospital to CHSs
VIETNAM COUNTRY PROFILE, CVD HEALTH BURDEN 11,847 patients were referred to district hospitals for treatment
16,455 (13.6%) (including newly and previously conditions)
5,110 (including newly and previously conditions)
FORWARD 6,727 (56.8%)
Not measured
N/A Not measured
Note: * Non of CHSs received dual projects at the same time. **Including people with unknown and known conditions.
Source: HCDC’s consolidated reports of HTN intervention projects from 2016 to 2021
HTN screened ** BP elevated HTN diagnosed HTN treated BP controlled
Project Year # of districts intervened*
Project Year
Abundant Health (Pfizer Foundation)
Abundant Health (Pfizer Foundation)
Community for Healthy Hearts (Novartis Foundation)
Transforming the NCD response (Access Accelerated)
Transforming the NCD response (Access Accelerated)
3/2016 3/2017 1 district (at 5 CHSs)
DIRECTIONS TO MOVE
# of districts intervened*
DM screened
HTN screened ** BP elevated HTN diagnosed HTN treated BP controlled
98,903 Not analyzed Newly: 1,414 (1.4%)
3/20163/2017 1 district (at 5 CHSs) 89,059 Not analyzed
6/2017 5/2018 1 district (at 11 CHSs)
9/2018 7/2019 24 districts (at 151 CHSs)
9/20187/2019 24 districts (at 151 CHSs)
8/2019 9/2020 23 districts (at 292 CHSs)
8/20199/2020 23 districts (at 292 CHSs)
6/2016 6/2019 4 districts (at 16 CHSs) 121,273 29,908 (for patients with known and unknown conditions)
6/2019 3/2021 1 district (at 16 CHSs) 16,739 7,940 (for patients with known and unknown conditions)
6/20203/2021 1 district (at 16 CHSs) 6,739 2,940 (for patients with known and unknown conditions)
Newly: 487 (0.5%)
VIETNAM COUNTRY PROFILE, CVD HEALTH BURDEN AND Not measured
Known: 5,029 (5.6%)
Previously: 18,412 (18.6%)
FORWARD 6/20175/2018 1 district (at 11 CHSs)
13,078 patients were treated at CHSs, including people screened by the CHSs and people who self-referred treatment from the hospital to CHSs
4,268 patients were treated at the CHSs including people diagnosed by the CHSs and people who self-referred treatment from the hospital to CHSs
Not measured
16,455 (13.6%) (including newly and previously conditions)
1,367 (including newly and known conditions)
5,110 (including newly and previously conditions)
11,847 patients were referred to district hospitals for treatment
6,727 (56.8%)
367 patients were referred to district hospitals for treatment
Not measured
N/A Not measured
Note: * Non of CHSs received dual projects at the same time. **Including people with unknown and known conditions. Source: HCDC’s consolidated reports of DM intervention projects from 2016 to 2021
** BS elevated DM diagnosed DM treated BS controlled
Points of service providers

Community health stations
Health facilities
Health collaborators Checkpoints

Families & Communities
Diabetes & Hypertension control among adults

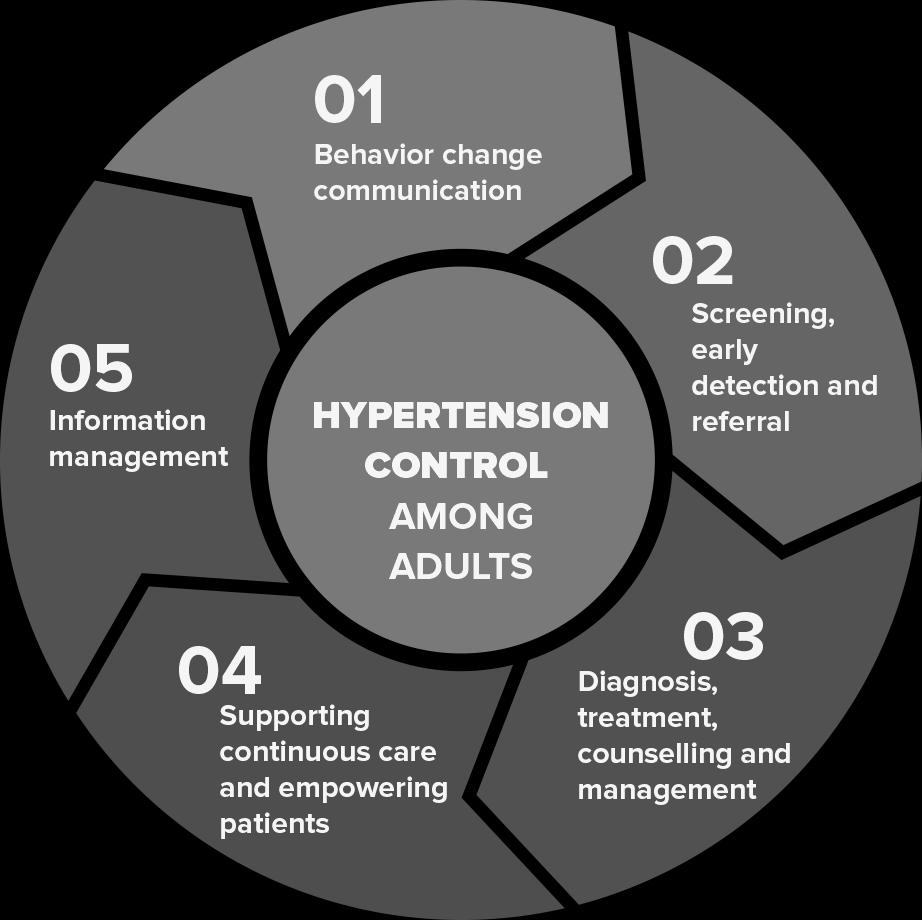
Approaches

1. Offer chronic care and support HTN and diabetes for patients along the patient journey

2. Enhance the quality of service provision
3. Increase patient awareness and empowerment, people centered-care approaches
4. Enhance e-tracking system for better patient management and support
5. Promote public private partnership
VIETNAM COUNTRY PROFILE, CVD HEALTH BURDEN AND DIRECTIONS TO MOVE FORWARD
VIETNAM COUNTRY PROFILE, CVD HEALTH BURDEN AND DIRECTIONS TO MOVE FORWARD 46.9% 63.6% Before (2016) After (2019) 121,273 29,908 16,455 11,847 6,727 Screened BP Elevated HTN Diagnosed HTN Treated BP controlled 24.7% 55% 71% 56.8% Chart 1: HTN Awareness* Chart 2: HTN control cascade** Chart 3: % Screened by various service points** 81.8% 5.5% 12.7% CC and Checkpoints Ses CHSs Chart 4: Number of HTN managed (not treated) at project CHSs** 800 16,455 Before intervention After intervention Source: *Community surveys before and after CH2 intervention, ** data extracted from CH2 eHTN.Tracker
Community awareness about HTN (early detection, diagnosis, treatment, and adherence to HTN treatment) is limited.
Many health stations do not yet have enough equipment and drugs to provide diagnostic and treatment services for patients.
Low capacity of commune NCD staff.
Coordination between health care levels and health facilities in managing NCDs and HTN is weak
High turnover rate of CCs and checkpoints.
Limits in support supervision, monitoring, and ensuring data quality.
Currently there is no mechanism in place to share data between medical examination and treatment facilities & health stations.
Diversifying communication channels (traditional and non-traditional) to reach the community better.
Collaborators, checkpoints, non-health sectors, and community organizations are important forces to support the prevention, screening, care, patient management in the community.
HTN screening in the community is an effective solution to raise people's awareness and detect HTN early.
The support and involvement of local authorities, mass organizations, social organizations, businesses, and the community is needed.
Information technology to manage HTN data should be applied synchronously at public and private health facilities to improve the efficiency of diagnosis, treatment, management of patients and improve follow-up rates.
VIETNAM COUNTRY PROFILE, CVD HEALTH BURDEN AND DIRECTIONS TO MOVE FORWARD
5: Population of
three prioritized
Total population: 1,969,4691
People aged ≥18: 1,480,3981
Estimation of people aged ≥25: 62%2
Source:
1. Census of the HCMC population reported by HCMC People’s Committee (No. 223/UBND VX, dated Jan 21,2022); 2. https://danso.org/viet nam/;
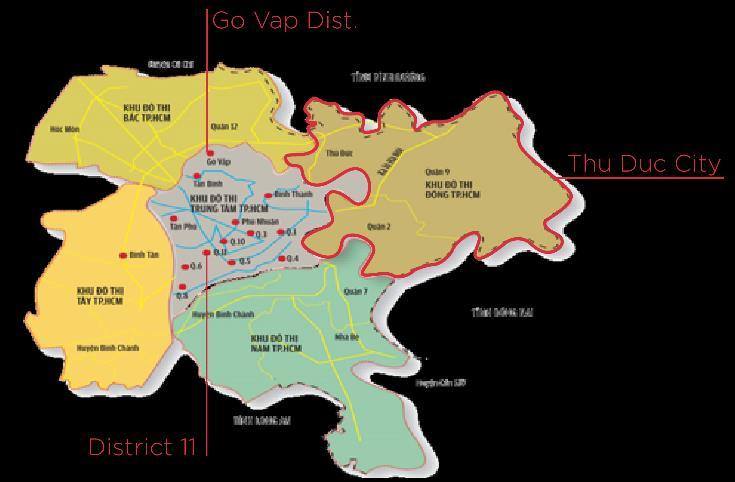
BASELINE ASSESSMENT OF EXISTING CVD SERVICES OF HEALTH FACILITIES IN THE THREE PRIORITY DISTRICTS 198,692 628,807 1,141,970 123,189 389,860 708,021 Dist. 11 Go Vap Dist. Thu Duc City Total population People aged ≥25 Chart
the
districts
64, 89% 3,4% 5,7% Commune Health Stations (CHS) District Health Centers (DHC) District Hospitals (DH) Chart 5: Seventy-two health facilities participate in the Population Health project 55% (35): insured CHSs 17% (11): one-stop-shop CHSs 67% (Go Vap and Thu Duc city): polyclinics with insured services 60%: in Thu Duc City 40%: level I 60%: level II
Chart 5: Seventy-two health facilities participate in the Population Health project
CHSs in Go Vap Dist.
CHSs in Dist.11
CHSs in Thu Duc city
CHSs
CHSs
Health workers
Doctors: 20.5% (87)
Assistant doctors: 29%
Nurses: 17% Pharmacists:13.9%
Midwives:14.2%
Others: 5.4%
of CHSs have doctors but without practicing license
Insured services for medical examination and treatment here are often interrupted
insured CHSs have doctors but without practicing license
16 16 5 5 16 5 7 32 14 1 5 1 Total
# of insured CHS # of
with no doctors #
# of
BASELINE ASSESSMENT OF EXISTING CVD SERVICES OF HEALTH FACILITIES IN THE THREE PRIORITY DISTRICTS
424
Chart 8: Health workers are trained on CV risk screening, HTN and DM treatment
Of CHSs
confirmed that booklets for CV risk screening, HTN, and DM diagnosis, and treatment are available. 24% of them could list out the correct documents issued by the MOH in December 2019
CHSs
Received the training in
Recommendations
Have new health workers delegated to NCD tasks recently
60%: received the training in 2020 40%: in 2021
Total facilities # of facilities had health workers received training
# of facilities had no health workers received training
1. Provide refresher training for key staff of CHSs and DHCs on CVD risk screening, first-line treatment for HTN and DM;
2. Extend the training topics to stroke, acute myocardial infarction, arteriosclerosis, and CVD with COVID-19.
86%
64 3 5 54 3 5 10
DHCs DHs
IMPROVE THE QUALITY OF CARE
1Role and responsibilities of CHS in prevention, early detection, diagnosis, treatment, and management of NCDs.
Clinical case discussion on HTN and DM out-patient treatment at CHSs.
Guidance on early detection of some NCDs.
Practice on counseling and prescribing of dietary choices and physical activities in the prevention and treatment of HTN and DM
Guidance on integrated management of HTN and DM applying the principles of family medicine at CHS.
Flow of sharing HTN and DM patient information from hospitals to CHSs.
Improving the NCDs quality management at CHSs.
Guidance on using NCD management software.
IMPROVE THE QUALITY OF CARE
2
3
4
5
6
7
8
Community collaborator network for the CV health program
100% of CHSs have collaborator networks (one in each neighborhood)
Collaborator networks mainly serve for population and reproductive health programs at each ward, managed by Ward PC.
100% of CHSs have limited financial capacity to incentivize collaborators
• 45% of CHSs have active collaborator networks.
• No dedicated collaborators for the CV health program.
Recommendations
1. Collaborators are the extension arm of the CHSs in public health communication and community mobilization, the HCMC authority should have an allocated budget to foster this force (this is also the recommendation of 72% of CHSs).


2. Advising the health authority to expand the scope of CV health/NCD program support to collaborators of the population program
.
IMPROVE THE QUALITY OF CARE
Community collaborator network for the CV health program
Patient registration



Measure height, weight, and calculate BMI
Take blood pressure & test for capillary blood glucose

Consult screening results & give followup visit appointment
Task-shifting in health care:
• Apply at 100% of CHSs
• Flexible in some CHSs with shortage of staff

Care coordination and patient referrals between providers and care levels
Integrate lifestyle screening in these steps
Collaborator/ Nurse Collaborator/ Nurse Assistant Doctor/ Nurse Doctor Doctor
Follow-up treatment & patient management at the station Confirm diagnosis
Team of doctors, physician assistants, nurses, and collaborators
Recommendations
• No priority on patient registration for referred patients from CHSs to DHs
• No data connecting & sharing (CHS-DH)
• Patients with stable HTN/DM at DHs are NOT REFERRED to CHSs
1. Reinforce the task-shifting practice at CHSs have new staff delegated for the NCD program.
2. Develop a procedure for receiving priority patients referred from CHSs to DHs to create favorable conditions for patients to maintain the treatment continuously;
3. Promote data connection between DHs and CHSs so that doctors at all care levels can monitor previous treatment processes and provide appropriate consultation to patients.
IMPROVE THE QUALITY OF CARE
Review of CVD
service performance at CHSs
Supportive supervision from the management level
Chart 9: Frequency of meeting review of CVD care service performance and take action
65% of them have recorded meeting minutes
2times/year
supportive supervision from HCDC/DoH to one selected CHS/district
4times/year
supportive supervision from DHCs to each CHS
IMPROVE THE QUALITY OF CARE
care
Recommendations 1. Orient CHSs using the PDCA improvement cycle; 2. Provide template of meeting minutes for CHSs to adopt; 3. Standardize the data review and improvement actions into the monitoring checklist of the NCD program. 59.4% 1.6% 1.6% 37.5% No review Weekly review Monthly review Quarterly review
Organize behavioral change communication (BCC) activities on CVD risk, HTN and DM
Chart 10: Places when CHSs normally conduct behavioral change communication sessions on HTN and DM during a calendar year
DHs DHC CHSs
At
100% in the hospital (through patient clubs on monthly or quarterly)
at the neighborhood
In & out of CHS facilities (integrated into local meetings or integrated with the health checkups held at CHSs)
quarters
Chart 11: Key challenges for CHSs to raising community awareness on CV risk prevention
Lack of leaflets
Lack of human resources
Lack of community collaborators
Language barrier (Chinese)
Community people is busy for livelihood
Lack of financial resources
Community awareness is low
EARLY ACCESS TO HEALTH AND CARE
51 51 42 34 2 1
CHS At quarters Loud speaker at ward At Ward PC Home visit At sub-
2/63 CHSs have no responses
20 14 13 7 5 5 5
Provide communication materials to HTN and DM patients




Communication materials are available at 100% of DHs, 67% of DHCs, and 84% of CHSs.

BCC leaflets are no longer preferred and often not distributed to CHSs.

Projects with interactive, practical communication activities such as projects by PATH, the Novartis Foundation, the Pfizer Foundation, helped improve NCD, CVD communication methods, and outcomes tremendously.
Leaflets on stroke (symptoms, causes, treatment) are not available at CHSs.


Recommendations
1. Producing leaflet/posters to educate community people on CV risk prevention and control, especially for the stroke event;


2. Promoting the use of mass media and social media and advocating the collaboration with private partners to accelerate the communication activities and generate demand of community on CV risk screening.
EARLY ACCESS TO HEALTH AND CARE
Organize HTN and DM screening activities at CHSs
Chart 12: When CHSs conduct HTN and DM screening events
For DM screening
Vaccination days
TB screening day
Blood donation days
For HTN screening
Mostly combined with other existing health programs
65% organize a screening in community
World diabetic day (Nov 14)
Elderly health check-up (from Jun to Oct)
Vietnam Women's day (Oct 20)
World heart day (Sep 29)
Vietnam's War Invalids and Martyrs Day…
World No-Tobacco Day (May 31)
World hypertension day (May 17)
Founded date of HCM Communist Youth…
International women's day (Mar 8)
Quarters, markets, pharmacy stores, schools would attract more
76% had challenges when mobilizing people to screen
Lack of funds to incentive people
Lack of HR to organize activity
Community people are busy during office hour
Language barrier to the Chinese community
0 5 10 15 20 25 30 35
Chart 13: The places where CHSs organized screening vs the places that would attract more community members
the places where CHSs organized the screening
the places where CHSs think that would be effective to attract more community members for screening
At quarters At markets At school Home visit At pharmacy store
At pogoda At church At CHS At Ward People's Committee
EARLY ACCESS TO HEALTH AND CARE
37 4 2 1 1 1 1 50 13 4 7 2 1
Perform HTN and DM screening, CVD risk estimation
Chart 14: where do CHSs record the blood pressure index?
Chart 15: where do CHSs record the blood sugar index?
Paper-based
Chart 16: where do CHSs record the CV risk index?
HTN/DM Screening CV risk estimation
100% of CHSs provide screening service (using screening device + paper based screening form)
Results are mainly stored in the paper based system
69% of CHSs incorporated CV risk estimation into the HTN/DM screening 33% DHCs & 80%DHs only done for patients who registered for the CVD examination
A paper-based chart is mainly used (except for Thu Duc and Le Van Thinh Hospital)
Recommendations
1. Upgrading the mobile NCD screening app with a tool for total estimation of CVD risk referencing the chart recommended by the MoH;
2. Promoting to use of the screening app and digital registry system at the CHS level so that data can be automatically connected and generated for reference in real-time.
Paper-based
EARLY ACCESS TO HEALTH AND CARE
6 5 5 1 15 1 1 1 24 8 5 2 1 Paper-based registry log Paper-based out patient's record Case management software Screening form NCD log (Excel file) CHSs in Go Vap Dist CHSs in Dist.11 CHSs in Thu Duc city 9/64 CHSs have no responses 5 5 5 2 1 15 1 3 1 20 10 4 4 1
registry log Paper-based out patient's record Case management software Screening form NCD log (Excel file)
2 2 2 1 1413 9 2 4 1
registry log Paper-based out patient's record Case management software Screening form NCD log (Excel file)
Chart
Reasons for drug insufficiency
Inaccurate drug forecast
Not order due to no qualified doctor
DHC stopped signing a sub-contract with DH
Insured drugs for dyslipidemia are not provided for use at the CHS
CV risk estimation
100% of CHSs haveanExceltoolto monitorandreportquarterlybloodpressureand bloodsugarindicesofpatientstreatedatCHSs.
100% DHC and DHs havea HIStostorebloodpressureandlabtestresults ofpatients►Nottoensurealldoctorswould enterdataintothesystem.
100% of CHSs havealistof HTN/DMpatientsinthelocalityformanagement
100% of health facilities haveNOautomatictooltosupportpatient adherencetotreatment ► remindpatient throughZalo/hotline
Recommendations
1. Advocating on providing sufficient insured drugs for CHSs & creating favorable conditions for junior doctors to receive a practicing license;
2. Working with the DHCs to improve CHS’s HIS on fully recording patient’s vital check results;
3. Promoting the use of mobile NCD screening app for reminding and tracking patient’s follow-up visits.
HTN&DM treatment and management at CHSs
EARLY ACCESS TO HEALTH AND CARE Provide
17: Insured drug status at 35 insured CHSs Chart 15: where do CHSs record the blood sugar index?
47% 50% 3% Sufficient Insufficient No respond 60% 40% Provided by DHCs Provided by DHs
Chart 19: The cascade of HTN care at CHSs in Thu Duc City
Screened High BP Newly diagnosed HTN Treated Controlled BP Reffered to
Chart 20: The cascade of HTN care at CHSs in Go Vap Dist.
Screened High BP Newly diagnosed HTN Treated Controlled BP Reffered to hospital
Chart 21: The cascade of HTN care at CHSs in Dist.11
Screened High BP Newly diagnosed HTN Treated Controlled BP Reffered to hospital
interrupted from Feb to Apr
due to
** Service interrupted from May to Dec 2021 due to Covid 19 (the
The reported data is very high compared to the AH project’s report ~ 1.4%.
3188 642 178 166 142 34 1174 251 73 53 53 3
hospital Year 2021 Year 2020 EARLY ACCESS TO HEALTH AND CARE Service indicators related to HTN care at CHS Year 2020* Year 2021** HTN screening 84% of CHSs 66% of CHSs 18% # of people screened 10,556 2,660 75% % of high BP 21% *** 20% *** % of newly diagnosed 8% 8% # of patients treated at CHS 714 382 46% % of patients with BP controlled 73% 94% # of patients referred to hospital for treatment 34 3
4315 997 417 462 299 0 554 120 63 222 206 0
3053 596 251 86 78 0 932 168 78 107 99 0
* Service
2020
Covid-19 (a first wave).
strongest hit). ***
4209 359 48 20 20 8 2199 114 29 4 4 6 Screened High BS Newly diagnosed DM Treated Controlled BS Reffered to hospital Year 2020 Year 2021 3289 398 88 46 35 0 290 64 41 31 29 0 Screened High BS Newly diagnosed DM Treated Controlled BS Reffered to hospital 3451 219 78 22 21 0 803 68 43 17 14 0 Screened High BS Newly diagnosed DM Treated Controlled BS Reffered to hospital EARLY ACCESS TO HEALTH AND CARE Service indicators related to HTN care at CHS Chart 22: The cascade of DM care at CHSs in Thu Duc City Chart 23: The cascade of DM care at CHSs in Go Vap Dist. Chart 24: The cascade of DM care at CHSs in Dist. 11 * Service interrupted from Feb to Apr 2020 due to Covid-19 (a first wave). ** Service interrupted from May to Dec 2021 due to Covid 19 (the strongest hit). *** The reported data is very high compared to the AH project’s report ~ 0.5%. Year 2020* Year 2021** DM screening 81% of CHSs 52% of CHSs 29% # of people screened 10,949 3,292 70% % of high BS 9% *** 7% *** % of newly diagnosed 2% 3% # of patients treated at CHS 88 52 41% % of patients with BS controlled 86% 90% # of patients referred to hospital for treatment 8 6
patients treated at DHC and DHs
Patients of CHSs and DH in Go Vap Dist. could opt to come to DHC to refill medicines.
of HTN and
2896 5727 9691 4501 8759 6041 2597 2371 571 1193 4910 2111 5035 3473 1525 1492 Year 2020 Year 2021 Year 2020 Year 2021 Year 2020 Year 2021 Year 2020 Year 2021 Go Vap DHC Go Vap DH Thu Duc General Hospital Le Van Viet Hospital HTN treated DM treated 164225 122379 66682 54386 18147 12185 21681 21427 Year 2020 Year 2021 Year 2020 Year 2021 Dist.11 Hospital Le Van Thinh Hospital 26% 14% EARLY ACCESS TO HEALTH AND CARE Service indicators related to HTN and DM care at DHC and DHs Chart 25: Number of follow-up visits of HTN and DM patients at DHs Chart 26: Number
DM
100% 55% 31% 6%
Service indicators related to HTN and DM care at DHC and DHs
Number of HTN patients with stroke in 2021 vs 2020
❖ Reduced 91% (968 ► 506) of HTN patients with stroke hospitalized
• Reduced 81% (520 ► 288) of HTN patients with stroke living locally
❖ Reduced 69% (27 ► 16) of in-hospital deaths of stroke patients
• Reduced 44% (13 ► 9) of in-hospital deaths of stroke patients living locally
Chart 27: Number of HTN patients died from stroke reported by 58 CHSs
from the
People’s Committee)
# of HTN patients with stroke hospitalized
# of HTN patients with stroke living locally hospitalized
# of in-hospital deaths of stroke patients
# of in-hospital deaths of stroke patients living locally
Chart 28: Number of patients with stroke hospitalized
EARLY ACCESS TO HEALTH AND CARE
94 39 4 26 29 8 CHSs in Go Vap Dist. CHSs in Dist.11 CHSs in Thu Duc City Year 2020 Year 2021
(Collected
Ward
494 30 189 156 7 6 278 314 230 30 135 98 5 6 150 154 27 1613 9 Year 2020 Year 2021 Year 2020 Year 2021 Year 2020 Year 2021 Year 2020 Year 2021 Go Vap DH Thu Duc General Hospital Le Van Viet Hospital Le Van Thinh Hospital
100% of health facilities have NO digital health tools for community people to do CV risks screening, referral of diagnosis, treatment selfmanagement, and health education
A dashboard with key CV health and non-health data does not exist at the health facilities
There is NO web provided by DOH/HCDC/DHC for online CME to upskill and reskill CHS's health workers
Data sharing is NOT made between CHSs and DHs
CHSs use Zalo to seek clinical consultation from experts* (except for one-stop-shop CHSs that have an established channel. They also use Zalo to offer clinical consultation and treatment follow-up to patients.

Recommendations

1. Promoting the use of mobile NCD screening app for the community people to self-screen CV risk and to self-manage their conditions,

2. Advocating and supporting data sharing at all care levels & building a dashboard for data real-time visualization reporting;

3. Building a webpage for continuously reinforcing and strengthening clinical knowledge & skills of CHS’s health care providers, and offering health education for community people;

4. Creating a clinical hub using the Zalo platform for clinical experts at the city and district level to offer clinical consultation to the CHS’s doctors.
LEVERAGE DATA AND DIGITAL TECHNOLOGY
No steering committee (SC) for CV health program established locally (except for Thu Duc city Health Center).
Current SCs: i) SC for Population Health Care, ii) SC for communicable disease prevention and control, iii) SC for Population and Family Planning.
The three SCs always have representatives of the health sector and other relevant sectors.
At the ward level, CHS Heads will have a monthly progress meeting with the Ward People’s Committee to share upcoming health activities
At the district level, there are quarterly and bi-annually socio-economic briefing meetings organized by the District People's Committee
Chart 29: Associations/Union are most active to support the health programs
Recommendations
Advise the HCMC DOH/PC to send official correspondence to district and ward PCs to establish an SC for non-communicable diseases or expand the scope of an annual action plan which will include details for the CV health program & NCDs.
Association of the Elderly Women Association Red Cross Association
Youth Union Veterans Association Fatherland Front
CREATE INTERSECTORAL COLLABORATION
23 11 10 7 5 3
The city always allocates a budget amount for the prevention and control of HTN and DM.
Most DHCs and CHSs are not sure whether nonhealth sectors have annual plans on CV risk prevention or not.
Chart 30: City’s annual budget for HTN and DM prevention program
USD 180,000
USD 160,000
USD 140,000
USD 120,000
USD 100,000
USD 80,000
USD 60,000
USD 40,000
USD 20,000
USD -
From20182020,theallocatedbudgetwas dramaticallybeingdecreasedduetohaving additionalfundingfromprojects.In2021(withno project),theaverageamountforeachCHSto conductscreeningwasonlyUS$64peryear
Thebudgetwasincreasingsignificantlybecause since2020allCHSswerebeingrequestedfor HTN/DMcasemanagementlocally
Behavioral change communication*
Note:
* For activities conducted by HCDC and CHSs;
** Mainly allocated for CHSs;
*** For activities performed by HCDC.
Screening ** Training ** Treatment management ** Monitoring*** Scientific research*** Other activities*** Total budget
Year 2017 Year 2018 Year 2019 Year 2020 Year 2021
In 2021, all preventive activities for HTN and DM were halted temporarily to prioritize resources for COVID-19 response
ENSURE LOCAL OWNERSHIP
