


At AultCare, You Matter!
Our commitment to teamwork alongside our network providers and hospital systems, allows us to offer convenient, local, personalized care to our members. Through teamwork, we provide YOU with excellent customer service, and quality cost-effective healthcare.
We are here for You!


Company representatives* should contact the Sales and Retention Department to request new enrollment packets and any other issues not listed below.
Phone | 330-363-6390
Fax | 330-454-7845
Company representatives and employees should contact the Service Center for questions regarding benefits that your plan covers or an outstanding claim. An AultCare Service Representative is available Monday through Friday 7:30 am to 5:00 pm.
Phone | 330-363-6360 or 800-344-8858
Fax | 330-438-9804
Online Chat at aultcare.com
Company representatives may contact the Billing Department with questions in regards to monthly invoices.
Phone | 330-363-6360 or 800-344-8858
Fax | 330-363-5012
Email | aultcarebilling@aultcare.com
Company representatives may contact the Member Services/Eligibility Department with enrollment questions.
Phone | 330-363-6360
Fax | 330-363-7746
Email | aultcareeligibility@aultcare.com
Visit our website www.aultcare.com
* Company representatives are individuals authorized to request information on behalf of the company.

to our AultCare family. Whether you are a new client, or have been with us for many years, we are proud to assist you in managing your employer account.
We have created an area on www.aultcare.com designed just for you. You can use the online account to retrieve monthly reporting and invoices, send us files, view your group’s eligibility, order ID cards, and more.
To get started, you and each authorized representative must register for a secured, online account. Once you have created an online account, use this document to learn how to retrieve files from your online account.
If you have questions you can contact your Account Coordinator, Account Executive, or for technical assistance, email the AultCare Web Team at AultConnect@aultcare.com.
Thank you,
Your AultCare Team
1. Open a web browser and go to ww w.aultcare.com
2. Click Account Login in the upper right corner and select “Employer” from the drop down menu.
• Then click on the “Register for a new account” link.
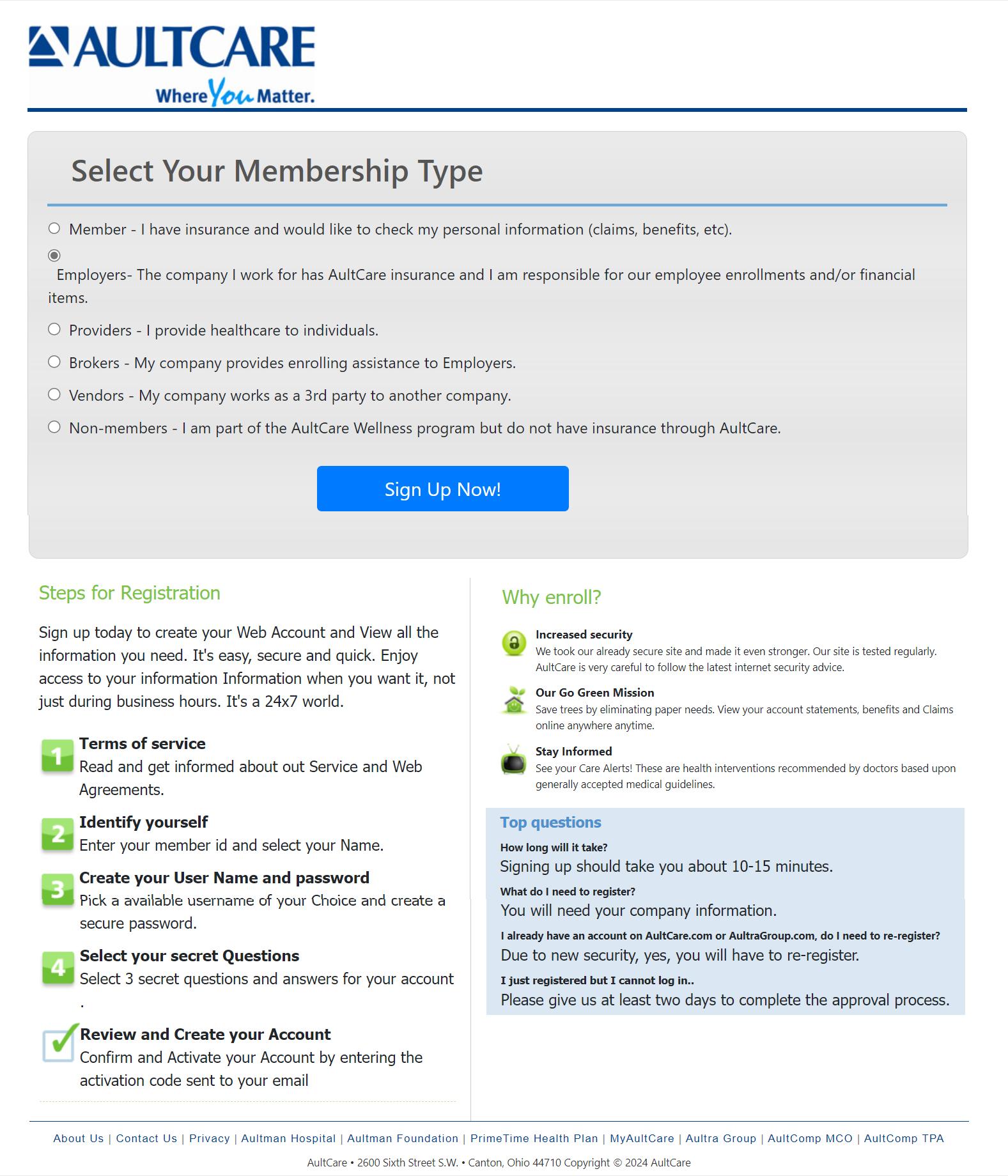
• Select “Employers” as your “Membership Type” and click on the “Sign Up Now!” button.

Step 1
You must agree with our “Terms of Service” before you can create an account with us.
1. Select “I Agree” to agree with the “Terms of service” outlined on this page.
2. By entering your name next to the “By” text-box, you are signing your signature.
3. Click on “CONTINUE” button to proceed.
Step 2
Enter the following information
• First Name
• Middle Initial
• Last Name
• A phone number where we can reach you
• The title of your position at your company
Click on “CONTINUE” button to proceed.
Step 3
1. Enter the 9 digit Tax ID number of your company (without the dash)
2. Enter the name of your company
3. Enter the street address, city and state of your company
Adding Group Numbers
1. Enter the Group Number of your company
2. Click “Add” button
3. The Group Number will then appear in a list box underneath
4. If you need to add more groups, repeat the steps in this section
Optional: If you already know someone at AultCare (e.g Account Coordinator), you can help us expedite the verification process for your employer account by supplying the following ”optional” information:
1. Enter your phone number
2. Enter the name of the person you know at AultCare; (e.g., Group Account Coordinator)
Click on “CONTINUE” button to proceed.
Step 4
Enter the following information
Username for your account
When you enter a username, the system will tell you if it is already taken or not. If the username is already taken, please choose and enter a different username.
Password for your account
The password you choose should consist of:
» 8 characters
» At least one uppercase character and one lowercase character
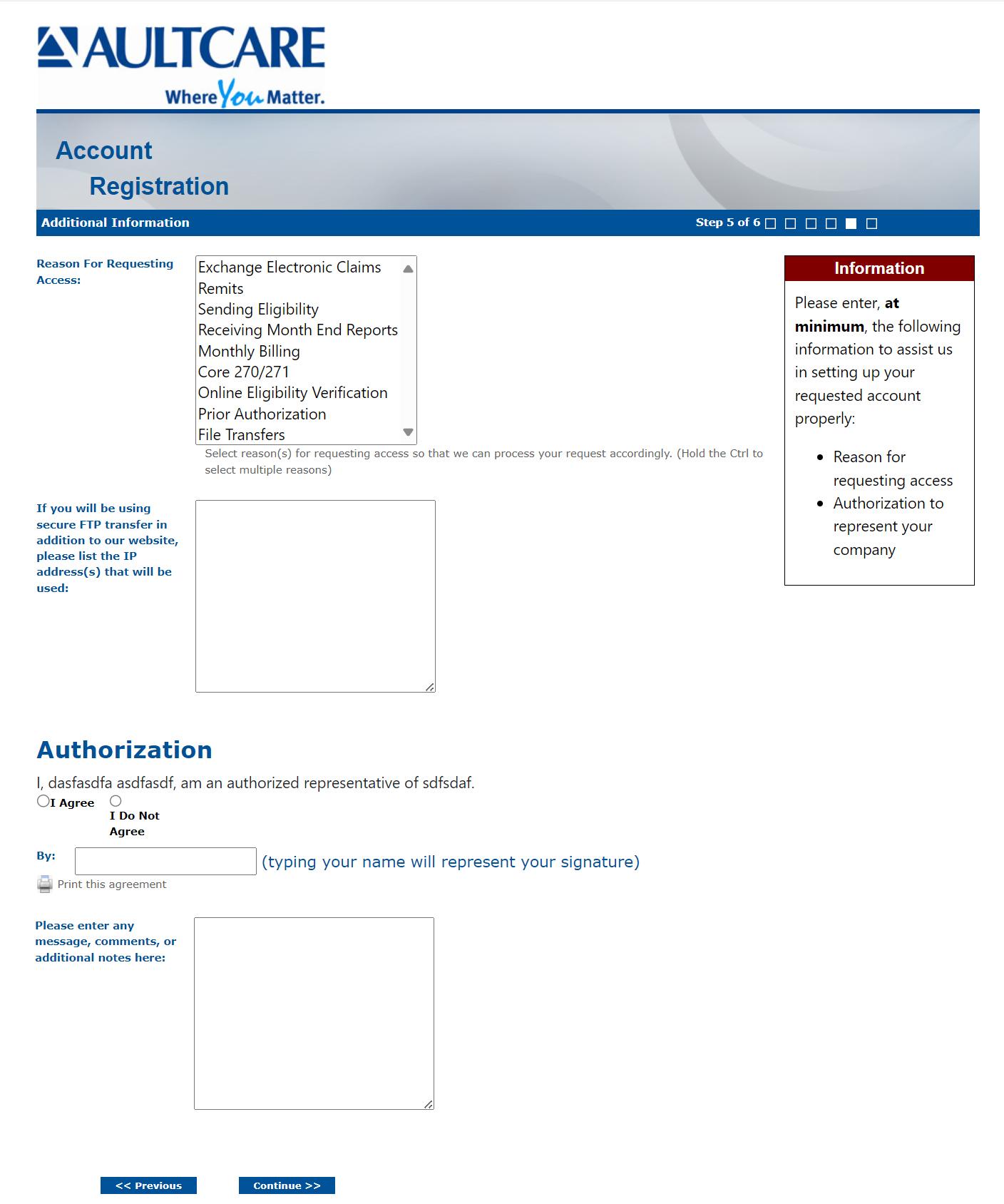
Step 5
1. Reason for requesting access
Select your reason(s) for requesting access. You can select more than one reason.
2. SFTP IP Addresses
If you will be using secure FTP transfer in addition to our website, please list the IP address(s) that will be used.
3. Authorization to represent your company
Select “I Agree” to state you are an authorized representative of the company you are applying for this account.
Optional on this page:
If you need to send us a message or have a question, enter it in the comments box.
Click on “CONTINUE” button to proceed.
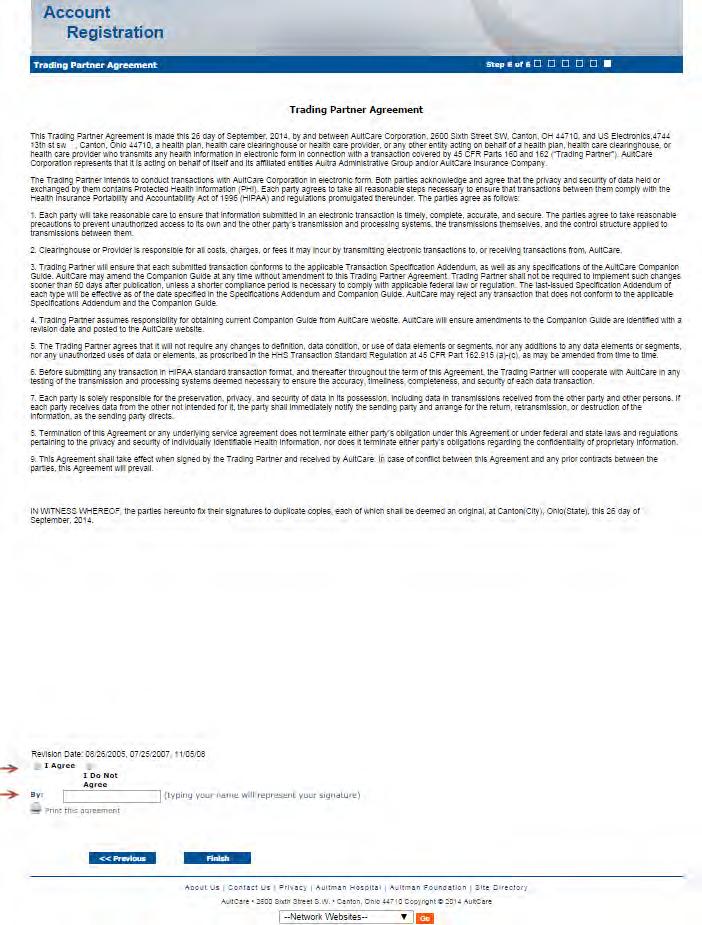
Step # 6
This is the final page of your account registration process. You must agree to the Trading Partner Agreement specified on this page. You can print this agreement by clicking on “Print this agreement.”
From this page:
1. Select “I Agree” to agree to the “Trading Partner Agreement” outlined on this page.
2. Indicate your approval by entering your name in “By:” textbox.
Click on the “FINISH” button to proceed.

Upon successful completion of your account registration, you will see the following message:
Upon successful completion of your account registration, you will see the following message:
Thank you for the submission of your registration request. You will receive an email advising on the next steps to complete the process.
Thank you for the submission of your registration request. You will receive an email advising on the next steps to complete the process.
What to expect next?
What to expect next?
• Upon completion of the registration process, you should receive an email stating the registration process has been completed. (Note: At this time, your account is not active yet)
• Upon completion of the registration process, you should receive an email stating the registration process has been completed. (Note: At this time, your account is not active yet)
• We will review the application and finish with the account setup process.
• We will review the application and finish with the account setup process.
• When your account setup has been completed, you will receive an email informing you your account has been set up and is ready for use. (Note: At this time, the process is complete, and you will be able to login to our website)
• When your account setup has been completed, you will receive an email informing you your account has been set up and is ready for use. (Note: At this time, the process is complete, and you will be able to login to our website)
If you have questions, you can contact your group coordinator, or for technical assistance, email the AultCare Web Team at aultconnect@aultcare.com
If you have questions, you can contact your group coordinator, or for technical assistance, email the AultCare Web Team at aultconnect@aultcare.com
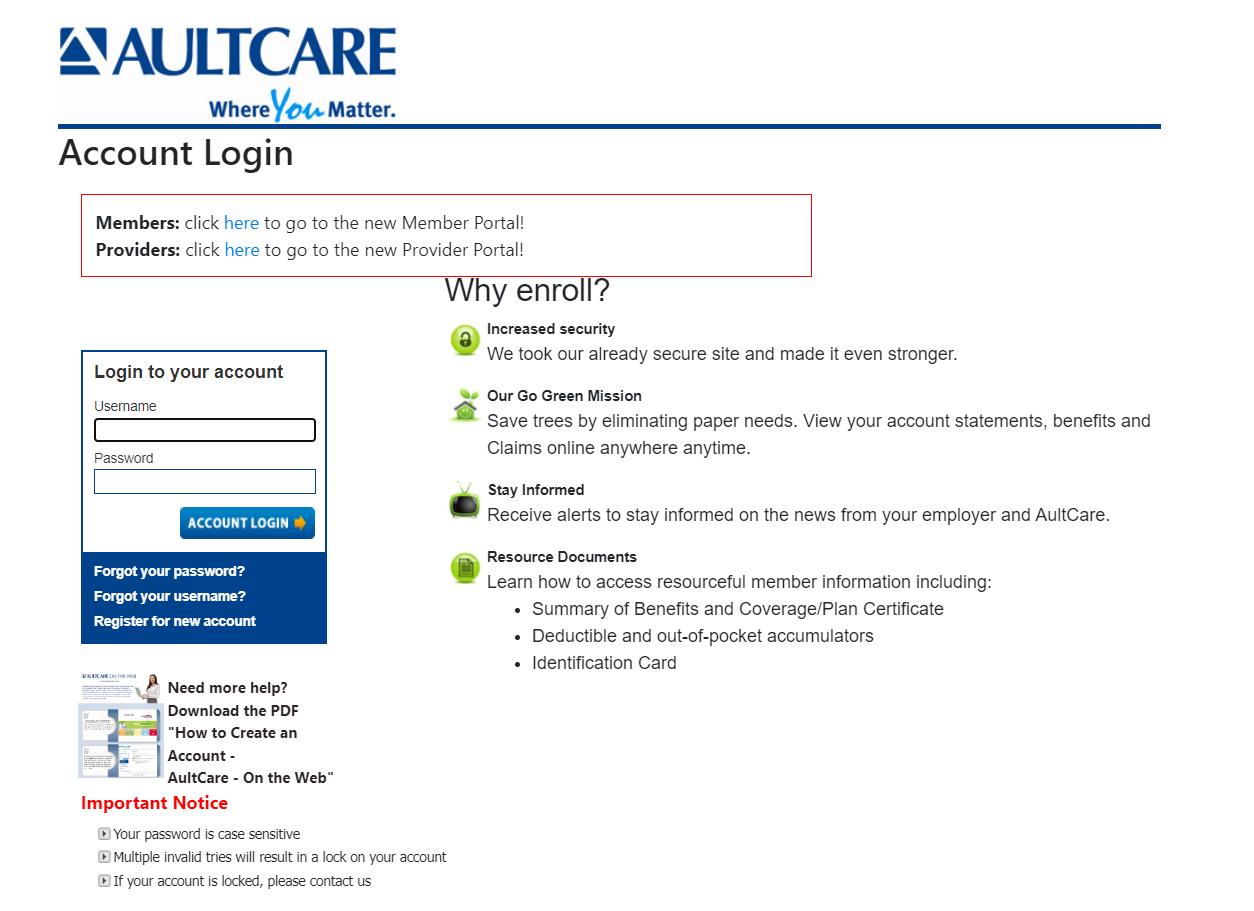
1. Open a web browser and go to ww w.aultcare.com
2. Click Account Login in the upper right corner and select “Employer” from the drop down menu.
3. Enter your username and password. Click Account Login to access your account.
4. You must have an online account to retrieve files. Select Register for new account if you do not have an account.
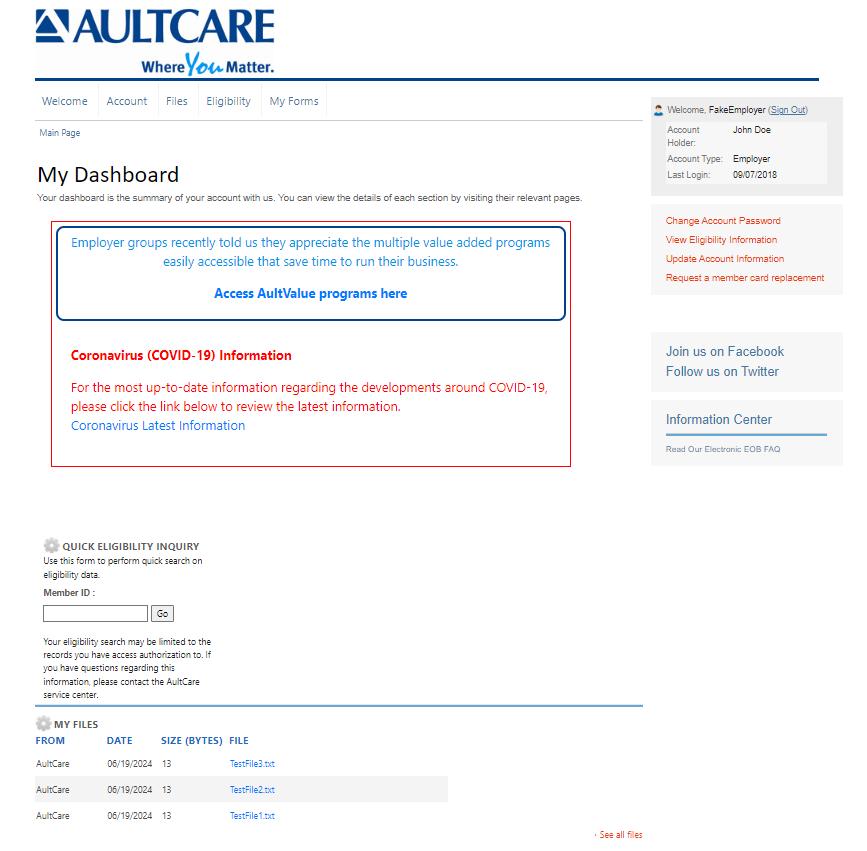
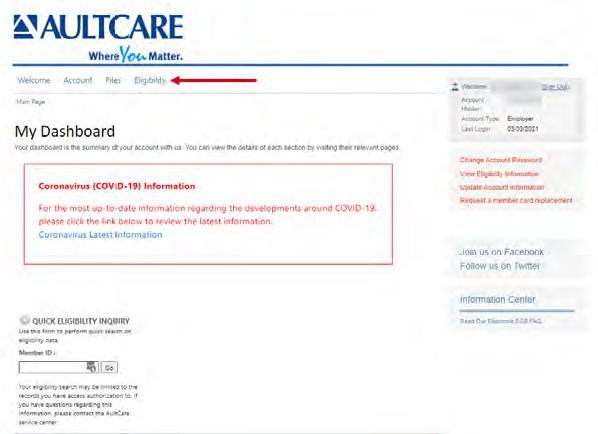
Once you are logged into your account, your dashboard will appear. All links associated to your account will be displayed.
In the screenshot below, three main areas have been identified.
• • • Once you are logged into your account, your dashboard will appear. All links associated to your account will be displayed. In the screenshot below, three main areas have been identified.
• Location A lists the last three (3) files AultCare has posted for you. These are on your dashboard so you can easily view these files.
• Location B is a link. This link will take you to your Secure FTP Center The FTP Center allows you to download all files AultCare uploaded to your account. This is where you can upload files to AultCare.
• Location C is a link similar to Area B. It will take you to the same place and files as Location B.

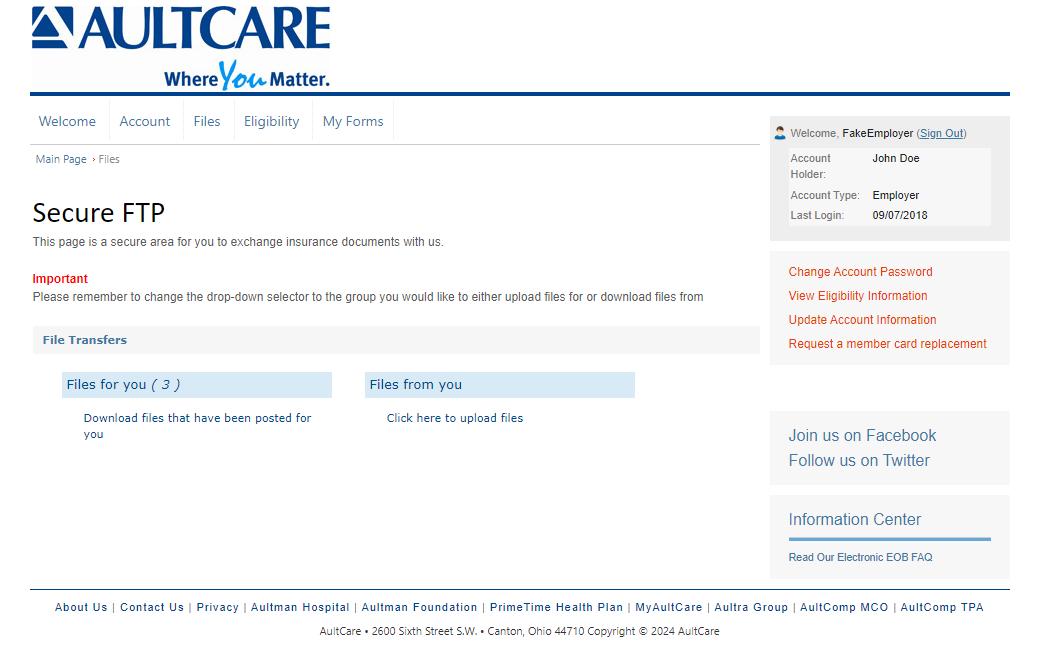
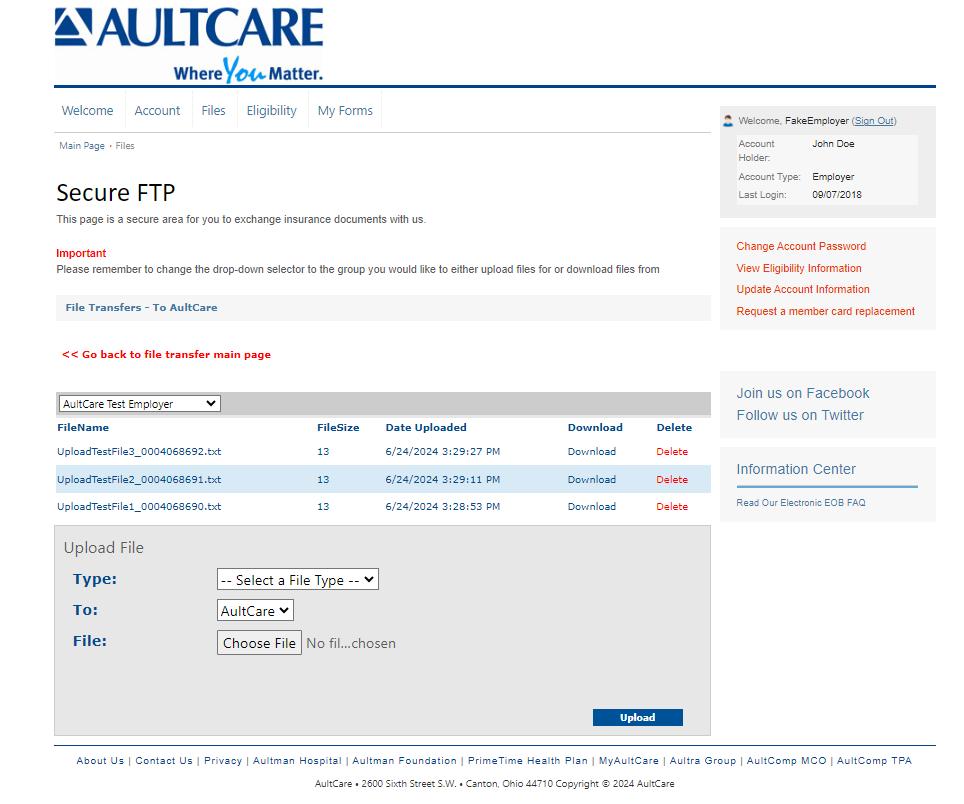
Secure FTP Center
When you click on the Files link from your dashboard (Location C in the example) you will be directed to the Secure FTP Center (see image below). You will see two links: Files for you and Files from you
VIEWING YOUR FILES
Files for you
This link will show all of the files AultCare uploaded to your account. Retrieve your files by clicking on this link. The number displayed is the number of available files.
UPLOADING FILES TO SEND TO AULTCARE
Files from you
This link will take you to a page where you can upload files to AultCare.
Step #1
on the text labeled Download files that have been posted for you.
Step #2
When you click the dropdown list appear. From list, select the name to view (Based on your authorization, only particular names will be displayed.)
Step #3
employers who more than one AultCare account, the appropriate account from the down box.
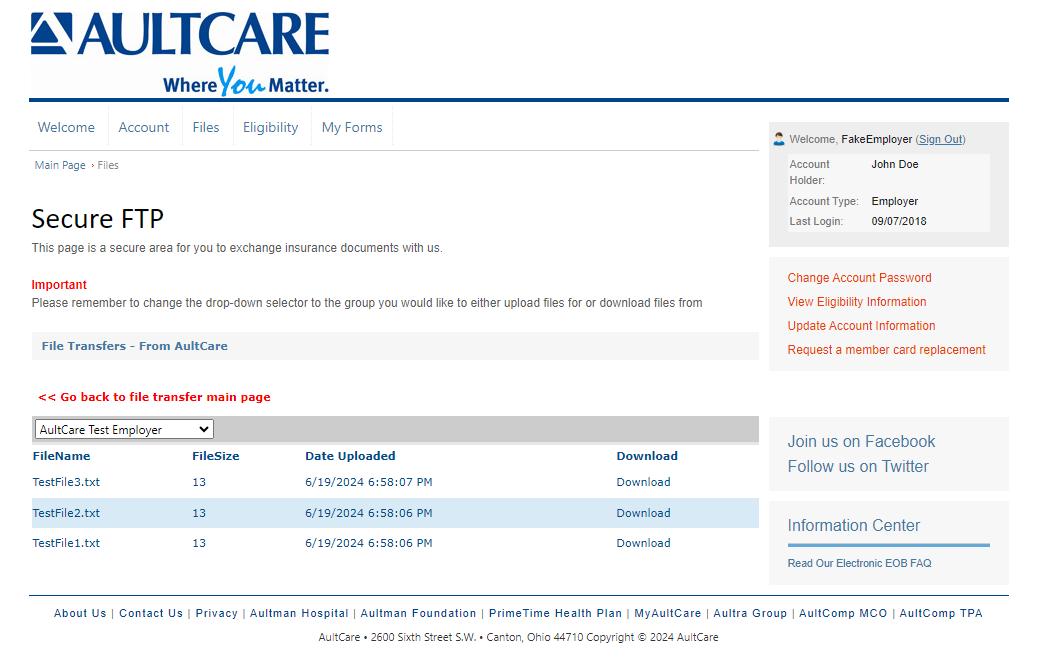
files. (Based on your authorization, only those particular group names will be displayed.)
3. For employers who have more than one AultCare account, select the appropriate account from the drop down box.
4
Once you see a list of files, click on the Download link to view/download it on your computer.
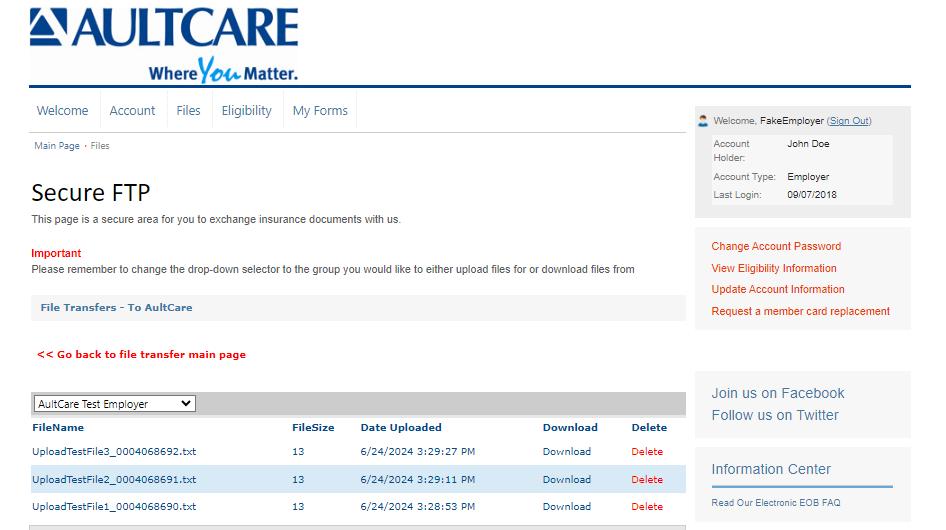

Uploading a File
1. Click the link labeled Click here to upload files
An example of the upload center is shown to the right.
An example of the upload center is shown to the right.
2.
3. Select the specific
4. Browse for the file you
5. Select
4. Browse for the file you want to upload on your computer.
2. Select the group number associated with your file upload.
3. Select the specific file type.
Previously Uploaded Files
5. Select Upload.
Previously Uploaded Files
4. Browse for the file you want to upload on your computer.
5. Select Upload
You can also see files previously uploaded.
Previously Uploaded Files
You can also see files previously uploaded.
If you have questions, contact your group coordinator, or for technical assistance, email the AultCare Web Team at AultConnect@AultCare.com
If you have questions, contact your group coordinator, or for technical assistance, email the AultCare Web Team at aultconnect@aultcare.com.
You can also see files previously uploaded.
If you have questions, contact your group coordinator, or for technical assistance, email the AultCare Web Team at AultConnect@AultCare.com
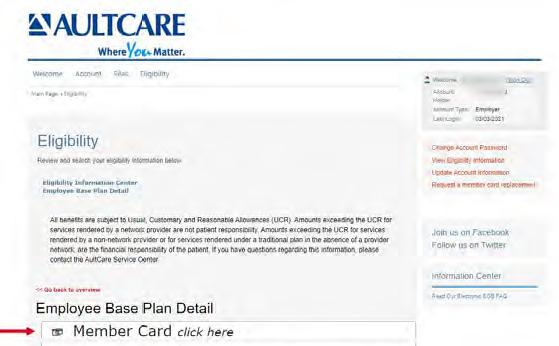
Log in to your employer secured account and select Eligibility
Step #2
Click Search to view a list of active members.

2. Click Search



The following information is provided to explain the process of enrolling and terminating employees and/or dependents. To ensure timely enrollment updates, please complete and return the Enrollment Application/Change Form or Cancellation and Continuation Form. If you would like information regarding electronic methods to complete enrollment changes, contact your Account Coordinator or Account Executive.
1. Step-By-Step Guide
This guide was created to assist with the completion of enrollment application/change form. The text denoted in red provides additional information to help understand what information is being requested.
2. Enrollment Application
All new employees and those employees requesting a change in their coverage, must complete this entire form, unless otherwise instructed. Spouse signature is required when waiving coverage.
3. Cancellation and Continuation Form
List all cancellations on this form. Utilize transaction codes for each change. Include enrollment form where indicated.
4. Important Information
All enrollment changes must be sent to AultCare within 31 days of qualifying event. Enrollment changes received before the 10th of the month will be reflected on the next monthly invoice.
Do not make enrollment changes on your monthly premium invoice.
Return completed enrollment forms to:
Email: aultcareeligibility@aultcare.com
Fax: 330-363-7746
Mail: AultCare Member Services
Questions may be directed to Customer Service 330-363-6360.

• Effective Dates:
> Members effective on the first day of the month, will be invoiced for the entire month.
> Members effective after the first of the month, will not be invoiced until the following month.
> Members with an effective date and termination date within the same month, will be invoiced for that month.
> Members with a termination date after the first of the month will be invoiced for the entire month.
• Newborns:
> Employee must enroll newborn, and Employer must submit enrollment paperwork to AultCare within 31 days of birth.
• Termination Dates:
> Coverage ends on the end of the month the member terminates.
> Coverage for dependents turning age 26 ends on the end of month.
• Reinstatement of coverage - Return to work rules:
> Employers with 50 or more employees - Members may be reinstated on the plan within 13 weeks with no waiting period.
> Employers with less than 50 employees on a Small Group Marketplace Plan - Members may be reinstated on the plan within 13 weeks with no waiting period.
> Employers with less than 50 employees on a Transitional Relief Plan - Members may be reinstated on the plan within 14 days with no waiting period.
Please complete this form in its entirety.
List all AultCare group numbers that apply. (Medical, Dental, Vision)
Employee Location/Job Classification
Use this section to designate an employee classification, if needed. These designations should be set-up as rate codes during the implementation of your plan. (Example: hourly vs. salary; executive or management; physical plant location.)
Designate if the employee is accessing an out-of-area network. (Cigna, First Health Network, etc.)
AultCare Effective Date
Provide the date the coverage is set to begin.
EMPLOYEE COVERAGE ELECTION
by the employee.
New Group
New Hire
Waiving Coverage
Open Enrollment
Designate the reason for applying for coverage or if coverage is being waived. If waiving coverage, a signature is required on the back of this form.
Qualifying Event — Explain:
If applying for coverage for a qualifying event, please provide a detailed explanation. (For example: spouse lost coverage, marriage, birth, adoption.)
If the original hire date is not available, please provide the month and year.
Coverage Type(s) Requested: Check All
Be sure to check all benefit options being elected.
Plan Requested: Plan Name
Use this section to designate the employee’s plan election. (Example: PPO, HDHP or OPT 1, OPT 2, etc.)
This section is to be completed by the employee.
A(dd), C(hange), D(elete)
Please provide the reason code for enrolling or disenrolling dependents.
Social Security Number
SSN are required for all dependents with coverage.
Benefits Selected (M,D,V,R)
List all that apply.
Other Insurance Coverage? (Y/N)
If yes, please complete the other coverage information on the back of this form.
This section is to be completed by the employee if any covered persons have other health insurance coverage.
This section is to be completed by the employee if any covered persons are enrolled in Medicare.
This section is to be completed by the employee to designate any specified needs.
Signature______________ Date __________
Employee must sign and date when electing coverage.
Employees Waiving Coverage
Reason for waiver of coverage: ______________
Employee and spouse must provide reason for waiving coverage.
Signature______________ Date __________
Employee and spouse must sign if either are waiving coverage.
Please submit this form to AultCare by one of the following methods:
Email: aultcareeligibility@aultcare.com |
Fax: 330-363-7746 | Mail: AultCare Member Services PO Box 6910 Canton, OH 44706
Employer to send completed form to AultCare by one of the following methods.
Upon your effective date with this plan, will you or any of your family members have other health insurance? YES NO
If yes, what is the name of the other insurance company?
If yes, what type(s) of other health insurance will you have? Check all that apply Medical Dental Rx Vision
Do you or your spouse or any enrolled dependents have Medicare coverage? YES NO If yes, please provide information below.
Medicare Medicare Hospital Effective Date Medical Effective Date Enrollee Name ID Number (Part A) (Part B)
Do you have Medicare Part D coverage? YES NO If yes, what is the effective date of your coverage?
Do you, or any of your dependents, have any cultural or linguistic needs? YES NO
If yes, what are they?
Ethnicity: Non-Hispanic/Latino Race: White Black American Indian/Alaska Native Language: English Spanish Hispanic/Latino Choose not to answer Asian Native Hawaiian/Pacific Islander
Choose not to answer
I am applying for group health coverage through AultCare Insurance Company and its related entities (“AultCare”). I acknowledge the coverage for which I am applying is subject to eligibility requirements and the terms of the policy. I acknowledge that I have read and understood all of the information contained within this document. Additionally, I acknowledge that all information that I have entered in this application, to the best of my knowledge, is complete, true, and accurate. I understand that any attempt to mislead or defraud AultCare is considered insurance fraud.
INSURANCE FRAUD WARNING: Any person who, with intent to defraud or knowing that he or she is facilitating a fraud against an insurer, submits an application or files a claim containing a false or deceptive statement is guilty of insurance fraud.
I acknowledge that AultCare may use and disclose my protected health information, as well as, the protected health information of my family for payment, treatment, and operations. This information may be disclosed to other insurance companies, third party administrators, state and federal agencies, health care providers and other organizations and persons that perform professional, business, or insurance functions for AultCare, as permitted by state and federal law.
The information may be used for, but not limited to, processing enrollment applications, risk classifications, detecting or preventing fraud, internal and external audits, claims administration, case management, quality improvement programs, public health reporting, law enforcement investigations, coordination of benefits, medical management programs, and subrogation.
Employees
I have read all of the statements contained in this application and declare that by signing this application the information I have provided is true and complete to the best of my knowledge. Electronic Signature Disclaimer: Please be advised that AultCare will not deny the enforceability or effect of an electronic signature solely because it is in an electronic format. Any valid signature provided in this section shall have the same legal effect and enforceability as a manually executed signature. I authorize deduction from my wages, as necessary, for any required premium for the coverage for which I have applied.
Signature Date
Employees Waiving Coverage
I have read all of the statements contained in this application and declare by signing that the information I have provided is true and complete to the best of my knowledge. I understand that I am eligible to apply for coverage through my employer. And I acknowledge that, subject to the terms and conditions of the policy, by waiving coverage at this time, I may not be able to enroll myself or my family again until the next annual enrollment period or a special enrollment period. I hereby decline coverage for (check all that apply): Myself Spouse Child(ren)
Reason for waiver of coverage:
Signature
Spouse Signature Date
Per the 2015 FTC TCPA, AultCare or a vendor of AultCare, may contact you for demographic, satisfaction, and/or medical care management information in accordance with its obligation under Federal Law.
EFFECTIVE DATE OF TRANSACTION EMPLOYEE NAME
Today’s Date:
Employer:
Group Numbers: Completed By:
COMMENTS
Please indicate all cancellations on this report. Do not make changes on the monthly premium statement. Utilize transaction codes for each change. Include enrollment form where indicated and provide within 31 days of event. *Signed enrollment forms must include spouse’s signature when applicable.
Cancellation of Coverage:
A. Cancellation – Left Employment/Termination (Include in Comments section Termination Date & if Voluntary, Involuntary or due to Gross Misconduct)
B. Cancellation – Deceased (Specify Date of Death in Comments section)
C. Cancellation – Layoff (Include in Comments section the Date of Layoff & if Voluntary or Involuntary)
D. Cancellation - Waiving (Specify in Comments if waiving coverage, include Enrollment Form with waiver section signed*.)
E. Cancellation – Reduction in hours: no longer meets minimum eligibility requirements
Continuation of Coverage:
F. COBRA Coverage Elected (Include Expiration Date, Copy of signed election form & proof of first payment) (This is not necessary if AultCare administers the COBRA)
G. State Continuation of Coverage (For employers under 20 – please indicate expiration date of State Continuation of Coverage in the Comments section. Please include a signed Continuation of Coverage Election Form.)
Other:
H. Other (Include detailed explanation)
I understand AultCare is relying on my answers to the above questions to ensure overall compliance for my group health plan. I certify the answers are true to the best of my knowledge and belief. I also understand I am responsible for promptly notifying AultCare if any information changes.
Please submit this form to AultCare by one of the following methods: Email: aultcareeligibility@aultcare.com | Fax: 330-363-7746 | Mail: AultCare Member Services PO Box 6910 Canton, OH 44706
6234/20
Please contact Customer Service with any questions: 330-363-6360
Q. What is the expected timeline for a Client/Employer to submit Open Enrollment changes once the Open Enrollment period has ended?
A. Submit Open Enrollment (OE) changes as soon as possible, but no later than 10 business days of the close of your OE period. Delays in OE submission will result in delays in member ID cards and coverage being in effect for prescription fills, as well as denied claims and incorrect monthly invoices. If this timeline is unattainable, contact your Account Coordinator or Eligibility Representative to establish an appropriate date for the submission of your OE changes.
Q. Can we send our OE changes in a different format than our standard process?
A. If you plan to send your OE in a format that you do not use currently, it is advisable to discuss this with your Account Coordinator to obtain approval before proceeding. Sending OE in a format that is not your standard could delay processing which will cause delays in getting ID cards to Employees.
Q. We are adding an ancillary product, i.e., dental, vision, life, etc. to our benefit package, how can we send enrollment to AultCare?
A. An enrollment election, within your standard enrollment process, is required to enroll the appropriate members into the new ancillary product.
Q. What is the expected time frame for our members to obtain ID cards?
A. Typically, it takes 7-10 business days for a member to receive their ID card once they are loaded into our system. At year end, enrollment must be delivered no later than the first Friday in December to guarantee ID card delivery by Jan. 1, otherwise, ID cards may be delayed.
Reminder: Members can view their ID cards on the website and mobile app once they have created a log in.
Q. Will all members receive new ID cards?
A. No, cards will only be issued to members on plans that have made benefit changes, i.e.: copayment, deductible, out of pocket.
Q. If we currently send paper applications for enrollment changes, is it necessary to send an application on every Employee during Open Enrollment?
A. No. If the Employee is not making plan election changes, adding or removing dependents/spouse, and/or does not have a demographic change, i.e. address change, then there is no need to complete and submit an enrollment application. Their current coverage will continue with no changes.
Q. Our current enrollment vendor has questions relating to the Open Enrollment process, who should they contact?
A. Please reach out to your Eligibility Representative or Account Coordinator for additional information.

We would like to take this opportunity to advise you of an important provision in your health care plan. To participate, you must complete an enrollment form. Dependent upon which specific plan you wish to enroll in, you may have to pay part of the premium through payroll deduction.
Additionally, HIPAA requires that we notify you of the “Special Enrollment Provision”.
Loss of Other Coverage. If you decline enrollment for yourself or for another eligible dependent (including your spouse) while other health insurance or group health plan coverage is in effect, you may be able to enroll yourself and your dependents in this plan if you or your dependents lose eligibility for that other coverage (or if the employer stops contributing toward your or your dependents’ other coverage). However, you must request enrollment within 30 days after your or your dependents’ other coverage ends (or after the employer stops contributing toward the other coverage).
New Dependent by Marriage, Birth, Adoption, or Placement for Adoption. In addition, if you have a new dependent as a result of marriage, birth, adoption, or placement for adoption, you may be able to enroll yourself and your new dependents. However, you must request enrollment within 30 days after the marriage, birth, adoption, or placement for adoption.
To request special enrollment or to obtain more information about the plan’s special enrollment provisions, contact your AultCare Service Center at 330-363-6360 or 1-800-344-8858
HIPAA requires that plan sponsors and/or insurers provide a Certificate of Creditable Coverage/Certificate of Health Plan Coverage (HIPAA Certificate) to each individual who requests one, so long as it is requested while the individual is covered under the AultCare Health Plan or within 24 months of the individual’s coverage under the AultCare Health Plan ending. The request also can be made by someone else’s behalf for an individual. For example, an individual who previously was covered under the AultCare Health Plan may authorize a new plan in which the individual enrolls to request a certificate of the individual’s Creditable Coverage/Health Plan Coverage from the AultCare Health Plan. An individual is entitled to receive a Certificate upon request even if the AultCare Health Plan has previously issued a Certificate to that individual.
Requests for Certificates should be directed to AultCare Corporation, Attn: Member Services, P.O. Box 6910, Canton, Ohio 44706-0910 or by calling your AultCare Service Center at 330-363-6360 or 1-800-3448858.
Telephone requests are accepted only if the Certificate is to be mailed to the address the plan has on file for the individual to who the request relates. Other requests must be made in writing.
All requests must include:
The name of the individual for whom the Certificate is requested;
AultCare Group Number and Identification Number
P.O. Box 6910 | Canton, OH 44706
PHONE: 330-363-6360 | TOLL FREE: 1-800-344-8858
TTY LINE: 711
WEBSITE: www.aultcare.com
The last date that the individual was covered under the plan;
The name of the participant that enrolled the individual in the plan; and
A telephone number to reach the individual for whom the Certificate is requested.
Required written request must also include:
The name of the person making the request and evidence of the person’s authority to request and receive the Certificate on behalf of the individual
The address to which the Certificate should be mailed.
The requester’s signature
After receiving a request that meets these requirements, the plan will act in a reasonable and prompt fashion to provide the Certificate.
(Note: A preexisting condition exclusion does not apply to enrollees of AultCare plans that have renewed effective January 1, 2014 and after.)
The Certificate of Creditable Coverage/Health Plan Coverage can be used as proof of loss of coverage.
P.O. Box 6910 | Canton, OH 44706
PHONE: 330-363-6360 | TOLL FREE: 1-800-344-8858
TTY LINE: 711
WEBSITE: www.aultcare.com

In regards to the Health Insurance Portability and Accountability Act of 1996 and the Omnibus Rule of 2013, employers who provide medical benefits to their employees using self-funded health plans need to be aware of their compliance responsibilities. This notification is intended to provide an overview for the employer sponsors of self-funded health plans. All employer health plans are regulated by the Health Insurance Portability and Accountability Act of 1996 (HIPAA). The Omnibus Rule of 2013 strengthened the privacy and security rules of HIPAA.
HIPAA-covered entities, including self-funded group health plans, and their “business associates,” should review their responsibilities under HIPAA and the Omnibus Rule.
When an employer purchases insurance through a group policy, exposures and risks from different Protected Health Information (PHI) may occur. It is usually limited to enrollment and summary information used to shop for insurance.
However, when an employer funds the benefits, instead of purchasing the insurance, the employer can directly, or through its agent (AultCare), access its employees’ medical information and is responsible for complying with privacy and security rules.
These rules include:
Requirements regarding uses and disclosures of health information
Notification of breaches
Preparation and distribution of notices of privacy practices and procedures
Updating business associate agreements
Training personnel who have access to PHI
For more comprehensive information on the HIPAA and the Omnibus Rules, please contact your company’s Benefits Counsel.
P.O. Box 6910 / Canton, OH 44706
PHONE: 330-363-6360 / TOLL FREE: 1-800-344-8858
TTY LINE: 330-363-2393 / 1-866-633-4752 for the hearing impaired
WEBSITE: www.aultcare.com
This Notice of Privacy Practices (NPP) describes how medical and claims information about you may be used and disclosed, how you can get access to your information, and your rights under HIPAA. Please review this NPP carefully. Feel free to share it with your family or personal representative.
AultCare Insurance Company (dba AultCare HMO), which is part of an Organized Health Care Arrangement with AultCare Corporation, AultCare Health Insuring Corporation dba PrimeTime Health Plan, and Aultra Administrative Group (AultCare or We) is a Group Health Plan Covered Entity under HIPAA.
We’re committed to safeguarding the Privacy and Security of Protected Health Information of its enrollees and their eligible dependents (you) in paper (PHI) or electronic form (ePHI).
This NPP describes our HIPAA-compliant policies and procedures for the Use and Disclosure of your PHI/ePHI, including the use of PHI/ePHI for eligibility, enrollment, underwriting, claims processing, coordination of benefits, and payment of treatment under your group health plan in compliance with HIPAA’s Privacy and Security Rules (updated by the Omnibus Rule of 2013), the HITECH Act, and the Genetic Information Nondiscrimination Act (GINA).
You may access this NPP on our website www.aultcare.com. If you do not have a computer or internet access, or if you want a paper copy of this NPP, please call our Service Center at 330-363-6361 or 1-800-344-8858.
Not every use or disclosure of PHI, with or without a signed Authorization, is listed in this NPP. Uses or disclosures not specified in this NPP often require an Authorization. Please contact our Privacy Officer if you have a question, concern, or need further guidance.
Accounting. An Accounting is a list of disclosures of your PHI/ePHI we have made.
Authorization. An Authorization is a document signed and dated by the individual who authorizes the use or disclosure of PHI/ePHI for purposes other than treatment, payment, or healthcare operations.
Business Associates. We contract with outside business associates that may access, use, or disclose PHI/ePHI to perform covered services for us. Examples include auditing, accounting, accreditation, actuarial services, and legal services. Business associates must protect the privacy and security of your PHI/ePHI to the same extent we do. If a business associate delegates services to a subcontractor or agent, that subcontractor or agent is also a business associate that must comply with HIPAA.
Covered Entities Covered Entities include health care providers (e.g. hospitals, doctors, nurses, nursing homes, home health agencies, durable medical equipment suppliers, other health care professionals and suppliers), and group health plans. AultCare is a group health plan covered entity.
Designated Record Set. A Designated Record set is a group of records containing PHI in paper or electronic form that we created and store. A Designated Record set includes medical, healthcare and service records, billing, claims and payment information, eligibility and enrollment information, and other information we use to make decisions
regarding the coverage and payment of medical care under your plan. Records created by others are not part of a designated record set.
Disclose. Disclose means our releasing, transferring, providing access to, or divulging PHI/ePHI to a third party, including covered entities and their business associates: (1) for treatment, payment, and health care operations; or (2) when you permit us by your signed authorization; or (3) as required by law.
Genetic Information. Genetic Information includes genetic testing of the individual or family members.
Health Plan. Health plan means an individual or group health plan that provides, or pays the cost of, medical care and includes a health insurance issuer, HMO, Part A or B of Medicare, Medicaid, voluntary prescription drug benefit program, issuer of Medicare supplemental policy, issuer or a long-term care policy, employee welfare benefit plan, plan for uniformed services, veterans’ health care program, CHAMPUS, Indian health service program, federal employee health benefit program, Medicare Advantage plan, approved state child health plan, high risk pool, and any other individual or group health plans or combination that provides or pays for the cost of medical care. AultCare is a group health plan.
Health Care Operations. Health Care Operations include quality assurance, performance improvement, utilization review, accreditation, licensing, legal compliance, provider/supplier credentialing, peer review, business management, auditing, enrollment, underwriting, stop-loss/reinsurance, and other functions related to your health plan, as well as offering and providing preventive, wellness, case management, and related services.
Individual. Individual means the enrollee or eligible dependent (including minors) to whom PHI belongs. It also applies to your family member or personal representative acting on your behalf.
Minimum Necessary. We will limit the use or disclosure of your PHI/ePHI to the minimum needed to accomplish the intended purpose of the use, disclosure, or request.
Payment. Payment means the activities by a group health plan to obtain premiums or to determine or fulfill its responsibility for coverage and the provisions of benefits under your plan and includes eligibility or coverage determination, coordination of benefits, adjudication and subrogation of health benefit claims, billing, claims management, EOBs, health care data processing, reinsurance (including stop-loss and excess), determination of medical necessity, utilization review (including pre-certification and retrospective review), and related activities.
Personal Representative. Personal Representative means a person acting on behalf of the individual, including family, spouse, guardian, attorney-in-fact under a durable or general power of attorney, or friend assisting the individual with healthcare and payment decisions.
Protected Health Information (PHI/ePHI). PHI/ePHI means individually identifiable medical and health information regarding your medical condition, treatment of your medical condition, and payment of your medical condition, and includes oral, written, and electronically generated and stored information. PHI/ePHI excludes de-identified information or health information regarding a person who has been deceased for more than 50 years.
Treatment. Treatment means the provision, coordination, and management of health care and services by one or more health care providers, including referrals and consultations between providers or suppliers.
Use. Use means our accessing, sharing, employing, applying, utilizing, examining, or analyzing your PHI/ePHI within the AultCare organization for payment and health care operation purposes. Your PHI/ePHI is accessible only to members of AultCare’s workforce who have been trained in HIPAA Privacy and have signed a confidentiality agreement
that limits their access and use of PHI/ePHI, according to the minimum necessary standard, to perform the authorized purpose.
Wellness Program. Wellness Program means a program that an employer has adopted to promote health and disease prevention, which is offered to employees as part of an employer-sponsored group health plan or separately as a benefit of employment.
When it comes to your health information, you have certain rights. This section explains some of your rights and our responsibilities.
You may get a copy or summary of your health and claims records:
• You may ask to see or get a copy of your health and claims records and PHI kept in a designated record set. Please call the Service Center to ask how to do this. There are some restrictions.
• We will get you a paper copy or electronic version of your health and claims records, or give you a summary, usually within 30 days of your request. We may charge reasonable, cost-based fees.
You may ask us to correct your health and claims records:
• You may ask us in writing to correct your health and claims records in a designated records set if you believe they are incorrect, inaccurate, or incomplete. Please call the Service Center or visit our website to get an amendment request form.
• We may say “no” to your request, but we’ll tell you why in writing within 60 days.
• You will have an opportunity to appeal. You may request confidential communications or communications by alternative means:
• You may ask us to contact you about claims, premiums, EOBs, or other matters about your health plan and coverage in a specific way, such as home phone, office phone, or cell phone, or by alternate means, such as an address different from your home or usual email address.
• Let us know if you do not want us to leave any voice mail message.
• Contact the Service Center to request. We will consider all reasonable requests.
You may ask us to limit (restrict) what we use or disclose:
• You may ask us in writing not to use or disclose certain health information for treatment, payment, or operations. We may honor your request if you pay for treatment in full out-of-pocket.
• Please call the Service Center for a restriction request form or visit our website.
• While we will consider reasonable requests, we are not required to agree to your request. We may say “no” if restricting information could affect your care or if disclosure is required by law. You may request a list (“Accounting”) of those to whom we’ve disclosed PHI/ePHI:
• You may ask in writing for a list of disclosures of your PHI/ePHI (Accounting) for the six years prior to your request.
• We will include all disclosures except for those about treatment, payment, and health care operations, and disclosures made to you or that you authorized us to make. We’ll provide one accounting a year for free but, will charge a reasonable, cost-based fee if you ask for another one within 12 months. You may get a copy of this NPP:
• You may ask for a paper copy of this NPP at any time, even if you have agreed to receive this NPP electronically. We will provide you with a paper copy promptly.
• You may access electronic copy of this NPP on our website at any time. You may choose someone to act for you:
• You may choose a family member or personal representative to receive PHI/ePHI from us, exercise your rights, and make choices for you.
• We will use reasonable efforts to confirm that the person is authorized to act on your behalf before we take any action.
You may file a complaint if you believe your rights have been violated:
• If you believe your privacy or your HIPAA rights have been violated, we urge you to contact our privacy officer, either by calling the Service Center or filing a written complaint at AultCare, P.O. Box 6029, Canton, OH 44706.
• We take all complaints very seriously. We will investigate and take appropriate action if needed.
• You also may file a complaint with the U.S. Department of Health and Human Services Office for Civil Rights by sending a letter to; 200 Independence Avenue, S.W., Washington, D.C. 20201, calling 1-877-6966775, or visiting Complaint Process | HHS.gov
• We will never retaliate against you for filing a complaint, asking a question, or expressing a concern.
This section describes how we may communicate with you, family members, or your personal representative.
Communicating with You:
We may communicate with you about claims, premiums, or other things regarding your health plan.
Communicating with Family or Others Involved In Your Care:
• We may disclose your PHI/ePHI to designated family, friends, guardians, persons named in a durable or general power of attorney, personal representatives, or others assisting in your care or payment of claims.
Minors and Emancipated Minors:
• We may disclose a minor’s PHI/ePHI to the minor’s parent(s) or guardian, unless there are legal or policy reasons not to do so.
• We will not disclose PHI/ePHI to the parent(s) or guardian of an emancipated minor. A minor is emancipated if he/she: (1) does not live with his/her parent(s); (2) is not covered by parental health insurance; (3) is financially independent of parent(s); (4) is married; (5) has children; or (6) is in the military.
Deceased Enrollees:
• If you die, we may disclose your PHI to the executor or administrator of your estate.
• We may disclose PHI/ePHI to your spouse, family, personal representative, or others who were involved in your care or management of your affairs, unless doing so would be inconsistent with your wishes made known to us.
This section describes how we typically use or disclose your PHI/ePHI with and without an Authorization.
No Authorization Needed:
• We will create, receive, or access your PHI/ePHI, which we may use or disclose to other covered entities for treatment, payment, and health care operations, without the need for you to sign an Authorization.
• We will disclose PHI/ePHI needed to treat or authorize treatment. For example, a doctor or health facility involved in your care may request your PHI/ePHI to make treatment decisions covered by the plan.
• We will use or disclose your PHI needed for payment. For example, we will use information about your medical procedures and treatment to process and pay claims, to determine whether services are medically necessary, and to pre-authorize or certify services covered by your health plan.
• We may disclose PHI/ePHI to governmental or commercial health plans that may be obligated under coordination of benefit rules to process and pay your claims.
• We will use and disclose your PHI/ePHI as necessary or required by law to administer your plan and for our health care operations. For example, we may use or disclose PHI/ePHI for underwriting purposes. We will not use or disclose genetic information for underwriting purposes.
• We may disclose PHI/ePHI to business associates to perform covered services. It is not necessary for you to sign an Authorization for us to share PHI/ePHI with our business associates for covered services.
• We will use PHI/ePHI gathered from our online enrollment tools to complete certain applications for enrollment. The use of these tools is voluntary and alternate methods of enrollment may be available should you choose not to provide all the requested information needed to complete the online enrollment.
Authorization Needed:
We will not use or disclose your PHI/ePHI for any purpose other than treatment, payment, or healthcare operations without your signed HIPAA-compliant Authorization, unless required by law.
• We will not disclose psychotherapy notes without a signed Authorization unless required by law.
• We will not disclose your PHI/ePHI to your employer without your signed Authorization. We may disclose PHI/ePHI to the plan sponsor of your health benefit plan on condition that the plan sponsor certifies that it will maintain the confidentiality of PHI/ePHI and will not use PHI to make employment-related decisions or employee benefit determinations.
• We will not release medical records if subpoenaed, unless you sign an Authorization, or the lawyers sign a qualified protective order, or if we receive a valid court or administrative order.
You may choose to receive information about health-related products or services or fundraising:
• We may use your PHI/ePHI if we believe you may be interested in, or benefit from, treatment alternatives, wellness, preventive disease management, or health-related programs, products or services that may be available to you as an enrollee or eligible beneficiary under your health plan. For example, we may use your PHI/ePHI to identify whether you have a particular illness, and contact you to let you know about a disease management program is available to help manage your illness.
• Let us know if you do not want to be contacted or receive information about these services and programs. Opting out will not affect coverage or services.
• We will not sell or disclose your PHI/ePHI to third-parties for marketing without your Authorization, which will indicate whether we are paid for selling PHI.
• We may contact you about charitable fundraising. If you do not want to be contacted or receive fundraising materials, let our Service Center know. Opting out will not affect coverage or services.
• If you voluntarily choose to participate in a Wellness Program, you may be asked to answer questions on a health risk assessment (HRA) and/or undergo biometric screenings for risk factors,
• Wellness Programs may also provide educational health-related information or services that may include nutrition classes, weight loss and smoking cessation programs, onsite exercise facilities, and/or health coaching to help employees meet their health goals.
• If your employer has entered or may enter into a contract with us to perform services, as well as receive, collect, use, disclose, and store data in connection with a Wellness Program. We will protect the privacy of your PHI.
We may use or disclose PHI/ePHI, without your Authorization, as required by law, including, but not limited to:
• Workers’ Compensation
• Public health agencies
• FDA and OSHA
• Ohio Department of Insurance and other regulatory and licensing agencies
• Armed Forces to assist in notifying family members of your location, general condition, or death
• Law Enforcement
• Homeland security
• Emergency and disaster
• Prevent threat of serious harm
• Proof of immunization
Breach Notification
• You have the right to notification if a breach of your PHI/ePHI occurs. We will promptly notify you by firstclass mail, at your last known address, or by email (if you prefer) if we discover a breach of unsecured PHI/ePHI, which includes the unauthorized acquisition, access, use, or disclosure of your PHI/ePHI, unless we determine through a risk analysis that a low probability exists that the compromise of your PHI would cause you financial, reputational, or other harm.
• We will include in the breach notification a brief description of what happened, a description of the types of unsecured PHI involved, steps you should take to protect yourself from potential harm, a brief description of what we are doing to investigate the breach and mitigate any potential harm, as well as contact information for you to ask questions and learn additional information.
This section describes how and when we make changes and how we will inform you of any material changes.
• We reserve the right to change this NPP at any time, which we may make effective for PHI/ePHI we already used or disclosed, and for any PHI/ePHI we may create, receive, use, or disclose in the future.
• We will make material amendments based on changes in the HIPAA laws.
• The revised NPP will be posted on our website www.aultcare.com. Copies of revised NPPs will be mailed to all enrollees covered by the plan, and copies may be obtained by mailing a request to: Privacy Coordinator, P.O. Box 6029, Canton, Ohio 44706.
If you have questions or need further assistance regarding this NPP, you may contact the Service Center at 330-363-6360 or 1-800-344-8858. If you are hearing impaired and have access to a TTY phone, you may reach us at our TTY line 711. Our Service Center hours are from 7:30 a.m. to 5:00 p.m., Monday-Friday.
Review Date: Dec 04, 2024
AultCare/Aultra General Tag Lines for the State of Ohio
English
If you, or someone you are helping, have questions about AultCare/Aultra you have the right to get help and information in your language at no cost. To speak with an interpreter, call Local: 330.363.6360 Outside Stark County: 1.800.344.8858 TTY Local: 711 Outside Stark County: 711
Spanish
Español
Si usted, o alguien a quien usted está ayudando, tiene preguntas acerca AultCare/Aultra tiene derecho a obtener ayuda e información en su idioma sin costo alguno. Para hablar con un intérprete, llame al Local : 330.363.6360
Fuera del condado de Stark : 1.800.344.8858 TTY Local : 711 Fuera del condado de Stark : 711
Chinese 中文
如果您,或是您正在協助的對象,有關於AultCare/Aultra保险公司
方面的問題,您有權利免費以您的母語得到幫助和訊息。洽詢一位翻譯員,請撥電話 本地: 330.363.6360
斯塔克縣外: 1.800.344.8858 TTY線 本地: 711斯塔克縣外: 711。
German
Deutsche Falls Sie oder jemand, dem Sie helfen, Fragen zum AultCare/Aultra haben, haben Sie das Recht, kostenlose Hilfe und Informationen in Ihrer Sprache zu erhalten. Um mit einem Dolmetscher zu sprechen, rufen Sie bitte die Nummer Local: 330.363.6360 Außerhalb von Stark County : 1.800.344.8858 TTY –Linie Local: 711
Außerhalb von Stark County : 711 an.
Arabic
1.800.344.8858
Pennsylvania Dutch
Deitsch
Wann du hoscht en Froog, odder ebber, wu du helfscht, hot en Froog baut AultCare/Aultra hoscht du es Recht fer Hilf un Information in deinre eegne Schprooch griege, un die Hilf koschtet nix. Wann du mit me Interpreter schwetze witt, kannscht du Local: 330.363.6360 Außerhalb von Stark County: 1.800.344.8858 TTY –Linie Local: 711 Außerhalb von Stark County : 711 uffrufe.
AultCare/Aultra
French Français
Si vous, ou quelqu'un que vous êtes en train d’aider, a des questions à propos de Compagnie d'Assurance
AultCare/Aultra, vous avez le droit d'obtenir de l'aide et l'information dans votre langue à aucun coût. Pour parler à un interprète, Appelez Locale 330.363.6360 En dehors du comté de Stark : 1.800.344.8858 ligne ATS Local : 711 En dehors du comté de Stark : 711.
Vietnamese
Việt Nam
Nếu quý vị, hay người mà quý vị đang giúp đỡ, có câu hỏi về Công ty Bảo hiểm AultCare/Aultra quý vị sẽ có quyền được giúp và có thêm thông tin bằng ngôn ngữ của mình miễn phí. Để nói chuyện với một thông dịch viên, xin gọi Địa phương: 330.363.6360 Bên ngoài của Stark County : 1.800.344.8858 TTY đường dây Địa phương: 711 Bên ngoài của Stark County : 711.
Cushite-Oromo
Isin yookan namni biraa isin deeggartan AultCare/Aultra, irratti gaaffii yo qabaattan, kaffaltii irraa bilisa haala ta’een afaan keessaniin odeeffannoo argachuu fi deeggarsa argachuuf mirga ni qabdu. Nama isiniif ibsu argachuuf, lakkoofsa bilbilaa Local: 330.363.6360 Outside of Stark County: 1.800.344.8858 TTY Line Local: 711 Outside of Stark County: 711 tiin bilbilaa.
Korean
한국어
만약 귀하 또는 귀하가 돕고 있는 어떤 사람이AultCare/Aultra 보험 회사 에 관해서 질문이 있다면 귀하는
그러한 도움과 정보를 귀하의 언어로 비용 부담없이 얻을 수 있는 권리가 있습니다. 그렇게 통역사와
얘기하기 위해서는 지역 : 330.363.6360 스타크 카운티 의 외부 : 1.800.344.8858 TTY 라인 지역 : 711 스타크
카운티 의 외부 : 711
로 전화하십시오
Italian
Italiano
Se tu o qualcuno che stai aiutando avete domande su AultCare/Aultra, hai il diritto di ottenere aiuto e informazioni nella tua lingua gratuitamente. Per parlare con un interprete, puoi chiamare Locale: 330.363.6360 Al di fuori di Stark County : 1.800.344.8858 TTY linea Locale: 711 Al di fuori di Stark County : 711.
Japanese 日本語
ご本人様、またはお客様の身の回りの方でもAultCare/Aultra保険会社についてご質問がございました ら、ご希望の言語でサポートを受けたり、情報を入手したりすることができます。料金はかかりませ ん。通訳とお話される場合、 ローカル: 330.363.6360 スターク郡の外: 1.800.344.8858 TTYライン ローカル: 711 スターク郡の外: 711までお電話ください。
Dutch Nederlands
Als u, of iemand die u helpt, vragen heeft over AultCare/Aultra, heeft u het recht om hulp en informatie te krijgen in uw taal zonder kosten. Om te praten met een tolk, bel Local : 330.363.6360 Buiten Stark County : 1.800.344.8858 TTY Line Local : 711 Buiten Stark County : 711.
Ukrainian
AultCare/Aultra,
County : 711. Romanian
Română
Dacă dumneavoastră sau persoana pe care o asistați aveți întrebări privind Compania de Asigurari
AultCare/Aultra, aveți dreptul de a obține gratuit ajutor și informații în limba dumneavoastră. Pentru a vorbi cu un interpret, sunați la Locale : 330.363.6360 In afara Stark Judet : 1.800.344.8858 TTY linie Locale : 711 In afara Stark Judet : 711.
Non-Discrimination Notice:
AultCare/Aultra complies with applicable Federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, or sex. AultCare/Aultra does not exclude people or treat them differently because of race, color, national origin, age, disability, or sex. AultCare/Aultra provides free aids and services to people with disabilities to communicate effectively with us, such as: Qualified sign language interpreters and written information in other formats (large print, audio, accessible electronic formats, other formats). AultCare/Aultra provides free language services to people whose primary language is not English, such as: Qualified interpreters and information written in other languages.
If you need these services, or if you believe that AultCare/Aultra has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, or sex, you can contact or file a grievance with the: AultCare/Aultra Civil Rights Coordinator, 2600 6th St. S.W. Canton, OH 44710, 330-3637456, CivilRightsCoordinator@aultcare.com. You can file a grievance in person or by mail, fax, or email. If you need help filing a grievance, our Civil Rights staff is available to help you.
You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office for Civil Rights electronically through the Office for Civil Rights Complaint Portal, available at https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at: U.S. Department of Health and Human Services 200 Independence Avenue, SW Room 509F, HHH Building Washington, D.C. 20201 1-800-368-1019, 800-537-7697 (TDD) Complaint forms are available at http://www.hhs.gov/ocr/office/file/index.html.
Various state and federal laws have requirements based on employee counts in determining how each regulatory guideline applies to an employer sponsored health plan, including; the Patient Protection and Affordable Care Act (ACA), COBRA, State Continuation, Medicare Secondary Payor, etc. Each year, AultCare will request employers to complete the Annual Determination of Group Size Demographics form, to assist employers with this responsibility. When counting employees, it’s important to conduct a related employer analysis. This section will assist you in counting your employees and determining your group size.
• Annual Group Size Demographics:
> Employers with 20 or more employees on at least half of the working days during the previous calendar year are eligible to offer COBRA.
• Medicare Coordination - Working Aged Employees:
> Medicare coordination rules for working age employees are based on the Employer size to determine whether the Employer plan or Medicare is primary.

Various state and federal laws have requirements based on employee counts. When counting employees, it’s important to conduct a related employer analysis.
The information detailed below does not constitute legal advice and is intended only for informational purposes. Please reach out to your benefits counsel to discuss your individual circumstances.
1. RELATED EMPLOYER ANALYSIS requires counting all employees of all members of the employers in a controlled group of companies or affiliated service group to determine employee count. Below is a summary of those groups.Bank Name
A controlled group may exist when two or more companies have any of the following:
• A Parent-Subsidiary Relationship: Exists when one or more chains of organizations are connected through ownership of a common parent company and 80% or more of the voting power or total value of each member of the group is owned by another member of the group, except for the common parent.
• A Brother-Sister Relationship: Exists when at least 50% of the voting power or total value of two or more organizations is owned by the same 5 or fewer persons taking into account only the ownership of each such organization that is identical for each other organization.
• A Combination Relationship: Exists when two or more organizations are members of a group that has common ownership which includes both parent-subsidiary relationships and brother-sister relationships, in which case all such organizations are considered the same controlled group of business.
An affiliated service group may exist when two or more organizations have a service relationship and/or ownership relationship with one another as satisfied by 1 of 3 tests (A-Org Test; B-Org Test; or Management Group Test).
More information about Controlled and Affiliated Service Groups can be found in the following IRS publication: https://www.irs.gov/pub/irs-tege/epchd704.pdf
Under Ohio law, a small, Ohio-based employer, for purposes of a group health plan and with respect to a calendar year and a plan year, is an employer who employed an average of at least two but no more than fifty eligible employees on business days during the preceding calendar year and who employs at least two employees on the first day of the plan year. With “Eligible Employee” being defined as an employee who works a normal work week of thirty or more hours. Eligible employee does not include a temporary or substitute employee, or a seasonal employee who works only part of the calendar year on the basis of natural or suitable times or circumstances. Ohio Rev. Code § 3924.01
COBRA generally applies to all private sector group health plans as well as plans sponsored by state and local governments. To be subject to COBRA, employers need to have at least 20 employees on more than 50% of their typical business days in the previous calendar year. When counting employees for COBRA purposes, both full- and part-time employees are counted, taking into consideration the above Related Employer Analysis. Each part-time employee counts as a fraction of a full-time employee. The fraction should be equal to the number of hours worked divided by the number of hours required to be considered full-time. (For example, a company requires a full-time employee work 40 hours a week. A part-time employee who works 20 hours a week is considered ½ of a full-time employee.) If you have fewer than 20 employees, you may be subject to state continuation of coverage requirements under ORC 3923.38 depending on whether your group health plan is subject to state regulation. These plans typically include Insured, MEWA plans, and self-funded public employers.
For more information, visit https://www.dol.gov/sites/dolgov/files/EBSA/about-ebsa/our-activities/resource-center publications/anemployers-guide-to-group-health-continuation-coverage-under-cobra.pdf
MSP is a federal law that requires Medicare pay secondary to group health plans unless certain circumstances apply. These exceptions are based on group size and the scenarios are listed below. This is not intended to be a comprehensive guide to the MSP law. As an employer group sponsoring a group health plan, you are required to maintain documentation regarding your total employee counts during the year. Please use the above Related Employer Analysis to report your employee count.
If Medicare requests a review of MSP status, AultCare will reach out to obtain information regarding your group size during the period in question. Medicare can inquire about claims that are several years old, so it’s imperative to maintain accurate records.
Age 65 or older (employee or spouse) and group health plan due to current employment of the Medicare beneficiary or the beneficiary’s spouse
Age 65 or older (employee or spouse) and group health plan not due to current employment (e.g. through a retiree health plan or COBRA) of the Medicare beneficiary or the beneficiary’s spouse
Disabled under age 65 (employee, spouse, or dependent) and group health plan due to current employment of the Medicare beneficiary or the beneficiary’s spouse or parent
Employer with fewer than 20 employees
Employer with at least 20 employees full or part-time in at least 20 weeks of the preceding or current year (the 20 weeks do not have to be consecutive)
All employers regardless of the number of employees
Disabled under age 65 (employee, spouse, or dependent) and group health plan not due to current employment (e.g. through a retiree health plan or COBRA) of the Medicare beneficiary of the beneficiary’s spouse or parent
ESRD patient (employee, spouse, or dependent) during the first 30 months of Medicare ESRD coverage
During at least half the year of the employer’s regular business days in the previous calendar year, the employer had:
Employer with fewer than 100 employees
Employer with at least 100 employees during at least half the year of the employer’s regular business days in the previous calendar year
All employers regardless of the number of employees
ESRD patient (employee, spouse, or dependent) regardless of age beginning with the 31st month of Medicare ESRD coverage
All employers regardless of the number of employees
If, when ESRD coverage begins, the employer plan is already primary payer according to MSP provisions
If, when ESRD coverage begins, the employer plan is correctly secondary payer because it is not subject to the applicable MSP provisions for working aged or for disability
and COBRA coverage)
All employers regardless of the number of employees Medicare, regardless of coverage for age 65 or disability, for the duration of ESRD coverage
COBRA coverage)
(Active and COBRA coverage)
Employer Name / Legal Name of Company
Group Number
Employer Identification Number (EIN/TIN)
Does the attached Related Employer Analysis define your company as part of a controlled group or affiliated service group? Yes No
a. If yes, list the other Related Employer name(s):_________________________________________________________
b. If yes, consider that fact when answering all of the questions below.
For Ohio-based employer plans, provide the number of employees in the preceding calendar year that worked at least 30 hours during a normal work week? (Note: If your answer is between 2 to 50 employees, you will be offered a Small Group or MEWA plan option.)
*Self-funded plans or employers outside Ohio may skip this question.
To determine the appropriate continuation of coverage (COBRA vs State Continuation) provide the following counts for 50% of the typical business days in the previous calendar year:
employee.)
a. Did you (including all Related Employers) have 100 or more full-time, part-time, seasonal employees or partners on 50 percent or more of your business days during:
The current calendar year? Yes No
The preceding calendar year? Yes No
b. Did you (including all Related Employers) have 20 or more full-time, part-time, seasonal employees, or partners for each working day in each of 20 or more calendar weeks (weeks do not have to be consecutive) during:
The current calendar year? Yes No
The preceding calendar year? Yes No
If you checked “Yes” for the current calendar year, and the 20-employee threshold was met during the current year, provide the date:_________________.
I understand AultCare is relying on my answers to the above questions to ensure overall compliance for my group health plan. I also understand the information submitted will be used to determine: whether Medicare will be the primary payer of claims for my Medicare-eligible insured(s), employer size for continuation of coverage, and employer size status under State and Federal regulations. I certify the answers are true to the best of my knowledge and belief. I also understand I am responsible for promptly notifying AultCare (as indicated above) if my answers to any of these questions change because our organization has increased or decreased the number of employees. I understand that CMS penalties may apply.
Signature of Company Officer or Authorized Representative Print Name
Title Daily Contact Email Address
Date Executive Email Address
• COBRA vs State Continuation:
> Employers with 20 or more employees on at least half of the working days during the previous calendar year are eligible to offer COBRA.
• Employer to determine COBRA administrator.
> Employers with fewer than 20 employees must offer State Continuation, for involuntary terminations, other than gross misconduct.
• Employer to administer.

Ohio’s law provides that an employee has a right to continue coverage under his or her employer’s group health plan upon involuntary termination of employment if certain requirements are met. All employer groups should be knowledgeable about Ohio’s continuation insurance laws; employers with fewer than 20 employees must be particularly aware of the requirements. For those employers, Ohio’s continuation coverage is the only continuation coverage available to their employees.
An employee is eligible for continuation of coverage if he or she satisfies all of the following requirements:
• Employee must have been continuously covered under the employer’s group health plan during the entire three months preceding his or her termination.
• Employee must have been involuntarily terminated for reasons other than gross misconduct.
• Employee is not eligible for or enrolled in Medicare or other group health coverage or COBRA.
If an employee satisfies these requirements, then the employer must offer that employee the right to continue coverage under its group health plan (even after the employee loses eligibility as a member of that group). The employer must inform the employee of his or her contribution amount in advance.
Important Notes:
• Coverage is only available for a maximum of twelve months.
• Coverage is not required to include benefits in addition to the hospital, surgical or major medical coverage, and prescription drug coverage if covered under the group policy. However, it may include dental, vision, or other benefits under the health plan.
• Payment is due from the employee to the employer in advance of each month of continuation coverage.
• Continuation coverage ceases if the employee fails to make timely premium payments. There is no grace period.
• Coverage ceases if the employee becomes eligible for or is covered under Medicare or any other group health plan.
This information is only intended to highlight the major requirements for the right to receive continuation of coverage and is not intended to offer legal guidance or advice regarding how an employer can comply with Ohio’s laws. There are many other significant requirements relating to continuation insurance not covered in this notice.
Employers are advised to consult with their tax professionals and attorneys to ensure compliance with these state laws. Employers may also call the Ohio Department of Insurance at 614-644-2658 or visit www.insurance.ohio.gov for additional information.
Termination of Employment
1) Covered by group health plan at least three months prior to termination;
2) Involuntary termination other than gross misconduct
Reservist called or ordered to active duty
3) Not eligible for or enrolled in Medicare or other group health coverage.
1) Employee is a reservist called or ordered to active duty; and
Employee Spouse Dependent Child(ren)
1) Employer must notify Employee of right of continuation at time Employee is notified of termination
2) Employer must notify Insurer of Employee’s continuation of coverage.
Employee must request continuation coverage and pay the first contribution to the Employer by the earliest of the following dates:
1) 31 days after date Employee’s coverage terminates
2) 10 days after date Employee’s coverage terminates, if Employer has notified Employee of right to continuation prior to that date
3) 10 days after date Employer notifies Employee of right to continuation if notice is given after Employee’s coverage terminates
1) Premium payments are not made on a timely basis.
NOTE: Payment can be made by parties other than the Employee.
2) Group policy is terminated by the Employer.
3) Period of 12 months expires after date Employee’s coverage would have terminated because of termination of employment.
4) Employee becomes eligible for or covered by Medicare or any group health plan.
Employee Spouse Dependent Child(ren)
2) Policy in effect covers eligible person at time of active duty.
18 months after date coverage would otherwise terminate with an option to extend to 36 months.
At the time reservist is called to duty, Employer notifies Employee about continuation.
Eligible person files a written election of continuation with the Employer and pays the first required contribution no later than 31 days after the date on which the coverage would otherwise terminate.
1) Premium payments are not made on a timely basis.
NOTE: Payment may be made by parties other than the enrollee.
2) Group policy is terminated by the Employer.
An example of the monthly invoice that each client receives is provided on the following page. The invoice you receive may differ in column headings and amounts.
Examples of column headings include: Medical, Dental, Vision, various PPO Access Fees, COBRA and HIPAA. The last column provides the total fees for each employee.
• The top portion of the invoice indicates the Run Date of the invoice and the Due Date of the payment. AultCare strives to have all invoices run by the 15th of each month and posted to the AultCare website, www.aultcare.com. Payment is then due by the date indicated. You will be notified by email when the invoices are available on your account.
Any adjustments made to enrollments, such as new additions or terminations, will be indicated in a section before the Grand Total. Eligibility changes that were received by the 10th of the month will be reflected on that month’s bill.
• It is your responsibility to review this monthly billing for accuracy.
• Please note: Payments must equal the Grand Total billed. Do not take adjustments to the amount due. Necessary adjustments due to enrollment changes will be made on next month’s invoice.
• Retrospective terminations will only be credited up to three months.
Please remit premium payment by:
• Electronic payments may be made to AultCare via ACH Transfer or AultCare may draft from your Account. To update your payment options, please contact your AultCare Account Management team for assistance.

The Statement Date is 15 days prior to the payment due.

This bottom portion of your Account Summary Statement is the Remittance Voucher. Every Remittance Voucher must be returned with your bill.
The Account Summary Statement is the name of your new bill(s).
Your group name will appear here.
Your group number will appear here. Each Account Summary Statement will have a unique Invoice Number.

COMPANY NAME: ________________________________
GROUP NUMBER:
MONTHLY INVOICE
(Pay as billed, enrollment adjustments will be made to subsequent invoices)
FUNDING ARRANGEMENT
Select and complete one option
ACH Transfer to AultCare Yes No
Huntington Bank: 800-480-4862
AultCare Corporation Account Number: 01039732131
Routing Code: 044115090
AultCare Draft from your Account: Yes No
Bank Name: __
Bank Contact & Phone Number: ___
Name on Account:_________________________________________________________
Tax Identification Number: __________________________________________________
Account Number: _____________________
Routing Code:
For quality assurance, please attach a copy of a voided check
Note: Automatic withdrawal on the 1st of every month
Completed by (printed name):
Signature:
Date:
The following section of information provides an explanation of various questionnaires that enrollees may receive if additional information is needed. Encourage employees to respond to any forms received in order to have their claims paid quickly and correctly.
1. Other Coverage Information Form (2-page form)
When other coverage information is needed, an Other Coverage Information form will be mailed to the employee for completion.
The Accident Questionnaire is mailed to a member to determine if an injury may be the responsibility of a third party. If a third party is at fault, AultCare will pursue reimbursement for the plan. Claims may be denied until the requested information is received.
The Designation of Authorized Representative Form is used to confirm permission to discuss with or disclose to a person’s protected health information (PHI).
Visit our website here to access important member forms.
Enrollee Name
Member ID #
Have you, your spouse, or any dependents covered under this AultCare plan had any other Medical, Dental, Vision, RX, or Medicare coverage in the past 24 months?
No: The rest of the form does not need to be completed. Please sign and date the second page and return to AultCare.
Yes: Please complete entire form, sign, date, and return to AultCare.
Do you have health insurance in which you are the enrollee/policyholder for other than this AultCare plan?
No: Previous Carrier Termination Date
Name
Yes: Complete below
Spouse’s Name Date of Birth Date of Marriage Is spouse employed?
No
Yes If Yes, Name of Employer
Please complete all information in this section for each child covered under your plan who have a different biological parent other than the enrollee and spouse listed on the first page. If not previously provided, court documentation and/or divorce decrees must be submitted to AultCare in order to accurately update your records.
Child’s Name Is their address the same as the enrollee? Yes No
If no, provide Address
If 17 or older, please provide date of graduation from high school
Name of Other Biological/Adoptive Parent
Other Parent’s Address
Parent’s Date of Birth
Does child(ren) have insurance coverage other than this AultCare plan? Yes No
Same as spouse’s coverage? Yes No If no, please complete the information below.
Policyholder’s Name
Insurance Name
Check
Child’s Name
Relationship to Child
Is insurance coverage available through adult child’s employer? Yes No
Policyholder’s Name
Relationship to Child Insurance
Part A Effective Date _______________
Part B Effective Date _______________
Part D Effective Date _______________
Reason for Medicare coverage: Age 65 or older Disabled End Stage Renal Disease (ESRD)
Date dialysis treatment began _______________ Dialysis started at Facility Self/home dialysis Date of kidney transplant _______________
Part A Effective Date _______________
Part B Effective Date _______________
Part D Effective Date _______________
Reason for Medicare coverage:
Age 65 or older Disabled
End Stage Renal Disease (ESRD)
Date dialysis treatment began _______________
Dialysis started at Facility Self/home dialysis
Date of kidney transplant _______________
FRAUD WARNING: Any person who, with intent to defraud or knowing that he or she is facilitating a fraud against an insurer, submits an application or files a claim containing a false or deceptive statement is guilty of insurance fraud. I acknowledge that AultCare may use and disclose my protected health information, as well as, the protected health information of my family for payment, treatment, and operations. This information may be disclosed to other insurance companies, third party administrators, state and federal agencies, health care providers and other organizations and persons that perform professional, business, or insurance functions for AultCare, as permitted by state and federal law. The information may be used for, but not limited to, processing enrollment applications, risk classifications, detecting or preventing fraud, internal and external audits, claims administration, case management, quality improvement programs, public health reporting, law enforcement investigations, coordination of benefits, medical management programs, and subrogation.
Enrollee’s Signature _______________________________________ __ Date ____________
Enrollee’s Phone Number _________________________ Email _____
Please mail, email, or fax this form to: AultCare Attn: COB, PO Box 6910 Canton, OH 44706 | email: aultcareeligibility@aultcare.com | or 330-363-7746 | Attn: COB Note: If any changes occur during the year, please notify AultCare at 330-363-6360 | 1-800-344-8858 | TTY: 711
Mail the completed form to: PO Box 6910 Canton, OH 44706
Group Number
Member Name
Member ID
Patient Name
All claims related to this injury/accident questionnaire will be DENIED until this questionnaire is fully completed and returned. If you have any questions, please contact AultCare at 330-363-6360 or 1-800-344-8858 (TTY: 711).
1. What was the date of your injury/accident?
2. How did your injury/accident occur? _____________________________________________________________
3. Where did the injury/accident occur? (Please select the appropriate box.)
Auto/motorized vehicle
Home
Business Property (Commercial)
Private Property
Medical treatment related
Work (If yes, was a workers’ compensation claim filed?) Yes No
There was no accident, sudden onset (Please contact AultCare)
Please sign and return form, or contact the Service Center.
Other, please specify ________________________________________________________________________
4. Automobile Accident Information
a. If an automobile accident, were you a driver, a passenger, a pedestrian?
b. If this was an auto accident, were all the covered family members involved wearing seatbelts at the time of the accident? Yes No
c. If accident involved a motorcycle or recreational vehicle, was a helmet worn at the time of the accident?
Yes No
d. If this was a motor vehicle accident, were you or a covered family member under the influence of drugs or alcohol? (Includes all motorized recreational vehicles, boats, etc.) Yes No
e. Is there a police report? Yes No
If yes, where can we obtain a copy? ______________________________________________________________
Member
5. Other insurance carrier information where a claim has been filed
Insurance name
Address
6. Were you responsible for the accident? Yes No
If yes, please sign and return the form. Do not complete questions 8-10.
7. Was another party responsible for your accident? Yes No
8. a. What is the name, address and telephone number of the party responsible for your accident?
Name
Address Phone number
b. What is the name, address and telephone number of the other party’s insurance carrier? What is the claim number and adjuster name?
Address Phone
9. Have any payments been made for expenses incurred as a result of this accident? Yes No
If yes, please explain. _________________________________________________________________________
10. Have you retained an attorney? Yes No
If yes, what is the name, address, and telephone number of your attorney?
Name
Address
INSURANCE FRAUD WARNING: Any person who, with intent to defraud or knowing that he or she is facilitating a fraud against an insurer, submits an application or files a claim containing a false or deceptive statement is guilty of insurance fraud. I acknowledge that AultCare may use and disclose my protected health information, as well as, the protected health information of my family for payment, treatment, and operations. This information may be disclosed to other insurance companies, third party administrators, state and federal agencies, health care providers and other organizations and persons that perform professional, business, or insurance functions for AultCare, as permitted by state and federal law. The information may be used for, but not limited to, processing enrollment applications, risk classifications, detecting or preventing fraud, internal and external audits, claims administration, case management, quality improvement programs, public health reporting, law enforcement investigations, coordination of benefits, medical management programs, and subrogation.
I hereby authorize the plan administrator is entitled to recover claim payments made on my behalf, from any future settlement in my favor, from the third party of other insurance carriers responsible for my accident and corresponding claim(s) outlined above. Recovery can also be made from me if I receive the settlement directly from the third party or other insurance carrier.
I hereby authorize the plan administrator to forward copies of claims to the insuring company and attorney.
I hereby authorize release of any information necessary to verify or investigate items pertaining to this accident.
Signature
You have the right to appoint a representative, including an attorney, to act on your behalf. This form is used to confirm permission to discuss with or disclose a person’s Protected Health Information (PHI) held by the affiliated entities AultCare Corporation, AultCare Health Insuring Corporation (AHIC) which also does business as PrimeTime Health Plan, Aultra Administrative Group (AAG), and AultCare Insurance Company (AIC) which also does business as AultCare HMO, to a particular individual who acts as the person’s personal representative. We are not always required to grant such access, but each request will be carefully reviewed and approved if warranted. Use of this information is strictly limited to that purpose.
Name Date of Birth
Member ID Number
Group Number
I hereby authorize the following person to act as my personal representative as indicated below (must fill out).
Name of Representative Relationship
Password the personal representative must provide to access PHI about me
OR No Password Needed
I understand I have the right to limit the information released under this authorization. For example, I may limit my personal representative’s access to information about a particular issue. Any such limitations must be described below in writing. However, if my authorization is for use/disclosure of substance abuse information, I understand the recipient may be prohibited from disclosing substance abuse information under the Federal Substance Abuse Confidentiality Requirements. Therefore, I release the affiliated entities AultCare Corporation, AultCare Insurance Company, and Aultra Administrative Group from all liability arising from this disclosure of my health information. Note: State law mandates that authorizations are limited to 12 months. This form will expire upon 12 months from the date of signature unless an earlier date is noted here. The following items must be checked to be included in the use and/or disclosure of health information pursuant to this Authorization (by leaving this section blank, I am imposing the following limitations on disclosure).
(a) HIV/AIDS related information and/or records (b) Mental health information and/or records
(c) Genetic testing information and/or records (d) Drug/alcohol diagnosis, treatment
Any other limitations described here:
I understand this authorization is voluntary and I may revoke this authorization at any time by providing written notice of such revocation to the health plan, except to the extent that action has been taken in reliance on this authorization.
I have had full opportunity to read and consider the content of this form. I understand this authorization is consistent with my request. I understand, by signing this form, I am confirming my authorization that the health plan may use and/or disclose my PHI to the person named as personal representative for the purpose as described above.
Signature
Date
Form must be signed by member. If form is signed by Power of Attorney or Legal Representative, a copy of documentation of position must be in AultCare’s receipt or attached to form. Please designate position held.
Please return the completed form to: ATTN: Privacy Coordinator, PO Box 6029, Canton, OH 44706.


SUMMARY OF BENEFITS AND COVERAGE
GLOSSARY OF HEALTH COVERAGE AND MEDICAL TERMS

On Feb. 14, 2012, the Departments of Treasury, Internal Revenue Service, Labor, Health and Human Services, and Employee Benefits Security Administration released a final rule that implemented disclosure requirements under section 2715 of the Public Health Service Act.
This health insurance market reform under the Patient Protection and Affordable Care Act requires group health plans and health insurance issuers in the group market to provide a summary of benefits and coverage and uniform glossary to members of their health plans.
Final Regulations were again issued in June 2015. A revised SBC template and uniform glossary was finalized for Plan Year 2021.
• What’s an SBC and a Uniform Glossary?
• What is Culturally and Linguistically Appropriate Manner?
• How do I meet the Electronic Disclosure requirements to distribute the SBC to my employees?
• What happens if I fail to comply?
• Who will provide me with the materials I need for distribution to my employees?
• When will I receive my SBC?
• Who should receive the SBC?
• When do I need to distribute the materials?
• FAQs

Is there an out–of–pocket limit on my expenses?
limit?
/ $5,000
non-participating
Premiums, balance-billed charges, and health care this plan doesn’t cover. Even though you pay these expenses, they don’t count toward the out-of-pocket limit
Is there an overall annual limit on what the plan pays? No. The chart starting on page 2 describes any limits on
Does this plan use a network of providers? Yes. See www.[insert].com or call 1-800-[insert] for a list of participating providers If you use an in-network doctor or other health
The Summary of Benefits and Coverage or “SBC” and Glossary of Health Coverage and Medical Terms or “Uniform Glossary” are designed to help consumers better understand their health coverage and allow for easy comparison of other coverage options when shopping, applying, enrolling and re-enrolling into a health plan. The SBC is a resource for your employees that will summarize your health plan options including:
• Deductible
• Out-of-pocket and annual limits
• In- and out-of-network provider coverage
• Coverage of common medical events
• Excluded services
• Common covered services
• Rights to continue coverage
• Member grievance and appeal rights
• Coverage examples for having a baby and managing type 2 diabetes
The “Uniform Glossary” lists commonly used terms in insurance coverage. You can access the glossary by logging on to www.aultcare.com.
This requirement provides employees and dependents the option to request their SBC in a non-English language if they reside in a county that meets or exceeds a 10 percent threshold of non-English speaking residents. The SBC that we provide will contain directions for non-English speaking individuals to receive further information in their non-English language.
Under the Department of Labor Electronic Disclosure requirement, if your employees are able to effectively access documents provided in electronic format at their worksite (i.e. e-mail) and this access is a part of their duties as an employee, you can send the SBC to them electronically. You can also allow the employees to elect to receive their SBC electronically.
Eligible employees (not currently enrolled) can receive the SBC electronically as long as a paper version option is available upon request. You can accomplish this by email, e-card, posting on your intranet or sending a postcard.
• Up to $1,000 per day (adjusted for inflation) for each instance of willing non-compliance
• A fine of $100 per day per affected individual until compliant
Who will provide me with the materials I need for
As your health issuer or third-party administrator, we are committed to providing you with the tools that you need to meet this regulatory requirement.
• We will provide you with an SBC master copy for distribution (electronically or paper copy) for your employees, dependents and eligible employees for health insurance coverage. This will include an SBC for each benefit package you offer and a new SBC when coverage changes.
• Continuously monitor changes to regulation that may impact you.
We will deliver your SBC to you at the following times:
• Upon my application for coverage or within 7 days
• Within 7 days upon my request
• If terms of my plan are not yet final, upon the first day of coverage
• Upon changes to my plan
• If automatically re-enrolled, a new SBC will be provided at that re-enrollment
If you have an employee and all of the dependents reside at one address, only one SBC is required to be distributed.
However, if an employee has dependents who have an alternate address, you are required to distribute an SBC to those alternate addresses.
You are also required to distribute an SBC to all of your employees who are eligible for health insurance coverage, even if they are not currently enrolled in your health plan.
You need to provide the SBC with open enrollment materials. If you do not hold an open enrollment period, provide the SBC no later than the first date your employees are eligible to enroll for coverage.
If you offer online enrollment, you are permitted to provide the SBC at the time of online enrollment or online renewal of coverage electronically but must provide the option to receive a paper copy.
If you have an automatic renewal, the SBC must be provided 30 days prior to the first day of the new plan year. This SBC will reflect the plan that the employee and dependents are currently enrolled.
If you have an employee or dependent who requests an SBC or Uniform Glossary, you must fulfill the request within seven business days. If the request is online, then you can deliver it electronically but you must provide the option to receive a paper copy.
If the SBC changes from what was distributed at enrollment, you must provide an updated SBC prior to the first day of coverage.
For Special Enrollment, you must provide an SBC within 90 days after they enrolled in your plan.
If you make a midyear change to your plan that changes the content of your SBC, you must provide a 60-day advance notice to employees. This can be complete via a new SBC or a separate notice (summary of material modification).
1. Does this regulation impact small and large groups?
Yes. Whether you are a small or large employer group, the SBC requirements apply to your health plan.
2. Does this apply to both fully insured and self-insured plans?
Yes, this impacts both fully insured and selfinsured plans.
3. Am I exempt because I am in a “grandfathered” plan?
No, the SBC requirement applies to both “grandfathered” and “non-grandfathered” plans.
4. Do I need an SBC for stand-alone dental or vision benefits?
No, the SBC regulations do not apply to standalone excepted benefits. Excepted benefits are generally benefits that require the individual to pay an additional premium.
5. Can I combine the SBC and Uniform Glossary with other documents?
Yes, as long as the SBC is displayed at the beginning.
6. Do COBRA enrollees receive SBCs?
Yes, COBRA enrollees have the same rights as other enrollees to receive SBCs.
7. Do I have to provide the SBC and Uniform Glossary in color?
No, you are permitted to provide in color or grayscale.


The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share the cost for covered health care services. NOTE: Information about the cost of this plan (called the premium) will be provided separately. This is only a summary. For more information about your coverage, or to get a copy of the complete terms of coverage, contact AultCare at 330-363-6360 or go to www.aultcare.com. For general definitions of common terms, such as allowed amount, balance billing, coinsurance, copayment, deductible, provider, or other underlined terms, see the Glossary. You can view the Glossary at www.aultcare.com or call 330-363-6360 or 1-800344-8858 to request a copy.
For network providers
What is the overall deductible?
Are there services covered before you meet your deductible?
Are there other deductibles for specific services?
$100 Individual / $300 Family
For out-of-network providers
$300 Individual / $900 Family
Yes. Network preventive care and services that apply a copayment are covered before you meet your deductible.
No.
For network medical providers
$600 Individual / $1,500 Family
Generally, you must pay all of the costs from providers up to the calendar year deductible amount before this plan begins to pay. If you have other family members on the plan, each family member must meet their own individual deductible until the total amount of deductible expenses paid by all family members meets the overall family deductible
This plan covers some items and services even if you haven’t yet met the deductible amount. But a copayment or coinsurance may apply. For example, this plan covers certain preventive services without cost sharing and before you meet your deductible. See a list of covered preventive services at https://www.healthcare.gov/coverage/preventive-care-benefits/.
You don’t have to meet deductibles for specific services.
What is the out-of-pocket limit for this plan?
What is not included in the out-of-pocket limit?
For out-of-network providers
$1,800 Individual/ $4,500 Family
For Prescription Drugs
$8,850 Individual/ $17,400 Family
Premiums, balance-billing charges, penalties, prescription medication coupon, discount, or other manufacturer assistance programs for Specialty or other qualified medications, and health care this plan doesn’t cover.
The out-of-pocket limit is the most you could pay in a calendar year for covered services. If you have other family members in this plan, they have to meet their own out-of-pocket limits until the overall family out-of-pocket limit has been met.
Even though you pay these expenses, they don’t count toward the out-of-pocket limit.
Will you pay less if you use a network provider?
Yes. See www.aultcare.com or call 330-363-6360 or 1-800-3448858 for a list of network providers
Do you need a referral to see a specialist? No.
This plan uses a provider network. You will pay less if you use a provider in the plan’s network. You will pay the most if you use an out-of-network provider, and you might receive a bill from a provider for the difference between the provider’s charge and what your plan pays (balance billing). Be aware, your network provider might use an out-of-network provider for some services (such as lab work). Check with your provider before you get services.
You can see the specialist you choose without a referral.
All coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common Medical Event Services You May Need
If you visit a health care provider’s office or clinic Primary care visit
Preventive care/screening/ immunization
If you have a test Diagnostic
(CT/PET
Preferred Generic drugs (Tier 1)
If you need drugs to treat your illness or condition
More information about prescription drug coverage is available at www.aultcare.com
This plan follows the Premium Managed Formulary.
Preferred Brand / NonPreferred Generic drugs (Tier 2)
Non-Preferred Brand / NonPreferred Generic drugs (Tier 3)
Retail 1-34 day supply: $10 copayment or 20% coinsurance, whichever is greater; Retail 35-60 day supply: $20 copayment or 20% coinsurance, whichever is greater; Mail order 90-day supply: $25 copayment or 20% coinsurance, whichever is greater
Retail 1-34 day supply: $30 copayment or 30% coinsurance, whichever is greater; Mail order 90-day supply: $85 copayment or 25% coinsurance, whichever is greater, up to a maximum of $200
Retail 1-34 day supply: $45 copayment or 50% coinsurance, whichever is greater; Mail order 90-day supply: $130 copayment or 45% coinsurance, whichever is greater, up to a maximum of $400
Limitations, Exceptions, & Other Important Information
Network office visits with an OB/GYN will apply a $5 copayment.
You may have to pay for services that aren’t preventive. Ask your provider if the services needed are preventive. Then check what your plan will pay for.
Preauthorization may be required.
Deductible does not apply.
Specialty Medications must be obtained from AultCare’s Preferred Specialty pharmacies.
If a prescription drug is purchased without using your card, this Plan will pay up to the allowed amount.
Certain Generic Medications may be subject to an incentive, which may reduce member cost share under the Generic Incentive Program.
Certain preventive medications may be covered at 100%, with no cost to you.
Certain classes of medications require Preauthorization or Step Therapy.
Common Medical Event Services You May Need What You Will Pay
Limitations, Exceptions, & Other Important Information Network Provider (You will pay the least) Out-of-Network Provider (You will pay the most)
If you have outpatient surgery
Specialty Generic (Tier 4)
**Limited to a 30-day fill
Retail or Mail order: $10 copayment or 20% coinsurance, whichever is greater
If you have a hospital stay
Specialty Brand (Tier 5)
***Limited to a 30-day fill Mail order 90-day supply: $125 copayment or 20% coinsurance, whichever is greater
Prescription medication coupon, discount, or other manufacturer assistance programs for Specialty or other qualified medications will not apply toward your Deductible or Out-ofPocket Maximum.
For a complete list of these medications and programs, visit the AultCare website at www.aultcare.com.
If you need mental health, behavioral
services Outpatient services Benefits paid based on the corresponding medical benefit.
paid based on the corresponding medical benefit. Services for Mental Health, Behavioral Health, or Substance Abuse are payable on the same basis as any other illness.
Common Medical Event Services You May Need
Office visits
Limitations, Exceptions, & Other Important Information Network Provider (You will pay the least)
Benefits paid based on the corresponding medical benefit.
Out-of-Network Provider (You will pay the most)
Benefits paid based on the corresponding medical benefit.
Cost sharing does not apply to certain preventive services. Depending on the type of service, a copayment, deductible or coinsurance may apply.
If you are pregnant
If you need help recovering or have other special health needs
Habilitation services
Benefits paid based on the corresponding medical benefit.
Benefits paid based on the corresponding medical benefit.
Preauthorization is required.
Preauthorization is required. Coverage is limited to 60 visits per calendar year.
Must be injury/illness related. Manipulation therapy is limited to 35 treatments per calendar year.
Coverage is limited to Autism Spectrum Disorder. Services are limited to the following: Speech/Language/Occupational Therapy - 20 visits per calendar year for each service; and Clinical Therapeutic Intervention including ABA at 20 hours per week; and Mental/ Behavioral Health Outpatient Services.
Preauthorization is required. Coverage is limited to 50 days per calendar year.
Preauthorization is required for a single item with a purchase price over $2,500.
Common Medical Event Services You May Need
What You Will Pay
Limitations, Exceptions, & Other Important Information Network Provider (You will pay the least)
Out-of-Network Provider (You will pay the most)
Children’s eye exam No cost share 35% coinsurance
If your child needs dental or eye care
Coverage is provided for vision screening for all children at least once through age 18 years, to detect the presence of amblyopia or its risk factors.
Children’s glasses Not covered Not covered
Children’s dental check-up Not covered Not covered
Excluded Services & Other Covered Services:
Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excluded services.)
• Abortion (except in cases of rape, incest, or when the life of the mother is endangered, as allowed under applicable law)
• Acupuncture
• Bariatric Surgery
• Cosmetic Surgery
• Dental Care (adult)
• Hearing Aids
• Long Term Care
• Non-Emergency care when traveling outside the U.S.
• Routine Eye Care (Adult)
• Routine Foot Care
• Weight Loss Programs
Other Covered Services (Limitations may apply to these services. This isn’t a complete list. Please see your plan document.)
• Chiropractic Care
• Habilitation Services
• Infertility Treatment
• Private Duty Nursing
Your Rights to Continue Coverage: There are agencies that can help if you want to continue your coverage after it ends. The contact information for those agencies is: for group health coverage subject to ERISA, contact Department of Labor’s Employee Benefits Security Administration at 1-866-444-EBSA(3272) or www.dol.gov/ebsa/healthreform; for non-federal governmental group health plans, contact Department of Health and Human Services, Center for Consumer Information and Insurance Oversight, at 1-877-267-2323 x61565 or www.cciio.cms.gov. Church plans are not covered by the Federal COBRA continuation coverage rules. If the coverage is insured, individuals should contact their State insurance regulator regarding their possible rights to continuation coverage under State law. Other coverage options may be available to you too, including buying individual insurance coverage through the Health Insurance Marketplace. For more information about the Marketplace, visit www.HealthCare.gov or call 1-800-318-2596.
Your Grievance and Appeals Rights: There are agencies that can help if you have a complaint against your plan for a denial of a claim. This complaint is called a grievance or appeal. For more information about your rights, look at the explanation of benefits you will receive for that medical claim. Your plan documents also provide complete information to submit a claim, appeal, or a grievance for any reason to your plan. For more information about your rights, this notice, or assistance, contact: for group health coverage subject to ERISA, contact Department of Labor’s Employee Benefits Security Administration at 1-866-444-EBSA(3272) or www.dol.gov/ebsa/healthreform or call the Ohio Department of Insurance 1-800-686-1526; for non-federal governmental group health plans and church plans that are group health plans, contact AultCare at 1-800-344-8858 or call the Ohio Department of Insurance 1-800-686-1526.
more information about limitations and exceptions, see the plan or policy document at www.aultcare.com.]
Does this plan provide Minimum Essential Coverage? Yes
Minimum Essential Coverage generally includes plans, health insurance available through the Marketplace or other individual market policies, Medicare, Medicaid, CHIP, TRICARE, and certain other coverage. If you are eligible for certain types of Minimum Essential Coverage, you may not be eligible for the premium tax credit. Does this plan meet the Minimum Value Standards? Yes If your plan doesn’t meet the Minimum Value Standards, you may be eligible for a premium tax credit to help you pay for a plan through the Marketplace.
Language Access Services:
[Spanish (Español): Para obtener asistencia en Español, llame al 330-363-6360 / 1-800-344-8858.]
[Tagalog (Tagalog): Kung kailangan ninyo ang tulong sa Tagalog tumawag sa 330-363-6360 / 1-800-344-8858.]
[Chinese (中文): 如果需要中文的帮助, 请拨打这个号码 330-363-6360 / 1-800-344-8858.]
[Navajo (Dine): Dinek'ehgo shika at'ohwol ninisingo, kwiijigo holne' 330-363-6360 / 1-800-344-8858.]
To see examples of how this plan might cover costs for a sample medical situation, see the next section.
PRA Disclosure Statement: According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is 0938-1146. The time required to complete this information collection is estimated to average 0.08 hours per response, including the time to review instructions, search existing data resources, gather the data needed, and complete and review the information collection. If you have comments concerning the accuracy of the time estimate(s) or suggestions for improving this form, please write to: CMS, 7500 Security Boulevard, Attn: PRA Reports Clearance Officer, Mail Stop C4-26-05, Baltimore, Maryland 212441850.

This is not a cost estimator. Treatments shown are just examples of how this plan might cover medical care. Your actual costs will be different depending on the actual care you receive, the prices your providers charge, and many other factors. Focus on the cost-sharing amounts (deductibles, copayments and coinsurance) and excluded services under the plan. Use this information to compare the portion of costs you might pay under different health plans. Please note these coverage examples are based on self-only coverage.
(9 months of in-network pre-natal care and a hospital delivery)
(a year of routine in-network care of a wellcontrolled condition)
Mia’s Simple Fracture (in-network emergency room visit and follow up care)
This EXAMPLE event includes services like:
Specialist office visits (prenatal care)
Childbirth/Delivery Professional Services
Childbirth/Delivery Facility Services
Diagnostic tests (ultrasounds and blood work)
Specialist visit (anesthesia)
This EXAMPLE event includes services like:
Primary care physician office visits (including disease education)
Diagnostic tests (blood work)
Prescription drugs
Durable medical equipment (glucose meter)
This EXAMPLE event includes services like: Emergency room care (including medical supplies)
Diagnostic test (x-ray)
Durable medical equipment (crutches)
Rehabilitation
The plan would be responsible for the other costs of these EXAMPLE covered services.
This glossary has many commonly used terms, but isn’t a full list. These glossary terms and definitions are intended to be educational and may be different from the terms and definitions in your plan. Some of these terms also might not have exactly the same meaning when used in your policy or plan, and in any such case, the policy or plan governs. (See your Summary of Benefits and Coverage for information on how to get a copy of your policy or plan document.)
Bold blue text indicates a term defined in this Glossary. Also, See page 60 for an example showing how deductibles, co-insurance and out-of-pocket limits work together in a real life situation.
Maximum amount on which payment is based for covered health care services. This may be called “eligible expense,” “payment allowance” or “negotiated rate.” If your provider charges more than the allowed amount, you may have to pay the difference. (See Balance Billing.)
A request for your health insurer or plan to review a decision or a grievance again.
When a provider bills you for the difference between the provider’s charge and the allowed amount. For example, if the provider’s charge is $100 and the allowed amount is $70, the provider may bill you for the remaining $30. A preferred provider may not balance bill you for covered services.

A fixed amount (for example, $15) you pay for a covered health care service, usually when you receive the service. The amount can vary by the type of covered health care service.
The amount you owe for health care services your health insurance or plan covers before your health insurance or plan begins to pay. For example, if your deductible is $1000, your plan won’t pay anything until you’ve met your $1000 deductible for covered health care services subject to the deductible. The deductible may not apply to all services.

Your share of the costs of a covered health care service, calculated as a percent (for example, 20%) of the allowed amount for the service. You pay co-insurance plus any deductibles (See page 4 for a detailed example.) you owe. For example, if the health insurance or plan’s allowed amount for an office visit is $100 and you’ve met your deductible, your co-insurance payment of 20% would be $20. The health insurance or plan pays the rest of the allowed amount.
Equipment and supplies ordered by a health care provider for everyday or extended use. Coverage for DME may include: oxygen equipment, wheelchairs, crutches or blood testing strips for diabetics.
An illness, injury, symptom or condition so serious that a reasonable person would seek care right away to avoid severe harm.
Ambulance services for an emergency medical condition.
Emergency Room Care
Emergency services you get in an emergency room.
Evaluation of an emergency medical condition and treatment to keep the condition from getting worse.
Health care services that your health insurance or plan doesn’t pay for or cover.
A complaint that you communicate to your health insurer or plan.
Habilitation Services
Health care services that help a person keep, learn or improve skills and functioning for daily living. Examples include therapy for a child who isn’t walking or talking at the expected age. These services may include physical and occupational therapy, speech-language pathology and other services for people with disabilities in a variety of inpatient and/or outpatient settings.
A contract that requires your health insurer to pay some or all of your health care costs in exchange for a premium
Home Health Care
Health care services a person receives at home.
Services to provide comfort and support for persons in the last stages of a terminal illness and their families.
Care in a hospital that requires admission as an inpatient and usually requires an overnight stay. An overnight stay for observation could be outpatient care.
Care in a hospital that usually doesn’t require an overnight stay.
The percent (for example, 20%) you pay of the allowed amount for covered health care services to providers who contract with your health insurance or plan. In-network co-insurance usually costs you less than out-of-network co-insurance.
A fixed amount (for example, $15) you pay for covered health care services to providers who contract with your health insurance or plan. In-network co-payments usually are less than out-of-network co-payments
Health care services or supplies needed to prevent, diagnose or treat an illness, injury, condition, disease or its symptoms and that meet accepted standards of medicine.
The facilities, providers and suppliers your health insurer or plan has contracted with to provide health care services.
A provider who doesn’t have a contract with your health insurer or plan to provide services to you. You’ll pay more to see a non-preferred provider. Check your policy to see if you can go to all providers who have contracted with your health insurance or plan, or if your health insurance or plan has a “tiered” network and you must pay extra to see some providers.
The percent (for example, 40%) you pay of the allowed amount for covered health care services to providers who do not contract with your health insurance or plan. Out-of-network co-insurance usually costs you more than in-network co-insurance.
A fixed amount (for example, $30) you pay for covered health care services from providers who do not contract with your health insurance or plan. Out-of-network co-payments usually are more than in-network co-payments
The most you pay during a policy period ( usually a year) before your health insurance or plan begins to pay I00% of the allowed amount This limit never includes your premium, balance-billed charges or (See page 4 for a detailed example.) health care your health insurance or plan doesn’t cover. Some health insurance or plans don’t count all of your co-payments, deductibles, co-insurance payments, out-of-network payments or other expenses toward this limit.
Health care services a licensed medical physician (M.D. -Medical Doctor or 0.0. - Doctor of Osteopathic Medicine) provides or coordinates.
A benefit your employer, union or other group sponsor provides to you to pay for your health care services.
A decision by your health insurer or plan that a health care service, treatment plan, prescription drug or durable medical equipment is medically necessary. Sometimes called prior authorization, prior approval or precertification. Your health insurance or plan may require preauthorization for certain services before you receive them, except in an emergency. Preauthorization isn’t a promise your health insurance or plan will cover the cost.
A provider who has a contract with your health insurer or plan to provide services to you at a discount. Check your policy to see if you can see all preferred providers or if your health insurance
or plan has a “tiered” network and you must pay extra to see some providers. Your health insurance or plan may have preferred providers who are also “participating” providers. Participating providers also contract with your health insurer or plan, but the discount may not be as great, and you may have to pay more.
The amount that must be paid for your health insurance or plan. You and/ or your employer usually pay it monthly, quarterly or yearly.
Health insurance or plan that helps pay for prescription drugs and medications.
Drugs and medications that by law require a prescription.
A physician (M.D. - Medical Doctor or 0.0. - Doctor of Osteopathic Medicine) who directly provides or coordinates a range of health care services for a patient.
A physician (M.D. - Medical Doctor or 0.0. - Doctor of Osteopathic Medicine), nurse practitioner, clinical nurse specialist or physician assistant, as allowed under state law, who provides, coordinates or helps a patient access a range of health care services.
A physician (M.D. - Medical Doctor or 0.0. - Doctor of Osteopathic Medicine), health care professional or health care facility licensed, certified or accredited as required by state law.
Surgery and follow-up treatment needed to correct or improve a part of the body because of birth defects, accidents, injuries or medical conditions.
Health care services that help a person keep, get back or improve skills and functioning for daily living that have been lost or impaired because a person was sick, hurt or disabled. These services may include physical and occupational therapy, speech-language pathology and psychiatric rehabilitation services in a variety of inpatient and/or outpatient settings.
Services from licensed nurses in your own home or in a nursing home. Skilled care services are from technicians and therapists in your own home or in a nursing home.
Specialist
A physician specialist focuses on a specific area of medicine or a group of patients to diagnose,
manage, prevent or treat certain types of symptoms and conditions. A non-physician specialist is a provider who has more training in a specific area of health care.
UCR (Usual, Customary and Reasonable)
The amount paid for a medical service in a geographic area based on what providers in the area usually charge for the same or similar medical service. The UCR amount sometimes is used to determine the allowed amount.
Care for an illness, injury or condition serious enough that a reasonable person would seek care right away, but not so severe as to require emergency room care.
Jane hasn’t reached her $1500 deductible yet. Her plan doesn’t pay any of the costs.
Office visit costs: $125
Jane pays: $125
Her plan pays: $0
Jane reaches her $1500 deductible, co-insurance begins.
Jane has seen a doctor several times and paid $1,500 in total. Her plan pays some of the costs for her next visit.
Office visit costs: $75
Jane pays: 20% of $75 = $15 Her plan pays: 80% of $75 = $60
Jane reaches her $5,000 out-of-pocket limit.
Jane has seen the doctor often and paid $5,000 in total. Her plan pays the full cost of her covered health care services for the rest of the year.
Office visit costs: $200
Jane pays: $0
Her plan
$200