Cohesion through competition in a large anaesthetic department: A role for fantasy sports selections
Rowing for Ukrainian medics
Reclaiming narratives
Why gain an accreditation in fTOE?
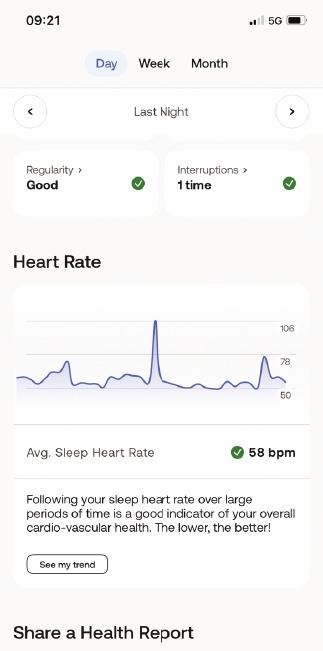
A measure of stress: How smart watches show the strain of on-call work
Welcome to the November issue of Anaesthesia News!
By the time this issue reaches your inbox, I will have completed my two-year term as the Association president and handed over to Tim Meek at our Annual Congress in Harrogate. It has been a very rewarding two years that I have thoroughly enjoyed. It has brought significant challenge that at times has felt all consuming, though considering the current challenges faced by us all in our workplaces you will not be surprised by that. I know I step back from the presidency leaving our organisation in very good hands with Tim as president and the excellent senior management team and staff at the helm.
Our advocacy work continues at pace as we will have been to four party conferences and hosted a health event at the Labour party conference focusing on inequality on health delivery. We continue to ensure we represent anaesthesia and our members at the COVID inquiry and by the time you read this we will have given our evidence as part of the joint RCOA/FICM/Association submission.
This issue of Anaesthesia News contains a variety of excellent articles and reports covering a broad range from topics. There is an article on fantasy rugby and how taking part in it can build camaraderie amongst departments and emphasise the importance of the team in all we do. There is a piece on the monumental challenge of rowing the Atlantic to raise money for Ukraine by Leonid Krivskiy, and some insightful reports exploring how students are spending their elective time.
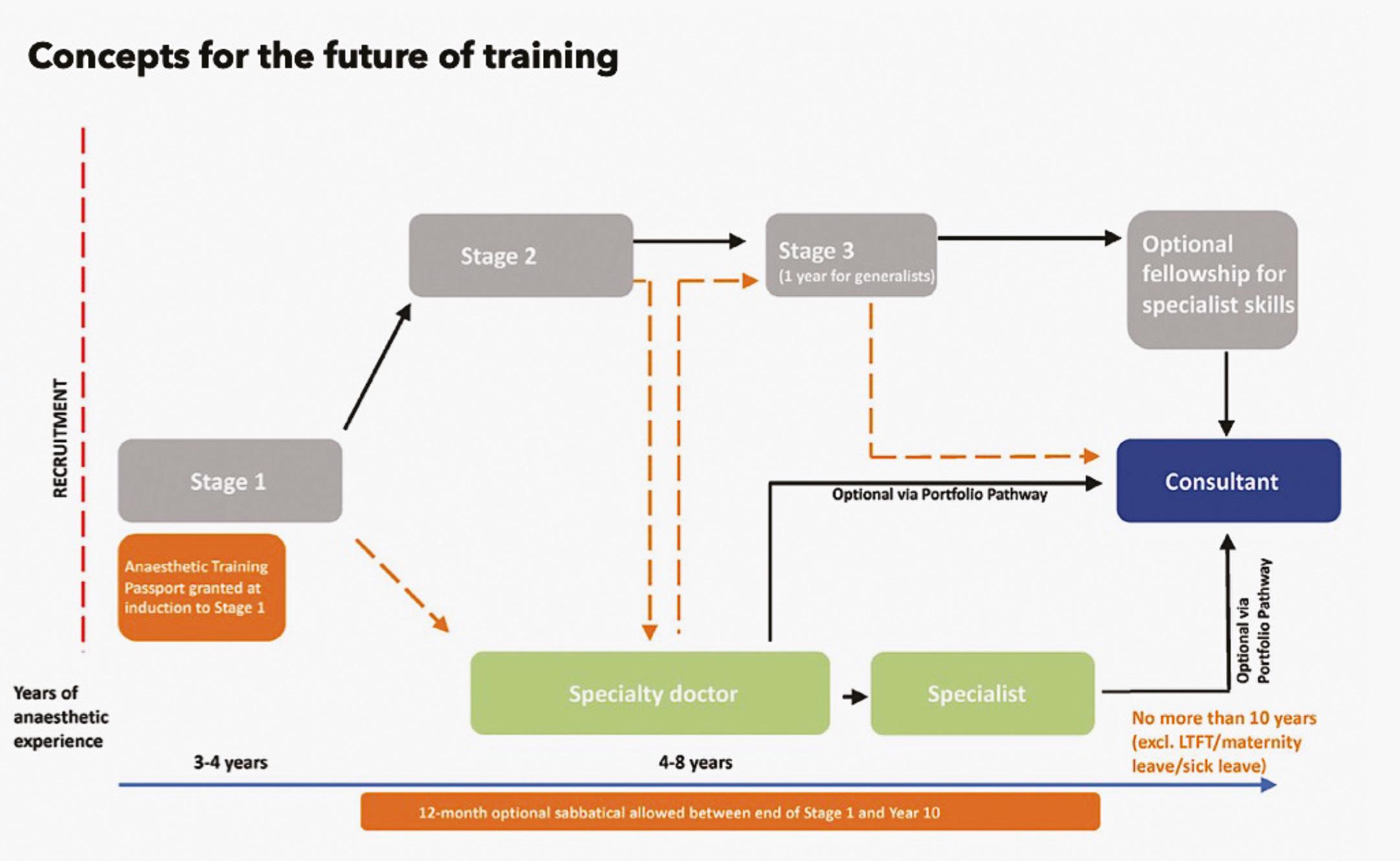
We look forward to the two-day hybrid Winter Scientific Meeting in January 2025 and our internal fTOE accreditation programme. Members of the Resident Doctors Committee have written on the topical subjects of what good anaesthesia training could look like and less than full-time training. This is just a snapshot of the excellent work the committee has produced in the last year to support resident doctors in their anaesthesia careers.
It is autumn now and the words ‘winter crisis in the NHS’ will be commonly heard. I do wonder how the proposed reforms may change the tone of those words? I know the Association will continue to inform, educate and represent you, the members, through these reforms to ensure that patients and staff remain at the centre of what may come.
I wish you all well.
Matt Davies Immediate Past President
ISSN 0959-2962
Association of Anaesthetists
21 Portland Place, London W1B 1PY
Telephone: 020 7631 1650
Website: www.anaesthetists.org
Editor: Francesca Cockshull
Address for all correspondence, advertising or submissions:
Editorial Assistant: Erin Taylor Email: anaenews.editor@anaesthetists.org
Design: Chris Steer, Digital Designer Telephone: 020 7631 8803 Email: chris@anaesthetists.org
Copyright 2024
Association of Anaesthetists
The Association cannot be responsible for the statements or views of the contributors. No part of this magazine may be reproduced without prior permission. Advertisements are accepted in good faith. Readers are reminded that Anaesthesia News cannot be held responsible in any way for the quality or correctness of products or services offered in advertisements.
Join us today and become part of a vibrant and supportive community of over 10,000 anaesthetists
Since 1932 the Association of Anaesthetists has proudly represented the thousands of individuals who work in the life-changing, life-saving specialty of anaesthesia.
We independently support and advocate for our members in the UK, Ireland and internationally. Informing and inspiring them to achieve their full potential at every stage of their career.
Join our vibrant and supportive community today.
You can enjoy exclusive member benefits and services, and wellbeing support. Find out more: https://anaesthetists.org/ Home/Membership/Benefits-of-membership
Follow us
@associationofanaesthetists
@Anaes_News
Association of Anaesthetists
Association of Anaesthetists
Cohesion through
competition in a large anaesthetic department: A role for fantasy sports selections
Cork University Hospital is among Ireland’s largest tertiary hospitals and continues to grow through optimism, patchwork and the judicious use of duct tape. Likewise, the department of Anaesthesia continues to grow - the current intake is the largest in the forty-five-year history of the regional centre and the single largest medical department in the country, with just over 100 members. The workload is distributed over three campuses and, obviously, all hours of the day and all days of the year. Shift work is essential to the system.
Doctors in training staff six call tiers. We have subgroups who, due to stages of training or professional interest, are often in the maternity hospital, intensive care, the block room or on pain rounds. It is not surprising that, one month down, I have only met about half of the current team of 70 or so trainees.
The department is becoming an increasingly cosmopolitan state, with doctors hailing from the UK, France, South Africa, Nigeria, Hungary, Romania, USA, several Asian and African countries, particularly Sudan, and of course Ireland and Cork, the latter a separate entity in and of itself. A truly eclectic mix of cultures and interests. Rumours that anyone arriving at the hospital can surrender their passport, no questions asked, and after three years’ service, leave with a new identity, a Cork accent and passport are hard to confirm. But the team is a large cross section of humanity, which due to the pressures of call, the reality of rosters and sheer size, is never all in one place at one time.
Throughout the year we have many events to boost collegiality and camaraderie with colleagues one might not necessarily see for weeks and, of course, other staff we spend our days with. Unsurprisingly, sport is a common spark for discussion and debate throughout the year.
At baseline, there is a significant rugby following at both international and club level in our group, predominantly following the red of Munster. However, there is usually a proud Leinster based group rotating through to act as a counterpoint (at least I think that’s why they’re there) and some English or French to keep us cultured. A few SouthAfrican doctors kindly and graciously remind everyone who keeps winning the World Cup. Full of optimism, we greet February warmly as a chance to enjoy the spectacle unfolding and try to showcase our knowledge and gut feeling with our Fantasy selections.
There are recurrent characters to our competition with eager efforts made to coerce new friends into the fold, both seasoned rugby followers new to Cork, and those trying to entice colleagues to give it a go. The bonus of having investment in a game you normally would switch away from is a great way to help people fall in love with the game. For the more cynical long-time followers, it can be a reason to watch a less than glamorous fixture. Italy playing Wales can be crucial if you’re in a close run off for top spot in the fantasy league, while without it, the game might be of little interest.
All in all, it provides an additional incentive to meet people outside of work and find a way to make it through bleak Irish winters or to claim departmental bragging rights for the coming year. If nothing else, one might find out the answers to the real difficult debates that are flowing at the emergency board: “Is Crowley going to be our third generational 10 in a row?”, “The Netflix series was all a bit much wasn’t it?” and of course “A Welshman making it in the NFL? Not a chance!”.
“A Welshman making it in the NFL? Not a chance!”
The tea-room television never once veered from the 2024 UEFA Euro football coverage over the summer; and the hospital was entirely bound in grief over the recent All-Ireland Hurling Final. Now we move on to catch snippets of the pentathlon in Paris while bluffing unsolicited expertise to anyone within earshot.
What has emerged as an annual tradition is to follow the 6 Nations tournament with a Fantasy League of current colleagues and alumni of CUH. Fantasy Leagues run online, with various rules to force strategic selections in different sports. Selecting players for the different team positions is the basis of it, and knowledge of who will play well, score, or exceed expectations is crucial. Most allocate a nominal budget to purchase players who valued based on perceived ability. In general, one is limited in how many one can pick from each real-world team, or country. You can’t just then pick France, say, if you think they will win. And if you pick the best players by reputation, you will probably find your budget runs out before you fill all positions.
The Fantasy Six Nations takes place alongside the actual event. Before each game, one selects a team of fifteen players and a substitute to try and score as many points as possible in that weekend’s fixtures. Fantasy points are accrued by scoring tries, kicking penalties, gaining meters and making tackles. You are given a strict player budget, and the value of each player is reflected in the price it costs to add them to your team.
As much as an Irishman would love to select a full fifteen playing in green jerseys, the game limits you to a maximum of four per nation. You can then have a go at guessing which teams are most likely to win over the weekend and therefore bring a significant haul of fantasy points. Leads swing over the month as your gamble over which French winger to select has rewarded you with a hat-trick of tries while Les Bleus romped to victory. However, titles and bragging rights are usually decided by astute decisions; the flanker with a gallant five turnovers in a game lost by half time, the hooker who mauled over from a lineout in a tight, messy and rainfilled affair or the scrum half that just can’t resist a snipe down the blindside gaining metres (and fantasy points) regardless of the strategies wisdom. Your choice of captain,
8
who wins double points, might keep you up at night; should you select a kicker to keep the score ticking over? Or do you play it safe and pick James Lowe?
Our own most recent league came down to a tight final weekend. Four players separated by a mere 20 points that a single try for your team could overturn. Leading into the final game, France v England, my hubris started to grow as my slender lead held on. However, my dreams came undone in the eighth minute, when Furbank went down and in comes my closest competitor’s haymaker secret weapon - Marcus Smith. That one substitute selection you made before the weekend? If they come off the bench and make the field in real life, they net you triple points.
As Smith racked up a try, an assist and countless metres, I could only concede defeat. Regardless of lost glory, the debrief along the corridor the following week was what it was all about. Strategies revealed, substitutions cursed, referee decisions questioned, but overwhelming satisfaction in the accomplished championship success, Grand Slam or not. Websites are bookmarked for the following season to get the latest squad updates while ignoring the thought that perhaps random selection may have bettered your painstaking selection process.
After running for over a decade in our department, prizes to date have included being bought a cup of coffee by a beaten rival. Perhaps we shall invest in a trophy for next year, being in Cork it would probably have to be named the ‘Ronan O’Gara Award for Rugby Excellence’. A big decision best deferred to an appropriately-attended departmental meeting.
As Fantasy leagues run online in a plethora of sports and formats, it may be worth considering them in other teams and departments. They are free and form a type of social event that can be squeezed into any available time. Literally anyone can do it. It can surprise you who turns out to be a keen fan - our department secretary, Eileen Kelly, is one of our most astute selectors. We had no idea of this until we ran the league. And for people who’ve left the department and are rotating elsewhere, it’s a good way to keep in touch. You can still sign up.
A speculative question is the degree to which actual sporting ability might correlate with fantasy sports selections. On the one hand, sport is a physical activity in which raw talent is often extremely obvious. Plus, knowledge and deep understanding of high-level competition might help in predicting outcomes or identifying patterns. Interestingly, over the many years of running a department six nations league we have had two Olympic athletes pass through the team, Paul Hession, a sprinter, and Carolyn Hayes, a triathlete who competed in Tokyo. Both won the fantasy competition by clear margins. It’s also well known that Magnus Carlson, perhaps the greatest chess player ever, is among the world’s best in fantasy football selections. So, maybe there’s something to be discerned from this pattern among our small sample.
As autumn comes in, many sports get started and leagues get going. A fantasy league is worth exploring as a backdrop to the working year and a source of rivalry and competition. Be careful though. They are oddly addictive.
Cathal Lee
Perennial CUH Fantasy 6 Nations Runner-Up, Cork, Ireland cathaljlee@gmail.com
Calling
SAS/NCHD doctors!
Unlock your potential with a £2000 grant for professional development
Are you looking to advance your career and develop new skills? The Association is pleased to offer a £2000 grant to support you to further your education or help with your professional development journey! The grant is designed to assist SAS doctors/NCHD in pursuing training, certifications, CPD courses, workshops, mentoring or any educational opportunities that will enhance their professional growth and career prospects.
The deadline for submission is: 23:59 on Wednesday 29 January 2025
Find out more here: anaesthetists.org/Home/Get-involved/Grants-awards -and-prizes/SAS-Professional-Development-Grant
Rowing for Ukrainian medics
My personal humanitarian project:
The why
I remember very clearly the day the war started. It did not come out of the blue – there had been a massive build-up of Russian troops along the Ukrainian border, there were provocations, there were clear warning signs of the things to come – but there was still a shock and disbelief when it started happening.
Kyiv was under attack! My beloved Kyiv that we had visited with the kids shortly beforehand; the city that my wife had been born in, the city that I visited as a child with my Ukrainian mum. I could not believe what I was seeing on the TV – attack helicopters flying overhead; rocket explosions in the city centre, tanks on the outskirts of the city, sketchy raw images and videos on social media channels showing civilians throwing Molotov cocktails into armoured vehicles from passing cars, then driving off at speed.
My wife’s parents were in Kyiv when the war started. We knew that they made the difficult decision to leave the city but we completely lost connection with them; it was only after one week that we discovered they were ok and managed to reach western Ukraine and cross the border another week later. This was all personal to me from the very beginning.
I was born in Moscow, then a capital of the USSR. I was 18 when it fell apart. I experienced the influence of Russian imperialism first-hand. The communist propaganda liked to talk about equality and ‘internationalism’, but life was bleak for the non-Russian population, just about bearable for those who accepted cultural norms, and awful for those who did not. The antipathy towards Ukrainians was particularly strong. Rebellious and freedom-loving, Ukrainians have always wanted to break away and have been paying a high price every time they have tried. As a child, I remember Ukrainian kids in my school being a constant subject of subtly racist jokes with an open consent and even encouragement of our teachers. They were trying to keep their heads down and shrug it all off, but I could tell it was affecting them. With time, they all became withdrawn, lonely and bitter, reinforcing the general prejudice against them.
I spent my childhood summers in my mother’s birthplace – a little village near Kyiv. While there I saw, and was forever fascinated by, the beauty of the place and the people. A lot of my formative experiences happened there and I have always felt a connection to it ever since. When Russians annexed the Crimea and invaded eastern Ukraine in 2014, I took it very personally. There was no question which side I was on. I wanted to help my Ukrainian colleagues, whom I knew were struggling. A lot of the civilian hospitals were getting overwhelmed with patients, both military and civilian, with blast injuries and there was an acute lack of expertise and experience in management of massive blood loss, airway injuries, and a multidisciplinary approach to major trauma in general. I understood the problems of the post-Soviet healthcare very well – I had initially trained and then worked as an anaesthetist in one of Moscow’s largest general hospitals in the 90s. There was a lot of enthusiastic and western-oriented young doctors who had to work in the hierarchical Soviet system, while learning new skills to deal with war injuries. It was clear to me that the most impactful help that I could offer was training the young generation of Ukrainian anaesthetists.
I had a few Ukrainian contacts from a time when I was involved with running an online educational platform for Russian-speaking anaesthetists mostly practicing in the post-Soviet countries, and I contacted them with an offer to help. I was then introduced to a head of anaesthetic department at a teaching hospital in Kyiv who invited me to speak at a conference and a few seminars on various key topics of particular interest to them, including difficult airway, major blood loss as well as vascular and thoracic anaesthesia, the specialities of my special interest here in the UK. Hence, very close professional relationships and friendships were born.
I organised seminars and workshops and went to Ukraine on a regular basis. My kids loved it too – it was an opportunity for them to see their grandparents as well as to attend theatre and ballet performances which they absolutely loved (and it did not break the parents’ bank!). By the time the big war started, I had developed multiple contacts in the Ukrainian medical world. When I learned about the war breaking out, my immediate reaction was to go all in and help my friends in any way that I could. I remember writing an emotional email to my consultant colleagues. I did not know what I was going to do but I had already made a contact with a few Ukrainian friends who had told me that the most acute need was felt at the frontline – good-quality tourniquets, Celox gauze, Israeli bandages were all in very high demand. I opened a JustGiving page and asked my colleagues for help. Within a few days I had £30,000 on my JustGiving account donated by my hospital colleagues. The people’s response was overwhelming – it inspired and motivated me to do everything I could to help.
I contacted a few of my Ukrainian colleagues and discovered that some of them had already volunteered with the territorial army and ended up being deployed at frontline stabilisation facilities and evacuation teams. I found out that the teams of frontline medics were
12
lacking good-quality TacMed as well as body armour, a scarce commodity at the beginning of the war as most of it was distributed among regular frontline troops, leaving medics vulnerable and exposed to blast injuries and sniper bullets. I sourced and bought all the items on the shopping list. It was nearly impossible to find Celox and tourniquets in the first months of the war and there were lots of volunteers with similar requests in the UK. There were no discounts offered and the companies selling TacMed undoubtedly made a good profit at the time. My house looked like a warehouse with all the boxes ready to go to Ukraine. Without giving it a second thought I decided to drive to Ukraine myself. A friend gave me his van and I was off to Ukraine one month after the war started.
I made it to Lviv without any major problems. The Polish-Ukrainian border crossing was not as bad as I had anticipated. It was the Polish customs officers, sternlooking young blonde women, who gave me a tough time – they searched through the boxes and demanded all the paperwork, especially for the body armour, and questioned me about the funny-looking van that did not belong to me. Finally, they released me into the arms of the Ukrainian border patrol officers, who had quite a cognitive dissonance looking at my British passport, which indicated Moscow as my place of birth and my UK car registration. I started speaking English to them, but they ended up speaking Russian to me. It was in my favour that the British were highly respected due to the support from our government. I was let into Ukraine without any hesitation, with a big smile and thumbs up.
underground in Lviv, so all you could do is sit in a basement, and hope that this one is just a nuisance too and pray that they will not hit the house above you. Because if they did, then nobody would stand a chance of getting out alive.
The first time I sat in the shelter was a strange experience. My family and I were having a meal with our hosts when we heard the sirens and just carried on downstairs as if nothing strange was happening. It was early evening, and having just met each other, we all had a lot of questions for each other and were genuinely interested in what the answers were. The kids were excited about their presents and the mood was cheery, not at all unpleasant. However, when I was woken up again at 2:00 am, and had to go down there, the atmosphere was quite different. Everyone just wanted it to be over so that they could go back to sleep but the sirens just kept going off every three hours, and with the novelty of a British visitor disappearing the heavy toll this was having on people’s mental health was palpable. Just the necessity of having to hide in the basement on a regular basis, even without actual explosions made us feel helpless. It took away any control we had over our own lives. It was a psychological warfare, and some people were clearly giving up without a fight. In one of the shelters, I saw parents completely withdrawn, scrolling their phones while their kids were left to their own devices trying to entertain themselves. Others were composed, leading their families as an epicentre of calm, which was quite infectious. It was a life lesson that I will never forget. Kids playing in bomb shelters is another image that will stay with me for a long time. I can tell you that there is nothing normal about that sight and should never be.
The gate was open, and there I was in a place where a brutal war was raging on, and it was only two days’ drive from home! I had to stop and let the thought sink in. There were lots of signs reminding me of where I was – there were tents where refugees could get basic medical help and some advice on their choices once in Poland, pop up shops selling snacks, and various everyday necessities, scores of women, elderly people, and children, either on foot, or inside their cars queuing up on the Ukrainian side, while vans, and lorries with number plates from all over Europe were getting in. I was the only vehicle with British plates.
I stayed with a colleague, whom I had never met in person before. A word had come out that I was paying a visit, and a stranger offered for me to stay in their house. There were no hotel rooms available, as they were all being used for housing internally displaced Ukrainians.
The bomb shelters were one of the most memorable experiences during my first visit. At the time, the city centre was not being bombed. However, there were a few rocket attacks at the infrastructure, including one just a day before I came when a power station on the outskirts of the city (and a few residential buildings) were targeted. The air sirens were heard up to 10 times per day, and you were supposed to go down to a shelter, which were mostly basements underneath the nearest building. There were probably ‘proper’ purpose-built bomb shelters somewhere, but I did not see one. In bigger cities, underground train systems were used as bomb shelters. There is no
My mission was a success on many levels – I brought much needed tactical medical disposables (tourniquets, Celox, compression bandages, IFAKs), which were delivered directly to the medics I had direct contact with on the southern, and eastern frontlines. I also brought some badly needed body armour for the medics supporting the troops who were pushing Russians out of the Kyiv region, which was one of the hottest spots at the time. The medics there were lacking bulletproof vests, and helmets, and were grateful for my delivery. I also brought a few boxes of airway kits, as well as cannulas for intravenous access, and needles for regional anaesthesia for local hospitals in Lviv. I had received a few specific requests from various hospitals that I was able to respond to. For example, a head of anaesthetic department in Vinnitsa, a big regional centre in the west of the country had asked for isoflurane vaporisers. Their hospital had received a large shipment of isoflurane but had no vaporisers to deliver it to their patients. I had managed to source four vaporisers with the help of our hospital’s engineering department. I bought the ones no longer in use due to an upgrade of our anaesthetic machines at a discounted price while they were on their way to a medical auction. The anaesthetists in Vinnitsa are now able to run four theatres using modern, and safe anaesthetic agents, which is a great result. It is a good illustration of what my mission is all about – a smallscale personalised help, which makes a real difference for those in need. Also, it is a good illustration of a lack of coordination between larger humanitarian organisations and the end users whose equipment is not compatible with the disposables that they receive.
Apart from delivering the medical supplies, I met new friends, and visited some old ones. I also visited a large hospital and delivered a few lectures on trauma-related care to their anaesthetists and intensivists. I was able to get a good idea of what was in greatest demand both in hospitals, and on the frontlines. I have made a few trips to Ukraine since then, including a three-week stay in Kyiv where I worked at a large tertiary centre.
Those missions have been effective and satisfying on many levels. I have been able to help real people with what they needed the most; I connected with people in ways only possible in times of war; I have been inspired to continue helping them. Coming back from my trips, I experienced a cognitive dissonance, a disconnect between my experience, and understanding of the Ukraine war, and its fading, often one-dimensional portrayal by the British media. Having heard a lot of survival stories about the physical and mental horrors of war, I felt that there was so much we could learn from people’s stories if we could only stop and listen to them through all the noise of superficial reporting, scare-mongering, and often frank parroting of propaganda.
I decided to start recording those stories. I first talked to my in-laws. This was the first time they were able to rationalise their harrowing experience of getting out of Kyiv under a heavy Russian bombardment on the first day of the war. It was clear that they wanted to tell their story, both to be heard, and to rationalise their painful experience. I wrote the first draft, but they did not like it. They wanted me to include some details to make their story more visual, more vivid for the readers. Like, when they were getting out of Kyiv, they did not use their GPS, but rather ’traffic updates’ from a local radio station broadcasting the exact locations of advancing Russian troops. Or, when they were staying at the border town, there was a big field where men were teaching their wives, and teenage children how to drive their cars before they could leave for the border. Men themselves were not allowed to leave the country due to new mobilisation laws. They wanted to connect with potential readers on a human level.
Those powerful images were important to our parents. They thought that without them my story would be too dry, too incomplete. I did make those corrections, and they loved the final version. I realised that people wanted to tell and hear war stories (and, any stories about something they have not experienced themselves) as if they look at the events through the eyes of the real people living through those experiences. That is how my idea of writing the ‘real stories of real people’ was born. We have a series of conversations with people who have a story to tell, then we discuss what it would be about with a particular emphasis on the important details that the author wants to include in it, then I write it up, and include some commentaries where I feel they are needed. Finally, I send it back to the author for corrections. I want stories to look and sound as if written by the people themselves. They are their stories, I am here to record, and adapt them for western audiences.
It is impossible to see what is really happening, the whole truth through ‘the fog of war’ - the sheer hatred, horrors, and war crimes being committed on an industrial scale right now. However, it is quite possible to see what is happening through the eyes of the people living through it, their different angles of vision, a collection of aerial photographs forming a composite picture of a large area on the ground.
Despite their sadness, the stories contain hope for humanity. A lot of the tactics used, such as bombings of the cities, war crimes against civilians, tortures, and executions of prisoners of war, are aimed at causing hatred towards a nation and parading the results of that hatred on propaganda media channels. Therefore, it is heart-warming for me to listen to and be able to record the stories of hope and love; love towards their families, their land, and their home.
I hope that after reading their stories you will be inspired by them as much as I have been.
The Ukrops charity
To amplify the impact of my efforts, I felt compelled to establish a charitable organisation. Thus, 'Ukrops' was born. The board comprises of three consultant anaesthetists of eastern European descent, sharing a profound understanding of the situation on the ground in Ukraine.
Together with Medical Lifelines Ukraine, we continue to send medical supplies and tactical kits to hospitals and front-line facilities across Ukraine. I'm also keeping up with my educational work, both online and in-person, and now we're bringing Ukrainian doctors to the UK for short clinical attachments. Thanks to the connections I've made between Ukrainian and Southampton doctors, there are active WhatsApp groups for real-time clinical advice. This collaboration has been lifesaving; for instance, it helped save a mother and her baby during a critical caesarean section in Zaporizhzhia, where Southampton surgeons provided vital guidance to Ukrainian obstetricians.
I have also brought a few Ukrainian doctors for short-term clinical attachments at our hospital and have been their clinical supervisor during their stay. This is important work, but it is quite costly for the Ukrainians as they must cover all the expenses, including the cost of their attachment. It would be good to be able to help them cover at least a part of that with allocated charity funds.
Through my personal connections, I can respond directly to the needs of the people in Ukraine. For my transatlantic row, I have chosen to focus on helping the individuals who are not just practicing clinicians, but also medical managers driving real change in their institutions.
Ocean rowing
‘Rowing the Atlantic is a daunting task; rowing it alone is downright crazy!’ That is exactly what I thought three years ago after finishing a rowing race across the Mediterranean, which did not exactly go according to plan. In fact, I did not want to have anything to do with ocean rowing after that experience. What I had planned as a little 50th birthday challenge turned out to be too much of a challenge, where our team of four strangers (who had only met for a couple of practice rows out in the Solent) had to face a brutal storm that blew us off course a few dozen miles. Rowing against those big 20 footers, which looked even bigger at night, was futile and we gave up rowing altogether and waited for the support boat to rescue us. There were other challenges, both physical and mental, which are inevitable when a group of strangers end up in a small boat and have to row in quite brutal round-the-clock shifts.
Despite all the difficulties, there were some unforgettable moments too when everything was just perfect. The sunrises and sunsets, the wildlife, and the team spirit and humanity at its best, and all of that with extreme discomfort, pain, and the brutality of Mother Nature in the background. There was something that struck a chord with me – the severe and uncontrollable nature of the environment versus the choices that we, as humans can make and how we react to it. Hence, the seed was sewn, and the bug of ocean rowing got through my immune system and infected my mind. I started looking for opportunities to join the right team. At
one point, I nearly made it with a group of Australians, but it fell apart at the last minute due to unforeseen circumstances. In August 2023, I was back at square one, but now absolutely determined to do it.
While I realised my crazy dream to row the Atlantic, the war in Ukraine continued. I spoke to a few ocean rowers, including Tom Mclean, who did the original solo transatlantic crossing in a fishing skiff in 1969, and I was humbled and inspired by his advice and support. I became convinced that going solo was the right choice for me. I also decided I would like to do it in a ’pure class’ boat and I was lucky to have acquired Happy Socks, a boat with quite a pedigree, which I will dedicate a separate article to in future. I have a mammoth task to tackle within less than a year, but I have a great land-support team who will be navigating me through the unknown terrain.
I am doing it both for personal reasons and for humanitarian ones, which do have much in common. A Ukrainian friend of mine, who is a military anaesthetist currently working at a frontline hospital summarised it perfectly:
“As an idle observer, it is like maintaining a sacred fire at the edge of the World in an abandoned church after the crowds have left, having given in to temptations and cheap entertainment, and abandoning the Truth. Only one person remains, unmoved by the Worldly temptations. He maintains the fire, holding the World at the edge of an opening abyss. To come off the common path and reach the edge of the World is the only way to find your own one. In times of chaos, uncertainty, and catastrophes, when you don’t know what to do, always move towards your fear. For me, the war is my Ocean now.”
I think this quote is beautiful and I will certainly be thinking about it when I am in the middle of the Atlantic being battered by big waves with no land in sight.
I am doing it to test myself, to be in a place where we rarely have an opportunity to find ourselves; to see if this experience will break me or make me a better man.
I am also doing it for my Ukrainian medical colleagues, both as a psychological support to show that they are remembered and cared for, and to raise money for my newly registered charity Ukrops, which will allow me to invest money in a bigger project aimed at changing their lives for the better in the long term.
Leo Krivskiy Consultant Anaesthetist, University Hospital Southampton
Facebook: Leo Krivskiy
Instagram: @Krivski
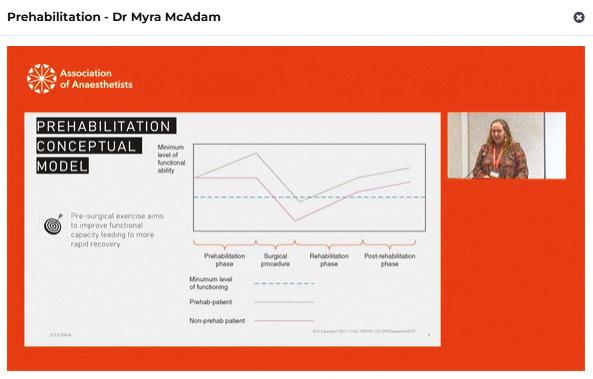
Harnessing technology to create individualised prehabilitation programmes
Increases elective bed capacity
Highly cost-effective
Improves patient outcomes
Reclaiming narratives
In October, this year’s Black History Month theme was Reclaiming Narratives. It offered us the perfect opportunity to shine a light on black contributors to healthcare who are perhaps lesser known.
First, let’s talk about Charles Drew. Drew significantly advanced practices around blood transfusion, especially in World War II, where he led the Blood for Britain project – an initiative that shipped plasma from the US to the UK to aid the wounded. Drew laid the foundations for our modern blood donation systems and his innovations included blood plasma preservation and the first large-scale blood bank. He was an important advocator for racial equality in healthcare and dedicated himself to the training of black doctors.
Another name we should remember is Cecil Clarke. Clarke was instrumental in improving maternal and infant health services, focussing on nutrition and prenatal care. Clark’s Rule, the mathematical formula to determine the safe dosage of medication to give to a child, is thanks to his legacy. Clarke was a prominent advocate for the UK civil rights movement and founded the pressure group ‘League of Coloured Peoples’, alongside black physician Harold Moody. The League was created in 1931, with the goal of racial equality around the world.
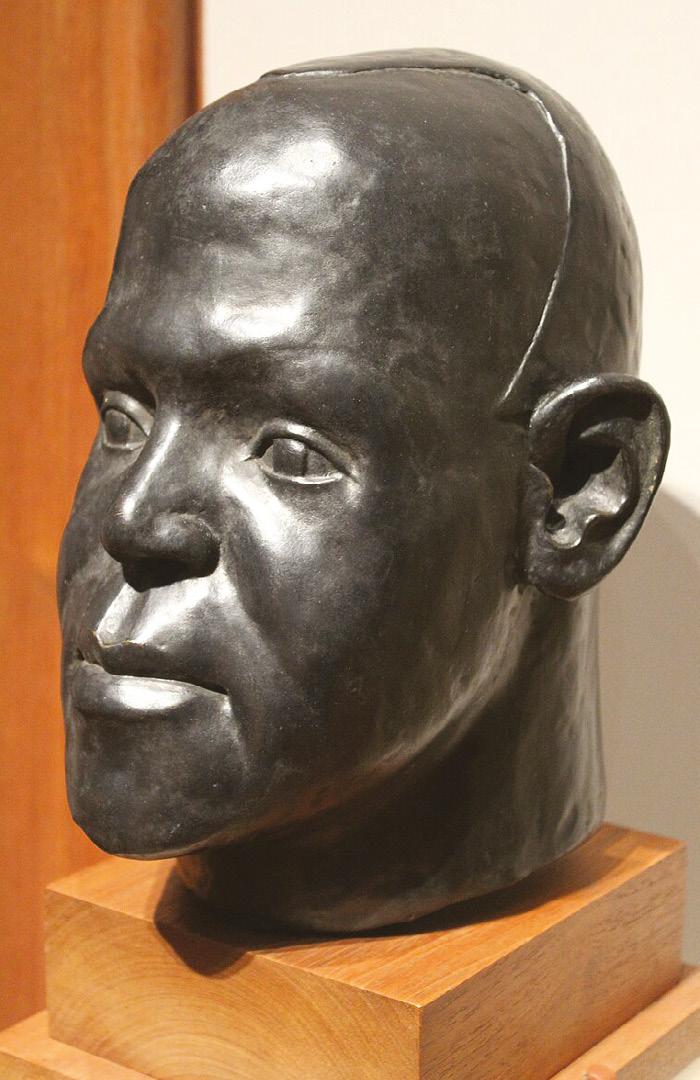
Harold Moody also deserves celebration. Despite racism which stopped him securing hospital positions, in 1913 he set up his own practice in Peckham, South London. His civil rights advocacy helped to implement the Race Relations Act 1965. This was the first legislation in the UK to prohibit racial discrimination in public places.
Charles Drew Cecil Belfield Clarke
Bronze bust of Harold Moody by Ronald Moody, National Portrait Gallery, London
There are so many more black contributors to healthcare, including Nurse Annie Brewster, who worked at the London Hospital in 1881-1902, Nurse Mary Seacole, a British nurse and prominent businesswoman, and Dame Elizabeth Anionwu, who is a British nurse, health visitor, lecturer, and Emeritus Professor of Nursing at the University of West London. The impact of their work to science as well as diversity, equality and inclusion is monumental.
Tami Cherrie-Rees
Digital Communications Officer, Association of Anaesthetists
Editor’s Note: We have also published this article on our Association website in the news section.
In there a doctor in the house? Snow and the societies of Marylebone and Mayfair
John Snow in Soho
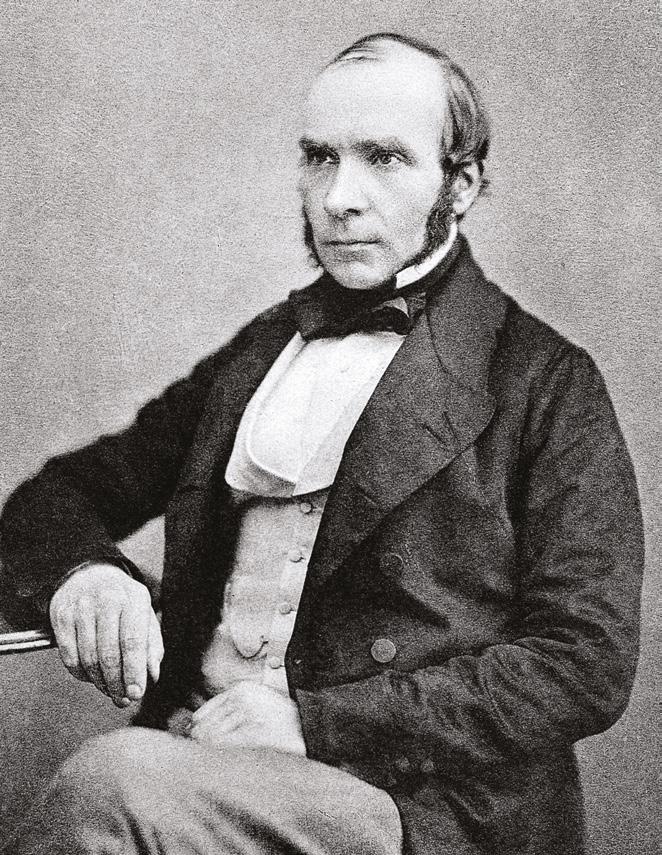
Previously we saw how London’s Early Modern medical institutions competed for superiority and advertised their authority with architectural frontispieces asserting institutional status. Today, we move west and south to the elegant Georgian streets of Marylebone and Mayfair, encountering the 19th century explosion of medical societies around Cavendish Square and Harley Street. Our guide is the eminent anaesthetist and epidemiologist John Snow (1813–1858) [1], whose career reflects those social and architectural changes. Born in York and trained near Newcastle where he first encountered Cholera, a disease that defined much of his professional life, in 1836 Snow moved to London as a qualified doctor. But where to locate?
London’s population had boomed; the fields and gardens of former aristocratic palaces and monasteries, west of the City, were developed - their history preserved in street names, like Blackfriars, still home to the Society of Apothecaries. In the 1630s King’s Surveyor Inigo Jones, laid out the Earl of Bedford’s gardens including those of the former nunnery of Westminster Abbey – the Convent Garden. Jones’ innovative Italianate Piazza and St Paul’s church, in Covent Garden, [2] offered architectural models. As appreciation for, and understanding of, classical architecture advanced, its strict symmetry and proportions became apparent in the creation of streets and garden squares, regarded as hallmarks of power and success.
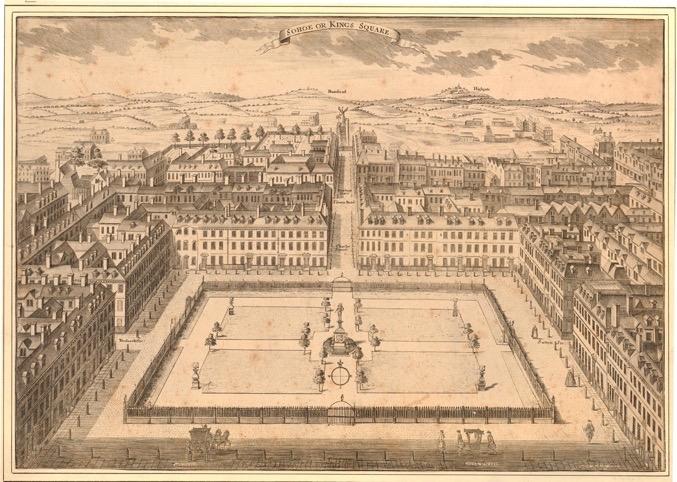
After the Great Fire (1666), building regulations specified fire-proof brick or stone, and imposed height and density restrictions to eliminate overcrowding. Houses reflected occupants’ rank while creating a sort of classical uniformity, from Spitalfields’ artisan houses in the east, to grand West End establishments. Often, builders, craftsmen, and architects developed land piecemeal, such as Soho Square where Snow first lodged in 1836, at 11 Bateman's Buildings. Soho Fields [3] were laid from 1677 to the designs of statistician Gregory King (1648–1712) by speculative builders Cadogan Thomas and Richard Frith, who subsequently developed Mayfair, Westminster, and St James’s. Frith parcelled out land in plots, personally oversaw some buildings and subcontracted others. Originally an aristocratic district, the lack of oversight from an overall landowner resulted in its social decline.
But Soho was professionally convenient: Doctors lived near the work. London’s medical world gradually expanded from the City’s principal hospitals: Bart’s, St Thomas’s, Guy’s and Bethlem, to include new voluntary hospitals like St Georges, the Middlesex, University College, Charing Cross, and the Royal Free, further west and south in Soho, Haymarket, and St James’s. Honorary hospital positions conferred status while introducing physicians to wealthy potential patients who were treated at home, particularly in fashionable Marylebone’s Georgian estate.
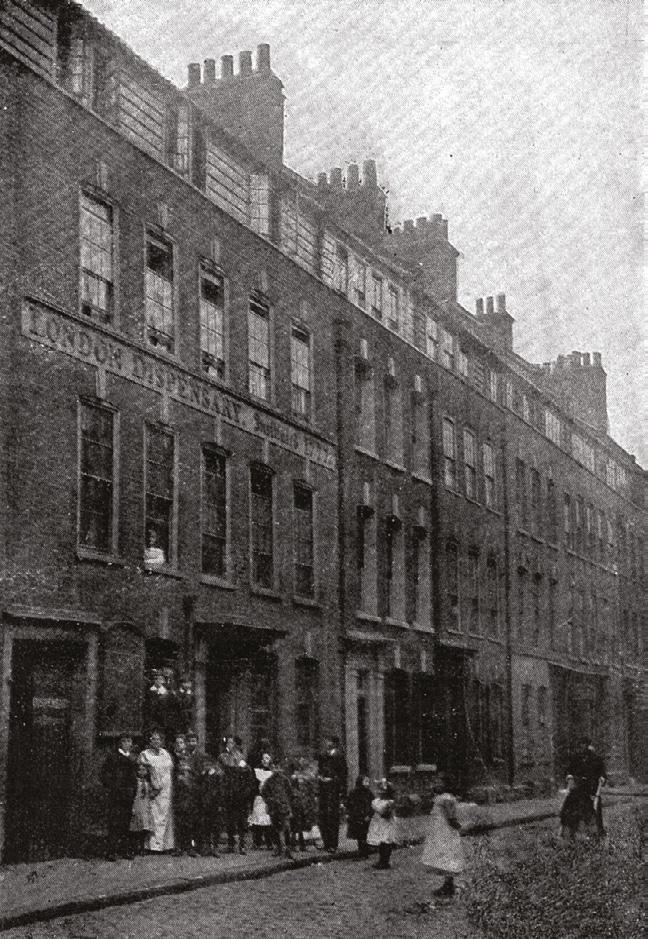
Politically radical clinicians staffed dispensaries serving poor communities, but they necessarily also tended private patients and Snow was no exception. In the 1830s he worked in the out-patient department of the West London Infirmary and Dispensary (1818) behind Soho’s Haymarket Theatre. Dispensaries [4] were benevolent institutions, offering shelter and medical attention to sick poor people, especially after the 19th century population explosion and punitive Poor Laws.
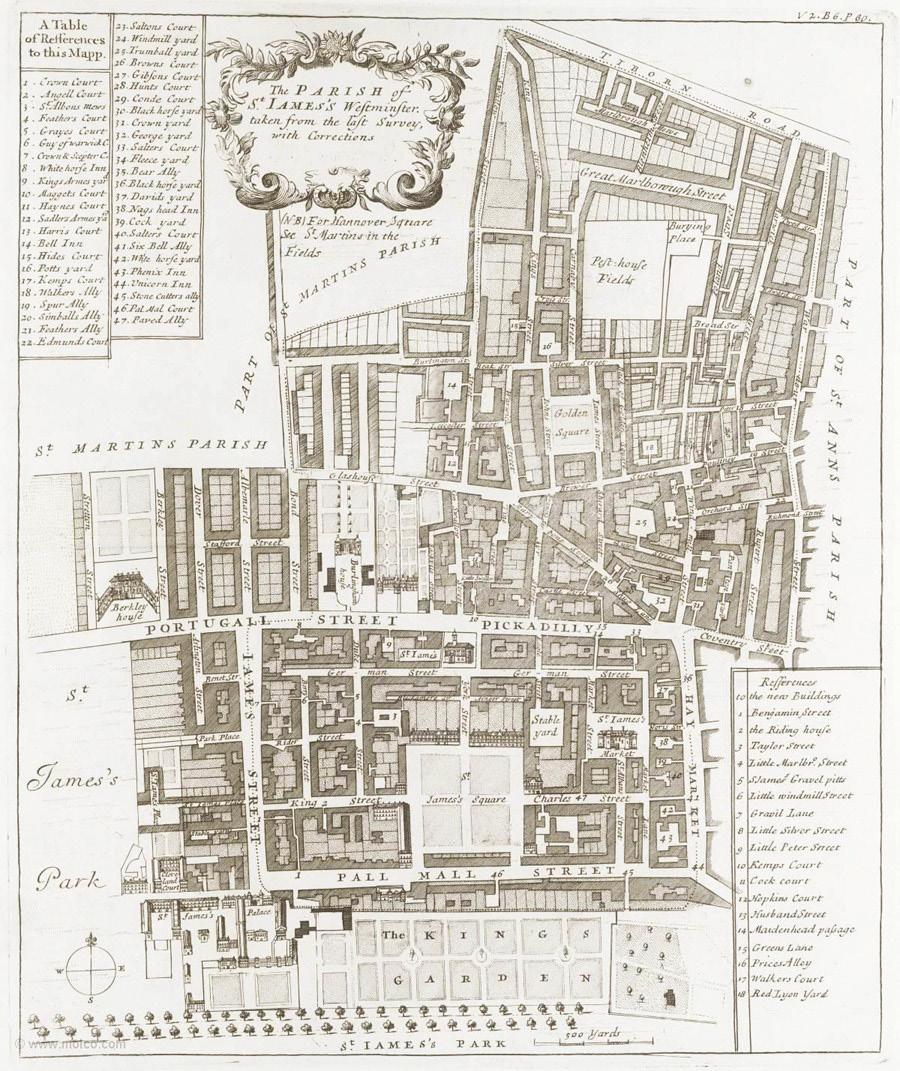
Snow also enrolled at the Great Windmill Street Medical School and after six months' surgical practice at Westminster Hospital, in 1838, he became a member of the Royal College of Surgeons, a licentiate of the Society of Apothecaries and established his practice at Soho’s 54 Frith Street (named for the developer). [5] This Soho era is globally significant: Snow’s reputation rests partly on his epidemiological work on cholera transmission. On the Mode of Communication of Cholera, (1849) was initially overlooked, but his 1855 edition gained traction after augmentation with statistics compiled from the August 1854 cholera outbreak in Broad Street (now Broadwick Street) that claimed over 500 lives in 10 days. Snow’s knowledge of the pump - five minutes’ walk from his practice - provoked suspicions of local water contamination and the pattern of deaths around the locality of which he was a longtime resident.
• Two jam-packed days of obstetric anaesthesia educational content, with expert speakers and plenty of time for discussion.
• Take part in our social event programme.
• View the latest abstracts in obstetric anaesthesia by visiting the e-poster boards and listen to your colleagues present in-person.
• Meet up with industry and get your hands on the latest equipment!
For more information and to book visit
The Oxford and Portland Estates
Not all London’s Georgian development created squares. Until the 18th century, the area north of Oxford Street was a royal hunting park. In 1708, the southern part was purchased for development by John Holles, Duke of Newcastle, and inherited by his daughter Lady Henrietta Cavendish, wife of Edward Harley, the Second Earl of Oxford – (hence the street names). In 1719 they commissioned surveyor John Prince for a masterplan; architect James Gibbs who’d worked at Wimpole, their Cambridgeshire estate; craftsmen, and speculative builders. As customary, architects, builders, and craftsmen leased plots, retaining some for personal use, subleasing others to patrons who shaped the design. Progress was piecemeal over 50 years, but accelerated under Britain’s richest woman, Margaret Cavendish Harley, Duchess of Portland [6] (hence the Portland Estate). In the early 1770s she released parcels of land including to the Adam brothers’ fashionable architectural practice that we’ll consider in the third part of this series.
Gradually, classical houses lined Harley Street, Wimpole Street, and Portland Place. [7] These elegant streets remained exclusive real estate for a century, but when the ton migrated to Belgravia and Mayfair, Cavendish Square became London’s supreme medical space. By the 19th century, together with Harley Street, it was so famously associated with fashionable doctors that Robert Louis Stevenson characterised it as a ‘citadel of medicine’ in The Strange Case of Dr Jekyll and Mr Hyde (1886). By 1905, nearly every house was occupied by leading practitioners or key medical organisations and - as medical historian Nick Black observes - “between 1840
and 1920 modern healthcare professions were defined and refined here, remaining the political centre of the healthcare professions”.
Medical societies
From the late 18th century, the medical profession established numerous societies promoting scientific, professional, and social networking as medical science created new specialisms, supported by societies like the Association of Anaesthetists. England’s first was the Medical Society of London, founded (1773) by the prolific Quaker physician and philanthropist John Coakley Lettsom (1744–1815), who also established free dispensaries. It aimed to unite medicine’s warring physicians, surgeons, and apothecaries as the only society where all professionals, irrespective of background, could meet on equal terms to exchange knowledge. Snow had joined while a student in 1837 and he later attributed his success to this early connection, eventually becoming President in 1855. The Hunterian Society (1819) and the Harveian Society of London (1831) still hold their meetings at the Medical Society of London’s premises at Lettsom House, Chandos Street, just off the prestigious Cavendish Square [8].
Medical societies and associations blossomed. Snow also joined the Medico-Chirurgical Society and was one of the first members of the Epidemiological Society of London (1850) founded to investigate the aetiology, progress, and prevention of epidemic diseases. Located in Hanover Square, near medical London’s epicentre, its activities reported in The Lancet, the British Medical Journal, The Medical Times, and The Sanitary Review before establishing its own Transactions. In 1907, it
merged with the Royal Medical and Chirurgical Society of London, becoming a part of the Royal Society of Medicine, now the Epidemiology and Public Health section.
Sackville Street, Piccadilly [9], adjacent to royal St James’s, was previously home to Sir Everard Home (1756-1832), sergeant-surgeon to George III, and the aural surgeon James Yearsley (1805–1869) established his clinic at No 29. It was appropriate, therefore, that in 1852 Snow established his final home at No 18. Snow's reputation for skilled safe practice led to the effective administration of chloroform to Queen Victoria during the births of Prince Leopold (1853) and Princess Beatrice (1857). Snow died in Sackville Street in 1858, a testament to how far he had travelled, not only from York to London, but across London’s medical geography and up the social ladder.
Ann-Marie Akehurst
Independent Scholar and Fellow of the Society of Antiquaries
Figures
1. Dr. John Snow (1813-1858), British physician. Public Domain, Wikimedia Commons
2. Piazza in Covent Garden, Wenceslaus Hollar (1647) (MET, 17.3.1166383). Metropolitan Museum of Art Collections, Public Domain, Creative Commons
4. Nineteenth-century photograph of the London Dispensary: Spitalfields. Wellcome Collection, Public Domain.
5. 38 Frith Street, Soho, engraved by Jonathan C. Sawyer
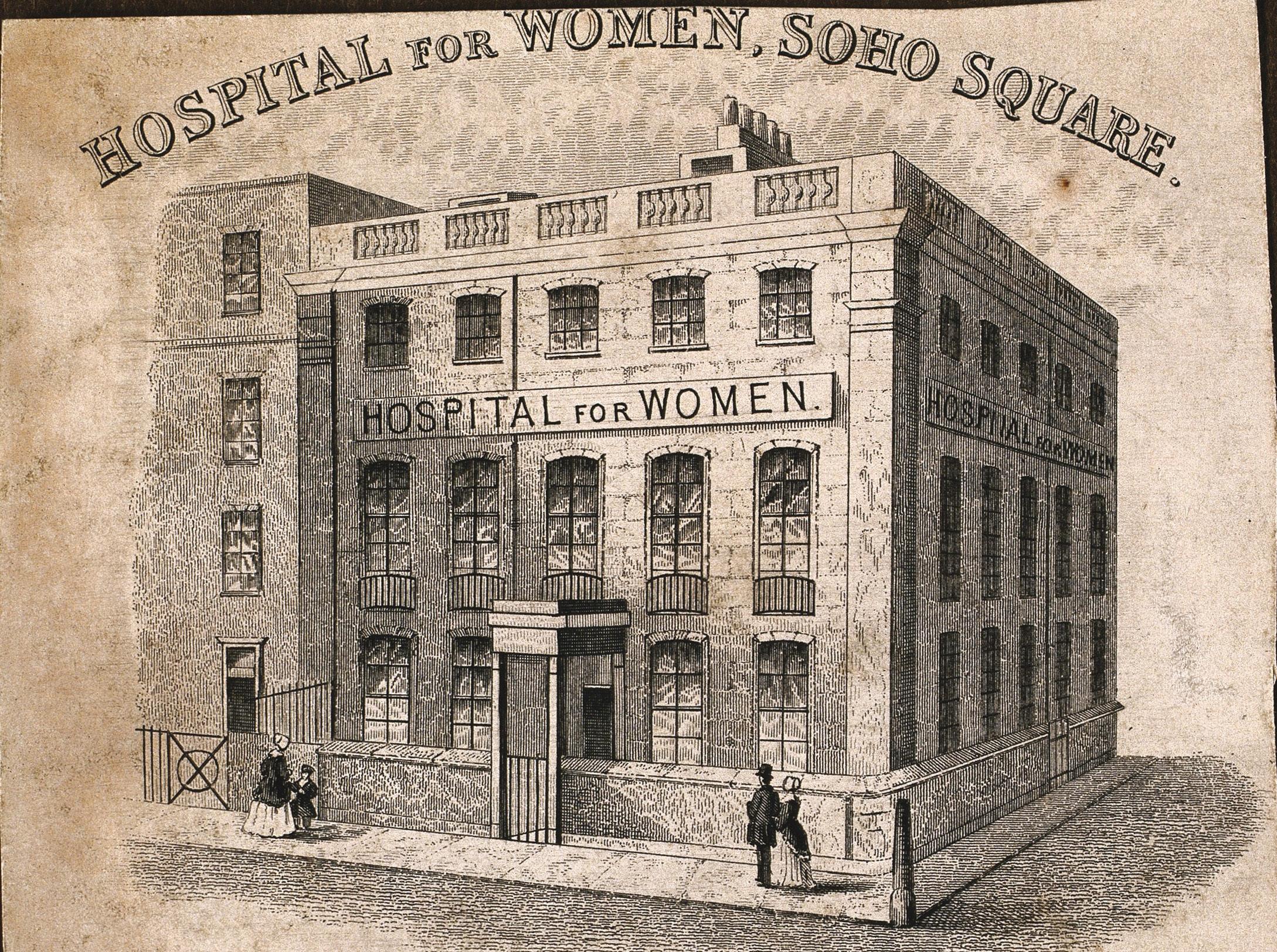
The Hospital for Women, founded at Red Lion Square in April 1843, moved to 30 Soho Square in 1852. Wellcome Collection. Source: Wellcome Collection Pubic Domain
6. Margaret Cavendish Bentinck, Duchess of Portland, Also known as Margaret Harley, Oil on canvas portrait, painted by Christian Friedrich Zincke, 1738. Christian Friedrich Zincke, Public domain, via Wikimedia Commons
9. The Parish of St James’s, Westminster from John Strype’s Survey of London (1720) showing Sackville Street, Great Windmill Street and – far right in Soho - Broad Street. https://www.dhi.ac.uk/ strype/figures.jsp courtesy of Motco Enterprises Limited, www.motco.com).
Acknowledgements
I am indebted for details regarding medical societies to Nick Black, Walking London’s Medical History (2012).
Now available on Sonosite ST
Now available on Sonosite ST
Hands-free control for optimal patient care
Hands-free control for optimal patient care
In situations where
In situations where you perform nerve blocks or during intricate procedures, Sonosite Voice Assist helps you deliver exceptional patient care without compromising efficiency.
Focus solely on your patients
Spend
Enhance flexibility
Control the system even across your
Spend less time fiddling with knobs and buttons, dedicating your full attention to patient care.
Control the system even across your patient’s bed, ensuring optimal positioning and comfort during procedures.
Any patient. Anywhere. Anytime.
Request
Maintain a sterile field
Maintain a sterile field
Minimise the risk of contamination and keep your environment sterile by using your voice.
Minimise the risk of contamination and keep your environment sterile by using your voice.
No assistant, no problem
No assistant, no problem
Have confidence to complete a procedure or exam without the need for an assistant.
Have confidence to complete a procedure or exam without the need for an assistant.
Ketamine to Kerabu: An elective in Malaysia
For my elective, I was based at Hospital Canselor Tuanku Muhriz (HCTM) in Kuala Lumpur, Malaysia. With more than 17,000 operations performed annually, I had the opportunity to be involved in a variety of procedures ranging from paediatric ear, nose and throat (ENT) surgery to complex oncological cases.
Paediatric anaesthesia
With no prior experience of paediatric anaesthesia, I was excited to explore the challenges of interacting with young children in what understandably is a daunting experience for some. It became apparent that adequate planning and communication was especially important in ensuring children were comfortable throughout the induction process. For example, the team would encourage parents to stay with their child and use playful distraction techniques such as allowing the child to hold the mask and bag. Additionally, pharmacological intervention in the form of pre-medication was often used as an adjunct to reduce anxiety.
During induction, I was able to carry out practical skills such as drawing up medication and airway management. One memorable moment was when I held the mask and carefully altered the flow settings under supervision during a gas induction for a small 8-month-old. This made me appreciate the precision with which paediatric anaesthetists work to provide a smooth anaesthetic. Personally, practising the CE grip technique on infants increased my confidence in creating a good seal, a skill which I had previously struggled with in adults.
During cases, I learnt about the anatomical and physiological differences between older children and young infants and the implications this has on anaesthetic practice. An example I observed was the use of a Miller over a Macintosh blade in infants due to their proportionally long and flaccid epiglottis.
Following surgery, I would head to recovery and help the team with monitoring vitals and assessing postoperative pain.
Obstetric anaesthesia
During my time on obstetrics, I saw a complex case of a 35-year-old lady with placenta percreta. The surgical team had decided to perform a hysterectomy following a caesarean section delivery. Due to the high risk of blood loss, the anaesthetists inserted an arterial and central line, with blood products ordered in advance. The team also worked alongside the interventional radiologists who had inflated a temporary balloon in the internal iliac artery to minimise bleeding. Thankfully, the large volume of blood that was lost during the case was replaced in a timely manner and the patient remained stable. The case again highlighted the need for sufficient planning to reduce the risk of complications associated with surgery.
However, the most impressive aspect was the clear and effective communication between the anaesthetists, radiologists and the surgical team, especially in a theatre filled with 28 people!
Related specialties
Outside of theatres, I had the opportunity to learn about and work with various teams related to anaesthesia. With the acute pain service, I understood the importance of function when deciding to reduce a patient’s analgesia post-op. In ICU, we discussed the concepts of treating tropical diseases such as dengue fever and the various ventilator modes used in respiratory pathology. Finally, in the electroconvulsive therapy (ECT) clinic, I pre-oxygenated patients and learnt about the factors affecting the dose of propofol administered.
During my elective, I was looking to explore how a patient’s anaesthetic journey differed in Malaysia. At HCTM, it was clear that the difference in healthcare provided was not as large as the difference in health spending per capita suggests (4.1% vs 12% in the UK [1]), though being a large teaching hospital may explain this. Equipment including the anaesthetic machines and optimisation in the form of pre-operative assessments were similar to those I have seen in the UK. However, I also observed notable differences, including the infrequent use of TIVA and medications such as remifentanil.
Conclusion
My time at HCTM has broadened my understanding of the differing facets of anaesthesia. I truly admired the vast knowledge base anaesthetists called upon to provide a safe and effective anaesthetic, alongside the composure with which they achieved this. The most enjoyable aspect of staying in Malaysia was the integration of multiple cultures, which gave rise to some of the best food I have ever had! I would like to thank Nizam Mokhtar and the anaesthetics department at HCTM for being so welcoming and eager to teach. I am also grateful to the Association for helping to fund an insightful and thoroughly enjoyable elective.
Mathun Kuganesan University College London
Reference
1. World Health Organisation. Global health expenditure database. https://apps.who.int/nha/database/country _profile/Index/en (accessed 24/05/2023).
Five weeks at Austin Health in Melbourne, Australia
Austin Health is a leading tertiary hospital in the suburbs of Melbourne. The primary aim of my elective was to understand the field of anaesthesia in greater detail and consolidate my cannulation skills, airway management and pre-op history taking.
Over my four clinical years in medical school so far, anaesthetists were always the doctors I admired for their in-depth understanding of physiology, for how stressful their jobs can be they always seem to be calm and in control. My elective cemented these preconceived opinions. I was fortunate to shadow different anaesthetists in various theatres such as orthopaedics, vascular, urology, endoscopy lists, gynaecology, cardiac and hepatobiliary surgery. This diverse range of procedures allowed me to truly appreciate the variability of the workload and stress anaesthetists encounter during different operations.
I witnessed some relatively straightforward cases from an anaesthetic perspective. This included colonoscopies that were managed with light sedation using propofol and airway support, knee and hip replacements under general anaesthesia and cystoscopies in the urology list. Although these procedures have few complications, the importance of a good history in pre-op clinic was stressed when there was a patient undergoing a left hip replacement with gastroparesis and acid reflux therefore, they had to undergo rapid sequence induction (RSI) to prevent the risk of aspiration. This provided some valued learning about the various indications and the process of RSI.
I also witnessed longer complex surgeries, particularly the atrial and mitral valve replacements and CABGs. This highlighted the complexity of anaesthetics, with the team inserting radial arterial lines, central lines and Swan Ganz catheters under ultrasound guidance prior to the start of surgery. During the surgery, I also learnt the importance of gathering images via the transoesophageal echo to determine heart function before replacement and was fortunate to be able to have a few attempts myself.
the various anaesthetic agents, muscle relaxants and antiemetics. My clinical and practical skills also developed considerably. I was routinely tasked with managing the patient’s airway – from maintaining an airway with a head tilt and chin lift or a jaw thrust. I also developed my preoxygenation skills by learning how to effectively achieve a good seal with the bag-valve mask using a two-handed approach, and occasionally with a onehanded approach. I also learnt how to analyse the end tidal CO2 trace to check the quality of the seal.
Furthermore, I familiarised myself with airway adjuncts by sizing and inserting Guedel’s, iGels and endotracheal tubes. At the start of the placement, I struggled with my cannulation, but after some further guidance from one of the anaesthetic fellows and further attempts, my success rate improved, and I subsequently feel more confident in my ability. The anaesthetic pre-op clinic allowed me to practice my history taking skills and provided me with the opportunity to listen to various murmurs such as aortic stenosis, aortic regurgitation and mitral stenosis. I learnt how to take an anaesthetic-focused history and was able to get feedback directly from the consultants.
Anaesthetists were always the doctors I admired for their in-depth understanding of physiology, for how stressful their jobs can be they always seem to be calm and in control.
Alongside the clinical aspect of anaesthetics, I was able to get involved in research by witnessing two ongoing studies (Citric-CPB and HepTemp) in cardio-pulmonary bypass patients. CITRIC-CPB was studying the effect of bypass on vitamin C levels, neuroinflammation, cerebral oxygenation and post-op confusion. HepTemp studied the effect of therapeutic hypothermia on heparin metabolism whilst on bypass. I was able to witness how these observational studies were conducted, the follow up of patients post op and the analysis of the results.
The management of blood pressure when going off pump and back on pump was particularly stressful as it is important to maintain an adequate mean arterial pressure. In most cases this was managed by metaraminol. During a liver transplant for a patient with liver cirrhosis, I was able to witness the preparation of the harvested liver prior to transplant. During this case the management of how to deal with the profound vasodilation that occurs during unclamping and how to pre-emptively manage this physiology was particularly interesting to note.
Overall, I witnessed many interesting cases and learnt vast amounts regarding the indications and benefits of
Overall, my elective was fantastically organised and provided great insight into a career in anaesthetics, whilst developing both my clinical and practical skills as well as my knowledge of physiology. I am very grateful to my supervisor, A/Prof Lachlan Miles (also an Editor for Anaesthesia) and the entire Anaesthetic Department at Austin for all their help and support during my five weeks. I would also like to thank the Association of Anaesthetists for their generous grant in enabling me to undertake this fantastic opportunity.
Nishant
Chaudhari Imperial College London n.chaudhari@nhs.net
Gunshots, stabbings and road traffic accidents: Another day in a Johannesburg major trauma centre
I
was fortunate enough to spend five weeks in the trauma unit of Charlotte Maxeke Johannesburg Academic Hospital; one of two state-funded level 1 trauma centres in the global capital of trauma.
“’A’ stands for securing the airway in the primary survey” was one of the first things drilled into me alongside fellow students from the University of the Witwatersrand in trauma tutorials led by the Head of Trauma Professor Moeng and his colleagues. It was important to him that students receive a firm foundation in trauma resuscitation before adding the intricacies of damage control surgery and other management in future teaching.
The primary and secondary survey was a routine that I became all too familiar with as ambulance trollies rolled in one after the other on day and night shifts loaded with priority one patients. These patients presented following mob assaults, gunshots, stabbings, road traffic collisions and falls from height. It was not uncommon that patients fulfilled the criteria for intubation and underwent rapid sequence intubation. Whilst we were busy applying monitoring devices, gaining IV access, and assessing breathing, circulation, disability and exposing the patient, the Medical Officer in the trauma resus unit stood at the head of the bed, calmly pre-oxygenating the patient with bag-valve-mask and taking lead to instruct the team on the next steps of sedation. The Medical Officers staffing trauma resus and managing complex airways were the equivalent of a UK core resident doctor and were remarkably proficient in their skills but were patient in teaching me and other students these skills too in a ‘see one, do one, teach one’ manner. After all, we were extra hands-on-deck, and were members of the team. Throughout the five weeks I was there, I performed countless arterial blood gases, wide-bore cannulations, and urinary catheterisations, I sutured, reduced fractures, learnt to perform E-FAST ultrasound scanning and placed chest drains and intubated under supervision.
Many patients had a prolonged requirement for sedation due to the extent of their injuries and the resus bay was certain to have several ventilated patients at any one time. Some of these patients were stepped from trauma resus to the trauma intensive care unit. On the daily rounds, I learnt a great deal about ventilator settings as well as standards of care within ICU. The cost of slipping standards was demonstrated on a separate occasion as I accompanied the anaesthetic team for an elective theatre case which involved the stenting of a tracheal stricture resulting from prolonged intubation with high cuff pressures following an organophosphate poisoning para-suicide.
‘see one, do one, teach one’
Through my work in the trauma unit, I managed to organise one day with the ambulance service. My last day in Johannesburg was spent in the responder car with an advanced life support (ALS) trained emergency care practitioner (ECP). It was just after midday when we received the call that we were required at a community clinic – no more information. After heading there with blue lights and sirens blaring, it was clear that paramedics were already on scene. The patient was having an acute life-threatening asthma exacerbation with a silent chest on auscultation. All medications from salbutamol nebulisers to magnesium sulphate and adrenaline had been administered with limited relief. The ECP and her colleague were ready to intubate, however, upon mandatory telephone consultation with senior clinicians they recommended against this and to bring the patient to the nearest hospital as they feared that it would be a difficult airway, and re-consult if she deteriorates. The patient did deteriorate, and after four consults and more than an hour on scene, a senior paramedic arrived and took the decision to perform rapid sequence intubation (RSI) in the
back of the ambulance. I bagged the patient for more than half an hour until we reached a hospital ventilator. For me, this was a chance to see the difficulties in pre-hospital care; whether to stabilise the patient before mobilising or transport to the hospital to provide definitive care as soon as possible. The situation revealed conflicting opinions between leadership, senior clinicians, and paramedics on scene, leading to overall delays in patient care, demonstrating the importance of one clear leader and followership of the rest of the team.
Julian Greig University of
Birmingham
I thank the Association of Anaesthetists for generously supporting the elective with a £500 grant. I have developed clinical skills and acumen in resuscitating a critically unwell trauma patient and learnt about the principles of safe sedation and its application in RSI. I am looking forward to exploring more anaesthetics and critical care medicine in my final year of medical studies.
Charlotte Maxeke Johannesburg Academic Hospital emergencies entrance
Frank Jennings, 1946-2023
A lifetime of family, friends and honing his craft
A longstanding Association member and reader of Anaesthesia News since 1999, Francis Oliver Jennings (Frank) was born in County Tipperary in rural Ireland in July 1946. His father was a forester, and the family moved frequently. He received his education in Co Galway, Wicklow, Tipperary and Cork. Frank was easy going, unassuming and a great conversationalist. He initially trained as a teacher, but then decided to become a doctor and completed his degree in Medicine at Trinity College in Dublin, later specialising in anaesthesia. Frank was able to work in many places during his training, in Dublin, St John’s in Newfoundland, Liverpool and many other locations.
Frank was an immensely talented individual and eventually took up a consultant post in Huddersfield where he was instrumental in setting up the Pain Clinic. His priority at all times was patient care and safety. For example, in 1980, the Faculty of Anaesthetists of the Royal College of Surgeons, Ireland created the Delaney Medal in honour of Edmund J Delaney, which was awarded to Frank, then a senior registrar who had worked closely with Edmund Delaney in chronic pain management prior to his death. Since 1980, this medal has been awarded to anaesthetists in training for work carried out in Ireland on a subject related to anaesthetic practice. Frank also authored and coauthored several academic papers during his career, including a significant article in the Journal of Anaesthesiology in December 1981, detailing how prolonged exposure to nitrous oxide inhibits bone marrow function.
Both inside and outside of work, Frank was known for his sense of humour and ability to tell a great story. Aside from his dedication to his work and his large and loving family, his other great passion was long distance walking. He was a member of the Long-Distance Walkers Association (LDWA) and through that, a group called The Irregulars, mainly made up of members from Yorkshire, Lancashire & Derbyshire and all counties in between. Frank would often be found on 20+ mile walks on the weekends with friends, and during the week when commitments allowed. Frank also completed marathons in Dublin, London, Paris and New York and was a keen follower of cycling and Gaelic games, such as hurling.
He was an avid music aficionado too, and particularly knowledgeable about Irish classical theatre and operatic genres. Always thinking about the welfare of others, Frank spent part of his holidays and retirement working for a charity in Chitrakoot in India, anaesthetising patients with cleft lip and palate who would otherwise have gone through life without an operation. He also volunteered on Mercy Ships, which uses modern hospital ships to bring world-class volunteer medical professionals directly to the places they’re needed most.
Frank passed away in Overgate Hospice, Halifax on 27th December 2023 in the company of his family. He was a true Irish gentleman and a dear friend to many. He is greatly missed by everyone who knew him. Frank is survived by his beloved wife, Ann, his brother John and his sister Mary, his five sons, one daughter and six grandchildren.
Why gain an accreditation in fTOE?
A collaboration between the Association of Anaesthetists (the Association) and the Intensive Care Society (ICS) led to the development of a Focused Transoesophageal Echo (fTOE) accreditation for both ICU and anaesthesia. But what is it and why would we encourage you to gain the accreditation?
fTOE is valuable when unexplained life-threatening circulatory instability persists despite corrective therapy, and whenever transthoracic echocardiography cannot or is unlikely to give an answer, such as during surgery or while a patient is intubated and ventilated in the ICU.
The concept of a focused (as opposed to comprehensive) echocardiogram to identify haemodynamic instability has revolutionised patient care. Point-of-care ultrasound (POCUS) using transthoracic scanning protocols, such as FATE [1] and FUSIC Heart [2], has empowered non-cardiologists – especially anaesthetists and intensivists – to rapidly assess cardiovascular status and treat the major causes of haemodynamic instability.
In 2022, to provide all acute care practitioners with the opportunity to acquire competency in focused transoesophageal echocardiography (TOE), the ICS and the Association launched a new accreditation pathway, known as fTOE. The aim of fTOE is to provide the practitioner with the necessary information to identify the aetiology of haemodynamic instability. Focused TOE can be taught in a shorter period, and teaching programmes are achievable with support from cardiothoracic anaesthetists, intensivists and cardiologists.
Traditionally, TOE has been performed by practitioners with advanced (so-called ‘level 2’) skills; their backgrounds were mainly in cardiology, cardiac anaesthesia and, less commonly, intensive care. However, the challenge remains that patients with haemodynamic instability are encountered in locations, such as the emergency department, intensive care unit and in non-cardiac theatres, where level 2 TOE practitioners are not always immediately available. There are several circumstances when a transoesophageal, rather than transthoracic approach, may be preferable such as during surgery and/or when a patient has a tracheal tube in situ. In these instances, it might be difficult to get to the patient’s chest or the view may be compromised because of mechanical ventilation. Examples include: the unstable patient in A&E, emergency trauma surgery, thoracic surgery, hepatic surgery including liver transplantation, and many patients in critical care.
The benchmark for acquiring basic echocardiography skills varies between 20 and 50 studies and can be significantly augmented with the use of simulators. Teaching programmes are achievable with support from cardiothoracic anaesthetists, intensivists, and cardiologists.
Registration for fTOE accreditation is via the ICS website; e-learning can then be accessed via the ICS learning portal. Learning materials include theoretical modules, clinical cases, and multiple-choice questions. The modules must be
completed prior to starting mentored practice and logbook collection. A suitable local supervisor can be contacted via the ICS learning team. The supervisor will be responsible for hands-on training, reviewing the scans, overseeing the logbook and recommendation for sign off after the final assessment. Completion of fTOE training is by a centralised assessment, run by the Association, after the sign-off by the supervisor and approval of the logbook by the exam commission. Eligibility as a fTOE supervisor requires level 2 TOE accreditation by the British Society of Echocardiography or European Association of Cardiovascular Imaging, or the ability to demonstrate equivalent knowledge and regular use of TOE by application to the fTOE accreditation committee.
Accreditation in fTOE represents a joint venture between the Intensive Care Society and Association of Anaesthetists and is endorsed by the Association of Cardiothoracic Anaesthetists and Critical Care. The process is led by TOE experts and represents a valuable expansion in the techniques available for acute care practitioners to assess haemodynamically unstable patients. While fTOE in invasive, its risks are mitigated by careful patient selection and clinical supervision, which are all built into the design of training and service delivery.
We hope this overview has whetted your appetite to consider developing an accreditation in fTOE. Comprehensive details, including how to perform a fTOE examination, can be found on the ICS website: https://ics.ac.uk
Jon Sacker Head of Communications, Intensive Care Society
1. Jensen MB, Sloth E, Larsen KM, et al. Transthoracic echocardiography for cardiopulmonary monitoring in intensive care. European Journal of Anaesthesiology 2004; 21: 700–707.
2. FUSIC, Intensive Care Society https://ics.ac.uk/learning/fusic.html.
3. Rubino A, Peck M, Miller A, et al. Focused transoesophageal TOE (fTOE): A new accreditation pathway. Journal of the Intensive Care Society, 2023; 24(4): 419-426. doi:10.1177/17511437231173350.
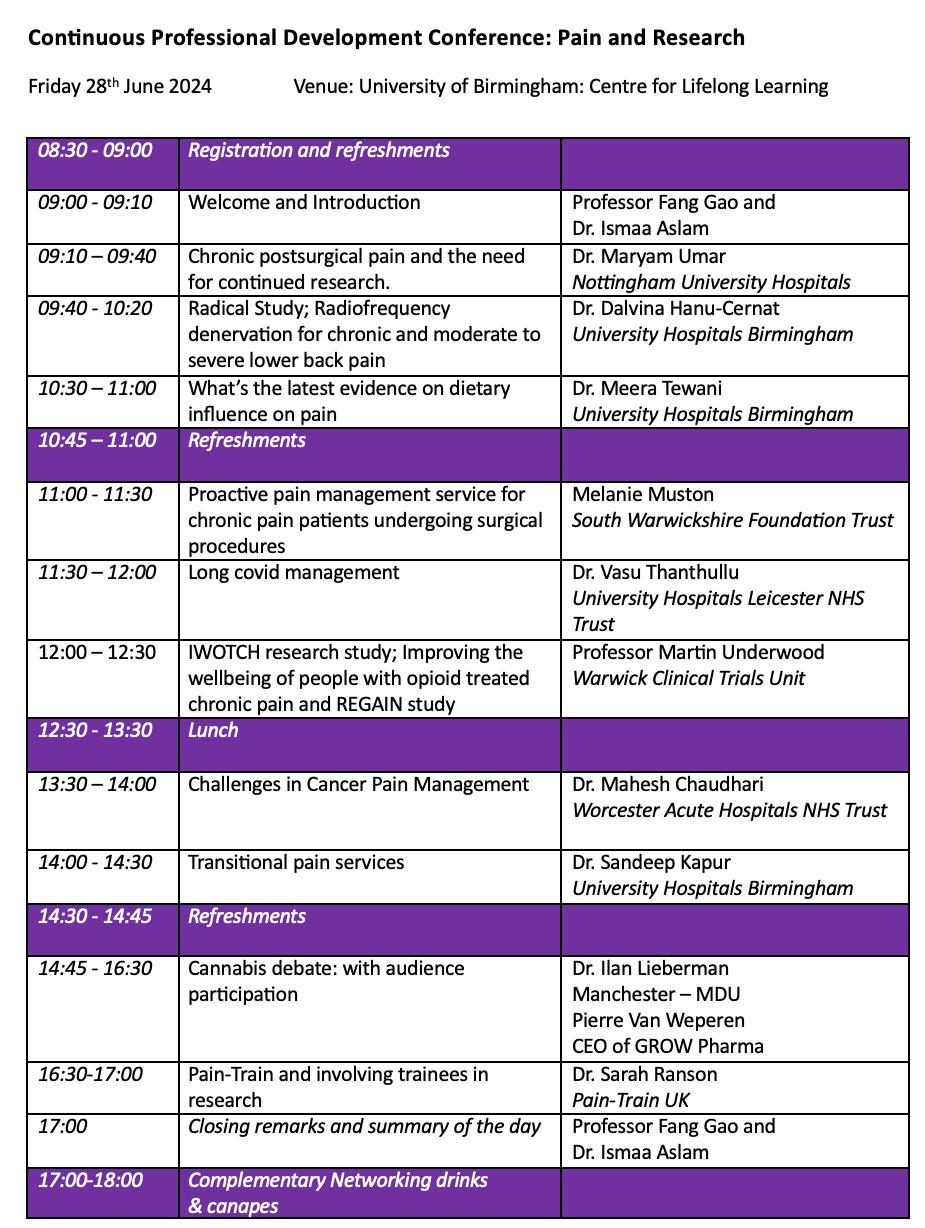
Resident doctor-led National Conference in Pain and Research
Our vision was to organise a national conference with the latest updates in pain and research from leading experts and a networking opportunity.
In June 2024, with the support of Fang Gao, I successfully organised the National Conference on Pain and Research at the University of Birmingham. This was the first resident doctor-led continuing professional development (CPD) course with speakers and delegates who support patients with acute or chronic pain.
Organising the conference
The vision was to have a one-day course that encouraged collaborative discussion and celebrated the multidisciplinary approaches to supporting patients with pain. In addition, we wanted the conference to act as a networking opportunity, facilitating collaboration between pre-clinical researchers, multi-disciplinary clinical staff and resident doctors.
In my role as an advanced pain specialist resident doctor, I liaised with local educators and discussed ideas with physiotherapists, clinical psychologists, and pain nurses about topics that should be covered in the conference. I also spoke to board members of the Pain-Train UK committee, offering the opportunity for other resident doctors to help organise the conference.
Whilst I have experience in organising and supporting local teaching programmes, this was my first opportunity to oversee a national conference. The College of Medicine and Health CPD lead and administrator at the University of Birmingham offered invaluable support, expertise and guidance on how to seek CPD accreditation.
The next task was to reach out to potential speakers. I was pleasantly surprised and honoured by the replies (as shown in Figure 1: Programme). Everyone I contacted went above and beyond to ensure that they could attend and if they could not, suggested alternative speakers. I was humbled by how downto-earth the speakers were and generous they were with their time.
Figure 1: Programme
With speakers confirmed and the programme set, my focus turned to ensuring the day ran smoothly. As a resident doctorled event, it was important to have the input of other resident doctors. The board members at Pain-Train UK supported the conference but were busy preparing for FRCA exams or organising a national audit, so, I went further afield. An anaesthetics specialist resident doctor with an interest in chronic pain, based in Trent Deanery, was keen to be involved, and an academic intensive care resident doctor in Mersey Deanery had experience with organising events. Together, we designed the posters for the conference, contacted sponsors, advertised the event, and had regular meetings to discuss logistics for the day.
We also wanted to ensure the course was economically viable. Whilst we were not expected to pay the speakers for their time, the nominal attendance fee enabled us to pay for their travel expenses and to provide lunch and refreshments for delegates. The University of Birmingham kindly allowed the use of a conference room free of charge. Through sponsorship and negotiation with the catering department, we offered a wine reception, canapés, and negotiated additional networking time at the end of the conference. We were grateful to the catering team for providing an excellent spread over lunch, of both hot and cold food. Left-overs were gratefully received by the busy Emergency Department of the neighbouring Queen Elizabeth Hospital Birmingham.
Challenges
A few challenges arose in the lead up to the conference. One of which was that the Faculty of Pain Medicine organised a national teaching event for resident doctors on the same day as the conference. The clash could have resulted in both events being affected. The Faculty of Pain Medicine’s event had the additional option of remote attendance, which we thought might have prompted more resident doctors to attend their event. However, after great deliberation, we decided it was too late to change the conference date due to the impact on speakers and delegates already signed up to attend.
Furthermore, I was about to enter the third trimester of a highrisk pregnancy and was nervous about going into labour and not being present on the day of the conference. Thankfully, I avoided any unplanned admissions to labour ward!
Two weeks before the conference, a doctor’s strike was scheduled for the same day as the conference. Our fears about whether speakers could attend were unfounded. Clinical commitments for a couple of speakers led us to rearrange the programme and we are very grateful to one speaker for agreeing at the eleventh-hour to talk. We were delighted that 72 delegates were able to attend.
Success
The energy on the day was great, thanks to the delegates and faculty. The presentations were inspiring and thoughtprovoking. Professionals from many disciplines shared their experiences, passions about the future of pain medicine and associated research, frustrations due to shortages in resources and the complex nature of pain and variations of services.
The environment was enriched by the presence of diverse professionals, including nurses, physiotherapists, clinical psychologists, PhD students, general practitioners, researchers, anaesthetists, palliative care consultants, resident doctors and authors of fundamental books within the field of pain.
The attendees travelled from across the country, including Liverpool, Glasgow, Manchester, and London. The feedback received was extremely positive and email exchanges have included job opportunities, setting up patient resources based on material presented and improvement in department and services. Attendees discussed opportunities for resident doctors to join clinical trials and how NHS staff can be involved in research. Feedback has been glowing with an average score of 9/10 of delegates finding the day to be very beneficial and relevant to their clinical practice.
Looking to the future
I had such a great experience organising this conference, with the support of the faculty. The talks and discussions were inspiring, and I intend to make this an annual conference. We hope to extend it to a two-day conference in 2025 and to have space to enable more delegates to attend.
Acknowledgements
I would like to offer my thanks to Fang Gao and Linda Lefievre for trusting me with this opportunity, Annabel Haylor-Giles for guiding me as the CPD administrator. I am particularly grateful to Annabel’s years of experience in supporting such conferences. She ensured catering, logistics and relevant paperwork were completed without any complications. My thanks also extend to the other faculty members, Maryam Umar, and Alicia Waite, who offered exceptional support leading up to and on the day of the conference. Lastly and most importantly, my thanks go to all our speakers and delegates without whom the day would not have been possible.
Ismaa Aslam
Warwickshire School of Anaesthesia
Ismaa.aslam1@nhs.net
Figure 2: CPD Conference
A week in the life of a consultant anaesthetist, NIHR regional specialty lead, research delivery lead and Anaesthesia Reports editor in Leeds
Monday
I spend alternate Mondays in a floor running role overseeing all lists rather than being allocated to one specific theatre. Today, I start by trouble-shooting a short-notice rota gap, and then I help reduce the anaesthetic time for a patient having a major colorectal case by scrubbing for the central line while my colleague does other procedures. We have staggered admissions, so later I let colleagues out to see their patients who have arrived over the course of the day. St James’ has several wings and a lot of stairs, so I always get my steps in on floor runner days! I am on call for obstetric anaesthesia tonight, so at around 17:30, I check in with the evening team and do joint handover with the obstetricians. There is an inpatient with placenta accreta who has a clear plan for elective delivery later in the week, but we make sure everyone is aware of her in case she becomes an emergency out of hours. When I get home, my husband and children (years 5 and 8) are back from work and school. My eldest asks for my advice about Spanish grammar, which is definitely not my forte!
Tuesday
My eldest goes to school by train, so I drop her at the station, take the youngest to breakfast club and head to work for a research day. I am the NIHR regional specialty lead, so I meet with our research delivery manager, and we look at recent studies in anaesthesia, perioperative medicine, and pain. We discuss each one and decide which are a good fit for our sites across the region. Not all can be run at all sites; it depends on the patient groups involved and resources to deliver research varies across sites. After this, I meet with a resident doctor who I am supervising on the NIHR associate principal investigator training scheme. They are part-way through their six-month training, so we ensure they are on track for sign-off and plan together to address a few gaps. Later, I meet with the research delivery team. A consultant colleague, three research nurses and I deliver a portfolio of studies in our department which we offer to our perioperative population. The meeting starts with the band 7 team leader, and we discuss the feasibility of potential recent studies. We are then joined by the band 6 research nurses, and discuss each study to review recruitment and solutions to problems. I am part of the national Perioperative Medicine Clinical Trials
Network research leaders' scheme, and this afternoon it is the board meeting. I have a brief update to present on a recently funded study. I take the kids to dancing and orchestra and go for a run while they’re busy. I’m presenting at a meeting in a few weeks’ time and as I find running useful thinking time, I consider how I might organise the talk.
Wednesday
My husband does the school run while I cycle to work. We live about 10km away and we’re lucky to have a lot of offroad routes near us. They’re great in summer although not so helpful for dark, winter commutes. I have a thoracic list today, and it’s a mixture of elective and acute cases. One of our research nurses let me know last week that there is a SINFONIA study patient today, and he is with the patient as I arrive for the pre-op visit. I let him know when we are approaching sending, and he phones me back to tell me which arm of the study they have been randomised to. I am Principal Investigator, so I know the protocol, and he leaves me some intra-op data collection forms to complete in theatre. We do two lobe resections and then two shorter acute cases. We are finished in theatre just after 17:00. I return the study paperwork to the research office and then as theatres either side of ours are still running, I check in to see if either of the anaesthetists need a break or help. My husband works in flood risk and his hours are more flexible than mine, which is immensely helpful especially with school run arrangements. They are home just ahead of me tonight and appear to be making dinner using every pan we have!
Thursday
On the bike again this morning. We have six women for elective caesareans on today’s list including two with placenta praevia. I was appointed in 2017, and over the years, the unit has become noticeably busier, with the section rate increasing each year. We have a slight delay to starting the list because the night team are finishing an emergency case. Nevertheless, we get going in reasonable time, and I have an excellent resident doctor with me. We have two obstetric theatres and when there are no acute cases, we have two ODPs which means that we can keep the list moving. One of us performs the neuraxial blocks in the anaesthetic room while the other
finishes the last case and transfers to recovery. I get home in time to take my eldest to hockey training. While she’s there, I do some work for Anaesthesia Reports. I issue a final accept decision for an article that has gone through several revisions in previous weeks. This is always a really good moment for me, and hopefully so for the authors too who have put in a lot of work to get it to this point. I review two new submissions and return initial thoughts to our Executive Editor who will then allocate them to me formally for further handling.
Friday
I get to the gym before work and then start the morning with a study meeting. I have recently been awarded NIHR funding to deliver a perioperative study on the use of non-steroidal anti-inflammatory drugs, and we aim to start recruitment next year. At the minute we are in the set-up phase and are writing study documents and getting approvals in place. I am working on various other projects at the minute including a systematic review with the help of some anaesthetic trainees and medical students. I make sure they are on track and happy with their current tasks, and then settle down to work on a narrative review.
Saturday
I cycle to work for a Saturday thoracic list. I have these as part of my job plan, but fewer than I did when I was first appointed. We usually have a full day list of acute cases, and it’s a good opportunity to get people to theatre and heading towards discharge as the new week begins. We have a typical list of people needing talc pleurodeses and pleural biopsies/drains. The last patient isn’t suitable for theatre today unfortunately, so we finish at 16:00. I head to the office to catch up on admin so I’m on top of my inbox before Monday. When I get home, the family have made dinner and after a re-run of my youngest’s new skills learned at gymnastics today, we all watch a film together.
Sunday
We try to keep today clear for family time. We live near the Leeds Liverpool canal, which is great for cycling, but because it’s raining today, the kids think the bouldering gym is a better idea. Next week, I have fewer clinical sessions, so I am looking forward to catching up with study work and other projects relating to my research role.
Caroline Thomas Consultant Anaesthetist, NIHR Regional Specialty Lead and Research Delivery Lead, Leeds Editor, Anaesthesia Reports
Hazy sunshine over the Leeds to Liverpool canal on a summer day.
A measure of stress: How smart watches show the strain of on-call work
On-call work is something of a bête noire topic throughout medical careers, with many doctors at the point of retirement feeling they might remain in practice but for the demands of out-of-hours work.
The associated stress is in many ways hard to quantify, and for those who don’t do it, hard to relate to. A recent event, combined with the insights of wearable technology gave me a useful snapshot of the physiological impact of being called late at night.
Having worked a full day in cardiac theatre, I was on call overnight for intensive care. This is separate from covering cardiac cases but a mix up is easy to imagine. Thus, I received a telephone call at 2:45 am asking if I was on duty for an aortic dissection - which I was not. I explained who was covering that service and over the next few minutes went back to sleep. I didn’t need to get up or go anywhere.
Looking at the analytics on my smart watch which records heart rate, the effects of even this brief disturbance are very obvious. At the time of the call, my pulse immediately doubled from 53 to 106 beats per minute (see image). As a simple measure of stress, a single call that was rapidly deflected is at the lowest end of the scale compared to the stress caused by calls that require further action. It is no surprise that, even decades later, doctors recoil in visceral horror from the sounds of pagers!
Brian O’Brien Consultant Anaesthetist and Intensivist, Cork University Hospital, Cork, Ireland
SCALE-Critical Care: The value of partnership visits
Alongside collaborative online working, partnership visits are vital for reciprocal relationships to develop and for both sides of the partnership to better understand the challenges of healthcare delivery in a different system.
SCALE-
Critical Care
SCALE is a collaborative health workforce capacity and educational development partnership between the Ugandan Ministry of Health and the UK NHS. SCALE focuses on several clinical specialties which have been targeted for specific development in Uganda, one of which is critical care. As in many countries, the Covid-19 pandemic exposed a severe lack of critical care capacity in Uganda. This project aims to support workforce development and bidirectional learning through initiatives such as remote and in-person learning, curriculum and training development, quality improvement, research, and reciprocal fellowships.
The SCALE conference: Opportunities for shared learning
After a successful visit to the UK from members of the SCALE team and the Permanent Secretary for Health, the UK partners visited Uganda in June 2022. This visit included spending time at several key partner hospitals in Kampala, to better understand the current resources and staffing and the differing needs of critical care. It was also timed so that we could attend the SCALE conference in person, at the Ministry of Health in Kampala. This was an excellent opportunity to have high level discussions about the future directions of the partnership, and to hear from other SCALE projects including maternity and emergency medicine. A formal memorandum of understanding was signed, which was an important step in ensuring the commitment to the partnership on both sides. We received positive feedback about the work SCALE critical care had done, including the speed at which the project had progressed, and the team focus on developing research capacity alongside clinical expertise. We also learnt from the challenges and successes of other SCALE Uganda partnerships during the conference and met collaborators from other specialities.
Ongoing partnership building: The importance of relationships
Since this visit, relationships between our colleagues and collaborators have grown immensely, and alongside anaesthetic and critical care doctors, critical care nurses have been undertaking some fantastic work including regular simulation training, medium term placements for UK nurses in Kampala, and a visit from one of the nursing leads to the UK to see our critical care units in Cambridge. The East of England Global Health fellowship programmehas now had three UK fellows working on the partnership since its conception – helping to provide continuity and dedicated time for projects. One project is the development of multidisciplinary hybrid high fidelity simulation training between Uganda and the UK.
As an ‘early adopter’ of SCALE we are regularly contacted by other units starting up similar programs in other African countries and specialities.
We have been able to support others with lessons learned from our experiences.
In November 2023, we conducted a pilot that revealed several technical issues but also underscored the value of reciprocal shared learning. Plans are in place to use a newly opened simulation centre in Mulago Hospital to expand on the concept for small groups of doctors and nurses. Additionally, we are implementing a programme to develop simulation debriefing skills.
We continue to run regular virtual grand rounds for both medical and nursing colleagues. These are shared learning events, open to all. Each grand round is chaired either by the Ugandan team or the UK team, alternating each time with speakers from both countries presenting cases on a named topic, with time for discussion. Topics are identified in advance by the clinical leads and are focused on important aspects of the critical care curriculum. The virtual grand rounds have been well received, with some sessions having over 200 participants attending online.
Successess and planning for the future
The SCALE critical care project has been a great success so far but has always had a long-term vision of increasing the workforce capacity in critical care in Uganda – so the work is ongoing. We currently have two Ugandan doctors completing rotations in two of our critical care units in Cambridge. They will spend a further year in the UK gaining extra experience before returning to Uganda to take up posts in Kampala with potentially another doctor joining us later in the year. Our aim is to support these doctors in expanding critical care training on their return home, utilising transferrable skills and system understanding.
The nursing arm of the program (not described here but integral to the SCALE ethos) has also been particularly successful in fostering remote and in-country teaching. In the last year the nursing team have focused on training the Ugandan team to run simulation sessions with a meaningful debrief. This program was collaboratively designed and conducted both virtually and in Uganda. We supported Mulago Hospital’s lead nurse visiting Cambridge for an observational placement where we exchanged knowledge and practice on trauma care. This year we are working towards hosting two long-term placements for Ugandan nurses with the opportunity to study at UEA and gain a PGcert in Critical Care. One of the most powerful take-home messages from the UK nursing team is that they gained many new skills including project management, flexibility and working differently, which they were able to transfer to their home units.
As an ‘early adopter’ of SCALE we are regularly contacted by other units starting up similar programs in other African countries and specialities. We have been able to support others with lessons learned from our experiences.
One of the most significant challenges facing this program is securing funding. Financial support is used to develop educators in both systems, facilitating bilateral visits (which although kept to a minimum are essential for mutual understanding of challenges) and for the development of online learning and technology support.
Next steps include recruitment of further fellows and nurses to undertake placements in the UK and integrating with other MDT members such as bioengineering and physiotherapy. The research arm of the SCALE critical care project includes a collaboration with the NIHR global health group on Acquired Brain and Spinal Injury (NIHR ABSI), to look at trauma care pathways in the country and the role of families and communities in acute illness. Building on the success of the Basic Assessment and Support in Intensive Care (BASIC) course held in November, plans are underway for a nationwide rollout. We are committed to supporting further course delivery, with Ugandan trainers leading the sessions. This approach aligns with our long-term goal of fostering sustainable workforce development.
Acknowledgements: We would like to thank the simulation team at Bedford Hospital for the use of their facilities to pilot our hybrid simulation, all the volunteers who work on the SCALE critical care project, the team at Cambridge Global Health Partnerships and Health Education England, without whom this work would not be possible. Our visit to the SCALE conference was funded through an Association of Anaesthetists IRC grant.
Laura Hobbs is supported by the NIHR Global Health Research Group on Acquired Brain and Spinal Injury ref NIHR132455. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Laura Hobbs
Consultant Anaesthetist, East and North Hertfordshire NHS Trust, Stevenage UK and NIHR Clinical Research Fellow, Cambridge, UK X: @global _neuro @ihsgcam
Sarah Loftus
ST4 Homerton University Hospital
Lisa Enoch
Education Lead Critical Care, Addenbrookes Hospital, Cambridge
Rowan Burnstein
Consultant in Anaesthesia and Critical Care, Addenbrookes Hospital Cambridge and Deputy Postgraduate Dean, NHSE WT&E, East of England
Annual Congress 2025
17-19 September 2025 | P&J Live, Aberdeen
Roc(k)
The 'Rapid Curonium' Sux' it is not But the best that we got Given our allegiance To a rapider sequence
The drug that came next On top of the podium ‘Sugammadex’ Is surely the best?
You have to admire The desire to respire
During the sign out
While the surgeons close Instrumenting the airway the issues arose…
Adductor contractions
Refractive to our actions
The glottis, rebellious anaesthetists perspiring with the pt expiring…
Total hellishness
The Brainiest Archie might attest How a few drops of local On the cords that are vocal
Could prevent an arrest
Aren’t ‘Old Friends’ the best? Whatever the block
Watch the clock
Isn’t Neostigmine our Rock?
Michael A Duncan
A Deeper Plane Ad Astra Per Aspera
Our mission was slow-moving to depart, For gravity held strong upon this world. The destination lay in light-years’ span, Failure never thought to be an option.
So much remains untouched and unexplored, An endless expanse stretches far beyond. I run tests on dark and silent matter— Is this a sight we’ve known from times before?
Arriving sooner than we had believed, Not even light can find a way to flee.
The event horizon now draws so near, Dimensions collide, all lost to entropy.
Phosphenes flicker with strange, elusive signs, As reference points begin to slip away.
I’ve crossed the bridge that bends both time and space, From motes of dust, the stars begin to form. The edge of tomorrow now shines brightly, Life examined and now once more made whole.
Michael Gibbons
Anaesthetic Registrar, Perth, Australia
Michael Gibbons’ contribution to ‘A Deeper Plane’ is inspired by his recent exam experience.
The use of personal smartphones for medical photography
We have all heard the phrase ‘can someone take a photo of this?’ as we go about our work. The evidence is that in most cases doctors reach for their personal smartphone. In this article we look at the scale of this practice, the specific issues of using smartphones for medical photography and the solutions we need to call for.
Smartphones are an invaluable resource for us at work and have without a doubt made our practice safer and more efficient. The benefits are countless, with quick access to guidelines, drug calculators, regional anaesthesia How-To's and, of course, a camera function. In an instant, our phones allow us to capture and communicate vital information that has a positive impact on patient care. Yet the practice of using smartphones for medical photography is still, for many reasons, extremely problematic.
In 2014 Chan et al surveyed responses from 147 Canadian plastic surgeons.[1]
They found:
• 89% had taken photos of patients with their personal smartphones
• 73% thought that verbal consent alone was sufficient
• 73% had images of patients stored amongst personal photos
• 26% had accidently shown clinical images to friends and family
In the UK, a study of orthopaedic clinicians in 2016 had similar findings: [2]
• 91% had patient images on their phone
• 83% of the images had been automatically saved to an online cloud
There are numerous other studies reporting similar results [3]. So, what are the problems with using phones for photographing patients and what are the possible consequences?
1. Confidentiality
In law any image documenting a patient's medical condition is considered part of their health record and therefore subject to the same standards of confidentiality and security as all other medical documentation. NHS professionals are legally and contractually obliged to maintain confidentiality when handling personal information. As well as causing significant distress to
patients, breaches of confidentiality involving images can result in serious consequences for both the employee taking the photograph and for the healthcare organisation involved.
2. Data protection
Data protection rules apply when a patient is identifiable from an image. Even if the face is not shown, any characteristic feature such as a tattoo, birthmark, or even distinctive clothing can cause a photograph to fall into this category. Noncompliance with General Data Protection Regulation (GDPR) can result in substantial fines for organisations, and these are considered particularly serious breaches where sensitive data are repeatedly communicated via unsecured platforms.
3. Consent
All consent, verbal or written, must be documented in the notes. When obtaining consent, two main factors should be covered; firstly, permission to take the photo (which includes an explanation for its purpose) and secondly, an explanation of how the image will be used and stored.
4. Professionalism
The use of phones at work has the potential to appear unprofessional. When anaesthetising for regional anaesthesia I often feel the need to reassure my patient (and surgeon) that I am completing my logbook and not idly scrolling through social media. It is possible that using our phones to photograph patients may make them anxious about what will be done with the image and how easily it could be shared.
5. Communication of images
Photographs are regularly communicated using apps such as WhatsApp. Despite the reassurance of end-to-end encryption, this app does not require a separate password once the phone has been unlocked. It also automatically saves images to both the sending and receiving device unless the settings are actively changed. Users should further be aware that when back-ups are enabled, data may be transferred to storage cloud areas outside of the European Economic Area (EEA).
Guidance, local policies, and current challenges
Numerous documents give guidance on creating and processing medical images. The Institute of Medical Illustrators has an excellent ‘Guide to Good Practice’ specifically addressing the use of mobile phones.[4] The GMC also has a ‘Making and using visual and audio recordings of patients’ document, opening with a reminder that “trust is an essential part of the doctor-patient relationship and confidentiality is central to this”.[5] As well as providing its own guidance, the GMC urges doctors to adhere to local policy.
Many local guidelines stipulate that consent should be in written form and that photos must only be taken using trust equipment. Keep in mind next time you lurk behind the ENT registrar scoping a dodgy-looking airway in ED that you will probably need written consent and a trust device before taking a photo.
Looking forward
This all calls into question what should be done to make an improvement? A challenge is that the technology currently available at work is not sufficient to support us to do things the right way, at any time of the day. Is it realistic to respond with a simple ‘don’t use your smartphone’? At the time of researching this article I made enquiries to see how easy it was to take a medical photograph at my hospital. The medical photography department was entirely uncontactable by
phone, both in and out of hours, and had no email address listed. In theatres I was informed that “there used to be a camera…but it was stolen.” Unlike a smartphone, it is likely this device was not password protected.
Organisations have several options for improving standards. As ever, none of these are free and we will need to convince finance managers that this serious issue is worth investing in. One answer would be for all doctors to be provided with trust devices. This would be expensive though and in the current NHS climate is unlikely to be enacted. My personal feeling is that a purpose-built, secure app for taking consent, creating, communicating, and uploading images to patients’ electronic notes would be a more viable solution. Apps offering some of these functions are already in existence - a good example being the Secure Clinical Image Transfer or ‘SCIT’ app developed by University Hospitals Birmingham.[6]
Let us hope that with time technology offering all these features will come. To any of you with a passion for quality improvement or medical technology – here is something to work on.
Take-home messages
• Valid consent to take a photograph or video must be documented in the patient’s notes. In many trusts this must be on a written consent form
• An image is part of a medical record. It should be kept confidential and added to the patient’s notes
• Check your local policy on what equipment is allowed for taking photographs
• If a distinctive feature such as a birthmark is included the image is considered as identifiable, and therefore GDPR rules apply
• Devices storing photos must be kept safe and secure, and images must not be backed-up to a storage cloud
Sarah Harrison ST7 Anaesthetics, Wessex Deanery
References
1. Chan N, Charette J, Dumestre DO, Fraulin FO. Should 'smart phones' be used for patient photography? Plastic Surgery 2016; 24(1): 32-4.
2. Nabulyato WM, Jeyaseelan L. Legal, ethical, and practical considerations of smartphone use in orthopaedics. The Bulletin of the Royal College of Surgeons of England 2016; 98(6): 252-257.
3. Kunde L, McMeniman E, Parker M. Clinical photography in dermatology: Ethical and medico-legal considerations in the age of digital and smartphone technology. Australasian College of Dermatologists 2013; 54(3): 192-7.
4. Institute of Medical Illustrators. Mobile phone and mobile apps for clinical photography – a guide to good practice, 2019. NG_Mobile_Devices_2_0.pdf (imi.org.uk) (accessed 25/08/2024).
5. General Medical Council. Professional standards for doctors – making and using visual and audio recordings of patients, 2011. Making-and-using-visual-and-audiorecordings-of-patients_pdf-58838365.pdf (gmc-uk.org) (accessed 20/08/2024).
Dermatology • General Practice • Plastic Surgery •Radiology • Trauma & Orthopaedics • Other Specialties
• Hands-on workshops
• Multidisciplinary lectures
• Satellite and joint sessions
• Bedside ultrasound course
• Contribution from allied specialities
• Keynote lectures by invited speakers
GASOC updates and unique opportunities
GASOC (Global Anaesthesia, Surgery and Obstetric Collaboration) was established in 2015 on the back of the Lancet Commission in Global Surgery. [1] It is a UK and Ireland based professional body that represents over 1,400 surgical, anaesthetic and obstetrics and gynaecology resident doctors with a global following online. Our goal is to increase equitable, ethical and effective resident doctor engagement in global surgery activity and in doing so, strengthen the partnerships we have with colleagues in LMICs and improve outcomes for patients through collaborative training and education.
Updates from 2023-24
Journal clubs
GASOC hosts a regular journal club every two months on the online platform, MedAll, rotating through the specialties of anaesthesia, surgery and obstetrics and gynaecology.
The most recent journal club on 21 August was anaesthesiafocused and looked at two papers on anaesthesia-related maternal mortality in resource-constrained environments and evaluation of practice following SAFE (Safe Anaesthesia for Education) courses in Tanzania [2, 3]. This work was presented by Kotutu Lombe Mulenga and Ayantu Hordofa Benti, anaesthesia residents from Zambia and Ethiopia respectively. All journal clubs have RCoA accreditation for CPD points and catch up content is available through MedAll (app.medall.org). We welcome authors and resident doctors from all over the world to suggest topics and present.
RCoA GASOC podcast series
In 2023, GASOC produced a Global Anaesthesia podcast mini-series with the RCoA, capturing the experiences of resident doctors who had worked with the charity Mercy Ships, GADP (Global Anaesthesia Development Partnerships) and a hospital in India (BKL Walawalkar). The final episode focused on medical capacity building, interviewing Michelle White, consultant anaesthetist at Great Ormond Street and long term volunteer with Mercy Ships. For senior resident doctors, an international anaesthetic placement can form part of their SIA (Special Interest Area). For consultants, there is the opportunity to become a Remote Educational Supervisor (RES) for resident doctors undergoing these placements and fellowships.
GASOC VRiMS anaesthesia courses
GASOC has been partnering with VRiMS (Virtual Reality in Medicine and Surgery) (vrims.net) since the inaugural VRiMS surgical hybrid teaching course run in Brighton and Kampala in 2022. VRiMS specialises in creating resources for medical training through extended reality technologies [4]. GASOC has organised anaesthetic workshops in Uganda (April 2023), Cameroon and Zambia (January 2024), focusing on advanced airway skills and ultrasound guided regional anaesthesia. This was taught by an all- African faculty including ambassadors from the African Society for Regional Anaesthesia (AFSRA). Plan A blocks were recorded using 360 degree VR technology in French and English. This is freely available from the VRiMS library and the hope going forwards is to have several global hubs live-streaming these workshops.
The feedback from the courses has been hugely positive with changes noted to knowledge, skills and practice from candidates. There is an upcoming workshop planned for Mbeya, Tanzania at the end of October 2024.
These projects have been made possible with the generous grant from the Association’s International Relations Committee and have been presented at the World Congress of Regional Anaesthesia meeting (ESRA, 2023), the AFSRA Annual Conference (2023), WFSA World Congress of Anaesthesiologists (2024) and the Association of Anaesthetists Annual Congress (2024).
Annual conference
GASOC organises an annual hybrid conference. This was attended by 346 delegates (over 70 in person) from 49 countries last year. It is always a great opportunity to hear from inspiring clinicians and organisations regarding their contributions to Global Surgery and to share innovative ideas through our scientific programme and international poster hall.
This year’s conference, ‘Creating Solutions in a Changing World’, was held on 18-19 October in Manchester. We were delighted to partner with the Association to host the inaugural essay prize. We focused on the ongoing efforts and challenges faced by clinicians to provide safe and effective medical care in a constantly evolving world with changes in political, environmental and humanitarian spheres. Our first day featured exciting interactive in-person workshops on a variety of themes (collaboration and emergency response, research in global health, education in global surgery, innovation and surgery in conflict settings). The second day was fully hybrid and all content was recorded and made available for registered delegates.
Regional events
GASOC has started to hold several hybrid regional events across the UK and Ireland to bring our events closer to you! Our most recent regional event was held in Leeds, Yorkshire, on 16 July with the theme of Innovation. We heard from our ex-GASOC President Will Bolton on frugal innovation, John Dalton and his Ugandan counterparts, Billy Ndiwalana and Henry Luweesi, on minimal access surgery in Mengo Hospital and Bishow Karki on low-cost laparoscopic simulation training in resource-poor settings. Our latest hybrid regional event was held in Dublin, Ireland, on 14 September, featuring talks from Irish doctors for the environment about the impact of climate change on global health. Catch up content is available on MedAll.
GASOC Global Frugal Innovation Skills course
An online, eight module innovation and research skills course, has been held on MedAll throughout 2023-2024. As part of this, the ‘Global Virtual Hackathon: AI and Digital Tech for Global Surgery’ was held on the 21 to 22 September, featuring leaders in AI, digital technology and global surgery, alongside dynamic global breakout sessions pitching live project proposals to win funding for a frugal innovations project. Funding is by the RCSEd and supported by Lifebox, MedAll, National MedTech Foundation and ASiT.
The future
EADP research methodology series
As part of an ongoing collaboration with GADP and EADP (Ethiopian Anaesthesia Development Program) we are working to produce a research methodology webinar series to meet the training needs that have been highlighted by clinicians there for their residents’ training. This will be run in conjunction with esteemed medical researchers from around the world through MedAll and is anticipated to go live in Spring 2025.
Working groups
Four multi-disciplinary, cross-continent working groups have been formed to invite enthusiastic training doctors in the field of research, education, innovation and international engagement. The working groups aim to encourage collaboration, sharing of experiences and engagement in sustainable change in specific areas. GASOC members can join a working group and engage with committee members on different projects. More information can be found on our webpage. https://www.gasocuk.co.uk/working-group
References
1. Meara JG, Leather AJM, Hagander L, et al. Global surgery 2030: Evidence and solutions for achieving health, welfare and economic development. Lancet 2015; 386: 569-624.
2. Sobhy S, Zamora J, Dharmarajah K, Arroyo-Manzano D, Wilson M, Navaratnarajah R, Coomarasamy A, Khan KS, Thangaratinam S. Anaesthesia-related maternal mortality in low-income and middle-income countries: A systematic review and meta-analysis. Lancet Global Health 2016; 4(5): e320-7. doi: 10.1016/S2214-109X (16) 30003-1. PMID: 27102195.
3. Lilaonitkul M, Zacharia A, Law TJ, Yusuf N, Saria P, Moore J. Evaluation of practice change following SAFE obstetric courses in Tanzania: A prospective cohort study. Anaesthesia 2023; 78(11):1354-1364. doi: 10.1111/ anae.16091. Epub 2023 Jul 10. PMID: 37431149.
4. Virtual reality in medicine and surgery (vrims.net)
Acknowledgements
We thank all our global partners who have made this work possible and so enjoyable!
Fiona Linton
UK Anaesthetic Representative, GASOC, ST5 Anaesthetics, Wessex
Pei Jean Ong
Join us
GASOC is always looking for new ideas and constantly recruiting to keep the committee vibrant, dynamic and fresh. Sign up to our mailing list to stay tuned for any future recruitment rounds.
www.gasocuk.co.uk | gasocuk@gmail.com | X @gasoc_2015
UK Anaesthetic representative, GASOC, ST7 Anaesthetics, London X: @wongjanman
Jules Harrington
UK Anaesthetic Representative (Elect), GASOC, ST6 Anaesthetics, London
Caren Chu
UK Anaesthetic Representative (Elect), GASOC, ST4 Anaesthetics, Wessex
Winter Scientific Meeting 2025
Thursday 9 and Friday 10 January 2025, QEII Centre, London, UK
With a jam-packed programme, 30+ hours of essential CPD and networking, don’t miss out on the Winter Scientific Meeting (WSM) 2025 this January.
Book your study leave and a place at Winter Scientific Meeting 2025. WSM delivers in-person and online anaesthesia education at the QEII Centre, Westminster, London. As an exciting hybrid conference, you have the option to join in online from the comfort of your home or workplace, anywhere in the world.
NEW for 2025
• All 3 streams to be live streamed online
Confirmed keynotes:
Prof Nicholas Levy, Consultant in Anaesthesia and Peri-operative medicine
Dr Rachel Clarke, Specialty doctor in palliative medicine, and author
Mr Chris Lemons, saturation diver and immortalised in hit Netflix/BBC documentary
'Last Breath'
• Newly innovated in exhibition learning hublecture theatre and demo zone
• Meet the experts
Reasons to attend
• Innovative ways of learning focused on interactivity and active learning
• A fully enhanced conference app
• Access first-class scientific content with two days of hot topics, live demonstrations and interactive debates
• A poster competition featuring e-posters, with an opportunity to present to colleagues at the venue
• Join our live symposia and meet our exhibitors
• Complimentary social event on Thursday evening for in-person delegates
Special member booking rates available, including exclusive early booking discounts.
*Based on delegate feedback from WSM 2024
Multiple streams of lectures, interactive sessions and panel
debates
• Anaesthetist or anaesthesiologist?
• Diversity
• POPPY: Patient reported outcomes, postoperative pain and pain relief after day case surgery
• Who is the most important person in the team?
• Ultrasound, pre-, intra- and postoperative use
• Emergency care for traumatically injured patients
• How to get the best anaesthetic and airway equipment for your department: a human factors approach
• Obstetric anaesthesia co-badged with OAA
• Peri-operative management of the surgical patient
• Regional anaesthesia
• Enhanced recovery
• Bleeding and transfusion
• Sedation
• Neurological monitoring
• Teamwork in an emergency situation
• New guidelines
• Diabetes
Plus much more! View the programme online.
Winter social
Join us on the evening of the first day for a lively winter social of canapés, drinks, great entertainment and great company. If you’re attending WSM 2025 in person, you’re already on the guest list as entry to the social is already included in your ticket price.
Book now
Save up to £100 by taking advantage of our early booking fee which is available until 23:59 on Thursday 28 November 2024
Delegate fees frozen at 2024 rates
Making the case for curriculum restructure
To anyone who was even laterally involved in the rolling out of the new Royal College of Anaesthetists (RCoA) 2021 curriculum, the sheer prospect of a new one is likely to induce a severe headache. However, the significant discontent among resident anaesthetists does serve as a springboard to re-examine how we train the anaesthetists of the future, and how we could do it better.
The recent ‘Exit Interviews’ project undertaken by the Association of Anaesthetists Resident Doctors Committee involved interviewing several individuals who had elected to leave the anaesthetic training programme for other pursuits. For some this was life as an SAS anaesthetist, a handful chose other specialties, and a few left medicine altogether. The reflections provided by these doctors are truly enlightening when it comes to examining the culture and way of life our curriculum enforces on those who go through it. Common themes included lack of agency, rigidity of training, burnout, lack of equity, and a long string of seemingly unnecessary hurdles.
Of note, not a single person interviewed mentioned that pay was a major factor in their decision to leave training. While it is clearly important, there are also many parts of our training infrastructure that could have been altered to improve their lives and increase retention.
While many local hospital-based initiatives to improve wellbeing of their workforce seem to centre around circumventing issues that make their staff unhappy (see: pizza parties, free yoga), it is worth taking a look at the real nuts and bolts of how we train anaesthetists to see if there is room for improvement.
If the changes do end up being monumental, then it is worth starting to think about them now for whenever the next future iteration of our curriculum is being written.
The problem
The elective surgical backlog in the NHS is naturally a major talking point at the moment. The 2022 RCoA UK State of the Nation report predicts that there will be a shortfall of 11,000 anaesthetists by 2040. 8.25 million elective operations would therefore be unable to take place due to shortage of anaesthetists alone. This document also stated that around 1 in 3 anaesthetists in training were considering not working for the NHS upon CCT [1].
The reduction in training numbers that we have seen in recent years (which are now steadily getting back to normal), coupled with the increasing issue of retention within our workforce creates a real concern for our future workforce.
Are there any elements of the training curriculum that could be altered to help address this?
1. Recruitment and run-through training
UK anaesthetic training is one of the few programmes around the world that decouples its training period. This has undergone several iterations in the past. Some of the reasons cited include that some people naturally wish to leave anaesthetic training after the Primary FRCA, or that people wish to transfer deaneries at this natural juncture.
In recent years, this further ST4 recruitment round has caused a series of bottlenecks and subsequent losses of anaesthetists. Furthermore, the last 5 years have been mired in significant administrative error and injustice through the recruitment process.
Stopping ST4 recruitment and creating a run-through programme would allow far less reliance on the national recruitment office, reduce numbers lost to recruitment bottlenecks, and improve the working lives of resident anaesthetists by reducing the necessary ‘arms race’ for point scoring in the run-up to applications.
Removing this unnecessary hurdle would give an ability for deaneries to plan each individual anaesthetist’s training journey much more in advance and give potentially greater certainty in workforce numbers.
2. Flexibility of training
Many resident anaesthetists comment on the rigidity of the training programme, and how it is difficult to combine with major life events or challenges. If run-through training were to be introduced, it may be feasible to have flexible entry and exit of the training programme at the end of Stage 1 and Stage 2 training (with prior agreement much ahead of time). This would allow individuals to plan life events and take
on other potentially more flexible roles (e.g. SAS) to help balance them.
A ‘Training Passport’ with a lifespan of 10 years FTE could be granted upon entry into CT1 which would record all the doctors training experience both in and out of formal training programmes.
3. Training duration
UK anaesthetic training is among the longest in duration globally. From starting medical school, it takes (at the absolute fastest possible) 14 years to train a consultant anaesthetist. With multiple necessary merits added in (e.g. intercalated degrees, teaching fellowships) for competitive applications, this is likely to be closer to 16 or 17 years.
The Australia and New Zealand College of Anaesthetists (ANZCA) has a 5-year training programme, while the USA has one lasting 4 years.
It is clear that we want to continue to train experienced, skilled, and well-rounded clinicians in the UK. However, is there an argument that this can be done in a programme lasting 6 FTE instead of 7? Some consolidation of clinical time (while keeping all subspecialty rotations) could potentially help to do this. This would not only help make the training journey less arduous and more streamlined, but also create more senior anaesthetists faster.
4. Rotational training
Frequency of rotations and their administrative burden are frequently cited as issues. Much good work has recently
been done to try and tackle this [2]. It is clear that resident anaesthetists value the different clinical experiences of multiple hospital sites, but feel they are currently being unnecessarily rotated far too frequently. A significant reduction of this in line with new guidance would be welcomed.
Conclusion
These concepts in no way aim to solve every issue in the training of an anaesthetist, but they do at least aim to spark a discussion for change. Many of these points can be found discussed in more detail in the Association’s new document ‘Anaesthetic training in the United Kingdom: Best practice for today and concepts for the future’ [3]. Figure 1 summarises some of these.
Stuart Edwardson
Anaesthesia and Intensive Care Medicine Registrar, Southeast Scotland
Immediate Past Chair, Association of Anaesthetists
Resident Doctors Committee
References
1. Royal College of Anaesthetists, The Anaesthetic Workforce: UK State of the Nation Report, February 2022.
2. Chambers J, Thornton S, Tuck M, Jackman S et al. Minimising the impact of rotational training within the anaesthetic training programme, August 2024.
3. Evans B, Gibney E, Agius CM, Ahmed N et al. Anaesthetic training in the United Kingdom: Best practice for today and concepts for the future, April 2024.
What is ‘full time’ anyway?
More resident anaesthetists are choosing to train less than full time, but why is this and what are the repercussions for the future workforce?
Increase in less than full time
Current resident anaesthetists are choosing to manage their time differently to previous generations. Nationally, over the past five years, the percentage of resident anaesthetists working less than full time (LTFT) has doubled, from 20% in 2019 to 39% in 2024, with only emergency medicine and paediatrics having a higher proportion of LTFT [1]. Our deanery, Health Education Southwest, has the highest proportion nationally of resident anaesthetists choosing to work LTFT (52% in 2024), and full time (FT) training is now the minority [1]. As well as an increase in numbers, the reasons for resident anaesthetists working LTFT have also changed. Prior to 2022, resident doctors had to justify working LTFT (e.g. for caring responsibilities, health, or other commitments). Since 2022, any ‘well-founded individual reason’ is now accepted [2] and although amongst resident anaesthetists childcare remains the most common reason, as of 2024 better work life balance was cited by 54% of LTFT resident anaesthetists [1].
What is full time?
This move away from FT training begs the question ‘what is full time?’. At the end of 2023, across all people in full-time employment in the UK, the average working week was 36.4 hours [3] whereas the FT resident anaesthetist works up to 48 hours per week. Another useful comparator is the typical consultant anaesthetist job plan working 10 programmed activities averaging 40 hours a week. As such, a resident anaesthetist working 0.8 whole time equivalent (WTE) could work an average of (0.8 x 48) 38.4 hours per week, which although classed as LTFT, is more hours than the average FT UK employee and nearly as much as a typical FT consultant job plan. When we also factor in the burden of resident unsociable hours, significant commute times, covering unfilled locum shifts, as well as college exams, job applications, portfolio, and non-clinical work projects (which often exceed the Education and Development Time allocation) we might go some way to understanding the decreasing popularity of ‘full time’ contracted hours.
Why are more resident anaesthetists working LTFT?
The high burden of hours dedicated either directly or indirectly to work is not unique to anaesthesia, however. LTFT working is on the increase amongst all resident doctors (from 13% in 2019 to 21% in 2024) [1], but there has been a disproportionate rise in LTFT amongst resident anaesthetists. Heavy workload and burnout are often suggested as reasons for resident anaesthetists to seek to work LTFT. Reflecting this, reported risk of burnout amongst Royal College of Anaesthetists (RCoA) members has increased from 8% to 14% between 2019 to 2024, however this remains below the average for all resident doctors (21%). Resident anaesthetists also report lower rates of heavy or very heavy workload compared to the average for all resident doctors (20% vs 43%) [1]. In a regional survey of LTFT resident anaesthetists in the Severn region (number of responses = 66, response rate = 68%) the most common reasons for opting for LTFT were childcare (58%) and wellbeing (30%), reflecting the national trend.
Impact on anaesthesia workforce planning
The full reasons behind the rapid uptake in LTFT amongst resident anaesthetists remains unclear but understanding this is crucial for future workforce planning in anaesthesia on both a local and nationwide level. In our survey, 71% of LTFT resident anaesthetists in the Severn area needed a fixed day off and 72% of those request Thursday and/or Fridays as non-working days. Creating a fair working pattern for FT and LTFT resident anaesthetists and providing a safe service is a constant challenge for rota writers. Whilst working LTFT allows great flexibility, it comes with added challenges; 71% of LTFT resident anaesthetists that we surveyed had problems with pay; 45% with rotas; and 26% with correct pro-rata bank holiday and study leave entitlement. Additionally, LTFT resident anaesthetists in Severn, despite just being in the majority, felt an inequality in various opportunities compared to their FT counterparts, especially with departmental induction and local departmental teaching.
The most recent workforce planning model by the RCoA dates from 2022, which whilst recent by some standards, does not account for the huge, latest changes in LTFT. Anaesthesia is predicted to have a shortfall of 11,000 staff by 2040 [4]. This is likely an under-estimate considering it now takes many resident anaesthetists longer than seven years to train due to LTFT working patterns. As a specialty we need to urgently address this shortfall and re-evaluate our workforce estimates to provide a sustainable workforce for the future.
Should 80% be the default?
So, are resident anaesthetists themselves indirectly calling for a change in their training programme? In our region, 80% WTE is the most common LTFT working pattern chosen (77% LTFT resident anaesthetists). Should this and a 38-hour week become the new default? This would permit more unity in rotations, inductions and ARCPs, as well as easier planning for Training Programme Directors and the future workforce; but what would the cost be? Either an increase in training time, or a decrease in clinical exposure. The 2021 curriculum describes training as outcome based rather than time based and the RCoA has no set logbook requirements for CCT. Despite this, training length remains fixed with only a flux of three months for ‘exceptional trainees’[5]. Although training in the UK is already two years longer than in Australia and New Zealand, allowing LTFT resident anaesthetists to drop hours but not increase training length is likely to be met with resistance, not least from FT resident anaesthetists. Particularly in view of the falling exposure to clinical cases: 30 years ago, a single speciality consultant would typically finish training with 7000 cases in their logbook, in 2016 an average of 3500 cases, and by 2019 less than 2500 cases [6]. Since Covid this is likely to have fallen further. In addition, non-clinical domains in the new 2021 curriculum mean that Education and Development Time and study leave are being used more for non-clinical activities. Completing the equivalent hours of the current training path at 80% (38 hours per week) would take 8.75 years, further prolonging one of the longest anaesthetics training programmes in the world.
Conclusion
Resident anaesthetists are choosing to train differently than previous generations and the proportion working LTFT is rapidly rising. The reasons behind this are likely multi-factorial: High burden of non-clinical requirements, cost and availability of childcare for shift work, and an increasing emphasis on life outside of work.
Changing training to a 38-hour week is not necessarily the answer and comes with its own challenges. Regardless of whether there is a formal change, more and more resident anaesthetists are moving away from FT training. If the current trajectory continues, the shortfall predicted in our future workforce will only worsen. Understanding this, re-evaluating our workforce estimates and addressing the shortfall is crucial.
For all our current and future resident anaesthetists, we need to ensure fairness in rotas, access to teaching and equality in
departmental induction. The challenges related to LTFT pay, pro-rata bank holiday and study leave entitlement need to be addressed to support this growing section of our workforce.
What is clear is what constitutes ‘full time’ is being redefined by the current generation of resident anaesthetists and our speciality needs to pro-actively adapt.
Claire Abeysekera
Anaesthetic Registrar (LTFT), University Hospitals Bristol and Weston NHS Foundation Trust
@ClaireAbeysekera1
Amy Baigent
Anaesthetic Registrar (LTFT), Gloucestershire Hospitals NHS Foundation Trust
James Brooks
Anaesthetic Registrar (FT), University Hospitals Bristol and Weston NHS Foundation Trust
@Jamesbrooks90
Editor’s Note: Tell us what you think about the points raised in this article by writing us a letter. Please send to anaenews.editor@anaesthetists.org.
References
1. General Medical Council. Educational data tool. 2024 https://edt.gmc-uk.org (accessed 30/09/2024).
2. Conference of Postgraduate Medical Deans. A reference guide for postgraduate foundation and specialty training in the UK: The gold guide, 9th Edition, 2022.
3. Gov.uk. Full time and part time employment, 2023. https://www.ethnicity-facts-figures.service.gov.uk/workpay-and-benefits/employment/full-time-and-part-timeemployment/latest/ (accessed 30/09/2024).
4. Royal College of Anaesthetists. The anaesthetic workforce: UKs State of the nation report 2022. https://www.rcoa.ac.uk/sites/default/files/ documents/2022-02/State-Nation2022.pdf (accessed 30/09/2024).
5. Royal College of Anaesthetists. Training time and calculation of CCT dates. https://www.rcoa.ac.uk/trainingcareers/training-hub/training-time-calculation-cct-dates (accessed 20/09/2024).
6. Perella P et al. Retrospective analysis of caseload and supervision from a large anaesthetic logbook database, Anaesthesia 2019; 74: 1524–1533.
Key
LTFT - Less than full time
FT - Full time
WTE - Whole time equivalent
RCoA - Royal College of Anaesthetists
Forthcoming seminars at our London headquarters,
21 Portland Place W1B 1PY
Perioperative point of care ultrasound
03 December 2024
Neurological disease and anaesthesia
11 February 2025
Total intravenous anaesthesia
20 February 2025
The principles of central venous access and best practice
4 March 2025
The ClearLite™ anaesthetic face mask shows a 72% reduction in environmental impact compared to a standard PVC mask.1
The ClearLite™ anaesthetic face mask shows a 72% reduction in environmental impact compared to a standard PVC mask.1
The ClearLite™ anaesthetic face mask shows a 72% reduction in environmental impact compared to a standard PVC mask.1
A clear choice to reduce your impact on the environment
A clear choice to reduce your impact on the environment
A clear choice to reduce your impact on the environment
For further information please visit: www.intersurgical.co.uk/info/anaestheticfacemasks-singleuse ClearLite™ anaesthetic face mask
For further information please visit: www.intersurgical.co.uk/info/anaestheticfacemasks-singleuse
For further information please visit: www.intersurgical.co.uk/info/anaestheticfacemasks-singleuse
Here, we present a selection of our best videos from our online learning platform Learn@.
Prehabilitation
Myra McAdam
VIDEOS
Fatal perioperative anaphylaxis
Guy Jackson
Avoiding the pitfalls of the prone position
Michelle Leemans
New diabetic drugsproblems and solutions
Jonathan Schofield
Emergency treatment of Perioperative anaphylaxis
Amy Dodd
Dissemination editors Maryann and Mike have a great discussion about some July papers in this episode. This July podcast covers some excellent studies, from a qualitative study on ‘successful return to work in anaesthesia after maternity leave’; to a ‘qualitative analysis of how gender affects a career in anaesthesia in Australia and Aotearoa New Zealand’; and a paper on the ‘impact of postoperative cardiovascular complications on 30-day mortality after major abdominal surgery’.
Episode 6: The Depth of the Problem
In the sixth episode of Ether/Or, Matthew Heron ends the series with a fitting exploration of new problems with modern inhaled anaesthetics. The risks of chloroform had finally been proved in 1911, but before this, it took doctors a long time to agree on whether it was safe or not.
Touching on Ted Eager’s research, Heron and his guests talk about how anaesthetics have been compared and measured in the past, and conclude with a reminder that engaging with the history of anaesthesia enriches the conversation we can have about anaesthesia’s future and looking back to the problems of the past can help us think harder about the problems we are trying to solve today.
https://www.etherorpod.com/episodes/six
Coffee and a Gas podcast
Episode 16: Equity in global anaesthesia
For this episode of Coffee and a Gas, hosts are joined by Tom Bashford and Rediet Shimeles Workneh to speak about the complex web of challenges and triumphs in the pursuit of global equity in anaesthesia. They discuss the achievements of the Association’s International Relations Committee and their efforts to bridge the gaps in the access of quality anaesthetic care. Don’t miss this special internationally-themed episode!
You must have prior experience as a Trustee and we are looking for someone who is interested in helping and educating students who wish to study in the UK to develop their skills, preferably from outside the UK.
www.afhill.co.uk
Undergraduate awards
Wylie Medal Undergraduate Essay Prize 2025
The Association of Anaesthetists invites medical students studying in Great Britain and Ireland to submit an essay on the topic 'Human factors is common sense dressed up as science?' to the Wylie Medal Undergraduate Essay Prize 2025.
Cash prizes of up to £500 will be awarded to the best three submissions. The overall winner will receive the Wylie Medal in memory of the late Dr W Derek Wylie, President of the Association 1980-82. The winning essay may also be published in our member magazine Anaesthesia News
For further information and to apply please visit our website: https://anaesthetists.org/Home/Get-involved/ Grants-awards-and-prizes/Wylie-Undergraduate-EssayPrize
If you are interested, please contact Andrew Hill at A F Hill Solicitor on 0203 612 4734 or andrew@afhill.co.uk
Undergraduate elective funding
Applications for funding towards a medical student elective period taking place between April and September 2025 are invited from medical students studying in Great Britain and Ireland (subject to confirmation of eligibility).
We invite applications for funding with a special emphasis on those demonstrating relevance to anaesthesia, intensive care, or pain relief. A key focus of the Association is support for projects in the developing world, hence elective placements supporting work in developing countries are given priority.
For further information and to apply please visit our website: https://anaesthetists.org/Home/Get-involved/ Grants-awards-and-prizes/Undergraduate-ElectiveFunding or email secretariat@anaesthetists.org
Closing date for applications: 23:59 on Wednesday 5 February 2025
H. Javanmard-Emamghissi, B. Doleman, J. N. Lund, S. Lockwood, S, Hare, L. Pearce, S. Moug, G. M. Tierney
Beyond high-risk: Analysis of the outcomes of extreme-risk patients in the National Emergency Laparotomy Audit
Anaesthesia 2023; 78: 1376–1385
Introduction
This study compared extreme risk surgeries, where National Emergency Laparotomy Audit (NELA) mortality is predicted to be >50% with high-risk surgeries, and how differentiating between these may broaden our understanding of what constitutes high risk surgery.
Methodology
Calculated NELA scores from laparotomies performed on adult patients were collected from December 2013 to November 2020 and categorised as extreme-risk or high-risk based on their 30- and 90-day mortality. Individual patient characteristics were labelled as confounding variables during data collection to reduce bias.
Results
In total, 161,337 patients were included in the study. Of these, 5,193 underwent extreme-risk surgery with a NELA risk score of ≥ 50%. The frequency of these extreme-risk surgeries decreased over the data collection period. Over half of the extreme-risk laparotomies were performed out of hours, where surgeons had greater input in patient management decisions than anaesthetists, as they were more readily available.
Patients undergoing extreme-risk surgery were less likely to have a computed tomography (CT) scan prior to surgery than those in the high-risk group. Post-operatively, only 5% of patients in the extreme-risk group were moved to a non-critical care ward. Of these patients, 40% had either
peri-operative findings of an inoperable pathology or a decision made to commence end of life care. All extreme risk procedures involved either an experienced surgical resident doctor or consultant, but the most senior anaesthetist present in some cases was a core resident doctor.
Discussion
Despite having a better functional baseline, patients undergoing extreme-risk surgeries were more likely to suffer from complications that required further intervention, and subsequent significantly prolonged length of stay, than those undergoing high-risk surgeries. There was not a significant increase in the number of patients admitted to critical care after having an extreme risk surgery. This may, in part, be due to an increased proportion of extreme-risk patients being commenced on end-of-life pathways.
The number of surgical procedures undertaken that are defined as extreme risk has lessened over time. This could be a result of increased utilisation of the shared-care approach in surgical decision making, where options and complications of surgeries are disclosed as per the reasonable patient test since the Montgomery Ruling (2015).
Conclusion
Further studies are required to determine whether extreme risk surgeries are improving patient outcomes. NELA scores are a prediction based on quantitative data; this score does not focus on gathering qualitative data of post-operative quality of life. This parameter could be seen as a more accurate reflection of the success of a surgery as it pertains to patient-centred care. Whilst this study accurately reflects surgical outcomes from emergency laparotomies using the NELA score, further prospective studies are required to investigate the long-term effects of such surgeries.
Ahmed Mahawish FY2 Doctor
Mruthunjaya Hulgur Consultant Anaesthetist, Wrightington, Wigan and Leigh NHS Foundation Trust
Safer Anaesthesia From Education (SAFE)
SAFE trains anaesthesia providers to deliver high-quality and safe care to patients, even in very low-resource settings, and creates a sustainable training model which can be embedded in national health systems.
Your donations make a huge difference to the education of anaesthetic providers around the world, and significantly improves patient care and safety.
Every pound you raise or donate helps us provide safe anaesthesia for patients every year. Donate now!
£20 pays for all training materials for one SAFE course, including a USB for each participant.
£50 pays for one rural anaesthetic provider to travel to a SAFE course.
£100 pays for a resuscitation manikin which can be used on the course and stay in country for future training courses.
£500 pays for five anaesthetic provider to complete a SAFE training course.
£750 pays for all training materials for a SAFE course for 32 participants.
AAGBI Foundation is registered as a charity in England & Wales No. 293575 and in Scotland No. SC040697