Harm Reduction… Beyond Narcan…Part 1
 Ashley Shukait, MPH, CHES®
Ashley Shukait, MPH, CHES®

Ashley Shukait, MPH, CHES®

Harm Reductionist
Patient w/ multiple-intersectionalities
• Overview of harm reduction services including syringe service programs and overdose prevention centers (Part 1)
• Current drug supply and drug checking capabilities (Part 2)
• Struggles, Barriers, Solutions for harm reduction in Michigan (Part 2)
• Provide strategies to strengthen and build more positive relationships between patients who use drugs & their healthcare providers (Part 3)


A movement for social justice built on a belief in and respect for, the rights of people who use drugs
• Focuses on shifting power & resources to people most vulnerable to structural violence through an anti-oppressive healing justice framework
• Recognizes realities of trauma, racial, social and structural inequities and – isms have various impacts on vulnerability and access to resources
Harm Reduction is rooted in Queer, Trans, Black & Brown PWUD & SW Survival Systems.
• Honors survival & healing without condemning or glorifying how people survive & heal
Credit: DQ Progressive Pride Flag
Perspective & set of practical strategies that promote “Any Positive Change” defined by the individual
Everyday Examples: Seatbelts, helmets, sunscreen, vaccines, and gait belts for fall precautions
Substance Specific: Nicotine patches to help quit smoking, designated drivers for alcohol, decaf coffee and sugar substitutes like Stevia
Gives us a code of ethics to follow to ensure we give a person compassion, love, and dignity; no matter if what they are doing makes sense to us
Credit: AS
• Our principles align, as a nurse's responsibility is to use critical inquiry and evidence-informed knowledge to protect and promote an individual's right to autonomy, respect, privacy, and dignity
• Our practices may differ because of prohibition, stigma, and oppressive policies that ban fully inclusive care and support
• Harm reduction is the missing link that can be applied to all levels of care- it is not an alternative to care
• Access to low-barrier, affordable, noncarceral healthcare services no matter if they are using drugs, involved in sex work, involved in the criminal legal system or experiencing a lack of housing
• Quality of life, well-being, and participantidentified goals are how we gauge whether interventions are successful
Nursing: Respect & Dignity
Person-Centered
• Non-judgmental, non-coercive
• Not a “one size fits all” approach
• Holds space & time for connection, learning, unlearning, and empowerment for people to identify their own goals and expectations
Nursing: Patient-Centered
Ensures PWUD are centered in the development, implementation, and evaluation of programs & policies designed to serve them • PAID for their expertise, time, and emotional labor
• May not be standard methods of formal economies
Affirms PWUD themselves as the primary agents of change and experts in their own lives
Empowers people to share information and support each other in strategies that meet their actual conditions of use
Look at people as human beings, not the substance they put in their body or how they use it Nursing: Autonomy
Accepts drug use as a complex, multi-faceted phenomenon that encompasses a continuum of behaviors and a natural part of life; Context is everything
Scientifically proven to reduce HIV/ HCV/ SSTIs and overdoses
Reduces crime and increases public safety
Nursing: Evidence-informed
• Recognizes realities of trauma, racial, social and structural inequities and – isms have various impacts on vulnerability and access to resources

• Honors survival & healing without condemning or glorifying how people survive & heal
Nursing: Justice
HIV/HCV & STI Testing, Treatment, and Care: PrEP/PEP, TB, COVID, HAV, HBV prevention & vaccinations
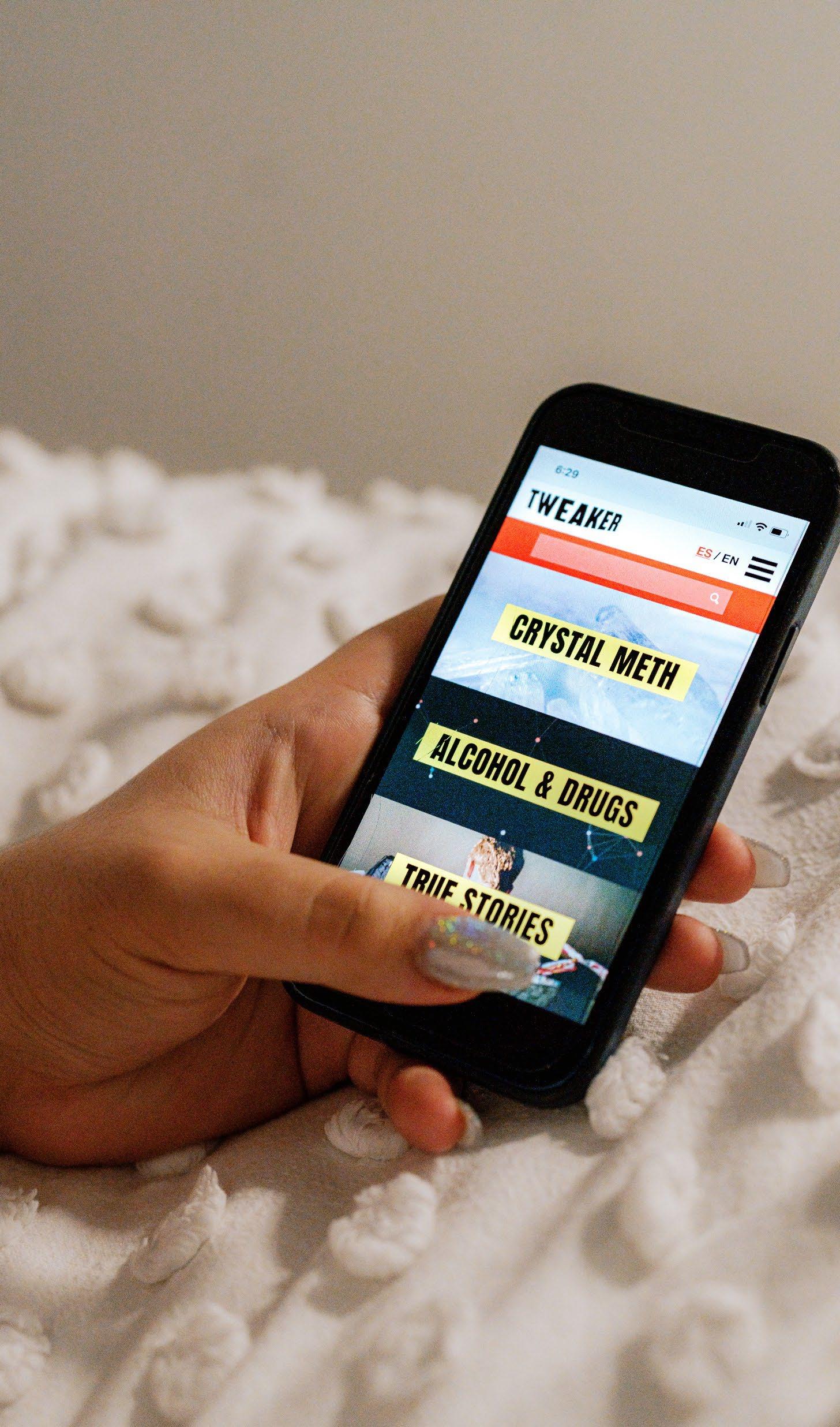
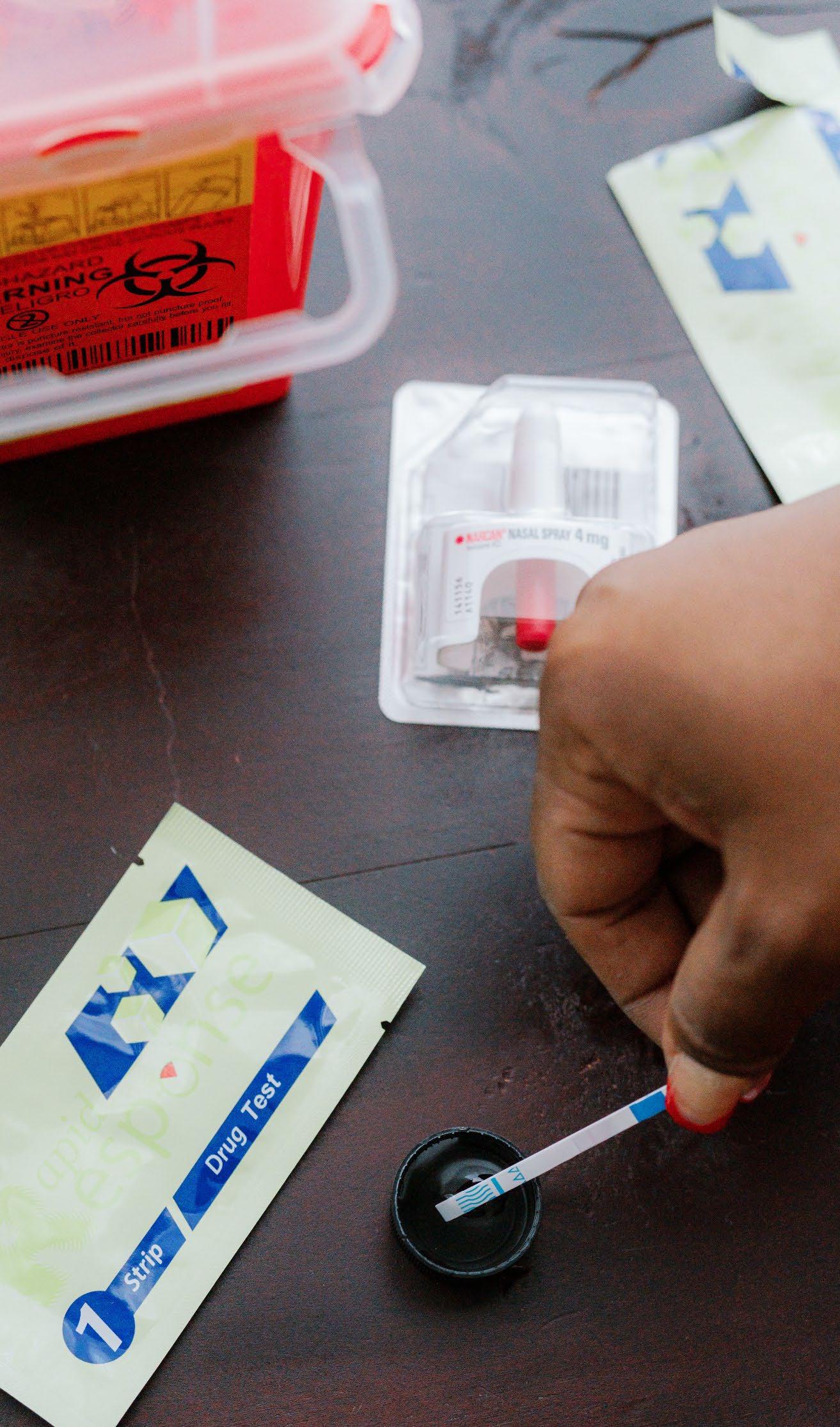
Supplies and Education for Safer Substance Use: Naloxone, drug checking, syringes, pipes, wound care, withdrawal mgmt supplies, etc
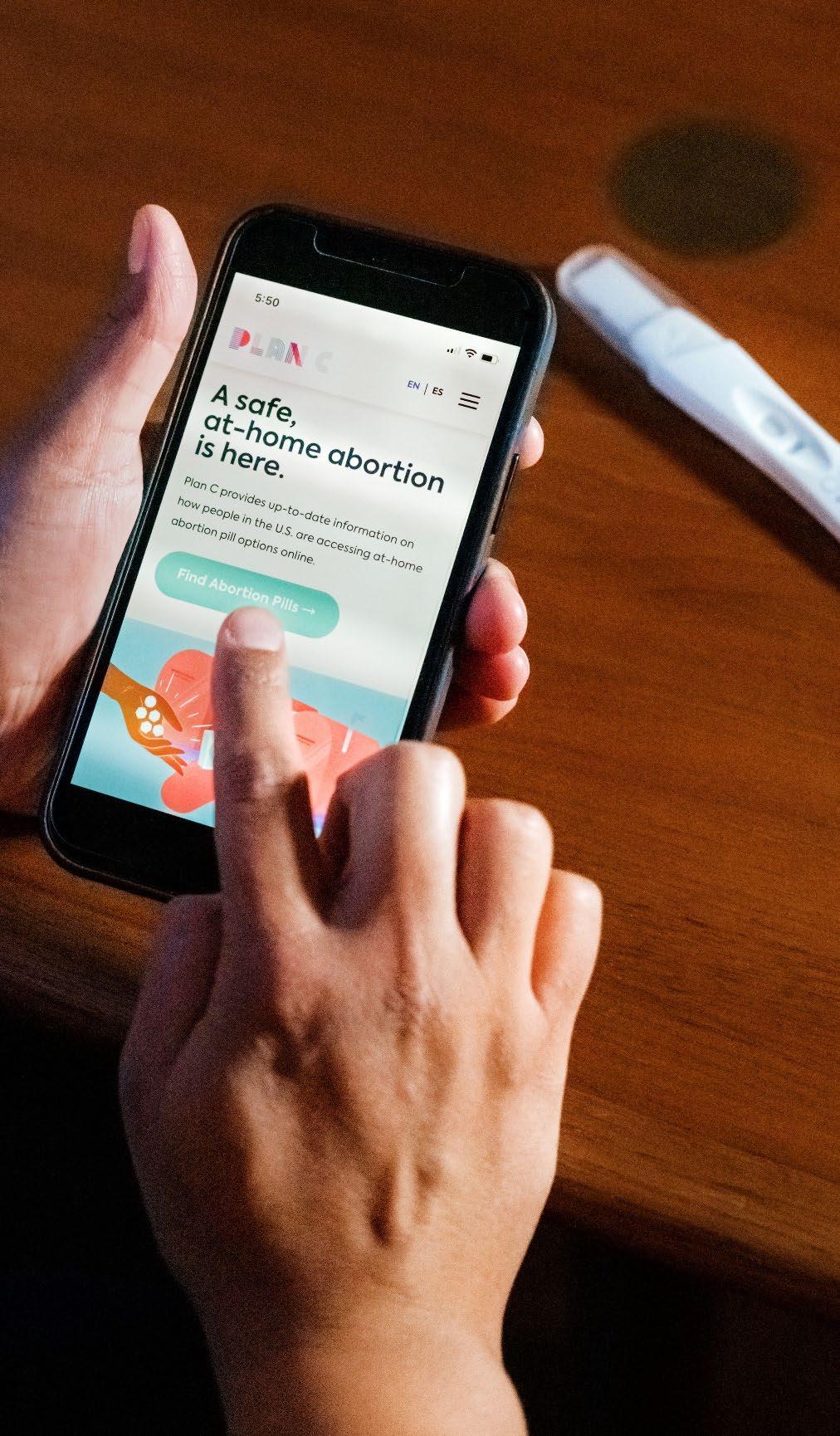
Sexual and Reproductive Health: Condoms, dental dam, lube, pregnancy tests, plan B, gender affirming care, etc
Overdose Prevention: Education, safety plans, response
Support Services: Case management, support groups, harm reduction therapy, substance use management and so much more!
• Official sites in Netherlands (1970s), Switzerland (1980s), and Germany (1994), then other European countries- 120 world-wide w/various models
• 2003 Insite opened in response to HIV/Overdoses in Vancouver and British Columbia in the 1990s (1st legally sanctioned in North America)

• Proven effective in reducing OD, infectious diseases & other health complications & improved community health & public safety Insite-Canada

• 1st organization to be sanctioned, but operated for years prior, like many other sites forced underground Washington Heights & Harlem
• Both are no-barrier walk-in spaces, where they offer coffee, snacks, showers, bathrooms, and laundry
• Health and Wellness Services: Massage and acupuncture
• Clinical Services: HIV and Hep-C testing, wound care, Medication for Opioid Use Disorder, medical assessments, and counseling

• Outreach and Public Safety: Hotline for community members to report syringe litter or public drug use, in which staff come and do clean- ups

• Community Education: Harm reduction, overdose prevention, and other services
• Case Managers: Conduct mental health services, benefits navigation, advocacy, health navigation, case conference sessions with various providers, drug education groups, individual counseling, and modalities for safer drug use
• Cool down room, garden, and beehives
• 3,890+ People served w/ 65k+ utilizations
• 820+ OD interventions -O2 usually & a small 15% w/Naloxone titrated
• Washington Heights: Younger population that tends to inject more; East Harlem: An older population that has a safer inhalation (smoking) room to accommodate
• One location is operated with “peers” that have extensive nurse training for OD intervention with medical personnel on staff; the other is run with medical staff who provide interventions

• Currently, there are many efforts across the US to make OPCs a reality!
• Canada has a Harm Reduction Nurses Association and extends the offer to the U.S to assist and support nurses advocating for services and human rights for people who use drugs and engage in sex work. (HRNA,2022)
• NYC became the 1st in the U.S. to have govsanctioned OPC where PWUD can bring their own drugs to use in a safe environment, it isn’t the only one, Several clinics in Canada & Europe have been rx pharmaceutical-grade heroin & fentanyl to keep them from using the street supply.
(CrossTown, 2022)
 Credit:
Credit:

For detailed access to references email Ashley
Shukait (ashleyshukaitconsulting@gmail.com) to be added to her Zotero account with an extensive list of publications and resources.