Incorporating Western Midwife

(left) Dr Sue Sinni, Director Midwifery and Nursing, King Edward Memorial Hospital, with (right) Romina Raschilla RN MBA, ANF State Secretary.




Nadine Mackay | Mobile Banker

ANF State Secretary Romina Raschilla

ANF State Secretary Romina Raschilla
Over the last few months, it’s been great reflecting on the challenges and triumphs we’ve experienced at the ANF over the past few years. It’s no secret that our journey has been marked by significant changes. I want to take this opportunity to thank you for your patience, resilience, and continued support during these transitions. Your commitment has been the foundation of my strength as your State Secretary, and I look forward to facing these and future challenges together.
This year, we’re turning a new page, with 2025 set to bring renewed growth and opportunity for our members. In this edition of The Western Nurse, you’ll find details about some of our new initiatives, including the ANF Career Compass and changes to the ANF holiday units. This groundbreaking service is designed to support members in navigating employment opportunities, enhancing job applications, and securing rewarding roles in the healthcare sector. Additionally, you’ll learn about our ANF Scholarships Program which will launch later this year, aimed at fostering professional development and lifelong learning. We’re also excited to share updates to the ANF holiday units, ensuring they remain a valued benefit for members seeking affordable and quality accommodation.
These initiatives represent only the beginning of our commitment to providing meaningful services for our members. As the healthcare landscape continues to evolve, the ANF remains steadfast in its dedication to addressing your needs and aspirations. We understand that our members work tirelessly in demanding and often underappreciated roles, and we’re determined to ensure your contributions are recognised and rewarded.
Following the historic Public Sector wage increase achieved in late 2024, I am focused on addressing the long-overdue Private Sector EBAs. With the Public Sector being seen as the ‘industry standard’ EBA, its conclusion means we can see fast movement in the Private Sector. While the ANF has recently secured a wellreceived win with the Ramsay RN EBA, many of our members employed at St John of God and smaller private practices have waited far too long for fair outcomes. Let me assure you that under my leadership, resolving these matters is a top priority. Negotiations are already underway, and we are committed to ensuring that every member sees tangible improvements in their wages and conditions in 2025. Your patience and perseverance during this process are deeply appreciated.
As we look ahead, it’s clear that 2025 will be a pivotal year for the ANF. Our strength lies in unity, and together, we can achieve incredible outcomes. With the backing of the Council, the dedication of our staff, and the unwavering determination of our members, I am confident we will continue to deliver the changes you deserve. Together, we will continue to make robust changes and reach new heights as a union, stronger and more united than ever before.
ANF State Secretary
The 2025 WA State Election has paved the way for a new approach to the infamously difficult Health portfolio.

Going forward, the Cook Government is going to split the heavy load historically managed solely by the Health Minister, to a range of new Ministerial portfolios aimed at better managing the sheer scale of WA’s health system.
ANF State Secretary Romina Raschilla said the ANF is looking forward to working with the new Health Minister and her team.
“I’m pleased to have had the opportunity to meet with the new Health Minister and passed on the shared concerns raised by our members.
“We had a constructive, robust discussion and covered a wide range of topics from member issues to the wider state of WA health.
“I look forward to working together to improve our health system and bettering working conditions for all ANF members.”


Hammat MLA Member for Girrawheen, Minister for Health, Mental Health
“I’m extremely proud to serve as the Minister for Health and Mental Health, and will work every day to do what’s right by WA.
“I’ve spent more than 20 years advocating for working people across the State and I know that nothing is more important to our health system than the nurses, doctors, and all health workers that keep our system running.
“The needs of Western Australians are changing, and, as our health workers know, so too are the demands on our health system.
“This new government is tackling these demands headon with our Health subcommittee.

“As Health Minister, I will lead our Health team to ensure our system is delivering affordable and accessible healthcare to all Western Australians.
“And I will drive collaboration between Ministers to ensure our health system continues to deliver for our community.
“Health Infrastructure Minister John Carey will build our hospitals.
“Aged Care and Seniors Minister Simone McGurk will lead efforts to reduce pressure on hospitals by improving access to aged care beds and supporting timely discharge of our largest cohort of patients.
“Preventative Health Minister Sabine Winton will drive long-term initiatives to keep people well and out of hospital.
“Medical Research Minister Stephen Dawson will lead health and medical research and innovation.
“The Premier and our team are determined to pursue every opportunity to make improvements, and we are throwing everything at changing the system for the better with this strong new approach.”

The Western Australian (WA) state election held on March 8, 2025, culminated in a decisive victory for the incumbent Labor Government, led by Premier Roger Cook. This triumph marked Labor’s third consecutive term in office, underscoring the party’s sustained dominance in the state’s political landscape.
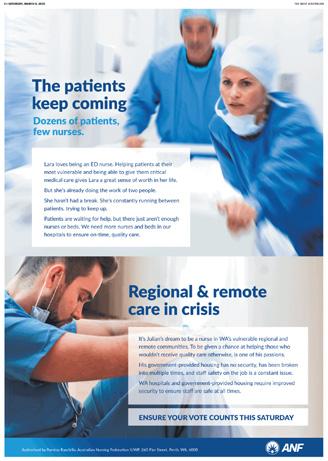
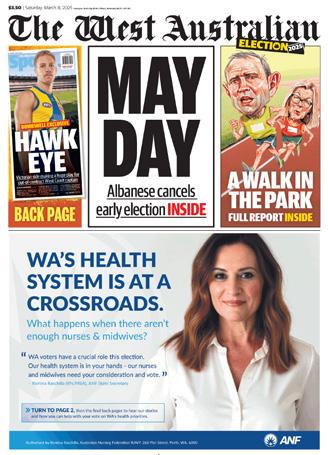
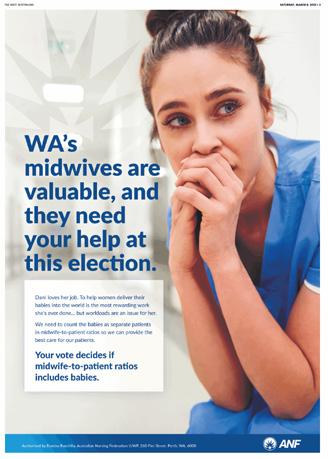
In the lead-up to the election, the Australian Nursing Federation Industrial Union of Workers Perth (ANFIUWP) embarked on a bold initiative to amplify the voices of nurses and midwives in the political arena. Health has always been a big election issue, though the costof-living struggles being felt worldwide had also been a main focal point for WA voters, as well as that we saw a big focus from parties on environmental, energy and regional policy.
To help keep nursing and midwifery issues at the forefront of the public’s mind, as well as the issues of our health
system in general, the ANF ran a series of advertisements on a range of mediums in the buildup to the election which included billboards, newspaper and digital.
are the ANF’s goals for the 42nd Parliament of Western Australia?
With the election now concluded, the ANFIUWP is poised to engage constructively with the newly elected Parliament to advocate for the interests of nurses and midwives. The union’s approach will focus on collaborative dialogue to ensure our members are heard.



The ANF is evolving – and our midwives are at the heart of it
The Australian Nursing Federation Industrial Union of Workers Perth is proud to announce that work is continuing to update our name to better reflect all of our incredible members – now finally including our highly valued midwives.
For far too long, the title of our union has failed to fully acknowledge the vital contribution of midwives. That’s about to change.
Under the leadership of Secretary Romina Raschilla, the ANF is taking real steps to ensure our name represents the full strength of our membership. The ANFIUWP Council is currently working on a shortlist that will incorporate midwifery in a meaningful way.
This long-overdue change is just one part of our ongoing mission to ensure every member feels seen, valued, and represented.
Stay tuned for more updates as we move toward this important milestone.

Midwives are absolutely covered and are entitled to all ANF services.
This includes the same robust insurance, legal support, and union advocacy, that every other ANF member is able to access.
got you covered.

The ANF is pleased to announce the introduction of an all-new service. Aimed at assisting members with clarifying employment opportunities. The ANF Career Compass is here to help broaden your horizons.
The new service will give ANF members the opportunity to obtain advice from employment and career experts to assist with CV/resume writing, interview techniques and how to best enhance your overall employment opportunities.
Group sessions will initially be available for ANF members to attend at the ANF office.
ANF State Secretary Romina Raschilla, who first came up with the idea for the
Career Compass, said it was always an aspiration of hers to expand the ANF’s member services.
“I have always believed unions are more than just enterprise bargaining and legal assistance.
“I believe your union should be with you every step of the way, that includes helping you enhance employment opportunities, whether that means straight out of university, or your next big promotional opportunity.
“The Career Compass will help members reach new career heights, by clarifying opportunities through marketing your best traits.
The new service will give ANF members the opportunity to receive advice from employment and career experts to enhance your overall employment opportunities.
“The Career Compass aims to help you reach new career heights, through clarifying opportunities in marketing your best traits.”

“However, I don’t just want to expand our services, but also bring on the best professionals needed to ensure maximum benefit to our members,” said Ms Raschilla.
The ANF Career Compass will be headed by human resources specialist and career coach, Gerry Gulla.
Gerry, who has a range of professional qualifications including Human Resources, Counselling and Professional Coaching, will be available to assist members with career management, confidence and resilience building, resumes, selection criteria, interview preparation and techniques.
Gerry’s established career makes her a great addition to the ANF team and an invaluable source of assistance to ANF members through her extensive experience in Human Resources and Coaching arena.
Also working in various international markets, Gerry has developed a comprehensive knowledge of both Corporate and Public Sectors in numerous industries including Health/Accounting/ Education/Insurance/Mining/Importing & Exporting.
Gerry said she is excited to be bringing her professional knowledge and years of experience to the ANF.
“When Romina approached me to help ANF members by providing this new service, I thought it was a great idea and way for the union to further get involved with WA’s hardworking nurses and midwives.
“With my previous experience in this field, I knew I had to accept, and offer my services and partner with ANF members in supporting them to clarify their career goals and aspirations,” said Gerry.
The ANF Career Compass will be launching over the next few months so stay tuned for more information on its rollout and how you can benefit!

The ANF is pleased to announce some critical changes to the way we do our bargaining in-house. Going forward, we are ensuring each EBA sees the same attention as the other, no matter how many members are employed at a certain workplace. ANF State Secretary Romina Raschilla is implementing these changes to ensure all of our members get the same equal and high-quality service when it comes to bargaining. The ANF is here to ensure these changes bring the service you deserve.
The recently negotiated Public Sector EBA has set a new benchmark across the industry, delivering improved pay rates, strengthened conditions, and key workplace reforms that ANF has fought hard to achieve. This agreement is now serving as a reference point in private sector negotiations.
• Ramsay Health Care RN EBA:
The ANF is happy to announce that Ramsay members have accepted the recent offer - with 79 per cent of those who voted being in favour of the offer!
• St John of God Health Care RN EBA:
With this agreement expiring in December 2024, the ANF has seen quick discussion with St John of God in order to see this agreement negotiated as soon as possible. As mentioned above, the Public Sector Agreement provides a good starting point that will allow us to set industry standard practices in this agreement. With the ANF pressing for wage parity with the public sector and stronger protections for employees, recent talks have also been focused on addressing other high priority EBA items of interest to our members. The ANF has rolling meetings with St John of God, and we are constantly seeking member feedback as negotiations continue.
The ANF remains committed to finalising these private sector agreements, as well as with other private sector workplaces as quickly as possible, ensuring that members receive the pay and conditions they deserve. Ongoing member engagement and collective action will be key in securing strong outcomes.
Members will be kept informed as negotiations progress, and further updates will be provided as we move closer to finalising these agreements.
In 2025, as part of the ANF’s expansion of services and opportunities, we are introducing the ANF Scholarship Program.

These scholarships, which will include a range of both undergraduate and postgraduate opportunities, are aimed at rewarding our longstanding members and encouraging others to follow in their footsteps.
The scholarships also make it easier to broaden your horizons with the ANF partially funding your study fees.
With cost-of-living concerns at an alltime high, the successful applicants will have the opportunity to better access and afford new study pathways.
Please stay tuned for more information in the coming months for details regarding the individual scholarships, when applications open, and how to apply.

In 2025, the ANF will introduce significant enhancements to our holiday units. Along with exciting upgrades that will be announced soon, there will be a series of changes aimed at improving our interactions with members and simplifying your experience.
Many members faced bans from accessing ANF holiday units for various reasons and the ANF State Secretary, Romina Raschilla, has announced that it’s time to start fresh. This means all members will once again have the chance

to enjoy this beloved ANF service, while still allowing for necessary restrictions for breaching our updated Holiday Unit Terms and Conditions.
Understanding the challenges of shift work, we are offering more flexible checkin and check-out options. You can now arrive and depart on any day, subject to availability, with a minimum stay of 3 nights and a maximum of 21 nights.
We are also abolishing the bond system for holiday unit bookings. We recognize
that the criteria for losing a bond have been overly strict, as expressed by several members. The ANF has heard your concerns and agree that the last thing you want is to learn that you've lost your bond over a minor issue. Our goal is to provide a benefit for you, not to risk your hard-earned money for something that wouldn’t normally affect your bond in other short-term accommodations. While no bond will be required, we will request a credit card number for any potential damages.
Our accommodation rates for the Holiday Units have not been increased in a long time, despite the rising costs of utilities, Kalbarri coastline.


strata levies, and the overall operation of the holiday units. To ensure that the holiday units remain a valuable asset for ANF members, we are implementing a modest fee increase. However, rest assured that these fees will still be very competitive in today’s market, along with the assurance of staying in a cleaner, improved unit for a more enjoyable holiday experience.
You’re on a well-deserved holiday –enjoy every moment! A cleaning fee will be applied, similar to other short-stay accommodations, and your unit will be serviced by professional cleaners, ensuring a significant improvement in

cleanliness. There’s no need to clean the unit upon arrival or departure, and you won’t even have to strip the beds! Just unwind and relax!
In addition to these changes, the ANF is actively working on more significant enhancements that members have requested. Please stay tuned for further communications via email and in the upcoming issue of Western Nurse, as we unveil these updates. State Secretary Romina Raschilla emphasized the importance of these changes:
“As both an ANF Councillor and State Secretary, addressing the concerns surrounding our holiday units has been a priority for me. For years, I’ve heard the demand for critical improvements, and I’m excited to unveil further changes in the coming months to ensure you receive great value for your money.”

Hello to all our Out ‘N’ About readers! It’s been a busy few months at the ANF. With the Public Sector EBA now wrapped up and Private Sector EBAs finally being negotiated and concluded too, we love celebrating our members who fight so hard to see their wages and conditions improved.













The Western Australian Industrial Relations Commission has ordered the ANF to amend its “meeting rules” and “control of funds” rules. The ANF has also changed Rule 35.
On 9th April 2025 the ANFIUWP Council endorsed the proposed changes and empowered the State Secretary to apply to the WAIRC to formally change the registered Rules. This application is made to the Registrar of the WAIRC.
The Industrial Relations Act requires that members be provided with the details of the rule changes; the reasons for the rule changes; and that members may object to the Registrar about the rule changes.
A copy of the initial rule, a “tracked change” version of the Rule and the amended version of each individual Rule is outlined below.
A copy of the initial rule, a “tracked change” version of the Rule and a PDF version of each amended Rule is available on the iFolio and the ANF website.
If you want to object to these Rule changes you can contact the Registrar of the WAIRC within 21 days, via email to registry@ wairc.wa.gov.au or via post to Level 17, 111 St Georges Terrace, Perth WA 6000.
Significant changes to this Rule as required by Chief Commissioner Kenner in Pres 2-6, 8-12 of 2023.
Changes clarify and set out consistent procedures for meetings as well as simplify the process and make it user friendly for everybody.
Four types of meetings - Annual General Meeting, General Meetings, Member Initiated Meeting, or Urgent General Meetings.
AGM: called by Council by 3rd week in November; Agenda to include Annual Report and financial position; notice to all members specifying date, time, place and agenda; notice by email to be sent no later than 14 days and placed on Union website; quorum is 50 members; adjourned if no quorum within ½ hour; new notice (as above) to be sent out; quorum is 50 members; lapses if no quorum within ½ hour, and matters referred to Council.
General meetings: called by Council; notice to all members specifying date, time, place and agenda; notice by email to be sent no later than 14 days and placed on Union website; quorum is 50 members; adjourned if no quorum within ½ hour; new notice (as above) to be sent out; quorum is 50 members; and lapses if no quorum within ½ hour.
MIM: called on written request of 350 members; President to convene MIM within 28 days of request; notice to all members specifying date, time, place and agenda; notice by email to be sent no later than 14 days and placed on Union website; quorum is 100 members calling the meeting; and if no quorum within ½ hour MIM lapses.
UGM: called by Executive with machinery provisions for calling meeting; notice to all members specifying date, time, place and agenda; notice by email to be sent no later than 72 hours and placed on Union website; quorum is 50 members; adjourned if no quorum within ½ hour; new notice (as above) to be sent out; quorum is 50 members; and lapses if no quorum within ½ hour.
General meeting provisions: President to chair meeting or ranked alternative; any meeting can direct Council; simple majority present to pass resolution; chairperson has deliberate and casting vote and can adjourn meeting with consent of members; financial member has one vote; and unfinancial and Honorary members have no voting rights.
Use of electronic funds transfer authorisation same as drawing cheques. This was required by Chief Commissioner Kenner in Pres 2.
Clarify that a member of Council, except Secretary can refer rule change to Secretary.
Removed notice to workplaces and in journal as slow and cumbersome. Notice of change changed to email, and on ANF website.
Secretary to notify members of changes, reasons for the changes and that they can object to WAIRC Registrar.
Changes take effect when certificate issued by Registrar.
(1) Regular meetings of the Council shall be held at such times and places as Council may decide from time to time.
(2) Meetings of the Union shall be the Annual General Meeting, General Meetings or Urgent General Meetings.
(3) The Annual General Meeting shall be held at a time and place determined by the Council.
(4) A General or urgent General Meeting may be called by Council as often as it sees necessary.
(5) The President shall, on the written request of at least five per cent (5%) of the members of the union, convene a General Meeting to be held within 28 days of that request being received, provided always that 75%
of those members calling the meeting shall attend otherwise the meeting shall be null and void.
(6) Such a request in writing shall state the object of the meeting to be convened and the business of the meeting shall be confined to that purpose alone.
(7) An Urgent General Meeting of the Union may be called by the Executive in circumstances where the Executive is satisfied the matter cannot wait for the deliberations of the Council.
(8) A decision of the Executive to call such an Urgent General Meeting may be made at a meeting of the Executive or by way of a telephone poll of Executive members or any other practical method which results in a majority decision of the Executive.
(9) Notification to members of an urgent General Meeting shall be as determined by the Executive and shall include the publication or broadcasting of the date, time and place of the meeting and the purpose or purposes for which the meeting has been called.
(10) Notification of other General Meetings and Annual General Meetings shall be either in writing to the members of the Union by publication in The West Australian newspaper or, time permitting, in the official journal 25 or newsletter of the Union. Notice concerning a General Meeting called under sub-rule (4) above shall include the business for which that meeting has been called.
(11) At any meeting of the Union 5% of the membership shall form a quorum. If within half an hour from the time appointed for the meeting a quorum of members is not present, the meeting shall lapse.
(12) At any meeting the President, if present, shall preside. In the absence of the President, the Senior Vice President shall preside. If neither the President nor Senior VicePresident are present, one of the Vice Presidents shall preside, and in the absence of the President or all the Vice Presidents a chairperson shall be elected by resolution of the majority of those present at the meeting.
(13) Any duly constituted meeting of the Union under this Rule shall have the power to direct the Council on matters of policy and administration and the Council shall carry into effect all decisions of such meetings.
(14) Every resolution proposed at any meeting of the Union shall be carried by a simple majority of those voting at the meeting and at any such meeting the chairperson shall have a deliberate as well as a casting vote.
(15) With the consent of the members present at any meeting, the Chairperson may adjourn the meeting from time to time and from place to place but no business shall be transacted at an adjourned meeting except that business left unfinished at the meeting from which the adjournment took place.
(16) Except as otherwise provided for in these Rules, every financial member shall have one vote at any meeting of the Union.
(17) Unfinancial and Honorary members of the Union shall have no voting rights whatsoever.
(1) Regular meetings of the Council shall be held at such times and places as Council may decide from time to time.
(12) Meetings of the Union shall be the Annual General Meeting, General Meetings Member Initiated Meeting or Urgent General Meetings.
(23) The Annual General Meeting shall be held no later than the end of the third week of November each year at a time and place determined by the Council.
(a4) The Agenda for the Annual General Meeting shall include a report on the Union’s activities for the past year and the Union’s financial position.
(b) A notice is to be issued to all members specifying the date, time, place and agenda for the Annual General Meeting.
(c) Notification of the Annual General Meeting shall be sent to members by email no later than 14 days prior to the date of proposed Annual General Meeting and by placing the notice on the Union website no later than 14 days prior to the date of proposed Annual General Meeting.
(d) The quorum for an Annual General Meeting shall be 50 members.
(
e) Where a quorum is not reached on the first meeting date, the meeting is to stand adjourned to a date within 14 days of the adjourned meeting, to be resumed, at which the quorum for the adjourned meeting is also to be 50 members, and if the resumed meeting is inquorate, the meeting should lapse.
(
f) A notice is to be issued to all members specifying the date, time, place and agenda for the adjourned Annual General Meeting.
(g) Where the Annual General Meeting is adjourned to a later date, member shall be notified by email and by a notice placed on the Union website no later than 7 days prior to the date of the proposed Annual General Meeting.
(h) Where an Annual General Meeting lapses due to a lack of quorum the report on the Union’s activities for the past year and the Union’s financial position shall be referred to the Council for approval.
(3) A General or urgent General Meeting may be called by Council as often as it sees necessary.
(
a) A notice is to be issued to all members specifying the date, time, place and purpose for the General Meeting.
(b) Notification of the General Meeting shall be sent to members by email no later than 14 days prior to the date of the proposed General Meeting and by placing the notice on the Union website no later than 14 days prior to the date of proposed General Meeting.
(
c) The quorum for a General Meeting shall be 50 members.
(d) Where a quorum is not reached on the first meeting date, the meeting is to stand adjourned to a date within 14 days of the adjourned meeting, to be resumed, at which the quorum for the adjourned meeting is also to be 50 members, and if the resumed meeting is inquorate, the meeting should lapse.
(5) The President shall, on the written request of at least five per cent (5%) of the members of the union, convene a General Meeting to be held within 28 days of that request being received, provided always that 75% of those members calling the meeting shall attend otherwise the meeting shall be null and void.
(6) Such a request in writing shall state the object of the meeting to be convened and the business of the meeting shall be confined to that purpose alone.
(4) A Member Initiated Meeting may be called on the written request of 350 members of the Union.
(a) Where a written request for a Member Initiated Meeting is made, the President shall convene a Member Initiated Meeting to be held within 28 days of the written request being received.
(
b) The written request shall state the purpose of the meeting to be convened and the business of the meeting shall be confined to that purpose.
(c) A notice is to be issued to all members specifying the date, time, place and purpose for the Member Initiated Meeting.
(d) Notification of the Member Initiated Meeting shall be sent to members by email no later than 14 days prior to the date of the proposed Member Initiated Meeting and by placing the notice on the Union website no later than 14 days prior to the date of proposed Member Initiated Meeting.
(e) The quorum for a Member Initiated Meeting shall be 100 members calling the meeting.
(
f) Where a quorum is not reached on the first meeting date, the meeting is to stand adjourned to a date within 14 days of the adjourned meeting, to be resumed, at which the quorum for the adjourned meeting is also to be 100 members calling the meeting, and if the resumed meeting is inquorate, the meeting should lapse.
(57) An Urgent General Meeting of the Union may be called by the Executive in circumstances where the Executive is satisfied the matter cannot wait for the deliberations of the Council.
(a8) A decision of the Executive to call such an Urgent General Meeting may be made at a meeting of the Executive or by way of a electronictelephone poll of Executive members or any other practical method which results in a majority decision of the Executive.
(b) A notice is to be issued to all members specifying the date, time, place and purpose for the Urgent General Meeting.
(
c) Notification of the Urgent General Meeting shall be sent to members by email no later than 72 hours prior to the proposed Urgent General Meeting and by placing the Notice on the Union website no later than 72 hours prior to the date of proposed Urgent General Meeting.
(6) If within half an hour from the time appointed for the initial meeting a quorum of members is not present, the meeting shall be adjourned.
(
a) If within half an hour from the time appointed for an adjourned meeting a quorum of members is not present, the meeting shall lapse.
(9) Notification to members of an urgent General Meeting shall be as determined by the Executive and shall include the publication or broadcasting of the date, time and place of the meeting and the purpose or purposes for which the meeting has been called.
(10) Notification of other General Meetings and Annual General Meetings shall be either in writing to the members of the Union by publication in The West Australian newspaper or, time permitting, in the official journal 25 or newsletter of the Union. Notice concerning a General Meeting called under sub-rule (4) above shall include the business for which that meeting has been called.
(11) At any meeting of the Union 5% of the membership shall form a quorum. If within half an hour from the time appointed for the meeting a quorum of members is not present, the meeting shall lapse.
(712) At any meeting the President, if present, shall preside. In the absence of the President, the Senior Vice President shall preside. If neither the President nor Senior Vice-President are present, one of the Vice Presidents shall preside, and in the absence of the President, Senior Vice President, and all the Vice Presidents, a chairperson shall be elected by resolution of the majority of those present at the meeting.
(813) Any duly constituted meeting of the Union under this Rule shall have the power to direct the Council on matters of policy and administration and the Council shall carry into effect all decisions of such meetings.
(914) Every resolution proposed at any meeting of the Union shall be carried by a simple majority of those voting at the meeting and at any such meeting the chairperson shall have a deliberate as well as a casting vote.
(10) At any AGM, General Meeting, Member Initiated Meeting or Urgent General Meeting the chairperson shall have a deliberate as well as a casting vote.
(1115) With the consent of the members present at any meeting, the Chairperson may adjourn the meeting from time to time and from place to place but no business shall be transacted at an adjourned meeting except that business left unfinished at the meeting from which the adjournment took place.
(1216) Except as otherwise provided for in these Rules, eEvery financial member shall have one vote at any meeting of the Union.
(1317) Unfinancial and Honorary members of the Union shall have no voting rights whatsoever.
(1) Meetings of the Union shall be the Annual General Meeting, General Meetings, Member Initiated Meeting, or Urgent General Meetings.
(2) The Annual General Meeting shall be held no later than the end of the third week of November each year at a time and place determined by the Council.
(a) The Agenda for the Annual General Meeting shall include a report on the Union's activities for the past year and the Union's financial position.
(b) A notice is to be issued to all members specifying the date, time, place and agenda for the Annual General Meeting.
(c) Notification of the Annual General Meeting shall be sent to members by email no later than 14 days prior to the date of proposed Annual General Meeting and by placing the notice on the Union website no later than 14 days prior to the date of proposed Annual General Meeting.
(d) The quorum for an Annual General Meeting shall be 50 members.
(e) Where a quorum is not reached on the first meeting date, the meeting is to stand adjourned to a date within 14 days of the adjourned meeting, to be resumed, at which the quorum for the adjourned meeting is also to be 50 members, and if the resumed meeting is inquorate, the meeting should lapse.
(f) A notice is to be issued to all members specifying the date, time, place and agenda for the adjourned Annual General Meeting.
(g) Where the Annual General Meeting is adjourned to a later date, member shall be notified by email and by a notice placed on the Union website no later than 7 days prior to the date of the proposed Annual General Meeting.
(h) Where an Annual General Meeting lapses due to a lack of quorum the report on the Union’s activities for the past year and the Union’s financial position shall be referred to the Council for approval.
(3) A General Meeting may be called by Council as often as it sees necessary.
(a) A notice is to be issued to all members specifying the date, time, place and purpose for the General Meeting.
(b) Notification of the General Meeting shall be sent to members by email no later than 14 days prior to the date of the proposed General Meeting and by placing the notice on the Union website no later than 14 days prior to the date of proposed General Meeting.
(c) The quorum for a General Meeting shall be 50 members.
(d) Where a quorum is not reached on the first meeting date, the meeting is to stand adjourned to a date within 14 days of the adjourned meeting, to be resumed, at which the quorum for the adjourned meeting is also to be 50 members, and if the resumed meeting is inquorate, the meeting should lapse.
(4) A Member Initiated Meeting may be called on the written request of 350 members of the Union.
(a) Where a written request for a Member Initiated Meeting is made, the President shall convene a Member Initiated Meeting to be held within 28 days of the written request being received.
(b) The written request shall state the purpose of the meeting to be convened and the business of the meeting shall be confined to that purpose.
(c) A notice is to be issued to all members specifying the date, time, place and purpose for the Member Initiated Meeting.
(d) Notification of the Member Initiated Meeting shall be sent to members by email no later than 14 days prior to the date of the proposed Member Initiated Meeting and by placing the notice on the Union website no later than 14 days prior to the date of proposed Member Initiated Meeting.
(e) The quorum for a Member Initiated Meeting shall be 100 members calling the meeting.
(f) Where a quorum is not reached on the first meeting date, the meeting is to stand adjourned to a date within 14 days of the adjourned meeting, to be resumed, at which the quorum for the adjourned meeting is also to be 100 members calling the meeting, and if the resumed meeting is inquorate, the meeting should lapse.
(5) An Urgent General Meeting may be called by the Executive in circumstances where the Executive is satisfied the matter cannot wait for the deliberations of the Council.
(a) A decision of the Executive to call an Urgent General Meeting may be made at a meeting of the Executive or by way of electronic poll of Executive members or any other practical method which results in a majority decision of the Executive.
(b) A notice is to be issued to all members specifying the date, time, place and purpose for the Urgent General Meeting.
(c) Notification of the Urgent General Meeting shall be sent to members by email no later than 72 hours prior to the proposed Urgent General Meeting and by placing the Notice on the Union website no later than 72 hours prior to the date of proposed Urgent General Meeting.
(6) If within half an hour from the time appointed for the initial meeting a quorum of members is not present, the meeting shall be adjourned.
(a) If within half an hour from the time appointed for an adjourned meeting a quorum of members is not present, the meeting shall lapse.
(7) At any meeting the President, if present, shall preside. In the absence of the President, the Senior Vice President shall preside. If neither the President nor Senior Vice-President are present, one of the Vice Presidents shall preside, and in the absence of the President, Senior Vice President, and all the Vice Presidents, a chairperson shall be elected by resolution of the majority of those present at the meeting.
(8) Any duly constituted meeting of the Union under this Rule shall have the power to direct the Council on matters of policy and administration and the Council shall carry into effect all decisions of such meetings.
(9) Every resolution proposed at any meeting of the Union shall be carried by a simple majority of financial members present and voting at the meeting.
(10) At any AGM, General Meeting, Member Initiated Meeting or Urgent General Meeting the chairperson shall have a deliberate as well as a casting vote.
(11) With the consent of the members present at any meeting, the Chairperson may adjourn the meeting from time to time and from place to place but no business shall be transacted at an adjourned meeting except that business left unfinished at the meeting from which the adjournment took place.
(12) Every financial member shall have one vote at any meeting of the Union.
(13) Unfinancial and Honorary members of the Union shall have no voting rights whatsoever.
(1) The Council shall control and administer the funds of the Union and cheques drawn on the Union's account shall be signed by any two of the President, Secretary, Senior Vice President and Vice Presidents.
(2) The books of the Union shall be audited annually. An audited report and balance sheet shall be presented at the Annual General Meeting of the Union.
(3) The funds of the Union shall be disbursed so that an amount equal to the capitation fees as determined from time to time by the Federal Council of the Australian Nursing Federation (a federally registered organisation) in accordance with its Rules shall be deposited to the credit of the W A Branch of the Australian Nursing Federation, and in addition to the foregoing such disbursements as the Council considers necessary for the effective operation of such organisation.
(1)(1) The Council shall control and administer the funds of the Union and cheques drawn on the Union’s account shall be signed by any two of the President, Secretary, Senior Vice President and Vice Presidents.
(2) Cheques drawn on the Union’s account shall be signed by any two of the President, Secretary, Senior Vice President and/or Vice Presidents.
(
3) Funds may be withdrawn by means of electronic funds transfer provided that the authorisation of any such electronic funds transfer shall be the same as that prescribed by these Rules for the signing of cheques. All accounts, other than petty expenses, shall be paid by means of cheque or electronic funds transfer.
(42) The books of the Union shall be audited annually. An audited report and balance sheet shall be presented at the Annual General Meeting of the Union.
(53) The funds of the Union shall be disbursed so that an amount equal to the capitation fees as determined from time to time by the Federal Council of the Australian Nursing and Midwifery Federation (a federally registered organisation) in accordance with its Rules shall be deposited to the credit of the W A Branch of the Australian Nursing and Midwifery Federation, and in addition to the foregoing such disbursements as the Council considers necessary for the effective operation of such organisation.
(1) The Council shall control and administer the funds of the Union.
(2) Cheques drawn on the Union’s account shall be signed by any two of the President, Secretary, Senior Vice President and/or Vice Presidents.
(3) Funds may be withdrawn by means of electronic funds transfer provided that the authorisation of any such electronic funds transfer shall be the same as that prescribed by these Rules for the signing of cheques. All accounts, other than petty expenses, shall be paid by means of cheque or electronic funds transfer.
(4) The books of the Union shall be audited annually. An audited report and balance sheet shall be presented at the Annual General Meeting of the Union.
(5) The funds of the Union shall be disbursed so that an amount equal to the capitation fees as determined from time to time by the Federal Council of the Australian Nursing and Midwifery Federation (a federally registered organisation) in accordance with its Rules shall be deposited to the credit of the W A Branch of the Australian Nursing and Midwifery Federation, and in addition to the foregoing such disbursements as the Council considers necessary for the effective operation of such organisation.
(1) The Union shall have the right to make Rules for its own use and guidance. Rules may be amended, added to, varied, repealed by notice of any proposed alteration to the Rules being given by any member to the Secretary in writing. The same shall be laid before the Council or before a meeting of the Union under
Rule 27 of these Rules, which may amend, add to, vary or repeal the Rules or any part of them in accordance with the proposal in the said notice or any reasonable amendment of same.
(2) No amendment, addition to variation, repeal, or substitution, of these Rules shall be made unless a notice of the proposed alteration, and the reasons therefore is:
(a) sent to each workplace for the attention of all members; or
(b) published in a Union magazine which shall be distributed to all members.
(3) In the notice referred to in sub-rule (2) members are to be informed that they or any of them may object to the proposed alteration by forwarding a written objection to the Registrar to reach him or her no later than 21 days after the date of issue of the notice in (2) (a) above or 21 days after the date of issue of the magazine as in (2) (b) above, as the case may be.
(1) The Union shall have the right to make Rules for its own use and guidance. Rules may be amended, added to, varied, repealed by notice of any proposed alteration to the Rules being given by any member to the Secretary in writing. The same shall be laid before the Council or before a meeting of the Union under Rule 27 of these Rules, which may amend, add to, vary or repeal the Rules or any part of them in accordance with the proposal in the said notice or any reasonable amendment of same.
(2) No amendment, addition to variation, repeal, or substitution, of these Rules shall be made unless a notice of the proposed alteration, and the reasons therefore is:
(a) sent to each workplace for the attention of all members; or
(b) published in a Union magazine which shall be distributed to all members.
(3) In the notice referred to in sub-rule (2) members are to be informed that they or any of them may object to the proposed alteration by forwarding a written objection to the Registrar to reach him or her no later than 21 days after the date of issue of the notice in (2) (a) above or 21 days after the date of issue of the magazine as in (2) (b) above, as the case may be.
(1) Rules may be amended, added to, varied or repealed by notice of any proposed alteration to the Rules being given by any financial member to the Secretary in writing.
(a) Financial member referred to in sub-rule (1) includes any member of Council but does not include the Secretary.
(2) The proposed alteration to the Rules shall be laid before the Council or before a Meeting of the Union under
(
Rule 27 of these Rules, which may amend, add to, vary or repeal the Rules or any part of them in accordance with the proposal or any reasonable amendment that does not change the original intention of the proposed alteration.
(3) The Secretary is to notify members of
(a) the changes endorsed by the Council or Meeting; and
(b) the reasons for the change; and
(c) any member may object to the proposed alteration, by forwarding a written objection to the Registrar, within twenty-eight (28) days of the issuing of notice to members.
(4) No amendment, addition to, variation or repeal of these Rules shall be made unless a notice is provided to members by:
(a) sending it to members by email to the email address provided by the member to the Union no later than 21 days after the date that the Council meeting or Meeting endorsed the alteration; and
(b) where no email address has been provided to the Union, the notice is to be posted to the home address provided by the member to the Union no later than 21 days after the date that the Council meeting or Meeting endorsed the alteration; and
(c) by placing the notice on the Union website no later than 21 days after the date that the Council meeting or Meeting endorsed the alteration.
5) Any alteration to these Rules shall not be effective until the Registrar has given to the Union a certificate that the alteration has been registered.
(1) Rules may be amended, added to, varied or repealed by notice of any proposed alteration to the Rules being given by any financial member to the Secretary in writing.
(a) Financial member referred to in sub-rule (1) includes any member of Council but does not include the Secretary.
(2) The proposed alteration to the Rules shall be laid before the Council or before a Meeting of the Union under Rule 27 of these Rules, which may amend, add to, vary or repeal the Rules or any part of them in accordance with the proposal or any reasonable amendment that does not change the original intention of the proposed alteration.
(3) The Secretary is to notify members of
(a) the changes endorsed by the Council or Meeting; and
(b) the reasons for the change; and
(c) any member may object to the proposed alteration, by forwarding a written objection to the Registrar, within twenty-eight (28) days of the issuing of notice to members.
(4) No amendment, addition to, variation or repeal of these Rules shall be made unless a notice is provided to members by:
(a) sending it to members by email to the email address provided by the member to the Union no later than 21 days after the date that the Council meeting or Meeting endorsed the alteration; and
(b) where no email address has been provided to the Union, the notice is to be posted to the home address provided by the member to the Union no later than 21 days after the date that the Council meeting or Meeting endorsed the alteration; and
(c) by placing the notice on the Union website no later than 21 days after the date that the Council meeting or Meeting endorsed the alteration.
(5) Any alteration to these Rules shall not be effective until the Registrar has given to the Union a certificate that the alteration has been registered.

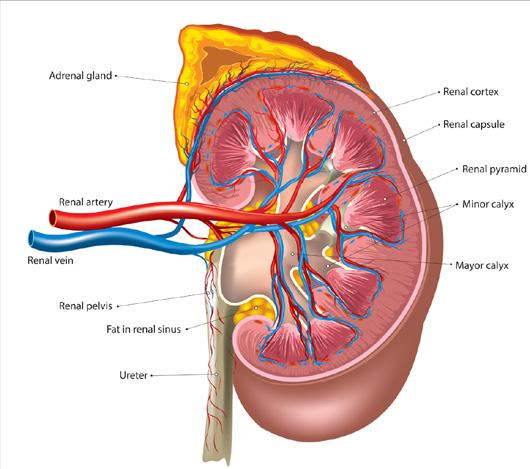
Acute pyelonephritis is a bacterial infection of the kidneys.1,2 It is an infection of the renal parenchyma (consisting of the renal cortex and the renal medulla), renal pelvis, and major and minor calyces (see Illustration 1).3,4,5
Acute pyelonephritis is a relatively common infection.4,5 It most commonly affects young, sexually active women due to the higher incidence of lower urinary tract infections experienced by this group.5,6
Most people with acute pyelonephritis, with prompt diagnosis and appropriate treatment, have a complete and uncomplicated recovery.5 However, acute pyelonephritis can be life threatening as it may cause renal failure, emphysematous pyelonephritis, septic shock, and multi-organ failure.7
Other complications associated with acute pyelonephritis include parenchymal renal scarring, renal abscess, perinephric abscess, chronic renal impairment, and renal vein thrombosis.4,5 Acute pyelonephritis during pregnancy is also associated with an increased risk of premature birth, low birth weight, and fetal mortality.5,7
TYPES OF ACUTE PYELONEPHRITIS
There are two main types of acute pyelonephritis: uncomplicated and complicated.5,6
Uncomplicated acute pyelonephritis is a bacterial kidney infection caused by a typical pathogen, in immunocompetent premenopausal women with no urological abnormalities or comorbidities, and who are not pregnant.5,7 Most cases of acute pyelonephritis are uncomplicated.5
Complicated acute pyelonephritis is a bacterial kidney infection in people who are immunocompromised or have increased susceptibility such that the infection is likely to be severe.5 Acute pyelonephritis is complicated if the infection occurs in:3,5,6
• Males
• Infants
• Older persons, over 60 years of age
• Pregnant women
• Patients with a history of recurrent urinary tract infections
• Patients with chronic renal disease
• Patients who have received a kidney transplant
• Patients with anatomic abnormalities of the urinary tract, such as double ureter, horseshoe kidney, ureterocele, vesicoureteric reflux, or polycystic kidney disease
• Patients who have recently undergone genitourinary procedures, such as cystoscopy
• Patients with diabetes mellitus
• Patients with advanced neurological disease
• Patients who are immunocompromised, such as patients with HIV or who are receiving chemotherapy or radiotherapy, or who are using corticosteroids
• Patients with a urinary catheter
• Patients with a urinary tract obstruction, such as benign prostatic hypertrophy, tumour, kidney stones, neurogenic bladder, or posterior ureteral valve.
Complicated pyelonephritis can also result from multi-drug-resistant pathogens.5,6
CAUSES AND RISK FACTORS
Acute pyelonephritis is generally caused by enteric bacteria ascending through the urinary tract to the kidneys.3,5,6
Most cases of acute pyelonephritis, more than 80%, are caused by the gramnegative bacteria Escherichia coli. Other gram-negative bacteria, Klebsiella species, Proteus species, Enterbacter species, and Pseudomonas species responsible for 5-20% of acute pyelonephritis cases.3,5 Acute pyelonephritis is less commonly caused by gram positive bacteria, such as Enterococcus faecalis, Staphylococcus saprophyticus, and Staphylococcus aureus.5
Acute pyelonephritis may also be caused by haematogenous seeding of the kidneys in patients with bacteraemia.3,5,6 Haematogenous
Read this article and complete the quiz to earn: 1 iFolio hour
seeding most commonly occurs in neonates and immunocompromised patients. The highly virulent Staphylococcus aureus is the most common cause of acute pyelonephritis occurring by haematogenous spread.3
RISK FACTORS
Factors that may increase the risk of acute pyelonephritis include:5,6
• Sex – women are more likely to develop acute pyelonephritis
• Previous urinary tract infections
• Family history of urinary tract infections
• Stress incontinence
• Diabetes mellitus
• Frequent sexual intercourse
• A new sexual partner in the previous year
• Recent spermicide use
• Urinary catheterisation
• Kidney stones
• Anatomical or functional urinary abnormality
• Immunosuppression.
SIGNS AND SYMPTOMS
Signs and symptoms of acute pyelonephritis include:1,2,5,7
• Flank pain (pain in the lower back, under the ribs, or to either side of the spine)
• Costovertebral angle tenderness
• Suprapubic tenderness
• Haematuria (blood in the urine)
• Cloudy or bad smelling urine
• Palpation of the abdomen to assess suprapubic tenderness.
Acute pyelonephritis is detected by urinalysis and confirmed with urine culture.5,8
Urinalysis, using a clean catch (midstream) sample, is recommended for all patients
pyelonephritis and the severity of the infection.5,7 Treatment generally involves antibiotics, analgesics, and antipyretics.6
Uncomplicated acute pyelonephritis can usually be treated in the community with oral antibiotics.4,5,7,10 Patients with
Paracetamol is pain and fever pyelonephritis. inflammatory drugs due to the potential injury.5
PREVENTION
Preventative risk of developing particularly for
• Maintaining adequate plenty of fluids the urinary tract
• Urinating without urinate is felt
• Wiping the genital after urinating
• Urinating as soon intercourse
• Avoiding the use deodorant sprays area.
REFERENCES
• Needing to pass urine often
• Burning or pain when passing urine
• Fever and chills
• Myalgia
• Nausea and vomiting.
Symptoms of acute pyelonephritis typically develop rapidly within a few hours or over the course of a day.5
Acute pyelonephritis is diagnosed using a combination of preliminary clinical assessment, including medical history and physical examination, and supportive laboratory tests.2,5
Physical examination should include:5
• Checking vital signs, including temperature, blood pressure, and respiration rate
• Palpation of the costovertebral angle to assess costovertebral angle tenderness (costovertebral angle tenderness is a key symptom of acute pyelonephritis and can help differentiate between acute pyelonephritis and kidney stones)
• Palpation of the abdomen to assess suprapubic tenderness.
Acute pyelonephritis is detected by urinalysis and confirmed with urine culture.5,8
Urinalysis, using a clean catch (midstream) sample, is recommended for all patients with suspected acute pyelonephritis.3,5,7,8 Acute pyelonephritis is indicated if the urinalysis is positive for leukocytes, red blood cells, or nitrites.5,8
Acute pyelonephritis is confirmed by urine microscopy and culture, using a clean catch (midstream) sample.3,5,7,8 Infection can be diagnosed if the leukocyte (white cell) count is more than 40 x 106/L and the bacterial colony count is more than 108/L (pure growth).9
Once acute pyelonephritis is confirmed, the susceptibility profile of the bacteria should be established to guide antimicrobial treatment.5,7
A full blood count (FBC) and electrolytes, urea and creatine (EUC) should be performed for all patients with suspected acute pyelonephritis. Blood culture should also be performed for febrile patients, or patients requiring hospital admission.3,5 Blood culture should not be routinely requested for patients with uncomplicated acute pyelonephritis.5
Diagnostic imaging is generally not required but may be used if local complications, such as renal abscess, renal infarct, hydronephrosis, or perinephric collections, are suspected. Imaging is also recommended if the diagnosis is equivocal after other investigations.3
Treatment of acute pyelonephritis varies depending on the type of pyelonephritis and the severity of the infection.5,7 Treatment
generally involves antibiotics, analgesics, and antipyretics.6
Uncomplicated acute pyelonephritis can usually be treated in the community with oral antibiotics.4,5,7,10 Patients with uncomplicated acute pyelonephritis requiring hospital admission, such as patients with a severe infection, should be treated initially with intravenous antibiotics and then with oral antibiotics.7,10
Patients with complicated acute pyelonephritis generally require hospital admission for antibiotic treatment and supportive care.5 Patients should be treated initially with intravenous antibiotics and then switched to oral antibiotics.7,10 Any urological abnormality, comorbidity or underlying complicating factor must also be appropriately managed.5,7
The initial selection of antibiotics for treating uncomplicated and complicated acute pyelonephritis should follow local protocols, considering the severity of symptoms, risk of complications, the patient’s previous antibiotic use, and local antibiotic resistance patterns.5,6 The shortest course of antibiotics that is likely to be effective in treating the infection should be used to minimise the risk of adverse effects and reduce the risk of antimicrobial resistance.5
The patient’s response to the antibiotic therapy should be assessed after 72 hours when the results of urine culture and sensitivity testing are available. The antibiotic therapy should be modified according to culture and susceptibility results and the patient’s response to treatment.5,11
Paracetamol is recommended to treat pain and fever associated with acute pyelonephritis.2,5 Nonsteroidal antiinflammatory drugs are not recommended due to the potential risk of acute kidney injury.5
Preventative measures to reduce the risk of developing acute pyelonephritis, particularly for women, include:1
• Maintaining adequate hydration – drinking plenty of fluids to help clear bacteria from the urinary tract
• Urinating without delay when the urge to urinate is felt
• Wiping the genital area from front to back after urinating or a bowel movement
• Urinating as soon as possible after sexual intercourse
• Avoiding the use of products, such as deodorant sprays or douches, in the genital area.
1. Mayo Clinic. Mayo Clinic Health Information [Internet]. Kidney infection; 2022 [cited 2024 Jul 6]. Available from: https://www.mayoclinic.org/diseasesconditions/kidney-infection
2. Healthdirect Australia. Healthdirect [Internet]. Kidney infection (pyelonephritis; 2022 [cited 2024 Jul 7]. Available from: https://www.healthdirect.gov.au/kidneyinfection
3. Agency for Clinical Innovation. Clinical tools [Internet]. Management of pyelonephritis in adults; 2022 [cited 2024 Jul 6]. Available from: https://aci.health.nsw.gov.au/ networks/eci/clinical/clinical-tools/renal/ pyelonephritis
4. Niknejad MT. Radiopaedia [Internet]. Acute pyelonephritis; 2024 [cited 2024 Jul 7]. Available from: https://radiopaedia.org/ articles/acute-pyelonephritis-1
5. BMJ Best Practice. Acute pyelonephritis [Internet]. London: BMJ Publishing Group Ltd; 2023 [cited 2024 Jul 7]. Available from: https://bestpractice.bmj.com/topics/ en-gb/3000111/pdf/3000111/Acute%20 pyelonephritis.pdf
6. Belyayeva M, Leslie SW, Jeong JM. Acute Pyelonephritis. 2024 [cited 2024 Jul 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing LLC. Available from: https://www.ncbi.nlm.nih.gov/books/ NBK519537
7. European Association of Urology. EAU Guidelines on Urological Infections [Internet]. 2024 [cited 2024 Jul 7]. Available from: https://d56bochluxqnz. cloudfront.net/documents/full-guideline/ EAU-Guidelines-on-UrologicalInfections-2024.pdf
8. Pathology Tests Explained. Pathology Tests Explained [Internet]. UTI (urinary tract infection) testing; 2023 [cited 2024 Jul 6]. Available from: https://www. pathologytestsexplained.org.au/ptests-pro. php?q=UTI+%28Urinary+tract+infection% 29+testing
9. Royal College of Pathologists of Australasia (RCPA). RCPA Manual. MCS Urine; 2024 [cited 2024 Jul 7]. Available from: https:// www.rcpa.edu.au/Manuals/RCPA-Manual/ Pathology-Tests/M/MCS-urine
10. Urinary infections. 2024 [cited 2024 Jul 6]. In: Australian Medicines Handbook [Internet]. Adelaide (Australia): Australian Medicines Handbook. Available from: https:// amhonline.amh.net.au/chapters/antiinfectives/tables/urinary-infections-table 11. Acute pyelonephritis in adults. 2019 [cited 2024 Jul 6]. In: Therapeutic Guidelines [Internet]. Melbourne (Australia): Therapeutic Guidelines Limited. Available from: https:// tgldcdp.tg.org.au/viewTopic?etgAccess=true &guidelinePage=Antibiotic&topicfile=acutepyelonephritis-adultsIllustration 1: Anatomy of the kidney

CSIRO, Australia’s national science agency, has issued a statement revealing plastic pollution littering Australian coastlines has dropped by more than a third over the last decade.
Six regions across Australia were surveyed by researchers, with a total of 8,383 debris items recorded within 100km of each city, by 1907 surveys.
The most found items were polystyrene and cigarette butts, followed by food wrappers, bottle lids and caps, with plastic fragments also frequently found.
Dr Denise Hardesty, Senior Research Scientist at CSIRO and co-author, noted that while up to 53 million metric tonnes of plastic waste are expected to enter aquatic ecosystems by 2030, it is encouraging to witness a significant decline in plastic pollution along Australia’s beaches and coastlines.
“Three-quarters of the rubbish we find on our beaches is plastic, and flexible plastics, such as food packaging, are the most harmful to wildlife,” Dr Hardesty said. “Decreases of plastic pollution in the coastal environment were observed in Newcastle, Perth, and the Sunshine Coast, with increases in Hobart and Port Augusta.”
The study, “Drivers of Environmental Debris in Metropolitan Areas: A Continental Scale Assessment”, published in Marine Pollution Bulletin, analyzes survey
data from a decade ago and expands on previous research that reported a 29% reduction in plastic waste across Australia. CSIRO is working towards an 80% reduction in plastic waste entering the environment by 2030 as part of its research to combat plastic pollution.
Dr Steph Brodie, CSIRO Research Scientist and co-author, stated that the surveys help pinpoint debris hotspots, analyze the impact of land use on environmental waste, and track how debris reaches coastal areas.
“Understanding the types and amount of plastic pollution in our environment provides critical data to develop strategies to stop it ending up there in the first place.
“These results will help to inform waste management and can be used to evaluate and measure the effectiveness of plastic waste policies, practices and education campaigns to reduce debris in metropolitan regions.”
The Federal Government’s Medical Research Future Fund (MRFF) has awarded Curtin University and WA
Country Health Service more than $3.6 million for their alliance-led research project aimed at improving healthcare outcomes for rural and remote communities.
Dr Sharmani Barnard from Curtin’s School of Population Health said, “People living in rural and remote areas often experience poorer health outcomes compared to those in metropolitan regions partly due to reduced access to primary and specialist care.”
The project will focus on developing the Rural and Remote Health Outcomes Monitoring Platform (RHOMP), with the aim of providing timely data to healthcare providers to improve service delivery.
De-identified data from multiple sources, including primary care, hospitals, aeromedical and ambulance services will be collated into a centralized platform.
Dr Barnard has said RHOMP will facilitate better allocation of resources by healthcare providers and policymakers by providing clearer insights into patient pathways and will improve care options closer to home.
Jeff Moffet, Chief Executive of WA Country Health Service said, “The collaborative project provides a digital platform for WA Country Health Service and our service partners to present insights into patient care pathways and clinical outcomes.”
“Importantly, it will support the provision of frontline care in hospitals and health services throughout country WA –allowing us to drive improvements across patient transfers.”
The monitoring program will incorporate two primary components:
• RHOMP Interactive – Designed to monitor patient care pathways and track clinical outcomes and,
• RHOMP Research Environment –designed to foster research to improve rural healthcare.
Key partners include WA Country Health Service, St John WA, The Royal Flying Doctor Service WA, Puntukurnu Aboriginal Medical Service and WA Primary Health Alliance.
Gastroscopy is an endoscopic procedure that allows direct visualisation of the upper gastrointestinal tract, including the oesophagus, stomach, and duodenum.1,2
Gastroscopy involves a gastroscope, a long thin flexible tube with a tiny camera, being passed through mouth into the oesophagus, stomach, and duodenum.1,3 The gastroscope captures video of the upper gastrointestinal tract and displays the images onto a screen so the healthcare professional can view the lining of the oesophagus, stomach, and duodenum.1,2,3
A gastroscope can also be used to obtain tissue and gastrointestinal fluid samples.2,3,4
INDICATIONS
Gastroscopy is used for diagnostic and therapeutic indications.1
Diagnostic indications for gastroscopy include:1,2,4
• Investigating upper gastrointestinal tractbleeding, persistent upper abdominal pain,intractable vomiting, recurring indigestion,and dysphagia
• Identifying diseases and health conditions,such as gastroesophageal reflux disease,oesophagitis, gastritis, duodenitis, celiacdisease, Crohn’s disease of the uppergastrointestinal tract, oesophageal andstomach cancer, tumours, oesophageal,stomach and duodenal ulcers, strictures, andoesophageal varices
• Assessing acute injury caused by causticsubstance ingestion
• Evaluating abnormalities detected onimaging studies
Screening for malignancy in patients with premalignant conditions such as polyposis syndromes or Barrett’s oesophagus.
Therapeutic indications for gastroscopy include:1,2,4
• Foreign body removal
• Polyp removal
• Dilation or stenting of strictures
• Oesophageal variceal ligation
• Treatment of bleeding ulcers
• Feeding or draining tube placement.
CONSENT AND PREPARATION
Gastroscopy is an invasive procedure. Before a gastroscopy the patient should be given information about the procedure and sedation, as well as the benefits, risks, and potential complications. The patient must consent to the gastroscopy.2,5
An empty stomach is critical for safe and effective visualisation of the upper gastrointestinal tract.3 The patient should not eat or drink for six hours before a gastroscopy.1,3
Patients taking blood thinning medications, such as warfarin, heparin, aspirin, and apixaban, or diabetes medications may need adjust the dose prior to the gastroscopy. The gastroenterologist will provide specific advice for the patient about dose adjustments.1,3,5
GASTROSCOPY PROCEDURE
A gastroscopy generally takes 15-30 minutes.3
Patient positioning
Patients are generally positioned in the left lateral position with their neck flexed forward.2,3,5
Sedation and anaesthesia
Most patients have a mild anaesthetic or sedation to minimise pain or discomfort during the gastroscopy.1,2,3,5
The patient’s suitability for sedation should be assessed before the gastroscopy by an appropriately trained healthcare professional.2 Sedation should be provided in accordance with the recommendations of the Australian and New Zealand College of Anaesthetists.6
Anaesthetic throat spray may minimise discomfort associated with inserting the gastroscope.2,3
Procedure
A small mouthguard is placed in the patient’s mouth prior to the insertion of the gastroscope to stop them from biting the gastroscope.2,3 Dentures may also be removed before insertion of the gastroscope.1,3
The gastroscope is passed through the patient’s mouth to the base of the tongue, where the tip of the gastroscope is gently angled down until the vocal cords, epiglottis, piriform sinuses, and cricoarytenoid cartilages are visualised. The gastroscope is then passed through the upper oesophageal sphincter, and advanced down the oesophagus allowing visualisation of the mucosa for inflammation, erythema, furrowing, varices, erosions, ulcerations, narrowing, or strictures.2,5
After careful and systematic examination of the oesophagus, the gastroscope is advanced past the esophagogastric junction into the stomach.2
The stomach is insufflated with air to improve visualisation, and the gastroscope is advanced along the lesser curvature towards the pylorus. After passing through the pylorus, the gastroscope enters the duodenum bulb. The duodenum bulb should be examined on insertion of the gastroscope, as passage of the scope may cause mucosal changes.2 After the duodenum bulb is examined, the gastroscope is advanced through the duodenal sweep and into the second portion of the duodenum. The scope is then slowly withdrawn.5 As the gastroscope is withdrawn the duodenum, pylorus, and stomach are carefully and systematically examined for inflammation, ulcerations, erosions, discolouration, nodules, cracks, and polyps.2,7
The oesophagus is re-examined as the gastroscope is withdrawn.2,5
Documentation
A report detailing the clinical findings, any polyps removed, biopsies taken, and therapeutic interventions should be documented in the health record.5
Read this article and complete the quiz to earn: 0.5 iFolio hour
RISKS AND CONTRAINDICATIONS
Gastroscopy is a safe procedure, and complications are rare.2,3,5 Possible complications include gastrointestinal tract perforation, excessive bleeding, infection, duodenal haematoma, and adverse events related to sedation, such as hypoxaemia, hypotension, arrhythmias, and aspiration.2-5
Complications are usually identified within 24 hours after the gastroscopy.2 Patients should seek medical attention immediately if they develop fever, dysphagia, or increasing throat, chest, or abdominal pain after the gastroscopy.1,3
Gastroscopy is contraindicated in patients with toxic megacolon, peritonitis, a known or suspected perforation, or severe coagulation abnormalities.2,5
1. Healthdirect Australia. Healthdirect [Internet]. Gastroscopy; 2024 [cited 2024 Jul 20]. Available from: https://www.healthdirect.gov.au/gastroscopy
2. Ahlawat R, Hoilat GJ, Ross AB. Esophagogastroduodenoscopy. 2023 [cited 2024 Jul 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing LLC. Available from: https:// www.ncbi.nlm.nih.gov/books/NBK532268
3. Gastroenterological Society of Australia. Information about Gastroscopy (Upper Endoscopy) [Internet]. Melbourne (Australia): Gastroenterological Society of Australia; 2022 [cited 2024 Jul 20]. Available from: https://www.gesa.org.au/public/13/files/ Education%20%26%20Resources/Patient%20 Resources/Gastroscopy/Gastroscopy_2022_ APPROVED.pdf
4. Johns Hopkins Medicine. Johns Hopkins Medicine [Internet]. Upper GI Endoscopy; c2024 [cited 2024 Jul 20]. Available from: https://www. hopkinsmedicine.org/health/treatment-tests-andtherapies/upper-gi-endoscopy
5. Cohen J, Greenwald DA. Overview of upper gastrointestinal endoscopy (esophagogastroduodenoscopy). 2022 [cited 2024 Jul 20]. In: UpToDate [Internet]. Waltham (MA): UpToDate Inc. Available from: https://www.uptodate. com/contents/overview-of-upper-gastrointestinalendoscopy-esophagogastroduodenoscopy
6. Australian Commission on Safety and Quality in Health Care. Colonoscopy: Clinical Care Standard [Internet]. Sydney (Australia): Australian Commission on Safety and Quality in Health Care; 2020 [cited 2024 Jul 20]. Available from: https://www. safetyandquality.gov.au/sites/default/files/2020-04/ colonoscopy_clinical_care_standard_updated_2020. pdf
7. Fujiwara Y, Tanoue K, Higashimori A, Nishida Y, Maruyama M, Itani S, et al. Endoscopic findings of gastric lesions in patients with eosinophilic gastrointestinal disorders. Endosc Int Open [Internet]. 2020 [cited 2024 Jul 20];8(12):E1817-E1825. doi: 10.1055/a-1268-7312

The CyberCX 2025 Threat Report highlights significant changes in the cyber threat landscape, with key findings including the increasing stealth of espionage attacks, the persistence of Business Email Compromise (BEC), and the growing sophistication of cyber extortion tactics.
• Espionage attacks remain undetected longer, with the average time to detect (TTD) rising to 404 days, compared to 390 in 2023. Financially motivated attacks, by contrast, had an average TTD of just 24 days.
• BEC remained the most common cyber incident, with 75% of attacks bypassing multi-factor authentication (MFA) using advanced phishing techniques.
• Healthcare was the most impacted sector, followed by financial services and education, reflecting attackers' focus on industries holding sensitive personal data.
• Financial motivation drives most cyber incidents (65%), with espionage accounting for 5%.
• Ransomware-only attacks surged, making up 38% of incidents in 2024, up from 13% in 2023, while data theft
extortion cases declined from 27% to 9%.
• Some stolen data is never leaked, with around 25% of data theft victims who refused to pay ransom never seeing their data published.
CyberCX’s Executive Director of Digital Forensics and Incident Response, Hamish Krebs, warned that cyber threats continue to evolve, with attackers increasingly targeting cloud infrastructure, exploiting weaknesses in Managed Service Providers (MSPs), and adapting to security measures like Endpoint Detection and Response (EDR). The report aims to help organisations allocate resources effectively to counter emerging cyber threats.
In a landmark move to defend Australians against cybercrime, the federal government has imposed targeted financial and travel sanctions on Russianbased cyber infrastructure company ZServers and five of its employees. These individuals were directly linked to the Medibank Private data breach, which
saw sensitive personal information stolen and leaked in a major 2022 cyberattack.
This is the first time Australia has used its autonomous cyber sanctions powers against a business — and the first time sanctions have been issued for providing services or infrastructure used in cybercrime. It’s a clear message: those who support or enable malicious cyber activity will be held accountable.
The sanctions were the result of sustained collaboration between the Australian Signals Directorate (ASD), federal agencies, and international partners. This action reinforces Australia's commitment to disrupting cybercriminal operations, particularly those targeting critical infrastructure, healthcare providers, government systems, and the broader community.
The Medibank attack was a confronting reminder of how vulnerable personal data — including health records — can be. Nurses and midwives understand better than most the importance of privacy in healthcare. Breaches like this can cause enormous distress to patients and damage public trust in the systems we rely on.
ASD continues to strongly discourage paying ransoms or extortion demands. Instead, they urge immediate reporting of cybercrime through their hotline at 1300 CYBER1 or online at cyber.gov.au/ report
For healthcare organisations and professionals, cyber vigilance is now part of the job. Protect yourself and your workplace by:
• Keeping software and devices up to date
• Backing up data regularly
• Avoiding suspicious links and emails
• Educating colleagues and staff on safe digital practices
As cyber threats evolve, so too must our defences — and that includes strong government action, robust digital hygiene, and a united commitment to safeguarding the personal information of all Australians.
Brand name: Betaloc, Metrol, Minax, Toprol-XL, Topreloc1
Drug class: beta-blockers1
MECHANISM OF ACTION
Metoprolol is a cardioselective beta-1-adrenergic receptor inhibitor that competitively blocks betareceptors in the heart, peripheral vasculature, bronchi, pancreas, uterus, kidney, brain, and liver.1,2,3 The inhibitory effects of metoprolol reduce heart rate, blood pressure, and cardiac contractility.1
ADMINISTRATION
Metoprolol is generally administered orally in tablet form but can be administered intravenously.1
INDICATIONS
Indications for metoprolol are:1
• Hypertension
• Angina
• Tachyarrhythmias
• Myocardial infarction
• Chronic heart failure with reduced ejection
CONTRAINDICATIONS
Metoprolol is contraindicated in patients with:1,2,3
• Hypersensitivity to metoprolol or other betablockers
• Bronchospasm
• Severe or poorly controlled asthma
• Allergic disorders that suggest a predisposition to bronchospasm
• Shock
• Second- and third-degree atrioventricular block
• Sinus bradycardia (less than 45-50 beats per minute)
• Right ventricular failure secondary to pulmonary hypertension
• Significant right ventricular hypertrophy
• Non-compensated congestive heart failure
• Sick-sinus syndrome (unless pacemaker is in place)
• Severe peripheral arterial circulatory disorders
• Myocardial infarction with heart rate of less than 45 beats per minute, PR interval of greater than 0.24 seconds, systolic blood pressure of less than 100mmHg, and/or moderate to severe non-compensated heart failure
• Hypotension
• Untreated phaeochromocytoma.
INTERACTIONS
Metoprolol has a number of clinically meaningful drug interactions. For example:4
• Paroxetine increases the concentration of metoprolol and may increase its adverse effects
• Metoprolol decreases the concentration of lercanidipine and may reduce its activity
• Rifampicin increases the metabolism of metoprolol and may reduce its therapeutic effect
• Metoprolol may reduce the metabolism of lidocaine, increasing the risk of lidocaine toxicity
• Amiodarone may increase the concentration of metoprolol, increasing the risk of severe bradycardia
• Metoprolol may reduce the pressor effects of noradrenaline.
Hypertension1
Read this article and complete the quiz to earn: 0.5 iFolio hour
Adult oral initially 50-100mg daily in 1-2 doses, usual maintenance dose of 50-100mg daily in 1-2 doses
Child (1 month–12 years) oral initially 1mg/kg twice daily, increased if required to 8mg/kg daily in 2-4 doses (maximum 200mg daily)
Angina1
Adult oral initially 25-50mg twice daily, usual maintenance dose of 50-100mg 2-3 times daily
Tachyarrhythmias1
Adult oral 25-100mg twice daily OR IV 5mg (1-2mg/minute) repeated if required at 5-minute intervals for up to 3 doses
Myocardial infarction1
Adult specialist advice should be sought for acute use oral usual maintenance dose 25-50mg twice daily
Heart failure1
Adult oral initially 23.75mg once daily for 14 days, then increased if tolerated to 47.5mg once daily for at least 14 days, then further increased to 95mg once daily for at least 14 days, then further increased to a maintained dose of 190mg once daily
Migraine prophylaxis1
Adult oral 50-75mg twice daily
The dosage of metoprolol should be individualised to the patient based on their response to treatment.2,3
PRECAUTIONS
Hepatic impairment
Metoprolol should be used with caution in patients with hepatic impairment.1,2,3 The dose should be carefully titrated according to response and adverse effects.1
Cardiovascular conditions
Metoprolol may impair peripheral circulation and exacerbate the symptoms of peripheral vascular disease.2,3 Metoprolol should be used with caution in patients with Raynaud’s phenomenon or severe peripheral arterial disease.1
Metoprolol should also be used with caution in patients with a first-degree atrioventricular block.1,2,3
Diabetes
Metoprolol may affect glucose metabolism and mask signs of acute hypoglycaemia and should be used with caution in patients with diabetes mellitus.1,2,3
Hyperthyroidism
Metoprolol may mask signs of developing or continuing hyperthyroidism and should be used with caution in patients who are hyperthyroid.1,2,3
Elderly population
Metoprolol should be used with caution in elderly patients. A lower initial dose should be used.1
Pregnancy and breastfeeding
Metoprolol should be used with caution during pregnancy.2,3,5 Metoprolol may cause neonatal bradycardia and transient hypoglycaemia, and may increase the risk of fetal loss, intrauterine growth restriction, pre-term birth, and low birth weight.2,3,5 Metoprolol should only be used during the second and third trimesters if the expected benefit is considered to outweigh the potential risks.2,3,5
If metoprolol is used during pregnancy, the lowest effective dose should be used and treatment should be discontinued at least two to three days before delivery to avoid increased uterine contractility and beta-blockade effects in the neonate.2,3
Metoprolol is considered safe to use while breastfeeding. However, as small amounts are excreted in breastmilk the infant should be monitored for signs of bradycardia or hypotension.5
ADVERSE EFFECTS
Common adverse effects associated with metoprolol include fatigue, headache, dizziness, nausea, diarrhoea, constipation, dyspnoea, bradycardia, palpitations, hypotension, and exacerbation of Raynaud’s phenomenon.2,3
Metoprolol may infrequently be associated with vomiting, paraesthesia, muscle cramps, weight gain, depression, insomnia, nightmares, impaired concentration, bronchospasm, rash, increased sweating, oedema, precordial pain, transient deterioration of heart failure symptoms, firstdegree atrioventricular block, and cardiogenic shock in patients with acute myocardial infarction.2,3
Rarely metoprolol may be associated with dry mouth, arthralgia, alopecia, photosensitivity, rhinitis, vision disturbances, dry eyes, conjunctivitis, tinnitus, taste disturbances, thrombocytopenia, liver function test abnormalities, hepatitis, anxiety, sexual dysfunction, amnesia, confusion, hallucinations, arrhythmias, disturbances of cardiac conduction, and gangrene in patients with severe peripheral circulatory disorders.2,3
REFERENCES
1. Metoprolol. 2024 [cited 2024 Feb 20]. In: Australian Medicines Handbook [Internet]. Adelaide (Australia): Australian Medicines Handbook. Available from: https://amhonline.amh.net.au/chapters/ cardiovascular-drugs/antihypertensives/beta-blockers/metoprolol
2. Therapeutic Goods Administration. Australian Product Information: Metrol Tablets [Internet]. Woden (Australia): TGA; 2024 [cited 2024 Feb 20]. Available from: https://www.ebs.tga.gov.au/ebs/ picmi/picmirepository.nsf/pdf?OpenAgent&id=CP-2024-PI-010631&d=20240218172310101
3. Therapeutic Goods Administration. Australian Product Information: Betaloc [Internet]. Woden (Australia): TGA; 2019 [cited 2024 Feb 20]. Available from: https://www.ebs.tga.gov.au/ebs/picmi/ picmirepository.nsf/pdf?OpenAgent&id=CP-2010-PI-046203&d=2 0240204172310101&d=20240218172310101
4. Drug interactions: Beta-blockers. 2024 [cited 2024 Feb 20]. In: Australian Medicines Handbook [Internet]. Adelaide (Australia): Australian Medicines Handbook. Available from: https://amhonline. amh.net.au/interactions/beta-blockers-inter#metoprolol-inter 5. Metoprolol. 2022 [cited 2024 Feb 20]. In: Pregnancy and Breastfeeding Medicines Guide [Internet]. Melbourne (Australia): The Royal Women’s Hospital. Available from: https://thewomenspbmg. org.au/medicines/metoprolol
Oxitec Australia, a new venture launched in collaboration between CSIRO and Oxitec Ltd, aims to combat the spread of deadly mosquito-borne diseases like dengue, Zika, and yellow fever in the Pacific region. The initiative uses Oxitec's Friendly™ platform, which involves genetically engineered male mosquitoes that carry a self-limiting gene, ensuring that only non-biting males survive and reducing the mosquito population. This technology will first target Aedes aegypti mosquitoes, followed by Aedes albopictus, which poses a significant risk to Australia.
Professor Brett Sutton, Director of Health & Biosecurity at CSIRO had this to say:
“Oxitec Australia offers a unique opportunity to help combat the growing threat of invasive and exotic pests, some of which are on mainland Australia’s doorstep like Aedes albopictus,” Professor Sutton said.
“Factors like climate change and growing pesticide resistance will only bring greater challenges to the health of Australians and our region via vector-borne diseases.
“By investing in new and innovative solutions that complement existing control programs, we can reduce the
public health impacts of these exotic and invasive mosquito species.
“This technology platform could also be used to develop solutions for a wide spectrum of pests that threaten livestock and crops and our food systems.”
Oxitec Australia is seeking partners to accelerate its efforts and address growing threats from invasive pests, exacerbated by climate change and pesticide resistance. The venture is also working on solutions for pests that threaten crops, such as the fall armyworm caterpillar. The program is already engaging with local communities in the Torres Strait to deploy these technologies in regions impacted by dengue outbreaks.
Grey Frandsen, CEO of Oxitec, said they were committed to transforming how pest threats to health, food security and ecosystems are addressed by collaborating with Indigenous Communities, leading scientific institutions, industry partners and farmers.
“In doing so, we aim to not only protect lives, livelihoods and biodiversity, but also empower Indigenous communities to take the lead in addressing their pest challenges,” Mr Frandsen said.


The City of Perth recently hosted Sunset Sounds, where they partnered with GO2CUP to introduce reusables and waste-sorting initiatives.
Sunset Sounds attracted around 500 community members and visitors to the stunning Derbarl Yerrigan (Swan River) foreshore. Thanks to the efforts of vendors and support of the community, less than 10 litres of landfill waste was generated from the entire event.
Two food vendors embraced the shift towards sustainability:
• That Little Gelato Cart served their delicious treats in reusable ice cream dishes, eliminating waste from their servings.
• Rio400 significantly reduced their environmental footprint by replacing 50% of their disposable serveware with reusable alternatives.
The City of Perth has stated: “This initiative was made possible thanks to funding support from the Plastic Free Riverpark program, run by the Department of Biodiversity, Conservation and Attractions. It aligns seamlessly with the City’s ongoing commitment to reducing waste and promoting environmentally responsible practices.”

Australia's peak nursing and midwifery groups call for immediate reform to improve access to affordable healthcare
A joint media statement from Australia’s Peak Nursing and Midwifery Groups calls on the major parties at this election to provide all Australians with quicker and more affordable access to health services.
The groups are advocating for immediate and effective nursing-led reform via seven actions to improve care, reduce waiting time, and deliver better health outcomes:
ACTION 1: Enable Nurse Practitioners and Endorsed Midwives to directly refer patients to relevant specialists, reducing waiting times for care.
ACTION 2: Introduce funding and regulatory reforms that support nurse and midwife-led clinics and innovative care models, particularly in rural, remote, and underserved communities, enabling nurses and midwives to take leadership roles in delivering community-based primary care.
ACTION 3: Work with State and Territory Governments to pass laws to support qualified Registered Nurses in every State and Territory to prescribe approved medications under the Pharmaceutical Benefits Scheme.
ACTION 4: Increase the Workforce Incentive Payment Practice Stream to cover up to seven healthcare professionals, and tie payments to higher scope clinical care.
ACTION 5: Authorise Nurse Practitioners, Endorsed Midwives and qualified Registered Nurses to order diagnostic tests such as mammograms, X-rays and DEXA scans. For Endorsed Midwives, this includes tests such as NIPT, pelvic ultrasound, multiple pregnancy items and iron studies.
ACTION 6: New and amended Medicare Benefit Schedule items for Endorsed Midwives to support pre-conception counselling, primary sexual and reproductive health, intrapartum care outside of a hospital setting (homebirth), and a general consult item for women’s health.
ACTION 7: Implement a primary healthcare workforce development strategy to unlock 15,000 extra education and training places for Registered Nurses, Nurse Practitioners and midwives in the places and settings that need them most.
The statement calls for the significant barriers preventing nursing and midwifery professionals from working to their full potential be removed, echoing sentiments and recommendations of the Unleashing the Potential of our Health Workforce – Scope of Practice Review – led by Professor Mark Cormack.
“Health reform is complex, but enabling these essential healthcare professionals to deliver the full range of care they are trained and qualified to provide must be a priority for the next government,” the statement reads.
The Perkins reaches major milestone in delivery of a Comprehensive Cancer Centre for WA
The Harry Perkins Institute of Medical Research (the Perkins) has reached a key milestone in advancing the Perkins WA Comprehensive Cancer Centre in Western Australia. The WA Government has accepted the Perkins’ Strategic Investment Plan (SIP), which outlines the preferred location and activities for the new cancer centre. This plan was endorsed by the Department of Health and delivered last year.
The State Government commended the thorough work done in the SIP, which assessed eight potential service delivery and location options. The cancer centre will be located on the QEIIMC campus, focusing on integrating existing cancer research with clinical care, with a core principle of equity of access.
The centre will include:
• Inpatient services:
» 90 multi-day beds (plus expansion for a further 30 beds)
» 40 same-day beds and chairs including chemotherapy and haematology
» 6-8 intensive care/high dependency beds
• Outpatient services:
» 36 ambulatory care/specialist clinics
» Space for two radiation oncology bunkers
» 4 operating theatres (plus space for 2 further theatres)
» 2 procedure rooms
» 7 imaging services (including CT, MRI and PET)
• Research and education services:
» Expanded clinical trial beds (in addition to the existing 18 beds in Linear Clinical Research)
» Wet lab and dry research spaces
» Function-specific embedded research units
» Cancer tissue biobank
• Cancer Care Coordination Centre (CCCC) providing:
» Care coordination
» Patient navigation
» Patient information services
» Virtual Health services providing support for regional, remote and Aboriginal patients living with cancer, and working with WA Country Health Service (WACHS) Command Centre.
• Other patient support services:
» Urgent review and rapid access service
» Family amenities co-located with multiday beds
» Supporting a transitional palliative care function for high-acuity palliative patients
» Supportive wellness and survivorship services for ongoing care and support
» Research training including for commercialisation
» Underpinned by strong multidisciplinary leadership and a culture of research
With the State Government having approved the Strategic Investment Plan, the Perkins can now finalise the detailed business case which will enable the State Government to make a final funding decision.
“In addition to the world-leading cancer research and treatment it would offer, the Perkins WA Comprehensive Cancer Centre at the QEIIMC could spearhead the State Government’s efforts to turn the broader site into a world-leading Biomedical Precinct,” said The Perkins CEO, Professor Peter Leedman AO.
Perkins Chair, Mr John Barrington AM said the Strategic Investment Plan had been the result of significant effort and that everyone involved can be proud of it, he went on to thank all collaborators.
“We also remain thankful to the Federal Government for maintaining its commitment to the Perkins WA Comprehensive Cancer Centre as it recognises West Australians should not miss out on world-first cancer treatment and care integrated with world leading discovery cancer research that is currently available in the eastern states but not yet available here in WA,” he continued.
The NSW Government has awarded a share of $5 million in grants to 10 researchers as part of the NSW Health Early-Mid Career Grant program.
According to a statement released by NSW Health, this round of the program is focused on advanced therapeutic impact, and awards researchers who are ready to take their career to the next level by building a multi-disciplinary team of expert researchers, clinicians and other key stakeholders.
“The latest round of funding will support research into gene therapy, precision medicine, RNA nanomedicine, advancing therapeutics in osteoporosis, cancers such as melanoma and immunotherapyresistant tumours, and more.”
Minister for Medical Research David Harris said The NSW Government is committed to supporting the best and brightest minds in medical research through this grant program, which aims to keep NSW at the forefront of medical research.
“This round of grants was highly competitive, and I would like to extend my congratulations to the 10 successful recipients and thank all those who applied.
"It is our hope the important work undertaken by these 10 talented researchers, their multi-disciplinary teams and collaborators, will make a real difference to the lives of people living in NSW and across the globe.”
Deputy Lead of the UNSW Pancreatic Cancer Translational Research Group, Dr George Sharbeen is one of the promising health researchers to be awarded a grant.
The statement from NSW Health reads:
“Dr Sharbeen and his expert team of researchers from the University of New South Wales will be testing their new RNA nanomedicine in cutting-edge models of pancreatic cancer.”
“The work includes forcing cancer cells to ‘self-destroy’ and a world-first 3D "tumour-ina-dish" model enabling researchers to grow and treat patient tumour tissue in the lab.”
Dr George Sharbeen said the funding from NSW Health would help develop new and more effective therapies for pancreatic cancer.
“Pancreatic cancer is a deadly disease with less than 13 per cent of patients surviving five years post-diagnosis and is predicted to become the second leading cause of cancerrelated deaths by 2030.”
“UNSW researchers have partnered with the UNSW RNA Institute to develop a new RNA nanomedicine suitable for clinical use, to treat pancreatic cancer by overcoming physical barriers to drug delivery and forcing tumour cells to release a signal to self-destroy.
“We hope that this therapeutic approach will have the potential to increase the survival of patients with pancreatic cancer, while offering a less toxic alternative to current chemotherapies.”
The people of New Zealand have elected their 2025 fish of the year with the blobfish triumphing over its deep sea rival, the orange roughy. Despite a strong start and healthy lead during the first half of the campaign, the orange roughy was ultimately overtaken by the worlds ugliest fish.
The blobfish’s iconic appearance is transformed when seen underwater, they have bulbous heads, large jaws, tapered tails, feathery pectoral fins and loose skin instead of scales. They rely on deep sea water pressure to hold their shape together instead of bones and muscles and when near the surface they collapse into a squishy mush.
The writing was on the waves for the orange roughy once More FM began campaigning for the blobfish. “We and the people of New Zealand had had enough of other fish getting all the headlines. The blobfish had been sitting patiently on the ocean floor, mouth open waiting for the next mollusc to come through to eat. He has been bullied his whole life and we thought, ‘stuff this, it’s time for the blobfish to have his moment in the sun’, and what a glorious moment it is!” say More FM Drive hosts Sarah and Flynny. Orange roughy sponsor Environmental Law initiative was buoyed by the
blobfish win nonetheless. “We have no bloblem with the blobfish winning,” says spokesperson Aaron Packard. “It’s still a win for deep sea ecosystems, and raises awareness about the environmental impacts of destructive bottom trawling.”
The competition drew a lot more attention this year, with 5,583 New Zealanders voting, compared to 1,021 in 2024. “More than ten thousand Kiwis visited the website to learn about freshwater and marine fish that call our waters home,” Mountains to Sea Conservation Trust Co-Director Kim Jones said. “We’re absolutely thrilled New Zealanders have taken such an interest in our native fish, and the conservation challenges affecting them.”
Nine of the ten Fish of the Year Nominees are considered vulnerable by conservation groups, including the blobfish.
“In some ways it was fitting blobfish and orange roughy were close at the end. They both live in deep sea environments close to New Zealand, and the blobfish is often incidentally caught during bottom trawling for orange roughy,” says Jones.
One thing is for certain, New Zealanders have declared that blob is beautiful.
Three cities honoured for public health achievements at 2025 Partnership for Healthy Cities Summit
The annual Partnership for Healthy Cities Summit was held in Paris this month, with three cities being celebrated for their achievements in preventing Non-communicable Diseases (NCDs) and injuries. The event, cohosted by Bloomburg Philanthropies, the World Health Organisation (WHO), Vital Strategies, and the City of Paris, brought together leaders from 61 cities in the global network to discuss effective strategies for saving lives and building healthier communities at the local level.
Córdoba, Argentina – Córdoba was honored for implementing a policy aiming to eliminate sugary and artificially sweetened beverages and ultraprocessed products from all schools by 2026. Currently 26 schools have benefitted from the program – reaching 15 000 of the cities 138 000 primary school children.
Fortaleza, Brazil – Fortaleza received recognition for establishing a legal framework for monitoring air quality. The decree, made in 2023, guarantees the local monitoring of air pollutants and their effects on residents’ health, with the installation of low-cost sensors to allow for the collection of reliable data which will help inform city policies.
Greater Manchester, United Kingdom –Greater Manchester was acknowledged for its efforts to reduce smoking rates by creating more outdoor smoke-free areas. The city opened its first smokefree park, covering 6.5 acres and engaged residents through a series of consultations and workshops on decision making. Additionally, it launched a smoke-free toolkit and communication guidance for NHS hospitals and is developing resources for other organizations and groups who wish to create smoke-free environments.
The Partnership for Healthy Cities is a network of 74 cities committed to
addressing NCDs—such as cancer, diabetes, heart disease, and chronic respiratory illnesses—and injuries through proven interventions. Each city selects one of 15 evidence-based measures to implement locally. The three winning cities are all part of the Partnership’s Policy Accelerator program, which provides training and support to help cities draft policies and develop political strategies for effective implementation.
Michael R. Bloomberg, founder of Bloomberg L.P. and Bloomberg Philanthropies, WHO Global Ambassador for Noncommunicable Diseases and Injuries, and 108th mayor of New York City said Noncommunicable diseases are responsible for more than 80% of all deaths globally, but the good news is, they are preventable.
“Cities are at the forefront of the fight against noncommunicable diseases and injuries. The progress made in Córdoba, Fortaleza, and Greater Manchester is not only improving health today but also setting a model for others to follow,” said WHO Director-General Dr Tedros Adhanom Ghebreyesus. “WHO is committed to working with cities to build healthier, safer and more resilient communities for all.”
“Local leadership has emerged as a powerful force for addressing the complex challenges presented by noncommunicable diseases and injuries,” said Dr Mary-Ann Etiebet, President and CEO, Vital Strategies. “We applaud the work of city leaders around the globe in their efforts to create healthier, safer environments for their populations. Their efforts are having a significant impact on people’s lives and well-being, while also demonstrating to national governments that there is significant support for these policy solutions.”
Launched in 2017, the Partnership aims to improve the health of 300 million people worldwide by reducing the prevalence of NCDs and injuries. Through initiatives like these, cities are demonstrating that strong leadership and evidence-based policies can help save lives and build healthier communities.
The Medicines and Healthcare products Regulatory Agency (MHRA) recently hosted an event in Westminster, London, bringing together key stakeholders to discuss the progress of the seven newly established Centres of Excellence in Regulatory Science and Innovation (CERSIs). The initiative aims to drive advancements in healthcare regulation and innovation, ensuring that new medical technologies and treatments reach patients safely and efficiently.
The event marked the first time that representatives from the MHRA, its funding partners – Innovate UK, the Office for Life Sciences, and the Medical Research Council (MRC) – as well as
government, industry, and academia, convened to hear directly from the CERSI leads. These centres, launched earlier this year, focus on key areas of regulatory science essential to modern healthcare.
Discussions during the event highlighted several critical themes, including:
• AI and MedTech – Ensuring artificial intelligence-driven tools are developed and integrated safely within healthcare systems.
• In silico trials – Exploring new approaches to streamline development while upholding safety standards.
• Pharmacogenomics and diagnostics –Moving healthcare towards prevention.

• Cell and gene therapies – Advancing laboratory approaches to tackle shared challenges in these cutting-edge therapies.
• Modernising manufacture – Leveraging digital tools to enhance the production of medicines and medical devices.
In addition to these focus areas, the event provided a platform to address broader cross-cutting issues:
• Data sharing – Promoting responsible and effective use of health data
• Skills and expertise – Ensuring regulatory scientists are equipped with the knowledge to keep pace with rapid medical advancements.
• Patient and public involvement –Embedding patient perspectives in innovation to shape its impact on healthcare experiences.
The collective impact of the CERSI initiative is set to accelerate the adoption of innovation in healthcare, ultimately benefiting patients by bringing new treatments to market more efficiently.
Keynote addresses were delivered by Science and Innovation Minister Lord Vallance and MHRA Chief Executive Dame June Raine. Emphasizing the importance of regulatory science, Dame June Raine remarked:
“At our CERSIs event this week, the depth of expertise was impressive and there was real excitement about the progress being made. The discussions highlighted a strong commitment to improving access to innovation for patients, shared with our partners Innovate UK, Office of Life Sciences, and the MRC. Through the CERSIs, we have a major opportunity to drive advances in regulatory science in the UK – now is the time to turn that potential into action.”
With continued collaboration and commitment, the CERSIs initiative represents a major step toward shaping the future of regulatory science, ensuring that healthcare innovations translate into tangible benefits for patients across the UK and beyond.

The World Health Organization (WHO) has introduced new guidance to help countries reform mental health policies and services. With mental health services globally underfunded and many people lacking access to care, the initiative aims to build inclusive, rights-based systems.
“Despite rising demand, quality mental health services remain out of reach for many people,” said Dr Tedros Adhanom Ghebreyesus, WHO Director-General.
“This new guidance gives all governments the tools to promote and protect mental health and build systems that serve everyone.”
Unfortunately, most people living with mental health conditions struggle to access the already existing prevention and treatment interventions. WHO aims to ensure mental health is promoted and protected while closing the gaps in access with the following:
• Upholding human rights – Aligning policies with international standards.
• Promoting holistic care – Integrating psychological, social, and economic support.
• Addressing social determinants –Considering employment, housing, and education.
• Implementing prevention strategies – Encouraging population-wide mental health and well-being.
• Empowering individuals with lived experience – Ensuring their involvement in policy design.
WHO has identified five key policy areas requiring urgent reform: leadership and governance, service organization, workforce development, person-centred interventions, and addressing social and structural determinants of mental health.
The guidance provides policymakers with strategic actions to customize mental health reforms based on their country’s specific needs, available resources, and operational frameworks.
Dr Michelle Funk, Unit Head, Policy, Law and Human Rights in the WHO Department for Mental Health and Substance Abuse states: “This new WHO guidance provides practical strategies for countries to build inclusive, responsive and resilient mental health systems. Designed to be flexible, it allows all countries – whether low- middle- or high-income – to adapt their approach to mental health care based on national context, needs, and priorities.”
The guidance has been developed with global experts and individuals with lived experience. It builds on WHO’s QualityRights initiative, promoting a person-centered, recovery-oriented and rights-based approach. The organization will support countries with technical assistance and capacity-building initiatives to ensure better mental health services worldwide.
Share your photos of yourself, your family or your team at work with any of our great ANF products and go in the running to win a range of great prizes.
A selection of the best photos will feature in the next edition of the Western Nurse. All entries must include your name and your membership number to be in the running.
If you think you have a winning photo, you can email your competition entry to us at Western.Nurse@anfiuwp.org.au

Long QT syndrome (LQTS) is a disorder of the heart’s conduction system.1,2 It is named after the distinctive pattern of QT interval prolongation seen on an electrocardiogram (ECG) (see Illustration 1).
The QT interval is defined from the beginning of the Q wave to the end of the T wave. It represents the duration of the ventricular action potential, that is, the time taken from the onset of ventricular depolarisation to the end of ventricular repolarisation.4 The QT interval is effectively the period of ventricular systole from ventricular isovolumetric contraction to isovolumetric relaxation.5
The duration of the ventricular action potential is dependent on the movement of sodium, potassium, and calcium via ion channels in the heart.4,5 Sodium channels are mainly responsible for ventricular depolarisation, calcium channels are important to maintain the plateau phase of the action potential, and potassium channels play a major role in ventricular repolarisation.4
Disturbances in the ion channels can have profound effects on the cardiac action potential.4 Any disturbances that lead to the intracellular accumulation of excess of positive ions will prolong the action potential, leading to QT interval prolongation and LQTS.5
TYPES OF LQTS
LQTS may be congenital or acquired.5,6
Congenital LQTS
Congenital LQTS is usually caused by mutations in three critical ion channels of the heart. Mutations in the genes coding for ion channel proteins results in malfunction, leading to excess intracellular positivity and prolonged QT interval.5 The mutation of 17 genes have been linked to LQTS.6,7
There are 17 subtypes of congenital LQTS based on the affected gene.6,7 Mutations of the genes associated with the subtypes LQT1, LQT2, and LQT3 account for 90-95% of cases where an affected gene has been identified.6 LQT1 is caused by loss-of-function mutations in the KCNQ1 gene, which encodes a potassium channel responsible for the slow component of the delayed rectifier current.6,7 The mutations of this gene lead to dysfunctional channels, resulting in dispersion of repolarisation from the epicardial to the endocardial surface.6 LQT1 accounts for up to 45% of cases of congenital LQTS.7
LQT2 is caused by loss-of-function mutations in the KCNH2 gene, which encodes a potassium channel responsible for the rapid component of the delayed rectifier current.6,7 The mutations of this gene lead to dysfunctional channels, resulting in slowed repolarisation and transmural dispersion of repolarisation.6 LQT2 accounts for 20-40% of cases of congenital LQTS.7
LQT3 is caused by gain-of-function mutations in the SCN5A gene, which encodes for rapidly inactivating sodium channels.6,7 The mutations of this gene allow an inward flow of sodium ions to persist long into the plateau phase of the action potential, prolonging ventricular repolarisation.6 LQT3 accounts for 5-10% of cases of congenital LQTS.7
It is estimated that at least 1 in 2500 people are affected by congenital LQTS worldwide.6
Acquired LQTS is most commonly caused by a reaction to medication.6 More than 100 medicines can prolong the QT interval, or cause depletion of potassium or magnesium leading to a prolonged QT interval.2,6
Other causes of acquired LQTS include:1,4,6
• Bradyarrhythmias
• Coronary artery disease
• Structural heart disease, suchas myocardial infarction and leftventricular hypertrophy
• Electrolyte disturbances, such ashypokalaemia, hypocalcaemia, andhypomagnesaemia
• Hypothermia
• Hypothyroidism
• Central nervous system lesions, suchas ischaemic stroke and intracranialhaemorrhage
• Pheochromocytoma (tumour of theadrenal gland)
• Malnutrition.
The overall incidence of acquired LQTS is not known.6
SIGNS AND SYMPTOMS
The most common symptom of LQTS is syncope.1,5,6 Other symptoms include fast or irregular heartbeats and seizures.1,7
Some types of LQTS are also associated with non-cardiac symptoms.5 For example:2,6
• LQT1, Jervell and Lange-Nielsensyndrome, is associated withsensorineural deafness
• LQT7, Andersen-Tawil syndrome, isassociated with periodic paralysis,ventricular tachyarrhythmias,and dysmorphic features, such asmicrognathia, widely spaced eyes,low-set ears, scoliosis, syndactyly, andclinodactyly
Read this article and complete the quiz to earn: 1 iFolio hour
• LQT8, Timothy syndrome, isassociated with syndactyly, cardiacmalformations, autism, and dysmorphicfeatures.
Some patients with LQTS are asymptomatic.2
Complications
Usually after an episode of QT prolongation the heart returns to a normal rhythm.1 However, LQTS can lead to serious episodes of arrhythmias, such as Torsades de Pointes and ventricular fibrillation, cardiac arrest, or sudden cardiac death.2-4
LQTS is diagnosed using a combination of preliminary clinical assessment, including medical history, family history and physical examination, and electrocardiogram (ECG).2,6,7
LQTS is diagnosed by ECG showing prolongation of the corrected QT interval (QTc).1,2,6
The QTc is used as the QT interval is affected by heart rate (the QT interval shortens at faster heart rates and lengthens at slower heart rates).3,6 The QTc estimates the QT interval at a standard heart rate of 60 beats per minute.4 The QT interval is prolonged if the QTc is more than 440ms in men or more than 460ms in women.3
An exercise stress ECG to identify QT interval prolongation during exercise and recovery or Holter monitoring to detect intermittent QT prolongation may be required for some patients.2,6,7
Genetic testing to identify specific gene mutations is recommended for all patients with a high probability of congenital LQTS.2,6
The goal of treatment for LQTS is the prevention of syncope, lethal arrhythmias, and sudden cardiac death.5,8
Congenital LQTS
The mainstay treatment for congenital LQTS is lifestyle modification and beta-blocker therapy.6 For some patients, placement of an implantable cardioverter defibrillator (ICD) may also be recommended.5,6,8
Lifestyle modification
In general, patients with congenital LQTS should avoid competitive sports or activities with similar extreme exertion.6
It is also important for patients with particular subtypes of congenital LQTS to avoid activities that increase sympathetic activation. For LQT1 it may include activities such as swimming, emotional stress, and exercise,
LQTS is diagnosed using a combination of preliminary clinical assessment, including medical history, family history and physical examination, and electrocardiogram (ECG).2,6,7
LQTS is diagnosed by ECG showing prolongation of the corrected QT interval (QTc).1,2,6
and patients with LQT2 are at high risk when woken from sleep or disturbed by a sudden noise.6
Beta-blockers
Beta-blockers help prevent ventricular arrhythmias in patients with congenital LQTS by stabilising ventricular action potential and inhibiting sympathetic surges associated with arrhythmias.5
Implantable cardioverter defibrillator
The QTc is used as the QT interval is affected by heart rate (the QT interval shortens at faster heart rates and lengthens at slower heart rates).3,6 The QTc estimates the QT interval at a standard heart rate of 60 beats per minute.4 The QT interval is prolonged if the QTc is more than 440ms in men or more than 460ms in women.3
An ICD is recommended for patients with congenital LQTS who have:5,6,8
• Experienced a previous a cardiac arrest
• Recurrent arrhythmic syncope or documented Torsades de Pointes despite optimally dosed beta-blocker therapy
• Contraindications to beta-blockers
An exercise stress ECG to identify QT interval prolongation during exercise and recovery or Holter monitoring to detect intermittent QT prolongation may be required for some patients.2,6,7
• Jervell and Lange-Nielsen syndrome.
Acquired LQTS
The cornerstone in treating patients with acquired LQTS is identifying and addressing the underlying cause of QT prolongation. This involves a comprehensive medication history to identify and cease the use of medications known to prolong the QT interval or cause the depletion of potassium or magnesium, as well as measuring serum electrolytes and correcting any electrolyte disturbances, such as hypokalaemia, hypocalcaemia, or hypomagnesaemia.6
Genetic testing to identify specific gene mutations is recommended for all patients with a high probability of congenital LQTS.2,6
The goal of treatment for LQTS is the prevention of syncope, lethal arrhythmias, and sudden cardiac death.5,8
Congenital LQTS
The mainstay treatment for congenital LQTS is lifestyle modification and beta-blocker therapy.6 For some patients, placement of an implantable cardioverter defibrillator (ICD) may also be
Lifestyle modification
In general, patients with congenital LQTS should avoid competitive sports or activities with similar extreme exertion. 6
It is also important for patients with particular subtypes of congenital LQTS to avoid activities that increase sympathetic activation. For LQT1 it may include activities such as swimming, emotional stress, and exercise, and patients with LQT2 are at high risk when woken from sleep or disturbed by a sudden noise. 6
1. Mayo Clinic. Mayo Clinic Health Information [Internet]. Long QT syndrome; 2024 [cited 2024 Jul 10]. Available from: https://www.mayoclinic.org/diseasesconditions/long-qt-syndrome
Beta-blockers
electrolytes and correcting any electrolyte disturbances, such as hypokalaemia, hypocalcaemia, or hypomagnesaemia. 6
1. Mayo Clinic. Mayo Clinic Health Information [Internet]. Long QT syndrome; 2024 [cited 2024 Jul 10]. Available from: https://www. mayoclinic.org/diseases-conditions/long-qtsyndrome
2. National Institutes of Health. National Heart, Lung, and Blood Institute Health Topics [Internet]. Long QT Syndrome; 2024 [cited 2024 Jul 10]. Available from: https://www. nhlbi.nih.gov/health/long-qt-syndrome
6. Ackerman MJ, Schwartz PJ. Congenital long QT syndrome: Pathophysiology and genetics. 2022 [cited 2024 Jul 10]. In: UpToDate [Internet]. Waltham (MA): UpToDate Inc. Available from: https:// www.uptodate.com/contents/congenitallong-qt-syndrome-pathophysiology-andgenetics
Beta-blockers help prevent ventricular arrhythmias in patients with congenital LQTS by stabilising ventricular action potential and inhibiting sympathetic surges associated with arrhythmias. 5
2. National Institutes of Health. National Heart, Lung, and Blood Institute Health Topics [Internet]. Long QT Syndrome; 2024 [cited 2024 Jul 10]. Available from: https://www.nhlbi.nih.gov/health/long-qtsyndrome
Implantable cardioverter defibrillator
3. Khatib R, Sabir FR, Omari C, Pepper C, Tayebjee MH. Managing drug-induced QT prolongation in clinical practice. Postgrad Med J [Internet]. 2021 [cited 2024 Jul 10];97(1149):452-458. doi: 10.1136/postgradmedj-2020-138661
4. Al-Akchar M, Siddique MS. Long QT Syndrome. 2022 [cited 2024 Jul 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing LLC. Available from: https://www. ncbi.nlm.nih.gov/books/NBK441860
7. Schwartz PJ, Ackerman MJ. Congenital long QT syndrome: Diagnosis. 2024 [cited 2024 Jul 10]. In: UpToDate [Internet]. Waltham (MA): UpToDate Inc. Available from: https://www.uptodate.com/ contents/congenital-long-qt-syndromediagnosis
An ICD is recommended for patients with congenital LQTS who have:5,6,8
• Experienced a previous a cardiac arrest
3. Khatib R, Sabir FR, Omari C, Pepper C, Tayebjee MH. Managing drug-induced QT prolongation in clinical practice. Postgrad Med J [Internet]. 2021 [cited 2024 Jul 10];97(1149):452-458. doi: 10.1136/ postgradmedj-2020-138661
• Recurrent arrhythmic syncope or documented Torsades de Pointes despite optimally dosed beta-blocker therapy
4. Al-Akchar M, Siddique MS. Long QT Syndrome. 2022 [cited 2024 Jul 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing LLC. Available from: https://www.ncbi.nlm.nih.gov/books/ NBK441860
• Contraindications to beta-blockers
• Jervell and Lange-Nielsen syndrome.
Acquired LQTS
5. BMJ Best Practice. Long QT syndrome [Internet]. London: BMJ Publishing Group Ltd; 2023 [cited 2024 Jul 10]. Available from: https://bestpractice.bmj.com/topics/ en-gb/829/pdf/829/Long%20QT%20 syndrome.pdf
The cornerstone in treating patients with acquired LQTS is identifying and addressing the underlying cause of QT prolongation. This involves a comprehensive medication history to identify and cease the use of medications known to prolong the QT
5. BMJ Best Practice. Long QT syndrome [Internet]. London: BMJ Publishing Group Ltd; 2023 [cited 2024 Jul 10]. Available from: https://bestpractice.bmj.com/topics/engb/829/pdf/829/Long%20QT%20syndrome. pdf
8. Schwartz PJ, Ackerman MJ. Congenital long QT syndrome: Treatment. 2022 [cited 2024 Jul 10]. In: UpToDate [Internet]. Waltham (MA): UpToDate Inc. Available from: https://www.uptodate.com/ contents/congenital-long-qt-syndrometreatment
6. Ackerman MJ, Schwartz PJ. Congenital long QT syndrome: Pathophysiology and genetics. 2022 [cited 2024 Jul 10]. In: UpToDate [Internet]. Waltham (MA): UpToDate Inc. Available from: https://www.uptodate.com/ contents/congenital-long-qt-syndromepathophysiology-and-genetics
7. Schwartz PJ, Ackerman MJ. Congenital long QT syndrome: Diagnosis. 2024 [cited 2024 Jul 10]. In: UpToDate [Internet]. Waltham (MA): UpToDate Inc. Available from: https://www. uptodate.com/contents/congenital-long-qtsyndrome-diagnosis
8. Schwartz PJ, Ackerman MJ. Congenital long QT syndrome: Treatment. 2022 [cited 2024 Jul 10]. In: UpToDate [Internet]. Waltham (MA): UpToDate Inc. Available from: https://www.

1 Food items such as chickpeas or kidney beans that provide protein and fibre (6)
5 Foot part that allows the foot to support the weight of the body (4)
9 --- Aviv, Israeli city (3)
10 Plant seed (5)
11 Evening meal (6)
13 Is not (contraction) (3’1)
15 French father (4)
16 Condition in which the corner or side of a foot cuticle grows into the flesh (7,7)
20 Against, opposed to (4)
22 Sugary treats (6)
24 Bonus (5)
25 Group of long, thin fibres that carry instructions or information from the brain to other body parts (5)
27 Care and protect a child as they are growing up (7)
28 Images (5)
30 Mexican flowering plant (5)
31 Devices for holding objects or parts together (6)
33 Deserve (4)
35 Range of nonverbal signals that you can use to communicate your feelings and intentions (4,8)
39 The M of BMI (4)
41 Largest organ of the body (4)
42 Leg/foot joints (6)
45 Remove hair with a razor (5)
46 Young goat (3)
47 Binds (4)
48 Causes to feel numb (6)
1 Liquid in infected tissue (3)
2 Mouth part (3)
3 Drinking tube (5)
4 --- palate, openings or splits in the roof of the mouth (5)
5 Not dead (5)
6 Feverish (3)
7 Physically unable to speak (4)
8 Type of asthma inhaler (8)
12 Footed vases (4)
14 Approaches (5)
15 Location (5)
17 Vital body parts such as the liver or heart (6)
18 Nose opening (7)
19 Lyrical poem (3)
21 --- von Bismarck, German chancellor (4)
23 Act of betraying one’s country (7)
24 Outer layer of 41 Across (10)
25 Capital of the Bahamas (6)
26 Temporary outbreak of red, bumpy, scaly or itchy patches on the body (4)
29 Religious sister (3)
31 Criminal (5)
32 Spanish sun (3)
34 Basic unit of hereditary (4)
36 Tugs, pulls (5)
37 Amino ---, protein forming molecules (5)
38 Endocrine, eg (5)
40 Mark left after a wound has healed (3)
41 Become firm (3)
43 Showed the way (3)
44 Male offspring (3)











