Free Education from the Education Universe and the ACG Annual Scientific Meeting that keeps you current on treatment, therapy and management of key GI conditions and disorders
Free Education from the Education Universe and the ACG Annual Scientific Meeting that keeps you current on treatment, therapy and management of key GI conditions and disorders
Free subscriptions to The American Journal of Gastroenterology, Clinical and Translational Gastroenterology, EvidenceBased GI: An ACG Publication and the unique ACG Case Reports Journal
Free subscriptions to The American Journal of Gastroenterology, Clinical and Translational Gastroenterology, EvidenceBased GI: An ACG Publication and the unique ACG Case Reports Journal
Practice management tools that help you improve efficiency and increase profitability in your practice
Practice management tools that help you improve efficiency and increase profitability in your practice
Prior Authorization Letter Generator gives members access to custom letters with relevant data and research that payors are requesting
Prior Authorization Letter Generator gives members access to custom letters with relevant data and research that payors are requesting
Leadership Training offers members Leadership YOU a weekend that brings together a community of established and emerging leaders to cultivate core competencies that drive effectiveness and impact
Leadership Training offers members Leadership YOU a weekend that brings together a community of established and emerging leaders to cultivate core competencies that drive effectiveness and impact
Tips from Dr. Patrick Young on how to be the best mentor (and mentee) you can be.
ACG MAGAZINE
MAGAZINE STAFF
Executive Director
Bradley C. Stillman, JD
Editor-in-Chief | Vice President, Communications
Brian C. Davis
Managing Editor | Senior Manager, Communications
Becky Abel
Art Director Emily Garel
BOARD OF TRUSTEES
President: William D. Chey, MD, MACG
President-Elect: Costas H. Kefalas, MD, MMM, MS-PopH, FACG
Vice President: Nicholas J. Shaheen, MD, MPH, MACG
Secretary: Jean-Paul Achkar, MD, FACG
Treasurer: Neil H. Stollman, MD, FACG
Immediate Past President: Amy S. Oxentenko, MD, MACG
Past President: Jonathan A. Leighton, MD, MACG
Director, ACG Institute: Neena S. Abraham, MD, MSc, MACG
Co-Editors, The American Journal of Gastroenterology:
Jasmohan S. Bajaj, MD, MS, FACG
Millie D. Long, MD, MPH, FACG
Chair, Board of Governors: Sita S. Chokhavatia, MD, MACG
Vice Chair, Board of Governors: Harish K. Gagneja, MD, MACG
Trustee for Administrative Affairs: Sunanda V. Kane, MD, MSPH, MACG
We'd love to hear from you. Send us your ideas, stories, and comments. ACGMag@gi.org
CONTACT ACG
American College of Gastroenterology 11333 Woodglen Drive, Suite 100 North Bethesda, MD 20852 (301) 263-9000 | gi.org
DIGITAL EDITIONS
American College of Gastroenterology is an organization with an international membership of over 21,000 individuals from 86 countries. The College's vision is to be the preeminent organization supporting health care professionals who provide compassionate, equitable, high-quality, state-of-the-art, and personalized care to promote digestive health. The mission of the College is to provide tools, services, and accelerate advances in patient care, education, research, advocacy, practice management, professional development, and clinician wellness, enabling our members to improve patients’ digestive health and to build personally fulfilling careers that foster wellbeing, meaning, and purpose.
CONTENTS
“It’s not enough to treat injuries; we must foster environments where individuals, families, and communities are equipped with the knowledge and tools to prevent violence before it occurs.”
—DR. CHRISTINA AWAD: MY GLOBAL JOURNEY IN VIOLENCE PREVENTION AND COMMUNITY EMPOWERMENT, PG 15
4 // MESSAGE FROM THE PRESIDENT
In his first message as ACG President, Dr. William Chey discusses his focus on elevating GI education and fostering innovation
6 // NOVEL & NOTEWORTHY
Recapping ACG 2025 awards, new ACG books, a podcast with ACG leadership, and more
8 // PATIENTS
COVID-19 Vaccination: What You Should Know
11 // ACG PERSPECTIVES
11 DANCING THROUGH THE DEMANDS
How dance helped Dr. Sumana Kumarappa focus on wellness, joy, and preventing burnout
13 INTERNATIONAL TRAINING GRANT
Dr. Coşkun Demirtaş reflects on his training experience at Yale University
15 PREVENTING VIOLENCE, EMPOWERING COMMUNITIES
Dr. Christina Awad shares her international service in violence prevention and community empowerment
18 // COVER STORY
MAXIMIZING MENTORSHIP
Dr. Patrick Young with tips for being the best mentor (and mentee) you can be
25 // TRAINEE HUB
CHOOSING A NON-ACGME FELLOWSHIP
Timing, pathways, and considerations by Dr. Eleazar Montalvan-Sanchez
29 // GETTING IT RIGHT
LAW MIND
What you need to know about private equity deals, by Ann Bittinger, Esq.
33 // INSIDE THE JOURNALS
AJG
Recent clinical guidance in the Red Journal: Global Consensus Statement on the Management of Pregnancy in IBD, Perioperative Risk Assessment and Management in Patients with Cirrhosis, and the ACG Monograph on Geriatrics & GI
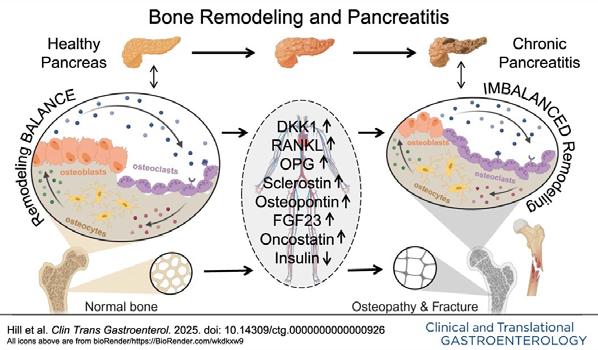
CTG
Circulating Molecular Drivers of Bone Remodeling in Pancreatitis by Hill, et al
ACGCRJ
Introducing the 2025–2026 Editorial Board, led by co-EICs Dr. Daniyal Abbas and Dr. Dushant Dahiya
37 ACG GUIDELINE HIGHLIGHTS
Ulcerative Colitis in Adults (June 2025)
38 ACG GUIDELINE HIGHLIGHTS
Malnutrition and Nutritional Recommendations in Liver Disease (May 2025)
ELEVATING GI EDUCATION & FOSTERING INNOVATION
William D. Chey, MD, MACG
I am humbled and grateful for the opportunity to serve as President of the American College of Gastroenterology. It is indeed a once-ina-lifetime opportunity to give back to an organization that has given so much to me, both professionally and personally.
As I start my presidential year, I want to thank the leaders and members of the College for having the confidence to indulge me the opportunity to lead the College for the next 12 months. I want to thank the Presidents who I have worked with during my 15 years on the Board of Trustees. Each has taught me about leadership, integrity, and serving our members and profession. I offer special thanks to Brad Stillman, Dr. Amy Oxentenko, Dr. Jonathan Leighton, Dr. Dan Pambianco, Dr. David Greenwald, and Dr. Irving Pike for helping to prepare me for this year and Dr. Costas Kefalas, Dr. Nick Shaheen, Dr. Neil Stollman, and the entire Board of Trustees for their support and guidance in the year to come.
I recently came to the realization that while it took many years to become ACG President, my time as President will come and go in the blink of an eye. As for my agenda—I plan to commission two task forces to explore how best to serve the educational needs of our members and how the ACG can best support and participate in medical innovation.
Our recently updated ACG Strategic Plan (gi.org/about/ governance/#strategic) identified education as a founding principle and key priority of ACG. The College has provided high-value education in digestive diseases for many decades. I see a chance for us to explore beyond traditional meetings and lectures and hybrid and hands-on learning opportunities. What opportunities exist in modern education concepts, such as personalized and adaptive learning, and new technologies, including virtual
and augmented reality to teach providerpatient communication skills or to help facilitate training in endoscopy? The other reality is that APPs are one of the fastestgrowing segments of the membership and likely have different educational needs. With this in mind, I plan to commission the ACG Education Task Force, which will:
1. Inventory our current education assets.
2. Identify gaps in our current teaching materials library.
3. Review the ways in which we provide education and ensure these methods are aligned with current medical education best practices.
4. Determine whether our education is meeting the diverse needs of the membership, from older vs. younger learners, learners from urban vs. rural settings, and MDs vs. APPs vs. RDNs vs. psychologists.
5. Identify the best way to assess ACG education’s impact on quality of care.
The ACG Education Task Force will prioritize its findings and make recommendations to the Board of Trustees on how best to address the highest-priority issues.
One of the most enjoyable and rewarding aspects of my career has been developing as a medical innovator. I have never had a shortage of ideas but for many years, I didn’t realize that those ideas could be more than just ideas. I am fortunate to be surrounded by many successful inventors and institutional infrastructure to support medical innovation at the University of Michigan. I have a number of patents and though most of my inventions have never made it to market, the “failures” have created the opportunity to learn about the innovation process and the “dos and don’ts” that can mean the difference between success and failure. One thing that I have learned is that having a good or even a great idea is not enough to be successful. There are so many ways that a very good idea can fail—it takes time, patience, and a village to succeed. We live in an unprecedented time in GI and hepatology—opportunities for
new devices, pharmaceuticals, digital therapeutics, and personalized medicine are, in the age of artificial intelligence, not even limited by our imaginations.
I plan to commission the ACG Medical Innovation Task Force—to be comprised of successful medical innovators from academics, private practice, and industry— and investors who will:
1. Review the innovation process and understand the key elements of successful inventions in GI and hepatology and the most common causes of failure.
2. Understand what other GI and non-GI societies are doing to participate in medical innovation and what has worked and what hasn’t worked.
3. Itemize and prioritize the ways in which ACG might participate in medical innovation.
4. Suggest how success might be measured.
5. Estimate the resources needed to stand up and sustain a medical innovation program.
Armed with this information, the ACG can become the home of medical innovation for clinical gastroenterologists. I started this discussion by acknowledging that my time as President will be short. I have always worried that the one-year term necessarily limits the types of projects that can be undertaken. In the hopes of encouraging a more blue skies mentality and creating the possibility of taking on larger, potentially transformative projects that will necessarily take more than a year to accomplish, I am initiating quarterly meetings with the other members of the Executive Leadership Team. These meetings will offer an opportunity to unlock our collective experiences and wisdom and allow us to think more strategically over a three-tofive-year time horizon. They will also create a more intentional runway for the next in line to take off in search of their own blue skies. We hope that this new process will allow the officers to better serve the College and ultimately, for the College to better serve its members.
Finally, I would be remiss if I failed to acknowledge the hard work and unwavering support provided by the entire ACG staff, with special props to Maria Susano, Meridith Phillips, Elaine McCubbin, Brad Conway, and Mario Scherhaufer. To all of them, I offer my heartfelt admiration and appreciation. At the end of the day, ACG is, above all else, my professional family and it is indeed an honor to sit at the head of the table for the coming year.
—Bill
JANUARY 30-FEBRUARY 1, 2026
MANDALAY BAY • LAS VEGAS, NEVADA
& NOTEWORTHY
[GUT
TALK]
Gut Talk Podcast with Dr. Chey and Dr. Oxentenko
ACG President William D. Chey, MD, MACG, and Immediate Past President Amy S. Oxentenko, MD, MACP, MACG, discuss Dr. Oxentenko’s experiences as ACG President and preview ACG 2025 during a recent Gut Talk podcast, published by Healio.
Listen to the conversation: bit.ly/gut-talk-podcast
Gut Talk, co-hosted by Dr. Chey and Sameer K. Berry, MD, MBA, explores the impact of health policy, technology, practice management, and research in gastroenterology.
[ON OUR SHELF]
Guide to the Guidelines, Vol. 3 launched at ACG 2025, completing the set of three books by co-authors Brennan Spiegel, MD, MSHS, FACG, and Hetal A. Karsan, MD, FACG. Volume 3 focuses on pancreaticobiliary and liver topics, complete with vignettes and author commentary providing practical application of the guideline recommendations.
Capsule Endoscopy by Case Study, Vol. 2 presents video capsule endoscopy (VCE) studies expertly curated by Daniel L. Raines, MD, FACG, reflecting advancements in capsule technology and the evolving understanding of small bowel disease. This case-based approach equips readers with essential interpretive skills for VCE and a comprehensive knowledge base in small bowel pathology. Each case is accompanied by expert commentary to aid in interpretation and clinical insight.
Both books (and more) are available in the ACG Store: members.gi.org/store
[BLAZING TRAILS]
New in 2025, the ACG Trailblazer Lecture recognizes a distinguished individual in the field of medicine, gastroenterology, or hepatology who has done groundbreaking work and is recognized as a pioneer in the field or in the life of the College. The inaugural lecture, “The Workforce of the Past and Present—Building Bridges Over Ever-Changing Waters for the Workforce of the Future,” was delivered by ACG’s first woman Trustee, Rosemarie L. Fisher, MD, MACG.
[TRAINEES ONLY]
ACG 2025 included many opportunities for trainees to connect and learn. The Fellows’ Fireside Chat featured professional and personal guidance from established GI leaders: ACG Trustees Dayna S. Early, MD, FACG, and Patrick E. Young, MD, MACG, as well as ACG Past Presidents Samir A. Shah, MD, MACG, and Lawrence R. Schiller, MD, MACG.
[CHAMPIONS]
Third-year fellow Ali Wakil, MD, and second-year fellow Oleksandr Shumeiko, MD, claimed the EndoTitans cup this year, demonstrating their speed and accuracy in the skills challenge.
The crowd-favorite GI Jeopardy concluded with two new champs representing the University of Missouri Columbia. Well done, Islam Mohamed, MD, and Mahmoud Mansour, MD!
[SCOPY AWARDS]
The 11th Annual SCOPY AWARDS recognized 26 applicants for their creative and impactful approaches to CRC awareness and prevention. These select projects may inspire your own March 2026 CRC Awareness Month activities!
Loving Your Guts: A Campaign to Improve the Colon Health of Our Community
Michelle L. Hughes, MD, FACG & Anne Mongiu, MD, PhD, FACS, FASCRS
A free virtual cooking class paired with recipes designed to highlight foods with colon health benefits.
A Single-Center, Nonrandomized Single Arm Investigation to Assess Colorectal Cancer Screening Rates Among Incarcerated Patients
FIT test distribution and follow-up colonoscopy for incarcerated individuals at Rikers Island.
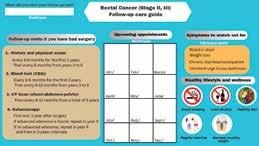
A Pilot Study to Develop a Follow-Up Care Guide for Colorectal Cancer Survivors
Pan African Organization for Health Education and Research
A follow-up care guide, tailored to colorectal cancer type, stage, and whether patients have had surgery. Pictured: Akwi W. Asombang, MD, MPH, FACG
Learn more about this year’s winning projects: gi.org/SCOPY
[DISRUPTIVE INNOVATORS]
CONGRATULATIONS to ACG Immediate Past President Amy S. Oxentenko, MD, MACP, MACG, and Bincy P. Abraham, MD, MS, FACG, for earning the Healio Lifetime Disruptor and Clinical Innovation awards, respectively, at the eighth annual Healio Disruptive Innovators Awards.
The Healio Lifetime Disruptor is awarded to a gastroenterologist or hepatologist who consistently elevated their field through innovative treatment, practice management, patient care, or research. ACG and Healio partner on the Clinical Innovation award, which is presented to a physician or institution that changed the face of the everyday gastroenterology practice, representing the core value of advancement.
The awards ceremony was held on October 26, 2025, in Phoenix, AZ, in conjunction with ACG 2025. More than 3,500 Healio readers cast their votes to determine the winners of the nine awards.
COVID-19 VACCINATION:
What You Should Know
Information from the American College of Gastroenterology & Current Centers for Disease Control and Prevention (CDC) Recommendations
The CDC recommends discussing COVID-19 vaccination for:
Adults aged 65 YEARS AND OLDER (discuss risks and benefits)
People ages SIX MONTHS TO 64 YEARS (shared decision-making)
Why Consider Vaccination?
COVID-19 can cause serious and long-lasting problems. One in five people ages 18–64 and one in four people aged 65 and older experience symptoms lasting months or years. These post-COVID conditions can affect the heart, lungs, digestive system, and brain.
ACG Recommendations for High-Risk Patients
The American College of Gastroenterology strongly recommends COVID-19 vaccination for:
• Individuals with inflammatory bowel disease (IBD), including Crohn's disease, ulcerative colitis, and pregnant women with IBD
• Liver transplant recipients: Talk to your transplant team about timing
• People with chronic liver disease, including cirrhosis and chronic hepatitis
• Adults aged 65 years and older: This group accounts for 70% of COVID-19 hospitalizations
Is the Vaccine Safe?
Yes. COVID-19 vaccines have been given safely to hundreds of millions of people. Vaccines do not worsen IBD or other digestive conditions. Serious side effects are rare, and the benefits of vaccination significantly outweigh the potential risks.
What Should You Do?
Talk to your gastroenterologist or primary care doctor about getting vaccinated. Your doctor understands your health situation and can help you make the best decision.
Dancing Through
the Demands
A Gastroenterologist’s Perspective on Wellness, Joy, and Preventing Burnout
By Sumana Kumarappa, MD
AS PHYSICIANS, WE LIVE AND WORK IN HIGH-STAKES ENVIRONMENTS—where our time, energy, and emotional reserves are constantly stretched. Like many of you, I entered medicine out of a deep sense of purpose. As a gastroenterologist, I find meaning in every patient interaction, every procedure, every moment of healing. But over time, I began to feel what many of us eventually do: the quiet creep of burnout. There were days when I felt like I was just moving through the motions— efficient and focused, but disconnected from joy. The emotional toll was subtle but persistent. I’d come home physically drained, mentally foggy, and somehow
still thinking about patients long after I left the hospital. It made me realize something had to change. I needed something that filled me back up.
And I found it through dance.
Dance has always been a part of my life, but recently it has evolved into something more than a hobby. It’s become therapy, expression, and joy—all rolled into one. What makes it even more special is that I share it with my daughter. We don’t just dance in the living room—though we love those spontaneous sessions—we also perform together with dance teams, rehearse regularly, and even film creative dance videos. It’s become a shared rhythm, a beautiful bond that keeps us both grounded.
In those moments, I’m not “Dr. so-andso.” I’m not thinking about consults, lab results, or my inbox. I’m fully present—with my daughter, with the music, with myself.
That space we create through dance has become sacred. It’s where I find energy again. It’s where I remember who I am outside of my professional role.
These moments are not just fun— they’re deeply restorative. After a week of complex procedures and emotional cases, a few hours of dancing can bring me back to myself. It reminds me that wellness isn’t about escaping the work, but about finding something that fills you up alongside it.
Sharing this joy with my daughter has been especially meaningful. She sees that her mom can care deeply for patients and carve out time for creative passion. She sees that joy and discipline don’t have to be separate. We learn from each other—she brings spontaneity, I bring structure, and together we create something that feeds both of our souls.
This connection to dance has made me a better physician. When I take care of myself, I show up more fully for others. I’m more present, more empathetic, and more attuned to my patients. It’s a reminder that we can't pour from an empty cup. Physician wellness isn’t a luxury—it’s a necessity.
I know how easy it is to push selfcare to the side. We delay hobbies, postpone rest, and convince ourselves we’ll get to it “after the next shift,” “once this stretch is over,” or “when things slow down.” But things rarely slow down. And we don’t need to earn joy—we need to claim it.
Wellness doesn’t have to mean taking weeks off or making drastic life changes. It can be small, meaningful investments in the things that light you up. Whether it’s painting, hiking, writing, or dancing—find the rhythm
that brings you back to yourself. And make space for it, unapologetically. We hear a lot about work-life balance, but I’ve started to think of it more as life rhythm. Dance gave me that rhythm—something steady and joyful to return to. It’s not about balancing everything perfectly. It’s about creating space for things that matter outside of medicine so we can keep thriving within it.
To my fellow physicians: if you’re feeling stretched thin, I see you. If you’re running on fumes, I’ve been there. You deserve to feel whole—not just as a caregiver, but as a human being. Find what recharges you, and don’t let go of it. That thing—your joy, your creative outlet, your passion—is not a distraction. It’s your medicine.
For me, wellness looks like spinning under stage lights, filming a dance video with my daughter, and remembering that I’m more than my white coat. And that joy? That joy is what sustains the healer.
“To my fellow physicians: if you’re feeling stretched thin, I see you. If you’re running on fumes, I’ve been there. You deserve to feel whole—not just as a caregiver, but as a human being. Find what recharges you, and don’t let go of it.”
Dr. Kumarappa practices at Austin Gastroenterology in Leander and Round Rock, TX.
EXPANDING GLOBAL HORIZONS
in Hepatology through the ACG International Training Grant at Yale University
By Coşkun Demirtaş, MD
LIVER DISEASES REMAIN A MAJOR GLOBAL HEALTH BURDEN, and with advancing tools in hepatology and an expanding network of international collaboration, we are better equipped than ever to meet these challenges. My clinical and research interests in portal hypertension and hepatocellular carcinoma (HCC) led me to seek specialized training opportunities that could build a bridge between academic excellence in the U.S. and ongoing work in Europe. I was honored to be selected as a 2024 recipient of the American College of Gastroenterology (ACG) International GI Training Grant, which made possible a research and clinical training program at the Yale University Liver Unit and Section of Digestive Diseases. I engaged in both
“These rotations offered an in-depth perspective on complex liver disease management and emphasized the value of multidisciplinary, integrated care in patients with advanced liver disease.”
academic and bedside activities, which expanded my clinical acumen and helped establish lasting collaborative ties.
During my training, I participated in daily GI rounds and rotated through the Klatskin Inpatient Hepatology Service and Medical Intensive Care Unit, where I had firsthand exposure to multidisciplinary liver disease management. These rotations offered an in-depth perspective on complex liver disease management and emphasized the value of multidisciplinary, integrated care in patients with advanced liver disease. The research experience was particularly transformative. Together with investigators from Yale and partner centers in Spain, France, and
“The research experience was particularly transformative...we launched an international, multicenter collaborative project to explore the usefulness of liver stiffness measurement in predicting hepatic venous pressure gradient in patients with HCC.”
Romania, we launched an international, multicenter collaborative project to explore the usefulness of liver stiffness measurement in predicting hepatic venous pressure gradient in patients with HCC. We successfully developed the study protocol and completed data collection, with plans to publish an original article in the upcoming year.
In addition to multicenter collaboration, I was involved in several research initiatives based at Yale and the affiliated Veterans Affairs Medical Center. These projects laid the foundation for an ongoing collaboration with Yale, and I am thrilled to continue our work as an Adjunct Assistant Professor at Yale University.
This remarkable opportunity would not have been possible without the ACG and its International Training Grant program. I am deeply grateful to the ACG International Relations Committee for its vision in promoting global medical education. My sincere thanks also go to my mentor, Professor Guadalupe Garcia-Tsao, whose leadership, generosity, and guidance were instrumental to the success of my training program. I am also profoundly grateful to Professor Tamar Taddei, whose support made my time at Yale both productive and enjoyable.
I look forward to the future with renewed enthusiasm, expanded knowledge, and strong academic partnerships that I believe will help shape the next chapter of my work in hepatology.
Dr. Demirtas is Director of the Gastroenterology Institute, Marmara University, Istanbul, Turkey, and Adjunct Assistant Professor, Yale University, New Haven, CT.
MY GLOBAL JOURNEY IN VIOLENCE PREVENTION AND COMMUNITY EMPOWERMENT
By Christina Awad, MD
FROM THE EARLIEST DAYS OF MY CAREER, I have held the fundamental belief that health and safety are universal human rights. As an immigrant, I developed a resilient work ethic that has driven my dedication to service and helping others.
Growing up in Egypt, I witnessed first hand the societal challenges surrounding women’s health and safety, including the high prevalence of female genital mutilation (FGM) in many communities. These early experiences left a lasting impression on me—shaping my awareness of how deeply cultural practices, gender norms, and limited access to education can intersect to harm women and girls. Seeing the emotional and physical trauma endured by many ignited my lifelong passion for violence prevention and intervention. It instilled in me a commitment to advocate for culturally sensitive, community-driven approaches that empower women, protect their dignity, and promote systemic change.
These formative experiences taught me that resilience is rooted in community, and that lasting change
often begins with education, empowerment, and culturally sensitive intervention. My journey into global health and violence prevention was fueled by a desire to create foundational shifts in communities that often faced systemic barriers. I realized quickly that violence—whether interpersonal or community based—is a major contributor to disease, mental health issues, socioeconomic disparities, and cycles of trauma that can span generations. Addressing these deep-rooted issues requires a multifaceted approach: engaging communities, training local providers, designing infrastructure, and fostering leadership from within.
Sex-based violence is insidious— claiming lives prematurely, impairing mental health, disrupting social cohesion, and perpetuating cycles of poverty and injustice. Its impacts are felt across all regions, but especially in resource-limited settings where healthcare systems are often overwhelmed and support services are scarce. Addressing violence isn’t just about responding to emergencies; it’s about prevention, education, and building resilient communities.
In my view, effective violence prevention integrates social, psychological, and health
pathways—meaning that collaboration is critical. It’s not enough to treat injuries; we must foster environments where individuals, families, and communities are equipped with the knowledge and tools to prevent violence before it occurs. This belief has shaped my approach—working closely with local partners, tailoring interventions culturally, and empowering communities to be active stakeholders in their safety and well-being.
My most comprehensive work in violence prevention was in Morocco, where we structured a multi-phase, sustainable initiative aimed at reducing violence and fostering community safety. The project unfolded in three fundamental phases, each building upon the last, culminating in a train-the-trainer model designed for lasting impact.
The first two phases involved extensive community engagement to understand the local context— collaborating with embassy officials, educators, and community leaders to identify gaps and intervention needs. This participatory approach uncovered critical insights: cultural
“I realized quickly that violence—whether interpersonal or community based—is a major contributor to disease, mental health issues, socioeconomic disparities, and cycles of trauma that can span generations.”
norms, economic stressors, and resource gaps that fueled cycles of violence and trauma. Armed with this knowledge, we developed culturally tailored training modules on early identification, de-escalation, trauma-informed care, and youth engagement. We ran workshops with community health workers, educators, and local leaders, equipping them with practical skills to intervene early, support survivors, and promote non-violent conflict resolution. These sessions emphasized respect for local customs and beliefs, ensuring that the interventions resonated with community values.
The third phase was designed to foster local ownership—training select leaders and health professionals as trainers who could sustain and expand the program independently throughout the region. We provided intensive instruction, mentorship, and resource
support, emphasizing adaptable strategies that aligned with local realities. Over time, these trainers will become champions, delivering workshops, mentoring peers, and raising awareness—creating a ripple effect that will begin changing community attitudes toward violence.
This approach proved highly effective. The community-oriented, culturally sensitive framework fostered trust and ownership, ensuring long-lasting change. It also demonstrated that community-led interventions can have profound, sustainable impacts. The success in Morocco strengthened my conviction that empowering local leaders is the cornerstone of effective violence prevention. This same effort was also carried out in Tunisia.
Building on this success, I expanded my global health efforts to Mauritius, where the urgent need was for integrated medical and mental health support for survivors of violence. In many parts of the
island, there is stigma around mental health and lack of specialized training hindered effective care. Recognizing this, I conducted a series of workshops aimed at health care providers, social workers, and community leaders.
The training focused on traumainformed care, recognizing signs of emotional and physical trauma and providing compassionate, culturally appropriate interventions. We emphasized the importance of mental health support alongside medical treatment, especially for survivors of domestic violence and abuse. The providers expressed a deep desire to implement trauma-informed practices, highlighting the importance of education as a catalyst for change.
Another significant chapter of my work in violence prevention took place in the Seychelles, where there was a critical need for safe, accessible spaces for survivors of violence. To address this gap, my team designed a comprehensive training program focused on the logistics, design, and management of community shelters— spaces that serve as safe havens for survivors and their families. The team spent some time touring and learning from one of the most successful and established shelters in the U.S., The Battered Women and Children’s Shelter in San Antonio, TX, and took some of those lessons learned to our partners in the Seychelles.
During this project, we trained local practitioners, community leaders, and government representatives on how to develop culturally appropriate and sustainable shelters. Topics covered included the principles of survivor-centered design, legal assistance, resource management, safety protocols, and staff training. Emphasizing community involvement, we collaborated with local stakeholders to ensure the shelters met their cultural norms and resource realities. Our goal was to empower Seychelles communities to independently develop and operate these safe spaces, thereby creating long-term resilience.
The training was highly impactful— participants engaged actively during workshops, sharing insights on local
customs and proposing solutions tailored to their societal context. We emphasized that these shelters are not just physical structures but symbols of hope and renewal, integral to healing and social cohesion. The success of this initiative underscored my belief that sustainable violence prevention depends on community ownership and culturally sensitive approaches.
Building these programs across diverse settings presented logistical and cultural challenges. Establishing trust with local communities, navigating language barriers, and aligning interventions with local policies required patience, cultural humility, and strategic planning. Our work emphasizes genuine partnerships—prioritizing local leadership, capacity building, and longterm sustainability in every project.
I had the opportunity to co-lead an annual comprehensive seminar on violence prevention and intervention in San Antonio, TX. The program brought together 40 participants from 23 countries, including military leaders, government officials, and community organizers. Over the weeklong course, attendees explored the complex power and control dynamics that underpin abusive relationships, examined relevant legal frameworks, and discussed culturally responsive approaches to survivor support. The seminar also included an onsite tour of a local women’s shelter, where participants observed first hand the coordinated community response that provides victims with safety, counseling, and empowerment resources. The diversity of perspectives in the room fostered rich dialogue and collaboration, reinforcing the universal importance of addressing genderbased violence through education, empathy, and sustainable systems of support.
One standout moment from the course involved an exercise where each participant is assigned to represent a person from different economic and social tiers in the community, i.e., one participant represents an illiterate farmer with no education, the next participant represents a well-to-do socialite from a large city. Instructors
“It’s not enough to treat injuries; we must foster environments where individuals, families, and communities are equipped with the knowledge and tools to prevent violence before it occurs.”
then read out a simple privilege—like having enough money for a newspaper, access to contraceptives, or saying no to sexual advances—and directed each participant to take one step forward if the person they were representing would have that privilege. One particular military general from Côte d’lvoire, who represented a 15-year-old girl, became emotional after not being able to take a single step during the exercise. He came face to face with the harsh realities of power and privilege. Our team’s overarching goal remains to expand these programs—training local practitioners, advocating for policy change, and integrating violence prevention into broader health and social systems worldwide. We aim to develop scalable models that respect cultural differences while maintaining core principles of trauma-informed, communitydriven intervention.
Looking Ahead
In addition to these field initiatives, we continue developing and teaching modules on violence prevention, trauma-informed care, and community safety at international workshops and conferences. We are committed to building a global network of practitioners and educators dedicated to creating safer, healthier communities. Our vision is a world where every community has the resources, knowledge, and leadership to prevent violence at its root—a future where safety and resilience are accessible to all.
Final Reflection
This work—addressing violence comprehensively and sustainably—is both challenging and profoundly rewarding. It entails not just addressing the immediate acts of violence, but transforming social attitudes, empowering local leaders, and fostering resilience from within communities. Every step, from Morocco, Tunisia, Mauritius, and the Seychelles, reinforces my belief that sustainable change begins with education, cultural humility, and genuine partnership.
As I move forward, I am committed to expanding this work, learning from each community, and sharing my experiences to inspire others. I see this journey not just as a profession but as a calling—a life-long mission to create a safer world, one community at a time.
Dr. Awad is a staff gastroenterologist and hepatologist at the San Antonio Uniformed Services Health Education Consortium, international health specialist and co-course director, Violence, Prevention and Intervention Courses with the Defense Institute for Medical Operations.
M A X I M IZ I N G MEN T O R S HI P
H OW T O B E TH E B E S T M E N T O R ( AN D ME N TE E ) TH AT YO U C A N B E
Patrick
E. Young, MD, MACP, FACG
RCompetence
REFLECTING ON MY CAREER IN
MEDICINE thus far, the number of people who have helped me become a better physician, a better leader, and perhaps even a better person, is staggering. I would not have gotten far without them. One of the greatest pleasures of my professional life is paying those gifts forward. In doing so, I have read, thought, and spoken much about the defining characteristics of the best mentors and mentees. In this article, I will summarize them for you in the hopes that they will facilitate your success as both a mentor and mentee.
HOW TO BE A GREAT MENTOR
Peruse any local bookstore—yes, these still exist—and you will find numerous treatises on mentorship. Go ahead, I’ll wait. If you are still reading this, I’ll assume that you decided you want a summary rather than a treatise. Perfect! You’re in the right place.
Like great leaders, great mentors are created rather than born. There are welldefined traits, skills, and behaviors which you can adopt to maximize the positive impact of your mentorship.
The Big Three Traits: Competence, Confidence/Vulnerability, Commitment
While there are numerous attributes a great mentor may exhibit, the “3 Cs” are the backbone which undergird the others.
This does not simply mean that the person is a competent physician. That is necessary, of course. How else would you respect the person? On its own, it is insufficient. One must also be emotionally competent. Mentoring relationships require openness and honesty. They require clarity and candor. If one does not feel fully seen and understood, effective mentorship becomes difficult.
Confidence/Vulnerability
Mentors and mentees often work in the same general focus area. In cases where the mentor and mentee are close in their career stages, jealousy may arise, particularly if the mentee’s career takes off and the mentor’s stalls. A good mentor has enough confidence to overcome this for the sake of the relationship.
On the flip side, in cases where the mentor is well established and the mentee is in an early career phase, mentees don’t see the struggles and setbacks the mentor has faced. They see the results but not all the hard work, failures, and learning it took to get there. Therefore, a great mentor must have enough vulnerability to share the difficult stories, the failures, the poor decisions we all have made and from which, if we are wise, we have learned. Additionally, we must be willing to share our contacts and networks—perhaps the most valuable asset we have—with our mentees. No one person can be all things to a mentee. When a different skillset or perspective is required, allowing them access to someone in our network with those traits is critical.
Commitment
Being an excellent mentor takes time and patience. The mentor and mentee must craft plans together. In turn, they must follow up at the appropriate interval to ensure that the actions taken are having the desired effect. If not, they must revise the plan. In an age where time is at a premium and every spare moment is precious, being a good mentor takes a deep commitment to your mentee. It means protecting time with your mentee from competing priorities.
A great mentor reflects on the mentee outside of their meetings. Therefore, the mentor often sees traits in the mentee that he or she does not recognize in themself. This allows the mentor to imagine a greater “future you.” I wholeheartedly agree with S. Kover’s assertion that if you leave a meeting with your mentor and your possibilities have shrunk rather than expanded, it is time to find a new mentor!
In addition to these traits, there are several key skills which a great mentor possesses.
CRITICAL MENTORSHIP SKILLS:
LISTENING AND DELIVERING FEEDBACK
Be an Excellent Listener
“...a great mentor must have enough vulnerability to share the difficult stories, the failures, the poor decisions we all have made and from which, if we are wise, we have learned.”
Being an outstanding listener is a core skill not only for mentors but for clinicians and leaders as well. Unfortunately, just as most drivers consider themselves to be above average when objective evidence proves otherwise, many people view themselves as better listeners than the data would support. So, what does it take to be a top-level listener? A 2016 study published in the Harvard Business Review provides some insight. In this study, the authors share data from the investigation of corporate leaders who were rated in surveys as being in the top 5% of all listeners. Here are the attributes and behaviors they evinced.
Set the Scene
We live in a world of near-constant distractions. Listening well means
removing these distractions. Find a quiet place. Put your cell phone away. The presence of a visible cell phone sends the message that, “This conversation is fine, but something may come along at any minute.”
Listening for Understanding
What is the person saying? What are they not saying? What do their body language, word choices, and tone connote? Listen aggressively to understand the deeper meaning of all the forms of communication.
Avoid Preparing a Response
Too often, we are constructing our response to what we are hearing rather than deeply listening to the speaker. Regrettably, the human brain can only attend to one thing at a time. Multitasking is a myth. At best, we can do rapid serial tasking, bouncing from listening to creating our response. In doing so, we inevitably miss potential key elements. Stop thinking about what you will say and listen to what they are saying.
Check for Accuracy
Once the speaker concludes, you must ensure that you fully understand them. Reflect on what you think you heard. “It seems that…” and, “What I heard you say was…” are useful phrases for reflection. Prepare to be corrected without taking offense. Use these corrections to refine your understanding. Once the other person says, “Exactly,” you are ready to move on.
Give Target Advice
Now that you and the speaker agree on the issues, you may give targeted advice. In our personal lives, it is certainly the case that people may simply want to be heard and understood rather than seeking solutions. In a professional setting, there is good evidence to suggest that mentees desire and appreciate advice.
Be a Master at Delivering Feedback
With all respect to Wheaties, I believe that feedback is the breakfast of champions. Practice does not make perfect; it makes permanent. Focused
“Too often, we are constructing our response to what we are hearing rather than deeply listening to the speaker...In doing so, we inevitably miss potential key elements. Stop thinking about what you will say and listen to what they are saying.”
feedback leading to thoughtful application creates improvement. Over time, improvement leads to mastery. In many ways, timely and thoughtful feedback is the greatest gift a mentor can give a mentee. Of course, it does not always feel like a gift. Most of us are high-achieving, type A+ people who are hyper self-critical. Even mildly negative feedback feels like a gut punch. That said, proper feedback delivery can help minimize the sting while maximizing the gains. Here are a few helpful tips.
Deliver the Truth With Grace
The truth can be difficult enough on its own. “Brutal honesty” should be erased from our lexicon. Many people receive even mildly corrective feedback as a hammer blow. While honesty is paramount, a great mentor recognizes that most people are trying. Sure, laziness is possible and must be addressed when present, but the issue is more often misplaced effort rather than a lack of it. This is an opportune moment to employ our listening skills to ensure that there are no competing priorities, personal struggles, etc., which better explain the mentee’s shortcomings. We must also refrain from holding the person to our standards—developed over years of practice and refinement—rather than a standard appropriate for their level of development.
Clarity Is Kindness
While we do not want the truth to be brutal, we do want it to be crystal clear. Defining the exact nature of the shortfall is critical. Reflective listening, which involves having the mentee restate the issue in their own words until understanding is achieved, is a useful tool.
Timing Is Everything
Corrective feedback is not a fine wine; it does not get better with time. Generally, giving feedback proximate to the action
allows for maximum clarity and facilitates effective communication. Moreover, it allows the mentee to make timely corrections rather than simply repeating the mistake(s). Sometimes, however, immediate feedback is illadvised. Corrective feedback should ideally be given in private. Thus, unless the action must be emergently corrected, waiting until you can get into a quiet, private setting is ideal. Some mistakes are so impactful—think of a highly morbid or fatal procedural complication—that immediate feedback is unhelpful. In such cases, the best first step is emotional and professional support. Once the shock has subsided, the person is better equipped to receive feedback.
Focus on Actions, Not Attributes
Focusing on actions, which are objective and observable, is the clearest and most practical form of feedback. By focusing on the behavior and its impact, we lessen the opportunity for misunderstandings and disagreements. The structure of such feedback is “When you did X, the impact was Y.” A better strategy is to “Z.” Even when expertly delivered, some will translate action-oriented feedback as attribute focused. They hear, “You are suboptimal,” rather than “You did something suboptimal.” While this reaction cannot be avoided entirely, action-oriented feedback helps minimize it.
A Word on Positive Feedback
While we tend to think of feedback as corrective, it may also be affirming. Often, the mentee displays actions which are positive and that we want to retain. In these instances, many of the principles outlined above still apply. Positive feedback should be:
“With all respect to Wheaties, I believe that feedback is the breakfast of champions. Practice does not make perfect; it makes permanent. Focused feedback leading to thoughtful application creates improvement. Over time, improvement leads to mastery.”
Clear
Statements such as “good job” and/ or “strong work” make the mentee feel good but are not actionable in that they do not tell the person which behaviors to retain. Be as specific as possible about what made the actions commendable.
Timely
As with corrective feedback, the closer the feedback is to the event, the more quickly it will be incorporated. For positive feedback, public delivery is appropriate and encouraged. In general, praise in public and criticize in private.
Action-Oriented
What actions do you want the mentee to retain and why?
HOW TO BE A GREAT MENTEE/ PROTÉGÉ
There are many things I wish I knew earlier in my career than I did. How many unnecessary struggles I could have avoided! How to be an excellent mentee is near the top of that list. When I was a fledgling physician, I thought if I simply showed up and listened carefully, I could maximize my mentorship experience. I now recognize that a bit of “pre-work” would have facilitated my growth. Here are a few tips to help you grow faster than I did.
Know Your Values
If you take one thing away from this article as a mentee, choose this—your values will guide every major decision in your career. There is no one-sizefits-all formula. The best advice is tailored to the things you care about most. If you don’t fully understand what those things are, your mentor will be much less effective, being
relegated to giving you generic advice. The wisest counsel, like the best suit, is tailor made. When determining your top values, stick with three. While many things may be important to you, going through the exercise of selecting your top three will hone your focus and jumpstart your success. Don’t know where to start? I highly recommend Brené Brown’s list from her book Dare to Lead; the list can be found at brenebrown.com
Be Clear About What You Are Optimizing
If you try to optimize for every factor, you end up optimized for none. Life is full of concessions. For example, when searching for a job, which of the following is most important to you: pay, location, nature of the work, prestige of the center, opportunity for advancement, or something else? There is not a universally “right” answer, but there is certainly a right answer for you. I strongly advise you to look within and not without when making this determination. Play your own game if you want to win. Comparison is a thief of joy.
Target
Specific Opportunities and Goals
Understanding where you want to go and what you want to be able to do when you get there will determine your growth and development strategy.
Identify Knowledge and Skill Gaps
This is closely knit to the previous discussion. To identify areas for improvement, I suggest the WIN principle—What’s Important Now? Based on your goals, values, and feedback, what are the most vital bits of knowledge and skills required to level up? Your mentor can help you figure this out but figure it out you must. Be intentional and focused as you grow.
Identify Your Work Style/Habits
Determining the answers to the following questions will help to capitalize on your mentee experience. How often do you want to communicate with your mentor? By what method? Understand that there may be some generational differences in communication styles and methods. For example, the “Facebook” generation may prefer email to texts, whereas the “TikTok” generation may want you to text before calling.
Master Managing Up
None of us is perfect, including your mentor. There will be times when you need to provide feedback to get things back on track. This can feel unnatural at best and dangerous at worst. Base your discussion on previously agreed-upon values, work styles, and timelines to facilitate the most productive interactions.
Have >1 Mentor (But Not Too Many)
Even the best mentor cannot meet all of a mentee’s needs. For instance, your mentor may be a highly skilled researcher who can help you prepare your first K grant but be ill-equipped to provide you advice on directing a large endoscopy unit. Having a few mentors who can guide you in the various aspects of your career is helpful. As with other relationships, it is possible to spread yourself too thin. If you cannot
“None of us is perfect, including your mentor. There will be times when you need to provide feedback to get
things back on track...
Base your discussion on previously agreed-upon values, work styles, and timelines to facilitate the most productive interactions.”
keep up your end of the mentor-mentee relationship, it may be a sign that you have too many mentors.
Be Excellent at Receiving Feedback
While training on feedback delivery is common, many fewer people are educated in the best way to receive feedback. These tips, while not specific to medicine, are incredibly helpful in maximizing the benefit of feedback.
General Principles
• Set a time: This allows your mentor to prepare quality feedback rather than coming up with something on the fly.
• Be specific and intentional: Let your mentor know on which elements of your performance you want feedback. Clarity begets quality.
• Ask guiding questions: If you are already a high-level performer, it may be difficult for your mentor to give you feedback on how to go from good to great. We are skilled at recognizing and correcting defective performance, but less skilled in seeing how a perfectly acceptable performance could become extraordinary. Guiding questions can help. They are, in essence, exercises in mental time travel to help the mentor see beyond the here and now. Here are a few examples.
• “What is one thing I could do better next time?”
• “Am I the best at “X” that you have ever seen? If not, what would it take to get me there?”
• “If you heard five years from now that I am not successful, are there things you see now which might explain it?”
• Get specific: When receiving generic positive feedback—which feels amazing—remember to dig a little deeper. If someone says, “Strong work,” for example, ask them what made it strong. This will help you retain and build upon the desired behaviors.
How to Receive Constructive Feedback
Like a Champ
• Stop your first reaction: Often, our first reaction is to become defensive (“But what about…”) or to shut down. Neither is helpful. Stay open and engaged.
“...your values will guide every major decision in your career. There is no one-size-fits-all formula. The best advice is tailored to the things you care about most. If you don’t fully understand what those things are, your mentor will be much less effective, being relegated to giving you generic advice.”
• Remember the benefit: The only way you will get better is to receive, process, and appropriately respond to feedback. It is a gift, even if it doesn't feel that way.
• Listen for understanding: Avoid preparing your response/defense and parse out what they are saying.
• Say “thank you”: This is for your benefit. Saying “thank you” provides a helpful reminder.
• Ask questions to deconstruct the feedback: Now that you’ve diffused your emotions, ask clarifying questions to make sure you understand what to work on.
• Decide what to do with the feedback: If someone spends the time and emotional/cognitive energy to give you feedback, critically consider that feedback. You may decide to keep all, some, or none. Some criticism will be practice-changing and even lifechanging. Some criticism simply needs to be discarded.
• Request time for follow-up: After you take actions to improve, you will need re-evaluation to make sure you are moving in the right direction.
While success is never guaranteed, following the advice above should set you, and keep you, on the path to a meaningful mentor-mentee relationship. Show grace as you grow, keep learning, and pass it on!
SUGGESTED READING
• Blanchard, K., & Diaz-Ortiz, C. (2017). One-Minute Mentoring: How to Find and Work with a Mentor—and Why You'll Benefit from Being One. William Morrow, an imprint of HarperCollins Publishers.
• Brown, B. (2018). Dare to Lead. Vermilion.
• Henley D. Handling feedback with a cool head. Forbes 2023. Dec 24.
• Hill SE, Ward WL, Seay A, et al. J Clin Psychol Med Settings. 2022 Jun 27;29(3):557–569.
• Koven S. What is a mentor? N Engl J Med 2024;390:683-685.
Dr. Young is Professor of Medicine and Director of the Division of Digestive Health at Uniformed Services University and serves as a Trustee of the College.
SUBMIT YOUR APPLICATION for the ACG 2026 International GI Training Grant Awards
The International Relations Commi ee of the American College of Gastroenterology is now accepting applications for the 2026 International GI Training Grants. The grants are to be used for travel to and from the training center and to the ACG Annual Meeting, as well as for incidental expenses related to the training. The training must take place between July 1, 2026, and June 30, 2027.
This $15,000 grant provides partial financial support to physicians outside the United States and Canada to receive clinical or clinical research training or education in Gastroenterology and Hepatology in selected medical training centers in North America.
WHO IS ELIGIBLE? Physicians who are not citizens or residents of the United States or Canada, and who are working in gastroenterology or related areas, are eligible
SUBMISSION DEADLINE April 15, 2026 APPLY HERE traininggrant.gi.org
This $10,000 grant provides partial financial support to United States and Canadian GI Fellows in training, or GI Physicians who have completed their training within the last five years, to receive clinical or clinical research training or education in Gastroenterology and Hepatology outside of North America.
WHO IS ELIGIBLE? GI Fellows in training who are enrolled in an accredited gastroenterology fellowship program, or GI Physicians who completed their training within the last five years, and are citizens of the United States or Canada, or have a U.S. green card, are eligible to apply together with their training institution.
SUBMISSION DEADLINE April 15, 2026 APPLY HERE traininggrant.gi.org
TRAINEE HUB
Choosing a Non-ACGME Fellowship: Timing, Pathways, and Considerations
By Eleazar Montalvan-Sanchez, MD
AT THE TIME OF WRITING THIS ARTICLE, I am in the first quarter of my second year of gastroenterology and hepatology fellowship at Yale University and beginning a nonACGME fellowship experience. After completing the first year of GI fellowship, many trainees begin exploring additional training opportunities. Unlike residency and ACGME-accredited fellowships, nonACGME fellowships do not follow a centralized match. Each program has its own process, requirements, and timeline, often requiring commitment nearly two years before the start date. For many, navigating this system can be daunting. This article provides a roadmap to help GI fellows decide which fellowship to pursue, when to reach out, and what the application process typically entails.
WHY CONSIDER A NON-ACGME FELLOWSHIP?
As gastroenterology continues to expand and subspecialize, nonACGME fellowships have emerged as important, highly focused training pathways. Although these programs are not accredited by the Accreditation Council for Graduate Medical Education (ACGME), they offer unique, customizable experiences that can be invaluable for academic advancement and career differentiation. A list of both ACGME-accredited fellowships— such as transplant hepatology and advanced endoscopy—and non-ACGME programs—such as inflammatory bowel disease (IBD), motility, and nutrition— can be found on the American College of Gastroenterology website (gi.org/ resident-resources).
“Benefits of Non-ACGME Fellowships
Non-ACGME fellowships share in common certain strengths and opportunities that are worth taking into account:
• Focused Expertise: Fellows can dedicate concentrated time to developing clinical, research, and procedural skills in a niche field.
• Mentorship and Networking: These programs are often small and mentorship-heavy, allowing close collaboration with national experts.
• Career Positioning: For trainees interested in academic careers, these fellowships can strengthen scholarly productivity and clinical reputation.
Non-ACGME fellowships have the flexibility to offer tailored advanced specialty training, working alongside experts in the field,” says Alexander Levy, MD, IBD Program Director at Yale University School of Medicine. “The additional year not only prepares fellows to become leading clinician-scientists but also helps them build career networks with lifelong mentors. These fellowships also provide a unique advantage to candidates when entering the job market, whether in academic or private practice settings.”
EXAMPLES OF NON-ACGME FELLOWSHIPS IN GASTROENTEROLOGY
Inflammatory
Bowel Disease
Approximately 25–30 of these programs are available in the United States, with most based at large academic centers. Here are a few important points to consider:
• Key Conferences: Advances in IBD, GUILD conference, Crohn’s & Colitis Congress, European Crohn’s and Colitis Organization Congress, Digestive Disease Week (AGA IBD sessions), and the ACG IBD School.
• When to Reach Out: Late in your first year or early in your second year of fellowship.
• Recommendation: Fellows considering an academic career in IBD should contact potential mentors by the fall of PGY-4 (first GI year). Additional opportunities for exposure and networking are available through the Crohn’s & Colitis Foundation, including the Visiting IBD Fellow Program and the REACH-IBD network for GI fellows and early-career faculty (crohnscolitisfoundation.org/scienceand-professionals/education-resources/ visiting-ibd-fellow-program).
“A dedicated fourth year can be invaluable for enhancing clinical expertise and building a strong research portfolio,” says Katherine Falloon, MD, of the Cleveland Clinic. “I encourage those planning to pursue an academic career in IBD or to focus their clinical practice on the care of patients with IBD to strongly consider this additional year of training.”
Pancreatology
Seven structured programs are available in the United States, often embedded within advanced endoscopy divisions (caper-pancreas.org/pancreatologyfellowships). Here are a few important points to consider:
• When to Reach Out: Late in your first year of fellowship; many programs expect early commitment.
• Recommendation: Highlight your procedural and clinical pancreas exposure early in your CV. For those interested in additional networking and mentorship, the Consortium for the Study of Pancreatitis, Diabetes, and Pancreatic Cancer (CAPER) offers pancreas mentorship opportunities through the CAPER Pancreas Scholars Program (caper-pancreas.org/caperpancreasscholars).
Medical pancreatology is a developing subspecialty focused on the diagnosis and medical management of pancreatic disorders. Traditionally, most patients with pancreatic diseases have been managed by interventional or pancreaticobiliary endoscopists. However, as these physicians increasingly specialize in bariatrics and third-space endoscopy, maintaining a concentrated focus on pancreatic disease has become more challenging.
Esophageal Diseases & Motility
Approximately six to eight dedicated programs are available in the United States. Here are a few important points to consider:
• Key Conferences: American Neurogastroenterology & Motility Society (ANMS), Digestive Disease Week (esophagus tracks), and ACG Esophagus School.
• When to Reach Out: Early in the second year of fellowship, though smaller programs may have rolling timelines.
• Recommendation: Consider attending the summer ANMS meeting for direct networking with program directors. ANMS also offers a career coaching program (motilitysociety.org/coachingprogram) and virtual clinical training opportunities (motilitysociety.org/ clinical_trainee_app.php) for interested fellows.
“Medical pancreatology is unique in that an individual has expertise across a broad spectrum of conditions—including acute pancreatitis, chronic pancreatitis, exocrine pancreatic insufficiency, pancreatic cysts, neuroendocrine tumors, autoimmune pancreatitis, complications following pancreatic surgery, genetics, and the prevention and management of complications related to these conditions. For many years, pancreatitis has lacked directed therapies, but this treatment landscape is changing. There are now FDA-approved therapies for various subtypes of pancreatitis with many more in the pipeline. The field of pancreatology is reminiscent of where IBD was about 15–20 years ago, with new opportunities in research, innovation, and clinical care. For those considering pancreatology as a career, I would strongly recommend additional subspecialty training in a center with dedicated pancreatology. One of the most rewarding things about being a pancreatologist is the opportunity to work in a multidisciplinary team to care for patients with these complex disorders.
For trainees early in their decision process, I recommend attending meetings such as PancreasFest, American Pancreatology Association, and even the CAPER Fellows’ Symposium. This allows one to gain more exposure to the type of clinical and research advancements being made as well as network with other adult and pediatric pancreatologists and learn about their practice.
In my experience, an individual with medical pancreatology training is highly valued within gastroenterology divisions. These patients often present with intricate and challenging conditions, and having a dedicated pancreatologist on the team significantly enhances both patient outcomes and institutional expertise.”
—Yasmin G. Hernandez-Barco, MD, Director, Massachusetts General Hospital Pancreas Program
“After years of medical school, internal medicine residency, and gastroenterology fellowship, it can be tough to stomach the idea of additional training (particularly without ACGME accreditation),” says Christopher Vélez, MD, of the Massachusetts General Hospital Center for Neurointestinal Health. “People want to begin their attending lives and may have families to support. But, as our advanced motility fellowship program director (and alumnus of the same training program), I attest to multiple advantages to pursuing such training. It can accelerate an academic career and offer a skill set that makes you highly attractive when seeking employment. Consider if it is right for you!”
Hereditary GI Cancer Syndromes
Limited: one dedicated program available; these are often tied to genetics departments. Here are a few important points to consider:
• Key Conferences: American Society of Clinical Oncology (GI Cancers Symposium), Digestive Disease Week (hereditary cancer sessions).
• When to Reach Out: Early in your second year; some recruit informally through genetics networks.
• Recommendation: Strengthen your CV with research or clinical exposure to hereditary cancer clinics.
Nutrition/Obesity Medicine (GI-Focused Tracks)
This is an emerging field, with select centers offering a GI-nutrition year. Here are a few important points to consider:
• Key Conferences: ASPEN (nutrition), Obesity Week, AGA Obesity/Nutrition sessions.
• When to Reach Out: Variable—some align with NIH training grants.
• Recommendation: Identify if your institution already offers internal nutrition exposure before seeking external fellowship.
GI Hospitalist Track
Still relatively rare but steadily growing, there are a handful of programs available based in high-volume hospitals. Here are a few important points to consider:
• Key Conferences: ACG and AGA Clinical Practice tracks and the DDW GI Hospitalist Session.
• When to Reach Out: Flexible—often depends on institutional needs and clinical volume.
• Recommendation: This track is ideal for fellows pursuing primarily clinical careers and may also appeal to educationminded individuals, given the extensive time GI hospitalists spend with residents and fellows. Many GI hospitalists also serve in educational leadership roles within fellowship programs.
“A career as a GI hospitalist can be an incredibly rewarding career. The work can be unpredictable and challenging, but there is ample opportunity to make a positive impact in the care of critically ill patients and foster the professional development of residents and fellows. A GI hospitalist is well positioned to have a role in education leadership or hospital/health system quality and patient safety roles due to the extensive time spent working with residents and fellows and the unique ability to experience multiple facets of inpatient care. Fellows who are interested in a career as a GI hospitalist should consider joining the ASGE’s GI Hospitalist Special Interest Group, gain ample exposure to inpatient care and associated procedures (gastrostomy tube placement, hemostasis), and feel free to contact GI hospitalists to gain their perspective on a career as a GI hospitalist.
—Kenneth Hung, MD, Yale University School of Medicine
Each of these fellowships provides additional skills that can shape future practice, open academic opportunities, or align with evolving healthcare needs.
TIPS FOR GI FELLOWS
START EARLY
Decide on a subspecialty by the middle of your first year.
LEVERAGE MENTORSHIP
Mentors often know informal timelines and unadvertised opportunities.
ATTEND SUBSPECIALTY MEETINGS
These are key venues for networking and recruitment.
STAY FLEXIBLE
Some programs recruit very early—being proactive is essential.
SEEK TESTIMONIALS
Hearing from program directors and fellows can help refine your approach.
WHEN TO REACH OUT
Most programs recruit 18–24 months before the start date. Applications may involve contacting program directors directly, networking at national meetings (ACG, AGA, DDW), or referrals through mentors. Some institutions use structured applications, while others rely heavily on personal communication.
What Programs Typically Request
• Updated CV highlighting GI fellowship training, scholarly work, and subspecialty interests
• Personal statement or letter of intent describing career goals and fellowship interest
• Letters of recommendation (often from fellowship program leadership or mentors in the field)
• Interview—usually virtual or on site, though some programs may coordinate interviews during major GI meetings such as DDW, ACG, or specialty conferences (e.g., Advances in IBD)
CONCLUSION
Non-ACGME fellowships offer GI trainees a unique opportunity to gain advanced clinical skills, enhance their academic profile, and align their training with long-term career goals. With early preparation, mentor guidance, and a strategic approach to networking, fellows can successfully navigate this individualized process.
As I conclude this article, I have just accepted a position at the Cleveland Clinic for an advanced IBD fellowship. I hope these insights help other fellows who are considering a fourth year of training and seeking the best path to align their education with their career aspirations.
Dr. Montalvan-Sanchez is a Gastroenterology and Hepatology Fellow at Yale University School of Medicine, New Haven, CT.
GETTING IT
MIND
Road Maps and Rainbows in Private Equity Deals
By Ann Bittinger, Esq.
AFTER NEARLY 30 YEARS PRACTICING as a healthcare transactions attorney, I have the discernment to say, “If you’ve seen one physician practice private equity deal, you have seen one physician practice private equity deal.” Every one is different. There are many shades of colors in a rainbow. Red might be fire red, maroon, cherry, cinnamon, and magenta. Blue might range from cobalt and navy, to azure, sapphire, and indigo. There is, however, a constant red or blue of some sort. This article aims to discuss some of the distinct colors that, as practicing gastroenterologists, you want to look for when evaluating proposed or current relationships between your practice, you, and private equity (PE).
LAW
WHO’S IN CHARGE?
First, understand who you work for. You might think that’s obvious. What’s the formal name of the company on your employment agreement? Where does that company fit within the organizational chart with its related entities? Sometimes the names of different entities within the PE organization are quite similar and confusing. Sometimes just one word or some letters distinguish the original physician practice that is sold to the PE firm to the new entity that they work for that is owned by the PE group. I’ve worked with physicians who think they own shares in the company that employs them but, it turns out, they own shares in a separate PE-owned company. You need a road map to know where you’re going. Ask for the “org chart” and use it to understand the larger organization. Find the management company. Find the parent company. Identify which company’s Tax Identification Number (TIN) is used to bill your services being billed to payers.
MONEY FLOW
Identify the company that your services are contracted or assigned to—the one under whose TIN your services are being billed to the payers. This may or may not be the company named on your employment agreement. You will then see where the money flows. Identifying that flow helps you understand a few things. First, if you are being offered or have ownership interests in one of the PE group’s companies, knowing how the money flows gives you an idea of the value of the stock that they are giving or selling to you. Look for whether the shares are in a shell company—one that doesn’t own much, or that doesn’t generate much income, or whose income is dependent on decisions made by owners of another company in the system. That gives you an idea of the true value of the shares that you buy or receive. Having shares in a company that owns nothing or that has little cash flow is a bit like holding an empty wine bottle. You can show people the bottle and think it’s wine, but it turns out to be empty. One of the main reasons I hear from physicians as to why they are interested in selling their practices to private equity and getting stock in the company is that the PE company will sell again in the
future, resulting in even more passive income. But that will happen only if the organization sells the company in which you own an interest. If the PE company sells the parent company of the entity that you own an interest in rather than the company you own, you may receive nothing. Understand the org chart and the money flow.
LOCAL GOVERNANCE
Generally, corporations have executives and boards of directors. When PE groups buy or take control as majority owners of physician groups, the local physicians do not usually serve as executives or directors of the company. Instead, they form a quasi-board, with local physicians appointed by the PE owners (not elected by their peers). That board might look like a formal board of directors, but instead its powers are limited to things that the PE investor approves. Review the list of duties and powers of this group, often called something like “the local governing board.” Look to see what actions under your employment agreement can be taken against you by the employer versus the local governing board. For example, look at
APP for Clinical Excellence ACADEMY
your employment agreement’s without cause termination provision. Can the company fire you without cause? Or is that firing subject to the vote of the local governing board. The more times you see references to the local governing board in your employment agreement, the greater indication you have that the PE investor has a more laissez faire approach to management of the practice because they are delegating decision-making to that local board. Generally, the PE investor almost always wants veto power on anything the local board does, but delegation to them of issues related to physician management and medicalrelated issues is a good sign for physician employees.
BREAKING UP
When evaluating the acquisition of your practice by a PE firm or joining one as an employee and receiving some ownership interests over time, plan for the divorce. What happens to your shares if you want to leave? Whereas with physician-owned practices we often see a mandatory buy-back by the practice of a physician’s shares upon termination of employment, retirement, disability, or death, with PE groups often the buyback is at the PE company’s discretion. That means you don’t get a return on your investment if you want to leave. You can’t cash out your shares and use the proceeds to retire like you might have in a private practice. It also makes it very difficult to plan your future if you are counting on seeing the fruits of that investment because you don’t control whether that fruit is picked from its tree, if you will.
COMMITMENT PERIOD
Similarly, many PE firms mandate that the physician shareholders of a practice who sell their shares to the PE firm in the original acquisition stay employed with the practice for quite some time, often five years. The PE firm’s rationale is akin to my empty wine bottle metaphor above: if all the physicians quit, the PE firm just paid a lot for nothing. The rationale
“Don’t assume that your contract is the same as a colleague’s who works in another city for the same PE group. There are many shades of terms and conditions to consider as each physician navigates his or her relationship with private equity employers.”
is continuity of physician services— frequently called “going concern value”— i.e., there’s value in buying an ongoing practice. Often there’s no right for the physician to leave except for cause. Other times, a large amount of the proceeds of the sale of their private practice shares to the PE firm are held back for a five-year period. Another shade of this color, so to speak, is for the PE entity to pay for the acquisition of the private practice with shares in a PE firm-owned company, but those shares don’t vest in full for five years. In both of these situations, the physician sells his or her shares to the PE firm but doesn’t see the payment for those shares for years, all while working for the new PE employer under the new PE employer’s terms and conditions. I’ve seen this lead to many uncomfortable situations. Not being able to quit your job is quite a freedom to give up.
NON-COMPETES
Employment non-competes are different than company-sale non-competes. State laws often allow for longer noncompetes tied to an asset or stock sale agreement for a company than they do for employment agreements. In a typical practice acquisition by a PE firm, it would be common to see the two-year noncompete in the employment agreement plus a five-year non-compete in the purchase agreement. I’ve worked with a number of physicians who want to leave the PE-owned practice, bring me their employment agreement non-compete, and are shocked to find out that, when they sold the practice years earlier, they signed a stock or asset purchase agreement that is much more stringent than the employment one. When a physician group sells to PE, the physician owner
takes on two new roles: employee of the firm’s physician enterprise and seller of shares (or assets) of the practice. Those roles are usually tethered to different restrictions upon competition.
No two private equity deals are alike, even when done by the same private equity group. Retain good counsel to help you navigate your onboarding to employment with the PE group. Don’t assume that your contract is the same as a colleague’s who works in another city for the same PE group. There are many shades of terms and conditions to consider as each physician navigates his or her relationship with private equity employers.
Ann Bittinger, Esq. is a healthcare attorney who focuses on physicians’ relationships with their employers, practices, and hospitals. She can be reached at ann@bittingerlaw.com.
Each chapter of the Guide to the Guidelines series includes carefully selected vignettes designed to illustrate key concepts from the guidelines, followed by a conversation-style discussion written to keep you awake and alert. The authors highlight noteworthy points and provide multiple-choice questions to test your knowledge of the material. Using their combined experience of managing GI and liver patients in both academic and private practice settings, they can help you provide high quality care to your patients.
Brennan Spiegel, MD, MSHS, FACG Hetal A. Karsan, MD, FACG
Inside the JOURNALS
THREE CLINICAL GUIDANCE DOCUMENTS WERE RECENTLY PUBLISHED IN THE RED JOURNAL: a global consensus statement on IBD in pregnancy, an ACG guideline on perioperative risk in cirrhosis, and the ACG Monograph on Geriatrics and GI. In CTG, we highlight a study of bone remodeling biomarkers in pancreatitis, and we introduce the 2025–2026 ACG Case Reports Journal Editorial Board, led by Co-EICs Dr. Daniyal Abbas and Dr. Dushyant Dahiya.
[THE AMERICAN JOURNAL OF GASTROENTEROLOGY]
GLOBAL CONSENSUS STATEMENT ON THE MANAGEMENT OF PREGNANCY IN
INFLAMMATORY BOWEL DISEASE
Mahadevan, et al
Pregnancy for women with inflammatory bowel disease (IBD) can be risky and lack of information on safe medications affects pregnancy rates, medication adherence, and outcomes, while varied practices and guidelines create challenges for providers. The Global Consensus Consortium, consisting of 39 IBD experts and seven patient advocates from six continents, developed 34 GRADE recommendations and 35 consensus statements focusing on best practices for maternal health to support infant health, to improve care for pregnant women with IBD globally.
READ: bit.ly/ibd-pregnancy-consensus
ACG CLINICAL GUIDELINE: PERIOPERATIVE RISK ASSESSMENT AND MANAGEMENT IN PATIENTS WITH CIRRHOSIS
Mahmud, et al
This guideline highlights the importance of assessing liver disease severity, other health issues, and surgery-specific risks before surgery in patients with cirrhosis. Key recommendations include optimizing preoperative health through nutrition, managing portal hypertension, correcting blood clotting issues, and addressing frailty and sarcopenia. The guideline stresses the value of surgeries at specialized centers, informed decision-making, and a team-based approach to improve outcomes.
READ: bit.ly/acg-periop-cirrhosis-2025
LISTEN: bit.ly/acg-periop-cirrhosis-podcast
SUMMARY: bit.ly/acg-periop-cirrhosis-highlights
[ACG MONOGRAPH] AMERICAN COLLEGE OF GASTROENTEROLOGY MONOGRAPH ON GERIATRICS & GI
Editors: Adam S. Faye, MD, MS; Sunanda V. Kane, MD, MSPH, MACG & Aasma Shaukat, MD, MPH, FACG
This monograph addresses the unique challenges and nuances of providing care to older patients with GI- and hepatology-related disorders and diseases. Topics covered include colonic conditions, inflammatory bowel disease, vaccinations, functional GI disorders, pancreatic diseases, hepatobiliary disorders, and gastroesophageal conditions.
READ: bit.ly/acg-monograph-geriatrics
[CLINICAL & TRANSLATIONAL GASTROENTEROLOGY] CIRCULATING MOLECULAR DRIVERS OF BONE REMODELING IN PANCREATITIS
Hill, et al
This study examined bone remodeling biomarkers in patients with recurrent acute pancreatitis and chronic pancreatitis (CP) compared with healthy controls. Eight of 10 biomarkers differed significantly, with elevated markers of bone resorption in pancreatitis, especially in CP. Osteopontin and oncostatin increased with disease severity, while insulin levels fell in CP. The findings suggest stage-specific disruption of bone metabolism, shifting toward greater bone loss as pancreatitis progresses. Larger studies are needed to guide strategies to prevent bone complications in these patients.
READ: bit.ly/ctg-bone-biomarkers-pancreatitis
Meet the 2025–2026 ACGCRJ EDITORIAL BOARD
Daniyal Abbas, MD Editor-in-Chief Harlem Hospital Center New York, NY
Hassam Ali, MD East Carolina University Health Medical Center Greenville, NC
Fouad Jaber, MD, MS Baylor College of Medicine Houston, TX
Dushyant Dahiya, MD Editor-in-Chief University of Kansas Kansas City, KS
Thanks to outgoing ACGCRJ Editorial Board members! We thank the outgoing members of the Editorial Board for their outstanding service to the Journal and wish them continued success in their careers.
Prateek Harne, MBBS, MD (Co-EIC)
Muhammad Nadeem Yousaf, MD (Co-EIC)
Sonya Bhaskar, MD
Tina Boortalary, MD
Vaishnavi Boppana, MD
Aastha Bharwad, MD University of Texas Health Sciences Center Houston, TX
Abel Joseph, MD Stanford University Stanford, CA
Harsimran Kalsi, MD
Lead Social Media Ambassador University of Central Florida / HCA North Florida Hospital Orlando, FL
Umer Farooq, MD St. Louis University St. Louis, MO
Rahul Karna, MD University of Minnesota Minneapolis, MN
Aya Akhras, MBBS
Associate Social Media Ambassador HCA Florida Aventura Hospital Aventura, FL
Faisal Nimri, MBBS Henry Ford Hospital Detroit, MI
Taha Bin Arif, MD
Associate Social Media Ambassador Sinai Hospital of Baltimore Baltimore, MD
MARCH 6-8, 2026
HILTON NEW ORLEANS RIVERSIDE
NEW ORLEANS, LOUISIANA
ACG GUIDELINE Highlights
Treatment of Helicobacter pylori Infection
Management of Ulcerative Colitis in Adults
Concept and Content: Erica Duh, MD | Reviewer: Millie D. Long, MD, MPH, FACG
William D. Chey, MD, FACG; Colin W. Howden, MD, FACG; Steven F. Moss, MD, FACG; Douglas R. Morgan, MD, MPH, FACG; Katarina B. Greer, MD, MSEpi; Shilpa Grover, MD, MPH; Shailja C. Shah, MD, MPH
Diagnosis, Assessment, Monitoring, and Prognosis
• Stool testing to rule out C. diff in those suspected of having UC
Epidemiology
• Do NOT use serologic antibody testing to establish, rule out, or determine prognosis of UC
• H. pylori prevalence in North America is 30%-40%
• Typically acquired in childhood
When to Test for H. pylori
Goals for Management
• Utilize treat-to-target with a goal of endoscopic improvement [Mayo endoscopic score 0 to 1]
• Use non-invasive markers such as fecal calprotectin and/or intestinal ultrasound to assess clinical response
• More prevalent among non-White races or ethnicities, those living in crowded or poor sanitary conditions, and early generation immigrants from endemic regions.
Benign Conditions
Proctitis (within 18 cm of anal verge, distal to rectosigmoid junction)
• Dyspepsia if <60 years without alarm features (GI bleeding, vomiting, unexplained weight loss, iron deficiency)
• Rectal 5-ASA therapies (1 g/day)
• Intolerant or nonresponsive? Tacrolimus suppository or topical steroid (suppository, budesonide foam)
Moderate UC:
• Adult household members of H. pylori positive individuals
• ITP
• Oral budesonide MMX is recommended
• Dyspepsia if <50 years with high risk for gastric cancer
Left-Sided Colitis (sigmoid to splenic flexure)
Treatment for H. pylori
• Rectal 5-ASA enemas (at least 1 g/day) + oral 5-ASA (2 g-4.8 g/day) compared to oral 5-ASA alone
• Unexplained IDA
Moderate to Severe UC:
• Current or prior history of PUD
• Oral systemic steroids
• Endoscopy with biopsies if dyspepsia and alarm features, NSAID use, family history of gastric cancer, immigration from high incidence region
• Intolerant or nonresponsive? Oral budesonide MMX 9 mg/day for induction
• PPI b.i.d.
Premalignant and Malignant Conditions
• High risk gastric premalignant condition
- Atrophy, intestinal metaplasia, dysplasia
• MALT lymphoma
• Test for C. diff
• Pharmacologic DVT
- Autoimmune gastritis
For Induction
• Gastric epithelial polyps WHO recognizes H. pylori as a group I (definite) carcinogen
Optimized bismuth quadruple
• Rectal 5-ASA enemas (at least 1 g/day) preferred over rectal steroids
Extensive Colitis (beyond splenic flexure, includes those with pancolitis or involvement of entire colorectum)
Rifabutin Triple
• Fail to respond? Oral systemic steroids
PCAB Dual
PCAB Triple
Levofloxacin Triple
Proctitis
• Rectal 5-ASA therapies (1 g/day)
• S1P receptor modulators (ozanimod, etrasimoid)
• IL12/23p40- antibody (ustekinumab)
• Chronically taking NSAID or starting daily aspirin therapies
• Infliximab is the preferred anti-TNF therapy for patients with moderately to severely active UC.
• Amoxicillin 1000 mg t.i.d.
• Omeprazole 40 mg t.i.d.
• In those who fail to reach remission with 5-ASA, pursue alternative therapies rather than alternating 5-ASA class.
If infliximab is used in induction, recommend combo therapy with a thiopurine
• Vonoprazan 20 mg b.i.d.
• Amoxicillin 1000 mg t.i.d.
• TPN for purpose of bowel rest
AVOID:
• Vonoprazan 20 mg b.i.d.
• Clarithromycin 500 mg b.i.d.
• Monotherapy with thiopurines or methotrexate
• Amoxicillin 1000 mg b.i.d.
• PPI b.i.d.
• Adding 5-ASA for clinical efficacy if previously failed 5-ASA and now on advanced therapies
• Amoxicillin 1000 mg b.i.d.
• Levofloxacin 500 mg q.d.
Thiopurines for maintenance of remission >> no treatment or steroid
Remission with infliximab
Recommended Suggested May be considered when no other options
• Left Sided Colitis/Extensive Colitis
• Oral 5ASA therapy (at least 1.5 g/ d)
Treatment Pearls
• All patients found to be infected with H. pylori should be treated
If induction was achieved using the same therapy, can continue the following:
• Continue infliximab
Remission with cyclosporine
• Complete test of cure at least four weeks after therapy with either:
• Urea breath test
• Fecal antigen test
Low dose (2-2.4 g) of 5-ASA should be used, as compared to the higher dose (4.8 g). No difference in remission rate! Dose based on patient preference!
• Biopsy-based test
Abx = antibiotic
b.i.d. = twice a day
GIM = gastric intestinal metaplasia
H. pylori = Helicobacter pylori
• Oral systemic steroids
• To avoid false negatives in test of cure – hold PPI x 2 weeks; bismuth and antibiotics x 4 weeks
• S1P receptor modulators (ozanimod, etrasimoid)
• IL12/23p40- antibody (ustekinumab)
• Suggest maintenance with thiopurines OR vedolizumab
• Avoid clarithromycin and levofloxacin-containing Rx unless demonstrated susceptibility
Recommend against systemic, budesonide MMX, or topical steroids for maintenance
Do not use methotrexate for maintenance
William D. Chey, MD, FACG; Colin W. Howden, MD, FACG; Steven F. Moss, MD, FACG; Douglas R. Morgan, MD, MPH, FACG; Katarina B. Greer, MD, MSEpi; Shilpa Grover, MD, MPH; Shailja C. Shah, MD, MPH The American Journal of Gastroenterology 119(9):p 1730-1753, September 2024. | DOI: 10.14309/ ajg.0000000000002968
5-ASA = 5-aminosalicylic acid
Anti-TNF = anti-tumor necrosis factor therapy
C. diff = Clostridioides difficile
cm = centimeter
T.
DVT = deep vein thrombosis
g = gram
IL12/23p40 = anti-interleukin 12/23p40
IL23p19
FACG. The American Journal of Gastroenterology DOI: 10.14309/ajg.0000000000003616
= once a day
= four
Concept and Content: Erica Duh, MD | Reviewers: William D. Chey, MD, FACG and Shailja C. Shah, MD, MPH
David
Rubin, MD, FACG; Ashwin N. Ananthakrishnan, MBBS, MPH, FACG; Corey A. Siegel, MD, MS; Edward L. Barnes, MD, MPH, FACG; Millie D. Long, MD, MPH,
ACG GUIDELINE Highlights
Treatment of Helicobacter pylori Infection
Malnutrition and Nutritional Recommendations in Liver Disease
Concept and
Content:
Epidemiology
Definitions
When to Test for H. pylori
Causes
William D. Chey, MD, FACG; Colin W. Howden, MD, FACG; Steven F. Moss, MD, FACG; Douglas R. Morgan, MD, MPH, FACG; Katarina B. Greer, MD, MSEpi; Shilpa Grover, MD, MPH; Shailja C. Shah, MD, MPH
Concept and Content: Erica Duh, MD | Reviewers: William D. Chey, MD, FACG and Shailja C. Shah, MD, MPH
Christina Awad, MD | Reviewer: Craig J. McClain, MD, FACG
• H. pylori prevalence in North America is 30%-40%
• Typically acquired in childhood
• More prevalent among non-White races or ethnicities, those living in crowded or poor sanitary conditions, and early generation immigrants from endemic regions.
• Malnutrition incudes both under- and over-nutrition
Benign Conditions
• Sarcopenia (including sarcopenic obesity) is the major consequent body composition change due to malnutrition
Dyspepsia if <60 years without alarm features (GI bleeding, vomiting, unexplained weight loss, iron deficiency)
Food-related
• Dyspepsia if <50 years with high risk for gastric cancer
Medical causes
• Endoscopy with biopsies if dyspepsia and alarm features, NSAID use, family history of gastric cancer, immigration from high incidence region
GI-related
Treatment for H. pylori
Complication of liver disease
• PPI b.i.d.
Treatment Team Approach
Optimized bismuth quadruple
• Adult household members of H. pylori positive individuals
• ITP
Premalignant and Malignant Conditions
• High risk gastric premalignant condition
• Poor availability/quality
• Unexplained IDA
• Current or prior history of PUD
- Atrophy, intestinal metaplasia, dysplasia
• Unpalatable (low Na, protein, etc.)
• Chronically taking NSAID or starting daily aspirin therapies
• Fasting for procedures
- Autoimmune gastritis
• MALT lymphoma
• Gastric epithelial polyps WHO recognizes H. pylori as a group I (definite) carcinogen
Abx = antibiotic
b.i.d. = twice a day
Rifabutin Triple
PCAB Dual
- Family history of gastric cancer
• Interruption of feeding
• Nausea/vomiting/diarrhea
- Foreign born with immigration from high incidence region
Subjective Global Assessment, hand grip strength, bioelectric impedance, and imaging are increasingly used assessment methods.
Encouraged for all, decreases adverse clinical outcomes in patients with MASH.
Dietary Recommendations
• Clarithromycin 500 mg b.i.d.
• Amoxicillin 1000 mg b.i.d.
• Low-fructose diet is recommended for all patients with chronic liver disease across the spectrum of disease.
Levofloxacin Triple
• PPI b.i.d.
• Amoxicillin 1000 mg b.i.d.
• Late evening snacks to improve lean muscle tissue and decrease risk for ascites/HE
• Levofloxacin 500 mg q.d.
• Nutritional supplementation for patients with alcohol-associated hepatitis and cirrhosis
Recommended Suggested May be considered when no other options
• In patients with non-cirrhosis MASH, consider daily supplementation of vitamin E 800 IU
Treatment Pearls
• All patients found to be infected with H. pylori should be treated
• In patients with chronic liver disease, drinking two or more cups of coffee per day can decrease risk for fibrosis progression or development of HCC.
• Complete test of cure at least four weeks after therapy with either:
• In patients with chronic liver disease, protein should not be restricted.
• Urea breath test
• Fecal antigen test
• To avoid false negatives in test of cure – hold PPI x 2 weeks; bismuth and antibiotics x 4 weeks
• Avoid clarithromycin and levofloxacin-containing Rx unless demonstrated susceptibility
• Biopsy-based test
GIM = gastric intestinal metaplasia
H. pylori = Helicobacter pylori
HCC = hepatocellular carcinoma
HE = hepatic encephalopathy
• For patients with cirrhosis and HE who need nutritional supplementation, ACG suggests a diet enriched with plant-based sources of protein
• ACG refrained from making a recommendation for or against rigorous restriction of dietary sodium among patients with cirrhosis and ascites who are managed with diuretic therapies.
William D. Chey, MD, FACG; Colin W. Howden, MD, FACG; Steven F. Moss, MD, FACG; Douglas R. Morgan, MD, MPH, FACG; Katarina B. Greer, MD, MSEpi; Shilpa Grover, MD, MPH; Shailja C. Shah, MD, MPH The American Journal of Gastroenterology 119(9):p 1730-1753, September 2024. | DOI: 10.14309/ ajg.0000000000002968
Ashwani K. Singal, MD, MS, FACG*; Robert J. Wong, MD, MS, FACG*; Srinivasan Dasarathy, MD; Manal F. Abdelmalek, MD, MPH, FACG; Brent A. Neuschwander-
Berkeley N.
READ THE GUIDELINE:
MD, PhD, FACG; Jessica Petrey, MSLS; Craig J. McClain, MD, FACG. The American Journal of Gastroenterology DOI: 10.14309/ajg.0000000000003379
READ THE GUIDELINE: bit.ly/acg-guideline-liver-nutrition