Dr Emma Hodge Committee of Doctors in Training Chair
Dr Lee Jones Committee of General Practice Chair
A/Prof Alka Kothari Greater Brisbane Area Representative
Craig Allen Skills Based Director
Grant Dearlove Skills Based Director *on Board and Council
Dr Jane MacLeod General Practitioner
Representative
Dr Robert Nayer North Area Representative, Committee of Consultant Specialists Chair
A/Prof Katie Panaretto Specialist Representative
Dr Bhavesh Patel Specialist
Representative
Dr Rachael PeryJohnston
Greater Brisbane Area Representative
Dr Siddhartha Sarmah General Practitioner
Representative Dr Sumaiya Sayed
International Medical Graduate Representative
AMA Queensland Secretariat
Dr Brett Dale Chief Executive Officer Filomena Ferlan General Manager –Corporate Services Katherine Gonzalez-Cork General Manager Member Services
Editor: Michelle Ford Russ
Phone: 07 3872 2222
Erin O’Donnell General Manager Policy
Address: PO Box 123, Red Hill QLD 4059
Email: amaq@amaq.com.au Website: ama.com.au/qld
Disclaimer – All material in Doctor Q remains the copyright of AMA Queensland and may not be reproduced or transmitted in any form without permission. While every care is taken to provide accurate information in this publication, the material within Doctor Q is for general information and guidance only and is not intended as advice. Readers are advised to make their own enquiries and/or seek professional advice as to the accuracy of the content of such articles and/or their applicability to any particular circumstances. AMA Queensland, its servants and agents exclude, to the maximum extent permitted by law, any liability which may arise as a result of the use of the material in Doctor Q
Editor’s desk
We’re pleased to welcome Dr Nick Yim back for another term, as well as Vice President Dr Emilia Dauway. The formidable Dr Eleanor Chew has returned as Board Chair and there is a great mix of experience and fresh ideas on the new Board and Council.
At the recent Dinner for the Profession, it was great to meet the AMA Queensland medal recipients:
Dr Mary Dunne, Gold Medal
Prof Sunil Lakhani, Excellence in Healthcare Award
Dr Matt Masel, Rural Health Medal
Dr Elise Witter, Doctor in Training Medal
Have a think about who you might like to nominate for these awards next year? Nominations will open later in the year.
Obituaries
The following AMA Queensland members have recently passed away. Our sincere condolences to their families.
Dr Robert George BOURNE
Radiation Oncologist Late of Yeronga Member for 63 years
Dr Glen BUCHANAN GP
Late of Stanthorpe Member for 66 years
We’re currently working behind the scenes to upgrade our website and database to provide the most up to date, secure and user-friendly experience for our members.
We recognise our responsibility in keeping your personal details secure and will be implementing the latest security features to ensure those details are as safe as possible.
In the next 4-6 weeks, you’ll notice some exciting new changes on our website, in our emails and within our Member Portal.
We don’t require anything from you at this stage, we just want to ensure you are aware of the upcoming changes.
We will reach out to you when this affects you or if access becomes limited while changes are underway.
AMA Queensland staff will be available to guide you through these changes to ensure a seamless transition.
Intensive Care – Excluding Neonatal, Neonatal Intensive Care, Nephrology, Neurology, Nuclear Medicine, Occupational Medicine, Oncology, Ophthalmology, Paediatrics – Excluding Neonatal Intensive Care, Pain Medicine, Palliative Care, Pharmacology, Psychiatry, Public Health & Preventative Medicine, Rehabilitation Medicine, Respiratory Medicine, Rheumatology, Skin Cancer Medicine, Sports Medicine, Surgical Specialties – Office Pract Only. Qantas Points will be credited to your Qantas Frequent Flyer or Qantas Business Rewards Account within 60 days of your first payment. Full Ts & Cs at https://www.miga.com.au/qantas-100kbonus-tc.
2 Travel insurance is available to members of Medical Defence Association of South Australia Limited (MDASA) (excluding student members) for journeys of up
President report
It was an honour to be re-elected AMA Queensland President for a second term at this year’s AGM. Thank you for placing your trust in me.
It was followed by our annual Dinner for the Profession, which celebrated four incredibly dedicated and hardworking members: Dr Mary Dunne (Gold Medal), Professor Sunil Lakhani (Excellent in Healthcare Medal), Dr Matt Masel (Rural Health Medal) and Dr Elise Witter (Doctor in Training Medal). Recipients of four AMA Queensland Foundation scholarships and three bursaries were also announced for deserving doctors at different stages of their careers.
We also recently celebrated our members Associate Professors Carol Douglas and David Rimmer who were honoured in the King’s Birthday List, and I visited Hawthorne Clinic in Brisbane’s east to celebrate its 100th year of service as a medical practice.
These are wonderful examples of the contributions AMA Queensland members make year-in, year-out.
It’s your dedication that inspires me in my medical advocacy work and I’m pleased to check in with some recent highlights.
State budget announcements
In addition to celebrating our members’ outstanding achievements, this edition places significant focus on the state budget, handed down on 24 June.
As Dr Brett Dale noted in his update, we are relieved by the significant investment in health. However, with patients waiting far too long for life-saving healthcare, the government must act on its proposals now.
This includes providing a clear plan that outlines how and when their workforce, bed, elective surgery, ramping and other targets will be met.
We also need reassurance that initiatives will be implemented sensibly and in alignment with long-term strategies that deliver permanent increases to public hospital capacity.
We reiterate our calls for Queensland Health to consult broadly with the medical profession about their proposals.
Workforce, workforce, workforce
The Queensland Government announced $24 million to retain a General Practice Training Incentive program. It means more than 550 doctors who begin their general practice training in Queensland in 2025 will receive $40,000 one-off payments.
This is a welcome step, and one AMA Queensland has long advocated for, as part of broader efforts to address the health workforce shortage.
Our Workforce Working Group has wrapped up, and I look forward to sharing more of its conclusions and
solutions with you – and the government. I also joined Health Minister Tim Nicholls and other health leaders on a Committee for Economic Development of Australia (CEDA) panel on 21 May to discuss the future of the health workforce.
Minister Nicholls has committed to outlining the government’s strategy to attract and retain healthcare professionals in the second half of this year and AMA Queensland will continue to advocate for the best outcomes for members and our patients.
Defunding Medicare items
I’ve had discussions with several members about Medicare changes to rebates for chronic disease and GP management plans and associated team care arrangements. While consolidating these into a single $156.55 payment will reduce red tape, it also means a reduction in the overall rebate for chronic disease and mental health patients.
GPs who have crunched the numbers report it will make employing practice nurses less viable – which could have the flow-on effect of reducing prevention and early intervention measures and eventually increasing pressure on our public hospitals.
The solution is clear: Medicare rebates must be increased and indexed appropriately. Complex care such as chronic disease, mental health and ultimately longer consultations need to be encouraged and supported. The Workforce Incentive Payments that support general practice to employ practice nurses and allied health workers to enhance team-based care have not kept up with rising costs. That must also be remedied.
Now, more than ever, we need to protect and strengthen general practice, not undermine it. Because when GPs can do their job properly, Australians stay healthier, longer.
I am passionate about our advocacy work, and I want to conclude by encouraging you to share your experiences and ideas with us.
We have a small but hardworking team that punches well above its weight in terms of using our public profile and goodwill to get better outcomes for clinicians, patients and the community.
Your membership fees underpin this work, but what makes it count is buy-in from you.
Tell us your stories, so we can tell everyone else.
Dr Nick Yim President
Read more on p17
CEO report
It’s my pleasure to begin this update by congratulating incumbent President Dr Nick Yim for his re-election to serve a second term as AMA Queensland President. His efforts over the past year have been nothing short of exemplary, marked by unwavering dedication and impactful leadership.
He was officially appointed to the role at the AMA Queensland AGM on Friday 30 May, alongside Vice President Dr Emilia Dauway who was re-elected unopposed and Dr Eleanor Chew OAM as Board Chair.
I also welcome new Board member Professor Paul Griffin and seven new Council members. I look forward to working closely with them throughout the year ahead. Together, we share a common goal — supporting Queensland doctors, creating better health.
State budget
AMA Queensland has been championing priority areas for reform and investment to improve health access and equity for all Queenslanders for some time.
In early March, we released our Budget Submission 2025-26 detailing these priorities, and in the lead-up to this year’s state budget, we ramped up our advocacy efforts to urge the LNP Government to invest in them.
Our calls were heard loud and clear, receiving strong media coverage across the state.
The budget was handed down on Tuesday 24 June and we were pleased to see a record investment in health. This includes funding for initiatives to improve patient flow and utilise private hospitals to reduce elective surgery backlogs, which were key recommendations in our Surgical Wait List Roundtable Action Plan
While it is a relief to see health remains a high priority, the government must now show how and when this funding will be delivered.
Digital upgrade
We’re currently working behind the scenes to upgrade our website and database to provide the most up to date, secure and user-friendly experience for our members.
We recognise our responsibility in keeping your personal details secure and will be implementing the latest security features to ensure those details are as safe as possible.
In the next 4-6 weeks, you’ll notice some exciting new changes on our website, in our emails and within our Member Portal.
We don’t require anything from you at this stage, we just want to ensure you are aware of the upcoming changes.
We will reach out to you when this affects you or if access becomes limited while changes are underway.
AMA Queensland staff will be available to guide you through these changes to ensure a seamless transition.
Private health
The viability of the private health sector is becoming an increasing challenge, and this is only exacerbated by the news of Healthscope’s collapse and Toowong Private Hospital’s recent closure.
With patients uncertain about treatment options and doctors scrambling to find alternatives, we’ve worked to keep our members informed throughout.
Healthscope has advised AMA Queensland that all its hospitals remain open and operational, with no current impacts on staff, doctors or patient care.
With Toowong Private Hospital’s closure, the administrators have informed us that they are working with hospital staff and other stakeholders to minimise disruptions to patients’ ongoing care.
As we move into the next quarter, we continue to advocate for a coordinated response from state and federal governments to support a sustainable private healthcare system.
Events
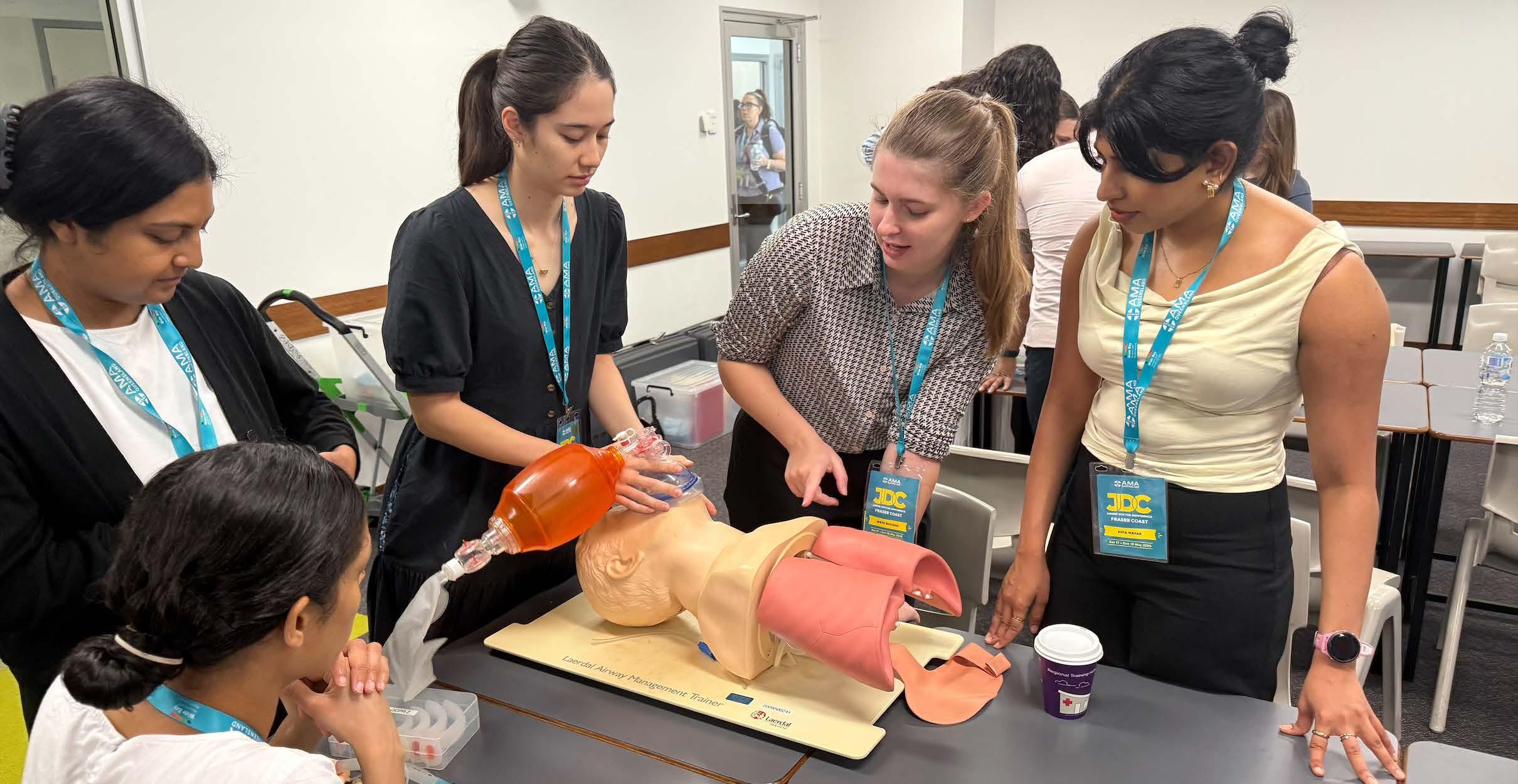
Our annual Junior Doctor Conference was once again a major success this year, bringing more than 200 medical students and doctors-in-training to the Fraser Coast for a weekend of inspiration and learning.
We’ve also hosted you at Medical Careers Expo, member networking events and our annual Dinner for the Profession, but our year is far from over.
This July, we’re heading to North Queensland and will be bringing one of our most popular functions, the Women in Medicine Breakfast , to Townsville. The breakfast will be preceded by a member networking event, offering a great opportunity to connect before the next morning.
In August, we are teaming up with the Australian Senior Active Doctors Association for our bi-annual Senior Doctor Conference. We are back with a dynamic program filled with expert speakers, discussions and opportunities to connect with colleagues.
Last, but certainly not least, we will be heading off to Vancouver, Canada this September for our Annual Conference 2025.
I look forward to reconnecting with familiar faces and welcoming new ones across our lineup of upcoming events.
See Board members See Council members
Dr Brett Dale Chief Executive Officer
AMA Queensland in the media
AMA Queensland joins Chief Health Officer to promote flu vaccinations
AMA Queensland Immediate Past President Dr Maria Boulton joined Chief Health Officer Dr Heidi Carroll at a Newmarket practice in April to call on more Queenslanders to roll up their sleeves before winter arrives.
Dr Carroll received her flu jab in front of the TV cameras to promote Queensland’s free vaccination program.
At the time of the event, more than 13,600 cases of influenza had been recorded across the state, a 35 per cent increase on 2024 – a trend Dr Boulton was already seeing at her own practice.
“If you’re thinking about getting the flu vaccine, now is the time to do it – don’t wait,” Dr Boulton said.
“The flu can affect anyone at any age, but people most at risk are people over the age of 65, young children, babies, people who are immune-compromised, people who have diabetes, heart disease, or lung disease, and also pregnant women.
“It is a yearly vaccine, so if you had your vaccine last year, that doesn’t count for this year.
“We know that flu vaccines reduce the risk of severe disease and reduce the risk that you’ll actually get the flu infection.”
Mass vaccination is also key to preventing extra strain on Queensland’s emergency departments during the winter season.
Investigating Lyme disease in Australia
To mark International Lyme Disease Awareness Month, AMA Queensland President Dr Nick Yim spoke to ABC Radio Sunshine Coast about the disease and the recommendations from a recent Senate inquiry into its prevalence in Australia.
“The Australian Government and the researchers, they state that there is no evidence of locally acquired Lyme disease,” Dr Nick Yim said.
“But without a doubt, there are many people in our community who have symptoms similar to Lyme disease.”
There is little recognition of the disease in Australia despite many people presenting with similar symptoms.
“People state they have been bitten by a tick locally, they get tested overseas, they have the symptoms,” he said.
“This is why we often call for increased research and education, so we can ensure that we have best practice for our country based on the evidence.”
Dr Yim also highlighted the need for evidence-based clinical pathways for doctors to best treat patients for their symptoms.
“We need diagnosis, we need management, because many people are suffering,” he said.
“This is the reason why we need to ensure we are investing into research to ensure that clinical pathways are in place.
“GPs are one of the first points of contact for people with rare diseases, such as tick-borne illnesses, and must be supported to investigate patients who present with such symptoms and signs that can be difficult to pinpoint.”
Investigating Lyme disease in Australia
AMA Queensland joins Chief Health Officer to promote flu vaccinations
AMA Queensland President speaks out on workforce challenges
Workforce has long been AMA Queensland’s top priority, but in the lead-up to the state budget, our efforts have been significantly amplified.
President Dr Nick Yim spoke to ABC Radio the morning of the Committee for Economic Development of Australia (CEDA) health workforce event about the importance of addressing our workforce crisis and what message he hoped to deliver as a panellist.
“We know patients are waiting longer and what that means is unfortunately sometimes our health conditions can deteriorate or we can have additional complications such as pain,” Dr Yim said.
“There is a state budget coming up and it’s great that there is a commitment for more hospital beds and health workforce, but we need to ensure there is a plan moving forward.”
Specifically, he highlighted the need for short-term, medium-term and long-term plans that are sustainable.
“Firstly, we know that we need to bring doctors into Queensland, but recruitment is currently quite competitive,” he said.
“The other key thing is training. We know that there are some areas that need more specialists and more GPs with additional skills… such as anaesthetics, obstetrics, mental health.
“One of the long-term solutions is to ensure that healthcare services and Queensland Health are educating from the top down to ensure that there are appropriate cultural supports across the whole system.
“If we have a system that promotes psychological safety, we know that it will minimise burnout among our colleagues… [and] prevent people from leaving the healthcare system.”
If you’d like to be a part of any upcoming social media campaigns, or would like us to highlight your workplace or practice, please call the Social Media Team on 07 3872 2222
AMA Queensland President Dr Nick Yim speaking at the Committee for Economic Development of Australia (CEDA)
Meeting Queensland’s future health workforce needs
Award winners Drs Matt Masel, Mary Dunne, Elise Witter and Professor Sunil Lakhani with AMA Queensland President Dr Nick Yim (centre)
AMA Queensland honours top doctors
Dr Mary Dunne
AMA Queensland Gold Medal
A Central Queensland doctor who has served the town of Woorabinda for nearly 30 years has been honoured with the Gold Medal at AMA Queensland’s annual Dinner for the Profession
Dr Mary Dunne has been a general practitioner in the First Nations community since 1998.
AMA Queensland President Dr Nick Yim praised Dr Dunne’s incredible contribution to the state’s medical profession and to regional Queensland.
“Dr Dunne exemplifies the passion, talent and hard work of truly great doctors,” he said.
“The Gold Medal is the highest honour AMA Queensland can bestow. It is given to a member who has rendered outstanding services to the association, to the practice of medicine, or to the community.
“Dr Dunne has done all three. She is the kind of person who would much rather work quietly in the background than stand in the spotlight. But the difference she has made in people’s lives has not gone unnoticed.”
After finishing her medical studies in 1982, Dr Dunne worked in Moranbah, then established a private practice in Clermont, where she worked until 1998, when she applied be the full-time doctor in Woorabinda.
“For the first 16 years Dr Dunne worked as a solo practitioner, on call seven days a week and up to 22 days at a time.
“She earned the community’s trust with her focus, availability and dedication to uncompromising care.”
Dr Dunne helped establish visiting services such as cardiology, gynaecology, paediatrics, and ENT clinics, which included yearly surgery for children’s ears. In the early days, during ENT surgery week, Mary would host up to 13 doctors and nurses on her own cattle farm to make sure services were delivered.
Dr Dunne is still practising in Woorabinda, running her farm, and spending as much time as possible with her nine grandchildren.
She was one of four incredible doctors honoured at AMA Queensland’s Dinner for the Profession
“The AMA Queensland Excellence in Healthcare Award went to breast cancer specialist Prof Sunil Lakhani, the Rural Health Medal to Dr Matt Masel and the Doctor in Training Medal to Dr Elise Witter.
“I congratulate these doctors on their phenomenal achievements throughout their careers so far,” Dr Yim said.
“They are an inspiration to the profession, and it was a delight to see them so warmly applauded by their peers.”
Prof Sunil Lakhani
AMA Queensland Excellence in Healthcare Award
After surviving a childhood in Uganda – which involved being expelled from the country by then-dictator Idi Amin – Dr Lakhani built an incredible medical career in London before moving to Brisbane in 2003 to head up the pathology department at the University of Queensland’s School of Medicine.
He has raised more than $20 million in grant funding for breast cancer research, written 12 books, and trained more than 100 students in research methodology and integrating research with clinical management.
He is currently a Clinical and Molecular Pathologist at The University of Queensland, Pathology Queensland and Sullivan Nicolaides Pathology.
Dr Matt Masel
Rural Health Medal
Dr Masel grew up in Brisbane, but he and wife Dr Sue Masel made Goondiwindi their home in 2001 and have since been tireless advocates for the border town community.
As well as being a rural GP, Dr Masel has worked as a visiting medical officer at Goondiwindi Hospital providing acute care and obstetric services. He is on the GP obstetric roster for the maternity service, and is interested in Aboriginal health, zoonoses and geriatrics. Matt provides senior input and teaching in the hospital ward rounds and on call assistance for emergencies and advice.
Dr Masel was also a leading participant in the first year of the COVID-19 pandemic response, and President of the Rural Doctors’ Association of Queensland from 2022 to 2023.
Dr Elise Witter
Doctor in Training Medal
Raised in Cairns, Dr Witter studied psychology before gaining her medical degree at the University of Queensland in 2019.
Returning to the far north, she has worked in Mareeba and around Cape York, including in remote Indigenous communities, all while becoming a strong and unrelenting advocate for doctors in training.
In 2023 she was nominated unopposed to the AMA Queensland Doctors in Training Chair position, and last year she became the Deputy Chair of the National DiT Committee – a testament to her leadership and passion for junior doctor wellbeing.
The Royal Australian College of General Practitioners (RACGP) Health of the Nation Survey collected information on the 3 most common reasons for patient presentation to primary care, as reported by GPs (RACGP 2023). In 2023 these were: psychological factors, including depression and anxiety
musculoskeletal conditions, including arthritis
endocrine and metabolic conditions, including diabetes.
Defunding chronic disease and mental health Medicare items hurts us all
General practice is the front line of Australia’s healthcare system. It’s where most people turn first—and most often— for long-term, whole-person care. GPs don’t just treat coughs and colds; they manage complex conditions, co-ordinate care plans and help keep people out of hospital. They are often the first point of contact for all mental health conditions too. But all of this relies on adequate funding – and right now, that’s under threat.
The Australian Government recently announced changes that reduce or remove patients’ chronic disease and mental health funding. These are changes that should concern us all deeply.
Firstly, the Medicare Benefits Scheme (MBS) will be indexed at 2.4% from 1 July 2025. Indexation is vital and welcome, but this modest increase does not account for the recurrent years of neglect when rebates were frozen. It also doesn’t match rising wage costs, including for practice nurses and allied health workers, which have increased three per cent annually over the last decade.
Secondly, rebates for chronic disease and GP management plans and associated team care arrangements will be rolled into a single $156.55 payment. While the government says the changes will reduce red tape, they will also lower the overall rebate many chronic disease and mental health patients currently receive.
With any changes to funding models, there must be appropriate lead time to allow GPs and practices to adapt their systems and workflow. Without, it can lead to significant angst. The government has given practices just one month to ready themselves.
GPs who have managed to crunch the figures report it will make employing practice nurses for chronic disease work less viable. This is despite GPs viewing practice nurses as essential in delivering care plans, coordinating
Dr Nick Yim President
appointments, following up results and supporting patients between visits. But if they can’t bill for these services, they can’t afford to keep these staff. That leaves patients with fewer services and longer waits.
For people living with ongoing health conditions, especially in rural, regional or lower-income communities, this means reduced access to care. Fewer follow up visits. Fewer mental health reviews. Fewer touchpoints to keep them well. The irony is stark: cutting these services will only increase pressure on hospitals and emergency departments down the track, at much greater cost to the health system.
Defunding key MBS items also doesn’t just devalue the work of GPs; it weakens the whole system. It’s not just a policy decision; it’s a decision that affects real people, in real communities, every day. Any health system funding changes must benefit all patients and not leave any worse off. This change does not achieve that aim – not by a long shot.
The removal or reduction of MBS items that cover chronic disease management plans and mental health care plans also sends a dangerous message – that this kind of care isn’t worth supporting. Yet it’s the cornerstone of prevention, early intervention and health equity.
The solution is clear: patients’ Medicare rebates must be increased and indexed appropriately. Complex care such as chronic disease, mental health and ultimately longer consultations need to be encouraged and supported. The Workforce Incentive Payments that support general practice to employ practice nurses and allied health workers to enhance team-based care have not kept up with rising costs. That must also be remedied.
Now, more than ever, we need to protect and strengthen general practice, not undermine it. Because when GPs can do their job properly, Australians stay healthier, longer.
Not part of the job
Emergency physicians expect many things during any given work day.
Anaphylaxis in a small child, cardiac arrests, young people critically injured in a road crash, patients in respiratory distress? Check.
Intoxicated or acutely mentally ill patients requiring the use of de-escalation techniques honed over years of training? No surprise.
Graveyard shifts, overtime and dinners scavenged from half-broken vending machines? Bring on the Burger Rings.
But aggression, verbal abuse and physical assault is not –and should never be part of the job.
Sadly, emergency department (ED) doctors report occupational violence is becoming commonplace, with incidents occurring at least weekly, if not multiple times per shift, in busy metropolitan hospitals.
The Australasian College for Emergency Medicine released a report in February calling for urgent action.
It specifically advocates for state governments to “take responsibility for the causative factors outside the control of EDs that contribute significantly to violent incidents”, including whole-of-system reforms to address ED overcrowding, access block and prolonged ED lengths of stay.
AMA Queensland has been similarly advocating for urgent action by Queensland Health to better protect ED staff and remove system factors contributing to patient frustration and aggression.
Those factors include the government’s new real-time data portal, retention of drug diversion, pill testing and alcohol-harm reduction laws and better regulation of medicinal cannabis products.
Real-time data portal
Queensland Health’s real-time data portal is a causative system factor that both doctors and nurses want fixed.
The portal prominently displays the ‘median waiting time – all patients’ for 25 Queensland Health public EDs and seven minor injury and illness clinics (see table of listed hospitals below).
Hospital ED ‘Median waiting time – all patients’
Royal Brisbane and Women’s Hospital 38 minutes
Princess Alexandra Hospital 13 minutes
Queensland Children’s Hospital 8 minutes
Queen Elizabeth II Jubilee Hospital 32 minutes
Logan Hospital 18 minutes
Redland Hospital 10 minutes
The Prince Charles Hospital 20 minutes
Caboolture Hospital 12 minutes
Redcliffe Hospital 17 minutes
Ipswich Hospital 24 minutes
Toowoomba Hospital 16 minutes
Mount Isa Hospital 47 minutes
Gold Coast University Hospital 19 minutes
Robina Hospital 12 minutes
Sunshine Coast University Hospital 22 minutes
Nambour Hospital 18 minutes
Gympie Hospital 8 minutes
Hervey Bay 26 minutes
Maryborough Hospital 75 minutes
Bundaberg Hospital 19 minutes
Cairns Hospital 25 minutes
Townsville University Hospital 27 minutes
Mackay Base Hospital 51 minutes
Rockhampton Hospital 20 minutes
Gladstone Hospital 28 minutes
Open Hospitals website 1 May 2025, approx. 2pm – 2.30pm
While the data does display median wait times, it is only the median waiting time from when a patient is assessed by a triage nurse until treatment is ‘commenced’.
Treatment is ‘commenced’ when ‘meaningful treatment’ is provided being the ‘active management of a patient following the completion of the initial triage process (e.g. when a patient is given pain medication to relieve their symptoms)’.
The portal’s disclaimer page also says patients may be asked to return to the waiting room once their treatment has commenced.
Clearly, this limited metric is not what patients or the community commonly mean or understand to be ED waiting time.
And the ‘real-time’ waiting times the portal displays are most certainly not the real wait times most patients are experiencing in our overcrowded ED waiting rooms.
Doctors report this is leading to frustration, with patients holding their phones up in front of clinicians and demanding to know why they have been waiting (sometimes hours) longer than the 24.2-minute average shown on the portal as per the above table.
Recent media reports stated ‘one nurse was struck by a phone when a patient lost their patience’.
Despite this, the Minister and Queensland Health have refused to change the metric reported to make it genuinely meaningful for patients – the median waiting time to see a doctor.
AMA Queensland will continue to urge the government to update the website with the wait time to see a doctor and accurate representations of the numbers of patients waiting in our EDs.
Substance-related harm
AMA Queensland is also dismayed that the government has walked away from life-saving substance use reforms that directly reduce ED presentations and clinician workloads.
Funding was not renewed for Queensland’s groundbreaking pill testing service which had already detected deadly nitazenes in the community, potentially saving multiple lives.
The Premier has likewise vowed to repeal drug diversion laws, introduced only last year and heralded as a vital and overdue reform by doctors, nurses, lawyers and police.
This may further increase ED presentations for avoidable drug harms and the risk of occupational violence linked to intoxication.
The government has also given clear indications it intends to walk back alcohol harm reduction laws, including safe night out precincts and lock out laws, which have been proven to reduce injuries and violence from alcohol use in pubs and clubs.
No ED doctor wants to treat patients harmed by alcoholfueled violence or become a victim of it themselves.
To date, neither the government nor opposition has responded to AMA Queensland’s appeal for retention of the legislation, sent both before and after the Queensland election.
More positively, AMA Queensland’s calls for better regulation of medicinal cannabis products alongside The Royal Australian and New Zealand College of Psychiatrists, Royal Australian College of General Practitioners and the Pharmacy Guild have been met with more open consideration.
ED physicians and psychiatrists have been alarmed at increasing rates of psychosis linked to highly potent medicinal cannabis products, including by patients who have never had mental ill health before.
Responsibility rests across jurisdictions, including the state and federal government, but meetings with agencies including the Therapeutic Goods Administration, have confirmed political leaders are also concerned about the issue.
AMA Queensland will continue to advocate for all reforms that reduce unnecessary ED presentations and, most importantly, the risk of occupational violence for our dedicated ED staff.
No one should have to accept that as part of the job.
The doctor’s dilemma: To speak, or stay comfortable in the age of AI
For most of my career, I’ve worked within the system — but not passively.
Inside clinics and policy circles, I’ve fought hard for patients and for truth. I’ve pushed against legacy thinking, challenged convenient silence and spoken plainly in rooms where plain speech wasn’t always welcome.
I’ve done this not to provoke, but because I believe the medical profession must do more than appear reasonable. It must act courageously.
Now, as the system nears irreversible change, I’m realising something else: being loud behind the scenes isn’t enough. We need to lead publicly.
What I saw early, and what I still see now
I grew up in Papua New Guinea. From a young age, I saw suffering up close. Not just illness, but the way distance, disconnection and under-resourcing turn treatable conditions into life-altering loss.
Now, working in Far North Queensland, I see many of the same structural failures here, just better dressed.
I’ve come to understand something confronting: our current health system is still failing Aboriginal and Torres Strait Islander communities.
We speak often about ‘Closing the Gap’, the national project to bring life expectancy and health outcomes for First Nations people in line with the rest of Australia.
But in practice, preventable diseases still go undetected, chronic illness is poorly managed, access is delayed or denied and outcomes remain generationally worse.
We are not closing the gap, we are administrating around it.
What we call Australia’s ‘world-leading’ healthcare system is still operating within a structure that was not built by, for or with First Nations communities in mind.
Dr Lee Jones Chair, Committee of General Practice
And it’s not just Indigenous health; it’s rural health more broadly.
Across regional Australia, doctors and healthcare workers are choosing not to stay. Many are retiring, burning out or quietly leaving the system. We have no sustained workforce strategy for these towns. No long-term plan for who will remain.
But there is a solution, and it’s not wishful thinking.
It’s artificial intelligence.
AI systems, deployed responsibly, could provide immediate diagnostic support, reduce dependence on overstretched staff, extend specialist care into the most remote communities and give patients real-time guidance when no clinician is physically present.
It will not replace human care, but it may be the only way to preserve access where human clinicians can no longer stay.
Inside the profession, and the courage we must find
There are many people in our profession who believe deeply in a system that serves patients, protects clinicians and improves health outcomes at scale.
But there is also drift.
Lobbying from external groups – many of whom fund both sides of politics – continues to distort healthcare priorities. It is structurally corrosive to good governance and it’s time to end it.
Government funding models reward throughput over quality, prioritising fast, reactive care over long-term, preventive outcomes.
Advocacy is too often reactive and lacks impact.
We should lead from a place that genuinely helps patients and not be pushed around by government agendas.
Meanwhile, healthcare policy is being shaped by short-term election optics, not predictive modelling or evidence-based roadmaps to a healthier Australia.
I’ve seen the pull of legacy – the instinct to preserve rather than transform.
I’ve also seen how easily good people become quiet when the cost of speaking up is career discomfort or institutional friction.
But healthcare is not a game of optics. It’s a moral contract.
I don’t want to play to maintain power. I want to play to win the future for patientss.
Artificial intelligence has arrived, and we are not ready
AI is no longer theoretical.
Right now there are systems that can: detect disease earlier and with greater accuracy, triage faster than emergency departments, support clinicians in low-resource areas, automate routine care and help patients understand their own health better than most explainers.
And yet, as a profession, we hesitate.
We tell ourselves, “It’s not real clinical reasoning”, “patients want a human touch”, “technology is just a tool, not a threat”.
But these responses miss the point.
This isn’t about replacing doctors. It’s about expanding care through access, equity and efficiency in ways we were never able to do before.
If we miss this moment, the cost won’t be our reputations. It will be the lives of those who continue to fall through the cracks.
Why I’m speaking now
Because I still believe in medicine.
I believe in governance, rigour and careful leadership.
But I also believe in clarity, and in courage.
I believe that we must shift from status preservation to system evolution, and that our peak bodies must lead on patient-first technology adoption, not follow reluctantly.
I believe that clinical excellence must include adaptability, not just tradition, and that speaking plainly is now an act of public service.
This is not disruption for the sake of novelty.
This is a call to realign medicine with the people it exists to serve.
What comes next, and who will lead it
We need doctors who can govern wisely and evolve quickly.
We need institutions that hold care above ego, and clarity above caution.
And we need to speak openly about what’s coming before others define it for us.
Because we are not decades away from change.
We are months to a few short years from artificial intelligence systems that can reason, diagnose and adapt at a level that will fundamentally alter clinical roles, patient expectations and healthcare delivery.
We are not preparing fast enough, and in the fog of denial, the cost is always borne by patients.
This is my first step forward.
Not with noise, but with conviction.
And with an open hand for anyone who’s been feeling the same but wasn’t sure when to speak.
Now is the time.
Election done and dusted: now is the time for real reform
Elections are always a chance to highlight the critical issues facing our nation, and this year health took centre stage in the federal campaign.
The major parties showed a real commitment to investing in the nation’s health system, particularly with historic funding announced for primary care.
We welcomed this focus — the quantum of funding committed is what we need — but sadly, a significant proportion of this money could have been better directed.
This election represented a missed opportunity for significant, structural reforms to the health system.
But now it’s time to look ahead. As the dust settles, we can get on with the job of pushing for meaningful reform in general practice, public hospitals, private health and more.
General practice and Medicare
The $8.5 billion for Medicare announced before the election was called, supported by the Coalition and locked into the budget, set the tone for the rest of the campaign.
While this funding is welcome and will help some patients and practices, we will continue to highlight through our Modernise Medicare campaign the need to rethink and redesign our out-of-date Medicare rebate structure.
Australia needs a new seven-tier GP consultation item structure designed to meet the challenges of an ageing population and the growing burden of complex and chronic disease.
Throughout the campaign, Prime Minister Anthony Albanese consistently said 90% of all GP visits will be bulk billed by 2030 under his policy to extend triple incentives to all patients.
While modelling in the years leading up to 2030 is not available, this 90% figure will be the figure this policy will be squarely judged on. We will do our best to ensure the government is held to account in improving affordable access to high quality GP services, while still pushing hard for the broader reforms we need to improve Medicare.
Dr Danielle McMullen AMA Federal President
Workforce
Some big wins came our way on workforce. Following years of AMA advocacy, both Labor and the Coalition made commitments to increase our GP workforce. Labor locked in funding in the budget to grow Australia’s specialist GP training places together with funding for additional training rotations in general practice for prevocational doctors, and to improve employment conditions for GP registrars, including the important addition of paid parental and study leave.
Looking forward, we will be vocal about the need for an independent national health workforce planning agency to guide new policies and provide a clearer picture about the state of our workforce, including in regional, rural and remote areas. It is crucial to ensure the medical workforce is distributed where it’s needed most — but this has been a huge blind spot since Health Workforce Australia was abolished in 2014.
Public hospitals
As we highlighted several times during the campaign, our public hospitals continue to be logjammed and our recent report found there is no end in sight to ambulance ramping.
There were some commitments to hospital funding made during the campaign, and indeed in the months before. But we know there is an urgent need to lock in a new National Health Reform Agreement. Without a new funding deal, these top-up commitments are little more than a nice idea.
We will be taking this government to task to ensure they expedite a new agreement for the sake of our patients, who are suffering, and our dedicated public hospital doctors.
Private health
The issue of private health sustainability was absent in this year’s federal election campaign. We know the system is demonstrating unprecedented vulnerability — just look at the recent closures of maternity wards and other private hospital services around the country.
This is proving to be one of Australia’s big sleeper issues, and if governments don’t act quickly, there will be devastating consequences for patients. We will engage with this government and continue to champion our proposal of a new independent authority that can create a platform for all the key players in the sector to create once-in-a-generation reforms. We will also be calling for a mandated minimum payout by insurers of 90% as a proportion of their premiums to encourage greater uptake of private health insurance.
Our Vice President A/Prof Julian Rait, a specialist ophthalmologist, sits on the Private Health CEO Forum created by Labor and will continue our strong representations on this platform.
Public health
We gained significant traction in the media for all our policy proposals throughout the course of the federal election campaign. And one of those was our proposal for a tax on sugar-sweetened beverages. This is a commonsense policy — backed by evidence and proven success around the world — that can address Australia’s obsession with sugar.
Sadly, no party committed to a sugar tax during the campaign, despite the clear need to help tackle Australia’s rising rates of chronic disease, and the opportunity to raise much needed funding, which could be used for preventive health activities.
Political analysts will continue dissecting this year’s election result. Our mission remains the same. Our commitment to advocating for doctors, patients and the health system is unwavering. We will continue to work tirelessly across the political divide, ensuring that the voices of medical professionals are heard and that meaningful reforms are achieved.
Grow your medical practice with expert insights
Are you looking to expand and strengthen your medical practice? Want to refresh your approach with sustainable strategies? AMA Queensland President Dr Nick Yim invites you to our Private Practice Refreshed Seminar series to gain the knowledge and tools needed to build a thriving, long-lasting practice.
Who should attend
GPs
Specialist Consultants
Private Practice Owners Practice Managers
Medical professionals looking for expert insights in finance, legal, and technology
Cost
FREE for AMA Queensland members (2 complimentary tickets per member)
$250 for non-members
Free for Toolkit subscribers
Discounts available for private practices purchasing multiple tickets, contact: registrations@amaq.com.au
Event dates and location
The Ville, Townsville – Friday 18 July QT Hotel, Gold Coast – Friday 5 December
Contact
Questions regarding registration: registrations@amaq.com.au or 07 3872 2222
AMA Queensland membership: membership@amaq.com.au
Our workforce: today, tomorrow and the future
I can’t think of a better way to begin my term as Chair of the Queensland Clinical Senate than to be part of a meeting focused on our workforce.
Having been a clinician for more than two decades, I am a huge advocate for our workforce and of working in healthcare. The work we all do each day makes a big difference to our patients, their loved ones and the community as a whole. Ensuring we have a workforce that can continue meeting these needs in a safe and caring way well into the future is an essential piece of work for the Senate.
One of the highlights of my career in medicine and medical administration has been the diverse range of people I have worked with, the friendships I have made and the people I have seen develop to take on new roles. This has made me passionate about our entire workforce; I want to see our workforce having opportunities for growth in an environment in which they feel safe, supported and love to work in.
So, to be part of a meeting about the healthcare workforce and the challenges we must face to ensure we have the workforce needed to provide safe healthcare across our vast state, was a real privilege for me.
Every one of the 150 clinicians, consumers and system leaders at that meeting wanted to be there—to interact and have their voice heard—and wants be part of the solution.
We talked about the challenges we face in retaining our workforce and what we can do about it: can we work in new ways, how can we better look after the wellbeing of our staff, how can we give clinicians more opportunities and more time with their patients? The conversations were thought provoking and bold.
Dr Kellie Wren
Chair, Queensland Clinical Senate and consultant anaesthetist
We heard from many talented clinicians about amazing pieces of work already underway across our system that we can learn from—initiatives that are working and with the potential to be scaled.
As a result of our discussions, we have developed a set of recommendations to present to Queensland Health to help contribute to solutions for a sustainable workforce for ‘today, tomorrow and the future’.
Our recommendations cover a range of areas from the use of digital systems to reduce the burden of administrative tasks for our staff, and leveraging partnerships to promote healthcare careers, to embedding high-level Aboriginal and Torres Strait Islander Health clinicians in every hospital and health service and exploring opportunities to optimise practice.
We are at a critical time for our workforce, and I am so pleased the Senate is part of the conversation and the solution. There are so many incredibly talented people in our healthcare system and the Senate enables their voices to be heard on the issues that matter.
I will work hard during my time as Chair of the Senate to make sure clinician and consumer voices continue to be heard and are front and centre for the future of our wonderful healthcare system.
You can learn more about the Queensland Clinical Senate and read the full set of recommendations (as they become available).
Queensland Clinical Senate
Meet a member
Dr Rob Nayer
We’re hundreds of doctors, and thousands of health workers in general, short of what we need and this puts pressure on the current workforce and leads to burn out.
Dr Rob Nayer didn’t always want to be a doctor. After finishing school in his native Canada, he completed a commerce degree to become an accountant, then finished a degree in health science.
While studying, he worked as a St Johns Ambulance emergency response volunteer and trained lifeguards. Realising he enjoyed this work far more than his chosen fields, he applied to the University of Queensland Medical School, always with a plan to do emergency medicine.
After graduating in 2016 and interning in Rockhampton, Dr Nayer then spent time as an RMO and registrar between Ipswich, Gold Coast and Robina hospitals.
Dr Nayer joined our Committee of Doctors in Training (CDT) in 2020 as the Industrial Relations Lead. It was a time when junior doctors were facing structural industrial challenges in Queensland, such as 12-month temporary contracts.
“I hoped that with better industrial protection we could also improve overall mental health and wellbeing. Doctors in training can be in precarious positions, and the interplay between employment and career progression/specialty training becomes incredibly stressful and I wanted to do what I could to help support DiTs industrially,” Dr Nayer said.
Dr Nayer went on to serve as CDT Chair, during which time the committee created a strategic plan and reorganised its structure to include more junior doctors and focus on areas of concern, such as climate and sustainability advocacy.
After making his mark in the Committee of Doctors in Training, Dr Rob Nayer is now fellowed and has set his sights on rallying consultant specialists together as Chair of AMA Queensland’s Committee of Consultant Specialists (CCS).
“We need strong senior doctor voices to drive professionled changes, because if we don’t take a leadership role, then government or other organisations will push for changes that may have a detrimental impact on doctors and our patients,” said Dr Nayer.
“Senior doctors still hold positions of immense power within our medical system.
“Doctors in training frequently cannot advocate for much needed change because the hierarchical nature of medical training combined with the competitiveness of being selected into training positions has a significant chilling effect.
“With CCS, I’m hoping to find one or two big ticket advocacy items we can rally senior doctors around,” he said.
In addition, Dr Nayer chairs AMA Queensland’s Workforce Working Group, where he sees two main problems.
“The first is a straight numbers issue. We’re hundreds of doctors, and thousands of health workers in general, short of what we need and this puts pressure on the current workforce and leads to burn out.
“It’s not just workforce numbers though, we also need appropriate spaces to do our work. I remember as a registrar roaming an emergency department for upwards of 60 minutes a shift trying to find a computer to use. Physical infrastructure (or lack thereof) becomes a workforce problem as well.
“The second issue is how we use our workforce. Doctors spend a lot of time on non-value-adding administrative tasks. A lot of time, energy and money goes into training doctors’ clinical skills and we need to make sure the jobs we’re asking them to do make use of that training appropriately.
“There are lots of examples of this throughout the different medical specialties, from primary care to private hospital workforces, and especially our public hospital workforce.”
The working group is finalising an action plan and is set to wrap up soon.
Dr Nayer is working as an emergency consultant at Mount Isa Hospital, flying in and out.
“I enjoy the variety and pace of emergency medicine. With my commerce education as well, I also appreciate the systems-based thinking that’s needed to be an effective emergency physician,” Dr Nayer said.
“The variety of patient presentations keeps me engaged, and I get a lot of professional satisfaction from helping people who frequently feel like they don’t have anywhere else in our health system they can access for care.
“I’m really enjoying working in remote Queensland. I find there’s less hospital politics, and I can focus on patient care and teaching doctors in training,” he said.
Outside of work in Mount Isa and his AMA Queensland roles, Dr Nayer also sits on the Queensland Doctors Health Programme Board and the ACEM Rural Regional and Remote Committee.
“It’s only been a little over a year since I finished my specialty training and it takes some time to re-adjust to life after constant studying. I’ve been working on finding some hobbies to keep me busy,” he said.
“I enjoy bushwalking/hiking and have a trip planned later this year to South America which I’m sure will include some great hiking opportunities.”
Research round up
Research Review Australia has more than 50,000 health professional subscribers across Australia. It provides clinical research updates and webinars that qualify for CPD points.
The updates cover more than 50 clinical areas and feature 10 papers from global journals with commentary by a local expert on the impact to everyday practice.
Sign up for Australian health professionals at no cost is available at researchreview.com.au
Severe obesity: a susceptibility factor for developing inflammatory bowel disease
Inflammatory Bowel Disease Research Review Issue 88
Reviewer: Dr Alex Barnes
The impact of bariatric surgery and severe obesity on the risk of developing IBD was examined in a populationbased study.
“This large public health system database study looked at obesity, super obesity and bariatric surgery and the incidence of IBD. Available confounders included smoking status, age and sex. Mortality was considerable, ranging from six per cent (bariatric surgery) to 19% (super obese).
The IBD incidence rates were similar for super obesity and bariatric surgery groups, with the obesity group having a lower incidence rate. The HRs (obesity as baseline) for severe obesity and bariatric surgery were similar to that of smoking in CD and in UC. Of note, smoking was associated with UC incidence here.
One would imagine that most of those with bariatric surgery were at one stage super obese. This study included a different population to others that have reported inconsistent associations between bariatric surgery and IBD incidence. I do not think the recommendation for non-invasive screening is warranted.”
Reference: J Crohns Colitis 2025;19:jjaf010
Inflammatory Bowel Disease Research Review Issue 88
Adolescent and adult transitions from major depressive disorder to bipolar disorder
Psychiatry Research Review Issue 89
Reviewer: Professor Nicholas Keks AM
The association between the age of major depressive disorder (MDD) onset and progression to bipolar disorder was examined in this retrospective cohort study. Data derived from the Stockholm MDD Cohort from 1997 to 2018, including 114 adults.
Following a bipolar disorder diagnosis, both groups experienced a significant reduction in inpatient care. These results indicate that adolescents may have a delayed progression to bipolar disorder compared to adults.
“This retrospective study from the Karolinska Institute in Sweden has made a significant finding, that adolescents who experience an initial bipolar depression are likely to experience their first manic episode significantly later than adults.
However, because of the unquestioning acceptance of the DSM-5’s (and earlier versions’) approach to bipolar diagnosis, the finding is conveyed in terms of conversion from the first episode of MDD to the diagnosis of bipolar disorder. DSM rules stipulate that bipolar diagnosis can only be made when there has been a manic episode.
The authors of the study take the DSM line that the initial MDD is not bipolar, when it is clearly the start of bipolar illness. Before the DSM, psychiatrists diagnosed any case of severe/melancholic/endogenous depression as manic-depressive, and treatment involved ECT and mood stabilisers. In the findings of this study, it is noted that once patients are properly diagnosed and treated, the need for antidepressants and hospitalisation decreases. Perhaps the real challenge is going back to the approach of diagnosing depressive illness as likely bipolar even if mania has not occurred. Poor response or worsening with antidepressants, melancholic characteristics, mixed states like agitation and family history, are among the indicators that a depression is likely to be due to bipolar mood disorder.”
Reference: JAMA Psychiatry. 2024;1;81(9):863-869.
Why the Doctor in Training voice matters
What does it mean to thrive as a doctor in training in 2025? For too long, success in medicine has been framed as surviving long hours, relentless pressure and constant relocation. As AMA Queensland’s Committee of Doctors in Training, we are challenging that narrative.
The primary goal of the CDT is to advocate for doctors in training across the state. While we all come from different hospitals, training programs and backgrounds, we are united by our passion for safe workplaces, fair conditions and genuine opportunities to thrive, rather than just survive, in the system.
Across Australia, doctors in training are managing increasing clinical loads, inflexible rosters and healthcare worker shortages. Amidst this, we are expected to plan our careers, pass high stakes exams and navigate systems that are too often opaque and inconsistent. The weight of those expectations is not only personal, but structural – and so must be the solution.
That’s why this year’s CDT is focusing not just on problems, but on system-level change. Ongoing MOCA 7 negotiations are an opportunity to reshape the industrial landscape and we are grateful to ASMOFQ for their persistent support of doctors in training. Alongside this industrial work is an equally urgent cultural shift: the increasing focus on wellbeing. It is encouraging to see wellbeing finally being treated as a core responsibility of our health services, rather than a personal responsibility to attend a yoga class or read a book on resilience. Wellbeing is not about individual doctors being better at self-care.
Dr Emma Hodge Chair, Committee of Doctors in Training
It is about the systems we work in being safer, fairer and more equipped to support the needs of doctors, as well as our patients. It is about ensuring that doctors can take sick leave without guilt, raise concerns without fear and access support without judgment. It is also about psychological safety, professional respect and the ability to progress through prevocational and vocational training with minimal obstacles.
As such, the CDT continues to advocate for reforms that address the root causes of burnout, such as lack of control over rosters, inflexible pathways into training, inconsistent supervision and the normalisation of overtime. Our goal is not just to prevent harm, but to build a culture where doctors in training are seen as people, not just a name on a roster.
Some of the most powerful wins recorded by the CDT in recent years have come directly from doctor in training voices: calling out unsafe rostering on ward call shifts, advocating for pathways to escalate concerns, or simply telling the truth about how hard it is to be a doctor in training in this current context. For those who have helped our work – thank you. For those who have yet to take part – this is your invitation to join us.
Whether you are an intern in your first few rotations or a senior registrar navigating fellowship, you have insights that can help shape policy, challenge outdated cultural norms and improve the experience for those who come after you. Reach out to your CDT representative. Join a Special Interest Group (SIG). Start a conversation with a colleague. The future of the medical profession is shaped by what happens in training. If we want a better system, it starts here.
2025 events calendar
July
Member Networking Event, Townsville – Thursday 17 July
Women in Medicine Breakfast, Townsville – Friday 18 July
Private Practice Seminar Series, Townsville – Friday 18 July
August
Senior Doctors Conference
– Saturday 9 August
Cutcher & Neale
Property and Finance
Hybrid Event – Thursday 21 August
September
International Annual Conference Vancouver, Canada – 21 to 27 September
October
Cutcher & Neale Hybrid Event – Thursday 23 October
Women in Medicine
Breakfast, Brisbane – Thursday 30 October
November
Intern Workshop, Brisbane – Thursday 27 November
December
Intern Workshop, Gold Coast – Thursday 4 December
Private Practice Seminar Series, Gold Coast – Friday 5 December
Member Networking Event, Gold Coast – Friday 5 December
Intern Workshop, Townsville – Wednesday 17 December
Visit the AMA Queensland website for more info about our events: ama.com.au/qld/events
The new financial year gives you an opportunity to reset, review and refocus. It’s the ideal time to put a plan in place that will secure your financial future.
We can help you:
Maximise your deductions and minimise your tax
Contribute to your super in an impactful way
Expand your investments and protect your assets
Kickstart your retirement planning
We help medical professionals turn tax-time insights into longterm gains. With the right planning, the new financial year can be a powerful springboard toward wealth creation.
988
Book your complimentary consultation with our trusted advisors today.
Nicole Brown Partner, Cutcher & Neale Specialist Medical Services
New financial year, plan ahead now
It’s hard to believe we’re already in a new financial year. Now’s the perfect time to hit refresh, tidy up your books, take stock of where you’re at and put plans in place for a stronger financial position this year.
Whether you’re a doctor or a practice manager, a little early preparation can go a long way.
For doctors: take the lead early.
Service fees – These are often one of your biggest expenses and the ATO is paying attention. Make sure your fees are in line with your agreement, paid in full and aligned with the Service Entity Guidelines.
Make the most of your super – You can contribute up to $30,000 in concessional contributions this financial year (inclusive of employer contributions). Use this time to not only maximise contributions but also review how your super is performing.
Update your logbook – If you use your car for work, a current logbook helps you claim fuel, registration, insurance and other running costs up to your businessuse percentage.
ATO payment arrangements – If you have one in place, from 1 July the interest is no longer tax deductible. Consider alternative ways to pay off your debt sooner rather than later to maximise your deductible debt.
Prepare your tax return early – If you are planning to buy property, most lenders will want your most recent tax return, so getting it done sooner gives you more flexibility when it comes to timing your loan application.
Earned income as a sole trader – Using a registered tax agent allows you to defer your tax bill until as late as June 2026.
For practice managers: these tasks are key.
Employee wages and superannuation – Award wages may have increased from 1 July and with the Super Guarantee now at 12%, your accounting software must reflect the correct rates to avoid underpayments or compliance issues.
Review your budget – Set realistic income and expense expectations for the year ahead. If you haven’t already, use your accounting software to map out a basic budget. This gives you a clear benchmark to track against as the months go on.
Sub-leased rooms – Now’s a good time to check that any rent reviews or updates have been completed. This helps you stay commercially aligned and avoid undercharging.
Make the most of your tax position.
Tax is likely one of your largest outgoings, so it’s well worth taking the time to get things right and maximise your available deductions. If you’re looking to get ahead this year, speak to our medical accounting specialists today.
For personalised advice contact us on 1800 988 522 or medical@cutcher.com.au
The information in this publication contains general advice only. It has been prepared without taking your personal objectives, financial situation or needs into account. You should consider whether the information contained within this publication is appropriate for you. Where we refer to a financial product you should obtain the relevant Product Disclosure Statement or offer document and consider it before making any decision about whether to acquire the product.
100 years of trust through the generations
2025 is a milestone year for MDA National for various reasons. While we celebrate our 100th anniversary of supporting members and promoting good medical practice, we also acknowledge a decade of collaboration with the Australian Medical Association Queensland (AMA Queensland), supporting the medical profession through advocacy, education and practical assistance across generations.
We’ve come a long way since 1925, when a small group of Western Australian doctors established an organisation to protect and support members when they needed it most. With strong leadership, dedication and member loyalty, we expanded nationally and proudly became a leading medical defence organisation — a trusted partner for thousands of doctors and medical students across the country.
But it hasn’t all been smooth sailing. Our history is marked by challenges such as the medical indemnity crisis, during which MDA National’s strong leadership and prudent financial management enabled us to continue providing uninterrupted support to our members without ever making a call on them.. Beyond strategic teamwork, our partnerships have played a crucial role in expanding our impact on our communities and offering enhanced support to members.
More than a banner in a newsletter
Over the past decade, the strategic alliance between MDA National and AMA Queensland has evolved to meet the needs of the profession. Through knowledge sharing and a joint commitment to education, AMA Queensland and MDA National have empowered doctors by providing them with the tools and confidence to navigate their careers as students, junior doctors or senior specialists.
“The partnership is beyond just an advertising banner in a newsletter. The more we know about what MDA National provides, the more we can inform our members,” said AMA Queensland CEO Dr Brett Dale.
The partnership also includes tangible benefits, such as the 50% premium reduction MDA National offers to AMA Queensland’s junior doctor members and coordinated initiatives that support doctors’ mental health and wellbeing.
From student engagement and intern workshops to campaigns focused on rural doctors, GPs, specialists, and senior medical officers, AMA Queensland and MDA National work side-by-side to offer education and practical resources.
“When they become interns, then GPs or specialists, they start to have that requirement of medical indemnity insurance and see the benefits of the long-term partnership with MDA National,” said Dr Dale.
He also highlighted the strength of the collaboration, especially when addressing challenges in accessing support and medical indemnity. A standout example was the campaign to support international medical graduates (IMGs), a group often navigating complex professional pathways. Together, both organisations provided clarity on coverage to make sure Queensland IMGs felt supported — an effort that continues to this day.
Towards the next century
As MDA National marks 100 years of service to the medical profession, we look towards our future as we continue to provide support and evolve our services to respond to the changing needs of our members. With a focus on making a positive impact on our communities, strategic alliances like the one with AMA Queensland play an important role in helping us deliver our purpose.
AMA Queensland celebrates alongside us.
“You don’t get to 100 years without knowing what you’re doing. It takes a great wealth of experience, perseverance and customer service. What a fantastic effort,” said Dr Dale.
Click to play MDA National’s 100 years video
Having
Your
Andrew Harrison Medical Insurance Adviser, Cutcher & Neale General Insurance
Is your business insurance ready for the new financial year?
A new financial year brings fresh opportunities and it’s the perfect time to take stock of your business insurance. Reviewing your cover now can save you a lot of headaches down the track.
Here are five smart steps to help make sure you’re properly protected for the 25/26 financial year ahead.
1. Start by documenting any business changes
A lot can change in a year! You might’ve launched new products, expanded your team or started working with new suppliers. These changes can impact the type and amount of insurance you need. So, step one is simple: jot down what’s changed. It’ll give you (and your broker) a clear picture of where your risks might have shifted.
2. Check what cover you already have
Most businesses hold a few key policies like public and product liability, property, motor and workers compensation insurance. But when was the last time you read the fine print?
Now’s a great time to review the limits on each policy (that’s the maximum you can claim) and look at any exclusions. Are they still relevant for how you operate now? While you’re at it, set calendar reminders for renewal dates — it’s easy to miss them and accidentally go without cover.
3. Don’t forget cyber protection
Cyber-crime isn’t just something that happens to big business. In fact, small and medium businesses are increasingly being targeted, and the cost of recovering from an attack can be significant. According to the Australian Cyber Security Centre, the average cost per
cyber-crime report is now $49,600. If you store sensitive customer data or rely on digital systems to run your business, cyber insurance is well worth a closer look.
4. Shop around
With rising costs putting pressure on all sides, business owners are understandably looking for value. When your policies come up for renewal, take the opportunity to compare providers. A better price doesn’t always mean better cover — but a quick check can often reveal gaps, overlaps or a better fit for your needs today.
5. Get advice from someone who knows
Business insurance can get complex quickly. That’s where a trusted advisor comes in. An experienced broker can review your current cover, flag any gaps and negotiate competitive premiums for you. It’s a simple way to save time and give you peace of mind that your business is properly protected.
Let’s make sure your cover is fit for purpose.
Getting your insurance sorted now can help you move through 2025 with confidence. If you’d like help reviewing your current policies or understanding where you might be underinsured, contact us on imedinsurance@cutcher.com.au or 1800 988 522
The information in this publication contains general advice only. It has been prepared without taking your personal objectives, financial situation or needs into account. You should consider whether the information contained within this publication is appropriate for you. Where we refer to a financial product you should obtain the relevant Product Disclosure Statement or offer document and consider it before making any decision about whether to acquire the product.
Investing in your future now has big payoffs later in life. Imagine looking back in 10, 20, or even 30 years and knowing you made the right financial moves early.
The secret? Compounding interest.
Compounding interest is like a snowball rolling down a hill – it starts small, but as it grows, it picks up more snow (interest) and gets bigger over time. For example, if you invest $1,000 at 10% interest, after one year you have $1,100, but in year two, you earn interest on $1,100, not just the original $1,000 – so your money keeps growing at an accelerating pace!
If you wait, compounding interest has less time to build your wealth.
Our advisors can help you get started with investing:
Setting clear financial goals
Developing a smart, tailored strategy
Assessing your risk tolerance
Maximising your investments
Continuously reviewing and improving your plan
Start your journey today.
SYDNEY | BRISBANE | NEWCASTLE
Take the first step to secure your financial future and speak to one of our trusted advisors today.
Johnson Partner, Cutcher & Neale Wealth Management
New financial year, new goals: retirement planning and wealth-building tips for doctors
For doctors, the start of a new financial year is more than just a fresh set of numbers. It’s the perfect time to reset your financial goals and refocus on your long-term aspirations.
Ask yourself – are you set up for a successful retirement? If the answer is no, now’s the time to start planning!
Why it pays to start early
When it comes to retirement planning, time is your greatest asset. The earlier you start, the more you benefit from the power of compounding, a force that can significantly grow your super and investment portfolio over the years.
Even small tweaks now can have a meaningful impact down the track.
Super strategies to consider
One of the smartest moves you can make early in the financial year is to review your superannuation contributions.
The concessional cap for FY26 remains at $30,000, and maximising this amount early allows those funds to work harder for longer.
If you’ve got unused concessional cap amounts from previous years and a total super balance below $500,000, you might also be eligible to make catch-up contributions. This is particularly powerful for doctors who’ve taken career breaks or had fluctuating income.
You can also look at non-concessional contributions which are capped at $120,000. Maximising these now can make a huge difference in the long run.
Is your investment strategy FY26-ready?
While superannuation is a cornerstone of retirement, it’s not the only piece of the puzzle. Reviewing your investment strategy is another important part of your FY26 planning.
Consider whether your current asset allocation still aligns with your goals, your risk tolerance and the market opportunities emerging this year.
You might be considering additional property, investing via a trust, or building out your portfolio with more international shares.
Whatever the path, the goal is the same: growing wealth in a way that’s sustainable, tax-effective and aligned with your timeline.
Your trusted advisor makes all the difference.
The reality is there’s no one-size-fits-all solution to retirement planning. That’s where a trusted advisor comes in. Not just to tick compliance boxes, but to guide you through the financial maze with clarity and confidence.
At Cutcher & Neale, we help doctors across all career stages develop clear, actionable roadmaps toward their ideal retirement. To speak with one of our trusted advisors, contact 1800 988 522 or at financialplanning@cutcher.com.au
The information in this publication contains general advice only. It has been prepared without taking your personal objectives, financial situation or needs into account. You should consider whether the information contained within this publication is appropriate for you. Where we refer to a financial product you should obtain the relevant Product Disclosure Statement or offer document and consider it before making any decision about whether to acquire the product.
Payroll tax and what it means for Queensland doctors
Payroll tax has become one of the most talked-about legal and financial issues facing health professionals in recent years. With increased scrutiny from state revenue authorities and changes in legal interpretation, doctors—whether early in their careers or well-established—need to understand how these developments could affect their practice models and income arrangements.
In this article, we focus on the evolving payroll tax landscape in Queensland and what it means for health practitioners across the state.
Why is payroll tax an issue?
Traditionally, where doctors operated under service agreements through medical centres or clinics, these arrangements were not subject to payroll tax. However, recent court decisions and updated guidance from the Queensland Revenue Office (QRO) have broadened how payroll tax laws are applied. In many cases, payments to contracted doctors are now treated as taxable ‘wages’ under the extended ‘relevant contract’ provisions.
This shift has raised alarm bells for practices and practitioners alike, prompting legal reviews of structures, agreements and compliance strategies.
The Queensland position
In Queensland, payroll tax is levied at 4.75% if a business’s annual taxable wages exceed $1.3 million.
On 22 December 2022, the QRO issued a Public Ruling (updated in February 2024), which clarified that agreements with contracted doctors — such as service agreements — may fall within the scope of taxable “relevant contracts” for payroll tax. This meant that many practices faced potential tax liabilities for payments made to independent GPs and other practitioners.
However, in a significant development, the Queensland Government passed the Revenue Legislation Amendment Bill 2024, confirming that from 1 December 2024, payments made by GP practices to GPs will be exempt from payroll tax—bringing welcome certainty for GPs and clinics alike.
Who qualifies for the GP exemption?
The exemption applies to:
doctors registered under the Health Practitioner Regulation National Law to practice in the specialty of general practice
practitioners listed in the federal Health Insurance (General Medical Services Table) Regulations 2021 (Cth), schedule 1, part 1, clause 1.1.3 prescribed medical practitioners who predominantly provide GP-style services.
This exemption does not extend to medical specialists or allied health practitioners, who must still assess their potential payroll tax obligations.
What doctors and practices should do
While the GP exemption offers relief, compliance obligations remain complex and vary depending on your practice model, specialty and financial thresholds. There are a few things to consider.
Know the law: understand current legislation and QRO rulings relevant to your specialty and business structure.
Assess your threshold: determine whether your practice is approaching or exceeding the payroll tax threshold.
Review contracts: revisit any service or independent contractor agreements with legal and accounting advisers.
Check eligibility: see if you or your practice qualifies for any exemptions or amnesties — and whether disclosure is required.
Seek advice: don’t delay in obtaining expert legal and tax advice tailored to your specific situation.
Looking ahead
While Queensland GPs now have greater clarity, specialists and allied health practitioners may still face uncertainty. Further updates will emerge as state revenue offices continue to scrutinise practitioner arrangements.
Practices and individuals alike should take a proactive approach to ensure they’re not caught off guard.
Need help?
Hillhouse Legal Partners can assist with reviewing or drafting agreements, assessing your payroll tax position and preparing for any future audits. We also provide advice to individual practitioners seeking to understand their personal exposure or contractual risks.
For tailored advice, contact Hillhouse Legal Partners, on 07 3220 1144 or via email at zac@hillhouse.com.au
Exclusive offer for AMA Queensland members
Receive a free 30-minute virtual consultation with Hillhouse Legal Partners to review your practice’s business structure and compliance strategies in preparation for the growing complexity of payroll tax obligations.
This is a valuable opportunity to ensure your practice is aligned with best-practice approaches and ready to navigate evolving regulatory requirements with confidence.
An SMSF loan with 90% LVR
A Commercial property loan with 100% LVR
Specialised access to Equipment and Fit-out Finance
But there’s a catch – these high-LVR loans are only available from a limited number of lenders.
That’s where we come in. We’ll walk you through every step, from assessing your eligibility, to working with your legal and accounting teams.
Own, don’t rent –your guide to financing a practice premises
For doctors in Australia, selecting the right place to set up your practice isn’t just important – it can define the success of your entire career.
You need to be aware of the financial considerations and careful planning that comes with owning your own practice.
With the recent RBA rate cut, borrowing just got a little easier – great news if you’re looking to buy your own practice premises.
Lower rates could mean lower repayments, making it a good time to explore your financing options.
Understanding what’s available in this shifting market can help you make the right move for your practice.
Commercial property loans
The most popular way to finance a practice premises is with a commercial property loan. These loans often come with lower interest rates than unsecured business loans because the property itself acts as security.
As a healthcare professional, you may be eligible for higher loan-to-value ratios (LVRs) than other borrowers. Depending on your financial structure, you could potentially secure:
up to 90 per cent of the property value through a Self-Managed Super Fund (SMSF).
up to 100 per cent of the property value through companies, trusts or personal names.
Given the recent RBA rate cut, lenders may offer more competitive terms, making now a perfect time to explore commercial property finance.
SMSF loans
If you have an SMSF, using an SMSF loan to buy commercial property can be a tax-effective strategy. You can get your practice premises up-and-running within your superannuation structure, while benefiting from lower capital gains tax rates and tax-deductible interest payments. It’s a win-win!
As a doctor, you may have access to an LVR of up to 90 per cent through SMSF lending! This is much higher than standard SMSF property loans, which typically require larger deposits.
However, these high-LVR SMSF loans are only available from a limited number of lenders, meaning expert guidance here is more important than ever.
Equipment and fit-out financing
So, you’ve purchased your state-of-the-art practice. What about your medical equipment and clinic fit-out?
This can be a big investment. Fortunately, equipment and fit-out financing solutions can help spread these costs while preserving cash flow.
Equipment finance covers essential items such as diagnostic machines, surgical tools, computers, and office furniture.
Fit-out finance assists with expenses related to making your practice fully operational, including interior modifications, cabinetry, lighting, and technology integration.
These financing options are often structured with flexible repayment terms and competitive interest rates, making them a key consideration when planning your practice setup.
Making the right choice
With the RBA’s recent decision to lower interest rates, now could be a strategic time to secure financing for your practice. However, choosing the right structure depends on many factors, including your financial position, long-term objectives, and risk tolerance.
At Cutcher & Neale, we specialise in helping healthcare professionals like you navigate the complexities of practice financing. For personalised advice contact us on 1800 988 522 or email finance@cutcher.com.au
The information in this publication contains general advice only. It has been prepared without taking your personal objectives, financial situation or needs into account. You should consider whether the information contained within this publication is appropriate for you. Where we refer to a financial product you should obtain the relevant Product Disclosure Statement or offer document and consider it before making any decision about whether to acquire the product.
Understanding the factors behind rising health insurance premiums
Health insurance is a cornerstone of financial security and peace of mind for millions of Australians. It ensures access to quality healthcare services without the burden of exorbitant out-of-pocket costs. However, one common concern among policyholders is the steady increase in health insurance premiums over time. If you’ve ever wondered why your health insurance costs more year after year, you’re not alone. In this article, we’ll explore the key factors driving these increases and provide insights into how you can navigate them.
Why do health insurance premiums increase?
The rising cost of health insurance premiums is influenced by a variety of interconnected factors. While it may seem like insurers are arbitrarily hiking prices, there are legitimate reasons behind these changes. Let’s break down some of the primary drivers.
1. Rising healthcare costs
One of the most significant contributors to increasing premiums is the escalating cost of medical care itself. Advances in medical technology, pharmaceuticals and treatments have revolutionised healthcare – but they come at a price. Cutting-edge procedures such as robotic surgeries, advanced diagnostic tools and new medications often require substantial investment. Hospitals and clinics pass these costs on to insurers, who then adjust their premiums accordingly.
Doctors’ Health Fund understands that while innovation saves lives, it also impacts affordability. That’s why we work closely with our network of healthcare providers to negotiate fair rates and ensure our members receive value for money without compromising on quality. Over the last decade, Doctors’ Health Fund has consistently kept premium increases below industry averages.1
2. Increased demand for services
Australia’s aging population plays a major role in the growing demand for healthcare services. As people live longer, they tend to require more frequent medical attention, including specialist consultations, hospital stays, and chronic disease management. This increased utilisation places pressure on the healthcare system and contributes to higher overall costs.
Additionally, lifestyle-related illnesses such as obesity, diabetes and heart disease are becoming more prevalent. These conditions often necessitate ongoing treatment and specialised care, further straining resources. At Doctors’ Health Fund, we support medically-evidenced treatments and don’t pay benefits for non-proven therapies.
3. Government policies and rebates
The Australian Government provides a rebate on private health insurance premiums to make coverage more affordable. However, the rebate percentage is indexed annually based on inflation, which means it doesn’t always keep pace with rising premiums. As a result, policyholders may see their out-of-pocket expenses increase even if the insurer hasn’t raised its base rates significantly.
Doctors’ Health Fund actively advocates for policies that support sustainable healthcare funding. We believe transparency and collaboration between insurers, policymakers and consumers are essential to maintaining equitable access to affordable health insurance.
4. Fraud and administrative costs
Unfortunately, fraudulent claims and administrative inefficiencies also contribute to rising premiums. Insurers must invest in robust fraud detection systems and maintain large customer service teams to handle enquiries and process claims. While these measures are necessary to protect both the insurer and its members, they add to operational expenses.
At Doctors’ Health Fund, we pride ourselves on efficient administration and ethical practices. Our streamlined processes help minimise overheads, allowing us to focus on delivering exceptional service and competitive pricing to our members.
5. Natural disasters and unforeseen events
Unpredictable events such as pandemics, natural disasters or economic downturns can disrupt the healthcare landscape and lead to unexpected spikes in claims. For example, during the COVID-19 pandemic, many insurers faced increased demand for mental health services, telehealth consultations and elective surgeries delayed due to lockdowns.
1800 226 126 doctorshealthfund.com.au
How can you manage rising premiums?
While some factors contributing to premium increases are beyond your control, there are steps you can take to manage your health insurance costs effectively:
Review your policy regularly: ensure your level of cover aligns with your current needs. If you no longer require extras like dental or optical, consider switching to a hospital-only policy or downgrade to save money.
Take advantage of discounts: many insurers, including Doctors’ Health Fund, offer discounts for paying annually, holding combined policies (e.g. hospital + extras), or being part of a loyalty program.
Optimise tax benefits: make use of the government rebate (e.g. LHC or youth discount) and any available tax deductions related to medical expenses.
Choose wisely when selecting extras: focus on benefits that truly matter to you, such as physiotherapy or chiropractic care, rather than opting for comprehensive policy with unnecessary inclusions or a junk policy that doesn’t offer any real benefits.
Why choose Doctors’ Health Fund?
Doctor’s Health Fund is the only health fund made for doctors, their families and the medical community. We provide our members with quality health cover that provides great value and prioritises member welfare above profit margins. Here’s what sets us apart:
Competitive pricing: our commitment to affordability ensures that our premiums remain competitive without sacrificing quality.
Tailored coverage options: whether you need basic hospital cover or an extensive package with extras, we offer flexible plans designed to suit diverse needs.
Strong provider networks: with agreements in place across Australia’s leading hospitals and specialists, we provide seamless access to top-tier care.
Member-centric approach: from personalised service to cover that pays up to the AMA list of medical services and fees, we go the extra mile to support our members’ wellbeing.
Industry leading gap cover: we cover more medical services with no gap than any other health fund, with 93% of medical services covered compared to an industry average of 88.3%.²
Part of Members Health: a member-owned organisation, we are owned by doctors, not public shareholders. Any profits are reinvested to benefit our members and the community.
Rising health insurance premiums are a complex issue shaped by numerous economic, social and systemic factors. While these increases can be frustrating, understanding the underlying causes empowers you to make informed decisions about your coverage. By partnering with a trusted provider like Doctors’ Health Fund, you can rest assured knowing that your health and your wallet is in safe hands.
For more information about our products and services, visit doctorshealthfund.com.au
2 Private Health Insurance Ombudsman, State of the health funds report 2023, Ombudsman’s website
Private health insurance products are issued by The Doctors’ Health Fund Pty Limited, ABN 68 001 417 527 (Doctors’ Health Fund), a member of the Avant Mutual Group. Cover is subject to the terms and conditions (including waiting periods, limitations and exclusions) of the individual policy, available at www.doctorshealthfund.com.au/our-cover
Read
Whisky Valley by Joan Sauers
WIN
All about you Watch House
From the intriguing Echo Lake, Rose McHugh, curious historian-turneddetective, returns to solve her next compelling mystery in the moody Southern Highlands.
A missing violinist. A rising flood. A race against time. Intrigue, music and danger collide in Whisky Valley
After nearly being murdered last year, Rose McHugh battles anxiety as she uses her investigative skills to find her son’s best friend, a famous violinist who is missing along with his priceless violin.
As floodwaters rise, Rose uncovers secrets and lies among the missing man’s fellow musicians, as well as their patron and her enigmatic psychologist husband.
But when a body is found, can Rose shield her son from suspicion?
House ran for eight seasons from 2004 – 2012 and features the life of Dr Gregory House (Hugh Laurie), an unconventional, misanthropic, cynical medical genius who, despite his dependence on pain medication, successfully leads a team of diagnosticians at the fictional Princeton-Plainsboro Teaching Hospital in New Jersey.
Yes, it’s an old show but all seasons are now on Netflix so it’s binge-ready material. What do real doctors think of House? From jaw-dropping rudeness to patients and a total disregard for hygiene, patient consent and human resources, it’s hard to believe he would ever be hired, let alone employed, to get away with what he does.
Most viewers watch House with the same understanding as someone watching it in a foreign language, not understanding the complex medical terms. A warning: several seasons in, the sexist comments, childish antics and god-complex does start to wear thin – but by then you’ll be committed.
Cutcher & Neale Seminar Series
Are you ready for the end of financial year? You might have missed our webinar with corporate partner Cutcher & Neale, in which they talked about what financial strategies you can put in place to start the next financial year with a plan in place.
Never fear – here’s a link to the recorded webinar to watch in your own time.
Topics included:
End of year tax planning: key deductions you should know about 2025 Budget updates and what they could mean for you
Superannuation tips that can lead to increased wealth in retirement
Refer 1 member 25% discount* Refer 4 members 1 year complimentary* Refer 2 members 50% discount* Refer 3 members 75% discount*
The Power of ‘Yes!’
Medical life is frequently about answering a series of yes-no questions. If ‘yes,’ then this. If ‘no,’ then that. It’s the essence of our diagnostic decision-making. We spend our whole careers weighing up these binary conundrums in our offices. Every ‘yes’ and ‘no’ has its own ramifications, actions and reactions. Our patients’ lives and lifestyles hang in the balance as each question is posed and answered.
Similarly, our own destinies are determined by our answers to various key questions, posed at pivotal times and by pivotal people. Each career and each life has its own sliding doors moments.
As my hair greys and my back aches, I become more nostalgic, and like to reflect on these times in my own life. I have been impulsive most of the time. When deciding to do general practice, the powers that be offered me a term in Dalby. “It’s only three months,” they said. Never having lived in the country, I leapt at the chance to experience something novel. I stayed for two years and had the best professional time of my whole career. The farming families were terrific people. I was out every night of the week playing cricket or footy or accepting some charming farming family’s invitation to dinner. I knew every breed of cattle and every crop. I wore RM Williams boots, a big buckle on my belt and talked a bit slower. But as a single bloke it was tough being away from my extended family and when I was offered a job back in Brisbane I again reflexively answered ‘yes’.
Then a mate suggested I join him working part-time for the army. I said ‘Yeah!’ The fun we had at Enoggera was unbelievable. What a fantastic bunch of men and women, all serving our nation and protecting the rest of us. I really loved their positive team vibe and I loved seeing all the tanks on base! Around this time I also answered ‘yes’ to a mate who asked me to cover him as doctor for the Souths Rugby Union Club’s home game the following Saturday. This one-off gig grew into 17 winters of continuous Magpies fun and glory.
Not long after starting at Souths, a drug rep suggested I join her in her new career. She was about to start presenting for a radio station and wanted a doctor for a weekly medical segment. I’d never thought about the media (even though my fantasy career was always to take over as the captain of the Channel Nine commentary team
Dr Matt Young General Practitioner, Inala Medical Centre
when Richie Benaud retired). My mates assured me I had a face for radio and so again I answered ‘Yeah!’. For two years I talked about medicine and even threw in some archaeology now and then. I’m sure my only audience was Mum and my wife, but the novelty and fun kept bubbling.
The AMA Queensland Registrar of the Year competition caught my eye back in 2014 and I thought my opening batting partner fitted the bill. Besides batting he could also operate, so I nominated him. Being the world’s smartest man, he naturally won the title and AMA Queensland asked me to write a quarterly article. Another ‘Yeah!’ and a decade later I still love doing it. This ‘yes’ led to another adventure, too. A medical travel company rang AMA Queensland looking for a doctor with some archaeological interests. AMA Queensland assured me it was my archaeology degree rather than my grey hair that prompted their recommendation and after another ‘yes,’ I now host a fortnight of ‘conference’ holidays for doctors annually. Great people, great destinations and great activities.
The best impulsive ‘yes’ I ever gave was actually to another drug rep, who offered to set me up on a blind date. I can’t remember which drug she sold but I certainly remember my first date with my wife. I just hope Medicines Australia never investigate.
Life offers so many opportunities. Sometimes you just have to fight against fear of the unknown, fear of failure and fear of extending yourself beyond your depth. Sometimes you will fall in a heap, as a blundering imbecile, but more often than not, you make your own luck and fortune favours the brave. My propensity to impulsively say ‘yes’ to the unknown has certainly caused me some hard times but these are too few to mention. Some might say I have a touch of ADHD, but my career and life have never been boring.
Vintage of the decade
If you’ve ever wondered what the future of wine tastes like, then grab a glass and get comfy, because the 2025 Australian wine vintage is set to be an unforgettable year for wine enthusiasts and curious sippers alike.
With a perfect blend of innovation and tradition (and great growing conditions), the best wines in 2025 are expected to dazzle with flavours that dance between classic elegance and bold new adventures. This year promises a tantalising array of flavour profiles that reflect the diverse Australian wine regions, each with its own unique story to tell.
Whether you’re a seasoned sommelier or someone who just likes a good drop with dinner, this vintage comparison will guide you through what to expect from Australia’s latest season. So, let’s uncork the excitement and explore what makes this year’s bottles a must-have addition to your collection!
Australian wine vintage 2025 overview
The 2025 Australian wine vintage is shaping up to be a year of remarkable innovation and quality. Let’s explore the key regions and climate factors that are influencing this exciting vintage.
Key regions to watch
The diverse Australian wine regions are set to shine in 2025, each bringing its unique character to the forefront.
Barossa Valley, known for its bold Shiraz, is expected to produce wines with unprecedented depth and complexity.
McLaren Vale is poised to deliver exceptional wines, with its signature Shiraz showcasing rich, velvety textures and vibrant blackberry notes, thanks to ideal ripening conditions. Expect Grenache to shine with bright, spicy elegance, while Cabernet Sauvignon should offer structured, dark-fruit-driven complexity, reflecting the region’s warm days and cool nights.
The cooler climate of Margaret River is likely to yield Chardonnays with a perfect balance of fruit and acidity. Tasmania’s sparkling wines are gaining momentum, with critics already buzzing about their potential to rival Champagne.
Meanwhile, the Hunter Valley is experiencing a renaissance, with its Semillon reaching new heights of refinement.
Yarra Valley and Adelaide Hills are pushing boundaries with their Pinot Noir, creating wines that are both delicate and intensely flavoured.
Common across all these regions is the fact that growing season was drier than normal, paving the way for intensely flavoured fruit, free from the pressures of disease and presented in perfect condition for their craftsmen to go to work.
Mademoiselle
Cherchez-vous un restaurant nouveau pour un repas très mémorable avec votre famille et amis? Il faut essayer Mademoiselle au Hamilton Portside! (Never fear dear reader, that’s as far as my Duolingo French lessons will take me at this stage!).
Portside’s new French offering comes from the makers of hit Hamilton bakery Rise and showcases a more provincial style of French cooking — envisage this as European ‘potato and bread’ style rather than ‘tomato and olive oil’ Mediterranean cooking. There is an inherent warmth and homeliness that accompanies this kind of food, even when served in a modern and fancy setting such as Mademoiselle’s. While we visited in summer, their offering of rich French favourites makes for perfect comfort eating during our cooler autumn and winter months.
Cast your eyes across the aperitifs menu if you’re inclined to start your meal with a Boulevardier or a Kir Royale, or a twist on a classic, like a Black Raspberry Margarita with Chambord and pomegranate or a Limonardier with Limoncello and Ricard. Their strawberry and rose flavoured mocktail is a lovely departure from the nonalcoholic menu that many other establishments seem to laden only with fruit juice and post-mix soft drinks. There is also an appropriately extensive wine menu, and a selection of spirits and beers.
To start your gastronomic journey, amuse-bouches include devilled egg with confit prawn, mussels in a garlic chervil butter sauce and charcuterie. The first breadbasket is complementary, but you can be forgiven for ordering a second (or third) — the bread sourced from their Rise bakery is divine and comes with a slightly addictive French cultured butter.
Next, entrees include ham hock terrine and tomato filled with pangrattato and goat cheese, but a standout is the Poulpe à la sauce vierge and Brochette de St Jacques. The WA octopus comes perfectly tender, with smooth hummus, zesty citrus and crispy crunchy chickpeas — an interesting bunch of ingredients to throw together, but one that just seems to work. The scallops on buttered leeks are melt-in-your-mouth, ingeniously paired with toasted hazelnuts, and with a seafood velouté that would rival many a southern French bouillabaisse in terms of its intense flavour profile.
The entrees may seem relatively small but don’t be fooled by this — the main meals are generously portioned, and you may find yourself accidentally over-ordering when there are so many tasty plates on offer. In addition, if you’ve ever watched My Kitchen Rules, you may have heard French celebrity chef Manu Fidel extoll the virtues of “THE SAUCE!” — and just like any good classic French kitchen, the sauces here are absolute standouts and really do make the mains marvellously memorable.
Plats principaux include a rôtisserie chicken to share, chuck tail flap with shallot jus, Steak Frites and a poached ‘catch of the day’ fish.
Magret de canard comes as a rare, cooked duck breast that’s not the least bit gamey, with the most intensely moreish blackberry and juniper reduction, served with carrots roasted and puréed. Even the puréed carrots have an essence of berries about them, which your palate may find intriguing at first but also delightful.
Daube à la provencale is served as a 300g slow cooked wagyu beef neck with crushed potatoes and black olives. Another decadently rich dish, with a tender cut of beef neck that can be gently pulled apart with a spoon. It’s so soft that it almost doesn’t need to be chewed (medically however, I advise you to please chew it).
The Gnocchi Parisienne au beurre blanc is a bit more heavy, very luxe and is really the ultimate comfort food. The gnocchi is made using a choux pastry style base instead of potatoes (like teeny-tiny savoury profiteroles pillows), served with a white onion cream with sweet and sour shallots and currants. Absolutely outstanding, but so rich that you could easily order it as a side for the entire table rather than a main meal on its own.
Due to the size of the mains, you may want to choose entrees or sides rather than both; but if you have the appetite, try the fragrant Dutch carrots with lavender honey. There’s also green beans with harissa and capers, potatoes with crème fraîche and a variety of sauces you can add on the side.
Dessert includes crème brûlée (bien sûr!), and a selection of cakes courtesy of Rise Bakery. Continuing with the theme, everything is wonderfully rich and delectable, especially the chocolate gateau, so it may be worthwhile sharing lest you walk out feeling like a blancmange yourself.
Indulge in the luxurious and make Mademoiselle’s your menu of choice for your next special occasion. Located at Portside Wharf Hamilton, open Tuesday to Saturday for lunch and dinner, bookings at mademoisellerestaurant.com.au
Dr Kat Gridley Emergency Medicine Staff Specialist, Mater Brisbane Hospital
Welcome to By Invitation — your access to extraordinary experiences
Imagine a journey crafted entirely around you — where extraordinary experiences, seamless service and exclusive benefits are simply part of the experience. Welcome to By Invitation, powered by Orbit World Travel.
By Invitation is a new era of travel: curated, personal and shaped around what matters most to discerning travellers. It is about more than just seeing the world — it is about experiencing it in ways few others can. From luxury cruises to immersive cultural adventures, every journey is handpicked for those who expect more.
Exceptional journeys, curated with care
Our team works closely with leading luxury travel providers to open doors to truly remarkable experiences — often with exclusive savings and privileges reserved just for By Invitation members. Whether you dream of iconic destinations or hidden treasures, our curated collection ensures your next escape is one to remember. Some of the exceptional journeys currently available include:
Africa — wildebeest migration safari
Embark on a once-in-a-lifetime 14-day safari through East Africa, perfectly timed for the wildebeest migration. Extend your adventure with options such as gorilla trekking in Rwanda or relaxing on Zanzibar’s pristine beaches — a seamless blend of culture, wildlife, and luxury.
Uniworld Boutique River Cruises — Christmas on the Rhine
Set sail from Cologne to Basel in December 2025, cruising past centuries-old Christmas markets, Gothic cathedrals, and storybook towns. Enjoy exclusive savings of up to $2,400 per person and special solo traveller offers. This is the perfect way to experience the magic of a European Christmas in style.
Explora Journeys — enchanting canals and Nordic delights
Journey from the UK to Denmark aboard the brand new EXPLORA III. Explore medieval Bruges, cruise Amsterdam’s famed canals, and marvel at Norway’s fjords before arriving in vibrant Copenhagen. Exclusive savings of up to $2,500 per cabin plus up to USD$700 onboard credit make this voyage even more enticing.
Regent Seven Seas Cruises — Alaska’s majestic beauty
Discover the wild frontier of Alaska with an all-inclusive luxury cruise from Seward to Vancouver. Witness snow-capped peaks, glaciers and incredible wildlife while enjoying bonus onboard spending of up to USD$1,200 per cabin.
Golden Eagle Luxury Trains — voyages of a lifetime
Step aboard a journey like no other. Golden Eagle Luxury Trains invites you to rediscover the art of slow travel — with every detail designed to inspire. From Europe’s regal landscapes to the mystical Silk Road and vibrant India, each journey offers a seamless blend of culture, comfort, and cinematic scenery. As a special bonus, receive two complimentary five-star hotel nights pre or post-tour (valued at $1,000).
Oceania Cruises — taste the world
Renowned for offering the finest cuisine at sea, Oceania Cruises combines rich culinary experiences with immersive insider tours and personal service. Enjoy up to 30% off select sailings, a free beverage package and up to USD$800 shipboard credit.
Coming Soon — Egypt 2026
Prepare for an unforgettable journey through time as we finalise an exclusive Egypt tour for November 2026. Highlights will include the Pyramids of Giza, a luxury cruise along the Nile and priority access to the magnificent Grand Egyptian Museum — the largest archaeological museum in the world.
Designed for you, with you
By Invitation is about creating journeys that feel personal, effortless and extraordinary. Your dedicated Luxury Travel Advisor takes the time to understand your interests, preferences and travel dreams — turning them into reality with tailored itineraries, privileged access and insider expertise.
Whether you are planning a once-in-a-lifetime adventure, a special celebration or a well-earned retreat, every detail is carefully considered to ensure your journey is truly unforgettable.
These are just a few of the many extraordinary experiences available through By Invitation. No matter where your imagination leads — from the Arctic to Africa, from ancient wonders to modern luxuries - we can make it happen.
Your invitation to travel in style
As an AMA Queensland member, you are warmly invited to experience the world through By Invitation. Explore bespoke journeys, enjoy exclusive savings and travel with the confidence that every detail has been curated with care.
The world awaits — and with By Invitation, Karen and I, you are not just travelling, you are accessing extraordinary experiences.
Four Queensland medical students awarded scholarships
AMA Queensland Foundation has awarded $10,000 scholarships to four Queensland medical students to support their medical studies and dreams of becoming doctors.
Rheannon Griffin, Alexandra Green and Noah Steel are the 2025 AMA Queensland Foundation Medical Student Scholarships recipients.
A fourth student, Ann Vincent, was awarded an AMA Queensland Foundation scholarship supported by the Indian Medical Association Queensland (IMAQ) under the Foundation’s Sponsor one Student (SoS) Program.
Financial support can be important while studying medicine, with rigorous workloads and placements required.
Without financial support, some medical students experience hardship significant enough to threaten their ability to complete their studies, and this is a need the Foundation seeks to fill with our scholarship program.
This year we were again overwhelmed with applications from deserving medical students, and it was an incredibly difficult task to narrow down our support to just four recipients.
With rising living costs, many medical students are doing it tougher than ever, and we are grateful to be able to help even a handful of individuals continue their journey.
The recipients were acknowledged recently at AMA Queensland’s doctors’ awards night, Dinner for the Profession.
The four doctors in training are outstanding examples of bright minds persevering under difficult circumstances.
It is an honour to award the scholarships to these four individuals who have continued through significant personal, financial and medical hurdles.
Their demonstrated passion for medicine and resilience will no doubt have a wonderful flow-on effect for the Queensland communities they eventually go on to serve.
Rheannon’s story
Rheannon is a sixth-year medical student studying at James Cook University (JCU). An aspiring rural generalist, she hopes to pursue a sub-specialty in obstetrics. As a mother of two young children, studying medicine has not been easy financially for Rheannon.
The scholarship will help her with relocation costs associated with her upcoming rural placement, as well as support expenses related to her daughter’s recent medical diagnosis and costs of care.
“This scholarship will make a huge difference in reducing the financial stress. The funds will cover travel, accommodation and childcare costs during my placement and enable me to complete my final year of medicine more comfortably, ensuring I can focus on my education and clinical responsibilities.”
Alexandra’s story
A fifth-year James Cook University (JCU) student, Alexandra has a goal to serve the North Queensland community as a rural generalist. Alexandra developed a passion for rural healthcare while working as a paramedic in Giru. Alongside her medical degree, she is studying a Masters of Public Health and Tropical Medicine, also at JCU.
Having exhausted her savings and being ineligible for Austudy, Alexandra was considering taking a leave of absence. The scholarship will help her stay on track and focus on her studies in the critical years of her degree so that she can pursue her intended rural pathway.
“This scholarship will allow me to focus entirely on my studies and clinical placements and fulfill my goal of becoming a dedicated rural medical practitioner in the North Queensland community.”
Noah’s story
Noah is a third-year medical student studying The University of Queensland Rural Medical Program in Bundaberg. He was drawn to study in a regional setting to be able to address the healthcare disparities in rural and regional communities.
Noah had previously been supported by a program for regional medical students, but this has now been discontinued, leaving him with a considerable shortfall in basic living costs. With the help of the scholarship, Noah can bridge the gap in finances and continue his studies without added financial pressure.
“The AMA Queensland Foundation scholarship will ensure that I can maintain stable housing and continue to meet the rigorous requirements of my medical education, ultimately allowing me to complete my studies and contribute to the healthcare needs of regional Queensland.”
Ann’s story
Sixth-year James Cook University (JCU) student Ann was awarded a scholarship supported by the Indian Medical Association Queensland under the Foundation’s Sponsor one Student (SoS) program. SoS is an initiative which sees the Foundation partner with individuals, companies and organisations to offer additional scholarships outside of the previous year’s fundraising efforts.
Ann’s inspiration for studying medicine was ignited due to her personal and family experience of illness. Diagnosed with tuberculosis at age five, and facing ongoing health and other challenges, Ann is determined to keep pursuing medicine against the odds.
She is driven by a desire to understand the medical conditions that have impacted the lives of her family, and to help others overcome the same struggles.
“This scholarship will be life changing, allowing me to independently cover essential living costs and enable me to afford my medications and other medical expenses. It will mean I can fully focus on my studies and placement during my final year, ultimately allowing me to work towards a future where I can provide for my family and give back to my community.”
See more about the benefits of partnering with us for the SoS initiative and supporting the next generation of doctors.
Support the Medical Student Scholarships EOFY Appeal
For every story like Rheannon’s, Alexandra’s, Noah’s or Ann’s, there are more medical students who also need support to finish their studies.
AMA Queensland Foundation is hoping to offer three or more scholarships in 2026, and with your support, we can get there.
Your donations help students experiencing financial disadvantage overcome the challenges they face and pursue their dreams of becoming doctors in Queensland.
Donate today through the 2025 End of Financial Year Tax Appeal. All donations over $2 are tax deductible. Every dollar that you donate will go directly to helping a student in their time of need, through the Medical Student Scholarships program.
There is also an option open to individuals, organisations and companies to partner with us under our Sponsor one Student (SoS) program and jointly name a scholarship in 2026. SoS helps you leave a legacy that has a profound impact both in one more student’s life and on the Queensland community they eventually serve.
Lange Endocrine Surgery: Clinical Diagnosis and Management
Packed with 800+ photos and illustrations, including CT scans, MRIs, X-rays and anatomic renderings, Lange Endocrine Surgery: Clinical Diagnosis and Management delivers high-yield descriptions of the latest diagnostic modalities and management protocols. Designed to foster quick recall of major diagnostic features, it provides clear, concise presentation of etiology, pathogenesis, clinical findings, differential diagnosis, and medical and surgical treatment.
Win this book: 30 July
WIN this book:
Lange Endocrine Surgery: Clinical Diagnosis and Management
Novel winner
Fill out the online form. Entries close 30 July
Enter now
InPrint winner
Dr Carmen Main has won a copy of The Bluff by Joanna Jenkins, thanks to Allen and Unwin Publishing.
Dr Lawrence Malisano has won a copy of Clinical Sports Medicine, thanks to McGraw Hill.
Helping support your business everyday
Make Officeworks your partner in business.
We’re here to support AMA QLD members with our trusted range of over 40,000 products, business services and specialist advice to keep your business running smoothly and help you get back to what you do best.
Register for a free Officeworks 30 Day Business Account to access your exclusive member business pricing on a select range of everyday office supplies, print, furniture and tech.
Along with your 30 Day Business Account you can also enjoy additional benefits to help you get on with business.
30 Day Business Account.†
Buy everything you need today and pay in 30 days. Use multiple cards linked to one account or a digital card in the Officeworks App to manage it all in one place.
Easy online ordering.
Shop the way that works for you with secure, 24/7 online ordering from wherever you are.
Flexible Delivery.
^‡Our flexible delivery options include 2 hour, same day and next day delivery within eligible metro areas.
Large store network.
When the unexpected happens, there’s always an Officeworks close by with 165+ stores across the country.
Click & Collect.
Save time by shopping online with free 2-hour Click & Collect# on stocked items in store.