• physician adult (18%), emergency medicine (15%) and general practice (14%) were the specialties with the most trainees
• of the trainees, 8% were interns, 24% prevocational and unaccredited trainees, 36% non-GP specialist trainees, 12% specialist GP trainees, and 20% IMGs.
The AMA commends the strong commitment once again of the doctors in training cohort who took the time to complete the survey, which supports advocacy to help them in the short and long term.
AMA SA’s Hospital Health Check
In recent years, the AMA SA Doctors in Training (DiT) Committee has used the MTS data to explore the prevalence of workplace cultural and safety issues affecting junior doctors in South Australia’s training hospitals. The data and commentary are summarised in the annual ‘Hospital Health Check’ (HHC), which reports on the working conditions across each of the major training locations in South Australia.
The HHC report is used to advocate for better workplace and training conditions for DiTs working locally in South Australia.
To ensure deidentified responses and valid results, a hospital needed to have at least 10
survey respondents working predominantly in that hospital for the period being investigated for its results to be examined.
The most significant change in demographic has been that 43% of DiTs now report having completed their primary medical degree outside of Australia or New Zealand, reflecting a significant shift in the medical workforce towards overseas-trained junior doctors at some hospitals: Modbury (28% to 47%), FMC (11% to 21%) and the LMH (14% to 21%).
There has been a 5% overall increase in South Australia in IMGs, up 16% from when pandemic lockdowns prevented IMGs entering South Australia and other Australian states.
The proportion of DiTs working fulltime, parttime and casually has remained constant among those not working in hospitals, and at FMC and the RAH, while there has been a slight increase in those working part-time at LMH and decrease at WCH.
All assessments throughout this publication are based on the proportions of junior doctors’ responses, as reported in the 2024 Medical Training Survey’s self-reported data, not on the numbers of doctors responding to any question.
Survey analysis
Workplace facilities
The availability of suitable workplaces, including desks and computers, has direct impacts on DiTs’ efficacy in delivering patient care and, if not up to standard, can lead to significant delays in treatment. Improving access to appropriate workspaces has become even more critical since the roll out of electronic medical records in South Australian public hospitals, with easy access to computers critical to tasks such as ordering and assessing blood tests and imaging, and charting medications.
There has been little change in access to these workspaces from 2023 to 2024. Between 55% (at the WCH) and 69% (at Modbury) of respondents rated their workplaces as ‘excellent or good’ in 2024, with FMC (60%), RAH (61%), LMH (62%) and QEH (65%). The result at the WCH was an improvement from 2023, when 46% of respondents considered their workspaces ‘excellent or good’. Modbury demonstrated the most improvement in the ‘excellent and good’ total, increasing by 10% from 59% the previous year. Modbury and the WCH demonstrated the largest decreases in the percentage of those junior doctors rating their workplaces as ‘terrible or poor’: at the WCH, 13% in 2024 compared to 25% in 2023, and at Modbury 4% in 2024 compared to 15% in 2023. At other hospitals, there were small reductions in the percentages rating their workplaces as ‘terrible or poor’ with the highest proportions in 2024 at FMC (16%) and the RAH (15%).
Workplace culture
The impact of bullying, harassment and discrimination on junior doctors can be profound, potentially affecting their mental health, job satisfaction, well-being and performance. Each can lead to increased stress, anxiety, depression, and even burnout, which in turn can affect patient care and the overall work environment in hospitals.
The unacceptably high rates of reported bullying, discrimination and harassment in both the ‘experienced’ and ‘witnessed’ categories have been a focus of HHC reporting for several years. DiTs have also noted in the past that they have not reported these behaviours because they feared repercussions or a lack of confidence that their reports would be followed up.
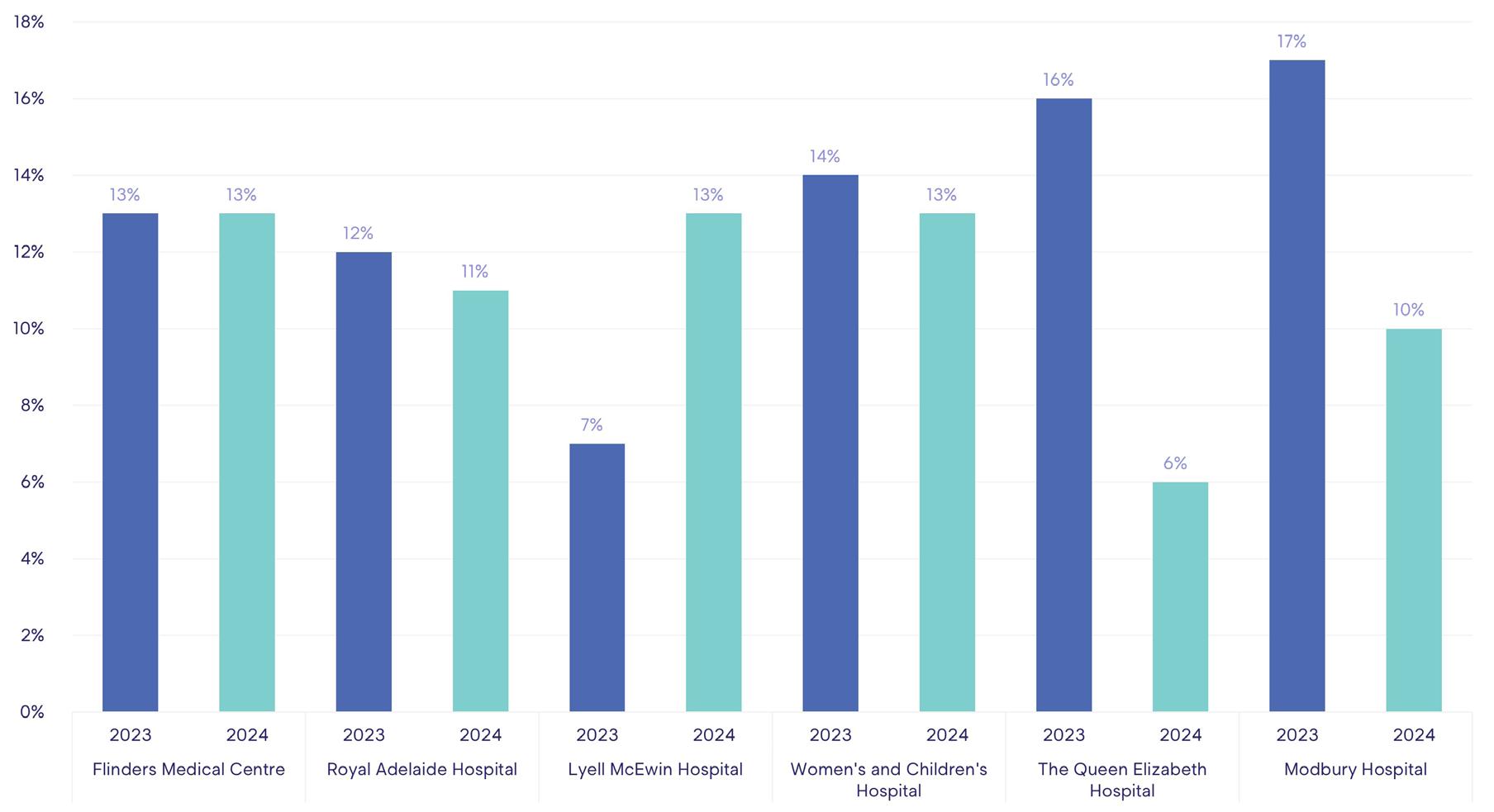
This year, there is a disappointing lack of improvement in the percentages of DiTs who reported they had experienced bullying. The percentage remained at 13% at FMC, decreased by 1% at both the RAH (11%) and WCH (13%), and concerningly increased by 6% to 13% at the LMH. However, there was a significant improvement of 10% to a system-best 6% at the QEH.
Have you experienced bullying in the past 12 months?
There were varying responses to the incidence of witnessed bullying. There were reductions in those who had witnessed bullying across multiple sites, with rates reducing by 11% at Modbury (to 23%), 6% at WCH (to 28%), 3% at RAH (to 18%) and 2% at FMC (to 16%).
Concerningly, the percentage of witnessed incidents increased by 4% (to 19%) at the LMH.
A zero-tolerance policy for bullying is crucial in healthcare settings. Such a policy ensures a safe and supportive environment for all employees, which is essential for their well-being, productivity and preparedness to support patient care and outcomes. By strictly enforcing a zero-tolerance policy, organisations can foster a culture of respect and inclusivity, which in turn enhances teamwork, communication, learning and performance.
DiTs’ views of whether bullying is not tolerated at their workplaces also varied. At Modbury there was a large increase in those who ‘strongly agreed’ or ‘agreed’ that bullying is not tolerated, from 56% in 2023 to 90% in 2024, and at WCH a 15% increase (from 63% in 2023 to 78% in 2024).
Harassment
Sexual harassment was reported as a separate category (from ‘harassment’) for the first time in 2024. While the aim is, of course, no sexual harassment at any workplace, it is pleasing that in this first reporting period levels of experienced sexual harassment are low, ranging from 0 to 3% at the major hospitals. Modbury Hospital reported the largest change in reporting of harassment more generally – 10% in 2023 to 2% in 2024; otherwise, there was little change, with improvements of 1% to 2% within single-figure percentages at the major hospitals.
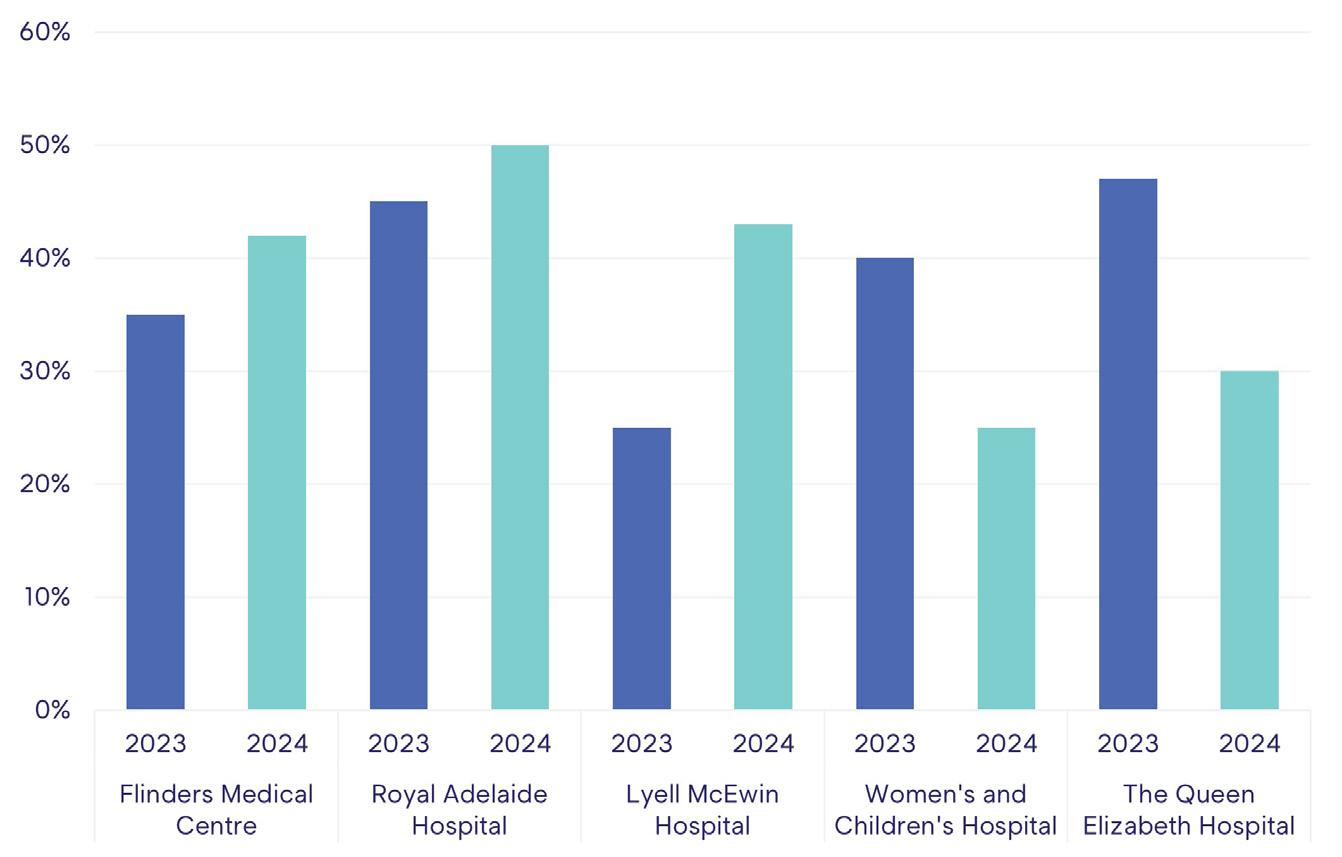
Has the report been followed up? Yes
There were notable changes in junior doctors’ perceptions of whether their reports of bullying were followed up across various hospitals from 2023 to 2024. There were marginal increases at FMC and the RAH, and more improvement (from 25% to 43%) at the LMH. However, there was a 17% drop at the QEH, to 30%.
Workload and overtime
The workload ratings of DiTs varied significantly between hospitals in 2023 and 2024. The reports of ‘very heavy’ or ‘heavy’ workloads at the WCH decreased markedly, from 66% in both 2022 and 2023 to 50% in 2024. Otherwise, there was little change in the major hospitals.
Hours worked and overtime
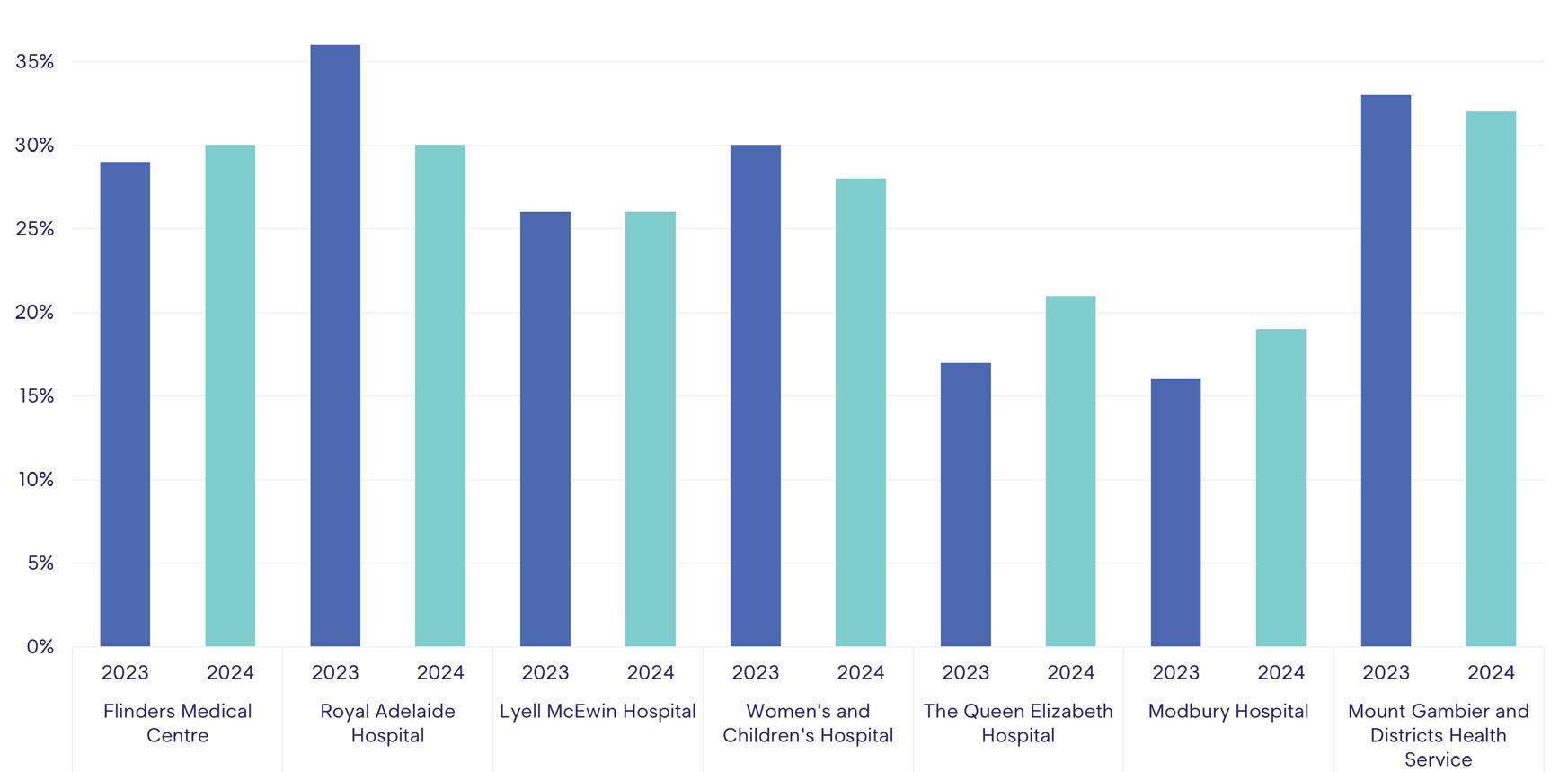
When examining the proportion of junior doctors working more than 50 hours a week, in 2024 the biggest change was the decrease of 6% (from 36 to 30%) at the RAH.
More than 50 hours/week
When combining reports of being paid for unrostered overtime ‘always’ or ‘most of the time’, percentages ranged from 75% at the WCH to 85% at FMC and Modbury. However, the WCH result is an improvement of about 10% from 2023.
There was also a decrease over time in the small number of respondents who reported ‘never’ being paid for unrostered overtime, with the highest proportion (among those specifying employers) 4% at the RAH and QEH – but that result was a noticeable decrease from the 13% of 2023.
The hospitals where there was noticeable change in junior doctors reporting being paid for unrostered overtime ‘most or the time’ or ‘always’ were LMH and Modbury, each with an increase of 11% (to 86% and 85% respectively), WCH (7% increase to 75%) and QEH (6% increase to 79%). At FMC and RAH the percentages remained higher, in the mid-80s, with little change.
Flexible arrangements
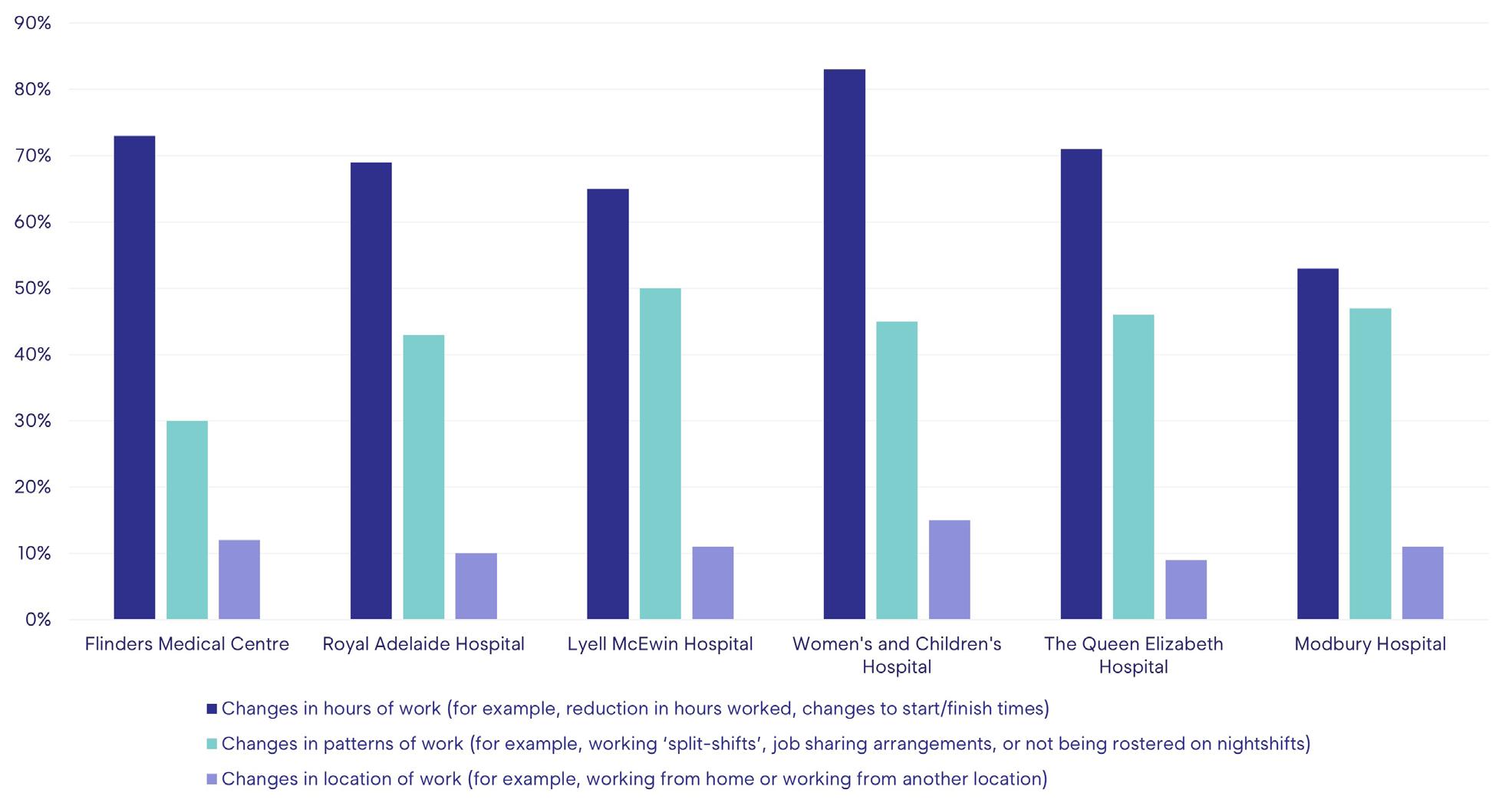
What sort of flexible arrangements did you access/would have liked to access?
Doctors were asked about the type of flexible working arrangements they would like to, or did, access. Among doctors at the major hospitals who accessed flexible arrangements, between 53% and 83% sought changes in hours worked (such as a reduction in hours, or changes to start and finish times). Job-sharing and other work-pattern arrangements were sought by between 30% and 50% – with all but FMC showing increases in the appeal of these arrangements. Changes in work location were sought by between 9 and 15%, with the highest percentage at the WCH.
Of those who noted they had sought or would like access to flexible hours of work, the highest percentage in 2024 was at the WCH, where 83% reported they had done so, with 73% at FMC, 69% at the RAH, 71% at the QEH and 65% at the LMH.
Training and workplace
Satisfaction with training positions
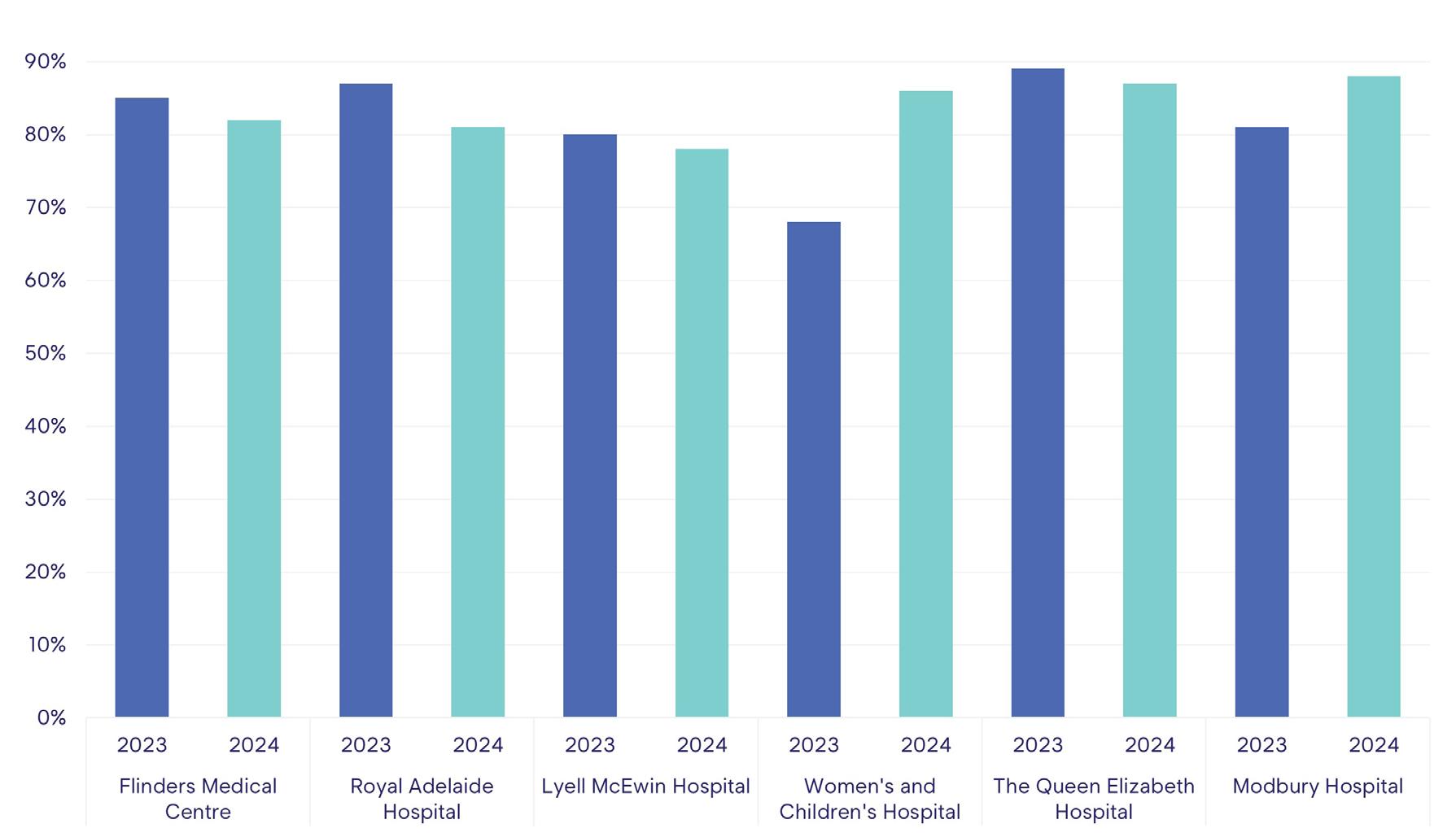
Junior doctors’ responses to whether they would recommend their current training position to other doctors show some notable trends and differences between 2023 and 2024. When considering the combined percentage of ‘strongly agree’ and ‘agree’ responses WCH achieved the most significant increase in satisfaction rates – 68% to 86% – with the 7% increase at Modbury and 6% drop at the RAH the other largest changes.
Satisfaction with training positions - net Strongly Agree + Agree
The WCH also improved markedly in reports of whether junior doctors would recommend their current workplace to other doctors: an increase of 19% to 86% in 12 months. There was also an increase at Modbury (74% to 81%) but little change elsewhere.
Professional development and training plans
Prevocational and unaccredited trainees were asked about their professional development or training plans. FMC, Modbury and the RAH had the largest increases in participants reporting they have plans, from 46% to 70% at FMC, Modbury 43% to 64%, and 44% to 62% at the RAH. LMH and WCH remained relatively static at 60%. QEH had the lowest rate at 46%.
It was pleasing to see that 100% of interns at FMC reported they had training plans, an increase of 20% on 2023 after reporting 100% in 2022. There were 100% results at each of the other major hospitals, too (no result recorded at Modbury).
The percentage of IMGs with training plans was higher than the proportions of prevocational and unaccredited trainees at the same sites. RAH reported a 93% rate. FMC decreased from 93% to 81%, while LMH dropped from 100% in 2022 to 93% in 2023 and 86% in 2024, and WCH from 93% in 2023 to 85% in 2024. The most marked 12-month decrease was at QEH, which
The worst result was at the LMH, where only 50% were satisfied with their research opportunities – down from 56% in 2023.
Survey participants were asked whether their job responsibilities prevented them meeting their training requirements. When ‘never’ and ‘rarely’ responses were combined, a less than satisfactory picture emerged, with the best result recorded at any of the hospitals 65% at the QEH. FMC, the RAH and Modbury recorded results of between 59% and 62%. At the WCH, the proportion was 58%, still the lowest but much improved from 37% in 2022 and 45% in 2023.
When asked whether they believed their formal education program had been useful in their development as doctors, agreement (agreed/strongly agreed) was between 81% and 94% at most sites. Modbury improved markedly from 71% in 2023 to record 94% in 2024. There was also improvement at the WCH (83% to 92%), with little change year-to-year at the other major hospital sites.
Bedside teaching or ‘hands on’ contact with patients is a time-honoured element of clinical training. As expected, there were high levels of recognition of its value across the sites, with agreement at about 90% at each hospital.
Conclusion
The range of concerns highlighted by the MTS and HHC gives administrators, staff and wouldbe employees much to ponder. However, the main issues continue to be related to workplace culture. The preponderance of bullying, harassment and discrimination continues to be of grave concern. The increasing numbers of perpetrators among the patients and carers group is a signal that the issues repeatedly highlighted in news headlines, including ramping, long waits in EDs, and lengthening elective surgery waiting lists, are affecting doctors at the ‘receiving end’ of those systemic issues.
Otherwise, it is pleasing that doctors’ reports of conditions at the Women’s and Children’s Hospital (WCH) indicate that measures to improve workplace safety and culture are finding success. AMA SA continues to advocate for appropriate workplaces for all clinicians in the design of the new WCH, with calls for plans to consider current and future IT needs.
Bullying, harassment and discrimination
Recent HHCs have demonstrated unacceptable levels of bullying, harassment and discrimination of trainee doctors in the state’s public hospitals. While there has been some change, there is much to be done. It is also concerning that the incidence of reported bullying among those doctors who chose not to specify where they are employed is increasing. This may indicate that bullying is continuing but that DiTs do not feel secure in nominating those responsible. In fact, it may be the most vulnerable DiTs who are electing to withhold any information they believe may identify them or lead to repercussions for themselves or their
peers. The survey’s anonymity and security must be improved if the data is to reveal the true picture of working conditions in the state’s hospitals.
While some hospitals have shown significant improvements, others have experienced mixed results, emphasising the need for continuous efforts and a system-wide monitoring and evaluation framework to foster respectful and supportive workplace environments in all public hospitals.
AMA SA advocacy to improve health workers’ psychosocial safety
For five years, HHCs and AMA SA advocacy have increased awareness of working conditions and their effect on doctors and patient health and safety. The issues have been discussed in parliament, prompting front-page headlines in The Advertiser. In 2020, the AMA SA Culture and Bullying Summit led to nation-leading legislative reform that now makes LHNs responsible for their employees’ psychosocial safety.
More recently, the AMA SA DiT Committee has identified barriers to the reporting of bullying, harassment and discrimination incidents and concerns. After a request for information from each LHN in late 2024, the DiT Committee has identified that while existing hospital policies outline the importance of safe workplaces, they do not clarify to whom reports should be submitted and discussed. The Committee has proposed a reporting pathway that clarifies who it is (or the positions among the hospital’s personnel) that the doctors can initially contact, safely and confidently, in South Australia’s hospitals. The pathway (see page 18) is being considered by individual hospitals.
AMA SA is also exploring ways to reduce bullying, harassment and discrimination at a system-wide level through a project proposed in conjunction with the UniSA Centre for Workplace Excellence and discussed with Health Minister Chris Picton and senior SA Health personnel.
The DiT Committee is concerned that patients and carers are responsible for more incidents of bullying, harassment and discrimination. AMA SA recognises the efforts of SA Health in alerting the public to this issue through its ED-focused campaign but suggests the stressors patients and carers are experiencing due to delays in surgeries and other care and long waiting times in clinics and EDs may be contributing to public responses.