Members, call 888.243.3368 and ask for a Member Services representative.
Mailing Lists
For information about ordering AGD mailing lists, call 888.243.3368 ext. 4097 or email advertising@agd.org.
All materials subject to copying and appearing in General Dentistry may be photocopied for the noncommercial purposes of scientific or educational advancement. Reproduction of any portion of General Dentistry for commercial purposes is strictly prohibited unless the publisher’s written permission is obtained.
AGD does not necessarily endorse opinions or statements contained in essays or editorials published in General Dentistry. The publication of advertisements in General Dentistry does not indicate endorsement for products and services. AGD approval for continuing education courses or course sponsors will be clearly stated.
General Dentistry (ISSN 0363-6771) is published bimonthly in 2025 by the AGD, 560 W Lake St, Sixth Floor, Chicago, IL 60661-6600.
Periodicals postage paid at Chicago, IL and additional mailing office. POSTMASTER: Send address changes to General Dentistry, 560 W Lake St, Sixth Floor, Chicago, IL 60661-6600. Email: subscriptions@agd.org.
Canadian mailing information: IPM Agreement number 40047941. Change of address or undeliverable copies should be sent to: Station A, PO Box 54, Windsor, Ontario, N9A 6J5, Canada. Email: subscriptions@agd.org.
AGD members receive General Dentistry as part of membership; annual subscription rates for nonmembers are $135 for individuals and $255 for institutions. Online-only subscriptions are $120 for individuals and $230 for institutions. All orders must be prepaid in US dollars. Single copies are available upon request. Please contact our Membership Services Center at 888.243.3368 for more information.
Starting with the end in mind: collaborative care by general dentists and endodontists
Today, the delivery of outstanding dental care for patients requires interdisciplinary cooperation between general dentists, often considered the gatekeepers for oral health, and other professionals. Among the most valued partners of general dentists are our endodontic colleagues, who focus on diagnosis, prevention, and treatment of pulpal and periapical diseases of the teeth and surrounding tissues. In multidisciplinary dental care, development of a comprehensive, successful treatment plan is easier when clinicians have a relationship founded on mutual respect and open communication.
Collaboration begins with the desired end in mind. Achieving the best possible outcome for the patient should be considered the end goal, and collegial communication is key to optimal results. For general dentists, feedback from endodontists after referral offers a great learning opportunity, allowing us to refine diagnostic and procedural skills. In any given case, interactions with an endodontist may provide new information about diagnosis, suggestions for restorative procedures, and, more importantly, a reasonable prognosis. Conversely, endodontists can learn from general dentists, gleaning techniques for restorative procedures and the specifics of patient preferences. Who better than the general dentist to provide details of a patient’s oral health history and treatment desires?
Another benefit of working with endodontists is taking advantage of their specialized training for cases involving nonspecific orofacial pain, retreatment of failed root canal therapy, and cracked teeth. Working with endodontists is also a tremendous help when dealing with the issue of access to care, especially for those of us in rural areas. The goal again,
and always, is to strive for the best possible outcome for the patient.
The relationship between endodontists and general dentists is highlighted in this issue of General Dentistry through a collaboration with the American Association of Endodontists (AAE). These partnerships are especially relevant in my family as my son, Daniel, is a board-certified endodontist, and his wife, Emily, is a general dentist. Now there’s a perfect example of collaboration—it’s enlightening to see them work together!
In 2024, Daniel invited me to attend the AAE meeting in Los Angeles. It was impressive to see like-minded endodontists pursuing new and advanced techniques to improve their professional skills. Attending the meeting also gave me the opportunity to connect with AAE leaders to talk further about the importance of this collaboration. I’m so pleased to be able to share it with our members and AAE members too.
By and large, AGD members are dedicated to obtaining high-quality continuing education and thus are more highly trained in general dentistry. This commitment is grounded in their desire to produce the best possible outcome for the patient, including when this goal means referring a patient to another professional. The lyrics of the 1978 song “The Gambler” have served me well since my practice began: “…you got to know when to hold ‘em, know when to fold ‘em.” Collaborating with endodontists, who have likewise devoted themselves to advanced education in their specialty, is “rooting” for everyone’s mutual success.
Bruce L. Cassis, DDS, MAGD Associate Editor
Partners in preservation: the value of endodontics in general practice
In every dental practice, we are reminded daily that patients value keeping their natural teeth. For decades, endodontics and endodontists have been central to helping general dentists honor that patient priority. Root canal treatment and related procedures have evolved dramatically, and today’s evidence-based, technologically advanced techniques give us more options than ever before to preserve teeth that, not long ago, could have been destined for extraction.
This special collaborative issue between the Academy of General Dentistry and the American Association of Endodontists highlights that shared commitment to tooth preservation. As colleagues in oral health, we recognize that endodontic specialty care does not stand apart from general dentistry; it is an integral part of it. Whether a patient presents with acute pain, a complex crack, or the need for a predictable long-term restoration, the decisions made in the operatory ripple forward into the patient’s overall well-being.
The articles gathered here provide insight into situations that every dentist encounters. One explores how careful attention to anatomy and canal morphology is essential in reducing the risk of extrusion-related injuries—an issue that, when understood fully, underscores the importance of thoughtful diagnosis and meticulous technique. Another addresses the restorative challenges of cracked teeth with deep radicular involvement, reminding us that even when root canal therapy is technically successful, the tooth’s long-term survival depends on the restorative strategy chosen. A third examines the coronal seal—a factor that may not receive as much attention as cleaning, shaping, and obturation, yet plays a critical role in preventing reinfection and ensuring long-term, durable outcomes.
Taken together, these contributions highlight a key theme: successful endodontic care is never just about what happens inside the root canal. It requires an integrated, whole-tooth perspective, blending surgical precision with restorative foresight. For general dentists, this means that endodontics should not be viewed as a separate specialty, but as part of a continuum of care that aligns with your daily mission to help patients keep healthy, functional teeth.
Our organizations share a vision of collaboration, education, and continuous improvement. General dentists are often the first to identify endodontic disease, provide urgent care, and determine when referral to a specialist is in the patient’s best interest. Endodontists, in turn, are partners in managing the most complex cases and advancing the science that makes treatment more predictable and less invasive. When we work together, we create the best environment for patients to make informed choices about their oral health.
We value the Academy of General Dentistry’s commitment to partner with the American Association of Endodontists and highlight this special topic in their journal. May the insights you find here reinforce the indispensable role of endodontics in your practice, spark reflection on treatment planning, and, most importantly, inspire renewed commitment to the patients we serve together.
Steven J. Katz, DDS, MS President
American Association of Endodontists
Beyond the apex: anatomical risk assessment to prevent extrusion injuries in endodontics
Gordon S. Lai, DDS, MSD
Extrusion of irrigants or obturation materials during endodontic therapy may result in significant complications, ranging from postoperative pain to nerve damage and chronic inflammation. Many of these adverse outcomes can be prevented through detailed anatomical assessment and thoughtful treatment planning. This article explores how anatomical complexities, including root apex morphology, proximity to vital structures, and apical resorption, contribute to extrusion risk.
Extrusion in endodontics refers to the unintended passage of materials such as irrigants, sealers, and obturation materials beyond the apical foramen. While some degree of extrusion may occur in routine endodontic therapy, the consequences can be severe when anatomical complexities are not adequately assessed. These complications can range from minor postoperative discomfort to severe tissue damage, persistent pain, infection, sinus involvement, and even irreversible nerve damage.1 One of the most commonly reported incidents in the endodontic literature is the “sodium hypochlorite accident,” a traumatic event caused by extrusion of irrigant into periapical tissues.2
An understanding of root canal anatomy is not only essential for effective cleaning and shaping but also critical to preventing iatrogenic injury. Risk factors for extrusion include the presence of complex root apex morphology, leading to overinstrumentation; close proximity of the root to anatomical structures such as the maxillary sinus or inferior alveolar nerve; and the presence of root resorption and external defects. Technological advancements, including cone beam computed tomography (CBCT), have improved the clinician’s ability to visualize these risks preoperatively. Nevertheless, the burden still remains on the clinician to interpret the anatomical information accurately and integrate it into clinical decision-making. This article provides a detailed exploration of anatomical variations contributing to extrusion injuries.
Factors contributing to extrusion risk
Complex anatomy and overinstrumentation
The apical third of the root canal system plays a pivotal role in the outcome of endodontic treatment. Numerous histologic studies have confirmed that microbial contamination in the apical third is strongly associated with persistent periapical lesions and posttreatment disease.3 Adequate cleaning and shaping of this region are essential to reduce microbial load, promote periapical healing, and achieve long-term treatment success. However, the complex apical region presents a paradox: it is both the area that most critically requires disinfection and the area most vulnerable to procedural mishaps, particularly overinstrumentation and extrusion. The ultimate goal of shaping and disinfection in endodontics is to eliminate apical irritants without mechanically or chemically violating periapical tissues.
Numerous studies have shown that mechanical instrumentation alone is insufficient for thorough canal debridement. Even with advanced rotary or reciprocating systems, only 35% to 55% of the canal walls in the apical third are typically contacted during instrumentation, leaving significant portions of the root canal system untouched.4 This limitation highlights the critical role of chemical disinfection and the importance of achieving a well-adapted obturation that seals the canal system effectively.
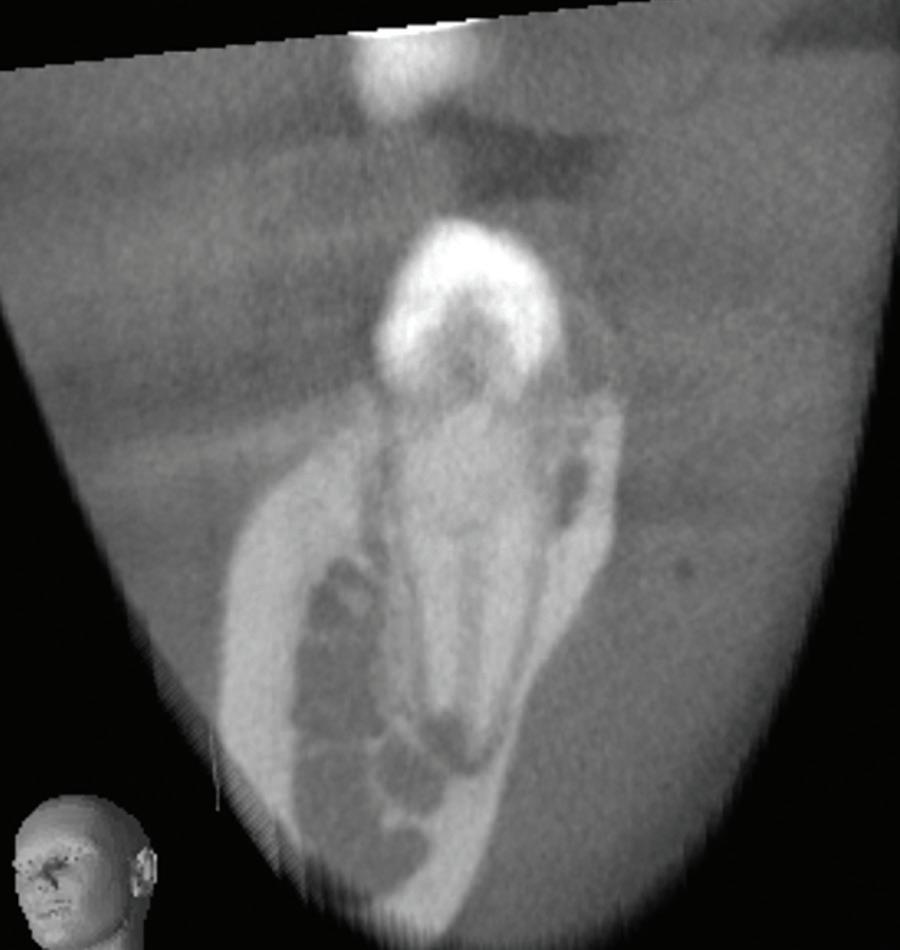
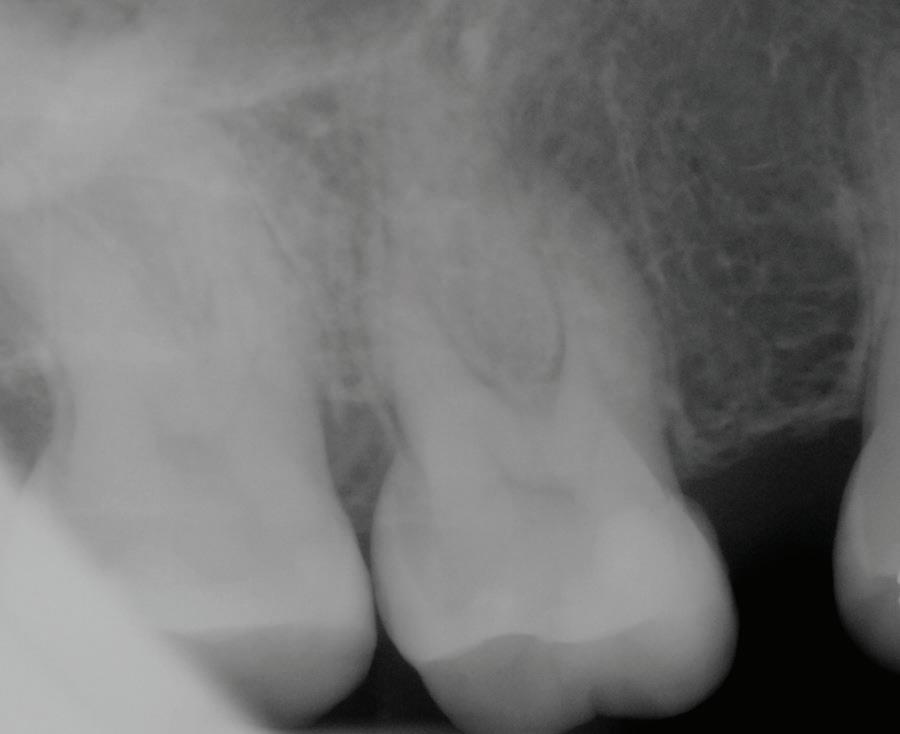
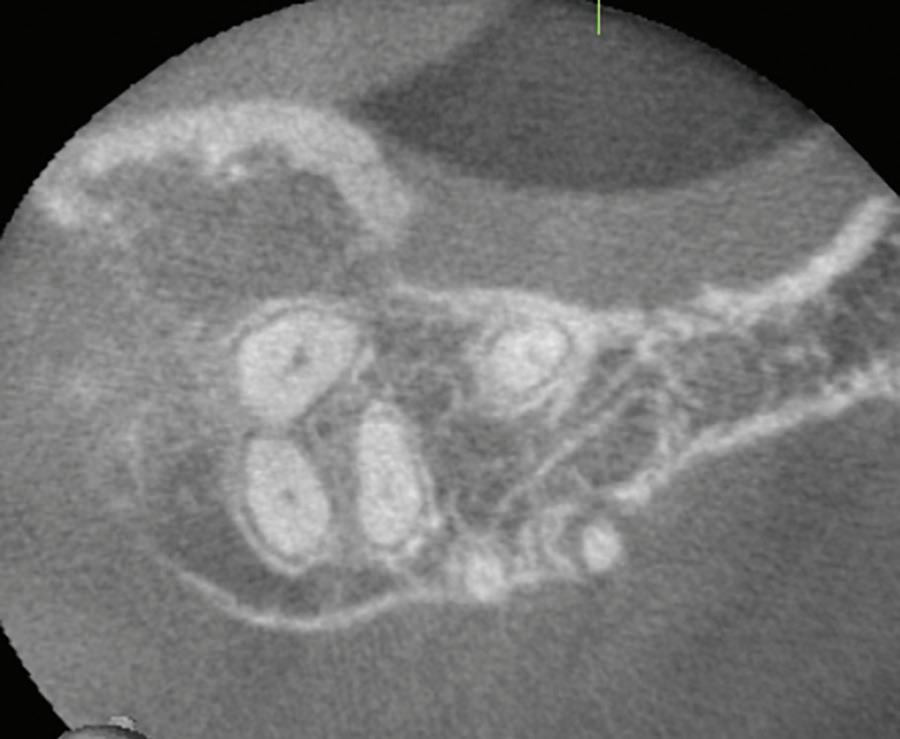
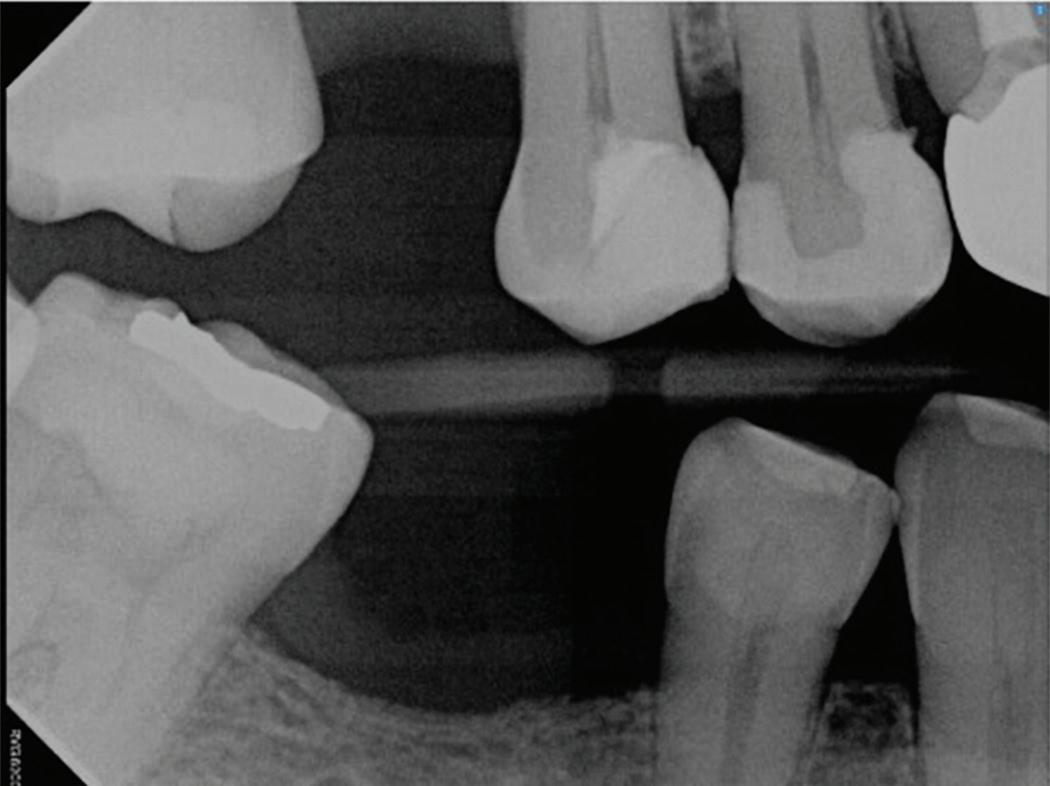
Fig 1. Proximity of root apices to vital structures. A. The periapical radiograph indicates that the apices of the mandibular right second molar and second premolar are in proximity to the inferior alveolar and mental nerves. B. A coronal CBCT image more clearly demonstrates the proximity of the molar apex to the inferior alveolar nerve. C. A coronal CBCT image more clearly demonstrates the proximity of the premolar apex to the mental nerve.
Extrusion of obturation material beyond the apex is consistently associated with reduced healing and unfavorable long-term outcomes.5,6 Complementary findings by Ricucci et al have further illustrated the biologic consequences of extrusion.7 Extrusion of irrigants or sealers beyond the apical foramen, particularly into anatomically sensitive areas such as the mandibular canal or maxillary sinus, can provoke intense inflammation, delayed periapical healing, or even permanent nerve injury.
Together, these findings highlight a clinical paradox: while optimal disinfection and obturation close to the apical terminus are essential for endodontic success, overinstrumentation or overfilling that violates periapical tissues may trigger foreign body reactions, persistent inflammation, and eventual treatment failure. This dichotomy underscores the importance of meticulous determination of the working length and controlled obturation, particularly in anatomically complex or high-risk regions.
Proximity of apex to vital structures
Proper preoperative planning, including clinical examination, radiographic interpretation, and CBCT when indicated, is essential to identify proximity to vital structures and reduce the risk of procedural complications associated with extrusion. Anatomical proximity of root apices to key neurovascular or sinus structures substantially increases the risk of iatrogenic extrusion injuries during endodontic procedures. In addition to the inferior alveolar nerve and maxillary sinus, the mental foramen and its associated neurovascular bundle, especially in relation to mandibular premolars, is a high-risk area often underestimated during treatment planning.
Inferior alveolar nerve
The inferior alveolar canal courses closely beneath the apices of mandibular molars, particularly second molars. Studies have shown that in more than 25% to 30% of patients, the inferior alveolar canal lies within 1 mm of the root apices of second molars; the prevalence is even higher in female and older patients due to reduced bone volume (Fig 1).8
This close proximity raises concern for chemical neuritis or neuropathic injury if obturation materials or irrigants are inadvertently forced through the apex. Extrusion of epoxy resin sealers, or even bioceramic materials, has been associated with persistent paresthesia and burning dysesthesia of the lower lip or chin. Although some cases eventually resolve, irreversible nerve damage has been reported in several cases, sometimes requiring surgical decompression.9,10
A lesser known risk is extrusion of calcium hydroxide (Ca[OH]2), commonly used as an intracanal medicament. This agent can also result in severe neurovascular injury when extruded into the periapical space. Its high pH (~12.5) can cause protein denaturation, fat necrosis, and chemical injury to nerve tissue.11,12 In a case series reported by Gluskin et al, 5 patients experienced persistent paresthesia and dysesthesia after Ca(OH) 2 was extruded into the inferior alveolar nerve space.13 These injuries were linked to direct chemical damage and potential ischemic necrosis, with radiographic evidence of radiopaque material near the mandibular canal. Beyond localized nerve injury, Ca(OH)2 extrusion can also result in more widespread vascular complications, such as Nicolau syndrome, a rare but severe ischemic event caused by intra-arterial or periarterial injection of irritants.14,15 The literature includes case reports of patients who received Ca(OH)2 injections mistakenly placed near arterial structures and developed cutaneous necrosis, severe tissue ischemia, and in some cases, permanent scarring or functional loss.11,14,15 These findings underscore that even small volumes of Ca(OH)2 can trigger vascular spasm, thrombosis, or embolic events, injuring tissues distant from the site of extrusion (Fig 2).
Mental foramen
In addition to the inferior alveolar nerve, the mental foramen is a critical anatomical landmark in the mandible, particularly due to its close proximity to the apices of the mandibular premolars, most notably the second premolars. Typically, studies have shown the mental foramen to be localized 5.0 mm from the closest root of the adjacent premolar.16
Dr Alan Gluskin, San Francisco, California.)
This proximity is clinically critical because extrusion of sealers or Ca(OH)2 during treatment of premolars may result in mental nerve paresthesia, manifesting as numbness or tingling of the lower lip and chin. Unlike injuries to the main inferior alveolar nerve trunk, mental nerve damage may initially appear minor but become long-standing if not recognized and managed appropriately.17
Maxillary sinus
In the maxillary arch, the area of most concern when it comes to extrusion injuries is the maxillary sinus region. The maxillary sinus is frequently in direct anatomical contact with the roots of the maxillary first and second molars, and sometimes in contact with premolars. Studies indicate that up to 70% of first molars have roots contacting or protruding into the sinus, especially the palatal or distobuccal roots.18
Extrusion of filling materials or sodium hypochlorite into the sinus may result in chemical sinusitis, chronic maxillary sinus infection, or oroantral communication. Such patients may present with postoperative congestion, facial pain, or foul nasal discharge, symptoms that often lead to referrals to an otolaryngologist and delayed diagnoses. Inflammatory sinus disease of dental origin may account for more than 40% of maxillary sinusitis cases.19
Apical root resorption and external defects
Beyond anatomical assessment, careful evaluation for root resorption and other external anomalies is also essential. Apical root resorption is a pathologic or iatrogenic process that can complicate endodontic treatment by eliminating the natural apical constriction, a key anatomical barrier against the
extrusion of materials. Resorptive processes alter the regular tapered architecture of the apical third, creating widened, irregular, or blunted root ends that are difficult to manage during cleaning, shaping, and obturation.
Resorbed apices are more prone to overinstrumentation, as they lack resistance to file advancement. The biggest concern with the loss of apical resistance is that sealers, irrigants, or thermoplastic gutta percha may be easily forced into periapical tissues, increasing the risk of inflammatory reactions, foreign body responses, and postoperative pain.20
Apical resorption can have various etiologies, including chronic periapical inflammation from long-standing infection; orthodontic tooth movement, particularly in response to excessive forces; trauma and revascularization attempts; and iatrogenic factors, including repeated overinstrumentation or overfilling in prior treatments.21 In teeth undergoing retreatment, especially those with prior extrusion of materials or necrotic infection, apical resorption is common and often undetected with conventional radiography.
One underrecognized anatomical risk factor closely associated with apical resorption is fenestration, a defect in the cortical plate where a portion of the root protrudes through the bone, often covered only by periosteum and mucosa. Fenestrations are most frequently observed in association with maxillary and mandibular incisors, due to the thin buccal cortical bone at those sites; mandibular premolars, where lingual cortical plates may be compromised; and teeth with severe apical curvatures or buccal root prominences.22
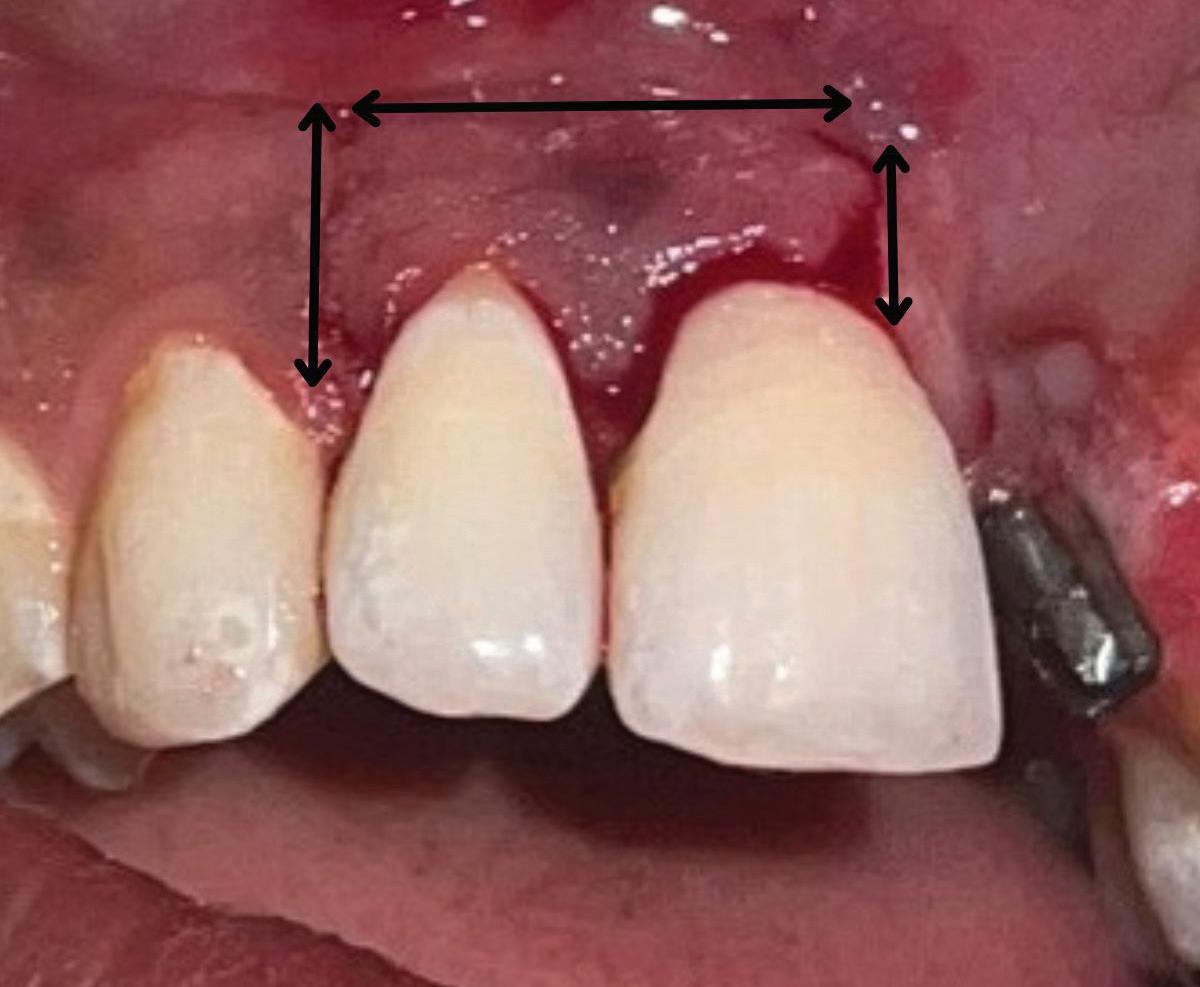
When endodontic irrigants or materials are extruded in teeth with fenestrations, they not only exit beyond the apex but also may enter directly into soft tissue or mucosal spaces, dramatically increasing the risk of postoperative swelling, pain, and delayed healing. In a recent retrospective case series investigating sodium hypochlorite extrusion injuries, fenestrations were identified in all 26 reported cases (Fig 3).23
Imaging tools to identify anatomical risk Periapical radiography
Proper diagnosis is essential to identifying cases at risk of extrusion. Conventional periapical radiography remains a fundamental diagnostic tool in endodontics, offering high-resolution, real-time imaging at low radiation exposure and minimal cost. However, the 2-dimensional (2D) nature of periapical radiographs presents inherent limitations when complex root anatomy is evaluated, especially in the apical third.
One of the most significant shortcomings of periapical radiography is its inability to provide information in the buccolingual dimension. This makes it difficult to detect resorptive lesions (internal or external) located on the buccal or lingual surfaces; fenestrations or dehiscences in the cortical plate; split canals, C-shaped canals, or isthmuses hidden in a single projection; and superimposed anatomical structures, including the zygomatic arch over maxillary molars or mental foramen overlapping premolar apices.
To improve diagnostic accuracy, clinicians are encouraged to take multiple angulated views. However, even with angulated views, the 2D limitation persists, and structures with significant buccolingual spread or overlap may still be misinterpreted. In cases in which a patient’s symptoms persist despite normal
Fig 2. Calcium hydroxide extrusion. During treatment of the mandibular left first molar, dysesthesia (burning pain) and paresthesia resulted from a substantial overfill of calcium hydroxide into the inferior alveolar nerve canal. (Courtesy of
radiographic findings, or an apical resorption, a fenestration, or an anatomical anomaly is suspected, reliance on periapical radiographs alone may result in missed diagnoses or mismanagement (Fig 4).
Additionally, periapical radiographs may underestimate the extent of periapical bone loss or resorption if confined to the cortical plate or masked by trabecular density. For instance, studies have shown that periapical radiolucencies must involve at least 30% mineral loss in the bone to be radiographically visible.24,25
Cone beam computed tomography
CBCT has revolutionized endodontic diagnostics by allowing practitioners to evaluate dental anatomy in 3 dimensions (3D). In contrast to traditional 2D radiographs, CBCT images can reveal nuances such as root canal curvature, apical deltas, external resorptions, fenestrations, and anatomical landmarks
that would otherwise go unnoticed. The ability to visualize the thickness of cortical bone, the position of the inferior alveolar canal, or the floor of the maxillary sinus can alter treatment decisions dramatically. For example, in cases where apical surgery is being considered, evaluation of CBCT images can determine whether the apex is embedded in the sinus or the mandibular canal is at risk of involvement.
The American Association of Endodontists and the American Academy of Oral and Maxillofacial Radiology jointly recommend the use of CBCT in select cases involving complex root canal anatomy, persistent periapical pathosis, or surgical planning.26 These guidelines emphasize CBCT as an adjunct, not a routine imaging modality, primarily to limit unnecessary radiation exposure and ensure judicious use of advanced diagnostics. Some clinicians have argued that concerns over CBCT radiation dosage may be overstated, particularly when weighed against the diagnostic and safety benefits in complex cases.27
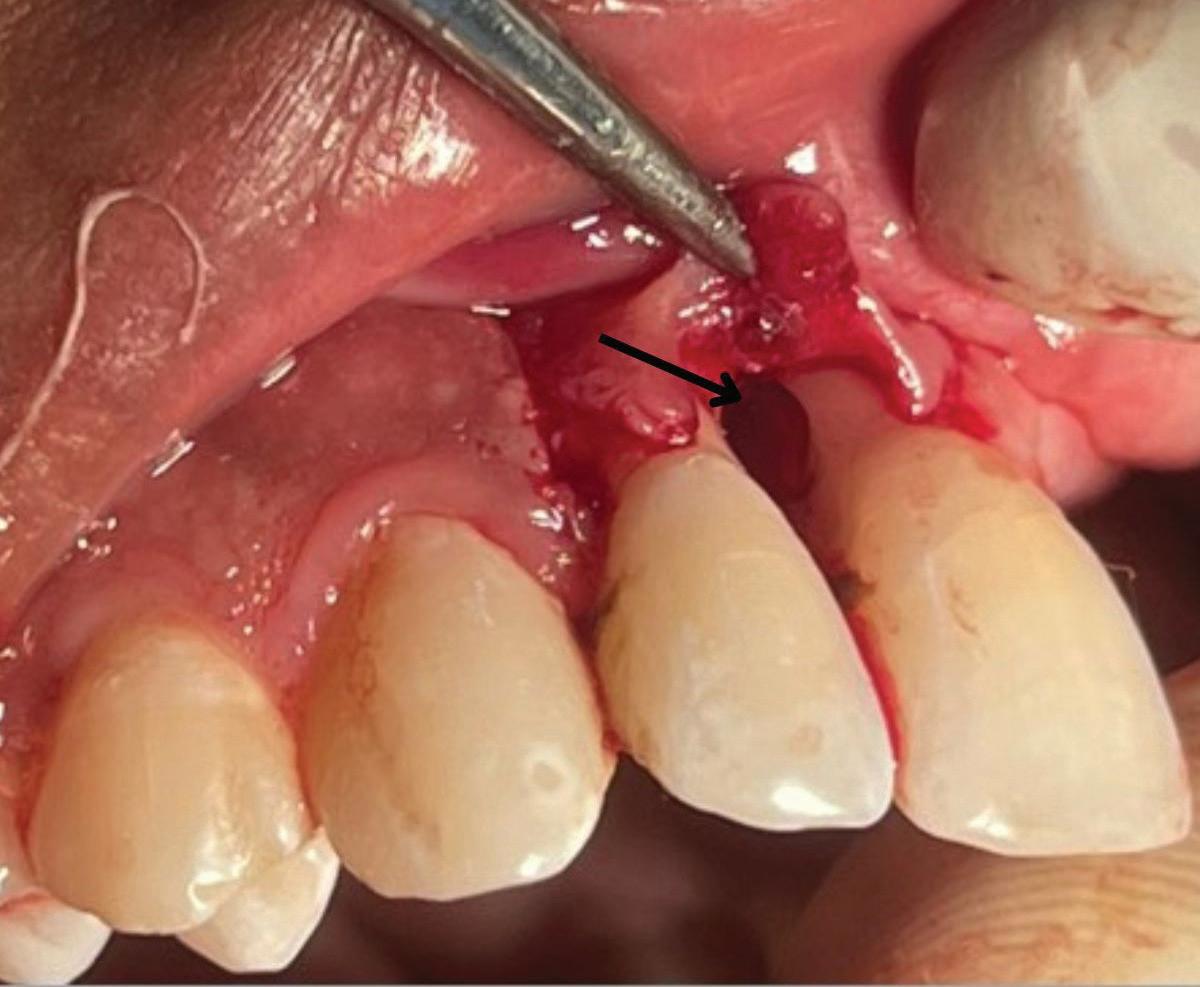
Fig 3. Sodium hypochlorite was extruded through a perforation that occurred during endodontic treatment of the maxillary left canine, causing immediate bruising, swelling, and pain.
A
Fig 4. Fenestration involving the maxillary right first molar. A. The periapical radiograph fails to demonstrate the presence of a fenestration at the mesiobuccal root. B. The axial CBCT image clearly depicts the fenestration. C. The coronal CBCT image also reveals the fenestration.
It also could be argued that the potential for iatrogenic complications, including extrusion-related nerve injuries or sinus involvement, supports a more universal application of preoperative CBCT, especially in posterior teeth or anatomically high-risk zones. For instance, bony fenestrations, which create direct communication between the root surface and soft tissue due to absence of cortical bone, are virtually invisible on standard 2D radiographs. These defects significantly increase the risk of overinstrumentation; endodontic irrigant and obturation material extrusion; and postoperative inflammation, particularly when the root apex lies adjacent to neurovascular structures or sinus cavities. CBCT is the only reliable tool to detect fenestrations preoperatively. It allows visualization of cortical bone thickness and can identify discontinuities in the buccal or lingual plate that predispose to soft tissue perforation (Fig 5).
In a CBCT-based study by Nalbantoğlu et al, fenestrations were identified in approximately 35.7% of maxillary anterior teeth, with the majority occurring in the apical third of the root. 28 Dehiscence was observed in 20% of teeth, and a significant proportion of cases were associated with thin buccal bone, particularly in patients with periodontal biotypes exhibiting bone thickness of 1 mm or less. These findings highlight the vulnerability of anterior teeth, especially in individuals with thin cortical bone, to structural defects such as fenestrations.
In this context, CBCT is not merely a luxury for complex cases; it becomes a predictive safety tool, offering 3D insight into risks that are otherwise undetectable by conventional means. While radiation exposure should always be balanced with diagnostic benefit, the potential for preventing irreversible complications in seemingly routine cases suggests that
broader adoption of preoperative CBCT may represent an evolution in the standard of care, particularly for molars, retreatments, or anatomically ambiguous presentations.
Conclusion
Anatomical complexity is a defining factor in endodontic diagnosis, treatment planning, and clinical execution. The success of root canal therapy depends not only on the elimination of microbial infection but also on the clinician’s ability to recognize and adapt to the nuances of root canal and periapical anatomy. From identifying atypical canal configurations and apical resorption to avoiding iatrogenic extrusion injuries near neurovascular structures or the maxillary sinus, thorough anatomical risk assessment is essential. Conventional radiography provides an initial overview, but the integration of advanced imaging modalities, including CBCT, enables more precise treatment planning. Ultimately, a proactive approach to anatomical risk that is grounded in the current literature, 3D imaging, and clinical experience can significantly reduce procedural errors, enhance patient safety, and improve long-term treatment outcomes in endodontics.
Author affiliation
Department of Endodontics, Arthur A. Dugoni School of Dentistry, University of the Pacific, San Francisco, California.
Correspondence
Gordon Lai, DDS, MSD (glai1@pacific.edu).
Conflicts of interest
None reported.
Fig 5. Fenestration involving the maxillary left central incisor. A. The periapical radiograph fails to demonstrate the apex protruding into the sinus. B. The CBCT 3D reconstructed volume clearly demonstrates the fenestration.
References
1. Gluskin AH. Anatomy of an overfill: a reflection on the process. Endod Top. 2007;16(1):6481. doi:10.1111/j.1601-1546.2009.00238.x
2. Guivarc’h M, Ordioni U, Ahmed HM, Cohen S, Catherine JH, Bukiet F. Sodium hypochlorite accident: a systematic review. J Endod. 2017;43(1):16-24. doi:10.1016/j.joen.2016.09.023. PMID: 27986099.
3. Siqueira JF Jr, Rôças IN. Clinical implications and microbiology of bacterial persistence after treatment procedures. J Endod. 2008;34(11):1291-1301.e3. doi:10.1016/j.joen.2008.07.028
4. Peters OA, Schönenberger K, Laib A. Effects of four Ni-Ti preparation techniques on root canal geometry assessed by micro computed tomography. Int Endod J. 2001;34(3):221-230. doi:10.1046/j.1365-2591.2001.00373.x
5. Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature, 2: influence of clinical factors. Int Endod J 2008;41(1):6-31. doi:10.1111/j.1365-2591.2007.01323.x
6. Ng YL, Mann V, Gulabivala K. Outcome of secondary root canal treatment: a systematic review of the literature. Int Endod J. 2008;41(12):1026-1046. doi:10.1111/j.13652591.2008.01484.x
7. Ricucci D, Siqueira JF Jr. Recurrent apical periodontitis and late endodontic treatment failure related to coronal leakage: a case report. J Endod. 2011;37(8):1171-1175. doi:10.1016/j. joen.2011.05.025
8. Denio D, Torabinejad M, Bakland LK. Anatomical relationship of the mandibular canal to its surrounding structures in mature mandibles. J Endod. 1992;18(4):161-165. doi:10.1016/ S0099-2399(06)81411-1
9. Pogrel MA. Damage to the inferior alveolar nerve as the result of root canal therapy. J Am Dent Assoc. 2007;138(1):65-69. doi:10.14219/jada.archive.2007.0022
10. Stanley E, Strother KK, Kirkpatrick T, Jeong JW. Calcium silicate–based sealer extrusion into the mandibular canal: 3 different recovery outcomes—a report of 3 cases. J Endod 2023;49(6):735-741. doi:10.1016/j.joen.2023.04.006
11. Ahlgren FK, Johannessen AC, Hellem S. Displaced calcium hydroxide paste causing inferior alveolar nerve paraesthesia: report of a case. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96(6):734-737. doi:10.1016/j.tripleo.2003.08.018
12. Shin Y, Roh BD, Kim Y, Kim T, Kim H. Accidental injury of the inferior alveolar nerve due to the extrusion of calcium hydroxide in endodontic treatment: a case report. Restor Dent Endod. 2016;41(1):63-67. doi:10.5395/rde.2016.41.1.63
13. Gluskin AH, Lai G, Peters CI, Peters OA. The double-edged sword of calcium hydroxide in endodontics: precautions and preventive strategies for extrusion injuries into neurovascular anatomy. J Am Dent Assoc. 2020;151(5):317-326. doi:10.1016/j.adaj.2020.01.026
14. Kang Q, Huang Z, Qian W. Nicolau syndrome with severe facial ischemic necrosis after endodontic treatment: a case report. J Endod. 2024;50(5):680-686. doi:10.1016/j. joen.2024.02.010
15. Al-Sheeb F, Al Mannai G, Tharupeedikayil S. Nicolau syndrome after endodontic treatment: a case report. J Endod. 2022;48(2):269-272. doi:10.1016/j.joen.2021.10.006
16. von Arx T, Friedli M, Sendi P, Lozanoff S, Bornstein MM. Location and dimensions of the mental foramen: a radiographic analysis by using cone-beam computed tomography. J Endod. 2013;39(12):1522-1528. doi:10.1016/j.joen.2013.07.033
17. Mohammadi Z. Endodontics-related paresthesia of the mental and inferior alveolar nerves: an updated review. J Can Dent Assoc. 2010;76:a117.
18. Regnstrand T, Ezeldeen M, Shujaat S, Ayidh Alqahtani K, Benchimol D, Jacobs R. Threedimensional quantification of the relationship between the upper first molar and maxillary sinus. Clin Exp Dent Res. 2022;8(3):750-756. doi:10.1002/cre2.561
19. Tataryn RW. Maxillary sinusitis of endodontic origin. Endodontics: Colleagues for Excellence Newsletter. American Association of Endodontists. 2018;Fall:1-8. https://www.aae.org/ specialty/wp-content/uploads/sites/2/2018/10/ecfe-fall-2018-final-002-1.pdf
20. Ricucci D, Siqueira JF Jr. Apical actinomycosis as a continuum of intraradicular and extraradicular infection: case report and critical review on its involvement with treatment failure. J Endod. 2008;34(9):1124-1129. doi:10.1016/j.joen.2008.06.002
21. Tronstad L. Root resorption—etiology, terminology and clinical manifestations. Endod Dent Traumatol. 1988;4(6):241-252. doi:10.1111/j.1600-9657.1988.tb00642.x
22. Sun L, Mu C, Chen L, Zhao B, Pan J, Liu Y. Dehiscence and fenestration of Class I individuals with normality patterns in the anterior region: a CBCT study. Clin Oral Investig 2022;26(5):4137-4145. doi:10.1007/s00784-022-04384-2
23. Cho-Kee D, Basrani BR, Vera J, Ordinola-Zapata R, Aguilar RR. Sodium hypochlorite accidents: a retrospective case-series analysis of CBCT imaging and clinician surveys. J Endod. 2025;51(10):1485-1489. doi:10.1016/j.joen.2025.05.024
24. Bender IB, Seltzer S. Roentgenographic and direct observation of experimental lesions in bone: I. 1961. J Endod. 2003;29(11):702-706. doi:10.1097/00004770-200311000-00005
25. Bender IB, Seltzer S. Roentgenographic and direct observation of experimental lesions in bone: II. 1961. J Endod. 2003;29(11):707-712. doi:10.1097/00004770-200311000-00006
26. Special Committee to Revise the Joint AAE/AAOMR Position Statement on Use of CBCT in Endodontics. AAE and AAOMR joint position statement: use of cone beam computed tomography in endodontics 2015 update. Oral Surg Oral Med Oral Pathol Oral Radiol 2015;120(4):508-512. doi:10.1016/j.oooo.2015.07.033
27. Azevedo BA. CBCT: dispelling the fear. AAE Communiqué. May 5, 2025. Accessed June 14, 2025. https://www.aae.org/specialty/cbct-dispelling-the-fear/
28. Nalbantoğlu AM, Yanık D. Fenestration and dehiscence defects in maxillary anterior teeth using two classification systems. Aust Dent J. 2023;68(1):48-57. doi:10.1111/adj.12950
Cracked teeth with radicular extension: an update on restorative procedures for endodontically treated deeply cracked teeth
Matthew C. Davis, DDS ¢ Suhaila S. Shariff, DMD, MPH
Cracked teeth with radicular extension have traditionally been considered nonrestorable; however, recent evidence supports a conservative treatment approach with favorable outcomes. This article outlines a protocol involving microscope-assisted endodontic therapy, placement of an intraradicular barrier, and timely fullcoverage restoration for endodontically treated deeply cracked teeth. When proper case selection guidelines are followed, these teeth show high survival and success rates comparable to those of noncracked teeth. The outlined protocol emphasizes preserving pericervical dentin, sealing the internal aspects of the crack to prevent bacterial contamination, and minimizing occlusal and parafunctional stresses. Although crack-associated isolated periodontal pocketing may persist, studies show these defects may remain stable and asymptomatic over time. A team approach for this protocol is recommended, with endodontists and restorative dentists each playing a role. This article encourages reconsideration of extraction as the default solution to deeply cracked teeth and highlights the importance of preserving natural dentition whenever possible.
Acracked tooth is defined as a tooth with one or more incomplete fractures originating in the clinical crown, extending through the enamel and dentin, and propagating apically. Cracks typically follow a mesiodistal orientation and, as they progress, may involve both the pulp and root surfaces. Cracked teeth represent a single category within the broader classification of longitudinal tooth fractures, which also includes craze lines, fractured cusps, split teeth, and vertical root fractures.1 Accurate differentiation among these fracture types is essential, as each carries specific prognoses and treatment protocols. While a detailed discussion of these distinctions is beyond the scope of this article, the Table provides a concise summary, including a recently defined category: cracked tooth with radicular extension.2-4 When these teeth are discussed, terms such as cracked root or radicular crack refer only to cracks that originate from the occlusal surface and extend onto the root, distinct from vertical root fractures, which originate within the root itself and represent a separate category of longitudinal tooth fracture. Although cracked teeth with radicular extension may present with any pulpal diagnosis, the depth of the crack greatly increases the likelihood of irreversible pulpal disease. For that reason, the following discussion will address only cracked teeth with radicular extension that require endodontic treatment. Effective management of cracks goes beyond treating the tooth itself. Since patients who present with one cracked tooth are at increased risk of having cracks in other teeth, there are likely unaddressed etiologic factors that predispose these patients to the development of cracked teeth.5 Rather than an isolated event, a crack is often a symptom of broader biomechanical imbalances or risk factors. Management of these cases should prioritize resolution of current symptoms in the affected tooth, followed by identification and control of contributing variables in an effort to prevent crack propagation, new crack formation, and additional cracked teeth. Two of the most common factors associated with cracked teeth are traumatic occlusion, such as heavy occlusal contacts and interferences, and parafunctional habits, such as bruxism and clenching.6
Historically, studies have shown that endodontically treated cracked teeth exhibit favorable prognoses, with outcomes comparable to those of noncracked teeth.7-10 In many studies of cracked teeth, however, researchers have found that success and survival rates are diminished in cracked teeth with radicular extension, typically identified by probing depths of 4 mm or greater.11-15 Extraction has traditionally been the treatment recommended for these teeth.16
Unlike in cracked teeth where the crack is limited to the clinical crown, in deeply cracked teeth, the cracks extend into
Table. Longitudinal tooth fracture types and appropriate endodontic and restorative treatment plans. a
Type of longitudinal tooth fracture Characteristics
Craze line Confined to enamel only
Transillumination: light transmits without interruption through a craze line
Cuspal fracture (complete and incomplete)
Initiates on the occlusal surface of the clinical crown; extends obliquely, undermining cusp(s); involves enamel and dentin; and may or may not involve the pulp:
• Incomplete cuspal fracture: a crack undermines cusp(s), but cusp(s) still present
• Complete cuspal fracture: the cusp is lost
Transillumination: light will stop at the fracture for incomplete cuspal fractures
Cracked tooth (confined to the clinical crown)
Cracked tooth with radicular extension
Initiates in the crown of the tooth, extending apically along the long axis of the tooth; typically oriented mesial to distal, involves enamel and dentin, may or may not involve the pulp, and is confined to coronal tooth structures; incomplete or greenstick fracture
Transillumination: light will stop at the fracture
Cracked tooth with further apical extension of a crack; involves enamel, dentin, root structure, and likely the pulp and periodontium
Transillumination: light will stop at the fracture
Endodontic treatment plan
No endodontic treatment
No endodontic treatment:
• If diagnosis is normal pulp or reversible pulpitis
• If no pulp exposure with complete cuspal fracture
Endodontic treatment:
• If diagnosis is irreversible pulpitis or pulpal necrosis
• If a post is necessary for complete cuspal fracture
• If the pulp is exposed in cases of complete cuspal fractures
Extraction:
• If extensive tooth structure is lost
No endodontic treatment:
• If diagnosis is normal pulp or reversible pulpitis
Endodontic treatment:
• If diagnosis is irreversible pulpitis or pulpal necrosis
Restorative treatment plan
Not necessary unless a cosmetic issue
No crown:
• If pulp is normal, the tooth is asymptomatic, and minimal tooth structure is lost
Crown ASAP:
• For all other pulpal diagnoses or if extensive tooth structure is compromised
Check and adjust occlusion; consider nightguard
Split tooth A cracked tooth with a complete fracture resulting in separate, mobile segments; extends deep into root structures with potentially significant destruction to the periodontium
Vertical root fracture Initiates in the root and propagates apically and coronally; typically seen in endodontically treated roots, usually oriented buccal to lingual
Transillumination: light will stop at the fracture
Abbreviation: ASAP, as soon as possible.
No endodontic treatment:
• If diagnosis is normal pulp or reversible pulpitis
Endodontic treatment:
• If diagnosis is irreversible pulpitis or pulpal necrosis
Microscopic visualization of the internal crack with placement of intraradicular barrier 2-3 mm apical to the extent of the crack
No endodontic treatment
No crown:
• An option if pulp is normal and the tooth is asymptomatic
Crown ASAP:
• If diagnosis is reversible pulpitis
• If root canal treatment is performed
Check and adjust occlusion; consider nightguard
Crown ASAP:
• If diagnosis is reversible pulpitis
• If root canal treatment is performed
Check and adjust occlusion; consider nightguard
Most will require extraction; however, root amputation, hemisection, and root resection are options in select cases
Extraction: restoration of the edentulous space may be considered
If extraction is selected: implant, fixed partial denture, or removable partial denture may be considered
a Adapted from Shariff SS, Davis MC. Cracked tooth with radicular extension. In: Shin Perry E, Patel S, Kanagasingam S, Hamer S, eds. Pitt Ford’s ProblemBased Learning in Endodontology. 2nd ed. Wiley; 2024:49-59. Reprinted with permission from Wiley. All rights reserved.
Box. Treatment protocols for restoring a cracked tooth with radicular extension.4
Intraoperative endodontic protocol
• Use a conservative endodontic technique, preserving pericervical dentin.
• Place an intraradicular barrier:
• Use an operating microscope to identify the deepest extent of the crack internally.
• Place a barrier material (eg, resin-modified glass ionomer cement or composite resin) 2 to 3 mm apical to the visual terminus of the fracture.
• Place orifice barriers 2 to 3 mm into the other canals.
• Place a composite resin core.
• Postoperative endodontic protocol (if immediate temporary or permanent crown is not placed)
• Reduce the tooth until it is entirely out of occlusion, eliminating all functional and excursive contacts.
• Instruct the patient to avoid chewing on the side with the cracked tooth.
Restorative protocol
• Place a full-coverage crown restoration within 3 weeks after endodontic treatment.
• Ensure optimal occlusion and the absence of excursive interferences.
Postrestorative protocol
• Consider whether patient should use a nightguard as a preventive measure against nocturnal bruxism.
• Address other possible etiologic factors for cracks (eg, parafunction or traumatic occlusion).
• Evaluate and adjust occlusion at 6-week, 6-month, and 1-year follow-up visits.
the canal spaces internally and the periodontium externally. Since all cracks in teeth harbor bacterial biofilms, any area in contact with the crack can potentially be affected by bacterial contamination.17 Internally, cracks place biofilms along the pulp chamber into canals, potentially giving bacteria access to the pulp space and periapical tissues. Externally, these cracks on the roots often manifest in the periodontium as asymptomatic, narrow, isolated areas of crestal bone loss, termed crackassociated isolated periodontal pocketing (CAIPP) defects. 18 Periodontal probing depths greater than 4 mm along a crack have been associated with an increased likelihood of pulpal necrosis; therefore, a considerable proportion of these teeth will require endodontic intervention.19
Shallower cracks can often be removed with operative procedures, effectively eliminating the biofilm.20,21 However, “chasing” or removing the crack in an endodontically treated deeply cracked tooth can further weaken the remaining tooth structure or disrupt a crown margin, rendering the tooth unrestorable. In fact, the greater the removal of deeper tooth structures, the more susceptible the tooth is to further crack propagation, new cracks, and vertical root fractures.22-24 Therefore, deep cracks should not be removed; instead endodontically treated cracked teeth with radicular extension should be restored with a core and crown to maintain as much supporting tooth structure as possible.
In cases where the crack is confined to the coronal tooth structure, placement of a core will seal the crack internally, while cementation of a crown seals the crack externally. However, in radicular cracks, a traditional core does not adequately seal the apical extent of the internal fracture as it extends into the radicular dentin and terminates within the obturated canal space. In these cases, bacterial contamination of the canal system and periapical tissues may occur, because gutta percha and sealer alone do not provide a sufficient barrier against microbial infiltration.25 Likewise, the external portion of the radicular crack lies apical to the crown margin in these cases, allowing for the ingress of periodontal bacteria in the crack and perpetuating a CAIPP defect. Bacteria can then travel through the crack pathway into the pulp space, contributing to the endodontic infection.
Given these differences between shallower and deeper cracks, it is reasonable to conclude that deeply cracked endodontically compromised teeth may require an alternative restorative strategy to address the weakened root and bacterial contamination resulting from the radicular crack. Recent studies have investigated a restorative protocol designed specifically for these teeth.4,26 Therefore, the purposes of this article are to detail a contemporary evidence-based technique for managing cracked teeth with radicular extension; examine the current evidence supporting this protocol; review the outcomes; and discuss other treatment planning considerations and limitations of the treatment strategy as they relate to clinical practice.
Restorative protocol
In 2019, Davis and Shariff published a prospective study introducing an evidence-based restorative technique specifically designed for managing those cracked teeth with radicular extension that require root canal treatment (Box).4 For the purposes of this article, orifice barriers are defined as restorative materials placed into all canal orifices routinely as a final step of endodontic obturation. In contrast, the term intraradicular barriers refers to restorative materials placed deeper into the canal space when a crack is present along the canal wall.
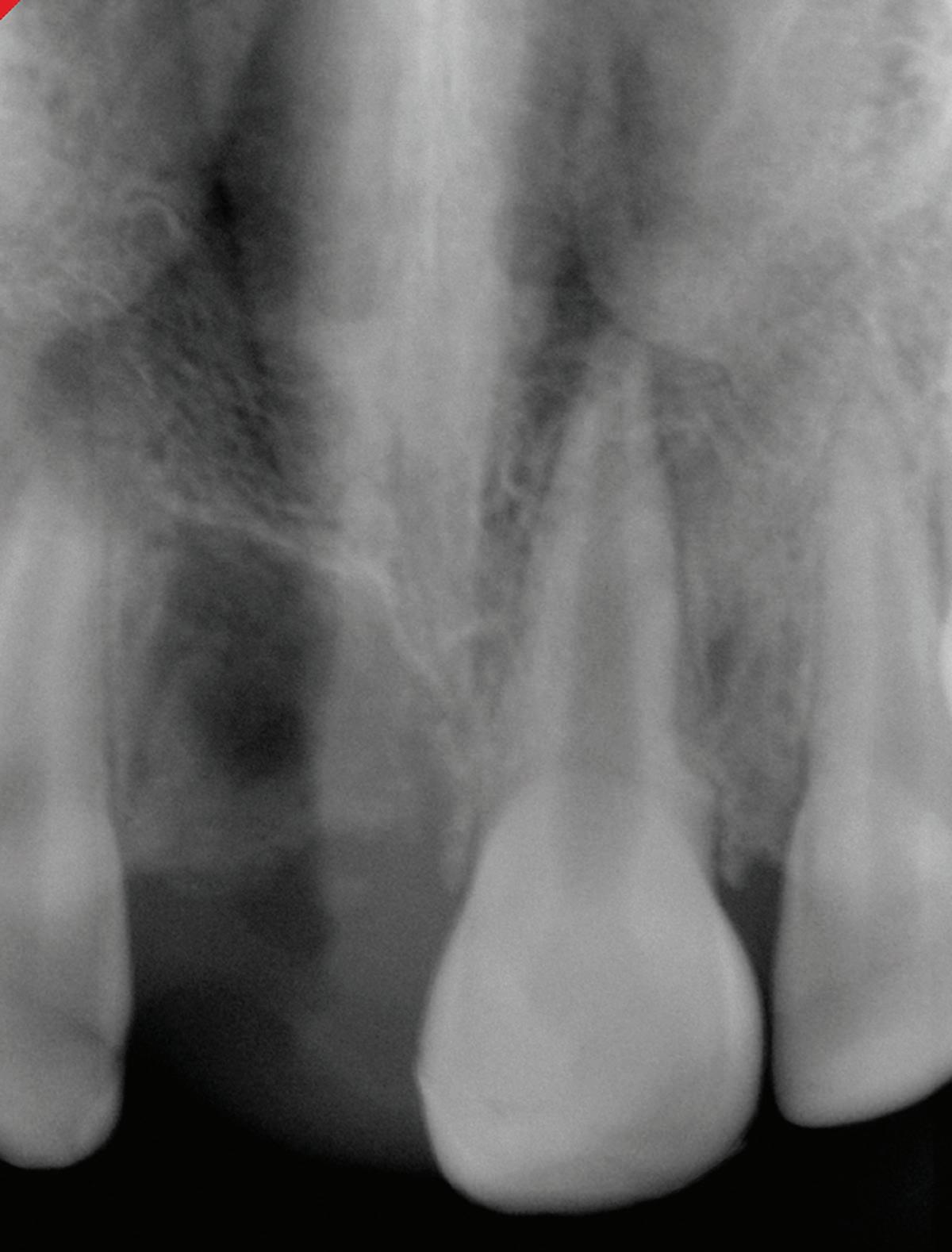
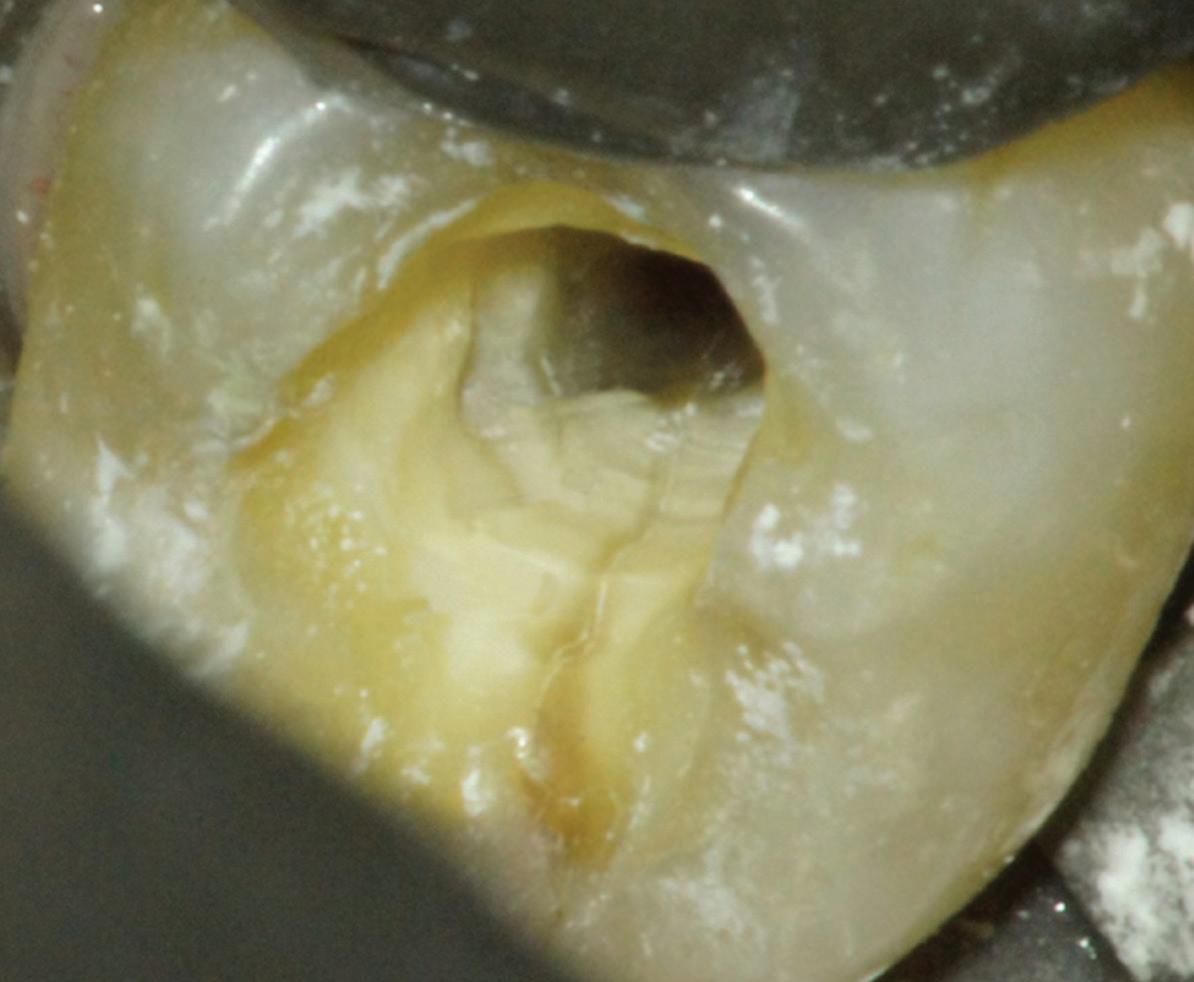
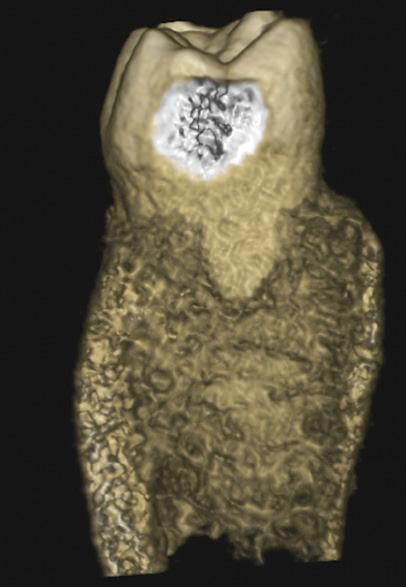
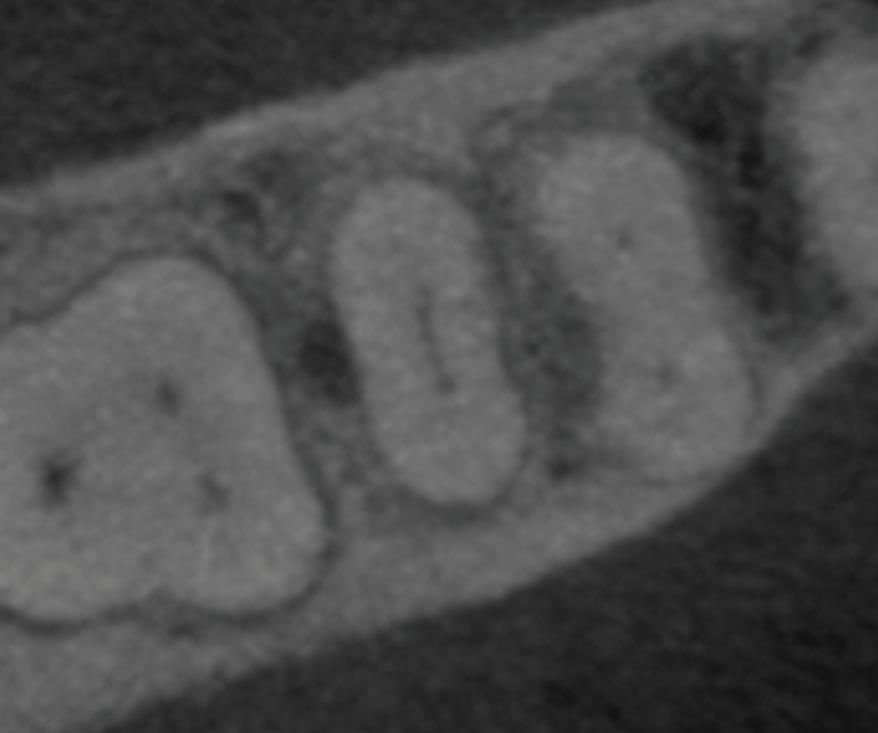
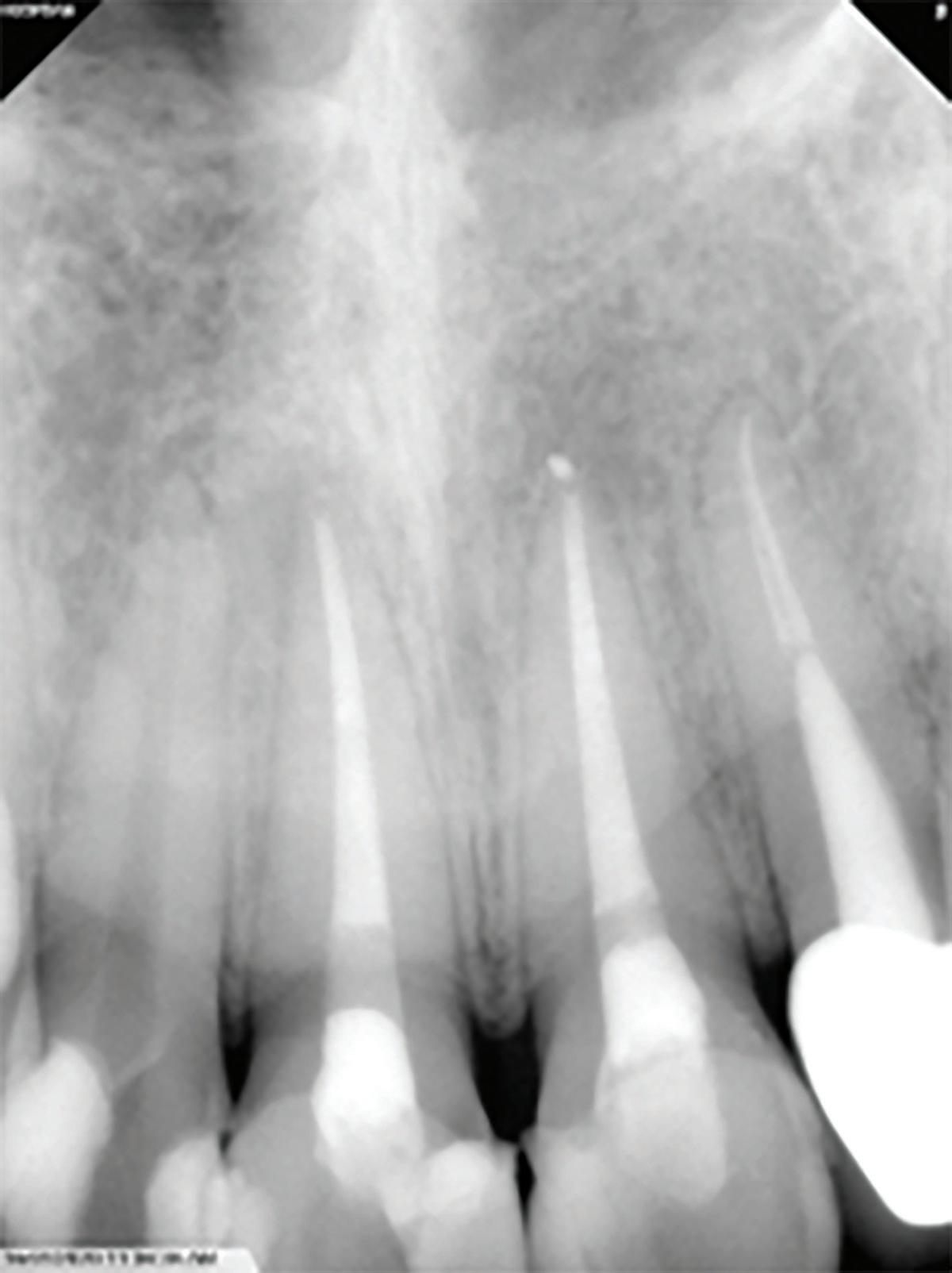
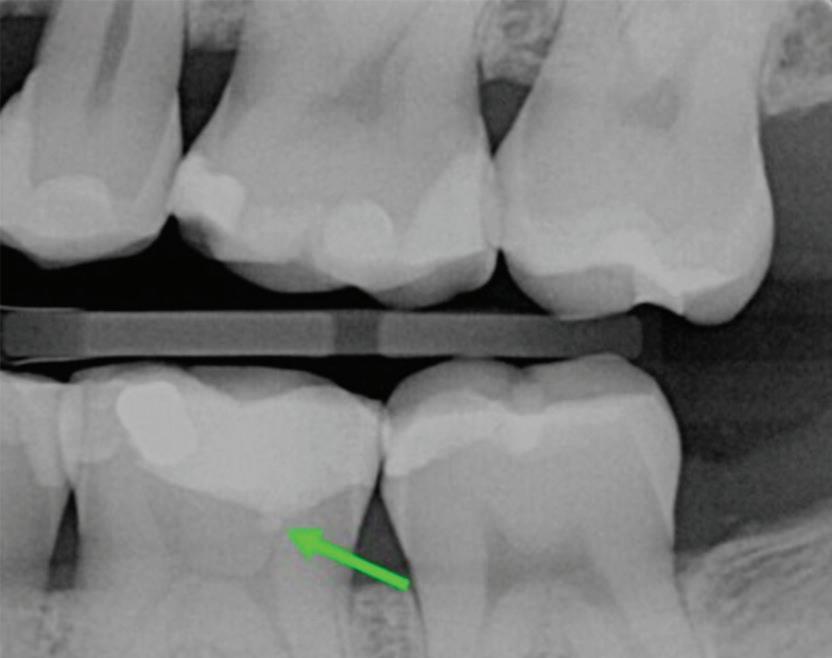
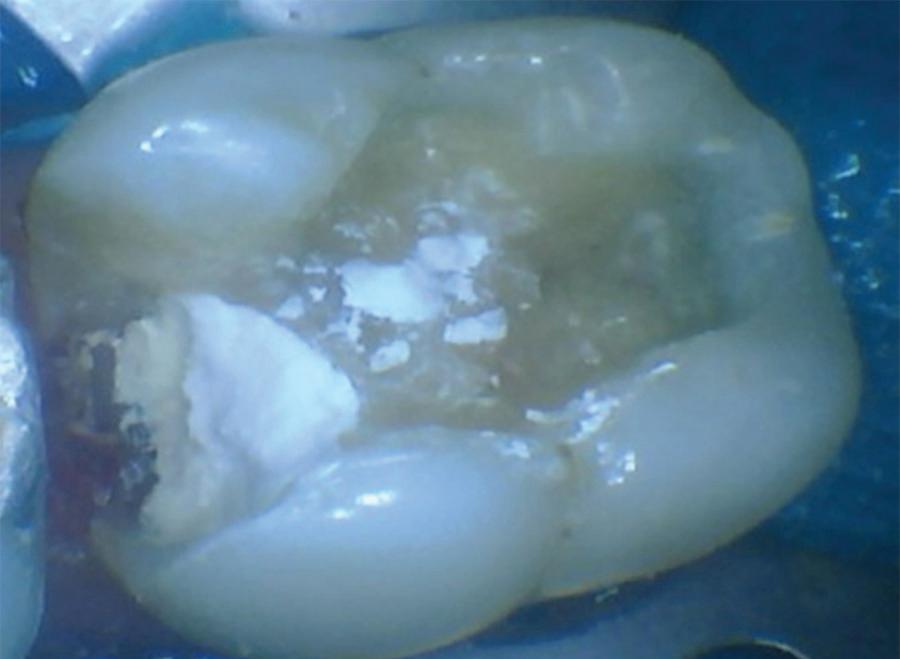
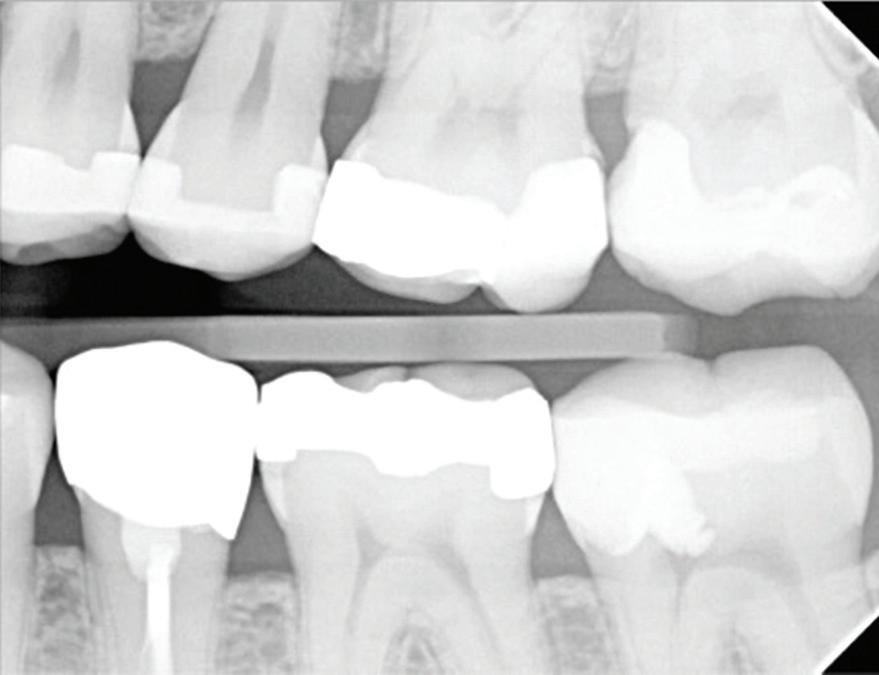
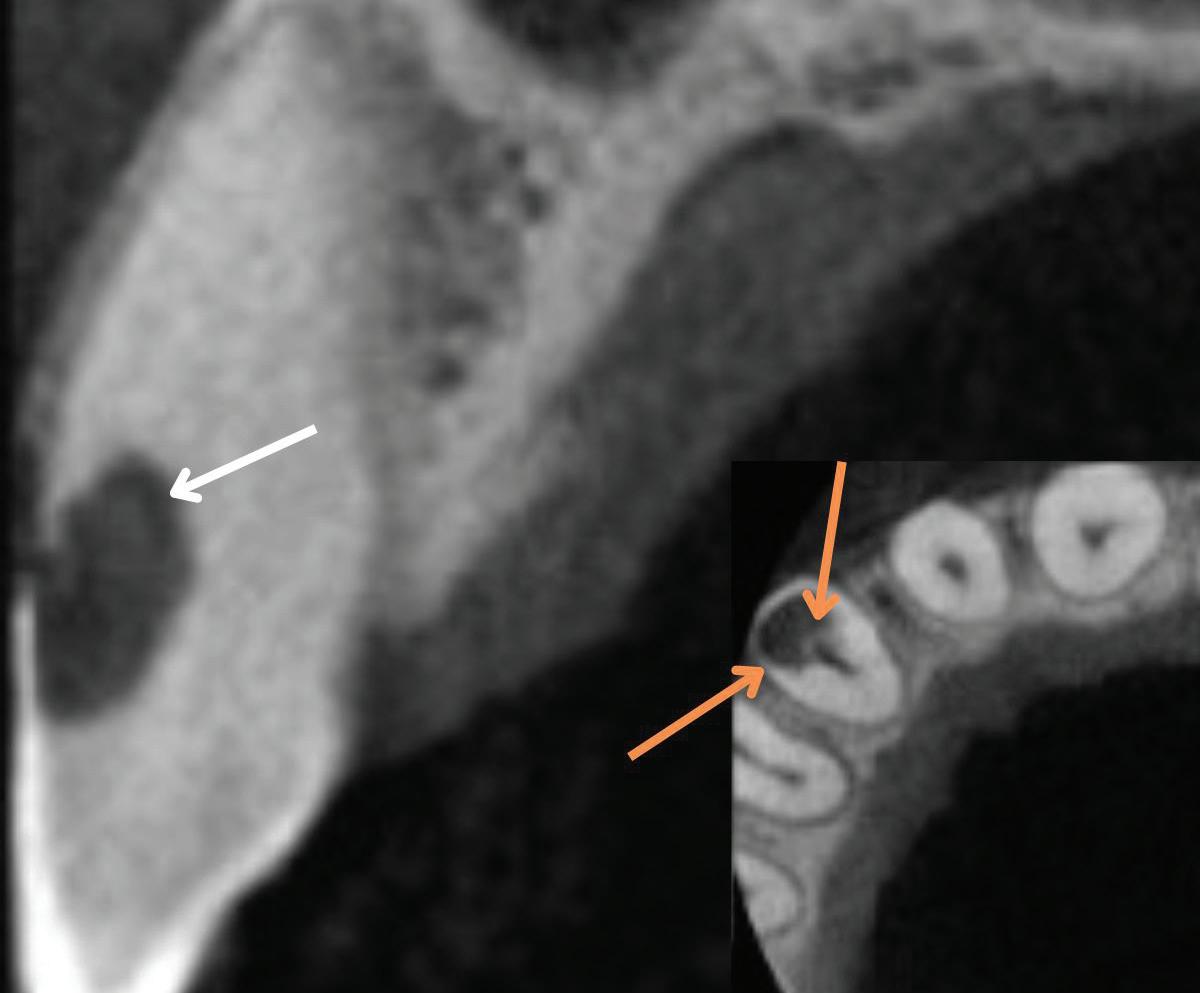
In the endodontic stage, conservative endodontic preparation and obturation with modern techniques are performed as they are for any tooth. All endodontic procedures are performed under an operating microscope to maximize visualization and illumination of the fracture line (Fig 1). The coronal portion of the newly placed gutta percha is removed 2 to 3 mm below the deepest extent of the crack in the affected canal to prepare for intraradicular barrier placement (Fig 2). Gutta percha is also removed 2 to 3 mm into the other noncracked canal orifices in the tooth to prepare for traditional orifice barriers. Microscopic transillumination with a fiber-optic light, in which an LED light probe is placed against buccal or lingual tissues overlying the roots, is utilized to illuminate the root and enhance visualization of the crack (Fig 3). A flowable resin-modified glassionomer or composite resin is then placed in this newly created void from the level of the gutta percha to the floor of the pulp chamber in all canal orifices (Fig 4). A composite resin core is then placed to permanently restore the endodontic access. If a temporary or permanent crown is not placed immediately after the endodontic procedures, the tooth is reduced
Periapical radiograph at the completion of the endodontic protocol. Resin-modified glass ionomer cement is placed as an intraradicular barrier in the distal canal, along the pulpal floor, and as an orifice barrier in the mesial canals.
completely out of occlusion, eliminating all functional and excursive contacts. The patient is instructed to chew exclusively on the contralateral side.
In the restorative stage, a full-coverage crown restoration is placed as soon as possible, ideally within 3 weeks. The occlusion of the final crown is evaluated and adjusted, if necessary, to eliminate heavy contacts and excursive interferences.
After completion of the restorative protocol, specific posttreatment modifiers are employed. Since endodontically treated and restored posterior teeth may shift during healing and over time, periodic occlusal evaluation and adjustment to eliminate interferences and malocclusion should be performed as necessary to neutralize any deleterious forces. Use of a nightguard, when appropriate, can moderate parafunctional habits that may pose an increased crack propagation risk in the treated cracked tooth as well as other teeth.
Evidence-based analysis of restorative protocol
Although not specific to cracked teeth with radicular extension, the use of conservative canal preparation and obturation techniques is essential to preserving the fracture resistance of root dentin in the critical pericervical region.27 This consideration is especially important in deeply cracked teeth.
The placement of intraradicular barriers in the described protocol is based on empirical data supporting their efficacy in improving both the seal and fracture resistance at the pericervical dentin. Studies on canal orifice barriers have noted that a minimum of 2 to 3 mm of material is necessary to create a coronal seal.28,29 In this protocol, removal of gutta percha to this depth was chosen to maximize the seal below the level of the crack on intact dentin. Studies have also shown that placement of these barriers can enhance the pericervical dentin’s
Fig 1. Microscopic visualization of the radicular extension of the crack (arrows) entering the canal.
Fig 4.
Fig 3. Microscopic transillumination. A. Canal space viewed under microscopy without transillumination. B, C. Same canal viewed at different angles with the aid of a fiber-optic light. Transillumination reveals a root fracture.
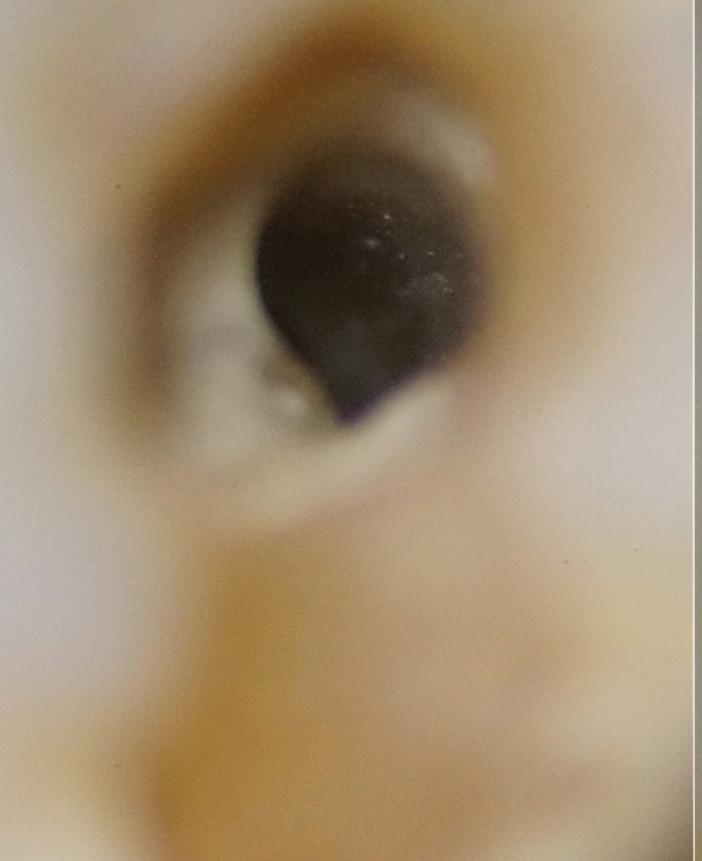
Fig 2. Gutta percha removed 2 mm apical to the terminus of the fracture (arrows).
resistance to fracture.30-32 Therefore, the recommendation in the protocol of placing these deep intracanal restorations maximizes both the seal internally and the fracture resistance of the root. A composite or glass ionomer core is placed after the intraradicular and orifice barriers to restore the endodontic access cavity and complete the internal seal of the crack. Posts should be avoided in cracked teeth as they decrease fracture resistance of pericervical dentin and have been linked to lower survival rates.15,27,33
Placement of a full-coverage restoration is the final step in managing these teeth. In a retrospective study, Chen et al reported a 93.6% success rate for cracked teeth restored with crowns, compared with just 20% for those that did not receive full-coverage restoration.15 They concluded that crown restoration was “the single most important factor for prognosis” of cracked teeth.15 Nguyen Thi and Jansson reported 5- and 10-year survival rates of endodontically treated cracked teeth that receive a full crown to be 97% and 95%, respectively, compared with 57% and 37%, respectively, for teeth that were restored with a composite resin crown or filling.34 Therefore, crown placement is highly predictive of both success and survival in cracked teeth.
Expeditious or immediate placement of the crown following endodontic treatment of cracked teeth is widely advocated to minimize the risk of interim fracture.4,33-36 The traditional practice of postponing restoration until the tooth is completely asymptomatic has been largely refuted. Advances in endodontic treatment, including microscopy, cone beam computed tomography (CBCT), and contemporary techniques, have increased success rates, making early endodontic failure uncommon. In contrast, deferring crown placement is associated with significantly higher rates of structural failure.35,36 This risk is likely compounded in teeth with existing cracks, especially cracks with radicular extension. Posttreatment discomfort is frequent and expected following root canal treatment of any tooth, with 19.5% of patients reporting severe pain within the first week and 6% experiencing persistent sensitivity at 6 months.37,38 Yet such symptoms generally resolve or lessen over time without compromising prognosis.39 Accordingly, immediate full-coverage restoration, accompanied by appropriate patient communication and reassurance, offers the most favorable risk-benefit profile.
Posttreatment modifiers to reduce the etiologic factors that can worsen existing cracks or promote the formation of new ones come into play both between the endodontic and crown placement procedures and after the permanent crown is cemented. Ratcliff et al correlated the presence of cracks with possible etiologic factors and found that excursive interferences and parafunctional habits further increase the risk of worsening cracks in teeth.40 Therefore, if a full-coverage restoration is not to be placed immediately after endodontic treatment, adjusting the cracked tooth out of occlusion and instructing the patient to chew on the unaffected side are of paramount importance.3,4
After the permanent crown is placed, risk factors have to be addressed again; although the crown offers protection against fracture propagation, it is still possible for the crack to worsen if contributing forces remain uncorrected. Excursive interferences and heavy contacts on the crown should be eliminated to
minimize risk.40 However, reducing occlusion on one tooth can impact the occlusion in other areas, so overall occlusal evaluation and adjustment may be necessary. In their previously mentioned study of restored cracked teeth, Davis and Shariff found that almost 80% of restorations required some level of occlusal adjustment over time.4 Occlusion is dynamic and shifts may occur during posttreatment healing or due to other new restorations or extractions; many of the teeth in the study exhibited new excursive interferences and heavy contacts at later examinations, which, especially for cracked teeth, can be catastrophic.4
Parafunctional habits, such as bruxism and clenching, also must be evaluated after crown placement. Existing nightguards should be retrofitted and adjusted to maintain proper fit and function. For patients without previous appliances, a parafunctional assessment is essential, and fabrication of a nightguard is recommended to minimize the risk of crack progression or the development of new cracks over time.4,26,40,41
Outcomes
Prognosis
The outcomes reported for the described treatment protocol are encouraging and suggest that this approach may improve retention rates for cracked teeth with radicular extension.4 The follow-up period for these teeth ranged from 2 to 4 years, with a success rate of 90.6% and survival rates of 100% at 2 years and 96.6% at 4 years, similar to rates found in noncracked endodontically treated teeth.9,42,43 However, the success rates reported by Davis and Shariff were higher than those previously reported for cracked teeth in general, lending some credibility to the modified restorative technique employed and the rationale behind it.4,7,8,11-14,44 A more recent study further validating this protocol utilized a similar method for treating deeply cracked teeth and a bioceramic material as the intraradicular barrier.26 At 1 to 3 years posttreatment, 100% of the teeth were asymptomatic and functional, showing no signs of treatment failure.26 Further prospective studies are needed, but the future of this protocol is promising.
Implications of a persistent CAIPP defect
A CAIPP defect can be expected to accompany the radicular crack or eventually develop. These bony dehiscences are not easily accessible and are not predictably amenable to current periodontal therapies because bacteria reside within the crack and not on the root surface. These defects are often missed by traditional radiography and probing due to their narrow width and interproximal location.
These CAIPP lesions are best identified and monitored with high-resolution CBCT scans (Fig 5). However, even advanced CBCT systems, with voxel sizes as small as 0.075 mm, are not capable of reliably detecting cracks, which are typically much narrower.45 Therefore, the presence of a CAIPP defect, combined with careful clinical diagnostics and evaluation, remains the most reliable indirect indicator of a crack with radicular extension.
The presumed clinical significance of a lingering CAIPP defect is that the persistent biofilm in the crack can lead to further periodontal breakdown and symptoms. However, the changes in these areas were monitored over the course of
previous studies, and these bony lesions did not progress over time and remained asymptomatic.4,26 Together, these studies demonstrated that the persistent bony defect adjacent to the cracks may remain stable and asymptomatic over time, making saving teeth with this technique a realistic option for patients.
Discussion
Treatment planning considerations
In light of the favorable outcomes reported with this protocol, several considerations should guide treatment planning for patients presenting with deeply cracked teeth. First, management of cracked teeth with radicular extension is highly technique sensitive and may be best approached through interdisciplinary collaboration. Endodontists, with access to magnification and experience in identifying crack lines, are well positioned to perform root canal therapy and place intraradicular barriers at the appropriate depth. A core build-up is ideally completed at the same appointment under rubber dam isolation to reduce the risk of microbial contamination. Following the core, patients should return to their restorative dentist promptly for definitive crown restoration. General dentists and prosthodontists responsible for the final crown restoration also play a critical role in addressing occlusion and parafunctional habits, ensuring that both the structural integrity of the tooth and the underlying etiologic factors are properly managed.
A second key consideration is case selection. Davis and Shariff successfully restored deeply cracked teeth but did so using strict inclusion criteria based on specific clinical findings.4 According to their method, 3 conditions should be met before proceeding: (1) the tooth must not be split—there should be no mobile or separable segments; (2) the crack must not traverse the pulpal floor; and (3) the internal extent of the crack within the canal must be visible under the operating microscope to allow precise placement of the intraradicular barrier.4
A split tooth is typically diagnosed during the initial clinical examination, excluding it early as a treatment candidate. However, the second and third conditions may only become evident after access is gained and the endodontic procedure has begun. This makes the clinician performing the root canal the most appropriate provider to determine whether the case
meets the criteria for this protocol and whether a predictable outcome can be achieved.
A third essential consideration is patient agreement and compliance. Because this is a relatively new treatment approach, patients must first accept its innovative nature and be fully informed of its limitations. They must also commit to following postoperative instructions, understanding that a persistent CAIPP defect may remain after the crown is placed. Ongoing management may include multiple follow-up visits for occlusal adjustments, periodic CBCT scans to monitor the defect, and consistent use of a nightguard or other protective appliance when parafunctional habits are present.
Patients should also be prepared for the financial implications of treatment. Managing a deeply cracked tooth may involve greater cost than treating noncracked or superficially cracked teeth due to the complexity of placing restorative materials into radicular structures, the need for periodic advanced imaging, and the clinical expertise required.
In the authors’ experience, when patients are presented with a realistic option to retain a deeply cracked tooth, particularly in light of the high success and survival rates reported in these studies, they are often motivated to pursue treatment to save their tooth. Clear communication of the risks, prognosis, and need for follow-up is essential to ensure realistic expectations. Given that maintaining natural dentition is consistently associated with improved quality of life, clinicians have an obligation to offer this protocol as an alternative to extraction and implant placement when appropriate.46,47
Limitations of implants as an alternative
It is increasingly important to recognize that dental implants are not an ideal tooth replacement. A growing body of literature highlights both biologic and mechanical complications associated with implants.48,49 While the prevalence of peri-implantitis is well established, recent studies have drawn attention to other concerns, particularly the loss of proximal contact due to mesial drift of natural teeth. Because implants are ankylosed, they do not adapt to this physiologic movement, often resulting in open contacts, food impaction, root caries, and localized periodontal breakdown.50
Fig 5. CBCT images of a crack-associated isolated periodontal pocketing defect associated with a distal crack in the mandibular right first molar. A. Sagittal view showing angular crestal bone loss (arrow) along a distal radicular crack at the cervical margin. B. CBCT 3-dimensional rendering showing the defect (arrow) at the distal root. C. Axial view showing the defect (arrow) at the distal root.
Emerging evidence also suggests that implants may negatively impact adjacent natural teeth. In one study, teeth located next to an implant were found to have a 13.4-fold increased risk of future tooth loss compared with those adjacent to natural teeth.51 These findings highlight the growing clinical imperative to retain natural dentition whenever possible.
While implants remain an excellent solution for restoring edentulous spaces, they are not ideal substitutes for natural teeth when those teeth are salvageable. Preserving a natural tooth, even temporarily, can offer long-term benefits. It may delay implant placement while technology and techniques continue to improve, and it may allow time for ongoing research to inform clinicians on how to better manage and mitigate implant-related complications. In this context, tooth preservation should remain a priority in modern dental practice.
Conclusion
Cracked teeth with radicular extension have historically been associated with a questionable prognosis and are often deemed nonrestorable. However, emerging evidence, including recent protocols and outcome studies, suggests that many of these teeth can be successfully retained when managed with an evidence-based, interdisciplinary approach.
The protocol reviewed addresses both the structural and microbial challenges of deep cracks through conservative endodontic therapy, placement of intraradicular barriers to reinforce the pericervical dentin, and timely full-coverage restorations. Success depends on proper case selection, collaboration between providers, and patient compliance. Endodontists are central to diagnosis and barrier placement, while restorative dentists manage occlusion and parafunction, critical factors in long-term stability.
Preserving the natural dentition should remain a primary goal of dental practice. This protocol offers a viable path for treating deeply cracked teeth and avoiding unnecessary extractions. Clinicians are encouraged to reconsider extraction as the default response to cracked teeth with radicular extension and evaluate their candidacy for this structured treatment approach in order to shift the focus toward retention, function, and longterm patient well-being.
1. Rivera E, Walton RE. Cracking the cracked tooth code: detection and treatment of various longitudinal tooth fractures. Endodontics: Colleagues for Excellence. American Association of Endodontists Newsletter. 2008;Summer:1-8. https://www.aae.org/specialty/wp-content/ uploads/sites/2/2017/07/crackedteethecfe_onlineversion.pdf
2. Patel S, Teng P, Liao W, Davis MC, et al. Position statement on longitudinal cracks and fractures of teeth. Int Endod J. 2025;58(3):379-390. doi:10.1111/iej.14186
3. Shariff SS, Davis MC. Cracked tooth with radicular extension. In: Shin Perry E, Patel S, Kanagasingam S, Hamer S, eds. Pitt Ford’s Problem-Based Learning in Endodontology. 2nd ed. Wiley; 2024:49-59. doi:10.1002/9781119565987
4. Davis MC, Shariff SS. Success and survival of endodontically treated cracked teeth with radicular extensions: a 2- to 4-year prospective cohort. J Endod. 2019;45(7):848-855. doi:10.1016/j.joen.2019.03.015
6. Banerji S, Mehta SB, Millar BJ. Cracked tooth syndrome, 1: aetiology and diagnosis. Br Dent J. 2010;208(10):459-463. doi:10.1038/sj.bdj.2010.449
7. Leong DJX, de Souza NN, Sultana R, Yap AU. Outcomes of endodontically treated cracked teeth: a systematic review and meta-analysis. Clin Oral Investig. 2020;24(1):465-473. doi:10.1007/s00784-019-03139-w
8. Olivieri JG, Elmsmari F, Miró Q, et al. Outcome and survival of endodontically treated cracked posterior permanent teeth: a systematic review and meta-analysis. J Endod. 2020;46(4):455463. doi:10.1016/j.joen.2020.01.006
9. Burns LE, Kim J, Wu Y, Alzwaideh R, McGowan R, Sigurdsson A. Outcomes of primary root canal therapy: an updated systematic review of longitudinal clinical studies published between 2003 and 2020. Int Endod J. 2022;55(7):714-731. doi:10.1111/iej.13736
10. Ng YL, Mann V, Gulabivala K. Tooth survival following non-surgical root canal treatment: a systematic review of the literature. Int Endod J. 2010;43(3):171-189. doi:10.1111/j.13652591.2009.01671.x
11. Krell KV, Caplan DJ. 12-month success of cracked teeth treated with orthograde root canal treatment. J Endod. 2018;44(4):543-548. doi:10.1016/j.joen.2017.12.025
12. Kang SH, Kim BS, Kim Y. Cracked teeth: distribution, characteristics, and survival after root canal treatment. J Endod. 2016;42(4):557-562. doi:10.1016/j.joen.2016.01.014
13. Kim SY, Kim SH, Cho SB, Lee GO, Yang SE. Different treatment protocols for different pulpal and periapical diagnoses of 72 cracked teeth. J Endod. 2013;39(4):449-452. doi:10.1016/ j.joen.2012.11.052
14. Tan L, Chen NN, Poon CY, Wong HB. Survival of root filled cracked teeth in a tertiary institution. Int Endod J. 2006;39(11):886-889. doi:10.1111/j.1365-2591.2006.01165.x
15. Chen YT, Hsu TY, Liu H, Chogle S. Factors related to the outcomes of cracked teeth after endodontic treatment. J Endod. 2021;47(2):215-220. doi:10.1016/j.joen.2020.11.024
16. Türp JC, Gobetti JP. The cracked tooth syndrome: an elusive diagnosis. J Am Dent Assoc 1996;127(10):1502-1507. doi:10.14219/jada.archive.1996.0060
17. Ricucci D, Siqueira JF, Loghin S, Berman LH. The cracked tooth: histopathologic and histobacteriologic aspects. J Endod. 2015;41(3):343-352. doi:10.1016/j.joen.2014.09.021
18. Shariff SS, Davis MC. Cracked teeth: to treat or not to treat? AAE Communique. October 30, 2023. Accessed July 9, 2025. https://www.aae.org/specialty/cracked-teeth-to-treat-or-notto-treat/
19. Yang SE, Jo AR, Lee HJ, Kim SY. Analysis of the characteristics of cracked teeth and evaluation of pulp status according to periodontal probing depth. BMC Oral Health. 2017;17(1):135. doi:10.1186/s12903-017-0434-x
20. Abbott P, Leow N. Predictable management of cracked teeth with reversible pulpitis. Aust Dent J. 2009;54(4):306-315. doi:10.1111/j.1834-7819.2009.01155.x
21. Abou-Rass M. Crack lines: the precursors of tooth fractures—their diagnosis and treatment. Quintessence Int Dent Dig. 1983;14(4):437-447.
22. Ossareh A, Rosentritt M, Kishen A. Biomechanical studies on the effect of iatrogenic dentin removal on vertical root fractures. J Conserv Dent. 2018;21(3):290-296. doi:10.4103/JCD. JCD_126_18
23. Majd H, Viray J, Porter JA, Romberg E, Arola D. Degradation in the fatigue resistance of dentin by bur and abrasive air-jet preparations. J Dent Res. 2012;91(9):894-899. doi:10.1177/0022034512455800
24. Ivancik J, Neerchal NK, Romberg E, Arola D. The reduction in fatigue crack growth resistance of dentin with depth. J Dent Res. 2011;90(8):1031-1036. doi:10.1177/0022034511408429
25. Swanson K, Madison S. An evaluation of coronal microleakage in endodontically treated teeth, I: time periods. J Endod. 1987;13(2):56-59. doi:10.1016/S0099-2399(87)80155-3
26. de Toubes KMS, Corrêa IS, Valadares RCL, Tonelli SQ, Bruzinga FFB, Silveira FF. Managing cracked teeth with root extension: a prospective preliminary study using Biodentine material. Int J Dent. 2024;2024:2234648. doi:10.1155/2024/2234648
27. Kishen A, Asundi A. Photomechanical investigations on post-endodontically rehabilitated teeth. J Biomed Opt. 2002;7(2):262-270. doi:10.1117/1.1463046
29. Ghulman MA, Gomaa M. Effect of intra-orifice depth on sealing ability of four materials in the orifices of root-filled teeth: an ex-vivo study. Int J Dent. 2012;2012:318108. doi:10.1155/2012/318108
30. Nagas E, Uyanik O, Altundasar E, et al. Effect of different intraorifice barriers on the fracture resistance of roots obturated with Resilon or gutta-percha. J Endod. 2010;36(6):1061-1063. doi:10.1016/j.joen.2010.03.006
31. Thota KS, Bhavya KL, Sreeha K, Deshpande S, Javvadi J, Avina A. Comparative evaluation of reinforcing effect of three different intraorifice barriers on pericervical dentin of endodontically treated teeth: an in vitro study. J Conserv Dent Endod. 2024;27(12):1276-1279. doi:10.4103/JCDE.JCDE_346_24
32. Gupta A, Arora V, Jha P, Nikhil V, Bansal P. An in vitro comparative evaluation of different intraorifice barriers on the fracture resistance of endodontically treated roots obturated with gutta-percha. J Conserv Dent. 2016;19(2):111-115. doi:10.4103/0972-0707.178682
33. de Toubes KMS, Soares CJ, Soares RV, et al. The correlation of crack lines and definitive restorations with the survival and success rates of cracked teeth: a long-term retrospective clinical study. J Endod. 2022;48(2):190-199. doi:10.1016/j.joen.2021.10.010
34. Nguyen Thi W, Jansson L. Survival rate after endodontic treatment in general dentistry for cracked teeth with different coronal restorations. Acta Odontol Scand. 2021;79(4):256-261. doi:10.1080/00016357.2020.1834615
35. Wu S, Lew HP, Chen NN. Incidence of pulpal complications after diagnosis of vital cracked teeth. J Endod. 2019;45(5):521-525. doi:10.1016/j.joen.2019.02.003
36. Yee K, Bhagavatula P, Stover S, et al. Survival rates of teeth with primary endodontic treatment after core/post and crown placement. J Endod. 2018;44(2):220-225. doi:10.1016/j.joen.2017.08.034
37. Law AS, Nixdorf DR, Aguirre AM, et al. Predicting severe pain after root canal therapy in the national dental PBRN. J Dent Res. 2015;94(3 Suppl):37S-43S. doi:10.1177/0022034514555144
38. Nixdorf DR, Moana-Filho EJ, Law AS, McGuire LA, Hodges JS, John MT. Frequency of nonodontogenic pain after endodontic therapy: a systematic review and meta-analysis. J Endod. 2010;36(9):1494-1498. doi:10.1016/j.joen.2010.06.020
39. Daline IH, Nixdorf DR, Law AS, Pileggi R. 3-Year outcome of patients with persistent pain after root canal treatment: The National Dental Practice-Based Research Network. J Endod 2020;46(5):619-626.e2. doi:10.1016/j.joen.2020.01.018
40. Ratcliff S, Becker IM, Quinn L. Type and incidence of cracks in posterior teeth. J Prosthet Dent. 2001;86(2):168-172. doi:10.1067/mpr.2001.116578
41. Banerji S, Mehta SB, Millar BJ. The management of cracked tooth syndrome in dental practice. Br Dent J. 2017;222(9):659-666. doi:10.1038/sj.bdj.2017.398
42. Paredes-Vieyra J, Enriquez FJJ. Success rate of single-versus two-visit root canal treatment of teeth with apical periodontitis: a randomized controlled trial. J Endod. 2012;38(9):11641169. doi:10.1016/j.joen.2012.05.021
43. Pontoriero DIK, Ferrari Cagidiaco E, Maccagnola V, Manfredini D, Ferrari M. Outcomes of endodontic-treated teeth obturated with bioceramic sealers in combination with warm gutta-percha obturation techniques: a prospective clinical study. J Clin Med. 2023;12(8): 2867. doi:10.3390/jcm12082867
44. Sim IG, Lim TS, Krishnaswamy G, Chen NN. Decision making for retention of endodontically treated posterior cracked teeth: a 5-year follow-up study. J Endod. 2016;42(2):225-229. doi:10.1016/j.joen.2015.11.011
45. Gao A, Cao D, Lin Z. Diagnosis of cracked teeth using cone-beam computed tomography: literature review and clinical experience. Dentomaxillofac Radiol. 2021;50(5):20200407. doi:10.1259/dmfr.20200407
46. Atanda AJ, Livinski AA, London SD, et al. Tooth retention, health, and quality of life in older adults: a scoping review. BMC Oral Health. 2022;22(1):185. doi:10.1186/s12903-02202210-5
47. Tan H, Peres KG, Peres MA. Retention of teeth and oral health-related quality of life. J Dent Res. 2016;95(12):1350-1357. doi:10.1177/0022034516657992
48. Derks J, Tomasi C. Peri-implant health and disease: a systematic review of current epidemiology. J Clin Periodontol. 2015;42(Suppl 16):S158-S171. doi:10.1111/jcpe.12334
49. Galarraga-Vinueza ME, Pagni S, Finkelman M, Schoenbaum T, Chambrone L. Prevalence, incidence, systemic, behavioral, and patient-related risk factors and indicators for periimplant diseases: an AO/AAP systematic review and meta-analysis. J Periodontol 2025;96(6):587-633 doi:10.1002/JPER.24-0154
50. Bento VAA, Gomes JML, Lemos CAA, Limirio JPJO, Rosa CDDRD, Pellizzer EP. Prevalence of proximal contact loss between implant-supported prostheses and adjacent natural teeth: a systematic review and meta-analysis. J Prosthet Dent. 2023;129(3):404-412. doi:10.1016/j. prosdent.2021.05.025
51. Chen HH, Lin GH, Kao RT, Yeh YT. Survival rate of teeth adjacent and nonadjacent to dental implants: a retrospective cohort study. J Periodontol. 2024;95(10):942-948. doi:10.1002/ JPER.23-0739
Coronal seal in endodontics: a critical but forgotten element
The success of root canal treatment depends greatly on maintaining asepsis throughout the procedure and achieving effective disinfection of the root canal system. In this context, the concept of the seal holds significant clinical importance. While the apical seal created by the root canal filling has traditionally received emphasis, the role of the coronal seal provided by a well-placed restoration has been a topic of ongoing discussion. This review aims to comprehensively examine the evidence from microbiologic, clinical, and materials science perspectives to highlight the importance of an integrated approach. Data from the scientific literature demonstrate that both a well-executed root canal filling and a timely, high-quality coronal restoration are essential for the long-term success and survival of endodontically treated teeth. This review also discusses the importance of timing in the placement of the coronal restoration and evaluates the properties of different materials used to achieve an effective coronal seal. The findings reinforce the need for clinicians to ensure that a permanent coronal seal is placed as soon as possible after root canal treatment.
The concept of a coronal seal is one of the most critical but underappreciated factors determining the longterm success of root canal treatment. The coronal seal refers to the ability of the coronal restoration, including the endodontic cavity restoration, to prevent the ingress of oral fluids, microbes, and their by-products into the treated root canal system. This protective barrier serves as the first line of defense against recontamination of the disinfected root canal space, making it an essential aspect of comprehensive endodontic therapy.1
Historically, endodontic success was thought to depend on achieving a “hermetic” apical seal, a goal we now recognize as practically unattainable; hence, the practically achievable goal is a fluid-tight seal. Decades of clinical observations and scientific investigations have highlighted the coronal seal as an equally critical determinant of outcome.2,3 Laboratory and clinical evidence show that a sound coronal restoration works synergistically with the root canal filling; when the coronal seal is of high quality, success rates are increased by more than 10%.3-5 Beginning in the late 1980s, landmark studies demonstrated that coronal leakage could occur independently of apical seal quality and severely compromise treatment outcomes. The pioneering work of Swanson and Madison—confirmed by numerous subsequent investigations—revealed that microbial contamination that enters the tooth coronally can negate even the most meticulously executed apical seal.6 This body of evidence has transformed our understanding of endodontic therapy and established the dual-seal concept of ensuring both coronal and apical integrity as a cornerstone of contemporary practice.
The clinical significance of coronal leakage is substantial; the literature highlights the rapid timeline during which coronal seal failure can lead to microbial and toxin penetration. Studies have shown that contamination through inadequate coronal restoration may occur within days to weeks following treatment.7-9 While the importance of the coronal seal has been questioned by some investigators who reported limited bacterial penetration in well-filled canals, these findings were based primarily on the detection of bacteria and signs of apical periodontitis.10,11 It is crucial to consider that the endodontic microenvironment and microbial selectivity play significant roles in the development of apical periodontitis—the mere absence of clinical or radiographic signs in teeth with compromised coronal restorations does not necessarily negate the importance of the coronal seal. In such cases, the lack of observed pathosis may reflect complex microbial dynamics rather than the irrelevance of coronal leakage.12
Despite extensive research on this topic, there remains a lack of consensus regarding the clinical relevance of the coronal seal as well as the optimal materials and timing for its placement following root canal treatment. The purpose of this review is to systematically examine the current understanding
of the coronal seal in endodontics, integrating evidence from microbiologic, clinical, and materials science perspectives. This review aims to emphasize the vital importance of the dual seal, both coronal and apical, in ensuring long-term success in treatment. Additionally, evidence-based recommendations are provided to support best practices in clinical endodontics.
Coronal leakage: mechanisms and pathways
Coronal leakage refers to the ingress of oral fluids, bacteria, and their by-products into the root canal system due to defects in the coronal restoration or interfacial failure between the restoration and tooth structure. This process is influenced by several factors, including the physical, chemical, and adhesive properties of the direct restorative materials; the design and marginal adaptation of the final indirect restoration; the integrity of the remaining tooth structure; and the progressive degradation of dentin over time.
Sources of leakage and anatomical considerations
The anatomical factors contributing to coronal leakage are complex and multifactorial. Microbial ingress commonly occurs through pathways such as caries, cracks, fractures, or structural defects in the tooth, particularly at the beveled dentin surface adjacent to the restoration-dentin interface.3 Access cavity preparation itself poses a significant risk for leakage, as the removal of sound tooth structure compromises the mechanical integrity of the coronal tooth structure and increases cuspal flexure.13 This increased flexure can predispose the restoration-dentin interface to interfacial failure. Additionally, the presence of accessory canals in the coronal third of the root canal system, along with furcation canals, provides further potential pathways for bacterial penetration when the coronal seal is inadequate.
Restoration quality and temporal nature of microbial ingress
Microleakage at the restoration-tooth interface occurs through several mechanisms, including the formation of an interfacial gap following polymerization shrinkage of resin-based materials, thermal expansion and contraction, mechanical loading, solubility of biomaterials, and chemical degradation of the bonding interfaces.14,15 The quality of the marginal seal is influenced by factors such as preparation design, enamel and dentin surface treatments, adhesive systems, and material handling techniques.16-18
Contemporary endodontic literature increasingly highlights the time-dependent degradation of the coronal seal. Bacterial penetration through inadequate coronal restorations can occur within days to weeks after treatment completion, much earlier than previously assumed, which has important clinical implications.7,19 Even restorations that are initially well-sealed and clinically acceptable may develop leakage pathways over time due to material degradation, mechanical fatigue, and/or chemical dissolution.20,21 Leakage varies significantly depending on the properties of the restorative material, and temporary materials exhibit increased leakage under thermocycling regardless
of thickness.22 Similarly, microbial contamination leading to periapical inflammation in endodontically treated teeth is not instantaneous; it requires time and is influenced by microenvironmental, microbial, and host immune factors.23 While the exact threshold of leakage that leads to clinical failure remains unclear, any degree of bacterial penetration into the root canal system has the potential to initiate reinfection.4
Impact of coronal seal on endodontic outcomes
Role of biofilms in endodontic diseases
Intracanal microbial colonization is a fundamental cause of apical periodontitis.24-27 The primary goal of endodontic therapy is to eliminate or significantly reduce microorganisms within the root canal system and prevent recontamination, thereby promoting periapical healing.28 Treatment success hinges on the principle that removing the bacterial reservoir disrupts the pathogen-associated molecular patterns that drive periapical inflammation.26 Achieving this outcome requires strict aseptic techniques, including rubber dam isolation, sterile instrumentation, and maintenance of a microbe-free environment throughout treatment.29 Importantly, asepsis must extend beyond the active treatment phase to the period between obturation and final restoration. This interim phase is particularly vulnerable to bacterial recontamination, which is often the result of inadequate temporary restorations or delays in placing the definitive restoration.20,30
The evidence linking microbial control to successful healing outcomes in apical periodontitis is robust. Numerous studies have shown significantly higher success rates when strict aseptic protocols are maintained during both the treatment and posttreatment phases.31,32 Most clinical cases of apical periodontitis can be effectively managed without systemic antibiotics—meticulous chemomechanical debridement of the root canal system is typically sufficient for resolution.33 Asepsis in endodontics should be understood as a continuous process spanning from the initiation of treatment to the final restoration rather than as an isolated event. While disinfection during root canal treatment is critical, the preservation of asepsis through a well-sealed coronal restoration is equally essential for long-term success.4 This reinforces the dual-seal concept, wherein both the apical seal provided by root canal obturation and the coronal seal established by the final restoration are indispensable for promoting and maintaining periapical healing.34
Endodontic infections are primarily driven by highly organized, surface-attached microbial communities known as biofilms. 27,35 Biofilms can form on both medicated and nonmedicated intracanal surfaces such as dentin and gutta percha, and they exhibit remarkable resistance and tolerance to antimicrobial strategies.36 Structural adaptations within root canal biofilms further complicate eradication, often requiring mechanical or physical activation for effective disruption.37 Despite advances in instrumentation and irrigation, the complete elimination of biofilms remains a clinical challenge due to anatomical complexities and the inherent resilience of these microbial communities.38
Persistent intraradicular infection is considered the principal cause of endodontic treatment failure.39 Bacteria may survive
within dentinal tubules, apical ramifications, and other inaccessible areas untouched by instrumentation.40 These organisms can penetrate dentinal tubules to depths exceeding 300 μm, creating reservoirs that are largely protected from conventional disinfection methods.41 Dormant or viable but nonculturable bacteria may persist and later serve as a nidus for biofilm recolonization when favorable conditions return. The patterns of biofilm recovery are influenced by the initial effectiveness of the disinfection, the presence of residual organic matter, and, critically, the integrity of the coronal seal.42-44 Compromised coronal restorations not only allow reentry of bacteria from the oral cavity but also enable saliva ingress, which provides nutrients that support the survival and regrowth of remnant microbes in the root canal system.7,30,44
Key studies on coronal leakage
In vitro studies
The foundation of our understanding of coronal leakage was established through pioneering in vitro investigations that demonstrated this phenomenon and posited its clinical significance. A series of studies systematically evaluated the temporal aspects of coronal leakage in endodontically treated teeth using dye penetration.6,34,45 All these studies suggested that significant coronal microleakage was evident within 3 days. While some root filling materials were more susceptible to dye leakage, every root filling showed signs of coronal leakage. However, the results of such dye leakage studies must be interpreted with caution, as they are not representative of bacterial or endotoxin leakage.
Building on this foundational work, Khayat et al conducted comprehensive time-based leakage studies to demonstrate that obturation technique (lateral condensation vs warm vertical condensation with gutta percha and a zinc oxide–eugenol [ZOE] sealer) did not influence the time taken to contaminate root canals with dye-stained saliva; regardless of the obturation technique, all filled canals were contaminated within 30 days. 8 Bacterial size, not motility, appears to be the primary driver in this process, with small, nonmotile bacteria such as Streptococcus epidermidis contaminating exposed root canals faster than large, motile bacteria such as Proteus vulgaris. 7 It has also been demonstrated that endotoxins can penetrate the entire depth of root canals, even those filled with gutta percha and a sealer, if they lack a coronal filling.11 Endotoxin leakage was significant after 8 days, whereas bacterial leakage was first identified after 43 days, demonstrating that rapid penetration of endotoxins due to coronal leakage can result in an early periapical reaction.11
The evolution of leakage-testing methods has been driven by the need for more clinically relevant assessment tools. Early studies primarily utilized dye penetration methods, which, while useful for identifying physical pathways of leakage, do not account for the biologic complexities of bacterial invasion.46 The subsequent development of bacterial leakage models marked a significant advancement, as these models better simulate clinical scenarios involving the microbial penetration of compromised restorations.47 However, emerging microbiologic insights have revealed that many salivary bacteria are not culturable under standard laboratory conditions
and that some biofilm bacteria can enter a viable but nonculturable state, which has potentially led to the underestimation of leakage in earlier studies.48 Contemporary approaches that incorporate polymicrobial communities, assessment of biofilm formation, and real-time monitoring offer a more nuanced understanding of leakage dynamics. Nevertheless, concerns have been raised about the validity of commonly used models; for example, the reliability of the 2-chamber system for evaluating coronal leakage has been questioned.49,50
In vivo and clinical studies
The role of coronal leakage in endodontic failure has been extensively investigated through in vivo animal models and clinical studies. As demonstrated by dye penetration in an investigation conducted using a monkey model, coronal leakage can occur regardless of the type of sealer used. 34 While the study used a physical tracer, it emphasized that an unsealed coronal interface facilitates leakage along the root canal filling. One of the most influential clinical investigations was a retrospective radiographic study by Ray and Trope, who assessed 1010 endodontically treated teeth. 30 Although the study could not standardize variables such as preoperative conditions or time since treatment, the results revealed a compelling association: teeth with a combination of high-quality root canal fillings and good coronal restorations showed absence of periapical inflammation in 91.4% of cases. Interestingly, when evaluated independently, the quality of the coronal restoration had a stronger correlation with periapical health than did the quality of the root canal filling. Contrasting these findings, Tronstad et al examined 1001 teeth in a similar retrospective study and concluded that the technical quality of the root canal filling had a greater impact on treatment success than the quality of the coronal restoration.4 Notably, the highest success rate (81%) was observed in teeth with both a good root filling and an adequate restoration. The authors emphasized that a well-placed coronal restoration could not compensate for a deficient root canal filling.
Beyond radiographic correlation, clinical studies have examined the influence of specific types of restorations on long-term outcomes. Aquilino and Caplan demonstrated that full-coverage crowns significantly improved the longevity of endodontically treated teeth when compared with direct restorations. 51 This benefit was attributed to superior marginal sealing and protection against coronal fracture, both of which safeguard the integrity of the root canal system.
Further evidence supporting the clinical impact of coronal leakage has come from microbiologic studies. Sundqvist et al found that Enterococcus faecalis, commonly associated with endodontic failures, was likely introduced during or between appointments, suggesting coronal leakage as a key pathway. 26 This was corroborated by Siren et al, who found higher failure rates in teeth colonized by enteric bacteria, indicating microbial ingress via compromised coronal restorations. 52 Pinheiro et al further showed that teeth lacking coronal seals had a higher prevalence of Streptococcus and Candida species. 53 These organisms are rarely found in primary infections but commonly associated with persistent lesions. 54,55
A particularly clinically relevant study by Hommez et al evaluated 745 teeth and found that restorations deemed unacceptable by radiographic criteria were associated with significantly higher rates of apical periodontitis (49.1%) than were restorations considered acceptable (23.8%).19 Moreover, teeth restored with a base beneath the coronal restoration—akin to contemporary orifice plugs—had significantly lower rates of apical periodontitis (25.9%) than those without a base (41.3%). This highlights the importance of layered barriers in preventing microbial leakage. Composite resin restorations were associated with higher rates of periapical pathosis (40.5%) than amalgam restorations (28.4%), likely due to polymerization shrinkage and increased marginal leakage in the former.
Adding high-level evidence, a prospective study by Ng et al involving more than 1400 teeth (702 with primary root canal treatment and 750 with retreatment) confirmed the prognostic value of a well-executed coronal restoration. 56 The quality of the restoration emerged as a strong predictor of periapical health, with an odds ratio of 10.73—significantly higher than reported in earlier meta-analyses. 57,58 Notably, when the quality of the restoration was adequate, the specific type of restoration (eg, crown vs direct filling) did not significantly influence outcomes.
Finally, bridging clinical and experimental research, an in vivo animal model demonstrated the functional efficacy of various endodontic filling techniques under conditions of bacterial challenge, providing a more biologically relevant framework for assessing coronal leakage than in vitro models alone.12 This model was designed to overcome the limitations of in vitro studies by allowing for evaluation of endodontic filling materials and techniques in a controlled clinical environment. Unlike standard usage tests, this model assesses both tissue compatibility and functional effectiveness, making it a valuable tool for advancing endodontic materials and methods.
Systematic reviews and meta-analyses
The seminal systematic review by Ng et al examined 63 studies on factors influencing endodontic treatment outcomes, 11 of which specifically assessed the impact of coronal restoration quality. 57 The findings were initially contradictory, likely due to variability in how restorations were evaluated across studies. However, a meta-analysis of 7 of these studies demonstrated that teeth with satisfactory coronal restorations had significantly higher odds of treatment success than did with those with unsatisfactory restorations.
In a related systematic review focused on retreatment outcomes, Ng et al performed a meta-analysis and found that teeth with adequate coronal restorations had significantly better outcomes than those with inadequate restorations. 58 Complementing these findings, Gillen et al concluded that both adequate root canal treatment and adequate coronal restoration significantly increased the odds of healing in cases of apical periodontitis. 3 Their analysis revealed no significant difference in healing outcomes between teeth with adequate root canal treatment but poor coronal restorations and those with inadequate root canal treatment but good coronal restorations. This suggests that both components are essential, and neither can reliably compensate for deficiencies in the other.
Materials and techniques for achieving coronal seal
Temporary restorative materials
The selection of appropriate temporary restorative materials represents a critical decision point in endodontic therapy, as these materials must provide adequate sealing properties during the interim period between treatment completion and placement of the definitive restoration. Temporary restorative materials have evolved considerably from the traditional ZOE formulations that dominated earlier decades of endodontic practice.
ZOE-based materials remain widely used due to their excellent sealing properties and ease of manipulation. The chemical setting reaction of ZOE creates a matrix that provides effective short-term bacterial barrier properties. However, these materials also exhibit substantial limitations, including poor mechanical properties, susceptibility to dissolution in oral fluids, and potential interference with resin-based bonding systems. The eugenol component can inhibit polymerization of methacrylate-based adhesives, necessitating complete removal before placement of resin-based restorations. Resinreinforced ZOE, such as Intermediate Restorative Material (IRM; Dentsply Sirona), is a widely used temporary filling material owing to its improved strength compared to ZOE. One study showed that IRM did not prevent salivary or bacterial penetration of root-filled teeth.20 This was likely the result of the less-than-optimal thickness of IRM required for an optimal seal (ie, 3 mm). 59,60
Glass ionomer cements (GICs) have been used effectively as temporary restorative materials during root canal treatment to maintain a coronal seal between appointments. Their chemical bonding to dentin, fluoride release, dimensional stability, and moisture tolerance make them superior to many conventional temporary materials such as Cavit (3M) or IRM. Studies have shown that GICs reduce microleakage and improve periapical outcomes when used as interim restorations or as an orifice barrier following obturation.19,21
Resin-modified GICs (RMGICs), in particular, have demonstrated enhanced sealing properties over the course of multiple weeks, making them well-suited for extended temporization in endodontics.9,61,62 These materials have gained popularity as temporary restorative materials due to their superior mechanical properties and chemical bonding to tooth structure, excellent marginal adaptation, and improved retention compared with conventional GICs. The fluoride-release properties of RMGICs may provide additional antimicrobial benefits, although the clinical significance of this effect remains debated.63,64 The dual-curing nature of RMGICs allows for both chemical and light-activated polymerization, ensuring complete curing even in areas with limited light access. Composite resin materials, while traditionally considered permanent restoratives, are also being increasingly used as temporary materials in specific clinical scenarios. Light-cured composite resins provide excellent mechanical properties and superior esthetics, making them particularly suitable for anterior teeth, where appearance is a primary concern. The bonding capabilities of composite materials to prepared tooth structures can provide better retention and marginal seal than conventional temporary materials.65
Composite resin can provide a high-quality coronal seal if placed under ideal conditions, but it may not be the ideal firstline material for temporization unless the operator can ensure strict moisture control and proper adhesive technique.16-18 Polymerization shrinkage and degradation of the resin-dentin interface over time may compromise the seal, especially under occlusal loading or if bonding protocols are suboptimal.14,21 For a short- to moderate-term coronal seal, RMGICs or layered restorations (eg, GIC base with composite resin overlay) are typically more reliable and less technique sensitive.19,21,62
Permanent restorations
The definitive coronal restoration represents the final barrier against bacterial recontamination of the treated root canal system. The selection of appropriate permanent restorative materials and techniques must consider factors such as remaining tooth structure, occlusal forces, esthetic requirements, and long-term durability. Direct composite resin restorations offer several advantages for endodontically treated teeth, including immediate placement, conservative preparation requirements, and excellent esthetic properties. Modern composite materials demonstrate superior physical properties compared with earlier generations, including improved wear resistance and reduced polymerization shrinkage.66 The key to successful direct composite restorations lies in proper isolation, adequate bonding techniques, and appropriate layering strategies to minimize the effects of polymerization shrinkage.
Indirect restorations, including inlays, onlays, and fullcoverage crowns, offer marginal sealing and mechanical properties that are superior to those provided by direct restorations. Their laboratory fabrication ensures optimal material properties and precise marginal adaptation. Ceramic materials, particularly feldspathic porcelain and lithium disilicate, provide excellent biocompatibility and sealing ability when properly bonded.67 The increased bulk and controlled thickness of indirect restorations contribute to improved resistance to fracture and marginal leakage. However, the type of indirect restoration is critical. Inlays, especially in endodontically treated premolars, may increase the risk of cusp fracture, while onlays that include cuspal coverage significantly reduce this risk.68
Full-coverage crowns placed within 4 months of root canal treatment are considered the gold standard for restoring endodontically treated teeth, particularly in posterior regions, where occlusal forces are substantial.69,70 Crown preparation also eliminates potential sources of marginal leakage by removing structurally compromised areas, such as fractured cusps, carious margins, defective restorations, and unsupported enamel. This enhances the adaptation and durability of the restoration while improving the long-term integrity of the coronal seal and resistance to bacterial ingress.51
Adhesive systems and bonding strategies
The evolution of dental adhesive systems has significantly advanced the ability to achieve a reliable coronal seal in endodontically treated teeth. Modern adhesives provide strong and durable bonds to both enamel and dentin, primarily through micromechanical retention, which enhances marginal seal integrity. Etch-and-rinse systems, which involve separate etching
and priming steps, allow for optimal adhesive penetration of tooth substrates. Etching the enamel generates micromechanical retention, while conditioning the dentin exposes collagen fibrils, facilitating the formation of a hybrid layer.71,72 Selective etching strategies recognize the differing requirements of enamel and dentin, optimizing the effectiveness of bonding to each.
Self-etching adhesive systems simplify the bonding process by combining etching and priming into a single step, reducing technique sensitivity and offering more consistent dentin bonding. Their mild acidity preserves the mineral content of dentin while still enabling effective surface modification for adhesive infiltration. Studies show that both etch-and-rinse and self-etching systems can achieve comparable marginal sealing when used appropriately.73
Universal adhesives represent the latest advancement in adhesive technology, offering flexibility by supporting both self-etching and etch-and-rinse techniques. Their inclusion of functional monomers promotes chemical bonding to both dental tissues and restorative materials, enhancing their versatility and performance. For optimal coronal sealing in endodontically treated teeth, 3-step etch-and-rinse adhesives and 2-step self-etching systems with selective enamel etching are considered the most reliable strategies. These systems provide superior bond strength, reduced microleakage, and enhanced long-term stability compared with simplified 1-step adhesives.74,75 While convenient, 1-step self-etching adhesives are more prone to hydrolytic degradation and generally offer inferior sealing performance, especially at enamel margins.76
When indirect restorations are placed, the use of resin cements in combination with high-performance adhesive systems further improves marginal adaptation and sealing. Additionally, the placement of a bonded orifice barrier using an RMGIC or flowable composite before final restoration has been shown to significantly reduce coronal leakage.21,62 Overall, the selection of an appropriate adhesive system, combined with careful moisture control and sound restorative protocols, is critical for maintaining the long-term success of root canal therapy.
Intraorifice barriers and orifice plugs
The strategic placement of intraorifice barriers is an effective method for enhancing the coronal seal in endodontically treated teeth. Any form of orifice sealing helps protect root canals from coronal leakage by providing an additional barrier against bacterial penetration, particularly when the quality of the coronal restoration is compromised.8,77
GICs are commonly preferred as intraorifice barriers because of their chemical bonding, favorable handling, and cost-effectiveness. However, effective sealing with GICs requires careful moisture control and adequate thickness. With the increasing use of tricalcium silicate–based sealers, bioactive materials such as mineral trioxide aggregate (MTA) are also employed as orifice barriers. MTA significantly reduces bacterial leakage, even when coronal restorations are compromised.78 The prevention of bacterial leakage obtained with a 3-mm thickness of either white or gray MTA is comparable to that offered by GIC.79 Proper placement technique, including attention to material consistency and condensation, is essential for optimal sealing.
It is important to consider the initial setting time of MTAbased materials, as immediate etching for composite resin placement is not recommended. Although a recent study showed that composite resins can be safely applied over set tricalcium silicate cements, including MTA, the timing between MTA placement and resin restoration was not specified.80 Onestep self-etching adhesives are suitable for bonding resin-based composites to white MTA immediately after placement, avoiding the need for a second appointment.81 Additionally, GIC can be safely placed over MTA after 45 minutes.82 Newer calcium silicate materials (eg, Biodentine, Septodont) and newer MTA formulations (eg, NeoMTA Plus, Avalon Biomed) show promise due to improved handling and mechanical properties, and, most importantly, absence of the discoloration associated with MTA, although their effectiveness as orifice barriers following root canal treatment remains to be thoroughly studied.83,84
Comparative studies consistently demonstrate that intraorifice barriers outperform temporary plugs in preventing coronal microleakage. Materials such as RMGICs, MTA, and bonded composite resins significantly enhance the seal when applied at the canal orifice, especially when combined with high-quality temporary or permanent coronal restorations. Consequently, a 2-layered approach is recommended: first, a bonded intraorifice barrier is placed; second, the access cavity is sealed with a temporary restoration until definitive coverage is placed. This combined method reduces coronal leakage more effectively than either technique alone.85
Recent advances
Recent technological advances have introduced innovative approaches to achieving a reliable coronal seal, showing promise for improving long-term endodontic outcomes. Bioactive materials containing antimicrobial agents offer enhanced resistance to bacterial colonization while maintaining effective sealing properties.86 In restorative dentistry, nanotechnology has led to the development of nanocomposite materials with superior physical properties and improved marginal adaptation. These materials exhibit reduced polymerization shrinkage, increased wear resistance, and enhanced mechanical strength due to the incorporation of nanofillers, all while preserving favorable handling characteristics.
The integration of digital workflows has transformed the fabrication of indirect restorations, enabling precise marginal adaptation and optimized material properties. Computer-aided design/computer-aided manufacturing systems facilitate same-day restoration placement, minimizing the time that temporary restorations may compromise the coronal seal. The precision of digital impressions and milling techniques results in better marginal fit than conventional methods.87 A detailed discussion of these materials and technologies is beyond the scope of this review.
Clinical recommendations
Best practices for ensuring coronal seal
Primary prevention of coronal leakage should focus on meticulous restoration placement and bonding procedures. The optimal approach is the immediate placement of definitive restorations following completion of endodontic treatment. The
authors recommend direct adhesive restorations for this purpose, as this strategy eliminates the vulnerable interim period during which temporary restorations may compromise seal integrity and increase the risk of bacterial recontamination. When immediate definitive restoration is not feasible, highquality temporary restorations with an appropriate orifice barrier must be placed, ensuring careful attention to marginal adaptation and material selection. Regardless of the restoration type, an orifice barrier is strongly recommended to protect the disinfected and filled root canal from coronal leakage caused by marginal gaps or unforeseen events such as restoration fracture or dislodgment. Glass ionomer–based cements are the preferred orifice barrier materials. When tricalcium silicate sealers are used to fill root canals, these bioactive materials may also serve effectively as orifice barriers. It is highly recommended that orifice barriers have a thickness of at least 2 to 3 mm apical to the orifice level.
Rubber dam isolation must be maintained throughout restoration placement to ensure optimal bonding conditions and prevent contamination. This controlled environment facilitates precise moisture control and enhances adhesive performance. Clinical studies consistently show that marginal seal properties are superior when bonding procedures are performed under rubber dam isolation.88,89 Quality assurance steps should include radiographic verification of restoration margins, clinical evaluation of marginal adaptation, and assessment of occlusion. Marginal discrepancies exceeding 100 μm are considered clinically unacceptable due to the increased risk of bacterial penetration. Regular recall evaluations are essential to monitor restoration integrity and enable early detection of marginal breakdown.
Interprofessional communication
Whenever clinical conditions permit, the definitive restoration should be placed on the same day that endodontic treatment is completed, as this represents the most effective approach. Accordingly, the authors recommend that the endodontist assume responsibility for placing the coronal restoration immediately following root canal treatment. Ideally, this would comprise an orifice plug followed by restoration of the access cavity (Figure). When same-day restoration is not feasible, such as in cases where a post and core will be placed by the referring dentist, the endodontist should place a well-adapted orifice barrier along with a high-quality temporary restoration. In such cases, the permanent restoration should be completed as soon as possible. Temporary restorations should ideally be replaced within 2 to 4 weeks, as coronal microleakage may begin within days and becomes significant after this period.6,8 In teeth with large access cavities or significant loss of tooth structure, such as cuspal loss in premolars, stainless steel bands may be placed to reduce cuspal flexure, prevent tooth fractures, and retain the interim restoration.90
Effective communication between endodontists and restorative or general dentists is essential for achieving optimal coronal seal outcomes. This interdisciplinary collaboration depends on clear and timely communication regarding treatment planning, material selection, and restoration timing. Pretreatment consultations should establish protocols for postendodontic
Orifice barrier/orifice plug with RMGIC
Access cavity restoration with composite resin
Figure. Periapical radiograph of endodontically treated teeth. Placement of an adequate thickness (at least 2 to 3 mm) of orifice barrier material (RMGIC) is followed by restoration of the access cavity with composite resin. (Courtesy of Dr F. C. Li, Toronto, Canada.)
restoration, including the type of restoration, materials to be used, and the timing of placement.
Posttreatment communication should include specific recommendations for restoration timing and any material or technique preferences. The endodontist should also convey the level of urgency for the definitive restoration based on the quality of the temporary restoration and patient-specific risk factors. This information enables the restorative dentist to appropriately prioritize scheduling and allocate sufficient appointment time.
Conclusion
The evidence presented in this review clearly demonstrates that the coronal seal is a critical determinant of endodontic treatment success, working in synergy with the apical seal to ensure optimal outcomes. The concept of a dual seal, encompassing both coronal and apical barriers, has emerged as a foundational principle in contemporary endodontic therapy, replacing the historical focus on the apical seal alone. This shift reflects decades of scientific investigation that have revealed the complex interactions among bacterial contamination pathways, biofilm persistence, and mechanisms of treatment failure. The timing of coronal seal failure underscores the urgency of
completing a durable coronal restoration immediately following endodontic treatment. Rapid salivary contamination and bacterial penetration through compromised restorations or at the restoration-tooth interface can occur within days of treatment completion, emphasizing that the coronal seal must not be treated as a secondary consideration.
The clinical message is clear: neither the coronal seal nor the apical seal alone is sufficient to ensure predictable endodontic success. A technically sound root canal filling cannot compensate for a compromised coronal seal, just as an excellent coronal restoration cannot overcome inadequate canal disinfection and obturation. This dual-seal requirement demands integrated treatment planning that addresses both components of the endodontic system with equal rigor and precision. Ultimately, the success of endodontic therapy depends on clinicians’ commitment to excellence throughout all phases of treatment, recognizing that the chain of endodontic success is only as strong as its weakest link.
Author affiliations
Faculty of Dentistry, University of Toronto, Canada; The Kishen Lab, Dental Research Institute, University of Toronto, Canada; and Department of Dentistry, Mount Sinai Hospital, Toronto, Canada (Kishen). Mike Petryk School of Dentistry, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Canada; The MICRO Lab, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Canada; Women and Children’s Health Research Institute, University of Alberta, Edmonton, Canada; Li Ka Shing Institute of Virology, University of Alberta, Edmonton, Canada; and Department of Medical Microbiology and Immunology, University of Alberta, Edmonton, Canada (Neelakantan).
The authors gratefully acknowledge the Canada Research Chair program, the Arthur Zwingenberger Decanal Chairship, and the Alberta Dental Association & College Chair in Oral Health Research.
References
1. Treatment standards. White paper. American Association of Endodontists; 2020. https:// www.aae.org/specialty/wp-content/uploads/sites/2/2018/04/TreatmentStandards_ Whitepaper.pdf
2. Dugas NN, Lawrence HP, Teplitsky PE, Pharoah MJ, Friedman S. Periapical health and treatment quality assessment of root-filled teeth in two Canadian populations. Int Endod J 2003;36(3):181-192. doi:10.1046/j.1365-2591.2003. 00640.x
3. Gillen BM, Looney SW, Gu LS, et al. Impact of the quality of coronal restoration versus the quality of root canal fillings on success of root canal treatment: a systematic review and meta-analysis. J Endod. 2011;37(7):895-902. doi: 10.1016/j.joen.2011.04.002
4. Tronstad L, Asbjørnsen K, Døving L, Pedersen I, Eriksen HM. Influence of coronal restorations on the periapical health of endodontically treated teeth. Endod Dent Traumatol 2000;16(5):218-221. doi:10.1034/j.1600-9657.2000.016005218
5. Salehrabi R, Rotstein I. Endodontic treatment outcomes in a large patient population in the USA: an epidemiological study. J Endod. 2004;30(12):846-850. doi: 10.1097/01. don.0000145031.04236.ca
6. Swanson K, Madison S. An evaluation of coronal microleakage in endodontically treated teeth, I: time periods. J Endod. 1987;13(2):56-59. doi:10.1016/S0099-2399(87)80155-3
7. Torabinejad M, Ung B, Kettering JD. In vitro bacterial penetration of coronally unsealed endodontically treated teeth. J Endod. 1990;16(12):566-569. doi:10.1016/S00992399(07)80198-1
8. Khayat A, Lee SJ, Torabinejad M. Human saliva penetration of coronally unsealed obturated root canals. J Endod. 1993;19(9):458-461. doi:10.1016/S0099-2399(06)80533-9
9. Wylie ME, Parashos P, Fernando JR, Palamara J, Sloan AJ. Biological considerations of dental materials as orifice barriers for restoring root-filled teeth. Aust Dent J. 2023;68(suppl 1): S82-S95. doi:10.1111/adj.12970
10. Ricucci D, Bergenholtz G. Bacterial status in root-filled teeth exposed to the oral environment by loss of restoration and fracture or caries—a histobacteriological study of treated cases. Int Endod J. 2003;36(11):787-802. doi:10.1046/j.1365-2591.2003. 00721.x
11. Alves J, Walton R, Drake D. Coronal leakage: endotoxin penetration from mixed bacterial communities through obturated, post-prepared root canals. J Endod. 1998;24(9):587-591. doi:10.1016/S0099-2399(98)80115-5
12. Friedman S, Torneck CD, Komorowski R, Ouzounian Z, Syrtash P, Kaufman A. In vivo model for assessing the functional efficacy of endodontic filling materials and techniques. J Endod 1997;23(9):557-561. doi:10.1016/S0099-2399(06)81120-9
13. Reeh ES, Messer HH, Douglas WH. Reduction in tooth stiffness as a result of endodontic and restorative procedures. J Endod. 1989;15(11):512-516. doi:10.1016/S00992399(89)80191-8
14. Davidson CL, de Gee AJ, Feilzer A. The competition between the composite-dentin bond strength and the polymerization contraction stress. J Dent Res. 1984;63(12):1396-1399. doi:10.1177/00220345840630121101
15. Zotti F, Falavigna E, Capocasale G, De Santis D, Albanese M. Microleakage of direct restorations—comparison between bulk-fill and traditional composite resins: systematic review and meta-analysis. Eur J Dent. 2021;15(4):755-767. doi:10.1055/s-0041-1724155
16. Hilton TJ. Can modern restorative procedures and materials reliably seal cavities? In vitro investigations. 1. Am J Dent. 2002;15(3):198-210.
17. Hilton TJ. Can modern restorative procedures and materials reliably seal cavities? In vitro investigations. 2. Am J Dent. 2002;15(4):279-289.
18. Spencer P, Ye Q, Song L, et al. Threats to adhesive/dentin interfacial integrity and next generation bio-enabled multifunctional adhesives. J Biomed Mater Res B Appl Biomater. 2019;107(8):2673-2683. doi:10.1002/jbm.b.34358
19. Hommez GM, Coppens CR, De Moor RJ. Periapical health related to the quality of coronal restorations and root fillings. Int Endod J. 2002;35(8):680-689. doi:10.1046/j.1365-2591.2002. 00546.x
20. Magura ME, Kafrawy AH, Brown CE Jr, Newton CW. Human saliva coronal microleakage in obturated root canals: an in vitro study. J Endod. 1991;17(7):324-331. doi:10.1016/S00992399(06)81700-0
21. Saunders WP, Saunders EM. Coronal leakage as a cause of failure in root-canal therapy: a review. Endod Dent Traumatol. 1994;10(3):105-108. doi:10.1111/j.1600-9657.1994. tb00533.x
22. Deveaux E, Hildelbert P, Neut C, Boniface B, Romond C. Bacterial microleakage of Cavit, IRM, and TERM. Oral Surg Oral Med Oral Pathol. 1992;74(5):634-643. doi:10.1016/00304220(92)90358-w
23. Hussein H, Kishen A. Local immunomodulatory effects of intracanal medications in apical periodontitis. J Endod. 2022;48(4):430-456. doi: 10.1016/j.joen.2022.01.003
24. Kakehashi S, Stanley HR, Fitzgerald RJ. The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral Surg Oral Med Oral Pathol. 1965;20:340349. doi:10.1016/0030-4220(65)90166-0
25. Möller AJ, Fabricius L, Dahlén G, Ohman AE, Heyden G. Influence on periapical tissues of indigenous oral bacteria and necrotic pulp tissue in monkeys. Scand J Dent Res 1981;89(6):475-484. doi:10.1111/j.1600-0722. 1981.tb01711.x
26. Sundqvist G, Figdor D, Persson S, Sjögren U. Microbiologic analysis of teeth with failed endodontic treatment and the outcome of conservative re-treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;85(1):86-93. doi:10.1016/s1079-2104(98)90404-8
27. Neelakantan P, Romero M, Vera J, et al. Biofilms in endodontics – current status and future directions. Int J Mol Sci. 2017;18(8):1748. doi:10.3390/ijms18081748
28. Siqueira JF Jr, Rôças IN. Clinical implications and microbiology of bacterial persistence after treatment procedures. J Endod. 2008;34(11):1291-1301.e3. doi: 10.1016/j. joen.2008.07.028
29. Klevant FJ, Eggink CO. The effect of canal preparation on periapical disease. Int Endod J 1983;16(2):68-75. doi:10.1111/j.1365-2591. 1983.tb01299.x
30. Ray HA, Trope M. Periapical status of endodontically treated teeth in relation to the technical quality of the root filling and the coronal restoration. Int Endod J. 1995;28(1):12-18. doi:10.1111/j.1365-2591. 1995.tb00150.x
31. Sjögren U, Figdor D, Persson S, Sundqvist G. Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. Int Endod J 1997;30(5):297-306. doi:10.1046/j.1365-2591.1997. 00092.x
32. Zahran S, Mannocci F, Koller G. Assessing the iatrogenic contribution to contamination during root canal treatment. J Endod. 2022;48(4):479-486. doi: 10.1016/j.joen.2022.01.007
33. Segura-Egea JJ, Martín-González J, Jiménez-Sánchez MDC, Crespo-Gallardo I, Saúco-Márquez JJ, Velasco-Ortega E. Worldwide pattern of antibiotic prescription in endodontic infections. Int Dent J. 2017;67(4):197-205. doi:10.1111/idj.12287
34. Madison S, Wilcox LR. An evaluation of coronal microleakage in endodontically treated teeth, III: in vivo study. J Endod. 1988;14(9):455-458. doi:10.1016/S0099-2399(88)80135-3
35. Kishen A, Shrestha A, Del Carpio-Perochena A. Validation of biofilm assays to assess antibiofilm efficacy in instrumented root canals after syringe irrigation and sonic agitation. J Endod 2018;44(2):292-298. doi: 10.1016/j.joen.2017.10.005
36. George S, Basrani B, Kishen A. Possibilities of gutta-percha-centered infection in endodontically treated teeth: an in vitro study. J Endod. 2010;36(7):1241-1244. doi: 10.1016/j. joen.2010.03.024
37. Kishen A, George S, Kumar R. Enterococcus faecalis–mediated biomineralized biofilm formation on root canal dentine in vitro. J Biomed Mater Res A. 2006;77(2):406-415. doi:10.1002/jbm.a.30622
38. Peters OA. Current challenges and concepts in the preparation of root canal systems: a review. J Endod. 2004;30(8):559-567. doi: 10.1097/01.don.0000129039.59003.9d
39. Siqueira JF Jr. Aetiology of root canal treatment failure: why well-treated teeth can fail. Int Endod J. 2001;34(1):1-10. doi:10.1046/j.1365-2591.2001. 00396.x
40. Love RM, Jenkinson HF. Invasion of dentinal tubules by oral bacteria. Crit Rev Oral Biol Med 2002;13(2):171-183. doi:10.1177/154411130201300207
41. Haapasalo M, Orstavik D. In vitro infection and disinfection of dentinal tubules. J Dent Res 1987;66(8):1375-1379. doi:10.1177/00220345870660081801
42. Brändle N, Zehnder M, Weiger R, Waltimo T. Impact of growth conditions on susceptibility of five microbial species to alkaline stress. J Endod. 2008;34(5):579-582. doi: 10.1016/j. joen.2008.02.027
43. Yang Y, Shen Y, Wang Z, et al. Evaluation of the susceptibility of multispecies biofilms in dentinal tubules to disinfecting solutions. J Endod. 2016;42(8):1246-1250. doi: 10.1016/j. joen.2016.05.011
44. Ali IAA, Cheung BPK, Matinlinna J, Lévesque CM, Neelakantan P. Trans-cinnamaldehyde potently kills Enterococcus faecalis biofilm cells and prevents biofilm recovery. Microb Pathog. 2020; 149:104482. doi: 10.1016/j.micpath.2020.104482
45. Madison S, Swanson K, Chiles SA. An evaluation of coronal microleakage in endodontically treated teeth, II: sealer types. J Endod. 1987;13(3):109-112. doi:10.1016/S00992399(87)80175-9
46. Wu MK, Wesselink PR. Endodontic leakage studies reconsidered, I: methodology, application and relevance. Int Endod J. 1993;26(1):37-43. doi:10.1111/j.1365-2591. 1993.tb00540.x
47. Barthel CR, Moshonov J, Shuping G, Orstavik D. Bacterial leakage versus dye leakage in obturated root canals. Int Endod J. 1999;32(5):370-375. doi:10.1046/j.1365-2591.1999. 00235.x
48. Williams JM, Trope M, Caplan DJ, Shugars DC. Detection and quantitation of E. faecalis by real-time PCR (qPCR), reverse transcription-PCR (RT-PCR), and cultivation during endodontic treatment. J Endod. 2006;32(8):715-721. doi: 10.1016/j.joen.2006.02.031
49. Rechenberg DK, De-Deus G, Zehnder M. Potential systematic error in laboratory experiments on microbial leakage through filled root canals: review of published articles. Int Endod J 2011;44(3):183-194. doi:10.1111/j.1365-2591.2010. 01821.x
50. Rechenberg DK, Thurnheer T, Zehnder M. Potential systematic error in laboratory experiments on microbial leakage through filled root canals: an experimental study. Int Endod J 2011;44(9):827-835. doi:10.1111/j.1365-2591.2011. 01888.x
51. Aquilino SA, Caplan DJ. Relationship between crown placement and the survival of endodontically treated teeth. J Prosthet Dent. 2002;87(3):256-263. doi:10.1067/mpr.2002.122014
52. Siren EK, Haapasalo MP, Ranta K, Salmi P, Kerosuo EN. Microbiological findings and clinical treatment procedures in endodontic cases selected for microbiological investigation. Int Endod J. 1997;30(2):91-95.
53. Pinheiro ET, Gomes BP, Ferraz CC, Sousa EL, Teixeira FB, Souza-Filho FJ. Microorganisms from canals of root-filled teeth with periapical lesions. Int Endod J. 2003;36(1):1-11. doi:10.1046/j.1365-2591.2003. 00603.x
54. Nair PN, Sjögren U, Krey G, Kahnberg KE, Sundqvist G. Intraradicular bacteria and fungi in root-filled, asymptomatic human teeth with therapy-resistant periapical lesions: a long-term light and electron microscopic follow-up study. J Endod. 1990;16(12):580-588. doi:10.1016/ S0099-2399(07)80201-9
55. Persoon IF, Crielaard W, Özok AR. Prevalence and nature of fungi in root canal infections: a systematic review and meta-analysis. Int Endod J. 2017;50(11):1055-1066. doi:10.1111/ iej.12730
56. Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment, 1: periapical health. Int Endod J. 2011;44(7):583-609. doi:10.1111/j.1365-2591.2011. 01872.x
57. Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature, 2: influence of clinical factors. Int Endod J 2008;41(1):6-31. doi:10.1111/j.1365-2591.2007. 01323.x
58. Ng YL, Mann V, Gulabivala K. Outcome of secondary root canal treatment: a systematic review of the literature. Int Endod J. 2008;41(12):1026-1046. doi:10.1111/j.1365-2591.2008. 01484.x
59. Webber RT, del Rio CE, Brady JM, Segall RO. Sealing quality of a temporary filling material. Oral Surg Oral Med Oral Pathol. 1978;46(1):123-130. doi:10.1016/0030-4220(78)90446-2
60. Bernstein DA, Todd MJ. IRM as an interappointment endodontic sealing agent. Gen Dent 1982;30(5):401-404.
61. Contardo MS, Muñoz-Sandoval C, Giacaman RA. Sealing dentin caries with resin-modified glass ionomer decreases lesion progression and bacterial survival in an experimental model. J Adhes Dent. 2015;17(3):207-212. doi: 10.3290/j.jad.a34056
62. Jensen AL, Abbott PV, Castro Salgado J. Interim and temporary restoration of teeth during endodontic treatment. Aust Dent J. 2007;52(1 Suppl): S83-S99. doi:10.1111/j.1834-7819. 2007.tb00528.x
63. Forss H, Widström E. Reasons for restorative therapy and the longevity of restorations in adults. Acta Odontol Scand. 2004;62(2):82-86. doi:10.1080/00016350310008733
64. Wiegand A, Buchalla W, Attin T. Review on fluoride-releasing restorative materials—fluoride release and uptake characteristics, antibacterial activity and influence on caries formation. Dent Mater. 2007;23(3):343-362. doi: 10.1016/j.dental.2006.01.022
65. Tjan AH, Grant BE, Dunn JR. Microleakage of composite resin cores treated with various dentin bonding systems. J Prosthet Dent. 1991;66(1):24-29. doi:10.1016/0022-3913(91) 90346.x
66. Ferracane JL. Resin composite—state of the art. Dent Mater. 2011;27(1):29-38. doi: 10.1016/j.dental.2010.10.020
67. Bindl A, Mörmann WH. Survival rate of mono-ceramic and ceramic-core CAD/CAM-generated anterior crowns over 2-5 years. Eur J Oral Sci. 2004;112(2):197-204. doi:10.1111/j.1600-0722.2004. 00119.x
68. Krejci I, Lieber CM, Lutz F. Time required to remove totally bonded tooth-colored posterior restorations and related tooth substance loss. Dent Mater. 1995;11(1):34-40. doi:10.1016/0109-5641(95)80006-9
69. Pratt I, Aminoshariae A, Montagnese TA, Williams KA, Khalighinejad N, Mickel A. Eight-year retrospective study of the critical time lapse between root canal completion and crown placement: its influence on the survival of endodontically treated teeth. J Endod 2016;42(11):1598-1603. doi: 10.1016/j.joen.2016.08.006
70. Yee K, Bhagavatula P, Stover S, et al. Survival rates of teeth with primary endodontic treatment after core/post and crown placement. J Endod. 2018;44(2):220-225. doi: 10.1016/j.joen.2017.08.034
71. Nakabayashi N, Kojima K, Masuhara E. The promotion of adhesion by the infiltration of monomers into tooth substrates. J Biomed Mater Res. 1982;16(3):265-273. doi:10.1002/ jbm.820160307
72. Breschi L, Maravic T, Mazzitelli C, et al. The evolution of adhesive dentistry: from etch-andrinse to universal bonding systems. Dent Mater. 2025;41(2):141-158. doi: 10.1016/j. dental.2024.11.011
73. Peumans M, Munck J, Van Landuyt K, Lambrechts P, Van Meerbeek B. Three-year clinical effectiveness of a two-step self-etch adhesive in cervical lesions. Eur J Oral Sci 2005;113(6):512-518. doi:10.1111/j.1600-0722.2005. 00256.x
74. Van Meerbeek B, Yoshihara K, Yoshida Y, Mine A, De Munck J, Van Landuyt KL. State of the art of self-etch adhesives. Dent Mater. 2011;27(1):17-28. doi: 10.1016/j.dental.2010.10.023
75. Perdigão J, Sezinando A, Monteiro PC. Laboratory bonding ability of a multi-purpose dentin adhesive. Am J Dent. 2012;25(3):153-158.
76. Van Landuyt KL, Snauwaert J, De Munck J, et al. Origin of interfacial droplets with one-step adhesives. J Dent Res. 2007;86(8):739-744. doi:10.1177/154405910708600810
77. Guerra JA, Skribner JE, Lin LM. Influence of a base on coronal microleakage of post-prepared teeth. J Endod. 1994;20(12):589-591. doi:10.1016/S0099-2399(06)80082-8
78. Torabinejad M, Rastegar AF, Kettering JD, Pitt Ford TR. Bacterial leakage of mineral trioxide aggregate as a root-end filling material. J Endod. 1995;21(3):109-112. doi:10.1016/s00992399(06)80433-4
79. Tselnik M, Baumgartner JC, Marshall JG. Bacterial leakage with mineral trioxide aggregate or a resin-modified glass ionomer used as a coronal barrier. J Endod. 2004;30(11):782-784. doi:10.1097/00004770-200411000-00008
80. Frankenberger R, Michalowski N, Amend S, Lücker S, Krämer N. Effect of indirect pulp capping materials on regional dentin seal. J Adhes Dent. 2025; 27:137-144. doi: 10.3290/j. jad.c_2109
81. Neelakantan P, Grotra D, Subbarao CV, Garcia-Godoy F. The shear bond strength of resinbased composite to white mineral trioxide aggregate. J Am Dent Assoc. 2012;143(8):e40e45. doi: 10.14219/jada.archive.2012.0302
82. Nandini S, Ballal S, Kandaswamy D. Influence of glass-ionomer cement on the interface and setting reaction of mineral trioxide aggregate when used as a furcal repair material using laser Raman spectroscopic analysis. J Endod. 2007;33(2):167-172. doi: 10.1016/j. joen.2006.10.010
83. Siboni F, Taddei P, Prati C, Gandolfi MG. Properties of NeoMTA Plus and MTA Plus cements for endodontics. Int Endod J. 2017;50(Suppl 2):e83-e94.doi:10.1111/iej.12787
84. Camilleri J. Staining potential of Neo MTA Plus, MTA Plus, and Biodentine used for pulpotomy procedures. J Endod. 2015;41(7):1139-1145. doi: 10.1016/j.joen.2015.02.032
85. Chen P, Chen Z, Teoh YY, Peters OA, Peters CI. Orifice barriers to prevent coronal microleakage after root canal treatment: systematic review and meta-analysis. Aust Dent J 2023;68(2):78-91. doi:10.1111/adj.12951
86. Del Carpio-Perochena A, Nicholson E, Singh CV, Camilleri J, Kishen A. Impact of dentin conditioning and sealer modification with chitosan-hydroxyapatite nanocomplexes on the antibacterial and mechanical characteristics of root dentin. J Endod. 2022;48(10):1319-1326. doi: 10.1016/j.joen.2022.06.014
87. Boitelle P, Mawussi B, Tapie L, Fromentin O. A systematic review of CAD/CAM fit restoration evaluations. J Oral Rehabil. 2014;41(11):853-874. doi:10.1111/joor.12205
88. Miao C, Yang X, Wong MC, et al. Rubber dam isolation for restorative treatment in dental patients. Cochrane Database Syst Rev. 2021;5(5):CD009858. doi: 10.1002/14651858. CD009858.pub3
89. Falacho RI, Melo EA, Marques JA, Ramos JC, Guerra F, Blatz MB. Clinical in-situ evaluation of the effect of rubber dam isolation on bond strength to enamel. J Esthet Restor Dent 2023;35(1):48-55. doi:10.1111/jerd.12979
90. Pane ES, Palamara JE, Messer HH. Stainless steel bands in endodontics: effects on cuspal flexure and fracture resistance. Int Endod J. 2002;35(5):467-471. doi:10.1046/j.1365-2591.2002. 00503.x
Failures and successes of vital pulp therapy in an undergraduate dental clinic
John F. Wisniewski, DMD, MS ¢ Mitchell Hogue, BA, MBA
Vital pulp therapy (VPT) has been the principal treatment option used to preserve pulp function during apical development of immature permanent teeth affected by caries and trauma. Advances in VPT protocols and bioactive materials have made this approach a possible treatment option for mature permanent teeth. This article presents a clinical VPT protocol for mature permanent teeth and compares 2 failed cases and 2 successful cases completed in the general dentistry clinic of a dental school. The objective is to allow general dentists to be more comfortable with providing VPT procedures as a treatment option. Four men underwent VPT in mature permanent teeth using established treatment protocols. In 2 treatments that failed, avascular pulp tissue removal was incomplete and/or inferior capping materials were used. In 2 treatments that were successful, all adversely affected pulp tissue was removed, and calcium silicate cements were used. The outcome differences in these cases support the application of advanced dental biomaterials and techniques to maintain pulpal vitality. Advanced VPT is more comprehensive than previous techniques, as it focuses on the removal of affected pulp tissue and the use of biomaterials to promote mineralized, hard tissue barriers. An accurate diagnosis, removal of inflamed necrotic/avascular pulp tissue, examination of the pulp tissue condition using magnification, and placement of calcium silicate cement directly on the exposed pulp tissue are critical to success.
Evidence-based techniques and methods are the driving force behind recent advancements in dentistry. Findings from current research encourage all dental professionals, in both clinical practice and educational environments, to remain cognizant of changing concepts and protocols.1 A paradigm shift has occurred among long-standing, traditional methods for treating and preserving vital pulp tissue.2 According to the American Association of Endodontists (AAE), “Vital pulp therapy (VPT) techniques are means of preserving the vitality and function of the dental pulp after injury resulting from trauma, caries, or restorative procedures.”2 Before 2021, there were several customary methods and some advanced treatments for the management of pulp exposure. The traditional methods of managing inflamed and exposed vital pulp tissue utilized various combinations of hard-setting calcium hydroxide (eg, Dycal [Dentsply Sirona]), glass ionomer cements, or a combination of both.3-5
Following publication of the AAE position statement on VPT, the advanced method recommends calcium silicate cements (CSCs) as the preferred material for teeth with exposed pulp.2,6 These inorganic cements, also classified as bioceramics, demonstrate osteogenic properties and have advantageous characteristics such as biocompatibility and chemical stability.7,8 CSCs and other bioceramics are responsible for the shift in using this treatment in mature permanent teeth as well as immature permanent teeth. When bioceramic dental materials are used in combination with the advanced VPT protocol and high magnification, success rates have the potential to approach 95%.9
This new VPT protocol is now recommended for the treatment of a variety of complex pulpal conditions. According to the AAE, teeth diagnosed with either reversible or irreversible pulpitis—the latter subdivided into symptomatic irreversible pulpitis or asymptomatic irreversible pulpitis—can be treated using VPT.2,6 These diagnoses can be determined by the patient’s pain history in conjunction with radiographic evidence, pulpal sensibility testing, and clinical findings. However, as previous studies have noted, these diagnostic tools do not always directly correlate with histopathologic findings of the pulp tissue.2,10,11
Traditional methods of VPT are recommended only for the treatment of primary or immature permanent teeth with open apices after pulp exposure.12 The advanced protocol can now be recommended to manage vital pulp exposure in mature permanent teeth.2,12 This suggests that VPT may be a valid alternative in teeth diagnosed with irreversible pulpitis, which conventionally has been treated with a nonsurgical root canal procedure.2,6 The purposes of this article are to (1) provide formative guidelines so that general dentists can become more confident using this procedure and understand the importance of each step; and (2) highlight common errors in VPT via a series of cases.
Advanced VPT protocols
Careful attention must be paid to avoid contamination of the pulp from saliva or other sources because the inadvertent introduction of bacteria can significantly reduce the likelihood of success. After local anesthesia is obtained, it is important to provide dental dam isolation to reduce microbial contamination and protect patients from direct sodium hypochlorite (NaOCl) exposure and other potential procedural mishaps.
Pulp assessment and management
When an unexpected pulp exposure occurs after complete caries excavation, hemostasis of hemorrhaging tissue should be achieved within 6 minutes using 3% NaOCl. The pulp exposure should then be examined to determine the pulp tissue status. Visual examination of the pulp tissue in the canal orifices with magnification is mandatory.
Scenario 1: visible bleeding
Whether or not bleeding has stopped, a new high-speed No. 4 round diamond bur should be used at high speed to selectively incise the pulp tissue, under copious water spray, to enlarge the exposure (2 mm deeper and 2 mm wider). The pulp tissue is observed for active bleeding or pooling of blood. If bleeding continues after 6 minutes of direct 3% NaOCl application via gentle irrigation or gentle placement of a cotton pellet saturated in 3% NaOCl, the incision step is repeated until healthy pulp tissue is reached, as evidenced by hemostasis. If segmental removal (2 mm deeper and 2 mm wider) of inflamed and nonvascular tissue is unsuccessful in locating healthy tissue, a complete pulpotomy is recommended. However, if bleeding stops after a single segmental incision of pulp tissue after 3% NaOCl is placed a second time, the procedure would be considered a partial pulpotomy.
In summary, a 3% NaOCl–based lavage is used to achieve hemostasis. If orifice bleeding is still uncontrolled after 6 minutes, a complete pulpectomy and nonsurgical root canal treatment are indicated.13
Scenario 2: no visible bleeding
If visible bleeding is not observed after pulp exposure, a new #4 high-speed round diamond bur with water coolant is used to segmentally remove (2 mm deeper and 2 mm wider) irreversibly inflamed and necrotic/avascular tissue until normal bleeding and healthy tissue have been encountered. Pulpal bleeding is then controlled using a cotton pellet soaked in 3% NaOCl (maximum exposure period of 6 minutes).13 After hemostasis and examination, direct capping can be initiated if the presence of healthy tissue is confirmed.11
Both scenarios
No artificial methods should be used to stop bleeding (eg, intrapulpal injection or placement of pellets soaked in products such as Hemodent [Premier Products] or ViscoStat [Ultradent Products]). It might be necessary to wait 5 to 10 minutes for bleeding to stop before more pulp tissue is removed. However, if bleeding has not stopped, a cotton pellet soaked in 3% NaOCl should be gently placed, without pressure, over the pulp exposure. This procedure should be repeated
intermittently until pulpal bleeding has stopped. This is necessary to disinfect the area and remove any blood clots. Capping a blood clot can worsen the prognosis.
When bleeding ceases and all inflamed or avascular pulp tissue is removed, a magnification-aided assessment of the pulp tissue condition must occur. This ensures that necrotic/ avascular tissue has been removed completely.
Placement of bioceramic material
After the area is rinsed and dried with a 2-way syringe—it is not necessary to excessively dry the tooth—a bioceramic material can be placed directly on the exposed pulp and surrounding dentin. If a partial pulpotomy was completed, the bioceramic material should be placed with a minimum thickness of 2 mm over the exposed pulp and should cover at least 2 mm of the noncarious dentin surrounding the exposure. If a full pulpotomy was executed, a minimum thickness of 2 mm of bioceramic material should be placed over the entire pulpal floor, covering all orifices.13
After placement of the bioceramic material, there are 2 ways to proceed. The first is to allow the bioceramic material to harden for about 10 minutes. After an adequate setting time, the cavity area can be restored in the conventional manner, avoiding dislodgment of the bioceramic material. If the bioceramic material exhibits a slow setting time, the second approach is to completely cover the material with a light-cured flowable composite resin or compomer and then restore the tooth with a bonded restoration. After either a complete or partial pulpotomy, it is critical that the area is restored promptly with a sealed adhesive restoration.
Case reports
Clinical disclosures
The treatments described in this article were performed in a general dentistry clinic at Roseman College of Dental Medicine, Roseman University of Health Sciences, South Jordan, Utah. Written informed consent was obtained from all patients. Cases 1 and 2 were each supervised by a different attending general dentistry faculty member. Neither of these individuals had received independent VPT calibration prior to performing the procedures. Case 3 was performed as a demonstration by an attending endodontic faculty member (J.F.W.). Case 4 was supervised by the same attending endodontist (J.F.W.) in conjunction with a general dentistry faculty member who had been calibrated independently on VPT procedures. All VPT clinical protocols and procedures were established by the Associate Dean of Clinical Affairs, who is currently the Executive Associate Dean as well as a diplomate of the American Board of Endodontics.
VPT preparation
All patients described in the case reports received either local infiltration anesthesia using articaine hydrochloride 4% with epinephrine 1:100,000 or block anesthesia using lidocaine hydrochloride 2% with epinephrine 1:100,000. The steps of the VPT procedure were completed under dental dam isolation. No endodontic surgical microscopes were available for use in the general dentistry clinic. Therefore, all cases were completed
using magnification loupes of ×2.5 to ×3.5. The clinical attending endodontist had loupes of ×4.5 magnification.
Unsuccessful cases
Case 1
A 19-year-old man presented for replacement of an occlusodistal restoration on the mandibular left first molar (tooth 19). Clinical examination revealed a fractured and defective amalgam restoration, and radiographic imaging showed recurrent caries below the margin of the distal gingival seat. The endodontic diagnosis was reversible pulpitis with normal apical tissue.
After dental dam isolation was confirmed, the restoration and recurrent caries were removed. This procedure resulted in a pinpoint pulp exposure with hemorrhaging that subsided without intervention. The cavity preparation and exposure were disinfected with NaOCl. A 2-mm-thick layer of fastsetting bioceramic putty (EndoSequence BC RRM Fast Set Putty, Brasseler USA) was placed over the exposure, including 2-mm coverage of the surrounding dentin. The tooth was restored with bonded composite resin (Scotchbond Universal Adhesive, 3M; Filtek One Bulk Fill Restorative, 3M) placed according to contemporary protocols.
One week later, the patient returned with a chief concern of ongoing pain and sensitivity. The tooth responded normally to cold testing; however, examination of occlusion revealed that the restoration was high. After occlusal adjustment, the patient was satisfied. Two weeks later (3 weeks after the initial visit), the patient returned with the same concern of pain in the restored tooth. The tooth was tested and found to have symptomatic irreversible pulpitis, as well as symptomatic apical periodontitis (Fig 1).
In this case, the VPT protocol was incorrectly followed because unidentified inflamed necrotic/avascular pulp tissue was present and not removed following the initial pinpoint pulp exposure.
Case 2
A 31-year-old man presented for an occlusodistal restoration on the maxillary right second premolar (tooth 4).
Radiographic imaging demonstrated advanced caries reaching half the distance to the pulp. The endodontic diagnosis was normal pulp and normal apical tissue.
A pinpoint pulp exposure was observed after cavity preparation and caries removal. The bleeding stopped quickly without intervention. Vitrebond light-curing glass ionomer cement (3M) was used to cap the exposure. The restoration was completed using conventional composite resin bonding techniques.
Six months later, the patient returned to the clinic with pain associated with tooth 4. Radiographic imaging showed the new restoration touching the distal pulp horn and a modest thickening of the periodontal ligament (Fig 2). The endodontic diagnosis was symptomatic irreversible pulpitis with symptomatic apical periodontitis. The patient opted for root canal treatment.
In this case, the VPT protocol was incorrectly followed because, after the initial pinpoint exposure, the inflamed pulp tissue was not removed to a level that was 2 mm deeper and 2 mm wider than the exposure. In addition, a glass ionomer material rather than a CSC was placed over the pinpoint exposure.
Successful cases
Case 3
A 31-year-old man presented for replacement of a mesioocclusal restoration on the mandibular left second molar (tooth 18). Clinical examination revealed leaking margins, and radiographic imaging indicated deep recurrent caries in close proximity to the pulp. Based on cold testing and imaging, the pulpal diagnosis was asymptomatic irreversible pulpitis with normal apical and supporting tissues.
Caries removal resulted in a pinpoint exposure in which blood was pooling. The tooth was managed according to treatment sequence 1 (Fig 3). A recall radiograph taken 37 months after treatment showed normal supporting structures (Fig 4). Tooth 18 exhibited a normal response to pulpal sensibility and apical tissue testing. The patient was asymptomatic. The tooth was in full function and demonstrated normal mobility and probing depths.
Fig 2. Case 2. Periapical radiograph of tooth 4 taken 6 months after initial restoration with a pulp cap.
Fig 1. Case 1. Bitewing radiograph of tooth 19 taken 3 weeks after initial restoration. Bioceramic material (arrow) was placed over the pinpoint exposure.
Case 4
A 38-year-old man presented for a mesio-occlusal restoration on the maxillary right second premolar (tooth 4). Clinical examination revealed a worn buccal cusp, and radiographic imaging identified deep caries in proximity to the pulp. The endodontic diagnosis was reversible pulpitis with normalappearing apical tissues.
The tooth was managed according to treatment sequence 1 (Fig 5). A recall radiograph obtained 31 months posttreatment showed normal supporting structures (Fig 6). Tooth 4 exhibited a normal response to pulpal sensibility and apical tissue testing. The patient was asymptomatic. The tooth was in full function and demonstrated normal mobility and probing depths.
Discussion
Establishing accurate pulpal and apical diagnoses is essential to correct application of the recommended AAE guidelines for treating pulp exposure in mature permanent teeth.2 The diagnoses of both the pulp and periapical tissues should be determined via initial patient report, direct clinical examination (including assessment of tooth restorability), diagnostic and sensibility testing, and radiographic examination. The AAE position statement on VPT contains current recommendations for teeth diagnosed with a normal pulp, reversible pulpitis, and irreversible pulpitis (symptomatic or asymptomatic).2 However, these recommendations require an accurate apical diagnosis confirming the absence of apical pathosis. The process to determine tooth treatment can vary, depending on the initial diagnosis (Chart).
Factors driving advanced VPT
According to the AAE VPT protocol, inflamed necrotic/ avascular tissue in which hemostasis is not achieved must be removed to increase the probability of successful treatment.2,13,14 This protocol is supported by a recent study of direct pulp capping that found a 7% pulp survival rate after 4 years without NaOCl hemostasis and a 55% rate when 2.5% NaOCl was used as the hemostatic agent.15 The contributing cause of unsuccessful cases in both groups was most likely the failure to remove irreversibly inflamed and necrotic/avascular tissue from the coronal pulp even after short-term NaOCl exposure and tissue examination.14,15 It is important to assess the condition of the pulp tissue under magnification and to remove affected tissue before placement of a capping material. These
Fig 6. Case 4. Bitewing radiograph at the 31-month recall.
Fig 5. Case 4. A. Two pinpoint exposures. B. Pulp exposures after stepwise pulp removal and hemostasis.
Fig 4. Case 3. Bitewing radiograph at the 37-month recall.
Fig 3. Case 3. A. Pinpoint exposure (arrow). B. Removal of inflamed pulp tissue. C. Calcium silicate cement placement.
Decision tree for the management of an inflamed vital pulp using the advanced vital pulp therapy method.
Pulpal diagnosis
Reversible pulpitis a
Normal apical tissue
Symptomatic irreversible pulpitis
Symptomatic apical periodontitis
Asymptomatic irreversible pulpitis
Vital pulp therapyb
a If decay results in pulp exposure.
b Provided that the final restorative treatment does not require a post for retention of the core placement.
recommendations are consistent with classic endodontic literature and current histologic evidence showing that coronal and radicular pulp tissues apical and proximal to areas affected by caries can remain vital.16,17
The development of bioceramic materials has been an essential component in elevating the advanced VPT protocol to the forefront of the dental field. Currently, CSCs are the most common bioceramic materials used in dentistry. These bioactive cements outperform a wide range of traditional materials previously used for VPT.2,7-9,13,18,19 This class of material produces a superior seal and reliably generates mineralized tissue barriers on healthy, exposed pulps.2,3,20 CSCs can chemically bond to dentin, produce hydroxyapatite, and provide a sustained alkaline pH after setting.7,8,21 These hydrophilic cements also exhibit osteogenic and microbial properties, have minimal linear expansion, demonstrate high compressive strength, and
feature intratubular crystallization during setting.7,8,21,22 They have shown improved clinical outcomes compared with zinc oxide–eugenol, resin-modified glass ionomer, and hard-setting calcium hydroxide cemens.7,8 The introduction of CSCs may be a major reason this advanced technique has provided improved clinical success rates.3,10,20
Comparison of unsuccessful and successful cases
The removal of inflamed micronecrotic pulp tissue and the placement of bioceramic materials in permanent teeth should be accomplished according to the recommended clinical protocol in treatment scenario 1 or 2. At subsequent recall appointments, sensibility testing should confirm a normal pulpal response if a partial pulpotomy is completed. If a full pulpotomy is performed, the tooth may not respond to cold testing.23 In either case, normal supporting tissues should be
Chart.
Pulpitis
Necrotic
Root canal treatment
radiographically evident after treatment that is performed according to the AAE guidelines.2 In a meta-analysis of direct pulp capping that compared the use of CSCs with that of hardsetting calcium hydroxide in permanent teeth with carious exposed pulp, Cushley et al found overall higher success rates for CSCs (84% to 86%) than calcium hydroxide (59%) at 2 to 3 years.24 A similar study of bioceramic materials used for pulpotomies of permanent teeth revealed an overall 1-year success rate of 93.2%.25 These results suggest that, when bioceramics are used for VPT, success rates are comparable to those of nonsurgical root canal treatment in teeth with inflamed pulps.6,26
In cases 1 and 2 of the present series, the conservative decision not to remove inflamed and affected pulp tissue (2 mm deeper and 2 mm wider) did not follow the guidelines in treatment scenario 1 or 2. The attending faculty members who managed these cases were not calibrated with the advanced VPT protocol. As noted through histologic studies, when inflamed avascular pulp tissue apical to the exposure is not removed completely, the pulp may not heal properly.11,14,16,17 Furthermore, the placement of glass ionomer cement materials directly over the pulp exposure did not correspond to the recommended placement of a CSC material per the AAE guidelines.2 The use of glass ionomer cement alone or in combination with hard-setting calcium hydroxide has led to lower success rates, as noted in past and current studies (58.7% to 80.1%) for pulp-capping procedures.7,13,18
There was a high probability in both failed cases that the pulpal inflammation was initially confined to the coronal pulp chamber, but the inflamed tissue was not adequately eliminated. Ultimately, the continued presence and growth of pathogenic microorganisms increased inflammatory responses that advanced through the pulp chamber and radicular pulp tissues. This resulted in increased intrapulpal pressure, sensitized afferent nerve fibers, pain for the patient, and changes in apical tissues.11,17
These example cases discuss the type of treatment provided in 2 failed cases compared with 2 of many successful cases completed by dental students at Roseman College of Dental Medicine. These treatment observations suggest that adherence to the advanced AAE VPT guidelines can improve patient outcomes.2
Removal of pulp tissue: a modified aggressive approach
Magnified examination of the pulp tissue is necessary and will improve the assessment of pulpal conditions throughout the procedure. Generally, ×12 to ×18 magnification is used to distinguish between necrotic and vital pulp tissue after a pinpoint exposure. However, the majority of general dentists and pediatric dentists use ×2.5 to ×4.5 loupes. From a practical viewpoint, therefore, treatment scenarios 1 and 2 recommend a modified aggressive approach. This approach allows for the removal of unidentified and presumably inflamed necrotic pulp tissue present at the exposure site. Pinpoint exposures should be managed in a slightly more aggressive manner, whether or not bleeding has stopped, with tissue removal automatically proceeding 2 mm deeper and 2 mm wider than the exposure site.
There are 3 important considerations for the modified aggressive approach: (1) establishment of an accurate pulpal
diagnosis combined with normal apical tissues, both clinically and radiographically; (2) removal of inflamed necrotic pulp tissue, as described by treatment scenarios 1 and 2; and (3) placement of CSC. Adherence to a strict clinical protocol in an aseptic environment can lead to a high success rate.9
Limitations
The results observed in the reported cases may not be generalizable to outcomes in all cases. Future clinical trials are needed to determine the overall success rate of VPT in undergraduate general dentistry teaching clinics. Comparative studies of VPT performed with endodontic surgical microscopes in comparison to the modified aggressive approach using lower magnification would be beneficial.
Conclusion
Based on the AAE position statement on VPT, a paradigm shift in treatment strategies has changed clinical management of pulp tissue exposed during caries excavation in mature permanent teeth.2 An accurate diagnosis, removal of inflamed necrotic/avascular pulp tissue, and examination of the pulp tissue condition using magnification are critical. The subsequent placement of CSCs directly on the exposed pulp tissue and proximal dentin, and completion with a permanent sealed restoration, are both equally important when using the modified aggressive approach for the management of exposed pulp tissues in VPT.
Author affiliations
Roseman College of Dental Medicine, Roseman University of Health Sciences, South Jordan, Utah.
Correspondence
John F. Wisniewski, DMD, MS (thewiz413@gmail.com).
Conflicts of interest
None reported.
Acknowledgments
The authors wish to thank Dr George Bogen, Senior Lecturer for the Department of Endodontics, University of Queensland School of Dentistry, Brisbane, Australia, for his support and invaluable editorial comments.
References
1. Versaci MB. Pathways to dentistry: researchers move dental profession forward. American Dental Association. June 12, 2022. Accessed September 5, 2025. https://adanews.ada.org/ ada-news/2022/june/pathways-to-dentistry-researchers-move-dental-profession-forward/
2. AAE position statement on vital pulp therapy. J Endod. 2021;47(9):1340-1344. doi:10.1016/j.joen.2021.07.015
3. Taha NA, Khazali MA. Partial pulpotomy in mature permanent teeth with clinical signs indicative of irreversible pulpitis: a randomized clinical trial. J Endod. 2017;43(9):1417-1421. doi:10.1016/j.joen.2017.03.033
4. Bergenholtz G. Evidence for bacterial causation of adverse pulpal responses in resin-based dental restorations. Crit Rev Oral Biol Med. 2000;11(4):467-480. doi:10.1177/ 10454411000110040501
5. de Souza Costa CA, do Nascimento AB, Teixeira HM. Response of human pulps following acid conditioning and application of a bonding agent in deep cavities. Dent Mater. 2002;18(7):543-551. doi:10.1016/s0109-5641(01)00089-6
6. Zhu L, Liu W, Deng X, Chen Z, Chen J, Qian W. Full pulpotomy versus root canal therapy in mature teeth with irreversible pulpitis: a randomized controlled trial. BMC Oral Health. 2024;24(1):1231. doi:10.1186/s12903-024-05011-0
7. Motwani N, Ikhar A, Nikhade P, et al. Premixed bioceramics: a novel pulp capping agent. J Conserv Dent. 2021;24(2):124-129. doi:10.4103/JCD.JCD_202_20
8. Raghavendra SS, Jadhav GR, Gathani KM, Kotadia P. Bioceramics in endodontics—a review. J Istanb Univ Fac Dent. 2017;51(3 Suppl 1):S128-S137. doi:10.17096/jiufd.63659
9. Bogen G, Kim JS, Bakland LK. Direct pulp capping with mineral trioxide aggregate: an observational study. J Am Dent Assoc. 2008;139(3):305-315. Erratum: 2008;139(5):541. doi:10.14219/jada.archive.2008.0160
10. Dummer PM, Hicks R, Huws D. Clinical signs and symptoms in pulp disease. Int Endod J. 1980;13(1):27-35. doi:10.1111/j.1365-2591.1980.tb00834.x
11. Ricucci D, Loghin S, Siqueira JF Jr. Correlation between clinical and histologic pulp diagnoses. J Endod. 2014;40(12):1932-1939. doi:10.1016/j.joen.2014.08.010
12. Aguilar P, Linsuwanont P. Vital pulp therapy in vital permanent teeth with cariously exposed pulp: a systematic review. J Endod. 2011;37(5):581-587. doi:10.1016/j.joen.2010.12.004
13. Bogen G. Clinical guidelines for vital pulp therapy. Endod Pract Today. 2019;13(4):283-286.
14. Bimstein E, Rotstein I. Cvek pulpotomy—revisited. Dent Traumatol. 2016;32(6):438-442. doi:10.1111/edt.12297
15. Ballal NV, Duncan HF, Wiedemeier DB, et al. 4-year pulp survival in a randomized trial on direct pulp capping. J Endod. 2024;50(1):4-9. doi:10.1016/j.joen.2023.10.008
16. Yamamura T. Differentiation of pulpal cells and inductive influences of various matrices with reference to pulpal wound healing. J Dent Res. 1985;64(Spec No):530-540. doi:10.1177/002203458506400406
17. Ricucci D, Siqueira JF Jr, Li Y, Tay FR. Vital pulp therapy: histopathology and histobacteriologybased guidelines to treat teeth with deep caries and pulp exposure. J Dent. 2019;86:41-52. doi:10.1016/j.jdent.2019.05.022
18. Iyer JV, Kanodia SK, Parmar GJ, Parmar AP, Asthana G, Dhanak NR. Comparative evaluation of different direct pulp capping agents in carious tooth: an in vivo study. J Conserv Dent. 2021;24(3):283-287. doi:10.4103/jcd.jcd_71_21
19. Cox CF, Bergenholtz G, Heys DR, Syed SA, Fitzgerald M, Heys RJ. Pulp capping of dental pulp mechanically exposed to oral microflora: a 1-2 year observation of wound healing in the monkey. J Oral Pathol. 1985;14(2):156-168. doi:10.1111/j.1600-0714.1985.tb00479.x
20. Asgary S, Ahmadyar M. Vital pulp therapy using calcium-enriched mixture: an evidencebased review. J Conserv Dent. 2013;16(2):92-98. doi:10.4103/0972-0707.108173
21. Han L, Okiji T. Uptake of calcium and silicon released from calcium silicate-based endodontic materials into root canal dentine. Int Endod J. 2011;44(12):1081-1087. doi:10.1111/j.13652591.2011.01924.x
22. Teoh YY, Liew KY, Siao J, Wong S, Chandler N, Bogen G. The effects of chelation on the intratubular penetration depth of mineral trioxide aggregate. Aust Endod J. 2023;49(3):483-491. doi:10.1111/aej.12766
23. Aravind A, R R, Sharma R, et al. Response to pulp sensibility tests after full pulpotomy in permanent mandibular teeth with symptomatic irreversible pulpitis: a retrospective data analysis. J Endod. 2022;48(1):80-86. doi:10.1016/j.joen.2021.10.005
24. Cushley S, Duncan HF, Lappin MJ, et al. Efficacy of direct pulp capping for management of cariously exposed pulps in permanent teeth: a systematic review and meta-analysis. Int Endod J. 2021;54(4):556-571. doi:10.1111/iej.13449
25. Silva EJNL, Pinto KP, Belladonna FG, Ferreira CMA, Versiani MA, De-Deus G. Success rate of permanent teeth pulpotomy using bioactive materials: a systematic review and metaanalysis of randomized clinical trials. Int Endod J. 2023;56(9):1024-1041. doi:10.1111/ iej.13939
26. Santos-Junior AO, De Castro Pinto L, Mateo-Castillo JF, Pinheiro CR. Success or failure of endodontic treatments: a retrospective study. J Conserv Dent. 2019;22(2):129-132. doi:10.4103/JCD.JCD_507_18
GENERAL DENTISTRY SELF-INSTRUCTION
Exercise No. GD552, 2 CE Credits
Endodontics
Subject Code: 070
The 15 questions for this exercise are based on the article “Failures and successes of vital pulp therapy in an undergraduate dental clinic” on pages 32-38. This exercise was developed by Hillary Homburg, DDS, in association with the General Dentistry Self-Instruction Committee
Reading the article and successfully completing this exercise will enable you to:
• understand current vital pulp therapy (VPT) protocols;
• identify the proper materials to use in the clinical management of exposed pulp tissues; and
• understand when VPT is indicated over root canal therapy.
Answers must be submitted online at agd.org/self-instruction by October 31, 2026.
1. VPT is indicated after injury to the pulp resulting from all of the following except one. Which is the exception?
A. trauma
B. caries
C. abscess
D. restorative procedure
2. The American Association of Endodontists recommends ________ as the preferred material for teeth with exposed pulp.
A. calcium hydroxide
B. calcium silicate cements
C. glass ionomer cements
D. a combination of calcium hydroxide and glass ionomer
3. If an unexpected pulp exposure occurs, hemostasis of tissue should be achieved within ___ minutes using ___% sodium hypochlorite.
A. 5; 0.5
B. 5; 3
C. 6; 0.5
D. 6; 3
4. Initial selective incision of pulp tissue should enlarge the exposure to __ mm deeper and __ mm wider.
A. 2; 2
B. 2; 3
C. 3; 2
D. 3; 3
5. If segmental removal of inflamed tissue is unsuccessful in locating healthy tissue, a ______ is recommended.
A. partial pulpotomy
B. complete pulpotomy
C. root canal therapy
D. direct pulp cap
6. If healthy pulp tissue is confirmed, ________ can be initiated.
A. VPT
B. complete pulpotomy
C. partial pulpotomy
D. direct pulp capping
7. Hemodent, ViscoStat, and other artificial methods can be used to stop bleeding if needed. It is necessary to remove any blood clots from the area before placing bioceramic materials.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
8. In a partial pulpotomy, bioceramic material should have a minimum thickness of __ mm and cover at least __ mm of noncarious dentin around the exposure.
A. 1; 1
B. 2; 1
C. 1; 2
D. 2; 2
9. Bioceramic material should be allowed to harden for ___ minutes.
A. 3
B. 6
C. 10
D. 12
10. Cases 1 and 2 were supervised by general dentistry faculty. All faculty had received independent calibration on VPT procedures.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
11. All cases were completed using ________.
A. surgical microscopes
B. magnification loupes of ×2.5 to ×3.5
C. magnification loupes of ×3.5 to ×4.5
D. a combination of surgical microscopes and magnification loupes
12. Case 1 involved tooth __ in a __ -year-old man.
A. 19; 31
B. 31; 19
C. 19; 19
D. 31; 31
13. All of the following steps were performed properly in case 1 except one. Which is the exception?
A. rubber dam isolation
B. selective removal of pulp tissue
C. achievement of pulpal hemostasis
D. placement of bioceramic material
14. The pulpal diagnosis in case 3 was ____________.
A. asymptomatic reversible pulpitis
B. symptomatic reversible pulpitis
C. asymptomatic irreversible pulpitis
D. symptomatic irreversible pulpitis
15. In case 4, the patient was asymptomatic at the ___-month recall.
A. 6
B. 26
C. 31
D. 37
Virtual Advocacy Conference
Nov. 21-22, 2025
Day 1: Noon to 4 p.m. CST
Day 2: 9 a.m. - 1 p.m. CST
Make an impact at both state and federal levels by participating in AGD’s free interactive workshop with our Advocacy Councils.
Gain essential information on crucial topics, including:
• Community Water Fluoridation
• Artificial Intelligence in Dentistry
• Dental Insurance Issues
• Insights from an AGD State Legislator
• Sedation in General Dentistry
• Updates on the CDT Code
Earn up to 8 hours of CE credits for free.
Combined endodontic and periodontal management of traumainduced tooth resorption: case reports and review of the literature
The objectives of this article are to report 2 cases of trauma-induced invasive cervical resorption (ICR) treated with surgical and nonsurgical restoration modalities and to review the literature on the clinical effectiveness of these approaches. Both surgical and nonsurgical techniques resulted in successful outcomes for 2 patients with trauma-induced ICR, classified as class 4 in the Heithersay classification and 3Bp in the 3-dimensional classification proposed by Patel et al. In the first case, the inapproachable resorptive lacuna was restored surgically, while in the second case, the large, approachable resorptive lacunae was treated nonsurgically. Treatment included root canal therapy, removal of granulation tissue, and placement of trichloroacetic acid and mineral trioxide aggregate to restore the resorptive lacuna. Follow-up examinations at 24 and 18 months for cases 1 and 2, respectively, indicated no recurrence, demonstrating successful management. Supporting the positive outcomes observed in these 2 clinical cases, the published literature suggests that the use of advanced diagnostic tools and appropriate treatment modalities tailored to each specific case can substantially increase the long-term retention of teeth affected by ICR.
Pathologic root resorption is a progressive clinical condition resulting in the breakdown of dental hard tissues such as dentin, cementum, and alveolar bone.1,2 It is difficult to identify the specific etiology of invasive cervical resorption (ICR), which is a form of external root resorption characterized by its typical location at the cervical margin and, in early lesions, an absence of pulpal involvement.2 The following have been identified as potential causes of ICR: destruction of cementoblasts from the external surface; exposure of dentin gaps at the cementoenamel junction; destruction of the odontoblastic layer; and/or loss of remnants of the epithelial rests of Malassez and cementoblasts, accompanied by necrosis or loss of the periodontal ligament.1,3
Clinically, ICR may range from a slight defect at the gingival margin to a major resorptive defect resulting in pink discoloration of the crown. The radiographic appearance of ICR lesions ranges from a well-defined radiolucency to a poorly defined lesion with irregular boundaries. However, advanced lesions are osseous in nature, with the possibility of having a mottled appearance.3,4 The Heithersay classification is commonly used for these lesions and proposes 4 distinct clinical categories for ICR: class 1, cervical area with modest invasion by a resorptive lesion and minor dentin involvement; class 2, well-defined resorptive lesion that affects the outer layers of dentin in close proximity to the pulp but not reaching the root dentin; class 3, deeper resorptive lesion invading both the coronal dentin and the coronal third of the root; and class 4, severe, invasive resorption that extends beyond the root’s coronal third.5
In a clinical study of 257 teeth, Heithersay studied potential predisposing factors for ICR.6 Although the most common single predisposing factor was orthodontics, reported in 24.1% of evaluated teeth, dental trauma was also identified as a significant risk factor for ICR, representing the sole predisposing factor in 15.1% of affected teeth. In an additional 10.6% of studied teeth, trauma was combined with another predisposing factor—intracoronal bleaching, orthodontic therapy, or delayed eruption.6 The gradual and asymptomatic character of ICR, which has an incidence that ranges from 0.02% to 2.3%, typically results in tooth loss.6,7 The resorptive process begins externally above the alveolar bone crest and involves loss of unmineralized precementum layers and inflammation with odontoclastic activities.8
While the Heithersay classification of ICR provides a useful framework for categorizing these lesions, it is important to note that relying solely on 2-dimensional radiographs for classification might result in limitations or inaccuracies in their
Fig 1. Case 1. Sagittal CBCT section (large-field-of-view, flat-panel detector, 11 × 5 cm in size; voxel size of 150 μm; operating at 90 kV, 14 mA, and 5.07 s) showing radiolucency (arrows) extending to the pulp.
identification; indeed, an ex vivo investigation showed that periapical radiography led to accurate classification in only 39.7% of cases, whereas cone beam computed tomography (CBCT) led to correct classification in about 70% of instances.9 The intraexaminer and interexaminer repeatability of classification accomplished via CBCT is also much greater than that of periapical radiography. Patel et al have developed a 3dimensional (3D) categorization technique for ICR lesions that uses CBCT to evaluate height, circumferential distribution, and closeness to the root canal.10 Lesion height is designated by grades ranging from 1 (cementoenamel junction) to 4 (apical third of root), circumferential distribution by grades ranging from A (≤ 90°) to D (> 270°), and closeness to the root canal by grade d (dentin) or p (pulp).
Multiple reports have described the complexity of managing class 4 ICR.11-13 The present article focuses on the potential of hydraulic calcium silicate–based materials to achieve biocompatible restoration and effective tissue repair of class 4 ICR in both surgical and nonsurgical techniques. This article presents 2 clinical cases of trauma-associated cervical resorption managed with combined endodontic and periodontal management procedures that included the use of mineral trioxide aggregate (MTA). In addition, existing research on surgical and nonsurgical management of root resorption is reviewed.
Case reports
Case 1
A 26-year-old woman reported to the Department of Conservative Dentistry and Endodontics, Sri Aurobindo College of Dentistry, Sri Aurobindo University, Indore, India, with chief concerns of pus discharge and mild pain in the
maxillary right anterior region that had lasted a few months. A review of the patient’s dental history revealed that 2 years previously she had sustained a traumatic injury in the maxillary anterior tooth region in a road accident, following which she underwent extraction of the maxillary left central and left lateral incisors (teeth 9 and 10, respectively). Teeth 9 and 10 were replaced with a provisional prosthesis that was still in use.
Removal of the provisional prosthesis revealed the presence of an implant in the position of tooth 9. To assess the vitality of the maxillary right central incisor (tooth 8), a thermal (cold) test (Endo-Frost, Coltene) was conducted. The tooth exhibited nonvitality, showing no reaction to pulp testing. Periodontal probing was within the physiologic limits at all locations around the tooth except for the distolabial surface, wherein a sinus tract was present.
Radiographic evaluation using a radiovisiograph (Kodak RVG 5200, Carestream Dental) revealed a root canal filling in the maxillary right lateral incisor (tooth 7), an implant abutment in position 9, and radiolucency at the distal aspect of tooth 8. The intraoral sinus was traced using No. 15 gutta percha, which showed that the origin of the sinus track was at the distal aspect of tooth 8 (subcrestal).
To gain comprehensive understanding of the clinical conditions, the patient underwent CBCT (CS 9300, Carestream Dental) with a field of view of 11 × 5 cm, a voxel size of 150 µm, and emission parameters of 90 kV, 14 mA, and 5.07 s. The CBCT images showed irregular canal morphology with scattered radiolucency indicative of ICR (Fig 1). An invasive resorptive lesion with pulpal involvement was evident close to the cervical area, which helped to establish the clinical classification of class 4 ICR (Heithersay classification). According to the 3D classification of ICR based on CBCT images, the lesion was class 3Bp, meaning the ICR extended into the mid-third of the root, showed a circumferential spread of > 90° and ≤ 180°, and had probable pulpal involvement.10
The fundamental objectives of ICR treatment are excavation of the resorptive defect, arrest of the resorptive process, and restoration of the hard tissue defect with a biocompatible and esthetic filling material to prevent recurrence. In this case, root canal treatment with debridement and surgical restoration of the resorptive lacuna (as the cavitation area was inaccessible) was considered as a treatment option. The patient received a detailed explanation of the proposed procedure, and verbal consent was obtained.
Endodontic treatment was initiated under rubber dam isolation. After local anesthesia (lidocaine with 1:200,000 epinephrine) was verified, a round bur was used to make the access opening. Patency was achieved using a No. 10 K-file. The working length was determined using an apex locator (E-PEX Pro, Eighteeth) and was confirmed using radiography. The canal was shaped with flexible nickel-titanium rotary files (Neoendo Flex, Orikam Healthcare) up to size 35/6, employing a crown-down technique with the assistance of an endo motor (E-Connect S, Eighteeth). Throughout the procedure, the canal was irrigated with a solution comprising 5.25% sodium hypochlorite (NaOCl) and saline in a 30-gauge side-vented needle. When shaping was completed, a 5.25% NaOCl solution was introduced into the canal and activated for 30 seconds with
incision performed with a No. 15 blade, starting from the distal end of tooth 7 and ending at the mesioproximal aspect of tooth 8, with 2 vertical releasing incisions for reflection of a full-thickness flap (represented by arrows).
an ultrasonic device. Calcium hydroxide paste (AvueCal, BLV Healthcare) was placed as an intracanal medication, and the access cavity was sealed using temporary cement (Cavit, 3M).
The calcium hydroxide paste was left in the canal for 10 days. During the second visit, the medication was removed, and the tooth was irrigated with NaOCl solution and saline. As the resorption lacuna was inaccessible, surgical intervention was planned. A sulcular incision was performed with a No. 15 blade, starting from the distal end of tooth 7 and ending at the mesioproximal aspect of tooth 8 (Fig 2). After 2 vertical releasing incisions were made, a full-thickness flap was reflected. A circular resorptive area containing granulation tissue was clearly visible in the surgical site (Fig 3).
The granulomatous tissue was removed from the resorption site with a spoon excavator. A cotton ball dipped in a aqueous solution of 90% trichloroacetic acid (TCA) was placed against the resorptive lacuna, which was then rinsed with saline. The canal was thoroughly dried, and gutta percha (No. 30/.06) was placed in the canal to maintain its patency during restoration of the resorptive lacuna. MTA Plus (Prevest DenPro) was placed to restore the defect (Fig 4).
The underside of the flap, in the depth of the fold between the mucoperiosteum and the alveolar bone, was thoroughly examined before the flap was repositioned. The repositioned flap was stabilized with 3-0 nonresorbable silk suture material placed with the single interrupted suturing technique (Fig 5). An immediate postoperative radiograph confirmed that the resorptive lacuna was completely filled (Fig 6).
Postendodontic surgery instructions to the patient included refraining from strenuous activities, maintaining a nutritious diet with adequate hydration, and avoiding inspection of the surgical site. The patient was informed that mild bleeding was normal and would be transient. Cold compresses were permissible for up to 8 hours. Additionally, the patient was
advised to rinse the mouth with chlorhexidine mouthwash twice daily for 5 days.
The patient returned after 10 days for suture removal, and complete healing of the intraoral sinus was observed. Thereafter, the patient was reevaluated on a regular basis. The tooth was asymptomatic and had no circumferential periodontal pockets. Regular recall examinations confirmed satisfactory gingival healing, and there was no recurrence at the 2-year follow-up.
Fig 2. Case 1. Sulcular
Fig 3. Case 1. Circular resorptive area (arrow) containing granulation tissue.
Fig 4. Case 1. Placement of MTA (arrows) to restore the resorptive lacuna.
Case 2
A 25-year-old man reported to the Department of Conservative Dentistry and Endodontics, Sri Aurobindo College of Dentistry, with chief concerns of bleeding gingivae, mild discomfort, and cavitation in the maxillary anterior tooth region that had developed in the last few months. The patient reported a history of trauma to the maxillary tooth region that had occurred 2 years prior. Since the initial injury, the patient had not experienced any provoked or spontaneous pain.
On clinical examination, the cervical third of the maxillary right canine (tooth 6) was found to have a cavitated lesion that appeared to originate subgingivally (Fig 7). Thermal and electric tests were conducted to assess the vitality of tooth 6, which exhibited a negative response. Periodontal probing was within the physiologic limits at all locations around the tooth except the labial surface. Probing of the cavitated area on the labial surface gave a fibrous sensation, and bleeding was observed. The periapical radiograph revealed radiolucency on the distal surface of the tooth.
To obtain a 3D view of the clinical conditions, the patient underwent CBCT with a field of view of 11 × 5 cm, a voxel size of 150 µm, and emission parameters of 90 kV, 14 mA, and 5.07 s. The CBCT images showed irregular canal morphology with scattered radiolucencies indicative of tooth resorption in tooth 6 (Fig 8). The resorptive lesion, which was invasive in nature with dentin penetration and pulpal involvement, was evidently close to the cervical area, contributing to a diagnosis of irreversible pulpitis with class 4 ICR. According to the 3D classification of ICR using CBCT, this case was consistent with 3Bp ICR.
A nonsurgical endodontic intervention with repair of the large resorptive lacuna was selected as the most conservative treatment for tooth 6. The patient received a detailed explanation of the proposed procedure and provided verbal consent.
After local anesthesia was obtained with 2% lidocaine with 1:200,000 epinephrine, endodontic treatment was initiated
under rubber dam isolation. A round bur was used to make the access opening. Patency was achieved with a No. 10 K-file. The granulation tissue in the cavitation site was removed with an endodontic spoon excavator. The working length was determined with hand K-files in conjunction with an apex locator. The canal was shaped up to No. 30/.06, employing a crown-down technique with the assistance of an endo motor. Throughout the procedure, irrigation was conducted with a solution comprising 5.25% NaOCl and saline.
After shaping of the canal, 30-second ultrasonic activation of a 5.25% NaOCl solution was performed. Calcium hydroxide paste was placed as intracanal medication for the subsequent 10 days, and the access cavity was sealed using temporary cement.
Ten days later, the medication was removed, the canal underwent cleaning with a warm 3% NaOCl solution, and final rinses were conducted using 17% ethylenediaminetetraacetic acid. Gutta percha (No. 30/.06) was placed in the canal to preserve its patency throughout the repair process. The resorptive lacuna was delicately treated with a 90% aqueous TCA solution for 1 minute, and MTA was employed for restoration (Fig 9). The endodontic access hole was sealed with composite resin (Filtek Z350, 3M).
Following treatment, evaluations of the tooth were performed regularly. Examination at the 18-month follow-up visit revealed no recurrence of the ICR or associated discomfort.
Fig 5. Case 1. Flap repositioned and stabilized with 3-0 nonresorbable silk sutures placed with the single interrupted suturing technique.
Fig 6. Case 1. Immediate postoperative radiograph showing the resorptive lacuna completely filled with MTA.
images (large-field-of-view, flat-panel detector; 11 × 5 cm in size; voxel size of 150 μm; operating at 90 kV, 14 mA, 5.07 s) showing radiolucency (arrows) extending to the pulp at the cervical third of the tooth. A. Sagittal section. B. Axial section.
Discussion
A systematic search of the PubMed and Google Scholar databases was conducted to identify case reports from January 2007 to August 2023 in which a surgical or nonsurgical approach was undertaken for the management of tooth resorption. The medical subject heading (MeSH) phrases utilized for the search were as follows: (“tooth resorption” OR “root resorption”) AND (“invasive” OR “external” OR “idiopathic”) AND (“therapeutics” OR “therapy” OR “management” OR “approach”). After abstracts and titles were screened, 38 case reports remained. Of these articles, 26 fulfilled the criteria and were considered for the final evaluation (Table).13-38
The reports comprised a total of 46 cases with follow-up periods ranging from 6 months to 6 years.13-38 Successful outcomes were reported in almost every case, with recurrence reported in only 1 case, in which 1 of 2 treated teeth in a single patient had a recurrence after 6 years.35 Several reports described successful management with a conservative approach.19,27,28 Umer et al reported a successful outcome with bone-like tissue infill 3 years after conservative management of class 2 ICR with orthograde root canal treatment that included calcium hydroxide as intracanal medicament.19 Both Schwartz et al and Johns et al emphasized the importance of early diagnosis and comprehensive management for successful outcomes.15,17
Class 4 ICR is a complex form of tooth resorption that extends beneath a tooth’s epithelial attachment at the cervical region. This resorptive process is characterized by its invasive and aggressive nature. While the mechanisms are poorly understood, it is generally accepted that resorption of the root dentin occurs when the cementum layer, which protects the dentin, is damaged or inadequate. Various terms, including odontoclastoma, peripheral cervical resorption, and supraosseous extracanal invasive resorption, have been used to describe ICR.8
The etiology of ICR is multifactorial, with numerous potential causes contributing to its growth. Predisposing
factors include dental trauma, orthodontic treatment, intracoronal bleaching, and surgery. Dental trauma, including luxation and avulsion injuries, accounts for a significant percentage of ICR cases. 6 Orthodontic treatment, particularly when excessive forces are applied to the cervical region of a tooth, may lead to tissue necrosis adjacent to exposed root dentin, stimulating odontoclasts and initiating resorption. Intracoronal bleaching, a common dental procedure, has been associated with ICR, with hydrogen peroxide denaturing dentin and creating an acidic environment that enhances osteoclastic activity. 3
Heithersay’s extensive investigation identified orthodontic treatment, dental trauma, and bleaching as the predisposing
Fig 9. Case 2. Intraoral postoperative periapical radiograph showing resorptive lacuna completely filled with MTA (arrows).
Fig 7. Case 2. Cavitated lesion with a subgingival origin at the cervical third of tooth 6.
Fig 8. Case 2. CBCT
Table. Summary of the literature on management of tooth resorption (2007-2023).
Study (year) Patients, n
Patel and Dawood (2007)13 1
Fernández and Rincón (2011)14 1
Schwartz et al (2011)15 3 None; orthodontic treatment; not reported
Vinothkumar et al (2011)16 1 Trauma
Johns et al (2013)17 1 Trauma
Tavares et al (2013)18 1 Trauma
Umer et al (2013)19 1 Trauma
Baranwal (2016)20 1 Trauma
Lo Giudice et al (2016)21 5 None (4 cases); orthodontic treatment (1 case)
Eftekhar et al (2017)22 1 Periodontal surgery
Fernandes et al (2017)23 1 Orthodontic treatment
Surgical endodontic management of class 4 ICR using MTA
Maxilla Nonsurgical treatment using internal debridement, endodontic treatment, and restoration; surgical exposure, debridement without endodontics, and restoration; “heroic efforts” using surgical exposure, debridement, and postsupported sandwich restoration
Maxilla Surgical management using reverse sandwich restoration technique for class 2 ICR and apical inflammation
Maxilla Early diagnosis, surgical elimination of resorption, and restorative management
y Successful
Maxilla Surgical management using resin-modified glass ionomer 1 y Successful
Maxilla Conservative management using orthograde root canal treatment including calcium hydroxide as intracanal medicament 3 y Successful
Maxilla Use of Biodentine under a dental operatory microscope
Maxilla (4); mandible (1)
Surgical management using mechanical debridement and composite resin restoration
Mandible Surgical management using Biodentine 2 y Successful
Surgical management using MTA, RMGIC, and composite resin
Karunakar et al (2018)24 2 Trauma Maxilla Surgical treatment with biocompatible restorative material
Mehra et al (2018)25 3 Trauma Maxilla Surgical management using Biodentine 18 mo–4 y Successful
Nagahara et al (2018)26 1 Abutment of 3-unit metal cantilever fixed partial denture Mandible Surgical management using MTA 3 y Successful
Alqedairi (2019)27 1 Orthodontic treatment Maxilla Nonsurgical endodontic therapy and MTA repair of class 3 ICR associated with secondary periodontal disease
Asgary et al (2019)28 6 Various, including extraction of adjacent tooth, restorative procedures, and poor oral hygiene Maxilla (1 case); mandible (5 cases) Conservative vital pulp therapy prioritizing excavation of lacuna and filling with calcium-enriched mixture cement 16 mo–3 y Successful
Table. Summary of the literature on management of tooth resorption (2007-2023) (continued).
Study (year) Patients, n Predisposing factors Location Approach and materials Follow-up Outcome
Ehlinger et al (2019)29 4 Not reported
Maxilla Surgical management of class 2 ICR using composite resin restoration; nonsurgical management of class 3 ICR using Biodentine and composite resin restoration; surgical management of class 4 ICR using post-supported crown; nonsurgical management of class 4 ICR using Biodentine and composite resin restoration
1-3 y Successful
Agrawal and Kapoor (2020)30 1 Trauma
Bachesk et al (2021)31 1 Orthodontic treatment
Gión-Guerra et al (2021)32 4 Not reported
Himasindhu et al (2021)33 1 Trauma
Tavares et al (2021)34 1 Not reported
Maxilla Surgical excision of granulation tissue and root reconstruction using Biodentine 1 y Successful
Maxilla Surgical management using RMGIC 1 y Successful
Maxilla Surgical management using MTA (3 cases) or Biodentine (1 case) 3 y Successful
Maxilla Surgical management using MTA 1 y Successful
Maxilla Surgical endodontics for class 4 ICR and subsequent endodontic retreatment with adjunctive antimicrobial photodynamic therapy 5 y Successfulb
AlAttas et al (2023)35 1 Orthodontic treatment Maxilla Nonsurgical endodontic treatment and surgical management of ICR using placement of bioceramic material in 2 teeth
Asgary (2023)36 1 None
da Cunha Isaltino et al (2023)37 1 Trauma
Asgary and Roghanizadeh (2024)38 1 None
6 y Successful (1 tooth); recurrence after 6 y (1 tooth)c
Mandible Surgical management of a large, perforated, asymptomatic class 4 ICR detected during routine radiographic examination 1 y Successful
Maxilla Endodontic and surgical management 1 y Successful
Maxilla Modified pulpotomy for typical class 3 ICR 1 y Successful
a Although the final recall examination was 9.5 years, it was reported that the tooth functioned normally until it fractured 20 years after treatment.15
bAfter initial surgical endodontic treatment resulted in incomplete sealing of the defect at 30 days, endodontic retreatment combined with antimicrobial photodynamic therapy resulted in successful healing.34
cThe patient failed to return for the 1-year follow-up, and recurrence was found during examination of a different symptomatic tooth 6 years posttreatment.35
factors most commonly associated with ICR. 6 Orthodontic treatment alone was a potential factor in almost one-quarter of teeth with ICR, with a diagnosis occurring years after the removal of appliances. Trauma, whether from accidents or orthodontic procedures, was a major contributor, and intracoronal bleaching was found to be associated with ICR in a significant percentage of cases. 6,7
The diagnosis of ICR can be challenging. Typically, it is identified in the cervical area of the tooth, manifesting as a pink spot caused by visible granulation tissue through thinned dentin and enamel. However, the condition is often painless, and early lesions may only be detected as incidental findings on radiographs.39 Radiographically, ICR lesions may vary in appearance, presenting as asymmetric radiolucencies with
irregular margins in the cervical region. CBCT has proven useful in assessing the extent and nature of ICR lesions.40
Histologically, ICR lesions resemble external inflammatory resorption, characterized by granulomatous tissue and the presence of osteoclasts.6 The predentin and innermost layers of dentin act as barriers, preventing the resorptive process from involving the pulp until the lesion is advanced. In long-standing lesions, there may be secondary bacterial colonization, leading to an inflammatory response in the associated periodontal or pulpal tissues.
Treatment of ICR poses challenges and depends on the extent of the lesion. The Heithersay classification categorizes lesions based on their depth and involvement. For smaller lesions (class 1 or 2), external approaches involve raising a full-thickness flap, removing granulomatous tissue, and using conservative filling materials. Internal approaches may utilize chemical agents such as TCA. For more extensive lesions (classes 3 or 4), treatment options include forced eruption, intentional reimplantation, or extraction with subsequent implant placement or a fixed prosthesis.41 However, although extraction is often recommended for advanced ICR lesions (Heithersay class 4/Patel 3Bp), repair was attempted in each of the present cases to preserve the natural tooth and its function. Both lesions were in single-rooted teeth, allowing complete debridement and sealing with biocompatible materials. While earlier studies reported poor outcomes (12.5% success for class 4), a few case reports have demonstrated long-term survival of class 4 lesions managed conservatively.6,14 Thus, repair was selected to avoid the functional and biologic disadvantages of extraction and prosthetic replacement.
Preventive measures involve avoiding indirect causes through careful orthodontic procedures, trauma prevention, and meticulous intracoronal bleaching techniques. Understanding the predisposing factors and adopting preventive strategies may decrease the occurrence of ICR.41
For the nonsurgical approach in the present study, chemicalmechanical debridement was combined with 90% aqueous TCA, calcium hydroxide, and NaOCl. Correct diagnosis is of utmost importance because the etiologies and treatment of internal and external resorption are different.42 It is imperative to differentiate between ICR and subgingival caries lesions, which are sticky when probed. When the ICR lesion is probed, extensive bleeding occurs due to the extremely vascular resorptive tissue underneath.42
The effectiveness of modern diagnostic technologies, particularly CBCT imaging, may contribute considerably to determining the optimal treatment approach.16 CBCT scanning reveals particular information about the extent, size, and position of ICR lesions.10 In 2018, Patel et al introduced a novel classification for external cervical resorption based on CBCT, which was adopted by the European Society of Endodontology.10
Calcium hydroxide is advised for treatment of ICR because studies suggest that it helps eliminate microbes, inactivate toxic products, and stimulate the establishment of a hard barrier.6,43 However, no material can meet the optimal parameters for restoration of a cavity located generally within the biologic width, where persistent periodontal issues might emerge. Bioactive
materials such as Biodentine (Septodont) and glass ionomer cement are more biocompatible with gingival tissues than composite resin and aid in establishing a long epithelial attachment.22,32,44,45 Despite the potential incompatibility with periodontal tissues, a well-polished nanohybrid composite resin was demonstrated to lessen plaque growth and produce acceptable clinical outcomes.46 In the present cases, a cotton pellet immersed in TCA was applied to the resorptive lesions, as TCA increases coagulative necrosis of infiltrating tissue by reaching smaller, less accessible recesses and resorptive channels.5,45 Some clinicians advise use of a bur to refresh the bonding surface, as the demineralization of dentin by TCA can affect the bonding procedure.47
In ICR, surgical intervention becomes the treatment of choice when elimination of the etiologic agent proves challenging despite conventional endodontic procedures.4 This involves curettage in the periradicular region, targeting the removal of pathologic tissue impeding repair, as evident radiographically. During curettage, the removal extends to the surrounding tissue infected by microorganisms, diminishing the risk of recurrence.48 The cavity walls are meticulously prepared and filled with biocompatible materials. However, surgical approaches are deemed invasive and potentially detrimental to the periodontal prognosis, as they necessitate substantial bone and dentin removal to expose the resorbed tissue.49
Conclusion
The management of class 4 ICR represents a complex and challenging task for dental professionals. The case reports in this article highlight the successful utilization of both surgical and nonsurgical approaches to address this condition. These cases underscore the importance of accurate diagnosis, aided by CBCT, in determining the appropriate treatment approach. Additionally, the choice of a biocompatible material, in these cases MTA, played a crucial role in achieving favorable outcomes. It is evident that a tailored approach considering factors such as lesion extent and the patient’s wishes can lead to successful outcomes, challenging the conventional notion of immediate extraction for such cases.
Author affiliations
Department of Conservative Dentistry and Endodontics, Government Dental College and Hospital, Jamnagar, India (Tripathi); Department of Conservative Dentistry and Endodontics, Sri Aurobindo College of Dentistry, Sri Aurobindo University, Indore, India (Patni, Jain, Raghuwanshi, Pandey).
The authors gratefully acknowledge the following individuals for their support and guidance in the preparation of this manuscript: Dr Vinod Bhandari, Sri Aurobindo Institute of Medical Sciences, Indore, India; and Dr Manjushri Bhandari, Sri Aurobindo University, Indore, India.
References
1. Trope M, Chivian N, Sigurdsson A, Vann WF. Traumatic injuries. In: Cohen S, Burns RC, eds. Pathways of the Pulp. 8th ed. Mosby; 2002:603-649.
2. Laux M, Abbott PV, Pajarola G, Nair PN. Apical inflammatory root resorption: a correlative radiographic and histological assessment. Int Endod J. 2000;33(6):483-493. doi:10.1046/ j.1365-2591.2000.00338.x
3. Patel S, Kanagasingam S, Pitt Ford T. External cervical resorption: a review. J Endod 2009;35(5):616-625. doi:10.1016/j.joen.2009.01.015
4. Heithersay GS. Management of tooth resorption. Aust Dent J. 2007;52(1 Suppl):S105-S121. doi:10.1111/j.1834-7819.2007.tb00519.x
5. Heithersay GS. Treatment of invasive cervical resorption: an analysis of results using topical application of trichloracetic acid, curettage, and restoration. Quintessence Int. 1999;30(2):96-110.
6. Heithersay GS. Invasive cervical resorption: an analysis of potential predisposing factors. Quintessence Int. 1999;30(2):83-95.
7. Irinakis E, Aleksejuniene J, Shen Y, Haapasalo M. External cervical resorption: a retrospective case-control study. J Endod. 2020;46(10):1420-1427. doi:10.1016/j.joen.2020.05.021
9. Vaz de Souza D, Schirru E, Mannocci F, Foschi F, Patel S. External cervical resorption: a comparison of the diagnostic efficacy using 2 different cone-beam computed tomographic units and periapical radiographs. J Endod. 2017;43(1):121-125. doi:10.1016/j. joen.2016.09.008
10. Patel S, Foschi F, Mannocci F, Patel K. External cervical resorption: a three-dimensional classification. Int Endod J. 2018;51(2):206-214. doi:10.1111/iej.12824
11. Hakki SS, Bozkurt SB, Hakki EE, Belli S. Effects of mineral trioxide aggregate on cell survival, gene expression associated with mineralized tissues, and biomineralization of cementoblasts. J Endod. 2009;35(4):513-519. doi:10.1016/j.joen.2008.12.016
12. Lovato KF, Sedgley CM. Antibacterial activity of EndoSequence root repair material and ProRoot MTA against clinical isolates of Enterococcus faecalis J Endod. 2011;37(11):15421546. doi:10.1016/j.joen.2011.06.022
13. Patel S, Dawood A. The use of cone beam computed tomography in the management of external cervical resorption lesions. Int Endod J. 2007;40(9):730-737. doi:10.1111/j.13652591.2007.01247.x
14. Fernández R, Rincón JG. Surgical endodontic management of an invasive cervical resorption class 4 with mineral trioxide aggregate: a 6-year follow-up. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;112(5):e18-e22. doi:10.1016/j.tripleo.2011.04.028
15. Schwartz RS, Robbins JW, Rindler E. Management of invasive cervical resorption: observations from three private practices and a report of three cases. Tex Dent J 2011;128(11):1173-1187.
16. Vinothkumar TS, Tamilselvi R, Kandaswamy D. Reverse sandwich restoration for the management of invasive cervical resorption: a case report. J Endod. 2011;37(5):706-710. doi:10.1016/j.joen.2011.02.005
17. Johns DA, Shivashankar VY, Maroli RK, Joseph R. Invasive cervical root resorption: engineering the lost tissue by regeneration. Contemp Clin Dent. 2013;4(4):536-539. doi:10.4103/0976-237X.123067
18. Tavares WL, Lopes RC, Oliveira RR, Souza RG, Henriques LC, Ribeiro-Sobrinho AP. Surgical management of invasive cervical resorption using resin-modified glass ionomer cement. Gen Dent. 2013;61(7):e16-e18.
19. Umer F, Adnan S, Raza Khan F. Conservative management of invasive cervical resorption: a case report. J Dent (Tehran). 2013;10(3):289-295.
20. Baranwal AK. Management of external invasive cervical resorption of tooth with Biodentine: a case report. J Conserv Dent. 2016;19(3):296-299. doi:10.4103/0972-0707.181952
21. Lo Giudice G, Matarese G, Lizio A, Lo Giudice R, Tumedei M, Zizzari VL, Tetè S. Invasive cervical resorption: a case series with 3-year follow-up. Int J Periodontics Restorative Dent 2016;36(1):103-109. doi:10.11607/prd.2066.
22. Eftekhar L, Ashraf H, Jabbari S. Management of invasive cervical root resorption in a mandibular canine using Biodentine as a restorative material: a case report. Iran Endod J 2017;12(3):386-389. doi:10.22037/iej.v12i3.16668
23. Fernandes M, Menezes L, De Ataide I. Management of invasive cervical resorption using a surgical approach followed by an internal approach after 2 months due to pulpal involvement. J Conserv Dent. 2017;20(3):214-218. doi:10.4103/0972-0707.218312
24. Karunakar P, Soloman RV, Anusha B, Nagarjun M. Endodontic management of invasive cervical resorption: report of two cases. J Conserv Dent. 2018;21(5):578-581. doi:10.4103/ JCD.JCD_119_18
25. Mehra N, Yadav M, Kaushik M, Roshni R. Clinical management of root resorption: a report of three cases. Cureus. 2018;10(8):e3215. doi:10.7759/cureus.3215. doi:10.7759/cureus.3215
26. Nagahara T, Takeda K, Aida Y, et al. Combined endodontic and periodontal management of a class 3 invasive cervical resorption in a mandibular first molar. Clin Case Rep 2018;6(10):2005-2010. doi:10.1002/ccr3.1785
27. Alqedairi A. Non-invasive management of invasive cervical resorption associated with periodontal pocket: a case report. World J Clin Cases. 2019;7(7):863-871. doi:10.12998/ wjcc.v7.i7.863
28. Asgary S, Nourzadeh M, Verma P, Hicks ML, Nosrat A. Vital pulp therapy as a conservative approach for management of invasive cervical root resorption: a case series. J Endod 2019;45(9):1161-1167. doi:10.1016/j.joen.2019.05.020
29. Ehlinger C, Ginies E, Bornert F, Bahi-Gross S, Schmittbuhl M, Minoux M. Decision criteria influencing the therapeutic approach to invasive cervical resorption: a case series. Quintessence Int. 2019;50(6):494-502. doi:10.3290/j.qi.a42479
30. Agrawal VS, Kapoor S. Management of root canal stenosis and external inflammatory resorption by surgical root reconstruction using Biodentine. J Conserv Dent. 2020;23(1):102-106. doi:10.4103/JCD.JCD_128_20
31. Bachesk AB, Queiroz AF, Bin LR, Bachesk AB, Pavan AJ. Clinical approach to external cervical resorption in the anterior teeth: a case report study. Iran Endod J. 2021;16(2):118-122. doi:10.22037/iej.v16i2.32373
32. Gión-Guerra B, Pérez-Lanza P, Almiñana-Pastor P, Micó-Martínez P, Alpiste-Illueca FM, López-Roldán A. Performance of the dentogingival junction with MTA and Biodentine on the treatment of invasive cervical resorptions. A literature review and case report. J Clin Exp Dent. 2021;13(1):e95-e98. doi:10.4317/jced.57410
33. Himasindhu U, Suneelkumar C, Lavanya A, Swapna S. Management of external cervical resorption using mineral trioxide aggregate. J Interdiscip Dent. 2021;11(1):40-43. doi:10.4103/jid.jid_13_20
34. Tavares WLF, Oliveira RR, Ferreira MVL, Sobrinho APR, Braga T, Amaral RR. The use of antimicrobial photodynamic therapy in the successful management of an invasive cervical resorption class 4: a case report with five years follow-up. Photodiagnosis Photodyn Ther 2021;33:102126. doi:10.1016/j.pdpdt.2020.102126
35. AlAttas MH, Edrees HY, Mohsin SF, Javed MQ. Recurrence of invasive cervical resorption after six years of nonsurgical and surgical management by bioceramic-material. Pak J Med Sci 2023;39(3):908-912. doi:10.12669/pjms.39.3.6959
36. Asgary S. Surgical management of large-perforated class 4 invasive cervical root resorption: a case report. J Dent Sci. 2023;18(1):484-485. doi:10.1016/j.jds.2022.07.012
37. da Cunha Isaltino M, da Silva Souza C, de Oliveira NG, de Melo Júnior PMR, Velozo Telles CT, de Albuquerque DS. Endodontic and surgical management of an invasive cervical resorption in a maxillary central incisor: a case report. Iran Endod J. 2023;18(3):168-173. doi:10.22037/ iej.v18i3.41385
38. Asgary S, Roghanizadeh L. Successful management of a typical class 3 invasive cervical root resorption with modified pulpotomy: a case report. Iran Endod J. 2024;19(1):56-60. doi:10.22037/iej.v19i1.44253
39. Bergmans L, Van Cleynenbreugel J, Verbeken E, Wevers M, Van Meerbeek B, Lambrechts P. Cervical external root resorption in vital teeth. J Clin Periodontol. 2002;29(6):580-585. doi:10.1034/j.1600-051x.2002.290615.x
40. Estrela C, Bueno MR, De Alencar AH, et al. Method to evaluate inflammatory root resorption by using cone beam computed tomography. J Endod. 2009;35(11):1491-1497. doi:10.1016/j.joen.2009.08.009
41. Abbott PV. Prevention and management of external inflammatory resorption following trauma to teeth. Aust Dent J. 2016;61(Suppl 1):82-94. doi:10.1111/adj.12400
42. Rodríguez G, Abella F, Durán-Sindreu F, Patel S, Roig M. Influence of cone-beam computed tomography in clinical decision making among specialists. J Endod. 2017;43(2):194-199. doi:10.1016/j.joen.2016.10.012
43. Gulabivala K, Searson LJ. Clinical diagnosis of internal resorption: an exception to the rule. Int Endod J. 1995;28(5):255-260. doi:10.1111/j.1365-2591.1995.tb00310.x
44. Santamaria MP, Suaid FF, Casati MZ, Nociti FH, Sallum AW, Sallum EA. Coronally positioned flap plus resin-modified glass ionomer restoration for the treatment of gingival recession associated with non-carious cervical lesions: a randomized controlled clinical trial. J Periodontol. 2008;79(4):621-628. doi:10.1902/jop.2008.070285
45. Martins TM, Bosco AF, Nóbrega FJ, Nagata MJ, Garcia VG, Fucini SE. Periodontal tissue response to coverage of root cavities restored with resin materials: a histomorphometric study in dogs. J Periodontol. 2007;78(6):1075-1082. doi:10.1902/jop.2007.060457
46. Garrido I, Abella F, Ordinola-Zapata R, Duran-Sindreu F, Roig M. Combined endodontic therapy and intentional replantation for the treatment of palatogingival groove. J Endod 2016;42(2):324-328. doi:10.1016/j.joen.2015.10.009
47. Heithersay GS, Wilson DF. Tissue responses in the rat to trichloracetic acid – an agent used in the treatment of invasive cervical resorption. Aust Dent J. 1988;33(6):451-461. doi:10.1111/j.1834-7819.1988.tb05849.x
48. Rotondi O, Waldon P, Kim SG. The disease process, diagnosis and treatment of invasive cervical resorption: a review. Dent J (Basel). 2020;8(3):64. doi:10.3390/dj8030064
49. Lima TFR, Silva EJNLD, Gomes BPFA, Almeida JFA, Zaia AA, Soares AJ. Relationship between initial attendance after dental trauma and development of external inflammatory root resorption. Braz Dent J. 2017;28(2):201-205. doi:10.1590/0103-6440201701299
GENERAL DENTISTRY SELF-INSTRUCTION
Exercise No. GD553, 2 CE Credits
Endodontics
Subject Code: 070
The 15 questions for this exercise are based on the article “Combined endodontic and periodontal management of trauma-induced tooth resorption: a case report and review of the literature” on pages 41-49. This exercise was developed by Jeffery B. Price, DDS, MS, MAGD, FICD, FACD, in association with the General Dentistry Self-Instruction Committee.
1. All of the following are potential etiologies for ICR except one. Which is the exception?
A. cementoblast destruction
B. cemental tears at the cementoenamel junction (CEJ)
C. odontoblast destruction
D. exposure of dentin gaps at the CEJ
2. Which of the following is considered a clinical sign of ICR?
A. spontaneous pain
B. tooth mobility
C. pink color of crown
D. severe halitosis
3. Which classification system is most commonly used for ICR?
A. Simon
B. Heithersay
C. Miller
D. Glickman
4. Dental trauma is a significant risk factor for the development of ICR. Other variables, such as orthodontic therapy and intracoronal bleaching, also increase the risk of developing ICR.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
5. The reported incidence of ICR is _____%.
A. < 0.02
B. 0.02 to 2.3
C. 2.4 to 5.3
D. > 5.3
Reading the article and successfully completing this exercise will enable you to:
• describe the leading theories of the etiology of invasive cervical resorption (ICR);
• recognize the most common clinical and radiographic features of ICR; and
• discuss how to manage the endodontic, periodontal, and restorative care of patients with ICR.
Answers must be submitted online at agd.org/self-instruction by October 31, 2026.
6. Which of the following best describes the past dental history of the patient in case 1?
A. failed endodontic therapy with retreatment
B. intracanal bleaching
C. orthodontic treatment as a child
D. trauma to the anterior maxilla
7. The resolution of the CBCT volumes acquired in both cases was ___ μm.
A. 5
B. 76
C. 100
D. 150
8. In an ex vivo study, periapical radiographs showed a 29.7% accuracy rate in classifying ICR lesions. The same study showed that CBCT had an accuracy rate of ~70%.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
9. Which of the following 3-dimensional classifications, as developed by Patel et al, describes the ICR lesions seen in both case reports?
A. 2Ap
B. 4Bp
C. 3Dp
D. 3Bp
10. Treatment objectives in cases of ICR include ____________ and ____________.
A. excavation of the resorptive defect; arrest of the resorptive process
B. excavation of the resorptive defect; prevention of future ICR lesions
C. composite restoration of the defect; arrest of the resorptive process
D. stannous fluoride treatment of the defect; glass ionomer restoration
11. Which of the following intracanal medicaments was used between endodontic therapy appointments in both case reports?
A. chlorhexidine
B. eugenol paste
C. calcium hydroxide
D. penicillin paste
12. Which of the following best describes the restoration sequence of the resorption defect in case 1?
A. 90% trichloroacetic acid (TCA) treatment, saline rinse, mineral trioxide aggregate (MTA)
B. water rinse, 37% phosphoric acid, bonding agent, composite
C. aluminum chloride for hemostasis, water rinse, glass ionomer
D. water rinse, glass ionomer liner, amalgam
13. All of the following may be considered synonyms for ICR except one. Which is the exception?
A. odontoclastoma
B. cementoblastoma
C. peripheral cervical resorption
D. supraosseous extracanal invasive resorption
14. All of the following are frequently recommended for managing extensive class 3 or 4 ICR lesions except one. Which is the exception?
A. forced eruption
B. intentional reimplantation
C. conservative restoration
D. extraction followed by implant or fixed prosthesis
15. TCA was used to treat the resorptive lesion before placement of MTA to achieve ________.
A. acid etching of the affected dentin
B. acid etching of the surrounding enamel
C. coagulative necrosis of resorptive tissues
D. stimulation of pulpal regeneration
Effect of the endodontic sealer on the bond strength of glass fiber posts
Rafael Coutinho Silva, DDS, MSc, PhD ¢ Mariana de Almeida Barbosa, DDS, MSc, PhD
This study aimed to evaluate the influence of 2 endodontic sealers on the bond strength between glass fiber posts and root canal dentin at different storage times (7 days or artificial aging), also considering the root canal region (cervical, middle, and apical). A total of 60 extracted single-rooted human teeth were divided randomly into 4 groups (n = 15) according to endodontic sealer (bioceramic sealer vs epoxy resin–based sealer) and storage time prior to cementation (7 days or artificial aging via thermocycling). Following root canal treatment and cementation of glass fiber posts, all groups were stored in distilled water for 7 days at 37°C. The bioceramic and epoxy resin sealer groups designated for artificial aging were then subjected to 10,000 thermocycles in a water bath alternating between 5°C and 55°C, with a dwell time of 30 seconds at each temperature. The roots were sectioned transversely, and a single slice (approximately 2 mm thick) per post/canal third was obtained and submitted to a push-out test in a universal testing machine at a speed of 5 mm/min. Data were analyzed using 3-way analysis of variance (α = 0.05). There was no statistically significant difference in the bond strength between the sealer groups (P = 0.619), regardless of the storage time (P = 0.933). Likewise, no significant differences were observed among the root canal thirds—cervical, middle, or apical (P = 0.665). In this in vitro study, none of the tested variables—type of sealer used (epoxy resin–based or bioceramic), storage time prior to cementation, or root canal third (cervical, middle, or apical)—affected the bond strength of glass fiber posts.
One of the most common concerns about weaker teeth after endodontic treatment is the appropriate restoration for rehabilitation.1 In certain circumstances, a prosthetic crown may be advised to avoid fractures.2 Glass fiber posts are commonly used as a retention system for the restorative material in endodontically treated teeth with significant coronal structure loss because they produce lower tension at the post-cement interface than metallic posts.3-5 Ideally, the post should avoid tension during fixation and require minimal root canal preparation for effective adaptation.6
Variations in dentinal tubule density pose a difficulty when the clinician is deciding which adhesive method to use to attach the post to the root dentin.1 Endodontic sealers can obliterate dentinal tubules, interfering with the adhesion of the resin cements used to cement the intraradicular retainers, especially since root space preparation does not completely remove the sealers.1,4 Endodontic sealers, depending on their composition, may affect the post’s durability and adherence to the root dentin.7-9 Dibaji et al found that the use of bioceramic EndoSequence BC Sealer (Brasseler USA) and zinc oxide–eugenol Dorifill (DoriDent) decreased the average bond strength of the fiber post to the root dentin in the cervical third when compared with the resin AH Plus sealer (Dentsply Sirona).10
In a 2018 study, the endodontic sealer AH Plus showed the least negative effect on the bond strength between the glass fiber post and a resin-based adhesive cement (RelyX ARC, 3M), whether cementation occurred immediately or 7 days after endodontic treatment.11 A more recent study showed that neither sealers based on zinc oxide and eugenol nor bioceramic sealers had positive outcomes, and they are not recommended in circumstances where a root retainer is required for tooth rehabilitation.12 In agreement with those findings, dos Santos et al reported that epoxy resin–based or calcium hydroxide−based sealers produced better results than a sealer based on zinc oxide and eugenol.13 Furthermore, the presence of endodontic sealer remnants reduced the bond strength between the root canal dentin and the post, particularly in the apical region.13
Composite cements (conventional and self-adhesive) differ in terms of bond strength when influenced by factors such as the type of endodontic sealer and interval between sealer placement and post cementation. Bohrer et al showed that the use of AH Plus sealer resulted in greater bond strength than did zinc oxide–eugenol sealer when posts were cemented after 24 hours and 6 months of storage and did not influence the degree of conversion of composite cements.4 Zinc oxide–eugenol sealer inhibited the adhesion between the fiber post and the root dentin, decreasing composite cement conversion.4
Another study found that the bond strength of glass fiber posts increased when they were cemented immediately after root canal treatment with bioceramic sealer.14
Intraradicular posts are commonly utilized to restore teeth with significant coronal loss after endodontic therapy, and various materials are employed to fill the root canal and cement the intraradicular posts with a goal of long-term success. Among the parameters required for successful restoration are root canal sealing and procedure durability, so knowledge of the properties of the materials employed and any potential interactions between them is important. Therefore, the aim of the present study was to evaluate the influence of 2 endodontic sealers on the bond strength of glass fiber posts depending on the root canal region and storage time. The null hypothesis was that there would be no differences in the bond strength between the glass fiber post and the root canal based on the endodontic sealer, root third, or storage time prior to cementation.
Methods
This study was approved by the Research Ethics Committee of Positivo University, Curitiba, Brazil (CAAE 36465920.3.0000.0093 and approval 4.404.952).
A total of 60 extracted single-rooted human teeth were used in this study. The teeth were cleaned and immersed in 0.5% chloramine-T at 4°C until use. The crowns were transversely sectioned using a carborundum disc (Dentorium Products) with constant water irrigation and then removed to create standard access to the root canal and root portions of 16 mm in length. The 60 roots were first randomly divided into 2 groups (n = 30) according to the endodontic sealer used (Bio-C Sealer, Angelus; or AH Plus). After root canal treatment and the initial 7-day storage period, each sealer group was further divided into 2 subgroups (n = 15) according to the storage condition: without aging or with artificial aging by thermocycling.
The same operator (M.A.B.) performed the root canal preparations, with the working length defined as 1 mm less than the root length, or 15 mm. The canals were prepared using reciprocating files with a 21-mm length (WaveOne Gold, Medium, 35/.05, Dentsply Sirona). After each 3-mm advancement of the file, the root canal was irrigated with 5 mL of 2.5% sodium hypochlorite. At the end of the working length, the canals were irrigated with 17% ethylenediaminetetraacetic acid for 3 minutes before being irrigated again with 2.5% sodium hypochlorite and dried with paper points.
The canals were then filled using 1 of 2 endodontic sealers (n = 30 per sealer): bioceramic (Bio-C Sealer) or epoxy resin (AH Plus). Each type of sealer was applied according to its manufacturer’s recommendations, and the canals were obturated with gutta percha (WaveOne Gold Conform Fit Medium, Dentsply Sirona) using the single-cone technique. Following root canal treatment, the cavities were sealed with a temporary restorative material based on zinc oxide and calcium sulfate (Restaurador Provisório, Villevie), and all roots were stored in distilled water at 37°C for 7 days.
After 7 days’ storage, the temporary restorative material was removed with a curette (Fava), and the glass fiber posts were prepared and cemented. First, the post space was prepared 11 mm deep to receive a fiber post (Exacto 1, Angelus) using
the corresponding bur of the system. The canals were then irrigated with distilled water for 5 seconds and dried with paper points. After the fiber posts were cleaned with 70% ethyl alcohol, resin cement (RelyX U200, 3M) was applied to the root canal from the apical third to the cervical third. The fiber post was inserted, excess cement was removed, and the cement was photoactivated for 20 seconds with an LED device operated at a power of 1000 mW/cm² (Demi LED, Kerr). The entirety of the cementation protocol was carried out according to the manufacturer’s instructions.
All specimens were stored in distilled water for 7 days at 37°C. For the subgroups without thermocycling, this was the only aging procedure performed. After this period, each sealer group (n = 30) was further divided into 2 subgroups (n = 15): without aging or with artificial aging. The specimens assigned to artificial aging were subjected to 10,000 cycles in a thermocycling machine (Odeme Dental Research) using water baths alternating between 5°C and 55°C with a dwell time of 30 seconds at each temperature. This protocol was chosen because 10,000 cycles are considered to simulate approximately 1 year of clinical function.15
After aging, the roots were sectioned transversely under water cooling using a diamond saw (IsoMet 1000 Precision Saw, Buehler). The first 1-mm cervical slice was discarded due to irregular cement amounts, and then 3 slices (2.0 ± 0.3 mm thick) were obtained per specimen, corresponding to the cervical, middle, and apical thirds. Thus, a total of 3 values (cervical, middle, and apical) per root were recorded for the push-out test. For the push-out test, each slice was placed on a metallic device with a central opening on a universal testing machine (Emic DL 2000, Instron Brasil Equipamentos Científicos). A metallic cylinder with a flat tip applied the load on the post in an apical to coronal direction without exerting pressure on the root portion of the slice. A 100-kN load cell was used at a speed of 0.5 mm/min until failure.
The data were statistically analyzed with 3-way analysis of variance (ANOVA) using the factors endodontic sealer, root third, and storage time prior to cementation. A significance level of 5% was used.
Results
The Table shows the mean and SD values for the bond strength of glass fiber posts according to the endodontic sealer used, root canal third, and storage time. Three-way ANOVA showed no statistically significant difference in the bond strength of glass fiber posts based on the sealer used (P = 0.619), storage time (P = 0.933), or root canal third (cervical, middle, or apical) (P = 0.665).
Discussion
Teeth that present extensive coronal destruction require rehabilitation through intraradicular retainers. The use of glass fiber posts relined with resin cement is the most conservative choice because it results in better stress distribution along the root.16 The longevity of endodontic treatment depends on several factors, including the tooth, the root, and the intracanal obturation technique. When resin cements are chosen to cement glass fiber posts, one concern is the gradual loss of
Table. Mean (SD) push-out bond strengths of glass fiber posts according to root canal sealer, root third, and storage time prior to cementation (n = 15 per sealer per storage time).
a Post cementation and push-out testing after 7 days of storage in distilled water at 37°C.
b Post cementation and push-out testing after 7 days of storage in distilled water at 37°C followed by 10,000 thermocycles in a water bath alternating between 5°C and 55°C, with a dwell time of 30 seconds at each temperature.
retention due to the sensitivity of the adhesive technique and polymerization of the resin cement.17
The objective of the present study was to evaluate the effect of 2 endodontic sealers on the bond strength of glass fiber posts to root dentin, considering different root canal thirds and storage times prior to testing. However, none of these factors resulted in a statistically significant difference in the retention of glass fiber posts. Therefore, the null hypothesis was not rejected.
Nesello et al evaluated the influence of calcium silicate–based sealer on the bond strength of glass fiber posts using conventional and self-adhesive cements, forming 6 different groups: AH Plus/RelyX ARC; AH Plus/RelyX U200; Bio-C Sealer/RelyX ARC; Bio-C Sealer/RelyX U200; Sealer Plus BC (MK Life)/RelyX ARC; and Sealer Plus BC/RelyX U200.18 The study concluded that AH Plus did not have a statistically significant detrimental effect (P > 0.05) on the union between the post and conventional cement (RelyX ARC) or self-adhesive cement (RelyX U200). The lowest bond strength was seen with calcium silicate–based cement associated with conventional resin cement (Bio-C Sealer/RelyX ARC and Sealer Plus BC/ RelyX ARC). All groups showed lower resistance in the apical portion, except for Sealer Plus BC/RelyX ARC.18
Vilas-Boas et al reported that the low bond strength of a glass fiber post to dentin can be avoided with the correct choice of endodontic sealer and appropriate timing of post cementation.11 They found that AH Plus sealer is the best choice for endodontic obturation and RelyX ARC cement the best choice for cementing glass fiber posts, which can be performed immediately or 7 days after completion of endodontic treatment. Another study found that the bond strength of glass fiber posts was greater when the post was cemented immediately after root canal treatment with bioceramic sealer.14
Bohrer et al evaluated the resistance of glass fiber posts using 2 different types of endodontic sealer; however, 2 different resin cements (RelyX U200 and Multilink Automix [Ivoclar Vivadent]) were used to cement the post, and different behaviors were found.4 The present study only evaluated different endodontic sealers, not different cements. The results showed no significant difference between the sealers regardless of the root third. Therefore, additional studies are required to evaluate the influence of these sealers on the push-out bond strength of glass fiber posts cemented with different resin cements.
Conclusion
In this in vitro study, the push-out bond strength of glass fiber posts was not affected by the endodontic sealer, root third, or storage time prior to cementation of the post.
Author affiliations
School of Health Sciences, Graduate Program in Dentistry, Positivo University, Curitiba, Brazil.
Correspondence
Flavia Sens Fagundes Tomazinho, DDS, MSc, PhD (flavia.tomazinho@gmail.com).
Conflicts of interest
None reported.
References
1. Teixeira CS, Pasternak-Junior B, Borges AH, Paulino SM, Sousa-Neto MD. Influence of endodontic sealers on the bond strength of carbon fiber posts. J Biomed Mater Res B Appl Biomater. 2008;84(2):430-435. doi:10.1002/jbm.b.30888
2. Apicella MJ, Loushine RJ, West LA, Runyan DA. A comparison of root fracture resistance using two root canal sealers. Int Endod J. 1999;32(5):376-380. doi:10.1046/j.13652591.1999.00240.x
3. Barjau-Escribano A, Sancho-Bru JL, Forner-Navarro L, Rodríguez-Cervantes PJ, PérezGónzález A, Sánchez-Marín FT. Influence of prefabricated post material on restored teeth: fracture strength and stress distribution. Oper Dent. 2006;31(1):47-54. doi:10.2341/04-169
4. Bohrer TC, Fontana PE, Wandscher VF, et al. Endodontic sealers affect the bond strength of fiber posts and the degree of conversion of two resin cements. J Adhes Dent. 2018;20(2): 165-172. doi:10.3290/j.jad.a40301
5. Santos AF, Meira JB, Tanaka CB, et al. Can fiber posts increase root stresses and reduce fracture? J Dent Res. 2010;89(6):587-591. doi:10.1177/0022034510363382
6. Musikant BL, Deutsch AS. Post design and its impact on the root and crown. Compend Contin Educ Dent. 2006;27(2):30-33.
7. Ngoh EC, Pashley DH, Loushine RJ, Weller RN, Kimbrough WF. Effects of eugenol on resin bond strengths to root canal dentin. J Endod. 2001;27(6):411-414. doi:10.1097/00004770200106000-00011
8. Schwartz RS, Robbins JW. Post placement and restoration of endodontically treated teeth: a literature review. J Endod. 2004;30(5):289-301. doi:10.1097/00004770-200405000-00001
9. Ortega MA, Rios L, Fraile-Martinez O, et al. Bioceramic versus traditional biomaterials for endodontic sealers according to the ideal properties. Histol Histopathol. 2024;39(3):279292. doi:10.14670/HH-18-664
10. Dibaji F, Mohammadi E, Farid F, Mohammadian F, Sarraf P, Kharrazifard MJ. The effect of BC Sealer, AH-Plus and Dorifill on push-out bond strength of fiber post. Iran Endod J 2017;12(4):443-448. doi:10.22037/iej.v12i4.15863
11. Vilas-Boas DA, Grazziotin-Soares R, Ardenghi DM, et al. Effect of different endodontic sealers and time of cementation on push-out bond strength of fiber posts. Clin Oral Invest 2018;22(3):1403-1409. doi:10.1007/s00784-017-2230-z
12. Hamdy TM, Galal MM, Ismail AG, Saber S. Physicochemical properties of AH Plus bioceramic sealer, Bio-C Sealer, and ADseal root canal sealer. Head Face Med. 2024;20(1):2. doi:10.1186/s13005-023-00403-z
13. dos Santos GL, Cardoso IV, Suzin SM, Ballarin A, Lopes GC, Teixeira CS. Influence of different endodontic sealers on bond strength of fiber posts to weakened roots after resin restoration. Clin Oral Investig. 2021;25(6):4125-4135. doi:10.1007/s00784-020-03744-0
14. Yuanli H, Juan W, Mengzhen J, et al. The effect of two endodontic sealers and interval before post-preparation and cementation on the bond strength of fiber posts. Clin Oral Investig 2021;25(11):6211-6217. doi:10.1007/s00784-021-03920-w
15. Gale MS, Darvell BW. Thermal cycling procedures for laboratory testing of dental restorations. J Dent. 1999;27(2):89-99. doi:10.1016/s0300-5712(98)00037-2
16. Santos-Filho PC, Veríssimo C, Raposo LH, Noritomi MecEng PY, Marcondes Martins LR. Influence of ferrule, post system, and length on stress distribution of weakened root-filled teeth. J Endod. 2014;40(11):1874-1878. doi:10.1016/j.joen.2014.07.015
17. Pulido CA, de Oliveira Franco AP, Gomes GM, et al. An in situ evaluation of the polymerization shrinkage, degree of conversion, and bond strength of resin cements used for luting fiber posts. J Prosthet Dent. 2016;116(4):570-576. doi:10.1016/j.prosdent.2016.02.019
18. Nesello R, Silva IA, Bem IA, et al. Effect of bioceramic root canal sealers on the bond strength of fiber posts cemented with resin cements. Braz Dent J. 2022;33(2):91-98. doi:10.1590/0103-6440202204529
GENERAL DENTISTRY SELF-INSTRUCTION
Exercise No. GD554, 2 CE Credits
Restorative Dentistry
Subject Code: 250
The 15 questions for this exercise are based on the article “Effect of the endodontic sealer on the bond strength of glass fiber posts” on pages 51-54. This exercise was developed by Sandra Montes, DDS, FAGD, in association with the General Dentistry Self-Instruction Committee.
1. To evaluate bond strength, the root specimens were subjected to a ________ test in a universal testing machine.
A. pull-in
B. tensile
C. push-out
D. compression
2. Glass fiber posts are commonly used as a retention system for the restorative material in endodontically treated teeth with significant coronal structure loss because they _______ than metallic posts.
A. produce a better esthetic result
B. produce lower tension at the post-cement interface
C. chemically bond to resin cements with less surface treatment
D. require more thermocycling to activate adhesive bonding
3. In a recent study, neither sealers based on ________ and eugenol nor bioceramic sealers showed positive outcomes where a root retainer is required for tooth rehabilitation, and they are not recommended in those circumstances.
A. calcium hydroxide
B. epoxy resin
C. glass ionomer
D. zinc oxide
4. Variations in __________ pose a difficulty for the selection of adhesive methods used to attach the post to the root dentin.
A. dentinal tubule density
B. post diameter
C. root canal morphology
D. dentin mineral content
5. Sixty single-rooted human teeth were used in this study. The teeth were cleaned and immersed in 0.9% sodium chloride at 4°C until use.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
Reading the article and successfully completing this exercise will enable you to:
• recognize the restorative challenges that arise in endodontically treated teeth with significant coronal loss;
• understand how endodontic sealers affect the bond strength of glass fiber posts; and
• select appropriate glass fiber post cementation protocols to improve treatment outcomes.
Answers must be submitted online at agd.org/self-instruction by October 31, 2026.
6. The same operator performed all root canal preparations, and the working length was defined as exactly 1 mm less than the root length, or ___ mm.
A. 13
B. 14
C. 15
D. 16
7. The canals were prepared with the _____ reciprocating system.
A. WaveOne Gold
B. ProTaper Gold
C. Reciproc Blue
D. XP-endo Shaper
8. At the end of the working length, the canals were irrigated with 17% ethylenediaminetetraacetic acid for exactly __ minutes before being irrigated again with 2.5% sodium hypochlorite.
A. 3
B. 5
C. 7
D. 9
9. The canals were obturated using the _______ technique.
A. lateral condensation
B. warm vertical compaction
C. carrier-based
D. single-cone
10. Following root canal therapy, the cavities were sealed with a ________ prior to fiber post placement.
A. cotton pellet
B. glass ionomer material
C. resin barrier
D. temporary restorative material
11. The post space was prepared ___ mm deep.
A. 10
B. 11
C. 12
D. 13
12. The fiber posts were cleaned with ________ before cementation.
A. ethyl alcohol
B. chlorhexidine
C. hydrogen peroxide
D. glutaraldehyde
13. Each specimen was subjected to thermocycling consisting of 5000 cycles. The temperature of the water alternated between 5°C and 55°C with a dwell time of 30 seconds at each temperature.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
14. The data were statistically analyzed using ________.
A. linear regression analysis
B. Wilcoxon signed-rank test
C. chi-square test
D. 3-way analysis of variance
15. The highest mean bond strength value (MPa) was observed in the ________ sealer group at the ________ root region.
A. AH Plus; apical
B. AH Plus; middle
C. Bio-C Sealer; apical
D. Bio-C Sealer; middle
Practical implementation of caries disease management in the era of CAMBRA: a guide for the general dentist
Douglas A. Young, DDS, EdD, MBA, MS ¢ Ryan L. Quock, DDS ¢ Susie Goolsby, DDS, MSHA
Martha McComas, RDH, MS ¢ Steven Powell, DDS ¢ Gregory G. Zeller, DDS, MS
Allen Wong, DDS, EdD ¢ Brian B. Nový, DDS
Although the philosophy of caries management by risk assessment (CAMBRA) is widely accepted as an essential part of comprehensive disease management, its implementation in daily clinical practice has historically been hindered by a lack of concise guidance that bridges the gap between scholarly research and the logistics of patient care. With the aim of guiding comprehensive disease management for dental caries by integrating available evidence-based systems such as the American Dental Association Caries Classification System (ADA CCS) and caries risk assessment (CRA), this review presents clinical strategies in a functional format. Clinical caries management strategies that integrate the ADA CCS with CRA were compiled and evaluated by clinicians representing a variety of practice settings. Examples of clinical protocols were selected to illustrate the use of CRA at the patient level and ADA CCS lesion classification at the tooth level to comprehensively manage caries lesions in a high-caries-risk population. Comprehensive caries management combines the clinical use of CRA and caries lesion classification to guide clinical decisions and to support tooth preservation in high-risk populations. These strategies should be individualized and fulfill evidence-based clinical practice criteria with oral health as the primary outcome. Person-centered comprehensive caries management integrating CRA and classification of caries lesions has the potential to improve patient outcomes by addressing the underlying causes of caries disease. Documenting and measuring the processes at the tooth, patient, and practice levels are essential for generating outcomes that will drive future approaches aimed at improving patient health.
The respect for comprehensive disease management as a whole, and caries management by risk assessment (CAMBRA) as a leading philosophy, has continued to increase among payers, educators, clinicians, organized oral healthcare, and the US Health Resources and Services Administration. Yet in an era of evidence-based clinical decisionmaking, the adoption of these concepts by more clinicians seems to be stalled by a lack of practical translational strategies that are urgently needed for the improvement of patient health. This is not to say that the underlying science is lacking or that research has failed to show any positive health outcomes from these approaches. Instead, the situation highlights the hurdles that make it difficult to evaluate and adopt the vast array of available information in the form of effective clinical protocols. Given that dental caries is one of the most common diseases treated in dentistry, it could be argued that every general dentist functions as a practical cariologist, requiring actionable information. This summary of clinical cariology based on the philosophy of CAMBRA is meant to provide guidance for general dentists to implement disease management concepts in daily practice and improve the oral health of the patients they treat.
Terminology
The term caries by itself is open to several interpretations, and caries is colloquially used to describe both the disease and the resulting symptomatic lesion; this may create confusing variations in diagnosis and treatment. Adoption of high-level consensus terminology, such as that described jointly by the International Association for Dental Research Cariology Research Group, the European Organization for Caries Research, and the International Caries Consensus Collaboration is recommended for more precise diagnosis, treatment, and communication.1-3 For example, the term dental caries is used to describe the actual disease process, while caries lesion describes the clinical manifestation of the disease; the 2 terms are closely related yet distinct.
Caries management is defined as “...actions taken to interfere with mineral loss at all stages of the caries disease, including nonoperative and operative interventions/treatments.”1 The term nonoperative refers to treating the lesion without tooth structure removal by employing the following strategies: surface protection (including barriers or sealants), biofilm modification, remineralization via chemotherapeutics, saliva supplementation, and behavioral modification, including changes in diet and lifestyle.
Because dental caries manifests on a spectrum, the term caries lesion alone lacks specificity and provides no information about the location, extent, severity, or activity of the caries lesion—all factors that influence appropriate caries management. Just as the disease of dental caries manifests on a scale, the response to caries lesions should be appropriately scaled. The American Dental Association Caries Classification System (ADA CCS) informs the evidence-based decision of when to treat a caries lesion nonoperatively with remineralization and/ or silver diamine fluoride (SDF) and when to treat operatively with restoration based on the presence or absence of full cavitation. If the tooth surface is fully cavitated through the enamel, an operative approach resulting in restoration may be indicated or the cavitated lesion can be treated with the appropriate SDF approach; by contrast, caries lesions that are active but not fully cavitated require a nonoperative approach.4
For scenarios that involve operative intervention, the term selective caries removal refers to the removal of demineralized or infected tooth structure from external walls and margins with judicious preservation of soft or leathery dentin in deeper areas of the lesion to maintain pulpal vitality.5-7 This approach is preferred over nonselective caries removal (also known as complete caries removal).5-7 The endpoint of selective caries removal differs based on the tactile quality of dentin and the depth of the lesion. Selective caries removal should stop in shallow or moderately deep lesions at firm (affected or demineralized) dentin when possible. In deep lesions radiographically extending into the pulpal third of dentin, selective removal may terminate at soft (infected) dentin rather than exposing a vital pulp.7-9
Comprehensive caries management
The effective management of the caries disease process encompasses more than addressing individual caries lesions. Caries lesions are simply the result (or sign) of dental caries, and treating individual caries lesions does not halt or reverse the overarching disease process.10
Dental caries management should be a disease-based approach directed at (1) performing a caries risk assessment (CRA) unique to the individual, (2) reducing pathologic factors, (3) enhancing protective factors to address the overall disease process, and (4) using a diagnostic classification such as the ADA CCS to drive appropriate, tooth-conserving nonoperative and operative interventions for individual caries lesions.11 In short, comprehensive caries management should address both the disease and its signs and symptoms while tracking the outcomes of the management strategy.12
Person-centered care
In person-centered disease management, the values and preferences of patients guide all aspects of their healthcare.13,14 The person-centered approach hinges on the ability of the provider and patient to communicate effectively so that the patient will change behavior related to oral disease. Motivational interviewing and shared decision making are 2 frameworks that can be used to communicate with patients and involve them in their preferred care path.14,15 CRA and lesion classification provide necessary insights that are critical to comprehensive person-centered care.12
Caries risk assessment
The comprehensive management of dental caries involves utilizing CRA to drive the decision-making process in choosing an appropriate level of care, including different treatment strategies for individual patients.16 CRA also establishes risk for future dental caries, elucidates hidden risk factors, and identifies any imbalance between risk factors and existing protective factors.11,17,18 Equipped with this information, the clinician can determine how to best decrease the pathogenic factors via medical management of dental caries and increase the protective factors via behavioral change strategies. Proper utilization of CRA also determines the caries management recall intervals for the individual and assesses the effectiveness of interventions.19
The chronic nature of dental caries indicates that CRA should permeate all patient interactions and be continually updated, not limited to specific types of appointments (eg, a comprehensive examination). Most third-party payers expect a documented caries risk assessment as part of the baseline visit after a comprehensive clinical examination (which includes a hard and soft tissue examination; radiographic examination; review of medical, dental, social, and nutritional histories; and biofilm/bacteria and saliva assessments) and then regular updates throughout life. 11,20 Documentation of active caries lesions (often called disease indicators ) during each examination complements CRA, as both processes support each other. Current active disease continues to remain the single most predictive factor for future caries lesion development. 21-24
CRA also includes a person-centered conversation with the patient to identify modifiable risk factors such as acidogenic biofilm behavior, destructive lifestyle habits (diet, frequency of snacking and sugar intake, use of xerostomic medications or illicit drugs, smoking), and absence of healthy saliva.13,14 In fact, some CRA tools consider the presence of abnormal saliva to represent extreme caries risk because without adequate saliva the patient may be lacking in naturally occurring calcium, phosphate, and pH neutralization.11 Thus, a CRA can be viewed as a way to assess the promoters of remineralization (calcium, phosphate, topical fluoride, pH neutralization, and biofilm modification). If any promoter is found deficient, therapeutic products may be considered to supplement missing chemistry. Any intervention should be based on the best available scientific evidence and the patient’s values and preferences.13,14
Creating a risk-based, personalized action plan will give the patient the best chance for halting, reversing, and preventing dental caries in both the present and future. This plan usually involves the use of oral care products and behavioral and/ or nutritional changes by the patient. Any caries management action plan should involve the patient’s feedback and participation, especially in the planning stage. The utility of motivational interviewing cannot be overstated in the risk assessment conversation, which often is poorly implemented as a yes-or-no question and answer session. The risk assessment process should manifest behavior change rather than simply fulfill data collection, since the act of collecting answers to questions is not synonymous with classifying the caries risk.12
Determining caries risk: The checked item farthest to the right determines overall caries risk
Low caries risk
No active caries lesion or radiolucency (cavitated or noncavitated) during past 24 mo
Healthy lifestyle habits, including diet with little to no consumption of simple sugars, infrequent snacking, and no drug or alcohol misuse
No visible plaque
Moderate
caries risk
No active caries lesion or radiolucency (cavitated or noncavitated) during past 12 mo
1-2 of the following:
Unhealthy lifestyle habits, including occasional (≤ 2 times per day) betweenmeal snacks of simple sugars, or drug or alcohol misuse
Inadequate oral hygiene or visible plaque
Wearing dental or orthodontic appliances
Susceptible pits and fissures
Exposed root surfaces
Saliva-reducing factors (medications, radiation, or systemic diseases)
High
caries risk
Any active caries lesion or radiolucency (cavitated or noncavitated) during the past 12 mo
High bacterial load by measurement or observation (heavy plaque)
3 or more of the following:
Unhealthy lifestyle habits, including frequent (≥ 3 times per day) between-meal snacks of simple sugars or drug or alcohol misuse
Inadequate oral hygiene
Wearing dental or orthodontic appliances
Susceptible pits and fissures
Exposed root surfaces
Saliva-reducing factors (medications, radiation, or systemic diseases)
Extreme
caries risk
High caries risk with hyposalivation by observation or measurement
High dependency on others for care
Recall interval 12 mo 6 mo 3 mo 3 mo Radiographs 24-36 mo 18-24 mo 6-18 mo
6 mo (until no new caries lesions)
aThis new tabular caries risk assessment form, adapted from the caries management by risk assessment form published in 2013 and revised in 2019, automatically incorporates the instructions and guidelines of those protocols.11,25 The checked item farthest to the right determines the overall caries risk level as well as the recommended recall and radiographic intervals. This form, completed after the comprehensive clinical examination, is meant to be fast and simple; clinicians should be able to complete it within 1 to 2 minutes. The user starts in the last column on the right and works to the left. Studies have validated that the instructions and guidelines used in this table lead to selection of the correct caries risk levels no matter who fills out the form. 25-27
An important note on evidence-based decision-making: Caries risk levels or perceived patient willingness to follow recommendations should not be used as a reason to intervene surgically with restoration if the lesion is not fully cavitated. A noncavitated lesion always has the potential for arrest and remineralization, regardless of current caries risk level. Every patient deserves the chance to change behaviors in the future, and some lesions will arrest on their own and may never progress to full cavitation. Stated another way: All currently noncavitated lesions are capable of arrest in the presence of the correct behavioral and environmental factors; in a worst-case scenario, a restorative intervention can be performed at a later time if full cavitation does eventually occur. In contrast, if a noncavitated lesion is prepared and restored immediately, the dental provider is creating the cavitation (via mechanical preparation), and the lesion never has the opportunity to remineralize. Furthermore, if the factors that caused the lesion are never addressed, that newly placed restoration remains at risk for secondary caries and an even larger replacement restoration down the line.
Table 1 presents a new CRA form adapted from the CAMBRA CRA form published in 2013 and later revised in
2019.11,25 The new form has been updated to automatically incorporate the instructions and guidelines and is completed after the comprehensive clinical examination so that all collected relevant disease data can accurately inform CRA. The checked item farthest to the right determines the overall caries risk level as well as the recommended recall and radiographic intervals. This form is meant to be fast and simple, and the clinician should be able to complete the assessment within 1 to 2 minutes. The user starts in the last column on the right and works to the left. There is no need to read or memorize instructions or guidelines, as they are built into the form. Studies have validated that the instructions and guidelines used in this table lead to the selection of correct/ same caries risk level no matter who completes the form.25-27
The selection of incorrect caries risk levels increases the possibility that the patient will not receive the most effective or correct treatment options. This tabular CRA can be modified to fit various clinical contexts.
Of course, the determination of caries risk level through CRA processes is not an endpoint; rather, it creates actionable patient-clinician collaboration that leads to disease
Table 1. Caries risk assessment form. a
Risk level Home care recommendations Recall interval, mo Radiographs, mo
Low Effective toothbrushing and interdental cleaning, oral hygiene instruction, individualized diet modification (eg, reduced frequency and exposure to sugary snacks), and, OTC fluoride toothpaste 12 24-36
Moderate All of the above plus:
• Xylitol chewing gum or mints throughout the day
• 0.05% sodium fluoride mouthrinse after meals, if possible
• Alternative therapy: 5000 ppm fluoride toothpaste twice daily (instead of OTC fluoride toothpaste) and no mouthrinse 6 18-24
High All the above plus:
• 5000 ppm fluoride toothpaste (instead of OTC toothpaste), morning and night
• Antibacterialb and pH neutralization strategies (eg, 0.2% hypochlorite rinse) before bedtime or topical office application of povidone iodine and fluoride varnish.
Extreme All the above plus:
• pH neutralization (neutralizing sprays, rinses, lozenges), xylitol gum, and/ or xylitol lollipops throughout the day
• Calcium and phosphate supplementation (eg, nano hydroxyapatite) throughout the day and right before bedtime
Abbreviations: AEGD, Advanced Education in General Dentistry; OTC, over-the-counter.
3 6 (until no new caries lesions)
aThis caries management strategy was adapted from the one used in the AEGD program at the University of the Pacific, San Francisco, California, and is based on the caries risk level (pathological risk factors vs protective factors) determined in the caries risk assessment. This caries management protocol is meant to be modified as needed to best fit the individual clinical context, and clinicians may use or recommend their products of choice.
b It is helpful to retest the bacteria about 1 month after initial antibacterial treatment to motivate behavioral change.
control (including disease risk mitigation). Table 2 presents an example caries risk management strategy used in the Advanced Education in General Dentistry program at the University of the Pacific, San Francisco, California. The protocol is based on the patient’s caries risk level (pathologic risk factors vs protective factors) determined in CRA. As in the case of the CRA form, the caries risk management protocol is meant to be modified as needed to best fit the individual clinical context.
ADA Caries Classification System
Caries risk management and therapeutic interventions, including effective communication and shared decisionmaking, lay the foundation for treating caries comprehensively as a disease at both the patient and tooth levels. From this global perspective, the focus is on etiology; therefore, caries risk is reduced, and protection and prevention of the disease are emphasized. To address specific, acute clinical manifestations of dental caries at the tooth level in tandem with the aforementioned approach, the ADA Council on Scientific Affairs published the ADA CCS.4 This system offers the clinician the capability to categorize all stages of caries lesions by the surfaces involved, site of origin, extent, and, when possible, activity level in a standardized, consistent manner over time.28 This emphasis on accurate detection and diagnosis of disease along its spectrum at the tooth level cannot be overstated because it has significant implications for treatment; noncavitated lesions are targeted chemically
for arrest and remineralization, while fully cavitated lesions may be considered for possible operative restoration.28
Contemporary person-centered caries management strategies integrate lesion classification to address the cause of the disease, the damage caused by the disease, and the most appropriate way to manage extant disease—this approach leverages both remineralization and minimally invasive operative strategies using selective caries removal.7
Table 3 presents the ADA CCS, in which the categories of sound, initial, moderate, and advanced lesions can be determined from careful visual and radiographic examination to provide information regarding the likelihood of the presence of infected dentin with full cavitation.4 The Box explains the components of the system. Establishing the degree of cavitation is crucial for accurate diagnosis and treatment planning, as full enamel cavitation is considered the threshold for operative intervention or the use of SDF with or without silver-modified atraumatic restorative treatment (SMART).28-34 For the majority of the clinical crown, cavitation is detectable via a careful visual examination; for less accessible areas, such as the approximal surfaces of the tooth, the ADA CCS integrates research correlating the likelihood of full clinical cavitation (infected dentin) to radiolucency.35-38
As the columns of the table progress from left to right, the severity characteristics of the individual lesions increase. Earlier stage noncavitated lesions can be addressed through chemical and medicinal therapies to arrest and remineralize active caries lesions. Later stage, cavitated lesions
Table 2. Example caries risk management strategy used at the University of the Pacific AEGD clinics. a
Table 3. American Dental Association Caries Classification System. a American Dental Association Caries Classification System Sound Initial Moderate Advanced
Clinical presentation No clinically detectable lesion.
Dental hard tissue appears normal in color, translucency, and gloss.
Other labels No surface change or adequately restored.
Earliest clinically detectable lesion compatible with mild demineralization. Lesion limited to enamel or to shallow demineralization of cementum/dentin. Mildest forms are detectable only after drying. When established and active, lesions may be white or brown and enamel has lost its normal gloss.
Visually noncavitated.
Visible signs of enamel breakdown or signs the dentin is moderately demineralized.
Enamel is fully cavitated and dentin is exposed. Dentin lesion is deeply and severely demineralized.
Established, early cavitated, shallow cavitation, microcavitation.
Spread/disseminated, late cavitated, deep cavitation. Infected dentin
Appearance of occlusal surfaces (pit and fissure)*†
Accessible smooth surfaces, including cervical and root‡
Radiographic presentation of the approximal surface§ E0¶ or R0# No radiolucency.
E1¶ or RA1# E2¶ or RA2# D1¶ or RA3# Radiolucency may extend to the dentinoenamel junction or outer one-third of the dentin. Note: radiographs are not reliable for mild occlusal lesions.
Abbreviation: ICDAS, International Caries Detection and Assessment System.
D2¶ or RB4# Radiolucency extends into the middle onethird of the dentin.
D3¶ or RC5# Radiolucency extends into the inner one-third of the dentin.
* Photographs of extracted teeth illustrate examples of pit and fissure caries.
†The ICDAS notation system links the clinical visual appearance of occlusal caries lesions with the histologically determined degree of dentinal penetration using the evidence collated and published by the ICDAS Foundation over the last decade; ICDAS also has a menu of options, including 3 levels of caries lesion classification; radiographic scoring; and an integrated, risk-based caries management system (ICCMS). Pitts NB, Ekstrand KR. International Caries Detection and Assessment System (ICDAS) and its International Caries Classification and Management System (ICCMS): methods for staging of the caries process and enabling dentists to manage caries. Community Dent Oral Epidemiol. 2013;41(1):e41-e52. Pitts NB, Ismail AI, Martignon S, Ekstrand K, Douglas GAV, Longbottom C. ICCMS Guide for Practitioners and Educators. December 2014. Accessed April 13, 2015. https://www.iccms-web.com/uploads/asset/59284654c0a6f822230100.pdf
‡ “Cervical and root” includes any smooth-surface lesion above or below the anatomical crown that is accessible through direct visual/tactile examination.
§Simulated radiographic images.
¶ E0-E2, D1-D3 notation system.4
# R0, RA1-RA3, RB4, and RC5-RC6 ICCMS radiographic scoring system (RC6 = into pulp). Pitts NB, Ismail AI, Martignon S, Ekstrand K, Douglas GAV, Longbottom C. ICCMS Guide for Practitioners and Educators. December 2014. Accessed April 13, 2015. https://www.iccms-web.com/uploads/ asset/59284654c0a6f822230100.pdf
Box. Understanding the ADA CCS.
The ADA (see Table 3) CCS is most easily understood by its key components—rows and columns. Columns: As demonstrated by the column headings, the ADA CCS uses the terms sound (no visible change), initial (first visible change), moderate (distinct change or microcavitation), and advanced (full cavitation with visible dentin).
Row 1: Clinical presentation. A sound surface has no clinically detectable lesion, appearing with normal translucency and gloss. An initial caries lesion is the earliest (first) detectable lesion, compatible with mild demineralization limited to enamel or shallow portions of the cementum/dentin. The earliest signs are not visible when wet and need to be air dried to be visible. Later signs of an initial lesion are more obvious. When active, the lesion may appear white or brown and may demonstrate loss of luster or normal gloss. A moderate caries lesion has visible signs of enamel breakdown or in later stages will have signs of moderate demineralization of the dentin (darkening or discoloration of the dentin). In an advanced caries lesion, the enamel is fully cavitated, exposing the dentin, which is deeply and severely demineralized.
Row 2: Other labels. A sound surface has no surface change or has an adequate restoration. An initial caries lesion appears visually nonactivated. A moderate caries lesion may be described as established, early cavitation, microcavitation, shallow cavitation, or partial cavitation. An advanced caries lesion may be described as spread/disseminated, late cavitation, or deep cavitation.
Row 3: Infected dentin. A sound surface has no possibility of infected dentin. An initial caries lesion is unlikely to have infected dentin. A moderate caries lesion may have infected dentin. An advanced caries lesion has infected dentin.
Row 4: Appearance of occlusal surface (pit and fissure). Based on published data, initial pit and fissure caries lesions (ICDAS 1 and 2) exhibit histologic dentin demineralization 9% to 50% of the time, and moderate pit and fissure caries lesions (ICDAS 3 and 4) demonstrate dentin demineralization histologically 50% to 88% of the time.39,40 Advanced pit and fissure caries lesions (ICDAS 5 and 6), because they are fully cavitated through enamel, would be expected to demonstrate histologic demineralization of the dentin 100% of the time. Even though expected histologic dentin penetration does not directly equate to enamel cavitation, the histologic data related to these probability ranges for dentin demineralization should be beneficial in any caries management system that includes treatment considerations (nonsurgical or surgical) based on the classification of the caries lesions.
Row 5: Accessible smooth surfaces, including cervical and root. Caries lesions on facial and lingual smooth surfaces, regardless of involvement of the cervical or root surfaces, are usually accessible for direct visual and tactile examination. This allows visual and tactile confirmation of surface changes and activity for easy classification of any caries lesion. To classify these lesions, the clinician simply describes an initial, moderate, or advanced caries lesion based on what is seen (eg, white or brown coloration, partial or microcavitation, or fully cavitated to dentin). When possible, an estimate of lesion activity is recorded as described in Table 4.
Row 6: Radiographic presentation of the approximal surface. Visual and tactile methods are also preferred on the approximal surfaces if possible. However, contact with an adjacent tooth often prevents direct access to the caries lesion. In that case, elastomeric tooth separation may be used to improve access for direct examination, and/or radiographs may be used to augment the examination. When sequential radiographs are available for an approximal caries lesion, row 6 may be used to determine the radiographic progression or regression and activity classification of the lesion over time.
Abbreviations: ADA CCS, American Dental Association Caries Classification System; ICDAS, International Caries Detection and Assessment System.
could likely benefit from either operative intervention to remove the bacterial niche and restore form, function, and cleansability to the tooth or the use of SDF with or without a SMART procedure. 29-34
Visual examination
The visual scale for clinical examination in the ADA CCS is informed by the International Caries Detection and Assessment System (ICDAS) and provides a reliable way to visually determine the relative extent of caries tooth destruction. The ICDAS was developed to facilitate epidemiologic caries research and appropriate clinical management.39 The ICDAS offers a helpful approach to clinical detection of caries, particularly of the occlusal surface, for which no metric was available to accurately classify occlusal caries lesions.40 This context contributed to cross-mapping of the ICDAS to the ADA CCS.4
Clinical significance of cavitation
The ADA CCS uses the likelihood of the presence of infected dentin as a metric to predict full cavitation through the
enamel. The term cavitation is best conceptualized as the irreversible loss of solid tooth structure at the macro level, resulting in a loss of surface integrity (ie, pitting or a hole) to some extent. For example, an advanced caries lesion can lead to a total loss of enamel at the surface (known as full cavitation), exposing the dentin to bacterial invasion (termed infected dentin).
However, it is important to note that many caries lesions present as only partial enamel loss at the surface, with some degree of enamel still remaining underneath (termed microcavitation, shallow cavitation, or partial cavitation).41 The remaining intact enamel in these moderate lesions prevents cariogenic bacteria from entering the dentin because the bacteria are physically too large to fit within the much smaller fluid-filled diffusion channels of enamel.42 An active caries lesion that is not fully cavitated through enamel can be treated chemically with fluorides that boost remineralization and create a more acid-resistant structure, or they can be treated with surface protection methods such as sealing with glass ionomer cement.43,44
Table 4. Characteristics of active and inactive caries lesions. a
Caries lesion activity assessment descriptors
Activity assessment factor
Location of the lesion
Plaque over the lesion
Likely to be inactive/ arrested
Lesion is not in a plaque stagnation area
Not thick or sticky
Surface appearance Shiny; color: brown-black
Tactile feeling Smooth, hard enamel/hard dentin
Gingival status (if the lesion is located near the gingiva)
No inflammation, no bleeding on probing
Likely to be active
Lesion is in a plaque stagnation area (pit/ fissure, approximal, gingival)
Radiographs do not provide absolute evidence of active caries lesions, much less clinical cavitation. Rather, the radiographic image simply demonstrates differences in mineral density. Thus, in addition to careful radiographic technique and interpretation, clinicians must rely on studies that correlate radiolucency depth to the likelihood of full clinical cavitation. On a related note, adoption of emerging technologies in this field, such as artificial intelligence, will require conscientious classification of lesion activity and full cavitation by clinicians to ensure that the most ethical treatment decisions are selected. In 1992, Pitts and Rimmer correlated approximal radiolucency depth to cavitation in posterior teeth, verifying their results through clinical elastomeric separation of the teeth and visual examination.35 Microcavitation and full cavitation were both classified as “cavitated.” Radiographic lesions limited to the enamel had, at most, a 10.5% likelihood of cavitation. If the radiolucency extended to the outer one-half of dentin, these percentages only increased to 40.9% in permanent teeth and 28.4% in primary teeth (thus both unlikely to be fully cavitated and need operative intervention).4 When the radiolucency extended to the inner one-half of the dentin, it was cavitated 100.0% of the time in permanent teeth and 95.5% in primary teeth.35 Since then, several studies have published similar results.36-38
The existing and compelling scientific evidence is therefore applied to the last row of the ADA CCS with slight modifications. Specifically, the ADA CCS nomenclature uses the categories E0, E1, E2, D1, D2, and D3 to define the depth of radiolucency on a radiograph. 4 The ADA CCS defines E0 as no radiolucency; E1 is a radiolucency in the outer half of the enamel; E2 is a radiolucency in the inner half of enamel. The dentin is divided into thirds, where D1 is a radiolucency in the outer third of the dentin (just inside the dentinoenamel junction); D2 is a radiolucency in the middle third of the dentin; and D3 is a radiolucency in the inner third of the dentin (nearest the pulp). Dividing the dentin into thirds instead of halves results in a finer gradation that allows specific attention to the D1 area, where full cavitation is less likely.
35-38,45
Caries lesion activity
Clinical application of any lesion classification relies on examinations conducted on a clean, dried tooth in a setting with adequate lighting. The ADA CCS scores visible changes in tooth structures; when there are visible changes of caries lesions over time, it is often possible to determine whether the lesion is active or arrested. Lesion activity, along with cavitation, is an important factor driving treatment options; an inactive or arrested caries lesion, especially if not fully cavitated, typically does not need further treatment. Table 4 summarizes work published by Ekstrand et al in 2009.46 It lists factors to consider when making a clinical determination of activity or inactivity in caries lesions. Beside pure visual examination, technique- and instrumentsensitive tactile approaches can add helpful data to clinical caries detection. A rounded (blunt or dull) explorer or a ball probe can be dragged over the surface in question to evaluate texture (rough vs smooth). An active lesion often presents with a rough surface, while a smooth hard surface typically identifies an inactive or arrested lesion. By contrast, forcing a sharp explorer into any site to detect a caries lesion can cause cavitation, inoculate the site with bacteria, and eliminate the chance to remineralize the previously intact surface; this approach should be avoided.47
Application of forceful inward pressure on the enamel with a sharp instrument is also contraindicated due to lack of diagnostic efficacy and potential damage to mineralizable enamel. Appropriately indicated radiographs should be available for the examination, especially to visualize any lesion progression or remineralization, which may be identified only by a lack of lesion progression.
There are nuances that make clinical detection of caries lesion activity in enamel distinct from that in dentin. Active, demineralized enamel lesions appear white and chalky due to a loss of translucency and feel rough when a dull probe is dragged across the surface. Demineralization appears and feels different in dentin, exhibiting a range of colors from yellow to brown and a soft, friable texture. Acids from the caries process that reach the dentin in lesions will increase when going from initial to moderate to advanced stages of the ADA CCS, but this does not mean the lesion cannot be arrested and remineralized to become even more acid resistant. Affected dentin is the term used to describe dentin
Chart. Decision tree
Tooth suitable for retention
• Caries lesion: noncleansable
• Pulp: vital (sensible) and not irreversibly inflamed
Primary tooth Permanent tooth
Lesion depth Lesion depth
Deep
Inner 1⁄3 or 1/4 dentin, risk of pulp exposure
• Selective removal to soft
Shallow/moderate
Not reaching inner 1⁄3 or 1/4 dentin, no risk of pulp exposure
that has previously undergone or is currently undergoing demineralization due to bacterial acids. Hardened, dark discolored affected dentin is arrested and acid resistant; it does not require surgical removal.48 As stated previously, infected dentin is found in advanced lesions where the enamel is fully cavitated, exposing the dentin to bacteria.
Restorative treatment
Traditionally, restorative treatment of caries lesions becomes necessary with fully cavitated lesions that are noncleansable and therefore likely to allow lesion progression. Currently, multiple applications of SDF can be considered as an option for cavitated lesions with or without a SMART procedure using glass ionomer restorative materials.29 This is the case for lesions categorized as advanced according to the ADA CCS.49 Active initial and moderate caries lesions confined to intact enamel surfaces can be managed therapeutically with sealants and/or chemical remineralization modalities such as topical fluoride and must be regularly monitored to ensure that prescribed chemical therapies are either slowing or halting lesion progression.
Successful caries management includes consideration of lesion activity, which guides clinical treatment decisions. Ultimately, options must be discussed between the clinician and the patient or caregiver, and the parties must mutually agree on the selected approach based on factors that best suit the patient’s abilities, preferences, and expectations.
Decision tree
The International Caries Consensus Collaboration created guidelines for the restoration of noncleansable caries lesions in retainable teeth with vital pulps. 50 The Chart presents a decision tree for restoration of primary and permanent teeth based on the depth of the caries lesion. Calling attention to the knowledge gaps in disease treatment strategies, the collaborative group urged researchers to report full details regarding lesion depth, activity, and extent; caries risk; and the treatment performed so as to inform future disease treatments. All clinical systems would benefit from more precise measurement of risk, lesions, treatment provided, and outcomes. 50
for noncleansable caries lesions in retainable teeth with vital pulps. a
Table 5. Example hard tissue preservation strategy based on the ADA CCS category using current tooth-preserving (tooth-level) and behavior management (patient-level) strategies.
Characteristics
Infected dentin (full cavitation)
Occlusal
presentation
Insidious caries
lesion; few lesions, slow progression
None
Rampant or aggressive caries lesion; multiple lesions, aggressive progression
Facial/lingual
Consider GIC sealant for primary prevention (no preparation)
Place GIC sealant (no preparation)
Place GIC sealant (no preparation)
Place GIC sealant (no preparation)
Place MID GIC restoration (selective caries removal)
Insidious caries lesion; few lesions, slow progression
Rampant or aggressive caries lesion; multiple lesions, aggressive progression
Approximal Clinical presentation
Difficult to assess insidious vs aggressive progression
Follow CRM protocol for primary prevention
Follow CRM protocol for primary prevention
Follow CRM protocol for primary prevention
Arrest with SDF; place GIC sealant (no preparation)
Arrest with SDF; place GIC sealant (no preparation)
Arrest and remineralize using riskbased CRM
Arrest and remineralize using CRM; consider GIC surface protection (no preparation) for deeper microcavitations and/ or SDF per patient wants
Consider SDF; place MID GIC restoration (selective caries removal)
Place MID GIC restoration (selective caries removal)
Arrest and remineralize using riskbased CRM; consider SDF
Arrest and remineralize using CRM; consider SDF
Arrest and remineralize using CRM; consider GIC surface protection (no preparation) and/or SDF
Consider SDF, orthodontic separation, surface protection with no preparation, and/or MID restoration with selective caries removal with or without SDF
Consider SDF; place GIC restoration (selective caries removal)
Place MID GIC restoration (selective caries removal) with or without SDF
CRM protocol: topical fluoride; pH neutralization; biofilm modification; saliva supplementation with calcium and phosphate based on caries risk; and behavioral modification (healthy diet and lifestyle choices and good oral hygiene).
Abbreviations: ADA CCS, American Dental Association Caries Classification System; CRM, caries risk management; GIC, glass ionomer cement; ICDAS, International Caries Detection and Assessment System; MID, minimally invasive dentistry; SDF, silver diamine fluoride.
Once treatment of dental caries at the patient level has begun, it is prudent to discuss tooth-level treatment. Table 5 presents a hard tissue preservation strategy for each ADA CCS category, incorporating current tooth-preserving (tooth-level) and behavior management (patient-level) approaches. Minimally invasive, tooth-preserving restorative procedures are limited to advanced caries lesions and involve selective caries removal.7-9 An example of selective caries removal is elimination of carious tissue confined to the outer perimeter of a fully cavitated (advanced) caries lesion, not to exceed about 1 mm past the dentinoenamel junction or 1 mm when there is no enamel (ie, root surfaces). The deeper areas of the axial and pulpal walls are left unexcavated to preserve vital pulp tissue. Selective caries removal was featured prominently in an ADA evidencebased clinical practice guideline on restorative treatments for caries lesions.7-9
For patients with high or extreme caries risk, the use of chemical treatments or surface protection is recommended for nonsurgical treatment of active initial or moderate caries lesions. Both glass ionomer restoratives and sealants, as well as silver diamine fluoride, are leveraged as additional chemical treatments (remineralization and caries prevention) at the tooth level.7,9,29,51 Additionally, the use of surface protection (a thin coat of glass ionomer cement placed with no preparation) or glass ionomer sealants is useful for microcavitations of the enamel surface. Elastomeric separation is also an exceptional tool to consider when a moderate approximal caries lesion is suspected of being cavitated, but the extent and activity are not known. Once the tooth is separated from the adjacent teeth, microcavitation can easily be accessed directly, and surface protection with a glass ionomer restorative material can be applied with no tooth preparation.45,52,53
Conclusion
Comprehensive caries management involves evidence-based control of dental caries at both the patient and tooth levels, with a management plan tailored to each individual and designed collaboratively by the clinician and patient. The primary goals of oral healthcare are to arrest current disease, prevent future disease, and provide optimally lasting, minimally invasive, and tooth-preserving restoration of irreversibly lost tooth structure. This process begins with and is framed by CRA that not only identifies the risk of developing future caries lesions but more importantly identifies the pathologic and etiologic factors affecting the patient—that is, the underlying cause of the disease. Subsequent management should address the disease factors through strategies known to modify negative health behaviors and implement protective factors.
The ADA CCS is used to inform management of dental caries at the tooth level. By defining and identifying graded, clinically significant changes to caries lesions, the ADA CCS terminology allows the clinician to discern between treatment of noncavitated lesions with tooth-preserving therapeutic modalities and treatment of advanced lesions with toothpreserving restorative best practices. For each nuanced stage of disease listed in the ADA CCS, a clinical strategy can be developed that includes patient-level care using behavioral change
and chemical therapeutics and tooth-level care using glass ionomer and silver diamine fluoride based on lesion progression and likelihood of cavitation. Leveraging CRA with lesion classification will lead to more personalized, prevention-focused, and comprehensive caries management to meet patients where they are. Outcome-based, person-centered care utilizing CRA and the ADA CCS can improve patients’ oral health by treating and preventing the cause of dental caries at the patient level as well as judiciously managing caries lesions at the tooth level.
Author affiliations
Department of Diagnostic Sciences, University of the Pacific, San Francisco, California (Young [Emeritus]); Department of Restorative Dentistry & Prosthodontics, The University of Texas School of Dentistry at Houston (Quock); Department of Restorative Dentistry, Oregon Health and Science University School of Dentistry, Portland (Goolsby); Department of Periodontics and Oral Medicine, Division of Dental Hygiene, University of Michigan, School of Dentistry, Ann Arbor (McComas); Division of General Dentistry, Loma Linda University, School of Dentistry, California (Powell); College of Dentistry, University of Kentucky, Lexington (Zeller [Emeritus]); Department of Diagnostic Sciences, University of the Pacific, San Francisco, California (Wong [Emeritus]); Department of General Practice, Virginia Commonwealth University, School of Dentistry, Richmond (Nový); Department of Oral Health Policy and Epidemiology, Harvard School of Dental Medicine, Boston, Massachusetts (Nový).
Correspondence
Douglas Young, DDS, EdD, MBA, MS (dyoung@pacific.edu).
Conflicts of interest
None reported.
Acknowledgments
The authors express their gratitude to Drs. Zahra Manan, Adel Rizkalla, and Daniel Jurgens for their contributions in reviewing, revising, technical editing, and proofreading.
References
1. Machiulskiene V, Campus G, Carvalho JC, et al. Terminology of Dental Caries and Dental Caries Management: Consensus Report of a Workshop Organized by ORCA and Cariology Research Group of IADR. Caries Res. 2020;54(1):7-14. doi:10.1159/000503309
2. Frencken JE, Innes NP, Schwendicke F. Managing carious lesions: why do we need consensus on terminology and clinical recommendations on carious tissue removal? Adv Dent Res. 2016;28(2):46-48. doi:10.1177/0022034516639272
3. Innes NP, Frencken JE, Bjørndal L, et al. Managing carious lesions: consensus recommendations on terminology. Adv Dent Res. 2016;28(2):49-57. doi:10.1177/0022034516639276
4. Young DA, Nový BB, Zeller GG, et al. The American Dental Association Caries Classification System for clinical practice: a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2015;146(2):79-86. doi:10.1016/j.adaj.2014.11.018
5. Ricketts D, Innes N, Schwendicke F. Selective removal of carious tissue. Monogr Oral Sci. 2018;27:82-91. doi:10.1159/000487838
6. Thompson V, Craig RG, Curro FA, Green WS, Ship JA. Treatment of deep carious lesions by complete excavation or partial removal: a critical review. J Am Dent Assoc. 2008;139(6):705712. doi:10.14219/jada.archive.2008.0252
7. Dhar V, Pilcher L, Fontana M, et al. Evidence-based clinical practice guideline on restorative treatments for caries lesions: a report from the American Dental Association. J Am Dent Assoc. 2023;154(7):551-566.e551. doi:10.1016/j.adaj.2023.04.011
8. Pilcher L, Pahlke S, Urquhart O, O’Brien KK, Carrasco-Labra A. Plain language summary for “Direct materials for restoring caries lesions: systematic review and meta-analysis—a report
of the American Dental Association Council on Scientific Affairs.” J Am Dent Assoc. 2023;154(2):171-173. doi:10.1016/j.adaj.2022.10.007
9. Pilcher L, Pahlke S, Urquhart O, et al. Direct materials for restoring caries lesions: systematic review and meta-analysis—a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2023;154(2):e1-e98. doi:10.1016/j.adaj.2022.09.012
10. Warreth A. Dental caries and its management. Int J Dent. 2023;2023:9365845. doi:10.1155/2023/9365845
11. Young DA, Featherstone JD. Caries management by risk assessment. Community Dent Oral Epidemiol. 2013;41(1):e1-e12. doi:10.1111/cdoe.12031
12. Fontana M, Gonzalez-Cabezas C, Tenuta LMA. Evidence-based approaches and considerations for nonrestorative treatments within modern caries management: integrating science into practice. J Am Dent Assoc. 2024;155(12):1000-1011. doi:10.1016/j. adaj.2024.09.007
13. Allen M. The value of values: shared decision-making in person-centered, value-based oral health care. J Public Health Dent. 2020;80(Suppl 2):S86-S88. doi:10.1111/jphd.12394
14. Elwyn G, Dehlendorf C, Epstein RM, Marrin K, White J, Frosch DL. Shared decision making and motivational interviewing: achieving patient-centered care across the spectrum of health care problems. Ann Fam Med. 2014;12(3):270-275. doi:10.1370/afm.1615
15. Sturgess J, Clapp JT, Fleisher LA. Shared decision-making in peri-operative medicine: a narrative review. Anaesthesia. 2019;74(Suppl 1):13-19. doi:10.1111/anae.14504
16. Fontana M, Young DA, Wolff MS. Evidence-based caries, risk assessment, and treatment. Dent Clin North Am. 2009;53(1):149-161. doi:10.1016/j.cden.2008.10.003
17. Featherstone JD. The caries balance: the basis for caries management by risk assessment. Oral Health Prev Dent. 2004;2(Suppl 1):259-264.
18. Featherstone JD. Caries prevention and reversal based on the caries balance. Pediatr Dent. 2006;28(2):128198.
19. Fontana M, Zero DT. Assessing patients’ caries risk. J Am Dent Assoc. 2006;137(9):12311239. doi:10.14219/jada.archive.2006.0380
20. Twetman S, Fontana M, Featherstone J. Risk assessment—can we achieve consensus? Community Dent Oral Epidemiol. 2013;41(1):e64-e70. doi:10.1111/cdoe.12026
21. Zero D, Fontana M, Lennon AM. Clinical applications and outcomes of using indicators of risk in caries management. J Dent Educ. 2001;65(10):1126-1132. doi:10.1002/j.0022-0337. 2001.65.10.tb03461.x
22. Riley JL 3rd, Gordan VV, Ajmo CT, et al. Dentists’ use of caries risk assessment and individualized caries prevention for their adult patients: findings from The Dental Practice-Based Research Network. Community Dent Oral Epidemiol. 2011;39(6):564-573. doi:10.1111/ j.1600-0528.2011.00626.x
24. Mejàre I, Axelsson S, Dahlén G, et al. Caries risk assessment: a systematic review. Acta Odontol Scand. 2014;72(2):81-91. doi:10.3109/00016357.2013.822548
25. Young DA, Goolsby SP, Rechmann P. Caries management by risk assessment—guidelines to improve caries risk level assignments. J Calif Dent Assoc. 2019;47(1):49-55. doi:10.1080/19 424396.2019.12220745
26. Goolsby SP, Young DA, Chiang HK, Carrico CK, Jackson LV, Rechmann P. The effects of faculty calibration on caries risk assessment and quality assurance. J Dent Educ. 2016;80(11):12941300. doi:10.1002/j.0022-0337.2016.80.11.tb06214.x
27. Young DA, Alvear Fa B, Rogers N, Rechmann P. The effect of calibration on caries risk assessment performance by students and clinical faculty. J Dent Educ. 2017;81(6):667-674. doi:10.21815/JDE.017.013
28. Zeller GG, Young DA, Novy BB. The American Dental Association Caries Classification System (ADA CCS). In: Ferreira Zandona A, Longbottom C, eds. Detection and Assessment of Dental Caries: A Clinical Guide. Springer; 2019:57-67.
29. Slayton RL, Urquhart O, Araujo MWB, et al. Evidence-based clinical practice guideline on nonrestorative treatments for carious lesions: a report from the American Dental Association. J Am Dent Assoc. 2018;149(10):837-849.e819. doi:10.1016/j.adaj.2018.07.002
30. Young DA, Quock RL, Horst J, et al. Clinical instructions for using silver diamine fluoride (SDF) in dental caries management. Compend Contin Educ Dent. 2021;42(6):e5-e9.
31. Duffin SR, Juhl J, Schwab J, Duffin ML, eds. SMART Oral Health: The Medical Management of Caries. Oral Health Outreach; 2019.
32. Ballikaya E, Ünverdi GE, Cehreli ZC. Management of initial carious lesions of hypomineralized molars (MIH) with silver diamine fluoride or silver-modified atraumatic restorative treatment (SMART): 1-year results of a prospective, randomized clinical trial. Clin Oral Investig. 2022;26(2):2197-2205. doi:10.1007/s00784-021-04236-5
33. Erbas Ünverdi G, Ballikaya E, Cehreli ZC. Clinical comparison of silver diamine fluoride (SDF) or silver-modified atraumatic restorative technique (SMART) on hypomineralised permanent molars with initial carious lesions: 3-year results of a prospective, randomised trial. J Dent. 2024;147:105098. doi:10.1016/j.jdent.2024.105098
34. Hegde D, Suprabha BS, Rao A. Silver modified atraumatic restorative treatment: a paradigm shift in dental caries management. Prim Dent J. 2024;13(2):29-35. doi:10.1177/20501684241249545
35. Pitts NB, Rimmer PA. An in vivo comparison of radiographic and directly assessed clinical caries status of posterior approximal surfaces in primary and permanent teeth. Caries Res. 1992;26(2):146-152. doi:10.1159/000261500
36. Akpata ES, Farid MR, al-Saif K, Roberts EA. Cavitation at radiolucent areas on proximal surfaces of posterior teeth. Caries Res. 1996;30(5):313-316. doi:10.1159/000262336
37. da Silva Neto JM, dos Santos RL, Sampaio MC, Sampaio FC, Passos IA. Radiographic diagnosis of incipient proximal caries: an ex-vivo study. Braz Dent J. 2008;19(2):97-102. doi:10.1590/s0103-64402008000200002
38. Muñoz-Sandoval C, Gambetta-Tessini K, Botelho JN, Giacaman RA. Detection of cavitated proximal carious lesions in permanent teeth: a visual and radiographic assessment. Caries Res. 2022;56(3):171-178. doi:10.1159/000525193
39. Pitts N. “ICDAS”—an international system for caries detection and assessment being developed to facilitate caries epidemiology, research and appropriate clinical management. Community Dent Health. 2004;21(3):193-198.
40. Ismail AI, Sohn W, Tellez M, et al. The International Caries Detection and Assessment System (ICDAS): an integrated system for measuring dental caries. Community Dent Oral Epidemiol. 2007;35(3):170-178. doi:10.1111/j.1600-0528.2007.00347.x
41. Longbottom CL, Huysmans MC, Pitts NB, Fontana M. Glossary of key terms. Monogr Oral Sci. 2009;21:209-216. doi:10.1159/000224225
42. González-Cabezas C. The chemistry of caries: remineralization and demineralization events with direct clinical relevance. Dent Clin North Am. 2010;54(3):469-478. doi:10.1016/j. cden.2010.03.004
43. Featherstone JD. The science and practice of caries prevention. J Am Dent Assoc. 2000;131(7):887-899. doi:10.14219/jada.archive.2000.0307
44. Ngo HC, Mount G, Mc Intyre J, Tuisuva J, Von Doussa RJ. Chemical exchange between glassionomer restorations and residual carious dentine in permanent molars: an in vivo study. J Dent. 2006;34(8):608-613. doi:10.1016/j.jdent.2005.12.012
45. Anusavice KJ. Present and future approaches for the control of caries. J Dent Educ. 2005;69(5):538-554. doi:10.1002/j.0022-0337.2005.69.5.tb03941.x
47. Stookey G. Should a dental explorer be used to probe suspected carious lesions? No—use of an explorer can lead to misdiagnosis and disrupt remineralization. J Am Dent Assoc. 2005;136(11):1527-1531. doi:10.14219/jada.archive.2005.0082
48. Kidd EA, Ricketts DN, Beighton D. Criteria for caries removal at the enamel-dentine junction: a clinical and microbiological study. Br Dent J. 1996;180(8):287-291. doi:10.1038/ sj.bdj.4809066
49. Kidd EA. Clinical threshold for carious tissue removal. Dent Clin North Am. 2010;54(3):541549. doi:10.1016/j.cden.2010.03.001
50. Schwendicke F, Frencken JE, Bjørndal L, et al. Managing carious lesions: consensus recommendations on carious tissue removal. Adv Dent Res. 2016;28(2):58-67. doi:10.1177/0022034516639271
51. Urquhart O, Tampi MP, Pilcher L, et al. Nonrestorative treatments for caries: systematic review and network meta-analysis. J Dent Res. 2019;98(1):14-26. doi:10.1177/0022034518800014
52. Mount GJ, Ngo H. Minimal intervention: early lesions. Quintessence Int. 2000;31(8):535-546.
53. Ngo H, Ruben J, Arends J, et al. Electron probe microanalysis and transverse microradiography studies of artificial lesions in enamel and dentin: a comparative study. Adv Dent Res. 1997;11(4):426-432. doi:10.1177/08959374970110040801
Color stability of composite resins with different photoinitiator systems when subjected to water aging: an in vitro study
Garima Poddar, BDS ¢ Suparna G. Saha, BDS, MDS ¢ Rolly S. Agarwal, BDS, MDS ¢ Manasi Kewlani, BDS, MDS
Anu Vashisht, BDS, MDS ¢ Ajay S. Rao, BDS, MDS
The objective of this study was to evaluate the color stability of composite resins with different photoinitiator systems when subjected to water aging for 28 days. A total of 48 disc-shaped specimens (1.5 mm in diameter × 2.0 mm thick) of 3 commercially available composite resins (n = 16 per group) were fabricated in custom acrylic molds. Each of the composite resins is formulated with a distinct photoinitiator system: diphenyl (2,4,6-trimethylbenzoyl) phosphineoxide (TPO), bis(4-methoxybenzoyl) diethylgermanium (Ivocerin), or camphorquinone (CQ). The specimens were polymerized with an LED curing unit and stored in a dark room for 24 hours. Baseline color measurements based on International Commission on Illumination (CIE) L*a*b* parameters were recorded with a spectrophotometer. To evaluate the effects of water aging, specimens were immersed in a thermostatic water bath at 37°C for 28 days; water was replaced every 7 days. Following immersion, specimens were remeasured spectrophotometrically to assess color change. Color differences between baseline values and values obtained after the aging procedures were calculated for each specimen and statistically analyzed using analysis of variance and post hoc Tukey tests. After 28 days of water aging, all specimens exhibited statistically significant (P < 0.001) overall color changes (ΔE*), underscoring a pronounced decline in color stability. A statistically significant difference (P < 0.001) in ΔE* was observed between the TPO and Ivocerin groups, with TPO presenting maximum preservation of color stability. No statistically significant difference (P > 0.05) was found between the TPO and CQ groups or the Ivocerin and CQ groups, suggesting somewhat comparable color stability in these groups. Despite color alterations across all materials, the TPO-based composite resin exhibited superior color stability when compared with the Ivocerin- and CQ-based resins in the study, suggesting that TPO may offer enhanced long-term esthetic durability in clinical applications.
The pursuit of esthetically pleasing and durable dental restorations has propelled remarkable innovations in restorative dentistry, where the hallmark of a truly successful restoration transcends mere surface esthetics. While achieving initial shade harmony is crucial, the longterm clinical outcome hinges on the restoration’s intrinsic durability—its ability to withstand color degradation amid the constant interplay of oral fluids, dietary pigments, and masticatory forces.1
Color stability in composite resins is directly linked to the material’s chemical composition, which encompasses factors such as filler content, activation mode, adsorption media, and the aging process.2 Over time, exposure to environmental factors such as oral fluids, dietary pigments, and masticatory forces can further exacerbate color changes, influencing both the esthetic and functional longevity of the restoration.1,2 Understanding these dynamic interactions is essential for improving the performance and durability of composite resins in clinical practice.
The propensity of composite resin to absorb water initiates a cascade of challenges, including chemical and mechanical degradation leading to polymer swelling; compromised bonding interfaces leading to microleakage and secondary caries; fracture propagation; and ultimately, clinically significant discoloration impacting esthetics.1 Central to this process lies the material’s photoinitiator, which is the catalyst directing the photopolymerization process. The photoinitiator is pivotal in determining the degree of cross-linking, which, in turn, influences the final properties of the composite resin.1
Camphorquinone (CQ), an α-diketone photoinitiator system, has long reigned as the gold standard for visible light photoinitiation in dental composite resins, owing to its efficient light absorption within the visible spectrum (approximately 468 nm).3 However, the inherent yellow hue of CQ poses challenges in achieving esthetically pleasing tooth-colored restorations.4 This inherent yellowness, which contributes to color instability, has spurred extensive research into alternative photoinitiators with the goals of enhancing polymerization kinetics, improving mechanical properties, and attaining superior color stability, paving the way for highly esthetic and durable dental restorations.
Diphenyl (2,4,6-trimethylbenzoyl) phosphineoxide (TPO), an acylphosphine oxide–based photoinitiator, is characterized by a distinct spectral profile, with peak absorption at 400 nm. This unique absorption spectrum closely mimics the optical properties of natural teeth, offering a promising solution to
enhance both the esthetic appeal and functional integrity of tooth-colored restorations.5
Bis(4-methoxybenzoyl)diethylgermanium (Ivocerin, Ivoclar Vivadent), a patented photoinitiator with a peak absorbance at 418 nm, not only demonstrates enhanced light absorption but also boasts a strong safety profile, exhibiting low cytotoxicity and absence of mutagenic effects.5 These characteristics position Ivocerin as an excellent candidate for improving both the esthetics and biocompatibility of dental restorations, offering a compelling alternative in the development of safe and highquality dental materials.
Costa et al highlighted that the color stability of dental materials can be evaluated by immersing them in aging solutions that simulate oral conditions and then performing colorimetric analysis with spectrophotometers.6 The International Commission on Illumination (CIE) CIE L*a*b* method, which accounts for changes in lightness (L*), the green-red axis (a*), and the blueyellow axis (b*), provides a quantitative assessment of total color differences.7 These differences are further contextualized by defined thresholds for perceptibility and acceptability, enabling clinicians to identify clinically significant color alterations.8 Despite growing interest in advanced photoinitiators, there remains a lack of substantial comparative data on the color stability of composite resins incorporating TPO, CQ, and Ivocerin before and after water aging to simulate oral conditions. To address this critical gap, the present in vitro study was undertaken to provide valuable insights into the comparative performance of these photoinitiators, emphasizing their ability to preserve the esthetic qualities of dental composites over time.
Methods
The study was conducted after approval by the Ethics Committee of the Index Institute of Dental Sciences, Indore, India (reference No. IIDS/IEC/2024/195(C)/CONS/02).
Specimen preparation
Three commercially available composite resins were selected based on the presence of different photoinitiators: Tetric EvoCeram (Ivoclar Vivadent), which uses TPO as a photoinitiator; Tetric N-Ceram Bulk Fill (Ivoclar Vivadent), which uses Ivocerin as a photoinitiator; and Filtek Supreme Ultra (3M), which uses CQ as a photoinitiator. A total of 48 discshaped specimens (1.5 mm in diameter × 2.0 mm thick) were fabricated from each composite resin (n = 16 per group), with the groups designated according to the photoinitiator: TPO, Ivocerin, or CQ.
The composite resin was placed in a custom acrylic mold positioned on a microscopic glass slide, which was supported by a glass slab. The material was adapted to the mold, covered with a polyester film strip, and gently pressed with another glass slide to remove excess material. The top surface of each material was then light cured with an LED curing unit (Bluephase N MC, Ivoclar Vivadent) at a power density of 1200 mW/cm² for 40 seconds. Following polymerization, the specimens were polished with a composite resin polishing system (PN0310B, Shofu) and subsequently stored at room temperature (37 ± 1°C) under dry conditions in darkness for 24 hours to continue postcure polymerization.
Color measurement
The color measurements of all specimens were recorded at baseline (after 24 hours of postcure storage) with a spectrophotometer (VITA Easyshade Advance, VITA Zahnfabrik). Measurements were recorded in the CIE L*a*b* color coordinate system. The measurement tip of the spectrophotometer was positioned perpendicular to the specimen in direct contact with the surface. A positioning device was used to ensure consistency in the measuring points on the different specimens.
The specimens subsequently underwent an aging process consisting of immersion in a digitally controlled thermostatic sterile water bath at 37°C for 28 days; the water was changed every 7 days. After aging, the specimens were cleaned in an ultrasonic bath for 3 minutes and dried with oil-free air, and the spectrophotometric measurements were repeated to evaluate any color changes that were present after aging.
The variation in color was established based on the coordinates L* (lightness, 0-100), a* (negative = green; positive = red) and b* (negative = blue; positive = yellow) of the CIE L*a*b* scale.7 The overall color change (ΔE*) of each specimen was calculated with the following formula:
∆E* = [(L* 1 − L*2)2 + (a* 1 − a*2)2 + (b* 1 − b*2)2 ]1/2, where L* 1, a*1, and b* 1 are the baseline values and L* 2, a*2, and b* 2 are the values after 28 days of water aging. The ΔE* value is the color change in the specimens that an observer can detect after water aging. This value is a more accurate representation of true color difference than the separate L*, a*, and b* values.
Statistical analysis
The data were entered into a spreadsheet and analyzed with SPSS software (version 21.0, IBM). The Kolmogorov-Smirnov test revealed that the data were normally distributed, so a parametric test of significance was applied. Intergroup comparisons of continuous variables were performed using 1-way analysis of variance (ANOVA) and post hoc Tukey test. A value of P < 0.05 was considered statistically significant.
Results
The mean (SD) difference in ΔL* was lowest in the Ivocerin group, at −10.03 (1.85), reflecting a significant shift toward a darker shade, while CQ exhibited the highest ΔL*, 8.81 (1.92), corresponding to the lightest shade among the 3 photoinitiators (Table 1). In the red-green axis, TPO exhibited a substantial shift toward a green hue, with a mean (SD) Δa* value of −1.93 (0.62), compared with the minimal change of −0.25 (0.54) observed in CQ. In the yellow-blue axis, Ivocerin demonstrated the most substantial shift toward blue, with a mean (SD) Δb* value of −5.75 (1.47), while CQ showed the least change in this axis, at −1.45 (1.45). These findings suggest the distinct photochemical behaviors of the photoinitiators, with Ivocerin driving a significant shift toward darker, bluer hues while TPO elicited a notable greenward trend after water aging.
After 28 days of water aging, all groups exhibited statistically significant (P = 0.001; 1-way ANOVA) overall color changes (ΔE*) from their baseline measurements. The TPO group showed the greatest color stability, followed by the CQ and Ivocerin groups. The analysis revealed a high F value (4.37) and
Table 1. Mean (SD) differences in color parameters of 3 composite resins with different photoinitiators after water aging (n = 16 per group).
Difference between baseline parameters and parameters after immersion in a thermostatic water bath at 37°C for 28 days (water replaced every 7 days).
relatively low P value (0.001) as well as a between-group sum of squares (163.60) that was substantially greater than the withingroup sum of squares (102.14). These findings suggest that the observed variations in color stability across the materials can be attributed to fundamental differences in material composition and the interaction of photoinitiators with water aging, rather than random variability.
Post hoc analysis with the Tukey test revealed a statistically significant difference (P = 0.001) in the ΔE* values of the TPO and Ivocerin groups (Table 2). No statistically significant differences were observed between TPO and CQ (P = 0.071) or Ivocerin and CQ (P = 0.137), suggesting comparable color stability among these groups after water aging.
Discussion
Composite resins have become indispensable in contemporary esthetic restorative dentistry due to their superior mechanical properties and ability to mimic the natural appearance of dental tissues. However, a significant limitation remains, which is their susceptibility to discoloration over time, primarily attributed to the frequent exposure to staining agents from food and beverages.1
Color stability, defined as the ability of a material to retain its original shade with minimal deviation under clinical conditions, is crucial for the longevity of esthetic restorations.9 Among the various factors contributing to color degradation, water aging is particularly influential, as it replicates hydrolytic degradation within the polymer matrix.10 Prolonged exposure to water induces swelling, expansion, and microcrack formation, which in turn facilitates increased pigment absorption and structural breakdown, leading to discoloration. The intrinsic composition of the resin matrix and the type of photoinitiator employed significantly influence the color stability of composite resins. The most widely used visible light photoinitiator in biomedical applications, CQ, has welldocumented limitations owing to its inherent yellow tint. This characteristic often poses challenges in achieving restorations with optimal esthetic outcomes.11
To overcome this drawback, alternative photoinitiators such as TPO and Ivocerin have been introduced to composite
formulations. The present spectrophotometric analysis confirmed statistically significant color changes in all experimental groups after water aging, with the material containing TPO exhibiting the least color alteration, followed by the material with CQ; the resin formulated with Ivocerin demonstrated the highest degree of discoloration. The difference in ΔE* values between TPO and Ivocerin was statistically significant (P < 0.05). The differences between the TPO and CQ groups and the Ivocerin and CQ groups were not statistically significant (P > 0.05), indicating comparable color shift values in these groups.
TPO, an acylphosphine oxide–based photoinitiator that is incorporated in Tetric Ceram, exhibits remarkable photobleaching properties. Unlike CQ, TPO eliminates the need for coinitiators, thus avoiding the presence of amine groups, which are known contributors to color instability over time. Miletic et al demonstrated that TPO, even at a low concentration of 0.22 wt%, achieves a polymerization efficiency of 68%.12 This rate is comparable to the 74% efficiency obtained with CQ at 0.86 wt%, indicating that TPO exhibits faster polymerization kinetics and a higher degree of conversion than CQ.12 Reinforcing these observations, Van der Laan et al found that TPO-based materials not only exhibit superior color retention but also possess optical properties that closely mimic those of natural dentition, making them a highly promising alternative in esthetic restorative formulations.13
In the present study, the CQ-based composite resin exhibited poorer color stability than TPO, which can be attributed to CQ’s intrinsic yellowish hue and its suboptimal bleaching on irradiation.1,3 While CQ undergoes some degree of color bleaching on polymerization, research suggests that its chromophore groups persist, postexposure, to blue light, leading to residual yellowish discoloration over time.3
The oxidation of amine coinitiators, which are often required to enhance CQ’s polymerization efficiency, further exacerbates color instability. This oxidative degradation contributes to persistent yellow staining, which may compromise the esthetic outcome of restorations in the long run. Despite its widespread use, CQ has a color change susceptibility that underscores the need for alternative photoinitiators, particularly in areas of esthetic concern such as the anterior dentition, where shade fidelity is paramount.
Among the 3 photoinitiators analyzed, Ivocerin specimens demonstrated the highest degree of color change after water
Table 2. Post hoc analysis of color difference values among 3 composite resins with different photoinitiators (n = 16 per group).
aging. This finding can be attributed due to the strong absorption and higher reactivity of the germanium compound, which generate a greater amount of residual radicals and secondary reactions on light activation. The unreacted photoinitiator components can further interact with resin matrix, increasing the water sorption and subsequent hydrolytic degradation and thereby contributing to color instability over time.14
These observations align with findings from studies emphasizing the crucial role of photoinitiator chemistry in color stability.15 The inherent properties of a photoinitiator—its reactivity, radical generation capacity, interaction with resin matrix, and susceptibility to hydrolytic processes—play a decisive role in determining the long-term esthetic stability of composite resins.15-17
Since water sorption can compromise the mechanical integrity, biocompatibility, and esthetic stability of composite resins, incorporation of alternative photoinitiators such as TPO can offer an optimal balance of reactivity and controlled radical generation, facilitating efficient polymerization while minimizing the formation of colored degradation products, resulting in a more stable polymer network, reduced water ingress, and enhanced long-term color retention. In contrast, composite resins formulated with Ivocerin demonstrate heightened reactivity, producing more radicals, which in turn can accelerate hydrolytic degradation and enhance water uptake, ultimately resulting in more pronounced color changes.
Conclusion
Within the limitations of this in vitro study, it may be concluded that water aging significantly impacts the color stability of composite resins, irrespective of the photoinitiator. Crucially, among the groups present in the study, the composite resin utilizing TPO demonstrated better color stability than its counterparts formulated with Ivocerin and CQ. The results suggest that although all of the tested materials are vulnerable to color shifts in aqueous environments over time, TPO-based composites may offer an advantage for maintaining long-term esthetic integrity.
Author affiliations
Department of Conservative Dentistry and Endodontics, Index Institute of Dental Sciences, Indore, India.
Correspondence
Garima Poddar, BDS (garimapoddar29@gmail.com).
Conflicts of interest
None reported.
References
1. Mazzitelli C, Paolone G, Sabbagh J, Scotti N, Vichi A. Color stability of resin cements after water aging. Polymers. 2023;15(3):655. doi:10.3390/polym15030655
2. Rai AV, Naik BD. The effect of saliva substitute on the color stability of three different nanocomposite restorative materials after 1 month: an in vitro study. J Conserv Dent 2021;24(1):50-56. doi:10.4103/JCD.JCD_444_20
3. Bertolo MV, Moraes RC, Pfeifer C, Salgado VE, Correr AR, Schneider LF. Influence of photoinitiator system on physical-chemical properties of experimental self-adhesive composites Braz Dent J. 2017;28(1):35-39. doi:10.1590/0103-6440201700841
4. Kowalska A, Sokolowski J, Bociong K. The photo-initiators used in resin based dental composite—a review and future perspectives. Polymers. 2021;13(3):470. doi:10.3390/ polym13030470
5. Topa-Skwarczyńska M, Jankowska M, Gruchała-Hałat A, Petko F, Galek M, Ortyl J. Highperformance photoinitiating systems for new generation dental fillings. Dent Mater 2023;39(8):729-742. doi:10.1016/j.dental.2023.06.003
6. Costa MP, Jacomine JC, Mosquim V, et al. Analysis of color stability and degree of conversion of different types of resin composites. Braz Oral Res. 2024;38:e003. doi:10.1590/18073107bor-2024.vol38.0003
7. Colorimetry. 4th ed. CIE 015:2018. International Commission on Illumination; 2018. doi:10.25039/TR.015.2018
8. Fathima JN, Hashir MM, Padmanabhan K. Spectrophotometric evaluation of color stability of composite resin after exposure to cold drinks: an in vitro study. J Conserv Dent Endod 2024;27(2):195-199. doi:10.4103/JCDE.JCDE_230_23
9. Prieto LT, Pimenta de Araújo CT, Araujo Pierote JJ, Salles de Oliveira DC, Coppini EK, Sartini Paulillo LAM. Evaluation of degree of conversion and the effect of thermal aging on the color stability of resin cements and flowable composite. J Conserv Dent. 2018;21(1): 47-51. doi:10.4103/JCD.JCD_128_17
10. Kolpakova A. Comparison of Monowave and Polywave Transmission and Curing Profile thru Various Composites. Honors thesis. Portland State University; 2015. doi:10.15760/ honors.173
11. Farzad A, Kasraei S, Haghi S, Masoumbeigi M, Torabzadeh H, Panahandeh N. Effects of 3 different light-curing units on the physico-mechanical properties of bleach-shade resin composites. Restor Dent Endod. 2022;47(1):e9. doi:10.5395/rde.2022.47.e9
12. Miletic V, Santini A. Optimizing the concentration of 2,4,6-trimethylbenzoyl diphenylphosphine oxide initiator in composite resins in relation to monomer conversion. Dent Mater J. 2012;31(5):717-723. doi:10.4012/dmj.2012-064
13. Van der Laan HL, Zajdowicz SL, Kuroda K, et al. Biological and mechanical evaluation of novel prototype dental composites. J Dent Res. 2019;98(1):91-97. doi:10.1177/0022034518795673
14. Bansal K, Acharya SR, Saraswathi V. Effect of alcoholic and non-alcoholic beverages on color stability and surface roughness of resin composites: an in vitro study. J Conserv Dent 2012;15(3):283-288. doi:10.4103/0972-0707.97961
15. Sideridou I, Achilias DS, Spyroudi C, Karabela M. Water sorption characteristics of light-cured dental resins and composites based on Bis-EMA/PCDMA. Biomaterials. 2004;25(2):367-376. doi:10.1016/s0142-9612(03)00529-5
16. Ahamed SAS, Raheel SA, Ajmal MB, et al. Evaluation of color stability of composite resin used to characterize acrylic teeth: an in vitro study. Appl Sci. 2023;13(3):1498. doi:10.3390/ app13031498
17. Hotwani K, Thosar N, Baliga S. Comparative in vitro assessment of color stability of hybrid esthetic restorative materials against various children’s beverages. J Conserv Dent 2014;17(1):70-74. doi:10.4103/0972-0707.124154
Antimicrobial efficacy of a novel antimicrobial 3D-printed denture base resin
Behailu B. Eshetea, PhD ¢ Maha Leila, MS ¢ Timothy Cho, BSc ¢ Maggie Xiaoxia Liu, PhD
Neil Park, DMD ¢ Jason A. Griggs, PhD, FADM ¢ Sreenivas Koka, DDS, MS, PhD, MBA, MAS
Colonizing microbes on denture resins can result in oral inflammation and infections associated with morbidity and mortality. The antibacterial activity of a denture base resin impregnated with silver sodium hydrogen zirconium phosphate and formulated for 3-dimensional (3D) printing was compared with that of a commonly used 3D-printed resin (negative control). A total of 336 disc-shaped specimens were 3D printed from the antimicrobial and control denture base resins (n = 168 per group). The ASTM E2180-07 standard test method was used to determine the shortterm and long-term in vitro antimicrobial properties of the materials against Streptococcus mutans, Streptococcus mitis, Staphylococcus aureus, methicillin-resistant S aureus (MRSA), vancomycin-resistant Enterococcus (VRE), Klebsiella pneumoniae, Escherichia coli, Candida albicans, Candida tropicalis, and Candida glabrata. The short-term testing assessed the number of colony-forming units (CFUs) of each species on test and control discs (n = 9 per group per species). The stability of antimicrobial activity against S mutans and C albicans was evaluated monthly on 78 discs of each material, which were stored in artificial saliva for up to 6 months under 3 conditions: real-time single-use (n = 18 group per species), real-time repeated-use (n = 3 per group per species), and accelerated tests (n = 18 per group per species). Analysis of variance and post hoc Tukey tests were used to measure the mean differences between the antimicrobial and control resins as well as among the microbes tested (α = 0.05). In the short-term testing, the antimicrobial resin demonstrated significantly fewer log10 CFUs/mL of all microbes than did the control resin (P < 0.05). In the long-term testing (6-month single-use, 6-month repeated-use, and 36-month accelerated tests), the antimicrobial resin exhibited a significantly decreased load of S mutans and C albicans compared with the control resin (P < 0.05). The results demonstrated that discs printed from an antimicrobial denture base resin had potent shortterm and long-term antimicrobial effects, including activity against microbes associated with pneumonia, candidiasis, stomatitis, and malodor.
Three-dimensional (3D) printing has emerged as a key element in the digital transformation of dental laboratory manufacturing. One area specifically showing a great deal of promise is the category of 3D-printed dentures. The evolution of resin and printing technology has made it possible to print denture bases quickly through a direct 3D printing process, using patient data acquired from digital intraoral scanning and computed tomography.1 However, printed dentures have shown limitations to date, with some studies showing a notable predisposition to hydrophobicity, surface porosity, and other issues that promote the surface adhesion of microorganisms, accelerating biofilm formation and growth as denture plaque.2-4
The presence of denture plaque and yeast-type fungi in the oral cavity promotes the formation of denture-induced stomatitis, which is an inflammatory reaction of the mucosa under dentures. Several studies suggest that many individuals wearing removable complete dentures suffer from stomatitis.5-8 Dentures also may be colonized by methicillinresistant Staphylococcus aureus (MRSA), a common cause of hospital infection–related deaths.9 Further, it has been shown that denture wearing during sleep is associated with a 2.3 times higher risk of contracting pneumonia in elderly patients.10
Based on the prevalence of denture-induced stomatitis and the risk that MRSA and pneumonia may cause infectionrelated death in an aging global population, it is highly desirable to mitigate or eliminate the propensity of dentures to cause infections. Various strategies have been developed to reduce the risk of infection, such as improved denturecleaning technologies and the incorporation of antimicrobial agents such as quaternary ammonium salts in denture materials.11,12 Denture materials treated or coated with an antimicrobial agent prevent microbial attachment, build-up, and accumulation in the oral cavity, averting denture-related infections such as stomatitis and candidiasis.13 Several types of antimicrobial agents have been used to treat or coat dentures, including metal ions (such as silver or zinc), polymers (triclosan or chitosan), and nanoparticles of silver or zinc oxide.13-15 Each of these agents has specific properties, and the effectiveness of antimicrobial denture materials varies depending on the type of antimicrobial agent used and the thickness of the coating.13
Scientists affiliated with Glidewell Laboratories have recently developed a novel denture material by incorporating an antimicrobial agent, silver sodium hydrogen zirconium phosphate (SSHZP), into a resin used for 3D-printed
dentures. The goal of this in vitro study was to investigate the effectiveness of this resin system in producing denture bases resistant to colonization by microbes that cause oral stomatitis and infection-associated death. The results were compared with the antimicrobial activity of a commonly used 3D-printed resin that served as a negative control.
Methods
Material preparation
A total of 336 disc-shaped specimens (30 × 30 × 1 mm) were prepared for the study. A commercially available denture base resin for 3D printing (Denture 3D+, NextDent) was used as a negative control, and 3DP Denture Base Resin (Glidewell) impregnated with SSHZP was used to prepare test discs. The control discs (n = 168) were printed, washed, and postcured following the manufacturer’s recommended procedure using NextDent 5100 3D Printer and NextDent LC-3DPrint Box.
The antimicrobial 3DP Denture Base Resin discs (n = 168) were printed with Asiga Max 3D printer (Asiga), washed with isopropanol alcohol in a cleaning unit (Form Wash, Formlabs) for 5 minutes, and postprocessed in a UV postcure unit (Form Cure, Formlabs) at 60°C for 30 minutes.
Microbes and growth media
The testing was performed with ready-to-use reference stock cultures (Kwik-Stiks, Microbiologics) of 10 microorganisms: Streptococcus mutans (ATCC 25175), Streptococcus mitis (NCIMB 13770), Staphylococcus aureus (ATCC 6538P), MRSA (ATCC 700699), vancomycin-resistant Enterococcus ([VRE] E faecium; ATCC 01143P), Klebsiella pneumoniae (ATCC 700603), Escherichia coli (ATCC 8739), Candida albicans (ATCC 14053), Candida tropicalis (ATCC 750), and Candida glabrata (also known as Nakaseomyces glabrata; ATCC 15126). Todd-Hewitt broth served as the culturing medium for S mutans and S mitis, while tryptic soy broth was used for cultured S aureus, MRSA, VRE, K pneumoniae, and E coli. Sabouraud dextrose broth was utilized for growing C albicans, C tropicalis, and C glabrata . Tryptic soy agar and Sabouraud dextrose agar were used as the plating media for the bacteria and Candida isolates, respectively. All of the culturing broth and plating media were produced by Hardy Diagnostics.
Short-term antimicrobial activity testing
The antimicrobial activity of the specimens was quantitatively determined according to the direct contact test method described in ASTM E2180-07.16 Sterilized discs of the control material and treated denture material were prepared for each of the 10 microbes tested (n = 9 per group per species). Separate discs were used for testing each microbe. Each disc was covered with 1.0 mL of molten agar slurry, which contained approximately 1.5 × 106 colony-forming units (CFUs)/ mL of the corresponding tested microbe.
After 24 hours of contact time with incubation at 37°C, the disc and agar were immersed in 10 mL of Dey-Engley neutralizing broth (Hardy Diagnostics) and vortexed to release agar inoculum. Serial dilutions were performed in sterile saline water, and 0.1 mL of solution was spread plated
onto the appropriate agar plates and incubated for 24 ± 2 hours. The viable CFUs for each dilution plate were counted and recorded, and the values were transformed into logarithmic counts for analysis.
Long-term antimicrobial activity testing
Comprehensive antimicrobial activity testing was implemented to assess the durability of the antimicrobial activity and monitor deterioration over time. Three types of tests were utilized (real-time or accelerated aging methods) to provide a robust measure of a material’s sustained antimicrobial efficacy following the methods recommended by ASTM F1980-16.17 The antimicrobial activity of the negative control and antibacterial denture base resins was monitored in all 3 long-term experiments by performing contact tests against S mutans and C albicans (n = 78 per group). The CFUs/mL on the control and antibacterial discs were compared at each timepoint. To establish the baseline antimicrobial activity, 3 discs per group per species were tested for their antimicrobial activity from the repeated-use experimental setup. The data obtained from this initial testing served as the month 0 reference point for all experimental conditions.
The first long-term experimental setting examined realtime antibacterial activity in a single-use scenario in a group of specimens with no antimicrobial additives (n = 36) and a group of antimicrobial resin specimens (n = 36). Following the baseline tests, the discs were inoculated with a microbial concentration of approximately 1.5 × 106 CFUs/mL of either S mutans or C albicans (n = 3 per group per species). The discs were transferred to 3 cups containing 18 mL of artificial saliva and incubated at 37°C. Antimicrobial activity was tested on 3 discs per group per species every month for 6 months.
In the second real-time long-term experimental setting, discs were reused after polishing and sterilizing to monitor the antimicrobial activity after repeated use. After specimen fabrication, a group of negative control discs (n = 6) and a group of antibacterial test specimens (n = 6) were stored in 18 mL of artificial saliva at 37°C. Each month for 6 months, the discs underwent a monthly treatment cycle in which the discs were removed from storage, disinfected with 70% isopropanol, and then inoculated with approximately 1.5 × 106 CFUs/mL of either S mutans or C albicans (n = 3 per group). After inoculation, the discs were disinfected again, polished to remove any surface buildup, and sterilized a third time to ensure cleanliness. Finally, they were placed in 18 mL of fresh artificial saliva and stored at 37°C until the next measurement.
In the third long-term experimental setting, a group of negative control specimens (n = 36) and a group of antimicrobial test specimens (n = 36) were stored in 18 mL of artificial saliva at a temperature of 50°C with 55% relative humidity to measure the effect of accelerated aging on the antimicrobial activity of the discs against S mutans and C albicans. At each timepoint, a new set of 6 discs from each group was removed from storage, sterilized with 70% isopropanol, and inoculated with a microbial concentration of approximately 1.5 × 106 CFUs/mL of C albicans or S mutans (n = 3 per group per species per timepoint). A total of 156 days in those conditions simulated 36 months of real-time activity.
Abbreviations: C albicans, Candida albicans ; C tropicalis, Candida tropicalis ; CFUs, colony-forming units; E coli, Escherichia coli ; K pneumoniae, Klebsiella pneumoniae; MRSA, methicillin-resistant Staphylococcus aureus ; C glabrata, Candida glabrata; S aureus, Staphylococcus aureus ; S mitis, Streptococcus mitis ; S mutans, Streptococcus mutans ; VRE, vancomycin-resistant Enterococcus
Error bars represent the standard deviation. The differences between the negative control and antibacterial resin groups are statistically significant for all species (P < 0.001; Tukey test).
Statistical analysis
The results of the ASTM contact test were analyzed using 3-way analysis of variance (ANOVA) blocked on the round or iteration of testing (substrate × strain × block). Results of the real-time tests were analyzed using repeated-measures 2-way ANOVA (substrate × time), where observing each bacterial culture over time was the repeated measure. ANOVA was followed by the Tukey test (α = 0.05). These tests assume that the data are normally distributed and that the groups have equal variances. After a logarithmic transformation was applied to the CFU data, the assumption of equal variances was met in every case (Brown-Forsythe; P > 0.05). The assumption of normality was met in all but 2 cases (Shapiro-Wilk test; P > 0.05), which were
C albicans and S mutans. Since the dataset contained many ties, it did not meet the assumption of few ties inherent to ANOVA on ranks; therefore, parametric ANOVA was used to analyze the results for all strains. Statistical tests were performed using SigmaPlot 14.0 (Grafiti) and Reliasoft Suite (Hottinger Brüel & Kjær).
Results
Short-term antimicrobial activity
The log10 reduction values of colony counts on discs printed from 3DP Denture Base Resin were compared against values on the control disks. The novel denture material showed statistically significant antimicrobial efficacy (P < 0.001; Tukey test)
Chart 1. Mean colony counts on negative control and antimicrobial denture resins (n = 9 per group).
Ctropicalis Cglabrata Calbicans
VRE MRSA Ecoli Kpneumoniae Saureus Smitis Smutans
2. Mean Streptococcus mutans colony counts on negative control and antimicrobial denture resins after a single use (n = 3 per group).
3. Mean Candida albicans colony counts on negative control and antimicrobial denture resins after a single use (n = 3 per group).
Abbreviation: CFUs, colony-forming units.
Error bars represent the standard deviation. The differences between the negative control and antibacterial resin groups are statistically significant at all timepoints (P < 0.05; Tukey test).
against all tested microorganisms (Chart 1). Compared with the negative control group, the antimicrobial-containing discs showed reductions of 7.44 and 5.57 log 10 CFUs/mL for S mutans and S mitis, respectively. The reductions in the cases of S aureus, K pneumoniae, and E coli were 8.13, 8.07, and 5.02 log10 CFUs/mL, respectively. The antibacterial 3D-printed disc also showed significant log10 CFUs/mL reductions in the tested VRE, MRSA, C albicans, and C glabrata isolates compared with the control material. Only C tropicalis in the test group showed a reduction of less than 3 log10 CFUs/mL compared with the control group.
Long-term antimicrobial activity
In the assessment of real-time single-use over 6 months, the S mutans and C albicans counts in the negative control group remained relatively stable, with values ranging from 4.52 to 5.70 and 5.70 to 7.85 log10 CFUs/mL, respectively (Charts 2 and 3). In contrast, the test group displayed 0 or imperceptible log10 CFUs/ mL of S mutans and C albicans throughout the study. The
Abbreviation: CFUs, colony-forming units.
Error bars represent the standard deviation. The differences between the negative control and antibacterial resin groups are statistically significant at all timepoints (P < 0.05; Tukey test).
differences between materials were statistically significant for both species at all timepoints (P < 0.05; Tukey test).
To simulate more realistic everyday use of a printed denture, the antimicrobial activity of discs against S mutans and C albicans was evaluated after repeated cleaning and disinfection over 6 months. The average S mutans load in the control group was 4.10 to 5.76 log10 CFUs/mL, and there was no growth observed in the test group for the 6-month study duration (Chart 4). Similarly, the mean C albicans load was 6.84 to 7.96 log10 CFUs/mL in the control group (Chart 5). No growth was observed on the test resin at any timepoint except at 6 months, when growth was measured as 4.57 log10 CFUs/mL. The differences between materials were statistically significant for both species at all timepoints (P < 0.05; Tukey test).
When the antimicrobial activity of the discs was evaluated in an accelerated aging protocol simulating 36 months of realtime use, the test discs demonstrated significantly reduced S mutans growth (P < 0.05; Tukey test) compared with the
Chart
Chart
Table 1. Mean
loads of Streptococcus mutans in negative control and antibacterial denture base resins subjected to accelerated aging (n = 3 per group).
Simulated time, moa
Negative control resin, log10 CFUs/mLb
Antibacterial resin, log10 CFUs/mLb
0c 4.77 (0.17) 0.00 (0.00)
6 4.54 (0.06) 0.00 (0.00)
Table 2. Mean (SD) loads of Candida albicans in negative control and antibacterial denture base resins subjected to accelerated aging (n = 3 per group).
Simulated time, moa
(0.01) 0.00 (0.00)
12 4.50 (0.03) 1.00 (1.41) 18
(0.04)
4.98 (0.14)
Abbreviation: CFUs, colony-forming units.
(0.00)
(1.56)
a A total of 156 days at 50°C and 55% relative humidity, simulating 36 months of real-time activity.
bThe differences between the negative control and antibacterial resin groups are statistically significant at all timepoints (P < 0.05; Tukey test).
cBaseline values were obtained from the real-time repeated-use test.
wearers; this is a concerning statistic given the increasing emergence and dissemination of MRSA strains.22 The notable reduction of S aureus, 8.13 log10 CFUs/mL, underscores the potential of innovative antimicrobial products to mitigate bacterial colonization in denture users.
Although E coli and K pneumoniae are not generally considered part of the normal oral microbiota, the prevalence of various species within the Enterobacteriaceae family was found to be 48.0% in the denture-wearing population.23 However, this figure may be higher in immunocompromised populations, in hospital environments, and intensive care units. In the present study, the antibacterial denture resin reduced E coli and K pneumoniae by 5.02 and 8.07 log10 CFUs/mL, respectively, compared with the control resin. The mitigation of E coli and K pneumoniae would be expected to decrease the incidence of opportunistic infections among immunocompromised individuals.
Another benefit observed in the present experiments is the reduction of VRE and MRSA on the test discs. It has been stated that approximately 20% of the US population wears some type of removable denture.24 As individuals age, their immunity declines and they develop health conditions that make them more vulnerable to infections and frequent visits to healthcare facilities. Both VRE and MRSA are significant concerns in healthcare settings, particularly in intensive care units. Reductions of 6.75 and 7.31 log10 CFUs/mL in VRE and MRSA in the present study have broader implications for public health and underscore the potential of this antimicrobial denture base resin to address one of the most pressing challenges in healthcare-associated infections.
Some studies have reported the loss of antimicrobial activity in medical devices, mainly due to leaching.25 Therefore, the long-term testing of the antimicrobial resin in the present
Abbreviation: CFUs, colony-forming units.
a A total of 156 days at 50°C and 55% relative humidity, simulating 36 months of real-time activity.
bThe differences between the negative control and antibacterial resin groups are statistically significant at all timepoints (P < 0.05; Tukey test). cBaseline values were obtained from the real-time repeated-use test.
study is important because it demonstrated that antimicrobial activity was maintained after 6 months, resulting in 5.00– and 5.70–log10 CFUs/mL reductions, respectively, in S mutans and C albicans, which are significant contributors to dentureassociated infections. The antimicrobial activity of the test discs was observed after repeated cleaning over 6 months, and a 5.64–log10 CFUs/mL reduction for S mutans was maintained. In the case of C albicans, the antibacterial disc showed a 2.27–log10 CFUs/mL reduction at 6 months after being cleaned 5 times. In the accelerated study, the discs maintained a reduction of at least 3.88 log10 CFUs/mL for S mutans and 5.69 log10 CFUs/mL for C albicans after a simulated 36 months, suggesting the long-term durability of the antimicrobial compound.
All studies have limitations, and the primary limitation of this study is the in vitro design, which prevents extrapolation to direct clinical application. Further studies are needed in the clinical setting to determine whether these in vitro findings are replicable in vivo. In addition, although 10 different and important microbial species were included in this study, many other species are commonly found in the oral cavity. These results cannot be extrapolated to include positive effects on all oral microbes.
Conclusion
Within the limitations of this in vitro study, the following conclusions are drawn:
1. Levels of microbes that cause denture-induced stomatitis are significantly reduced by the use of a denture resin impregnated with SSHZP.
2. Levels of microbes associated with patient death from denture-related hospital and nursing home infections are significantly reduced by the use of a denture resin impregnated with SSHZP.
(SD)
3. Further research is needed to determine if in vitro findings from this study translate into clinical patient care settings.
Author affiliations
Research and Development, Glidewell Dental Laboratories, Irvine, California (Eshetea, Leila, Cho, Liu); Clinical Education, Glidewell Dental Laboratories, Irvine, California (Park); University of Mississippi Medical Center School of Dentistry, Jackson (Griggs; Koka [formerly]); formerly, Department of Dental Specialties, Mayo Clinic, Rochester, Minnesota (Koka); now with Executive Leadership Enterprises, LLC (Koka).
Correspondence
Sreenivas Koka, DDS, MS, PhD, MBA, MAS (skoka66@gmail.com).
Conflicts of interest
Behailu B. Eshetea, Maha Leila, Timothy Cho, Maggie Xiaoxia Liu, and Neil Park are employees of Glidewell Dental Laboratories. Sreenivas Koka has received speaker honoraria and travel reimbursement from Glidewell Dental Laboratories in the past 12 months. Jason A. Griggs reports no conflicts of interest.
Funding
Glidewell Laboratories funded the research described in this article.
Acknowledgments
The authors wish to thank Raj Malyala, John Bernhard, and Ryan Stein for facilitating this study and Kevin Duong for his assistance in preparing 3D-printed test specimens.
References
1. Goodacre BJ. 3D printing of complete dentures: a narrative review. Int J Prosthodont. 2024;37(7):159-164. doi:10.11607/ijp.8832
2. Silva MDDD, Nunes TSBS, Viotto HEDC, Coelho SRG, Souza RF, Pero AC. Microbial adhesion and biofilm formation by Candida albicans on 3D-printed denture base resins. PLoS One. 2023;18(10):e0292430. doi:10.1371/journal.pone.0292430
3. Freitas RFCP, Duarte S, Feitosa S, et al. Physical, mechanical, and anti-biofilm formation properties of CAD-CAM Milled or 3D printed denture base resins: in vitro analysis. J Prosthodont. 2023;32(S1):38-44. doi:10.1111/jopr.13554
4. Osman RB, Khoder G, Fayed B, Kedia RA, Elkareimi Y, Alharbi N. Influence of fabrication technique on adhesion and biofilm formation of Candida albicans to conventional, milled, and 3D-printed denture base resin materials: a comparative in vitro study. Polymers (Basel). 2023;15(8):1836. doi:10.3390/polym15081836
5. Hannah VE, O’Donnell L, Robertson D, Ramage G. Denture stomatitis: causes, cures and prevention. Prim Dent J. 2017;6(4):46-51. doi:10.1308/205016817822230175
7. Ramage G, Tomsett K, Wickes BL, López-Ribot JL, Redding SW. Denture stomatitis: a role for Candida biofilms. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;98(1):53-59. doi:10.1016/j.tripleo.2003.04.002
8. Budtz-Jörgensen E. The significance of Candida albicans in denture stomatitis. Eur J Oral Sci. 1974;82(2):151-190. doi:10.1111/j.1600-0722.1974.tb00378.x
9. Rossi T, Peltonen R, Laine J, Eerola E, Vuopio-Varkila J, Kotilainen PJ. Eradication of the long-term carriage of methicillin-resistant Staphylococcus aureus in patients wearing dentures: a follow-up of 10 patients. Hosp Infect. 1996;34(4):311-320. doi:10.1016/s0195-6701(96)90111-5
10. Iinuma T, Arai Y, Abe Y, et al. Denture wearing during sleep doubles the risk of pneumonia in the very elderly. J Dent Res. 2015;94(3 Suppl):28S-36S. doi:10.1177/0022034514552493
11. Rao S, Nandish BT, Preman NK, et al. Synthesis, characterization, and evaluation of quaternary ammonium-based polymerizable antimicrobial monomers for prosthodontic applications. Heliyon. 2022;8(8):e10374. doi:10.1016/j.heliyon.2022. e10374
12. Patel M, Barrera L, Chu L, Whang K. Development of an antimicrobial, 3D printable denture base material with K18 quaternary ammonium silane-functionalized methyl methacrylate and filler. J Prosthet Dent. 2024;131(6):1251.e1-1251.e8. doi:10.1016/j.prosdent.2024.03.013
13. Mirizadeh A, Atai M, Ebrahimi S. Fabrication of denture base materials with antimicrobial properties. J Prosthet Dent. 2018;119(2):292-298. doi:10.1016/j. prosdent.2017.03.011
14. Corrêa JM, Mori M, Sanches HL, da Cruz AD, Poiate E Jr, Poiate IA. Silver nanoparticles in dental biomaterials. Int J Biomater. 2015;2015:485275. doi:10.1155/2015/485275
15. Kwon JS, Kim JY, Mangal U, et al. Durable oral biofilm resistance of 3D-printed dental base polymers containing zwitterionic materials. Int J Mol Sci 2021;22(1):417. doi:10.3390/ijms22010417
16. ASTM E2180-07. Standard Test Method for Determining the Activity of Incorporated Antimicrobial Agent(s) in Polymeric or Hydrophobic Materials. ASTM; 2007. doi:10.1520/E2180-07
17. ASTM F1980-16. Standard Guide for Accelerated Aging of Sterile Barrier Systems for Medical Devices. ASTM; 2016. doi:10.1520/F1980-16
18. Gendreau L, Loewy ZG. Epidemiology and etiology of denture stomatitis. J Prosthodont. 2011;20(4):251-260. doi:10.1111/j.1532-849X.2011.00698.x
19. Abaci O, Haliki-Uztan A, Ozturk B, Toksavul S, Ulusoy M, Boyacioglu H. Determining Candida spp. incidence in denture wearers. Mycopathologia. 2010;169(5):365-372. doi:10.1007/s11046-010-9275-8
20. Hassan Y, Chew SY, Than LTL. Candida glabrata: pathogenicity and resistance mechanisms for adaptation and survival. J Fungi (Basel). 2021;7(8):667. doi:10.3390/jof7080667
21. Cheng L, Zhang K, Weir MD, Liu H, Zhou X, Xu HH. Effects of antibacterial primers with quaternary ammonium and nano-silver on Streptococcus mutans impregnated in human dentin blocks. Dent Mater. 2013;29(4):462-472. doi:10.1016/j. dental.2013.01.011
22. Lee D, Howlett J, Pratten J, et al. Susceptibility of MRSA biofilms to denturecleansing agents. FEMS Microbiol Lett. 2009;291(2):241-246. doi:10.1111/j.15746968.2008.01463.x
23. Goldberg S, Cardash H, Browning H, Sahly H, Rosenberg M. Isolation of Enterobacteriaceae from the mouth and potential association with malodor. J Dent Res 1997;76(11):1770-1775. doi:10.1177/00220345970760110801
24. Slade G, Akinkugbe A, Sanders A. Projections of U.S. edentulism prevalence following 5 decades of decline. J Dent Res. 2014;93(10):959-965. doi:10.1177/0022034514546165
25. Bruenke J, Roschke I, Agarwal S, Riemann T, Greiner A. Quantitative comparison of the antimicrobial efficiency of leaching versus nonleaching polymer materials. Macromol Biosci 2016;16(5):647-654. doi:10.1002/mabi.201500266
Galal Omami, BDS, MSc, MDentSc, FRCD(C)
Cigar-shaped radiopacity
A 64-year-old man presented for dental evaluation and treatment. Clinical examination showed multiple missing and carious teeth. The patient’s medical history was remarkable for tremor and ataxia. A panoramic radiograph revealed a large, cigar-shaped radiopacity superimposed
Panoramic radiograph showing a large, cigar-shaped radiopacity superimposed on the mandibular alveolar process. Note the position and the homogenous internal pattern.
Unusual root abnormality
A 65-year-old woman presented for dental evaluation and treatment. The patient’s medical history was significant for hypertension and osteoarthritis. Clinical examination revealed severe periodontitis with marked tooth mobility and attrition.
Figure. Periapical radiograph showing advanced periodontal lesions, eggshelllike calcification along the distal surface of the first premolar root, and wear facets on the incisal edges of the canine and lateral incisor.
over the right side of the mandibular alveolar process (Figure). The patient did not recall any history of trauma but reported episodic pain and swelling below the mandible. Palpation of the floor of the mouth revealed a hard mass beneath the mucosa.
Which of the following is the most appropriate diagnosis?
A. foreign body
B. osseous choristoma
C. sialolithiasis
D. lingual tori
Diagnosis is on page 80.
A full-mouth series of intraoral radiographs showed generalized severe periodontal bone loss. A thin calcification with an eggshell-like appearance was observed along the distal root surface of the maxillary right first premolar (Figure).
Which of the following is the most appropriate diagnosis?
A. external root resorption
B. cemental tear
C. vertical root fracture
D. hypercementosis
Diagnosis is on page 80.
Author affiliation
Department of Oral Health Practice, University of Kentucky College of Dentistry, Lexington.
Figure.
GENERAL DENTISTRY SELF-INSTRUCTION ANSWERS
Exercise No. GD536
November/December 2024, p. 25
1. A
2. C
3. D
4. C
5. B
6. C 7. B 8. B 9. D 10. C 11. A 12. D 13. A 14. B 15. B
Exercise No. GD537
November/December 2024, p. 46
1. C 2. C
3. D
4. A 5. C 6. A 7. C 8. C 9. A 10. A 11. C 12. D 13. B 14. B 15. A
Exercise No. GD538
November/December 2024, p. 53
1. D
2. B
3. A
4. B
5. D
6. C 7. B 8. A 9. A 10. C 11. D 12. C 13. B 14. A 15. A
HAVE YOU MOVED?
If you have recently moved, or plan to in the near future, please make sure to update your AGD profile. Log into the AGD website today! We want to make sure you receive AGD publications and other important information from us! View or update your profile, check the status of your membership dues, manage your email subscriptions and change your password.
Please contact the AGD Membership Services Center with any questions at 888.243.3368 (toll-free) or 312.440.4300. Our member representatives are available to assist you Monday through Friday from 7:30 a.m. to 5:30 p.m. CST.
UPDATE YOUR PROFILE agd.org/my-agd
Coming next issue
Look for these articles and more in the January/February 2026 issue of General Dentistry:
• Knowledge, practices, and attitudes of pregnant women regarding maternal and child oral health: questionnaire development, psychometric properties, and associated factors
• Recurrence of clinical symptoms on endodontically treated tooth following COVID-19 vaccination: a case report
• Comparing the shade stability of lithium disilicate veneers bonded with a light-cured or dual-cured resin cement: a narrative review
In the November issue of AGD Impact
• Student Debt Success Stories
• Restoring Heroes: The Legacy of the Air Force Maxillofacial Prosthetics Fellowship Program
In the December issue of AGD Impact
• Latest in Cosmetic Dentistry
• To Be Continued: DSO-Provided Continuing Education
• President’s Profile on Dr. Marc J. Worob
as above Names and Mailing Addresses of Publisher, Editor, and
Dentistry, 560 W Lake St, Sixth Floor, Chicago, IL, 60661-6600 Editor:
of
F. Kosinski, DDS, MAGD, address same as above Executive Editor: Tiffany Slade, address same as above Owner: Academy of General Dentistry, address same as above Known Bondholders, Mortgagees, and Other Security Holders: None Tax Status: Has not changed during preceding 12 months Issue Date for Circulation Data Below: 09/01/2025.
Publication of Statement of Ownership: November/December 2025 issue Signature and Title: Tiffany Slade, Executive Editor Date: 09-26-2025
and Nature of Circulation
Cigar-shaped radiopacity
Diagnosis
C. sialolithiasis
Sialolithiasis is a condition characterized by the formation of calcified stones, known as sialoliths, within the salivary glands. About 85% of salivary stones occur within the submandibular gland, and about 85% of the submandibular gland stones occur within the submandibular duct, also known as Wharton’s duct. The increased incidence of sialolithiasis in the submandibular gland can be attributed to the viscous, mucous nature of its secretions and the long, tortuous, uphill course of the submandibular duct. Sialoliths frequently cause obstruction of the salivary ductal system and result in intermittent pain or swelling of the affected gland, particularly at mealtimes when salivation is increased. Salivary obstruction can ultimately lead to secondary infection. Radiographically, sialoliths appear as round, oval, or cylindrical calcified masses that have a homogenous radiopaque internal pattern. Sialoliths in the submandibular duct may appear on panoramic and periapical views as radiopacities superimposed over the mandible, giving the appearance of a dense bone island.
Unusual root abnormality
Diagnosis
B. cemental tear
Cemental tear is a rare condition characterized by a partial or complete detachment of a fragment of cementum from the root surface. The cause of this condition is unknown, but local trauma, occlusal trauma, and aging have been suggested as possible etiologic factors. Incisor teeth are affected most frequently. Cemental tear is associated with rapidly progressive periodontal breakdown. The clinical and radiographic features of cemental tears can resemble those of marginal periodontitis, periapical periodontitis, or combined endodontic-periodontal lesions.1
Radiographic detection of a cemental tear depends on the angulation of the incident X-ray beam and the degree of separation of the torn cemental fragments. The utility of CBCT imaging can be limited by streaking artifacts caused by
When sialolithiasis is suspected, the modality of choice for imaging is either cone beam computed tomography (CBCT) or medical computed tomography (CT). If this imaging is not available, a mandibular occlusal view can be helpful in visualizing stones in the submandibular duct. In addition to CT imaging, several advanced techniques are also available to evaluate sialolithiasis, including ultrasonography, sialography, and magnetic resonance imaging.
In general, stones within the distal portion of the duct are removed by simple surgical excision, while stones within the proximal portion of the duct or glandular parenchyma usually require excision of the salivary gland. Minimally invasive techniques, such as shock wave lithotripsy and sialendoscopy, have been shown to be effective in the treatment of sialolithiasis in select patients.
Reference
White SC, Pharoah MJ, eds. Oral Radiology: Principles and Interpretation. 7th ed. Mosby; 2014:529-531.
root canal filling materials and metallic restorations. In many instances, a definitive diagnosis of cemental tear can only be made after surgical biopsy.
Successful treatment depends on early diagnosis and removal of the torn fragments, often combined with regenerative periodontal procedures. 2
References
1. Pedercini A, Weitz DF, Heyse JD Jr, et al. Cemental tear: an overlooked finding associated with rapid periodontal destruction. A case series. Aust Dent J. 2021;66(Suppl 1):S82-S87. doi:10.1111/adj.12844
2. Lee AHC, Neelakantan P, Dummer PMH, Zhang C. Cemental tear: literature review, proposed classification and recommendations for treatment. Int Endod J 2021;54(11):2044-2073. doi:10.1111/iej.13611
Your Circle Has Power. Use it.
Each Referral Could Earn You $50 in Rewards!
AGD Referral Rewards Program
Shifting policies are impacting dentistry. By referring colleagues to AGD, you can help grow a stronger community that remains grounded in science, protects patients and ensures oral health is guided by those who understand it best—dentists.
You’ll both also earn $50 in Referral Rewards once they join!
Recruiter Tip: Share the News New members get the rest of 2025 free when joining now for 2026
Purchase Power
Use rewards to pay for Fellowship Review Course study materials.
Cut the Cost
Apply your rewards toward your membership renewal—easy savings.
Top the Charts
Earn bragging rights on the recruiter leaderboard for every colleague who joins.
Endless Rewards
Keep recruiting. Keep earning. There’s no limit to how much you can rack up.