Fracture resistance of a bulk-fill composite hybrid
ENDODONTICS
Giving the pulp another chance
ETHICS
Ethical considerations for medical tourism
PSYCHOSOCIAL ANXIETY AND FEAR IN DENTISTRY
Effects of a therapy dog intervention
REFER A COLLEAGUE, GET REWARDED
“By recruiting colleagues to join AGD, I’ve not only lowered my membership renewal cost, I’m also helping my fellow dentists.”
Filippo Marchello, DDS, MAGD Member since 1992
AGD Referral Rewards Program
Refer your colleagues to join AGD now, and they’ll pay only half of 2024 headquarters membership dues.*
You’ll both also earn $50 in Referral Rewards once they join!
LEARN MORE agd.org/member-center
*Half-year rate does not apply towards constituent and component portion of dues. Half-year rate does not apply for memberships that expired on Dec. 31, 2023, residents, or new dentists who graduated in 2023 or 2024. Members who pay half year dues may record CE starting on July 1, 2024.
17 - 20 AGD2024.ORG
ATTEND THE PREMIER MEETING FOR GENERAL DENTISTRY
Expand your knowledge and grow professionally with AGD2024’s numerous education offerings:
• Network with more than 2,500 fellow dentists and AGD members.
• Have the opportunity to earn more than 54 CE credits.
• Participate in interactive courses.
• Gain best practices from industry thought leaders.
• Attend free New Dentist Lounge lectures.
• Attend cutting-edge learning lab presentations.
Make the Most of Your Stay in Minneapolis
With its beautiful lakes, expansive park system, thriving arts scene, plentiful shopping and great food, Minneapolis offers a great backdrop for AGD2024 and is a great destination whether you plan on bringing guests or traveling solo.
DEPARTMENTS CLINICAL ARTICLES
6 Editorial
The added value of mentorship
7 Ethics
Medical tourism: ethical considerations for patients and dentists
78
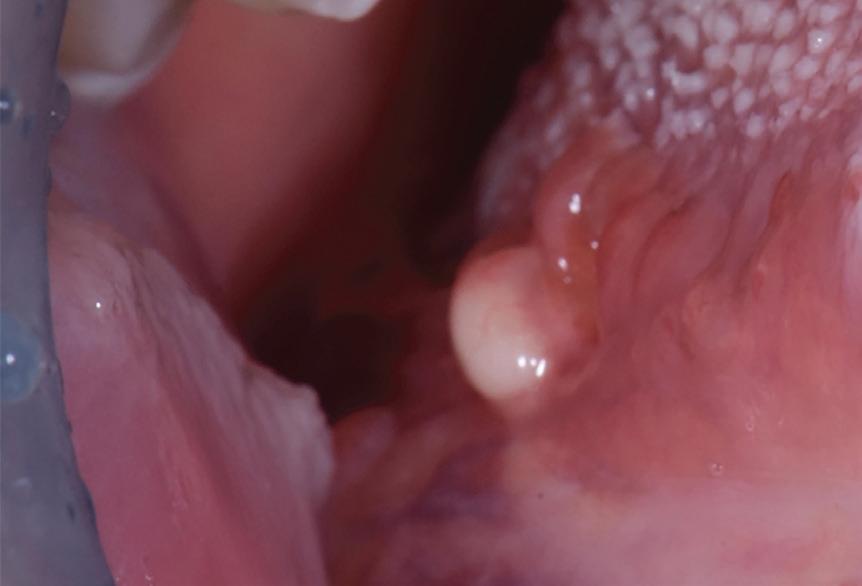
Oral Diagnosis
Yellowish tongue nodule and White tongue plaque
79
Self-Instruction Answers
Exercises No. GD513 and GD514
10 Endodontics
Incidence of missed canals during endodontic treatment of maxillary first and second molars
Michael Rodillo
Patricia Ann Bauer
Bruno Cavalcanti
Rodrigo Sanches-Cunha
Suncica Travan
Neville McDonald
SELF-INSTRUCTION EXERCISE GD530, 2 CE CREDITS, P. 15
16 Endodontics
Giving the pulp another chance: a case report of vital pulp therapy retreatment
Hataichanok Machareonsap
Nattakan Chaipattanawan
23 Endodontics
Papimon Chompu-inwai
Chanika Manmontri
Performance of a novel self-adhesive bulk-fill composite hybrid in endodontically treated maxillary premolars: analysis of fracture resistance and failure mode
Fereshteh Shafiei
Zahra Fattah
Shadi Tivay
SELF-INSTRUCTION EXERCISE GD531, 2 CE CREDITS, P. 30
31 Oral Medicine, Oral Diagnosis, Oral Pathology
Globe-shaped central incisors in a patient with otodental syndrome
Daniel Adrian Silva Souza
Rebeca Brasil Oliveira
André Wilson Machado
37 Basic Science
Candice Belchior Duplat
Frederico Sampaio Neves
Jean Nunes dos Santos
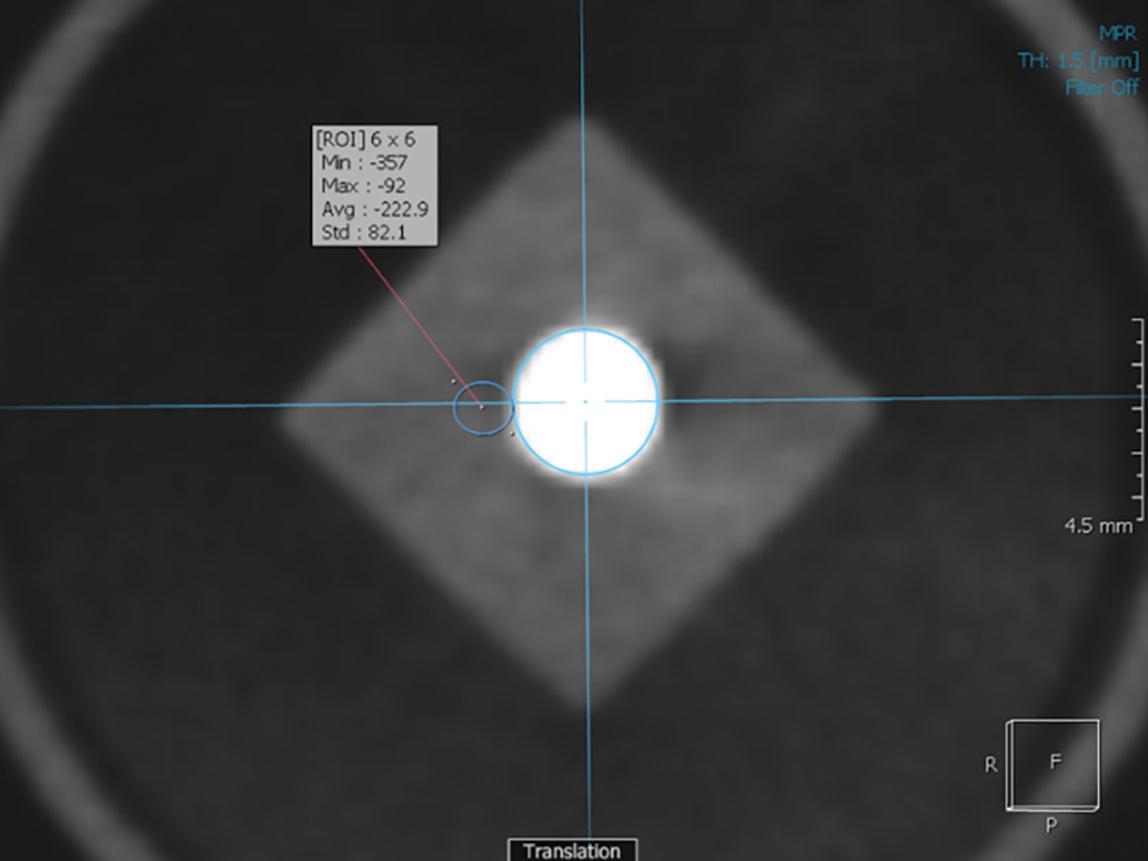
Evaluation of artifacts produced by conventional dental materials in standard and high-resolution CBCT imaging
Solmaz Valizadeh
Zahra Sahebnasagh
Mitra Ghazizadeh Ahsaie
SELF-INSTRUCTION EXERCISE GD532, 2 CE CREDITS, P. 43
44 Psychosocial Anxiety and Fear in Dentistry
The effects of a therapy dog intervention on dental fear and anxiety in adult patients undergoing dental procedures: a pilot study
Doris Lam
Sara A. Chilcutt
Andrew J. Avillo
John E. Schmidt
50 Restorative Dentistry
Dominique A. D’Anthony
Amy O’Connor
Nicholas J. Hamlin
Clinical guidelines for posterior semidirect composite resin restorations: a case report with a 17-month follow-up
Franco Naoki Mezarina-Kanashiro Fernanda Furuse Ventura dos Santos
Adilson Yoshio Furuse
54 Restorative Dentistry
Tribochemical silicoating of amalgam promotes effective amalgam-resin repairs
Terence A. Imbery
Peter C. Moon
58 Orofacial Pain
Anna Pitz
Caroline K. Carrico
Ectopic sulcular pain: detection and treatment
James V. Potter
62 Basic Science
Pilot, open-label, randomized controlled clinical trial evaluating 4 oral hygiene regimens using a manual toothbrush, toothpaste, and mouthwash
Serban Rosu
Salvatore Bianco
Vincenzo Nobile
Dario Cattaneo
72 Basic Science
Paola Benatti
Dionisio Franco Barattini
Marta Mellai
ChatGPT and dentistry: a step toward the future
Lucas Lacerda de Souza
Manoela Domingues Martins
Fernanda Viviane Mariano Brum Corrêa
Syed Ali Khurram
Alan Roger Santos-Silva
Márcio Ajudarte Lopes
Helder Antônio Rebelo Pontes
Felipe Paiva Fonseca
Fábio Luiz Coracin
Ahmed Hagag
Pablo Agustin Vargas
Cover image inspired by: Performance of a novel self-adhesive bulk-fill composite hybrid in endodontically treated maxillary premolars: analysis of fracture resistance and failure mode, on p. 23
Members, call 888.243.3368 and ask for a Member Services representative.
Mailing Lists
For information about ordering AGD mailing lists, call 888.243.3368 ext. 4097 or email advertising@agd.org.
All materials subject to copying and appearing in General Dentistry may be photocopied for the noncommercial purposes of scientific or educational advancement. Reproduction of any portion of General Dentistry for commercial purposes is strictly prohibited unless the publisher’s written permission is obtained.
AGD does not necessarily endorse opinions or statements contained in essays or editorials published in General Dentistry. The publication of advertisements in General Dentistry does not indicate endorsement for products and services. AGD approval for continuing education courses or course sponsors will be clearly stated.
General Dentistry (ISSN 0363-6771) is published bimonthly in 2024 by the AGD, 560 W Lake St, Sixth Floor, Chicago, IL 60661-6600. AGD members receive GeneralDentistry as part of membership.
Periodicals postage paid at Chicago, IL and additional mailing office. POSTMASTER: Send address changes to General Dentistry, 560 W Lake St, Sixth Floor, Chicago, IL 60661-6600. Email: subscriptions@agd.org.
Canadian mailing information: IPM Agreement number 40047941. Change of address or undeliverable copies should be sent to: Station A, PO Box 54, Windsor, Ontario, N9A 6J5, Canada. Email: subscriptions@agd.org.
The nonmember individual subscription rate for General Dentistry is $120 for the print version, $120 for the online version, and $200 for print and online versions; the nonmember institution rate is $355 (add $5 for Canada). Single copies of General Dentistry are available to nonmember individuals for $22.50 and nonmember institutions for $27.
Editor
Timothy F. Kosinski, DDS, MAGD
Associate Editor
Bruce L. Cassis, DDS, MAGD
Director, Communications
Kristin S. Gover, CAE
Executive Editor
Tiffany Nicole Slade, MFA
Technical Editor Barbara Holmstrom
Associate Editor Emily Parenti-Lopez
Manager, Production/Design
Timothy J. Henney
Graphic Designers
Robert Ajami Eric Grawe
Advertising Bill Spilman
Advertising and Exhibit Sales 309.483.6467 advertising@agd.org
Subscriptions
888.243.3368 subscriptions@agd.org
Reprints scsreprints@sheridan.com
AGD Corporate Sponsors
• AGD Supply Discount: Automatically access your membership’s savings benefit of up to 30% off standard industry retail.
• Authorized Access: Order with confidence! No gray market. No fraudulent products.
• FREE Shipping: Consolidate your supply sources and eliminate shipping fees within the continental United States.
• Save Time: Order all of your dental supplies from one easy-to-use online dental supply store.
• Support: Our dedicated account managers review every order for accuracy and apply qualifying manufacturer discounts and deals.
The added value of mentorship
What do we expect when we attend a CE program? Most courses we register for have some significance to a personal or professional goal, but others are completed to fulfill a mandatory state requirement and may not interest us that much. However, participation programs can be relatively costly in terms of tuition, travel, hotel, and time away from our practice. We must remember that each course is likely to provide us with at least a few nuggets of practical information that will advance our skills, enhance clinical outcomes, or improve practice management. The goal is to learn something that can be taken back to our practice to develop clinical experience and foster proficiency.
We can get more out of the CE programs we attend by participating in a mentoring relationship. When I’m a speaker, it feels rewarding to share accumulated knowledge, but I also gain insight and new perspectives from the pertinent questions asked during the program or from one-on-one conversations afterward. As an attendee, I often seek out recent graduates at CE events so that we can share ideas and viewpoints. I take the opportunity to encourage lifelong learning, since continual dental education is the best investment we can make as dentists. For dentists who are newer to practice, it’s beneficial to develop relationships with experienced colleagues who can offer guidance during participation courses or after a webinar, sharing tips on how to incorporate demonstrations into real-world situations.
What better way to grow in this dynamic, ever-advancing profession than to share educational experiences with colleagues? Throughout my career, other dentists have challenged me, watched over me, elevated me, and shared their hard-earned wisdom. Meeting with contemporaries at local or national CE events
offers benefits for everyone involved. Having the desire to continue accumulating knowledge is critical to success, regardless of our years in practice. Any form of education works—from webinars and study clubs to evening programs offered by suppliers or dentists in the community—all are viable pathways to improving clinical aptitude.
However, true scholarship involves much more than attending a class, taking notes, or watching a YouTube video. One of the benefits of membership in our AGD is the opportunity to meet highly motivated, highly educated colleagues who are interested in advancing not only their own practice but the profession as a whole. For less experienced dentists, a mentor is an invaluable resource who can serve as a guide through challenging situations or provide advice on practical matters. For mentors, having to explain why or how we do something can be eye opening, sometimes reinforcing our choices and sometimes making us consider other approaches. And just as important to us as gaining clinical knowledge, many life lessons are learned from exchanging ideas with contemporaries. Take advantage of the mentoring opportunities offered by your AGD membership and reach out to others at CE courses, conferences, and other professional events. All of us have unique talents and skills that we have chosen to utilize for the benefit of our patients. While we all have strengths as individuals, we can fly even higher when we connect with colleagues.
Timothy F. Kosinski, DDS, MAGD Editor
Medical tourism: ethical considerations for patients and dentists
Toni M. Roucka, RN, DDS, MA
Medical tourism, or the practice of traveling to foreign countries for healthcare services, has grown in popularity as patients seek less expensive alternatives to costly treatments. Dentistry is a major sector of this industry. Globalization and regional disparities in healthcare costs contribute to this practice.1 Although practices that cater to travelers may provide major economic advantages to destination nations and cost savings for consumers, medical tourism poses serious ethical concerns. This column will investigate these ethical challenges, evaluating the impact on patients, home-country providers, participating communities, and governments. For the sake of this column, the terms medical tourism and healthcare tourism will apply to individual sectors of care, including dentistry.
The medical tourism market
The magnitude of the medical tourism industry worldwide is significant. Patients Beyond Borders estimated the medical tourism market size to be between $74 billion and $92 billion in 2019, based on an approximate range of 21 million to 26 million crossborder patients worldwide, spending an average of $3550 per visit, including procedure-related costs, cross-border and local transport, inpatient stay, and accommodations.2 Numbers decreased during the pandemic but are now rising again. The dental sector of the market is
expected to exceed $5 billion by 2025.3 The most common medical procedures sought abroad include cancer treatment, fertility treatment, organ and tissue transplantation, and various forms of surgery, including bariatric, cosmetic, and noncosmetic (eg, orthopedic). Other care sought includes physician-assisted suicide and addiction treatment.4 For US residents, popular destinations include Argentina, Brazil, Canada, Colombia, Costa Rica, Cuba, Dominican Republic, Ecuador, Germany, India, Malaysia, Mexico, Nicaragua, Peru, Singapore, and Thailand, where the cost of care can be a fraction of what it is in the United States, Canada, and Western Europe.4 These countries advertise high-quality care at reduced prices, often coupling healthcare with appealing vacation packages.
Patient motivations
Dental tourism attracts patients due to the lower cost of dental procedures. According to the Dental Tourism Association, the most common destinations for care include Mexico, Dominican Republic, Turkey, Columbia, Costa Rica, India, Thailand, and Puerto Rico. 5 Popular treatments include implants, all-on-X prostheses, veneers, crowns, fullmouth reconstruction, and dentures. 5 It would be easy to assume that everyone who travels for healthcare abroad does so to receive quick and affordable care. Data analysis suggests otherwise. According to a survey by Ehrbeck et al,
40% of respondents sought high-tech operations performed by professionals with advanced training unavailable in their home country; 32% said they want better, more personalized medical attention; and 15% prioritized prompt treatment without lengthy wait times.6 The remaining 13% cited cheaper costs as their key justification for traveling for care.6 Most healthcare tourists pay for their care at the time of service, and they frequently use private firms or concierge services to find overseas healthcare facilities. Some US health insurance companies and corporations have formed relationships with healthcare institutions outside the United States to control costs.4 Dental care is the most popular type of medical tourism among US citizens, due largely to the escalating costs of dental treatment in the United States and the fact that many Americans have inadequate coverage or lack dental insurance altogether.4,7 A study by Stoney et al found that dentistry accounted for 55% of medical tourism treatments.7
Impact on patients and home-country providers
The foremost ethical concern in medical tourism involves the quality of care provided and patient safety. While some destinations offer world-class facilities and highly skilled practitioners, others may lack adequate regulation, potentially leading to substandard treatment and patient risks. Standards of practice vary
widely between countries, and care that is considered acceptable in one place might not meet the rigorous health and safety protocols of another. This discrepancy can pose significant risks to the health of patients. For instance, the use of nonapproved materials or differing protocols for sterilization and infection control can lead to severe complications, ranging from ineffective treatments to life-threatening infections. Several infectious disease outbreaks have been documented among medical tourists, including carbapenemresistant Enterobacterales, fungal infections (eg, Candida auris), nontuberculous mycobacteria in cosmetic surgery patients treated in Dominican Republic, and Q fever in patients who received fetal sheep cell injections in Germany.4
Informed consent is a cornerstone of ethical healthcare practice, requiring that patients understand the risks, benefits, and alternatives of any treatment. However, in the context of medical tourism, language barriers and differing cultural expectations about the disclosure of healthcare information can lead to inadequate informed consent. Patients might not fully understand their procedures, and confusion might be exacerbated by the pressure of limited time frames and immediate financial transactions. 8 Such situations can undermine the ethical principles of respect for patient autonomy (“selfgovernance”), nonmaleficence (“do no harm”), and veracity (“truthfulness”), leading to potential exploitation.9
The transient nature of the patientprovider relationship in medical tourism further complicates these issues, often leaving little recourse for patients who experience posttreatment complications once they return home. The American Medical Association Code of Medical Ethics (AMA Code) states10 :
Medical tourism can leave home country physicians in problematic positions: faced with the reality that medical tourists often need followup when they return, even if only to monitor the course of an uneventful recovery; confronted with the fact that returning medical tourists often do not have records of the procedures they underwent and the medications they received or contact information
for the foreign health care professionals who provided services; asked to make right what went wrong when patients experience complications as a result of medical travel, often having not been informed about, let alone part of the patient’s decision to seek healthcare abroad. Physicians need to be aware of the implications of medical tourism for individual patients and the community.
Dentists managing the care of dental tourists in their practice may face the same issues.
The American Dental Association Council on Ethics, Bylaws and Judicial Affairs white paper on dental tourism acknowledges that patients have freedom of choice when considering where to seek care, including abroad.11 They also acknowledge that there are very capable dentists in other countries who provide quality care, implying that we should not assume that care abroad is always substandard. The council’s guidance to US dentists is the following11:
The ethical dentist will treat the patient who has received dental treatment outside the United States in the same manner as he/she would treat a patient who has transferred their care from any other practice, irrespective of the fact that the treatment performed outside of the United States might or might not be substandard and, in some instances, a possible detriment to the patient’s health. A dentist should consult applicable state law to determine the definition of “patient of record.” Failure to treat such a patient may raise ethical concerns.
Furthermore, the council states11:
Where there is an emergency situation that develops as a result of dental tourism and the patient is not—or is no longer—one of record, dentists are obliged, at the least, to make reasonable arrangements for emergency care.
Impact on destination communities and governments
Tourism is critical to both urban and rural development programs around
the world, and many disciplines have recognized tourism as a powerful means of economic and social development. Previous research has identified that tourism both benefits and costs a community.8 While it generates revenue and creates jobs in host countries, healthcare tourism can also profoundly impact local healthcare systems, potentially diverting resources away from local populations. Medical tourism may turn locals’ access to traditional healthcare into a commercial opportunity. This could have several counterintuitive effects, such as small towns crammed with tourists, increased service costs, embezzlement of public funds, higher local taxes, restricted access to healthcare for locals, and strained ties between locals and visitors—all of which would diminish the quality of life for locals.8
While Americans may not think about their home country as a popular medical tourism destination, some cities in the United States are considering promoting medical tourism to boost their local economies. 8 Additionally, according to the Medical Tourism Review, many travelers already come to the United States for care, with the largest groups visiting from the Caribbean, Europe, and Central America.12 Common treatments sought in the United States include stem cell treatment, cancer treatment, Lutetium 177 treatment for motor neuron disease, vitiligo treatment, retinitis pigmentosa treatment, and psoriasis treatment. Even though medical care in the United States can be more expensive than in other nations, many foreign patients seeking specialty care choose to receive their treatment in the United States because of its state-of-the-art healthcare facilities and expertise.12
Responding to patient interest in dental tourism
Although US dentists may feel betrayed or upset over the potential loss of a patient to dental tourism, they are positioned to offer valuable guidance to such patients before they go. If the patient’s reason is financial—and for dental care it usually is—dentists can explore other options with patients1:
• Offering a payment plan or other financial arrangements
• Connecting patients with charitable
organizations, such as a local Donated Dental Services provider
• Offering a referral to a local dental school where fees are often discounted and follow-up care is highly accessible
If none of these suggestions suits the patient, dentists should emphasize a critical point with their patients instead of outright discouraging the notion of dental tourism: thorough preparation is paramount. Individuals considering healthcare services abroad should conduct comprehensive research. This includes investigating medication availability, infection control protocols, and the prevalence of antibiotic-resistant microorganisms in the destination locale. Furthermore, patients should ascertain the credentials of their providers and whether the chosen facility holds appropriate accreditation for the desired procedures in the respective country.4 Additionally, patients should proactively explore their recourse options in the event of unfavorable outcomes. This encompasses understanding the procedures for seeking retreatment, addressing post-treatment complications, and pursuing potential refunds or restitution. Different countries offer diverse avenues for grievances, ranging from health ministries to dedicated complaint forums. Patients may simplify the process by working with a reputable healthcare tourism concierge service that will manage the travel arrangements and most of the appointment details. Patients
can navigate dental tourism with greater confidence and security by meticulously preparing and understanding their rights and options.1,4
Conclusion
Healthcare tourism presents opportunities and challenges for patients seeking care abroad. While it offers the allure of cost savings and access to treatments not readily available domestically, it also entails risks associated with varying healthcare standards, regulatory frameworks, and recourse mechanisms. Dentists play a pivotal role in guiding patients through the decision-making process, emphasizing the importance of thorough research, verification of credentials, and awareness of recourse options. As the landscape of healthcare continues to evolve globally, informed decisionmaking remains paramount in optimizing patient outcomes and experiences in the realm of dental tourism.
Author affiliation
Marquette University School of Dentistry, Milwaukee, Wisconsin.
Conflicts of interest
None reported.
References
1. Newman E. Worth the trip? A look at dental tourism. AGD Impact. 2020;48(1):26-29.
2. Patients beyond borders. Accessed May 8, 2024. https://www.patientsbeyondborders.com/media
3. Khorsandi J. Dental tourism – make sure it is worth the trip. Byte. March 1, 2022. Accessed May 4, 2024. https://www.byte.com/community/resources/article/ dental-tourism
4. Crist M, Appiah G, Leidel L, Stoney R. Health care abroad. In: Centers for Disease Control, Nemhauser JB, eds. CDC Yellow Book 2024: Health Information for International Travel. Oxford University Press; 2024. https://wwwnc.cdc.gov/travel/yellowbook/2024/ health-care-abroad/medical-tourism
5. Dental Tourism Association. Accessed April 29, 2024. https://dentaltourismassociation.com/
6. Ehrbeck T, Guevara C, Mango PD. Mapping the market for medical travel. The McKinsey Quarterly. May 2008. https://www.lindsayresnick.com/Resource_Links/ MedicalTravel.pdf
7. Stoney RJ, Kozarsky PE, Walker AT, Gaines JL. Population-based surveillance of medical tourism among US residents from 11 states and territories: findings from the behavioral risk factor surveillance system. Infect Control Hosp Epidemiol. 2022;43(7):870-875. doi:10.1017/ice.2021.245
8. Suess C, Baloglu S, Busser JA. Perceived impacts of medical tourism development on community wellbeing. Tour Manage. 2018;69(4):232-245. doi:10.1016/j.tourman.2018.06.006
9. Principles of Ethics & Code of Professional Conduct. American Dental Association. Updated March 2023. Accessed May 14, 2024. https://www.ada.org/-/ media/project/ada-organization/ada/ada-org/files/ about/ada_code_of_ethics.pdf
10. American Medical Association Code of Medical Ethics. Opinion 1.2.13. Medical Tourism. Accessed April 25, 2024. https://code-medical-ethics.ama-assn.org/ ethics-opinions/medical-tourism
11. American Dental Association. Statement of the ADA Council on Ethics, Bylaws and Judicial Affairs on dental tourism - ethical obligations of dentists. Updated November 2009. Accessed May 7, 2024. https://www.ada.org/-/media/project/ ada-organization/ada/ada-org/files/about/ principles/cebja-statements-and-white-papers/ statement_ethics_dental_tourism_2009.pdf
12. Health tourism in the United States. MedicalTourism. Review. Accessed May 5, 2024. https://medicaltourism. review/countries/united-states
Incidence of missed canals during endodontic treatment of maxillary first and second molars
Michael Rodillo, DDS, MS ¢ Rodrigo Sanches-Cunha, DDS, MS ¢ Patricia Ann Bauer, DDS, MS
Suncica Travan, DDS, MS ¢ Bruno Cavalcanti, DDS, MS, PhD ¢ Neville McDonald, DDS, MS
Untreated canals are a primary cause of persistent apical periodontitis, and the inability to identify and adequately treat canals has been considered a major cause of failure of root canal therapy in maxillary molars. The purpose of this retrospective study was to use cone beam computed tomography (CBCT) to quantify the number of missed canals in maxillary first and second molars needing endodontic retreatment after treatment by general dentists. A total of 401 CBCT scans of maxillary first and second molars were examined. A total of 214 scan sets (53.37% [95% CI, 48.48%-58.25%]) showed evidence of an untreated canal, with the highest rate (49.38%; n = 198) observed in the second mesiobuccal canal. Imaging revealed that multiple canals were missed in some patients, for a total of 225 missed canals. The examinations showed untreated first mesiobuccal canals in 2.99% of CBCT scan sets (n = 12), untreated distobuccal canals in 2.99% of CBCT scan sets (n = 12), and untreated palatal canals in 0.75% of CBCT scan sets (n = 3). Preoperative CBCT imaging should be considered prior to initial root canal treatment of maxillary molars. When the risks and limitations of CBCT are taken into consideration, the additional information it provides can improve diagnostic accuracy, increase confidence in decision-making, and positively impact treatment planning.
Untreated canals are a primary cause of persistent apical periodontitis due to their potential to harbor bacteria.1 It is possible that a high proportion of canals are missed during endodontic treatment, in particular the second mesiobuccal canal (MB2).2 In maxillary molars, the inability to identify all canals and treat them appropriately is a main cause of endodontic treatment failure.3 Canals may be missed during treatment for multiple reasons, including an operator’s limited knowledge of the tooth anatomy, complexities of canal configuration, procedural errors, and/or inadequate preoperative radiographic imaging.4-6
A systematic review obtained data on the mesiobuccal roots of 15,285 first molars and 8641 second molars using cone beam computed tomography (CBCT).3 An MB2 canal was present in 69.6% (64.5% to 74.8%) of maxillary first molars and 39.0% (31.1% to 46.9%) of maxillary second molars. Wolcott et al evaluated disparities in locating MB2 canals between initial endodontic treatment and retreatment in maxillary first and second molars.7 With only the use of magnification (×3.5 or greater) and fiber-optic headlamps, the authors identified the presence of an MB2 canal in 67.4% (178/264) of cases in first molar retreatment compared with 58.8% (546/929) of cases during initial treatment. In second molars, MB2 canals were found in 43.6% (27/62) of retreatment cases compared with 35.3% (218/618) of cases during initial treatment. The difference in frequencies of MB2 canal identification during initial treatment and retreatment was statistically significant. However, using only magnification and a dental operating microscope may limit the clinician’s ability to identify MB2 canals. A clinical study in which 10 endodontic residents evaluated 200 maxillary molars determined that there was no significant increase in the number of MB2 canals located in maxillary molars when a microscope was used vs access modification without the use of a microscope.8 Therefore, other methods of identifying MB2 canals must be utilized.
CBCT is a valuable tool for the investigation of root canal morphology.9 It has been suggested that small–field-of-view (FOV) CBCT can be used routinely before endodontic treatment and retreatment of maxillary molars.10 It has also been shown that an MB2 canal was found more often during treatment when a preoperative CBCT scan was available than when it was not available, identified in 76% vs 54.5% of cases, respectively.10 CBCT imaging has been found to be an accurate tool for locating MB2 canals in maxillary molars because it provides 3-dimensional reconstruction of the canal anatomy.11-13 This ability reinforces the suggestion that the use of preoperative CBCT should be considered to ensure correct diagnostics and improve the treatment prognosis.14,15
Abbreviations: CBCT, cone beam computed tomography; DB, distobuccal canal; F, female; M, male; MB1, first mesiobuccal canal; MB2, second mesiobuccal canal; P, palatal canal.
CBCT scanning allows for in vivo dental investigation in the axial, sagittal, and coronal planes simultaneously, which can improve the clinician’s ability to see the entire root canal system and thus improve the quality of endodontic treatment in maxillary molars by reducing the likelihood that canals will be missed during treatment.16,17 The purpose of this retrospective study was to evaluate 401 CBCT scans to quantify the number of missed canals in maxillary first and second molars needing endodontic retreatment after treatment by general dentists.
Methods
The present study was reviewed and authorized by the Institutional Review Board of the University of Michigan School of Dentistry (HUM00198726).
This retrospective study examined preoperative small-FOV CBCT images of maxillary molars requiring endodontic retreatment. Images were deidentified and reviewed by 2 examiners, an endodontist (R.S.-C.) and an endodontic resident (M.R.). The examiners were trained together to ensure consistency during assessment. The CBCT scans were obtained with the Veraview X800 imaging system (J. Morita USA) with the following specifications: 90 kV, 7 mA, 17.9 seconds of exposure time, and a 40 × 40-mm voxel size.
Inclusion criteria were maxillary first and second molars previously treated by general dentists and requiring endodontic retreatment. The previous records and radiographs of all cases referred for retreatment were reviewed, and, to the best of the authors’ knowledge, no CBCT was performed for any of the cases included in this study. Participants were excluded if teeth had no evidence of previous root canal treatment (ie, intracanal radiopaque filling material); if the teeth were previously treated by an endodontist or a dental student; or if the CBCT scans had artifacts affecting the diagnostic quality of the images.
All CBCT scans were viewed with Digital Imaging and Communications in Medicine (DICOM) software (i-Dixel 1.0, J. Morita USA), which is the standard format for CBCT-based data sets.18 The examiners had full access to the software features to manipulate images in 3 orthogonal planes (axial, coronal, and sagittal) by selecting and moving the cursor to change the center of view on the reconstructed slices. The examiners used these views to inspect the root canal system by
carefully scrolling downward through the images in the axial perspective, from the pulp chamber to the apex.9 If there was any indication of an unfilled canal at any point along the path, from the cementoenamel junction to the apex, the canal was recorded as untreated.15
The power analysis for determining the sample size needed to estimate the proportion of missed canals was based on the formula n ≈ [z 2 α/2 ∙ p ∙ (1 − p)]/d2 , where n represents the sample size; z 2 α/2 is a constant associated with the confidence interval and margin of error; p represents the population proportion; and d represents the margin of error. With the use of an online sample size calculator set to a 95% CI, margin of error of 5%, and a population proportion of 50%, this study required evaluation of a minimum of 387 maxillary molars. Statistical analysis was done using a logistic regression model (SPSS, version 28.7, IBM).
Results
A total of 401 maxillary first molars (n = 298) and second molars (n = 103) were obtained. The dates of the CBCT scans ranged from December 20, 2019, to October 10, 2021. The sample comprised 160 male and 198 female patients ranging in age from 15 to 92 years (mean, 52.87 years). Of the 401 CBCT scans reviewed, 214 (53.37% [95% CI, 48.48%-58.25%]) showed a canal that was missed during previous treatment ( Table 1). Imaging revealed that multiple canals were missed in some patients, for a total of 225 missed canals. The highest incidence of missed canals involved MB2 canals, with 49.38% (95% CI, 44.48%-54.27%; 198/401) of all CBCT image sets revealing an MB2 canal that was missed ( Table 2).
CBCT scans of the maxillary right first molars revealed that 77.58% (128/165) had an MB2 canal, with 56.97% (94/165) being untreated. Among the maxillary left first molars, 72.18% (96/133) had an MB2 canal, with 50.38% (67/133) untreated. For the maxillary right second molars, 54.55% (18/33) had an MB2 canal, with 39.39% (13/33) untreated. For the maxillary left second molars, 65.71% (46/70) had an MB2 canal, with 34.29% (24/70) untreated. Overall, maxillary first molars showed the highest rate of untreated MB2 canals (54.03% [95% CI, 48.36%-59.69%]; 161/298). In second molars, this rate was 35.92% (95% CI, 26.66%-45.19%; 37/103). For the preceding analyses, all molars were included in the percentage
Table 1. Frequency of missed canals in endodontically treated maxillary molars as determined by CBCT (N = 401 scans).
Table 2. Frequency of missed MB2 canals in endodontically treated maxillary molars as determined by CBCT (N = 401 scans).
Teeth Total, n Missed, n (%)
First molars
Second molars
298 161 (54.03)
103 37 (35.92)
Total 401 198 (49.38)
Abbreviations: CBCT, cone beam computed tomography; MB2, second mesiobuccal canal.
calculations, regardless of whether or not an MB2 canal was identified. This approach was selected because it is possible that these teeth had an MB2 canal (eg, very calcified) that was not detected by the examiners. In addition, as the other canals were obturated, scattering in the CBCT could have influenced the analysis.
A logistic regression model was created based on the data and showed a statistically significant correlation between age and the presence of an untreated MB2 canal ( Table 3). The average age of patients with a missed canal was 50.51 years, and the average age of patients with a treated canal was 55.18 years. As patient age increased by each year, the likelihood of missing an MB2 canal decreased by 2.38%. There was also a statistically significant correlation between a missed MB2 canal and sex, with a significant difference in the number of untreated MB2 canals between male and female patients (56.88% vs 44.40%, respectively; P < 0.05). Statistical analysis was not possible for the other canals (first mesiobuccal [MB1], distobuccal [DB], and palatal [P] canals) because the proportions were too low.
Discussion
Observational studies describing the incidence of missed canals during endodontic treatment have shown that the rate is highest for the MB2 canal of maxillary molars.3,4,10 The present study aimed to use CBCT methodology to assess the identification of untreated canals in maxillary molars requiring endodontic retreatment, with an emphasis on the MB2 canal in particular. The findings confirmed that preoperative CBCT imaging can increase the likelihood that all canals in maxillary molars will be identified prior to endodontic treatment.
Of the 401 CBCT scans included in the present study, 198 (49.38%) showed evidence of an untreated MB2 canal. In maxillary first molars, this frequency was 54.03% (right first molar, 56.97%; left first molar, 50.38%), while in second molars, it was 35.92% (right second molar, 39.39%; left second molar, 34.29%).
A similar retrospective cohort study that used CBCT imaging to evaluate missed canals found that the rates of a missed canal were 41.3% in 121 maxillary right first molars, 46.5% in 144 maxillary left first molars, 33.3% in 51 maxillary right second molars, and 27.7% in 47 maxillary left second molars.15 It was concluded that the most frequently missed canal was the MB2 canal (65%). However, it is unknown who performed the initial endodontic treatment in that study.15
a Regression coefficient divided by the standard error (SE).
b P value associated with the Z value.
c Statistically significant (P < 0.05).
Another retrospective study collected data on consecutive nonsurgical retreatments of maxillary and mandibular molars (n = 133) for a duration of 1 year.19 With the use of standard straight-on and distal angled periapical radiographs, untreated canals were identified in 48% (64/133) of the previously treated teeth. The study further identified untreated canals in 60.87% (28/46) of previously treated maxillary first molars and 58.33% (7/12) of previously treated maxillary second molars. The fact that the study did not utilize CBCT imaging but resulted in higher frequencies of missed canals is most likely due to its smaller sample size in comparison to the present study. Based on the sample size calculation and the actual sample size collected in this study, it can be determined with 95% confidence that 48.36% to 59.69% of maxillary first molars and 26.66% to 45.19% of maxillary second molars had an untreated MB2 canal. Overall, the incidence of an untreated MB2 canal in all maxillary molars was 44.48% to 54.27%.
A retrospective study by Shetty et al utilized CBCT scans to evaluate MB2 canals in endodontically treated permanent maxillary molars.20 The investigators determined that, for teeth with an MB2 canal present, 77.19% (44/57) of maxillary first molars and 90.00% (9/10) of maxillary second molars had an unfilled MB2 canal.20 However, the sample size of Shetty et al was also small, and, unlike the present study, they calculated the percentage of missed canals based only on the numbers of teeth in which an MB2 canal was present rather than on the total numbers of molars examined.20 Thus, selection bias may have affected their results.
A study by do Carmo et al gathered data on missed canals, including those other than the MB2 canal, and revealed frequencies of 6.48% (41/633) for missed MB1 canals, 7.11% (45/633) for missed DB canals, and 1.26% (8/633) for missed P canals.13 In the present study, these rates were 2.99% (12/401), 2.99% (12/401), and 0.75% (3/401), respectively. In the study by do Carmo et al, it was unknown whether the initial root canal treatment was performed by dental students, general dentists, or endodontists, and the reasons for CBCT evaluation were not specified.13 These factors could explain the differences in the results.
As a person ages, the continued production and mineralization of secondary or tertiary dentin can result in pulp canal calcification, making the identification of canals difficult.21 The logistic regression model in this study showed that the likelihood of missing an MB2 canal decreased by 2.38% for each
Table 3. Logistic regression model.
year of increased patient age. It is possible that, as MB2 canals become increasingly difficult to identify with age, they become difficult to identify in CBCT scans as well. In such cases, older patients would not present with a missed MB2 canal because the canal would be completely calcified.
Another factor to note is that the age distribution in this sample size was not specifically designed for the investigation of age. The present data are skewed because there was a larger proportion of patients over the age of 50 years compared with those under the age of 50 years. As a result, this study does not appropriately represent the under-50 demographic. Of the 401 patients, 246 were 50 years or older, and 43.09% of these patients showed a missed MB2. Of the 155 patients younger than 50 years, 59.35% showed a missed MB2. The present data set included patients who required endodontic retreatment, and there was no statistical structuring of the study to allow for precise statistical inferences as to the effects of age on missed canals.
Another study found a similar correlation regarding sex and the frequency of a missed MB2 canal.22 Pan et al determined that missed MB2 canals in maxillary second molars were more common in men (13.4%) than in women (4.9%) (P < 0.05).22
The logistic regression model in the present study also demonstrated a statistically significant difference, showing men to have a greater number of untreated MB2 canals. Although the present data set had an uneven ratio of 160 molars from male patients (39.90%) to 241 molars from female patients (60.10%), the ratio is similar to that in Pan et al (90 [43.3%] and 118 [56.7%], respectively).22 Further studies are needed to obtain accurate data regarding the correlation between sex and missed MB2 canals.
Conventional radiography is limited because it provides a restricted 2-dimensional image in the mesiodistal plane of a 3-dimensional anatomy. Conventional radiography often hinders accurate portrayal of the spatial relationships between anatomical complexities. Geometric distortion accounts for a minimum magnification of 5% of the object being radiographed and will rarely reproduce an image with complete accuracy.23 Maintaining patient stability during imaging is essential because the images may be easily distorted by subtle movements, which could decrease their quality.24 Another complicating factor is the anatomical noise caused by the overlying features of alveolar bone, such as the cortical plate, trabeculae, and marrow spaces, which can interfere with diagnostic interpretation.23 The presence of metallic restorations (eg, amalgam, posts, crowns, and implants) or even gutta percha can also significantly compromise details of the root canal anatomy due to radiographic beam hardening or artifacts.24 Last, there may be a financial burden on the patient, which should be taken into consideration.25
Dutra et al determined that the accuracy of CBCT imaging was excellent and that it can overcome the limitations of conventional radiography.26 Studebaker et al proposed that small-FOV CBCT imaging of maxillary molars be routinely used for initial endodontic treatment and nonsurgical retreatment.10 However, it is essential to keep patient radiation exposure as low as reasonably achievable (the ALARA principle), because CBCT imaging comes at the expense of an increased radiation dose.27,28
One limitation of the present study is that the data obtained were not randomized. Only cases referred for endodontic retreatment due to initial treatment failure were selected and examined, and this inclusion criterion does not take into consideration maxillary molars that had been endodontically treated and were asymptomatic, unreported, or not referred for retreatment. However, the selection bias in this study was still limited because all CBCT scans that fit the inclusion criteria within a specific time frame were included. Another limitation is that the teeth were not standardized; thus, it was unknown whether they had a full-coverage crown prior to initial treatment, which could have interfered with the visualization of the canals. Last, it cannot be determined if an untreated canal was the sole reason for endodontic retreatment. Along with untreated MB2 canals, this study identified the incidence of untreated MB1 canals (2.99%), DB canals (2.99%), and P canals (0.75%). Further studies are required to examine possible reasons canals are untreated during initial root canal treatment and the possible outcomes of treatment failure, such as periapical involvement or thickening of the sinus mucosa adjacent to the affected roots.29,30
Conclusion
Within the limitations of this study, it can be determined that failure to perform CBCT imaging prior to initial endodontic treatment of maxillary molars resulted in a 53.37% incidence of untreated canals, with the highest frequency of missed canals (49.38%) involving the MB2 canal. Preoperative CBCT images should be considered for examination prior to endodontic treatment of maxillary molars because this visual preoperative aid appears to increase the likelihood that the clinician will identify all canals. When the risks and limitations of CBCT are taken into consideration, the additional information it provides can improve diagnostic accuracy, increase confidence in decision-making, and positively impact treatment planning.
Author affiliations
Department of Cariology, Restorative Sciences and Endodontics, University of Michigan School of Dentistry, Ann Arbor (Rodillo, Bauer, Cavalcanti, McDonald); Private practice, Winnipeg, Canada (Sanches-Cunha); Department of Periodontics and Oral Medicine, University of Michigan School of Dentistry, Ann Arbor (Travan).
Correspondence
Bruno Cavalcanti, DDS, MS, PhD (brunocav@umich.edu).
Conflicts of interest
None reported.
References
1. Costa FFNP, Pacheco-Yanes J, Siqueira JF Jr, et al. Association between missed canals and apical periodontitis. Int Endod J. 2019;52(4):400-406. doi:10.1111/iej.13022
2. Buhrley LJ, Barrows MJ, BeGole EA, Wenckus CS. Effect of magnification on locating the MB2 canal in maxillary molars. J Endod. 2002;28(4):324-327. doi:10.1097/00004770200204000-00016
3. Martins JNR, Marques D, Silva EJNL, Caramês J, Mata A, Versiani MA. Second mesiobuccal root canal in maxillary molars—a systematic review and meta-analysis of prevalence studies using cone beam computed tomography. Arch Oral Biol. 2020;113:104589. doi:10.1016/ j.archoralbio.2019.104589
4. Baruwa AO, Martins JNR, Meirinhos J, et al. The influence of missed canals on the prevalence of periapical lesions in endodontically treated teeth: a cross-sectional study. J Endod 2020;46(1):34-39.e1. doi:10.1016/j.joen.2019.10.007
5. Song M, Kim HC, Lee W, Kim E. Analysis of the cause of failure in nonsurgical endodontic treatment by microscopic inspection during endodontic microsurgery. J Endod 2011;37(11):1516-1519. doi:10.1016/j.joen.2011.06.032
6. Tabassum S, Khan FR. Failure of endodontic treatment: the usual suspects. Eur J Dent 2016;10(1):144-147. doi:10.4103/1305-7456.175682
7. Wolcott J, Ishley D, Kennedy W, Johnson S, Minnich S. Clinical investigation of second mesiobuccal canals in endodontically treated and retreated maxillary molars. J Endod. 2002;28(6):477-479. doi:10.1097/00004770-200206000-00016
8. Sempira HN, Hartwell GR. Frequency of second mesiobuccal canals in maxillary molars as determined by use of an operating microscope: a clinical study. J Endod. 2000;26(11):673674. doi:10.1097/00004770-200011000-00010
9. Lee JH, Kim KD, Lee JK, et al. Mesiobuccal root canal anatomy of Korean maxillary first and second molars by cone-beam computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;111(6):785-791. doi:10.1016/j.tripleo.2010.11.026
10. Studebaker B, Hollender L, Mancl L, Johnson JD, Paranjpe A. The incidence of second mesiobuccal canals located in maxillary molars with the aid of cone-beam computed tomography. J Endod. 2018;44(4):565-570. doi:10.1016/j.joen.2017.08.026
11. Mirmohammadi H, Mahdi L, Partovi P, Khademi A, Shemesh H, Hassan B. Accuracy of cone-beam computed tomography in the detection of a second mesiobuccal root canal in endodontically treated teeth: an ex vivo study. J Endod. 2015;41(10):1678-1681. doi:10.1016/j.joen.2015.06.011
12. Huumonen S, Kvist T, Gröndahl K, Molander A. Diagnostic value of computed tomography in re-treatment of root fillings in maxillary molars. Int Endod J. 2006;39(10):827-833. doi:10.1111/j.1365-2591.2006.01157.x
13. do Carmo WD, Verner FS, Aguiar LM, et al. Missed canals in endodontically treated maxillary molars of a Brazilian subpopulation: prevalence and association with periapical lesion using cone-beam computed tomography. Clin Oral Investig. 2021;25(4):2317-2323. doi:10.1007/ s00784-020-03554-4
14. Parker J, Mol A, Rivera EM, Tawil P. CBCT uses in clinical endodontics: the effect of CBCT on the ability to locate MB2 canals in maxillary molars. Int Endod J. 2017;50(12):1109-1115. doi:10.1111/iej.12736
15. Karabucak B, Bunes A, Chehoud C, Kohli MR, Setzer F. Prevalence of apical periodontitis in endodontically treated premolars and molars with untreated canal: a cone-beam computed tomography study. J Endod. 2016;42(4):538-541. doi:10.1016/j.joen.2015.12.026
16. Zhang R, Yang H, Yu X, Wang H, Hu T, Dummer PM. Use of CBCT to identify the morphology of maxillary permanent molar teeth in a Chinese subpopulation. Int Endod J. 2011;44(2): 162-169. doi:10.1111/j.1365-2591.2010.01826.x
17. Mashyakhy M, Ali Hadi F, Alhazmi HA, et al. Prevalence of missed canals and their association with apical periodontitis in posterior endodontically treated teeth: a CBCT study. Int J Dent 2021;2021:9962429. doi:10.1155/2021/9962429
18. Spin-Neto R, Marcantonio E Jr, Gotfredsen E, Wenzel A. Exploring CBCT-based DICOM files. A systematic review on the properties of images used to evaluate maxillofacial bone grafts. J Digit Imaging. 2011;24(6):959-966. doi:10.1007/s10278-011-9377-y
19. Witherspoon DE, Small JC, Regan JD. Missed canal systems are the most likely basis for endodontic retreatment of molars. Tex Dent J. 2013;130(2):127-139.
20. Shetty H, Sontakke S, Karjodkar F, Gupta P, Mandwe A, Banga KS. A cone beam computed tomography (CBCT) evaluation of MB2 canals in endodontically treated permanent maxillary molars. A retrospective study in Indian population. J Clin Exp Dent. 2017;9(1):e51-e55. doi:10.4317/jced.52716
21. Kiefner P, Connert T, ElAyouti A, Weiger R. Treatment of calcified root canals in elderly people: a clinical study about the accessibility, the time needed and the outcome with a three-year follow-up. Gerodontology. 2017;34(2):164-170. doi:10.1111/ger.12238
22. Pan JYY, Parolia A, Chuah SR, Bhatia S, Mutalik S, Pau A. Root canal morphology of permanent teeth in a Malaysian subpopulation using cone-beam computed tomography. BMC Oral Health. 2019;19(1):14. doi:10.1186/s12903-019-0710-z
23. Durack C, Patel S. Cone beam computed tomography in endodontics. Braz Dent J 2012;23(3):179-191. doi:10.1590/S0103-64402012000300001
24. Patel S, Brown J, Pimentel T, Kelly RD, Abella F, Durack C. Cone beam computed tomography in endodontics—a review of the literature. Int Endod J. 2019;52(8):1138-1152. doi:10.1111/ iej.13115
25. Aung NM, Myint KK. Diagnostic accuracy of CBCT for detection of second canal of permanent teeth: a systematic review and meta-analysis. Int J Dent. 2021;2021:1107471. doi:10.1155/ 2021/1107471
26. Dutra KL, Haas L, Porporatti AL, et al. Diagnostic accuracy of cone-beam computed tomography and conventional radiography on apical periodontitis: a systematic review and metaanalysis. J Endod. 2016;42(3):356-364. doi:10.1016/j.joen.2015.12.015
27. Portelli M, Militi A, Lo Giudice A, et al. 3D assessment of endodontic lesions with a low-dose CBCT protocol. Dent J (Basel). 2020;8(2):51. doi:10.3390/dj8020051
28. Farman A. ALARA still applies. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;100(4):395-397. doi:10.1016/j.tripleo.2005.05.055
29. Maillet M, Bowles WR, McClanahan SL, John MT, Ahmad M. Cone-beam computed tomography evaluation of maxillary sinusitis. J Endod. 2011;37(6):753-757. doi:10.1016/ j.joen.2011.02.032
30. Aksoy U, Orhan K. Association between odontogenic conditions and maxillary sinus mucosal thickening: a retrospective CBCT study. Clin Oral Investig. 2019;23(1):123-131. doi:10.1007/ s00784-018-2418-x
GENERAL DENTISTRY SELF-INSTRUCTION
Exercise No. GD530, 2 CE Credits
Endodontics
Subject Code: 070
The 15 questions for this exercise are based on the article “Incidence of missed canals during endodontic treatment of maxillary first and second molars” on pages 10-14. This exercise was developed by Jeffery B. Price, DDS, MS, MAGD, FICD, FACD, in association with the General Dentistry Self-Instruction committee.
1. What is the exact number of CBCT scans used in this study?
A. 198
B. 214
C. 401
D. 582
2. All of the following statements describe causes of endodontic failure in maxillary molars except one. Which is the exception?
A. operator’s limited knowledge of tooth anatomy
B. inadequate laser-assisted canal sterilization
C. complexity of root canal configuration
D. inadequate preoperative radiographic imaging
3. A systematic review revealed that a second mesiobuccal (MB2) canal was present in 69.6% of maxillary first molars. This same study reported that the incidence of untreated distobuccal canals in endodontically treated molars was 39.0%.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
4. Clinicians utilizing magnification and fiberoptic headlamps detected more MB2 canals in maxillary first and second molars at the time of endodontic retreatment than at initial treatment. Endodontic residents were not able to detect MB2 canals in maxillary molars at a higher rate when using a dental operating microscope.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
5. The use of preoperative CBCT allowed for the detection of MB2 canals in ____% of maxillary molars during endodontic treatment.
A. 76
B. 78
C. 86
D. 96
Reading the article and successfully completing this exercise will enable you to:
• understand a major contributing factor to the failure of endodontic treatment in maxillary molars;
• describe diagnostic and treatment techniques that, when used properly, can improve the outcomes of endodontic treatment in maxillary molars; and
• discuss the role of dental cone beam computed tomography (CBCT) in aiding endodontic diagnosis.
Answers must be submitted online at agd.org/self-instruction by June 30, 2025.
6. All of the following terms describe the available planar views while using CBCT to evaluate a tooth for radiographic diagnosis except one. Which is the exception?
A. axial
B. sagittal
C. coronal
D. superior
7. In the present study, CBCT scans of teeth that had been endodontically treated by _________ were reviewed.
A. endodontic residents
B. general dentists
C. dental students
D. AEGD residents
8. The power analysis performed to determine the number of teeth needed in the study indicated that a minimum of ____ maxillary molars should be evaluated.
A. 98
B. 214
C. 387
D. 401
9. The mean age of the patients was 62.87 years, and there were more women than men. A missed canal was noted in 53.37% of the scans.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
10. Maxillary first molars had a frequency of untreated MB2 canals of ____%.
A. 35.92
B. 54.03
C. 59.69
D. 65.71
11. Maxillary second molars had a frequency of untreated MB2 canals of ____%.
A. 35.92
B. 45.19
C. 54.03
D. 59.69
12. Which of the following best describes the effect of age on the accuracy of detecting MB2 canals?
A. Age has no effect on the detection of MB2 canals.
B. MB2 canals are less likely to be missed in older adults.
C. MB2 canals are more likely to be missed in older adults.
D. The effect of age on the detection of MB2 canals is unknown.
13. Shetty et al found that the incidence of untreated _____ canals was greater in maxillary _____ molars.
A. MB2; second
B. MB1; first
C. MB2; first
D. MB1; second
14. Ensuring that radiation exposure is as low as possible is known as ___________.
A. good image quality
B. low anatomical noise
C. beam hardening
D. the ALARA principle
15. Which of the following statements is supported by the study’s conclusion concerning radiographic examination before molar endodontic treatment?
A. Use periapical imaging only.
B. Always use CBCT.
C. Consider use of CBCT.
D. Use bitewing radiographs.
Giving the pulp another chance: a case report of vital pulp therapy retreatment
Hataichanok Machareonsap, DDS, MS ¢ Papimon Chompu-inwai, DDS, MS ¢ Nattakan Chaipattanawan, DDS, MS Chanika Manmontri, DDS, MS
Vital pulp therapy (VPT) has been increasingly advocated due to its advantages in preserving tooth vitality. While VPT is often successful, failures can occur, and traditional root canal therapy is often recommended following VPT failure. This case report provides an example of successful preservation of tooth vitality using coronal pulpotomy (CP), a more invasive type of VPT, after failure of partial pulpotomy (PP) that had been performed in a healthy 10-year-old boy. A mandibular right first molar with a diagnosis of reversible pulpitis was initially treated with PP, which included the use of tricalcium silicate cement as a pulp dressing and a resin-modified glass ionomer cement base, followed by placement of a composite resin restoration. The restoration dislodged after 34 months without complaints from the patient or radiographically detectable lesions. A stainless steel crown was placed on the tooth; however, 15 months after crown placement, the patient returned with symptoms in the treated tooth. The tooth was diagnosed with irreversible pulpitis and asymptomatic apical periodontitis but responded positively to cold testing, and the pulp appeared clinically vital upon direct inspection. The tooth was re-treated with CP, including the use of mineral trioxide aggregate as a dressing material, and examination 21 months posttreatment revealed successful resolution of the periapical lesion. When a tooth remains vital, a more invasive type of VPT may be an alternative to root canal therapy for treating failures in more conservatively treated teeth. Moreover, regular periodic recalls are essential for ensuring tooth survival and early detection of problems (ie, restoration failure) that may worsen treatment outcomes.
Vital pulp therapy (VPT) can be a promising alternative to traditional root canal treatment in vital teeth challenged by deep dental caries, trauma, or mechanical insults.1 This procedure aims to preserve tooth vitality, allowing the pulp to maintain its functions, including protective, reparative, proprioceptive, and pain mechanisms; dentinogenesis; and apexogenesis.2,3 However, despite its high success rates, posttreatment failure can occur due to inadequate removal of infected pulp tissue or reinfection.2,4,5 Previous studies have reported the need to perform root canal treatment in teeth where VPT has failed.6-8 The present case report describes the failure of partial pulpotomy (PP) in a first molar that was successfully re-treated with coronal pulpotomy (CP), a more invasive type of VPT, emphasizing the importance of accurate diagnosis, a sealed restoration, and periodic recall after VPT to the treatment outcome.
Case report
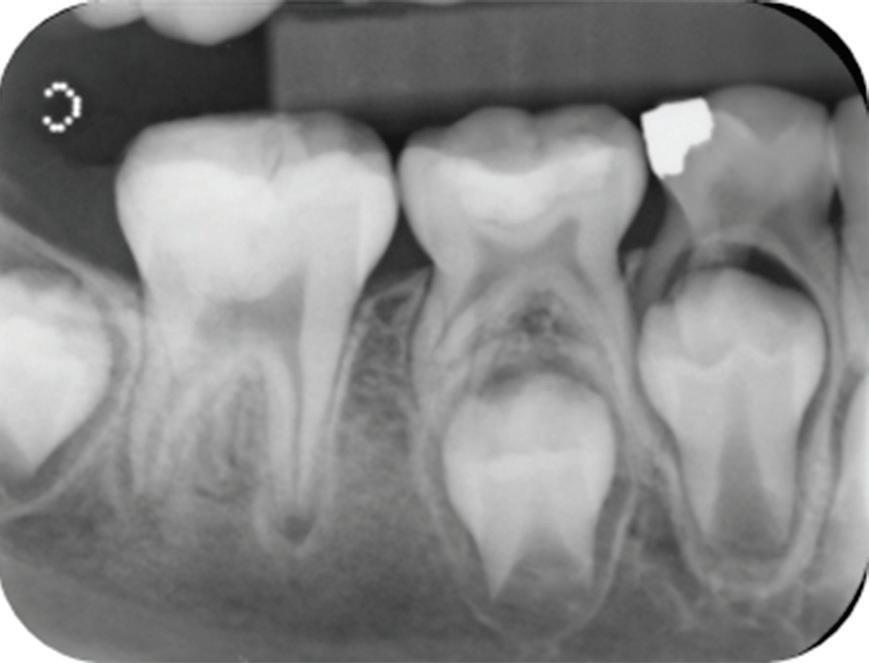
A healthy 10-year-old boy, accompanied by his mother, sought treatment of his mandibular right first molar because of pain in response to cold stimuli but reported no spontaneous pain in this tooth. Clinical examination revealed a carious lesion involving the occlusobuccal surfaces, and the tooth also appeared hypomineralized on the affected surfaces (Fig 1). The tooth responded positively to sensitivity tests, including the electric pulp test and cold test (Endo-Frost, Coltene), and there was no lingering pain or pain on percussion. A preoperative radiograph showed a large carious lesion extending to the pulp, incomplete root formation, and no pathologic periapical lesions (Fig 2). Therefore, the initial preoperative diagnosis was reversible pulpitis. The patient and parent were informed of possible pulp exposure, and VPT treatment after pulp exposure was explained in detail. Written consent for VPT was obtained from the parent.
Under local anesthesia and rubber dam isolation, nonselective caries removal resulted in a pulp exposure of 2 mm in diameter. The exposure site was irrigated with 2.5% sodium hypochlorite (NaOCl), and 2 mm of the inflamed pulp tissue at the exposure site was removed with a sterile high-speed round bur. Hemostasis was achieved within 2 minutes. After direct clinical evaluation of the remaining pulp tissue showed it to be healthy, the tooth was treated using PP with tricalcium silicate cement (Biodentine, Septodont) as a pulp dressing material and a resin-modified glass ionomer cement (RMGIC) as a base (Vitrebond Light Cure Glass Ionomer Liner, 3M). The tooth was then restored with composite resin (Filtek Z350 XT, 3M; Fig 3). An immediate postoperative radiograph was taken (Fig 4).
of a mandibular right first molar with caries affecting the occlusobuccal surfaces, which appear hypomineralized.
resin restoration following partial pulpotomy with a tricalcium silicate cement dressing and a resin-modified glass ionomer cement base.
deep caries, exposed pulp, and incomplete root formation but no pathologic periapical lesion.
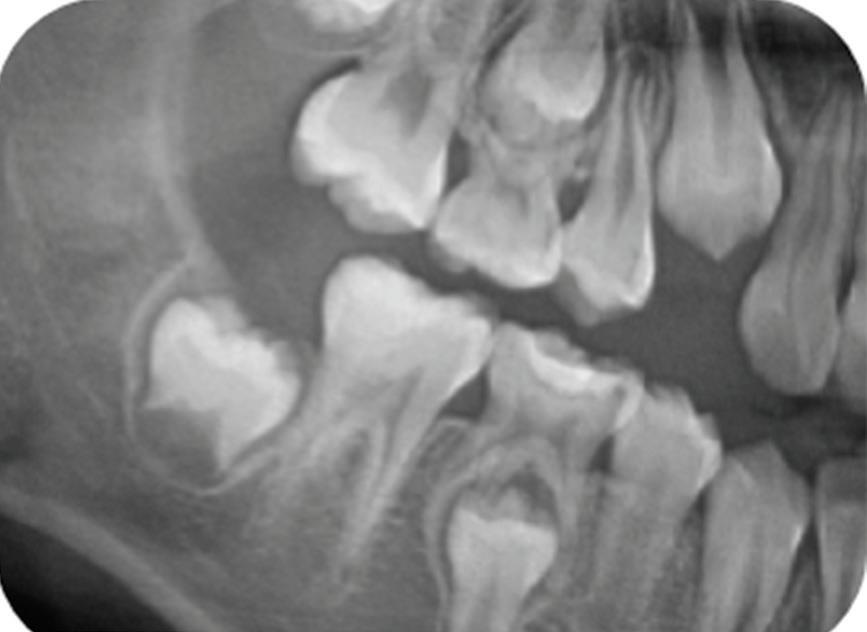
The patient did not present for the 6-month recall but did present 19 months after partial pulpotomy for an orthodontic consultation at the orthodontic clinic of the same institution. At this visit, the patient reported no complaints of spontaneous or stimulated pain. Continued root development of the mandibular right first molar was noticeable in the panoramic radiograph ordered by the orthodontist, indicating that the treatment was successful (Fig 5).
At 34 months after PP, the composite resin and RMGIC base had dislodged, though some parts of the Biodentine layer remained (Fig 6). The patient could not recall precisely when the restoration had failed but reported cold sensitivity. The first molar showed no signs of clinical failure, exhibiting a normal response to the cold test, a positive response to the electric pulp test, and a negative response to the percussion test. A periapical radiograph showed that the condition had remained stable since the orthodontic consultation visit. Therefore, it was decided that the tooth should be restored with a stainless steel crown (SSC). Vitrebond was placed over the remaining Biodentine layer, and an SSC was placed, causing accidental damage to the mesial aspect of the unerupted mandibular right second molar.
The patient presented for recall 6 months after SSC placement, and there were no signs or symptoms of irreversible pulpitis or pulpal necrosis in the PP-treated tooth. The results of the electric pulp test and cold tests were positive, and the result of the percussion test was negative. A periapical radiograph showed possible widening of the periodontal ligament space (Fig 7). Moreover, the patient reported sometimes feeling brief sensitivity after drinking cold water. However, the emerging mandibular right second molar that had been accidentally damaged during SSC placement was considered the potential cause of sensitivity, and a further follow-up of the treated tooth was scheduled. However, the patient did not return for these recall visits.
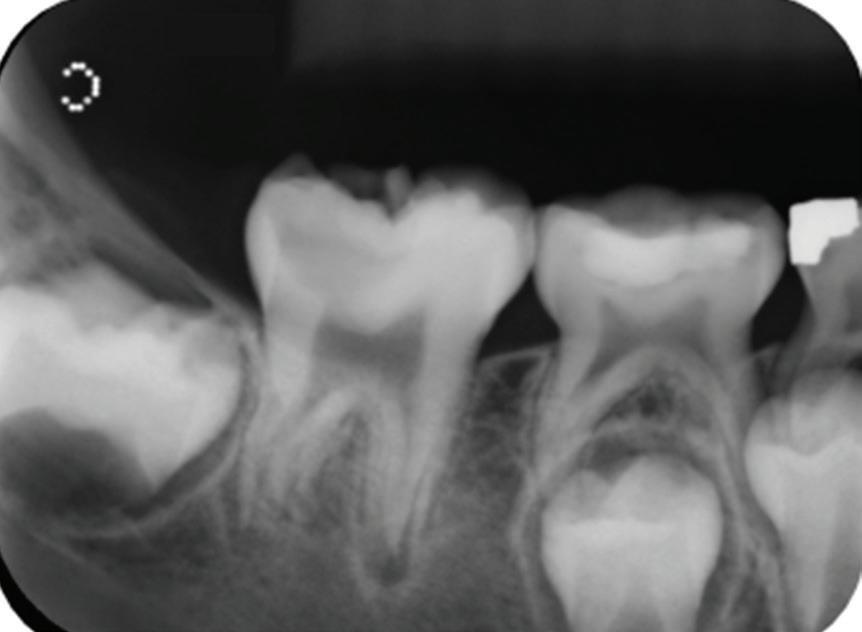
Approximately 15 months after SSC placement (49 months after PP), the patient returned with a complaint of sensitivity to cold stimuli in the treated tooth. Cold testing elicited sharp pain lasting approximately 10 seconds, but the results of the electric pulp test and percussion test were negative. Radiographic examination of the first molar showed a periapical radiolucency with a periapical index score of 3 (Fig 8).9 The tooth was diagnosed with irreversible pulpitis and asymptomatic apical periodontitis.
Fig 1. Preoperative clinical photograph
Fig 2. Preoperative radiograph showing
Fig 3. Composite
Fig 4. Immediate postoperative radiograph.
Radiograph 15 months after stainless steel crown placement, showing periapical radiolucency that indicates vital pulp therapy failure 49 months after partial pulpotomy.
The same radiograph also showed impaction of the mandibular right second molar. Root canal treatment and CP were offered as treatment options for the first molar and explained to the patient and his parent. They preferred CP due to its reduced invasiveness and lower cost.
After establishment of local anesthesia and rubber dam isolation, the SSC, the Vitrebond layer, and the Biodentine layer were removed. A hard tissue barrier was found, and an access opening into the pulp chamber was created with a high-speed round diamond bur used with water coolant. Slight bleeding from the visually pale pulp tissue was observed; therefore, CP was performed by removing the pulp tissue from the orifices using a sterile high-speed round diamond bur with water coolant and spoon excavation. The radicular pulp tissue had a resilient texture and bright red blood with continuous flow, suggesting that the pulp was healthy and vital (Fig 9). Next, 2.5% NaOCl was used for pulp wound irrigation, and hemostasis was achieved within 6 minutes by applying cotton pellets soaked in 2.5% NaOCl. Afterward, the pulp tissue and coronal portion of the tooth were irrigated with normal saline solution
followed by 17% ethylenediaminetetraacetic acid (EDTA) as the final irrigant.
Mineral trioxide aggregate (ProRoot MTA, Dentsply Sirona) was used as the dressing material, and the tooth was temporarily restored with RMGIC (Vitremer, 3M) to allow evaluation of the treatment outcome before placement of the final restoration. An orthodontic elastic separator was placed between the mandibular right first and second molars. Composite resin restoration of the second molar that was damaged during SSC placement was performed 1 week later.
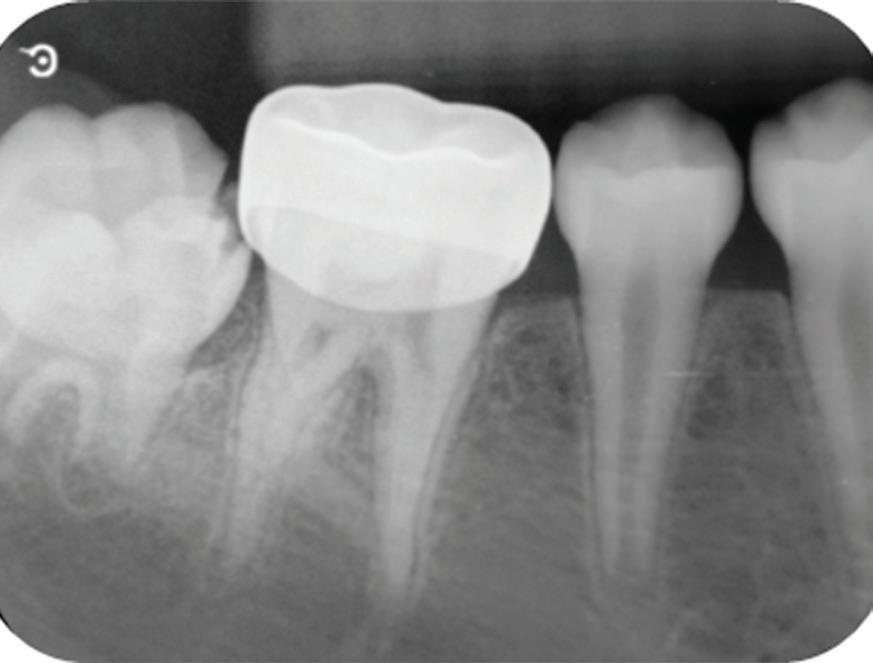
At the 3-month recall, the re-treated first molar was asymptomatic, and the periapical lesion had resolved. Therefore, the tooth underwent final preparation for a new SSC. The occlusion was checked before the SSC was fixed with RMGIC (RelyX Luting Plus Cement, 3M). The composite restoration on the mandibular right second molar was intact, and the patient had no complaints of sensitivity.
At 21 months following retreatment, the patient and parent were satisfied with the final treatment outcome, as all complaints were resolved. The follow-up radiograph showed an
Fig 5. Cropped panoramic radiograph 19 months after partial pulpotomy, revealing continued root development.
Fig 6. Dislodgment of the composite resin restoration 34 months after partial pulpotomy. Some parts of the tricalcium silicate cement layer remain.
Fig 7. Periapical radiograph 6 months after placement of a stainless steel crown, showing possible widening of the periodontal ligament space.
Fig 8.
improved periapical index score of 1, reduced from the immediate postoperative score of 3 (Fig 10).
Discussion
Young permanent teeth have unique characteristics, including thin dentinal walls and incomplete root formation.10 These properties, along with incomplete settling of the tooth position and occlusion, may present challenges for endodontic treatment and restorative plans in teeth with deep carious lesions in these young patients.11 Despite these drawbacks, advantages such as higher stem cell amounts and greater blood supply within the pulp compared with adults could facilitate increased healing ability in these teeth.10,12,13 Therefore, a conservative treatment method such as VPT should be a preferred choice for young permanent teeth in pediatric patients because it promotes further tooth development and increases tooth survivability by delaying invasive endodontic and restorative treatments.14
Initially, PP was preferred in this young patient because it is more conservative than CP. A systematic review and metaanalysis showed that PP in cariously exposed posterior permanent teeth had a 92% success rate after 2 years.15 Moreover, PP using calcium silicate–based cement in teeth with irreversible pulpitis has also been shown to have high success rates (83% to 92%).6,16 However, subjective clinical assessment of the remaining pulp tissue during PP may make it more difficult to determine the precise extent of infection and inflammation compared with complete removal of the entire coronal pulp with CP. Nevertheless, preserving the coronal, cell-rich pulp tissues can be advantageous since this facilitates healing, enabling hard tissue formation and cervical dentin deposition to continue.17,18 Moreover, the absence of physiologic properties in the coronal pulp following CP may result in reduced or no response to sensitivity tests after treatment.17,19
Baranwal et al found that PP and CP procedures provided similarly high success rates (80.7% after PP and 92.8% after CP) in teeth with irreversible pulpitis.18 However, CP resulted in more cases of root canal calcification than PP. An earlier study by Linsuwanont et al also found up to a 30% incidence of pulp canal obliteration after CP, contrasting with other studies that
found no pulp canal obliteration.20-22 However, in the present case, PP failure was presumably caused by reinfection due to microleakage after restoration failure and not by the inadequate removal of infected pulp tissue, as there was evidence of continued root formation. Tan et al found that a good coronal seal was essential for the long-term success of VPT, while misjudgment of the extent of pulp inflammation would likely result in early failures within 6 months after treatment.21
Although the tooth in the present case had complete root formation when the PP failure occurred, CP was offered to the patient and his parent as an alternative to root canal treatment. Traditional root canal treatment is a challenging procedure requiring sound theoretical knowledge and continuing professional development to avoid treatment errors or malpractice claims.23 In complicated cases, consultation with or referral to specialists should be considered, since the long-term (10-year) survival rate of endodontically treated teeth has been reported to be significantly higher when an endodontist performs the root canal treatment.23,24 In addition, endodontically treated teeth have decreased longevity compared with vital teeth, as the overall hazard ratio for tooth extraction has been reported to be up to 7.4 in endodontically treated molars.25 Moreover, Peretz et al showed that the long-term treatment success of endodontically treated teeth in patients aged 8 to 16 years was only 36%.26
A more conservative and less challenging procedure such as VPT is considered to be more cost-effective than root canal treatment in young patients.27 A study using a Markov simulation model to compare the annual failure probability of carious exposed teeth in children and adolescents treated by pulp capping vs root canal treatment found that the costs of initial pulp capping, including possible posttreatment procedures, and the likelihood of posttreatment tooth extraction were lower than those associated with teeth initially treated by root canal treatment.27 Moreover, a retrospective cohort study found that a patient’s age at root canal treatment significantly impacted survival of the treated teeth, whereby the risk of failure was elevated in younger patients, with an estimated 5-year survival probability of 46.4% in patients aged 6 to 11 years compared with 80.0% in those aged 15 to 18 years.28 Based on the results of these studies
Fig 9. Clinical evaluation showing bright red bleeding, suggesting a resilient pulp.
Fig 10. Radiograph 21 months after retreatment with coronal pulpotomy, revealing resolution of the periapical lesion.
and the suggestion that root canal treatment should be deferred as long as possible in children to increase tooth survival, CP was offered as an alternative to root canal treatment and was shown to be beneficial in the present case.23-28
Despite the diagnosis of symptomatic irreversible pulpitis and the presence of a periapical lesion (periapical index score of 3), the first molar in the present study was suitable for CP 49 months after PP because it still had vital pulp. Clinical studies have shown that VPT can provide successful outcomes in both immature and mature permanent teeth with a diagnosis of irreversible pulpitis and early periapical lesions.6,16,18,20,22,29 A recent systematic review and meta-analysis showed high success rates after pulpotomy (partial and coronal) in teeth with symptomatic (84%) and asymptomatic (91%) irreversible pulpitis.30 Histologic findings have shown that infection and inflammation in teeth diagnosed with irreversible pulpitis can be confined to a portion of the pulp and may not extend to the tooth’s radicular portion.31 Moreover, a periapical lesion should not be the sole criterion for assessing tooth vitality. Besides the successful VPT outcomes in teeth with periapical lesions that have been shown in clinical studies, a histologic study showed that a periapical lesion does not necessarily indicate an entirely inflamed or necrotic pulp.6,16,22,29,32 Therefore, VPT can be considered a viable treatment option for teeth with irreversible pulpitis and periapical lesions once infection and inflammation are adequately addressed, provided the remaining pulp appears healthy and modern materials such as calcium silicate–based cement (eg, ProRoot MTA and Biodentine) are used, as in the present case.33 These materials have many beneficial properties that can enhance pulp healing, including antibacterial effects, excellent biocompatibility, and bioactive properties.34,35
One essential factor affecting VPT outcome is an excellent coronal seal. Coronal leakage can lead to VPT failure due to bacterial invasion and reinfection of the pulp.19 Therefore, restoration integrity significantly affects treatment success. While restoration with composite resin over an RMGIC is recommended for teeth affected by hypomineralization, the poor bond strength between the restoration and the tooth might still cause restoration failure.36,37 Although dentin bonding is unaltered in hypomineralized teeth, the bond strength is significantly lower in hypomineralized enamel than in normal enamel, which could eventually cause cracks and marginal fractures.37,38 In addition, in the present case, because the restoration was located on a functional cusp (the buccal cusp of a mandibular posterior tooth), the loading force on the poorly bonded area may have been another factor contributing to restoration failure. Moreover, bacterial invasion might have advanced further into the pulp after restoration dislodgment because the exposed Biodentine would not be able to provide an effective coronal seal, as its mechanical properties and bond strength to intraradicular dentin are significantly decreased in acidic environments.39 In this patient, composite resin failure likely caused reinfection of the pulp, with symptoms manifesting 15 months after SSC placement and warranting retreatment of the symptomatic tooth.
Restoration of young permanent teeth can be challenging since the occlusion has not yet settled. In addition to direct composite resin restorations, SSCs are widely used as an interim restoration
for teeth with multisurface or extensive cavities and in teeth treated with VPT. Nevertheless, this prefabricated restoration also has disadvantages, such as its association with periodontal defects and impaction of the adjacent erupting tooth, as in the present case.11,16,29,40 Other drawbacks include poor marginal adaptation and occlusal perforation, which could potentially lead to microleakage, plaque retention, and recurrent caries, which may in turn eventually compromise the outcome of VPT.11,41,42 Therefore, replacement of an SSC may be required since the longevity of this restoration is limited.11
The events described in this case report highlight the importance of periodic evaluation of teeth treated by VPT. Although VPT was initially successful, the treatment failed when a defective coronal seal was found after a long period with no follow-up. While a tentative prognosis after VPT can be established 3 months posttreatment, further recalls at 6 and 12 months, annual visits posttreatment, and/or follow-ups at regular intervals for at least 1 year are suggested to ensure healing of the pulp and periapical tissues, because failure may result from remaining infection or reinfection.2,5,43 Regular recalls could detect early signs and symptoms of treatment failure or problems that may affect treatment success, enabling timely interventions to preserve the remaining vital tissues.
A notable feature of this case report is the use of 17% EDTA in the VPT procedure. Previous clinical studies on VPT have used various irrigants, with many using NaOCl, while some use normal saline solution.23 The American Association of Endodontists' position statement on VPT indicates that NaOCl can be used as an irrigant and for hemorrhage control after pulp exposure.44 While NaOCl has the advantages of antibacterial effects and the ability to dissolve tissues, it has also shown cytotoxicity to dental pulp stem cells in vitro.45-47 On the other hand, despite its lack of antibacterial effects, normal saline solution has excellent biocompatibility, which may facilitate pulpal healing, and is commonly used between other irrigants to prevent the occurrence of undesirable chemical interactions by elimination of the residual components of each irrigant.45,47,48 Despite its less common use in VPT, EDTA is widely used in endodontic procedures such as root canal treatment and regenerative endodontics.48,49 Dentin demineralization caused by the chelating ability of EDTA results in the release of enclosed cytokines and growth factors into the dentin matrix, which can facilitate dentinogenesis by inducing dental mesenchymal cells and odontoblast differentiation.50,51 Additionally, in vitro studies have shown that EDTA has good biocompatibility, causing no harm to stem cells.47 Given these properties, Bahcall et al suggested using 17% EDTA instead of NaOCl after hemostasis and cryotherapy in VPT.52 Nevertheless, the evidence regarding the use of 17% EDTA in VPT is scarce, with no published clinical studies of its use, to the authors’ knowledge. The present case report demonstrates successful VPT using EDTA and NaOCl as irrigants, with normal saline solution used in between, which may encourage further laboratory or clinical studies on this subject.
Conclusion
Treatment failure after conservative VPT methods such as PP may not be an absolute indication for root canal treatment when the tooth still has vital pulp, especially in pediatric
patients with high potential for pulpal healing. Therefore, preservation of the pulp may be feasible if the tooth is given a second chance to survive via the further removal of infection and inflammation, placement of a bioactive pulp dressing material on the remaining healthy pulp, and establishment of an effective coronal seal to foster successful healing. In addition, regular examinations of the treated tooth must be performed to ensure tooth survival and early detection of problems that may adversely affect treatment outcomes.
Author affiliations
Department of Dentistry, Fang Hospital, Chiang Mai, Thailand (Machareonsap); Division of Pediatric Dentistry, Department of Orthodontics and Pediatric Dentistry, Faculty of Dentistry, Chiang Mai University, Chiang Mai, Thailand (Chompu-inwai, Chaipattanawan, Manmontri).
Correspondence
Papimon Chompu-inwai DDS, MS (papimon.c@cmu.ac.th).
Conflicts of interest
None reported.
References
1. Li Y, Sui B, Dahl C, et al. Pulpotomy for carious pulp exposures in permanent teeth: a systematic review and meta-analysis. J Dent. 2019;84:1-8. doi:10.1016/j.jdent.2019.03.010
2. Dammaschke T, Galler K, Krastl G. Current recommendations for vital pulp treatment. Scientific communication. Dtsch Zahnärztl Z Int. 2019;1(1):43-52. doi:10.3238/dzz-int.2019. 0043-0052
3. Bjørndal L, Simon S, Tomson PL, Duncan HF. Management of deep caries and the exposed pulp. Int Endod J. 2019;52(7):949-973. doi:10.1111/iej.13128
4. Aguilar P, Linsuwanont P. Vital pulp therapy in vital permanent teeth with cariously exposed pulp: a systematic review. J Endod. 2011;37(5):581-587. doi:10.1016/j.joen.2010.12.004
5. European Society of Endodontology. Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. Int Endod J. 2006;39(12):921-930. doi:10.1111/j.1365-2591.2006.01180.x
6. Taha NA, Khazali MA. Partial pulpotomy in mature permanent teeth with clinical signs indicative of irreversible pulpitis: a randomized clinical trial. J Endod. 2017;43(9):1417-1421. doi:10.1016/j.joen.2017.03.033
7. Ballal NV, Duncan HF, Rai N, Jalan P, Zehnder M. Sodium hypochlorite reduces postoperative discomfort and painful early failure after carious exposure and direct pulp capping—initial findings of a randomized controlled trial. J Clin Med. 2020;9(8):2408. doi:10.3390/ jcm9082408
8. Özgür B, Uysal S, Güngör HC. Partial pulpotomy in immature permanent molars after carious exposures using different hemorrhage control and capping materials. Pediatr Dent. 2017; 39(5):364-370.
9. Orstavik D, Kerekes K, Eriksen HM. The periapical index: a scoring system for radiographic assessment of apical periodontitis. Endod Dent Traumatol. 1986;2(1):20-34. doi:10.1111/ j.1600-9657.1986.tb00119.x
10. Fuks A, Peretz B, eds. Pediatric Endodontics. Current Concepts in Pulp Therapy for Primary and Young Permanent Teeth. Springer International Publishing; 2016.
11. Chaipattanawan N, Chompu-inwai P, Nirunsittirat A, Phinyo P, Manmontri C. Longevity of stainless steel crowns as interim restorations on young permanent first molars that have undergone vital pulp therapy treatment in children and factors associated with their treatment failure: a retrospective study of up to 8.5 years. Int J Paediatr Dent. 2022;32 (6):925-937. doi:10.1111/ipd.12971
12. Bernick S, Nedelman C. Effect of aging on the human pulp. J Endod. 1975;1(3):88-94. doi:10.1016/S0099-2399(75)80024-0
13. Morse DR. Age-related changes of the dental pulp complex and their relationship to systemic aging. Oral Surg Oral Med Oral Pathol. 1991;72(6):721-745. doi:10.1016/0030-4220(91) 90019-9
14. Bogen G, Chandler NP. Pulp preservation in immature permanent teeth. Endod Top 2010;23(1):131-152. doi:10.1111/j.1601-1446.2012.00286.x
15. Elmsmari F, Ruiz XF, Miró Q, Feijoo-Pato N, Durán-Sindreu F, Olivieri JG. Outcome of partial pulpotomy in cariously exposed posterior permanent teeth: a systematic review and metaanalysis. J Endod. 2019;45(11):1296-1306.e3. doi:10.1016/j.joen.2019.07.005
16. Uesrichai N, Nirunsittirat A, Chuveera P, Srisuwan T, Sastraruji T, Chompu-inwai P. Partial pulpotomy with two bioactive cements in permanent teeth of 6- to 18-year-old patients with signs and symptoms indicative of irreversible pulpitis: a noninferiority randomized controlled trial. Int Endod J. 2019;52(6):749-759. doi:10.1111/iej.13071
17. Fong CD, Davis MJ. Partial pulpotomy for immature permanent teeth, its present and future. Pediatr Dent. 2002;24(1):29-32.
18. Baranwal HC, Mittal N, Yadav J, Rani P, Naveen Kumar PG. Outcome of partial pulpotomy verses [sic] full pulpotomy using Biodentine in vital mature permanent molar with clinical symptoms indicative of irreversible pulpitis: a randomized clinical trial. J Conserv Dent 2022;25(3):317-323. doi:10.4103/jcd.jcd_118_22
19. Taha NA, About I, Sedgley CM, Messer HH. Conservative management of mature permanent teeth with carious pulp exposure. J Endod. 2020;46(9S):S33-S41. doi:10.1016/j.joen. 2020.06.025
20. Linsuwanont P, Wimonsutthikul K, Pothimoke U, Santiwong B. Treatment outcomes of mineral trioxide aggregate pulpotomy in vital permanent teeth with carious pulp exposure: the retrospective study. J Endod. 2017;43(2):225-230. doi:10.1016/j.joen.2016.10.027
21. Tan SY, Yu VSH, Lim KC, et al. Long-term pulpal and restorative outcomes of pulpotomy in mature permanent teeth. J Endod. 2020;46(3):383-390. doi:10.1016/j.joen.2019.11.009
22. Qudeimat MA, Alyahya A, Hasan AA. Mineral trioxide aggregate pulpotomy for permanent molars with clinical signs indicative of irreversible pulpitis: a preliminary study. Int Endod J. 2017;50(2):126-134. doi:10.1111/iej.12614
23. Alrahabi M, Zafar MS, Adanir N. Aspects of clinical malpractice in endodontics. Eur J Dent. 2019;13(3):450-458. doi:10.1055/s-0039-1700767
24. Burry JC, Stover S, Eichmiller F, Bhagavatula P. Outcomes of primary endodontic therapy provided by endodontic specialists compared with other providers. J Endod. 2016;42(5): 702-705. doi:10.1016/j.joen.2016.02.008
25. Caplan DJ, Cai J, Yin G, White BA. Root canal filled versus non-root canal filled teeth: a retrospective comparison of survival times. J Public Health Dent. 2005;65(2):90-96. doi:10.1111/j.1752-7325.2005.tb02792.x
26. Peretz B, Yakir O, Fuks AB. Follow up after root canal treatment of young permanent molars. J Clin Pediatr Dent. 1997;21(3):237-240.
27. Brodén J, Davidson T, Fransson H. Cost-effectiveness of pulp capping and root canal treatment of young permanent teeth. Acta Odontol Scand. 2019;77(4):275-281. doi:10. 1080/00016357.2018.1538536
28. Bufersen S, Jones J, Shanmugham J, et al. Survival of endodontically treated permanent teeth among children: a retrospective cohort study. BMC Oral Health. 2021;21(1):589. doi:10.1186/s12903-021-01952-y
29. Parinyaprom N, Nirunsittirat A, Chuveera P, et al. Outcomes of direct pulp capping by using either ProRoot Mineral Trioxide Aggregate or Biodentine in permanent teeth with carious pulp exposure in 6- to 18-year-old patients: a randomized controlled trial. J Endod 2018;44(3):341-348. doi:10.1016/j.joen.2017.10.012
30. Ather A, Patel B, Gelfond JAL, Ruparel NB. Outcome of pulpotomy in permanent teeth with irreversible pulpitis: a systematic review and meta-analysis. Sci Rep. 2022;12(1):19664. doi:10.1038/s41598-022-20918-w
31. Ricucci D, Loghin S, Siqueira JF Jr. Correlation between clinical and histologic pulp diagnoses. J Endod. 2014;40(12):1932-1939. doi:10.1016/j.joen.2014.08.010
32. Lin L, Langeland K. Light and electron microscopic study of teeth with carious pulp exposures. Oral Surg Oral Med Oral Pathol. 1981;51(3):292-316. doi:10.1016/0030-4220 (81)90060-8
33. Asgary S, Parhizkar A. The role of vital pulp therapy in the management of periapical lesions. Letter. Eur Endod J. 2021;6(1):130-131. doi:10.14744/eej.2020.04706
34. Wang Z. Bioceramic materials in endodontics. Endod Top. 2015;32(1):3-30. doi:10.1111/ etp.12075
35. Parirokh M, Torabinejad M. Mineral trioxide aggregate: a comprehensive literature review, III: clinical applications, drawbacks, and mechanism of action. J Endod. 2010;36(3):400-413. doi:10.1016/j.joen.2009.09.009
36. Arab M, Al-Sarraf E, Al-Shammari M, Qudeimat M. Microshear bond strength of different restorative materials to teeth with molar-incisor-hypomineralisation (MIH): a pilot study. Eur Arch Paediatr Dent. 2019;20(1):47-51. doi:10.1007/s40368-018-0384-2
37. Krämer N, Bui Khac NN, Lücker S, Stachniss V, Frankenberger R. Bonding strategies for MIH-affected enamel and dentin. Dent Mater. 2018;34(2):331-340. doi:10.1016/j. dental.2017.11.015
38. William V, Burrow MF, Palamara JE, Messer LB. Microshear bond strength of resin composite to teeth affected by molar hypomineralization using 2 adhesive systems. Pediatr Dent 2006;28(3):233-241.
39. Elnaghy AM. Influence of acidic environment on properties of Biodentine and white mineral trioxide aggregate: a comparative study. J Endod. 2014;40(7):953-957. doi:10.1016/ j.joen.2013.11.007
40. Randall RC. Preformed metal crowns for primary and permanent molar teeth: review of the literature. Pediatr Dent. 2002;24(5):489-500.
41. Yilmaz Y, Kara NB, Yilmaz A, Sahin H. Wear and repair of stainless steel crowns. Eur J Paediatr Dent. 2011;12(1):25-30.
42. Mulder R, Medhat R, Mohamed N. In vitro analysis of the marginal adaptation and discrepancy of stainless steel crowns. Acta Biomater Odontol Scand. 2018;4(1):20-29. doi:10.1080/23337931.2018.1444995
43. Matsuo T, Nakanishi T, Shimizu H, Ebisu S. A clinical study of direct pulp capping applied to carious-exposed pulps. J Endod. 1996;22(10):551-556. doi:10.1016/S00992399(96)80017-3
44. AAE Position Statement on Vital Pulp Therapy. J Endod. 2021;47(9):1340-1344. doi: 10.1016/j.joen.2021.07.015
45. Heling I, Chandler NP. Antimicrobial effect of irrigant combinations within dentinal tubules. Int Endod J. 1998;31(1):8-14.
46. Rosenfeld EF, James GA, Burch BS. Vital pulp tissue response to sodium hypochlorite. J Endod. 1978;4(5):140-146. doi:10.1016/S0099-2399(78)80129-0
47. Sutimuntanakul S, Sritanaudomchai H, Lerdarksornpaiboon W, Songtrakul K. Effect of root canal irrigants on attachment and survival of dental pulp stem cells. Mahidol Dent J 2016;36:375-392. https://dt.mahidol.ac.th/en/wp-content/uploads/2018/05/7-Effect-ofroot-canal-lrrigants-on-attachement-and-survival-of-dental-pulp-stem.pdf
48. Haapasalo M, Shen Y, Wang Z, Gao Y. Irrigation in endodontics. Br Dent J. 2014;216(6): 299-303. doi:10.1038/sj.bdj.2014.204
49. American Association of Endodontists. Root canal irrigants and disinfectants. Endodontics: Colleagues for Excellence Newsletter. 2011;Winter:1-7. https://www.aae.org/specialty/ wp-content/uploads/sites/2/2017/07/rootcanalirrigantsdisinfectants.pdf
50. Smith AJ, Matthews JB, Hall RC. Transforming growth factor- β1 (TGF- β1) in dentine matrix. Ligand activation and receptor expression. Eur J Oral Sci. 1998;106 Suppl 1:179-184. doi:10.1111/j.1600-0722.1998.tb02173.x
51. Tziafas D, Alvanou A, Panagiotakopoulos N, et al. Induction of odontoblast-like cell differentiation in dog dental pulps after in vivo implantation of dentine matrix components. Arch Oral Biol. 1995;40(10):883-893. doi:10.1016/0003-9969(95)00069-2
52. Bahcall J, Xie Q, Baker M, Weeks S. New approach in endodontics: cryotherapy for vital pulp treatment. Decis Dent. 2019;5(9):14-18.
Performance of a novel self-adhesive bulk-fill composite hybrid in endodontically treated maxillary premolars: analysis of fracture resistance and failure mode
Fereshteh Shafiei, DDS, MS ¢ Shadi Tivay, DDS ¢ Zahra Fattah, DDS, MS
This study evaluated the fracture resistance of endodontically treated maxillary premolars restored with a new self-adhesive composite hybrid material (Surefil one [SO]) using different protocols. A total of 72 maxillary premolars were divided into 6 groups (n = 12). The control group included intact teeth, and the other 5 groups included teeth in which disto-occlusal cavities were prepared and endodontic treatment was performed. The prepared cavities were assigned to groups that were based on the restorative procedures: bulk-fill group, universal adhesive plus conventional bulk-fill composite resin plus a layer of conventional composite resin; SO-SC group, self-cured SO; SO-LC group, light-cured SO; SO-UA group, universal adhesive plus SO; or SO-core group, a 4.0-mm layer of SO covered by a layer of conventional composite resin. Specimens in each group underwent thermocycling and load cycling to test the fracture strength and fracture mode. The results were analyzed using analysis of variance and the Tukey test (α = 0.05). The SO-core group showed the highest mean (SD) fracture resistance, 959.9 (171.8) N, among the restored groups. The SO-core group did not differ significantly from the control group (P > 0.05) but did show significantly higher strength than all other test groups (P < 0.05) except SO-SC (P = 0.364). No significant differences were found between the bulk-fill, SO-SC, SO-LC, and SO-UA groups (P > 0.05). The SO-core group showed the highest number of unrestorable fractures, while the main fracture mode for the other groups was restorable fracture. Although the use of SO as a core material restored the fracture strength of endodontically treated premolars to the level of intact teeth, it also resulted in a higher incidence of unrestorable fractures. The SO-SC group demonstrated a high fracture resistance comparable to that of the SO-core group and had a greater tendency to experience restorable fractures.
Endodontically treated teeth are more susceptible to biomechanical failure than vital teeth due to diminished structural integrity resulting from caries removal and restorative procedures.1 Such failures are especially common in endodontically treated maxillary premolars due to their anatomy, unfavorable crown to root ratio, and position in the dental arch, which can result in cuspal flexure when they are subjected to compressive and shearing forces.2 Because the preservation of tooth structure is crucial for restorative treatment, conservative techniques are the preferred approach to restoring endodontically treated teeth.3 Although cuspal coverage is typically recommended for weakened teeth, some studies suggest using adhesive restorations without reduction of the cusps because the adhesion is expected to provide sufficient retention and to strengthen the tooth structure by splinting the cusps intracoronally.4-7 This approach is thought to be especially effective for 3-wall cavities, where the mesial and/or distal marginal ridges protect the tooth from catastrophic fracture.8,9
Today, resin-based composites facilitate minimally invasive restorations with maximum esthetics.10 However, there are concerns regarding the shrinkage stress of composite resins, especially in larger and deeper cavities. Shrinkage stress can lead to stress accumulation at the tooth-composite interface, adhesive-composite interface, or both, which can contribute to a higher risk of tooth fracture. To reduce accumulated stress, the recommended approach is to place and cure composite resin in layers that are 1.5 to 2.0 mm thick.11 However, this technique still presents several challenges, including increased chair time, higher risk of contamination, potential void formation, and an absence of union between layers.11-13 To address these challenges, bulk-fill composite resins were developed to enable clinicians to place composite resin in 4.0-mm-thick layers, leading to lower polymerization shrinkage stress. These resins are classified either as a flowable base material to be covered with 2.0 mm of posterior composite or as a final paste-like composite that does not require an overlying occlusal layer.14 Despite their acceptable performance, bulk-fill composites still require surface preparation and a separate adhesive layer.15
A new self-adhesive bulk-fill composite hybrid material, Surefil one (SO; Dentsply Sirona), has been recently introduced to address this limitation. According to the manufacturer, this product exhibits all the advantages of self-adhesive, bulk-fill, dual-curing, and fluoride-releasing filling materials. Accordingly, it obviates the need for etching, bonding, and layering and can restore all types of
cavities when the tooth does not require cuspal coverage.16 A key ingredient of this material is the modified polyacid system (MOPOS), a patented monomer that enhances selfadhesive properties.17 Additionally, the acidic components in SO may have an etching effect, leading to the creation of a hydroxyapatite-rich hybrid layer on a submicron level that further facilitates adhesion.18 Therefore, based on the claim that SO combines the self-adhesive and easy-handling properties of glass ionomer–based materials with the strength of composite resins, this new material would simplify the restorative procedure for deep cavities, reducing chair time and technique sensitivity.19 Recent studies comparing different self-adhesive materials have found that SO exhibited the highest shear bond strength to untreated dentin surfaces and had a good marginal quality, highlighting its favorable bonding ability.10,16,20 Several studies have also showed the fracture behavior of SO to be similar to that of conventional composites and its wear resistance to be acceptable.10,21,22 These reports indicate the potential for SO to be used in posterior stress-bearing areas.
According to some investigations, an effective approach to filling large cavities is to apply a flowable bulk-fill composite resin base as a stress-decreasing intermediate layer and cover it with a layer of conventional nanohybrid composite resin, thereby combining the advantages of low stress, low shrinkage values, and adequate mechanical properties.14 This restoration method has resulted in intact, tooth-level fracture resistance in both endodontically treated and vital teeth.14,23 Accordingly, SO can also be used as a base in large cavities because it may be able to decrease the shrinkage stress due to its self-curing properties.
Studies conducted on this self-adhesive restorative material are limited. So far, there has been no study on the performance of this material in endodontically treated teeth. Therefore, the present study aimed to evaluate the fracture resistance of endodontically treated maxillary premolars restored with SO used as a base material in different protocols and compare the results of the various protocols with the fracture resistance of another bulk-fill composite material. The null hypothesis was that there would be no difference between the fracture resistance values of endodontically treated maxillary premolars restored by SO with different methods.
Methods
Tooth selection and preparation
Following approval of the research protocol by the local ethics committee of Shiraz University of Medical Sciences, Shiraz, Iran, 72 intact maxillary premolars without caries or restorations were collected. The teeth had been extracted for orthodontic purposes. They were approximately similar in shape and size (ie, buccolingual and mesiodistal width) as measured in millimeters with a digital caliper (Mitutoyo Digimatic, Mitutoyo) with 0.1-mm sensitivity for the standardization of cavity dimensions.
Any soft or hard tissues attached to the teeth were separated with periodontal curettes, disinfected in 0.5% chloramine solution, and then stored in distilled water at 4°C. The cleaned teeth were carefully observed under a
stereomicroscope (Carl Zeiss Microscopy) at ×20 magnification, and those with any defects, such as fracture lines, were excluded from the study.
Endodontic access cavities were prepared in all teeth except those in the control group. High-speed, coarse, parallel-sided, flat-end diamond burs (Teeskavan) were used under constant water cooling to prepare disto-occlusal cavities down to the canal orifice. The cavities had buccolingual dimensions of 3.5 mm in the gingival area and 3.0 mm in the occlusal area and a 2.0-mm-thick mesial marginal ridge. 8 The gingival margin was placed 1.0 mm coronal to the cementoenamel junction (CEJ), producing a total cavity depth of 6.0 mm. The bur was replaced every 10 preparations, and all of the preparations were done by the same operator (F.S.).
Endodontic treatment was accomplished using the ProTaper nickel-titanium rotary system (Dentsply Sirona) with the master file F2. The canals were irrigated with 2.5% sodium hypochlorite solution, dried with paper points, and obturated with laterally condensed gutta percha cones and AH 26 sealer (Dentsply Maillefer). The specimens were then stored at 100% humidity for 1 week.
Specimen
grouping and restoration
Table 1 shows the materials used in this study. The teeth were randomly divided into 6 groups according to restoration method (n = 12): control, bulk-fill, SO-SC, SO-LC, SO-UA, or SO-core. The control group consisted of intact teeth without any cavity preparation.
In the bulk-fill group, the surfaces of the specimens underwent selective enamel etching with 37% phosphoric acid (Condac 37, FGM Dental Group) for 20 seconds and were then rinsed and gently air dried to avoid dentin desiccation. Then, universal adhesive (Futurabond U, VOCO) was applied according to the manufacturer’s instructions and cured for 10 seconds with a halogen light-curing unit (VIP Junior, Bisco) at 600 mW/cm2. The cavities were restored by placing a single 4.0-mm layer of bulk-fill flowable composite resin (X-tra base shade universal, VOCO) and covering it with a single 2.0-mm covering layer of conventional composite resin (GrandioSO, VOCO). Each layer was light cured for 20 seconds.
In the SO-SC group, the specimens were not etched but were rinsed and dried similar to the bulk-fill group. The cavities were restored with a single 6.0-mm-thick layer of SO according to the manufacturer’s instructions. The specimens were allowed to self-cure for 6 minutes at room temperature.
In the SO-LC group, after restoration following the same protocol used for the SO-SC group, the surface layer was light cured for 20 seconds.
In the SO-UA group, after selective enamel etching with 37% phosphoric acid for 20 seconds, the cavities were treated with a universal adhesive (Prime&Bond active, Dentsply Sirona), which was light cured for 10 seconds. The cavities were restored with a single 6.0-mm-thick layer of SO, and light cured at the surface layer for 20 seconds.
In the SO-core group, after rinsing and drying of the prepared tooth, a 4.0-mm layer of SO was placed as a core material. It was inserted into the cavity depth and then light cured for 20 seconds. Next, the enamel margin was selectively etched,
rinsed, gently air dried, and restored with a 2.0-mm layer of conventional composite resin (TPH Spectra ST, Dentsply Sirona), which was light cured for 20 seconds. After storage in distilled water at 37ºC for 24 hours, the groups were submitted to finishing procedures (Sof-Lex Finishing and Polishing Discs, 3M).
Aging and fracture testing
The root surfaces were covered with a 0.2- to 0.3-mm layer of melted wax (Renfert) and then embedded in cylindrical molds filled with self-polymerized acrylic resin (Acropars 200, Marlic) up to 2.0 mm below the CEJ. Thereafter, the roots were
removed from the acrylic resin blocks, and the wax surfaces were replaced with light-body polyvinyl siloxane (Hydrorise Extra Light Body, Zhermack) to mimic the periodontal ligament.2 The specimens were placed so that the long axis of the tooth was perpendicular to the base of the cylinder.
All specimens were thermocycled (TC300, Vafaei) following a regimen of 5000 cycles alternating between 5°C and 55°C (dwell time: 30 seconds). Then, a mastication simulation machine (Chewing Stimulator CS-4, SD Mechatronik) was used to apply 50,000 loading cycles at a frequency of 2 Hz with a load ranging from 0 to 100 N, representing a range of approximately 3 to 12 months of clinical use.2 The mechanical
Table 1. Materials used in this study.
A.
specimen from the SO-core group (layer of SO plus occlusal layer of conventional composite). C. Restorable specimen from the SO-LC group (light-cured SO). D. Restorable specimen from the SO-SC group (self-cured SO).
Table 2. Mean (SD) fracture resistance of endodontically treated maxillary premolars (n = 12 per group).
Group
Control
Table 3. Frequency of failure modes in endodontically treated maxillary premolars (n = 12 per group).
Fracture resistance, N
1023.6 (128.2)a Bulk-fill 764.8 (129.1)b SO-SC
Group
829.3 (122.4)bc
(161.2)b
(161.9)b
(171.8)ac
Groups: Control, intact teeth; Bulk-fill, universal adhesive, X-tra base, and conventional composite resin occlusal layer; SO-SC, self-cured Surefil one (SO); SO-LC, light-cured SO; SO-UA, universal adhesive plus SO; SO-core, layer of SO plus occlusal layer of conventional composite.
Groups with different superscript letters are significantly different (P < 0.001; 1-way analysis of variance).
load was applied to the center of the occlusal surface, in contact with both cusp ridges, using a stainless steel rounded-end antagonist that was 6.0 mm in diameter. During testing, all specimens were immersed in 37º C distilled water.
After the aging procedures, a universal testing machine (model Z020, ZwickRoell) was used to apply a compressive load parallel to the long axis of each restored tooth. The load was applied with a stainless steel cylinder, 6.0 mm in diameter, at a crosshead speed of 1.0 mm/min until fracture. The antagonist cylinder was placed in the center of the tooth with contacts only on the buccal and palatal cuspal inclines. The load to failure was recorded in Newtons as the fracture resistance value.
The type of fracture was determined by visual inspection with the aid of transillumination and recorded as unrestorable when the fracture line was more than 1.0 mm below the CEJ (Figure). The fracture was recorded as restorable when the fracture line was above the CEJ or no more than 1.0 mm below the CEJ.
Statistical analysis
The Kolmogorov-Smirnov test showed that the data were normally distributed. Statistical analyses were performed using
4 (33.3) 8 (66.6)
Groups: Control, intact teeth; Bulk-fill, universal adhesive, X-tra base, and conventional composite resin occlusal layer; SO-SC, self-cured Surefil one (SO); SO-LC, light-cured SO; SO-UA, universal adhesive plus SO; SO-core, layer of SO plus occlusal layer of conventional composite.
1-way analysis of variance (ANOVA) followed by post hoc Tukey tests to compare group differences at a significance level of α = 0.05. All analyses were conducted using SPSS software (version 11.5, IBM).
Results
One-way ANOVA revealed statistically significant differences (P < 0.001) in mean and SD fracture resistance values between groups (Table 2).
Among the restored groups, SO-core showed the highest mean (SD) fracture resistance, 959.9 (171.8) N, and was the only group that did not statistically differ from the control group, which had a fracture resistance of 1023.6 (128.2) N. The SO-core group also demonstrated significantly higher strength than all other groups (P < 0.05; Tukey test) except for the SO-SC group (P = 0.364). There were no significant differences between the bulk-fill, SO-SC, SO-LC, and SO-UA groups (P > 0.05); however, the SO-UA group had the lowest mean (SD) fracture resistance, 697.2 (161.9) N, and showed significant differences from the control and SO-core groups (P = 0.001 and P = 0.003, respectively).
Figure. Different types of fracture.
Unrestorable specimen from the SO-UA group (universal adhesive plus Surefil one [SO]). B. Unrestorable
All specimens in the control group displayed restorable fractures (Table 3). Most of the fractures (66.6% to 75.0%) in the bulk-fill, SO-SC, and SO-LC groups were restorable. However, the SO-UA specimens were evenly distributed between restorable and unrestorable, and 66.6% of the fractures in the SO-core group were unrestorable.
Discussion
Successful endodontic treatment is highly dependent on a restoration that is stable and durable. When a restorative technique is selected, the remaining tooth structure and occlusal loading forces are of great importance. 24 If the marginal ridge is preserved after endodontic treatment and the occlusal conditions are normal, the first restorative treatment option should be composite resin because it is timesaving and cost effective. 8 This approach can prevent the excessive removal of sound tooth structure while providing adequate esthetics. However, it is essential that the composite resin have an effective bonding ability for restabilizing the strength of endodontically treated teeth. 25
To the authors’ knowledge, this study is the first to investigate the performance of SO for the restoration of endodontically treated teeth. Analysis showed that different simplified restorative techniques significantly affected the strength of treated premolars; thus, the null hypothesis was rejected. The simplified protocols of the SO-SC and SO-LC groups were evaluated to determine their efficacy in restoring endodontically treated teeth while minimizing chair time, following the manufacturer’s instructions. The most simplified technique was the SO-SC group, in which the SO was placed in bulk and did not require light curing. This group showed no significant difference from the SO-LC group. Two studies indicated that SO in light-curing mode provided effective and durable bonding to flat dentin; however, when bonded in Class I cavities, SO in self-curing mode demonstrated a stronger bonding ability.18,26 This result was attributed to the fact that self-curing produces lower polymerization shrinkage stress due to the slower rate of polymerization.27 In the present study, because SO was applied in bulk and light curing was performed only on the surface layer in the SO-LC group, it is possible that both SO curing-mode groups (SO-SC and SO-LC) benefitted from the low polymerization stress at the depth of the cavity, which had a high configuration factor (C-factor). It appeared that light curing mainly improved the mechanical properties at the surface of the restoration. Furthermore, cavity preparations were completed using fine diamonds, a method that prevents the formation of a thick smear layer. This allowed for better penetration and interaction of the self-adhesive SO with the underlying dentin, leading to the creation of a submicron hydroxyapatite-rich hybrid layer.18,20
Due to the high viscosity and paste-like consistency of SO, it would be reasonable to expect that achieving self-adhesiveness might be problematic and that a separately applied adhesive would be beneficial for resistance to polymerization shrinkage stress. Thus, the present study also included the SO-UA group, in which a universal adhesive in self-etching mode was applied to the cavity surfaces before the SO. Theoretically, the increased wettability caused by the adhesive could improve
both the micromechanical retention and the chemical bond between the acidic functional monomer in the universal adhesive and the calcium in the dentin.28 Moreover, the resinous content in SO might enhance the co-curing process with the adhesive. However, the SO-UA group showed fracture behavior similar to that of the groups without adhesive (SO-SC and SO-LC), confirming that the self-adhesiveness of SO is adequate. The similar fracture strength result may also be attributed to the low polymerization stress produced in the bulk of SO due to its slow self-curing process in deep cavities. In agreement with these findings, a study by Latta et al reported that the bond strength of SO to enamel and flat dentin after thermomechanical loading was similar to that of a combination of conventional composite resin and universal adhesive used in self-etching mode after thermocycling.29 This similarity was also reported for flat dentin and cavity-bottom dentin.18 However, another study reported that the initial bond strength of SO was lower than that of universal adhesive in self-etching mode used with conventional composite.20
The bonding ability of an adhesive plays a critical role in enhancing the efficacy of a composite restoration and increasing the fracture resistance in restored teeth.25,30,31 Adhesive bonding should be able to overcome the polymerization shrinkage stress of a composite resin, thus increasing the strength of the restored teeth.31 In light of the present results, the use of SO alone appears to be sufficient for achieving adequate fracture resistance in restored maxillary premolars without the need for an extra adhesive application. The strength recovery for the SO-UA group was only 68% when compared to intact premolars, while the SO-SC and SO-LC groups exhibited strength recovery rates of 81% and 69%, respectively. The recovery rate of the SO-core group was 93%; however, a higher rate of unrestorable fracture was observed in this group. Furthermore, in the bulk-fill group, where a universal adhesive in self-etching mode was used with a bulk-fill flowable composite, the fracture resistance value fell within the range observed in 3 of the other groups (SO-SC, SO-LC, and SO-UA), with a recorded strength recovery of 74%.
The present study also evaluated the efficacy of SO as a stress-absorbing base material, especially in comparison to X-tra base, an established bulk-fill flowable composite indicated for use as a 4.0-mm-thick restoration base. However, the self-adhesiveness of SO facilitates a simplified restoration, especially when combined with its bulk-fill advantages. Both the SO-core and bulk-fill groups, which utilized SO and X-tra base, respectively, as 4.0-mm-thick bases, were treated with their manufacturers’ universal adhesives and covered with a layer of their corresponding conventional nanohybrid composites to make them suitable for stress-bearing areas.32 In the bulk-fill group, the effect of polymerization shrinkage stress at the adhesive interface appeared negligible despite the fact the X-tra base was light cured in a single step.
This finding is in agreement with a previous study showing that the bonding efficacy of a flowable bulk-fill composite was insensitive to the C-factor, while the paste-like bulk-fill composites showed higher shrinkage stress in cavities with a high C-factor.33 This result could be expected, as flowable bulk-fill composites are known to exhibit lower polymerization
shrinkage, reduced cuspal deflection, lower elastic modulus, and good cavity adaptation while maintaining an increased degree of cure.34-36 X-tra base has been reported to significantly reduce cuspal deflection in Class II cavities.37 This product has a low total polymerization shrinkage due to its high filler content (60% volume), and its high translucency allows for greater polymerization depth.38 With its low elastic modulus, this base may serve as a stress-absorbing layer, potentially dissipating stress and increasing fracture strength.39 However, it might not support masticatory loads in stress-bearing areas.32 To protect the base from occlusal load and ensure satisfactory mechanical performance in addition to improved esthetics, a layer of conventional nanohybrid-microhybrid composite resin is recommended.32,40
The present study utilized the concept of a covering layer in the bulk-fill group, which showed a similar performance to that found in other fracture resistance studies employing a combination of flowable bulk-fill composite and conventional composite resin to restore endodontically treated teeth.2,25,30 The fracture resistance values in teeth with mesio-occlusodistal restorations did not reach the level of intact teeth in 2 studies.2,30 However, for mesio-occlusal cavities, the values were comparable to those of intact teeth.25
An interesting finding in the current study was that, among the different restorative techniques, the use of SO as a core material restored the strength of endodontically treated premolars to the level of intact teeth. The restorative technique for this group differed from the SO-SC and SO-LC groups, as the enamel margins were acid etched and a universal adhesive was applied prior to placement of a conventional composite as an occlusal covering layer. The strong and durable bonding caused by selective enamel etching might be responsible for the increased fracture strength in this group.41 Although this restorative technique could benefit from the desirable properties of SO as the bulk of the restoration, it contradicted the simplification and time-saving advantages of the SO-SC and SO-LC groups, in which no acid etchant or adhesive was applied. A short-term clinical study on the performance of SO in Class II cavities similarly revealed improved bonding when enamel etching was performed.42 The researchers also reported that universal adhesive/bulk-fill and SO restorations exhibited significantly increasing marginal discoloration/staining over time. This observation was attributed to the lack of enamel acid etching in those restorations.42 Atalay et al highlighted the importance of adhesive efficacy in providing a strong enamel bond and therefore higher fracture resistance for teeth restored with composite resin.30
In addition to the importance of fracture resistance for predicting the prognosis of restored teeth, the fracture mode of different restored groups may provide valuable information. Consistent with previous studies, the primary fracture mode of the intact teeth and bulk-fill specimens in this study was restorable fracture.2,30 This was also observed in the SO-LC and SO-SC groups, which could be clinically desirable. Although the SO-core group exhibited the highest fracture resistance values, this group also showed an increased risk of unrestorable fracture. The SO-SC group showed a fracture resistance similar to that of the SO-core group but had a higher tendency for restorable fractures.
It has been anticipated that the strengthening effect of a composite restoration on the remaining tooth structure could diminish remarkably over the years in clinical function. 30 Thus, the present study applied cyclic loading, water storage, and thermocycling to the specimens to simulate intraoral conditions. However, this experimental study did not completely mimic the several factors involved in the degradation of the adhesive interface in vivo. The restored teeth were subjected to static compressive loading in a vertical direction until fracture occurred. While the strength testing used in this study may not exactly mimic functional loads during mastication, this approach has been demonstrated to be a useful method for comparing the effectiveness of various restorative techniques.2,24 Long-term clinical trials should be conducted to evaluate the behavior of this simplified composite hybrid restorative material in endodontically treated maxillary premolars.
Conclusion
The use of SO as a core material was the most effective approach for recovering the fracture strength of endodontically treated premolars to the level of intact teeth (93% recovery). However, specimens prepared with this method also showed an increased risk of unrestorable fracture. For achieving both a higher fracture resistance and a lower risk of unrestorable fracture, the most favorable approach in a Class II cavity that has a single remaining marginal ridge may be to fill the entire cavity with SO and use the self-curing mode.
Author affiliations
Oral and Dental Disease Research Center, Department of Operative Dentistry, School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran (Shafiei, Fattah); Postgraduate Program in Operative Dentistry, Department of Operative Dentistry, School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran (Tivay).
Correspondence
Zahra Fattah, DDS, MS (fattahz@sums.ac.ir).
Conflicts of interest
None reported.
Acknowledgments
This article is based on a thesis by Dr Shadi Tivay. The authors thank Dr Naeimehossadat Asmarian for the statistical analyses.
Funding
This research was supported by the Vice-Chancellery of Research, Shiraz University of Medical Sciences (grant 26362).
References
1. Karzoun W, Abdulkarim A, Samran A, Kern M. Fracture strength of endodontically treated maxillary premolars supported by a horizontal glass fiber post: an in vitro study. J Endod. 2015;41(6):907-912. doi:10.1016/j.joen.2015.01.022
2. Mergulhão VA, de Mendonça LS, de Albuquerque MS, Braz R. Fracture resistance of endodontically treated maxillary premolars restored with different methods. Oper Dent. 2019;44(1):E1-E11. doi:10.2341/17-262-L
3. Roperto R, Sousa YT, Dias T, et al. Biomechanical behavior of maxillary premolars with conservative and traditional endodontic cavities. Quintessence Int. 2019;50(5):350-356. doi:10.3290/j.qi.a42369
4. Mincik J, Urban D, Timkova S, Urban R. Fracture resistance of endodontically treated maxillary premolars restored by various direct filling materials: an in vitro study. Int J Biomater. 2016;2016:9138945. doi:10.1155/2016/9138945
5. Chen Y, Chen D, Ding H, Chen Q, Meng X. Fatigue behavior of endodontically treated maxillary premolars with MOD defects under different minimally invasive restorations. Clin Oral Investig. 2022;26(1):197-206. doi:10.1007/s00784-021-03991-9
6. Scotti N, Scansetti M, Rota R, Pera F, Pasqualini D, Berutti E. The effect of the post length and cusp coverage on the cycling and static load of endodontically treated maxillary premolars. Clin Oral Investig. 2011;15(6):923-929. doi:10.1007/s00784-010-0466-y
7. Kantardžić I, Vasiljević D, Lužanin O, Maravić T, Blažić L. Influence of the restorative procedure factors on stress values in premolar with MOD cavity: a finite element study. Med Biol Eng Comput. 2018;56(10):1875-1886. doi:10.1007/s11517-018-1824-1
8. Shahrbaf S, Mirzakouchaki B, Oskoui SS, Kahnamoui MA. The effect of marginal ridge thickness on the fracture resistance of endodontically-treated, composite restored maxillary premolars. Oper Dent. 2007;32(3):285-290. doi:10.2341/06-83
9. Rocca GT, Krejci I. Crown and post-free adhesive restorations for endodontically treated posterior teeth: from direct composite to endocrowns. Eur J Esthet Dent. 2013;8(2):156-179.
10. Frankenberger R, Dudek MC, Winter J, et al. Amalgam alternatives critically evaluated: effect of long-term thermomechanical loading on marginal quality, wear, and fracture behavior. J Adhes Dent. 2020;22(1):107-116. doi:10.3290/j.jad.a44001
11. Soto-Montero J, Giannini M, Sebold M, et al. Comparison of the operative time and presence of voids of incremental and bulk-filling techniques on Class II composite restorations. Quintessence Int. 2022;53(3):200-208. doi:10.3290/j.qi.b2218737
12. Kaisarly D, El Gezawi M, Kessler A, Rösch P, Kunzelmann KH. Shrinkage vectors in flowable bulk-fill and conventional composites: bulk versus incremental application. Clin Oral Investig. 2021;25(3):1127-1139. doi:10.1007/s00784-020-03412-3
13. Pardo Díaz C, Shimokawa C, Sampaio C, Freitas AZ, Turbino ML. Characterization and comparative analysis of voids in Class II composite resin restorations by optical coherence tomography. Oper Dent. 2020;45(1):71-79. doi:10.2341/18-290-L
14. Taha NA, Maghaireh GA, Ghannam AS, Palamara JE. Effect of bulk-fill base material on fracture strength of root-filled teeth restored with laminate resin composite restorations. J Dent. 2017;63:60-64. doi:10.1016/j.jdent.2017.05.016
15. Boaro LCC, Lopes DP, de Souza ASC, et al. Clinical performance and chemical-physical properties of bulk fill composites resin [sic] —a systematic review and meta-analysis. Dent Mater. 2019;35(10):e249-e264. doi:10.1016/j.dental.2019.07.007
16. François P, Remadi A, Le Goff S, Abdel-Gawad S, Attal JP, Dursun E. Flexural properties and dentin adhesion in recently developed self-adhesive bulk-fill materials. J Oral Sci. 2021;63(2):139-144. doi:10.2334/josnusd.20-0448
17. Rathke A, Pfefferkorn F, McGuire MK, Heard RH, Seemann R. One-year clinical results of restorations using a novel self-adhesive resin-based bulk-fill restorative. Sci Rep. 2022;12(1):3934. doi:10.1038/s41598-022-07965-z
18. Yao C, Ahmed MH, Okazaki Y, Van Landuyt KL, Huang C, Van Meerbeek B. Bonding efficacy of a new self-adhesive restorative onto flat dentin vs Class-I cavity-bottom dentin. J Adhes Dent. 2020;22(1):65-77. doi:10.3290/j.jad.a43999
19. Francois P, Fouquet V, Attal J-P, Dursun E. Commercially available fluoride-releasing restorative materials: a review and a proposal for classification. Materials (Basel) 2020;13(10):2313. doi:10.3390/ma13102313
20. Latta MA, Radniecki SM. Bond strength of self-adhesive restorative materials affected by smear layer thickness but not dentin desiccation. J Adhes Dent. 2020;22(1):79-84. doi:10.3290/j.jad.a.43932
21. Lohbauer U, Belli R. The mechanical performance of a novel self-adhesive restorative material. J Adhes Dent. 2020;22(1):47-58. doi:10.3290/j.jad.a.43997
22. Latta MA, Tsujimoto A, Takamizawa T, Barkmeier WW. In vitro wear resistance of selfadhesive restorative materials. J Adhes Dent. 2020;22(1):59-64. doi:10.3290/j. jad.a.43998
23. Leyton BS, Rached RN, Igná cio SA, Souza EM. Fracture strength of extended Class I composite restorations with different restorative techniques. Odontology. 2022;110(2):269-277. doi:10.1007/s10266-021-00656-7
24. Shafiei F, Tavangar MS, Ghahramani Y, Fattah Z. Fracture resistance of endodontically treated maxillary premolars restored by silorane-based composite with or without fiber or nano-ionomer. J Adv Prosthodont. 2014;6(3):200-206. doi:10.4047/jap.2014.6.3.200
25. Thongbai-On N, Chotvorrarak K, Banomyong D, Burrow MF, Osiri S, Pattaravisitsate N. Fracture resistance, gap and void formation in root-filled mandibular molars restored with bulk-fill resin composites and glass-ionomer cement base. J Investig Clin Dent. 2019;10(4):e12435. doi:10.1111/jicd.12435
26. Yao C, Ahmed MH, Zhang F, et al. Structural/chemical characterization and bond strength of a new self-adhesive bulk-fill restorative. J Adhes Dent. 2020;22(1):85-97. doi:10.3290/ j.jad.a44000
27. Kinomoto Y, Torii M, Takeshige F, Ebisu S. Comparison of polymerization contraction stresses between self- and light-curing composites. J Dent. 1999;27(5):383-389. doi:10.1016/s0300-5712(98)00065-7
28. Chen C, Niu LN, Xie H, et al. Bonding of universal adhesives to dentine—old wine in new bottles? J Dent. 2015;43(5):525-536. doi:10.1016/j.jdent.2015.03.004
29. Latta MA, Tsujimoto A, Takamizawa T, Barkmeier WW. Enamel and dentin bond durability of self-adhesive restorative materials. J Adhes Dent. 2020;22(1):99-105. doi:10.3290/ j.jad.a43996
30. Atalay C, Yazici AR, Horuztepe A, Nagas E, Ertan A, Ozgunaltay G. Fracture resistance of endodontically treated teeth restored with bulk fill, bulk fill flowable, fiber-reinforced, and conventional resin composite. Oper Dent. 2016;41(5):E131-E140. doi:10.2341/15-320-L
31. Moosavi H, Afshari S, Manari F. Fracture resistance of endodontically treated teeth with different direct corono-radicular restoration methods. J Clin Exp Dent. 2017;9(3):e454e459. doi:10.4317/jced.53160
32. Rosatto CM, Bicalho AA, Veríssimo C, et al. Mechanical properties, shrinkage stress, cuspal strain and fracture resistance of molars restored with bulk-fill composites and incremental filling technique. J Dent. 2015;43(12):1519-1528. doi:10.1016/j.jdent.2015.09.007
33. Van Ende A, De Munck J, Van Landuyt KL, Poitevin A, Peumans M, Van Meerbeek B. Bulkfilling of high C-factor posterior cavities: effect on adhesion to cavity-bottom dentin. Dent Mater. 2013;29(3):269-277. doi:10.1016/j.dental.2012.11.002
34. Ilie N, Keßler A, Durner J. Influence of various irradiation processes on the mechanical properties and polymerisation kinetics of bulk-fill resin based composites. J Dent. 2013;41(8):695-702. doi:10.1016/j.jdent.2013.05.008
35. Leprince JG, Palin WM, Vanacker J, Sabbagh J, Devaux J, Leloup G. Physico-mechanical characteristics of commercially available bulk-fill composites. J Dent. 2014;42(8):9931000. doi:10.1016/j.jdent.2014.05.009
36. Floriani DH, Rached RN, Ignácio SA, Souza EM. Internal adaptation of cusp-weakened Class I preparations restored with bulk-fill, bi-layered, and incremental restorative techniques: a micro-CT analysis. Oper Dent. 2022;47(5):527-534. doi:10.2341/20-244-L
37. Moorthy A, Hogg CH, Dowling AH, Grufferty BF, Benetti AR, Fleming GJP. Cuspal deflection and microleakage in premolar teeth restored with bulk-fill flowable resin-based composite base materials. J Dent. 2012;40(6):500-505. doi:10.1016/j.jdent.2012.02.015
38. Marovic D, Tauböck TT, Attin T, Panduric V, Tarle Z. Monomer conversion and shrinkage force kinetics of low-viscosity bulk-fill resin composites. Acta Odontol Scand. 2015;73(6):474-480. doi:10.3109/00016357.2014.992810
39. El-Damanhoury H, Platt J. Polymerization shrinkage stress kinetics and related properties of bulk-fill resin composites. Oper Dent. 2014;39(4):374-382. doi:10.2341/13-017-L
40. Ilie N, Bucuta S, Draenert M. Bulk-fill resin-based composites: an in vitro assessment of their mechanical performance. Oper Dent. 2013;38(6):618-625. doi:10.2341/12-395-L
41. Szesz A, Parreiras S, Reis A, Loguercio A. Selective enamel etching in cervical lesions for self-etch adhesives: a systematic review and meta-analysis. J Dent. 2016;53:1-11. doi:10.1016/j.jdent.2016.05.009
42. Cieplik F, Scholz KJ, Anthony JC, et al. One-year results of a novel self-adhesive bulk-fill restorative and a conventional bulk-fill composite in Class II cavities—a randomized clinical split-mouth study. Clin Oral Investig. 2022;26(1):449-461. doi:10.1007/s00784-02104019-y
GENERAL DENTISTRY SELF-INSTRUCTION
Exercise No. GD531, 2 CE Credits
Endodontics
Subject Code: 070
The 15 questions for this exercise are based on the article “Performance of a novel self-adhesive bulk-fill composite hybrid in endodontically treated maxillary premolars: analysis of fracture resistance and failure mode” on pages 23-29. This exercise was developed by Millie K. Tannen, DDS, MAGD, in association with the General Dentistry Self-Instruction committee.
1. All of the following factors contribute to the high incidence of fracture in endodontically treated maxillary premolars except one. Which is the exception?
A. prevalence of accessory canals
B. unfavorable crown to root ratio
C. position in the arch
D. cuspal flexure
2. The most ideal conservative restoration for an endodontically treated tooth is a composite resin restoration, if a marginal ridge is preserved. This study hypothesized that when these premolars were restored with SO using a variety of techniques, no significant difference in fracture resistance would be found among them.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
3. To reduce shrinkage stress, the recommended approach is to place and cure the composite in ______-mm-thick layers.
A. 0.5 to 1.0
B. 1.5 to 2.0
C. 2.5 to 3.0
D. 3.5 to 4.0
4. All of the following are challenges of incremental resin placement except one. Which is the exception?
A. void formation
B. lack of union between layers
C. partially uncured resin
D. contamination
5. Bulk-fill composite resins were developed to allow the placement of composite in ___-mm increments.
A. 3.0
B. 4.0
C. 5.0
D. 6.0
Reading the article and successfully completing this exercise will enable you to:
• familiarize yourself with the self-adhesive properties of the new hybrid composite resin Surefil one (SO);
• evaluate the fracture resistance of endodontically treated maxillary premolars following restoration with SO in combination with a variety of adhesive techniques and materials; and
• evaluate the effect of various restorative techniques on the restorability of the premolars following fracture.
Answers must be submitted online at agd.org/self-instruction by June 30, 2025.
6. Bulk-fill composite resins are available as both flowable and paste-like materials. Both types require occlusal coverage with a layer of hybrid composite.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
7. According to the manufacturer’s claim, SO exhibits all the following advantages except one. Which is the exception?
A. long-term esthetics
B. bulk fill
C. dual cure
D. self-adhesion
8. Tooth preparations in the experimental groups included a ___-mm-thick mesial marginal ridge and a ___-mm cavity depth.
A. 2.0; 4.0
B. 2.0; 6.0
C. 3.0; 4.0
D. 3.0; 6.0
9. Restoration of the teeth in the study groups included some composites placed with __________.
A. selective enamel etching for 10 seconds
B. total etching for 10 seconds
C. total etching for 20 seconds
D. no etching
10. In the SO-SC group, restoration with SO included ______ of ______ thickness for ______.
A. self-curing; 4.0-mm; 4 minutes
B. self-curing; 6.0-mm; 6 minutes
C. light curing; 4.0-mm; 40 seconds
D. light curing; 6.0-mm; 40 seconds
11. To test fracture resistance, the mastication simulation machine applied ______ loading cycles to represent a range of ____ months of clinical service.
A. 20,000; 1 to 3
B. 20,000; 3 to 6
C. 50,000; 3 to 12
D. 50,000; 3 to 18
12. The degree of fracture was determined with cone beam computed tomography. A tooth was recorded as unrestorable when the fracture line was more than 2 mm below the cementoenamel junction.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
13. Results of the fracture resistance testing determined that the ______ group was the only experimental group that did not differ significantly from the control group.
A. SO-SC
B. SO-LC
C. SO-UA
D. SO-core
14. Among the study groups, the ____ group exhibited the lowest fracture resistance.
A. SO-SC
B. SO-LC
C. SO-UA
D. SO-core
15. In the SO-core group, ____% of the fractures were unrestorable.
A. 20.5
B. 33.4
C. 45.8
D. 66.6
Globe-shaped central incisors in a patient with otodental syndrome
Daniel Adrian Silva Souza, MSc ¢ Candice Belchior Duplat, DDS ¢ Rebeca Brasil Oliveira, MSc
Frederico Sampaio Neves, PhD ¢ André Wilson Machado, PhD ¢ Jean Nunes dos Santos, PhD
Hearing impairments and dental anomalies are found in many genetic syndromes. Otodental syndrome is a rare combination of hearing loss and the presence of a pathognomonic dental phenotype known as globodontia, in which the tooth exhibits an abnormal globe shape. There is no histologic evidence of structural anomalies in the enamel, dentin, or pulp. This report describes the case of a 12-year-old boy who had hearing loss and 2 supernumerary globe-shaped teeth in the sites of the permanent maxillary central incisors. The diagnosis of otodental syndrome was established based on the clinical, radiographic, and histologic features, but other conditions, including dens evaginatus, talon cusp, dens invaginatus, and compound odontoma, should be included in the differential diagnosis. Dental treatment consisted of the extraction of both anomalous teeth, allowing spontaneous eruption of the impacted permanent central incisors. Early diagnosis of otodental syndrome permits a multidisciplinary approach to prevent other pathologic conditions, reduce functional damage, and avoid social problems.
Hearing impairments and dental anomalies are found in many genetic syndromes. Globodontia, an abnormal crown morphology manifesting as globe-shaped teeth, is a pathognomonic dental phenotype of the rare condition known as otodental syndrome or otodental dysplasia, which is associated with high-frequency hearing loss.1-3 The dental features were described in 1969 by Denes and Csiba, who reported their presence in a mother and son.1 Subsequently, Levin and Jorgenson identified a family in which 28 members had similar dental anomalies in addition to hearing loss.4 The existence of this syndromic combination has since been validated by additional reports.3-5
The otologic finding in patients with otodental syndrome consists of sensorineural hearing loss for frequencies above 1000 Hz.6 Sensorineural bilateral hearing loss has been reported to start as early as infancy and progress to a plateau.6 When the affected individual also presents an ocular phenotype known as coloboma, in which there is an absence or defect of eye tissue, the condition is termed oculo-otodental syndrome. The eye abnormality is described as a keyhole-shaped defect in the inferior iris caused by a deficiency in the iris pigment epithelium.7,8 Otodental syndrome is an autosomal dominant condition with variable penetrance and expressivity.3,7,9,10
Teeth affected by globodontia can demonstrate anomalies of eruption, number, size, shape, and structure.2 Globodontia can affect both the primary and permanent dentitions, causing delays in eruption. Clinically, globodontia manifests as canines and/or molars with an unusual number of well-developed cusps and an absence of developmental grooves and fossa on the cusps.10,11 Histologically, there is no evidence of structural anomalies in the enamel, dentin, or pulp.12,13
The aim of this article is to describe an unusual case of a young patient with morphologic and histologic manifestations of globodontia affecting the permanent central incisors, which is not usually a feature of otodental syndrome. The features of the case are also compared with those described in the literature.
Case report
The patient and his legal guardian provided informed consent for publication of the details of diagnosis and treatment. No institutional review board approval was indicated, as the patient provided consent and this case report meets the standard of care for the patient.
A 12-year-old boy was referred to the School of Dentistry, Federal University of Bahia, Salvador, Brazil, for general dental assessment. His main concern was the shape of his maxillary central incisors. Intraoral examination revealed that the patient was in the permanent dentition stage and had an Angle Class II molar relationship characterized by a severe lack of space in the maxillary arch. Bulbous globe- or flower
bud–shaped teeth were present in the sites of the permanent maxillary central incisors (Fig 1). The patient had no previous history of involvement in the primary dentition. The anomalous teeth had a large central cusp surrounded by multiple isomorphic cusps.
Periapical radiographs showed that each anomalous tooth had a single root and single canal. Panoramic radiography revealed the presence of unerupted, impacted maxillary central incisors with normal morphology (Fig 2). The third molars were also unerupted and all adjacent bone structure was normal. A cephalometric radiograph also showed a hyperdivergent growth pattern consisting of proclined maxillary and mandibular anterior teeth, compatible with a convex profile.
The patient’s medical records revealed early hearing loss. The patient had no history of drug treatments in early childhood, and his family had no history of congenital disorders.
On radiographic analysis, both teeth were considered to be supernumerary, and it was thought that the impacted maxillary central incisors could attain occlusion through spontaneous eruption or orthodontic traction. Therefore, the supernumerary teeth were extracted and submitted to histopathologic examination.
The hematoxylin-eosin–stained sections were evaluated by an experienced pathologist. Analysis of the sections showed teeth with a punctate dentin surface as well as the usual presence of cementum and pulp tissue. Marked chronic inflammation was present in areas near the apex. Remnants
of enamel matrix on the tooth surface, especially among the punctate structures, were also observed. A diagnosis of otodental syndrome was rendered based on the clinical, radiographic, and histopathologic features.
Dental treatment consisted of the extraction of both anomalous teeth. The patient was referred for follow-up by a specialized medical team that included an ophthalmologist and otolaryngologist. Ophthalmologic examination of the patient did not show any deficits.
Approximately 2 years 2 months after extraction of the globe-shaped teeth, the impacted central incisors erupted spontaneously (Fig 3). The panoramic radiograph revealed that the patient’s osseous and dental features were normal (Fig 4). Although orthodontic treatment was suggested after the patient’s central incisors erupted, his family lacked the financial means to seek care.
Discussion
This article reports a case of otodental syndrome in which the presence of globodontia affecting supernumerary maxillary central incisors helped to establish the diagnosis in a 12-year-old boy. This syndrome is a rare and severe autosomal dominant anomaly characterized by abnormal, globe-shaped teeth in association with hearing loss and, in some individuals, visual problems.2,3 When colobomas are present in addition to hearing loss, the condition is called oculo-otodental syndrome. 1,8 In the present case, the patient had no ocular or vision anomalies.
Fig 1. Two bulbous globe- or flower bud–shaped teeth occupy the space of the central incisors in a 12-year-old boy. A. Extraoral view. B. Intraoral view. C. Occlusal view.
Fig 2. The permanent central incisors are impacted but show normal morphology.
The diagnosis of otodental syndrome was based on the clinical, radiographic, and histologic features, but other pathologic conditions should be included in the differential diagnosis. Dens evaginatus, or evaginated odontoma, is a developmental alteration characterized by the presence of an abnormal elevation or an accessory tubercle resembling a cusp.6,9 This condition projects from the cingulum or cementoenamel junction and is mainly found on the occlusal surface of mandibular premolars and lingual surface of anterior teeth.6,9 The anomaly in the present case resembled dens evaginatus in the premolars.
The talon cusp is a well-delimited extra cusp that is found only on the surface of an anterior tooth and projects at least half of the distance from the cementoenamel junction to the incisal edge. This type of accessory cusp projects from the lingual surface and resembles an eagle’s talon.9 The present case did not meet the description of this condition.
Dens invaginatus, or dens in dente, is a dental anomaly in which invagination of the enamel organ begins in the crown and extends to the root during soft tissue development.6 During formation of the hard tissues, the invaginated enamel organ produces a small tooth inside the developing pulp chamber.7 This condition was not observed radiographically in the present case.
Compound odontoma is a benign tumor arising from odontogenic tissues and consists of a unilocular conglomerate of
multiple tooth-like structures.6,9 The epithelial and mesenchymal cells of an odontoma may appear normal but have a flawed structural arrangement.6,10 The size and conformation of the dental tissues are altered, giving rise to multiple small teeth.6,10 Although compound odontomas are commonly found in the maxillary anterior region, they rarely erupt, as the teeth in the present case did, and they seldom have a cusp shape. However, this condition may occur after traumatic injury in this area.9
Otodental syndrome may also be confused with congenital syphilis. Tooth defects related to congenital syphilis were first described by Hutchinson in 1858, as part of a triad that includes corneal keratitis and sensorineural hearing loss.9 In this condition, the teeth are smaller, round, and well separated. Some teeth are notched at the incisal edge and the enamel has a grayish color.6 So-called Hutchinson incisors have a smaller incisal edge with mesial and distal bulging.6 These features differ from the condition of the incisors observed in the present case. The mulberry shape with hypoplastic features is commonly associated with the molars in patients with congenital syphilis; in the present case, globodontia was only observed in the maxillary incisors.7
The Table summarizes cases reported in the English literature, including the present case.2,6,7,9,10,14-16 Otodental syndrome affects both sexes and children aged 3 years and older. These teeth are easily detected when they erupt with a shape anomaly. The present case differed from previously reported
Fig 4. Normal anterior osseous and dental features are evident 2 years 2 months after extraction of the anomalous teeth.
Fig 3. Permanent central incisors with normal morphology have spontaneously erupted 2 years 2 months after extraction of the anomalous teeth. A. Extraoral view. B. Intraoral view. C. Occlusal view.
Table. Comparison of previously reported cases of otodental syndrome and the present case.
Patient
Study and location
Examination findings
Sex Age, y Radiographic Otolaryngologic Ophthalmologic
Enright et al (2015)2; United Kingdom F 8 Taurodontism; irregular pulp chambers; spherical crowns; single, small, eccentrically placed cusp on molars
Sedano et al (2001)6; Brazil M 5
Vieira et al (2002)7; UK 2 M; 7 F 2-50
Globe-shaped molars with enlarged pulp chambers
Delayed primary tooth eruption; posterior globodontia and anomalous crowns in permanent dentition
Santos-Pinto et al (1998)9; Brazil 5 M; 5 F NR Roots shorter than their crowns
Liu et al (2017)10; China F 9
Su et al (2019)14; China M 3
Paglia et al (2022)15; Italy M 7
Van Doorne et al (1998)16; Belgium M 12
Molars with larger pulp chambers and short root length; absence of mandibular permanent premolars and complex odontomas
Globe-shaped molars and canines with enlarged pulp chambers; short roots on molars
Globe-shaped molars and canines
Primary canines with bulbous morphology; primary maxillary first molars with multiple bubbleshaped cusps; other primary molars with a globe shape
Present case (2024); Brazil M 12 Impacted central incisors
Abbreviations: F, female; M, male; NR, not reported; UK, United Kingdom.
cases in that the central incisors were affected. In addition, the altered incisors were identified as supernumerary teeth. Santos-Pinto et al and Liu et al each described cases of possible fusion between a supernumerary and a globe-shaped tooth, but such teeth with altered anatomy are not generally considered to be supernumerary teeth.9,10
Genetic testing was only performed in about half of the previously reported cases and therefore was not always the determining factor for diagnosis. Genetic testing is still expensive and may not be available at centers in lower income areas. However, genetic testing would facilitate the diagnosis, especially in patients without a family history or certain clinical features. In addition, variable gene expression and penetrance are observed in otodental syndrome.6,9 The Fas-associated death domain (FADD) gene was found to be deleted in a family with coloboma, and haploinsufficiency is likely responsible for this ocular problem. 3 Screening of the genome of 2 families revealed overlapping
Bilateral hearing loss No coloboma No
Moderate bilateral sensorineural hearing loss NR No
Hearing loss Coloboma Yes
Hearing loss No coloboma No
Bilateral hearing loss No coloboma Yes
Hearing loss No coloboma No
Bilateral mild-tomoderate hearing loss No coloboma Yes
Bilateral hearing loss No coloboma Yes
Hearing loss No coloboma No
hemizygous microdeletions and subsequent haploinsufficiency of the fibroblast growth factor 3 (FGF3) gene, which was implicated as the probable cause of otodental syndrome. 3,7
A combination of hearing loss and dental anomalies is found in more than 100 genetic syndromes of variable severity.17 The association of ocular problems with dental defects is less common and may be mild in oculo-otodental syndrome. In the absence of ocular involvement, the syndrome has been called otodental syndrome, otodental dysplasia, familial otodentodysplasia, or globodontia-deafness syndrome. 7,9 Hearing and vision tests are indicated for patients who are suspected to have this diagnosis, and medical follow-up should be continued for the early detection of hearing and vision problems that may arise during the child’s development.
Dental anomalies have been reported as significant characteristics of many syndromes and provide an important clue for the identification of some of them. An abnormal crown
Affected teeth
Family involvement
Primary canines and molars NR
Primary canines and molars NR
Various 1 family; 5 generations; 9 cases
Primary and permanent canines and molars 1 family; 3 generations; 10 cases
Primary canines and molars NR
Primary canines and molars NR
Primary canines and molars NR
Primary and permanent canines and molars NR
Permanent maxillary central incisors NR
morphology in selected tooth types is the most consistent anatomical finding in otodental syndrome.9 Histologic analysis suggests that the overall structure of enamel, dentin, cementum, and pulp is normal, as observed in the present case.6,9 However, immature dental tissue, in the form of enamel matrix, was observed in the histopathologic specimens.
The facial esthetics of the patient in the present case were compromised because vertical maxillary excess resulted in gingival exposure, revealing the morphologically altered teeth. The child therefore felt insecure about his smile, and this factor was the main reason that the patient sought care, which led to the unexpected diagnosis. The earlier the diagnosis, the better will be the treatment, permitting a multidisciplinary approach to prevent other pathologic conditions, reduce functional damage, and avoid social problems.9
Regular monitoring of the patient was a treatment strategy. Tooth migration was observed after space was created by tooth
removal. If the oral conditions include sufficient space, favorable positioning, and an absence of opposing forces, the teeth will move to achieve interocclusal contact.6 This conservative approach reduces biological and financial costs and offers a less invasive treatment to patients with systemic conditions.
Conclusion
This case report describes a rare case of otodental syndrome involving hearing loss and globodontia that affected supernumerary central incisors. The findings highlight the importance of obtaining a complete medical history as well as performing clinical evaluations, histopathologic investigations, and, if possible, genetic testing for affected individuals. Early diagnosis was particularly important for this patient, considering his age and stage of dental development, which offered the possibility of dental treatment. Spontaneous eruption occurred after extraction of the affected teeth, and this conservative approach
will facilitate corrective orthodontic treatment in the future. Functional and esthetic rehabilitation to facilitate social integration were other benefits of an early diagnosis.
Author affiliations
Department of Propaedeutics and Integrated Clinic, Division of Oral Radiology, School of Dentistry, Federal University of Bahia, Salvador, Brazil (Souza, Duplat, Neves); School of Dentistry, Federal University of Bahia, Salvador, Brazil (Oliveira); Department of Social Dentistry, Division of Orthodontics, School of Dentistry, Federal University of Bahia, Salvador, Brazil (Machado); Department of Pathology, School of Dentistry, Federal University of Bahia, Salvador, Brazil (dos Santos).
Correspondence
Daniel Adrian Silva Souza, MSc (danieladrian.doc@gmail.com).
Conflicts of interest
None reported.
Funding
Daniel Adrian Silva Souza was supported by a research scholarship from the Research Support Foundation of Bahia State (FAPESB), Brazil.
References
1. Denes J, Csiba A. An unusual case of hereditary developmental anomalies of the cuspids and molars. Article in Hungarian. Fogorv Sz. 1969;62(7):208-212.
2. Enright S, Humphrys AK, Rea G, James JA. Globodontia in the otodental syndrome: a rare defect of tooth morphology occurring with hearing loss in an eight-year-old. Dent Update 2015;42(10):927-932. doi:10.12968/denu.2015.42.10.927
3. Gregory-Evans CY, Moosajee M, Hodges MD, et al. SNP genome scanning localizes oto-dental syndrome to chromosome 11q13 and microdeletions at this locus implicate FGF3 in dental and inner-ear disease and FADD in ocular coloboma. Hum Mol Genet 2007;16(20):2482-2493. doi:10.1093/hmg/ddm204
4. Levin LS, Jorgenson RJ. Familial otodentodysplasia: a “new” syndrome. Abstract 61a. Presented at: Annual Meeting of the American Society of Human Genetics; October 11-14, 1972; Philadelphia.
5. Colter JD, Sedano HO. Otodental syndrome: a case report. Pediatr Dent. 2005;27(6):482485.
6. Sedano HO, Moreira LC, de Souza RA, Moleri AB. Otodental syndrome: a case report and genetic considerations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;92(3):312317. doi:10.1067/moe.2001.116818
7. Vieira H, Gregory-Evans K, Lim N, Brookes JL, Brueton LA, Gregory-Evans CY. First genomic localization of oculo-oto-dental syndrome with linkage to chromosome 20q13.1. Invest Ophthalmol Vis Sci. 2002;43(8):2540-2545.
8. Winter G. The association of ocular defects with the otodental syndrome. J Int Assoc Dent Child. 1983;14(2):83-87.
9. Santos-Pinto L, Oviedo MP, Santos-Pinto A, Iost HI, Seale NS, Reddy AK. Otodental syndrome: three familial case reports. Pediatr Dent. 1998;20:208-211.
10. Liu A, Wu M, Guo X, et al. Clinical, pathological, and genetic evaluations of Chinese patient with otodental syndrome and multiple complex odontoma: case report. Medicine (Baltimore). 2017;96(5):e6014. doi:10.1097/MD.0000000000006014
11. Cook RA, Cox JR, Jorgenson RJ. Otodental dysplasia: a five year study. Ear Hear 1981;2(2):90-94. doi:10.1097/00003446-198103000-00007
12. Beck-Mannagetta J, Müller H, Richter E, Donath K. Odontomas and pan-tonal hearing loss in the otodental syndrome. Article in German. Dtsch Zahnarztl Z. 1984;39(3):232-241.
13. Bausells H, Vono R, Rocca R. Rare multiple dental anomaly in 3 brothers. Report of case. Article in Portuguese. Rev Fac Farm Odontol Araraquara. 1971;5(2):207-214.
14. Su JM, Zeng SJ, Ye XW, Wu ZF, Huang XW, Pathak JL. Three years of follow-up of otodental syndrome in 3-year-old Chinese boy: a rare case report. BMC Oral Health. 2019;19(1):164. doi:10.1186/s12903-019-0860-z
15. Paglia M, Giani G, Pisoni L, Paglia L. Otodental syndrome: case report and differential diagnosis with Treacher Collins syndrome. Eur J Paediatr Dent. 2022;23(1):66-58. doi:10.23804/ejpd.2022.23.01.12
16. Van Doorne L, Wackens G, De Maeseneer M, Deron P. Otodental syndrome. A case report. Int J Oral Maxillofac Surg. 1998;27(2):121-124. doi:10.1016/s0901-5027(98)80309-3
17. London Medical Databases. Face2Gene Library. Accessed April 26, 2024. https://www. face2gene.com/ lmd-library-london-medical-database-dysmorphology/
Evaluation of artifacts produced by conventional dental materials in standard and high-resolution CBCT imaging
The aim of this study was to identify and quantify artifacts produced by commonly used dental restorative materials in both standard and high-resolution cone beam computed tomographic imaging. In this in vitro study, 25 different dental materials were placed in holes (3 mm in diameter × 2 mm thick) prepared in the center of 10 × 10-mm polymethyl methacrylate plates. The specimens, along with a control plate prepared with an unfilled hole, were scanned at standard and high resolutions. The gray values (GVs) of the specimens were measured at 1-, 2-, 4-, and 8-mm distances from the material surfaces, and in 8 different directions, resulting in 32 measurements per specimen. The absolute value of the difference (ΔGV) between the GV of each measurement point on the specimen disc and the GV of the corresponding point on the control disc was considered to be the number of artifacts at that point. The median ΔGV of each material was calculated, and the materials were then ranked in terms of artifact formation using the Kruskal-Wallis test. At standard resolution, the greatest numbers of artifacts were caused by AH 26 root canal sealer and Heraenium S nickel-chromium alloy, and the fewest were caused by Whitepost DC #3 glass fiber post and ChemFil Superior glass ionomer cement. At high resolution, the greatest numbers of artifacts were found in amalgam (admix; SDI) and Heraenium S, and the fewest in Whitepost DC and GC Initial enamel porcelain. The median ΔGV values at standard and high resolutions were 46.0 and 57.0, respectively. High and standard resolutions were significantly different in terms of artifact formation (P = 0.001; Wilcoxon test). AH 26 sealer was the only material that demonstrated a statistically significant reduction in artifact formation at high resolution compared with standard resolution (P = 0.05; Wilcoxon test). The number of artifacts produced by dental materials at both resolutions decreased with an increasing distance from the surface of the material.
Received: April 25, 2023
Accepted: June 14, 2023
Keywords: artifact, cone beam computed tomography, dental materials, high resolution, standard resolution
Application of cone beam computed tomography (CBCT) in dentistry has increased rapidly given its ability to provide detailed cross-sectional images with submillimeter resolution with shorter scan time, lower radiation doses, and lower costs compared to conventional multidetector computed tomography (MDCT).1-3 However, like MDCT, CBCT is prone to producing artifacts from dental materials.4 The presence of metal objects with high attenuation, such as dental restorations, orthodontic bands, surgical plates, and pins, can cause artifacts.5 These artifacts can significantly influence the quality of CBCT images and reduce their diagnostic value by distorting the images of anatomical structures and reducing the contrast between adjacent objects.6
CBCT can be used to capture images of maxillofacial structures with various voxel sizes. Smaller voxel sizes produce higher image resolution but also require higher radiation doses.7 According to the principle of ALARA (as low as reasonably achievable), patient exposure should be considered when a CBCT system is used, and the overall diagnostic advantage should be greater than the radiation exposure to the patient.8-12
The recognition of CBCT artifacts associated with different filling materials is of high importance. Exposure parameters such as tube voltage, tube current, field of view (FOV) size, and voxel size may also affect the quality of CBCT images, especially if the patient has various dental restorations.13,14 Safi et al indicated that a higher tube current results in a higher signal to noise ratio and therefore enhances the quality of a CBCT image.15 The effect of spatial resolution, which is directly related to the selected voxel size, is still controversial.15
The purpose of this in vitro study was to identify and quantify artifacts produced by 25 conventional dental materials (metallic and nonmetallic) in CBCT images at standard and high resolutions. The number of artifacts produced at different distances from the material surface and in different directions were also assessed at both resolutions.
Methods
Specimen preparation
In this in vitro study, artifacts produced by 25 common dental materials were assessed (Box). A hole 3 mm in diameter × 2 mm thick was made in 10 × 10-mm polymethyl methacrylate (PMMA) plates (Fig 1). In total, 26 plates were prepared. One was chosen as the control plate; in the remaining 25 plates, a dental material was placed in the hole according to its manufacturer’s instructions. Each plate was fixed to a piece of cardboard to stabilize the plates during scanning. The plates were then placed horizontally into 2 cylindrical vessels, 1 holding
13 specimens and the other 12 specimens, with 13-mm-thick discs of red wax inserted between specimens as a separator (Fig 2). Each cylindrical vessel was then fixed in a plastic container filled with water to simulate soft tissue.
Scanning procedure
A laser guide was used to position the plastic containers full of water on the chin rest of the CBCT machine (VGi, NewTom) so that the specimens were in the center of a 12 × 8-cm FOV. The control plate and the 25 specimens were each analyzed twice, once at standard resolution and once at high resolution (a total of 52 scans for the sample). The standard and highresolution scans were carried out with the following parameters: acceleration voltage of 110 kV (both resolutions); beam current of 0.58 mA (both resolutions); FOV of 12 × 8 cm (both resolutions); voxel sizes of 0.25 mm and 0.15 mm, respectively; and scan times of 3.6 seconds and 5.4 seconds, respectively.
Image analysis
Images with a thickness of 0.5 mm were reconstructed in axial sections using NNT Viewer software (version 2.21, NewTom). The gray value (GV) of each disc (control plus 25 experimental specimens) was assessed at 1-, 2-, 4-, and 8-mm distances from the surface of the specimen and recorded in 8 directions (upper, lower, left, right, upper right, upper left, lower right, and lower left), resulting in 32 measurements per specimen
per resolution (64 total per specimen). These directions were fixated with respect to 4 lines drawn perpendicular to the borders of the red wax separator and a line at a 45° angle to each perpendicular line (Fig 3).
The obtained information was recorded as DICOM (digital imaging communications in medicine) files using
Fig 1. Polymethyl methacrylate plate (10 × 10 mm) with a 3-mm hole in the middle for placement of a dental material.
Fig 2. Preparation of specimens for CBCT imaging. A. Polymethyl methacrylate plates containing specimens fixed on cardboard. B. Stacked specimens with 13-mm red wax separators.
Fig 3. Assessment of the mean gray value on an axial CBCT image .
Table 1. Median absolute values of ΔGV (artifacts)a of restorative materials (n = 32 per material).
aThe absolute value of the difference (ΔGV) between the GV of each measurement point on the specimen disc and the GV of the corresponding point on the control disc was considered to be the number of artifacts at that point.
OnDemand3D software (version 1.0.9.1332, Dexis). The GVs from the different distances and directions were calculated in circular areas with 1-mm diameters.
The GV was measured at 32 sites for each specimen by an experienced oral and maxillofacial radiologist (Z.S.). The mean value was automatically calculated by the software and employed for ΔGV calculation. The absolute value of the difference (ΔGV) between the GV of each measurement point on the specimen disc and the GV of the corresponding point on the control disc was considered to be the number of artifacts at that point. This formula was applied for both standard and high resolutions.
Table 2. Median absolute values of ΔGV (artifacts)a at different distances from the material surface (n = 200 per resolution).
aThe absolute value of the difference (ΔGV) between the GV of each measurement point on the specimen disc and the GV of the corresponding point on the control disc was considered to be the number of artifacts at that point.
bStatistically significant difference from standard resolution at 2 mm (P = 0.05; Wilcoxon test).
Table 3. Median absolute value of ΔGV (artifacts)a produced in different directions (n = 100 per direction).
aThe absolute value of the difference (ΔGV) between the GV of each measurement point on the specimen disc and the GV of the corresponding point on the control disc was considered to be the number of artifacts at that point.
Statistical analysis
Intraclass correlation coefficient (ICC) testing was performed with 10 specimens to assess the intraoperator reliability. The studied materials (n = 25) were ranked by the Kruskal-Wallis test using SPSS version 18.0 (IBM) in terms of artifact formation. The simultaneous effects of the type of material, distance from the surface, and direction of the artifact were examined using multivariate regression analysis (Wilcoxon test).
Results
Measures for the first and second replicates of 10 specimens were recorded, and ICC values were established for all
measurements. Most measurements demonstrated a high degree of reliability between the first and second replicates, with ICC values ranging from 0.83 to 0.98.
At standard resolution, the greatest numbers of artifacts were caused by AH 26 root canal sealer and Heraenium S nickelchromium alloy, with medians of 175.5 and 129.5, respectively (Table 1). The fewest artifacts were reported in Whitepost DC #3 glass fiber post and ChemFil Superior glass ionomer cement specimens, with medians of 13.0 and 20.0, respectively.
At high resolution, the greatest numbers of artifacts were caused by amalgam (admix, SDI) and Heraenium S nickel-chromium alloy, with median values of 181.5 and 136.0, respectively. The fewest artifacts resulted from Whitepost DC #3 glass fiber post and GC Initial enamel porcelain, with medians of 23.0 and 24.0, respectively.
The Wilcoxon test was used to compare the median ΔGV values of standard and high resolutions within each material and found a significantly greater number of artifacts in highresolution images for 5 materials: Fuji II LC glass ionomer (P = 0.002), zinc phosphate cement (P = 0.003), ProTaper Universal rotary nickel-titanium file (P = 0.008), amalgam (P = 0.03), and ChemFil Superior glass ionomer (P = 0.05). The greater number of artifacts in high-resolution imaging of Whitepost DC #3 glass fiber post had borderline significance (P = 0.07). In contrast, other materials produced a greater number of artifacts at standard resolution than at high resolution: Z100 restorative composite, AH 26 root canal sealer, gutta percha (Aria Dent brand), GC Initial enamel porcelain, and GC Initial dentin porcelain. However, this difference was statistically significant only for AH 26 (P = 0.05; Wilcoxon test).
Analysis of the ΔGV at different distances from the specimen surface showed that, at both resolutions, increasing the distance usually resulted in a reduction in the ΔGV (Table 2). At standard resolution, a small increase in the ΔGV was reported when the distance increased from 2 to 4 mm; however, this increase was statistically insignificant. The numbers of artifacts identified were greater for each distance at high resolution compared with standard resolution; however, this change was only statistically significant at the 2-mm distance (P = 0.03; Wilcoxon test).
Evaluation of the frequency distribution of artifacts in the various directions at both resolutions indicated that the frequency was greater in high-resolution images in the following directions: upper, upper right, right, lower right, lower, and lower left (Table 3). In contrast, in the left and upper left directions, fewer artifacts were observed at high resolution than at standard resolution.
According to multivariate regression analysis (Wilcoxon test) for determining the relationship between the ΔGV and the type of material, distance from the surface of the material, and direction of the artifact, the only variable that showed a significant negative correlation at standard resolution was distance from the surface (β = −0.3; P < 0.001). There was also a significant negative correlation between ΔGV and distance from the surface in high-resolution images (β = −0.17; P < 0.001). In high-resolution images, the median ΔGV values had a positive correlation with the left or right direction that was borderline significant (β = 0.06; P < 0.06).
The Wilcoxon test was used to investigate the difference between the results of standard and high-resolution imaging. The
median ΔGV values at standard and high resolutions were 46.0 and 57.0, respectively. There was a statistically significant difference between the resolutions in terms of artifact formation (P = 0.001).
Discussion
Many different types of materials with known properties are used in dental treatment, including dental composites, metal alloys, porcelain materials, ceramics, root canal filling materials, cement, and temporary materials.16,17 Some of these materials are prone to producing artifacts in CBCT images. Artifacts produced by dental materials can significantly reduce the quality of CBCT images and decrease their diagnostic value.18
Based on the results of this study, the greatest numbers of artifacts at standard resolution were produced by AH 26 root canal sealer and Heraenium S nickel-chromium alloy. The fewest were caused by the Whitepost DC #3 glass fiber post and ChemFil Superior glass ionomer. At high resolution, the greatest numbers of artifacts were produced by amalgam and Heraenium S, and the fewest were caused by Whitepost DC #3 and GC Initial enamel porcelain.
At standard resolution, AH 26 sealer produced more artifacts than amalgam. Bismuth is the major component of AH 26 (60%) and can lead to beam hardening because of its high atomic number (83) and high mass density (9.78 g/cm3), caused by its high absorption of X-ray beams. However, at high resolution, significant artifacts were observed adjacent to the amalgam restorations. This difference could be related to the fact that, clinically, the thickness of sealer is typically 0.05 to 0.3 mm, while the thickness of amalgam as a restorative material should be at least 1.5 to 2.0 mm. Most amalgam restorations have a thickness of more than 2 mm, which could be expected to cause the presence of more significant artifacts in CBCT images compared with those produced by a root canal sealer.
The analysis of the present results revealed that 5 materials caused significantly more artifacts at high resolution than at standard resolution. Pauwels et al evaluated 1 MDCT and 12 CBCT devices to compare the artifacts resulting from titanium and lead present in dental materials.12 Comparing the results of high-dose and low-dose exposure protocols, they found that some devices had fewer metal artifacts in high-dose protocols, although none of the decreases were statistically significant. This disagreement between the studies could be attributed to differences in the study designs; Pauwels et al tested numerous devices and altered multiple exposure factors, including the FOV, kilovoltage peak, milliamps, exposure time, voxel size, and type of material.12
An increase in the amount of artifacts at high resolution compared with standard resolution was observed for 20 dental materials. The difference was statistically significant for Fuji II LC glass ionomer, zinc phosphate cement, ProTaper Universal rotary nickel-titanium file, amalgam, and ChemFil Superior, and it was borderline significant for the Whitepost DC #3 glass fiber post. For Z100 restorative composite, AH 26 root canal sealer, gutta percha (Aria Dent), GC Initial enamel porcelain, and GC Initial dentin porcelain, the number of artifacts was reduced at high resolution compared with standard resolution, although this reduction was only significant for AH 26.
The numbers of artifacts produced at 1-, 2-, 4-, and 8-mm distances from the surface of the dental materials were also
evaluated. The numbers of artifacts showed a significant negative correlation with distance at both resolutions. The number of artifacts also increased at high resolution compared to standard resolution for each distance, but this change was only significant at the 2-mm distance (P < 0.05). Overall, at both resolutions and regardless of the material type, the number of artifacts was usually reduced with increasing distance from the surface of the material.
These findings are consistent with results reported by Benic et al.4 In their laboratory evaluation of artifacts produced by titanium dental implants in CBCT, they showed that the artifacts were always adjacent to the titanium implants regardless of the implant location. There was also a significant decrease in the intensity of artifacts when the distance from the implant surface increased.4 Similarly, in the present study, a significant reduction in artifacts was observed in both standard and highresolution imaging when the distance from the surface of the material increased.
Among the 3 evaluated variables (type of material, distance from the surface, and direction of the artifact), at standard resolution, the direction did not have a significant impact on artifact formation in comparison to the other 2 factors. No significant correlation was observed at high resolution, although the artifacts increased to some degree in the left or right direction.
In a study by Brito-Júnior et al, which evaluated the rate of streaking artifacts produced by different sealers in CBCT images of different voxel resolutions, sealers played a major role in the formation of artifacts.6 In fact, more artifacts were produced by the AH 26 sealer and Endofill with higher voxel sizes. In the present study, the rate of artifacts in AH 26 sealer was higher at standard resolution (higher voxel size) compared with high resolution
To evaluate and compare beam-hardening artifacts between 2 CBCT systems, Esmaeili et al utilized a method that described artifacts based on the percentage of objects accurately imaged.19 The results showed that the NewTom System produced fewer beam-hardening artifacts and provided higher-quality images than the Planmeca Promax 3D Max System. The authors suggested that the NewTom System is preferable for CBCT examinations of patients with extensive dental restorations, dentures, and dental implants.19 The present study also used the NewTom System for scanning materials (DICOM files).
Klinke et al studied artifacts produced by different dental materials using CT and magnetic resonance imaging (MRI).20 They reported that the use of ceramic materials such as zirconium dioxide in crowns, fixed partial dentures, and permanent restorations produced significant artifacts in both CT and MRI images of the maxillofacial region. They also indicated that Z100 restorative composite produced streak artifacts smaller than 15.0 mm in CT images. Among the temporary filling materials they tested, only Cavit produced artifacts in MRI images; these artifacts were smaller than 30.0 mm. Cavit and gutta percha also produced streak artifacts of 15.0 to 30.0 mm in CT images. Furthermore, metallic materials produced artifacts larger than 30.0 mm.20 These results were similar to the findings of the current study.
In vitro studies like the present study enable precise control of variables and the isolation of specific factors. Consequently, when the study was conducted, no unresolvable issues were encountered. Although in vitro studies do not accurately represent the variability found in clinical practice, they can serve as a reference point for future clinical studies. Within the boundaries of ethical research, studies should be performed to measure the artifacts caused by materials in vivo. Further investigations also should be carried out to analyze the effects of different dental materials on CBCT image quality using different CBCT systems, DICOM viewers, FOVs, resolutions, voltages, and currents.
Conclusion
The numbers of artifacts produced were lower at standard resolution than at high resolution for 20 of 25 tested materials; the difference was statistically significant for 5 materials and borderline significant for another. AH 26 root canal sealer was the only material that caused significantly more artifacts at standard resolution. The number of artifacts produced by dental materials at both standard and high resolutions decreased with increasing distance from the surface of the material, with one exception, which was not statistically significant. Unlike the type of material and the distance from the surface, the direction of the artifact was not affected by changing the resolution.
The results of the study suggest that standard resolution can be used in CBCT examinations to reduce radiation exposure of patients who have common dental materials in their mouth. The findings of this research can help dentists select the most suitable exposure voxel size based on patients’ existing dental materials, as these artifacts can negatively affect image quality and reduce the reliability of clinical diagnoses. With knowledge of the number of artifacts produced at different resolutions, practitioners can also reduce the amount of image distortion by employing different measures (such as voxel size or resolution selection, or adjusting patient positioning).
Author affiliations
Department of Oral and Maxillofacial Radiology, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran (Valizadeh, Ghazizadeh Ahsaie); Private practice, Tehran, Iran (Sahebnasagh).
The authors would like to thank S. Marjan Arianezhad, DDS, MSc, Shahid Beheshti University of Medical Sciences, Tehran, Iran, for providing extremely valuable supervision and shaping the final version of the manuscript.
References
1. Safi Y, Amid R, Zadbin F, Ghazizadeh Ahsaie M, Mortazavi H. The occurrence of dental implant malpositioning and related factors: a cross-sectional cone-beam computed tomography survey. Imaging Sci Dent. 2021;51(3):251-260. doi:10.5624/isd.20200331
2. Scarfe WC, Farman AG, Sukovic P. Clinical applications of cone-beam computed tomography in dental practice. J Can Dent Assoc. 2006;72(1):75-80.
3. Moshfeghi M, Abedian B, Ghazizadeh Ahsaie M, Tajdini F. Prevalence of nasal septum deviation using cone-beam computed tomography: a cross-sectional study Contemp Clin Dent. 2020;11(3):223-228. doi:10.4103/ccd.ccd_110_19
4. Benic GI, Sancho-Puchades M, Jung RE, Deyhle H, Hämmerle CHF. In vitro assessment of artifacts induced by titanium dental implants in cone beam computed tomography. Clin Oral Implants Res. 2013;24(4):378-383. doi:10.1111/clr.12048
5. Queiroz PM, Santaella GM, Groppo FC, Freitas DQ. Metal artifact production and reduction in CBCT with different numbers of basis images. Imaging Sci Dent. 2018;48(1):41-44. doi:10.5624/isd.2018.48.1.41
6. Brito-Júnior M, Santos LAN, Faria-e-Silva AL, Pereira RD, Sousa-Neto MD. Ex vivo evaluation of artifacts mimicking fracture lines on cone-beam computed tomography produced by different root canal sealers. Int Endod J. 2014;47(1):26-31. doi:10.1111/iej.12121
7. Farman AG. ALARA still applies. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;4(100):395-397. doi:10.1016/j.tripleo.2005.05.055
8. Martin C. The importance of radiation quality for optimisation in radiology. Biomed Imaging Interv J. 2007;3(2):e38. doi:10.2349/biij.3.2.e38
9. Harrison JD, Streffer C. The ICRP protection quantities, equivalent and effective dose: their basis and application. Radiat Prot Dosimetry. 2007;127(1-4):12-18. doi:10.1093/rpd/ ncm248
10. Thilander-Klang A, Helmrot E. Methods of determining the effective dose in dental radiology. Radiat Prot Dosimetry. 2010;139(1-3):306-309. doi:10.1093/rpd/ncq081
11. Pedram A, Torkzadeh A, Ghaffari R, Aryanezhad SS. Assessing olfactory fossa depth and its relationship with the variations in adjacent anatomical structures by using cone beam computed tomography (CBCT). Indian J Otolaryngol Head Neck Surg. 2023;75(4):2862-2869.
12. Pauwels R, Stamatakis H, Bosmans H, et al. Quantification of metal artifacts on cone beam computed tomography images. Clin Oral Implants Res. 2013;24(Suppl A100):94-99. doi:10.1111/j.1600-0501.2011.02382.x
13. Mallya SM, Lam EWN, eds. White and Pharoah’s Oral Radiology: Principles and Interpretation. 8th ed. 2018: Elsevier Health Sciences.
14. Rabelo KA, Cavalcanti YW, de Oliveira Pinto MG, et al. Quantitative assessment of image artifacts from root filling materials on CBCT scans made using several exposure parameters. Imaging Sci Dent. 2017;47(3):189-197. doi:10.5624/isd.2017.47.3.189
15. Safi Y, Moshfesghi M, Vasegh Z, Aghdasi MM, Haghani J, Afsahi M. Evaluating the affect [sic] of tube current’s [sic] on different dental material artifacts in cone beam computed tomography using signal difference to noise ratio index. Iran J Radiol. 2017;14(2):e38620. doi:10.5812/iranjradiol.38620
16. Omar G, Abdelsaiam Z, Hamed W. Quantitative analysis of metallic artifacts caused by dental metallic restorations: comparison between four CBCT scanners. Future Dent J. 2016;2(1):1521. doi:10.1016/j.fdj.2016.04.001
17. Bezerra IS, Neves FS, Vasconcelos TV, Ambrosano GMB, Freitas DQ. Influence of the artefact reduction algorithm of Picasso Trio CBCT system on the diagnosis of vertical root fractures in teeth with metal posts. Dentomaxillofac Radiol. 2015;44(6):20140428. doi:10.1259/ dmfr.20140428
18. Cebe F, Aktan AM, Ozsevik AS, Ciftci ME, Surmelioglu HD. The effects of different restorative materials on the detection of approximal caries in cone-beam computed tomography scans with and without metal artifact reduction mode. Oral Surg Oral Med Oral Pathol Oral Radiol. 2017;123(3):392-400. doi:10.1016/j.oooo.2016.11.008
19. Esmaeili F, Johari M, Haddadi P, Vatankhah M. Beam hardening artifacts: comparison between two cone beam computed tomography scanners. J Dent Res Dent Clin Dent Prospects. 2012;6(2):49-53. doi:10.5681/joddd.2012.011
20. Klinke T, Daboul A, Maron J, et al. Artifacts in magnetic resonance imaging and computed tomography caused by dental materials. PLoS One. 2012;7(2):e31766. doi:10.1371/journal. pone.0031766
GENERAL DENTISTRY SELF-INSTRUCTION
Exercise No. GD532, 2 CE Credits
Basic Science
Subject Code: 010
The 15 questions for this exercise are based on the article “Evaluation of artifacts produced by conventional dental materials in standard and high-resolution CBCT imaging” on pages 37-42. This exercise was developed by Ralph Pruette, DDS, in association with the General Dentistry Self-Instruction committee.
1. Cone beam computed tomography (CBCT) has shorter scan times and higher radiation doses than multidetector computed tomography (MDCT). CBCT produces artifacts from dental materials, similar to MDCT.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
2. Smaller voxel sizes produce ______ image resolution and require ______ radiation doses.
A. higher; higher
B. higher; lower
C. lower; higher
D. lower; lower
3. A study by Safi et al indicated that a higher tube current results in a ______ signal to noise ratio and therefore ______ the quality of a CBCT image.
A. higher; diminishes
B. lower; enhances
C. higher; enhances
D. lower; diminishes
4. A total of ___ common dental materials were included to assess produced artifacts.
A. 10
B. 15
C. 20
D. 25
5. The materials were placed in 3-mm holes in _______ plates.
A. red wax
B. polymethyl methacrylate
C. cardboard
D. agar gel
Reading the article and successfully completing this exercise will enable you to:
• understand how exposure parameters of CBCT affect the quality of images;
• identify and quantify artifacts produced by dental materials in CBCT; and
• be aware of how distance and direction from the material affect artifacts at standard and high resolutions.
Answers must be submitted online at agd.org/self-instruction by June 30, 2025.
6. Each specimen was imaged a total of ___ times (standard and high resolutions).
A. 2
B. 4
C. 6
D. 8
7. The gray value of the discs was assessed at all of the following distances except one. Which is the exception?
A. 1 mm
B. 3 mm
C. 4 mm
D. 8 mm
8. The gray value was recorded from ___ directions from each distance.
A. 2
B. 4
C. 6
D. 8
9. At standard resolution, the greatest numbers of artifacts were caused by _______ and _______.
A. amalgam; zinc phosphate cement
B. Coltosol; calcium hydroxide cement
C. AH 26; nickel-chromium alloy
D. glass fiber post; glass ionomer cement
10. At standard resolution, the fewest artifacts were caused by _______ and _______.
A. gutta percha; zinc oxide–eugenol paste
B. glass fiber post; glass ionomer cement
C. Temp-Bond NE; Z100 restorative composite
D. dentin porcelain; enamel porcelain
11. At high resolution, the greatest numbers of artifacts were caused by _______ and _______.
A. amalgam; nickel-chromium alloy
B. AH 26 root canal sealer; nickel-chromium alloy
C. Coltosol; calcium hydroxide
D. dentin porcelain; enamel porcelain
12. At high resolution, only _______ showed a statistically significant reduction in number of artifacts compared with standard resolution.
A. Z100 restorative composite
B. AH 26 root canal sealer
C. gutta percha
D. enamel porcelain
13. At each of the studied distances, the number of artifacts increased at high resolution compared with standard resolution. The amount was statistically significant at all distances.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
14. A reduction in artifacts was observed in both the _______ and _______ directions at high resolution compared with standard resolution.
A. left; upper left
B. right; upper right
C. left; lower left
D. right; lower right
15. An increase in the number of artifacts at high resolution compared with standard resolution was observed for ___ materials.
A. 20
B. 21
C. 23
D. 25
The effects of a therapy dog intervention on dental fear and anxiety in adult patients undergoing dental procedures: a pilot study
Doris Lam, DDS, MS ¢ Dominique A. D’Anthony, DMD, MS ¢ Sara A. Chilcutt, DDS, MS ¢ Amy O’Connor, LCSW, PMP
Andrew J. Avillo, DDS, MS ¢ Nicholas J. Hamlin, PhD, DDS, MS ¢ John E. Schmidt, PhD, MS
Dental anxiety poses challenges for providing effective oral healthcare. While therapy dogs have shown promise in various medical and mental health contexts, their use for alleviating dental anxiety in adults remains underexplored. This study aimed to investigate the emotional and physiologic effects of therapy dogs on self-reported dental anxiety. Adults with dental anxiety were randomly assigned to an intervention group (DOG; n = 19) or a standard care group (SC; n = 14). Standard self-report measures were used to assess dental anxiety (Index of Dental Anxiety and Fear [IDAF-4C+]), depression (Patient Health Questionnaire 9), and generalized anxiety (Generalized Anxiety Disorder 7) prior to the intervention. Participants in the DOG group received a 10-minute therapy dog intervention before dental procedures in sessions 1 and 2, while participants in the SC group rested quietly for 10 minutes before their procedure. The SC participants received the 10-minute therapy dog intervention before dental procedures in the third and final session, while patients in the DOG group received no intervention prior to their third procedure. After the dental procedures, patients completed a questionnaire about their satisfaction with the dog therapy (Therapy Satisfaction Scale) and recorded their anxiety and comfort levels on visual analog scales. Continuous electrocardiographic recording measured heart rate variability during the intervention and dental procedure. Prior to the intervention, most participants (90.9%) met the IDAF-4C+ criteria for dental anxiety, with 7 (21.2%) meeting the criteria for dental phobia. The DOG group participants expressed high satisfaction with the therapy dog intervention. No significant differences in heart rate variability were observed between the groups during dental procedures. Therapy dogs can effectively manage dental anxiety in adults with mild to moderate dental anxiety, offering potential benefits for oral healthcare.
Received: November 10, 2023
Accepted: February 4, 2024
Keywords: animal-assisted therapy, dental anxiety, dental fear, dog, pet therapy
Dental anxiety encompasses apprehension before or during dental procedures, often triggered by factors such as needles or dental handpiece noise. The collective term dental fear and anxiety (DFA) denotes strong negative feelings associated with dental treatment.1 DFA affects up to 20% of adults, with a higher prevalence in women.2,3 This anxiety can lead to treatment avoidance, eliminating some options for conservative treatment as diseases progress. In a study on procrastination and dental attendance, moderate to severe DFA was correlated with delays in care, increasing the probability of such delays by threefold.4
Early identification and management of DFA are crucial. Physiologic markers such as heart palpitations, tachycardia, increased blood pressure, and hyperventilation, among others, can help identify DFA. Factors such as predisposition to anxiety, other phobias, mental illness, depression, stress, or substance abuse can contribute to its severity.5,6 Assessment can be subjective (self-reports) or objective (physiologic responses).
Current interventions for DFA include behavioral therapy, pharmacologic agents, distraction techniques, and emerging methods like aromatherapy.7 Cognitive behavioral therapy modifies beliefs and gradually exposes patients to triggers while they are in a relaxed state.8 Pharmacologic options have drawbacks, including cost, onset time, dependency, and side effects.9 Animal-assisted therapy is a potential anxiolytic without these drawbacks.
Animal-assisted therapy involves animals in goaloriented interventions for therapeutic gain.10 It has shown benefits in managing mental health conditions such as depression, dementia, and posttraumatic stress disorder.11 Physiologically, human-dog interactions can improve heart rate variability (HRV), increase oxytocin levels, and reduce cortisol, likely via the parasympathetic nervous system and oxytocinergic system.12
Considering the role dogs can play in providing comfort in medicine, therapy dogs could reduce DFA in an economic and noninvasive manner.10,13 While the use of therapy dogs in dentistry has been suggested, formal research on their efficacy is lacking.
This pilot study aimed to assess the efficacy of a therapy dog as an intervention in patients with DFA by evaluating participants’ self-reported anxiety and comfort levels and physiologic reactivity during dental care. It was expected that increased comfort, reduced anxiety, and improved HRV would be observed in patients receiving therapy dog intervention compared with patients in a control group.
Methods
Study participants
This study received approval from the Walter Reed National Military Medical Center Institutional Review Board (IRB 20160016). Eligible participants were patients at the Naval Postgraduate Dental School, Bethesda, Maryland, including active-duty service members, retirees, and dependents. Participants required a minimum of 3 treatment appointments from 2017 to 2023 and reported dental anxiety. Patients were recruited from a clinic dedicated to advanced treatments such as endodontic therapy, crown preparation, implant preparation, and dental extractions. The typical appointments for this cohort lasted approximately 2 hours. Exclusion criteria were dog-related issues, psychiatric disorders, pregnancy, and age under 18 years, ensuring eligible participants were able to provide informed consent.
Study design
Participants were randomly assigned to the intervention (DOG) or standard care (SC) group. The SC group served as a waitlist control condition, but the SC participants were allowed to interact with therapy dogs before dental procedures in the third session. The therapy dogs, which included golden retrievers, a yellow labrador, a black labrador, and a German shepherd, were provided by the Facility Dog Program of the Walter Reed National Military Medical Center. These dogs, initially trained as service dogs, aimed to reduce stress and enhance well-being among patients and staff.
Intervention
The therapeutic intervention occurred before the first 2 dental procedures (sessions 1 and 2). Participants in both groups completed self-report measures and had their heart rate monitored using a heart rate device (Bodyguard, Firstbeat Technologies). Both groups completed a demographics and health history questionnaire prior to the intervention in session 1.
In sessions 1 and 2, both groups completed the Index of Dental Anxiety and Fear (IDAF-4C+), the Generalized Anxiety Disorder 7 (GAD-7) for generalized anxiety, and the Patient Health Questionnaire 9 (PHQ-9) for depressive symptoms.14-16 After these self-report measures were completed, patients in the DOG group spent 10 minutes with a therapy dog and handler before the dental procedure as their intervention, with instructions regarding interaction with the dog. The SC control group rested quietly in the operatory for 10 minutes before the dental procedure. After the procedure, both groups recorded their anxiety and comfort levels using a visual analog scale (VAS), and the DOG group also completed the Therapy Satisfaction Scale (TSS), a modified version of the scale proposed by Oei and Shuttlewood.14,17
In session 3, after both groups completed the IDAF-4C+, GAD-7, and PHQ-9, the SC participants interacted with a therapy dog for 10 minutes prior to the dental procedure. The members of the DOG group did not interact with the therapy dogs before the third session, instead resting quietly in the operatory before dental care began. In this session, the SC group completed the TSS and the DOG group did not. All other interventions and data collection procedures remained the same for both groups at session 3.
a All characteristics were self-reported on a questionnaire.
Self-report measures
Prior to session 1, all of the participants completed a demographics and health history questionnaire. Prior to all 3 sessions, they also completed the IDAF-4C+, the GAD-7, and the PHQ-9.14-16 The IDAF-4C+ consists of 8 items in which 2 items each assess the emotional, behavioral, physiologic, and cognitive components of the dental anxiety and fear response. All items are on a 5-point Likert scale of scores that range from 1 to 5, with 5 indicating more severe symptoms. Higher scores indicate higher dental anxiety and fear.
The VAS measures for comfort and anxiety were assessed at the end of each dental procedure. The VAS for comfort level was a 100-mm line anchored with “very uncomfortable” and “very comfortable” at the 0-mm and 100-mm ends, respectively. The VAS for anxiety level was a 100-mm line anchored
Table 1. Demographic characteristics (N = 33). a
Session DOG group (n = 19),
Item mean (SD)b
1
2 3.21 (1.23)
3
Total mean (SD)c 1
2
3
SC group (n = 14),
Abbreviations: DOG, intervention (therapy dog); IDAF-4C+, Index of Dental Anxiety and Fear; SC, standard care.
aThe Dental Anxiety and Fear module (IDAF-4C+) consists of 8 items in which 2 items each assess the emotional, behavioral, physiologic, and cognitive components of the dental anxiety and fear response. All items are on a 5-point Likert scale of scores that range from 1 to 5, with 5 indicating more severe symptoms. Higher scores indicate higher dental anxiety and fear.
b Group means for the 8 items.
c Group means for the total score (all 8 items summed). There were no statistically significant differences between groups at any session (P > 0.05; univariate analysis of variance).
with “no anxiety” and “worst anxiety” at the 0-mm and 100-mm ends, respectively. The TSS, completed by the DOG group after sessions 1 and 2 and the SC group after session 3, measured satisfaction with the intervention.17
Physiologic measures
Continuous electrocardiographic data were recorded using the heart rate device from the start of the intervention to 45 minutes into the dental procedure. The HRV time and frequency domain indices were calculated using aHRV software (version 13.4.0, Nevrokard). The fast Fourier transform nonparametric HRV values (low-frequency [LF] to highfrequency [HF] ratio) and the time domain measure root mean square successive difference (RMSSD) were reported. The RMSSD is a statistical calculation measuring variation in the intervals between heartbeats. Higher RMSSD values are indicative of higher parasympathetic nervous system activity.
Statistical analysis
SPSS software (version 25.0, IBM) was used for data analysis. Demographics, self-report measures, and HRV variables were expressed as mean and SD. Univariate analysis of variance (ANOVA) tests were used to compare groups at each visit, with a significance threshold set at α = 0.05.
Results
Patient demographics
Table 3. Mean (SD) anxiety and comfort levels at the end of each dental procedure.
Abbreviations: DOG, intervention (therapy dog); SC, standard care, VAS, visual analog scale.
a Each VAS consisted of a 100-mm line anchored with verbal descriptors.
bVAS anchored with “very uncomfortable” and “very comfortable” at the 0- and 100-mm ends, respectively.
cVAS anchored with “no anxiety” and “worst anxiety” at the 0- and 100-mm ends, respectively.
There were no statistically significant differences between groups at any session (P > 0.05; univariate analysis of variance).
Between April 2017 and October 2022, 37 participants were initially enrolled in the study, and there were 4 withdrawals, primarily due to the COVID-19 pandemic. The final sample comprised 19 participants in the DOG group and 14 in the SC group. The average ages of the participants were 32.5 years (SD, 11.1) in the DOG group and 36.9 years (SD, 11.5) in the SC group. Most participants were female (78.8%), White (72.7%), and married or partnered (54.4%). There were no significant demographic differences between groups (Table 1).
Self-report measures
The mean DFA scores (IDAF-4C+) for the DOG group ranged from 3.21 to 3.64, while those for the SC group ranged from 2.30 to 3.10 (Table 2). No statistically significant differences were observed between groups in the IDAF-4C+ mean or total scores at any assessment (P > 0.05; univariate ANOVA). Nearly all participants (30/33; 90.9%) met the IDAF-4C+ criteria for dental anxiety, with 4 patients in the DOG group and 3 patients in the SC group (total, 7/33; 21.2%) meeting the criteria for probable dental phobia. No significant differences were noted between groups in anxiety triggers.
No statistically significant differences between groups were found for VAS anxiety or comfort scores following the interventions (P > 0.05; univariate ANOVA) (Table 3). Likewise, there were no significant differences between groups in symptoms of generalized anxiety (GAD-7) or depression (PHQ-9) at any assessment. Participants generally scored in the mild range on these psychological measures.
Participants in the DOG group reported high satisfaction with the intervention on the TSS (mean [SD] at session 1,
Table 2. Dental fear and anxiety scores before intervention or control.
Session
DOG group (n = 19), RMSSDa SC group (n = 14), RMSSDa F P
Intervention (10 min)
1 33.08 (11.12) 40.66 (15.14) 2.317 0.140
2 35.81 (20.12) 29.76
3
Dental procedure (45 min)
2
3
Abbreviations: DOG, intervention (therapy dog); HRV, heart rate variability; RMSSD, root mean square of successive differences between normal heartbeats; SC, standard care.
aThe RMSSD is a statistical calculation measuring variation in the time intervals between heartbeats. Higher RMSSD values are indicative of higher parasympathetic nervous system activity.
There were no statistically significant differences between groups at any session (P > 0.05; univariate analysis of variance).
32.64 [4.65]; session 2, 33.36 [3.30]). The SC group participants, who received the therapy dog intervention before the third procedure, also reported high satisfaction on the TSS (mean [SD], 33.55 [3.42]).
Physiologic measures
The HRV was assessed during the 10-minute intervention and up to the first 45 minutes of dental procedure, using time domain (RMSSD) and frequency domain (LF/HF ratio) indices.18-20 No significant differences were found between groups in RMSSD at any session (P > 0.05; univariate ANOVA) (Table 4). The DOG group had a significantly higher mean [SD] LF/HF HRV during the session 1 intervention (DOG, 4.19 [1.97]; SC, 1.99 [2.08]; P = 0.008) but not during the session 2 intervention (DOG, 3.94 [1.69]; SC, 2.51 [2.97]; P = 0.201) (Chart 1). There were no statistically significant differences in LF/HF HRV during the dental procedures at any session (P > 0.05; univariate ANOVA) (Chart 2).
Discussion
This pilot study aimed to assess the efficacy and practicality of a therapy dog intervention in patients with DFA, as determined by IDAF-4C+ scores. Most participants met the criteria for significant dental anxiety, with some meeting criteria for dental phobia, confirming the enrollment of appropriate patients. No significant differences were found in self-report measures between the DOG and SC groups, although there was a trend toward lower anxiety in the DOG group. Interestingly, the DOG group reported lower anxiety during the third session, even without the dog’s presence, possibly indicating a lingering positive impact on perception of the dental experience. Conversely, the SC group experienced reduced anxiety when a dog was present before the third dental
Abbreviations: DOG, intervention (therapy dog); HF, high-frequency; HRV, heart rate variability; LF, low-frequency; SC, standard care. Mean LF/HF HRV recorded during the 10-minute intervention prior to the dental procedure. Error bars represent the standard deviation. There was a statistically significant difference at session 1 but not session 2 (univariate analysis of variance).
Abbreviations: DOG, intervention (therapy dog); HF, high-frequency; HRV, heart rate variability; LF, low-frequency; SC, standard care. Mean LF/HF HRV recorded during the first 45 minutes of dental treatment. Error bars represent the standard deviation. There were no statistically significant differences at either session (univariate analysis of variance).
procedure. Although no significant differences were noted in HRV measures between groups, the DOG group exhibited higher LF/HF values during the first intervention, likely due to active engagement with the therapy dogs.
The TSS results indicated high satisfaction with the intervention, suggesting that therapy dogs can effectively manage DFA. Participants expressed that the intervention’s duration could be longer, and some felt anxiety returning after the dog left. To enhance the effectiveness of therapy dogs, the use of dogs specifically trained for dental patient
Chart 2. Mean LF/HF HRV during the dental procedure.
Chart 1. Mean LF/HF HRV during the intervention.
Table 4. Mean (SD) time domain HRV comparisons between groups.
interaction—such as remaining still during dental work— may be considered.
Among the limitations of this study are the fact that recruiting active-duty members of the military, their dependents, and retirees posed challenges due to the obligations to attend appointments, as frequent duty station changes and deployments complicated scheduling, and missed appointments could result in ineligibility for inclusion. The COVID-19 pandemic further disrupted recruitment and appointments and may have heightened dental anxiety due to social distancing and reluctance to schedule routine dental care.21,22
Future research should involve larger sample sizes, varying intervention protocols, and analysis of ideal therapy dog characteristics in dental settings. Additionally, assessing the health and safety risks of this approach and developing evidence-based guidelines for therapy dog use in dental settings are essential to implementation of animal-assisted therapy. Most states lack regulations regarding therapy dogs, prompting concerns about zoonotic pathogens, allergies, and adverse behavior.10,23,24 North Carolina recently mandated training requirements for dental therapy dogs that emphasize safety precautions, but widespread adoption of such protocols is needed.23
Conclusion
This study demonstrates the feasibility and positive patient reception of introducing therapy dogs into dental settings, improving the dental experience for those with mild to moderate dental anxiety. High satisfaction levels and appointment adherence suggest that therapy dogs may incentivize patients to keep appointments. Future steps include establishing clinical guidelines for therapy dog use in dental settings and exploring the possibility of dogs remaining with patients throughout dental procedures.
Author affiliations
21st Dental Company, Marine Corps Base, Kaneohe Bay, Hawaii (Lam); USS Essex, LHD-2, San Diego, California (D’Anthony); Dental Services, Navy Medicine Readiness and Training Command Oak Harbor, Washington (Chilcutt); Office of the Assistant Chief of Staff, Walter Reed National Military Medical Center, Bethesda, Maryland (O’Connor); Primary Care Dentistry Department, Walter Reed National Military Medical Center, Bethesda, Maryland (Avillo); Postgraduate Dental College, Uniformed Services University of the Health Sciences, Bethesda, Maryland (Avillo, Hamlin, Schmidt); Research Department, Naval Postgraduate Dental School, Naval Medical Leader & Professional Development Command, Bethesda, Maryland (Hamlin); Department of Psychology, Naval Postgraduate Dental School, Naval Medical Leader & Professional Development Command, Bethesda, Maryland (Schmidt).
Correspondence
John E. Schmidt, PhD, MS (john.e.schmidt.civ@health.mil).
Conflicts of interest
None reported.
Disclaimer
The views expressed in this article reflect the results of research conducted by the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, Uniformed Services University of the Health Sciences, or the US government.
The authors are military service members of the US government. This work was prepared as part of their official duties. Title 17 USC §105 provides that copyright protection under this title is not available for any work of the US government. Title 17 USC §101 defines a US government work as work prepared by a military service member or employee of the US government as part of that person’s official duties.
Acknowledgments
The authors thank the following for their support and contributions to the successful completion of this study: Dr Catherine Daniel, Dr Wonil Chong, and Dr Patrick Fox. We also gratefully acknowledge the support of the Comprehensive Dentistry Department, Naval Postgraduate Dental School, and the Facility Dog Program at the Walter Reed National Military Medical Center. We are especially grateful for the Walter Reed facility dogs and their handlers for the incredible support and work they do every day for our service members.
References
1. Armfield JM, Heaton LJ. Management of fear and anxiety in the dental clinic: a review. Aust Dent J. 2013;58(4):390-407. doi:10.1111/adj.12118
2. White AM, Giblin L, Boyd LD. The prevalence of dental anxiety in dental practice settings. J Dent Hyg. 2017;91(1):30-34.
3. Carter AE, Carter G, Boschen M, AlShwaimi E, George R. Pathways of fear and anxiety in dentistry: a review. World J Clin Cases. 2014;2(11):642-653. doi:10.12998/wjcc.v2.i11.642
4. Steinvik LM, Svartdal F, Johnsen JK. Delay of dental care: an exploratory study of procrastination, dental attendance, and self-reported oral health. Dent J (Basel). 2023;11(2):56. doi:10.3390/dj11020056
5. De Stefano R, Bruno A, Muscatello MR, Cedro C, Cervino G, Fiorillo L. Fear and anxiety managing methods during dental treatments: a systematic review of recent data. Minerva Stomatol. 2019;68(6):317-331. doi:10.23736/S0026-4970.19.04288-2
6. Eaton WW, Bienvenu OJ, Miloyan B. Specific phobias. Lancet Psychiatry. 2018;5(8):678686. doi:10.1016/S2215-0366(18)30169-X
7. Arslan I, Aydinoglu S, Karan NB. Can lavender oil inhalation help to overcome dental anxiety and pain in children? A randomized clinical trial. Eur J Pediatr. 2020;179(6):985-992. doi:10.1007/s00431-020-03595-7
8. Anthonappa RP, Ashley PF, Bonetti DL, Lombardo G, Riley P. Non-pharmacological interventions for managing dental anxiety in children. Cochrane Database Syst Rev. 2017;(6): CD012676. doi:10.1002/14651858.CD012676
9. Fiorillo L. Conscious sedation in dentistry. Medicina (Kaunas). 2019;55(12):778. doi:10.3390/medicina55120778
10. Barchas D, Melaragni M, Abrahim H, Barchas E. The best medicine: personal pets and therapy animals in the hospital setting. Crit Care Nurs Clin North Am. 2020;32(2):167-190. doi:10.1016/j.cnc.2020.01.002
11. Charry-Sánchez JD, Pradilla I, Talero-Gutiérrez C. Animal-assisted therapy in adults: a systematic review. Complement Ther Clin Pract. 2018;32:169-180. doi:10.1016/ j.ctcp.2018.06.011
12. Teo JT, Johnstone SJ, Römer SS, Thomas SJ. Psychophysiological mechanisms underlying the potential health benefits of human-dog interactions: a systematic literature review. Int J Psychophysiol. 2022;(180):27-48. doi:10.1016/j.ijpsycho.2022.07.007
13. Jones MG, Rice SM, Cotton SM. Incorporating animal-assisted therapy in mental health treatments for adolescents: a systematic review of canine assisted psychotherapy. PLoS One. 2019;14(1):e0210761. doi:10.1371/journal.pone.0210761
14. Armfield JM. A comparison of three continuous scales used to determine the prevalence of clinically significant dental fear. Community Dent Oral Epidemiol. 2011;39(6):554-563. doi:10.1111/j.1600-0528.2011.00628.x
15. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092-1097. doi:10.1001/ archinte.166.10.1092
16. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606-613. doi:10.1046/j.1525-1497.2001. 016009606.x
17. Oei TP, Shuttlewood GJ. Development of a satisfaction with therapy and therapist scale. Aust N Z J Psychiatry. 1999;33(5):748-753. doi:10.1080/j.1440-1614.1999.00628.x
18. Shaffer F, McCraty R, Zerr CL. A healthy heart is not a metronome: an integrative review of the heart’s anatomy and heart rate variability. Front Psychol. 2014;5:1040. doi:10.3389/ fpsyg.2014.01040
19. Shaffer F, Ginsberg JP. An overview of heart rate variability metrics and norms. Front Public Health. 2017;5:258. doi:10.3389/fpubh.2017.00258
20. Nunan D, Sandercock GR, Brodie DA. A quantitative systematic review of normal values for short-term heart rate variability in healthy adults. Pacing Clin Electrophysiol. 2010;33(11): 1407-1417. doi:10.1111/j.1540-8159.2010.02841.x
21. Peloso RM, Pini NIP, Sundfeld Neto D, et al. How does the quarantine resulting from COVID-19 impact dental appointments and patient anxiety levels? Braz Oral Res 2020;34:e84. doi:10.1590/1807-3107bor-2020.vol34.0084
22. De Stefano R. Psychological factors in dental patient care: odontophobia. Medicina (Kaunas) 2019;55(10):678. doi:10.3390/medicina55100678
23. Crouch M. A dog day at the dentist’s: North Carolina regulates pups in dentistry. March 1, 2022. Accessed May 17, 2023. https://kffhealthnews.org/news/article/dentist-dogsregulate-north-carolina/
24. Gussgard AM, Weese JS, Hensten A, Jokstad A. Dog-assisted therapy in the dental clinic: part A - hazards and assessment of potential risks to the health and safety of humans. Clin Exp Dent Res. 2019;5(6):692-700. doi:10.1002/cre2.240
Clinical guidelines for posterior semidirect composite resin restorations: a case report with a 17-month follow-up
Patients are always looking for conservative, esthetic, and long-lasting dental restorations, and the technique used directly influences the longevity of the treatment. The location of the restoration in the mouth and the extent of the decay influence the treatment choice. The larger the dimensions of the cavity preparation, the greater the difficulties in restoring the tooth using direct techniques. The semidirect technique, when indicated, can achieve satisfactory results. It is a relatively easy procedure, consisting of tooth preparation to receive an indirect restoration, fabrication of an alginate impression, fabrication of the composite resin restoration on a flexible cast, cementation, removal of excess cement, and occlusal adjustment. The aim of this case report is to present a viable alternative to direct and indirect restorations for posterior teeth with extensive decay. The article describes the extraoral semidirect technique for fabricating a composite resin restoration, highlighting its indications and discussing advantages and disadvantages.
Traditionally accepted esthetic restorative approaches include direct and indirect techniques, while the semidirect technique is poorly understood. In Class II cavities with easy access, proximal slots, visible margins on either enamel or dentin, and no loss of cusps, the direct composite resin technique is indicated. In the direct technique, the restoration is fabricated directly on the prepared tooth, relying only on the adhesive system for retention. This technique is less expensive than other approaches. However, the more cavity walls that are involved and the larger the buccolingual extension, the more difficult it is to perform the direct technique. In cases involving weakened tooth structure and a wide intercuspal distance, indirect restorations are preferable.
Cavity configurations with large buccolingual widths are more prone to fracture. When the preparation involves more than one-third of the intercuspal distance, the fracture strength is substantially decreased.1 In addition, weakened tooth structure must be evaluated to determine whether cuspal coverage is necessary. Loss of reinforcement structures such as marginal ridges, the pulp chamber floor, and the oblique ridge leads to cuspal deflection and stress concentrations that could result in a premature fracture. In such cases, an indirect restoration is indicated.1,2
For the indirect technique, after preparation of the tooth with tapered walls, an impression is made with a polyvinyl siloxane (PVS) material or digitally by means of an intraoral scanner. With the conventional approach, after the PVS impression is taken, a temporary restoration is fabricated, and the final restoration is made on a plaster cast by the laboratory. This technique is more time consuming than the direct approach and increases the cost of the procedure.3 When using a digital workflow, the clinician can produce the indirect restoration quickly in a chairside procedure. However, high-cost equipment and well-trained staff are needed.
Semidirect and indirect restorations have similar indications, but the semidirect technique consists of intraoral and extraoral phases that can be performed in 2 ways: either the restoration is made directly inside the mouth—this method is also referred to as a direct-indirect technique—or the restoration is made in a flexible silicone cast obtained from the impression.4,5 The major advantages of this technique are as follows: the dentist can prepare a restoration in a single visit; it is a low-cost procedure; the chances of contamination are reduced; polishing of the gingival margin is excellent; the interproximal contact point is improved; the bond strength is enhanced because the restoration generates less stress at the interface than the direct technique; and the mechanical properties of the restoration may
be improved because of an additional polymerization process, which increases the monomers’ degree of conversion.3,6,7
The aim of this case report is to describe the step-by-step procedures involved in restoring an extensively decayed posterior tooth using the extraoral semidirect technique, focusing on the indications, contraindications, advantages, and disadvantages.
Case report
A 21-year-old woman was referred for treatment of a large mesio-occlusodistopalatal restoration on the maxillary right first molar that needed to be replaced because of fracture (Fig 1). The treatment plan consisted of removal of the fractured restoration, tooth preparation with tapered walls, and restoration by means of a chairside semidirect technique. A radiograph was obtained to verify the extent of the restoration and to assess for possible secondary caries. No periapical alterations or secondary caries was observed.
The fractured restoration was removed with round diamond burs (No. 2135, KG Sorensen), and the tooth was prepared with rounded internal angles and tapered walls to receive an indirect restoration. Surrounding margins were well defined and slightly divergent. The clinician also checked the insertion axis. Prior to the impression procedure, a retraction cord (No. 000, Ultrapak, Ultradent) was inserted into the gingival sulcus (Fig 2). An impression was taken with alginate (Jeltrate Plus, Dentsply Sirona). The flexible cast was made with a regularbody PVS impression material (Express XT, 3M) (Fig 3). To improve visualization of the gingival contour and obtain a better interproximal contact point, the cast was then partially sectioned with a No. 15 surgical blade (Fig 4). This procedure
not only helped to expose the preparation interproximal finishing line, but also facilitated adaptation of the composite resin at the proximal slots.
The restoration was fabricated on the PVS flexible cast with a nanohybrid composite resin (Vittra APS, FGM Dental Group). Each layer was light cured for 40 seconds with an LED unit (Valo, Ultradent). The first layer was placed using dentin shade A3. An enamel A2 shade was then inserted, also in a single layer (Fig 5). After the final anatomy was achieved, a brown flowable composite resin (Allure Artcolor, Yller Biomaterials) was applied to the fissures for color characterization (Fig 6). The postcure procedure was completed by heating the restoration in a microwave at 440 W for 3 minutes (MEF33, Electrolux). The objective was to enhance the curing properties of the restoration.8
The final restoration was seated in the preparation to check the fit. The clinician then polished the restoration using polishing discs (Sof-Lex, 3M), polishing points (Enhance, Dentsply Sirona), and a silicon carbide brush (Astrobrush, Ivoclar Vivadent) (Fig 7). The inner surface of the restoration was then sandblasted with 25-μm aluminum oxide for 10 seconds at a distance of 5 cm from the surface to cleanse it and increase its superficial roughness. Care was taken not to damage the external margins. An adhesive layer (Scotchbond Multi-Purpose, 3M ESPE) was then applied but not light activated. The surface of the cavity was sandblasted with 25-μm aluminum oxide, cleaned with an air-water spray, and blot dried. A 3-step etchand-rinse adhesive (Scotchbond Multi-Purpose, 3M) was then applied according to the manufacturer’s instructions.
As soon as the restoration and tooth were ready to receive the luting agent, a dual-cured resin cement (AllCem, FGM Dental Group) was placed on the inner surface of the
Fig 1. Large fractured mesio-occlusodistopalatal restoration.
Fig 2. Prepared tooth with No. 000 retraction cord inserted into the gingival sulcus.
Fig 3. Insertion of polyvinyl siloxane into the alginate impression to fabricate a cast.
Fig 4. Partial sectioning of the polyvinyl siloxane cast at the interproximal contact point to improve adaptation in the cervical area.
Fig 5. Restoration with a final layer of enamel shade A2.
Fig 6. Characterization of the fissures with brown flowable composite resin.
restoration (Fig 8). The excess cement was removed with a microbrush and dental floss after 3 seconds of activation with a PointCure lens attachment (Valo, Ultradent). The final light activation was performed for 40 seconds per surface. After cementation was completed, the clinician checked the occlusion with articulating paper and proximal contacts with dental floss (Fig 9). The restoration was then repolished. At the 17-month follow-up appointment, the restoration was still in good condition and was repolished (Fig 10).
Discussion
Indirect restorations are often used to restore extensively decayed teeth. When direct restorations are placed in posterior teeth, it is difficult to achieve a tight interproximal contact point when one or more cusps have been lost. At the same time, use of a rubber dam is not always feasible because of the gingival extension of the restoration. Although the idea is not new, semidirect composite resin restorations may be a viable treatment option for these cases because the procedure is performed chairside at a lower cost than that of indirect restorations and without the limitations related to direct restorations. Polymerization shrinkage in direct restorations may cause cracks in the remaining tooth structure, discomfort in the postoperative period, and recurrence of caries via marginal infiltration.9 The semidirect technique is advantageous with respect to polymerization shrinkage. Because the composite resin restoration is light cured outside the mouth, shrinkage stress on the cavity walls is reduced, as it occurs only on the line where the luting resin cement is placed. Thus, this technique may reduce marginal gaps and microleakage, which are the main causes of restoration failure. Composite resin restorations made using the semidirect technique have demonstrated higher bond
strength than direct restorations made with either bulk fill or incremental filling materials.7
A simple impression technique with an alginate material was used in the present case. Although the flexible cast was made with a PVS material, the impression could be made with other materials such as polydimethylsiloxanes or polyether silicones. 5,10,11 When alginate is used, marginal gaps may occur. When gaps are detected between the restoration and the cavity wall, cementation is enhanced by use of a preheated composite resin.12-14
In the present case, a postcure process was conducted in a microwave oven. This procedure is based on the findings of several research groups, who reported different thermal treatments, such as use of a microwave, an autoclave, and a highintensity light source.8,10,15,16 In 1992, Ferracane and Condon observed that postcure heating of a light-activated composite resin material significantly reduced the quantity of unreacted monomers, even at low cure temperatures (50°C), thereby improving surface hardness, tensile strength, bending strength, and color stability.17 Several studies have shown that indirect and semidirect composite resin restorations have better mechanical properties after undergoing a thermal treatment; in addition, Class II and onlay restorations have superior marginal adaptation, and clinical performance is similar to that of direct composite resin restorations and indirect ceramic restorations.8,10,15,16 Finishing and polishing are also improved because these steps are performed outside the mouth.4
After 17 months of follow-up, the restoration in this patient remained in good condition; nevertheless, longer follow-up is needed to ensure clinical success. Notwithstanding the relatively brief follow-up in this case, the semidirect technique offers practical advantages that make it an excellent option
Fig 7. Final polishing of the cervical area of the restoration.
Fig 8. Cementation of the restoration with a dual-cured resin cement.
Fig 9. Final appearance of the restoration after occlusal adjustment and before repolishing.
Fig 10. Restoration at the 17-month followup appointment.
when indicated. In the short term (up to 3 years), low-quality evidence suggests no difference in tooth survival or restoration quality between direct composite resin and indirect restorations when used in endodontically treated posterior teeth.18
As with any composite resin restoration, the material will experience surface degradation over time.19 Several risk factors play a role in the longevity of composite resin restorations, and the patient should be aware that periodic maintenance and repolishing appointments are necessary. Further, depending on the patient’s diet, composite resins will exhibit decreased color stability.20 Although multiple composite resin–based materials are available, Demarco et al recently reported that differences between them played only a minor role in restoration durability.9 They found that patient factors (eg, caries risk, parafunctional habits) played an important role in the longevity of the restoration.9
Conclusion
Use of semidirect composite resin restorations may be a reliable approach when indicated; they offer the advantages of composite resin and fulfill the biomechanical requirements of an extensively decayed posterior tooth. The semidirect technique has other clinical advantages as well, such as low cost; a brief chairside procedure; better finishing and polishing, especially at the gingival margins; an easier way to create tooth anatomy; effective interproximal contact points; and the possibility of performing postpolymerization thermal treatment.
Author affiliations
Department of Operative Dentistry, Endodontics and Dental Materials, Bauru School of Dentistry, University of São Paulo, Bauru, Brazil.
Correspondence
Fernanda Furuse Ventura dos Santos (ferfuruse@usp.br).
Conflicts of interest
None reported.
Funding
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior of Brasil (CAPES)—finance code 001.
Acknowledgments
The authors thank Gustavo de Oliveira Lima for his technical assistance during preparation of the case report.
References
1. Teixeira ESS, Rizzante FAP, Ishikiriama SK, et al. Fracture strength of the remaining dental structure after different cavity preparation designs. Gen Dent. 2016;64(2):33-36.
2. Mondelli RF, Ishikiriama SK, de Oliveira Filho O, Mondelli J. Fracture resistance of weakened teeth restored with condensable resin with and without cusp coverage. J Appl Oral Sci. 2009;17(3):161-165. doi:10.1590/s1678-77572009000300006
3. Azeem RA, Sureshbabu NM. Clinical performance of direct versus indirect composite restorations in posterior teeth: a systematic review. J Conserv Dent. 2018;21(1):2-9. doi:10.4103/ JCD.JCD_213_16
4. Fahl N, Jr, Ritter AV. Composite veneers: the direct-indirect technique revisited. J Esthet Restor Dent. 2021;33(1):7-19. doi:10.1111/jerd.12696
5. Torres CRG, Zanatta RF, Huhtala M, Borges AB. Semidirect posterior composite restorations with a flexible die technique: a case series. J Am Dent Assoc. 2017;148(9):671-676. doi:10.1016/j.adaj.2017.02.032
6. Caneppele TMF, Meirelles LCF, Rocha RS, et al. A 2-year clinical evaluation of direct and semidirect resin composite restorations in non-carious cervical lesions: a randomized clinical study. Clin Oral Investig. 2020;24(3):1321-1331. doi:10.1007/s00784-019-03011-x
7. Ribeiro AEL, Dias JDN, Melo A, Borges BCD, de Assunção IV. Direct and semi-direct resin composite restoration in large cavity preparations: analysis of dentin bond strength stability and bottom/top microhardness ratio in a cavity model. Odontology. 2022;110(3):482-488. doi:10.1007/s10266-021-00680-7
8. Poskus LT, Latempa AMA, Chagas MA, da Silva EM, Leal MPS, Guimarães JGA. Influence of post-cure treatments on hardness and marginal adaptation of composite resin inlay restorations: an in vitro study. J Appl Oral Sci. 2009;17(6):617-622. doi:10.1590/s167877572009000600015
9. Demarco FF, Cenci MS, Montagner AF, et al. Longevity of composite restorations is definitely not only about materials. Dent Mater. 2023;39(1):1-12. doi:10.1016/j.dental.2022.11.009
10. Alharbi A, Rocca GT, Dietschi D, Krejci I. Semidirect composite onlay with cavity sealing: a review of clinical procedures. J Esthet Restor Dent. 2014;26(2):97-106. doi:10.1111/ jerd.12067
11. Papazoglou E, Diamantopoulou S. The modified semidirect onlay technique with articulated elastic model. Eur J Prosthodont Restor Dent. 2015;23(4):207-212. doi:10.1922/ EJPRD_1470Papazoglou06
12. Lopes LCP, Terada RSS, Tsuzuki FM, et al. Heating and preheating of dental restorative materials—a systematic review. Clin Oral Investig. 2020;24:4225-4235. doi:10.1007/s00784020-03637-2
13. Poubel DLN, Zanon AEG, Almeida JCF, Rezende LVML, Garcia FCP. Composite resin preheating techniques for cementation of indirect restorations. Int J Biomater. 2022;2022:5935668. doi:10.1155/2022/5935668
14. Sampaio CS, Barbosa JM, Cáceres E, et al. Volumetric shrinkage and film thickness of cementation materials for veneers: an in vitro 3D microcomputed tomography analysis. J Prosthet Dent. 2017;117(6):784-791. doi:10.1016/j.prosdent.2016.08.029
15. Almeida-Chetti VA, Macchi RL, Iglesias ME. Effect of post-curing treatment on mechanical properties of composite resins. Acta Odontol Latinoam. 2014;27(2):72-76. doi:10.1590/ S1852-48342014000200005
16. Gresnigt MM, Kalk W, Özcan M. Randomized clinical trial of indirect resin composite and ceramic veneers: up to 3-year follow-up. J Adhes Dent. 2013;15:181-190. doi:10.3290/j.jad. a28883
17. Ferracane JL, Condon JR. Post-cure heat treatments for composites: properties and fractography. Dent Mater. 1992;8(5):290-295. https://www.sciencedirect.com/science/article/abs/ pii/010956419290102I
18. de Kuijper MCFM, Cune MS, Özcan M, Gresnigt MMM. Clinical performance of direct composite resin versus indirect restorations on endodontically treated posterior teeth: a systematic review and meta-analysis. J Prosthet Dent. 2023;130(3):295-306. doi:10.1016/j. prosdent.2021.11.009
19. Elnour M, Krejci I, Bortolotto T. Surface degradation of composite resins for direct restorations: effects on wear and gloss retention. Gen Dent. 2021;69(2):34-39.
20. Ramalho LO, de Souza Oliveira LP, Valente LD, Cohen-Carneiro F, Regalado DF, Pontes DG. Effect of hydroelectrolytic and energy beverages on the color stability and fluorescence of composite resins. Gen Dent. 2021;69(2):40-46.
Tribochemical silicoating of amalgam promotes effective amalgam-resin repairs
Terence A. Imbery, DDS ¢ Anna Pitz, DDS, MS ¢ Peter C. Moon, PhD ¢ Caroline K. Carrico, PhD
The purpose of this study was to determine the most effective method for bonding composite resin to artificially aged amalgam. A spherical amalgam alloy was triturated and condensed by hand into cylindrical plastic molds (6 mm in diameter and 4 mm in height) to create 90 specimens, which were then aged for 2 weeks in closed plastic containers at 23°C. The amalgam surfaces underwent 1 of 3 surface treatments (n = 30 per treatment): (1) air particle abrasion (APA) with 50-µm aluminum oxide particles applied with a force of 45 psi from a 10-mm distance, followed by rinsing with deionized water for 60 seconds; (2) APA following the same protocol with subsequent application of a metal primer (Alloy Primer); or (3) coating with 30-μm silica (CoJet) at a force of 45 psi from a 10-mm distance until the surface turned black. Specimens were then treated with 1 of 3 adhesives (n = 10 per adhesive per surface treatment): (1) 2-step total-etch adhesive (OptiBond Solo Plus), (2) 1-step self-etching adhesive (Scotchbond Universal), or (3) dual-cured resin cement (Panavia F 2.0). Each adhesive was applied to the treated amalgam surfaces following its manufacturer’s instructions. The specimens were placed in a bonding clamp, and nanocomposite resin columns, 2.38 mm in diameter and 2.00 mm in height, were photocured (40 seconds, 500 mW/cm2) against the treated amalgam surfaces. The specimens were stored for 24 hours in 37°C deionized water and underwent shear bond strength testing at a crosshead speed of 0.5 mm/min. Data were analyzed using 2-way analysis of variance and post hoc analysis with the Tukey test at 95% confidence. The mean (SD) shear bond strength values ranged from 12.3 (1.2) MPa for aluminum oxide–treated surfaces bonded with OptiBond Solo Plus to 25.9 (4.6) MPa for silicoated surfaces bonded with Panavia F 2.0. All bonding agents produced the highest shear bond strength when the amalgam surface was silicoated. These results indicate that composite can be effectively bonded to amalgam via silicoating.
Received: June 2, 2023
Accepted: August 30, 2023
Keywords: amalgam, bond strengths, composite resins, repair, silicoating
Cuspal-coverage amalgam restorations, especially in the maxillary premolar region, may be esthetically unacceptable. Porcelain-fused-to-metal crowns or allceramic restorations are sometimes preferable esthetic treatment options, but many patients with limited finances may be unable to select this treatment. Case reports have documented the successful veneering of aged amalgam restorations with composite resin.1-5 Another indication for amalgam veneered with composite is the repair of cuspal fractures in teeth with large amalgam restorations. Fracture of nonfunctional cusps in teeth restored with amalgam restorations is a common clinical occurrence, with the prevalence of fractured cusps reported to be 4% to 8% in premolars and 5% to 15% in molars.6-9
An important aspect of veneering amalgam with composite resin is the formation of an interfacial bond between the 2 materials. Several systems are commercially available to facilitate bonding to alloy surfaces. One such product is CoJet (3M), which abrasively embeds a 30-µm ceramic (silicon dioxide) layer on the alloy surface. This process is referred to as tribochemical silica coating, or silicoating. After silanization with ESPE Sil (3M), the ceramic layer on the amalgam enables coupling with composite for a true chemical bond. Another product used to enhance the bond strength between metals and resin-based materials is the metal-conditioning agent Alloy Primer (Kuraray America), which contains complex proprietary molecules better known by their abbreviations, VBATDT (6-[4-vinylbenzyl-Npropyl] amino-1,3,5-triazine-2,4-dithiol) and MDP (10-methacryloyloxydecyl dihydrogen phosphate). These molecules purportedly enhance the bond strength of resins to both noble and base metal alloys. A third alloy surface treatment is micromechanical retention created by microabrasion using 50-µm aluminum oxide (Al 2 O3). Pilo et al demonstrated adequate shear bond strength of composite to amalgam treated with Al 2 O3 abrasion and various adhesives and resins.10
The purpose of this in vitro study was to find the best combination of surface treatment and adhesive agent for bonding composite resin to an amalgam surface. The study evaluated 3 surface treatments and 3 adhesive agents for a total of 9 approaches. Amalgam specimens underwent 1 of the following surface treatments: (1) air particle abrasion (APA) with 50-µm Al2O3, (2) APA followed by application of Alloy Primer, or (3) silicoating with CoJet. The specimens were treated with 1 of the following adhesive agents: (1) OptiBond Solo Plus (OBSP; Kerr), a 2-step, total-etch-and-rinse adhesive; (2) Scotchbond Universal Adhesive (SUA; 3M), a 1-step self-etching adhesive that is purported to bond to all substrates and can also be used as a selective-etch or total-etch adhesive; or (3) Panavia F 2.0 (PF; Kuraray America), a resin cement that can bond to enamel, dentin, composite, and noble and base metal alloys that have
Table. Mean (SD) bond strength values of composite resin to amalgam (n = 10 per adhesive per surface treatment).
Shear bond strength, MPa
Adhesive
Abbreviation: APA, air particle abrasion.
Values followed by the same superscript letter are not significantly different (
Tukey test).
been tin plated or primed with Alloy Primer. The null hypothesis was that there would be no differences in the shear bond strength of composite to amalgam among the different combinations of surface treatments and adhesive agents tested.
Methods
A spherical amalgam alloy (Tytin, Kerr) was triturated for 8 seconds in an amalgamator and condensed by hand into plastic molds measuring 6 mm in diameter and 4 mm in depth. The amalgam was over condensed and carved level and parallel to the external surface of the mold using operative hand instruments. Specimens (n = 90) were sealed in plastic containers for 7 days at 23°C.
After storage, the specimens were removed from the containers, and the amalgam surfaces were treated with 1 of the 3 surface treatments (n = 30 per treatment). In the APA group, specimens were abraded with 50-µm Al 2O 3 using a force of 45 psi from a distance of 10 mm and rinsed for 60 seconds with deionized water. In the APA plus Alloy Primer group, specimens were treated as described for the APA group, and then 2 drops of Alloy Primer were applied to the treated surface and allowed to evaporate. In the CoJet group, specimens were abrasively sprayed with CoJet Sand using a force of 45 psi from a distance of 10 mm until the surface turned uniformly black. Two drops of ESPE Sil were then applied and allowed to evaporate.
After the surface treatments were completed, the adhesive protocol was applied. Specimens in each surface treatment group were divided into subgroups and treated with one of the 3 adhesives (n = 10 per adhesive per surface treatment). In the OBSP subgroups, the adhesive was applied with a scrubbing motion for 20 seconds and then gently air thinned for 10 seconds to evaporate the solvent. The application and air-thinning process was then repeated, and subsequently the adhesive was photocured for 20 seconds. In the SUA subgroups, the adhesive was applied with a rubbing action for 20 seconds and then gently air thinned for 5 seconds to evaporate the solvent. The adhesive was then photocured for 10 seconds. In the PF
subgroups, equal amounts of the catalyst and base were mixed for 30 seconds. A thin layer of cement was applied evenly to the amalgam surface and photocured for 5 seconds. All photopolymerization was accomplished with a curing unit (SmartLite IQ, Dentsply Sirona) with an intensity of 500 mW/cm2.
After application of the adhesive agents, the specimens were placed in a bonding clamp (Ultradent Products), and a column of nanocomposite resin (Filtek Supreme Ultra, 3M), 2.00 mm in height and 2.38 mm in diameter, was photocured for 40 seconds against the amalgam surface. Excess resin around the column of composite was removed with a No. 25 blade (Miltex). A completed specimen is shown in Fig 1.
Specimens were stored in deionized water for 48 hours at 37°C, and then subjected to shear force testing in a universal testing machine (model TTC, Instron). A 1-mm chiseled bar was used to apply force at a crosshead speed of 0.5 mm/ min. The forces resulting in failure were recorded in megapascals. The specimens were assessed at ×5 magnification to determine the failure mode, which was recorded as adhesive, cohesive, or mixed.
The parametric data were analyzed using 2-way analysis of variance with surface treatment and bonding agent as independent variables. Significant differences among experimental groups were assessed with the Tukey test (P < 0.05). All analyses were performed using SAS Enterprise (version 6.1, SAS Institute).
Results
The mean (SD) shear bond strength values ranged from a low of 12.3 (1.2) MPa for APA-treated amalgam bonded using OBSP to a high of 25.9 (4.6) MPa for CoJet-treated (silicoated) amalgam bonded using PF (Table). The silicoated amalgam surfaces produced the highest shear bond strength, and the 3 adhesive agents showed no statistical differences (P > 0.05) when the surface treatment was silicoating.
The use of Alloy Primer on APA-treated amalgam significantly increased the shear bond strength for OBSP from 12.3 to 17.6 MPa (P < 0.05; Tukey test). Similarly, Alloy Primer
Fig 1. Specimen with a column of composite resin bonded to amalgam.
increased the shear bond strength of PF from 14.5 to 21.4 MPa (P < 0.05). However, using Alloy Primer on APA-treated amalgam with SUA did not significantly improve the bond strength.
The majority of failures in the silicoated specimens were cohesive, with a large portion of the amalgam fracturing (Fig 2). All of the other failures in the experimental groups were adhesive.
Discussion
The null hypothesis was rejected, as there were differences in the shear bond strength of composite to amalgam among the different combinations of surface treatments and adhesive agents. The bonding of composite to amalgam is not a novel idea; however, there is no consensus of how to treat the amalgam surface for bonding. APA with Al2O3 cleans the alloy surface, increases the surface area, and creates micromechanical retention. Studies evaluating Al2O3 APA showed that this protocol provided superior results compared with the use of a crosscut fissure carbide bur.11-14 Surfaces treated with burs provide excessive macromechanical retention, and these macroretentive features provide centers from which crack propagation may occur in the adhesive, ultimately leading to earlier failure.14-16
Silicoating and APA with Al 2O3 are considered to be forms of micromechanical retention.14 Silicoating embeds a 30-µm ceramic layer on the amalgam surface, which dramatically enhances bond strength. The embedded ceramic layer enables silane coupling (using ESPE Sil) with the composite for a true chemical bond with the amalgam. The results of the present study reflect those reported by Özcan et al in that silicoating produced the highest bond strength, followed by Al 2O3 APA with Alloy Primer.16 However, although the highest shear bond strength in this study was produced with silicoating, this procedure requires an additional armamentarium and may be messy when used intraorally.
Alloy Primer contains 2 proprietary chemicals: VBATDT and MDP (Fig 3). The phosphoric acid group of MDP
purportedly creates a strong chemical bond to hydroxyapatite, oxides of noble and base metal alloys, zirconia, alumina, and titanium.17-20 The vinyl group on the other end of the molecule (C=C) is available to copolymerize with the resin monomers. In VBATDT, the sulfur atoms bond chemically to the atoms in precious metals, while its vinyl group on the opposite end of the molecule copolymerizes with the resin monomers. The 4 elements in Tytin amalgam alloy are silver, tin, copper, and mercury. Of these 4 elements, only silver is a precious element, and it constitutes approximately 25% to 35% of the alloy. The increase in bond strength when Alloy Primer is used may be due to the reaction of VBATDT with any available silver atoms and the reaction of MDP with any available copper or tin ions or their oxides. Compared to CoJet, the main advantage of Alloy Primer is its simplicity.
SUA was chosen for this study because the manufacturer states that it bonds to all surfaces, including enamel, dentin, glass ceramics, zirconia, noble and base metal alloys, and composites without additional primers. 21
The results indicate chemical adhesion between SUA and the amalgam alloy because there were statistically significant differences between APA-treated specimens bonded with SUA (21.8 MPa) and those bonded with PF (14.5 MPa) and OBSP (12.3 MPa). PF was selected for this study because this material may be used for bonding resin-bonded fixed partial dentures (ie, Maryland bridges) to enamel and dentin. Like Alloy Primer, the resin component of PF contains MDP. Thus, it should be able to form a chemical bond with available oxides on amalgam treated with Al 2O 3 APA. However, there was no significant difference between the results for APA-treated amalgam bonded with OBSP vs PF.
The highest bond strengths obtained in this study (23.4 to 25.9 MPa) are comparable to the dentin-composite and enamel-composite shear bond strength values obtained in previous studies undertaken by the same research group using OBSP with the same methodology. 22,23 If the
Fig 3. Molecular structures of the primary polymers present in Alloy Primer.
A. VBATDT (6-[4-vinylbenzyl-N-propyl] amino-1,3,5-triazine-2,4-dithiol).
B. MDP (10-methacryloyloxydecyl dihydrogen phosphate).
Fig 2. Adhesive failure of a silicoated amalgam surface.
amalgam-composite bond strength is comparable to the dentin-composite bond strength, then repairing amalgam with composite may be successful.
In select clinical cases, it may be more conservative to repair an amalgam restoration than to replace it. Complete restoration replacement results in increased preparation and restoration size. This repetitive restoration cycle in turn results in additional expense, time, removal of tooth structure, possible detrimental pulpal effects, and potential damage to adjacent teeth. When restoration repair is being considered as a treatment approach, silicoating amalgam may provide an effective method of surface treatment prior to bonding composite to aged amalgam.
This investigation was a pilot study to determine whether a strong interfacial bond can be created between amalgam and composite resin. Thus, future inquiries should investigate the effects of additional aging of amalgam, the corrosion products of amalgam, amalgam type (spherical vs admixed), and thermocycling of the repaired restoration.
Conclusion
Within the limitations of this study, silicoating of the amalgam surface provided the highest bond strength among the combination of surface treatments and adhesive agents tested. These results indicate that composite can be effectively bonded to amalgam via silicoating.
Author affiliations
Department of General Practice, Virginia Commonwealth University, School of Dentistry, Richmond (Imbery, Moon); Private practice, Boulder, Colorado (Pitz); Department of Dental Public Health and Policy, Oral Health Services Research Core, Philips Institute for Oral Health Research, Virginia Commonwealth University, School of Dentistry, Richmond (Carrico).
Correspondence
Terence A. Imbery, DDS (taimbery@vcu.edu).
Conflicts of interest
None reported.
Funding
Dr Anna Pitz was a student at the time of the study, and she received funding from the A.D. Williams Fellowship Foundation at Virginia Commonwealth University, School of Dentistry. The Kerr Corporation donated the Tytin amalgam alloy.
References
1. Roda RS, Zwicker PF. The combined composite resin and amalgam restoration for posterior teeth: a clinical report. Quintessence Int. 1992;23(1):9-13.
2. Meiers JC. Salvaging a compromised tooth using a combination amalgam core/composite window technique. Oper Dent. 2004;29(4):477-480.
4. Plasmans PJ, Reukers EA. Esthetic veneering of amalgam restorations with composite resin— combining the best of both worlds? Oper Dent. 1993;18(2):66-71.
5. Gordon M, Laufer BZ, Metzger Z. Composite-veneered amalgam restorations. J Prosthet Dent. 1985;54(6):759-762. doi:10.1016/0022-3913(85)90464-0
6. Bader JD, Martin JA, Shugars DA. Preliminary estimates of the incidence and consequences of tooth fracture. J Am Dent Assoc. 1995;126(12):1650-1654. doi:10.14219/jada. archive.1995.0113
7. Heft MW, Gilbert GH, Dolan TA, Foerster U. Restoration fractures, cusp fractures and root fragments in a diverse sample of adults: 24-month incidence. J Am Dent Assoc. 2000;131(10):1459-1464. doi:10.14219/jada.archive.2000.0057
8. Fennis WM, Kuijs RH, Kreulen CM, Roeters FJ, Creugers NH, Burgersdijk RC. A survey of cusp fractures in a population of general dental practices. Int J Prosthodont. 2002;15(6):559-563.
9. Van Nieuwenhuysen JP, D’Hoore W, Carvalho J, Qvist V. Long-term evaluation of extensive restorations in permanent teeth. J Dent. 2003;31(6):395-405. doi:10.1016/s03005712(03)00084-8
10. Pilo R, Nissan J, Shafir H, Shapira G, Alter E, Brosh T. The influence of long term water immersion on shear bond strength of amalgam repaired by resin composite and mediated by adhesives or resin modified glass ionomers. J Dent. 2012;40(7):594-602. doi:10.1016/ j.jdent.2012.04.001
11. Machado C, Sanchez E, Alapati S, Seghi R, Johnston W. Shear bond strength of the amalgamresin composite interface. Oper Dent. 2007;32(4):341-346. doi:10.2341/06-100
12. Sperber RL, Watson PA, Rossouw PE, Sectakof PA. Adhesion of bonded orthodontic attachments to dental amalgam: in vitro study. Am J Orthod Dentofacial Orthop. 1999;116(5):506513. doi:10.1016/s0889-5406(99)70180-0
13. Ruse ND, Sekimoto RT, Feduik D. The effect of amalgam surface preparation on the shear bond strength between composite and amalgam. Oper Dent. 1995;20(5):180-185.
14. Blum IR, Hafiana K, Curtis A, et al. The effect of surface conditioning on the bond strength of resin composite to amalgam. J Dent. 2012;40(1):15-21. doi:10.1016/j.jdent.2011.10.019
15. Fruits TJ, Duncanson MG Jr, Coury TL. Interfacial bond strength of amalgam bonded to amalgam and resin composite bonded to amalgam. Quintessence Int. 1998;29(5):327-334.
16. Özcan M, Vallittu PK, Huysmans MC, Kalk W, Vahlberg T. Bond strength of resin composite to differently conditioned amalgam. J Mater Sci Mater Med. 2006;17(1):7-13. doi:10.1007/ s10856-006-6324-4
17. Kadoma Y. Chemical structures of adhesion promoting monomers for precious metals and their bond strengths to dental metals. Dent Mater J. 2003;22(3):343-358. doi:10.4012/dmj.22.343
18. Choo SS, Huh YH, Cho LR, Park CJ. Effect of metal primers and tarnish treatment on bonding between dental alloys and veneer resin. J Adv Prosthodont. 2015;7(5):392-399. doi:10.4047/ jap.2015.7.5.392
19. Bulbul M, Kesim B. The effect of primers on shear bond strength of acrylic resins to different types of metals. J Prosthet Dent. 2010;103(5):303-308. doi:10.1016/S0022-3913(10)60063-7
20. Shimizu H, Kurtz KS, Tachii Y, Takahashi Y. Use of metal conditioners to improve bond strengths of autopolymerizing denture base resin to cast Ti-6Al-7Nb and Co-Cr. J Dent. 2006;34(2):117122. doi:10.1016/j.jdent.2005.05.002
22. Moon PC, Weaver J, Brooks CN. Review of matrix metalloproteinases’ effect on the hybrid dentin bond layer stability and chlorhexidine clinical use to prevent bond failure. Open Dent J. 2010;4:147-152. doi:10.2174/1874210601004010147
23. Imbery TA, Kennedy M, Janus C, Moon PC. Evaluating EDTA as a substitute for phosphoric acidetching of enamel and dentin. Gen Dent. 2012;60(2):e55-e61.
Ectopic sulcular pain: detection and treatment
James V. Potter, DDS
Patients who present with acute or chronic posterior dental pain but cannot identify the tooth from which the pain originates may suffer from a common but often unrecognized condition. The present article introduces a new term for this disorder, ectopic sulcular pain (ESP), derived from its unusual presentation, location, and defining symptom. It is tempting to call ESP an infection, but this has not been confirmed. In ESP, oral examination reveals no visual abnormalities, and there are no evident fractures, caries, periodontitis, attachment loss, traumatic occlusion, or periapical abscesses. This confusing symptomatology often leads to incorrect diagnosis and, consequently, treatment that fails to relieve the patient’s pain. This article discusses ESP and reports 13 cases in which the condition was identified via intraligamental or topical application of an anesthetic agent to numb the gingiva. In 12 patients, ESP was successfully treated with meticulous oral hygiene, chlorhexidine rinses, and, in some cases, oral antibiotics.
Received: June 12, 2023
Revised: October 9, 2023
Accepted: November 29, 2023
Keywords: cracked tooth syndrome, differential diagnosis, ectopic sulcular pain, local anesthesia, referred pain
Oral pain frequently presents with confusing symptoms that make identifying the cause difficult, often resulting in incorrect diagnosis and treatment.1,2 The present article introduces a new term for one such condition, ectopic sulcular pain (ESP), so named because of its unusual presentation, location in the gingival sulcus, and primary symptom, pain. Because ESP is a painful condition, it is important to identify and treat as soon as possible.
It is widely understood that gingivitis and periodontitis can occur without pain.3 In ESP, pain is the primary symptom and usually the reason the patient seeks care. In the case series that will be presented in this article, pain was observed in 100% of patients with ESP, while bleeding on probing and other signs and symptoms were observed only sporadically. Some patients exhibited radiographic bone loss and attachment loss on probing, but it was not determined whether the attachment loss resulted from ESP or a previous condition. Although pockets were frequently found when other quadrants of the oral cavity were examined, the patients were not experiencing pain in those areas.
When patients report pain, they should be asked to describe the area involved, the severity, the time when the pain started, and other standard information needed to formulate a diagnosis. Unfortunately, the pain symptoms of ESP are common across a wide range of dental issues, making it a challenge to identify the etiology of this condition.4 Once the clinician is aware of ESP and how to diagnose it, correct treatment can be provided, resulting in successful outcomes.
In the author’s clinical experience, ESP almost always appears in the posterior area distal to the second premolar, and it can occur in either the maxilla or mandible. Patients report that the pain comes and goes and seems more prevalent when they are trying to sleep. The pain is throbbing, not sharp, and frequently occurs after eating a meal, and then may subside.3 The pain develops slowly but increases to an intolerable level, which causes patients to seek care. Patients frequently describe the pain as coming from an area, not a specific tooth, and rub the painful side of the face with an open hand rather than point to the painful area with a finger.
With ESP, there are no fractured teeth or abscesses. Percussion and cold testing reveal no periodontal disease or sinus infection.5-7 Radiographs reveal normal conditions. A frequent misdiagnosis after all options are seemingly exhausted is cracked tooth syndrome, because cracked teeth often result in complicated symptoms.8 However, if the condition is misdiagnosed and incorrect treatment is provided, the ESP patient will report persistent pain that is intense enough for the individual to seek professional care.
This series of case reports from a single private dental practice describes a diagnostic method and therapeutic regimen that resulted in resolution of ESP.
Case reports
Diagnostic process
Case 1
A 44-year-old man presented for a limited examination, complaining of increasing pain in the posterior region of the maxilla. The pain came and went but frequently kept him up at night. Acetaminophen helped him, but the pain would return. The pain had started several months previously but was worsening at the time of presentation. Radiographic and clinical examinations showed nothing that contributed to the symptoms.
When asked which tooth was causing pain, the patient rubbed the upper right region of his cheek and guessed that it was the first molar but added that both molars were hurting at that moment. Direct examination of the maxillary right second molar (tooth 2) and the maxillary right first molar (tooth 3) revealed no fractures or previous restorations, and a periapical radiograph showed no opacities or bone loss. The results of the percussion test were negative, and the teeth were not mobile. All teeth in the maxillary right quadrant had a positive response to a cold test with a cotton pellet and refrigerant. The patient did not report any history of sinus infections or hay fever.
Although the patient reported current pain, he also reported that the teeth had not been hurting when he first came to the appointment. A periodontal probe was used to lightly probe the maxillary left first and second molars on the mesial, facial, and distal gingival margins to demonstrate to the patient what a “normal” condition should feel like. The patient reported no sensitivity. Next, the mesial, facial, and distal gingival margins of teeth 2 and 3 were probed. When the interproximal areas were probed, the patient jumped, and repeat probing on the lingual aspects of teeth 2 and 3 produced a similar pain response in the same interproximal areas.
An intraligamental syringe was used to inject a small amount of local anesthetic (lidocaine 2% with epinephrine 1:100,000) carefully into the gingival tissues surrounding teeth 2 and 3 to anesthetize only the gingiva without numbing the teeth. In 1 minute, the patient reported that the pain had disappeared. This response indicated that the correct diagnosis was ESP.
Case 2
A 50-year-old woman presented with emergency pain that had kept her awake all night. The patient was rubbing her face in the area of the mandibular right first molar (tooth 30). The patient’s records showed that she had reported mild discomfort over the past 6 months, but previous examinations found nothing remarkable, and the lack of specific symptoms could not produce a definitive diagnosis. At the time of presentation, the pain had intensified significantly.
The pain had developed slowly over a long period of time. The patient reported that the pain came and went, and she could not identify a stimulus for the painful episodes. The patient also reported that the pain was migrating to teeth 2 and 3. For all of the teeth, the cold test was positive, and the percussion test was negative. The radiograph did not show abnormality, and all tissues appeared pink, with no swelling or erythema. The patient indicated that tooth 30 had started hurting again after the appointment began.
On periodontal probing of the facial gingiva around tooth 30, the patient jumped. There was no response to probing of any other area. After a small amount of anesthetic (lidocaine 2% with epinephrine 1:100,000) was administered to the gingiva around tooth 30 via intraligamental injection, the patient reported that the pain had disappeared, including the maxillary pain, even though no anesthetic had been applied in that area. The diagnosis was established as ESP with referred pain.
Case 3
A 28-year-old woman complained of pain in the left side of the mandible for several days. She was unable to locate the exact tooth causing the pain and reported that the source seemed to move around. At the time of presentation, she indicated that the pain affected the mandibular left first molar (tooth 19) and second molar (tooth 18). The pain had started a few days previously and was sporadic but worse at night.
The results of percussion tests were negative, and examination showed a well-maintained dentition with no caries. Periodontal probing of the facial marginal tissues of teeth 18 through 21 produced sensitivity interproximal to teeth 18 and 19.
The sensitive interproximal gingiva was swabbed with a 20% benzocaine topical anesthetic. After 3 minutes, the patient reported the pain was gone. A diagnosis of ESP was established.
Case 4
A 30-year-old woman presented with tooth pain in the right side of the maxilla that had persisted for several days. Clinical examination and periapical radiographs found a nonproductive fistula tract buccal to tooth 3, which had undergone endodontic treatment 5 years previously. The radiograph showed no radiolucency, and the tooth was negative to percussion.
Periodontal probing produced sensitivity on the buccal surfaces of the maxillary right second premolar (tooth 4) and the maxillary right first premolar (tooth 5). An intraligamental injection of an anesthetic (lidocaine 2%, with 1:100,000 epinephrine) was administered along the gingival margins of teeth 4 and 5. After 1 minute, the patient reported that the pain had disappeared. A diagnosis of ESP was given.
Treatment
The treatment prescribed for ESP was meticulous oral hygiene, including brushing, flossing, and a 0.12% chlorhexidine gluconate rinse with instructions for use (swish 1 capful for 30 seconds and spit, without rinsing, twice a day). A follow-up assessment was conducted in 7 days. If the pain had not resolved by that time, an oral antibiotic was added to the treatment.9 The drug, dosage, frequency, and duration were tailored to the patient’s needs, including consideration of the patient’s history of antibiotic use, allergic reactions, and tolerance. Patients received amoxicillin or clindamycin, and both were effective.
Outcomes
The records of all patients who were examined from April through September 2022 were reviewed to determine the effectiveness of the described protocols for diagnosis and treatment of ESP. During that period, a total of 13 patients were diagnosed with ESP. Each patient completed a
therapeutic regimen of meticulous oral hygiene with chlorhexidine rinses. Five patients needed to take an oral antibiotic before the pain was resolved.
Of the 13 patients who received a diagnosis of ESP, 12 reported that the pain had resolved after completion of the treatment regimen. The patients continued to be pain-free and were simply recalled for annual examinations after the successful completion of treatment. No relapses were reported. One patient who received oral hygiene instruction and a chlorhexidine prescription failed to return for the 7-day followup examination. When contacted, she reported that she had sought a second opinion from another dentist, who diagnosed a fractured tooth and performed an extraction.
Discussion
Episodic oral pain that presents in a nonspecific location in the region of the molars and premolars and increases in severity with no apparent cause should be systematically investigated for ESP. First, the standard investigative tools of dentistry should be used to identify other possible causes of pain. The presence of periapical abscesses can be verified or ruled out with a percussion test, and the existence of radiolucency can be verified or ruled out with a radiograph. A cold test should be used to assess tooth vitality.10 A light source can be placed against the tooth to identify possible fractures via indirect lighting. Recently placed dental restorations may have poor occlusal contacts, so the occlusion should be checked with articulating paper.
At this point in the examination, clinicians frequently make a mistaken diagnosis because ESP symptoms are common and associated with a variety of causes. However, if no apparent cause of pain is found, ESP should be considered in the differential diagnosis. In the author’s clinical experience of treating patients with this condition, ESP is most prevalent around the maxillary and mandibular molars and premolars. Patients report that symptoms begin as mild to moderate throbbing pain that affects an area, not a specific tooth. The pain usually comes and goes, often after a meal, and dissipates slowly. The pain is often greater at night and can cause sleep disruption. There may be cold sensitivity. These symptoms are common to fractures, periapical abscesses, irritation from caries, and other conditions.
Some of the patients in the present case series displayed bleeding on probing in the affected area, but others did not. In those patients, bleeding on probing was also observed in areas not affected by ESP. In all 13 patients with ESP, the only constant symptom was pain. Bleeding had little to do with the diagnosis. Bleeding is considered a prominent factor in gingivitis and periodontal disease. However, analysis of the literature demonstrates a disparity in associating bleeding and periodontal disease. Multiple periodontal classification systems were examined by Benamghar et al as well as by Wei and Lang.11,12 Neither Glavind and Löe’s classification, based on probing depth and loss of attachment, nor the Navy Periodontal Disease Index includes bleeding among the criteria.13,14 Other systems consider bleeding only after periodontal disease advances along a given scale of signs and symptoms; the Gingival Periodontal Index by O’Leary, the Periodontal Disease Index by Ramfjord,
and the Gingivitis Index by Suomi and Barbano consider bleeding after periodontal disease has progressed.15-17
ESP should only be considered after no other potential causes of pain are found. The investigation should begin with gentle gingival probing in an area not suspected as the source of pain. This step is intended to show the patient what “normal” feels like. Then, probing should proceed to the area that is the suspected source of pain, and the patient should be asked if he or she is experiencing any sensitivity. If sensitivity is found, there is a high probability of ESP.
The clinician can establish definitive proof of ESP by applying topical benzocaine gel or injecting a small amount of lidocaine or a similar anesthetic in the gingival area. If the pain resolves, the diagnosis is ESP. Periodontal probing will produce a sensitive response in the painful area in patients with ESP, and relief of the pain after the application of anesthetic clearly demonstrates the origin of the pain to the patient. However, applying a small amount of anesthetic to the painful area is not therapy; it is a diagnostic procedure.
Once a diagnosis is established, a home-care program of meticulous oral hygiene, including brushing, flossing, and rinsing with 0.12% chlorhexidine gluconate, should be initiated. This program should be supplemented with an oral antibiotic if the pain is not relieved after 7 days. The antibiotic should be selected based on the clinician’s training and experience and tailored to the patient’s needs, including consideration of any history of antibiotic use, allergic reactions, and tolerance. In the author’s experience, either amoxicillin or clindamycin can be effective. Deeper investigation is needed to establish the cause of ESP. ESP could be classified as a precursor to periodontitis; however, ESP often lacks the symptoms of sulcular destruction, bleeding, and loss of periodontal structures that characterize periodontitis. It is tempting to call ESP an infection, but infection has not been established as a source. Nevertheless, the evidence for an infectious component is strong, given that antibiotic therapy resulted in a successful treatment outcome for all 5 of the patients in the present case series who did not respond to the initial oral hygiene and chlorhexidine regimen. If infection is found to be the cause, studies to determine prevalent bacteria and the most appropriate antibiotic would be helpful.
ESP also could be a form of peripheral neuropathy. However, if that were the case, nerve endings would be dying.18 Morever, the speed at which the tissues in ESP respond to antibiotics likely rules out nerve death since nerve regeneration is a lengthy process.
Conclusion
When the clinician does not recognize ESP, the incorrect diagnosis is followed by incorrect treatment, and the patient suffers from persistent pain. This case series has described a procedure for definitive diagnosis of the condition as well as a therapeutic regimen that has shown positive results. A larger study with controls to validate the described protocols would strengthen this report.
Author affiliation
Private practice, Austin, Texas.
Correspondence
James V. Potter, DDS (bazooka@ix.netcom.com).
Conflicts of interest
None reported.
References
1. Moule AJ, Hicks ML, eds. Diagnosing Dental and Orofacial Pain: A Clinical Manual. WileyBlackwell; 2016.
2. Miranda-Rius J, Brunet-Llobet L, Lahor-Soler E. The periodontium as a potential cause of orofacial pain: a comprehensive review. Open Dent J. 2018;12:520-528. doi:10.2174/1874210601812010520
3. Gaurilcikaite E, Renton T, Grant AD. The paradox of painless periodontal disease. Oral Dis 2017;23(4):451-463. doi:10.1111/odi.12537
4. Lineberry J. When patients present with confusing pain. Spear Education. June 11, 2021. Accessed May 23, 2024. https://www.speareducation.com/spear-review/2012/09/whenpatients-present-with-confusing-pain
5. Balto K. Using a cold test to assess pulpal anesthesia. Is a cold test effective in determining whether a patient will experience pain during root canal therapy? Evid Based Dent. 2007;8(4):102. doi:10.1038/sj.ebd.6400522
6. Peters DD, Baumgartner JC, Lorton L. Adult pulpal diagnosis, I: evaluation of the positive and negative responses to cold and electrical pulp tests. J Endod. 1994;20(10):506-511. doi:10.1016/S0099-2399(06)80048-8
7. Lin S. Can tooth pain be a symptom of sinusitis? Verywell Health. Updated September 8, 2022. Accessed May 23, 2024. https://www.verywellhealth.com/is-your-toothache-a-signof-sinusitis-1059305
8. Banerji S, Mehta SB, Millar BJ. Cracked tooth syndrome, 1: aetiology and diagnosis. Br Dent J. 2010;208(10):459-463. doi:10.1038/sj.bdj.2010.449
9. Kapoor A, Malhotra R, Grover V, Grover D. Systemic antibiotic therapy in periodontics. Dent Res J (Isfahan). 2012;9(5):505-515. doi:10.4103/1735-3327.104866
10. Weisleder R, Yamauchi S, Caplan DJ, Trope M, Teixeira FB. The validity of pulp testing: a clinical study. J Am Dent Assoc. 2009;140(8):1013-1017. doi:10.14219/jada.archive. 2009.0312
11. Benamghar L, Penaud J, Kaminsky P, Abt F, Martin J. Comparison of gingival index and sulcus bleeding index as indicators of periodontal status. Bull World Health Organ. 1982;60(1):147151.
12. Wei SH, Lang KP. Periodontal epidemiological indices for children and adolescents, I: gingival and periodontal health assessments. Pediatr Dent. 1981;3(4):353-360.
13. Glavind L, Löe H. Errors in the clinical assessment of periodontal destruction. J Periodontal Res. 1967;2(3):180-184. doi:10.1111/j.1600-0765.1967.tb01887.x
14. Grossman FD, Fedi PF Jr. Navy periodontal screening examination. J Am Soc Prev Dent. 1973;3(6):41-45.
15. O’Leary T. The periodontal screening examination. J Periodontol. 1967;38(6):617-624. doi:10.1902/jop.1967.38.6_part2.617
16. Ramfjord SP. The Periodontal Disease Index (PDI). J Periodontol. 1967;38(6):602-610. doi:10.1902/jop.1967.38.6.602
17. Suomi JD, Barbano JP. Patterns of gingivitis. J Periodontol. 1968;39(2):71-74. doi:10.1902/ jop.1968.39.2.71
18. Salomon SH. What is neuropathy? Symptoms, causes, diagnosis, treatment, and prevention. Everyday Health. Updated January 14, 2023. Accessed May 23, 2024. https://www.everydayhealth.com/neuropathy/guide/
Pilot, open-label, randomized controlled clinical trial evaluating 4 oral hygiene regimens using a manual toothbrush, toothpaste, and mouthwash
Serban Rosu, Dr Prof, PhD, MD ¢ Paola Benatti, PharmD ¢ Salvatore Bianco, Dr Prof, MD
In this prospective pilot study, 84 patients with a history of poor oral hygiene were enrolled in an open-label, interventional, randomized controlled clinical trial. The aim was to provide preliminary clinical data on a new line of oral hygiene products containing a prebiotic and a paraprobiotic based on Lactobacillus plantarum. The recruitment rate and patient satisfaction were analyzed to estimate resources for the future primary study, and descriptive data on rebalancing of the oral microbiota were collected. The population was divided into 5 groups based on the products assigned to the patients: 1, delicate mint toothpaste (n = 20); 2, mint toothpaste (n = 12); 3, mint mouthwash (n = 20); 4, delicate mint toothpaste, mint mouthwash, and an antimicrobial toothbrush (n = 20); and 5, continued use of their usual oral care products and routine (control group; n = 12). The study duration was 28 days. All patients tolerated the products well, and there were no adverse events. The recruitment capability and procedures allowed for a realistic estimation for the future main trial. The products did not cause any changes in tooth color. The participants in group 4, who completed the treatment consisting of delicate mint toothpaste, mint mouthwash, and an antimicrobial toothbrush, reported the greatest reduction in gingival sensitivity (P ≤ 0.000; Wilcoxon signed rank test). Analysis with the Wilcoxon signed rank test revealed that all products induced a statistically significant decrease in plaque (P ≤ 0.002) and a reduction in gingival sensitivity (delicate mint toothpaste, P ≤ 0.005; mint toothpaste, P ≤ 0.015; and mint mouthwash, P ≤ 0.015). All products were effective in stabilizing the oral microbiota. The tested products showed an optimal safety profile and a statistically significant efficacy in reducing gingival sensitivity and plaque. They also stabilized the biodiversity of the oral microbiota, making it less susceptible to microbial fluctuations than the control group. Trial registration: ClinicalTrials.gov (NCT05999175).
The oral cavity offers several habitats for microbial colonization, such as the saliva, teeth, tongue, gingival sulcus, palate, and other epithelial surfaces of the oral mucosa.1 Knowledge of the oral microbiota has sharply increased after the development of culture-independent study methods, such as 16S ribosomal RNA (rRNA) gene community profiling, which revolutionized the detection and identification of microorganisms in the oral microbiome.2 The oral microbiota consist mainly of bacteria, fungi, and viruses; archaea and protozoa are also present but in lower proportions.3 Over 700 bacterial species have been identified, making the oral microbiota the second most diverse microbiota in humans. Streptococcus is the genus found in the greatest quantity in the microbiome of adults, followed by Gemella, Veillonella, Prevotella, Fusobacterium, Porphyromonas, Neisseria, Capnocytophaga, Corynebacterium, and Actinomyces.4 The bacteria of the oral microbiome form dental plaque biofilm, which is embedded in an extracellular matrix at the interface between the tooth surface and the saliva or gingival crevicular fluid.5 A balanced and stable state of the microbiota (ie, symbiosis) is essential for maintaining oral health.6 Changes in the oral environment and the interference of certain lowabundance microbial pathogens with the host immune system may alter the diversity and relative proportions of species or taxa within the microbiota, leading to the overgrowth of pathogenic species. Consequently, the lack of stability and the disequilibrium of the oral microbiota (ie, dysbiosis) can lead to conditions such as caries, gingivitis, and periodontitis, which are among the most prevalent diseases globally.7,8
Proper oral hygiene is essential for symbiosis of the oral microbiota. The ability and willingness of the individual to maintain plaque control are the foundation for the prevention and treatment of oral diseases.9 Toothbrushing is the mainstay of oral hygiene, although several procedures are available for the mechanical removal of plaque, such as interdental cleaning devices (including dental floss, interdental brushes, oral irrigators, and woodsticks) and scaling.10-12 Manual and battery-powered toothbrushes have been shown to effectively reduce the amount of dental plaque.13 Proper use and storage of toothbrushes are crucial to avoid gingival recession and contamination from several sources, including the oral cavity, the environment, hands, aerosols, blood, skin, and containers.
Toothpastes, mouthwashes, gels, and/or sprays are used as adjuvants to conventional toothbrushing.14,15 These products
may contain ingredients with antimicrobial action (eg, chlorhexidine, cetylpyridinium chloride, fluorides, and natural substances) that exert antiplaque and/or antigingivitis and antiperiodontitis actions.16 However, oral cleansing products should not abrade the tooth enamel or alter its color.17 Moreover, they should be accepted by the user (ie, with a favorable flavor, texture, and feeling of freshness).
Recently, interest in prebiotic and probiotic supplementation for the prevention and treatment of oral diseases has emerged. Supplementation with viable microorganisms favors symbiosis of the oral microbiota and has shown promising results for reducing dental plaque and the risk of caries, improving clinical periodontal parameters.18-20 Products based on Lactobacillus plantarum demonstrated beneficial effects on the oral microbiota in preclinical studies and in a randomized controlled clinical trial.21-23
The complete line of consumer oral hygiene products Tau-Marin Protezione e Prevenzione (owner and distributor, Alfasigma; cosmetics manufacturing site, Biokosmes) with an innovative formula containing a prebiotic (Bioecolia, Solabia Group) and a paraprobiotic based on Lactobacillus plantarum (SymReboot OC, Symrise) was launched on the Italian market in 2023.24,25 The products include mint (Tau-Marin Dentifricio Gel Menta Delicata) and delicate mint toothpastes (Tau-Marin Dentifricio Gel Menta) and mint mouthwash (Tau-Marin Collutorio Menta). Alfasigma, which owns and distributes these products, recommends that they be used with a proprietary antimicrobial toothbrush (Tau-Marin Scalare 33) that can reportedly eliminate Staphylococcus aureus, methicillinresistant Staphylococcus aureus, Pseudomonas aeruginosa, and Escherichia coli bacteria because the bristles, handle, and toothbrush head are infused with silver ions.26,27 The probiotic Bioecolia is an α-glucan oligosaccharide that is a preferential substrate for commensal bacteria and selectively stimulates their growth. SymReboot OC is a paraprobiotic, which is a nonviable microbial cell (either intact or broken) or a crude cell extract that can confer health benefits to the user when administered in adequate amounts.28 SymReboot OC is composed of heat-treated L plantarum HEAL19. Preclinical studies have shown that SymReboot OC favors the expression of antimicrobial peptides, soothes the oral cavity, and promotes a healthy oral microbiota (data on file, Alfasigma). Moreover, SymReboot OC supports the production of filaggrin, a protein that facilitates the aggregation of keratin filaments, thus strengthening the oral mucosa barrier.29 The combined action of prebiotics and paraprobiotics restored symbiosis.30 The microbiota stability and results of preclinical tests confirmed the safety of these products (data on file, Alfasigma).
The aim of this pilot study was to provide preliminary clinical data (efficacy of plaque removal, effect on gingival sensitivity, and the safety and tolerability of the products), the monthly recruitment rate, and patient acceptance, as well as descriptive data on the effects of the products on rebalancing the oral microbiota. An additional objective was to verify whether the subjective evaluations of the subjects using the traditional mint toothpaste would be different from those of the group using the new delicate mint toothpaste formulation. The data obtained from this study will form the basis for a future larger
confirmatory study on the feasibility of a standard daily hygiene model including the use of the toothpaste, mouthwash, and toothbrush marketed with the claim of improving oral prevention and protection.
Methods
This study was conducted in accordance with the Declaration of Helsinki (as amended by the 64th World Medical Association General Assembly, Fortaleza, Brazil, October 2013) and following Italian regulations for clinical trials on cosmetics.31 The study followed the guidelines of the CONSORT (Consolidated Standards of Reporting Trials) pilot and feasibility trials checklist.32 The protocol was approved by the Internal Ethics Committee of Complife Italia. The study protocol was also registered on ClinicalTrials.gov (NCT05999175). The first participant was enrolled on May 17, 2022, and the end of the enrollment period was on June 28, 2022, with the last participant’s final visit performed on July 26, 2022. The tested products were provided by Biokosmes.
Study design and participants
This was a 28-day, prospective, open-label, interventional, randomized, parallel-group study in 84 healthy volunteers who had a history of poor oral hygiene. All patients who attended a routine dental visit at a private clinic in San Genesio ed Uniti, Italy, between May and July 2022, were screened by a single dental practitioner (D.C.) for the inclusion and exclusion criteria and evaluated for oral hygiene compliance. Only patients who signed the informed consent form could potentially be included in the study.
Patients were first interviewed and assigned scores with regard to their oral health habits, including frequency of toothbrushing (0, more than once a day; 1, once a day or less), self-diagnosis of oral malodor (0, rarely or never self-conscious; 1, sometimes; 2, often), and self-assessment of compliance with regular oral hygiene (0, optimal; 1, mild; 2, bad). For inclusion in the study, the patient had to have a total score of 4 or greater on this self-assessment questionnaire. In addition, the Simplified Oral Hygiene Index (OHI-S) proposed by Greene and Vermillion was applied.33 An OHI-S score of 2 or greater was necessary for inclusion in the trial. Patients who met the eligibility criteria and assured they would not change their daily routine or lifestyle during the study period were enrolled.
To be enrolled in the study, patients had to meet the following inclusion criteria: healthy White men and women aged between 18 and 65 years; history of and current poor oral hygiene, as verified by an OHI-S score of 2 or greater and a self-assessment score of 4 or greater on the questionnaire on oral habits; signed informed consent form; registration with the Italian National Health Service; ability to understand the language used in the investigation center and to comply with the study procedures; certification of the truthfulness of the personal data disclosed to the investigator; stability of any pharmacologic therapy with the exception of excluded pharmaceuticals (ie, proton pump inhibitors, metformin, antibiotics, thyroxine, and statins34); and a commitment not to change daily routine or lifestyle. As the patients were recruited from a township in northern Italy where almost the entire population is White,
inclusion was limited to White patients to ensure homogeneity with the location of the study.
Patients were excluded from the study if they met any of the following criteria: allergies or sensitivity to oral care products, cosmetic products, drugs, patches, and/or medical devices; any condition of the oral cavity inappropriate for participation (ie, ulcers or lesions of the oral mucosa, gingival lesions or recession, periodontitis); gingival bleeding due to pathologic conditions or pharmacologic treatment; antibiotic therapy in the week before baseline or during the 28 days of the study; a smoking habit (5 or more cigarettes a day); acute, chronic, or progressive diseases, illnesses, or conditions that could interfere with the outcome of the study or that were considered dangerous or incompatible with the study requirements; pathologic staining of teeth; breastfeeding, pregnancy, or, in women of childbearing age, an unwillingness to take the necessary precautions to avoid pregnancy during the study; the intention to participate in a different clinical trial or participation in other clinical trials within the previous 3 months; hospitalization or planned hospitalization; deprivation of freedom by administrative or legal decision, or under guardianship; or an inability to be contacted in case of emergency.
When recruiting a patient, the investigator called the central randomization service located at the Complife Italia clinical center, San Martino Siccomario, Italy, to obtain basic patient information and then assign treatment following a computergenerated list. Randomization was not stratified by age or sex. The patients were allocated to one of the following groups: group 1 (n = 20) used Tau-Marin delicate mint toothpaste; group 2 (n = 12) used Tau-Marin mint toothpaste; group 3 (n = 20) used TauMarin mint mouthwash (1 tbsp of undiluted product swished around the mouth for 1 minute) 3 times a day after toothbrushing with their routine toothpaste; and group 4 (n = 20) used Tau-Marin mint mouthwash and Tau-Marin delicate mint toothpaste, applied with the Tau-Marin Scalare 33 medium toothbrush, 3 times a day (after meals) for 28 days. Groups 1 to 3 were provided with a standard toothbrush to be used 3 times a day after meals for 28 days. Group 5 (n = 12) was included as a control group, and these patients continued to use their routine oral hygiene products for 28 days 3 times a day after meals.
As this was a pilot study, and for logistical reasons, the size of the treatment groups was not equal. Thus, the number of patients included in group 2 was reduced for economic reasons, considering that the aim of comparing groups 1 and 2 (traditional mint versus delicate mint flavor) was only to determine differences in the subjective evaluations of the products on the self-assessment questionnaire. Finally, the 12 patients in the control group were included only to assess the variations in the oral microbiota. The patients and investigator were not blinded to the treatment allocations.
As reported previously, the screening visit (TS) was performed at the private clinic of a single dental practitioner (D.C.), while the patients underwent the examinations required by the study protocol at the Complife Italia clinical center (T0 visit).
Data collection
A routine oral health assessment was performed in each patient at all visits for the presence of caries; tartar; gingival
recession, lesions, or irritations (reddening, burning sensation, swelling, or bleeding); and ulcers or lesions of the oral mucosa. The presence or absence of any sign was recorded in the case report of each patient.
The clinical data required by the study protocol were collected immediately before use of the product (baseline [T0]) and after 14 (T14) and 28 (T28) days of use. Visits were performed at least 4 hours after the patient’s most recent oral activity (eating, drinking, brushing teeth, etc). A specific evaluation was made immediately after first use of the products (TImm) to assess the amount of dental plaque and complete the product assessment questionnaire.
Clinical parameters at T14, T28, and TImm were assessed only for the treatment groups 1 to 4; participants in group 5 only underwent the oral microbiota analyses at T0 and T28. Data were collected at planned timepoints as described in the following paragraphs.
Dental plaque was assessed at T0 (4 hours after the most recent toothbrushing) and TImm using an erythrosine-based disclosing tablet. The total plaque score was calculated by determining the area of the tooth surface covered, and the following scores were possible: 0 to 3, excellent; 4 to 7, good; 8 to 11, fairly good; and 12 to 18, poor.33
Gingival sensitivity was evaluated at T0, T14, and T28 using a visual analog scale where 0 represented no sensitivity and 10 represented the highest sensitivity.
Tooth color was assessed by a single evaluator (V.N.) at T0 and T28 using the Vitapan (VITA Zahnfabrik) scale, which has 4 families of shades: reddish brownish (A1, A2, A3, A3.5, A4), reddish yellowish (B1, B2, B3, B4), grayish (C1, C2, C3, C4), and reddish gray (D2, D3, D4).
To assess the stability of the oral microbiota, samples were collected at T0 and T28 from 12 patients each in groups 1, 3, and 4 (selected according to a randomization list) as well as all patients in groups 2 and 5 (n = 12 each). The samples were analyzed by the Laboratory of Genomics & Transcriptomics, Translational Research Centre for Autoimmune and Allergic Diseases, Department of Health Sciences, University of Eastern Piedmonte, Novara, Italy, via metagenomic analysis of the 16S rRNA gene. A microbiota sample was collected by brushing the surface of the oral mucosa with a swab. Bacterial DNA was isolated from the components of the sample, purified, and subjected to 16S rRNA gene amplification. Analysis was completed by sequencing the 16S rRNA gene pool using bioinformatics tools. The effect of the treatment products on the diversity within samples (alpha diversity) was evaluated using a biodiversity index (Shannon index).35 Beta diversity analysis was used to compare the compositions of the microbial communities between groups by generating a dissimilarity matrix.
A product questionnaire was completed by the participants in the treatment groups at TImm, T14, and T28 to evaluate their opinions on the tested products. The 18-item questionnaire was focused on each patient’s perception of the efficacy and sensory properties of the products. The questionnaire was administered to the patients in groups 1, 2, 3, and 4 at TImm, T14, and the final visit (T28). Each item was rated by patients on a 4-point scale, ranging from 1 (very unsatisfied) to 4 (very satisfied). Scores 3 and 4 were considered positive responses.
Screening/patient informationa
Eligibility criteria
Informed consent form
Age/sex
Simplified Oral Hygiene Index (OHI-S)
Self-assessment questionnaire on oral habits X
Oral health assessmentc
Caries, tartar, and gingival recession
Gingival lesions or irritation
Ulcers or lesions of the oral mucosa
Study outcomes
Dental plaqued
Gingival sensitivityd
Tooth colord
Oral microbiotae
Product assessment questionnaired
Diaryf Continuous
Abbreviations: TS , screening visit; T0 , immediately before first use of the designated product (baseline); TImm , immediately after first use of the designated product; T14 , after 14 days of product use; T28 , after 28 days of product use.
aThe screening assessments were performed in groups 1 through 5.
bThe inclusion criteria were reverified.
cThe oral health assessments were performed in groups 1 through 5.
dThese assessments were performed in groups 1, 2, 3, and 4.
eThe analyses of oral microbiota at T0 and T28 were performed in groups 1 through 5.
f Patients used the diary throughout the study to record product applications, study deviations, and adverse events.
The participants were also provided with a diary in which they recorded product applications, study deviations, and adverse events. Participants were instructed to discontinue use of the products and contact the investigator immediately if undesirable side effects or discomfort occurred.
The study schedule is shown in Table 1.
Study outcomes
The study outcomes were gingival sensitivity, dental plaque reduction, monthly recruitment rate, oral microbiota analysis, patient satisfaction with the tested products, tolerability, and tooth color. Adverse events were described by the participants in their diaries.
Statistical analysis
It was planned to include a minimum of 12 participants per group. Given the descriptive nature of this pilot study, neither a formal estimate of the sample size nor intergroup comparisons were planned. The exception was a comparison of the product
assessment responses of patients in groups 1 and 2 to analyze their reactions to different product flavors. The data were analyzed and interpreted using both descriptive and inferential statistical procedures. Statistical analysis was performed using NCSS 10 statistical software (2015).
Intragroup variations in gingival sensitivity and dental plaque were analyzed using nonparametric Wilcoxon signed rank test. Differences between the questionnaire responses of groups 1 and 2 were analyzed with the chisquare test. Statistical significance was set at P < 0.05. For the clinical evaluations, a positive effect of the product on the evaluated parameter was confirmed if more than 50% of the participants registered an improvement. The sensation of effective cleaning and the agreeability of the products were considered positive if perceived in this way by at least 60% of the participants. Regarding analysis of the oral microbiota, the Shannon index and statistics were calculated using MicrobiomeAnalyst software (Xia Lab, https:// www.microbiomeanalyst.ca).
Table 1. Study schedule.
Characteristic Data
Sex Female: n = 64; male: n = 20
Age Mean (SD): 44.04 (15.56) y
Range: 18-64 y
Oral hygiene habits
OHI-S score ≥ 2: n = 84
Inadequate oral hygiene habits (score ≥ 4)a: n = 84
Frequent use of sugar and processed foodsa: n = 84
Smoking
Pharmaceutical use
Oral mucosal lesions in the last 12 mob
≥ 5 cigarettes/day: n = 0
< 5 cigarettes/day: n = 84
Antibiotic treatment in last 7 days: n = 0
Frequent supplementation with probiotics: n = 0
Use of drugs potentially disrupting oral microbiome in the last 30 days (ie, proton pump inhibitors, metformin): n = 0
bTissue injury, ulcers, aphthous stomatitis, or infection.
Results
Patient demographics and baseline characteristics
A total of 84 patients, 20 men and 64 women, aged between 18 and 64 years, participated in this study. All of the participants completed the study in its entirety. The characteristics of the enrolled patients at baseline are reported in Table 2.
Monthly recruitment rate
Participants were recruited from May 17, 2022, to June 28, 2022; the date of the final visit of the last patient was on July 26, 2022. Therefore, the enrollment rate was 14 patients per week, a result obtained in a standard practice without any advertising. This value was consistent with the monthly site recruitment rate planned for the future main randomized controlled trial (between 40 and 45 patients per month per site) and indicates that the proposed study is feasible.
Dental plaque
Each treatment group showed a statistically significant decrease in dental plaque at TImm (Chart 1).
Gingival sensitivity
The use of the products resulted in a statistically significant decrease in the visual analog scale score for gingival sensitivity at
Chart 1. Total mean plaque scores of the treatment groups at T0 and TImm
Abbreviations: T0 , immediately before first use of the designated product (baseline); TImm , immediately after first use of the designated product.
Groups: 1, delicate mint toothpaste; 2, mint toothpaste; 3, mint mouthwash; 4, delicate mint toothpaste, mint mouthwash, and antimicrobial toothbrush.
Plaque scores: 0 to 3, excellent; 4 to 7, good; 8 to 11, fairly good; 12 to 18, poor.32
aStatistically significant difference between T0 and TImm (P ≤ 0.000; nonparametric Wilcoxon signed rank test).
bStatistically significant difference between T0 and TImm (P ≤ 0.002; nonparametric Wilcoxon signed rank test)
both T14 and T28 compared to baseline in each treatment group (Table 3). The study protocol did not include any comparisons between groups, but group 4 reported the greatest reduction in gingival sensitivity (P ≤ 0.000; Wilcoxon signed rank test).
Tooth color
The tested products did not show an effect on tooth color after 28 days of use compared to baseline.
Oral microbiota
Six phyla, 12 classes, 15 orders, 23 families, and 37 genera were detected in the oral microbiota of 60 participants across the 5 groups. Bacillota (formerly Firmicutes), Actinomycetota (formerly Actinobacteria), Candidatus Saccharibacteria, Pseudomonadota (formerly Proteobacteria), and Fusobacteriota accounted for over 80% of all phyla present in the oral microbiota. Bacillota exhibited the highest relative abundance over time. The abundance profiles of the 10 most represented genera confirmed the trends observed for the phyla (Chart 2). Genera belonging to the phylum Bacillota (Streptococcus, Gemella, Granulicatella, Veillonella, Abiotrophia) were the most abundant, followed by genera in the phyla Actinomycetota (Actinomyces and Rothia), Pseudomonadota (Haemophilus), Candidatus Saccharibacteria (genera incertae sedis), and Fusobacteriota (Fusobacterium). Analysis of the Shannon Index indicated a significant variation in alpha diversity for the control patients (group 5, P < 0.01)
Table 2. Patient characteristics at baseline (T0)
Group !
3 (n = 20)
4 (n = 20)
Abbreviations: T0 , immediately before first use of the designated product (baseline); T14 , after 14 days of product use; T28 , after 28 days of product use.
Groups: 1, delicate mint toothpaste; 2, mint toothpaste; 3, mint mouthwash; 4, delicate mint toothpaste, mint mouthwash, and antimicrobial toothbrush.
a Gingival sensitivity scored by patients on a visual analog scale where 0 indicated no sensitivity and 10 indicated the highest sensitivity.
bSignificantly different from T0 (P ≤ 0.05; nonparametric Wilcoxon signed rank test).
!Streptococcus
!Gemella
!Granulicatella !Veillonella !Abiotrophia
!Other Bacillota
!Actinomyces !Rothia
!Other Actinomycetota !Haemophilus
!Other Pseudomonadota
!Candidatus Saccharibacteria genera incertae sedis
Abbreviations: T0 , immediately before first use of the designated product (baseline); T28 , after 28 days of product use.
Color groups according to phylum: greens, Bacillota; blues, Actinomycetota; yellows, Candidatus Saccharibacteria; reds, Pseudomonadota; oranges, Fusobacteriota; purples, Bacteroidota.
(Chart 3). However, all treatment groups were statistically stable over time (group 1, P < 0.44; group 2, P < 0.44; group 3, P < 0.62; group 4, P < 0.58).
Analysis of the beta diversity revealed that the composition of the oral microbiota in the treatment groups was similar before and after product use. Small variations over time were observed in groups 1 and 2, and almost none were observed in groups 3 and 4. In contrast, significant differences in terms of taxa richness, abundance, and bacterial composition were detected from T0 to T28 in group 5 (Table 4).
Product assessment
Globally, participants in all treatment groups positively evaluated the test items during the product assessment questionnaire. The percentage of positive answers (score 3 or 4) ranged from 70.0% to 100.0% at the different timepoints. Table 5 displays the answers to a selection of questions at T28. Analysis of the responses of groups 1 and 2 showed no statistically significant difference in responses to the traditional mint and delicate mint toothpaste flavors (P > 0.05; chi-square test).
Chart 2. Most abundant genera in the microbiome analysis and corresponding parent phyla.
T28
T0
Table 3. Gingival sensitivity at T0 , T14 , and T28 in the treatment groups. a
Chart 3. Shannon index (alpha diversity) scores of all groups at T0 and T28
5 1 2 3 4 (n
Abbreviations: T0 , immediately before first use of the designated product (baseline); T28 , after 28 days of product use.
Groups: 1, delicate mint toothpaste; 2, mint toothpaste; 3, mint mouthwash; 4, delicate mint toothpaste, mint mouthwash, and antimicrobial toothbrush; 5, continued use of their routine oral hygiene products (control).
The lines within the boxes indicate the median. The Xs within the boxes indicate the mean. The lower and upper bounds of the boxes indicate the first and third quartiles, respectively. The lower and upper whiskers indicate the minimum and maximum values, respectively. The open circles represent the individual values of the analyzed patients (n = 12 per group). The open circles overlap in several cases.
aStatistically significant difference between T0 and T28 (P < 0.01; Wilcoxon signed rank test).
Study diary
The tested products were well tolerated by all participants. No adverse reactions or effects occurred during the study period.
Discussion
This pilot study was planned to avoid starting the future clinical trial with unresolved critical logistic issues or potential bias in the selection of endpoints. The data collected on recruitment capability (14 patients per week per site) and study procedures allowed for a realistic estimation of time and will be used for the budget calculation of the main study. The extremely positive evaluation of the tested products is also a promising factor for the future study; in clinical trials, high patient satisfaction with the tested product is associated with a low dropout rate.
This pilot study showed that the tested products induced a significant reduction in plaque immediately after their first use. The magnitude of this result appears consistent across products. However, without formal comparison to a control group, it cannot be determined how much is attributable to the individual products (delicate mint toothpaste, mint toothpaste, and mint mouthwash) vs the physical action of a toothbrush. This bias will be eliminated in the future large-population clinical trial, which should also allow for identification of the possible adjuvant actions of the products under study.
For alpha diversity, only the control patients (those with inadequate oral hygiene) showed a significant increase in the number of taxa from T0 to T28 . In addition, the trends in beta diversity from T0 to T28 diverged in the treated and control patients; the bacterial composition of the oral microbiota showed a significant difference only in the control group (group 5; P < 0.00), while the microbiota in the patients in groups 1 to 4 appeared very similar before and after treatment. These trends support a possible correlation between proper oral hygiene and stability of the oral microbiota.
The population enrolled in this study had a history of poor oral hygiene but no periodontal disease. The medical literature has demonstrated the beneficial effects of different types of toothpaste and mouthwash on the oral microbiota in patients with periodontal disease or removable partial dentures. 36-39 Chhaliyil et al introduced the concept of “frequent biofilm disruption” to improve oral hygiene; the cleansing protocol proposed included the use of the index finger to clean the teeth, a process known as GIFTS ( g um and tooth rubbing with index f inger, tongue cleaning, and water s wishing), but this protocol proved to be difficult to follow for an adequate period of time.40 An alternative approach may be frequent brushing and thus frequent biofilm disruption using a mildly flavored toothpaste, such as delicate mint toothpaste, combined with frequent rinsing (with mint mouthwash) when brushing is difficult, such as at the workplace or during outdoor activities. This could be a pragmatic and effective strategy even in the long term, given the positive feedback obtained from this study.
The reduction in gingival sensitivity observed during the study visits was consistent with effective plaque removal. The subjective evaluation by the self-assessment questionnaire showed no statistically significant difference for any item between the group of patients using the traditional mint toothpaste and the group using the new delicate mint toothpaste formulation. User acceptance is particularly important because it ensures continuity in oral hygiene practices.
The limitations of this study are related to its descriptive nature, as no formal comparisons were made between products. However, considering that the tested products should act in a preventive rather than a curative way, the results demonstrating efficacy for plaque removal and stabilization of the microbiota are of particular interest. Despite the limitations of the small sample size and the descriptive methods used for analysis, the main value of this study is the finding of no variability between the baseline and final data in the population that was treated with the tested products. This
Table 4. Beta diversity analysis (within-group P values) comparing numbers of taxa at T0 and T28
Group
1 (n = 20)
2 (n = 12)
3 (n = 20)
4 (n = 20)
5 (n = 12)
Abbreviations: T0 , immediately before first use of the designated product (baseline); T28 , after 28 days of product use.
Groups: 1, delicate mint toothpaste; 2, mint toothpaste; 3, mint mouthwash; 4, delicate mint toothpaste, mint mouthwash, and antimicrobial toothbrush; 5, continued use of their routine oral hygiene products (control).
Table 5. Results of the product assessment questionnaire. a
1 (n = 20)b
2 (n = 12)b
3 (n = 20)
4 (n = 20)
Abbreviation: NP, not present in questionnaire (group 4).
Groups: 1, delicate mint toothpaste; 2, mint toothpaste; 3, mint mouthwash; 4, delicate mint toothpaste, mint mouthwash, and antimicrobial toothbrush.
a Percentage of patients reporting a score of 3 (satisfied) or 4 (very satisfied) on these questionnaire items at the final visit (T28).
bThere is no statistically significant difference between groups 1 and 2 for any item (P > 0.05; chi-square test).
suggests that the future final study may show substantial stabilization of the microbiota as a result of these cleaning methods in a population of individuals without pathologic oral conditions.
Conclusion
This study showed that regular oral hygiene with delicate mint toothpaste, mint toothpaste, mint mouthwash, and an antimicrobial toothbrush reduced plaque and stabilized the oral microbiota, thereby promoting symbiosis and helping to prevent clinical inflammatory conditions. It is reasonable to hypothesize that these results are related to the specific formulations of the tested products and are in line with previous literature reports on prebiotics, which are the defining elements of the tested product line. The authors believe that
a pragmatic clinical trial in a real-world setting can be successfully planned to compare these products to alternative hygiene strategies and other products for the prevention of diseases in the oral mucosa. An adequate sample size larger than the population enrolled in this study would be needed.
Author affiliations
Department of Clinical Research, Oral and Maxillofacial Surgery, Victor Babeş University of Medicine and Pharmacy of Timişoara, Timișoara, Romania (Rosu); Corporate Research & Development, Alfasigma, Rome, Italy (Benatti); Faculty of Biology, Tor Vergata University of Rome, Rome, Italy (Bianco); Tigermed (formerly Opera CRO Romania), Timișoara, Romania (Barattini); Research & Development, Complife Italia, Italy (Nobile); Laboratory of Genomics
& Transcriptomics, Translational Research Centre for Autoimmune and Allergic Diseases, Department of Health Sciences, University of Eastern Piedmonte, Novara, Italy (Mellai); Private practice, San Genesio ed Uniti, Italy (Cattaneo).
Correspondence
Serban Rosu, Dr Prof, PhD, MD (serbanrosu@gmail.com).
Conflicts of interest
Dionisio Franco Barattini is employed at Tigermed (formerly Opera CRO Romania), the contract research organization that performed data management for the study. Paola Benatti is employed at Alfasigma, owner and distributor of the Tau-Marin products line tested in this study. The other authors report no potential conflicts of interest.
Acknowledgments
The authors extend a special thanks to Diana Koprivec, MD, PhD, for her valuable feedback throughout the project.
Funding
Grant support was received from Biokosmes, Lecco, Italy, and the company also donated the products under study. The funder had no role in the study design; data collection, analysis, or interpretation; or decision to submit the study results for publication.
References
1. Costalonga M, Herzberg MC. The oral microbiome and the immunobiology of periodontal disease and caries. Immunol Lett. 2014;162(2 Pt A):22-38. doi:10.1016/j. imlet.2014.08.017
2. Willis JR, Gabaldón T. The human oral microbiome in health and disease: from sequences to ecosystems. Microorganisms. 2020;8(2):308. doi:10.3390/microorganisms8020308
3. Radaic A, Kapila YL. The oralome and its dysbiosis: new insights into oral microbiome-host interactions. Comput Struct Biotechnol J. 2021;19:1335-1360. doi:10.1016/j. csbj.2021.02.010
4. Sedghi L, DiMassa V, Harrington A, Lynch SV, Kapila YL. The oral microbiome: role of key organisms and complex networks in oral health and disease. Periodontol 2000 2021;87(1):107-131. doi:10.1111/prd.12393
5. Valm AM. The structure of dental plaque microbial communities in the transition from health to dental caries and periodontal disease. J Mol Biol. 2019;431(16):2957-2969. doi:10.1016/ j.jmb.2019.05.016
6. Abdulkareem AA, Al-Taweel FB, Al-Sharqi AJB, Gul SS, Sha A, Chapple ILC. Current concepts in the pathogenesis of periodontitis: from symbiosis to dysbiosis. J Oral Microbiol 2023;15 (1):2197779. doi:10.1080/20002297.2023.2197779
7. Kilian M, Chapple IL, Hannig M, et al. The oral microbiome—an update for oral healthcare professionals. Br Dent J. 2016;221(10):657-666. doi:10.1038/sj.bdj.2016.865
8. Peres MA, Macpherson LMD, Weyant RJ, et al. Oral diseases: a global public health challenge. Lancet. 2019;394(10194):249-260. doi:10.1016/S0140-6736(19)31146-8
9. Carra MC, Detzen L, Kitzmann J, Woelber JP, Ramseier CA, Bouchard P. Promoting behavioural changes to improve oral hygiene in patients with periodontal diseases: a systematic review. J Clin Periodontol. 2020;47(Suppl 22):72-89. doi:10.1111/jcpe.13234
10. Toshniwal SH, Reche A, Bajaj P, Maloo LM. Status quo in mechanical plaque control then and now: a review. Cureus. 2022;14(8):e28613. doi:10.7759/cureus.28613
11. Amarasena N, Gnanamanickam ES, Miller J. Effects of interdental cleaning devices in preventing dental caries and periodontal diseases: a scoping review. Aust Dent J 2019;64(4):327-337. doi:10.1111/adj.12722
12. Zhang X, Hu Z, Zhu X, Li W, Chen J. Treating periodontitis—a systematic review and metaanalysis comparing ultrasonic and manual subgingival scaling at different probing pocket depths. BMC Oral Health. 2020;20(1):176. doi:10.1186/s12903-020-01117-3
13. Sälzer S, Graetz C, Dörfer CE, Slot DE, Van der Weijden FA. Contemporary practices for mechanical oral hygiene to prevent periodontal disease. Periodontol 2000. 2020;84(1): 35-44. doi:10.1111/prd.12332
14. Fatima F, Taha Mahmood H, Fida M, Hoshang Sukhia R. Effectiveness of antimicrobial gels on gingivitis during fixed orthodontic treatment: a systematic review and meta-analysis. Int Orthod. 2020;18(1):10-21. doi:10.1016/j.ortho.2019.10.002
15. Zhang J, Ab Malik N, McGrath C, Lam O. The effect of antiseptic oral sprays on dental plaque and gingival inflammation: a systematic review and meta-analysis. Int J Dent Hyg 2019;17(1):16-26. doi:10.1111/idh.12331
16. Rajendiran M, Trivedi HM, Chen D, Gajendrareddy P, Chen L. Recent development of active ingredients in mouthwashes and toothpastes for periodontal diseases. Molecules 2021;26(7):2001. doi:10.3390/molecules26072001
17. Aspinall SR, Parker JK, Khutoryanskiy VV. Oral care product formulations, properties and challenges. Colloids Surf B Biointerfaces. 2021;200:111567. doi:10.1016/j.colsurfb.2021. 111567
18. Patel RM, Denning PW. Therapeutic use of prebiotics, probiotics, and postbiotics to prevent necrotizing enterocolitis: what is the current evidence? Clin Perinatol. 2013;40(1):11-25. doi:10.1016/j.clp.2012.12.002
19. Sivamaruthi BS, Kesika P, Chaiyasut C. A review of the role of probiotic supplementation in dental caries. Probiotics Antimicrob Proteins. 2020;12(4):1300-1309. doi:10.1007/ s12602-020-09652-9
20. Gheisary Z, Mahmood R, Harri Shivanantham A, et al. The clinical, microbiological, and immunological effects of probiotic supplementation on prevention and treatment of periodontal diseases: a systematic review and meta-analysis. Nutrients. 2022;14(5):1036. doi:10.3390/nu14051036
21. Kistler J PM, Goetz M, Wade W. The effect of probiotic treatments on the composition of in-vitro oral biofilms. Paper presented at: IADR/AADR/CADR General Session; March 25, 2017; San Francisco.
22. Schmitter T, Fiebich BL, Fischer JT, et al. Ex vivo anti-inflammatory effects of probiotics for periodontal health. J Oral Microbiol. 2018;10(1):1502027. doi:10.1080/20002297.2018. 1502027
23. Volgenant CMC, van der Waal SV, Brandt BW, et al. The evaluation of the effects of two probiotic strains on the oral ecosystem: a randomized clinical trial. Front Oral Health 2022;3:825017. doi:10.3389/froh.2022.825017
25. Symrise launches SymReboot OC, its first processed probiotic dedicated to oral care. News release. August 7, 2021. Accessed April 29, 2024. https://www.symrise.com/newsroom/ article/symrise-launches-symrebootTM-oc-its-first-processed-probiotic-dedicated-to-oralcare/
26. Talapko J, Matijević T, Juzbašic M, Antolović-Požgain A, Škrlec I. Antibacterial activity of silver and its application in dentistry, cardiology and dermatology. Microorganisms 2020;8(9):1400. doi:10.3390/microorganisms8091400
28. Siciliano RA, Reale A, Mazzeo MF, Morandi S, Silvetti T, Brasca M. Paraprobiotics: a new perspective for functional foods and nutraceuticals. Nutrients. 2021;13(4):1225. doi: 10.3390/nu13041225
29. De Benedetto A, Qualia CM, Baroody FM, Beck LA. Filaggrin expression in oral, nasal, and esophageal mucosa. J Invest Dermatol. 2008;128(6):1594-1597. doi:10.1038/ sj.jid.5701208
30. Martyniak A, Medyńska-Przęczek A, Wędrychowicz A, Skoczeń S, Tomasik PJ. Prebiotics, probiotics, synbiotics, paraprobiotics and postbiotic compounds in IBD. Biomolecules 2021;11(12):1903. doi:10.3390/biom11121903
31. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191-2194. doi:10.1001/jama.2013.281053
32. Eldridge SM, Chan CL, Campbell MJ, et al. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. Pilot Feasibility Stud. 2016;2:64. doi:10.1186/ s40814-016-0105-8
33. Greene JC, Vermillion JR. The Simplified Oral Hygiene Index. J Am Dent Assoc. 1964;68:713. doi:10.14219/jada.archive.1964.0034
34. DeClercq V, Nearing JT, Langille MGI. Investigation of the impact of commonly used medications on the oral microbiome of individuals living without major chronic conditions. PLoS One. 2021;16(12):e0261032. doi:10.1371/journal.pone.0261032
35. Lahti L, Borman T, Ernst FGM, et al. Orchestrating Microbiome Analysis with Bioconductor [beta version] 2021. Accessed April 29, 2024. https://microbiome.github.io/OMA/docs/ devel/
36. Silin AV, Satygo EA, Reutskaya KV. Effectiveness of Paradontax toothpaste in patients undergoing orthodontic treatment. Article in Russian. Stomatologiia (Mosk) 2017;96(4):20-22. doi:10.17116/stomat201796420-22
37. Prêcheur I, Rolland Y, Hasseine L, Orange F, Morisot A, Landreau A. Solidago virgaurea L. plant extract targeted against Candida albicans to reduce oral microbial biomass: a double blind randomized trial on healthy adults. Antibiotics (Basel). 2020;9(4):137. doi:10.3390/ antibiotics9040137
38. Saeed MA, Khabeer A, Faridi MA, Makhdoom G. Effectiveness of propolis in maintaining oral health: a scoping review. Can J Dent Hyg. 2021;55(3):167-176.
39. Wiatrak K, Morawiec T, Rój R, et al. Evaluation of effectiveness of a toothpaste containing tea tree oil and ethanolic extract of propolis on the improvement of oral health in patients using removable partial dentures. Molecules. 2021;26(13):4071. doi:10.3390/molecules26134071
40. Chhaliyil P, Fischer KF, Schoel B, Chhalliyil P. A novel, simple, frequent oral cleaning method reduces damaging bacteria in the dental microbiota. J Int Soc Prev Community Dent 2020;10(4):511-519. doi:10.4103/jispcd.JISPCD_31_20.
EARN CE AT YOUR CONVENIENCE WITH SELF-INSTRUCTION
Now is the time to take advantage of AGD’s Self-Instruction program that includes exercises based on AGD Impact articles. These exercises contain 10 questions and are worth 1 CE credit. It’s the perfect complement to General Dentistry
AGD Impact
1 exercise = $15
2 exercises = $25 (save $5)
4 exercises = $50 (save $10)
General Dentistry
1 exercise = $30
3 exercises = $70 (save $20)
6 exercises = $120 (save $60)
12 exercises = $180 (save $180)
LEARN MORE
agd.org/self-instruction
ChatGPT and dentistry: a step toward the future
Lucas Lacerda de Souza, DDS, MSc ¢ Helder Antônio Rebelo Pontes, DDS, PhD
This article aims to explore the integration of ChatGPT, an advanced conversational artificial intelligence model, in the field of dentistry. The review primarily consists of information related to the capabilities and functionalities of ChatGPT and how these abilities can aid dental professionals. This study includes data from research papers, case studies, and relevant literature on language models, as well as papers on dentistry, patient communication, dental education, and clinical decision-making. A systematic approach was used to select relevant studies and literature. The selection criteria focused on papers that specifically discussed the integration of language models, ChatGPT in particular, in dentistry and their applications. The study findings revealed that ChatGPT has significant potential to revolutionize dentistry by offering various applications and benefits. It can enhance patient engagement and understanding through personalized oral health information and guidance. In dental education, ChatGPT can provide interactive learning, case studies, and virtual patient simulations. ChatGPT can also assist researchers in analyzing dental literature, identifying patterns, and generating insights. Moreover, it supports dentists with evidence-based recommendations, treatment options, and diagnostic support. Integrating ChatGPT in dentistry can be highly beneficial, but it is crucial to address ethical considerations, accuracy, and privacy concerns. Responsible implementation and continuous improvement of its functionalities are necessary to ensure that patient care and outcomes are improved.
Received: August 7, 2023
Accepted: November 29, 2023
Keywords: artificial intelligence, ChatGPT, dentistry, large language model, robotics
Large language models are advanced artificial intelligence (AI) systems that process and generate humanlike text.1 Built using deep learning techniques and trained on vast amounts of text data, these models can understand and generate coherent and contextually relevant text across various topics and writing styles.1,2 They excel at language-related tasks such as translation, answering questions, summarization, and creative writing. The training process for these models involves exposing them to extensive text data from diverse sources, enabling them to learn grammar, semantics, and facts.3 Once trained, the models can be finetuned for specific applications, adapting their language generation capabilities accordingly.1,3
ChatGPT is an advanced conversational AI model developed by OpenAI. It is built on generative pre-trained transformer (GPT) architecture and is designed to engage in interactive and dynamic conversations with users.4 ChatGPT leverages a vast amount of training data to generate humanlike responses and provide helpful information across a wide range of topics. This language model is capable of understanding and generating coherent and contextually relevant text, which allows it to handle various conversational tasks. 5,6 It can provide answers to questions, engage in natural dialogue, offer suggestions, and even simulate different personalities and writing styles. 5
ChatGPT has significant potential in dentistry because it can assist with patient communication, dental education, research, and clinical decision-making.7-9 ChatGPT generates informative materials for patients and can thus improve understanding and compliance. This model can also aid in creating interactive learning resources, case studies, and virtual patient simulations for dental education.7,8 It analyzes extensive dental literature, helping researchers identify trends and advances, and provides up-todate information for accurate diagnosis and treatment planning.
ChatGPT has the potential to revolutionize the way dental treatment is delivered, improving efficiency, accuracy, and patient outcomes.5,7-9 However, ethical considerations and ongoing research are important considerations when ChatGPT is integrated into the field of dentistry. The aim of the current article is to give an overview about the functionalities of ChatGPT as related to dental practice, education, and research.
Methods Search strategy
To assess the integration of ChatGPT in dental practices, a detailed literature search was conducted using the PubMed, Scopus, Web of Science, and Google Scholar databases. The
search included terms such as “ChatGPT,” “artificial intelligence,” “dentistry,” “dental practice,” “patient communication,” “diagnostic support,” and “treatment planning.” These keywords were combined with Boolean operators to ensure comprehensive coverage and retrieval of relevant studies.
Inclusion criteria
The inclusion criteria were peer-reviewed articles published in English; studies focusing on the use of ChatGPT or conversational AI in dental contexts; and articles published from January 2015 through December 2023, capturing recent developments in AI within dentistry.
Exclusion criteria
Articles were excluded from the review if they were not written in English; were non–peer-reviewed documents, including editorials, commentaries, and conference abstracts; or reported on studies that did not focus on ChatGPT or its applications in dentistry.
Article selection process
The search initially identified 421 articles. Following a screening of titles and abstracts for relevance based on the defined inclusion and exclusion criteria, 280 articles were excluded for not meeting the criteria. The remaining 141 full-text articles were thoroughly reviewed by one reviewer. Of these, 108 articles were excluded for reasons such as not focusing on evolution of large language models and ChatGPT specifically or lacking empirical data. This left 33 articles for inclusion in the review.
Data extraction and synthesis
Data from the included studies were extracted, which included author information, publication year, study design, sample size, type of AI technology employed, specific dental specialties involved, key findings, and conclusions. This extracted information was organized into a structured format to facilitate a comprehensive synthesis and to elucidate the implications and potential of ChatGPT in enhancing dental practice efficiency and patient care.
History of large language models
The history of large language models can be traced back to the early development of natural language processing and AI.1 While the concept of language models has been studied for decades, the emergence of deep learning techniques and the availability of vast amounts of text data revolutionized the field and led to the creation of large-scale language models.10 This process began in 1950, when Alan Turing laid the foundation for AI with his groundbreaking work in computational machines and intelligent behavior.11 The 1960s saw the emergence of early examples of conversational agents, ELIZA and PARRY, showcasing the potential for human-like interaction through natural language processing.12 The 1970s and 1980s marked an “AI winter,” a downturn in AI research due to limited progress and unmet expectations that in turn led to reduced funding and interest in the field.13 In 1997, IBM’s Deep Blue made history by defeating world chess champion Garry Kasparov, highlighting the power of AI in complex strategy games.14
The year 2011 witnessed significant advancements with the introduction of Apple’s Siri, a virtual assistant that brought AI-powered voice recognition and natural language understanding to mobile devices.15 In the same year, IBM’s Watson made headlines by winning the Jeopardy! quiz show, showcasing the ability of AI systems to understand and process human language and knowledge.16 In 2013, the Word2vec model revolutionized word embeddings and distributed representations, enabling AI systems to capture semantic relationships and meaning in language.17 Amazon’s Alexa then made its debut in 2014, bringing AI-powered voice assistants to homes and introducing a new era of voice-controlled smart devices.15 Microsoft’s Tay, introduced in 2016, aimed to showcase the potential of AI in social media interactions but faced controversy when the system learned and reproduced inappropriate content from users.18 That same year, AlphaGo, developed by DeepMind, defeated world champion Go player Lee Sedol, marking a significant milestone in AI’s ability to master complex games with intuitive strategy.19
In 2018, OpenAI released GPT-1, a large-scale language model that demonstrated the power of pre-training for language understanding and generation. OpenAI unveiled GPT-2, a significantly larger language model, in 2019, which pushed the boundaries of language generation and captured widespread attention for its potential impacts and ethical considerations.20 The year 2020 witnessed the release of GPT-3, a groundbreaking language model with 175 billion parameters showcasing remarkable capabilities in language comprehension and generation across diverse tasks and domains.20 OpenAI introduced the GPT-3 API (application programming interface) in 2021, providing developers with access so they could integrate the model into their applications and services, expanding its practical applications across industries.21 GPT-4 was implemented in 2022 and showed significant advancements in diverse categories of specialties.22 The development of AI and language models demonstrates the continuous progress and transformative impact of AI technology.
ChatGPT and dental practice
ChatGPT can serve as a valuable tool for dental professionals due to its vast knowledge base and natural language-processing capabilities. It can assist dentists by answering patient questions, providing information on various dental procedures, explaining oral health recommendations, and even offering personalized treatment suggestions based on patient symptoms or conditions.7-9 Moreover, ChatGPT can contribute to patient education, helping patients understand dental terminology, preventive measures, and posttreatment care instructions. Dentists can use ChatGPT to enhance patient interactions, improve access to accurate dental information, and ultimately deliver better oral healthcare services.8,9 However, considerations relating to ethical concerns, accuracy, and privacy must also be considered to ensure optimal clinical decision-making and patient outcomes.8,9
Dental professionals
ChatGPT can serve as a valuable tool for dental professionals to augment their practice and improve patient care. Dental
professionals can utilize ChatGPT as an on-demand knowledge resource, accessing information on dental procedures, treatment options, and oral health conditions.8,23 However, it is important for dental professionals to exercise caution and remember that ChatGPT is an AI model, not a substitute for professional judgment or individual patient assessment.24 While ChatGPT can provide general information, it is crucial for dental professionals to validate and contextualize the information it provides by cross-referencing against reliable sources and considering the specific needs and circumstances of each patient.8 Dental professionals should also be aware of the limitations of AI technology and ensure that the information obtained from ChatGPT is used as a complement to their own expertise rather than rely solely on its suggestions. By utilizing ChatGPT responsibly and integrating it into their practice with appropriate care, dental professionals can harness its potential to enhance patient education, treatment planning, and overall dental care outcomes.24
Dental telemedicine
Dental telemedicine can also leverage the power of ChatGPT to enhance remote patient consultations and improve access to oral healthcare. Dental professionals can use ChatGPT as an aid to communicate with patients virtually, address their concerns, provide guidance, and answer their dental-related questions.8,24 ChatGPT can assist in triaging patients by evaluating their symptoms or conditions and offer initial recommendations for self-care or further evaluation. However, it is essential for dental telemedicine practitioners to exercise caution and consider the limitations of AI.24 Dental telemedicine providers must establish clear communication channels with patients to ensure they understand the limitations of the technology and that they are guided appropriately. By utilizing ChatGPT responsibly and in conjunction with best practices in telemedicine, dental professionals can leverage its capabilities to enhance remote patient care and improve oral health outcomes.25
Clinical decision-making
Dental clinical decision-making can be augmented by integrating ChatGPT into the process, providing dental professionals with a valuable tool to support their expertise. ChatGPT can assist in the evaluation of patient symptoms, suggest potential diagnoses or treatment options, and offer insights into evidence-based guidelines and research findings.9,26 However, as with its other uses, it is crucial for dental professionals to exercise caution and maintain critical thinking when using AI for these purposes. While ChatGPT can provide helpful suggestions, it should not replace a thorough clinical examination, patient history review, or professional judgment.26 Dental professionals must validate the information provided by ChatGPT, cross-referencing it against reliable sources and considering the unique characteristics and circumstances of each patient. They should be aware of the limitations of AI technology and use ChatGPT as an aid, not a substitute, in the decision-making process.8,26 It is essential to ensure that final clinical decisions are based on a comprehensive assessment, taking into account patient preferences, individual factors, and the most up-to-date clinical evidence.8
By utilizing ChatGPT as a complementary tool and incorporating it into the decision-making process with care and critical thinking, dental professionals can enhance their clinical practice and provide optimal care for their patients.24
Patient support
ChatGPT can be a valuable resource for patient support in the field of dentistry, providing accessible and reliable information to empower individuals in managing their oral health. Patients can utilize ChatGPT to seek guidance on common dental concerns, oral hygiene practices, or posttreatment care instructions.8 ChatGPT can also serve as a virtual assistant, addressing patient questions and offering educational materials to promote oral health literacy.
However, it is important for patients to be aware that ChatGPT is an AI-based tool and should not replace direct communication with dental professionals. Patients should exercise caution and understand that the information provided by ChatGPT is general in nature and may not account for their unique medical history or specific circumstances.8,25,27 It is crucial to directly contact dental professionals for personalized advice and treatment recommendations. For their part, dental professionals should guide patients in the appropriate use of ChatGPT, ensuring they understand its limitations and encouraging them to seek professional care for individualized assessment and treatment.25,27 By utilizing ChatGPT as a supplement to professional guidance and engaging in open communication with dental professionals, patients can enhance their oral health knowledge and make informed decisions about their dental care.25
Patient privacy
Patient privacy is a critical consideration when ChatGPT or any other AI-powered tool is used in healthcare, including dentistry. Dental professionals and organizations must prioritize safeguarding patient information and adhering to privacy regulations and ethical guidelines.25,27 When ChatGPT is used, it is essential to ensure that patient data are protected, encrypted, and securely transmitted. Dental professionals should use secure communication channels and platforms that comply with privacy standards to exchange patient information.28 It is important to be cautious about sharing personally identifiable information during interactions with ChatGPT because the AI model may not have the same level of confidentiality as a human professional.8,28 Patients should also be aware of the potential risks and exercise discretion when sharing personal health information. Dental professionals and organizations should thoroughly vet their chosen technology providers to ensure that these entities follow mandated data privacy practices and have adequate security measures in place.28 By prioritizing patient privacy, implementing robust security measures, and adhering to applicable privacy regulations, dental professionals can ensure the safe and responsible use of ChatGPT while protecting patient confidentiality.27,28
Ethical challenges
The use of ChatGPT in dentistry brings with it important ethical considerations and challenges. One key aspect is the
responsibility of ensuring that ChatGPT operates ethically and avoids bias in its responses.28,29 Developers and dental professionals should be vigilant in monitoring and addressing any potential biases or inaccuracies in the information provided by ChatGPT.28 Additionally, transparency is crucial. Patients interacting with ChatGPT should be made aware they are engaging with an AI model and not a human professional. Informed consent should be obtained, and patients should be informed about the limitations and potential risks of relying solely on AI-generated information.28,30 Patient autonomy and privacy must be respected with a clear understanding of how patient data are handled and protected. Dental professionals need to exercise caution in using ChatGPT as a supplemental tool, not relying solely on its suggestions and ensuring that their own professional judgment and expertise remain central to decision-making.30 By addressing these ethical challenges, promoting transparency, and maintaining patient-centered care, dental professionals can navigate the use of ChatGPT in a responsible and ethically sound manner.25,30
Dental education
ChatGPT can play a valuable role in dental education and could prove to be an innovative tool for students, educators, and dental professionals to enhance their learning experience. It can provide a platform for interactive and dynamic learning, where students can ask questions and receive immediate responses.31 ChatGPT can serve as a virtual mentor, offering explanations of complex dental concepts, assisting in case discussions, and providing access to a vast repository of dental knowledge. However, it is important to approach ChatGPT as a supplementary resource and not a replacement for comprehensive dental education.32
As the model has disadvantages as well as advantages, dental educators should guide students in utilizing ChatGPT responsibly, emphasizing critical thinking and validation of the information provided (Box). Students must understand the limitations of AI and recognize that professional judgment and human interaction are indispensable in dental education and practice.31,32 By integrating ChatGPT into dental education curricula with caution, educators can harness its potential to engage students, foster curiosity, and facilitate deeper understanding of dental concepts, ultimately preparing them for successful careers in dentistry.31
Scientific writing
ChatGPT can be a valuable aid in scientific writing, supporting researchers and scholars in various aspects of the writing process. It can assist in generating ideas, offering suggestions for structuring research articles, and providing access to relevant scientific literature.9,23 ChatGPT can also help researchers find appropriate terminology, improve sentence structure, and enhance the overall clarity of their scientific manuscripts.23 However, it is important to exercise caution and critically evaluate the suggestions provided by ChatGPT. While it can offer valuable insights, it should not replace the researcher’s own expertise or peer review. Researchers must ensure the accuracy and validity of the information obtained from ChatGPT by cross-referencing against reliable sources and conducting
Box. Advantages and disadvantages of ChatGPT in dental education.
Advantages
• Enhanced learning experience
• Access to information
• Around-the-clock availability
• Standardized information
• Practice-based scenarios
• Reinforcement of concepts
• Personalized assessment
• Proficiency development
• Learning support
• Evidence-based practice
Disadvantages
• Lack of clinical experience
• Limited ability to perform examinations.
• Possibility of misleading information
• Inability to adapt to learning
• Lack of real-time feedback
• Ethical concerns and bias
• Absence of emotions
• Technical limitations
• Incomplete understanding
• Reduced interpersonal skills thorough literature reviews.3,32 Additionally, proper citation and acknowledgment of sources are essential when incorporating information from ChatGPT into scientific writing. By using ChatGPT as a complementary tool, researchers can streamline the writing process and improve the quality of their scientific manuscripts while maintaining academic integrity.3,30
Research
ChatGPT can be a valuable asset for researchers as an additional tool to aid in various stages of the research process. It can assist in literature reviews by quickly summarizing and identifying relevant studies based on specified keywords or topics and help researchers generate hypotheses, explore different research methodologies, and offer insights into potential data analysis techniques.9,23 However, it is crucial for researchers to exercise caution and critically evaluate the information provided by ChatGPT.23,32 While ChatGPT can offer valuable suggestions and guidance, researchers must independently verify and validate the information obtained, ensuring its accuracy and reliability. Additionally, researchers need to be aware of any biases or limitations that may exist within the underlying training data of ChatGPT and carefully consider the ethical implications of using AI-generated content in research.3,30,32 By incorporating ChatGPT as a supportive tool alongside rigorous research practices and peer review, researchers can enhance the efficiency of their work, explore new perspectives, and contribute to the advancement of knowledge in their respective fields.30 Areas of dental research
where using the information provided by ChatGPT could be helpful include geographic data, evidence-based medicine, electronic health records, radiologic aspects, and clinical, microscopic, and molecular analysis.
Limitations
ChatGPT can process information rapidly and support healthcare professionals by offering an objective and evidence-based approach to clinical decision-making, reducing the likelihood of human errors. Nonetheless, it is important to acknowledge that ChatGPT has potential drawbacks in addition to its strengths. It may generate inaccurate content or pose risks such as bias, prejudice, and privacy concerns, which need to be taken seriously.28-30 ChatGPT has even been found to fabricate literature references, including falsified PubMed ID numbers, making suspect content look more legitimate.1,6 Careful consideration of these limitations is necessary when ChatGPT and other AI technologies are integrated into healthcare workflows, and it is advisable to involve human professionals in the process to monitor and verify the output, minimizing the risk of errors.23,30,33 In the context of dental education, it is crucial to ensure high accuracy to prevent potential harm to patient safety. Students with limited knowledge may struggle to identify incorrect information provided by ChatGPT, so clear guidelines and verification procedures should be established and tested.31,32 Additionally, measures such as plagiarism detection technologies can help address concerns of overreliance on AI-generated content.
Conclusion
AI has made significant progress in dental practice, and ChatGPT has the potential to revolutionize the dental and healthcare systems by offering services such as treatment planning and monitoring of oral health. However, it is crucial to proceed with caution and to establish policies that mitigate potential risks. Furthermore, consistent monitoring of this chatbot is advisable, particularly in research settings, to address ethical concerns and ensure the accuracy of the information and referencing generated during use.
Author affiliations
Department of Oral Diagnosis, Piracicaba Dental School, University of Campinas, Piracicaba, Brazil (de Souza, Pontes, Martins, Fonseca, Corrêa, Santos-Silva, Vargas, Lopes); Department of Oral Pathology, University Hospital João de Barros Barreto, Belém, Brazil (Pontes); Department of Oral Pathology, School of Dentistry, Federal University of Rio Grande do Sul, Porto Alegre, Brazil (Martins); Department of Oral Surgery and Pathology, School of Dentistry, Federal University of Minas Gerais, Belo Horizonte, Brazil (Fonseca); Department of Pathology, Faculty of Medical Sciences, State University of Campinas, Campinas, Brazil (Corrêa); Department of Pathology, Barretos Cancer Hospital, Barretos, Brazil (Coracin); Unit of Oral and Maxillofacial Pathology, School of Clinical Dentistry, University of Sheffield, Sheffield, England (Khurram); Scientific Computing Department, Faculty of Computers and Artificial Intelligence, Benha University, Benha, Egypt (Hagag).
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES), Finance Code 001; São Paulo State Research Foundation (FAPESP 22/03123-5); and Minas Gerais State Research Foundation (FAPEMIG).
References
1. Shen Y, Heacock L, Elias J, et al. ChatGPT and other large language models are doubleedged swords. Radiology. 2023;307(2):e230163. doi:10.1148/radiol.230163
2. De Angelis L, Baglivo F, Arzilli G, et al. ChatGPT and the rise of large language models: the new AI-driven infodemic threat in public health. Front Public Health. 2023;11:1166120. doi:10.3389/fpubh.2023.1166120
3. Kim YG, Schatschneider C. Expanding the developmental models of writing: a direct and indirect effects model of developmental writing (DIEW). J Educ Psychol. 2017;109(1):3550. doi:10.1037/edu0000129
4. Gao CA, Howard FM, Markov, NS, et al. Comparing scientific abstracts generated by ChatGPT to real abstracts with detectors and blinded human reviewers. NPJ Digit Med 2023;6(1):75. doi:10.1038/s41746-023-00819-6
5. Biswas S. ChatGPT and the future of medical writing. Radiology. 2023;307(2):e223312. doi:10.1148/radiol.223312
6. Alkaissi H, McFarlane SI. Artificial hallucinations in ChatGPT: implications in scientific writing. Cureus. 2023;15(2):e35179. doi:10.7759/cureus.35179
7. Eggmann F, Blatz MB. ChatGPT: chances and challenges for dentistry. Compend Contin Educ Dent. 2023;44(4):220-224.
8. Eggmann F, Weiger R, Zitzmann NU, Blatz MB. Implications of large language models such as ChatGPT for dental medicine. J Esthet Restor Dent. 2023;35(7):1098-1102. doi:10.1111/jerd.13046
9. Cascella M, Montomoli J, Bellini V, Bignami E. Evaluating the feasibility of ChatGPT in healthcare: an analysis of multiple clinical and research scenarios. J Med Syst. 2023;47(1):33. doi:10.1007/s10916-023-01925-4
10. de Souza LL, Fonseca FP, Araújo ALD, et al. Machine learning for detection and classification of oral potentially malignant disorders: a conceptual review. J Oral Pathol Med. 2023;52(3):197-205. doi:10.1111/jop.13414
11. Mintz Y, Brodie R. Introduction to artificial intelligence in medicine. Minim Invasive Ther Allied Technol. 2019;28(2):73-81. doi:10.1080/13645706.2019.1575882
12. Shum HY, He XD, Li D. From Eliza to XiaoIce: challenges and opportunities with social chatbots. Front Inform Technol Electron Eng. 2018;19:10-26. doi:10.1631/FITEE.1700826
13. van de Sande D, Van Genderen ME, Smit JM, et al. Developing, implementing and governing artificial intelligence in medicine: a step-by-step approach to prevent an artificial intelligence winter. BMJ Health Care Inform. 2022;29(1):e100495. doi:10.1136/ bmjhci-2021-100495
14. Kasparov G. Strategic intensity: a conversation with world chess champion Garry Kasparov. Harv Bus Rev. 2005;83(4):49-53,132.
15. Shih J. Voice revolution. Libr Technol Rep. 2020;56(4):5-13. doi:10.5860/ltr.56n4
16. Ferrucci D, Brown E, Chu-Carroll J, et al. Building Watson: an overview of the DeepQA project. AI Magazine. 2010;31(3):59-79. doi:10.1609/aimag.v31i3.2303
17. Adjuik TA, Ananey-Obiri D. Word2vec neural model-based technique to generate protein vectors for combating COVID-19: a machine learning approach. Int J Inf Technol. 2022;14(7):3291-3299. doi:10.1007/s41870-022-00949-2
18. Criado N, Such JM. Digital discrimination. In: Yeung K, Lodge M, eds. Algorithmic Regulation. Oxford; 2019:82-97.
19. Bory P. Deep new: the shifting narratives of artificial intelligence from Deep Blue to AlphaGo. Convergence. 2019;25(4):627-642. doi:10.1177/1354856519829679
20. Yenduri G, Ramalingam M, Chemmalar Selvi G, et al. GPT (generative pre-trained transformer)—a comprehensive review on enabling technologies, potential applications, emerging challenges, and future directions. IEEE Access. 2024;12:54608-54649. doi:10.1109/ACCESS.2024.3389497
21. Sezgin E, Sirrianni J, Linwood SL. Operationalizing and implementing pretrained, large artificial intelligence linguistic models in the US health care system: outlook of generative pretrained transformer 3 (GPT-3) as a service model. JMIR Med Inform. 2022;10(2):e32875. doi:10.2196/32875
22. Temsah MH, Jamal A, Aljamaan F, Al-Tawfiq JA, Al-Eyadhy A. ChatGPT-4 and the global burden of disease study: advancing personalized healthcare through artificial intelligence
in clinical and translational medicine. Cureus. 2023;15(5):e39384. doi:10.7759/ cureus.39384
23. Badruddin Bin Ghazali A. Utilising ChatGPT. Letter. BDJ Student. 2023;30(5). doi:10.1038/ s41406-023-0959-1
24. Huang H, Zheng O, Wang D, et al. ChatGPT for shaping the future of dentistry: the potential of multi-modal large language model. Int J Oral Sci. 2023;15(1):29. doi:10.1038/ s41368-023-00239-y
25. Tiwari A, Kumar A, Jain S, et al. Implications of ChatGPT in public health dentistry: a systematic review. Cureus. 2023;15(6):e40367. doi:10.7759/cureus.40367
26. Dorri M. AI and clinical decision making. Br Dent J. Letter. 2023;234(10):711. doi:10.1038/ s41415-023-5928-0
27. Sciberras M, Farrugia Y, Gordon H, et al. Accuracy of information given by ChatGPT for patients with inflammatory bowel disease in relation to ECCO guidelines. J Crohns Colitis 2023;17(4):453-462. doi:10.1093/ecco-jcc/jjae040
28. Derner E, Batistič K. Beyond the safeguards: exploring the security risks of ChatGPT. arXiv. 2023;2305.08005. Published May 2023. doi:10.48550/arXiv.2305.08005
29. Alhaidry HM, Fatani B, Alrayes JO, Almana AM, Alfhaed NK. ChatGPT in dentistry: a comprehensive review. Cureus. 2023;15(4):e38317. doi:10.7759/cureus.38317
30. Wang C, Liu S, Yang H, Guo J, Wu Y, Liu J. Ethical considerations of using ChatGPT in health care. J Med Internet Res. 2023;25:e48009. doi:10.2196/48009
31. Abbas M, Jam FA, Khan TI. Is it harmful or helpful? Examining the causes and consequences of generative AI usage among university students. Int J Educ Technol High Educ 2024;21:10. https://doi.org/10.1186/s41239-024-00444-7
32. Khurana S, Vaddi A. ChatGPT from the perspective of an academic oral and maxillofacial radiologist. Editorial. Cureus. 2023;15(6):e40053. doi:10.7759/cureus.40053
33. Kim SG. Using ChatGPT for language editing in scientific articles. Editorial. Maxillofac Plast Reconstr Surg. 2023;45(1):13. doi:10.1186/s40902-023-00381-x
ORAL DIAGNOSIS
Tanya M. Gibson, DDS
Yellowish tongue nodule
(Case courtesy of Dr Peter Domagala, Durango, Colorado.)
A 34-year-old woman presented to the dental office for a new patient examination. Intraoral examination revealed an asymptomatic, smooth, 5-mm, yellowish nodule on the
White tongue plaque
A 57-year-old man presented to the dental office for a new patient examination. He reported that he had smoked a pack of cigarettes daily for the past 30 years. The patient did not report a history of repeated trauma to the area. Intraoral
posterior right lateral surface of the tongue (Figure). No other lesions were noted.
Which of the following is the most appropriate diagnosis?
A. aphthous stomatitis
B. Fordyce granules
C. granular cell tumor
D. lymphoepithelial cyst
Diagnosis is on page 80.
examination revealed an asymptomatic, homogenous white plaque on the right lateral and ventral surfaces of the tongue (Figure). No other clinical lesions were noted during the oral examination, and the white lesion could not be wiped off.
Which of the following is the most appropriate diagnosis?
A. leukoplakia
B. lichen planus
C. morsicatio linguarum
D. pseudomembranous candidiasis
Diagnosis is on page 80.
Author affiliations
Department of Oral Pathology, Radiology and Medicine, School of Dentistry and School of Graduate Studies, University of Missouri – Kansas City.
Figure. Smooth, yellowish nodule measuring 5 mm in diameter.
Figure. Homogenous, translucent, 4.0 × 0.5-cm white plaque.
GENERAL DENTISTRY SELF-INSTRUCTION ANSWERS
Exercise No. GD513
July/August 2023, p. 23
1. C
2. B
3. C
4. C
5. C
6. A 7. A 8. C 9. C 10. B 11. B 12. A 13. D 14. A 15. D
Exercise No. GD514
July/August 2023, p. 30
1. B
2. C
3. C
4. A
5. D 6. B 7. C 8. A 9. D 10. D 11. D 12. D 13. B 14. B 15. D
Coming next issue
Look for these articles and more in the September/October 2024 issue of General Dentistry:
• Effect of mouthwashes on the color stability of a nanohybrid composite
• Nonsurgical management of large perforated bony lesions
• Treatment of gingival recession with a laterally positioned flap and grafting
In the July issue of AGD Impact
• Chronicling the Paths of Internationally Educated Dentists
• Doing It Right the First Time: A Look at Implant Surgical Guides
• Spotlight on 2024 FAGD, MAGD and LLSR Recipients
In the August issue of AGD Impact
• Improving Your Relationship with Your Dental Lab
• Where Artistry Meets Exceptional Skills: Profiling Master Ceramists
• What Dentists Can Learn from Other Business Models
HAVE YOU
MOVED?
If you have recently moved, or plan to in the near future, please make sure to update your AGD profile.
Log into the AGD website today! We want to make sure you receive AGD publications and other important information from us! View or update your profile, check the status of your membership dues, manage your email subscriptions and change your password.
Please contact the AGD Membership Services Center with any questions at 888.243.3368 (toll-free) or 312.440.4300. Our member representatives are available to assist you Monday through Friday from 7:30 a.m. to 5:30 p.m. CST.
Yellowish tongue nodule
Diagnosis
D. lymphoepithelial cyst
An oral lymphoepithelial cyst is a developmental intramucosal lesion of unknown etiology that occurs in areas that contain accessory lymphoid tissue or areas where lymphoid tissue is plentiful, like the Waldeyer ring.1 Common intraoral locations include the floor of the mouth, ventral surface of the tongue, posterior lateral border of the tongue, soft palate, and oropharynx.1 Clinically, it appears as a firm compressible yellowish nodule that often contains a creamy material. They are usually smaller than 1.0 cm and rarely exceed 1.5 cm.1
Lymphoepithelial cysts are typically asymptomatic unless secondarily traumatized. The oral lymphoepithelial cyst is histologically identical to the cervical lymphoepithelial cyst (brachial cleft cyst) found in the neck, anterior to the sternocleidomastoid muscle. A biopsy is curative and confirms the clinical diagnosis. Recurrence is not expected.1
Aphthous stomatitis (canker sore) occurs on the freely movable nonkeratinized soft tissue and classically presents as a yellowish ulcerative lesion surrounded by an erythematous halo. It may present as a solitary or multiple lesions. Aphthous stomatitis is not a proliferative or mass-forming lesion; it is an ulceration that represents a break in the continuity of the
White tongue plaque Diagnosis
A. leukoplakia
A leukoplakia is a white patch that cannot be wiped off and is clinically classified as a pathologic entity. It most often presents as an isolated lesion. In general, there is a male predilection; however, a female predilection is seen in areas where there is a higher incidence of tobacco use among women.1
Leukoplakias are most commonly found in individuals over the age of 40 years, and the prevalence increases with age.1
A leukoplakia is a potentially premalignant lesion, and a biopsy is required for a definitive diagnosis. The microscopic diagnosis can range from hyperkeratosis to epithelial dysplasia to squamous cell carcinoma. These lesions are especially concerning when they occur on the tongue, lip vermilion, or floor of the mouth, because these represent 90% of the leukoplakias that show dysplasia or carcinoma.1 Treatment and prognosis are dependent on the histologic diagnosis.
Lichen planus is a bilateral mucocutaneous disorder of unknown etiology. The reticular form is usually asymptomatic and presents as a classic, white lace–like appearance, or Wickham striae, on multiple mucosal surfaces. Lichen planus can be differentiated clinically from a leukoplakia based on its
epithelium. The clinical presentation of aphthous stomatitis is usually characteristic enough that a biopsy is not warranted to make a diagnosis.
Fordyce granules are ectopic sebaceous glands. They present as multiple small, yellowish submucosal granules, most commonly located on the bilateral buccal mucosa but found throughout the oral cavity. Their clinical presentation is usually characteristic enough that a biopsy is not warranted to make a diagnosis.
A granular cell tumor is a benign soft tissue tumor that may occur intraorally or on the skin. The favored intraoral site is the dorsal surface of the tongue. It presents as a firm submucosal mass that may have a yellowish clinical appearance. It does not contain a cystic cavity or fluid, so it will not be fluctuant on compression. A biopsy is curative and required for diagnosis.
Reference
1. Neville BW, Damm DD, Allen CM, Chi AC. Oral and Maxillofacial Pathology. 5th ed. Saunders/Elsevier; 2024:36-37.
multifocal and lace-like presentation. A biopsy is usually not indicated when lichen planus presents with Wickham striae. Morsicatio linguarum results from habitual biting of the tongue and is often supported by the patient’s report of the habit. Clinically, it appears as a diffuse, irregular, ragged appearance of the mucosa. It may be difficult to differentiate between a milder clinical presentation of morsicatio linguarum and a leukoplakia. If the area does not resolve after cessation of the biting habit, a biopsy is indicated to rule out a potentially premalignant lesion.
Pseudomembranous candidiasis, commonly referred to as thrush, is an infectious disease that can affect the oral mucosa. It presents as a white cottage cheese appearance on the mucosa and can easily be wiped away with gauze, leaving behind an erythematous background. The clinical diagnosis can be confirmed with a culture or cytologic smear.
Reference
1. Neville BW, Damm DD, Allen CM, Chi AC. Oral and Maxillofacial Pathology. 5th ed. Saunders/Elsevier; 2024:381-390.
AGD PREMIUM PLUS MEMBERSHIP
Take advantage of membership tailored to you!
For an additional $158, you can receive the following:
• Free Early-Bird Scientific Session Registration
• Free CE Library PLUS 4 On-Demand Webinars of Your Choice
• 20% Discount off Fall Fellowship Review Course
• 20% Discount off Fellowship Study Guide
“I wanted to take advantage of all the lectures and classes that the scientific session offers, so, to get the best value, Premium Plus membership was the obvious choice.”