Lymphadenopathy in a patient with mucous membrane pemphigoid
ORAL MEDICINE, ORAL DIAGNOSIS, ORAL PATHOLOGY
Malignant transformation of oral lichen planus
ORAL AND MAXILLOFACIAL SURGERY
Root migration after coronectomy
BASIC SCIENCE
Bond strength of Bis-GMA–free adhesive
PEER-REVIEWED JOURNAL OF THE ACADEMY OF GENERAL DENTISTRY
DEPARTMENTS CLINICAL ARTICLES
5 Editorial
Cutting-edge dentistry
6 Pharmacology
Doxycycline: 3 new things about an old drug
11
Orofacial Pain
Understanding cracked tooth syndrome: diagnosing nondental pain in dentistry
14
Prosthodontics
The crucial second appointment in full-arch removable prosthesis cases
17
Public Health
Understanding and preparing for our aging patient population
20 Implants
Tooth replacement from extraction to restoration.
3. Second-stage and impression procedures
78
Oral Diagnosis
Heart-shaped radiolucency and Gingival yellow spot
79
Self-Instruction Answers
Exercises No. GD533, GD534, and GD536
25 Oral Medicine, Oral Diagnosis, Oral Pathology
What every dentist needs to know about cannabis use and head and neck cancer
John K. Brooks
Maureen A. Fitzpatrick
28 Periodontics
Muhammad Hamza
Nasir Bashirelahi
A comparative evaluation of serum and salivary levels of apelin in chronic periodontitis associated with obesity and type 2 diabetes mellitus
Jammula Surya Prasanna
SELF-INSTRUCTION
Duddukuri Hema
36 Oral Medicine, Oral Diagnosis, Oral Pathology
Nonodontogenic cysts and pseudocysts of the oral cavity: a retrospective study of 218 cases
Saede Atarbashi-Moghadam
Seyed Sepehr Mirebeigi-Jamasbi
SELF-INSTRUCTION
42 Basic Science
Nastaran Niknam
Influence of a Bis-GMA–free universal adhesive system on enamel bond strength to ceramic brackets
Aline Júnia Oliveira
Jurandir Antonio Barbosa
Victor Angelo Martins Montalli
Roberta Tarkany Basting
48 Oral Medicine, Oral Diagnosis, Oral Pathology
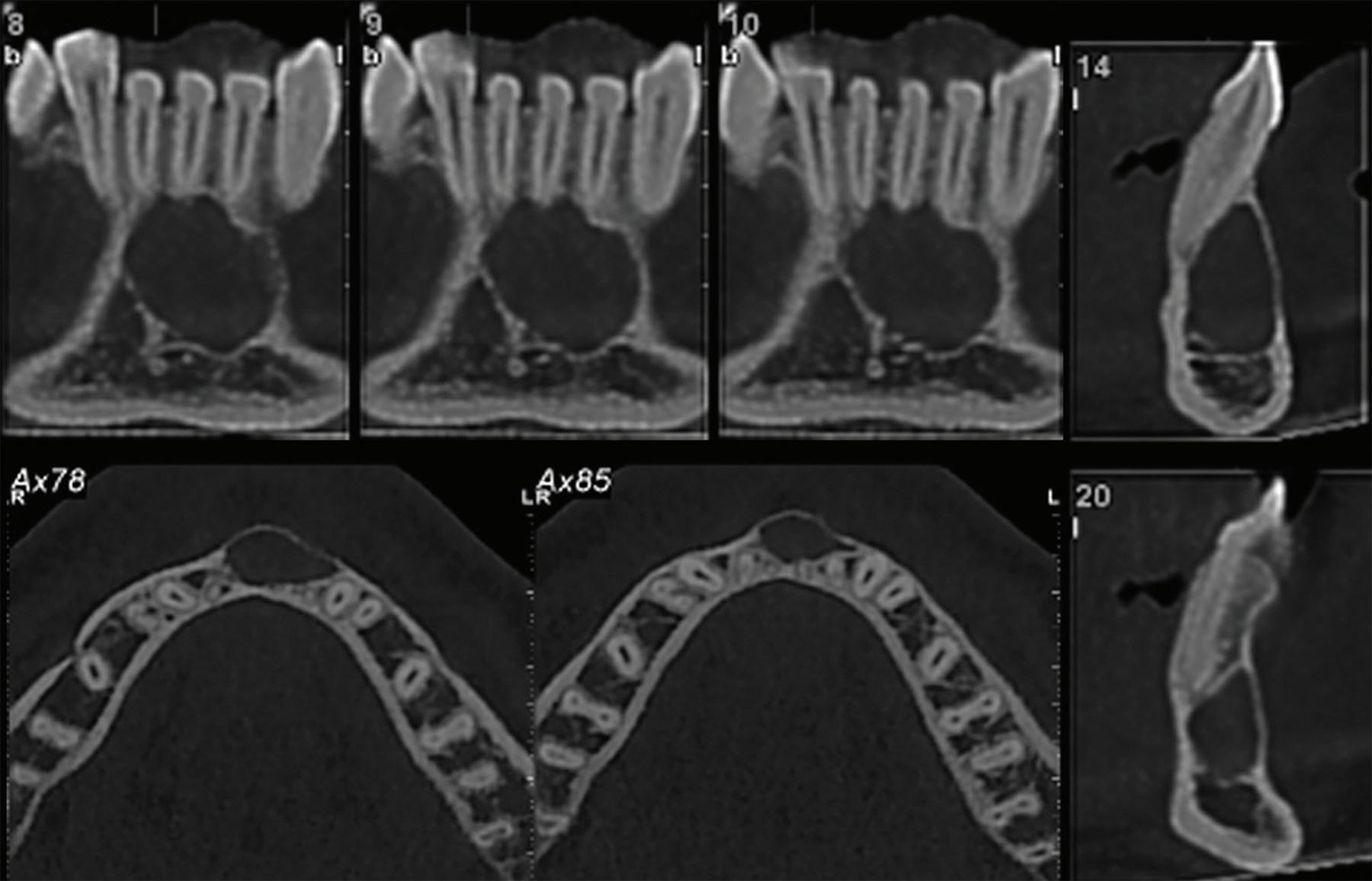
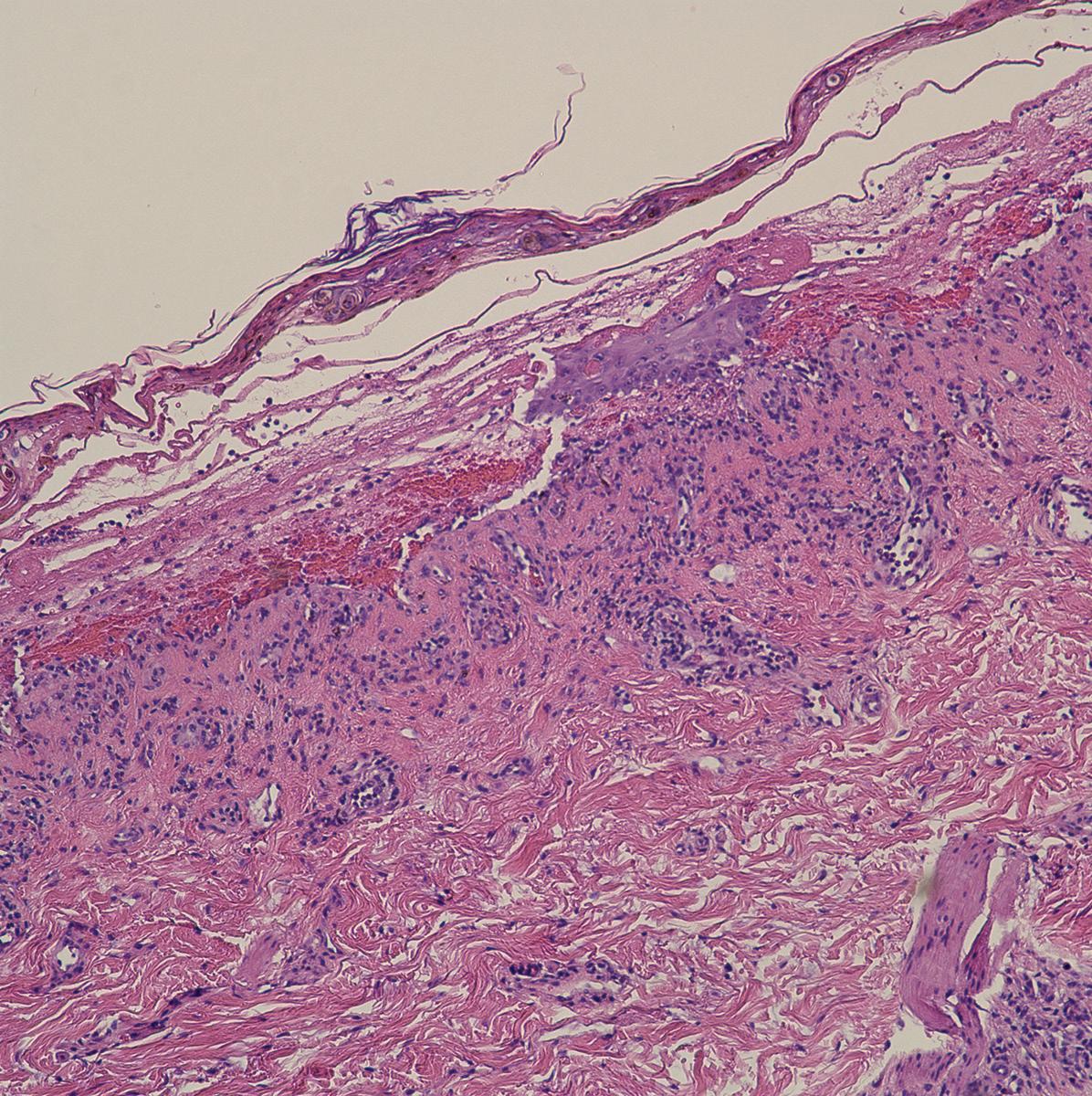
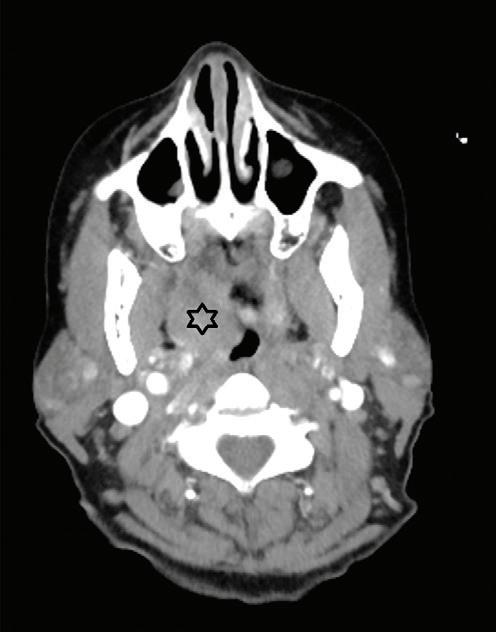
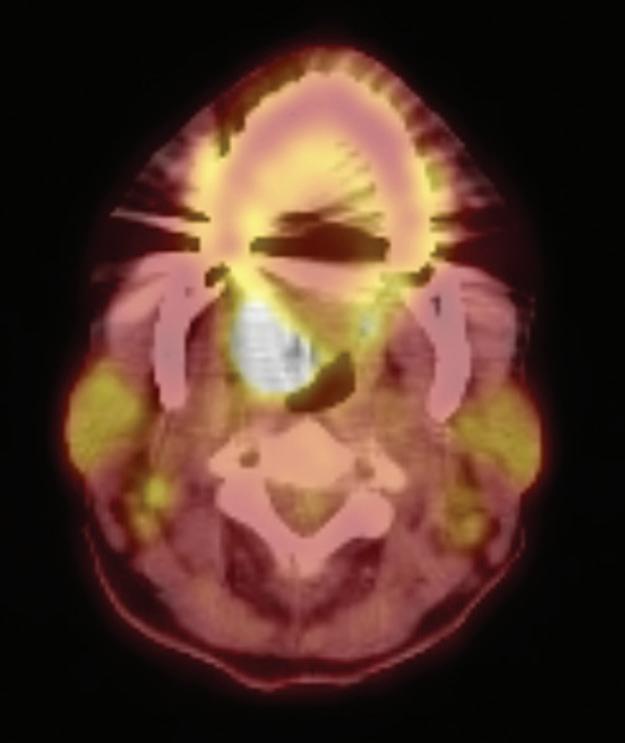
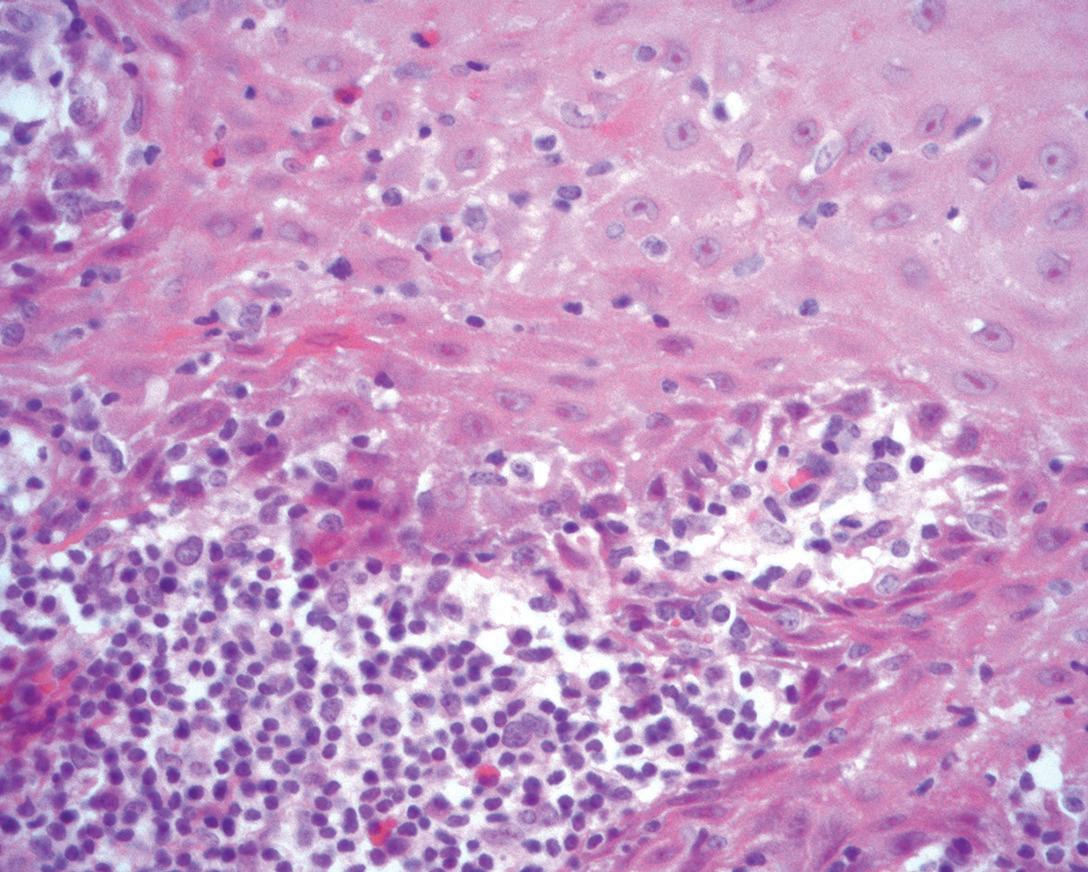
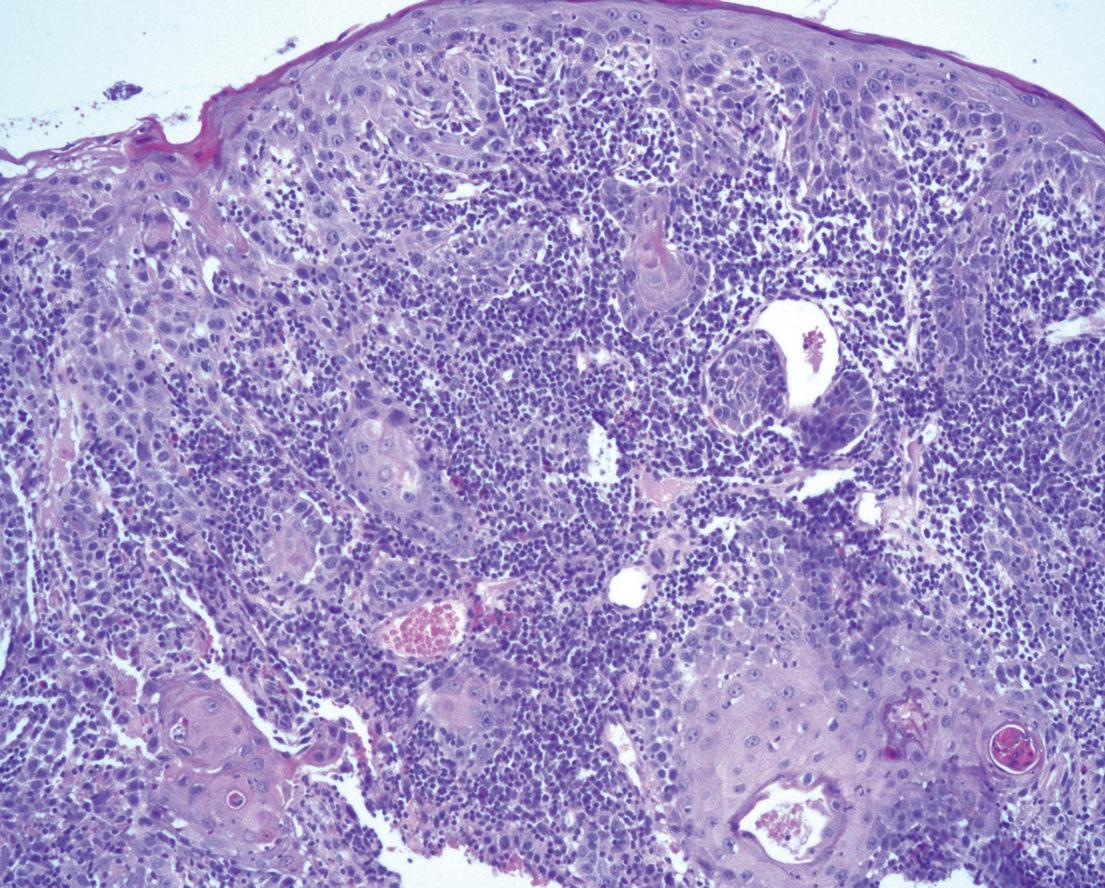
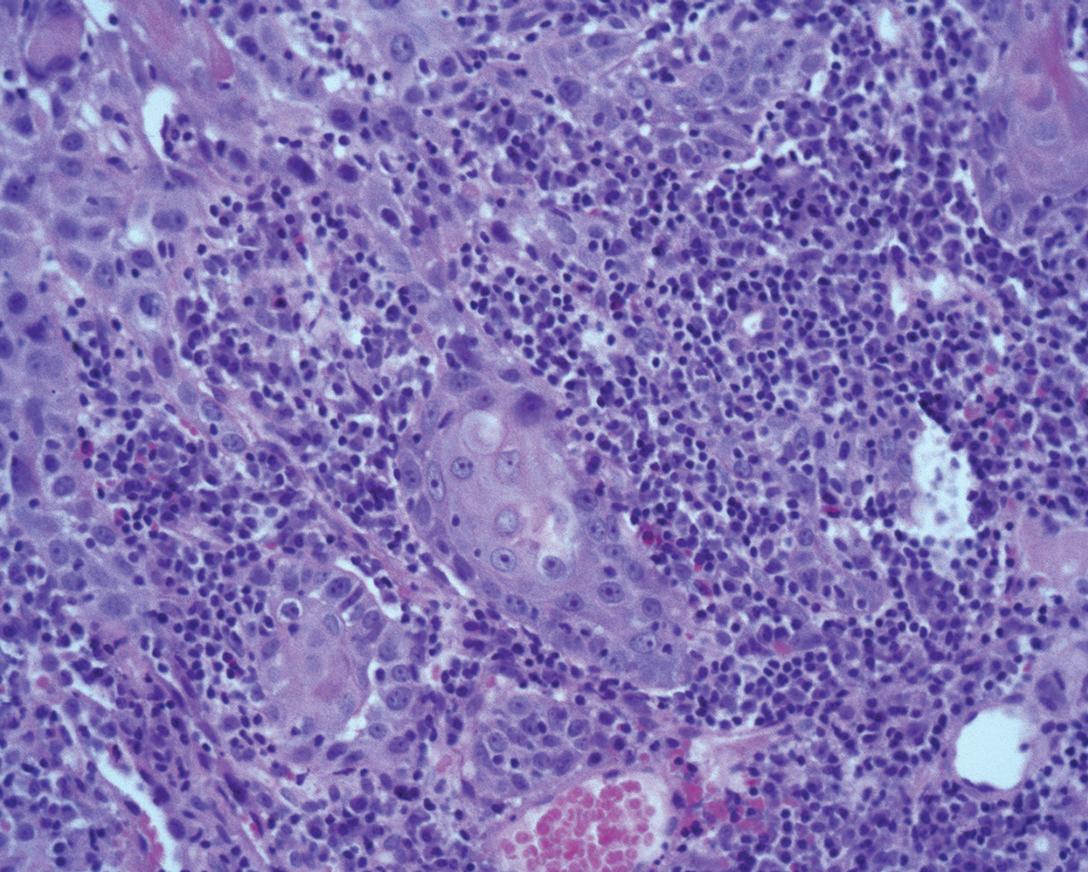
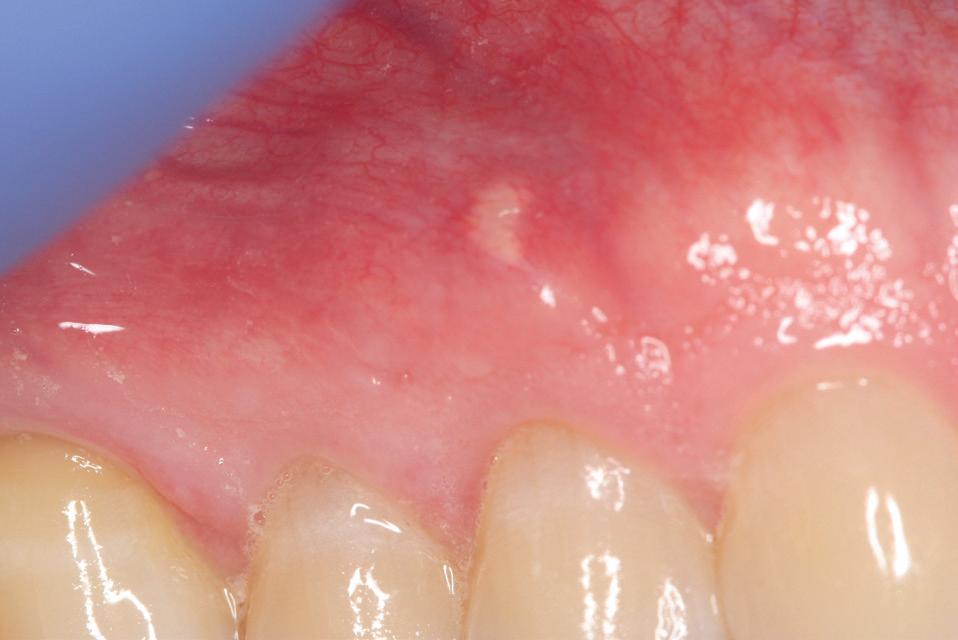
Multidisciplinary approach to diagnosis and management of lymphadenopathy in a patient with mucous membrane pemphigoid: a case report
Heba Turkstani
Eric T. Stoopler
Temitope T. Omolehinwa
Eman Alamodi
Mel Mupparapu
54 Oral and Maxillofacial Surgery
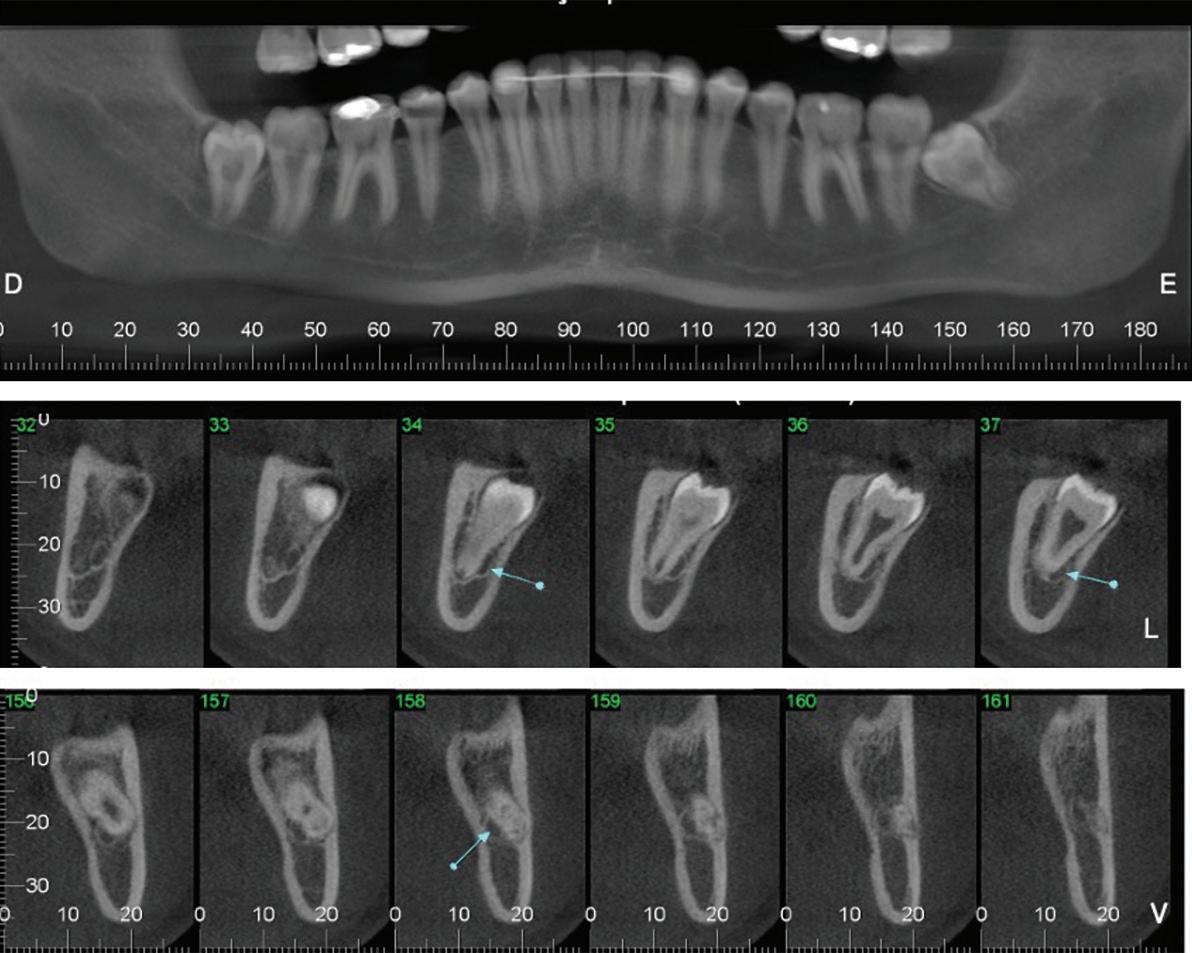
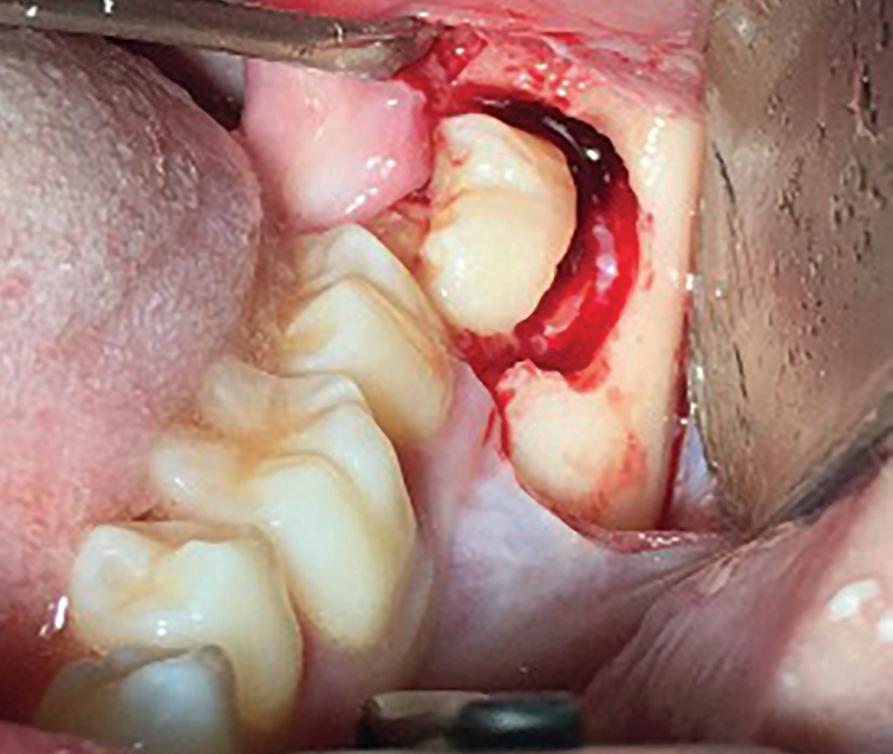
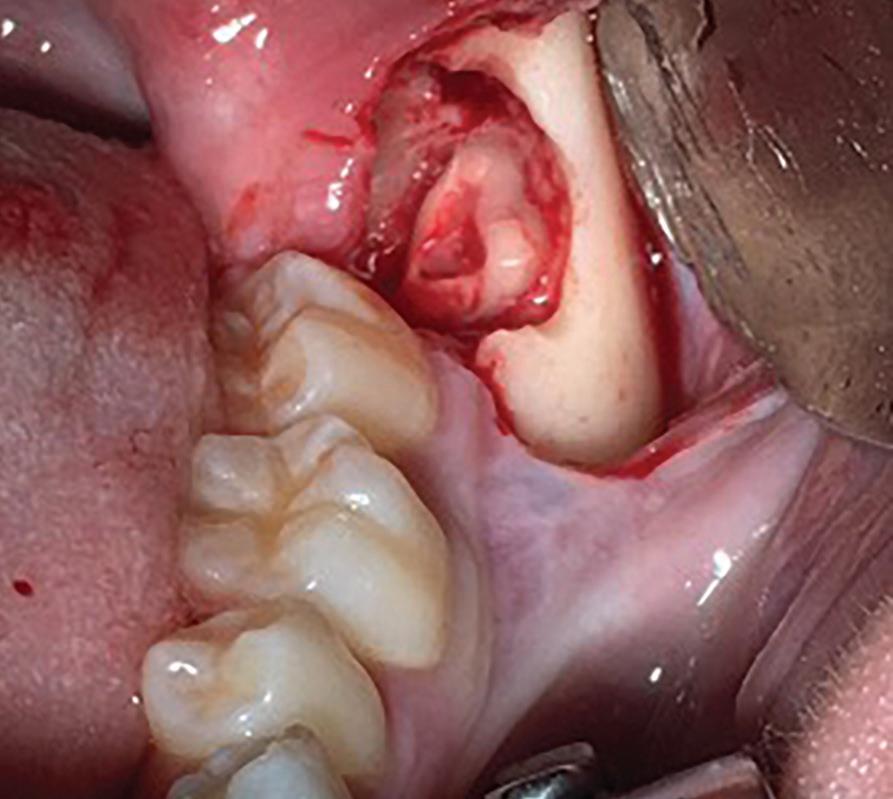
Root migration after coronectomy of impacted mandibular third molars: case reports
Gustavo Henrique de Souza Silva Enzo Balestrero
Jéssica Lemos Gulinelli
Pâmela Leticia dos Santos
59 Oral Medicine, Oral Diagnosis, Oral Pathology
Malignant transformation of oral lichen planus after 6 years: a case report
Patrícia Peres Iucif Pereira
João Adolfo Costa Hanneman
Henrique de Carvalho Petean
Alessandro Antônio Costa Pereira
64 Special Patient Care
Amanda Bandeira de Almeida
Eduardo Pereira Guimarães
Daiana Moreira Mendes Rozendo
Oral health in relation to manifestations and severity of cystic fibrosis: a cross-sectional study
Ana Carolina Evangelista Colafêmina Aline Cristina Gonçalves
Cecília Regina Frazatto
Antônio Fernando Ribeiro
Márcio Ajudarte Lopes
72 Fixed Prosthodontics
Camila Real Delegá Rodrigues
José Dirceu Ribeiro
Influence of beverage solutions on the microhardness and surface roughness of provisional fixed denture materials
Eduardo Comeron Pieralini
Henrico Badaoui Strazzi-Sahyon
Paulo Henrique Dos Santos
Renan Aparecido Fernandes
Anelise Rodolfo Ferreira Pieralini
Sabrina Pavan
Cover image inspired by: Multidisciplinary approach to diagnosis and management of lymphadenopathy in a patient with mucous membrane pemphigoid: a case report, on p. 48
Members, call 888.243.3368 and ask for a Member Services representative.
Mailing Lists
For information about ordering AGD mailing lists, call 888.243.3368 ext. 4097 or email advertising@agd.org.
All materials subject to copying and appearing in General Dentistry may be photocopied for the noncommercial purposes of scientific or educational advancement. Reproduction of any portion of General Dentistry for commercial purposes is strictly prohibited unless the publisher’s written permission is obtained.
AGD does not necessarily endorse opinions or statements contained in essays or editorials published in General Dentistry. The publication of advertisements in General Dentistry does not indicate endorsement for products and services. AGD approval for continuing education courses or course sponsors will be clearly stated.
General Dentistry (ISSN 0363-6771) is published bimonthly in 2025 by the AGD, 560 W Lake St, Sixth Floor, Chicago, IL 60661-6600.
Periodicals postage paid at Chicago, IL and additional mailing office. POSTMASTER: Send address changes to General Dentistry, 560 W Lake St, Sixth Floor, Chicago, IL 60661-6600. Email: subscriptions@agd.org.
Canadian mailing information: IPM Agreement number 40047941. Change of address or undeliverable copies should be sent to: Station A, PO Box 54, Windsor, Ontario, N9A 6J5, Canada. Email: subscriptions@agd.org.
AGD members receive General Dentistry as part of membership; annual subscription rates for nonmembers are $135 for individuals and $255 for institutions. Online-only subscriptions are $120 for individuals and $230 for institutions. All orders must be prepaid in US dollars. Single copies are available upon request. Please contact our Membership Services Center at 888.243.3368 for more information.
Innovations in dentistry—particularly the integration of artificial intelligence for diagnosis and treatment planning— are rapidly elevating our profession and reshaping how we learn, plan, and deliver care. While new technologies often come with a hefty price tag, dentists who embrace and master them often find greater proficiency, precision, and efficiency.
It’s an exciting time to be a dentist. Our practice recently incorporated a biofluorescence detection device that visualizes demineralization and biofilm, even projecting images onto our iPhones for patient education. Oral cancer screening devices have improved detection and are very much appreciated by the patients in our hygiene chair.
AI-driven X-ray detection devices provide both dentists and patients with visual insight into necessary treatment, reducing the risk of overtreatment. CBCT allows us to view vital anatomy before intervention. Digital scanning has refined our tooth preparation techniques, and in-office printing and milling can provide same-day restorations. These tools don’t just streamline care—they enhance it.
Orthodontic aligners have made tooth movement more patient-friendly, though a very clear understanding of anatomy and biomechanics remains essential. Similarly, guided implant surgery and robotics have made these procedures more predictable, but their success hinges on thoughtful design and awareness of potential complications. Technology is a tool, not a replacement for clinical judgment.
Today’s younger dentists are naturally more adept at digital workflows, thanks to updated dental school curricula. Still, many practices operate with a hybrid approach: scanning digitally in-office while working with labs to complete design and fabrication. Some begin with analog and convert to digital off-site. Regardless of the method, a thorough understanding of the principles of occlusion and esthetics must guide treatment.
Digital tools help us plan restorations with greater accuracy, but we must understand
every step of the workflow. Evaluating biological health, tooth structure, condylar path, and protrusive contacts ensures the best outcomes. CBCT, intraoral and facial scanners, and virtual articulators allow us to “stack” datasets and plan with unprecedented detail. Digital wax-ups are now often completed before preparation and tooth reductions. Esthetic veneers and full-arch restorations can be designed and printed chairside, sometimes using shrink-wrap techniques. Once mastered, these tools can be incredibly accurate and save time. Facial recognition scanners, virtual waxups, surgical guides, orthotics, and diagnostic mock-ups are making “trial smiles” easier to design and present.
Digital bite registrations, virtual mounting, and occlusion analysis—whether in centric relation or maximum intercuspation—are more accurate than ever. CBCT even allows us to evaluate condylar paths and merge anatomical landmarks like the Bonwill triangle into treatment planning. All our planning is now prosthetically driven. We aren’t here to promote specific products, but dentists must evaluate all the options and get proper training and education. The transition from analog to digital isn’t optional—it’s happening. And there’s a learning curve. Those with years of experience in this space are invaluable mentors. Technology is only worthwhile when it is fully integrated into practice. It can set you apart. A hygiene-driven general practice, with focused niche procedures, can lead to professional growth and financial success. Aspire to be the “super GP” in your community—the go-to provider for comprehensive care.
From single crowns to full-mouth reconstructions, treatment planning is an art, and technology is our greatest tool in getting it right.
Timothy F. Kosinski, DDS, MAGD Editor
PHARMACOLOGY
Doxycycline: 3 new things about an old drug
Mark Donaldson, BSP, ACPR, PHARMD, FASHP, FACHE ¢ Jason H. Goodchild, DMD
Doxycycline is a long-established tetracycline antibiotic that continues to play a key role in treating a range of infectious diseases, particularly in dental medicine. Doxycycline was patented in 1957 and approved by the US Food and Drug Administration for commercial use in 1967.1 With activity against many gram-positive, gram-negative, and atypical bacteria, as well as certain parasites, it was originally marketed as Pfizer’s first once-aday, broad-spectrum antibiotic under the brand name Vibramycin.1,2 Doxycycline has also been on the World Health Organization’s List of Essential Medicines since the inaugural publication in 1977.3
Recent clinical data and updated guidelines have refined the understanding of the optimal use and safety profile of doxycycline as well as its emerging resistance patterns. This column provides an updated overview of its pharmacology, mechanism of action, and antimicrobial spectrum, highlighting 3 specific changes related to dental practice: infective endocarditis (IE) prophylaxis, long-term periodontal therapy, and local delivery of peri-implantitis therapy (Table 1).
Pharmacology, mechanism of action, and spectrum of activity
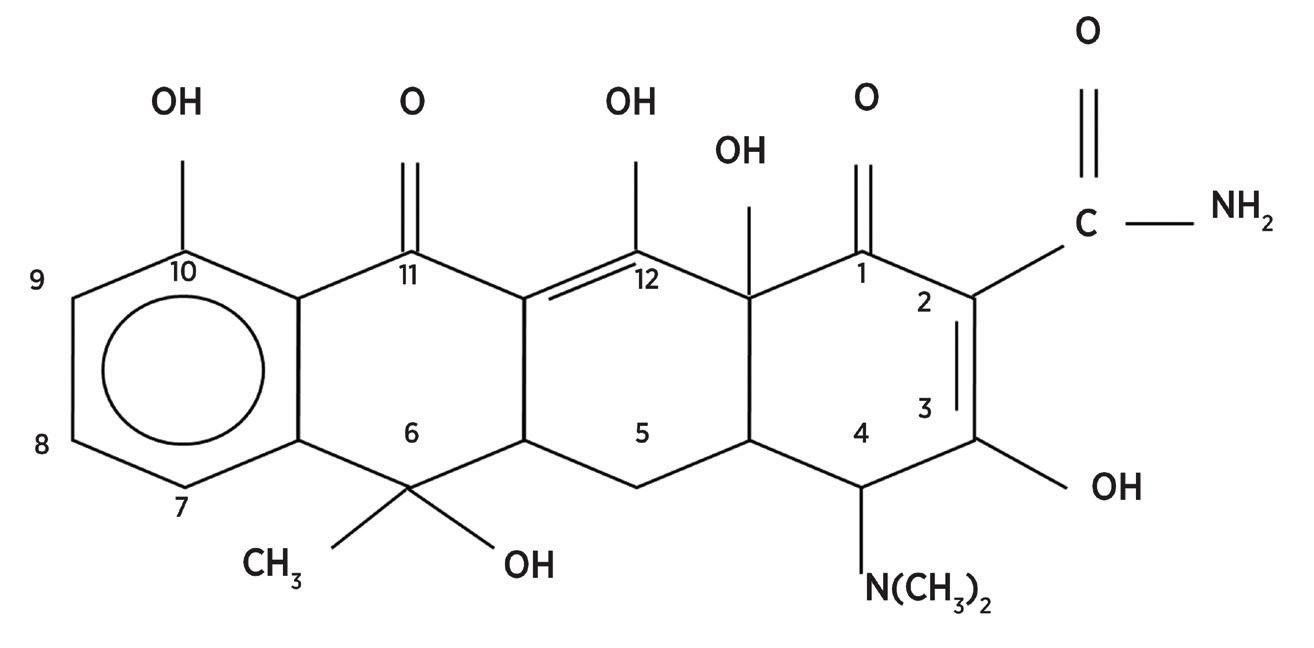
The family of tetracycline antibiotics available in the United States consists of demeclocycline, tetracycline, oxytetracycline, minocycline, and doxycycline (Figure). Doxycycline is a semisynthetic, second-generation tetracycline that exerts bacteriostatic effects by inhibiting bacterial protein synthesis.1,2 It binds to the 30S ribosomal subunit of bacteria
Clinical area
Infective endocarditis prophylaxis
Long-term periodontal therapy
Local delivery of periimplantitis therapy
Overview of change
Doxycycline has been added as an alternative to clindamycin in AHA/ADA guidelines for patients allergic to penicillin who require preprocedure prophylaxis.21,23
The ADA endorses low-dose systemic doxycycline (20 mg twice daily for 3 to 9 months) as a host-modulating adjunct to scaling and root planing for moderate to severe disease.24
There is growing interest in local doxycycline gels as a nonsurgical adjunct, supported by emerging reviews.27-30
Abbreviations: ADA, American Dental Association; AHA, American Heart Association.
Figure. Structural formulas of the tetracycline family.
Children (> 8 y): 7 to 13 mg/kg/d orally, divided into 2 to 4 doses
Maximum dose: 600 mg/d
Adults and children > 8 y and ≥ 45 kg: 100 mg every 12 h
Children > 8 y and < 45 kg: 4 to 5 mg/kg/d in 2 divided doses the first day, then 2 to 2.5 mg/kg given 1 to 2 times/d
Adults: 200 mg initially, followed by 100 mg every 12 h
Children > 8 y: 4 mg/kg initially, followed by 2 mg/kg every 12 h, not to exceed the usual adult dose
Adults: 250 to 500 mg every 12 h
Children > 8 y: 6.25 to 12.5 mg/kg every 6 h, maximum 500 mg
Adults: 125 to 500 mg every 6 to 8 h
Children < 12 y: 25 to 50 mg/kg every 6 to 8 h
Adults and children ≥ 40 kg: 250 to 500 mg every 8 to 12 h
Children < 40 kg: 25 to 50 mg every 8 to 12 h
Adults and children ≥ 40 kg: 250 to 500 mg every 8 h
Alternative dosing: 875 mg every 12 h
Adults and children ≥ 15 y: 250 to 1000 mg every 6 h (maximum 4 g/d)
Children 1 to 14 y: 25 to 100 mg/kg/d, taken in 3 to 4 divided doses
Z-Pak
500 mg on day 1; 250 mg on days 2 to 5
Z-Max extended-release suspension
Adults: single 2-g dose
Children > 6 mo: 60 mg/kg as a single dose, up to a maximum of 2g
Clindamycin (Cleocin)
With or without food
Metronidazole (Flagyl) With food
and blocks the attachment of aminoacyl–transfer RNA to the ribosome acceptor site, thereby halting peptide chain elongation. This mechanism of action prevents bacteria from producing essential proteins, effectively suppressing growth. This is also the mechanism by which doxycycline prevents the development of IE in at-risk patients.4 In addition to its antimicrobial actions, doxycycline, like other tetracyclines, has ancillary anti-inflammatory properties, such as inhibition of metalloproteinases and suppression of proinflammatory cytokines, which may contribute to its therapeutic effects in certain conditions like periodontitis and peri-implantitis.5,6
Adults: 150 to 450 mg every 8 h
Children ≥ 11 kg: 8 to 20 mg/kg/d as hydrochloride in 3 to 4 divided doses; 8 to 25 mg/kg/d as pamoate in 3 to 4 divided doses
Adults: 250 to 500 mg every 12 h for up to 10 d
Children < 45 kg: 35 to 50 mg/kg/d, divided into 3 doses, for 10 d
Doxycycline’s spectrum of activity is broad, covering a wide range of organisms. It is active against many grampositive bacteria (eg, Staphylococcus aureus, including many communityacquired, methicillin-resistant S aureus [MRSA] strains; Streptococcus pneumoniae; and Bacillus anthracis), gramnegative bacteria (eg, Haemophilus influenzae, Moraxella catarrhalis, and Vibrio species), and numerous atypical and zoonotic pathogens.2 Doxycycline is also highly effective against intracellular bacteria like Chlamydia trachomatis, Mycoplasma pneumoniae, and Chlamydia psittaci, as well as Rickettsiae, the agents responsible for
causing spotted fevers and typhus. It is also a first-line treatment for diseases caused by spirochetes such as Borrelia burgdorferi (Lyme disease) and Treponema pallidum (syphilis; used in patients allergic to penicillin). Other susceptible organisms include Brucella species (brucellosis), Coxiella burnetii (Q fever), and even malaria parasites (doxycycline is commonly used for malarial prophylaxis).
This broad spectrum of activity— which encompasses typical respiratory and odontogenic pathogens, sexually transmitted bacteria, tick-borne organisms, and others—makes doxycycline a versatile agent in clinical practice.
Table 2. Antibiotics used in dentistry for bacterial infection and their treatment doses.
However, like all antibiotics, its activity is limited by patterns of resistance. Thus, susceptibility testing and knowledge of local resistance patterns are important when treating certain organisms.
The oral absorption of doxycycline is high, and its bioavailability of more than 95% makes it very effective when administered by mouth.2,4 For adults and children over the age of 8 years (and weighing 45 kg or more), the dose of doxycycline is 100 mg 12 hours apart on the first day, followed by 100 mg once or twice daily when severe infection is present. For children who are older than 8 years but weigh less than 45 kg, the dose is 4 to 5 mg/kg/d in 2 divided doses the first day, followed by 2 to 2.5 mg/kg given once or twice daily. It is not typically recommended in children younger than 8 years old. The effectiveness of doxycycline with once or twice daily dosing is possible because of the drug’s 16-hour half-life.
Table 2 provides an overview of the tetracycline antibiotics and other agents commonly used in dental practice, detailing their standard dosages and recommended administration relative to food intake.
Emerging resistance patterns
Although doxycycline is an older antibiotic, it remains effective against many pathogens. However, resistance is increasingly a concern in some settings.2,3 Bacterial resistance to tetracyclines typically occurs via efflux pumps such as tet(A) or tet(K) or via ribosomal protection proteins like tet(M), mechanisms that can render doxycycline ineffective.7,8 For example, S aureus, particularly MRSA, has shown rising resistance to tetracyclines. A study of US outpatient MRSA isolates noted tetracycline resistance had increased from 3.6% in 2010 to 12.8% in 2019.9 Still, the majority of community MRSA strains remain susceptible to doxycycline, making it a valuable oral option for skin and soft tissue infections. Oral healthcare practitioners are encouraged to contact their local hospital laboratories to check local susceptibility based on current antibiograms (in many areas, the doxycycline susceptibility of MRSA often ranges from 85% to 95%).
Novel resistance genes have emerged globally, including the tet(X) family of
tetracycline-destroying enzymes identified in the late 2010s.10 These enzymes can inactivate doxycycline, and variants like tet(X3) and tet(X4) were identified in animal and human bacterial isolates in China, conferring high-level resistance to all tetracyclines.11 The emergence of tet(X) genes, frequently plasmid-mediated, is of significant concern due to their potential to disseminate among human pathogens and compromise the efficacy of doxycycline, a last-resort tetracycline. Although these genes have not yet become prevalent in clinical isolates, sustained surveillance is imperative.
Safety profile and tolerability
Doxycycline is generally well-tolerated and its safety profile well-characterized, though certain adverse effects and precautions warrant attention.1,2
Gastrointestinal irritation
Gastrointestinal irritation is the most common side effect of doxycycline, often causing epigastric discomfort, nausea, and diarrhea. To minimize gastrointestinal upset and the risk of esophageal ulceration, patients should take doxycycline with adequate fluids and remain upright for at least 30 minutes after dosing. Although doxycycline may be taken with or without food, taking it with food can help reduce gastrointestinal side effects. Esophagitis from doxycycline pills getting lodged in the esophagus is a known issue; taking it with a full glass of water and avoiding taking it at bedtime are advised preventive measures. As with any antibiotic, Clostridioides difficile infection is a consideration if severe diarrhea occurs, although tetracyclines show a somewhat lower risk for C difficile than some broader-spectrum agents.
Photosensitivity
Doxycycline can cause an exaggerated sunburn reaction in skin exposed to sunlight or UV light. Patients taking doxycycline should be counseled to use sun protection measures such as sunscreen and protective clothing and to avoid tanning beds. This phototoxicity is dose related and can affect individuals who spend time in strong sunlight even after a short duration of therapy.
Tooth and bone effects
Although tetracyclines are traditionally avoided for children younger than 8 years and during pregnancy due to concerns about tooth discoloration and inhibited bone growth, doxycycline binds less strongly than older tetracyclines to calcium. Short courses have not been linked to significant dental staining in children.12 Current guidelines support its use in young children when necessary for serious infections like Rocky Mountain spotted fever, as the benefits outweigh the theoretical risks.13,14 When used in such short courses (eg, 5 days or less), the development of permanent teeth is usually not affected.15 Use of tetracyclines during pregnancy should still generally be avoided; a recent review continues to advise against it unless no alternative exists.16,17
Unique or rare adverse effects
While older tetracyclines at high doses were linked to fatty liver in pregnant women, hepatotoxicity with doxycycline is rare—at standard doses, there are only isolated case reports of hepatic injury.18 Doxycycline is primarily excreted nonrenally via feces or bile, so it does not tend to accumulate with renal impairment. This makes it safe for use in patients with kidney dysfunction without needing to adjust the dose.2
Like other tetracyclines, doxycycline can cause benign intracranial hypertension (pseudotumor cerebri) in rare cases, especially in young women.19 Symptoms include headache and blurred vision. If raised intracranial pressure is suspected, doxycycline should be stopped. This condition is typically reversible after the antibiotic is discontinued.
Doxycycline is generally well-tolerated, with few significant adverse effects in most patients. Taking doxycycline with food can help reduce stomach upset; food may slightly lower absorption, but the effect is minimal. Unlike with older tetracyclines, the absorption of doxycycline is less affected by dairy or moderate calcium intake; however, it is best to avoid taking it at the same time as highdose mineral supplements or antacids, which can bind to the drug.
New clinical data and guidelines
In recent years, new clinical data and guidelines have refined the
understanding of doxycycline’s optimal uses, highlighting 3 specific changes related to dental practice: IE prophylaxis; long-term periodontal therapy; and local delivery of peri-implantitis therapy.
IE prophylaxis
In 2007, the American Heart Association (AHA) published updated evidence-based guidelines on the recommended use of antibiotic prophylaxis to prevent viridans group streptococcal IE in cardiac patients undergoing invasive procedures.20 The 2007 guidelines significantly reduced the underlying conditions for which antibiotic prophylaxis was recommended, leaving only 4 categories thought to confer the highest risk of an adverse outcome: prosthetic cardiac valve or prosthetic material used for cardiac valve repair; previous IE; congenital heart disease; and cardiac transplantation recipients who develop cardiac valvulopathy.
In 2021, a scientific statement published by the AHA and adapted for publication in the Journal of the American Dental Association recommended no changes to the 2007 viridans group streptococcal IE prevention guidelines but added doxycycline (100 mg for adults and children weighing 45 kg or more [2.2 mg/kg for children weighing less than 45 kg], 30 to 60 minutes prior to the dental procedure) as another alternative for patients with penicillin allergy undergoing dental procedures involving the manipulation of gingival tissue or the periapical region of teeth/perforation of the oral mucosa.21-23
Long-term periodontal therapy
The American Dental Association’s 2015 clinical practice guideline on the nonsurgical treatment of chronic periodontitis was in favor of systemic subantimicrobial doxycycline (20 mg twice a day for 3 to 9 months) as a recommendation alongside scaling and root planing (SRP) for moderate to severe disease.24 This doxycycline regimen targets matrix metalloproteinases and inflammatory mediators rather than microbes, offering small but significant clinical improvements with a favorable safety profile.
The clinical practice guideline from 2015 was founded on a systematic review of the evidence that included 72 research articles providing clinical attachment
level data from trials of at least 6 months' duration.24 The strength of each recommendation (strong, in favor, weak, expert opinion for, expert opinion against, and against) was based on assessment of the level of certainty of the evidence for treatment benefit in combination with assessment of the balance between the magnitude of that benefit and the potential for adverse effects. The authors concluded that SRP should be the initial nonsurgical treatment for patients with chronic periodontitis, although subantimicrobial doxycycline showed magnitudes of benefit similar to those of other therapies adjunctive to SRP. Two recent studies have evaluated the use of doxycycline as an adjunct to nonsurgical periodontal treatment in patients with diabetes.25,26 The studies confirmed that doxycycline combined with SRP conferred subtle benefits such as reduced inflammation, measured as bleeding on probing, and reduction of periodontal probing depths.
Local delivery of periimplantitis therapy
A systematic review published in May 2025 highlighted growing interest in the use of locally applied doxycycline gel as a nonsurgical adjunct for treating peri-implantitis.27 While the current evidence is still preliminary and should be interpreted with caution, antimicrobial agents like doxycycline show potential benefits. These include improved probing depth reduction, better biofilm control, and effective decontamination of titanium implant surfaces without the need for systemic antibiotic exposure.28,29 A 2024 meta-analysis also supported the use of systemic or locally delivered antibiotics in reducing probing depth in peri-implantitis cases, although it emphasized the need for careful and selective application.30
A recent long-term study found that approximately 50% of patients with dental implants developed peri-implant diseases over a 10-year follow-up period. Smoking and a history of periodontal disease were identified as major risk factors for both peri-implant mucositis and peri-implantitis.31 Based on these findings, continued research into the local application of doxycycline for the treatment of peri-implantitis is warranted.
Conclusion
Doxycycline remains a cornerstone antimicrobial agent with broad-spectrum activity and versatile clinical applications. Recent literature and updated guidelines continue to support its effectiveness in dentistry, particularly in 3 key areas: prophylaxis for IE, long-term periodontal therapy, and local delivery of peri-implantitis therapy. Its safety profile is generally favorable, with most adverse effects being mild or preventable. Emerging evidence also supports its short-term safety in children when clinically indicated.
In an era marked by rising antibiotic resistance and increasing cost pressures, doxycycline stands out as a well-tolerated, affordable, and broadly effective treatment option. Current evidence confirms that doxycycline continues to play a vital role in modern antimicrobial therapy.
Author affiliations
Kaufman Hall, a Vizient Company, Pharmacy Advisory Solutions, Irving, Texas; Skaggs School of Pharmacy, University of Montana, Missoula, Montana; School of Dentistry, Oregon Health & Sciences University, Portland, Oregon; and Faculty of Dentistry, University of British Columbia, Vancouver, Canada (Donaldson); Premier Dental Products Company, Plymouth Meeting, Pennsylvania; Department of Oral and Maxillofacial Surgery, Creighton University School of Dentistry, Omaha, Nebraska; and Division of Oral Diagnosis, Department of Diagnostic Sciences, Rutgers School of Dental Medicine, Newark, New Jersey (Goodchild).
Conflicts of interest
None reported.
Disclaimer
The views expressed in this column are those of the authors and do not necessarily reflect those of their affiliated institutions.
References
1. Label: Doxycycline hyclate—doxyclycline hyclate tablet, coated. September 18, 2023. Accessed July 28, 2025. https://dailymed.nlm.nih.gov/dailymed/drugInfo. cfm?setid=2cffb084-2b25-4e1b-846b-8681de7ea666
2. MacDougall C. Protein synthesis inhibitor. In: Brunton LL, Hilal-Dandan R, Knollmann BC, eds. Goodman & Gilman’s: The Pharmacological Basis of Therapeutics. 14th ed. McGraw-Hill Medical; 2022:1179-1192.
3. World Health Organization Expert Committee. The selection of essential drugs. Technical Report Series 615. World Health Organization; 1977. https://list.essentialmeds. org/files/trs/sC1L9Ib4I8o8cDqlyfhnKyoa8MGm7XUFDffFVNUc.pdf
4. Ibrahim AM, Siddique MS. Subacute bacterial endocarditis prophylaxis. In: StatPearls. StatPearls Publishing; February 10, 2024. https://www.ncbi.nlm.nih.gov/books/ NBK532983/
5. Nath S, Pulikkotil SJ, Dharmarajan L, Arunachalam M, Jing KT. Effect of locally delivered doxycycline as an adjunct to scaling and root planing in the treatment of periodontitis in smokers: a systematic review of randomized controlled trials with meta-analysis and trial sequential analysis. Dent Res J (Isfahan). 2020;17(4):235-243.
6. Passarelli PC, Netti A, Lopez MA, et al. Local/topical antibiotics for peri-implantitis treatment: a systematic review. Antibiotics (Basel). 2021;10(11):1298. doi:10.3390/ antibiotics10111298
7. Rothstein DM, McGlynn M, Bernan V, et al. Detection of tetracyclines and efflux pump inhibitors. Antimicrob Agents Chemother. 1993;37(8):1624-1629. doi:10.1128/ AAC.37.8.1624
8. Beheshti M, Ardebili A, Beheshti F, et al. Tetracycline resistance mediated by tet efflux pumps in clinical isolates of Acinetobacter baumannii. Rev Inst Med Trop Sao Paulo. 2020;62:e88. doi:10.1590/S1678-9946202062088
9. Carrel M, Smith M, Shi Q, et al. Antimicrobial resistance patterns of outpatient Staphylococcus aureus isolates. JAMA Netw Open. 2024;7(6):e2417199. doi:10.1001/ jamanetworkopen.2024.17199
10. Gasparrini AJ, Markley JL, Kumar H, et al. Tetracyclineinactivating enzymes from environmental, human commensal, and pathogenic bacteria cause broad-spectrum tetracycline resistance. Commun Biol. 2020;3(1):241. doi:10.1038/s42003-020-0966-5
11. Yang J, Xiao G, Xiao N, et al. Characteristics of tet(X4)producing Escherichia coli in chicken and pig farms in Hunan Province, China. Antibiotics (Basel). 2023;12(1):147. doi:10.3390/antibiotics12010147
12. Cross R, Ling C, Day NP, McGready R, Paris DH. Revisiting doxycycline in pregnancy and early childhood—time to rebuild its reputation? Expert Opin Drug Saf. 2016;15(3):367382. doi:10.1517/14740338.2016.1133584
13. Biggs HM, Behravesh CB, Bradley KK, et al. Diagnosis and management of tickborne rickettsial diseases: Rocky Mountain spotted fever and other spotted fever group
rickettsioses, ehrlichioses, and anaplasmosis - United States. MMWR Recomm Rep. 2016;65(2):1-44. doi:10.15585/mmwr.rr6502a1
14. Todd SR, Dahlgren FS, Traeger MS, et al. No visible dental staining in children treated with doxycycline for suspected Rocky Mountain spotted fever. J Pediatr. 2015;166(5):12461251. doi:10.1016/j.jpeds.2015.02.015
15. Hemphill ME, Mollanazar NK, Hsu S. Doxycycline is safe for short-term use in children of all ages. Skinmed. 2019;17(5):322.
16. Ghanshani R, Lee K, Crew AB, Shi VY, Hsiao JL. A guide to the management of hidradenitis suppurativa in pregnancy and lactation. Am J Clin Dermatol. 2025;26(3):345-360. doi:10.1007/s40257-025-00935-x
17. Bontsevich RA, Zarudskaya OM, Adonina AV. Doctors’ preferences in the choice of antibacterial drugs in pregnant women (PIKAP study). Int J Risk Saf Med. 2025;9246479251327814. doi:10.1177/09246479251327814
18. Varma S, Nathanson J, Dowlatshahi M, Del Portillo A, Ramirez I, Garcia-Carrasquillo R. Doxycycline-induced cholestatic liver injury. Clin J Gastroenterol. 2021;14(5):15031510. doi:10.1007/s12328-021-01475-7
19. Friedman DI, Gordon LK, Egan RA, et al. Doxycycline and intracranial hypertension. Neurology. 2004;62(12):22972299. doi:10.1212/wnl.62.12.2297
20. Wilson W, Taubert KA, Gewitz M, et al. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation. 2007;116(15):1736-1754. doi:10.1161/CIRCULATIONAHA.106.183095
21. Wilson WR, Gewitz M, Lockhart PB, et al. Prevention of viridans group streptococcal infective endocarditis: a scientific statement from the American Heart Association. Circulation. 2021;143(20):e963-e978. doi:10.1161/ CIR.0000000000000969
22. Goodchild JH, Donaldson M. Antibiotic prophylaxis guidelines: is there new information for 2021? Gen Dent. 2021;69(6):6-9.
23. Wilson WR, Gewitz M, Lockhart PB, et al. Adapted from: Prevention of viridans group streptococcal infective endocarditis: a scientific statement from the American Heart
Association. J Am Dent Assoc. 2021;152(11):886-902.e2. doi:10.1016/j.adaj.2021.09.003
24. Smiley CJ, Tracy SL, Abt E, et al. Evidence-based clinical practice guideline on the nonsurgical treatment of chronic periodontitis by means of scaling and root planing with or without adjuncts. J Am Dent Assoc. 2015;146(7):525-535. doi:10.1016/j.adaj.2015.01.026
25. de Molon RS, Rodrigues JVS, Deroide MB, da Silva Barbirato D, Garcia VG, Theodoro LH. The efficacy of topical or systemic antibiotics as adjuvants to non-surgical periodontal treatment in diabetic patients
26. : a systematic review and meta-analysis of randomized clinical trials. J Clin Med. 2024;13(16):4763. doi:10.3390/ jcm13164763
27. Zhang Z, Zhang Z, Zhang G. Systemic doxycycline as an adjunct to nonsurgical periodontal therapy in diabetic patients with periodontitis: a systematic review and metaanalysis. Front Physiol. 2025;15:1479152. doi:10.3389/ fphys.2024.1479152
28. Corbella S, Vendrame A, Tedeschi L, Ashurko I, Francetti L. The application of local doxycycline gel for the nonsurgical treatment of peri-implant diseases: a systematic review of the literature. Appl Sci. 2025;15(10):5357. doi:10.3390/ app15105357
29. Büchter A, Meyer U, Kruse-Lösler B, Joos U, Kleinheinz J. Sustained release of doxycycline for the treatment of periimplantitis: randomised controlled trial. Br J Oral Maxillofac Surg. 2004;42(5):439-444. doi:10.1016/j. bjoms.2004.06.005
30. Neely AL, Thompson TN, Gupta V, Kinaia B. Successful management of peri-implantitis using a titanium brush and a doxycycline-saline slurry for surface detoxification with guided bone regeneration: a 5-year follow-up. Clin Adv Periodontics. 2020;10(3):118-122. doi:10.1002/ cap.10085
31. Lu Y, Bao S, Luo H, Chen Q, Si M. Efficacy of adjunctive systemic or local antibiotic therapy in peri-implantitis: a systematic review and meta-analysis of randomized controlled clinical trials. J Zhejiang Univ Sci B. 2024;26(2):145-157. doi:10.1631/jzus.B2300730
32. Galarraga-Vinueza ME, Pagni S, Finkelman M, Schoenbaum T, Chambrone L. Prevalence, incidence, systemic, behavioral, and patient-related risk factors and indicators for peri-implant diseases: an AO/AAP systematic review and meta-analysis. J Periodontol. 2025;96(6)587-633. doi:10.1002/JPER.24-0154
Understanding cracked tooth syndrome: diagnosing nondental pain in dentistry
Stanley Markman, DDS, Dip ABOP ¢ Amey G. Patil, BDS, MSD, Dip ABOP, Dip ABAD
Cracked tooth syndrome (CTS) is a recognized entity with characteristic clinical and radiographic findings; however, this condition is often diagnosed in patients who present with atypical orofacial pain lacking these supporting features.1,2 This practice, driven by “nociceptive mania”—the tendency to attribute all orofacial pain to dental causes—can lead to unnecessary dental interventions, including root canal treatments and extractions.
This column highlights the limitations of current diagnostic methods for CTS, particularly in cases without clear clinical or radiographic evidence. The importance of a thorough patient history that includes previous dental treatments and pain experiences in order to differentiate between true CTS and other pain conditions is emphasized. The concept of neuropathic pain, with characteristic symptoms such as burning, tingling, and allodynia, is discussed as a potential alternative diagnosis in cases where typical CTS findings are absent. Increased awareness of nonodontogenic pain and referral to orofacial pain specialists when pain presentations are atypical or unresponsive to conventional dental treatment can prevent unnecessary dental procedures and improve outcomes by addressing the true source of the patient’s pain.
Cracked tooth syndrome
About 60 years ago, Cameron proposed an explanation for an atypical form of tooth pain.3 He suggested that
anomalous pain complaints are likely to be caused by cracks in the roots of teeth. Cameron referred to this phenomenon as cracked tooth syndrome. 3 As time progressed, this assessment gained acceptance among dental professionals, especially when verified by a typical J-shaped radiographic image hugging the offending tooth. Other radiographic findings include J-shaped radiolucencies in the periapical regions of teeth with small restorations, in the absence of periodontal bone loss.4,5 Cone beam computed tomography (CBCT) is now also used to verify the diagnosis of CTS; however, irregular pain complaints cannot always be verified with CBCT imaging.6
Nociceptive mania
Patients see dentists for multiple reasons, including pain. When dental-presenting pain does not conform to its usual signs and symptoms, dentists pursue an alternative dental diagnosis, often CTS.1,7 A confirmed cracked tooth illustrates common findings, including temperature responses, a positive bite test (wherein the release of occlusal pressure can cause pain), and supporting imaging that suggests pathosis.5 Yet, even in the absence of such findings, CTS is often a soughtout diagnosis, with clinicians considering the possibility that the crack might be invisible even if it is located in the root.7,8 The literature on CTS reports that this pain is difficult to diagnose and has vague symptoms and that complaints fail to correspond to usual findings; instead, symptoms such as sudden unprovoked
pain or tingling more often point toward nonodontogenic causation.1,4,7 Essentially, the pain reports fail to match expected dental symptoms.1,4
There are several proposed reasons why CBCT may fail to reveal a crack.9 After extraction of a cracked tooth, a crack may not be visible, even on close examination of the root.8,10 Some suggest there are very small, not-yet-visible, or microscopic cracks in portions of the root and that bone changes that cannot be seen have occurred.1,4 When a diagnosis cannot be confirmed, the patient who reports pain that fails to match expected dental symptoms might visit other dentists for an opinion, especially if the tooth has undergone endodontic treatment.11
If a patient presents with pain in a tooth that has undergone root canal treatment, an initial question to ask is why the procedure was performed. One answer from a patient might be: “Because the dentist said I needed it.” This answer suggests that an asymptomatic tooth has been converted into a symptomatic tooth, which can be verified with additional questions.12
Diagnosis
A good test to identify the source of pain is the administration of local anesthesia. If the patient’s pain disappears after injection of an anesthetic agent, the likely diagnosis is a dental problem—specifically, nociceptive pain. If the patient’s response is equivocal, the dentist should expect that the source of the pain is not dental; how can there be a diagnosis of
dental pain when an odontogenic cause is not verified? It is possible that many teeth are extracted with the label of CTS without true verification or with an unsupported diagnosis.8 The thought that the vague pain described by patients could be of nondental origin seldom enters dentists’ minds for 2 reasons: dental pain is 100% nociceptive pain, and all dental school programs focus on the treatment of nociceptive pain.
No literature exists that explains the mechanisms behind the pain response in the bite test used to confirm CTS.4 In the absence of a positive bite response, significant temperature responses, and supporting radiographic findings, how can the clinician diagnose a cracked root? What we should conclude is that the tooth in question has pain of a nonodontogenic origin.9
When examining a patient who might have been previously diagnosed with a cracked tooth, dentists should assess the history of the tooth at the beginning rather than the end of the appointment.5,11 The main focus should be on obtaining an accurate history through careful questioning:
• If there was a root canal procedure, why was it done? Was it done because of pain? If yes, was the pain relieved, or did the nature of the pain become different?
• Was any dental treatment performed on the tooth in question prior to the root canal treatment?
• Did pain induce the patient to go to a dentist, and then did the dentist suggest that root canal treatment was needed?
• Was the root canal treatment done once, or has the treatment been done more than once?
Without knowledge of the patient’s pain history, the dentist will not be aware if the pain is related to a previous problem. The patient’s pain history may reveal a long-term problem with a tooth, but the focus on the patient’s immediate pain may prevent an accurate diagnosis. The tooth pain history may indicate that the current diagnosis is not simple or obvious.
Neuropathic pain
If the patient does not have CTS, what could be the source of the pain? In dental
school, students are trained to identify different sources of dental pain: pulpal, periodontal, or postsurgical. All fall into the category of nociceptive pain, where primary afferent nociceptors interpret action potentials that are sent through the central nervous system to the somatosensory cortex.13
Another kind of pain that some dentists are less familiar with, neuropathic pain, is caused by damage to the nervous system. This damage can occur in the brain, spinal cord, or nerves throughout the body. When nerves are damaged, signals are forwarded to the somatosensory cortex, which interprets such action potentials as pain. Neuropathic pain can be chronic or intermittent, and it can vary in intensity. Neuropathic pain is typified by the following characteristics:
• Abnormal sensations: pain that often presents with unusual sensations, such as burning, tingling, shooting, stabbing, or electric shock–like pain
• Spontaneous pain: pain with no obvious provocation
• Allodynia: pain from light touch or temperature changes that do not normally cause pain
• Numbness: loss of feeling
• Hyperalgesia: exaggerated pain response to painful stimuli
• Emotional distress: anxiety, depression, and difficulty sleeping
In 2020, the American Dental Association recognized a new dental specialty: orofacial pain.14,15 This discipline might be more recognizable to dentists if it was named oral and facial pain. Dentists with this specialty are trained to recognize patients with nonodontogenic pain and provide continuing education to other dentists to illustrate the concepts. Yet, when presented with a tooth or tooth area where such a condition exists, some dentists ignore information about this newly recognized pain specialty. Nociceptive mania sets in, and they try very hard to transform nondental symptoms into nociceptive pain. A tooth diagnosed with CTS that lacks the expected signs and symptoms requires a change in the thought process—perhaps no nociceptive pain is present, and the pain has a nonodontogenic origin.7
Diagnostic confusion may arise when the patient uses uncommon descriptors, such as tingling, burning, continuous, episodic, or unprovoked, to describe the pain that the dentist suspects is odontogenic in origin. However, misdiagnosis of the condition as nociceptive pain results in unnecessary root canal treatment or extraction. Sometimes the resulting root canal treatment can become excessive, such as when a well-intentioned dentist attempts to relieve neuropathic pain with a series of unsuccessful endodontic treatments across an entire quadrant.
Conclusion
Orofacial pain exists because of a cause. If the dentist cannot definitively identify the reason, dental treatment should be avoided. Referral to an orofacial pain specialist should be considered, especially when pain symptoms do not match expected or known nociceptive signs and symptoms.
Author affiliations
Center for Temporomandibular Disorders and Orofacial Pain, Department of Diagnostic Sciences and Department of Restorative Dentistry, Rutgers School of Dental Medicine, Newark, New Jersey.
Conflicts of interest
None reported.
References
1. Li F, Diao Y, Wang J, et al. Review of cracked tooth syndrome: etiology, diagnosis, management, and prevention. Pain Res Manag. 2021;2021:3788660. doi:10.1155/2021/3788660
2. Lynch CD, McConnell RJ. The cracked tooth syndrome. J Can Dent Assoc. 2002;68(8):470-475.
4. Hasan S, Singh K, Salati N. Cracked tooth syndrome: overview of literature. Int J Appl Basic Med Res. 2015;5(3):164-168. doi:10.4103/2229-516X.165376
5. Mathew S, Thangavel B, Mathew CA, Kailasam S, Kumaravadivel K, Das A. Diagnosis of cracked tooth syndrome. J Pharm Bioallied Sci. 2012;4(Suppl 2):S242-S244. doi:10.4103/0975-7406.100219
6. Alaugaily I, Azim AA. CBCT patterns of bone loss and clinical predictors for the diagnosis of cracked teeth and teeth with vertical root fracture. J Endod. 2022;48(9):11001106. doi:10.1016/j.joen.2022.06.004
7. John K, Pepper T. Cracked tooth syndrome. In: StatPearls. StatPearls Publishing; May 7, 2024. https://www.ncbi. nlm.nih.gov/books/NBK606115/
8. Yu M, Li J, Liu S, Xie Z, Liu J, Liu Y. Diagnosis of cracked tooth: clinical status and research progress. Jpn Dent Sci Rev. 2022;58:357-364. doi:10.1016/j. jdsr.2022.11.002
9. Gao A, Cao D, Lin Z. Diagnosis of cracked teeth using cone-beam computed tomography: literature review and clinical experience. Dentomaxillofac Radiol. 2021;50(5):20200407. doi:10.1259/dmfr.20200407
10. Kakka A, Gavriil D, Whitworth J. Treatment of cracked teeth: a comprehensive narrative review. Clin Exp Dent Res. 2022;8(5):1218-1248. doi:10.1002/cre2.617
11. Obadan-Udoh E, Howard R, Valmadrid LC, Walji M, Mertz E. Patients’ experiences of dental diagnostic failures:
a qualitative study using social media. J Patient Saf. 2024;20(3):177-185. doi:10.1097/ PTS.0000000000001198
12. Segura-Egea JJ, Cisneros-Cabello R, Llamas-Carreras JM, Velasco-Ortega E. Pain associated with root canal treatment. Int Endod J. 2009;42(7):614-620. doi:10.1111/ j.1365-2591.2009.01562.x
13. Renton T, Wilson NH. Understanding and managing dental and orofacial pain in general practice. Br J Gen Pract. 2016;66(646):236-237. doi:10.3399/bjgp16X684901
14. Fricton J, Crandall JA. Orofacial pain as a new dental specialty. Cranio. 2020;38(2):69-72. doi:10.1080/088696 34.2020.1716140
15. Heir GM. Orofacial pain, the 12th specialty: the necessity. J Am Dent Assoc. 2020;151(7):469-471. doi:10.1016/j. adaj.2020.05.002
PROSTHODONTICS
The crucial second appointment in full-arch removable prosthesis cases
Samuel M. Strong, DDS
The standard or traditional sequence of appointments for full dentures and overdentures is a 4-appointment protocol.1 At the first appointment, a master impression is made, lip ruler measurements are collected, and photographs of existing restorations or dentition are taken. At the second appointment, the clinician inserts the baseplate with a wax rim; marks the midline, the alae of the nose, high smile, and resting lip lines; and records the centric relation at the approved vertical dimension of occlusion. The third appointment is for try-in of denture teeth that are either set in wax, solid milled, or printed. Approval by the patient and the dentist is needed to proceed with the final appointment, which is made for the delivery of the finished prosthesis.
This article will focus on the critical items a dentist must obtain at the second appointment. Capturing this data is very important in providing accurate information to the laboratory technician producing a suitable try-in. Having success at this appointment is crucial to avoiding unnecessary additional appointments.
As a review, the first appointment requires a highly accurate master impression of the existing edentulous arch. This impression traditionally is obtained using a well-fitted impression tray and polyvinyl siloxane impression material, or a virtual impression can be taken using a handheld intraoral scanner.
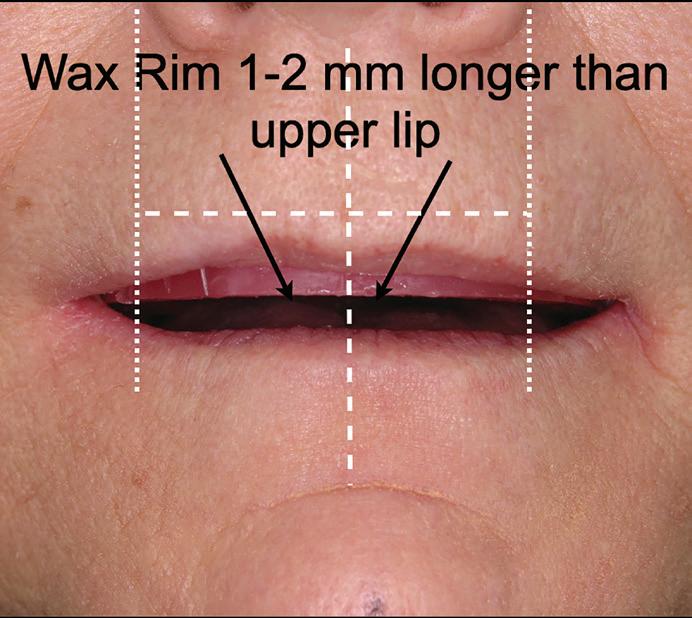
A lip ruler measurement is highly recommended to identify the desired positioning of the wax rim. The lip ruler is positioned under the upper lip with the lip
draped at rest. This ruler has gradations of millimeters inscribed on the facial aspect to confirm the distance from the edentulous ridge to the resting lip line.
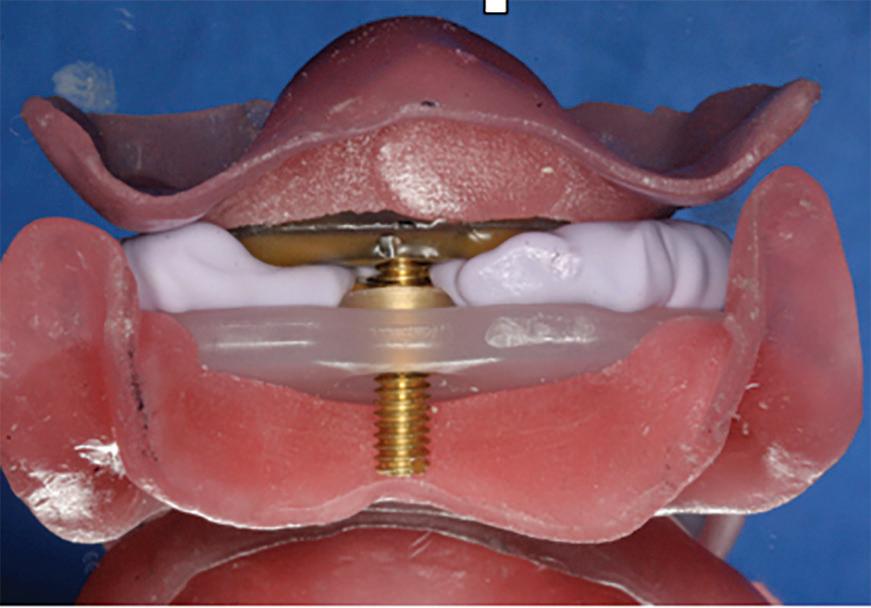
At the second appointment, the baseplate/wax rim is seated in the mouth. First, retention of the baseplate must be evaluated intraorally. If the milled or printed baseplate remains firmly seated on the maxilla or mandible without loss of retention, we can expect the same degree of retention in the final prosthesis. Note that this retention level will only be duplicated in a milled or printed final prosthesis and cannot be replicated exactly in a traditionally processed appliance.
The seated baseplate and wax rim are then subjected to critical evaluations and adjustments as needed. First, the incisal length of the baseplate is reduced or extended to produce a length 1 to 2 mm longer than the maxillary lip line at rest. This position will be used by the laboratory technician to set the incisal edge positions of the maxillary central incisors. The border of the maxillary lip at rest is marked into the wax rim with a horizontal line. For a mandibular prosthesis, the wax rim is fabricated to correspond evenly with the lower lip line at rest.
The high smile line is then observed by instructing the patient to produce an animated smile, exposing more of the wax rim length. This maxillary lip position should be maintained by the patient long enough to mark a horizontal line in the wax along the lip border.
Next, the midline is marked with a vertical line using an instrument to crease
Fig 1. The maxillary wax rim is marked to show the midline, resting lip position, high smile line, alae of the nose, and the buccal corridor.
Fig 2. Use of the Fox plane. A. A Fox plane is placed on the wax rim to confirm the profile plane of occlusion. B. The frontal view confirms that the maxillary rim is parallel to the floor.
Fig 3. Tooth shells applied to the facial aspect of a maxillary wax rim serve as a guide to the laboratory technician for setting denture teeth.
the wax. I suggest enlisting the patient’s opinion about this designated midline mark. The idea is to create a line of demarcation with half of the face on each side of the line, not necessarily using the middle of the nose as a midline indicator.
Then the alae of the nose, left and right, are identified in the wax rim with vertical lines. These lines are used by the laboratory technician to establish the distal contact points of the maxillary canine denture teeth. This guideline for canine denture tooth position can vary among men and women or among various racial demographics.2 Some disagreement also exists about the significance or accuracy of using this facial landmark.3 However, many (if not most) laboratory technicians use the interalar width as a starting point for establishing canine teeth positions.
The buccal corridor—represented by the rounded extent of the wax rim from canines to the corners of the lips—is then adjusted in the wax rim. The dentist should envision the facial contour of the
wax rim duplicating the facial surfaces of the denture teeth to be set in wax (Fig 1).
The use of a Fox plane instrument is valuable to obtain an acceptable plane of occlusion in the wax rim. The Fox plane is held against the occlusal surface of the wax rim. The wax is adjusted to create a level, balanced rim as observed on profile and frontal views of the patient (Fig 2).
A valuable alternative to using only a wax rim with markings for the laboratory technician’s instruction is the use of tooth shells (Global Dental Impression Trays [GDIT]). These shells come in a card that replicates maxillary tooth arrangement from first premolar to first premolar. They are available in various sizes and shapes, similar to full denture teeth cards. These shells can be heated in a water bath and arranged on the facial aspect of the wax rim to visualize where the definitive denture teeth can be set in wax for the try-in appointment (Fig 3). The patient can obtain a preliminary view of how the final prosthetic teeth will look and provide immediate feedback to the dentist.
Photographs of the markings in the wax rim or the tooth shells in place should be obtained and sent to the laboratory technician. These photographs will be invaluable to the technician in setting the denture teeth in wax in preparation for the next appointment. This set-up of denture teeth will be evaluated by the patient and clinician at the try-in appointment for esthetics, phonetics, and occlusion. All of these issues must be approved by the patient and dentist before proceeding to the final milling, printing, or conventional processing. Perhaps the most challenging issue in all of dentistry is the task of obtaining a repeatable centric relation or centric occlusion record. The accuracy of this record will completely determine how successful the final prosthesis will be. A poorly determined bite registration will translate into additional appointments to reset denture teeth in wax until an acceptable occlusion is achieved.
The gothic arch tracing technique has been found by many clinicians to produce the most accurate centric relation record, and it has the added benefit of being made at the correct vertical dimension of occlusion.4 The patient is fitted with a maxillary striking plate and a mandibular ball bearing pin (Massad Jaw Recorder, Global Dental Impressions Trays.) The correct vertical dimension of occlusion is determined with the maxillary plate and mandibular pin placed intraorally. When the patient closes so that the mandibular pin touches the maxillary plate and rubs the pin anteriorly and laterally (left and right), an arrow or gothic arch tracing is inscribed on the plate. The tip of this arrow represents the patient’s true centric relation (Fig 4). The maxillary striking plate and mandibular pin are then joined together at this arrow tip, producing an extremely accurate jaw relation record (Fig 5). The maxillary and mandibular casts are mounted on the articulator using this jaw relation record (Fig 6).
The patient’s preferred shade for the final restoration must be obtained at the second appointment. Photographs or diagrams of different arrangements for the smile design should also be presented for the patient to designate a preference.
All of this information and the prosthetic items are returned to the laboratory for fabrication of a try-in appliance.
Fig 4. The tip of the gothic arch tracing represents the patient’s centric relation made at the correct vertical dimension of occlusion.
Fig 5. The maxillary tracing plate and mandibular tracing pin are connected.
Fig 6. The maxillary and mandibular casts are mounted on the articulator using the jaw relation record.
The try-in has traditionally consisted of denture teeth set in wax, called a wax-up or try-in. The denture teeth are positioned in wax after selection of the appropriate mold size, shape, and shade. This item is inserted intraorally at the third appointment for evaluation of occlusion, midline, buccal corridor, positions of the cervical and incisal teeth edges at rest and at a high smile position, and phonetics (Fig 7). In a digital mode, the setup of teeth is created by computer and usually sent by email to the dentist for evaluation and approval. However, a newer option is to request the laboratory to return a solid acrylic try-in, milled or printed, for evaluation at the next appointment. This offers the unique advantage of allowing the patient and dentist a longer period of time for evaluation before committing to final production of the prosthesis. I have often allowed the patient to use the try-in for a few days or even weeks to confirm approval of the appliance before finishing the case (Fig 8).
Conclusion
The second appointment uses a baseplate with wax rim, tooth shells, and markings to indicate critical data, which pave the way for a successful completion of the case. In my experience, spending significant time and effort at the second appointment to obtain measurements of the midline as well as resting and high smile lines; accurate recording of centric relation; and shade and tooth size selections is more than worth the effort, helping dentists avoid frustrating and labor-intensive corrections at later appointments or after delivery of a poorly finished prosthesis.
Author affiliation
Private practice, Little Rock, Arkansas.
Conflicts of interest
None reported.
References
1. Daher T, El Sherif M, Davis WJ, et al. Successful and predictable custom complete dentures. Dent Today. 2016;35(3):86.
2. Srimaneekam N, Arayapisit T, Pookuantong O, Cheng HR, Soonsawad P. Determining of canine position by multiple facial landmarks to achieve natural esthetics in complete
8. Milled solid acrylic try-in provides longer term evaluation than a denture setup in wax. The solid appliance can be used for days or weeks to confirm approval by the patient or determine any adjustments that are needed.
3. Varjão FM, Nogueira SS. 2006: Nasal width as a guide for the selection of maxillary complete denture anterior teeth in four racial groups. J Prosthodont. 2006;15:353-358. doi:10.1111/j.1532-849X.2006.00134.x
4. Massad JM, Connelly ME, Rudd KD, Cagna DR. Occlusal device for diagnostic evaluation of maxillomandibular relationships in edentulous patients: a clinical technique. J Prosthet Dent. 2004;91(6):586-590. doi:10.1016/j.prosdent.2004.03.008
Fig
Fig 7. A to D. Data from the second appointment are used to fabricate the denture setup for evaluation intraorally at the third appointment.
Understanding and preparing for our aging patient population
Larry N. Williams, DDS, MPH
It has long been an adage that it is cheaper to prevent disease than it is to treat it. This adage is reinforced today by 2 important findings. The first is the aging population of baby boomers (people born between 1945 and 1965), known as the “silver tsunami.” According to the US Census Bureau, by the year 2030, all baby boomers will have turned 65 years old.1 The census data predict that, in 2034, the number of people aged 65 years and older (hereafter referred to as 65+) will outnumber people under the age of 18 years.1
The second is the health status of the aging population. According to a 2010 publication by Yong et al, 40% of all premature deaths in the aging population in the United States were related to unhealthy and preventable behaviors.2 These behaviors included tobacco and alcohol use, lack of vaccinations, and lack of cancer screening. Any oral health provider with 65+ patients knows that many of these behaviors are also likely to influence the patient’s oral health, thus affecting patient care.2
As the 65+ population grows, we must be aware that some of the health issues patients are likely to develop are preventable. This article will provide some basic, up-to-date information on our aging patient population, then discuss how information gathered via health questionnaire screenings in patient records can help us better treat our patients, allowing us to find and address preventable health issues and avert premature deaths.2
A look at our aging population
It is a fact that our population is aging. According to the Population Reference Bureau, the number of 65+ Americans is expected to grow to 82 million by 2050, which will account for nearly 25% of the US population.3 Additionally, the median age of the US population today is older than it has ever been, rising from 30 to nearly 40 years between 1980 and 2022.
As the population ages, it’s becoming more racially and ethnically diverse, among other changes.3 Education levels are increasing in the 65+ population; the proportion with 4 or more years of college increased from 5% in 1965 to 33% in 2023. In addition, more of the 65+ population is working longer. In 2022, 24% of men and 15% of women aged 65+ were in the US workforce. These rates are predicted to rise to 25% of men and 17% of women by 2032. Finally, more 65+ adults today can perform basic activities of daily living (ADLs), such as bathing, dressing, and feeding themselves, and fewer reside in assisted living and nursing homes.3 This can be attributed to better health among older adults as well as the availability of assistive devices and home modifications.3 It can be inferred that the number of individuals who can perform instrumental ADLs, which require more complex thinking (eg, shopping, cooking, and making appointments), has also increased; however, people often require assistance with instrumental ADLs before they need help with basic ADLs.4
A look at the health of the 65+ population
According to a 2024 report from the National Council on Aging summarizing data from 2022, members of our 65+ potential patient population are likely have at least 1 chronic health condition, and many older adults are affected by multiple health problems.5 Among the chronic conditions evident in the 65+ population is heart disease, which is the leading cause of death among Americans. Heart disease can affect people of all ages but is most prevalent in those aged 75 years and older. The report also noted that arthritis is a frequent finding in 65+ adults, present in about 45% of this cohort. Additionally, 1 in 5 adults aged 65+ have a diagnosis of diabetes. Obesity is also common among this cohort, as almost 42% of Americans aged 60 years and older are considered obese.5
In addition to health issues, members of the 65+ population often have some degree of financial insecurity, which is a pressing issue for older adults. In 2022, approximately 1 in 10 Americans aged 65+ had an income below the official poverty line.3 According to data from the US Census Bureau, that proportion increased to 14% of the 65+ population when calculated using the criteria of the Supplemental Poverty Measure—an alternative measure that provides a more comprehensive picture of economic hardship by incorporating noncash benefits, subtracting necessary expenses (such as taxes), and making geographic adjustments for variations in the cost of living.6
In recent years, the older population has also been struggling with higher prices associated with inflation, which affects the cost of necessities such as housing, groceries, utilities, and healthcare. A single health emergency or unforeseen expense can quickly deplete the savings of those on a fixed income.5
Poverty and hunger go hand in hand, and too many older adults don’t have enough to eat. In 2022, nearly 1 in 10 households with an older adult were food insecure, with a higher rate seen among those 65+ living alone. Hunger has a profound impact on older adults’ health and nutrition, increasing their risks for diabetes, depression, asthma, and, possibly, poor oral health.5
Older adults living with disability have nearly triple the rate of food insecurity as their peers without disability. Although the Supplemental Nutrition Assistance Program (SNAP) is available for households with older adults, millions remain unenrolled in the benefit, which means that many people are missing out on vital assistance.5
A look at the caregivers
The individuals helping our 65+ population directly impact our role as oral healthcare providers. We need to make sure that family caregivers are trained to help older adults with oral health as well as other areas of care. We must also remember that most of these family caregivers have other responsibilities to manage, such as jobs and childcare. Approximately 37.1 million individuals provided unpaid care to someone aged 65+ in the period from 2021 to 2022.7 About 41% of these family caregivers were aged 45 to 64 years.
Conversely, older Americans may be family caregivers as well. From 2021 to 2022, 15% of those providing care to an older family member were in the 65+ cohort themselves.7 Moreover, those who were aged 65+ were the most likely of any caregiver group to deliver care on any given day. In addition, about 1.1 million grandparents aged 60 years and older were providing the majority of basic care for grandchildren who lived with them. In 2019, 1.3 million people with intellectual and developmental disabilities lived with a family caregiver who was 60 years or older.7 How many
of these older caregivers are aware of the importance of oral health and its link to systemic disease?
Aging and oral health
Although many 65+ adults living today have more remaining teeth than previous generations, many are also suffering from limited access to care and limited funds for treating oral problems, including caries and periodontal disease as well as oral and oropharyngeal cancers. Added to the difficulty obtaining care is the fact that Medicare excludes dental benefits except for special circumstances. With the loss of dental insurance and lower levels of income after retirement, the growing population of older Americans is more at risk for untreated oral disease.
According to the National Institute of Dental and Craniofacial Research, almost 17% of 65+ adults have untreated caries.8 Rates of untreated caries are higher in certain subgroups of this cohort, including non-Hispanic Black and Mexican American individuals as well as those living in poverty. Root caries in particular is more prevalent in the aging population, although other factors, such poor plaque control, tobacco use, and low socioeconomic status, also increase risk. Periodontitis is also prevalent, with approximately 60% of those aged 65+ having some degree of gingivitis or periodontal disease. Edentulism among older Americans has decreased in recent decades; approximately 17% of this age group are without teeth, compared with nearly 50% in 1960. However, people who live in poverty are 3 times more likely to be edentulous than are those whose incomes exceed the federal poverty guidelines by 200% or more. Finally, the older adult population is at increased risk for oropharyngeal cancer due to the prevalence of human papillomavirus infection among this cohort.8
What can dentists do?
What can we do to improve the oral and general health of our patients? Here’s a synopsis of the issues we face:
• The population is aging; soon, 65+ adults will account for 25% of the US population.3
• Among the 65+ population, 40% of premature deaths are due to a preventable cause.2
• 65+ adults suffer from chronic diseases, hunger, and poverty, and many provide caregiving for grandchildren and adults with disabilities.3,5-7
• Older adults often have limited resources for oral healthcare and are thus at risk of caries, tooth loss, periodontal disease, and oral cancer.8
My first recommendation would be to make sure that all of our patients receive our full attention regarding their oral and systemic health issues. While we cannot provide physician-level care for systemic conditions, we can utilize health questionnaires, review prescribed and over-the-counter medications, measure vital signs such as blood pressure and heart rate, and ask open-ended questions about health issues we find when reviewing questionnaires or vital sign measurements.
For our 65+ patients, we need to be aware of changes that may have occurred during the aging process and over the course of our clinical care. We also need to make sure we consult our patients when we feel we need more information. It is important to remember that the health of the patient we saw in our 30s is probably not the same as that of the patient we are seeing 35 years later. Unfortunately, as our patients age, so do we—and so we may find that we unconsciously accommodate subtle changes in our patients, such as cognitive and mobility issues, without directly discussing them. Here are some examples I have encountered when treating older patients:
• The patient repeats the same questions during care.
• The patient demonstrates a personality change since the last appointment (eg, suddenly irritable or withdrawn).
• The patient exhibits an undesirable change in dress and hygiene (body odor, unkempt appearance, etc).
• The patient has new mobility difficulties.
These types of changes must be documented. Problems that are observed may require follow-up to see if additional resources or people need to be involved in the patient’s care, although such follow-up must maintain compliance with the requirements of
the Health Insurance Portability and Accountability Act. Many areas of the country have help available for the 65+ population. In addition, the new 988 mental health crisis telephone line is available to all Americans.
An additional and important source of 65+ health information is the plan created after the patient’s Medicarefunded yearly wellness visit. While this information may not be available to dentists firsthand, we can certainly ask our 65+ patients if they use Medicare, have received the results of their annual wellness visit, and are willing to provide a copy so that the information is in our records. If a copy is not available, then we can ask about and document some of the information typically included in the wellness records. The following items covered by the annual wellness visit could be easily included in a dental health questionnaire or screening9:
• Screening schedule (eg, a checklist) for appropriate oral health preventive services
Conclusion
The bottom line is that our aging patients, especially those 65+, may benefit from some extra attention when visiting our dental practices. We can provide better care for our patients aged 65+ if we consider the following questions:
• Do we need to modify our health questionnaire to help recognize the needs of our older patients?
• Do we need to address the preventive needs or physical needs of our older patients?
• Do we have a mechanism in place to notify someone (caregiver, family member, or individual with healthcare power of attorney) if changes are noted and help is needed?
Those of us with older parents, friends, and loved ones—and those of us who are getting up there ourselves—know that most people need extra help as they age. As oral health professionals, we can and should be part of that support system.
Author affiliation
Midwestern University College of Dental Medicine-Illinois, Downers Grove, Illinois.
Conflicts of interest
None reported.
References
1. Older people projected to outnumber children for first time in U.S. history. Revised October 8, 2019. Accessed May 27, 2025. https://www.census.gov/newsroom/ press-releases/2018/cb18-41-population-projections. html
2. Yong PL, Saunders RS, Olsen LA, eds. The Healthcare Imperative. Lowering Costs and Improving Outcomes: Workshop Series Summary. National Academies Press; 2010:219-237. https://www.ncbi.nlm.nih.gov/books/ NBK53914/
3. Population Reference Bureau. Fact sheet: aging in the United States. January 9, 2024. Accessed May 27, 2025. https://www.prb.org/resources/fact-sheet-aging-in-theunited-states/
4. Edemekong PF, Bomgaars DL, Sukumaran S, Schoo C. Activities of daily living. In: StatPearls. StatPearls Publishing; May 4, 2025. https://www.ncbi.nlm.nih.gov/books/ NBK470404/
5. National Council on Aging. Aging in America. Get the facts on older Americans. June 1, 2024. Accessed May 27, 2025. https://www.ncoa.org/article/get-the-facts-on-olderamericans/
6. Shrider EA, Creamer J. Poverty in the United States: 2022. Report no. P60-280. US Census Bureau; 2023. https:// www.census.gov/data/tables/2023/demo/incomepoverty/p60-280.html
7. Administration for Community Living, US Department of Health and Human Services. 2023 Profile of Older Americans. May 2024. https://acl.gov/sites/default/files/ Profile%20of%20OA/ACL_ProfileOlderAmericans2023_508.pdf
8. Section 3B. Oral health across the lifespan: older adults. In: Oral Health in America: Advances and Challenges. National Institute of Dental and Craniofacial Research; 2021. https://www.ncbi.nlm.nih.gov/books/ NBK578296/
9. US Centers for Medicare and Medicaid Services. Yearly “wellness” visits. Accessed May 27, 2025. https://www. medicare.gov/coverage/yearly-wellness-visits
Tooth replacement from extraction to restoration. 3. Second-stage and impression procedures
Marcus Cowan, DMD
The third part of this series reviews uncovering of implants that were buried in a 2-stage approach, provisionalization of the implant, and impression and scanning techniques.1 These techniques are all crucial for the final restorative outcome of the implant. The uncovering and second-stage procedures set the foundation for the shape and position of the soft tissue, which are very important esthetic factors. This information must also be properly transferred to the laboratory via a highly accurate impression so the laboratory has as much information as possible. If these steps are done properly, the result will be implant crowns that are easy to seat, biologically ideal, and esthetically pleasing.
Second-stage procedures
Anesthesia
Similar to the implant placement protocol, the patient is given a preoperative rinse with 0.12% chlorhexidine for 60 seconds at the beginning of the appointment to help reduce the bacterial load in the mouth.2
After the chlorhexidine rinse, betadine is applied locally to the area where the incision is to be made, and the area is rinsed thoroughly with sterile saline.
Local anesthesia for second-stage implant uncovering is less complicated than for implant placement as there is little to no bone manipulation during this appointment.3 Although a small amount of bone may need to be removed with a
profiling drill due to bone growth over the cover screw, even that is typically superficial and does not cause patients the same discomfort as an osteotomy. Therefore, buccal and lingual infiltration with 4% articaine with 1:100,000 epinephrine is typically sufficient.
After the buccal and lingual anesthesia is allowed to take effect for a few minutes, it is helpful to infiltrate additional anesthesia directly on the crest of the ridge. The hydraulic pressure from the anesthetic will help lift the periosteum off the bone, making it easier to raise the flap; however, this must be done immediately before any incisions are made, because the pressure will only lift the tissue for a moment.
To be prepared, it is important to have the prosthetic kit for the implant system that is being used. A surgical kit can be used but is not always necessary since no osteotomy drills will be applied; nevertheless a surgical kit and the profiling drill it includes can come in handy if bone is present over the cover screw and bone profiling is needed.
A 15C blade is used to make the initial incision, and a Woodson elevator or periosteal elevator can be used to hold the flap. A Minnesota or Buser cheek retractor is also helpful for retracting the patient’s cheek.
Implant uncovering
Four different techniques for uncovering the implant will be discussed. Each
has its nuances, and the appropriate approach must be chosen to avoid complications. For all of the techniques, if bone grew over the cover screw, bone profiling must be performed before any attempts are made to remove the cover screw and seat the healing abutment. Also, the implant sites should be copiously irrigated to remove any debris from the internal connection of the implant prior to seating of the components.
Tissue punch
If there is ample tissue thickness and attached gingiva at the implant site, a tissue punch can be performed.4 A tissue punch is a circular blade that removes the tissue just above the implant platform so the components can be seated. If a surgical guide was used, the tissue punch can be performed through the guide sleeve to ensure that the punch is applied in the right location.
Typically, a tissue punch is the least traumatic way to uncover an implant since no flap is raised, and patients experience little to no discomfort. The downside is that the procedure removes healthy soft tissue, and the presence of adequate soft tissue volume around implants is crucial for long-term success. Clinicians should be very selective when deciding to use a tissue punch because once the tissue is gone, it will be challenging to get back.
Once the tissue is completely removed, the healing abutment is seated. The
diameter of the tissue punch and the diameter of the healing abutment must match to avoid excessive tissue impingement and issues in proper seating of the healing abutment. No sutures are needed if the tissue punch and the healing abutment are chosen appropriately. This is my least preferred method of uncovering.
Midcrestal incision
A midcrestal incision is a common technique used in second-stage procedures (Fig 1).5 A size 15C blade is used, and an incision is made directly in the middle of the crest of the ridge. This typically splits the keratinized tissue in the middle so there is an equal amount of keratinized tissue on the buccal and lingual sides of the flap. Typically, only the crestal portion of the flap is reflected; it is usually not necessary to reflect the flap far enough to expose the buccal and lingual portions of the bone. This is a good technique to use if there is ample keratinized tissue; in fact, because the
tissue is being split, a midcrestal incision can result in a slight gain in keratinized tissue width. Once the healing abutment is seated, 2 simple interrupted sutures are performed on the mesial and distal aspects of the healing abutment. My preference is a 6-0 PGCL (poly[glycolide-co-ε-caprolactone]) monofilament resorbable suture.
Lingually biased incision
A variation of the midcrestal incision, the lingually (palatally) biased incision uses the size 15C blade to make a cut that is off-center from the crest of the ridge, erring toward the lingual (Fig 2). The remainder of the technique for a lingually biased incision is the same as for the midcrestal incision. The difference between the 2 techniques is that a lingually biased incision allows for more tissue to be pushed to the buccal aspect of the implant, which can be helpful because the tissue and bone buccal to the implant are important for esthetics.
Roll flap
In the roll flap technique, rather than a straight incision, the size 15C blade is used to make a tissue-sparing incision in the papilla that is rounded in the outline of the tooth being replaced.6 My dental laboratory has fabricated incision guides that allow the location of the incision for a roll flap to be perfectly marked (Fig 3). The incision guide is seated, and the size 15C blade follows the contours of the guide so the location is in the perfect position relative to the healing component that is going to be used. The tissue in the middle of the flap is deepithelialized; then, this deepithelialized tissue is tucked under the buccal flap, thickening the tissue (Fig 4). This tissue now acts as a connective tissue graft and augments the buccal soft tissue profile without requiring a donor site as in a palatal connective tissue harvest. This will result in improved bulk and buccal corridor volume of the soft tissue, which is good for long-term stability of the implant.
The rolled, deepithelialized tissue is stabilized with a single horizontal mattress suture on the midbuccal aspect of the flap, and the healing abutment is seated. Two interrupted sutures are then placed, one on the mesial and one on the distal aspect of the healing abutment, with 6-0 PGCL (Fig 5). There must be ample keratinized gingiva for this technique—if a wide band of keratinized gingiva is not present, this approach may result in the removal of all keratinized gingiva from around the implant, leaving only mucosal tissue, which is not good for the implant in the long term. This method is my preferred technique in both anterior and posterior healed sites.
Fig 1. Midcrestal incision.
Fig 2. Lingually biased incision.
Fig 3. Incision guide in place for roll flap technique.
Fig 4. Roll flap incision.
Fig 5. Roll flap incision with sutures.
Healing components
Clinicians have several options for healing components to place during the second-stage appointment: stock healing abutments, anatomical healing abutments, custom healing abutments, and provisional crowns. Each of these healing abutments has its pros and cons, but all can be helpful in obtaining a good clinical result.7
Stock healing abutments are prefabricated healing abutments that are manufactured to fit the implant connection. They are circular and come in varying diameters and heights to suit each case. An advantage of stock healing abutments is that they are typically easier to have available during procedures, as a single size can be used in multiple different areas in the mouth. A disadvantage is that teeth are rarely circular in shape; as a result, there will be some difference in the shape of the intaglio of the healing abutment and the intaglio of the final restoration. This difference, depending on its size, can cause issues with the delivery of the final restoration.
Anatomical healing abutments are also prefabricated and manufactured to fit the implant connection; however, these healing abutments follow the shape of the tooth they are replacing. They typically come in molar, premolar, canine, and incisor forms, which provide an intaglio shape that is much closer to the shape of the tooth the healing component is replacing. Anatomical healing abutments, similar to custom healing abutments, result in an improved emergence profile when compared with the emergence profile of a stock healing abutment. Not all systems have anatomical healing abutments available, so make sure to check with your system's representative.
Custom healing abutments are similar to anatomical healing abutments in that they are manufactured to fit the implant connection and are shaped like the tooth that needs replacing. The difference is that custom healing abutments are patient-specific, and the abutment is designed to fit only in one particular implant site. These can be made chairside or in the laboratory. If done chairside, a common fabrication method is to engage a metal temporary cylinder on
the implant and add flowable composite resin to form the ideal intaglio shape. Having the aid of a template can also be helpful, especially if it is a healed site. As described in part 2 of this series, there are techniques that can be used to ensure that a laboratory-fabricated custom healing abutment is available for the second-stage appointment.1 For instance, if a scan body is placed on the implant and scanned on the day of implant placement, the exact position of the implant is known, and a custom abutment can be fabricated prior to the second-stage appointment. This custom healing abutment can be milled out of titanium or generated in a 3-dimensional (3D) printer and luted to a titanium base. A 3D-printed abutment is much more cost-effective to fabricate, and, when the abutment is well-polished, the tissue attaches well to both titanium and resin surfaces. This hemidesmosomal attachment forms a protective seal around the implant during healing.8
Provisional crowns are used in the same fashion as custom abutments. They can be made chairside with a template or fabricated in the laboratory. The implant will be osseointegrated at this stage, so the restoration will be functional without risk of damaging the implant as long as the restoration has a balanced occlusion. Due to the minimally invasive nature of the second-stage appointment, the patient is not usually seen for a postoperative appointment prior to the impression appointment. Resorbable sutures are used, so there is typically no need for suture removal.
Impression procedures
After the second-stage appointment, the patient is allowed to heal for 1 month before impressions are made for the implant restoration. If significant tissue manipulation or any grafting was performed, up to 12 weeks of healing may be needed.
The point of the impression or scan is to tell the laboratory the exact locations of the implant platform, the soft tissue around the implant, and the adjacent and opposing teeth. This can be accomplished via analog or digital methods. The analog method requires either an open-tray or a closed-tray coping and a polyvinyl siloxane (PVS) impression.
The digital method requires the use of a scan body and intraoral scanner. Both analog and digital techniques are able to produce accurate results if used appropriately, although digital impressions have a slight edge as far as accuracy and operator ease of use.9,10 Either way, it is important to minimize distortions during the impression step to avoid later fit issues with the restoration.
A particularly important step in the restorative process is that shade matching should be performed at the beginning of the appointment, before any components have been removed—the longer the patient’s mouth is open, the more the teeth become dehydrated, thus becoming lighter in color and higher in value. If this is not accounted for, the cosmetics of the case could be compromised. It is recommended to obtain shades for the incisal, middle, and gingival thirds of at least the adjacent teeth to ensure a good match.
Analog impressions
Both closed-tray and open-tray impressions are analog impressions taken intraorally with PVS and a tray. For all impression types, the component that is currently on the implant (stock, custom, or anatomical healing abutment or provisional crown) must be removed. It is recommended to irrigate the internal implant components with chlorhexidine to clean the area of any debris or plaque anytime the implant components are removed. After the impression coping is seated, it is important to take a radiograph to verify full seating of the coping. For a closed-tray impression, the impression coping is placed in the
Fig 6. Custom impression coping (analog).
patient’s mouth. Once seating is verified, a small amount of wax is placed over the screwhead portion of the coping because the small, intricate details of the screwhead can be hard to capture and can become distorted, causing inaccuracies in the impression. An impression is then taken, with light-body PVS placed on the gingiva around the impression coping and in the occlusal grooves of the posterior teeth. Light-body PVS can capture details of up to approximately 20 μm, while heavy-body PVS captures details of up to approximately 50 μm.11 However, putting light-body PVS in the occlusal grooves of the posterior teeth allows for a more accurate bite. After the appropriate setting time, the PVS impression is removed. With a closedtray impression, the impression coping stays in the patient’s mouth when the impression is removed; the coping is then removed and sent to the laboratory for crown fabrication.
For an open-tray impression, in contrast with a closed-tray impression, the impression coping stays fixed in the impression when the PVS tray is removed from the mouth. To accomplish this, the tray being used to take the impression must be modified before PVS is placed in the tray. A hole must be cut in the impression tray to allow for the screw to be accessible after the impression is seated.
One technique to accomplish this is as follows: First, the open-tray coping is seated the patient’s mouth, and full seating is verified. Then, the empty tray is tried in the patient’s mouth and adjusted as needed to allow for the head of the open-tray coping to stick out of the tray without binding anywhere. Once this is done, the tray is removed, and tape is placed over the access hole. This keeps the PVS from spilling while the
trays are loaded. A portion of the tape should be left easily accessible so it can be removed once the tray is reseated. The PVS is now placed on the gingiva around the coping and on the occlusal surfaces of the teeth, and the tray is seated. Once fully seated, the head of the open-tray coping will hit the tape. At this point, the tape is removed and the PVS is wiped off the coping with a gloved finger. This will provide access to the screw of the coping, which must be removed after the PVS sets. After adequate setting time per the manufacturer’s specifications, the open-tray coping is unscrewed and the impression is removed. The coping will come out in the impression.
With an impression, in addition to capturing the position of the implant platform, it is also important to capture the soft tissue around the implant. It influences the emergence of the final restoration and the esthetics of the case. To capture the tissue accurately, it must be rigidly supported or else it begins to collapse as soon as its support is removed. This is the reason that the tissue can be completely closed up in just a few days if a healing abutment falls off. If a stock healing abutment was used, typically there are impression copings that match the emergence of the healing abutment. This means that when the coping is seated, the peri-implant soft tissue is fully supported during the impression and no tissue collapse occurs.
If an anatomical healing abutment, custom healing abutment, or provisional crown was used to shape the tissue during the healing period, the peri-implant soft tissue is larger and shaped differently than is the case with stock impression components. If stock impression components are used in cases like this, some of the soft tissue
is unsupported and will collapse, compromising the tissue contours that have formed. To compensate for this, an additional step is needed to obtain an accurate soft tissue impression.
A custom impression coping can be fabricated by flowing flowable composite around the impression coping after it is seated in the mouth.12 Once cured, this composite will support the tissue, allowing the laboratory to see accurate soft tissue dimensions (Fig 6). This composite will remain attached to the impression coping and be sent to the laboratory. I recommend using a narrow emergence impression coping when fabricating custom impression copings. If a wide emergence impression coping is used, the coping itself takes up more space and there is less room for flowable composite to capture the customized tissue shape.
Digital impressions
Digital impressions are taken with a scan body and intraoral scanner. A scan body is the digital workflow version of an impression coping. It is seated in a similar fashion to the impression coping, and a radiograph is also needed to verify seating (Fig 7). If custom tissue shaping was done before scanning, special steps must be taken to accurately capture the tissue. As previously discussed, the soft tissue begins to collapse immediately when the healing abutment or provisional crown is removed. Adding flowable composite to the sulcus would block the scanner from being able to scan the tissue and ruin the scan body; therefore, the healing abutment or provisional restoration must be removed and the soft tissue of the implant sulcus immediately scanned (Fig 8). This is an additional scan that will also be sent to the laboratory, and the full quadrant must also be scanned so the laboratory can appropriately align this scan with subsequent scans.
Once the soft tissue scan is captured, the normal scanning protocol can proceed. The internal components of the implant are irrigated with chlorhexidine, the scan body is seated, a radiograph is taken to ensure full seating, and then the implant is scanned.
After scanning or impression-taking is completed, the internal components
Fig 7. Seated scan body.
Fig 8. Healed roll flap site shaped with custom healing abutment.
Tooth replacement from extraction to restoration. 3. Second-stage and impression procedures
of the implant are irrigated again with 0.12% chlorhexidine, and the healing component that was in place prior to impression procedures is reseated. If possible, while the healing component is not attached to the implant, it should be cleaned ultrasonically in a chlorhexidine solution to remove plaque or debris. Once the component is reseated, a final radiograph is taken to ensure seating, and the patient is dismissed until the restoration comes back from the laboratory.
Author affiliation
Private practice, Hudson, Massachusetts.
Conflicts of interest
The author owns CowTech Dental Lab, Lithonia, Georgia, which produces incision guides and custom healing abutments for implants.
References
1. Cowan M. Tooth replacement from extraction to restoration. 2. Implant planning and placement. Gen Dent. 2025;73(3):6-11.
2. Young MP, Korachi M, Carter DH, Worthington HV, McCord JF, Drucker DB. The effects of an immediately pre-surgical chlorhexidine oral rinse on the bacterial contaminants of bone debris collected during dental implant surgery. Clin Oral Implants Res. 2002;13(1):20-29. doi:10.1034/j.16000501.2002.130102.x
3. Cowan M. Tooth replacement from extraction to restoration. 1. Extraction and socket preservation. Gen Dent. 2025;73(1):6-9.
4. Deeb GR, Deeb JG. Soft tissue grafting around teeth and implants. Oral Maxillofac Surg Clin North Am. 2015;27(3):425-448. doi:10.1016/j.coms.2015.04.010
5. Kamakshi LNVA, Uppoor AS, Nayak DG, Pralhad S. Evaluation of papilla levels following three different techniques for the second stage of implants—a clinical and radiographic study. J Indian Soc Periodontol. 2021;25(2):120127. doi:10.4103/jisp.jisp_60_20. Erratum: 2021;25(3):270. doi:10.4103/0972-124X.315467
6. Lisi L. Soft tissue thickening around implants using the roll flap technique. C-Tech Implant. Accessed July 23, 2025. https://www.c-tech-implant.com/en/clinical-cases/softtissue-thickening-around-implants-using-the-roll-flaptechnique.html
7. Chokaree P, Poovarodom P, Chaijareenont P, Yavirach A, Rungsiyakull P. Biomaterials and clinical applications of customized healing abutment—a narrative review. J Funct Biomater. 2022;13(4):291. doi:10.3390/jfb13040291
8. Teślak M, Ziemlewski A, Foltyn I, Ordyniec-Kwaśnica I, Drogoszewska B. Development of custom anatomic healing abutment based on cone-beam computer tomography measurement on human teeth cross-section. Materials (Basel). 2021;14(16):4570. doi:10.3390/ma14164570
9. Park JS, Alshehri YFA, Kruger E, Villata L. Accuracy of digital versus conventional implant impressions in partially dentate patients: a systematic review and meta-analysis. J Dent. 2025;160:105918. doi:10.1016/j. jdent.2025.105918
10. Fathi A, Rismanchian M, Yazdekhasti A, Salamati M. Accuracy of tooth-implant impressions: comparison of five different techniques. Clin Exp Dent Res. 2023;9(3):526534. doi:10.1002/cre2.737
11. Tousignant G. Dual arch impressions: clinically acceptable vs. quality results! OralHealth. November 1, 2007. Accessed July 23, 2025. https://www.oralhealthgroup. com/features/dual-arch-impressions-clinically-acceptable-vs-quality-results/
12. Polack MA. Simple method of fabricating an impression coping to reproduce peri-implant gingiva on the master cast. J Prosthet Dent. 2002;88(2):221-223. doi:10.1067/ mpr.2002.127895
What every dentist needs to know about cannabis use and head and neck cancer
John K. Brooks, DDS ¢ Muhammad Hamza, BS ¢ Maureen A. Fitzpatrick, MSN, CRNP ¢ Nasir Bashirelahi, PhD
Cannabis use is widespread, raising concerns about a myriad of health problems, notably regarding pulmonary disease and head and neck cancer (HNC). The objective of this review is to examine the association between cannabis exposure and HNC, including a discussion of epidemiologic findings and molecular mechanisms. A recent cohort study established that individuals with cannabis-related disorder have a significantly increased risk for HNC, including laryngeal, oral, nasal, sinus, and oropharyngeal cancers. Moreover, molecular studies suggest that cannabis smoke upregulates carcinogenetic pathways. Dental healthcare providers should inform their patients that heavy cannabis use may be associated with an increased risk of HNC.
Received: September 30, 2024
Accepted: March 10, 2025
Keywords: cannabis, epidemiology, head and neck cancer, oropharyngeal neoplasms
Cannabis smoking and the use of cannabis-based products have risen globally following greater social acceptance and legalization, offering an array of medical benefits such as lessening the adverse effects of antineoplastic agents, alleviating cancer pain, relieving chronic noncancer pain, reducing opioid-related burden, and treating refractory epilepsy.1-4 As a result, understanding the potential long-term deleterious health impacts of cannabis use has become increasingly important. A variety of health disturbances have been associated with cannabis use, including addiction, psychological disorders, neurodevelopmental disturbances, and poisoning.5-8
Tobacco and alcohol consumption and human papillomavirus infection are well-established risk factors for the development of head and neck cancer (HNC).9 Cannabis smoke mainly contains the bioactive ingredient Δ-9-tetrahydrocannabinol (THC), which effectuates enzymatic conversion of complex hydrocarbons into carcinogenic substances similar to tobacco.10 However, its oncogenic role in the promotion of aerodigestive and lung cancer has remained unclear. The present article summarizes recent findings about cannabis use and its potential correlation with cancers of the oral cavity, nasal and sinus mucosa, larynx, and oropharynx. Investigations involving the molecular basis for cancer induction will also be discussed.
Epidemiologic evidence
Although the earliest records of cannabis use date back to antiquity, a conspicuous surge began in the mid 1960s in the United States. In 1972, Henderson et al documented findings in 200 hashish smokers, aged 18 to 23 years, who developed various respiratory symptoms, mostly pharyngitis.11 There were also cases of rhinitis, bronchitis, and asthma. Hashish is a cannabis derivative that contains 5 to 10 times more THC than marijuana.11
Donald raised concerns about the effects of cannabis smoking after the diagnosis of head and neck cancers in 6 young adults, sites typically not predisposed to malignancy in this age group.12 In 1999, Zhang et al reviewed the risk factors among 173 patients with previously untreated biopsy-proven squamous cell carcinoma of the head and neck and had 176 control patients without a history of head and neck cancer.13 Among the cancer patients, 13.9% (24) were marijuana users, mainly with cancers of the larynx and tongue, whereas 9.7% (17/176) of controls were marijuana users. Although the number of marijuana users was small in both cohorts, there was a 2-fold increased risk for squamous cell carcinoma among those who smoked marijuana once per day and 4.9 times greater risk among those who smoked marijuana more frequently.
In contrast, in a 2008 case-control study, Aldington et al investigated 75 patients diagnosed with HNC and a control group of 319 individuals without HNC and found no statistically significant association between cannabis use and increased cancer risk, even for heavy cannabis smokers (more than 8.3 joint-years of use, with 1 joint-year representing 1 marijuana cigarette smoked per day for 1 year).14 The investigators emphasized that the existence of minimal or long-term effects could not be ruled out due to the limited median duration of cannabis use, the small sample size, particularly in the case group, and confounding factors of concurrent tobacco and alcohol use. In 2019, Ghasemiesfe et al published a systematic review and meta-analysis seeking to determine whether there was any etiologic association between cannabis use and the development of head and neck, pulmonary, urogenital, and other cancers.15 The authors stipulated that there was low-strength evidence to establish an association between cannabis smoking and testicular cancer, but the results for other cancers were unclear. Recently, Gallagher et al analyzed a 20-year data set containing the clinical records of 116,076 adults with a diagnosis of cannabis-related disorder and a cohort of 3,985,286 adults without such a diagnosis to ascertain whether there was a link between cannabis use and HNC.16 The cohort with cannabisrelated disorder consisted of 61,434 (52.9%) men and 51,646 (44.5%) women and had a mean age of 46.4 years. The investigation revealed that the group with cannabis-related disorder had a significantly higher relative risk (RR) of new HNC diagnoses (RR, 3.49; 95% CI, 2.78-4.39), including laryngeal cancer (RR, 8.39; 95% CI, 4.72-14.90), oropharyngeal cancer (RR, 4.90; 95% CI, 2.99-8.02), oral cancer (RR, 2.51; 95% CI, 1.81-3.47), and salivary gland cancer (RR, 2.70; 95% CI, 1.31-5.58). According to the investigators, this represents the largest study to date to establish the oncogenic potential of cannabis. Of note, the authors did not correlate the modality of cannabis usage (smoking, ingestion [edibles or beverages], or vaping) with the sites of cancer transformation. As the most common manner of cannabis use is smoking, it may be presumed that the majority of affected patients also smoked cannabis.17 Additional studies are warranted to confirm the potential of cannabis to promote head and neck cancer by segregating based on the manner of use. Although the literature lacks data as to whether edible cannabis products are associated with cancers of the gastrointestinal tract, there is a preliminary report that cannabis (unspecified type of use) significantly reduces the lifetime risk of esophageal, gastric, pancreatic, liver and intrahepatic duct, colon, rectosigmoid, and rectal cancers but is marginally associated with an increased risk for small intestine cancer.18
In apparent contradiction to studies associating cannabis use with increased cancer risks, some studies have shown that coadministration of various active compounds of cannabis may enhance the efficacy of antineoplastic agents for a range of cancers, such as triple-negative breast cancer, colorectal cancer, prostate cancer, and cholangiocarcinoma.19-23 Cannabis extracts have also demonstrated in vitro cytotoxicity to human oral cancer cell populations.24 There are also published data that cannabis use may activate various oral mucosal receptors that confer anti-inflammatory, antimicrobial, and antioxidant bioactivity, potentially offering an ameliorative effect on periodontal disease and pulpitis.25
Molecular evidence
Molecular studies suggest that cannabis smoke may trigger carcinogenic pathways in the upper aerodigestive tract.26-28 Like tobacco smoke, cannabis smoke contains polycyclic aromatic hydrocarbons and acetaldehyde, which are implicated in initiation of DNA damage and activation of cancer-promoting pathways.26,27 Metabolized alcohol (ethanol) also leads to acetaldehyde formation.26 Thus, the synergistic effects of metabolites of cannabis and tobacco smoke and/or consumed alcohol may promote an even greater risk for carcinogenesis.26 Gallagher et al noted that cannabis is typically smoked unfiltered and the smoke is usually inhaled more deeply than tobacco smoke, potentially resulting in even greater exposure to harmful carcinogenic compounds for users.16 Bhattacharyya et al found that cannabis smokers exhibit elevated levels of epidermal growth factor receptor, protein kinase B, nuclear factor κB, and cyclooxygenase 2, which promote cell proliferation and inflammation and contribute to the development of early-onset laryngeal cancer.28
Patient education
Teaching patients methods to improve their oral hygiene and offering dietary counseling are fundamental components of preventive dental practice. Oral healthcare practitioners have the opportunity to inform their patients that use of tobacco products and cannabis smoking pose increased risks for the development of several cancers of the head and neck.29 Clinicians should also utilize routine dental visits to discuss published findings of the potential associations between cancer and cannabis use. Such conversations will strengthen informed decision-making among patients who use cannabis. Further, government agencies should require that cannabis products contain labels specifying that chronic smoking may promote head and neck cancer, similar to the health warnings mandated for tobacco products.30
Conclusion
Current epidemiologic evidence has established a link between heavy cannabis use and pathogenesis of laryngeal, oral, oropharyngeal, and salivary gland cancers. In addition, molecular studies support the theory that cannabis smoke upregulates cancer-promoting pathways. Given the increasing legalization and use of cannabis, an understanding of the health risks of cannabis is essential to implementing greater surveillance for head and neck cancers. Oral healthcare practitioners should advise their patients about potential adverse consequences of using cannabis, particularly emphasizing the increased risk for head and neck cancer.
Author affiliations
Department of Oncology and Diagnostic Sciences, University of Maryland School of Dentistry, Baltimore, Maryland (Brooks, Bashirelahi); University of Maryland School of Dentistry, Baltimore, Maryland (Hamza); Private practice, Baltimore, Maryland (Fitzpatrick).
Correspondence
John K. Brooks, DDS (jbrooks@umaryland.edu).
Conflicts of interest
None reported.
References
1. Carter GT, Flanagan AM, Earleywine M, Abrams DI, Aggarwal SK, Grinspoon L. Cannabis in palliative medicine: improving care and reducing opioid-related morbidity. Am J Hosp Palliat Care. 2011;28(5):297-303. doi:10.1177/1049909111402318
2. Wright P, Walsh Z, Margolese S, et al. Canadian clinical practice guidelines for the use of plant-based cannabis and cannabinoid-based products in the management of chronic non-cancer pain and co-occurring conditions: protocol for a systematic literature review. BMJ Open. 2020;10(5):e036114. doi:10.1136/bmjopen-2019-036114
3. Pessar SC, Smart R, Naimi T, et al. The association between state cannabis policies and cannabis use among adults and youth, United States, 2002-2019. Addiction. 2025;120 (1):164-170. doi:10.1111/add.16663
4. Chico SFV, Diaz DAM, Contreras-Puentes N. Use of cannabidiol in the treatment of drugrefractory epilepsy in children and young adults: a systematic review. J Neurosci Rural Pract 2024;15(2):203-210. doi:10.25259/JNRP_618_2023
5. Seddon JL, Birchwood M, Copello A, et al. Cannabis use is associated with increased psychotic symptoms and poorer psychosocial functioning in first-episode psychosis: a report from the UK National EDEN Study. Schizophr Bull. 2016;42(3):619-625. doi:10.1093/schbul/ sbv154
6. Hammig B, Jones C, Haldeman S. Pediatric poisonings associated with ingestion of marijuana products. J Emerg Med. 2023;64(2):181-185. doi:10.1016/j.jemermed. 2022.12.025
7. Hoch E, Volkow ND, Friemel CM, Lorenzetti V, Freeman TP, Hall W. Cannabis, cannabinoids and health: a review of evidence on risks and medical benefits. Eur Arch Psychiatry Clin Neurosci. 2025;275(2):281-292. doi:10.1007/s00406-024-01880-2
8. Karatayev O, Collier AD, Targoff SR, Leibowitz SF. Neurological disorders induced by drug use: effects of adolescent and embryonic drug exposure on behavioral neurodevelopment. Int J Mol Sci. 2024;25(15):8341. doi:10.3390/ijms25158341
9. Xu H, Gao Z, Liu H, et al. Associations of lifestyle factors with oral cancer risk: an umbrella review. J Stomatol Oral Maxillofac Surg. 2025;126(3S):102234. doi:10.1016/j. jormas.2025.102234
10. Hall W, Christie M, Currow D. Cannabinoids and cancer: causation, remediation, and palliation. Lancet Oncol. 2005;6(1):35-42. doi:10.1016/S1470-2045(04)01711-5
11. Henderson RL, Tennant FS, Guerry R. Respiratory manifestations of hashish smoking. Arch Otolaryngol. 1972;95(3):248-251. doi:10.1001/archotol.1972.00770080390012
12. Donald PJ. Marijuana smoking—possible cause of head and neck carcinoma in young patients. Otolaryngol Head Neck Surg. 1986;94(4):517-521. doi:10.1177/ 019459988609400420
13. Zhang ZF, Morgenstern H, Spitz MR, et al. Marijuana use and increased risk of squamous cell carcinoma of the head and neck. Cancer Epidemiol Biomarkers Prev. 1999;8(12):1071-1078.
14. Aldington S, Harwood M, Cox B, et al. Cannabis use and cancer of the head and neck: casecontrol study. Otolaryngol Head Neck Surg. 2008;138(3):374-380. doi:10.1016/j. otohns.2007.12.002
15. Ghasemiesfe M, Barrow B, Leonard S, Keyhani S, Korenstein D. Association between marijuana use and risk of cancer: a systematic review and meta-analysis. JAMA Netw Open 2019;2(11):e1916318. doi:10.1001/jamanetworkopen.2019.16318. Erratum: 2020;3(1):e1921065. doi:10.1001/jamanetworkopen.2019.21065
16. Gallagher TJ, Chung RS, Lin ME, Kim I, Kokot NC. Cannabis use and head and neck cancer. JAMA Otolaryngol Head Neck Surg. 2024;150(12):1068-1075. doi:10.1001/ jamaoto.2024.2419. Erratum: 2025;151(4):416. doi:10.1001/jamaoto.2025.0242
17. Subbaraman MS, Kerr WC. Cannabis use frequency, route of administration, and co-use with alcohol among older adults in Washington state. J Cannabis Res. 2021;3(1):17. doi:10.1186/ s42238-021-00071-3
18. Waris SA, Raiker R, Siva N, Boustany O, Pakhchanian H, Khalid AA. Assessing the risk of gastrointestinal cancers among cannabis users compared to nicotine users. Abstract 10571. J Clin Oncol. 2023;41(16 suppl). doi:10.1200/JCO.2023.41.16_suppl.10571
19. Kim BG, Kim BR, Kim DY, et al. Cannabidiol enhances atezolizumab efficacy by upregulating PD-L1 expression via the cGAS-STING pathway in triple-negative breast cancer cells. Cancer Immunol Res. 2024;12(12):1796-1807. doi:10.1158/2326-6066.CIR-23-0902
20. Yu H, Chen Y, Deng J, et al. Integrated metabolomics and proteomics analyses to reveal anticancer mechanism of hemp oil extract in colorectal cancer. J Pharm Biomed Anal 2024;249:116379. doi:10.1016/j.jpba.2024.116379
21. Shalata W, Abu Saleh O, Tourkey L, et al. The efficacy of cannabis in oncology patient care and its anti-tumor effects. Cancers (Basel). 2024;16(16):2909. doi:10.3390/ cancers16162909
22. Erzurumlu Y, Catakli D. Cannabidiol enhances the anticancer activity of etoposide on prostate cancer cells. Cannabis Cannabinoid Res. 2025;10(2):258-276. doi:10.1089/can.2023.0284
23. Pongking T, Thongpon P, Intuyod K, et al. Cannabidiol exhibits potent anti-cancer activity against gemcitabine-resistant cholangiocarcinoma via ER-stress induction in vitro and in vivo. BMC Complement Med Ther. 2024;24(1):325. doi:10.1186/s12906-024-04610-2
24. Huang CC, Chiu SC, Chao SC, et al. Real-time monitoring of the cytotoxic and antimetastatic properties of cannabidiol in human oral squamous cell carcinoma cells using electric cellsubstrate impedance sensing. Int J Mol Sci. 2022;23(24):15842. doi:10.3390/ijms232415842
25. Hu Z, Qin Z, Xie J, Qu Y, Yin L. Cannabidiol and its application in the treatment of oral diseases: therapeutic potentials, routes of administration and prospects. Biomed Pharmacother. 2024;176:116271. doi:10.1016/j.biopha.2024.116271
26. Lopes CF, de Angelis BB, Prudente HM, de Souza BV, Cardoso SV, de Azambuja Ribeiro RI. Concomitant consumption of marijuana, alcohol and tobacco in oral squamous cell carcinoma development and progression: recent advances and challenges. Arch Oral Biol 2012;57(8):1026-1033. doi:10.1016/j.archoralbio.2012.05.006
27. Bando JM, Tashkin DP, Barjaktarevic IZ. Impact of marijuana use on lung health. Semin Respir Crit Care Med. 2024;45(5):548-559. doi:10.1055/s-0044-1785679
28. Bhattacharyya S, Mandal S, Banerjee S, Mandal GK, Bhowmick AK, Murmu N. Cannabis smoke can be a major risk factor for early-age laryngeal cancer—a molecular signaling-based approach. Tumour Biol. 2015;36(8):6029-6036. doi:10.1007/s13277-015-3279-4
29. Gonzalez YM, Lozier EB. Smoking cessation practices in the dental setting. Gen Dent 2014;62(1):e13-e16.
30. US Food and Drug Administration. Cigarette labeling and health warning requirements. Updated January 15, 2025. Accessed June 19, 2025. https://www.fda.gov/tobaccoproducts/labeling-and-warning-statements-tobacco-products/cigarette-labeling-andhealth-warning-requirements
A comparative evaluation of serum and salivary levels of apelin in chronic periodontitis associated with obesity and type 2 diabetes mellitus
Jammula Surya Prasanna, MDS ¢ Duddukuri Hema, MDS
Periodontitis is an inflammatory destructive condition influenced by obesity and type 2 diabetes mellitus (T2DM). Apelin, a bioactive peptide, is linked to periodontitis, obesity, and T2DM. This study aimed to investigate apelin levels in individuals with periodontitis who are affected by obesity and T2DM. This cross-sectional observational study included 84 participants categorized into 3 main groups of 24 patients based on their periodontal status, body mass index (BMI), and glycated hemoglobin (HbA1c) levels. Group 1 comprised systemically healthy participants, group 2 comprised individuals with obesity (BMI of 30.0 to 39.0 kg/m2), and group 3 comprised individuals with both obesity and T2DM (HbA1c of 6.5% to 8.5%). Each group was subcategorized based on the presence or absence of chronic periodontitis (CP), resulting in 6 subgroups with 14 participants each. The clinical parameters assessed included the Sulcus Bleeding Index (SBI), probing depth (PD), clinical attachment loss (CAL), BMI, and HbA1c level. Apelin levels in serum and saliva were quantified using enzyme-linked immunosorbent assay. Data were analyzed using 1-way analysis of variance and independent samples t test. Pearson correlation coefficients were calculated to assess relationships between different parameters. Within groups, individuals with CP had lower serum and salivary levels of apelin than those without CP, and the differences were statistically significant except in the case of salivary levels in patients with obesity (P < 0.05). Individuals with obesity, as well as those with both T2DM and obesity, had elevated levels of serum apelin compared with systemically healthy individuals. A significant negative correlation was observed between serum apelin and periodontal parameters (SBI, PD, and CAL) in specific subgroups. Apelin could be a valuable biomarker for evaluating periodontal disease affected by obesity and T2DM. However, further longitudinal research with a larger patient sample is needed. Trial registration: Clinical Trials Registry – India No. CTRI/2019/02/017522.
Received: December 11, 2024
Accepted: April 11, 2025
Keywords: adipokines, apelin, biomarker, obesity, periodontitis, type 2 diabetes mellitus
Periodontitis is an inflammatory condition caused by an alteration in the bacteria that live in the mouth, leading to destruction of the soft tissue and bones that support the teeth. Numerous factors, including environmental and/or systemic conditions, can influence this condition and modify the course and nature of the host’s response to the bacterial challenge.1 Recent studies have found a relationship among obesity, diabetes, and periodontal disease whereby the conditions influence each other, with inflammation the crucial factor connecting them.
It has been proposed that diabetes worsens the inflammatory response to plaque build-up through various mechanisms.2 Periodontal disease can affect fat metabolism by elevating cytokine levels, which induces inflammatory changes in adipose tissue. This results in increased secretion of adipokines, which leads to impaired glycemic control and increased expression of advanced glycation end products. These advanced glycation end products in turn impact periodontal inflammation by increasing the formation of cytokines, suggesting a bidirectional relationship between the conditions.3
Adipose tissue secretes pleiotropic molecules known as adipokines, which have various biologic functions. One of these adipokines is apelin, a novel bioactive peptide that regulates physiologic functions and pathologic processes.4 This adipokine has been shown to exacerbate periodontal inflammation via modulation of the inflammatory response in periodontal ligament cells by elevating markers such as cyclooxygenase 2, chemokine ligand 2, and tumor necrosis factor α (TNF-α). Apelin levels are often dysregulated in obesity or diabetes; furthermore, these altered levels are associated with insulin resistance and chronic inflammation, 2 hallmarks of these metabolic disorders.5
Given these correlations, apelin may be used as a marker to monitor inflammatory conditions that are frequently aggravated by systemic inflammation. A study examining the relationships between apelin levels and inflammatory markers across periodontal inflammation, obesity, and diabetes may provide important insights into common pathogenic mechanisms, thereby informing treatment strategies targeting systemic inflammation in these interrelated conditions. The present study aimed to examine the possible role of apelin in periodontitis as well as its viability as a biomarker for periodontitis impacted by type 2 diabetes mellitus (T2DM) and obesity.
Methods
This cross-sectional observational study was conducted at the Department of Periodontics, Panineeya Institute of Dental Sciences and Research Centre, Hyderabad,
Abbreviations: CP, chronic periodontitis; T2DM, type 2 diabetes mellitus.
India. Before the study commenced, approval was obtained from the Institutional Ethical Committee (IEC No. PMVIDS & RC /IEC /PERIO /DN/0172-17), and the study was recorded in the Clinical Trials Registry - India (CTRI/2019/02/017522). The protocol was explained to all participants, and written informed consent was obtained. The study was performed by a qualified periodontist (D.H.) and was conducted in a single center.
Study sample
The required sample size was computed for a power (1 − β) of 0.85, indicating a total sample size of 84, translating to 14 per group. Patients aged 25 to 55 years who had at least 20 natural teeth and had not undergone periodontal therapy in the last 6 months were included in the study. Patients with or without chronic periodontitis (CP), which was defined as probing depths of ≥ 5 mm or attachment loss of ≥ 3 mm, were recruited from the outpatient clinic at the Department of Periodontics, Panineeya Institute of Dental Sciences and Research Centre, Hyderabad, India. Patients with a body mass index (BMI) of 30.0 to 39.0 kg/m2 and those with T2DM (glycated hemoglobin [HbA1c] level of 6.5% to 8.5%) were included according to their respective groups. Patients were excluded from the study if they had certain health conditions, such as cardiovascular diseases or autoimmune disorders; were taking medications such as corticosteroids or anticonvulsants; were undergoing immunosuppressive or radiation therapy; had a history of bruxism or sleep apnea; had a history of smoking/alcohol consumption; or were pregnant or lactating.
Of 100 patients actively recruited for the study, 10 ultimately did not meet the study criteria and 6 were not interested in participating in the investigation. A total of 84 patients were categorized into 3 equal groups (n = 28) based on their BMI and HbA1c (Chart). Each group of patients was subdivided into equal subgroups (n = 14) based on the absence (A) or presence (B) of CP. Group 1 comprised systemically healthy individuals, group 2 comprised individuals with obesity (BMI of 30.0 to
39.0 kg/m2), and group 3 comprised individuals with obesity and T2DM (HbA1c of 6.5% to 8.5%).
Sample collection and preparation
The clinical parameters assessed were Sulcus Bleeding Index (SBI), probing depth (PD), clinical attachment loss (CAL), BMI, and HbA1c level.6-9 All clinical measurements were performed by a single calibrated examiner using a UNC-15 periodontal probe.
Apelin levels were measured in serum and saliva. For assessment of serum levels, blood was collected from the antecubital fossa using a 20-G needles and 2-mL syringes and then transferred to red-capped serum clot activator vacuum tubes (I M Tubes Healthcare). The tubes were left to stand for 30 minutes and then centrifuged at 3000 rpm for 10 minutes. The serum was transferred into sterile Eppendorf tubes (I M Tubes Healthcare) with droppers and labeled.
Saliva was collected via unstimulated passive drool in sterile tubes, then centrifuged at 3000 rpm for 10 minutes (model R-8C Plus, REMI) to remove sediment. The supernatant was then transferred to labeled Eppendorf tubes. Patients were instructed not to use mouthrinses on the day of saliva collection.
All collected samples were stored at −20°C until the assay time. The samples were assayed with a highly sensitive enzymelinked immunosorbent assay apelin kit (Human AP13 ELISA Kit, No. E-EL-H0458, Elabscience).
Statistical analysis
The data were analyzed using SPSS software (version 23, IBM). The normality of the data was assessed with the Shapiro-Wilk test. One-way analysis of variance was used to compare all of the groups, while the independent samples t test was used to compare the subgroups. Pearson correlation coefficients were calculated to assess relationships between different parameters. A value of P < 0.05 was considered statistically significant.
Chart. Study groups.
Patients (N = 84)
Group 1
healthy (n = 28)
Group 3
and T2DM (n = 28)
Subgroup 1A
Subgroup 1B
Subgroup 2A
Subgroup 2B
Subgroup 3A
Subgroup 3B
Group 2
(n = 28)
(group 1; n = 14 per subgroup).
Parameter
(0.82) 0.011b
Abbreviations: BMI, body mass index; CAL, clinical attachment loss; PD, probing depth; SBI, Sulcus Bleeding Index.
Subgroups: 1A, systemically healthy patients without chronic periodontitis; 1B, systemically healthy patients with chronic periodontitis.
aStatistically significant difference between subgroups (P < 0.01; independent samples t test).
bStatistically significant difference between subgroups (P < 0.05; independent samples t test).
Table 3. Statistical comparison of clinical and biochemical parameters in patients with obesity and type 2 diabetes mellitus (group 3; n = 14 per subgroup).
Parameter Subgroup, mean (SD) P 3A 3B
Age, y 37.93 (5.51) 42.64 (6.44) 0.047a
SBI 1.31 (0.45) 3.81 (0.66) 0.000b
PD, mm 2.61 (0.34) 6.87 (1.02) 0.000b CAL, mm 0.00 (0.00) 4.00 (0.68) 0.000b
Abbreviations: BMI, body mass index; CAL, clinical attachment loss; HbA1c, glycated hemoglobin; PD, probing depth; SBI, Sulcus Bleeding Index.
Subgroups: 3A, patients with obesity and type 2 diabetes mellitus and without chronic periodontitis; 3B, patients with obesity, type 2 diabetes mellitus, and chronic periodontitis.
aStatistically significant difference between subgroups (P < 0.05; independent samples t test).
bStatistically significant difference between subgroups (P < 0.01; independent samples t test).
Table 2. Statistical comparison of clinical and biochemical parameters in patients with obesity (group 2; n = 14 per subgroup).
Abbreviations: BMI, body mass index; CAL, clinical attachment loss; PD, probing depth; SBI, Sulcus Bleeding Index.
Subgroups: 2A, patients with obesity and without chronic periodontitis; 2B, patients with obesity and chronic periodontitis.
aStatistically significant difference between subgroups (P < 0.01; independent samples t test).
Results
Of 84 patients participating in the study, 40 were men (47.6%) and 44 were women (52.4%). Tables 1 to 3 present the results of clinical and biochemical assessments in systemically healthy patients (group 1), patients with obesity (group 2), and patients with obesity and T2DM (group 3), respectively. Participants ranged in age from 25 to 55 years, and in all 3 groups the mean ages of the patients were significantly different based on periodontal health, with higher mean ages among patients in the B subgroups (patients with CP).
The mean BMI values were 24.45 kg/m2 in group 1, 34.73 kg/m2 in group 2, and 34.76 kg/m2 in group 3. Within-group comparison revealed no statistically significant difference in the mean BMIs of any group according to subgroups A (patients without CP) and B. However, there was a statistically significant difference in the mean HbA1c levels in group 3 (P = 0.036), with a higher level observed in subgroup 3B.
The periodontal parameters (SBI, PD, and CAL) were also analyzed within each group according to the presence of CP or absence of CP. In each group, the values were significantly higher in patients with CP (P < 0.01).
Within group 1, there were statistically significant differences in the mean serum (P < 0.01) and salivary (P < 0.05) apelin levels, with higher levels seen in subgroup 1A than in 1B. Within group 2, a significant difference was found only for serum apelin levels, with higher levels in subgroup 2A than in 2B (P < 0.01). Within group 3, both serum (P < 0.01) and salivary (P < 0.05) apelin levels significantly differed between subgroups 3A and 3B, with higher values for both in 3A.
Table 4 shows comparisons of the periodontal parameters among all of the subgroups without CP (A subgroups). The mean SBI and PD values did not show any statistically significant differences (P = 0.096 and 0.220, respectively), but the highest PD values were observed in group 2A. No patients in the A subgroups showed CAL.
Table 1. Statistical comparison of clinical and biochemical parameters in systemically healthy patients
Table 4. Intergroup comparison of clinical and biochemical parameters in patients without periodontitis (n = 14 per subgroup). Parameter
Abbreviations: BMI, body mass index; CAL, clinical attachment loss; NA, not applicable; PD, probing depth; SBI, Sulcus Bleeding Index.
Subgroups: 1A, systemically healthy patients without chronic periodontitis; 2A, patients with obesity and without chronic periodontitis; 3A, patients with obesity and type 2 diabetes mellitus and without chronic periodontitis.
aStatistically significant difference between subgroups (P < 0.01; 1-way analysis of variance).
Table 5. Intergroup comparison of clinical and biochemical parameters in patients with periodontitis (n = 14 per subgroup).
Abbreviations: BMI, body mass index; CAL, clinical attachment loss; PD, probing depth; SBI, Sulcus Bleeding Index.
Subgroups: 1B, systemically healthy patients with chronic periodontitis; 2B, patients with obesity and chronic periodontitis; 3B, patients with obesity, type 2 diabetes mellitus, and chronic periodontitis.
aStatistically significant difference between subgroups (P < 0.01; 1-way analysis of variance).
bStatistically significant difference between subgroups (P < 0.05; 1-way analysis of variance).
Comparison of the mean salivary and serum apelin levels between all A subgroups revealed no statistically significant difference in mean apelin levels; however, the highest serum levels were seen in subgroup 3A and the highest salivary levels in subgroup 1A.
Table 5 shows comparisons of the periodontal parameters among all of the subgroups with CP (B subgroups). As in the A subgroups, there were no statistically significant differences in mean SBI, PD, or CAL (P = 0.802, 0.494, and 0.377, respectively). The highest mean values in all 3 variables were in subgroup 2B. Comparison of mean serum and salivary apelin levels in all the B subgroups showed that both values were higher in group 3B, but a significant difference was observed only for serum apelin levels (P = 0.024).
Table 6 shows the correlations between the periodontal parameters and apelin levels. In group 1, patients with CP (subgroup 1B) showed a high negative and significant correlation between serum apelin levels and all periodontal parameters (SBI, r = −0.951; PD, r = −0.934; CAL, r = −0.757). In group 2, the SBI showed a high negative and significant correlation with serum apelin levels in both subgroups (2A, r = 0.718; 2B, r = −0.632), while PD and CAL revealed a high negative and significant correlation with serum apelin levels only in subgroup 2B (r = −0.711 and −0.707, respectively). In group 3, the PD showed a high negative and significant correlation with serum apelin levels in both subgroups (3A, r = −0.711; 3B, r = −0.889), while SBI and CAL showed significant correlations only in subgroup 3B (r = −0.872 and −0.887, respectively).
Parameter
Serum apelin
Salivary apelin
Abbreviations: BMI, body mass index; CAL, clinical attachment loss; HbA 1c , glycated hemoglobin; NA, not applicable; PD, probing depth; SBI, Sulcus Bleeding Index.
Subgroups: 1A, systemically healthy patients without chronic periodontitis; 1B, systemically healthy patients with chronic periodontitis; 2A, patients with obesity and without chronic periodontitis; 2B, patients with obesity and chronic periodontitis; 3A, patients with obesity and type 2 diabetes mellitus and without chronic periodontitis; 3B, patients with obesity, type 2 diabetes mellitus, and chronic periodontitis.
aStatistically significant difference between subgroups (P < 0.01; Pearson correlation).
bStatistically significant difference between subgroups (P < 0.05; Pearson correlation).
Salivary apelin levels did not show any significant correlation with the periodontal parameters in any of the 3 groups.
Significant positive correlations were identified between serum apelin levels and BMI in subgroups 2A, 3A, and 3B. In addition, a significant positive correlation between the mean serum apelin level and HbA1c was observed in patients with obesity, T2DM, and CP (subgroup 3B).
Discussion
Periodontitis is a complex and multifactorial disease, with many systemic and local risk factors contributing to its development. While plaque is the harbinger, other systemic factors can also increase the intensity of periodontal disease.10 Obesity can affect the onset and progression of periodontitis, wherein chronic inflammation, oxidative stress, and tissue damage may cause insulin resistance to develop.11 Additionally, adipocytes secrete proinflammatory cytokines and other molecules such as leptin, adiponectin, and resistin, which play various roles in this relationship.12,13 Moreover, periodontitis contributes to insulin resistance and altered lipid and glucose metabolism, further linking it to obesity and diabetes. Thus, the connection of periodontitis, obesity, and diabetes is considered to be bidirectional, where each condition influences the others.
Biomarkers are quantifiable indicators of pathogenic processes, physiologic health, and response to treatment. The discovery of biomarkers in several sources, including gingival
crevicular fluid, biofilm, saliva, and serum, among others, has facilitated new therapeutic approaches. Nevertheless, molecular biomarkers that may accurately detect and forecast periodontitis activity are scarce. Current research suggests that the endogenous peptide ligand apelin and its receptor (APJ) play a significant role in physiologic and pathologic conditions.14 By upregulating the extracellular signal-regulated kinase 1 and 2 pathway and downregulating the nuclear factor κB pathway, the apelin/APJ system may reduce the inflammatory response. Furthermore, as inflammation is a necessary physiologic defense mechanism and a potential modulator of organ damage, either too little or too much apelin might exacerbate the condition.14
According to recent clinical research by Mund et al, people who have both T2DM and obesity typically have increased levels of apelin in their plasma and serum.15 In the present study, a significant positive correlation was observed between serum apelin levels and BMI in subgroups 3A and 3B and between serum apelin and HbA1c in subgroup 3B. This rise in apelin is thought to be a compensatory mechanism that enhances the body’s sensitivity to insulin. The precise function of apelin in controlling inflammation is still debatable, with some research indicating that it may contribute to inflammation-related disorders via the Janus kinase 3/signal transducer and activator of transcription 3 pathway.14 The discovery of small chemical agonists and antagonists that target APJ suggests that this receptor may be a viable therapeutic target for many apelin-regulated disorders.15
Table 6. Correlation between apelin levels and clinical and biochemical parameters (n = 14 per subgroup).
Despite its crucial role in several pathophysiologic processes, the potential connection between periodontitis and apelin has not been thoroughly explored. The present study investigated whether periodontitis affects apelin levels and whether apelin can be used as a biomarker for periodontitis influenced by obesity and T2DM. This study included a similar number of male (47.6%) and female (52.4%) participants and specifically chose patients within the age group of 25 to 55 years to minimize the possible effects of age and sex on apelin concentrations.
The present study observed no significant differences in any of the periodontal parameters (SBI, PD, and CAL) between the systemically healthy, obesity, and obesity and T2DM groups, regardless of the CP subgroup. This outcome may have been influenced by various factors. First, sample size limitations could have reduced the power to detect moderate differences across groups. Additionally, shared inflammatory pathways in obesity and diabetes and individual variations in health behaviors and genetics may have contributed to overlapping periodontal outcomes. Periodontitis is influenced by a complex interplay of systemic and environmental factors, and it might not vary drastically solely due to systemic conditions. Finally, measurement limitations and variability in immune responses could have further obscured any differences in periodontal health among the groups. Some studies have highlighted that consistent blood sugar management and individual health practices may influence periodontal health outcomes more than diabetes or obesity alone.16-18
A comparison of serum and salivary apelin levels between groups revealed higher levels among patients in groups 2 and 3 than in group 1, but a significant difference was noted only for serum levels in patients with CP (groups 1B, 2B, and 3B). In line with the findings of the present study, Boucher et al, Castan-Laurell et al, and Sörhede Winzell et al observed that serum apelin levels are significantly raised in obesity and may be involved in its pathophysiology, while other studies failed to detect this association.19-23 The varied findings could be the result of methodologic differences among studies. Habchi et al also demonstrated that plasma apelin concentrations were greater in patients with diabetes than in a nondiabetic control group.24 The apelin levels were greater in patients with type 1 diabetes mellitus than in those with T2DM, indicating that obesity may not be the primary determinant of plasma apelin levels. In contrast, Erdem et al discovered that plasma apelin levels are reduced in newly diagnosed and untreated patients with T2DM.25
In the present study, a significant positive correlation was observed between serum apelin levels and BMI in patients with obesity (subgroup 2A) or obesity and T2DM (subgroup 3A) who did not have CP. In patients with obesity, T2DM, and CP (subgroup 3B), there were significant positive correlations between serum apelin levels and both BMI and HbA1c. Similarly, Motawi et al also observed that serum apelin levels were positively correlated with BMI and HbA1c.26 In contrast, other studies have found no association between apelin and BMI, suggesting that adiposity may not be a major determinant in some conditions and that different mechanisms regulate apelin.22,25,27 Additionally, Erdem et al found a negative correlation between apelin levels and Homeostatic Model Assessment indices, indicating that the association between insulin and
apelin might not always be in the same direction under physiologic or pathologic conditions.25
Koguchi et al postulated a possible anti-inflammatory role of apelin and observed that apelin could decrease the expression of proinflammatory cytokines such as TNF-α and interleukin 1β 28 However, in all 3 groups in the present study, the mean serum and salivary apelin levels were higher in patients without CP than with CP. This difference was statistically significant in all comparisons except salivary levels of apelin in subgroups 2A and 2B. Similar findings were also observed by Lee et al, where there was a decrease in apelin expression in the gingival tissues of periodontitis patients.29 In contrast to the present study findings, Sarhat et al observed significantly higher levels of salivary apelin among patients with T2DM and CP, but the mechanism remains unclear.30 Hirani et al also observed that patients with both periodontitis and diabetes had the highest salivary apelin level compared with healthy controls and patients who had periodontitis but not diabetes.31
The variations in apelin levels observed in periodontitis studies could be due to differences in study designs, sample populations, and inflammatory assessment methods. Apelin is a proinflammatory adipokine, and elevated levels are expected in chronic inflammatory conditions such as periodontitis. However, factors such as disease severity, participants’ metabolic status, and measurement techniques can influence results. Some studies may not observe a consistent increase in apelin if the inflammatory response is milder or if metabolic factors are not thoroughly taken into consideration.
Conclusion
The present study found that serum apelin levels were higher in patients with obesity and T2DM than in the healthy group; this difference was statistically significant in the subgroups with CP. In contrast, healthy individuals without CP had higher salivary levels of apelin than those with obesity and T2DM, but the difference was not significant. Furthermore, serum apelin levels were significantly higher among patients without periodontitis, regardless of obesity or T2DM status, but differences in salivary levels were not consistently significant. A significant negative correlation was observed between serum apelin and periodontal parameters (SBI, PD, and CAL) in specific subgroups.
Author affiliations
Department of Periodontics, Panineeya Institute of Dental Sciences and Research Centre, Hyderabad, India.
3. Li S, Li H, Kong H, Wu SY, Cheng CK, Xu J. Endogenous and microbial biomarkers for periodontitis and type 2 diabetes mellitus. Front Endocrinol (Lausanne). 2023;14:1292596. doi:10.3389/fendo.2023.1292596
4. Yeganeh-Hajahmadi M, Moosavi-Saeed Y, Rostamzadeh F. Apelin receptor dimerization and oligomerization. Curr Mol Pharmacol. 2024;17(1):e180823219999. doi:10.2174/187446721 7666230818113538
5. Li C, Cheng H, Adhikari BK, et al. The role of apelin-APJ system in diabetes and obesity. Front Endocrinol (Lausanne). 2022;13:820002. doi:10.3389/fendo.2022.820002
6. Gutin I. In BMI we trust: reframing the body mass index as a measure of health. Soc Theory Health. 2018;16(3):256-271. doi:10.1057/s41285-017-0055-0
7. Health Quality Ontario. Point-of-care hemoglobin A1c testing: an evidence-based analysis. Ont Health Technol Assess Ser. 2014;14(8):1-30.
8. Newbrun E. Indices to measure gingival bleeding. J Periodontol. 1996;67(6):555-561. doi:10.1902/jop.1996.67.6.555
9. Kour A, Kumar A, Puri K, Khatri M, Bansal M, Gupta G. Comparative evaluation of probing depth and clinical attachment level using a manual probe and Florida probe. J Indian Soc Periodontol. 2016;20(3):299-306. doi:10.4103/0972-124X.181241
10. Salhi L, Reners M. Update on the bidirectional link between diabetes and periodontitis. Adv Exp Med Biol. 2022;1373:231-240. doi:10.1007/978-3-030-96881-6_12
11. Arbildo-Vega HI, Cruzado-Oliva FH, Coronel-Zubiate FT, et al. Association between periodontal disease and obesity: umbrella review. Medicina (Kaunas). 2024;60(4):621. doi:10.3390/medicina60040621
12. Zhu M, Nikolajczyk BS. Immune cells link obesity-associated type 2 diabetes and periodontitis. J Dent Res. 2014;93(4):346-352. doi:10.1177/0022034513518943
13. Lavigne SE, Forrest JL. An umbrella review of systematic reviews examining the relationship between type 2 diabetes and periodontitis: position paper from the Canadian Dental Hygienists Association. Can J Dent Hyg. 2021;55(1):57-67.
14. Wang X, Zhang L, Li P, Zheng Y, Yang Y, Ji S. Apelin/APJ system in inflammation. Int Immunopharmacol. 2022;109:108822. doi:10.1016/j.intimp.2022.108822
15. Mund C, Kellellu CK, Rattan R, Mahapatra S, Lamare AA, Jena S. Study of serum apelin and insulin resistance in type 2 diabetes mellitus patients with or without obesity. Cureus. 2023;15(8):e43401
16. Solis Soto J, Meester I, Lopez Villarreal SM, et al. A complex relationship among periodontal disease, obesity and diabetes. Int J Appl Dent Sci. 2024;10(2):402-406. doi:10.22271/oral.2024.v10.i2f.1968
17. Saxlin T, Ylöstalo P, Suominen-Taipale L, Aromaa A, Knuuttila M. Overweight and obesity weakly predict the development of periodontal infection. J Clin Periodontol. 2010;37(12):1059-1067. doi:10.1111/j.1600-051X.2010.01633.x
18. Kongstad J, Hvidtfeldt UA, Grønback M, Stoltze K, Holmstrup P. The relationship between body mass index and periodontitis in the Copenhagen City Heart Study. J Periodontol. 2009;80(8):1246-1253. doi:10.1902/jop.2009.080559
19. Boucher J, Masri B, Daviaud D, et al. Apelin, a newly identified adipokine up-regulated by insulin and obesity. Endocrinology. 2005;146(4):1764-1771. doi:10.1210/en.2004-1427
20. Castan-Laurell I, Vítkova M, Daviaud D, et al. Effect of hypocaloric diet-induced weight loss in obese women on plasma apelin and adipose tissue expression of apelin and APJ. Eur J Endocrinol. 2008;158(6):905-910. doi:10.1530/EJE-08-0039
21. Sörhede Winzell M, Magnusson C, Ahrén B. The apj receptor is expressed in pancreatic islets and its ligand, apelin, inhibits insulin secretion in mice. Regul Pept. 2005;131(1-3):12-17. doi:10.1016/j.regpep.2005.05.004
22. Tasci I, Dogru T, Naharci I, et al. Plasma apelin is lower in patients with elevated LDLcholesterol. Exp Clin Endocrinol Diabetes. 2007;115(7):428-432. doi:10.1055/s-2007-971067
23. Heinonen MV, Purhonen AK, Miettinen P, et al. Apelin, orexin-A and leptin plasma levels in morbid obesity and effect of gastric banding. Regul Pept. 2005;130(1-2):7-13. doi:10.1016/j.regpep.2005.05.003
24. Habchi M, Duvillard L, Cottet V, et al. Circulating apelin is increased in patients with type 1 or type 2 diabetes and is associated with better glycaemic control. Clin Endocrinol (Oxf). 2014;81(5):696-701. doi:10.1111/cen.12404
25. Erdem G, Dogru T, Tasci I, Sonmez A, Tapan S. Low plasma apelin levels in newly diagnosed type 2 diabetes mellitus. Exp Clin Endocrinol Diabetes. 2008;116(5):289-292. doi:10.1055/s-2007-1004564
26. Motawi TMK, Mahdy SG, El-Sawalhi MM, Ali EN, El-Telbany RFA. Serum levels of chemerin, apelin, vaspin, and omentin-1 in obese type 2 diabetic Egyptian patients with coronary artery stenosis. Can J Physiol Pharmacol. 2018;96(1):38-44. doi:10.1139/cjpp-2017-0272
27. Chong KS, Gardner RS, Morton JJ, Ashley EA, MacDonagh TA. Plasma concentrations of the novel peptide apelin are decreased in patients with chronic heart failure. Eur J Heart Fail. 2006;8(4):355-360. doi:10.1016/j.ejheart.2005.10.007
28. Koguchi W, Kobayashi N, Takeshima H, Ishikawa M, Sugiyama F, Ishimitsu T. Cardioprotective effect of apelin-13 on cardiac performance and remodeling in end-stage heart failure. Circ J. 2012;76(1):137-144. doi:10.1253/circj.cj-11-0689
29. Lee G, Song WH, Kim SJ, Kim YG, Ryu JH. Apelin-APJ axis inhibits TNF-alpha-mediated expression of genes involved in the inflammatory response in periodontal ligament cells. Int J Oral Biol. 2019;44(4):182-190. doi:10.11620/IJOB.2019.44.4.182
30. Sarhat ER, Rmaid ZJ, Jabir TH. Changes of salivary interleukine-17, apelin, omentin and vaspin levels in normal subjects and diabetic patients with chronic periodontitis. Ann Trop Med & Pub Health. 2020;23(1):S404. doi:10.36295/ASRO.2020.23118
31. Hirani T, Haq MA, Shetty NJ, et al. Evaluating salivary apelin level among chronic periodontitis patients, with and without type 2 diabetes mellitus utilizing enzyme linked immunosorbent assay: a comparative study. Bangladesh J Med Sci. 2023;22(2):305-315. doi:10.13140/ RG.2.2.13400.37125
GENERAL DENTISTRY SELF-INSTRUCTION
Exercise No. GD550, 2 CE Credits
Periodontics
Subject Code: 490
The 15 questions for this exercise are based on the article “A comparative evaluation of serum and salivary levels of apelin in chronic periodontitis associated with obesity and type 2 diabetes mellitus” on pages 28-34. This exercise was developed by Douglas P. Rockwood, DDS, MAGD, ABGD, in association with the General Dentistry Self-Instruction Committee.
Reading the article and successfully completing this exercise will enable you to:
• appreciate the difficulties in identifying a specific marker for periodontal disease;
• gain insight into the many systemic variables associated with the development of periodontal disease; and
• understand the interaction between apelin and metabolic functions.
Answers must be submitted online at agd.org/self-instruction by August 31, 2026.
1. Within groups, individuals with chronic periodontitis (CP) had ________ serum and salivary apelin levels than did individuals without CP; obese and diabetic subgroups had ________ serum apelin levels than healthy individuals.
A. lower; higher
B. higher; lower
C. lower; lower
D. higher; higher
2. Studies have found a relationship between obesity, diabetes, and periodontal disease, and ________ is a crucial factor connecting them.
A. diet
B. lifestyle
C. immunocompromisation
D. inflammation
3. Periodontal disease can affect carbohydrate metabolism by elevating cytokine levels. This induces inflammatory changes in connective tissue.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
4. Apelin is secreted by ________ and has been shown to ________ periodontal inflammation.
A. adipose tissue; exacerbate
B. adipose tissue; reduce
C. connective tissue; exacerbate
D. connective tissue; reduce
5. Apelin levels are altered in obesity and diabetes and are associated with ________.
A. decreased cyclooxygenase 2 markers
B. insulin resistance
C. diminished immunologic response
D. increased production of other adipokines
6. The sample size consisted of ___ individuals divided into 6 equal groups of ___.
A. 72; 12
B. 84; 14
C. 96; 16
D. 108; 18
7. For the purposes of this study, CP was defined as probing depths of > __ mm or attachment loss of > __ mm.
A. 4; 3
B. 5; 3
C. 6; 4
D. 7; 4
8. Body mass index for the group with obesity ranged from ______________.
A. 22.4 to 34.2
B. 30.0 to 39.0
C. 33.8 to 42.5
D. 36.1 to 44.6
9. All of the following health conditions resulted in exclusion from the study except one. Which is the exception?
A. immunosuppressive therapy
B. history of smoking/alcohol consumption
C. hemoglobin A1c > 7.5%
D. radiation therapy
10. A(n) ____________ was used to compare the subgroups in the study.
A. independent samples t test
B. Shapiro-Wilk test
C. 1-way analysis of variance
D. Pearson correlation
11. Which of the following B subgroups (CP) demonstrated the highest serum level of apelin?
A. 3B (obesity and type 2 diabetes)
B. 2B (obesity)
C. 1B (systemically healthy)
D. none
12. Relative to all groups, higher serum apelin levels were seen in group 3 (patients with obesity and type 2 diabetes mellitus). Salivary apelin revealed a significant correlation with the periodontal parameters in all 3 groups.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
13. The connection between periodontitis, obesity, and diabetes is considered to be ________.
A. symbiotic
B. bidirectional
C. codependent
D. cause and effect
14. The mean clinical attachment loss for all 3 groups with periodontitis (B subgroups) was in the range of ________ mm.
A. 3.50 to 3.99
B. 4.00 to 4.49
C. 4.50 to 4.99
D. 5.00 to 5.49
15. Serum apelin levels were greater than salivary levels in all 6 subgroups. Serum levels in all of the periodontitis groups were higher than in any of the nonperiodontitis groups.
A. Both statements are true.
B. The first statement is true; the second is false.
C. The first statement is false; the second is true.
D. Both statements are false.
Nonodontogenic cysts and pseudocysts of the oral cavity: a retrospective study of 218 cases
Nonodontogenic cysts and pseudocysts pose diagnostic challenges due to their similarity to other maxillofacial lesions in clinical and radiographic appearance. However, these lesions are studied less frequently than odontogenic lesions. This retrospective cross-sectional study aimed to evaluate the frequencies and characteristics of nonodontogenic lesions in an Iranian population over a 20-year period. Archived records of 7036 patients referred to the Department of Oral and Maxillofacial Pathology, Shahid Beheshti University Faculty of Dentistry, Tehran, were reviewed. Data on the age and sex of the patients and the type, clinical and radiographic features, and histopathologic diagnoses of the lesions were collected. Statistical analyses included Fisher exact, Kruskal-Wallis, and chi-square tests, and a value of P < 0.05 was considered statistically significant. Nonodontogenic cysts were found in 0.5% of all referred patients, while pseudocysts were identified in 2.6%. After a review of records, 218 patients with a confirmed diagnosis of oral pseudocysts or nonodontogenic cysts were included in a more detailed analysis. Mucocele was the most common lesion (63.8%), followed by simple bone cyst (13.8%) and nasopalatine duct cyst (11.9%). The mean (SD) age of these patients was 30.5 (15.7) years, and 53.7% of all the lesions occurred in men. Statistically significant relationships were observed between cyst type and sex (P = 0.001; Fisher exact test), age (P < 0.001; Kruskal-Wallis test), and location (P < 0.001; chi-square test). Most pseudocysts occurred on the lower lip, while nonodontogenic cysts and intraosseous pseudocysts were predominantly found in the maxilla and mandible, respectively. The results of this study highlight the varied demographics and clinical and radiographic presentations of nonodontogenic cysts and pseudocysts, emphasizing the need for thorough radiographic and histopathologic analyses to guide appropriate treatment strategies.
Cysts are cavity-like structures lined with epithelium, and those found in the maxillofacial region are categorized as 2 types: odontogenic and nonodontogenic.1 Nonodontogenic cysts can develop from structures within the jaw and facial region, such as salivary glands, nasopalatine ducts, and nasolabial ducts, or they may be found in other parts of the body. Examples of this group include dermoid cyst and lymphoepithelial cyst. Pseudocysts of the oral cavity, which represent a significant aspect of maxillofacial pathology, lack an epithelial lining but may exhibit clinical and radiographic features that closely resemble those of true cysts.2 Common pseudocysts of the oral cavity include mucocele/ranula and cysts arising from bone, such as simple bone cyst (SBC) and aneurysmal bone cyst (ABC).3
Nasopalatine duct cyst (NPDC) is the most frequently occurring nonodontogenic cyst, affecting approximately 1% of individuals, followed by nasolabial cyst, comprising 0.7% of all oral cavity cysts.1,4 NPDC typically presents as a painless swelling in the palate originating from proliferation of the epithelium of the nasopalatine duct and is most commonly observed in middle-aged individuals.1,4 Mucocele is the most common pseudocyst of the oral cavity, affecting 0.24% of the population, followed by SBC and ABC, which represent 0.2% and 0.07% of all oral lesions, respectively.5-7
On radiographic images, intraosseous cysts or pseudocysts usually appear as radiolucencies with well-defined borders; for instance, NPDC often presents as a well-defined heartshaped radiolucency. Despite similarities in radiographic features, the treatment and prognosis of cysts can vary depending on their origin. Histopathologic analysis provides crucial diagnostic information.1,8 Patients with nonodontogenic cysts often do not exhibit specific symptoms such as pain, although they may report issues such as a bad taste in the mouth, trismus, and dental or gingival problems. Treatment for oral cysts varies based on their type, size, and impact on the surrounding structures, but it typically includes enucleation, curettage, or marsupialization.2
While numerous studies have explored the frequency of odontogenic lesions, the epidemiology of nonodontogenic cysts has been less frequently examined.9 Despite their relatively low prevalence, the study of these lesions is crucial.10 The present study therefore aimed to assess the frequency, anatomical location, and clinical and radiographic characteristics of nonodontogenic cysts and pseudocysts as well as the sex and age distribution of affected patients at a major Iranian oral and maxillofacial pathology center over a 20-year period.
Methods
This cross-sectional study received ethical approval from the Ethics Committee of Shahid Beheshti University of Medical Sciences, Tehran, Iran (IR.SBMU.DRC.REC.1402.038). A comprehensive review was conducted using the archived records of the Department of Oral and Maxillofacial Pathology, School of Dentistry, from the years 2004 to 2024, covering 20 years. All patients with a confirmed diagnosis of oral pseudocyst or nonodontogenic cyst were included in the analysis, and patients with incomplete records or without a definitive histopathologic diagnosis were excluded.
After the eligible cases were selected, data were collected, including the age and sex of the patients and the type, location, clinical characteristics, and microscopic diagnosis of the lesions. Radiographs were evaluated for any radiographic alterations associated with the lesions, and these changes were categorized based on their type.
The Fisher exact, Kruskal-Wallis, and chi-square tests were applied for data analysis. The Fisher exact test was applied to assess the association between lesion type and sex. The Kruskal-Wallis test was used to compare patient age across different lesion types. The chi-square test was used for analyzing lesion location and age group. The analyses were conducted using SPSS software (version 21, IBM), and a value of P < 0.05 was considered statistically significant.
Results
Among 7036 patients referred to the center for oral biopsies, 218 with a confirmed diagnosis of oral pseudocysts or nonodontogenic cysts were included in the analysis. Nonodontogenic cysts, including NPDCs, nasolabial cysts, and surgical ciliated cysts, were identified in 35 patients, representing 0.5% of the total oral biopsies. Oral pseudocysts, consisting of mucoceles, SBCs, ABCs, antral pseudocysts, and Stafne cysts, were detected in 183 patients, accounting for 2.6% of all biopsy results. In the 218 patients included in the analysis, the most prevalent lesions were mucoceles (n = 139; 63.8%), SBCs (n = 30; 13.8%), and NPDCs (n = 26; 11.9%). Figure 1 shows representative cone beam computed tomography (CBCT) images of an NPDC.
Among the patients with oral pseudocysts or nonodontogenic cysts, 117 (53.7%) were male and 101 (46.3%) were female, representing a male to female ratio of 1.16 (Table 1). The Fisher exact test revealed a statistically significant association between sex and cyst type (P = 0.001). Specifically, 70.0% of SBCs and all of the nasolabial cysts occurred in female patients, while 77.8% of ABCs and 65.4% of NPDCs were found in male patients.
The patients’ ages ranged from 2 to 69 years, and the mean (SD) age was 30.5 (15.7) years. The Kruskal-Wallis test indicated a statistically significant correlation between age and lesion type (P < 0.001); patients with ABCs had the lowest mean (SD) age, 19.0 (11.4) years, while those with Stafne and nasolabial cysts had the highest mean ages, 57.0 (7.1) and 44.5 (14.6) years, respectively. Pairwise comparisons of lesion types using the Bonferroni method showed that the mean ages of patients with SBCs, ABCs, or mucoceles were not significantly different from each other, but these 3 groups had significantly
different mean ages compared with patients with all other lesion types (P < 0.05).
Additionally, the chi-square test demonstrated a significant relationship between the patients’ age decade and lesion type (P < 0.001); specifically, NPDCs, nasolabial cysts, mucoceles, SBCs, and ABCs were most frequently observed in the seventh, fourth, third, second, and first decades of life, respectively. Nonodontogenic cysts were most prevalent in the fourth and seventh decades of life (22.9% for each decade), whereas 37.7% of pseudocysts were observed in the third decade.
The most common anatomical location for pseudocysts was the lower lip, accounting for 100 cases (54.6%), while 23 cases of nonodontogenic cysts occurred in the maxilla (65.7%). The chi-square test confirmed a significant association between the lesion location and cyst type (P < 0.001). Notably, 78.0% of mucoceles were located on the lower lip, and 96.6% of SBCs and all of the ABCs were located in the mandible. Figure 2 shows representative CBCT images of a simple bone cyst.
Clinically, the most common presentation of pseudocysts and nonodontogenic cysts was painless swelling, reported in 76.3% of the cases, followed by asymptomatic lesions detected incidentally on routine radiographs in 16.0% of the patients. Tenderness or pain was infrequently reported.
The lesion location was not documented in the records of 13 patients; therefore, analyses related to lesion location were conducted for the remaining 205 patients. Among the lesions included in the analysis, 62.0% were in soft tissue, while 38.0% were intraosseous. Radiographic images were available for 59 intraosseous lesions. Radiolucencies with well-defined borders were observed in 96.6% of this subset, with 44.1% causing bone expansion and 18.6% leading to bone perforation. Root resorption or divergence was noted in 27.1% of intraosseous lesions with imaging records. All NPDCs, surgical ciliated cysts, antral pseudocysts, and Stafne cysts presented as well-defined unilocular radiolucencies (Table 2).
Discussion
The frequency of nonodontogenic cysts in this study was 0.5% of all biopsies, aligning with the findings of several studies, although Oner and Semiz reported a frequency of 0.7%.2,5,8,11 The most prevalent nonodontogenic cysts were NPDCs and nasolabial cysts, which is in agreement with the findings of other studies.5,9 Conversely, Passos et al identified dermoid cysts and epidermoid cysts as the most common nonodontogenic cysts, possibly due to their inclusion of cutaneous samples alongside intraoral samples in their research.11
The present study found pseudocysts to comprise 2.6% of diagnoses among all biopsies, and the most common of these lesions were mucoceles, SBCs, and ABCs. This is comparable to the findings of Wang et al, who observed a 2.16% prevalence of ABCs and SBCs in the jaws, and Francischetto et al, who reported a 1.77% frequency of mucoceles in both adult and pediatric populations.12,13 However, Flores et al and Passos et al documented lower frequencies of pseudocysts, ranging from 0.18% to 0.27%.11,14 This discrepancy could be attributed to their separate categorization of soft tissue pseudocysts from those with an intraosseous presentation. Wang et al reported SBC as the most frequently encountered intraosseous pseudocyst in the
Lesion Patient age, mean (SD), y Patient sex, n (%)
Nonodontogenic cysts (n = 35)
aThe lesion location was not documented in the records of 13 patients; therefore, analyses related to lesion location were conducted for the remaining 205 patients.
maxilla and mandible, similar to the present study.12 The results of the present study are also consistent with the findings of Menditti et al, in that the most common pseudocyst with a soft tissue appearance was the mucocele.3
The average age of patients with nonodontogenic cysts was 43.2 years, with the highest incidence occurring in the fifth decade of life. This finding aligns with previous studies, such as the one conducted by Philbert and Sandhu, which also identified the fifth decade as the most common age range for nonodontogenic cysts.1 However, Grossmann et al reported the third decade as the most frequent age, a difference that may be attributed to the inclusion of both odontogenic and nonodontogenic cysts in their analysis.5
Over the 20-year study period, the sex distribution of patients with nonodontogenic cysts was relatively equal.
Nevertheless, all nasolabial cysts were found in women. In addition, NPDCs exhibited a slight male predominance, similar to findings by Jones and Dillon.6 Similarly, Naini et al found that NPDC showed a slight male predominance.9
The most common location for nonodontogenic cysts was the maxilla, consistent with studies conducted in various countries.1,2,6 Mucoceles accounted for 1.9% of all oral cavity biopsies, with the highest occurrence in the third decade of life. There were fewer mucoceles in women than in men. The lower lip was the most common site, the location of 78.0% of all mucoceles. These findings are consistent with previous studies, including those of More et al, Francischetto et al, and Miranda et al.13,15,16 However, Miranda et al, as well as other studies, reported a female predominance, which could be attributed to racial differences and variations in sample sizes.13,16
Fig 1. CBCT images of a nasopalatine duct cyst showing a well-defined radiolucency associated with buccal cortical thinning, palatal perforation, root divergence, and central incisor resorption.
Table 1. Patient demographics and lesion location according to lesion type.
Lesion
(n = 27)
cyst (n = 2)
pseudocyst (n = 2)
Surgical ciliated cyst (n = 2)
(n = 21)
The frequencies of SBC and ABC in the present study were 0.4% and 0.1% of all histopathologically examined samples (7036), respectively. These frequencies are consistent with those reported in previous studies.2,14 The mandible was the most common location for these 2 pseudocysts, as observed in prior research, including the study by Wang et al.12 In the present study, the average ages of patients with SBC and ABC were 26.6 years and 19.0 years, respectively, which aligns with the typical age range of approximately 20 years reported in other countries. Wang et al noted a higher prevalence of ABCs in female subjects (50.0%); this discrepancy with the present findings (22.2%) could be due to the smaller number of ABCs in their sample.12
The present study identified only 2 cases of Stafne cyst among all biopsied lesions, representing a frequency of 0.03%.
This finding aligns with the results of a meta-analysis of 54 articles on this lesion.17 Among the 3 cases of antral pseudocyst observed in the present study, all were found in middle-aged men and were located in the maxilla. Kara et al also suggested a male predilection for this cyst.18 Surgical ciliated cysts, another rare finding, were predominantly observed in the maxilla of patients in the fourth decade of life. However, there have also been reports of such cysts occurring in the mandible.19
According to the present radiographic findings, nonodontogenic cysts were predominantly observed in the maxilla as radiolucencies with well-defined borders that frequently affected the roots of teeth. This observation is consistent with that of Philbert and Sandhu, who reported that the nonodontogenic cysts they evaluated were well-defined radiolucencies with intact lamina dura, often associated with root divergence.1 For pseudocysts,
Fig 2. CBCT images of a simple bone cyst showing a well-defined, corticated radiolucency in the anterior mandible associated with cortical bone thinning.
Table 2. Features of intraosseous lesions with available radiographic images (n = 59).
the radiographic findings revealed that most lesions (93.2%) appeared as unilocular radiolucencies with regular, well-defined borders. This finding aligns with the study by Flores et al, which also characterized these lesions as radiolucencies with regular margins. The main difference noted was the lower percentage of multilocular SBCs in the present study compared to Flores et al.14 While the present study provides valuable insights, there are a few limitations to note. The sample sizes of certain lesion groups were small, which is not uncommon in studies of this nature. However, these low-frequency findings may not generalize to other populations or settings. Additionally, as this was a retrospective study, there was no interaction with the patients, which restricted the ability to directly assess the presence or severity of clinical symptoms. In a few cases, patient files were incomplete or lacked radiographic images.
Conclusion
Although pseudocysts and nonodontogenic cysts constitute a small group of oral cavity lesions, knowledge of the demographic data of affected patients and clinical and radiographic features of the lesions will help to ensure a correct diagnosis. In this Iranian population, the most common clinical presentation was painless swelling, and the majority of the intraosseous lesions showed well-defined radiolucencies. Bone expansion, cortical perforation, and root resorption or divergence were also observed in varying percentages of the sample.
Author affiliations
Department of Oral and Maxillofacial Pathology, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran (Atarbashi-Moghadam); Research Committee, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran (Niknam, Mirebeigi-Jamasbi).
1. Philbert RF, Sandhu NS. Nonodontogenic cysts. Dent Clin North Am. 2020;64(1):63-85. doi:10.1016/j.cden.2019.08.006
2. Ruslin M, van Trikt KN, Yusuf AS, et al. Epidemiology, treatment, and recurrence of odontogenic and non-odontogenic cysts in South Sulawesi, Indonesia: a 6-year retrospective study. J Clin Exp Dent. 2022;14(3):e247-e253. doi:10.4317/jced.59309
3. Menditti D, Laino L, Di Domenico M, et al. Cysts and pseudocysts of the oral cavity: revision of the literature and a new proposed classification. In Vivo. 2018;32(5):999-1007. doi:10.21873/invivo.11340
4. Al-Shamiri HM, Elfaki S, Al-Maweri SA, Alaizari NA, Tarakji B. Development of nasopalatine duct cyst in relation to dental implant placement. N Am J Med Sci. 2016;8(1):13-16. doi:10.4103/1947-2714.175187
5. Grossmann SM, Machado VC, Xavier GM, et al. Demographic profile of odontogenic and selected nonodontogenic cysts in a Brazilian population. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104(6):e35-e41. doi:10.1016/j.tripleo.2007.05.028
6. Jones RS, Dillon J. Nonodontogenic cysts of the jaws and treatment in the pediatric population. Oral Maxillofac Surg Clin North Am. 2016;28(1):31-44. doi:10.1016/j.coms.2015.08.001
7. Senthilkumar B, Mahabob MN. Mucocele: an unusual presentation of the minor salivary gland lesion. J Pharm Bioallied Sci. 2012;4(Suppl 2):S180-S182. doi:10.4103/0975-7406.100265
8. Oner B, Semiz H. Retrospective evaluation of odontogenic and nonodontogenic cysts in the jaws in the series of 147 cases. Oral Health Dent Sci. 2020;4(4). doi:10.33425/26399490.1065
9. Naini FB, Aminishakib P, Ghorbanpour M, Vakili MM, Kharazifard MJ. Demographic profile of non-odontogenic jaw lesions in an Iranian population: a 30-year archive review. J Dent (Tehran). 2017;14(3):132-137.
10. Hghighat A, Shirani AM, Mirahmadi R, Hosseinian M. A study on the prevalence of benign, bony, odontogenic and non-odontogenic cysts and tumors among patients admitted to Esfahan Dental School and Al-Zahra Hospital (1995-2010). J Isfahan Dent Sch 2011;6(4):663-672.
11. Passos K, Silva P, Leonel A, et al. Nonodontogenic cysts and pseudocysts of the jaws: a clinicopathologic analysis of a case series. Oral Surg Oral Med Oral Pathol Oral Radiol 2020;129(1):e162. doi:10.1016/j.oooo.2019.06.693
12. Wang Y, Tang F, Li Z, Chen Q. Pseudocysts of the jaw: a retrospective study of 41 cases from a single institution. BMC Oral Health. 2023;23(1):87. doi:10.1186/s12903-023-02741-5
13. Francischetto M, Gonçalvez Gomez F, Rocha P, et al. Prevalence of oral mucocele in children and adolescents: systematic review and meta-analysis. Res Soc Dev. 2022;11(10): e458111032933. doi:10.33448/rsd-v11i10.32933
14. Flores IL, Hamilton ME, Zanchin-Baldissera E, Uchoa-Vasconcelos AC, Chaves-Tarquinio SB, Neutzling-Gomes AP. Simple and aneurysmal bone cyst: aspects of jaw pseudocysts based on an experience of Brazilian pathology service during 53 years. Med Oral Patol Oral Cir Bucal. 2017;22(1):e64-e69. doi:10.4317/medoral.21551
15. More CB, Bhavsar K, Varma S, Tailor M. Oral mucocele: a clinical and histopathological study. J Oral Maxillofac Pathol. 2014;18(Suppl 1):S72-S77. doi:10.4103/0973-029X.141370
16. Miranda GGB, Chaves-Junior SC, Lopes MP, et al. Oral mucoceles: a Brazillian multicenter study of 1,901 cases. Braz Dent J. 2022;33(5):81-90. doi:10.1590/0103-6440202204965
17. Chaweeborisuit P, Yurasakpong L, Kruepunga N, Tubbs RS, Chaiyamoon A, Suwannakhan A. The prevalence of Stafne bone cavity: a meta-analysis of 355,890 individuals. J Dent Sci 2023;18(2):594-603. doi:10.1016/j.jds.2022.08.022
18. Kara MI, Kirmali O, Ay S. Clinical evaluation of lateral and osteotome techniques for sinus floor elevation in the presence of an antral pseudocyst. Int J Oral Maxillofac Implants. 2012;27(5):1205-1210.
19. Atarbashi-Moghadam S, Latifi F, Atarbashi-Moghadam F, Gholami S. A mandibular lesion four years after orthognathic surgery. J Stomatol Oral Maxillofac Surg. 2023;124(3):101377. doi:10.1016/j.jormas.2022.101377
GENERAL DENTISTRY SELF-INSTRUCTION
Exercise No. GD551, 2 CE Credits
Oral Medicine, Oral Diagnosis, Oral Pathology
Subject Code: 730
The 15 questions for this exercise are based on the article “Nonodontogenic cysts and pseudocysts of the oral cavity: a retrospective study of 218 cases” on pages 36-40. This exercise was developed by Ralph Pruette, DDS, in association with the General Dentistry SelfInstruction Committee.
Reading the article and successfully completing this exercise will enable you to:
• be aware of the frequency of nonodontogenic cysts and pseudocysts;
• identify their anatomical locations and sex and age distributions; and
• understand their clinical and radiographic characteristics.
Answers must be submitted online at agd.org/self-instruction by August 31, 2026.
1. Nonodontogenic cysts and pseudocysts were evaluated for frequency and characteristics from records covering a ___-year period.
A. 10
B. 15
C. 20
D. 25
2. All of the following are typical treatments for pseudocysts except one. Which is the exception?
A. enucleation
B. curettage
C. marsupialization
D. resection
3. Nonodontogenic cysts were identified in ____% of patients.
A. 0.3
B. 0.4
C. 0.5
D. 0.6
4. Oral pseudocysts accounted for _____% of lesions.
A. 2.6
B. 3.2
C. 4.9
D. 5.2
5. The most prevalent lesion in the analyzed patients was _________.
A. mucocele
B. simple bone cyst (SBC)
C. nasopalatine duct cyst (NPDC)
D. aneurysmal bone cyst (ABC)
6. On analysis of sex distribution by cyst type, _____% of SBCs were found in female patients, and _____% of ABCs were found in male patients.
A. 64.5; 70.0
B. 64.5; 77.8
C. 70.0; 77.8
D. 77.8; 70.0
7. NPDCs were most frequently observed in the ________ decade of life.
A. second
B. third
C. fifth
D. seventh
8. The ________ was the most common anatomical location for pseudocysts.
A. lower lip
B. upper lip
C. buccal mucosa
D. floor of the mouth
9. The mandible was the location of ____% of SBCs.
A. 65.7
B. 76.3
C. 84.5
D. 96.6
10. What was the most common clinical presentation of the lesions?
A. painful swelling
B. painless swelling
C. altered sensation
D. bony expansion
11. Among the lesions included in the location analysis, 62.0% were ______, and 38.0% were_______.
A. in soft tissue; intraosseous
B. intraosseous; in soft tissue
C. mucoceles; NPDCs
D. NPDCs; mucoceles
12. The highest incidence of nonodontogenic cysts was in the ________ decade of life.
A. second
B. third
C. fourth
D. fifth
13. All ________ were found in women.
A. NPDCs
B. nasolabial cysts
C. mucoceles
D. ABCs
14. All of the following are true for most of the pseudocysts in the study except one. Which is the exception?
A. well-defined borders
B. unilocular
C. multilocular
D. radiolucent
15. Bone expansion was observed in ____% of ABCs.
A. 20.0
B. 40.0
C. 60.0
D. 80.0
Influence of a Bis-GMA–free universal adhesive system on enamel bond strength to ceramic brackets
Jurandir Antonio Barbosa, DDS, MSc, PhD ¢ Roberta Tarkany Basting, DDS, MSc, PhD
The aim of this study was to evaluate the shear bond strength and Adhesive Remnant Index (ARI) of ceramic brackets bonded to enamel using a universal adhesive system free of bisphenol A glycidyl methacrylate (Bis-GMA). A total of 100 bovine incisors were divided into 2 groups (n = 50) that received ceramic brackets (Morelli Ceramic or Ice Clear) bonded after acid etching and application of 1 of 5 adhesive systems (n = 10): Adper Single Bond 2, a conventional adhesive system (control group); Scotchbond Universal Plus, a BisGMA–free universal adhesive system; and Single Bond Universal, BeautiBond Xtreme, and BeautiOrtho Bond II, all Bis-GMA–containing universal adhesives. Shear bond strength was tested in a universal testing machine (50-kgf load cell; 0.5 mm/min crosshead speed), and the ARI was analyzed under ×20 magnification. Statistical analysis included a generalized linear model with Fisher exact test, Kruskal-Wallis test with post hoc Dunn test, and Mann-Whitney U test; the significance level was set at 5%. No statistically significant differences in shear bond strength were observed among the adhesive systems (P = 0.7821) or their interactions with bracket type (P = 0.5449). A significant difference was found when bracket types were compared (P < 0.0001), with the Morelli Ceramic bracket groups showing the highest bond strengths regardless of the adhesive system used. A significant association between adhesives and the Morelli Ceramic bracket was observed for the ARI score (P = 0.0018), with 100% of specimens in the Scotchbond Universal Plus adhesive group retaining more than half of the resin on the tooth. The Bis-GMA–free universal adhesive system achieved the highest percentage of adhesive retention on the tooth for both bracket types.
Received: February 13, 2025
Accepted: June 30, 2025
Keywords: bisphenol A glycidyl methacrylate, ceramic brackets, dental adhesives, dental enamel, shear bond strength
Orthodontic treatment with ceramic brackets enables mechanical adjustments without significantly affecting the esthetics of a patient’s smile. This makes ceramic brackets a preferred material, especially for adult patients.1-3
Polycrystalline brackets in particular are manufactured through a simplified and cost-effective process that involves heating aluminum oxide particles with a binder.4 The bracket bases vary in design and can include mesh, microspheres, or elevations, with more retentive bases providing greater mechanical adhesion.5-7 Additionally, procedures such as the use of acidic agents to increase enamel roughness and surface energy, or the use of bonding materials containing functional monomers (eg, 10-methacryloyloxydecyl dihydrogen phosphate [10-MDP], phosphonic acid, carboxylic acid, and phosphoric acid monomers), can facilitate chemical bonding to the enamel substrate. However, despite the potential of universal adhesive systems, their application for bracket bonding has yet to be thoroughly investigated.8,9 Bisphenol A glycidyl methacrylate (Bis-GMA) serves as the structural monomer and primary component of the organic matrix of resin-based materials, providing mechanical strength and a high molecular weight.10-12 Additional components, such as hydroxyethyl methacrylate (HEMA) and triethylene glycol dimethacrylate (TEGDMA), are incorporated to counteract the high viscosity of Bis-GMA and increase fluidity.13 Despite the favorable physical properties of Bis-GMA, studies have pointed out potential adverse biologic interactions due to its derivation from bisphenol A (BPA).11,14 These interactions include endocrine disruptions such as alterations in estrogen receptors, cytotoxicity, and cell death. Consequently, Bis-GMA–free materials are being developed to minimize BPA exposure.11,14 While some adhesives are formulated without Bis-GMA, comparative studies between these materials and those containing Bis-GMA remain limited. Thus, the present study aimed to evaluate the shear bond strength and Adhesive Remnant Index (ARI) of ceramic brackets bonded to a preconditioned enamel surface using a BisGMA–free universal adhesive system in comparison with other Bis-GMA–containing universal adhesives. The null hypotheses tested were as follows: (1) the different adhesives would not affect the bond strength to enamel for any bracket type evaluated; (2) the different adhesives would not influence the ARI for any bracket studied; and (3) the type of ceramic bracket would not affect the bond strength of the universal adhesive systems.
Methods
A total of 100 bovine maxillary incisors that were free of cracks and fractures were selected. The vestibular surfaces of the tooth crowns were lightly abraded to eliminate irregularities without exposing dentin. Abrasion was performed using
Table 1. Material compositions and instructions for use.
Product, batch No.
Ceramic brackets
Ceramic brackets (Morelli Ortodontia), 2877962
Ice Clear brackets (Orthometric), 167875001
Bis-GMA–free adhesive
Scotchbond Universal Plus universal adhesive system (3M), 2307400387
Composition
Polycrystalline alumina ceramic15
Polycrystalline alumina ceramic16
10-MDP; 2-propenoic acid, 2-methyl-, diesters with 4,6-dibromo-1,3-benzenediol 2-(2-hydroxyethoxy)ethyl 3-hydroxypropyl diethers; HEMA; 2-propenoic acid, 2-methyl-, reaction products with 1,10-decanediol and phosphorus oxide (P2O5); 2-propenoic acid, 2-methyl-, 3-(triethoxysilyl)propyl ester, reaction products with silica and 3-(triethoxysilyl)-1-propanamine; ethanol; water; synthetic amorphous silica, crystalline-free; methacrylic acid, 3-(triethoxysilyl)propyl ester; camphorquinone; acrylic and itaconic acid copolymer, N,N-dimethylbenzocaine; acetic acid, copper(2+) salt, monohydrate17
Instructions for use
NA
NA
Shake the bottle to homogenize, apply with an applicator for 20 s, lightly volatilize with an air jet for 5 s, and photoactivate for 20 s.
Bis-GMA adhesives
Adper Single Bond 2 conventional adhesive system (3M), 2311000966
Single Bond Universal adhesive system (3M), 2220700710
BeautiBond Xtreme universal adhesive system (Shofu Dental), 122235
BeautiOrtho Bond II universal adhesive system (Shofu Dental), 072002
400- and 600-μm silicon carbide sandpaper (3M) under water irrigation with a rotary electric polisher (Aropol 2V, Arotec). The teeth were then embedded in polyvinyl chloride tubes filled with polyether resin so that the clinical crowns were
exposed and the vestibular surfaces were oriented perpendicular to the horizontal plane. Prophylaxis of the vestibular surface of the crowns was carried out with rubber cups (KG Sorensen) and an extrafine pumice stone (SS White) used at low speed.
Table 2. Shear bond strengths of adhesive system and ceramic bracket combinations (n = 10 per group).
Adhesive system
Mean (SD) bond strength, MPa Morelli Ceramic Ice Clear
Scotchbond Universal Plus 28.28 (9.30)Aa 18.94 (3.15)Ba
Adper Single Bond 2 29.10 (7.94)Aa 20.63 (5.39)Ba
Single Bond Universal 24.01 (7.96)Aa 18.97 (10.49)Ba
BeautiBond Xtreme 31.95 (8.37)Aa 17.40 (3.68)Ba
BeautiOrtho Bond II 28.72 (11.45)Aa 16.86 (5.38)Ba
Different uppercase letters within rows indicate statistically significant differences between brackets (P ≤ 0.05; Mann-Whitney U test). Different lowercase letters within columns indicate statistically significant differences between adhesives (P ≤ 0.05; Dunn test).
Adhesive tape was applied to delineate the bracket bonding area, thus preventing material leakage.
The teeth were divided into 2 groups (n = 50) based on the type of ceramic bracket: Ceramic (Morelli Ortodontia), hereafter known as Morelli Ceramic, or Ice Clear (Orthometric). Each group was then subdivided into 5 equal groups (n = 10) according to the adhesive system: Adper Single Bond 2 (3M), a conventional universal adhesive system containing Bis-GMA serving as the control group; Scotchbond Universal Plus (3M), a Bis-GMA–free universal adhesive system; and Single Bond Universal (3M), BeautiBond Xtreme (Shofu Dental), and BeautiOrtho Bond II (Shofu Dental), all of which are universal adhesive systems that contain Bis-GMA.
The bonding protocol involved enamel conditioning with 37% phosphoric acid (Condac 37, FGM Dental Group) for 30 seconds followed by rinsing with water for 30 seconds. The respective adhesive systems were applied to each group according to the manufacturer instructions (Table 1).15-23 The brackets were positioned using bracket tweezers and bonded with a microhybrid composite resin (Z100 Universal Restorative, 3M) that was applied to the bracket. The bracket was placed on the enamel surface, and the composite resin was photopolymerized for 40 seconds with an LED curing light with a standard irradiance of 1000 mW/cm2 (Valo, Ultradent Products). The specimens were subsequently stored in an oven at 37°C, and shear bond strength was tested after 24 hours.
Shear bond strength tests were conducted on a universal testing machine (Emic DL 2000, Instron Brasil Equipamentos Científicos) equipped with a 50-kgf load cell. A chisel tip was applied at a crosshead speed of 0.5 mm/min to the interface between the ceramic bracket and the enamel surface until the bracket was dislodged.
Following bracket detachment, the test specimens were examined under a stereomicroscope ( EK3ST, CQA Comercial Química Americana) at ×20 magnification to assess the ARI according to the following scores: 0 = no adhesive remaining on the tooth; 1 = less than half of the adhesive remaining on the tooth; 2 = more than half of the adhesive remaining on the
Table 3. Adhesive Remnant Index (ARI) scores for adhesive system and ceramic bracket combinations. Adhesive system
Bond II
Clear Scotchbond Universal Plus
Single Bond 2
Bond Universal
Xtreme
Bond
ARI scores: 0, no adhesive remaining on the tooth; 1, less than half the adhesive remaining on the tooth; 2, more than half of the adhesive remaining on the tooth; 3, all adhesive remaining on the tooth. aStatistically significant difference (P ≤ 0.05; Fisher exact test).
tooth; and 3 = all adhesive remaining on the tooth, with a clear impression of the bracket base.24
Descriptive and exploratory analyses were conducted for the collected data. Bond strength values were evaluated using a generalized linear model to account for the effects of the adhesive system and bracket type as well as the interaction between them. The ARI data were analyzed using the Fisher exact test to assess associations with adhesive systems; Kruskal-Wallis and post hoc Dunn tests to compare scores among adhesive systems; and Mann-Whitney U test to compare scores between bracket types. Statistical analyses were performed using the R software program (2024, R Core Team), with the significance level set at 5%.
Results
No statistically significant difference was observed among the adhesive systems (P = 0.7821) (Table 2). However, the bond strength was significantly higher when Morelli Ceramic brackets were used, regardless of the adhesive system (P < 0.0001). The interaction between the adhesive system and bracket type was not significant (P = 0.5449).
A significant association between adhesive system and ARI was observed for both bracket types (P < 0.05) (Table 3). When the Morelli Ceramic bracket was used, Single Bond Universal and Scotchbond Universal Plus retained more than half (score 2) or all of the adhesive (score 3) on the tooth in 60% and 100% of test specimens, respectively. In contrast, Adper Single Bond 2, BeautiBond Xtreme, and BeautiOrtho Bond II accounted for 60%, 70%, and 80% of test specimens, respectively, with no adhesive (score 0) or less than half the adhesive (score 1) remaining on the tooth. Additionally, Scotchbond Universal Plus specimens exhibited a significantly higher mean ARI score than BeautiOrtho Bond II specimens, specifically when Morelli Ceramic brackets were used (P < 0.05). When Ice Clear brackets were used, 70%, 90%, 70%, 60%, and 60% of the specimens bonded using Single Bond Universal, Scotchbond Universal Plus, Adper Single Bond 2, BeautiBond Xtreme, and BeautiOrtho Bond II, respectively, retained more than half (score 2) or all of the adhesive (score 3) on the tooth. Notably, no significant difference in ARI was observed between the bracket types (P > 0.05).
Discussion
To meet orthodontic demands, the enamel surface must be properly prepared for bracket adhesion, which includes selecting an appropriate bonding agent.25 Adhesive systems often contain acidic functional monomers that facilitate bonding with the calcium (Ca) present in dental substrates.26 Two of the adhesive systems evaluated in this study, Scotchbond Universal Plus and Single Bond Universal, are formulated with 10-MDP, a phosphoric acid derivative capable of forming an ionic bond with hydroxyapatite, resulting in the stable and insoluble 10-MDP–Ca salt.27 In addition to enhancing micromechanical retention through mild demineralization due to its acidic nature (pH ~ 2.7), the 10-MDP–Ca salt stabilizes the adhesivesubstrate bond via nanolayer formation.28,29 However, the present study demonstrated that the bond strength of different ceramic brackets adhered to enamel did not statistically differ among adhesives containing various functional monomers, supporting the failure to reject the first null hypothesis.
BeautiBond Xtreme and BeautiOrtho Bond II adhesives, in contrast, contain a combination of functional monomers, including carboxylic acid and organophosphorus acid monomer in BeautiBond Xtreme and phosphoric acid monomer in BeautiOrtho Bond II.9,28 These monomers also chemically bond to the Ca in dental hydroxyapatite, but their bonding is more discrete and less stable than that of 10-MDP derivatives.30 The pH values of these adhesives are approximately 2.3 for BeautiBond Xtreme and 2.2 for BeautiOrtho Bond II.28,31 In the present study, no significant differences were observed in bond strength between these adhesives and those containing 10-MDP. However, significant differences were identified in the ARI depending on the bracket type, resulting in rejection of the second null hypothesis.
Selective acid etching increases surface roughness, enhances the flow of the adhesive on the enamel surface, and raises surface energy, thereby improving adhesive penetration into the enamel surface.32 In this regard, the conventional adhesive used as a control group (Adper Single Bond) has a pH
of approximately 4.7 and does not contain acidic functional monomers.33 Consequently, bonding to enamel relies only on the micromechanical retention created by phosphoric acid etching, where the resin monomers fill the etched retentive spaces.10 This differs from the chemical bonding achieved by the other adhesive systems evaluated in the present study, all of which contain acidic functional monomers.27
The highest shear bond strength values were observed for the Morelli Ceramic bracket, leading to rejection of the third null hypothesis. The Morelli Ceramic bracket features a regular mesh that covers its entire base, which may enhance the mechanical interlocking of the adhesive within the mesh irregularities, thereby improving bond strength. In contrast, the Ice Clear bracket has projections of varying shapes that do not fully cover the bracket base, thus impacting the ARI observed in this study.
Scotchbond Universal Plus and Single Bond Universal adhesives use a combination of water and ethanol as solvents, whereas BeautiBond Xtreme and BeautiOrtho Bond II utilize a combination of water and acetone. These solvent compositions, along with the types of functional acid monomers present in these adhesives, may have influenced the ARI, as previously discussed. When used with the Morelli Ceramic bracket, adhesives containing 10-MDP and solvents based on water and ethanol (Scotchbond Universal Plus and Single Bond Universal) predominantly resulted in half or more of the resin remaining on the tooth. In contrast, adhesives derived from phosphoric and carboxylic acid monomers predominantly resulted in less than half of the resin remaining on the tooth.
Monomers are the fundamental components of adhesives, classified into 2 major categories: functional monomers and cross-linked monomers. Among the latter, Bis-GMA is one of the most well-known. It is a derivative of BPA and glycidyl methacrylate (GMA), characterized by high viscosity and molecular weight, which contribute to enhanced mechanical resistance.14 Despite the widespread use of Bis-GMA, its biocompatibility remains a topic of significant concern. Studies have reported its potential endocrine-disrupting effects in rats, including alterations in fertility.10 Other studies have linked it to adverse effects on organs such as the kidneys and liver as well as skin hypersensitivity reactions.11 Additionally, Bis-GMA has been associated with cell necrosis, further raising questions regarding its safety.14,34
Scotchbond Universal Plus does not contain derivatives of BPA or GMA, relying instead on 10-MDP as its primary component.27 The group treated with Scotchbond Universal Plus exhibited the highest levels of adhesive residue, highlighting the influence of the adhesive system on residue levels. During debonding, the failure of this adhesive predominantly occurred at the interface between the bracket and the adhesive, with 90% to 100% of the resin remaining on the tooth. This indicates strong bonding to the tooth enamel, which may be advantageous since it minimizes damage to the substrate.5 However, this also poses challenges for orthodontists, since the removal of residual resin can be time-consuming and difficult.
The shear bond strength values reported for Scotchbond Universal Plus (20 MPa) in a previous study align closely with the results of the present study, which found mean values of
28.28 MPa for the Morelli Ceramic bracket and 18.94 MPa for the Ice Clear bracket.35 Although significant differences were observed between the mean bond strength values of the brackets in this study, all values exceeded the range recommended in the literature (6 to 8 MPa).36 This suggests that the combination of ceramic brackets and acid etching of the enamel provides high bond strength values irrespective of the adhesive used.8,37 The microhybrid composite resin (Z100 Universal Restorative) that was used for bonding between the bracket base and the adhesive systems in all groups contributed to the observed bond strength values; this may be a reason for the absence of significant differences among adhesive systems within each type of bracket.
Based on the results, adhesive systems containing functional monomers are recommended for bonding ceramic brackets. All groups demonstrated shear bond strength values significantly higher than those reported in the literature and the minimum recommended threshold.36-38 Additionally, the ARI scores favored enamel substrate preservation during debonding. The design of the bracket base, particularly a well-distributed mesh, also plays a crucial role in enhancing mechanical retention and bond strength, as observed with the Morelli Ceramic bracket.5
Conclusion
The type of adhesive system (Bis-GMA–free or Bis-GMA–containing) did not influence the shear bond strength of ceramic brackets bonded to enamel. The Morelli Ceramic bracket exhibited higher bond strength to enamel than the Ice Clear bracket irrespective of the adhesive used. The Bis-GMA–free adhesive system (Scotchbond Universal Plus) demonstrated higher ARI scores, with a greater percentage of resin remaining bonded to the tooth with both brackets that were evaluated.
Author affiliations
São Leopoldo Mandic School of Dentistry, Campinas, Brazil.
Correspondence
Roberta Tarkany Basting, DDS, MSc, PhD (rbasting@yahoo.com).
Conflicts of interest
None reported.
References
1. Mocuta DE, Miron MI, Lungeanu D, Mateas M, Ogodescu E, Todea CD. Laser Er:YAG-assisted debonding may be a viable alternative to the conventional method for monocrystalline ceramic brackets. Int J Environ Res Public Health. 2022;19(21):14564. doi:10.3390/ ijerph192114564
2. Rosvall MD, Fields HW, Ziuchkovski J, Rosenstiel SF, Johnston WM. Attractiveness, acceptability, and value of orthodontic appliances. Am J Orthod Dentofacial Orthop. 2009;135(3):276.e1-276.e12. doi:10.1016/j.ajodo.2008.09.020
3. Malkiewicz K, Jastrzebska A, Janas-Naze A, Boryczko W, Bartczak J. Assessment of the susceptibility of aesthetic orthodontic brackets to discoloration. Coatings. 2022;12(10):1080. doi:10.3390/coatings12081080
4. Aldossary MS, Abu Hajia SS, Santini A. Light energy transmission through six different makes of ceramic orthodontic brackets. Int Orthod. 2018;16(4):638-651. doi:10.1016/j. ortho.2018.09.005
5. Kilponen L, Varrela J, Vallittu PK. Priming and bonding metal, ceramic and polycarbonate brackets. Biomater Investig Dent. 2019;6(1):61-72. doi:10.1080/26415275.2019.1684823
6. Kang DY, Choi SH, Cha JY, Hwang CJ. Quantitative analysis of mechanically retentive ceramic bracket base surfaces with a three-dimensional imaging system. Angle Orthod. 2013;83(4):705-711. doi:10.2319/100412-782.1
7. Zheng BW, Cao S, Al-Somairi MAA, He J, Liu Y. Effect of enamel-surface modifications on shear bond strength using different adhesive materials. BMC Oral Health. 2022;22(1):224. doi:10.1186/s12903-022-02254-7
8. Saito H, Miyagawa Y, Endo T. Effects of plastic bracket primer on the shear bond strengths of orthodontic brackets. J Dent Sci. 2021;16(4):424-430. doi:10.1016/j.jds.2020.07.014
9. Yuasa T, Iijima M, Ito S, Muguruma T, Saito T, Mizoguchi I. Effects of long-term storage and thermocycling on bond strength of two self-etching primer adhesive systems. Eur J Orthod. 2010;32(3):285-290. doi:10.1093/ejo/cjp118
10. Van Landuyt KL, Snauwaert J, De Munck J, et al. Systematic review of the chemical composition of contemporary dental adhesives. Biomaterials. 2007;28(26):3757-3785. doi:10.1016/j.biomaterials.2007.04.044
11. He J, Kopperud HM. Preparation and characterization of bis-GMA-free dental composites with dimethacrylate monomer derived from 9,9-bis[4-(2-hydroxyethoxy)phenyl]fluorene. Dent Mater. 2018;34(7):1003-1013. doi:10.1016/j.dental.2018.03.007
12. Pouyanfar H, Golshah A, Shekarbeigi M. Shear bond strength of metal and ceramic brackets to composite using single bond and universal adhesive. Open Access Maced J Med Sci. 2020;8(D):1-6. doi:10.3889/oamjms.2020.3118
13. Yang J, Liao M, Hong G, et al. Effect of APTES- or MPTS-conditioned nanozirconia fillers on mechanical properties of bis-GMA-based resin composites. ACS Omega. 2020;5(50):3254032550. doi:10.1021/acsomega.0c04762
14. Assery MK, Ajwa N, Alshamrani A, Alanazi BJ, Durgesh BH, Matinlinna JP. Titanium dioxide nanoparticles reinforced experimental resin composite for orthodontic bonding. Mater Res Express. 2019;6(12):125098. doi:10.1088/2053-1591/ab5a93
15. Morelli Ortodontia. Bráquetes. Accessed July 25, 2025. https://www.morelli.com.br/loja/ departamento/departamento.aspx?categoria=braquetes&subcategoria=estetico
16. Orthometric. New Ice Clear. Accessed July 25, 2025. https://www.orthometric.com.br/ produtos/new-ice-clear/
17. 3M. Scotchbond Universal Plus. Safety data sheet. January 5, 2023. https://multimedia.3m. com/mws/mediawebserver?mwsId=SSSSSuUn_zu8l00xNx_1OY_v4v70k17zHvu9lxtD7SSSSSS--
18. 3M. Adper Single Bond 2. Safety data sheet. May 11, 2023. https://multimedia.3m.com/ mws/mediawebserver?mwsId=SSSSSuUn_zu8l00x4YtGlx21Ov70k17zHvu9lxtD7SSSSSS--
19. 3M. Single Bond Universal. Safety data sheet. March 9, 2020. https://multimedia.3m. com/mws/mediawebserver?mwsId=SSSSSuUn_zu8l00xMY_eMYtGlv70k17zHvu9lxtD7SSSSSS--
20. Shofu Dental. BeautiBond Extreme. Safety data sheet. December 19, 2022. https://www. shofu.com/wp-content/uploads/BeautiBond-Xtreme-SDS-US-Version-2.pdf
21. Saito H, Miyagawa Y, Endo T. Effects of plastic bracket primer on the shear bond strengths of orthodontic brackets. J Dent Sci. 2021;16(1):424-430. doi:10.1016/j.jds.2020.07.014
22. FGM Dental Group. Condac 37. Ficha de informação de segurança de produtos químicos. April 11, 2020. https://fgmdentalgroup.com/wp-content/uploads/2022/12/ SDS-Condac-37-PT1.pdf
23. 3M. Z100 Restorative Paste. Safety data sheet. June 9, 2021. https://multimedia.3m.com/ mws/mediawebserver?mwsId=SSSSSuUn_zu8l00xl8_ZOx_9lv70k17zHvu9lxtD7SSSSSS--
24. Artun J, Bergland S. Clinical trials with crystal growth conditioning as an alternative to acid-etch enamel pretreatment. Am J Orthod. 1984;85(4):333-340. doi:10.1016/00029416(84)90190-8
25. Cevik P, Karacam N, Eraslan O, Sari Z. Effects of different surface treatments on shear bond strength between ceramic systems and metal brackets. J Adhes Sci Tech. 2016;30(17):11051115. doi:10.1080/01694243.2016.1245074
26. Barceleiro MO, Lopes LS, Tardem C, et al. Thirty-six-month follow-up of cervical composite restorations placed with an MDP-free universal adhesive system using different adhesive protocols: a randomized clinical trial. Clin Oral Investig. 2022;26(6):4337-4350. doi:10.1007/ s00784-022-04397-x
27. Fehrenbach J, Isolan CP, Münchow EA. Is the presence of 10-MDP associated to higher bonding performance for self-etching adhesive systems? A meta-analysis of in vitro studies. Dent Mater. 2021;37(10):1463-1485. doi:10.1016/j.dental.2021.08.014
28. Yuan Y, Intajak P, Islam R, et al. Effect of sodium hypochlorite on bonding performance of universal adhesives to pulp chamber dentin. J Dent Sci. 2023;18(3):1116-1124. doi:10.1016/j.jds.2022.11.007
29. Maciel Pires P, Dávila-Sánchez A, Faus-Matoses V, Nuñez Martí JM, Lo Muzio L, Sauro S. Bonding performance and ultramorphology of the resin-dentine interface of contemporary universal adhesives. Clin Oral Investig. 2022;26(6):4391-4405. doi:10.1007/s00784-02204402-3
30. Van Landuyt KL, Yoshida Y, Hirata I, et al. Influence of the chemical structure of functional monomers on their adhesive performance. J Dent Res. 2008;87(8):757-761. doi:10.1177/154405910808700804
31. Flores T, Mayoral JR, Giner L, Puigdollers A. Comparison of enamel-bracket bond strength using direct- and indirect-bonding techniques with a self-etching ion releasing S-PRG filler. Dent Mater J. 2015;34(1):41-47. doi:10.4012/dmj.2014-138
32. Wong J, Tsujimoto A, Fischer NG, et al. Enamel etching for universal adhesives: examination of enamel etching protocols for optimization of bonding effectiveness. Oper Dent. 2020;45(1):80-91. doi:10.2341/18-275-L
33. Jaberi Ansari Z, Panahandeh N, Tabatabaei Shafiei ZS, Akbarzadeh Baghban A. Effect of selfetching adhesives on the bond strength of glass-ionomer cements. J Dent (Tehran). 2014;11(6):680-686.
34. Klauer E, Belli R, Petschelt A, Lohbauer U. Mechanical and hydrolytic degradation of an Ormocer-based bis-GMA-free resin composite. Clin Oral Investig. 2019;23(5):2113-2121. doi:10.1007/s00784-018-2651-3
35. Jäggi M, Karlin S, Zitzmann NU, Rohr N. Shear bond strength of universal adhesives to human enamel and dentin. J Esthet Restor Dent. 2024;36(5):804-812. doi:10.1111/ jerd.13204
36. Reynolds IR. A review of direct orthodontic bonding. Br J Orthod. 1975;2(3):171-178. doi:10.1080/0301228X.1975.11743666
37. Costa AC, Sabóia V, Marçal F, et al. In vitro evaluation of experimental self-adhesive orthodontic composites used to bond ceramic brackets. Materials (Basel). 2019;12(3):419. doi:10.3390/ma12030419
38. Arash V, Naghipour F, Ravadgar M, Karkhah A, Barati MS. Shear bond strength of ceramic and metallic orthodontic brackets bonded with self-etching primer and conventional bonding adhesives. Electron Physician. 2017;9(1):3584-3591. doi:10.19082/3584
Multidisciplinary approach to diagnosis and management of lymphadenopathy in a patient with mucous membrane pemphigoid: a case report
Heba Turkstani, BDS ¢ Eman Alamodi, BDS ¢ Eric T. Stoopler, DMD, FDSRCS, FDSRCPS
Autoimmune blistering diseases (AIBDs) can present concurrently with solid or hematologic malignancies. This concomitant finding is believed to be associated with paraneoplastic syndrome, and management typically requires a multidisciplinary approach. This case report describes diagnosis and treatment of a patient previously diagnosed with mucous membrane pemphigoid of the skin who was referred to an oral medicine clinic for evaluation of oral mucosal blisters and gingival bleeding of 8 months’ duration. Routine head and neck examination revealed incidental findings of a unilateral large palatine tonsil and fixed submandibular lymph node. A biopsy of the right tonsil was performed, and immunohistochemical analyses revealed markers consistent with mantle cell lymphoma, which was later determined to be stage III. The patient was started on a regimen of acalabrutinib and rituximab. At the 3-month follow-up, the patient’s skin and oral blisters had cleared, and she was completely asymptomatic. To ensure timely referral and better patient outcomes, careful attention should be paid to subtle cues that can lead to early detection of malignancies in persons with AIBDs.
Autoimmune blistering diseases (AIBDs) are a group of disorders marked by autoantibodies that attack structural proteins on the skin and mucous membrane.1 Mucous membrane pemphigoid (MMP), a type of AIBD, is a chronic and rare disease with a female predilection.2 It is more common in older adults aged 60 to 80 years.3 Autoantibodies in MMP specifically attack the basement membrane zone of the epithelium and epidermis. On histologic examination, MMP appears as subepithelial blistering at the basement membrane zone, seen as separation between the epithelium and connective tissue in mucosal sites or separation between the epidermis and dermis in the skin.4 Also noted within the connective tissue is an abundance of chronic inflammatory cells, especially lymphocytes and sometimes histiocytes and eosinophils.5
MMP primarily affects mucosal surfaces, and the oral mucosa is the most affected site.6 Oral mucosa sites frequently affected include the gingiva, buccal and labial mucosae, tongue, and palate.7 Commonly affected nonoral sites include the ocular conjunctiva, skin, genitals, and pharynx.8
The clinical presentation of MMP can vary from mild erosions and subepithelial blistering to more severe erosions, ulcerations, blindness, and strictures, which can be life-threatening.1,2 The presentation is dependent on disease severity and the mucosal surface affected.
The definitive diagnosis of MMP is made from a combination of a thorough patient-based history of the present illness, review of system and clinical examination findings, and biopsy. Occasionally, blood (serum) sample collection may be needed. Hematoxylin and eosin staining and direct immunofluorescence are carried out on the biopsy specimen. In cases where the epithelium is lost during biopsy, indirect immunofluorescence assays or enzyme-linked immunosorbent assays that detect circulating anti–basement membrane antibodies in the serum aid in making a diagnosis.4 Direct immunofluorescence shows linear immunoglobulin G (IgG), immunoglobulin A, and/or C3 staining along the basement membrane zone in 70% to 100% of cases.9 In contrast, indirect immunofluorescence shows IgG antibody localization along the basement membrane zone, supporting the diagnosis of bullous pemphigoid (BP) or MMP. Enzyme-linked immunosorbent assays detect elevated levels of circulating IgG antibodies against BP-180 and BP-230 in patients with both MMP and BP, but BP-180 antibodies are more frequently associated with MMP.9
The presence of anti–laminin-322 (anti–LM-332) antibodies has been linked to the diagnosis of cancers in persons
The Lugano classification is used for staging MCL.19 This classification considers the number of lymph nodes involved, the presence of extranodal disease, and the involvement of organs such as the spleen or liver.19
This case report describes a patient who presented with MMP and incidental findings during the routine head and neck examination that led to a diagnosis of MCL.
Case report
diagnosed with MMP.6 These include B- and T-cell lymphomas and solid tumors.6 It is possible to test for the presence of anti–LM-332 and collagen VII antibodies, but this is currently limited to specialized centers and for research purposes, partly due to the widespread unavailability of testing facilities for LM-332 autoantibodies.6,10
B-cell lymphoma, a type of non-Hodgkin lymphoma, is a common hematologic malignancy of white blood cells that originates from B lymphocytes.11 It accounts for up to 85% of lymphomas in the United States and has many subtypes.12 An example is mantle cell lymphoma (MCL), an uncommon and fast-growing lymphoma that develops from B cells in the mantle zone of lymphoid tissue.13 The incidence of MCL in the United States is estimated to range from 4 to 8 cases per million individuals annually.14 The median age at diagnosis of MCL is 68 years, and there is a male to female preponderance of 3:1.14
Mantle cell lymphoma demonstrates considerable clinical and biologic heterogeneity, varying from a slowly developing, nonnodal leukemic form to an aggressive, rapidly proliferating blastoid variation.15 The distinctive genetic characteristic of this lymphoma is the chromosome translocation t(11;14) (q13;q32) involving the immunoglobulin H gene and the cyclin D1 (CCND1) gene.16 This abnormality leads to the overexpression of the CCND1 protein, which can be readily detected through immunohistochemistry.16
The immunophenotypes most commonly linked with MCL are positive CD20, CD5, and CCND1 surface markers and negative CD23 and CD10. 17 Also, SOX11, a transcription factor, is frequently overexpressed in the majority of MCL cases and is considered a specific oncogene driving the pathology of MCL. 18
A 65-year-old woman with an 8-month history of oral blisters and gingival bleeding was referred by her dermatologist to the Oral Medicine Clinic at the Hospital of the University of Pennsylvania, Philadelphia. She had previously seen a general dentist for evaluation of the oral lesions and was treated with amoxicillin for suspected dental infection without benefit.
Four months prior to coming to the clinic, the patient had presented to a dermatologist with skin blisters and a rash affecting her face, neck, and arms. An incisional biopsy was performed on a lesion on her neck. Analysis of the specimen resulted in histologic findings of subepidermal bulla formation with mixed inflammation and linear IgG and C3 staining on hematoxylin and eosin staining and direct immunofluorescence (Fig 1). The enzyme-linked immunosorbent assay was negative for BP-180, BP-230, desmoglein 1, and desmoglein 3 antigens. Based on these findings, the patient was diagnosed with MMP. Before the patient visited the oral medicine clinic, the dermatologist prescribed a prednisone taper of 40 mg for 5 weeks and 25 mg of dapsone, along with topical clobetasol gel, 0.05%, for the skin lesions.
The patient had no significant medical or medication history, no known drug allergies, and unremarkable social and family histories. A review of systems revealed dysphagia, odynophagia, and nasal bleeding. On examination of the head and neck, no facial asymmetry or swelling was noted. However, the submandibular lymph nodes were hard on the right side and palpable but freely mobile on the left side, each measuring approximately 1.5 cm in diameter. Erosions were also observed on the left side of her neck, and a blister was present on the upper left eyelid (Fig 2).
The intraoral examination showed moderate erythema, erosions, blistering, and ulcerations on the maxillary gingiva,
Fig 1. Specimen from a skin biopsy of the neck revealing subepidermal bulla formation (hematoxylin and eosin stain; original magnification ×10).
Fig 2. Extraoral clinical images. A. Blistering on the upper left eyelid. B. Erosion on the left side of the neck.
Fig 5. Positron emission tomography/CT image showing glucose uptake in the right palatine tonsil, evidenced by enhanced contrast in the region (arrow).
Table 1. Results of hematologic testing of the patient with corresponding reference ranges.
Laboratory value Result Reference range
White
Hematocrit,
Mean corpuscular volume, fL 83 80-100
Mean corpuscular hemoglobin, pg 27 27-33
Mean corpuscular hemoglobin concentration, g/dL 33 31-36
MMP. The differential diagnosis for the incidental findings of the enlarged right palatine tonsil and palpable lymph nodes included reactive lymph nodes and possible malignancy. The patient was referred for computed tomography (CT) and to the otorhinolaryngologist for further investigation of the findings on head and neck examination. She was also prescribed dexamethasone oral rinse, 0.5 mg/5 mL, and 100,000 U of nystatin oral suspension (swish and spit twice a day) to manage the MMP and prevent yeast infection from prolonged steroid use. A 3-month follow-up was scheduled.
The CT scan images showed significant enlargement of the right palatine tonsil as well as bilateral submandibular, right supraclavicular, and right retropharyngeal lymphadenopathy (Fig 4). Diagnostic considerations included neoplasm, lymphoid hypertrophy, and an inflammatory process.
Basophil count, × 103/μL
Abbreviations: H, high; L, low.
The patient was a 65-year-old woman with an 8-month history of oral blisters and gingival bleeding.
mandibular labial mucosa, and buccal mucosae bilaterally (Fig 3). Her right palatine tonsil was also enlarged.
The results of hematology investigations were within normal limits except for low hemoglobin (10.7 g/dL), hematocrit (33%), and neutrophil levels (1.7 × 103/μL), as well as marginally high red cell distribution width (14.6%) (Table 1).
Based on history, clinical examination, and previous diagnosis from the skin biopsy, the oral lesions were consistent with
A biopsy of the right tonsil was done, and staining revealed normal squamous epithelium over a dense infiltrate of small- to medium-sized atypical lymphoid cells. These cells had oval to mildly irregular nuclei, condensed chromatin, inconspicuous nucleoli, and scant cytoplasm. Immunophenotyping showed a dominant population of λ-restricted B cells, comprising 89% of lymphocytes, with low forward and side scatter, suggesting small size. These B cells had the following markers: CD5+ (dim), CCND1+ (dim), CD10 , CD23 , CD20+ (moderate), CD200 , CD38+ (variable), and CD22+. These findings are consistent with MCL.
The patient was referred to a hematology-oncology specialist for management of the MCL. A positron emission tomography/CT scan was ordered and showed hypermetabolic lymphadenopathy both above and below the diaphragm, including the bilateral cervical, subclavicular/supraclavicular, bilateral axillary, mediastinal, pelvic, and inguinal nodal stations, along with enlargement of the right palatine tonsil, which demonstrated marked fluorodeoxyglucose avidity (Fig 5). The hematologist diagnosed stage III MCL characterized by an ataxia-telangiectasia mutated gene.
The patient was started on a regimen of acalabrutinib, 100 mg, taken orally twice daily, and rituximab, 375 mg/m2, administered
Fig 3. Intraoral clinical images. A. Erythema and erosion on the maxillary gingiva. B. Large area of mucosal erosion on the mandibular left labial mucosa.
Fig 4. Axial contrast-enhanced CT image, obtained in soft tissue windows at the level of the pharynx, showing the enlarged right palatine tonsil (star).
intravenously weekly for 4 weeks. The treatment plan included maintenance rituximab, administered monthly for 12 months, followed by every other month for another 12 to 24 months, and indefinite acalabrutinib use. The patient’s complete blood count was monitored monthly due to the potential hematologic side effects of the medications.
At the 3-month follow-up with the oral medicine clinic, the patient reported significant improvement. Her skin and oral blisters had cleared, and she was completely asymptomatic after starting the systemic treatment for MCL. It was recommended that she use the dexamethasone and nystatin rinse only as needed for flare-up of oral mucosal lesions.
Discussion
This case report, which to the best of the authors’ knowledge is the first reported case highlighting a rare instance of MMP associated with MCL, reinforces the importance of thorough, routine head and neck examinations by oral medicine specialists and all healthcare providers managing patients with AIBDs. The incidental finding of hematologic malignancy in this patient underscores the critical role of comprehensive evaluations in identifying such conditions.
Dysphagia in patients with AIBDs can result from mucosal involvement or tumors, whether benign or malignant. Other potential causes include infections, inflammatory conditions, structural abnormalities, neuromuscular disorders, trauma, or medication side effects. Each possible cause should be carefully evaluated.20
A comprehensive review of articles published within a span of 24 years found a total of 344 recorded cases of anti–LM-332–type MMP, and 75 of the patients (21.8%) had malignancies that occurred either before diagnosis or during treatment of MMP.8 In addition, a study of 520 individuals with BP-180–positive MMP evaluated the correlation between anti–LM-332 autoantibodies and malignancy. Of the 116 patients who tested positive for anti–LM-332 autoantibodies, 19 (16.4%) had malignant tumors, compared with 39 (9.7%) of 404 patients who tested negative for anti–LM-332, suggesting a possible association between anti–LM-332–type MMP and malignancy.21 A retrospective study on 133 cases of anti–LM-332–type MMP also showed that 22 patients developed malignancies.22
None of the previously mentioned studies report a case of MCL in a patient with MMP, although 2 published cases described co-occurrence of BP and MCL (Table 2). 23,24 However, the relationship between BP and malignancy is controversial, with some studies indicating an increased risk of various cancers, particularly lymphoma. 25 Other researchers suggest that the observed association may be related to the patient’s age rather than a direct connection between BP and malignancy. 26
The paraneoplastic phenomenon of mucous membrane pemphigoid is characterized by chronic mucosal erosions and fibrosis. It is typically triggered by an immune response to LM-332 and is frequently associated with underlying malignancies such as B-cell chronic lymphocytic leukemia, non-Hodgkin lymphoma, and acute myeloid leukemia.27 The risk of neoplastic association is substantially increased in MMP patients due to
Table 2. Summary of clinical presentation, diagnosis, and outcomes in 2 published cases of concomitant bullous pemphigoid and mantle cell lymphoma.
Characteristic Iranzo et al23
Md Radzi and Kasim24
Age, y 39 29
Sex Male Male
Symptoms Severe odynophagia resulting in weight loss (3-mo history); tense blisters and painful oral ulcers (6-wk history)
Generalized skin itchiness, night sweats, and weight loss (5-mo history); tense blisters over face, trunk, and limbs (3-d history)
Hematologic results Normal complete blood counts Leukocytosis
Skin biopsy results Subepidermal bulla with eosinophils; linear deposition of immunoglobulin G and C3 along the basement membrane zone
Lymph node biopsy results
Diagnosis
Effacement of nodal architecture; small lymphocytes
Bullous pemphigoid with mantle cell lymphoma (stage IVA)
Treatment Oral prednisone, bone marrow transplant, and cytoreductive chemotherapy
Outcome Full remission after 48 mo; no recurrence of bullous pemphigoid or mantle cell lymphoma
Subepidermal bullae with acantholytic cells; deposition of immunoglobulin G, C3, and C1q along the basement membrane zone
Effacement of nodal architecture; small lymphocytes with irregular nuclei
Bullous pemphigoid with mantle cell lymphoma
Rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone
Died after 2 wk due to neutropenic sepsis
the presence of LM-332 autoantibodies, necessitating prompt investigation of the underlying cancers.27
Patients diagnosed with MCL typically exhibit advanced stage III or IV disease, marked by widespread swollen lymph nodes, involvement of blood and bone marrow, and splenomegaly.13 Some patients may also exhibit pancytopenia or a leukemic presentation with significant leukocytosis. Additional extranodal regions involve the gastrointestinal tract or Waldeyer ring.28
The treatment for MCL includes monitoring, chemotherapy, and consolidation therapy with transplantation, which varies based on the patient’s age and health and whether they are symptomatic.29 Pharmacologic interventions include inhibitors of
Bruton tyrosine kinase, such as acalabrutinib, ibrutinib, and zanubrutinib, as well as immunomodulatory medicines such as lenalidomide. Additionally, venetoclax is a medication that inhibits B-cell lymphoma 2. Immunotherapy options include CD20-directed monoclonal antibodies such as rituximab or chimeric antigen receptor T-cell treatment utilizing brexucabtagene autoleucel.29
In the present case, due to the advanced stage of her disease, the patient began a regimen of acalabrutinib, a Bruton tyrosine kinase inhibitor, and rituximab, an anti-CD20 monoclonal antibody. After treatment with rituximab and acalabrutinib was initiated, she experienced complete resolution of skin and oral blisters, demonstrating a positive response to therapy. Complete blood counts should be regularly monitored in patients taking these medications because of the associated risks of thrombocytopenia, neutropenia, and anemia.30 Long-term follow-up is necessary, even if the lymphoma is in remission, to monitor for potential recurrence or late-onset complications.
Conclusion
This case underscores the complex relationship between MMP and associated malignancies, particularly MCL. The variability in disease presentation, from systemic involvement to localized manifestations, highlights the need for thorough diagnostic evaluations. The standard approach in the Department of Oral Medicine at the University of Pennsylvania (both Penn Medicine and Penn Dental Medicine) involves ensuring ageand sex-appropriate cancer screening. Symptoms, physical examination, and routine screening results guide further evaluation for malignancy.
This case also reinforces the importance of routine head and neck examinations in assessment of patients with AIBD, as well as the value of a multidisciplinary approach to management, which can lead to early detection of concurrent malignancies and improved patient outcomes.
Author affiliations
Department of Oral Medicine, Penn Dental Medicine, University of Pennsylvania, Philadelphia (Turkstani, Stoopler, Mupparapu, Omolehinwa); Department of Oral and Diagnostic Sciences, Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia (Turkstani); Department of Oral Diagnostic Sciences, College of Dentistry, King Khalid University, Abha, Saudi Arabia (Alamodi).
Correspondence
Temitope T. Omolehinwa, BDS, DMD, DScD (omote@upenn.edu).
Conflicts of interest
None reported.
References
1. Cowan TL, Huang C, Murrell DF. Autoimmune blistering skin diseases triggered by COVID-19 vaccinations: an Australian case series. Front Med (Lausanne). 2023;9:1117176. doi:10.3389/fmed.2022.1117176
2. Rashid H, Lamberts A, Borradori L, et al. European guidelines (S3) on diagnosis and management of mucous membrane pemphigoid, initiated by the European Academy of Dermatology
and Venereology. I. J Eur Acad Dermatol Venereol. 2021;35(9):1750-1764. doi:10.1111/ jdv.17395
3. Leisti P, Huilaja L, Jokelainen J, Varpuluoma O, Tasanen K. Epidemiology and comorbidities of mucous membrane pemphigoid: a national cohort study. J Invest Dermatol. 2024;144(9):2078-2080. doi:10.1016/j.jid.2024.02.008
4. Kamaguchi M, Iwata H. The diagnosis and blistering mechanisms of mucous membrane pemphigoid. Front Immunol. 2019;10:34. doi:10.3389/fimmu.2019.00034
5. Dharman S, Muthukrishnan A. Oral mucous membrane pemphigoid—two case reports with varied clinical presentation. J Indian Soc Periodontol. 2016;20(6):630-634. doi:10.4103/jisp. jisp_155_16
6. Du G, Patzelt S, van Beek N, Schmidt E. Mucous membrane pemphigoid. Autoimmun Rev. 2022; 21(4):103036. doi:10.1016/j.autrev.2022.103036
7. Martins NF, Dos Santos RTN, Azevêdo ABF, de Sousa Duda Júnior LG, de Vasconcelos AJA, Sobral APV. Comparative analysis of the prevalence of oral manifestations between pemphigus vulgaris and mucous membrane pemphigoid: scoping review. Arch Dermatol Res. 2024;316(5):166. doi:10.1007/s00403-024-02925-1
8. Shi L, Li X, Qian H. Anti-laminin 332-type mucous membrane pemphigoid. Biomolecules. 2022;12(10):1461. doi:10.3390/biom12101461
9. Sárdy M, Kostaki D, Varga R, Peris K, Ruzicka T. Comparative study of direct and indirect immunofluorescence and of bullous pemphigoid 180 and 230 enzyme-linked immunosorbent assays for diagnosis of bullous pemphigoid. J Am Acad Dermatol. 2013;69(5):748-753. doi:10.1016/j.jaad.2013.07.009
10. Ahmed AR, Kalesinskas M, Kooper-Johnson S. Paraneoplastic autoimmune laminin-332 syndrome (PALS): anti-laminin-332 mucous membrane pemphigoid as a prototype. Autoimmun Rev. 2023;22(10):103444. doi:10.1016/j.autrev.2023.103444
11. Shingleton J, Wang J, Baloh C, et al. Non-Hodgkin lymphomas: malignancies arising from mature B cells. Cold Spring Harb Perspect Med. 2021;11(3):a034843. doi:10.1101/ cshperspect.a034843
12. American Cancer Society. Types of B-cell lymphoma. Revised February 15, 2024. Accessed September 8, 2024. https://www.cancer.org/cancer/types/non-hodgkin-lymphoma/ about/b-cell-lymphoma
13. Jain P, Wang ML. Mantle cell lymphoma in 2022—a comprehensive update on molecular pathogenesis, risk stratification, clinical approach, and current and novel treatments. Am J Hematol. 2022;97(5):638-656. doi:10.1002/ajh.26523.
14. Teras LR, DeSantis CE, Cerhan JR, Morton LM, Jemal A, Flowers CR. 2016 US lymphoid malignancy statistics by World Health Organization subtypes. CA Cancer J Clin. 2016;66(6):443459. doi:10.3322/caac.21357
15. Kumar A ET, Lewis KL, Thompson MC, Cheah CY. New directions for mantle cell lymphoma in 2022. Am Soc Clin Oncol Educ Book. 2022;42:1-15. doi:10.1200/EDBK_349509.
16. Aqil B, Triska G, Frater J, et al. Immunophenotypic variations in mantle cell lymphoma and their impact on clinical behavior and outcome. Arch Pathol Lab Med. 2018;142(10):12681274. doi:10.5858/arpa.2017-0368-OA
17. Mishra P, Padhi S, Ayyanar P, et al. Clinicopathological and immunohistochemical profile of mantle cell lymphoma: an institutional experience. Cureus. 2021;13(7):e16534. doi:10.7759/ cureus.16534
18. Kuo PY, Jatiani SS, Rahman AH, et al. SOX11 augments BCR signaling to drive MCL-like tumor development. Blood. 2018;131(20):2247-2255. doi:10.1182/blood-2018-02-832535
19. Cheson BD, Fisher RI, Barrington SF, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol. 2014;32(27):3059-3068. doi:10.1200/jco.2013.54.8800
20. Malagelada JR, Bazzoli F, Boeckxstaens G, et al. World Gastroenterology Organisation global guidelines: dysphagia—global guidelines and cascades update September 2014. J Clin Gastroenterol. 2015;49(5):370-378. doi:10.1097/mcg.0000000000000307
21. Li X, Pas HH, Qian H, et al. Potential correlation between anti-laminin 332 autoantibodies and malignant tumours in anti-BP180-type mucous membrane pemphigoid. Letter. Clin Exp Dermatol. 2024;49(9):1075-1076. doi:10.1093/ced/llae124
22. Qian H, Natsuaki Y, Koga H, et al. The second study of clinical and immunological findings in anti-laminin 332-type mucous membrane pemphigoid examined at Kurume University— diagnosis criteria suggested by summary of 133 cases. Front Immunol. 2021;12:771766. doi:10.3389/fimmu.2021.771766
23. Iranzo P, López I, Robles MT, Mascaró JM Jr, Campo E, Herrero C. Bullous pemphigoid associated with mantle cell lymphoma. Arch Dermatol. 2004;140(12):1496-1499. doi:10.1001/ archderm.140.12.1496
24. Md Radzi AB, Kasim SS. A case report of paraneoplastic bullous pemphigoid associated with mantle cell lymphoma: a rare presentation. Medicine (Baltimore). 2023;102(4):e32822. doi:10.1097/md.0000000000032822
25. Lucariello RJ, Villablanca SE, Mascaró JM Jr, Reichel M. Association between bullous pemphigoid and malignancy: a meta-analysis. Australas J Dermatol. 2018;59(4):253-260. doi:10.1111/ajd.12764
26. Baum S, Steinberg S, Tzanani I, Barzilai A, Lyakhovitsky A. Prevalence, spectrum and clinical implications of malignancies in patients with bullous pemphigoid. Acta Derm Venereol. 2023;103:adv00888. doi:10.2340/actadv.v103.3979
27. Kartan S, Shi VY, Clark AK, Chan LS. Paraneoplastic pemphigus and autoimmune blistering diseases associated with neoplasm: characteristics, diagnosis, associated neoplasms,
proposed pathogenesis, treatment. Am J Clin Dermatol. 2017;18(1):105-126. doi:10.1007/ s40257-016-0235-z
28. Morello L, Rattoti S, Giordano L, et al. Mantle cell lymphoma of mucosa-associated lymphoid tissue: a European Mantle Cell Lymphoma Network study. Hemasphere. 2019;4(1):e302. doi:10.1097/HS9.0000000000000302
29. Silkenstedt E, Dreyling M. Mantle cell lymphoma—update on molecular biology, prognostication and treatment approaches. Hematol Oncol. 2023;41(Suppl 1):36-42. doi:10.1002/ hon.3149
30. O’Brien SM, Brown JR, Byrd JC, et al. Monitoring and managing BTK inhibitor treatmentrelated adverse events in clinical practice. Front Oncol. 2021;11:720704. doi:10.3389/ fonc.2021.720704
Root migration after coronectomy of impacted mandibular third molars: case reports
Coronectomy is recommended for third molars that require extraction and are located near the inferior alveolar nerve (IAN) or the mandibular base. The procedure is aimed at reducing the risk of complications, but root migration is among the possible sequelae of this surgical technique. This report describes 3 clinical cases of root migration after coronectomy of impacted mandibular third molars. All 3 cases involved women aged 21 to 31 years and followed the surgical principles recommended for the technique: local anesthesia, periodontal ligament detachment, pericoronal ostectomy, sectioning of the dental crown, and crown removal with complete elimination of enamel from the roots, which remain impacted below 3 mm of bone. The patients were followed up with clinical and imaging examinations for 1 year. Panoramic radiographs at 1 year revealed root migration of 3 to 5 mm. None of the patients opted for removal of the residual root fragments because they were not causing any pain. Root migration after coronectomy cannot be perceived as a failure of this relatively safe alternative to extracting mandibular third molars near the IAN because the root always moves away from the nerve and usually causes no additional symptoms. Secondary surgery to remove the residual root should only be performed if migration results in root exposure, pain, or infection.
Received: May 31, 2024
Revised: July 18, 2024
Accepted: September 4, 2024
Keywords: coronectomy, oral surgery, paresthesia, third molar, tooth extraction
In 1989, Knutsson et al introduced the coronectomy technique (also known as intentional partial odontectomy) for mandibular third molars that require extraction and are located near the inferior alveolar nerve (IAN) or the mandibular base.1 The method involves sectioning and removing the dental crown, with enamel, and retaining the roots of the tooth inside the alveolar socket (2 to 3 mm below the bone crest) to induce bone formation.2,3 The principal advantage of this surgical technique is that it significantly reduces the risk of IAN injuries.2,4-8 However, the procedure does have potential disadvantages—it may require reoperation due to infection, root exposure, or residual root enamel that delays bone healing, and it can cause short-term postoperative complications such as alveolitis and pain.2,6,8,9
Migration of the retained root is common after coronectomy. The majority of root fragment movement, approximately 3 to 4 mm of total migration, occurs up to 6 months after extraction.3 After that period, movement gradually decreases, with additional mean migration of 0.4 mm between 6 and 12 months and 0.2 mm between 12 and 24 months.3 The slowing of root migration may be attributable to bone formation over the roots.3,8
Considering the value of reducing the risk of paresthesia after mandibular third molar extraction, the present report describes 3 clinical cases of coronectomy and subsequent root migration.
Case reports
This case study was approved by the ethics committee of Sacred Heart University (UNISAGRADO), Bauru, Brazil.
Case 1
A 25-year-old woman attended the postgraduate clinic at the School of Dentistry, UNISAGRADO, Bauru, Brazil, to undergo mandibular third molar extraction. The patient answered a medical health questionnaire and did not report systemic health changes.
A clinical examination revealed that both mandibular third molars were impacted, which was verified by panoramic radiography and computed tomography (Fig 1). The roots of both third molars were located near the IAN, and coronectomy was proposed to the patient. After a thorough discussion of the advantages and potential drawbacks of the procedure as well as alternative treatment options, the patient chose to undergo coronectomy. The surgical procedure for the mandibular left third molar started with intraoral and extraoral antisepsis with 0.12% and 2% chlorhexidine digluconate, respectively. Then, 3 sites were injected with an anesthetic solution of 2% mepivacaine with 1:100,000 epinephrine to block the buccal, lingual, and inferior alveolar nerves (Fig 2). After successful local anesthesia
was confirmed, an incision was made in the bone crest with a No. 15C blade in a No. 3 scalpel handle. Next, a relaxing incision (Neumann incision) was placed, a full-thickness mucoperiosteal flap was reflected, and the periodontal ligament was detached, exposing the area.
A tapered fissure bur (No. 702 XXL) in a high-speed handpiece was used under constant irrigation to perform a pericoronal ostectomy that exposed the crown of the mandibular third molar up to the cementoenamel junction (Fig 3). The crown of the tooth was sectioned at the cervical margin with the same bur, which was held at approximately 45° and used under constant sterile saline solution irrigation. The crown was then removed with an extractor. After the coronectomy, the remaining dental root was reduced to approximately 3 mm below the alveolar bone crest so that it was completely submerged and surrounded by bone tissue (Fig 4). As is the case in most coronectomy procedures, the enamel was almost completely removed along with the dental crown. The No. 702 XXL bur was used to remove any residual enamel. After the remaining bone was smoothed and curettage was performed to remove soft tissue from the bony defect, the site was thoroughly irrigated with 0.9% saline, and the flap was closed with 4-0 nylon suture.
Antibiotic (amoxicillin, 500 mg every 8 hours), nonsteroidal anti-inflammatory (nimesulide, 100 mg every 12 hours), and analgesic (dipyrone, 500 mg every 6 hours) medications were
Fig 1. Case 1. A. Initial computed tomograph showing mandibular canal (arrows).
Fig 4. Case 1. Clinical appearance after excision of the crown.
Fig 3. Case 1. Clinical appearance after ostectomy and odontosection.
Fig 2. Case 1. Impacted mandibular third molar region after local anesthesia.
Case 3
A healthy 21-year-old woman who reported no systemic changes attended the postgraduate clinic at UNIARA for mandibular third molar extraction. Clinical examination and a panoramic radiograph resulted in a diagnosis of impacted mandibular third molars. The roots of both molars were near the IAN, and bilateral coronectomy was proposed to the patient (Fig 8), who provided informed consent for the procedures.
The surgical procedures followed the protocol described in case 1. The left molar crown was removed first; at the 15-day postoperative evaluation, the patient had no complaints of pain, the surgical sites were healing normally, and there was no paresthesia. Coronectomy of the right molar was performed 2 months after the procedure on the left side, and healing progressed normally.
prescribed for the immediate postoperative period. The patient was also requested to rinse with a 0.12% chlorhexidine digluconate mouthwash 3 times a day after oral hygiene procedures for 7 days after the second postoperative day. After 15 days, the patient returned for postoperative evaluation and had no complaints of pain. Clinical evaluation showed that the surgical site was undergoing normal tissue repair processes and demonstrated no paresthesia. Coronectomy of the mandibular right third molar was performed in a similar manner 2 months after the procedure on the left side, and healing progressed normally.
The patient was followed up with clinical and imaging examinations for 1 year, and root migration was observed (Fig 5). The extent of movement was measured on the panoramic radiograph by drawing a line parallel to the occlusal plane up to the mandibular ramus and a second line that ran longitudinally through the middle of the root apex and extended to the first line. The distance between the root apex and the intersection of the 2 lines was measured pretreatment and after 1 year, revealing migration of 4 mm bilaterally.3 The patient was scheduled for continued follow-up because she did not report painful symptoms or show evidence of root exposure.
Case 2
A 31-year-old woman attended the postgraduate clinic at University of Araraquara (UNIARA), Araraquara, Brazil, for mandibular third molar extraction. The patient answered a medical health questionnaire and reported no systemic changes. Clinical and radiographic examinations confirmed the diagnosis of impacted third molars. The roots of the mandibular right third molar were near the IAN, and coronectomy was proposed to the patient (Fig 6). The left third molar was to be extracted through a conventional surgical procedure.
The patient provided informed consent, and the coronectomy procedure followed the protocol described in case 1. After 15 days, the patient returned for postoperative evaluation without pain complaints, and the surgical site was found to be at the expected stage of repair and without paresthesia. The patient was followed up with imaging examinations for 1 year, and the retained root demonstrated migration of 5 mm (Fig 7). The patient did not report painful symptoms and preferred not to undergo removal of the root fragment.
The patient was followed up with imaging examinations for 1 year, and root migration of 3 and 4 mm occurred on the left and right sides, respectively (Fig 9). The patient did not report pain and preferred to retain the root fragments.
Discussion
As previously mentioned, the principal benefit of coronectomy as an alternative to third molar extraction is that the technique minimizes the risks of neurosensory loss or changes. Nevertheless, although reported complication rates are low, this approach does not exempt patients from adverse effects that may arise during surgery and the postoperative period.4,5,6,8 The technique is indicated for impacted teeth near the IAN and/or mandibular cortical bone, and patients must be aware of the possibility that additional surgery to remove the roots from the socket may be required.6 Contraindications include active infections in the tooth root, mobility of the tooth or root, and horizontal impaction of the tooth near the mandibular canal, which presents a high risk of inadvertent sectioning of the vascular nerve bundle during the procedure.6
Radiographic and computed tomographic imaging are crucial for establishing a correct diagnosis and confirming that coronectomy is the correct treatment choice in each case, based on higher success rates and a decrease in potential transoperative and postoperative risks and complications.10 Among the potential complications that must be considered by dentists and patients when choosing the technique are development of periodontal pockets, root migration (with or without the need for a second surgical intervention), alveolitis, local postoperative infection, pain, and inadvertent root removal.11
Root migration is specifically beneficial for impacted third molars in close contact with the IAN because it occurs toward the coronal region; as a result, if a second surgery is needed to remove the root fragment, the procedure has a lower risk of causing paresthesia and temporary and potentially permanent neurosensory changes.12,13 Approximately 30% of roots move away from the mandibular canal after coronectomy, migrating by as much as 4 mm over the first 2 years. Most show reduced or no additional movement between the second and third postoperative years.9 A 3-year study by Leung and Cheung showed that 75% of roots stopped migrating between 12 and 24 postoperative months, without any migration between 24 and 36 months.14 Moreover, they reported no increased
Fig 5. Case 1. Panoramic radiograph at 1 year postsurgery.
incidence of infection, pain, abnormalities, or root exposure after 12 months. Gady and Fletcher noted that the literature suggests that root fragment movement primarily occurs up to 6 months after extraction, with potential total migration of 3 to 4 mm.15 This assertion was corroborated in a more recent study by Hamad, who observed mean migration of 3.85 mm at 12 months.16 Simons et al reported a slightly higher rate, with mean values of 3.30 mm at 2 months and 5.27 mm at 6 months.17 Dolanmaz et al found that movement gradually decreases after 6 months, with mean additional fragment migration of 0.4 mm between 6 and 12 months and 0.2 mm between 12 and 24 months.3 Corroborating the literature, the present cases showed root migration of 3 to 5 mm among 3 patients studied for a period of 1 year.
Kohara et al noted the possible association of the age and sex of patients with root migration rates, as they are distinctly higher in younger female patients because cancellous bone density in the mandible is lower in women and younger people.18 In the present case series, the 3 patients were women aged 21 to 31 years.
Deceleration of root migration is probably due to bone formation over root fragments. Root migration that is not associated with pain or root exposure is not a reason for reoperation, as the surviving roots may remain in situ without the risk of complications as long as root mobilization is limited and causes no symptoms or infection.15 All 3 patients in the present clinical study experienced significant root migration
in the first year of follow-up, with the result that the root fragments were no longer near the IAN. None of the patients had pain complaints or signs of infection, and they all decided not to undergo a second surgery to remove the residual roots. The patients were instructed to continue to attend regular followup appointments.
After performing 43 coronectomies, Monaco et al concluded that all root migration cases induced bone regeneration distal to the second molars, similar to the regeneration observed after root migration caused by orthodontic extrusion.19
Corroborating that finding, Goto et al stated that a healthy and noninflamed periodontal condition was observed distal to the second molar in 99.2% of cases.20
It is worth noting that coronectomy is not an alternative that should be adopted to salvage a failed extraction procedure. Rather, it is a useful technique for managing impacted third molars near the IAN; coronectomy must be selected in advance as the treatment option and requires detailed planning. The surgical skills and experience of the clinician are among the main risk factors for the development of permanent sensory deficit in the IAN after coronectomy—the greater the dentist’s knowledge, the lesser the risk of paresthesia.7,20,21
Conclusion
Root migration after coronectomy cannot be perceived as a failure of this relatively safe alternative to extracting mandibular third molars near the IAN because the root always
Fig 7. Case 2. Panoramic radiograph at 1 year postsurgery.
Fig 6. Case 2. Initial panoramic radiograph.
Fig 9. Case 3. Panoramic radiograph at 1 year postsurgery.
Fig 8. Case 3. Initial panoramic radiograph.
moves away from the nerve and usually causes no additional symptoms. Coronectomy shows low rates of complications, as long as it is well planned and executed. Secondary surgery to remove the residual root should only be performed if migration results in root exposure, pain, or infection.
Author affiliations
Araraquara School of Dentistry, São Paulo State University (FOAr/UNESP), Araraquara, Brazil (Silva); School of Dentistry, University of Araraquara (UNIARA), Araraquara, Brazil (Balestrero, Santos); School of Dentistry, State University of Londrina (UEL), Londrina, Brazil (Gulinelli).
Correspondence
Pâmela Letícia dos Santos, DDS, MSc, PhD (pamelalsantos@hotmail.com).
Conflicts of interest
None reported.
References
1. Knutsson K, Lysell L, Rohlin M. Postoperative status after partial removal of the mandibular third molar. Swed Dent J. 1989;13(1-2):15-22.
2. Cervera-Espert J, Pérez-Martínez S, Cervera-Ballester J, Peñarrocha-Oltra D, Peñarrocha-Diago M. Coronectomy of impacted mandibular third molars: a meta-analysis and systematic review of the literature. Med Oral Patol Oral Cir Bucal. 2016;21(4):e505-e513. doi:10.4317/medoral.21074
3. Dolanmaz D, Yildirim G, Isik K, Kucuk K, Ozturk A. A preferable technique for protecting the inferior alveolar nerve: coronectomy. J Oral Maxillofac Surg. 2009;67(6):1234-1238. doi:10.1016/j.joms.2008.12.031
4. Cilasun U, Yildirim T, Guzeldemir E, Pektas ZO. Coronectomy in patients with high risk of inferior alveolar nerve injury diagnosed by computed tomography. J Oral Maxillofac Surg 2011;69(6):1557-1561. doi:10.1016/j.joms.2010.10.026
5. Geisler S. Coronectomy is an effective strategy for treating impacted third molars in close proximity to the inferior alveolar nerve. J Am Dent Assoc. 2013;144(10):1172-1173. doi:10.14219/jada.archive.2013.0036
7. Agbaje JO, Heijsters G, Salem AS, et al. Coronectomy of deeply impacted lower third molar: incidence of outcomes and complications after one year follow-up. J Oral Maxillofac Res 2015;6(2):e1. doi:10.5037/jomr.2015.6201
8. Dias-Ribeiro E, Rocha JF, Corrêa APS, Song F, Sonoda CK, Noleto JW. Coronectomia em terceiro molar inferior: relato de casos. Rev Cir Traumatol Buco-Maxilo-Fac. 2015;15(2):4954. https://www.revistacirurgiabmf.com/2015/2/08-Coronectomia.pdf
9. Barcellos BM, Velasques BD, Moura LB, Xavier CB. What are the parameters for reoperation in mandibular third molars submitted to coronectomy? A systematic review. J Oral Maxillofac Surg. 2019;77(6):1108-1115. doi:10.1016/j.joms.2019.01.013
10. Gay-Escoda C, Sánchez-Torres A, Borrás-Ferreres J, Valmaseda-Castellón E. Third molar surgical difficulty scales: systematic review and preoperative assessment form. Med Oral Patol Oral Cir Bucal. 2022;27(1):e68-e76. doi:10.4317/medoral.24951
11. Leizerovitz M, Leizerovitz O. Modified and grafted coronectomy: a new technique and a case report with two-year follow-up. Case Rep Dent. 2013;2013:914173. doi:10.1155/2013/914173
12. Hatano Y, Kurita K, Kuroiwa Y, Yuasa H, Ariji E. Clinical evaluations of coronectomy (intentional partial odontectomy) for mandibular third molars using dental computed tomography: a case-control study. J Oral Maxillofac Surg. 2009;67(9):1806-1814. doi:10.1016/j. joms.2009.04.018
13. Salgado-Peralvo ÁO, Kewalramani N, Madruga-González D, Garcia-Sanchez A, Barbi-Actis J, Pérez-Sayáns M. Coronectomy of lower third molars in intimate relation to the inferior alveolar nerve: a report of two cases. J Clin Exp Dent. 2024;16(2):e223-e228. doi:10.4317/ jced.60335
14. Leung YY, Cheung LK. Coronectomy of the lower third molar is safe within the first 3 years. J Oral Maxillofac Surg. 2012;70(7):1515-1522. doi:10.1016/j.joms.2011.12.029
15. Gady J, Fletcher MC. Coronectomy: indications, outcomes, and description of technique. Atlas Oral Maxillofac Surg Clin North Am. 2013;21(2):221-226. doi:10.1016/j. cxom.2013.05.008
16. Hamad SA. Outcomes of coronectomy and total odontectomy of impacted mandibular third molars. Int Dent J. 2024;74(2):195-198. doi:10.1016/j.identj.2023.07.015
17. Simons RN, Tuk JG, Ho JTF, Su N, Lindeboom JA. Early root migration after a mandibular third molar coronectomy. Oral Maxillofac Surg. 2023;27(2):353-364. doi:10.1007/s10006022-01072-z
18. Kohara K, Kurita K, Kuroiwa Y, Goto S, Umemura E. Usefulness of mandibular third molar coronectomy assessed through clinical evaluation over three years of follow-up. Int J Oral Maxillofac Surg. 2015;44(2):259-266. doi:10.1016/j.ijom.2014.10.003
19. Monaco G, de Santis G, Gatto MR, Corinaldesi G, Marchetti C. Coronectomy: a surgical option for impacted third molars in close proximity to the inferior alveolar nerve. J Am Dent Assoc 2012;143(4):363-369. doi:10.14219/jada.archive.2012.0178
20. Goto S, Kurita K, Kuroiwa Y, et al. Clinical and dental computed tomographic evaluation 1 year after coronectomy. J Oral Maxillofac Surg. 2012;70(5):1023-1029. doi:10.1016/j. joms.2011.09.037
21. Nowak SM, Justice J, Aslam A, Suida MI. The success rates and outcomes of mandibular third molar coronectomy: 167 cases. Oral Maxillofac Surg. 2024;28(3):1227-1239. doi:10.1007/ s10006-024-01244-z
Malignant transformation of oral lichen planus after 6 years: a case report
Patrícia Peres Iucif Pereira, DDS, PhD ¢ Amanda Bandeira de Almeida, DDS, PhD
João Adolfo Costa Hanneman, DDS, PhD ¢ Eduardo Pereira Guimarães, DDS, MSc
Lichen planus (LP) is a chronic or recurrent autoimmune mucocutaneous inflammatory disease. The etiology is uncertain, and it is considered to originate from a multifactorial process. A diagnosis can be made clinically if the disease presents with classic patterns of oral or skin lesions; if these patterns are absent, a biopsy is necessary to establish a diagnosis. Although the World Health Organization has classified oral LP (OLP) as an oral potentially malignant disorder, there is controversy in the literature. Malignancy usually occurs around 60 years of age, with a slight predilection for women. The objective of this case report is to describe a possible occurrence of this process. A 53-year-old woman who sought treatment for oral lesions in 2018 was diagnosed with OLP with epithelial dysplasia and underwent standard treatment with a topical corticosteroid. After ceasing to attend follow-up examinations, the patient continued periodontal treatment with different providers. In 2024, she developed a lesion on the maxillary right alveolar ridge that led to tooth loss in the region. A biopsy was performed, and histopathologic evaluation of the specimen led to a diagnosis of squamous cell carcinoma. There are several differential diagnoses for the clinical forms of OLP, in addition to the possibility of manifestation of concomitant pathoses, and the final diagnosis must reflect a combination of clinical and histopathologic examinations. Patients should be advised about the importance of returning for follow-up appointments, as malignant transformation of OLP may occur.
Lichen planus (LP) is a chronic or recurrent autoimmune mucocutaneous inflammatory disease. Its prevalence is variable, being more common in the oral mucosa and in women aged 40 years or older.1,2 The ratio of women to men with LP is 4:1, and it affects 0.5% to 2.2% of the total population, rarely being found in pediatric patients.1,2
The etiology of the disease is not certain, but it is believed that it develops through a multifactorial pathologic process with different triggers.3-9 These include biochemical factors, psychological causes, mechanical trauma, stress from a variety of causes, endocrine disorders and disturbances, pathoses of the salivary system, immunologic diseases, malnutrition, genetic susceptibility, and viral infection (eg, in patients infected with hepatitis B or C virus, who are twice as likely to develop LP as uninfected individuals).3-9
A clinical diagnosis can be made if the disease presents with classic patterns such as concomitant lesions in the oral mucosa and skin. In the absence of these patterns, clinical diagnosis may be difficult, and a biopsy is necessary to establish a diagnosis. LP undergoes periods of exacerbation and remission, and manifestations are related to stress, anxiety, or mechanical trauma.5,10-15
Although the World Health Organization (WHO) has classified oral LP (OLP) as a premalignant condition (oral potentially malignant disorder), there is controversy in the literature.15,16 In 2003, van der Meij and van der Waal suggested changes to the diagnostic criteria for OLP defined by Kramer et al (WHO Collaborating Centre for Oral Precancerous Lesions) in 1978 in order to distinguish OLP from the so-called lichenoid lesion, an entity that likely has a greater potential for malignancy.9,16,17 Malignancy generally occurs around the age of 60 years, with a slightly greater prevalence in women; the tongue is the most common site of involvement.17 The objective of this clinical report is to describe a case in which a patient with oral lesions diagnosed microscopically as OLP presented, years later, with a lesion diagnosed as squamous cell carcinoma.
Case report
A 53-year-old woman was referred to the stomatology clinic of the School of Dentistry, Federal University of Alfenas, Alfenas, Brazil, in 2018 because she had oral lesions that did not respond to treatment. The results of the extraoral examination were within normal limits, but intraoral examination revealed several lesions. A white plaque with an irregular surface, the appearance of cracked clay, and poorly defined limits was present on the dorsum of the tongue (Fig 1). White
are erythematous and edematous but nonbleeding, and there are areas of atrophy and erosion. A. Maxillary vestibular gingiva. B. Mandibular vestibular gingiva.
streaks were present on the buccal mucosa bilaterally; the left side also had a white plaque with a corrugated surface and, contiguously, an area of ulceration (Fig 2). The maxillary and mandibular vestibular gingivae were edematous and erythematous; they were nonbleeding but atrophic in some areas and erosive in others (Fig 3). White streaks and small white plaques were also observed on the palatal gingiva, mainly in the molar region.
The diagnostic hypotheses were OLP and pemphigoid. The patient underwent an incisional biopsy of the left buccal mucosa. A specimen was submitted for histopathologic analysis, and the diagnosis was OLP with dysplasia (Fig 4). The results of immunofluorescence were inconclusive.
Topical 0.2% triamcinolone acetonide (4 times a day for 30 days) was prescribed, and the patient was referred to a dermatologist. The patient returned for follow-up 4 months later, and
the condition showed significant improvement. The patient did not return for long-term follow-up and remained under periodontal treatment by a private dentist.
Five years after treatment for OLP, she was referred to the Center for Dental Specialties in Varginha, Brazil. During periodontal treatment, she had developed a submandibular abscess without an evident cause. After the infection had subsided, the oral and maxillofacial surgeon detected an ulcerated lesion on the maxillary right alveolar ridge as well as significant mobility of the right first premolar, which was later extracted (Fig 5).
A biopsy of the lesion was performed, and the histopathologic examination revealed squamous cell carcinoma (Fig 6). The patient was referred to the Oncology Center of Bom Pastor Hospital in Varginha and is currently undergoing radiotherapy and chemotherapy. The patient chose not to undergo a surgical procedure.
Fig 2. The left buccal mucosa shows white streaks, white plaque with a corrugated and homogenous surface, and an area of ulceration.
Fig 1. A white plaque with a nonhomogenous surface, a cracked clay appearance, and poorly defined limits is present on the dorsum of the tongue.
Fig 3. The alveolar gingivae
A B
Fig 4. Histopathologic findings in a fragment of oral mucosa (hematoxylin and eosin stain). A. The tissue consists of stratified orthokeratinized and parakeratinized squamous epithelium, sometimes atrophic, sometimes hyperplastic, with irregular ridges (original magnification ×20). B. In some areas, the epithelium is partially destroyed by exocytosis and includes mitotic figures and underlying epithelial microinfiltration. The lamina propria consists of dense fibrous connective tissue with intense bands of mononuclear inflammatory infiltrate, predominantly lymphocytic, as well as numerous small hyperemic blood vessels. Intraepithelial eosinophils are also present (original magnification ×40).
Discussion
Reports of malignant transformation of lesions previously diagnosed as OLP are undeniably present in the literature.18 Several studies have reported that OLP has a malignant transformation rate of 0.07% to 5.8%, while others have found no potential for malignancy.19-23 Leite et al suggested that some cases of oral squamous cell carcinoma attributed to malignant transformation might result from an initial diagnostic error, where lesions were labeled OLP despite the absence of epithelial dysplasia, as in the case they reported.23
Several risk factors for malignant transformation of OLP have been identified, such as erosive or ulcerative clinical forms, tongue lesions, female sex, and age between the sixth and seventh decades of life.20 However, some of these aspects are the subject of disagreement among researchers.24 Therefore, it is prudent for oral healthcare providers to seek greater understanding and recommend continued clinical monitoring of patients with OLP, which can assist in the implementation of a long-term management plan.25 In some
Fig 5. An infiltrative ulcer is present on the right maxillary alveolar ridge. A. The ulcer has raised edges and a lowered center. B. The lesion extends to the hard palate and buccal gingiva.
Fig 6. Histopathologic findings in a fragment of oral mucosa (hematoxylin and eosin stain). A. The tissue consists of stratified parakeratinized squamous epithelium, sometimes atrophic, sometimes hyperplastic. Areas of ulceration and dysplasia are present (original magnification ×20). B. The underlying lamina propria demonstrates infiltration of neoplastic epithelial cells arranged in sheets and small nests as well as intense dysplasia, characterized by mitoses, pleomorphism, hyperchromatism, loss of the nucleus to cytoplasm ratio, and formation of discrete keratin pearls. There is intense mononuclear inflammatory infiltrate (original magnification ×40).
cases, plaque-like OLP lesions have been relevant, sometimes arising alone or associated with atrophic-erosive lesions.23 The reported mean interval between the diagnosis of OLP and the diagnosis of cancer varies widely, from 20.8 months to 10.1 years, although the greatest risk is reportedly 3 to 6 years after the diagnosis of LP.11 Candida albicans is also thought to represent a risk factor in the malignant transformation of OLP, probably because of the production of N-nitroso benzylmethylamine, a known carcinogen. Therefore, treatment of oral fungal infections has been specifically recommended for patients with OLP.11
In addition, due to the long-term chronic nature of OLP and the discomfort associated with its symptoms, psychosocial interventions and support are also considered important. However, the role of psychological factors, particularly acute stress and/or anxiety, in the onset of OLP is controversial.26 For symptomatic lesions, treatment is largely based on the use of topical immunosuppressants, particularly corticosteroids. Although new therapeutic modalities have been introduced, the clinical evidence for their use remains inconclusive.27
In a systematic review, Giuliani et al evaluated 21 publications including 6559 patients with OLP or oral lichenoid lesions and calculated a combined malignant potential rate of 1.40% (1.37% for OLP and 2.43% for oral lichenoid lesions).4 This was a higher rate than was found by Fitzpatrick et al, Aghbari et al, and Bermejo-Fenoll et al, who reported malignant potential rates of 1.09%, 1.1%, and 0.9%, respectively.28-30 In a study including 67 patients with a diagnosis of OLP and 125 patients with oral lichenoid lesions, van der Meij et al observed no malignant transformation in patients with OLP, although 4 patients with lichenoid lesions developed oral squamous cell carcinoma.20 Giuliani et al suggested that to assess the true rate of malignant transformation of OLP, it is necessary to base the differential
diagnosis between OLP and lichenoid lesion on the WHO criteria modified by van der Meij and van der Waal in 2003.4,16 They also consider that aspects that could significantly influence the diagnosis would consequently influence the method of the review and that changes in the criteria since 1978 could considerably modify the calculated malignancy rate.4
Some authors suggest that the potential for malignant transformation is related to the chronic inflammation present in OLP, indicating that increased oxidative stress in inflamed sites due to the release of free radicals, as well as the release of a large number of growth factors and inflammation mediators, may predispose patients to DNA damage that leads to cancer.31,32 On the other hand, DNA analysis for 2 specific genetic alterations (loss of heterozygosity and microsatellite instability) showed that OLP presents with characteristics more similar to those of benign lesions of the oral mucosa than to those associated with dysplasias and malignant lesions.33 Therefore, the malignancy potential of OLP has not been definitively established.
Conclusion
Potentially malignant oral disorders are lesions that have an increased potential for malignant transformation. Early diagnosis makes it possible to monitor such lesions and possibly detect cancer at an early stage, increasing the chances of a better prognosis. When the clinical characteristics of a lesion suspected to be OLP are not sufficient to determine the diagnosis, the dentist should perform a biopsy and send the specimen for histopathologic examination.
In asymptomatic cases of OLP, the procedure is to monitor the lesions at least every 6 months. When the patient has symptoms, topical and systemic corticosteroids are the most commonly used forms of drug therapy. In addition, the oral
healthcare provider should advise the patient on how to control stress and anxiety as ways to prevent exacerbations of the disease. The patient should be referred to a dermatologist when there are lesions on the skin. If the patient reports experiencing stress or anxiety, psychological evaluation is warranted. The patient should be advised about the importance of returning for recommended follow-up appointments, as malignant transformation of OLP may occur.
Author affiliations
School of Dentistry, Federal University of Alfenas, Alfenas, Brazil (P.P.I. Pereira, Almeida, Hanneman, Rozendo); Oral and Maxillofacial Surgery, Bom Pastor Hospital, Varginha, Brazil (Guimarães, Petean); Institute of Biomedical Sciences, Federal University of Alfenas, Alfenas, Brazil (A.A.C. Pereira).
1. Garcia de Sousa FAC, Paradella TC. Malignant potential of oral lichen planus: a meta-analysis. Rev Odonto Cienc. 2009;24(2):194-197. https://revistaseletronicas.pucrs.br/fo/article/ view/4337
2. van der Waal I. Oral lichen planus and oral lichenoid lesions: a critical appraisal with emphasis on the diagnostic aspects. Med Oral Patol Oral Cir Bucal. 2009;14(7):E310-E314.
3. Larsen KR, Johansen JD, Reibel J, Zachariae C, Rosing K, Pedersen AML. Oral symptoms and salivary findings in oral lichen planus, oral lichenoid lesions and stomatitis. BMC Oral Health 2017;17(1):103. doi:10.1186/s12903-017-0393-2
4. Giuliani M, Troiano G, Cordaro M, et al. Rate of malignant transformation of oral lichen planus: a systematic review. Oral Dis. 2019;25(3):693-709. doi:10.1111/odi.12885
5. Chiang CP, Yu-Fong Chang J, Wang YP, Wu YH, Lu SY, Sun A. Oral lichen planus—differential diagnoses, serum autoantibodies, hematinic deficiencies, and management. J Formos Med Assoc. 2018;117(9):756-765. doi:10.1016/j.jfma.2018.01.021
6. Jaafari-Ashkavandi Z, Aslani E. Caveolin-1 expression in oral lichen planus, dysplastic lesions and squamous cell carcinoma. Pathol Res Pract. 2017;213(7):809-814. doi:10.1016/j. prp.2017.03.006
7. Peng Q, Zhang J, Ye X, Zhou G. Tumor-like microenvironment in oral lichen planus: evidence of malignant transformation? Expert Rev Clin Immunol. 2017;13(6):635-643. doi:10.1080/ 1744666X.2017.1295852
8. Ghazi N, Khorasanchi M. Markers associated with malignant transformation of oral lichen planus: a review article. Arch Oral Biol. 2021;127:105158. doi:10.1016/j.archoralbio. 2021.105158
9. Abati S, Bramati C, Bondi S, Lissoni A, Trimarchi M. Oral cancer and precancer: a narrative review on the relevance of early diagnosis. Int J Environ Res Public Health 2020;17(24):9160. doi:10.3390/ijerph17249160
10. García-Pola MJ, González-Álvarez L, Garcia-Martin JM. Treatment of oral lichen planus: systematic review and therapeutic guide. Med Clin (Barc). 2017;149(8):351-362. doi:10.1016/j.medcli.2017.06.024
11. Alrashdan MS, Cirillo N, McCullough M. Oral lichen planus: a literature review and update. Arch Dermatol Res. 2016;308(8):539-551. doi:10.1007/s00403-016-1667-2
12. Dillenburg CS, Martins MAT, Almeida LO, et al. Epigenetic modifications and accumulation of DNA double-strand breaks in oral lichen planus lesions presenting poor response to therapy. Medicine (Baltimore). 2015;94(30):e997. doi:10.1097/MD.0000000000000997
13. Cruz AF, Vitório JG, Duarte-Andrade FF, et al. Reticular and erosive oral lichen planus have a distinct metabolomic profile: a preliminary study using gas chromatography-mass spectrometry. J Oral Pathol Med. 2019;48(5):400-405. doi:10.1111/jop.12842
14. Nosratzehi T. Oral lichen planus: an overview of potential risk factors, biomarkers and treatments. Asian Pac J Cancer Prev. 2018;19(5):1161-1167. doi:10.22034/APJCP.2018.19.5. 1161
15. González-Moles MÁ, Ruiz-Ávila I, González-Ruiz L, Ayén Á, Gil-Montoya JA, Ramos-García P. Malignant transformation risk of oral lichen planus: a systematic review and comprehensive meta-analysis. Oral Oncol. 2019;96:121-130. doi:10.1016/j.oraloncology.2019.07.012
16. van der Meij EH, van der Waal I. Lack of clinicopathologic correlation in the diagnosis of oral lichen planus based on the presently available diagnostic criteria and suggestions for modifications. J Oral Pathol Med. 2003;32(9):507-512. doi:10.1034/j.1600-0714.2003.00125.x
17. Kramer IR, Lucas RB, Pindborg JJ, Sobin LH; WHO Collaborating Centre for Oral Precancerous Lesions. Definition of leukoplakia and related lesions: an aid to studies on oral precancer. Oral Surg Oral Med Oral Pathol. 1978;46(4):518-539. doi:10.1016/0030-4220(78)90383-3
18. van der Meij EH, Schepman KP, Smeele LE, van der Wal JE, Bezemer PD, van der Waal I. A review of the recent literature regarding malignant transformation of oral lichen planus. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88(3):307-310. doi:10.1016/s10792104(99)70033-8
19. Rode M, Kogoj-Rode M. Malignant potential of the reticular form of oral lichen planus over a 25-year observation period in 55 patients from Slovenia. J Oral Sci. 2002;44(2):109-111.
20. van der Meij EH, Mast H, van der Waal I. The possible premalignant character of oral lichen planus and oral lichenoid lesions: a prospective five-year follow-up study of 192 patients. Oral Oncol. 2007;43(8):742-748. doi:10.1016/j.oraloncology.2006.09.006
21. Oliveira Alves MG, Almeida JD, Balducci I, Guimarães Cabral LA. Oral lichen planus: a retrospective study of 110 Brazilian patients. BMC Res Notes. 2010;3:157. doi:10.1186/17560500-3-157
22. Radochova V, Drizhal I, Slezak R. A retrospective study of 171 patients with oral lichen planus in the East Bohemia–Czech Republic—single center experience. J Clin Exp Dent. 2014;6(5): e556-e561. doi:10.4317/jced.51784
23. Leite AC, Assay NT, Ito FA, de Lima HG, Takahama Junior A. Descoberta de carcinoma de células escamosas em lesão previamente diagnosticada como líquen plano oral: malignização ou erro de diagnóstico inicial? Arch Health Investig. 2019;8(4):178-181. doi:10.21270/archi.v8i4.3296
25. de França GM, Júnior JF, Severo MLB, et al. Líquen plano oral: relato de caso com diferentes aspectos clínicos. Braz J Health Rev. 2019;2(6):5996-6003. doi:10.34119/bjhrv2n6-092
26. Al-Hashimi I, Schifter M, Lockhart PB, et al. Oral lichen planus and oral lichenoid lesions: diagnostic and therapeutic considerations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;103(Suppl):S25.e1-S25.e12. doi:10.1016/j.tripleo.2006.11.001
27. Kurago ZB. Etiology and pathogenesis of oral lichen planus: an overview. Oral Surg Oral Med Oral Pathol Oral Radiol. 2016;122(1):72-80. doi:10.1016/j.oooo.2016.03.011
28. Fitzpatrick SG, Hirsch SA, Gordon SC. The malignant transformation of oral lichen planus and oral lichenoid lesions: a systematic review. J Am Dent Assoc. 2014;145(1):45-56. doi:10.14219/jada.2013.10
29. Aghbari SMH, Abushouk AI, Attia A, et al. Malignant transformation of oral lichen planus and oral lichenoid lesions: a meta-analysis of 20095 patient data. Oral Oncol. 2017;68:92-102. doi:10.1016/j.oraloncology.2017.03.012
30. Bermejo-Fenoll A, Sánchez-Siles M, López-Jornet P, Camacho-Alonso F, Salazar-Sánchez N. A retrospective clinicopathological study of 550 patients with oral lichen planus in southeastern Spain. J Oral Pathol Med. 2010;39(6):491-496. doi:10.1111/j.16000714.2010.00894.x
31. Chaiyarit P, Ma N, Hiraku Y, et al. Nitrative and oxidative DNA damage in oral lichen planus in relation to human oral carcinogenesis. Cancer Sci. 2005;96(9):553-559. doi:10.1111/j.13497006.2005.00096.x
32. Georgakopoulou EA, Achtari MD, Achtaris M, Foukas PG, Kotsinas A. Oral lichen planus as a preneoplastic inflammatory model. J Biomed Biotechnol. 2012;2012:759626. doi:10.1155/2012/759626
33. Accurso BT, Warner BM, Knobloch TJ, et al. Allelic imbalance in oral lichen planus and assessment of its classification as a premalignant condition. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;112(3):359-366. doi:10.1016/j.tripleo.2011.03.042
Oral health in relation to manifestations and severity of cystic fibrosis: a cross-sectional study
Cecília Regina Frazatto, DDS, MSc ¢ Camila Real Delegá Rodrigues, DDS, MSc
Antônio Fernando Ribeiro, DDS, MSc, PhD ¢ José Dirceu Ribeiro, DDS, MSc, PhD
Márcio Ajudarte Lopes, DDS, MSc, PhD
Cystic fibrosis (CF) is an autosomal recessive disorder characterized by defective ion transport in epithelial cells, leading to the development of viscous mucus and glandular duct obstruction. Individuals with CF often present with gingival inflammation, dental enamel defects (DEDs), caries, and reduced salivary flow. This cross-sectional study of 82 patients with CF investigated the population’s oral health in relation to systemic CF manifestations. Clinical oral examinations and medical record analyses were conducted for the entire sample, and panoramic radiographs were obtained for 26 patients. Data on oral hygiene practices, DEDs, gingival inflammation (gingival index [GI] score), caries, malocclusion, breathing pattern, and systemic health parameters were collected. The sample included 44 female and 38 male patients with a mean age of 11.5 years (range 8 months to 26 years). DEDs, predominantly affecting the permanent maxillary anterior teeth, were observed in 47.6% of the patients. Gingival inflammation was noted in 57.3% of the patients, and patients with higher GI scores reported reduced brushing frequency, experienced longer hospitalizations, and were more likely to develop exacerbation of pulmonary symptoms. Dental caries affected 17.1% of the cohort. Panoramic radiographs revealed nasal septum deviation (46.2% of the cohort), sinus opacification (38.5%), and dental agenesis (19.2%), primarily involving the premolars and the maxillary lateral incisors. Oral or mixed breathing was identified in 41.5% of the sample, and malocclusions were present in 28.0%. Fifteen patients with advanced lung disease exhibited infrequent toothbrush replacement, high plaque index scores, and severe gingival inflammation. While the prevalence of caries was relatively low in this small sample, the proportions of CF patients exhibiting DEDs, gingival inflammation, and occlusal abnormalities were high, particularly among those with advanced systemic disease. These findings underscore the importance of integrating dental care into the multidisciplinary management of CF to address patients’ specific oral health challenges and improve overall quality of life.
Cystic fibrosis (CF) is a monogenic autosomal recessive disease with a multisystemic and heterogenous phenotype that primarily affects the respiratory and digestive tracts.1,2 It is estimated that approximately 105,000 individuals worldwide are diagnosed with CF, and about 1000 new cases are reported annually. In Brazil, the 2021 registry identified 6427 individuals with CF. 3
Progressive loss of lung function resulting from chronic colonization by pathogenic microorganisms such as Staphylococcus aureus and Pseudomonas aeruginosa remains the leading cause of morbidity and mortality in this population.4 Other pathogenic microorganisms associated with CF include Haemophilus influenzae, Burkholderia cepacia complex, Aspergillus fumigatus, and nontuberculous mycobacteria. 5 Patients with CF undergo recurrent antibiotic treatment and are monitored for the emergence of pathogenic strains to reduce the pulmonary microbial load, ideally resulting in a smaller number of pulmonary lesions, which are irreversible. 5,6
Beyond systemic complications, people with CF frequently exhibit oral health alterations. These alterations have been studied since 1960, when Zegarelli et al observed a color change in the teeth of patients with CF due to prolonged use of tetracycline.7 The cystic fibrosis transmembrane conductance regulator (CFTR) gene acts on the salivary glands and dental enamel, and genetic variants in patients with CF compromise salivary flow and cause enamel defects. 8 In addition, individuals with CF require a high-energy, high-fat diet to compensate for malabsorption of nutrients and increased energy expenditure, and they frequently meet these caloric requirements by consuming energy-dense nutrition-poor foods. The combination of this cariogenic diet and poor oral hygiene habits can lead to the development of gingival inflammation and periodontal pockets that are reservoirs of microorganisms.9
As advances in treatment increase the life expectancy of individuals with CF, the integration of dental care into the multidisciplinary management of CF becomes even more essential. Recognizing and addressing oral manifestations may play a critical role in improving the overall health outcomes and quality of life for individuals with CF.10 Given that different CFTR gene variants are classified into functional groups associated with varying levels of disease severity, this cross-sectional study aimed to investigate the oral health of a cohort of patients with CF in relation to systemic CF manifestations.
Methods
The present study was approved by the Institutional Ethics Committee, Piracicaba Dental School, University of Campinas, Piracicaba, Brazil, ensuring that all procedures complied with the ethical guidelines for research involving human subjects, as established by Resolution No. 466/12 of the National Health Council. The study protocol was reviewed and authorized, guaranteeing adherence to the ethical principles of autonomy, beneficence, nonmaleficence, and justice.
A total of 82 patients who had a diagnosis of CF and were regularly seen at the Hospital de Clínicas, State University of Campinas, Campinas, Brazil, were included in this study. Data were collected between August 2021 and December 2023. Participants required an established diagnosis of CF confirmed by the identification of 2 pathogenic variants in the CFTR gene or 2 sweat tests showing a chloride concentration of 60 mEq/L or greater. The exclusion criterion was the patient’s refusal to participate in the study. The CFTR gene variants were categorized into different classes according to their functional consequences. Class I, II, and III variants are typically linked to more severe disease, as these mutations result in the absence of functional CFTR protein (due to defective synthesis) or the production of proteins that, although present in the cell membrane, remain inactive. In contrast, Class IV, V, and VI variants allow for some residual CFTR activity or partially preserved protein synthesis and are generally associated with milder clinical presentations.11
Exacerbations of pulmonary disease and hospitalizations over the preceding 3 years were evaluated, as well as their possible relationships with the severity of pulmonary involvement, classified according to lung function. In addition, because the patients frequently used dornase alfa, an inhaled medication for thinning mucus, lung function was evaluated with the spirometry test to establish the forced expiratory volume (FEV1) of patients aged 6 years and older. Lung function was classified according to the degree of obstruction: normal/none, %FEV1 ≥ 90% of predicted volume; mild, %FEV1 ≥ 70% and < 90% of predicted volume; moderate, %FEV1 ≥ 40% and < 70% of predicted volume; or severe, %FEV1 < 40% of predicted volume.12
Medical data, including laboratory test results, treatment data, follow-up information, and the presence of gastrointestinal and pulmonary involvement, were obtained from the patients’ medical records. Microbiologic data were collected through cultures using swab samples of sputum obtained during routine clinical appointments. If patients presented with oral or dental alterations, their systemic condition, as represented by test results, was analyzed to investigate possible associations with the dental findings.
For dental data, the patients underwent clinical oral examination to assess the presence of caries, dental enamel defects (DEDs), gingival inflammation, bacterial plaque, type of occlusion or malocclusion, and breathing pattern. The clinical examinations to evaluate enamel defects and caries were performed by previously calibrated examiners (A.C.E.C. and C.R.D.R.). Whenever doubts arose during the evaluations, a more experienced dentist (A.C.G.) was consulted to ensure uniformity and accuracy in the diagnoses.
Additionally, data were collected through a questionnaire administered during the dental appointments, including information on oral hygiene habits (such as the frequency of toothbrushing, toothbrush replacement, and flossing) as well as self-reported deleterious habits. For younger patients, parents or caregivers reported oral hygiene practices (supervised or assisted toothbrushing and flossing routines).
Bacterial plaque was measured by staining the tooth surface with a revealing solution and assigning a plaque index (PI) score of 0 to 3 according to the amount of dental biofilm.13 The gingival index (GI) was also scored from 0 to 3.14
For permanent teeth, the phase of dental eruption was assessed through clinical examination and panoramic radiography using the Nolla stage as reference. Panoramic radiographs were analyzed to evaluate the chronology of dental eruption as well as specific anatomical structures, including nasal turbinates, maxillary sinuses, the coronoid process of the mandible, and the mandibular condyle.
No statistical analysis was performed because the study design was primarily descriptive, and there was no significant variation among the groups that would allow for meaningful statistical comparisons. The small sample size and the lack of variability in several clinical variables further limited the possibility of conducting meaningful statistical analyses.
Results
Among the cohort, there were 1 infant (younger than 1 year), 3 toddlers (1 to 2 years), and 16 preschoolers (3 to 5 years) who did not have a full set of primary or permanent teeth. The sample included 44 female patients (53.7%) and 38 male patients (46.3%) with a mean age of 11.5 years. There was consanguinity between the parents in only 1 patient.
Molecular research for CFTR variants was performed according to the routine of the pediatric clinic, in which oral swabs from all patients were collected for genetic sequencing. Genetic sequencing was available for most participants. However, in 3 children, the results had not yet been confirmed because their analyses were still in progress at the time of the study. In this sample, 79.3% of the patients had at least one F508del allele, with 35.4% of the participants being homozygous (F508del/F508del) and 43.9% heterozygous (F508del/other variants) for that variant. F508del is the most common CFTR variant worldwide and is classified as a Class II variant, leading to defective protein folding and degradation before reaching the cell surface.
Pulmonary function was assessed in 41 patients aged 6 years and older. According to the classification based on FEV1, 13 patients (31.7%) had normal lung function, and an equal proportion (31.7%) presented with mild impairment. Additionally, 10 patients (24.4%) exhibited moderate pulmonary involvement, while 5 patients (12.2%) were classified as having severe impairment.
Regarding oral hygiene habits, 13.4% and 45.1% of the patients brushed their teeth once a day and twice a day, respectively. Regarding dental floss, only 9.8% of patients used it daily ( Table 1). For younger children, these practices were performed or supervised by parents or caregivers.
DEDs were present in 39 patients, or 47.6% of the entire sample. Considering only the 78 patients aged 3 years and older with
Table 1. Distribution of the sample (patients with cystic fibrosis) according to self-reported oral hygiene habits.
Hygiene habit
Brushing frequency, times/d (n = 82)
Frequency n (%) 1 11 (13.4) 2 37 (45.1) 3 34 (41.5)
Toothbrush replacement (n = 82) 15 d 3 (3.7)
Monthly 23 (28.0)
Every 2 mo 25 (30.49)
Every 3 mo 18 (22.0)
Every 5 mo 2 (2.4)
Every 6 mo 6 (7.3)
Do not know 5 (6.1)
Flossing (n = 82) Yes 23 (28.0) No 59 (72.0)
Flossing frequency (n = 23) 1 time/d 8 (34.8)
Rarely 15 (65.2)
sufficient erupted teeth for assessment, the prevalence was 50.0%. Defects were more prevalent in the permanent dentition, mainly the maxillary central incisors (n = 29 teeth affected), lateral incisors (n = 18), canines (n = 13), and first premolars (n = 12). In the permanent dentition, the maxillary teeth were more affected by enamel defects than the mandibular teeth (Chart).
When DEDs were analyzed according to type, it was found that white/cream opacity was the most prevalent category, affecting 76.9% of patients with DEDs (n = 30). Other changes in tooth enamel included diffuse line opacity (23.1% of patients with DEDs; n = 9), yellow/brown demarcated opacity (5.1% of patients; n = 2), and diffuse confluent opacity (2.6%; n = 1).
Three patients had more than 1 type of defect. The prevalence of DEDs was greater in female patients than in male patients (62.5% and 37.5%, respectively).
Analysis of bacterial plaque in relation to oral hygiene practices revealed that patients with higher PI score levels had a lower frequency of toothbrushing per day ( Table 2). Regarding gingival inflammation, the majority of patients with PI scores of 2 or 3 exhibited a GI score of 1, indicating mild inflammation, while fewer patients had GI scores of 2 or 3.
The highest mean ages at the time of the first positive cultures were observed in patients with a PI score of 0 for both S aureus (53.0 months) and P aeruginosa (60.4 months). In contrast, patients with PI scores of 1 had the lowest mean ages at first culture for both organisms. Regarding hospitalization, patients with PI scores of 1 and 2 had higher mean durations of stay (73.2 and 65.3 days, respectively), while those with a PI score of 0 had the lowest mean duration (9.3 days).
The frequency of toothbrushing was lower among patients with GI scores 2 and 3, with mean values of 1.7 and 2.0 times
daily, respectively ( Table 3). The frequency of toothbrush replacement was also lower among the groups with GI scores 2 and 3, recorded as means of 112.5 and 30.0 days between replacements, respectively. The groups with GI scores 2 and 3 each had a greater mean number of days of hospitalization (107.0 and 162.0 days, respectively) than was observed for patients with a GI score of 0 (25.7 days) or 1 (39.6 days). In contrast, higher PI scores did not show a consistent association with longer hospitalization times.
Dental carious lesions were present in 17.1% of patients (14 patients with a mean age of 12.3 years). Genetic analysis of these patients showed the following CFTR variants: F508del homozygous (n = 6); F508del heterozygous combined with another variant (n = 5); and no F508del alleles (n = 3), including 1 with class I/I, 1 with class I/IV, and 1 with class II/II variants. All patients had gastrointestinal involvement; only 2 were not colonized by S aureus, while 4 were chronically colonized by P aeruginosa. Only 1 patient did not have pulmonary involvement and therefore did not use inhaled corticosteroids or dornase alfa.
Radiographic evaluation of 26 patients was conducted to assess various craniofacial and dental characteristics. These patients were selected based on clinical need, as radiographic examinations were requested when there was an indication related to dental development, suspected anomalies, or other specific dental conditions requiring imaging evaluation. Six patients reported bruxism or a tooth clenching habit, although only 1 reported associated temporomandibular joint pain. Additionally, 2 patients without a history of bruxism or clenching experienced temporomandibular joint pain. Nasal septum deviation was identified in 12 patients (46.2%), while 10 patients (38.5%) exhibited opacification of the maxillary sinuses.
Prolonged tooth retention was observed in 6 (23.1%) of the 26 patients who underwent radiographic evaluation. Among these 6 patients, 4 with class II variants also had dental agenesis. Of these 4 patients with agenesis, 1 showed delayed eruption of all 4 first premolars, and another had delayed eruption of 1 second premolar.
Dental agenesis was identified in 5 of 26 patients, corresponding to 19.2% of the subsample. The most commonly affected teeth were the maxillary lateral incisors and maxillary or mandibular first premolars and second premolars. These 5 patients also demonstrated class I and II genetic variants, sinusopathy (n = 4), mixed breathing pattern (n = 2), and malocclusion, including open bite (n = 2) and crossbite (n = 1).
Finally, deleterious habits, such as lip biting, object biting, and nail biting, were found in 29.3% of the sample. Of these patients, 24.4% had pulmonary exacerbations in the last 3 years. Furthermore, half of these patients had a nasal breathing pattern, and 8 had an open bite.
Among the sample as a whole, 34 patients (41.5%) demonstrated oral or mixed oral and nasal breathing, and 23 of these used a bottle or pacifier. Of these 23 patients, 13 had discontinued the habit, with a mean age at cessation of 3.8 years. The other 10 patients, with a mean age of 5.1 years, were still using a bottle or pacifier at the time of the study. Malocclusions were detected in 23 patients (28.0%), 15 of whom demonstrated nasal or mixed breathing, and 2 patients had a high palate.
type
Discussion
Of the 82 patients analyzed in the present study, 65 had at least one F508del allele, corroborating the finding that this is the most frequent CF variant found in Brazil (in approximately 51.9% of individuals).12 In addition, the female to male ratio was relatively balanced (1.16 to 1), as expected from an autosomal recessive disease.
Pulmonary exacerbations affected 61 patients in this study, 20 of whom had deleterious oral habits, including nail biting, lip biting, or biting objects. However, when the presence of the F508del allele was analyzed, it was noticed that the variant was present in 57 of the 61 patients, contributing to the assertion that classes I and II determine the severity of the disease.
Of the 15 patients who had moderate or severe lung disease, only 4 changed their toothbrush every 15 days or monthly. There is evidence that prolonged use of the same toothbrush can result in contamination by various microorganisms, including S aureus and Candida albicans, contributing to the worsening of lung disease.15,16 Furthermore, oral bacteria related to dental and periodontal diseases can also colonize the lungs, increasing the risk of complications.17,18
In addition, in this group of 15 patients, 11 had a PI score of 2 or 3, and only 1 was not chronically colonized by S aureus, which tends to be the first bacteria to infect the airways of pediatric CF patients.19 These 15 patients had some positive cultures for P aeruginosa, which chronically colonizes up to 80% of adolescents and young adults with CF.19
Chart. Prevalence of dental enamel defects in the permanent dentition of patients with cystic fibrosis.
Tooth
PI (n = 74)
Toothbrushing habits (n = 74)
Staphylococcus aureus colonization (n = 73)
Pseudomonas aeruginosa colonization (n = 73)
index (n = 74)
Abbreviation: CF, cystic fibrosis.
a Plaque index was not assessed in 8 patients (4 homozygous, 3 heterozygous, and 1 other variant) due to factors such as young age, lack of cooperation with the dental examination, and, in 1 case, absence of dentition. Mean and median values are based on the total number of affected patients within each PI group. Some patients did not undergo some of the tests or did not experience a particular event (eg, hospitalization). Percentages are based on the total number of tested patients within each PI group.
b F508del/F508del.
cF508del/other variants.
Passarelli Mantovani et al noted that the nasal and oral cavities are bacterial reservoirs, and they favor the transmission of potentially pathogenic microorganisms to the lower airways.20 The passage of bacteria from the oral cavity to the lungs can occur by aspiration of pathogens present in saliva or during examinations with devices such as bronchoscopes or endotracheal tubes. It can also result from contact with daily hygiene objects, such as a toothbrush, or objects of common use in nonnutritive sucking habits.20-22
Coffey et al observed that 63% of patients with CF brushed their teeth twice a day or more, 36% used dental floss, and
a considerable proportion did not change their toothbrush regularly (5.6% changed monthly, 38% changed between 1 and 3 months, and 22.5% changed after 6 months).23 In addition, 53.7% of the patients did not go to the dentist with the recommended frequency. The results of the present study indicated that dental care, including replacing the toothbrush within a short period of time, is important for preventing or minimizing the worsening of CF lung disease, in agreement with the findings of another study by Passarelli Mantovani et al.22
Another important oral finding in CF patients is the high prevalence of DEDs, which may have some esthetic impact.24,25
Table 2. Characterization of patients with CF according to plaque index (PI). a
GI (n = 74)
Variant F508del (n = 65)
Toothbrushing habits (n = 74)
= 23)
(n = 20)
Abbreviations: CF, cystic fibrosis; NA, not applicable.
a Gingival index was not assessed in 8 patients (4 homozygous, 3 heterozygous, and 1 other variant) due to factors such as young age, lack of cooperation with the dental examination, and, in 1 case, absence of dentition. Mean and median values are based on the total number of affected patients within each GI group. Some patients did not undergo some of the tests or did not experience a particular event (eg, hospitalization). Percentages are based on the total number of tested patients within each GI group.
b F508del/F508del.
cF508del/other variants.
These defects may be the result of metabolic disease and continuous use of pancreatic enzymes and antibiotics. Another possibility is that the CFTR protein supports mineral deposition by participating in the buffering of dental enamel, and CF is characterized by CFTR deficiency.26 Bronckers et al observed that bone- and dentin-forming cells express CFTR protein, mainly intracellularly, suggesting that this is the explanation for the greater frequency of DEDs in people diagnosed with CF.26 These data are in accordance with the present results, which demonstrated a high frequency of DEDs, especially in patients who had at least one F508del allele. Another notable observation is that DEDs were more frequent in permanent teeth, mainly in the maxillary anterior dentition.
DEDs can cause changes in the enamel that may predispose teeth to the development of carious lesions and tooth sensitivity. Regular visits to the dentist can minimize this damage and prevent future discomfort.25
Analysis of the PI revealed that scores of 2 and 3 were associated with a lower frequency of toothbrushing per day. However, when the medical records of patients with PI scores of 3 were analyzed, this group showed a shorter mean length of hospitalization than patients with PI scores of 1 or 2. Patients with a PI of 3 also had a higher mean age at first positive culture for S aureus, which is the most prevalent bacteria in children and
adolescents and the main cause of hospitalization, and this difference could explain the shorter hospitalizations.
The present results showed a high prevalence of gingival inflammation, affecting 57.3% of patients. This high prevalence could be correlated with hospitalization. Higher GI scores were associated with longer mean hospital stays for intravenous antibiotic therapy. They were also linked to higher percentages of patients experiencing pulmonary exacerbations. However, because the numbers of patients with GI scores of 2 and 3 were low, these findings should be interpreted cautiously. These data support the results of prior studies that concluded that adequate oral hygiene could reduce the number of exacerbations in chronic obstructive pulmonary disease, which is the lung disease associated with CF.27,28
The levels of gingival inflammation were measured in 2 studies that found that children with CF had increased levels of gingivitis compared with control groups and exhibited greater bleeding on periodontal probing.29,30 On the other hand, in their systematic review, Pawlaczyk-Kamieńska et al reported no significant differences in dental plaque accumulation between patients with CF and healthy controls.9
Although the frequency of dental caries was low in the studied population, agreeing with the studies carried out by Ferrazanno et al, exposure to sugars was not assessed.24,25
Table 3. Characterization of patients with CF according to gingival index (GI). a
However, all patients in the present study had at least one class I or class II allele. These alleles result in a significant change in the quantity and function of the CFTR protein, which can cause porosity on the surface of the tooth enamel.31,32 Such surface defects favor the presence of DEDs, a condition present in 10 of 14 patients with caries in the present study.
Other alterations that may be present in patients with CF include nasal obstruction and maxillary sinus opacification, which can be observed radiographically. According to Batsakis and El-Naggar, the histopathologic modifications observed in these patients suggest susceptibility of the paranasal sinuses to anatomical changes and mucociliary dysfunction.33 Similarly, Blacharsh reported that CF patients might present with nasal obstruction and maxillary sinus opacification due to repeated respiratory infections, which can result in oral or mixed oral and nasal breathing.34 In the present study, panoramic radiographs of 26 patients were evaluated, and sinusopathy was observed in 12 patients (who had a combination of class I and II variants). However, among these 12 patients, only 3 (25.0%) exhibited oral or mixed breathing patterns.
Dental agenesis is considered the most common dental developmental anomaly in humans.35 The estimated prevalence in the global population ranges from 0.3% to 36.5%, with variations across the sexes and ethnic groups. The most frequently absent teeth are the mandibular second premolars followed by the maxillary lateral incisors.36,37 In the present study, 19.2% of the 26 patients with panoramic radiographs demonstrated dental agenesis, observed exclusively with first and second premolars. It was also found that dental agenesis affected patients with class I and II variant combinations. Prolonged retention was present in 23.1% of the patients, most of whom had 2 distinct variants within Class II. These findings emphasize the high prevalence of craniofacial and dental anomalies in patients with CF, highlighting a notable association between specific genetic variants and the radiographic alterations identified.
Malocclusions were detected in 23 patients, of whom 15 had nasal or mixed breathing and 2 had a high palate. Mouth breathing can influence facial growth, which will consequently alter dental occlusion. Although malocclusion is considered multifactorial, genetics, ethnicity, and the environment are the main contributors to the condition.38
Deleterious oral habits were detected in 24 patients, only half of whom demonstrated nasal breathing, and 8 had an open bite. These data are consistent with the findings of Almeida et al, who reported that the main causes of open bite are parafunctional habits, deleterious oral habits, mouth breathing, and tongue displacement.39 In a systematic review and meta-analysis, Gois-Santos et al noted that there is an association between deleterious oral habits and asthma, which, like CF, is a chronic obstructive pulmonary disease.40
This study has some limitations. Its cross-sectional design does not allow causal inferences, and the lack of a control group without CF restricts direct comparisons with healthy individuals. The sample was limited to patients from a single reference center, which may affect generalizability. Some information was self-reported by patients or caregivers, introducing potential recall bias. In addition, no statistical analyses were conducted due to limited variability among clinical variables.
Future longitudinal studies with larger samples are needed to confirm these observations.
Conclusion
The present study highlights the significant oral health challenges faced by patients with CF. DEDs were the most prevalent finding, affecting 47.6% of patients, particularly in the maxillary anterior teeth. Gingivitis was frequently observed and was more common in patients with prolonged hospitalizations for acute lung disease exacerbations. While the prevalence of dental caries was low, radiographic findings revealed dental agenesis, primarily of the second premolars and maxillary lateral incisors, along with craniofacial anomalies such as nasal septum deviation and maxillary sinus opacification. Additionally, irregular toothbrush replacement in patients with moderate or severe lung disease may contribute to contamination by pathogenic microorganisms, although further studies are needed to confirm this hypothesis.
The observations in this cohort underscore the multifaceted impact of CF on oral health, emphasizing the importance of early diagnosis, preventive strategies, and the integration of dental care into multidisciplinary management to enhance the overall quality of life for these patients.
Author affiliations
Department of Oral Diagnosis, Piracicaba Dental School, University of Campinas, Piracicaba, Brazil (Colafêmina, Frazatto, Rodrigues, Lopes); Faculty of Medical Sciences, State University of Campinas, Campinas, Brazil (Gonçalves, A.F. Ribeiro, J.D. Ribeiro).
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), finance code 001, and by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), process No. 303548/2022-3.
References
1. De Boeck K, Amaral MD. Progress in therapies for cystic fibrosis. Lancet Respir Med 2016;4(8):662-674. doi:10.1016/S2213-2600(16)00023-0
3. Grupo Brasileiro de Estudos de Fibrose Cística (GBEFC). Registro Brasileiro de Fibrose Cística ano 2021. Accessed May 12, 2025. https://portalgbefc.org.br/ckfinder/userfiles/files/ Rebrafc_2021_REV_fev24.pdf
4. Qvist T, Pressles VO, Thomsen M, Skov M, Iversen M, Katzenstein TL. Nontuberculous mycobacterial disease is not a contraindication to lung transplantation in patients with cystic fibrosis: a retrospective analysis in a Danish patient population. Transplant Proc 2013;45(1):342-345. doi:10.1016/j.transproceed.2012.02.035
5. Gilligan PH. Infections in patients with cystic fibrosis: diagnostic microbiology update. Clin Lab Med. 2014;34(2):197-217. doi:10.1016/j.cll.2014.02.001
6. Lutz L, de-Paris F, Vieira MI, Marques E de A, Barth AL. Bacteriologia da fibrose cística. Clin Biomed Res. 2011;31(2):168-184.
7. Zegarelli EV, Kutscher AH, Denning CR, Saporito R, Slaughter TW, Fahn B. Coloration of teeth in patients with cystic fibrosis of the pancreas. 2. Oral Surg Oral Med Oral Pathol 1962;15(8):929-933. doi:10.1016/0030-4220(62)90086-5
8. da Silva Modesto KB, de Godói Simões JB, de Souza AF, et al. Salivary flow rate and biochemical composition analysis in stimulated whole saliva of children with cystic fibrosis. Arch Oral Biol. 2015;60(11):1650-1654. doi:10.1016/j.archoralbio.2015.08.007
9. Pawlaczyk-Kamieńska T, Borysewicz-Lewicka M, Śniatała R, Batura-Gabryel H, Cofta S. Dental and periodontal manifestations in patients with cystic fibrosis—a systematic review. J Cyst Fibros. 2019;18(6):762-771. doi:10.1016/j.jcf.2018.11.007
10. Myer H, Chupita S, Jnah A. Cystic fibrosis: back to the basics. Neonatal Netw. 2023;42(1):2330. doi:10.1891/NN-2022-0007
11. Cutting GR. Cystic fibrosis genetics: from molecular understanding to clinical application. Nat Rev Genet. 2015;16(1):45-56. doi:10.1038/nrg3849
12. Grupo Brasileiro de Estudos de Fibrose Cística (GBEFC). Registro Brasileiro de Fibrose Cística ano 2019. Accessed May 12, 2025. http://portalgbefc.org.br/ckfinder/userfiles/files/ REBRAFC_2019.pdf
13. O’Leary TJ, Drake RB, Naylor JE. The plaque control record. J Periodontol. 1972;43(1):38-40.
14. Silness J, Loe H. Periodontal disease in pregnancy, II: correlation between oral hygiene and periodontal condition. Acta Odontol Scand. 1964;22(1):121-135. doi:10.3109/00016356408993968
15. Wetzel WE, Schaumburg C, Ansari F, Kroeger T, Sziegoleit A. Microbial contamination of toothbrushes with different principles of filament anchoring. J Am Dent Assoc 2005;136(6):758-765. doi:10.14219/jada.archive.2005.0259
16. Karibasappa GN, Nagesh L, Sujatha BK. Assessment of microbial contamination of toothbrush head: an in vitro study. Indian J Dent Res. 2011;22(1):2-5. doi:10.4103/09709290.79965
17. Bansal M, Khatri M, Taneja V. Potential role of periodontal infection in respiratory diseasesa review. J Med Life. 2013;6(3):244-248.
18. Coffey N, O’Leary F, Burke F, Roberts A, Hayes M. Periodontal and oral health status of people with cystic fibrosis: a systematic review. J Dent. 2020;103:103509. doi:10.1016/j. jdent.2020.103509
19. Oliver A. Mutators in cystic fibrosis chronic lung infection: prevalence, mechanisms, and consequences for antimicrobial therapy. Int J Med Microbiol. 2010;300(8):563-572. doi:10.1016/j.ijmm.2010.08.009
20. Passarelli Mantovani R, Sandri A, Boaretti M, et al. Longitudinal monitoring of sinonasal and oral bacterial reservoirs to prevent chronic lung infection in people with cystic fibrosis. ERJ Open Res. 2020;6(3):00115-2020. doi:10.1183/23120541.00115-2020
21. Rivas Caldas R, Boisramé S. Upper aero-digestive contamination by Pseudomonas aeruginosa and implications in cystic fibrosis. J Cyst Fibros. 2015;14(1):6-15. doi:10.1016/j. jcf.2014.04.008
22. Passarelli Mantovani R, Sandri A, Boaretti M, et al. Toothbrushes may convey bacteria to the cystic fibrosis lower airways. J Oral Microbiol. 2019;11(1):1647036. doi:10.1080/ 20002297.2019.1647036
23. Coffey N, O’Leary F, Burke F, Plant B, Roberts A, Hayes M. Self-reported dental attendance, oral hygiene habits, and dietary habits of adults with cystic fibrosis. Spec Care Dentist 2023;43(4):401-408. doi:10.1111/scd.12773
24. Ferrazzano GF, Orlando S, Sangianantoni G, Cantile T, Ingenito A. Dental and periodontal health status in children affected by cystic fibrosis in a southern Italian region. Eur J Paediatr Dent. 2009;10(2):65-68.
25. Ferrazzano GF, Sangianantoni G, Cantile T, Amato I, Orlando S, Ingenito A. Dental enamel defects in Italian children with cystic fibrosis: an observational study. Community Dent Health. 2012;29(1):106-109.
26. Bronckers A, Kalogeraki L, Jorna HJ, et al. The cystic fibrosis transmembrane conductance regulator (CFTR) is expressed in maturation stage ameloblasts, odontoblasts and bone cells. Bone. 2010;46(4):1188-1196. doi:10.1016/j.bone.2009.12.002
27. Liu Z, Zhang W, Zhang J, et al. Oral hygiene, periodontal health and chronic obstructive pulmonary disease exacerbations. J Clin Periodontol. 2012;39(1):45-52. doi:10.1111/j.1600051X.2011.01808.x
28. Fernandez Fernandez E, De Santi C, De Rose V, Greene CM. CFTR dysfunction in cystic fibrosis and chronic obstructive pulmonary disease. Expert Rev Respir Med. 2018;12(6):483-492. doi:10.1080/17476348.2018.1475235
29. Narang A, Maguire A, Nunn JH, Bush A. Oral health and related factors in cystic fibrosis and other chronic respiratory disorders. Arch Dis Child. 2003;88(8):702-707. doi:10.1136/ adc.88.8.702
30. Duruel O, Berker E, Özşin-Özler C, et al. Levels of pro- and anti-inflammatory cytokines in cystic fibrosis patients with or without gingivitis. Cytokine. 2020;127:154987. doi:10.1016/j. cyto.2020.154987
31. Mishra A, Greaves R, Massie J. The limitations of sweat electrolyte reference intervals for the diagnosis of cystic fibrosis: a systematic review. Clin Biochem Rev. 2007;28(2):60-76.
32. Lopes-Pacheco M. CFTR modulators: the changing face of cystic fibrosis in the era of precision medicine. Front Pharmacol. 2020;10:1662. doi:10.3389/fphar.2019.01662
33. Batsakis JG, El-Naggar AK. Cystic fibrosis and the sinonasal tract. Ann Otol Rhinol Laryngol 1996;105(4):329-330. doi:10.1177/000348949610500418
34. Blacharsh C. Dental aspects of patients with cystic fibrosis: a preliminary clinical study. J Am Dent Assoc. 1977;95(1):106-110.
35. Chhabra N, Goswami M, Chhabra A. Genetic basis of dental agenesis—molecular genetics patterning clinical dentistry. Med Oral Patol Oral Cir Bucal. 2014;19(2):e112-e119. doi:10.4317/medoral.19158
36. Polder BJ, Van’t Hof MA, Van der Linden FP, Kuijpers-Jagtman AM. A meta-analysis of the prevalence of dental agenesis of permanent teeth. Community Dent Oral Epidemiol 2004;32(3):217-226. doi:10.1111/j.1600-0528.2004.00158.x
37. Mattheeuws N, Dermaut L, Martens G. Has hypodontia increased in Caucasians during the 20th century? A meta-analysis. Eur J Orthod. 2004;26(1):99-103. doi:10.1093/ejo/26.1.99
38. Heimer MV, Tornisiello Katz CR, Rosenblatt A. Non-nutritive sucking habits, dental malocclusions, and facial morphology in Brazilian children: a longitudinal study. Eur J Orthod 2008;30(6):580-585. doi:10.1093/ejo/cjn035
39. Almeida RR, Garib DG, Henriques JFC, Almeida MR. Ortodontia preventiva e interceptora: mito ou realidade? Rev Dent Press Ortodon Ortop Facial. 1999;4(6):87-108.
40. Gois-Santos VT, Santos VS, Tavares CSS, et al. Association between deleterious oral habits and asthma in children: a systematic review and meta-analysis. Braz Oral Res. 2022;36:e039. doi:10.1590/1807-3107bor-2022.vol36.0039
Influence of beverage solutions on the microhardness and surface roughness of provisional fixed denture materials
Paulo Henrique Dos Santos, DDS, MS, PhD ¢ Sabrina Pavan, DDS, MS, PhD
This in vitro study examined the influence of aging in different beverage solutions on the Knoop hardness and surface roughness of provisional fixed denture materials. A total of 160 resin blocks were created and divided into 4 groups (n = 40) based on the provisional material: Structur 2 SC bis-acrylic resin, Protemp 4 bis-acrylic resin, Z350 XT nanoparticle composite resin, or Acri
Duralay acrylic resin. The material groups were subdivided into 4 groups (n = 10) according to the beverage solution used to simulate aging: distilled water (control), red wine, orange juice, or soda (Coca-Cola). After 24 hours, the specimens were polished, and the initial microhardness and surface roughness were measured using a microhardness tester and profilometer, respectively. The specimens were then submerged in different beverage solutions for 4 weeks, and microhardness and surface roughness measurements were taken again.
Two-way repeated-measures analysis of variance and Fisher least significant difference test were performed (α = 0.05). The aging process with different beverage solutions resulted in significantly lower hardness values compared with baseline for both Z350 XT and Acri
Duralay materials (P < 0.05); however, Z350 XT still demonstrated significantly higher hardness values than all other materials regardless of the aging condition (P < 0.05). In general, Protemp 4 and Z350 XT exhibited lower surface roughness values than Structur 2 SC and Acri Duralay regardless of the solution used (P < 0.05). Beverage solutions significantly influenced the mechanical properties of the materials, with Protemp 4 bis-acryl–based resin material demonstrating hardness and surface roughness values that were less affected by aging.
Provisional restorations play a crucial role in the success of oral rehabilitations. Their primary function is to safeguard prepared teeth against mechanical, thermal, and biologic risks during the fabrication of a definitive prosthesis, which is especially vital in cases of extended prosthodontic treatments.1-4 These resin materials also help to stabilize the tooth position, ensuring satisfactory masticatory function, phonetics, and esthetics. 2 To meet these requirements, interim materials must maintain satisfactory mechanical properties, including hardness and surface roughness, to prevent fractures from occlusal forces and plaque accumulation. 5-8 This, in turn, helps prevent potential periodontal and esthetic damage. 2,9-11
Several resin-based materials are currently available for the fabrication of provisional restorations. These materials can generally be categorized into 2 main groups based on their compositions: unfilled methacrylate and filled dimethacrylate composite resins. Compared with conventional provisional restorations made of acrylic resins, bis-acrylic resins have garnered clinical acceptance as a provisional material.12 This shift is attributed to the advantages of bis-acrylic resins, including low polymerization contraction, reduced exothermic reaction, improved mechanical properties, esthetic enhancements, and simplified handling and polishing procedures.4,13-16 While acrylic resins were once widely used for provisional restorations due to their mechanical properties and costeffectiveness, their polymerization, characterized by an exothermic reaction, poses challenges.17 When in contact with dental tissue, acrylic resins may transfer a significant amount of heat to the pulp, potentially causing irreversible pulp damage.1,12,18
The detrimental impact of consuming beverages with dyes and low pH values extends beyond dental tissue erosion; it can also expedite the degradation of resin-based restorative materials.19-24 When provisional restorative materials come into contact with chemical agents in low-pH environments, their filler compounds may become dislodged from the resin matrix, leading to a decline in material properties.25-27
Hence, the aim of this in vitro study was to assess the impact of various beverage solutions on the Knoop hardness and surface roughness of provisional fixed denture materials. The null hypotheses tested were as follows: (1) there would be no differences in Knoop hardness or surface roughness among different provisional resin materials; and (2) there would be no differences in Knoop hardness or surface roughness based on immersion in the different beverage solutions.
Methods
Specimen preparation
The resin materials utilized in this study are detailed in Table 1. A nanoparticle composite resin (Filtek Z350 XT, shade A2, 3M), 2 bis-acrylic resins (Protemp 4, shade A2, 3M; and Structur 2 SC, shade A2, VOCO), and a methyl methacrylate acrylic resin (Acri Duralay, shade 66, Reliance Dental) were used. A metallic matrix (6.0 mm in diameter and 1.5 mm in thickness) was used to fabricate 40 specimens of each material. Each resin material was manipulated according to the manufacturer’s recommendations. The bis-acrylic resins were inserted into the metallic matrix with a specific dispenser and automixing tips, while the composite resin and acrylic resin were placed with a spatula (Thompson, Quinelato).
Transparent polyester film strips and glass microscope slides were utilized to cover the materials, flattening the surface and preventing bubble formation. The composite resin specimens were light activated with a light-curing unit (Optilux 501, Kerr) operated at 600 mW/cm² for 40 seconds. The other materials, classified as chemically cured resin materials, were kept in the polyester matrix until complete polymerization according to their respective manufacturer’s recommendations. All specimens were stored in distilled water at 37°C for 24 hours in light-protected containers.
The experimental design and preparation protocols were informed by relevant aspects of International Organization for Standardization (ISO) guidelines (ISO 4049 and ISO/TR 11405).28,29 While this study did not aim to follow a specific ISO guideline in its entirety, procedures such as specimen conditioning, storage, and immersion aging were aligned with recommendations for testing the mechanical properties and degradation behaviors of polymer-based dental materials.
Hardness analysis
Knoop microhardness measurements were conducted atop the resin specimens using a microhardness tester (Micromet 5104, Buehler). For each specimen, 5 initial indentations were made 1 mm apart under a static load of 50 g for 15 seconds. The arithmetic mean of these values was then calculated to obtain the representative microhardness for each specimen.19,30
Surface roughness analysis
The initial surface roughness measurements (micrometers) were assessed using a profilometer (model SJ-401, Mitutoyo). Three measurements were taken on each specimen while the specimen was rotated 120°, employing a cutoff length of 0.25 mm. The surface roughness value represents the arithmetic average of the roughness profile.
Aging procedures
Following the initial measurements, 10 specimens from each experimental group underwent the aging process. The specimens were immersed in 1 of 4 different solutions: distilled water (pH ~ 6.4), red wine (cabernet sauvignon, Concha y Toro; pH ~ 3.7), orange juice (Del Valle; pH ~ 3.5), or soda (Coca-Cola; pH ~ 2.7). The resin specimens were stored at 37 °C in light-proof containers with these solutions for 4 weeks with weekly solution changes. After the aging
Table 1. Composition of the materials investigated.
procedure was complete, the microhardness and surface roughness analyses were repeated following the previously described methods.
Statistical analysis
Hardness and surface roughness analyses were conducted using 2-way repeated-measures analysis of variance, with Fisher least significant difference test applied for both analyses, maintaining a significance level of α = 0.05.
Results
Table 2 presents the results of the hardness analysis, which revealed a significantly higher hardness value for Z350 XT than for all other materials at baseline and after aging, regardless of beverage solution (P < 0.0001). The statistical evaluation showed that Structur 2 SC and Protemp 4 groups both exhibited significantly higher hardness values than the Acri Duralay material regardless of the aging involving the beverage solution (P < 0.05), except at baseline, where Protemp 4 and Acri Duralay materials revealed no significant difference (P > 0.05).
Structur 2 SC aged with red wine or orange juice exhibited a higher mean hardness than the same material at baseline or after immersion in distilled water (P < 0.05). Protemp 4 aged
Coca-Cola.
Different uppercase letters within columns indicate statistically significant differences between fixed denture materials (P < 0.05; Fisher least significant difference test).
Different lowercase letters within rows indicate statistically significant differences between beverage solutions (P < 0.05; Fisher least significant difference test).
Table 3. Surface roughness as a function of provisional fixed denture material and beverage solution (n = 10 per material per solution).
(SD) surface roughness, μm
Material
Different uppercase letters within columns indicate statistically significant differences between fixed denture materials (P < 0.05; Fisher least significant difference test).
Different lowercase letters within rows indicate statistically significant differences between beverage solutions (P < 0.05; Fisher least significant difference test).
with soda had higher a hardness value than it did at baseline and after aging in all other solutions (P < 0.05). For Z350 XT, the aging process, regardless of beverage solution, led to lower hardness values than were found at baseline (P < 0.05). For Acri Duralay, aging with red wine and soda solutions resulted in lower hardness values compared with baseline (P < 0.05).
Results of the surface roughness analysis are shown in Table 3. Structur 2 SC exhibited higher surface roughness values than the other resin materials at baseline and regardless of aging solution, except for the red wine group, in which Acri Duralay showed higher surface roughness values (P < 0.05). Acri Duralay specimens also exhibited significantly higher surface roughness values than Protemp 4 and Z350 XT specimens regardless of beverage solution (P < 0.05), except for the distilled water group, where no statistically significant differences were observed between Acri Duralay and Protemp 4 (P > 0.05).
Structur 2 SC showed significantly lower surface roughness measurements at baseline than after aging, regardless of the beverage solution (P < 0.05). For Protemp 4 and Z350 XT, aging with red wine, orange juice, or soda did not result in a statistically significant difference in surface roughness compared with their baseline groups ( P > 0.05). However, for both materials, specimens aged in distilled water exhibited higher surface
roughness values than were found at baseline ( P < 0.0001). Acri Duralay showed higher surface roughness after aging in red wine compared with baseline ( P = 0.0033) and the other solution groups ( P < 0.0001).
Discussion
The provisional material exerted a significant influence on the hardness and surface roughness of the resin materials, leading to rejection of the first null hypothesis. Analysis of the aging effects of the beverage solutions resulted in rejection of the second null hypothesis.
The evaluation of both hardness and surface roughness in this study was essential to assess the overall mechanical performance and surface integrity of provisional fixed denture materials under the influence of common beverage solutions. Hardness is a key indicator of a material’s resistance to localized deformation and surface wear, which are both critical for maintaining occlusal form and function during the provisional phase. Although not directly preventing fractures, higher hardness values suggest improved durability under masticatory forces. Surface roughness, on the other hand, is directly associated with plaque accumulation, susceptibility to staining, and patient comfort. A smoother surface contributes to better oral hygiene and
outcomes while minimizing
Table 2. Hardness as a function of provisional fixed denture material and beverage solution (n = 10 per material per solution).
the risk of microbial colonization. By analyzing both parameters, this study provides a more comprehensive understanding of how exposure to acidic and pigmented beverages may compromise the clinical performance and longevity of provisional restorations.12,14,19,31-35
The tested bis-acrylic composite–based materials generally demonstrated higher hardness values than the methyl methacrylate–based resin. This distinction can be attributed to their constituent monomers. Bis-acryl–based resins incorporate dimethacrylate monomers such as bisphenol A glycidyl methacrylate (Bis-GMA) or triethylene glycol dimethacrylate (TEGDMA), enhancing strength through cross-linking with other monomers and the presence of load particles.6-8,12 This combination promotes heightened strength and hardness in the resin material.
Conversely, methyl methacrylate–based resins possess a lower molecular weight and form a linear polymer network, resulting in less rigidity and resistance, making them more susceptible to water sorption.6,7,12 The mechanical properties of acrylic resins can vary based on composition, with the concentration of benzoyl peroxide initiator and dimethyl-p-toluidine activator significantly influencing material properties.7,12 This influence is mitigated in dimethacrylates, as these materials present a stiff central structure that allows them to absorb only 0.8 wt% of water.12 Moreover, dimethacrylates are available in a self-mixing cartridge system, minimizing air entrapment and providing control over compound proportions.6,16 The mode of provisional crown fabrication, whether automixed or hand-mixed, influences surface porosities and the formation of defects.36 Incorporation of bubbles and/or unreacted monomer during the fabrication process can impact the mechanical properties, color stability, and water sorption of the restorations.4,37
In the present study, Protemp 4 bis-acrylic resin and Z350 XT composite resin exhibited significantly lower surface roughness values. This outcome can be attributed to the specific composition of each resin material employed. Filtek Z350 includes ethoxylated bisphenol A dimethacrylate (Bis-EMA), Bis-GMA, and nanoparticles. This composite resin is recommended for direct restorations in both anterior and posterior teeth owing to its high mechanical resistance and exceptional surface smoothness.19
Although both Protemp 4 and Structur 2 are bis-acryl–based resin materials, there were significant differences in surface roughness values between them. Structur 2 specimens exhibited higher surface roughness values than Protemp 4 at baseline and regardless of which beverage solution was used for aging. According to Schwantz et al, Protemp 4 incorporates smaller particles compared with other bis-acrylic composite resins, and these fillers are likely silica nanoparticles.14 The intrinsic material chemistry, initiator, matrix composition of the resin materials, and presence of filler particles, along with their distribution and size, directly influence material smoothness.13 These factors may contribute to the observed differences in surface roughness values in the present study.25,32,33
In addition to the particle size in the resin materials, the higher surface roughness values of Duralay and Structur 2 materials could be attributed to the solubility of the resin components, which may exhibit unsatisfactory clinical behavior
under hydrolytic degradation.38 According to Strazzi-Sahyon et al, resin materials containing TEGDMA release large quantities of monomers in an aqueous medium.38 When TEGDMA is combined with Bis-GMA, water sorption is directly proportional to the TEGDMA concentration in the material.38 The release of monomers from the resinous matrix creates irregularities on the material surface, providing an environment conducive to bacterial adhesion, plaque accumulation, and gingival inflammation, as well as a alterations in color and deterioration of mechanical properties.4,9
Considering the clinical relevance of these parameters, it is generally accepted that provisional materials should exhibit a Knoop hardness number greater than 18 to ensure adequate resistance to occlusal wear and deformation during function, as reported by Diaz-Arnold et al.39 Additionally, surface roughness values less than 0.2 µm are considered ideal to minimize bacterial adhesion and plaque accumulation, thereby contributing to better periodontal health and patient comfort.40
The aging process employed in this study did not involve thermocycling. Instead, a chemical aging protocol was used via immersion of the specimens in different beverage solutions over a continuous 4-week period with weekly solution replacement. This approach was selected to focus on the chemical effects of pigment-rich and low-pH beverages on provisional restorative materials, particularly their potential to cause hydrolytic degradation, monomer leaching, and surface erosion.
The beverage solutions significantly affected the mechanical properties of the specimens. The alterations in mechanical properties observed after the specimens were immersed in distilled water can be attributed to the softening of the polymer resin component, resulting from network swelling and a reduction in frictional forces between polymeric chains.41 According to Catelan et al, low-pH beverages exert a considerable influence on resin-based materials, leading to compound solubility after a 28-day immersion period.19 This solubility induces surface erosion and dissolution, adversely impacting hardness and surface integrity due to matrix softening and the loss of structural ions.13,19,21,22
An interesting finding in the present study was that Structur 2 SC specimens aged in red wine and orange juice exhibited higher hardness values than those aged in soda, even higher than the baseline. One possible explanation is the difference in pH and chemical composition among the solutions. Coca-Cola, with the lowest pH (~2.7) and the presence of phosphoric acid and carbonation, may induce more aggressive polymer matrix degradation than the organic acids found in red wine (tartaric acid) and orange juice (citric acid). Moreover, substances such as the tannins in wine or the natural sugars in juice may influence the surface chemistry differently, potentially leading to reduced leaching or even surface precipitation effects that temporarily enhance hardness.42 Additionally, prolonged exposure to aqueous acidic environments can contribute to postpolymerization or the leaching of unreacted monomers, resulting in a denser, more cross-linked surface with improved hardness. This effect could explain why all 3 immersion groups—red wine, orange juice, and soda—exhibited higher hardness values than were recorded at
baseline, which was only stored in distilled water for 24 hours, possibly allowing incomplete polymerization or higher plasticizer content to persist on the surface.13,19
Some limiting factors in this study warrant consideration. It is crucial to interpret the results cautiously, recognizing that resin materials may be exposed to other influences not assessed by the in vitro methodology employed, such as interactions with saliva, proteins, and enzymes; temperature changes resulting from food and drinks; toothbrushing; and occlusal function. Future studies should address these aspects to provide clearer clinical recommendations, exploring additional parameters such as optical properties, degree of conversion, fracture strength, and bacterial adhesion on resin materials. Investigations could also examine the impact of various beverage solutions on other provisional fixed denture materials fabricated using computer-aided design/computer-aided manufacturing and 3-dimensional printing technology. Furthermore, assessing the long-term maintenance of restorations could provide valuable insights into clinical applicability.
Conclusion
From the results obtained in this in vitro study, it can be concluded that beverage solutions exerted an influence on the mechanical properties of resin materials. Notably, Protemp 4 bis-acryl–based resin demonstrated more stable mechanical properties after aging, making it a suitable choice for provisional restorations.
Author affiliations
Department of Prosthodontics, Adamantina School of Dentistry, Adamantina Integrated Faculty, Adamantina, Brazil (E.C. Pieralini, A.R.F. Pieralini); Department of Dental Materials and Prosthodontics, Araçatuba School of Dentistry, São Paulo State University, Araçatuba, Brazil (Fernandes, Strazzi-Sahyon); Department of Prosthodontics and Periodontology, Bauru School of Dentistry, University of São Paulo, Bauru, Brazil (Strazzi-Sahyon); Division of Biomaterial and Biomedical Sciences, Department of Oral Rehabilitation and Biosciences, Oregon Health & Science University, Portland (Strazzi-Sahyon); Dental Research Institute – Restorative Dentistry, Faculty of Dentistry, University of Toronto, Canada (Dos Santos); Faculty of Dentistry, University of Toronto, Canada (Pavan).
Correspondence
Paulo Henrique Dos Santos, DDS, MS, PhD (pauloh.dossantos@utoronto.ca).
Conflicts of interest
None reported.
Funding
This study was supported by grant No. 2022/12118-5, São Paulo Research Foundation (FAPESP).
References
1. Seelbach P, Finger WJ, Ferger P, Balkenhol M. Temperature rise on dentin caused by temporary crown and fixed partial denture materials: influencing factors. J Dent. 2010;38(12):964-973. doi:10.1016/j.jdent.2010.08.008
2. Libecki W, Elsayed A, Freitag-Wolf S, Kern M. Reducing the effect of polymerization shrinkage of temporary fixed dental prostheses by using different materials and fabrication techniques. Dent Mater. 2016;32(12):1464-1471. doi:10.1016/j.dental.2016.09.020
3. Juntavee N, Juntavee A, Srisontisuk S. Flexural strength of various provisional restorative materials for rehabilitation after aging. J Prosthodont. 2023;32(S1):20-28. doi:10.1111/ jopr.13549
4. Cakan U, Kara HB. Effect of liquid polishing materials on the stainability of bis-acryl interim restorative material in vitro. J Prosthet Dent. 2015;113(5):475-479. doi:10.1016/j. prosdent.2014.09.020
5. Revilla-León M, Meyers MJ, Zandinejad A, Özcan M. A review on chemical composition, mechanical properties, and manufacturing work flow of additively manufactured current polymers for interim dental restorations. J Esthet Restor Dent. 2019;31(1):51-57. doi:10.1111/jerd.12438
7. Nejatidanesh F, Momeni G, Savabi O. Flexural strength of interim resin materials for fixed prosthodontics. J Prosthodont. 2009;18(6):507-511. doi:10.1111/j.1532849X.2009.00473.x
8. Rosentritt M, Behr M, Lang R, Handel G. Flexural properties of prosthetic provisional polymers. Eur J Prosthodont Restor Dent. 2004;12(2):75-79.
9. Ozel GS, Guneser MB, Inan O, Eldeniz AU. Evaluation of C. albicans and S. mutans adherence on different provisional crown materials. J Adv Prosthodont. 2017;9(5):335-340. doi:10.4047/jap.2017.9.5.335
10. Şahin O, Dede DÖ, Köroğlu A, Yılmaz B. Influence of surface sealant agents on the surface roughness and color stability of artificial teeth. J Prosthet Dent. 2015;114(1):130-137. doi:10.1016/j.prosdent.2015.02.009
11. Parakaw T, Ruangsawasdi N, Dararat P, Phruksaniyom C, Srihirun S, Petchmedyai P. Biocompatibility and biofilm formation on conventional and CAD/CAM provisional implant restorations. BMC Oral Health. 2023;23(1):718. doi:10.1186/s12903-023-03468-z
12. Astudillo-Rubio D, Delgado-Gaete A, Bellot-Arcís C, Montiel-Company JM, Pascual-Moscardó A, Almerich-Silla JM. Mechanical properties of provisional dental materials: a systematic review and meta-analysis. PLoS One. 2018;13(2):e0193162. doi:10.1371/journal.pone.0193162
13. Macedo MGFP, Volpato CAM, Henriques BAPC, Vaz PCS, Silva FS, Silva CFCL. Color stability of a bis-acryl composite resin subjected to polishing, thermocycling, intercalated baths, and immersion in different beverages. J Esthet Restor Dent. 2018;30(5):449-456. doi:10.1111/ jerd.12404
14. Schwantz JK, Oliveira-Ogliari A, Meereis CT, Leal FB, Ogliari FA, Moraes RR. Characterization of bis-acryl composite resins for provisional restorations. Braz Dent J. 2017;28(3):354-361. doi:10.1590/0103-6440201601418
15. Rayyan MM, Aboushelib M, Sayed NM, Ibrahim A, Jimbo R. Comparison of interim restorations fabricated by CAD/CAM with those fabricated manually. J Prosthet Dent. 2015;114(3):414-419. doi:10.1016/j.prosdent.2015.03.007
16. Young HM, Smith CT, Morton D. Comparative in vitro evaluation of two provisional restorative materials. J Prosthet Dent. 2001;85(2):129-132. doi:10.1067/mpr.2001.112797
17. Mazurek-Popczyk J, Nowicki A, Arkusz K, Pałka Ł, Zimoch-Korzycka A, Baldy-Chudzik K. Evaluation of biofilm formation on acrylic resins used to fabricate dental temporary restorations with the use of 3D printing technology. BMC Oral Health. 2022;22(1):442. doi:10.1186/ s12903-022-02488-5
18. Michalakis K, Pissiotis A, Hirayama H, Kang K, Kafantaris N. Comparison of temperature increase in the pulp chamber during the polymerization of materials used for the direct fabrication of provisional restorations. J Prosthet Dent. 2006;96(6):418-423. doi:10.1016/j. prosdent.2006.10.005
19. Catelan A, Briso ALF, Sundfeld RH, Dos Santos PH. Effect of artificial aging on the roughness and microhardness of sealed composites. J Esthet Restor Dent. 2010;22(5):324-330. doi:10.1111/j.1708-8240.2010.00360.x
20. Badra VV, Faraoni JJ, Ramos RP, Palma-Dibb RG. Influence of different beverages on the microhardness and surface roughness of resin composites. Oper Dent. 2005;30(2):213-219.
21. Arocha MA, Mayoral JR, Lefever D, Mercade M, Basilio J, Roig M. Color stability of siloranes versus methacrylate-based composites after immersion in staining solutions. Clin Oral Investig. 2013;17(6):1481-1487. doi:10.1007/s00784-012-0837-7
22. Gaglianone LA, Martins JD, Rossi TR, Saraiva LO, Cavalcanti AN, Mathias P. Changes on the color parameters of air-abraded resin composite exposed to different colored beverages. J Investig Clin Dent. 2011;2(3):201-206. doi:10.1111/j.2041-1626.2011.00063.x
23. Almejrad L, Yang CC, Morton D, Lin WS. The effects of beverages and surface treatments on the color stability of 3D-printed interim restorations. J Prosthodont. 2022;31(2):165-170. doi:10.1111/jopr.13377
24. Ribera OK, Mendes JM, Mendes J, Barreiros P, Aroso C, Silva AS. Influence of popular beverages on the fracture resistance of implant-supported bis-acrylic resin provisional crowns: an in vitro study. Polymers (Basel). 2023;15(16):3411. doi:10.3390/polym15163411
25. Köroğlu A, Sahin O, Dede DÖ, Yilmaz B. Effect of different surface treatment methods on the surface roughness and color stability of interim prosthodontic materials. J Prosthet Dent. 2016;115(4):447-455. doi:10.1016/j.prosdent.2015.10.005
26. Yannikakis SA, Zissis AJ, Polyzois GL, Caroni C. Color stability of provisional resin restorative materials. J Prosthet Dent. 1998;80(5):533-539. doi:10.1016/s0022-3913(98)70028-9
27. Burns DR, Beck DA, Nelson SK; Committee on Research in Fixed Prosthodontics of the Academy of Fixed Prosthodontics. A review of selected dental literature on contemporary provisional fixed prosthodontic treatment: report of the Committee on Research in Fixed Prosthodontics of the Academy of Fixed Prosthodontics. J Prosthet Dent. 2003;90(5):474497. doi:10.1016/s0022-3913(03)00259-2
28. ISO 4049:2019. Dentistry – polymer-based restorative materials. Geneva: International Organization for Standardization; 2019.
29. ISO/TR 11405:1994. Dental materials – guidance on testing of adhesion to tooth structure. Geneva: International Organization for Standardization; 1994.
30. Sahyon HBS, Guedes APA, Godas AGL, Suzuki TYU, Briso ALF, Dos Santos PH. Effect of fluoride-releasing adhesive systems in control of dental enamel hardness subjected to acid challenge. Arch Health Invest. 2017;6(5):192-196. doi:10.21270/archi.v6i5.2075
31. Moda MD, Godas AGL, Fernandes JC, et al. Comparison of different polishing methods on the surface roughness of microhybrid, microfill, and nanofill composite resins. J Investig Clin Dent. 2018;9(1):e12287. doi:10.1111/jicd.12287
32. Reis AF, Giannini M, Lovadino JR, Ambrosano GM. Effects of various finishing systems on the surface roughness and staining susceptibility of packable composite resins. Dent Mater. 2003;19(1):12-18. doi:10.1016/s0109-5641(02)00014-3
33. Sarac D, Sarac YS, Kulunk S, Ural C, Kulunk T. The effect of polishing techniques on the surface roughness and color change of composite resins. J Prosthet Dent. 2006;96(1):33-40. doi:10.1016/j.prosdent.2006.04.012
34. Franco LM, Machado LS, Salomão FM, Dos Santos PH, Briso ALF, Sundfeld RH. Surface effects after a combination of dental bleaching and enamel microabrasion: an in vitro and in situ study. Dent Mater J. 2016;35(1):13-20. doi:10.4012/dmj.2014-334
35. Catelan A, Suzuki TYU, Becker F Jr, Briso ALF, Dos Santos PH. Influence of surface sealing on color stability and roughness of composite submitted to ultraviolet-accelerated aging. J Investig Clin Dent. 2017;8(2):e12203. doi:10.1111/jicd.12203
37. Nomoto R, McCabe JF. Effect of mixing methods on the compressive strength of glass ionomer cements. J Dent. 2001;29(3):205-210. doi:10.1016/s0300-5712(01)00010-0
38. Strazzi-Sahyon HB, Chimanski A, Yoshimura HN, Dos Santos PH. Effect of previous photoactivation of the adhesive system on the color stability and mechanical properties of resin components in ceramic laminate veneer luting. J Prosthet Dent. 2018;120(4):631.e1-631.e6. doi:10.1016/j.prosdent.2018.06.014
39. Diaz-Arnold AM, Dunne JT, Jones AH. Microhardness of provisional fixed prosthodontic materials. J Prosthet Dent. 1999;82(5):525-528. doi:10.1016/s0022-3913(99)70050-8
40. Bollen CM, Lambrechts P, Quirynen M. Comparison of surface roughness of oral hard materials to the threshold surface roughness for bacterial plaque retention: a review of the literature. Dent Mater. 1997;13(4):258-269. doi:10.1016/s0109-5641(97)80038-3
41. Da Fonte Porto Carreiro A, Dos Santos Cruz CA, Vergani CE. Hardness and compressive strength of indirect composite resins: effects of immersion in distilled water. J Oral Rehabil. 2004;31(11):1085-1089. doi:10.1111/j.1365-2842.2004.01147.x
42. Okte Z, Villalta P, García-Godoy F, Lu H, Powers JM. Surface hardness of resin composites after staining and bleaching. Oper Dent. 2006;31(5):623-628. doi:10.2341/05-124
ORAL DIAGNOSIS
Tanya M. Gibson, DDS
Heart-shaped radiolucency
(Case courtesy of Dr Albana Simoni, O’Fallon, Missouri.)
An 18-year-old man presented with an asymptomatic unilocular radiolucency of the anterior maxilla that was present for more than 1 year. A panoramic radiograph revealed a welldefined, heart-shaped radiolucency located in the midline of
the maxilla between the central incisors (Figure). Both teeth tested vital. There was no evidence of expansion noted on clinical examination.
Gingival yellow spot
(Case courtesy of Dr Nabil Beaini, Columbia, Missouri.)
A 61-year-old man presented for evaluation of an asymptomatic yellowish submucosal granule located in the buccal gingiva apical to the maxillary right first premolar (Figure). The patient noticed it several months prior. The area was firm to clinical
Figure. Firm, yellowish submucosal granule located on the buccal gingiva apical to the right first premolar.
Which of the following is the most appropriate diagnosis?
A. incisive canal
B. nasopalatine duct cyst
C. median palatine cyst
D. primordial cyst
Diagnosis is on page 80.
palpation. The patient did not report any history of trauma to that area, nor were any gross carious lesions present. Radiographic examination did not reveal any abnormalities.
Which of the following is the most appropriate diagnosis?
A. Fordyce granule
B. parulis
C. pseudomembranous candidiasis
D. sialolith
Diagnosis is on page 80.
Author affiliation
Department of Oral Pathology, Radiology and Medicine, School of Dentistry and School of Graduate Studies, University of Missouri – Kansas City.
Figure. Well-defined heart shaped radiolucency located in the midline of the maxilla between the vital central incisors.
GENERAL DENTISTRY SELF-INSTRUCTION ANSWERS
Exercise No. GD533
September/October 2024, p. 19
1. B
2. C
3. A 4. D
5. C 6. C 7. A 8. C 9. A 10. B 11. D 12. C 13. B 14. B 15. B
Exercise No. GD534
September/October 2024, p. 26
1. C
2. C
3. A
4. C
5. B
6. D 7. C 8. C 9. B 10. A 11. C 12. D 13. B 14. D 15. C
Exercise No. GD535
September/October 2024, p. 42
1. D
2. C 3. B 4. A 5. D 6. A 7. D 8. D 9.
Look for these articles and more in the November/December 2025 issue of General Dentistry:
• Failures and successes of vital pulp therapy in an undergraduate dental clinic
• Recurrence of clinical symptoms in an endodontically treated tooth following COVID-19 vaccination: a case report
• Practical implementation of caries disease management in the era of CAMBRA: a guide for the general dentist
In the September issue of AGD Impact
• Exploring the Overlap of Personal and Professional Lives in Dentistry
• What Dentists Need to Know About New Tax Laws in 2026
In the October issue of AGD Impact
• Testing the Tools: Green Products
• Debunking the Latest Dental Hacks: Why You Should Never DIY Your Smile
HAVE YOU MOVED?
If you have recently moved, or plan to in the near future, please make sure to update your AGD profile.
Log into the AGD website today! We want to make sure you receive AGD publications and other important information from us! View or update your profile, check the status of your membership dues, manage your email subscriptions and change your password.
Please contact the AGD Membership Services Center with any questions at 888.243.3368 (toll-free) or 312.440.4300. Our member representatives are available to assist you Monday through Friday from 7:30 a.m. to 5:30 p.m. CST.
Heart-shaped radiolucency
Diagnosis
B. nasopalatine duct cyst
The nasopalatine duct cyst, also referred to as an incisive canal cyst, is the most common developmental nonodontogenic cyst, affecting approximately 1% of the population.1 It can develop at any age but is mostly seen in patients between the ages of 30 and 59.1 Due to its developmental origin, it will only be found in the midline of the maxilla near the incisive canal between the maxillary central incisors. It is usually asymptomatic and discovered on routine radiographic examination. The nasopalatine duct cyst presents as an oval or round radiolucency and rarely causes expansion or root resorption.1 On occasion, superimposition of the nasal spine can be observed, yielding the classic heart-shaped radiolucency.1
The vitality of the adjacent teeth should be confirmed, because inflammatory odontogenic pathoses, such as periapical cyst and periapical granuloma, can mimic the radiographic presentation of a nasopalatine duct cyst. Surgical enucleation is curative, and recurrence is not expected. Biopsy is warranted to rule out other gnathic pathoses.
The incisive canal is an anatomical landmark located in the midline of the anterior maxilla. This bony canal serves as a passageway for nasopalatine nerves and vessels and contains remnants of the epithelial nasopalatine duct, which can give
Gingival yellow spot
Diagnosis
A. Fordyce granule
Fordyce granules are ectopic sebaceous glands: adnexal structures that are typically found in the skin. When sebaceous glands are located in the oral cavity they are referred to as Fordyce granules or ectopic sebaceous glands. Fordyce granules are considered a variation of normal, affecting more than 80% of the population.1 They present as small, yellowish granules located just beneath the mucosal surface, most commonly on the buccal mucosa and the lateral vermilion of the upper lip, but they can be found throughout the oral cavity.1
Fordyce granules are asymptomatic, and patients are usually unaware of their presence. When they present as multiple submucosal granules or are multifocal, their clinical presentation is usually characteristic enough that a biopsy is not required to make a diagnosis. However, when the gland presents as a solitary granule, it can pose a diagnostic challenge, necessitating a biopsy to confirm the diagnosis.
A parulis, commonly referred to as a gum boil, is the intraoral terminal end of a draining sinus tract, which can occur as a result of pulpal disease. Often pus can be extruded clinically from the parulis, and periapical pathosis associated with the offending nonvital tooth can be visualized on radiographs as a periapical radiolucency. If there is any doubt as to which tooth is the offending tooth, gutta percha can be used to
rise to the epithelium lining of the nasopalatine duct cyst.1 Radiographically, it presents as a well-defined or ill-defined radiolucent area that typically measures around 6 mm. If the width exceeds 1 cm or there is evidence of enlargement, it should be considered pathologic, and a biopsy is warranted.
The median palatine cyst has a similar radiographic presentation to the nasopalatine duct cyst, but it is more posteriorly located. It presents as a radiolucency in the palatal midline, and is not intimately associated with the roots of the maxillary central incisors. Often, it will present with clinical enlargement of the palate. A biopsy is required for diagnosis, and recurrence is not expected following surgical removal.
The term primordial cyst is primarily used as a radiographic diagnosis. This term is applicable to a well-defined, radiolucent lesion that occurs in lieu of a congenitally missing tooth. To determine the exact gnathic pathosis, a biopsy is required, and the likelihood of recurrence and required treatment would be based on the microscopic diagnosis.
Reference
1. Neville BW, Damm DD, Allen CM, Chi AC. Oral and Maxillofacial Pathology. 5th ed. Saunders/Elsevier; 2024:172-173.
trace the route of the infection from the parulis orifice to the offending tooth. Treatment with appropriate medications and surgical and/or nonsurgical management of the affected tooth are required. If tissue is removed as part of the management strategy, histologic analysis should be performed.
Pseudomembranous candidiasis is an infection on the surface of the epithelium and presents with a white, “cottage cheese” appearance that wipes off, leaving an erythematous background. Most often it is diagnosed by its clinical appearance, or a culture or cytology smear can be used to confirm the diagnosis. It does not present as a submucosal granule.
Pseudomembranous candidiasis requires treatment with the appropriate antifungal medication.
A sialolith is a calcification that occurs in association with the salivary gland ductal system. It is often accompanied by a history of pain or episodic swelling, requiring surgical or nonsurgical intervention to relieve the blockage and symptoms. A sialolith is not expected within the gingival tissue, because there is an absence of salivary gland tissue.
Reference
1. Neville BW, Damm DD, Allen CM, Chi AC. Oral and Maxillofacial Pathology. 5th ed. Saunders/Elsevier; 2024:86-87.
Refer a Colleague, Get Rewarded
AGD Referral Rewards Program
Refer your colleagues to join AGD now, and they’ll get 50% off AGD’s 2025 dues.*
You’ll both also earn $50 in Referral Rewards once they join!
Learn More agd.org/refer
“AGD has been pivotal in shaping my career through its quality education and relationships among the members. I wouldn’t be where I am today without AGD!”
Amanda Sonntag, DDS, MAGD
Wyomissing, PA Member since 2014
*Half-year rate does not apply towards constituent and component portion of dues. Half-year rate does not apply for memberships that expired on Dec. 31, 2024, residents or new dentists who graduated in 2024 or 2025. Members who pay half year dues may record CE starting on July 1, 2025.